RU2707433C1 - Method for lower occlusion treatment by prosthetic repair - Google Patents
Method for lower occlusion treatment by prosthetic repair Download PDFInfo
- Publication number
- RU2707433C1 RU2707433C1 RU2019104434A RU2019104434A RU2707433C1 RU 2707433 C1 RU2707433 C1 RU 2707433C1 RU 2019104434 A RU2019104434 A RU 2019104434A RU 2019104434 A RU2019104434 A RU 2019104434A RU 2707433 C1 RU2707433 C1 RU 2707433C1
- Authority
- RU
- Russia
- Prior art keywords
- treatment
- jaw
- jaws
- compression
- force
- Prior art date
Links
Images


Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61C—DENTISTRY; APPARATUS OR METHODS FOR ORAL OR DENTAL HYGIENE
- A61C7/00—Orthodontics, i.e. obtaining or maintaining the desired position of teeth, e.g. by straightening, evening, regulating, separating, or by correcting malocclusions
Landscapes
- Health & Medical Sciences (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Dentistry (AREA)
- Epidemiology (AREA)
- Life Sciences & Earth Sciences (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Dental Tools And Instruments Or Auxiliary Dental Instruments (AREA)
Abstract
Description
Изобретение относится к медицине, а именно к стоматологии, и предназначено для лечения больных с дисфункцией жевательной мускулатуры.The invention relates to medicine, namely to dentistry, and is intended for the treatment of patients with masticatory muscular dysfunction.
По литературным данным дисфункцией жевательной мускулатуры страдают до 85% населения. В основе нарушений мышечных функций лежат изменения сократительных процессов в мускулатуре. Нарушение функции жевательной мускулатуры приводит к развитию генерализованных форм пародонтита, повышенной стираемости твердых тканей зубов, осложняющихся снижением высоты прикуса и болевой дисфункцией височно-нижнечелюстного сустава.According to published data, up to 85% of the population suffer from masticatory musculature dysfunction. The basis of violations of muscle functions are changes in contractile processes in the musculature. A violation of the function of the masticatory muscles leads to the development of generalized forms of periodontitis, increased abrasion of hard tooth tissues, complicated by a decrease in the height of the bite and pain dysfunction of the temporomandibular joint.
Известно большое разнообразие методов лечения стоматологических больных с дисфункцией жевательной мускулатуры. К ним относятся медикаментозная терапия, мануальная терапия, иглорефлексотерапия, ортопедическое лечение (протезирование) и физиотерапия. Предлагаемый способ относится к комплексному лечению, включающему протезирование.A wide variety of treatment methods for dental patients with masticatory muscular dysfunction are known. These include drug therapy, manual therapy, acupuncture, orthopedic treatment (prosthetics) and physiotherapy. The proposed method relates to complex treatment, including prosthetics.
Для разработки эффективного лечения предварительно проводят диагностику пациентов с различной степенью поражения жевательных мышц. Разработана классификация различных типов дисфункции и разработаны методики лечения для каждого типа нарушений.To develop effective treatment, patients with various degrees of masticatory muscle damage are pre-diagnosed. A classification of various types of dysfunction has been developed and treatment methods have been developed for each type of disorder.
Существуют различные способы определения центрального соотношения челюстей у больных со сниженным прикусом перед окончательным протезированием. По результатам определения центрального соотношения челюстей с применением аппарата «АОЦО-М» пациенты делятся на три группы по виду распределения усилий сжатия челюстей (Войтяцкая И.В., 2017. Анатомо-физиологическое обоснование объема и тактики лечения стоматологических больных со сниженным прикусом: диссертация д-ра. мед наук: 14.01.14 - Стоматология: СПБ, СЗГМУ им. И.И. Мечникова, 338., стр. 140-142, 187, 209-213). Три вида графиков центрального соотношения челюстей у больных со сниженным прикусом представлены в таблице 1.There are various methods for determining the central jaw ratio in patients with reduced occlusion before the final prosthetics. According to the results of determining the central correlation of the jaws using the AOTsO-M apparatus, patients are divided into three groups according to the type of distribution of the jaw compression efforts (I.Voityatskaya, 2017. Anatomical and physiological substantiation of the volume and tactics of treatment of dental patients with reduced occlusion: thesis -ra. honey of sciences: 01/14/14 - Dentistry: St. Petersburg, SZGMU named after II Mechnikov, 338., pp. 140-142, 187, 209-213). Three types of graphs of the central ratio of the jaws in patients with a reduced occlusion are presented in table 1.

Однопиковый вариант зависимости силовых показателей усилий сжатия челюстей характеризует сохранное функциональное состояние зубочелюстного аппарата. Лечение больных с однопиковым вариантом графика следует проводить по одноэтапной схеме, описанной в диссертации Войтяцкой И.В.The one-peak version of the dependence of the force indicators of the jaw compression forces characterizes the preserved functional state of the dentition. Treatment of patients with a single-peak schedule option should be carried out according to the one-stage scheme described in the thesis of I.V.
Беспиковый вариант зависимости силовых показателей усилий сжатия челюстей характеризует сниженное функциональное состояние зубочелюстного аппарата и требует перед протезированием изготовления лечебной каппы и лечение на каппе. Только после лечения на каппе возможно окончательное протезирование.The peakless version of the dependence of the force indicators of the jaw compression forces characterizes the reduced functional state of the dentofacial apparatus and requires the manufacture of a medical mouthguard and treatment on the mouthguard before prosthetics. Only after treatment on the mouth guard is final prosthetics possible.
Двухпиковый вариант зависимости силовых показателей усилий сжатия челюстей характеризует резко сниженное функциональное состояние зубочелюстного аппарата и требует длительного комплексного лечения.The two-peak variant of the dependence of the force indicators of the jaw compression forces characterizes a sharply reduced functional state of the dentition and requires a long complex treatment.
Таким образом, лечение больных с двумя последними вариантами силовых показателей усилий сжатия челюстей существенно сложнее и дольше, чем протезирование больных с первым вариантом. Сложность состоит в дополнительном этапе протезирования (с применением лечебной каппы), который может занимать от нескольких недель до нескольких месяцев и в ряде случаев в дополнительном лечении у врачей других специальностей (невролог, остеопат, эндокринолог и др.)Thus, the treatment of patients with the last two options for strength indicators of jaw compression efforts is much more complicated and longer than prosthetics for patients with the first option. The difficulty lies in the additional stage of prosthetics (using therapeutic mouthguards), which can take from several weeks to several months and in some cases in additional treatment by doctors of other specialties (neurologist, osteopath, endocrinologist, etc.)
Многолетние исследования и опыт протезирования больных показал, что у части больных с беспиковым вариантом силовых показателей усилий сжатия челюстей возможно восстановление функционального состояния зубочелюстного аппарата более простым способом по одноэтапной схеме.Long-term studies and the experience of prosthetics of patients showed that in some patients with a peakless version of the force indicators of the jaw compression efforts, the functional state of the dentition can be restored in a simpler way according to a one-stage scheme.
Прототипом предлагаемого способа лечения можно считать лечение больных с беспиковым вариантом зависимости силовых показателей усилий сжатия челюстей, описанный в диссертации Войтяцкой И.В (Войтяцкая И.В., 2017. Анатомо-физиологическое обоснование объема и тактики лечения стоматологических больных со сниженным прикусом: диссертация д-ра. мед наук: 14.01.14 - Стоматология: СПБ, СЗГМУ им. И.И. Мечникова, стр. 234-236. Учебное пособие «Функционально-физиологический метод определения соотношения челюстей» СПБ Человек. 2017, стр. 27).The prototype of the proposed method of treatment can be considered the treatment of patients with a peakless version of the dependence of the strength indicators of the jaw compression efforts, described in the dissertation by I.Voityatskaya (I.V. Voitatskaya, 2017. Anatomical and physiological rationale for the volume and tactics of treatment of dental patients with a reduced bite: dissertation Doctor of Medical Sciences: 01/14/14 - Dentistry: St. Petersburg, North-Western State Medical University named after II Mechnikov, pp. 234-236. Textbook "Functional-physiological method for determining the ratio of the jaws" St. Petersburg Man. 2017, p. 27).
Техническим результатом предлагаемого решения является упрощение лечения сниженного прикуса и повышение эффективности лечения.The technical result of the proposed solution is to simplify the treatment of reduced occlusion and increase the effectiveness of treatment.
Для достижения заявленного результата в способе лечения сниженного прикуса путем протезирования, включающем определение центрального соотношение челюстей и измерение аппаратом АОЦО-М силы сжатия челюстей, меняют процедуру лечения перед окончательным протезированием. При выявлении беспикового варианта зависимости силовых показателей усилий сжатия челюстей проводят чрескожную электронейростимуляцию, после которой повторно проводят измерение аппаратом АОЦО-М силы сжатия челюстей, при получении в процессе повторного измерения однопикового вида графика силовых показателей усилий сжатия челюстей переходят к протезированию.To achieve the claimed result in the method of treating a reduced occlusion by means of prosthetics, which includes determining the central jaw ratio and measuring the jaw compression force by the AOCO-M apparatus, the treatment procedure is changed before the final prosthesis. If a peakless variant of the dependence of the force indicators of the jaw compression efforts is detected, percutaneous electroneurostimulation is performed, after which the AOZO-M apparatus measures the jaw compression forces again, when a single-peak view of the graph of the force indicators of the jaw compression forces is transferred to prosthetics during repeated measurement.
Замена лечения на каппе, включающее изготовление лечебной каппы и многодневное лечение с каппой, определением функциональных возможностей жевательных мышц путем одноэтапного лечения чрескожной электронейростимуляцией существенно упрощает процесс лечения дисфункции и ускоряет процесс протезирования.Replacing the treatment on the mouthguard, including the manufacture of therapeutic mouthguard and multi-day treatment with mouthguard, determining the functionality of the masticatory muscles by one-stage treatment of percutaneous electroneurostimulation significantly simplifies the treatment of dysfunction and speeds up the prosthetics process.
Способ осуществляют следующим образом.The method is as follows.
Больные с некомпенсированными формами проявлений общесоматической патологии перед началом протезирования проходят этап функциональной диагностики центрального соотношения челюстей с применением аппарата АОЦО-М.Patients with uncompensated forms of manifestations of general somatic pathology before the start of prosthetics go through the stage of functional diagnostics of the central ratio of the jaws using the apparatus AOTsO-M.
При первом посещении врача у стоматологического больного получают альгинатные оттиски с верхней и нижней челюстей, отливают модели и изготавливают жесткие индивидуальные ложки из пластмассы. Особенностью верхней индивидуальной ложки является наличие опорной площадки в области твердого неба, расположенной от резцового сосочка до уровня первых моляров. На нижней индивидуальной ложке создается площадка, на которой располагается тензометрический датчик прибора АОЦО-М (рисунок 1). Нижняя индивидуальная ложка с перекидными кламмерами позволяет «выключить» периодонто-мускулярный рефлекс, что дает возможность учитывать только морфофункциональное состояние жевательных мышц и элементов ВНЧС.At the first doctor’s visit, the dental patient receives alginate impressions from the upper and lower jaws, models are cast, and individual hard plastic spoons are made. A feature of the upper individual spoon is the presence of a support site in the area of the hard palate, located from the incisal papilla to the level of the first molars. On the lower individual spoon, a platform is created on which the AOCO-M strain gauge sensor is located (Figure 1). The lower individual spoon with flipping clasps allows you to "turn off" the periodontal-muscular reflex, which makes it possible to take into account only the morphofunctional state of the masticatory muscles and TMJ elements.
Во время второго посещения врача проводят этап определения центрального соотношения челюстей с использованием прибора АОЦО-М. При этом путем последовательного разобщения прикуса с применением штифтов различной высоты оценивают значения интегрированного показателя максимального усилия сжатия челюстей, определяют величину уменьшения межальвеолярного расстояния (MAP) и смещения нижней челюсти в сагиттальной и горизонтальной плоскостях (рисунок 2). Для этого на опорную площадку нижней индивидуальной ложки устанавливают датчик с измерительным штифтом минимальной высоты, который фиксирует привычное положение челюстей. Затем определяют диапазон измерений, в котором будет проводиться исследование. Рабочим считается диапазон, в котором стрелка прибора находится в зоне шкалы. Если стрелка выходит за пределы шкалы диапазона, следует перейти на следующий диапазон с помощью нажатия на кнопку второго или третьего диапазонов. В процессе измерений высоту штифта поступательно увеличивают на 1,0 мм. Показания прибора заносят в таблицу карты обследования пациента (таблица 2).During the second visit to the doctor, the stage of determining the central ratio of the jaws is carried out using the AOCO-M device. At the same time, by sequentially dissociating the bite using pins of various heights, the values of the integrated index of the maximum compression force of the jaws are estimated, the magnitude of the decrease in the interalveolar distance (MAP) and the displacement of the lower jaw in the sagittal and horizontal planes are determined (Figure 2). To do this, a sensor with a measuring pin of minimum height is installed on the supporting platform of the lower individual spoon, which fixes the usual position of the jaws. Then determine the range of measurements in which the study will be conducted. The working range is the range in which the arrow of the device is in the area of the scale. If the arrow goes beyond the range scale, go to the next range by pressing the button of the second or third ranges. During measurements, the height of the pin is progressively increased by 1.0 mm. The readings of the device are entered in the table of the patient examination card (table 2).
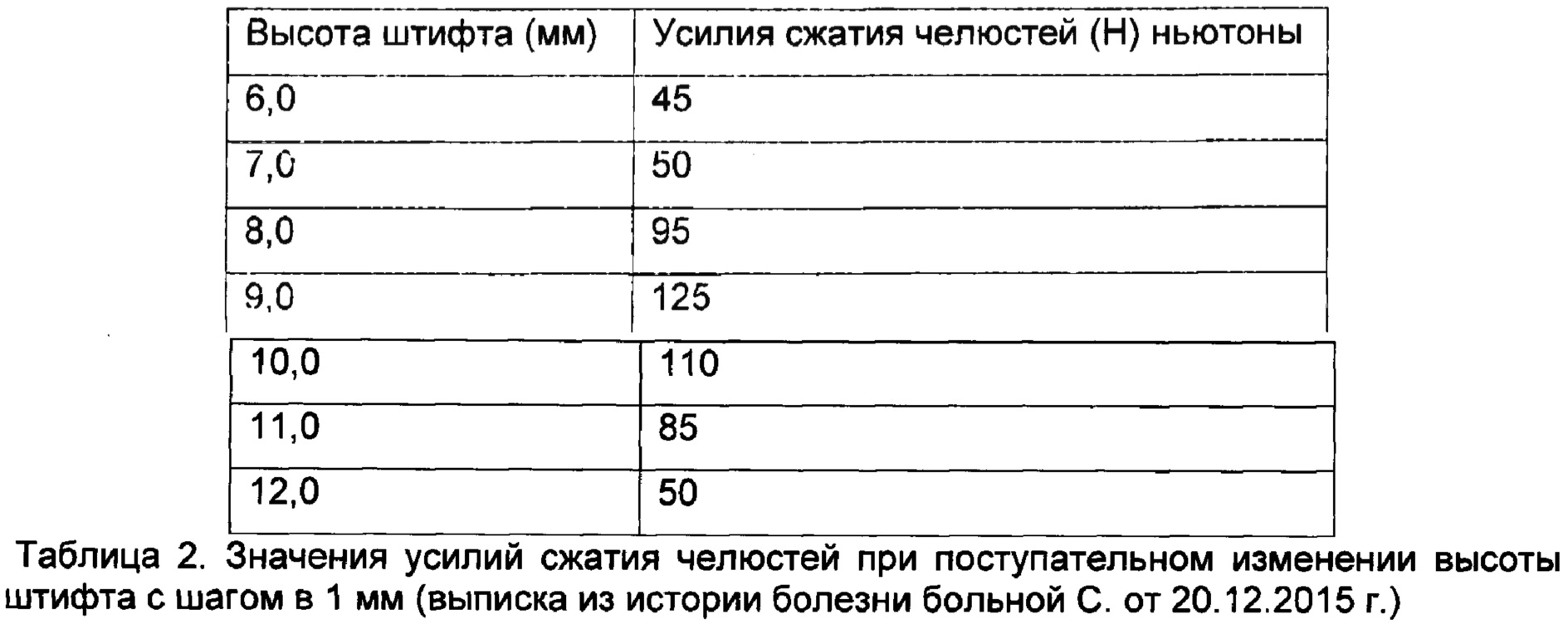
Из таблицы 2 видно, что при поступательном изменении высоты штифтов максимальное значение усилия сжатия челюстей в 125 Н определяется при высоте штифта 9,0 мм.From table 2 it is seen that with a progressive change in the height of the pins, the maximum value of the compression force of the jaws of 125 N is determined at a pin height of 9.0 mm.
Анализируя результаты первой серии измерений, которые проводились с шагом в 1 мм, выбирают высоту штифта, при которой регистрируется максимальное усилие сжатия. Для уточнения найденного положения необходимо повторить серию измерений. Абсолютные значения могут не повторяться при выборе высоты штифта, фиксирующего максимальное значение усилия сжатия челюстей. На этом этапе необходимо уточнить усилия сжатия челюстей при изменении высоты штифта с шагом в 0,5 мм.Analyzing the results of the first series of measurements, which were carried out with a step of 1 mm, select the pin height at which the maximum compression force is recorded. To clarify the found position, it is necessary to repeat a series of measurements. Absolute values may not be repeated when choosing the height of the pin, fixing the maximum value of the compression force of the jaws. At this stage, it is necessary to clarify the compression forces of the jaws when changing the height of the pin in increments of 0.5 mm.
После выбора штифта, фиксирующего максимальное значение следует повторить измерения, проводя их с шагом в 0,5 мм (таблица 3)After selecting the pin that fixes the maximum value, repeat the measurements, taking them in increments of 0.5 mm (table 3)

По мере увеличения высоты штифта регистрируемые усилия сжатия челюстей будут нарастать с последующим их снижением, либо повтором максимального значения (таблица 3).As the pin height increases, the recorded jaw compression forces will increase with their subsequent decrease, or by repeating the maximum value (table 3).
Определив высоту штифта, при котором было выявлено максимальное усилие сжатия челюстей, осуществляют фиксацию конструктивного взаимоотношения челюстей с помощью силиконового материала класса «С» и получают силиконовые регистраты (рисунок 2, 3; 4)Having determined the height of the pin at which the maximum compression force of the jaws was revealed, a structural relationship between the jaws is fixed using silicone material of class “C” and silicone registers are obtained (Figure 2, 3; 4)
У больных с беспиковым вариантом силовых показателей усилий сжатия челюстей выявлены различные дефекты зубных рядов, повышенная стираемость твердых тканей зубов, генерализованный пародонтит. Для этой категории больных наибольший лечебный эффект был выявлен при использовании чрескожной электронейростимуляции импульсами с частотой 15-30 Гц и силой тока 8-10 мА, в течение 15 мин. Т.о., после определения центрального соотношения челюстей проводят чрескожную электронейростимуляцию импульсным током с частотой 15-30 Гц и силой тока 8-10 мА, в течение 15 мин, а затем повторно осуществляют определения центрального соотношения челюстей с использованием аппарата «АОЦО-М» и выбирают алгоритм лечения в зависимости от полученного вида графика.In patients with a peakless version of the force indicators of the jaw compression efforts, various defects in the dentition, increased abrasion of the hard tissues of the teeth, and generalized periodontitis were revealed. For this category of patients, the greatest therapeutic effect was revealed when using percutaneous electroneurostimulation with pulses with a frequency of 15-30 Hz and a current strength of 8-10 mA, for 15 minutes. Thus, after determining the central ratio of the jaws, percutaneous electroneurostimulation is carried out by a pulsed current with a frequency of 15-30 Hz and a current strength of 8-10 mA for 15 minutes, and then the central ratio of the jaws is re-performed using the AOCO-M and choose a treatment algorithm depending on the type of schedule obtained.
ПРИМЕРЫ ЛЕЧЕНИЯ.EXAMPLES OF TREATMENT.
Одноэтапная схема лечения.One-stage treatment regimen.
Сохранные возможности жевательного аппарата и сохранный реабилитационный ресурс.Preserving capabilities of the masticatory apparatus and safe rehabilitation resource.
Больной П., 44 лет, обратился на кафедру ортопедической стоматологии СЗГМУ им. И.И. Мечникова с жалобами на неудобство при жевании, неудовлетворительную эстетичность внешнего вида лица.Patient P., 44 years old, turned to the Department of Orthopedic Dentistry, North-Western Medical University named after I.I. Mechnikov with complaints of inconvenience when chewing, unsatisfactory aesthetics of the appearance of the face.
Объективно. Отсутствие 16-, 17-, 18-, 25-, 26-, 27-, 28-го зубов на верхней челюсти; отсутствие 31-, 35-го зубов на нижней челюсти. Прикус ортогнатический, слизистая оболочка полости рта бледно-розовая, влажная, без видимых патологических изменений. Смещение резцовой линии в привычной окклюзии влево на 1,5 мм. При открывании рта выявлена девиация нижней челюсти влево. Амплитуда открывания рта в норме. Пальпация жевательной мышцы справа вызывает боль. Патологический шум при движениях в ВНЧС справа. По клиническому индексу дисфункции ВНЧС (М. Helkimo) - легкая степень дисфункции D I (2 балла).Objectively. Lack of 16-, 17-, 18-, 25-, 26-, 27-, 28th teeth on the upper jaw; lack of 31-, 35th teeth on the lower jaw. The bite is orthognathic, the mucous membrane of the oral cavity is pale pink, moist, with no visible pathological changes. Displacement of the incisal line in the usual occlusion to the left by 1.5 mm. When opening the mouth revealed deviation of the lower jaw to the left. The amplitude of the opening of the mouth is normal. Palpation of the chewing muscle on the right causes pain. Pathological noise during movements in the TMJ on the right. According to the clinical index of TMJ dysfunction (M. Helkimo) - mild degree of dysfunction D I (2 points).
Сопутствующие заболевания, по данным анамнеза: хронический гастрит, остеохондроз шейного отдела позвоночника.Associated diseases, according to the anamnesis: chronic gastritis, osteochondrosis of the cervical spine.
Стоматологический диагноз при направлении: Повышенная стираемость твердых тканей зубов, генерализованная форма, 3-й степени. Частичная потеря зубов: дефекты зубного ряда верхней челюсти (1-й класс по Кеннеди), нижней челюсти (3-й класс по Кеннеди). Дисфункция ВНЧС.Dental diagnosis with direction: Increased abrasion of hard tooth tissue, generalized form, 3rd degree. Partial tooth loss: defects in the dentition of the upper jaw (Kennedy 1st grade), lower jaw (Kennedy 3rd grade). TMJ dysfunction.
С помощью функционально-физиологического метода (ФФМ) с одновременной регистрацией электромиограммы (ЭМГ) при определении межальвеолярного расстояния (MAP) выявлен беспиковый вид зависимости усилий сжатия челюстей, уменьшение MAP величиной 3,0 мм, при высоте штифта 9,0 мм. Величина смещения нижней челюсти в горизонтальной плоскости 2,0 мм, в сагиттальной плоскости 0,5 мм (таблица 4).Using the functional physiological method (FFM) with simultaneous recording of an electromyogram (EMG) when determining the interalveolar distance (MAP), a peakless dependence of the jaw compression forces was revealed, a decrease in MAP of 3.0 mm, with a pin height of 9.0 mm. The magnitude of the displacement of the lower jaw in the horizontal plane of 2.0 mm, in the sagittal plane of 0.5 mm (table 4).

Из таблицы 4 следует, что при оптимизации MAP на штифте 9 мм с одновременным применением ФФМ и электромиографии выявлено повышение амплитуды биоэлектрической активности (БЭА) жевательных мышц справа и слева (от 0,7 и 0,6 мВ исходно до 1,12 и 1,16 мВ соответственно), амплитуда БЭА височных мышц также повысилась (от 1,21 и 1,19 мВ исходно до 1,35 и 1,32 мВ соответственно).From table 4 it follows that when optimizing MAP on a 9 mm pin with the simultaneous use of FFM and electromyography, an increase in the amplitude of bioelectric activity (BEA) of the masticatory muscles on the right and left (from 0.7 and 0.6 mV initially to 1.12 and 1, 16 mV, respectively), the amplitude of the BEA of the temporal muscles also increased (from 1.21 and 1.19 mV initially to 1.35 and 1.32 mV, respectively).
При проведении жевательной пробы реакция мышц шеи на изменение MAP отсутствует. Выявлена асимметрия амплитуд биоэлектрической активности жевательных и височных мышц.When conducting a chewing test, there is no reaction of neck muscles to a change in MAP. The asymmetry of the amplitudes of the bioelectric activity of the masticatory and temporal muscles was revealed.
Наблюдалось наличие патологических феноменов (ПФ) в виде веретен парафункций, выпадений активности электрогенеза в мышцах, одиночных нециклических всплесков биоэлектрической активности. Реабилитационные возможности жевательного аппарата сохранны.The presence of pathological phenomena (PF) was observed in the form of spindles of parafunctions, loss of activity of electrogenesis in the muscles, single non-cyclic bursts of bioelectric activity. The rehabilitation capabilities of the chewing apparatus are preserved.
Диагноз поставлен на основании наличия уменьшения MAP, мышечной дисфункции и признаков, подтверждающих верхнезаднюю асимметричную дислокацию головок нижней челюсти в суставной впадине ВНЧС, и признаков, отражающих компрессию биламинарной зоны.The diagnosis was made on the basis of the presence of a decrease in MAP, muscle dysfunction, and signs confirming an upper-posterior asymmetric dislocation of the heads of the lower jaw in the articular cavity of the TMJ, and signs reflecting compression of the bilaminar zone.
Диагноз: Повышенная стираемость твердых тканей зубов 3-й степени, генерализованная форма, декомпенсированная. Частичная потеря зубов: дефекты зубного ряда на верней челюсти - 1-й класс по Кеннеди, дефекты зубного ряда на нижней челюсти - 3-й класс по Кеннеди. Реабилитационный ресурс сохранен. «Синдром сниженного прикуса», 1-й степени тяжести.Diagnosis: Increased abrasion of hard tissues of teeth of the 3rd degree, generalized form, decompensated. Partial tooth loss: defects in the dentition on the upper jaw - Kennedy Grade 1, defects in the dentition in the lower jaw - Kennedy Grade 3. Rehabilitation resource saved. "Reduced bite syndrome", 1st degree of severity.
По данным функциональных нагрузочных проб и исследования вариабельности сердечного ритма (ВСР), констатировались сохранные реабилитационные возможности жевательного аппарата и сохранный реабилитационный ресурс, что обеспечивает хороший реабилитационный потенциал больного. Реабилитационный прогноз у больного П. хороший, возможна полная морфофункциональная реабилитация.According to the data of functional stress tests and studies of heart rate variability (HRV), the safe rehabilitation capabilities of the masticatory apparatus and the safe rehabilitation resource were established, which ensures a good rehabilitation potential of the patient. The rehabilitation prognosis of patient P. is good, complete morphofunctional rehabilitation is possible.
Планируемая продолжительность лечебно-реабилитационных мероприятий 3 месяца. На основании сохранного реабилитационного потенциала выбрана одноэтапная схема лечения.The planned duration of treatment and rehabilitation measures is 3 months. Based on the preserved rehabilitation potential, a one-stage treatment regimen was selected.
Подготовительное лечение у физиотерапевта. Для компенсации мышечной дисфункции применяли чрескожную электронейростимуляцию прибором «Электроника ЭПБ 50.01». Использовали импульсы частотой 15-30 Гц и силой тока 8-10 мА. При чрескожной электронейростимуляции отрицательный электрод накладывали на область козелка уха, а положительный электрод закрепляли на наиболее выступающей части собственно жевательной мышцы. Процедуры проводили ежедневно по 15 минут. Всего выполнено 10 процедур.Preparatory treatment at the physiotherapist. To compensate for muscle dysfunction, transdermal electroneurostimulation was used with the EPB 50.01 Electronics device. Used pulses with a frequency of 15-30 Hz and a current strength of 8-10 mA. During percutaneous electroneurostimulation, a negative electrode was placed on the ear tragus region, and a positive electrode was fixed on the most prominent part of the chewing muscle proper. The procedures were performed daily for 15 minutes. A total of 10 procedures were performed.
Повторное определение соотношения челюстей с применением аппарата «АОЦО-М» выявило наличие однопикового вида графика усилия сжатия челюстей.Re-determination of the ratio of the jaws using the apparatus "AOCO-M" revealed the presence of a one-peak view of the graph of the compression force of the jaws.
После чего осуществлялось протезирование.After which prosthetics was carried out.
Зубное протезирование включало в себя наложение на верхнюю челюсть металлокерамического мостовидного протеза и бюгельного протеза с замковыми Dental prosthetics included the application of a ceramic-metal bridge-like denture and a clasp prosthesis to the upper jaw
креплениями; на нижнюю челюсть металлокерамических мостовидных протезов, продолжительность лечения составила 2 месяца.fixtures; on the lower jaw of ceramic-metal bridges, the duration of treatment was 2 months.
На этапе адаптации к зубным протезам использовали мягкую силиконовую каппу для профилактики мышечной дисфункции (продолжительность применения каппы определяли по данным ЭМГ жевательных мышц). Пациент полностью адаптировался к зубным протезам. Жалоб не предъявлял.At the stage of adaptation to dentures, a soft silicone mouthguard was used to prevent muscle dysfunction (the duration of mouthguard use was determined according to the EMG of the masticatory muscles). The patient is fully adapted to the dentures. No complaints.
С помощью лечебно-реабилитационного комплекса была достигнута полная морфофункциональная реабилитация пациента П.With the help of the treatment and rehabilitation complex, a complete morphofunctional rehabilitation of patient P. was achieved.
Состояние зубных рядов до и после лечения представлены на рисунках 5, 6, 7, 8.The condition of the dentition before and after treatment is shown in Figures 5, 6, 7, 8.
Двухэтапная схема лечения.The two-stage treatment regimen.
Снижены реабилитационные возможности и реабилитационный ресурс.Rehabilitation opportunities and rehabilitation resources have been reduced.
Больная С., 56 лет, преподаватель средней школы, обратилась на кафедру ортопедической стоматологии СЗГМУ им. И.И. Мечникова с жалобами: на затрудненное жевание, нарушение внешнего вида лица и состояние зубов, отмечает усталость в мышцах во время разговора, иногда ощущает дискомфорт в области жевательных мышц, особенно после нагрузки.Patient S., 56 years old, a high school teacher, turned to the Department of Orthopedic Dentistry, North-Western Medical University named after I.I. Mechnikova with complaints: difficulty in chewing, violation of the appearance of the face and condition of the teeth, notes fatigue in the muscles during a conversation, and sometimes feels discomfort in the masticatory muscles, especially after exercise.
Объективно: отсутствие 25-, 26-, 27-, 35-, 46-го зубов. Прикус ортогнатический. Деформация окклюзионной поверхности верхнего зубного ряда. Зубы 11, 12 покрыты пластмассовыми коронками. Амплитуда открывания рта в полном объеме, 45 мм. Девиация нижней челюсти при открывании рта вправо. Пальпаторно определяется боль в собственно жевательных мышцах справа.Objectively: the absence of the 25-, 26-, 27-, 35-, 46th teeth. Orthognathic bite. Deformation of the occlusal surface of the upper dentition. Teeth 11, 12 are covered with plastic crowns. The amplitude of the opening of the mouth in full, 45 mm. Deviation of the lower jaw when opening the mouth to the right. Palpation is determined by pain in the chewing muscles of the right.
По клиническому индексу дисфункции ВНЧС (Helkimo) - легкая степень дисфункции D I (3 балла).According to the clinical index of TMJ dysfunction (Helkimo) - mild degree of dysfunction D I (3 points).
Сопутствующие заболевания в анамнезе - заболевание щитовидной железы зубного ряда на верней челюсти - 3-й класс по Кеннеди, на нижней челюсти - 3-й класс по Кеннеди); деформация верхнего зубного ряда. Дисфункция височно-нижнечелюстного сустава.A history of concomitant diseases is a disease of the thyroid gland of the dentition in the upper jaw — Kennedy grade 3, Kennedy grade 3 in the lower jaw); deformation of the upper dentition. Temporomandibular joint dysfunction.
Функционально-физиологический метод позволил выявить беспиковый вид графика, уменьшение MAP 3,0 мм, при высоте штифта 9,0 мм (таблица 1). вправо, в сагиттальной плоскости 1,5 мм.The functional-physiological method revealed a peakless graph, a decrease in MAP of 3.0 mm, with a pin height of 9.0 mm (table 1). to the right, in the sagittal plane of 1.5 mm.
Из данных таблицы 1 следует, что при увеличении MAP с одновременными ФФМ и электромиографией выявлен беспиковый вид графика. При высоте штифта 9,0 мм - оптимальная высота. На этой высоте разобщения происходило повышение амплитуды БЭА жевательных мышц справа и слева (от 0,72 мВ и 0,41 мВ исходно до 1,25 мВ и 0,67 мВ соответственно), амплитуда БЭА височных мышц незначительно повысилась (от 0,18 мВ и 0,21 мВ исходно до 0,31 мВ и 0,50 мВ соответственно).From the data of table 1 it follows that with an increase in MAP with simultaneous FFM and electromyography, a peakless graph is detected. With a pin height of 9.0 mm, the optimum height. At this separation height, an increase in the amplitude of BEA of chewing muscles on the right and left (from 0.72 mV and 0.41 mV initially to 1.25 mV and 0.67 mV, respectively), the amplitude of BEA of the temporal muscles slightly increased (from 0.18 mV and 0.21 mV initially up to 0.31 mV and 0.50 mV, respectively).
При выполнении жевательной пробы выявлена асимметрия амплитуд БЭА жевательных и височных мышц на высоте привычной окклюзии и при разобщении. Также определялась реакция мышц шеи на изменение MAP в виде повышения амплитуды БЭА грудинноключично-сосцевидных мышц с двух сторон (от 1,25 мВ и 1,21 мВ исходно до 1,42 мВ и 1,35 мВ соответственно).When performing a chewing test, an asymmetry of the amplitudes of BEA of the chewing and temporal muscles at the height of the usual occlusion and during separation was revealed. The neck muscle response to a change in MAP was also determined in the form of an increase in the amplitude of BEA of the sternocleidomastoid muscles on both sides (from 1.25 mV and 1.21 mV initially to 1.42 mV and 1.35 mV, respectively).

Диагноз: Частичная потеря зубов; дефекты зубного ряда на верхней челюсти (3-й класс по Кеннеди), на нижней челюсти (3-й класс по Кеннеди). Деформация зубных рядов. Реабилитационный ресурс снижен. «Синдром сниженного прикуса», 2-й степени тяжести.Diagnosis: Partial tooth loss; defects in the dentition on the upper jaw (Kennedy 3rd grade), on the lower jaw (Kennedy 3rd grade). Deformation of the dentition. The rehabilitation resource is reduced. “Reduced occlusion syndrome”, 2nd degree of severity.
По данным функциональных нагрузочных проб и исследования вариабельности сердечного ритма (ВСР), констатировались низкие реабилитационные возможности жевательного аппарата и низкий реабилитационный ресурс, что отражало снижение реабилитационного потенциала больной С. Это обстоятельство позволило сделать реабилитационный прогноз о возможности полной морфофункциональной реабилитации при использовании двухэтапной схемы лечения. Общая продолжительность лечебно-реабилитационных мероприятий составила 6 месяцев.According to the data of functional stress tests and studies of heart rate variability (HRV), low rehabilitation capabilities of the chewing apparatus and low rehabilitation resource were detected, which reflected a decrease in the rehabilitation potential of patient C. This circumstance made it possible to make a rehabilitation forecast about the possibility of complete morphofunctional rehabilitation using a two-stage treatment regimen. The total duration of treatment and rehabilitation measures was 6 months.
Проведено подготовительное лечение у физиотерапевта. Для компенсации мышечной дисфункции использовалась чрескожная электронейростимуляция. Использовали импульсы частотой 15-30 Гц и силой тока 8-10 мА. При чрескожной электронейростимуляции отрицательный электрод накладывали на область козелка уха, а положительный электрод закрепляли на наиболее выступающей части собственно жевательной мышцы. Процедуры проводили ежедневно по 15 минут. Всего выполнено 10 процедур.Preparatory treatment was carried out by a physiotherapist. Percutaneous electroneurostimulation was used to compensate for muscle dysfunction. Used pulses with a frequency of 15-30 Hz and a current strength of 8-10 mA. During percutaneous electroneurostimulation, a negative electrode was placed on the ear tragus region, and a positive electrode was fixed on the most prominent part of the chewing muscle proper. The procedures were performed daily for 15 minutes. A total of 10 procedures were performed.
Повторное определение соотношения челюстей выявило наличие беспикового вида графика усилия сжатия челюстей.Re-determination of the ratio of the jaws revealed the presence of a peakless graph of the compression force of the jaws.
Принято решение провести лечение с наложением жесткой пластмассовой каппы.A decision was made to conduct treatment with a rigid plastic mouthguard.
В этот период наложена жесткая пластмассовая каппа на нижний зубной ряд с разобщением на 1,5-2 мм от найденного оптимального MAP. В течение 1 месяца проводилось пришлифовывание каппы. На протяжении этапа необходимо добиваться уменьшения высоты пластмассовой каппы до оптимального двустороннего контакта на высоту, определенную с помощью ФФМ.During this period, a rigid plastic mouthguard was placed on the lower dentition with a separation of 1.5-2 mm from the found optimal MAP. For 1 month, the mouthguards were ground. Throughout the stage, it is necessary to achieve a decrease in the height of the plastic mouthguard to the optimal bilateral contact to the height determined using the FFM.
Предложенная методика лечебных мероприятий направлена на установление головок нижней челюсти в оптимальное положение для комфортной деятельности элементов ВНЧС и восстановления электрогенеза жевательной мускулатуры и мышцах шеи. Критерием положительного эффекта использования каппы являлось отсутствие патологической феноменологии на ЭМГ и включения мышц шеи в покое и в момент проведения специфических проб. Достижение положительного результата являлось показанием для проведения окончательного ортопедического лечения. На следующем этапе проводилось протезирование на оптимальном MAP.The proposed methodology of therapeutic measures is aimed at establishing the heads of the lower jaw in an optimal position for comfortable activity of TMJ elements and restoration of electrogenesis of chewing muscles and neck muscles. The criterion for the positive effect of the use of mouthguards was the absence of pathological phenomenology on EMG and the inclusion of neck muscles at rest and at the time of specific tests. Achieving a positive result was an indication for the final orthopedic treatment. At the next stage, prosthetics were performed at the optimal MAP.
Зубное протезирование осуществляли при оптимальном MAP: на верхнюю челюсть - металлокерамический мостовидный протез, на нижнюю - металлокерамические мостовидные протезы.Dental prosthetics was performed with optimal MAP: on the upper jaw - a ceramic-metal bridge, on the lower - metal-ceramic bridges.
Продолжительность лечебных мероприятий составила 2 месяца.The duration of treatment was 2 months.
На этапе адаптации к зубным протезам использовали мягкую силиконовую каппу для профилактики мышечной дисфункции. В связи с профессиональной нагрузкой рекомендовано длительное использование мягкой каппы. Пациентка полностью адаптировалась к зубным протезам. Жалоб не предъявляла. Эффективность лечебно-реабилитационных мероприятий определяли по данным функциональной диагностики.At the stage of adaptation to dentures, soft silicone mouthguards were used to prevent muscle dysfunction. In connection with professional work, prolonged use of soft mouthguards is recommended. The patient fully adapted to the dentures. No complaints. The effectiveness of treatment and rehabilitation measures was determined according to the functional diagnostics.
На ЭМГ жевательных мышц была выявлена нормализация амплитуды БЭА жевательных мышц в покое и при функционировании. Показатель асимметрии соответствовал физиологическому коридору, патологическая феноменология (ПФ) не выявлена. Данные ЭМГ после лечения представлены в таблице 6.On EMG of the masticatory muscles, normalization of the amplitude of the BEA of the masticatory muscles at rest and during functioning was revealed. The asymmetry index corresponded to the physiological corridor, pathological phenomenology (PF) was not detected. EMG data after treatment are presented in table 6.

По данным компьютерной стабилометрии, нарушения функции статокинетической системы не выявлены.According to computer stabilometry, no dysfunction of the statokinetic system was detected.
При использовании данного лечебно-реабилитационного комплекса была достигнута полная морфофункциональная реабилитация пациентки С. Исходное состояние и результат лечебных мероприятий представлен на рисунках 9, 10, 11, 12. При использовании данного лечебно-реабилитационного комплекса была достигнута полная морфофункциональная реабилитация пациентки С.When using this treatment and rehabilitation complex, a complete morphofunctional rehabilitation of patient C was achieved. The initial state and result of treatment measures are shown in Figures 9, 10, 11, 12. When using this treatment and rehabilitation complex, a complete morphofunctional rehabilitation of patient C was achieved.
Таким образом, предлагаемое решение после диагностики определения соотношения челюстей, среди пациентов с беспиковым вариантом силовых показателей усилий сжатия челюстей позволяет выявить больных, которые после дополнительной процедуры черескожной электронейростимуляции могут быть отнесены к пациентам однопикового варианта силовых показателей усилий сжатия челюстей. Это позволило существенно упростить и сократить время лечения больных со сниженным прикусом.Thus, the proposed solution, after diagnosing the determination of the jaw ratio, among patients with a peakless version of the force indicators of the jaw compression forces, it is possible to identify patients who, after an additional procedure of percutaneous electroneurostimulation, can be assigned to patients with a one-peak version of the force indicators of the jaw compression efforts. This made it possible to significantly simplify and reduce the treatment time for patients with reduced occlusion.
Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2019104434A RU2707433C1 (en) | 2019-02-18 | 2019-02-18 | Method for lower occlusion treatment by prosthetic repair |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2019104434A RU2707433C1 (en) | 2019-02-18 | 2019-02-18 | Method for lower occlusion treatment by prosthetic repair |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2707433C1 true RU2707433C1 (en) | 2019-11-26 |
Family
ID=68653224
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2019104434A RU2707433C1 (en) | 2019-02-18 | 2019-02-18 | Method for lower occlusion treatment by prosthetic repair |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2707433C1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2737252C1 (en) * | 2020-03-18 | 2020-11-26 | ЮАБ "Теманик" | Method for determining a central ratio of jaws |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2070001C1 (en) * | 1993-08-24 | 1996-12-10 | Медицинская академия постдипломного образования | Method for determining optimum occlusion |
| RU2093108C1 (en) * | 1992-05-20 | 1997-10-20 | Александр Викторович Цимбалистов | Apparatus for determining central relationship of jaws |
| RU2489114C1 (en) * | 2012-02-17 | 2013-08-10 | Мукатдес Ибрагимович Садыков | Method of determining optimal position of lower jaw |
| US20180093091A1 (en) * | 2015-02-26 | 2018-04-05 | Rb Patents Sarl | Device for functional electrical stimulation and measurement of electromyogram, comprising means for short-circuiting and earthing a pair of electrodes, and associated transcutaneous electrode |
-
2019
- 2019-02-18 RU RU2019104434A patent/RU2707433C1/en not_active IP Right Cessation
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2093108C1 (en) * | 1992-05-20 | 1997-10-20 | Александр Викторович Цимбалистов | Apparatus for determining central relationship of jaws |
| RU2070001C1 (en) * | 1993-08-24 | 1996-12-10 | Медицинская академия постдипломного образования | Method for determining optimum occlusion |
| RU2489114C1 (en) * | 2012-02-17 | 2013-08-10 | Мукатдес Ибрагимович Садыков | Method of determining optimal position of lower jaw |
| US20180093091A1 (en) * | 2015-02-26 | 2018-04-05 | Rb Patents Sarl | Device for functional electrical stimulation and measurement of electromyogram, comprising means for short-circuiting and earthing a pair of electrodes, and associated transcutaneous electrode |
Non-Patent Citations (2)
| Title |
|---|
| ВОЙТЯЦКАЯ И. В. Анатомо-физиологическое обоснование объема и тактики лечения стоматологических больных со сниженным прикусом: диссертация на соискание ученой степени доктора медицинских наук. Санкт-Петербург, СЗГМУ им. И.И. Мечникова, * |
| ВОЙТЯЦКАЯ И. В. Анатомо-физиологическое обоснование объема и тактики лечения стоматологических больных со сниженным прикусом: диссертация на соискание ученой степени доктора медицинских наук. Санкт-Петербург, СЗГМУ им. И.И. Мечникова, 2016. * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2737252C1 (en) * | 2020-03-18 | 2020-11-26 | ЮАБ "Теманик" | Method for determining a central ratio of jaws |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Haraldson et al. | Functional state, bite force and postural muscle activity in patients with osseointegrated oral implant bridges | |
| Rivera-Morales et al. | Relationship of occlusal vertical dimension to the health of the masticatory system | |
| Hayakawa et al. | Changes in the masticatory function of complete denture wearers after relining the mandibular denture with a soft denture liner. | |
| Pisani et al. | Electromyography of masticatory muscles after denture relining with soft and hard denture liners | |
| Wafa’a et al. | Effect on patient satisfaction of mandibular denture tooth arrangement in the neutral zone | |
| Maria de Felicio et al. | Clinical validity of the protocol for multi-professional centers for the determination of signs and symptoms of temporomandibular disorders. Part II | |
| Abdelnabi et al. | Influence of denture adhesives on occlusion and disocclusion times | |
| Amorim et al. | Analysis of the condyle/fossa relationship before and after prosthetic rehabilitation with maxillary complete denture and mandibular removable partial denture | |
| Soo et al. | A technique for measurement of intraoral lip pressures with lip bumper therapy | |
| RU182370U1 (en) | Kappa palatal plate | |
| Smaglyuk et al. | EMG-characteristic of masticatory muscles in patients with class II malocclusion and temporomandibular disorders | |
| Ribeiro et al. | Effect of short-term increase in occlusal vertical dimension on masticatory muscle electrical activities and pressure-to-pain threshold: A crossover clinical study | |
| Maddalone et al. | Treatment of temporomandibular disorders of muscular origin with a silicon oral device (Alifix®): electromyographic analysis | |
| RU2707433C1 (en) | Method for lower occlusion treatment by prosthetic repair | |
| Shinogaya et al. | A new approach to evaluating occlusal support by analyzing the center of the bite force | |
| Tzakis et al. | Evaluation of masticatory function before and after treatment in patients with craniomandibular disorders. | |
| Shah et al. | An alternative technique to determine vertical dimension of occlusion from anthropometric study done in Gujarati population | |
| Achmad et al. | Detection of Temporomandibular Muscle Disorders in Children. Development of Android-Based Electromyography Tools (EMG Dentosmart) | |
| Shanahan | Dental physiology for dentures: The direct application of the masticating cycle to denture occlusion | |
| Bianco et al. | Restoration of the vertical posterior dimension in a grinding patient before orthodontic treatment: A case-report with electromyographic evaluation of masticatory muscles balance | |
| RU2489114C1 (en) | Method of determining optimal position of lower jaw | |
| RU2805020C1 (en) | Method for determining central position of lower jaw | |
| Mouhibi et al. | The means of determining the Vertical Occlusion Dimention | |
| Bertolino et al. | Functional Significance of the Curve of Spee: Electro-myographic Analysis of Young Adults-A Preliminary Study | |
| Abdel-Salam et al. | Effect of occlusal vertical dimension of complete denture on maximum biting force |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees |
Effective date: 20210219 |