RU2595863C2 - Method of evaluating state of human health in prediction of clinical course of infectious disease - Google Patents
Method of evaluating state of human health in prediction of clinical course of infectious disease Download PDFInfo
- Publication number
- RU2595863C2 RU2595863C2 RU2014152102/15A RU2014152102A RU2595863C2 RU 2595863 C2 RU2595863 C2 RU 2595863C2 RU 2014152102/15 A RU2014152102/15 A RU 2014152102/15A RU 2014152102 A RU2014152102 A RU 2014152102A RU 2595863 C2 RU2595863 C2 RU 2595863C2
- Authority
- RU
- Russia
- Prior art keywords
- patients
- cfu
- microbiocenosis
- biotope
- group
- Prior art date
Links
- 208000015181 infectious disease Diseases 0.000 title claims abstract description 61
- 238000000034 method Methods 0.000 title claims abstract description 48
- 208000035473 Communicable disease Diseases 0.000 title claims abstract description 21
- 230000036541 health Effects 0.000 title claims abstract description 14
- 230000008569 process Effects 0.000 claims description 34
- 230000002458 infectious effect Effects 0.000 claims description 28
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 claims description 27
- 230000001717 pathogenic effect Effects 0.000 claims description 27
- 201000010099 disease Diseases 0.000 claims description 20
- 244000052769 pathogen Species 0.000 claims description 18
- 210000004400 mucous membrane Anatomy 0.000 claims description 17
- 230000001684 chronic effect Effects 0.000 claims description 10
- 230000002349 favourable effect Effects 0.000 claims description 10
- 238000012795 verification Methods 0.000 claims description 9
- 208000037048 Prodromal Symptoms Diseases 0.000 claims description 7
- 230000000694 effects Effects 0.000 abstract description 10
- 239000003814 drug Substances 0.000 abstract description 5
- 239000000126 substance Substances 0.000 abstract 1
- 230000001936 parietal effect Effects 0.000 description 38
- 208000027244 Dysbiosis Diseases 0.000 description 30
- 230000007140 dysbiosis Effects 0.000 description 29
- 238000011282 treatment Methods 0.000 description 29
- 244000005700 microbiome Species 0.000 description 27
- 244000005706 microflora Species 0.000 description 27
- 206010006451 bronchitis Diseases 0.000 description 25
- 230000001154 acute effect Effects 0.000 description 20
- 241000606161 Chlamydia Species 0.000 description 18
- 241000186660 Lactobacillus Species 0.000 description 18
- 210000003300 oropharynx Anatomy 0.000 description 16
- 230000007423 decrease Effects 0.000 description 15
- 238000002560 therapeutic procedure Methods 0.000 description 15
- 241000222120 Candida <Saccharomycetales> Species 0.000 description 14
- 241001591005 Siga Species 0.000 description 14
- 241000894006 Bacteria Species 0.000 description 13
- 238000001514 detection method Methods 0.000 description 13
- 238000011161 development Methods 0.000 description 12
- 230000018109 developmental process Effects 0.000 description 12
- 241000202898 Ureaplasma Species 0.000 description 11
- 241000186000 Bifidobacterium Species 0.000 description 10
- 230000009257 reactivity Effects 0.000 description 10
- 230000001018 virulence Effects 0.000 description 10
- 241000233866 Fungi Species 0.000 description 9
- 241000295644 Staphylococcaceae Species 0.000 description 9
- 241000894007 species Species 0.000 description 9
- 208000004926 Bacterial Vaginosis Diseases 0.000 description 8
- 206010006458 Bronchitis chronic Diseases 0.000 description 8
- 230000002924 anti-infective effect Effects 0.000 description 8
- 230000015572 biosynthetic process Effects 0.000 description 8
- 208000007451 chronic bronchitis Diseases 0.000 description 8
- 230000001900 immune effect Effects 0.000 description 8
- 230000005764 inhibitory process Effects 0.000 description 8
- 230000007246 mechanism Effects 0.000 description 8
- 230000007170 pathology Effects 0.000 description 8
- 108090000623 proteins and genes Proteins 0.000 description 8
- 210000003296 saliva Anatomy 0.000 description 8
- 241000701806 Human papillomavirus Species 0.000 description 7
- 108060003951 Immunoglobulin Proteins 0.000 description 7
- 231100000749 chronicity Toxicity 0.000 description 7
- 208000035475 disorder Diseases 0.000 description 7
- 102000018358 immunoglobulin Human genes 0.000 description 7
- 230000004054 inflammatory process Effects 0.000 description 7
- 208000003322 Coinfection Diseases 0.000 description 6
- 241000305071 Enterobacterales Species 0.000 description 6
- 241000588724 Escherichia coli Species 0.000 description 6
- 206010035664 Pneumonia Diseases 0.000 description 6
- 239000003795 chemical substances by application Substances 0.000 description 6
- 230000003247 decreasing effect Effects 0.000 description 6
- 230000007613 environmental effect Effects 0.000 description 6
- 238000011156 evaluation Methods 0.000 description 6
- 230000005713 exacerbation Effects 0.000 description 6
- 238000009343 monoculture Methods 0.000 description 6
- 210000000056 organ Anatomy 0.000 description 6
- 230000001681 protective effect Effects 0.000 description 6
- 239000000829 suppository Substances 0.000 description 6
- 241000207202 Gardnerella Species 0.000 description 5
- 206010062106 Respiratory tract infection viral Diseases 0.000 description 5
- 230000004888 barrier function Effects 0.000 description 5
- 230000003862 health status Effects 0.000 description 5
- 230000036039 immunity Effects 0.000 description 5
- 229940072221 immunoglobulins Drugs 0.000 description 5
- 201000006747 infectious mononucleosis Diseases 0.000 description 5
- 230000003993 interaction Effects 0.000 description 5
- 238000010899 nucleation Methods 0.000 description 5
- 230000007918 pathogenicity Effects 0.000 description 5
- 238000002360 preparation method Methods 0.000 description 5
- 235000018102 proteins Nutrition 0.000 description 5
- 102000004169 proteins and genes Human genes 0.000 description 5
- 241001453172 Fusobacteria Species 0.000 description 4
- 208000037273 Pathologic Processes Diseases 0.000 description 4
- 230000002411 adverse Effects 0.000 description 4
- 230000001580 bacterial effect Effects 0.000 description 4
- 238000006243 chemical reaction Methods 0.000 description 4
- 229940079593 drug Drugs 0.000 description 4
- 230000008030 elimination Effects 0.000 description 4
- 238000003379 elimination reaction Methods 0.000 description 4
- 238000005516 engineering process Methods 0.000 description 4
- 230000006870 function Effects 0.000 description 4
- 230000004807 localization Effects 0.000 description 4
- 230000002906 microbiologic effect Effects 0.000 description 4
- 239000000203 mixture Substances 0.000 description 4
- 230000009054 pathological process Effects 0.000 description 4
- 238000003786 synthesis reaction Methods 0.000 description 4
- 230000001225 therapeutic effect Effects 0.000 description 4
- 206010044008 tonsillitis Diseases 0.000 description 4
- 102000009027 Albumins Human genes 0.000 description 3
- 108010088751 Albumins Proteins 0.000 description 3
- 241000701022 Cytomegalovirus Species 0.000 description 3
- 206010061598 Immunodeficiency Diseases 0.000 description 3
- 241000589517 Pseudomonas aeruginosa Species 0.000 description 3
- 241000191940 Staphylococcus Species 0.000 description 3
- 241000194017 Streptococcus Species 0.000 description 3
- 206010046914 Vaginal infection Diseases 0.000 description 3
- 201000008100 Vaginitis Diseases 0.000 description 3
- 230000003115 biocidal effect Effects 0.000 description 3
- 230000006378 damage Effects 0.000 description 3
- 230000013632 homeostatic process Effects 0.000 description 3
- 210000000987 immune system Anatomy 0.000 description 3
- 238000011081 inoculation Methods 0.000 description 3
- 230000003902 lesion Effects 0.000 description 3
- 239000003550 marker Substances 0.000 description 3
- 244000000010 microbial pathogen Species 0.000 description 3
- 230000035755 proliferation Effects 0.000 description 3
- 230000000241 respiratory effect Effects 0.000 description 3
- 230000004044 response Effects 0.000 description 3
- 230000001052 transient effect Effects 0.000 description 3
- 230000007704 transition Effects 0.000 description 3
- 241001148471 unidentified anaerobic bacterium Species 0.000 description 3
- 206010061041 Chlamydial infection Diseases 0.000 description 2
- 241000498849 Chlamydiales Species 0.000 description 2
- 208000036649 Dysbacteriosis Diseases 0.000 description 2
- 108090000790 Enzymes Proteins 0.000 description 2
- 102000004190 Enzymes Human genes 0.000 description 2
- 208000029462 Immunodeficiency disease Diseases 0.000 description 2
- 241000588748 Klebsiella Species 0.000 description 2
- 241001430197 Mollicutes Species 0.000 description 2
- 241000588653 Neisseria Species 0.000 description 2
- 206010028980 Neoplasm Diseases 0.000 description 2
- 241000700605 Viruses Species 0.000 description 2
- 230000006978 adaptation Effects 0.000 description 2
- 230000000844 anti-bacterial effect Effects 0.000 description 2
- 201000000902 chlamydia Diseases 0.000 description 2
- 208000012538 chlamydia trachomatis infectious disease Diseases 0.000 description 2
- 239000000824 cytostatic agent Substances 0.000 description 2
- 230000001085 cytostatic effect Effects 0.000 description 2
- 229940088598 enzyme Drugs 0.000 description 2
- 210000002919 epithelial cell Anatomy 0.000 description 2
- 210000000981 epithelium Anatomy 0.000 description 2
- 239000012634 fragment Substances 0.000 description 2
- 230000014509 gene expression Effects 0.000 description 2
- 230000002949 hemolytic effect Effects 0.000 description 2
- 230000004727 humoral immunity Effects 0.000 description 2
- 230000007813 immunodeficiency Effects 0.000 description 2
- 239000002955 immunomodulating agent Substances 0.000 description 2
- 229940121354 immunomodulator Drugs 0.000 description 2
- 230000003308 immunostimulating effect Effects 0.000 description 2
- 230000003834 intracellular effect Effects 0.000 description 2
- 230000007108 local immune response Effects 0.000 description 2
- 230000000813 microbial effect Effects 0.000 description 2
- 230000001575 pathological effect Effects 0.000 description 2
- 238000001228 spectrum Methods 0.000 description 2
- 230000001629 suppression Effects 0.000 description 2
- 208000024891 symptom Diseases 0.000 description 2
- 210000001519 tissue Anatomy 0.000 description 2
- 210000001215 vagina Anatomy 0.000 description 2
- XMAYWYJOQHXEEK-ZEQKJWHPSA-N (2S,4R)-ketoconazole Chemical compound C1CN(C(=O)C)CCN1C(C=C1)=CC=C1OC[C@H]1O[C@](CN2C=NC=C2)(C=2C(=CC(Cl)=CC=2)Cl)OC1 XMAYWYJOQHXEEK-ZEQKJWHPSA-N 0.000 description 1
- 102000040650 (ribonucleotides)n+m Human genes 0.000 description 1
- 201000001320 Atherosclerosis Diseases 0.000 description 1
- 102100024222 B-lymphocyte antigen CD19 Human genes 0.000 description 1
- 241000193830 Bacillus <bacterium> Species 0.000 description 1
- 102000004127 Cytokines Human genes 0.000 description 1
- 108090000695 Cytokines Proteins 0.000 description 1
- 241000194033 Enterococcus Species 0.000 description 1
- 241000588722 Escherichia Species 0.000 description 1
- 241000282412 Homo Species 0.000 description 1
- 101000980825 Homo sapiens B-lymphocyte antigen CD19 Proteins 0.000 description 1
- 108010003272 Hyaluronate lyase Proteins 0.000 description 1
- 102000009066 Hyaluronoglucosaminidase Human genes 0.000 description 1
- 206010061218 Inflammation Diseases 0.000 description 1
- 108010063045 Lactoferrin Proteins 0.000 description 1
- 102100032241 Lactotransferrin Human genes 0.000 description 1
- 208000017170 Lipid metabolism disease Diseases 0.000 description 1
- IPWKIXLWTCNBKN-UHFFFAOYSA-N Madelen Chemical compound CC1=NC=C([N+]([O-])=O)N1CC(O)CCl IPWKIXLWTCNBKN-UHFFFAOYSA-N 0.000 description 1
- 241001465754 Metazoa Species 0.000 description 1
- 241000736262 Microbiota Species 0.000 description 1
- 241000192041 Micrococcus Species 0.000 description 1
- 102000016943 Muramidase Human genes 0.000 description 1
- 108010014251 Muramidase Proteins 0.000 description 1
- 108010062010 N-Acetylmuramoyl-L-alanine Amidase Proteins 0.000 description 1
- 102000005348 Neuraminidase Human genes 0.000 description 1
- 108010006232 Neuraminidase Proteins 0.000 description 1
- 241000206591 Peptococcus Species 0.000 description 1
- 241000191992 Peptostreptococcus Species 0.000 description 1
- 201000007100 Pharyngitis Diseases 0.000 description 1
- 241000588769 Proteus <enterobacteria> Species 0.000 description 1
- 102400001107 Secretory component Human genes 0.000 description 1
- 241000700584 Simplexvirus Species 0.000 description 1
- 241001505901 Streptococcus sp. 'group A' Species 0.000 description 1
- 241000223996 Toxoplasma Species 0.000 description 1
- 241001502500 Trichomonadida Species 0.000 description 1
- 206010046367 Ureaplasma infections Diseases 0.000 description 1
- 241000202921 Ureaplasma urealyticum Species 0.000 description 1
- 230000003213 activating effect Effects 0.000 description 1
- 230000004913 activation Effects 0.000 description 1
- 206010001093 acute tonsillitis Diseases 0.000 description 1
- 230000003044 adaptive effect Effects 0.000 description 1
- 230000016571 aggressive behavior Effects 0.000 description 1
- 238000004458 analytical method Methods 0.000 description 1
- 239000003242 anti bacterial agent Substances 0.000 description 1
- 230000000843 anti-fungal effect Effects 0.000 description 1
- 229940124350 antibacterial drug Drugs 0.000 description 1
- 229940088710 antibiotic agent Drugs 0.000 description 1
- 229940121375 antifungal agent Drugs 0.000 description 1
- 230000000890 antigenic effect Effects 0.000 description 1
- 238000013459 approach Methods 0.000 description 1
- 230000003385 bacteriostatic effect Effects 0.000 description 1
- 210000000481 breast Anatomy 0.000 description 1
- 201000011510 cancer Diseases 0.000 description 1
- 239000000969 carrier Substances 0.000 description 1
- 210000004027 cell Anatomy 0.000 description 1
- 230000008859 change Effects 0.000 description 1
- 201000001883 cholelithiasis Diseases 0.000 description 1
- 230000008576 chronic process Effects 0.000 description 1
- 206010009887 colitis Diseases 0.000 description 1
- 210000001072 colon Anatomy 0.000 description 1
- 238000010835 comparative analysis Methods 0.000 description 1
- 230000021615 conjugation Effects 0.000 description 1
- 238000011109 contamination Methods 0.000 description 1
- 230000002596 correlated effect Effects 0.000 description 1
- 238000010219 correlation analysis Methods 0.000 description 1
- 230000007123 defense Effects 0.000 description 1
- 230000007812 deficiency Effects 0.000 description 1
- 238000002405 diagnostic procedure Methods 0.000 description 1
- 230000004069 differentiation Effects 0.000 description 1
- 229940063123 diflucan Drugs 0.000 description 1
- 230000001079 digestive effect Effects 0.000 description 1
- 231100000676 disease causative agent Toxicity 0.000 description 1
- 229960003722 doxycycline Drugs 0.000 description 1
- XQTWDDCIUJNLTR-CVHRZJFOSA-N doxycycline monohydrate Chemical compound O.O=C1C2=C(O)C=CC=C2[C@H](C)[C@@H]2C1=C(O)[C@]1(O)C(=O)C(C(N)=O)=C(O)[C@@H](N(C)C)[C@@H]1[C@H]2O XQTWDDCIUJNLTR-CVHRZJFOSA-N 0.000 description 1
- 239000002158 endotoxin Substances 0.000 description 1
- 230000029142 excretion Effects 0.000 description 1
- RFHAOTPXVQNOHP-UHFFFAOYSA-N fluconazole Chemical compound C1=NC=NN1CC(C=1C(=CC(F)=CC=1)F)(O)CN1C=NC=N1 RFHAOTPXVQNOHP-UHFFFAOYSA-N 0.000 description 1
- 229940124307 fluoroquinolone Drugs 0.000 description 1
- 210000001035 gastrointestinal tract Anatomy 0.000 description 1
- 210000004392 genitalia Anatomy 0.000 description 1
- 244000005709 gut microbiome Species 0.000 description 1
- 230000009931 harmful effect Effects 0.000 description 1
- 229960002773 hyaluronidase Drugs 0.000 description 1
- 230000007124 immune defense Effects 0.000 description 1
- 230000028993 immune response Effects 0.000 description 1
- 208000026278 immune system disease Diseases 0.000 description 1
- 230000000951 immunodiffusion Effects 0.000 description 1
- 229940099472 immunoglobulin a Drugs 0.000 description 1
- 230000000686 immunotropic effect Effects 0.000 description 1
- 230000001771 impaired effect Effects 0.000 description 1
- 230000000977 initiatory effect Effects 0.000 description 1
- 230000010354 integration Effects 0.000 description 1
- 230000000968 intestinal effect Effects 0.000 description 1
- 230000035987 intoxication Effects 0.000 description 1
- 231100000566 intoxication Toxicity 0.000 description 1
- 238000001990 intravenous administration Methods 0.000 description 1
- 230000009545 invasion Effects 0.000 description 1
- CSSYQJWUGATIHM-IKGCZBKSSA-N l-phenylalanyl-l-lysyl-l-cysteinyl-l-arginyl-l-arginyl-l-tryptophyl-l-glutaminyl-l-tryptophyl-l-arginyl-l-methionyl-l-lysyl-l-lysyl-l-leucylglycyl-l-alanyl-l-prolyl-l-seryl-l-isoleucyl-l-threonyl-l-cysteinyl-l-valyl-l-arginyl-l-arginyl-l-alanyl-l-phenylal Chemical compound C([C@H](N)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CS)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC(C)C)C(=O)NCC(=O)N[C@@H](C)C(=O)N1CCC[C@H]1C(=O)N[C@@H](CO)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CS)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(O)=O)C1=CC=CC=C1 CSSYQJWUGATIHM-IKGCZBKSSA-N 0.000 description 1
- 235000021242 lactoferrin Nutrition 0.000 description 1
- 229940078795 lactoferrin Drugs 0.000 description 1
- 210000000265 leukocyte Anatomy 0.000 description 1
- 210000004698 lymphocyte Anatomy 0.000 description 1
- 235000010335 lysozyme Nutrition 0.000 description 1
- 229960000274 lysozyme Drugs 0.000 description 1
- 239000004325 lysozyme Substances 0.000 description 1
- 239000000463 material Substances 0.000 description 1
- 210000004877 mucosa Anatomy 0.000 description 1
- 210000003097 mucus Anatomy 0.000 description 1
- 210000000440 neutrophil Anatomy 0.000 description 1
- 229940064438 nizoral Drugs 0.000 description 1
- 239000002773 nucleotide Substances 0.000 description 1
- 125000003729 nucleotide group Chemical group 0.000 description 1
- 230000035764 nutrition Effects 0.000 description 1
- 235000016709 nutrition Nutrition 0.000 description 1
- 229960000988 nystatin Drugs 0.000 description 1
- VQOXZBDYSJBXMA-NQTDYLQESA-N nystatin A1 Chemical compound O[C@H]1[C@@H](N)[C@H](O)[C@@H](C)O[C@H]1O[C@H]1/C=C/C=C/C=C/C=C/CC/C=C/C=C/[C@H](C)[C@@H](O)[C@@H](C)[C@H](C)OC(=O)C[C@H](O)C[C@H](O)C[C@H](O)CC[C@@H](O)[C@H](O)C[C@](O)(C[C@H](O)[C@H]2C(O)=O)O[C@H]2C1 VQOXZBDYSJBXMA-NQTDYLQESA-N 0.000 description 1
- 231100000590 oncogenic Toxicity 0.000 description 1
- 230000002246 oncogenic effect Effects 0.000 description 1
- 230000005868 ontogenesis Effects 0.000 description 1
- 230000000242 pagocytic effect Effects 0.000 description 1
- 210000002741 palatine tonsil Anatomy 0.000 description 1
- 230000000803 paradoxical effect Effects 0.000 description 1
- 231100000255 pathogenic effect Toxicity 0.000 description 1
- 230000035699 permeability Effects 0.000 description 1
- 210000001539 phagocyte Anatomy 0.000 description 1
- 238000013081 phylogenetic analysis Methods 0.000 description 1
- 230000037081 physical activity Effects 0.000 description 1
- 239000013612 plasmid Substances 0.000 description 1
- 230000035935 pregnancy Effects 0.000 description 1
- 239000006041 probiotic Substances 0.000 description 1
- 230000000529 probiotic effect Effects 0.000 description 1
- 235000018291 probiotics Nutrition 0.000 description 1
- 238000004393 prognosis Methods 0.000 description 1
- 238000001959 radiotherapy Methods 0.000 description 1
- 238000011084 recovery Methods 0.000 description 1
- 230000007363 regulatory process Effects 0.000 description 1
- 230000003248 secreting effect Effects 0.000 description 1
- 230000028327 secretion Effects 0.000 description 1
- 238000012163 sequencing technique Methods 0.000 description 1
- 210000002966 serum Anatomy 0.000 description 1
- 230000035939 shock Effects 0.000 description 1
- 230000000392 somatic effect Effects 0.000 description 1
- 230000006641 stabilisation Effects 0.000 description 1
- 238000011105 stabilization Methods 0.000 description 1
- 230000000638 stimulation Effects 0.000 description 1
- 230000031068 symbiosis, encompassing mutualism through parasitism Effects 0.000 description 1
- 230000009885 systemic effect Effects 0.000 description 1
- 230000026683 transduction Effects 0.000 description 1
- 238000010361 transduction Methods 0.000 description 1
- 238000012546 transfer Methods 0.000 description 1
- 230000009466 transformation Effects 0.000 description 1
- 230000032258 transport Effects 0.000 description 1
- 238000011269 treatment regimen Methods 0.000 description 1
- 241000701161 unidentified adenovirus Species 0.000 description 1
- 241001515965 unidentified phage Species 0.000 description 1
- 210000000605 viral structure Anatomy 0.000 description 1
- 230000003612 virological effect Effects 0.000 description 1
- 235000019154 vitamin C Nutrition 0.000 description 1
- 239000011718 vitamin C Substances 0.000 description 1
- 235000019165 vitamin E Nutrition 0.000 description 1
- 239000011709 vitamin E Substances 0.000 description 1
Images


Landscapes
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Abstract
Description
Изобретение относится к микроэкологии и иммунологии и может использоваться для интегральной оценки состояния здоровья человека при прогнозировании инфекционного заболевания.The invention relates to microecology and immunology and can be used for integrated assessment of human health in predicting an infectious disease.
Реактивность организма - способность организма отвечать на воздействия внешней среды изменением своей жизнедеятельности, что обеспечивает его адаптацию к различным условиям обитания. Резистентность тесно связана с реактивностью организма, представляя собой одно из основных ее следствий и выражений. Реализация механизмов резистентности организма обеспечивается, как правило, не одним каким-либо органом или системой, а взаимодействием комплекса различных органов и физиологических систем, включая все звенья регуляторных процессов. Резистентность организма может определяться относительно стабильными свойствами различных органов, тканей и физиологических систем, в т.ч. не связанными с активными реакциями на данное воздействие. Значительные колебания индивидуальной резистентности могут быть связаны с особенностями реактивности организма во время его взаимодействия с повреждающим агентом. Резистентность может понижаться при недостатке, избытке или качественной неадекватности биологически значимых факторов (питания, двигательной активности, трудовой деятельности, информационной нагрузки и стрессовых ситуаций, различных интоксикаций, экологических факторов и др.). В формирования резистентности решающее значение занимают активные защитно-приспособительные реакции, направленные на сохранение гомеостаза при потенциально вредных воздействиях факторов внешней среды или неблагоприятных сдвигах во внутренней среде организма. Эффективность таких реакций и, следовательно, степень резистентности к различным факторам зависит от врожденных и приобретенных индивидуальных особенностей организма. Резистентность изменяется в процессе онтогенеза, причем ее возрастная динамика по отношению к различным воздействиям неодинакова, однако в целом она оказывается наиболее высокой в зрелом возрасте и снижается по мере старения организма. Различают неспецифическую и специфическую резистентность. Под неспецифической резистентностью понимают способность организма противостоять воздействию разнообразных по своей природе факторов. Специфическая резистентность характеризует высокую степень противодействия организма воздействию определенных факторов или их близких групп, устойчивость против различных болезнетворных воздействий [1].An organism’s reactivity is the body’s ability to respond to environmental influences by changing its life activity, which ensures its adaptation to various living conditions. Resistance is closely related to the reactivity of the body, representing one of its main consequences and expressions. The implementation of the mechanisms of resistance of an organism is ensured, as a rule, not by a single organ or system, but by the interaction of a complex of various organs and physiological systems, including all parts of regulatory processes. The resistance of the body can be determined by the relatively stable properties of various organs, tissues and physiological systems, including not associated with active reactions to this effect. Significant fluctuations in individual resistance can be associated with the characteristics of the reactivity of the body during its interaction with a damaging agent. Resistance can decrease with a deficiency, excess or qualitative inadequacy of biologically significant factors (nutrition, physical activity, labor, information load and stressful situations, various intoxications, environmental factors, etc.). In the formation of resistance, active protective and adaptive reactions are crucial, aimed at maintaining homeostasis under the potentially harmful effects of environmental factors or adverse shifts in the internal environment of the body. The effectiveness of such reactions and, therefore, the degree of resistance to various factors depends on the innate and acquired individual characteristics of the body. Resistance changes in the process of ontogenesis, and its age dynamics in relation to various influences is not the same, however, in general, it turns out to be the highest in adulthood and decreases as the body ages. Distinguish non-specific and specific resistance. By non-specific resistance is understood the ability of an organism to withstand the effects of factors of various nature. Specific resistance characterizes a high degree of body resistance to the influence of certain factors or their close groups, resistance to various pathogenic effects [1].
Известен способ прогнозирования частоты развития у детей острых инфекционных заболевания на первом году жизни (патент РФ №2431147) с определением на первые и пятые сутки после рождения иммунного статуса: абсолютного числа лимфоцитов, носителей маркеров дифференцировки CD3, CD4, CD8, CD19, СД56, СД95, фагоцитарный показатель, концентрации IgA, IgM, IgG и после определения индекса прогнозирования с помощью уравнения судят о вероятности возникновения того или иного количества инфекционных заболеваний.A known method for predicting the incidence of acute infectious diseases in children in the first year of life (RF patent No. 2431147) with determination of the immune status on the first and fifth days after birth: the absolute number of lymphocytes, carriers of differentiation markers CD3, CD4, CD8, CD19, SD56, SD95 , phagocytic index, concentrations of IgA, IgM, IgG, and after determining the prognosis index using the equation, they judge the likelihood of a certain number of infectious diseases.
Известен способ прогнозирования тяжести течения инфекционных заболеваний ротоглотки у детей, (патент РФ №2231073 предусматривающий определение количества секреторного иммуноглобулина А в слюне методом радиальной иммунодиффузии в геле и при значении sIgA ниже 0,4 мг/мл прогнозируют тяжелое течение заболевания.A known method for predicting the severity of infections of the oropharynx in children, (RF patent No. 2231073 providing for determining the amount of secretory immunoglobulin A in saliva by radial immunodiffusion in a gel and with a sIgA value below 0.4 mg / ml, a severe course of the disease is predicted.
Недостатком обоих способов изобретения является отсутствие микроэкологических факторов оценки состояния здоровья, учитываемых при прогнозе течения или частоты возникновения инфекционных заболеваний.The disadvantage of both methods of the invention is the lack of microecological factors for assessing the health status, taken into account when predicting the course or frequency of occurrence of infectious diseases.
Задачей настоящего изобретения является способ оценки состояния здоровья человека при прогнозировании течения инфекционного заболевания.The objective of the present invention is a method for assessing the state of human health in predicting the course of an infectious disease.
Сущность изобретения состоит в следующем:The invention consists in the following:
Для оценки состояния здоровья при прогнозировании течения инфекционного заболевания оценивают показатели микробиотопа слизистых открытых полостей. На их основе определяют степень нарушения микробиотопа слизистых открытых полостей как показатель степени нарушения микробиоценоза биотопа слизистых открытых полостей. В зависимости от полученного результата судят о состоянии здоровья человека и прогнозируют течение инфекционного заболевания. При этом, полноценное здоровье прогнозируют при отсутствии верификации возбудителя и клинических проявлений инфекционного процесса и регистрации первой или второй степени микробиоценоза биотопа слизистых открытых полостей;To assess the state of health in predicting the course of an infectious disease, the microbiotope of open mucous membranes is evaluated. On their basis, the degree of violation of the microbiotope of the mucous open cavities is determined as an indicator of the degree of violation of the microbiocenosis of the biotope of the mucous open cavities. Depending on the result, they judge the state of human health and predict the course of the infectious disease. In this case, full health is predicted in the absence of verification of the pathogen and clinical manifestations of the infectious process and registration of the first or second degree of microbiocenosis of the biotope of mucous open cavities;
- продромальный период инфекционного заболевания прогнозируют при отсутствии верификации возбудителя и клинических проявлений инфекционного процесса и регистрации третьей или четвертой степени микробиоценоза биотопа слизистых открытых полостей;- the prodromal period of an infectious disease is predicted in the absence of verification of the pathogen and clinical manifestations of the infectious process and registration of the third or fourth degree microbiocenosis of the biotope of mucous open cavities;
- благоприятное течение заболевания прогнозируют при наличии клинических проявлений инфекционного процесса и/или верификации возбудителя и регистрации третьей или четвертой степени микробиоценоза биотопа слизистых открытых полостей;- a favorable course of the disease is predicted in the presence of clinical manifestations of the infectious process and / or verification of the pathogen and registration of the third or fourth degree microbiocenosis of the biotope of mucous open cavities;
- хроническое течение заболевания прогнозируют при наличии клинических проявлений инфекционного процесса и/или верификации возбудителя и регистрации первой или второй степени микробиоценоза биотопа слизистых открытых полостей.- the chronic course of the disease is predicted in the presence of clinical manifestations of the infectious process and / or verification of the pathogen and registration of the first or second degree of microbiocenosis of the biotope of mucous open cavities.
В настоящее время накоплен большой фактический материал о роли микрофлоры в жизнедеятельности человека и в формировании его реактивности и антиинфекционной резистентности. Нормальная микрофлора способствует поддержанию необходимого барьерного уровня слизистых оболочек, кожи и образует первую линию защиты от инфекций, а также выполняет ряд других важных функций в организме человека. Изменения в видовом составе микрофлоры не только свидетельствуют о нарушении бактериального равновесия в разных микробиотопах, но и являются показателями функциональных и анатомических повреждений определенных структурно-физиологических мест организма [2]. Микробиоценоз является весьма чувствительным индикатором, реагирующим количественными и качественными изменениями на любые сдвиги внешней и внутренней среды [3]. Известно, что исследование микрофлоры организма- это высокоинформативный и доступный метод оценки состояния здоровья человека, коррелирующий с другими клиническими и лабораторными показателями. Разрабатываются региональные значения норм микрофлоры, которые отличаются от общероссийских, показана зависимость микробиоценоза от возраста. Установлено, что в процессе развития человека наблюдаются определенные критические периоды, когда на антигенное воздействие иммунная система дает неадекватный или парадоксальный ответ [4]. Было показано, что каждому периоду критического развития иммунной системы детей соответствует определенная микрофлора кишечника. При этом во всех периодах отмечается угнетение индигенной микрофлоры и увеличение условно-патогенной микрофлоры (УПМ) [5].Currently, a great deal of factual material has been accumulated on the role of microflora in human life and in the formation of its reactivity and anti-infectious resistance. Normal microflora helps maintain the necessary barrier level of mucous membranes, skin and forms the first line of defense against infections, and also performs a number of other important functions in the human body. Changes in the species composition of microflora not only indicate a violation of bacterial equilibrium in different microbiotopes, but also are indicators of functional and anatomical damage to certain structural and physiological places of the body [2]. Microbiocenosis is a very sensitive indicator that responds by quantitative and qualitative changes to any shifts in the external and internal environment [3]. It is known that the study of the microflora of the body is a highly informative and affordable method for assessing human health, correlating with other clinical and laboratory parameters. Regional values of microflora norms are being developed, which differ from the all-Russian ones, and the dependence of microbiocenosis on age is shown. It has been established that in the process of human development, certain critical periods are observed when the immune system gives an inadequate or paradoxical response to antigenic effects [4]. It was shown that each period of critical development of the children's immune system corresponds to a certain intestinal microflora. Moreover, in all periods, inhibition of indigenous microflora and an increase in conditionally pathogenic microflora (UPM) are noted [5].
Любое заболевание, по сути, является следствием нарушенного гомеостаза. Дисбиотические нарушения появляются задолго до клинических проявлений болезни и являются отражением иммунологической реактивности макроорганизма. В этой связи микрофлора является его важнейшим фактором и патологию любой локализации следует рассматривать в связи с состоянием микробиоценозов. Изменения качественного и количественного состава микрофлоры толстой кишки в виду иммуностимулирующей функции индигенной микрофлоры, в свою очередь, ведет к снижению иммунологической реактивности организма [6, 7]. В связи с этим, возникает вопрос, что является первичным: либо процесс начинается с изменения микрофлоры и ведет к развитию иммунодефицита, отражаясь на течении основной болезни, либо снижение иммунологической реактивности макроорганизма под влиянием неблагоприятных факторов среды провоцирует развитие дисбактериоза. С современных позиций нарушение нормальной микрофлоры, состояние иммунного статуса и проявление болезни рассматривается в единстве, причем роль пускового механизма в каждом конкретном случае может принадлежать любому из этих компонентов триады: дисбактериозу, иммунному статусу и патологическому процессу. Дисбактериоз может быть следствием развития иммунодефицитов или сопровождать болезнь [5]. В свете взаимообусловленности микроэкологических и иммунологических сдвигов макроорганизма актуальным являются работы по экологической иммунологии. Микроэкологические нарушения в организме человека, в определенной степени, можно считать пусковыми механизмами при нарушениях липидного обмена и патологических процессов, связанных с ними, таких как атеросклероз, желчнокаменная болезнь, функциональные расстройства органов пищеварения и другие. Микроэкологические подходы к пониманию их развития могут явиться отправной точкой создания новых методов лечения. Человеку свойственен только ему присущий микроэкологический гомеостаз, поэтому возможны и другие проявления микроэкологического кризиса. Отсутствие четкого разграничения между условным патогеном и комменсалом дает основание полагать, что неограниченная колонизация организма любым видом бактерий, способным выживать в организме человека, может приводить к развитию патологии. Ведущую роль в развитии таких осложнений играет, по-видимому, не вирулентность самого возбудителя, а состояние иммунологической реактивности организма. Так у иммунокомпрометированных лиц слабовирулентные или авирулентные микроорганизмы (кандиды и пневмоцисты) могут вызывать тяжелые и часто фатальные поражения. Ряд заболеваний, в том числе и опухолевый процесс, или цитостатическая терапия могут нарушить баланс между микробом и хозяином. Повреждение кожи, слизистых или иммунной системы при онкологическом заболевании, а также использование цитостатиков, лучевой терапии, наличие различных устройств, таких как внутривенные катетеры являются факторами риска для возникновения нозокомиальных (внутрибольничных, госпитальных) инфекций. Разнообразные неблагоприятные воздействия вызывают изменения иммунного ответа и поэтому могут влиять на качественные и количественные характеристики микробиоценозов открытых полостей. У детей, находившихся на искусственном вскармливании, аутофлора кишечника чаще вызывает эндогенные инфекционные процессы. Инфекции могут быть вызваны как нормальной эндогенной микрофлорой, так и экзогенными микроорганизмами, колонизирующими больных в процессе нахождения в клинике. Антибиотики, подавляющие анаэробную микрофлору ЖКТ, увеличивают риск последующей колонизации как УПМ, так и патогенной микрофлорой. Во взаимоотношениях макроорганизма с его микрофлорой в неблагоприятных условиях, вызванных различными воздействиями на организм (например, стресс) или на микробиоту (массивная антибиотикотерапия), симбиоз может превращаться в отношения взаимной агрессии. При этом оба участника обладают достаточным потенциалом, чтобы нанести друг другу существенный ущерб или «расчистить дорогу» для внедрения в организм настоящих патогенных микроорганизмов. В частности, эпителий может вырабатывать бактериостатические и бактерицидные ферменты (лизоцим, лактоферрин), в него начинают проникать активированные фагоцитирующие клетки (нейтрофилы). В свою очередь, это вызывает ответ в форме активации «ударного» ферментативного аппарата бактерий (нейраминидазы, гиалуронидазы), высвобождение эндотоксина и синтез прочих атрибутов вирулентности. Является доказанным фактом, что нарушение экологического баланса и возникновение дисбактериозов приводят не только к увеличению возможности заражения "официальными" патогенами, но и возникновению инфекционного заболевания, вызываемого представителями как факультативной, так и облигатной части нормальной микрофлоры [5]. В настоящее время возрастает удельный вес инфекционных заболеваний, этиологическими агентами которых являются условно-патогенные микроорганизмы (УПМ) нормальной микрофлоры человеческого организма, такие как стафилококки, стрептококки, эшерихии, серрации, клебсиеллы, энтеробактеры, протеи. Приобретение ими патогенных свойств в определенной степени обусловлено появлением у них островков патогенности (ОП). Под ОП принято понимать фрагменты DNA, размерами от 1 до 10 kb («островки») или от 10-20 до 200 kb («острова»), включающие дискретные гены вирулентности и обнаруживаемые только у патогенных микроорганизмов. Указанные фрагменты DNA отличаются от «core genome» по содержанию % G+C, как правило, фланкированы малыми прямыми нуклеотидными повторами (DR-directly repead) и часто ассоциированы с 3′ областью локусов различных транспортных RNA (tRNA). Детерминанты ОП способны распространяться среди родственных видов бактерий при конъюгации, трансдукции или трансформации. Такая мобильность ОП связана с тем, что они могут входить в состав бактериофагов, транспозонов или плазмид. Именно интеграция, стабилизация и экспрессия генов вирулентности, входящих в состав ОП, и лежит в основе формирования новых свойств, в том числе вирулентных, у родственных непатогенных видов бактерий различных таксономических групп [8]. Регистрация и нарастание инфицированности УПМ при дисбактериозах являются объективными критериями их выраженности. Следовательно, дисбактериоз - любые качественные и количественные изменения типичной для данного биотопа микрофлоры человека и животных, возникающие в результате воздействия на макро- и микроорганизм различных факторов экзогенного и эндогенного характера, влекущие за собой клинические проявления со стороны макроорганизма или являющиеся следствием каких-либо патологических процессов в организме. Дисбиоз-микробиологический дисбаланс в организме, который со временем проявляет себя местными симптомами, а затем и общими нарушениями, которые отягощают течение различных заболеваний. Дисбактериозы различной локализации, как правило, обусловлены микроэкологическими и иммунологическими нарушениями, способствующими развитию инфекционных процессов. Любой инфекционный процесс в слизистой оболочке, независимо от этиологии, развивается по одному и тому же сценарию. Первый этап - это адгезия микробов в пристеночном муцине или на эпителиальных клетках, которая обеспечивается специальными структурами возбудителя. Закрепившись, микроорганизмы начинают размножаться, что приводит к патологической колонизации слизистой - это второй этап инфекционного процесса (дисбактериоз). Следующий, третий этап инфекционного процесса - это инвазия микроорганизмов, когда они преодолевают защитный барьер слизистой оболочки и проникают в эпителиальные клетки или подлежащую ткань, вызывая при этом местную иммунную реакцию (колит, вагинит, фарингит и др.). При преодолении местного защитного барьера возможна генерализация инфекции. Патогенность отдельных видов бактерий зависит от наличия или отсутствия представителей других видов [9]. Поэтому при оценке микробиоценозов биотопов слизистых открытых полостей необходимо учитывать количественный и видовой состав как микроорганизмов, свободно располагающихся в просвете, так и адгезированных к эпителиальным поверхностям (пристеночная область).Any disease, in fact, is a consequence of impaired homeostasis. Dysbiotic disorders appear long before the clinical manifestations of the disease and are a reflection of the immunological reactivity of the macroorganism. In this regard, microflora is its most important factor and the pathology of any localization should be considered in connection with the state of microbiocenoses. Changes in the qualitative and quantitative composition of the colon microflora in view of the immunostimulating function of indigenous microflora, in turn, lead to a decrease in the immunological reactivity of the organism [6, 7]. In this regard, the question arises which is primary: either the process begins with a change in microflora and leads to the development of immunodeficiency, affecting the course of the underlying disease, or a decrease in the immunological reactivity of the macroorganism under the influence of adverse environmental factors provokes the development of dysbiosis. From modern perspectives, the disturbance of normal microflora, the state of the immune status and the manifestation of the disease are considered in unity, and the role of the triggering mechanism in each case can belong to any of these components of the triad: dysbiosis, immune status and the pathological process. Dysbacteriosis can be a consequence of the development of immunodeficiencies or accompany the disease [5]. In light of the interdependence of microecological and immunological shifts of a macroorganism, works on environmental immunology are relevant. Microecological disturbances in the human body, to a certain extent, can be considered triggering mechanisms for lipid metabolism disorders and pathological processes associated with them, such as atherosclerosis, cholelithiasis, digestive disorders and others. Microecological approaches to understanding their development may be the starting point for creating new treatment methods. Only the intrinsic microecological homeostasis is peculiar to a person; therefore, other manifestations of a microecological crisis are possible. The lack of a clear distinction between the conditional pathogen and commensal suggests that unlimited colonization of the body by any type of bacteria that can survive in the human body can lead to the development of pathology. The leading role in the development of such complications is apparently played not by the virulence of the pathogen itself, but by the state of the immunological reactivity of the organism. So in immunocompromised individuals, weakly virulent or avirulent microorganisms (candida and pneumocysts) can cause severe and often fatal lesions. A number of diseases, including the tumor process, or cytostatic therapy can upset the balance between the microbe and the host. Damage to the skin, mucous membranes or the immune system in cancer, as well as the use of cytostatics, radiation therapy, the presence of various devices, such as intravenous catheters, are risk factors for nosocomial (nosocomial, hospital) infections. A variety of adverse effects cause changes in the immune response and therefore can affect the qualitative and quantitative characteristics of the microbiocenoses of open cavities. In children who were breast-fed, intestinal autoflora often causes endogenous infectious processes. Infections can be caused both by normal endogenous microflora and by exogenous microorganisms that colonize patients in the process of being in the clinic. Antibiotics that suppress the anaerobic microflora of the gastrointestinal tract increase the risk of subsequent colonization of both UPM and pathogenic microflora. In the relationship of a macroorganism with its microflora under adverse conditions caused by various effects on the body (e.g. stress) or on microbiota (massive antibiotic therapy), symbiosis can turn into a relationship of mutual aggression. At the same time, both participants have sufficient potential to cause significant damage to each other or to “clear the way” for the introduction of real pathogenic microorganisms into the body. In particular, the epithelium can produce bacteriostatic and bactericidal enzymes (lysozyme, lactoferrin), activated phagocytic cells (neutrophils) begin to penetrate into it. In turn, this causes a response in the form of activation of the “shock” enzyme apparatus of bacteria (neuraminidase, hyaluronidase), the release of endotoxin and the synthesis of other attributes of virulence. It is a proven fact that the violation of the ecological balance and the occurrence of dysbiosis lead not only to increase the possibility of infection with "official" pathogens, but also to the occurrence of an infectious disease caused by representatives of both the optional and obligate parts of normal microflora [5]. At present, the proportion of infectious diseases is increasing, the etiological agents of which are opportunistic microorganisms (UPM) of the normal microflora of the human body, such as staphylococci, streptococci, Escherichia, serrations, Klebsiella, enterobacteria, and Proteus. The acquisition of pathogenic properties to a certain extent is due to the appearance of pathogenicity islands (OP) in them. By OD, it is customary to understand DNA fragments ranging in size from 1 to 10 kb ("islands") or from 10-20 to 200 kb ("islands"), including discrete virulence genes and found only in pathogenic microorganisms. These DNA fragments differ from the “core genome” in% G + C content, as a rule, are flanked by small direct nucleotide repeats (DR-directly repead) and are often associated with the 3 ′ region of loci of different transport RNAs (tRNAs). The determinants of OP are able to spread among related bacterial species during conjugation, transduction, or transformation. Such mobility of OP is due to the fact that they can be part of bacteriophages, transposons or plasmids. It is the integration, stabilization and expression of virulence genes that make up the OP that underlies the formation of new properties, including virulent ones, in related non-pathogenic bacterial species of various taxonomic groups [8]. The registration and increase in the infection of UPM with dysbiosis are objective criteria for their severity. Therefore, dysbacteriosis is any qualitative and quantitative changes in the microflora of humans and animals that are typical of a given biotope that arise as a result of exposure to a macro- and microorganism of various exogenous and endogenous factors, entailing clinical manifestations by the macroorganism, or resulting from any pathological processes in the body. Dysbiosis is a microbiological imbalance in the body, which over time manifests itself as local symptoms, and then general disorders that aggravate the course of various diseases. Dysbacterioses of various localization, as a rule, are caused by microecological and immunological disorders that contribute to the development of infectious processes. Any infectious process in the mucous membrane, regardless of etiology, develops according to the same scenario. The first stage is the adhesion of microbes in the parietal mucin or on epithelial cells, which is provided by special structures of the pathogen. Having fixed themselves, microorganisms begin to multiply, which leads to pathological colonization of the mucosa - this is the second stage of the infectious process (dysbiosis). The next, third stage of the infectious process is the invasion of microorganisms, when they overcome the protective barrier of the mucous membrane and penetrate the epithelial cells or underlying tissue, causing a local immune response (colitis, vaginitis, pharyngitis, etc.). When overcoming the local protective barrier, generalization of the infection is possible. The pathogenicity of certain types of bacteria depends on the presence or absence of representatives of other species [9]. Therefore, when assessing the microbiocenoses of biotopes of mucous open cavities, it is necessary to take into account the quantitative and species composition of both microorganisms freely located in the lumen and adhered to epithelial surfaces (parietal region).
Микробиоценоз биотопов слизистых открытых полостей макроорганизма - динамическая микроэкологическая система, компонентами которой является макроорганизм, его микрофлора (совокупность типичных для определенного биологического вида и конкретного биотопа ассоциаций микроорганизмов) и окружающая среда, характеризующаяся способностью к саморегуляции, которая является интегральной частью организма («дополнительным органом») хозяина и местного иммунитета, в частности, и выполняет или регулирует многочисленные функции макроорганизма. Показатели состояния микробиоценозов биотопов слизистых открытых полостей отражают состояние реактивности макроорганизма - способность организма отвечать на воздействия внешней среды изменением своей жизнедеятельности, что обеспечивает его адаптацию к различным условиям обитания. Слизистые открытых полостей макроорганизма представляют собой единую систему. Состояние микробиоценоза и барьерной функции слизистых можно оценивать по выраженности колонизационной резистентности (КР) открытых полостей организма - физиологический феномен - способности микрофлоры и макроорганизма в кооперации защищать экосистему слизистых от патогенных микроорганизмов.The microbiocenosis of biotopes of mucous open cavities of a macroorganism is a dynamic microecological system, the components of which are the macroorganism, its microflora (a set of associations of microorganisms typical for a particular biological species and a particular biotope) and an environment characterized by the ability to self-regulation, which is an integral part of the body ("additional organ" ) the host and local immunity, in particular, and performs or regulates the numerous functions of the macroorganism. Indicators of the state of microbiocenoses of biotopes of mucous open cavities reflect the state of reactivity of a macroorganism - the body's ability to respond to environmental influences by changing its life activity, which ensures its adaptation to various living conditions. The mucous open cavities of a macroorganism represent a single system. The state of microbiocenosis and the barrier function of the mucous membranes can be assessed by the severity of colonization resistance (CR) of the open cavities of the body - a physiological phenomenon - the ability of microflora and macroorganisms in cooperation to protect the mucous ecosystem from pathogenic microorganisms.
Оценка микробиоценоза биотопа слизистых открытых полостей может быть проведена согласно методологии, изложенной в пособии утвержденном Учебно-методическим объединением (10), а также согласно новой медицинской технологии (11). Заявляемое изобретение подтверждается на следующих примерах.The evaluation of the microbiocenosis of the biotope of mucous open cavities can be carried out according to the methodology described in the manual approved by the Educational and Methodical Association (10), as well as according to new medical technology (11). The invention is confirmed by the following examples.
Пример 1. Оценка состояния здоровья по состоянию микробиоценоза биотопа ротоглотки при бронхитах у детей.Example 1. Assessment of the health status of the microbiocenosis of the oropharynx biotope for bronchitis in children.
Клинически обследовано 194 ребенка в возрасте от 3 до 10 лет: из них 51 ребенок - с острым и 15 детей - с хроническим бронхитом (средний возраст больных детей - 4,0±2,2 года); группу контроля составили 128 клинически здоровых детей в возрасте 3-10 лет (средний возраст - 5,0±2,9 года). Всего было обследовано 49 мальчиков и 47 девочек. Оценку микробиоценоза биотопа ротоглотки проводили согласно методологии, изложенной в пособии утвержденном Учебно-методическим объединением (10).Clinically examined 194 children aged 3 to 10 years: of which 51 children - with acute and 15 children - with chronic bronchitis (the average age of sick children is 4.0 ± 2.2 years); the control group consisted of 128 clinically healthy children aged 3-10 years (mean age - 5.0 ± 2.9 years). A total of 49 boys and 47 girls were examined. The evaluation of the microbiocenosis of the oropharynx biotope was carried out according to the methodology described in the manual approved by the Educational and Methodological Association (10).

При бронхитах у детей при анализе ассоциации патогенных вирусных и внутриклеточных бактериальных агентов выявлено (табл. 1), что частота инфицированности ими была наивысшей при остром бронхите и достоверные различия по χ2 по сравнению с хроническим бронхитом и клинически здоровыми пациентами выявлены при инфицировании аденовирусами (P<0,05). Различия в обсемененности слизистой задней стенки глотки (ЗСГ) индигенными микроорганизмами в контрольной группе и больных бронхитами детей не достоверны как по количественному содержанию, так и по частоте встречаемости; однако они превышали показатели нормоценоза. По частоте выявляемости УПМ при бронхитах у детей выявлены достоверные различия (χ2) по частоте инфицирования S. aureus и грибами рода Candida при остром бронхите по сравнению с хроническим бронхитом и клинически здоровыми пациентами (p<0,05). Увеличение интенсивности колонизации задней стенки глотки УПМ также достоверно выше было при остром бронхите по сравнению с хроническим бронхитом и клинически здоровыми пациентами (p<0,05). Высеваемость УПМ в титре 6 lg КОЕ/г и выше может свидетельствовать о приобретении ею вирулентности.In bronchitis in children, when analyzing the association of pathogenic viral and intracellular bacterial agents, it was revealed (Table 1) that the frequency of infection with them was highest in acute bronchitis and significant differences in χ 2 compared with chronic bronchitis and clinically healthy patients were detected with infection with adenoviruses (P <0.05). Differences in the colonization of the mucous membrane of the posterior pharyngeal wall (CHH) by indigenous microorganisms in the control group and children with bronchitis of children are not significant both in quantitative content and in frequency of occurrence; however, they exceeded the values of normocenosis. According to the frequency of detection of UPM in bronchitis in children, significant differences (χ 2 ) were revealed in the frequency of infection with S. aureus and fungi of the genus Candida in acute bronchitis compared with chronic bronchitis and clinically healthy patients (p <0.05). The increase in the intensity of colonization of the posterior pharyngeal wall of the UPM was also significantly higher in acute bronchitis compared with chronic bronchitis and clinically healthy patients (p <0.05). Inoculation of UPM in a titer of 6 lg CFU / g and above may indicate the acquisition of virulence by it.
У 13 детей было выявлено (табл. 2) достоверное (p<0,05) увеличение уровня IgM в слюне. Это свидетельствует о том, что на начальной стадии заболевания при остром бронхите на слизистых идет активная стимуляция местного иммунного ответа. Значения IgM были 1,0±0,8 мкг/мг общего белка. Отличительной особенностью детей с острым бронхитом являлась более высокая, чем у здоровых, концентрация IgG в слюне, которая составила 8,6±5,6 мкг/мг общего белка. Достоверное (p<0,001) повышение уровня IgG в слюне было выявлено у 32 больных детей. Это говорит о прямой взаимосвязи количества IgG в слюне со степенью выраженности воспалительного процесса, которое имеет место при остром бронхите, так как относительно высокие концентрации уровня IgG в слюне обусловлены просачиванием IgG плазменного происхождения через поверхность воспаленного эпителия.In 13 children, a significant (p <0.05) increase in the level of IgM in saliva was revealed (Table 2). This suggests that at the initial stage of the disease with acute bronchitis on the mucous membranes, there is an active stimulation of the local immune response. IgM values were 1.0 ± 0.8 μg / mg total protein. A distinctive feature of children with acute bronchitis was a higher than normal concentration of IgG in saliva, which amounted to 8.6 ± 5.6 μg / mg of total protein. A significant (p <0.001) increase in the level of IgG in saliva was detected in 32 sick children. This suggests a direct relationship between the amount of IgG in saliva and the severity of the inflammatory process that occurs in acute bronchitis, since relatively high concentrations of IgG in saliva are due to leakage of plasma-derived IgG through the surface of the inflamed epithelium.

У 28 детей выявлено достоверное (p<0,001) повышение уровня sIgA, которое составило 29,0±25,6 мкг/мг общего белка и у 5 детей было обнаружено достоверное (p<0,05) повышение уровня IgA в слюне, которое составило 0,5±0,2 мкг/мг общего белка. Это может указывать на возможность активирующего действия вирусов, бактерий и внутриклеточных патогенов на синтез иммуноглобулинов, так как данные иммуноглобулины в слизи действуют как первая линия иммунной защиты слизистых, нейтрализующая патогены. Особенно их количество увеличивается при возникновении острой формы бронхита. Также достоверно (p<0,001) увеличивался уровень свободного секреторного компонента (sc) - у 21 больного ребенка по сравнению с детьми контрольной группы. Он составил 35,2±25,0 мкг/мг общего белка. Показатели нарушения проницаемости слизистой ротоглотки у детей с острым бронхитом также были достоверно увеличены по сравнению со здоровыми детьми, у которых соотношение sIgA/IgG слюны составляло 1,04. Соотношение sIgA/IgG слюны у детей с острым бронхитом составляло 3,7 (p<0,001), а соотношение sIgA/альбумин увеличивалось до 0,05 (p<0,001) по сравнению со здоровыми детьми, у которых оно составляло 0,01. Выраженное увеличение показателей соотношений sIgA/IgG, sIgA/альбумин и содержания альбумина указывает на местный синтез иммуноглобулинов и одновременное поступление IgG и IgM из сыворотки крови, а выявление sIgA и sc обусловлено их местным синтезом.In 28 children, a significant (p <0.001) increase in sIgA level was detected, which amounted to 29.0 ± 25.6 μg / mg of total protein, and in 5 children a significant (p <0.05) increase in IgA level in saliva was found, which amounted to 0.5 ± 0.2 μg / mg total protein. This may indicate the possibility of the activating effect of viruses, bacteria and intracellular pathogens on the synthesis of immunoglobulins, since these immunoglobulins in mucus act as the first line of mucosal immune defense that neutralizes pathogens. Especially their number increases when an acute form of bronchitis occurs. The level of the free secretory component (sc) also increased significantly (p <0.001) - in 21 sick children compared with children in the control group. It amounted to 35.2 ± 25.0 μg / mg of total protein. Indicators of violation of the permeability of the mucous membrane of the oropharynx in children with acute bronchitis were also significantly increased in comparison with healthy children, in which the sIgA / IgG saliva ratio was 1.04. The salivary sIgA / IgG ratio in children with acute bronchitis was 3.7 (p <0.001), and the sIgA / albumin ratio increased to 0.05 (p <0.001) compared with healthy children in whom it was 0.01. A marked increase in the ratios of sIgA / IgG, sIgA / albumin and albumin content indicates a local synthesis of immunoglobulins and simultaneous intake of IgG and IgM from blood serum, and the detection of sIgA and sc is due to their local synthesis.
При сопоставлении частоты определения типа микробиоценоза биотопа (табл. 3) ротоглотки у детей с острым и хроническим бронхитом по сравнению с клинически здоровыми детьми (нормоценоз - у 48,1% пациентов, промежуточный тип - у 44,4% пациентов, дисбиоз - у 7,4% пациентов) выявлены достоверные различия. При остром бронхите нормоценоз регистрировался у 21,6% (p<0,05), промежуточный тип микробиоценоза - у 11,8% (р<0,01), дисбиоз - у 35,3% (р<0,05), выраженный воспалительный процесс - у 31,4% (р<0,01) пациентов. При хроническом бронхите нормоценоз регистрировался у 20,0% (р<0,05), промежуточный тип микробиоценоза - у 20,0% (р<0,01), дисбиоз- у 33,3% (р<0,05), выраженный воспалительный процесс - у 26,7% (р<0,01) пациентов. Достоверных различий по типу микробиоценоза ротоглотки между острым и хроническим бронхитом не выявлено. Патогенетическое действие ассоциации обусловлено суммированием воздействий каждого из ассоциатов с разнонаправленными механизмами их влияния на клетки макроорганизма.When comparing the frequency of determining the type of biotope microbiocenosis (Table 3) of the oropharynx in children with acute and chronic bronchitis compared with clinically healthy children (normocenosis in 48.1% of patients, the intermediate type in 44.4% of patients, dysbiosis in 7 , 4% of patients) revealed significant differences. In acute bronchitis, normocenosis was recorded in 21.6% (p <0.05), an intermediate type of microbiocenosis in 11.8% (p <0.01), dysbiosis in 35.3% (p <0.05), severe inflammatory process - in 31.4% (p <0.01) of patients. In chronic bronchitis, normocenosis was recorded in 20.0% (p <0.05), an intermediate type of microbiocenosis in 20.0% (p <0.01), dysbiosis in 33.3% (p <0.05), severe inflammatory process - in 26.7% (p <0.01) of patients. There were no significant differences in the type of oropharyngeal microbiocenosis between acute and chronic bronchitis. The pathogenetic effect of the association is due to the summation of the effects of each of the associates with differently directed mechanisms of their influence on the cells of the macroorganism.
У клинически здоровых детей: I или II тип (степень) микробиоценоза биотопа задней стенки глотки (табл. 3) превалирует, выявление у них III и IV типов микробиценоза биотопа задней стенки глотки свидетельствует о продромальном периоде заболевания инфекционного заболевания (продромальном состоянии макроорганизма). При остром бронхите: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки превалирует (благоприятное течение), выявление I или II типа (степени) микробиоценоза биотопа задней стенки глотки (неблагоприятное течение) свидетельствует об угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса. При хроническом бронхите: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки (благоприятное течение) указывает на обострение инфекционного процесса, выявление I или II типа (степени) микробиоценоза биотопа задней стенки (неблагоприятное течение) свидетельствует об угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса.In clinically healthy children: I or II type (degree) of the microbiocenosis of the biotope of the posterior pharyngeal wall (Table 3) prevails; the identification of the III and IV types of microbiocenosis of the biotope of the posterior pharyngeal wall indicates the prodromal period of the disease of the infectious disease (prodromal state of the macroorganism). In acute bronchitis: III or IV type (degree) of the microbiocenosis of the biotope of the posterior pharyngeal wall prevails (favorable course), the identification of I or II type (degree) of the microbiocenosis of the biotope of the posterior pharyngeal wall (unfavorable course) indicates the suppression of anti-infectious resistance and possible chronicity of the infectious process. In chronic bronchitis: III or IV type (degree) of microbiocenosis of the biotope of the posterior pharyngeal wall (favorable course) indicates an aggravation of the infectious process, identification of I or II type (degree) of microbiocenosis of the biotope of the posterior pharyngeal (unfavorable course) indicates inhibition of anti-infectious resistance and possible chronicity infectious process.

При проведении терапии установление степени нарушений микробиоценоза биотопа задней стенки глотки повышает информативность оценки ее эффективности за счет выявления механизмов ее лечебного эффекта: при клинической эффективности проводимой терапии регистрировался переход к показателям физиологической нормы - выявлялись I или II типы (степени) микробиоценоза биотопа задней стенки глотки; продолжение регистрации у части больных III и IV типов микробиоценоза биотопа задней стенки глотки указывало на необходимость продолжения лечения.During therapy, the degree of disturbance of the microbiocenosis of the biotope of the posterior pharyngeal wall increases the information content of assessing its effectiveness by identifying the mechanisms of its therapeutic effect: during the clinical effectiveness of the therapy, a transition to the physiological norm was recorded - I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall were detected; continued registration in some patients of types III and IV of the microbiocenosis of the biotope of the posterior pharyngeal wall indicated the need for continued treatment.
Пример 2. Оценка состояния здоровья по состоянию микробиоценоза биотопа ротоглотки при респираторной патологии.Example 2. Assessment of the health status of the microbiocenosis of the oropharynx biotope for respiratory pathology.
Обследован 351 ребенок в возрасте от 2 месяцев до 15 лет (в том числе: клинически здоровые дети - 128, острый тонзиллит (ангина) - 58, ОРВИ - 128, пневмония - 20, инфекционный мононуклеоз с гнойно-воспалительным поражением ротоглотки - 47). Оценку микробиоценоза биотопа ротоглотки проводили согласно методологии, изложенной в пособии утвержденном Учебно-методическим объединением (10).351 children aged 2 months to 15 years were examined (including: clinically healthy children - 128, acute tonsillitis (tonsillitis) - 58, acute respiratory viral infections - 128, pneumonia - 20, infectious mononucleosis with purulent-inflammatory lesions of the oropharynx - 47). The evaluation of the microbiocenosis of the oropharynx biotope was carried out according to the methodology described in the manual approved by the Educational and Methodological Association (10).
Постоянная (облигатная) микрофлора данного биотопа в основном представлена альфа- и гамма-гемолитическими стрептококками (105-106 КОЕ/мл) и нейссериями (102-104 КОЕ/мл). Добавочную группу составляют стафилококки, коринебактерии и гемофилы, выделяемые у 26,9-46,2% здоровых детей, в количестве 101-104 КОЕ/мл. К случайным (транзиторным) микроорганизмам отнесены Bacillus, грибы рода Candida, Micrococcus, синегнойная палочка, грамотрицательные энтеробактерии в количестве не выше 101-102 КОЕ/мл, в 1,9-25,0%). У подавляющего числа здоровых детей (99%) на задней стенке глотки (ЗСГ) был зарегистрирован рост альфа-гемолитического стрептококка в ассоциации с нейссериями. Причем у половины из них другие виды микробов не обнаруживались. При гнойном или катаральном воспалительном процессе в ротоглотке обнаружено угнетение облигатной ассоциации альфа-гемолитического стрептококка и нейссерий, образующих защитную биопленку. Дисбиоз локуса развивался в 75-100% случаев. Он имел определенные особенности в зависимости от характера инфекционного процесса. Наиболее выраженное угнетение пролиферации облигатных бактерий было обусловлено местным гнойно-воспалительным процессом при ангине и системным поражением при пневмонии (рис. 1). Именно при данной патологии чаще всего отсутствовали микробы, выделялись монокультуры или ассоциации микроорганизмов, состоящие только из добавочных и/или транзиторных представителей с высокой вероятностью их этиологической значимости, обнаруживались отрицательные посевы (рис. 2). Наиболее устойчивым компонентом облигатной ассоциации был стрептококк, отсутствие нейссерий либо снижение их количества наблюдалось значительно чаще.The constant (obligate) microflora of this biotope is mainly represented by alpha and gamma hemolytic streptococci (10 5 -10 6 CFU / ml) and neysseries (10 2 -10 4 CFU / ml). An additional group is made up of staphylococci, corynebacteria and hemophils, excreted in 26.9-46.2% of healthy children, in an amount of 10 1 -10 4 CFU / ml. Random (transient) microorganisms included Bacillus, fungi of the genus Candida, Micrococcus, Pseudomonas aeruginosa, gram-negative enterobacteria in an amount not exceeding 10 1 -10 2 CFU / ml, 1.9-25.0%). In the vast majority of healthy children (99%), an increase in alpha-hemolytic streptococcus in association with neysseries was recorded on the posterior pharyngeal wall (CHH). Moreover, half of them did not show other types of microbes. With a purulent or catarrhal inflammatory process in the oropharynx, inhibition of the obligate association of alpha-hemolytic streptococcus and neisseria, forming a protective biofilm, was found. Locus dysbiosis developed in 75-100% of cases. He had certain features depending on the nature of the infectious process. The most pronounced inhibition of obligate bacteria proliferation was due to local purulent-inflammatory process in tonsillitis and systemic lesion in pneumonia (Fig. 1). It was with this pathology that microbes were most often absent, monocultures or associations of microorganisms were isolated, consisting only of additional and / or transient representatives with a high probability of their etiological significance, negative crops were detected (Fig. 2). The most stable component of obligate association was streptococcus, the absence of neysseries or a decrease in their number was observed much more often.
Сравнительный анализ полученных результатов обнаружил достоверные различия в состоянии микроэкологии задней стенки глотки в группах клинически здоровых детей и пациентов с респираторной патологией (табл. 1). Инициация инфекционного процесса респираторными вирусами способствовала преимущественной пролиферации грамотрицательных бактерий (особенно клебсиеллы) в больших количествах (более 104 КОЕ/мл), а также их ассоциаций (р=0,000, рис. 2, табл. 1.). Синегнойная палочка выделялась только у часто болеющих детей (ЧБД) либо больных пневмонией. Лечение в стационаре способствовало нарастанию частоты обнаружения грамотрицательных микробов в 2-3 раза вне зависимости от этиологии инфекционного процесса. Обнаружение грамотрицательных бактерий у клинически здоровых детей являлось следствием перенесенной ОРВИ (20% против 0, р<0,001) и сохранялось до двух месяцев. Наиболее часто грамотрицательные бактерии высевались со слизистой ротоглотки у детей первого года жизни (р=0,002) или часто болеющих (р=0,004). Пролиферация грибов рода Candida, особенно в больших количествах (более 102 КОЕ/мл), была характерна для больных инфекционным мононуклеозом, пневмонией, ЧБД - особенно младших возрастных групп (р=0,000), активировалась на фоне антибактериальной терапии и расценивалась как неблагоприятный фактор, поскольку отсутствовала у здоровых детей из группы эпизодически болеющих.A comparative analysis of the results found significant differences in the state of microecology of the posterior pharyngeal wall in groups of clinically healthy children and patients with respiratory pathology (Table 1). The initiation of the infectious process by respiratory viruses facilitated the preferential proliferation of gram-negative bacteria (especially Klebsiella) in large quantities (more than 10 4 CFU / ml), as well as their associations (p = 0,000, Fig. 2, Table 1.). Pseudomonas aeruginosa was isolated only in frequently ill children (FBI) or in patients with pneumonia. Inpatient treatment contributed to an increase in the detection rate of gram-negative microbes by 2-3 times, regardless of the etiology of the infectious process. The detection of gram-negative bacteria in clinically healthy children was the result of acute respiratory viral infections (20% versus 0, p <0.001) and lasted up to two months. Most often, gram-negative bacteria were seeded from the mucous membrane of the oropharynx in children of the first year of life (p = 0.002) or often sick (p = 0.004). The proliferation of Candida fungi, especially in large quantities (more than 10 2 CFU / ml), was characteristic of patients with infectious mononucleosis, pneumonia, FBI - especially younger age groups (p = 0,000), was activated against antibiotic therapy, and was regarded as an unfavorable factor, since it was absent in healthy children from the group of episodically ill.

Стафилококки, в том числе S. aureus, на слизистой ротоглотки с равной частотой встречались у здоровых и больных детей (за исключением пациентов с пневмонией, у которых они обнаруживались достоверно реже). Чаще S. aureus (47,4 против 9,4%, р<0,01) высевался при гнойно-воспалительном процессе в ротоглотке у детей с массивными наложениями на миндалинах или сопутствующими гнойными очагами инфекции. Назначение антибактериальной терапии не снижало частоту выделения и среднюю обсемененность S. aureus после лечения (22% и 17,8%, 4,17±0,52 и 5,06±0,55 lg КОЕ/мл). На наш взгляд, его обнаружение на слизистой ротоглотки не должно рассматриваться как однозначное показание к лечению при отсутствии клинических признаков болезни либо при инфекционном процессе, если одновременно присутствуют облигатные бактерии. Значение следует придавать обнаружению монокультуры стафилококка, особенно S. aureus, при условии наличия гнойно-воспалительного процесса в ротоглотке. Установлено, что отсутствие альфа-гемолитических стрептококков и/или нейссерий, обнаружение синегнойной палочки, грибов рода Candida и спорообразующих анаэробов, а также грамотрицательных бактерий нескольких видов или их монокультур является признаком глубокого дисбиоза и требует внимания педиатра. Оценка выраженности дисбиоза ротоглотки у детей, не имеющих признаков острой инфекции на момент обследования, должна проводиться с учетом клинического состояния пациентов их преморбидного состояния и анамнеза. Внимание следует уделять частоте эпизодов ОРВИ в году, срокам и тяжести последнего заболевания, а также наличию хронической патологии ЛОР-органов, поскольку именно наличие этих клинических признаков коррелировало с глубиной дисбиотических нарушений в ротоглотке.Staphylococci, including S. aureus, on the mucous membrane of the oropharynx were found with equal frequency in healthy and sick children (with the exception of patients with pneumonia, in which they were detected significantly less often). More often S. aureus (47.4 versus 9.4%, p <0.01) was sown during a purulent-inflammatory process in the oropharynx in children with massive overlays on the tonsils or concomitant purulent foci of infection. The administration of antibacterial therapy did not reduce the frequency of excretion and the average contamination of S. aureus after treatment (22% and 17.8%, 4.17 ± 0.52 and 5.06 ± 0.55 log CFU / ml). In our opinion, its detection on the mucous membrane of the oropharynx should not be considered as an unambiguous indication for treatment in the absence of clinical signs of the disease or in the infectious process if obligate bacteria are present at the same time. Importance should be given to the detection of staphylococcus monoculture, especially S. aureus, provided that there is a purulent-inflammatory process in the oropharynx. It was established that the absence of alpha-hemolytic streptococci and / or neisseria, the detection of Pseudomonas aeruginosa, Candida fungi and spore-forming anaerobes, as well as gram-negative bacteria of several species or their monocultures is a sign of deep dysbiosis and requires the attention of a pediatrician. Assessment of the severity of oropharyngeal dysbiosis in children who do not have signs of acute infection at the time of the examination should be carried out taking into account the clinical condition of patients with their premorbid state and history. Attention should be paid to the frequency of acute respiratory viral infections per year, the timing and severity of the last disease, as well as the presence of chronic pathology of ENT organs, since it is the presence of these clinical signs that correlated with the depth of dysbiotic disorders in the oropharynx.
В состав комплексного лечения и реабилитации пациентов включались иммунотропные средства. В качестве одного из современных иммуномодуляторов использован препарат Кипферон® суппозитории для вагинального или ректального введения. Кипферон® представляет собой композицию из комплексного иммуноглобулинового препарата (КИП) с высоким содержанием специфических IgG, IgA и IgM и рекомбинантного человеческого IFN-α-2b. Содержащийся в препарате рекомбинантный человеческий IFN-α-2b вызывает активацию местного иммунитета, позволяет эффективно устранять очаги воспаления, а КИП - уменьшает количество УПМ и устойчиво восстанавливает нормальную микрофлору, как минимум на протяжении 2-3 месяцев. У детей с ОРВИ, получавших Кипферон®, после лечения в 3 раза снизилась частота высева S. aureus (от 33,3% до 10%, р<0,05). Не отмечено угнетения облигатных микроорганизмов. В 2 раза реже регистрировалась транзиторная микрофлора. В группе сравнения, в динамике лечения, возросло число несвойственных для данного биотопа микроорганизмов, в том числе выявлялись ранее отсутствовавшие гемолизирующая кишечная палочка и грибы рода Candida. У больных тонзиллитом после лечения в 6 раз уменьшилась частота высева S. aureus (от 20% до 3,3%, р<0,05), реже (6,6% против 24,2%, р<0,05), чем в контроле, обнаруживались грамотрицательные энтеробактерии. У больных инфекционным мононуклеозом лечение Кипфероном® способствовало улучшению микробиологических показателей, в том числе снижению числа детей с высоким уровнем (3-6) микробных ассоциантов на слизистой ротоглотки, элиминации S. aureus (от 53,3% до 23,1%), грибов рода Candida, бета-гемолитического стрептококка группы А (от 20% до 0%, р<0,05).The complex treatment and rehabilitation of patients included immunotropic drugs. Kipferon® suppositories for vaginal or rectal administration were used as one of the modern immunomodulators. Kipferon® is a composition of a complex immunoglobulin preparation (CIP) with a high content of specific IgG, IgA and IgM and recombinant human IFN-α-2b. The recombinant human IFN-α-2b contained in the preparation activates local immunity, effectively eliminates foci of inflammation, and CIP reduces the number of UPM and stably restores normal microflora for at least 2-3 months. In children with acute respiratory viral infections who received Kipferon®, after treatment, the frequency of seeding of S. aureus decreased 3 times (from 33.3% to 10%, p <0.05). No inhibition of obligate microorganisms was noted. Transient microflora was registered 2 times less frequently. In the comparison group, in the treatment dynamics, the number of microorganisms unusual for a given biotope increased, including previously absent hemolytic Escherichia coli and fungi of the genus Candida. In patients with tonsillitis after treatment, the frequency of seeding of S. aureus decreased by 6 times (from 20% to 3.3%, p <0.05), less often (6.6% against 24.2%, p <0.05), than in the control, gram-negative enterobacteria were detected. In patients with infectious mononucleosis, treatment with Kipferon® improved microbiological parameters, including a decrease in the number of children with a high level (3-6) of microbial associates in the oropharynx, elimination of S. aureus (from 53.3% to 23.1%), fungi genus Candida, beta-hemolytic group A streptococcus (20% to 0%, p <0.05).
У клинически здоровых детей: I или II тип (степень) микробиоценоза биотопа задней стенки глотки (табл. 2) превалирует, выявление у них III и IV типов микробиоценоза биотопа задней стенки глотки может рассматриваться как маркер продромального периода инфекционного заболевания. При остром ОРВИ: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки (благоприятное течение), выявление I или II типов (степеней) микробиоценоза биотопа задней стенки глотки за счет вирусного компонента заболевания (неблагоприятное течение) свидетельствует о угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса. При тонзиллите: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки превалирует (благоприятное течение), выявление I или II типов (степеней) микробиоценоза биотопа задней стенки глотки (неблагоприятное течение) свидетельствует о угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса. При пневмонии: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки превалирует (благоприятное течение), выявление I или II типов (степеней) микробиоценоза биотопа задней стенки глотки (неблагоприятное течение) свидетельствует об угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса. При инфекционном мононуклеозе: III или IV тип (степень) микробиоценоза биотопа задней стенки глотки превалирует (благоприятное течение), выявление I или II типов (степеней) микробиоценоза биотопа задней стенки глотки (неблагоприятное течение) свидетельствует о угнетении антиинфекционной резистентности и возможной хронизации инфекционного процесса.In clinically healthy children: I or II type (degree) of the microbiocenosis of the biotope of the posterior pharyngeal wall (Table 2) prevails; the identification of the III and IV types of microbiocenosis of the biotope of the posterior pharyngeal wall can be considered as a marker of the prodromal period of the infectious disease. In acute acute respiratory viral infections: III or IV type (degree) of microbiocenosis of the biotope of the posterior pharyngeal wall (favorable course), identification of I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall due to the viral component of the disease (unfavorable course) indicates inhibition of anti-infection resistance and possible chronicity of the infectious process. In tonsillitis: III or IV type (degree) of microbiocenosis of the biotope of the posterior pharyngeal wall prevails (favorable course), identification of I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall (unfavorable course) indicates inhibition of anti-infectious resistance and possible chronicity of the infectious process. In pneumonia: III or IV type (degree) of microbiocenosis of the biotope of the posterior pharyngeal wall prevails (favorable course), identification of I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall (unfavorable course) indicates inhibition of anti-infection resistance and possible chronicity of the infectious process. In infectious mononucleosis: III or IV type (degree) of microbiocenosis of the biotope of the posterior pharyngeal wall prevails (favorable course), identification of I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall (unfavorable course) indicates the suppression of anti-infectious resistance and possible chronicity of the infectious process.

![]()
![]()
При проведении терапии установление степени нарушений микробиоценоза биотопа-задней стенки глотки повышает информативность оценки ее эффективности за счет выявления механизмов ее лечебного эффекта: при клинической эффективности проводимой терапии регистрировался переход к показателям физиологической нормы - выявлялись I или II типы (степени) микробиоценоза биотопа задней стенки глотки; продолжение регистрации у части больных III и IV типов микробиоценоза биотопа задней стенки глотки указывало на необходимость продолжения лечения.During therapy, establishing the degree of microbiocenosis of the biotope-posterior pharyngeal wall increases the informativeness of assessing its effectiveness by identifying the mechanisms of its therapeutic effect: during the clinical effectiveness of the therapy, a transition to physiological norm indicators was detected - I or II types (degrees) of microbiocenosis of the biotope of the posterior pharyngeal wall were detected ; continued registration in some patients of types III and IV of the microbiocenosis of the biotope of the posterior pharyngeal wall indicated the need for continued treatment.
Пример 3. Оценка состояния здоровья по состоянию микробиоценоза биотопа влагалища при уреаплазмозе.Example 3. Assessment of the health status of the microbiocenosis of the biotope of the vagina with ureaplasmosis.
Обследовано 50 женщин с установленной уреаплазменной моно- и микст-инфекцией. Лечение больных I группы (25 пациентов) включало только антибактериальные препараты широкого спектра действия (тиберал, доксициклин, вильпрофен, фторхинолоны), противогрибковые препараты (нистатин, низорал, дифлюкан), витамины С и Е, местное лечение (свечи "Тержинан"). Во II группе (25 больных) в приведенный выше курс лечения был включен препарат "Кипферон, суппозитории". Контрольная группа (группа сравнения) включала 81 клинически здоровых женщин. Оценку микробиоценоза влагалища (Вл) проводили согласно методологии(10), а также согласно новой медицинской технологии (11).50 women with established ureaplasma mono- and mixed infections were examined. Treatment of group I patients (25 patients) included only broad-spectrum antibacterial drugs (tiberal, doxycycline, vilprofen, fluoroquinolones), antifungal drugs (nystatin, nizoral, diflucan), vitamins C and E, local treatment (Terzhinan suppositories). In group II (25 patients), the drug “Kipferon, suppositories” was included in the above course of treatment. The control group (comparison group) included 81 clinically healthy women. The evaluation of the vaginal microbiocenosis (VL) was carried out according to the methodology (10), as well as according to the new medical technology (11).
Исследованием на наличие уреаплазм выявлен высокий титр возбудителя >104 КОЕ/мл - у 100% больных. Установлены у 6 больных уреаплазменная моноинфекция и у 44 больных - сочетанный характер инфицирования. При микст-инфекциях наблюдалось образование 2-7 - компонентных ассоциаций патогенных агентов.A study for the presence of ureaplasmas revealed a high titer of the pathogen> 10 4 CFU / ml in 100% of patients. Ureaplasma monoinfection was established in 6 patients and the combined nature of infection in 44 patients. In mixed infections, the formation of 2-7-component associations of pathogenic agents was observed.
В контрольной (табл. 1 ) группе клинически здоровых женщин нормоценоз определялся у 70%, промежуточный тип и дисбиоз - у 20% и 10% обследованных, соответственно. При нормоценозе в контрольной группе при I степени чистоты мазка в просветной и в пристеночной областях доминировали лактобациллы, выделявшиеся в 100% случаев в количестве 6,8±0,2 lg КОЕ/г и 7,9±0,3 lg КОЕ/г, соответственно. Бифидобактерии выявлялись в 42% случаев в количестве 3,2±04 lg КОЕ/г - в просветной области, и в количестве 4,6±0,6 lg КОЕ/г - в пристеночной области. Количество УПМ, представленной аэробными и анаэробными стрептококками, не превышало 3 lg КОЕ/г, при средних значениях 1,7±0,2 lg КОЕ/г и 2,6±0,3 lg КОЕ/г - в просветной области, 1,3±0,4 lg КОЕ/г и 3,4±0,2 lg КОЕ/г - в пристеночной области, соответственно. При промежуточном типе микробиоценоза биотопа Вл при II степени чистоты мазка в просветной и пристеночной области Вл обнаруживались факультативно-анаэробные стрептококки в количестве 2,6±0,2 lg КОЕ/г и 1,7±0,3 lg КОЕ/г и пептострептококки - в количестве 2,7±0,3 lg КОЕ/г и 3,5±0,4 lg КОЕ/г, соответственно. Количество лактобацилл снижалось до 4,3±0,3 lg КОЕ/г в просветной и до 6,2±0,6 lg КОЕ/г в пристеночной области, бифидобактерии не выделялись.In the control (Table 1) group of clinically healthy women, the normocenosis was determined in 70%, the intermediate type and dysbiosis in 20% and 10% of the examined, respectively. In case of normocenosis, in the control group with I degree of smear purity, lactobacilli dominated in the luminal and parietal regions, which were released in 100% of cases in the amount of 6.8 ± 0.2 lg CFU / g and 7.9 ± 0.3 lg CFU / g, respectively. Bifidobacteria were detected in 42% of cases in an amount of 3.2 ± 04 lg CFU / g in the luminal region, and in an amount of 4.6 ± 0.6 lg CFU / g in the parietal region. The number of UPM represented by aerobic and anaerobic streptococci did not exceed 3 lg CFU / g, with average values of 1.7 ± 0.2 lg CFU / g and 2.6 ± 0.3 lg CFU / g in the lumen, 1, 3 ± 0.4 lg CFU / g and 3.4 ± 0.2 lg CFU / g in the parietal region, respectively. With the intermediate type of microbiocenosis of the VL biotope at II degree of smear purity in the luminal and parietal region of VL, facultative anaerobic streptococci were detected in the amount of 2.6 ± 0.2 lg CFU / g and 1.7 ± 0.3 lg CFU / g and peptostreptococci - in the amount of 2.7 ± 0.3 log CFU / g and 3.5 ± 0.4 log CFU / g, respectively. The number of lactobacilli decreased to 4.3 ± 0.3 lg CFU / g in the lumen and to 6.2 ± 0.6 lg CFU / g in the parietal region; no bifidobacteria were isolated.

Дисбиоз Вл сопровождался значительным снижением количества лактобацилл (интенсивность колонизации просветной области - 2,5±0,2 lg КОЕ/г, пристеночной области - 3,5±0,4 lg КОЕ/г). На фоне снижения уровня лактобацилл при II степени чистоты мазка в просветной и пристеночной областях выявлялись коагулазо-отрицательный стафилококк в концентрации 5 lg КОЕ/г и 3 lg КОЕ/г, Е. coli и грибы рода Candida- в концентрации 4 lg КОЕ/г и 2 lg КОЕ/г и пептострептококки - в концентрации 2,3±0,3 lg КОЕ/г и 5,2±0,7 lg КОЕ/г, соответственно. Процент встречаемости УПМ в контрольной группе составлял для пептострептококков - 52,5%, аэробных стрептококков - 32,5%, стафилококк, кишечная палочка и грибы рода Candida выявлялись у 7,5% обследованных. УПМ при промежуточном типе и дисбиозе выявлялись в монокультуре или в 2-х компонентных ассоциациях. В контрольной группе содержание лактобацилл при промежуточном II типе микробиоценоза (у 20% пациентов) при р≤0,05 и дисбиозе (III тип; у 10% пациентов) при р≤0,01 было достоверно ниже по сравнению с нормоценозом (I тип микробиоценоза; у 70% пациентов), а по сравнению с типом II при дисбиозе при р≤0,05. Содержание УПМ достоверно выше по сравнению с типом I при типе II (р≤0,05) и типе III (р≤0,01), а по сравнению с типом II при типе III (р≤0,05). Содержание факультативных анаэробов достоверно выше в просветной области (р≤0,05), а облигатных анаэробов достоверно выше в пристеночной области (р≤0,05).Vl dysbiosis was accompanied by a significant decrease in the number of lactobacilli (the intensity of the colonization of the luminal region was 2.5 ± 0.2 lg CFU / g, the parietal region was 3.5 ± 0.4 lg CFU / g). Against the background of a decrease in the level of lactobacilli with a II degree of smear purity in the luminal and parietal regions, coagulase-negative staphylococcus at a concentration of 5 lg CFU / g and 3 lg CFU / g, E. coli and Candida-fungi at a concentration of 4 lg CFU / g and 2 lg CFU / g and peptostreptococcus - at a concentration of 2.3 ± 0.3 lg CFU / g and 5.2 ± 0.7 lg CFU / g, respectively. The percentage of UPM in the control group was 52.5% for peptostreptococci, 32.5% for aerobic streptococci, staphylococcus, Escherichia coli and fungi of the genus Candida were detected in 7.5% of the examined. UPM in the intermediate type and dysbiosis were detected in monoculture or in 2 component associations. In the control group, the content of lactobacilli with intermediate type II microbiocenosis (in 20% of patients) at p≤0.05 and dysbiosis (type III; in 10% of patients) at p≤0.01 was significantly lower compared to normocenosis (type I microbiocenosis ; in 70% of patients), and compared with type II with dysbiosis at p≤0.05. The content of UPM is significantly higher in comparison with type I with type II (p≤0.05) and type III (p≤0.01), and compared with type II with type III (p≤0.05). The content of facultative anaerobes is significantly higher in the luminal region (p≤0.05), and obligate anaerobes are significantly higher in the parietal region (p≤0.05).
При анализе микробиоценоза (табл. 2) биотопа Вл больных уреаплазменной микст-инфекцией нормоценоз не выявлен ни у одной пациентки, у 10% определялся промежуточный тип микробиоценоза биотопа Вл, у 44% - дисбиоз биотопа Вл и у 46% диагностирован бактериальный вагинит). При промежуточном типе микробиоценоза биотопа Вл (II степень чистоты мазка) в его просветной и пристеночной области обнаруживались факультативно-анаэробные стрептококки в количестве 3,8±0,2 lg КОЕ/г и 2,3±0,4 lg КОЕ/г и пептострептококки- в количестве 3,2±0,6 lg КОЕ/г и 4,5±0,4 lg КОЕ/г, соответственно. Количество лактобацилл снижалось до 4,3±0,2 lg КОЕ/г в просветной и до 5,8±0,4 lg КОЕ/г в пристеночной области. Бифидобактерии выявлялись в количестве 3,2±1,2 lg КОЕ/г и 4,2±0,8 lg КОЕ/г в просветной и пристеночной областях, соответственно. При дисбиозе и бактериальном вагините выявлялась III-IV степень чистоты мазка, расширялся видовой спектр условно-патогенной факультативно-анаэробной и облигатно-анаэробной микрофлоры.When analyzing the microbiocenosis (Table 2) of the VL biotope in patients with a ureaplasma mixed infection, no normocenosis was detected in any patient, in 10% the intermediate type of VB biotope microbiocenosis was determined, in 44% - VL biotope dysbiosis, and in 46% bacterial vaginitis was diagnosed). In the intermediate type of microbiocenosis of the VL biotope (grade II smear purity), facultative anaerobic streptococci in the amount of 3.8 ± 0.2 lg CFU / g and 2.3 ± 0.4 lg CFU / g and peptostreptococci were found in its luminal and parietal region - in an amount of 3.2 ± 0.6 lg CFU / g and 4.5 ± 0.4 lg CFU / g, respectively. The number of lactobacilli decreased to 4.3 ± 0.2 lg CFU / g in the luminal and to 5.8 ± 0.4 lg CFU / g in the parietal region. Bifidobacteria were detected in the amount of 3.2 ± 1.2 log CFU / g and 4.2 ± 0.8 log CFU / g in the luminal and parietal regions, respectively. With dysbiosis and bacterial vaginitis, a III-IV degree of purity of the smear was detected, the species spectrum of conditionally pathogenic facultative anaerobic and obligate anaerobic microflora expanded.


Содержание факультативных анаэробов: энтеробактерий, стрептококков, стафилококков и грибов рода Candida достигало в просветной области 7,8±2,4 lg КОЕ/г, в пристеночной области - 6,4±1,8 lg KOE/г. Облигатные анаэробы: пептострептококки, гарднереллы, бактероиды, фузобактерии выявлялись в просветной области в количестве 6,2±1,4 lg КОЕ/г, в пристеночной области- в количестве 8,2±1,2 lg КОЕ/г. Наиболее часто при уреаплазменной микст-инфекции выявлялись пептострептококки, стрептококки, энтерококки, стафилококки и грибы рода Candida - от 42% до 56%. Частота выявления β-гемолитических стрептококков составляла 4%, пептококков, пропионибактерий, коринебактерий, кишечной палочки, бактериодов и фузобактерий находилась в пределах 8-20%, гарднереллы выявлялись у 22% обследованных. Содержание лактобацилл у больных достоверно ниже по сравнению с промежуточным типом (II тип микробиоценоза; у 10% пациентов) при дисбиозе (III тип; у 44% пациентов) при р<0,05, вагините (IV тип; у 46% пациентов) при р<0,01, а по сравнению с типом III при вагините при р<0,05. Содержание УПМ достоверно выше по сравнению с типом II при типе III (р<0,05) и типе IV (р<0,01), а по сравнению с типом III при типе IV (р<0,05). Содержание факультативных анаэробов достоверно выше в просветной области (р≤0,05), а облигатных анаэробов достоверно выше в пристеночной области (р≤0,05). Следовательно, при дисбиотических нарушениях биотопа Вл у больных с уреаплазмозом наблюдалось доминирование факультативно-анаэробной флоры в просветной области или облигатно-анаэробной флоры в пристеночной области Вл при общем снижении уровня протективной флоры - лактобацилл по сравнению с нормоценозом.The content of facultative anaerobes: enterobacteria, streptococci, staphylococci and fungi of the genus Candida reached 7.8 ± 2.4 lg CFU / g in the luminal region and 6.4 ± 1.8 lg KOE / g in the parietal region. Obligatory anaerobes: peptostreptococci, gardnerella, bacteroids, fusobacteria were detected in the luminal region in the amount of 6.2 ± 1.4 lg CFU / g, in the parietal region in the amount of 8.2 ± 1.2 lg CFU / g. Most often, with ureaplasma mixed infection, peptostreptococci, streptococci, enterococci, staphylococci, and fungi of the genus Candida were detected - from 42% to 56%. The detection rate of β-hemolytic streptococci was 4%, peptococci, propionibacteria, corynebacteria, E. coli, bacteriodes and fusobacteria were in the range of 8-20%, gardnerella was detected in 22% of the examined. The content of lactobacilli in patients is significantly lower compared with the intermediate type (type II microbiocenosis; in 10% of patients) with dysbiosis (type III; in 44% of patients) with p <0.05, vaginitis (type IV; in 46% of patients) with p <0.01, and compared with type III with vaginitis at p <0.05. The content of UPM is significantly higher compared with type II with type III (p <0.05) and type IV (p <0.01), and compared with type III with type IV (p <0.05). The content of facultative anaerobes is significantly higher in the luminal region (p≤0.05), and obligate anaerobes are significantly higher in the parietal region (p≤0.05). Consequently, with dysbiotic disorders of the VL biotope in patients with ureaplasmosis, facultative anaerobic flora in the luminal region or obligate anaerobic flora dominated in the parietal region of Vl with a general decrease in the level of protective flora - lactobacilli compared to the normocenosis.
При сопоставлении пациенток I и II групп микробиоценоза биотопа Вл с обследованными пациентками контрольной группы не выявлено существенных различий микробиологических характеристик просветной и пристеночной областей биотопа Вл при промежуточном типе микробиоценоза. УПМ была представлена стрептококками и пептострептококками, выделявшимися в небольших количествах, преимущественно, в монокультурах. Вместе с тем, при дисбиозе у больных определялся более широкий спектр и увеличивалось число ассоциантов УПМ. Так, если в группе контроля при дисбиозе УПМ была представлена преимущественно монокультурами факультативно-анаэробных бактерий стрептококками, стафилококками, кишечной палочкой, преобладающими в просветной области, то у больных выявлялись 2-4-компонентные ассоциации факультативно- и облигатно-анаэробных микроорганизмов пептострептококков, гарднерелл, пропионибактерий, стрептококков, энтерококков, стафилококков, энтеробактерий. Следовательно, при одинаковой степени воспалительного процесса, у больных выявлялись более выраженные изменения микроэкологии биотопа Вл по сравнению с контрольной группой. При бактериальном вагините у больных выявлялись 3-х и более компонентные ассоциации УПМ. Ассоциации, вызывающие выраженные дисбиотические нарущения биотопа Вл, были представлены энтеробактериями и энтерококками, стрептококками, стафилококками и грибами рода Candida, облигатно-анаэробными бактериями. Наблюдалось преобладание факультативных анаэробов в просветной области и облиганых анаэ-робов в пристеночной области Вл. Высеваемость УПМ в титре 5 lg КОЕ/г и выше может указывать на приобретение ею фенотипических маркеров вирулентности.When comparing patients of groups I and II of the microbiocenosis of the VL biotope with the examined patients of the control group, no significant differences were found in the microbiological characteristics of the luminal and parietal regions of the VL biotope with an intermediate type of microbiocenosis. UPM was represented by streptococci and peptostreptococci, secreted in small quantities, mainly in monocultures. However, with dysbiosis in patients, a wider spectrum was determined and the number of UPM associates increased. So, while in the control group with dysbiosis, UPM was predominantly represented by monocultures of facultative anaerobic bacteria streptococci, staphylococci, Escherichia coli, prevailing in the luminal region, then 2-4-component associations of facultative and obligate-anaerobic microorganisms peptostreptococci, guards were revealed propionibacteria, streptococci, enterococci, staphylococci, enterobacteria. Therefore, with the same degree of the inflammatory process, more pronounced changes in the microecology of the VL biotope were revealed in patients compared with the control group. With bacterial vaginitis, 3 or more component associations of UPM were detected in patients. Associations causing pronounced dysbiotic disturbances of the Vl biotope were represented by enterobacteria and enterococci, streptococci, staphylococci and fungi of the genus Candida, obligate-anaerobic bacteria. There was a predominance of facultative anaerobes in the luminal region and licked anaerobes in the parietal region of Vl. Inoculation of UPM in a titer of 5 lg CFU / g and above may indicate the acquisition by it of phenotypic markers of virulence.
Корреляционный анализ (r>0,5; табл. 3) микробиологических и иммунологических показателей с учетом типа микробиоценоза биотопа Вл у здоровых женщин и больных уреаплазмозом показал, что при нормоценозе и промежуточном типе микробиоценоза биотопа Вл не наблюдалось достоверной корреляционной зависимости между количеством УПМ просветной и пристеночной и показателями гуморального иммунитета (r<0,3). Однако, у больных с дисбиозом и бактериальным вагинитом наблюдалась выраженная корреляция содержания УПМ просветной и пристеночной локализации и уровней иммуноглобулинов классов М, А и G, а также sIgA и sc в секрете Вл. У больных с сочетанной уреаплазменной инфекцией значительно возрастало содержание в отделяемом Вл IgG, уровень которого при бактериальных вагинитах уреаплазменной этиологии достоверно превышал контрольные значения нормоценоза более чем в 30 раз.Correlation analysis (r> 0.5; Table 3) of microbiological and immunological parameters taking into account the type of microbiocenosis of the Biotope Vl in healthy women and patients with ureaplasmosis showed that with normocenosis and the intermediate type of microbiocenosis of the Biotope Vl, there was no significant correlation between the number of UPM of the luminal and parietal and indicators of humoral immunity (r <0.3). However, in patients with dysbiosis and bacterial vaginitis, there was a pronounced correlation of the UPM content of the luminal and parietal localization and the levels of immunoglobulins of classes M, A and G, as well as sIgA and sc in the secret of Vl. In patients with combined ureaplasma infection, the IgG content in the separated Vl significantly increased, the level of which with bacterial vaginitis of the ureaplasma etiology significantly exceeded the control values of the normocenosis by more than 30 times.


Элиминация уреаплазм и разрешение клинических симптомов смешанной инфекции после однократного курса антибиотикотерапии наблюдалась у 24% (6 больных) больных контрольной группы и у 56% (14 больных) II группы, получавших препарат "Кипферон, суппозитории" (р≤0,05; χ2=5,23). Элиминация уреаплазм и других возбудителей инфекций, передаваемых половым путем (ИППП) после первого курса лечения по сравнению с их верификацией до лечения была выявлена у 12 (48%) при р≤0,001 (χ2=15,47) пациентов I группы и у 18 (72%) пациентов II группы при р≤0,001 (χ2=27,56). У 13 пациентов I группы и 7 пациентов II группы не наблюдалось полной элиминации уреаплазм в сочетании с другими возбудителями ИППП после первого курса лечения. Не выявлено достоверных различий содержания патогенных агентов у этих больных после первого курса лечения (р>0,05). Вместе с тем, общее количество больных с 2-7-компонентными ассоциациями после первого курса лечения во II группе было достоверно меньшим (р≤0,001), чем в первой.Elimination of ureaplasmas and resolution of clinical symptoms of mixed infection after a single course of antibiotic therapy was observed in 24% (6 patients) of the control group patients and in 56% (14 patients) of the II group treated with Kipferon suppositories (p≤0.05; χ 2 = 5.23). Elimination of ureaplasmas and other causative agents of sexually transmitted infections (STIs) after the first course of treatment compared with their verification before treatment was detected in 12 (48%) with p≤0.001 (χ 2 = 15.47) of group I patients and 18 (72%) patients of group II with p≤0.001 (χ 2 = 27.56). In 13 patients of group I and 7 patients of group II, complete elimination of ureaplasmas was not observed in combination with other STI pathogens after the first course of treatment. There were no significant differences in the content of pathogenic agents in these patients after the first course of treatment (p> 0.05). At the same time, the total number of patients with 2-7 component associations after the first course of treatment in the II group was significantly lower (p≤0.001) than in the first.
При повторном обследовании больных после первого курса лечения (табл. 4) нормоценоз был выявлен у 10 (20%) пациентов (2- из I группы и 8 - из II группы; при р≤0,05 и χ2=4,41), промежуточный тип микробиоценоза биотопа Вл - у 10 (20%) пациентов (4 - из I группы и 6 - из II группы), дисбиоз - у 23 (46%) больных (15 - из I группы и 8 - из II группы; при р≤0,05 и χ2=3,87), бактериальный вагинит - у 7 (14%) больных (4 - из I группы и 3 - из II группы). При 100% встречаемости в обеих группах, у больных II группы наблюдалось достоверно более высокое по сравнению с I группой (р≤0,05) содержание лактобацилл как в просветной, так и в пристеночной областях Вл. Так, содержание лактобацилл у больных II группы составляло 6,8±1,2 lg КОЕ/г - в пристеночной области и 4,6±0,8 lg КОЕ/г - в просветной. У больных I группы содержание лактобацилл не превышало 4,2±0,6 lg КОЕ/г - в пристеночной области и 2,8±0,4 lg КОЕ/г - в просветной. Бифидобактерии, не выявлявшиеся у больных до лечения, верифицировались после лечения у 20% больных II группы и у 4% больных I группы. Содержание бифидобактерий у больных II группы после лечения составляло 3,8±0,2 lg КОЕ/г в пристеночной области и 2,4±0,4 lg КОЕ/г - в просветной. У больных I группы бифидобактерии выявлялись в пристеночной области в количестве 2,8±0,2 lg КОЕ/г и 1,4±0,6 lg КОЕ/г - в просветной.When re-examining patients after the first course of treatment (Table 4), normocenosis was detected in 10 (20%) patients (2 from group I and 8 from group II; with p≤0.05 and χ 2 = 4.41) , the intermediate type of microbiocenosis of the VL biotope is in 10 (20%) patients (4 from group I and 6 from group II), dysbiosis in 23 (46%) patients (15 from group I and 8 from group II; at p≤0.05 and χ 2 = 3.87), bacterial vaginitis - in 7 (14%) patients (4 from group I and 3 from group II). At 100% occurrence in both groups, in patients of group II, a significantly higher content of lactobacilli was observed in comparison with group I (p≤0.05) in both the luminal and parietal regions of Vl. So, the content of lactobacilli in patients of group II was 6.8 ± 1.2 lg CFU / g in the parietal region and 4.6 ± 0.8 lg CFU / g in the lumen. In patients of group I, the content of lactobacilli did not exceed 4.2 ± 0.6 lg CFU / g in the parietal region and 2.8 ± 0.4 lg CFU / g in the lumen. Bifidobacteria, not detected in patients before treatment, were verified after treatment in 20% of patients of group II and in 4% of patients of group I. The content of bifidobacteria in patients of group II after treatment was 3.8 ± 0.2 lg CFU / g in the parietal region and 2.4 ± 0.4 lg CFU / g in the lumen. In patients of group I, bifidobacteria were detected in the parietal region in the amount of 2.8 ± 0.2 lg CFU / g and 1.4 ± 0.6 lg CFU / g in the lumen.
У больных I группы после первого курса лечения (табл. 4) наблюдалась достоверно более высокая (р<0,05), по сравнению с группой II, частота встречаемости и значительное содержание факультативно-анаэробных бактерий и грибов рода Candida. Стафилококки и стрептококки (2% β-гемолитические) выявлялись у 48% больных I группы при интенсивности колонизации просветной области 4,6±0,8 lg КОЕ/г и 5,8±1,2 lg КОЕ/г, пристеночной области 3,8±1,6 lg КОЕ/г и 5,4±1,2 lg КОЕ/г, соответственно, и у 24% и 28% больных II группы при интенсивности колонизации просветной области 2,3±0,1 lg КОЕ/г и 4,2±0,8 lg КОЕ/г, пристеночной области - 1,8±0,2 lg КОЕ/г и 3,2±1,3 lg КОЕ/г, соответственно. Энтерококки и кишечная палочка выявлялись у 20% и 12% больных I группы в количестве 5,2±1,3 lg КОЕ/г и 4,8±1,4 lg КОЕ/г - в просветной области и 4,6±1,8 lg КОЕ/г и 3,8±1,4 lg КОЕ/г - пристеночной области; у 8% и 4% больных II группы в количестве 4,2±0,2 lg КОЕ/г и 3,8±0,4 lg КОЕ/г в просветной области, 3,2±0,6 lg КОЕ/г и 2,4±0,4 lg КОЕ/г - в пристеночной области, соответственно. Коринебактерии и пропионибактерии у больных I группы после лечения выявлялись в 12% и 16% случаев в количестве 3,8±1,2 lg КОЕ/г и 4,2±1,6 lg КОЕ/г - в просветной области, и 4,6±1,4 lg КОЕ/г и 5,2±1,2 lg КОЕ/г - в пристеночной области, у больных II группы - 8% и 12% случаев в количестве 2,8±0,2 lg КОЕ/г и 3,8±1,4 lg КОЕ/г - в просветной области, и 3,2±0,4 lg КОЕ/г и 4,2±0,8 lg КОЕ/г - в пристеночной области. Грибы рода Candida были выделены у 36% больных I группы и у 16% больных II группы в количестве 6,2±0,8 lg KOE/г и 4,8±1,2 - в просветной области, и 4,2±0,2 lg КОЕ/г и 3,8±0,4 lg КОЕ/г - в пристеночной области, соответственно.In patients of group I after the first course of treatment (Table 4), a significantly higher (p <0.05), compared with group II, frequency of occurrence and a significant content of facultative anaerobic bacteria and fungi of the genus Candida were observed. Staphylococci and streptococci (2% β-hemolytic) were detected in 48% of patients of group I with an intensity of colonization of the luminal region of 4.6 ± 0.8 lg CFU / g and 5.8 ± 1.2 lg CFU / g, parietal region 3, 8 ± 1.6 lg CFU / g and 5.4 ± 1.2 lg CFU / g, respectively, and in 24% and 28% of patients of group II with an intensity of colonization of the luminal region 2.3 ± 0.1 lg CFU / g and 4.2 ± 0.8 log CFU / g, of the parietal region - 1.8 ± 0.2 log CFU / g and 3.2 ± 1.3 log CFU / g, respectively. Enterococci and Escherichia coli were detected in 20% and 12% of patients of group I in the amount of 5.2 ± 1.3 lg CFU / g and 4.8 ± 1.4 lg CFU / g in the lumen and 4.6 ± 1, 8 lg CFU / g and 3.8 ± 1.4 lg CFU / g of the parietal region; in 8% and 4% of patients of group II in the amount of 4.2 ± 0.2 lg CFU / g and 3.8 ± 0.4 lg CFU / g in the lumen, 3.2 ± 0.6 lg CFU / g and 2.4 ± 0.4 lg CFU / g - in the parietal region, respectively. Corynebacteria and propionibacteria in patients of group I after treatment were detected in 12% and 16% of cases in the amount of 3.8 ± 1.2 lg CFU / g and 4.2 ± 1.6 lg CFU / g in the lumen, and 4, 6 ± 1.4 lg CFU / g and 5.2 ± 1.2 lg CFU / g in the parietal region, in patients of group II - 8% and 12% of cases in an amount of 2.8 ± 0.2 lg CFU / g and 3.8 ± 1.4 log CFU / g in the luminal region, and 3.2 ± 0.4 log CFU / g and 4.2 ± 0.8 log CFU / g in the parietal region. Candida fungi were isolated in 36% of patients of group I and in 16% of patients of group II in the amount of 6.2 ± 0.8 lg KOE / g and 4.8 ± 1.2 in the lumen, and 4.2 ± 0 , 2 lg CFU / g and 3.8 ± 0.4 lg CFU / g - in the parietal region, respectively.

У больных I группы в пристеночной области (табл. 4) выявлялись в значительном количестве облигатно-анаэробные бактерии: пептострептококки - 5,2±1,4 lg КОЕ/г, пептококки - 4,8±0,3 lg КОЕ/г и гарднереллы - 6,2±1,8 lg КОЕ/г, в просветной области количество этих микрооганизмов снижалось до 4,8±1,7 lg КОЕ/г, 3,6±0,4 lg КОЕ/г и 5,2±1,6 lg КОЕ/г, соответственно. Частота обнаружения пептострептококков достигала 68%, пептококков и гарднерелл - 12%. У больных II группы пептострептококки выявлялись в 44% случаев в количестве 3,8±1,2 lg КОЕ/г - в пристеночной области и 2,4±0,8 lg КОЕ/г - в просветной, пептококки и гарднереллы - у 8% обследованных, при интенсивности колонизации пристеночной области - 2,8±0,4 lg КОЕ/г и 4,2±0,6 lg КОЕ/г, просветной области - 1,2±0,2 lg КОЕ/г и 3,4±0,8 lg КОЕ/г, соответственно. Частота обнаружения грамотрицательных облигатно-анаэробных бактерий: бактероидов и фузобактерий, у больных I группы составляла 16% и 14%, при интенсивности колонизации пристеночной области Вл - 5,2±1,2 lg КОЕ/г и 4,6±0,8 lg КОЕ/г, просветной области - 4,2±1,4 lg КОЕ/г и 3,4±1,2 lg КОЕ/г, соответственно. У больных II группы бактероиды и фузобактерии выявлялись в 12% и 10% случаев при интенсивности колонизации пристеночной области - 4,2±0,4 lg КОЕ/г и 3,5±1,3, просветной области - 2,4±0,6 lg КОЕ/г и 1,7±0,3 lg КОЕ/г, соответственно. Анализ динамики содержания IgA, IgM, IgG, sIgA и sc в отделяемом Вл выявил значительное достоверное снижение концентрации IgG (р≤0,01) и sc (р≤0,05) у больных II группы по сравнению с I группой после первого курса лечения. Так, средние значения IgG и sc составляли для I группы 134,8±15,4 мкг/мл и 54,6±8,2 мкг/мл, а для II - 78,4±6,3 мкг/мл и 32,4±4,6 мкг/мл, соответственно. У больных II группы также более интенсивно снижался уровень IgM (р≤0,01), концентрация которого составляла 22,4±1,7 мкг/мл в I группе и 12,3±1,2 мкг/мл - во II. Вместе с тем, уровни IgA и sIgA были достоверно выше (р≤0,05) во II группе больных по сравнению с первой I. Концентрация IgA после лечения в I группе составляла 12,4±1,6 мкг/мл, во II - 18,6±2,4 мкг/мл, a sIgA - 20,4±3,2 мкг/мл в I группе и 28,6±2,6 мкг/мл - во II. Содержание достоверно ниже во II группе, чем в I для IgG и IgM при р<0,01, для sc при р<0,05. Содержание IgA и sIgA достоверно ниже в I группе, чем во II при р<0,05. Следовательно, у больных, получавших в составе комплексной терапии иммунобиологический препарат "Кипферон, суппозитории" наблюдалось выраженное снижение интенсивности воспалительного процесса (более низкие уровни IgM, IgG по сравнению с контрольной группой) и высокая активность местного иммунитета - повышение уровней IgA и sIgA в секрете Вл.Obligatory anaerobic bacteria were detected in significant numbers in patients of group I in the parietal region (table 4): peptostreptococci - 5.2 ± 1.4 lg CFU / g, peptococci - 4.8 ± 0.3 lg CFU / g and gardnerella - 6.2 ± 1.8 log CFU / g, in the luminal region, the number of these microorganisms decreased to 4.8 ± 1.7 log CFU / g, 3.6 ± 0.4 log CFU / g and 5.2 ± 1 , 6 lg CFU / g, respectively. The detection rate of peptostreptococci reached 68%, peptococci and gardnerella - 12%. In patients of group II, peptostreptococci were detected in 44% of cases in the amount of 3.8 ± 1.2 lg CFU / g in the parietal region and 2.4 ± 0.8 lg CFU / g in the luminal, peptococcus and gardnerella in 8% examined, with the intensity of colonization of the parietal region - 2.8 ± 0.4 lg CFU / g and 4.2 ± 0.6 lg CFU / g, luminal region - 1.2 ± 0.2 lg CFU / g and 3.4 ± 0.8 lg CFU / g, respectively. The detection rate of gram-negative obligate-anaerobic bacteria: bacteroids and fusobacteria, in patients of group I was 16% and 14%, with colonization of the parietal region Vl - 5.2 ± 1.2 lg CFU / g and 4.6 ± 0.8 lg CFU / g, lumen - 4.2 ± 1.4 log CFU / g and 3.4 ± 1.2 log CFU / g, respectively. In group II patients, bacteroids and fusobacteria were detected in 12% and 10% of cases with a colonization of the parietal region of 4.2 ± 0.4 lg CFU / g and 3.5 ± 1.3, and the luminal region of 2.4 ± 0, 6 lg CFU / g and 1.7 ± 0.3 lg CFU / g, respectively. Analysis of the dynamics of the content of IgA, IgM, IgG, sIgA and sc in the separated VL revealed a significant significant decrease in the concentration of IgG (p≤0.01) and sc (p≤0.05) in patients of group II compared with group I after the first course of treatment . So, the average values of IgG and sc were 134.8 ± 15.4 μg / ml and 54.6 ± 8.2 μg / ml for group I, and 78.4 ± 6.3 μg / ml for group II and 32, 4 ± 4.6 μg / ml, respectively. In patients of group II, the IgM level also decreased more intensively (p≤0.01), the concentration of which was 22.4 ± 1.7 μg / ml in group I and 12.3 ± 1.2 μg / ml in group II. At the same time, the levels of IgA and sIgA were significantly higher (p≤0.05) in the II group of patients compared with the first I. The IgA concentration after treatment in the I group was 12.4 ± 1.6 μg / ml, in II - 18.6 ± 2.4 μg / ml, and sIgA - 20.4 ± 3.2 μg / ml in group I and 28.6 ± 2.6 μg / ml in II. The content is significantly lower in group II than in group I for IgG and IgM at p <0.01, for sc at p <0.05. The content of IgA and sIgA is significantly lower in group I than in II at p <0.05. Therefore, in patients receiving the Kipferon, suppositories immunobiological preparation as a part of complex therapy, a marked decrease in the intensity of the inflammatory process was observed (lower levels of IgM, IgG compared with the control group) and a high activity of local immunity - an increase in IgA and sIgA levels in the secretion of Vl .
Таким образом, применение в составе комплексной терапии уреаплазмоза "Кипферон, суппозитории" обеспечивало более быстрое восстановление КР биотопа Вл, сопровождающееся восстановлением нормального соотношения автохтонных и аллохтонных микроорганизмов.Thus, the use of Kipferon suppositories as part of the complex therapy of ureaplasmosis ensured a more rapid restoration of the VL biotope, accompanied by the restoration of the normal ratio of autochthonous and allochthonous microorganisms.
У клинически здоровых женщин превалируют I и II типы (степени) микробиоценоза биотопа влагалища (табл. 5); выявление у них III и IV типов микробиоценоза биотопа влагалища может рассматриваться как маркер продромального периода инфекционного заболевания. При остром уреаплазмозе: в основном регистрируются (в 90% случаев) III и IV типы микробиоценоза биотопа влагалища (благоприятное течение); выявление у больных I и II типов (степеней) микробиоценоза биотопа влагалища (не благоприятное течение) свидетельствует о низком уровне антиинфекционной резистентности, возможной хронизации инфекционного процесса и о необходимости включения в лечебные схемы иммуномодуляторов.In clinically healthy women, I and II types (degrees) of vaginal biotope microbiocenosis prevail (Table 5); identification of the III and IV types of microbiocenosis of the vaginal biotope in them can be considered as a marker of the prodromal period of the infectious disease. In acute ureaplasmosis: mainly registered (in 90% of cases) III and IV types of vaginal biotope microbiocenosis (favorable course); the detection of vaginal biotope in microbiocenosis of types I and II (degrees) (an unfavorable course) indicates a low level of anti-infectious resistance, a possible chronicity of the infectious process, and the need to include immunomodulators in treatment regimens.

При проведении терапии установление степени нарушений микробиоценоза биотопа влагалища повышает информативность оценки ее эффективности за счет выявления механизмов ее лечебного эффекта: достоверно подтверждена целесообразность подключения к комплексной терапии препарата «Кипферон®», ускоряющего выздоровление пациентов; продолжение регистрации у части больных III и IV типов микробиоценоза биотопа влагалища указывает на необходимость продолжения лечения.During the course of therapy, the degree of violations of the microbiocenosis of the vaginal biotope increases the information content of evaluating its effectiveness by identifying the mechanisms of its therapeutic effect: the feasibility of connecting the Kipferon ® drug to the complex therapy, accelerating the recovery of patients, has been confirmed; continued registration in some patients of types III and IV of the microbiocenosis of the vaginal biotope indicates the need for continued treatment.
Пример 4. Оценка состояния здоровья по состоянию микробиоценоза биотопа влагалища при урогенитальном хламидиозе (УГХ).Example 4. Assessment of the health status of the microbiocenosis of the vaginal biotope with urogenital chlamydia (UHC).
Отобранные 149 пациенток с УГХ и 32 клинически здоровых женщин были разбиты на 4 группы: группу I (острый хламидиоз) составила 41 пациентка; группу II (хронический хламидиоз) составляли 29 пациентки; в группу III (группа сравнения, переболевшие) вошли 30 пациенток, в анамнезе которых ранее диагностировался УГХ; в группу IV (контрольная, группа сравнения) включили 81 клинически здоровые женщины. Оценку микробиоценоза биотопа влагалища (Вл) проводили согласно методологии, изложенной в пособии утвержденном Учебно-методическим объединением (10), а также согласно новой медицинской технологии (11).Selected 149 patients with UHF and 32 clinically healthy women were divided into 4 groups: group I (acute chlamydia) was 41 patients; group II (chronic chlamydia) comprised 29 patients; group III (comparison group, who had been ill) included 30 patients whose history had previously been diagnosed with UHF; Group IV (control, comparison group) included 81 clinically healthy women. The evaluation of the microbiocenosis of the vaginal biotope (VL) was carried out according to the methodology described in the manual approved by the Educational and Methodical Association (10), as well as according to new medical technology (11).
Чаще всего хламидийная инфекция протекает в смешанной форме, в ассоциации с патогенными и УПМ. Тяжесть смешанных инфекций и разнообразие их вариантов определяется исходом взаимодействия двух и более возбудителей, результатом их взаимоотношения могут стать независимое размножение, экзальтация (усиление размножения одного или всех ассоциатов), комплементация (специфическая зависимость размножения одного ассоцианта от другого).Most often, chlamydial infection occurs in a mixed form, in association with pathogenic and UPM. The severity of mixed infections and the diversity of their variants is determined by the outcome of the interaction of two or more pathogens, the result of their relationship can be independent reproduction, exaltation (increased reproduction of one or all associates), complementation (a specific dependence of the reproduction of one associate on the other).
У 17,1% (7 пациенток) больных I группы в цервикальном канале (Цк) выявлена (табл. 1, 2) хламидийная моноинфекция, а у 82,9% (34 пациенток) - в сочетании с другими возбудителями инфекций, передаваемых половым путем, (ИППП): уреаплазмами, микоплазмами, вирусом папилломы человека (ВПЧ), вирусом простого герпеса (ВПГ0, цитомегаловирусом(ЦМВ), трихомонадами и токсоплазмами). Выявлено одновременное доминирование двух биоваров U. urealyticum Parvo и Т-960, что значительно усугубляло течение УГХ. У 31,7% установлено наличие ВПЧ низкой онкогенности (типы 6 и 11), и у 9,8% человек ВПЧ с ЦМВ или сразу несколько типов ВПЧ (16, 18 и 35) с высокой онкогенной способностью, что также является неблагоприятным патогенетическим фактором. Наличие УПМ установлено в I группе во влагалище (Вл) - у 51,2% пациенток (11 родов микроорганизмов). Исследования во II группе на наличие возбудителей ИППП в Цк выявили у 37,9% больных хламидийную моноинфекцию, у остальных - сочетанный характер инфицирования. УПМ во Вл - у 48,3% пациенток (5 родов микроорганизмов). В III группе у 36,6% женщин из Вл выделялись УПМ (4 рода микроорганизмов). В IV группе не выявлены ИППП. УПМ выявлялись у трех пациенток - во Вл - (4 рода микроорганизмов).In 17.1% (7 patients) of patients of group I in the cervical canal (CK), chlamydial monoinfection was detected (Table 1, 2), and in 82.9% (34 patients) - in combination with other pathogens of sexually transmitted infections , (STI): ureaplasmas, mycoplasmas, human papillomavirus (HPV), herpes simplex virus (HSV0, cytomegalovirus (CMV), trichomonads and toxoplasmas). The simultaneous dominance of two biovars U. urealyticum Parvo and T-960 was revealed, which significantly aggravated the course of UHC. In 31.7%, the presence of HPV of low oncogenicity (types 6 and 11) was found, and in 9.8% of people HPV with CMV or several types of HPV (16, 18 and 35) with high oncogenic ability, which is also an unfavorable pathogenetic factor . The presence of UPM was established in group I in the vagina (VL) in 51.2% of patients (11 genera of microorganisms). Studies in group II for the presence of STIs in the Central Committee revealed in 37.9% of patients chlamydial monoinfection, in the rest - the combined nature of the infection. UPM in Vl - in 48.3% of patients (5 genera of microorganisms). In group III, 36.6% of women from VL were allocated UPM (4 kinds of microorganisms). In group IV, no STIs were detected. UPM was detected in three patients - in Vl - (4 kinds of microorganisms).
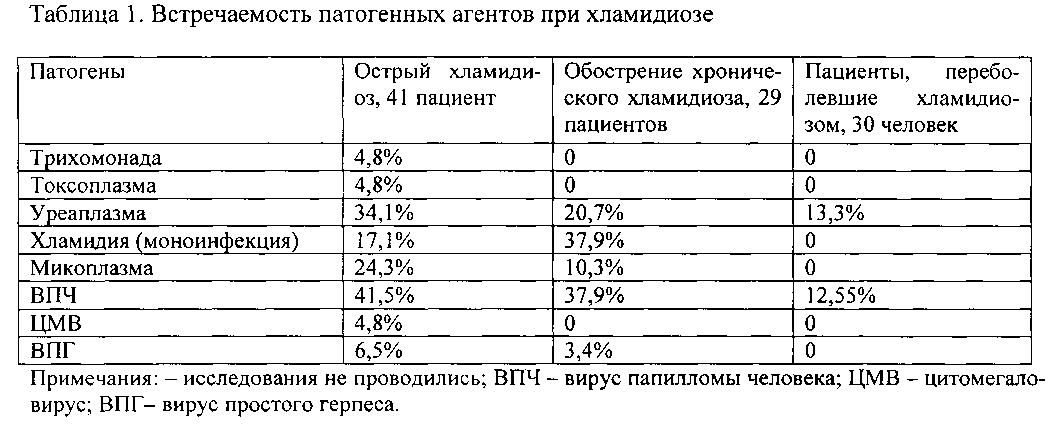
При остром хламидиозе (табл. 1), включая обострение хронического процесса, выявлено, что из всех верифицированных патогенных агентов достоверно (по сравнению с группой переболевших хламидиозом пациентов) наиболее часто выявлялись уреаплазмы (χ2=4,471, р<0,05), микоплазмы (χ2=7,098, р<0,01), ВПЧ (χ2=6,012, р<0,05), при хроническом хламидиозе - ВПЧ (χ2=4,023, р<0,05).In acute chlamydia (Table 1), including an exacerbation of the chronic process, it was found that of all verified pathogenic agents, ureaplasmas (χ 2 = 4.471, p <0.05), mycoplasmas were most often detected reliably (compared with the group of patients with chlamydia) (χ 2 = 7.098, p <0.01), HPV (χ 2 = 6.012, p <0.05), with chronic chlamydia - HPV (χ 2 = 4.023, p <0.05).
УПМ во Вл при остром хламидиозе определялись в количестве 8,1±0,4 lg КОЕ/мл, при обострении хронического хламидиоза - 4,6±1,0 lg КОЕ/мл, у переболевших - 2,5±1,2 lg КОЕ/мл, у клинически здоровых пациентов - 2,74±0,94 lg КОЕ/мл. Уровни выявления УПМ при остром хламидиозе достоверно (при р<0,05) отличались от таковых других сравниваемых групп пациентов. При хламидиозе дисбиотические нарушения во Вл (табл. 2, 3) сопровождались повышением частоты встречаемости семи УПМ. Высеваемость Enterococcus spp. у больных острым хламидиозом достоверно выше чем при обострении хронического хламидиоза (χ2=3,854, р<0,05), у переболевших (χ2=16,405, р<0,001) и клинически здоровых (χ2=17,527, р<0,001), а при обострении хронического хламидиоза достоверно выше по сравнению с переболевшими (χ2=4,964, р<0,05) и клинически здоровыми пациентами (χ2=5,423, р<0,05); уровни показателей высеваемости Candida spp. у больных острым хламидиозом и обострением хронического хламидиоза достоверно не различались, однако они достоверно выше чем у переболевших хламидиозом (χ2=4,254 при р<0,05 и χ2=4,278 при р<0,05, соответственно) и у клинически здоровых пациентов (χ2=6,701 при р<0,01 и χ2=6,730 при р<0,01, соответственно). Следовательно, наблюдается относительно сниженная реакция слизистых УГТ на УПМ.UPM in VL in acute chlamydia was determined in the amount of 8.1 ± 0.4 lg CFU / ml, with exacerbation of chronic chlamydia - 4.6 ± 1.0 lg CFU / ml, in patients - 2.5 ± 1.2 lg CFU / ml, in clinically healthy patients - 2.74 ± 0.94 lg CFU / ml. The levels of detection of UPM in acute chlamydia significantly (at p <0.05) differed from those of the other compared groups of patients. With chlamydia, dysbiotic disorders in VL (Tables 2, 3) were accompanied by an increase in the frequency of occurrence of seven UPM. Inoculation of Enterococcus spp. in patients with acute chlamydia, significantly higher than with exacerbation of chronic chlamydia (χ 2 = 3.854, p <0.05), in patients with illness (χ 2 = 16.405, p <0.001) and clinically healthy (χ 2 = 17.527, p <0.001), and at exacerbation of chronic chlamydia is significantly higher compared to convalescents (χ 2 = 4.964, p <0.05) and a clinically healthy patients (χ 2 = 5.423, p <0.05); Candida spp. in patients with acute chlamydia and exacerbation of chronic chlamydia did not significantly differ, however, they are significantly higher than in patients with chlamydia (χ 2 = 4.254 at p <0.05 and χ 2 = 4.278 at p <0.05, respectively) and in clinically healthy patients (χ 2 = 6.701 at p <0.01 and χ 2 = 6.730 at p <0.01, respectively). Consequently, a relatively reduced response of mucous UGT to UPM is observed.


По частоте выявляемости УПМ (табл. 2, 3) во Вл достоверные различия выявлены между I и II группами (χ2=7,540, р<0,01), I и III группами (χ2=13,240, р<0,001), I и IV группами (χ2=27,010, р<0,001), II и III группами (χ2=4,940, р<0,01), II и IV группами (χ2=20,530, р<0,001), III и IV группами (χ2=5,120, р<0,01), а между группами I и II различия не достоверны.According to the frequency of detection of UPM (Tables 2, 3) in VL, significant differences were revealed between groups I and II (χ 2 = 7.540, p <0.01), groups I and III (χ 2 = 13.240, p <0.001), I and groups IV (χ 2 = 27.010, p <0.001), groups II and III (χ 2 = 4.940, p <0.01), groups II and IV (χ 2 = 20.530, p <0.001), groups III and IV (χ 2 = 5.120, p <0.01), and between groups I and II the differences are not significant.
Несмотря на относительную стабильность микробных ассоциаций нормальной микрофлоры УГТ, нередко наблюдаются ее изменения, обусловленные как состоянием макроорганизма, так и различными экзогенными воздействиями. Одним из таких факторов является наличие ИППП, которые, попадая на гениталии, могут нарушать защитные барьеры, обеспечивающие динамическое равновесие между макроорганизмом и микрофлорой. Оценивалась нормофлора Вл. Обнаружено достоверное снижение (χ2=16,353, р<0,001) количества лактобацилл в I группе (выявлялись у 56,1% пациента; интенсивность колонизации 6,5±1,0 lg КОЕ/г) по сравнению с IV группой (выявлялись у 100% пациентов; интенсивность колонизации 7,5±1,5 lg КОЕ/г), также достоверно различие по сравнению со II (χ2=4,272, р<0,01; выявлялись у 72,10% пациентов; интенсивность колонизации 6,2±1,0 lg КОЕ/г), с III группами (χ2=6,200, р<0,01; выявлялись у 87,00%) пациентов; интенсивность колонизации 7,2±0,6 lg КОЕ/г). Бифидобактерии не выявлялись: достоверно различие по сравнению с III группой (χ2=9,790, р<0,001; выявлялись у 26,6% пациентов; интенсивность колонизации 5,2±0,7 lg КОЕ/г) и IV группами (χ2=17,580, р<0,001; выявлялись у 50,0% пациентов; интенсивность колонизации 6,1±0,9 lg КОЕ/г), а со II группой различия не достоверны). У обследованных II группы имело место достоверное снижение (χ2=7,880, р<0,01) количества лактобацилл по сравнению с IV группой, а с группой III - не достоверны. Бифидобактерии выявлялись у двух пациентов (интенсивность колонизации 3,5±1,0 lg КОЕ/г; различия достоверны по сравнению с III - χ2=7,364, р<0,01 и IV группами χ2=7,600, р<0,001, а с группой III - не достоверны). По содержанию лактобацилл и бифидобактерий различия между III и IV группами не достоверны. Во Вл у II группы пациенток выявлена обратная корреляционная зависимость между УПМ и лакто-бациллами (rs=-0,7). Следовательно, хламидийная инфекция сопровождается выраженными нарушениями (уменьшением) в содержании лактобацилл на слизистых гениталий женщин. Динамика содержания лактобацилл и бифидобактерий отражает состояние микробиоценоза УГТ женщин при УГХ. Оценивались уровни иммуноглобулинов (табл. 4).Despite the relative stability of the microbial associations of the normal microflora of UGT, its changes are often observed due to both the state of the macroorganism and various exogenous influences. One of these factors is the presence of STIs, which, getting on the genitals, can violate protective barriers that provide a dynamic balance between the macroorganism and microflora. The normoflora of Vl was estimated. A significant decrease (χ 2 = 16.353, p <0.001) of the number of lactobacilli in group I was detected (detected in 56.1% of the patient; colonization intensity 6.5 ± 1.0 lg CFU / g) compared with group IV (detected in 100 % of patients; colonization rate 7.5 ± 1.5 log CFU / g), also a significant difference compared to II (χ 2 = 4.272, p <0.01; detected in 72.10% of patients; colonization rate 6.2 ± 1.0 lg CFU / g), with III groups (χ 2 = 6,200, p <0,01; were detected in 87.00%) patients; colonization intensity 7.2 ± 0.6 log CFU / g). Bifidobacteria were not detected: a significant difference compared with group III (χ 2 = 9.790, p <0.001; were detected in 26.6% of patients; colonization intensity 5.2 ± 0.7 log CFU / g) and group IV (χ 2 = 17.580, p <0.001; were detected in 50.0% of patients; the colonization rate was 6.1 ± 0.9 lg CFU / g), and the differences were not significant with group II). In the examined group II there was a significant decrease (χ 2 = 7.880, p <0.01) of the number of lactobacilli compared with group IV, and with group III they were not significant. Bifidobacteria were detected in two patients (colonization intensity 3.5 ± 1.0 lg CFU / g; differences are significant compared with III - χ 2 = 7.364, p <0.01 and group IV χ 2 = 7.600, p <0.001, and with group III - not reliable). According to the content of lactobacilli and bifidobacteria, the differences between groups III and IV are not significant. In Vl, in the II group of patients, an inverse correlation was found between UPM and lactobacilli (r s = -0.7). Therefore, chlamydial infection is accompanied by severe disorders (decrease) in the content of lactobacilli on the mucous membranes of women. The dynamics of the content of lactobacilli and bifidobacteria reflects the state of microbiocenosis of UGT in women with UHC. The levels of immunoglobulins were evaluated (table. 4).

Сопоставляя содержание нормофлоры с количеством лейкоцитов в мазках и уровнями УПМ в сравниваемых группах пациенток и учитывая разработанную ранее систему оценки нарушений микробиоценоза биотопа Вл, можно констатировать (табл. 5) в I группе у 43,9% пациенток III степень нарушения микробиоценоза биотопа (бактериальный вагинит) и у 56,1% - II степень нарушения (дисбиоз), во II группе у 27,5% пациенток - III степень нарушения (бактериальный вагинит) и у 72,4% - II степень нарушения (дисбиоз), в III и IV группа у всех пациенток - нормоценоз.Comparing the content of normoflora with the number of leukocytes in smears and the levels of UPM in the compared groups of patients and taking into account the previously developed system for assessing violations of the microbiocenosis of the Biotope Vl, we can state (Table 5) in group I in 43.9% of patients the III degree of violation of the microbiocenosis of the biotope (bacterial vaginitis ) and in 56.1% - II degree of violation (dysbiosis), in II group, 27.5% of patients - III degree of violation (bacterial vaginitis) and 72.4% - II degree of violation (dysbiosis), in III and IV group in all patients - normocenosis.
У клинически здоровых женщин и переболевших ранее превалируют I и II типы (степени) микробиоценоза биотопа влагалища (табл. 5); выявление у них III и IV типов микробиоценоза биотопа влагалища может рассматриваться как маркер продромального периода инфекционного заболевания. При остром хламидиозе и при обострении хронического хламидиоза в основном регистрируются (в 90% случаев) III и IV типы микробиоценоза биотопа влагалища, свидетельствующие о благоприятном течении заболевания.In clinically healthy women and those who have been ill previously, I and II types (degrees) of vaginal biotope microbiocenosis prevail (Table 5); identification of the III and IV types of microbiocenosis of the vaginal biotope in them can be considered as a marker of the prodromal period of the infectious disease. In acute chlamydia and exacerbation of chronic chlamydia, III and IV types of microbiocenosis of the vaginal biotope are mainly recorded (in 90% of cases), indicating a favorable course of the disease.

При проведении терапии установление степени нарушений микробиоценоза биотопа влагалища повышает информативность оценки ее эффективности за счет выявления механизмов ее лечебного эффекта: при клинической эффективности проводимой терапии регистрировался переход к показателям нормально протекающей беременности - выявлялись I или II типы (степени) микробиоценоза биотопа влагалища; продолжение регистрации у части больных III и IV типов микробиоценоза биотопа влагалища указывало на необходимость продолжения лечения.During the course of therapy, the degree of violations of the microbiocenosis of the vaginal biotope increases the informativeness of evaluating its effectiveness by identifying the mechanisms of its therapeutic effect: with the clinical effectiveness of the therapy, a transition to normal pregnancy was recorded - I or II types (degrees) of microbiocenosis of the vaginal biotope were detected; continued registration in some patients of types III and IV of the microbiocenosis of the vaginal biotope indicated the need for continued treatment.
Таким образом, на различных примерах из клинической практики показано, что микробиоценозы биотопов слизистых открытых полостей макроорганизма чутко реагируют на разнообразные изменения во внешней среде обитания, а также реагируют и участвуют в развитии инфекционной и не инфекционной патологии. Реакция на внешние и внутренние воздействия проявляется развитием дисбактериоза, появлением в биотопах слизистых микроорганизмов, не свойственных для них в нормальных условиях жизни; приобретением ими за счет возможного взаимовлияния микроорганизмов различных родов и видов новых генотипических (обмен генами - горизонтальный перенос, секвенстипирование) и фенотипических свойств; повышением частоты высеваемости отдельных микроорганизмов(высеваемости в титре ≥5,0-6,0 lg КОЕ/г), повышением патогенетических свойств (повышение вирулентности - приобретение островков патогенности, структурных и биохимических показателей вирулентности, филогенетический анализ). Все это способствует развитию инфекционного процесса, а также утяжеляет течение, провоцирует и обеспечивает возникновение соматических заболеваний. Во всех случаях выраженность генотипических и фенотипических изменений микроорганизмов биотопа слизистых коррелирует с интенсивностью внешних воздействий и с тяжестью клинических проявлений, а при их исчезновении и/или снижении их выраженности генотипические и фенотипические показатели микроорганизмов возвращаются к исходным уровням, в том числе, и благодаря взаимовлиянию микроорганизмов в биотопе слизистых, а также воздействию цитокинового и иммуноглобулинового звеньев иммунитета.Thus, using various examples from clinical practice, it was shown that microbiocenoses of biotopes of mucous open cavities of a macroorganism sensitively respond to various changes in the external environment, as well as react and participate in the development of infectious and non-infectious pathologies. The reaction to external and internal influences is manifested by the development of dysbiosis, the appearance in the biotopes of mucous microorganisms that are not typical for them in normal living conditions; their acquisition, due to the possible interaction of microorganisms of various genera and species, of new genotypic (gene exchange - horizontal transfer, sequencing) and phenotypic properties; increasing the frequency of seeding of individual microorganisms (seeding in the titer ≥ 5.0-6.0 lg CFU / g), increasing pathogenetic properties (increasing virulence - the acquisition of islands of pathogenicity, structural and biochemical indicators of virulence, phylogenetic analysis). All this contributes to the development of the infectious process, and also complicates the course, provokes and ensures the occurrence of somatic diseases. In all cases, the severity of genotypic and phenotypic changes in the mucous biotope microorganisms correlates with the intensity of external influences and the severity of clinical manifestations, and when they disappear and / or their severity decreases, the genotypic and phenotypic indicators of microorganisms return to their initial levels, including due to the interaction of microorganisms in the biotope of the mucous membranes, as well as the effects of cytokine and immunoglobulin immunity.
Установление генотипических и фенотипических свойств микроорганизмов биотопов слизистых открытых полостей макроорганизма, частоты высеваемости и их патогенетических свойств (вирулентности - приобретение островков патогенности, структурных и биохимических показателей вирулентности) наряду с общепринятыми для конкретного заболевания лабораторно-диагностическими исследованиями ускоряет и повышает информативность лабораторной диагностики. Критерии оценки состояния микробиоценозов биотопов слизистых открытых полостей как показателя общей реактивности макроорганизма позволяют судить и о состоянии здоровья обследуемого.Establishing the genotypic and phenotypic properties of microorganisms of biotopes of mucous open cavities of a macroorganism, the frequency of seeding and their pathogenetic properties (virulence - the acquisition of pathogenicity islands, structural and biochemical indicators of virulence) along with laboratory diagnostic tests generally accepted for a specific disease accelerates and increases the informativeness of laboratory diagnostics. Criteria for assessing the state of microbiocenoses of biotopes of mucous open cavities as an indicator of the general reactivity of a macroorganism make it possible to judge the state of health of the subject.
Впервые показано, что слизистые открытых полостей организма (рис. 3) функционируют как единый орган, а потому независимо от биотопа слизистых открытых полостей одновременно регистрируются однотипные изменения (одинаковые типы - степени) их микробиоценозов; локализация патологического процесса в конкретном биотопе слизистых открытых полостей определяет выраженность изменения микробиоценоза в нем, по сравнению с другими биотопами слизистых открытых полостей макроорганизма.It was shown for the first time that the mucous membranes of the open cavities of the body (Fig. 3) function as a single organ, and therefore, regardless of the biotope of the mucous open cavities, the same type of changes (the same types and degrees) of their microbiocenoses are simultaneously recorded; localization of the pathological process in a particular biotope of mucous open cavities determines the severity of changes in microbiocenosis in it, compared with other biotopes of mucous open cavities of a macroorganism.
ЛитератураLiterature
1. Хаитов P.M., Пинегин Б.В. Иммуномодуляторы: механизмы действия и клиническое применение // Аллергология и иммунология. - 2000. - Т. 1., №2. - С. 14-15.1. Khaitov P.M., Pinegin B.V. Immunomodulators: mechanisms of action and clinical application // Allergology and Immunology. - 2000. - T. 1., No. 2. - S. 14-15.
2. Козлова В.И., Пухнер А.Ф. Вирусные, хламидийные и микоплазменные заболевания гениталий // Руководство для врачей, издание 6-е, обновленное и дополненное. - М.: Триада-Х. - 2003.2. Kozlova V.I., Pukhner A.F. Viral, chlamydial and mycoplasma diseases of the genitals // Guide for physicians, 6th edition, updated and updated. - M .: Triad-X. - 2003.
3 Грачев С.В., Несвижский Ю.В., ![]()
![]()
4. Петров Р.В., Хаитов P.M. Основы иммунитета и иммунная биотехнология // Вестн. РАМН. - 2000. - №11. - С. 18-21.4. Petrov R.V., Khaitov P.M. The basics of immunity and immune biotechnology // Vestn. RAMS. - 2000. - No. 11. - S. 18-21.
5. Иммунобиологические препараты, перспективы применения в инфектологии. Г.Г. Онищенко, В.А. ![]()
![]()
6. Богданова Е.А., Несвижский Ю.В., Зверев В.В. Пристеночный микробиоценоз желудочно-кишечного тракта человека (учебное пособие). - М.: Издательский дом «Русский врач». - 2009.6. Bogdanova EA, Nesvizhsky Yu.V., Zverev V.V. Parietal microbiocenosis of the human gastrointestinal tract (study guide). - M .: Publishing House "Russian Doctor". - 2009.
7. Караулов А.В., Лахтин М.В., ![]()
![]()
8. Бондаренко В.М., Рубакова Э.И., Лаврова В.А. Иммуностимулирующее действие лактобактерий, используемых в качестве основы препаратов-пробиотиков // Журн. микробиол. - 1998. - №5. - С. 107-112.8. Bondarenko V.M., Rubakova E.I., Lavrova V.A. The immunostimulating effect of lactobacilli used as the basis for probiotic preparations // Zh. microbiol. - 1998. - No. 5. - S. 107-112.
9. Бондаренко В.М. «Острова» патогенности бактерий // Журн. микробиол. - 2001. - №4. - С. 67-74.9. Bondarenko V.M. "Islands" of pathogenicity of bacteria // Zh. microbiol. - 2001. - No. 4. - S. 67-74.
10. Зверев В.В., Несвижский Ю.В., Воропаева Е.А. и др. Микроэкология и гуморальный иммунитет слизистых открытых полостей человека в норме и при патологических состояниях. Учебное пособие для системы послевузовского профессионального образования врачей. - М. Астрахань. - 2011.10. Zverev V.V., Nesvizhsky Yu.V., Voropaeva E.A. and others. Microecology and humoral immunity of the mucous membranes of open human cavities in normal and pathological conditions. Textbook for the system of postgraduate professional education of doctors. - M. Astrakhan. - 2011.
11. Воропаева Е.А., Караулов А.В., Афанасьев С.С. и др. Оценка микробиоценоза влагалища при акушерской и гинекологической патологии (новая медицинская технология). Серия АА. №0001997. ФС №2009/187 от 17.07.2009 г. - Москва-Астрахань. - 2012).11. Voropaeva E.A., Karaulov A.V., Afanasyev S.S. et al. Evaluation of vaginal microbiocenosis in obstetric and gynecological pathology (new medical technology). AA series. No. 0001997. FS No. 2009/187 dated July 17, 2009 - Moscow-Astrakhan. - 2012).
Claims (1)
- полноценное здоровье при отсутствии верификации возбудителя и клинических проявлений инфекционного процесса и регистрации первой или второй степени микробиоценоза биотопа слизистых открытых полостей;
- продромальный период инфекционного заболевания при отсутствии верификации возбудителя и клинических проявлений инфекционного процесса и регистрации третьей или четвертой степени микробиоценоза биотопа слизистых открытых полостей;
- благоприятное течение заболевания при наличии клинических проявлений инфекционного процесса и/или верификации возбудителя и регистрации третьей или четвертой степени микробиоценоза биотопа слизистых открытых полостей;
- хроническое течение заболевания при наличии клинических проявлений инфекционного процесса и/или верификации возбудителя и регистрации первой или второй степени микробиоценоза биотопа слизистых открытых полостей. A method for assessing the state of human health in predicting the course of an infectious disease, characterized in that the microbiotope indices of the open mucous membranes are evaluated and the degree of violation of the microbiotope of the mucous open cavities is determined on their basis as an indicator of the degree of violation of the microbiocenosis of the biotope of the mucous open cavities, depending on the result, the state human health and predict the course of an infectious disease:
- full health in the absence of verification of the pathogen and clinical manifestations of the infectious process and registration of the first or second degree of microbiocenosis of the biotope of mucous open cavities;
- the prodromal period of an infectious disease in the absence of verification of the pathogen and the clinical manifestations of the infectious process and registration of the third or fourth degree microbiocenosis of the biotope of mucous open cavities;
- the favorable course of the disease in the presence of clinical manifestations of the infectious process and / or verification of the pathogen and registration of the third or fourth degree microbiocenosis of the biotope of mucous open cavities;
- the chronic course of the disease in the presence of clinical manifestations of the infectious process and / or verification of the pathogen and registration of the first or second degree of microbiocenosis of the biotope of mucous open cavities.
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2014152102/15A RU2595863C2 (en) | 2014-12-23 | 2014-12-23 | Method of evaluating state of human health in prediction of clinical course of infectious disease |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2014152102/15A RU2595863C2 (en) | 2014-12-23 | 2014-12-23 | Method of evaluating state of human health in prediction of clinical course of infectious disease |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| RU2014152102A RU2014152102A (en) | 2016-07-10 |
| RU2595863C2 true RU2595863C2 (en) | 2016-08-27 |
Family
ID=56372627
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2014152102/15A RU2595863C2 (en) | 2014-12-23 | 2014-12-23 | Method of evaluating state of human health in prediction of clinical course of infectious disease |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2595863C2 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2644831C1 (en) * | 2017-02-08 | 2018-02-14 | Федеральное государственное бюджетное научное учреждение "Дальневосточный научный центр физиологии и патологии дыхания" | Method for predicting the tightening of acute nazofaringetic in women with reactivation of chronic mixed-herpesvirus infection in the second trimester of pregnancy |
| RU2770433C1 (en) * | 2021-09-23 | 2022-04-18 | Елена Алексеевна Беседина | Method for choosing an algorithm for providing medical care to children with acute respiratory pathology |
Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2362808C1 (en) * | 2008-02-13 | 2009-07-27 | Государственное образовательное учреждение дополнительного профессионального образования Российская медицинская академия последипломного образования Федерального агентства по здравоохранению и социальному развитию (ГОУ ДПО РМАПО Росздрава) | Way of diagnostics of microbiota disbalance of various human biotopes and degree of its expression |
| RU2381504C1 (en) * | 2008-07-29 | 2010-02-10 | Федеральное государственное учреждение науки Центральный научно-исследовательский институт эпидемиологии Роспотребнадзора РФ | Method of estimating condition colonisation resistance of human biotope microbiocenosis (versions) |
| RU2535406C1 (en) * | 2013-10-01 | 2014-12-10 | Государственное бюджетное образовательное учреждение высшего профессионального образования "Самарский государственный медицинский университет" Министерства здравоохранения Российской Федерации | Method for monitoring of individual's health |
| RU2556958C1 (en) * | 2014-03-28 | 2015-07-20 | Федеральное бюджетное учреждение науки "Московский научно-исследовательский институт эпидемиологии и микробиологии им. Г.Н. Габричевского" Федеральной службы по надзору в сфере защиты прав потребителей и благополучия человека | Method for assessing mucosal immunity state of open cavities of different localisation accompanying prediction of clinical course of infectious-inflammatory processes, and method for correcting infectious-inflammatory processes |
-
2014
- 2014-12-23 RU RU2014152102/15A patent/RU2595863C2/en active
Patent Citations (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2362808C1 (en) * | 2008-02-13 | 2009-07-27 | Государственное образовательное учреждение дополнительного профессионального образования Российская медицинская академия последипломного образования Федерального агентства по здравоохранению и социальному развитию (ГОУ ДПО РМАПО Росздрава) | Way of diagnostics of microbiota disbalance of various human biotopes and degree of its expression |
| RU2381504C1 (en) * | 2008-07-29 | 2010-02-10 | Федеральное государственное учреждение науки Центральный научно-исследовательский институт эпидемиологии Роспотребнадзора РФ | Method of estimating condition colonisation resistance of human biotope microbiocenosis (versions) |
| RU2535406C1 (en) * | 2013-10-01 | 2014-12-10 | Государственное бюджетное образовательное учреждение высшего профессионального образования "Самарский государственный медицинский университет" Министерства здравоохранения Российской Федерации | Method for monitoring of individual's health |
| RU2556958C1 (en) * | 2014-03-28 | 2015-07-20 | Федеральное бюджетное учреждение науки "Московский научно-исследовательский институт эпидемиологии и микробиологии им. Г.Н. Габричевского" Федеральной службы по надзору в сфере защиты прав потребителей и благополучия человека | Method for assessing mucosal immunity state of open cavities of different localisation accompanying prediction of clinical course of infectious-inflammatory processes, and method for correcting infectious-inflammatory processes |
Non-Patent Citations (1)
| Title |
|---|
| АЛЕШКИН В.А. и др. Микробиоценозы и здоровье человека. Из-во Династия. 2015, с.548. * |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2644831C1 (en) * | 2017-02-08 | 2018-02-14 | Федеральное государственное бюджетное научное учреждение "Дальневосточный научный центр физиологии и патологии дыхания" | Method for predicting the tightening of acute nazofaringetic in women with reactivation of chronic mixed-herpesvirus infection in the second trimester of pregnancy |
| RU2770433C1 (en) * | 2021-09-23 | 2022-04-18 | Елена Алексеевна Беседина | Method for choosing an algorithm for providing medical care to children with acute respiratory pathology |
Also Published As
| Publication number | Publication date |
|---|---|
| RU2014152102A (en) | 2016-07-10 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| De Seta et al. | Lactobacillus plantarum P17630 for preventing Candida vaginitis recurrence: a retrospective comparative study | |
| D’Incà et al. | Rectal administration of Lactobacillus casei DG modifies flora composition and Toll-like receptor expression in colonic mucosa of patients with mild ulcerative colitis | |
| Verdenelli et al. | Impact of probiotic SYNBIO® administered by vaginal suppositories in promoting vaginal health of apparently healthy women | |
| Park et al. | A sporadic outbreak of human brucellosis in Korea | |
| Dausset et al. | Comparative phase I randomized open-label pilot clinical trial of Gynophilus®(Lcr regenerans®) immediate release capsules versus slow release muco-adhesive tablets | |
| Yun et al. | Effects of oral florfenicol on intestinal structure, function and microbiota in mice | |
| AL et al. | Isolation of Proteus mirabilis and Proteus vulgaris from different clinical sources and study of some virulence factors | |
| Burgos-Portugal et al. | The role of autophagy in the intracellular survival of Campylobacter concisus | |
| Vivekanandan et al. | VagiBIOM Lactobacillus suppository improves vaginal health index in perimenopausal women with bacterial vaginosis: a randomized control trial | |
| RU2595863C2 (en) | Method of evaluating state of human health in prediction of clinical course of infectious disease | |
| Acherjya et al. | Pattern of antimicrobial resistance to Escherichia coli among the urinary tract infection patients in Bangladesh | |
| LEE et al. | Reevaluation of the role of T-mycoplasmas in nongonococcal urethritis | |
| RU2578028C1 (en) | Method of evaluating state of women's health when predicting physiological and complicated course of pregnancy at early stages of gestation | |
| US9962416B2 (en) | Probiotics for treating neuropathic bladder associated urinary tract infection | |
| Dickson et al. | The effect of enterococci on feline Tritrichomonas foetus infection in vitro | |
| Lu et al. | Effect of mixed probiotics on pulmonary flora in patients with mechanical ventilation: an exploratory randomized intervention study | |
| CN115590892A (en) | Female private probiotic bacteria inhibiting powder containing probiotic bacteria composite powder and preparation method | |
| RU2556958C1 (en) | Method for assessing mucosal immunity state of open cavities of different localisation accompanying prediction of clinical course of infectious-inflammatory processes, and method for correcting infectious-inflammatory processes | |
| Mykhailyshyn et al. | The Effect of Probiotic Therapy on the Vagina Microbiota and the Humoral Link of Immunity in Bacterial Vaginosis | |
| Das et al. | Higher vaginal pH is associated with Chlamydia trachomatis infection in women: a prospective case–controlled study | |
| Mian et al. | Efficacity of ternidazole-neomycin sulfate-nystatin and prednisolone association in syndromic management of vaginitis in low and middle incomes countries | |
| MYKHAILYSHYN et al. | THE EFFECT OF PROBIOTIC THERAPY ON THE VAGINA MICROBIOTA AND THE HUMORAL LINK OF IMMUNITY IN BACTERIAL VAGI. | |
| Chou et al. | Primary lung abscess caused by Staphylococcus lugdunensis | |
| Farhana et al. | Effectiveness of Probiotics for the Treatment of Urinary Tract Infection among Women in Bangladesh | |
| Kumar et al. | An RCT for efficacy of oral probiotics in treatment of cases with symptomatic white discharge per vagina in rural population |