RU2675398C1 - Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers - Google Patents
Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers Download PDFInfo
- Publication number
- RU2675398C1 RU2675398C1 RU2018105880A RU2018105880A RU2675398C1 RU 2675398 C1 RU2675398 C1 RU 2675398C1 RU 2018105880 A RU2018105880 A RU 2018105880A RU 2018105880 A RU2018105880 A RU 2018105880A RU 2675398 C1 RU2675398 C1 RU 2675398C1
- Authority
- RU
- Russia
- Prior art keywords
- lens
- cataract
- opacities
- diffuse
- ultrasonic wave
- Prior art date
Links
Images




Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B8/00—Diagnosis using ultrasonic, sonic or infrasonic waves
- A61B8/10—Eye inspection
Abstract
Description
Изобретение относится к офтальмологии и предназначено для измерения толщины хрусталика (ТХ) у пациентов со зрелой катарактой до операции с целью наиболее точного расчета оптической силы ИОЛ.The invention relates to ophthalmology and is intended to measure the thickness of the lens (TX) in patients with mature cataract before surgery in order to most accurately calculate the optical power of the IOL.
Известно, что формула Barrett Universal II является наиболее точной современной формулой для расчета оптический силы интраокулярной линзы (ИОЛ), в которой учитывается показатель ТХ пациента [Jack X. Kane, Anton Van Heerden, Alp Atik,, Constantinos Petsoglou. Accuracy of 3 new methods for intraocular lens power selection // J Cataract Refract Surg. - 2017. Vol. - 43 (3). P. 333 - 339]; [Olga Reitblat, Adi Levy, Guy Kleinmann, Tsahi T. Lerman, Ehud I. Assia. Intraocular lens power calculation for eyes with high and low average keratometry readings: Comparison between various formulas // J Cataract Refract Surg. - 2017. Vol. - 43 (9). P. 1149-1156]; [David L. Cooke, Timothy L. Cooke. Comparison of 9 intraocular lens power calculation formulas // J Cataract Refract Surg. - 2016. Vol. - 42 (8). P. 1157-1164].It is known that the Barrett Universal II formula is the most accurate modern formula for calculating the optical power of an intraocular lens (IOL), which takes into account the patient's TX [Jack X. Kane, Anton Van Heerden, Alp Atik ,, Constantinos Petsoglou. Accuracy of 3 new methods for intraocular lens power selection // J Cataract Refract Surg. - 2017. Vol. - 43 (3). P. 333 - 339]; [Olga Reitblat, Adi Levy, Guy Kleinmann, Tsahi T. Lerman, Ehud I. Assia. Intraocular lens power calculation for eyes with high and low average keratometry readings: Comparison between various formulas // J Cataract Refract Surg. - 2017. Vol. - 43 (9). P. 1149-1156]; [David L. Cooke, Timothy L. Cooke. Comparison of 9 intraocular lens power calculation formulas // J Cataract Refract Surg. - 2016. Vol. - 42 (8). P. 1157-1164].
В настоящее время оптическая биометрия остается наиболее достоверным методом для измерения ТХ ГН. John Shammas, Maya С. Shammas. Measuring the cataractous lens // J Cataract Refract Surg. - 2015. Vol. - 41 (9). P. 1875-1879], однако его применение ограничено техническими возможностями приборов и снижением прозрачности оптических сред глаза. Кроме того, существует прямая взаимосвязь между возникновением помутнений хрусталика, увеличением плотности катаракты и снижением точности расчетов оптической силы ИОЛ [Ueda T.I., Taketani F., Ota T, Hara Y. Impact of nuclear cataract density on postoperative refractive outcome: IOL Master versus ultrasound // Ophthalmologica - 2007. Vol.- 221(6). P. 384-387].Currently, optical biometry remains the most reliable method for measuring TX GN. John Shammas, Maya S. Shammas. Measuring the cataractous lens // J Cataract Refract Surg. - 2015. Vol. - 41 (9). P. 1875-1879], however, its use is limited by the technical capabilities of the devices and reducing the transparency of the optical media of the eye. In addition, there is a direct relationship between the occurrence of lens opacities, an increase in cataract density and a decrease in the accuracy of calculating the optical power of the IOL [Ueda TI, Taketani F., Ota T, Hara Y. Impact of nuclear cataract density on postoperative refractive outcome: IOL Master versus ultrasound / / Ophthalmologica - 2007. Vol. 221 (6). P. 384-387].
Универсальным методом определения ТХ у всех пациентов независимо от состояния оптических сред глаза является ультразвуковая биометрия. Измерение может проводиться как контактным, так и иммерсионным способами. Контактный метод А - эхографии широко распространен в офтальмологической практике, однако, его точность ограничена разрешающей способностью прибора, эхосигнал от роговицы локализуется в «мертвой зоне» датчика. Точность и воспроизводимость данных иммерсионной биометрии значительно выше по сравнению с контактным методом за счет фиксации датчика в насадке Прагера и наличия иммерсионной среды между датчиком и роговицей [Michael Р Hennessy, Derek G Chan. Contact versus immersion biometry of axial length before cataract surgery // J Cataract Refract Surg. - 2003. Vol. - 29 (11). P. 2195-2198].A universal method for determining TX in all patients, regardless of the state of the optical media of the eye, is ultrasound biometry. Measurement can be carried out both by contact and immersion methods. The contact method of A ultrasound imaging is widespread in ophthalmic practice, however, its accuracy is limited by the resolution of the device, the echo signal from the cornea is localized in the "dead zone" of the sensor. The accuracy and reproducibility of immersion biometric data is significantly higher compared to the contact method due to the fixation of the sensor in the Prager nozzle and the presence of an immersion medium between the sensor and the cornea [Michael P Hennessy, Derek G Chan. Contact versus immersion biometry of axial length before cataract surgery // J Cataract Refract Surg. - 2003. Vol. - 29 (11). P. 2195-2198].
S.T. Fontana и R.F. Brubaker установили, что среднее значение ТХ составляет 4,01 мм для детей 1 года и 4,8 мм для лиц старше 80 лет [S.T. Fontana, R.F. Brubaker. Volume and depth of the anterior chamber in the normal aging human eye // Arch Ophthalmol. - 1980. Vol. - 98. P. 1803-1808]. G. Bellows предложил определять ТХ по формуле: 4+ значение возраста пациента, выраженное в сотых долях. Например, согласно формуле, у пациента в 52 года ТХ должна составлять 4,52 мм [G. Bellows. Cataract and anomalies of the lens: growth, structure, composition, metabolism, development, growth disorders and treatment of the crystalline Lens // St Louis, MO, CV Mosby. - 1944. P. 60-86].S.T. Fontana and R.F. Brubaker found that the average value of TX is 4.01 mm for
Кроме того, значение скорости ультразвуковой волны варьирует по мере созревания катаракты. Изменение скорости ультразвука в хрусталике на 50 м/с приводит к средней ошибке в расчете оптической силы ИОЛ до 0,5 Дптр [G.L. Vanderheijde, J. Weber. Accommodation used to determine ultrasound velocity in the human lens // Optom Vis Sci. 1989. - Vol. 66(12) - P. 830-833].In addition, the speed of the ultrasonic wave varies as the cataract ripens. A change in the speed of ultrasound in the lens by 50 m / s leads to an average error in calculating the optical power of the IOL up to 0.5 Dptr [G.L. Vanderheijde, J. Weber. Accommodation used to determine ultrasound velocity in the human lens // Optom Vis Sci. 1989. - Vol. 66 (12) - P. 830-833].
В опубликованных работах результаты измерения скорости ультразвуковой волны в помутневшем хрусталике вариабельны. D.J. Coleman с соавторами в 1975 году провели исследование 4 глаз у детей и 50 глаз у взрослых пациентов с катарактой и определили, что показатель скорости ультразвуковой волны в хрусталике составляет в среднем 1659 м/с в возрасте 1 года и достигает значения 1629 м/с к 72 годам. [D.J. Coleman, F.L. Lizzi, L.A. Franzen, D.H. Abramson. A Determination of the velocity of ultrasound in cataractous lenses. // Ultrasonography in Ophthalmology. - Bibl. Ophthalmol. 1975. - Vol. 83. P. 246-251]. В 1962 году F. Jansson и E. Kock получили среднее значение скорости ультразвука, равное 1640,5 м/с, причем у лиц молодого возраста в прозрачном хрусталике - 1641 м/с, при начальном помутнении - 1628 м/с, при зрелой катаракте - 1589 м/с, однако данное исследование включало всего 12 глаз [F. Jansson, Е. Kock. Determination of the velocity of ultrasound in the human lens and vitreous. // Acta Ophthalmol. 1962. - 40. - P. 420-433]. D.J. Coleman с соавторами в 1975 году опубликовали данные, в которых скорость ультразвуковой волны в зрелой катаракте составила 1670 м/с. [D.J. Coleman, F.L. Lizzi, R.L. Jack Ultrasonography of the Eye and Orbit. Philadelphia: Lea & Febiger; 1977]In published works, the results of measuring the speed of an ultrasonic wave in a clouded lens are variable. D.J. Coleman et al. In 1975 conducted a study of 4 eyes in children and 50 eyes in adult patients with cataracts and determined that the rate of ultrasonic wave velocity in the lens is on average 1659 m / s at the age of 1 year and reaches a value of 1629 m / s to 72 years. [D.J. Coleman, F.L. Lizzi, L.A. Franzen, D.H. Abramson A Determination of the velocity of ultrasound in cataractous lenses. // Ultrasonography in Ophthalmology. - Bibl. Ophthalmol. 1975 .-- Vol. 83. P. 246-251]. In 1962, F. Jansson and E. Kock obtained an average ultrasound velocity of 1640.5 m / s, with 1641 m / s for young people in a clear crystalline lens, 1628 m / s for an initial clouding, and mature cataract - 1589 m / s, however, this study included a total of 12 eyes [F. Jansson, E. Kock. Determination of the velocity of ultrasound in the human lens and vitreous. // Acta Ophthalmol. 1962. - 40. - P. 420-433]. D.J. Coleman et al. Published data in 1975 in which the velocity of an ultrasonic wave in a mature cataract was 1670 m / s. [D.J. Coleman, F.L. Lizzi, R.L. Jack Ultrasonography of the Eye and Orbit. Philadelphia: Lea &Febiger; 1977]
Ближайшим аналогом предлагаемого изобретения является способ измерения толщины хрусталика с помутнениями с помощью стандартного метода ультразвуковой иммерсионной А - биометрии [Renu Jivrajka, Maya С. Shammas, Teresa Boenzi, Mike Swearingen, H. John Shammas. Variability of axial length, anterior chamber depth, and lens thickness in the cataractous eye // J Cataract Refract Surg. - 2008. Vol. - 34 (2). P. 289-294]. Измерение ПЗО и ТХ глаз с прозрачными хрусталиками, а также глаз с начальной и заднекапсулярной катарактой, проводится в стандартном режиме «Phackic», подрамевающий использование известной скорости распространения ультразвуковой волны в хрусталике - 1641 м/с. У пациентов с плотной катарактой и диффузными помутнениями хрусталика проводится измерение в режиме «Dence cataract», который использует стандартное значение ТХ - 4,7 мм без учета скорости распространения скорости ультразвуковой волны в хрусталике. Таким образом, несмотря на развитие ультразвуковых и оптических методов биометрии, до сих пор остается актуальным вопрос точного измерения ТХ у пациентов с зрелой катарактой.The closest analogue of the invention is a method of measuring the thickness of the lens with opacities using the standard method of ultrasonic immersion A - biometry [Renu Jivrajka, Maya C. Shammas, Teresa Boenzi, Mike Swearingen, H. John Shammas. Variability of axial length, anterior chamber depth, and lens thickness in the cataractous eye // J Cataract Refract Surg. - 2008. Vol. - 34 (2). P. 289-294]. The measurement of PZO and TX eyes with transparent lenses, as well as eyes with initial and posterior capsular cataracts, is carried out in the standard “Phackic” mode, which implies the use of the known ultrasonic wave propagation velocity in the lens - 1641 m / s. In patients with dense cataracts and diffuse opacities of the lens, the measurement is performed in the “Dens cataract” mode, which uses a standard TX value of 4.7 mm without taking into account the speed of propagation of the ultrasonic wave velocity in the lens. Thus, despite the development of ultrasonic and optical methods of biometry, the issue of accurate measurement of TX in patients with mature cataracts still remains an issue.
Задачей предлагаемого изобретения является разработка более точного ультразвукового определения толщины хрусталика при диффузных помутнениях ядра и кортикальных слоев.The task of the invention is to develop a more accurate ultrasound determination of the thickness of the lens with diffuse opacities of the nucleus and cortical layers.
Техническим результатом предлагаемого способа является возможность наиболее точного расчета оптической силы ИОЛ, имплантируемой после факоэмульсификации катаракты.The technical result of the proposed method is the possibility of the most accurate calculation of the optical power of the IOL implanted after cataract phacoemulsification.
Технический результат достигается за счет проведения иммерсионной А-биометрии с использованием скорости ультразвуковой волны равной 1629 м/с и определения задней границы хрусталика с диффузными помутнениями с установкой метки при активации функции «Gate» для локализации задней капсулы хрусталика на эхограмме.The technical result is achieved by performing immersion A-biometry using an ultrasonic wave velocity of 1629 m / s and determining the posterior border of the lens with diffuse opacities with the setting of a mark when the “Gate” function is activated to localize the posterior lens capsule on the echogram.
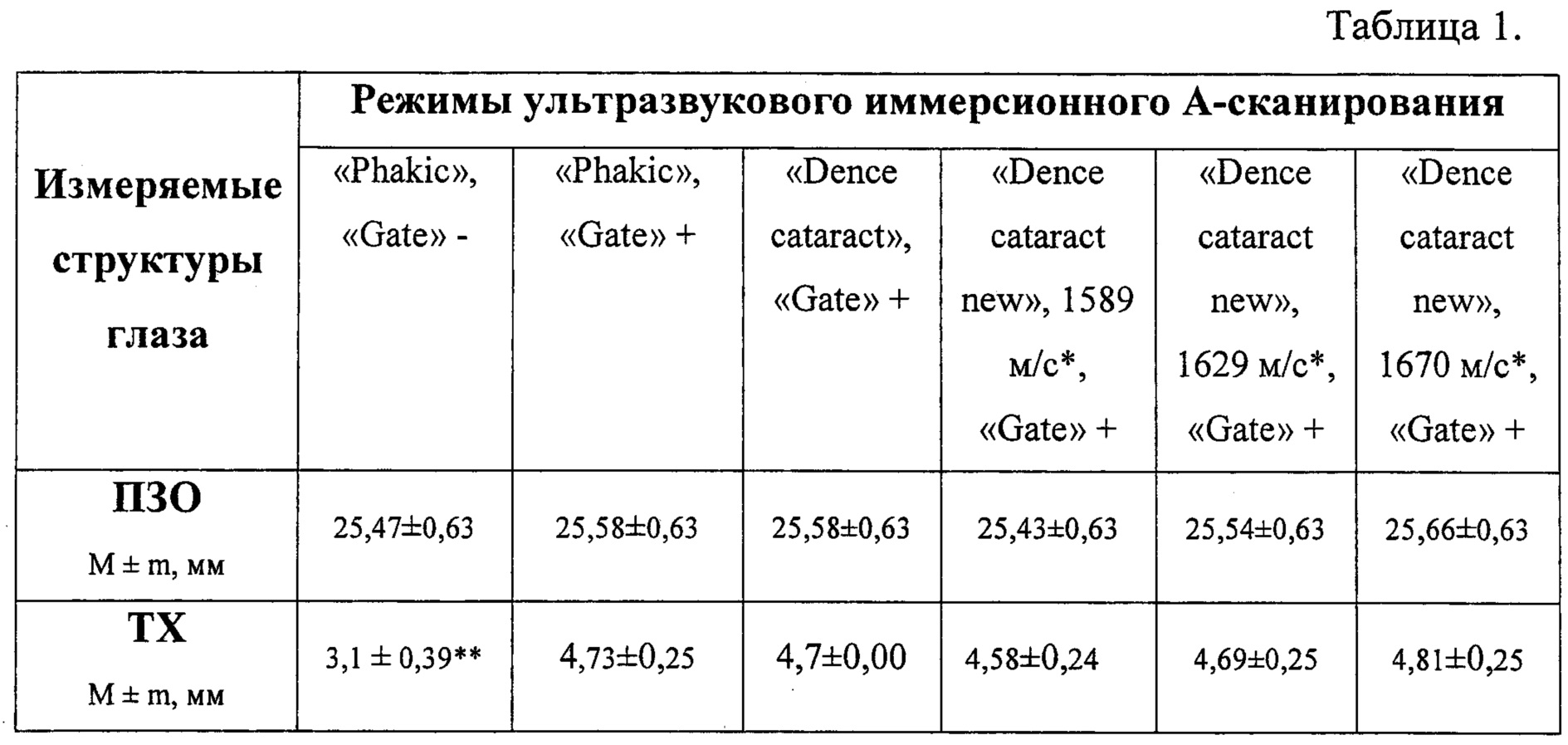
Мы провели исследование, в котором определили оптимальное значение скорости ультразвуковой волны для биометрии помутневшего хрусталика. Нами проведено измерение ПЗО и ТХ у пациентов со зрелой набухающей катарактой (36 глаз) с использованием различных диагностических режимов ультразвукового скана. Во-первых, выполнено иммерсионное А-сканирование глаз в стандартном режиме «Phakic», проведено измерение ПЗО и ТХ, затем те же параметры определены после активации функции «Gate» и локализации эхосигнала задней капсулы хрусталика. Во-вторых, измерение ПЗО и ТХ выполнено в режиме «Dence cataract», рекомендованном производителями ультразвукового оборудования для использования у пациентов со зрелой катарактой. В-третьих, после создания нами режима «Dence cataract new», в котором последовательно использованы скорости ультразвуковой волны для помутневшего хрусталика 1589 м/с, 1629 м/с, 1670 м/с, были определены значения ПЗО и ТХ. Результаты биометрии представлены в Таблице 1.We conducted a study in which we determined the optimal value of the ultrasonic wave velocity for the biometrics of a clouded lens. We measured PZO and TX in patients with mature swelling cataract (36 eyes) using various diagnostic modes of the ultrasound scan. First, immersion A-scan of the eyes was performed in the standard “Phakic” mode, the PZO and TX measurements were performed, then the same parameters were determined after the “Gate” function was activated and the echo signal of the posterior lens capsule was localized. Secondly, the measurement of PZO and TX was carried out in the "Dens cataract" mode recommended by manufacturers of ultrasound equipment for use in patients with mature cataract. Thirdly, after we created the “Dense cataract new” mode, in which the ultrasonic wave velocities for a clouded lens 1589 m / s, 1629 m / s, 1670 m / s were used sequentially, the values of PZO and TX were determined. The results of biometrics are presented in Table 1.
Примечание:Note:
* - разработанные нами режимы ультразвукового сканирования со скоростью ультразвуковой волны для измерения ТХ 1589 м/с, 1629 м/с и 1670 м/с* - the ultrasonic scanning modes developed by us with the speed of an ultrasonic wave for measuring TX 1589 m / s, 1629 m / s and 1670 m / s
** - различия статистически достоверны (р<0,05)** - differences are statistically significant (p <0.05)
«Gate» + - активирована функция «Gate», измерения проведены с учетом локализации сигнала от задней капсулы хрусталика.“Gate” + - the “Gate” function is activated, measurements are taken taking into account the localization of the signal from the posterior lens capsule.
«Gate» - - не активирована функция «Gate», измерения проведены без учета локализации сигнала от задней капсулы хрусталика.“Gate” - - the “Gate” function is not activated, measurements were taken without taking into account the localization of the signal from the posterior lens capsule.
Статистически достоверных различий между полученными значениями ПЗО при проведении иммерсионной А-биометрии с использованием всех выше описанных режимов не выявлено (р>0,05), несмотря на клинически значимые различия между значениями с использованием функции «Gate» и без нее. Выявлены статистически достоверные различия между результатами измерения ТХ без активации функции «Gate» и с ней. Скорость распространения ультразвуковой волны в набухающем хрусталике вариабельна, однако измерения ТХ, полученные при использовании значения 1629 м/с, оказались идентичными с используемыми в режиме «Dence cataract» и составили 4,69±0,25 и 4,7±0,0 соответственно. Следовательно, режим «Dence cataract new» со скоростью ультразвуковой волны для измерения ТХ равной 1629 м/с в наибольшей степени подходит для измерения ТХ у пациентов с зрелой набухающей катарактой, использование значений 1589 м/с и 1670 м/с для проведения биометрии не целесообразно. Физические свойства ультразвука также предполагают уменьшение скорости ультразвуковой волны по мере нарастания структурных изменений набухающего хрусталика.There were no statistically significant differences between the obtained PZO values during immersion A-biometry using all the above-described modes (p> 0.05), despite clinically significant differences between the values using the Gate function and without it. Statistically significant differences were found between the results of measuring TX without activating the “Gate” function and with it. The propagation velocity of an ultrasonic wave in a swelling lens is variable, however, the measurements of TX obtained using a value of 1629 m / s turned out to be identical to those used in the "Dense cataract" mode and amounted to 4.69 ± 0.25 and 4.7 ± 0.0, respectively . Therefore, the “Dense cataract new” mode with an ultrasonic wave velocity for measuring TX equal to 1629 m / s is most suitable for measuring TX in patients with mature swelling cataract, using the values of 1589 m / s and 1670 m / s for biometrics . The physical properties of ultrasound also suggest a decrease in the speed of the ultrasonic wave as structural changes of the swelling lens increase.
Следовательно, для точного измерения толщины хрусталика у пациента с зрелой набухающей катарактой ультразвуковым способом следует активировать функцию «Gate» и использовать скорость ультразвуковой волны для измерения толщины хрусталика, равную 1629 м/с.Therefore, to accurately measure the thickness of the lens in a patient with mature swelling cataracts by ultrasound, the “Gate” function should be activated and the ultrasonic wave velocity used to measure the thickness of the lens equal to 1629 m / s.
Таким образом, нами разработан новый режим «Dence cataract new» (Фиг. 1 - Режим «Dense cataract new», при проведении А-сканирования установлено значение скорости ультразвука для мутного хрусталика - 1629 м/с), учитывающий среднюю скорость ультразвука 1629 м/с для хрусталика с диффузными помутнениями, которая является оптимальной, и соответствует морфологическим изменениям плотного хрусталика на фоне зрелой катаракты. Способ определения ТХ при зрелой катаракте включает проведение иммерсионной ультразвуковой А-биометрии с получением максимально высоких эхосигналов от роговицы, передней и задней поверхности хрусталика, сетчатки и склеры с последующим убывающим по амплитуде эхокомплексом сигналов от ретробульбарной клетчатки в разработанном режиме, учитывающем среднюю скорость ультразвуковой волны в помутневшем хрусталике, равную 1629 м/с, с дальнейшим определением расстояния между амплитудами А - эхосигнала от передней до задней поверхности хрусталика с установкой и активацией функции «Gate» на эхограмме.Thus, we have developed a new “Dense cataract new” mode (Fig. 1 - “Dense cataract new” mode, when conducting A-scan, the ultrasound speed for a cloudy lens was set to 1629 m / s), taking into account the average ultrasound speed of 1629 m / c for a lens with diffuse opacities, which is optimal and corresponds to the morphological changes of the dense lens against the background of mature cataract. A method for determining TX during mature cataract includes immersion ultrasound A-biometry with obtaining the highest possible echo signals from the cornea, anterior and posterior surfaces of the lens, retina and sclera, followed by a decrease in amplitude of the echocomplex of signals from retrobulbar fiber in a developed mode that takes into account the average speed of the ultrasonic wave in clouded lens equal to 1629 m / s, with further determination of the distance between the amplitudes A - of the echo signal from the front to the back surface of the crystal This is the installation and activation of the “Gate” function on the echogram.
Способ осуществляют следующим образом.The method is as follows.
У пациента с диффузными помутнениями ядра и кортикальных слоев проводят ультразвуковую иммерсионную А-биометрию. Используют среднюю скорость ультразвуковой волны, равную 1629 м/с, определяют расстояние между амплитудами А-эхосигнала от передней до задней поверхности хрусталика, при этом заднюю границу хрусталика с диффузными помутнениями определяют с установкой и активацией функции «Gate» для локализации задней капсулы хрусталика на эхограмме.In a patient with diffuse opacities of the nucleus and cortical layers, ultrasound immersion A-biometry is performed. Using the average speed of the ultrasonic wave, equal to 1629 m / s, determine the distance between the amplitudes of the A-echo signal from the front to the back surface of the lens, while the posterior border of the lens with diffuse opacities is determined by setting and activating the “Gate” function to localize the posterior lens capsule on the echogram .
Клинический пример.Clinical example.
Пациентка К., 49 лет.При поступлении острота зрения левого глаза - 0,02 н/к, авторефрактометрию выполнить не удалось. Результаты кератометрии левого глаза по данным прибора IOL-Master составили: R1 - 44,87 Дптр ах 45°; R2 - 44,37 Дптр ах 135°; cyl -0,5 Дптр ах 5°, ACD - 2,7 мм, WTW - 12,0 мм. Пневмотонометрия - 17 мм рт.ст.При проведении ультразвукового исследования в стекловидном теле визуализировались плавающие помутнения, задняя отслойка стекловидного тела; отслойка сетчатки не определялась. При объективном исследовании: глаз был спокоен, передняя камера мельче средней (2,7 мм), выявлена деструкция пигментной каймы радужки 1-2 ст., выраженные диффузные помутнения хрусталика. По данным обследования поставлен диагноз: зрелая катаракта левого глаза. Запланировано выполнение факоэмульсификации катаракты левого глаза. При выполнении А-сканирования глазного яблока в режиме «Phakic» без активации функции «Gate» ТХ составила 3,43 мм, ПЗО - 23,65 мм. (Фиг. 2 - А-сканирование глазного яблока у пациентки К., 49 лет со зрелой катарактой: режим «Phakic», функция «Gate» для задней капсулы хрусталика не активирована, толщина хрусталика - 3,43 мм).Patient K., 49 years old. Upon receipt of the visual acuity of the left eye - 0.02 n / a, failed to perform autorefractometry. The results of keratometry of the left eye according to the IOL-Master device were: R1 - 44.87 Dptr ah 45 °; R2 - 44.37 Dptr ax 135 °; cyl -0.5
При использовании функции «Gate» в режиме «Phakic» толщина хрусталика составила 5,58 мм, ПЗО - 23,79 мм, что на 0,14 мм больше, чем в предыдущем измерении (Фиг. 3 - А-сканирование глазного яблока у пациентки К., 49 лет со зрелой катарактой: режим «Phakic», активирована функция «Gate» для задней капсулы хрусталика, толщина хрусталика - 5,58 мм). В режиме «Dense cataract» измерение толщины хрусталика не проводится, поскольку используется стандартная величина 4,7 мм, значение ПЗО - 23,74 мм (Фиг. 4 - А-сканирование глазного яблока у пациентки К., 49 лет со зрелой катарактой: режим «Dense cataract», толщина хрусталика стандартна - 4,7 мм;). Таким образом, измерение биометрических параметров глаза у пациентов со зрелой катарактой в режиме «Phakic» с использованием скорости для оптически прозрачного хрусталика 1641 м/с не корректно. Применение режима «Dense cataract new» позволило наиболее точно измерить и ТХ (5,54 мм) и длину глаза (23,75 мм) у пациента со зрелой катарактой. (Фиг. 5 - А-сканирование глазного яблока у пациентки К., 49 лет со зрелой катарактой: режим «Dence cataract new», активирована функция «Gate» для задней капсулы хрусталика, толщина хрусталика - 5,54 мм.) Значения ПЗО, полученные в режиме «Dense cataract» и «Dense cataract new» оказались практически одинаковыми, 23,74 и 23,75 соответственно. На Фиг. 6 (А-сканирование глазного яблока у пациентки К., 49 лет со зрелой катарактой: в режиме «Dence cataract new» установлена скорость ультразвуковой волны для зрелого хрусталика 1670 м/с, активирована функция «Gate» для задней капсулы хрусталика, толщина хрусталика - 5,68 мм, ПЗО 23,89) представлено А-сканирование левого глазного яблока в режиме «Dence cataract new» при установленой скорости ультразвуковой волны для зрелого хрусталика, равной 1670 м/с (Фиг. 7 - Режим «Dense cataract new», при проведении А-сканирования установлено значение скорости ультразвука для мутного хрусталика - 1670 м/с), активирована функция «Gate» для задней капсулы хрусталика, ТХ составила 5,68 мм, ПЗО - 23,89, что наглядно показывает отличия от полученных значений при применении режима «Dense cataract new» со скоростью ультразвуковой волны для помутневшего хрусталика 1629 м/с.When using the “Gate” function in the “Phakic” mode, the lens thickness was 5.58 mm, the PZD was 23.79 mm, which is 0.14 mm more than in the previous measurement (Fig. 3 - A-scan of the eyeball in the patient K., 49 years old with mature cataract: “Phakic” mode, the “Gate” function for the posterior lens capsule is activated, the thickness of the lens is 5.58 mm). In the "Dense cataract" mode, the lens thickness is not measured, since a standard value of 4.7 mm is used, the PZO value is 23.74 mm (Fig. 4 - A-scan of the eyeball in patient K., 49 years old with mature cataract: mode "Dense cataract", the thickness of the lens is standard - 4.7 mm;). Thus, the measurement of biometric parameters of the eye in patients with mature cataract in the Phakic mode using the speed for an optically transparent lens of 1641 m / s is not correct. The use of the Dense cataract new regime allowed the most accurate measurement of both TX (5.54 mm) and eye length (23.75 mm) in a patient with mature cataract. (Fig. 5 - A-scan of the eyeball in patient K., 49 years old with mature cataract: “Dence cataract new” mode, the “Gate” function for the posterior lens capsule is activated, the lens thickness is 5.54 mm.) those obtained in the Dense cataract and Dense cataract new modes turned out to be almost the same, 23.74 and 23.75, respectively. In FIG. 6 (A-scan of the eyeball in patient K., 49 years old with mature cataract: in the “Dens cataract new” mode, the ultrasonic wave speed for the mature lens is set at 1670 m / s, the “Gate” function for the posterior lens capsule is activated, the lens thickness is 5.68 mm, PZO 23.89) presents an A-scan of the left eyeball in the "Dense cataract new" mode at a set ultrasonic wave speed for the mature lens equal to 1670 m / s (Fig. 7 - "Dense cataract new" mode, when conducting A-scan, the ultrasound speed value for a cloudy lens was established - 1670 m / s), the “Gate” function for the posterior lens capsule was activated, the TX was 5.68 mm, the PZO was 23.89, which clearly shows the differences from the obtained values when applying the “Dense cataract new” mode with the speed of the ultrasonic wave for clouded lens 1629 m / s.
На основании полученных данных проведен расчет ИОЛ по формуле Barrett Universal II, полученное значение оптической силы ИОЛ Domilens Nidek NS-60YG Aktis SP составило +19,0 Дптр при расчете на эмметропию (расчетное значение сфероэквивалента послеоперационной рефракции -0,26 Дптр). На следующий день у пациентки максимальная некоррегированная острота зрения составила 0,9, через 1 неделю - 1,0.Based on the obtained data, the IOL was calculated using the Barrett Universal II formula; the obtained optical power value of the Domilens Nidek NS-60YG Aktis SP IOL was +19.0 Dptr when calculating for emmetropia (the calculated value of the spheroequivalent of postoperative refraction is -0.26 Dptr). The next day, the patient's maximum uncorrected visual acuity was 0.9, after 1 week - 1.0.
Таким образом, предложенный способ обеспечивает повышение информативности измерения ТХ для точного расчета ИОЛ у пациентов со зрелой катарактой за счет проведения иммерсионной А - биометрии глаза с учетом изменения скорости ультразвуковой волны в плотном помутневшем хрусталике, что является одним из главных аспектов достижения рефракции цели после оперативного лечения катаракты.Thus, the proposed method provides an increase in the informational content of TX measurement for the accurate calculation of IOL in patients with mature cataract due to immersion A-biometry of the eye, taking into account changes in the speed of the ultrasonic wave in a dense clouded lens, which is one of the main aspects of achieving refraction of the target after surgical treatment cataracts.
Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2018105880A RU2675398C1 (en) | 2018-02-16 | 2018-02-16 | Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2018105880A RU2675398C1 (en) | 2018-02-16 | 2018-02-16 | Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2675398C1 true RU2675398C1 (en) | 2018-12-19 |
Family
ID=64753461
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2018105880A RU2675398C1 (en) | 2018-02-16 | 2018-02-16 | Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2675398C1 (en) |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2577235C1 (en) * | 2015-04-06 | 2016-03-10 | Федеральное государственное бюджетное учреждение "Московский научно-исследовательский институт глазных болезней имени Гельмгольца" Министерства здравоохранения Российской Федерации | Method of measuring length of eye in patients with mature cataract |
| WO2017019117A1 (en) * | 2015-07-27 | 2017-02-02 | Amo Wavefront Sciences, Llc | Optical imaging and measurement systems and methods for cataract surgery and treatment planning |
-
2018
- 2018-02-16 RU RU2018105880A patent/RU2675398C1/en not_active IP Right Cessation
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2577235C1 (en) * | 2015-04-06 | 2016-03-10 | Федеральное государственное бюджетное учреждение "Московский научно-исследовательский институт глазных болезней имени Гельмгольца" Министерства здравоохранения Российской Федерации | Method of measuring length of eye in patients with mature cataract |
| WO2017019117A1 (en) * | 2015-07-27 | 2017-02-02 | Amo Wavefront Sciences, Llc | Optical imaging and measurement systems and methods for cataract surgery and treatment planning |
Non-Patent Citations (1)
| Title |
|---|
| RHOND G WALDRON A-Scan Biometry, помещено на сайт в Интернет: https://emedicine.medscape.com/article/1228447-overview > 07.10.2017; дата размещения подтверждена по адресу Интернет-архива < https://web.archive.org/web/*/https://emedicine.medscape.com/article/1228447-overview > . RENU JIVRAJKA et al. Variability of axial length, anterior chamber depth, and lens thickness in the cataractous eye. J Cataract Refract Surg. 2008, vol. 34, pp 289-294 [L1-L2, fig. 1]. * |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Ehlers et al. | Corneal thickness: measurement and implications | |
| Shammas | A comparison of immersion and contact techniques for axial length measurement | |
| Reinstein et al. | Correlation of anterior chamber angle and ciliary sulcus diameters with white-to-white corneal diameter in high myopes using artemis VHF digital ultrasound | |
| RU2675398C1 (en) | Method of measurement of the thickness of a lens with diffuse opacities of a nucleus and cortical layers | |
| RU2548503C1 (en) | Method of determining indications for ablation of presbyopic crystalline lens with implantation of intraocular lens in case of hypermetropia | |
| Zhan et al. | Significance of axial length monitoring in children with congenital cataract and update of measurement methods | |
| RU2577235C1 (en) | Method of measuring length of eye in patients with mature cataract | |
| Storey et al. | Ultrasonic measurement of transverse lens diameter during accommodation | |
| Freudiger et al. | Influence of intraocular lenses on ultrasound axial length measurement: in vitro and in vivo studies | |
| RU2407442C1 (en) | Method of early pre-clinical diagnostics of lens cataract capsule state | |
| Holladay | Ultrasound and optical biometry | |
| Olsen | Calculating axial length in the aphakic and the pseudophakic eye | |
| Stoiber et al. | Ex vivo evaluation of Tono-Pen and pneumotonometry in cat eyes | |
| RU2388437C1 (en) | Method of determining dimensions of posterior chamber phakic intraocular lens | |
| Fang et al. | Advanced intraocular lens power calculations | |
| RU2576784C1 (en) | Method for ultrasonic scanning of vitreous body and retina (versions) | |
| RU2455938C1 (en) | Method of determining indications for ablation of transparent lens in case of primary closed-angle glaucoma with presence of cyclovitreolenticular unit | |
| Dutta et al. | 26 Determination of Intraocular Lens Implant Power | |
| Leary | Ultrasonographic assessment of the implant lens required to produce emmetropia after implantation | |
| Martin et al. | Asteroid hyalosis affecting the choice of intraocular lens implant | |
| Ganapathi Rajesh | Reliability of biometry. | |
| Li et al. | Comparison of intraocular pressures at different points in human’s cornea before and after laser in situ keratomileusis with tono-pen tonometer | |
| Lewis et al. | Effect of soft contact lenses on optical measurements of axial length and keratometry for biometry in eyes with corneal irregularities | |
| Rabie et al. | Pupil size in relation to ultrasonic anterior chamber depth measurements in pseudophakic eyes | |
| Savitha | Accuracy of Intraocular Lens Power Calculation in Eyes with Axial Length Less Then 22.00 mm |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees |
Effective date: 20200217 |