WO2018003995A1 - 免疫チェックポイント阻害薬使用における免疫関連副作用の予測方法 - Google Patents
免疫チェックポイント阻害薬使用における免疫関連副作用の予測方法 Download PDFInfo
- Publication number
- WO2018003995A1 WO2018003995A1 PCT/JP2017/024244 JP2017024244W WO2018003995A1 WO 2018003995 A1 WO2018003995 A1 WO 2018003995A1 JP 2017024244 W JP2017024244 W JP 2017024244W WO 2018003995 A1 WO2018003995 A1 WO 2018003995A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- antibody
- administration
- scd163
- cxcl5
- side effects
- Prior art date
Links
Images


Classifications
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2818—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against CD28 or CD152
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/435—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- C07K14/52—Cytokines; Lymphokines; Interferons
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K14/00—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- C07K14/435—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- C07K14/705—Receptors; Cell surface antigens; Cell surface determinants
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/24—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against cytokines, lymphokines or interferons
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2827—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against B7 molecules, e.g. CD80, CD86
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/15—Medicinal preparations ; Physical properties thereof, e.g. dissolubility
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/5005—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving human or animal cells
- G01N33/5008—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving human or animal cells for testing or evaluating the effect of chemical or biological compounds, e.g. drugs, cosmetics
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6893—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids related to diseases not provided for elsewhere
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/52—Assays involving cytokines
- G01N2333/521—Chemokines
- G01N2333/522—Alpha-chemokines, e.g. NAP-2, ENA-78, GRO-alpha/MGSA/NAP-3, GRO-beta/MIP-2alpha, GRO-gamma/MIP-2beta, IP-10, GCP-2, MIG, PBSF, PF-4 or KC
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/70596—Molecules with a "CD"-designation not provided for elsewhere in G01N2333/705
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/52—Predicting or monitoring the response to treatment, e.g. for selection of therapy based on assay results in personalised medicine; Prognosis
Definitions
- the present invention relates to a novel method for predicting the onset of side effects resulting from administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof.
- Cancer cells prevent the attack of immune cells by reducing the activity of immune cells that attack the cancer cells. This mechanism is called “immune checkpoint”. Therefore, by inhibiting this “immune checkpoint”, the action of immune cells can be activated again to attack cancer cells.
- An immune checkpoint inhibitor is a drug that activates immune cells whose activity has been lowered by cancer cells and attacks cancer cells.
- immune checkpoint inhibitors include anti-PD-1 antibody and anti-CTLA4 antibody.
- Nivolumab and pembrolizumab which are anti-PD-1 antibodies, are known to be useful for the treatment of malignant melanoma, and have also been reported to have therapeutic effects on non-small cell lung cancer and renal cell carcinoma (Patent Document 1).
- anti-CTLA4 antibodies ipilimumab or tremelimumab are useful for the treatment of melanoma and other malignant tumors (Patent Document 2).
- autoimmune-related side effects caused by administration of immune checkpoint inhibitors are more frequent than conventional drugs.
- the incidence of Grade 3 or higher adverse events when anti-PD-1 antibody (nivolumab) or anti-CTLA4 antibody (ipilimumab) is administered to patients with unresectable malignant melanoma is 16.3% for nivolumab alone
- ipilimumab alone is 27.3%
- ipilimumab and ipilimumab are used in combination is 55.0% (Non-patent Document 1).
- the present invention relates to the development of side effects in subjects administered with at least one antibody drug selected from anti-PD-1 antibodies, anti-PD-L1 antibodies, anti-CTLA4 antibodies and antigen-binding fragments thereof, which are immune checkpoint inhibitors.
- the purpose is to provide a new technical means for predicting the possibility (risk) of this.
- the present inventors have identified sCD163 in a biological sample collected from a subject administered with at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof. It was also found that by measuring the level of at least one marker selected from CXCL5, the onset of side effects caused by administration of the antibody drug can be predicted.
- the following inventions are provided.
- a method Measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject administered the antibody drug.
- the marker is a combination of sCD163 and CXCL5.
- the level of the marker in a biological sample collected from a subject administered with the antibody drug and the level of the corresponding marker in a biological sample collected from the subject prior to administration of the antibody drug The method according to any one of (1) to (6), comprising obtaining comparison data.
- the method according to (7), wherein the level of the marker or the comparison data in a biological sample collected from a subject to which the antibody drug is administered serves as an index for developing a side effect.
- a method for monitoring side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof Measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject administered the antibody drug.
- side effects caused by administration of the antibody drug A marker comprising sCD163 or CXCL5 for predicting onset.
- Anti-sCD163 antibody for predicting the onset of side effects resulting from administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof
- a diagnostic agent comprising at least one component selected from anti-CXCL5 antibodies and antigen-binding fragments thereof.
- Anti-sCD163 antibody for predicting the onset of side effects resulting from administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof
- a diagnostic kit comprising at least one component selected from anti-CXCL5 antibodies and antigen-binding fragments thereof.
- the method of the present invention is advantageous in that the occurrence of a side effect is predicted in advance and a drug is administered to prevent, suppress or delay the occurrence of the side effect, or reduce the side effect. Moreover, by using the method of the present invention, it is possible to predict the occurrence of side effects and reduce the damage caused by side effects. Moreover, by using the method of the present invention, it is possible to predict the onset of side effects resulting from the administration of the antibody drug by simple means.
- A is a graph showing changes in serum sCD163 concentration before and after nivolumab administration for each patient who received nivolumab.
- B is a graph showing changes in serum CXCL5 concentration before and after nivolumab administration for each patient who received nivolumab.
- concentration is shown.
- the method of the present invention comprises at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof.
- One feature is measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from an administered subject.
- the marker used is preferably a combination of sCD163 and CXCL5. According to such a method, it is possible to predict the onset of side effects based on the obtained data.
- the method of the present invention comprises the level of the marker in a biological sample collected from a subject administered with the antibody drug, and the corresponding marker in the biological sample collected from the subject prior to administration of the antibody drug.
- Obtaining comparison data with the level refers to, for example, the level difference or ratio.
- the level of the marker or the comparison data in a biological sample collected from a subject to which the antibody drug is administered is an index for developing a side effect.
- the level of the marker or the comparative data in a biological sample collected from a subject to which the antibody drug has been administered is an index for administering a drug, preferably a steroid, to the subject.
- the above comparative data is preferable as an index for developing the above-mentioned side effects or an index for administering a drug, preferably a steroid, to a subject.
- the marker level will be described later.
- sCD163, CXCL5 Side effects caused by administration of the antibody drug in a subject administered with at least one antibody drug selected from the anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof of the present invention
- Markers for predicting onset comprise sCD163 or CXCL5.
- CD163 in the present invention is a single-chain transmembrane protein, a member of the scavenger receptor cysteine-rich family, and is used interchangeably with “M130”.
- sCD163 (soluble CD163)” is obtained by cutting CD163 into a soluble type.
- SCD163 in the present invention may include variants, isoforms, and species homologs of sCD163.
- CXCL5 in the present invention is a neutrophil / monocyte chemotactic protein, and is a member of the ELR + group having the ELR motif on the N-terminal side of the CXC motif, “LIX” and “GCP-2” And may include CXCL5 variants, isoforms, and species homologs.
- the level of at least one marker selected from sCD163 and CXCL5 in the biological sample is, for example, the concentration or amount of the marker in the biological sample, and preferably the concentration of sCD163 in the biological sample. Or the concentration of CXCL5.
- the concentration of sCD163 to be measured includes, for example, a concentration in the range of 1 ng / mL to 500 ng / mL.
- the concentration of CXCL5 to be measured includes, for example, concentrations in the range of 10 pg / mL to 10000 pg / mL, 10 pg / mL to 5000 pg / mL.
- the “antibody” in the present invention is a full-length antibody, and comprises at least two heavy chains (H) and two light chains linked by disulfide bonds.
- Each heavy chain is composed of a heavy chain variable region (hereinafter sometimes abbreviated as V H ) and a heavy chain constant region.
- the heavy chain constant region is comprised of three domains, C H 1, C H 2 and C H 3.
- Each light chain is composed of a light chain variable region (hereinafter sometimes abbreviated as VL ) and a light chain constant region.
- the light chain constant region is comprised of one domain C L.
- V H and V L regions are further subdivided into regions of high variability called complementarity determining regions (CDRs), which are called framework regions (FR) and are more conserved regions Are scattered.
- CDRs complementarity determining regions
- FR framework regions
- the variable regions of the heavy and light chains contain a binding domain that interacts with an antigen.
- antibodies include monoclonal antibodies, polyclonal antibodies, bispecific antibodies, low molecular weight antibodies, domain antibodies, synthetic antibodies, chimeric antibodies, humanized antibodies, human antibodies, antibody conjugates, single chain antibodies. , Antibody derivatives, antibody analogs, and respective antigen-binding fragments thereof.
- an “antigen-binding fragment” (or simply referred to as “antibody fragment”) of an antibody in the present invention refers to one or more fragments of an antibody that retains the ability to specifically bind to an antigen (eg, PD-1). It is shown.
- binding fragments included in an “antigen-binding fragment” of an antibody include (i) a Fab fragment that is a monovalent fragment composed of V L , V H , C L and C H 1 domains, and (ii) a hinge region F (ab ′) 2 fragment, which is a divalent fragment containing two Fab fragments linked by a medium disulfide bridge, (iii) Fd fragment composed of V H and C H 1 domains, (iv) Single antibody Fv fragments composed of VL and VH domains of arms, (v) dAb fragments composed of VH domains, or (vi) isolated complementarity determining regions (CDRs).
- a Fab fragment that is a monovalent fragment composed of V L , V H , C L and C H 1 domains
- a hinge region F (ab ′) 2 fragment which is a divalent fragment containing two Fab fragments linked by a medium disulfide bridge
- Fd fragment composed of V H and C H 1 domains
- the two domains of the Fv fragment, VL and VH are encoded by separate genes, they can be linked by a synthetic linker that can be made as a single protein chain using recombinant techniques; In this chain, the VL and VH regions can be paired to form a monovalent molecule (single chain Fv (scFv)).
- single chain Fv single chain Fv
- Such single chain antibodies are also included in “antigen-binding fragments” of antibodies.
- PD-1 is an immune receptor that mediates a signal for regulating an immune response, and is a type I membrane protein belonging to the CD28 / CTLA-4 family.
- PD-1 in the present invention is used interchangeably with “Programmed Death 1”, “Programmed Cell Death 1”, “Protein PD-1”, “PD1”, “PDCD1”, and “hPD-1”, and modification of PD-1 Bodies, isoforms, species homologs, and analogs having at least one common epitope with PD-1.
- the “anti-PD-1 antibody” in the present invention is not particularly limited as long as it does not interfere with the effects of the present invention, and may be an antibody that specifically binds to PD-1.
- Such an antibody may be an antibody that specifically recognizes part of the structure of the amino acid sequence, or may be an antibody that specifically recognizes the entire structure.
- the antibody is not particularly limited, and examples thereof include nivolumab, pembrolizumab, and lambrolizumab, preferably nivolumab or pembrolizumab.
- CTLA4 in the present invention is a regulatory factor that suppresses activation of T cells, and includes “cytotoxic T lymphocyte-associated antigen-4”, “CTLA-4”, “CTLA-4 antigen” and “CD152”. And may include human CTLA4 variants, isoforms, species homologs, and analogs having at least one common epitope with CTLA4.
- the “anti-CTLA4 antibody” in the present invention is not particularly limited as long as the effects of the present invention are not hindered, and may be an antibody that specifically binds to CTLA4.
- Such an antibody may be an antibody that specifically recognizes part of the structure of the amino acid sequence, or may be an antibody that specifically recognizes the entire structure.
- the antibody is not particularly limited, but is preferably ipilimumab or tremelimumab.
- PD-L1 in the present invention is a ligand of PD-1, and is used interchangeably with “CD274”, “ProgrammedCellDeath1Ligand1”, “PDCD1L1”, “B7-H”, and “B7H1”. Variants, isoforms, species homologues, and analogs having at least one common epitope with PD-L1.
- the “anti-PD-L1 antibody” in the present invention is not particularly limited as long as the effects of the present invention are not hindered, and may be an antibody that specifically binds to PD-L1.
- Such an antibody may be an antibody that specifically recognizes part of the structure of the amino acid sequence, or may be an antibody that specifically recognizes the entire structure.
- the antibody is not particularly limited, but is preferably MPDL3280A (RG7446) or atezolizumab.
- the “antibody drug” in the present invention is at least one selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody, and antigen-binding fragments thereof. Only one type of the antibody or antigen-binding fragment thereof may be administered to the subject, or two or more types may be combined and administered to the subject simultaneously or separately. Examples of combinations of two or more include a combination of an anti-PD-1 antibody and an anti-CTLA4 antibody.
- the method for administering the antibody is not particularly limited, but intravenous administration is preferred.
- the subject of the present invention is preferably a human, more preferably treated by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof.
- treatment includes not only treating an established pathological condition but also preventing a pathological condition that may be established in the future.
- the antibody drug may be an anticancer agent.
- cancersarcoma, or malignant mesothelioma include malignant melanoma (eg, metastatic malignant malignant melanoma, unresectable malignant melanoma), cutaneous squamous cell carcinoma, extramammary Paget Disease, or skin cancer such as Merkel cell carcinoma; kidney cancer (eg, renal cell carcinoma, clear cell carcinoma); prostate cancer (eg, hormone refractory prostate adenocarcinoma); breast cancer; colon cancer; lung cancer (eg, non-small) Bone cancer; Pancreatic cancer; Head and neck cancer; Skin or orbital malignant melanoma; Uterine cancer; Ovarian cancer; Rectal cancer; Anal cancer; Gastric cancer; Testicular cancer; Uterine carcinoma; Cervical carcinoma; vaginal carcinoma; vulvar carcinoma; esophageal carcinoma; small intestine cancer; colon cancer; endocrine cancer; thyroid cancer; parathyroid cancer; adrenal cancer; soft tissue sarcoma; multiple mye
- the side effect resulting from the administration of the antibody drug in the present invention is not particularly limited, but immune-related side effects (side effects presumed to be related to immunity: irAE) are preferable (for example, pharmaceutical interview form Opdivo®).
- the side effect of the present invention include interstitial lung disease, myasthenia gravis, myositis, colitis, type 1 diabetes, liver dysfunction (liver disorder), hepatitis (for example, autoimmunity)
- Pulmonary disorders such as pneumonia, hypopituitarism, pituitary dysfunction such as hypophysitis, thyroid dysfunction such as hypothyroidism, neuropathy, renal disorder, encephalitis, adrenal dysfunction such as adrenal insufficiency, severe Skin disorders, venous thromboembolism, infusion reaction, psoriasis, psoriatic rash, diarrhea (eg, severe diarrhea), rheumatoid arthritis, uveitis, episclerosis, synovial bursitis, exacerbation of radioactive dermatitis, Chronic inflammatory demyelinating polyneuritis (hereinafter also referred to as demyelinating polyneuritis), biliary dysfunction or nephritis can be mentioned, and pituit
- irAE immune-related side effects
- grade or “irAE assessment”.
- irAE evaluation is an index representing the severity of a disease and is represented by 1 to 3. 1 indicates a state that “additional treatment intervention is not necessary for irAE”, and 2 indicates “drug intervention is required for irAE but hospitalization treatment is not required, or treatment interruption is required. 3 indicates a state that “drug intervention with hospitalization is necessary for irAE, and that treatment is interrupted”.
- grade irAE evaluation” is an index representing the severity of a disease and is represented by 1 to 3. 1 indicates a state that “additional treatment intervention is not necessary for irAE”, and 2 indicates “drug intervention is required for irAE but hospitalization treatment is not required, or treatment interruption is required. 3 indicates a state that “drug intervention with hospitalization is necessary for irAE, and that treatment is interrupted”. The correspondence between “irAE evaluation” and “grade” varies depending on each disease.
- the biological sample examples include serum, plasma, blood, urine and the like, preferably serum.
- the biological sample is collected before the onset of the side effect from the viewpoint of preventing the onset of the side effect.
- the occurrence of the side effect include before the administration of the antibody drug, after the administration of the antibody drug, or both.
- the antibody drug may be included at the time of administration or immediately after administration.
- after administration of the antibody drug for example, within 12 weeks after administration of the antibody drug, preferably within 8 weeks, more preferably within 6 weeks.
- the antibody drug may be administered before the first administration and after the first administration, respectively.
- the collection time of the biological sample is not limited from the viewpoint of monitoring and confirmation of the effects of the drug described later, and the period after administration of the antibody drug is not limited, after administration of the antibody drug, Furthermore, you may measure 2 times or more after administration.
- any currently known method can be employed to measure sCD163 or CXCL5.
- immunoassay electrophoresis, western blotting, mass spectrometry and the like can be mentioned, and immunoassay is preferable.
- the immunoassay examples include an immunoturbidimetric assay and an enzyme immunoassay.
- the immunoassay is an immunoassay for measuring protein or the like as an antigen, and the antibody is not particularly limited as long as it does not interfere with the effects of the present invention.
- At least one selected component can be used, and preferably a polyclonal antibody or a monoclonal antibody thereof can be used.
- a commercially available antibody can be used, and it can also be produced by a known method.
- the anti-sCD163 antibody or the anti-CXCL5 antibody is not particularly limited as long as it can specifically bind to sCD163 or CXCL5, respectively, and may be an antibody that specifically recognizes part of the structure of the amino acid sequence. It may be an antibody that specifically recognizes.
- sCD163 or CXCL5 in a biological sample is reacted with at least one component selected from anti-sCD163 antibody, anti-CXCL5 antibody and their antigen-binding fragments, and an antigen-antibody reaction is carried out.
- at least one component selected from anti-sCD163 antibody, anti-CXCL5 antibody and their antigen-binding fragments and an antigen-antibody reaction is carried out.
- an antigen-antibody reaction is carried out.
- TIA method is a method for measuring the degree of turbidity at a specific absorbance in an immunoturbidimetric assay.
- the latex immunoturbidimetric method is a method in which at least one component selected from an anti-sCD163 antibody, an anti-CXCL5 antibody and an antigen-binding fragment thereof is bound to latex particles in an immunoturbidimetric assay. It is a method of measuring.
- the nepherometry method is a method for measuring the degree of turbidity in the immunoturbidimetric method by collecting light scattered to a magnitude of a certain angle or more and measuring it as scattered light.
- Examples of the enzyme immunoassay include EIA methods such as ELISA using a plate as a support.
- EIA methods such as ELISA using a plate as a support.
- a solid phase as a primary antibody.
- sCD163 or CXCL5 is measured by enzyme immunoassay, for example, a biological sample for measuring sCD163 or CXCL5 is added to the primary antibody bound to the solid phase and reacted. After reacting for a certain period of time, the solid phase is washed and a secondary labeled antibody is added to carry out a secondary reaction. The solid phase is washed again and the labeled moiety bound to the solid phase is measured.
- an enzyme such as horseradish peroxidase (HRP) alkaline phosphatase can be used as the labeling substance.
- HRP horseradish peroxidase
- the labeling substance is not only an enzyme such as gold colloid, europium, but also various chemical and biological fluorescent substances such as FITC, rhodamine, Texas Red, Alexa, GFP, 32 P, 51 Any substance that can be labeled, such as a radioactive substance such as Cr, can be mentioned.
- an avidin-biotin system or a streptavidin-biotin system can also be used.
- streptavidin or avidin labeled with an enzyme such as HRP can be used together with a secondary labeled antibody labeled with biotin.
- chemiluminescence immunoassay using a luciferase-labeled antibody fluorescent immunoassay using a fluorescent dye-labeled antibody, flow cytometry, and the like can be given.
- an SDS-PAGE method can be generally used.
- Protein staining includes Coomassie brilliant blue, Ponceau S staining, amide black staining, and a method using direct enzyme activity.
- the electrophoresed gel is transferred to a nitrocellulose membrane, a PVDF membrane or the like, and then at least one component selected from anti-sCD163 antibody, anti-CXCL5 antibody and their antigen-binding fragments as primary antibodies,
- the next labeled antibody such as HRP-labeled anti-IgG
- HRP color reagent an HRP color reagent
- sCD163 or CXCL5 can be measured by the degree of color development of a band corresponding to sCD163 or CXCL5.
- mass spectrometry examples include an analysis method using a mass analyzer.
- a mass analyzer For example, surface enhanced laser desorption ionization (Surface Enhanced Laser Desorption / Ionization) time-of-flight mass spectrometer (SELDI-TOF MS method), matrix-assisted laser ionization (Matrix-Assisted Laser Desorption / Ionization) time-of-flight mass spectrometer Examples thereof include a method using MALDI-TOF MS method) and ESI method (Electrospray Ionization).
- the SELDI-TOF MS method is preferable because an ion spectrum with a high reproducible S / N ratio is obtained because impurities are removed while the target substance is uniformly trapped on the functional group on the chip surface and ionized with laser light. .
- the anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody, and at least one antibody drug selected from antigen-binding fragments thereof are collected from a subject who has been administered (ie, after administration). It is preferred to compare the level of at least one marker selected from sCD163 and CXCL5 in a biological sample with the level of the corresponding marker in a biological sample taken from the subject prior to administration.
- the present invention is collected from a subject prior to administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof.
- the level of at least one marker selected from sCD163 and CXCL5 in a biological sample can be measured by the above measurement method, and measurement by the ELISA method is preferable.
- the prediction step does not include judgment by a doctor.
- the prediction of the occurrence of a side effect means that, in addition to predicting the occurrence of a side effect before the side effect occurs, the side effect has occurred when the grade of the side effect is low Including forecasts.
- the low grade of side effects is preferably 1 to 2.
- predicting the occurrence of a side effect includes predicting that a side effect has occurred when the immune-related side effect (irAE) rating is low.
- the low irAE evaluation is preferably 1 to 2.
- the difference or ratio of the level of at least one marker selected from sCD163 and CXCL5 in the biological sample before and after administration of the antibody drug in the subject (group) that has developed side effects, and the occurrence of side effects Statistical differences may be performed by comparing the differences or ratios of the levels of corresponding markers in non-subject subjects (groups). Moreover, when the level of the marker is measured twice or more after administration of the antibody drug, the difference or ratio of the marker levels at any two measurement points may be compared.
- the difference or ratio in the level of the marker used was determined as the possibility of the occurrence of side effects.
- Prediction of the onset of side effects caused by administration of the antibody drug of the present invention is, for example, that the level of sCD163 in a biological sample collected from a subject after administration of the antibody drug is the biological level of the subject before administration.
- the level of sCD163 in the sample it can be performed based on an index that the possibility of developing a side effect is high.
- the level of sCD163 in the biological sample collected from the subject after administration of the antibody drug is preferably 1.2 times or more compared to the level of sCD163 in the biological sample collected from the subject before administration, More preferably 1.5 times or more, even more preferably 1.6 times or more, even more preferably 1.8 times or more, and even more preferably 2 times or more, it is predicted that there is a high possibility of developing a side effect be able to.
- the sCD163 concentration in the biological sample collected from the subject after administration of the antibody drug is preferably 10 ng / mL, more preferably 15 ng / mL, compared to the sCD163 concentration in the subject biological sample before administration. More preferably, when it is 20 ng / mL, even more preferably 40 ng / mL or more, it can be predicted that there is a high possibility of developing a side effect.
- Prediction of the onset of side effects caused by administration of the antibody drug of the present invention is, for example, that the level of CXCL5 in a biological sample collected from a subject after administration of the antibody drug is the biological level of the subject before administration. When it is higher than the CXCL5 level in the sample, it can be performed based on an index that the possibility of developing a side effect is high.
- the CXCL5 level in the biological sample collected from the subject after administration of the antibody drug is preferably 1.05 times or more, more preferably compared to the CXCL5 level in the subject biological sample before administration. Is 1.1 times or more, more preferably 1.2 times or more, and even more preferably 1.3 times or more, it can be predicted that the possibility of developing a side effect is high.
- the concentration of CXCL5 in the biological sample collected from the subject after administration of the antibody drug is preferably 50 pg / mL, more preferably 100 pg, compared to the concentration of CXCL5 in the subject biological sample before administration. / ML, more preferably when it is higher than 150 pg / mL, it can be predicted that there is a high possibility of developing a side effect.
- the level of at least one marker selected from sCD163 and CXCL5 measured in a subject is a preset threshold for the onset of side effects caused by administration of the antibody drug. If it deviates from the above, it can be predicted that there is a high possibility of developing a side effect.
- the case of deviating from the preset threshold value means, for example, a case where the level of the marker is the same as or higher than the preset threshold value, and when the threshold value has an upper limit value and a lower limit value as will be described later. A case where the level of the marker is the same as or higher than the upper limit value, or the same as the lower limit value or lower than the upper limit value.
- the threshold value can be set in advance.
- a threshold can be set in advance based on the difference or ratio of the marker levels at any two measurement points. Prediction of the onset of a side effect may be performed by comparing the threshold value with a level difference or level ratio of a corresponding marker of a subject who predicts the onset of a side effect.
- the threshold value can be appropriately set based on the level difference or level ratio of markers selected from sCD163 and CXCL5 before and after administration of the antibody drug.
- the threshold value is not particularly limited.
- the average value of the level difference or ratio of the above markers in the subject (group) who developed side effects, the subject (group) who does not develop side effects, or all subjects (group), and the center Value, X percentile value can be used, preferably an average value.
- any numerical value can be selected for X, and 3, 5, 10, 15, 20, 30, 40, 60, 70, 80, 85, 90, 95, and 97 can be appropriately used.
- the threshold may be one, or a plurality of thresholds may be set according to the type of side effect, the type of antibody drug to be administered, the condition of the subject to which the antibody drug is administered, the type of marker to be measured, or a combination thereof.
- the threshold value for example, the average value of the level difference or ratio of the markers in biological samples collected from subjects (groups) that develop side effects, subjects (groups) that do not develop side effects, or all subjects (groups), A specific numerical value range can be provided around the median value and the X percentile value.
- the numerical range is the level difference or ratio of the marker before and after administration of the antibody drug in the subject (group) who developed side effects, and the level difference or ratio of the marker before and after administration of the antibody drug in the subject (group) that does not develop side effects. And can be determined based on the ratio. Alternatively, the numerical value range can be determined based on the level difference or ratio of the marker before and after administration of the antibody drug in all subjects (group). As the numerical value range, for example, the standard deviation or standard error of the level difference or ratio of the marker before and after administration of the antibody drug for all subjects (group) can be used.
- an ROC curve may be created using the level difference or ratio of the marker before and after administration of the antibody drug for all subjects (group), and an upper limit value and a lower limit value may be set.
- the said threshold value has a numerical value range, there exists an upper limit and a lower limit.
- the level difference or ratio of the marker before and after administration of the antibody drug in the subject (group) that developed side effects and the level difference of the marker before and after administration of the antibody drug in the subject (group) that does not develop side effects Alternatively, specific upper and lower limits can be set based on the ratio or based on the level difference or ratio of the markers before and after administration of the antibody drug to all subjects (group).
- the upper limit value and the lower limit value may be set independently, or may be set so that the absolute values of the upper limit value and the lower limit value are the same.
- an ROC curve may be created using all objects (groups), and an upper limit value and a lower limit value may be set.
- any two X percentile values (values of X are different for all objects (groups)). May be set as an upper limit value and a lower limit value.
- the ratio of the level of CXCL5 after administration of the antibody drug to the level of CXCL5 before administration of the antibody drug is preferably 1.05 times or more, more preferably 1.1 times or more, and still more preferably The case of 1.3 times or more, and even more preferably 1.5 times or more is considered significant, and the ratio can be used as a threshold value.
- the ratio of the level of sCD163 after administration of the antibody drug to the level of the corresponding sCD163 before administration of the antibody drug is preferably 1.3 times or more, more preferably 1.5 times or more, and even more preferably 1 .Times.6 times or more, even more preferably 1.8 times or more, and even more preferably 2 times or more is considered significant, and the ratio can be used as a threshold value.
- the threshold value is a value having a specific numerical range centered on the average value of all subjects (groups) of the ratio of the CXCL5 level after administration of the antibody drug to the CXCL5 level before antibody drug administration
- the numerical value range is, for example, 20 to 75%, preferably 30 to 60%, particularly preferably 40 to 50%.
- the threshold value is a value with a specific numerical range centered on the average value of all subjects (group) of the difference between the CXCL5 level after administration of the antibody drug and the CXCL5 level before antibody drug administration
- the numerical range is, for example, 50 to 400 pg / mL, preferably 70 to 200 pg / mL, particularly preferably 100 to 150 pg / mL.
- the threshold value is a value provided with a specific numerical range centering on the average value of all subjects (groups) of the ratio of the level of sCD163 after administration of the antibody drug to the level of sCD163 before administration of the antibody drug
- the numerical value range is, for example, 15 to 50%, preferably 20 to 40%, more preferably 25 to 35%.
- the threshold value is a value with a specific numerical range centered on the average value of all subjects (group) of the difference between the level of sCD163 after administration of the antibody drug and the level of sCD163 before administration of the antibody drug
- the numerical value range is, for example, 1 to 25 ng / mL, preferably 2 to 10 ng / mL, more preferably 2.5 to 5 ng / mL.
- the upper limit value is, for example, 20
- the lower limit is, for example, ⁇ 60 to ⁇ 20%, preferably ⁇ 50 to ⁇ 30%.
- the upper limit value is, for example, 50 to 300 pg.
- the lower limit is, for example, ⁇ 300 to ⁇ 50 pg / mL, preferably ⁇ 200 to ⁇ 100 pg / mL.
- the upper limit value is, for example, 20
- the lower limit value is, for example, ⁇ 40 to 0%, ⁇ 30 to ⁇ 10%, preferably ⁇ 25 to ⁇ 15%.
- the upper limit value is, for example, 7 0.5 to 25 ng / mL, preferably 7.5 to 12.5 ng / mL
- the lower limit is, for example, ⁇ 15 to 2.5 ng / mL, preferably ⁇ 2.5 to 2.5 ng / mL. is there.
- the level of at least one marker selected from sCD163 and CXCL5 after administration of the antibody drug in a subject (group) that has developed a side effect or a subject (group) that does not develop a side effect is determined in advance.
- a threshold can be set. Prediction of the onset of a side effect may be performed by comparing the above threshold value with the level of a corresponding marker of a subject that predicts the onset of a side effect.
- a person skilled in the art appropriately sets a threshold value based on the level of at least one marker selected from sCD163 and CXCL5 after administration of the antibody drug in a subject (group) that develops side effects or a subject (group) that does not develop side effects. be able to.
- the threshold value is not particularly limited. For example, the average value, the median value, and the X percentile value of the marker level of the subject (group) that develops side effects or the subject (group) that does not develop side effects are used.
- the average value is preferable.
- any numerical value can be selected for X, and 3, 5, 10, 15, 20, 30, 40, 60, 70, 80, 85, 90, 95, and 97 can be appropriately used.
- the threshold may be one, or a plurality of thresholds may be set according to the type of side effect, the type of antibody drug to be administered, the condition of the subject to which the antibody drug is administered, the type of marker to be measured, or a combination thereof. .
- the threshold value for example, the average value, median value, and X percentile value of the level of the marker in the biological sample after administration of the antibody drug in the subject (group) that develops side effects or the subject (group) that does not develop side effects
- a specific numerical value range can be provided centering on.
- An average value is preferably used as the central numerical value.
- the numerical range is determined based on the level of the marker after administration of the antibody drug in the subject (group) that developed side effects and the level of the marker after administration of the antibody drug in the subject (group) that does not develop side effects. it can.
- the said threshold value has a numerical value range, there exists an upper limit and a lower limit.
- the threshold is based on the level of the marker after administration of the antibody drug in the subject (group) that developed side effects and the level of the marker before and after administration of the antibody drug in the subject (group) that does not develop side effects.
- Specific upper and lower limits can be set.
- the upper limit value and the lower limit value may be set independently, or may be set so that the absolute values of the upper limit value and the lower limit value are the same.
- side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof are monitored.
- a method comprising measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject administered an antibody drug.
- Such a method can be carried out by a method similar to the method of acquiring data and the method of predicting the onset of side effects.
- Such monitoring is advantageous in confirming the occurrence of side effects or the grade of side effects or irAE evaluation over time in a subject.
- a marker comprising sCD163 or CXCL5 for predicting onset.
- sCD163 alone or CXCL5 alone may be used, sCD163 and CXCL5 may be combined, and further, other markers may be combined.
- the mode of such a marker can be carried out according to the description relating to the method for obtaining data and the method for predicting the onset of side effects.
- diagnostic agents that detect or measure the level of at least one marker selected from sCD163 and CXCL5 to predict the onset.
- diagnostic agent for example, various measurement methods described above can be performed. Examples of the measurement method include immunoassay, electrophoresis, western blotting, mass spectrometry and the like, and immunoassay is preferable.
- immunochromatography is also included as an immunoassay.
- the diagnostic agent can contain, for example, at least one component selected from anti-sCD163 antibody, anti-CXCL5 antibody, and antigen-binding fragments thereof.
- at least one component selected from the anti-sCD163 antibody, anti-CXCL5 antibody and antigen-binding fragments thereof the same antibodies as those in the above-described immunoassay can be used.
- Such an embodiment of the diagnostic agent can be carried out according to the description relating to the method for obtaining data and the method for predicting the onset of side effects.
- kits that detects or measures the level of at least one marker selected from sCD163 and CXCL5 to predict onset.
- these kits can contain various reagents as constituent components according to the measurement method. Examples of the measurement method include immunoassay, electrophoresis, western blotting, mass spectrometry and the like, and immunoassay is preferable.
- immunochromatography is also included as an immunoassay.
- the diagnostic kit can contain, for example, at least one component selected from anti-sCD163 antibody, anti-CXCL5 antibody, and antigen-binding fragments thereof.
- the kit may further contain a well-known reagent according to the measurement method to be performed, such as a coloring reagent for the labeling substance.
- a well-known reagent according to the measurement method to be performed, such as a coloring reagent for the labeling substance.
- the above-described diagnostic kit can be carried out in accordance with the description relating to the method for obtaining data, the method for predicting the onset of side effects, or the diagnostic agent.
- the diagnostic kit can be used for determination of preventive administration of a drug, which will be described later, or for confirming the effect of the administered drug.
- the diagnostic kit comprises at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody, and antigen-binding fragments thereof described below. It can also be used to obtain data for adjusting or determining a test plan for predicting the onset of side effects due to administration.
- collected from a subject administered with at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof collected from a subject administered with at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof.
- a method of maintaining a low grade or irAE rating of low, or a method of improving onset side effects is provided.
- an effective amount of a drug is administered. Or a reduction in the amount of the antibody drug being administered, or cessation or cessation of administration of the antibody drug.
- a drug to be administered a drug that is predicted to develop or is useful for a side effect that has developed is selected.
- steroids such as corticosteroids and immunosuppressive agents can be mentioned.
- steroids include cortisol (hydrocortisone, cortisone), prednisolone (methylprednisolone, prednisolone), triamcinolone.
- the administered drug is preferably an intermediate steroid having a blood half-life of about 3 hours and a biological half-life of 12 to 36 hours, more preferably methylprednisolone or prednisolone.
- the method comprises measuring a level of at least one marker selected from sCD163 and CXCL5 in a biological sample, and determining whether or not to prophylactically administer the drug based on a predicted result of occurrence of a side effect.
- the anti-PD-1 antibody, the anti-PD-L1 antibody, the anti-CTLA4 antibody, and an antigen-binding fragment thereof are collected from a subject administered with at least one antibody drug.
- a method for preventing, suppressing or delaying the onset of the side effect based on the predicted result of the onset of the side effect, by measuring the level of at least one marker selected from sCD163 and CXCL5 in the biological sample A method of maintaining a low side effect grade or irAE rating, or a method of improving onset side effects, comprising the step of administering an effective amount of a drug to a subject in need thereof.
- a method for confirming the effect of an administered drug which is selected from sCD163 and CXCL5 in a biological sample collected from a subject to which the aforementioned drug is administered.
- a method comprising measuring the level of at least one marker.
- the method for confirming the effect of the drug can be performed according to the description relating to the method for predicting the onset of side effects.
- the marker in the biological sample from the subject after the drug administration in the subject whose drug effect is confirmed.
- the level and the level of the marker in a biological sample collected from the subject prior to administration of the antibody drug may be used.
- the drug After administration of the drug, for example, within 12 weeks after administration of the drug, preferably within 9 weeks, more preferably within 6 weeks.
- Examples of the effect of the drug include preventing, suppressing or delaying the onset of side effects, maintaining a low grade of ill side effects or irAE evaluation, or improving onset side effects.
- the effective amount of the drug is not particularly limited, and is appropriately determined by those skilled in the art according to the type, purity, side effect type, degree, target type, nature, sex, age, symptom, and the like of the drug.
- the effective amount includes 0.1 to 20 mg / kg body weight / day, preferably 1.0 to 20 mg / kg body weight / day once or several times.
- the subject of the present invention is a mammal, such as a rodent, dog, cat, cow, primate, etc., preferably a human, more preferably a human suffering from cancer, sarcoma, or malignant mesothelioma It is. It may also be a human administered with a drug, preferably a steroid.
- the occurrence of side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof is a method for assisting in the prediction of blood pressure, comprising measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject administered with the antibody drug. Provided.
- the occurrence of side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof is provided.
- a method comprising measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject to which the antibody drug has been administered.
- the occurrence of side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof comprising measuring the level of at least one marker selected from sCD163 and CXCL5 in a biological sample collected from a subject to which the antibody drug has been administered.
- sCD163 or CXCL5 as a marker for predicting the onset of side effects resulting from administration of an antibody drug.
- the sCD163 or CXCL5 is preferably contained in a biological sample collected from the subject.
- sCD163 or CXCL5 in a subject administered with at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof, there is provided the use of sCD163 or CXCL5 in the manufacture of a marker for predicting the development of side effects due to administration of an antibody drug.
- the occurrence of side effects caused by administration of at least one antibody drug selected from anti-PD-1 antibody, anti-PD-L1 antibody, anti-CTLA4 antibody and antigen-binding fragments thereof is provided.
- a method of obtaining data for adjusting or determining a test plan for prediction of at least one selected from sCD163 and CXCL5 in a biological sample collected from a subject administered with the antibody drug A method comprising measuring the level of one marker is provided. Usually, clinical examinations are performed every 2-3 weeks, which is the dosing interval of the antibody drug.
- the interval can be changed to a shorter interval than usual, for example, every week to twice a week. Furthermore, clinical test items can be changed from normal clinical test items in accordance with the prediction that there is a high possibility of developing side effects.
- Protocol treatment Week 0 (before administration)
- Physical findings ECOG, PS
- Skin findings Presence / absence, size, number of skin metastases
- Blood test blood count: Red blood cells, white blood cells, platelets, hemoglobin level, hematocrit, leukocyte fractionation
- Biochemical tests AST, ALT, ⁇ -GTP, ALP , LDH, total bilirubin, BUN, creatinine, CK, TSH, T3, T4, KL6, cortisol / combination therapy / support therapy: Record the details of the combination therapy / support therapy performed during protocol treatment.
- ⁇ Self-finding findings Grade is determined by CTCAE v4.0-JCOG for the following items. Gastrointestinal disorders, skin and subcutaneous tissue disorders, mental disorders, respiratory organs, thorax and mediastinal disorders Protocol treatment: 3 weeks , physical findings: ECOG, PS ⁇ Skin findings: Presence / absence, size, number of skin metastases ⁇ Blood test (blood count): Red blood cells, white blood cells, platelets, hemoglobin level, hematocrit, leukocyte fractionation ⁇ Biochemical tests: AST, ALT, ⁇ -GTP, ALP , LDH, total bilirubin, BUN, creatinine, CK, TSH, T3, T4, KL6, cortisol / combination therapy / support therapy: Record the details of the combination therapy / support therapy performed during protocol treatment.
- Grade is determined by CTCAE v4.0-JCOG for the following items. Gastrointestinal disorders, skin and subcutaneous tissue disorders, mental disorders, respiratory organs, thorax and mediastinal disorders At the end of protocol treatment (6 weeks) ⁇ Physical findings: ECOG, PS ⁇ Skin findings: Presence / absence, size, number of skin metastases ⁇ Blood test (blood count): Red blood cells, white blood cells, platelets, hemoglobin level, hematocrit, leukocyte fractionation ⁇ Biochemical tests: AST, ALT, ⁇ -GTP, ALP , LDH, total bilirubin, BUN, creatinine, CK, TSH, T3, T4, KL6, cortisol / thoracic CT: Existence of interstitial pneumonia, presence of pleural effusion. Grade is judged by .0-JCOG. Gastrointestinal disorders, skin and subcutaneous tissue disorders, mental disorders, respiratory organs, thorax and mediastinal disorders
- the method of diagnosing the method of assisting the diagnosis of the development of side effects, the use as a marker, the use for the manufacture of markers, the method of obtaining data for determining the plan of the test for the prediction of the development of side effects
- Any aspect can be implemented by the same method as the method of acquiring data and the method of predicting the onset of side effects.
- Test Example 1 Measurement of sCD163 and CXCL5 in serum of patients before and after nivolumab administration
- Eight patients suffering from malignant melanoma administered nivolumab were used as subjects. Of the 8 patients who received nivolumab, 7 had no side effects due to nivolumab administration. On the other hand, one patient had side effects caused by nivolumab administration. Patients with side effects had melanoma metastases and were given 2 mg / kg nivolumab once every 3 weeks.
- Six months after administration of nivolumab metastasis to the brain was examined by MRI, and metastasis to the whole body was examined by CT scan.
- thyroid stimulating hormone (TSH) levels began to increase (2.84 ⁇ IU / mL), and it was confirmed that serum TSH levels were 7.07 ⁇ IU / mL 8 months after nivolumab administration. Suspected of suffering from hypopituitarism. Therefore, when a corticotropin releasing hormone (CRH) tolerance test was performed on the above patients, serum corticotropin (ACTH) decreased (less than 1.0 ng / mL) and cortisol decreased (0.8 ⁇ g / dL). As a result, the patient was diagnosed with ACTH deficiency.
- CSH corticotropin releasing hormone
- sCD163 and CXCL5 in the serum were measured by ELISA.
- the sCD163 concentration in serum was measured according to the protocol using a kit Human CD163 DuoSet (catalog number: DY1607) (R and D system, Minneapolis, MN) containing an antibody that specifically binds to sCD163.
- CXCL5 concentration in serum was measured using a Human CXCL5 / ENA-78 DuoSet ELISA (catalog number: DY254) (R and D system, Minneapolis, MN) according to the protocol.
- TNF ⁇ concentration of TNF ⁇
- sera before and 6 weeks after administration of nivolumab were collected, and the concentration of TNF ⁇ in the serum was measured by ELISA.
- the serum TNF ⁇ concentration was measured according to the protocol using Human TNFa DuoSet (catalog number: DY210) (R and D system, Minneapolis, MN).
- sCD163 and CXCL5 in sCD163 and CXCL5 in serum were higher in one patient with side effects attributable to nivolumab administration than in seven patients with no side effects attributable to nivolumab administration.
- was up-regulated (when the number of specimens n 3, there is a significant difference at the corresponding t-test, p ⁇ 0.05). TNF ⁇ was not detected in all patients.
- Test Example 2 Measurement of sCD163 and CXCL5 in serum of patients before and after nivolumab administration (46 cases) 46 patients suffering from malignant melanoma to which nivolumab was administered as in Test Example 1 were used as subjects. Specifically, patients 1-46 were administered 2 mg / kg once every 3 weeks or 3 mg / kg nivolumab once every 2 weeks. For the 46 patients, sera before and 6 weeks after administration of nivolumab were collected, and the concentrations of sCD163 and CXCL5 in the serum were measured by ELISA. Of the 46 patients described above, patients 1 to 8 were the same patients as those of Test Example 1 and were examined continuously after Test Example 1. The results are shown in Table 1.
- a positive predictive value, a negative predictive value, and a predictive value were obtained according to the following criteria. Specifically, among patients who actually had side effects, if it was determined that there was a high possibility of developing side effects in this study, it was determined to be “positive”, and it was determined that there was a high possibility of developing side effects. The case where there was no “false negative”. Among patients who did not actually have any side effects, the case where it was determined that the possibility of developing a side effect was not high in this study was ⁇ negative '', and the case where it was determined that the possibility of developing a side effect was high “False positive”.
- the percentage of patients who actually had side effects was defined as a positive predictive value.
- Sensitivity was defined as the proportion of patients who were determined to have a high possibility of developing side effects in this study among patients who actually had side effects.
- Specificity was the proportion of patients who did not actually have any side effects and were not determined to have a high possibility of developing side effects in this study.
- the ratio of positive and negative patients to all patients was the hit rate in this study.
- the average value of sCD163 was 10.8%, and the average value of CXCL5 was 0.0%.
- the standard deviation of sCD163 was 30.8%, and the standard deviation of CXCL5 was 40.5%.
- Threshold setting based on the standard deviation of sCD163 and CXCL5
- the threshold was set within ⁇ 1 ⁇ from the standard deviation ( ⁇ ) with the average value of the increase / decrease ratio data of sCD163 and CXCL5 as the center.
- Set thresholds sCD163 upper limit 42% lower limit ⁇ 20%, CXCL5 upper limit 41% lower limit ⁇ 41%)
- patients whose CXCL5 increase / decrease ratio measured is greater than or equal to the upper limit value of the threshold value or less than the lower limit value, or whose measured increase / decrease ratio of sCD163 is greater than or equal to the upper limit value of the threshold value or less than the lower limit value
- Patients were highly likely to develop side effects. Based on the above criteria, the hit rate was determined. The results are shown in Table 2.
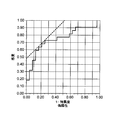
- FIG. 2 shows the ROC curve.
- the horizontal axis of the ROC curve represents (1-specificity), which increases with the rate of false positives.
- the vertical axis represents sensitivity.
- irAE 1 is set to “positive”.
- the point at which “sensitivity ⁇ (1 ⁇ specificity)” was maximum in this ROC curve was 0.231, and the area under the ROC curve (AUC) was 0.746.
- a threshold was set at ⁇ 21.3% centered on the average value of sCD163.
- the set threshold is the upper limit 32% lower limit-11% of sCD163)
- a patient whose measured increase / decrease ratio data of sCD163 is greater than or equal to the upper limit value or less than the lower limit value of the threshold value is defined as a patient who is highly likely to develop side effects. Based on the above criteria, the hit rate was determined. The results are shown in Table 3.
- Threshold setting based on ROC curve of sCD163 and CXCL5 Further, similar to sCD163 described in 2, the ROC curve is created based on the absolute value of the difference between the increase / decrease ratio data of CXCL5 and the average value, and the threshold of CXCL5 is also set Set.
- the threshold values set were upper limit 32% lower limit ⁇ 11% for sCD163 and upper limit 48% lower limit ⁇ 48% for CXCL5.
- patients whose CXCL5 increase / decrease ratio measured is greater than or equal to the upper limit value of the threshold value or less than the lower limit value, or whose measured increase / decrease ratio of sCD163 is greater than or equal to the upper limit value of the threshold value or less than the lower limit value
- Patients were highly likely to develop side effects.
- the hit rate was determined.
- the positive predictive value was 71.4%
- the negative predictive value was 88.9%
- the sensitivity was 90.9%
- the predictive value was 78.3%.
- the specificity was almost the same as that in the case of sCD163 of 2 above.
Abstract
本発明は、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するためのデータを取得する新規方法または該副作用の発症を予測する新規方法を提供する。 より詳細には、本発明は、上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる、副作用の発症を予測するためのデータを取得する方法または該副作用の発症を予測する方法を提供する。
Description
本特許出願は、2016年7月1日に出願された日本国特許出願2016-131913号に基づく優先権の主張を伴うものであり、かかる先の特許出願における全開示内容は、引用することにより本明細書の一部とされる。
本発明は、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測する新規な方法に関する。
ガン細胞は、ガン細胞を攻撃する免疫細胞の活性を下げることにより、免疫細胞の攻撃を阻止している。この仕組みは「免疫チェックポイント」と呼ばれている。したがって、この「免疫チェックポイント」を阻害することにより、免疫細胞の働きを再び活発にしてガン細胞を攻撃することができる。免疫チェックポイント阻害薬は、ガン細胞により活性の下げられた免疫細胞を活性化させ、ガン細胞を攻撃させる薬である。
免疫チェックポイント阻害薬として、具体的には、抗PD-1抗体、抗CTLA4抗体等が挙げられる。抗PD-1抗体であるニボルマブおよびペムブロリズマブは、悪性黒色腫の治療に有用であることが知られており、また、非小細胞肺癌や腎細胞癌に対する治療効果も報告されている(特許文献1、非特許文献1)。また、抗CTLA4抗体であるイピリムマブまたはトレメリムマブも、黒色腫および他の悪性腫瘍の治療に有用であることが知られている(特許文献2)。
一方、免疫チェックポイント阻害薬の投与に起因する自己免疫関連の副作用の出現は従来の薬剤に比して多いことが知られている。例えば、抗PD-1抗体(ニボルマブ)または抗CTLA4抗体(イピリムマブ)を根治切除不能悪性黒色腫の患者に投与した場合のグレード3以上の有害事象の発生率が、ニボルマブ単独では16.3%、イピリムマブ単独では27.3%、ニボルマブとイピリムマブとの併用では55.0%であることが報告されている(非特許文献1)。
免疫チェックポイント阻害薬の投与に起因する副作用には、下垂体機能障害、自己免疫性大腸炎、間質性肺炎、重度肝障害等の生命にかかわる重篤な副作用が存在する。これら副作用の出現時期、進行速度等は予測できないため、患者が自宅で発症に気付かずに、受診時には致命的な状況であることも少なくない。
したがって、免疫チェックポイント阻害薬の投与に起因する副作用の発症前において、発症の可能性(危険性)を予測できる技術的手段の開発が求められている。
Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med 2015; 373: p.23-34.
本発明は、免疫チェックポイント阻害薬である、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象における副作用の発症の可能性(危険性)を予測する新たな技術的手段を提供することを目的とする。
本発明者らは、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することにより、前記抗体医薬の投与に起因する副作用の発症を予測しうることを見出した。
本発明によれば、以下の発明が提供される。
(1)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するためのデータを取得する方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(2)上記抗PD-1抗体がニボルマブである、(1)に記載の方法。
(3)上記抗CTLA4抗体がイピリムマブである、(1)または(2)に記載の方法。
(4)上記抗体医薬が抗癌剤である、(1)~(3)のいずれか一つに記載の方法。
(5)上記副作用が免疫関連副作用である、(1)~(4)のいずれか一つに記載の方法。
(6)上記マーカーがsCD163およびCXCL5の組み合わせである、(1)~(5)のいずれか一つに記載の方法。
(7)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルと、上記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとの比較データを取得することを含んでなる、(1)~(6)のいずれか一つに記載の方法。
(8)上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、副作用を発症する指標となる、(7)に記載の方法。
(9)上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、対象にステロイドを投与する指標となる、(7)に記載の方法。
(10)前記比較データが副作用を発症する指標となる、請求項8または9に記載の方法。
(11)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測する方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(12)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルと、上記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとを比較することを含んでなる、(11)に記載の方法。
(13)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルが、あらかじめ設定された閾値から外れた場合には副作用を発症する可能性が高いと予測する、(12)に記載の方法。
(14)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用をモニタリングする方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(15)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された対象において、該抗体医薬の投与に起因する副作用の発症を予測するための、sCD163またはCXCL5を含んでなるマーカー。
(16)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断薬。
(17)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断用キット。
(1)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するためのデータを取得する方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(2)上記抗PD-1抗体がニボルマブである、(1)に記載の方法。
(3)上記抗CTLA4抗体がイピリムマブである、(1)または(2)に記載の方法。
(4)上記抗体医薬が抗癌剤である、(1)~(3)のいずれか一つに記載の方法。
(5)上記副作用が免疫関連副作用である、(1)~(4)のいずれか一つに記載の方法。
(6)上記マーカーがsCD163およびCXCL5の組み合わせである、(1)~(5)のいずれか一つに記載の方法。
(7)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルと、上記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとの比較データを取得することを含んでなる、(1)~(6)のいずれか一つに記載の方法。
(8)上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、副作用を発症する指標となる、(7)に記載の方法。
(9)上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、対象にステロイドを投与する指標となる、(7)に記載の方法。
(10)前記比較データが副作用を発症する指標となる、請求項8または9に記載の方法。
(11)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測する方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(12)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルと、上記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとを比較することを含んでなる、(11)に記載の方法。
(13)上記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルが、あらかじめ設定された閾値から外れた場合には副作用を発症する可能性が高いと予測する、(12)に記載の方法。
(14)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用をモニタリングする方法であって、
上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。
(15)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された対象において、該抗体医薬の投与に起因する副作用の発症を予測するための、sCD163またはCXCL5を含んでなるマーカー。
(16)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断薬。
(17)抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断用キット。
本発明によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することにより、上記抗体医薬の投与に起因する副作用の発症を予測することができる。本発明の方法は、予め副作用の発症を予測して薬剤を投与し、副作用の発症を防止、抑制もしくは遅延、または副作用を軽減する上で有利である。また、本発明の方法を用いることにより、副作用の発症を予測して、副作用による障害を減らすことができる。また、本発明の方法を用いることにより、簡便な手段で、上記抗体医薬の投与に起因する副作用の発症を予測することができる。
データを取得する方法/副作用の発症を予測する方法
本発明の方法は、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを一つの特徴としている。ここで、用いるマーカーはsCD163およびCXCL5の組み合わせが好ましい。かかる方法によれば、得られたデータに基づいて、副作用の発症を予測することができる。
本発明の方法は、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを一つの特徴としている。ここで、用いるマーカーはsCD163およびCXCL5の組み合わせが好ましい。かかる方法によれば、得られたデータに基づいて、副作用の発症を予測することができる。
本発明の方法は、上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルと、前記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとの比較データを取得することを含んでなる。ここで、比較データとは、例えば、上記レベルの差または比をいう。また、上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、副作用を発症する指標となる。さらに、上記抗体医薬を投与された対象から採取された生物学的試料における上記マーカーのレベルまたは上記比較データが、対象に薬剤、好ましくはステロイド、を投与する指標となる。上記副作用を発症する指標または対象に薬剤、好ましくはステロイド、を投与する指標としては、上記比較データが好ましい。マーカーのレベルについては後述する。
sCD163、CXCL5
本発明の、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象における、該抗体医薬の投与に起因する副作用の発症を予測するためのマーカーは、sCD163またはCXCL5を含んでなる。
本発明における「CD163」は、1本鎖の膜貫通型タンパク質で、スカベンジャーレセプターシステイン-リッチファミリーのメンバーであり、「M130」と相互に使用される。また、「sCD163(可溶型CD163)」は、CD163が切断されて可溶型となったものである。本発明における「sCD163」は、sCD163の改変体、アイソフォーム、および種ホモログを含んでよい。
本発明における「CXCL5」は、好中球/単球走化性タンパク質であって、CXCモチーフのN末端側にELRモチーフを有するELR+グループのメンバーであり、「LIX」および「GCP-2」と相互に使用され、CXCL5の改変体、アイソフォーム、および種ホモログを含んでよい。
本発明の、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象における、該抗体医薬の投与に起因する副作用の発症を予測するためのマーカーは、sCD163またはCXCL5を含んでなる。
本発明における「CD163」は、1本鎖の膜貫通型タンパク質で、スカベンジャーレセプターシステイン-リッチファミリーのメンバーであり、「M130」と相互に使用される。また、「sCD163(可溶型CD163)」は、CD163が切断されて可溶型となったものである。本発明における「sCD163」は、sCD163の改変体、アイソフォーム、および種ホモログを含んでよい。
本発明における「CXCL5」は、好中球/単球走化性タンパク質であって、CXCモチーフのN末端側にELRモチーフを有するELR+グループのメンバーであり、「LIX」および「GCP-2」と相互に使用され、CXCL5の改変体、アイソフォーム、および種ホモログを含んでよい。
また、生物学的試料におけるsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルとは、例えば、生物学的試料における上記マーカーの濃度または量であり、好ましくは、生物学的試料におけるsCD163の濃度、またはCXCL5の濃度である。なお、測定するsCD163の濃度としては、例えば、1ng/mL~500ng/mLの範囲の濃度が挙げられる。また、測定するCXCL5の濃度としては、例えば、10pg/mL~10000pg/mL、10pg/mL~5000pg/mLの範囲の濃度が挙げられる。
抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体
本発明における「抗体」は、全長抗体であって、ジスルフィド結合で連結された少なくとも2個の重鎖(H)と2個の軽鎖(L)を含む糖タンパク質を含む。各重鎖は、重鎖可変領域(以下、VHと略すこともある。)と重鎖定常領域とから構成されている。重鎖定常領域は、3個のドメインCH1、CH2およびCH3から構成されている。各軽鎖は、軽鎖可変領域(以下、VLと略すこともある。)と軽鎖定常領域から構成されている。軽鎖定常領域は、1個のドメインCLで構成されている。VHおよびVL領域はさらに、相補性決定領域(CDR)と称される変異性の高い領域に小分割され、それらには、フレームワーク領域(FR)と称され、より保存性の高い領域が散在している。上記重鎖および軽鎖の可変領域は、抗原と相互作用する結合ドメインを含んでいる。
かかる「抗体」としては、例えば、モノクローナル抗体、ポリクローナル抗体、二重特異性抗体、低分子化抗体、ドメイン抗体、合成抗体、キメラ抗体、ヒト化抗体、ヒト抗体、抗体複合体、一本鎖抗体、抗体誘導体、抗体類似体、およびそのそれぞれの抗原結合断片が挙げられる。
本発明における「抗体」は、全長抗体であって、ジスルフィド結合で連結された少なくとも2個の重鎖(H)と2個の軽鎖(L)を含む糖タンパク質を含む。各重鎖は、重鎖可変領域(以下、VHと略すこともある。)と重鎖定常領域とから構成されている。重鎖定常領域は、3個のドメインCH1、CH2およびCH3から構成されている。各軽鎖は、軽鎖可変領域(以下、VLと略すこともある。)と軽鎖定常領域から構成されている。軽鎖定常領域は、1個のドメインCLで構成されている。VHおよびVL領域はさらに、相補性決定領域(CDR)と称される変異性の高い領域に小分割され、それらには、フレームワーク領域(FR)と称され、より保存性の高い領域が散在している。上記重鎖および軽鎖の可変領域は、抗原と相互作用する結合ドメインを含んでいる。
かかる「抗体」としては、例えば、モノクローナル抗体、ポリクローナル抗体、二重特異性抗体、低分子化抗体、ドメイン抗体、合成抗体、キメラ抗体、ヒト化抗体、ヒト抗体、抗体複合体、一本鎖抗体、抗体誘導体、抗体類似体、およびそのそれぞれの抗原結合断片が挙げられる。
本発明における抗体の「抗原結合断片」(または、単に「抗体断片」ともいう)とは、特異的に抗原(例えば、PD-1)に結合する能力を保持する抗体の1個以上の断片を示すものである。抗体の「抗原結合断片」に含まれる結合断片の例として、(i)VL、VH、CLおよびCH1ドメインから構成される1価の断片であるFab断片、(ii)ヒンジ領域中ジスルフィド架橋で結合した2個のFab断片を含む2価の断片であるF(ab´)2断片、(iii)VHおよびCH1ドメインから構成されるFd断片、(iv)抗体のシングルアームのVLおよびVHドメインで構成されるFv断片、(v)VHドメインから構成されるdAb断片、または(vi)単離相補性決定領域(CDR)が挙げられる。さらに、Fv断片の2個のドメインであるVLおよびVHは別々の遺伝子によりコードされているが、それらは、組み換え技術を用いてそれらを単一タンパク質鎖として作製できる合成リンカーにより連結でき、この鎖中では、VLおよびVH領域が対となって1価の分子を形成できる(単一鎖のFv(scFv))。このような単一鎖の抗体も、抗体の「抗原結合断片」に含まれる。
本発明における「PD-1」は、免疫応答調節のシグナルを介する免疫レセプターであって、CD28/CTLA-4ファミリーに属するI型膜タンパク質である。本発明における「PD-1」は、「ProgrammedDeath1」、「ProgrammedCellDeath1」、「タンパク質PD-1」、「PD1」、「PDCD1」、および「hPD-1」と相互に使用され、PD-1の改変体、アイソフォーム、種ホモログ、およびPD-1と少なくとも1個の共通エピトープを有するアナログを含んでよい。
本発明における「抗PD-1抗体」とは、本発明の効果を妨げない限り、特に限定されず、PD-1に特異的に結合する抗体であってよい。かかる抗体は、アミノ酸配列の構造の一部を特異的に認識する抗体でもあってもよく、全体構造を特異的に認識する抗体でもよい。また、上記抗体としては、特に限定されるものではないが、ニボルマブ、ペムブロリズマブ、またはラムブロリズマブが挙げられ、好ましくはニボルマブ、またはペムブロリズマブである。
本発明における「CTLA4」は、T細胞の活性化を抑制する調節因子であって、「細胞毒性Tリンパ球関連抗原-4」、「CTLA-4」、「CTLA-4抗原」および「CD152」と相互に使用され、ヒトCTLA4の改変体、アイソフォーム、種ホモログ、およびCTLA4と少なくとも1個の共通エピトープを有するアナログを含んでよい。
本発明における「抗CTLA4抗体」とは、本発明の効果を妨げない限り、特に限定されず、CTLA4に特異的に結合する抗体であってよい。かかる抗体は、アミノ酸配列の構造の一部を特異的に認識する抗体でもあってもよく、全体構造を特異的に認識する抗体でもよい。また、上記抗体としては、特に限定されるものではないが、好ましくは、イピリムマブ、またはトレメリムマブである。
本発明における「PD-L1」は、PD-1のリガンドであって、「CD274」、「ProgrammedCellDeath1Ligand1」、「PDCD1L1」、「B7-H」、および「B7H1」と相互に使用され、PD-L1の改変体、アイソフォーム、種ホモログ、およびPD-L1と少なくとも1個の共通エピトープを有するアナログを含んでよい。
本発明における「抗PD-L1抗体」とは、本発明の効果を妨げない限り、特に限定されず、PD-L1に特異的に結合する抗体であってよい。かかる抗体は、アミノ酸配列の構造の一部を特異的に認識する抗体でもあってもよく、全体構造を特異的に認識する抗体でもよい。また、上記抗体としては、特に限定されるものではないが、好ましくは、MPDL3280A(RG7446)、またはアテゾリズマブである。
本発明における「抗体医薬」は、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つのものである。上記抗体またはその抗原結合断片は、1種のみを対象に投与してもよく、2種以上を組み合わせて同時にまたは別々に対象に投与してもよい。2種以上の組み合わせの例としては、抗PD-1抗体と抗CTLA4抗体との組み合わせ等が挙げられる。上記抗体の投与方法としては、特に限定されるものではないが、静脈投与が好ましい。
本発明の対象は、好ましくはヒトであり、より好ましくは、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与により治療されうる疾患に罹患しているか、または該疾患に罹患する可能性のあるヒトである。ここで、「治療」には、確立された病態を治療することだけでなく、将来確立される可能性のある病態を予防することをも含む。
抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与により治療されうる疾患としては、特に限定されるものではないが、癌、肉腫、または悪性中皮腫が挙げられる。したがって、上記抗体医薬は、抗癌剤であってよい。癌、肉腫、または悪性中皮腫としては、具体的には、悪性黒色腫(メラノーマ)(例えば、転移性悪性悪性黒色腫、根治切除不能悪性黒色腫)、皮膚有棘細胞癌、乳房外パジェット病、またはメルケル細胞癌等の皮膚癌;腎癌(例えば、腎細胞癌、透明細胞カルシノーマ);前立腺癌(例えば、ホルモン難治性前立腺アデノカルシノーマ);乳癌;結腸癌;肺癌(例えば、非小細胞肺癌);骨癌;膵癌;頭頚部癌;皮膚若しくは眼窩内悪性メラノーマ;子宮癌;卵巣癌;直腸癌;肛門部癌;胃癌;精巣癌;子宮癌;卵管のカルシノーマ;子宮内膜カルシノーマ;子宮頚部カルシノーマ;膣カルシノーマ;外陰部カルシノーマ;食道癌;小腸癌;大腸癌;内分泌系癌;甲状腺癌;副甲状腺癌;副腎癌;柔組織肉腫;多発性骨髄腫;尿道癌;陰茎癌;慢性若しくは急性白血病(例えば、急性骨髄性白血病、慢性骨髄性白血病、急性リンパ芽球性白血病、慢性リンパ球性白血病);小児固形癌;進行性固形癌;膀胱癌;腎臓若しくは尿管の癌;腎盂カルシノーマ;尿路上皮癌;中枢神経系(CNS)腫瘍;リンパ腫(例えば、リンパ球性リンパ腫、原発性CNSリンパ腫、非ホジキンリンパ腫、ホジキンリンパ腫(ホジキン病)、T細胞リンパ腫);胸膜悪性中皮腫;心膜悪性中皮腫;腹膜悪性中皮腫;腫瘍新脈管形成;脊椎腫瘍;脳幹グリオーム;下垂体アデノーマ;カポシ肉腫;扁平上皮癌;扁平細胞癌;アスベスト誘発癌を含む環境誘発癌;またはそれらの組み合わせが挙げられ、好ましくは、皮膚癌、より好ましくは、悪性黒色腫、皮膚有棘細胞癌、乳房外パジェット病、またはメルケル細胞癌である。
本発明における抗体医薬の投与に起因する副作用としては、特に限定されるものではないが、免疫関連副作用(免疫に関連すると推察される副作用:irAE)が好ましい(例えば、医薬品インタビューフォーム オプジーボ(R)点滴静注20mg・100mg、2016年4月改訂(第9版)、日本皮膚科学会悪性黒色腫の新薬に関する安全性検討委員会、抗CTLA-4抗体イピリムマブ(ヤーボイ(R))の特性と副作用への対応について、平成27年8月24日参照)。また、本発明の上記副作用の具体的な態様としては、間質性肺疾患、重症筋無力症、筋炎、大腸炎、1型糖尿病、肝機能障害(肝障害)、肝炎(例えば、自己免疫性肺炎)等の肺障害、下垂体機能低下症、下垂体炎等の下垂体機能障害、甲状腺機能低下症等の甲状腺機能障害、神経障害、腎障害、脳炎、副腎機能不全等の副腎障害、重度の皮膚障害、静脈血栓塞栓症、infusion reaction、乾癬、乾癬様皮疹、下痢(例えば、重度の下痢)、関節リウマチ、ブドウ膜炎、上強膜炎、滑膜包炎、放射性皮膚炎の増悪、慢性炎症性脱髄性多発神経炎(以下、脱髄性多発神経炎ともいう)、胆道障害または腎炎が挙げられ、好ましくは下垂体機能障害である。
また、免疫関連副作用(irAE)は例えば投与後8週以降、または8~12週後に発症することが知られている。
免疫関連副作用は、「グレード」または「irAE評価」により評価される。ここで、「irAE評価」は、疾患の重篤度を表す指標であり、1~3で表される。1とは、「irAEのため追加で治療介入を必要としない」という状態を示し、2とは、「irAEのため薬剤介入等が必要だが入院治療を必要としない、もしくは治療の中断を必要としない」という状態を示し、3とは、「irAEのため入院を伴う薬剤介入等が必要かつ治療の中断を要する」という状態を示す。なお、「irAE評価」と「グレード」との対応は各疾患により異なる。
また、免疫関連副作用(irAE)は例えば投与後8週以降、または8~12週後に発症することが知られている。
免疫関連副作用は、「グレード」または「irAE評価」により評価される。ここで、「irAE評価」は、疾患の重篤度を表す指標であり、1~3で表される。1とは、「irAEのため追加で治療介入を必要としない」という状態を示し、2とは、「irAEのため薬剤介入等が必要だが入院治療を必要としない、もしくは治療の中断を必要としない」という状態を示し、3とは、「irAEのため入院を伴う薬剤介入等が必要かつ治療の中断を要する」という状態を示す。なお、「irAE評価」と「グレード」との対応は各疾患により異なる。
測定方法
本発明で用いることができる生物学的試料としては、血清、血漿、血液、または尿等が挙げられ、好ましくは血清である。
また、上記生物学的試料の採取時期は、副作用の発症を予防する観点から、上記副作用の発症前が挙げられる。上記副作用の発症前としては、例えば、上記抗体医薬の投与前、上記抗体医薬の投与後またはその両者が挙げられる。ここで、上記抗体医薬の投与前としては、上記抗体医薬を投与する前に加え、上記抗体医薬の投与時または投与直後も含んでいてもよい。さらに、上記抗体医薬の投与後としては、例えば、上記抗体医薬を投与してから12週以内が挙げられ、好ましくは8週以内、さらに好ましくは6週以内である。また、上記抗体医薬の投与前、投与後は、それぞれ上記抗体医薬の1回目の投与前、1回目の投与後としてよい。
さらに、上記生物学的試料の採取時期は、モニタリングや後述の薬剤の効果の確認等の観点から、上記抗体医薬の投与後としては、上記抗体医薬を投与してからの期間は制限されず、さらに、投与後に2回以上測定してもよい。
本発明で用いることができる生物学的試料としては、血清、血漿、血液、または尿等が挙げられ、好ましくは血清である。
また、上記生物学的試料の採取時期は、副作用の発症を予防する観点から、上記副作用の発症前が挙げられる。上記副作用の発症前としては、例えば、上記抗体医薬の投与前、上記抗体医薬の投与後またはその両者が挙げられる。ここで、上記抗体医薬の投与前としては、上記抗体医薬を投与する前に加え、上記抗体医薬の投与時または投与直後も含んでいてもよい。さらに、上記抗体医薬の投与後としては、例えば、上記抗体医薬を投与してから12週以内が挙げられ、好ましくは8週以内、さらに好ましくは6週以内である。また、上記抗体医薬の投与前、投与後は、それぞれ上記抗体医薬の1回目の投与前、1回目の投与後としてよい。
さらに、上記生物学的試料の採取時期は、モニタリングや後述の薬剤の効果の確認等の観点から、上記抗体医薬の投与後としては、上記抗体医薬を投与してからの期間は制限されず、さらに、投与後に2回以上測定してもよい。
sCD163またはCXCL5を測定するためには現在既知のあらゆる方法を採用することができる。例えば、免疫測定法、電気泳動法、ウエスタンブロッティング法、質量分析法等が挙げられ、好ましくは免疫測定法である。
免疫測定法としては、例えば、免疫比濁測定法、酵素免疫測定法等が挙げられる。免疫測定法は、タンパク質等を抗原として測定する免疫測定法であって、抗体としては、本発明の効果を妨げない限り特に限定されないが、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を用いることができ、好ましくはそのポリクローナル抗体やモノクローナル抗体を用いることができる。抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分としては、市販品の抗体を用いることができ、また、周知の方法により、製造することもできる。また、抗sCD163抗体または抗CXCL5抗体はそれぞれ、sCD163またはCXCL5に特異的に結合しうる限り特に限定されず、アミノ酸配列の構造の一部を特異的に認識する抗体でもあってもよく、全体構造を特異的に認識する抗体でもよい。
免疫比濁測定法としては、生物学的試料におけるsCD163またはCXCL5と、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分とを反応させて抗原抗体反応させ、その結果、発生する濁りの度合いからsCD163またはCXCL5のレベルを測定するものであれば、とくに限定されない。そのような方法として、TIA法、ラテックス免疫比濁法、ネフェロメトリー法を例示することができる。TIA法は、免疫比濁測定法において濁りの度合いを特定の吸光度において測定する方法である。また、ラテックス免疫比濁法は、免疫比濁測定法において、抗体として抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分をラテックス粒子に結合させたものを用いて測定する方法である。さらに、ネフェロメトリー法は、免疫比濁測定法において濁りの度合いを、一定角度以上の大きさに散乱した光を集めて散乱光として測定する方法である。
酵素免疫測定法としては、プレートを支持体とした、ELISA法等のEIA法を挙げることが出来る。はじめに固相に直接または間接的に抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を一次抗体として結合させる。
sCD163またはCXCL5を酵素免疫測定法で測定する場合には、例えば、固相に結合した一次抗体に、sCD163またはCXCL5を測定するための生物学的試料を加えて反応させる。一定時間反応させた後、固相を洗浄し二次標識抗体を加えて二次反応させる。固相を再度洗浄し、固相に結合した標識部分を測定する。
sCD163またはCXCL5を酵素免疫測定法で測定する場合には、例えば、固相に結合した一次抗体に、sCD163またはCXCL5を測定するための生物学的試料を加えて反応させる。一定時間反応させた後、固相を洗浄し二次標識抗体を加えて二次反応させる。固相を再度洗浄し、固相に結合した標識部分を測定する。
上記二次標識抗体を用いる免疫測定法において、標識物質としては西洋ワサビペルオキシダーゼ(HRP)アルカリホスファターゼ等の酵素を用いることができる。例えば、HRP標識抗体を利用した場合には基質に既知のDAB、TMB、OPD等を用いることができる。また、標識物質には、HRPのような酵素だけではなく、金コロイド、ユーロピウム等の標識金属やFITC、ローダミン、Texas Red、Alexa、GFP等の化学的、生物的各種蛍光物質、32P、51Cr等の放射性物質等標識可能なあらゆる物質が挙げられる。また、本発明で標識物質を用いる場合、アビジン-ビオチン系またはストレプトアビジン-ビオチン系を用いることもできる。その場合には、例えば、ビオチンで標識された二次標識抗体とともに、HRP等の酵素で標識されたストレプトアビジンまたはアビジンを用いることができる。また、ルシフェラーゼ標識抗体による化学発光イムノアッセイ、蛍光色素標識抗体による蛍光イムノアッセイ、フローサイトメトリー法等を挙げることができる。
電気泳動法としては、一般的にはSDS-PAGE法を挙げることができる。そのほかにもセルロース・アセテートを支持体としたもの等がある。タンパク質の染色にはクマシー・ブリリアント・ブルー、ポンソーS染色、アミドブラック染色、直接酵素活性を利用する方法等がある。
また、ウエスタンブロッティング法による検出も有効である。すなわち、電気泳動をしたゲルをニトロセルロース膜やPVDF膜等に転写し、次いで、一次抗体である抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分、さらに、二次標識抗体であるHRP標識抗IgG等を反応させ、次いで、HRP発色試薬で発色させ、sCD163またはCXCL5に相当するバンドの発色度合いにより、sCD163またはCXCL5を測定することができる。
質量分析法としては、例えば、質量分析器を使用した分析方法を挙げることができる。例えば、表面増強レーザー脱離イオン化(Surface Enhanced Laser Desorption/Ionization)飛行時間型質量分析計(SELDI-TOF MS法)、マトリックス支援レーザーイオン化(Matrix-Assisted Laser Desorption/Ionization)飛行時間型質量分析計(MALDI-TOF MS法)、ESI法(Electrospray Ionization)を用いる方法を例示できる。SELDI-TOF MS法は、チップ表面の官能基に目的物質を均一に捕捉したまま不純物を除去し、レーザー光でイオン化するため、再現性のあるS/N比の高いイオンスペクトルが得られるので好ましい。
副作用の発症の予測
また、本発明においては、上述のような測定により得られたデータを用いて、上記抗体医薬の投与に起因する副作用の発症を予測することができる。上記予測工程では、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された(すなわち、投与後の)対象から採取された生物学的試料におけるsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルと、投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとを比較することが好ましい。
また、本発明においては、上述のような測定により得られたデータを用いて、上記抗体医薬の投与に起因する副作用の発症を予測することができる。上記予測工程では、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された(すなわち、投与後の)対象から採取された生物学的試料におけるsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルと、投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとを比較することが好ましい。
したがって、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与する前の対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定する工程を含んでもよい。また、上記抗体医薬投与後に2回以上上記マーカーのレベルを測定している場合は、任意の2つの測定ポイントにおける上記マーカーのレベルを比較してもよい。
また、生物学的試料におけるsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルは、上記の測定方法により測定でき、ELISA法による測定が好ましい。
さらに、本発明の好ましい態様によれば、上記予測工程は、医師による判断を含まない。
さらに、本発明の別の態様によれば、副作用の発症の予測とは、副作用が発症する前にその発症を予測することに加えて、副作用のグレードが低い場合において副作用が発症していることの予測も含む。ここで、副作用のグレードが低いとは、好ましくは1~2である。本発明の別の態様によれば、副作用の発症の予測とは、免疫関連副作用(irAE)評価が低い場合において副作用が発症していることの予測も含む。ここで、irAE評価が低いとは、好ましくは1~2である。
副作用の発症の予測に際し、副作用を発症した対象(群)における上記抗体医薬の投与前後の生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルの差または比と、副作用を発症しない対象(群)における対応するマーカーのレベルの差または比について比較し、統計学的処理を行ってもよい。また、上記抗体医薬投与後に2回以上上記マーカーのレベルを測定している場合は、任意の2つの測定ポイントにおける上記マーカーのレベルの差または比を比較してもよい。その結果、副作用を発症した対象(群)と副作用を発症しない対象(群)との間に有意差がある場合には、用いた前記マーカーのレベルの差または比を、副作用の発症の可能性を予測する指標とすることができる。上記統計処理としては、U検定(ノンパラメトリカル)、または対応のあるt-検定(正規分布の場合)が挙げられる。
本発明の上記抗体医薬の投与に起因する副作用の発症の予測は、例えば、上記抗体医薬を投与後の対象から採取された生物学的試料におけるsCD163のレベルが、投与前の対象の生物学的試料におけるsCD163のレベルに比べて高い場合、副作用を発症する可能性が高いとの指標に基づいて行うことができる。
また、上記抗体医薬投与後の対象から採取された生物学的試料におけるsCD163のレベルが、投与前の対象から採取された生物学的試料におけるsCD163のレベルに比べて好ましくは1.2倍以上、より好ましくは1.5倍以上、さらに好ましくは1.6倍以上、さらにより好ましくは1.8倍以上、さらにより一層好ましくは2倍以上高い場合、副作用を発症する可能性が高いと予測することができる。また、上記抗体医薬投与後の対象から採取された生物学的試料におけるsCD163濃度が、投与前の対象の生物学的試料におけるsCD163濃度に比べて好ましくは10ng/mL、より好ましくは15ng/mL、さらに好ましくは20ng/mL、さらにより好ましくは40ng/mL以上高い場合、副作用を発症する可能性が高いと予測することができる。
本発明の上記抗体医薬の投与に起因する副作用の発症の予測は、例えば、上記抗体医薬を投与後の対象から採取された生物学的試料におけるCXCL5のレベルが、投与前の対象の生物学的試料におけるCXCL5のレベルに比べて高い場合、副作用を発症する可能性が高いとの指標に基づいて行うことができる。
また、上記抗体医薬投与後の対象から採取された生物学的試料におけるCXCL5のレベルが、投与前の対象の生物学的試料におけるCXCL5のレベルに比べて、好ましくは1.05倍以上、より好ましくは1.1倍以上、さらに好ましくは1.2倍以上、さらにより好ましくは1.3倍以上高い場合、副作用を発症する可能性が高いと予測することができる。また、上記抗体医薬投与後の対象から採取された生物学的試料におけるCXCL5の濃度が、投与前の対象の生物学的試料におけるCXCL5の濃度に比べて、好ましくは50pg/mL、より好ましくは100pg/mL、さらに好ましくは150pg/mL以上高い場合、副作用を発症する可能性が高いと予測することができる。
また、本発明の一つの態様によれば、対象において測定されたsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルが、上記抗体医薬の投与に起因する副作用の発症について、予め設定された閾値から外れる場合には、副作用を発症する可能性が高いと予測することができる。予め設定された閾値から外れる場合とは、例えば、上記マーカーのレベルが予め設定された閾値と同じもしくは該閾値より高い場合をいい、後述のように閾値が上限値と下限値を有する場合には、上記マーカーのレベルが該上限値と同じもしくは該上限値より高い、または下限値と同じもしくは該上限値より低い場合をいう。
上記の別の態様によれば、副作用を発症した対象(群)または副作用を発症しない対象(群)における上記抗体医薬投与前後のsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベル差またはレベル比から予め閾値を設定することができる。また、上記抗体医薬投与後に2回以上上記マーカーのレベルを測定している場合は、任意の2つの測定ポイントにおける上記マーカーのレベルの差または比に基づいて予め閾値を設定することができる。副作用の発症の予測は、上記閾値と、副作用の発症を予測する対象の対応するマーカーのレベル差またはレベル比とを比較することにより行ってもよい。
当業者であれば、副作用を発症した対象(群)、副作用を発症しない対象(群)または副作用を発症した対象(群)および副作用を発症しない対象(群)(以下、全対象(群)ともいう)の上記抗体医薬投与前後のsCD163およびCXCL5から選択されるマーカーのレベル差またはレベル比から、閾値を適宜設定することができる。閾値としては、特に限定されるものではないが、例えば副作用を発症した対象(群)、副作用を発症しない対象(群)または全対象(群)の上記マーカーのレベル差または比の平均値、中央値、Xパーセンタイル値を使用することができ、好ましくは平均値である。ここでXは任意の数値を選択することができ、3、5、10、15、20、30、40、60、70、80、85、90、95、97を適宜使用することができる。閾値は1つであってもよいし、副作用の種類、投与する抗体医薬の種類、抗体医薬を投与する対象の状態、測定するマーカーの種類等またはそれらの組合せに応じて複数設定することもできる。
また、閾値としては、例えば副作用を発症した対象(群)、副作用を発症しない対象(群)または全対象(群)から採取された生物学的試料における上記マーカーのレベル差または比の平均値、中央値、Xパーセンタイル値を中心に、特定の数値幅を設けることができる。中心の数値としては、平均値を用いることが好ましい。上記数値幅は、副作用を発症した対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比と、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比とに基づいて決定できる。または、上記数値幅は、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比に基づいて決定できる。上記数値幅として、例えば、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比の標準偏差、標準誤差を用いることができる。また、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比を用いてROC曲線を作成し上限値および下限値を設定してもよい。また、上記閾値は、数値幅を有することから、上限値と下限値とが存在する。
また、閾値としては、副作用を発症した対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差もしくは比と、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差もしくは比とに基づいて、または全対象(群)上記抗体医薬投与前後の上記マーカーのレベル差または比に基づいて特定の上限値および下限値を設定できる。ここで、前記上限値および前記下限値はそれぞれ独立して設定してもよく、前記上限値と下限値の絶対値が同じになるように設定してもよい。例えば、全対象(群)を用いてROC曲線を作成し上限値および下限値を設定してもよく、また、全対象(群)における任意の2つのXパーセンタイル値(Xの値は異なるものである)を上限値および下限値と設定してもよい。
当業者であれば、副作用を発症した対象(群)、副作用を発症しない対象(群)または副作用を発症した対象(群)および副作用を発症しない対象(群)(以下、全対象(群)ともいう)の上記抗体医薬投与前後のsCD163およびCXCL5から選択されるマーカーのレベル差またはレベル比から、閾値を適宜設定することができる。閾値としては、特に限定されるものではないが、例えば副作用を発症した対象(群)、副作用を発症しない対象(群)または全対象(群)の上記マーカーのレベル差または比の平均値、中央値、Xパーセンタイル値を使用することができ、好ましくは平均値である。ここでXは任意の数値を選択することができ、3、5、10、15、20、30、40、60、70、80、85、90、95、97を適宜使用することができる。閾値は1つであってもよいし、副作用の種類、投与する抗体医薬の種類、抗体医薬を投与する対象の状態、測定するマーカーの種類等またはそれらの組合せに応じて複数設定することもできる。
また、閾値としては、例えば副作用を発症した対象(群)、副作用を発症しない対象(群)または全対象(群)から採取された生物学的試料における上記マーカーのレベル差または比の平均値、中央値、Xパーセンタイル値を中心に、特定の数値幅を設けることができる。中心の数値としては、平均値を用いることが好ましい。上記数値幅は、副作用を発症した対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比と、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比とに基づいて決定できる。または、上記数値幅は、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比に基づいて決定できる。上記数値幅として、例えば、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比の標準偏差、標準誤差を用いることができる。また、全対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差または比を用いてROC曲線を作成し上限値および下限値を設定してもよい。また、上記閾値は、数値幅を有することから、上限値と下限値とが存在する。
また、閾値としては、副作用を発症した対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差もしくは比と、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベル差もしくは比とに基づいて、または全対象(群)上記抗体医薬投与前後の上記マーカーのレベル差または比に基づいて特定の上限値および下限値を設定できる。ここで、前記上限値および前記下限値はそれぞれ独立して設定してもよく、前記上限値と下限値の絶対値が同じになるように設定してもよい。例えば、全対象(群)を用いてROC曲線を作成し上限値および下限値を設定してもよく、また、全対象(群)における任意の2つのXパーセンタイル値(Xの値は異なるものである)を上限値および下限値と設定してもよい。
上記閾値としては、例えば、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する比が、好ましくは1.05倍以上、より好ましくは1.1倍以上、さらに好ましくは1.3倍以上、さらにより好ましくは1.5倍以上である場合を有意とし、その比を閾値として用いることができる。また、例えば、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前の対応するsCD163のレベルに対する比が、好ましくは1.3倍以上、より好ましくは1.5倍以上、さらに好ましくは1.6倍以上、さらにより好ましくは1.8倍以上、さらにより一層好ましくは2倍以上である場合を有意とし、その比を閾値として用いることができる。
さらに、閾値が、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する比の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、20~75%、好ましくは30~60%、特に好ましくは40~50%である。閾値が、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する差の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、50~400pg/mL、好ましくは70~200pg/mL、特に好ましくは100~150pg/mLである。また、閾値が、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する比の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、15~50%、好ましくは20~40%、より好ましくは25~35%である。閾値が、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する差の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、1~25ng/mL、好ましくは2~10ng/mL、より好ましくは2.5~5ng/mLである。
また、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する比を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、20~60%、好ましくは30~50%であり、該下限値は、例えば、-60~-20%、好ましくは-50~-30%である。上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する差を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、50~300pg/mL、好ましくは100~200pg/mLであり、該下限値は、例えば、-300~-50pg/mL、好ましくは-200~-100pg/mLである。また、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する比を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、20~60%、30~50%、好ましくは35~45%であり、該下限値は、例えば、-40~0%、-30~-10%、好ましくは-25~-15%である。また、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する差を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、7.5~25ng/mL、好ましくは7.5~12.5ng/mLであり、該下限値は、例えば、-15~2.5ng/mL、好ましくは-2.5~2.5ng/mLである。
予め設定された閾値と、対象のレベル差またはレベル比とを比較することにより、対象が副作用を発症する可能性を予測、判定または決定することが可能になる。
さらに、閾値が、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する比の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、20~75%、好ましくは30~60%、特に好ましくは40~50%である。閾値が、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する差の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、50~400pg/mL、好ましくは70~200pg/mL、特に好ましくは100~150pg/mLである。また、閾値が、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する比の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、15~50%、好ましくは20~40%、より好ましくは25~35%である。閾値が、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する差の全対象(群)の平均値を中心に特定の数値幅を設けた値である場合には、該数値幅は、例えば、1~25ng/mL、好ましくは2~10ng/mL、より好ましくは2.5~5ng/mLである。
また、上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する比を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、20~60%、好ましくは30~50%であり、該下限値は、例えば、-60~-20%、好ましくは-50~-30%である。上記抗体医薬投与後のCXCL5のレベルの、抗体医薬投与前のCXCL5のレベルに対する差を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、50~300pg/mL、好ましくは100~200pg/mLであり、該下限値は、例えば、-300~-50pg/mL、好ましくは-200~-100pg/mLである。また、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する比を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、20~60%、30~50%、好ましくは35~45%であり、該下限値は、例えば、-40~0%、-30~-10%、好ましくは-25~-15%である。また、上記抗体医薬投与後のsCD163のレベルの、抗体医薬投与前のsCD163のレベルに対する差を用いる場合の閾値として特定の上限値と下限値を設定する場合は、該上限値は、例えば、7.5~25ng/mL、好ましくは7.5~12.5ng/mLであり、該下限値は、例えば、-15~2.5ng/mL、好ましくは-2.5~2.5ng/mLである。
予め設定された閾値と、対象のレベル差またはレベル比とを比較することにより、対象が副作用を発症する可能性を予測、判定または決定することが可能になる。
また、上記の別の態様によれば、副作用を発症した対象(群)または副作用を発症しない対象(群)における上記抗体医薬投与後のsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルから予め閾値を設定することができる。副作用の発症の予測は、上記閾値と、副作用の発症を予測する対象の対応するマーカーのレベルとを比較することにより行ってもよい。
当業者であれば、副作用を発症した対象(群)または副作用を発症しない対象(群)の上記抗体医薬投与後のsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルから、閾値を適宜設定することができる。閾値としては、特に限定されるものではないが、例えば副作用を発症した対象(群)または副作用を発症しない対象(群)の上記マーカーのレベルの平均値、中央値、Xパーセンタイル値を使用することができ、好ましくは平均値である。ここでXは任意の数値を選択することができ、3、5、10、15、20、30、40、60、70、80、85、90、95、97を適宜使用することができる。閾値は1つであってもよいし、副作用の種類、投与する抗体医薬の種類、抗体医薬を投与する対象の状態、測定するマーカーの種類等またはそれらの組合せに応じて複数設定することもできる。
また、閾値としては、例えば副作用を発症した対象(群)または副作用を発症しない対象(群)における上記抗体医薬投与後の生物学的試料における上記マーカーのレベルの平均値、中央値、Xパーセンタイル値を中心に、特定の数値幅を設けることができる。中心の数値としては、平均値を用いることが好ましい。上記数値幅は、副作用を発症した対象(群)の上記抗体医薬投与後の上記マーカーのレベルと、副作用を発症しない対象(群)の上記抗体医薬投与後の上記マーカーのレベルとに基づいて決定できる。また、上記閾値は、数値幅を有することから、上限値と下限値とが存在する。
また、閾値としては、副作用を発症した対象(群)の上記抗体医薬投与後の上記マーカーのレベルと、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベルとに基づいて、特定の上限値および下限値を設定できる。ここで、前記上限値および前記下限値はそれぞれ独立して設定してもよく、前記上限値と下限値の絶対値が同じになるように設定してもよい。
予め設定された閾値と、対象のレベルとを比較することにより、対象が副作用を発症する可能性を予測、判定または決定することが可能になる。
当業者であれば、副作用を発症した対象(群)または副作用を発症しない対象(群)の上記抗体医薬投与後のsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルから、閾値を適宜設定することができる。閾値としては、特に限定されるものではないが、例えば副作用を発症した対象(群)または副作用を発症しない対象(群)の上記マーカーのレベルの平均値、中央値、Xパーセンタイル値を使用することができ、好ましくは平均値である。ここでXは任意の数値を選択することができ、3、5、10、15、20、30、40、60、70、80、85、90、95、97を適宜使用することができる。閾値は1つであってもよいし、副作用の種類、投与する抗体医薬の種類、抗体医薬を投与する対象の状態、測定するマーカーの種類等またはそれらの組合せに応じて複数設定することもできる。
また、閾値としては、例えば副作用を発症した対象(群)または副作用を発症しない対象(群)における上記抗体医薬投与後の生物学的試料における上記マーカーのレベルの平均値、中央値、Xパーセンタイル値を中心に、特定の数値幅を設けることができる。中心の数値としては、平均値を用いることが好ましい。上記数値幅は、副作用を発症した対象(群)の上記抗体医薬投与後の上記マーカーのレベルと、副作用を発症しない対象(群)の上記抗体医薬投与後の上記マーカーのレベルとに基づいて決定できる。また、上記閾値は、数値幅を有することから、上限値と下限値とが存在する。
また、閾値としては、副作用を発症した対象(群)の上記抗体医薬投与後の上記マーカーのレベルと、副作用を発症しない対象(群)の上記抗体医薬投与前後の上記マーカーのレベルとに基づいて、特定の上限値および下限値を設定できる。ここで、前記上限値および前記下限値はそれぞれ独立して設定してもよく、前記上限値と下限値の絶対値が同じになるように設定してもよい。
予め設定された閾値と、対象のレベルとを比較することにより、対象が副作用を発症する可能性を予測、判定または決定することが可能になる。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用をモニタリングする方法であって、抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。かかる方法は、データを取得する方法、副作用の発症を予測する方法と同様の手法により実施することができる。かかるモニタリングは、対象における副作用の発症状況または副作用のグレードまたはirAE評価を経時的に確認する上で有利である。
本発明では、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象において、該抗体医薬の投与に起因する副作用の発症を予測するための、sCD163またはCXCL5を含んでなるマーカーも提供される。上記マーカーはsCD163単独またはCXCL5単独を用いてもよく、また、sCD163とCXCL5とを組み合わせてもよく、さらに、他のマーカーと組み合わせてもよい。かかるマーカーの態様は、データを取得する方法、副作用の発症を予測する方法に関する記載に準じて実施することができる。
本発明では、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象において、該抗体医薬の投与に起因する副作用の発症を予測するためにsCD163およびCXCL5から選択される少なくとも一つのマーカーを検出またはそのレベルを測定する診断薬も提供される。上記診断薬を用いることにより、例えば、上記に説明した各種の測定方法を行うことができる。上記測定方法としては、例えば、免疫測定法、電気泳動法、ウエスタンブロッティング法、質量分析法等が挙げられ、好ましくは免疫測定法である。ここで、免疫測定法としては、イムノクロマトグラフィー法も含まれる。
したがって、上記診断薬としては、例えば、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含有させることができる。抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分としては、上記免疫測定法における抗体と同様のものを使用することができる。
かかる診断薬の態様は、データを取得する方法、副作用の発症を予測する方法に関する記載に準じて実施することができる。
したがって、上記診断薬としては、例えば、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含有させることができる。抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分としては、上記免疫測定法における抗体と同様のものを使用することができる。
かかる診断薬の態様は、データを取得する方法、副作用の発症を予測する方法に関する記載に準じて実施することができる。
また、本発明では、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象において、該抗体医薬に起因する副作用の発症を予測するために、sCD163およびCXCL5から選択される少なくとも一つのマーカーを検出またはそのレベルを測定する診断用キットも提供される。これらのキットには、上記に説明した各種の測定方法を行うために、測定方法に応じて、各種の試薬を構成成分として含有させることができる。上記測定方法としては、例えば、免疫測定法、電気泳動法、ウエスタンブロッティング法、質量分析法等が挙げられ、好ましくは免疫測定法である。ここで、免疫測定法としては、イムノクロマトグラフィー法も含まれる。
したがって、上記診断用キットとしては、例えば、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含有させることができる。上記キットには、更に、標識物質の発色系試薬等、実施する測定方法に応じて、周知の試薬を含有させることができる。
上記の診断用キットの態様は、データを取得する方法、副作用の発症を予測する方法または診断薬に関する記載に準じて実施することができる。
本発明の別の態様によれば、上記診断キットは、後述の、薬剤の予防投与の判断に用いるため、または投与した薬剤の効果を確認するために用いることもできる。本発明の別の好ましい態様によれば、上記診断キットは、後述の、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症の予測のための検査の計画を調整または決定するためのデータを取得するために用いることもできる。
したがって、上記診断用キットとしては、例えば、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含有させることができる。上記キットには、更に、標識物質の発色系試薬等、実施する測定方法に応じて、周知の試薬を含有させることができる。
上記の診断用キットの態様は、データを取得する方法、副作用の発症を予測する方法または診断薬に関する記載に準じて実施することができる。
本発明の別の態様によれば、上記診断キットは、後述の、薬剤の予防投与の判断に用いるため、または投与した薬剤の効果を確認するために用いることもできる。本発明の別の好ましい態様によれば、上記診断キットは、後述の、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症の予測のための検査の計画を調整または決定するためのデータを取得するために用いることもできる。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定し、得られた副作用の発症の予測結果に基づき、該副作用の発症を予防、抑制もしくは遅延する方法、発症した副作用のグレードまたはirAE評価を低く保持する方法、または、発症した副作用を改善する方法が提供される。ここで、副作用のグレードまたはirAE評価が低いとは、好ましくは1~2である。上述の、副作用の発症を予防、抑制もしくは遅延する方法、発症した副作用のグレードまたはirAE評価を低く保持する方法、または、発症した副作用を改善する方法としては、例えば、有効量の薬剤を投与すること、または、投与している上記抗体医薬の量の低減または上記抗体医薬の投与の中止または休止が挙げられる。投与される薬剤は、発症が予測された、または、発症した副作用に有用な薬剤が選択される。例えば、副作用が免疫関連副作用の場合には、副腎皮質ホルモン等のステロイド、免疫抑制剤が挙げられ、ステロイドとして、具体的には、コルチゾール(ヒドロコルチゾン、コルチゾン)、プレドニゾロン(メチルプレドニゾロン、プレドニゾロン)、トリアムシノロン、デキサメタゾン、ベタメタゾンまたはそれらの塩等が挙げられる。投与される薬剤としては、好ましくは、血中半減期が3時間程度、生物学的半減期が12~36時間である、中間型のステロイド、より好ましくはメチルプレドニゾロン、プレドニゾロンである。上記いずれかの別の好ましい態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定し、副作用の発症の予測結果に基づき、薬剤を予防投与するか否かの判断に用いる方法を含んでなる。
したがって、本発明の別の好ましい態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与した対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定し、得られた副作用の発症の予測結果に基づき、該副作用の発症を予防、抑制もしくは遅延する方法、発症した副作用のグレードまたはirAE評価を低く保持する方法、または、発症した副作用を改善する方法であって、有効量の薬剤を、それを必要とする対象に投与する工程を含むものである。
また、本発明の別の好ましい態様によれば、投与した薬剤の効果を確認する方法であって、上述の薬剤が投与された対象から採取された生物学的試料において、sCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。上記薬剤の効果を確認する方法は、副作用の発症を予測する方法に関する記載に準じて実施することができる。ここで、薬剤の効果を確認するために、マーカーのレベル差またはレベル比を用いる場合には、薬剤の効果を確認する対象における、上記薬剤投与後の対象からの生物学的試料における上記マーカーのレベルと、上記抗体医薬投与前の対象から採取された生物学的試料における上記マーカーのレベルとを用いてよい。上記薬剤の投与後としては、例えば、上記薬剤を投与してから12週以内が挙げられ、好ましくは9週以内、さらに好ましくは6週以内である。上記薬剤の効果としては、例えば、副作用の発症を予防、抑制もしくは遅延すること、発症した副作用のグレードまたはirAE評価を低く保持すること、または、発症した副作用を改善することが挙げられる。
上記薬剤の有効量は、特に限定されず、薬剤の種類、純度、副作用の種類、程度、対象の種類、性質、性別、年齢、症状等に応じて当業者によって、適宜決定される。例えば、かかる有効量としては、0.1~20mg/体重kg/日、好ましくは1.0~20mg/体重kg/日を1回または数回等が挙げられる。
本発明の対象は、哺乳動物、例えば、げっ歯類、イヌ、ネコ、ウシ、霊長類などであり、好ましくはヒトであり、より好ましくは、癌、肉腫、または悪性中皮腫に罹患したヒトである。また、薬剤、好ましくはステロイド、を投与されたヒトであってもよい。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症の予測を補助する方法であって、上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を診断する方法であって、上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症の診断を補助する方法であって、上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つ抗体医薬を投与された対象における、該抗体医薬の投与に起因する副作用の発症を予測するためのマーカーとしての、sCD163またはCXCL5の使用が提供される。また、上記sCD163またはCXCL5は、好ましくは、上記対象から採取された生物学的試料中に含まれるものである。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つ抗体医薬を投与された対象において、該抗体医薬の投与に起因する副作用の発症を予測するためのマーカーの製造における、sCD163またはCXCL5の使用が提供される。
また、本発明の別の態様によれば、抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症の予測のための検査の計画を調整または決定するためのデータを取得する方法であって、上記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定することを含んでなる方法が提供される。通常、臨床検査は、上記抗体医薬の投薬間隔である2~3週間毎に行われている。上記方法において、得られたデータに基づき、副作用を発症する可能性が高いと予測された場合には、通常より短い間隔、例えば、1週間毎~週2回、に変更することができる。さらに、臨床検査項目も、副作用を発症する可能性が高いとの予測に伴い、通常の臨床検査項目から変更することができる。
上記の通常の臨床検査項目を以下に例示する。
プロトコル治療:0週(投与前)
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・併用治療・支持療法:プロトコル治療中に実施した併用療法・支持療法の内容を記録する。
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
プロトコル治療:3週
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・併用治療・支持療法:プロトコル治療中に実施した併用療法・支持療法の内容を記録する。
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
プロトコル治療終了時(6週)
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・胸部CT:間質性肺炎の有無、胸水の有無を検証
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
プロトコル治療:0週(投与前)
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・併用治療・支持療法:プロトコル治療中に実施した併用療法・支持療法の内容を記録する。
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
プロトコル治療:3週
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・併用治療・支持療法:プロトコル治療中に実施した併用療法・支持療法の内容を記録する。
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
プロトコル治療終了時(6週)
・身体所見:ECOG, PS
・皮膚所見:皮膚転移巣の有無、大きさ、個数
・血液検査(血算):赤血球、白血球、血小板、ヘモグロビン値、ヘマトクリット、白血球分画
・生化学検査:AST、ALT、γ-GTP、ALP、LDH、総ビリルビン、BUN、クレアチニン、CK、TSH、T3、T4、KL6、コルチゾール
・胸部CT:間質性肺炎の有無、胸水の有無を検証
・自他覚所見:以下の項目について、CTCAE v4.0-JCOGでGradeを判定する。
胃腸障害、皮膚および皮下組織障害、精神障害、呼吸器、胸郭および縦隔障害
上記の「副作用を発症する可能性が高いと予測された場合」に短い間隔で測定する臨床検査項目を例示する。
末梢血、白血球分画、CRP
末梢血、白血球分画、CRP
上述の、副作用の発症を予防、抑制または遅延する方法、発症した副作用のグレードまたはirAE評価を低く保持する方法、発症した副作用を改善する方法、副作用の発症の予測を補助する方法、副作用の発症を診断する方法、副作用の発症の診断を補助する方法、マーカーとしての使用、マーカーの製造のための使用、副作用の発症の予測のための検査の計画を決定するためのデータを取得する方法の態様はいずれも、データを取得する方法、副作用の発症を予測する方法と同様の手法により実施することができる。
以下、実施例により、本発明をより具体的に説明するが、本発明の技術範囲は、これらの例示に限定されるものではない。なお、特に記載しない限り、本明細書に記載の単位や測定方法はJIS規格による。
試験例1:ニボルマブ投与前後の患者の血清中のsCD163およびCXCL5の測定
ニボルマブを投与した悪性黒色腫に罹患した患者8名を対象として行った。ニボルマブを投与した患者8名のうち7名には、ニボルマブ投与に起因する副作用は認められなかった。一方、1名の患者にはニボルマブ投与に起因する副作用が認められた。副作用の認められた患者は、黒色腫転移巣を有しており、3週間に一度2mg/kgのニボルマブが投与された。ニボルマブ投与6ヶ月後に、MRIにて脳への転移、CTスキャンにて全身への転移を検査した結果、脳に転移していると診断された。同時期に、甲状腺刺激ホルモン(TSH)レベルが増加し始め(2.84μIU/mL)、ニボルマブ投与8ヶ月後に血清中のTSHレベルが7.07μIU/mLであることが確認され、上記患者は下垂体機能性低下症に罹患していることが疑われた。そのため、上記患者に関し、コルチコトロピン放出ホルモン(CRH)負荷試験を行ったところ、血清中副腎皮質刺激ホルモン(ACTH)の低下(1.0ng/mL未満)およびコルチゾールの低下(0.8μg/dL)が認められたことから、上記患者はACTH欠損症と診断された。
ニボルマブを投与した悪性黒色腫に罹患した患者8名を対象として行った。ニボルマブを投与した患者8名のうち7名には、ニボルマブ投与に起因する副作用は認められなかった。一方、1名の患者にはニボルマブ投与に起因する副作用が認められた。副作用の認められた患者は、黒色腫転移巣を有しており、3週間に一度2mg/kgのニボルマブが投与された。ニボルマブ投与6ヶ月後に、MRIにて脳への転移、CTスキャンにて全身への転移を検査した結果、脳に転移していると診断された。同時期に、甲状腺刺激ホルモン(TSH)レベルが増加し始め(2.84μIU/mL)、ニボルマブ投与8ヶ月後に血清中のTSHレベルが7.07μIU/mLであることが確認され、上記患者は下垂体機能性低下症に罹患していることが疑われた。そのため、上記患者に関し、コルチコトロピン放出ホルモン(CRH)負荷試験を行ったところ、血清中副腎皮質刺激ホルモン(ACTH)の低下(1.0ng/mL未満)およびコルチゾールの低下(0.8μg/dL)が認められたことから、上記患者はACTH欠損症と診断された。
上記患者8名について、ニボルマブの投与前および投与6週後の血清を採取し、血清中のsCD163およびCXCL5の濃度をELISA法にて測定した。具体的には、血清中のsCD163濃度測定はsCD163に特異的に結合する抗体を含むキットHuman CD163 DuoSet(カタログ番号:DY1607)(R and D system、Minneappolis,MN)を用いて、プロトコールに従い行った。血清中のCXCL5濃度測定はHuman CXCL5/ENA-78 DuoSet ELISA(カタログ番号:DY254)(R and D system、Minneappolis,MN)を用いて、プロトコールに従い行った。
また、TNFαの濃度に関しても、ニボルマブの投与前および投与6週後の血清を採取し、血清中のTNFαの濃度を、ELISA法にて測定した。具体的には、血清中のTNFα濃度測定はHuman TNFa DuoSet(カタログ番号:DY210)(R and D system、Minneappolis,MN)を用いて、プロトコールに従い行った。
図1A、Bに示される通り、ニボルマブ投与に起因する副作用が認められた1名の患者では、ニボルマブ投与に起因する副作用が認められなかった7名の患者に比べて、血清中のsCD163およびCXCL5の濃度がアップレギュレートされた(検体数 n=3の場合、対応のあるt検定、p<0.05で有意差有り)。
なお、TNFαについては全ての患者で検出されなかった。
なお、TNFαについては全ての患者で検出されなかった。
試験例2:ニボルマブ投与前後の患者の血清中のsCD163およびCXCL5の測定(46症例)
試験例1と同様にニボルマブを投与した悪性黒色腫に罹患した患者46名を対象とした。具体的には、患者1~46に、3週間に一度2mg/kgまたは2週間に一度3mg/kgニボルマブを投与した。上記患者46名について、ニボルマブの投与前および投与6週後の血清を採取し、血清中のsCD163およびCXCL5の濃度をELISA法にて測定した。なお、上記46名の患者のうち、患者1~8は試験例1の患者と同じ患者であり、試験例1の後に継続して診察を行った。
結果を表1に示す。
試験例1と同様にニボルマブを投与した悪性黒色腫に罹患した患者46名を対象とした。具体的には、患者1~46に、3週間に一度2mg/kgまたは2週間に一度3mg/kgニボルマブを投与した。上記患者46名について、ニボルマブの投与前および投与6週後の血清を採取し、血清中のsCD163およびCXCL5の濃度をELISA法にて測定した。なお、上記46名の患者のうち、患者1~8は試験例1の患者と同じ患者であり、試験例1の後に継続して診察を行った。
結果を表1に示す。

患者4、5、および7は、試験例1の診察時点ではニボルマブ投与に起因する副作用が確認されていなかった。その後の診察により、患者4はニボルマブ投与8週後に、患者5はニボルマブ投与60週後に、患者7はニボルマブ投与16週後に、表1の副作用の発症が認められた。また、患者8はニボルマブ投与30週後に下垂体炎の発症が認められた。
上記表1の結果に基づき予め設定したカットオフ値(閾値)を指標として、以下の基準に従い陽性的中率、陰性的中率、および的中率を求めた。
具体的には、実際に副作用が認められた患者のうち、本試験においても副作用を発症する可能性が高いと判定された場合を「陽性」とし、副作用を発症する可能性が高いと判定されなかった場合を「偽陰性」とした。
実際に副作用が認められかった患者のうち、本試験においても副作用を発症する可能性が高いと判定されなかった場合を「陰性」とし、副作用を発症する可能性が高いと判定された場合を「偽陽性」とした。
本試験において副作用を発症する可能性が高いと判定された患者のうち実際に副作用が認められた患者、すなわち、陽性患者、の割合を陽性的中率とした。
本試験において副作用を発症する可能性が高いと判定されなかった患者のうち実際に副作用が認められなかった患者、すなわち、陰性患者、の割合を陰性的中率とした。
実際に副作用が認められた患者のうち、本試験において副作用を発症する可能性が高いと判定された患者の割合を感度とした。
実際に副作用が認められかった患者のうち、本試験において副作用を発症する可能性が高いと判定されなかった患者の割合を特異度とした。
全患者に対する陽性患者および陰性患者の割合を本試験における的中率とした。
具体的には、実際に副作用が認められた患者のうち、本試験においても副作用を発症する可能性が高いと判定された場合を「陽性」とし、副作用を発症する可能性が高いと判定されなかった場合を「偽陰性」とした。
実際に副作用が認められかった患者のうち、本試験においても副作用を発症する可能性が高いと判定されなかった場合を「陰性」とし、副作用を発症する可能性が高いと判定された場合を「偽陽性」とした。
本試験において副作用を発症する可能性が高いと判定された患者のうち実際に副作用が認められた患者、すなわち、陽性患者、の割合を陽性的中率とした。
本試験において副作用を発症する可能性が高いと判定されなかった患者のうち実際に副作用が認められなかった患者、すなわち、陰性患者、の割合を陰性的中率とした。
実際に副作用が認められた患者のうち、本試験において副作用を発症する可能性が高いと判定された患者の割合を感度とした。
実際に副作用が認められかった患者のうち、本試験において副作用を発症する可能性が高いと判定されなかった患者の割合を特異度とした。
全患者に対する陽性患者および陰性患者の割合を本試験における的中率とした。
全46症例の増減比データについて、sCD163の平均値は10.8%、CXCL5での平均値は0.0%であった。平均値を中心とした増減比データについて、sCD163の標準偏差は30.8%、CXCL5での標準偏差は40.5%であった。
1.sCD163およびCXCL5の標準偏差を基にした閾値設定
sCD163およびCXCL5の増減比データの平均値を中心に標準偏差(σ)から±1σで閾値を設定した。(設定された閾値:sCD163の上限42%下限-20%、CXCL5の上限41%下限-41%)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表2に示す。

sCD163およびCXCL5の増減比データの平均値を中心に標準偏差(σ)から±1σで閾値を設定した。(設定された閾値:sCD163の上限42%下限-20%、CXCL5の上限41%下限-41%)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表2に示す。
2.sCD163のROC曲線を基にした閾値設定
46症例のsCD163の増減比データとその平均値の差分の絶対値に基づいてROC曲線を作成した。図2にROC曲線を示す。
ROC曲線の横軸は、(1-特異度)を表し、これは、偽陽性の割合と共に増大する。縦軸は、感度を表す。なお、作成にあたり、irAE=1を「陽性」としている。このROC曲線で「感度-(1-特異度)」が最大となる点は0.231で、ROC曲線下の面積(AUC)は0.746であった。
sCD163の平均値を中心に±21.3%で閾値を設定した。
(設定された閾値は、sCD163の上限32%下限-11%)
測定されたsCD163の増減比データが、上記閾値の上限値以上または下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表3に示す。

46症例のsCD163の増減比データとその平均値の差分の絶対値に基づいてROC曲線を作成した。図2にROC曲線を示す。
ROC曲線の横軸は、(1-特異度)を表し、これは、偽陽性の割合と共に増大する。縦軸は、感度を表す。なお、作成にあたり、irAE=1を「陽性」としている。このROC曲線で「感度-(1-特異度)」が最大となる点は0.231で、ROC曲線下の面積(AUC)は0.746であった。
sCD163の平均値を中心に±21.3%で閾値を設定した。
(設定された閾値は、sCD163の上限32%下限-11%)
測定されたsCD163の増減比データが、上記閾値の上限値以上または下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表3に示す。
3.sCD163およびCXCL5のROC曲線を基にした閾値設定
さらに、2に記載のsCD163と同様に、CXCL5の増減比データとその平均値の差分の絶対値に基づいてROC曲線を作成し、CXCL5の閾値も設定した。
(設定された閾値としては、sCD163の上限32%下限-11%、CXCL5の上限48%下限-48%であった。)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
その結果、陽性的中率は71.4%、陰性的中率は88.9%、感度は90.9%、的中率は78.3%であり、上記2のsCD163のみの場合に比べて上昇した。一方、特異度は、上記2のsCD163のみの場合と同程度であった。
さらに、2に記載のsCD163と同様に、CXCL5の増減比データとその平均値の差分の絶対値に基づいてROC曲線を作成し、CXCL5の閾値も設定した。
(設定された閾値としては、sCD163の上限32%下限-11%、CXCL5の上限48%下限-48%であった。)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
その結果、陽性的中率は71.4%、陰性的中率は88.9%、感度は90.9%、的中率は78.3%であり、上記2のsCD163のみの場合に比べて上昇した。一方、特異度は、上記2のsCD163のみの場合と同程度であった。
4.sCD163およびCXCL5で同じ閾値幅にて設定
sCD163およびCXCL5の閾値を、平均値を中心に±32%に設定した。(閾値は、sCD163の上限43%下限-21%、CXCL5上限32%下限-32%であった。)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表4に示す。
sCD163およびCXCL5の閾値を、平均値を中心に±32%に設定した。(閾値は、sCD163の上限43%下限-21%、CXCL5上限32%下限-32%であった。)
ここで、測定されたCXCL5の増減比が上記閾値の上限値以上もしくは下限値以下であるか、または、測定されたsCD163の増減比が上記閾値の上限値以上もしくは下限値以下である患者を、副作用を発症する可能性が高い患者とした。
上記基準に基づき、的中率等を求めた。
この結果を表4に示す。

Claims (15)
- 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するためのデータを取得する方法であって、
前記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。 - 前記抗PD-1抗体がニボルマブである、請求項1に記載の方法。
- 前記抗CTLA4抗体がイピリムマブである、請求項1または2に記載の方法。
- 前記抗体医薬が抗癌剤である、請求項1~3のいずれか一項に記載の方法。
- 前記副作用が免疫関連副作用である、請求項1~4のいずれか一項に記載の方法。
- 前記マーカーがsCD163およびCXCL5の組み合わせである、請求項1~5のいずれか一項に記載の方法。
- 前記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルと、前記抗体医薬投与前の対象から採取された生物学的試料における、対応するマーカーのレベルとの比較データを取得することを含んでなる、請求項1~6のいずれか一項に記載の方法。
- 前記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルまたは前記比較データが、副作用を発症する指標となる、請求項7に記載の方法。
- 前記抗体医薬を投与された対象から採取された生物学的試料における前記マーカーのレベルまたは前記比較データが、対象にステロイドを投与する指標となる、請求項7に記載の方法。
- 前記比較データが副作用を発症する指標となる、請求項8または9に記載の方法。
- 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測する方法であって、
前記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。 - 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用をモニタリングする方法であって、
前記抗体医薬を投与された対象から採取された生物学的試料においてsCD163およびCXCL5から選択される少なくとも一つのマーカーのレベルを測定すること
を含んでなる、方法。 - 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬を投与された対象において、該抗体医薬の投与に起因する副作用の発症を予測するための、sCD163またはCXCL5を含んでなるマーカー。
- 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断薬。
- 抗PD-1抗体、抗PD-L1抗体、抗CTLA4抗体およびそれらの抗原結合断片から選択される少なくとも一つの抗体医薬の投与に起因する副作用の発症を予測するための、抗sCD163抗体、抗CXCL5抗体およびそれらの抗原結合断片から選択される少なくとも一つの成分を含んでなる診断用キット。
Priority Applications (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US16/314,474 US11359017B2 (en) | 2016-07-01 | 2017-06-30 | Method of altering an antibody-related adverse event based on SCD163 and/or CXCL5 levels |
| JP2018525312A JP6910653B2 (ja) | 2016-07-01 | 2017-06-30 | 免疫チェックポイント阻害薬使用における免疫関連副作用の予測方法 |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2016131913 | 2016-07-01 | ||
| JP2016-131913 | 2016-07-01 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2018003995A1 true WO2018003995A1 (ja) | 2018-01-04 |
Family
ID=60785137
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2017/024244 WO2018003995A1 (ja) | 2016-07-01 | 2017-06-30 | 免疫チェックポイント阻害薬使用における免疫関連副作用の予測方法 |
Country Status (3)
| Country | Link |
|---|---|
| US (1) | US11359017B2 (ja) |
| JP (1) | JP6910653B2 (ja) |
| WO (1) | WO2018003995A1 (ja) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2020101039A1 (ja) * | 2018-11-16 | 2020-05-22 | 国立大学法人東北大学 | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果判定 |
| WO2020218322A1 (ja) * | 2019-04-23 | 2020-10-29 | 国立大学法人東北大学 | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果予測 |
| WO2022149410A1 (ja) | 2021-01-05 | 2022-07-14 | 公立大学法人横浜市立大学 | 妊孕性を判定するためのバイオマーカー及びそれを用いた判定方法 |
| WO2023127543A1 (ja) * | 2021-12-28 | 2023-07-06 | 国立大学法人大阪大学 | 免疫チェックポイント阻害剤による重篤な有害事象の発生の予測を補助する方法、予測補助装置 |
Families Citing this family (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2023140713A1 (ko) * | 2022-01-20 | 2023-07-27 | 재단법인 아산사회복지재단 | 면역항암제 유도 면역관련 이상반응의 발병 예측을 위한 snp 기반 모델 |
| EP4252766A1 (en) * | 2022-04-01 | 2023-10-04 | The Healthy Aging Company | Hip/pap protein or a derivative thereof for treating and/or preventing a disorder characterized by a high cxcl5 serum level in an individual |
Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2002040990A1 (fr) * | 2000-11-15 | 2002-05-23 | Akiko Itai | Procede permettant de determiner le profil d'une proteine |
| WO2015036499A1 (en) * | 2013-09-11 | 2015-03-19 | Medimmune Limited | Anti-b7-h1 antibodies for treating tumors |
| US20150118245A1 (en) * | 2012-05-08 | 2015-04-30 | H. Lee Moffitt Cancer Center And Research Institute, Inc. | Predictive Biomarkers for CTLA-4 Blockade Therapy and for PD-1 Blockade Therapy |
| EP2937698A1 (en) * | 2014-04-25 | 2015-10-28 | ImmunID | Use of immune combinatorial diversity as a predictive marker for identifying patients likely to respond to an anti-CTLA-4 treatment |
| WO2015190538A1 (ja) * | 2014-06-11 | 2015-12-17 | Idacセラノスティクス株式会社 | 免疫チェックポイント制御剤の副作用低減方法 |
| WO2016081947A2 (en) * | 2014-11-21 | 2016-05-26 | Memorial Sloan Kettering Cancer Center | Determinants of cancer response to immunotherapy by pd-1 blockade |
| WO2016100975A1 (en) * | 2014-12-19 | 2016-06-23 | Massachsetts Institute Ot Technology | Molecular biomarkers for cancer immunotherapy |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EA201590451A1 (ru) | 2012-08-30 | 2016-05-31 | Эмджен Инк. | Способ лечения меланомы с применением вируса простого герпеса и ингибитора иммунной контрольной точки |
| JP2016064989A (ja) | 2014-09-22 | 2016-04-28 | 国立研究開発法人国立がん研究センター | 癌を治療するための医薬組成物、およびpd−1阻害剤による治療に対する感受性を評価する方法 |
-
2017
- 2017-06-30 JP JP2018525312A patent/JP6910653B2/ja active Active
- 2017-06-30 US US16/314,474 patent/US11359017B2/en active Active
- 2017-06-30 WO PCT/JP2017/024244 patent/WO2018003995A1/ja active Application Filing
Patent Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2002040990A1 (fr) * | 2000-11-15 | 2002-05-23 | Akiko Itai | Procede permettant de determiner le profil d'une proteine |
| US20150118245A1 (en) * | 2012-05-08 | 2015-04-30 | H. Lee Moffitt Cancer Center And Research Institute, Inc. | Predictive Biomarkers for CTLA-4 Blockade Therapy and for PD-1 Blockade Therapy |
| WO2015036499A1 (en) * | 2013-09-11 | 2015-03-19 | Medimmune Limited | Anti-b7-h1 antibodies for treating tumors |
| EP2937698A1 (en) * | 2014-04-25 | 2015-10-28 | ImmunID | Use of immune combinatorial diversity as a predictive marker for identifying patients likely to respond to an anti-CTLA-4 treatment |
| WO2015190538A1 (ja) * | 2014-06-11 | 2015-12-17 | Idacセラノスティクス株式会社 | 免疫チェックポイント制御剤の副作用低減方法 |
| WO2016081947A2 (en) * | 2014-11-21 | 2016-05-26 | Memorial Sloan Kettering Cancer Center | Determinants of cancer response to immunotherapy by pd-1 blockade |
| WO2016100975A1 (en) * | 2014-12-19 | 2016-06-23 | Massachsetts Institute Ot Technology | Molecular biomarkers for cancer immunotherapy |
Non-Patent Citations (1)
| Title |
|---|
| KITANO, SHIGEHISA: "Gan Men'eki Ryoho no Breakthrough, Clinical development of immune check point inhibitors", JOURNAL OF CLINICAL AND EXPERIMENTAL MEDICINE, vol. 256, no. 7, 13 February 2016 (2016-02-13), pages 793 - 797 * |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2020101039A1 (ja) * | 2018-11-16 | 2020-05-22 | 国立大学法人東北大学 | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果判定 |
| WO2020218322A1 (ja) * | 2019-04-23 | 2020-10-29 | 国立大学法人東北大学 | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果予測 |
| WO2022149410A1 (ja) | 2021-01-05 | 2022-07-14 | 公立大学法人横浜市立大学 | 妊孕性を判定するためのバイオマーカー及びそれを用いた判定方法 |
| WO2023127543A1 (ja) * | 2021-12-28 | 2023-07-06 | 国立大学法人大阪大学 | 免疫チェックポイント阻害剤による重篤な有害事象の発生の予測を補助する方法、予測補助装置 |
Also Published As
| Publication number | Publication date |
|---|---|
| JPWO2018003995A1 (ja) | 2019-05-16 |
| JP6910653B2 (ja) | 2021-07-28 |
| US11359017B2 (en) | 2022-06-14 |
| US20190202915A1 (en) | 2019-07-04 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| WO2018003995A1 (ja) | 免疫チェックポイント阻害薬使用における免疫関連副作用の予測方法 | |
| WO2021164713A1 (zh) | 与肿瘤免疫治疗效果相关的生物标志物及其应用 | |
| US9535074B2 (en) | Immunoassay for soluble PD-L1 | |
| JP5963005B2 (ja) | 膵臓癌の治療のためのベバシズマブ組合せ療法のための血漿バイオマーカー | |
| RU2679913C2 (ru) | Способ диагностики или мониторинга почечной функции или диагностики почечной дисфункции | |
| US20220332828A1 (en) | Anti-pd-l1 antibody treatment of bladder cancer | |
| KR102395580B1 (ko) | 동반진단용 바이오마커 조성물 및 이를 포함하는 동반진단용 키트 | |
| CN108496084B (zh) | 通过测量血浆生物标记的水平预测疑似患有癌症的患者使用阿柏西普的治疗的结果的方法 | |
| KR20220062239A (ko) | 동반진단용 바이오마커 조성물 및 이를 포함하는 동반진단용 키트 | |
| US20220390450A1 (en) | Method of detecting or monitoring minimal residual disease in a monoclonal gammopathy patient | |
| KR102159538B1 (ko) | 폐암 환자의 면역항암제에 대한 치료 반응성 예측용 il-6 마커 및 이의 용도 | |
| EP3861347B1 (en) | Biomarkers for a combination therapy comprising lenvatinib and everolimus | |
| WO2020218322A1 (ja) | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果予測 | |
| WO2020101039A1 (ja) | 血中ケモカインを用いた免疫チェックポイント阻害薬の治療効果判定 | |
| US20230310499A1 (en) | Plasma exchange removal of spd-l1 | |
| EP4014045B1 (en) | Diagnosis of cancer using detection of auto-antibodies directed against pd1 and pd-l1 | |
| Liu et al. | Therapeutic drug monitoring of immune checkpoint inhibitors: based on their pharmacokinetic properties and biomarkers | |
| Hutcherson et al. | Monoclonal gammopathy detection and current technologies | |
| WO2023056387A1 (en) | Diagnosing multiple sclerosis (ms) | |
| Boekhout et al. | Concise Drug Monograph: trastuzumab |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 17820349 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2018525312 Country of ref document: JP Kind code of ref document: A |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 17820349 Country of ref document: EP Kind code of ref document: A1 |