RU2594512C1 - Method for intraportal ozone therapy in patients with widespread peritonitis - Google Patents
Method for intraportal ozone therapy in patients with widespread peritonitis Download PDFInfo
- Publication number
- RU2594512C1 RU2594512C1 RU2015121148/14A RU2015121148A RU2594512C1 RU 2594512 C1 RU2594512 C1 RU 2594512C1 RU 2015121148/14 A RU2015121148/14 A RU 2015121148/14A RU 2015121148 A RU2015121148 A RU 2015121148A RU 2594512 C1 RU2594512 C1 RU 2594512C1
- Authority
- RU
- Russia
- Prior art keywords
- peritonitis
- intraportal
- ozone
- patients
- days
- Prior art date
Links
Images


Landscapes
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
Abstract
Description
Изобретение относится к брюшной хирургии и может быть использовано для лечения больных с острой патологией органов брюшной полости, осложнившейся развитием распространенного перитонита как метод коррекции функциональной недостаточности печени в комплексном лечении.The invention relates to abdominal surgery and can be used to treat patients with acute abdominal organs pathology complicated by the development of peritonitis widespread as a method for correcting liver functional insufficiency in complex treatment.
В настоящее время считается общепризнанным, что в механизме сложных общепатофизиологических реакций при распространенном перитоните ведущая роль отводится эндогенной интоксикации. Несмотря на системный характер нарушений, их многогранность и взаимосвязанность, главными источниками эндотоксикоза при перитоните являются брюшная полость и кишечник, находящийся в состоянии стойкого пареза в условиях нарушения его защитно-барьерной функции [1, 2].At present, it is generally recognized that in the mechanism of complex general pathophysiological reactions with widespread peritonitis, the leading role is given to endogenous intoxication. Despite the systemic nature of the disorders, their versatility and interconnectedness, the main sources of endotoxicosis in peritonitis are the abdominal cavity and intestines, which are in a state of persistent paresis in conditions of violation of its protective and barrier function [1, 2].
Печень является одной из главных детоксицирующих систем организма. Решающая роль в патогенезе повреждения высокоспециализированных гепатоцитов принадлежит нарушениям внутрипеченочного кровообращения и гипоксии, тогда как поражение печеночных макрофагов в наибольшей степени связано с массивным поступлением в печень по портальному руслу инфекционно-токсических агентов из гастроинтестинального тракта [3].The liver is one of the main detoxifying systems of the body. A decisive role in the pathogenesis of damage to highly specialized hepatocytes belongs to impaired intrahepatic circulation and hypoxia, while damage to the hepatic macrophages is most associated with a massive inflow of toxic agents from the gastrointestinal tract into the liver through the portal channel [3].
Повреждение гепатоцитов и развитие печеночно-клеточной недостаточности приводит, главным образом, к нарушению метаболической функции печени, что характеризуется уменьшением синтеза белка (прежде всего альбуминов), повышением продукции белков острой фазы, угнетением окисления энергетических субстратов, сопровождающееся активацией глюконеогенеза и накоплением недоокисленных токсических метаболитов [4]. Поражение значительной части звездчатых ретикулоэндотелиоцитовцитов в условиях портальной бактериемии и токсинемии приводит к формированию макрофагальной печеночной недостаточности, характеризующейся нарушением ретикулоэндотелиального барьера печени, «прорывом» инфекционно-токсических агентов в системную гемоциркуляцию, что предопределяет развитие токсико-септического шока, прогрессирование эндотоксикоза и органных повреждений. В этом случае нарушение барьерной (макрофагальной) функции печени в условиях истощения резервов ее ретикулоэндотелиальной системы в настоящее время расценивается как более опасная форма печеночной недостаточности и рассматривается в качестве одного из главных критериев в оценке прогноза течения и исхода распространенного перитонита [5].Damage to hepatocytes and the development of liver cell failure leads mainly to a violation of the metabolic function of the liver, which is characterized by a decrease in protein synthesis (primarily albumin), an increase in the production of acute phase proteins, inhibition of oxidation of energy substrates, accompanied by activation of gluconeogenesis and the accumulation of under-oxidized toxic metabolites [ four]. The defeat of a significant part of stellate reticuloendotheliocytocytes under conditions of portal bacteremia and toxinemia leads to the formation of macrophage liver failure, characterized by a violation of the reticuloendothelial barrier of the liver, a “breakthrough” of toxic agents into systemic hemocirculation, which determines the development of toxic-septic shock and progression of endotoxin. In this case, a violation of the barrier (macrophage) function of the liver under conditions of depletion of the reserves of its reticuloendothelial system is currently regarded as a more dangerous form of liver failure and is considered as one of the main criteria in assessing the prognosis of the course and outcome of peritonitis [5].
В настоящее время патогенетическую основу программы реабилитации детоксицирующей системы печени при распространенном перитоните составляют методы внутрипортальной (трансумбиликальной) терапии. При этом осуществляется целенаправленное внутрипортальное введение различных лекарственных препаратов (антибиотиков, антикоагулянтов, дезагрегантов, антиоксидантов, антигипоксантов, аминокислот и пр.), воздействующих на различные патогенетические механизмы повреждения печени [6, 7].Currently, the pathogenetic basis of the program for the rehabilitation of the detoxifying system of the liver with widespread peritonitis is made up of the methods of intraportal (transumbilical) therapy. In this case, targeted intraportal administration of various drugs (antibiotics, anticoagulants, antiplatelet agents, antioxidants, antihypoxants, amino acids, etc.) is carried out, affecting various pathogenetic mechanisms of liver damage [6, 7].
Одним из перспективных направлений в комплексном лечении распространенного перитонита является применение лекарственных средств, воздействующих одновременно на несколько наиболее значимых звеньев патогенеза развития функциональной недостаточности печени, среди которых важнейшими являются гипоксия, нарушения внутрипеченочного кровотока, портальная бактериемия и эндотоксинемия. К таким лекарственным средствам относится отечественный препарат на основе перфторуглеродных эмульсий - перфторан.One of the promising directions in the complex treatment of common peritonitis is the use of drugs that simultaneously affect several of the most significant links in the pathogenesis of the development of functional liver failure, among which the most important are hypoxia, impaired intrahepatic blood flow, portal bacteremia and endotoxinemia. Such drugs include the domestic product based on perfluorocarbon emulsions - perfluorane.
Перфторуглеродные препараты первоначально разрабатывались для использования в качестве кровезаменителей с газотранспортными функциями. В дальнейшем у этих препаратов обнаружились дополнительные биологические свойства, позволяющие расширить сферу применения этих лекарственных средств. Одним из дополнительных их свойств явилась способность оказывать лечебное воздействие на течение инфекционно-воспалительных процессов при регионарном применении. Большое количество экспериментально-клинических исследований свидетельствует о высокой эффективности внутрибрюшинного введения перфторана в комплексном лечении распространенного перитонита [8-14]. Имеются также указания на возможность коррекции интестинальных нарушений при энтеральном применении перфторана у больных с распространенным перитонитом [15]. По мнению большинства исследователей, перфторан в комплексной терапии распространенного перитонита оказывает многоплановое воздействие: осуществляет транспортировку кислорода и углекислого газа, улучшает периферический кровоток и микроциркуляцию в органах, уменьшает тканевую гипоксию, а также активирует систему мононуклеарных фагоцитов и факторы неспецифического гуморального иммунитета [16].Perfluorocarbon preparations were originally developed for use as blood substitutes with gas transport functions. In the future, these drugs revealed additional biological properties that expand the scope of use of these drugs. One of their additional properties was the ability to exert a therapeutic effect on the course of infectious and inflammatory processes with regional use. A large number of experimental and clinical studies indicate the high efficiency of intraperitoneal administration of perftoran in the complex treatment of common peritonitis [8-14]. There are also indications of the possibility of correcting intestinal disturbances in the case of enteral use of perftoran in patients with advanced peritonitis [15]. According to most researchers, perftoran in the complex therapy of peritonitis widespread has a multifaceted effect: it carries oxygen and carbon dioxide, improves peripheral blood flow and microcirculation in organs, reduces tissue hypoxia, and also activates the system of mononuclear phagocytes and factors of non-specific humoral immunity [16].
В настоящее время появились исследования, указывающие на возможность повышения лечебной эффективности перфторана путем насыщения его медицинским озоном. Как известно, воздействие озона на организм заключается в улучшении транспортных механизмов кислорода и повышении его утилизации, уменьшении тканевой гипоксии, активации мононуклеарных клеток и стимуляции фагоцитоза, усилении специфического и неспецифического иммунного ответа, а также в дезинтоксикационном, бактерицидном и противовоспалительном эффектах [17]. При этом проведен ряд исследований, свидетельствующих о высокой растворимости и физико-химической стабильности озона в перфторорганических соединениях [18, 19]. В этом случае перфторан, насыщенный озоном, за счет суммарного синергического эффекта обеих лекарственных средств оказывает более продолжительное и активное воздействие на биологические субстраты. По данным многочисленных исследователей, перфузия брюшной полости озонированным перфтораном при распространенном гнойном перитоните оказывает выраженный санирующий, дезинтоксикационный и противовоспалительный эффект, сопровождается активацией перитонеальных макрофагов и факторов неспецифической резистентности [20-24].Currently, studies have appeared that indicate the possibility of increasing the therapeutic effectiveness of perftoran by saturating it with medical ozone. As is known, the effect of ozone on the body consists in improving the transport mechanisms of oxygen and increasing its utilization, reducing tissue hypoxia, activating mononuclear cells and stimulating phagocytosis, enhancing a specific and non-specific immune response, as well as detoxifying, bactericidal and anti-inflammatory effects [17]. At the same time, a number of studies have been carried out indicating the high solubility and physicochemical stability of ozone in organo perfluorine compounds [18, 19]. In this case, perfluoran saturated with ozone, due to the total synergistic effect of both drugs, has a longer and more active effect on biological substrates. According to numerous researchers, perfusion of the abdominal cavity with ozonized perfluorane with widespread purulent peritonitis has a pronounced sanitizing, detoxification and anti-inflammatory effect, accompanied by activation of peritoneal macrophages and non-specific resistance factors [20-24].
Учитывая многостороннее и выраженное воздействие озонированных растворов, в большей степени перфторана, на различные звенья метаболизма и патогенетические механизмы при инфекционно-воспалительной патологии, представляется вполне обоснованным и целесообразным применение этих лекарственных средств путем их внутрипортального введения с целью детоксикации и коррекции функциональной недостаточности печени при проведении комплексной интенсивной терапии у больных с распространенным перитонитом. Несмотря на логичность такого предположения, сведения о применении озонированных растворов и перфторана посредством его введения непосредственно в портальное русло печени при лечении больных с распространенным перитонитом в литературе отсутствуют.Given the many-sided and pronounced effect of ozonated solutions, to a greater extent perfluorane, on various metabolic links and pathogenetic mechanisms in infectious and inflammatory pathologies, it seems quite reasonable and appropriate to use these drugs by introducing them intraportally in order to detoxify and correct functional liver failure during complex intensive care in patients with advanced peritonitis. Despite the consistency of such an assumption, there is no literature data on the use of ozonized solutions and perfluorane through its introduction directly into the portal channel of the liver in the treatment of patients with advanced peritonitis.
Из патентной литературы, известен способ озонотерапии при перитоните. Согласно данному способу, во время операции вводят в брюшную полость физиологический раствор. Барботируют раствор озоном непосредственно в брюшной полости до достижения терапевтической концентрации. В послеоперационном периоде вводят озонированный физиологический раствор через дренажную трубку, расположенную в полости малого таза, 2-4 раза в сутки и внутривенно в терапевтических концентрациях на протяжении 8-10 дней (см. патент России №2122835, опубл. 10.12.1998, кл. А61В 17/00).From the patent literature, a method of ozone therapy for peritonitis is known. According to this method, saline is injected into the abdominal cavity during surgery. The solution is bubbled with ozone directly in the abdominal cavity until a therapeutic concentration is reached. In the postoperative period, ozonized saline is administered through a drainage tube located in the pelvic cavity 2-4 times a day and intravenously at therapeutic concentrations for 8-10 days (see Russian patent No. 2122835, publ. 10.12.1998, cl. A61B 17/00).
На наш взгляд, основным недостатком данного способа является то, что озонированные растворы вводят интраоперационно в брюшную полость с дальнейшим использованием озонированных растворов внутривенно, так как доказано, что наибольшее значение в регуляции активности ретикулоэндотелиальной системы печени при распространенном перитоните принадлежит синдрому портальной бактериотоксемии [25].In our opinion, the main disadvantage of this method is that ozonated solutions are administered intraoperatively into the abdominal cavity with the subsequent use of ozonated solutions intravenously, since it has been proven that the greatest significance in the regulation of the activity of the reticuloendothelial system of the liver with widespread peritonitis belongs to the portal bacteriotoxemia syndrome [25].
Печень является первым барьером и органом-мишенью на пути различных токсических продуктов, поступающих из брюшной полости и просвета кишечника в системный кровоток. Нарастающее токсическое воздействие на печень при прогрессировании абдоминального инфекционно-воспалительного процесса приводит к развитию печеночной недостаточности и сопровождается значительным снижением антитоксической функции этого органа. В связи с чем, предложенный нами способ внутрипортального введения озонированных физиологических растворов и перфторана является патогенетически обоснованным.The liver is the first barrier and target organ in the path of various toxic products coming from the abdominal cavity and intestinal lumen into the systemic circulation. The increasing toxic effect on the liver with the progression of the abdominal infectious and inflammatory process leads to the development of liver failure and is accompanied by a significant decrease in the antitoxic function of this organ. In this connection, the method of intraportal administration of ozonized physiological solutions and perfluorane proposed by us is pathogenetically substantiated.
Преимущества внутрипортального введения препаратов обусловлены следующим: препараты подводятся к паренхиме печени в химически неизмененном виде в достаточно высокой концентрации; достигается непосредственный контакт лекарственных препаратов с печеночными клетками; на уровне паренхимы печени происходит связывание токсических продуктов как образующихся в печени, так и поступающих из просвета кишечника.The advantages of intraportal administration of drugs are due to the following: drugs are brought to the liver parenchyma in a chemically unchanged form in a sufficiently high concentration; direct contact of drugs with liver cells is achieved; at the level of the liver parenchyma, toxic products are bound both to those formed in the liver and from the intestinal lumen.
Задача изобретения: улучшение эффективности лечения больных с распространенным перитонитом путем интрапортального введения озонированного перфторана и физраствора.Object of the invention: improving the effectiveness of treatment of patients with advanced peritonitis by intraportal administration of ozonated perftoran and saline.
Техническим результатом изобретения является улучшение спланхнической гемодинамики и оксигенации портальной крови, а также снижение эндогенной интоксикации у больных с распространенным перитонитом.The technical result of the invention is to improve splanchnic hemodynamics and oxygenation of portal blood, as well as reducing endogenous intoxication in patients with advanced peritonitis.
Поставленная задача решается тем, что способ внутрипортальной озонотерапии при распространенном перитоните, включающий комплексное лечение, характеризуется интрапортальным введением озонированного перфторана и физиологического раствора.The problem is solved in that the method of intraportal ozone therapy for common peritonitis, including complex treatment, is characterized by the intraportal administration of ozonated perftoran and physiological saline.
При этом озонирование проводят посредством медицинского озонатора, с концентрацией озона в озоно-кислородной смеси не менее 1000 мкг/л. После устранения источника перитонита, проведения назоинтестинальной интубации, лаважа и дренирования брюшной полости перед ушиванием срединной раны выполняют реканализацию и катетеризацию пупочной вены с ее канюлированием для проведения внутрипортальной инфузии озонированным перфтораном в 1-2 сутки после операции капельным способом по 40 капель в 1 мин. После этого проводят мониторинг портальной крови с целью оценки функционального состояния печени: билирубина, белка, альбуминов, активности АлТ и АсТ. Также проводят насыщение кислородом портальной крови и УЗ-контроль с оценкой скорости печеночного кровотока. Далее на 3-5 сутки проводят внутрипортальную инфузию озонированным физиологическим раствором, с вышеуказанной схемой мониторинга.In this case, ozonation is carried out by means of a medical ozonator, with an ozone concentration in the ozone-oxygen mixture of at least 1000 μg / L. After eliminating the source of peritonitis, conducting nasointestinal intubation, lavage and drainage of the abdominal cavity before suturing the median wound, recanalization and catheterization of the umbilical vein with its cannulation for intraportal infusion with ozonated perfluorane in 1-2 days after the operation is carried out dropwise in drops of 40 drops in 1 min. After that, portal blood is monitored to assess the functional state of the liver: bilirubin, protein, albumin, ALT and ACT activity. Portal blood oxygenation and ultrasound control are also carried out with an assessment of the rate of hepatic blood flow. Then, for 3-5 days, intraportal infusion is carried out with ozonized physiological saline, with the above monitoring scheme.
Использование интрапортального введения озонированного перфторана в раннем послеоперационном периоде у пациентов с распространенным гнойным перитонитом, приводит к улучшению спланхнической гемодинамики и оксигенации портальной крови в большей степени, чем введение обычных озононасыщенных растворов в систему верхней полой вены и системный кровоток, а также ведет к нивелированию клинико-лабораторных проявлений эндотоксикоза, что способствует реабилитации функциональной недостаточности печени и позволяет улучшить непосредственные результаты хирургического лечения.The use of intraportal administration of ozonated perftoran in the early postoperative period in patients with advanced purulent peritonitis leads to an improvement in splanchnic hemodynamics and oxygenation of portal blood to a greater extent than the introduction of conventional ozone-saturated solutions into the superior vena cava system and systemic blood flow, and also leads to the leveling of clinical and laboratory manifestations of endotoxemia, which contributes to the rehabilitation of functional liver failure and improves direct e results of surgical treatment.
Заявляемое изобретение иллюстрируется следующими чертежами, где:The invention is illustrated by the following drawings, where:
На фиг. 1 изображена мобилизация пупочной вены.In FIG. 1 shows the mobilization of the umbilical vein.
На фиг. 2 - реканализация пупочной вены.In FIG. 2 - recanalization of the umbilical vein.
На фиг. 3 - пупочный катетер.In FIG. 3 - umbilical catheter.
На фиг. 4 - окончательный вид послеоперационной раны с фиксированным катетером к передней брюшной стенке.In FIG. 4 - the final view of the postoperative wound with a fixed catheter to the anterior abdominal wall.
На фиг. 5 - способ озонирования физиологического раствора и перфторана.In FIG. 5 - a method of ozonation of saline and perfluorane.
Подробное описание способа и пример его клинического примененияA detailed description of the method and an example of its clinical application
Оперативное пособие проводят под эндотрахеальным наркозом. После выполнения широкой срединной или поперечной лапаротомии производят тщательную ревизию брюшинной полости и забрюшинного пространства со стороны живота.Surgical allowance is carried out under endotracheal anesthesia. After performing a wide median or transverse laparotomy, a thorough revision of the peritoneal cavity and retroperitoneal space from the abdomen is performed.
После устранения источника перитонита, проведения назоинтестинальной интубации, лаважа и дренирования брюшной полости перед ушиванием срединной раны из круглой связки печени выделяют пупочную вену, идущей к воротам печени. После рассечения брюшины выполняется мобилизация пупочной вены на протяжении не менее 3 см (фиг. 1). Под вену подводят две капроновые нити, между которыми, в поперечном направлении на ![]()
![]()
Далее в раннем послеоперационном периоде (1-3 сутки), нами выполнялась инфузия озонированных растворов и перфторана по следующей методике.Further, in the early postoperative period (1-3 days), we infused ozonated solutions and perfluorane according to the following procedure.
Озонирование физиологического раствора и перфторана осуществляют путем барботирования его озоно-кислородной смесью (т.е. озоно-кислородная смесь пропускается через физиологический раствор и перфторан по полихлорвиниловой трубке, фиг. 5-2) в течение 15-20 минут со скоростью 0,5 л/мин с концентрацией озона 800-1000 мкг/л. Для данной процедуры использованы заводские флаконы с перфтораном и физиологическим раствором (фиг. 5-3), еще один стерильный пустой флакон (фиг. 5-5) емкостью 400 мл, укупоренный резиновой крышкой и обжатый алюминиевым колпачком. Для этого использовался обычный флакон с физиологическим раствором, предварительно опорожнив его стерильным шприцем. Флакон с перфтораном соединялся с пустым стерильным флаконом с помощью полихлорвиниловой трубки с двумя иглами на концах (фиг. 5-4), вводя иглы: одну во флакон с перфтораном, а другую - в пустой, стерильный флакон. В этом случае трубка для отведения в деструктор озона использованной газовой смеси выходит не из флакона с раствором, а из другого, соединенного с ним пустого флакона, как показано на фиг. 5 (фиг. 5-4 и 5-5), что предотвращает попадание озонированного раствора и перфторана в деструктор (фиг. 5-6). Для получения озонированного раствора и перфторана использован озонатор «Медозонс-БМ» фирмы ОАО «Арзамасский приборостроительный завод».Ozonation of saline and perfluorane is carried out by bubbling it with an ozone-oxygen mixture (i.e., the ozone-oxygen mixture is passed through saline and perfluorane through a polyvinyl chloride tube, Fig. 5-2) for 15-20 minutes at a rate of 0.5 l / min with an ozone concentration of 800-1000 μg / l. For this procedure, factory bottles with perfluorane and physiological saline were used (Fig. 5-3), another sterile empty bottle (Fig. 5-5) with a capacity of 400 ml, corked with a rubber cap and crimped with an aluminum cap. To do this, we used an ordinary bottle with physiological saline, after emptying it with a sterile syringe. The perfluorane vial was connected to an empty sterile vial using a polyvinyl chloride tube with two needles at the ends (Fig. 5-4), introducing needles: one into the vial with perfluorane and the other into an empty, sterile vial. In this case, the tube for discharging the used gas mixture to the ozone destructor does not exit from the solution bottle, but from another empty bottle connected to it, as shown in FIG. 5 (Figs. 5-4 and 5-5), which prevents the ozonized solution and perfluorane from entering the destructor (Figs. 5-6). To obtain the ozonized solution and perfluorane, the Medozons-BM ozonizer of the company Arzamas Instrument-Making Plant OJSC was used.
При подсчете дозы введенного пациенту озона учитывалось, что концентрация растворенного в физиологическом растворе озона в среднем составляет 20% от концентрации озона в барботирующей раствор газовой смеси, то есть коэффициент пересчета равен 0,2. Это означает, что, например, при концентрации озона в озоно-кислородной смеси 1000 мкг/л в 1 литре физиологического раствора растворится 0,2×1000=200 мкг О3 (ошибка подсчета не более 10%).When calculating the dose of ozone introduced to the patient, it was taken into account that the concentration of ozone dissolved in physiological saline is on average 20% of the concentration of ozone in the bubbling solution of the gas mixture, i.e., the conversion factor is 0.2. This means that, for example, when the concentration of ozone in the ozone-oxygen mixture is 1000 μg / L in 1 liter of physiological solution, 0.2 × 1000 = 200 μg O3 will dissolve (calculation error is not more than 10%).
Внутрипортальная инфузия озонированным перфтораном проводилась в 1-2 сутки после операции капельным способом по 40 капель в 1 мин. Соответственно проводился мониторинг портальной крови с целью оценки функционального состояния печени: билирубина, белка, альбуминов, активности АлТ и АсТ, насыщение кислородом портальной крови, а также УЗ-контроль с оценкой скорости печеночного кровотока. Далее на 3-5 сутки проводилась внутрипортальная инфузия озонированным физиологическим раствором, с вышеуказанной схемой мониторинга. При улучшении общего состояния пациента, отрицательном результате бактериологического исследования крови из портальной системы на анаэробные микроорганизмы (через 5-6 дней после операции) введение озонированных растворов прекращалось. Катетер в пупочной вене сохранялся для введения глюкозо-электролитных растворов, витаминов, кровезаменителей, а затем извлекали с соблюдением правил асептики и мер, предупреждающих кровотечение из реканализированной пупочной вены.Intraportal infusion with ozonated perfluorane was carried out 1-2 days after the operation by the drip method of 40 drops per 1 min. Accordingly, portal blood was monitored to assess the functional state of the liver: bilirubin, protein, albumin, ALT and ACT activity, oxygen saturation of portal blood, as well as ultrasound control with an assessment of the speed of hepatic blood flow. Then, for 3-5 days, intraportal infusion was carried out with ozonized physiological saline, with the above monitoring scheme. With an improvement in the general condition of the patient, a negative result of bacteriological blood tests from the portal system for anaerobic microorganisms (5-6 days after surgery), the introduction of ozonated solutions was stopped. The umbilical vein catheter was stored for the administration of glucose-electrolyte solutions, vitamins, blood substitutes, and then removed in compliance with aseptic rules and measures to prevent bleeding from the recanalized umbilical vein.
Оценка эндотоксикоза проводилась на основе клинических параметров и лабораторных критериев (ЛИИ, СМП, миоглобин, содержание мочевины и креатинина). Выраженность системной воспалительной реакции оценивалась по уровню содержания белков острой фазы воспаления (СРБ, фибриноген). Оценка функционального состояния печени проводилась по показателям уровня общего билирубина, белка, альбуминов, активности АлТ и АсТ.Evaluation of endotoxemia was carried out on the basis of clinical parameters and laboratory criteria (LII, SMP, myoglobin, urea and creatinine content). The severity of the systemic inflammatory reaction was evaluated by the level of protein content of the acute phase of inflammation (CRP, fibrinogen). Assessment of the functional state of the liver was carried out by indicators of the level of total bilirubin, protein, albumin, ALT and AcT activity.

Как видно из таблицы 1, исходные проявления эндогенной интоксикации в исследуемых группах были максимальными, что соответствовало выраженным явлениям эндотоксикоза и печеночной недостаточности. На фоне проведения патогенетически направленных лечебных мероприятий, включающих интрапортальную инфузию озонированного физиологического раствора, отмечается отчетливая положительная динамика, начиная с первых послеоперационных суток и достигающая максимума к пятым суткам. Так, С-реактивный белок у пациентов I группы к 5 суткам достигал 164,9±3,1 мг/л, а во II исследуемой группе, составлял 123,5±2,9 мг/л.As can be seen from table 1, the initial manifestations of endogenous intoxication in the studied groups were maximum, which corresponded to the pronounced phenomena of endotoxemia and liver failure. Against the background of pathogenetically directed therapeutic measures, including intraportal infusion of ozonized physiological saline, a distinct positive dynamics is noted, starting from the first postoperative days and reaching a maximum by the fifth day. So, C-reactive protein in patients of group I by

Судя по результатам, представленным в таблице 2, на фоне проведения патогенетически направленной терапии макрофагальной печеночной недостаточности, имело место выраженное снижение уровня «шлаков» крови у пациентов II группы, по сравнению с контрольной исследуемой группой. Так, на 5 сутки послеоперационного течения, уровень креатинина у больных I группы достигал в среднем 121,2±4,0 мкмоль/л, тогда как у пациентов II группы данный показатель снизился до 98,9±3,1 мкмоль/л. Мочевина у больных I группе на 3 сутки послеоперационного периода достигала 16,4±0,3 мкмоль/л, а во II-ой, исследуемой группе снижалась до 11,2±0,1 мкмоль/л.Judging by the results presented in table 2, against the background of pathogenetically directed therapy of macrophage liver failure, there was a pronounced decrease in the level of "blood slag" in patients of group II, compared with the control study group. So, on the 5th day of the postoperative course, the creatinine level in patients of group I reached an average of 121.2 ± 4.0 μmol / l, while in patients of group II this indicator decreased to 98.9 ± 3.1 μmol / l. Urea in patients of group I on the 3rd day of the postoperative period reached 16.4 ± 0.3 μmol / l, and in the second, studied group, it decreased to 11.2 ± 0.1 μmol / l.
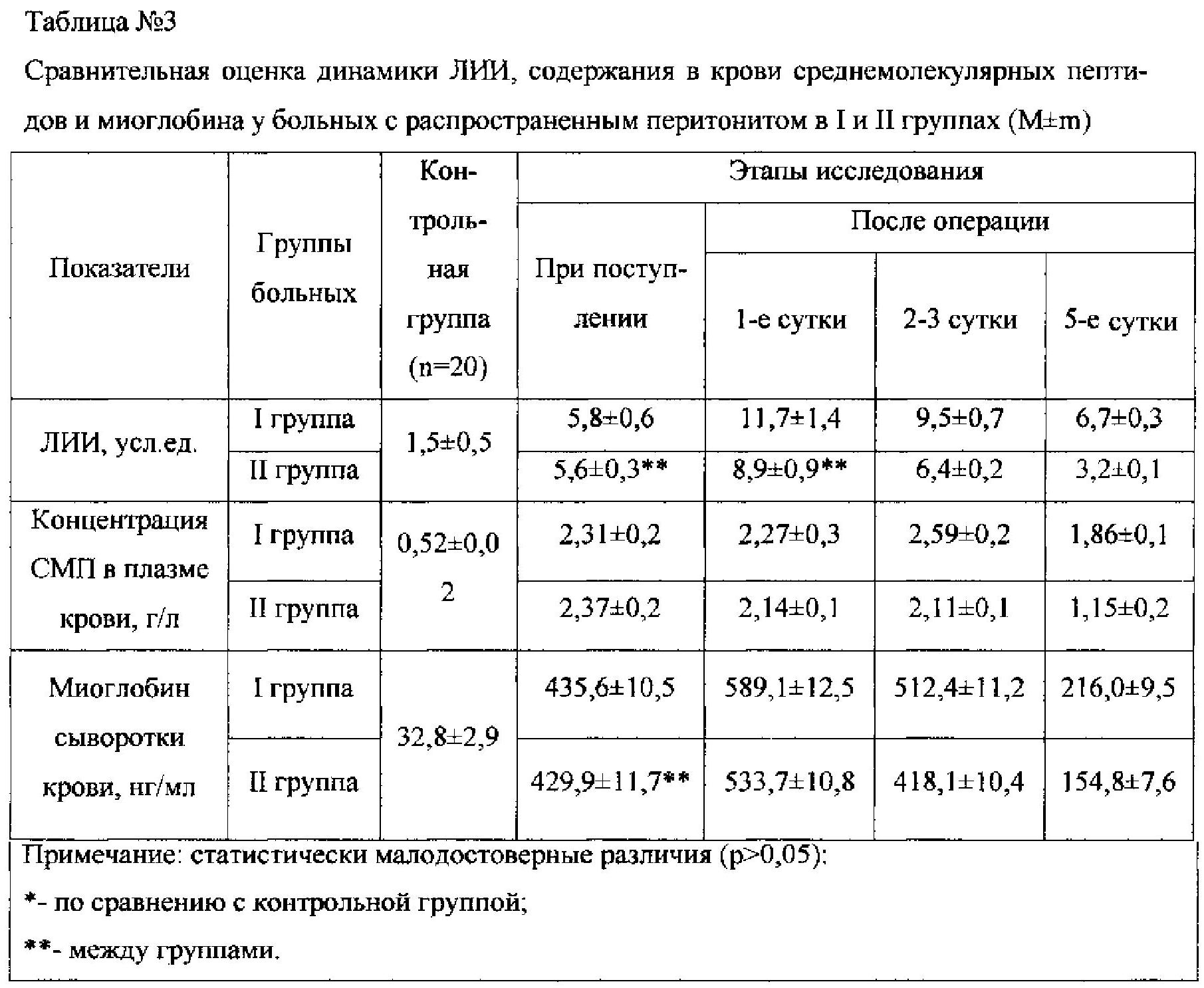
Из данных, представленных в таблице 3, следует, что на фоне введения озонированного физиологического раствора, имело место отчетливое снижение показателей эндогенной интоксикации, в контрольной группе более чем в 2 раза к пятым послеоперационным суткам.From the data presented in table 3, it follows that against the background of the introduction of ozonized physiological saline, there was a clear decrease in the indicators of endogenous intoxication, in the control group more than 2 times by the fifth postoperative day.
Клинический пример. Больной А., 75 лет, поступил в клинику на 8-е сутки от начала заболевания с диагнозом: Острый деструктивный аппендицит? перитонит? ОКН?, эндотоксикоз II степени, с-г мочевого пузыря T1N0M0, состояние после ТУР. ХИБС, коронарокардиосклероз. При поступлении состояние больного тяжелое (по шкале SAPS 5-9 баллов, прогностическая летальность 7,9%, оценка тяжести по шкале Глазго - 14), больной вял, кожные покровы бледно-розовой окраски, покрыты холодным потом. В легких с обеих сторон жесткое, дыхание, хрипов нет. ЧДД 19 в минуту. Артериальное давление 130/90 мм рт. ст., ЧСС 90 в минуту. Язык сухой, обложен серым налетом, живот равномерно вздут. При пальпации живот резко болезненный во всех отделах, преимущественно в нижних отделах (левая и правая подвздошные области), напряжен. Определяются положительные симптомы раздражения брюшины. Перкуторно над всей поверхностью живота определяется тимпанит, аускультативно - перистальтика резко ослаблена. В общем анализе крови лейкоцитоз 15,2×10%, ЛИИ=10,1 расч. ед., мочевина 12,5 ммоль/л, креатинин 224 мкмоль/л, билирубин 34,1 мкмоль/л. При лапаротомии в брюшинной полости до 2000 мл гнойно-фибринозного выпота, обращают на себя внимание спаянные между собой рыхлыми спайками, расширенные до 6 см, петли тонкой кишки, в просвете отмечается наличие секвестрированной жидкости, перистальтика отсутствует. В правой подвздошной ямке визуализирован червеобразный отросток, увеличен в размерах, напряжен, у основания перфорация до 0,2 см. Выполнена аппендэктомия. После блокады корня брыжейки тонкой кишки 0,25% раствором новокаина в количестве 100 мл выполнена тотальная назоинтестинальная интубация с интраоперационной энтеросорбцией. Проведена реканализация и катетеризация пупочной вены с ее канюлированием. На вторые сутки после операции проведена внутрипортальная инфузия озонированным перфтораном капельным способом по 40 капель в 1 мин. Соответственно проводился мониторинг портальной крови с целью оценки функционального состояния печени: билирубина, белка, альбуминов, активности АлТ и АсТ, насыщение кислородом портальной крови, а также УЗ-контроль с оценкой скорости печеночного кровотока. Далее на третьи сутки провели внутрипортальную инфузию озонированным физиологическим раствором, с вышеуказанной схемой мониторинга.Clinical example. Patient A., 75 years old, was admitted to the clinic on the 8th day from the onset of the disease with a diagnosis of Acute destructive appendicitis? peritonitis? OKN ?, endotoxicosis of the II degree, c-g of the bladder T1N0M0, condition after TUR. HIBS, coronary cardiosclerosis. Upon admission, the patient's condition is severe (on a SAPS scale of 5–9 points, prognostic mortality of 7.9%, Glasgow severity rating is 14), the patient is sluggish, the skin is pale pink in color, covered with cold sweat. In the lungs on both sides, hard breathing, no rales. NPV 19 per minute. Blood pressure 130/90 mm RT. Art., heart rate of 90 per minute. The tongue is dry, coated with a gray coating, the stomach is evenly swollen. On palpation, the abdomen is sharply painful in all departments, mainly in the lower sections (left and right iliac regions), tense. The positive symptoms of peritoneal irritation are determined. Percussion over the entire surface of the abdomen is determined by tympanitis, auscultatory - peristalsis is sharply weakened. In the general analysis of blood leukocytosis 15.2 × 10%, LII = 10.1 calc. units, urea 12.5 mmol / L, creatinine 224 μmol / L, bilirubin 34.1 μmol / L. With laparotomy in the peritoneal cavity up to 2000 ml of purulent-fibrinous effusion, attention is paid to soldered together by loose adhesions, expanded to 6 cm, loops of the small intestine, the presence of sequestered fluid is noted in the lumen, there is no peristalsis. In the right iliac fossa, the vermiform appendix is visualized, enlarged, strained, perforation at the base up to 0.2 cm. Appendectomy was performed. After blockade of the mesentery root of the small intestine with 0.25% novocaine solution in an amount of 100 ml, total nasointestinal intubation with intraoperative enterosorption was performed. Recanalization and catheterization of the umbilical vein with its cannulation was performed. On the second day after the operation, intraportal infusion was carried out by the drip method with ozonized perfluorane, 40 drops per 1 min. Accordingly, portal blood was monitored to assess the functional state of the liver: bilirubin, protein, albumin, ALT and ACT activity, oxygen saturation of portal blood, as well as ultrasound control with an assessment of the speed of hepatic blood flow. Then, on the third day, intraportal infusion was carried out with ozonized physiological saline, with the above monitoring scheme.
Больной переведен в отделение реанимации для проведения интенсивной инфузионной, антибактериальной, дезинтоксикационной терапии, лаваж кишечника с энтеросорбентами, раннее энтеральное зондовое питание. К 4-м суткам состояние больного стабилизировалось, значительно уменьшились признаки эндогенной интоксикации (АД 131/89 мм рт. ст., ЧСС 91 в минуту, ЧДД 22 в минуту, ЛИИ 5,25 расч. ед., мочевина 11,1 ммоль/л., креатинин 97 мкмоль/л, билирубин 7,5 мкмоль), парез кишечника сохранялся. К 6-м суткам состояние больного значительно улучшилось (АД 130/80 мм рт. ст., ЧСС 80 в минуту, ЧДД 16 в минуту, ЛИИ 5,0 расч. ед., мочевина 10,0 ммоль/л., креатинин 121 мкмоль/л), перистальтика активная, газы отходят. Количество отделяемого по назоинтестинальному зонду значительно уменьшилось. Зонд удален. Дренажные трубки удалены на 5 сутки от момента операции. Больной выписан на 15 сутки после операции. Исход - выздоровление.The patient was transferred to the intensive care unit for intensive infusion, antibacterial, detoxification therapy, intestinal lavage with enterosorbents, early enteral tube feeding. By the 4th day, the patient's condition stabilized, signs of endogenous intoxication significantly decreased (BP 131/89 mm Hg, heart rate 91 per minute, NPV 22 per minute, LII 5.25 calculation units, urea 11.1 mmol / l., creatinine 97 μmol / l, bilirubin 7.5 μmol), intestinal paresis persisted. By the 6th day, the patient's condition improved significantly (blood pressure 130/80 mm Hg. Art., Heart rate 80 per minute, NPV 16 per minute, LII 5.0 calculated units, urea 10.0 mmol / l., Creatinine 121 μmol / l), active peristalsis, gases go away. The amount of discharge through the nasointestinal probe decreased significantly. The probe has been deleted. Drainage tubes removed 5 days from the time of surgery. The patient was discharged 15 days after surgery. The outcome is recovery.
Предлагаемый способ лечения апробирован нами на 17 больных с распространенным перитонитом, семи из которых в 1-2 послеоперационные сутки вводился озонированный перфторан, при этом летальность в данной группе составила всего лишь 12,5%, что значительно превышает среднестатистические показатели при данной патологии.The proposed method of treatment was tested by us for 17 patients with peritonitis, seven of whom ozonated perfluorane was administered on the 1-2 postoperative day, while the mortality in this group was only 12.5%, which significantly exceeds the average statistics for this pathology.
Предложенный способ позволяет улучшить результаты лечения больных с распространенным перитонитом.The proposed method allows to improve the treatment results of patients with advanced peritonitis.
Заявляемый способ лечения в комплексной терапии у больных с распространенным перитонитом апробирован на достаточном клиническом материале, показал эффективность применения и может быть рекомендован к использованию в специализированных хирургических стационарах.The claimed method of treatment in complex therapy in patients with advanced peritonitis has been tested on sufficient clinical material, has shown its effectiveness and can be recommended for use in specialized surgical hospitals.
Список использованной литературы List of references
1. Ерюхин И.А., Петров В.П., Ханевич М.Д. Кишечная непроходимость: руководство для врачей, 1999.1. Eryukhin I.A., Petrov V.P., Kanevich M.D. Intestinal Obstruction: A Guide for Physicians, 1999.
2. Авдовенко А.Л., Гостищев В.К., Сажин В.П. Перитонит: Монография, 2002.2. Avdovenko A.L., Gostishchev V.K., Sazhin V.P. Peritonitis: Monograph, 2002.
3. Жадкевич М.М., Матвеев Д.В., Мишнев О.Д. и др. Печеночная недостаточность у больных перитонитом // Вестник хирургии, 1989.3. Zhadkevich M.M., Matveev D.V., Mishnev O.D. et al. Hepatic insufficiency in patients with peritonitis // Herald of surgery, 1989.
4. Гологорский В.А., Гельфанд Б.Р., Багдатьев В.Е., Топазова Е.Н. Синдром полиорганной недостаточности у больных с перитонитом // Хирургия. 1988. №2.4. Gologorsky V.A., Gelfand B.R., Bagdatiev V.E., Topazova E.N. Syndrome of multiple organ failure in patients with peritonitis // Surgery. 1988. No. 2.
5. Жадкевич М.М., Бурневич С.З. Ретикулоэндотелиальная система печени у больных перитонитом // Вестник хирургии, 1989.5. Zhadkevich M.M., Burnevich S.Z. Reticuloendothelial system of the liver in patients with peritonitis // Bulletin of surgery, 1989.
6. Беляев С.А. Применение озона для коррекции функциональной активности печени и системы гемостаза при внепеченочном холестазе. - Саранск, 2004.6. Belyaev S.A. The use of ozone to correct the functional activity of the liver and hemostasis system with extrahepatic cholestasis. - Saransk, 2004.
7. Исследование гепатопротекторного действия озонотерапии при остром панкреатите / Ю.С. Винник и др. // Анналы хирургической гепатологии. - 2003. Т. 8. №2.7. The study of the hepatoprotective effect of ozone therapy in acute pancreatitis / Yu.S. Vinnik et al. // Annals of surgical hepatology. - 2003. T. 8. No. 2.
8. Г.Р. Аскерханов, А.М. Голубев, А.Г. Гусейнов и др. // Хирургия, 2000.8. G.R. Askerkhanov, A.M. Golubev, A.G. Huseynov et al. // Surgery, 2000.
9. В.В. Мороз // Хирургия, 2000.9. V.V. Frost // Surgery, 2000.
10. В.В. Мороз, Г.Р. Аскерханов, А.Г. Гусейнов // Пущино, 2001.10. V.V. Frost, G.R. Askerkhanov, A.G. Huseynov // Pushchino, 2001.
11. И.В. Ярема, М.А. Магомедов // Бюлл. экспер. биологии и медицины, 2003.11. I.V. Yarema, M.A. Magomedov // Bull. expert. Biology and Medicine, 2003.
12. Р.Д. Мустафин, Ю.В. Кучин, А.А. Анферов // Мат. Всеросс. научн. конф. // СПб., 2004.12.R.D. Mustafin, Yu.V. Kuchin, A.A. Anferov // Mat. All-Russian. scientific conf. // St. Petersburg, 2004.
13. А.М. Лабазанова, Б.И. Шипиев // Известия Дагестан, гос. пед. ун-та. - 2011.13. A.M. Labazanova, B.I. Shipiev // News of Dagestan, state. ped un-that. - 2011.
14. А.А. Белогривцев, Р.Д. Мустафин, И.З. Китиашвили, Кучин Ю.В. // Общая реаниматология. - 2009.14. A.A. Belogrivtsev, R.D. Mustafin, I.Z. Kitiashvili, Kuchin Yu.V. // General resuscitation. - 2009.
15. Иваницкий Г.Р. Как перфторан обеспечивает газотранспорт // Перфторорганические соединения в биологии и медицине. Пущино, 1999.15. Ivanitsky G.R. How perfluorane provides gas transport // Organofluorine compounds in biology and medicine. Pushchino, 1999.
16. С.П. Алехина, Т.Г. Щербатюк // Н. Новгород: изд-во «Литтера», - 2003.16. S.P. Alekhina, T.G. Shcherbatyuk // N. Novgorod: Litter Publishing House, - 2003.
17. С.Д. Разумовский, В.В.Подмастерьев // Мат. IV науч.-практ. конф. - Н. Новгород, 2000.17. S.D. Razumovsky, V.V. Podmasteriev // Mat. IV scientific and practical. conf. - N. Novgorod, 2000.
18. Е.И. Мохов, С.И. Воробьев, А.Р. Армасов // Вестн. экспер. и клин. хирургии. - 2012.18. E.I. Mokhov, S.I. Vorobiev, A.R. Armasov // Vestn. expert. and wedge. surgery. - 2012.
19. Р.М. Рагимов, Т.С. Гусейнов, Ш.К. Таймазова и др. // Мат. Всеросс. науч. конф. -СПб., 2004.19. R.M. Ragimov, T.S. Huseynov, Sh.K. Taymazova et al. // Mat. All-Russian. scientific conf. -SPb., 2004.
20. А.М. Голубев, Р.М.Рагимов, З.Ш. Манасова, М.З. Саидов // Общая реаниматология. - 2008.20. A.M. Golubev, R.M. Ragimov, Z.S. Manasova, M.Z. Saidov // General resuscitation. - 2008.
21. З.Ш. Манасова // Автореф. дисс. канд. мед. наук. - Ростов-на-Дону, 2009.21. Z.Sh. Manasova // Abstract. diss. Cand. honey. sciences. - Rostov-on-Don, 2009.
22. Р.М. Рагимов, А.М.Голубев, А О.Османов, Б.К.Омаров // Астраханский мед. журнал.- 2010; З.Ш. Манасова, Е.А.Цадкин // Электронный научн.-образоват. вестн. «Здоровье и образование в XXI веке». - 2010.22. R.M. Ragimov, A.M. Golubev, A.O. Osmanov, B.K. Omarov // Astrakhan honey. Journal. - 2010; Z.S. Manasova, E.A. Tsadkin // Electronic Scientific-Educational. Vestn. "Health and education in the XXI century." - 2010.
23. Р.М. Рагимов // Автореф. дисс. докт. мед. наук. - Махачкала, 2010.23. R.M. Ragimov // Author. diss. Doct. honey. sciences. - Makhachkala, 2010.
24. А.О. Османов, Р.М. Рагимов, А.М. Голубев и др. // Вестн. Дагестан. госуд. мед. академии. - 2012.24. A.O. Osmanov, R.M. Ragimov, A.M. Golubev et al. // Vestn. Dagestan. gos. honey. academy. - 2012.
25. Н.А. Локтев и соавтор., 2005; J.W.B. Bradfield, 1974; M. Prytz et al., 1976; K.S. Bermion et al., 1984.25. N.A. Loktev et al., 2005; J.W.B. Bradfield, 1974; M. Prytz et al., 1976; K.S. Bermion et al., 1984.
Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015121148/14A RU2594512C1 (en) | 2015-06-03 | 2015-06-03 | Method for intraportal ozone therapy in patients with widespread peritonitis |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015121148/14A RU2594512C1 (en) | 2015-06-03 | 2015-06-03 | Method for intraportal ozone therapy in patients with widespread peritonitis |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2594512C1 true RU2594512C1 (en) | 2016-08-20 |
Family
ID=56697099
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2015121148/14A RU2594512C1 (en) | 2015-06-03 | 2015-06-03 | Method for intraportal ozone therapy in patients with widespread peritonitis |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2594512C1 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2634630C1 (en) * | 2016-11-11 | 2017-11-02 | Борис Михайлович Белик | Method for intestine peristalsis stimulation in complex treatment of abdominal infection |
| RU2758124C1 (en) * | 2021-04-15 | 2021-10-26 | Общество с ограниченной ответственностью "Гардлайнер" | Device for intravenous infusions in ozone therapy |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2154997C1 (en) * | 1999-03-12 | 2000-08-27 | Чернов Виктор Николаевич | Method of treating generalized peritonitis |
| RU2199326C2 (en) * | 1999-08-18 | 2003-02-27 | Красноярская медицинская государственная академия | Treating endotoxicosis in patients with destructive pancreatitis |
| UA53059U (en) * | 2010-03-04 | 2010-09-27 | Игорь Андреевич Криворучко | method for correction of blood circulation at purulent-necrotic diseases and damages of abdominal cavity bodies |
| RU2445130C2 (en) * | 2009-05-04 | 2012-03-20 | Государственное образовательное учреждение высшего профессионального образования "Дагестанская государственная медицинская академия федерального агентства по здравоохранению и социальному развитию" | Method for prevention of postoperative enteroparesis |
-
2015
- 2015-06-03 RU RU2015121148/14A patent/RU2594512C1/en not_active IP Right Cessation
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2154997C1 (en) * | 1999-03-12 | 2000-08-27 | Чернов Виктор Николаевич | Method of treating generalized peritonitis |
| RU2199326C2 (en) * | 1999-08-18 | 2003-02-27 | Красноярская медицинская государственная академия | Treating endotoxicosis in patients with destructive pancreatitis |
| RU2445130C2 (en) * | 2009-05-04 | 2012-03-20 | Государственное образовательное учреждение высшего профессионального образования "Дагестанская государственная медицинская академия федерального агентства по здравоохранению и социальному развитию" | Method for prevention of postoperative enteroparesis |
| UA53059U (en) * | 2010-03-04 | 2010-09-27 | Игорь Андреевич Криворучко | method for correction of blood circulation at purulent-necrotic diseases and damages of abdominal cavity bodies |
Non-Patent Citations (1)
| Title |
|---|
| БЕЛЯЕВ С.А. и др. "Влияние внутрипортальной озонотерапии на функциональное состояние печени в комплексном лечении обтурационного холестаза" // "Медицинский альманах", N3 (27) август 2013, стр.96-98. ABDULLAEV IA "Effect on performance ozonized perftoran cytokine profile in generalized peritonitis". Khirurgiia (Mosk). 2014;(9):30-2, реферат, найдено 02.03.2016 из PubMed PMID: 25327742. * |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2634630C1 (en) * | 2016-11-11 | 2017-11-02 | Борис Михайлович Белик | Method for intestine peristalsis stimulation in complex treatment of abdominal infection |
| RU2758124C1 (en) * | 2021-04-15 | 2021-10-26 | Общество с ограниченной ответственностью "Гардлайнер" | Device for intravenous infusions in ozone therapy |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Potapov et al. | Guidelines for the diagnosis and treatment of severe traumatic brain injury. Part 2. Intensive care and neuromonitoring | |
| RU2594512C1 (en) | Method for intraportal ozone therapy in patients with widespread peritonitis | |
| RU2400259C1 (en) | Method of preperitoneal blocade in post-operation period | |
| RU2445130C2 (en) | Method for prevention of postoperative enteroparesis | |
| Tivers et al. | Gastric dilation‐volvulus syndrome in dogs 1. Pathophysiology, diagnosis and stabilisation | |
| RU2496493C1 (en) | Method for prevention of acute postoperative pancreatitis | |
| RU2348415C2 (en) | Method of adhesion therapy following thoracic and abdominal organs surgery | |
| RU2460552C2 (en) | Method for preoperative preparation of patients suffering extensive peritonitis | |
| RU2432944C2 (en) | Method of preventing postoperative commissural process in abdominal cavity | |
| Adamantos et al. | Emergency care of the cat with multi‐trauma | |
| RU2523822C1 (en) | Method for postoperative prevention of colocolonic anastomotic leakage | |
| RU2634630C1 (en) | Method for intestine peristalsis stimulation in complex treatment of abdominal infection | |
| RU2428191C1 (en) | Method of local dosed ozone therapy following gall bladder and/or bile passages surgery | |
| RU2699919C1 (en) | Method for determining indications for operation of programmed sanation relaparotomy in peritonitis | |
| RU2190412C2 (en) | Method for body detoxication | |
| RU2265455C1 (en) | Method for treating chemical esophageal burns | |
| RU2199326C2 (en) | Treating endotoxicosis in patients with destructive pancreatitis | |
| RU2446756C1 (en) | Method of treating purulent-necrotic pancreonecrosis | |
| RU2212852C2 (en) | Surgical method for preventing pancreonecrosis development | |
| RU2341269C1 (en) | Method of surgical endotoxicosis treatment | |
| RU2154505C1 (en) | Method for treating abdominal cavity in acute peritonitis cases | |
| SU1421317A1 (en) | Method of treatment of acute purulent peritonitis | |
| RU2340367C1 (en) | Method of treatment of intestinal insufficiency in postoperative period | |
| RU2197972C2 (en) | Method for indirect intestinal electrochemical detoxication in patients with intestinal obstruction | |
| RU1780751C (en) | Method for treating vertebrogenous paint syndrome |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees |
Effective date: 20170604 |