WO2019172427A1 - Marcksのリン酸化を指標にしたad(アルツハイマー病)、ftld(前頭側頭葉変性症)、als(筋萎縮性側索硬化症)、pd(パーキンソン病)およびdlb(レビー小体型認知症)の検出 - Google Patents
Marcksのリン酸化を指標にしたad(アルツハイマー病)、ftld(前頭側頭葉変性症)、als(筋萎縮性側索硬化症)、pd(パーキンソン病)およびdlb(レビー小体型認知症)の検出 Download PDFInfo
- Publication number
- WO2019172427A1 WO2019172427A1 PCT/JP2019/009370 JP2019009370W WO2019172427A1 WO 2019172427 A1 WO2019172427 A1 WO 2019172427A1 JP 2019009370 W JP2019009370 W JP 2019009370W WO 2019172427 A1 WO2019172427 A1 WO 2019172427A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- marcks
- phosphorylated
- disease
- pser46
- amount
- Prior art date
Links
Images











































Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6893—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids related to diseases not provided for elsewhere
- G01N33/6896—Neurological disorders, e.g. Alzheimer's disease
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12Q—MEASURING OR TESTING PROCESSES INVOLVING ENZYMES, NUCLEIC ACIDS OR MICROORGANISMS; COMPOSITIONS OR TEST PAPERS THEREFOR; PROCESSES OF PREPARING SUCH COMPOSITIONS; CONDITION-RESPONSIVE CONTROL IN MICROBIOLOGICAL OR ENZYMOLOGICAL PROCESSES
- C12Q1/00—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions
- C12Q1/48—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving transferase
- C12Q1/485—Measuring or testing processes involving enzymes, nucleic acids or microorganisms; Compositions therefor; Processes of preparing such compositions involving transferase involving kinase
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/573—Immunoassay; Biospecific binding assay; Materials therefor for enzymes or isoenzymes
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2440/00—Post-translational modifications [PTMs] in chemical analysis of biological material
- G01N2440/14—Post-translational modifications [PTMs] in chemical analysis of biological material phosphorylation
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/28—Neurological disorders
- G01N2800/2814—Dementia; Cognitive disorders
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/28—Neurological disorders
- G01N2800/2814—Dementia; Cognitive disorders
- G01N2800/2821—Alzheimer
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/28—Neurological disorders
- G01N2800/2835—Movement disorders, e.g. Parkinson, Huntington, Tourette
Definitions
- the present invention relates to a method for detecting AD (Alzheimer's disease), FTLD (frontotemporal lobar degeneration), ALS (amyotrophic lateral sclerosis), PD (Parkinson's disease) and DLB (Lewy body dementia).
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- DLB Lewy body dementia
- AD Alzheimer's disease
- amyloid hypothesis based on the cytotoxicity of amyloid fibrils produced by extracellular accumulation of amyloid ⁇ peptide (A ⁇ ).
- a ⁇ has emerged as a major therapeutic target for AD.
- Treatment strategies including antibody therapies such as Bapineuzumab and Solanezumab have reduced A ⁇ aggregation in the brain of human AD patients in clinical trials after dementia, but cognition in previous clinical symptoms Recovery from the disease was inadequate.
- antibody therapies such as Bapineuzumab and Solanezumab have reduced A ⁇ aggregation in the brain of human AD patients in clinical trials after dementia, but cognition in previous clinical symptoms Recovery from the disease was inadequate.
- research interest has shifted to early molecular events in AD before onset of symptoms where similar or new therapies may be more effective.
- the present inventors performed comprehensive phosphoprotein analysis of brain tissue from mouse AD models and human AD patients. 17 core proteins with aberrant phosphorylation were identified in multiple AD mouse models. Interestingly, these changes occurred before onset, and abnormal phosphorylation was detected in several core proteins, even before A ⁇ aggregation was detected immunohistologically in the model mouse brain, It was suggested to play an important role in the early stage of AD pathology (see Non-Patent Document 1).
- MARCKS myristoylated alanine-rich C kinase substrate
- PLC protein kinase C
- Non-Patent Document 2 MARRCKS phosphorylation at Ser46 destabilizes dendritic spines and causes neurite degeneration.
- the present invention is highly sensitive and highly specific with human AD (Alzheimer's disease), FTLD (frontotemporal lobar degeneration), ALS (Amyotrophic lateral sclerosis), PD (Parkinson's disease) and DLB (Lewy body type).
- the object is to provide a method for detecting a neurodegenerative disease selected from the group consisting of dementia or Lewy body disease.
- the inventors previously have increased phosphorylated MARCKS even before the formation of histological amyloid ⁇ (A ⁇ ) aggregates in an Alzheimer's disease (AD) mouse model, and that change is due to human postmortem AD Found to persist in the brain.
- Ser46-phosphorylated MARCKS pSer46-MARCKS was detected in degenerate neurites surrounding A ⁇ aggregates in mouse models of human patients and senile plaques.
- CSF cerebrospinal fluid
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- the present inventors quantified pSer46-MARCKS and non-phosphorylated MARCKS in cerebrospinal fluid (CSF) from human patients with AD and other neurodegenerative diseases by mass spectrometry.
- CSF cerebrospinal fluid
- the present inventors have developed a new parameter based on the integration of pSer46-MARCKS and non-phosphorylated MARCKS to further increase its value as a diagnostic parameter did.
- the parameters made it possible to distinguish multiple neurodegenerative diseases from healthy controls with high sensitivity and high specificity.
- pathological analysis revealed that pSer46-MARCKS reflects neurite degeneration throughout neurodegenerative diseases. Based on these results, the integration of pSer46-MARCKS and non-phosphorylated MARCKS developed a new parameter called “DO (Distance from origin)” as a more sensitive and definitive biomarker for all neurodegenerative diseases.
- step (iii) The DO value calculated for the subject is compared with a predetermined cutoff value, and when it is higher than the cutoff value, it is determined that a neurodegenerative disease is detected.
- step (iii) the DO value calculated for the subject is compared with a predetermined cutoff value, and when it is higher than the cutoff value, it is determined that a neurodegenerative disease is detected.
- [6] The method of [5], wherein the DO value cutoff value is 50 to 55.
- [7] Selected from the group consisting of human FTLD (frontotemporal lobar degeneration), ALS (amyotrophic lateral sclerosis), PD (Parkinson's disease) and DLB (Lewy body dementia), including the following steps: Methods for detecting neurodegenerative diseases that are: (i) a step of measuring MARCKKS protein phosphorylated at position 46 in a specimen sample collected from a subject; (ii) comparing the amount of MARCKS protein phosphorylated at position 46 in a sample sample collected from a subject with the amount of MARCKS protein phosphorylated at position 46 in a sample sample collected from a healthy person; and (iii) When the amount of MARCKS protein phosphorylated at position 46 in the sample sample collected from the subject is greater than the amount of MARCKS protein phosphorylated at position 46 in the sample sample collected from a healthy person,
- a method comprising the step of
- the amount of MARCKS protein phosphorylated at position 46 normalized the measured value of MARCKS protein phosphorylated at position 46 by the total protein amount in the sample sample or the total MARCKS protein amount in the sample sample.
- human AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinsoninson's disease
- DLB Lewy body dementia
- FIG. 1-1A shows the amount of pSer46-MARCKS in each neurodegenerative disease group normalized by total protein.
- FIG. 1-1B shows sensitivity and specificity. It is a figure which shows the evaluation result as a biomarker for the diagnosis of cS cerebrospinal fluid (CSF) pSer46-MARCKS.
- FIG. 1-2A shows the amount of pSer46-MARCKS in each neurodegenerative disease group normalized by the total MARCKS protein.
- FIG. 1-2B shows sensitivity and specificity.
- FIG. 2-1A shows the amount of non-phosphorylated MARCKS in each neurodegenerative disease group normalized by the total protein.
- FIG. 2-1B shows sensitivity and specificity. It is a figure which shows the evaluation result as a biomarker for the diagnosis of the non-phosphorylated MARCKS of cerebrospinal fluid (CSF).
- FIG. 2-2A shows the amount of non-phosphorylated MARCKS in each neurodegenerative disease group normalized by the total MARCKS protein.
- FIG. 2-2B shows sensitivity and specificity.
- FIG. 3-1A shows the amount normalized by the total protein
- FIG. 3-1B shows the value normalized by the total MARCKS amount.
- FIG. 3-2A shows the amount normalized by the total protein
- FIG. 3-2B shows the value normalized by the total MARCKS amount.
- FIG. 4 is a diagram showing all the relationships A to D in FIG. 4-1. It is a figure which shows the relationship between pSer46-MARCKS and non-phosphorylated MARCKS when normalized by the total amount of MARCKS in AD, FTLD and ALS patients, and shows for each disease group (A: control, B: AD, C : FTLD, D: ALS).
- FIG. 4 is a diagram showing all the relationships A to D in FIG. 4-3.
- pSer129- ⁇ -Syn staining revealed multiple cytoplasmic inclusions (Lewy bodies) in the same patient group. It is a figure which shows the immunohistochemistry of a human DLB brain, and is a figure which shows the result of the simultaneous dyeing
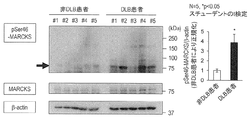
- FIG. 6 shows the results of Western blot analysis of occipital lobes from non-DLB control patients and DLB patients with antibodies to pSer46-MARCKS, total MARCKS and ⁇ -actin.
- the graph shows the quantitative results of pSer46-MARCKS from 5 patients and 5 non-neurologic disease controls. Band intensity was normalized to ⁇ -actin.
- Statistical analysis was performed using Student's t-test. * Indicates p ⁇ 0.05. It is a figure which shows the time-sequential change of pSer46-MARCKS in a human.
- ⁇ -Syn-BAC-Tg / GBA-hetero KO mice pSer46-MARCKS and pSer129- ⁇ -Syn are human normal ⁇ -Syn-BAC- at 1, 6 and 24 months of age (3 male mice at each time point) Tg ⁇ / glucocerebrosidase (GBA)-hetero-KO mice were co-stained. Images were obtained by Olympus FV1200 IX83 confocal microscopy. All bar graphs show mean values and S.E.M. Three mice were used for each group, and signal intensity (average pixel intensity) was quantitatively analyzed in 10 visual fields (100 ⁇ 100 ⁇ m) randomly selected from the brain region.
- Ubiquitin was co-stained as a dot-like structure or cytoplasmic aggregate in a subset of cells (yellow arrows), but pSer129- ⁇ -Syn positive / ubiquitin negative dots or aggregates were also observed.
- the immunohistochemistry of the parietal lobe of ⁇ -Syn-BAC-Tg / GBA-hetero KO mice is shown.
- pSer46-MARCKS and pSer129- ⁇ -Syn were co-stained on the outer and inner pyramid cell layers at 24 months of age.
- pSer46-MARCKS stained with both apical dendrites and cell bodies, whereas pSer129- ⁇ -Syn stained with cytoplasmic aggregates.
- the immunohistochemistry of the parietal lobe of ⁇ -Syn-BAC-Tg / GBA-hetero KO mice is shown, and the staining of the wall side cortical tissue derived from human ⁇ -Syn-BAC-Tg / GBA-hetero KO mice is shown.
- FIG. 16A shows anti-pSer46-MARCKS or anti-pSer129- ⁇ -Syn antibody immunoprecipitation from brain samples of ⁇ -Syn-BAC-Tg / GBA-hetero KO mice at 1, 6 and 24 months.
- FIG. 16B shows the results of examining similar coprecipitates from the occipital cortex of human DLB patients. It is a figure which shows activation of Erk1 (R) / (R) 2 in a mouse
- the right graph shows quantitative analysis of pErk1 / 2 signal intensity in 3 mice (10 fields for each mouse average). Statistical analysis was performed using 2-way ANOVA followed by Student's t-test. * P ⁇ 0.05, ** p ⁇ 0.01.
- FIG. 6 shows the results of Western blot analysis of whole cortical tissue from / AGBA-hetero KO (Tg) or non-transgenic sibling control (non-Tg) mice.
- FIG. 6 shows pSer46-MARCKS in 6-month-old human ⁇ -Syn-BAC-Tg / GBA-hetero KO mice.
- pSer46-MARCKS and pSer129- ⁇ -Syn were co-stained in 1 month old human normal ⁇ -Syn-BAC-Tg / glucocerebrosidase-hetero KO mice (3 per group).
- the signal intensity was significantly higher in the yellow area. It is a figure which shows pSer46-MARCKS in 24-month-old human ⁇ -Syn-BAC-Tg / GBA-hetero KO mouse. pSer46-MARCKS and pSer129- ⁇ -Syn were co-stained in 1 month old human normal ⁇ -Syn-BAC-Tg / glucocerebrosidase-hetero KO mice (3 per group). The signal intensity was significantly higher in the yellow area.
- PSer46- between peripheral blood cells (PBC) and whole cerebral cortex (brain) of 6-month-old ⁇ -Syn-BAC-Tg / GBA-hetero KO (Tg) mice or non-transgenic sibling control (non-Tg) mice It is a figure which shows the comparison of the protein level of MARCKS.
- the present invention is a method for detecting a neurodegenerative disease.
- detection of a neurodegenerative disease refers to determining that a subject is suffering from a neurodegenerative disease or determining that a subject is at risk of developing a neurodegenerative disease.
- the present invention also includes a method for acquiring auxiliary data for detecting a neurodegenerative disease.
- neurodegenerative diseases include Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD), amyotrophic lateral sclerosis (ALS), Parkinson's disease (ALS).
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- LLB Lewy body dementia
- Alzheimer's disease is a neurodegenerative disease also called Alzheimer's dementia, which is caused by genetic factors such as “familial Alzheimer's disease” and “hereditary Alzheimer's disease” and environmental factors such as lifestyle and stress. “Spontaneous Alzheimer's disease” is also included.
- Frontotemporal lobar degeneration also called FTLD
- FTLD frontotemporal lobar degeneration
- PNFA progressive non-fluent aphasia
- SD semantic dementia
- FTLD-Tau is classified into 3R Tau type, 4R Tau type, and 3 / 4R Tau type according to the number of repeats of the microtubule binding region in tau protein that accumulates predominantly in cells.
- 3R Tau type includes FTLD (Pick disease) with Pick sphere, FTLD (FTLD-17) with MAPT (microtubule-related protein tau) gene mutation, etc.
- 4R Tau type has cerebral cortex basal Nuclear degeneration, progressive supranuclear palsy, multisystem tauopathy with dementia, addiction-granular dementia (additional-granule disease), FTLD with MAPT gene mutation (FTLD-17), etc.
- FTLD-U neurofibrillary tangle dementia
- FTLD-U FTLD with MAPT gene mutation
- FTLD-FUS FTLD-FUS
- FTLD-TDP refers to a disease that is positive for TDP-43 among FTLD-U, and includes PGLD (progranulin (progranulin) gene) FTLD, sporadic FTLD-TDP / FTLD-U, FTLD with TARDBP (TDP-43 gene) mutation, FTLD with VCP (valosin-containing protein gene) mutation, FTLD linked to chromosome 9 and the like are included.
- PGLD progranulin (progranulin) gene
- FTLD sporadic FTLD-TDP / FTLD-U
- FTLD with TARDBP TDP-43 gene
- VCP valosin-containing protein gene
- FTLD-FUS means a disease in which FTLD-U is negative for TDP-43 and positive for FUS (fused in sarcoma), and the disease includes neuronal intermediate filament inclusion body disease, Atypical FTLD-U, basophilic inclusion body disease, FTLD with FUS mutation, etc. are included.
- TLD-UPS is a type of FTLD-U that is negative for TDP-43, and the disease includes FTLD with CHMP2B (charged multivesicular protein 2B gene) mutation.
- CHMP2B charged multivesicular protein 2B gene
- Amyotrophic lateral sclerosis is a type of motor neuron disease and is a neurodegenerative disease characterized by severe muscle atrophy and muscle weakness. Approximately 20 types of genes have been reported as causative genes for amyotrophic lateral sclerosis, and the cause is abnormal accumulation of TDP-43.
- “Parkinson's disease” is a progressive degenerative disease mainly composed of degeneration of nigral dopamine neurons. There is depigmentation of the substantia nigra and the locus coeruleus, and neuronal loss occurs in the substantia nigra, locus coeruleus, dorsal nucleus of the vagus nerve, hypothalamus, sympathetic ganglia, and the transmitter dopamine is deficient. Characteristic inclusion bodies called Lewy bodies are observed in the remaining neurons and part of their processes.
- Lewy body dementia is a degenerative dementia in which Lewy bodies appear throughout the cerebral cortex, and in addition to progressive cognitive impairment, hallucinations and Parkinson's syndrome.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- HD Huntington's disease
- SCA spinocerebellar ataxia
- amyotrophic lateral sclerosis It is a recognized feature of neurodegenerative disorders including ALS.
- disease-related proteins are thought to have a misfolded structure, which is then converted to a structure that tends to aggregate, including ⁇ -sheets.
- the phosphorylation of MARCKS at Ser46 is induced by TLR4-mediated damage-related molecular pattern (DAMP), especially HMGB1 (Fujita et al, (2016) Sci Rep 6: 31895).
- DAMP damage-related molecular pattern
- PSer46-MARCKS can be used as a biomarker that can detect molecular pathology in PD / DLB at the very early stage (preaggregation / preclinical).
- Detection of neurodegenerative disease based on the amount of MARCKS phosphorylated with serine at position 46 the subject is treated with AD by using phosphorylation of MARCKS in a human biological sample as an index. Detect if you have FTLD or ALS. “Detect” is also referred to as “determining” and “evaluating”.
- MARCKS is a myristoylated alanine-rich protein-kinase-C substrate and includes a human-derived protein identified by RefSeq ID: NP_002347 (NP_002347.5).
- a typical human-derived nucleic acid encoding MARCKS includes a nucleic acid containing the coding region (CDS) described in RefSeqRefID: NM_002356 (NM_002356.6).
- Biological samples used as specimen samples include body fluids, tissues, cells, etc. collected from the subject's body (eg, cerebrospinal fluid, cranial nerve tissue (particularly neurological biopsy tissue), blood, plasma, serous fluid, lymph fluid, urine) Cerebrospinal fluid is preferable among them.
- body fluids, tissues, cells, etc. collected from the subject's body eg, cerebrospinal fluid, cranial nerve tissue (particularly neurological biopsy tissue), blood, plasma, serous fluid, lymph fluid, urine
- Cerebrospinal fluid is preferable among them.
- phosphorylation of serine (Ser) at position 46 of MARCKS is used as an index.
- the detection method of phosphorylated MARCKS is not limited, and any known method can be used. Examples include mass spectrometry and immunological measurement methods.
- Mass spectrometry can be performed using a mass spectrometer.
- the mass spectrometer includes a sample introduction unit, an ionization chamber, an analysis unit, a detection unit, a recording unit, and the like.
- a matrix-assisted laser desorption ionization (MALDI) method, an electrospray ionization (ESI) method, or the like may be used.
- Analytical units include double-focusing mass spectrometer, quadrupole mass spectrometer (QMS), time-of-flight mass spectrometer (TOF), Fourier transform mass spectrometer (FT), ion cyclotron mass spectrometer (ICR), etc. Is used.
- a tandem mass spectrometer in which two mass spectrometers are combined for precise analysis can also be used.
- the mass spectrometer may be used alone, or may be connected to a separation instrument such as liquid chromatography or a measuring instrument.
- Liquid chromatography mass spectrometry LC / MS, LC / MS
- high performance liquid chromatography MS / MS high performance liquid chromatography MS / MS.
- the immunoassay can be performed by an immunoassay using an anti-pSer46-MARCKS antibody capable of recognizing MARCKS (pSer46-MARCKS) phosphorylated with serine at position 46.
- the immunological assay include solid phase immunoassay (RIA, EIA, FIA, CLIA, etc.), dot blotting, latex agglutination (LA: Latex Agglutination-Turbidimetric Immunoassay), and immunochromatography.
- the antibody can be immobilized on a substrate and used.
- the ELISA (Enzyme-Linked ImmunoSorbent Assay) method which is one of the EIA (Enzyme Immunoassay) methods is preferable from the viewpoint of quantitativeness.
- a specimen is added to a well of a microtiter plate on which an antibody is immobilized, an antigen / antibody reaction is performed, an enzyme-labeled antibody is further added, an antigen / antibody reaction is performed, and after washing, an enzyme substrate
- the color of the protein or partial peptide in the sample can be calculated from the measured value.
- fluorescence may be measured after an antigen-antibody reaction using a fluorescently labeled antibody.
- the antigen-antibody reaction can be performed at 4 ° C.
- the antibody used in the immunological method may be a monoclonal antibody or a polyclonal antibody, and a binding active fragment such as Fab, F (ab ′), F (ab ′) 2 or the like of the monoclonal antibody can also be used.
- MARCKS pSer46-MARCKS
- PET positron emission tomography
- a tracer for imaging pSer46-MARCKS may be administered to the subject, and pSer46-MARCKS in the subject may be detected by PET (Positron Emission Tomography).
- PET Positron Emission Tomography
- Examples of the tracer for imaging pSer46-MARCKS include an antibody PET tracer in which an antibody against MARCKS protein phosphorylated at position 46 is labeled with a positron nuclide.
- a sample collected from a healthy person may be measured simultaneously as a negative control.
- “healthy” means that the subject has Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD), amyotrophic lateral sclerosis (ALS), PD (Parkinson's disease), and DLB (Lewy body type).
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- DLB Lewy body dementia
- the degree of phosphorylation at the serine at position 46 of MARCKS in the subject's specimen is higher than in healthy individuals. That is, the amount of pSer46-MARCKS in the specimen of the subject is higher than that of a healthy person.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- pSer46-MARCKS may be quantified by the above method, and the obtained quantified value may be normalized and judged.
- the pSer46-MARCKS concentration may be divided by the total protein concentration in the sample.
- the amount of pSer46-MARCKS can be expressed as a concentration (ppm) with respect to the total protein amount.
- the pSer46-MARCKS concentration may be quantified and divided by the total MARCKS (total amount of phosphorylated MARCKS and non-phosphorylated MARCKS) in the specimen. In this case, the amount of pSer46-MARCKS can be expressed as a percentage of the total MARCKS.
- the value of pSer46-MARCKS in the sample of the subject is 1.3 times or more, preferably 1.5 times or more, more preferably 2.0 times or more, particularly preferably 3.0 times or more of the amount in the sample of a healthy person Detects neurodegeneration such as Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD), amyotrophic lateral sclerosis (ALS) or Parkinson's disease (PD) and dementia with Lewy bodies (DLB) Can be determined.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- DLB dementia with Lewy bodies
- the amount of pSer46-MARCKS in the sample of a healthy person may be measured in advance, and a cut-off value (threshold value) may be determined for the measured value of the pSer46-MARCKS amount based on the measured value.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- DLB dementia with Lewy bodies
- the cut-off value is set to, for example, the average of normal control group + 2SD, and when this value is exceeded, in subjects, Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD), muscle atrophic side It can be determined that neurodegeneration such as cord sclerosis (ALS) or Parkinson's disease (PD) and dementia with Lewy bodies (DLB) has been detected.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS cord sclerosis
- PD Parkinson's disease
- DLB dementia with Lewy bodies
- DO distance from origin
- DO distance from origin
- Detection of neurodegenerative diseases based on DO (Distance from origin) value is used as an index.
- DO distance from origin
- Detect neurodegenerative diseases such as Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD) or amyotrophic lateral sclerosis (ALS).
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- DO is a parameter obtained by integrating the amounts of pSer46-MARCKS and non-phosphorylated MARCKS and using both as indices.
- DO is the value reflecting the distance from the origin of the coordinates of the plotted point when the amount of pSer46-MARCKS and the amount of non-phosphorylated MARCKS protein are plotted on (x, y) coordinates
- DO is the value of pSer46-MARCKS
- “pSer46-MARCKS” indicates the amount of MARCKS protein phosphorylated at position 46
- non-phosphorylated-MARCKS indicates the amount of non-phosphorylated MARCKS protein.
- DO values are more sensitive and more specific than those using pSer46-MARCKS alone as an indicator, with Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD), or amyotrophic lateral sclerosis (ALS). And other neurodegenerative diseases can be detected.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
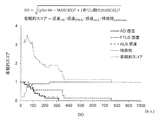
- the DO value can be set to a normal upper limit value (cutoff value) at which sensitivity and specificity are good by performing a numerical simulation. As shown in the numerical simulation shown in FIG.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- the cut-off value of DO value is 50 to 55 (ppm)
- the sensitivity is 0.8 to 1.0
- the specificity is 0.8 or more, preferably 0.8.
- the amount of pSer46-MARCKS and the amount of non-phosphorylated MARCKS in the sample of a healthy person are measured in advance, the DO value is calculated for the healthy person, and the DO value is cut off based on the calculated value.
- a value (threshold value) may be determined.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- PD Parkinson's disease
- DLB Lewy body dementia
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- PD Parkinson's disease
- LLB Lewy Body Dementia
- AD Alzheimer's disease
- drugs that promote information transmission between neurons such as donepezil, rivastigmine, galantamine, and memantine
- antibody drugs such as bapineuzumab and solanezumab that can remove amyloid ⁇ that causes Alzheimer's disease from the brain Treatment by administration.
- Frontotemporal lobar degeneration Treatment with selective serotonin reuptake inhibitors, targeted genes such as the tau gene, TDP-43 gene, and progranulin gene.
- ALS Amyotrophic lateral sclerosis
- drugs such as riluzole, edaravone, methylcobalamin, retigabine, BIIB067, MN-166
- treatment targeting genes such as SOD1 gene, TDP-43 gene, FUS gene, C9orf72 gene reported as causative genes
- human Treatment such as regenerative treatment in which nerve cells are regenerated using pluripotent stem cells.
- Parkinson's disease There are drug treatment, surgical treatment, physical therapy, oral administration of L-dopa and dopamine agonist as drug treatment, deep brain stimulation therapy (subthalamic nucleus stimulation, pallidal stimulation, thalamic stimulation) and stereotaxy as surgical treatment Destruction (thalamic destruction, pallidum destruction) or deep brain stimulation (DBS).
- DBS deep brain stimulation
- DLB Lewy bodies
- Example 1 Methods for studying Alzheimer's disease (AD), frontotemporal lobar degeneration (FTLD) and amyotrophic lateral sclerosis (ALS) Human patients Clinical and electrophysiological studies at Nagoya University and Tohoku University Cerebrospinal fluid from 8 AD patients, 7 FTLD patients and 10 ALS patients diagnosed by neuroimaging including examination, MRI, SPECT and PET were used.
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- MMSE Mini-mental state test
- CSF cerebrospinal fluid
- the mean and range of MMSE scores for these patients were 18.1 and 7-30, and the mean and range of FAB scores were 8.6 and 3-16.
- Sample Preparation Samples were prepared from cerebrospinal fluid (CSF) for proteomic analysis. Specifically, 50 ⁇ l of cerebrospinal fluid derived from a human patient was added to 5 ⁇ l of a buffer containing 100 mM Tris-HCl (pH 7.5), 2% SDS and 1 mM DTT, and incubated at 100 ° C. for 15 minutes.
- CSF cerebrospinal fluid
- SWATH-Cerebrospinal Fluid Mass Spectrometry A C18 column (0.1 mm x 100 mm, KYA Technologies Corporation) containing solution A (0.1% formic acid) with a 30 ⁇ l aliquot of a gradient from 2 to 41% solution A and B (99.9% acetonitrile and Analysis was performed with an Eksigent NanoLC-Ultra 1D Plus system (Sciex Inc.) at a flow rate of 300 nl / min in 0.1% formic acid and subjected to a Triple TOF 5600 system (Sciex) with an ion spray voltage of 2.3 kV.
- IDA information-dependent acquisition
- SWATH® sequential window acquisition of all theoretical mass spectra
- SWATH acquisition of MS / MS spectral data was performed with Analyst TF1.6 software (Sciex Inc.) at 100 ms / window
- an MS / MS spectral library was prepared with Protein Pilot software (version 4.5).
- MS / MS spectral data were correlated with peptide data and LC retention time using Peakview software (version 1.2.0.3, Sciex Inc.). MS / MS product ions from the same peptide were summed and used as the amount of peptide.
- Mass Data Analysis Using the SWATH 1.0 application of PeavView 1.2 software, process the raw MS / MS spectrum data for 5 minutes in the extracted ion chromatogram (XIC) extraction window and the XIC width of 0.01 Da, A spectrum of clearly identified species was extracted.
- XIC was shown as the curve shown in the LC retention time and relative ionic strength graphs in the small m / z range. Fragment ions XIC were summed to obtain the peptide peak area, and the areas of multiple peptides per protein were summed to obtain the protein area.
- Peptide mass spectral data was normalized for each individual subject by the total amount of all proteins detected or the total amount of peptide correlated with MARCKS protein (these are “total protein” or “total MARCKS”, respectively) Called). In order to calculate sensitivity and specificity, abnormal phosphorylation was determined by the mean amount of the control group ⁇ 2SD.
- pSer46-MARCKS antibody was prepared. Primary antibodies from similar host species (rabbit anti-phospho-MARCKS and anti-phospho-TDP43 antibodies) were labeled with Zenon Rabbit IgG Labeling Kits (Thermo Fisher Scientific, IL) and used for double immunostaining. VECTASTAIN Elite ABC standard kit (Vector Laboratories, PK-6100 CA) and DAB peroxidase substrate kit (Vector Laboratories, SK-4100) were used for enzymatic detection of phospho-TDP43 or MAP2.
- CSF cerebrospinal fluid
- AD Alzheimer's disease
- FTLD frontotemporal lobar degeneration
- ALS amyotrophic lateral sclerosis
- Fluid (CSF) pSer46-MARCKS was quantified as well as from controls. To compare the relative amount of phosphorylated peptide in disease groups or individual subjects, the amount was normalized for each subject by the amount of total protein detected by mass spectrometry or the total MARCKS protein. Peptides were determined with greater than 95% confidence.
- FIG. 1-1A is a diagram in which the values of pSer46-MARCKS are plotted for each disease group, and the values are normalized by the total protein amount of each subject.
- FIG. 1-2A is a graph in which the values of pSer46-MARCKS are plotted for each disease group, and the values are normalized by the total MARCKS protein amount of each subject. The rectangular box portion below FIGS.
- FIGS. 1-1A and 1-2A shows the mean number of control groups ⁇ 2SD, and the line in the box shows the mean of healthy controls.
- FIGS. 1-1B and 1-2B show sensitivity and specificity. A patient's value was judged abnormal when it exceeded the mean + 2SD of the control group. In this state, pSer46-MARCKS was found to be very specific in all three groups of neurodegenerative diseases (FIGS. 1-1B and 1-2B). This means that if pSer46-MARCKS exceeds the control mean + 2SD, the subject is definitely abnormal.
- the sensitivity of pSer46-MARCKS for diagnosis was relatively low in all disease groups.
- the sensitivity was 0.50 for AD, 0.57 for FTLD, and 0.40 for ALS (FIG. 1-1B).
- the value was smaller (FIGS. 1-2B). Therefore, it was considered appropriate at this stage of analysis to limit the use of pSer46-MARCKS, such as progression biomarkers rather than disease-specific or screening biomarkers.
- FIG. 2-1A is a plot of the amount of unphosphorylated MARCKS in each disease group, and the values are normalized by the total protein.
- FIG. 2-2A is a plot of the amount of non-phosphorylated MARCKS in each disease group, and the values are normalized by the total MARCKS protein amount.
- the rectangular box portion below FIGS. 2-1A and 2-2A shows the mean number of control groups ⁇ 2SD, and the line in the box shows the mean of healthy controls.
- Figures 2-1B and 2-2B show sensitivity and specificity. In this case, the specificity did not reach 100% in AD and ALS, and the sensitivity was 0. Thus, non-phosphorylated MARCKS alone was clearly not suitable for diagnostic biomarkers.
- FIG. 3-1 shows the amount of pSer46-MARCKS of each subject
- FIG. 3-2 shows the amount of non-phosphorylated MARCKS of each subject.
- the amounts in FIGS. 3-1A and 3-2A were normalized by the total protein amount
- the amounts in FIGS. 3-1B and 3-2B were normalized by the total MARCKS amount.
- the line in the figure shows the median value of each group.
- FIG. 4-1 is a diagram in which values normalized by total protein amount are plotted for each of AD, FTLD, and ALS disease groups
- FIG. 4-2 is a diagram in which the respective plots in FIG. 4-1 are merged.
- FIG. 4-3 is a diagram in which values normalized by the total MARCKS amount are plotted for each of AD, FTLD, and ALS disease groups
- FIG. 4-4 is a diagram in which the plots in FIG. 4-3 are merged. .
- the control group showed a clear positive relationship between pSer46-MARCKS and non-phosphorylated MARCKS (FIGS. 4-1 and 4-3), while the AD group showed a weak negative relationship, the FTLD and ALS groups Did not show any relationship. This result may mean that the phosphorylation of MARCKS at Ser46 is pathologically affected in AD and FTLD.
- HMGB1 which is a representative molecule belonging to the damage-related molecular pattern (DAMP)
- DAMP damage-related molecular pattern
- HMGB1-ELISA sensitivity threshold There is a technical limit of HMGB1-ELISA sensitivity threshold, and HMGB1 value was below detection level in most patients, but clearly more than expected between cerebrospinal fluid (CSF) and PSER46-MARCKS in AD patients A large positive correlation was seen (FIGS. 5-1 and 5-2).
- FIG. 6-1 is a pTDP-43-stained image of human FTLD. TDP43 staining revealed abnormal distribution of TDP43 and cytoplasmic inclusion of TDP43.
- 6-2A and B show immunohistochemical methods using anti-pSer46-MARCKS antibodies.
- FIG. 6-2A neurite degeneration was observed in the FTLD occipital lobe (occipital cortex) and frontal lobe (frontal cortex) (layer IV).
- occipital cortex occipital cortex
- frontal lobe frontal cortex
- dendrites and cell bodies at the apex of the occipital lobe were well stained.
- FIG. 6-2B almost no staining was observed in the most severely affected frontal lobe.
- FIG. 6-3A shows the result of co-staining of MAP2 and pSer46-MARCKS in human FTLD occipital lobe, and neurons were stained with anti-pSer46-MARCKS antibody.
- processes and cell bodies stained with pSer46-MARCKS are also positive for MAP2, indicating that they are neurons and neurites (FIG. 6-3A).
- FIG. 6-3B shows that neurons with cytoplasmic phosphorylated TDP43 were co-stained with pSer46-MARCK.
- pSer46-MARCKS and phosphate TDP43 were co-stained with cytoplasmic aggregates (FIG. 6-3C).
- FIG. 7A In human FTLD, Nissl staining hardly detected frontal neurons, and only a spongy degeneration was observed in the vacuolar mass (FIG. 7A). On the other hand, neurons having abnormal characteristics such as chromatin melting and no pigment were observed in the occipital lobe (FIG. 7B). In control brains that were not neurodegenerative diseases, such abnormal changes were not observed in neuron density, neural network morphology, etc. (FIG. 7C).
- the DO value was statistically increased in the three neurodegenerative disease groups compared with the control group, and the difference by the Wilcoxson test was confirmed (FIG. 8-2). Exceptionally, one control subject had a large DO. The subject may be in the preclinical stage of dementia, as judged by the sharp decline in ADAS score (-3.216949153 / year).
- FIG. 8-2 shows the DO value in each disease.
- DO values are shown as box plots.
- the upper limit of normality was determined by numerical simulation.
- Each group box represents a lower to higher value.
- the median is also displayed in the box.
- FIG. 8-3 shows the number of cases judged to be abnormal in the control, AD, FTLD, and ALS groups, the target score, and the sensitivity and specificity values at the time of maximum optimization in the DO range.
- FIG. 8-1 was temporarily shown with a DO of 50.262, but the sensitivity and specificity did not change in the range of 50.262 to 54.239 DO.
- FIG. 8-3 by setting the upper limit of the normal value to 50.26, it was possible to determine an abnormal value with sensitivity of 0.875, 0.857, and 1.00 in AD, FTLD, and ALS (FIG. 8-3, FIG. 9).
- the specificity was 0.800 in all diseases (FIGS. 8-3 and 9).
- the specificity increased to 0.889 by judging abnormal cases from the control group and excluding cases with rapid cognitive decline (in parentheses in FIG. 8-3).
- CSF cerebrospinal fluid
- pSer46-MARCKS was very specific but not very sensitive (FIGS. 1-1 and 1-2).
- the values of unphosphorylated MARCKS and pSer46-MARCKS were integrated to generate a new parameter called DO (FIG. 8-1).
- DO is a good parameter with both high sensitivity and high specificity, and DO reflects well disease severity in AD and FTLD.
- the best value of the normal upper limit of DO was further searched to optimize sensitivity and specificity in the three neurodegenerative diseases.
- DO changed in common in multiple neurodegenerative diseases.
- DO and pSer46-MARCKS itself were higher in FTLD than AD. This result indicates that DO and pSer46-MARCKS are not disease-specific markers, but they are indicators of a common pathological process across three neurodegenerative diseases.
- Example 2 Examination method in Parkinson's disease (PD) and dementia with Lewy bodies (DLB) Mouse PD / DLB model Normal human ⁇ -Syn-BAC-Tg mice were treated with Yamakado et al (2012) Neurosci Res 73: 173- It was produced by the method described in 177.
- the BAC-Tg construct (PAC AF163864 and BAC AC097478, including all human genes plus 28kb 5'-flanking sequence and 50kb 3'-flanking sequence) in C57BL6 / J ova Microinjected homozygous ⁇ -Syn-Tg mice were produced.
- GBA-hetero KO mice were purchased from The Jackson Laboratory (B6.129S6-Gbatm1Nsb / J, stock number 003321) and mated with human ⁇ -Syn-BAC-Tg mice.
- the obtained normal human ⁇ -Syn-BAC-Tg / GBA-hetero-KO (homo / hetero) mice were maintained as a strain.
- mice or human brains were fixed with 4% paraformaldehyde and embedded in paraffin.
- Paraffin-embedded brain sections were deparaffinized, rehydrated and antigens activated (10 mM citrate buffer, pH 6.0, microwaved for 5 minutes at 100 ° C. This process was repeated 3 times) And cooled to room temperature (RT). Sections were further activated with 98% formic acid (WAKO, 066-00461) for 5 minutes at room temperature for staining for phospho- ⁇ -Syn.
- PBST PBS containing 0.1% Tween-20
- PBS containing 0.5% Triton® X-100 PBS containing 0.5% Triton® X-100
- mice anti-phospho- ⁇ -Syn (Ser129) (1: 2000, WAKO, 015 -25191)) for 60 minutes at 37 ° C; mouse anti- ⁇ -Syn (1: 1000, Abcam, ab27766) for 12 hours at 4 ° C; rabbit antiphospho-MARCKS (Ser46) (1: 1000, GL Biochem (Shanghai) ), Or mouse anti-ubiquitin antibody (1: 1000, Cell Signaling Technology, 3936S) for 120 minutes at 37 ° C; mouse Thr203 / Tyr205-ERK1 // Thr183 // Tyr185-ERK2 and human Thr202 // Tyr204-ERK1 // Thr185 // Tyr187 -ERK2 (1: 250, Cell Signaling Technology, # 4370) Rabbit anti-phospho-ERK1z / 2, mouse anti-MAP2 (1: 100, santa cruz, sc-32791) or mouse anti-GF
- anti-pSer129- ⁇ -Syn antibody was labeled with Zenon-Alexa-Fluor-488 mouse IgG1 labeling kit (Z-25002, Invitrogen). Nuclei were stained with DAPI (Dojin Laboratories, D523). Images were acquired by confocal microscopy: Olympus FV1200 IX83 (Olympus).
- the crude extract was centrifuged at 16,000 g for 10 minutes at 4 ° C., and an equal volume of sample buffer (0.1 M Tris-HCl pH 7.5, 4% SDS, 20% glycerol, 12% ⁇ -mercaptoethanol, and Separation on 1% SDS-PAGE, transfer to polyvinylidene difluoride membrane (Immobilon-P, Merck Millipore) using semi-dry method and block with 5% milk or 2% broth.
- TBST (10 mM Tris / HCl pH 8. 0,150 mM NaCl, and 0.05% Tween-20) in BSA (% BSA) and reacted with the following primary and secondary antibodies diluted with Can Get Signal solution (Toyobo).
- mice anti-phospho- ⁇ -Syn (Ser129) (1: 5000, WAKO, 015-25191); mouse anti- ⁇ -Syn (1: 5000, Abcam, ab27766) for 12 hours at 4 ° C; Rabbit anti-phospho-MARCKS (Ser46) (1: 200,000, GL Biochem (Shanghai) Ltd.) at 37 ° C.
- mouse anti-ubiquitin antibody (1: 5000, Cell Signa ling Technology, 3936S) 12 hours at 4 ° C; Rabbit anti-phospho-ERK1 / 2 (Thr203 / Tyr205 (mouse) -ERK1 / Thr183 / Tyr185 (mouse) -ERK2, Thr202 / Tyr204 (human) -ERK1 / Thr185 / Tyr187 ( (Human) -ERK2) (1: 10,000, Cell Signaling Technology, # 4370); or rabbit anti-ERK1 / 2 (1: 5,000, Cell Signaling Technology, # 4695S); anti-mouse IgG HRP conjugate (1: 3000, GE Healthcare, NA931VA) and anti-rabbit IgG (1: 3000, GE Healthcare, NA934VS) to detect bands using LAS4000 (GE Healthcare), ECL Prime (GE Healthcare, RPN2232) or SCL Select (GE Healthcare, RPN2235) was used.
- TNE buffer (10 mM Tris-HCl (pH 7.5), 10 mM NaCl, 1 mM EDTA, 1% NP-40, 0.5% protease inhibitor cocktail, 0.5% phosphatase inhibitor cocktail) did.
- An aliquot was incubated with a 50% slurry of Protein G Sepharose beads (GE Healthcare) followed by centrifugation (2000 ⁇ g) for 3 minutes. The supernatant was incubated overnight at 4 ° C. with 1 ⁇ g of rabbit anti-pSer46-MARCKS or rabbit anti-pSer129- ⁇ -synuclein antibody.
- protein G Sepharose beads (GE Healthcare) for 4 hours, washed with TNE buffer and eluted with sample buffer.
- Peripheral blood cells (polymorphonuclear leukocytes (PMN) and mononuclear cells (MC)) were collected using Polymorphprep solution (Alere Technologies AS) according to the manufacturer's protocol. Briefly, 1 mL venous blood containing EDTA (final concentration 2.0 mM) was carefully layered over 1 mL Polymorphprep in a 15 mL tube. After centrifugation at 500 ⁇ g for 30 minutes at room temperature, plasma was removed to obtain a layer containing PMN and MC. Collected aliquots were diluted with 0.45% NaCl and cell pellets were obtained by centrifugation at 400 ⁇ g for 10 minutes.
- PMN polymorphonuclear leukocytes
- MC mononuclear cells
- the pellet is lysed with lysis buffer (10 mM Tris-HCl (pH 7.5), 0.2% SDS, 0.5% protease inhibitor cocktail, and 0.5% phosphatase inhibitor cocktail), 62.5 mM Tris-HCl, pH 6.8, 2 SDS-PAGE was performed by adding to a mixture of SDS, 2.5% (v / v) 2-mercaptoethanol, 5% (v / v) glycerol and 0.0025% (w / v) bromophenol blue.
- lysis buffer 10 mM Tris-HCl (pH 7.5), 0.2% SDS, 0.5% protease inhibitor cocktail, and 0.5% phosphatase inhibitor cocktail
- brain extracts from mouse and human cerebral cortex were denatured by surfactant and heat treatment, then cysteine residues were reduced and blocked by alkylation. Protein samples were digested with trypsin.
- the tolerance of peptide search by ProteinPilot was set to 0.05 Da for MS and 0.10 Da for MS / MS analysis. Redundantly identified proteins were excluded using the Pro Group algorithm (AB SCIEX).
- the confidence score for protein or peptide identification was calculated by ProteinPilot and used as a confidence threshold.
- the threshold for detection was set at 95% confidence, and peptides with> 95% confidence were accepted as identified peptides.
- Quantification of the protein was performed through analysis of iTRAQ reporter groups in MS / MS spectra generated during fragmentation in a mass spectrometer.
- bias correction was used to normalize signals between different iTRAQ reporters, assuming that the total amount of signal from each iTRAQ must be equal.
- a bias correction option was used to normalize the different iTRAQ signals.
- the peptide ratio was calculated as the ratio of the reporter signal in the disease model to the control model after bias correction. Details of this formulation are described in the AB SCIEX manual.
- the peptide summary results from ProteinPilot were output as an Excel file for further data analysis.
- the amount of peptide fragment was calculated as the geometric mean of the signal intensity of multiple MS / MS fragments including phosphorylation sites.
- Temporal and occipital pole human brain samples used for human brain proteome analysis were dissected from 5 AD, 5 DLB and 5 age-matched normal control patients and deep within 1 hour after death Frozen (-80 ° C).
- pSer46-MARCKS levels increased in the temporal lobe but not in the DLB occipital lobe, but increased in the opposite pattern (ie, occipital but not temporal lobe) in AD (FIG. 10B).
- the increase in pSer46-MARCKS level in the early stage of disease was normalized in the late stage (Fujita et al., (2016) Sci Rep 6: 31895).
- this brain region contained pSer129- ⁇ -Syn cytoplasmic inclusion bodies (FIG. 11B) that were mostly ubiquitinated (FIG. 11C). Since cytoplasmic staining of pSer46-MARCKS appeared to be aggregates (FIG. 11A), we examined whether they were ⁇ -Syn aggregates and half of the neuronal cytoplasmic pSer46-MARCKS positive structure was pSer129- ⁇ -Syn. The yellow arrow was found to be stained with However, the other half of them did not stain strongly with pSer129- ⁇ -Syn (FIG. 11D, red arrow).
- pSer46-MARCKS positive / pSer129- ⁇ -Syn negative cells can correspond to surrounding neurons indirectly affected by HMGB1 released from damaged neurons that accumulate pSer129- ⁇ -Syn, even in the late stage of DLB Suggests that the pathology continues to progress in the brain.
- the present inventors performed Western blotting of pSer46-MARCKS and total MARCKS with the occipital lobe of human postmortem DLB patients and non-DLB control patients (FIG. 11E).
- pSer46-298 MARCKS levels increased in DLB patients.
- mice slightly increased the signal of pSer46RC-MARCKS in the olfactory bulb, frontal cortex, and parietal cortex in 1 month (FIGS. 12 and 18). Thereafter, the area of pSer46S-MARCKS positive staining expanded to the parietal and occipital cortex at 6 months (FIGS. 12 and 19), but did not increase in the hippocampus before 24 months (FIGS. 12 and 20).
- FIGS. 13A-C show high magnification images of olfactory bulbs of human ⁇ -Syn-BAC-Tg / GBA-hetero KO mice co-stained with antibodies against pSer46-MARCKS and pSer129- ⁇ -Syn.
- FIG. 14A cytoplasmic ⁇ -Syn aggregates were also detected in the wall cortex.
- FIG. 14B The relationship between pMARCKS and p- ⁇ -Syn, p- ⁇ -Syn and ubiquitin in aging cortical neurons was similar to that of olfactory neurons (FIG. 14B).
- the inventor also tested the level of pSer46-MARCKS in peripheral blood cells and found it to be much lower than that of the brain (FIG. 21).
- MARCKS is a representative substrate for PKC known as a myristoylated alanine-rich C kinase substrate.
- PKA ⁇ has been reported to phosphorylate Ser159, Ser163 and Ser170.
- MAPK MAPK3 / MAPK1
- the immunohistochemical staining pattern of pSer46 -MARCKS was similar in AD and PD / DLB lesions.
- neurite degeneration revealed by pSer46 -MARCKS was first detected in the olfactory bulb and then became prominent in the occipital and temporal cortex (Table 1).
- Table 1 summarizes the pSer46-MARCKS, pSer129- ⁇ -syn and ubiquitin staining patterns in human ⁇ -Syn-BAC-TgT / GBA-hetero KO mice.
- pSer46MA-MARCKS is not a severely affected area (DLB occipital lobe, AD temporal lobe) but disease (DLB temporal lobe, AD occipital lobe) ) Increased in brain areas relatively unaffected.
- pSer46 -MARCKS as a biomarker that can detect molecular pathology in PD / DLB at the very early stage (preaggregation / preclinical) stage.
- peripheral blood cells such as erythrocytes, granule cells or lymphocytes express pSer46-MARCKS. If so, it would be difficult to identify the brain from PBC-derived pSer46-MARCKS, and using pSer46-MARCKS as a biomarker for extra-cerebral diagnosis would require some additional tricks. Fortunately, PBC did not express detectable levels of pSer46-MARCKS comparable to the brain tissue of 5xFAD mice ( Figure 21). It supports the possibility of developing pSer46-MARCKS as a blood biomarker.
- PBC peripheral blood cells
- the present inventors found co-localization in cytoplasmic aggregates (FIG. 13, FIG. 14A, FIG. 14B) and biochemical interaction (FIG. 16) of pSer46-MARCKS and pSer129- ⁇ -Syn.
- ⁇ -Syn and MARCKS appear to be intrinsically disordered proteins (IDPs).
- IDPs intrinsically disordered proteins
- the increase in pSer46-MARCKS and DO quantifies the in vivo activity of neurodegeneration, as the pathological cycle from neurite degeneration to cell death occurs repeatedly in brains with neurodegenerative disease until all neurons in the brain are necrotic Symptomatic and possibly non-syndromic tests, as well as GOT and GPT, which are general quantitative indicators of hepatocellular injury in non-disease-specific but multiple liver disease, which can also be used as potential biomarkers The same applies to the body.
- This example provides a new biomarker that reflects neurite degeneration in neurodegenerative diseases.
- the method of the present invention comprises human AD (Alzheimer's disease), FTLD (frontotemporal lobar degeneration), ALS (amyotrophic lateral sclerosis), PD (Parkinson's disease) and DLB (Lewy body dementia). It can be used for the detection of neurodegenerative diseases selected from the group. All publications, patents and patent applications cited herein are hereby incorporated by reference in their entirety.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Engineering & Computer Science (AREA)
- Chemical & Material Sciences (AREA)
- Biomedical Technology (AREA)
- Immunology (AREA)
- Molecular Biology (AREA)
- Hematology (AREA)
- Urology & Nephrology (AREA)
- Biochemistry (AREA)
- Analytical Chemistry (AREA)
- Microbiology (AREA)
- Biotechnology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- General Health & Medical Sciences (AREA)
- Physics & Mathematics (AREA)
- Medicinal Chemistry (AREA)
- Cell Biology (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Food Science & Technology (AREA)
- Organic Chemistry (AREA)
- Neurosurgery (AREA)
- Neurology (AREA)
- Zoology (AREA)
- Wood Science & Technology (AREA)
- Biophysics (AREA)
- Bioinformatics & Cheminformatics (AREA)
- General Engineering & Computer Science (AREA)
- Genetics & Genomics (AREA)
- Investigating Or Analysing Biological Materials (AREA)
- Other Investigation Or Analysis Of Materials By Electrical Means (AREA)
Abstract
高感度かつ高い特異性でヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)からなる群から選択される神経変性疾患を検出する方法の提供。 以下の工程を含む、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)からなる群から選択される神経変性疾患を検出する方法: (i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質および非リン酸化MARCKSタンパク質を測定する工程; (ii) (i)で得られた測定値から以下の式で表されるDO値を算出する工程;および [式1] [式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す] (iii) DO値を指標に神経変性疾患を検出する工程 を含む方法。
Description
本発明は、AD(アルツハイマー病)、FTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)の検出法に関する。
神経変性疾患の前臨床病理学は大きな注目を集めており、そのような早期病態を測定する定量的バイオマーカーが必要とされている。
アルツハイマー病(AD)は、最も一般的な神経変性疾患であり、よく知られた認知症の原因である。
ADの病因において最も支持されているモデルの1つは、アミロイドβペプチド(Aβ)の細胞外蓄積によって産生されるアミロイド原線維の細胞傷害性を前提とするアミロイド仮説である。
この仮説に基づいて、AβはADの主要な治療ターゲットとして浮上した。バピネオズマブ(Bapineuzumab)やソラネズマブ(Solanezumab)のような抗体療法を含む治療戦略は、認知症発症後の臨床試験においてヒトAD患者の脳におけるAβ凝集を低下させたが、これまでの臨床的症状における認知症の回復は不十分であった。結果として、類似または新しい治療法がより効果的である可能性がある症状発生前のADの初期の分子事象に研究関心が移っている。
本発明者らは、マウスADモデルおよびヒトAD患者からの脳組織の包括的なリン酸化タンパク質分析を行った。複数のADマウスモデルにおいて異常なリン酸化を有する17のコアタンパク質を同定した。興味深いことに、これらの変化は発症前に生じており、しかもAβ凝集がモデルマウスの脳において免疫組織学的に検出される前でさえ、いくつかのコアタンパク質において異常なリン酸化が検出され、AD病理の初期段階において重要な役割を果たすことが示唆された(非特許文献1を参照)。
特に、定量的な質量分析では、Ser46でリン酸化されたMARCKS(ミリストイル化アラニンリッチCキナーゼ基質)の増加は、ADモデルマウスにおけるAβ凝集の組織学的検出の1ヶ月前に始まり、ヒトAD患者の死後も脳に残った(非特許文献1および2を参照)。MARCKSは、アクチン細胞骨格ネットワークとプロテインキナーゼC(PKC)の代表的な基質を固定するサブメンブランタンパク質である。抗pSer46-MARCKSを用いた免疫組織化学法により、ADモデルマウスにおいて症状の発症のはるか前の変性神経突起が検出され、またヒト剖検AD脳の老人斑を取り囲む変性神経突起が検出された(非特許文献2を参照)。さらに、Ser46でのMARCKSリン酸化が樹状突起棘を不安定化させ、神経突起変性を引き起こすことを明らかにした(非特許文献2を参照)。これらの結果は、pSer46-MARCKSが、ADの末期段階まで、そして恐らくは他の神経変性疾患において、超早期または前臨床段階から利用可能な神経突起変性の代用バイオマーカーであり得るという仮説を提供した。
Tagawa, K. et al., Hum. Mol. Genet. 24, 540-58 (2015).
Fujita, K. et al., Sci. Rep. 6, 31895 (2016).
本発明は、高感度かつ高い特異性でヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症またはレビー小体病)からなる群から選択される神経変性疾患を検出する方法の提供を目的とする。
上記のように、本発明者らは以前に、アルツハイマー病(AD)マウスモデルにおける組織学的アミロイドβ(Aβ)凝集体の形成前でさえもリン酸化MARCKSが増加し、その変化がヒト死後AD脳で持続することを見出した。特に、Ser46でリン酸化されたMARCKS(pSer46-MARCKS)は、ヒト患者のマウスモデルおよび老人斑におけるAβ凝集体を取り囲む変性神経突起において検出された。
本発明者らは、これらの知見に基づき、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)の脳脊髄液(CSF)におけるpSer46-MARCKSの量を定量化した。予期せぬことに、最も顕著な変化が前頭側頭葉変性症(FTLD)で検出され、神経突起変性がpSer46-MARCKSの免疫組織化学法によって確認された。脳脊髄液(CSF)のpSer46-MARCKSに関する特異性は1.0であり、これは明らかに神経変性を正常な症例と区別することができた。
また、MARCKSにおける同様の変化が、マウスモデルおよびヒト患者の両方において、パーキンソン病とレビー小体病による認知症で生じることがわかった。
ヒトα-Syn-BAC-Tg/GBA-hetero-KOマウスが症状を示さない時点で、α-シヌクレイン凝集体形成の前にpSer46 - MARCKSレベルの上昇が始まり、老化の間持続し、ヒトの死後の脳のパターンと一致した。
この結果は、ADおよびPD/DLB病変における前凝集神経突起変性の共通メカニズムを強く示唆している。
また、パーキンソン病(PD)およびレビー小体型認知症(DLB)のマウスモデルおよびヒト患者の両方において同様の変化が確認された。
さらに、本発明者らは、ADのヒト患者および質量分析による他の神経変性疾患からの脳脊髄液(CSF)のpSer46-MARCKSおよび非リン酸化MARCKSを定量した。pSer46-MARCKSはそれ自身で感度・特異度ともに十分に高いが、本発明者らは、さらに診断パラメータとしての価値を高めるために、pSer46-MARCKSと非リン酸化MARCKSの統合に基づく新しいパラメータを開発した。そのパラメータにより、高感度かつ高い特異性で、複数の神経変性疾患を健常対照と区別することができた。さらに、病理学的分析により、pSer46-MARCKSが神経変性疾患全体の神経突起変性を反映することが明らかになった。これらの結果より、pSer46-MARCKSと非リン酸化MARCKSの統合により、すべての神経変性疾患のより感受性の高い決定的なバイオマーカーとして、「DO(Distance from origin)」と呼ばれる新しいパラメータを開発した。
すなわち、本発明は以下のとおりである。
[1] 以下の工程を含む、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)からなる群から選択される神経変性疾患を検出する方法:(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質および非リン酸化MARCKSタンパク質を測定する工程;
(ii) (i)で得られた測定値から以下の式で表されるDO値を算出する工程;および
[式1]
 [式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す]
[式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す]
(iii) DO値を指標に神経変性疾患を検出する工程
を含む方法。
[2] 検体試料が脳脊髄液である、[1]の方法。
[3] 「pSer46-MARCKS」および「non-phosphorylated-MARCKS」の測定を質量分析法により行う[1]又は[2]の方法。
[4] 式中の「pSer46-MARCKS」および「non-phosphorylated-MARCKS」が、検体試料中の全タンパク質量で正規化した値である、[1]~[3]のいずれかの方法。
[5] 工程(iii)において、被験体について算出されたDO値とあらかじめ定めたカットオフ値と比較し、カットオフ値より高い場合に、神経変性疾患が検出されたと判断する、[1]~[4]のいずれかの方法。
[6] DO値のカットオフ値が、50~55である、[5]の方法。
[7] 以下の工程を含む、ヒトFTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。
[8] 検体試料が脳脊髄液である、[7]の方法。
[9] 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う[7]又は[8]の方法。
[10] 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、[7]~[9]のいずれかの方法。
[11] 以下の工程を含む、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。
[12] 検体試料が脳脊髄液である、[11]の方法。
[13] 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う[11]又は[12]の方法。
[14] 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、[11]~[13]のいずれかの方法。
[15] 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーを用い、46位でリン酸化されたMARCKSタンパク質の測定をPET(陽電子放射断層撮影)により行う[11]の方法。
[16] 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーが、46位でリン酸化されたMARCKSタンパク質に対する抗体をポジトロン核種でラベルした抗体PETトレーサーである[15]の方法。
本明細書は本願の優先権の基礎となる日本国特許出願番号2018-043641号、2018-138785号の開示内容を包含する。
[1] 以下の工程を含む、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)からなる群から選択される神経変性疾患を検出する方法:(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質および非リン酸化MARCKSタンパク質を測定する工程;
(ii) (i)で得られた測定値から以下の式で表されるDO値を算出する工程;および
[式1]
(iii) DO値を指標に神経変性疾患を検出する工程
を含む方法。
[2] 検体試料が脳脊髄液である、[1]の方法。
[3] 「pSer46-MARCKS」および「non-phosphorylated-MARCKS」の測定を質量分析法により行う[1]又は[2]の方法。
[4] 式中の「pSer46-MARCKS」および「non-phosphorylated-MARCKS」が、検体試料中の全タンパク質量で正規化した値である、[1]~[3]のいずれかの方法。
[5] 工程(iii)において、被験体について算出されたDO値とあらかじめ定めたカットオフ値と比較し、カットオフ値より高い場合に、神経変性疾患が検出されたと判断する、[1]~[4]のいずれかの方法。
[6] DO値のカットオフ値が、50~55である、[5]の方法。
[7] 以下の工程を含む、ヒトFTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。
[8] 検体試料が脳脊髄液である、[7]の方法。
[9] 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う[7]又は[8]の方法。
[10] 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、[7]~[9]のいずれかの方法。
[11] 以下の工程を含む、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。
[12] 検体試料が脳脊髄液である、[11]の方法。
[13] 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う[11]又は[12]の方法。
[14] 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、[11]~[13]のいずれかの方法。
[15] 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーを用い、46位でリン酸化されたMARCKSタンパク質の測定をPET(陽電子放射断層撮影)により行う[11]の方法。
[16] 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーが、46位でリン酸化されたMARCKSタンパク質に対する抗体をポジトロン核種でラベルした抗体PETトレーサーである[15]の方法。
本明細書は本願の優先権の基礎となる日本国特許出願番号2018-043641号、2018-138785号の開示内容を包含する。
本発明の方法により、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を高感度かつ高い特異性で検出することができる。
以下、本発明を詳細に説明する。
本発明は、神経変性疾患を検出する方法である。本発明において、神経変性疾患の検出とは、被験体が神経変性疾患に罹患していると判断すること、あるいは、被験体が神経変性疾患を発症するリスクがあると判断することをいう。
また、本発明は、神経変性疾患を検出するための補助的データを取得する方法も含む。 本発明において、神経変性疾患は、アルツハイマー病(AD:Alzheimer disease)、前頭側頭葉変性症(FTLD:Frontotemporal lobar degeneration)、筋萎縮性側索硬化症(ALS:Amyotrophic lateral sclerosis)、パーキンソン病(PD:Parkinson's disease)およびレビー小体型認知症(DLB:dementia with Lewy body)を含む。
「アルツハイマー病」とは、アルツハイマー型認知症とも称される神経変性疾患であり、遺伝子の変異に起因する「家族性アルツハイマー病」および「遺伝性アルツハイマー病」や、生活習慣やストレスといった環境因子による「孤発性アルツハイマー病」も含まれる。
「前頭側頭葉変性症」とは、FTLDとも称される、早期には前頭葉・側頭葉に萎縮を呈し、晩期には脳全体の萎縮に至る、非アルツハイマー病型の神経変性疾患のことである。すなわち、前頭側頭葉変性症には、臨床的特徴上分類される3種の疾患、前頭側頭型認知症(FTD)、進行性非流暢性失語(PNFA)および意味性認知症(SD)が含まれ、また病理学上においては、細胞内に異常タンパク質として蓄積されるタンパク質の種類に応じ、FTLD-Tau、FTLD-TDP、FTLD-UPSおよびFTLD-FUSに分類される4種の疾患が含まれる。
さらに、FTLD-Tauは、細胞内に優位に蓄積されるtauタンパク質中の微小管結合領域のリピート数に応じ、3R Tau型、4R Tau型および3/4R Tau型に分類される。また、3R Tau型には、Pick球を伴うFTLD(ピック病)、MAPT(微小管関連蛋白tau)遺伝子変異を伴うFTLD(FTLD-17)等が含まれ、4R Tau型には、大脳皮質基底核変性症、進行性核上性麻痺、認知症を伴う多系統タウオパチー、嗜銀顆粒性認知症(嗜銀顆粒病)、MAPT遺伝子変異を伴うFTLD(FTLD-17)等が含まれ、3/4R Tau型には、神経原線維変化型認知症、MAPT遺伝子変異を伴うFTLD(FTLD-17)等が含まれる。一方、tauが陰性であり、ユビキチン陽性封入体を有するFTLD群は、FTLD-Uと称され、上記FTLD-TDP、FTLD-UPSおよびFTLD-FUSが含まれる。
FTLD-TDPは、FTLD-Uのうち、TDP-43が陽性の疾患を意味し、該疾患には、PGRN(progranulin(プログラニュリン)遺伝子)変異を伴うFTLD、孤発性のFTLD-TDP/FTLD-U、TARDBP(TDP-43遺伝子)変異を伴うFTLD、VCP(valosin含有蛋白遺伝子)変異を伴うFTLD、9番染色体に連鎖するFTLD等が含まれる。また、FTLD-FUSは、FTLD-Uのうち、TDP-43が陰性であり、FUS(fused in sarcoma)が陽性の疾患を意味し、該疾患には、神経細胞性中間径フィラメント封入体病、非典型的FTLD-U、好塩基性封入体病、FUS変異を伴うFTLD等が含まれる。
また、「TLD-UPSは、TDP-43が陰性であるFTLD-Uの1種であり、該疾患には、CHMP2B(荷電多発空胞体蛋白2B遺伝子)変異を伴うFTLD等が含まれる。
「筋萎縮性側索硬化症」とは、運動ニューロン病の一種であり、重篤な筋肉の委縮と筋力低下を特徴とする神経変性疾患である。筋萎縮性側索硬化症の原因遺伝子として約20種類の遺伝子が報告されており、また、TDP-43の異常蓄積が原因とされている。
「パーキンソン病」とは、黒質のドーパミン神経細胞の変性を主体とする進行性変成疾患である。中脳の黒質・青斑核の色素脱失がみられ、黒質や青斑、迷走神経背側核、視床下部、交感神経節などの神経細胞脱落が生じて伝達物質ドーパミンが不足する。残存神経細胞やその突起の一部にレビー小体(Lewy body)という特徴的な封入体が認められる。
「レビー小体型認知症」とは、大脳皮質全体にレビー小体が現れるもので、進行性の認知機能障害に加えて、幻視症状とパーキンソン症候群を示す変性性認知症である。
プロテイン凝集は、アルツハイマー病(AD)、パーキンソン病、レビー小体型認知症、前頭側頭葉変性(FTLD)、ハンチントン病(HD)、脊髄小脳失調(SCA)、および筋萎縮性側索硬化症(ALS)を含む神経変性障害の広く認められた特徴である。一般に、疾患関連タンパク質はミスフォールド構造をとると考えられ、その後、β-シートを含む凝集しやすい構造に変換される。
しかし、これらの構造の年代的および/または確率的変化の詳細は、ほとんど知られておらず、真の毒性種の正体と、凝集タンパク質または可溶性タンパク質が毒性であるかどうかについての議論を引き起こす。
AD治療の臨床試験は、これらの議論に大きな影響を与えてきた。抗Aβ抗体による受動免疫は、脳における細胞外Aβプラークの存在量を減少させることに大いに成功している。
しかしながら、これらの試験においては、Aβ-PET(陽電子放射断層撮影)の改善と臨床症状の改善との間に相違があることが報告されている。
したがって、早期段階の病態の解明は、ADの病因の解明と治療法の開発にとって緊急の課題であり、状況はPD / DLBを含む他の神経変性疾患においてほぼ同様である。
マウスADモデルおよびヒトAD患者からの脳サンプルの包括的なリンタンパク質分析は、細胞外Aβプラークが組織学的に検出可能になる前にいくつかのタンパク質のリン酸化の変化が開始されることを明らかにした(Tagawa et al. (2015) Hum Mol Genet 24:540-558)。
マウスADモデルおよびヒトAD患者からの脳サンプルの包括的なリンタンパク質分析は、細胞外Aβプラークが組織学的に検出可能になる前にいくつかのタンパク質のリン酸化の変化が開始されることを明らかにした(Tagawa et al. (2015) Hum Mol Genet 24:540-558)。
Ser46でのMARCKSのリン酸化は、TLR4を介した損傷関連分子パターン(DAMP)、特にHMGB1によって誘発される(Fujita et al, (2016) Sci Rep 6:31895)。
今回、グルコセレブロシダーゼ(GBA) - ヘテロ接合ノックアウト(KO)バックグラウンド(ヒトα-Syn-BAC-T細胞)中のヒト正常α-シヌクレイン(α-Syn)を過剰発現するBAC-Tgマウスにおいて、ヒトDLB患者における観察と同様のSer46でのMARCKSのリン酸化を検出した。セリン46(pSer46-MARCKS)上のMARCKSのリン酸化の組織学的特徴および脳における時系列進行は、ADおよびPD / DLBにおいて同様であった。興味深いことに、神経変性のこのマーカーは、組織学的に検出可能なα-Syn凝集体の形成前に陽性になった。
これらの結果は、ニューロン変性とタンパク質凝集との間の関係を明示し、神経突起変性の開始がタンパク質凝集体の形成に先行することを明らかにした。
pSer46-MARCKSは、超早期(前凝集/前臨床)段階でPD / DLBにおける分子病理を検出することができるバイオマーカーとして利用できる。
1.46位のセリンでリン酸化されたMARCKS(pSer46-MARCKS)の量に基づいた神経変性疾患の検出
本発明においては、ヒト生体試料中のMARCKSのリン酸化を指標にして、被験体がAD、FTLDまたはALSに罹患しているかどうかを検出する。「検出する」を「判定する」、「評価する」ともいう。
本発明においては、ヒト生体試料中のMARCKSのリン酸化を指標にして、被験体がAD、FTLDまたはALSに罹患しているかどうかを検出する。「検出する」を「判定する」、「評価する」ともいう。
MARCKSとは、ミリストイル化アラニンリッチCキナーゼ基質(myristoylated alanine rich protein kinase C substrate)であり、RefSeq ID:NP_002347(NP_002347.5)で特定されるヒト由来のタンパク質が挙げられる。また、MARCKSをコードする核酸のヒト由来の典型例としては、RefSeq ID:NM_002356(NM_002356.6)に記載のコーディング領域(CDS)を含む核酸が挙げられる。
検体試料として用いる生体試料としては、被験体の身体から採取した体液、組織、細胞等(例えば、脳脊髄液、脳神経組織(特に神経学的生検組織)、血液、血漿、漿液、リンパ液、尿、唾液)が挙げられ、この中でも脳脊髄液が好ましい。
本発明においては、MARCKSの46位のセリン(Ser)のリン酸化を指標にする。
リン酸化MARCKSの検出法は限定されず、公知のいかなる方法も用い得る。例えば、質量分析法、免疫学的測定法が挙げられる。
リン酸化MARCKSの検出法は限定されず、公知のいかなる方法も用い得る。例えば、質量分析法、免疫学的測定法が挙げられる。
質量分析法は、質量分析計を用いて行うことができる。質量分析計は、試料導入部、イオン化室、分析部、検出部、記録部等を含む。イオン化法としては、matrix-assisted laser desorption ionization(MALDI)法、エレクトロスプレーイオン化(ESI)法等を用いればよい。分析部は、二重収束質量分析計、四重極型質量分析計(QMS)、飛行時間型質量分析計(TOF)、フーリエ変換質量分析計(FT)、イオンサイクロトロン質量分析計(ICR)等が用いられる。精密な分析のために質量分析計を2台結合した、タンデム質量分析計(MS/MS)を用いることもできる。質量分析計は単独で用いられてもよいし、液体クロマトグラフィーなどの分離機器や測定機器などと接続してもよく、高速液体クロマトグラフィーと組み合わせた液体クロマトグラフ質量分析(LC/MS、LC/MS/MS)で分析することができる。
免疫学的測定法は、46位のセリンでリン酸化されたMARCKS(pSer46-MARCKS)を認識し得る抗pSer46-MARCKS抗体を用いた免疫学的測定法により行うことができる。免疫学的測定法としては、例えば、固相免疫測定法(RIA、EIA、FIA、CLIA等)、ドット・ブロッティング法、ラテックス凝集法(LA:Latex Agglutination-Turbidimetric Immunoassay)、イムノクロマト法などが挙げられる。抗体は基板上に固定化し用いることができる。この中でも、定量性の観点からEIA(Enzyme Immunoassay)法の1種であるELISA(Enzyme-Linked ImmunoSorbent Assay)法が好ましい。ELISA法では、抗体を固相化したマイクロタイタープレートのウェルに検体を添加し、抗原・抗体反応を行わせ、さらに酵素標識した抗体を添加し、抗原・抗体反応をさせ、洗浄後、酵素基質と反応・発色させ、吸光度を測定してサンプル中のマーカータンパク質または部分ペプチドを検出すると共に、その測定値から検体中のタンパク質または部分ペプチド濃度を算出することができる。また、蛍光標識した抗体を用いて、抗原抗体反応をさせた後に蛍光を測定してもよい。抗原抗体反応は4℃~45℃、より好ましくは20℃~40℃、さらに好ましくは25℃~38℃で行うことができ、また、反応時間は、10分~18時間、より好ましくは10分~1時間、さらに好ましくは30分~1時間程度である。免疫学的方法において用いられる抗体は、モノクローナル抗体でも、ポリクローナル抗体でもよく、モノクローナル抗体のFab、F(ab')、F(ab')2等の結合活性断片を用いることもできる。
さらに、46位のセリンでリン酸化されたMARCKS(pSer46-MARCKS)をPET(陽電子放射断層撮影)により検出することもできる。PETで検出する場合、pSer46-MARCKSをイメージングするためのトレーサーを被験体に投与し、被験体中のpSer46-MARCKSをPET(陽電子放射断層撮影)により検出すればよい。pSer46-MARCKSをイメージングするためのトレーサーとしては、例えば、46位でリン酸化されたMARCKSタンパク質に対する抗体をポジトロン核種でラベルした抗体PETトレーサーが挙げられる。
本発明においては、健常人から採取した検体を陰性対照として同時に測定してもよい。ここで、「健常」とは、被験体がアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)、PD(パーキンソン病)およびDLB(レビー小体型認知症)等の神経変性症に罹患していない状態をいう。この場合、被験体がアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)またはパーキンソン病(PD)およびレビー小体型認知症(DLB)等の神経変性症に罹患しているか、神経変性疾患を発症するリスクがある場合、被験体の検体中のMARCKSの46位のセリンにおけるリン酸化の程度が健常人に比べ高くなる。すなわち、被験体の検体中のpSer46-MARCKSの量が健常人に比べ高くなる。従って、被験体の検体中のMARCKSの46位のセリンにおけるリン酸化の程度が健常人よりも高い場合、pSer46-MARCKSは陽性と判断され、被験体においてアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)または筋萎縮性側索硬化症(ALS)等の神経変性症が検出された、すなわち、被験体がアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)またはパーキンソン病(PD)およびレビー小体型認知症(DLB)等の神経変性症に罹患しているか、あるいは神経変性疾患を発症するリスクがあると判断することができる。
この際、上記の方法により、pSer46-MARCKSを定量し、得られた定量値を正規化して判断してもよい。正規化は、例えば、pSer46-MARCKS濃度を検体中の全タンパク質濃度で除すればよい。この場合、例えば、pSer46-MARCKS量を全タンパク質量に対する濃度(ppm)で表すことができる。また、pSer46-MARCKS濃度を定量し、検体中の総MARCKS(リン酸化MARCKSと非リン酸化MARCKSの総量)で除してもよい。この場合、pSer46-MARCKS量を総MARCKSに対する%で表すことができる。
例えば、被験体の検体中のpSer46-MARCKSの値が健常人の検体中の量の1.3倍以上、好ましくは1.5倍以上、さらに好ましくは2.0倍以上、特に好ましくは3.0倍以上の場合に被験体において、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)またはパーキンソン病(PD)およびレビー小体型認知症(DLB)等の神経変性症が検出されたと判断することができる。
また、あらかじめ健常人の検体中のpSer46-MARCKSの量を測定しておき、該測定値に基づいてpSer46-MARCKS量の測定値についてカットオフ値(閾値)を定めておいてもよい。該カットオフ値を基準とし、カットオフ値を超えた場合に、被験体から採取した検体試料中のpSer46-MARCKS量が健常人から採取した検体試料中のpSer46-MARCKS量よりも多いと判断し、該被験体において、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)またはパーキンソン病(PD)およびレビー小体型認知症(DLB)等の神経変性症が検出されたと判断することができる。
カットオフ値は、例えば、健常人対照群の平均+2SDに設定し、この値を超えたときに被験体において、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)またはパーキンソン病(PD)およびレビー小体型認知症(DLB)等の神経変性症が検出されたと判断することができる。
2.DO(Distance from origin)値に基づいた神経変性疾患の検出
さらに、本発明においては、pSer46-MARCKSと非リン酸化MARCKSの統合により得られた新しいパラメータであるDO(Distance from origin)値を指標として、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)または筋萎縮性側索硬化症(ALS)等の神経変性疾患を検出する。DOは、pSer46-MARCKSと非リン酸化MARCKS量を統合して、両者を指標とするパラメータである。DOはpSer46-MARCKSの量と非リン酸化MARCKSタンパク質の量を(x、y)座標上にプロットしたときのプロットした点の座標の原点からの距離を反映した値であり、DOはpSer46-MARCKS量の2乗と非リン酸化MARCKS量の2乗を足した値の平方根、すなわち以下の式で表される。
[式1]
 式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す。
式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す。
さらに、本発明においては、pSer46-MARCKSと非リン酸化MARCKSの統合により得られた新しいパラメータであるDO(Distance from origin)値を指標として、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)または筋萎縮性側索硬化症(ALS)等の神経変性疾患を検出する。DOは、pSer46-MARCKSと非リン酸化MARCKS量を統合して、両者を指標とするパラメータである。DOはpSer46-MARCKSの量と非リン酸化MARCKSタンパク質の量を(x、y)座標上にプロットしたときのプロットした点の座標の原点からの距離を反映した値であり、DOはpSer46-MARCKS量の2乗と非リン酸化MARCKS量の2乗を足した値の平方根、すなわち以下の式で表される。
[式1]
DO値は、pSer46-MARCKSのみを指標とした場合よりも、より高感度かつ高い特異性でアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)または筋萎縮性側索硬化症(ALS)等の神経変性疾患を検出することができる。DO値は、図8-1に示すように、数値シミュレーションを行うことにより、感度および特異性が良好となる正常の上限値(カットオフ値)を定めることができる。図8-1に示す数値シミュレーションのように、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)および筋萎縮性側索硬化症(ALS)の3つの疾患の感度(各疾患において最大= 1.0、したがって3つの疾患において最大=3.0)と3つの疾患に共通する特異性(3つの疾患の代表として最大=1.0)の合計である「客観的スコア」という別のパラメータを使用し、最も高い客観的スコアを生成するDOの範囲を選択すればよい。例えば、pSer46-MARCKSおよび非リン酸化MARCKSの量として、検体中の全タンパク質濃度で正規化した値を用いる場合、DO値のカットオフ値は、50~55(ppm)となり、感度は、0.8~1.0となり、特異性は0.8以上、好ましくは0.8となる。
また、あらかじめ健常人の検体中の検体中のpSer46-MARCKSの量と非リン酸化MARCKSの量を測定しておき、健常人についてDO値を算出し、該算出値に基づいてDO値についてカットオフ値(閾値)を定めておいてもよい。該カットオフ値を基準としDO値がカットオフ値を超えた場合に、該被験体においてアルツハイマー病(AD)、前頭側頭葉変性症(FTLD)または筋萎縮性側索硬化症(ALS)等の神経変性症が検出されたと、すなわち、該被験体は神経変性疾患に罹患しているか、あるいは神経変性疾患を発症するリスクがあると判断することができる。
さらに、アルツハイマー病(AD)および前頭側頭葉変性症(FTLD)において、疾患の重篤度とDO値は関連しており、DO値が高いほど疾患の重篤度が高いと判断することができる。
PD(パーキンソン病)およびDLB(レビー小体型認知症)においても、アルツハイマー病(AD)および前頭側頭葉変性症(FTLD)と同様に脳組織中のpSer46 -MARCKSレベルは上昇する。従って、PD(パーキンソン病)およびDLB(レビー小体型認知症)においても検体中のpSer46 -MARCKSレベル上昇により、神経変性を検出し、重症度を反映できる。
3.神経変性疾患の治療
本発明の方法で神経変性疾患が検出された場合、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)、パーキンソン病(PD)またはレビー小体型認知症(DLB)は以下の方法により治療あるいは症状の改善ができる可能性がある。
本発明の方法で神経変性疾患が検出された場合、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)、筋萎縮性側索硬化症(ALS)、パーキンソン病(PD)またはレビー小体型認知症(DLB)は以下の方法により治療あるいは症状の改善ができる可能性がある。
アルツハイマー病(AD)
ドネペジル、リバスチグミン、ガランタミン、メマンチンなどのニューロン間の情報伝達を促進する医薬の投与、脳からアルツハイマー病の原因とされるアミロイドβを除去し得るバピネオズマブ(Bapineuzumab)やソラネズマブ(Solanezumab)のような抗体医薬の投与等による治療。
ドネペジル、リバスチグミン、ガランタミン、メマンチンなどのニューロン間の情報伝達を促進する医薬の投与、脳からアルツハイマー病の原因とされるアミロイドβを除去し得るバピネオズマブ(Bapineuzumab)やソラネズマブ(Solanezumab)のような抗体医薬の投与等による治療。
前頭側頭葉変性症(FTLD)
選択的セロトニン再取り込み阻害薬の投与、原因遺伝子とされるタウ遺伝子、TDP-43遺伝子、プログラニュリン遺伝子などの遺伝子を標的とした治療。
選択的セロトニン再取り込み阻害薬の投与、原因遺伝子とされるタウ遺伝子、TDP-43遺伝子、プログラニュリン遺伝子などの遺伝子を標的とした治療。
筋萎縮性側索硬化症(ALS)
リルゾール、エダラボン、メチルコバラミン、レチガビン、BIIB067、MN-166などの医薬の投与、原因遺伝子として報告されているSOD1遺伝子、TDP-43遺伝子、FUS遺伝子、C9orf72遺伝子等の遺伝子を標的とした治療、ヒト多能性幹細胞を用いて神経細胞を再生させる再生治療等による治療。
リルゾール、エダラボン、メチルコバラミン、レチガビン、BIIB067、MN-166などの医薬の投与、原因遺伝子として報告されているSOD1遺伝子、TDP-43遺伝子、FUS遺伝子、C9orf72遺伝子等の遺伝子を標的とした治療、ヒト多能性幹細胞を用いて神経細胞を再生させる再生治療等による治療。
パーキンソン病(PD)
薬物治療、外科治療、理学療法があり、薬物治療としてL-ドパとドパミンアゴニストの内服、外科治療として脳深部刺激療法(視床下核刺激術、淡蒼球刺激術、視床刺激術)と定位的破壊術(視床破壊術、淡蒼球破壊術)または脳深部刺激療法(DBS)。
薬物治療、外科治療、理学療法があり、薬物治療としてL-ドパとドパミンアゴニストの内服、外科治療として脳深部刺激療法(視床下核刺激術、淡蒼球刺激術、視床刺激術)と定位的破壊術(視床破壊術、淡蒼球破壊術)または脳深部刺激療法(DBS)。
レビー小体型認知症(DLB)
ドネペジルなどの医薬の投与。
ドネペジルなどの医薬の投与。
本発明を以下の実施例によって具体的に説明するが、本発明はこれらの実施例によって限定されるものではない。
[実施例1] アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)および筋萎縮性側索硬化症(ALS)についての検討
方法
ヒト患者
名古屋大学および東北大学において、臨床症状、電気生理学的検査、MRI、SPECTおよびPETを含む神経イメージングにより診断された8人のAD患者、7人のFTLD患者および10人のALS患者からの脳脊髄液を使用した。
方法
ヒト患者
名古屋大学および東北大学において、臨床症状、電気生理学的検査、MRI、SPECTおよびPETを含む神経イメージングにより診断された8人のAD患者、7人のFTLD患者および10人のALS患者からの脳脊髄液を使用した。
対照被験体は、男性6名(平均年齢72.6歳、55~83歳)および女性4名(平均年齢75.5歳、69~79歳)であった。ミニメンタルステート検査(MMSE)スコアは、脳脊髄液(CSF)を採取した時点で25以上(平均28.3、26~30)であった。AD患者は男性2名(54歳および80歳)および女性6名(平均64.5歳、57~75歳)であった。これらの患者のMMSEスコアは25を超えず(平均17.1、4~25)、FABスコアの平均および範囲は9.3および6~13であった。FTLD患者は男性5人、女性2人であった。これらの患者のMMSEスコアの平均および範囲は18.1および7~30であり、FABスコアの平均および範囲は8.6および3~16であった。ALS患者は男性8人、女性2人であった。これらの患者のALSFR-Rスコアの平均および範囲は40.5および24~47であった。9例のALS症例が「確定」と診断され、1例が「可能性のある」ALS症例と診断された。
サンプルの調製
プロテオーム分析のために、脳脊髄液(CSF)から試料を調製した。すなわち、ヒト患者由来の脳脊髄液50μlを、100mM Tris-HCl(pH7.5)、2%SDSおよび1mM DTTを含有する5μlの緩衝液に添加し、100℃で15分間インキュベートした。
プロテオーム分析のために、脳脊髄液(CSF)から試料を調製した。すなわち、ヒト患者由来の脳脊髄液50μlを、100mM Tris-HCl(pH7.5)、2%SDSおよび1mM DTTを含有する5μlの緩衝液に添加し、100℃で15分間インキュベートした。
サンプル溶液を16,000g、4℃で10分間遠心分離し、上清を0.22μmPVDFフィルター(Millipore)を用いて濾過した。アリコート(55μL)を25μLの1Mトリエチルアンモニウム重炭酸塩(TEAB)(pH8.5)、0.75μLの10%SDSおよび7.5μLの50mMトリス-2-カルボキシエチルホスフィンに添加し、60℃で1時間インキュベートした。システイン残基を10mMメチルメタンチオスルホネートを用いて10分間25℃でブロックした。次いで、サンプルを24mM CaCl2中の1.5μgのトリプシン(10:1=タンパク質:酵素、w/w)で37℃で24時間消化し、C18スピンカラム(MonoSpin C18、GL Sciences Inc.)により脱塩し、乾燥させ、0.1%ギ酸35μlに溶解した。
SWATH-脳脊髄液の質量分析
溶液A(0.1%ギ酸)を含むC18カラム(0.1mm×100mm、KYA Technologies Corporation)に30μlのアリコートを2~41%の溶液AおよびBの勾配(99.9%アセトニトリルおよび0.1%ギ酸)中で300nl /分の流速でEksigent NanoLC-Ultra 1D Plusシステム(Sciex Inc.)で分析し、2.3kVのイオンスプレー電圧でTriple TOF 5600システム(Sciex)に供した。IDA(information-dependent acquisition)は、2~5回の荷電で400~1000m/zに設定し、生成イオンのMS/MSスキャン範囲は100~1600Daであり、スペクトルライブラリーの蓄積時間は100msであった。SWATH(登録商標)(sequential window acquisition of all theoretical mass spectra)は、400Daから1000Daにまたがる25Daの24の連続ウィンドウによって行われた。MS/MSスペクトルデータのSWATH取得をAnalyst TF1.6ソフトウェア(Sciex Inc.)により100ms /ウィンドウで行い、MS/MSスペクトルライブラリーをProtein Pilotソフトウェア(バージョン4.5)により調製した。MS/MSスペクトルデータは、Peakviewソフトウェア(バージョン1.2.0.3、Sciex Inc.)を用いて、ペプチドデータおよびLC保持時間と相関させた。同じペプチドからのMS/MS生成物イオンを合計し、ペプチドの量として使用した。
溶液A(0.1%ギ酸)を含むC18カラム(0.1mm×100mm、KYA Technologies Corporation)に30μlのアリコートを2~41%の溶液AおよびBの勾配(99.9%アセトニトリルおよび0.1%ギ酸)中で300nl /分の流速でEksigent NanoLC-Ultra 1D Plusシステム(Sciex Inc.)で分析し、2.3kVのイオンスプレー電圧でTriple TOF 5600システム(Sciex)に供した。IDA(information-dependent acquisition)は、2~5回の荷電で400~1000m/zに設定し、生成イオンのMS/MSスキャン範囲は100~1600Daであり、スペクトルライブラリーの蓄積時間は100msであった。SWATH(登録商標)(sequential window acquisition of all theoretical mass spectra)は、400Daから1000Daにまたがる25Daの24の連続ウィンドウによって行われた。MS/MSスペクトルデータのSWATH取得をAnalyst TF1.6ソフトウェア(Sciex Inc.)により100ms /ウィンドウで行い、MS/MSスペクトルライブラリーをProtein Pilotソフトウェア(バージョン4.5)により調製した。MS/MSスペクトルデータは、Peakviewソフトウェア(バージョン1.2.0.3、Sciex Inc.)を用いて、ペプチドデータおよびLC保持時間と相関させた。同じペプチドからのMS/MS生成物イオンを合計し、ペプチドの量として使用した。
質量データ分析
PeavView1.2ソフトウェアのSWATH 1.0アプリケーションを使用して、抽出されたイオンクロマトグラム(XIC)抽出ウィンドウの5分間およびXIC幅の0.01Daの条件で、MS/MSスペクトル生データを処理し、明確に同定された種のスペクトルを抽出した。XICは、小さなm/z範囲において、LC保持時間および相対イオン強度のグラフに示される曲線として示された。フラグメントイオンXICを合計してペプチドピーク領域を得、タンパク質当たりの複数のペプチドの面積を合計してタンパク質面積を得た。ペプチドの質量スペクトルデータは、個々の被験体ごとに、検出されたすべてのタンパク質の総量またはMARCKSタンパク質と相関するペプチドの総量によって正規化された(これらはそれぞれ、「全タンパク質」または「総MARCKS」と呼ぶ)。感度および特異性を計算するために、異常なリン酸化を対照群の平均量±2SDにより判定した。
PeavView1.2ソフトウェアのSWATH 1.0アプリケーションを使用して、抽出されたイオンクロマトグラム(XIC)抽出ウィンドウの5分間およびXIC幅の0.01Daの条件で、MS/MSスペクトル生データを処理し、明確に同定された種のスペクトルを抽出した。XICは、小さなm/z範囲において、LC保持時間および相対イオン強度のグラフに示される曲線として示された。フラグメントイオンXICを合計してペプチドピーク領域を得、タンパク質当たりの複数のペプチドの面積を合計してタンパク質面積を得た。ペプチドの質量スペクトルデータは、個々の被験体ごとに、検出されたすべてのタンパク質の総量またはMARCKSタンパク質と相関するペプチドの総量によって正規化された(これらはそれぞれ、「全タンパク質」または「総MARCKS」と呼ぶ)。感度および特異性を計算するために、異常なリン酸化を対照群の平均量±2SDにより判定した。
免疫組織化学法
免疫組織化学法のために、パラフィン包埋したヒト脳切片を脱パラフィンし、再水和させ、10mMクエン酸緩衝液(pH6.0、100℃)中で5回マイクロ波処理し、次いでPBSで5分間、2回洗浄した。ブロッキング(10%FBS、60分間)後、切片を2%FBSおよび0.1%Triton X-100を含有するPBSおよび一次抗体:ウサギ抗ホスホ-TDP43(pS409 / 410-2)(1:4000、Cosmo Bio Co.,LTD、TIP-PTD-P02)、ウサギ抗ホスホ-MARCKS(Ser46)(1:1000、GL Biochem(Shanghai)Ltd.)、マウス抗MAP2(AP20)(1:100、Santa Cruz Biotechnology)と4℃で一晩または二晩、最後に二次抗体:Alexa Fluor 488標識抗マウスIgG(1:1000、Invitrogen)、Cy3標識抗ウサギIgG(1:500、Jackson ImmunoResearch)、ビオチン化抗ウサギIgG(1:200、Vector Laboratories、BA-10009)、ビオチン化抗マウスIgG(1:200、Vector Laboratories、BA-2000)と室温(RT)で60分間、インキュベートした。pSer46-MARCKS抗体を作製した。同様の宿主種(ウサギ抗ホスホ-MARCKSおよび抗ホスホ-TDP43抗体)由来の一次抗体を、Zenon Rabbit IgG Labeling Kits(Thermo Fisher Scientific、IL)によって標識し、二重免疫染色に使用した。ホスホ-TDP43またはMAP2の酵素的検出のために、VECTASTAIN Elite ABC標準キット(Vector Laboratories、PK-6100 CA)およびDABペルオキシダーゼ基質キット(Vector Laboratories、SK-4100)を使用した。DAB染色の場合、切片を、Carrazzi's Hematoxylin溶液(1.15938.0025、Merck)を用いて室温で10分間対比染色し、水道水で10分間洗浄し、室温で5分間エオシン溶液(80%エタノールで希釈した0.25%エオシン、Wako)で染色し、エタノールで脱水した。キシレンで洗浄した後、切片を覆った。核はDAPI(同仁研究所、D523)で染色した。画像は、共焦点顕微鏡(Olympus、FV1200 IX83)および光学顕微鏡(Olympus、BX53)により得られた。
免疫組織化学法のために、パラフィン包埋したヒト脳切片を脱パラフィンし、再水和させ、10mMクエン酸緩衝液(pH6.0、100℃)中で5回マイクロ波処理し、次いでPBSで5分間、2回洗浄した。ブロッキング(10%FBS、60分間)後、切片を2%FBSおよび0.1%Triton X-100を含有するPBSおよび一次抗体:ウサギ抗ホスホ-TDP43(pS409 / 410-2)(1:4000、Cosmo Bio Co.,LTD、TIP-PTD-P02)、ウサギ抗ホスホ-MARCKS(Ser46)(1:1000、GL Biochem(Shanghai)Ltd.)、マウス抗MAP2(AP20)(1:100、Santa Cruz Biotechnology)と4℃で一晩または二晩、最後に二次抗体:Alexa Fluor 488標識抗マウスIgG(1:1000、Invitrogen)、Cy3標識抗ウサギIgG(1:500、Jackson ImmunoResearch)、ビオチン化抗ウサギIgG(1:200、Vector Laboratories、BA-10009)、ビオチン化抗マウスIgG(1:200、Vector Laboratories、BA-2000)と室温(RT)で60分間、インキュベートした。pSer46-MARCKS抗体を作製した。同様の宿主種(ウサギ抗ホスホ-MARCKSおよび抗ホスホ-TDP43抗体)由来の一次抗体を、Zenon Rabbit IgG Labeling Kits(Thermo Fisher Scientific、IL)によって標識し、二重免疫染色に使用した。ホスホ-TDP43またはMAP2の酵素的検出のために、VECTASTAIN Elite ABC標準キット(Vector Laboratories、PK-6100 CA)およびDABペルオキシダーゼ基質キット(Vector Laboratories、SK-4100)を使用した。DAB染色の場合、切片を、Carrazzi's Hematoxylin溶液(1.15938.0025、Merck)を用いて室温で10分間対比染色し、水道水で10分間洗浄し、室温で5分間エオシン溶液(80%エタノールで希釈した0.25%エオシン、Wako)で染色し、エタノールで脱水した。キシレンで洗浄した後、切片を覆った。核はDAPI(同仁研究所、D523)で染色した。画像は、共焦点顕微鏡(Olympus、FV1200 IX83)および光学顕微鏡(Olympus、BX53)により得られた。
Nissl染色
ヒト脳のパラフィン包埋切片を脱パラフィンし、再水和した。蒸留水で洗浄した後、切片をクレシルバイオレット溶液(300mLの0.1%クレシルバイオレットを蒸留水に5滴の10%酢酸溶液と共に加え、次いで使用前に濾過した)を37℃で15分間浸漬した。次いで、切片をエタノールで脱水し、キシレンで洗浄し、カバーガラスで覆った。画像は光学顕微鏡(Olympus、BX53)により得た。
ヒト脳のパラフィン包埋切片を脱パラフィンし、再水和した。蒸留水で洗浄した後、切片をクレシルバイオレット溶液(300mLの0.1%クレシルバイオレットを蒸留水に5滴の10%酢酸溶液と共に加え、次いで使用前に濾過した)を37℃で15分間浸漬した。次いで、切片をエタノールで脱水し、キシレンで洗浄し、カバーガラスで覆った。画像は光学顕微鏡(Olympus、BX53)により得た。
数値シミュレーション
正常の上限の数値シミュレーションで最大化するためのパラメータとして、3つの疾患(各疾患において最大= 1.0、3つの疾患において最大= 3.0)からの感度値および3つの疾患(3つの疾患の代表として最大= 1.0)によって共有される特異値の3つの疾患の合計を採用した。また、Rプログラム言語(バージョン3.4.0、R統計学コンピューティング、https://www.R-project.org/)を使用したオリジナルの数値シミュレーションプログラムを開発し、パラメータを最大化する正常の上限を最適化した。DO値とそのカテゴリーの主部をプログラムに入れた。最初の試行では、本質的な解析範囲を決定するためにプログラムを実行し、3つの疾患の感度スコアが0になったときのシミュレーションのDOの上限を1,000と決定した。この範囲内で、数値シミュレーションを繰り返して客観的スコアを最大化する最適なDOを見出した。
正常の上限の数値シミュレーションで最大化するためのパラメータとして、3つの疾患(各疾患において最大= 1.0、3つの疾患において最大= 3.0)からの感度値および3つの疾患(3つの疾患の代表として最大= 1.0)によって共有される特異値の3つの疾患の合計を採用した。また、Rプログラム言語(バージョン3.4.0、R統計学コンピューティング、https://www.R-project.org/)を使用したオリジナルの数値シミュレーションプログラムを開発し、パラメータを最大化する正常の上限を最適化した。DO値とそのカテゴリーの主部をプログラムに入れた。最初の試行では、本質的な解析範囲を決定するためにプログラムを実行し、3つの疾患の感度スコアが0になったときのシミュレーションのDOの上限を1,000と決定した。この範囲内で、数値シミュレーションを繰り返して客観的スコアを最大化する最適なDOを見出した。
統計的解析
疾患群と対照群との間の生物学的距離をウィルコクソンの順位和検定によって試験した。各被験体におけるpSer46と非リン酸化ペプチドとの間の相関を評価するために、ピアソンの相関係数を算出した。Pearsonの相関係数を用いて、各被験体におけるHMGB1濃度とpSer46-MARCKSシグナルとの相関も算出した。
疾患群と対照群との間の生物学的距離をウィルコクソンの順位和検定によって試験した。各被験体におけるpSer46と非リン酸化ペプチドとの間の相関を評価するために、ピアソンの相関係数を算出した。Pearsonの相関係数を用いて、各被験体におけるHMGB1濃度とpSer46-MARCKSシグナルとの相関も算出した。
結果
神経変性疾患の脳脊髄液(CSF)におけるpSer46-MARCKS
質量分析を用いて、ヒトの患者から、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)および筋萎縮性側索硬化症(ALS)の3つの神経変性疾患のヒト患者由来の脳脊髄液(CSF)のpSer46-MARCKSを定量した、ならびに対照から定量化した。疾患群または個々の被験体におけるリン酸化ペプチドの相対量を比較するために、各被験体について、質量分析で検出された全タンパク質の量または総MARCKSタンパク質によって量を正規化した。ペプチドは、95%以上の信頼性で決定された。
神経変性疾患の脳脊髄液(CSF)におけるpSer46-MARCKS
質量分析を用いて、ヒトの患者から、アルツハイマー病(AD)、前頭側頭葉変性症(FTLD)および筋萎縮性側索硬化症(ALS)の3つの神経変性疾患のヒト患者由来の脳脊髄液(CSF)のpSer46-MARCKSを定量した、ならびに対照から定量化した。疾患群または個々の被験体におけるリン酸化ペプチドの相対量を比較するために、各被験体について、質量分析で検出された全タンパク質の量または総MARCKSタンパク質によって量を正規化した。ペプチドは、95%以上の信頼性で決定された。
脳脊髄液(CSF)のpSer46-MARCKSを診断のためのバイオマーカーとして評価するために、3つの疾患群における全タンパク質(図1-1AおよびB)または総MARCKSタンパク質(図1-2AおよびB)によって正規化されたpSer46-MARCKSの感度および特異性を計算した。図1-1AはpSer46-MARCKSの値を各疾患群ごとにプロットした図であり、値はそれぞれの被験体の全タンパク質量により正規化してある。図1-2AはpSer46-MARCKSの値を各疾患群ごとにプロットした図であり、値はそれぞれの被験体の総MARCKSタンパク質量により正規化してある。図1-1Aおよび図1-2Aの下の長方形のボックス部分は対照群の平均数±2SDを示し、ボックス中の線は健常対照の平均を示す。図1-1Bおよび1-2Bは、感度および特異性を示す。患者の値が対照群の平均+ 2SDを超えたときに異常と判断した。この状態では、神経変性疾患の3つのグループすべてにおいてpSer46-MARCKSの特異性が非常に高いことが判明した(図1-1Bおよび図1-2B)。これは、pSer46-MARCKSが対照の平均+ 2SDを上回った場合、被験体は確実に異常であることを意味する。
一方、診断のためのpSer46-MARCKSの感度は、すべての疾患群において比較的低かった。pSer46-MARCKSがタンパク質全体で正規化された場合、感度はADでは0.50、FTLDでは0.57、ALSでは0.40であった(図1-1B)。総MARCKSにより正規化されたpSer46-MARCKSの場合、値はより小さかった(図1-2B)。したがって、この分析段階では、疾患特異的バイオマーカーまたはスクリーニングバイオマーカーではなく進行バイオマーカーのように、pSer46-MARCKSの使用を制限することが適切であると考えられた。
同様の方法で、3つの神経変性疾患(図2-1および2-2)のヒト患者由来の脳脊髄液(CSF)の非リン酸化MARCKSを定量した。図2-1Aは各疾患群の非リン酸化MARCKSの量をプロットした図であり、値は全タンパク質により正規化してある。図2-2Aは各疾患群の非リン酸化MARCKSの量をプロットした図であり、値は総MARCKSタンパク質量により正規化してある。図2-1Aおよび図2-2Aの下の長方形のボックス部分は対照群の平均数±2SDを示し、ボックス中の線は健常対照の平均を示す。図2-1Bおよび2-2Bは、感度および特異性を示す。この場合、ADおよびALSでは特異性が100%に達しておらず、感度は0であった。したがって、非リン酸化MARCKS単独は、明らかに診断バイオマーカーには適していなかった。
脳脊髄液(CSF)のpSer46-MARCKSのAD、FTLDおよびALSにおける上昇
次に、疾患群と対照との間のpSer46-MARCKSの値を比較した。図3-1に各被験体のpSer46-MARCKSの量を、図3-2に各被験体の非リン酸化MARCKSの量を示す。図3-1Aおよび3-2Aの量は全タンパク質量により正規化し、図3-1Bおよび3-2Bの量は総MARCKS量で正規化した。図中の線は各群の中央値を示す。疾患群で認められた以上に高い値を考慮し、各群の値を比較するためにノンパラメトリックなウィルコクソンの順位和検定を行い、AD患者と対照(p = 0.02941)、FTLDと対照(p = 0.00358)、およびALSと対照(p = 0.0007)の間に統計的な差があることを見出した(図3-1A)。pSer46-MARCKSの正規化の方法によって結果は変わったが、pSer46-MARCKSを総MARCKS(図3-1B)で正規化すると、FTLD患者と対照(p = 0.0128)の差は維持された。さらに、非リン酸化MARCKSの値は、AD患者と対照(p = 0.0455)およびALS患者と対照(p = 0.0212)の間で、全タンパク質によって値が正規化された場合にも統計的に差があることがわかった(図3-2A)。さらに、総MARCSによって値が正規化された場合にFTLD患者と対照(p = 0.0217)との間で統計的に差があることがわかった(図3-2B)。
次に、疾患群と対照との間のpSer46-MARCKSの値を比較した。図3-1に各被験体のpSer46-MARCKSの量を、図3-2に各被験体の非リン酸化MARCKSの量を示す。図3-1Aおよび3-2Aの量は全タンパク質量により正規化し、図3-1Bおよび3-2Bの量は総MARCKS量で正規化した。図中の線は各群の中央値を示す。疾患群で認められた以上に高い値を考慮し、各群の値を比較するためにノンパラメトリックなウィルコクソンの順位和検定を行い、AD患者と対照(p = 0.02941)、FTLDと対照(p = 0.00358)、およびALSと対照(p = 0.0007)の間に統計的な差があることを見出した(図3-1A)。pSer46-MARCKSの正規化の方法によって結果は変わったが、pSer46-MARCKSを総MARCKS(図3-1B)で正規化すると、FTLD患者と対照(p = 0.0128)の差は維持された。さらに、非リン酸化MARCKSの値は、AD患者と対照(p = 0.0455)およびALS患者と対照(p = 0.0212)の間で、全タンパク質によって値が正規化された場合にも統計的に差があることがわかった(図3-2A)。さらに、総MARCSによって値が正規化された場合にFTLD患者と対照(p = 0.0217)との間で統計的に差があることがわかった(図3-2B)。
pSer46-MARCKSと非リン酸化MARCKSの関係
次に、各群におけるpSer46-MARCKSと非リン酸化MARCKSとの関係(比)を解析した(図4-1~4-3)。図4-1はAD、FTLDおよびALS疾患群のそれぞれについて、全タンパク質量で正規化した値をプロットした図であり、図4-2は図4-1のそれぞれのプロットをマージした図である。図4-3はAD、FTLDおよびALS疾患群のそれぞれについて、総MARCKS量で正規化した値をプロットした図であり、図4-4は図4-3のそれぞれのプロットをマージした図である。対照群は、pSer46-MARCKSと非リン酸化MARCKS(図4-1および4-3)との間に明らかな正の関係を示したが、AD群は弱い負の関係を示し、FTLDおよびALS群はいずれの関係も示さなかった。この結果は、Ser46におけるMARCKSのリン酸化が、ADおよびFTLDにおいて病理学的に影響を受けることを意味し得る。
次に、各群におけるpSer46-MARCKSと非リン酸化MARCKSとの関係(比)を解析した(図4-1~4-3)。図4-1はAD、FTLDおよびALS疾患群のそれぞれについて、全タンパク質量で正規化した値をプロットした図であり、図4-2は図4-1のそれぞれのプロットをマージした図である。図4-3はAD、FTLDおよびALS疾患群のそれぞれについて、総MARCKS量で正規化した値をプロットした図であり、図4-4は図4-3のそれぞれのプロットをマージした図である。対照群は、pSer46-MARCKSと非リン酸化MARCKS(図4-1および4-3)との間に明らかな正の関係を示したが、AD群は弱い負の関係を示し、FTLDおよびALS群はいずれの関係も示さなかった。この結果は、Ser46におけるMARCKSのリン酸化が、ADおよびFTLDにおいて病理学的に影響を受けることを意味し得る。
もう1つの注目すべき点は、疾患群のプロットが、ほとんどが座標グラフ(x、y =非リン酸化MARCKS、pSer46-MARCKS)の対照群から決定された回帰直線の上に位置することであった(図4-2および4-4)。これは、pSer46-MARCKSが全タンパク質または全MARCKS(図4-1~4-4)のどちらによって正規化されたかどうかにかかわらず、AD、FTLDおよびALS患者において、非リン酸化MARCKSに対するpSer46-MARCKSの比が増加する傾向を有することを意味する。これらの分析に基づいて、非リン酸化MARCKSに対するpSer46-MARCKSの比が病理学的変化のバイオマーカーとなり得るかどうかを試験した。しかし、群間の差は統計的に有意ではなかった(図4-1~4-4)。スコアの相違が大きかったので(図4-1~4-4)、これは、初期および後期の疾患相が混在した患者群の不均一性に起因する可能性がある。
脳脊髄液(CSF)におけるHMGB1とpSer46-MARCKSとの関係
本発明者らは以前に、ダメージ関連分子パターン(DAMP)に属する代表的な分子であるHMGB1が、TLR4のシグナル伝達経路の下流のSer46でMARCKSリン酸化を誘発し、HMGB1に対する抗体がAD13の発症を遅らせる可能性があることを明らかにした。一連のアイデアに基づき、以前のデータを用いて、AD患者の脳脊髄液(CSF)におけるHMGB1とpSer46-MARCKSとの関係を試験した(図5-1および5-2)。図5-1は全タンパク質量に対するpSer46-MARCKSであり、図5-2は総MARCKS量に対するpSer46-MARCKSである。HMGB1およびpSer46-MARCKSに関する仮説が実際にインビボで適用されるかどうかを知るために、以前に公表されたデータ(別の試験者による)による遡及分析は非バイアス試験でなければならない。
本発明者らは以前に、ダメージ関連分子パターン(DAMP)に属する代表的な分子であるHMGB1が、TLR4のシグナル伝達経路の下流のSer46でMARCKSリン酸化を誘発し、HMGB1に対する抗体がAD13の発症を遅らせる可能性があることを明らかにした。一連のアイデアに基づき、以前のデータを用いて、AD患者の脳脊髄液(CSF)におけるHMGB1とpSer46-MARCKSとの関係を試験した(図5-1および5-2)。図5-1は全タンパク質量に対するpSer46-MARCKSであり、図5-2は総MARCKS量に対するpSer46-MARCKSである。HMGB1およびpSer46-MARCKSに関する仮説が実際にインビボで適用されるかどうかを知るために、以前に公表されたデータ(別の試験者による)による遡及分析は非バイアス試験でなければならない。
HMGB1-ELISA感度の閾値という技術的限界があり、HMGB1値はほとんどの患者で検出レベル以下であったが、AD患者の脳脊髄液(CSF)とPSER46-MARCKSの間に明らかに予想したよりも大きな正の相関が見られた(図5-1および5-2)。
ヒトFTLDの変性神経突起中でのpSer46-MARCKSの上昇
次に、ADマウスモデルおよびADヒト患者において、変性神経突起のようなヒトFTLD脳における神経突起においてpSer46-MARCKSが増加したかどうかを試験した(Fujita, K. et al.,Sci. Rep. 6, 31895 (2016))。病理学的に診断されたヒトFTLDの脳(図6-1)を抗pSer46-MARCKS抗体による免疫組織化学法に用いた(図6-2AおよびB)。図6-1はヒトFTLDのpTDP-43染色像であり、TDP43染色により、TDP43の異常な分布およびTDP43の細胞質封入が明らかになった。また、図6-2AおよびBは、抗pSer46-MARCKS抗体による免疫組織化学法を示す。図6-2Aに示すように、FTLD後頭葉(後頭皮質)および前頭葉(前頭皮質)における神経突起変性が認められた(第IV層)。また、後頭葉の頂端の樹状突起および細胞体はよく染色されていた。しかし、図6-2Bに示すように、最も重篤に冒された前頭葉では染色はほとんど認められなかった。抗pSer46-MARCKS抗体と二次Cy3標識抗ウサギIgG抗体を用いて単一染色した後、552nmの励起光および570nmの蛍光で可視であったが、498nmの励起光および520nmの蛍光(図6-2B)、または552nmの励起光および520nmの蛍光(データは示されていない)では可視でなく、これは、これは染色が特異的であり、自己蛍光が発せられなかったことを示している。染色パターンは先の報告(Fujita, K. et al., Sci. Rep. 6, 31895 (2016))におけるヒトADの染色に非常に類似していた。FTLDにおいては比較的免れていた後頭葉において、pSer46-MARCKS陽性神経突起が頻繁に観察されたが、最も強く影響を受けた前頭葉ではほとんど観察されなかった。この議論を引き起こす発見は、pSer46-MARCKSは初期段階特異的マーカーであり、病期が進むと消失することを示している。図6-3AはヒトFTLD後頭葉におけるMAP2およびpSer46-MARCKSの共染色の結果を示し、抗pSer46-MARCKS抗体によってニューロンが染色された。ヒトFTLDの脳において、pSer46-MARCKSによって染色された突起および細胞体は、MAP2についても陽性であり、このことはそれらがニューロンおよび神経突起であることを示している(図6-3A)。次に、pSer46-MARCKS陽性細胞が、凝集体を有するニューロンまたはTDP43の異常な細胞質分布を示すことを確認した。すなわち、図6-3Bは、細胞質リン酸化TDP43を有するニューロンはpSer46-MARCKと共染色されたことを示す。興味深いことに、pSer46-MARCKSおよびリン酸TDP43は、細胞質凝集体で共染色された(図6-3C)。
次に、ADマウスモデルおよびADヒト患者において、変性神経突起のようなヒトFTLD脳における神経突起においてpSer46-MARCKSが増加したかどうかを試験した(Fujita, K. et al.,Sci. Rep. 6, 31895 (2016))。病理学的に診断されたヒトFTLDの脳(図6-1)を抗pSer46-MARCKS抗体による免疫組織化学法に用いた(図6-2AおよびB)。図6-1はヒトFTLDのpTDP-43染色像であり、TDP43染色により、TDP43の異常な分布およびTDP43の細胞質封入が明らかになった。また、図6-2AおよびBは、抗pSer46-MARCKS抗体による免疫組織化学法を示す。図6-2Aに示すように、FTLD後頭葉(後頭皮質)および前頭葉(前頭皮質)における神経突起変性が認められた(第IV層)。また、後頭葉の頂端の樹状突起および細胞体はよく染色されていた。しかし、図6-2Bに示すように、最も重篤に冒された前頭葉では染色はほとんど認められなかった。抗pSer46-MARCKS抗体と二次Cy3標識抗ウサギIgG抗体を用いて単一染色した後、552nmの励起光および570nmの蛍光で可視であったが、498nmの励起光および520nmの蛍光(図6-2B)、または552nmの励起光および520nmの蛍光(データは示されていない)では可視でなく、これは、これは染色が特異的であり、自己蛍光が発せられなかったことを示している。染色パターンは先の報告(Fujita, K. et al., Sci. Rep. 6, 31895 (2016))におけるヒトADの染色に非常に類似していた。FTLDにおいては比較的免れていた後頭葉において、pSer46-MARCKS陽性神経突起が頻繁に観察されたが、最も強く影響を受けた前頭葉ではほとんど観察されなかった。この議論を引き起こす発見は、pSer46-MARCKSは初期段階特異的マーカーであり、病期が進むと消失することを示している。図6-3AはヒトFTLD後頭葉におけるMAP2およびpSer46-MARCKSの共染色の結果を示し、抗pSer46-MARCKS抗体によってニューロンが染色された。ヒトFTLDの脳において、pSer46-MARCKSによって染色された突起および細胞体は、MAP2についても陽性であり、このことはそれらがニューロンおよび神経突起であることを示している(図6-3A)。次に、pSer46-MARCKS陽性細胞が、凝集体を有するニューロンまたはTDP43の異常な細胞質分布を示すことを確認した。すなわち、図6-3Bは、細胞質リン酸化TDP43を有するニューロンはpSer46-MARCKと共染色されたことを示す。興味深いことに、pSer46-MARCKSおよびリン酸TDP43は、細胞質凝集体で共染色された(図6-3C)。
ヒトFTLDのニッスル(Nissl)染色では、前頭葉のニューロンをほとんど検出できず、液胞塊では海綿状の変性しか認められなかった(図7A)。一方、後頭葉には染色質融解や無色素などの異常な特徴を持つニューロンが認められた(図7B)。神経変性疾患ではない対照の脳では、ニューロン密度および神経網の形態等について、このような異常な変化は見られなかった(図7C)。
バイオマーカーとしてのpSer46-MARCKSと非リン酸化MARCKSの統合値
プロットグラフ(図4-2および4-4)を見ると、対照被験体の(x、y)座標位置は原点(0,0)に比較的近いことがわかる。したがって、pSer46-MARCKSと非リン酸化型MARCKSを統合した変化の程度が、病理学的変化を正常対照と区別すると予測し、対照および疾患におけるpSer46-MARCKSの2乗+非リン酸化MARCKSの2乗の平方根(DO:Distance from origin)を算出した(図8-1)。すなわち、対照群と比較して3つの神経変性疾患群でDO値が統計的に増加し、Wilcoxson検定による差異が確認された(図8-2)。例外的に、一人の対照被験体は大きなDOを有していた。被験体は、ADASスコアの急激な低下(-3.216949153 /年)から判断すると、認知症の前臨床段階にある可能性がある。
プロットグラフ(図4-2および4-4)を見ると、対照被験体の(x、y)座標位置は原点(0,0)に比較的近いことがわかる。したがって、pSer46-MARCKSと非リン酸化型MARCKSを統合した変化の程度が、病理学的変化を正常対照と区別すると予測し、対照および疾患におけるpSer46-MARCKSの2乗+非リン酸化MARCKSの2乗の平方根(DO:Distance from origin)を算出した(図8-1)。すなわち、対照群と比較して3つの神経変性疾患群でDO値が統計的に増加し、Wilcoxson検定による差異が確認された(図8-2)。例外的に、一人の対照被験体は大きなDOを有していた。被験体は、ADASスコアの急激な低下(-3.216949153 /年)から判断すると、認知症の前臨床段階にある可能性がある。
病理学的DO値を正常DO値と効率的に区別するために、最大感度および特異性の両方を生み出すことができる「DOの正常の上限」が必要であった。数値シミュレーションにより最良の「DOの正常の上限」を探索した(図8-1)。ここでは、3つの疾患の感度(各疾患において最大= 1.0、したがって3つの疾患において最大=3.0)と3つの疾患に共通する特異性(3つの疾患の代表として最大=1.0)の合計である「客観的スコア(objective score)」という別のパラメータを使用し、最も高い客観的スコアを生成するDOの範囲を見つけようとした(図8-1)。図8-1のグラフは、0~1000までのDOの客観的スコアを示している。その結果、上限値が50.26から54.24の場合のDOにおいて、3.532という最高の客観的スコアが得られることがわかった(図8-1および8-2)。図8-2は、各疾患におけるDO値を示す。図中、DO値をボックスプロットで示した。正常の上限は数値シミュレーションによって決定した。各グループのボックスは、下位から上位の値を表わす。中央値もボックス内に表示されている。図8-3はコントロール、AD、FTLD、ALS群で異常と判断された症例数、対象スコアとDO範囲での最大限の最適化時の感度と特異度の値を示す。図8-1の閾値は、50.262のDOで一時的に示されたが、50.262から54.239のDOの範囲では感度および特異度は変化しなかった。図8-3に示すように、正常値の上限を50.26に設定することで、AD、FTLD、ALSにおいて0.875、0.857、1.00の感度で異常値を判定することができた(図8-3、図9)。特異性はすべての疾患において0.800であった(図8-3、図9)。特異度は、コントロール群から異常例を判断することにより、急速な認知低下を伴う症例を除外すると、0.889まで上昇した(図8-3の括弧内)。
DOと疾患の重症度との相関
最後に、臨床症状におけるDOと疾患重症度との相関を調べた(図9)。AD(図9AおよびB)およびFTLD(図9CおよびD)では、MMSEとDO(図9AおよびC)またはFAB(Frontal Assessment Battery)とDO(図9BおよびD)では負の相関が認められ、これはDOがこれらの認知症における臨床症状の重篤度を反映することを示している。しかし、ALS機能評価スケール-R(ALSFRS-R)とDO(図9E)との間にALSにおける相関は検出されなかった。その理由は明らかではないが、ADとFTLDよりも速いALSの急速な進行が関連している可能性がある。例えば、病理学における実際の進行速度は、ALSの特定の時点における運動障害の重症度を反映しないことがある。
最後に、臨床症状におけるDOと疾患重症度との相関を調べた(図9)。AD(図9AおよびB)およびFTLD(図9CおよびD)では、MMSEとDO(図9AおよびC)またはFAB(Frontal Assessment Battery)とDO(図9BおよびD)では負の相関が認められ、これはDOがこれらの認知症における臨床症状の重篤度を反映することを示している。しかし、ALS機能評価スケール-R(ALSFRS-R)とDO(図9E)との間にALSにおける相関は検出されなかった。その理由は明らかではないが、ADとFTLDよりも速いALSの急速な進行が関連している可能性がある。例えば、病理学における実際の進行速度は、ALSの特定の時点における運動障害の重症度を反映しないことがある。
本実施例の結果より以下のことが判明した。
Ser46でのMARCKSのリン酸化は、ADの非常に初期の段階で、近傍の細胞内Aβの細胞内蓄積を伴うニューロンから放出されるダメージ警告分子HMGB1によって誘導されるHMGB1-TLR4シグナル伝達経路を介して神経突起に起こることが報告されている(Fujita, K. et al.、Sci. Rep. 6, 31895 (2016))。本実施例では、これまでの知見に基づいて、AD、FTLDおよびALSの3つの脳脊髄液(CSF)において、初期の病理学的段階において利用可能な神経突起の変性の指標となるバイオマーカーとなることを期待して、Ser46でリン酸化されたMARCKSを評価した。
Ser46でのMARCKSのリン酸化は、ADの非常に初期の段階で、近傍の細胞内Aβの細胞内蓄積を伴うニューロンから放出されるダメージ警告分子HMGB1によって誘導されるHMGB1-TLR4シグナル伝達経路を介して神経突起に起こることが報告されている(Fujita, K. et al.、Sci. Rep. 6, 31895 (2016))。本実施例では、これまでの知見に基づいて、AD、FTLDおよびALSの3つの脳脊髄液(CSF)において、初期の病理学的段階において利用可能な神経突起の変性の指標となるバイオマーカーとなることを期待して、Ser46でリン酸化されたMARCKSを評価した。
すべての神経変性疾患において、脳脊髄液(CSF)のpSer46-MARCKSは非常に特異的であったが、感度はそれほどでもなかった(図1-1および1-2)。バイオマーカーとしてのpSer46-MARCKSの困難性を克服するために、非リン酸化MARCKSとpSer46-MARCKSの値を統合し、DOという新しいパラメータを生み出した(図8-1)。DOが高感度および高特異性の両方を有する良好なパラメータであり、DOはADおよびFTLDにおいて疾患重症度を良好に反映することを確認した。数値シミュレーションを用いて、3つの神経変性疾患における感度と特異度を最適化するために、DOの正常上限値の最良値をさらに検索した。その結果、50.26~54.24の「正常のDOの上限」を用いて、AD、FTLD、ALSの感度はそれぞれ0.875、0.857、1.00となり、すべての疾患において0.800の特異性が得られた(図8-1~8-3および図9)。
意外にも、DOは複数の神経変性疾患において共通して変化した。また、DOとpSer46-MARCKSそれ自体はADよりもFTLDにおいて高かった。この結果は、DOおよびpSer46-MARCKSが疾患特異的マーカーではないが、それらは3つの神経変性疾患にわたる共通の病理学的プロセスの指標であることを示している。以前の研究は、組織学的Aβ凝集体の形成前でさえも、pSer46-MARCKSが異常に増加していることを明らかにしたので(Tagawa, K. et al., Hum. Mol. Genet. 24, 540-58 (2015); Fujita, K. et al.、Sci. Rep. 6, 31895 (2016))、ADおよびFTLDおよびALSの早期段階でDOおよびpSer46-MARCKSはおそらく神経突起変性を反映している。
より良いバイオマーカーを生成するために非リン酸化MARCKSの値が統合されるべきである生物学的意味は明確ではない。しかし、pSer46-MARCKSと非リン酸化MARCKSの両方が分解された神経突起から放出され、MARCKSの活性リン酸化は末端段階のニューロンでは起こらないので、非リン酸化MARCKSとの統合で得られるDO値はより良いマーカーはpSer-MARCKS単独よりも良好なマーカーである。
[実施例2] パーキンソン病(PD)およびレビー小体型認知症(DLB)における検討
方法
マウスPD / DLBモデル
正常ヒトα-Syn-BAC-TgマウスをYamakado et al (2012) Neurosci Res 73:173-177に記載の方法で作製した。
方法
マウスPD / DLBモデル
正常ヒトα-Syn-BAC-TgマウスをYamakado et al (2012) Neurosci Res 73:173-177に記載の方法で作製した。
具体的には、BAC-Tg構築物(PAC AF163864およびBAC AC097478、全部のヒト遺伝子に加えて、28kbの5'-フランキング配列および50kbの3'-フランキング配列を含む)をC57BL6 / J卵子にマイクロインジェクションしたホモ接合型α-Syn-Tgマウスを産生した。GBA-ヘテロKOマウスをThe Jackson Laboratory(B6.129S6-Gbatm1Nsb / J、ストック番号003321)から購入し、ヒトα-Syn-BAC-Tgマウスと交配させた。得られた正常ヒトα-Syn-BAC-Tg/GBA-hetero-KO(ホモ/ヘテロ)マウスを系統として維持した。
α-Syn-BAC-Tg/GBA-hetero-KOマウスを10世代以上交配し、免疫組織化学および生物学的分析のために1、6および24ヶ月齢(N = 3)で使用した。
免疫組織化学
免疫組織化学のために、マウスまたはヒトの脳を4%パラホルムアルデヒドで固定し、パラフィンに包埋した。
免疫組織化学のために、マウスまたはヒトの脳を4%パラホルムアルデヒドで固定し、パラフィンに包埋した。
パラフィン包埋された脳切片を脱パラフィンし、再水和し、抗原を活性化し(10mMクエン酸緩衝液、pH6.0、100℃で5分間マイクロ波処理した。このプロセスを3回繰り返した)、室温(RT)に冷却した。ホスホ-α-Synに対する染色のために、切片を室温で5分間98%ギ酸(WAKO、066-00461)によってさらに活性化した。
切片をPBST(0.1%Tween-20を含むPBS)で5分間2回洗浄し、0.5%Triton X-100を含有するPBSで20分間処理した後、PBSTで5分間3回洗浄した。ブロッキング(10%FBSにより37%℃で30分間)後、切片を、2%FBSおよび0.1%Triton X-100、一次抗体(マウス抗ホスホ-α-Syn(Ser129)(1 :2000、WAKO、015-25191))と共に37℃で60分間;マウス抗α-Syn(1:1000、Abcam、ab27766)と共に4℃で12時間;ウサギ抗ホスホ-MARCKS(Ser46)(1:1000、GL Biochem(Shanghai)Ltd.)、またはマウス抗ユビキチン抗体(1:1000、Cell Signaling Technology、3936S)と共に37℃で120分間;マウスThr203 / Tyr205-ERK1 / Thr183 / Tyr185-ERK2およびヒトThr202 / Tyr204-ERK1 / Thr185 / Tyr187-ERK2(1:250、Cell Signaling Technology、#4370)を検出するウサギ抗ホスホ-ERK1 /2、マウス抗MAP2(1:100、santa cruz、sc-32791)またはマウス抗GFAP(1:2000、sigma、C9205)と共に4℃で12時間 、そして二次抗体(Alexa Fluor標識抗マウスIgG(1:1000、Invitrogen)またはCy3標識抗ウサギIgG(1:500、Jackson ImmunoResearch)を用いてRTで60分間、連続的にインキュベートした。 pSer46-MARCKS抗体が生成され、Fujita et al.,(2016) Sci Rep 6:31895に記載の方法で品質を評価した。
pSer129-α-Synおよびユビキチンの二重標識のために、抗pSer129-α-Syn抗体をZenon Alexa Fluor 488マウスIgG1標識キット(Z-25002、Invitrogen)で標識した。核はDAPI(同仁研究所、D523)で染色した。共焦点顕微鏡法により画像を取得した:Olympus FV1200 IX83(オリンパス)。
ウエスタンブロッティング
マウス大脳皮質およびヒト側頭葉組織を、2%SDS、1mM DTT、および10mM Tris-HCl(pH7.5)を含有する抽出緩衝液に溶解し、20ストロークのDounceガラスホモジナイザーを用いて氷上でホモジナイズした。この粗製抽出物を、16,000gで4℃で10分間遠心分離し、等容積のサンプル緩衝液(0.1M Tris-HCl pH7.5,4%SDS、20%グリセロール、12% β-メルカプトエタノール、および1% SDS-PAGEで分離し、セミドライ法を用いてポリビニリデンジフルオライド膜(Immobilon-P、Merck Millipore)に移し、5%ミルクまたは2%ブロスでブロックした。TBST(10mM Tris / HCl pH8.0,150mM NaCl、および0.05%Tween-20)中のBSA(%BSA)に溶解し、Can Get Signal溶液(東洋紡)で希釈した次の一次および二次抗体と反応させた。一次および二次抗体を以下のように希釈した:マウス抗ホスホ-α-Syn(Ser129)(1:5000、WAKO、015-25191); マウス抗-α-Syn(1:5000、Abcam、ab27766)4℃で12時間; ウサギ抗ホスホ-MARCKS(Ser46)(1:200,000、GL Biochem(Shanghai)Ltd.)37℃で120分間; マウス抗ユビキチン抗体(1:5000、Cell Signaling Technology、3936S)4℃で12時間; ウサギ抗ホスホ-ERK1 / 2(Thr203 / Tyr205(マウス)-ERK1 / Thr183 / Tyr185(マウス)-ERK2、Thr202 / Tyr204(ヒト)-ERK1 / Thr185 / Tyr187(ヒト)-ERK2)(1:10,000、Cell Signaling Technology、#4370);またはウサギ抗ERK1 / 2(1:5,000、Cell Signaling Technology、#4695S); 抗マウスIgG HRP conjugate(1:3000、GE Healthcare、NA931VA)および抗ウサギIgG (1:3000、GE Healthcare、NA934VS)。LAS4000(GE Healthcare)を使用してバンドを検出するために、ECLプライム(GEヘルスケア、RPN2232)またはSCLセレクト(GEヘルスケア、RPN2235)を使用した。
マウス大脳皮質およびヒト側頭葉組織を、2%SDS、1mM DTT、および10mM Tris-HCl(pH7.5)を含有する抽出緩衝液に溶解し、20ストロークのDounceガラスホモジナイザーを用いて氷上でホモジナイズした。この粗製抽出物を、16,000gで4℃で10分間遠心分離し、等容積のサンプル緩衝液(0.1M Tris-HCl pH7.5,4%SDS、20%グリセロール、12% β-メルカプトエタノール、および1% SDS-PAGEで分離し、セミドライ法を用いてポリビニリデンジフルオライド膜(Immobilon-P、Merck Millipore)に移し、5%ミルクまたは2%ブロスでブロックした。TBST(10mM Tris / HCl pH8.0,150mM NaCl、および0.05%Tween-20)中のBSA(%BSA)に溶解し、Can Get Signal溶液(東洋紡)で希釈した次の一次および二次抗体と反応させた。一次および二次抗体を以下のように希釈した:マウス抗ホスホ-α-Syn(Ser129)(1:5000、WAKO、015-25191); マウス抗-α-Syn(1:5000、Abcam、ab27766)4℃で12時間; ウサギ抗ホスホ-MARCKS(Ser46)(1:200,000、GL Biochem(Shanghai)Ltd.)37℃で120分間; マウス抗ユビキチン抗体(1:5000、Cell Signaling Technology、3936S)4℃で12時間; ウサギ抗ホスホ-ERK1 / 2(Thr203 / Tyr205(マウス)-ERK1 / Thr183 / Tyr185(マウス)-ERK2、Thr202 / Tyr204(ヒト)-ERK1 / Thr185 / Tyr187(ヒト)-ERK2)(1:10,000、Cell Signaling Technology、#4370);またはウサギ抗ERK1 / 2(1:5,000、Cell Signaling Technology、#4695S); 抗マウスIgG HRP conjugate(1:3000、GE Healthcare、NA931VA)および抗ウサギIgG (1:3000、GE Healthcare、NA934VS)。LAS4000(GE Healthcare)を使用してバンドを検出するために、ECLプライム(GEヘルスケア、RPN2232)またはSCLセレクト(GEヘルスケア、RPN2235)を使用した。
免疫沈降
マウスおよびヒト脳試料をTNE緩衝液(10mM Tris-HCl(pH7.5)、10mM NaCl、1mM EDTA、1%NP-40、0.5%プロテアーゼ阻害剤カクテル、0.5%ホスファターゼ阻害剤カクテル)で溶解した。アリコートをプロテインGセファロースビーズ(GEヘルスケア)の50%スラリーとインキュベートし、続いて3分間遠心分離(2000×g)した。上清を1μgのウサギ抗-pSer46-MARCKSまたはウサギ抗-pSer129-τ-シヌクレイン抗体と共に4℃で一晩インキュベートした。プロテインGセファロースビーズ(GEヘルスケア)と共に4時間インキュベートし、TNE緩衝液で洗浄し、サンプルバッファーで溶出した。
マウスおよびヒト脳試料をTNE緩衝液(10mM Tris-HCl(pH7.5)、10mM NaCl、1mM EDTA、1%NP-40、0.5%プロテアーゼ阻害剤カクテル、0.5%ホスファターゼ阻害剤カクテル)で溶解した。アリコートをプロテインGセファロースビーズ(GEヘルスケア)の50%スラリーとインキュベートし、続いて3分間遠心分離(2000×g)した。上清を1μgのウサギ抗-pSer46-MARCKSまたはウサギ抗-pSer129-τ-シヌクレイン抗体と共に4℃で一晩インキュベートした。プロテインGセファロースビーズ(GEヘルスケア)と共に4時間インキュベートし、TNE緩衝液で洗浄し、サンプルバッファーで溶出した。
ADモデルマウスからの末梢血細胞の収集
Polymorphprep溶液(Alere Technologies AS)を使用して、製造業者のプロトコールに従って、末梢血細胞(多形核白血球(PMN)および単核細胞(MC))を収集した。簡潔には、EDTA(最終濃度2.0mM)を含む1mLの静脈血を、15mLのチューブ中の1mLのPolymorphprep上に注意深く重層した。室温で500×gで30分間遠心分離した後、血漿を除去し、PMNおよびMCを含む層を得た。収集したアリコートを0.45%NaClで希釈し、400×gで10分間の遠心分離によって細胞ペレットを得た。ペレットを溶解緩衝液(10mM Tris-HCl(pH7.5)、0.2%SDS、0.5%プロテアーゼ阻害剤カクテル、および0.5%ホスファターゼ阻害剤カクテル)で溶解し、62.5mM Tris-HCl、pH6.8、2 SDS、2.5%(v / v)2-メルカプトエタノール、5%(v / v)グリセロールおよび0.0025%(w / v)ブロモフェノールブルーの混合物に添加し、SDS-PAGEを行った。
Polymorphprep溶液(Alere Technologies AS)を使用して、製造業者のプロトコールに従って、末梢血細胞(多形核白血球(PMN)および単核細胞(MC))を収集した。簡潔には、EDTA(最終濃度2.0mM)を含む1mLの静脈血を、15mLのチューブ中の1mLのPolymorphprep上に注意深く重層した。室温で500×gで30分間遠心分離した後、血漿を除去し、PMNおよびMCを含む層を得た。収集したアリコートを0.45%NaClで希釈し、400×gで10分間の遠心分離によって細胞ペレットを得た。ペレットを溶解緩衝液(10mM Tris-HCl(pH7.5)、0.2%SDS、0.5%プロテアーゼ阻害剤カクテル、および0.5%ホスファターゼ阻害剤カクテル)で溶解し、62.5mM Tris-HCl、pH6.8、2 SDS、2.5%(v / v)2-メルカプトエタノール、5%(v / v)グリセロールおよび0.0025%(w / v)ブロモフェノールブルーの混合物に添加し、SDS-PAGEを行った。
質量分析
リンタンパク質分析のために、Fujita et al.,(2016) Sci Rep 6:31895やTagawa et al., (2015) Hum Mol Genet 24:540-558に記載された方法でリン酸化ペプチドを調製した。
リンタンパク質分析のために、Fujita et al.,(2016) Sci Rep 6:31895やTagawa et al., (2015) Hum Mol Genet 24:540-558に記載された方法でリン酸化ペプチドを調製した。
具体的には、マウスおよびヒト大脳皮質由来の脳抽出物を界面活性剤および熱処理によって変性させ、次いでシステイン残基を還元し、アルキル化によりブロックした。タンパク質試料をトリプシンで消化した。
iTRAQ Reagentマルチプレックスキット(SCIEX Ins.)を用いて標識し、強力な陽イオン交換クロマトグラフィーで分画して、Titansphere Phos-TiOキット(GL Sciences Inc.)を用いてホスホペプチドを富化させた。LC-MS / MSシステム(Triple TOF 5600システム、Eksigent LCシステム、SCIEX Ins.)およびC18カラム(0.1×100mm; KYA Technologies Corporation)を用いて各画分を分析した。イオン噴霧電圧は2.3kVであり、IDA(information dependent acquisition)設定は400-1250m / zであった。
データ分析
ペプチドの質量スペクトルデータを取得し、Analyst TF(バージョン1.6)(AB SCIEXA)によって分析した。結果に対応するタンパク質は、UniProtKB / Swiss-Prot(2010年6月22日にhttp://www.uniprot.orgからダウンロード)を検索し、Paragonアルゴリズムを採用したProteinPilot(バージョン4)(AB SCIEX) (Shilov et al. (2007) Mol421 Cell Proteomics 6:1638-1655)。
ペプチドの質量スペクトルデータを取得し、Analyst TF(バージョン1.6)(AB SCIEXA)によって分析した。結果に対応するタンパク質は、UniProtKB / Swiss-Prot(2010年6月22日にhttp://www.uniprot.orgからダウンロード)を検索し、Paragonアルゴリズムを採用したProteinPilot(バージョン4)(AB SCIEX) (Shilov et al. (2007) Mol421 Cell Proteomics 6:1638-1655)。
ProteinPilotによるペプチド検索の許容差は、MSについては0.05Da、MS / MS分析については0.10Daに設定した。冗長に同定されたタンパク質はPro Groupアルゴリズム(AB SCIEX)を用いて除外した。
タンパク質またはペプチド同定の信頼スコアは、ProteinPilotによって計算され、信頼閾値として用いられた。検出のための閾値は95%の信頼度に設定され、> 95%の信頼性を有するペプチドは同定されたペプチドとして受け入れられた。
タンパク質の定量は、質量分析計におけるフラグメンテーション時に生成されたMS / MSスペクトルにおけるiTRAQレポーター基の分析を介して行った。ペプチドおよびタンパク質の定量のために、各iTRAQからのシグナルの合計量が等しくなければならないと仮定して、異なるiTRAQレポーター間でシグナルを正規化するためにバイアス補正を用いた。ペプチドの定量のために、異なるiTRAQシグナルを正規化するためにバイアス補正オプションを使用した。
ペプチド比は、バイアス補正後の対照モデルに対する疾患モデルにおけるレポーターシグナルの比として計算した。この製剤の詳細は、AB SCIEXのマニュアルに記載されている。
ProteinPilotからのペプチドサマリーの結果は、さらなるデータ分析のためのExcelファイルとして出力された。ペプチド断片の量を、リン酸化部位を含む複数のMS / MS断片のシグナル強度の幾何平均として計算した。
すべての疾患群について、対照群との生物学的差異をウェルチの試験によって評価した。複数試験の補正のために、Benjamini-Hochberg手順を用いてp値を調整した。
複数の疾患群で変化したホスホペプチドを同定し、さらなる分析のために選択した。
人間の脳プロテオーム解析に使用された側頭極および後頭極のヒト脳サンプルを、5人のAD、5人のDLBおよび5人の年齢適合正常対照患者から解剖し、死亡後1時間以内に深冷凍した(-80℃)。
人間の脳プロテオーム解析に使用された側頭極および後頭極のヒト脳サンプルを、5人のAD、5人のDLBおよび5人の年齢適合正常対照患者から解剖し、死亡後1時間以内に深冷凍した(-80℃)。
結果
ヒトADおよびDLBのリン酸化プロテオームにおけるpSer46-MARCKSレベルの上昇
ADマウスモデルおよびヒトAD患者からの脳サンプルの以前の分析(Tagawa et al., (2015) Hum Mol Genet 24:540-558)に続いて、死後のヒトDLB患者を用いて包括的なリン酸化タンパク質分析を行った。病理学的に純粋なAD(5人の男性)およびDLB(5人の女性)の脳の後頭部および側頭部の先端を用いた。
ヒトADおよびDLBのリン酸化プロテオームにおけるpSer46-MARCKSレベルの上昇
ADマウスモデルおよびヒトAD患者からの脳サンプルの以前の分析(Tagawa et al., (2015) Hum Mol Genet 24:540-558)に続いて、死後のヒトDLB患者を用いて包括的なリン酸化タンパク質分析を行った。病理学的に純粋なAD(5人の男性)およびDLB(5人の女性)の脳の後頭部および側頭部の先端を用いた。
この場合、純粋な病理を有する死後の脳を選択したが、細胞内α-Syn凝集体はニューロン内にあるが、細胞外Aβ凝集体または細胞質タウ/ TDP43病変はなかった。この比較により、ADサンプルとDLBサンプルとの間でリン酸化部位が共有されることが明らかになった。
このような修飾の1つであるpSer46 -MARCKSは、ADマウスモデルおよび死後ヒトAD脳(Fujita et al.,(2016) Sci Rep 6:31895)(図10A)において上昇した。
興味深いことに、pSer46-MARCKSレベルはDLBの後頭葉ではなく側頭葉で上昇したが、AD(図10B)では逆のパターン(すなわち、後頭葉ではあるが側頭葉ではない)で上昇した。5×FADマウスでは、疾患の初期段階(前臨床/前凝集段階)でのpSer46-MARCKSレベルの上昇は後期段階で正常化した(Fujita et al.,(2016) Sci Rep 6:31895)。
したがって、2つの葉の間のpSer46 -MARCKSレベルの相違は、各疾患の神経変性の葉の優先を反映している可能性がある。質量分析結果は、ADおよびPD / DLBヒト脳において共通の変化が起こったことを示唆しており、pSer46-MARCKSがPD / DLBにおける前臨床/前凝集段階を反映するかどうかの調査が必要であることを示した。
ヒトDLBの免疫組織化学におけるpSer46-MARCKSの増加
次に、ヒト死後DLB脳においてpSer46-MARCKSが上昇したかどうかを調べた。この目的のために、本発明者らは、DLB患者から後頭葉サンプルを染色し、MAP2でマークされた頂端の樹状突起がpSer46-MARCKSによって共染色されたことを見出した(図11A)。
次に、ヒト死後DLB脳においてpSer46-MARCKSが上昇したかどうかを調べた。この目的のために、本発明者らは、DLB患者から後頭葉サンプルを染色し、MAP2でマークされた頂端の樹状突起がpSer46-MARCKSによって共染色されたことを見出した(図11A)。
一方、この脳領域には、ほとんどがユビキチン化されたpSer129-α-Syn細胞質封入体(図11B)が含まれることが確認された(図11C)。pSer46-MARCKSの細胞質染色は凝集物のように思われたため(図11A)、それらがα-Syn凝集体であるかどうかを調べ、ニューロンの細胞質pSer46-MARCKS陽性構造の半分がpSer129-α-Synで染色されていることを見出した、黄色の矢印)。しかし、それらのもう半分は、pSer129-α-Synで強く染色されなかった(図11D、赤矢印)。
pSer46-MARCKS陽性/ pSer129-α-Syn陰性細胞は、pSer129-α-Synを蓄積する損傷ニューロンから放出されたHMGB1によって間接的に影響される周囲ニューロンに対応し得、DLBの末期においてさえもヒトの脳において病理が進行し続けることを示唆する。
免疫組織化学の上記の結果を確認するために、本発明者らは、ヒト死後DLB患者および非DLB対照患者の後頭葉とのpSer46-MARCKSおよび全MARCKSのウエスタンブロッティングを行った(図11E)。pSer46-298 MARCKSレベルはDLB患者で増加した。
ヒト化α-Syn-TgマウスにおけるpSer46 -MARCKSの増加
脳におけるpSer46-MARCKSの増加の初期時点を決定するために、動物が運動機能障害または行動異常を示さなかった1、6および24ヶ月齢のヒトα-Syn-BAC-Tg/GBA-hetero-KOマウスを分析した。
脳におけるpSer46-MARCKSの増加の初期時点を決定するために、動物が運動機能障害または行動異常を示さなかった1、6および24ヶ月齢のヒトα-Syn-BAC-Tg/GBA-hetero-KOマウスを分析した。
マウスは、嗅球、前頭皮質、および頭頂皮質におけるpSer46 -MARCKSのシグナルを1ヶ月でわずかに上昇させた(図12、図18)。その後、pSer46 -MARCKS陽性染色の面積は、6ヶ月で頭頂および後頭皮質に拡大したが(図12、図19)、24ヶ月前では海馬で増加しなかった(図12、図20)。
24ヶ月齢まで内胚葉層および嗅球の僧帽細胞層のニューロンにおいて、抗リン酸化α-Syn(pSer129-α-Syn)抗体によって染色された明確な細胞質α-Syn凝集物は検出されなかった(図13A~C)。図13A~Cは、pSer46-MARCKSおよびpSer129-α-Synに対する抗体で共染色したヒトα-Syn-BAC-Tg / GBA-ヘテロKOマウスの嗅球の高倍率像を示す。1ヶ月齢からpSer46-MARCKS(白矢印)およびpSer129-α-Syn(星印)のドット様染色の細胞質染色が検出されたが、pSer129-α-Synの細胞質凝集物は24ヶ月でのみ検出された。α-Syn-skein- またはLewy神経突起-様構造は、1ヶ月齢からこれらの層に存在し、高齢化の過程で豊富に増加した。これらの構造は1ヶ月で抗ユビキチン抗体で同時染色されなかったが、6ヶ月後から共染色が明白であった(図13D)。
興味深いことに、pSer46 -MARCKS陽性神経突起はp-α-Syn-共染色神経突起よりも多かった。
まとめると、これらの結果は、少なくともこのPD / DLBマウスモデルにおいて、pSer46 -MARCKSによって検出された神経突起変化がα-Synのユビキチン陽性凝集体の形成に先行することを示した(表1)。
24ヶ月齢では、細胞質α-Syn凝集体も壁側皮質で検出された(図14A)。老化中の皮質ニューロンにおけるpMARCKSとp-α-Syn、p-α-Synとユビキチンの関係は、嗅覚ニューロンと同様であった(図14B)。
これらの結果を確認するために、本発明者らは、1、6、および24ヶ月齢の大脳皮質組織を有するpSer46 -MARCKS、pSer129-α-Synおよびユビキチンのウエスタンブロット分析を行った(図15)。リン酸化されたMARCKSのレベルは、1、6、および24ヶ月齢で上昇したが、6ヶ月後にリン酸化されたα-Synおよびユビキチンが発生し、十分に増加した(図15)。
本発明者はまた、末梢血細胞中のpSer46-MARCKSのレベルを試験し、脳のそれよりもはるかに低いことを見出した(図21)。
DLB脳におけるMARKCSとα-Synとの相互作用
細胞質凝集体の半分がpSer46-MARCKSおよびpSer129-α-Syn(図11D)に対して二重陽性であることを考慮して、本発明者らは2つのリンタンパク質の生化学的相互作用を調べた。24ヶ月齢のα-Syn-BAC-Tg / GBA-ヘテロKOマウス(図16A)の脳サンプル(全大脳皮質)(図16A)およびヒトDLB患者(図16B)からの抗pSer46-MARCKSとpSer129-a-Synとの同時沈降による免疫沈降を行った。抗pSer129-a-Syn抗体による逆沈殿はまた、マウスモデルおよびヒト患者の両方においてpSer46-MARCKSを共沈させた(図16AおよびB)。この結果は、2つのリンタンパク質の生化学的相互作用を示す。
細胞質凝集体の半分がpSer46-MARCKSおよびpSer129-α-Syn(図11D)に対して二重陽性であることを考慮して、本発明者らは2つのリンタンパク質の生化学的相互作用を調べた。24ヶ月齢のα-Syn-BAC-Tg / GBA-ヘテロKOマウス(図16A)の脳サンプル(全大脳皮質)(図16A)およびヒトDLB患者(図16B)からの抗pSer46-MARCKSとpSer129-a-Synとの同時沈降による免疫沈降を行った。抗pSer129-a-Syn抗体による逆沈殿はまた、マウスモデルおよびヒト患者の両方においてpSer46-MARCKSを共沈させた(図16AおよびB)。この結果は、2つのリンタンパク質の生化学的相互作用を示す。
DLB脳における上流キナーゼの活性化
最後に、Ser46でMARCKSをリン酸化する上流のキナーゼを調べた。MARCKSは、ミリストイル化アラニンリッチCキナーゼ基質として知られているPKCの代表的な基質である。PKAαはSer159、Ser163およびSer170をリン酸化することが報告されている。一方、PKCの代わりにErk1 / Erk2(= MAPK3 / MAPK1)がSer46においてMARCKSをリン酸化することが明らかになった。一貫して、別のグループはまた、MAPKが海馬ニューロンにおいてMARCKSをリン酸化することを示したが、MAPKによる正確なリン酸化部位はそれらの研究で決定された。
最後に、Ser46でMARCKSをリン酸化する上流のキナーゼを調べた。MARCKSは、ミリストイル化アラニンリッチCキナーゼ基質として知られているPKCの代表的な基質である。PKAαはSer159、Ser163およびSer170をリン酸化することが報告されている。一方、PKCの代わりにErk1 / Erk2(= MAPK3 / MAPK1)がSer46においてMARCKSをリン酸化することが明らかになった。一貫して、別のグループはまた、MAPKが海馬ニューロンにおいてMARCKSをリン酸化することを示したが、MAPKによる正確なリン酸化部位はそれらの研究で決定された。
したがって、Thr202 / Tyr204でのErk1リン酸化およびThr185 / Tyr187でのErk2リン酸化を検出するウサギモノクローナル抗体を用いて、免疫組織化学およびウエスタンブロットによるErk1 / 2の活性化を調べた(図17A)。
予想通り、pErk1 / 2の免疫染色は、α-Syn-BAC-Tg / GBA-ヘテロKOマウス(図17A)の大脳皮質において増加した。細胞はMAP2で同時染色されたが、GFAPでは共染色されず、ニューロンであることが示された(図17B)。pErk1 / 2の染色は、それらの酵素 - 基質の関係と一貫して同じニューロン(図8A)中のpSer46-MARCKSと共局在した。DLB患者の後頭葉皮質において、pSer46-MARCKSおよびpErk1 / 2の増加した同様の共染色が確認された(図17C)。ウエスタンブロット分析はまた、α-Syn-BAC-Tg / GBA-ヘテロKOマウス(図17D)およびDLB患者(図17E)の大脳皮質におけるpErk1 / 2の増加を確認した。これらの分析は、PD / DLB病理の下でErk1 / 2リン酸化の異常な増加および皮質ニューロンにおける年齢依存性増強をまとめて明らかにした(図17A~E)。
上記実施例の結果より以下のことが判明した。
AD病理の前凝集段階における神経突起変性の特徴であるpSer46でリン酸化されたMARCKSのレベルもマウスモデルとヒト患者両方においてPD / DLB病状において上昇することを明らかにした。
AD病理の前凝集段階における神経突起変性の特徴であるpSer46でリン酸化されたMARCKSのレベルもマウスモデルとヒト患者両方においてPD / DLB病状において上昇することを明らかにした。
pSer46 -MARCKSの免疫組織化学的染色パターンも、ADおよびPD / DLB病変において類似していた。マウスモデルでは、pSer46 -MARCKSによって明らかにされた神経突起変性が、嗅球において最初に検出され、その後、後頭部および側頭皮質において顕著になった(表1)。表1は、ヒトα-Syn-BAC-Tg / GBA-ヘテロKOマウスにおけるpSer46-MARCKS、pSer129-α-synおよびユビキチン染色パターンのまとめを示す。「+/-」は、バックグラウンドマウスでは陽性染色が細胞の10%未満で観察されなかったことを示し、「+」は、Tgマウスの細胞の10~50%において陽性染色が観察されたことを示し、「++」は、陽性染色がTgマウスの細胞の50%以上で観察されたことを示す。
このパターンは、ヒトPD / DLB病理における神経変性の提案された進行と一致し、最も初期の病変が嗅球に現れ、後頭葉が最終的に優勢である。

この研究の第2の重要な結論は、神経突起変性が、組織学的レベルで疾患関連タンパク質凝集に先行することである。マウスモデルにおいて、pSer46 -MARCKSの増加は、ユビキチン化α-Syn凝集物の形成に先行した(表1)。
pSer46 -MARCKSが組織学的凝集体形成に先行するPD / DLBマウスモデルの時系列は、pSer46 -MARCKSがニューロンの細胞質および神経突起で検出されたADモデルマウスにおける以前の観察と類似していた細胞外Aβ凝集体の染色が明らかになる。
このモデルを用いて、本発明者らは生化学レベルでpSer46 -MARCKSの重要性を確認した。これらの結果は、凝集体よりむしろ単量体またはオリゴマー形態の細胞内ミスフォールドα-Synが神経突起変性の開始においてより重要な役割を果たすことを強く示唆している。
興味深いことに、ヒト死後の脳において、pSer46 -MARCKSは、重篤な影響を受けた領域(DLBの後頭葉、ADの側頭葉)ではなく、疾患(DLBの側頭葉、ADの後頭葉)に比較的影響されない脳領域において上昇した。
この理由はまだ決定されていない。1つの可能性は、重篤な脳領域の神経突起が代謝的に「燃え尽きており、高レベルのpSer46-MARCKSを維持できない」ということである。
これらの観察に基づいて、超早期(前凝集/前臨床)段階でPD / DLBにおける分子病理を検出することができるバイオマーカーとしてpSer46 -MARCKSを開発することは価値がある。
さらに、質量分析に基づくアッセイおよびELISAに基づくアッセイおよび/またはPETを開発することが有用であろう。このように高感度のアッセイシステムが利用可能になると、神経変性疾患のリスクのある人々の超早期病態の検出に直接つながると考えられる。
予備的に、本発明者らは、赤血球、顆粒細胞またはリンパ球などの末梢血細胞(PBC)がpSer46-MARCKSを発現するかどうかウエスタンブロットによって調べた。そうであれば、PBC由来のpSer46-MARCKS由来の脳由来の識別が困難になり、脳外診断用のバイオマーカーとしてpSer46-MARCKSを使用するには、いくつかの追加のトリックが必要となる。幸いにも、PBCは、5xFADマウスの脳組織に匹敵する検出可能なレベルのpSer46-MARCKSを発現しなかった(図21)。pSer46-MARCKSを血液バイオマーカーとして開発する可能性を支持している。
本発明者らは、pSer46-MARCKSおよびpSer129-α-Synの細胞質凝集体(図13、図14A、図14B)および生化学的相互作用(図16)における共局在を見出した。興味深いことに、α-SynとMARCKSの両方が本質的に無秩序なタンパク質(IDP)と思われる。以前の研究では、α-Synが自然に変性する性質を有することが明らかになった。
一方、利用可能なアルゴリズム(RONN v3.2、https://www.strubi.ox.ac.uk/RONNおよびIUPred、http://iupred.enzim.hu)によるバイオインフォマティクス分析は、MARCKSがIDPであると予測した以前のいくつかの報告は構造生物学実験によってこの考えを支持した。α-SynとMARCKSの同様の変性傾向は、それらの生化学的相互作用の基礎をなしている可能性がある。また、α-SynとMARCKSの両方が変性神経突起に局在していることも注目されている軸索成長およびアクチンネットワーク調節のような軸索末端機能において重要である。
脳の全てのニューロンが壊死するまで、神経変性疾患を患う脳では神経突起変性から細胞死への病理学的サイクルが繰り返し起こるので、pSer46-MARCKSおよびDOの上昇は、神経変性のインビボ活性の定量的バイオマーカーとしても使用することができる、疾患特異的ではないが多発性肝疾患における肝細胞障害の一般的な定量的指標であるGOTおよびGPTと同様に、症候性患者および恐らく非症候性被験体においても同様である。本実施例は、神経変性疾患の神経突起変性を反映する新しいバイオマーカーを提供している。
本発明の方法は、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患の検出のために利用することができる。
本明細書で引用した全ての刊行物、特許及び特許出願はそのまま引用により本明細書に組み入れられるものとする。
本明細書で引用した全ての刊行物、特許及び特許出願はそのまま引用により本明細書に組み入れられるものとする。
Claims (16)
- 以下の工程を含む、ヒトAD(アルツハイマー病)、FTLD(前頭側頭葉変性症)およびALS(筋萎縮性側索硬化症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質および非リン酸化MARCKSタンパク質を測定する工程;
(ii) (i)で得られた測定値から以下の式で表されるDO値を算出する工程;および
[式1]
[式中、「pSer46-MARCKS」は46位でリン酸化されたMARCKSタンパク質の量を示し、「non-phosphorylated-MARCKS」は非リン酸化MARCKSタンパク質の量を示す]
(iii) DO値を指標に神経変性疾患を検出する工程
を含む方法。 - 検体試料が脳脊髄液である、請求項1記載の方法。
- 「pSer46-MARCKS」および「non-phosphorylated-MARCKS」の測定を質量分析法により行う請求項1又は2に記載の方法。
- 式中の「pSer46-MARCKS」および「non-phosphorylated-MARCKS」が、検体試料中の全タンパク質量で正規化した値である、請求項1~3のいずれか1項に記載の方法。
- 工程(iii)において、被験体について算出されたDO値とあらかじめ定めたカットオフ値と比較し、カットオフ値より高い場合に、神経変性疾患が検出されたと判断する、請求項1~4のいずれか1項に記載の方法。
- DO値のカットオフ値が、50~55である、請求項5に記載の方法。
- 以下の工程を含む、ヒトFTLD(前頭側頭葉変性症)、ALS(筋萎縮性側索硬化症)、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。 - 検体試料が脳脊髄液である、請求項7記載の方法。
- 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う請求項7又は8に記載の方法。
- 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、請求項7~9のいずれか1項に記載の方法。
- 以下の工程を含む、PD(パーキンソン病)およびDLB(レビー小体型認知症)からなる群から選択される神経変性疾患を検出する方法:
(i) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質を測定する工程;
(ii) 被験体の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量を健常人の後頭葉および側頭葉からそれぞれ採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量と比較する工程;および
(iii) 被験体の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量が健常人の側頭葉から採取した検体試料中の46位でリン酸化されたMARCKSタンパク質の量よりも多い場合に、被験体において神経変性疾患が検出されたと判断する工程
を含む方法。 - 検体試料が脳脊髄液である、請求項11記載の方法。
- 46位でリン酸化されたMARCKSタンパク質の測定を質量分析法により行う請求項11又は12に記載の方法。
- 46位でリン酸化されたMARCKSタンパク質の量が、46位でリン酸化されたMARCKSタンパク質の測定値を、検体試料中の全タンパク質量または検体試料中の総MARCKSタンパク質量で正規化した値である、請求項11~13のいずれか1項に記載の方法。
- 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーを用い、46位でリン酸化されたMARCKSタンパク質の測定をPET(陽電子放射断層撮影)により行う請求項11の方法。
- 46位でリン酸化されたMARCKSタンパク質イメージング用PETトレーサーが、46位でリン酸化されたMARCKSタンパク質に対する抗体をポジトロン核種でラベルした抗体PETトレーサーである請求項15記載の方法。
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US16/978,959 US20200408783A1 (en) | 2018-03-09 | 2019-03-08 | Detection of alzheimer's disease (ad), frontotemporal lobar degeneration (ftld), amyotrophic lateral schlerosis (als), parkinson's disease (pd), and dementia with lewy bodies (dlb) indicated by phosphorylation of marcks |
| JP2020504057A JP7329497B2 (ja) | 2018-03-09 | 2019-03-08 | Marcksのリン酸化を指標にしたad(アルツハイマー病)、ftld(前頭側頭葉変性症)、als(筋萎縮性側索硬化症)、pd(パーキンソン病)およびdlb(レビー小体型認知症)の検出 |
| EP19764930.4A EP3764102A4 (en) | 2018-03-09 | 2019-03-08 | DETECTION OF ALZHEIMER'S DISEASE (MA), FRONTOTEMPORAL LOBAR DEGENERATION (FRONTOTEMPORAL LOBAR DEGENERATION), AMYOTROPHIC LATERAL SCLEROSIS (ALS), PARKINSON'S DISEASE (PD) AND INDICATED LEWY-BODY DEMENTIA (PARL) MARCKS PHOSPHORYLATION |
| CN201980018335.7A CN111886500A (zh) | 2018-03-09 | 2019-03-08 | 以marcks磷酸化为指标的ad(阿尔茨海默病)、ftld(额颞叶变性症)、als(肌萎缩侧索硬化症)、pd(帕金森病)和dlb(路易小体型痴呆)的检测 |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2018043641 | 2018-03-09 | ||
| JP2018-043641 | 2018-03-09 | ||
| JP2018-138785 | 2018-07-24 | ||
| JP2018138785 | 2018-07-24 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2019172427A1 true WO2019172427A1 (ja) | 2019-09-12 |
Family
ID=67846634
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2019/009370 WO2019172427A1 (ja) | 2018-03-09 | 2019-03-08 | Marcksのリン酸化を指標にしたad(アルツハイマー病)、ftld(前頭側頭葉変性症)、als(筋萎縮性側索硬化症)、pd(パーキンソン病)およびdlb(レビー小体型認知症)の検出 |
Country Status (5)
| Country | Link |
|---|---|
| US (1) | US20200408783A1 (ja) |
| EP (1) | EP3764102A4 (ja) |
| JP (1) | JP7329497B2 (ja) |
| CN (1) | CN111886500A (ja) |
| WO (1) | WO2019172427A1 (ja) |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20130196925A1 (en) * | 2010-07-09 | 2013-08-01 | Translational Genomics Research Institute | Compositions and methods useful in enhancement of memory |
| WO2015099094A1 (ja) * | 2013-12-27 | 2015-07-02 | 国立大学法人東京医科歯科大学 | アルツハイマー病及び前頭側頭葉変性症の診断方法、診断薬、治療薬、及びこれら薬剤のスクリーニング方法 |
| JP2018043641A (ja) | 2016-09-14 | 2018-03-22 | 株式会社ブリヂストン | タイヤ |
| JP2018138785A (ja) | 2013-01-17 | 2018-09-06 | ムライエ, ニールマルMULYE, Nirmal | 内部冷却される内燃エンジンおよびその方法 |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2004066943A2 (en) * | 2003-01-27 | 2004-08-12 | Baylor College Of Medicine | Methods for diagnosis anf monitoring of neurological disease by detection of an encephalotoxin |
-
2019
- 2019-03-08 CN CN201980018335.7A patent/CN111886500A/zh active Pending
- 2019-03-08 WO PCT/JP2019/009370 patent/WO2019172427A1/ja unknown
- 2019-03-08 JP JP2020504057A patent/JP7329497B2/ja active Active
- 2019-03-08 US US16/978,959 patent/US20200408783A1/en active Pending
- 2019-03-08 EP EP19764930.4A patent/EP3764102A4/en active Pending
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20130196925A1 (en) * | 2010-07-09 | 2013-08-01 | Translational Genomics Research Institute | Compositions and methods useful in enhancement of memory |
| JP2018138785A (ja) | 2013-01-17 | 2018-09-06 | ムライエ, ニールマルMULYE, Nirmal | 内部冷却される内燃エンジンおよびその方法 |
| WO2015099094A1 (ja) * | 2013-12-27 | 2015-07-02 | 国立大学法人東京医科歯科大学 | アルツハイマー病及び前頭側頭葉変性症の診断方法、診断薬、治療薬、及びこれら薬剤のスクリーニング方法 |
| JP2018043641A (ja) | 2016-09-14 | 2018-03-22 | 株式会社ブリヂストン | タイヤ |
Non-Patent Citations (9)
| Title |
|---|
| FUJITA ET AL., SCI REP, vol. 6, 2016, pages 31895 |
| FUJITA, K. ET AL., SCI. REP., vol. 6, 2016, pages 31895 |
| FUJITA, K. ET AL.: "HMGB1, a pathogenic molecule that induces neurite degeneration via TLR4-MARCKS, is a potential therapeutic target for Alzheimer' s disease", SCIENTIFIC REPORTS, vol. 6, no. 31895, 25 August 2016 (2016-08-25), pages 1 - 15, XP055463477 * |
| KIMURA, T. ET AL.: "Phosphorylation of MARCKS in Alzheimer disease brains", NEUROREPORT, vol. 11, no. 4, 20 March 2000 (2000-03-20), pages 869 - 873, XP008184615, doi:10.1097/00001756-200003200-00042 * |
| SHILOV ET AL., MOL421 CELL PROTEOMICS, vol. 6, 2007, pages 1638 - 1655 |
| TAGAWA ET AL., HUM MOL GENET, vol. 24, 2015, pages 540 - 558 |
| TAGAWA, K. ET AL., HUM. MOL. GENET., vol. 24, 2015, pages 540 - 58 |
| TAGAWA, K. ET AL.: "Comprehensive phosphoproteome analysis unravels the core signaling network that initiates the earliest synapse pathology in preclinical Alzheimer' s disease brain", HUMAN MOLECULAR GENETICS, vol. 24, no. 2, 17 September 2014 (2014-09-17), pages 540 - 558, XP055640705 * |
| YAMAKADO ET AL., NEUROSCI RES, vol. 73, 2012, pages 173 - 177 |
Also Published As
| Publication number | Publication date |
|---|---|
| CN111886500A (zh) | 2020-11-03 |
| JP7329497B2 (ja) | 2023-08-18 |
| EP3764102A4 (en) | 2021-12-15 |
| EP3764102A1 (en) | 2021-01-13 |
| US20200408783A1 (en) | 2020-12-31 |
| JPWO2019172427A1 (ja) | 2021-03-25 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Gkanatsiou et al. | A distinct brain beta amyloid signature in cerebral amyloid angiopathy compared to Alzheimer’s disease | |
| JP6954839B2 (ja) | アルツハイマー病の診断及び治療のための材料及び方法 | |
| US10914749B2 (en) | Biomarkers of cognitive dysfunction | |
| Ho Kim et al. | Proteome-wide characterization of signalling interactions in the hippocampal CA4/DG subfield of patients with Alzheimer’s disease | |
| US20170184614A1 (en) | Methylated Peptides Derived from Tau Protein and their Antibodies for Diagnosis and Therapy of Alzheimer's Disease | |
| Villar-Conde et al. | The human hippocampus in Parkinson’s disease: an integrative stereological and proteomic study | |
| Oglesby et al. | Scleral fibroblast response to experimental glaucoma in mice | |
| Mueller et al. | The heme degradation pathway is a promising serum biomarker source for the early detection of Alzheimer's disease | |
| Shultz et al. | Temporal proteomics of human cerebrospinal fluid after severe traumatic brain injury | |
| Montero-Calle et al. | Proteomics analysis of prefrontal cortex of Alzheimer’s disease patients revealed dysregulated proteins in the disease and novel proteins associated with amyloid-β pathology | |
| Wen et al. | Proteomic characterization of secretory granules in dopaminergic neurons indicates chromogranin/secretogranin-mediated protein processing impairment in Parkinson’s disease | |
| Schedin-Weiss et al. | Proteomics Time-Course Study of App Knock-In Mice Reveals Novel Presymptomatic Aβ 42-Induced Pathways to Alzheimer’s Disease Pathology | |
| EP3835424A1 (en) | Diagnostic drug and diagnostic method for alzheimer's disease | |
| Ning et al. | Comparative proteomic analysis of urine and laser microdissected glomeruli in IgA nephropathy | |
| Gnanapavan et al. | Progression in multiple sclerosis is associated with low endogenous NCAM | |
| Park et al. | Hornerin deposits in neuronal intranuclear inclusion disease: direct identification of proteins with compositionally biased regions in inclusions | |
| EP2817632B1 (en) | New dual biomarker of neurodegeneration and of neuroregeneration | |
| WO2019172427A1 (ja) | Marcksのリン酸化を指標にしたad(アルツハイマー病)、ftld(前頭側頭葉変性症)、als(筋萎縮性側索硬化症)、pd(パーキンソン病)およびdlb(レビー小体型認知症)の検出 | |
| JP2014071016A (ja) | 神経系の変性疾患の検出方法 | |
| US20230349924A1 (en) | Determination agent and determination method for tauopathy and dementia-related diseases | |
| Chen et al. | Proteomics reveals defective peroxisomal fatty acid oxidation during the progression of acute kidney injury and repair | |
| Fujita et al. | Ser46-phosphorylated MARCKS is a marker of neurite degeneration at the pre-aggregation stage in PD/DLB pathology | |
| Darricau et al. | Tau seeds from Alzheimer's disease brains trigger tau spread in macaques while oligomeric‐Aβ mediates pathology maturation | |
| US12000844B2 (en) | Diagnostic drug and diagnostic method for Alzheimer's disease | |
| WO2023058627A1 (ja) | 認知症の検査方法 |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 19764930 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2020504057 Country of ref document: JP Kind code of ref document: A |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2019764930 Country of ref document: EP Effective date: 20201009 |