RU2598960C1 - Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children - Google Patents
Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children Download PDFInfo
- Publication number
- RU2598960C1 RU2598960C1 RU2015137368/14A RU2015137368A RU2598960C1 RU 2598960 C1 RU2598960 C1 RU 2598960C1 RU 2015137368/14 A RU2015137368/14 A RU 2015137368/14A RU 2015137368 A RU2015137368 A RU 2015137368A RU 2598960 C1 RU2598960 C1 RU 2598960C1
- Authority
- RU
- Russia
- Prior art keywords
- ellipse
- width
- children
- statokinesiogram
- formation
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/103—Detecting, measuring or recording devices for testing the shape, pattern, colour, size or movement of the body or parts thereof, for diagnostic purposes
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Biomedical Technology (AREA)
- Heart & Thoracic Surgery (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Biophysics (AREA)
- Pathology (AREA)
- Engineering & Computer Science (AREA)
- Dentistry (AREA)
- Physics & Mathematics (AREA)
- Medical Informatics (AREA)
- Molecular Biology (AREA)
- Surgery (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Measurement Of The Respiration, Hearing Ability, Form, And Blood Characteristics Of Living Organisms (AREA)
Abstract
Description
Изобретение относится к медицине, а именно к детской неврологии, и позволяет диагностировать формирование нарушения моторного развития у детей 3-6 месяцев жизни.The invention relates to medicine, namely to children's neurology, and allows you to diagnose the formation of motor development disorders in children 3-6 months of life.
Актуальность заявляемого способа определяется высокой частотой поражений центральной нервной системы в перинатальном периоде (80% среди патологии нервной системы в детском возрасте) и их тяжелых последствий. Двигательные нарушения являются наиболее частым проявлением этих поражений (68,5% в структуре синдромов перинатальных поражений нервной системы и их последствий). (Хачатрян Л.Г. Ранние и отдаленные проявления перинатальных поражений нервной системы у детей раннего возраста: автореф. дис… канд. мед. наук. - М., 2003. - 49 с.). Дети с данной патологией подвержены высокому риску формирования детского церебрального паралича (ДЦП), ведущего к инвалидизации ребенка. В этой ситуации очень важным является ранняя диагностика и вовремя начатое лечение нарушения моторного развития (Барашнев Ю.А. Клинико-морфологическая характеристика и исходы церебральных расстройств при гипоксически-ишемических энцефалопатиях // Акушерство и гинекология. - 2007. - №5. - С. 39-42.). Предлагаемый нами способ позволяет диагностировать нарушение моторного развития на стадии формирования первых антигравитационных поз, которые имеют базовое значение для дальнейшего развития двигательных функций ребенка. Возможность ранней и точной диагностики нарушения моторного развития в возрасте 3-6 месяцев жизни позволит своевременно начать лечение и предотвратить формирование инвалидизирующих последствий.The relevance of the proposed method is determined by the high frequency of lesions of the central nervous system in the perinatal period (80% of the pathology of the nervous system in childhood) and their severe consequences. Movement disorders are the most frequent manifestation of these lesions (68.5% in the structure of the syndromes of perinatal lesions of the nervous system and their consequences). (Khachatryan L.G. Early and long-term manifestations of perinatal lesions of the nervous system in young children: abstract of thesis ... candidate of medical sciences. - M., 2003. - 49 p.). Children with this pathology are at high risk for the formation of cerebral palsy (cerebral palsy), leading to disability of the child. In this situation, early diagnosis and timely treatment of impaired motor development is very important (Barashnev Yu.A. Clinical and morphological characteristics and outcomes of cerebral disorders in hypoxic-ischemic encephalopathies // Obstetrics and gynecology. - 2007. - No. 5. - P. 39-42.). Our proposed method allows us to diagnose a violation of motor development at the stage of formation of the first anti-gravity postures, which are of fundamental importance for the further development of the motor functions of the child. The possibility of early and accurate diagnosis of motor development disorders at the age of 3-6 months of life will allow timely initiation of treatment and prevent the formation of disabling consequences.
По данным литературы известны способы диагностики задержки психомоторного развития детей раннего возраста которые основаны на применении разработанных в разное время шкал психомоторного развития: "Таблицы развития" А. Гезелла, 1925; шкалы Н. Бейли, 1969; денверская шкала, 1973; мюнхенская функциональная диагностика, 1985; шкала, предложенная Л.Т. Журбой и Е.М. Мастюковой, 1981; шкала, разработанная О.В. Баженовой, 1986. Недостатками данных способов диагностики являются: субъективность оценки, возможность провести только качественную оценку моторного развития.According to the literature, there are known methods for diagnosing delays in the psychomotor development of young children, which are based on the use of psychomotor development scales developed at different times: "Development Tables" by A. Gesell, 1925; Scales of N. Bailey, 1969; Denver scale, 1973; Munich functional diagnostics, 1985; scale proposed by L.T. Zhurboy and E.M. Mastyukova, 1981; scale developed by O.V. Bazhenova, 1986. The disadvantages of these diagnostic methods are: subjectivity assessment, the ability to conduct only a qualitative assessment of motor development.
Раняя диагностика нарушения моторного развития у детей первого полугодия жизни осуществлялась путем неврологического осмотра с определением мышечного тонуса, сухожильных рефлексов, безусловных рефлексов, асимметричного шейно-тонического рефлекса, цепных симметрических реакций, сенсорно-моторного поведения. При этом проводили только качественную оценку определяемых показателей (Л.Т. Журба Е.М. Мастюкова. «Нарушение психомоторного развития детей первого года жизни» - М. «Медицина». - 1981).Early diagnosis of motor development disorders in children in the first half of life was carried out by neurological examination with the definition of muscle tone, tendon reflexes, unconditioned reflexes, an asymmetric neck-tonic reflex, symmetrical chain reactions, and sensory-motor behavior. In this case, only a qualitative assessment of the indicators was carried out (L.T. Zhurba E.M. Mastyukova. "Violation of the psychomotor development of children in the first year of life" - M. "Medicine". - 1981).
Известен способ, используемый для диагностики и оценки прогноза задержки психомоторного развития у детей с перинатальным поражением центральной нервной системы путем определения в крови уровня активности лейкоцитарной эластазы (ЛЭ) и уровня активности ее антагониста - 1-протеазного ингибитора (1-ПИ). При этом сочетание исходного уровня ЛЭ>225 нм/мин/мл и исходного уровня активности 1-ПИ>30 ИЕ/мл свидетельствует о положительном прогнозе психомоторного развития детей с задержкой психомоторного развития и перинатальным поражением центральной нервной системы гипоксически-ишемического генеза в анамнезе. Чем выше показатель активности ЛЭ и ниже показатель активности 1-протеазного ингибитора, тем о более выраженной задержке психомоторного развития данной категории детей это свидетельствует. (Патент №2475747. Российская Федерация. Способ прогнозирования психомоторного развития детей с перинатальным поражением центральной нервной системы/ Каримова Х.М., Намазова-Баранова Л.С., Клюшник Т.П., Мамедьяров A.M., Турти Т.В. // Изобретения. Полезные модели. - 2013. - №5).A known method is used to diagnose and evaluate the prognosis of delayed psychomotor development in children with perinatal damage to the central nervous system by determining the level of activity of leukocyte elastase (LE) in the blood and the level of activity of its antagonist, a 1-protease inhibitor (1-PI). Moreover, the combination of the initial level of LE> 225 nm / min / ml and the initial level of activity of 1-PI> 30 IE / ml indicates a positive prognosis of psychomotor development of children with delayed psychomotor development and perinatal damage to the central nervous system with a history of hypoxic-ischemic origin. The higher the activity indicator of LE and the lower the activity indicator of a 1-protease inhibitor, the more pronounced the delay in the psychomotor development of this category of children is indicated. (Patent No. 2475747. Russian Federation. A method for predicting the psychomotor development of children with perinatal damage to the central nervous system / Karimova Kh.M., Namazova-Baranova LS, Klyushnik TP, Mamedyarov AM, Turty TV // Inventions. Utility models. - 2013. - No. 5).
Недостатки способа:The disadvantages of the method:
1. Способ применялся у детей с установленным диагнозом нарушения моторного развития.1. The method was used in children with a diagnosis of impaired motor development.
2. Способ является инвазивным.2. The method is invasive.
3. Требует для своего проведения большого количества времени.3. It takes a lot of time to spend.
4. Способ требует наличия специальных реактивов.4. The method requires special reagents.
5. Реализация способа сопряжена с техническими сложностями.5. The implementation of the method involves technical difficulties.
Наиболее близким по техническому решению к заявляемому способу является способ диагностики нарушения моторного развития у детей первого года жизни с помощью проведения интерференционной электромиографии, с определением нелинейных параметров, а именно фрактальной размерности, корреляционной размерности и корреляционной энтропии. При значении корреляционной размерности у детей первого месяца жизни в пределах 7,21-7,84, диагностируют двигательные нарушения (Зарипова Ю.Р. Клинико-нейрофизиологические особенности двигательной системы у детей раннего возраста с отягощенным перинатальным анамнезом: автореф. дис… док. мед. наук. М., 2014. - 43 с.).Closest to the technical solution to the claimed method is a method for diagnosing motor development disorders in children of the first year of life using interference electromyography, with the determination of non-linear parameters, namely fractal dimension, correlation dimension and correlation entropy. When the value of the correlation dimension in children of the first month of life is in the range of 7.21-7.84, motor disorders are diagnosed (Zaripova Yu.R. Clinical and neurophysiological features of the motor system in young children with a burdened perinatal history: abstract of dissertation ... doc. Honey Science. M., 2014 .-- 43 p.).
Недостатки способа:The disadvantages of the method:
1. Способ применялся у детей с установленным диагнозом нарушения моторного развития.1. The method was used in children with a diagnosis of impaired motor development.
2. Требует наложения электродов на тело ребенка (возможна аллергическая реакция от контакта с дезинфицирующими средствами и гелями для усиления электропроводности).2. Requires the application of electrodes to the child’s body (an allergic reaction from contact with disinfectants and gels is possible to enhance electrical conductivity).
3. Не указана точность метода.3. The accuracy of the method is not indicated.
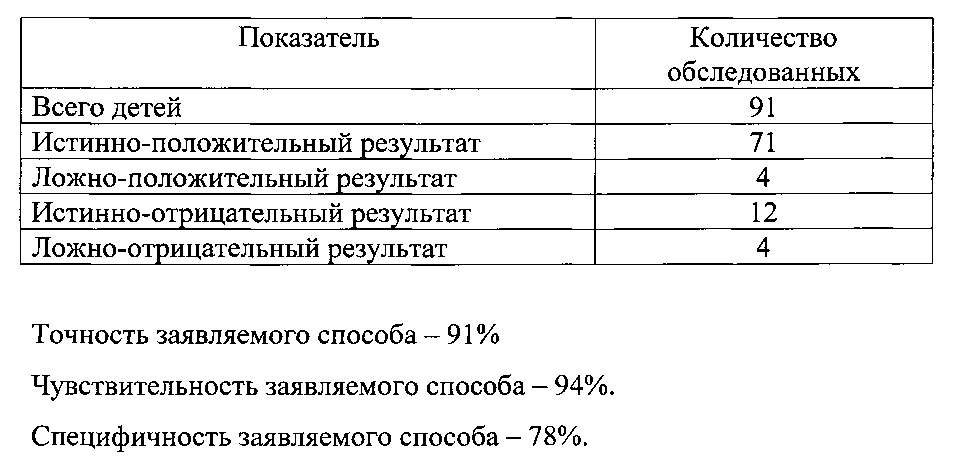
Технический результат заявляемого способа достигается тем, что детям 3-6 месяцев жизни выполняют функциональную компьютерную стабилометрию на стабилоплатформе с высокой чувствительностью для малого веса. Пациента укладывают в антигравитационной позе лежа на животе с опорой на предплечья или ладони и определяют производные параметры: скорость перемещения центра давления (ЦД), ширину эллипса статокинезиограммы, разность длины и ширины эллипса статокинезиограммы. При значениях хотя бы одного из показателей: скорости перемещения центра давления ниже 40,0 мм/с или выше 120,0 мм/с, ширины эллипса статокинезиограммы ниже 12,0 мм, разности длины и ширины эллипса статокинезиограммы выше 1,3 мм диагностируют нарушение моторного развития с точностью 91%.The technical result of the proposed method is achieved in that children 3-6 months of age perform functional computer stabilometry on a stabilized platform with high sensitivity for low weight. The patient is placed in an anti-gravity posture lying on his stomach resting on his forearms or palms and the derived parameters are determined: the velocity of the center of pressure (CD), the width of the ellipse of the statokinesiogram, the difference in length and width of the ellipse of the statokinesiogram. With values of at least one of the indicators: the velocity of the center of pressure is lower than 40.0 mm / s or higher than 120.0 mm / s, the width of the ellipse of the statokinesiogram is lower than 12.0 mm, the difference in length and width of the ellipse of the statokinesiogram is greater than 1.3 mm motor development with an accuracy of 91%.
Новизна способа заключается в том, что впервые для диагностики нарушения моторного развития у детей первого года жизни в процессе перехода к вертикализации используют количественную оценку показателей компьютерной стабилометрии.The novelty of the method lies in the fact that for the first time for the diagnosis of motor development disorders in children of the first year of life, in the process of transition to verticalization, a quantitative assessment of the indicators of computer stabilometry is used.
Метод компьютерной стабилометрии применяли у детей в возрасте старше 5 лет для диагностики нарушений равновесия, патологий опорно-двигательного аппарата и абилитации детей с детским церебральным параличом с использованием принципа биологической обратной связи. Все исследования проводились в положении стоя и были направлены на выявление патологического стереотипа опоры в основной стойке (Киселев Д.А. Стабилометрия в диагностике и лечении детей с гемипаретической формой детского церебрального паралича: ав-тореф. канд. мед. наук. - М., 2007. - 28 с.; Погосян И.А. Система диагностики и комплексного лечения нарушений опорно-двигательного аппарата у детей с мультифакторной патологией: автореф. док. мед. наук. - Пермь, 2007. - 39 с.; Савельев М.Ю. Физиологическое обоснование стабилометрии в оценке статического равновесия у детей младшего школьного возраста в норме и при нарушениях двигательной функции: автореф. канд. мед. наук. - Архангельск, 2005. - 19 с.).The method of computer stabilometry was used in children over the age of 5 years for the diagnosis of imbalances, pathologies of the musculoskeletal system and the habilitation of children with cerebral palsy using the principle of biological feedback. All studies were carried out in a standing position and were aimed at identifying a pathological stereotype of support in the main stance (Kiselev D.A. Stabilometry in the diagnosis and treatment of children with a hemiparetic form of cerebral palsy: author-candidate of medical science. - M., 2007. - 28 p .; IA Poghosyan. System for the diagnosis and complex treatment of musculoskeletal disorders in children with multifactorial pathology: abstract of a doctor of medical sciences. - Perm, 2007. - 39 p.; M. Savelyev The physiological justification of stabilometry in the assessment of static equals weight in children of primary school age is normal and with impaired motor function: abstract of Candidate of Medical Sciences. - Arkhangelsk, 2005. - 19 p.).
Однако у детей первого полугодия жизни поддержание данной позы еще не сформировано. Предлагаемый нами способ позволяет диагностировать формирование нарушения моторного развития на основании количественной оценки колебательных движений тела ребенка при поддержании первой антигравитационной позы, характерной для данного возраста (в положении лежа на животе). Ребенок должен удерживать позу, лежа на животе, приподнимая голову, опираясь на предплечья или ладони. На характеристики колебательных движений (скорость перемещения центра давления, ширина эллипса статокинезиограммы, разность длины и ширины эллипса статокинезиограммы) основное влияние оказывает состояние мышечного тонуса ребенка (гипотония, гипертонус или дистония).However, in children of the first half of life, the maintenance of this posture has not yet been formed. Our proposed method allows us to diagnose the formation of motor development disorders based on a quantitative assessment of the vibrational movements of the child’s body while maintaining the first anti-gravity posture that is typical for a given age (lying on the stomach). The child should hold the pose, lying on his stomach, raising his head, resting on his forearms or palms. The characteristics of the vibrational movements (the speed of the center of pressure, the width of the ellipse of the statokinesiogram, the difference in length and width of the ellipse of the statokinesiogram) are mainly influenced by the state of the child’s muscle tone (hypotension, hypertonicity or dystonia).
Способ осуществляется следующим образом: исследование проводят на стабилометрическом компьютеризированном комплексе, состоящем из персонального компьютера и стабилометрической платформы (фирма МБН, рег. удостоверение №29/03010403/5416-03 от 02.07.2003 г., Комплекс стабилометрический компьютеризированный «СТАБИЛО-МБН»: руководство по эксплуатации.- М., 2004.). Дополнительно использовался утяжелитель платформы с целью повышения чувствительности для проведения исследования у пациентов с малым весом, позволяющий проводить компьютерную стабилометрию у детей 3-6 месяцев жизни. Ребенка 3-6 месяцев жизни укладывают на стабилометрическую платформу с высокой чувствительностью для малого веса в антигравитационной позе лежа на животе с опорой на предплечья или ладони. Стабилоплатформа должна находиться на твердой, ровной горизонтальной поверхности. Выдерживают временной промежуток до принятия ребенком устойчивого положения. Далее активируют на компьютере команду записи, и начинается время регистрации длительностью 20 секунд. Затем проводится обработка зарегистрированных данных с определением скорости перемещения центра давления (измеряется в миллиметрах в секунду), ширины эллипса статокинезиограммы (измеряется в миллиметрах), разности длины и ширины эллипса статокинезиограммы (измеряется в миллиметрах). При значениях хотя бы одного из показателей: скорости перемещения центра давления ниже 40,0 мм/с или выше 120,0 мм/с, ширины эллипса статокинезиограммы ниже 12,0 мм, разности длины и ширины эллипса статокинезиограммы выше 1,3 мм диагностируют нарушение моторного развития.The method is as follows: the study is carried out on a stabilometric computerized complex consisting of a personal computer and a stabilometric platform (MBN company, reg. Certificate No. 29/03010403 / 5416-03 from 07/02/2003, the stabilized computerized complex "STABILO-MBN": operation manual.- M., 2004.). In addition, a platform weighting agent was used to increase sensitivity for conducting research in patients with low weight, which allows computer stabilization in children 3-6 months of life. A child of 3-6 months of life is laid on a stabilometric platform with high sensitivity for low weight in an anti-gravity pose lying on his stomach, resting on his forearms or palms. The platform must be on a firm, level, horizontal surface. They withstand the time period until the child takes a stable position. Next, the recording command is activated on the computer, and the registration time of 20 seconds begins. Then the registered data are processed to determine the velocity of the center of pressure (measured in millimeters per second), the width of the ellipse of the statokinesiogram (measured in millimeters), the difference in the length and width of the ellipse of the statokinesiogram (measured in millimeters). With values of at least one of the indicators: the velocity of the center of pressure is lower than 40.0 mm / s or higher than 120.0 mm / s, the width of the ellipse of the statokinesiogram is lower than 12.0 mm, the difference in length and width of the ellipse of the statokinesiogram is greater than 1.3 mm motor development.
Отличительными признаками способа является то, что проводят компьютерную стабилометрию на стабилоплатформе с высокой чувствительностью для малого веса, при этом укладывают пациента в антигравитационной позе лежа на животе с опорой на предплечья или ладони и определяют следующие производные параметры: скорость перемещения центра давления, ширину эллипса статокинезиограммы, разность длины и ширины эллипса статокинезиограммы и при значениях, хотя бы одного из показателей: скорости перемещения центра давления ниже 40,0 мм/с или выше 120,0 мм/с, ширины эллипса статокинезиограммы ниже 12,0 мм, разности длины и ширины эллипса статокинезиограммы выше 1,3 мм диагностируют формирование нарушения моторного развития.Distinctive features of the method is that they perform computer stabilometry on a stable platform with high sensitivity for low weight, while laying the patient in an anti-gravity pose lying on his stomach resting on his forearms or palms and determine the following derived parameters: the speed of the center of pressure, the width of the ellipse of the statokinesiogram, the difference between the length and width of the ellipse of the statokinesiogram and for values of at least one of the indicators: the velocity of the center of pressure is lower than 40.0 mm / s or higher than 120.0 mm / s, the width of the statokinesiogram ellipse below 12.0 mm, the difference in the length and width of the statokinesiogram ellipse above 1.3 mm diagnose the formation of motor development disorders.
Для объективизации данных, параллельно с применением заявляемого способа проводилось клиническое обследование детей 3-6 месяцев жизни.To objectify the data, in parallel with the application of the proposed method, a clinical examination of children 3-6 months of life was carried out.
Существо способа поясняется следующими примерами:The essence of the method is illustrated by the following examples:
Пример 1.Example 1
Ребенок М., 4 мес. рожденный от 3 беременности 2 родов в сроке 40 недель с оценкой по шкале Апгар 7/8 баллов в удовлетворительном состоянии. Неврологический статус: окружность головы 41,5 см., большой родничок 1,5×1,5 см, не выбухает. Черепные нервы без патологии. Мышечный тонус удовлетворительный. Сухожильные рефлексы живые, симметричные. Лежа на животе голову удерживает. При тракции за руки группируется недостаточно. Шаговый рефлекс не вызывается. Хватательный рефлекс выражен слабо. Вызывается рефлекс Моро - 1 фаза. Выпрямляющая реакция с туловища на голову выражена слабо. Эмоциональный тонус положительный. На основании клинических данных диагноз нарушения моторного развития сомнителен. Согласно предлагаемому способу получены следующие значения стабилометрических показателей: скорость перемещения ЦД - 34,5 мм/с, ширина эллипса статокинезиограммы - 8,62 мм, разность длины и ширины эллипса статокинезиограммы - 0,75 мм соответствуют заявленным параметрам нарушения моторного развития. При повторном осмотре ребенка в возрасте 5 мес. в неврологическом статусе: окружность головы 42,5 см., большой родничок 1,5×1,5 см, не выбухает. Черепные нервы без патологии. Мышечный тонус снижен в плечевом отделе. Сухожильные рефлексы живые, симметричные. Лежа на животе опора на предплечья. При тракции за руки не группируется. Ребенок не переворачивается. Хватательный рефлекс выражен слабо. Вызывается рефлекс Моро - 1 фаза. Выпрямляющая реакция с туловища на голову выражена слабо. Эмоциональный тонус положительный. На основании клинических данных (понижение мышечного тонуса в плечевом отделе, задержка развития цепных симметрических рефлексов, задержка редукции безусловных рефлексов) диагностируется нарушение моторного развитияBaby M., 4 months born from 3 pregnancies of 2 births in a period of 40 weeks with an Apgar score of 7/8 points in satisfactory condition. Neurological status: head circumference 41.5 cm, large fontanel 1.5 × 1.5 cm, does not swell. Cranial nerves without pathology. Muscle tone is satisfactory. Tendon reflexes are lively, symmetrical. Lying on his stomach holds his head. When traction for hands is not grouped enough. The step reflex is not called. The grasping reflex is weakly expressed. Moro reflex is triggered - phase 1. The straightening reaction from the trunk to the head is poorly expressed. Emotional tone is positive. Based on clinical data, the diagnosis of impaired motor development is uncertain. According to the proposed method, the following values of stabilometric indicators were obtained: the displacement speed of the central nervous system is 34.5 mm / s, the width of the ellipse of the statokinesiogram is 8.62 mm, the difference in length and width of the ellipse of the statokinesiogram is 0.75 mm corresponds to the declared parameters of impaired motor development. When re-examining a child aged 5 months. in neurological status: head circumference 42.5 cm, large fontanel 1.5 × 1.5 cm, does not swell. Cranial nerves without pathology. Muscle tone is reduced in the shoulder. Tendon reflexes are lively, symmetrical. Lying on his stomach resting on his forearms. When traction is not grouped by hand. The child does not roll over. The grasping reflex is weakly expressed. Moro reflex is triggered - phase 1. The straightening reaction from the trunk to the head is poorly expressed. Emotional tone is positive. On the basis of clinical data (decrease in muscle tone in the shoulder, delayed development of symmetrical chain reflexes, delayed reduction of unconditioned reflexes), motor development is diagnosed
Заключение: диагностировано нарушение моторного развития.Conclusion: a motor development disorder was diagnosed.
Пример 2.Example 2
Ребенок Д., 3 мес., рожденный от 1 беременности в сроке 39 недель с оценкой по шкале Апгар 8/9 баллов в удовлетворительном состоянии. Неврологический статус: окружность головы 40,0 см., большой родничок 1,5×2,0 см, не выбухает. Черепные нервы без патологии. Мышечный тонус дистоничный. Сухожильные рефлексы живые, симметричные. Лежа на животе голову удерживает. При тракции за руки группируется слабо. Реакция опоры положительная. Шаговый рефлекс не вызывается. Хватательный рефлекс выражен слабо. Вызывается рефлекс Моро - 1 фаза. Выпрямляющая реакция с туловища на голову положительная. Эмоциональный тонус положительный. На основании клинических данных диагноз нарушения моторного развития сомнителен. Согласно предлагаемому способу получены следующие значения стабилометрических показателей: скорость перемещения ЦД - 75,33 мм/с, ширина эллипса статокинезиограммы - 25,21 мм, разность длины и ширины эллипса статокинезиограммы - 3,02 мм соответствуют заявленным параметрам нарушения моторного развития. При повторном осмотре ребенка в возрасте 4 мес. в неврологическом статусе: окружность головы 41,0 см., большой родничок 1,5×1,5 см, не выбухает. Черепные нервы без патологии. Мышечный тонус повышен в разгибателях нижних конечностей. Сухожильные рефлексы повышены, симметричные. Лежа на животе голову удерживает. При тракции за руки группируется недостаточно. Реакция опоры положительная, опора на носочки. Шаговый рефлекс не вызывается. Хватательный рефлекс выражен слабо. Вызывается рефлекс Моро - 1 фаза. На основании клинических данных (повышение мышечного тонуса в разгибателях нижних конечностей, повышение сухожильных рефлексов, задержка редукции безусловных рефлексов) диагностируется нарушение моторного развития.Baby D., 3 months old, born from 1 pregnancy in a period of 39 weeks with an Apgar score of 8/9 points in satisfactory condition. Neurological status: head circumference 40.0 cm, large fontanel 1.5 × 2.0 cm, does not swell. Cranial nerves without pathology. Muscular tone is dystonic. Tendon reflexes are lively, symmetrical. Lying on his stomach holds his head. When traction by hand is grouped weakly. The support reaction is positive. The step reflex is not called. The grasping reflex is weakly expressed. Moro reflex is triggered - phase 1. The straightening reaction from the trunk to the head is positive. Emotional tone is positive. Based on clinical data, the diagnosis of impaired motor development is uncertain. According to the proposed method, the following values of stabilometric indicators were obtained: the displacement speed of the central displacement is 75.33 mm / s, the width of the ellipse of the statokinesiogram is 25.21 mm, the difference in length and width of the ellipse of the statokinesiogram is 3.02 mm corresponds to the declared parameters of impaired motor development. When re-examining a child aged 4 months. in neurological status: head circumference 41.0 cm, large fontanel 1.5 × 1.5 cm, does not swell. Cranial nerves without pathology. Muscle tone is increased in the extensors of the lower extremities. Tendon reflexes are elevated, symmetrical. Lying on his stomach holds his head. When traction for hands is not grouped enough. The support reaction is positive, the support on the socks. The step reflex is not called. The grasping reflex is weakly expressed. Moro reflex is triggered - phase 1. Based on clinical data (increased muscle tone in the extensors of the lower extremities, increased tendon reflexes, delayed reduction of unconditioned reflexes), motor development is diagnosed.
Заключение: диагностировано нарушение моторного развития.Conclusion: a motor development disorder was diagnosed.
Пример 3.Example 3
Ребенок К., 6 мес. рожденный от 2 беременности 2 родов в сроке 39 недель с оценкой по шкале Апгар 7/8 баллов в удовлетворительном состоянии. Неврологический статус: окружность головы 43,5 см., большой родничок 1,0×1,0 см, не выбухает. Черепные нервы без патологии. Мышечный тонус удовлетворительный. Сухожильные рефлексы живые, симметричные. Лежа на животе опора на предплечья. При тракции за руки группируется. Лежа на спине, тянет руки к игрушке, но не захватывает ее. Шаговый рефлекс не вызывается. Рефлекс Моро - не вызывается. Эмоциональный тонус положительный. На основании клинических данных диагноз нарушения моторного развития сомнителен. Согласно предлагаемому способу получены следующие значения стабилометрических показателей: скорость перемещения ЦД - 126,1 мм/с, ширина эллипса статокинезиограммы - 34,7 мм, разность длины и ширины эллипса статокинезиограммы - 8,62 мм соответствуют заявленным параметрам нарушения моторного развития. При повторном осмотре ребенка в возрасте 7 мес. в неврологическом статусе: окружность головы 44,5 см., большой родничок 1,0×1,0 см, не выбухает. Черепные нервы без патологии. Мышечный тонус умеренно повышен в верхних конечностях. Сухожильные рефлексы живые, симметричные. При тракции за руки присаживается. Ребенок не садиться. Лежа на спине, тянет руки к игрушке, захватывает ее не уверенно. Эмоциональный тонус положительный. На основании клинических данных (повышение мышечного тонуса, задержка развития цепных симметрических рефлексов, нарушение сенсорно-моторного поведения) диагностируется нарушение моторного развития.Baby K., 6 months born from 2 pregnancies of 2 births in a period of 39 weeks with an Apgar score of 7/8 points in satisfactory condition. Neurological status: head circumference 43.5 cm, large fontanel 1.0 × 1.0 cm, does not swell. Cranial nerves without pathology. Muscle tone is satisfactory. Tendon reflexes are lively, symmetrical. Lying on his stomach resting on his forearms. When traction is grouped by hand. Lying on his back, pulls his hands to the toy, but does not grab it. The step reflex is not called. Reflex Moro - not called. Emotional tone is positive. Based on clinical data, the diagnosis of impaired motor development is uncertain. According to the proposed method, the following values of the stabilometric indicators were obtained: the displacement speed of the CP is 126.1 mm / s, the width of the ellipse of the statokinesiogram is 34.7 mm, the difference in length and width of the ellipse of the statokinesiogram is 8.62 mm corresponds to the declared parameters of impaired motor development. When re-examining a child aged 7 months. in neurological status: head circumference 44.5 cm, large fontanel 1.0 × 1.0 cm, does not swell. Cranial nerves without pathology. Muscle tone is moderately elevated in the upper limbs. Tendon reflexes are lively, symmetrical. When traction sits down by the hands. The child does not sit down. Lying on his back, pulls his hands to the toy, captures it with uncertainty. Emotional tone is positive. Based on clinical data (increased muscle tone, delayed development of symmetrical chain reflexes, impaired sensory-motor behavior), impaired motor development is diagnosed.
Заключение: диагностировано нарушение моторного развития.Conclusion: a motor development disorder was diagnosed.
Пример 4.Example 4
Ребенок А., 3 мес. рожденный от 2 беременности 2 родов в сроке 39 недель с оценкой по шкале Апгар 8/9 баллов в удовлетворительном состоянии. Неврологический статус: окружность головы 39,5 см., большой родничок 2×1,5 см, не выбухает. Черепные нервы без патологии. Мышечный тонус удовлетворительный. Сухожильные рефлексы живые, симметричные. Лежа на животе голову удерживает. При тракции за руки группируется удовлетворительно. Переворачивается со спины на бок. Шаговый рефлекс не вызывается. Рефлекс Моро не вызывается. Эмоциональный тонус положительный. На основании клинических данных: нарушение моторного развития не диагностируются. Согласно предлагаемому способу получены следующие значения стабилометрических показателей: скорость перемещения ЦД - 63,93 мм/с, ширина эллипса статокинезиограммы - 15,3 мм, разность длины и ширины эллипса статокинезиограммы - 0,4 мм соответствуют состоянию ребенка при отсутствии нарушения моторного развития.Baby A., 3 months born from 2 pregnancies of 2 births in a period of 39 weeks with an Apgar score of 8/9 points in satisfactory condition. Neurological status: head circumference 39.5 cm, large fontanel 2 × 1.5 cm, does not swell. Cranial nerves without pathology. Muscle tone is satisfactory. Tendon reflexes are lively, symmetrical. Lying on his stomach holds his head. When traction by hand is grouped satisfactorily. Flips from back to side. The step reflex is not called. Reflex Moro is not caused. Emotional tone is positive. Based on clinical data: motor development disorders are not diagnosed. According to the proposed method, the following values of stabilometric indicators were obtained: the displacement speed of the central displacement is 63.93 mm / s, the width of the ellipse of the statokinesiogram is 15.3 mm, the difference in length and width of the ellipse of the statokinesiogram is 0.4 mm corresponds to the state of the child in the absence of impaired motor development.
Заключение: нарушение моторного развития не диагностируется. При повторном осмотре в 4 месяца моторное развитие не нарушено.Conclusion: impaired motor development is not diagnosed. When re-examined at 4 months, motor development is not impaired.
Преимущества данного способа:The advantages of this method:
1. Возможность объективно (количественно) выявить формирование нарушения моторного развития у детей 3-6 месяцев жизни.1. The ability to objectively (quantitatively) identify the formation of impaired motor development in children 3-6 months of life.
2. Высокая точность - 91%, чувствительность - 94%, специфичность - 78%.2. High accuracy - 91%, sensitivity - 94%, specificity - 78%.
3. Не требует специальной подготовки ребенка для исследования.3. Does not require special preparation of the child for research.
4. Не требует наложения датчиков или электродов на тело ребенка4. Does not require the application of sensors or electrodes to the child’s body
5. Неинвазивность способа, его нетравматичность.5. Non-invasiveness of the method, its non-invasiveness.
6. Требует для своего проведения малое количество времени (20 сек).6. Requires a small amount of time (20 seconds) for its conduct.
7. Проводится однократно, не требует исследования в динамике.7. It is carried out once, does not require research in dynamics.
8. Позволяет своевременно проводить коррекцию лечебных мероприятий для предупреждения неблагоприятных исходов.8. Allows timely correction of therapeutic measures to prevent adverse outcomes.
9. Способ позволяет проводить скрининговое исследование у детей 3-6 месяцев для выявления нарушения моторного развития.9. The method allows a screening study in children 3-6 months to detect impaired motor development.
Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015137368/14A RU2598960C1 (en) | 2015-09-01 | 2015-09-01 | Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015137368/14A RU2598960C1 (en) | 2015-09-01 | 2015-09-01 | Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2598960C1 true RU2598960C1 (en) | 2016-10-10 |
Family
ID=57127366
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2015137368/14A RU2598960C1 (en) | 2015-09-01 | 2015-09-01 | Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2598960C1 (en) |
Cited By (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2689918C1 (en) * | 2018-06-07 | 2019-05-29 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for predicting formation of infantile cerebral paralysis in children 3-6 months of age |
| RU2719655C1 (en) * | 2019-06-25 | 2020-04-21 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for assessing clinical effectiveness of children 3-6 months of age with consequences of perinatal central nervous system affection in form of motor development disorder |
| CN113499074A (en) * | 2021-07-13 | 2021-10-15 | 李焰 | Muscle tension detecting apparatus for infants |
| RU2758478C1 (en) * | 2021-04-14 | 2021-10-28 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for diagnosing motor development disorders in children age 3 - 5 months |
| RU2804646C1 (en) * | 2023-03-14 | 2023-10-03 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method of diagnosis of motor development disorders in premature children |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2475747C1 (en) * | 2011-12-15 | 2013-02-20 | Учреждение Российской академии медицинских наук Научный центр здоровья детей РАМН (НЦЗД РАМН) | Method of predicting psychomotor development of children with perinatal affection of central nervous system |
| RU2497451C1 (en) * | 2012-06-14 | 2013-11-10 | Федеральное государственное бюджетное учреждение "Уральский научно-исследовательский институт травматологии и ортопедии имени В.Д. Чаклина" Министерства здравоохранения и социального развития Российской Федерации | Method of diagnosing functional impairment of locomotor system |
-
2015
- 2015-09-01 RU RU2015137368/14A patent/RU2598960C1/en active
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2475747C1 (en) * | 2011-12-15 | 2013-02-20 | Учреждение Российской академии медицинских наук Научный центр здоровья детей РАМН (НЦЗД РАМН) | Method of predicting psychomotor development of children with perinatal affection of central nervous system |
| RU2497451C1 (en) * | 2012-06-14 | 2013-11-10 | Федеральное государственное бюджетное учреждение "Уральский научно-исследовательский институт травматологии и ортопедии имени В.Д. Чаклина" Министерства здравоохранения и социального развития Российской Федерации | Method of diagnosing functional impairment of locomotor system |
Non-Patent Citations (2)
| Title |
|---|
| ЗАРИПОВА Ю.Р. Клинико-нейрофизиологические особенности двигательной системы у детей раннего возраста с отягощенным перинатальным анамнезом. Автореф. на соиск. уч. ст. к. м. н., М., 2014. * |
| САВЕЛЬЕВ М.Ю. Физиологическое обоснование стабилометрии в оценке статического равновесия у детей младшего школьного возраста в норме и при нарушениях двигательной функции. Автореф. на соиск. уч. ст. к.м.н., Архангельск, 2005. CULTRERA P. et al. Evaluation with stabilometric platform of balance disorders in osteoporosis patients. A proposal for a diagnostic protocol. Clin Cases Miner Bone Metab. 2010 May; 7(2):123-5. * |
Cited By (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2689918C1 (en) * | 2018-06-07 | 2019-05-29 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for predicting formation of infantile cerebral paralysis in children 3-6 months of age |
| RU2719655C1 (en) * | 2019-06-25 | 2020-04-21 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for assessing clinical effectiveness of children 3-6 months of age with consequences of perinatal central nervous system affection in form of motor development disorder |
| RU2758478C1 (en) * | 2021-04-14 | 2021-10-28 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method for diagnosing motor development disorders in children age 3 - 5 months |
| CN113499074A (en) * | 2021-07-13 | 2021-10-15 | 李焰 | Muscle tension detecting apparatus for infants |
| RU2804646C1 (en) * | 2023-03-14 | 2023-10-03 | Федеральное государственное бюджетное учреждение "Ивановский научно-исследовательский институт материнства и детства имени В.Н. Городкова" Министерства здравоохранения Российской Федерации | Method of diagnosis of motor development disorders in premature children |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Isroilovich et al. | Analysis of Risk Factors in the Etiopatogenesis of Congenital Myopathy Syndrome | |
| Quinsey et al. | Penile circumference, skin conductance, and ranking responses of child molesters and “normals” to sexual and nonsexual visual stimuli | |
| RU2598960C1 (en) | Diagnostic technique for disturbance formation of motor expansion in 3-6 months old children | |
| Lorentzen et al. | Distinguishing active from passive components of ankle plantar flexor stiffness in stroke, spinal cord injury and multiple sclerosis | |
| Futagi et al. | The grasp reflex and moro reflex in infants: hierarchy of primitive reflex responses | |
| Gupta et al. | Premorbid adjustment as a predictor of phenomenological and neurobiological indices in schizophrenia | |
| Aneja | Evaluation of a child with cerebral palsy | |
| Chmielewska et al. | Static postural stability in women with stress urinary incontinence: Effects of vision and bladder filling | |
| Harris-Love et al. | Assessing function and endurance in adults with spinal and bulbar muscular atrophy: validity of the adult myopathy assessment tool | |
| Stadelmaier et al. | Exposure to sodium valproate during pregnancy: facial features and signs of autism | |
| Kusaka et al. | Large calf circumference indicates non-sarcopenia despite body mass | |
| Greene et al. | Quantitative assessment of multiple sclerosis using inertial sensors and the TUG test | |
| Labanca et al. | Vestibular-evoked myogenic potential triggered by galvanic vestibular stimulation may reveal subclinical alterations in human T-cell lymphotropic virus type 1-associated myelopathy | |
| Kim et al. | Pyramidal and extrapyramidal scale (PEPS): a new scale for the assessment of motor impairment in vascular cognitive impairment associated with small vessel disease | |
| Matsukiyo et al. | Relationship between muscle-tendon length, range of motion, and resistance to passive movement in children with normal and increased tone | |
| RU2719655C1 (en) | Method for assessing clinical effectiveness of children 3-6 months of age with consequences of perinatal central nervous system affection in form of motor development disorder | |
| Turk et al. | Reliability and sensitivity of a wrist rig to measure motor control and spasticity in poststroke hemiplegia | |
| RU2585142C1 (en) | Method of analysing equilibrium function in children aged 3-6 months | |
| RU2804646C1 (en) | Method of diagnosis of motor development disorders in premature children | |
| RU2689918C1 (en) | Method for predicting formation of infantile cerebral paralysis in children 3-6 months of age | |
| Pinkhardt et al. | The combination of dopa-responsive parkinsonian syndrome and motor neuron disease | |
| RU2758478C1 (en) | Method for diagnosing motor development disorders in children age 3 - 5 months | |
| RU2581519C1 (en) | Method for diagnosing spinal disorders in newborns | |
| Dafkin et al. | Kinematic and kinetic analysis of the inter-and intra-applicator assessment of the Babinski reflex | |
| RU2804797C1 (en) | Method of predicting cerebral palsy in premature children |