WO2007081744A2 - Methods and compositions for administration of iron - Google Patents
Methods and compositions for administration of iron Download PDFInfo
- Publication number
- WO2007081744A2 WO2007081744A2 PCT/US2007/000176 US2007000176W WO2007081744A2 WO 2007081744 A2 WO2007081744 A2 WO 2007081744A2 US 2007000176 W US2007000176 W US 2007000176W WO 2007081744 A2 WO2007081744 A2 WO 2007081744A2
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- iron
- complex
- grams
- carbohydrate
- disease
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7135—Compounds containing heavy metals
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/715—Polysaccharides, i.e. having more than five saccharide radicals attached to each other by glycosidic linkages; Derivatives thereof, e.g. ethers, esters
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/715—Polysaccharides, i.e. having more than five saccharide radicals attached to each other by glycosidic linkages; Derivatives thereof, e.g. ethers, esters
- A61K31/716—Glucans
- A61K31/721—Dextrans
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K33/00—Medicinal preparations containing inorganic active ingredients
- A61K33/24—Heavy metals; Compounds thereof
- A61K33/26—Iron; Compounds thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0019—Injectable compositions; Intramuscular, intravenous, arterial, subcutaneous administration; Compositions to be administered through the skin in an invasive manner
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P1/00—Drugs for disorders of the alimentary tract or the digestive system
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P13/00—Drugs for disorders of the urinary system
- A61P13/12—Drugs for disorders of the urinary system of the kidneys
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P19/00—Drugs for skeletal disorders
- A61P19/02—Drugs for skeletal disorders for joint disorders, e.g. arthritis, arthrosis
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P3/00—Drugs for disorders of the metabolism
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
- A61P35/02—Antineoplastic agents specific for leukemia
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/06—Antianaemics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
- A61P9/04—Inotropic agents, i.e. stimulants of cardiac contraction; Drugs for heart failure
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07H—SUGARS; DERIVATIVES THEREOF; NUCLEOSIDES; NUCLEOTIDES; NUCLEIC ACIDS
- C07H23/00—Compounds containing boron, silicon, or a metal, e.g. chelates, vitamin B12
Definitions
- the present invention generally relates to treatment of iron-related conditions with iron carbohydrate complexes.
- Parenteral iron therapy is known to be effective in a variety of diseases and conditions including, but not limited to, severe iron deficiency, iron deficiency anemia, problems of intestinal iron absorption, intestinal iron intolerance, cases where regular intake of an oral iron preparation is not guaranteed, iron deficiency where there is no response to oral therapy (e.g., dialysis patients), and situations where iron stores are scarcely or not at all formed but would be important for further therapy (e.g., in combination with erythropoietin).
- erythropoietin e.g., in combination with erythropoietin.
- Geisser et al., Arzneiffenforschung (1992) 42(12), 1439-1452 There exist various commercially available parenteral iron formulations. But many currently available parenteral iron drugs, while purportedly effective at repleting iron stores, have health risks and dosage limitations associated with their use.
- Iron dextran the first parenteral iron product available in the United States (US) has been associated with an incidence of anaphylactoid-type reactions (i.e., dyspnea, wheezing, chest pain, hypotension, urticaria, angioedema).
- anaphylactoid-type reactions i.e., dyspnea, wheezing, chest pain, hypotension, urticaria, angioedema.
- Negative characteristics include high pH, high osmolarity, low dosage limits (e.g., maximum 500 mg iron once per week, not exceeding 7 mg iron/kg body weight), and the long duration of administration (e.g., 100 mg iron over at least 5 minutes as an injection; 500 mg iron over at least 3.5 hours as a drip infusion). Furthermore, injectable high molecular mass substances produce more allergic reactions than the corresponding low molecular mass substances. Geisser et al. (1992) Arzneiffenbachforschung 42: 1439-1452.
- Ferumoxytol is a newer parenteral iron formulation but limited information is available as to its efficacy and administration. See e.g., Landry et al. (2005) Am J Nephrol 25, 400-410, 408; and Spinowitz et al. (2005) Kidney lntl 68, 1801-1807; U.S. Patent No. 6,599,498.
- the present invention is directed to use of iron carbohydrate complexes that can be administered parenterally at relatively high single unit dosages, thereby providing a safe and efficient means for delivery of a total dose of iron in fewer sessions over the course of therapeutic treatment.
- the present teachings include methods of treating a disease, disorder, or condition characterized by iron deficiency or dysfunctional iron metabolism through the administration of at least 0.6 grams of elemental iron via a single unit dosage of an iron carbohydrate complex to a subject that is in need of such therapy.
- the method treats anemia.
- the anemia is an iron deficiency anemia, such as that associated with chronic blood loss; acute blood loss; pregnancy; childbirth; childhood development; psychomotor and cognitive development in children; breath holding spells; heavy uterine bleeding; menstruation; chronic recurrent hemoptysis; idiopathic pulmonary siderosis; chronic internal bleeding; gastrointestinal bleeding; parasitic infections; chronic kidney disease; dialysis; surgery or acute trauma; and chronic ingestion of alcohol, chronic ingestion of salicylates, chronic ingestion of steroids; chronic ingestion of non-steroidial anti-inflammatory agents, or chronic ingestion of erythropoiesis stimulating agents.
- the anemia is anemia of chronic disease, such as rheumatoid arthritis; cancer; Hodgkins leukemia; non-Hddgkins leukemia; cancer chemotherapy; inflammatory bowel disease; ulcerative colitis thyroiditis; hepatitis; systemic lupus erythematosus; polymyalgia rheumatica; scleroderma; mixed connective tissue disease; Sojgren's syndrome; congestive heart failure / cardiomyopathy; or idiopathic geriatric anemia.
- chronic disease such as rheumatoid arthritis; cancer; Hodgkins leukemia; non-Hddgkins leukemia; cancer chemotherapy; inflammatory bowel disease; ulcerative colitis thyroiditis; hepatitis; systemic lupus erythematosus; polymyalgia rheumatica; scleroderma; mixed connective tissue disease; Sojgren's syndrome; congestive heart failure / cardiomyopathy
- the anemia is due to impaired iron absorption or poor nutrition, such as anemia associated with ' Crohn's Disease; gastric surgery; ingestion of drug products that inhibit iron absorption; and chronic use of calcium.
- the method treats restless leg syndrome; blood donation; Parkinson's disease; hair loss; or attention deficit disorder.
- the single dosage unit of elemental iron is between at least about 0.6 grams and 2.5 grams. In some embodiments, the single dosage unit of elemental iron is at least about 0.7 grams; at least about 0.8 grams; at least about 0.9 grams; at least about 1.0 grams; at least about 1.1 grams; at least about 1.2 grams; at least about 1.3 grams; at least about 1 A grams; at least about 1.5 grams; at least about 1.6 grams; at least about 1.7 grams; at least about 1.8 grams; at least about 1.9 grams; at least about 2.0 grams; at least about 2.1 grams; at least about 2.2 grams; at least about 2.3 grams; at least about 2.4 grams; or at least about 2.5 grams.
- the single dosage unit of elemental iron is administered in about 15 minutes or less. In some embodiments, the single dosage unit of elemental iron is administered in about 10 minutes or less, about 5 minutes or less, or about 2 minutes or less.
- the subject does not experience a significant adverse reaction to the single dosage unit administration.
- the iron carbohydrate complex has a pH between about 5.0 to about 7.0; physiological osmolarity; an iron core size no greater than about 9 nm; a mean diameter particle size no greater than about 35 nm; a blood half-life of between about 10 hours to about 20 hours; a substantially non-immunogenic carbohydrate component; and substantially no cross reactivity with anti-dextran antibodies.
- the iron carbohydrate complex contains about 24% to about 32% elemental iron; contains about 25% to about 50% carbohydrate; has a molecular weight of about 90,000 daltons to about 800,000 daltons, or some combination thereof.
- the iron carbohydrate complex is an iron monosaccharide complex, an iron disaccharide complex, or an iron polysaccharide complex.
- the iron carbohydrate complex is iron carboxymaltose complex, iron mannitol complex, iron polyisomaltose complex, iron polymaltose complex, iron gluconate complex, iron sorbitol complex, or an iron hydrogenated dextran complex.
- the iron carbohydrate complex is an iron polyglucose sorbitol carboxymethyl ether complex.
- the iron carboxymaltose complex contains about 24% to about 32% elemental iron, about 25% to about 50% carbohydrate, and is about 100,000 daltons to about 350,000 daltons.
- the iron carboxymaltose complex is obtained from an aqueous solution of iron (III) salt and an aqueous solution of the oxidation product of one or more maltodextrins using an aqueous hypochlorite solution at a pH value within the alkaline range, wherein, when one maltodextrin is applied, its dextrose equivalent lies between 5 and 20, and when a mixture of several maltodextrins is applied, the dextrose equivalent lies between 5 and 20 and the dextrose equivalent of each individual maltodextrin contained in the mixture lies between 2 and 20.
- the iron carboxymaltose complex has a chemical formula of [FeO x (OH) y (H 2 O) 2 I n [ ⁇ (C 6 H 10 O 5 ) m (C 6 H 12 O 7 )Ji ] k , where n is about 103, m is about 8, 1 is about 11, and k is about 4; contains about 28% elemental iron; and has a molecular weight of about 150,000 Da.
- the iron carboxymaltose complex is polynuclear iron (lll)-hydroxide 4(R)-(poly-(1 ⁇ 4)-0- ⁇ -glucopyranosyl)-oxy-2(R),3(S),5(R),6- tetrahydroxy-hexanoate.
- the iron carbohydrate complex comprises an iron core with a mean iron core size of no greater than about 9 nm.
- the mean iron core size is at least about 1 nm but no greater than about 9 nm; at least about 3 nm but no greater than about 7 nm; or at least about 4 nm but not greater than about 5 nm.
- the mean size of a particle of the iron carbohydrate complex is no greater than about 35 nm. In some embodiments, the particle mean size is no greater than about 30 nm. In some embodiments, the particle mean size is no greater than about 25 nm. In some embodiments, the particle mean size is no greater than about 20 nm; no greater than about 15 nm; no greater than about 10 nm; or at least about 6 nm but no greater than about 7 nm.
- the iron carbohydrate complex is administered parenterally, for example intravenously or intramuscularly.
- the iron carbohydrate complex is intravenously infused.
- the single unit dose of iron carbohydrate complex is intravenously infused at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, for example, about 250 ml of diluent or about 215 ml of diluent.
- the iron carbohydrate complex is intravenously injected as a bolus.
- the iron carbohydrate complex is intravenously injected as a bolus at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, for example, about 250 ml of diluent or about 215 ml of diluent. In some embodiments, the iron carbohydrate complex is intramuscularly infused at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, for example, about 250 ml of diluent or about 215 ml of diluent. In some embodiments, the iron carbohydrate complex is intramuscularly infused at a concentration of about 500 mg elemental iron in less than about 10 ml diluent.
- the method also includes a second administration of the iron carbohydrate complex upon recurrence of at least one symptom of the treated disease, disorder, or condition.
- the method also includes a second administration of the iron carbohydrate complex after 1 day to 12 months after the first administration.
- the method of treating a disease, disorder, or condition characterized by iron deficiency or dysfunctional iron metabolism comprises intravenously administering to a subject in need thereof an iron carboxymaltose complex in a single dosage unit of at least about 1000 mg of elemental iron in about 200 ml to about 300 ml of diluent in about 5 minutes or less; wherein the iron carboxymaltose complex comprises an iron core with a mean iron core size of at least about 1 nm but no greater than about 9 nm; mean size of a particle of the iron carboxymaltose complex is no greater than about 35 nm; and the iron carboxymaltose complex is administered intravenously infused or intravenously injected at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent.
- the iron carboxymaltose complex is polynuclear iron (lll)-hydroxide 4(R)-(poly-(1— >4)-0-a-glucopyranosyl)-oxy-2(R),3(S),5 ⁇ R),6-tetrahydroxy-hexanoate.
- the iron carboxymaltose complex is obtained from an aqueous solution of iron (III) salt and an aqueous solution of the oxidation product of one or more maltodextrins using an aqueous hypochlorite solution at a pH value within the alkaline range, wherein, when one maltodextrin is applied, its dextrose equivalent lies between about 5 and about 20, and when a mixture of several maltodextrins is applied, the dextrose equivalent lies between about 5 and about 20 and the dextrose equivalent of each individual maltodextrin contained in the mixture lies between about 2 and about 20.
- FIG I is a series of electron micrographs that depict the particle size of three iron carbohydrate complexes.
- FIG 1 A is an electron micrograph depicting the particle size of Dexferrum (an iron dextran).
- FIG 1 B is an electron micrograph depicting the particle size of Venofer (an iron sucrose).
- FIG 1C is an electron micrograph depicting the particle size of polynuclear iron (lll)-hydroxide 4(R)-(poly-(1 ⁇ 4)-O- ⁇ -glucopyranosyl)-oxy-2(R),3(S),5(R),6- tetrahydroxy-hexanoate ("VIT-45", an iron carboxymaltose complex).
- FIG 2 is a schematic representation of an exemplary iron carboxymaltose complex.
- the present invention makes use of iron carbohydrate complexes that can be administered parenterally at relatively high single unit dosages for the therapeutic treatment of a variety of iron-associated diseases, disorders, or conditions.
- states indicative of a need for therapy with high single unit dosages of iron carbohydrate complexes include, but are not limited to iron deficiency anemia, anemia of chronic disease, and states characterized by dysfunctional iron metabolism.
- Efficacious treatment of these, and other, diseases and conditions with parenteral iron formulations (supplied at lower single unit dosages than those described herein) is generally known in the art. See e.g.. Van Wyck et al. (2004) J Am Soc Nephrol 15, S91-S92.
- the present invention is directed to use of iron carbohydrate complexes that can be administered parenterally at relatively high single unit dosages, thereby providing a safe and efficient means for delivery of a total dose of iron in fewer sessions over the course of therapeutic treatment.
- Iron deficiency anemia is associated with, for example, chronic blood loss; acute blood loss; pregnancy; childbirth; childhood development; psychomotor and cognitive development in children; breath holding spells; heavy uterine bleeding; menstruation; chronic recurrent hemoptysis; idiopathic pulmonary siderosis; chronic internal bleeding; gastrointestinal bleeding; parasitic infections; chronic kidney disease; dialysis; surgery or acute trauma; and chronic ingestion of alcohol, chronic ingestion of salicylates, chronic ingestion of steroids; chronic ingestion of non-steroidial anti-inflammatory agents, or chronic ingestion of erythropoiesis stimulating agents.
- Anemia of chronic disease is associated with, for example, rheumatoid arthritis; cancer; Hodgkins leukemia; non-Hodgkins leukemia; cancer chemotherapy; inflammatory bowel disease; ulcerative colitis thyroiditis; hepatitis; systemic lupus erythematosus; polymyalgia rheumatica; scleroderma; mixed connective tissue disease; Sojgren's syndrome; congestive heart failure / cardiomyopathy; and idiopathic geriatric anemia.
- Anemia is also associated with, for example, Crohn's Disease; gastric surgery; ingestion of drug products that inhibit iron absorption; and chronic use of calcium.
- States characterized by dysfunctional iron metabolism and treatable with the single unit dosages of iron carbohydrate complexes described herein include, but are not limited to, restless leg syndrome; blood donation; Parkinson's disease; hair loss; and attention deficit disorder.
- each of the above listed states, diseases, disorders, and conditions, as well as others, can benefit from the treatment methodologies described herein.
- treating a state, disease, disorder, or condition includes preventing or delaying the appearance of clinical symptoms in a mammal that may be afflicted with or predisposed to the state, disease, disorder, or condition but does not yet experience or display clinical or subclinical symptoms thereof.
- Treating can also include inhibiting the state, disease, disorder, or condition, e.g., arresting or reducing the development of the disease or at least one clinical or subclinical symptom thereof. Furthermore, treating can include relieving the disease, e.g., causing regression of the state, disease, disorder, or condition or at least one of its clinical or subclinical symptoms.
- the benefit to a subject to be treated is either statistically significant or at least perceptible to the patient or to the physician.
- Measures of efficacy of iron replacement therapy are generally based on measurement of iron-related parameters in blood.
- the aim of treatment is usually to return both Hb and iron stores to normal levels.
- efficacy of iron replacement therapy can be interpreted in terms of the ability to normalise Hb levels and iron stores.
- the effectiveness of treatment with one or more single unit doses of iron carbohydrate complex, as described herein can be demonstrated, for example, by improvements in ferritin and transferrin saturation, and in raising hemoglobin levels in anemic patients.
- Iron stores can be assessed by interpreting serum ferritin levels. TfS is frequently used, in addition, to diagnose absolute or functional iron deficiencies. In patients with iron deficiency, serum transferrin is elevated and will decrease following successful iron treatment.
- Methods of treatment of various diseases, disorders, or conditions with iron complex compositions comprise the administration of the complex in single unit dosages of at least 0.6 grams of elemental iron to about at least 2.5 grams of elemental iron.
- Administration of single unit dosages can be, for example, over pre-determined time intervals or in response to the appearance and/or reappearance of symptoms.
- the iron carbohydrate complex can be re-administered upon recurrence of at least one symptom of the disease or disorder.
- the iron carbohydrate complex can be re-administered at some time period after the initial administration (e.g., after 4 days to 12 months).
- any route of delivery of the single unit dose of iron carbohydrate complex is acceptable so long as iron from the iron complex is released such that symptoms are treated.
- the single unit dose of iron carbohydrate complex can be administered parenterally, for example intravenously or intramuscularly. Intravenous administration can be delivered as a bolus or preferably as an infusion.
- the single unit dose of iron carbohydrate complex can be intravenously infused at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, preferably about 215 ml of diluent or about 250 ml of diluent.
- the iron carbohydrate complex can be intravenously injected as a bolus.
- the iron carbohydrate complex can be intravenously injected as a bolus at a concentration of about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, preferably about 215 ml of diluent or about 250 ml of diluent.
- the iron carbohydrate complex can be intramuscularly infused at a concentration of, for example, about 1000 mg elemental iron in about 200 ml to about 300 ml of diluent, preferably, about 250 ml of diluent or about 215 ml of diluent.
- the iron carbohydrate complex can be diluted with sterile saline (e.g., polynuclear iron (Hl)- hydroxide 4(R)-(poly-(1— f-4)-O- ⁇ -glucopyranosyl)-oxy-2(R),3(S),5(R),6-tetrahydroxy-hexanoate ("VIT-45") 0.9% m/V NaCI or 500 mg iron in up to 250 mL NaCI).
- the iron carbohydrate complex can be intravenously injected as a bolus without dilution.
- the iron carbohydrate complex can be intramuscularly injected at a concentration of about 500 mg elemental iron in less than about 10 ml diluent, preferably about 5 ml.
- total iron dosage will depend on the iron deficit of the patient.
- One skilled in the art can tailor the total iron dose required for a subject while avoiding iron overload, as overdosing with respect to the total required amount of iron has to be avoided, as is the case for all iron preparations.
- the total iron dosage can be delivered as a single unit dosage or a series of single unit dosages.
- An appropriate single unit dosage level will generally be at least 0.6 grams of elemental iron, particularly at least 0.7 grams; at least 0.8 grams; at least 0.9 grams; at least 1.0 grams; at least 1.1 grams; at least 1.2 grams; at least 1.3 grams; at least 1.4 grams; at least 1.5 grams; at least 1.6 grams; at least 1.7 grams; at least 1.8 grams; at least 1.9 grams; at least 2.0 grams; at least 2.1 grams; at least 2.2 grams; at least 2.3 grams; at least 2.4 grams; or at least 2.5 grams.
- a single unit dosage is at least 1.0 grams of elemental iron.
- a single unit dosage is at least 1.5 grams of elemental iron.
- a single unit dosage is at least 2.0 grams of elemental iron.
- a single unit dosage is at least 2.5 grams of elemental iron.
- an appropriate single unit dosage level can also be determined on the basis of patient weight.
- an appropriate single unit dosage level will generally be at least 9 mg of elemental iron per kg body weight, particularly at least 10.5 mg/kg, at least 12 mg/kg, at least 13.5 mg/kg, at least 15 mg/kg, at least 16.5 mg/kg, at least 18 mg/kg, at least 19.5 mg/kg, at least 21 mg/kg, at least 22.5 mg/kg, at least 24 mg/kg, at least 25.5 mg/kg, at least 27 mg/kg, at least 28.5 mg/kg, at least 30 mg/kg, at least 31.5 mg/kg, at least 33 mg/kg, at least 34.5 mg/kg, at least 36 mg/kg, or at least 37.5 mg/kg.
- a single unit dosage can be administered in 15 minutes or less.
- the single unit dosage can be administered in 14 minutes or less, 13 minutes or less, 12 minutes or less, 11 minutes or less, 10 minutes or less, 9 minutes or less, 8 minutes or less, 7 minutes or less, 6 minutes or less, 5 minutes or less, 4 minutes or less, 3 minutes or less, or 2 minutes or less.
- Administration of iron can occur as a one-time delivery of a single unit dose or over a course of treatment involving delivery of multiple single unit doses.
- Multiple single unit doses can be administered, for example, over pre-determined time intervals or in response to the appearance and reappearance of symptoms.
- the frequency of dosing depends on the disease or disorder being treated, the response of each individual patient, and the administered amount of elemental iron.
- An appropriate regime of dosing adequate to allow the body to absorb the iron from the bloodstream can be, for example, a course of therapy once every day to once every eighteen months.
- Such consecutive single unit dosing can be designed to deliver a relatively high total dosage of iron over a relatively low period of time.
- a single unit dose e.g., 1000 mg
- a total dose of 2000, 2500, 3000, 3500, 4000, 4500, or 5000 mg of elemental iron can be delivered via consecutive daily single unit doses of about 600 mg to about 1000 mg of elemental iron.
- a single unit dose of 1000 mg can be intravenously introduced into a patient in a concentrated form over, for example, two minutes, such administrative protocol provides a practitioner and patient with an effective, efficient, and safe means to deliver elemental iron.
- a single unit dose can be administered every 3-4 days.
- a single unit dose can be administered once per week.
- the single unit doses of iron complex may be administered ad hoc, that is, as symptoms reappear, as long as safety precautions are regarded as practiced by medical professionals.
- Iron carbohydrate complex can be given as a single unit dose for the treatment of Restless Leg Syndrome.
- 1000 mg of elemental iron from an iron carboxymaltose e.g., polynuclear iron (lll)-hydro ⁇ ide 4(R)-(poly-(1 ⁇ 4)-0- ⁇ -glucopyranosyl)-oxy- 2(R),3(S),5(R),6-tetrahydroxy-hexanoate
- a single dose e.g., 1.5-5 mg iron/ml in normal saline
- a single intravenous treatment can provide relief of symptoms for an extended period of time.
- post- infusion changes in central nervous system iron status can be monitored using measurements of cerebral spinal fluid (CSF) ferritin (and other iron-related proteins) and of brain iron stores using MRI.
- CSF cerebral spinal fluid
- Post-infusion changes in Restless Leg Syndrome are assessed using standard subjective (e.g., patient diary, rating scale) and objective (e.g., P50, SlT, Leg Activity Meters) measures of clinical status.
- CSF and serum iron values MRI measures of brain iron and full clinical evaluations with sleep and immobilization tests are obtained prior to treatment, approximately two weeks after treatment, and again twelve months later or when symptoms return. Clinical ratings, Leg Activity Meter recordings and serum ferritin are obtained monthly after treatment. CSF ferritin changes can also be used to assess symptom dissipation.
- Iron carbohydrate complex can be given as a single unit dose for the treatment of iron deficiency anemia secondary to heavy uterine bleeding.
- a single unit dose of 1 ,000 mg of elemental iron from an iron carboxymaltose in about 250 cc normal saline can be intravenously injected into a subject suffering from iron deficiency anemia secondary to heavy uterine bleeding over 15 minutes every week until a calculated iron deficit dose has been administered.
- the iron deficit dose can be calculated as follows:
- Iron carbohydrate complex can be given as a single unit dose for the treatment of iron deficiency anemia.
- a subject diagnosed as suffering from iron deficiency anemia can be, for example, intravenously injected with a dose of 1 ,000 mg of iron as VIT- 45 (or 15 mg/kg for weight ⁇ 66 kg) in 250 cc of normal saline over 15 minutes.
- Subjects with iron deficiency anemia secondary to dialysis or non-dialysis dependent-Chronic Kidney Disease (CKD) as per K/DOQI guidelines will generally have Hgb ⁇ 12 g/dL; TSAT ⁇ 25%; and Ferritin ⁇ 300 ng/mL.
- CKD non-dialysis dependent-Chronic Kidney Disease
- Subjects with iron deficiency anemia secondary to Inflammatory Bowel Disease will generally have Hgb ⁇ 12 g/dL; TSAT ⁇ 25%; and Ferritin ⁇ 300 ng/mL.
- Subjects with iron deficiency anemia secondary to other conditions will generally have Hgb ⁇ 12 g/dL-; TSAT ⁇ 25%; and Ferritin ⁇ 100 ng/mL.
- Single unit dosages of intravenous iron described herein can be administered to a subject where there is a clinical need to deliver iron rapidly or in higher doses and/or in subjects with functional iron deficiency such as those on erythropoietin therapy.
- a determination of the need for treatment with parenteral iron is within the abilities of one skilled in the art. For example, need can be assessed by monitoring a patient's iron status. The diagnosis of iron deficiency can be based on appropriate laboratory tests, for example, haemoglobin (Hb), serum ferritin, serum iron, transferrin saturation (TfS), and hypochromic red cells.
- a determination of the need for treatment with high dosages of parenteral iron can be also be determined through diagnosis of a patient as suffering from a disease, disorder, or condition that is associated with iron deficiency or dysfunctional iron metabolism. For example, many chronic renal failure patients receiving erythropoietin will require intravenous iron to maintain target iron levels. As another example, most hemodialysis patients will require repeated intravenous iron administration, due to dialysis-associated blood loss and resulting negative iron balance.
- Monitoring frequency can depend upon the disease, disorder, or condition the patient is afflicted with or at risk for. For example, in a patient initiating erythropoietin therapy, iron indices are monitored monthly. As another example, in patients who have achieved target range Hb or are receiving intravenous iron therapy, TSAT and ferritin levels can be monitored every 3 months.
- a patient's iron status can be indicative of an absolute or a functional iron deficiency, both of which can be treated with the compositions and methods described herein.
- An absolute iron deficiency occurs when an insufficient amount of iron is available to meet the body's requirements.
- the insufficiency may be due to inadequate iron intake, reduced bioavailability of dietary iron, increased utilization of iron, or chronic blood loss.
- Prolonged iron deficiency can lead to iron deficiency anemia — a microcytic, hypochromic anemia in which there are inadequate iron stores.
- Absolute iron deficiency is generally indicated where TSAT ⁇ 20% and Ferritin ⁇ 100 ng/mL.
- Functional iron deficiency can be characterized by the following characteristics: Inadequate hemoglobin response to erythropoietin; Serum ferritin may be normal or high; Transferrin saturation (TSAT) usually ⁇ 20%; and/or reduced mean corpuscular volume (MCV) or mean corpuscular hemoglobin concentration (MCHC) in severe cases.
- Functional iron deficiency i.e., iron stores are thought to be adequate but unavailable for iron delivery
- TSAT ⁇ 20% and Ferritin >100 ng/mL.
- the target hemoglobin level of a patient can be selected as 11.0 g/dL to 12.0 g/dL (hematocrit approximately 33% to 36%).
- sufficient iron supplied via an iron carbohydrate complex, is provided to maintain TSAT ⁇ 20% and ferritin ⁇ 100 ng/mL.
- TSAT levels are below 20%, the likelihood that hemoglobin will rise or erythropoietin doses fall after iron administration is high. Achievement of target hemoglobin levels with optimum erythropoietin doses is associated with providing sufficient iron to maintain TSAT above 20%.
- Iron therapy can be given to maintain target hemoglobin while preventing iron deficiency and also preventing iron overload. Adjusting dosage of iron to maintain target levels of hemoglobin, hematocrit, and laboratory parameters of iron storage is within the normal skill in the art. For example, where a patient is anemic or iron deficient, intravenous iron can be administered when a patient has a ferritin ⁇ 800, a TSAT ⁇ 50, and/or a Hemoglobin ⁇ 12. Iron overload can be avoided by withholding iron for TSAT >50% and/or ferritin >800 ng/mL.
- Iron carbohydrate complexes are commercially available, or have well known syntheses.
- iron carbohydrate complexes include iron monosaccharide complexes, iron disaccharide complexes, iron oligosaccharide complexes, and iron polysaccharide complexes, such as: iron carboxymaltose, iron sucrose, iron polyisomaltose (iron dextran), iron polymaltose (iron dextrin), iron gluconate, iron sorbitol, iron hydrogenated dextran, which may be further complexed with other compounds, such as sorbitol, citric acid and gluconic acid (for example iron dextrin-sorbitol-citric acid complex and iron sucrose-gluconic acid complex), and mixtures thereof.
- iron carbohydrate complexes for use in the methods described herein are those which have one or more of the following characteristics: a nearly neutral pH (e.g., about 5 to about 7); physiological osmolality; stable carbohydrate component; an iron core size no greater than about 9 nm; mean diameter particle size no greater than about 35 nm, preferably about 25 nm to about 30 nm; slow and competitive delivery of the complexed iron to endogenous iron binding sites; serum half-life of over about 7 hours; low toxicity; non- immunogenic carbohydrate component; no cross reactivity with anti-dextran antibodies; and/or low risk of anaphylactoid / hypersensitivity reactions.
- a nearly neutral pH e.g., about 5 to about 7
- physiological osmolality e.g., about 9 nm
- mean diameter particle size no greater than about 35 nm, preferably about 25 nm to about 30 nm
- slow and competitive delivery of the complexed iron to endogenous iron binding sites
- Useful techniques to assess physical and electronic properties include absorption spectroscopy, X-ray diffraction analysis, transmission electron microscopy, atomic force microscopy, and elemental analysis. See Kudasheva et al. (2004) J lnorg Biochem 98, 1757-1769. Pharmacokinetics can be assessed, for example, by iron tracer experiments. Hypersensitivity reactions can be monitored and assessed as described in, for example, Bailie et al. (2005) Nephrol Dial Transplant, 20(7), 1443-1449. Safety, efficacy, and toxicity in human subjects can be assessed, for example, as described in Spinowitz et al. (2005) Kidney lntl 68, 1801-1807.
- a particularly preferred iron carbohydrate complex will have a pH between 5.0- 7.0; physiological osmolarity; an iron core size no greater than 9 nm; mean diameter particle size no greater than 30 nm; serum half-life of over 10 hours; a non-immunogenic carbohydrate component; and no cross reactivity with anti-dextran antibodies.
- iron carbohydrate complex for use in the methods described herein is an iron carboxy-maltose complex (e.g., polynuclear iron (lll)-hydroxide 4(R)-(poly-(1— »4)-O- ⁇ -glucopyranosyl)-oxy- 2(R),3(S),5(R),6-tetrahydroxy-hexanoate, "VIT-45").
- an iron carboxy-maltose complex e.g., polynuclear iron (lll)-hydroxide 4(R)-(poly-(1— »4)-O- ⁇ -glucopyranosyl)-oxy- 2(R),3(S),5(R),6-tetrahydroxy-hexanoate, "VIT-45”
- Another example of a preferred iron carbohydrate complex for use in the methods described herein is a carboxyalkylated reduced polysaccharide iron oxide complex (e.g., ferumoxytol, described in U
- an iron carbohydrate complex for use in methods disclosed herein, contains about 24% to about 32% elemental iron, more preferably about 28% elemental iron.
- an iron carbohydrate complex for use in methods disclosed herein, contains about 25% to about 50% carbohydrate (e.g., total glucose).
- an iron carbohydrate complex, for use in methods disclosed herein is about 90,000 daltons to about 800,000 daltons, more preferably 100,000 daltons to about 350,000 daltons.
- Iron carboxymaltose complex [0065] One preferred iron carbohydrate complex for use in the methods described herein is an iron carboxymaltose complex.
- An example of an iron carboxymaltose complex is polynuclear iron (lll)-hydroxide 4(R)-(poly-(1 ⁇ 4)-O- ⁇ -glucopyranosyl)-oxy-2(R),3(S),5(R),6- tetrahydroxy-hexanoate ("VIT-45").
- VIT-45 is a Type I polynuclear iron (III) hydroxide carbohydrate complex that can be administered as parenteral iron replacement therapy for the treatment of various anemi.a-related conditions as well as other iron-metabolism related ⁇ conditions.
- VIT-45 can be represented by the chemical formula: [FeOx(OH)y(H2O)z]n [ ⁇ (C6H10O5)m (C6H12O7) ⁇ ! ]k, where n is about 103, m is about 8, 1 is about 11, and k is about 4).
- the molecular weight of VIT-45 is about 150,000 Da.
- An exemplary depiction of VIT-45 is provided in Figure 2.
- the degradation rate and physicochemical characteristics of the iron carbohydrate complex make it an efficient means of parenteral iron delivery to the body stores. It is more efficient and less toxic than the lower molecular weight complexes such as iron sorbitol/citrate complex, and does not have the same limitations of high pH and osmolarity that leads to dosage and administration rate limitations in the case of, for example, iron sucrose and iron gluconate.
- the iron carboxymaltose complex (e.g., VIT-45) generally does not contain dextran and does not react with dextran antibodies; therefore, the risk of anaphylactoid /hypersensitivity reactions is very low compared to iron dextran.
- the iron carboxymaltose complex (e.g., VIT-45) has a nearly neutral pH (5.0 to 7.0) and physiological osmolarity, which makes it possible to administer higher single unit doses over shorter time periods than other iron- carbohydrate complexes.
- the iron carboxymaltose complex (e.g., VIT-45) can mimic physiologically occurring ferritin.
- the carbohydrate moiety of iron carboxymaltose complex (e.g., VIT-45) is metabolized by the glycolytic pathway. Like iron dextran, the iron carboxymaltose complex ⁇ e.g., VIT-45) is more stable than iron gluconate and sucrose. The iron carboxymaltose complex (e.g., VIT-45) produces a slow and competitive delivery of the complexed iron to endogenous iron binding sites resulting in an acute toxicity one-fifth that of iron sucrose.
- These characteristics of the iron carboxymaltose complex (e.g., VIT-45) allow administration of higher single unit doses over shorter periods of time than, for example, iron gluconate or iron sucrose. Higher single unit doses can result in the need for fewer injections to replete iron stores, and consequently is often better suited for outpatient use.
- the iron carboxymaltose complex (e.g., VIT- 45) is mainly found in the liver, spleen, and bone marrow.
- Pharmacokinetic studies using positron emission tomography have demonstrated a fast initial elimination of radioactively labeled iron (Fe) 52 Fe/ 59 Fe VIT-45 from the blood, with rapid transfer to the bone marrow and rapid deposition in the liver and spleen. See e.g., Beshara et al. (2003) Br J Haematol 2003; 120(5): 853-859.
- Eight hours after administration 5 to 20% of the injected amount was observed to be still in the blood, compared with 2 to 13% for iron sucrose.
- the projected calculated terminal half-life (iy,) was approximately 16 hours, compared to 3 to 4 days for iron dextran and 6 hours for iron sucrose.
- the iron in the iron carboxymaltose complex (e.g., VIT-45) slowly dissociates from the complex and can be efficiently used in the bone marrow for Hgb synthesis.
- red cell utilization followed for 4 weeks, ranged from 61% to 99%.
- the reticuloendothelial uptake of this complex reflects the safety of polysaccharide complexes.
- VIT-45 demonstrated a monoexponential elimination pattern with a t 1/2 in the range 7 to 18 hours, with negligible renal elimination.
- VIT-45 is clastogenic, mutagenic, or causes chromosomal damage or bone marrow cell toxicity. There were no specific responses to VIT-45 in a dextran antigenicity test.
- VIT-45 iron carboxymaltose complex
- Ferumoxytol is a polyglucose sorbitol carboxymethyl ether-coated non-stoichiometric magnetite (e.g., "ferumoxytol"). Ferumoxytol is known in the art to be effective for treating anemia (at single unit doses lower than described herein). See e.g., Spinowitz et al. (2005) Kidney lntl 68, 1801-1807'. Ferumoxytol is a superparamagnetic iron oxide that is coated with a low molecular weight semisynthetic carbohydrate, polyglucose sorbitol carboxymethyl ether.
- Ferumoxytol and its synthesis are described in U.S. Patent No.6,599,498, incorporated herein by reference. Safety, efficacy, and pharmacokinetics of ferumoxytol are as described, for example, in Landry et al. (2005) Am J Nephrol 25, 400-410, 408; and Spinowitz et al. (2005) Kidney lntl 68, 1801-1807.
- the iron oxide of ferumoxytol is a superparamagnetic form of non- stoichiometric magnetite with a crystal size of 6.2 to 7.3 nm. Average colloidal particle size can be about 30 nm, as determined by light scattering. Molecular weight is approximately 750 kD. The osmolarity of ferumoxytol is isotonic at 297 m ⁇ sm/kg and the pH is neutral. The blood half- life of ferumoxytol is approximately 10-14 hours. It has been previously reported that ferumoxytol can be given by direct intravenous push over 1-5 minutes in doses up to 1,800 mg elemental iron per minute, with maximal total dose up to 420 mg per injection. Landry et al. (2005) Am J Nephrol 25, 400-410, 408.
- Intravenous iron agents are generally spheroidal iron-carbohydrate nanoparticles. At the core of each particle is an iron-oxyhydroxide gel. The core is surrounded by a shell of carbohydrate that stabilizes the iron-oxyhydroxide, slows the release of bioactive iron, and maintains the resulting particles in colloidal suspension. Iron agents generally share the same core chemistry but differ from each other by the size of the core and the identity and the density of the surrounding carbohydrate. See Table 1 ; Figure 1.
- Differences in core size and carbohydrate chemistry can determine pharmacological and biological differences, including clearance rate after injection, iron release rate in vitro, early evidence of iron bioactivity in vivo, and maximum tolerated dose and rate of infusion.
- One of the primary determinants of iron bioactivity is the size of the core and the surface area to volume ratio. Generally, the rate of labile iron release in each agent is inversely related to the size of its iron core. Van Wyck (2004) J. Am. Soc. Nephrology 15, S 107- S111 , S109. Furthermore, in vitro iron donation to transferrin is inversely related to core size. Core size can depend upon the number of iron atoms contained within. For example, the number of iron atoms contained within a 1 nm core is calculated to be 13, while a 10 nm core is calculated to contain 12770 iron atoms.
- the rate of iron release per unit surface area is likely similar, differing perhaps by the strength of the carbohydrate ligand-core iron bound. But for the same total amount of core iron, surface area available for iron release increases dramatically as core radius decreases. That is to say, for equal amounts of iron, the smaller the core, the greater the surface area available for iron release. Of course, the explanation for this non-linear trend is the fact that volume is radius cubed. In short, a collection of many small spheres exposes a greater total surface area than does a collection of an equal mass of fewer, larger spheres.
- a smaller iron core size of an iron complex administered for the treatment of various diseases, disorders, or conditions allows wider distribution through tissues, a greater rate of labile iron release, and increased in vitro iron donation to transferrin. Furthermore, the iron complex is more evenly distributed and metabolizes faster due to the smaller core size. But if the core size is too small, the iron complex can move into cells unable to metabolize iron. In one embodiment, an iron complex with a mean iron core size of no greater than about 9 nm is administered.
- mean iron core size is less than about 9 nm but greater than about 1 nm, about 2 nm, about 3 nm, about 4 nm, about 5 nm, about 6 nm, about 7 nm, or about 8 nm.
- Mean iron core size can be, for example, between about 1 nm and about 9 nm; between about 3 nm and about 7 nm; or between about 4 nm and about 5 nm.
- the molecular weight (i.e., the whole molecular weight of the agent) is considered a primary determinant in the pharmacokinetics, or in other words, how quickly it Is cleared from the blood stream.
- the amount of labile (i.e., biologicaly available) iron is inversely correlated with the molecular weight of the iron-carbohydrate complex. Van Wyck (2004) J. Am. Soc. Nephrology 15, S107-S111 , S109. That is to say, the magnitude of labile iron effect is greatest in iron-carbohydrate compounds of lowest molecular weight and least in those of the highest molecular weight.
- the mean diameter size of a particle of the iron carbohydrate complex is no greater than about 35 nm.
- the particle mean size can be no greater than about 30 nm.
- the particle mean size can be no greater than about 25 nm.
- the particle mean size can be no greater than about 20 nm.
- the particle mean size can be no greater than about 15 nm.
- the particle mean size can be no greater than about 10 nm.
- the particle mean size can be no greater than about 7 nm.
- a safe and effective amount of an iron carbohydrate complex is, for example, that amount that would cause the desired therapeutic effect in a patient while minimizing undesired side effects.
- the dosage regimen will be determined by skilled clinicians, based on factors such as the exact nature of the condition being treated, the severity of the condition, the age and general physical condition of the patient, and so on.
- treatment- emergent adverse events will occur in less than about 5% of treated patients.
- treatment-emergent adverse events will occur in less than 4% or 3% of treated patients.
- treatment-emergent adverse events will occur in less than about 2% of treated patients.
- minimized undesirable side effects can include those related to hypersensitivity reactions, sometimes classified as sudden onset closely related to the time of dosing, including hypotension, bronchospasm, layngospasm, angioedema or uticaria or several of these together.
- Hypersensitivity reactions are reported with all current intravenous iron products independent of dose. See generally Bailie et al. (2005) Nephrol Dial Transplant, 20(7), 1443-1449.
- minimized undesirable side effects can include those related to labile iron reactions, sometimes classified as nausea, vomiting, cramps, back pain, chest pain, and/or hypotension. Labile iron reactions are more common with iron sucrose, iron gluconate, and iron dextran when doses are large and given fast.
- a single unit dose of iron carbohydrate complex may be delivered as a simple composition comprising the iron complex and the buffer in which it is dissolved.
- other products may be added, if desired, for example, to maximize iron delivery, preservation, or to optimize a particular method of delivery.
- a "pharmaceutically acceptable carrier” includes any and all solvents, dispersion media, coatings, antibacterial and anti-fungal agents, isotonic and absorption delaying agents, and the like, compatible with pharmaceutical administration (see e.g., Banker, Modern Pharmaceutics, Drugs and the Pharmaceutical Sciences, 4th ed. (2002) ISBN 0824706749; Remington The Science and Practice of Pharmacy, 21st ed. (2005) ISBN 0781746736).
- Preferred examples of such carriers or diluents include, but are not limited to, water, saline, Finger's solutions and dextrose solution. Supplementary active compounds can also be incorporated into the compositions.
- the iron carbohydrate complex is preferably diluted in normal saline to approximately 2-5 mg/ml. The volume of the pharmaceutical solution is based on the safe volume for the individual patient, as determined by a medical professional.
- An iron complex composition of the invention for administration is formulated to be compatible with the intended route of administration, such as intravenous injection.
- Solutions and suspensions used for parenteral, intradermal or subcutaneous application can include a sterile diluent, such as water for injection, saline solution, polyethylene glycols, glycerine, propylene glycol or other synthetic solvents; antibacterial agents such as benzyl alcohol or methyl parabens; antioxidants such as ascorbic acid or sodium bisulfite; buffers such as acetates, citrates or phosphates, and agents for the adjustment of tonicity such as sodium chloride or dextrose.
- the pH can be adjusted with acids or bases, such as hydrochloric acid or sodium hydroxide. Preparations can be enclosed in ampules, disposable syringes or multiple dose vials made of glass or plastic.
- compositions suitable for injection include sterile aqueous solutions or dispersions for the extemporaneous preparation of sterile injectable solutions or dispersion.
- suitable carriers include physiological saline, bacteriostatic water, Cremophor EL TM (BASF; Parsippany, NJ.) or phosphate buffered saline (PBS).
- the composition must be sterile and should be fluid so as to be administered using a syringe.
- Such compositions should be stable during manufacture and storage and must be preserved against contamination from microorganisms, such as bacteria and fungi.
- the carrier can be a dispersion medium containing, for example, water, polyol (such as glycerol, propylene glycol, and liquid polyethylene glycol), and other compatible, suitable mixtures.
- polyol such as glycerol, propylene glycol, and liquid polyethylene glycol
- Various antibacterial and anti-fungal agents for example, parabens, chlorobutanol, phenol, ascorbic acid, and thimerosal, can contain microorganism contamination.
- Isotonic agents such as sugars, polyalcohols, such as manitol, sorbitol, and sodium chloride can be included in the composition.
- Compositions that can delay absorption include agents such as aluminum monostearate and gelatin.
- Sterile injectable solutions can be prepared by incorporating an iron complex in the required amount in an appropriate solvent with a single or combination of ingredients as required, followed by sterilization.
- Methods of preparation of sterile solids for the preparation of sterile injectable solutions include vacuum drying and freeze-drying to yield a solid containing the iron complex and any other desired ingredient.
- Active compounds may be prepared with carriers that protect the compound against rapid elimination from the body, such as a controlled release formulation, including implants and microencapsulated delivery systems.
- Biodegradable or biocompatible polymers can be used, such as ethylene vinyl acetate, polyanhydrides, polyglycolic acid, collagen, polyorthoesters, and polylactic acid. Such materials can be obtained commercially from ALZA Corporation (Mountain View, CA) and NOVA Pharmaceuticals, Inc. (Lake Elsinore, CA) 1 or prepared by one of skill in the art.
- a single unit dose of iron carbohydrate complex may be intravenously administered in a volume of pharmaceutically acceptable carrier of, for example, about 1000 mg of elemental iron in about 200 ml to about 300 ml of diluent.
- a single unit dose of iron carbohydrate complex may be intravenously administered in a volume of pharmaceutically acceptable carrier of about 1000 mg of elemental iron in about 250 ml of diluent.
- a single unit dose of iron carbohydrate complex may be intravenously administered in a volume of pharmaceutically acceptable carrier of about 1000 mg of elemental iron in about 215 ml of diluent.
- a preferred pharmaceutical composition for use in the methods described herein contains VIT-45 as the active pharmaceutical ingredient (API) with about 28% weight to weight (m/m) of iron, equivalent to about 53% m/m iron (lll)-hydroxide, about 37% m/m of ligand, ⁇ 6% m/m of NaCI, and ⁇ 10% m/m of water.
- API active pharmaceutical ingredient
- Iron complex compositions can be included in a kit, container, pack or dispenser, together with instructions for administration according to the methods described herein.
- the different components of the composition may be packaged in separate containers, such as ampules or vials, and admixed immediately before use. Such packaging of the components separately may permit long-term storage without losing the activity of the components. Kits may also include reagents in separate containers that facilitate the execution of a specific test, such as diagnostic tests.
- kits can be supplied in containers of any sort such that the life of the different components are preserved and are not adsorbed or altered by the materials of the container.
- sealed glass ampules or vials may contain lyophilized iron complex or buffer that have been packaged under a neutral non-reacting gas, such as nitrogen.
- Ampules may consist of any suitable material, such as glass, organic polymers, such as polycarbonate, polystyrene, etc., ceramic, metal or any other material typically employed to hold reagents.
- suitable containers include bottles that are fabricated from similar substances as ampules, and envelopes that consist of foil-lined interiors, such as aluminum or an alloy.
- Containers include test tubes, vials, flasks, bottles, syringes, etc.
- Containers may have a sterile access port, such as a bottle having a stopper that can be pierced by a hypodermic injection needle.
- Other containers may have two compartments that are separated by a readily removable membrane that, upon removal, permits the components to mix.
- Removable membranes may be glass, plastic, rubber, etc.
- Kits may also be supplied with instructional materials. Instructions may be printed on paper or other substrate, and/or may be supplied on an electronic-readable medium, such as a floppy disc, CD-ROM, DVD-ROM, mini-disc, SACD, Zip disc, videotape, audio tape, etc. Detailed instructions may not be physically associated with the kit; instead, a user may be directed to an internet web site specified by the manufacturer or distributor of the kit, or supplied as electronic mail.
- Nonclinical toxicity of VIT-45 is very low, as is normal for Type I polynuclear iron (lll)-hydroxide carbohydrate complexes.
- the single dose toxicity is so low that the LD 50 could not be estimated and is higher than 2000 mg iron/kg b.w.
- the highest non- lethal dose level of 1000 mg iron/kg b.w. in mice and rats is also very high in comparison to a single unit dose of, for example, 15 mg iron/kg b.w. once per week in humans.
- VIT-45 15 for VIT-45 was calculated to be approximately 16 hours, compared to about 6 hours for iron sucrose.
- pharmacokinetic analyses revealed increases in exposure roughly proportional with VIT-45 dose (Cmax approximately 150 ⁇ g/mL and 320 ⁇ g/mL following 500 mg and 1000 mg doses, respectively).
- VIT-45 demonstrated a monoexponential elimination pattern with a t 1/2 in the range 7 to 18 hours. There was negligible
- VIT-45 The main pharmacodynamic effects of VIT-45 were transient elevations of serum iron levels, TfS and serum ferritin. These effects were seen in all studies (where measured), following both single doses and repeated doses. The increase in serum ferritin levels
- VIT-45 A total of 2429 subjects were treated with VIT-45 or control agents over 10 studies that provide safety data for VIT-45. Of these, 1709 subjects received VIT-45 (1095 in completed multicenter studies, 584 in placebo-controlled, single-dose, crossover studies and 30 in pharmacokinetic studies). The mean total dose of VIT-45 administered among the 1095 subjects in the completed multicenter studies was approximately 1300 mg; however, some subjects received VlT-45 closes as high as 3400 mg. The majority of the subjects treated were able to receive their calculated iron requirement in only 1 or 2 doses.
- Table 2 provides a summary of VIT-45 studies described in this example.
- Study A was a single-center, single-dose escalation, randomized, double- blind, placebo-controlled pharmacokinetic study. Subjects were male and female, between 18 and 45 years of age, inclusive, with mild iron-deficiency anemia. Treatment was a single IV bolus injection of VIT-45 at 100 mg, 500 mg, 800 mg, or 1000 mg.
- Examined pharmacokinetic parameters included total serum iron and pharmacodynamic (serum ferritin and transferrin, iron binding capacity, %TSATpost, hemoglobin, reticulocyte, and serum transferrin receptor concentrations) endpoints.
- Examined safety parameters included adverse events, clinical laboratory evaluations, vital signs, ECG, and physical examinations.
- Study B was a single-center, single-dose, open label, uncontrolled pharmacokinetic study. Subjects were between 18 and 75 years of age with iron-deficiency or renal anemia with no other cause of anaemia. Inclusion criteria included hemoglobin concentration between 9 and 13 g/dL, no blood transfusions in the previous 3 months, and no history of treatment with intravenous iron in the last 2 weeks. Treatment was a single IV bolus injection of VIT-45 at 100 mg labelled with 52 Fe and 59 Fe. Examined primary pharmacokinetic parameters included the distribution of 52 Fe and incorporation of 59 Fe into red blood cells. Examined safety parameters included adverse events, clinical laboratory evaluations, vital signs, and physical examinations.
- TSAT screening serum transferrin saturation
- dosage prepregnancy weight (kg) x (15-baseline hemoglobin [g/dL]) x 2.4 + 500 mg.
- Study D was a multicenter, open-label, randomized, active-controlled, multiple- dose postpartum anemia study. Subjects were adult women >18 years old with postpartum anaemia within 6 days after delivery. Treatment was administered once-weekly for a maximum of 3 infusions.
- ECG electrocardiogram
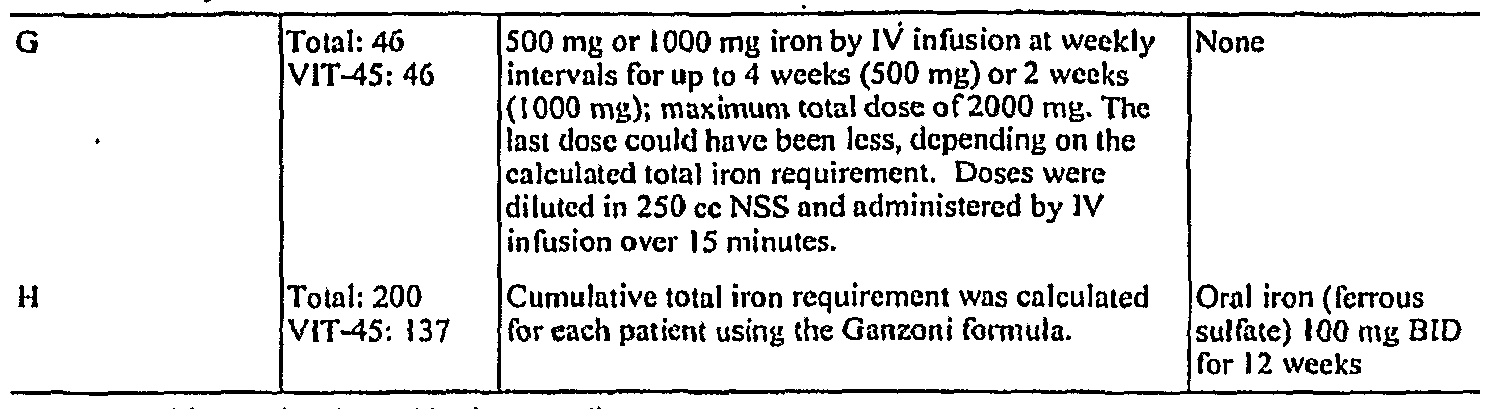
- Study E was a multicenter, open-label, randomized, active-controlled, multiple- dose hemodialysis-associated anemia study. Subjects were adult male or female subjects between the ages of 18 and 80 years (inclusive) requiring haemodialysis with iron deficiency secondary to chronic renal failure. Dosing started on Day 1 , Week 0 for both treatment arms and continued 2 or 3 times weekly until the individual calculated cumulative dose was reached. Patients received 200 mg VIT-45 during their scheduled haemodialysis sessions (2-3 sessions/week) until the calculated cumulative dose was reached. Cumulative total iron requirement was calculated for each patient using the Ganzoni formula. Primary Efficacy was examined as the percentage of patients reaching an increase in hemoglobin >10 g/L at 4 weeks after baseline. Examined safety parameters included adverse events, vital signs, 12-lead ECG, physical examinations, and clinical laboratory evaluations.
- Study F was a multicenter, open-label, multiple dose, uncontrolled hemodialysis-associated anemia study. Subjects were male and female patients 18-65 years of age, inclusive, with haemodialysis-associated anaemia undergoing maintenance haemodialysis. Treatment duration was a maximum of six weeks. Patients received 200 mg VIT-45 during their scheduled haemodialysis sessions (2-3 sessions/week) until the calculated cumulative dose was reached. Cumulative total iron requirement was calculated for each patient using the Ganzoni formula. Efficicacy was examined as correction of iron deficiency and hemoglobin concentration of the patient. Examined safety parameters included adverse events, vital signs, 12-lead ECG, physical examinations, haematology and blood chemistry profiles, and urea reduction ratio.
- Study G was a multicenter, multiple-dose open-label, uncontrolled gastrointestinal disorder-associated anemia study. Subjects were males and females between 18 and 60 years of age, inclusive, with moderate stable iron-deficiency anemia secondary to a gastrointestinal disorder and a calculated total iron requirement >1000 mg; >50% of patients in each cohort were to require ⁇ 1500 mg total iron. Duration of treatment was single doses at weekly intervals for up to 4 weeks (Cohort 1 ) or 2 weeks (Cohort 2). Administration of VIT-45 was by IV bolus injection of 500 mg (Cohort 1) or 1000 mg (Cohort 2), where total iron requirement for each patient, which determined how many weekly infusions were received, was calculated using the formula of Ganzoni.
- Examined pharmacokinetic parameters included total serum iron and pharmacodynamic (hemoglobin, ferritin, TSAT) endpoints.
- Examined safety parameters included adverse events, clinical laboratory evaluations, vital signs, ECG, physical examinations, and elevated serum ferritin (>500 ⁇ g/L) AND elevated TSAT (>45%).
- Study H was a multicenter, multiple-dose randomized, open-label, active-controlled gastrointestinal disorder-associated anemia study. Subjects were males and females aged 18 to 80 years, inclusive, with iron-deficiency anaemia secondary to chronic inflammatory bowel disease (ulcerative colitis or Crohn's disease) and a calculated total iron requirement of at least 1000 mg total iron. Treatment was weekly VIT-45 infusions, with a maximum of 3 infusions permitted in a single treatment cycle. Administration consisted of an infusion on Day 1 , with subsequent infusions at weekly intervals up to a maximum of 1000 mg iron per dose. The doses were continued until the patient received the cumulative dose based on their individual requirement for iron. Primary efficacy was examined as change from baseline to Week 12 in hemoglobin. Examined safety parameters included adverse events, vital signs, 12-lead ECG, physical examinations, and clinical laboratory evaluations.
- Study I was an open label, multiple-dose, multicenter, randomized, active- control anemia due to heavy uterine bleeding study. Subjects were females at least 18 years of age with iron-deficiency anemia secondary to heavy uterine bleeding. Duration of treatment was six weeks.
- ⁇ 200 mg was administered as an undiluted IVP over 1-2 minutes; 300-400 mg was administered in 100 cc NSS over 6 minutes; and 500-1 ,000 mg was administered in 250 cc NSS over 15 minutes.
- Study J was a multicenter, single-dose blinded, randomized, placebo- controlled crossover iron deficiency anemia study.
- Subjects were male or female, at least 18 years of age, with a hemoglobin ⁇ 12 g/dL, TSAT ⁇ 25%, and ferritin ⁇ 300 ng/mL (iron- deficiency anemia due to dialysis or non-dialysis dependent chronic kidney disease or inflammatory bowel disease), or ferritin ⁇ 100 ng/mL (iron-deficiency anemia due to other conditions).
- Treatment was two single doses seven days apart.
- Administration of VIT-45 occurred over 15 minutes and was ⁇ 1000 mg (15 mg/kg for weight ⁇ 66 kg).
- Examined safety parameters included adverse events, clinical laboratory evaluations, vital signs, and physical examinations.
- I Total 456 ⁇ IOOO mg/week (15 mg/kg for weight ⁇ 66 kg); Oral iron (ferrous VIT-45: 230 patients received VIT-45 infusions once weekly sulfate) 325 mg TID until the calculated cumulative dose was reached or for 6. weeks a maximum of 2500 mg had been administered.
- Doses ⁇ 200 mg were administered IV push over 1- 2 minutes; doses of 300-400 mg were diluted in 100 cc NSS and administered over 6 minutes; doses of 500-1000 mg were diluted in 250 cc NSS and administered over 15 minutes.
- VIT-45 The majority of the subjects who received VIT-45 completed the study. The incidence of premature discontinuations in the completed multicenter studies was 10% in the VIT-45 group which is comparable to that observed in the oral iron (9.6%) and Venofer (13.6%) groups. Reasons for premature discontinuation were generally comparable among the treatment groups, except that the incidence of adverse events leading to discontinuation were higher in the Venofer group (5.9%) compared to the VIT-45 (1.8%) and oral iron (2.1%) groups, demonstrating the overall tolerability of VIT-45.
- VIT-45 gastrointestinal disorders
- greater proportions of subjects in the oral iron group than the VIT-45 group experienced constipation, nausea, diarrhoea, and vomiting, while a greater proportion of VIT-45 subjects experienced abdominal pain than oral iron subjects.
- greater proportions of VIT-45 subjects experienced blood phosphate decreased and GGT increased than oral iron subjects.
- greater proportions of VIT-45 subjects experienced rash and pruritus than oral iron subjects.
- VIT-45 There were no deaths in the study attributed to VIT-45. The incidence of other serious adverse events among VIT-45 subjects was low (3% in all completed multicenter studies and 0.3% in the placebo-controlled, single-dose crossover study) and none were considered related to study drug. The incidence of premature discontinuation due to adverse events was comparable between the VIT-45 group (2.1%) and the other active treatment groups (3.1% oral iron and 2.5% Venofer). The incidence of drug-related treatment-emergent adverse events of hypersensitivity was 0.2%, the same as that observed with oral iron (0.2%). Drug-related mild or moderate hypotension was observed in 4 (0.2%) VIT-45 subjects, none of which were considered serious, led to premature discontinuation, or were symptomatic. Treatment-emergent adverse events indicative of potential allergic reactions including rash, pruritus, and urticaria were reported by ⁇ 2% of subjects who were treated with VIT-45; none of these events was considered serious and few led to premature discontinuation.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Organic Chemistry (AREA)
- Molecular Biology (AREA)
- Epidemiology (AREA)
- Engineering & Computer Science (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Genetics & Genomics (AREA)
- Biotechnology (AREA)
- Biochemistry (AREA)
- Hematology (AREA)
- Cardiology (AREA)
- Diabetes (AREA)
- Dermatology (AREA)
- Inorganic Chemistry (AREA)
- Rheumatology (AREA)
- Physical Education & Sports Medicine (AREA)
- Obesity (AREA)
- Urology & Nephrology (AREA)
- Oncology (AREA)
- Orthopedic Medicine & Surgery (AREA)
- Hospice & Palliative Care (AREA)
- Heart & Thoracic Surgery (AREA)
- Immunology (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Abstract
Description

Claims
Priority Applications (12)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| ES07716309.5T ES2602433T3 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for iron administration |
| EP07716309.5A EP1973549B1 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| AU2007205167A AU2007205167B2 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| CN2007800020060A CN101365458B (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| KR1020187018660A KR20180077337A (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| CA2635894A CA2635894C (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| DK07716309.5T DK1973549T3 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of the iron |
| KR1020177005732A KR101905340B1 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| LTEP07716309.5T LT1973549T (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| KR1020147024469A KR20140117678A (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
| HK09103049.6A HK1125044A1 (en) | 2006-01-06 | 2009-03-31 | Methods and compositions for administration of iron |
| CY20161101047T CY1118780T1 (en) | 2006-01-06 | 2016-10-19 | METHODS AND COMPOSITIONS FOR IRON SUPPLY |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US75711906P | 2006-01-06 | 2006-01-06 | |
| US60/757,119 | 2006-01-06 | ||
| US11/620,986 | 2007-01-08 | ||
| US11/620,986 US7754702B2 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| WO2007081744A2 true WO2007081744A2 (en) | 2007-07-19 |
| WO2007081744A3 WO2007081744A3 (en) | 2007-11-08 |
Family
ID=38233459
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2007/000176 WO2007081744A2 (en) | 2006-01-06 | 2007-01-08 | Methods and compositions for administration of iron |
Country Status (11)
| Country | Link |
|---|---|
| US (11) | US7754702B2 (en) |
| EP (3) | EP2626074A1 (en) |
| KR (4) | KR101905340B1 (en) |
| CN (1) | CN101365458B (en) |
| AU (1) | AU2007205167B2 (en) |
| CA (2) | CA2953964A1 (en) |
| CY (1) | CY1118780T1 (en) |
| DK (1) | DK1973549T3 (en) |
| HK (1) | HK1125044A1 (en) |
| PT (1) | PT1973549T (en) |
| WO (1) | WO2007081744A2 (en) |
Cited By (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2011523866A (en) * | 2008-05-23 | 2011-08-25 | ホスピラ・インコーポレイテツド | Packaged iron sucrose products |
| ITMI20101028A1 (en) * | 2010-06-09 | 2011-12-10 | Biofer Spa | NEW COMPLEXES AT LOW MOLECULAR WEIGHT BETWEEN IRON AND MALTOBIONIC ACID, USE OF THESE FOR INTRAMUSCULAR OR SUBCUTANEOUS ADMINISTRATION IN ANEMIC STATE THERAPY, AND NEW PHARMACEUTICAL COMPOSITIONS SUITABLE FOR THESE USES. |
| EP2420243A1 (en) | 2010-08-18 | 2012-02-22 | Inovativo Biomedicinas Tehnologiju Instituts, SIA | Compositions obtainable from bred beetroot juice to promote iron absorption and blood forming |
| EP2626074A1 (en) | 2006-01-06 | 2013-08-14 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron |
| US9376505B2 (en) | 2002-10-23 | 2016-06-28 | Vifor (International) Ag. | Aqueous iron carbohydrate complexes, their production and medicaments containing them |
| US9657098B2 (en) | 2013-03-15 | 2017-05-23 | Intrinsic Lifesciences, Llc | Anti-hepcidin antibodies and uses thereof |
| US10323088B2 (en) | 2014-09-22 | 2019-06-18 | Intrinsic Lifesciences Llc | Humanized anti-hepcidin antibodies and uses thereof |
| US10414831B2 (en) | 2009-03-25 | 2019-09-17 | Pharmacosmos Holding A/S | Stable iron oligosaccharide compound |
| WO2020089227A1 (en) | 2018-10-29 | 2020-05-07 | Pharmacosmos Holding A/S | Treating iron deficiency with ferric carboxymaltose |
Families Citing this family (35)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20060116349A1 (en) * | 2003-03-14 | 2006-06-01 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron for the treatment of restless leg syndrome |
| EP1790356A1 (en) * | 2005-11-24 | 2007-05-30 | Vifor (International) Ag | Preparation containing iron(III)-complexes and redox substances |
| JP2011516419A (en) * | 2008-03-28 | 2011-05-26 | カイナ エルエルシー | Use of ferritin to treat iron deficiency disorders |
| GB0808835D0 (en) * | 2008-05-15 | 2008-06-18 | Vitra Pharmaceuticals Ltd | Therapeutic compositions |
| US9913806B2 (en) | 2008-06-25 | 2018-03-13 | Fe3 Medical, Inc. | Patches and methods for the transdermal delivery of a therapeutically effective amount of iron |
| KR101017432B1 (en) * | 2008-11-06 | 2011-02-28 | (주)유케이케미팜 | Manufacturing method for Iron Oxide Saccharated |
| US8058076B2 (en) * | 2009-03-31 | 2011-11-15 | Astron Research Limited | In-vitro method for testing bioequivalence of iron-sucrose formulation |
| US8821945B2 (en) | 2009-04-25 | 2014-09-02 | Fe3 Medical, Inc. | Method for transdermal iontophoretic delivery of chelated agents |
| KR20140016438A (en) | 2009-07-21 | 2014-02-07 | 케릭스 바이오파마슈티컬스 인코포레이티드 | Ferric citrate dosage forms |
| CN106176808A (en) | 2010-10-19 | 2016-12-07 | 长春纳米生技公司 | Metal ion nanocluster composition |
| US20120184894A1 (en) * | 2010-12-31 | 2012-07-19 | Mir Imran | Patches and Methods for the Transdermal Delivery of Agents to Treat Hair Loss |
| CN102153651B (en) * | 2011-01-21 | 2012-11-14 | 厦门大学 | Anti-dextran single-chain antibody and preparation method of anti-dextran single-chain antibody |
| WO2013102054A1 (en) | 2011-12-30 | 2013-07-04 | Sloiron, Llc | Methods for isolation, use and analysis of ferritin |
| ES2970050T3 (en) * | 2012-06-21 | 2024-05-24 | Keryx Biopharmaceuticals Inc | Use of ferric citrate in the treatment of patients with chronic kidney disease |
| CN107890472A (en) * | 2012-07-27 | 2018-04-10 | 本质生命科学有限公司 | The method for treating hypoferric anemia |
| US9370202B2 (en) | 2013-03-15 | 2016-06-21 | LG Bionano, LLC | Encapsulated metal ion nanoclusters |
| JP6049194B2 (en) * | 2013-03-28 | 2016-12-21 | 富士フイルム株式会社 | Graph display device, method of operating graph display device, and graph display program |
| EP2856941B1 (en) * | 2013-10-01 | 2020-11-25 | Fresenius Medical Care Deutschland GmbH | Method and apparatuses for determining a patient's daily loss of iron |
| KR101536325B1 (en) | 2013-10-16 | 2015-07-14 | 주식회사 지니스 | The thermosensitizer composition for electromagnetic wave-based hyperthermia and its use to treat cancer |
| KR20150078375A (en) * | 2013-12-30 | 2015-07-08 | 한화케미칼 주식회사 | Pharmaceutical composition for prevention or treatment of iron deficiency comprising iron oxide nanoparticle |
| TWI689310B (en) | 2014-07-11 | 2020-04-01 | 巨生生醫股份有限公司 | Method of treating iron deficiency |
| EP2913054A1 (en) * | 2015-03-19 | 2015-09-02 | Pharmacosmos Holding A/s | Iron carbohydrate complex for treatment of restless leg syndrome (rls) |
| WO2016196274A1 (en) * | 2015-05-29 | 2016-12-08 | Luitpold Pharmaceuticals, Inc. | Compositions and methods for treatment of fibromyalgia |
| ES2892488T3 (en) | 2015-06-22 | 2022-02-04 | Pharmacosmos Holding As | Iron and carbohydrate complex for the treatment of iron deficiency in a fetus or infant |
| CA2932075C (en) * | 2015-09-01 | 2020-11-17 | Particle Dynamics International, Llc | Iron-polysaccharide complexes and methods for the preparation thereof |
| US10258647B2 (en) | 2015-09-01 | 2019-04-16 | Particle Dynamics International, Llc | Iron-polysaccharide complexes and methods for the preparation thereof |
| EP3347025A4 (en) * | 2015-09-11 | 2019-04-24 | Memorial Sloan-Kettering Cancer Center | Methods and compositions for cancer treatment |
| CN105520955B (en) * | 2015-12-21 | 2018-05-11 | 南京生命能科技开发有限公司 | A kind of carboxyl maltose iron Pharmaceutical composition and preparation method thereof |
| CN105708805A (en) * | 2016-01-28 | 2016-06-29 | 山西普德药业股份有限公司 | Reduced carboxy alkyl dextriferron and preparation method thereof |
| CN105708792A (en) * | 2016-01-28 | 2016-06-29 | 山西普德药业股份有限公司 | Reduced carboxy alkyl dextriferron injection and preparation method thereof |
| CN105616372A (en) * | 2016-01-28 | 2016-06-01 | 山西普德药业股份有限公司 | Reduced-type carboxyl alkyl dextriferron tablet |
| CN105726569A (en) * | 2016-03-02 | 2016-07-06 | 东南大学 | Application of glycan superpara magnetism ferric oxide to preparation of medicine for treating cardiovascular disease |
| WO2019152618A1 (en) * | 2018-01-31 | 2019-08-08 | University Of Maryland, Baltimore | A comprehensive method to quantify iron distribution in plasma |
| WO2021226087A1 (en) * | 2020-05-04 | 2021-11-11 | Amphastar Pharmaceuticals, Inc. | Small angle x-ray scattering methods for characterizing the iron core of iron carbohydrate colloid drug products |
| CN115364114B (en) * | 2021-05-21 | 2023-12-01 | 武汉科福新药有限责任公司 | Iron carboxyl maltose medicinal composition and preparation method thereof |
Family Cites Families (87)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CA623411A (en) | 1961-07-04 | Muller Arthur | Process for the manufacture of iron-polyisomaltose complex for therapeutical purposes | |
| DE370194C (en) | 1923-02-28 | Therese Rocksch Geb Laschet | Electrolytic tin bath for the representation of sponge-free tin crystals | |
| US1199951A (en) | 1915-11-06 | 1916-10-03 | Robert E Leigh | Lubricating device. |
| CH123744A (en) | 1925-09-04 | 1927-12-16 | Anode Rubber Company Limited | Process for the production of homogeneous precipitates from aqueous dispersions of rubber-like substances on metallic precipitate substrates. |
| GB335965A (en) | 1929-06-05 | 1930-10-06 | Ig Farbenindustrie Ag | Process for the manufacture of complex iron compounds |
| US2807610A (en) | 1952-02-15 | 1957-09-24 | Baker Chem Co J T | Hydrogenated dextran |
| GB748024A (en) | 1953-02-27 | 1956-04-18 | Benger S Ltd | Improved therapeutic preparations of iron |
| GB879441A (en) | 1959-05-25 | 1961-10-11 | Crookes Lab Ltd | Improved injectable iron preparations |
| US3065138A (en) | 1959-10-09 | 1962-11-20 | Warren Teed Products Company | Therapeutic preparations of elemental iron |
| US3100202A (en) * | 1960-06-17 | 1963-08-06 | Muller Arthur | Process for preparing an iron hydroxide polyisomaltose complex and the resulting product |
| US3151107A (en) | 1960-12-22 | 1964-09-29 | Central Pharmacal Company | Water-soluble iron complexes of carboxymethyl dextran |
| US3076798A (en) | 1961-02-23 | 1963-02-05 | Hausmann Lab Ltd | Process for preparing a ferric hydroxide polymaltose complex |
| GB985206A (en) | 1961-12-20 | 1965-03-03 | Hausmann Ag Labor | Improvements in or relating to therapeutic iron preparation |
| ES282099A1 (en) | 1962-11-02 | 1963-01-01 | Rocador Sa | Procedure for the preparation of a complex of iron oxide and dextranic acids (Machine-translation by Google Translate, not legally binding) |
| FR1451203A (en) | 1964-01-31 | 1966-01-07 | Rocador Sa | Process for the manufacture of a complex of ferric oxide and polysaccharide |
| GB1183940A (en) | 1966-10-22 | 1970-03-11 | Fisons Pharmaceuticals Ltd | Ferric Hydroxide Complexes |
| US3639588A (en) | 1966-10-22 | 1972-02-01 | Fisons Pharmaceuticals Ltd | Pharmaceutical compositions containing ferric hydroxide complexed with dextran or dextrin heptonic acids |
| GB1199951A (en) | 1967-05-13 | 1970-07-22 | Fisons Pharmaceuticals Ltd | Modified Dextran and Derivatives Thereof |
| GB1200902A (en) | 1967-05-13 | 1970-08-05 | Fisons Pharmaceuticals Ltd | Iron-dextran complexes |
| US3395229A (en) | 1967-07-03 | 1968-07-30 | Mattox And Moore Inc | Process and product for combatting iron deficiency anemia in suckling pigs |
| US3821192A (en) | 1971-08-18 | 1974-06-28 | Central Pharmacal Co | Process for preparing an iron-saccharide complex |
| SE359447B (en) | 1971-10-06 | 1973-09-03 | Astra Laekemedel Ab | |
| US3928581A (en) | 1972-09-13 | 1975-12-23 | Astra Laekemedel Ab | Certain polymer-iron complexes for treatment of iron deficiency |
| US3969395A (en) | 1972-10-04 | 1976-07-13 | Astra Lakemedel Aktiebolag | Polymers of hydroxy carboxylic acid and a polyhydric alcohol |
| US3965133A (en) | 1972-10-04 | 1976-06-22 | Astra Lakemedel Aktiebolag | Polymer |
| US4056672A (en) | 1973-03-22 | 1977-11-01 | Astra Lakemedel Aktiebolag | Polymer prepared by cyanhydrin method |
| JPS6039681B2 (en) | 1976-01-01 | 1985-09-07 | 日本臓器製薬株式会社 | Dextrin-citric acid-ferric polynuclear complex and parenteral iron preparation containing the complex |
| US4180567A (en) | 1977-09-02 | 1979-12-25 | Pharmachem Corporation | Iron preparations and methods of making and administering the same |
| US4370476A (en) | 1979-07-17 | 1983-01-25 | Usher Thomas C | Dextran polycarboxylic acids, ferric hydroxide complexes |
| DE3026868C2 (en) | 1980-07-16 | 1986-03-13 | Laboratorien Hausmann AG, St. Gallen | Process for the preparation of iron (III) hydroxide-dextran complexes and pharmaceutical sterile aqueous solution containing them |
| US4335116A (en) | 1980-10-07 | 1982-06-15 | University Patents, Inc. | Mineral-containing therapeutic compositions |
| EP0051707A1 (en) | 1980-11-12 | 1982-05-19 | Thomas Clemens Usher | Dextran polycarboxylic acids, ferric hydroxide complexes thereof, pharmaceutical compositions containing them and methods for their manufacture |
| US4788281A (en) | 1984-01-04 | 1988-11-29 | Tosoni Anthony L | Dextran hexonic acid derivative, ferric hydroxide complex and method manufacture thereof |
| US4689235A (en) | 1984-01-31 | 1987-08-25 | Scm Corporation | Encapsulation matrix composition and encapsulate containing same |
| US4612284A (en) | 1984-09-28 | 1986-09-16 | A. E. Staley Manufacturing Company | Process for the enzymatic hydrolysis of non-gelatinized granular starch material directly to glucose |
| US5102652A (en) | 1986-07-03 | 1992-04-07 | Advanced Magnetics Inc. | Low molecular weight carbohydrates as additives to stabilize metal oxide compositions |
| US5160726A (en) | 1990-02-15 | 1992-11-03 | Advanced Magnetics Inc. | Filter sterilization for production of colloidal, superparamagnetic MR contrast agents |
| KR880012235A (en) | 1987-04-10 | 1988-11-26 | 벤자민 에프.람버트 | How to increase hematocrit in normal mammals |
| GB8902894D0 (en) | 1989-02-09 | 1989-03-30 | Fisons Plc | Compositions |
| JP2726520B2 (en) | 1989-10-20 | 1998-03-11 | 名糖産業株式会社 | Organic magnetic composite |
| DE10199064I2 (en) | 1991-06-11 | 2004-07-12 | Meito Sangyo Kk | Oxidized composition containing a water-soluble carboxypolysaccharide and magnetic iron oxide. |
| TW293036B (en) | 1992-11-27 | 1996-12-11 | Takeda Pharm Industry Co Ltd | |
| EP0634174A1 (en) | 1993-07-13 | 1995-01-18 | Takeda Chemical Industries, Ltd. | Antianemic composition for veterinary use |
| US5624668A (en) * | 1995-09-29 | 1997-04-29 | Luitpold Pharmaceuticals, Inc. | Iron dextran formulations |
| ES2195023T3 (en) | 1995-11-09 | 2003-12-01 | Abbott Lab | CRYSTAL IRON-DEXTRAN PREPARATION PROCEDURE. |
| US5756715A (en) | 1996-11-08 | 1998-05-26 | Abbott Laboratories | Process for making crystalline iron dextran |
| CA2195283C (en) | 1997-01-16 | 2008-07-22 | Thomas C. Usher | Process for manufacturing iron dextran using ultrafiltration |
| US6219440B1 (en) | 1997-01-17 | 2001-04-17 | The University Of Connecticut | Method and apparatus for modeling cellular structure and function |
| US6010719A (en) | 1997-09-16 | 2000-01-04 | Universiteit Gent | Freeze-dried disintegrating tablets |
| DK172860B1 (en) | 1998-03-25 | 1999-08-16 | Pharmacosmos Holding As | Iron dextran compound for use as a component of a therapeutic agent for the prevention or treatment of iron man |
| DE19833548A1 (en) | 1998-07-25 | 2000-02-03 | Messer Griesheim Gmbh | Supercritical fluorination |
| US6587550B2 (en) | 1998-09-02 | 2003-07-01 | Michael O. Council | Method and apparatus for enabling a fee to be charged to a party initiating an electronic mail communication when the party is not on an authorization list associated with the party to whom the communication is directed |
| DK173138B1 (en) | 1998-11-20 | 2000-02-07 | Pharmacosmos Holding As | Process for Preparing an Iron Dextran Compound, Iron Dextran Compound Prepared by the Process, Pharmaceutical |
| DE60043188D1 (en) * | 1999-04-09 | 2009-12-03 | Amag Pharmaceuticals Inc | HEAT-RESISTANT WRAPPED COLLOIDAL ICE OXIDE |
| US7871597B2 (en) | 1999-04-09 | 2011-01-18 | Amag Pharmaceuticals, Inc. | Polyol and polyether iron oxide complexes as pharmacological and/or MRI contrast agents |
| US6495177B1 (en) | 1999-08-13 | 2002-12-17 | Warner Chilcott Laboratories Ireland Limited | Orally dissolvable nutritional supplement |
| AT500063A1 (en) | 1999-11-23 | 2005-10-15 | Sandoz Ag | COATED TABLETS |
| US20020119174A1 (en) | 2000-07-26 | 2002-08-29 | Gardlik John Michael | Compositions useful for regulating hair growth containing metal complexes of oxidized carbohydrates |
| RU2003121403A (en) | 2000-12-07 | 2004-12-27 | АД "ЗДРАВЛЬЕ" Фармасеутско-кемийска индустри , Сентар за истразиванье и развой (YU) | POLYNUCLEAR COMPLEX FE (III) WITH PULULANAN OLIGOMERS, METHOD OF ITS PRODUCTION AND PHARMACEUTICAL PRODUCTS ON ITS BASIS |
| JP2002260951A (en) | 2000-12-28 | 2002-09-13 | Denso Corp | Laminated dielectric element and its manufacturing method and paste material for electrode |
| US20030023208A1 (en) | 2001-07-24 | 2003-01-30 | Osypka Thomas P. | Apparatus for vascular access |
| MXPA04009770A (en) | 2002-04-09 | 2004-12-13 | Pharmacosmos Holding As | Iron dextrin compounds for the treatment of iron deficiency anaemia. |
| JP2005533812A (en) | 2002-06-21 | 2005-11-10 | ユニバーシティ オブ ピッツバーグ オブ ザ コモンウェルス システム オブ ハイヤー エデュケイション | Pharmaceutical use of nitric oxide, heme oxygenase-1 and heme degradation products |
| DE10249552A1 (en) | 2002-10-23 | 2004-05-13 | Vifor (International) Ag | Water-soluble iron-carbohydrate complexes, their preparation and medicaments containing them |
| US20060116349A1 (en) | 2003-03-14 | 2006-06-01 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron for the treatment of restless leg syndrome |
| US6960571B2 (en) * | 2003-03-14 | 2005-11-01 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron for the treatment of restless leg syndrome |
| US8614204B2 (en) | 2003-06-06 | 2013-12-24 | Fibrogen, Inc. | Enhanced erythropoiesis and iron metabolism |
| WO2005041928A1 (en) | 2003-10-31 | 2005-05-12 | Alza Corporation | Compositions and dosage forms for ehnanced absorption of iron |
| US20060134227A1 (en) | 2004-12-22 | 2006-06-22 | Bortz Jonathan D | Compositions including iron |
| EP1848446B1 (en) | 2005-02-09 | 2009-10-14 | Vifor (International) Ag | Use of iron(iii) complex compounds |
| EP1757299A1 (en) | 2005-08-25 | 2007-02-28 | Vifor (International) Ag | Complexes of iron III for treating iron deficiencies in patients with inflammatory bowel disease |
| KR101905340B1 (en) | 2006-01-06 | 2018-10-05 | 루이트폴드 파머수티컬스, 인코퍼레이티드 | Methods and compositions for administration of iron |
| US8071542B2 (en) | 2007-01-29 | 2011-12-06 | Chyna, LLC | Use of ferritin to treat iron deficiency disorders |
| US8778878B2 (en) | 2007-01-29 | 2014-07-15 | Chyna, LLC | Use of ferritin to treat iron disorders |
| EP2155850B1 (en) | 2007-05-18 | 2014-04-16 | Raffinerie Notre Dame - Orafti S.A. | Method for providing fragrance to a substrate; fragrance-containing substrate |
| EP1997833A1 (en) | 2007-05-29 | 2008-12-03 | Vifor (International) Ag | Water-soluble ferric carbohydrate derivative complexes, their manufacture and medicines containing these |
| FR2934272B1 (en) | 2008-07-24 | 2013-08-16 | Roquette Freres | PROCESS FOR THE PREPARATION OF COMPOSITIONS BASED ON AMYLACEOUS MATERIAL AND SYNTHETIC POLYMER |
| US8815301B2 (en) | 2009-03-25 | 2014-08-26 | Pharmacosmos Holding A/S | Stable iron oligosaccharide compound |
| FR2951177B1 (en) | 2009-10-09 | 2012-12-21 | Roquette Freres | PROCESS FOR THE PREPARATION OF ACETYLATED DERIVATIVES OF AMYLACEOUS MATERIAL |
| WO2011055374A2 (en) | 2009-11-04 | 2011-05-12 | Symed Labs Limited | Process for the preparation of iron (iii) carboxymaltose complex |
| WO2012145392A2 (en) | 2011-04-18 | 2012-10-26 | Curators Of The University Of Missouri | Saccharide conjugates |
| CN107890472A (en) | 2012-07-27 | 2018-04-10 | 本质生命科学有限公司 | The method for treating hypoferric anemia |
| WO2014071194A2 (en) | 2012-11-01 | 2014-05-08 | Katz Robert S | Methods for treating fibromyalgia |
| CN104918486B (en) | 2012-11-30 | 2017-12-15 | 法玛科思莫斯股份公司 | The composition of cryoprotection reagent, cryoprotection and freezen protective, its purposes, and freezing and storing method |
| WO2016151367A1 (en) | 2015-03-23 | 2016-09-29 | Suven Life Sciences Limited | Preparation of water soluble trivalent iron carbohydrate complexes |
| WO2016181195A1 (en) | 2015-05-08 | 2016-11-17 | Suven Life Sciences Limited | Improved process for water soluble iron carbohydrate complexes |
| EP3339329A1 (en) | 2016-12-22 | 2018-06-27 | LEK Pharmaceuticals d.d. | Selective oxidation of maltodextrin and its use in the preparation of water-soluble iron (iii) carboxymaltose complexes |
-
2007
- 2007-01-08 KR KR1020177005732A patent/KR101905340B1/en active IP Right Grant
- 2007-01-08 WO PCT/US2007/000176 patent/WO2007081744A2/en active Application Filing
- 2007-01-08 EP EP13166988.9A patent/EP2626074A1/en not_active Withdrawn
- 2007-01-08 DK DK07716309.5T patent/DK1973549T3/en active
- 2007-01-08 KR KR1020147024469A patent/KR20140117678A/en not_active Application Discontinuation
- 2007-01-08 CN CN2007800020060A patent/CN101365458B/en not_active Ceased
- 2007-01-08 CA CA2953964A patent/CA2953964A1/en not_active Withdrawn
- 2007-01-08 CA CA2635894A patent/CA2635894C/en not_active Expired - Fee Related
- 2007-01-08 EP EP07716309.5A patent/EP1973549B1/en not_active Revoked
- 2007-01-08 EP EP16172826.6A patent/EP3081219A1/en active Pending
- 2007-01-08 AU AU2007205167A patent/AU2007205167B2/en active Active
- 2007-01-08 KR KR1020187018660A patent/KR20180077337A/en not_active Application Discontinuation
- 2007-01-08 KR KR1020087016352A patent/KR20080082674A/en not_active Application Discontinuation
- 2007-01-08 US US11/620,986 patent/US7754702B2/en active Active
- 2007-01-08 PT PT77163095T patent/PT1973549T/en unknown
-
2009
- 2009-03-31 HK HK09103049.6A patent/HK1125044A1/en not_active IP Right Cessation
-
2010
- 2010-05-25 US US12/787,283 patent/US8431549B2/en active Active
-
2013
- 2013-03-19 US US13/847,254 patent/US20130230565A1/en not_active Abandoned
- 2013-12-09 US US14/100,717 patent/US8895612B2/en active Active
-
2015
- 2015-04-10 US US14/683,415 patent/US10478450B2/en active Active
-
2016
- 2016-10-19 CY CY20161101047T patent/CY1118780T1/en unknown
-
2018
- 2018-04-20 US US15/958,930 patent/US11433091B2/en active Active
- 2018-11-15 US US16/192,681 patent/US11406656B2/en active Active
-
2019
- 2019-06-11 US US16/438,340 patent/US11478502B2/en active Active
-
2020
- 2020-03-20 US US16/825,121 patent/US11344568B2/en active Active
- 2020-03-20 US US16/825,337 patent/US11364260B2/en active Active
-
2022
- 2022-06-16 US US17/842,483 patent/US20230008240A1/en active Pending
Non-Patent Citations (1)
| Title |
|---|
| See references of EP1973549A2 * |
Cited By (28)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US9376505B2 (en) | 2002-10-23 | 2016-06-28 | Vifor (International) Ag. | Aqueous iron carbohydrate complexes, their production and medicaments containing them |
| US11291645B2 (en) | 2002-10-23 | 2022-04-05 | Vifor (International) Ag | Aqueous iron carbohydrate complexes, their production and medicaments containing them |
| US11123321B2 (en) | 2002-10-23 | 2021-09-21 | Vifor (International) Ag | Aqueous iron carbohydrate complexes, their production and medicaments containing them |
| US10519252B2 (en) | 2002-10-23 | 2019-12-31 | Vifor (International) Ag. | Aqueous iron carbohydrate complexes, their production and medicaments containing them |
| US10478450B2 (en) | 2006-01-06 | 2019-11-19 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron |
| US11433091B2 (en) | 2006-01-06 | 2022-09-06 | American Regent, Inc. | Methods and compositions for administration of iron |
| US20150297630A1 (en) | 2006-01-06 | 2015-10-22 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron |
| EP2626074A1 (en) | 2006-01-06 | 2013-08-14 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron |
| EP1973549B1 (en) | 2006-01-06 | 2016-07-20 | Luitpold Pharmaceuticals, Inc. | Methods and compositions for administration of iron |
| US11344568B2 (en) | 2006-01-06 | 2022-05-31 | American Regent, Inc. | Methods and compositions for administration of iron |
| US11478502B2 (en) | 2006-01-06 | 2022-10-25 | American Regent, Inc. | Methods and compositions for administration of iron |
| US11364260B2 (en) | 2006-01-06 | 2022-06-21 | American Regent, Inc. | Methods and compositions for administration of iron |
| US11406656B2 (en) | 2006-01-06 | 2022-08-09 | American Regent, Inc. | Methods and compositions for administration of iron |
| JP2011523866A (en) * | 2008-05-23 | 2011-08-25 | ホスピラ・インコーポレイテツド | Packaged iron sucrose products |
| US10414831B2 (en) | 2009-03-25 | 2019-09-17 | Pharmacosmos Holding A/S | Stable iron oligosaccharide compound |
| US10865255B2 (en) | 2009-03-25 | 2020-12-15 | Pharmacosmos Holding A/S | Stable iron oligosaccharide compound |
| US12030962B2 (en) | 2009-03-25 | 2024-07-09 | Pharmacosmos Holding A/S | Stable iron oligosaccharide compound |
| US8828967B2 (en) | 2010-06-09 | 2014-09-09 | Biofer S.P.A. | Low molecular weight complexes between iron and maltobionic acid, use thereof for intramuscular or subcutaneous administration in the treatment of anemic states, and new pharmaceutical compositions adapted for these uses |
| ITMI20101028A1 (en) * | 2010-06-09 | 2011-12-10 | Biofer Spa | NEW COMPLEXES AT LOW MOLECULAR WEIGHT BETWEEN IRON AND MALTOBIONIC ACID, USE OF THESE FOR INTRAMUSCULAR OR SUBCUTANEOUS ADMINISTRATION IN ANEMIC STATE THERAPY, AND NEW PHARMACEUTICAL COMPOSITIONS SUITABLE FOR THESE USES. |
| WO2011154452A1 (en) | 2010-06-09 | 2011-12-15 | Biofer S.P.A. | New low molecular weight complexes between iron and maltobionic acid, use thereof for intramuscular or subcutaneous administration in the treatment of anemic states, and new pharmaceutical compositions adapted for these uses |
| EP2420243A1 (en) | 2010-08-18 | 2012-02-22 | Inovativo Biomedicinas Tehnologiju Instituts, SIA | Compositions obtainable from bred beetroot juice to promote iron absorption and blood forming |
| US10239941B2 (en) | 2013-03-15 | 2019-03-26 | Intrinsic Lifesciences Llc | Anti-hepcidin antibodies and uses thereof |
| US9803011B2 (en) | 2013-03-15 | 2017-10-31 | Intrinsic Lifesciences Llc | Anti-hepcidin antibodies and uses thereof |
| US9657098B2 (en) | 2013-03-15 | 2017-05-23 | Intrinsic Lifesciences, Llc | Anti-hepcidin antibodies and uses thereof |
| US10323088B2 (en) | 2014-09-22 | 2019-06-18 | Intrinsic Lifesciences Llc | Humanized anti-hepcidin antibodies and uses thereof |
| US11020369B2 (en) | 2018-10-29 | 2021-06-01 | Pharmacosmos Holding A/S | Treating iron deficiency with ferric carboxymaltose |
| WO2020089227A1 (en) | 2018-10-29 | 2020-05-07 | Pharmacosmos Holding A/S | Treating iron deficiency with ferric carboxymaltose |
| US11806329B2 (en) | 2018-10-29 | 2023-11-07 | Pharmacosmos Holding A/S | Treating iron deficiency with ferric carboxymaltose |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US11364260B2 (en) | Methods and compositions for administration of iron | |
| Kalra et al. | Iron isomaltoside 1000: a new high dose option for parenteral iron therapy | |
| AU2018202715A1 (en) | Methods and compositions for administration of iron | |
| AU2013206429B2 (en) | Methods and compositions for administration of iron | |
| EP2822574A1 (en) | Methods for modulation of phosphorus and fgf23 | |
| HUE029259T2 (en) | Methods and compositions for administration of iron | |
| Maladkar et al. | From Tradition to Innovation: The Clinical Edge of Ferric Carboxymaltose in Managing Iron Deficiency Anemia. |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application | ||
| WWE | Wipo information: entry into national phase |
Ref document number: 2007205167 Country of ref document: AU |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2635894 Country of ref document: CA |
|
| ENP | Entry into the national phase |
Ref document number: 2007205167 Country of ref document: AU Date of ref document: 20070108 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 1020087016352 Country of ref document: KR |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 200780002006.0 Country of ref document: CN |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REEP | Request for entry into the european phase |
Ref document number: 2007716309 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2007716309 Country of ref document: EP |