RU2612861C1 - Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde - Google Patents
Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde Download PDFInfo
- Publication number
- RU2612861C1 RU2612861C1 RU2016110493A RU2016110493A RU2612861C1 RU 2612861 C1 RU2612861 C1 RU 2612861C1 RU 2016110493 A RU2016110493 A RU 2016110493A RU 2016110493 A RU2016110493 A RU 2016110493A RU 2612861 C1 RU2612861 C1 RU 2612861C1
- Authority
- RU
- Russia
- Prior art keywords
- formaldehyde
- phenol
- toluene
- benzene
- children
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
Landscapes
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
Abstract
Description
Изобретение относится к медицине, а именно к пульмонологии, кардиологии и токсикологии, и может быть использовано для ранней диагностики морфофункциональных нарушений миокарда у детей старше 5 лет с заболеваниями органов дыхания, в частности с бронхообструкцией, проживающих в условиях среды обитания с повышенным аэрогенным воздействием токсических соединений: толуола, бензола, фенола, формальдегида.The invention relates to medicine, namely to pulmonology, cardiology and toxicology, and can be used for early diagnosis of morphofunctional myocardial disorders in children over 5 years old with respiratory diseases, in particular with bronchial obstruction, living in a living environment with increased aerogenic exposure to toxic compounds : toluene, benzene, phenol, formaldehyde.
Изобретение может быть использовано для выявления нарушений миокарда, ассоциированных с ингаляционным воздействием указанных органических соединений, и направлено на раннее выявление кардиальных нарушений, с целью предотвращения прогрессирования осложнений хронических заболеваний органов дыхания.The invention can be used to detect myocardial disorders associated with the inhalation effect of these organic compounds, and is aimed at early detection of cardiac disorders, in order to prevent the progression of complications of chronic respiratory diseases.
Сердечно-сосудистая и дыхательная система морфологически и функционально связаны между собой, поэтому в развитии респираторных заболеваний определенную роль играют изменения сердца. Разнообразие сердечно-сосудистых нарушений в период обострения бронхолегочных заболеваний у детей изучалось многими исследователями, однако до сих пор имеются определенные диагностические трудности.The cardiovascular and respiratory systems are morphologically and functionally interconnected; therefore, changes in the heart play a role in the development of respiratory diseases. A variety of cardiovascular disorders during exacerbation of bronchopulmonary diseases in children has been studied by many researchers, but there are still some diagnostic difficulties.
Болезни органов дыхания детей стабильно занимают ведущее место в структуре общей заболеваемости и, например, в 2013 году составили 12561,7 случаев на 100000 детского населения Российской Федерации. За последние пять лет отмечается небольшое снижение заболеваемости хронических бронхитов, хронических обструктивных болезней, бронхиальной астмы у детей с 1521,2 до 1325,6 случаев на 100000 детского населения. Согласно данным Государственного доклада в 2013 году напряженная ситуация по уровню загрязнения атмосферного воздуха складывалась в Сибирском, Уральском и Дальневосточном округах. Распространенными загрязняющими веществами от промышленных предприятий и автотранспорта явились взвешенные вещества, оксид углерода, диоксид азота, ароматические углеводороды, формальдегид. При этом 5,6% заболеваний органов дыхания являются ассоциированными с загрязнением атмосферного воздуха.Diseases of the respiratory organs of children consistently occupy a leading place in the structure of the general incidence rate and, for example, in 2013 amounted to 12,561.7 cases per 100,000 children in the Russian Federation. Over the past five years, there has been a slight decrease in the incidence of chronic bronchitis, chronic obstructive diseases, bronchial asthma in children from 1521.2 to 1325.6 cases per 100,000 children. According to the State Report in 2013, the tense situation regarding the level of atmospheric air pollution developed in the Siberian, Ural and Far Eastern districts. Common pollutants from industrial enterprises and vehicles were suspended solids, carbon monoxide, nitrogen dioxide, aromatic hydrocarbons, formaldehyde. At the same time, 5.6% of respiratory diseases are associated with air pollution.
В настоящее время остаются недостаточно освещенными вопросы развития морфофункциональных изменений миокарда у детей с хроническими заболеваниями органов дыхания, которые связаны с аэрогенным воздействием неблагоприятных факторов среды обитания.Currently, the issues of the development of morphofunctional changes in the myocardium in children with chronic respiratory diseases, which are associated with the aerogenic impact of adverse environmental factors, remain insufficiently covered.
В настоящее время известны способы диагностики поражений миокарда, в том числе и у пациентов, страдающих легочными заболеваниями, на основе клинических, инструментальных и лабораторных данных.Currently, there are known methods for diagnosing myocardial lesions, including in patients suffering from pulmonary diseases, based on clinical, instrumental and laboratory data.
Известен способ диагностики некоронарогенного повреждения миокарда у больных туберкулезом легких (патент РФ №2475746), согласно которому у одного и того же пациента до и во время проведения противотуберкулезной терапии в сыворотке крови определяют концентрацию сердечного белка, связывающего жирные кислоты (СБСЖК), и при увеличении концентрации СБСЖК диагностируют некоронарогенное повреждение миокарда. Известное изобретение обеспечивает раннюю доклиническую диагностику некоронарогенного повреждения миокарда у указанной группы больных.A known method for the diagnosis of non-coronarogenic myocardial damage in patients with pulmonary tuberculosis (RF patent No. 2475746), according to which the same patient before and during anti-tuberculosis therapy in the blood serum determines the concentration of heart protein that binds fatty acids (SBLC), and with an increase Concentrations of SBSS are diagnosed with non-coronarogenic myocardial damage. The known invention provides early preclinical diagnosis of non-coronarogenic myocardial damage in this group of patients.
Однако его недостатком является то, что СБСЖК, располагаясь в цитолизе кардиомиоцита в свободном виде, быстро освобождается вне зависимости от воздействующего фактора в результате ишемии миокарда, ведущей к некрозу, что снижает точность метода. Кроме того, он не учитывает модифицирующего влияния факторов среды обитания на формирование заболеваний легких (туберкулеза).However, its drawback is that SBLC, located in the free form of the cardiomyocyte, is rapidly released regardless of the acting factor as a result of myocardial ischemia leading to necrosis, which reduces the accuracy of the method. In addition, it does not take into account the modifying effect of environmental factors on the formation of lung diseases (tuberculosis).
Из уровня техники известен способ диагностики гипертрофии правого желудочка сердца у больных хроническим обструктивным бронхитом (патент РФ №2216270). При его реализации у больных хроническим обструктивным бронхитом регистрируют электрокардиограмму (ЭКГ) по стандартной методике. Анализируют следующие показатели: амплитуда зубца S в первом стандартном отведении, сумма амплитуды зубцов R в первом грудном и S в пятом грудном отведениях, амплитуда зубца R в усиленном отведении от правой руки, амплитуда зубца Т в первом и втором грудных отведениях, учитывают возраст пациента и длительность заболевания. Вышеперечисленные параметры подставляют в оригинальную математическую формулу. Наличие гипертрофии правого желудочка сердца диагностируют по значению вычисленного показателя Z.The prior art method for the diagnosis of right ventricular hypertrophy in patients with chronic obstructive bronchitis (RF patent No. 2216270). When it is implemented in patients with chronic obstructive bronchitis, an electrocardiogram (ECG) is recorded according to a standard technique. The following indicators are analyzed: the amplitude of the S wave in the first standard lead, the sum of the amplitude of the R waves in the first chest and S in the fifth chest leads, the amplitude of the R wave in the strengthened lead from the right hand, the amplitude of the T wave in the first and second chest leads, take into account the patient’s age and the duration of the disease. The above parameters are substituted into the original mathematical formula. The presence of right ventricular hypertrophy is diagnosed by the value of the calculated indicator Z.
Недостатком этого способа является возможность проведения диагностики только у взрослого населения, имеющего длительный стаж заболевания хроническим обструктивным бронхитом; а также исключение из обследования пациентов с наличием на ЭКГ признаков блокад ножек пучка Гиса и/или инфаркта миокарда любой локализации.The disadvantage of this method is the ability to diagnose only in the adult population with a long history of chronic obstructive bronchitis; and also the exclusion from examination of patients with the presence on the ECG of signs of blockade of the legs of the bundle of His and / or myocardial infarction of any location.
Также известен способ диагностики ишемической болезни сердца (ИБС) у больных с хроническими обструктивными заболеваниями легких (ХОБЛ) (патент РФ №2187240). Больным с ХОБЛ проводят провокационную фармакологическую пробу. Проба заключается в ингаляции сальбутамола в дозе 5 мг или фенотерола 1 мг через небулайзер. Проводят мониторирование ЭКГ в течение часа после ингаляции. При возникновении клиники стенокардии и/или регистрации электрокардиографических признаков ишемии миокарда продолжительностью более 1 мин пробу считают положительной. Способ позволяет выявить сопутствующую ИБС у лиц с ХОБЛ и одновременно улучшить бронхиальную проводимость.Also known is a method for diagnosing coronary heart disease (CHD) in patients with chronic obstructive pulmonary disease (COPD) (RF patent No. 2187240). A patient with COPD is given a provocative pharmacological test. The test consists in the inhalation of salbutamol in a dose of 5 mg or fenoterol 1 mg through a nebulizer. ECG is monitored for an hour after inhalation. If there is a clinic of angina pectoris and / or registration of electrocardiographic signs of myocardial ischemia lasting more than 1 min, the sample is considered positive. The method allows to identify concomitant coronary heart disease in patients with COPD and at the same time improve bronchial conduction.
Однако и этот известный способ не лишен недостатков, а именно: выявление признаков стенокардии, которая в детском возрасте не встречается; проведение фармакологических провокационных проб у детей ограничено.However, this known method is not without drawbacks, namely: the identification of signs of angina pectoris, which in childhood does not occur; conducting pharmacological provocative tests in children is limited.
В известном способе ранней диагностики стенокардии напряжения типичного и атипичного течения при хронической обструктивной болезни легких (патент РФ №2414847) реализация осуществляется путем лабораторного исследования крови больных с ХОБЛ. Оценивают цитолейкограмму гранулоцитосвязывающих лимфоцитов. Вычисляют индекс розеткообразования (ИРО) как соотношение между ЛСГ-1 (лимфоцит + 1 гранулоцит), ЛСГ-2 (лимфоцит + 2 гранулоцита), ЛСГ-3 (лимфоцит + 3 гранулоцита) и свободнолежащими лимфоцитами. При увеличении ИРО ЛСГ-3 более 0,03, уменьшении ИРО ЛСГ-2 менее 0,11 у больных ХОБЛ диагностируют стенокардию напряжения. Его недостатком является инвазивность, возможность разнонаправленных сдвигов гранулоцитосвязывающих лимфоцитов, обусловленных более выраженным иммунодефицитом и аутоиммунными механизмами, а также наличием выраженного воспалительного процесса в организме, что приводит к недостаточной специфичности, так как на розеткообразование оказывает влияние целый ряд факторов.In the known method for the early diagnosis of angina pectoris of a typical and atypical course in chronic obstructive pulmonary disease (RF patent No. 2414847), the implementation is carried out by laboratory testing of blood of patients with COPD. The cytoleukogram of granulocyte-binding lymphocytes is evaluated. The Rosette Index (IRO) is calculated as the ratio between LSH-1 (lymphocyte + 1 granulocyte), LSH-2 (lymphocyte + 2 granulocyte), LSH-3 (lymphocyte + 3 granulocyte) and free-lying lymphocytes. With an increase in the RTI of LSH-3 more than 0.03, a decrease in the RTI of LSH-2 less than 0.11, patients with COPD are diagnosed with angina pectoris. Its disadvantage is invasiveness, the possibility of multidirectional shifts of granulocyte-binding lymphocytes due to more pronounced immunodeficiency and autoimmune mechanisms, as well as the presence of a pronounced inflammatory process in the body, which leads to insufficient specificity, as a number of factors affect the formation of rosettes.
Из уровня техники также известен ряд технических решений, направленных на установление кардиологических изменений у детей.The prior art also known a number of technical solutions aimed at establishing cardiological changes in children.
Например, известен способ диагностики нарушений деятельности сердечно-сосудистой системы в остром периоде бронхиальной обструкции у детей (Гнусаев С.Ф. Значение малых аномалий развития сердца (МАРС) у здоровых детей и при сердечно-сосудистой патологии по данным клинико-эхокардиографических исследований. Автореферат диссертации докт. мед. наук. - Москва, 1996. - 53 с.), включающий проведение эхокардиографического (ЭХОкг) исследования с использованием ультразвуковых диагностических приборов «SSD-600 ALOKA» в М и В режимах. На основании оценки ультраструктуры сердечной мышцы при ее визуализации определяют малые аномалии развития сердца (МАРС). Исследование систолической и диастолической функций левых отделов сердца и проведение измерений определенных показателей позволяет оценить: конечно-диастолический и конечно-систолический объем левого желудочка (КДО и КСО ЛЖ, мл) по формуле 1. TEICHHOLS; ударный объем (УО): КДО-КСО (мл); минутный объем кровообращения (МОК): УОХЧСС (л/мин); фракцию выброса УО: КДО (%). По наличию МАРС судят о функциональных изменениях сердца, а при снижении систолодиастолических показателей - о нарушении сократительной деятельности миокарда и кардиальной дисфункции в острый период бронхиальной обструкции.For example, there is a method for diagnosing disorders of the cardiovascular system in the acute period of bronchial obstruction in children (Gnusaev SF. The value of small cardiac abnormalities (MARS) in healthy children and cardiovascular disease according to clinical and echocardiographic studies. Abstract of dissertation Doctor of Medical Sciences - Moscow, 1996. - 53 pp.), including conducting an echocardiographic (ECHO) study using ultrasonic diagnostic devices "SSD-600 ALOKA" in M and B modes. Based on the assessment of the ultrastructure of the heart muscle during its visualization, small abnormalities of the development of the heart (MARS) are determined. The study of systolic and diastolic functions of the left heart and the measurement of certain indicators allows you to evaluate: end-diastolic and end-systolic volume of the left ventricle (BWW and CSR LV, ml) according to the formula 1. TEICHHOLS; shock volume (UO): KDO-KSO (ml); minute volume of blood circulation (IOC): UOCHCHSS (l / min); EO emission fraction: BWW (%). By the presence of MARS, functional changes in the heart are judged, and with a decrease in systolodiastolic indices, a violation of the contractile activity of the myocardium and cardiac dysfunction in the acute period of bronchial obstruction is judged.
Недостатком указанного известного способа является то, что:The disadvantage of this known method is that:
- он не является патогенетически обоснованным и позволяет диагностировать лишь наличие нарушения функции левых отделов сердца;- it is not pathogenetically substantiated and allows you to diagnose only the presence of dysfunction of the left heart;
- отсутствие объективных показателей для оценки топических особенностей его повреждения не дает возможности дифференцировать варианты поражения миокарда;- the lack of objective indicators for assessing the topical features of its damage does not make it possible to differentiate the options for myocardial damage;
- патологические изменения, как правило, выявляются данным методом в остром периоде заболевания или при тяжелом течении болезни;- pathological changes, as a rule, are detected by this method in the acute period of the disease or in severe cases of the disease;
- способ не является точным, даже при тяжелой патологии показатели могут не иметь отклонений от нормы.- the method is not accurate, even with severe pathology, indicators may not have deviations from the norm.
Еще известен способ дифференциальной диагностики поражений миокарда у новорожденных (патент РФ №2089900). Он может быть использован для дифференциальной диагностики поражений миокарда у новорожденных, перенесших перинатальное поражение центральной нервной системы. У новорожденных детей проводят биохимическое исследование сыворотки крови, определяют активность кардиоспецифического изофермента креатинфосфокиназы /КФК-МВ/, и при увеличении активности КФК-МВ от 10 до 50% диагностируют постгипоксическую кардиопатию, свыше 51% - ишемическое повреждение миокарда. К недостаткам данного способа диагностики можно отнести то, что у детей, перенесших перинатальную гипоксию, в периоде новорожденности повышение активности кардиоспецифических ферментов обусловлено перестройкой метаболизма миокарда (В.А. Таболин, Н.П. Котлукова, Л.В. Симонова, Н.В. Гайдукова, Н.А. Чернявская, 2001). Кроме того, у данного метода отсутствуют доклинические диагностические маркеры дисфункции сердечно-сосудистой системы у новорожденных.Another known method for the differential diagnosis of myocardial lesions in newborns (RF patent No. 2089900). It can be used for the differential diagnosis of myocardial lesions in newborns after a perinatal lesion of the central nervous system. In newborns, a biochemical study of blood serum is carried out, the activity of the cardiospecific creatine phosphokinase isoenzyme (KFK-MV) is determined, and with an increase in KFK-MV activity from 10 to 50%, posthypoxic cardiopathy is diagnosed, over 51% ischemic myocardial damage. The disadvantages of this diagnostic method include the fact that in children undergoing perinatal hypoxia, in the neonatal period, an increase in the activity of cardiospecific enzymes is due to a restructuring of myocardial metabolism (V.A. Tabolin, N.P. Kotlukova, L.V. Simonova, N.V. Gaidukova, N.A. Chernyavskaya, 2001). In addition, this method lacks preclinical diagnostic markers of cardiovascular dysfunction in newborns.
Известен способ диагностики ишемических поражений миокарда у детей (авт. свид. СССР №1749833), согласно которому исследуют биохимически сыворотку крови, определяя активность фермента пирофосфатазы, отражающего изменения энергетического обмена, спектрофотометрическим методом и при значениях показателей активности, превышающих 11,92 ммоль/л относительно нормы, диагностируют ранние ишемические поражения миокарда у детей с нарушением ритма и проводимости сердца. Его недостатки заключаются в том, что пирофосфатаза присутствует в разных структурах клеток и осуществляет контрольную функцию во многих важных обменных процессах организма, поэтому ее использование не делает способ селективным. Кроме того, известный метод предполагает исследования детей с нарушениями ритма и проводимости и не учитывает влияния техногенных факторов среды обитания.A known method for the diagnosis of ischemic myocardial lesions in children (ed. Certificate of the USSR No. 1749833), according to which blood serum is examined biochemically, determining the activity of the pyrophosphatase enzyme, reflecting changes in energy metabolism, spectrophotometrically and with values of activity indicators exceeding 11.92 mmol / l relatively normal, diagnosed with early ischemic myocardial damage in children with rhythm and cardiac conduction. Its disadvantages are that pyrophosphatase is present in different cell structures and performs a control function in many important metabolic processes of the body, so its use does not make the method selective. In addition, the known method involves the study of children with rhythm and conduction disorders and does not take into account the influence of technogenic environmental factors.
Из уровня техники было найдено только одно техническое решение, позволяющее диагностировать нарушение миокарда от токсического воздействия окружающей среды. В авт. свид. СССР №1784923 «Способ диагностики кобальтовой миокардиопатии» описано изобретение, позволяющее диагностировать профессиональное поражение сердечной мышцы при воздействии кобальта и его соединений. Его сущность заключается в том, что в крови пациента определяют концентрацию гормона кальмодулина и при его значении 300 мг/мл и более диагностируют патологию. Его недостатки заключаются в том, что на концентрацию кальмодулина могут оказывать влияние разнообразные факторы, так как он участвует во всех процессах, регулируемых ионами кальция, в том числе в поперечно-полосатой скелетной мускулатуре. Поэтому такой диагностический критерий не обеспечивает точность диагноза.From the prior art, only one technical solution was found to diagnose myocardial impairment from toxic environmental effects. In auth. testimonial. USSR No. 1784923 "A method for the diagnosis of cobalt myocardiopathy" describes an invention that allows you to diagnose professional damage to the heart muscle when exposed to cobalt and its compounds. Its essence lies in the fact that the concentration of the hormone calmodulin is determined in the patient’s blood and, with its value of 300 mg / ml or more, pathology is diagnosed. Its disadvantages are that a variety of factors can influence the calmodulin concentration, since it is involved in all processes regulated by calcium ions, including the striated skeletal muscle. Therefore, such a diagnostic criterion does not ensure the accuracy of the diagnosis.
При этом из уровня техники не были выявлены известные способы диагностики нарушений миокарда у детей с заболеваниями органов дыхания, ассоциированными с токсическим воздействием ароматических соединений и формальдегида, поэтому сделать выбор ближайшего аналога к заявляемому объекту не представляется возможным.Moreover, the known methods for diagnosing myocardial disorders in children with respiratory diseases associated with the toxic effects of aromatic compounds and formaldehyde have not been identified from the prior art; therefore, it is not possible to choose the closest analogue to the claimed object.
Технический результат, достигаемый предлагаемым изобретением, заключается в создании информативного и доказательного способа диагностики морфофункциональных нарушений системы миокарда у детей при наличии у них бронхолегочных заболеваний, вызванных воздействием фенола, толуола, бензола и формальдегида, позволяющего на ранних стадиях заболевания назначить адекватную терапию и предупредить развитие осложнений.The technical result achieved by the present invention is to create an informative and evidence-based method for the diagnosis of morphofunctional disorders of the myocardial system in children with bronchopulmonary diseases caused by exposure to phenol, toluene, benzene and formaldehyde, which allows prescribing adequate therapy in the early stages of the disease and preventing the development of complications .
Поставленный технический результат достигается предлагаемым способом диагностики морфофункциональных нарушений миокарда у детей старше 5 лет с бронхолегочными заболеваниями, ассоциированными с воздействием бензола, толуола, фенола и формальдегида, включающим определение в пробе крови ребенка концентрации бензола, толуола, фенола и формальдегида, и при превышении ее выше фоновой осуществляют определение функциональных и лабораторных показателей, при этом в качестве функциональных показателей определяют: электрофизиологическую функцию миокарда путем проведения электрокардиографии; вариабельность сердечного ритма под влиянием вегетативной нервной системы по данным кардиоинтервалографии, и сократительную функцию сердца и внутрисердечную гемодинамику с определением основных параметров кровотока в сердечных камерах и функции клапанного аппарата при эхокардиографии; а в качестве лабораторных показателей устанавливают: уровень лейкоцитов; уровень антиоксидантной активности АОА; уровень малонового диальдегида МДА; уровень высокочувствительного С-реактивного белка; и состояние антиатерогенной защиты - аполипротеины; и при наличии синусовой брадикардии/тахикардии при проведении электрокардиографии; при эйтоническом исходном вегетативном тонусе, сопровождающемся преобладанием активности парасимпатического отдела автономной нервной системы, асимпатикотонической/гиперсимпатикотонической реактивности по данным кардиоинтервалографии; при наличии повышения систолического давления в легочной артерии, преходящей диастолической дисфункции правого желудочка при эхокардиографии; а также при превышении относительно возрастной физиологической нормы уровня лейкоцитов на 20% и более, МДА - в 1,3 раза и более, высокочувствительного С-реактивного белка - в 1,8 раза и более, и снижения АОА в 1,2 раза и более и при изменении факторов антиатерогенной защиты, заключающихся в повышении относительно возрастной физиологической нормы Аполипротеина А1 и снижения коэффициента «Аполипротеин В/Аполипротеин А1», диагностируют морфофункциональные нарушения миокарда у детей старше 5 лет с бронхолегочными заболеваниями, ассоциированными с воздействием бензола, толуола, фенола и формальдегида.The technical result is achieved by the proposed method for the diagnosis of morphofunctional myocardial disorders in children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde, including determining the concentration of benzene, toluene, phenol and formaldehyde in a child’s blood sample, and if it is exceeded the background carry out the determination of functional and laboratory parameters, while the following are determined as functional indicators: electrophysiological function myocardial lumen by electrocardiography; heart rate variability under the influence of the autonomic nervous system according to cardiointervalography, and contractile function of the heart and intracardiac hemodynamics with determination of the main parameters of blood flow in the heart chambers and valve function during echocardiography; and as laboratory indicators establish: the level of leukocytes; the level of antioxidant activity of AOA; MDA malondialdehyde level; level of highly sensitive C-reactive protein; and the state of anti-atherogenic defense - apoliproteins; and in the presence of sinus bradycardia / tachycardia during electrocardiography; with an ejtonic initial vegetative tone, accompanied by a predominance of activity of the parasympathetic department of the autonomic nervous system, asymptaticotonic / hypersympathicotonic reactivity according to cardiointervalography; in the presence of an increase in systolic pressure in the pulmonary artery, transient diastolic dysfunction of the right ventricle with echocardiography; as well as when the relative physiological norm is exceeded, the level of leukocytes is 20% or more, MDA is 1.3 times or more, highly sensitive C-reactive protein is 1.8 times or more, and AOA is reduced by 1.2 times or more and when the anti-atherogenic defense factors change, which consists in increasing the relative physiological norm of Apoliprotein A1 and decreasing the Apoliprotein B / Apoliprotein A1 coefficient, morphofunctional myocardial disorders in children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde.
Указанный технический результат достигается за счет следующего.The specified technical result is achieved due to the following.
Для понимания существа вопроса, следует пояснить что сердечно-сосудистая и дыхательная системы морфологически и функционально связаны между собой, поэтому в развитии респираторных заболеваний определенную роль играют изменения сердца. Установлено, что хроническое аэрогенное комбинированное воздействие бензола, толуола, фенола и формальдегида вызывает развитие местного хронического воспалительного процесса в слизистой оболочке дыхательного тракта с нарушением мукоцилиарного клиренса и развитием дистрофических процессов.To understand the essence of the issue, it should be clarified that the cardiovascular and respiratory systems are morphologically and functionally interconnected, therefore, changes in the heart play a role in the development of respiratory diseases. It was established that the chronic aerogenic combined effect of benzene, toluene, phenol and formaldehyde causes the development of a local chronic inflammatory process in the mucous membrane of the respiratory tract with impaired mucociliary clearance and the development of dystrophic processes.
Наряду с дыхательной системой в патологический процесс вовлекается и сердечно-сосудистая система, что связано как с прямым кардиотоксичным действием бензола и фенола, так и с опосредованным, обусловленным нарушением функции внешнего дыхания и изменением функционирования вегетативной нервной системы под действием техногенных химических факторов. Кроме того, длительное воздействие бензола, толуола, фенола и формальдегида нарушает процессы тканевого метаболизма, что в дальнейшем приводит к хронической интоксикации. В результате у детей с бронхообструкцией возникает гипоксическая вазоконстрикция, приводящая к повышению сопротивления в легочных сосудах и давления в легочных тканях с развитием в дальнейшем легочной гипертензии.Along with the respiratory system, the cardiovascular system is also involved in the pathological process, which is associated both with the direct cardiotoxic effect of benzene and phenol, as well as indirect, due to impaired respiratory function and a change in the functioning of the autonomic nervous system under the influence of technogenic chemical factors. In addition, prolonged exposure to benzene, toluene, phenol and formaldehyde disrupts the processes of tissue metabolism, which subsequently leads to chronic intoxication. As a result, in children with bronchial obstruction, hypoxic vasoconstriction occurs, leading to increased resistance in the pulmonary vessels and pressure in the lung tissue with the development of further pulmonary hypertension.
Благодаря расширению в предлагаемом способе информационных показателей (одновременное использование функциональных и лабораторных), связанных с сердечно-сосудистой системой и одновременно с количеством химического токсиканта - толуола, бензола, фенола и формальдегида, в крови, и будет обеспечена точность оценки диагностики влияния этих соединений на развитие указанной патологии.Due to the expansion in the proposed method of information indicators (the simultaneous use of functional and laboratory) associated with the cardiovascular system and at the same time with the amount of chemical toxicant - toluene, benzene, phenol and formaldehyde in the blood, the accuracy of the diagnosis of the impact of these compounds on development will be ensured specified pathology.
Благодаря тому что в предлагаемом способе, наряду с результатами указанной диагностики, дополнительно используют информацию о содержании бензола, толуола, фенола и формальдегида в крови ребенка и заявляемые конкретные совокупные показатели (функциональные: электрофизиологическая функция миокарда, вариабельность сердечного ритма под влиянием вегетативной нервной системы, сократительная функция сердца и внутрисердечная гемодинамика с определением основных параметров кровотока в сердечных камерах и функции клапанного аппарата; лабораторные показатели: уровни лейкоцитов; АОА; МДА; высокочувствительного С-реактивного белка и состояние антиатерогенной защиты - аполипротеины), клиническая значимость которых доказана методом корреляционно-регрессионного анализа, обеспечивается дополнительная информационная связь изменений указанных совокупных показателей с превышением над фоновым уровнем содержания в крови указанных ароматических соединений и формальдегида, что делает предлагаемый способ точным и достоверным.Due to the fact that in the proposed method, along with the results of this diagnosis, information on the content of benzene, toluene, phenol and formaldehyde in the blood of the child and the claimed specific aggregate indicators (functional: electrophysiological function of the myocardium, heart rate variability under the influence of the autonomic nervous system, contractile cardiac function and intracardiac hemodynamics with determination of the main parameters of blood flow in the heart chambers and valve function; factor indicators: leukocyte levels; AOA; MDA; highly sensitive C-reactive protein and the state of anti-atherogenic defense - apoliproteins), the clinical significance of which has been proved by the method of correlation and regression analysis, provides additional information linkage of changes in these aggregate indicators with excess above the background level in blood levels of these aromatic compounds and formaldehyde, which makes the proposed method accurate and reliable.
Исходя из вышеизложенного, можно сделать вывод, что поставленный технический результат обеспечивается за счет совокупности всех операций предлагаемого способа, их последовательности и режимов его реализации.Based on the foregoing, we can conclude that the technical result is achieved due to the totality of all operations of the proposed method, their sequence and modes of implementation.
При реализации предлагаемого способа осуществляют следующие операции в нижеуказанной последовательности:When implementing the proposed method, the following operations are carried out in the following sequence:
- выбирают экологически неблагополучную территорию по высокой нагрузке химических факторов среды обитания с неудовлетворительным качеством атмосферного воздуха по санитарно-химическим показателям (превышение содержания бензола, толуола, фенола и формальдегида более 1,0 ПДК м.р., ПДК с.с.).- choose an ecologically unfavorable territory for a high load of chemical environmental factors with unsatisfactory atmospheric air quality for sanitary and chemical indicators (excess of benzene, toluene, phenol and formaldehyde in excess of 1.0 MPC m.r., MPC s.s.).
Результаты исследования качества атмосферного воздуха получают на основании данных социально-гигиенического мониторинга в рамках Постановления правительства РФ от 02.02.2006 г. №60 «Положение о проведении социально-гигиенического мониторинга» (с изменениями от 04.09.2012 г.) с учетом требований ГН 2.1.6.1338-03 «Предельно-допустимые концентрации (ПДК) загрязняющих веществ в атмосферном воздухе населенных мест» (с изменениями от 3 ноября 2005 г., 4 февраля 2008 г., 27 января 2009 г.).The results of a study of atmospheric air quality are obtained on the basis of socio-hygienic monitoring data in the framework of the Decree of the Government of the Russian Federation of 02.02.2006 No. 60 "Regulation on the conduct of socio-hygienic monitoring" (as amended on 04.09.2012), taking into account the requirements of GN 2.1 .6.1338-03 "Maximum allowable concentrations (MPC) of pollutants in the atmospheric air of populated areas" (as amended on November 3, 2005, February 4, 2008, January 27, 2009).
Данные о наличие риска возникновения патологии органов дыхания у населения, подвергающегося воздействию бензола, толуола, фенола и формальдегида, оценивают по стандартизованной методике в соответствии с «Руководством по оценке риска для здоровья населения при воздействии химических веществ, загрязняющих окружающую среду» (Р 2.1.10.1920-04):Data on the presence of a risk of respiratory pathology in a population exposed to benzene, toluene, phenol and formaldehyde are evaluated according to a standardized method in accordance with the Guidelines for assessing the risk to public health when exposed to chemicals polluting the environment (R 2.1.10.1920 -04):
- проводят отбор детей старше 5 лет, проживающих на территории с загрязнением атмосферного воздуха бензолом, толуолом, фенолом и формальдегидом, с установленным диагнозом бронхиальная астма (МКБ10: J45.0) и рецидивирующий бронхит (МКБ10: J44.8) вне обострения; проводят их клинический осмотр;- carry out the selection of children over 5 years old, living in the territory with atmospheric air pollution with benzene, toluene, phenol and formaldehyde, with a diagnosis of bronchial asthma (ICD10: J45.0) and recurrent bronchitis (ICD10: J44.8) without exacerbation; conduct their clinical examination;
- производят отбор пробы крови у каждого ребенка и определение в ней концентрации бензола, толуола, фенола и формальдегида;- take a blood sample from each child and determine the concentration of benzene, toluene, phenol and formaldehyde in it;
- и при превышении ее выше фонового уровня осуществляют дальнейшие медико-биологические исследования ребенка, заключающиеся в установлении определенных функциональных и лабораторных показателей.- and when it is exceeded above the background level, further biomedical studies of the child are carried out, consisting in the establishment of certain functional and laboratory indicators.
При этом в качестве функциональных показателей определяют:Moreover, as functional indicators determine:
- электрофизиологическую функцию миокарда путем проведения электрокардиографии;- electrophysiological function of the myocardium by conducting electrocardiography;
- вариабельность сердечного ритма под влиянием вегетативной нервной системы по данным кардиоинтервалографии;- heart rate variability under the influence of the autonomic nervous system according to cardiointervalography;
- и сократительную функцию сердца и внутрисердечную гемодинамику с определением основных параметров кровотока в сердечных камерах и функции клапанного аппарата при эхокардиографии.- and contractile function of the heart and intracardiac hemodynamics with the determination of the main parameters of blood flow in the heart chambers and the function of the valve apparatus during echocardiography.
В качестве лабораторных показателей устанавливают:As laboratory indicators establish:
- уровень лейкоцитов;- white blood cell count;
- уровень АОА сыворотки крови;- serum AOA level;
- уровень МДА в плазме крови;- the level of MDA in blood plasma;
- уровень высокочувствительного С-реактивного белка в сыворотке крови;- the level of highly sensitive C-reactive protein in blood serum;
- состояние антиатерогенной защиты - аполипротеины;- state of anti-atherogenic defense - apoliproteins;
- а морфофункциональные нарушения миокарда у ребенка с бронхолегочным заболеванием, ассоциированным с воздействием бензола, толуола, фенола и формальдегида, диагностируют в том случае, если одновременно у ребенка наблюдаются отклонения как в функциональных, так и в лабораторных показателях, а именно:- and morphofunctional myocardial disorders in a child with a bronchopulmonary disease associated with exposure to benzene, toluene, phenol and formaldehyde are diagnosed if at the same time the child has deviations in both functional and laboratory parameters, namely:
- наличие синусовой брадикардии/тахикардии при проведении электрокардиографии;- the presence of sinus bradycardia / tachycardia during electrocardiography;
- эйтонический исходный вегетативный тонус, сопровождающийся повышением активности парасимпатического отдела автономной нервной системы,- aytonic initial vegetative tone, accompanied by an increase in the activity of the parasympathetic department of the autonomic nervous system,
- повышение асимпатикотонической/гиперсимпатикотонической реактивности;- increase in asymptaticotonic / hypersympathicotonic reactivity;
- повышение систолического давления в легочной артерии, преходящей диастолической дисфункции правого желудочка;- increased systolic pressure in the pulmonary artery, transient diastolic dysfunction of the right ventricle;
- превышение относительно возрастной физиологической нормы уровня лейкоцитов на 20% и более; МАД - в 1,2 раза и более; высокочувствительного С-реактивного белка - в 1,8 раза и более,- excess of the age-related physiological norm of the level of leukocytes by 20% or more; MAD - 1.2 times or more; highly sensitive C-reactive protein - 1.8 times or more,
- снижение АОА в 1,2 раза и более,- reduction of AOA by 1.2 times or more,
- изменение липидного обмена, заключающегося в повышении Аполипротеина А1 и снижении коэффициента «Аполипротеин В/Аполипротеин А1».- change in lipid metabolism, which consists in increasing Apoliprotein A1 and lowering the coefficient "Apoliprotein B / Apoliprotein A1".
При диагностическом обследовании предлагаемым способом используют оборудование, указанное в таблице 1.When a diagnostic examination of the proposed method use the equipment specified in table 1.
В качестве критериев оценки отклонений функциональных и лабораторных показателей используются возрастные физиологические уровни, а для содержания бензола, толуола, фенола, формальдегида - фоновые уровни.The physiological levels are used as criteria for assessing deviations of functional and laboratory parameters, and background levels are used for the content of benzene, toluene, phenol, formaldehyde.
Для доказательства правомерности применяемых в предлагаемом способе диагностических критериев был использован корреляционный анализ между полученными функциональными и лабораторными показателями и содержанием бензола, толуола, фенола и формальдегида в крови ребенка с использованием модели логистической регрессии, согласно которой рассчитывают вероятность негативного изменения маркера ответа организма (вышеуказанные показатели) при воздействии на организм маркера экспозиции (указанных токсикантов, поступающих ингаляционным путем). Выявление и оценка связи между изменением функциональных и лабораторных показателей у детей и концентрацией бензола, толуола, фенола и формальдегида в крови выполняется на основании расчета показателя отношения шансов (OR) и его доверительного интервала (DI). Критерием наличия связи «концентрация бензола, толуола, фенола и формальдегида в крови - показатель ответа» является OR≥1. Обоснование маркеров ответа осуществляется на основании оценки параметров зависимости изменения показателя отношения шансов от концентрации бензола, толуола, фенола и формальдегида в крови, описываемой регрессионной моделью в виде экспоненциальной функции. В качестве критерия для проверки статистических гипотез используется критерий Фишера (F). Различия считаются статистически значимыми при вероятности p≤0,05.To prove the validity of the diagnostic criteria used in the proposed method, a correlation analysis was used between the obtained functional and laboratory parameters and the content of benzene, toluene, phenol and formaldehyde in the child’s blood using the logistic regression model, according to which the probability of a negative change in the response marker of the body is calculated (the above indicators) when exposed to an exposure marker (specified toxicants received by inhalation eat). The identification and assessment of the relationship between changes in functional and laboratory parameters in children and the concentration of benzene, toluene, phenol and formaldehyde in the blood is performed based on the calculation of the odds ratio (OR) indicator and its confidence interval (DI). The criterion for the presence of the relationship "the concentration of benzene, toluene, phenol and formaldehyde in the blood - an indicator of the response" is OR≥1. The justification of response markers is based on the assessment of the parameters of the dependence of the odds ratio on the concentration of benzene, toluene, phenol and formaldehyde in the blood, described by the regression model in the form of an exponential function. The Fisher test (F) is used as a criterion for testing statistical hypotheses. Differences are considered statistically significant with a probability of p≤0.05.
Пример конкретной реализации предлагаемого способаAn example of a specific implementation of the proposed method
1. Выбирают экологически неблагополучную территорию по высокой нагрузке химических факторов среды обитания с неудовлетворительным качеством атмосферного воздуха по санитарно-химическим показателям (превышение содержания бензола, толуола, фенола и формальдегида более 1,0 ПДК м.р., ПДК с.с.). ПДК - предельно-допустимая концентрация.1. Choose an ecologically unfavorable territory for a high load of chemical environmental factors with unsatisfactory atmospheric air quality for sanitary and chemical indicators (excess of benzene, toluene, phenol and formaldehyde in excess of 1.0 MPC MP, MPC SS). MPC - maximum permissible concentration.
2. Для обоснования критериев диагностики кардиальных нарушений у детей с хроническими заболеваниями органов дыхания, ассоциированными с воздействием бензола, толуола, фенола и формальдегида, было проведено углубленное клиническое, функциональное, инструментальное и лабораторное обследование.2. To substantiate the criteria for the diagnosis of cardiac disorders in children with chronic respiratory diseases associated with exposure to benzene, toluene, phenol and formaldehyde, an in-depth clinical, functional, instrumental and laboratory examination was carried out.
Группу наблюдения составили 43 человека с бронхиальной астмой и рецидивирующим бронхитом вне обострения в возрасте 6-13 лет (средний возраст 9,8±0,53 лет; 47,6% мальчиков и 52,4% девочек), проживающих на территориях Пермского края с неудовлетворительным качеством атмосферного воздуха по санитарно-химическим показателям (превышение содержания бензола, толуола, фенола и формальдегида более 1,0 ПДК м.р., ПДК с.с.).The observation group consisted of 43 people with bronchial asthma and recurrent bronchitis without exacerbation at the age of 6-13 years (average age 9.8 ± 0.53 years; 47.6% of boys and 52.4% of girls) living in the Perm Territory with unsatisfactory air quality for sanitary and chemical indicators (excess of benzene, toluene, phenol and formaldehyde more than 1.0 MPC MP, MPC SS).
Группу сравнения составили 39 детей (средний возраст 9,3±0,55 года; 53,5% мальчиков и 46,5% девочек) с бронхиальной астмой и рецидивирующим бронхитом в периоде ремиссии, проживающие в условиях санитарно-гигиенического благополучия.The comparison group consisted of 39 children (average age 9.3 ± 0.55 years; 53.5% of boys and 46.5% of girls) with bronchial asthma and recurrent bronchitis in remission, living in conditions of sanitary and hygienic well-being.
При анализе медико-социальных анкет достоверных различий между группами по социальным показателям не выявлено.When analyzing medical and social questionnaires, there were no significant differences between groups by social indicators.
3. В ходе химико-аналитического исследования у детей группы наблюдения установлено присутствие в крови бензола (0,013±0,0024 мг/дм3) и толуола (0,025±0,0047 мг/дм3), которые отсутствовали у детей сравниваемой группы (р=0,001) (табл. 1). Концентрация фенола в крови детей группы наблюдения была в 3,2 раза достоверно выше показателя группы сравнения (0,013±0,005 мг/дм3 и 0,0041±0,004 мг/дм3 соответственно, р=0,01). Содержание формальдегида в крови определялось на уровне 0,0057±0,0016 мг/дм3, что статистически значимо превышало показатель группы сравнения (0,0025±0,0011 мг/дм3, р=0,001). Данные о содержании токсикантов в крови обследованных детей приведены в таблице 2.3. In the course of a chemical-analytical study in children of the observation group, the presence in the blood of benzene (0.013 ± 0.0024 mg / dm 3 ) and toluene (0.025 ± 0.0047 mg / dm 3 ), which were absent in children of the compared group (p = 0.001) (table. 1). The phenol concentration in the blood of children in the observation group was 3.2 times significantly higher than the comparison group (0.013 ± 0.005 mg / dm 3 and 0.0041 ± 0.004 mg / dm 3, respectively, p = 0.01). The formaldehyde content in the blood was determined at the level of 0.0057 ± 0.0016 mg / dm 3 , which statistically significantly exceeded the indicator of the comparison group (0.0025 ± 0.0011 mg / dm 3 , p = 0.001). Data on the content of toxicants in the blood of the examined children are shown in table 2.
4. При проведении клинических исследований было установлено, что сравнительный анализ частоты встречаемости жалоб показал, что родители детей группы наблюдения достоверно чаще указывали на перенесенную ранее пневмонию (27,9% и 10,3% в группе сравнения, р=0,034), простудные заболевания 4-6 раза в год и более (25,6% и 12,8% соответственно, ОШ=2,4, р=0,08, при этом ОШ - это отношение шансов, характеризует собой отношение вероятности того, что событие произойдет к вероятности того, что событие не произойдет). У 23,3% детей группы наблюдения отмечался эпизодический сухой кашель ночью (в группе сравнения 12,8%, ОШ=2,14, р=0,23); у 13,9% - постоянный кашель в течение трех месяцев (в группе сравнения 5,1%, ОШ=2,72, р=0,16); у 27,9% - шумное дыхание (в группе сравнения 12,8%, ОШ=2,63, р=0,08).4. During clinical trials, it was found that a comparative analysis of the frequency of complaints showed that the parents of the children in the observation group reliably more often indicated previous pneumonia (27.9% and 10.3% in the comparison group, p = 0.034), colds 4-6 times a year or more (25.6% and 12.8%, respectively, OS = 2.4, p = 0.08, while OS is the odds ratio, characterizes the ratio of the probability that the event will occur to the likelihood that the event will not happen). In 23.3% of the children of the observation group there was an episodic dry cough at night (in the comparison group 12.8%, OS = 2.14, p = 0.23); 13.9% had a persistent cough for three months (in the comparison group 5.1%, OS = 2.72, p = 0.16); 27.9% had noisy breathing (in the comparison group 12.8%, OR = 2.63, p = 0.08).
Кроме того, у детей группы наблюдения достоверно чаще встречались жалобы вегетативного характера в виде быстрой утомляемости (46,5% и 23,1% соответственно, р=0,027); головных болей (37,2% и 17,9% соответственно, р=0,03); слабости (37,2% и 15,4% соответственно, р=0,02); повышенной раздражительности (34,8% и 20,5% соответственно, ОШ=1,59, р=0,07) и тревожности (16,3% и 7,7% соответственно, ОШ=2,33, р=0,14). Относительный риск появления жалоб вегетативного характера был в 2,9 раза выше в группе наблюдения (OR=2,9; DI=1,11-7,54; р=0,047).In addition, in children of the observation group, complaints of a vegetative nature in the form of rapid fatigue were significantly more common (46.5% and 23.1%, respectively, p = 0.027); headaches (37.2% and 17.9%, respectively, p = 0.03); weaknesses (37.2% and 15.4%, respectively, p = 0.02); increased irritability (34.8% and 20.5%, respectively, OSH = 1.59, p = 0.07) and anxiety (16.3% and 7.7%, respectively, OSH = 2.33, p = 0, fourteen). The relative risk of vegetative complaints was 2.9 times higher in the observation group (OR = 2.9; DI = 1.11-7.54; p = 0.047).
Вместе с этим 23,3% детей, проживающих на территории с загрязнением атмосферного воздуха бензолом, толуолом, фенолом и формальдегидом, беспокоили боли в области сердца или перебои ритма при физической нагрузке, что в 2,2 раза чаще по отношению к сравниваемой группе (10,3%, ОШ=2,72, р=0,07).At the same time, 23.3% of children living in the territory with atmospheric air pollution with benzene, toluene, phenol, and formaldehyde were worried about pain in the heart or rhythm interruptions during physical activity, which is 2.2 times more often in relation to the compared group (10 , 3%, OR = 2.72, p = 0.07).
В анамнезе у каждого третьего ребенка, проживающего на территории аэрогенного воздействия формальдегида, отмечалось наличие аллергического ринита (30,2% против 10,3% в группе сравнения, р=0,025).In the history of every third child living on the territory of the aerogenic exposure to formaldehyde, allergic rhinitis was noted (30.2% versus 10.3% in the comparison group, p = 0.025).
При объективном обследовании у детей группы наблюдения отмечалась бледность кожных покровов с мраморным рисунком (48,8% и 20,5% в группе сравнения, р=0,007), темные круги вокруг глаз (30,2% и 12,8% соответственно, р=0,04).An objective examination of children in the observation group showed pale skin with a marble pattern (48.8% and 20.5% in the comparison group, p = 0.007), dark circles around the eyes (30.2% and 12.8%, respectively, p = 0.04).
По данным спирографии выявлено, что показатели жизненной емкости легких находились в пределах нормативных значений, но имели достоверное снижение до 95,46±13,22% у детей группы наблюдения относительно группы сравнения (118,36±13,07%, р=0,012). Данные об этом приведены в таблице 3. Эти данные показывают, что получено достоверное снижение объемных скоростных показателей, отражающих проходимость средних и мелких бронхов (MEF 50, MEF 25, MEF 25-75), у детей группы наблюдения по отношению к сравниваемой группе (р=0,001-0,002).According to spirography data, it was found that the indicators of lung capacity were within the normative values, but had a significant decrease to 95.46 ± 13.22% in children of the observation group relative to the comparison group (118.36 ± 13.07%, p = 0.012) . The data on this are shown in Table 3. These data show that a significant decrease in volumetric speed indicators was obtained, reflecting patency of the middle and small bronchi (MEF 50, MEF 25, MEF 25-75) in children of the observation group in relation to the compared group (p = 0.001-0.002).
Отмечено, что у 25,4% детей группы наблюдения выявлялись нарушения внешнего дыхания обструктивного или смешанного характера, которые регистрировались в 1,5 раза реже в группе сравнения (16,7%, р=0,27).It was noted that in 25.4% of the children in the observation group, obstructive or mixed breathing disorders were detected, which were recorded 1.5 times less often in the comparison group (16.7%, p = 0.27).
Результаты импульсной осциллометрии свидетельствовали о достоверном повышении дыхательного импеданса (Zrs), резистанса (R5), что свидетельствует о наличии обструкции на уровне мелких и средних бронхов у детей группы наблюдения по отношению к группе сравнения (р=0,04) (таблица 4).The results of pulsed oscillometry showed a significant increase in respiratory impedance (Zrs), resistance (R5), which indicates the presence of obstruction at the level of small and medium bronchi in the children of the observation group relative to the comparison group (p = 0.04) (table 4).
Выявлено, что каждый четвертый ребенок, проживающий в условиях аэрогенного воздействия бензола, толуола, фенола и формальдегида, имел признаки периферической обструкции дыхательных путей в период ремиссии хронических заболеваний органов дыхания (23,8% и 7,5% в группе сравнения, р=0,028). Относительный риск развития периферической обструкции был в 3,84 раза выше в группе наблюдения (OR=3,84; DI=1,04-14,31; р=0,06).It was revealed that every fourth child living under the conditions of aerogenic exposure to benzene, toluene, phenol and formaldehyde had signs of peripheral airway obstruction during the remission of chronic respiratory diseases (23.8% and 7.5% in the comparison group, p = 0.028 ) The relative risk of developing peripheral obstruction was 3.84 times higher in the observation group (OR = 3.84; DI = 1.04-14.31; p = 0.06).
5. При проведении функциональных исследований сердца было установлено, что для всех обследованных детей физиологические параметры временных показателей электрокардиограммы (зубец Р, интервал PQ, комплекс QRS, интервала Q-T) находились в пределах возрастной нормы (таблица 5). Установлена прямая корреляционная зависимость укорочения зубца Р при наличии в крови повышенного содержания фенола (r=-0,29, р=0,027). У 17,2% детей группы наблюдения зарегистрировано отклонение электрической оси сердца вправо, что было в 3,4 раза чаще группы сравнения (5,1%, р=0,05).5. When conducting functional studies of the heart, it was found that for all the children examined, the physiological parameters of the time parameters of the electrocardiogram (P wave, PQ interval, QRS complex, Q-T interval) were within the age norm (table 5). A direct correlation was established for shortening of the P wave in the presence of an increased phenol content in the blood (r = -0.29, p = 0.027). In 17.2% of children in the observation group, a deviation of the electrical axis of the heart to the right was registered, which was 3.4 times more often than the comparison group (5.1%, p = 0.05).
Нарушения синусового ритма встречались более чем у половины всех обследованных детей (таблица 6). Причем данные, приведенные в таблице 6, показывают, что нарушения автоматизма синусового узла у детей группы наблюдения в виде синусовой тахикардии и синусовой брадикардии встречались в 3,1-1,6 раза чаще, чем в сравниваемой группе (р=0,14-0,001).Sinus rhythm disturbances occurred in more than half of all examined children (table 6). Moreover, the data shown in table 6 show that violations of the automatism of the sinus node in children of the observation group in the form of sinus tachycardia and sinus bradycardia were found 3.1-1.6 times more often than in the compared group (p = 0.14-0.001 )
Анализ вариабельности сердечного ритма показал, что преобладающим типом исходного вегетативного тонуса у детей группы наблюдения являлась эйтония, у обследованных сравниваемой группы - ваготония (таблица 7).Analysis of heart rate variability showed that eutonia was the predominant type of initial vegetative tone in children of the observation group, and vagotonia was in the examined group (table 7).
Однако у детей обеих групп отмечалось усиление активности парасимпатического звена вегетативной регуляции (Дх, RMSSD, pNN50), более выраженное у детей группы сравнения (р=0,83-0,0002) (таблица 8). При этом у детей, проживающих в условиях аэрогенного воздействия бензола, толуола, фенола и формальдегида, наблюдалось уменьшение мощности волн высокой частоты (HF%) и повышение мощности очень низкочастотного компонента спектра (VLF%), что свидетельствует о снижении активности парасимпатического отдела автономной нервной системы и повышении роли центральных регуляторных влияний (нейро-гуморального и метаболического уровня) на деятельность сердца. В то время как у детей группы сравнения преобладал парасимпатический тип автономной нервной регуляции сердечного ритма (HF% и LF %).However, in children of both groups there was an increase in the activity of the parasympathetic link of autonomic regulation (Dx, RMSSD, pNN50), more pronounced in children of the comparison group (p = 0.83-0.0002) (table 8). At the same time, children living under the aerogenic effects of benzene, toluene, phenol and formaldehyde showed a decrease in the power of high-frequency waves (HF%) and an increase in the power of the very low-frequency component of the spectrum (VLF%), which indicates a decrease in the activity of the parasympathetic department of the autonomic nervous system and increasing the role of central regulatory influences (neuro-humoral and metabolic levels) on the activity of the heart. While in the children of the comparison group the parasympathetic type of autonomic nervous regulation of the heart rhythm prevailed (HF% and LF%).
Оценка вегетативной реактивности по данным клиноортостатической пробы показала, что в группе наблюдения в 60,5% случаев отмечался симпатикотонический тип ответной реакции (таблица 9). Причем приведенные данные показывают, что асимпатикотоническая реактивность, характеризовавшаяся напряжением адаптационно-компенсаторных механизмов и нарушением ответа всех звеньев вегетативной регуляции, выявлена только у 5,3% детей, проживающих в условиях аэрогенного воздействия бензола, толуола, фенола и формальдегида.Assessment of vegetative reactivity according to the clinostatostatic test data showed that in the observation group in 60.5% of cases there was a sympathicotonic type of response (table 9). Moreover, the data presented show that asymptaticotonic reactivity, characterized by a strain of adaptive-compensatory mechanisms and a violation of the response of all parts of the autonomic regulation, was detected only in 5.3% of children living under the conditions of aerogenic exposure to benzene, toluene, phenol and formaldehyde.
Спектральный анализ вегетативной регуляции ритма в клиноортостатической пробе выявил снижение вагусной активности (HF) при усилении симпатической автономной нервной системы (LF) и гуморально-метаболических механизмов регуляции сердечного ритма (VLF) у детей группы наблюдения (таблица 10), а в группе сравнения уровень центральных эрготропных влияний и гуморальной регуляции был в 1,2 раза достоверно выше (р=0,023).A spectral analysis of the autonomic rhythm regulation in a clino-orthostatic test revealed a decrease in vagal activity (HF) with an increase in the sympathetic autonomic nervous system (LF) and humoral-metabolic mechanisms of heart rhythm regulation (VLF) in children of the observation group (table 10), and in the comparison group the level of central ergotropic influences and humoral regulation was 1.2 times significantly higher (p = 0.023).
Таким образом, у детей, имеющих повышенное содержание в крови бензола, толуола, фенола и формальдегида, выявлены нарушения регуляторно-компенсаторных механизмов вегетативной нервной системы в виде снижения функционирования гуморально-метаболического звеньев при активации парасимпатического звена вегетативной регуляции, что говорит о напряжении адаптационно-компенсаторных реакций организма на изменение условий внешней и внутренней среды.Thus, in children with high blood levels of benzene, toluene, phenol and formaldehyde, violations of the regulatory-compensatory mechanisms of the autonomic nervous system in the form of a decrease in the functioning of the humoral-metabolic links upon activation of the parasympathetic link of the autonomic regulation are revealed, which indicates the tension of adaptive-compensatory body reactions to changes in the conditions of the external and internal environment.
При анализе данных эхокардиографии показатели левого и правого желудочков у обследованных детей находились в пределах физиологических нормативов (таблица 11). Однако было выявлено повышение систолического давления в легочной артерии у детей группы наблюдения по отношению к группе сравнения (9,78±1,09 мм рт.ст. и 8,35±1,07 мм рт.ст. соответственно, р=0,05), что свидетельствовало о повышенной нагрузке в малом круге кровообращения.When analyzing echocardiography data, the indicators of the left and right ventricles in the examined children were within the physiological standards (table 11). However, an increase in systolic pressure in the pulmonary artery was revealed in children of the observation group relative to the comparison group (9.78 ± 1.09 mm Hg and 8.35 ± 1.07 mm Hg, respectively, p = 0, 05), which indicated an increased load in the pulmonary circulation.
Показатели диастолической функции левого желудочка в группах находились в пределах нормы и не имели достоверных различий (таблица 12). При этом у детей группы наблюдения отмечено увеличение максимальной скорости раннего диастолического наполнения правого желудочка по отношению к показателю сравниваемой группы (0,56±0,036 м/с и 0,52±0,03 м/с соответственно, р=0,08). Индекс Е/А (отношение скоростей диастолического наполнения и предсердной систолы) был достоверно выше в группе наблюдения (1,68±0,22 у.е. против 1,42±0,096 у.е. группы сравнения, р=0,031), что свидетельствовало о функциональных изменения правого желудочка сердца в период клинической ремиссии.Indicators of diastolic function of the left ventricle in the groups were within normal limits and did not have significant differences (table 12). At the same time, in children of the observation group, an increase in the maximum speed of early diastolic filling of the right ventricle with respect to the indicator of the compared group was noted (0.56 ± 0.036 m / s and 0.52 ± 0.03 m / s, respectively, p = 0.08). The E / A index (the ratio of the rates of diastolic filling and atrial systole) was significantly higher in the observation group (1.68 ± 0.22 cu against 1.42 ± 0.096 cu of the comparison group, p = 0.031), which testified to functional changes in the right ventricle of the heart during clinical remission.
Кроме того, у 17,9% детей группы наблюдения выявлена преходящая диастолическая дисфункция правого желудочка, которая отсутствовала в группе сравнения (р=0,046).In addition, in 17.9% of the children of the observation group, transient diastolic dysfunction of the right ventricle was revealed, which was absent in the comparison group (p = 0.046).
6. При проведении лабораторных исследований устанавливали следующие показатели: уровень лейкоцитов; уровень антиоксидантной активности АОА сыворотки крови; уровень МДА в плазме крови; уровень высокочувствительного С-реактивного белка в сыворотке крови и состояние липидного обмена.6. When conducting laboratory tests, the following indicators were established: white blood cell count; the level of antioxidant activity of serum AOA; the level of MDA in blood plasma; the level of highly sensitive C-reactive protein in serum and the state of lipid metabolism.
Сравнительный анализ результатов лабораторного исследования показал, что для детей группы наблюдения, в отличие от группы сравнения, характерно повышение в общем анализе крови содержания лейкоцитов (6,7±0,42⋅109/л против 5,69±0,50⋅109/л, р=0,001), у 62,3% выявлен лимфоцитоз (46,3±1,46%). Установлена прямая корреляционная зависимость повышения содержания лейкоцитов крови при увеличения в крови фенола (r=0,253, р=0,05). Превышение уровня лейкоцитов составило 20% от физиологической нормы.A comparative analysis of the results of a laboratory study showed that for children in the observation group, in contrast to the comparison group, an increase in the total blood count of leukocytes is characteristic (6.7 ± 0.42⋅10 9 / L versus 5.69 ± 0.50⋅10 9 / L, p = 0.001), 62.3% revealed lymphocytosis (46.3 ± 1.46%). A direct correlation was established between the increase in the blood leukocyte count with an increase in phenol in the blood (r = 0.253, p = 0.05). Excess leukocyte count was 20% of the physiological norm.
Анализ биохимических показателей крови детей группы наблюдения свидетельствовал об интенсивном накоплении продуктов усиленной пероксидации, так, содержание МДА в плазме крови составило 3,31±0,37 мкмоль/см3, что в 1,3 раза выше физиологического предела (нормы) и показателя группы сравнения (2,73±0,17 мкмоль/см3, р=0,005). Причем получена прямая корреляционная зависимость увеличения содержания МДА при повышении в крови фенола (r=0,397, р=0,004).Analysis of biochemical blood parameters of children in the observation group showed an intensive accumulation of products of enhanced peroxidation, for example, the MDA content in blood plasma was 3.31 ± 0.37 μmol / cm 3 , which is 1.3 times higher than the physiological limit (norm) and the group indicator comparison (2.73 ± 0.17 μmol / cm 3 , p = 0.005). Moreover, a direct correlation dependence of the increase in the content of MDA with an increase in the blood phenol (r = 0.397, p = 0.004) was obtained.
Оценка окислительно-восстановительных резервов установила, что средний уровень АОА сыворотки крови детей группы наблюдения составил 33,30±1,89%, что достоверно ниже показателя группы сравнения (36,28±1,74%, р=0,02) и физиологической нормы в 1,2 раза.Assessment of redox reserves found that the average level of AOA in the blood serum of children in the observation group was 33.30 ± 1.89%, which was significantly lower than the value of the comparison group (36.28 ± 1.74%, p = 0.02) and physiological norms are 1.2 times.
В ходе исследования липидного обмена у детей группы наблюдения был установлен достоверно более высокий показатель аполипротеина А1 относительно группы сравнения (1,65±0,18 г/см3 против 1,37±0,1 г/дм3, р=0,01). Одновременно у детей, проживающих в условиях аэрогенного воздействия бензола, толуола, фенола и формальдегида, выявлено достоверное снижение коэффициента «Аполипротеин В/Аполипротеин А1» (0,39±0,05 у.е. против 0,47±0,06 у.е., р=0,05), что свидетельствовало о повышении синтеза кардиопротективных защитных факторов при наличии внешнесредовой химической нагрузки.During the study of lipid metabolism in children of the observation group, a significantly higher indicator of apoliprotein A1 was established relative to the comparison group (1.65 ± 0.18 g / cm 3 versus 1.37 ± 0.1 g / dm 3 , p = 0.01 ) At the same time, in children living under the aerogenic effects of benzene, toluene, phenol and formaldehyde, a significant decrease in the Apoliprotein B / Apoliprotein A1 coefficient (0.39 ± 0.05 cu versus 0.47 ± 0.06 c. e., p = 0.05), which indicated an increase in the synthesis of cardioprotective protective factors in the presence of an external chemical load.
Кроме того, в группе наблюдения высокочувствительный С-реактивный белок в сыворотке крови, являющийся индикатором хронического вялотекущего сосудистого воспаления, составил 5,32±0,5 мг/дм3, что было в 1,8 раза выше физиологической нормы и уровня группы сравнения (2,74±0,55 мг/дм3, р=0,001). Установлена корреляционная зависимость увеличения количества высокочувствительного С-реактивного белка при повышении в крови фенола, формальдегида, толуола (r=0,275-0,462, р=0,048-0,001).In addition, in the observation group, the highly sensitive C-reactive protein in serum, which is an indicator of chronic sluggish vascular inflammation, was 5.32 ± 0.5 mg / dm 3 , which was 1.8 times higher than the physiological norm and level of the comparison group ( 2.74 ± 0.55 mg / dm 3 , p = 0.001). The correlation dependence of the increase in the amount of highly sensitive C-reactive protein with an increase in the blood phenol, formaldehyde, toluene (r = 0.275-0.462, p = 0.048-0.001) was established.
Таким образом, проведенные исследования показали, что у детей с хроническими заболеваниями органов дыхания, ассоциированными с воздействием бензола, толуола, фенола и формальдегида, морфофункциональные нарушения сердца проявляются вегетативными нарушениями (повышенная утомляемость, раздражительность, головные боли, слабость, тревожность, боли в области сердца или перебои ритма при физической нагрузке; наличие синусовой бради-, тахикардии; изменения регуляторно-компенсаторных механизмов вегетативной нервной системы в виде снижения функционирования гуморально-метаболического и симпатического звеньев при активации парасимпатического отдела вегетативной регуляции), повышением систолического давления в легочной артерии, преходящей диастолической дисфункцией правого желудочка и сопровождаются воспалительной реакцией в виде повышения уровня лейкоцитов в крови с относительным лимфоцитозом, увеличения высокочувствительного С-реактивного белка; нарушением факторов антиатерогенной защиты (повышение аполипротеина А1, снижение коэффициента «Аполипротеин В/Аполипротеин Al»); дисбалансом оксидантных и антиокислительных реакций (увеличение содержания МДА в сыворотке крови на фоне снижения АОА сыворотки крови).Thus, the studies showed that in children with chronic respiratory diseases associated with exposure to benzene, toluene, phenol and formaldehyde, morphofunctional heart disorders are manifested by autonomic disorders (increased fatigue, irritability, headaches, weakness, anxiety, pain in the heart or interruptions in rhythm during physical exertion; the presence of sinus brady, tachycardia; changes in the regulatory and compensatory mechanisms of the autonomic nervous system in the form of a decrease in functions of the humoral-metabolic and sympathetic links upon activation of the parasympathetic division of autonomic regulation), increased systolic pressure in the pulmonary artery, transient diastolic dysfunction of the right ventricle and are accompanied by an inflammatory reaction in the form of an increase in the level of leukocytes in the blood with relative lymphocytosis, an increase in the highly sensitive C-reactive protein; violation of anti-atherogenic defense factors (increased apoliprotein A1, decreased coefficient "Apoliprotein B / Apoliprotein Al"); an imbalance of oxidative and antioxidant reactions (an increase in the content of MDA in blood serum against the background of a decrease in serum AOA).
ПримерExample
Больной Е., 9 лет, с диагнозом: Бронхиальная астма, атопическая, легкая, вне обострения. Аллергический ринит, ремиссия.Patient E., 9 years old, with a diagnosis of Asthma, atopic, lung, without exacerbation. Allergic rhinitis, remission.
Химико-аналитическое исследование содержания химических соединений в крови установило присутствие бензола (0,003 мг/дм3), толуола (концентрация фенола составила 0,015 мг/дм3, содержание формальдегида определялось на уровне 0,004 мг/дм3.A chemical-analytical study of the content of chemical compounds in the blood established the presence of benzene (0.003 mg / dm 3 ), toluene (phenol concentration was 0.015 mg / dm 3 , the formaldehyde content was determined at the level of 0.004 mg / dm 3 .
В общем анализе крови уровень лейкоцитов составил 7,4⋅109/л (физиологическая норма 4,5-6,5⋅109/л).In the general blood test, the leukocyte count was 7.4⋅10 9 / L (physiological norm 4.5-6.5⋅10 9 / L).
Анализ биохимических показателей показал повышение содержания МДА в плазме крови до 2,8 мкмоль/см3, снижение среднего уровня АОА сыворотки крови до 23,16%. Установлены высокий показатель аполипротеина А1 (2,67 г/см3 при физиологической норме 0,93-1,72 г/дм3) и снижение коэффициента «Аполипротеин В/Аполипротеин А1» до 0,26 у.е. (0,52-0,73 у.е. нормативные значения). Уровень высокочувствительного С-реактивного белка в сыворотке крови составил 3,97 мг/дм3 (физиологическая норма 0-3 мг/дм3).Analysis of biochemical parameters showed an increase in the content of MDA in blood plasma to 2.8 μmol / cm 3 , a decrease in the average level of AOA in blood serum to 23.16%. A high apoliprotein A1 value (2.67 g / cm 3 with a physiological norm of 0.93-1.72 g / dm 3 ) and a decrease in the Apoliprotein B / Apoliprotein A1 coefficient to 0.26 cu were established. (0.52-0.73 cu standard values). The level of highly sensitive C-reactive protein in blood serum was 3.97 mg / dm 3 (physiological norm 0-3 mg / dm 3 ).
По данным спирографии вентиляционная способность находилась в пределах условной нормы (FVC - 88,5%; FEV1 - 89,7%; PEF - 80,4%; MEF50 - 66,1%; MEF25 - 72,6%; MEF25-75 - 80,7%).According to spirography data, the ventilation ability was within the conventional norm (FVC - 88.5%; FEV1 - 89.7%; PEF - 80.4%; MEF50 - 66.1%; MEF25 - 72.6%; MEF25-75 - 80.7%).
Осциллометрия с оценкой бронхиального сопротивления показала повышение бронхиального сопротивления и признаки периферийной обструкции (Rocc - 286,8%; Frs - 16,70%; Z - 137,1%; R5 - 70,6%; R20 - 122,8%; Х5 - 254,9%).Oscillometry with an assessment of bronchial resistance showed an increase in bronchial resistance and signs of peripheral obstruction (Rocc - 286.8%; Frs - 16.70%; Z - 137.1%; R5 - 70.6%; R20 - 122.8%; X5 - 254.9%).
Проведенная электрокардиография выявила легкую синусовую брадикардию (ЧСС 72 уд. в мин, угол альфа - 67°, зубец Р - 0,08 сек, интервал PQ - 0,12 сек, комплекс QRS - 0,12 сек, интервал QT - 0,35 сек).The performed electrocardiography revealed mild sinus bradycardia (heart rate of 72 beats per minute, angle alpha - 67 °, P wave - 0.08 sec, PQ interval - 0.12 sec, QRS complex - 0.12 sec, QT interval - 0.35 sec).
По данным кардиоинтервалографии зарегистрирован ваготонический исходный вегетативный тонус (ИН=25,3 у.е.). Структура вариабельности сердечного ритма отражала преобладание волн медленного периода (LF-компонента) и обусловлена усилением симпатического влияния на модуляцию сердечного ритма. Общая мощность спектра нейрогуморальной модуляции высокая. Оценка вегетативной реактивности по данным клиноортостатической пробы показала гиперсимпатикотонический тип ответной реакции (ИН2/ИН1=3,29).According to cardiointervalography, a vagotonic initial vegetative tone was recorded (IN = 25.3 cu). The structure of heart rate variability reflected the predominance of waves of a slow period (LF component) and is due to an increase in the sympathetic effect on heart rate modulation. The total power of the neurohumoral modulation spectrum is high. Assessment of vegetative reactivity according to the clinostatic test showed a hypersympathicotonic type of response (IN2 / IN1 = 3.29).
При анализе данных эхокардиографии показатели левого и правого желудочков находились в пределах физиологических нормативов (Ао - 21 мм; КДР ЛЖ - 43 мм; КСР ЛЖ - 29 мм; КДО ЛЖ - 83 мл; КСО ЛЖ - 31 мл, ММЛЖ - 118 г; УО - 52 мл; ФВ - 62%; ПЖ - 15 мм).When analyzing the data of echocardiography, the indicators of the left and right ventricles were within physiological standards (Ao - 21 mm; CRD of the LV - 43 mm; CSR of the LV - 29 mm; BWC of the LV - 83 ml; CSR of the LV - 31 ml, MML - 118 g; UO - 52 ml; PV - 62%; RV - 15 mm).
Показатели диастолической функции левого желудочка находились в пределах нормы (Ем 0,8 м/с, Ам 0,37 м/с, Ем/Ам 2 у.е.). При этом отмечена диастолическая дисфункция правого желудочка (Етр 0,5 м/с, Атр 0,37 м/с, Етр/Атр 0,82 у.е.).Indicators of diastolic function of the left ventricle were within normal limits (Em 0.8 m / s, Am 0.37 m / s, Em / Am 2 cu). At the same time, diastolic dysfunction of the right ventricle was noted (Etr 0.5 m / s, Apr 0.37 m / s, Etr / Apr 0.82 cu).
В данном случае у пациента были выявлены отклонения как функциональных, так и лабораторных показателей, которые предлагаются заявляемым способом.In this case, the patient revealed deviations of both functional and laboratory parameters, which are proposed by the claimed method.
Проведение эхокардиографии позволило выявить признаки морфофункциональных нарушений миокарда в виде диастолической дисфункции правого желудочка. Полученные данные свидетельствовали о наличии у больного с бронхиальной астмой и аллергическим ринитом проявлений вегетативной дисфункции по кардиальному типу. А значит, это подтверждает точность предлагаемого способа.Echocardiography revealed signs of morphofunctional myocardial disorders in the form of diastolic dysfunction of the right ventricle. The data obtained indicated the presence of a cardiac type of vegetative dysfunction in a patient with bronchial asthma and allergic rhinitis. So, this confirms the accuracy of the proposed method.
Разработанный способ диагностики позволяет получить достоверные данные, не требует дефицитных реактивов, дорогостоящих приборов (доплероэхокардиограф это дорогой аппарат со специальными датчиками), прост в исполнении, экономичен и не имеет противопоказаний.The developed diagnostic method allows you to obtain reliable data, does not require scarce reagents, expensive instruments (the Doppleroechocardiograph is an expensive device with special sensors), it is simple to perform, economical and has no contraindications.










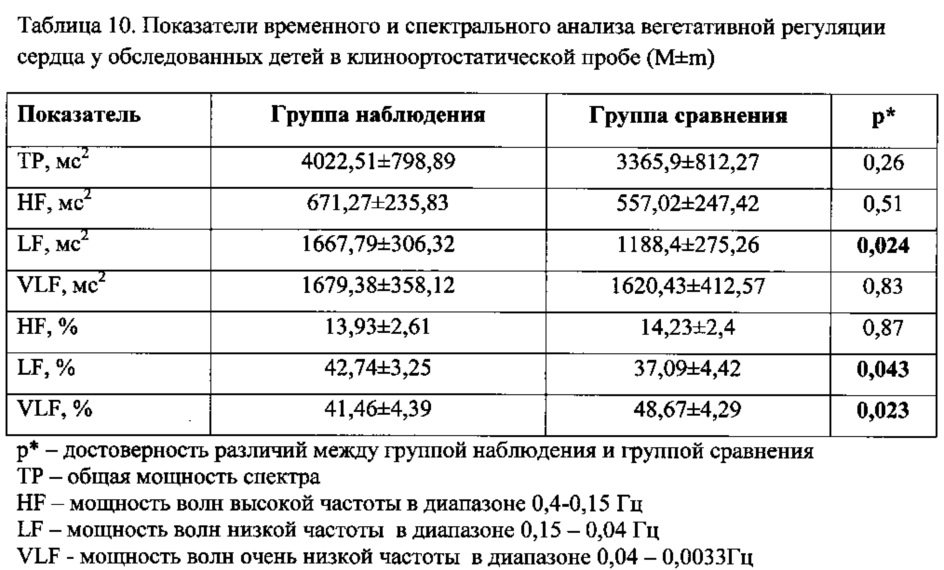


Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2016110493A RU2612861C1 (en) | 2016-03-22 | 2016-03-22 | Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2016110493A RU2612861C1 (en) | 2016-03-22 | 2016-03-22 | Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2612861C1 true RU2612861C1 (en) | 2017-03-13 |
Family
ID=58458185
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2016110493A RU2612861C1 (en) | 2016-03-22 | 2016-03-22 | Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2612861C1 (en) |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2089900C1 (en) * | 1994-08-23 | 1997-09-10 | Ростовский научно-исследовательский институт акушерства и педиатрии | Method of differential diagnosis of myocardium damage in newborns |
| RU2140639C1 (en) * | 1998-07-10 | 1999-10-27 | Нижегородская государственная медицинская академия | Method of diagnosis of myocardium diseases |
| UA34580U (en) * | 2008-04-15 | 2008-08-11 | Харьковский Национальный Медицинский Университет | Method for diagnostics of myocarditis in children with distortions of cardiac rate |
-
2016
- 2016-03-22 RU RU2016110493A patent/RU2612861C1/en not_active IP Right Cessation
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2089900C1 (en) * | 1994-08-23 | 1997-09-10 | Ростовский научно-исследовательский институт акушерства и педиатрии | Method of differential diagnosis of myocardium damage in newborns |
| RU2140639C1 (en) * | 1998-07-10 | 1999-10-27 | Нижегородская государственная медицинская академия | Method of diagnosis of myocardium diseases |
| UA34580U (en) * | 2008-04-15 | 2008-08-11 | Харьковский Национальный Медицинский Университет | Method for diagnostics of myocarditis in children with distortions of cardiac rate |
Non-Patent Citations (3)
| Title |
|---|
| GOWER S. Development of a health effects-based priority ranking system for air emissions reductions from oil refineries in Canada. J Toxicol Environ Health A. 2008;71(1):81-5 - . * |
| GOWER S. Development of a health effects-based priority ranking system for air emissions reductions from oil refineries in Canada. J Toxicol Environ Health A. 2008;71(1):81-5 - реферат. * |
| МАКЛАКОВА О.А. Особенности вегетативных нарушений у детей, проживающих в условиях загрязнения атмосферного воздуха бензолом и толуолом. Фундаментальные исследования, N 11-1, 2013, с.74-78. * |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Daniel et al. | Risk factors and markers for acute myocardial infarction with angiographically normal coronary arteries | |
| RU2573499C1 (en) | Method for prediction of risk of unfavourable outcome in patients with acute coronary syndrome and concomitant type 2 diabetes mellitus | |
| RU2612861C1 (en) | Method for diagnosis of myocardium morphofunctional disturbances for children older than 5 years with bronchopulmonary diseases associated with exposure to benzene, toluene, phenol and formaldehyde | |
| RU2539990C2 (en) | Method of complex evaluation of indications for administration of cardiometabolic therapy in case of infectious diseases | |
| Koyama et al. | Evaluation of QT interval prolongation in dogs with heart failure | |
| Ghosh et al. | Steroids in sudden sensorineural hearing loss | |
| RU2806726C1 (en) | Method for predicting probability of death in patients with covid-19 hospitalized on basis of laboratory and instrumental studies | |
| RU2436091C1 (en) | Method of estimation of microvascular endothelium status in patients with bronchial asthma | |
| RU2193341C2 (en) | Method for determining human cardiovascular system aging rate | |
| RU2410021C2 (en) | Method for prediction of acute coronary syndrome | |
| RU2601661C1 (en) | Method of clinical assessment of the probability of non-massive pulmonary artery thromboembolia in female patients taking combined oral contraceptives | |
| Maklakova et al. | Features of cardiac disorders in children with chronic respiratory diseases associated with aerogenic exposure to chemical environmental factors | |
| RU2826852C1 (en) | Method for determining risk of developing and progression of chronic kidney disease of variable aetiology in adults | |
| Butler et al. | Lignocaine as a pretreatment to rapid sequence intubation in patients with status asthmaticus | |
| RU2796385C1 (en) | Method for determination of bronchial destruction degree in patients with bronchial asthma | |
| RU2663935C1 (en) | Method for predicting development of cardiovascular complications in the late period after acute coronary syndrome | |
| RU2781565C1 (en) | Method for predicting risk of death at hospital stage in patients without st-segment elevation myocardial infarction who have undergone new covid-19 coronavirus infection, taking into account their immunological status | |
| RU2805263C1 (en) | Method for predicting onset of death in covid-19 patients aged 60 years and older | |
| SU1425548A1 (en) | Method of analysing dilatation cardiomyopathy | |
| Terraneo et al. | Distinct mechanical properties of the respiratory system evaluated by forced oscillation technique in acute exacerbation of COPD and acute decompensated heart failure. Diagnostics (Basel). 2021; 11 (3): 554 | |
| RU2596056C1 (en) | Method for clinical assessment of probability non-massive pulmonary artery thromboembolia in patients receiving menopausal hormone therapy | |
| RU2391905C1 (en) | Method of early diagnostics of diabetic autonomous cardial neuropathy in children and teenagers | |
| Khotijah et al. | The measurement of malondialdehyde level in heart tissue of hyperlipidemic rats after intervention of combination of Jicama (Pachyrhizus erosus) concentrate and kefir milk as a syn | |
| UA120481C2 (en) | METHOD FOR PREDICTING RISK OF HEART RATE DISORDERS IN ISCHEMIC HEART DISEASE | |
| RU2160045C2 (en) | Method for diagnosing disturbed bronchial patency |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees |
Effective date: 20180323 |