WO2023013764A1 - 非アルコール性脂肪性肝炎における線維化進行度および/または前記肝疾患の活動性を推定する方法 - Google Patents
非アルコール性脂肪性肝炎における線維化進行度および/または前記肝疾患の活動性を推定する方法 Download PDFInfo
- Publication number
- WO2023013764A1 WO2023013764A1 PCT/JP2022/030093 JP2022030093W WO2023013764A1 WO 2023013764 A1 WO2023013764 A1 WO 2023013764A1 JP 2022030093 W JP2022030093 W JP 2022030093W WO 2023013764 A1 WO2023013764 A1 WO 2023013764A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- igfals
- reference value
- fibrosis
- antibody
- blood
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Ceased
Links
Images

















Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/543—Immunoassay; Biospecific binding assay; Materials therefor with an insoluble carrier for immobilising immunochemicals
Definitions
- the present disclosure relates to a method for estimating the degree of fibrosis progression and/or activity of the liver disease in non-alcoholic steatohepatitis.
- the disclosure also relates to compositions and kits for use in such methods.
- non-alcoholic steatohepatitis NASH
- development of a method capable of non-invasively monitoring fibrosis is strongly desired, since progress of liver fibrosis determines patient prognosis.
- NASH is a pathological condition in which the liver becomes inflamed with non-alcoholic fatty liver (NAFL) and liver fibrosis progresses. If NASH progresses, there is a risk of developing liver cirrhosis or liver cancer.
- NASH was characterized by (i) macrovesicular/vesicular fatty deposits, (ii) inflammatory cell infiltration, (iii) balloon-like hepatocytes, and and (iv) fibrosis around hepatocytes in the center of the hepatic lobule, and 3) viral hepatitis (viruses include, for example, HBV and HCV) and autoimmune hepatitis. Diagnosis is based on no other liver disease.
- liver biopsy is a standard method for evaluating liver fibrosis in patients, but due to its high invasiveness and cost, it is difficult to perform routinely and repeatedly. In addition, since liver biopsy can only provide information on a small area of the liver tissue, it has been pointed out that sampling errors occur in NASH, which has heterogeneous intrahepatic lesions. . On the other hand, although several blood biomarkers for liver fibrosis in NASH have been developed and applied, many of them have problems in terms of performance.
- Patent Document 1 and Non-Patent Document 1 disclose that circulating insulin-like growth factor-binding protein acid-labile subunit (IGFALS) levels are reduced in patients with HCV-induced hepatitis.
- WO 2005/010102 also discloses that blood IGFALS levels are reduced in patients with HCV-induced hepatitis.
- Patent Document 2 discloses that blood IGFALS decreases in end-stage HCV-induced hepatitis patients and severe liver fibrosis cases (grade 4 or later). Disclosed are diagnostics based on marker levels.
- NASH is diagnosed on the basis that the patient does not have viral hepatitis such as HCV, and NASH and HCV-induced hepatitis are different diseases.
- the present disclosure relates to a method for estimating the degree of fibrosis progression and/or activity of the liver disease in non-alcoholic steatohepatitis.
- the disclosure also provides compositions and kits for use in such methods.
- the present inventors have extensively studied a method for early detection of liver fibrosis in patients with non-alcoholic steatohepatitis, and found that serum IGFALS protein levels in patients with non-alcoholic steatohepatitis are at an early stage such as grade 1-2. It was found to be a good biomarker of fibrosis, including fibrosis (see, eg, Figure 2C). Serum IGFALS levels were unchanged in patients with alcoholic steatohepatitis (ASH) compared to healthy controls (see Figure 3D), and the difference was not clear in HCV-induced hepatitis.
- ASH alcoholic steatohepatitis
- the serum IGFALS level is not necessarily a biomarker showing efficacy in general liver fibrosis, but was thought to be a specific biomarker for estimating liver fibrosis grade in NASH patients.
- the inventors further demonstrated that non-alcoholic steatohepatitis activity can be estimated by serum IGFALS levels (see FIGS. 6A-7).
- a method for estimating the progression of liver fibrosis and/or the activity of said liver disease in a subject with non-alcoholic fatty liver disease comprising: measuring the protein level of insulin-like growth factor binding protein (acid-labile subunit, IGFALS) in a blood sample obtained from the subject; (i) blood IGFALS protein levels in said subject; (ii) (a) reference value in healthy subjects (first reference value), or (ii) (b) reference value in subjects with fibrosis grade 2-3 liver fibrosis (second reference value), or (ii)(c) comparing to a reference value for blood IGFALS levels; A method, including (2) (i) comparing the blood IGFALS protein level of said subject with (ii) (a) a reference value (first reference value) of a healthy subject; A subject from whom a blood sample in which the ratio of said level to a first reference value (said level/first reference value) is less than a first reference value has
- the method according to (1) above further comprising (3) (i) comparing the subject's blood IGFALS protein level to a reference value (second reference value) for a subject with (ii)(b) fibrosis grade 2-3 liver fibrosis; A subject from whom a blood sample in which the ratio of said level to a second reference value (said level/second reference value) is less than a second reference value has fibrosis with a liver fibrosis grade of 2 or higher , or presumed to be likely, and/or A subject from whom a blood sample in which the ratio of said level to a second reference value (said level/second reference value) is equal to or greater than a second reference value has fibrosis with a liver fibrosis grade of 2 or higher.
- the second reference value is a value of 1.5 or less.
- the reference value for the blood IGFALS level is lower than the reference value (first reference value) in healthy subjects, and the reference value (second reference value) in subjects with fibrosis grade 2-3 liver fibrosis.
- NAFLD non-alcoholic steatohepatitis
- the means for measuring blood IGFALS levels comprises an antibody that binds to IGFALS or a protein complex containing IGFALS.
- the means for measuring blood IGFALS levels comprises an antibody that binds to IGFALS.
- the means for measuring blood IGFALS levels comprises an antibody that binds to a protein complex containing IGFALS.
- the antibody that binds to a protein complex comprising IGFALS comprises an antibody that binds to IGFALS and an antibody that binds to IGF1 or IGFBP-3 or IGFBP-5.
- a means for measuring IGFALS levels includes a first antibody that binds to IGFALS or a protein complex containing IGFALS immobilized on a support, and a labeled IGFALS or a protein complex containing IGFALS that binds to the first antibody.
- a protein complex comprising the first antibody, the second antibody, and IGFALS or IGFALS, comprising a second antibody, comprising the first antibody, the second antibody, and IGFALS or a protein complex comprising IGFALS The kit according to (13) above, which is capable of forming a complex.
- the means for measuring IGFALS levels includes test strips for immunochromatography;
- a test strip is a strip comprising a sample pad for introducing a blood sample, a conjugate pad, an area containing a test line and a control line, and a waste pad.
- the conjugate pad comprises a substance (first binding substance) that binds to IGFALS or a protein complex comprising IGFALS, the first binding substance being labeled;
- the test line contains a binding substance (second binding substance) that binds to IGFALS or a protein complex containing IGFALS, the second binding substance is immobilized on the test line,
- a control line did not contain any substance that binds to IGFALS, the first binding agent and the second binding agent are capable of simultaneously binding to IGFALS or a protein complex comprising IGFALS;
- IGFALS or a protein complex containing IGFALS contained in the blood sample binds to the first binding substance labeled on the conjugate pad to form a complex, and the complex is immobilized on the test line.
- the amount of label bound to the phased second binding agent and detected on the test line is indicative of the amount of IGFALS in the blood sample; 14.
- the means for measuring IGFALS levels comprises immunochromatographic test strips;
- a test strip is a strip comprising a sample pad for introducing a blood sample, a conjugate pad, an area containing a test line and a control line, and a waste pad.
- the conjugate pad comprises a substance that binds to IGFALS (the first binding substance), the first binding substance being labeled;
- the test line contains a binding substance (second binding substance) that binds to IGFALS, the second binding substance is immobilized on the test line, A control line did not contain any substance that binds to IGFALS, the first binding agent and the second binding agent can simultaneously bind to IGFALS;
- IGFALS contained in the blood sample binds to the first binding substance labeled on the conjugate pad to form a complex, and the complex is immobilized on the test line to form a second binding substance.
- the means for measuring IGFALS levels comprises immunochromatographic test strips;
- a test strip is a strip comprising a sample pad for introducing a blood sample, a conjugate pad, an area containing a test line and a control line, and a waste pad.
- the conjugate pad comprises a substance (first binding substance) that binds to a protein complex comprising IGFALS, the first binding substance being labeled;
- the test line contains a binding substance (second binding substance) that binds to the protein complex containing IGFALS, the second binding substance is immobilized on the test line,
- a control line did not contain any substance that binds to IGFALS, the first binding agent and the second binding agent are capable of simultaneously binding to a protein complex comprising IGFALS;
- the protein complex containing IGFALS contained in the blood sample binds to the first binding substance labeled on the conjugate pad to form a complex, and the complex is immobilized on the test line.
- each of the first binding substance and the second binding substance is an antibody that binds to IGFALS or an antibody that binds to a protein complex comprising IGFALS.
- each of the first binding substance and the second binding substance is an antibody that binds to IGFALS.
- each of the first binding agent and the second binding agent is an antibody that binds to a protein complex comprising IGFALS.
- one of the first binding substance and the second binding substance is an antibody that binds to IGFALS and the other is an antibody that binds to IGF1 or IGFBP-3 or IGFBP-5 (17) or The kit according to (17B).
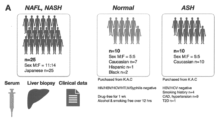
- FIG. 1A represents the subject population of this example.
- Subjects were non-alcoholic fatty liver (NAFL), non-alcoholic steatohepatitis (NASH), healthy subjects, and alcoholic steatohepatitis (ASH) based on Liver Biopsy and other clinical data.
- a population diagnosed as In this example, the serum biomarker levels of these subjects were examined.
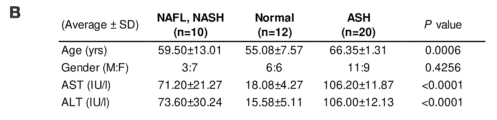
- FIG. 1B shows age, gender, AST values, and ALT values in each subject group.
- FIG. 1C shows IGF1 levels in the NAFL/NASH group with grades 1-3 fibrosis graded according to Table 1, the normal group, and the ASH group.
- FIG. 1D shows serum IGFALS levels in the NAFL/NASH group with grades 1-3 fibrosis, the healthy group, and the ASH group, graded according to Table 1.
- FIG. FIG. 2A shows a comparison of ROC curves based on each diagnostic index. The vertical axis in FIG. 2A represents sensitivity (%) and the horizontal axis represents 100-specificity (%).
- FIG. 2B shows the area under the curve (AUC) of the ROC curve based on each diagnostic index, the cutoff value, the sensitivity and specificity at that cutoff value, and the p-value.
- FIG. 2C shows the ROC curve in the NAFL/NASH group with grade 2 fibrosis in the low fibrosis group plus healthy subjects.
- FIG. 3A shows a comparison of AST values in healthy subjects, NAFL/NASH group and ASH group.
- FIG. 3B shows a comparison of ALT values in the healthy subject group, NAFL/NASH group and ASH group.
- FIG. 3C is a diagram plotting the AST and ALT values of each subject in the healthy subject group, NAFL/NASH group, and ASH group.
- FIG. 3D shows that serum IGFALS levels are not significantly different between healthy and ASH groups.
- FIG. 3 shows that serum IGFALS levels do not respond to fibrosis in general, but specifically to fibrosis in the NAFL/NASH group.
- FIG. 3E is a diagram showing the relationship between each subject group and age.
- FIG. 4 shows ROC curves for each biomarker for diagnosing subjects with greater than grade 1 fibrosis. The vertical axis represents sensitivity (%) and the horizontal axis represents 100-specificity (%).
- FIG. 5 shows ROC curves for each biomarker for diagnosing subjects with greater than grade 2 fibrosis (ie, between grades 2 and 3, and grade 3). The vertical axis represents sensitivity (%) and the horizontal axis represents 100-specificity (%).
- FIG. 4 shows ROC curves for each biomarker for diagnosing subjects with greater than grade 1 fibrosis. The vertical axis represents sensitivity (%) and the horizontal axis represents 100-specificity (%).
- FIG. 5 shows ROC curves for each biomarker for diagnosing subjects with greater than grade 2 fibro
- FIG. 6A shows blood levels of each factor in the healthy subject group (Normal), ASH group, and NASH group.
- FIG. 6B shows the correlation between the blood IGFALS level and the blood IGF1 level in the healthy subject group (Normal), ASH group, and NASH group.
- FIG. 6C shows the correlation (Pearson correlation coefficient) of the parameters obtained from the analysis of the three groups of the healthy subject group (Normal), ASH group, and NASH group.
- FIG. 7 shows blood levels of each factor in the active NASH group and the other control groups.
- FIG. 8 shows ROC curves in detecting active NASH groups based on blood levels of each factor.
- a "subject” can be a mammal, e.g., primates such as humans and chimpanzees, laboratory animals such as rats, mice, rabbits, domesticated animals such as pigs, cows, horses, sheep, and goats, and companion animals such as dogs and cats, preferably humans.
- patient means a subject with a disease, preferably a human with a disease.
- non-alcoholic fatty liver disease is defined as a condition in which fat accumulates in the liver (fatty liver) in people who have never been or rarely drink alcohol (30 g in men). /day, less than 20g/day for women (converted to ethanol). The intake of alcohol can be calculated by alcohol content (%) x amount of alcohol (mL) x specific gravity of alcohol (0.8 g/mL).
- NAFLD is a general term for a series of diseases including non-alcoholic fatty liver, progressing to steatohepatitis and cirrhosis.
- Causes of NAFLD include lifestyle diseases such as obesity, diabetes, dyslipidemia, and hypertension, as well as diseases such as sleep apnea, polycystic ovarian syndrome, hypothyroidism, and hypopituitarism. , pancreaticoduodenectomy, central parenteral nutrition after surgery such as jejuno-ileal bypass, and administration of drugs (tamoxifen, valproic acid, amiodarone, etc.) are known.
- Diagnosis of non-alcoholic fatty liver disease is based on 1) no history of alcohol consumption or very little alcohol consumption (less than 30 g/day for men and less than 20 g/day for women); (i) macrovesicular/vesicular fat deposition, (ii) inflammatory cell infiltration, (iii) hepatocyte ballooning, and (iv) perihepatocyte fibrosis in the central hepatic lobule. and 3) not viral hepatitis (viruses include, for example, HBV and HCV) and other liver diseases such as autoimmune hepatitis. NAFLD is therefore distinct from hepatitis caused by HCV and HBV.
- MAFLD metabolic-related fatty liver disease
- the diagnostic criteria for MAFLD are, in addition to the presence of hepatic steatosis, 1) a BMI value of 25 kg/m 2 or more, 2) the presence of type 2 diabetes, or 3) the following seven metabolic risk criteria (metabolic at- by the presence of two or more of the risk criteria).
- NAFL non-alcoholic fatty liver
- Treatments for subjects with NAFL include diet and/or exercise regimens and weight loss thereby. Treatment of the underlying disease, such as those listed above, may also be effective.
- non-alcoholic steatohepatitis is a pathological condition in which NAFL causes liver inflammation and liver fibrosis progresses.
- NASH non-alcoholic steatohepatitis
- subjects can develop cirrhosis and liver cancer. It can be diagnosed by a liver biopsy, which examines liver tissue.
- the diagnosis of NASH is NAFLD, and 2) histological findings from liver biopsy show either (iii) hepatocyte ballooning and (iv) perihepatocyte fibrosis in the central hepatic lobules.
- NASH can be diagnosed when:
- ASH alcoholic steatohepatitis
- liver tissue lesions are mainly degeneration or necrosis of hepatocytes, 1) significant swelling of hepatocytes mainly in the center of the lobule (ballooning, ballooning), and 2) Varying degrees of hepatocyte necrosis and 3) Mallory's body (alcoholic vitreous), or 4) polynuclear leukocyte infiltration.
- confirmation of drinking history e.g., drinking an average of 60 g (ethanol equivalent) or more per day for 5 years or more
- exclusion of liver damage due to causes other than alcohol e.g., hepatitis virus marker negative, anti-mitochondrial antibody negative, and antinuclear antibody negative.
- hepatic fibrosis refers to a state in which connective tissue accumulates in the liver. Connective tissue accumulates, for example, due to repair of damage in the liver. In particular, when the damage is chronic, repair occurs repeatedly, resulting in accelerated accumulation of connective tissue and progression of fibrosis.
- Pathologically, fibrosis is initiated by the activation of perivascular stellate cells in the liver. These cells can participate in the inflammatory response and overproduce extracellular matrix (such as collagen) and matrixcellular proteins while producing fibrosis-inducing factors such as TGF- ⁇ .
- the fibrosis grade can be determined, for example, based on Table 1 below (see NASH clinical research network historical scoring system (Keliner et al., Hepatology, 2005)).
- Fibrosis can be improved or prevented from progressing by removing the cause.
- Medicaments to treat fibrosis include PPAR agonists (e.g., thiazolidine derivatives), bile acid nuclear receptor agonists (e.g., bile acid analogs, e.g., obeticholic acid), CCR2 or CCR5 antagonists (e.g., Senicriviroc), kinase inhibitors. agents (eg, sorafenib), ASK1 antagonists (eg, seronsertib), collagen-specific chaperone inhibitors (eg, siRNA or antisense oligos against HSP47).
- PPAR agonists e.g., thiazolidine derivatives
- bile acid nuclear receptor agonists e.g., bile acid analogs, e.g., obeticholic acid
- CCR2 or CCR5 antagonists e.g., Senicriviroc
- IGFALS insulin-like growth factor-binding protein acid-labile subunits
- IGF1 insulin-like growth factor 1
- IGFBP1-6 IGF binding proteins
- Human IGFALS is registered with the US National Center for Biotechnology Information (NCBI) as GENE ID: 3483, and its amino acid sequence is not particularly limited, but for example, the amino acid sequence registered in NCBI Reference Sequence: NP_001139478.1. could be.
- a "blood sample” can be whole blood, serum, and plasma.
- Whole blood may contain an anticoagulant.
- Serum is the liquid component obtained by centrifugation after drawing blood into an anticoagulant-free container and allowing the blood to clot.
- Plasma is the supernatant obtained by centrifuging blood mixed with an anticoagulant to sediment blood cell components.
- the term "antibody” refers to an immunoglobulin, a protein having a structure in which two heavy chains (H chains) and two light chains (L chains) stabilized by disulfide bonds are associated.
- the heavy chain consists of a heavy chain variable region VH, heavy chain constant regions CH1, CH2, CH3, and a hinge region located between CH1 and CH2, and the light chain consists of a light chain variable region VL and a light chain constant region CL.
- a variable region fragment (Fv) consisting of VH and VL is a region that directly participates in antigen binding and imparts diversity to antibodies.
- the antigen-binding region consisting of VL, CL, VH and CH1 is called the Fab region, and the region consisting of the hinge region, CH2 and CH3 is called the Fc region.
- the regions that directly contact the antigen undergo particularly large changes and are called complementarity-determining regions (CDRs).
- CDRs complementarity-determining regions
- a portion other than the CDRs with relatively few mutations is called a framework region (FR).
- FR framework region
- the light chain and heavy chain variable regions each have three CDRs, which are referred to as heavy chain CDRs 1-3 and light chain CDRs 1-3 in order from the N-terminus. Each CDR is integrated into framework regions.
- the heavy chain variable region of the antibody consists of, from the N-terminal side to the C-terminal side, heavy chain framework region 1, heavy chain CDR1, heavy chain framework region 2, heavy chain CDR2, heavy chain framework region 3, heavy chain It has CDR3, and heavy chain framework region 4, in that order.
- the light chain variable region of the antibody consists of, from the N-terminal side to the C-terminal side, light chain framework region 1, light chain CDR1, light chain framework region 2, light chain CDR2, light chain framework region 3, light chain It has CDR3, and light chain framework region 4, in that order.
- Antibodies can be recombinant proteins (recombinant antibodies) and can be produced in animal cells, such as Chinese hamster ovary cells (CHO cells).
- the origin of the antibody is not particularly limited, but examples thereof include non-human animal antibodies, non-human mammal antibodies (eg, mouse antibodies, rat antibodies, camel antibodies), and human antibodies.
- Antibodies may also be chimeric, humanized, and fully humanized antibodies.
- Antibodies may be polyclonal antibodies or monoclonal antibodies, preferably monoclonal antibodies.
- Antibodies can be isolated antibodies or purified antibodies.
- Antibodies can be, for example, IgG.
- Antibodies can be, for example, IgG1, IgG2, IgG3, or IgG4.
- variable regions of immunoglobulin chains consist of relatively conserved framework regions (FR) joined by three hypervariable regions (more often called “complementarity determining regions” or CDRs). generally exhibit the same overall structure, including
- the CDRs from the two chains of each heavy/light chain pair described above are represented by framework regions to form structures that specifically bind to specific epitopes on target proteins (e.g., PCSK9).
- target proteins e.g., PCSK9
- FR1, CDR1, FR2, CDR2, FR3, CDR3 and FR4 parallel to From N-terminus to C-terminus, both naturally occurring light and heavy chain variable regions typically conform to the following order of these elements.
- FR1, CDR1, FR2, CDR2, FR3, CDR3 and FR4 A numbering system, such as that of Kabat, has been devised to assign numbers to the amino acids that occupy positions in each of these domains.
- Heavy chain CDRs 1-3 and light chain CDRs 1-3 can be determined based on the amino acid sequences of the heavy and light chain variable regions, respectively, for example, by the numbering system according to Kabat.
- a "protein complex” is a complex comprising multiple proteins, each associated with at least one other protein.
- An “antibody-protein complex” is a protein complex that includes an antibody and a protein, and the antibody is bound to the protein. Protein complexes include protein complexes found in blood samples (protein complexes in blood samples) and complexes that do not contain antibodies, such as artificially produced antibodies (such as monoclonal antibodies) ( antibody-free protein complexes).
- liver fibrosis level (or liver fibrosis progression, liver fibrosis grade, or liver fibrosis) in a subject with or likely to have non-alcoholic fatty liver disease (NAFLD) score) is provided.
- NAFLD non-alcoholic fatty liver disease
- the methods of the present disclosure involve measuring the protein level (ie, concentration) of IGFALS in a biological sample (eg, body fluid sample, preferably blood sample) obtained from a subject.
- a biological sample may preferably be a blood sample.
- the use of blood samples allows for minimally invasive and repeatable tests, which can be beneficial in that liver biopsies, previously required for diagnosis, can be avoided. Measurements can be made with either serum or plasma.
- the average protein level of IGFALS in blood can be, for example, less than half of the average in healthy individuals.
- the subject may be a NASH patient who does not have fibrosis (has grade 0 fibrosis) or who may have fibrosis.
- the patient can be a NASH patient who has or is likely to have grade 1 fibrosis (eg, a grade selected from the group consisting of grades 1A, 1B and 1C).
- the subject can be a NASH patient with or at risk of having grade 2 fibrosis. In certain aspects of the present disclosure, the subject has or may have grade 3 fibrosis. Can be a NASH patient. In certain aspects of the present disclosure, the subject may be a NASH patient with or at risk of having grade 4 fibrosis. In one preferred aspect, the subject is a NASH patient without fibrosis (with grade 0 fibrosis) or with possible fibrosis, grade 1 (e.g., grades 1A, 1B and 1C selected from the group consisting of ) and one or more NASH patients selected from the group consisting of NASH patients with or with the potential for grade 2 fibrosis.
- grade 1 e.g., grades 1A, 1B and 1C selected from the group consisting of
- the subject with said grade of fibrosis has NASH or NAFL, e.g., diagnosed by alcohol history and liver biopsy, and ruled out for hepatitis due to other causes, such as viral hepatitis, as described above.
- NASH or NAFL e.g., diagnosed by alcohol history and liver biopsy, and ruled out for hepatitis due to other causes, such as viral hepatitis, as described above.
- the subject can be one that has been determined to have a fibrosis grade. Therefore, in one embodiment, the liver fibrosis grade can be estimated by body fluid biopsy (liquid biopsy) for a patient whose presence or absence of liver fibrosis and liver fibrosis grade have been determined by liver biopsy or the like.
- the method of the present disclosure comprises comparing (i) the subject's blood IGFALS protein level (measurement) with (ii) (a) a reference value (first reference value) in a healthy subject. can further include If the measured value of (i) (the measured value) is lower than the first reference value, the subject has or is likely to have fibrosis of fibrosis grade 2 or higher. Accordingly, the methods of the present disclosure further comprise presuming that a subject with a blood IGFALS protein level lower than the first reference value has, or is likely to have, fibrosis grade 2 or greater. You can stay.
- the method of the present disclosure comprises: (i) comparing the blood IGFALS protein level (measured value) of the subject with (ii) (a) a reference value (first reference value) of a healthy subject;
- the ratio of the subject's blood IGFALS protein level (measured value) to a first reference value (said measured value/first reference value) is equal to or less than a first reference value (i.e., a predetermined cutoff value), or It can further include presuming that the subject from whom the blood sample is less than has or is likely to have fibrosis with a liver fibrosis grade of 2 or greater.
- the method of the present disclosure comprises: (i) comparing the blood IGFALS protein level (measured value) of the subject with (ii) (a) a reference value (first reference value) of a healthy subject; A subject from which a blood sample in which the ratio of the measured value to the first reference value (the measured value/first reference value) is equal to or greater than the first reference value (i.e., a predetermined cutoff value) is Presuming that there is no fibrosis with a fibrosis grade of 2 or higher, or that there is a possibility thereof (i.e., the possibility of not having fibrosis with a liver fibrosis grade of 2 or higher); can further include
- the first reference value is, for example, the mean value of the IGFALS level (preferably blood IGFALS level) in a biological sample (e.g., body fluid sample, preferably blood sample) from healthy subjects, the first quartile value, or a minimum value, or a value in between.
- a biological sample e.g., body fluid sample, preferably blood sample
- the first reference value (that is, the predetermined cutoff value) is, for example, less than 1.0, 0.9 or less, 0.8 or less, 0.7 or less, 2/3 or less, 0.6 or less, 0.6 or less. It can be a value of 55 or less, 0.5 or less, 0.45 or less, or 0.4 or less.
- the first reference value (ie, the predetermined cutoff value) can be a value of 0.4 or greater, 0.45 or greater, 0.5 or greater, or 0.55 or greater.
- the first reference value ie, the predetermined cutoff value
- the first reference value can be the average blood IGFALS level in healthy subjects, and the first reference value (i.e., cutoff value) can be a value of 2/3 or less, e.g. , may be in the range of 0.4 to 0.7, preferably in the range of 0.5 to 0.6.
- the first reference value can be the first quartile of blood IGFALS levels in healthy subjects, and the first reference value (ie, cutoff value) is 0.9 or less, 0.9 or less, It can be a number of 8 or less, 0.7 or less, 2/3 or less.
- the first reference value can be the minimum blood IGFALS level in healthy subjects, and the first reference value (ie, cutoff value) can be a number less than one.
- the method of the present disclosure comprises: (i) the subject's blood IGFALS protein level (measurement) is compared to (ii) (b) a reference value for a subject with fibrosis grade 2-3 liver fibrosis (second reference value) can include
- the method of the present disclosure comprises: (i) the subject's blood IGFALS protein level (measurement) is compared to (ii) (b) a reference value for a subject with fibrosis grade 2-3 liver fibrosis (second reference value) including A subject from which a blood sample in which the ratio of the measured value to a second reference value (said measured value/second reference value) is less than a second reference value (i.e., a predetermined cutoff value) is treated with liver It may further comprise assuming that the fibrosis grade has or is likely to have fibrosis of 2 or more.
- the method of the present disclosure comprises: (i) the subject's blood IGFALS protein level (measurement) is compared to (ii) (b) a reference value for a subject with fibrosis grade 2-3 liver fibrosis (second reference value) including A subject from which a blood sample in which the ratio of the measured value to the second reference value (said measured value/second reference value) is equal to or greater than the second reference value (i.e., a predetermined cutoff value) is It may further include estimating that there is no fibrosis with a fibrosis grade of 2 or greater, or that there is a likelihood of having fibrosis with a fibrosis grade of 2 or greater (ie, the likelihood of having no fibrosis with a liver fibrosis grade of 2 or greater).
- the second reference value can be the mean, third quartile, or maximum blood IGFALS level in subjects with fibrosis grade 2-3 liver fibrosis, or a value therebetween.
- the second reference value (i.e. cutoff value) is 1.8 or less, 1.7 or less, 1.6 or less, 1.5 or less, 1.4 or less, 1.3 or less, 1.2 or less, 1 .1 or less, or can be a number of 1 or less.
- the second reference value (ie, cutoff value) can be, for example, a numerical value greater than or equal to 1, greater than or equal to 1.1, greater than or equal to 1.2, greater than or equal to 1.3, or greater than or equal to 1.4.
- the second reference value (ie, cutoff value) can be, for example, a numerical value in the range of 1-1.8, and can be a numerical value in the range of 1-1.5.
- the second reference value is the mean blood IGFALS level in subjects with fibrosis grade 2-3 liver fibrosis, and the second reference value (i.e., cutoff value) is 1 It can be a number of 0.8 or less, a number of 1.5 or less, or a number in the range of 1 to 1.8, preferably in the range of 1 to 1.5.
- the method of the present disclosure comprises: (i) comparing the subject's blood IGFALS protein level (measurement) with (ii)(c) a reference value (ie, a predetermined cut-off value) for blood IGFALS levels.
- the method of the present disclosure comprises: (i) comparing the subject's blood IGFALS protein level (measurement) to (ii)(c) a predetermined cut-off value for blood IGFALS level; A subject from whom a blood sample for which the measured value is less than a reference value (i.e., a predetermined cutoff value) for blood IGFALS levels is defined as having or likely to have fibrosis with a liver fibrosis grade of 2 or greater. It may further include estimating that
- the method of the present disclosure comprises: (i) comparing the blood IGFALS protein level (measurement) of said subject with (ii)(c) a reference value (i.e., a predetermined cut-off value) for the blood IGFALS level; A subject from whom a blood sample for which the measured value is equal to or greater than a reference value (i.e., a predetermined cut-off value) for blood IGFALS level is free of, or likely to have, fibrosis with a liver fibrosis grade of 2 or higher. It can further include assuming that there is.
- the blood IGFALS protein level (measurement) of said subject including comparing Methods are provided further comprising assuming that a subject from whom a blood sample from which said measured value is equal to or less than said reference value has or may have active NAFL/NASH.
- Reference values (i.e., predetermined cut-off values) for blood IGFALS levels are, for example, values below 7 ⁇ g/mL, values below 6.9 ⁇ g/mL, values below 6.8 ⁇ g/mL, values below 6.7 ⁇ g/mL 6.6 ⁇ g/mL or less, 6.5 ⁇ g/mL or less, 6.4 ⁇ g/mL or less, 6.3 ⁇ g/mL or less, 6.2 ⁇ g/mL or less, 6 .1 ⁇ g/mL or less, 6.0 ⁇ g/mL or less, 5.9 ⁇ g/mL or less, 5.8 ⁇ g/mL or less, 5.7 ⁇ g/mL or less, 5.6 ⁇ g/mL or less , 5.5 ⁇ g/mL or less, 5.4 ⁇ g/mL or less, 5.3 ⁇ g/mL or less, 5.2 ⁇ g/mL or less, 5.1 ⁇ g/mL or less, or 5 0 ⁇ g
- Reference values (i.e., predetermined cut-off values) for blood IGFALS levels are, for example, values greater than or equal to 5.0 ⁇ g/mL, values greater than or equal to 5.1 ⁇ g/mL, values greater than or equal to 5.2 ⁇ g/mL, 5.3 ⁇ g /mL or more, 5.4 ⁇ g/mL or more, 5.5 ⁇ g/mL or more, 5.6 ⁇ g/mL or more, 5.7 ⁇ g/mL or more, 5.8 ⁇ g/mL or more , a value of 5.9 ⁇ g/mL or greater, or a value of 6.0 ⁇ g/mL or greater.
- the reference value (i.e., predetermined cutoff value) for blood IGFALS levels can be, for example, 4 ⁇ g/mL to 7 ⁇ g/mL, more preferably 5 ⁇ g/mL to 6 ⁇ g/mL. .
- the reference values for blood IGFALS levels for assessment of active NAFL/NASH are similar, but the lower the blood IGFALS level, the more likely is active NAFL/NASH. Therefore, it can be assumed that subjects with blood IGFALS levels below the lower reference value are more likely to have active NAFL/NASH.
- the reference value for blood IGFALS levels for active NAFL/NASH assessment may preferably be between 4 ⁇ g/mL and 7 ⁇ g/mL, more preferably between 5 ⁇ g/mL and 6 ⁇ g/mL. Those skilled in the art can appropriately set the reference value.
- a method as described above comprising: said subject has grade 0 or 1 liver fibrosis at the first time the method is performed; performing the method of any one of claims 1 to 11 using each blood sample obtained from the subject at multiple time points; determining that a subject presumed to have grade 2 or greater liver fibrosis in each blood sample obtained after a specified time point has transitioned from grade 0 or 1 liver fibrosis to grade 2 or greater; estimating when liver fibrosis transitioned from grade 0 or 1 to grade 2 or greater in a subject with grade 2 or greater liver fibrosis; A method is provided.
- the method comprises presuming the subject does not have or is likely to have fibrosis with a liver fibrosis grade of 2 or greater, wherein said After the subject has fibrosis of grade 2 or greater, it would include presuming that the subject has or is likely to have fibrosis of liver fibrosis grade 2 or greater. Then, when the subject's hepatic fibrosis grade progresses to 2 or higher, it can be determined that the subject's fibrosis has transitioned to grade 2 or higher.
- the time when the last blood sample when the liver fibrosis grade was 0 or 1 and the first when the liver fibrosis grade became 2 It can be estimated that the liver fibrosis transitioned from grade 0 or 1 to grade 2 or later between the time points of collecting blood samples. In this way, it is possible to estimate when liver fibrosis transitioned from grade 0 or 1 to grade 2 or later in the subject.
- the method of the present disclosure is a blood sample technique that is less invasive and can be performed repeatedly. Therefore, the methods of the present disclosure are suitable for monitoring liver fibrosis grade over time.
- blood IGFALS protein levels can be estimated by serum or plasma IGFALS protein levels. Serum or plasma IGFALS protein levels can be determined by an enzyme-linked immunosorbent assay (ELISA). Blood samples may be subjected to gel filtration or the like to separate IGFALS from other contaminants prior to measurement.
- ELISA enzyme-linked immunosorbent assay
- ELISA includes direct method, indirect method, sandwich method, and competitive method.
- IGFALS are immobilized on a support (for example, plate surface), and after washing, the immobilized IGFALS are detected with a labeled antibody.
- IGFALS are immobilized on a support (for example, a plate surface), and after washing, the immobilized IGFALS are allowed to bind to antibodies. It is detected by an antibody.
- the sandwich method the first antibody is immobilized on a support (e.g., plate surface), and after washing, IGFALS is allowed to bind to the immobilized first antibody, and after further washing, IGFALS is labeled. It is detected with a second antibody.
- an antibody is immobilized on a support (for example, a plate surface), and after washing, the immobilized antibody is brought into contact with a sample containing a certain concentration of labeled IGFALS. It estimates the concentration of IGFALS in the sample by measuring the amount of label that remains in the sample. In either case, an antibody that binds to IGFALS can be used as the antibody.
- the antibody that binds IGFALS can be specific for IGFALS.
- the antibody that binds to IGFALS is 10 ⁇ 7 M or less, 10 ⁇ 8 M or less, 10 ⁇ 9 M or less, 10 ⁇ 10 M or less, 10 ⁇ 11 M or less, or 10 ⁇ 12 M or less to IGFALS. It can bind with a KD value of M or less.
- the first antibody and the second antibody are capable of binding IGFALS simultaneously.
- the first antibody, second antibody and IGFALS can form a complex (protein-antibody complex) comprising the first antibody, second antibody and IGFALS.
- IGFALS can form protein complexes with IGF1 and/or IGFBP-3, particularly with IGF1 and IGFBP-3, in a sample.
- IGFALS may form protein complexes with IGF1 and/or IGFBP-5, particularly IGF1 and IGFBP-5, in a sample. Therefore, IGFALS may be measured by detecting the protein complexes described above. In this case, the protein complex can be detected with an antibody that binds to IGFALS and an antibody that binds to IGF1 and/or IGFBP-3 (or IGFBP-5).
- the protein complex is adsorbed to the solid phase surface with an antibody that binds to immobilized IGFALS, and then the protein complex is adsorbed with an antibody that binds to IGF1 and/or an antibody that binds to IGFBP-3 (or IGFBP-5).
- the protein complex is adsorbed to the solid phase surface by the immobilized antibody that binds to IGF1 and/or the antibody that binds to IGFBP-3 (or IGFBP-5), and then by the antibody that binds to IGFALS. Protein complexes can also be detected.
- the first antibody comprises an antibody that binds IGFALS and the second antibody comprises an antibody that binds IGF1 and/or an antibody that binds IGFBP-3 (or IGFBP-5).
- the first antibody comprises an antibody that binds to IGF1 and/or an antibody that binds to IGFBP-3 (or IGFBP-5) and the second antibody comprises an antibody that binds to IGFALS.
- the protein complex may be detected using the above antibody by a sandwich assay, or may be detected using the above antibody by an immunochromatographic method described below.
- IGFALS levels can be measured by a chemiluminescent enzyme immunoassay (CLEIA).
- IGFALS or a protein complex containing IGFALS eg, a protein complex with IGF1 and IGF3 (or IGFBP-5)
- the solid phase can be a plate surface or a bead (eg, magnetic bead) surface.
- IGFALS or multimers containing IGFALS adsorbed to the solid surface can be detected with a second antibody.
- the magnetic beads can be washed by bringing a magnet into contact with the container from outside the container, trapping the magnetic beads on the inner surface of the contact portion, and exchanging the solution.
- IGFALS can be captured on the solid phase directly by the first antibody, or by an additional antibody that recognizes the immobilized first antibody and the non-immobilized first antibody. good. In this case, a complex is formed that binds in the order solid phase-further antibody-first antibody.
- the complex can be an antibody complex comprising a solid phase-further antibody-first antibody-IGFALS or a protein complex comprising IGFALS.
- Antibody complexes comprising the first antibody-IGFALS or-or protein complexes comprising IGFALS are obtained by washing after antibody complex formation and then cleaving the bond between the additional antibody and the first antibody. It can be released into the clear water. This antibody complex can also be recovered, captured on another solid surface, and detected with a second antibody.
- a further antibody may recognize the first antibody via a labeling molecule attached to the first antibody.
- the labeling molecule can be disassociated from further antibody binding, for example, by introducing an excess amount of free labeling molecule into the system. In this way the bond between the further antibody and the first antibody can be cleaved.
- the labeling molecule is not particularly limited, but for example, 2,4-dinitrophenyl (DNP) can be used.
- the additional antibody may be an antibody that recognizes DNP.
- the first antibody and the second antibody can be monoclonal antibodies.
- the first antibody and the second antibody each replace the heavy chain CDRs 1-3 and light chain CDRs 1-3, respectively, of the anti-human IGFALS antibody produced from clone M6005C04. 3, and the antibody having the heavy chain CDRs 1-3 and light chain CDRs 1-3 of the anti-human IGFALS antibody produced from clone M6001E07 as heavy chain CDRs 1-3 and light chain CDRs 1-3, respectively.
- the first antibody and the second antibody each replace the heavy chain CDRs 1-3 and light chain CDRs 1-3, respectively, of the anti-human IGFALS antibody produced from clone M6001E07.
- CDRs are numbered by Kabat et al. , AbM, contact, IMGT, Aho, or Martin (Enhanced Chothia).
- the first antibody and the second antibody respectively have the heavy and light chain variable regions of the anti-human IGFALS antibody produced from clone M6005C04 and the anti-human IGFALS produced from clone M6001E07. It can be an antibody having a heavy chain variable region and a light chain variable region of an antibody. In certain aspects, the first antibody and the second antibody respectively have the heavy and light chain variable regions of the anti-human IGFALS antibody produced from clone M6001E07 and the anti-human IGFALS produced from clone M6005C04. It can be an antibody having a heavy chain variable region and a light chain variable region of an antibody.
- the first antibody and the second antibody can be an anti-human IGFALS antibody produced from clone M6005C04 and an anti-human IGFALS antibody produced from clone M6001E07, respectively. In one aspect, the first antibody and the second antibody can be an anti-human IGFALS antibody produced from clone M6001E07 and an anti-human IGFALS antibody produced from clone M6005C04, respectively.
- Enzymes used in the enzyme antibody method can be used as labels.
- Substrates for the above enzymes chromogenic substrates, fluorescent substrates, and luminescent substrates
- biotin can be used as the label
- an avidin-labeled enzyme can be used when detecting the biotinylated antibody.
- avidin, streptavidin, neutravidin and the like can be used.
- IGFALS levels are measured or estimated based on the amount of substrate conversion by an enzyme linked to an antibody bound to IGFALS.
- Substrates that are colored or discolored by enzymes are preferably used.
- a calibration method for estimation and specific estimation can be performed by a conventional method.
- a person skilled in the art can label the antibody using a conventional method. Labeling can, for example, be covalent. A labeled antibody can be obtained in this manner.
- horseradish peroxidase can be used as the peroxidase.
- Horseradish peroxidase produces color, fluorescence or chemiluminescence upon addition of a chromogenic, fluorogenic or luminescent substrate. Therefore, the presence of labeled capture molecules can be detected using chromogenic, fluorescent or chemiluminescent indicators.
- Chromogenic substrates for horseradish peroxidase include, for example, tetramethylbenzidine (TMB), o-phenylenediamine (OPD), 2,2-azinobis[3-ethylbenzo-thiazoline-6-sulfonic acid (ABTS), and Amplex ( Trademark) Red, which can be used to detect labeled molecules in the presence of hydrogen peroxide.
- TMB tetramethylbenzidine
- OPD o-phenylenediamine
- ABTS 2,2-azinobis[3-ethylbenzo-thiazoline-6-sulfonic acid
- Amplex Trademark
- Luminescent substrates for alkaline phosphatase include p-nitrophenyl phosphate (pNPP), 4-methylumbelliferyl phosphate (4-MUP), and AttoPhos (trademark), and can be used to detect capture molecules.
- pNPP p-nitrophenyl phosphate
- 4-MUP 4-methylumbelliferyl phosphate
- AttoPhos trademark
- Glucose oxidase oxidizes glucose to generate gluconic acid and hydrogen peroxide.
- Hydrogen peroxide can be readily detected, for example, using a colorimetric probe for detecting hydrogen peroxide (eg, peroxidase).
- Hydrogen peroxide can be developed, for example, in the presence of peroxidase and its chromogenic substrate.
- the sensitivity and specificity can each be 70% or higher, 75% or higher, 80% or higher, 85% or higher, or 90% or higher.
- blood biomarker levels other than blood IGFALS may not be considered. That is, in the above method of the present disclosure, only the blood IGFALS level can be used for evaluation.
- the blood IGFALS level can be estimated from the serum IGFALS level.
- blood IGFALS levels can be determined by mass spectrometry.
- Mass spectrometry can be performed appropriately by those skilled in the art. Mass spectrometry includes, for example, matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry, electrospray ionization (ESI) mass spectrometry, surface-enhanced laser desorption ionization time-of-flight (SELDI-TOF) mass spectrometry.
- MALDI-TOF matrix-assisted laser desorption ionization time-of-flight
- ESI electrospray ionization
- SELDI-TOF surface-enhanced laser desorption ionization time-of-flight
- the method of the present disclosure is an in vitro method.
- the "method for estimating the level of liver fibrosis” refers to the “method for estimating the level of liver fibrosis", the “method for determining the level of liver fibrosis”, or the “diagnosis of the level of liver fibrosis”.
- method for obtaining preliminary information for The methods of the present disclosure do not involve diagnosing humans.
- compositions, kits or articles of manufacture for use in the disclosed methods are provided.
- a composition, kit or article of manufacture of the present disclosure comprises at least a means for measuring IGFALS levels.
- a composition, kit or article of manufacture of the disclosure may further comprise instructions for performing the methods of the disclosure with the means for measuring IGFALS levels.
- the means for measuring the IGFALS level is not particularly limited as long as it can identify the IGFALS level.
- it can be an antibody or lectin that binds to IGFALS or a protein complex containing IGFALS.
- Antibodies or lectins that bind to IGFALS can be prepared by those skilled in the art by routine methods. So are antibodies that bind to protein complexes containing IGFALS.
- Antibodies that bind to protein complexes containing IGFALS can be obtained as antibodies that bind to each component of the complex.
- Antibodies can be obtained, for example, by immunizing a non-human mammal or the like with IGFALS as an immunogen and cloning the resulting antibody-producing cells.
- Antibodies can also be produced from antibody-producing cells into which a gene encoding the antibody has been introduced. As antibody-producing cells, for example, Cheney's hamster ovary cells (CHO cells) can be used.
- compositions, kit or article of manufacture for use in the methods of the present disclosure can comprise an antibody that binds to IGFALS.
- the antibody can be labeled.
- the compositions, kits or articles of manufacture for use in the methods of the present disclosure can be compositions, kits or articles of manufacture for ELISA (direct method).
- compositions, kits or articles of manufacture for use in the methods of the present disclosure can contain unlabeled antibodies that bind IGFALS. Unlabeled antibody can be detected by a labeled secondary antibody.
- a composition, kit or article of manufacture for use in the methods of the present disclosure may further comprise a labeled secondary antibody in addition to the unlabeled antibody that binds IGFALS.
- the compositions, kits or articles of manufacture for use in the methods of the present disclosure can be compositions, kits or articles of manufacture for ELISA (indirect method).
- kits or articles of manufacture for use in the methods of the present disclosure can include an unlabeled antibody that binds IGFALS and a labeled antibody that binds IGFALS.
- An unlabeled antibody that binds to IGFALS can be immobilized on the surface of an assay plate, or immobilized on the surface of an assay plate. Immobilization can be appropriately carried out by a person skilled in the art by a conventional method. Accordingly, kits or articles of manufacture for use in the disclosed methods may further comprise assay plates.
- antibodies can be used to detect IGFALS, eg, by Western blotting.
- Western blotting can be performed by methods well known to those skilled in the art.
- an unlabeled antibody that binds to IGFALS is reacted with a membrane onto which proteins are transferred from a gel after electrophoresis, followed by washing, followed by detection with a labeled antibody that recognizes the labeled antibody.
- labels include substrates (chromogenic substrates, fluorescent substrates, and luminescent substrates) and enzymes used in enzyme-antibody methods (eg, peroxidase, glucose oxidase, and alkaline phosphatase).
- a label can be detected by a known method or the like.
- antibodies can be used to prepare samples for mass spectrometry. That is, the antibody can be used to prepare a sample for mass spectrometry by enriching or purifying IGFALS in the sample using its affinity with the antibody. Antibodies may thereby be useful in the detection of IGFALS in mass spectrometry.
- IGFALS can form complexes with IGF1 and/or IGFBP-3, particularly protein complexes with IGF1 and IGFBP-3, in a sample.
- IGFALS may form complexes with IGF1 and/or IGFBP-5, particularly protein complexes with IGF1 and IGFBP-5, in a sample. Therefore, IGFALS may be measured by detecting the protein complexes described above. In this case, the protein complex can be detected with an antibody that binds to IGFALS and an antibody that binds to IGF1 and/or IGFBP-3 (or IGFBP-5).
- the protein complex is adsorbed to the solid phase surface with an antibody that binds to immobilized IGFALS, and then the protein complex is adsorbed with an antibody that binds to IGF1 and/or an antibody that binds to IGFBP-3 (or IGFBP-5).
- the protein complex is adsorbed to the solid phase surface by the immobilized antibody that binds to IGF1 and/or the antibody that binds to IGFBP-3 (or IGFBP-5), and then by the antibody that binds to IGFALS. Protein complexes can also be detected.
- a kit may include, for example, an antibody that binds to IGFALS and an antibody that binds to IGF1 and/or an antibody that binds to IGFBP-3 (or IGFBP-5).
- the protein complex may be detected using the above antibody by a sandwich assay, or may be detected using the above antibody by an immunochromatographic method described below.
- a kit or article of manufacture for use in the methods of the disclosure comprises an antibody that binds IGFALS and an antibody that binds IGF1 and/or an antibody that binds IGFBP-3 (or IGFBP-5). obtain.
- Kits or products for use in these methods of the present disclosure may further include a substrate that develops color based on the label.
- kits or articles of manufacture for use in a method of the present disclosure, comprising: Kits or products are provided in which means for measuring IGFALS levels include a detection system in an immunochromatographic method (lateral flow method).
- kits or product comprising a means for measuring IGFALS levels or a detection system in immunochromatography (lateral flow method),
- the detection system including test strips for immunochromatography (e.g., the substrate can be a cellulose membrane);
- a test strip is a strip comprising a sample pad for introducing a blood sample, a conjugate pad, an area containing a test line and a control line, and a waste pad.
- the conjugate pad contains a substance that binds to IGFALS (the first binding substance) and the first binding substance is labeled ⁇ wherein the first binding substance is directed from the conjugate pad to the test line is movable on the strip ⁇
- the test line contains a binding substance (second binding substance) that binds to IGFALS, the second binding substance is immobilized on the test line
- the control line contains no substance that binds to IGFALS (eg, may contain an isotype control antibody), the first binding agent and the second binding agent can simultaneously bind to IGFALS;
- IGFALS contained in the blood sample binds to the first binding substance labeled on the conjugate pad to form a complex, migrates onto the test line, and forms a complex on the test line.
- the amount of label bound to the immobilized second binding substance and detected on the test line indicates the amount of IGFALS in the blood sample;
- kits or product comprising a means for measuring IGFALS levels or a detection system in immunochromatography (lateral flow method),
- the detection system including test strips for immunochromatography (e.g., the substrate can be a cellulose membrane);
- a test strip is a strip comprising a sample pad for introducing a blood sample, a conjugate pad, an area containing a test line and a control line, and a waste pad.
- the conjugate pad contains a substance (first binding substance) that binds to a protein complex comprising IGFALS, the first binding substance being labeled ⁇ wherein the first binding substance is from the conjugate pad is movable on the strip towards the test line ⁇ ,
- the test line contains a binding substance (second binding substance) that binds to the protein complex, the second binding substance is immobilized on the test line,
- a control line does not contain a substance that binds to the protein complex (for example, it may contain an isotype control antibody), the first binding substance and the second binding substance can simultaneously bind to the protein complex;
- the protein complex contained in the blood sample binds to the first binding substance labeled on the conjugate pad to form a complex, migrates onto the test line, and moves onto the test line.
- a protein complex comprising IGFALS can comprise IGFALS, IGF1 and IGFBP-3. In one aspect, a protein complex comprising IGFALS can comprise IGFALS, IGF1 and IGFBP-5. In certain aspects, one of the first binding agent and the second binding agent binds to IGFALS. In some aspects, the other of the first binding agent and the second binding agent binds to IGF1. In some aspects, the other of the first binding agent and the second binding agent binds to IGFBP-3. In some aspects, the other of the first binding agent and the second binding agent binds to IGFBP-5.
- the binding substance is preferably an antibody, more preferably a monoclonal antibody.
- kits or articles of manufacture of this disclosure can be for use in a method of this disclosure.
- the protein level of IGFALS can be measured or estimated based on measurements by an absorption method or a fluorescence method using a reader for quantification of the protein level of IGFALS. Correlations between absorbance or fluorescence measurements and IGFALS protein levels can be determined according to conventional methods. Thus, the protein level of IGFALS can be estimated from the measured value by calibrating the measured value and the protein level.
- a label suitable for the absorption method or fluorescence method using a reader (such as an enzyme that can use a dye, a fluorescent dye, etc. as a substrate) can be used as the label.
- a substance that binds to IGFALS or a protein complex containing IGFALS in the kit or product of the present disclosure can be an antibody or a lectin.
- the agents that bind to IGFALS or a protein complex comprising IGFALS are the first antibody and the second antibody described above, respectively. It can be an antibody, or a second antibody and a first antibody.
- one of the first antibody and the second antibody binds to IGFALS.
- the other of the first antibody and the second antibody binds to IGF1.
- the other of the first antibody and the second antibody binds to IGFBP-3.
- the other of the first antibody and the second antibody binds to IGFBP-5.
- NASH non-alcoholic steatohepatitis
- NASH non-alcoholic steatohepatitis
- Serum Samples from Healthy Individuals and ASH Patients Serum samples from healthy individuals were obtained from HBV/HCV/HIV-negative healthy donors of known age, sex, and race, and obtained from KAC Co., Ltd. , Ltd. purchased from.
- KAC Co., Ltd. , Ltd. purchased from for alcoholic steatohepatitis patient sera, those derived from patients diagnosed as ASH who are HBV/HCV-negative with clear age, sex, race, height, weight, AST, ALT, medical history, and medications taken are KAC. Co. , Ltd. purchased from.
- the detection antibody is biotinylated and detected by horseradish peroxidase coupled to avidin.
- the kit contains 3,3',5,5'-tetramethylbenzidine (TMB substrate) and develops a yellow color (maximum absorption wavelength 450 nm) by horseradish peroxidase treatment followed by sulfuric acid or phosphoric acid treatment.
- IGF1 insulin-like growth factors
- IGF1 is a peptide growth factor mainly produced in the liver, and its production is maintained at a high level by good nutritional conditions and growth hormone stimulation.
- IGF1 is known to be a hormone having various physiological actions such as individual development/growth, regulation of substance metabolism, and aging.
- IGF1 forms a complex with a binding protein in blood, and is characterized by having a long half-life in blood and maintaining a high concentration.
- IGF binding proteins 1-6 Six types of IGF binding proteins (IGF binding proteins 1-6, IGFBP1-6) are known to exist in IGF1, but most of IGF1 circulating in the blood is associated with IGFBP3 or IGFBP5. In addition to either, it exists in the form of protein complexes (trimers) with acid-labile subunits (ALS or IGFALS), which are glycoproteins (Baxter, Nat Rev Cancer 2014).
- FIG. 6A blood IGFALS levels were significantly lower in the NAFL/NASH group than in healthy subjects.
- FIG. 6B blood IGF1 level and blood IGFALS level showed a certain positive correlation.
- FIG. 6C blood IGFALS levels showed a negative correlation with blood type IV collagen 7S levels or blood M2BPGi levels.
- NAFL/NASH specimens were grouped according to the degree of fibrosis progression in the liver biopsy (fibrosis grade 0-3).
- IGFALS may be a biomarker to detect some fibrosis in MAFLD (or fibrosis in NASH).
- blood IGF1 levels are known to decrease with age after adulthood. (Fig. 3E), the effect of age on IGFALS values seen in the NASH group with fibrosis grade 2 and above was considered negligible.
- IGFALS is superior in both sensitivity and specificity to existing fibrosis markers.
- Type IV collagen 7s T4 Col7s
- Mac-2 binding protein glycosylation isomer M2BPGi
- platelet count age, AST, ALT Calculated based on the following formula (1) Therefore, ROC (receiver operating characteristic) analysis was performed based on each of the Fib-4 indexes.
- fibrosis grade 1A or lower in liver biopsy was classified as a low fibrosis group, and grade 2 or higher was classified as a high fibrosis group, and the sensitivity and specificity of each marker for fibrosis were analyzed.
- the serum IGFALS level was 0.9026 in AUC (area under curve), and other markers (Fib-4, 0.8442; HA, 0.6993; T4 Col7s, 0.5455; M2BPGi, 0 .5035) (Fig. 2A, B; Cutoff ⁇ 0.5587, Sensitivity 100, Specificity 81.82).
- the AUC reached 0.940, and the low fibrosis group and the high fibrosis group with a cutoff value of 5.587 (about half of the healthy subject group) (Fig. 2C).
- the ROC curve for >Grade 1 fibrosis was shown in FIG. 4 and the ROC curve for >Grade 2 fibrosis was as shown in FIG. Tables 3 to 5 below show the results of AUC and P value for each marker. In Tables 3-5, cutoffs were determined by the Youden Index.
- liver fibrosis is an urgent issue.
- Liver biopsy is a standard method for evaluating liver fibrosis in NASH patients, but it is difficult to perform routinely and repeatedly due to its high invasiveness and cost.
- sampling errors occur in NASH, which has heterogeneous intrahepatic lesions, since information on only a small area of the liver tissue can be obtained.
- liver fibrosis in NASH Although several blood biomarkers for liver fibrosis in NASH have been developed/applied, there are many markers that are uncertain regarding their positioning in diagnosis and the setting of cutoff values, and there is no evidence as to whether they can be used to determine therapeutic effects. is insufficient. In this study, it was revealed that serum IGFALS shows a low value in NASH with fibrosis grade 2 or later, and that both sensitivity and specificity are superior to existing HA, T4 Col7s, and M2BPGi. Based on this knowledge, it is possible to establish a blood diagnostic method that is superior to existing liver fibrosis markers, and a method to manage the liver fibrosis state of NASH patients without invasive diagnosis such as liver biopsy. can be established.
- IGFALS-producing organ in humans is the liver, and the producing cells are hepatocytes. Therefore, in NASH, HCV hepatitis, and hepatic fibrosis, it is suggested that the production of IGFALS from the liver decreases due to specific loads on hepatocytes such as metabolic changes. In addition, it is interesting that reduction in IGFALS can sensitively detect fibrosis of grade 2 and beyond.
- NAFL / NASH a group of patients with NAS4 points or more and fibrosis level of 2 points or more is defined as active NAFL / NASH, and patients in the active NAFL / NASH group and the inactive NAFL / NASH group categorized.
- the blood IGFALS level, blood IGF1 level, blood hyaluronic acid level, blood type IV collagen 7S level, and blood M2BPGi level of each group were measured. The results were as shown in FIG. As shown in FIG. 7, blood IGFALS levels were significantly different between the active NAFL/NASH group and the inactive NAFL/NASH group.
- the blood hyaluronic acid level which is an existing marker, was high in the activated NAFL/NASH group.
- the blood IGFALS level could effectively discriminate between the active NAFL/NASH group and others. As a result, for example, it may be possible to identify patients at high risk of transition to liver cirrhosis using the blood IGFALS level as an index.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Immunology (AREA)
- Engineering & Computer Science (AREA)
- Molecular Biology (AREA)
- Biomedical Technology (AREA)
- Chemical & Material Sciences (AREA)
- Hematology (AREA)
- Urology & Nephrology (AREA)
- Biotechnology (AREA)
- Microbiology (AREA)
- Cell Biology (AREA)
- Food Science & Technology (AREA)
- Medicinal Chemistry (AREA)
- Physics & Mathematics (AREA)
- Analytical Chemistry (AREA)
- Biochemistry (AREA)
- General Health & Medical Sciences (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Investigating Or Analysing Biological Materials (AREA)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2023540425A JPWO2023013764A1 (https=) | 2021-08-06 | 2022-08-05 |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2021-129760 | 2021-08-06 | ||
| JP2021129760 | 2021-08-06 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2023013764A1 true WO2023013764A1 (ja) | 2023-02-09 |
Family
ID=85154604
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2022/030093 Ceased WO2023013764A1 (ja) | 2021-08-06 | 2022-08-05 | 非アルコール性脂肪性肝炎における線維化進行度および/または前記肝疾患の活動性を推定する方法 |
Country Status (2)
| Country | Link |
|---|---|
| JP (1) | JPWO2023013764A1 (https=) |
| WO (1) | WO2023013764A1 (https=) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2024185901A1 (ja) * | 2023-03-09 | 2024-09-12 | 国立大学法人 東京医科歯科大学 | 脂肪性肝疾患を処置することに用いるための組成物 |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2009090882A1 (ja) * | 2008-01-18 | 2009-07-23 | The University Of Tokyo | 非アルコール性脂肪性肝疾患の診断方法 |
| US20130225428A1 (en) * | 2011-11-30 | 2013-08-29 | Institute For Systems Biology | Liver disease markers |
| CN110577998A (zh) * | 2019-01-31 | 2019-12-17 | 上海交通大学医学院附属仁济医院 | 预测肝癌术后早期复发风险分子模型的构建及其应用评估 |
| CN110914689A (zh) * | 2017-05-10 | 2020-03-24 | 首尔大学校产学协力团 | 肝癌高危人群的肝癌发病监视或诊断用生物标记物及其用途 |
-
2022
- 2022-08-05 JP JP2023540425A patent/JPWO2023013764A1/ja active Pending
- 2022-08-05 WO PCT/JP2022/030093 patent/WO2023013764A1/ja not_active Ceased
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2009090882A1 (ja) * | 2008-01-18 | 2009-07-23 | The University Of Tokyo | 非アルコール性脂肪性肝疾患の診断方法 |
| US20130225428A1 (en) * | 2011-11-30 | 2013-08-29 | Institute For Systems Biology | Liver disease markers |
| CN110914689A (zh) * | 2017-05-10 | 2020-03-24 | 首尔大学校产学协力团 | 肝癌高危人群的肝癌发病监视或诊断用生物标记物及其用途 |
| CN110577998A (zh) * | 2019-01-31 | 2019-12-17 | 上海交通大学医学院附属仁济医院 | 预测肝癌术后早期复发风险分子模型的构建及其应用评估 |
Non-Patent Citations (1)
| Title |
|---|
| JEFFERS, THOMAS ET AL.: "Proteomics Signature of Advanced Fibrosis in Non-alcoholic Steatohepatitis (NASH) using Data-independent Acquisition (DIA) Mass Spectrometry", JOURNAL OF HEPATOLOGY, ELSEVIER, AMSTERDAM, NL, vol. 75, no. Suppl. 2, 1 July 2021 (2021-07-01) - 26 June 2021 (2021-06-26), AMSTERDAM, NL , pages S592, XP009543292, ISSN: 0168-8278 * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2024185901A1 (ja) * | 2023-03-09 | 2024-09-12 | 国立大学法人 東京医科歯科大学 | 脂肪性肝疾患を処置することに用いるための組成物 |
Also Published As
| Publication number | Publication date |
|---|---|
| JPWO2023013764A1 (https=) | 2023-02-09 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US8889366B2 (en) | Marker for graft failure and mortality | |
| US12399186B2 (en) | Method for diagnosing or monitoring kidney function or diagnosing kidney dysfunction | |
| CN107667294A (zh) | 用于预测慢性肾病发生风险的方法 | |
| EP3919906B1 (en) | Method for immunologically analyzing free aim in biological specimen, and method for detecting nash in subject | |
| US20180143208A1 (en) | Diagnostic of Heart Failure | |
| WO2023013764A1 (ja) | 非アルコール性脂肪性肝炎における線維化進行度および/または前記肝疾患の活動性を推定する方法 | |
| JP5518836B2 (ja) | 肺動脈高血圧を診断するための方法 | |
| JP7271442B2 (ja) | 腎機能を診断またはモニターする方法、または腎機能障害を診断することを補助する方法 | |
| JP5524241B2 (ja) | 腎症と関連するバイオマーカー | |
| KR20260003222A (ko) | 말기 간세포 암종의 진단 | |
| JP7307479B2 (ja) | IgA腎症診断用キット | |
| WO2024242058A1 (ja) | 三次リンパ組織の検査方法、及び三次リンパ組織の検査用キット | |
| JP4423426B2 (ja) | アドレノメデュリン前駆体c末端ペプチドの濃度の上昇を循環器疾患又は炎症性疾患の指標とする方法 | |
| US20230053658A1 (en) | Circulating nedd9 is increased in pulmonary arterial hypertension | |
| CN115639371A (zh) | 一种反映脂联素质量浓度的试剂盒及其使用方法 | |
| JP2011257147A (ja) | データ収集方法、キット及び腫瘍マーカー | |
| HK1212436B (en) | A method for diagnosing or monitoring kidney function or diagnosing kidney dysfunction | |
| HK1250779B (zh) | 用於预测慢性肾病发生风险的方法 | |
| HK1212762B (zh) | 预测女性对象患癌症风险或诊断其癌症的方法 |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 22853182 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2023540425 Country of ref document: JP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 22853182 Country of ref document: EP Kind code of ref document: A1 |