KR20220133243A - Method of treating cancer using anti-TIGIT antagonist antibody - Google Patents
Method of treating cancer using anti-TIGIT antagonist antibody Download PDFInfo
- Publication number
- KR20220133243A KR20220133243A KR1020227029306A KR20227029306A KR20220133243A KR 20220133243 A KR20220133243 A KR 20220133243A KR 1020227029306 A KR1020227029306 A KR 1020227029306A KR 20227029306 A KR20227029306 A KR 20227029306A KR 20220133243 A KR20220133243 A KR 20220133243A
- Authority
- KR
- South Korea
- Prior art keywords
- subject
- dose
- weeks
- subjects
- antibody
- Prior art date
Links
Images



























Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/335—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin
- A61K31/337—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin having four-membered rings, e.g. taxol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/335—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin
- A61K31/365—Lactones
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/555—Heterocyclic compounds containing heavy metals, e.g. hemin, hematin, melarsoprol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7042—Compounds having saccharide radicals and heterocyclic rings
- A61K31/7052—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides
- A61K31/706—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom
- A61K31/7064—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines
- A61K31/7068—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines having oxo groups directly attached to the pyrimidine ring, e.g. cytidine, cytidylic acid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K33/00—Medicinal preparations containing inorganic active ingredients
- A61K33/24—Heavy metals; Compounds thereof
- A61K33/243—Platinum; Compounds thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2827—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against B7 molecules, e.g. CD80, CD86
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
- A61K2039/507—Comprising a combination of two or more separate antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/54—Medicinal preparations containing antigens or antibodies characterised by the route of administration
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/545—Medicinal preparations containing antigens or antibodies characterised by the dose, timing or administration schedule
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K2300/00—Mixtures or combinations of active ingredients, wherein at least one active ingredient is fully defined in groups A61K31/00 - A61K41/00
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/90—Immunoglobulins specific features characterized by (pharmaco)kinetic aspects or by stability of the immunoglobulin
Abstract
본 발명은 암(예컨대, 폐암; 자궁경부암; 유방암; 두경부암; 간암; 위암; 방광암; 식도암; 췌장암; 신장암; 흑색종; 난소암; 또는 결장직장암)의 치료를 위한 방법, 사용 및 조성물에 관한 것이다. 더 구체적으로, 본 발명은 병용 요법에서의 항 TIGIT 길항제 항체를 이용한 치료를 포함하여, 암을 가진 환자를 항 TIGIT 길항제 항체를 이용해 치료하는 것에 관한 것이다. The present invention provides methods, uses and compositions for the treatment of cancer (e.g., lung cancer; cervical cancer; breast cancer; head and neck cancer; liver cancer; stomach cancer; bladder cancer; esophageal cancer; pancreatic cancer; kidney cancer; melanoma; ovarian cancer; or colorectal cancer). it's about More specifically, the present invention relates to the treatment of patients with cancer with anti-TIGIT antagonist antibodies, including treatment with anti-TIGIT antagonist antibodies in combination therapy.
Description
관련 출원에 대한 상호 참조CROSS-REFERENCE TO RELATED APPLICATIONS
본 출원은 2020년 1월 27일에 출원한 미합중국 특허 출원 제62/966,448호; 2020년 3월 5일에 출원한 미합중국 특허 출원 제62/985,822호; 2020년 3월 24일에 출원한 미합중국 특허 출원 제62/994,272호; 2020년 3월 24일에 출원한 국제 출원 제PCT/US2020/024526호; 2020년 7월 30일에 출원한 미합중국 특허 출원 제63/059,054호; 2020년 7월 31일에 출원한 미합중국 특허 제63/059,960호; 2020년 9월 4일에 출원한 미합중국 특허 제63/074,807호; 2020년 9월 4일에 출원한 미합중국 특허 제63/074,827호; 2020년 9월 4일에 출원한 국제 출원 제PCT/US2020/049415호; 2020년 9월 30일에 출원한 미합중국 특허 출원 제63/085,890호; 2020년 10월 23일에 출원한 미합중국 특허 출원 제63/105,198호; 2020년 11월 16일에 출원한 미합중국 특허 출원 제63/114,517호; 2020년 12월 11일에 출원한 미합중국 특허 출원 제63/124,693호; 및 2020년 12월 17일에 출원한 미합중국 특허 출원 제63/127,109호의 우선권 이익을 주장하며, 그 각각의 내용은 전체가 본원에 원용된다.This application is filed on January 27, 2020 in U.S. Patent Application Serial Nos. 62/966,448; US Patent Application No. 62/985,822, filed March 5, 2020; US Patent Application No. 62/994,272, filed March 24, 2020; International Application No. PCT/US2020/024526, filed March 24, 2020; U.S. Patent Application Serial No. 63/059,054, filed July 30, 2020; U.S. Patent Nos. 63/059,960, filed July 31, 2020; U.S. Patent Nos. 63/074,807, filed September 4, 2020; U.S. Patent Nos. 63/074,827, filed September 4, 2020; International Application No. PCT/US2020/049415 filed on September 4, 2020; U.S. Patent Application Serial No. 63/085,890, filed September 30, 2020; U.S. Patent Application Serial No. 63/105,198, filed October 23, 2020; U.S. Patent Application Serial No. 63/114,517, filed on November 16, 2020; U.S. Patent Application Serial No. 63/124,693, filed December 11, 2020; and U.S. Patent Application No. 63/127,109, filed on December 17, 2020, the contents of each of which are incorporated herein by reference in their entirety.
서열 목록sequence list
본 출원은 ASCII 포맷으로 전자적으로 제출된 서열 목록을 포함하며, 이의 내용은 그 전체가 본원에 원용된다. 2021년 01월 25일 생성된 상기 ASCII 사본의 파일명은 50474-206WO2_Sequence_Listing_1_25_2021_ST25이며 30,641 바이트 크기이다. This application contains a sequence listing submitted electronically in ASCII format, the contents of which are incorporated herein by reference in their entirety. The file name of this ASCII copy, created on January 25, 2021, is 50474-206WO2_Sequence_Listing_1_25_2021_ST25 and is 30,641 bytes in size.
본 발명은 암의 치료를 위한 방법, 사용, 및 조성물에 관한 것이다. 더 구체적으로, 본 발명은 항 TIGIT 길항제 항체를 이용한 암을 가진 환자의 치료(예컨대, 단일요법 또는 병용 요법으로서 항 TIGIT 길항제 항체를 이용한 치료)에 관한 것이다. The present invention relates to methods, uses, and compositions for the treatment of cancer. More specifically, the present invention relates to treatment of a patient with cancer with an anti-TIGIT antagonist antibody (eg, treatment with an anti-TIGIT antagonist antibody as monotherapy or combination therapy).
암은 세포 소집단의 통제되지 않은 성장을 특징으로 한다. 암은 선진국에서 주요 사망 원인이자 개발도상국에서 두 번째 주요 사망 원인으로, 매년 1,400만 건 이상의 새로운 암 사례가 진단되고 800만 명이 넘는 암 사망이 발생한다. 따라서, 암 치료는 유의적이고 지속적으로 증가하는 사회적 부담이 되고 있다.Cancer is characterized by the uncontrolled growth of subpopulations of cells. Cancer is the leading cause of death in developed countries and the second leading cause of death in developing countries, with over 14 million new cancer cases diagnosed each year and over 8 million cancer deaths. Therefore, cancer treatment has become a significant and continuously increasing social burden.
따라서, 암 치료를 위한 효과적인 면역요법 및 이를 투여하는 방법의 개발 분야에서 충족되지 않은 요구가 있다.Accordingly, there is an unmet need in the field of development of effective immunotherapy for cancer treatment and methods of administering the same.
일 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In one aspect, the present invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, the PD-1 axis at a dose of about 900 mg to about 1500 mg every 3 weeks. A method is provided, comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and PD-1 axis binding at a dose of about 1400 mg to 2000 mg every 4 weeks A method is provided comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the antagonist.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and the PD-1 axis at a dose of about 600 mg to about 1200 mg every two weeks. A method is provided comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the binding antagonist.
다른 양태에서, 본 발명은 본원에 제공된 방법에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한 항 TIGIT 길항제 항체를 포함하는, 키트를 제공한다.In another aspect, the invention provides a kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to the methods provided herein.
다른 양태에서, 본 발명은 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서, 상기 방법은 본원에 제공된 방법에 따르는, 항 TIGIT 길항제 항체 및 항 PD-1 축 결합 길항제를 제공한다.In another aspect, the invention provides an anti TIGIT antagonist antibody and an anti-PD-1 axis binding antagonist for use in a method of treating a subject having cancer, said method comprising an anti-TIGIT antagonist antibody and anti-PD-1 according to a method provided herein. Axial binding antagonists are provided.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용되는 항 TIGIT 길항제 항체의 사용으로서, 상기 치료는 본원에 제공된 방법에 따르는, 사용을 제공한다.In another aspect, the invention provides the use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, wherein said treatment is according to a method provided herein. .
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and PD-1 axis binding at a dose of about 1400 mg to 2000 mg every 4 weeks A method is provided comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the antagonist.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and the PD-1 axis at a dose of about 600 mg to about 1200 mg every two weeks. A method is provided comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the binding antagonist.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis at a dose of about 900 mg to about 1500 mg every 3 weeks. A method is provided, comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 100 mg 내지 약 300 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and anti-PD-1 at a dose of about 100 mg to about 300 mg every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the antagonist antibody, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 티라골루맙 및 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 300 mg 내지 약 500 mg의 용량으로 투여되는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer comprising administering to the subject a dosing regimen comprising at least one dosing cycle of tiragolumab and pembrolizumab, wherein said pembrolizumab is administered at a dose of about 300 mg to about 500 mg every 6 weeks.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, the PD-1 axis at a dose of about 900 mg to about 1500 mg every 3 weeks a dosing regimen comprising one or more dosing cycles of the combination antagonist, and an antimetabolite at a dose of about 10 mg/m 2 to about 10000 mg/m 2 orally twice daily every 3 weeks of a 2 week dosing/1 week washout. A method is provided, comprising administering to the subject.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 젬시타빈, 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis at a dose of about 900 mg to about 1500 mg every 3 weeks. Provided is a method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a binding antagonist, gemcitabine, and nap-paclitaxel.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg 용량의 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having cancer, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis at a dose of about 900 mg to about 1500 mg every 3 weeks. A method is provided, comprising administering to the subject a dosing regimen comprising a binding antagonist and one or more dosing cycles of a VEGF antagonist at a dose of about 1 mg/kg to about 35 mg/kg every three weeks.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 상기 유도기는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고 (b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer, comprising administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein: (a) the induction phase is from about 500 mg to about every 3 weeks Anti-TIGIT antagonist antibody at a dose of about 700 mg, PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, platinum-based chemotherapeutic agent every 3 weeks, and non-platinum-based chemotherapeutic agent once every 3 weeks comprising more than one dosing cycle; and (b) said maintenance phase comprises one or more additional dosing cycles of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said The maintenance phase does not include administration of the platinum-based chemotherapeutic agent.
다른 양태에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 상기 유도기는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고 (b) 상기 유지기는 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cancer, comprising administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein: (a) the induction phase is from about 500 mg to about every 3 weeks Anti-TIGIT antagonist antibody at a dose of about 700 mg, PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, platinum-based chemotherapeutic agent every 3 weeks, and non-platinum-based chemotherapeutic agent once every 3 weeks comprising more than one dosing cycle; and (b) the maintenance phase comprises one or more additional dosing cycles of the anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and the PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. and wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent.
다른 양태에서, 본 발명은 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장시키는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having lung cancer, comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a single dose of a topoisomerase II inhibitor. administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle, wherein the treatment is a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II in the absence of the anti-TIGIT antagonist antibody. A method of prolonging progression-free survival (PFS) in the subject as compared to treatment with an inhibitor is provided.
다른 양태에서, 본 발명은 폐암을 가진 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 약 8.2개월 내지 약 9.2개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a population of subjects having lung cancer, comprising one or more administrations of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. A method is provided, comprising administering to the subject population a dosing regimen comprising a cycle, wherein the treatment results in a median PFS in the subject population of from about 8.2 months to about 9.2 months.
다른 양태에서, 본 발명은 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 OS를 연장시키는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having lung cancer, comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a single dose of a topoisomerase II inhibitor. administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle, wherein the treatment is a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II in the absence of the anti-TIGIT antagonist antibody. A method of prolonging OS in the subject as compared to treatment with an inhibitor is provided.
다른 양태에서, 본 발명은 폐암을 가진 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 약 15.3개월 내지 약 17.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a population of subjects having lung cancer, comprising one or more administrations of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. A method is provided, comprising administering to the subject population a dosing regimen comprising a cycle, wherein the treatment results in a median OS of the subject population of from about 15.3 months to about 17.6 months.
다른 양태에서, 본 발명은 SCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having SCLC, comprising: on
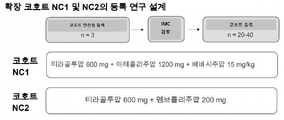
다른 양태에서, 본 발명은 ES-SCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 4회의 초기 투약 주기에 이어서 1회 이상의 추가적인 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서: (a) 상기 4회의 초기 투약 주기는 각 초기 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 초기 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 초기 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 초기 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드를 투여하는 단계를 포함하고; 그리고 (b) 상기 1회 이상의 추가적인 투약 주기는 각각의 추가적인 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각각의 추가적인 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙을 투여하는 단계를 포함하고, 여기서 상기 4회의 초기 투약 주기 및 상기 1회 이상의 추가적인 투약 주기는 각각의 21일 투약 주기이고, 여기서 상기 치료는 상기 티라골루맙 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having ES-SCLC, comprising administering to said subject or population of subjects four initial dosing cycles followed by one or more additional dosing cycles, wherein : (a) said four initial dosing cycles are tiragolumab at a dose of about 600 mg on
다른 양태에서, 본 발명은 암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제인 제1 화학요법제, 및 비백금계 화학요법제인 제2 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having cancer, comprising an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent, and a second agent that is a non-platinum-based
다른 양태에서, 본 발명은 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg 용량으로 투여되고, 상기 카보플라틴은 3주마다 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되거나, 또는 상기 시스플라틴은 3주마다 75 mg/m2 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2 용량으로 투여되는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects with advanced nonsquamous NSCLC comprising four 21 day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed. administering to the subject or population of subjects a dosing regimen comprising The carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min every 3 weeks, or the cisplatin is administered at a dose of 75 mg/m 2 every 3 weeks, and the pemetrexed is administered in 4 doses of 21 and administered at a dose of about 500 mg/m 2 every 3 weeks on each day of the dosing cycle.
다른 양태에서, 본 발명은 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 상기 대상체 또는 대상체 집단에: (i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및 (ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/㎡ 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고, 여기서 상기 대상체 또는 대상체 집단은 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having advanced nonsquamous NSCLC, wherein said subject or population of subjects: (i) tyragolumab at a dose of about 600 mg every 3 weeks, about 1200 every 3
다른 양태에서, 본 발명은 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다. In another aspect, the invention provides a method of treating a subject with resectable lung cancer, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and PD- at a dose of about 900 mg to about 1500 mg every 3 weeks. A method is provided comprising administering to the subject one or more dosing cycles of a uniaxial binding antagonist.
다른 양태에서, 본 발명은 폐암을 가진 대상체를 치료하는 방법으로서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having lung cancer, comprising administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein during said dosing cycles administering as neoadjuvant treatment a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody at least once every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks , provides a method.
다른 양태에서, 본 발명은 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는 (ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및 (b) (i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject with resectable lung cancer, comprising: tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (a) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) cisplatin at a dose of about 75 mg/m 2 every 3 weeks; and (b) (i) pemetrexed at a dose of about 500 mg/m 2 every 3 weeks or gemcitabine at a dose of about 1000 mg/m 2 or about 1250 mg/m 2 on
다른 양태에서, 본 발명은 폐암을 가진 대상체를 치료하는 방법으로서, 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게 (a) 3주마다 약 1200 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; 그리고 (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 티라골루맙 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having lung cancer, comprising administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein (I) at least one of said dosing cycles One time is neoadjuvant treatment and the subject is given (a) tyragolumab at a dose of about 1200 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m 2 on
다른 양태에서, 본 발명은 PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,In another aspect, the invention provides a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1, the method comprising:
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method is provided, comprising the steps of:
다른 양태에서, 본 발명은 자궁경부암을 가진 대상체를 위한 요법을 선별하기 위한 방법으로서, (a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및 (b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 약 500 mg 내지 약 700 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 투여되는 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method for selecting a therapy for a subject having cervical cancer, comprising (a) PD on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining. - detecting the protein expression level of L1; and (b) an anti-TIGIT antagonist antibody administered at a dose of about 500 mg to about 700 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1; selecting a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist administered at a dose of about 900 mg to about 1500 mg every three weeks.
다른 양태에서, 본 발명은 PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject having cervical cancer having a detectable expression level of PD-L1, wherein the tiragolumab at a dose of about 600 mg every 3 weeks and atezoli at a dose of about 1200 mg every 3 weeks Provided is a method comprising administering to the subject one or more dosing cycles of zumab.
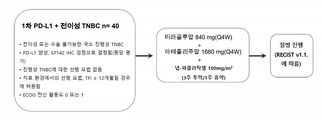
다른 양태에서, 본 발명은 유방암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 4주마다 약 840 mg 용량의 티라골루맙, 4주마다 약 1680 mg 용량의 아테졸리주맙, 및 3주 투약/1주 휴약의 약 100 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having breast cancer, comprising tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and dosing for 3 weeks/1 A method is provided, comprising administering to the subject or population of subjects a dosing regimen comprising one or more dosing cycles of nap-paclitaxel at a dose of about 100 mg/m 2 of a weekly break.
다른 양태에서, 본 발명은 초기 삼중 음성 유방암(eTNBC)을 가진 대상체를 치료하는 방법으로서, 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject with early stage triple negative breast cancer (eTNBC) comprising an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and about 600 mg to about 1200 mg every two weeks. A method is provided comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a dose of a PD-1 axis binding antagonist.
다른 양태에서, 본 발명은 eTNBC를 가진 대상체를 치료하는 방법으로서, 2주마다 약 420 mg 용량의 티라골루맙, 2주마다 약 840 mg 용량의 아테졸리주맙, 및: (a) (i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및 (ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/ m2 용량의 독소루비신, 2주마다 약 600 mg/ m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는 (b) (i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/ m2 용량의 냅-파클리탁셀; 및 (ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/ m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고; 여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject with eTNBC, comprising: tiragolumab at a dose of about 420 mg every two weeks, atezolizumab at a dose of about 840 mg every two weeks, and: (a) (i) dosing Nap-paclitaxel at a dose of about 125 mg/m 2 every week for the first 12 weeks of therapy and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and (ii) doxorubicin at a dose of about 60 mg/m 2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m 2 every 2 weeks, and G-CSF every 2 weeks for
다른 양태에서, 본 발명은 PD-L1의 검출 가능한 단백질 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,In another aspect, the present invention provides a method of treating a subject or population of subjects having SCCHN having a detectable protein expression level of PD-L1, the method comprising:
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method is provided, comprising the steps of:
다른 양태에서, 본 발명은 SCCHN을 가진 대상체 또는 대상체 집단를 위한 요법을 선택하는 방법으로서: (a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체 또는 대상체 집단으로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및 (b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체 또는 대상체 집단에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of selecting a therapy for a subject or population of subjects having SCCHN: (a) PD in a tumor sample from said subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining. - detecting the protein expression level of L1; and (b) a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks based on PD-L1 expression detected for said subject or population of subjects having a detectable expression level of PD-L1; A method is provided, comprising selecting a regimen comprising at least one dosing cycle of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg per week.
다른 양태에서, 본 발명은 PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. administering to the subject one or more dosing cycles of
다른 양태에서, 본 발명은 간세포 암종(HCC)을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체 집단은 HCC에 대해 선행 전신 요법을 받은 적이 없는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having hepatocellular carcinoma (HCC) comprising administering to said subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist. wherein the subject or population of subjects has not received prior systemic therapy for HCC.
다른 양태에서, 본 발명은 HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having HCC, comprising administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist. A method is provided, comprising the steps of:
다른 양태에서, 본 발명은 HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having HCC, comprising a dose of about 600 mg tiragolumab every 3 weeks, a dose of about 1200 mg atezolizumab every 3 weeks, and about 15 every 3 weeks Provided is a method comprising administering to the subject one or more dosing cycles of bevacizumab at a dose of mg/kg.
다른 양태에서, 본 발명은 MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects with MIBC, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and PD at a dose of about 900 mg to about 1500 mg every 3 weeks. - administering to the subject one or more dosing cycles of a -1 axis binding antagonist, wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
다른 양태에서, 본 발명은 MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects with MIBC, comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and PD at a dose of about 900 mg to about 1500 mg every 3 weeks. - administering to the subject one or more dosing cycles of the -1 axis binding antagonist, wherein the treatment is perioperative treatment.
다른 양태에서, 본 발명은 MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체들은 시스플라틴 부적격인, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects with MIBC comprising one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. administering to the subject or population of subjects, wherein the subject or subjects are cisplatin ineligible.
다른 양태에서, 본 발명은 MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects with MIBC comprising one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. administering to the subject or population of subjects, wherein the treatment is perioperative treatment.
다른 양태에서, 본 발명은 mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having mUC, wherein the anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and PD at a dose of about 900 mg to about 1500 mg every 3 weeks - administering to the subject or population of subjects a dosing regimen comprising one or more dosing cycles of the -1 axis binding antagonist.
다른 양태에서, 본 발명은 mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having mUC, comprising one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. and administering to the subject or population of subjects.
다른 양태에서, 본 발명은 mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: (a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having mUC, comprising administering to said subject or population of subjects a first dosing regimen followed by a second dosing regimen, wherein: (a) said the first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and (b) said second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin is administered weekly of 2 weeks on / 1 week off. is administered at a dose of 1.25 mg/kg, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg of 2 weeks of dosing/weekly off, wherein the second dosing regimen is administered to the subject or population of subjects and to the subject or population of subjects after experiencing disease progression or unacceptable toxicity during said first dosing regimen.
다른 양태에서, 본 발명은 췌장암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having pancreatic cancer, comprising: tyragolumab at a dose of about 420 mg on
다른 양태에서, 본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, wherein on
다른 양태에서, 본 발명은 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법을 제공한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having esophageal cancer, wherein the anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg on
다른 양태에서, 본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 방법을 제공한다.In another aspect, the invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising: tyragolumab at a dose of about 600 mg on
다른 양태에서, 본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서, 제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: (a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함한다.In another aspect, the present invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, the method comprising administering to the subject or population of subjects a first dosage regimen and a second dosage regimen, wherein: (a ) said first dosing regimen is cisplatin at a dose of about 80 mg/m 2 on
다른 양태에서, 본 발명은 본원에 제공된 방법에 따라 암을 가진 대상체를 치료하기 위한 PD-1 축 결합 길항제 및/또는 항 TIGIT 길항제 항체를 포함하는, 키트를 제공한다.In another aspect, the invention provides a kit comprising a PD-1 axis binding antagonist and/or anti TIGIT antagonist antibody for treating a subject having cancer according to the methods provided herein.
다른 양태에서, 본 발명은 본원에 제공된 방법에 따라 암을 가진 대상체를 치료하기 위해 항 TIGIT 길항제 항체와 병용으로 사용하기 위한 PD-1 축 결합 길항제를 포함하는, 키트를 제공한다.In another aspect, the invention provides a kit comprising a PD-1 axis binding antagonist for use in combination with an anti TIGIT antagonist antibody to treat a subject having cancer according to the methods provided herein.
다른 양태에서, 본 발명은 본원에 제공된 방법에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한 항 TIGIT 길항제 항체를 포함하는, 키트를 제공한다.In another aspect, the invention provides a kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to the methods provided herein.
다른 양태에서, 본 발명은 암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서, 상기 방법은 본원에 제공된 방법에 따르는, 항 TIGIT 길항제 항체 및 항 PD-1 축 결합 길항제를 제공한다.In another aspect, the present invention provides an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cancer, said method comprising an anti TIGIT antagonist antibody and an anti-TIGIT antagonist antibody according to the methods provided herein. PD-1 axis binding antagonists are provided.
다른 양태에서, 본 발명은 암을 가진 대상체 또는 대상체 집단을 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용되는 항 TIGIT 길항제 항체의 사용으로서, 상기 치료는 본원에 제공된 방법에 따르는, 사용을 제공한다.In another aspect, the invention provides the use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or population of subjects having cancer, wherein the treatment is according to a method provided herein. provides
도 1은 Ib상 화학요법 확장 및 Ib상 Q4W 투약 확장을 도시한 흐름도이다.
도 2는 Ib상 실험 계획의 흐름도이다. EOCG = 이스턴 코퍼레이티브 종양학 그룹(Eastern Cooperative Oncology Group); IHC = 면역조직화학(immunohistochemistry); PD-L1+ = 예정된 세포사멸 리간드(programmed death-ligand) 1 양성; Q4W = 4주마다; RECIST v1.1 = 고형 종양의 반응 기준(Response Criteria in Solid Tumors), 버전 1.1; TFI = 무치료 간격(treatment-free interval); TNBC = 삼중음성 유방암(triple-negative breast cancer).
도 3은 Ia상 연구 설계의 흐름도이다. CRC = 결장직장암, DLT = 용량 제한 독성, GC = 위암, HNSCC = 두경부 편평 세포 암종, IV = 정맥내, MAD = 최대 투여 용량, MSI = 미세 위성 불안정, MSS = 미세 위성 불안정, MTD = 최대 허용 용량, NSCLC = 비소세포 폐암, OC = 난소암, PD = 질병의 진행, PK = 약동학, RCC = 신세포 암종, TNBC = 삼중음성 유방암, UBC = 요로상피 방광암.
도 4는 Ib상 티라골루맙 및 아테졸리주맙 확장 코호트, 연속 생검 코호트, 및 Q4W 투약 확장 코호트 연구 설계의 흐름도이다. CIT = 암 면역요법; DLT = 용량 제한 독성; HNSCC = 두경부 편평 세포 암종, IV = 정맥내, MAD = 최대 투여 용량, MSI = 미세 위성 불안정성, MSS = 미세 위성 안정, MTD = 최대 허용 용량, NSCLC = 비소세포 폐암, PD = 질병 진행; PD 1 = 예정된 세포사멸-1; PD-L1 = 예정된 세포사멸 리간드 1; PK = 약동학, TIGIT = Ig 및 ITIM 도메인을 갖는 세포 면역수용체. 비고: PD-L1 선택 및/또는 TIGIT 선택 종양이 있는 환자로 제한된다. a 진행성, 난치성, 불응성 종양. 3주마다 티라골루맙 IV 및 아테졸리주맙 1200 mg IV. Ia상의 안전성 데이터에 대한 IMC 검토 후에만 등록한다. DLT 기간이 21일인 3+3 용량 증량. MTD를 초과하지 않는 경우 티라골루맙의 다른 중간 용량을 연구할 수 있다. 추가적인 안전성, PK 및 PD 데이터를 얻기 위해, 환자가 선택적 연속 생검에 동의하는 경우 환자를 다시 등록할 수 있다. 1200 mg 티라골루맙을 초과하는 용량 수준의 평가는 뒷받침하는 근거와 함께 프로토콜 수정이 필요할 것이다. b 확장은 MTD 또는 MAD 이하의 용량에서 시작할 수 있다. c 최대 약 절반의 환자가 선택적인 연속 생검에 동의할 것이다. 이에 대한 항 PD-L1/PD-1 제제가 지역 규제 당국의 승인을 받은 종양(예컨대, NSCLC 흑색종, 신세포 암종)을 가진 환자는 항 PD-L1과 병용한 연구용 제제에 대한 임상시험이 허용 가능한 치료 옵션으로 간주되는 경우에만 확장 코호트(적응증 확장 또는 연속 생검)에 등록할 수 있다. d 선택적 연속 생검(허용가능한 샘플은 중심부 바늘, 절제, 절개, 펀치, 및/또는 포셉 생검을 포함함)에 동의한 환자로 제한된다. e Q4W 투약 확장 코호트에서, 약 3명의 환자에 대한 안전성 탐색이 완료될 것이다. 안전성 탐색의 모든 관련 안전 데이터는 등록을 계속하기 전에 IMC 및 조사관이 철저히 검토해야 한다.
도 5는 Ib상 화학요법 확장 코호트 연구 설계의 흐름도이다.
도 6은 Ib상 비화학요법 확장 코호트 연구 설계의 흐름도이다.
도 7은 진행을 넘어 연구 치료를 계속하기 위한 조건을 도시한 흐름도이다. EOCG = 이스턴 코퍼레이티브 종양학 그룹(Eastern Cooperative Oncology Group); RECIST = 고형 종양의 반응 기준(Response Criteria in Solid Tumors),
도 8은 Ia상에서 Ib상으로의 전환을 도시한 흐름도이다. AE = 유해 사례, DLT = 용량 제한 독성, PD = 질병 진행.
도 9는 티라골루맙의 약동학을 도시한 그래프이다.
도 10은 티라골루맙의 약동학을 도시한 일련의 그래프이다.
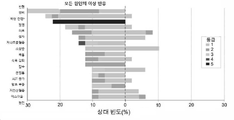
도 11은 Ia상 티라골루맙 용량 증량 연구에서 10% 이상인 모든 유해 사례를 도시한 그래프이다. * 등급 5의 AE는 악성 신생물 진행(n=3)이었고, 티라골루맙과 관련이 없었다.
도 12는 Ib상 티라골루맙 및 아테졸리주맙 용량 증량 연구에서 10% 이상인 모든 유해 사례를 도시한 그래프이다. * 등급 5의 AE는 악성 신생물 진행(n=12) 및 폐 색전증(n=2)이었고, 연구 약물(들)과 관련이 없었다.
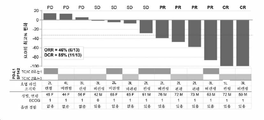
도 13은 Ia상 티라골루맙 용량 증량 연구에서 종양 크기 감소를 도시한 그래프이다.
도 14는 Ib상 티라골루맙 및 아테졸리주맙 용량 증량 연구에서 종양 크기 감소를 도시한 그래프이다.
도 15는 Ib상 티라골루맙 및 아테졸리주맙 용량 증량 연구에서 CIT 미경험 PD-L1 양성 NSCLC 종양 크기 감소를 도시한 그래프이다.
도 16은 Ib상 티라골루맙 및 아테졸리주맙 용량 증량 연구에서 시간에 따른 CIT 미경험 PD-L1 양성 NSCLC 종양 크기 감소를 도시한 그래프이다.
도 17은 3상 실험 계획의 흐름도이다. 1L = 1차; CE = 카보플라틴 및 에토포시드; ECOG PS = 이스턴 코퍼레이티브 종양학 그룹 전신 활동도; ES-SCLC = 확장기 소세포 폐암; LDH = 락타아제 탈수소효소; RECIST = 고형 종양의 반응 평가 기준; ITT= 치료 의향; PP = 1차 모집단.
도 18은 대상체의 선택, 계층화 기준, 치료군의 무작위 배정, 및 치료 평가변수에 관한 매개변수를 도시한 연구 설계의 개략도이다.
도 19는 GO42501 임상 II상 단계 연구의 연구 설계의 계통도이다. 활성화 EGFR 돌연변이(EGFR-)가 없고, ALK 융합 종양 유전자(ALK-)가 없고, ECOG 전신 활동도가 0 또는 1로 선택되는 절제 가능한 II기, IIIA기 또는 선택 IIIB(T3N2) 비소세포폐암(NSCLC) 환자. 코호트 A는 PD-L1이 높은 환자로 구성된다. 코호트 A의 환자는 4회 주기 동안 3주마다(Q3W) 아테졸리주맙(아테조) 및 티라골루맙(티라)으로 치료한다. 코호트 B는 임의의 PD-L1 상태를 갖는 환자로 구성된다. 코호트 B의 환자는 4회 주기 동안 아테조, 티라 및 백금계 이중 화학요법(화학(Chemo)) Q3W로 치료한다. 2주기 및 4주기 후에 흉부 컴퓨터 단층촬영(CT)을 실시한다. 두 코호트의 환자에 대해 수술을 실시하고, 주요 병리학적 반응(MPR) 및 병리학적 완전 반응(pCR)을 평가한다. 수술 후, 코호트 A의 환자는 16회 주기 동안 아테조 및 티라 Q3W 또는 4회 주기 동안 화학 Q3W로 치료한다. 코호트 B의 환자는 16회 주기 동안 아테조 및 티라 Q3W로 치료한다. 수술 후 방사선 요법(PORT)은 보조제 투여 전 R1/R2 절제 및/또는 ypN2에 대해 선택 사항이다. 생존 추적을 실시한다.
도 20은 GO42501 II상 임상 시험에서의 환자 등록을 도시한 흐름도이다. 코호트 A(PD-L1이 높은 환자; PD-L1 종양 비율 점수(TPS) ≥ 50%)의 경우, 6명의 환자를 활용하여 안전성 도입을 실시한다. 수술 안전성 기준이 충족되지 않으면, 코호트 A의 등록을 중단한다. 수술 안전성 기준이 충족되면, 코호트 A의 등록을 계속한다. 코호트 B(임의의 PD-L1 상태를 가진 환자)의 경우, PD-L1 TPS가 50% 미만인 6명의 환자를 활용하여 안전 도입을 실시한다. 수술 안전성 기준이 충족되지 않으면, 코호트 B의 등록을 중단한다. 수술 안전성 기준이 충족되면, 코호트 B의 등록을 계속하며, PD-L1 TPS가 50% 미만이고 PD-L1 TPS가 50% 이상인 환자를 등록한다. PD-L1 ≥ 50%를 발현하는 종양을 가진 8명의 환자를 코호트 B에 등록한 후, PD-L1 TPS ≥ 50%를 갖는 환자의 코호트 A 등록을 계속한다.
도 21은 II상 실험 계획의 흐름도이다. 1L = 1차; CDx = 동반 진단; ECOG PS = 이스턴 코퍼레이티브 종양학 그룹 전신 활동도; IHC = 면역조직화학; IRC = 독립 검토 위원회; PD-L1 = 예정된 세포 사멸 리간드 1; Q3W = 3주마다; R = 무작위화; s/p = 이후의 상태; IV = 정맥 주사.
도 22는 Ib상 실험 계획의 흐름도이다. TNBC = 삼중 음성 유방암; G-CSF = 과립구 집락 자극 인자; GM-CSF = 과립구-대식세포 집락 자극 인자; Rand. = 무작위화, pCR = 병리학적 완전 반응, QW = 주 1회, Q2W = 2주마다, Q3W = 3주마다.
도 23은 2b상 실험 계획의 흐름도이다. HPV = 인유두종 바이러스; IHC = 면역조직화학; IV = 정맥 주사; Q3W = 3주마다; PD-L1 낮음 = TIC 10%-49%; PD-L1 높음 = TIC ≥ 50%; SCCHN = 두경부의 편평세포 암종; RECIST = 고형 종양 반응 평가 기준.
도 24는 WO39613 Ib/II상 임상 시험의 근육 침윤성 방광암(MIBC) 코호트의 설계를 도시하는 개략도이다. 스크리닝 단계에서, 시스플라틴 부적격이고 PD-L1 양성(+)(위) 또는 PD-L1 음성(-)(아래) 중 하나인 MIBC 환자를 식별한다. 무작위 배정(R) 후, 환자는 아테졸리주맙(아테조; 대조군) 또는 아테졸리주맙 및 티라골루맙(티라)으로 치료한다.
도 25는 WO39613 Ib/II상 임상 시험의 전이성 요로 상피암(mUC) 코호트의 설계를 도시하는 개략도이다. 스크리닝 단계에서, 백금 함유 요법 중 또는 이후에 진행되고 암 면역요법(CIT) 경험이 없는 2차 국소 진행성 또는 전이성 UC 환자를 식별한다. 무작위 배정(R) 후, 환자는 아테졸리주맙(아테조; 대조군); 아테졸리주맙 및 엔포르투맙 베도틴(EV); 아테졸리주맙 및 니라파립(니라); 아테졸리주맙 및 Hu5F9-G4; 아테졸리주맙 및 티라골루맙(티라); 아테졸리주맙 및 사시투주맙 고비테칸(SG); 아테졸리주맙 및 토실리주맙(TCZ); 아테졸리주맙 및 RO7122290(FAP-4-1BBL); 또는 RO7121661(PD1/TIM-3)으로 1단계 동안 치료된다. a1단계 동안, 시험자가 결정한 바와 같이 임상적 이점의 상실 또는 허용할 수 없는 독성을 경험한 환자는 적격 기준을 충족하는 경우 2단계 동안 상이한 치료 조합을 받는 데에 적격일 수 있다. b아테조니라 군에는 40명의 환자가 있다. c1 단계에서 엔포르투맙 베도틴을 투여받은 환자는 2단계에서 엔포르투맙 베도틴을 투여받지 않고, 1단계에서 사시투주맙 고비테칸을 투여받은 환자는 2단계에서 사시투주맙 고비테칸을 투여받지 않고; 하나 초과의 치료군에 적격인 다른 환자는 시험자에 의해 치료군을 할당받는다. 일단 아테조SG 군이 개방되면, 아테조EV 군의 등록이 폐쇄된다. d아테조RO7122290(FAP-4-1BBL) 군은 미국 이외의 국가에서만 개방된다.
도 26은 팜Dx 22C3 IHC 분석(높은 TPS ≥ 50%; 낮은 TPS 1~49%)에 의해 평가된 바와 같이 낮거나 높은 PD-L1 TPS, 또는 CE-IVD VENTANA SP263 IHC 분석(높은 TC ≥ 50%; 낮은 TC 1~49%)로 평가된 바와 같이 낮거나 높은 PD-L1 종양 함량(TC)을 갖는 CITYSCAPE 시험으로부터의 환자를 대상으로 객관적 반응률(ORR)(완전 반응/부분 반응(CR/PR); 안정한 질병/진행성 질병(SD/PD); 또는 평가 불가(NE))을 도시하는 도면이다.
도 27a는 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상인 CITYSCAPE 시험의 환자에 대하여 반응률(95% 신뢰 구간(CI))을 도시하는 막대 그래프이다.
도 27b는 SP263 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상(및 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상)인 CITYSCAPE 시험의 환자에 대하여 반응률(95% CI)을 도시하는 막대 그래프이다.
도 28a는 티라골루맙 및 아테졸리주맙(티라 + 아테조) 또는 위약 + 아테조로 치료를 받고 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상인 CITYSCAPE 시험의 환자에 대한 무진행 생존(퍼센트)을 도시하는 그래프이다. 삽입된 표는 월(월) 및 위험 비율(HR)의 PFS 중앙값을 나타낸다.
도 28b는 티라골루맙 및 아테졸리주맙(티라 + 아테조) 또는 위약 + 아테조로 치료를 받고 SP263 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상(및 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 1% 이상)인 CITYSCAPE 시험의 환자에 대한 무진행 생존(퍼센트)을 도시하는 그래프이다. 삽입된 표는 PFS 중앙값(월) 및 HR을 나타낸다.
도 29a는 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 50% 이상인 CITYSCAPE 시험의 환자에 대하여 반응률(95% 신뢰 구간(CI))을 도시하는 막대 그래프이다.
도 29b는 SP263 IHC 분석을 사용하여 측정한 바와 같이 TC가 50% 이상인 CITYSCAPE 시험의 환자에 대하여 반응률(95% CI)을 도시하는 막대 그래프이다.
도 30a는 티라골루맙 및 아테졸리주맙(티라 + 아테조) 또는 위약 + 아테조로 치료를 받고 22C3 IHC 분석을 사용하여 측정한 바와 같이 TPS가 50% 이상인 CITYSCAPE 시험의 환자에 대한 무진행 생존(퍼센트)을 도시하는 그래프이다. 삽입된 표는 PFS 중앙값(월) 및 HR을 나타낸다.
도 30b는 티라골루맙 및 아테졸리주맙(티라 + 아테조) 또는 위약 + 아테조로 치료를 받고 SP263 IHC 분석을 사용하여 측정한 바와 같이 TC가 50% 이상인 CITYSCAPE 시험의 환자에 대한 무진행 생존(퍼센트)을 도시하는 그래프이다. 삽입된 표는 PFS 중앙값(월) 및 HR을 나타낸다.1 is a flow chart depicting Phase Ib Chemotherapy Expansion and Phase Ib Q4W Dosing Expansion.
2 is a flow chart of the phase Ib experimental design. EOCG = Eastern Cooperative Oncology Group; IHC = immunohistochemistry; PD-L1+ = programmed death-
3 is a flow chart of the Phase Ia study design. CRC = colorectal cancer, DLT = dose limiting toxicity, GC = gastric cancer, HNSCC = head and neck squamous cell carcinoma, IV = intravenous, MAD = maximum dose administered, MSI = microsatellite instability, MSS = microsatellite instability, MTD = maximum tolerated dose , NSCLC = non-small cell lung cancer, OC = ovarian cancer, PD = disease progression, PK = pharmacokinetics, RCC = renal cell carcinoma, TNBC = triple negative breast cancer, UBC = urothelial bladder cancer.
4 is a flowchart of the study design of the Phase Ib Tiragolumab and Atezolizumab Expansion Cohort, Serial Biopsy Cohort, and Q4W Dosing Expansion Cohort. CIT = cancer immunotherapy; DLT = dose limiting toxicity; HNSCC = head and neck squamous cell carcinoma, IV = intravenous, MAD = maximal dose, MSI = microsatellite instability, MSS = microsatellite stable, MTD = maximally tolerated dose, NSCLC = non-small cell lung cancer, PD = disease progression;
5 is a flow diagram of a phase Ib chemotherapy expansion cohort study design.
6 is a flow chart of a phase Ib non-chemotherapy expansion cohort study design.
7 is a flow chart illustrating conditions for continuing study treatment beyond progression. EOCG = Eastern Cooperative Oncology Group; RECIST = Response Criteria in Solid Tumors,
8 is a flow chart illustrating the transition from phase Ia to phase Ib. AE = adverse event, DLT = dose limiting toxicity, PD = disease progression.
9 is a graph depicting the pharmacokinetics of tiragolumab.
10 is a series of graphs depicting the pharmacokinetics of tiragolumab.
11 is a graph depicting all adverse events ≥ 10% in a phase la tiragolumab dose escalation study. *
12 is a graph depicting all adverse events ≥ 10% in a phase Ib tiragolumab and atezolizumab dose escalation study. *
13 is a graph depicting tumor size reduction in a phase Ia tyragolumab dose escalation study.
14 is a graph depicting tumor size reduction in a phase Ib tiragolumab and atezolizumab dose escalation study.
15 is a graph depicting CIT-naive PD-L1 positive NSCLC tumor size reduction in a phase Ib tiragolumab and atezolizumab dose escalation study.
16 is a graph depicting CIT-naive PD-L1 positive NSCLC tumor size reduction over time in a phase Ib tiragolumab and atezolizumab dose escalation study.
17 is a flowchart of a three-phase experimental design. 1L = primary; CE = carboplatin and etoposide; ECOG PS = Eastern Corporate Oncology Group Systemic Activity; ES-SCLC = diastolic small cell lung cancer; LDH = lactase dehydrogenase; RECIST = response criteria for solid tumors; ITT = intent to treat; PP = primary population.
18 is a schematic of a study design depicting parameters regarding subject selection, stratification criteria, randomization of treatment groups, and treatment endpoints.
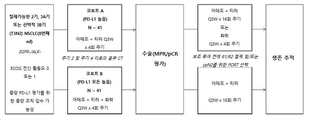
19 is a schematic diagram of the study design of the GO42501 Phase II clinical study. Resectable stage II, IIIA or selection IIIB (T3N2) non-small cell lung cancer (NSCLC) without an activating EGFR mutation (EGFR-), without an ALK fusion oncogene (ALK-), and with ECOG systemic activity of 0 or 1 selected ) patient. Cohort A consists of patients with high PD-L1. Patients in Cohort A are treated with atezolizumab (Atezo) and tiragolumab (Tira) every 3 weeks (Q3W) for 4 cycles. Cohort B consists of patients with any PD-L1 status. Patients in Cohort B are treated with Artezo, Tyra and Platinum-based dual chemotherapy (Chemo) Q3W for 4 cycles. After
20 is a flowchart illustrating patient enrollment in the GO42501 Phase II clinical trial. For Cohort A (patients with high PD-L1; PD-L1 Tumor Rate Score (TPS) ≥ 50%), a safety introduction is performed using 6 patients. If surgical safety criteria are not met, discontinue enrollment in Cohort A. If surgical safety criteria are met, continue enrollment in Cohort A. For Cohort B (patients with any PD-L1 status), a safety introduction is performed utilizing 6 patients with PD-L1 TPS <50%. If surgical safety criteria are not met, discontinue enrollment in Cohort B. If surgical safety criteria are met, continue enrollment in Cohort B, enrolling patients with a PD-L1 TPS of <50% and a PD-L1 TPS of >50%. Eight patients with tumors expressing PD-L1 > 50% will be enrolled in Cohort B, then continue with Cohort A enrollment of patients with PD-L1 TPS > 50%.
21 is a flow chart of the Phase II experimental design. 1L = primary; CDx = companion diagnosis; ECOG PS = Eastern Corporate Oncology Group Systemic Activity; IHC = immunohistochemistry; IRC = independent review committee; PD-L1 = programmed
22 is a flow chart of the phase Ib experimental design. TNBC = triple negative breast cancer; G-CSF = granulocyte colony stimulating factor; GM-CSF = granulocyte-macrophage colony stimulating factor; Rand. = randomized, pCR = pathological complete response, QW = once weekly, Q2W = every 2 weeks, Q3W = every 3 weeks.
23 is a flowchart of the phase 2b experimental design. HPV = human papillomavirus; IHC = immunohistochemistry; IV = intravenous; Q3W = every 3 weeks; PD-L1 low =
24 is a schematic diagram depicting the design of the muscle invasive bladder cancer (MIBC) cohort of the WO39613 Phase Ib/II clinical trial. At the screening stage, MIBC patients who are cisplatin ineligible and either PD-L1 positive (+) (top) or PD-L1 negative (-) (bottom) are identified. After randomization (R), patients are treated with either atezolizumab (Atezo; control) or atezolizumab and tiragolumab (Tira).
25 is a schematic diagram depicting the design of the metastatic urothelial carcinoma (mUC) cohort of WO39613 Phase Ib/II clinical trial. In the screening phase, patients with secondary locally advanced or metastatic UC who have progressed on or after platinum-containing therapy and who are not cancer immunotherapy (CIT) are identified. After randomization (R), patients were treated with atezolizumab (atezo; control); atezolizumab and enfortumab vedotin (EV); atezolizumab and niraparib (Nira); atezolizumab and Hu5F9-G4; atezolizumab and tiragolumab (Tira); atezolizumab and sacituzumab gobitecan (SG); atezolizumab and tocilizumab (TCZ); atezolizumab and RO7122290 (FAP-4-1BBL); or RO7121661 (PD1/TIM-3) during
26 is a low or high PD-L1 TPS, or CE-IVD VENTANA SP263 IHC assay (high TC > 50%) as assessed by the PalmDx 22C3 IHC assay (high TPS ≥ 50%; low TPS 1-49%). ; objective response rate (ORR) (complete response/partial response (CR/PR)) in patients from the CITYSCAPE trial with low or high PD-L1 tumor content (TC) as assessed as low TC 1-49%). Stable disease/progressive disease (SD/PD); or non-evaluative (NE)).
FIG. 27A is a bar graph depicting response rates (95% confidence intervals (CI)) for patients in the CITYSCAPE trial with a TPS greater than or equal to 1% as measured using the 22C3 IHC assay.
27B shows response rates (95% CI) for patients in the CITYSCAPE trial with TPS ≥1% (and TPS ≥1% as measured using the 22C3 IHC Assay) as determined using the SP263 IHC assay. It is a bar graph showing.
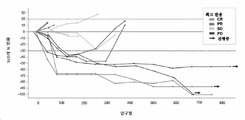
FIG. 28A shows progression-free survival (percentage) for patients in the CITYSCAPE trial treated with tiragolumab and atezolizumab (Tira + atezo) or placebo + atezo and had a TPS of 1% or greater as measured using the 22C3 IHC assay. ) is a graph showing The inset table shows the median PFS of month (month) and hazard ratio (HR).
FIG. 28B shows a TPS greater than or equal to 1% (and as measured using the 22C3 IHC assay) treated with tiragolumab and atezolizumab (Tira + atezo) or placebo + atezo and as measured using the SP263 IHC assay. A graph depicting progression-free survival (percent) for patients in the CITYSCAPE trial with a TPS equal to or greater than 1%). The inset table shows the median PFS (months) and HR.
29A is a bar graph depicting response rates (95% confidence intervals (CI)) for patients in the CITYSCAPE trial with a TPS of 50% or greater as measured using the 22C3 IHC assay.
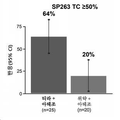
29B is a bar graph depicting response rates (95% CI) for patients in the CITYSCAPE trial with a TC greater than or equal to 50% as determined using the SP263 IHC assay.
30A shows progression-free survival (percentage) for patients in the CITYSCAPE trial treated with tiragolumab and atezolizumab (Tira + atezo) or placebo + atezo and had a TPS greater than or equal to 50% as measured using the 22C3 IHC assay. ) is a graph showing The inset table shows the median PFS (months) and HR.
30B shows progression-free survival (percentage) for patients in the CITYSCAPE trial treated with tiragolumab and atezolizumab (Tira + atezo) or placebo + atezo and had a TC greater than or equal to 50% as measured using the SP263 IHC assay. ) is a graph showing The inset table shows the median PFS (months) and HR.
본 발명은 암(예컨대, 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC))의 치료를 위한 치료 방법 및 조성물을 제공한다. 본 발명은 PD-1 축 결합 길항제, VEGF 길항제, 및/또는 화학요법제와 병용한 항 TIGIT 항체(예컨대, 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 면역요법이 암 치료에 유용할 수 있다는 발견에 적어도 부분적으로 기초한다. 상기 조합 및/또는 투약 요법을 포함하는 조성물, 사용, 및 키트가 또한 본원에 제공된다.The present invention relates to cancers (eg, lung cancer (eg, early stage lung cancer (eg, resectable lung cancer)), SCLC (eg ES-SCLC), NSCLC (eg, squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB) NSCLC, relapsed or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., the subject has not been previously treated for stage IV NSCLC) if absent); )) or HER2 positive breast cancer); head and neck cancer (eg, SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); liver cancer (eg, HCC, such as locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (such as , MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; ovarian cancer; stomach cancer (eg, gastroesophageal junction cancer); or CRC ( (e.g., MSS or low MSI CRC)).The present invention provides an anti-TIGIT antibody (e.g., anti-TIGIT antibody) in combination with a PD-1 axis binding antagonist, a VEGF antagonist, and/or a chemotherapeutic agent. It is based at least in part on the discovery that immunotherapy comprising TIGIT antagonist antibody (such as tiragolumab) can be useful for cancer treatment.Composition, use, and kit comprising the combination and/or dosing regimen are also described herein. is provided
I.I. 일반적인 기술general technique
본원에 기재되거나 참조된 기술 및 절차는 해당 분야의 숙련가에 의하여 통상적인 방법, 예컨대, 예를 들어, 하기에 기재된 널리 이용되는 방법들을 사용하여 일반적으로 잘 이해되고 통상적으로 사용될 것이다: Sambrook et al., Molecular Cloning: A Laboratory Manual 3d edition (2001) Cold Spring Harbor Laboratory Press, Cold Spring Harbor, N.Y.; Current Protocols in Molecular Biology (F.M. Ausubel, et al. eds., (2003)); the series Methods in Enzymology (Academic Press, Inc.): PCR 2: A Practical Approach (M.J. MacPherson, B.D. Hames and G.R. Taylor eds. (1995)), Harlow and Lane, eds. (1988) Antibodies, A Laboratory Manual, and Animal Cell Culture (R.I. Freshney, ed. (1987)); Oligonucleotide Synthesis (M.J. Gait, ed., 1984); Methods in Molecular Biology, Humana Press; Cell Biology: A Laboratory Notebook (J.E. Cellis, ed., 1998) Academic Press; Animal Cell Culture (R.I. Freshney), ed., 1987); Introduction to Cell and Tissue Culture (J.P. Mather and P.E. Roberts, 1998) Plenum Press; Cell and Tissue Culture: Laboratory Procedures (A. Doyle, J.B. Griffiths, and D.G. Newell, eds., 1993-8) J. Wiley and Sons; Handbook of Experimental Immunology (D.M. Weir and C.C. Blackwell, eds.); Gene Transfer Vectors for Mammalian Cells (J.M. Miller and M.P. Calos, eds., 1987); PCR: The Polymerase Chain Reaction, (Mullis et al., eds., 1994); Current Protocols in Immunology (J.E. Coligan et al., eds., 1991); Short Protocols in Molecular Biology (Wiley and Sons, 1999); Immunobiology (C.A. Janeway and P. Travers, 1997); Antibodies (P. Finch, 1997); Antibodies: A Practical Approach (D. Catty., ed., IRL Press, 1988-1989); Monoclonal Antibodies: A Practical Approach (P. Shepherd and C. Dean, eds., Oxford University Press, 2000); Using Antibodies: A Laboratory Manual (E. Harlow and D. Lane (Cold Spring Harbor Laboratory Press, 1999); The Antibodies (M. Zanetti and J. D. Capra, eds., Harwood Academic Publishers, 1995); and Cancer: Principles and Practice of Oncology (V.T. DeVita et al., eds., J.B. Lippincott Company, 1993).The techniques and procedures described or referenced herein will be generally well understood and commonly used by those skilled in the art using conventional methods, such as, for example, the widely used methods described below: Sambrook et al. , Molecular Cloning: A Laboratory Manual 3d edition (2001) Cold Spring Harbor Laboratory Press, Cold Spring Harbor, NY; Current Protocols in Molecular Biology (FM Ausubel, et al. eds., (2003)); the series Methods in Enzymology (Academic Press, Inc.): PCR 2: A Practical Approach (MJ MacPherson, BD Hames and GR Taylor eds. (1995)), Harlow and Lane, eds. (1988) Antibodies, A Laboratory Manual , and Animal Cell Culture (RI Freshney, ed. (1987)); Oligonucleotide Synthesis (MJ Gait, ed., 1984); Methods in Molecular Biology , Humana Press; Cell Biology: A Laboratory Notebook (JE Cellis, ed., 1998) Academic Press; Animal Cell Culture (RI Freshney), ed., 1987); Introduction to Cell and Tissue Culture (JP Mather and PE Roberts, 1998) Plenum Press; Cell and Tissue Culture: Laboratory Procedures (A. Doyle, JB Griffiths, and DG Newell, eds., 1993-8) J. Wiley and Sons; Handbook of Experimental Immunology (DM Weir and CC Blackwell, eds.); Gene Transfer Vectors for Mammalian Cells (JM Miller and MP Calos, eds., 1987); PCR: The Polymerase Chain Reaction , (Mullis et al., eds., 1994); Current Protocols in Immunology (JE Coligan et al., eds., 1991); Short Protocols in Molecular Biology (Wiley and Sons, 1999); Immunobiology (CA Janeway and P. Travers, 1997); Antibodies (P. Finch, 1997); Antibodies: A Practical Approach (D. Catty., ed., IRL Press, 1988-1989); Monoclonal Antibodies: A Practical Approach (P. Shepherd and C. Dean, eds., Oxford University Press, 2000); Using Antibodies: A Laboratory Manual (E. Harlow and D. Lane (Cold Spring Harbor Laboratory Press, 1999); The Antibodies (M. Zanetti and JD Capra, eds., Harwood Academic Publishers, 1995); and Cancer: Principles and Practice of Oncology (VT DeVita et al., eds., JB Lippincott Company, 1993).
II.II. I.정의I. Definition
본원에서 설명된 발명의 양상과 구체예는 “포함하는”, “구성되는” 및 “본질적으로 구성되는” 양상과 구체예를 포함하는 것으로 이해되어야 한다. 본원에서 사용되는, 단수 형태 "하나" 및 "그것"은 달리 지시되지 않는 한 복수의 지칭을 포함한다.Aspects and embodiments of the invention described herein are to be understood to include aspects and embodiments “comprising”, “consisting of” and “consisting essentially of”. As used herein, the singular forms “a” and “the” include plural references unless otherwise indicated.
본원에서 사용된 바와 같이, 용어 “약”은 당업자에게 용이하게 공지된 개별 값에 대한 통상의 오차 범위를 지칭한다. 본원의 값 또는 매개변수에 대한 "약"의 지칭은 그 값 또는 매개변수 그 자체(per se)에 관한 양상들을 포함 (및 설명)한다. 예를 들면, "약 X"를 지칭하는 기재는 "X"의 기재를 포함한다.As used herein, the term “about” refers to a common error range for an individual value readily known to one of ordinary skill in the art. Reference to “about” to a value or parameter herein includes (and describes) aspects relating to that value or parameter per se. For example, a description referring to “about X” includes a description of “X”.
일반적으로 용어 "발현의 수준" 또는 "발현 수준"은 호환적으로 사용되며 일반적으로 생물학적 샘플에서 바이오마커의 양을 지칭한다. "발현"은 일반적으로, 정보 (예를 들어, 유전자-인코드된 및/또는 후성유전적 정보)가 세포에 존재하고 작동하는 구조로 전환되는 과정을 지칭한다. 따라서, 본원에서 사용되는 "발현"은 폴리뉴클레오티드로의 전사, 폴리펩티드로의 번역, 또는 심지어 폴리뉴클레오티드 및/또는 폴리펩티드 변형 (예를 들어, 폴리펩티드의 번역 후 변형)을 지칭 할 수 있다. 전사된 폴리뉴클레오티드의 단편, 번역된 폴리펩티드 또는 폴리뉴클레오티드 및/또는 폴리펩티드 변형 (예를 들어, 폴리펩티드의 번역 후 변형)은 또한 이들이 대체 스플라이싱 또는 분해된 전사체에 의해 생성된 전사체들로부터 유래되었는지 또는 예를 들어 단백질 분해에 의한 폴리펩티드의 번역 후 프로세싱으로부터 유래되었는지 여부에 따른 발현으로 간주되어야 한다. "발현된 유전자"는 mRNA와 같은 폴리뉴클레오티드로 전사된 후 폴리펩티드로 번역된 유전자, 및 또한 RNA로 전사되지만 폴리펩티드로 번역되지 않는 유전자 (예를 들어, 전달 및 리보솜 RNA)를 포함한다. 바이오마커의 “양” 및 “수준”(예컨대, 발현 수준)은 당업자에게 공지되고, 또한 본원에 개시된 방법에 의해 측정할 수 있다. 개체에 대해 증가된 임상 이익과 관련하여 바이오마커의 양 또는 수준은, 예를 들어 생물학적 샘플에서 검출가능한 수준일 수 있다. 일부 양태들에서, 바이오마커의 발현 수준 또는 양은 특정 요법(예컨대, PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 포함한 1회 이상의 투약 주기를 포함하는 요법 또는 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함하는 요법)에 반응하거나, 또는 이로부터 이익을 얻을 가능성이 있을 수 있는 암을 갖는 대상체를 식별/특성화하는 데 사용할 수 있다.In general, the terms “level of expression” or “expression level” are used interchangeably and generally refer to the amount of a biomarker in a biological sample. "Expression" generally refers to the process by which information (eg, gene-encoded and/or epigenetic information) is converted into structures present and functioning in a cell. Thus, as used herein, “expression” may refer to transcription into a polynucleotide, translation into a polypeptide, or even modification of a polynucleotide and/or a polypeptide (eg, post-translational modification of a polypeptide). Fragments of transcribed polynucleotides, translated polypeptides or polynucleotides and/or polypeptide modifications (eg, post-translational modifications of a polypeptide) are also derived from transcripts in which they are produced by alternative splicing or digested transcripts. expression according to whether or not it is derived from post-translational processing of the polypeptide, for example by proteolysis. "Expressed genes" include genes that are transcribed into polynucleotides such as mRNA and then translated into polypeptides, and also genes that are transcribed into RNA but not translated into polypeptides (eg, transfer and ribosomal RNA). “Amount” and “level” (eg, expression level) of a biomarker are known to those of skill in the art and can also be determined by the methods disclosed herein. The amount or level of a biomarker with respect to an increased clinical benefit to an individual may be, for example, a detectable level in a biological sample. In some aspects, the expression level or amount of a biomarker is dependent on a specific therapy (eg, a therapy comprising one or more dosing cycles comprising a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody or one or more dosing cycles of an anti-TIGIT antagonist antibody. to identify/characterize a subject having cancer who may be likely to respond to, or benefit from, a therapy comprising
"증가된 발현", "증가된 발현 수준", "증가된 수준", "상승된 발현", "상승된 발현 수준" 또는 "상승된 수준"은 대조군, 예컨대, 질병 또는 장애(예컨대, 암)를 앓고 있지 않은 개체 또는 개체들 또는 내부 대조군(예컨대, 하우스키핑 바이오마커)에 비해 개체에서 바이오마커의 증가된 발현 또는 증가된 수준을 지칭한다."Increased expression", "increased expression level", "increased level", "elevated expression", "elevated expression level" or "elevated level" refers to a control, such as a disease or disorder (eg, cancer). refers to increased expression or increased level of a biomarker in an individual or individuals not suffering from or compared to an internal control (eg, a housekeeping biomarker).
"감소된 발현", "감소된 발현 수준", "감소된 수준", "저하된 발현", "저하된 발현 수준" 또는 "저하된 수준"은 대조군, 예컨대 질병 또는 장애(예컨대, 암)를 앓고 있지 않은 개체 또는 개체들 또는 내부 대조군(예컨대, 하우스키핑 바이오마커)에 비해 개체에서 바이오마커의 감소된 발현 또는 감소된 수준을 지칭한다. 일부 양태들에서, 감소된 발현은 발현이 거의 또는 전혀 없는 것이다."Decreased expression", "reduced expression level", "reduced level", "decreased expression", "decreased expression level" or "decreased level" refers to a control, such as a disease or disorder (eg, cancer). Refers to reduced expression or reduced level of a biomarker in an individual compared to an individual or individuals not suffering from or an internal control (eg, a housekeeping biomarker). In some aspects, reduced expression is little or no expression.
샘플 내에서 본원에서 기재된 다양한 바이오마커의 존재 및/또는 발현 수준/양은 다수의 방법론에 의해 분석될 수 있고, 면역조직화학(“IHC”), 웨스턴 블롯 분석, 면역침전, 분자 결합 분석, ELISA, ELIFA, 형광 활성화된 세포 분류(“FACS”), MassARRAY, 단백질체학, 정량적 혈액 기반 분석(예컨대, 혈청 ELISA), 생화학적 효소 활성 분석, 제자리 혼성화, 형광 제자리 혼성화(FISH), 서던 분석, 노던 분석, 전체 유전체 염기서열분석, 대량의 병렬 DNA 염기서열분석(예컨대, 차세대 염기서열분석), NANOSTRING®, 정량적 실시간 PCR(qRT-PCR)을 포함한 중합효소 연쇄 반응(PCR), 및 다른 증폭 유형 검출 방법, 예컨대 예를 들어 분지된 DNA, SISBA, TMA 등, RNA-seq, 마이크로어레이 분석, 유전자 발현 프로파일링 및/또는 유전자 발현의 연속 분석(“SAGE”) 뿐만 아니라 단백질, 유전자 및/또는 조직 어레이 분석에 의해 실시될 수 있는 매우 다양한 분석 중에서 어느 하나를 포함하지만 이에 제한되지는 않는, 이들 중 다수는 당해 분야에서 공지되고 당업자에 의해 이해된다. 유전자 및 유전자 산물의 상태를 평가하기 위한 일반적인 프로토콜은, 예를 들어 Ausubel et al., eds., 1995, Current Protocols In Molecular Biology, Units 2 (Northern Blotting), 4 (Southern Blotting), 15 (Immunoblotting) and 18 (PCR Analysis)에서 찾을 수 있다. Rules Based Medicine 또는 Meso Scale Discovery("MSD")에서 입수 가능한 것과 같은 다중 면역분석법도 사용할 수 있다.The presence and/or expression level/amount of the various biomarkers described herein in a sample can be analyzed by a number of methodologies, including immunohistochemistry (“IHC”), Western blot analysis, immunoprecipitation, molecular binding assay, ELISA, ELIFA, Fluorescence Activated Cell Sorting (“FACS”), MassARRAY, Proteomics, Quantitative Blood Based Assays (eg, Serum ELISA), Biochemical Enzyme Activity Assay, In Situ Hybridization, Fluorescence In Situ Hybridization (FISH), Southern Assay, Northern Assay , whole genome sequencing, massively parallel DNA sequencing (e.g., next-generation sequencing), NANOSTRING ® , polymerase chain reaction (PCR) including quantitative real-time PCR (qRT-PCR), and other amplification types detection methods , such as for example branched DNA, SISBA, TMA, etc., RNA-seq, microarray analysis, gene expression profiling and/or serial analysis of gene expression (“SAGE”) as well as protein, gene and/or tissue array analysis Many of these are known in the art and understood by one of ordinary skill in the art, including but not limited to any one of the wide variety of assays that can be performed by General protocols for assessing the status of genes and gene products are, for example, Ausubel et al., eds., 1995, Current Protocols In Molecular Biology , Units 2 (Northern Blotting), 4 (Southern Blotting), 15 (Immunoblotting). and 18 (PCR Analysis). Multiple immunoassays such as those available from Rules Based Medicine or Meso Scale Discovery (“MSD”) may also be used.
“상관시키다” 또는 “상관시키는”은 제1 분석 또는 프로토콜의 성과 및/또는 결과를 제2 분석 또는 프로토콜의 성과 및/또는 결과와 어떤 방식으로든 비교하는 것으로 의미된다. 예를 들어, 제2 프로토콜을 실시할 때 제1 분석 또는 프로토콜의 결과를 사용할 수 있고, 그리고/또는 제2 분석 또는 프로토콜을 실시해야 하는지 여부를 결정하기 위해 제1 분석 또는 프로토콜의 결과를 사용할 수 있다. 폴리펩티드 분석 또는 프로토콜의 양태와 관련하여, 특정 치료 요법이 실시되어야하는지 여부를 결정하기 위해 폴리펩티드 발현 분석 또는 프로토콜의 결과를 사용할 수 있다. 폴리뉴클레오티드 분석 또는 프로토콜의 양태와 관련하여, 특정 치료 요법이 실시되어야하는지 여부를 결정하기 위해 폴리뉴클레오티드 발현 분석 또는 프로토콜의 결과를 사용할 수 있다.By “correlate” or “correlating” is meant comparing in any way the performance and/or results of a first analysis or protocol with the performance and/or results of a second analysis or protocol. For example, the results of a first analysis or protocol may be used when conducting a second protocol, and/or the results of a first analysis or protocol may be used to determine whether a second analysis or protocol should be performed. have. With respect to aspects of a polypeptide assay or protocol, the results of a polypeptide expression assay or protocol can be used to determine whether a particular treatment regimen should be administered. With respect to aspects of a polynucleotide assay or protocol, the results of a polynucleotide expression assay or protocol may be used to determine whether a particular treatment regimen should be administered.
본원에서 사용된 문구 "실질적으로 감소된" 또는 "실질적으로 상이한"은 는 문구는 2개의 수치 값(일반적으로 하나는 분자와 관련되고 다른 하나는 참조/비교 분자와 관련됨) 사이에 충분히 높은 정도의 상이함을 나타내므로, 당업자는 상기 값(예컨대, KD 값)에 의해 측정되는 생물학적 특성의 맥락에서 이들 2개 값 간의 차이가 통계적 유의성이 있는 것으로 간주할 것이다. 상기 2개의 값의 차이는, 예를 들어 참조/비교 분자에 대한 값의 함수로서 약 10% 초과, 약 20% 초과, 약 30% 초과, 약 40% 초과, 및/또는 약 50% 초과이다.As used herein, the phrase "substantially reduced" or "substantially different" means that there is a sufficiently high degree of between two numerical values (generally one associated with a molecule and the other associated with a reference/comparator molecule). Indicative of a difference, one of ordinary skill in the art would consider a difference between these two values to be statistically significant in the context of the biological property measured by said value (eg, K D value). The difference between the two values is, for example, greater than about 10%, greater than about 20%, greater than about 30%, greater than about 40%, and/or greater than about 50% as a function of the value for the reference/comparison molecule.
본원에서 사용된 용어 "실질적으로 유사한" 또는 "실질적으로 동일한"은 2개의 수치 값(예를 들어, 하나는 본 발명의 항체와 관련되고 다른 하나는 참조/비교 항체와 관련됨) 사이에 충분히 높은 정도의 유사성을 나타내므로, 당업자는 상기 값(예컨대, KD 값)에 의해 측정되는 생물학적 특성의 맥락에서 이들 2개 값 간의 차이가 생물학적 및/또는 통계적 유의성이 거의 또는 전혀 없는 것으로 간주할 것이다. 상기 2개의 값의 차이는, 예를 들어 참조/비교 값의 함수로서 약 50% 미만, 약 40% 미만, 약 30% 미만, 약 20% 미만, 및/또는 약 10% 미만이다.As used herein, the term "substantially similar" or "substantially identical" refers to a sufficiently high degree between two numerical values (eg, one associated with an antibody of the invention and the other associated with a reference/comparison antibody). Because of the similarity of The difference between the two values is, for example, less than about 50%, less than about 40%, less than about 30%, less than about 20%, and/or less than about 10% as a function of the reference/comparison value.
본원에서 사용되느 문구 “에 근거하여”는 하나 이상의 바이오마커에 관한 정보가 치료 결정, 포장 삽입물 상에 제공된 정보, 또는 마케팅/홍보 지침 등을 통지하는 데 이용된다는 것을 의미한다.As used herein, the phrase “based on” means that information regarding one or more biomarkers is used to inform treatment decisions, information provided on a package insert, or marketing/promotional guidelines, etc.
본원에서 사용된 용어 “TIGIT” 또는 “Ig 및 ITIM 도메인을 갖는 T 세포 면역수용체"는 달리 지시되지 않는 한, 영장류(예컨대, 인간) 및 설치류(예컨대, 마우스 및 랫트)와 같은 포유동물을 포함한 임의의 척추동물 출처의 임의의 고유 TIGIT를 지칭한다. TIGIT는 또한 당업계에서 DKFZp667A205, FLJ39873, V 세트 및 면역글로불린 도메인 함유 단백질 9, V 세트 및 막횡단 도메인 함유 단백질 3, VSIG9, VSTM3, 및 WUCAM으로 공지되어 있다. 이 용어는 "전장", 미처리 TIGIT(예컨대, 서열번호 30의 아미노산 서열을 갖는 전장 인간 TIGIT) 및 세포 내 처리로부터 발생한 임의의 TIGIT 형태(예컨대, 서열번호 31의 아미노산 서열을 갖는 신호 서열이 없는 처리된 인간 TIGIT)를 포함한다. 이 용어는 또한 TIGIT의 자연 발생 변이체, 예컨대 스플라이스 변이체 또는 대립유전자 변이체를 포함한다. 예시적인 인간 TIGIT의 아미노산 서열은 유니프롯(UniProt) 수탁 번호 Q495A1에서 찾을 수 있다.
As used herein, the term “TIGIT” or “T cell immunoreceptor having Ig and ITIM domains” refers to any, unless otherwise indicated, including mammals such as primates (eg, humans) and rodents (eg, mice and rats). refers to any native TIGIT of vertebrate origin. TIGIT is also known in the art as DKFZp667A205, FLJ39873, V set and immunoglobulin
용어 “예정된 세포사멸 1” 및 “PD-L1”은 본원에서 천연 서열 인간 PD-L1 폴리펩티드를 지칭한다. 천연 서열 PD-L1 폴리펩티드는 유니프롯 수탁 번호 Q9NZQ7(서열 번호 32) 하에 제공된다. 예를 들어, 천연 서열 PD-L1은 유니프롯 수탁 번호 Q9NZQ7-1(이소형 1)에 기재된 아미노산 서열을 가질 수 있다. 다른 예에서, 천연 서열 PD-L1은 유니프롯 수탁 번호 Q9NZQ7-2(이소형 2)에 기재된 아미노산 서열을 가질 수 있다. 또 다른 예에서, 천연 서열 PD-L1은 유니프롯 수탁 번호 Q9NZQ7-3(이소형 3)에 기재된 아미노산 서열을 가질 수 있다. 상기 용어는 또한 PD-L1의 자연 발생 변이체, 예컨대 스플라이스 변이체 또는 대립유전자 변이체를 포함한다. PD-L1은 또한 당업계에서 “예정된 세포 사멸 1 리간드 1,” “PDCD1LG1,” “CD274,” “B7-H,” 및 “PDL1"로 지칭된다.The terms “
본원에서 용어 “PD-1” 또는 “예정된 세포 사멸 리간드 1”은 달리 지시가 없는 한, 영장류(예컨대, 인간) 및 설치류(예컨대, 마우스 및 랫트)와 같은 포유동물을 포함한 임의의 척추동물 출처의 임의의 고유 PD-L1을 지칭한다. PD-1은 또한 CD279, PDCD1, 및 예정된 세포 사멸 1로서 당업계에 공지되어 있다. 상기 용어는 또한 PD-1의 자연 발생 변이체, 예컨대, 스플라이스 변이체 또는 대립형질 변이체를 포괄한다. 예시적인 인간 PD-1의 아미노산 서열은 유니프롯 수탁 번호 Q15116에서 찾을 수 있다.As used herein, the term “PD-1” or “programmed
본원에서 용어 “PD-L2” 또는 “세포 예정사 1 리간드 2”은 달리 지시가 없는 한, 영장류(예컨대, 인간) 및 설치류(예컨대, 마우스 및 랫트)와 같은 포유동물을 포함한 임의의 척추동물 출처의 임의의 고유 PD-L2를 지칭한다. PD-L2는 또한 CD273 분자, B7DC 및 PDCD1L2로서 당업계에 공지되어 있다. 상기 용어는 또한 PD-L2의 천연 발생 변이체, 예컨대 스플라이스 변이체 또는 대립유전자 변이체를 수반한다. 예시적인 인간 PD-L2의 아미노산 서열은 유니프롯 수탁 번호 Q9BQ51에서 찾을 수 있다.As used herein, the term “PD-L2” or “
"길항제"라는 용어는 가장 넓은 의미로 사용되며, 본원에 개시된 천연 폴리펩타이드의 생물학적 활성을 부분적으로 또는 완전히 차단, 억제 또는 중화하는 임의의 분자를 포함한다. 적합한 길항제 분자는 길항제 항체 또는 항체 단편(예컨대, 항원 결합 단편), 선천적 폴리펩티드의 단편 또는 아미노산 서열 변이체, 펩티드, 안티센스 올리고뉴클레오티드, 작은 유기 분자 등을 특이적으로 포함한다. 폴리펩티드의 길항제를 확인하기 위한 방법은 폴리펩티드를 후보 길항제 분자와 접촉시키고, 폴리펩티드와 정상적으로 연관된 하나 또는 그 이상의 생물학적 활성에서 검출 가능한 변화를 측정하는 단계를 포함할 수 있다.The term “antagonist” is used in its broadest sense and includes any molecule that partially or fully blocks, inhibits or neutralizes the biological activity of a native polypeptide disclosed herein. Suitable antagonist molecules specifically include antagonist antibodies or antibody fragments (eg, antigen binding fragments), fragments of native polypeptides or amino acid sequence variants, peptides, antisense oligonucleotides, small organic molecules, and the like. A method for identifying an antagonist of a polypeptide may comprise contacting the polypeptide with a candidate antagonist molecule and measuring a detectable change in one or more biological activities normally associated with the polypeptide.
용어 "PD-1 축 결합 길항제"는 상기 PD-1 신호전달 축에서 신호전달로 인한 T 세포 기능이상을 제거하기 위하여, PD-1 축 결합 짝과 이의 하나 이상의 결합 짝과의 상호작용을 억제하는 분자를 지칭하며, 그 결과 T 세포 기능(예컨대, 증식, 사이토카인 생산, 및/또는 표적 세포 사멸)이 복원 또는 강화된다. 본원에서 사용되는 PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제 및 PD-L2 결합 길항제를 포함한다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제 또는 PD-1 결합 길항제를 포함한다. 일 양태에서, 상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제이다. 다른 양태에서, 상기 PD-1 축 결합 길항제는 PD-1 결합 길항제이다. 다른 양태에서, 상기 PD-1 축 결합 길항제는 PD-L2 결합 길항제이다.The term "PD-1 axis binding antagonist" refers to an agent that inhibits the interaction of a PD-1 axis binding partner with one or more binding partners thereof in order to eliminate T cell dysfunction due to signaling in the PD-1 signaling axis. molecule, whereby T cell function (eg, proliferation, cytokine production, and/or target cell death) is restored or enhanced. PD-1 axis binding antagonists as used herein include PD-L1 binding antagonists, PD-1 binding antagonists and PD-L2 binding antagonists. In some cases, the PD-1 axis binding antagonist comprises a PD-L1 binding antagonist or a PD-1 binding antagonist. In one embodiment, the PD-1 axis binding antagonist is a PD-L1 binding antagonist. In another embodiment, the PD-1 axis binding antagonist is a PD-1 binding antagonist. In another embodiment, the PD-1 axis binding antagonist is a PD-L2 binding antagonist.
용어 "PD-1 결합 길항제"는, PD-1이 이의 결합 짝들 중 하나 이상, 예컨대 PD-L1 및/또는 PD-L2와 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 폐지 또는 방해하는 분자를 지칭한다. Pd-1(예정된 사멸 1)은 또한 당업계에서 “예정된 세포 사멸 1”, “PDCD1”, “CD279”, 및 “SLEB2”로도 지칭된다. 예시적인 인간 PD-1은 유니프롯KB/스위스-프롯(Swiss-Prot) 수탁 번호 Q15116에 나타나 있다. 일부 경우들에서, 상기 PD-1 결합 길항제는 PD-1이 이의 하나 이상의 결합 짝에 결합하는 것을 억제하는 분자다. 특정 양태에서, 상기 PD-1 결합 길항제는 PD-1이 PD-L1 및/또는 PD-L2에 결합하는 것을 억제한다. 예를 들어, PD-1 결합 길항제는 PD-1의 PD-L1 및/또는 PD-L2와의 상호작용으로부터 발생하는 신호 변환을 감소시키거나, 차단하거나, 억제하거나, 제거하거나 또는 방해하는 항 PD-1 항체, 이의 항원 결합 단편, 면역부착소, 융합 단백질, 올리고펩티드 및 기타 분자를 포함한다. 한 경우에서, PD-1 결합 길항제는 PD-1을 통하여 T 림프구 매개된 신호 전달에서 발현된 세포 표면 단백질에 의해 또는 이를 통하여 매개된 음성 공동 자극 신호를 감소시켜, 이상기능 T 세포의 기능 이상을 더 적게 한다(예컨대, 항원 인지에 대한 작동체 반응을 강화). 일부 경우들에서, 상기 PD-1 결합 길항제는 PD-1에 결합한다. 일부 경우들에서, 상기 PD-1 결합 길항제는 항 PD-1 항체(예컨대, 항 PD-1 길항제 항체)이다. 예시적인 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680(AMP 514), PDR001(스파르탈리주맙), REGN2810(세미플리맙), BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 및 hAb21을 포함한다. 특정 양태에서, PD-1 결합 길항제는 MDX-1106(니볼루맙)이다. 다른 특정 양태에서, PD-1 결합 길항제는 MK-3475 (펨브롤리주맙, 이전에 람브롤리주맙으로도 공지됨)이다. 다른 특정 양태에서, PD-1 결합 길항제는 PD-L2 Fc 융합 단백질, 예컨대, AMP-224이다. 다른 특정 양태에서, PD-1 결합 길항제는 MEDI-0680이다. 다른 특정 양태에서, PD-1 결합 길항제는 PDR001(스파르탈리주맙)이다. 다른 특정 양태에서, PD-1 결합 길항제는 REGN2810(세미플리맙)이다. 다른 특정 양태에서, PD-1 결합 길항제는 BGB-108이다. 다른 특정 양태에서, PD-1 결합 길항제는 프롤골리맙이다. 다른 특정 양태에서, PD-1 결합 길항제는 캄렐리주맙이다. 다른 특정 양태에서, PD-1 결합 길항제는 신틸리맙이다. 다른 특정 양태에서, PD-1 결합 길항제는 티슬렐리주맙이다. 다른 특정 양태에서, PD-1 결합 길항제는 토리팔리맙이다. 다른 추가의 예시적인 PD-1 결합 길항제는 BION-004, CB201, AUNP-012, ADG104, 및 LBL-006을 포함한다.The term "PD-1 binding antagonist" refers to reducing, blocking, inhibiting, abrogating or abrogating signal transduction resulting from the interaction of PD-1 with one or more of its binding partners, such as PD-L1 and/or PD-L2. interfering molecules. Pd-1 (programmed death 1) is also referred to in the art as “
용어 "항 PD-1 길항제 항체"는 PD-1의 생물학적 활성을 실질적으로 또는 완전히 억제하기에 충분한 친화도로 PD-1에 결합할 수 있는 항체 또는 이의 항원 결합 단편 또는 변이체를 지칭한다. 예를 들어, 항 PD-1 길항제 항체는 PD-1이 이의 결합 짝들 중 하나 이상, 예컨대 PD-L1 및/또는 PD-L2와 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 폐지 또는 방해하는 분자를 지칭한다. 일부 경우들에서, 항 PD-1 길항제 항체가 다른 PD-1 활성에 영향을 미치지 않으면서 하나의 PD-1 활성을 길항할 수 있다는 것이 당업자에 의해 이해될 것이다. 예를 들어, 본원에 기재된 특정 방법 또는 용도에 사용하기 위한 항 PD-1 길항제 항체는 다른 PD-1 상호작용들 중 임의의 것에 영향을 미치지 않거나 최소한으로 영향을 미치면서 이의 결합 짝(예컨대, PD-L1 또는 PD-L2) 중 하나에 반응하여 PD-1 활성을 길항하는 항 PD-1 길항제 항체이다. 일 양태에서, 관련되지 않은 비 PD-1 단백질에 대한 항 PD-1의 길항제 항체의 결합 정도는, 예컨대, 방사면역분석(RIA)에 의해 측정된 바와 같이 PD-1에 대한 항체의 결합의 약 10% 미만이다. 특정 양태들에서, PD-1에 결합하는 항 PD-1 길항제 항체는 ≤ 1μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, 또는 ≤ 0.001 nM(예컨대, 10-8 M 이하, 예컨대, 10-8 M 내지 10-13 M, 예컨대, 10-9 M 내지 10-13 M)의 해리 상수(KD)를 갖는다. 특정 양태들에서, 항 PD-1 길항제 항체는 상이한 종으로부터 PD-1 사이에 보존된 PD-1의 에피토프 또는 종간 교차 반응성을 허용하는 PD-1 상의 에피토프에 결합한다. 일 양태에서, 상기 항 PD-1 길항제 항체는 펨브롤리주맙(이전에 람브롤리주맙으로 공지됨)이다. 일 양태에서, 상기 항 PD-1 길항제 항체는 니볼루맙이다.The term “anti-PD-1 antagonist antibody” refers to an antibody, or antigen-binding fragment or variant thereof, capable of binding to PD-1 with sufficient affinity to substantially or completely inhibit the biological activity of PD-1. For example, an anti-PD-1 antagonist antibody reduces, blocks, inhibits, abrogates, signal transduction resulting from the interaction of PD-1 with one or more of its binding partners, such as PD-L1 and/or PD-L2. or interfering molecules. It will be understood by those of skill in the art that in some cases, an anti-PD-1 antagonist antibody may antagonize one PD-1 activity without affecting the other PD-1 activity. For example, an anti-PD-1 antagonist antibody for use in a particular method or use described herein can have its binding partner (eg, PD) with no or minimal effect on any of the other PD-1 interactions. It is an anti-PD-1 antagonist antibody that antagonizes PD-1 activity in response to either -L1 or PD-L2). In one aspect, the extent of binding of the antagonist antibody of anti-PD-1 to an unrelated non-PD-1 protein is about the same as that of the binding of the antibody to PD-1 as measured by radioimmunoassay (RIA). less than 10%. In certain aspects, the anti-PD-1 antagonist antibody that binds PD-1 is ≤ 1 μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, or ≤ 0.001 nM (e.g., 10 - It has a dissociation constant (K D ) of 8 M or less, such as 10 -8 M to 10 -13 M, such as 10 -9 M to 10 -13 M). In certain embodiments, the anti-PD-1 antagonist antibody binds to an epitope of PD-1 that is conserved between PD-1 from different species or an epitope on PD-1 that allows cross-species reactivity. In one aspect, the anti-PD-1 antagonist antibody is pembrolizumab (previously known as lambrolizumab). In one embodiment, said anti-PD-1 antagonist antibody is nivolumab.
용어 "PD-L1 결합 길항제"는 PD-L1이 이의 결합 짝들 중 하나 이상, 예컨대 PD-1 및/또는 B7-1과 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 폐지 또는 방해하는 분자를 지칭한다. 일부 경우들에서, PD-L1 결합 길항제는 PD-L1이 이의 결합 짝에 결합하는 것을 억제하는 분자다. 특정 양태에서, 상기 PD-L1 결합 길항제는 PD-L1이 PD-1 및/또는 B7-1에 결합하는 것을 억제한다. 일부 경우들에서, 상기 PD-L1 결합 길항제들은 PD-L1이 이의 결합 짝들 중 하나 이상, 예컨대 PD-1 및/또는 B7-1과 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 소멸 또는 간섭하는 항 PD-L1 항체, 이의 항원 결합 단편, 면역접합체, 융합 단백질, 올리고펩티드 및 기타 분자를 포함한다. 한 경우에서, PD-L1 결합 길항제는 PD-L1을 통하여 T 림프구 매개된 신호 전달에서 발현된 세포 표면 단백질에 의해 또는 이를 통하여 매개된 음성 공동 자극 신호를 감소시켜, 이상기능 T 세포의 기능이상을 더 적게 한다(예컨대, 항원 인지에 대한 작동체 반응을 강화). 일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-1에 결합한다. 일부 경우들에서, PD-L1 결합 길항제는 항 PD-L1 항체(예컨대, 항 PD-L1 길항제 항체)이다. 예시적인 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, MEDI4736(더발루맙), MSB0010718C(아벨루맙), SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 및 Hs-636을 포함한다. 일부 양태들에서, 상기 항 PD-L1 항체는 아테졸리주맙, MDX-1105, MEDI4736(더발루맙), 또는 MSB0010718C(아벨루맙)이다. 일 특정 양태에서, 상기 PD-L1 결합 길항제는 MDX-1105이다. 다른 특정 양태에서, 상기 PD-L1 결합 길항제는 MEDI4736 (더발루맙)이다. 다른 특정 양태에서, 상기 PD-L1 결합 길항제는 MSB0010718C(아벨루맙)이다. 다른 양태들에서, 상기 PD-L1 결합 길항제는 소분자, 예컨대, GS-4224, INCB086550, MAX-10181, INCB090244, CA-170 또는 ABSK041일 수 있으며, 이는 일부 경우들에서 경구 투여될 수 있다. 다른 예시적인 PD-L1 결합 길항제들은 AVA-004, MT-6035, VXM10, LYN192, GB7003, 및 JS-003을 포함한다. 바람직한 양태에서, 상기 PD-L1 결합 길항제는 티센트릭(TECENTRIQ)™으로 시판되는 아테졸리주맙이다. 아테졸리주맙은 WHO 약물 정보(Drug Information)(제약 물질에 대한 국제 일반명칭(International Nonproprietary Names for Pharmaceutical Substances)), Proposed INN: List 112, Vol. 28, No. 4(2015년 1월 16일에 공개, 485 페이지 참조)에 기재되어 있다. 다른 특정 양태에서, 항 PD-L1 항체는 MSB0015718C이다.The term “PD-L1 binding antagonist” refers to reducing, blocking, inhibiting, abrogating or interfering with signal transduction resulting from the interaction of PD-L1 with one or more of its binding partners, such as PD-1 and/or B7-1. refers to molecules that In some cases, a PD-L1 binding antagonist is a molecule that inhibits the binding of PD-L1 to its binding partner. In certain embodiments, the PD-L1 binding antagonist inhibits the binding of PD-L1 to PD-1 and/or B7-1. In some cases, the PD-L1 binding antagonists decrease, block, inhibit, anti-PD-L1 antibodies, antigen-binding fragments thereof, immunoconjugates, fusion proteins, oligopeptides and other molecules that abrogate or interfere. In one case, the PD-L1 binding antagonist reduces the dysfunction of dysfunctional T cells by reducing negative costimulatory signals mediated by or through cell surface proteins expressed in T lymphocyte mediated signaling through PD-L1. less (eg, enhance effector response to antigen recognition). In some cases, the PD-L1 binding antagonist binds PD-1. In some cases, the PD-L1 binding antagonist is an anti-PD-L1 antibody (eg, an anti-PD-L1 antagonist antibody). Exemplary anti-PD-L1 antagonist antibodies are atezolizumab, MDX-1105, MEDI4736 (durvalumab), MSB0010718C (avelumab), SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX- 072, IMC-001, KL-A167, APL-502, Cosibelimab, Rhodapoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, and Hs-636. In some aspects, the anti-PD-L1 antibody is atezolizumab, MDX-1105, MEDI4736 (durvalumab), or MSB0010718C (avelumab). In one particular embodiment, the PD-L1 binding antagonist is MDX-1105. In another specific embodiment, said PD-L1 binding antagonist is MEDI4736 (durvalumab). In another specific embodiment, said PD-L1 binding antagonist is MSB0010718C (avelumab). In other aspects, the PD-L1 binding antagonist may be a small molecule, such as GS-4224, INCB086550, MAX-10181, INCB090244, CA-170 or ABSK041, which in some cases may be administered orally. Other exemplary PD-L1 binding antagonists include AVA-004, MT-6035, VXM10, LYN192, GB7003, and JS-003. In a preferred embodiment, the PD-L1 binding antagonist is atezolizumab marketed as TECENTRIQ™. Atezolizumab is prescribed in the WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN: List 112, Vol. 28, No. 4 (published January 16, 2015, see page 485). In another specific embodiment, the anti-PD-L1 antibody is MSB0015718C.
용어 "항 PD-L1 길항제 항체"는 PD-L1의 생물학적 활성을 실질적으로 또는 완전히 억제하기에 충분한 친화도로 PD-L1에 결합할 수 있는 항체 또는 이의 항원 결합 단편 또는 변이체를 지칭한다. 예를 들어, 항 PD-L1 길항제 항체는 PD-L1이 이의 결합 짝들 중 하나 이상, 예컨대 PD-1 및/또는 B7-1과 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 폐지 또는 방해하는 분자를 지칭한다. 일부 경우들에서, 항 PD-L1 길항제 항체가 다른 PD-L1 활성에 영향을 미치지 않으면서 하나의 PD-L1 활성을 길항할 수 있다는 것이 당업자에 의해 이해될 것이다. 예를 들어, 본원에 기재된 특정 방법 또는 용도에 사용하기 위한 항 PD-L1 길항제 항체는 다른 PD-L1 상호작용들 중 임의의 것에 영향을 미치지 않거나 최소한으로 영향을 미치면서 이의 결합 짝(예컨대, PD-1 또는 B7-1) 중 하나에 반응하여 PD-L1 활성을 길항하는 항 PD-L1 길항제 항체이다. 일 양태에서, 관련되지 않은 비 PD-L1 단백질에 대한 항 PD-L1의 길항제 항체의 결합 정도는, 예컨대, 방사면역분석(RIA)에 의해 측정된 바와 같이 PD-L1에 대한 항체의 결합의 약 10% 미만이다. 특정 양태들에서, PD-1에 결합하는 항 PD-L1 길항제 항체는 ≤ 1μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, 또는 ≤ 0.001 nM(예컨대, 10-8 M 이하, 예컨대, 10-8 M 내지 10-13 M, 예컨대, 10-9 M 내지 10-13 M)의 해리 상수(KD)를 갖는다. 특정 양태들에서, 항 PD-L1 길항제 항체는 상이한 종으로부터 PD-L1 사이에 보존된 PD-L1의 에피토프 또는 종간 교차 반응성을 허용하는 PD-L1 상의 에피토프에 결합한다. 일 양태에서, 상기 항 PD-L1 길항제 항체는 아테졸리주맙이다.The term “anti-PD-L1 antagonist antibody” refers to an antibody, or antigen-binding fragment or variant thereof, capable of binding to PD-L1 with sufficient affinity to substantially or completely inhibit the biological activity of PD-L1. For example, an anti-PD-L1 antagonist antibody reduces, blocks, inhibits, abrogates, signal transduction resulting from the interaction of PD-L1 with one or more of its binding partners, such as PD-1 and/or B7-1. or interfering molecules. It will be understood by those of skill in the art that in some cases, an anti-PD-L1 antagonist antibody may antagonize one PD-L1 activity without affecting the other PD-L1 activity. For example, an anti-PD-L1 antagonist antibody for use in a particular method or use described herein may have its binding partner (eg, PD) with minimal or no effect on any of the other PD-L1 interactions. It is an anti-PD-L1 antagonist antibody that antagonizes PD-L1 activity in response to either -1 or B7-1). In one aspect, the extent of binding of an antagonist antibody of anti-PD-L1 to an unrelated non-PD-L1 protein is about the extent of binding of the antibody to PD-L1 as measured, eg, by radioimmunoassay (RIA). less than 10%. In certain aspects, an anti-PD-L1 antagonist antibody that binds PD-1 is ≤ 1 μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, or ≤ 0.001 nM (e.g., 10 - It has a dissociation constant (K D ) of 8 M or less, such as 10 -8 M to 10 -13 M, such as 10 -9 M to 10 -13 M). In certain aspects, the anti-PD-L1 antagonist antibody binds to an epitope of PD-L1 that is conserved between PD-L1 from different species or an epitope on PD-L1 that allows cross-species reactivity. In one embodiment, said anti-PD-L1 antagonist antibody is atezolizumab.
용어 "PD-L2 결합 길항제"는 PD-L2가 이의 결합 짝들 중 하나 이상, 예컨대 PD-1과 상호작용하는 것으로부터 유발된 신호 변환을 감소, 차단, 억제, 폐지 또는 방해하는 분자를 지칭한다. PD-L2(예정된 사멸 리간드 2)는 또한 당업계에서 “예정된 세포 사멸 1 리간드 2,” “PDCD1LG2,” “CD273,” “B7-DC,” “Btdc,” 및 “PDL2”로 지칭된다. 예시적인 인간 PD-L2는 유니프롯KB/스위스-프롯 수탁 번호 Q9BQ51에 나타내었다. 일부 경우들에서, PD-L2 결합 길항제는 이의 결합 짝들 중 하나 이상에 대한 PD-L2의 결합을 억제하는 분자이다. 특정 양태에서, 상기 PD-L2 결합 길항제는 PD-1에 대한 PD-L2의 결합을 억제한다. 예시적인 PD-L2 길항제들은 PD-L2가 이의 결합 짝들 중 하나 이상, 예컨대 PD-1과 상호작용하는 것으로 인하여 유발된 신호 변환을 감소, 차단, 억제, 소멸 또는 간섭하는 항 PD-L2 항체, 이의 항원 결합 단편들, 면역접합체, 융합 단백질, 올리고펩티드 및 기타 분자를 포함한다. 일 양태에서, PD-L2 결합 길항제는 PD-L2를 통하여 T 림프구 매개된 신호 전달에서 발현된 세포 표면 단백질에 의해 또는 이를 통하여 매개된 음성 공동 자극 신호를 감소시켜, 이상기능 T 세포의 기능이상을 더 적게 한다(예컨대, 항원 인지에 대한 작동체 반응을 강화). 일부 양태들에서, 상기 PD-L2 결합 길항제는 PD-L2에 결합한다. 일부 양태들에서, PD-L2 결합 길항제는 면역접합체이다. The term "PD-L2 binding antagonist" refers to a molecule that reduces, blocks, inhibits, abrogates or interferes with signal transduction resulting from the interaction of PD-L2 with one or more of its binding partners, such as PD-1. PD-L2 (predetermined death ligand 2) is also referred to in the art as “
PD-1 축 결합 길항제의 추가적인 예들에는 세미플리맙, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티스렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 스파탈리주맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, 짐베렐리맙, 발스틸리맙, 게놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, CX-072, IMC-001, KL-A167, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, APL-502, 코시벨리맙, 로다폴리맙, GS-4224, INCB086550, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, MAX-10181, RC98, BION-004, AM0001, CB201, ENUM 244C8, ENUM 388D4, AUNP-012, STI-1110, ADG104, AK-103, LBL-006, hAb21, AVA-004, PDL-GEX, INCB090244, KD036, KY1003, LYN192, MT-6035, VXM10, YBL-007, ABSK041, GB7003, JS-003, 및 HS-636이 포함된다.Additional examples of PD-1 axis binding antagonists include semiplimab, prolgolimab, camrelizumab, scintilimab, tisrelizumab, torifalimab, dostalimab, retipanrimab, spatalizumab, sasanrimab, fen fulimab, CS1003, HLX10, SCT-I10A, SHR-1316, CS1001, envafoliumab, TQB2450, ZKAB001, LP-002, gimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL- 006, BAT1306, HX008, CX-072, IMC-001, KL-A167, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, APL-502, cosibelimab , rhodafoliumab, GS-4224, INCB086550, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, MAX-10181, RC98, BION-004, AM0001, CB201 , ENUM 244C8, ENUM 388D4, AUNP-012, STI-1110, ADG104, AK-103, LBL-006, hAb21, AVA-004, PDL-GEX, INCB090244, KD036, KY1003, LYN192, MT-6035, VXM10, YBL -007, ABSK041, GB7003, JS-003, and HS-636.
본원의 목적을 위해, "아테졸리주맙"은 PD-L1에 결합하는 Fc 조작, 인간화, 비당화 IgG1 카파 면역글로불린이고, 서열번호 28의 중쇄 서열 및 서열번호 29의 경쇄 서열을 포함한다. 아테졸리주맙은 Fc 영역 아미노산 잔기의 EU 넘버링을 사용하여 중쇄(N297A)의 위치 297에서 단일 아미노산 치환(아스파라긴에서 알라닌으로)을 포함하며, 이는 Fc 수용체에 대한 최소 결합을 갖는 비당화된 항체를 발생시킨다. 아테졸리주맙은 또한 WHO 약물 정보(제약 물질에 대한 국제 일반명칭), Proposed INN: List 112, Vol. 28, No. 4(2015년 1월 16일에 공개, 485 페이지 참조)에 기재되어 있다. For the purposes herein, "Atezolizumab" is an Fc engineered, humanized, aglycosylated IgGl kappa immunoglobulin that binds to PD-L1 and comprises the heavy chain sequence of SEQ ID NO: 28 and the light chain sequence of SEQ ID NO: 29. Atezolizumab contains a single amino acid substitution (asparagine to alanine) at position 297 of the heavy chain (N297A) using EU numbering of Fc region amino acid residues, resulting in an aglycosylated antibody with minimal binding to the Fc receptor. make it Atezolizumab is also described in the WHO Drug Information (International Common Name for Pharmaceutical Substances), Proposed INN: List 112, Vol. 28, No. 4 (published January 16, 2015, see page 485).
본원에 사용된 "펨브롤리주맙"은 인간 세포 표면 수용체 PD-1에 대해 지시된 재조합 인간화 단일클론 IgG4 항체이다. 펨브롤리주맙은 WHO 약물 정보(제약 물질에 대한 국제 일반명칭), Proposed INN: List 72, Vol. 28, No. 3(2014년에 공개, 407 페이지 참조)에 기재되어 있다.As used herein, “pembrolizumab” is a recombinant humanized monoclonal IgG4 antibody directed against the human cell surface receptor PD-1. Pembrolizumab is listed in the WHO Drug Information (International Common Name for Pharmaceutical Substances), Proposed INN:
본원에 사용된 "티라골루맙"은 TIGIT에 결합하는 오픈 모노클로날 테크놀로지(Open Monoclonal Technology, OMT) 래트에서 유래된 완전 인간 IgG1/카파 Mab이고, 서열번호"Tiragolumab," as used herein, is a fully human IgG1/kappa Mab derived from Open Monoclonal Technology (OMT) rats that binds TIGIT, SEQ ID NO:
33의 중쇄 서열 및 서열번호 34의 경쇄 서열을 포함한다. 티라골루맙은 Fc 도메인에서 2개의 N 연결 당화 부위(N306)를 포함한다. 티라골루맙은 WHO 약물 정보(제약 물질에 대한 국제 일반명칭), Proposed INN: List 117, Vol. 31, No. 2(2017년 7월 7일에 공개, 343 페이지 참조)에 기재되어 있다. 33 and the light chain sequence of SEQ ID NO: 34. Tiragolumab contains two N-linked glycosylation sites (N306) in the Fc domain. Tiragolumab is listed in the WHO Drug Information (International Common Name for Pharmaceutical Substances), Proposed INN: List 117, Vol. 31, No. 2 (published 7 July 2017, see page 343).
본원에 사용된 "베바시주맙"은 VEGF의 모든 동형을 인식하는 재조합 인간화 단일 항체이고, 이는 WHO 약물 정보(제약 물질에 대한 국제 일반명칭), Proposed INN: List 83, Vol. 14, No. 2(2000년에 공개, 107 페이지 참조)에 기재되어 있다. 베바시주맙은 서열번호 X의 중쇄 가변 영역 서열 및 서열번호 X의 경쇄 가변 영역 서열을 포함한다.As used herein, "bevacizumab" is a recombinant humanized single antibody that recognizes all isoforms of VEGF, which is described in WHO Drug Information (International Common Name for Pharmaceutical Substances), Proposed INN: List 83, Vol. 14, No. 2 (published in 2000, see p. 107). Bevacizumab comprises a heavy chain variable region sequence of SEQ ID NO: X and a light chain variable region sequence of SEQ ID NO: X.
용어 "항 TIGIT 길항제 항체"는 TIGIT의 생물학적 활성을 실질적으로 또는 완전히 억제하기에 충분한 친화도로 TIGIT에 결합할 수 있는 항체 또는 이의 항원 결합 단편 또는 변이체를 지칭한다. 예를 들어, 항 TIGIT 길항제 항체는 기능장애 상태에서부터 항원 자극까지 T 세포(예컨대, 증식, 사이토킨 생성, 표적 세포 사멸)에 의해 기능 반응을 회복하기 위하여PVR, PVRL2, 및/또는 PVRL3을 통하여 신호전달을 차단할 수 있다. 예를 들어, 항 TIGIT 길항제 항체는 PVR-CD226 상호작용에 영향을 미치지 않으면서 PVR을 통한 신호전달을 차단할 수 있다. 일부 경우들에서, 항 TIGIT 길항제 항체가 다른 TIGIT 활성에 영향을 미치지 않으면서 하나의 TIGIT 활성을 길항할 수 있다는 것이 당업자에 의해 이해될 것이다. 예를 들어, 본원에 기재된 특정 방법 또는 용도에 사용하기 위한 항 TIGIT 길항제 항체는, 예컨대, 다른 TIGIT 상호작용들 중 임의의 것에 영향을 미치지 않거나 최소한으로 영향을 미치면서 PVR 상호 작용, PVRL3 상호 작용 또는 PVRL2 상호 작용 중 하나 중 하나에 반응하여 TIGIT 활성을 길항하는 항 TIGIT 길항제 항체이다. 일 양태에서, 관련되지 않은 비 TIGIT 단백질에 대한 항 TIGIT의 길항제 항체의 결합 정도는, 예컨대, 방사면역분석(RIA)에 의해 측정된 바와 같이 TIGIT에 대한 항체의 결합의 약 10% 미만이다. 특정 양태예들에서, TIGIT에 결합하는 항 TIGIT 길항제 항체는 ≤ 1μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, 또는 ≤ 0.001 nM (예컨대, 10-8 M 또는 그 미만, 예컨대, 10-8 M 내지 10-13 M, 예컨대, 10-9 M 내지 10-13 M)의 해리 상수 (KD)를 갖는다. 특정 양태들에서, 항 TIGIT 길항제 항체는 상이한 종으로부터 TIGIT 사이에 보존된 TIGIT의 에피토프 또는 종간 교차 반응성을 허용하는 TIGIT 상의 에피토프에 결합한다. 일부 양태들에서, 상기 항 TIGIT 결합 항체는 원형 Fc 매개 작동체 기능(예컨대, 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448 또는 TJ-T6)을 갖는다. 일부 양태들에서, 상기 항 TIGIT 결합 항체는 강화된 Fc 매개 작동체 기능(예컨대, SGN-TGT)을 갖는다. 다른 양태들에서, 상기 항 TIGIT 길항제 항체는 Fc 매개 작동체 기능이 결여되었다(예를 들어, 돔바날리맙, BMS-986207, ASP8374, 또는 COM902). 일부 양태들에서, 상기 항 TIGIT 결합 항체는 IgG1 부류 항체(예컨대, 티라골루맙, 비보스톨리맙, 돔바날리맙, BMS-986207, 에티길리맙, BGB-A1217, SGN-TGT, EOS084448(EOS-448), TJ-T6, 또는 AB308)이다. 다른 양태들에서, 상기 항 TIGIT 결합 항체는 IgG 부류 항체(예컨대, ASP8374 또는 COM902)이다. 일 양태에서, 상기 항 TIGIT 길항제 항체는 티라골루맙이다.The term “anti-TIGIT antagonist antibody” refers to an antibody or antigen-binding fragment or variant thereof capable of binding TIGIT with sufficient affinity to substantially or completely inhibit the biological activity of TIGIT. For example, an anti-TIGIT antagonist antibody may signal through PVR, PVRL2, and/or PVRL3 to restore a functional response by T cells (eg, proliferation, cytokine production, target cell death) from a dysfunctional state to antigen stimulation. can be blocked. For example, an anti-TIGIT antagonist antibody can block signaling through the PVR without affecting the PVR-CD226 interaction. It will be appreciated by those of skill in the art that in some cases, an anti-TIGIT antagonist antibody may antagonize one TIGIT activity without affecting the other TIGIT activity. For example, an anti-TIGIT antagonist antibody for use in a particular method or use described herein may contain, for example, a PVR interaction, a PVRL3 interaction, or It is an anti-TIGIT antagonist antibody that antagonizes TIGIT activity in response to one of the PVRL2 interactions. In one aspect, the extent of binding of the antagonist antibody of anti-TIGIT to an unrelated non-TIGIT protein is less than about 10% of the binding of the antibody to TIGIT as measured, eg, by radioimmunoassay (RIA). In certain embodiments, an anti-TIGIT antagonist antibody that binds TIGIT is ≤ 1 μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, or ≤ 0.001 nM (eg, 10 −8 M or It has a dissociation constant (K D ) of less than that, such as 10 -8 M to 10 -13 M, such as 10 -9 M to 10 -13 M). In certain embodiments, an anti-TIGIT antagonist antibody binds to an epitope of TIGIT that is conserved between TIGITs from different species or an epitope on TIGIT that permits cross-species cross-reactivity. In some aspects, the anti-TIGIT binding antibody has a prototypical Fc mediated effector function (eg, tyragolumab, bivostolimab, etigilimab, EOS084448 or TJ-T6). In some aspects, the anti-TIGIT binding antibody has enhanced Fc-mediated effector function (eg, SGN-TGT). In other aspects, the anti-TIGIT antagonist antibody lacks Fc-mediated effector function (eg, dombanalimab, BMS-986207, ASP8374, or COM902). In some aspects, the anti-TIGIT binding antibody is an IgG1 class antibody (e.g., tiragolumab, bivostolimab, dombanalimab, BMS-986207, ethigilumab, BGB-A1217, SGN-TGT, EOS084448 (EOS-448) ), TJ-T6, or AB308). In other embodiments, the anti-TIGIT binding antibody is an IgG class antibody (eg, ASP8374 or COM902). In one embodiment, said anti-TIGIT antagonist antibody is tyragolumab.
본원에서 사용된 "투여하는"은 화합물(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체), VEGF 길항제, 또는 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드)), 탁산(예컨대, 파클리탁셀, 예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 또는 조성물(예컨대, 약학적 조성물, 예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체), 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)) 및/또는 하나 또는 추가 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)), 항체-약물 접합체(ADC)(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/또는 집락 자극 인자(CSF)(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀)를 포함하는 약학적 조성물)의 투여량을 대상체에게 제공하는 방법을 의미한다. 본원에 기재된 방법에 사용되는 화합물 및/또는 조성물은, 예를 들어, 정맥내(예컨대, 정맥내 주입에 의해), 피하, 근육내, 피내, 경피, 동맥내, 복강내, 병변내, 두개내, 동맥내, 전립선내, 흉막내, 기관내, 비강내, 유리체내, 질내, 직장내, 국소적으로, 종양내, 복막내, 결막하, 방광내, 점막내, 심낭내, 탯줄내, 안구내, 경구, 국소, 국부, 흡입으로, 주사로, 주입으로, 연속 주입으로, 직접적으로 표적 세포들을 약욕시키는 국부화 관류로, 카테터로, 세정으로, 크림으로, 또는 지질 조성물로 투여될 수 있다. 투여 방법은 다양한 인자들(예컨대, 투여되는 화합물 또는 조성물 및 치료되는 상태, 질병 또는 장애의 중증도)에 따라 가변될 수 있다.As used herein, “administering” refers to a compound (eg, an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antibody), a VEGF antagonist, or a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent) eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide)), a taxane (eg, paclitaxel such as nap-paclitaxel), and/or topoiso merase II inhibitors (eg, doxorubicin)) or compositions (eg, pharmaceutical compositions such as anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists (eg anti-PD-L1 antibodies), chemotherapeutic agents (eg, platinum-based) a chemotherapeutic agent (such as carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (such as an alkylating agent (such as cyclophosphamide), a taxane (such as paclitaxel such as nap-paclitaxel), and/or a topoisomerase II inhibitor (eg, doxorubicin), an antibody-drug conjugate (ADC) (eg, enfortumab vedotin or sacituzumab gobitecan), and/or a colony stimulating factor (CSF) ( For example, pegfilgrastim, filgrastim or sagramostim) refers to the method of providing to the subject a dose of a pharmaceutical composition).The compound and/or composition used in the method described herein can For example, intravenous (eg, by intravenous infusion), subcutaneous, intramuscular, intradermal, transdermal, intraarterial, intraperitoneal, intralesional, intracranial, intraarterial, intraprostatic, intrapleural, intratracheal, intranasal , intravitreal, vaginal, rectal, topically, intratumoral, intraperitoneal, subconjunctival, intravesical, intramucosal, intrapericardial, intraumbilical, intraocular, oral, topical, topical, by inhalation, by injection, infusion It can be administered by means of continuous infusion, by localized perfusion that directly bathes the target cells, by catheter, by irrigation, by cream, or by lipid composition.The method of administration depends on a variety of factors (such as the compound or composition being administered). and the severity of the condition, disease or disorder being treated).
치료제(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체), VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀))의 “고정” 또는 “일정” 용량은 환자의 체중이나 체표면적(BSA)에 관계없이 상기 환자에게 투여되는 용량을 지칭한다. 따라서, 고정 또는 일정 용량은 mg/kg 용량 또는 mg/m2 용량으로서 제공되지 않고, 오히려 치료제의 절대량(예컨대, mg인 치료제의 절대량)으로서 제공된다.Therapeutic agents (eg, anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists (eg, anti-PD-L1 antibodies), VEGF antagonists, chemotherapeutic agents (eg, platinum-based chemotherapeutic agents or non-platinum-based chemotherapeutic agents), ADCs (eg, , enfortumab vedotin or sacituzumab govitecan), or a “fixed” or “constant” dose of CSF (eg, pegfilgrastim, filgrastim, or sagramostim)) depends on the patient's weight or body surface area. (BSA) refers to the dose administered to the patient. Thus, a fixed or constant dose is not provided as a mg/kg dose or a mg/m 2 dose, but rather as an absolute amount of therapeutic agent (eg, absolute amount of therapeutic agent in mg).
본원에 사용된 용어 "치료" 또는 "치료하는"은 임상 병리 과정 동안 치료되는 개체 또는 세포의 자연 과정을 변경하도록 설계된 임상 개입을 지칭한다. 치료의 바람직한 효과에는 질병 진행의 지연 또는 감소, 질병 상태의 개선 또는 완화, 관해 또는 예후 개선이 포함된다. 예를 들어, 암세포의 증식의 감소(또는 파괴), 질병으로 인한 증상 감소, 질병을 앓고 있는 사람의 삶의 질 증가, 질병 치료에 필요한 다른 약물의 용량 감소, 질병의 진행 지연, 및/또는 개체의 생존 연장을 포함하지만 이에 제한되지는 않는 암과 관련된 하나 이상의 증상이 완화되거나 제거되는 경우, 개체는 성공적으로 "치료된다". 예를 들어, 치료하는 것은 유효량의 치료제(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사르그라모스팀)) 또는 치료제들의 조합을 이용한 효과적인 암 치료를 포함한다. 본원에서 치료하는 것은 특히 보조 요법, 신보조 요법, 비전이성 암 요법(예컨대, 국소 진행성 암 요법), 및 전이성 암 요법을 포함한다. 치료는 1차 치료(예컨대, 환자가 이전에 치료를 받지 않았거나, 또는 선행 전신 요법을 받지 않았을 수 있음), 또는 2차 또는 이후의 치료일 수 있다.As used herein, the term “treatment” or “treating” refers to a clinical intervention designed to alter the natural course of the individual or cell being treated during the course of a clinical pathology. Desirable effects of treatment include delaying or reducing disease progression, ameliorating or ameliorating the disease state, and improving remission or prognosis. For example, reducing the proliferation (or destruction) of cancer cells, reducing symptoms caused by the disease, increasing the quality of life of a person with the disease, reducing the dose of other drugs needed to treat the disease, delaying the progression of the disease, and/or the individual A subject is successfully "treated" when one or more symptoms associated with the cancer, including, but not limited to, prolonging survival of the cancer are alleviated or eliminated. For example, treating may include an effective amount of a therapeutic agent (eg, an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a VEGF antagonist, a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent or a non-platinum-based chemotherapeutic agent), an ADC (eg, , enfortumab vedotin or sacituzumab govitecan), and/or CSF (eg, pegfilgrastim, filgrastim or sargramostim) or combinations of therapeutic agents. Treating herein includes, inter alia, adjuvant therapy, neoadjuvant therapy, non-metastatic cancer therapy (eg, locally advanced cancer therapy), and metastatic cancer therapy. Treatment may be primary treatment (eg, the patient may not have previously received treatment, or may not have received prior systemic therapy), or secondary or subsequent treatment.
본원에 사용된, "~와 병용으로" 또는 "~와 함께”는 한 치료 양식에 더하여 다른 치료 양식을 투여하는 것, 예를 들어, PD-1 축 결합 길항제(예컨대, 아테졸리주맙), VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀), 및 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 투여를 포함하는 치료 요법을 지칭한다. 이처럼, "~와 함께"는 환자에게 다른 치료 양식의 투여 이전, 동안 또는 이후에 한 치료 양식을 투여하는 것을 지칭한다. As used herein, “in combination with” or “with” refers to administration of one treatment modality in addition to another treatment modality, e.g., a PD-1 axis binding antagonist (e.g., atezolizumab), VEGF Antagonists, chemotherapeutic agents (eg, platinum-based chemotherapeutic agents or non-platinum-based chemotherapeutic agents), ADCs (eg, enfortumab vedotin or sacituzumab govitecan), and/or CSF (eg, pegfilgrastim) , filgrastim or sagramostim), and an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab). As such, "with "Conjointly" refers to administration of one treatment modality to a patient before, during, or after administration of the other treatment modality.
하나 이상의 다른 약물과 “동시에” 투여되는 약물은 동일한 치료 주기 동안, 하나 이상의 다른 약물과 동일한 치료 일자에, 그리고 임의적으로, 상기 하나 이상의 다른 약물과 동일한 시간에 투여된다. 예를 들어, 3주마다 제공되는 암 요법의 경우에, 동시에 투여되는 약물은 각각 3주 주기의 제 1일에 투여된다.A drug administered “concurrently” with one or more other drugs is administered during the same treatment cycle, on the same treatment day as the one or more other drugs, and optionally, at the same time as the one or more other drugs. For example, in the case of cancer therapy given every three weeks, the concurrently administered drugs are each administered on
본원에서 사용되는, 용어 "수술 전후 치료"는 수술 전후에 투여되는 치료를 지칭한다. 수술 전후 치료는 수술 전 신보조 요법(예컨대, 방광 절제술) 및 수술 후 요법(예컨대, 보조 요법)의 투여를 포함할 수 있다. 예를 들어, 수술 전후 치료는 진단 후 및 수술(예컨대, 방광절제술) 및 상기 수술 후(예컨대, 상기 수술 후 약 1주, 2주, 3주, 4주, 5주, 6주, 7주, 8주, 9주, 12주, 13주, 14주, 15주 또는 그 이상) 요법(예컨대, 보조 요법(예컨대, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제 보조 요법)) 전에(예컨대, 약 1주, 2주, 3주, 4주, 5주, 6주, 7주, 8주, 9주, 12주, 13주, 14주, 15주 또는 그 이상 전에) 투여되는 신보조 요법(예컨대, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제 신보조 요법)을 포함할 수 있다.As used herein, the term “perioperative treatment” refers to treatment administered before or after surgery. The perioperative treatment may include administration of preoperative neoadjuvant therapy (eg, cystectomy) and postoperative therapy (eg, adjuvant therapy). For example, perioperative treatment may include post-diagnosis and surgery (eg, cystectomy) and post-surgery (eg, about 1 week, 2 weeks, 3 weeks, 4 weeks, 5 weeks, 6 weeks, 7 weeks, after the surgery); 8 weeks, 9 weeks, 12 weeks, 13 weeks, 14 weeks, 15 weeks or more) before therapy (eg, adjuvant therapy (eg, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist adjuvant therapy)) (eg, about Neoadjuvant therapy (e.g., 1 week, 2 weeks, 3 weeks, 4 weeks, 5 weeks, 6 weeks, 7 weeks, 8 weeks, 9 weeks, 12 weeks, 13 weeks, 14 weeks, 15 weeks or more) administered before , anti-TIGIT antagonist antibody and PD-1 axis binding antagonist neoadjuvant therapy).
"장애" 또는 "질병"은 어느 정도의 비정상적인 세포 증식과 관련된 장애, 예컨대, 암을 포함하지만 이에 제한되지는 않는 치료로부터 이익을 얻을 수 있는 임의의 상태이다.A “disorder” or “disease” is any condition that would benefit from treatment, including, but not limited to, a disorder associated with some degree of abnormal cell proliferation, such as cancer.
면역 기능장애와 관련하여 용어 "기능장애"는 항원 자극에 대한 면역 반응이 감소된 상태를 의미한다.The term “dysfunction” in the context of immune dysfunction refers to a state in which the immune response to antigenic stimulation is reduced.
본원에서 사용되는 용어 “기능장애”는 또한 항원 인식에 대한 불응성 또는 비반응성, 구체적으로, 항원 인식을 하류 T-세포 기능, 가령, 증식, 사이토카인 생성 (예컨대, 감마 인터페론) 및/또는 표적 세포 사멸로 번역하는 능력 손상을 포함한다.As used herein, the term “dysfunction” also refers to refractory or non-responsiveness to antigen recognition, specifically, antigen recognition that is associated with downstream T-cell functions, such as proliferation, cytokine production (eg, gamma interferon) and/or targeting. including impaired ability to translate into apoptosis.
"암" 및 "암성"이라는 용어는 전형적으로 조절되지 않은 세포 성장을 특징으로 하는 포유동물의 생리학적 병태를 지칭하거나 설명한다. 암에는 고형 종양 암 및 비고형 종양 암 및 국소 진행성 또는 전이성 암(예컨대, 국소 진행성 또는 전이성 종양)이 포함된다. 암의 예는 암종, 림프종, 모세포종, 육종, 및 백혈병 또는 림프성 악성종양을 포함하지만, 이에 제한되지는 않는다. 상기 암의 더 특정한 예는: 국소 진행성 및 전이성 UC(mUC)를 포함한 요로상피암(UC); 방광암(예컨대, 근육 침습성 방광암(MIBC) 및 비근육 침습성 방광암(NMIBC), 예컨대, BCG 불응성 NMIBC), MIBC 요로상피 방광암(UBC); 신장 또는 신장암(예컨대, 신장 세포 암종(RCC)); 요로암; 폐암, 예컨대, 확장기 SCLC(ES-SCLC)를 포함하는 소세포 폐암(SCLC); 국소 진행성 절제 불가능한 NSCLC(예컨대, IIIB기 NSCLC), 또는 재발성 또는 전이성 NSCLC(예컨대, IV기 NSCLC), 폐의 선암종, 또는 편평세포암(예컨대, 상피 편평세포암(예컨대, 폐의 편평상피암)을 포함한 편평 NSCLC 또는 비편평 NSCLC를 포함하는 비소세포 폐암(NSCLC); 췌장암(예컨대, 췌장관 선암종(PDAC), 예컨대, 전이성 PDAC)); 두경부암(예컨대, SCCHN, 예컨대, 재발성/전이성 PD-L1 양성 SCCHN, 및 두경부 편평세포암(HNSCC); 난소암(OC); 식도암; 복막암; 간세포암; 위암(GC)(예컨대, 위식도 접합부(GEJ) 암) 또는 위암(위암 및 위장관 기질암 포함); 교모세포종; 요로암; 간암; 유방암(예컨대, HER2+ 유방암 및 삼중 음성 유방암(TNBC(예컨대, 초기 TNBC(eTNBC)), 에스트로겐 수용체(ER-), 프로게스테론 수용체(PgR-) 및 HER2(HER2-) 음성임); 거세 저항성 전립선암(CRPC)과 같은 전립선암; 복막암; 간세포암; 위장암 및 위장관 기질암을 포함하는 위암; 췌장암(예컨대, 췌장관 선암종(PDAC)); 교모세포종; 자궁경부암(예컨대, IVB기, 전이성, 재발성 또는 지속성 자궁경부암, 예컨대, 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 난소암; 간암(예컨대, 간세포 암종(HCC), 예컨대, 국소 진행성 또는 전이성 HCC 및/또는 절제불가능한 HCC); 간암; 대장암; 직장암; 결장직장암(CRC; 예컨대, 미세위성 안정성(MSS) 및 미세위성 불안정성(MSI)이 낮은(MSI-낮음) CRC); 자궁내막암 또는 자궁암; 타액선 암종; 전립선암; 외음부암; 갑상선 암; 간암; 항문 암종; 음경 암종; 표재성 확산 흑색종, 악성 분석사마귀 흑색종, 말단흑자흑색종 및 결절성 흑색종을 포함하는 흑색종; 다발성 골수종 및 B 세포 림프종(저등급/여포성 비호지킨 림프종(NHL) 포함); 소림프구성(SL) NHL; 중급/여포성 NHL; 중간 등급 확산 NHL; 고급 면역모세포 NHL; 고급 림프모구 NHL; 고급 소형 비절단 세포 NHL; 거대 종양 NHL; 외투 세포 림프종; AIDS 관련 림프종; 및 발텐스트롬마크로 거대글로불린혈증); 만성 림프구성 백혈병(CLL); 급성 림프구성 백혈병(ALL); 급성 골수성 백혈병(AML); 모세포 백혈병; 만성 골수성 백혈병(CML); 이식후 림프증식성 장애(PTLD); 및 골수이형성 증후군(MDS), 뿐만 아니라 모반증, 부종(뇌종양과 관련됨), Meigs 증후군, 뇌암, 두경부암 및 관련 전이와 관련된 비정상적인 혈관 증식을 포함하지만 이에 제한되지는 않는다. The terms “cancer” and “cancerous” refer to or describe a physiological condition in mammals that is typically characterized by unregulated cell growth. Cancers include solid and non-solid tumor cancers and locally advanced or metastatic cancers (eg, locally advanced or metastatic tumors). Examples of cancer include, but are not limited to, carcinoma, lymphoma, blastoma, sarcoma, and leukemia or lymphoid malignancy. More specific examples of such cancers include: urothelial cancer (UC), including locally advanced and metastatic UC (mUC); bladder cancer (eg, muscle invasive bladder cancer (MIBC) and non-muscle invasive bladder cancer (NMIBC), such as BCG refractory NMIBC), MIBC urothelial bladder cancer (UBC); kidney or kidney cancer (eg, renal cell carcinoma (RCC)); urinary tract cancer; lung cancer such as small cell lung cancer (SCLC), including advanced stage SCLC (ES-SCLC); Locally advanced unresectable NSCLC (eg, stage IIIB NSCLC), or relapsed or metastatic NSCLC (eg, stage IV NSCLC), adenocarcinoma of the lung, or squamous cell carcinoma (eg, epithelial squamous cell carcinoma (eg, squamous cell carcinoma of the lung) non-small cell lung cancer (NSCLC), including squamous NSCLC or non-squamous NSCLC, pancreatic cancer (eg, pancreatic ductal adenocarcinoma (PDAC), eg, metastatic PDAC); Head and neck cancers (eg, SCCHN, eg, recurrent/metastatic PD-L1 positive SCCHN, and head and neck squamous cell carcinoma (HNSCC); ovarian cancer (OC); esophageal cancer; peritoneal cancer; hepatocellular carcinoma; gastric cancer (GC) (eg, gastric cancer) junctional junction (GEJ) cancer) or stomach cancer (including gastric and gastrointestinal stromal cancer); glioblastoma; urinary tract cancer; liver cancer; breast cancer (eg, HER2+ breast cancer and triple negative breast cancer (TNBC (eg, early TNBC (eTNBC))), estrogen receptor (ER-), progesterone receptor (PgR-) and HER2 (HER2-) negative); prostate cancer such as castration resistant prostate cancer (CRPC); Pancreatic cancer (eg, pancreatic ductal adenocarcinoma (PDAC)); glioblastoma; cervical cancer (eg, stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); liver cancer (eg, hepatocellular carcinoma (HCC), such as locally advanced or metastatic HCC and/or unresectable HCC); liver cancer; colorectal cancer; rectal cancer; colorectal cancer (CRC; such as microsatellite stability (MSS) and microsatellite instability) (MSI-low) CRC); endometrial or uterine cancer; salivary gland carcinoma; prostate cancer; vulvar cancer; thyroid cancer; liver cancer; anal carcinoma; penile carcinoma; superficial diffuse melanoma, malignant analyte melanoma; Melanoma, including lentiginous melanoma and nodular melanoma; Multiple myeloma and B-cell lymphoma (including low-grade/follicular non-Hodgkin's lymphoma (NHL)); Small lymphocytic (SL) NHL; Intermediate/follicular NHL; Medium Grade diffuse NHL; high-grade immunoblastic NHL; high-grade lymphoblastic NHL; high-grade small uncut cell NHL; large tumor NHL; mantle cell lymphoma; AIDS-related lymphoma; and Waltenstrommacromacroglobulinemia); chronic lymphocytic leukemia (CLL) ; acute lymphocytic leukemia (ALL); acute myeloid leukemia (AML); blastic leukemia; chronic myelogenous leukemia (CML); post-transplant lymphoproliferative disorder (PTLD); and myelodysplastic syndrome ( MDS), as well as abnormal vascular proliferation associated with nevus, edema (associated with brain tumors), Meigs syndrome, brain cancer, head and neck cancer and related metastases.
본원에 사용된, 용어 "지속성 자궁경부암"은 이전 요법 후 검출 불가능하거나 양성이 되지 않은 자궁경부암을 지칭한다.As used herein, the term “persistent cervical cancer” refers to cervical cancer that is undetectable or not benign after previous therapy.
본원에 사용된 "IVB기 자궁경부암"은 자궁경부암 병기결정 시스템(예컨대, 국제 산부인과 연맹(International Federation of Gynecology and Obstetrics, FIGO) 병기 시스템)을 사용하여 그 자체로 분류되는 자궁경부암을 지칭한다. 일부 양태들에서, 자궁경부암은 원거리 기관(비장 또는 간 실질을 포함) 또는 사타구니 및 복부 외 림프절로 전이된 경우 IVB기로 분류된다.As used herein, "stage IVB cervical cancer" refers to cervical cancer that is classified as such using the cervical cancer staging system (eg, the International Federation of Gynecology and Obstetrics (FIGO) staging system). In some aspects, cervical cancer is classified as stage IVB if it has metastasized to distant organs (including the spleen or liver parenchyma) or to inguinal and extra-abdominal lymph nodes.
본원에 사용된, 용어 "재발성 자궁경부암"은 수술, 방사선 요법 및/또는 화학요법에 의한 초기 치료 후에 발견되거나 재발한 자궁경부암을 지칭한다.As used herein, the term “recurrent cervical cancer” refers to cervical cancer that is discovered or relapsed after initial treatment with surgery, radiation therapy, and/or chemotherapy.
용어 "TNBC"는 ER, PR 및 HER2의 발현이 결여된 유방암을 지칭한다. 용어 "eTNBC"는 T2-4d TNBC(예컨대, cT2-cT4, cN0-cN3 및 cM0)를 지칭한다. The term “TNBC” refers to breast cancer that lacks expression of ER, PR and HER2. The term “eTNBC” refers to T2-4d TNBC (eg, cT2-cT4, cN0-cN3 and cM0).
두경부암은 상부 호흡소화관의 점막 표면에서 시작하여 구강, 구강인두, 후두, 하인두 및 비인두에 영향을 미치는 암들을 포함한다.Head and neck cancers include cancers that start on the mucosal surface of the upper aerodigestive tract and affect the oral cavity, oropharynx, larynx, hypopharynx, and nasopharynx.
본원에 사용된, "요로상피암" 및 "UC"는 비뇨기계에서 전형적으로 발생하는 암의 유형을 지칭하며, 근육 침습성 방광암(MIBC) 및 근육 침습성 요로상피암(UTUC)을 포함한다. UC는 또한 당업계에서 이행 세포 암종(TCC)으로 지칭된다. As used herein, "urothelial cancer" and "UC" refer to types of cancer that typically occur in the urinary system and include muscle invasive bladder cancer (MIBC) and muscle invasive urothelial cancer (UTUC). UC is also referred to in the art as transitional cell carcinoma (TCC).
"종양"이란 악성 또는 양성이건 간에 모든 신생물 세포 성장과 증식, 그리고 모든 전-암성 및 암 세포와 조직을 지칭한다. 용어 “암”, “암성”, “세포 증식성 질병”, “증식성 질병” 및 “종양”은 본원에서 이용된 바와 같이, 상호 배타적이지 않다."Tumor" refers to all neoplastic cell growth and proliferation, whether malignant or benign, and all pre-cancerous and cancerous cells and tissues. The terms “cancer”, “cancerous”, “cell proliferative disease”, “proliferative disease” and “tumor”, as used herein, are not mutually exclusive.
본원에 사용된 "종양 세포"는 종양 또는 이의 샘플에 존재하는 임의의 종양 세포를 지칭한다. 종양 세포는 당해 분야에서 공지된 및/또는 본원에서 설명된 방법을 이용하여, 종양 표본 내에 존재할 수 있는 다른 세포, 예를 들면, 간질 세포 및 종양 침윤 면역 세포로부터 구별될 수 있다.As used herein, “tumor cell” refers to any tumor cell present in a tumor or sample thereof. Tumor cells can be distinguished from other cells that may be present in a tumor specimen, such as stromal cells and tumor infiltrating immune cells, using methods known in the art and/or described herein.
"종양 면역성"은 종양이 면역 인식 및 제거를 회피하는 과정을 의미한다. 따라서 치료 개념으로서 종양 면역성은 이러한 회피가 약화되고 이러한 종양이 면역계에 의해 인식되고 공격받을 때 "치료"된다. 종양 인식의 예로는 종양 결합, 종양 수축 및 종양 제거가 포함된다."Tumor immunity" refers to the process by which a tumor evades immune recognition and clearance. Thus, as a therapeutic concept, tumor immunity is “treated” when this evasion is weakened and these tumors are recognized and attacked by the immune system. Examples of tumor recognition include tumor binding, tumor shrinkage, and tumor removal.
본원에서 사용되는, "전이"는 암의 원발성 부위로부터 신체의 다른 부위로의 전이를 의미한다. 암세포는 원발성 종양에서 떨어져 나와 림프관과 혈관으로 침투하고 혈류를 통해 순환하고 신체 다른 곳의 정상 조직에서 원거리 초점으로 성장할 수 있다 (전이). 전이는 국소적이거나 원격일 수 있다. 전이는 종양 세포가 원발성 종양에서 떨어져 나와 혈류를 따라 이동하고 먼 부위에서 멈추는 순차 과정이다. 새로운 부위에서 세포는 혈액 공급을 확립시키고 성장하여 생명을 위협하는 덩어리를 형성할 수 있다. 종양 세포 내의 자극 및 억제 분자 경로는 모두 이러한 거동을 조절하며, 종양 세포와 원거리에 있는 숙주 세포 사이의 상호 작용 또한 중요하다.As used herein, “metastasis” refers to metastasis from the primary site of cancer to other parts of the body. Cancer cells can break away from the primary tumor, penetrate into lymphatic and blood vessels, circulate through the bloodstream, and grow to distant foci in normal tissue elsewhere in the body (metastasize). Metastases may be local or distant. Metastasis is a sequential process in which tumor cells break away from the primary tumor, migrate through the bloodstream, and stop at distant sites. In the new site, cells can establish a blood supply and grow to form life-threatening masses. Both stimulatory and inhibitory molecular pathways within tumor cells regulate this behavior, and interactions between tumor cells and distant host cells are also important.
본원에서 사용된, 용어 “세포독성 작용제”는 세포에게 유해한(예컨대, 세포 사멸 또는 파괴를 유발하거나, 증식을 저해하거나, 또는 만약 그렇지 않으면 세포 기능을 방지하는) 임의의 작용제를 지칭한다. 세포독성 작용제는 방사성동위원소(예컨대, At211, I131, I125, Y90, Re186, Re188, Sm153, Bi212, P32, Pb212 및 Lu의 방사성동위원소); 화학요법제 또는 약물 (예를 들면, 메토트렉사트, 아드리아마이신, 빈카 알칼로이드 (빈크리스틴, 빈블라스틴, 에토포시드), 독소루비신, 멜팔란, 미토마이신 C, 클로람부실, 다우노루비신 또는 다른 삽입 작용제); 성장 저해제; 효소 및 이들의 단편, 예컨대 핵산분해 효소; 항생제; 및 독소, 예컨대 소형 분자 독소, 또는 세균, 진균, 식물 또는 동물 기원의 효소적으로 활성 독소뿐만 아니라 이들의 단편 및/또는 변이체; 그리고 아래에 개시된 다양한 항종양 또는 항암 작용제를 포함하지만 이들에 한정되지 않는다. 예시적인 세포독성 작용제는 항미소관 작용제, 백금 배위 복합체, 알킬화제, 국소이성화효소 II 저해제, 대사길항물질, 국소이성화효소 I 저해제, 호르몬 및 호르몬 유사체, 신호 전달 경로 저해제, 비-수용체 티로신 키나아제 혈관신생 저해제, 면역치료제, 친아폽토시스성 작용제, LDH-A의 저해제, 지방산 생합성의 저해제, 세포 주기 신호전달 저해제, HDAC 저해제, 프로테아좀 저해제, 그리고 암 물질대사의 저해제에서 선택될 수 있다. 한 경우에서, 상기 세포독성제는 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)이다. 한 경우에서, 상기 세포독성제는 EGFR의 길항제, 예컨대, N-(3-에티닐페닐)-6,7-비스(2-메톡시에톡시)퀴나졸린-4-아민(예컨대, 에를로티닙)이다. 한 경우에서, 상기 세포독성제는 RAF 억제제, 예컨대, BRAF 및/또는 CRAF 억제제이다. 한 경우에서, 상기 RAF 저해제는 베무라페닙이다. 한 경우에서, 상기 세포독성 작용제는 PI3K 저해제이다. As used herein, the term “cytotoxic agent” refers to any agent that is detrimental to a cell (eg, causes cell death or destruction, inhibits proliferation, or otherwise prevents cell function). Cytotoxic agents include radioisotopes (eg, At 211 , I 131 , I 125 , Y 90 , Re 186 , Re 188 , Sm 153 , Bi 212 , P 32 , Pb 212 and radioisotopes of Lu); Chemotherapeutic agents or drugs (eg, methotrexate, adriamycin, vinca alkaloids (vincristine, vinblastine, etoposide), doxorubicin, melphalan, mitomycin C, chlorambucil, daunorubicin or other insertion agents); growth inhibitors; enzymes and fragments thereof, such as nucleases; Antibiotic; and toxins, such as small molecule toxins, or enzymatically active toxins of bacterial, fungal, plant or animal origin, as well as fragments and/or variants thereof; and various anti-tumor or anti-cancer agents disclosed below. Exemplary cytotoxic agents include anti-microtubule agents, platinum coordination complexes, alkylating agents, topoisomerase II inhibitors, antimetabolites, topoisomerase I inhibitors, hormones and hormone analogs, signal transduction pathway inhibitors, non-receptor tyrosine kinase angiogenesis inhibitors , immunotherapeutic agents, pro-apoptotic agents, inhibitors of LDH-A, inhibitors of fatty acid biosynthesis, cell cycle signaling inhibitors, HDAC inhibitors, proteasome inhibitors, and inhibitors of cancer metabolism. In one case, the cytotoxic agent is a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin). In one case, the cytotoxic agent is an antagonist of EGFR, such as N-(3-ethynylphenyl)-6,7-bis(2-methoxyethoxy)quinazolin-4-amine (eg, erlotinib). )to be. In one case, the cytotoxic agent is a RAF inhibitor, such as a BRAF and/or CRAF inhibitor. In one case, the RAF inhibitor is vemurafenib. In one case, the cytotoxic agent is a PI3K inhibitor.
"화학요법제"는 암의 치료에 유용한 화학적 화합물을 포함한다. 화학요법제의 예는 엘로티닙 (TARCEVA®, Genentech/OSI Pharm.), 보르테조밉(VELCADE®, Millennium Pharm.), 디설피람, 에피갈로카테킨 갈레이트, 살리노스포라미드 A, 카르필조밉, 17-AAG(겔다나마이신), 라디시콜, 젖산 탈수소효소 A (LDH-A), 풀베스트란트(FASLODEX®, AstraZeneca), 수니티브(SUTENT®, Pfizer/Sugen), 레트로졸(FEMARA®, Novartis), 이마티닙 메실레이트(GLEEVEC®, Novartis), 피나수네이트(VATALANIB®, Novartis), 옥살리플라틴(ELOXATIN®, Sanofi), 5-FU(5-플루오로우라실), 류코보린, 라파마이신(Sirolimus, RAPAMUNE®, Wyeth), 라파티닙(TYKERB®, GSK572016, Glaxo Smith Kline), 로나파밉 (SCH 66336), 소라페닙 (NEXAVAR®, Bayer Labs), 게피티닙 (IRESSA®, AstraZeneca), AG1478, 알킬화제, 예를 들어, 티오테파 및 CYTOXAN® 시클로포스파미드; 알킬 술포네이트, 예를 들어, 부술판, 임프로술판 및 피포술판; 아지리딘, 예를 들어, 벤조도파, 카르보쿠온, 메투레도파, 우레도파; 알트레타민, 트리에틸렌멜라민, 트리에틸렌포스포르아미드, 트리에틸렌티오포스포르아미드 및 트리메틸로멜라민을 포함하는 에틸렌이민 및 메틸라멜라민; 아세토게닌 (특히 불라타신 및 불라타시논); 캄토테신 (토포테칸 및 이리노테칸 포함); 브리오스타틴; 칼리스타틴; CC-1065 (아도젤레신, 카르젤레신 및 비젤레신 합성 유사체 포함); 크립토피신 (특히 크립토파이신 1 및 크립토파이신 8); 부신피질호르몬제 (프레드니손 및 프레드니솔론 포함); 사이프로테론 아세테이트; 피나스테리드 및 두타스테리드를 포함하는 5a-환원효소); 보리노스타트, 로미뎁신, 파노비노스타트, 발프로산, 모세티노스타트 돌라스타틴; 알데스류킨, 탈크 듀오카르마이신 (합성 유사체, KW-2189 및 CB1-TM1 포함); 엘류테로빈; 판크라티스타틴; 사르코딕틴; 스폰지스타틴; 질소 머스타드, 예를 들어, 클로람부실, 클로마파진, 클로로포스파미드, 에스트라무스틴, 이포스파미드, 메클로레타민, 메클로레타민 옥사이드 하이드로클로라이드, 멜팔란, 노벤비친, 페네스테린, 프레드니무스틴, 트로포스파미드, 우라실 머스타드; 니트로소우레아, 예를 들어, 카르무스틴, 클로로조토신, 포테무스틴, 로무스틴, 니무스틴 및 라님누스틴; 항생제, 예를 들어, 에네다이인 항생제 (예를 들어, 칼리케아마이신, 특히, 칼리케아마이신 γ1I 및 칼리케아마이신 ω1I (Angew Chem. Intl. Ed. Engl. 1994 33:183186); 다이네미신 A를 포함하는 다이네미신; 클로드로네이트와 같은 비스포스포네이트; 에스페라미신; 뿐만 아니라 네오카르지노스타틴 발색단 및 관련 발색단백 엔디인 항생제 발색단), 아클라시노마이신, 악티노마이신, 아우트라마이신, 아자세린, 블레오마이신, 칵티노마이신, 카라비신, 카미노마이신, 카르지노필린, 크로모마이신, 닥티노마이신, 다우노루비신, 데토루비신, 6-디아조-5-옥소-L-노르류신, ADRIAMYCIN®(독소루비신), 모르폴리노-독소루비신, 시아노모르폴리노-독소루비신, 2-피롤리노-독소루비신 및 데옥시독소루비신), 에피루비신, 에소루비신, 에베롤리무스, 소트라타우린, 이다루비신, 마르셀로마이신, 미토마이신, 예를 들어, 미토마이신 C, 마이코페놀산, 노갈라마이신, 올리보마이신, 페플로마이신, 포르피로마이신, 퓨로마이신, 켈라마이신, 로도루비신, 스트렙토니그린, 스트렙토조신, 투베르시딘, 우베니멕스, 지노스타틴, 조루비신; 메토트렉세이트 및 5-플루오로우라실(5-FU)과 같은 항대사물질; 데놉테린, 메토트렉세이트, 프테롭테린, 트리메트렉세이트와 같은 엽산 유사체; 플루다라빈, 6-메르캅토퓨린, 티아미프린, 티오구아닌과 같은 퓨린 유사체; 안시타빈, 아자시티딘, 6-아자우리딘, 카르모푸르, 시타라빈, 디데옥시우리딘, 독시플루리딘, 에노시타빈, 플록수리딘과 같은 피리미딘 유사체; 칼루스테론, 드로모스타놀론 프로피오네이트, 에피티오스타놀, 메피티오스탄, 테스토락톤과 같은 안드로겐; 아미노글루테티미드, 미토탄, 트리로스탄과 같은 항부신; 프롤린산과 같은 엽산 보충제; 아세글라톤; 알도포스파미드 글리코시드; 아미노레불린산; 에닐루라실; 암사크린; 베스트라부실; 비산트렌; 에다트락세이트; 데포파민; 데메콜신; 디아지쿠온; 엘포미틴; 엘립티늄 아세테이트; 에포틸론; 에토글루시드; 갈륨 니트레이트; 하이드록시우레아; 렌티난; 로니다이닌; 메이탄신 및 안사미토신과 같은 메이탄시노이드; 미토구아존; 미톡산트론; 모피담놀; 니트라에린; 펜토스타틴; 페나멧; 피라루비신; 로속산트론; 포도필린산; 2-에틸하이드라지드; 프로카바진; PSK® 다당류 복합체(JHS Natural Products, Eugene, Oreg.); 라족산; 리족신; 시조푸란; 스피로게르마늄; 테누아존산; 트리아지쿠온; 2,2',2''-트리클로로트리에틸아민; 트리코테센(특히 T-2 독소, 베라쿠린 A, 로리딘 A 및 안구이딘); 우레탄; 빈데신; 다카르바진; 만노무스틴; 미토브로니톨; 미토락톨; 피포브로만; 가시토신; 아라비노사이드("Ara-C"); 시클로포스파미드; 티오테파; 탁산(탁소이드), 예컨대, TAXOL®(파클리탁셀; Bristol-Myers Squibb Oncology, Princeton, N.J.), ABRAXANE®(무-크레모포어), 파클리탁셀의 알부민-조작된 나노입자 제제(예컨대, 나노입자 알부민 조작된 파클리탁셀(냅-파클리탁셀))(American Pharmaceutical Partners, Schaumberg, Ill.), 및 TAXOTERE®(도세탁셀, 독세탁셀; Sanofi-Aventis); 클로람부실; GEMZAR®(젬시타빈); 6-티오구아닌; 머캅토퓨린; 메토트렉세이트; 시스플라틴 및 카보플라틴과 같은 백금 유사체; 빈블라스틴; 에토포시드(VP-16); 이포스파미드; 미톡산트론; 빈크리스틴; NAVELBINE® (비노렐빈); 노반트론; 테니포사이드; 에다트렉세이트; 다우노마이신; 아미노프테린; 카페시타빈 (XELODA®); 이반드로네이트; CPT-11; 토포이소머라제 억제제 RFS 2000; 디플루오로메틸오르니틴(DMFO); 레티노산과 같은 레티노이드; 및 상기 어느 하나의 약학상 허용되는 염, 산 및 유도체; 뿐만 아니라 상기 둘 이상의 복합물, 예를 들어, 시클로포스파미드, 독소루비신, 빈크리스틴, 및 프레드니솔론의 복합 요법의 약어 CHOP, 및 옥살리플라틴 (ELOXATINTM)을 5-FU 및 류코보린과 복합하여 사용하는 치료 요법의 약어 FOLFOX를 포함하나 이에 제한되는 것은 아니다."Chemotherapeutic agent" includes chemical compounds useful in the treatment of cancer. Examples of chemotherapeutic agents include erlotinib (TARCEVA ® , Genentech/OSI Pharm.), bortezomib (VELCADE ® , Millennium Pharm.), disulfiram, epigallocatechin gallate, salinosporamide A, carfilzomib , 17-AAG (geldanamycin), radicicol, lactate dehydrogenase A (LDH-A), fulvestrant (FASLODEX ® , AstraZeneca), SUTENT ® , Pfizer/Sugen, letrozole (FEMARA) ® , Novartis), imatinib mesylate (GLEEVEC ® , Novartis), pinasunate (VATALANIB ® , Novartis), oxaliplatin (ELOXATIN ® , Sanofi), 5-FU (5-fluorouracil), leucovorin, rapamycin ( Sirolimus, RAPAMUNE ® , Wyeth), lapatinib (TYKERB ® , GSK572016, Glaxo Smith Kline), lonapamib (SCH 66336), sorafenib (NEXAVAR ® , Bayer Labs), gefitinib (IRESSA ® , AstraZeneca), AG1478 , for example thiotepa and CYTOXAN ® cyclophosphamide; alkyl sulfonates such as busulfan, improsulfan and piposulfan; aziridines such as benzodopa, carboquone, meturedopa, uredopa; ethyleneimine and methyllamelamine, including altretamine, triethylenemelamine, triethylenephosphoramide, triethylenethiophosphoramide and trimethyllomelamine; acetogenins (especially bullatacin and bullatacinone); camptothecin (including topotecan and irinotecan); bryostatin; callistatin; CC-1065 (including adozelesin, carzelesin and bizelesin synthetic analogs); cryptophycins (especially cryptophycin 1 and cryptophycin 8); corticosteroids (including prednisone and prednisolone); cyproterone acetate; 5a-reductase including finasteride and dutasteride); vorinostat, romidepsin, panobinostat, valproic acid, mostinostat dolastatin; aldesleukin, talc duocarmycin (including synthetic analogs, KW-2189 and CB1-TM1); eluterobin; pancratistatin; sarcodictin; spongestatin; Nitrogen mustards such as chlorambucil, clomaphazine, chlorophosphamide, estramustine, ifosfamide, mechlorethamine, mechlorethamine oxide hydrochloride, melphalan, novenvicin, phenesterine , prednimustine, trophosphamide, uracil mustard; nitrosoureas such as carmustine, chlorozotocin, potemustine, lomustine, nimustine and ranimnustine; Antibiotics such as enedyin antibiotics (eg, calicheamicin, in particular calicheamicin γ1I and calicheamicin ω1I (Angew Chem. Intl. Ed. Engl. 1994 33:183186); dynemycin A dynemycin, including; bisphosphonates such as clodronate; esperamicin; as well as neocarzinostatin chromophore and related chromoprotein endyin antibiotic chromophore), aclasinomycin, actinomycin, outramycin, azaserine , Bleomycin, Cactinomycin, Carabicin, Caminomycin, Carginophylline, Chromomycin, Dactinomycin, Daunorubicin, Detorubicin, 6-diazo-5-oxo-L-norleucine, ADRIAMYCIN® (doxorubicin), morpholino-doxorubicin, cyanomorpholino-doxorubicin, 2-pyrrolino-doxorubicin and deoxydoxorubicin), epirubicin, esorubicin, everolimus, sotrataurine, idarubicin , marcelomycin, mitomycin, for example mitomycin C, mycophenolic acid, nogalamicin, olibomycin, peplomycin, porphyromycin, puromycin, kelamicin, rhodorubicin, streptonigrin, strepto zocin, tubersidine, ubenimex, ginostatin, zorubicin; antimetabolites such as methotrexate and 5-fluorouracil (5-FU); folic acid analogs such as denopterin, methotrexate, pteropterin, trimetrexate; purine analogs such as fludarabine, 6-mercaptopurine, thiamiprine, thioguanine; pyrimidine analogs such as ancitabine, azacitidine, 6-azauridine, carmofur, cytarabine, dideoxyuridine, doxyfluridine, enocitabine, floxuridine; androgens such as calusterone, dromostanolone propionate, epithiostanol, mepitiostan, testolactone; antiadrenal such as aminoglutethimide, mitotane, trirostan; folic acid supplements such as prolinic acid; aceglatone; aldophosphamide glycoside; aminolevulinic acid; eniluracil; amsacrine; bestlabucil; bisantrene; edatraxate; depopamine; demecholcin; diagequoon; elformitin; elliptinium acetate; epothilone; etoglucide; gallium nitrate; hydroxyurea; lentinan; Ronidinine; maytansinoids such as maytansine and ansamitocin; mitoguazone; mitoxantrone; fur wall; nitraerin; pentostatin; phennamet; pyrarubicin; losoxantrone; podophyllic acid; 2-ethylhydrazide; procarbazine; PSK ® polysaccharide complex (JHS Natural Products, Eugene, Oreg.); Lazoxic acid; lyzoxine; sizofuran; spirogermanium; tenuazonic acid; triaziquone; 2,2',2''-trichlorotriethylamine; trichothecenes (especially T-2 toxins, veracurin A, loridine A and anguidin); urethane; vindesine; dacarbazine; mannomustine; mitobronitol; mitolactol; pipobroman; gastocin; arabinoside ("Ara-C");cyclophosphamide;thiotepa; Taxanes (taxoids) such as TAXOL ® (paclitaxel; Bristol-Myers Squibb Oncology, Princeton, NJ), ABRAXANE ® (creamophor-free), albumin-engineered nanoparticle formulations of paclitaxel (eg, nanoparticulate albumin engineering) paclitaxel (Nap-paclitaxel)) (American Pharmaceutical Partners, Schaumberg, Ill.), and TAXOTERE® (docetaxel, docetaxel; Sanofi-Aventis); chlorambucil; GEMZAR ® (gemcitabine); 6-thioguanine; mercaptopurine; methotrexate; platinum analogs such as cisplatin and carboplatin; vinblastine; etoposide (VP-16); ifosfamide; mitoxantrone; vincristine; NAVELBINE ® (vinorelbine); novantron; teniposide; edatrexate; daunomycin; aminopterin; Capecitabine (XELODA ® ); ibandronate; CPT-11; topoisomerase inhibitor RFS 2000; difluoromethylornithine (DMFO); retinoids such as retinoic acid; and pharmaceutically acceptable salts, acids and derivatives of any of the above; as well as the abbreviation CHOP for combination therapy of two or more of the above compounds, for example, cyclophosphamide, doxorubicin, vincristine, and prednisolone, and oxaliplatin (ELOXATINTM) in combination with 5-FU and leucovorin in combination with treatment regimens. including but not limited to the abbreviation FOLFOX.
화학요법제는 또한, (i) 예를 들면, 타목시펜 (NOLVADEX®; 타목시펜 구연산염 포함), 랄록시펜, 드롤록시펜, 요오독시펜, 4-히드록시타목시펜, 트리녹시펜, 케옥시펜, LY117018, 오나프리스톤 및 FARESTON® (토레미핀 구연산염)을 비롯하여, 종양에 대한 호르몬 작용을 조절하거나 또는 저해하는 작용을 하는 항호르몬 작용제 예컨대 항에스트로겐 및 선택적 에스트로겐 수용체 조절인자 (SERMs); (ii) 부신에서 에스트로겐 생산을 조절하는 효소 아로마타아제를 저해하는 아로마타아제 저해제, 예컨대 예를 들면, 4(5)-이미다졸, 아미노글루테티미드, MEGASE® (메게스트롤 아세트산염), AROMASIN® (엑세메스테인; Pfizer), 포르메스타니, 파드로졸, RIVISOR® (보로졸), FEMARA® (레트로졸; Novartis) 및 ARIMIDEX® (아나스트로졸; AstraZeneca); (iii) 항안드로겐 예컨대 플루타미드, 닐루타미드, 비칼루타미드, 류프롤라이드 및 고세렐린; 부세렐린, 트립테렐린, 메드록시프로게스테론 아세트산염, 디에틸스틸베스트롤, 프레마린, 플루오시메스테론, 모든 트랜스레티노산, 펜레티나이드뿐만 아니라 트록사시타빈 (1,3-디옥솔란 뉴클레오시드 시토신 유사체); (iv) 단백질 키나아제 저해제 (예를 들면, 역형성 림프종 키나아제 (Alk) 저해제, 예컨대 AF-802 (CH-5424802 또는 알렉티닙으로서 또한 알려져 있음)); (v) 지질 키나아제 저해제; (vi) 안티센스 올리고뉴클레오티드, 특히 일탈적 세포 증식에 연루된 신호전달 경로에서 유전자, 예컨대 예를 들면, PKC-알파, Ralf 및 H-Ras의 발현을 저해하는 것들; (vii) 리보자임 예컨대 VEGF 발현 저해제 (예를 들면, ANGIOZYME®) 및 HER2 발현 저해제; (viii) 백신 예컨대 유전자 요법 백신, 예를 들면, ALLOVECTIN®, LEUVECTIN® 및 VAXID®; PROLEUKIN®, rIL-2; 국소이성화효소 1 저해제 예컨대 LURTOTECAN®; ABARELIX® rmRH; 그리고 (ix) 전술한 것들 중 어느 것의 제약학적으로 허용되는 염, 산 및 유도체를 포함한다.Chemotherapeutic agents may also include (i), for example, tamoxifen (NOLVADEX ® ; including tamoxifen citrate), raloxifene, droloxifene, iodoxifen, 4-hydroxytamoxifen, trioxifene, keoxifene, LY117018, antihormonal agents such as antiestrogens and selective estrogen receptor modulators (SERMs) that act to modulate or inhibit the action of hormones on tumors, including onapristone and FARESTON ® (toremipine citrate); (ii) aromatase inhibitors that inhibit the enzyme aromatase that regulates estrogen production in the adrenal gland, such as, for example, 4(5)-imidazole, aminoglutethimide, MEGASE® (megestrol acetate), AROMASIN ® (exemestein; Pfizer), formestani, fadrozole, RIVISOR ® (vorozol), FEMARA ® (retrozole; Novartis) and ARIMIDEX ® (anastrozole; AstraZeneca); (iii) anti-androgens such as flutamide, nilutamide, bicalutamide, leuprolide and goserelin; Buserellin, tripterelin, medroxyprogesterone acetate, diethylstilbestrol, premarin, fluocimesterone, all transretinoic acids, fenretinide as well as troxacitabine (1,3-dioxolane nucleoside) cytosine analogs); (iv) protein kinase inhibitors (eg, anaplastic lymphoma kinase (Alk) inhibitors such as AF-802 (also known as CH-5424802 or alectinib)); (v) lipid kinase inhibitors; (vi) antisense oligonucleotides, particularly those that inhibit the expression of genes in signaling pathways implicated in aberrant cell proliferation, such as, for example, PKC-alpha, Ralf and H-Ras; (vii) ribozymes such as VEGF expression inhibitors (eg ANGIOZYME ® ) and HER2 expression inhibitors; (viii) vaccines such as gene therapy vaccines such as ALLOVECTIN ® , LEUVECTIN ® and VAXID ® ; PROLEUKIN®, rIL-2; Topoisomerase 1 inhibitors such as LURTOTECAN ® ; ABARELIX ® rmRH; and (ix) pharmaceutically acceptable salts, acids and derivatives of any of the foregoing.
화학요법제는 또한 백금을 분자의 필수적인 부분으로 함유하는 유기 화합물을 포함하는, 또한 본원에서 “백금제”라고도 하는, "백금계" 화학요법제를 포함한다. 전형적으로, 백금계 화학요법제는 백금의 배위 착물이다. 백금계 화학요법제는 당해 분야에서 때때로 "플라틴(platin)"으로 불린다. 백금계 화학요법제의 예는 시스플라틴, 카보플라틴, 옥살리플라틴, 네다플라틴, 트리플라틴 테트라니트레이트, 페난트리플라틴, 피코플라틴, 리포플라틴 및 사트라플라틴을 포함하지만 이에 제한되지는 않는다. 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴)는 하나 이상의 추가 화학요법제, 예를 들어 뉴클레오시드 유사체(예컨대, 젬시타빈), 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈), 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)과 병용으로 투여될 수 있다. Chemotherapeutic agents also include "platinum-based" chemotherapeutic agents, also referred to herein as "platinum agents", including organic compounds containing platinum as an integral part of the molecule. Typically, platinum-based chemotherapeutic agents are coordination complexes of platinum. Platinum-based chemotherapeutic agents are sometimes referred to in the art as "platin". Examples of platinum-based chemotherapeutic agents include, but are not limited to, cisplatin, carboplatin, oxaliplatin, nedaplatin, triplatin tetranitrate, phenantriplatin, picoplatin, lipoplatin and satraplatin. Platinum-based chemotherapeutic agents (eg, cisplatin or carboplatin) may include one or more additional chemotherapeutic agents, such as nucleoside analogs (eg, gemcitabine), antimetabolites (eg, pemetrexed or gemcitabine), or in combination with a taxane (eg, paclitaxel or nap-paclitaxel).
용어 "백금계 화학요법를 이용한 치료에 적격"은 담당 임상의의 판단에 따라 또는 당업계에 공지된 백금계 화학요법에 대한 적격성에 대한 표준화된 기준에 따라 대상체가 백금계 화학요법을 이용한 치료에 적격인 것을 의미한다.The term “eligible for treatment with platinum-based chemotherapy” means that a subject is eligible for treatment with platinum-based chemotherapy according to the judgment of the attending clinician or according to standardized criteria for eligibility for platinum-based chemotherapy known in the art. means to be
화학요법제는 또한 본원에서 사용되는 바와 같이 "백금계"가 아닌 화학요법제를 지칭하는 "비백금계 화학요법제"를 포함한다. 본원에 사용된 용어 "비백금계 화학요법제" 및 "비백금제"는 상호교환적으로 사용된다. 예시적인 비백금계 화학요법제는 항대사물질(예컨대, 페메트렉시드 및 젬시타빈), 토포이소머라제 II 억제제(예컨대, 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331), 탁산(예컨대, 파클리탁셀(예컨대, 나노입자-알부민 결합 파클리탁셀(냅-파클리탁셀l)이라고도도 하는 알부민 조작 파클리탁셀), 도세탁셀, 라로탁셀, 카바지탁셀, 밀라탁셀, 테세트탁셀 및/또는 오라탁셀)을 포함한다. 예시적인 비백금계 화학요법제는 또한 알킬화제(예컨대, 시클로포스파미드)를 포함한다.Chemotherapeutic agents also include “non-platinum-based chemotherapeutic agents,” which as used herein refer to chemotherapeutic agents that are not “platinum-based”. As used herein, the terms "non-platinum-based chemotherapeutic agent" and "non-platinum agent" are used interchangeably. Exemplary non-platinum chemotherapeutic agents include antimetabolites (eg, pemetrexed and gemcitabine), topoisomerase II inhibitors (eg, etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsa krine, ellipticin, aurintricarboxylic acid, or HU-331), taxanes (eg, paclitaxel (eg, albumin-engineered paclitaxel, also known as nanoparticle-albumin-bound paclitaxel (nap-paclitaxel)), docetaxel, larotaxel , cabazitaxel, milataxel, tessetaxel, and/or orataxel). Exemplary non-platinum-based chemotherapeutic agents also include alkylating agents (eg, cyclophosphamide).
본원에 사용된 "뉴클레오시드 유사체"는 핵산 유사체 및 당을 포함하는 뉴클레오시드를 지칭한다. 뉴클레오시드 유사체는 항대사물질로서 작용할 수 있다. 예시적인 뉴클레오시드 유사체는 젬시타빈, 시타라빈, 플루다라빈 및 클라드리빈을 포함하지만 이에 제한되지는 않는다.As used herein, "nucleoside analog" refers to nucleic acid analogs and nucleosides comprising sugars. Nucleoside analogs can act as antimetabolites. Exemplary nucleoside analogs include, but are not limited to, gemcitabine, cytarabine, fludarabine, and cladribine.
본원에 사용된 바와 같이, 탁산은, 미세소관 조립 및 안정화를 촉진하는 튜불린에 결합할 수 있고/있거나 미세소관 탈중합을 예방할 수 있는 디터펜이다. 본원에 포함된 탁산은 탁소이드 10-데아세틸바카틴 III 및/또는 이의 유도체를 포함한다. 예시적인 탁산은 파클리탁셀(즉, 탁솔(TAXOL)®, CAS # 33069-62-4), 도세탁셀(즉, 탁소테레(TAXOTERE)®, CAS # 114977-28-5), 라로탁셀, 카바지탁셀, 밀라탁셀, 테세트탁셀 및/또는 오라탁셀을 포함하지만, 이에 제한되지는 않는다. 일부 양태들에서, 상기 탁산은 알부민 코팅된 나노입자(예컨대, 냅-파클리탁셀, 즉 아브락산(ABRAXANE)® 및/또는 냅-도세탁셀, ABI-008)이다. 일부 양태들에서, 상기 탁산은 냅-파클리탁셀(아브락산®)이다. 일부 양태들에서, 상기 탁산은 크레모포어(CREMAPHOR)®(예컨대, 탁솔(TAXOL)®) 및/또는 트윈(Tween), 예컨대, 폴리소르베이트 80(예컨대, 탁소테레®)으로 제형화된다. 일부 양태들에서, 상기 탁산은 리포좀 캡슐화된 탁산이다. 일부 양태들에서, 상기 탁산은 탁산의 전구약물 형태 및/또는 접합된 형태(예컨대, 파클리탁셀, 파클리탁셀 폴리글루멕스, 및/또는 리놀레일 카보네이트-파클리탁셀에 공유적으로 접합된 DHA)이다. 일부 양태들에서, 상기 파클리탁셀은 실질적으로 계면활성제의 부재하에서(예컨대, 크레모포어(CREMAPHOR) 및/또는 트윈(Tween)-예컨대 토코솔(TOCOSOL)® 파클리탁셀의 부재 하에서) 제형화된다.As used herein, taxanes are diterpenes that can bind tubulin to promote microtubule assembly and stabilization and/or prevent microtubule depolymerization. Taxanes included herein include the taxoid 10-deacetylbaccatin III and/or derivatives thereof. Exemplary taxanes are paclitaxel (ie, TAXOL ® , CAS # 33069-62-4), docetaxel (ie, TAXOTERE ® , CAS # 114977-28-5), larotaxel, cabazitaxel, mila taxel, tessetaxel and/or orataxel. In some embodiments, the taxane is an albumin coated nanoparticle (eg, nap-paclitaxel, ie, ABRAXANE ® and/or nap-docetaxel, ABI-008). In some embodiments, the taxane is nap-paclitaxel (Abraxane ® ). In some embodiments, the taxane is formulated with CREMAPHOR ® (eg, TAXOL ® ) and/or Tween, such as polysorbate 80 (eg, Taxotere ® ). In some embodiments, the taxane is a liposomal encapsulated taxane. In some embodiments, the taxane is a prodrug form and/or a conjugated form of the taxane (eg, paclitaxel, paclitaxel polyglomex, and/or DHA covalently conjugated to linoleyl carbonate-paclitaxel). In some embodiments, the paclitaxel is formulated substantially in the absence of a surfactant (eg, in the absence of CREMAPHOR and/or Tween-such as TOCOSOL ® paclitaxel).
본원에서 사용된 “항대사물질”은 세포(예컨대, 암세포) 내의 내인성(정상) 대사 과정을 (전체적으로 또는 부분적으로)방해하고 억제하는 화학요법제이다. 항대사물질은 젬시타빈, 페메트렉시드, 카페시타빈, 히드록시우레아, 메토트렉세이트, 플루오로우라실, 클라드리빈, 머캅토퓨린 및 프랄라트렉세이트를 포함한다. As used herein, “antimetabolites” are chemotherapeutic agents that interfere (in whole or in part) and inhibit endogenous (normal) metabolic processes within cells (eg, cancer cells). Antimetabolites include gemcitabine, pemetrexed, capecitabine, hydroxyurea, methotrexate, fluorouracil, cladribine, mercaptopurine and pralatrexate.
화학요법제는 또한 덱사메타손, 인터페론, 콜히친, 메토프린, 시클로스포린, 암포테리신, 메트로니다졸, 알렘투주맙, 알리트레티노인, 알로퓨리놀, 아미포스틴, 아르세닉 트라이옥사이드, 아스파라기나제, 생 BCG, 베바쿠지맙, 벡사로텐, 클라드리빈, 클로파라빈, 다르베포에틴 알파, 데닐루킨, 덱스라족세인, 에포에틴 알파, 엘로티닙, 필그라스팀, 히스트렐린 아세테이트, 이브리투모맙, 인터페론 알파- 2a, 인터페론 알파-2b, 레날리도마이드, 레바미솔, 메스나, 메톡살렌, 난드롤론, 넬라라빈, 노페투모맙, 오프렐베킨, 팔리퍼민, 파미드로네이트, 페가데마제, 페가스파르가제, 페그필그라스팀, 페메트렉시드 다이소듐, 플리마카이신, 포르피머 소듐, 퀴나크린, 라스부리카제, 사르그라모스팀, 테모졸로마이드, VM-26, 6-TG, 토레미펜, 트레티노인, ATRA, 발루비신, 졸레드로네이트, 및 졸레드로닉 애시드, 및 이의 약학적으로 허용되는 염을 포함한다.Chemotherapeutic agents also include dexamethasone, interferon, colchicine, methoprine, cyclosporine, amphotericin, metronidazole, alemtuzumab, alitretinoin, allopurinol, amifostine, arsenic trioxide, asparaginase, raw BCG, bevacuzi. Mab, bexarotene, cladribine, clofarabine, darbepoetin alfa, denilukin, dexrazoxane, epoetin alfa, erlotinib, filgrastim, histrelin acetate, ibritumomab, interferon alfa- 2a, interferon alpha-2b, lenalidomide, levamisole, mesna, methoxsalen, nandrolone, nelarabine, nofetumomab, ofrelbekin, palipermine, pamidronate, pegademase, pegaspar Gauze, pegfilgrastim, pemetrexed disodium, plimacycin, porfimer sodium, quinacrine, rasburicase, sargramostim, temozolomide, VM-26, 6-TG, toremifene, tretinoin , ATRA, valrubicin, zoledronate, and zoledronic acid, and pharmaceutically acceptable salts thereof.
화학요법제는 또한 하이드로코르티손, 하이드로코르티손 아세테이트, 코르티손 아세테이트, 틱소코르톨 피발레이트, 트라이암시놀론 아세토나이드, 트라이암시놀론 알콜, 모메타손, 암시노나이드, 부데소나이드, 데소나이드, 플루오시노나이드, 플루오시놀론 아세토나이드, 베타메타손, 베타메타손 소듐 포스페이트, 덱사메타손, 덱사메타손 소듐 포스페이트, 플루오코르톨론, 하이드로코르티손-17-부티레이트, 하이드로코르티손-17-발러레이트, 아클로메타손 다이프로피오네이트, 베타메타손 발러레이트, 베타메타손 다이프로피오네이트, 프레드니카르베이트, 클로베타손-17-부티레이트, 클로베타솔-17-프로피오네이트, 플루오코르톨론 카프로에이트, 플루오코르톨론 피발레이트 및 플루프레드니덴 아세테이트; 면역 선택적 항 염증 펩티드 (ImSAIDs), 가령, 페닐알라닌-글루타민-글리신 (FEG) 및 이의 D-이성질체 형태 (feG) (IMULAN BioTherapeutics, LLC); 항 류마티스 약물, 가령, 아자티오프린, 사이클로스포린 (사이클로스포린 A), D-페니실라민, 금 염, 하이드록시클로로퀸, 레플루노미데미노사이클린, 설파살라진, 종양 괴사 인자 알파 (TNFα) 차단제, 가령, 에타네르셉트 (Enbrel), 인플릭시맙(Remicade), 아달리무맙 (Humira), 세르톨리주맙 페골 (Cimzia), 골리무맙 (Simponi), 인터루킨 1 (IL-1) 차단제, 가령, 아나킨라 (Kineret), T 세포 공자극 차단제, 가령, 아바타셉트 (Orencia), 인터루킨 6 (IL-6) 차단제, 가령, 토실리주맙 (ACTEMERA®); 인터루킨 13 (IL-13) 차단제, 가령, 레브리키주맙; 인터페론 알파 (IFN) 차단제, 가령, 론탈리주맙; 베타 7 인테그린 차단제, 가령, rhuMAb Beta7; IgE 경로 차단제, 가령, 항 M1 프라임; 분비된 동종삼량체 LTa3 및 막 결합 이종삼량체 LTa1/β2 차단제, 가령, 항 림프독소 알파 (LTa); 방사성 동위원소 (예컨대, At211, I131, I125, Y90, Re186, Re188, Sm153, Bi212, P32, Pb212 및 Lu의 방사성 동위원소); 기타 연구 물질, 가령, 티오플라틴, PS-341, 페닐부티레이트, ET-18- OCH3, 또는 파르네실 전달효소 억제제 (L-739749, L-744832); 폴리페놀, 가령, 쿠에르세틴, 레스베라트롤, 에피갈로카테킨 갈레이트, 테아플라빈, 플라바놀, 프로시아니딘, 베툴리닉 애시드 및 이의 유도체; 오토파지 억제제, 가령, 클로로퀸; 델타-9-테트라하이드로칸나비놀 (드로나비놀, MARINOL®); 베타-라파콘; 라파콜; 콜히친; 베툴리닉 애시드; 아세틸캄프토테신, 스코포레틴, 및 9-아미노캄프토테신); 포도필로톡신; 테가푸르 (UFTORAL®); 벡사로텐 (TARGRETIN®); 비스포스포네이트, 가령, 클로드로네이트 (예를 들면, BONEFOS® 또는 OSTAC®), 에티드로네이트 (DIDROCAL®), NE-58095, 졸레드로닉 애시드/졸레드로네이트 (ZOMETA®), 알렌드로네이트 (FOSAMAX®), 파미드로네이트 (AREDIA®), 틸루드로네이트 (SKELID®), 또는 리세드로네이트 (ACTONEL®); 및 표피 성장 인자 수용체 (EGF-R); 백신, 가령, THERATOPE® 백신; 페리포신, COX-2 억제제 (예컨대 셀레콕시브 또는 에토리콕시브), 프로테오좀 억제제 (예컨대 PS341); CCI-779; 티피파르닙 (R11577); 오라페닙, ABT510; Bcl-2 억제제, 가령, 오블리메르센 소듐 (GENASENSE®); 픽산트론; 파르네실전달효소 억제제, 가령, 로나파르닙 (SCH 6636, SARASARTM); 및 상기 어느 하나의 약학적으로 허용가능한 염, 산 또는 유도체; 뿐만 아니라 상기 둘 이상의 조합, 가령, 사이클로포스파미드, 독소루비신, 빈크리스틴, 및 프레드니솔론의 조합 치료제 약자인 CHOP; 및 5-FU 및 류코보린과 조합된 옥살리플라틴 (ELOXATINTM)을 이용한 치료 요법제 약자인 FOLFOX를 포함한다.Chemotherapeutic agents also include hydrocortisone, hydrocortisone acetate, cortisone acetate, thixocortol pivalate, triamcinolone acetonide, triamcinolone alcohol, mometasone, amcinonide, budesonide, desonide, fluocinonide. , fluocinolone acetonide, betamethasone, betamethasone sodium phosphate, dexamethasone, dexamethasone sodium phosphate, fluocortolone, hydrocortisone-17-butyrate, hydrocortisone-17-valerate, aclomethasone dipropionate, betamethasone valerate , betamethasone dipropionate, prednicarbate, clobetasone-17-butyrate, clobetasol-17-propionate, fluocortolone caproate, fluocortolone pivalate and flupredniden acetate; immunoselective anti-inflammatory peptides (ImSAIDs) such as phenylalanine-glutamine-glycine (FEG) and its D-isomer form (feG) (IMULAN BioTherapeutics, LLC); Antirheumatic drugs such as azathioprine, cyclosporine (cyclosporin A), D-penicillamine, gold salt, hydroxychloroquine, leflunomideminocycline, sulfasalazine, tumor necrosis factor alpha (TNFα) blockers such as etaner Sept (Enbrel), infliximab (Remicade), adalimumab (Humira), certolizumab pegol (Cimzia), golimumab (Simponi), interleukin 1 (IL-1) blockers such as anakinra (Kineret) , T cell costimulatory blockers such as abatacept (Orencia), interleukin 6 (IL-6) blockers such as tocilizumab (ACTEMERA®); interleukin 13 (IL-13) blockers such as lebrikizumab; interferon alpha (IFN) blockers such as rontalizumab; beta 7 integrin blockers such as rhuMAb Beta7; IgE pathway blockers such as anti M1 prime; secreted homotrimeric LTa3 and membrane bound heterotrimeric LTa1/β2 blockers such as anti-lymphotoxin alpha (LTa); radioactive isotopes (eg, At211, I131, I125, Y90, Re186, Re188, Sm153, Bi212, P32, Pb212 and radioactive isotopes of Lu); other research substances such as thioplatin, PS-341, phenylbutyrate, ET-18-OCH3, or farnesyltransferase inhibitors (L-739749, L-744832); polyphenols such as quercetin, resveratrol, epigallocatechin gallate, theaflavin, flavanol, procyanidin, betulinic acid and derivatives thereof; autophagy inhibitors such as chloroquine; delta-9-tetrahydrocannabinol (dronabinol, MARINOL®); beta-rapacon; Raphacol; colchicine; betulinic acid; acetylcamptothecin, scoporetin, and 9-aminocamptothecin); podophyllotoxin; Tegafur (UFTORAL®); bexarotene (TARGRETIN®); Bisphosphonates such as clodronate (eg BONEFOS® or OSTAC®), etidronate (DIDROCAL®), NE-58095, zoledronic acid/zoledronate (ZOMETA®), alendronate (FOSAMAX) ®), pamidronate (AREDIA®), tiludronate (SKELID®), or risedronate (ACTONEL®); and epidermal growth factor receptor (EGF-R); vaccines, such as THERATOPE® vaccine; perifosine, COX-2 inhibitors (such as celecoxib or etoricoxib), proteosome inhibitors (such as PS341); CCI-779; Tipifarnib (R11577); aurafenib, ABT510; Bcl-2 inhibitors such as oblimersen sodium (GENASENSE®); pixantrone; farnesyltransferase inhibitors such as lonafarnib (SCH 6636, SARASARTM); and a pharmaceutically acceptable salt, acid or derivative of any one of the above; as well as combinations of two or more of the above, such as CHOP, which is an abbreviation for combination therapeutics of cyclophosphamide, doxorubicin, vincristine, and prednisolone; and FOLFOX, a treatment regimen with oxaliplatin (ELOXATINTM) in combination with 5-FU and leucovorin.
화학요법제는 또한 진통 해열, 및 항 염증 효과를 가진 비 스테로이드 항 염증 약물을 포함한다. NSAID는 상기 효소 시클로옥시게나제의 비-선택적 억제제를 포함한다. NSAID들의 구체적인 예는 아스피린, 프로피온산 유도체, 예컨대, 이부프로펜, 페노프로펜, 케토프로펜, 플루르비프로펜, 옥사프로진 및 나프록센, 아세트산 유도체, 예컨대, 인도메타신, 설린닥, 에토돌락, 디클로페낙, 에놀산 유도체, 예컨대, 피록시캄, 멜록시캄, 테녹시캄, 드록시캄, 로르녹시캄 및 이속시캄, 페남산 유도체, 예컨대, 메페남산, 메클로페남산, 플루페남산, 톨페남산, 및 COX-2 억제제, 예컨대, 셀레콕십, 에토리콕십, 루미라콕십, 파레콕십, 로페콕십, 및 발데콕십을 포함한다. NSAID는 류마티스성 관절염, 골관절염, 염증성 관절병, 강직성 척추염, 건선성 관절염, 라이타 증후군, 급성 통풍, 월경 곤란증, 전이성 골 통증, 두통 및 편두통, 수술후 통증, 염증 및 조직 손상으로 인한 경통증 내지 중통증, 발열, 장폐색, 및 신장 산통과 같은 병태의 증상 완화를 위해 권고될 수 있다.Chemotherapeutic agents also include non-steroidal anti-inflammatory drugs that have analgesic, antipyretic, and anti-inflammatory effects. NSAIDs include non-selective inhibitors of the enzyme cyclooxygenase. Specific examples of NSAIDs include aspirin, propionic acid derivatives such as ibuprofen, fenoprofen, ketoprofen, flurbiprofen, oxaprozin and naproxen, acetic acid derivatives such as indomethacin, sulindac, etodolac, Diclofenac, enolic acid derivatives such as piroxicam, meloxicam, tenoxicam, droxicam, loroxicam and isoxicam, fenamic acid derivatives such as mefenamic acid, meclofenamic acid, flufenamic acid , tolfenamic acid, and COX-2 inhibitors such as celecoxib, etoricoxib, lumiracoxib, parecoxib, rofecoxib, and valdecoxib. NSAIDs include rheumatoid arthritis, osteoarthritis, inflammatory arthritis, ankylosing spondylitis, psoriatic arthritis, Reita's syndrome, acute gout, dysmenorrhea, metastatic bone pain, headache and migraine, postoperative pain, mild to moderate pain due to inflammation and tissue damage. , for symptomatic relief of conditions such as fever, intestinal obstruction, and renal colic.
화학요법제는 또한, “EGFR 저해제”를 포함하는데, 이들은 EGFR에 결합하거나 또는 만약 그렇지 않으면 이것과 직접적으로 상호작용하고 이의 신호전달 활성을 예방하거나 또는 감소시키는 화합물을 지칭하고, 그리고 “EGFR 길항제”로서 대체 지칭된다. 이러한 제제들의 예들에는 EGFR에 결합하는 저분자들이 포함된다. EGFR 길항제는 저분자, 예컨대 미국 특허 제5,616,582호, 5,457,105호, 5,475,001호, 5,654,307호, 5,679,683호, 6,084,095호, 6,265,410호, 6,455,534호, 6,521,620호, 6,596,726호, 6,713,484호, 5,770,599호, 6,140,332호, 5,866,572호, 6,399,602호, 6,344,459호, 6,602,863호, 6,391,874호, 6,344,455호, 5,760,041호, 6,002,008호, 및 5,747,498호 뿐만 아니라 하기의 PCT 공보들: WO98/14451, WO98/50038, WO99/09016, 및 Wo99/24037에 기재되는 화합물을 포함한다. 특히 저분자 EGFR 길항제는 OSI-774(CP-358774, 에를로티닙, TARCEVA® 제넨텍(Genentech)/OSI 제약); PD 183805(CI 1033, 2-프로펜아미드, N-[4-[(3-클로로-4-플루오로페닐)아미노]-7-[3-(4-모르폴리닐)프로폭시]-6-퀴나졸리닐]-, 디히드로클로라이드, 화이자(Pfizer Inc.); ZD1839, 제피티닙(IRESA®) 4-(3'-클로로-4'-플루오로아닐리노)-7-메톡시-6-(3-모르폴리노프로폭시)퀴나졸린, 아스트라제네카(AstraZeneca)); ZM 105180((6-아미노-4-(3-메틸페닐아미노)-퀴나졸린, 제네카(Zeneca)); BIBX-1382(N8-(3-클로로-4-플루오로-페닐)-N2-(1-메틸-피페리딘-4-일)-피리미도[5,4-d]피리미딘-2,8-디아민, 베링거인겔하임), PKI-166((R)-4-[4-[(1-페닐에틸)아미노]-1H-피롤로[2,3-d]피리미딘-6-일]-페놀); (R)-6-(4-히드록시페닐)-4-[(1-페닐에틸)아미노]-7H-피롤로[2,3-d]피리미딘); CL-387785(N-[4-[(3-브로모페닐)아미노]-6-퀴나졸리닐]-2-부틴아미드); EKB-569(N-[4-[(3-클로로-4-플루오로페닐)아미노]-3-시아노-7-에톡시-6-퀴놀리닐]-4-(디메틸아미노)-2-부텐아미드)(와이어스); AG1478(화이자); AG1571(SU 5271, 화이자); 이중 EGFR/HER2 티로신 키나아제 억제제, 예컨대, 라파티닙(TYKERB®, GSK572016 또는 N-[3-클로로-4-[(3 플루오로페닐)메톡시]페닐]-6[5[[[2메틸술포닐)에틸]아미노]메틸]- 2-푸라닐]-4-퀴나졸린아민)을 포함한다.Chemotherapeutic agents also include "EGFR inhibitors," which refer to compounds that bind to or otherwise interact directly with EGFR and prevent or reduce its signaling activity, and "EGFR antagonists" alternatively referred to as Examples of such agents include small molecules that bind EGFR. EGFR antagonists are small molecules, such as US Pat. , 6,399,602, 6,344,459, 6,602,863, 6,391,874, 6,344,455, 5,760,041, 6,002,008, and 5,747,498 as well as the following PCT publications: WO98/14451, WO98/50038, WO99/24037, compounds as described. In particular, small molecule EGFR antagonists include OSI-774 (CP-358774, erlotinib, TARCEVA® Genentech/OSI Pharmaceuticals); PD 183805 (CI 1033, 2-propenamide, N-[4-[(3-chloro-4-fluorophenyl)amino]-7-[3-(4-morpholinyl)propoxy]-6- Quinazolinyl]-, dihydrochloride, Pfizer Inc.; ZD1839, gefitinib (IRESA ® ) 4-(3'-chloro-4'-fluoroanilino)-7-methoxy-6- (3-morpholinopropoxy)quinazoline, AstraZeneca); ZM 105180((6-amino-4-(3-methylphenylamino)-quinazoline, Zeneca); BIBX-1382(N8-(3-chloro-4-fluoro-phenyl)-N2-(1- Methyl-piperidin-4-yl)-pyrimido[5,4-d]pyrimidine-2,8-diamine, Boehringer Ingelheim), PKI-166((R)-4-[4-[( 1-phenylethyl)amino]-1H-pyrrolo[2,3-d]pyrimidin-6-yl]-phenol);(R)-6-(4-hydroxyphenyl)-4-[(1- phenylethyl)amino]-7H-pyrrolo[2,3-d]pyrimidine); CL-387785 (N-[4-[(3-bromophenyl)amino]-6-quinazolinyl]-2-butinamide); EKB-569 (N-[4-[(3-chloro-4-fluorophenyl)amino]-3-cyano-7-ethoxy-6-quinolinyl]-4-(dimethylamino)-2- butenamide) (Wires); AG1478 (Pfizer); AG1571 (SU 5271, Pfizer); Dual EGFR/HER2 tyrosine kinase inhibitors such as lapatinib ( TYKERB® , GSK572016 or N-[3-chloro-4-[(3-fluorophenyl)methoxy]phenyl]-6[5[[[2methylsulfonyl] ethyl]amino]methyl]-2-furanyl]-4-quinazolinamine).
화학요법제는 또한 선행하는 단락에서 언급된 EGFR 표적화된 약물을 포함하는 "티로신 키나아제 억제제"; 역형성 림프종 키나제(Alk) 억제제를 포함한 인슐린 수용체 티로신 키나아제의 억제제, 예컨대, AF-802(CH-5424802 또는 알렉티닙으로도 공지됨), ASP3026, X396, LDK378, AP26113, 크리조티닙(XALKORI®) 및 세리티닙(ZYKADIA®); 다케다(Takeda)로부터 입수가능한 TAK165와 같은 저분자 HER2 티로신 키나아제 억제제; ErbB2 수용체 티로신 키나아제의 경구 선택적 억제제인 CP-724,714(화이자 및 OSI); EGFR에 우선적으로 결합하지만 HER2 및 EGFR 과발현 세포 둘 다를 억제하는 EKB-569(와이어스로부터 입수가능)와 같은 이중 HER 억제제; 경구 HER2 및 EGFR 티로신 키나제 억제제인 라파티닙(GSK572016; 글락소 스미스클라인(Glaxo-SmithKline)에서 입수 가능); PKI-166(노바티스로부터 입수가능); 카네르티닙(CI-1033; 파마시아(Pharmacia)와 같은 범 HER 억제제; Raf-1 신호전달을 억제하는 ISIS 제약으로부터 입수가능한 안티센스 제제 ISIS-5132와 같은 Raf-1 억제제; 이마티닙 메실레이트(글리백(GLEEVEC)®, 글락소 스미스클라인에서 입수가능)와 같은 비 HER 표적 TK 억제제; 수니티닙(SUTENT®, 화이자로부터 입수가능)과 같은 다중 표적 티로신 키나제 억제제; VEGF 수용체 티로신 키나아제 억제제, 예컨대, 바탈라닙(PTK787/ZK222584, 노바티스/쉐링(Novartis/Schering) AG로부터 입수가능); MAPK 세포외 조절된 키나아제 I 억제제 CI-1040(파마시아에서 입수 가능); PD 153035,4-(3-클로로아닐리노) 퀴나졸린과 같은 퀴나졸린; 피리도피리미딘; 피리미도피리미딘; CGP 59326, CGP 60261 및 CGP 62706과 같은 피롤로피리미딘; 피라졸로피리미딘, 4-(페닐아미노)-7H-피롤로[2,3-d]피리미딘; 커큐민(디페룰로일 메탄, 4,5-비스(4-플루오로아닐리노)프탈이미드); 니트로티오펜 모이어티를 함유하는 티르포스틴; Pd-0183805(워너-램버); 안티센스 분자(예컨대, HER 암호화 핵산에 결합하는 분자); 퀴녹살린(미국 특허 제5,804,396호); 트리포스틴(미국 특허 제5,804,396호); ZD6474(아스트라 제네카); PTK-787(노바티스/쉐링 AG); CI-1033(화이자)과 같은 범 HER 억제제; 아피니탁(Affinitac)(ISIS 3521; 이시스/릴리(Isis/Lilly)); 이마티닙 메실레이트(GLEEVEC®); PKI 166(노바티스); GW2016(글락소 스미스클라인); CI-1033(화이자); EKB-569(와이어스); 세막시닙(화이자); ZD6474(아스트라제네카); PTK-787(노바티스/쉐링 AG); INC-1C11(임클론), 라파마이신(시롤리무스, 라마뮨(RAPAMUNE)®); 또는 하기의 특허 공보들: 미국 특허 제5,804,396호; WO 1999/09016(아메리칸 시아나미드(American Cyanamid)); WO 1998/43960(아메리칸 시아나미드); WO 1997/38983(워너 램버트(Warner Lambert)); WO 1999/06378(워너 램버트); WO 1999/06396(워너 램버트); WO 1996/30347(화이자); WO 1996/33978(제네카); WO 1996/3397(제네카) 및 WO 1996/33980(제네카) 중 임의의 것에 기재된 바를 포함한다.Chemotherapeutic agents also include "tyrosine kinase inhibitors", including EGFR targeted drugs mentioned in the preceding paragraph; Inhibitors of insulin receptor tyrosine kinases, including anaplastic lymphoma kinase (Alk) inhibitors, such as AF-802 (also known as CH-5424802 or alectinib), ASP3026, X396, LDK378, AP26113, crizotinib ( XALKORI® ) and ceritinib (ZYKADIA ® ); small molecule HER2 tyrosine kinase inhibitors such as TAK165 available from Takeda; CP-724,714, an oral selective inhibitor of ErbB2 receptor tyrosine kinase (Pfizer and OSI); dual HER inhibitors such as EKB-569 (available from Wires) that preferentially binds to EGFR but inhibits both HER2 and EGFR overexpressing cells; lapatinib, an oral HER2 and EGFR tyrosine kinase inhibitor (GSK572016; available from Glaxo-SmithKline); PKI-166 (available from Novartis); Canertinib (CI-1033; pan-HER inhibitors such as Pharmacia; Raf-1 inhibitors such as the antisense agent ISIS-5132 available from ISIS Pharmaceuticals that inhibits Raf-1 signaling; Imatinib mesylate (Gleevac ( Non-HER targeted TK inhibitors such as GLEEVEC® , available from Glaxo SmithKline); multi-targeted tyrosine kinase inhibitors such as sunitinib ( SUTENT® , available from Pfizer); VEGF receptor tyrosine kinase inhibitors such as batalanib (PTK787/ZK222584, available from Novartis/Schering AG); MAPK extracellular regulated kinase I inhibitor CI-1040 (available from Pharmacia); PD 153035,4-(3-chloroanilino) quina quinazolines such as zoline; pyridopyrimidines; pyrimidopyrimidines; pyrrolopyrimidines such as CGP 59326, CGP 60261 and CGP 62706; pyrazolopyrimidines, 4-(phenylamino)-7H-pyrrolo[2] ,3-d]pyrimidine; curcumin (diferuloyl methane, 4,5-bis(4-fluoroanilino)phthalimide); tyrphostine containing a nitrothiophene moiety; Pd-0183805 ( Warner-Lamber); Antisense molecules (e.g., molecules that bind HER encoding nucleic acids); Quinoxaline (US Pat. No. 5,804,396); Tripostin (US Pat. No. 5,804,396); ZD6474 (AstraZeneca); Novartis/Schering AG); Pan HER inhibitors such as CI-1033 (Pfizer); Affinitac (ISIS 3521; Isis/Lilly); Imatinib mesylate ( GLEEVEC® ); PKI 166 (Novatis) ); GW2016 (Glaxo SmithKline); CI-1033 (Pfizer); EKB-569 (Wiers); Semaxinib (Pfizer); ZD6474 (AstraZeneca); PTK-787 (Novatis/Schering AG); INC-1C11 ( Imclone), rapamycin (sirolimus, RAPAMUNE ® ) or the following patent publications: US 5,804,396; WO 1999/09016 (American Cyanamid); WO 1998/43960 (American Cyanamide); WO 1997/38983 (Warner Lambert); WO 1999/06378 (Warner Lambert); WO 1999/06396 (Warner Lambert); WO 1996/30347 (Pfizer); WO 1996/33978 (Zeneca); WO 1996/3397 (Zeneca) and WO 1996/33980 (Zeneca).
용어 "안트라사이클린"은 화학요법제, 바람직하게는 토포이소머라제 II에서 DNA의 재결합을 억제함으로써 세포자멸사를 유도하는 항암제에 관한 것이다. 이의 예는 독소루비신(아드리아마이신), 다우노루비신(다우노마이신), 에피루비신, 이다루비신, 로도마이신, 피라루비신, 발루비신, N-트리플루오로-아세틸 독소루비신-14-발레레이트, 아클라시노마이신, (모르폴리노-DOX), 시아노모르폴리노-독소루비신(시아노모르폴리노-DOX), 2-피롤리노-독소루비신(2-PDOX), 5-이미노다우노마이신, 미톡산트론 및 아클라시노마이신 A(아클라루비신)를 포함한다. 일부 양태들에서, 안트라사이클린은 알킬화제, 예컨대 시클로포스파미드와 조합된 독소루비신(AC를 사용한 치료)과 병용으로 투여된다.The term "anthracycline" relates to a chemotherapeutic agent, preferably an anticancer agent that induces apoptosis by inhibiting DNA recombination in topoisomerase II. Examples thereof include doxorubicin (adriamycin), daunorubicin (daunomycin), epirubicin, idarubicin, rhodomycin, pyrarubicin, valrubicin, N-trifluoro-acetyl doxorubicin-14-valerate, Aclasinomycin, (morpholino-DOX), cyanomorpholino-doxorubicin (cyanomorpholino-DOX), 2-pyrrolino-doxorubicin (2-PDOX), 5-iminodaunomycin, mitoxantrone and aclasinomycin A (aclarubicin). In some embodiments, the anthracycline is administered in combination with doxorubicin (treatment with AC) in combination with an alkylating agent such as cyclophosphamide.
본원에 사용된 "알킬화제"는 DNA에 알킬기를 부착함으로써 DNA 손상을 일으키는 화학요법제이다. 알킬화제는 시클로포스파미드 및 N,N',N''-트리에틸렌티오포스포르아미드를 포함한다.As used herein, an “alkylating agent” is a chemotherapeutic agent that causes DNA damage by attaching an alkyl group to the DNA. Alkylating agents include cyclophosphamide and N,N',N''-triethylenethiophosphoramide.
화합물의 "유효량", 예를 들어, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체), VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸) 또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀)의 유효량은 원하는 치료적 결과, 예컨대, 특정 질병 또는 장애(예컨대, 암)의 전체 생존 또는 무진행 생존의 측정 가능한 증가를 달성하는데 필요한 적어도 최소량이다. 본원에서 유효량은 환자의 질병 상태, 연령, 성별 및 체중, 및 대상체에서 원하는 반응을 유도하는 항체의 능력과 같은 인자에 따라 가변될 수 있다. 유효량은 또한 치료의 임의의 독성 또는 유해한 효과가 치료학적으로 유익한 효과보다 더 큰 양이다. 예방적 사용에 있어서, 유익한 또는 원하는 결과는 위험의 제거 또는 감소, 중증도 감소, 또는 질병의 생화학적, 조직학적 및/또는 행동 증상, 질병의 발달 중 나타나는 합병증 및 중간 병리학적 표현형을 비롯한, 질병의 발병 지연과 같은 결과를 포함한다. 치료적 사용에 있어서, 유익한 또는 원하는 결과에는, 질병으로 인한 하나 이상의 증상 감소 (예를 들어, 암 관련 통증, 증상성 골격 관련 사건(SSE)의 감소 또는 지연, 유럽 암 연구 치료 기구 삶의 질 설문지에 따른 증상 (EORTC QLQ-C30, 예를 들어, 피로, 메스꺼움, 구토, 통증, 호흡곤란, 불면증, 식욕 상실, 변비, 설사 또는 일반적인 수준 신체적 정서적, 인지적 또는 사회적 기능)의 감소, 예를 들어, 10-포인트 통증 중증도 (최악에서 측정됨) 수치 등급 척도(NRS)에 의해 측정된 통증 감소, 및/또는 질병을 앓고 있는 사람들의 삶의 질 증가, 질병을 치료함에 필요한 다른 약물들의 용량 감소, 또 다른 약물의, 예를 들어, 표적화를 통한 효과 향상, 질병의 진행 지연 (예를 들어 무진행 생존 또는 방사선학적 무진행 생존 (rPFS); 명백한 임상 진행의 지연(예를 들어, 암 관련 통증 진행, 증상이 있는 골격 관련 사건, 동부 협력 종양 학회 (ECOG) 전신 활동도 (PS)의 악화 (예를 들어, 질병이 환자의 일상 생활 능력에 어떤 영향을 미치는지), 및/또는 다음 전신 항암 요법의 시작), 및/또는 생존 연장과 같은 임상 결과들이 포함된다. 암 또는 종양의 경우, 유효량의 약물은 암 세포수 감소; 종양 크기 감소; 말초 기관으로의 암 세포 침윤 억제 (즉, 어느 정도 둔화 또는 바람직하게는 정지); 종양 전이를 억제 (즉, 어느 정도 느리게하고 바람직하게는 정지); 종양 성장을 어느 정도 억제; 및/또는 질병과 관련된 하나 이상의 증상을 어느 정도 경감시키는 효과를 가질 수 있다. 유효량은 1회 이상의 투여로 투여될 수 있다. 본 발명의 목적과 관련하여, 약물, 화합물 또는 약학 조성물의 유효량은 직접 또는 간접적으로 예방 또는 치료적 치료를 달성하기에 충분한 양이다. 임상적 맥락에서 이해되는 바와 같이, 약물, 화합물 또는 약학 조성물의 유효량은 다른 약물, 화합물 또는 약학 조성물과 함께 조합되어 달성되거나 달성되지 않을 수 있다. 따라서, "유효량"은 하나 이상의 치료제 투여와 관련하여 고려될 수 있으며, 그리고 만약 하나 이상의 다른 제제와 함께 바람직한 결과가 달성될 수 있거나 달성되면 단일 제제는 유효량으로 제공되는 것으로 간주될 수 있다. 일부 양태들에서, 유익하거나 바람직한 결과는 폐암(SILC) 척도의 증상(예컨대, 기침 및 흉통의 악화까지의 시간(TTD))에 의해 평가된 바와 같이 건강 관련 삶의 질(HRQoL) 설문에 따라 폐암과 관련된 증상의 감소, 및/또는 폐 특이적 항원 진행까지의 시간 지연이다.An “effective amount” of the compound, e.g., an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (e.g., an anti-PD-Ll antibody), a VEGF antagonist, a chemotherapeutic agent (e.g., a platinum-based chemotherapeutic agent or a non-platinum-based chemotherapeutic agent) agent), an effective amount of an ADC (eg, enfortumab vedotin or sacituzumab govitecan) or a CSF (eg, pegfilgrastim, filgrastim or sagramostim) may result in a desired therapeutic outcome, such as a specific disease. or at least the minimum amount necessary to achieve a measurable increase in overall survival or progression-free survival of a disorder (eg, cancer). An effective amount herein may vary depending on factors such as the disease state, age, sex and weight of the patient, and the ability of the antibody to elicit a desired response in the subject. An effective amount is also an amount in which any toxic or deleterious effect of the treatment is greater than the therapeutically beneficial effect. For prophylactic use, beneficial or desired outcomes are the elimination or reduction of risk, reduction in severity, or biochemical, histological and/or behavioral symptoms of the disease, complications during development of the disease and intermediate pathological phenotypes of the disease. including consequences such as delayed onset. For therapeutic use, beneficial or desired outcomes include, but are not limited to, reduction of one or more symptoms due to disease (e.g., cancer-related pain, reduction or delay of symptomatic skeletal-related events (SSE), European Cancer Research Treatment Organization Quality of Life Questionnaire) reduction of symptoms (EORTC QLQ-C30, e.g. fatigue, nausea, vomiting, pain, dyspnea, insomnia, loss of appetite, constipation, diarrhea or general level physical, emotional, cognitive or social functioning), e.g. , reducing pain as measured by the 10-point pain severity (measured at worst) Numerical Rating Scale (NRS), and/or increasing the quality of life of people with the disease, reducing the dose of other drugs needed to treat the disease, Improving the effectiveness of another drug, e.g., through targeting, delaying disease progression (e.g., progression-free survival or radiological progression-free survival (rPFS); delaying apparent clinical progression (e.g., cancer-related pain progression) , symptomatic skeletal-related events, deterioration of the Eastern Cooperative Oncology Society (ECOG) systemic activity (PS) (e.g., how the disease affects the patient's ability to live daily), and/or the following systemic chemotherapy initiation), and/or prolong survival.In the case of cancer or tumors, an effective amount of the drug reduces the number of cancer cells; reduces the size of the tumor; preferably arrest); inhibit (ie, slow to some extent and preferably arrest) tumor metastasis; inhibit to some extent tumor growth; and/or relieve to some extent one or more symptoms associated with the disease. An effective amount can be administered in one or more administrations.For the purposes of the present invention, an effective amount of a drug, compound or pharmaceutical composition is an amount sufficient to directly or indirectly achieve prophylactic or therapeutic treatment. As will be understood, an effective amount of a drug, compound or pharmaceutical composition may or may not be achieved in combination with another drug, compound or pharmaceutical composition. can be Thus, an “effective amount” may be contemplated in connection with the administration of one or more therapeutic agents, and a single agent may be considered to be provided in an effective amount if a desired result can be or is achieved with one or more other agents. In some aspects, a beneficial or desirable outcome is lung cancer according to a health-related quality of life (HRQoL) questionnaire as assessed by symptoms on the lung cancer (SILC) scale (eg, time to exacerbation of cough and chest pain (TTD)). reduction of symptoms associated with, and/or delay in time to lung-specific antigen progression.
"면역원성"은 특정 물질이 면역 반응을 유발하는 능력을 지칭한다. 종양은 면역원성이며 종양 면역원성을 향상시키는 것은 면역 반응에 의한 종양 세포의 제거를 보조한다. 종양 면역원성 향상의 예에는 TIGIT 및/또는 PD-L1 길항제(예컨대, 항 TIGIT 길항제 항체 및/또는 항 PD-L1 항체)를 이용한 치료를 포함하지만 이제 제한되지는 않는다.“Immunogenicity” refers to the ability of a particular substance to elicit an immune response. Tumors are immunogenic and enhancing tumor immunogenicity aids in the clearance of tumor cells by an immune response. Examples of enhancing tumor immunogenicity include, but are not limited to, treatment with a TIGIT and/or PD-L1 antagonist (eg, an anti-TIGIT antagonist antibody and/or an anti-PD-L1 antibody).
"개별 반응" 또는 "반응"은 하기를 포함하지만 이에 제한되지는 않는 대상체에게 이점을 나타내는 임의의 평가변수를 사용하여 평가할 수 있다: (1) 질병 진행의 어느 정도 억제(예컨대, 암, 예컨대, 폐암(예컨대, 확장기 SCLC(ES-SCLC)을 포함한 소세포 폐암(SCLC)의 진행); 국소 진행성 절제 불가능한 NSCLC(예컨대, IIIB기 NSCLC) 또는 재발성 또는 전이성 NSCLC(예컨대, IV기 NSCLC), 폐 선암종을 포함하는 편평 NSCLC 또는 비편평 NSCLC 포함하는 비소세포 폐암(NSCLC), UC, 예컨대, 방광암(예컨대, MIBC), 요로상피 방광암(UBC), 췌장암(예컨대, 췌관 선암종(PDAC), 예컨대, 전이성 PDAC)), 신장 또는 신장암(예컨대, 신세포암(RCC), 흑색종, 두경부암(예컨대, 두경부 편평세포암(HNSCC)), 난소암(OC), 위암(GC)(예컨대, 위식도 접합부(GEJ) 암), 간세포 암종(HCC), 결장직장암(CRC, 예컨대, 미세위성 안정(MSS) 및 미세위성 불안정(MSI)이 있는(MSI-낮음) CRC), 또는 유방암(예컨대, 에스트로겐 수용체(ER-), 프로게스테론 수용체(PgR-) 및 HER2(HER2-) 음성인 HER2+ 유방암 및 삼중 음성 유방암(TNBC)) - 지연 및 완전한 저지를 포함; (2) 종양 크기의 감소; (3) 인접한 말초 기관 및/또는 조직으로의 암 세포 침윤의 억제(즉, 감소, 감속 또는 완전한 중지); (4) 전이의 억제(즉, 감소, 감속 또는 완전한 중지); (5) 질병 또는 장애(예컨대, 암)와 관련된 하나 이상의 증상의 어느 정도 경감; (6) 전체 생존 및 무진행 생존을 포함하는 생존 기간의 증가 또는 연장; 및/또는 (9) 치료 후 주어진 시점에서 사망률 감소. An “individual response” or “response” can be assessed using any endpoint that shows benefit to a subject, including but not limited to: (1) inhibition of disease progression to some extent (eg, cancer, such as, Lung cancer (e.g., progression of small cell lung cancer (SCLC), including advanced stage SCLC (ES-SCLC)); locally advanced unresectable NSCLC (e.g., stage IIIB NSCLC) or recurrent or metastatic NSCLC (e.g., stage IV NSCLC), lung adenocarcinoma Non-small cell lung cancer (NSCLC), including squamous NSCLC or non-squamous NSCLC, including UC, such as bladder cancer (eg, MIBC), urothelial bladder cancer (UBC), pancreatic cancer (eg, pancreatic ductal adenocarcinoma (PDAC), such as metastatic PDAC) )), kidney or kidney cancer (eg, renal cell carcinoma (RCC), melanoma, head and neck cancer (eg, head and neck squamous cell carcinoma (HNSCC)), ovarian cancer (OC), gastric cancer (GC) (eg, gastroesophageal junction) (GEJ) cancer), hepatocellular carcinoma (HCC), colorectal cancer (CRC, e.g., CRC with microsatellite stable (MSS) and microsatellite instability (MSI) (MSI-low)), or breast cancer (e.g., estrogen receptor ( HER2+ breast cancer and triple negative breast cancer (TNBC) negative for ER-), progesterone receptor (PgR-) and HER2 (HER2-) - including delayed and complete arrest; (2) reduction in tumor size; (3) adjacent peripheral organs and/or inhibiting (ie, reducing, slowing, or completely stopping) cancer cell infiltration into a tissue; (4) inhibiting metastasis (ie, reducing, slowing or completely stopping); (5) a disease or disorder (eg, cancer) relief to some extent of one or more symptoms associated with: (6) an increase or prolongation of survival, including overall survival and progression-free survival; and/or (9) a decrease in mortality at a given time point after treatment.
본원에서 사용된 "병리학적 완전 반응"(pCR)은 완전한 절제된 표본의 잔류 침습성 암이 없는 환자의 비율로 정의된다. 유방암과 관련하여, "병리학적 완전 반응" 또는 "pCR"은 유방 및 림프절 모두에서 종양의 근절을 의미한다(ypT0/ypN0).As used herein, “pathological complete response” (pCR) is defined as the proportion of patients free of residual invasive cancer in a completely resected specimen. In the context of breast cancer, "pathological complete response" or "pCR" refers to eradication of the tumor in both breast and lymph nodes (ypT0/ypN0).
요로상피암(UC)의 맥락에서 본원에 사용된 "병리학적 하향병기율"은 방광 절제술 시 ≤ pT1pN0에 도달하는 환자의 비율로 정의된다.As used herein in the context of urothelial cancer (UC), "pathological down-staging" is defined as the proportion of patients achieving ≤ pT1pN0 upon cystectomy.
본원에서 사용되는 “완전 관해” 또는 “CR”은 모든 표적 병변들이 사라짐을 지칭한다.As used herein, “complete remission” or “CR” refers to the disappearance of all target lesions.
본원에서 사용되는 “부분 관해” 또는 “PR”은 기준선 SLD를 기준으로 하여 표적 병변의 최장 직경의 합 (SLD)의 적어도 30% 감소를 지칭한다.As used herein, “partial remission” or “PR” refers to at least a 30% reduction in the sum of the longest diameters (SLD) of the target lesion relative to the baseline SLD.
본원에서 사용되는 "객관적 반응율 (ORR)"은 완전 관해 (CR) 비율과 부분 관해 (PR) 비율의 합을 지칭한다.As used herein, “objective response rate (ORR)” refers to the sum of the complete remission (CR) rate and the partial remission (PR) rate.
본원에서 사용된 "객관적 반응의 지속기간"(DOR)은 기록된 객관적 반응의 최초 발생시부터 질병 진행 또는 치료제 최종 투약 후 30일 이내 임의의 원인으로 인한 사망 (어느 것이든 먼저 발생하는 것)까지의 시간으로 정의된다."Duration of objective response" (DOR), as used herein, is from the first occurrence of a documented objective response to disease progression or death from any cause within 30 days of the last dose of therapeutic agent, whichever occurs first. defined as time.
"지속적인 반응"은 치료 중단 후 종양 성장 감소에 대한 지속적인 효과를 지칭한다. 예를 들어, 종양 크기는 투여 단계 초기의 크기와 비교하여 동일하거나 더 작게 유지 될 수 있다. 일부 양태들, 지속 반응은, 치료 기간의 적어도 1.5x, 2.0x, 2.5x, 또는 3.0x 길이의 치료 기간과 적어도 동일한 기간을 가진다."Persistent response" refers to a lasting effect on reducing tumor growth after discontinuation of treatment. For example, the tumor size may remain the same or smaller compared to the size at the beginning of the administration phase. In some aspects, a sustained response has a duration of treatment that is at least equal to a treatment period that is at least 1.5x, 2.0x, 2.5x, or 3.0x the length of the treatment period.
대상체의 “효과적인 반응” 또는 약제를 이용한 치료에 대한 대상체의 “반응성” 및 유사한 용어는 질병 또는 장애, 예컨대 암의 위험에 처해 있거나, 또는 이것을 앓는 환자에게 부여된 임상적 또는 치료적 유익성을 지칭한다. 일 양태에서, 이런 유익성은 생존(전체 생존 및 무진행 생존을 포함)의 연장; 객관적인 반응(CR 또는 PR 포함)의 유발; 또는 암의 징후 또는 증상 향상 중에서 임의의 하나 이상을 포함한다."Effective response" of a subject or "response" of a subject to treatment with a medicament and similar terms refer to a clinical or therapeutic benefit conferred to a patient at risk of, or suffering from, a disease or disorder, such as cancer. do. In one aspect, such benefits include prolonging survival (including overall survival and progression-free survival); eliciting an objective response (including CR or PR); or improving any one or more of the signs or symptoms of cancer.
치료에 대한 “효과적인 반응을 갖지 않는” 대상체는 생존(전체 생존 및 무진행 생존을 포함)의 연장; 객관적인 반응 (CR 또는 PR 반응을 포함)의 유발; 또는 암의 징후 또는 증상 향상 중에서 어느 것도 갖지 않는 환자를 지칭한다. Subjects who “do not have an effective response” to treatment are characterized by prolongation of survival (including overall survival and progression-free survival); induction of objective responses (including CR or PR responses); or patients who do not have any improvement in signs or symptoms of cancer.
본원에서 사용되는 "생존"은 살아남은 환자를 말하며 전체 생존 및 무진행 생존을 포함한다.As used herein, “survival” refers to a patient who survives and includes overall survival and progression-free survival.
본원에서 사용된, "전체 생존" 및 "OS"는 환자가 여전히 살아있는 질병(예컨대, 암)에 대한 진단일 또는 치료 시작으로부터의 기간을 의미한다. 예를 들어, OS는 무작위 배정으로부터 임의의 원인으로 인한 사망까지의 시간으로서 정의될 수 있다.As used herein, "overall survival" and "OS" refer to the period from the date of diagnosis or initiation of treatment for a disease (eg, cancer) in which the patient is still alive. For example, OS may be defined as the time from randomization to death from any cause.
본원에서 사용된 “전체 생존율”은 특정 지속 기간, 예컨대, 진단 또는 치료의 시점으로부터 6개월, 1년 또는 5년 후 살아있는, 군에서 개체의 백분율을 지칭한다. As used herein, “overall survival” refers to the percentage of individuals in a group that are alive after a certain duration, eg, 6 months, 1 year, or 5 years from the time of diagnosis or treatment.
본원에 사용된 "무재발 생존"(RFS)은 수술 후 제1 주기의 제 1일부터 질병의 최초 문서화된 재발 또는 임의의 원인으로 인한 사망까지의 시간으로 정의된다.As used herein, “relapse-free survival” (RFS) is defined as the time from
본원에 사용된 "무사건 생존"(EFS)은 무작위 배정으로부터 하기의 사건(이 중 먼저 발생하는 것)까지의 시간으로 정의된다: 질병 진행(예컨대, 시험자가 평가한 바와 같이 수술을 배제하는 진행); 국소 또는 원거리 질병 재발; 또는 임의의 원인으로 인한 사망.As used herein, “event-free survival” (EFS) is defined as the time from randomization to the event (whichever occurs first): disease progression (e.g., progression excluding surgery as assessed by the investigator) ); local or distant disease recurrence; or death from any cause.
본원에서 사용된, “무진행 생존”(PFS)은 치료 중인 질환(예컨대, 암)이 악화되지 않는 치료 중 및 치료 후 시간의 길이를 지칭한다. 무진행 생존은 환자가 CR 또는 PR을 경험한 시간의 양뿐만 아니라 환자가 안정적 질환을 경험한 시간의 양을 포함할 수 있다.As used herein, “progression-free survival” (PFS) refers to the length of time during and after treatment that the disease being treated (eg, cancer) does not worsen. Progression-free survival can include the amount of time the patient has experienced CR or PR as well as the amount of time the patient has stable disease.
본원에서 사용된 "안정한 질병" 또는 "SD"는 치료 시작 이후 최소 SLD를 기준으로 하여, CR 또는 PR에 적합한 충분한 표적 병변의 수축도, PD에 적합한 충분한 증가를 의미하지 않는다.As used herein, "stable disease" or "SD" does not mean a sufficient increase in contractility of the target lesion suitable for CR or PR, or sufficient increase for PD, based on the minimum SLD since initiation of treatment.
본원에서 사용된 “진행성 질환” 또는 “PD”는 치료가 시작되거나, 또는 하나 이상의 새로운 병변의 존재 이후로 기록된 가장 작은 SLD(가장 긴 지름의 합)를 기준으로서 간주할 때, 표적 병변의 SLD에서 적어도 20% 증가를 지칭한다. As used herein, “progressive disease” or “PD” refers to the SLD of a target lesion, taken as a criterion for the smallest SLD (sum of longest diameters) recorded since treatment was initiated, or the presence of one or more new lesions. refers to an increase of at least 20% in
본원에 사용된 "주요 병리학적 반응"(MPR)은 원발성 종양에서 외과적 절제 시점에 ≤ 10%의 잔여 생존 종양으로 정의된다.As used herein, a “major pathological response” (MPR) is defined as a residual viable tumor of <10% at the time of surgical resection in the primary tumor.
본원에서 사용된, 질환 또는 질병의 "진행 지연"은 질환 또는 질병(예컨대, 암)의 진행을 보류, 방해, 지체, 저지, 안정화, 및/또는 연기하는 것을 지칭한다. 이러한 지연은 질병의 이력 및/또는 치료받는 대상체에 따라 시간의 길이가 다양할 수 있다. 당업자에게 명백한 바와 같이, 충분한 또는 유의미한 지연은, 효과에 있어서, 대상체에서 질병이 발병하지 않는다는 점에서, 예방을 포함할 수 있다. 예를 들어, 말기 암에서, 중추 신경계 (CNS) 전이의 발병이 지연될 수 있다.As used herein, “delaying progression” of a disease or disorder refers to withholding, impeding, retarding, arresting, stabilizing, and/or delaying the progression of a disease or disorder (eg, cancer). This delay may vary in length of time depending on the history of the disease and/or the subject being treated. As will be apparent to those skilled in the art, a sufficient or significant delay, in effect, may include prevention, in that the subject does not develop the disease. For example, in terminal cancer, the onset of central nervous system (CNS) metastases may be delayed.
본원에서 사용되는 용어 "암 재발 감소 또는 억제"는 종양 또는 암 재발 또는 종양 또는 암 진행을 감소 또는 억제하는 것을 의미한다.As used herein, the term “reducing or inhibiting cancer recurrence” means reducing or inhibiting tumor or cancer recurrence or tumor or cancer progression.
“감소시키거나 또는 저해한다”는 20%, 30%, 40%, 50%, 60%, 70%, 75%, 80%, 85%, 90%, 95%, 또는 그 이상의 전반적인 감소를 유발하는 능력인 것으로 의미된다. 감소시키거나 또는 저해한다는 치료되는 장애(예컨대, 암)의 증상, 전이의 존재 또는 크기, 또는 일차 종양의 크기를 지칭할 수 있다. “Reducing or inhibiting” means an overall reduction of 20%, 30%, 40%, 50%, 60%, 70%, 75%, 80%, 85%, 90%, 95%, or more. It means ability. Reducing or inhibiting may refer to the symptoms of the disorder (eg, cancer) being treated, the presence or size of metastases, or the size of the primary tumor.
"생존 연장"은 치료받지 않은 환자(예컨대, 약물로 치료받지 않은 환자에 비해) 또는 지정된 수준으로 바이오마커를 발현하지 않는 환자에 비해, 및/또는 승인된 항암제로 치료받은 환자에 비해, 치료받은 환자에서 전체 또는 무진행 생존의 증가를 의미한다. "객관적 반응"은 CR 또는 PR을 포함하여 측정가능한 반응을 지칭한다."Prolonging survival" refers to a treated patient compared to an untreated patient (eg, compared to a patient not treated with a drug) or a patient not expressing a biomarker at a designated level, and/or compared to a patient treated with an approved anticancer agent. means an increase in overall or progression-free survival in a patient. “Objective response” refers to a measurable response, including CR or PR.
용어 "검출하는 것" 및 "검출"은 표적 분자의 정성적 및 정량적 측정을 모두 포함하는 가장 넓은 의미로 본원에서 사용된다. 검출은 단순히 샘플 내 표적 분자의 존재를 식별하는 것, 뿐만 아니라 표적 분자가 검출가능한 수준으로 샘플 내 존재하는지 여부를 결정하는 것을 포함한다. 검출은 직접적이거나 간접적일 수 있다. The terms “detecting” and “detecting” are used herein in their broadest sense to include both qualitative and quantitative measurement of a target molecule. Detection includes not only identifying the presence of a target molecule in a sample, but also determining whether the target molecule is present in the sample at a detectable level. Detection may be direct or indirect.
본원에서 사용되는 “PD-L1-양성 종양 세포 분율”은 항체 SP142, SP263, 22C3, 또는 28-8을 사용한 PD-L1 염색에 대한 면역조직화학 (IHC) 분석법, 예를 들어, IHC 분석법과 관련하여 샘플 염색 후, 샘플에 존재하는 모든 생존가능한 종양 세포들에 대한, 임의의 강도에서 부분 또는 완전 막 염색 (세포질 염색 제외)을 보여주는 생존가능한 종양 세포들의 백분율이다. 따라서 PD-L1-양성 종양 세포 분율은 PD-L1 IHC SP263(Ventana) 분석을 사용하여 예를 들어, 식 PD-L1-양성 종양 세포 분율 = (PD-L1-양성 종양의 수 세포)/(PD-L1 양성 및 PD-L1 음성 종양 세포의 전체 수)에 의해 계산될 수 있으며, 이때 종양 세포 및 모든 비종양 세포(예를 들어, 종양 침윤 면역 세포, 정상 세포, 괴사 세포, 파편)의 PD-L1 세포질 염색은 평가 및 점수화 대상에서 제외된다. 임의의 주어진 진단 PD-L1 항체는 PD-L1-양성 종양 세포 분율을 유도하기 위해 사용될 수 있는 특정 IHC 분석 프로토콜 및/또는 점수화 용어에 상응할 수 있음이 이해될 것이다. 예를 들어, PD-L1 양성 종양 세포 분획은 SP263, 22C3, SP142, 또는 28-8로 염색된 종양 세포 샘플로부터, 각각, 벤치마크(Benchmark) ULTRA에서의 OPTIVIEW® 검출, 오코스테이너링크(AutostainerLink) 48에서의 엔비전 플렉스(EnVision Flex), 벤치마크 ULTRA에서의 옵티뷰(OPTIVIEW)® 검출 및 증폭, 또는 오코스테이너링크 48에서의 엔비전 플렉스를 사용하여 유도될 수 있다. 다른 예에서, PD-L1-양성 종양 세포 분율은 상기 식에 따라 PD-L1 IHC 22C3 pharmDx 분석(Dako)을 사용하여 계산될 수 있다. 당업자는 IHC 분석에 사용되는 상이한 PD-L1 항체들 간에 민감도가 달라질 수 있음을 이해할 것이다. 예를 들어, 28-8 또는 22C3 및 SP263으로 염색함으로써 각각 정의된 1% TC 또는 25% TC 임계값을 충족하는 샘플의 약 64%만이 SP142를 사용하여 염색할 때 임계값을 충족한다. Hirsch et al., Journal of Thoracic Oncology 2016, 12(2): 208-222. 본원에서 사용되는 용어 PD-L1-양성 종양 세포 분율 및 "종양 비율 점수"(TPS)는 상호교환적으로 사용된다.As used herein, “PD-L1-positive tumor cell fraction” refers to an immunohistochemical (IHC) assay, eg, an IHC assay, for PD-L1 staining using antibodies SP142, SP263, 22C3, or 28-8. is the percentage of viable tumor cells showing partial or complete membrane staining (excluding cytoplasmic staining) at any intensities relative to all viable tumor cells present in the sample after staining the sample. Thus, the PD-L1-positive tumor cell fraction can be calculated using the PD-L1 IHC SP263 (Ventana) assay, e.g., expression PD-L1-positive tumor cell fraction = (number of PD-L1-positive tumor cells)/(PD -L1 positive and total number of PD-L1 negative tumor cells), where PD- of tumor cells and all non-tumor cells (e.g., tumor infiltrating immune cells, normal cells, necrotic cells, debris) L1 cytoplasmic staining is excluded from evaluation and scoring. It will be appreciated that any given diagnostic PD-L1 antibody may correspond to specific IHC assay protocols and/or scoring terms that may be used to derive a fraction of PD-L1-positive tumor cells. For example, a PD-L1-positive tumor cell fraction can be obtained from tumor cell samples stained with SP263, 22C3, SP142, or 28-8, respectively, with OPTIVIEW® detection at Benchmark ULTRA, AutostainerLink ) 48, OPTIVIEW® detection and amplification on benchmark ULTRA, or EnVision Flex on
본원에 사용된 "벤타나 SP142 IHC 분석"은 벤타나 PD-L1(SP142) 분석 패키지 삽입에 따라 실시되고(투손(Tucson), AZ: 벤타나 메디컬 시스템즈(Ventana Medical Systems, Inc.)), 이는 그 전체가 본원에 원용된다.As used herein, "Ventana SP142 IHC assay" is performed according to the Ventana PD-L1 (SP142) assay package insert (Tucson, AZ: Ventana Medical Systems, Inc.), which The entirety is incorporated herein by reference.
본원에 사용된 "벤타나 SP263 IHC 분석"은 벤타나 PD-L1(SP263) 분석 패키지 삽입에 따라 실시되고(투손, AZ: 벤타나 메디컬 시스템즈), 이는 그 전체가 본원에 원용된다.As used herein, "Ventana SP263 IHC Assay" is performed according to the Ventana PD-L1 (SP263) Assay Package Insert (Tucson, AZ: Ventana Medical Systems), which is incorporated herein in its entirety.
본원에 사용된 "팜(pharm)Dx 22C3 IHC 분석"은 PD-L1 IHC 22C3 팜Dx 분석 패키지 삽입에 따라 실시되고(카핀테리아(Carpinteria), CA: 다코(Dako), 애질런트 파톨로지 솔루션(Agilent Pathology Solutions)), 이는 그 전체가 본원에 원용된다.As used herein, "pharmDx 22C3 IHC assay" is performed according to the PD-L1 IHC 22C3 PharmDx assay package insert (Carpinteria, CA: Dako, Agilent Pathology) Solutions), which is incorporated herein in its entirety.
본원에 사용된 "팜(pharm)Dx 28-8 IHC 분석"은 PD-L1 IHC 28-8 팜Dx 분석 패키지 삽입에 따라 실시되고(카핀테리아, CA: 다코(Dako), 애질런트 파톨로지 솔루션(Agilent Pathology Solutions)), 이는 그 전체가 본원에 원용된다.As used herein, “pharmDx 28-8 IHC assay” is performed according to the PD-L1 IHC 28-8 PharmDx assay package insert (Carpinteria, CA: Dako, Agilent Patology Solutions (Agilent). Pathology Solutions), which is incorporated herein in its entirety.
본원에서 사용되는 "종양-침윤 면역 세포"는 종양 또는 이의 샘플에 존재하는 임의의 면역 세포를 지칭한다. 종양-침윤 면역 세포는 종양내 면역 세포, 종양주위 면역 세포, 다른 종양 기질 세포 (예를 들어, 섬유아세포) 또는 이들의 임의의 조합을 포함하지만 이에 제한되지는 않는다. 이러한 종양-침윤 면역 세포는, 예를 들어, T 림프구 (가령, CD8+ T 림프구 및/또는 CD4+ T 림프구), B 림프구, 또는, 과립구를 포함한 기타 골수 계통 세포 (예컨대, 호중구, 호산구 및 호염기구), 단핵구, 대식세포, 수지상 세포 (예컨대, 깍지낀 수지상 세포), 조직구 및 자연 살해 세포일 수 있다.As used herein, “tumor-infiltrating immune cell” refers to any immune cell present in a tumor or sample thereof. Tumor-infiltrating immune cells include, but are not limited to, intratumoral immune cells, peritumoral immune cells, other tumor stromal cells (eg, fibroblasts), or any combination thereof. Such tumor-infiltrating immune cells include, for example, T lymphocytes (eg, CD8+ T lymphocytes and/or CD4+ T lymphocytes), B lymphocytes, or other myeloid lineage cells including granulocytes (eg, neutrophils, eosinophils and basophils). , monocytes, macrophages, dendritic cells (eg, interdigitated dendritic cells), histocytes and natural killer cells.
본원에 사용된 용어 "바이오마커"는 샘플, 예를 들어, PD-L1, ctDNA, 또는 사이토카인(예컨대, T 세포 활성화 및/또는 림프구 하위집단과 관련된 사이토카인)에서 검출될 수 있는 지표, 예컨대, 예측, 진단 및/또는 예후를 지칭한다. 바이오마커는 특정, 분자, 병리, 조직 및/또는 임상 특징으로 특성화되는 질병 또는 장애(예컨대, 암)의 특정 아형의 지표로서 기능할 수 있다. 일부 양태들에서, 바이오마커는 유전자이다. 바이오마커는 폴리펩티드, 폴리뉴클레오티드(예컨대, DNA(예컨대, ctDNA)및/또는 RNA), 폴리뉴클레오티드 복제수 변경(예컨대, DNA 복제수), 폴리펩티드 및 폴리뉴클레오티드 변형(예컨대, 번역후 변형), 탄수화물, 및/또는 당지질 기반의 분자 마커를 포함하지만 이에 제한되지는 않는다. 일부 양태들에서, 상기 바이오마커는 PD-L1이다. 일부 양태들에서, 상기 바이오마커는 ctDNA이다. 일부 양태들에서, 상기 바이오마커는 하나 이상의 사이토카인(예컨대, T 세포 활성화 및/또는 림프구 하위집단과 관련된 하나 이상의 사이토카인)이다. 일부 양태들에서, 상기 바이오마커는 세포(예컨대, 면역 세포, 예컨대, T 세포, 예컨대, T 세포 하위집합, 예컨대, 활성화된 T 세포)이다. 일부 양태들에서, 상기 바이오마커는 인유두종바이러스(HPV) 상태의 직접적 또는 간접적 지표이다. 일부 양태들에서, 상기 바이오마커는 p16이다. 일부 양태들에서, 상기 바이오마커는 HPV 단백질 또는 핵산이다.As used herein, the term “biomarker” refers to an indicator that can be detected in a sample, e.g., PD-L1, ctDNA, or a cytokine (eg, a cytokine associated with T cell activation and/or lymphocyte subpopulations), such as , prediction, diagnosis and/or prognosis. A biomarker may serve as an indicator of a particular subtype of a disease or disorder (eg, cancer) characterized by a particular, molecular, pathology, tissue and/or clinical feature. In some aspects, the biomarker is a gene. Biomarkers include polypeptides, polynucleotides (eg, DNA (eg, ctDNA) and/or RNA), polynucleotide copy number alterations (eg, DNA copy number), polypeptides and polynucleotide modifications (eg, post-translational modifications), carbohydrates, and/or glycolipid-based molecular markers. In some aspects, the biomarker is PD-L1. In some aspects, the biomarker is ctDNA. In some aspects, the biomarker is one or more cytokines (eg, one or more cytokines associated with T cell activation and/or lymphocyte subpopulations). In some aspects, the biomarker is a cell (eg, an immune cell, eg, a T cell, eg, a subset of T cells, eg, an activated T cell). In some aspects, the biomarker is a direct or indirect indicator of human papillomavirus (HPV) status. In some aspects, the biomarker is p16. In some aspects, the biomarker is an HPV protein or nucleic acid.
용어 “하우스키핑 바이오마커”는 전형적으로 모든 세포 유형에서 유사하게 존재하는 바이오마커 또는 바이오마커의 군(예컨대, 폴리뉴클레오티드 및/또는 폴리펩티드)을 지칭한다. 일부 양태들에서, 상기 하우스키핑 바이오마커는 “하우스키핑 유전자”이다. “하우스키핑 유전자”는 본원에서 세포 기능의 유지를 위해 활성이 필수적인 단백질을 부호화하고, 전형적으로 모든 세포 유형에서 유사하게 존재하는 유전자 또는 유전자의 군을 지칭한다.The term “housekeeping biomarker” refers to a biomarker or group of biomarkers (eg, polynucleotides and/or polypeptides) that are typically similarly present in all cell types. In some aspects, the housekeeping biomarker is a “housekeeping gene”. “Housekeeping gene” herein refers to a gene or group of genes that encode proteins essential for activity for maintenance of cellular function, and are typically similar in all cell types.
본원에 사용된 "순환하는 종양 DNA" 및 "ctDNA"는 세포와 연관되지 않은 순환계의 종양 유래 DNA를 지칭한다. ctDNA는 종양 세포 또는 순환 종양 세포(CTC)에서 유래할 수 있는 일종의 무세포 DNA(cfDNA)이다. ctDNA는, 예컨대, 환자의 혈류 또는 환자로부터 수득한 생물학적 샘플(예컨대, 혈액, 혈청, 혈장 또는 소변)에서 발견될 수 있다. 일부 양태들에서, ctDNA는 비정상적인 돌연변이(예컨대, 환자 특이적 변이체) 및/또는 메틸화 패턴을 포함할 수 있다. As used herein, “circulating tumor DNA” and “ctDNA” refer to tumor-derived DNA in the circulation that is not associated with a cell. ctDNA is a type of cell-free DNA (cfDNA) that can be derived from tumor cells or circulating tumor cells (CTCs). ctDNA can be found, for example, in the bloodstream of a patient or in a biological sample obtained from the patient (eg, blood, serum, plasma or urine). In some aspects, the ctDNA may comprise aberrant mutations (eg, patient-specific variants) and/or methylation patterns.
용어 “항체”는, 이들이 원하는 생물학적 활성을 나타내는 한, 단일클론 항체(면역글로불린 Fc 영역을 갖는 전장 항체 포함), 다중클론 항체, 폴리에피토프 특이성을 갖는 항체 조성물, 다중특이적 항체(예컨대, 이중특이적 항체), 이중체, 그리고 단일 사슬 분자뿐만 아니라 항원 결합 단편, 예컨대 Fab, F(ab’)2 및 Fv를 포함한 항체 단편을 포함한다. 용어 "면역글로불린"(Ig)은 본원에서 "항체"와 상호교환적으로 사용된다. 일 양태에서, 상기 항체는 전장 단일클론 항체이다.The term “antibody” refers to monoclonal antibodies (including full-length antibodies having an immunoglobulin Fc region), polyclonal antibodies, antibody compositions having polyepitopic specificity, multispecific antibodies (e.g., bispecific antibodies), so long as they exhibit the desired biological activity. antibody fragments), duplexes, and single chain molecules as well as antigen binding fragments such as Fab, F(ab′) 2 and Fv. The term “immunoglobulin” (Ig) is used interchangeably herein with “antibody”. In one embodiment, the antibody is a full length monoclonal antibody.
본원에서 이용된 바와 같이, 용어 IgG “아이소타입” 또는 “하위부류”는 그들의 불변 영역의 화학적 및 항원성 특징에 의해 규정되는 면역글로불린의 임의의 하위부류인 것으로 의미된다. As used herein, the term IgG “isotype” or “subclass” is meant to be any subclass of immunoglobulins defined by the chemical and antigenic characteristics of their constant regions.
중쇄의 불변 도메인의 아미노산 서열에 따라서, 항체 (면역글로불린)는 상이한 부류에 배정될 수 있다. 면역글로불린의 5가지 주요 부류인: IgA, IgD, IgE, IgG, 및 IgM, 그리고 이들 중 몇몇은 하위부류(동형), 예컨대, IgG1, IgG2, IgG3, IgG4, IgA1, 및 IgA2로 더욱 세분화될 수 있다. 면역글로불린의 상이한 부류에 상응하는 중쇄 불변 도메인은 각각, α, γ, ε, γ 및 μ로 불린다. 면역글로불린의 상이한 클래스의 하부단위 구조 및 3-차원 입체배치는 잘 알려지고 일반적으로, 예를 들어, 하기에 기술된다: Abbas et al. Cellular and Mol. Immunology, 4th ed. (W.B. Saunders, Co., 2000)에 기재되어 있다. 항체는 항체 및 하나 또는 그 이상의 다른 단백질 또는 펩티드의 공유 또는 비공유 연관에 의해 형성되는, 더 큰 융합 분자의 부분일 수 있다.Depending on the amino acid sequence of the constant domain of the heavy chain, antibodies (immunoglobulins) can be assigned to different classes. There are five major classes of immunoglobulins: IgA, IgD, IgE, IgG, and IgM, and some of these can be further subdivided into subclasses (isotypes), e.g., IgG1, IgG2, IgG3, IgG4, IgA1, and IgA2. have. The heavy chain constant domains corresponding to the different classes of immunoglobulins are called α, γ, ε, γ and μ, respectively. The subunit structures and three-dimensional configurations of the different classes of immunoglobulins are well known and generally described, for example, in Abbas et al. Cellular and Mol. Immunology , 4 th ed. (WB Saunders, Co., 2000). An antibody may be part of a larger fusion molecule, formed by covalent or non-covalent association of the antibody and one or more other proteins or peptides.
기본 4-사슬 항체 단위는 2개의 동일한 경쇄(L)와 2개의 동일한 중쇄(H)로 구성된 이종사량체 당단백질이다. IgM 항체는 J 쇄로 불리우는 추가 폴리펩티드와 함께 염기성 이종사량체 단위 중 5개로 구성되고, 10개의 항원 결합 부위를 함유하며, 한편 IgA 항체는 중합하여 J 쇄와 조합된 다가 집합체를 형성할 수 있는 염기성 4-쇄 단위의 2 내지 5개를 포함한다. IgG의 경우, 4-사슬 단위는 일반적으로 약 150,000 달톤이다. 각 L 쇄는 하나의 공유 이황화 결합에 의해 H 쇄에 연결되지만, 두 개의 H 쇄는 H 쇄 아이소형에 따라 하나 이상의 이황화 결합에 의해 서로에 연결된다. 각 H 및 L 쇄는 또한 규칙적 간격의 사슬내 다이설파이드 다리를 가진다. 각 H 쇄는 N-말단에, 가변 도메인 (VH)을 가지며, 이어서 α 및 γ 사슬 각각에 대해서는 세 개의 불변 도메인 (CH)을 그리고 μ 및 ε 아이소형에 대해서는 네 개의 CH 도메인을 수반한다. 각 L 쇄는 N-말단에, 가변 도메인 (VL)을 가지며 이어서 다른 단부에 불변 도메인을 수반한다. VL은 VH와 함께 정렬되고 CL은 중쇄의 제 1 불변 도메인 (CH1)과 함께 정렬된다. 특정 아미노산 잔기는 경쇄와 중쇄 가변 도메인들 사이의 경계면을 형성하는 것으로 생각된다. VH와 VL의 페어링은 하나의 항원- 결합 부위를 함께 형성한다. 항체의 상이한 부류의 구조와 성질에 대해, 예를 들면 Basic and Clinical Immunology, 8th Edition, Daniel P. Sties, Abba I. Terr and Tristram G. Parsolw (eds), Appleton & Lange, Norwalk, CT, 1994, page 71 및 Chapter 6을 참조한다. 임의의 척추동물 종으로부터의 L 쇄는 이들의 불변 도메인의 아미노산 서열들에 기초하여, 카파 및 람다로 불리는 두 가지 명확히 상이한 유형들 중 하나에 할당될 수 있다. 그 중쇄의 불변 도메인 (CH)의 아미노산 서열에 따라, 면역글로불린은 상이한 클래스 또는 아이소형에 할당될 수 있다. 5개 주요 부류의 면역글로불린이 있다: 각각 α, δ, ε, γ, 및 μ로 지정된 중쇄를 갖는 IgA, IgD, IgE, IgG 및 IgM. γ 및 α 부류는 CH 서열 및 기능에서의 상대적으로 작은 차이에 기초하여 하위부류로 더 분류되며, 예컨대, 인간은 하기 하위부류를 발현한다: IgG1, IgG2A, IgG2B, IgG3, IgG4, IgA1 및 IgA2.The basic four-chain antibody unit is a heterotetrameric glycoprotein composed of two identical light (L) chains and two identical heavy (H) chains. IgM antibodies are made up of 5 of the basic heterotetrameric units, with an additional polypeptide called the J chain, and contain 10 antigen binding sites, while IgA antibodies are basic 4 capable of polymerizing to form a multivalent aggregate combined with the J chain. - contains 2 to 5 chain units. For IgG, a four-chain unit is generally about 150,000 daltons. Each L chain is linked to the H chain by one covalent disulfide bond, but the two H chains are linked to each other by one or more disulfide bonds, depending on the H chain isotype. Each H and L chain also has regularly spaced intrachain disulfide bridges. Each H chain has, at the N-terminus, a variable domain (V H ) followed by three constant domains ( CH ) for each of the α and γ chains and four CH domains for the μ and ε isoforms. do. Each L chain has, at the N-terminus, a variable domain (V L ) followed by a constant domain at the other end. V L is aligned with V H and CL is aligned with the first constant domain of the heavy chain ( CH 1 ). Certain amino acid residues are believed to form the interface between the light and heavy chain variable domains. The pairing of V H and V L together forms one antigen-binding site. For the structure and properties of the different classes of antibodies, see, for example, Basic and Clinical Immunology , 8th Edition, Daniel P. Sties, Abba I. Terr and Tristram G. Parsolw (eds), Appleton & Lange, Norwalk, CT, 1994 , page 71 and
본원에서 사용되는 용어 “초가변 영역” 또는 “HVR”은 서열에서 초가변적이고, 항원 결합 특이성을 결정하는 항체 가변 도메인의 영역들 각각, 예를 들어, "상보성 결정 영역" ("CDR")을 지칭한다.As used herein, the term “hypervariable region” or “HVR” refers to each of the regions of an antibody variable domain that are hypervariable in sequence and that determine antigen binding specificity, e.g., a “complementarity determining region” (“CDR”). refers to
일반적으로, 항체는 6개 CDR을 포함한다: VH에서 3개(CDR-H1, CDR-H2, CDR-H3), 및 VL에서 3개(CDR-L1, CDR-L2, CDR-L3). 본원에서 예시적인 CDR은 하기를 포함한다: Generally, antibodies comprise six CDRs: three in the VH (CDR-H1, CDR-H2, CDR-H3), and three in the VL (CDR-L1, CDR-L2, CDR-L3). Exemplary CDRs herein include:
(a) 아미노산 잔기 26-32(L1), 50-52(L2), 91-96(L3), 26-32(H1), 53-55(H2), 및 96-101(H3)에서 발생하는 초가변 루프(Chothia and Lesk, J. Mol. Biol. 196:901-917 (1987));(a) occurring at amino acid residues 26-32 (L1), 50-52 (L2), 91-96 (L3), 26-32 (H1), 53-55 (H2), and 96-101 (H3) hypervariable loops (Chothia and Lesk, J. Mol. Biol. 196:901-917 (1987));
(b) 아미노산 잔기 24-34(L1), 50-56(L2), 89-97(L3), 31-35b(H1), 50-65(H2), 및 95-102(H3)에서 발생하는 CDR(Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, MD (1991)); 및(b) occurring at amino acid residues 24-34 (L1), 50-56 (L2), 89-97 (L3), 31-35b (H1), 50-65 (H2), and 95-102 (H3) CDR (Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, MD (1991)); and
(c) 아미노산 잔기 27c-36(L1), 46-55(L2), 89-96(L3), 30-35b(H1), 47-58(H2), 및 93-101(H3)에 발생하는 항원 접촉(MacCallum et al. J. Mol. Biol. 262: 732-745 (1996)).(c) occurring at amino acid residues 27c-36 (L1), 46-55 (L2), 89-96 (L3), 30-35b (H1), 47-58 (H2), and 93-101 (H3) antigen contact (MacCallum et al. J. Mol. Biol. 262: 732-745 (1996)).
별도로 지시되지 않으면, CDR은 Kabat et al., 위와 같음에 따라서 결정된다. 당업자는 CDR 지정이 Chothia, 위와 같음, McCallum, 위와 같음, 또는 임의의 다른 과학적으로 용인된 명명법 시스템에 따라서 또한 결정될 수 있다는 것을 이해할 것이다.Unless otherwise indicated, CDRs are determined according to Kabat et al., supra. Those of skill in the art will appreciate that CDR designations may also be determined according to Chothia, supra, McCallum , supra , or any other scientifically accepted system of nomenclature.
"프레임워크" 또는 "FR"은 상보성 결정 영역(CDR) 이외의 가변 도메인 잔기를 지칭한다. 가변 도메인의 FR은 일반적으로 4개의 FR 도메인들로 구성된다: FR1, FR2, FR3, 및 FR4. 따라서, CDR 및 FR 서열들은 일반적으로 VH (또는 VL)에서 다음의 순서로 나타난다: FR1-CDR-H1(CDR-L1)-FR2- CDR-H2(CDR-L2)-FR3- CDR-H3(CDR-L3)-FR4. “Framework” or “FR” refers to variable domain residues other than complementarity determining regions (CDRs). The FRs of a variable domain generally consist of four FR domains: FR1, FR2, FR3, and FR4. Thus, CDR and FR sequences generally appear in the following order in VH (or VL): FR1-CDR-H1(CDR-L1)-FR2-CDR-H2(CDR-L2)-FR3-CDR-H3(CDR) -L3)-FR4.
표현 “Kabat에서처럼 가변 도메인 잔기-넘버링” 또는 “Kabat에서처럼 아미노산-위치 넘버링” 및 이들의 변이는 Kabat et al., 위와 같음에서 항체의 편집의 중쇄 가변 도메인 또는 경쇄 가변 도메인에 이용된 넘버링 시스템을 지칭한다. 이 넘버링 체계를 사용하여, 실제 선형 아미노산 서열은 가변 도메인의 FR 또는 HVR의 단축 또는 삽입에 상응하도록 몇개 더 적은 수의 아미노산을, 또는 추가의 아미노산을 함유할 수 있다. 예를 들면, 중쇄 가변 도메인은 H2의 잔기 52 뒤에 단일 아미노산 삽입물 (예컨대, 카바트에 따른 잔기 52a), 그리고 중쇄 FR 잔기 82 뒤에 삽입된 잔기 (예를 들면, Kabat에 따른 잔기 82a, 82b 및 82c 등)를 포함할 수 있다. Kabat의 잔기 넘버링은 "표준" Kabat 넘버링 서열과 항체의 서열의 상동성 영역을 정렬하여 주어진 항체에 대하여 결정될 수 있다.The expressions “variable domain residue-numbering as in Kabat” or “amino acid-position numbering as in Kabat” and variations thereof refer to the numbering system used for heavy chain variable domains or light chain variable domains of compilation of antibodies in Kabat et al ., supra do. Using this numbering system, an actual linear amino acid sequence may contain a few fewer amino acids, or additional amino acids to correspond to shortening or insertions of FRs or HVRs of the variable domain. For example, a heavy chain variable domain may have a single amino acid insertion after residue 52 of H2 (eg, residue 52a according to Kabat) and a residue inserted after heavy chain FR residue 82 (eg, residues 82a, 82b and 82c according to Kabat) etc.) may be included. Residue numbering of Kabat can be determined for a given antibody by aligning regions of homology of the antibody's sequence with a "standard" Kabat numbering sequence.
상기 카밧 넘버링 시스템은 가변 도메인 내 잔기(대략 경쇄의 잔기 1-107 및 중쇄의 잔기 1-113)에 대하여 지칭할 때 일반적으로 사용된다 (예를 들어, Kabat et al., Sequences of Immunological Interest. 5th Ed. Public Health Service, National Institutes of Health, Bethesda, Md. (1991)). "EU 넘버링 체계" 또는 "EU 색인"은 면역글로불린 중쇄 불변 영역에서 잔기를 지칭할 때 일반적으로 사용된다 (예컨데, 상기 Kabat 외의 문헌에서 보고된 EU 색인). “Kabat의 경우에서와 같은 EU 색인”은 인간 IgG1 EU 항체의 잔기 넘버링을 지칭한다.The Kabat numbering system is generally used when referring to residues in the variable domain (approximately residues 1-107 of the light chain and residues 1-113 of the heavy chain) (eg, Kabat et al. , Sequences of Immunological Interest . 5th Ed. Public Health Service, National Institutes of Health, Bethesda, Md. (1991). "EU numbering system" or "EU index" is commonly used when referring to residues in the immunoglobulin heavy chain constant region (eg, the EU index as reported in Kabat et al., supra). “EU index as in the case of Kabat” refers to the residue numbering of the human IgG1 EU antibody.
용어 "가변"은 가변 도메인의 특정 분절들이 항체들 간 서열에 있어 광범위하게 다름을 의미한다. V 도메인은 항원 결합을 매개하고 특정 항원에 대한 특정 항체의 특이성을 정의한다. 그러나 가변성은 가변 도메인의 전체 범위에 걸쳐 고르게 분포되지 않는다. 대신 이는 경쇄 및 중쇄 가변 도메인 모두에서 초가변 영역 (HVR)이라고 불리는 3개의 분절에 집중되어 있다. 가변 도메인들 중 보다 많이 보존되는 부분들을 프레임워크 영역 (FR)이라 한다. 고유의 중쇄 및 경쇄의 각 가변 도메인들은 3개의 HVR에 의해 연결된, 대체로 베타-쉬트 배위를 취하는 4개의 FR 영역들을 포함하며, 루프 연결을 만들고, 일부 경우에는 베타-쉬트 구조의 일부가 된다. 각 쇄에서 HVRs은 FR 영역들에 의해 근접하게, 그리고 다른 쇄의 HVRs과 함께 유지되며, 항체의 항원-결합 부위 형성에 기여한다 (Kabat 외, Sequences of Immunological Interest, Fifth Edition, National Institute of Health, Bethesda, MD (1991)). 불변 도메인은 항체와 항원의 결합에 직접적으로 관여하지는 않지만, 항체 의존성 세포 독성에서의 항체의 참여와 같은 다양한 효과기 기능을 나타낸다.The term “variable” means that certain segments of a variable domain differ widely in sequence between antibodies. The V domain mediates antigen binding and defines the specificity of a particular antibody for a particular antigen. However, the variability is not evenly distributed over the entire range of the variable domain. Instead, it is concentrated in three segments called hypervariable regions (HVRs) in both the light and heavy chain variable domains. The more conserved portions of the variable domains are called framework regions (FR). Each variable domain of the native heavy and light chains comprises four FR regions, usually in beta-sheet configuration, joined by three HVRs, forming loop links, and in some cases becoming part of the beta-sheet structure. The HVRs in each chain are held in close proximity by the FR regions and together with the HVRs of the other chain, contributing to the formation of the antigen-binding site of the antibody (Kabat et al., Sequences of Immunological Interest , Fifth Edition, National Institute of Health, Bethesda, Md. (1991)). The constant domains are not directly involved in antibody-antigen binding, but exhibit various effector functions, such as participation of the antibody in antibody-dependent cytotoxicity.
항체의 "가변 영역" 또는 "가변 도메인"은 항체의 중쇄 또는 경쇄의 아미노-말단 도메인을 지칭한다. 중쇄 및 경쇄의 가변 도메인은 각각 "VH" 및 "VL"로 지칭될 수 있다. 이러한 도메인은 일반적으로 (동일 클래스의 다른 항체들에 비해) 해당 항체의 가장 가변적인 부분이며 항원 결합 부위를 포함한다.A “variable region” or “variable domain” of an antibody refers to the amino-terminal domain of the heavy or light chain of an antibody. The variable domains of the heavy and light chains may be referred to as "VH" and "VL", respectively. This domain is generally the most variable part of the antibody (relative to other antibodies of the same class) and contains the antigen binding site.
“프레임워크” 또는 “FR”은 초가변 영역 (HVR) 잔기 이외의 가변 도메인 잔기를 지칭한다. 가변 도메인의 FR은 일반적으로 4개의 FR 도메인들로 구성된다: FR1, FR2, FR3, 및 FR4. 따라서, HVR 및 FR 서열들은 일반적으로 VH (또는 VL)에서 다음의 순서로 나타난다: FR1-H1(L1)-FR2-H2(L2)-FR3-H3(L3)-FR4.“Framework” or “FR” refers to variable domain residues other than hypervariable region (HVR) residues. The FRs of a variable domain generally consist of four FR domains: FR1, FR2, FR3, and FR4. Thus, HVR and FR sequences generally appear in the following order in VH (or VL): FR1-H1(L1)-FR2-H2(L2)-FR3-H3(L3)-FR4.
본원에서 사용된 용어들 "전장 항체", "무손상 항체" 및 "전체 항체"는 항체 단편과 반대로, 실질적으로 무손상 형태의 항체를 상호교환적으로 지칭한다. 구체적으로, 전체 항체는 Fc 영역을 포함하는 중쇄 및 경쇄를 갖는 항체들을 포함한다. 불변 도메인은 고유 서열 불변 도메인 (예컨대, 인간 고유 서열 불변 도메인) 또는 이의 아미노산 서열 변이체 일 수 있다. 일부 경우, 무손상 항체는 하나 이상의 효과기 기능을 가질 수 있다.As used herein, the terms “full length antibody,” “intact antibody,” and “whole antibody” refer interchangeably to an antibody in its substantially intact form, as opposed to antibody fragments. Specifically, whole antibodies include antibodies having heavy and light chains comprising an Fc region. The constant domain may be a native sequence constant domain (eg, a human native sequence constant domain) or an amino acid sequence variant thereof. In some cases, an intact antibody may have more than one effector function.
“네이키드(naked) 항체”는 이종 모이어티(예컨대, 세포독성 모이어티) 또는 방사성표지에 접합되지 않은 항체를 지칭한다. 상기 네이키드 항체는 약학 조성물에 존재할 수 있다.A “naked antibody” refers to an antibody that is not conjugated to a heterologous moiety (eg, a cytotoxic moiety) or a radiolabel. The naked antibody may be present in a pharmaceutical composition.
“항체 단편”은 무손상 항체의 일부분, 바람직하게는 무손상 항체의 항원 결합 및/또는 가변 영역을 포함한다. 항체 단편의 예는 Fab, Fab', F(ab')2 및 Fv 단편을 포함하고; 이중체; 선형 항체(미국 특허 5,641,870, 실시예 2; Zapata et al., Protein Eng. 8(10): 1057-1062[1995]를 참조); 단일쇄 항체 분자 및 항체 단편으로부터 형성된 다중특이적 항체를 포함한다. 항체들을 파파인으로 절단하면 2개의 동일한 항원-결합 단편, 소위 “Fab” 단편, 그리고 용이하게 결정화할 수 있는 능력을 반영하는 명칭인 잔부 “Fc” 단편이 생성되었다. 상기 Fab 단편은 전적으로 경(L) 쇄와 상기 중(H) 쇄의 가변 영역 도메인 (VH), 그리고 하나의 중쇄의 제 1 불변 도메인 (CH1)으로 구성된다. 각 Fab 단편은 항원 결합과 관련하여 일가이다, 즉, 이 단편은 하나의 항원-결합 부위를 가진다. 항체를 펩신 처리하면, 상이한 항원-결합 활성을 갖는 2개의 다이설파이드로 연결된 Fab 단편에 대체로 상응하며 여전히 항원과 가교(cross-linking)하는 단일한 큰 F(ab’)2 단편이 수득된다. Fab’ 단편은 항체 힌지(hinge)의 영역으로부터의 하나 또는 그 이상의 시스테인을 포함하여 CH1 도메인의 카르복시 말단의 추가적인 몇 개 잔기를 가지므로, Fab 단편과 상이하다. Fab'-SH는 본원에서 불변 도메인의 시스테인 잔기(들)이 유리 티올기를 보유하는 Fab’를 표시한다. F(ab’)2 항체 단편은 최초에 이들 사이에 힌지 시스테인을 보유하는 Fab’ 단편 쌍으로서 생성되었다. 항체 단편의 다른 화학적 커플링 또한 공지되어 있다.An “antibody fragment” comprises a portion of an intact antibody, preferably the antigen binding and/or variable region of an intact antibody. examples of antibody fragments include Fab, Fab', F(ab') 2 and Fv fragments; duplex; linear antibody (see US Pat. No. 5,641,870, Example 2; Zapata et al., Protein Eng. 8(10): 1057-1062 [1995]); single chain antibody molecules and multispecific antibodies formed from antibody fragments. Papain cleavage of the antibodies produced two identical antigen-binding fragments, a so-called “Fab” fragment, and a residual “Fc” fragment, a name reflecting its ability to crystallize readily. The Fab fragment consists entirely of the light (L) chain and the variable region domain of the heavy (H) chain (V H ), and the first constant domain of one heavy chain ( CH 1 ). Each Fab fragment is monovalent with respect to antigen binding, ie, it has one antigen-binding site. Pepsin treatment of the antibody yields a single large F(ab′) 2 fragment that largely corresponds to two disulfide linked Fab fragments with different antigen-binding activities and still cross-links the antigen. Fab' fragments differ from Fab fragments by having an additional few residues at the carboxy terminus of the
Fc 단편은 다이설파이드에 의해 서로 함께 지지되는 두 개의 H쇄 모두의 카르복시-말단 부분을 포함한다. 항체들의 효과기 기능은 Fc 영역 내 서열들에 의해 결정되는데, 이 영역 또한 특정 유형의 세포에서 발견되는 Fc 수용체 (FcR)에 의해 인식된다.Fc fragments contain the carboxy-terminal portions of both H chains supported together by disulfides. The effector function of antibodies is determined by sequences in the Fc region, which is also recognized by the Fc receptor (FcR) found in certain types of cells.
본 발명의 항체의 "기능적 단편"은 일반적으로 무손상 항체의 항원 결합 또는 가변 영역 또는 변형된 FcR 결합 능력을 보유하거나 갖는 항체의 Fc 영역을 포함하는 무손상 항체의 일부를 포함한다. 항체 단편의 예는 선형 항체, 단일 쇄 항체 분자 및 항체 단편들로부터 형성된 다중특이적 항체를 포함한다.A “functional fragment” of an antibody of the invention generally comprises a portion of an intact antibody comprising the antigen-binding or variable region of an intact antibody or the Fc region of an antibody that retains or has altered FcR-binding ability. Examples of antibody fragments include linear antibodies, single chain antibody molecules, and multispecific antibodies formed from antibody fragments.
"Fv"는 완전한 항원 인식 및 결합 부위를 포함하는 최소 항체 단편이다. 이 단편은 단단하게 비공유 결합된, 하나의 중쇄 및 하나의 경쇄 가변 영역 도메인의 이량체로 구성된다. 이 두 도메인의 폴딩으로부터 아미노산 잔기들을 항원 결합하게 하고 항체에 항원 결합 특이성을 부여하는 6개의 초가변 루프(각각 H 및 L 쇄에서 3개의 루프)가 나온다. 그러나, 단일 가변 도메인 (또는 항원에 특이적인 3개의 HVR만을 포함하는 Fv의 절반)은 비록 전체 결합 부위보다 친화도가 더 낮기는 하지만, 여전히 항원을 인식하고, 이에 결합하는 능력을 갖는다. An “Fv” is the smallest antibody fragment comprising a complete antigen recognition and binding site. This fragment consists of a dimer of one heavy and one light chain variable region domain, bound tightly, non-covalently. From the folding of these two domains arise six hypervariable loops (three loops in the H and L chains, respectively) that allow antigen binding of amino acid residues and confer antigen binding specificity to the antibody. However, a single variable domain (or half of an Fv comprising only three HVRs specific for an antigen) still has the ability to recognize and bind antigen, albeit with a lower affinity than the entire binding site.
"sFv" 또는 "scFv"로도 약칭되는 "단일쇄 Fv"는 단일 폴리펩티드 사슬에 연결된 VH 및 VL 항체 도메인을 포함하는 항체 단편이다. 바람직하게는, sFv 폴리펩티드는 상기 VH와 VL 도메인 사이에 폴리펩티드 링커를 더 포함하는데, 이 링커는 상기 sFv가 항원 결합에 바람직한 구조를 형성하도록 한다. scFv의 내용에 관하여, 예를 들어, Pluckthun in The Pharmacology of Monoclonal Antibodies, vol. 113, Rosenburg and Moore eds., Springer-Verlag, New York, pp. 269-315 (1994)를 참조하라.A “single chain Fv”, also abbreviated as “sFv” or “scFv”, is an antibody fragment comprising V H and V L antibody domains linked to a single polypeptide chain. Preferably, the sFv polypeptide further comprises a polypeptide linker between said V H and V L domains, which linker allows said sFv to form the desired structure for antigen binding. For the content of scFv, see, eg, Pluckthun in The Pharmacology of Monoclonal Antibodies , vol. 113, Rosenburg and Moore eds., Springer-Verlag, New York, pp. 269-315 (1994).
본원에서 용어 “Fc 영역”은 불변 영역의 적어도 일부를 함유하는 면역글로불린 중쇄의 C 말단 영역을 규정하는 데 이용된다. 상기 용어는 선천적 서열 Fc 영역 및 변이체 Fc 영역을 포함한다. 한 양상에서, 인간 IgG 중쇄 Fc 영역은 중쇄의 Cys226으로부터, 또는 Pro230으로부터 카르복실 말단까지 걸친다. 하지만, 숙주 세포에 의해 생산되는 항체는 중쇄의 C 말단으로부터 하나 또는 그 이상, 특히 1개 또는 2개의 아미노산의 번역후 개열을 겪을 수 있다. 이런 이유로, 전장 중쇄를 인코딩하는 특이적 핵산 분자의 발현에 의해 숙주 세포에 의해 생산되는 항체는 전장 중쇄를 포함할 수 있거나, 또는 이것은 전장 중쇄의 개열된 변이체를 포함할 수 있다. 이는 중쇄의 최종 2개의 C-말단 아미노산이 글리신(G446) 및 리신(K447)인 경우일 수 있다. 이런 이유로, Fc 영역의 C 말단 리신 (Lys447), 또는 C 말단 글리신 (Gly446) 및 리신 (Lys447)은 존재하거나 존재하지 않을 수 있다. 본원에서 Fc 영역을 포함하는 중쇄의 아미노산 서열은 별도로 지시되지 않으면, C 말단 리신(Lys447) 없이 표시된다. 일 양태에서, 본원에 개시된 항체 내에 포함된, 본원에서 특정된 바와 같은 Fc 영역을 포함하는 중쇄는 추가의 C 말단 글리신-리신 디펩티드(G446 및 K447)를 포함한다. 일 양태에서, 본원에 개시된 항체 내에 포함된, 본원에서 특정된 바와 같은 Fc 영역을 포함하는 중쇄는 추가의 C 말단 글리신 잔기(G446 및 K447)를 포함한다. 일 양태에서, 본원에 개시된 항체 내에 포함된, 본원에서 특정된 바와 같은 Fc 영역을 포함하는 중쇄는 추가의 C 말단 리신 잔기(K447)를 포함한다. 일 양태에서, 상기 Fc 영역은 중쇄의 단일 아미노산 치환 N297A를 함유한다. 본원에서 다르게 명시되지 않는 한, Fc 영역 또는 불변 영역에서 아미노산 잔기의 넘버링은 Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, MD, 1991에 기재된 바와 같이 EU 인덱스라고도 하는 EU 넘버링 시스템에 따른다.The term “Fc region” is used herein to define the C-terminal region of an immunoglobulin heavy chain that contains at least a portion of the constant region. The term includes native sequence Fc regions and variant Fc regions. In one aspect, the human IgG heavy chain Fc region spans from Cys226, or from Pro230, to the carboxyl terminus of the heavy chain. However, antibodies produced by the host cell may undergo post-translational cleavage of one or more, in particular one or two amino acids, from the C terminus of the heavy chain. For this reason, an antibody produced by a host cell by expression of a specific nucleic acid molecule encoding a full-length heavy chain may comprise a full-length heavy chain, or it may comprise a cleaved variant of the full-length heavy chain. This may be the case when the last two C-terminal amino acids of the heavy chain are glycine (G446) and lysine (K447). For this reason, the C-terminal lysine (Lys447), or the C-terminal glycine (Gly446) and lysine (Lys447) of the Fc region may or may not be present. The amino acid sequence of a heavy chain comprising an Fc region herein is shown without a C-terminal lysine (Lys447), unless otherwise indicated. In one aspect, a heavy chain comprising an Fc region as specified herein, comprised within an antibody disclosed herein, comprises additional C-terminal glycine-lysine dipeptides (G446 and K447). In one aspect, a heavy chain comprising an Fc region as specified herein, comprised within an antibody disclosed herein, comprises additional C-terminal glycine residues (G446 and K447). In one aspect, a heavy chain comprising an Fc region as specified herein, comprised within an antibody disclosed herein, comprises an additional C-terminal lysine residue (K447). In one embodiment, said Fc region contains the single amino acid substitution N297A of the heavy chain. Unless otherwise specified herein, the numbering of amino acid residues in the Fc region or constant region is described in Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. It follows the EU numbering system, also known as the EU index, as described in Public Health Service, National Institutes of Health, Bethesda, MD, 1991.
"Fc 수용체" 또는 "FcR"은 항체의 Fc 영역에 결합하는 수용체를 기재한다. 바람직한 FcR은 천연 서열 인간 FcR이다. 더욱이, 바람직한 FcR은 IgG 항체(감마 수용체)에 결합하고 대립형질 변이체 및 대안적으로 이들 수용체의 스플라이싱된 형태를 포함하는 FcγRI, FcγRII 및 FcγRIII 서브클래스의 수용체를 포함하는 FcR이고, FcγRII는 FcγRIIA (“활성화 수용체”) 및 FcγRIIB (“억제 수용체”)를 포함하며, 이들은 유사한 아미노산 서열들을 가지는데, 이 서열들은 주로 이들의 세포질 도메인들에서 상이하다. 활성화 수용체 FcγRIIA는 세포질 도메인에 면역 수용체 티로신 기반 활성화 모티프(ITAM)를 포함한다. 억제 수용체 FcγRIIB는 세포질 도메인에서 면역수용체 티로신 기반 억제 모티프(ITIM)를 함유한다(M. Da![]()
![]()
용어 "이중체"는 VH 및 VL 도메인 사이에 짧은 링커(약 5~10개의 잔기)를 갖는(선행 단락을 참조) sFv 단편을 작제함으로써, V 도메인의 사슬내가 아닌 사슬간 쌍형성이 달성되어, 2가 단편, 즉, 2개 항원 결합 부위를 갖는 단편을 발생시킴으로써 제조되는 소형 항체 단편을 지칭한다. 이중특이적 이중체는 2개의 항체의 VH 및 VL 도메인이 상이한 폴리펩티드 사슬에 존재하는 2개의 "교차" sFv 단편의 이종이량체이다. 이중체는, 예를 들어 EP 404,097; WO 93/11161; Hollinger et al., Proc. Natl. Acad. Sci. USA 90: 6444-6448 (1993)에 상세히 기재되어 있다.The term "duplex" refers to the construction of an sFv fragment (see the preceding paragraph) with a short linker (about 5-10 residues) between the V H and V L domains, whereby interchain pairing of the V domain is achieved, rather than intrachain. It refers to small antibody fragments prepared by generating bivalent fragments, ie, fragments with two antigen binding sites. A bispecific duplex is a heterodimer of two “crossover” sFv fragments in which the V H and V L domains of the two antibodies are in different polypeptide chains. Duplexes are described, for example, in EP 404,097; WO 93/11161; Hollinger et al. , Proc. Natl. Acad. Sci. USA 90: 6444-6448 (1993).
본원의 단일클론 항체는 구체적으로 “키메라” 항체(면역글로불린)를 포함하고, 중쇄 및/또는 경쇄 부분은 특정 종으로부터 유래되거나 특정 항체 부류 또는 하위부류에 속하는 항체 내 상응하는 서열과 동일하거나 상동성인 반면, 상기 쇄(들)의 나머지는 다른 종으로부터 유래되거나 다른 항체 부류 또는 하위부류에 속하는 항체 뿐만 아니라 이들이 목적하는 생물학적 활성을 나타내는 한 상기 항체의 단편 내에서 상응하는 서열과 동일하거나 상동성이다(미국 특허 제4,816,567호; Morrison et al., Proc. Natl. Acad. Sci. USA, 81:6851-6855 (1984)). 본원의 관심이 되는 키메라성 항체에는 PRIMATIZED® 항체가 포함되며, 여기서 항체의 항원 결합 영역은, 예컨대, 관심 항원으로 마카크 원숭이를 면역화하여 생산된 항체로부터 유도된다. 본원에 사용된 "인간화 항체"는 "키메라 항체"의 하위 집합으로 사용된다.Monoclonal antibodies herein specifically include "chimeric" antibodies (immunoglobulins), wherein the heavy and/or light chain portions are identical to or homologous to the corresponding sequence in an antibody derived from a particular species or belonging to a particular antibody class or subclass. On the other hand, the rest of the chain(s) are identical or homologous to the corresponding sequences in antibodies derived from other species or belonging to other antibody classes or subclasses as well as fragments of said antibodies so long as they exhibit the desired biological activity ( U.S. Patent No. 4,816,567; Morrison et al., Proc. Natl. Acad. Sci. USA , 81 :6851-6855 (1984)). Chimeric antibodies of interest herein include PRIMATIZED ® antibodies, wherein the antigen binding region of the antibody is derived from an antibody produced, for example, by immunizing a macaque monkey with an antigen of interest. As used herein, “humanized antibody” is used as a subset of “chimeric antibody”.
항체의 “부류”는 이의 중쇄에 의해 소유된 불변 도메인 또는 불변 영역의 유형을 지칭한다. 항체에는 5가지 주요 분류가 있다: IgA, IgD, IgE, IgG, 및 IgM, 그리고 이들중 몇몇은 서브클래스(아이소형), 예컨대, IgG1, IgG2, IgG3, IgG4, IgA1, 및 IgA2로 더욱 세분될 수 있다. 상이한 클래스의 면역글로불린에 해당하는 중쇄 불변 도메인들은 각각 a, d, e, g, 및 m로 불린다.A “class” of an antibody refers to the type of constant domain or constant region possessed by its heavy chain. There are five main classes of antibodies: IgA, IgD, IgE, IgG, and IgM, and some of these subclasses (isotypes), such as IgG 1 , IgG 2 , IgG 3 , IgG 4 , IgA 1 , and It can be further subdivided into IgA 2 . The heavy chain constant domains corresponding to the different classes of immunoglobulins are called a, d, e, g, and m, respectively.
“친화성”은 분자(예컨대, 항체)의 단일 결합 부위 및 이의 결합 짝(예컨대, 항원, 예컨대 TIGIT, PD-L1, 또는 VEGF) 사이의 비공유 상호작용의 총합의 강도를 지칭한다. 달리 표시되지 않은 한, 본원에 기재된 "결합 친화도"는 결합쌍(예를 들면, 항체 및 항원)의 구성원 간의 1:1 상호작용을 반영하는 고유 결합 친화도를 의미한다. 파트너 Y에 대한 분자 X의 친화성은 일반적으로, 해리 상수 (KD)에 의해 표현될 수 있다. 친화도는 본원에 기재된 것을 포함하여 당업계에 공지된 일반적인 방법에 의해 측정될 수 있다. 결합 친화도를 측정하기 위한 구체적인 설명적 및 예시적 양상들은 아래에 기재되어 있다.“Affinity” refers to the strength of the sum total of non-covalent interactions between a single binding site of a molecule (eg, an antibody) and its binding partner (eg, an antigen, such as TIGIT, PD-L1, or VEGF). Unless otherwise indicated, "binding affinity" as used herein refers to intrinsic binding affinity that reflects a 1:1 interaction between members of a binding pair (eg, antibody and antigen). The affinity of a molecule X for its partner Y can generally be expressed by the dissociation constant (K D ). Affinity can be measured by general methods known in the art, including those described herein. Specific illustrative and exemplary aspects for determining binding affinity are described below.
"인간 항체"는 인간에 의해 생성된 항체에 상응하는 아미노산 서열을 보유하고 및/또는 본원에 개시된 인간 항체를 제조하는 임의의 기술을 사용하여 제조된 항체이다. 인간 항체의 이러한 정의는 비인간 항원 결합 잔기를 포함하는 인간화 항체를 특정적으로 배제한다. 인간 항체는 파지-디스플레이 라이브러리를 비롯하여 해당 분야에 공지된 다양한 기술을 사용하여 생성 될 수 있다. Hoogenboom and Winter, J. Mol. Biol., 227:381 (1991); Marks et al., J. Mol. Biol., 222:581 (1991). 인간 단일클론 항체의 제조를 위해, Cole et al., Monoclonal Antibodies and Cancer Therapy , Alan R. Liss, p. 77 (1985); Boerner et al., J. Immunol ., 147(1):86-95 (1991)에서 설명된 방법이 또한 입수 가능하다. 또한, van Dijk and van de Winkel, Curr. Opin. Pharmacol., 5: 368-74 (2001)를 참조한다. 인간 항체는 항원 유발접종에 반응하여 상기 항체를 생성하기 위해 개질되었지만, 그 내인성 유전자좌가 불활성화된 형질전환(transgenic) 동물, 예컨대 면역화된 제노마우스(예컨대, XENOMOUSE™ 기술에 관한 미국 특허 제6,075,181호 및 6,150,584호를 참조)에 항원을 투여함으로써 제조될 수 있다. 또한, 예를 들어 인간 B 세포 하이브리도마 기술을 통해 생성된 인간 항체에 관한 Li et al., Proc. Natl. Acad. Sci. USA, 103:3557-3562 (2006)를 참조한다.A “human antibody” is an antibody that possesses an amino acid sequence corresponding to an antibody produced by a human and/or is prepared using any technique for making human antibodies disclosed herein. This definition of a human antibody specifically excludes a humanized antibody comprising non-human antigen-binding residues. Human antibodies can be generated using a variety of techniques known in the art, including phage-display libraries. Hoogenboom and Winter, J. Mol. Biol ., 227:381 (1991); Marks et al. , J. Mol. Biol ., 222:581 (1991). For the preparation of human monoclonal antibodies, see Cole et al., Monoclonal Antibodies and Cancer Therapy, Alan R. Liss, p. 77 (1985); The method described in Boerner et al., J. Immunol., 147(1):86-95 (1991) is also available. See also van Dijk and van de Winkel, Curr. Opin. Pharmacol., 5: 368-74 (2001). Human antibodies have been modified to produce such antibodies in response to antigen challenge, but transgenic animals whose endogenous loci have been inactivated, such as immunized xenomouses (e.g., US Pat. No. 6,075,181 for XENOMOUSE™ technology) and 6,150,584). See also, for example, Li et al. , Proc. Natl. Acad. Sci. USA , 103:3557-3562 (2006).
비인간 (예를 들어, 쥐과) 항체의 "인간화된" 형태는 비인간 면역글로불린으로부터 유래된 최소 서열을 포함하는 키메라 항체이다. 한 양상에서, 인간화 항체는 수용자의 HVR (아래에 규정됨)로부터 잔기가 원하는 특이성, 친화성 및/또는 수용력을 갖는, 비인간 종 (공여자 항체), 예컨대 생쥐, 쥐, 토끼 또는 비인간 영장류의 HVR로부터 잔기에 의해 대체되는 인간 면역글로불린 (수용자 항체)이다. 일부 경우에서, 상기 인간 면역글로불린의 프레임워크 ("FR") 잔기는 대응하는 비-인간 잔기에 의해 대체된다. 게다가, 인간화 항체는 수용자 항체에서 또는 공여자 항체에서 발견되지 않는 잔기를 포함할 수 있다. 이들 변형은 항체 성능, 예를 들어, 결합 친화도를 추가로 개선하기 위해 이루어질 수 있다. 일반적으로, 비록 FR 영역이 항체 성과, 예컨대 결합 친화성, 이성화, 면역원성 등을 향상시키는 하나 또는 그 이상의 개별 FR 잔기 치환을 포함할 수 있긴 하지만, 인간화 항체는 적어도 1개, 그리고 전형적으로 2개의 가변 도메인을 실제적으로 모두 포함할 것이고, 여기서 초가변 루프 중에서 전부 또는 실제적으로 전부가 비인간 면역글로불린 서열의 것들에 상응하고, 그리고 FR 영역 중에서 전부 또는 실제적으로 전부가 인간 면역글로불린 서열의 것들이다. FR에서 이들 아미노산 치환의 수는 전형적으로, H 사슬에서 6개 이내이고 L 사슬에서 3개 이내이다. 인간화 항체는 또한 선택적으로 면역글로불린 불변 영역(Fc), 전형적으로 인간 면역글로불린의 불변 영역의 적어도 일부를 포함할 것이다. 추가적인 세부사항에 대해서는, 예컨대, Jones et al., Nature, 321:522-525 (1986); Reichmann et al., Nature, 332:323-329 (1988); and Presta, Curr. Op. Struct. Biol. 2:593-596 (1992)을 참조한다. 또한, 예를 들어 하기를 참고한다: Vaswani and Hamilton, Ann. Allergy, Asthma & Immunol. 1:105-115 (1998); Harris, Biochem. Soc. Transactions 23:1035-1038 (1995); Hurle and Gross, Curr. Op. Biotech. 5:428-433 (1994); 및 미국 특허 제6,982,321호 및 제7,087,409호를 참조한다."Humanized" forms of non-human (eg, murine) antibodies are chimeric antibodies that contain minimal sequence derived from non-human immunoglobulin. In one aspect, the humanized antibody is derived from the HVR of a non-human species (donor antibody), such as a mouse, rat, rabbit or non-human primate, wherein residues from the recipient's HVR (defined below) have the desired specificity, affinity and/or capacity. It is a human immunoglobulin (recipient antibody) replaced by a residue. In some cases, framework (“FR”) residues of the human immunoglobulin are replaced by corresponding non-human residues. Furthermore, humanized antibodies may contain residues that are not found in the recipient antibody or in the donor antibody. These modifications can be made to further improve antibody performance, eg, binding affinity. In general, humanized antibodies contain at least one, and typically two variable domains, wherein all or substantially all of the hypervariable loops correspond to those of non-human immunoglobulin sequences, and all or substantially all of the FR regions are those of human immunoglobulin sequences. The number of these amino acid substitutions in the FR is typically within 6 in the H chain and within 3 in the L chain. The humanized antibody will also optionally comprise at least a portion of an immunoglobulin constant region (Fc), typically that of a human immunoglobulin. For further details, see, eg, Jones et al. , Nature , 321:522-525 (1986); Reichmann et al. , Nature, 332:323-329 (1988); and Presta, Curr. Op. Struct. Biol. 2:593-596 (1992). See also, for example, Vaswani and Hamilton, Ann. Allergy, Asthma & Immunol . 1:105-115 (1998); Harris, Biochem. Soc. Transactions 23:1035-1038 (1995); Hurle and Gross, Curr. Op. Biotech . 5:428-433 (1994); and US Pat. Nos. 6,982,321 and 7,087,409.
본원에 개시된 다양한 항체를 설명하기 위해 사용될 때 용어 "단리된 항체"는 그것이 발현된 세포 또는 세포 배양물로부터 식별 및 분리 및/또는 회수된 항체를 의미한다. 자연 환경의 오염 성분은 해당 폴리펩티드에 대한 진단 또는 치료적 사용을 통상적으로 방해하는 물질이며, 효소, 호르몬 및 기타 단백질성 또는 비단백질성 용질을 포함 할 수 있다. 일부 양상에서, 항체는 예를 들면, 전기이동 (예를 들면, SDS-PAGE, 등전위 초점 (IEF), 모세관 전기이동) 또는 크로마토그래피 (예를 들면, 이온 교환 또는 역상 HPLC)에 의해 결정될 때, 95% 또는 99% 이상의 순도로 정제된다. 항체 순도를 평가하는 방법들을 검토하려면, 예컨대 Flatman et al., J. Chromatogr. B 848:79-87 (2007)을 참조한다. 바람직한 양상에서, 항체는 (1) 스피닝 컵 서열분석기의 이용에 의해 N 말단 또는 내부 아미노산 서열의 적어도 15개 잔기를 획득하는 데 충분한 정도까지, 또는 (2) 쿠마시 블루 또는 바람직하게는, 은 염색을 이용하여 비환원 또는 환원 조건하에 SDS-PAGE에 의해 균질성까지 정제될 것이다. 단리된 항체는 폴리펩티드 자연 환경의 최소한 하나의 성분이 존재하지 않기 때문에, 재조합 세포 내에 인시튜(in situ) 항체를 포함한다. 그러나, 통상적으로, 단리된 폴리펩티드는 최소한 하나의 정제 단계에 의해 제조될 것이다.The term “isolated antibody” when used to describe the various antibodies disclosed herein refers to an antibody that has been identified and isolated and/or recovered from the cell or cell culture in which it is expressed. Contaminant components of the natural environment are substances that would normally interfere with diagnostic or therapeutic uses for the polypeptide, and may include enzymes, hormones, and other proteinaceous or nonproteinaceous solutes. In some aspects, the antibody is determined by, e.g., electrophoresis (e.g., SDS-PAGE, isopotential focus (IEF), capillary electrophoresis) or chromatography (e.g., ion exchange or reverse phase HPLC), Purified to greater than 95% or 99% purity. For a review of methods for assessing antibody purity, see, eg, Flatman et al., J. Chromatogr. B 848:79-87 (2007). In a preferred aspect, the antibody is either (1) to an extent sufficient to obtain at least 15 residues of the N-terminal or internal amino acid sequence by use of a spinning cup sequencer, or (2) Coomassie blue or, preferably, silver staining was purified to homogeneity by SDS-PAGE under non-reducing or reducing conditions. An isolated antibody includes the antibody in situ in recombinant cells, since at least one component of the polypeptide's natural environment is absent. However, ordinarily, an isolated polypeptide will be prepared by at least one purification step.
본 명세서에서 사용되는 용어 "단클론 항체"는 실질적으로 동질성 항체 집단으로부터 획득된 항체를 지칭한다, 즉, 해당 집단을 포함하는 개별 항체들은 동일하며 및/또는 동일한 에피토프에 결합하며, 다만, 예를 들어, 자연 발생적 돌연변이를 내포하는 또는 단클론 항체 제재를 만드는 동안 발생되는 변이체 항체들이 있을 수 있으며, 이러한 변이체들은 일반적으로 소량으로 존재한다. 상이한 결정인자 (에피토프)에 대해 지향된 상이한 항체를 전형적으로 포함하는 다중클론 항체 제조물과 대조적으로, 단일클론 항체 제조물의 각 단일클론 항체는 항원 상에서 단일 결정인자에 대해 지향된다. 따라서, 수식어 “단일클론”은 항체의 실제적으로 균질한 모집단으로부터 획득되는 것으로서 항체의 특징을 표시하고, 그리고 임의의 특정 방법에 의한 항체의 생성을 필요로 하는 것으로 해석되지 않는다. 예를 들어, 본 발명에 따른 단일클론 항체는 하이브리도마 방법, 재조합 DNA 방법, 파지 전시 방법, 및 인간 면역글로불린 좌위 중에서 전부 또는 일부를 내포하는 유전자도입 동물을 활용하는 방법을 포함하지만 이들에 한정되지 않는 다양한 기술에 의해 만들어질 수 있다.As used herein, the term "monoclonal antibody" refers to an antibody obtained from a population of substantially homogeneous antibodies, i.e., the individual antibodies comprising the population are identical and/or bind the same epitope, provided that, for example, There may be variant antibodies, which contain naturally occurring mutations, or which arise during the making of monoclonal antibody preparations, and such variants are generally present in small amounts. In contrast to polyclonal antibody preparations that typically include different antibodies directed against different determinants (epitopes), each monoclonal antibody of a monoclonal antibody preparation is directed against a single determinant on an antigen. Accordingly, the modifier "monoclonal" indicates the character of the antibody as being obtained from a substantially homogeneous population of antibodies, and is not to be construed as requiring production of the antibody by any particular method. For example, monoclonal antibodies according to the present invention include, but are not limited to, hybridoma methods, recombinant DNA methods, phage display methods, and methods utilizing transgenic animals containing all or part of a human immunoglobulin locus. It can be made by a variety of technologies that are not available.
본원에서 사용된, 용어 "~에 특이적으로 결합하는" 또는 "~에 특이적인"은, 표적 및 항체 간의 결합과 같은 측정가능하고 재현가능한 상호작용을 지칭하며, 이는 생물학적 분자를 비롯한 분자의 이종성 집단의 존재하에서 표적의 존재를 결정한다. 예를 들면, 표적 (에피토프일 수 있음)에 특이적으로 결합하는 항체는 다른 표적에 결합하는 것보다 더 큰 친화도, 결합력으로, 더욱 쉽게, 및/또는 더 긴 지속시간으로 상기 표적에 결합하는 항체이다. 한 양상에서, 관련 없는 표적에 항체의 결합의 정도는 예를 들면, 방사면역분석 (RIA)에 의해 계측될 때 표적에 대한 상기 항체의 결합의 약 10%보다 적다. 일정한 양상에서, 표적에 특이적으로 결합하는 항체는 ≤ 1 μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, 또는 ≤ 0.1 nM의 해리 상수 (KD)를 갖는다. 일정한 양상에서, 항체는 상이한 종으로부터 단백질 사이에서 보존되는 단백질 상에 에피토프에 특이적으로 결합한다. 다른 양상에서, 특이적 결합은 배타적 결합을 포함할 수 있지만, 이를 필요로 하지는 않는다. 본원에서 사용되는 이 용어는, 예를 들어, 표적에 대해 10-4 M 이하, 대안적으로 10-5 M 이하, 대안적으로 10-6 M 이하, 대안적으로 10-7 M 이하, 대안적으로 10-8 M 이하, 대안적으로 10-9 M 이하, 대안적으로 10-10 M 이하, 대안적으로 10-11 M 이하, 대안적으로 10-12 M 이하의 KD 또는 10-4 M 내지 10-6 M 또는 106M 내지 1010M 또는 107 M 내지 109M 범위의 KD를 가지는 분자에 의해 나타낼 수 있다. 당업자에 의해 이해되는 바와 같이, 친화도 및 KD 값은 반비례한다. 항원에 대한 높은 친화도는 낮은 KD 값으로 측정된다. 한 양상에서, 용어 “특이적 결합”은 분자가 임의의 다른 폴리펩티드 또는 폴리펩티드 에피토프에 실제적으로 결합하지 않으면서, 특정 폴리펩티드 또는 특정 폴리펩티드 상에서 에피토프에 결합하는 결합을 지칭한다.As used herein, the term "specifically binds to" or "specific Determine the presence of a target in the presence of a population. For example, an antibody that specifically binds to a target (which may be an epitope) binds to that target with greater affinity, avidity, more readily, and/or longer duration than it binds to another target. is an antibody In one aspect, the extent of binding of the antibody to an unrelated target is less than about 10% of the binding of the antibody to the target as measured, for example, by radioimmunoassay (RIA). In certain aspects, an antibody that specifically binds a target has a dissociation constant (K D ) of < 1 μM, < 100 nM, < 10 nM, < 1 nM, or < 0.1 nM. In certain aspects, an antibody specifically binds to an epitope on a protein that is conserved among proteins from different species. In another aspect, specific binding can include, but does not require, exclusive binding. As used herein, this term includes, for example, 10 -4 M or less, alternatively 10 -5 M or less, alternatively 10 -6 M or less, alternatively 10 -7 M or less, alternatively, for a target or less as 10 -8 M or less, alternatively 10 -9 M or less, alternatively 10 -10 M or less, alternatively 10 -11 M or less, alternatively 10 -12 M or less K D or 10 -4 M to 10 -6 M or 10 6 M to 10 10 M or 10 7 M to 10 9 M. As will be understood by one of ordinary skill in the art, affinity and K D values are inversely proportional. A high affinity for an antigen is measured by a low K D value. In one aspect, the term “specific binding” refers to binding in which the molecule binds to a particular polypeptide or epitope on a particular polypeptide without substantially binding to any other polypeptide or polypeptide epitope.
기준 폴리펩티드 서열에 대한 "퍼센트(%) 아미노산 서열 동일성"은 기준 폴리펩티드 서열의 아미노산 잔기와 동일한 후보 서열의 아미노산 잔기들의 백분율로 정의되는데, 이때 서열을 정렬시킨 후 최대 서열 동일성 백분율을 달성하기 위하여 필요하다면 갭을 도입하며, 임의의 보존적 치환은 상기 서열의 동일성의 일부로서 간주하지 않는다. 아미노산 서열 동일성 퍼센트를 결정하기 위한 정렬은 예를 들어 BLAST, BLAST-2, ALIGN 또는 Megalign (DNASTAR) 소프트웨어와 같은 공개적으로 이용가능한 컴퓨터 소프트웨어를 사용하여 해당 업계의 기술 범위에 속하는 다양한 방법으로 구현될 수 있다. 당업자는 비교되는 서열들의 전체 길이에 걸쳐 최대 정렬을 구현하는 데 필요한 임의의 알고리즘을 포함하여 서열들을 정렬하기 위한 적절한 매개변수를 결정할 수 있다. 그러나, 본원의 목적을 위해, 아미노산 서열 동일성 % 값은 서열 비교 컴퓨터 프로그램 ALIGN-2를 사용하여 생성된다. ALIGN-2 서열 비교 컴퓨터 프로그램은 Genentech, Inc.에서 제작되었으며 소스 코드는 미국 워싱턴 D.C., 20559에 소재한 미국 저작권청에 사용자 문서와 함께 제출되었으며, 미국 저작권 등록 번호 TXU510087로 등록되었다. ALIGN-2 프로그램은 캘리포니아주 사우스 샌프란시스코에 소재한 Genentech, Inc.사로부터 공개적으로 이용가능하거나 소스 코드로부터 컴파일될 수 있다. ALIGN-2 프로그램은 디지털 UNIX V4.0D를 포함한 UNIX 운영 체제에서 사용되도록 컴파일해야 한다. 모든 서열 비교 매개변수는 ALIGN-2 프로그램에 의해 설정되며 변경되지 않는다. "Percent (%) amino acid sequence identity" to a reference polypeptide sequence is defined as the percentage of amino acid residues in a candidate sequence that are identical to the amino acid residues in the reference polypeptide sequence, if necessary to achieve the maximum percent sequence identity after aligning the sequences. Gaps are introduced, and any conservative substitutions are not considered as part of the identity of the sequences. Alignment to determine percent amino acid sequence identity can be implemented in a variety of ways within the skill of the art using publicly available computer software such as, for example, BLAST, BLAST-2, ALIGN or Megalign (DNASTAR) software. have. One of ordinary skill in the art can determine appropriate parameters for aligning sequences, including any algorithms necessary to achieve maximal alignment over the entire length of the sequences being compared. However, for purposes herein, % amino acid sequence identity values are generated using the sequence comparison computer program ALIGN-2. The ALIGN-2 sequence comparison computer program was produced by Genentech, Inc., the source code was submitted with user documentation to the United States Copyright Office, Washington, D.C., 20559, United States, and registered under the United States Copyright Registration No. TXU510087. The ALIGN-2 program is publicly available from Genentech, Inc. of South San Francisco, CA or may be compiled from source code. The ALIGN-2 program must be compiled for use on UNIX operating systems, including digital UNIX V4.0D. All sequence comparison parameters are set by the ALIGN-2 program and are not changed.
ALIGN-2가 아미노산 서열 비교에 사용되는 경우, 주어진 아미노산 서열 B에, 이와 관련한, 또는 이에 대한 주어진 아미노산 서열 A의 아미노산 서열 동일성 %는 (다른 방식으로, 주어진 아미노산 서열 B에, 이와 관련한, 또는 이에 대한 특정 아미노산 서열 동일성 %를 가지는 또는 포함하는 주어진 아미노산 서열 A로 표현될 수 있음) 다음과 같이 계산된다:When ALIGN-2 is used for amino acid sequence comparison, the percent amino acid sequence identity of a given amino acid sequence A to, with respect to, or with respect to a given amino acid sequence B is (which can be expressed as a given amino acid sequence A having or comprising a specific % amino acid sequence identity to) is calculated as follows:
100 x 분율 X/Y100 x fraction X/Y
이때 X는 A와 B의 프로그램 정렬에서 서열 정렬 프로그램 ALIGN-2에 의해 동일한 매치로 기록되는 아미노산 잔기의 수를 말하며, Y는 B의 전체 아미노산 잔기 수가 된다. 아미노산 서열 A의 길이는 아미노산 서열 B의 길이와 동일하지 않는 경우, B에 대한 A의 아미노산 서열 동일성 %는 A에 대한 B의 아미노산 서열 동일성 %와 동일하지 않은 것으로 인정된다. 달리 특정 언급이 없는 한, 본원에서 이용된 모든 아미노산 서열 동일성 % 값은 ALIGN-2 컴퓨터 프로그램을 이용하여 바로 전 단락에서 설명된 바와 같이 수득된다.In this case, X refers to the number of amino acid residues recorded as the same match by the sequence alignment program ALIGN-2 in the program alignment of A and B, and Y is the total number of amino acid residues in B. If the length of amino acid sequence A is not equal to the length of amino acid sequence B, it is recognized that the % amino acid sequence identity of A to B is not equal to the % amino acid sequence identity of B to A. Unless otherwise specified, all amino acid sequence identity % values used herein are obtained as described in the immediately preceding paragraph using the ALIGN-2 computer program.
본원에 사용된 "대상체" 또는 "개체"는 인간 또는 비인간 포유동물, 예컨대 소, 말, 개, 양 또는 고양이를 포함하나 이에 제한되지 않는 포유동물을 의미한다. 일부 양태들에서, 상기 대상체는 인간이다. 본원에서 환자 또한 대상체이다. As used herein, “subject” or “individual” means a mammal, including, but not limited to, a human or non-human mammal, such as a cow, horse, dog, sheep, or cat. In some aspects, the subject is a human. A patient herein is also a subject.
용어 "환자"는 인간 환자를 지칭한다. 예를 들어, 상기 환자는 성인이다.The term “patient” refers to a human patient. For example, the patient is an adult.
용어 "진단"은 분자 또는 병리학적 상태, 질병 또는 병태(예컨대, 암)의 식별 또는 분류를 지칭하기 위해 본원에서 사용된다. 예를 들어, "진단"은 특정 유형의 암의 식별을 지칭 할 수 있다. "진단"은 또한 예를 들어, 조직병리학적 기준 또는 분자 특징 (예를 들어, 바이오마커 (예를 들어, 특정 유전자 또는 상기 유전자들에 의해 인코드된 단백질) 하나 또는 이들의 조합의 발현을 특징으로하는 아형)에 의한, 암의 특정 아형의 분류를 지칭 할 수 있다.The term “diagnosis” is used herein to refer to the identification or classification of a molecular or pathological condition, disease or condition (eg, cancer). For example, “diagnosing” may refer to the identification of a particular type of cancer. "Diagnosis" also characterizes the expression of one or a combination of, e.g., histopathological criteria or molecular characteristics (e.g., biomarkers (e.g., specific genes or proteins encoded by said genes). It can refer to the classification of a specific subtype of cancer by subtype).
본원에서 사용된 바와 같이, 용어 "샘플"은, 예를 들어 물리적, 생화학적, 화학적 및/또는 생리학적 특성을 기준으로 특성화되고/되거나 식별되어야만 하는 세포 및/또는 다른 분자 실체를 함유하는 목적하는 대상체 및/또는 개체로부터 수득되거나 유래된 조성물을 지칭한다. 예를 들어, 문구 "종양 샘플", "질병 샘플" 및 이의 변화형은 특성화되는 세포 및/또는 분자 실체를 함유하는 것으로 공지된 또는 예상되는 관심 대상체로부터 수득된 임의의 샘플을 지칭한다. 표본은 조직 표본, 일차 또는 배양된 세포 또는 세포주, 세포 상층액, 세포 용해물, 혈소판, 혈청, 혈장, 유리체액, 림프액, 윤활액, 여포액, 정액, 양수, 유액, 전혈, 혈액 유래된 세포, 소변, 뇌척수액, 타액, 객담, 눈물, 땀, 점액, 종양 용해물, 그리고 조직 배양 배지, 조직 추출물, 예컨대 균질화된 조직, 종양 조직, 세포 추출물, 그리고 이들의 조합을 포함하지만 이들에 한정되지 않는다. As used herein, the term "sample" refers to a desired target containing cellular and/or other molecular entities that must be characterized and/or identified based, for example, on physical, biochemical, chemical and/or physiological properties. Refers to a composition obtained or derived from a subject and/or individual. For example, the phrases "tumor sample", "disease sample" and variants thereof refer to any sample obtained from a subject of interest known or expected to contain the cellular and/or molecular entity being characterized. Specimens may include tissue samples, primary or cultured cells or cell lines, cell supernatants, cell lysates, platelets, serum, plasma, vitreous humor, lymph fluid, synovial fluid, follicular fluid, semen, amniotic fluid, fluid, whole blood, blood-derived cells, urine, cerebrospinal fluid, saliva, sputum, tears, sweat, mucus, tumor lysates, and tissue culture media, tissue extracts such as homogenized tissue, tumor tissue, cell extracts, and combinations thereof.
"조직 샘플" 또는 "세포 샘플"은 대상자 또는 개체의 조직으로부터 수득된 유사한 세포의 수집물을 의미한다. 조직 또는 세포 샘플의 출처는 신선한, 동결된 및/또는 보존된 장기, 조직 표본, 생검 및/또는 흡인물로부터 얻은 고형 조직; 혈액 또는 임의의 혈액 성분, 예컨대 혈장; 체액, 예컨대 뇌척수액, 양수, 복막액, 또는 사이질액; 대상자의 임신 또는 발생에 있어서의 임의의 시점에서 얻은 세포일 수 있다. 조직 표본은 또한, 일차 또는 배양된 세포 또는 세포주일 수 있다. 임의적으로, 조직 또는 세포 표본은 질환 조직/장기로부터 획득된다. 예를 들어, "종양 샘플"은 종양 또는 기타 암 조직에서 얻은 조직 샘플이다. 조직 샘플은 세포 유형들 (예컨대, 종양 세포 및 비 종양 세포, 암 세포 및 비암 세포)이 혼합된 집단을 포함 할 수 있다. 조직 표본은 자연에서 조직과 자연적으로 혼합되지 않는 화합물, 예컨대 보존제, 항응고제, 완충액, 고정제, 영양소, 항생제, 또는 기타 유사한 것을 내포할 수 있다. 일부 양태들에서, 상기 샘플은 종양 조직 샘플이다. 일부 양태들에서, 상기 종양 조직 샘플은 UC 종양 조직 샘플(예컨대, 방광암 종양 조직 샘플(예컨대, MIBC 종양 조직 샘플))이다. 일부 양태들에서, 상기 샘플은 방광 종양의 경요도 절제술(TURBT) 샘플이다. 일부 양태들에서, 상기 샘플은 방광 절제술 또는 신장 절제술 샘플이다. 다른 양태들에서, 상기 종양 조직 샘플은 폐암 종양 조직 샘플(예컨대, 조기 폐암 조직 샘플(예컨대, NSCLC 종양 조직 샘플(예컨대, II기, IIIA기, 또는 IIIB기 NSCLC 종양 조직 샘플)), 예컨대, 편평 또는 비편평 NSCLC 종양 조직 샘플, 예컨대, 절제 가능한 NSCLC 종양 조직 샘플))이다. 일부 양태들에서, 상기 샘플은 국소 진행성 절제불가능한 NSCLC 종양 조직 샘플(예컨대, IIIB기 NSCLC 종양 조직 샘플), 또는 재발성 또는 전이성 NSCLC 종양 조직 샘플(예컨대, IV기 NSCLC 종양 조직 샘플), 췌장암 종양 조직 샘플(예컨대, PDAC 종양 조직 샘플), 예컨대, 전이성 PDAC 종양 조직 샘플), 또는 유방암 종양 조직 샘플(예컨대, HER2+ 유방암 종양 조직 샘플 또는 TNBC 종양 조직 샘플)이다. "Tissue sample" or "cell sample" means a collection of similar cells obtained from the tissue of a subject or individual. Sources of tissue or cell samples include solid tissue obtained from fresh, frozen and/or preserved organs, tissue specimens, biopsies and/or aspirates; blood or any blood component such as plasma; bodily fluids such as cerebrospinal fluid, amniotic fluid, peritoneal fluid, or interstitial fluid; The cells may be obtained at any point in the subject's pregnancy or development. The tissue sample may also be primary or cultured cells or cell lines. Optionally, the tissue or cell sample is obtained from a diseased tissue/organ. For example, a “tumor sample” is a tissue sample obtained from a tumor or other cancerous tissue. A tissue sample may comprise a population of a mixture of cell types (eg, tumor cells and non-tumor cells, cancer cells and non-cancer cells). A tissue sample may contain compounds that do not naturally mix with the tissue in nature, such as preservatives, anticoagulants, buffers, fixatives, nutrients, antibiotics, or the like. In some aspects, the sample is a tumor tissue sample. In some aspects, the tumor tissue sample is a UC tumor tissue sample (eg, a bladder cancer tumor tissue sample (eg, a MIBC tumor tissue sample)). In some aspects, the sample is a transurethral resection (TURBT) sample of a bladder tumor. In some aspects, the sample is a cystectomy or nephrectomy sample. In other aspects, the tumor tissue sample is a lung cancer tumor tissue sample (eg, an early lung cancer tissue sample (eg, a NSCLC tumor tissue sample (eg, a stage II, IIIA, or IIIB NSCLC tumor tissue sample)), such as a squamous or a non-squamous NSCLC tumor tissue sample, such as a resectable NSCLC tumor tissue sample)). In some aspects, the sample is a locally advanced unresectable NSCLC tumor tissue sample (eg, stage IIIB NSCLC tumor tissue sample), or a recurrent or metastatic NSCLC tumor tissue sample (eg, stage IV NSCLC tumor tissue sample), pancreatic cancer tumor tissue a sample (eg, a PDAC tumor tissue sample), eg, a metastatic PDAC tumor tissue sample), or a breast cancer tumor tissue sample (eg, a HER2+ breast cancer tumor tissue sample or a TNBC tumor tissue sample).
본원의 목적을 위해, 조직 샘플의 "절편"은 조직 샘플의 단일 부분 또는 조각, 예를 들어, 조직 샘플 (예를 들어, 종양 샘플)로부터 절단된 조직 또는 세포의 얇은 슬라이스를 의미한다. 조직 샘플의 동일한 섹션이 양쪽 형태적 및 분자적 수준에서 분석될 수 있거나, (예를 들면, 면역조직화학에 의해) 폴리펩타이드 및/또는 (예를 들면, 원 위치에서 하이브리드화에 의해) 폴리뉴클레오타이드에 관하여 분석될 수 있다는 것이 이해된다면, 조직 샘플의 다중 섹션이 얻어질 수 있고 분석에 적용될 수 있다는 것이 이해되어야 한다.For purposes herein, a “section” of a tissue sample means a single portion or piece of a tissue sample, eg, a thin slice of tissue or cells cut from a tissue sample (eg, a tumor sample). The same section of a tissue sample can be analyzed at both morphological and molecular levels, or polypeptides and/or polynucleotides (e.g., by in situ hybridization) (e.g., by immunohistochemistry) It is to be understood that multiple sections of a tissue sample can be obtained and subjected to analysis, if it is understood that they can be analyzed with respect to
본원에서 사용되는, "참조 샘플", "참조 세포", "참조 조직", "대조 표본", "대조 세포", 또는 "대조 조직"은 비교 목적으로 이용되는 표본, 세포, 조직, 표준, 또는 수준을 지칭한다. 일 구체예에서, 참조 샘플, 참조 세포, 참조 조직, 대조 샘플, 대조 세포, 또는 대조 조직은, 동일한 대상자 또는 개체의 신체 (예를 들어, 조직 또는 세포)의 건강한 및/또는 비-질병 부분으로부터 수득될 수 있다. 예를 들어, 참조 샘플, 참조 세포, 참조 조직, 대조 샘플, 대조 세포 또는 대조 조직은 질환에 걸린 세포 또는 조직 (예컨대, 종양에 인접한 세포 또는 조직)에 인접한 건강한 및/또는 비-질환 세포 또는 조직 일 수 있다. 또 다른 구체예에서, 참조 샘플은 동일한 대상자 또는 개체의 신체의 비처리된 조직 및/또는 세포로부터 수득된다. 또한 또 다른 구체예에서, 참조 샘플, 참조 세포, 참조 조직, 대조군 샘플, 대조군 세포, 또는 대조군 조직은, 상기 대상자 또는 개체가 아닌 개체의 신체(예를 들어, 조직 또는 세포)의 건강하고/하거나 비-질병 부분으로부터 수득될 수 있다. 추가의 또 다른 구체예에서, 참조 샘플, 참조 세포, 참조 조직, 대조 샘플, 대조 세포, 또는 대조 조직은, 상기 대상자 또는 개체가 아닌 개체의 신체의 비처리된 조직 및/또는 세포로부터 수득될 수 있다.As used herein, “reference sample”, “reference cell”, “reference tissue”, “control sample”, “control cell”, or “control tissue” refers to a sample, cell, tissue, standard, or refers to the level. In one embodiment, the reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is from a healthy and/or non-diseased portion of the body (eg, tissue or cell) of the same subject or individual. can be obtained. For example, a reference sample, reference cell, reference tissue, control sample, control cell or control tissue is a healthy and/or non-diseased cell or tissue adjacent to a diseased cell or tissue (eg, a cell or tissue adjacent to a tumor). can be In another embodiment, the reference sample is obtained from untreated tissues and/or cells of the body of the same subject or individual. In yet another embodiment, a reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is a healthy and/or It can be obtained from non-disease parts. In yet another embodiment, a reference sample, reference cell, reference tissue, control sample, control cell, or control tissue may be obtained from untreated tissue and/or cells of the body of an individual other than the subject or individual. have.
본원에서 사용되는 용어 "단백질"은, 달리 지시가 없는 한, 영장류 (예컨대, 인간) 및 설치류 (예컨대, 마우스 및 랫트)와 같은 포유동물을 포함한 임의의 척추동물 출처의 임의의 고유 단백질을 지칭한다. 이 용어는 "전장"의, 비처리 단백질, 뿐만 아니라 세포에서 처리된 임의의 형태의 단백질을 포함한다. 이 용어는 또한 단백질의 자연 발생 변이체, 예를 들어, 스플라이스 변이체 또는 대립유전자 변이체를 포함한다. The term "protein," as used herein, unless otherwise indicated, refers to any native protein of any vertebrate origin, including mammals such as primates (eg, humans) and rodents (eg, mice and rats). . The term includes "full length", untreated proteins, as well as any form of protein that has been processed in a cell. The term also includes naturally occurring variants of a protein, eg, splice variants or allelic variants.
본원에서 호환적으로 사용되는 "폴리뉴클레오티드" 또는 "핵산"은 임의의 길이의 뉴클레오티드의 중합체를 지칭하고, DNA 및 RNA를 포함한다. 뉴클레오티드는 데옥시리보뉴클레오티드, 리보뉴클레오티드, 변형된 뉴클레오티드 또는 염기 및/또는 이들의 유사체, 또는 DNA 또는 RNA 중합효소에 의해 또는 합성 반응에 의해 중합체에 통합 될 수 있는 임의의 기질 일 수 있다. 따라서, 예를 들어, 본원에 정의된 폴리뉴클레오티드는 제한없이 단일- 및 이중-가닥 DNA, 단일- 및 이중-가닥 영역을 포함하는 DNA, 단일- 및 이중-가닥 RNA, 및 단일- 및 이중-가닥 영역을 포함하는 RNA, 단일-가닥 또는, 보다 일반적으로 이중-가닥이거나 또는 단일- 및 이중-가닥 영역을 포함 할 수 있는 DNA 및 RNA를 포함하는 하이브리드 분자를 포함한다. 또한, 본원에 사용된 용어 "폴리뉴클레오티드"는 RNA 또는 DNA 또는 RNA 및 DNA모두를 포함하는 삼중-가닥 영역들을 지칭한다. 이러한 영역들의 가닥들은 동일한 분자 또는 다른 분자로부터 유래할 수 있다. 이들 영역들은 하나 이상의 분자들 모두를 포함 할 수 있지만, 보다 일반적으로 분자들 중 일부 영역만을 포함한다. 삼중-나선 영역의 분자들 중 하나는 종종 올리고뉴클레오티드이다. 용어 "폴리뉴클레오티드" 및 "핵산"은 구체적으로 mRNA 및 cDNA를 포함한다. "Polynucleotide" or "nucleic acid," as used interchangeably herein, refers to a polymer of nucleotides of any length, and includes DNA and RNA. A nucleotide can be a deoxyribonucleotide, a ribonucleotide, a modified nucleotide or base and/or analogs thereof, or any substrate that can be incorporated into a polymer by DNA or RNA polymerase or by a synthetic reaction. Thus, for example, polynucleotides as defined herein include, without limitation, single- and double-stranded DNA, DNA comprising single- and double-stranded regions, single- and double-stranded RNA, and single- and double-stranded DNA. RNA comprising a region, single-stranded or, more generally, double-stranded, or hybrid molecule comprising DNA and RNA, which may comprise single- and double-stranded regions. Also, as used herein, the term “polynucleotide” refers to triple-stranded regions comprising RNA or DNA or both RNA and DNA. The strands of these regions may be from the same molecule or from different molecules. These regions may contain all of one or more molecules, but more generally contain only some regions of the molecules. One of the molecules of the triple-helix region is often an oligonucleotide. The terms “polynucleotide” and “nucleic acid” specifically include mRNA and cDNA.
폴리뉴클레오티드는 변형된 뉴클레오티드, 가령, 메틸화된 뉴클레오티드 및 이의 유사체를 포함할 수 있다. 존재하는 경우, 뉴클레오티드 구조에 대한 변형들은 중합체 어셈블리 전 또는 이후에 부여될 수 있다. 뉴클레오티드들의 서열은 비-뉴클레오티드 성분들에 의해 불연속될 수 있다. 폴리뉴클레오티드는 합성 후, 가령, 표지와의 접합에 의해 추가로 변형 될 수 있다. 다른 유형의 변형들은, 예를 들면, “캡”, 하나 이상의 자연-발생 뉴클레오티드를 유사체로 치환, 뉴클레오티드간 변형, 가령, 예를 들면, 비하전된 연결부 (예컨대, 메틸 포스포네이트, 포스포트리에스테르, 포스포라미데이트, 카바메이트, 등) 및 하전된 연결부 (예컨대, 포스포로티오에이트, 포스포로디티오에이트, 등)로 변형, 부속 모이어티, 가령, 예를 들면, 단백질 (예컨대, 뉴클레아제, 독소, 항체, 신호 펩티드, 폴리-L-리신, 등)로 변형, 인터칼레이터 (예컨대, 아크리딘, 소랄렌, 등)로 변형, 킬레이터 (예컨대, 금속, 방사성 금속, 붕소, 산화성 금속, 등)를 포함한 변형, 알킬화제를 포함한 변형, 변형된 연결부 (예컨대, 알파 아노머 핵산)로 변형, 뿐만 아니라 폴리뉴클레오티드(들)의 비변형 형태를 포함한다. 또한, 당에 통상적으로 존재하는 임의의 하이드록실 그룹은, 예를 들어, 포스포네이트 그룹, 포스페이트 그룹으로 대체되거나, 표준 보호 그룹에 의해 보호되거나, 또는 활성화되어, 추가 뉴클레오티드에 대한 추가 연결부를 제조할 수 있으며, 또는 고체 또는 반-고체 지지체에 접합될 수 있다. 5' 및 3' 말단 OH는 인산화되거나 아민 또는 1 내지 20개 탄소 원자의 유기 캡핑 그룹 모이어티로 치환 될 수 있다. 다른 하이드록실기는 표준 보호 그룹들로 유도 될 수도 있다. 폴리뉴클레오티드는 또한, 예를 들어, 2'-O-메틸-, 2'-O-알릴-, 2'-플루오로-, 또는 2'-아지도-리보스, 카보사이클릭 당 유사체, α-아노머 당, 에피머 당, 가령, 아라비노스, 자일로스 또는 릭소스, 피라노스 당, 푸라노스 당, 세도헵툴로스, 아사이클릭 유사체 및 비염기성 뉴클레오시드 유사체, 가령, 메틸 리보시드를 비롯한, 당업계에 일반적으로 공지된 리보스 또는 데옥시리보스 당의 유사 형태들을 포함할 수 있다. 하나 이상의 포스포디에스테르 연결부는 다른 연결 그룹으로 대체 될 수 있다. 이들 대안적 연결 기는 인산염이 P(O)S (“티오에이트”), P(S)S (“디티오에이트”), (O)NR2 (“아미데이트”), P(O)R, P(O)OR’, CO 또는 CH2 (“포름아세탈”)에 의해 대체되는 양상을 포함하지만 이들에 한정되지 않는데, 여기서 각 R 또는 R’은 독립적으로 H, 또는 에테르 (-O-) 연쇄, 아릴, 알케닐, 시클로알킬, 시클로알케닐 또는 아르알딜을 임의적으로 내포하는 치환되거나 치환되지 않은 알킬 (1-20 C)이다. 폴리뉴클레오티드의 모든 연결부들이 동일 할 필요는 없다. 상기 설명은 RNA 및 DNA를 비롯하여 본원에서 언급된 모든 폴리뉴클레오티드에 적용된다.Polynucleotides may include modified nucleotides, such as methylated nucleotides and analogs thereof. If present, modifications to the nucleotide structure may be imparted before or after polymer assembly. The sequence of nucleotides may be discontinuous by non-nucleotide components. The polynucleotide may be further modified after synthesis, such as by conjugation with a label. Other types of modifications include, for example, “caps”, substitution of one or more naturally-occurring nucleotides with analogs, internucleotide modifications, such as, for example, uncharged linkages (eg, methyl phosphonates, phosphotriesters). , phosphoramidates, carbamates, etc.) and charged linkages (eg, phosphorothioates, phosphorodithioates, etc.), modified with accessory moieties, such as, for example, proteins (eg, nucleas). agents, toxins, antibodies, signal peptides, poly-L-lysine, etc.), modified with intercalators (eg acridine, psoralen, etc.), chelators (eg metals, radioactive metals, boron, oxidizing metals, etc.), modifications with alkylating agents, modifications with modified linkages (eg, alpha anomeric nucleic acids), as well as unmodified forms of the polynucleotide(s). In addition, any hydroxyl groups ordinarily present in sugars can be replaced with, for example, phosphonate groups, phosphate groups, protected by standard protecting groups, or activated to create additional linkages to additional nucleotides. may be, or may be bonded to a solid or semi-solid support. The 5' and 3' terminal OH may be phosphorylated or substituted with an amine or an organic capping group moiety of 1 to 20 carbon atoms. Other hydroxyl groups can also be derivatized with standard protecting groups. Polynucleotides can also be, for example, 2'-O-methyl-, 2'-O-allyl-, 2'-fluoro-, or 2'-azido-ribose, carbocyclic sugar analogs, α-ano Mer sugars, epimeric sugars such as arabinose, xylose or lyxose, pyranose sugar, furanose sugar, sedoheptulose, acyclic analogs and abasic nucleoside analogs such as sugars, including methyl riboside similar forms of ribose or deoxyribose sugars generally known in the art. One or more phosphodiester linkages may be replaced by other linkages. These alternative linking groups include P(O)S (“thioate”), P(S)S (“dithioate”), (O)NR 2 (“amidate”), P(O)R, P(O)OR′, CO or CH 2 (“formacetal”), wherein each R or R′ is independently H, or an ether (-O-) linkage. , substituted or unsubstituted alkyl (1-20 C) optionally containing aryl, alkenyl, cycloalkyl, cycloalkenyl or araldyl. Not all linkages of a polynucleotide need be identical. The above description applies to all polynucleotides mentioned herein, including RNA and DNA.
본원에 사용된 "담체"는 사용되는 투여량 및 농도에서 노출될 세포 또는 포유동물에 비독성인 약학적으로 허용되는 담체, 부형제 또는 안정화제를 포함한다. 종종 생리학적으로 허용되는 담체는 수성 pH 완충액이다. 생리학적으로 허용되는 담체의 예에는 완충액, 예를 들어, 포스페이트, 시트레이트, 및 다른 유기산; 아스코르브산을 포함하는 항산화제; 저분자량 (약 10개 잔기 미만) 폴리펩티드; 단백질, 예컨대 혈청 알부민, 젤라틴, 또는 면역글로불린; 친수성 중합체, 예컨대 폴리비닐피롤리돈; 아미노산, 예컨대 글리신, 글루타민, 아스파라긴, 아르기닌, 또는 라이신; 단당류, 이당류, 및 글루코스, 만노스, 또는 덱스트린을 비롯한 다른 탄수화물; 킬레이트제, 예컨대 EDTA; 당류, 예컨대, 만니톨 또는 소르비톨; 염 형성 짝이온, 예컨대 나트륨; 및/또는 비이온성 계면활성제, 예를 들어, TWEEN™, 폴리에틸렌 글리콜 (PEG), 및 PLURONICS™가 포함된다.As used herein, "carrier" includes pharmaceutically acceptable carriers, excipients or stabilizers that are nontoxic to the cells or mammals to be exposed at the dosages and concentrations employed. Often the physiologically acceptable carrier is an aqueous pH buffer. Examples of physiologically acceptable carriers include buffers such as phosphate, citrate, and other organic acids; antioxidants including ascorbic acid; low molecular weight (less than about 10 residues) polypeptides; proteins such as serum albumin, gelatin, or immunoglobulins; hydrophilic polymers such as polyvinylpyrrolidone; amino acids such as glycine, glutamine, asparagine, arginine, or lysine; monosaccharides, disaccharides, and other carbohydrates including glucose, mannose, or dextrins; chelating agents such as EDTA; sugars such as mannitol or sorbitol; salt forming counterions such as sodium; and/or nonionic surfactants such as TWEEN™, polyethylene glycol (PEG), and PLURONICS™.
어구 “약제학적으로 허용가능한”은 서브스턴스 또는 조성물이, 제형을 포함하는 다른 성분, 및/또는 그와 함께 치료될 포유동물과, 화학적으로 및/또는 독물학적으로 양립가능해야 하는 것을 나타낸다. The phrase “pharmaceutically acceptable” indicates that the substance or composition must be chemically and/or toxicologically compatible with the other ingredients comprising the formulation, and/or the mammal being treated therewith.
용어 "약제학적 제제" 또는 "약제학적 조성물"은 여기에 함유된 활성 성분의 생물학적 활성이 효과적이게 허용하게 하는 형태이고, 제제가 투여되는 대상체에게 허용 불가능하게 독성인 추가적인 성분을 함유하지 않는 제제를 의미한다.The term "pharmaceutical preparation" or "pharmaceutical composition" refers to a preparation that is in a form that allows the biological activity of the active ingredient contained therein to be effective, and which does not contain additional ingredients that are unacceptably toxic to the subject to which the preparation is administered. it means.
용어 "패키지 삽입물"은 적응증, 사용법, 투여량, 투여, 병용 요법, 포장된 제품과 결합되는 기타 약물, 및/또는 그러한 치료 제품 또는 약물의 사용에 관한 금기 및/또는 경고을 포함하는, 치료 제품 또는 약물의 상업적 패키지에 통상적으로 포함된 지침을 지칭하기 위해 사용된다.The term "package insert" refers to a therapeutic product or product, including contraindications and/or warnings regarding the indications, directions for use, dosage, administration, combination therapy, other drugs in combination with the packaged product, and/or the use of such therapeutic products or drugs. Used to refer to instructions commonly included in commercial packages of drugs.
본원에 사용된 용어 "유도기"는 대상체에게 투여되는 하나 이상의 치료제(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제 및/또는 화학요법제)에 대한 일련의 1회 이상의 투약 주기(예컨대, 약 4 내지 6회 주기)를 지칭하고, 여기서 상기 1회 이상의 투약 주기는 선택적으로 유지기가 뒤따른다. As used herein, the term “induction phase” refers to a series of one or more dosing cycles (e.g., about 4 to 6 cycles), wherein said one or more dosing cycles are optionally followed by a maintenance phase.
본원에 사용된 용어 "유지기"는 유도기 이후에 대상체에게 투여되는 하나 이상의 치료제(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제 및/또는 화학요법제)에 대한 일련의 1회 이상의 투약 주기를 지칭한다. 일부 경우들에서, 상기 유지기는 대상체가 유도기 동안 질병 진행 또는 허용할 수 없는 독성을 경험하지 않은 경우에만 개시된다. 상기 유도기 및 유지기는 동일한 치료제의 사용을 포함하거나 포함하지 않을 수 있다. 예를 들어, 일부 경우들에서, 상기 유도기는 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제 및 비백금계 화학요법제의 사용을 포함하고, 상기 유지기는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함한다. As used herein, the term “maintenance phase” refers to a series of one or more dosing cycles for one or more therapeutic agents (eg, anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, and/or chemotherapeutic agents) administered to a subject after an induction phase. refers to In some cases, the maintenance phase is initiated only when the subject does not experience disease progression or unacceptable toxicity during the induction phase. The induction and maintenance phases may or may not involve the use of the same therapeutic agent. For example, in some cases, the induction phase comprises the use of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, and the maintenance phase comprises an anti-TIGIT antagonist antibody and a PD -Including the use of -1 axis binding antagonists.
방광암과 관련하여, "백금계 화학요법에 부적격" 또는 "백금계 화학요법을 이용한 치료에 부적합"이라는 용어는 담당 임상의의 판단에 따라 또는 당업계에 공지된 백금계 화학요법에 대한 적격성에 대한 표준화된 기준에 따라 대상체가 백금계 화학요법을 이용한 치료에 부적격 또는 부적합인 것을 의미한다. 예를 들어, 그 전체가 본원에서 원용된 Galsky et al. Lancet Oncol. 12(3):211-4, 2011에 제시된 기준은 대상체가 시스플라틴 기반 화학요법에 적합한지 여부를 결정하는 데 사용될 수 있다. Galsky et al.은 하기 중 하나 이상을 충족하는 환자가 시스플라틴 기반 화학요법에 적합하지 않은 것으로 간주되는 전이성 UC(mUC) 환자에 대한 합의된 정의를 설명한다: (i) WHO(세계보건협회) 또는 ECOG 전신 활동도의 2 또는 카르노프스키 수행 상태 60~70%, (ii) 1 mL/s 미만의 크레아티닌 청소율(계산 또는 측정); (iii) 국립 암 연구소의 이상 반응에 대한 공통 용어 기준(CTCAE) v4.0 등급 ≥ 2 청력 상실; (iv) CTCAE v.4.0 등급 ≥ 2 말초 신경병증; 및/또는 뉴욕 심장 협회(NYHA) 부류 III 심부전. 일례에서, 환자는 하기 중 하나 이상을 갖는 경우 시스플라틴 기반 화학요법에 부적합한 것으로 간주된다: 신장 기능 장애(예컨대, 사구체 여과율(GFR) >30, <60 mL/분); GFR이 직접 측정(즉, 크레아티닌 청소율 또는 에틸데디아민테트라아세테이트), 또는 입수 가능하지 않은 경우 혈청/혈장 크레아티닌(콕크로프트-가울트 공식)으로부터 계산하여 평가할 수 있음; 청력 상실(예컨대, NCI CTCAE v4.0 등급 ≥ 2 청력학적 청력 상실, 2개의 인접한 주파수에서 25 데시벨); 말초 신경병증(예컨대, NCI CTCAE v4.0 등급 ≥ 2 말초 신경병증(즉, 감각 변화 또는 감각 이상, 따끔거림 포함)); 및/또는 ECOG 전신 활동도 평가(참조: Oken et al. Am. J. Clin. Oncol. 5:649-655, 1982, 이는 그 전체가 본원에 원용됨)(예컨대, ECOG 전신 활동도 2). 일부 양태에서, 하기 중 하나를 갖는 대상체는 카보플라틴 기반 화학요법에 적격일 수 있다: 신장 기능 장애(예컨대, GFR >30, <60 mL/분); GFR이 직접 측정(즉, 크레아티닌 청소율 또는 에틸데디아민테트라아세테이트), 또는 입수 가능하지 않은 경우 혈청/혈장 크레아티닌(콕크로프트-가울트 공식)으로부터 계산하여 평가할 수 있음; 청력 상실(예컨대, NCI CTCAE v4.0 등급 ≥ 2 청력학적 청력 상실, 2개의 인접한 주파수에서 25 데시벨); 말초 신경병증(예컨대, NCI CTCAE v4.0 등급 ≥ 2 말초 신경병증(즉, 감각 변화 또는 감각 이상, 따끔거림 포함)); 및/또는 ECOG 전신 활동도 평가(예컨대, ECOG 전신 활동도 2). 예를 들어, 시스플라틴 부적격은 하기의 기준들 중 임의의 하나로 정의될 수 있다: (i) 손상된 신장 기능(GFR <60 mL/분); GFR은 직접 측정(예컨대, 크레아티닌 청소율 또는 에틸데디아민테트라아세테이트), 또는 입수 가능하지 않은 경우 혈청/혈장 크레아티닌(콕크로프트-가울트 공식)에서 계산하여 평가할 수 있음; (ii) 두 개의 인접한 주파수에서 25dB의 청력 손실(청력 측정으로 측정); (iii) 2등급 이상의 말초 신경병증(즉, 감각 변화 또는 따끔거림을 포함한 마비); 및 (iv) ECOG 전신 활동도 2.In the context of bladder cancer, the terms “ineligible for platinum-based chemotherapy” or “not suitable for treatment with platinum-based chemotherapy” are used at the discretion of the attending clinician or as an indication of eligibility for platinum-based chemotherapy known in the art. means ineligible or ineligible for treatment with platinum-based chemotherapy according to standardized criteria. See, for example, Galsky et al. Lancet Oncol. The criteria set forth in 12(3):211-4, 2011 can be used to determine whether a subject is eligible for cisplatin-based chemotherapy. Galsky et al. describe an agreed definition of a patient with metastatic UC (mUC) who is considered ineligible for cisplatin-based chemotherapy in which one or more of the following are met: (i) WHO (World Health Association) or
III. 치료 및 진단 방법 및 사용III. Treatment and diagnostic methods and use
A.A. 암과 관련된 치료 방법 및 사용 Treatment methods and uses associated with cancer
치료 방법 및 사용Treatment methods and use
본원에서는 암(예컨대, 고형 종양 및/또는 국소 진행성 또는 전이성 암, 예컨대 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암)), 소세포 폐암(SCLC)(예컨대, 확장기(ES)-SCLC), 비소세포폐암(NSCLC)(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)), 자궁경부암(예컨대, 4B기, 전이성, 재발성 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암), 유방암(예컨대, 삼중음성 유방암(TNBC)(예컨대, 에스트로겐 수용체 음성(ER-), 프로게스테론 수용체 음성(PR-), 및 HER2 음성(HER2-) 유방암, 예컨대 초기 TNBC(eTNBC)) 또는 HER2-양성 유방암); 두경부암(예컨대, 두경부의 편평 세포 암종(SCCHN), 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, 간세포 암종(HCC), 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, 근육 침습성 방광암(MIBC) 또는 국소 진행성 또는 전이성 요로상피암(mUC)); 식도암; 췌장암(예컨대, 췌장관 선암종(PDAC), 예컨대 전이성 PDAC); 신장암(예컨대, 신장 세포 암종(RCC)); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 유효량의 항 TIGIT 길항제 항체(예컨대, 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 또는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 조합(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 대상체에게 투여하는 단계를 포함하는 결장직장암(CRC; 예컨대 미세위성-안정성(MSS)이거나 또는 또는 미세위성 불안정성(MSI)이 낮은 (MSI-Low) CRC)의 치료를 위한 방법 및 사용이 제공된다. Cancers (e.g., solid tumors and/or locally advanced or metastatic cancers such as lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer)), small cell lung cancer (SCLC) (e.g., expanded stage (ES)-SCLC), Non-small cell lung cancer (NSCLC) (e.g., squamous or nonsquamous NSCLC, locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC) NSCLC)), or stage IV NSCLC (eg, if the subject has not been previously treated for stage IV NSCLC), cervical cancer (eg, stage 4B, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or persistent) or recurrent PD-L1 positive cervical cancer), breast cancer (eg, triple negative breast cancer (TNBC) (eg, estrogen receptor negative (ER-), progesterone receptor negative (PR-), and HER2 negative (HER2-) breast cancer), such as Early TNBC (eTNBC)) or HER2-positive breast cancer); locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (such as muscle invasive bladder cancer (MIBC) or locally advanced or metastatic urothelial cancer (mUC)); esophageal cancer; pancreatic cancer (such as pancreatic ductal adenocarcinoma (PDAC), such as metastatic) PDAC); renal cancer (eg, renal cell carcinoma (RCC)); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); lumab), or a combination of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab). colorectal comprising administering a cycle to the subject Cancer (CRC; Methods and uses are provided, such as for the treatment of microsatellite-stable (MSS) or low microsatellite instability (MSI) (MSI-Low) CRC).
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이를 필요로 하는 대상체에게 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 제공한다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 완전 반응(CR) 또는 부분 반응(PR)을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 무진행 생존 기간(PFS) 또는 객관적 반응 기간(DOR)의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 전체 생존(OS)의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 OS의 증가를 발생시킨다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or Provided are methods and uses that involve administering an anti-PD-1 antagonist antibody, such as pembrolizumab) to a subject in need thereof every 4 weeks (eg, on
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체에게 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대, 예를 들어 펨브롤리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 DOR의 증가를 발생시킨다. 일부 예들경우들에서에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체에서 OR를 연장시킨다.The present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject in need thereof every 4 weeks (eg, on
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대, 예를 들어 펨브롤리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이를 필요로 하는 대상체에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 제공한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 OS의 증가를 발생시킨다.The present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject in need thereof every two weeks (eg, on the first day of each 28-day dosing cycle, and on day 15) and methods and uses involving administration. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered every two weeks (eg, on
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체에게 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대, 예를 들어 펨브롤리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 특정 경우들에서, 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체에게 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체에서 OR를 연장시킨다. 일부 경우들에서, 본 발명은 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법을 포함한다. 일부 경우들에서, 상기 방법은 3주마다 500 mg 내지 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 900 mg 내지 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject in need thereof every 3 weeks (eg, on
특정 경우들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 화학요법제 없이 투여된다(예컨대, 임의의 화학요법제 없이, 예컨대 전체 투약 요법에는 상기 대상체에 대한 화학요법제의 투여가 없다). In certain instances, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered without a chemotherapeutic agent (eg, without any chemotherapeutic agent, eg, the total dosing regimen includes administration of the chemotherapeutic agent to the subject). none).
일부 구현예들에서, 상기 대상체는 이전에 암에 대한 요법(예컨대, 암 면역요법 및/또는 화학요법제)으로 치료받은 적이 없다. 일부 구현예들에서, 상기 대상체는 이전에 암에 대한 선행 치료(예컨대, 암 면역요법 및/또는 화학요법제)를 받은 적이 없다. 일부 경우들에서, 상기 대상체는 선행 전신 요법(예컨대, 치료 목적으로 선행 전신 요법, 예컨대 화학요법)을 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체의 투여 전 적어도 해당 월 이내에(예컨대, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체의 투여 전 2개월 이내, 3개월 이내, 4개월 이내, 6개월 이내, 1년 이내, 2년 이내, 3년 이내, 4년 이내, 5년 이내, 또는 10년 이내에) 받지 않았다. 일부 경우들에서, 상기 대상체는 화학요법에 대한 치료 경험이 없다.In some embodiments, the subject has not been previously treated with therapy for cancer (eg, cancer immunotherapy and/or chemotherapeutic agents). In some embodiments, the subject has not previously received prior treatment for cancer (eg, cancer immunotherapy and/or chemotherapeutic agents). In some cases, the subject receives prior systemic therapy (eg, prior systemic therapy for therapeutic purposes, such as chemotherapy) at least within the month prior to administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (eg, the Within 2 months, within 3 months, within 4 months, within 6 months, within 1 year, within 2 years, within 3 years, within 4 years, within 5 years prior to administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody , or within 10 years). In some cases, the subject is naive to chemotherapy.
일부 구현예들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 화학요법과 함께 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체의 2주 1회(Q2W), 3주 1회(Q3W), 또는 4주 1회(Q4W) 투약 요법은 하나 이상의 화학요법제와 함께 투여될 수 있다. 상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체(Q2W, Q3W, 또는 Q4W)의 투여 빈도와 동일한 빈도로 또는 상이한 빈도(예컨대, 3주 투약/1주 휴약 일정(예컨대, 각 28일 주기의 제 1일 및 15일)로 투여될 수 있다. 예를 들어, 일부 구현예들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 2주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 3주 투약/1주 휴약, 2주마다, 3주마다, 또는 4주마다 투여된다. 대안적으로, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 3주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 2주마다, 3주마다, 또는 4주마다 투여된다. 대안적으로, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 4주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 3주 투약/1주 휴약, 2주마다, 3주마다, 또는 4주마다 투여된다. 특정 예들에서, 화학요법제는 주당 수회(예컨대, 주당 2, 3, 4, 5, 6 또는 7회(예컨대, 투약 주기의 제 1일, 2일, 및 3일에) 투여된다. In some embodiments, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered in combination with chemotherapy. For example, the once every two weeks (Q2W), once every three weeks (Q3W), or once every four weeks (Q4W) dosing regimen of the PD-1 axis binding antagonist and/or the anti-TIGIT antagonist antibody comprises one or more chemical agents. It may be administered with a therapeutic agent. The one or more chemotherapeutic agents are administered at the same frequency or at a different frequency than the dosing frequency of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (Q2W, Q3W, or Q4W) (e.g., on a 3-week dosing/1 week off schedule eg, on days 1 and 15 of each 28-day cycle).For example, in some embodiments, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered every two weeks, The one or more chemotherapeutic agents are administered weekly, every 3 weeks dosing/1 week off, every 2 weeks, every 3 weeks, or every 4 weeks Alternatively, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered every 3 weeks, and said one or more chemotherapeutic agents are administered every week, every 2 weeks, every 3 weeks, or every 4 weeks Alternatively, said PD-1 axis binding antagonist and said anti-TIGIT antagonist antibody are administered every 4 weeks and the one or more chemotherapeutic agents are administered every week, every 3 weeks dosing/1 week off, every 2 weeks, every 3 weeks, or every 4 weeks In certain instances, the chemotherapeutic agent is administered several times per week (eg, weekly 2, 3, 4, 5, 6 or 7 (eg, on days 1, 2, and 3 of the dosing cycle).
일부 구현예들에서, 화학요법제의 용량은 1회 이상의 초기 용량 후(예컨대, 1회, 2회, 3회, 4회 또는 그 이상의 초기 용량 후) 감소된다. 예를 들어, 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드)), 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신))의 후속 용량는 초기 용량의 약 95%, 90%, 85%, 80%, 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, 20%, 15%, 10% 또는 5%로 투여될 수 있다. 예를 들어, 125 mg/m2의 냅-파크리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 100 mg/m2 또는 75 mg/m2으로 감소될 수 있고; 100 mg/m2의 냅-파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 75 mg/m2으로 감소될 수 있고; 약 175 mg/m2의 파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 150 mg/m2, 125 mg/m2, 100 mg/m2, 또는 75 mg/m2으로 감소될 수 있고; 약 200 mg/m2의 파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 175 mg/m2, 150 mg/m2, 125 mg/m2, 100 mg/m2, 또는 75 mg/m2으로 감소될 수 있고; 약 1000 mg/m2의 젬시타빈의 초기 용량은 후속 용량에 대해, 예컨대 900 mg/m2, 800 mg/m2, 750 mg/m2, 700 mg/m2, 600 mg/m2, 또는 500 mg/m2으로 감소될 수 있고; 약 75 mg/m2의 시스플라틴의 초기 용량은 후속 용량에 대해, 예컨대 70 mg/m2, 65 mg/m2, 60 mg/m2, 55 mg/m2, 50 mg/m2 또는 45 mg/m2으로 감소될 수 있고; 약 500 mg/m2의 페메트렉시드의 초기 용량은 후속 용량에 대해, 예컨대 450 mg/m2, 400 mg/m2, 350 mg/m2, 300 mg/m2, 250 mg/m2, 또는 200 mg/m2으로 감소될 수 있고; 그리고/또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴의 초기 용량은 후속 용량에 대해, 예컨대 AUC = 5.5 mg/ml/분, 5.0 mg/ml/분, 4.5 mg/ml/분 또는 4.0 mg/ml/분을 달성하기에 충분한 용량으로 감소될 수 있다. 일부 경우들에서, 125 mg/m2의 냅-파크리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 100 mg/m2 또는 75 mg/m2으로 감소될 수 있고; 100 mg/m2의 냅-파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 75 mg/m2으로 감소될 수 있고; 175 mg/m2의 파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 150 mg/m2, 125 mg/m2, 100 mg/m2, 또는 75 mg/m2으로 감소될 수 있고; 200 mg/m2의 파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 175 mg/m2, 150 mg/m2, 125 mg/m2, 100 mg/m2, 또는 75 mg/m2으로 감소될 수 있고; 1000 mg/m2의 젬시타빈의 초기 용량은 후속 용량에 대해, 예컨대 900 mg/m2, 800 mg/m2, 750 mg/m2, 700 mg/m2, 600 mg/m2, 또는 500 mg/m2으로 감소될 수 있고; 75 mg/m2의 시스플라틴의 초기 용량은 후속 용량에 대해, 예컨대 70 mg/m2, 65 mg/m2, 60 mg/m2, 55 mg/m2, 50 mg/m2 또는 45 mg/m2으로 감소될 수 있고; 500 mg/m2의 페메트렉시드의 초기 용량은 후속 용량에 대해, 예컨대 450 mg/m2, 400 mg/m2, 350 mg/m2, 300 mg/m2, 250 mg/m2, 또는 200 mg/m2으로 감소될 수 있고; 그리고/또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴의 초기 용량은 후속 용량에 대해, 예컨대 AUC = 5.5 mg/ml/분, 5.0 mg/ml/분, 4.5 mg/ml/분 또는 4.0 mg/ml/분을 달성하기에 충분한 용량으로 감소될 수 있다.In some embodiments, the dose of the chemotherapeutic agent is reduced after one or more initial doses (eg, after 1, 2, 3, 4 or more initial doses). For example, a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide)), a taxane ( For example, subsequent doses of paclitaxel, such as nap-paclitaxel), and/or topoisomerase II inhibitors (eg, doxorubicin)) may be administered at about 95%, 90%, 85%, 80%, 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, 20%, 15%, 10% or 5%. For example, an initial dose of nap-paclitaxel of 125 mg/m 2 may be reduced for subsequent doses, such as 100 mg/m 2 or 75 mg/m 2 ; The initial dose of nap-paclitaxel of 100 mg/m 2 may be reduced for subsequent doses, eg to 75 mg/m 2 ; The initial dose of paclitaxel of about 175 mg/m 2 may be reduced for subsequent doses, such as 150 mg/m 2 , 125 mg/m 2 , 100 mg/m 2 , or 75 mg/m 2 ; The initial dose of paclitaxel of about 200 mg/m 2 is reduced for subsequent doses, such as 175 mg/m 2 , 150 mg/m 2 , 125 mg/m 2 , 100 mg/m 2 , or 75 mg/m 2 . can be; An initial dose of gemcitabine of about 1000 mg/m 2 for subsequent doses, such as 900 mg/m 2 , 800 mg/m 2 , 750 mg/m 2 , 700 mg/m 2 , 600 mg/m 2 , or can be reduced to 500 mg/m 2 ; An initial dose of cisplatin of about 75 mg/m 2 is for subsequent doses, such as 70 mg/m 2 , 65 mg/m 2 , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 or 45 mg. can be reduced to /m 2 ; An initial dose of pemetrexed of about 500 mg/m 2 is for subsequent doses, such as 450 mg/m 2 , 400 mg/m 2 , 350 mg/m 2 , 300 mg/m 2 , 250 mg/m 2 , or 200 mg/m 2 ; and/or an initial dose of carboplatin in a dose sufficient to achieve AUC=6 mg/ml/min for subsequent doses, such as AUC=5.5 mg/ml/min, 5.0 mg/ml/min, 4.5 mg/min. ml/min or a dose sufficient to achieve 4.0 mg/ml/min. In some cases, the initial dose of nap-paclitaxel of 125 mg/m 2 may be reduced for a subsequent dose, such as 100 mg/m 2 or 75 mg/m 2 ; The initial dose of nap-paclitaxel of 100 mg/m 2 may be reduced for subsequent doses, eg to 75 mg/m 2 ; The initial dose of paclitaxel at 175 mg/m 2 may be reduced for subsequent doses, such as 150 mg/m 2 , 125 mg/m 2 , 100 mg/m 2 , or 75 mg/m 2 ; The initial dose of 200 mg/m 2 paclitaxel may be reduced for subsequent doses, such as 175 mg/m 2 , 150 mg/m 2 , 125 mg/m 2 , 100 mg/m 2 , or 75 mg/m 2 . can; The initial dose of gemcitabine of 1000 mg/m 2 is for subsequent doses, such as 900 mg/m 2 , 800 mg/m 2 , 750 mg/m 2 , 700 mg/m 2 , 600 mg/m 2 , or 500 can be reduced to mg/m 2 ; An initial dose of cisplatin of 75 mg/m 2 is for subsequent doses, such as 70 mg/m 2 , 65 mg/m 2 , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 or 45 mg/
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예커대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 화학요법 조합은 유효량의 제1 비백금계 화학치료제 및 유효량의 제2 비백금계 화학치료제를 포함한다. 일부 경우들에서, 상기 제1 비백금계 화학요법제는 항대사물질이고 제2 비백금계 화학요법제는 탁산이다. 일부 구현예들에서, 상기 화학요법 조합(예컨대, 항대사물질(예컨대, 젬시타빈, 페메트렉시드 또는 카페시타빈) 및 탁산(예컨대, 냅-파클리탁셀 및 파클리탁셀)은 매주, 격주, 또는 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일 및 15일에) 투여된다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or methods and uses involving administering to a subject in need thereof an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapy combination. In some embodiments, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, Yeckerdae Arte) Zolizumab) is administered every 2 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 젬시타빈, 및 파클리탁셀을 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)은 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여되고, 상기 화학요법 조합(예컨대, 항대사물질 및 탁산(예컨대, 젬시타빈 및 파클리탁셀)은 더 자주 투여된다(예컨대, 4주마다 3회(예컨대, 각 28일 투약 주기의 1, 8 및 15일에).In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), gemcitabine, and paclitaxel to a subject in need thereof, wherein said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and said A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) is administered every two weeks (eg, on
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 항대사물질(예컨대, 젬시타빈), 및 탁산(예컨대, 파클리탁셀)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 항대사물질(예컨대, 젬시타빈), 및 탁산(예컨대, 파클리탁셀)의 투여는 상기 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 항대사물질(예컨대, 젬시타빈), 및 탁산(예컨대, 파클리탁셀)의 투여는 상기 대상체에서 OS를 연장시킨다. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), antimetabolites (eg gemcitabine), and taxanes (eg paclitaxel) result in CR or PR. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), antimetabolites (eg gemcitabine), and taxanes (eg paclitaxel) result in an increase in PFS in the subject. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), antimetabolites (eg gemcitabine), and taxanes (eg paclitaxel) prolong OS in the subject.
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용을 포함하고, 여기서 상기 화학요법 조합은 유효량의 백금계 화학요법제 및 유효량의 비백금계 화학요법제를 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예커대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 항대사물질(예컨대, 페메트렉시드)이다. 일부 구현예들에서, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제 및 상기 항대사물질(예컨대, 페메트렉시드))은 매주, 2주마다, 4주마다, 또는 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일, 및 15일에) 투여된다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or methods and uses comprising administering to a subject in need thereof an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapeutic combination, wherein the chemotherapy combination comprises an effective amount of a platinum-based chemotherapeutic agent and and an effective amount of a non-platinum-based chemotherapeutic agent. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody, e.g. Atezoli) Zumab) every 2 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 항대사물질(예컨대, 페메트렉시드)를 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 상기 항대사물질(예컨대, 페메트렉시드)는 동일한 빈도(예컨대, 3주마다, 예컨대 각 21일 투약 주기의 제 1일에)로 투여된다. 일부 경우들에서, 상기 투약은 4회 내지 6회 유도 투약 주기 동안 계속된다(예컨대, 4회의 유도 투약 주기, 5회의 유도 투약 주기, 또는 6회의 유도 투약 주기). 상기 유도 투약 주기 후에, 유지 요법은 1회 이상의 후속(유지) 투약 주기로 투여될 수 있다. 특정 구현예들에서, 상기 1회 이상의 유지 투약 주기는 상기 백금계 화학요법제를 포함하지 않는다. In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and an antimetabolite (eg, pemetrexed) to a subject in need thereof, wherein said anti-TIGIT antagonist An antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) are administered every 3 weeks (eg, each on day 1 of a 21 day dosing cycle), the chemotherapy combination (eg, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and the antimetabolite (eg, pemetrexed)) are administered at the same frequency (eg, every 3 weeks, eg, on Day 1 of each 21 day dosing cycle) In some cases, the dosing is continued for 4 to 6 induction dosing cycles (eg, 4 induction dosing cycles) , 5 induction dosing cycles, or 6 induction dosing cycles).After said induction dosing cycle, maintenance therapy can be administered in one or more subsequent (maintenance) dosing cycles.In certain embodiments, said one or more maintenance dosing cycles The cycle does not include the platinum-based chemotherapeutic agent.
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 상기 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 상기 대상체의 OS를 연장시킨다. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg carboplatin or cisplatin), and the antimetabolites (eg pemetrexed) result in CR or PR. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the antimetabolite (eg, pemetrexed) result in an increase in PFS in the subject. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the antimetabolite (eg, pemetrexed) prolong the OS in the subject.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)을 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있다. 추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the antimetabolite (eg, pemetrexed) are being treated for a solid tumor or locally advanced or metastatic cancer. Additionally or alternatively, the cancer is lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), SCLC (eg, ES-SCLC), NSCLC (eg, squamous or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (eg, stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (eg, TNBC (eg, early TNBC) (eTNBC)) or HER2-positive breast cancer); (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; ovarian cancer; stomach cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or low MSI CRC).
본 발명은 또한 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법(예컨대, 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예커대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 구현예들에서, 상기 화학요법은 매주, 2주마다, 4주마다, 또는 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일, 및 15일에) 투여된다. 일부 구현예들에서, 상기 화학요법은 매주 투여된다.The present invention also provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab; or an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapy, such as a taxane (eg, paclitaxel or nap-paclitaxel), to a subject in need thereof. In instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, ecker vs. atezolizumab) ) every 2 weeks (eg, on
일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법(예컨대, 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법(예컨대, 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 기준 PFS와 비교하여 상기 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법(예컨대, 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 DOR의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법(예컨대, 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 대상체의 OS를 연장시킨다.In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) , or administration of an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapy, such as a taxane (eg, paclitaxel or nap-paclitaxel), results in CR or PR. In some cases, an effective amount of anti-TIGIT an antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody; Administration of such as pembrolizumab) and chemotherapy (such as taxanes (such as paclitaxel or nap-paclitaxel) results in an increase in PFS in the subject compared to baseline PFS. In some cases, an effective amount of an anti-TIGIT antagonist an antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as Administration of pembrolizumab) and chemotherapy (eg, taxane (eg, paclitaxel or nap-paclitaxel) results in an increase in DOR. In some cases, an effective amount of an anti-TIGIT antagonist antibody (eg, as disclosed herein) An anti TIGIT antagonist antibody such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody such as atezolizumab, or an anti PD-1 antagonist antibody such as pembrolizumab), and chemotherapy ( For example, administration of a taxane (eg, paclitaxel or nap-paclitaxel) prolongs the subject's OS.
본 발명은 또한 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용을 포함하고, 여기서 상기 화학요법 조합은 유효량의 백금계 화학요법제 및 유효량의 비백금계 화학요법제를 포함하고, 여기서 상기 비백금계 화학요법제는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예커대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)은 매주, 2주마다, 4주마다, 또는 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일, 및 15일에) 투여된다.The present invention also provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab; or an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapeutic combination comprising administering to a subject in need thereof, wherein the chemotherapy combination comprises an effective amount of a platinum-based chemotherapeutic agent. and an effective amount of a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is a taxane (eg, paclitaxel or nap-paclitaxel). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, e.g. Atezoli) Zumab) every 2 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)을 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)은 동일한 빈도(예컨대, 3주마다, 예컨대 각 21일 투약 주기의 제 1일에)로 투여된다. 일부 경우들에서, 상기 투약은 4회 내지 6회 유도 투약 주기 동안 계속된다(예컨대, 4회의 유도 투약 주기, 5회의 유도 투약 주기, 또는 6회의 유도 투약 주기). 상기 유도 투약 주기 후에, 유지 요법은 1회 이상의 후속(유지) 투약 주기로 투여될 수 있다. 특정 구현예들에서, 상기 1회 이상의 유지 투약 주기는 상기 백금계 화학요법제를 포함하지 않는다. In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a taxane (eg, paclitaxel or nap-paclitaxel) to a subject in need thereof, wherein said anti-TIGIT antagonist An antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) are administered every 3 weeks (eg, each on day 1 of a 21 day dosing cycle), the chemotherapy combination (eg, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and the taxane (eg, paclitaxel or nap-paclitaxel)) are administered at the same frequency (eg, every 3 weeks, eg, on Day 1 of each 21 day dosing cycle) In some cases, the dosing is continued for 4 to 6 induction dosing cycles (eg, 4 induction dosing cycles) , 5 induction dosing cycles, or 6 induction dosing cycles).After the induction dosing cycle, maintenance therapy can be administered in one or more subsequent (maintenance) dosing cycles.In certain embodiments, the one or more maintenance dosing cycles The cycle does not include the platinum-based chemotherapeutic agent.
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 상기 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)의 투여는 상기 대상체의 OS를 연장시킨다. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the taxane (eg, paclitaxel or nap-paclitaxel) result in CR or PR. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the taxane (eg, paclitaxel or nap-paclitaxel) result in an increase in PFS in the subject. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the taxane (eg, paclitaxel or nap-paclitaxel) prolong OS in the subject.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)을 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있다. 추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the taxane (eg, paclitaxel or nap-paclitaxel) are being treated for a solid tumor or locally advanced or metastatic cancer. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (eg, stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (eg, TNBC (eg, early TNBC) (eTNBC)) or HER2-positive breast cancer); (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; ovarian cancer; stomach cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or low MSI CRC).
또한 본원에서는 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용이 제공되고, 여기서 상기 화학요법 조합은 유효량의 백금계 화학요법제 및 유효량의 비백금계 화학요법제를 포함하고, 여기서 상기 비백금계 화학요법제는 토포이소머라제 II 억제제(예컨대, 에토포시드)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예커대 아테졸리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 구현예들에서, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드))는 매주, 2주마다, 4주마다, 또는 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일, 및 15일에) 투여된다. 일부 구현예들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 상기 백금계 화학요법제보다 더 빈번하게 투여된다(예컨대, 주당 3회, 예컨대 각 투약 주기의 제 1일, 2일, 및 3일에).Also disclosed herein is an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or Methods and uses are provided that involve administering an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapeutic combination to a subject in need thereof, wherein the chemotherapy combination comprises an effective amount of a platinum-based chemotherapeutic agent and An effective amount of a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is a topoisomerase II inhibitor (eg, etoposide). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody, e.g. Atezoli) Zumab) every 2 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)를 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 동일한 빈도(예컨대, 3주마다, 예컨대 각 21일 투약 주기의 제 1일에)로 투여된다. 일부 경우들에서, 상기 투약은 4회 내지 6회 유도 투약 주기 동안 계속된다(예컨대, 4회의 유도 투약 주기, 5회의 유도 투약 주기, 또는 6회의 유도 투약 주기). 상기 유도 투약 주기 후에, 유지 요법은 1회 이상의 후속(유지) 투약 주기로 투여될 수 있다. 특정 구현예들에서, 상기 1회 이상의 유지 투약 주기는 상기 백금계 화학요법제 또는 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)를 포함하지 않는다. In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide) to a subject in need thereof, wherein said An anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) are administered every 3 weeks ( For example, on Day 1 of each 21 day dosing cycle), the chemotherapy combination (eg, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin)) and the topoisomerase II inhibitor (eg, eto Forsyd) is administered at the same frequency (eg, every 3 weeks, eg, on Day 1 of each 21-day dosing cycle) In some cases, the dosing is continued for 4 to 6 induction dosing cycles (eg, , 4 induction dosing cycles, 5 induction dosing cycles, or 6 induction dosing cycles).After the induction dosing cycle, maintenance therapy can be administered in one or more subsequent (maintenance) dosing cycles. In certain embodiments, The one or more maintenance dosing cycles do not include the platinum-based chemotherapeutic agent or the topoisomerase II inhibitor (eg, etoposide).
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 (a) CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 상기 대상체에서 PFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 상기 대상체의 OS를 연장시킨다.In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg carboplatin or cisplatin), and the topoisomerase II inhibitor (eg etoposide) (a) generate CR or PR. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the topoisomerase II inhibitor (eg, etoposide) result in an increase in PFS in the subject. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the topoisomerase II inhibitor (eg, etoposide) prolong OS in the subject.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)를 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있다. 추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the topoisomerase II inhibitor (eg, etoposide) are treated for solid tumors or locally advanced or metastatic cancer. are receiving Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (eg, stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (eg, TNBC (eg, early TNBC) (eTNBC)) or HER2-positive breast cancer); (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; ovarian cancer; stomach cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or low MSI CRC).
또한 본원에서는 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용을 제공한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여된다. Also disclosed herein is an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or Provided are methods and uses that involve administering an anti-PD-1 antagonist antibody, such as pembrolizumab), and a VEGF antagonist (eg, an anti-VEGF antibody, such as bevacizumab) to a subject in need thereof. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered every 3 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 대상체에서 OS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 대상체에서 PFS의 증가를 발생시킨다.In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), and the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) to a subject in need thereof, wherein the anti-TIGIT antagonist antibody (eg, as disclosed herein) anti-TIGIT antagonist antibodies, such as tyragolumab), the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody, such as atezolizumab), and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizu) mob)) every 3 weeks (eg, on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있다. 추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, TNBC(예컨대, eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), and the subject receiving the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is being treated for a solid tumor or locally advanced or metastatic cancer. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer); eTNBC) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); bladder cancer (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; or CRC (eg, MSS or low MSI CRC).
본 발명은 아테졸리주맙, 베바시주맙 및 티라골루맙의 조합을 암 치료에 효과적인 양으로 환자에게 투여하는 단계를 포함하는, 암 환자에서 암을 치료하는 방법을 포함한다.The present invention includes a method of treating cancer in a cancer patient comprising administering to the patient a combination of atezolizumab, bevacizumab and tiragolumab in an amount effective to treat the cancer.
또한 본원에서는 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 항 PD-1 길항제 항체, 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용이 제공되고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 항 PD-1 길항제 항체, 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다.Also disclosed herein is an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), an anti-PD-1 antagonist antibody, and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) ))) to a subject in need thereof, wherein the anti-PD-1 antagonist antibody is pembrolizumab. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), an anti-PD-1 antagonist antibody, and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevaciz) Mab)) is administered every 3 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 항 PD-L1 길항제 항체, 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 항 PD-L1 길항제 항체, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 항 PD-1 길항제 항체, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 대상체에서 OS의 증가를 발생시키고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 항 PD-1 길항제 항체, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 대상체에서 PFS의 증가를 발생시키고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다.In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), an anti-PD-L1 antagonist antibody, and a VEGF antagonist (eg, an anti-VEGF antibody). (eg, bevacizumab)) to a subject in need thereof, wherein said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), said anti-PD- The L1 antagonist antibody, and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) are administered every 3 weeks (eg, on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 항 PD-1 길항제 항체, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, TNBC(예컨대, eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다.In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), the anti-PD-1 antagonist antibody, and the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is being treated for a solid tumor or locally advanced or metastatic cancer, wherein the anti-PD-1 antagonist antibody is pembrolizumab. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer); eTNBC) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); bladder cancer (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; or CRC (eg, MSS or low MSI CRC).
또한 본원에서는 유효량의 티라골루맙 및 펨브롤리주맙을 이를 필요로 하는 대상체에게 투여하는 것을 수반한 방법 및 사용이 제공된다. 일부 경우들에서, 티라골루맙은 3주마다(예컨대, 각 42일 투약 주기의 제 1일 및 22일에) 투여되고 펨브롤리주맙은 6주마다(예컨대, 각 42일 투약 주기의 제 1일에) 투여된다. Also provided herein are methods and uses that involve administering to a subject in need thereof effective amounts of tiragolumab and pembrolizumab. In some cases, tiragolumab is administered every 3 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 티라골루맙 및 펨브롤리주맙을 이를 필요로 하는 대상체에게 투여하는 것을 수반하고, 여기서 티라골루맙은 3주마다(예컨대, 각 42일 투약 주기의 제 1일 및 22일에) 투여되고 펨브롤리주맙은 6주마다(예컨대, 각 42일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 유효량의 티라골루맙 및 펨브롤리주맙은 상기 대상체의 OS의 증가를 발생시키고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 일부 경우들에서, 상기 유효량의 티라골루맙 및 펨브롤리주맙은 상기 대상체의 PFS의 증가를 발생시키고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다.In certain embodiments, the method involves administering to a subject in need thereof an effective amount of tiragolumab and pembrolizumab, wherein tiragolumab is administered every 3 weeks (eg, the first of each 42-day dosing cycle). days and 22) and pembrolizumab is administered every 6 weeks (eg, on
일부 경우들에서, 티라골루맙 및 펨브롤리주맙을 투여받은 대상체는 고형 종양 또는 국소 진행성 또는 전이성 암에 대해 치료를 받고 있고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다.In some cases, the subject receiving tiragolumab and pembrolizumab is being treated for a solid tumor or locally advanced or metastatic cancer, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
추가적으로 또는 대안적으로, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, TNBC(예컨대, eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)일 수 있다. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, Stage IIIB NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously received treatment for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer); eTNBC) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); bladder cancer (eg, MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; or CRC (eg, MSS or low MSI CRC).
또한 본원에서는 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법이 제공된다. 일부 경우들에서, 상기 방법은 유도기 및 유지기를 포함한다. 일부 경우들에서, 상기 유도기 및 유지기는 각각 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는다. 일부 경우들에서, 상기 유지기는 상기 비백금계 화학요법제의 투여를 포함하지 않는다. 일부 경우들에서, 상기 유지기는 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한다.Also disclosed herein is a method of treating a subject having cancer, comprising: an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, 3 A method is provided, comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a platinum-based chemotherapeutic agent per week, and one or more dosing cycles of a non-platinum-based chemotherapeutic agent every three weeks. In some cases, the method includes an induction phase and a maintenance phase. In some cases, the induction and maintenance phases each comprise one or more dosing cycles. In some cases, the maintenance phase does not include administration of the platinum-based chemotherapeutic agent. In some cases, the maintenance phase does not include administration of the non-platinum-based chemotherapeutic agent. In some cases, the maintenance phase comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and the PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. do.
또한 본원에서는 암을 가진 대상체를 치료하는 방법으로서, 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 100 mg 내지 약 300 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 방법이 제공된다. Also disclosed herein is a method of treating a subject having cancer, comprising one of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and an anti-PD-1 antagonist antibody at a dose of about 100 mg to about 300 mg every 3 weeks. There is provided a method comprising administering to the subject a dosing regimen comprising at least one dosing cycle, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
또한 본원에서는 암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 제공되고, 여기서 상기 방법은 본원에 제공된 방법에 따른다. Also provided herein is an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cancer, wherein the method is according to a method provided herein.
또한 본원에서는 암을 가진 대상체 또는 대상체 집단을 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용으로 항 TIGIT 길항제 항체의 사용이 제공되고, 여기서 상기 치료는 본원에 제공된 방법에 따른다. 일부 양태들에서, 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공된다. 다른 양태들에서, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공된다. 일부 양태들에서, 티라골루맙 및 아테졸리주맙은 투여 이전에 IV 백(bag)에 결합된다.Also provided herein is the use of an anti TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or population of subjects having cancer, wherein said treatment is according to a method provided herein. In some embodiments, the PD-1 axis binding antagonist is provided in a separate formulation. In other embodiments, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form. In some aspects, tiragolumab and atezolizumab are combined in an IV bag prior to administration.
제제의 투약dosing of the formulation
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, VEGF 길항제, 및 화학요법제의 투약은 섹션 III(K)에 기재되어 있다. Dosing of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, VEGF antagonists, and chemotherapeutic agents is described in Section III(K).
암 특성화 및 선택Cancer characterization and selection
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 암은 고형 종양 또는 국소 진행성 또는 전이성 암일 수 있다. 일부 경우들에서, 상기 암은 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)이다. 상기 대상체가 유방암을 가진 일부 경우들에서, 상기 대상체는 전이성 유방암에 대한 선행 전신 요법을 받은 적이 없다.In any of the methods, uses, or compositions for use described herein, the cancer may be a solid tumor or a locally advanced or metastatic cancer. In some cases, the cancer is lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), SCLC (eg, ES-SCLC), NSCLC (eg, squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, IIIB) Stage NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously been treated for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (e.g., TNBC (e.g., early TNBC) eTNBC)) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); liver cancer (eg, HCC, such as locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer ( e.g., MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; (eg, MSS or low MSI CRC) In some cases where the subject has breast cancer, the subject has not received prior systemic therapy for metastatic breast cancer.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는다. 일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 감작성 EGFR 유전자 돌연변이 또는 ALK 유전자 재배열을 갖지 않는다. 일부 경우들에서, 상기 대상체는 0 또는 1의 이스턴 코퍼레이티브 종양학 그룹(ECOG) 전신 활동도(PS)를 가진다. In some cases, in a method, use, or compositions for use described herein, the subject does not have an epidermal growth factor receptor (EGFR) or an anaplastic lymphoma kinase (ALK) genomic tumor abnormality. In some cases, in a method, use, or compositions for use described herein, the subject does not have a sensitizing EGFR gene mutation or ALK gene rearrangement. In some cases, the subject has an Eastern Corporate Oncology Group (ECOG) systemic activity (PS) of 0 or 1.
돌연변이 상태 EGFR 및 ALK를 검출하는 방법은 당업계에 일반적으로 공지되어 있으며, 임상 샘플(예컨대, 종양 생검 또는 혈액 샘플(예컨대, 혈액 중 순환 종양 DNA)로부터의 DNA를 차세대 서열분석 방법을 사용하여, 예컨대 본원에 그 전체가 원용된 Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013)에 기재된 표적화된 유전자 풀다운 및 서열분석 방법을 사용하여 서열분석하는 것을 포함하지만 이에 제한되지는 않는다. 이러한 차세대 시퀀싱 방법은 다양한 돌연변이(예를 들어, 삽입, 결실, 염기 치환, 국소 유전자 증폭 및/또는 동형 접합 유전자 결실)를 검출하기 위해 본원에 개시된 임의의 방법과 함께 사용될 수 있으며, 동시에 소형 샘플들 (예를 들어, 작은 코어 바늘 생검, 미세 바늘 흡인 및/또는 세포 블록들) 또는 고정된 샘플들 (예를 들어, 포르말린-고정 및 파라핀 포매(FFPE) 샘플)을 사용할 수 있게 한다. EGFR 및 ALK의 돌연변이 상태를 검출하기 위한 다른 방법에는 형광 인시튜 혼성화(FISH) 및 면역조직화학(IHC) 방법이 포함된다. ALK의 돌연변이 상태의 검출을 위한 예시적인 방법은 미국 특허 제 9,651,555에 개시되며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, VENTANA® 항 ALK (D5F3) IHC 분석은 ALK 유전자의 돌연변이 상태를 결정하기 위해 사용한다.Methods for detecting the mutant state EGFR and ALK are generally known in the art, and DNA from a clinical sample (e.g., a tumor biopsy or a blood sample (e.g., circulating tumor DNA in blood)) can be analyzed using next-generation sequencing methods; including, but not limited to, sequencing using, for example, targeted gene pulldown and sequencing methods described in Frampton et al. ( Nature Biotechnology . 31(11): 1023-1033, 2013), which is incorporated herein in its entirety. This next-generation sequencing method can be used in conjunction with any of the methods disclosed herein to detect a variety of mutations (e.g., insertions, deletions, base substitutions, local gene amplifications and/or homozygous gene deletions), while at the same time compact Allows the use of samples (eg, small core needle biopsy, fine needle aspiration and/or cell blocks) or fixed samples (eg, formalin-fixed and paraffin-embedded ( FFPE ) samples). and other methods for detecting the mutant status of ALK include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods.Exemplary methods for detecting the mutant status of ALK are disclosed in US Pat. No. 9,651,555, , which is incorporated herein in its entirety In some cases, the VENTANA® anti- ALK (D5F3) IHC assay is used to determine the mutation status of the ALK gene.
본원에 기재된 임의의 방법의 일부 경우들에서, 상기 돌연변이는 감작성 EGFR 돌연변이이다. 감작성 EGFR 돌연변이는 당업계에 일반적으로 공지되어 있으며 미국 특허 공보 제 US 2018/0235968 및 in Juan et al. (Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18-21 중 어느 하나에서의 돌연변이(예컨대, 엑손 18, 엑손 19, 엑손 20, 및/또는 엑손 21에서의 돌연변이)이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 19에서의 결실(del19)이다. 다른 예들에서, 상기 감작성 EGFR 돌연변이는 엑손 21에서의 L858R 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 C, A, 또는 S이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719S 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 G719A 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 S720F 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861Q 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861R 점 돌연변이이다. 다른 경우들에서, 감작성 EGFR 돌연변이는 T790M 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 E709X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 K, A, 또는 H이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 S768I 점 돌연변이이다.In some cases of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are generally known in the art and described in US Patent Publication Nos. US 2018/0235968 and in Juan et al. ( Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017), which is incorporated herein by reference in its entirety. In some cases, the sensitizing EGFR mutation is a mutation in any one of exon 18-21 (eg, a mutation in
본원에 기재된 방법들 중 임의의 것의 일부 경우들에서, 상기 돌연변이는 ALK 유전자 재배열이다. ALK 유전자 재배열은 당업계에 일반적으로 공지되어 있으며 미국 특허 제 9,651,555 및 in Du et al. (Thoracic Cancer. 9: 423-430, 2018)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, ALK 유전자 재배열은 하류 신호전달 경로를 활성화하여 세포 증식 및 생존을 증가시키는 발암성 ALK 티로신 키나제의 생성을 초래한다. 일부 경우들에서, ALK 유전자 재배열은 EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC, TMP4, 및 MSN로 구성된 그룹에서 선택된 유전자와의 ALK 재배열이며, 융합 종양유전자를 형성시킨다. 일부 경우들에서, ALK 유전자 재배열은 ALK 와의 EML4 재배열이며 융합 종양유전자 EML4-ALK를 형성한다.In some cases of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are generally known in the art and described in US Pat. Nos. 9,651,555 and in Du et al. ( Thoracic Cancer. 9: 423-430, 2018), which is incorporated herein by reference in its entirety. In some cases, ALK gene rearrangement results in the production of oncogenic ALK tyrosine kinases that activate downstream signaling pathways to increase cell proliferation and survival. In some cases, the ALK gene rearrangement is a gene selected from the group consisting of EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A , BIRC6, RANBP2, ATIC, CLTC, TMP4, and MSN . ALK rearrangement with and forms a fusion oncogene. In some cases, the ALK gene rearrangement is an EML4 rearrangement with ALK and forms the fusion oncogene EML4-ALK .
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 대상체는 NSCLC의 폐 림프상피종 유사 암종 하위유형이 없다. NSCLC의 하위유형을 검출하는 방법은 당업계에 널리 공지이며, 조직병리적 기준에 의한, 또는 분자 특징 (예를 들면, 바이오마커 (예를 들면, 상기 유전자에 의해 인코딩된 특정한 유전자 또는 단백질)의 하나 또는 조합의 발현에 의해 특성규명된 하위유형)에 의한 결정 방법을 포함하나 이에 제한되는 것은 아니다. 일부 경우들에서, 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 조직 샘플은 종양 샘플이다. In some instances, in a method, use, or compositions for use described herein, the subject is free of the lung lymphothelioma-like carcinoma subtype of NSCLC. Methods for detecting subtypes of NSCLC are well known in the art and are based on histopathological criteria, or by molecular characteristics (e.g., biomarkers (e.g., specific genes or proteins encoded by said genes)). subtypes characterized by expression of one or a combination). In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample.
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 대상체는 활동성 엡스타인-바 바이러스(EBV) 감염 또는 알려진 또는 의심되는 만성 활동성 EBV 감염이 없다. 본원에 기재된 방법에 사용하기 위한 활동성 또는 만성 활동성 EBV 감염의 지표는, 대상체의 샘플(예컨대, 혈액 또는 혈청 샘플)에서 검출된 EBV IgM, EBV IgG, 엡스타인-바 핵 항원 (EBNA), 및 엡스타인-바 바이러스 입자들을 포함할 수 있으나 이에 제한되는 것은 아니다. 대상체의 샘플에서 EBV IgM, EBV IgG, 엡스타인-바 핵 항원(EBNA), 및 엡스타인-바 바이러스 입자들을 포함하는 활동성 또는 만성 활동성 EBV 감염의 하나 이상의 지표의 존재를 검출하는 방법은 당업계에 널리 공지이며, 혈청학적 진단(예컨대, EBV DNA의 검출(예컨대, EBV 바이러스 입자 검출을 위한 혈액 샘플의 PCR 분석에 의함) 또는 EBV 항원 또는 항 EBV 항체의 검출(예컨대, 이종성 항체를 사용한 EBNA, EBV IgM 또는 EBV IgG의 검출))을 포함하는 방법들을 포함하지만, 이에 제한되지는 않는다. 일부 경우들에서, 샘플은 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 경우들에서, 대상체는 EBV IgM에 대해 음성이고 및/또는 EBV PCR에 의해 음성이다. 일부 경우들에서, 대상체는 EBV IgM에 대해 음성이고 및/또는 EBV PCR에 의해 음성이며 EBV IgG에 대해 양성이고 및/또는 엡스타인-바 핵 항원 (EBNA)에 대해 양성이다. 다른 경우들에서, 대상체는 EBV IgG에 대해 음성이고 및/또는 EBNA에 대해 음성이다. In some cases, in a method, use, or compositions for use described herein, the subject does not have an active Epstein-Barr virus (EBV) infection or a known or suspected chronic active EBV infection. An indicator of active or chronic active EBV infection for use in the methods described herein is EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein- bar virus particles, but are not limited thereto. Methods for detecting the presence of one or more indicators of active or chronic active EBV infection comprising EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein-Barr virus particles in a sample of a subject are well known in the art. serological diagnosis (e.g., detection of EBV DNA (e.g., by PCR analysis of a blood sample for detection of EBV virus particles) or detection of EBV antigen or anti-EBV antibody (e.g., EBNA, EBV IgM or detection of EBV IgG))). In some cases, the sample is selected from the group consisting of a whole blood sample, a serum sample, and a plasma sample. In some cases, the subject is negative for EBV IgM and/or is negative by EBV PCR. In some cases, the subject is negative for EBV IgM and/or negative by EBV PCR and positive for EBV IgG and/or positive for Epstein-Barr nuclear antigen (EBNA). In other cases, the subject is negative for EBV IgG and/or negative for EBNA.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체는 PD-L1 선택된 종양(예컨대, SP263 또는 22C3 항체를 이용한 IHC에 의해 결정된 바와 같이 최소 PD-L1 양성 종양 세포 분획 또는 TPS가 ≥ 30%(예컨대, ≥ 50%)인 종양 PD-L1 발현 또는 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 SP142 항체를 이용한 IHC에 의해 결정된 바와 같이 1% 이상인 경우)을 갖는다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 양성 종양 세포 분획 또는 PD-L1 TPS가 면역조직화학적(IHC) 분석법에 의해 30% 이상(예컨대, 50% 이상)인 것으로 결정된 종양이다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 발현 면역 세포(IC)에 의해 차지하는 종양 면적의 비율이 면역조직화학적(IHC) 분석법에 의해 1% 이상인 것으로 결정된 종양이다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP263, 22C3, SP142, 또는 28-8을 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP263를 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 22C3를 사용한다. 일부 경우들에서, 종양 샘플은 50% 이상의 TPS를 갖는 것으로 결정되었다. 일부 경우들에서, PD-L1-양성 종양 세포 분율은 (예를 들어, 항 PD-L1 항체 SP263을 사용한 양성 염색에 의해 결정 시 (예를 들어, Ventana 분석법 사용), 항 PD-L1 항체 22C3을 사용한 양성 염색에 의해 결정 시 (예를 들어, pharmDx 분석법 사용), 또는 항 PD-L1 항체 28-8을 사용한 양성 염색에 의해 결정 시) 50% 이상이다. 일부 구현예들에서, PD-L1-양성 종양 세포 분율은 항 PD-L1 항체 SP142를 사용한 양성 염색에 의해 결정 시 30% 이상이다. 일부 경우들에서, 상기 IC는 1% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 5% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 10% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 50% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 30% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). In some cases, in any of the methods, uses, or compositions for use described herein, the subject has a PD-L1 selected tumor (eg, minimal PD-L1 positive tumor as determined by IHC using SP263 or 22C3 antibody) As determined by IHC with SP142 antibody, the fraction of cells or the proportion of tumor area occupied by tumor PD-L1-expressing or PD-L1-expressing tumor infiltrating immune cells (IC) with TPS ≥ 30% (eg ≥ 50%) 1% or more). In some cases, the PD-L1 selected tumor is a tumor that has been determined to be at least 30% (eg, at least 50%) by immunohistochemical (IHC) analysis of a PD-L1 positive tumor cell fraction or PD-L1 TPS. In some cases, the PD-L1-selected tumor is a tumor in which the proportion of tumor area occupied by PD-L1-expressing immune cells (IC) is determined by immunohistochemical (IHC) analysis to be greater than or equal to 1%. In some cases, the IHC assay uses anti-PD-L1 antibodies SP263, 22C3, SP142, or 28-8. In some cases, the IHC assay uses the anti-PD-L1 antibody SP263. In some cases, the IHC assay uses the anti-PD-L1 antibody SP142. In some cases, the IHC assay uses anti-PD-L1 antibody 22C3. In some cases, the tumor sample was determined to have a TPS of 50% or greater. In some cases, the PD-L1-positive tumor cell fraction (eg, as determined by positive staining with anti-PD-L1 antibody SP263 (eg, using a Ventana assay)) is determined by using anti-PD-L1 antibody 22C3 greater than 50% as determined by positive staining used (eg, using pharmDx assay), or as determined by positive staining with anti-PD-L1 antibody 28-8. In some embodiments, the fraction of PD-L1-positive tumor cells is greater than or equal to 30% as determined by positive staining with anti-PD-L1 antibody SP142. In some cases, the IC was determined to be greater than or equal to 1% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 5% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 10% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 50% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 30% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay).
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 개체로부터 얻은 종양 샘플은 PD-L1의 검출 가능한 단백질 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출 가능한 단백질 발현 수준은 IHC 분석법에 의해 결정되었다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 1% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 1% 이상 5% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 5% 이상 50% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 50% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 1% 이상을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 1% 이상 5% 미만을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 5% 이상 10% 미만을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 10% 이상을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. In some cases, in a method, use, or compositions for use described herein, the tumor sample obtained from the individual has a detectable protein expression level of PD-L1. In some cases, detectable protein expression levels of PD-L1 were determined by IHC assay. In some cases, the IHC assay uses the anti-PD-L1 antibody SP142. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% and less than 5% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 5% and less than 50% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 50% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 1% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 1% and less than 5% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 5% and less than 10% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 10% of the tumor sample.
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 개체로부터 얻은 종양 샘플은 PD-L1의 검출 가능한 핵산 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 경우들에서, 조직 샘플은 종양 샘플이다. 일부 경우들에서, 종양 샘플은 종양-침윤 면역 세포, 종양 세포, 간질 세포 및 이들의 임의의 조합을 포함한다. In some cases, in a method, use, or compositions for use described herein, the tumor sample obtained from the individual has a detectable nucleic acid expression level of PD-L1. In some cases, the detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. became In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample. In some cases, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
치료에 대한 반응response to treatment
본원에 기재된 임의의 방법의 일부 구현예들에서, 요법에 대한 대상체의 반응은 하나 이상의 측정에 의해 특징지어질 수 있다. 일부 구현예들에서, 치료는 CR 또는 PR을 발생시킨다. 일부 구현예들에서, 상기 치료는 PFS 또는 DOR의 증가를 발생시킨다. In some embodiments of any of the methods described herein, the subject's response to therapy can be characterized by one or more measures. In some embodiments, the treatment results in CR or PR. In some embodiments, the treatment results in an increase in PFS or DOR.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 PFS의 증가를 발생시킨다. 예를 들어, 화학요법제가 투여되지 않는 구현예들에서(예컨대, PD-1 축 결합 길항제(예컨대, 아테졸리주맙)와 병용한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)만이 투여됨), 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 PFS의 증가를 발생시킨다. 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀(예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신))와 병용하여 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)가 투여된 구현예들에서, 상기 치료는 (i) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제 및 하나 이상의 화학요법제를 이용한 치료와 비교하거나; (ii) PD-1 축 결합 길항제가 없이 항 TIGIT 길항제 항체 및 하나 이상의 화학요법제를 이용한 치료와 비교하거나; 및/또는 (iii) 하나 이상의 화학요법제 없이 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 PFS의 증가를 발생시킨다.In some cases, the treatment increases the subject's PFS, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. causes For example, in embodiments where no chemotherapeutic agent is administered (eg, only an anti TIGIT antagonist antibody (eg, tyragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), the Treatment results in an increase in the subject's PFS, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide), a taxane (eg, paclitaxel)) An anti-TIGIT antagonist antibody (eg, tyragolumab) and a PD-1 axis binding antagonist (eg, atezolizumab) in combination with (eg, nap-paclitaxel), and/or a topoisomerase II inhibitor (eg, doxorubicin)) ) is administered, the treatment is compared to (i) treatment with a PD-1 axis binding antagonist and one or more chemotherapeutic agents in the absence of an anti-TIGIT antagonist antibody; (ii) in the absence of a PD-1 axis binding antagonist of PFS in a subject compared to treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents; and/or (iii) treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody in the absence of one or more chemotherapeutic agents. causes an increase.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 OS를 연장시킨다. 예를 들어, 화학요법제가 투여되지 않는 구현예들에서(예컨대, PD-1 축 결합 길항제(예컨대, 아테졸리주맙)와 병용한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)만이 투여됨), 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 OS의 증가를 발생시킨다. 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드, 젬시타빈, 또는 카페시타빈), 탁산(예컨대, 파클리탁셀(예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 에토포시드))와 병용하여 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)가 투여된 구현예들에서, 상기 치료는 (i) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제 및 하나 이상의 화학요법제를 이용한 치료와 비교하거나; (ii) PD-1 축 결합 길항제가 없이 항 TIGIT 길항제 항체 및 하나 이상의 화학요법제를 이용한 치료와 비교하거나; 및/또는 (iii) 하나 이상의 화학요법제 없이 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체에서 OS의 증가를 발생시킨다.In some cases, the treatment prolongs the subject's OS, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. make it For example, in embodiments where no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tyragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), the Treatment results in an increase in the subject's OS, eg, as compared to treatment with a PD-1 axis binding antagonist without an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody without a PD-1 axis binding antagonist. one or more chemotherapeutic agents (eg, platinum-based chemotherapeutic agents (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin)) and/or one or more non-platinum-based chemotherapeutic agents (eg, antimetabolites (eg, peme) Trexed, gemcitabine, or capecitabine), a taxane (e.g., paclitaxel (e.g., nap-paclitaxel), and/or a topoisomerase II inhibitor (e.g., etoposide)), an anti-TIGIT antagonist antibody ( In embodiments in which tiragolumab) and a PD-1 axis binding antagonist (eg, atezolizumab) are administered, the treatment comprises (i) a PD-1 axis binding antagonist and one or more chemotherapy without an anti-TIGIT antagonist antibody. (ii) treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents in the absence of a PD-1 axis binding antagonist; and/or (iii) PD- without one or more chemotherapeutic agents. results in an increase in OS in a subject compared to treatment with a uniaxial binding antagonist and an anti-TIGIT antagonist antibody.
상기 대상체의 무진행 생존은 Eisenhauer et al., Eur. J. Cancer. 2009, 45:228-47에 기재된 바와 같이 RECIST v1.1 기준에 따른 측정할 수 있다. 일부 구현예들에서, PFS는 RECIST v1.1 기준에 의해 결정된 바와 같이 치료 시작부터 질병 진행의 최초 발생까지의 기간으로서 측정된다 일부 구현예들에서, PFS는 치료 시작부터 사망까지의 시간으로서 측정된다. The progression-free survival of the subject was determined by Eisenhauer et al., Eur. J. Cancer . 2009, 45:228-47, it can be measured according to the RECIST v1.1 standard. In some embodiments, PFS is measured as the period from initiation of treatment to the first occurrence of disease progression as determined by the RECIST v1.1 criteria. In some embodiments, PFS is measured as the time from initiation of treatment to death. .
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체의 PFS를 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 PFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 치료는 상기 대상체의 PFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein reduces the subject's PFS by at least about 2.4 months (eg, by 2.4-120 months, by 2.5-100 months, by 3.0-80 months, by 4.0-60 months, by 5.0- by 48 months, by 6.0 to 36 months, by 8.0 to 24 months, or by 10 to 12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's PFS by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months) by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment reduces the subject's PFS by at least about 2 months (eg, by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, by 8 to 48 months) , by 9-36 months, by 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months , 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 (by months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) make it
일부 구현예들에서, 치료는 상기 대상체의 DOR을 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 DOR을 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 치료는 상기 대상체의 DOR을 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, treatment increases the subject's DOR by at least about 2.4 months (eg, by 2.4-120 months, by 2.5-100 months, by 3.0-80 months, by 4.0-60 months, by 5.0-48 months) , by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0, 5.1, 5.2, 5.3, 5.4, 5.5, 5.6, 5.7, 5.8, 5.9, 6.0, 6.5, 7.0, 7.5, 8.0, 8.5, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment increases the subject's DOR by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months) by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment increases the subject's DOR by at least about 2 months (eg, by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, by 8 to 48 months) , by 9-36 months, by 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months , 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 (by months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) make it
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월,4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, OS is measured as the period from initiation of treatment to death. In some cases, the treatment reduces the subject's OS by at least about 2 months (eg, by 2-120 months, by 3-110 months, by 4-100 months, by 5-80 months, by 6-60 months) , by 7-48 months, by 8-36 months, by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months , 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 Months, 20 Months, 21 Months, 22 Months, 23 Months, 24 Months, 25 Months, 26 Months, 27 Months, 28 Months, 29 Months, 30 Months, 31 Months, 32 Months, 33 Months, 34 Months, 35 Months, or by 36 months). In some cases, the treatment reduces the subject's OS by at least about 3.3 months (eg, by 3.3-120 months, by 4-100 months, by 5-80 months, by 6-60 months, by 7-48 months) , by 8-36 months, or by 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months , 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, by 34 months, 35 months, or 36 months). In some cases, the treatment reduces the subject's OS by at least about 5.3 months (eg, by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months). by, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months , by 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
B.B. 폐암과 관련된 치료 방법 및 사용Treatment methods and uses associated with lung cancer
폐암은 계속 전 세계적으로 암 사망의 주요 원인이다. 미국에서는, 남성과 여성 모두에게 가장 흔한 암이며 모든 새로운 암 사례의 12%~14%를 차지한다. 2020년에는, 약 228,820명의 새로운 폐암 사례가 발생하여 미국에서 135,720명이 사망할 것으로 예상된다(Siegel et al. CA Cancer J Clin. 70:7-30 (2020)).Lung cancer continues to be the leading cause of cancer death worldwide. In the United States, it is the most common cancer in both men and women, accounting for 12% to 14% of all new cancer cases. By 2020, approximately 228,820 new cases of lung cancer will occur and 135,720 deaths are expected in the United States (Siegel et al. CA Cancer J Clin. 70:7-30 (2020)).
비소세포 폐암non-small cell lung cancer
비소세포폐암(NSCLC)은 모든 사례의 약 85%를 차지하는 폐암의 주요 하위유형이다. Non-small cell lung cancer (NSCLC) is the major subtype of lung cancer, accounting for approximately 85% of all cases.
비소세포폐암(NSCLC)은 모든 사례의 약 80%~85%를 차지하는 폐암의 주요 하위유형이다(Osmani et al. Semin Cancer Biol. 52 (Pt 1):103-9 (2018)). NSCLC는 두 가지 주요 조직학적 유형으로 나눌 수 있다: 선암종 및 편평 세포 암종(Travis et al. 2011). 선암종 조직학은 모든 NSCLC의 약 40%~50%를 차지하는 반면, 편평 세포 조직학은 NSCLC의 약 20%~30%를 차지한다(Osmani et al. Semin Cancer Biol. 52 (Pt 1):103-9 (2018)). NSCLC의 나머지 사례는 대세포 암종, 신경내분비 종양, 육종양 암종으로 대표되며, 조직학이 잘 분화되지 않는다.Non-small cell lung cancer (NSCLC) is the major subtype of lung cancer, accounting for approximately 80%-85% of all cases (Osmani et al. Semin Cancer Biol. 52 (Pt 1):103-9 (2018)). NSCLC can be divided into two main histological types: adenocarcinoma and squamous cell carcinoma (Travis et al. 2011). Adenocarcinoma histology accounts for about 40% to 50% of all NSCLCs, whereas squamous cell histology accounts for about 20% to 30% of NSCLCs (Osmani et al. Semin Cancer Biol. 52 (Pt 1):103-9 ( 2018)). The remaining cases of NSCLC are represented by large cell carcinomas, neuroendocrine tumors, and sarcoma carcinomas, with poorly differentiated histology.
초기 단계에서, NSCLC는 치료 목적으로 외과적으로 치료된다. 하지만, 절제술을 받은 환자의 30~70%가 재발하여 질병 진행의 결과로서 사망한다(Siegel et al. Cancer Statistics. CA Cancer J Clin. 70:7-30 (2020)). 따라서, 초기 NSCLC에 대한 개선된 의학적 개입에 대한 충족되지 않은 요구가 높다.In the early stages, NSCLC is treated surgically for therapeutic purposes. However, 30-70% of patients undergoing resection recur and die as a result of disease progression (Siegel et al. Cancer Statistics. CA Cancer J Clin. 70:7-30 (2020)). Therefore, there is a high unmet need for improved medical interventions for early NSCLC.
진행성 질병의 경우, 전체 5년의 생존율은2%-4%이다. NSCLC 환자의 생존에 대한 불량한 예후 인자에는 초기 진단시 질병의 진행 단계, 전신 활동도 및 의도하지 않은 체중 감소의 병력이 포함된다. NSCLC 환자의 절반 이상이 원격 질병으로 진단되고, 이는 좋지 않은 생존 전망의 직접적 원인이 된다.For advanced disease, the overall 5-year survival rate is 2%-4%. Poor prognostic factors for survival in patients with NSCLC include disease progression at initial diagnosis, systemic activity, and a history of unintended weight loss. More than half of NSCLC patients are diagnosed with a distant disease, which is a direct cause of poor survival prospects.
진행성 NSCLC 환자의 1차 치료가 개선되어 생존 기간이 연장되고 질병 관련 증상이 감소했음에도 불구하고 거의 모든 환자가 질병 진행을 경험한다. 특히, 암 면역 요법은 장기적인 질병 통제의 가능성을 제공한다. 전이성 NSCLC 설정에서 PD-L1/PD-1 차단 항체(예를 들어, 아테졸리주맙, 니볼루맙, 펨브롤리주맙)는 선택되지 않은 또는 PD-L1-선택된 진행성 NSCLC 환자에게 임상적으로 의미 있는 이점을 제공하였다; 그러나 상당한 비율의 환자가 항 PD-L1/PD-1 치료에 여전히 무반응이거나 진행성인 상태로 남아있으며 이러한 치료에 대한 탈출 메커니즘은 잘 이해되지 않고 있다. Almost all patients experience disease progression, despite improvements in first-line treatment of patients with advanced NSCLC, prolonging survival and reducing disease-related symptoms. In particular, cancer immunotherapy offers the potential for long-term disease control. In the setting of metastatic NSCLC, PD-L1/PD-1 blocking antibodies (e.g., atezolizumab, nivolumab, pembrolizumab) offer clinically meaningful benefits in patients with unselected or PD-L1-selected advanced NSCLC. provided; However, a significant proportion of patients still remain unresponsive or advanced to anti-PD-L1/PD-1 therapy, and the mechanisms of escape for these therapies are not well understood.
따라서, 보다 유리한 이익-위험 프로파일 달성하는 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))의 치료(예컨대, 1차 치료)를 위한 효과적인 면역요법 및 이를 투약하는 방법을 개발하는 분야에서 충족되지 않은 요구가 있다.Thus, treatment (e.g., first line There is an unmet need in the field of developing effective immunotherapy for treatment) and methods of administering the same.
소세포 폐암small cell lung cancer
소세포폐암(SCLC)은 전체 폐암 사례의 약 15%를 차지한다. 소세포 폐암(SCLC) 환자의 대다수(약 70%)는 생존 가능성이 낮은 확장 병기의 소세포 폐암(ES-SCLC)으로 진단된다(OS 중앙값이 약 10~12개월). 화학요법만으로도 확장 병기의 소세포 폐암(ES-SCLC) 환자의 증상을 완화하고 생존을 연장시킬 수 있지만, 장기 생존은 드물다. I기 SCLC 환자의 5년 상대 생존율은 약 31%이다. IV기에서는, 5년 상대생존율은 약 2%로 감소한다. Small cell lung cancer (SCLC) accounts for about 15% of all lung cancer cases. The majority (approximately 70%) of patients with small cell lung cancer (SCLC) are diagnosed with expanded-stage small cell lung cancer (ES-SCLC) with low survival rates (median OS of approximately 10 to 12 months). Chemotherapy alone can relieve symptoms and prolong survival in patients with expanded-stage small cell lung cancer (ES-SCLC), but long-term survival is rare. The 5-year relative survival rate for patients with stage I SCLC is approximately 31%. In stage IV, the 5-year relative survival rate decreases to about 2%.
따라서, 폐암(예컨대, SCLC, 예컨대 ES-SCLC)에 대한 개선된 치료가 현장에서 필요하다. Therefore, there is a need in the field for improved treatments for lung cancer (eg, SCLC, such as ES-SCLC).
i. 폐암 치료를 위한 방법 및 사용 i. Methods and uses for the treatment of lung cancer
본원에서는 폐암을 가진 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하는 방법이 제공되고, 여기서 상기 치료는 적어도 약 6개월(예컨대, 적어도 약 6개월(예컨대, 적어도 약 6개월(예컨대, 6개월 내지 24개월)(예컨대, 약 6개월 내지 약 15개월(예컨대, 6개월, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 14개월 또는 15개월), 예컨대 약 6개월 내지 약 13개월(예컨대, 6개월, 6.5개월, 7개월, 7.5개월, 8개월, 8.5개월, 9개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 12.5개월, 13개월)), 예컨대, 약 8개월 내지 약 10개월(예컨대, 8.1개월, 8.2개월, 8.3개월, 8.4개월, 8.5개월, 8.6개월, 8.7개월, 8.8개월, 8.9개월, 9.0개월, 9.1개월, 9.2개월, 9.3개월, 9.4개월, 9.5개월, 9.6개월, 9.7개월, 9.8개월, 9.9개월, 10.0개월))의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 치료는 약 8.2개월 내지 약 9.2개월(예컨대, 약 8.2개월, 8.4개월, 8.6개월, 8.8개월, 9.0개월, 또는 9.2개월, 예컨대 8.2~8.4개월, 8.4~8.6개월, 8.6~8.8개월, 8.8~9.0개월, 또는 9.0~9.2개월)의 대상체 집단의 PFS 중앙값을 발생시킨다.Disclosed herein is a method of treating a population of subjects with lung cancer, comprising a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. Provided is a method comprising administering to said subject population, wherein said treatment is for at least about 6 months (eg, at least about 6 months (eg, at least about 6 months (eg, 6 months to 24 months) (eg, about 6 months to about 15 months (e.g., 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months or 15 months), such as about 6 months to about 13 months ( For example, 6 months, 6.5 months, 7 months, 7.5 months, 8 months, 8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 12.5 months, 13 months)), such as , from about 8 months to about 10 months (eg, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8.5 months, 8.6 months, 8.7 months, 8.8 months, 8.9 months, 9.0 months, 9.1 months, 9.2 months, 9.3 months, 9.4 months, 9.5 months, 9.6 months, 9.7 months, 9.8 months, 9.9 months, 10.0 months), in some cases, treatment is from about 8.2 months to about 9.2 months (e.g., about 8.2 months, 8.4 months, 8.6 months, 8.8 months, 9.0 months, or 9.2 months, such as 8.2-8.4 months, 8.4-8.6 months, 8.6-8.8 months, 8.8-9.0 months, or 9.0-9.2 months) Generates the median PFS.
본원에서는 또한 폐암을 가진 대상체 집단을 치료하는 방법으로서, 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하는 방법이 제공되고, 여기서 상기 치료는 적어도 약 12개월(예컨대, 적어도 약 12개월 내지 약 40개월(예컨대, 약 12개월 내지 약 30개월(예컨대, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 또는 30개월), 예컨대 약 12개월 내지 약 20개월(예컨대, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 또는 20개월))의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 약 15.3개월 내지 약 17.6개월(예컨대, 약 15.5개월, 16개월, 16.5개월, 17개월, 17.5개월, 또는 17.6개월, 예컨대 15.3~16개월, 16~17개월, 또는 17~17.6개월)의 대상체 집단의 PFS 중앙값을 발생시킨다.Also disclosed herein is a method of treating a population of subjects having lung cancer, comprising administering an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and one or more dosing cycles of a topoisomerase II inhibitor. Provided is a method comprising administering therapy to said population of subjects, wherein said treatment is for at least about 12 months (eg, at least about 12 months to about 40 months (eg, about 12 months to about 30 months (eg, 12 months)). months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, or 30 months), such as from about 12 months to about 20 months (eg, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, or 20 months)) In some cases, the treatment is about 15.3 months to about 17.6 months (e.g., about 15.5 months, 16 months, 16.5 months, 17 months, 17.5 months, or 17.6 months, such as 15.3-16 months) months, 16-17 months, or 17-17.6 months).
ii. 소세포 폐암 치료를 위한 방법 및 사용 ii. Methods and uses for the treatment of small cell lung cancer
본원에서는 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 상기 대상체 또는 대상체 집단에서 폐암(예컨대, 소세포 폐암(SCLC), 예컨대 확장기 SCLC(ES-SCLC))을 치료하기 위한 방법 및 사용이 제공된다. Disclosed herein is an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), platinum a subject or a population of subjects comprising administering to the subject or population of subjects one or more dosing cycles of a chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide) Methods and uses are provided for treating lung cancer (eg, small cell lung cancer (SCLC), such as diastolic SCLC (ES-SCLC)) in a subject population.
투약 요법, 투여, 및 치료에 대한 반응Dosing regimen, administration, and response to treatment
일 양태에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 폐암(예컨대, SCLC, 예컨대 ES-SCLC)을 가진 대상체 또는 대상체 집단에게 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 백금계 화학요법제, 및 토포이소머라제 II 억제제를 투여하는 단계를 포함하고, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 무진행 생존(PFS)을 연장함으로써, 상기 대상체 또는 대상체 집단을 치료한다. 일부 경우들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)을 연장시킨다.In one aspect, the treatment methods and uses of the invention described herein are administered to a subject or population of subjects having lung cancer (eg, SCLC, such as ES-SCLC) in an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist as disclosed herein). administering an antibody such as tyragolumab), a PD-1 axis binding antagonist (such as an anti-PD-L1 antagonist antibody (such as atezolizumab)), a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor and wherein said treatment is compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody ( PFS), thereby treating said subject or population of subjects. In some cases, the treatment comprises overall survival (OS) of the subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. ) is extended.
일부 구현예들에서, 상기 개체의 PFS는 Eisenhauer et al., Eur. J. Cancer. 2009, 45:228-47에 기재된 바와 같이 RECIST v1.1 기준에 따른 측정한다. 일부 구현예들에서, PFS는 RECIST v1.1 기준에 의해 결정된 바와 같이 치료 시작부터 질병 진행의 최초 발생까지의 기간으로서 측정된다 일부 구현예들에서, PFS는 치료 시작부터 사망까지의 시간으로서 측정된다. In some embodiments, the subject's PFS is described in Eisenhauer et al., Eur. J. Cancer . 2009, 45:228-47 according to RECIST v1.1 criteria as described. In some embodiments, PFS is measured as the period from initiation of treatment to the first occurrence of disease progression as determined by the RECIST v1.1 criteria. In some embodiments, PFS is measured as the time from initiation of treatment to death. .
일부 구현예들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 양태들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3개월 내지 약 4개월 만큼 연장시킨다. In some embodiments, the treatment is compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody in the subject or population of subjects. PFS by at least about 2.4 months (e.g., by 2.4-120 months, by 2.5-100 months, by 3.0-80 months, by 4.0-60 months, by 5.0-48 months, by 6.0-36 months, by 8.0-24 months by, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months , 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months , by 35 months, or by 36 months). In some embodiments, the treatment is compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody in the subject or population of subjects. PFS by at least about 4 months (e.g., by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months, by 9 to 36 months, or by 10 to 24 months) by months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months. , 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 Months, 20 Months, 21 Months, 22 Months, 23 Months, 24 Months, 25 Months, 26 Months, 27 Months, 28 Months, 29 Months, 30 Months, 31 Months, 32 Months, 33 Months, 34 Months, 35 Months, or by 36 months). In some embodiments, the treatment is compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody in the subject or population of subjects. PFS by at least about 2 months (e.g., by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, by 8 to 48 months, by 9 to 36 months, or by 10 to 24 months) by months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months. , 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months , by 33 months, 34 months, 35 months, or 36 months). In some aspects, said treatment is PFS of said subject or population of subjects compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. to at least about 3 months to about 4 months.
일부 경우들에서, 폐암(예컨대, SCLC, 예컨대 ES-SCLC)을 가진 대상체 또는 대상체 집단을 치료하는 방법 및 사용은 상기 대상체 또는 대상체 집단에게 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)를 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 연장시킨다. In some cases, the methods and uses of treating a subject or population of subjects having lung cancer (eg, SCLC, such as ES-SCLC) include administering to the subject or population of subjects an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist as disclosed herein). TIGIT antagonist antibodies, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies, such as atezolizumab), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin), and topoiso and administering a merase II inhibitor (eg, etoposide), wherein said treatment is without said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase. prolongs the OS of the subject or population of subjects as compared to treatment with a II inhibitor.
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some embodiments, OS is measured as the period from initiation of treatment to death. In some instances, the treatment reduces the OS of the subject or population of subjects as compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody. by at least about 2 months (e.g., by 2 to 120 months, by 3 to 110 months, by 4 to 100 months, by 5 to 80 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months; or by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months , 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, said treatment is an OS of said subject or population of subjects compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. by at least about 3.3 months (e.g., by 3.3 to 120 months, by 4 to 100 months, by 5 to 80 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months by, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months , 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, said treatment is an OS of said subject or population of subjects compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. by at least about 5.3 months (e.g., by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months, such as by at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months , by 34 months, 35 months, or 36 months).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 600 mg(예컨대, 약 50 mg 내지 약 600 mg, 예컨대, 약 60 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 550 mg, 예컨대, 약 250 mg 내지 약 500 mg, 예컨대, 약 300 mg 내지 약 450 mg, 예컨대, 약 350 mg 내지 약 400 mg, 예컨대, 약 375 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 600 mg의 용량(예컨대, 고정 용량)이다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about 1100) every 3 weeks. mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, For example, a dose (eg, a fixed dose) of 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 30 mg to about 600 mg (eg, from about 50 mg to about) every 3 weeks. 600 mg, such as about 60 mg to about 600 mg, such as about 100 mg to about 600 mg, such as about 200 mg to about 600 mg, such as about 200 mg to about 550 mg, such as about 250 mg to about A dose (eg, a fixed dose) of 500 mg, such as about 300 mg to about 450 mg, such as about 350 mg to about 400 mg, such as about 375 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose (eg, a fixed dose) of about 600 mg every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 30 mg 내지 600 mg(예컨대, 50 mg 내지 600 mg, 예컨대, 60 mg 내지 600 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 200 mg 내지 600 mg, 예컨대, 200 mg 내지 550 mg, 예컨대, 250 mg 내지 500 mg, 예컨대, 300 mg 내지 450 mg, 예컨대, 350 mg 내지 400 mg, 예컨대, 375 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 600 mg의 용량(예컨대, 고정 용량)이다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 30 mg to 1200 mg (eg, 30 mg to 1100 mg, eg, 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as , 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 30 mg to 600 mg (eg, 50 mg to 600 mg, such as every 3 weeks) , 60 mg to 600 mg, such as 100 mg to 600 mg, such as 200 mg to 600 mg, such as 200 mg to 550 mg, such as 250 mg to 500 mg, such as 300 mg to 450 mg, such as 350 mg to 400 mg, such as 375 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg (eg, a fixed dose) every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 600 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 토포이소머라제 II 억제제(예컨대, 에토포시드), 및/또는 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)와의 병용 치료)으로 투여되는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량(예컨대, 고정 용량)은 단일요법으로 투여되는 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg (eg, a fixed dose) every 3 weeks. In some cases, combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), a topoisomerase II inhibitor (eg, etoposide), and/or platinum A dose (e.g., a fixed dose) of the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tyragolumab) administered in combination therapy with a chemotherapeutic agent (e.g., carboplatin or cisplatin) ) may be reduced compared to the standard dose of the anti-TIGIT antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 1600 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1600 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 약 840 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 1200 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 1600 mg, 예컨대, 200 mg 내지 1600 mg, 예컨대, 300 mg 내지 1600 mg, 예컨대, 400 mg 내지 1600 mg, 예컨대, 500 mg 내지 1600 mg, 예컨대, 600 mg 내지 1600 mg, 예컨대, 700 mg 내지 1600 mg, 예컨대, 800 mg 내지 1600 mg, 예컨대, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 840 mg의 용량(예컨대, 고정 용량)이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 3 weeks. 1600 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1600 mg, such as about 400 mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg , eg, 1200±2.5 mg, eg, 1200±1.0 mg, eg, 1200±0.5 mg, eg, 1200 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of about 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 1600 mg, such as every 3 weeks) , 200 mg to 1600 mg, such as 300 mg to 1600 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to A dose (e.g., 1225 mg, such as 1190 mg to 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg) fixed capacity). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of 840 mg every two weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 1400 mg 내지 2000 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 1400 mg 내지 2000 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주 마다 약 1680 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주 마다 1680 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 토포이소머라제 II 억제제(예컨대, 에토포시드), 및/또는 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴과의 병용 치료)으로 투여되는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량(예컨대, 고정 용량)은 단일요법으로 투여되는 상기 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of about 1400 mg to 2000 mg every 3 weeks. . In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of 1400 mg to 2000 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, a fixed dose) of 1680 mg every 4 weeks. In some cases, combination therapy (eg, an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab), a topoisomerase II inhibitor (eg, etoposide), and/or platinum-based chemistry A dose (eg, a fixed dose) of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) administered as a therapy (eg, combination treatment with carboplatin or cisplatin) can be reduced compared to a standard dose of the PD-1 axis binding antagonist administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대 약 1 mg/kg 내지 약 35 mg/kg, 예컨대 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대 약 5 mg/kg 내지 약 25 mg/kg, 예컨대 약 10 mg/kg 내지 약 20 mg/kg, 예컨대 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 투여되는 약 15 mg/kg의 용량이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 50 mg/kg of the subject's body weight every 3 weeks. kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg /kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 15 mg/kg of the subject's body weight every 3 weeks. (e.g., about 0.1 mg/kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, such as about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 10 mg/kg to about 15 mg/kg, such as , about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, such as about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 15 mg/kg administered every 3 weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대 0.1 mg/kg 내지 40 mg/kg, 예컨대 1 mg/kg 내지 35 mg/kg, 예컨대 2.5 mg/kg 내지 30 mg/kg, 예컨대 5 mg/kg 내지 25 mg/kg, 예컨대 10 mg/kg 내지 20 mg/kg, 예컨대 12.5 mg/kg 내지 15 mg/kg, 예컨대 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대 0.5 mg/kg 내지 15 mg/kg, 예컨대 1 mg/kg 내지 15 mg/kg, 예컨대 2.5 mg/kg 내지 15 mg/kg, 예컨대 5 mg/kg 내지 15 mg/kg, 예컨대 7.5 mg/kg 내지 15 mg/kg, 예컨대 10 mg/kg 내지 15 mg/kg, 예컨대 12.5 mg/kg 내지 15 mg/kg, 예컨대 14 mg/kg 내지 15 mg/kg, 예컨대 15 ± 1 mg/kg, 예컨대 15 ± 0.5 mg/kg, 예컨대 15 ± 0.2 mg/kg, 예컨대 15 ± 0.1 mg/kg, 예컨대 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 투여되는 15 mg/kg의 용량이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 50 mg/kg of body weight of the subject every 3 weeks ( For example, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 15 mg/kg of body weight of the subject every 3 weeks ( For example, 0.1 mg/kg to 15 mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 15 mg/kg, such as 10 mg/kg to 15 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 14 mg/kg to 15 mg/kg, for example 15 ± 1 mg/kg, such as 15 ± 0.5 mg/kg, such as 15 ± 0.2 mg/kg, such as 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 15 mg/kg administered every 3 weeks.
일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 토포이소머라제 II 억제제(예컨대, 에토포시드), 및/또는 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴과의 병용 치료)으로 투여되는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 상기 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다.In some cases, combination therapy (eg, an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab), a topoisomerase II inhibitor (eg, etoposide), and/or platinum-based chemistry The dose of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) administered as a therapy (eg, combination treatment with carboplatin or cisplatin) is administered as a monotherapy. may be reduced compared to a standard dose of the PD-1 axis binding antagonist.
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 1~50 mg/ml/분(예컨대, 2~25 mg/ml/분, 3~15 mg/ml/분, 4~10 mg/ml/분, 또는 5 mg/ml/분, 예컨대 2 mg/ml/분, 3 mg/ml/분, 4 mg/ml/분, 5 mg/ml/분, 6 mg/ml/분, 7 mg/ml/분, 8 mg/ml/분, 9 mg/ml/분, 10 mg/ml/분, 11 mg/ml/분, 12 mg/ml/분, 13 mg/ml/분, 14 mg/ml/분, 15 mg/ml/분, 20 mg/ml/분, 25 mg/ml/분, 30 mg/ml/분, 35 mg/ml/분, 40 mg/ml/분, 45 mg/ml/분, 50 mg/ml/분)의 AUC를 달성하기에 충분한 용량이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 AUC = 5 mg/ml/분을 달성하기에 충분한 용량이다.In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 1-50 mg/ml/min (eg, 2-25 mg/ml/min, 3-15 mg/ml/min) min, 4-10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml/min, 6 mg /ml/min, 7 mg/ml/min, 8 mg/ml/min, 9 mg/ml/min, 10 mg/ml/min, 11 mg/ml/min, 12 mg/ml/min, 13 mg/ ml/min, 14 mg/ml/min, 15 mg/ml/min, 20 mg/ml/min, 25 mg/ml/min, 30 mg/ml/min, 35 mg/ml/min, 40 mg/ml /min, 45 mg/ml/min, 50 mg/ml/min). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is a dose sufficient to achieve AUC=5 mg/ml/min.
AUC는 칼버트(Calvert) 공식을 사용하여 계산할 수 있다(Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):AUC can be calculated using the Calvert formula (Calvert et al., J. Clin. Oncol . 1989, 7:1748-56):
총 용량(mg) =(목표 AUC) ´(사구체 여과율[GFR] +25)Total dose (mg) =(target AUC) ´(glomerular filtration rate [GFR] +25)
일부 경우들에서, 예를 들어, 아테졸리주맙의 1200 mg은 평균 체중 기반 용량의 15 m/kg과 같다.In some cases, for example, 1200 mg of atezolizumab is equal to 15 m/kg of an average body weight based dose.
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 200 mg~1500 mg(예컨대, 300 mg~1200 mg, 400 mg~1100 mg, 또는 500 mg~1000 mg, 예컨대 300 mg~400 mg, 400 mg~500 mg, 500 mg~600 mg, 600 mg~700 mg, 700 mg~750 mg, 750 mg~800 mg, 800 mg~900 mg, 900 mg~1000 mg, 1000 mg~1100 mg, 또는 1100 mg~1200 mg, 예컨대 약 200 mg, 약 300 mg, 약 400 mg, 약 500 mg, 약 600 mg, 약 700 mg, 약 800 mg, 약 900 mg, 약 1000 mg, 약 1100 mg, 약 1200 mg, 약 1300 mg, 약 1400 mg, 또는 약 1500 mg)이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 약 500 mg~1000 mg(예컨대, 약 500 mg, 약 600 mg, 약 700 mg, 약 800 mg, 약 900 mg, 또는 약 1000 mg)이다.In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, For example 300 mg-400 mg, 400 mg-500 mg, 500 mg-600 mg, 600 mg-700 mg, 700 mg-750 mg, 750 mg-800 mg, 800 mg-900 mg, 900 mg-1000 mg, 1000 mg-1100 mg, or 1100 mg-1200 mg, such as about 200 mg, about 300 mg, about 400 mg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, about 1000 mg, about 1100 mg, about 1200 mg, about 1300 mg, about 1400 mg, or about 1500 mg). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is between about 500 mg and 1000 mg (eg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg). mg, or about 1000 mg).
일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 10~1000 mg/m2(예컨대, 20~800 mg/m2, 30~700 mg/m2, 40~500 mg/m2, 50~300 mg/m2, 75~200 mg/m2, 또는 80~150 mg/m2, 예컨대, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 또는 약 1000 mg/m2)이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 약 100 mg/m2이다.In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40- 500 mg/m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg /m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/ m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 ). In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 .
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 200 mg~1500 mg(예컨대, 300 mg~1200 mg, 400 mg~1100 mg, 또는 500 mg~1000 mg, 예컨대 300 mg~400 mg, 400 mg~500 mg, 500 mg~600 mg, 600 mg~700 mg, 700 mg~750 mg, 750 mg~800 mg, 800 mg~900 mg, 900 mg~1000 mg, 1000 mg~1100 mg, 또는 1100 mg~1200 mg, 예컨대 200 mg, 300 mg, 400 mg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, 1000 mg, 1100 mg, 1200 mg, 1300 mg, 1400 mg, 또는 1500 mg)이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 500 mg~1000 mg(예컨대, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, 또는 1000 mg)이다.In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, For example 300 mg-400 mg, 400 mg-500 mg, 500 mg-600 mg, 600 mg-700 mg, 700 mg-750 mg, 750 mg-800 mg, 800 mg-900 mg, 900 mg-1000 mg, 1000 mg-1100 mg, or 1100 mg-1200 mg, such as 200 mg, 300 mg, 400 mg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, 1000 mg, 1100 mg, 1200 mg, 1300 mg, 1400 mg, or 1500 mg). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is between 500 mg and 1000 mg (eg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, or 1000 mg). to be.
일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 10~1000 mg/m2(예컨대, 20~800 mg/m2, 30~700 mg/m2, 40~500 mg/m2, 50~300 mg/m2, 75~200 mg/m2, 또는 80~150 mg/m2, 예컨대, 20 mg/m2, 30 mg/m2, 40 mg/m2, 50 mg/m2, 60 mg/m2, 70 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 250 mg/m2, 300 mg/m2, 400 mg/m2, 500 mg/m2, 600 mg/m2, 700 mg/m2, 800 mg/m2, 900 mg/m2, 또는 1000 mg/m2)이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 100 mg/m2이다.In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40- 500 mg/m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg/m 2 , 130 mg/m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/ m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , or 1000 mg/m 2 ) is. In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is 100 mg/m 2 .
본 발명의 임의의 방법 및 사용에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)는 1회 이상의 투약 주기(예컨대, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 또는 50회 이상의 투약 사이클)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))(백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)을 포함 또는 미포함) 및/또는 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망, 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 18 내지 24일(예컨대, 15일, 16일, 17일, 18일, 19일, 20일, 21일, 22일, 23일, 또는 24일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 28일이다. In any of the methods and uses of the invention, said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) (eg, atezolizumab)), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide) are administered in one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycle). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab)) (with or without a platinum-based chemotherapeutic agent (eg carboplatin or cisplatin)) and/or the dosing cycle of the topoisomerase II inhibitor (eg etoposide) results in loss of clinical benefit (eg, , disease progression, drug resistance, death, or unacceptable toxicity). In some cases, the length of each dosing cycle is about 18 to 24 days (eg, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, or 24 days). to be. In some cases, the length of each dosing cycle is about 21 days. In some cases, the length of each dosing cycle is about 14 days. In some cases, the length of each dosing cycle is about 28 days.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기, 예컨대 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기, 예컨대 각 21일 주기의 제 1일에 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여된다. 유사하게, 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 고정 용량으로 (즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 다른 예들에서, 예컨대 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 고정 용량으로 (즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 고정 용량으로 (즉, 3주마다 1200 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 둘 모두는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 일부 경우들에서, 상기 백금계 화학요법제는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 일부 경우들에서, 상기 토포이소머라제 II 억제제는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로 정맥내 투여되고(즉, 3주마다 약 600 mg의 용량으로), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량) 정맥내 투여되고, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 AUC = 5mg/ml/분을 달성하기에 충분한 용량으로 4회 초기 투약 주기 각각의 1일에 투여되며, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 4회의 초기 투약 주기의 각각의 1일, 2일 및 3일에 100 mg/m2의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로 정맥내 투여되고(즉, 3주마다 600 mg의 용량으로), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량) 정맥내 투여되고, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 AUC = 5mg/ml/분을 달성하기에 충분한 용량으로 4회 초기 투약 주기의 각 1일에 투여되며, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 4회의 초기 투약 주기의 각각의 1일, 2일 및 3일에 100 mg/m2의 용량으로 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about day 1 (eg,
일부 경우들에서, 상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각에서 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 약 30 mg 내지 약 1200 mg의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 약 30 mg 내지 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 4회의 초기 투약 주기의 각 1일에 약 80 mg 내지 약 1600 mg의 용량으로 투여된다(예컨대, 4회의 초기 투약 주기의 각 1일에 약 1200 mg의 용량으로). 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 30 mg 내지 1200 mg의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 30 mg 내지 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 4회의 초기 투약 주기의 각 1일에 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 4회의 초기 투약 주기의 각 1일에 80 mg 내지 1600 mg의 용량으로 투여된다(예컨대, 4회의 초기 투약 주기의 각 1일에 1200 mg의 용량으로). 일부 경우들에서, 상기 백금계 화학요법제는 4회의 초기 투약 주기의 각 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되고, 그리고/또는 상기 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각의 1일, 2일 및 3일에 100 mg/m2의 용량으로 투여된다. In some cases, the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered in each of the four initial dosing cycles. In some cases, the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg on
일부 경우들에서, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 제4 초기 투약 주기 이후에 1회 이상의 추가 주기로 더 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 1회 이상의 추가적인 투약 주기의 각 1일에 약 30 mg 내지 약 1200 mg의 용량으로 투여된다(예컨대, 1회 이상의 추가적인 투약 주기의 각 1일에 약 30 mg 내지 약 600 mg의 용량으로). 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 1회 이상의 추가적인 투약 주기의 각 1일에 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 1회 이상의 추가적인 투약 주기의 각 1일에 약 80 mg 내지 약 2000 mg의 용량으로 투여된다(예컨대, 1회 이상의 추가적인 투약 주기의 각 1일에 약 840 mg, 1200 mg, 또는 1680 mg의 용량으로). 일부 경우들에서, 상기 추가적인 투약 주기는 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)를 2주마다 약 840 mg, 3주마다 약 1200 mg, 또는 4주마다 약 1680 mg의 용량으로 투여하는 것을 포함한다. 예를 들어, 일부 경우들에, 상기 1회 이상의 투약 주기의 각각은 약 14일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 약 840 mg의 용량으로 투여된다. 일부 경우들에서, 상기 1회 이상의 투약 주기의 각각은 약 21일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 약 1200 mg의 용량으로 투여된다. 일부 경우들에서, 상기 1회 이상의 투약 주기의 각각은 약 28일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 약 1680 mg의 용량으로 투여된다. In some cases, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are further administered in one or more additional cycles after the fourth initial dosing cycle. In some cases, the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg on each day of one or more additional dosing cycles (eg, about 30 on each day of one or more additional dosing cycles). mg to about 600 mg). In some cases, the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg on each day of one or more additional dosing cycles. In some cases, the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg on each day of one or more additional dosing cycles (eg, on each day of one or more additional dosing cycles) at a dose of about 840 mg, 1200 mg, or 1680 mg). In some cases, the additional dosing cycle comprises administering the PD-1 axis binding antagonist (eg, atezolizumab) at a dose of about 840 mg every 2 weeks, about 1200 mg every 3 weeks, or about 1680 mg every 4 weeks includes doing For example, in some cases, each of the one or more dosing cycles is about 14 days, and the PD-1 axis binding antagonist (eg, atezolizumab) is administered on
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 1회 이상의 추가적인 투약 주기의 각 1일에 30 mg 내지 1200 mg의 용량으로 투여된다(예컨대, 상기 1회 이상의 추가적인 투약 주기의 각 1일에 30 mg 내지 600 mg의 용량으로). 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 80 mg 내지 2000 mg의 용량으로 투여된다(예컨대, 1회 이상의 추가적인 투약 주기의 각 1일에 840 mg, 1200 mg, 또는 1680 mg의 용량으로). 일부 경우들에서, 상기 추가적인 투약 주기는 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)를 2주마다 840 mg, 3주마다 1200 mg, 또는 4주마다 1680 mg의 용량으로 투여하는 것을 포함한다. 예를 들어, 일부 경우들에, 상기 1회 이상의 투약 주기의 각각은 14일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 840 mg의 용량으로 투여된다. 일부 경우들에서, 상기 1회 이상의 투약 주기의 각각은 21일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 1200 mg의 용량으로 투여된다. 일부 경우들에서, 상기 1회 이상의 투약 주기의 각각은 28일이고, 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 상기 1회 이상의 추가적인 투약 주기의 각 1일에 1680 mg의 용량으로 투여된다. In some cases, the anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg on each day of one or more additional dosing cycles (eg, 30 mg to 1200 mg on each day of one or more additional dosing cycles) at a dose of 600 mg). In some cases, the anti-TIGIT antagonist antibody is administered at a dose of 600 mg on each day of the one or more additional dosing cycles. In some cases, the PD-1 axis binding antagonist is administered at a dose of 80 mg to 2000 mg on each
일부 경우들에서, 폐암(예컨대, SCLC, 예컨대, ES-SCLC)을 가진 대상체 또는 대상체의 집단은 상기 대상체 또는 대상체 집단에게 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대 약 60 mg 내지 약 1000 mg, 예컨대 약 100 mg 내지 약 900 mg, 예컨대 약 200 mg 내지 약 800 mg, 예컨대 약 300 mg 내지 약 800 mg, 예컨대 약 400 mg 내지 약 800 mg, 예컨대 약 400 mg 내지 약 750 mg, 예컨대 약 450 mg 내지 약 750 mg, 예컨대 약 500 mg 내지 약 700 mg, 예컨대 약 550 mg 내지 약 650 mg, 예컨대 600 mg ± 10 mg, 예컨대 600 ± 6 mg, 예컨대 600 ± 5 mg, 예컨대 600 ± 3 mg, 예컨대 600 ± 1 mg, 예컨대 600 ± 0.5 mg, 예컨대 600 mg) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 각 투약 주기의 제 1일에 약 80 mg 내지 약 2000 mg(예컨대 약 100 mg 내지 약 1600 mg, 예컨대 약 200 mg 내지 약 1600 mg, 예컨대 약 300 mg 내지 약 1600 mg, 예컨대 약 400 mg 내지 약 1600 mg, 예컨대 약 500 mg 내지 약 1600 mg, 예컨대 약 600 mg 내지 약 1600 mg, 예컨대 약 700 mg 내지 약 1600 mg, 예컨대 약 800 mg 내지 약 1600 mg, 예컨대 약 900 mg 내지 약 1500 mg, 예컨대 약 1000 mg 내지 약 1400 mg, 예컨대 약 1050 mg 내지 약 1350 mg, 예컨대 약 1100 mg 내지 약 1300 mg, 예컨대 약 1150 mg 내지 약 1250 mg, 예컨대 약 1175 mg 내지 약 1225 mg, 예컨대 약 1190 mg 내지 약 1210 mg, 예컨대 1200 mg ± 5 mg, 예컨대 1200 ± 2.5 mg, 예컨대 1200 ± 1.0 mg, 예컨대 1200 ± 0.5 mg, 예컨대 1200 mg) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 각 투약 주기의 제 1일에(예컨대 약 30 mg 내지 1200 mg 용량의(예컨대 30 mg 내지 1100 mg, 예컨대 60 mg 내지 1000 mg, 예컨대 100 mg 내지 900 mg, 예컨대 200 mg 내지 800 mg, 예컨대 300 mg 내지 800 mg, 예컨대 400 mg 내지 800 mg, 예컨대 400 mg 내지 750 mg, 예컨대 450 mg 내지 750 mg, 예컨대 500 mg 내지 700 mg, 예컨대 550 mg 내지 650 mg, 예컨대 600 mg ± 10 mg, 예컨대 600 ± 6 mg, 예컨대 600 ± 5 mg, 예컨대 600 ± 3 mg, 예컨대 600 ± 1 mg, 예컨대 600 ± 0.5 mg, 예컨대 600 mg), 각 투약 주기의 제 1일에 80 mg 내지 2000 mg 용량의(예컨대 100 mg 내지 1600 mg, 예컨대 200 mg 내지 1600 mg, 예컨대 300 mg 내지 1600 mg, 예컨대 400 mg 내지 1600 mg, 예컨대 500 mg 내지 1600 mg, 예컨대 600 mg 내지 1600 mg, 예컨대 700 mg 내지 1600 mg, 예컨대 800 mg 내지 1600 mg, 예컨대 900 mg 내지 1500 mg, 예컨대 1000 mg 내지 1400 mg, 예컨대 1050 mg 내지 1350 mg, 예컨대 1100 mg 내지 1300 mg, 예컨대 1150 mg 내지 1250 mg, 예컨대 1175 mg 내지 1225 mg, 예컨대 1190 mg 내지 1210 mg, 예컨대 1200 mg ± 5 mg, 예컨대 1200 ± 2.5 mg, 예컨대 1200 ± 1.0 mg, 예컨대 1200 ± 0.5 mg, 예컨대 1200 mg) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 각 투약 주기의 제 1일에 1~50 mg/ml/분의(예컨대 2~25 mg/ml/분, 3~15 mg/ml/분, 4~10 mg/ml/분, 또는 5 mg/ml/분, 예컨대 2 mg/ml/분, 3 mg/ml/분, 4 mg/ml/분, 5 mg/ml/분, 6 mg/ml/분, 7 mg/ml/분, 8 mg/ml/분, 9 mg/ml/분, 10 mg/ml/분, 11 mg/ml/분, 12 mg/ml/분, 13 mg/ml/분, 14 mg/ml/분, 15 mg/ml/분, 20 mg/ml/분, 25 mg/ml/분, 30 mg/ml/분, 35 mg/ml/분, 40 mg/ml/분, 45 mg/ml/분, 50 mg/ml/분, 예컨대 5 mg/ml/분) AUC를 달성하기에 충분한 용량의 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 각 투약 주기의 각각의 1일, 2일, 및 3일에 100 mg/m2 용량의 토포이소머라제 II 억제제(예컨대, 에토포시드)의 1회 이상의 투약 주기(예컨대, 21일 투약 주기)를 투여함으로써 치료하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시킨다.In some cases, a subject or population of subjects with lung cancer (eg, SCLC, eg, ES-SCLC) is administered to the subject or population of subjects at a dose (eg, from about 30 mg to about 1200 mg on Day 1 of each dosing cycle) , about 30 mg to about 1100 mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tyra goluumab), about 80 mg to about 2000 mg (such as about 100 mg to about 1600 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1600 mg, such as about 400, on Day 1 of each dosing cycle) mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg , such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg) PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) )), on the first day of each dosing cycle (such as at a dose of about 30 mg to 1200 mg (such as 30 mg to 1100 mg, such as 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg), at a dose of 80 mg to 2000 mg ( such as 100 mg to 1600 mg, such as 200 mg to 1600 mg, such as 300 mg to 1600 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg) PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) at 1-50 mg/ml/min (eg 2-25 mg/ml/min, 3- 15 mg/ml/min, 4-10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml /min, 6 mg/ml/min, 7 mg/ml/min, 8 mg/ml/min, 9 mg/ml/min, 10 mg/ml/min, 11 mg/ml/min, 12 mg/ml/ min, 13 mg/ml/min, 14 mg/ml/min, 15 mg/ml/min, 20 mg/ml/min, 25 mg/ml/min, 30 mg/ml/min, 35 mg/ml/min , 40 mg/ml/min, 45 mg/ml/min, 50 mg/ml/min, such as 5 mg/ml/min) a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and one or more dosing cycles (eg, 21 one dosing cycle), wherein the treatment is a PD-1 axis binding antagonist (e.g., anti-PD- the subject as compared to treatment with an L1 antagonist antibody (eg, atezolizumab), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide); or prolong the PFS and/or OS of the subject population.
일부 경우들에서, 폐암(예컨대, SCLC, 예컨대, ES-SCLC)을 가진 대상체 또는 대상체의 집단은 상기 대상체 또는 대상체 집단에게 각 투약 주기의 제 1일에 30 mg 내지 1200 mg 용량의(예컨대, 30 mg 내지 1100 mg, 예컨대 60 mg 내지 1000 mg, 예컨대 100 mg 내지 900 mg, 예컨대 200 mg 내지 800 mg, 예컨대 300 mg 내지 800 mg, 예컨대 400 mg 내지 800 mg, 예컨대 400 mg 내지 750 mg, 예컨대 450 mg 내지 750 mg, 예컨대 500 mg 내지 700 mg, 예컨대 550 mg 내지 650 mg, 예컨대 600 mg ± 10 mg, 예컨대 600 ± 6 mg, 예컨대 600 ± 5 mg, 예컨대 600 ± 3 mg, 예컨대 600 ± 1 mg, 예컨대 600 ± 0.5 mg, 예컨대 600 mg) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 각 투약 주기의 제 1일에 80 mg 내지 2000 mg(예컨대 100 mg 내지 1600 mg, 예컨대 200 mg 내지 1600 mg, 예컨대 300 mg 내지 1600 mg, 예컨대 400 mg 내지 1600 mg, 예컨대 500 mg 내지 1600 mg, 예컨대 600 mg 내지 1600 mg, 예컨대 700 mg 내지 1600 mg, 예컨대 800 mg 내지 1600 mg, 예컨대 900 mg 내지 1500 mg, 예컨대 1000 mg 내지 1400 mg, 예컨대 1050 mg 내지 1350 mg, 예컨대 1100 mg 내지 1300 mg, 예컨대 1150 mg 내지 1250 mg, 예컨대 1175 mg 내지 1225 mg, 예컨대 1190 mg 내지 1210 mg, 예컨대 1200 mg ± 5 mg, 예컨대 1200 ± 2.5 mg, 예컨대 1200 ± 1.0 mg, 예컨대 1200 ± 0.5 mg, 예컨대 1200 mg) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 각 투약 주기의 제 1일에 1~50 mg/ml/분의(예컨대 2~25 mg/ml/분, 3~15 mg/ml/분, 4~10 mg/ml/분, 또는 5 mg/ml/분, 예컨대 2 mg/ml/분, 3 mg/ml/분, 4 mg/ml/분, 5 mg/ml/분, 6 mg/ml/분, 7 mg/ml/분, 8 mg/ml/분, 9 mg/ml/분, 10 mg/ml/분, 11 mg/ml/분, 12 mg/ml/분, 13 mg/ml/분, 14 mg/ml/분, 15 mg/ml/분, 20 mg/ml/분, 25 mg/ml/분, 30 mg/ml/분, 35 mg/ml/분, 40 mg/ml/분, 45 mg/ml/분, 50 mg/ml/분, 예컨대 5 mg/ml/분) AUC를 달성하기에 충분한 용량의 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 각 투약 주기의 각각의 1일, 2일, 및 3일에 100 mg/m2 용량의 토포이소머라제 II 억제제(예컨대, 에토포시드)의 1회 이상의 투약 주기(예컨대, 21일 투약 주기)를 투여함으로써 치료하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시킨다.In some cases, a subject or population of subjects with lung cancer (eg, SCLC, eg, ES-SCLC) is administered to the subject or population of subjects at a dose (eg, 30 mg to 1200 mg on Day 1 of each dosing cycle) mg to 1100 mg, such as 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), 80 mg to 2000 mg (eg 100 mg to 1600 mg, such as 200 mg to 1600 mg, such as 300 mg to 1600 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg , such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg) PD-1 axis binding antagonists (such as , anti-PD-L1 antagonist antibody (eg, atezolizumab) at 1-50 mg/ml/min (eg 2-25 mg/ml/min, 3-15 mg/ml on Day 1 of each dosing cycle) /min, 4-10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml/min, 6 mg/ml/min, 7 mg/ml/min, 8 mg/ml/min, 9 mg/ml/min, 10 mg/ml/min, 11 mg/ml/min, 12 mg/ml/min, 13 mg /ml/min, 14 mg/ml/min, 15 mg/ml/min, 20 mg/ml/min, 25 mg/ml/min, 30 mg/ml/min, 35 mg/ml/min, 40 mg/ ml/min, 45 mg/ml/min, 50 mg/ml/min, such as 5 mg/ml/min) a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) in a dose sufficient to achieve an AUC, and One or more dosing cycles (eg, a 21 day dosing cycle) of a 100 mg/m 2 dose of a topoisomerase II inhibitor (eg, etoposide) on each day 1, 2, and 3 of each dosing cycle. wherein the treatment comprises administering a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, an anti-PD-L1 antagonist antibody) PFS of the subject or population of subjects as compared to treatment with a chemotherapeutic agent (eg, carboplatin or cisplatin), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide))) and/or extend the OS.
일부 경우들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some cases, said treatment is an OS of said subject or population of subjects compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. by at least about 3.3 months (e.g., by 3.3 to 120 months, by 4 to 100 months, by 5 to 80 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months by, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months , 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, said treatment is an OS of said subject or population of subjects compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. by at least about 5.3 months (e.g., by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months, such as by at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months , by 34 months, 35 months, or 36 months).
일부 구현예들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some embodiments, the treatment is compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody in the subject or population of subjects. PFS by at least about 2.4 months (e.g., by 2.4-120 months, by 2.5-100 months, by 3.0-80 months, by 4.0-60 months, by 5.0-48 months, by 6.0-36 months, by 8.0-24 months by, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months , 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months , by 35 months, or by 36 months). In some embodiments, the treatment is compared to treatment with the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor without the anti-TIGIT antagonist antibody in the subject or population of subjects. PFS by at least about 4 months (e.g., by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months, by 9 to 36 months, or by 10 to 24 months) by months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months. , 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 Months, 20 Months, 21 Months, 22 Months, 23 Months, 24 Months, 25 Months, 26 Months, 27 Months, 28 Months, 29 Months, 30 Months, 31 Months, 32 Months, 33 Months, 34 Months, 35 Months, or by 36 months).
일부 구현예들에서, 상기 대상체 또는 대상체 집단은 각 추가적인 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 추가적인 투약 주기의 제 1일에 약 80 mg 내지 약 2000 mg 용량의 아테졸리주맙의 1회 이상의 추가적인 21일 투약 주기를 투여 받고, 여기서 카보플라틴 및 에토포시드는 상기 1회 이상의 추가적인 투약 주기의 각각으로부터 생략된다.In some embodiments, the subject or population of subjects comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 60 ± 15분(예컨대, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 또는 약 70분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 60 ± 15 minutes (eg, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes , about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered in about 60 ± 15 minutes (eg, about 45 minutes, about 46 minutes, about 47 minutes, About 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, to the subject or population of subjects by intravenous infusion over about 73 minutes, about 74 minutes, or about 75 minutes).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 투여 이후 및 상기 PD-1 축 결합 길항제 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제 투여 후 제2 관찰 기간을 더 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체 투여 이후 제1 관찰 기간 및 상기 PD-1 축 결합 길항제 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우, 상기 방법은 상기 제1 및 제2 관찰 기간 중 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is combined with the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli). Zumab)) previously administered to said subject or population of subjects. In some cases, for example, after administration of the anti-TIGIT antagonist antibody and prior to administration of the PD-1 axis binding antagonist, the method comprises an intermediate first observation period. In some cases, the method further comprises a second observation period following administration of the PD-1 axis binding antagonist. In some cases, the method includes both a first observation period following administration of the anti-TIGIT antagonist antibody and a second observation period following administration of the PD-1 axis binding antagonist. In some cases, the first and second observation periods are each between about 30 minutes and about 60 minutes in length. In cases where the first and second observation periods are each about 60 minutes in length, the method comprises about 30 ± after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist during the first and second observation periods. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) at 10 minutes. When the first and second observation periods are each about 30 minutes in length, the method comprises about 15 ± 10 minutes after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist during the first and second observation periods. and recording vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) of the subject.
다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 PD-1 축 결합 길항제 투여 이후 및 상기 항 TIGIT 길항제 항체 투여 이전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체 투여 이후 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제 투여 이후 제1 관찰 기간 및 상기 항 TIGIT 길항제 항체 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우, 상기 방법은 상기 제1 및 제2 관찰 기간 중 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In other instances, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as Tyra). gorumab) prior to said subject or population of subjects. In some cases, for example, after administration of the PD-1 axis binding antagonist and prior to administration of the anti-TIGIT antagonist antibody, the method comprises an intermediate first observation period. In some cases, the method comprises a second observation period following administration of the anti-TIGIT antagonist antibody. In some cases, the method includes both a first observation period following administration of the PD-1 axis binding antagonist and a second observation period following administration of the anti-TIGIT antagonist antibody. In some cases, the first and second observation periods are each between about 30 minutes and about 60 minutes in length. In cases where said first and second observation periods are each about 60 minutes in length, the method comprises about 30 ± after administration of said PD-1 axis binding antagonist and said anti-TIGIT antagonist antibody during said first and second observation periods recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) at 10 minutes. When the first and second observation periods are each about 30 minutes in length, the method comprises about 15 ± 10 minutes after administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody during the first and second observation periods. and recording vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) of the subject.
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1(아테졸리주맙) 길항제 항체)는 상기 대상체 또는 대상체 집단에게 동시에 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체)의 투여 이후, 상기 방법은 관찰 기간을 포함한다. 일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 중 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체) 및 상기 항 TIGIT 길항제 항체 투여 이후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 관찰 기간이 약 30분의 길이인 경우, 상기 방법은 상기 관찰 기간 중 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체) 및 상기 항 TIGIT 길항제 항체 투여 이후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다.In other cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, anti PD-L1 (atezolizumab) antagonist antibody) ) are administered to the subject or population of subjects simultaneously. In some cases, for example, following administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody), the method comprises an observation period. In some cases, the observation period is between about 30 minutes and about 60 minutes in length. In instances where the observation period is about 60 minutes in length, the method comprises about 30 ± 10 following administration of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) and the anti-TIGIT antagonist antibody during the observation period. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) in minutes. When the observation period is about 30 minutes in length, the method comprises administering the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) and the anti-TIGIT antagonist antibody at about 15 ± 10 minutes during the observation period. The method may include recording vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) of the subject.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체(예컨대, 아테졸리주맙)), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)), 또는 이의 약제는, 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA에서 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대 CTLA-4 길항제, 예컨대 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)), 또는 하나 이상의 면역 공동-자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동-자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대 OX-40 작용제, 예컨대 OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In any of the methods, uses, or compositions for use described herein, said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti a PD-L1 antibody (eg, atezolizumab)), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and a topoisomerase II inhibitor (eg, etoposide)), or an agent thereof, one or more additional anti-cancer therapeutic agent(s) (e.g., an immunomodulatory agent (e.g., one or more immune co-suppressive receptors (e.g., selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that decreases or inhibits one or more immune co-suppression receptors, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab (YERVOY®)), or one or more immune co-stimulatory receptors (eg, Agents that increase or activate one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR, such as OX-40 agonists, such as OX-40 agonist antibodies), chemistries Therapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or together) may be administered.
일부 경우들에서, 상기 폐암은 소세포 폐암(SCLC), 특히 확장기 SCLC(ES-SCLC)이다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 ES-SCLC에 대해 치료 경험이 없다(예컨대, ES-SCLC에 대해 화학요법 경험이 없다). In some cases, the lung cancer is small cell lung cancer (SCLC), particularly diastolic SCLC (ES-SCLC). In some cases, the subject or population of subjects is treatment naive for ES-SCLC (eg, chemotherapy naive for ES-SCLC).
일부 경우들에서, 상기 폐암은 PD-L1 발현에 대해 선택되지 않는다. 일부 경우들에서, 상기 폐암은 PD-L1 발현에 대해 선택된다. 일부 경우들에서, 상기 폐암은 항 PD-L1 항체, 예컨대 SP263, 22C3, SP142, 또는 28-8로 염색하는 단계를 포함한 면역조직화학적(IHC) 분석에 의해 PD-L1 발현에 대해 선택된다. 일부 경우들에서, 상기 항 PD-L1 항체는 SP263이고 상기 IHC 분석은 벤타나(Ventana) SP263 IHC 분석이고; 상기 항 PD-L1 항체는 22C3이고 상기 IHC 분석은 팜(pharm)Dx 22C3 IHC 분석이고; 상기 항 PD-L1 항체는 SP142이고 상기 IHC 분석은 벤타나 SP142 IHC 분석이거나, 또는 상기 항 PD-L1 항체는 28-8이고 상기 IHC 분석은 팜Dx 28-8 IHC 분석이다. In some cases, the lung cancer is not selected for PD-L1 expression. In some cases, the lung cancer is selected for PD-L1 expression. In some cases, the lung cancer is selected for PD-L1 expression by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody, such as SP263, 22C3, SP142, or 28-8. in some cases, said anti-PD-L1 antibody is SP263 and said IHC assay is a Ventana SP263 IHC assay; the anti-PD-L1 antibody is 22C3 and the IHC assay is a pharmDx 22C3 IHC assay; wherein the anti-PD-L1 antibody is SP142 and the IHC assay is a Ventana SP142 IHC assay, or the anti-PD-L1 antibody is 28-8 and the IHC assay is a PalmDx 28-8 IHC assay.
일부 예들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 개체로부터 얻은 종양 샘플은 PD-L1의 검출 가능한 핵산 발현 수준을 갖는다. 일부 예들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 예들에서, 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 예들에서, 조직 샘플은 종양 샘플이다. 일부 예들에서, 종양 샘플은 종양-침윤 면역 세포, 종양 세포, 간질 세포 및 이들의 임의의 조합을 포함한다. In some embodiments, in a method, use, or compositions for use described herein, a tumor sample obtained from an individual has a detectable nucleic acid expression level of PD-L1. In some instances, the detectable nucleic acid expression level of PD-L1 was determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. . In some examples, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
일부 구체예에서, 폐암은 소세포 폐암 (SCLC)이다. 일부 구현예들에서, 상기 소세포 폐암(SCLC)은 4(IV)기 소세포 폐암(SCLC)으로도 지칭되는 확장병기의 소세포 폐암(ES-SCLC)이다. 일부 구현예들에서, 상기 소세포 폐암(SCLC)은 미국보훈부폐연구그룹(Veterans Administration Lung Study Group: VALG)의 병기 체계(예컨대, Micke et al. Lung Cancer 2002, 37:271-6을 참조)에 따라서 또는 이에 정의된 바와 같이 조직학적 또는 세포학적으로 확인되었다. 일부 구현예들에서, 소세포 폐암(SCLC)은 상기 개체가 수술이 불가능하고, 제한된 또는 제한된 병기의 소세포 폐암(L-SCLC 또는 LS-SCLC)을 갖는 것으로 분류될 수 없는 경우, 확장병기의 소세포 폐암(ES-SCLC)으로 분류된다. 일부 구현예들에서, 상기 확장병기의 소세포 폐암(ES-SCLC)은 검출 가능하고/거나 최초로 암이 발생한 폐의 외부로 퍼져 나갔다. 일부 구현예들에서, 상기 확장병기의 소세포 폐암(ES-ESSCLC)은 검출 가능하고/거나, 기타(예컨대, 먼) 기관, 예컨대(이에 제한되지는 않는), 간, 부신, 림프절 및/또는 뇌로 추가로 퍼져 나갔다. 일부 구현예들에서, 상기 확장병기의 소세포 폐암(ES-ESSCLC)은 치료하기 어렵다.In some embodiments, the lung cancer is small cell lung cancer (SCLC). In some embodiments, the small cell lung cancer (SCLC) is advanced stage small cell lung cancer (ES-SCLC), also referred to as stage 4 (IV) small cell lung cancer (SCLC). In some embodiments, the small cell lung cancer (SCLC) is on the Veterans Administration Lung Study Group (VALG) staging system (see, eg, Micke et al. Lung Cancer 2002, 37:271-6). thus or as defined histologically or cytologically. In some embodiments, small cell lung cancer (SCLC) is an expanded stage small cell lung cancer when the subject is inoperable and cannot be classified as having limited or limited stage small cell lung cancer (L-SCLC or LS-SCLC). (ES-SCLC). In some embodiments, the advanced stage small cell lung cancer (ES-SCLC) is detectable and/or has spread outside of the lung where the cancer first developed. In some embodiments, the advanced stage small cell lung cancer (ES-ESSCLC) is detectable and/or directed to other (eg, distant) organs such as, but not limited to, liver, adrenal glands, lymph nodes and/or brain. further spread out. In some embodiments, the expanded stage small cell lung cancer (ES-ESSCLC) is difficult to treat.
일부 구현예들에서, 상기 대상체 또는 대상체 집단은 예후가 좋지 않다. 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 치료 경험이 없는 대상체 또는 대상체의 집단(예컨대, 화학요법 경험이 없는 대상체 또는 대상체의 집단)이다. 일부 구현예들에서, 치료 경험이 없는 대상체는, 예컨대, 암, 소세포 폐암(SCLC) 또는 확장 병기의 소세포 폐암(ES-SCLC)에 대한 선행 치료를 받지 않은 대상체이다. 일부 구현예들에서, 상기 치료 경험이 없는 대상체는 확장 병기의 소세포 폐암(ES-SCLC)에 대한 선행 치료를 받지 않은 대상체이다. 일부 구현예들에서, 상기 치료 경험이 없는 대상체는 화학요법 경험이 없는, 예컨대, 암, 소세포 폐암(SCLC) 및/또는 확장 병기의 소세포 폐암(ES-SCLC)의 치료를 위해 선행 화학요법을 받지 않은 대상체이다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 확장 병기의 소세포 폐암(ES-SCLC)에 대한 치료를 받지 않았다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 확장 병기의 소세포 폐암(ES-SCLC)에 대한 선행 전신 치료를 받지 않았다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 치료 목적으로 제한된 병기의 소세포 폐암(LS-SCLC)에 대한 선행 화학방사선 요법을 받았으며, 확장 병기의 소세포 폐암(ES-SCLC) 진단으로부터 마지막 In some embodiments, the subject or population of subjects has a poor prognosis. In some embodiments, the subject or population of subjects is a treatment naive subject or population of subjects (eg, a chemotherapy naive subject or population of subjects). In some embodiments, a treatment naive subject is a subject who has not received prior treatment, eg, for cancer, small cell lung cancer (SCLC) or expanded stage small cell lung cancer (ES-SCLC). In some embodiments, the treatment naive subject has not received prior treatment for expanded stage small cell lung cancer (ES-SCLC). In some embodiments, the treatment naive subject has not received prior chemotherapy for the treatment of chemotherapy naive, e.g., cancer, small cell lung cancer (SCLC) and/or expanded stage small cell lung cancer (ES-SCLC). object that is not In some embodiments, the subject or population of subjects has not received treatment for expanded stage small cell lung cancer (ES-SCLC). In some embodiments, the subject or population of subjects has not received prior systemic treatment for expanded stage small cell lung cancer (ES-SCLC). In some embodiments, the subject or population of subjects has received prior chemoradiation therapy for limited-stage small cell lung cancer (LS-SCLC) for therapeutic purposes, and last
화학요법, 방사선 요법 또는 화학방사선 요법 주기 이후 6개월 이상의 무치료 주기를 경험하였다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 무증상 상부 또는 소뇌 중추 신경계(CNS) 전이를 갖는다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 중뇌, 뇌교, 수질 또는 척수로의 전이를 갖지 않는다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 중추 신경계(CNS) 질환을 가지며, 중추 신경계(CNS) 질환에 대한 코르티코스테로이드 치료를 필요로 하지 않는다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 새로운 무증상 전이를 가지며, 중추 신경계(CNS) 전이에 대한 방사선 요법 및/또는 수술을 받았다. 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 RECIST v1.1 기준에 따라/에 의해 정의된 바와 같은 측정가능한 질병을 갖는다(예컨대, Eisenhauer et al., Eur. J. Cancer 2009, 45: 228-247을 참조). 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 CD137 작용제 또는 면역 관문 차단 요법을 사용한 선행 치료를 받지 않았다.After a cycle of chemotherapy, radiation therapy, or chemoradiation, a treatment-free cycle of at least 6 months was experienced. In some embodiments, the subject or population of subjects has asymptomatic upper or cerebellar central nervous system (CNS) metastases. In some embodiments, the subject or population of subjects does not have metastasis to the midbrain, pons, medulla or spinal cord. In some embodiments, the subject or population of subjects has a central nervous system (CNS) disease and does not require corticosteroid treatment for the central nervous system (CNS) disease. In some embodiments, the subject or population of subjects has new asymptomatic metastases and has undergone radiation therapy and/or surgery for central nervous system (CNS) metastases. In some embodiments, the subject or population of subjects has a measurable disease according to/as defined by RECIST v1.1 criteria (eg, Eisenhauer et al., Eur. J. Cancer 2009, 45: 228). -247). In some embodiments, the subject or population of subjects has not received prior treatment with a CD137 agonist or immune checkpoint blockade therapy.
일부 구현예들에서, 상기 치료는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 상기 대상체 또는 대상체 집단의 무진행 생존(PFS)은 기준 PFS 시간과 비교하여 증가된다. 일부 경우들에서, 상기 기준 PFS 시간은 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 없이 (예컨대, 항 PD-L1 항체(예컨대, 아테졸리주맙)), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 토포이소머라제 II 억제제(예컨대, 에토포시드)로 치료를 받은 대상체 집단의 PFS 시간 중앙값이다.In some embodiments, the treatment results in CR or PR. In some cases, progression-free survival (PFS) of the subject or population of subjects is increased as compared to a baseline PFS time. In some cases, the baseline PFS time is in the absence of an anti-TIGIT antagonist antibody (eg, tyragolumab) (eg, an anti-PD-L1 antibody (eg, atezolizumab)), a platinum-based chemotherapeutic agent (eg, carboplatin) or cisplatin), and the median PFS time of a population of subjects treated with a topoisomerase II inhibitor (eg, etoposide).
일부 경우들에서, 상기 방법들은 추가 요법을 더 포함한다. 상기 추가 요법은 방사선 요법, 수술(예컨대, 종양절제술 및 유방절제술), 화학요법, 유전자 요법, DNA 요법, 바이러스 요법, RNA 요법, 면역 요법, 골수 이식, 나노 요법, 단일클론 항체 요법, 또는 이들의 조합일 수 있다. 상기 추가 요법은 보조 또는 신보조 요법의 형태일 수 있다. 일부 구현예들에서, 상기 추가 요법은 소분자 효소 억제제 또는 항 전이성 제제의 투여이다. 일부 구현예들에서, 상기 추가 요법은 부작용 제한 제제(예컨대, 치료의 부작용의 발생 및/또는 중증도를 줄이고자 하는 제제, 예컨대 항 메스꺼움 제제 등)의 투여이다. 일부 구현예들에서, 상기 추가 요법은 방사선 요법이다. 일부 구현예들에서, 상기 추가 요법은 수술이다. 일부 구현예들에서, 상기 추가 요법은 방사선 요법 및 수술의 병용이다. 일부 구현예들에서, 상기 추가 요법은 감마선 조사이다.In some cases, the methods further comprise an additional therapy. The additional therapy may include radiation therapy, surgery (eg, tumor resection and mastectomy), chemotherapy, gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, or a combination thereof. It can be a combination. The additional therapy may be in the form of adjuvant or neoadjuvant therapy. In some embodiments, the additional therapy is administration of a small molecule enzyme inhibitor or an anti-metastatic agent. In some embodiments, the additional therapy is the administration of a side-effect limiting agent (eg, an agent intended to reduce the occurrence and/or severity of side effects of treatment, such as an anti-nausea agent, etc.). In some embodiments, the additional therapy is radiation therapy. In some embodiments, the additional therapy is surgery. In some embodiments, the additional therapy is a combination of radiation therapy and surgery. In some embodiments, the additional therapy is gamma irradiation.
본원에서의 사용을 위해 고려되는 다른 추가적인 치료 항체들은 알렘투 주맙(캠패트(Campath)), 베바시주맙(아바스틴(AVASTIN)®, 제넨텍); 세툭시맙(얼비툭스(ERBITUX)®, 임클론); 파니투무맙(벡티빅스(VECTIBIX)®, 암젠), 리툭시맙(리툭산(RITUXAN)®, 제넨텍/바이오젠 아이덱), 퍼투주맙(옴니타그(OMNITARG)®, 2C4, 제넨텍), 트라스투주맙(헤셉틴(HERCEPTIN)®, 제넨텍), 토시투모맙(벡사, 코릭시아), 항체 약물 접합체, 젬투주맙 오조가미신(마일로타그(MYLOTARG)®, 와이어쓰), 아폴리주맙, 아셀리주맙, 아틀리주맙, 바피뉴주맙, 비바투주맙 메르탄신, 칸투주맙 메르탄신, 세델리주맙, 세르톨리주맙 페골, 시드푸시투주맙, 시드투주맙, 다클리주맙, 에쿨리주맙, 에팔리주맙, 에프라투주맙, 에를리주맙, 펠비주맙, 폰톨리주맙, 젬투주맙 오조가미신, 이노투주맙 오조가미신, 이필리무맙, 라베투주맙, 린투주맙, 마투주맙, 메폴리주맙, 모타비주맙, 모토비주맙, 나탈리주맙, 니모투주맙, 놀로비주맙, 누마비주맙, 오크렐리주맙, 오말리주맙, 팔리비주맙, 파스콜리주맙, 펙푸시투주맙, 펙투주맙, 펙셀리주맙, 랄리비주맙, 라니비주맙, 레슬리비주맙, 레슬리주맙, 레시비주맙, 로벨리주맙, 루플리주맙, 시브로투주맙, 시플리주맙, 손투주맙, 타카투주맙 테트락세탄, 타도시주맙, 탈리주맙, 테피바주맙, 토실리주맙, 토랄리주맙, 투코투주맙 셀모류킨, 투쿠시투주맙, 우마비주맙, 유르톡사주맙, 유스테키누맙, 비실리주맙, 및 항 인터류킨-12(ABT-874/J695, 와이어쓰 리써치 앤드 애보트 래보러토리즈)를 포함하지만, 이에 제한되지는 않는다. Other additional therapeutic antibodies contemplated for use herein include alemtuzumab (Campath), bevacizumab ( AVASTIN® , Genentech); cetuximab (ERBITUX ® , Imclone); Panitumumab (VECTIBIX ® , Amgen), Rituximab (RITUXAN ® , Genentech/Biogen IDec), Pertuzumab (OMNITARG ® , 2C4, Genentech), Trastuzumab ( Heceptin (HERCEPTIN ® , Genentech), tositumomab (bexa, corixia), antibody drug conjugate, gemtuzumab ozogamicin (MYLOTARG ® , Wyeth), apolizumab, celizumab, ah tlizumab, bafinuzumab, vibatuzumab mertansine, cantuzumab mertansine, cedelizumab, certolizumab pegol, sidfucituzumab, sidtuzumab, daclizumab, eculizumab, efalizumab, epratuzumab Zumab, erlizumab, felbizumab, pontolizumab, gemtuzumab ozogamicin, inotuzumab ozogamicin, ipilimumab, rabetuzumab, lintuzumab, matuzumab, mepolizumab, motavizumab, moto vizumab, natalizumab, nimotuzumab, nolovizumab, numivizumab, ocrelizumab, omalizumab, palivizumab, pascolizumab, pekfucituzumab, pectuzumab, pexelizumab, ralivizumab, rani vizumab, reslibizumab, reslizumab, resivizumab, lobelizumab, luflizumab, cibrotuzumab, ciflizumab, sontuzumab, takatuzumab tetraxetane, tadozumab, talizumab, tefiva Zumab, tocilizumab, toralizumab, tucotuzumab celmorleukin, tucusituzumab, umavizumab, urtoxazumab, eustekinumab, vicilizumab, and anti-interleukin-12 (ABT-874/J695) , Wires Research and Abbott Laboratories).
일부 구현예들에서, 상기 추가 요법은 PI3K/AKT/mTOR 경로, HSP90 억제제, 튜불린 억제제, 세포자멸사 억제제, 및/또는 화학예방적 제제를 표적한 요법이다. 일부 구현예들에서, 상기 추가 요법은 CTLA-4(CD152로도 공지됨), 예컨대, 차단 항체, 이필리무맙(MDX-010, MDX-101, 또는 예르보이(Yervoy)®로도 공지됨), 트레멜리무맙(티실리무맙 또는 CP-675,206으로도 공지됨), B7-H3에 대해 지향된 길항제(CD276으로도 공지됨), 예컨대, 차단 항체, MGA271, TGF 베타에 대해 지향된 길항제, 예컨대, 메테리무맙(CAT-192로도 공지됨), 프레소리무맙(GC1008로도 공지됨), 또는 LY2157299, 키메라 항원 수용체(CAR)를 발현하는 T 세포(예컨대, 세포독성 T 세포 또는 CTL)의 입양 전이를 포함한 치료, 우성-음성 TGF 베타 수용체, 예컨대, 우성-음성 TGF 베타 II형 수용체를 포함하는 T 세포의 입양 전이를 포함한 치료, HERCREEM 프로토콜(예컨대, ClinicalTrials.gov Identifier NCT00889954를 참조)을 포함한 치료, CD137에 대해 지향된 작용제(TNFRSF9, 4-1BB, 또는 ILA로도 공지됨), 예컨대, 활성 항체, 우렐루맙(BMS-663513으로도 공지됨), CD40에 대해 지향된 작용제, 예컨대, 활성 항체, CP-870893, OX40에 대해 지향된 작용제(CD134로도 공지됨), 예컨대, 상이한 항 OX40 항체(예컨대, AgonOX)와 병용으로 투여되는 활성 항체, CD27에 대해 지향된 작용제, 예컨대, 활성 항체, CDX-1127, 인돌아민-2,3-디옥시게나제(IDO), 1-메틸-D-트립토판(1-D-MT로도 공지됨), 항 약물 접합체(일부 구현예들에서, 메르탄신 또는 모노메틸 아우리스타틴 E(MMAE)를 포함), 항 NaPi2b 항체-MMAE 접합체(DNIB0600A 또는 RG7599로도 공지됨), 트라스투주맙 엠탄신(TDM1, 아도-트라스투주맙 엠탄신, 또는 케싸일라(KADCYLA)®, 제넨텍으로 공지됨), DMUC5754A, 엔도텔린 B 수용체(EDNBR)를 표적하는 항 약물 접합체, 예컨대, MMAE와 접합된 EDNBR에 대해 지향된 항체, 혈관신생 억제제, VEGF, 예컨대, VEGF-A에 대해 지향된 항체, 베바시주맙(아바스틴®, 제넨텍으로도 공지됨), 안지오포이에틴 2(Ang2로도 공지됨)에 대해 지향된 항체, MEDI3617 항종양성 제제, CSF-1R(M-CSFR 또는 CD115로도 공지됨)을 표적하는 제제, 항 CSF-1R(IMCCS4로도 공지됨), 인터페론, 예를 들어, 인터페론 알파 또는 인터페론 감마, 로페론(Roferon)-A, GM-CSF(재조합 인간 과립구대식구집락자극인자, rhu GM-CSF, 사그라모스팀, 또는 류카인(Leukine)®으로도 공지됨), IL-2(알데스루킨 또는 프로류킨(Proleukin)®으로도 공지됨), IL-12, CD20을 표적하는 항체(일부 구현예들에서, CD20을 표적하는 상기 항체는 오비누투주맙(GA101 또는 가싸이바(Gazyva)®로도 공지됨) 또는 리툭시맙임), GITR를 표적하는 항체(일부 구현예들에서, GITR을 표적하는 상기 항체는 TRX518임), 암 백신과 병용(일부 구현예들에서, 상기 암 백신은 펩티드 암 백신이며, 일부 구현예들에서, 맞춤형 펩티드 백신이고; 일부 구현예들에서, 상기 펩티드 암 백신은 다가 긴 펩티드, 멀티-펩티드, 혼합 펩티드, 잡종 펩티드, 또는 펩티드로 감작된 수지상 세포(예컨대, Yamada et al., Cancer Sci, 104:14-21, 2013을 참조)), 보강제인 TLR 작용제와 병용, 예컨대, 폴리-ICLC(힐토놀(Hiltonol)®로도 공지됨), LPS, MPL, 또는 CpG ODN, 종양괴사인자(TNF) 알파, IL-1, HMGB1, IL-10 길항제, IL-4 길항제, IL-13 길항제, HVEM 길항제, ICOS 작용제, 예컨대, ICOS-L의 투여, 또는 ICOS에 대해 지향된 작용 항체, CX3CL1표적 치료, CXCL10 표적 치료, CCL5 표적 치료, LFA-1 또는 ICAM1 작용제, 셀렉틴(Selectin) 작용제, 표적 치료, B-Raf의 억제제, 베뮤라페닙(젤보라프(Zelboraf)®로도 공지됨), 다브라페닙(타핀라(Tafinlar)®로도 공지됨), 엘로티닙(타쎄바(Tarceva)®로도 공지됨), MEK, 예컨대 MEK1(MAP2K1로도 공지됨) 또는 MEK2(MAP2K2로도 공지됨)의 억제제, 코비메티닙(GDC-0973 또는 XL-518로도 공지됨), 트라메티닙(메키니스트(Mekinist)®으로도 공지됨), K-Ras의 억제제, c-Met의 억제제, 오나투주맙(메트맙(MetMAb)으로도 공지됨), Alk의 억제제, AF802(CH5424802 또는 알렉티닙으로도 공지됨), 포스파티딜이노시톨 3-키나제(PI3K)의 억제제, BKM120, 이델라리십(GS-1101 또는 CAL-101로도 공지됨), 페리포신(KRX-0401로도 공지됨), Akt, MK2206, GSK690693, GDC-0941, mTOR의 억제제, 시롤리무스(라파마이신으로도 공지됨), 템시롤리무스(CCI-779 또는 토리셀(Torisel)®로도 공지됨), 에베로리무스(RAD001로도 공지됨), 리다포롤리스(AP-23573, MK-8669 또는 데포롤리무스로도 공지됨), OSI-027, AZD8055, INK128, 이중 PI3K/mTOR 억제제, XL765, GDC-0980, BEZ235(NVP-BEZ235로도 공지됨), BGT226, GSK2126458, PF-04691502, PF-05212384 (PKI-587로도 공지됨)이다. 상기 추가 요법은 본원에 기재된 화학치료제들 중 하나 이상일 수 있다.In some embodiments, the additional therapy is a therapy targeting the PI3K/AKT/mTOR pathway, an HSP90 inhibitor, a tubulin inhibitor, an apoptosis inhibitor, and/or a chemopreventive agent. In some embodiments, the additional therapy is CTLA-4 (also known as CD152), such as a blocking antibody, ipilimumab (also known as MDX-010, MDX-101, or Yervoy® ), Tre Melimumab (also known as ticilimumab or CP-675,206), antagonists directed against B7-H3 (also known as CD276), such as blocking antibodies, MGA271, antagonists directed against TGF beta, such as meth Rimumab (also known as CAT-192), presolimumab (also known as GC1008), or LY2157299, including adoptive transfer of T cells (e.g., cytotoxic T cells or CTLs) expressing a chimeric antigen receptor (CAR). treatment, treatment including adoptive transfer of T cells comprising a dominant-negative TGF beta receptor, such as a dominant-negative TGF beta type II receptor, treatment including the HERCREEM protocol (see, e.g., ClinicalTrials.gov Identifier NCT00889954), to CD137 Agents directed against (also known as TNFRSF9, 4-1BB, or ILA), such as an active antibody, urelumab (also known as BMS-663513), an agent directed against CD40, such as an active antibody, CP-870893 , an agonist directed against OX40 (also known as CD134), such as an active antibody administered in combination with a different anti OX40 antibody (eg, AgonOX), an agonist directed against CD27, such as an active antibody, CDX-1127, indole Amine-2,3-dioxygenase (IDO), 1-methyl-D-tryptophan (also known as 1-D-MT), anti-drug conjugate (in some embodiments, mertansine or monomethyl auristatin E) (MMAE)), anti-NaPi2b antibody-MMAE conjugate (also known as DNIB0600A or RG7599), trastuzumab emtansine (TDM1, ado-trastuzumab emtansine, or KADCYLA ® , also known as Genentech) ), DMUC5754A, anti-drug conjugates targeting the endothelin B receptor (EDNBR), e.g. For example, an antibody directed against EDNBR conjugated with MMAE, an angiogenesis inhibitor, an antibody directed against VEGF such as VEGF-A, bevacizumab (Avastin ® , also known as Genentech), angiopoietin 2 ( Antibodies directed against Ang2), MEDI3617 anti-tumor agents, agents targeting CSF-1R (also known as M-CSFR or CD115), anti-CSF-1R (also known as IMCCS4), interferons, e.g. , interferon alpha or interferon gamma, Roferon-A, GM-CSF (also known as recombinant human granulocyte macrophage colony-stimulating factor, rhu GM-CSF, sagramostim, or Leukine ® ), IL -2 (also known as aldesleukin or Proleukin®), IL-12, an antibody targeting CD20 (in some embodiments, the antibody targeting CD20 is obinutuzumab (GA101 or Ga (also known as Gazyva® ) or rituximab), an antibody that targets GITR (in some embodiments, the antibody that targets GITR is TRX518), in combination with a cancer vaccine (in some embodiments, The cancer vaccine is a peptide cancer vaccine, and in some embodiments, a customized peptide vaccine; In some embodiments, the peptide cancer vaccine is a multivalent long peptide, multi-peptide, mixed peptide, hybrid peptide, or dendritic cell sensitized to a peptide (eg, Yamada et al., Cancer Sci, 104:14-21, 2013). )), in combination with adjuvant TLR agonists, such as poly-ICLC (also known as Hiltonol® ), LPS, MPL, or CpG ODN, tumor necrosis factor (TNF) alpha, IL-1, HMGB1 , IL-10 antagonist, IL-4 antagonist, IL-13 antagonist, HVEM antagonist, ICOS agonist, such as ICOS-L, or agonistic antibody directed against ICOS, CX3CL1 targeted therapy, CXCL10 targeted therapy, CCL5 targeted therapy , LFA-1 or ICAM1 agonists, Selectin agonists, targeted therapy, inhibitors of B-Raf, vemurafenib (also known as Zelboraf ® ), dabrafenib (also known as Tafinlar ® ) erlotinib (also known as Tarceva ® ), an inhibitor of MEKs such as MEK1 (also known as MAP2K1) or MEK2 (also known as MAP2K2), cobimetinib (GDC-0973 or XL-518) ), trametinib (also known as Mekinist ® ), inhibitor of K-Ras, inhibitor of c-Met, onatuzumab (also known as MetMAb), of Alk inhibitor, AF802 (also known as CH5424802 or alectinib), inhibitor of phosphatidylinositol 3-kinase (PI3K), BKM120, idelarisib (also known as GS-1101 or CAL-101), perifosine (also known as KRX-0401) known), Akt, MK2206, GSK690693, GDC-0941, inhibitor of mTOR, sirolimus (also known as rapamycin), temsirolimus (also known as CCI-779 or Torisel ® ), ebe Lolimus (also known as RAD001), ridaforolis (also known as AP-23573, MK-8669 or deforolimus), OSI-027, AZD8055, INK128, dual PI3K/mTOR inhibitors, XL765, GDC-0980, BEZ235 (also known as NVP-BEZ235), BGT226, GSK2126458, PF-04691502, PF-05212384 (also known as PKI-587) . The additional therapy may be one or more of the chemotherapeutic agents described herein.
iii. 국소 진행성 절제 불가능한 또는 전이성 폐암을 치료하기 위한 방법 및 사용iii. Methods and uses for treating locally advanced unresectable or metastatic lung cancer
본원에서는 대상체 또는 대상체 집단에서 폐암(예컨대, 확장 병기 SCLC(ES-SCLC) 및 폐 선암종을 포함하는 국소 진행성 절제 불가능한 NSCLC(예컨대, IIIB기 NSCLC), 또는 재발성 또는 전이성 NSCLC(예컨대, IV기 NSCLC), 소세포 폐암(SCLC)을 포함하는 편평 NSCLC 또는 비편평 NSCLC를 포함하는 비소세포 폐암(NSCLC)을 치료하는 방법 및 사용으로서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 제1 및 제2 화학요법제(예컨대, 백금계 화학요법제 및 비백금계 화학요법제)의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는 방법 및 사용이 제공된다. Provided herein are lung cancer (eg, expanded stage SCLC (ES-SCLC) and locally advanced unresectable NSCLC including lung adenocarcinoma (eg, stage IIIB NSCLC), or recurrent or metastatic NSCLC (eg, stage IV NSCLC) in a subject or population . an antibody such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody such as atezolizumab), and a first and a second chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent) Methods and uses are provided comprising administering to the subject or population of subjects one or more dosing cycles of a chemotherapeutic agent).
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여된다. 일부 양태들에서, 본 발명은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 대상체 또는 대상체 집단의 체중(BW) 또는 체표면적(BSA)을 기준으로 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 투여하는 것을 수반한 방법 및 사용을 제공한다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), and methods and uses involving administering a chemotherapy combination to a subject or population of subjects in need thereof. In some embodiments, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as artezoli) Zumab) is administered every 3 weeks (eg, on
일부 양태들에서, 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화합요법 조합을 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반한 방법 및 사용을 포함하고, 여기서 상기 화학요법 조합은 유효량의 백금계 화학요법제 및 유효량의 비백금계 화학요법제를 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 항대사물질(예컨대, 페메트렉시드)이다. In some aspects, the present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), and methods and uses involving administering to a subject or population of subjects in need thereof, a chemotherapeutic combination, wherein the chemotherapy combination comprises an effective amount of a platinum-based chemotherapeutic agent and an effective amount of a non-platinum-based chemotherapeutic agent. including remedies. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) are administered every 3 weeks (eg, on
특정 구현예들에서, 상기 방법은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 항대사물질(예컨대, 페메트렉시드)를 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반하고, 여기서 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여되고, 상기 화학요법 조합(예컨대, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 상기 항대사물질(예컨대, 페메트렉시드)는 동일한 빈도(예컨대, 3주마다, 예컨대 각 21일 투약 주기의 제 1일에)로 투여된다. 일부 경우들에서, 상기 투약은 4회 내지 6회 유도 투약 주기 동안 계속된다(예컨대, 4회의 유도 투약 주기, 5회의 유도 투약 주기, 또는 6회의 유도 투약 주기). 상기 유도 투약 주기 후에, 유지 요법은 1회 이상의 후속(유지) 투약 주기로 투여될 수 있다. 특정 구현예들에서, 상기 1회 이상의 유지 투약 주기는 상기 백금계 화학요법제를 포함하지 않는다. In certain embodiments, the method comprises an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg atezolizumab), a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and an antimetabolite (eg, pemetrexed) to a subject or population in need thereof, wherein said An anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) are administered every 3 weeks ( For example, on
일부 경우들에서, 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 제공한다. In some cases, the invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) to a subject or population in need thereof every 4 weeks (eg, on
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 PFS 또는 DOR의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 OS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 무진행 생존의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 Os를 연장시킨다.In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab) results in CR or PR. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in PFS or DOR. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in OS. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) increases progression-free survival in a subject or population of subjects as compared to, for example, treatment with a PD-1 axis binding antagonist without the anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without the PD-1 axis binding antagonist. causes In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) prolongs the Os of a subject or population of subjects as compared to, for example, treatment with a PD-1 axis binding antagonist without the anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without the PD-1 axis binding antagonist.
일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제의 조합(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 페메트렉시드))을 이를 필요로 하는 대상체 또는 대상체 집단에 투여하는 것은 펨브롤리주맙 및 상기 화학요법 조합(예컨대, 항대사물질(예컨대, 페메트렉시드) 및 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴))를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 중앙값의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3.5개월 또는 약 4.7개월(예컨대, 적어도 약 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 또는 4.7개월, 예컨대 적어도 약 3.5~3.7개월, 3.7~3.9개월, 3.9~4.1개월, 4.1~4.3개월, 4.3~4.5개월, 또는 4.5~4.7개월) 만큼 연장시킨다.In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), and a chemotherapeutic combination (eg, a combination of platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and an antimetabolite (eg, pemetrexed)) to a subject or population of subjects in need thereof of the subject or population of subjects compared to treatment with pembrolizumab and the chemotherapy combination (eg, an antimetabolite (eg, pemetrexed) and the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin)). This results in an increase in the median PFS. In some cases, the treatment reduces the PFS of the subject or population of subjects by at least about 3.5 months or about 4.7 months (eg, at least about 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, or 4.7 months, such as at least about 3.5-3.7 months, 3.7-3.9 months, 3.9-4.1 months, 4.1-4.3 months, 4.3-4.5 months, or 4.5- 4.7 months).
일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 8.8개월 초과(예컨대, 적어도 8.9개월, 적어도 9.0개월, 적어도 9.2개월, 적어도 9.5개월, 적어도 10개월, 적어도 11개월, 적어도 12개월, 적어도 13개월, 적어도 14개월, 적어도 15개월, 적어도 16개월, 적어도 17개월, 적어도 18개월, 적어도 20개월, 적어도 24개월, 적어도 30개월, 적어도 36개월, 적어도 42개월, 적어도 48개월, 적어도 54개월, 또는 그 이상, 예컨대 약 8.9개월, 약 9.0개월, 약 9.2개월, 약 9.5개월, 약 10개월, 약 11개월, 약 12개월, 약 13개월, 약 14개월, 약 15개월, 약 16개월, 약 17개월, 약 18개월, 약 20개월, 약 24개월, 약 30개월, 약 36개월, 약 42개월, 약 48개월, 약 54개월 또는 그 이상)의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 8개월(예컨대, 8개월 내지 36개월, 예컨대 8개월 내지 24개월(예컨대, 8개월, 9개월, 10개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 또는 24개월)의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 약 12.5개월 내지 약 14.7개월(예컨대, 12.5개월, 12.7개월, 12.9개월, 13.1개월, 13.3개월, 13.5개월, 13.7개월, 13.9개월, 14.1개월, 14.3개월, 14.5개월, 또는 14.7개월, 예컨대 약 12.5~13개월, 13~13.5개월, 13.5~14개월, 또는 14~14.7개월)의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 10개월의 PFS 중앙값을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 12개월의 PFS 중앙값을 발생시킨다. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) for greater than 8.8 months (e.g., at least 8.9 months, at least 9.0 months, at least 9.2 months, at least 9.5 months, at least 10 months, at least 11 months, at least 12 months, at least 13 months , at least 14 months, at least 15 months, at least 16 months, at least 17 months, at least 18 months, at least 20 months, at least 24 months, at least 30 months, at least 36 months, at least 42 months, at least 48 months, at least 54 months, or longer, such as about 8.9 months, about 9.0 months, about 9.2 months, about 9.5 months, about 10 months, about 11 months, about 12 months, about 13 months, about 14 months, about 15 months, about 16 months, about 17 months, about 18 months, about 20 months, about 24 months, about 30 months, about 36 months, about 42 months, about 48 months, about 54 months or more). In some cases, the treatment lasts for at least about 8 months (eg, 8 to 36 months, such as 8 to 24 months (eg, 8 months, 9 months, 10 months, 12 months, 13 months, 14 months, 15 months). , 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, or 24 months). to about 14.7 months (eg, 12.5 months, 12.7 months, 12.9 months, 13.1 months, 13.3 months, 13.5 months, 13.7 months, 13.9 months, 14.1 months, 14.3 months, 14.5 months, or 14.7 months, such as about 12.5-13 months , 13 to 13.5 months, 13.5 to 14 months, or 14 to 14.7 months of the subject population.In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist as disclosed herein) An antibody, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), and a chemotherapy combination (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) ) and an antimetabolite (eg, pembrolizumab) in accordance with any of the methods described herein to a subject or population of subjects with lung cancer (eg, NSCLC) results in a median PFS of at least 10 months. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) results in a median PFS of at least 12 months.
일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제의 조합(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 페메트렉시드))을 폐암을 가진 대상체 또는 대상체 집단에 투여하는 것은 펨브롤리주맙 및 상기 화학요법 조합(예컨대, 항대사물질(예컨대, 페메트렉시드) 및 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴))를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS 중앙값의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 4개월(예컨대, 4 내지 12개월(예컨대, 4개월, 5개월, 6개월, 7개월, 8개월, 9개월, 10개월, 11개월 또는 12개월)) 만큼 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.5개월 내지 약 8.0개월(예컨대, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 또는 8.0개월, 예컨대 5.5~6.5개월, 6.5~7.5개월, 또는 7.5~8.0개월) 만큼 연장시킨다.In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), and a chemotherapy combination (eg, a combination of platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and an antimetabolite (eg, pemetrexed)) to a subject or population of subjects with lung cancer OS of the subject or population of subjects compared to treatment with rolizumab and the chemotherapy combination (eg, an antimetabolite (eg, pemetrexed) and the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin)) causes an increase in the median value. In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 4 months (eg, 4-12 months (eg, 4 months, 5 months, 6 months, 7 months, 8 months, 9 months, 10 months). , 11 months or 12 months))). In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 5.5 months to about 8.0 months (eg, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, or 8.0 months, such as 5.5-6.5 months). months, 6.5 to 7.5 months, or 7.5 to 8.0 months).
일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 22개월 초과(예컨대, 적어도 23개월, 적어도 24개월, 적어도 25개월, 적어도 26개월, 적어도 27개월, 적어도 28개월, 적어도 29개월, 적어도 30개월, 적어도 31개월, 적어도 32개월, 적어도 33개월, 적어도 34개월, 적어도 35개월, 적어도 36개월, 적어도 42개월, 적어도 48개월, 적어도 54개월, 적어도 60개월, 적어도 70개월, 적어도 80개월, 적어도 90개월, 적어도 100개월, 적어도 110개월, 적어도 120개월, 적어도 130개월, 적어도 140개월, 적어도 150개월, 적어도 160개월, 적어도 170개월, 적어도 180개월, 적어도 190개월, 또는 적어도 200개월, 예컨대 약 23개월, 약 24개월, 약 25개월, 약 26개월, 약 27개월, 약 28개월, 약 29개월, 약 30개월, 약 31개월, 약 32개월, 약 33개월, 약 34개월, 약 35개월, 약 36개월, 약 40개월, 약 42개월, 약 48개월, 약 54개월, 약 60개월, 약 70개월, 약 80개월, 약 90개월, 약 100개월, 약 110개월, 약 120개월, 약 130개월, 약 140개월, 약 150개월, 약 160개월, 약 170개월, 약 180개월, 약 190개월, 약 200개월)의 OS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 24개월(예컨대, 24개월 내지 42개월(예컨대 24개월 내지 36개월(예컨대, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월)의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 치료는 약 27.5개월 내지 약 32.0개월(예컨대, 27.5개월, 28.0개월, 28.5개월, 29.0개월, 29.5개월, 30.0개월, 30.5개월, 31.0개월, 31.5개월, 또는 32.0개월(예컨대, 27.5~28.5개월, 28.5~29.5개월, 29.5~30.5개월, 30.5~31.5개월, 또는 31.5~32개월)의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 24개월의 OS 중앙값을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 36개월의 OS 중앙값을 발생시킨다. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) for greater than 22 months (e.g., at least 23 months, at least 24 months, at least 25 months, at least 26 months, at least 27 months, at least 28 months, at least 29 months, at least 30 months) , at least 31 months, at least 32 months, at least 33 months, at least 34 months, at least 35 months, at least 36 months, at least 42 months, at least 48 months, at least 54 months, at least 60 months, at least 70 months, at least 80 months, at least 90 months, at least 100 months, at least 110 months, at least 120 months, at least 130 months, at least 140 months, at least 150 months, at least 160 months, at least 170 months, at least 180 months, at least 190 months, or at least 200 months, such as about 23 months, about 24 months, about 25 months, about 26 months, about 27 months, about 28 months, about 29 months, about 30 months, about 31 months, about 32 months, about 33 months, about 34 months, about 35 months , about 36 months, about 40 months, about 42 months, about 48 months, about 54 months, about 60 months, about 70 months, about 80 months, about 90 months, about 100 months, about 110 months, about 120 months, about 130 months, about 140 months, about 150 months, about 160 months, about 170 months, about 180 months, about 190 months, about 200 months). In some embodiments, the treatment lasts for at least about 24 months (eg, 24-42 months (eg, 24-36 months (eg, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months) months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months of the subject population.In some embodiments, the treatment is from about 27.5 months to about 32.0 months (e.g., 27.5 months, 28.0 months, 28.5 months, 29.0 months, 29.5 months, 30.0 months, 30.5 months, 31.0 months, 31.5 months, or 32.0 months (eg, 27.5 to 28.5 months, 28.5 to 29.5 months, 29.5 to 30.5 months, 30.5 to 31.5 months, or 31.5-32 months) of the subject population.In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), and a chemotherapy combination (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolites (eg, pembrolizumab) in accordance with any of the methods described herein, to a subject or population of subjects with lung cancer (such as NSCLC) results in a median OS of at least 24 months. An anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), and a chemotherapy combination ( For example, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab) is administered to a subject or subject having lung cancer (eg, NSCLC) according to any of the methods described herein. Dosing to a population results in a median OS of at least 36 months.
일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것은 펨브롤리주맙 및 상기 화학요법 조합(예컨대, 항대사물질(예컨대, 페메트렉시드) 및 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴))를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 반응률(ORR)의 증가, 예컨대 펨브롤리주맙 및 상기 화학요법 조합(예컨대, 항대사물질(예컨대, 페메트렉시드) 및 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴))을 이용한 치료와 비교하여 적어도 10%(예컨대, 적어도 15%, 적어도 20%, 적어도 25%, 적어도 30%, 적어도 35%, 또는 적어도 40%)의 ORR 증가를 발생시킨다.In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) to a subject or population in need thereof. compared to treatment with pembrolizumab and the chemotherapy combination (eg, an antimetabolite (eg, pemetrexed) and a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin)) in the subject or population of subjects. an increase in overall response rate (ORR), such as treatment with pembrolizumab and the chemotherapy combination (eg, an antimetabolite (eg, pemetrexed) and a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin)) and compared to an ORR increase of at least 10% (eg, at least 15%, at least 20%, at least 25%, at least 30%, at least 35%, or at least 40%).
일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 47.5% 초과(예컨대, 적어도 48%, 적어도 49%, 적어도 50%, 적어도 55%, 적어도 60%, 적어도 65%, 적어도 70%, 적어도 75%, 적어도 80 %, 적어도 85%, 적어도 90%, 적어도 95%, 또는 100%, 예컨대 약 48%, 약 49%, 약 50%, 약 55%, 약 60%, 약 65%, 약 70%, 약 75%, 약 80%, 약 85%, 약 90%, 약 95%, 또는 약 100%)의 ORR을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 50%의 ORR을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 60%의 ORR을 발생시킨다. 일부 구현예들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법 조합(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 항대사물질(예컨대, 펨브롤리주맙)의 조합)을 본원에 기재된 임의의 방법에 따라 폐암(예컨대, NSCLC)을 가진 대상체 또는 대상체 집단에게 투여하는 것은 적어도 70%의 ORR을 발생시킨다. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) is greater than 47.5% (eg, at least 48%, at least 49%, at least 50%, at least 55%, at least 60%, at least 65%, at least 70%, at least 75%). , at least 80%, at least 85%, at least 90%, at least 95%, or 100%, such as about 48%, about 49%, about 50%, about 55%, about 60%, about 65%, about 70%, about 75%, about 80%, about 85%, about 90%, about 95%, or about 100%). In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) results in an ORR of at least 50%. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) Zumab), and a chemotherapy combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in lung cancer (eg, , NSCLC) results in an ORR of at least 60%. In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezoli) zumab), and a chemotherapeutic combination (eg, a combination of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and an antimetabolite (eg, pembrolizumab)) in accordance with any of the methods described herein. , NSCLC) results in an ORR of at least 70%.
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체 또는 대상체 집단에서 무진행 생존의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 DOR의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체 또는 대상체 집단에서 OR를 연장시킨다.The present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject or population of subjects in need thereof every 4 weeks (eg, the first of each 28-day dosing cycle). per day) and methods and uses involving administration. In some cases, administration of an effective amount of said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) results in a CR or PR. In some cases, administration of an effective amount of said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) results in an increase in progression-free survival in a subject or population of subjects as compared to baseline PFS. make it In some cases, administration of an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) results in an increase in DOR. In some cases, administration of an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) prolongs the OR in a subject or population of subjects.
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 제공한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 무진행 생존의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 투여하는 것은, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 Os를 연장시킨다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab). Methods and uses are provided that involve administering to a subject or population in need thereof every two weeks (eg, on
특정 경우들에서, 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체 또는 대상체 집단에서 무진행 생존의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체 또는 대상체 집단에서 OR를 연장시킨다.In certain instances, the present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject or population of subjects in need thereof every two weeks (eg, each 28 on
일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 전신 요법(예컨대, 치료 목적으로 선행 전신 요법, 예컨대 화학요법)을 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체의 투여 전 해당 월 이내에(예컨대, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체의 투여 전 2개월 이내, 3개월 이내, 4개월 이내, 6개월 이내, 1년 이내, 2년 이내, 3년 이내, 4년 이내, 5년 이내, 또는 10년 이내에) 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 화학요법에 대한 치료 경험이 없다.In some cases, the subject or population of subjects receives prior systemic therapy (eg, prior systemic therapy for therapeutic purposes, such as chemotherapy) within the month prior to administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (eg, , Within 2 months, within 3 months, within 4 months, within 6 months, within 1 year, within 2 years, within 3 years, within 4 years, 5 before administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody within one year, or within 10 years). In some cases, the subject or population of subjects is naive to chemotherapy.
일부 구현예들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 화학요법과 함께 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체의 2주 1회(Q2W), 3주 1회(Q3W), 또는 4주 1회(Q4W) 투약 요법은 하나 이상의 화학요법제와 함께 투여될 수 있다. 상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체(Q2W, Q3W, 또는 Q4W)의 투여 빈도와 동일한 빈도로 또는 상이한 빈도(예컨대, 3주 투약/1주 휴약 일정)로 투여될 수 있다. 예를 들어, 일부 구현예들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 2주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 3주 투약/1주 휴약, 2주마다, 3주마다, 또는 4주마다 투여된다. 대안적으로, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 3주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 2주마다, 3주마다, 또는 4주마다 투여된다. 대안적으로, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 4주마다 투여되고, 상기 하나 이상의 화학요법제는 매주, 3주 투약/1주 휴약, 2주마다, 3주마다, 또는 4주마다 투여된다. 특정 예들에서, 화학요법제는 주당 수회(예컨대, 주당 2, 3, 4, 5, 6 또는 7회(예컨대, 투약 주기의 제 1일, 2일, 및 3일에)) 투여된다. In some embodiments, the PD-1 axis binding antagonist and the anti TIGIT antagonist antibody are administered in combination with chemotherapy. For example, the once every two weeks (Q2W), once every three weeks (Q3W), or once every four weeks (Q4W) dosing regimen of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody may include one or more chemotherapeutic agents. can be administered together with The one or more chemotherapeutic agents are administered at the same frequency or different from the dosing frequency of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (Q2W, Q3W, or Q4W) (eg, a 3-week dosing/1 week washout schedule). can be administered. For example, in some embodiments, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered every two weeks, and the one or more chemotherapeutic agents are administered every week, 3 weeks on/off, every 2 weeks , every 3 weeks, or every 4 weeks. Alternatively, said PD-1 axis binding antagonist and said anti TIGIT antagonist antibody are administered every 3 weeks and said one or more chemotherapeutic agents are administered every week, every 2 weeks, every 3 weeks, or every 4 weeks. Alternatively, said PD-1 axis binding antagonist and said anti-TIGIT antagonist antibody are administered every 4 weeks, and said one or more chemotherapeutic agents are administered weekly, 3 weeks dosing/weekly off, every 2 weeks, every 3 weeks, or It is administered every 4 weeks. In certain instances, the chemotherapeutic agent is administered several times per week (eg, 2, 3, 4, 5, 6, or 7 times per week (eg, on
일부 구현예들에서, 화학요법제의 용량은 1회 이상의 초기 용량 후(예컨대, 1회, 2회, 3회, 4회 또는 그 이상의 초기 용량 후) 감소된다. 예를 들어, 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 후속 용량는 초기 용량의 약 95%, 90%, 85%, 80%, 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, 20%, 15%, 10% 또는 5%로 투여될 수 있다. 예를 들어, 75 mg/m2의 시스플라틴의 초기 용량은 후속 용량에 대해, 예컨대 70 mg/m2, 65 mg/m2, 60 mg/m2, 55 mg/m2, 50 mg/m2, 또는 45 mg/m2으로 감소될 수 있고; 500 mg/m2의 페메트렉시드의 초기 용량은 후속 용량에 대해, 예컨대 75 mg/m2으로 감소될 수 있고; 약 175 mg/m2의 파클리탁셀의 초기 용량은 후속 용량에 대해, 예컨대 450 mg/m2, 400 mg/m2, 350 mg/m2, 300 mg/m2, 250 mg/m2, 또는 200 mg/m2으로 감소될 수 있고; 그리고/또는 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴의 초기 용량은 후속 용량에 대해, 예컨대 AUC = 4.5 mg/ml/분, 4.0 mg/ml/분, 3.5 mg/ml/분 또는 3.0 mg/ml/분을 달성하기에 충분한 용량으로 감소될 수 있다.In some embodiments, the dose of the chemotherapeutic agent is reduced after one or more initial doses (eg, after 1, 2, 3, 4 or more initial doses). For example, a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an antimetabolite (eg, pemetrexed or gemcitabine)) Subsequent doses of approximately 95%, 90%, 85%, 80%, 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25% of the initial dose %, 20%, 15%, 10% or 5% For example, an initial dose of cisplatin of 75 mg/m 2 for subsequent doses, such as 70 mg/m 2 , 65 mg/m 2 , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 , or 45 mg/m 2 ; an initial dose of 500 mg/m 2 pemetrexed for subsequent doses, may be reduced to eg 75 mg/m 2 ; an initial dose of about 175 mg/m 2 paclitaxel for subsequent doses, eg 450 mg/m 2 , 400 mg/m 2 , 350 mg/m 2 , 300 mg/m 2 , 250 mg/m 2 , or 200 mg/m 2 ; and/or an initial dose of carboplatin sufficient to achieve AUC=5 mg/ml/min for subsequent doses, For example, AUC = 4.5 mg/ml/min, 4.0 mg/ml/min, 3.5 mg/ml/min or 3.0 mg/ml/min.
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 상기 대상체 또는 대상체 집단에서 무진행 생존의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)의 투여는 상기 대상체 또는 대상체 집단의 OS를 연장시킨다. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg carboplatin or cisplatin), and the antimetabolites (eg pemetrexed) result in CR or PR. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the antimetabolite (eg, pemetrexed) result in an increase in progression-free survival in the subject or population of subjects. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab), the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin), and the antimetabolite (eg, pemetrexed) prolong OS in the subject or population of subjects.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴), 및 상기 항대사물질(예컨대, 페메트렉시드)을 투여받은 대상체 또는 대상체 집단은 폐암, 예컨대 NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))에 대해 치료를 받고 있다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), the platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and the antimetabolite (e.g. pemetrexed) , are being treated for locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC).
제제의 투약dosing of the formulation
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 화학요법제의 투약은 섹션 III(K)에 기재되어 있다. Dosing of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, and chemotherapeutic agents is described in Section III(K).
암의 특성화 Characterization of Cancer
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 폐암은 NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))일 수 있다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 폐암에 대한 선행 전신 요법을 받지 않았다.In any of the methods, uses, or compositions for use described herein, the lung cancer can be NSCLC (e.g., nonsquamous NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)). In some embodiments, the subject or population of subjects has not received prior systemic therapy for lung cancer.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는다. 일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 EGFR 유전자 돌연변이(예컨대, 감작성 EGFR 유전자 돌연변이) 또는 ALK 유전자 재배열을 갖지 않는다. 일부 경우들에서, 상기 대상체는 0 또는 1의 이스턴 코퍼레이티브 종양학 그룹(ECOG) 전신 활동도(PS)를 가진다. In some cases, in a method, use, or compositions for use described herein, the subject does not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality. In some cases, in a method, use, or compositions for use described herein, the subject does not have an EGFR gene mutation (eg, a sensitizing EGFR gene mutation) or an ALK gene rearrangement. In some cases, the subject has an Eastern Corporate Oncology Group (ECOG) systemic activity (PS) of 0 or 1.
돌연변이 상태 EGFR 및 ALK를 검출하는 방법은 당업계에 일반적으로 공지되어 있으며, 임상 샘플(예컨대, 종양 생검 또는 혈액 샘플(예컨대, 혈액 중 순환 종양 DNA)로부터의 DNA를 차세대 서열분석 방법을 사용하여, 예컨대 본원에 그 전체가 원용된 Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013)에 기재된 표적화된 유전자 풀다운 및 서열분석 방법을 사용하여 서열분석하는 것을 포함하지만 이에 제한되지는 않는다. 이러한 차세대 시퀀싱 방법은 다양한 돌연변이(예를 들어, 삽입, 결실, 염기 치환, 국소 유전자 증폭 및/또는 동형 접합 유전자 결실)를 검출하기 위해 본원에 개시된 임의의 방법과 함께 사용될 수 있으며, 동시에 소형 샘플들 (예를 들어, 작은 코어 바늘 생검, 미세 바늘 흡인 및/또는 세포 블록들) 또는 고정된 샘플들 (예를 들어, 포르말린-고정 및 파라핀 포매(FFPE) 샘플)을 사용할 수 있게 한다. EGFR 및 ALK의 돌연변이 상태를 검출하기 위한 다른 방법에는 형광 인시튜 혼성화(FISH) 및 면역조직화학(IHC) 방법이 포함된다. ALK의 돌연변이 상태의 검출을 위한 예시적인 방법은 미국 특허 제 9,651,555에 개시되며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, VENTANA® 항 ALK (D5F3) IHC 분석은 ALK 유전자의 돌연변이 상태를 결정하기 위해 사용한다.Methods for detecting the mutant states EGFR and ALK are generally known in the art, and DNA from a clinical sample (e.g., a tumor biopsy or a blood sample (e.g., circulating tumor DNA in blood)) can be analyzed using next-generation sequencing methods; including, but not limited to, sequencing using, for example, targeted gene pull-down and sequencing methods described in Frampton et al. ( Nature Biotechnology . 31(11): 1023-1033, 2013), which is incorporated herein in its entirety. This next-generation sequencing method can be used in conjunction with any of the methods disclosed herein to detect a variety of mutations (e.g., insertions, deletions, base substitutions, local gene amplifications and/or homozygous gene deletions), while at the same time compact Allows the use of samples (eg, small core needle biopsy, fine needle aspiration and/or cell blocks) or fixed samples (eg, formalin-fixed and paraffin-embedded ( FFPE ) samples). and other methods for detecting the mutant state of ALK include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods.Exemplary methods for detecting the mutant state of ALK are disclosed in US Pat. No. 9,651,555 , which is incorporated herein in its entirety In some cases, the VENTANA® anti- ALK (D5F3) IHC assay is used to determine the mutation status of the ALK gene.
본원에 기재된 임의의 방법의 일부 경우들에서, 상기 돌연변이는 감작성 EGFR 돌연변이이다. 감작성 EGFR 돌연변이는 당업계에 일반적으로 공지되어 있으며 미국 특허 공보 제 US 2018/0235968 및 in Juan et al. (Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18-21 중 어느 하나에서의 돌연변이(예컨대, 엑손 18, 엑손 19, 엑손 20, 및/또는 엑손 21에서의 돌연변이)이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 19에서의 결실(del19)이다. 다른 예들에서, 상기 감작성 EGFR 돌연변이는 엑손 21에서의 L858R 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 C, A, 또는 S이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719S 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 G719A 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 S720F 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861Q 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861R 점 돌연변이이다. 다른 경우들에서, 감작성 EGFR 돌연변이는 T790M 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 E709X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 K, A, 또는 H이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 S768I 점 돌연변이이다.In some cases of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are generally known in the art and described in US Patent Publication Nos. US 2018/0235968 and in Juan et al. ( Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017), which is incorporated herein by reference in its entirety. In some cases, the sensitizing EGFR mutation is a mutation in any of exon 18-21 (eg, a mutation in
본원에 기재된 방법들 중 임의의 것의 일부 경우들에서, 상기 돌연변이는 ALK 유전자 재배열이다. ALK 유전자 재배열은 당업계에 일반적으로 공지되어 있으며 미국 특허 제 9,651,555 및 in Du et al. (Thoracic Cancer. 9: 423-430, 2018)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, ALK 유전자 재배열은 하류 신호전달 경로를 활성화하여 세포 증식 및 생존을 증가시키는 발암성 ALK 티로신 키나제의 생성을 초래한다. 일부 경우들에서, ALK 유전자 재배열은 EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC, TMP4, 및 MSN로 구성된 그룹에서 선택된 유전자와의 ALK 재배열이며, 융합 종양유전자를 형성시킨다. 일부 경우들에서, ALK 유전자 재배열은 ALK 와의 EML4 재배열이며 융합 종양유전자 EML4 In some cases of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are generally known in the art and described in US Pat. Nos. 9,651,555 and in Du et al. ( Thoracic Cancer. 9: 423-430, 2018), which is incorporated herein by reference in its entirety. In some cases, ALK gene rearrangement results in the production of oncogenic ALK tyrosine kinases that activate downstream signaling pathways to increase cell proliferation and survival. In some cases, the ALK gene rearrangement is a gene selected from the group consisting of EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A , BIRC6, RANBP2, ATIC, CLTC, TMP4, and MSN . ALK rearrangement with and forms a fusion oncogene. In some cases, the ALK gene rearrangement is an EML4 rearrangement with ALK and the fusion oncogene EML4
ALK를 형성한다. ALK is formed.
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 대상체는 NSCLC의 폐 림프상피종 유사 암종 하위유형이 없다. NSCLC의 하위유형을 검출하는 방법은 당업계에 널리 공지이며, 조직병리적 기준에 의한, 또는 분자 특징 (예를 들면, 바이오마커 (예를 들면, 상기 유전자에 의해 인코딩된 특정한 유전자 또는 단백질)의 하나 또는 조합의 발현에 의해 특성규명된 하위유형)에 의한 결정 방법을 포함하나 이에 제한되는 것은 아니다. 일부 예들에서, 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 예들에서, 조직 샘플은 종양 샘플이다. In some cases, in a method, use, or compositions for use described herein, the subject is free of the lung lymphothelioma-like carcinoma subtype of NSCLC. Methods for detecting subtypes of NSCLC are well known in the art and are based on histopathological criteria, or by molecular characteristics (e.g., biomarkers (e.g., specific genes or proteins encoded by said genes)). subtypes characterized by expression of one or a combination). In some examples, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some examples, the tissue sample is a tumor sample.
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 대상체는 활동성 엡스타인-바 바이러스(EBV) 감염 또는 알려진 또는 의심되는 만성 활동성 EBV 감염이 없다. 본원에 기재된 방법에 사용하기 위한 활동성 또는 만성 활동성 EBV 감염의 지표는, 대상체의 샘플(예컨대, 혈액 또는 혈청 샘플)에서 검출된 EBV IgM, EBV IgG, 엡스타인-바 핵 항원 (EBNA), 및 엡스타인-바 바이러스 입자들을 포함할 수 있으나 이에 제한되는 것은 아니다. 대상체의 샘플에서 EBV IgM, EBV IgG, 엡스타인-바 핵 항원 (EBNA), 및 엡스타인-바 바이러스 입자들을 포함하는 활동성 또는 만성 활동성 EBV 감염의 하나 이상의 지표의 존재를 검출하는 방법은 당업계에 널리 공지이며, 혈청학적 진단 (예를 들어, EBV DNA의 검출 (예를 들어, EBV 바이러스 입자 검출을 위한 혈액 샘플의 PCR 분석에 의함) 또는 EBV 항원 또는 항 EBV 항체의 검출 (예를 들어, 이종성 항체를 사용한 EBNA, EBV IgM 또는 EBV IgG의 검출))을 포함하는 방법들을 포함하나 이에 제한되는 것은 아니다. 일부 경우들에서, 샘플은 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 경우들에서, 대상체는 EBV IgM에 대해 음성이고 및/또는 EBV PCR에 의해 음성이다. 일부 경우들에서, 대상체는 EBV IgM에 대해 음성이고 및/또는 EBV PCR에 의해 음성이며 EBV IgG에 대해 양성이고 및/또는 엡스타인-바 핵 항원 (EBNA)에 대해 양성이다. 다른 경우들에서, 대상체는 EBV IgG에 대해 음성이고 및/또는 EBNA에 대해 음성이다. 일부 경우들에서, 상기 대상체는 PD-L1 선택된 종양(예컨대, SP263 또는 22C3 항체를 이용한 IHC에 의해 결정된 바와 같이 최소 PD-L1 양성 종양 세포 분획 또는 TPS가 ≥ 30%(예컨대, ≥ 50%)인 종양 PD-L1 발현 또는 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 SP142 항체를 이용한 IHC에 의해 결정된 바와 같이 1% 이상인 경우)을 갖는다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 양성 종양 세포 분획 또는 PD-L1 TPS가 면역조직화학적(IHC) 분석법에 의해 30% 이상(예컨대, 50% 이상)인 것으로 결정된 종양이다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 발현 면역 세포(IC)에 의해 차지하는 종양 면적의 비율이 면역조직화학적(IHC) 분석법에 의해 1% 이상인 것으로 결정된 종양이다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP263, 22C3, SP142, 또는 28-8을 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP263를 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 22C3를 사용한다. 일부 경우들에서, 종양 샘플은 50% 이상의 TPS를 갖는 것으로 결정되었다. 일부 경우들에서, PD-L1-양성 종양 세포 분율은 (예를 들어, 항 PD-L1 항체 SP263을 사용한 양성 염색에 의해 결정 시 (예를 들어, Ventana 분석법 사용), 항 PD-L1 항체 22C3을 사용한 양성 염색에 의해 결정 시 (예를 들어, pharmDx 분석법 사용), 또는 항 PD-L1 항체 28-8을 사용한 양성 염색에 의해 결정 시) 50% 이상이다. 일부 구현예들에서, PD-L1-양성 종양 세포 분율은 항 PD-L1 항체 SP142를 사용한 양성 염색에 의해 결정 시 30% 이상이다. 일부 경우들에서, 상기 IC는 1% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 5% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 10% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 50% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 30% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이).In some cases, in a method, use, or compositions for use described herein, the subject does not have an active Epstein-Barr virus (EBV) infection or a known or suspected chronic active EBV infection. An indicator of active or chronic active EBV infection for use in the methods described herein is EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein- bar virus particles, but are not limited thereto. Methods for detecting the presence of one or more indicators of active or chronic active EBV infection comprising EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein-Barr virus particles in a sample of a subject are well known in the art. serological diagnosis (e.g., detection of EBV DNA (e.g., by PCR analysis of a blood sample for detection of EBV virus particles) or detection of EBV antigen or anti-EBV antibody (e.g., heterologous antibody detection of EBNA, EBV IgM or EBV IgG used)). In some cases, the sample is selected from the group consisting of a whole blood sample, a serum sample, and a plasma sample. In some cases, the subject is negative for EBV IgM and/or is negative by EBV PCR. In some cases, the subject is negative for EBV IgM and/or negative for EBV PCR and positive for EBV IgG and/or positive for Epstein-Barr nuclear antigen (EBNA). In other cases, the subject is negative for EBV IgG and/or negative for EBNA. In some cases, the subject has a PD-L1 selected tumor (eg, minimal PD-L1 positive tumor cell fraction or TPS as determined by IHC using SP263 or 22C3 antibody > 30% (eg > 50%) If the proportion of tumor area occupied by tumor PD-L1-expressing or PD-L1-expressing tumor infiltrating immune cells (IC) is greater than or equal to 1% as determined by IHC using SP142 antibody). In some cases, the PD-L1 selected tumor is a tumor that has been determined to be at least 30% (eg, at least 50%) by immunohistochemical (IHC) analysis of a PD-L1 positive tumor cell fraction or PD-L1 TPS. In some cases, the PD-L1-selected tumor is a tumor in which the proportion of tumor area occupied by PD-L1-expressing immune cells (IC) is determined by immunohistochemical (IHC) analysis to be greater than or equal to 1%. In some cases, the IHC assay uses anti-PD-L1 antibodies SP263, 22C3, SP142, or 28-8. In some cases, the IHC assay uses the anti-PD-L1 antibody SP263. In some cases, the IHC assay uses the anti-PD-L1 antibody SP142. In some cases, the IHC assay uses anti-PD-L1 antibody 22C3. In some cases, the tumor sample was determined to have a TPS of 50% or greater. In some cases, the PD-L1-positive tumor cell fraction (eg, as determined by positive staining with anti-PD-L1 antibody SP263 (eg, using a Ventana assay)) is determined by using anti-PD-L1 antibody 22C3 greater than 50% as determined by positive staining used (eg, using pharmDx assay), or as determined by positive staining with anti-PD-L1 antibody 28-8. In some embodiments, the fraction of PD-L1-positive tumor cells is greater than or equal to 30% as determined by positive staining with anti-PD-L1 antibody SP142. In some cases, the IC was determined to be greater than or equal to 1% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 5% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 10% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 50% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 30% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay).
일부 경우들에서, 본원에 기재된 방법, 용도, 또는 용도를 위한 조성물들에서, 개체로부터 얻은 종양 샘플은 PD-L1의 검출 가능한 단백질 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출 가능한 단백질 발현 수준은 IHC 분석법에 의해 결정되었다. 일부 경우들에서, IHC 분석법은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 1% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 1% 이상 5% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 5% 이상 50% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플 내 종양 세포의 50% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 1% 이상을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 1% 이상 5% 미만을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 5% 이상 10% 미만을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 종양 샘플은 종양 샘플의 10% 이상을 포함하는 종양-침윤 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. In some cases, in a method, use, or compositions for use described herein, the tumor sample obtained from the individual has a detectable protein expression level of PD-L1. In some cases, detectable protein expression levels of PD-L1 were determined by IHC assay. In some cases, the IHC assay uses the anti-PD-L1 antibody SP142. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% and less than 5% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 5% and less than 50% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 50% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 1% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 1% and less than 5% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 5% and less than 10% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 10% of the tumor sample.
일부 경우들에서, 상기 대상체는 PD-L1 발현으로부터 평가되지 않은 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진다. 예를 들어, 일부 경우들에서, 폐암을 가진 대상체는 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않았다(예컨대, 상기 대상체는 PD-L1 양성 종양 세포 분획이 45%, 40%, 35%, 또는 30% 이상인 것으로 결정되지 않았다). 예를 들어, 일부 경우들에서, 상기 대상체는, 예컨대 본원에 기재되거나 해당 기술 분야에 공지된 임의의 IHC 방법을 사용하여 평가된 바와 같이, TPS가 50% 이상 PD-L1 양성인 것으로 결정되지 않았다(예컨대, 상기 대상체는 TPS가 45% 이상 PD-L1 양성, 40% 이상 PD-L1 양성, 35% 이상 PD-L1 양성, 또는 30% 이상 PD-L1 양성인 것으로 결정되지 않았다).In some cases, the subject has lung cancer that has not been assessed from PD-L1 expression (eg, NSCLC (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC))). For example, in some cases, the subject with lung cancer has not been determined to have a PD-L1 positive tumor cell fraction greater than or equal to 50% (eg, the subject has a PD-L1 positive tumor cell fraction of 45%, 40% , 35%, or 30%).For example, in some cases, the subject is assessed using any IHC method, such as described herein or known in the art, The TPS was not determined to be at least 50% PD-L1 positive (eg, the subject has a TPS of at least 45% PD-L1 positive, at least 40% PD-L1 positive, at least 35% PD-L1 positive, or at least 30% PD not determined to be -L1 positive).
일부 경우들에서, 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체는 PD-L1 양성 종양 세포 분획이 50% 미만인 것으로 결정되었다(예컨대, 1% 내지 50%, 1% 내지 49%, 5% 내지 45%, 10% 내지 40%, 15% 내지 35%, 또는 20% 내지 30%, 예컨대 1% 내지 5 %, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40% , 40% 내지 45%, 또는 45% 내지 49%, 예컨대 49% 미만, 45% 미만, 40% 미만, 35% 미만, 30% 미만, 25% 미만, 20% 미만, 15% 미만, 10% 미만, 9% 미만, 8% 미만, 7% 미만, 6% 미만, 5% 미만, 4% 미만, 3% 미만, 2% 미만, 1% 미만, 또는 약 0%). 예를 들어, 특정 경우들에서, 폐암을 가진 대상체는 PD-L1 양성 종양 세포 분획이 1% 내지 49% 미만인 것으로 결정되었다(예컨대, 1% 내지 5%, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40%, 40% 내지 45%, 또는 45% 내지 49%). 다른 경우들에서, 폐암을 가진 대상체는 PD-L1 양성 종양 세포 분획이 1% 미만인 것으로 결정되었다(예컨대, 0%, 또는 검출 불가능한 PD-L1 발현).In some cases, a subject with lung cancer (eg, NSCLC (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)) has a PD-L1-positive tumor cell fraction was determined to be less than 50% (eg, 1% to 50%, 1% to 49%, 5% to 45%, 10% to 40%, 15% to 35%, or 20% to 30%, such as 1% to 5%, 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45% , or from 45% to 49%, such as less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15%, less than 10%, less than 9%, 8 %, less than 7%, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than 1%, or about 0%).For example, in certain cases, subjects with lung cancer was determined to have a fraction of PD-L1 positive tumor cells between 1% and less than 49% (eg, between 1% and 5%, between 5% and 10%, between 10% and 15%, between 15% and 20%, between 20% and 25%). , 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49%) In other cases, the subject with lung cancer has a PD-L1 positive tumor cell fraction was determined to be less than 1% (eg, 0%, or undetectable PD-L1 expression).
예를 들어, 일부 경우들에서, 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체는 TPS가 50%미만 PD-L1 양성인 것으로 결정되었다(예컨대, 1% 내지 50%, 1% 내지 49%, 5% 내지 45%, 10% 내지 40%, 15% 내지 35%, 또는 20% 내지 30% PD-L1 양성, 예컨대 1% 내지 5 %, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40% , 40% 내지 45%, 또는 45% 내지 49% PD-L1 양성, 예컨대 49% 미만, 45% 미만, 40% 미만, 35% 미만, 30% 미만, 25% 미만, 20% 미만, 15% 미만, 10% 미만, 9% 미만, 8% 미만, 7% 미만, 6% 미만, 5% 미만, 4% 미만, 3% 미만, 2% 미만, 1% 미만, 또는 약 0% PD-L1 양성). 예를 들어, 특정 경우들에서, 폐암을 가진 대상체는 TPS가 1% 내지 49% PD-L1 양성인 것으로 결정되었다(예컨대, 1% 내지 5%, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40%, 40% 내지 45%, 또는 45% 내지 49% PD-L1 양성). 다른 경우들에서, 폐암을 가진 대상체는 TPS가 1% 미만 PD-L1 양성인 것으로 결정되었다(예컨대, 약 0%, 또는 검출 불가능한 PD-L1 발현).For example, in some cases, a subject with lung cancer (eg, NSCLC (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)) has a TPS of 50% was determined to be less than PD-L1 positive (eg, between 1% and 50%, between 1% and 49%, between 5% and 45%, between 10% and 40%, between 15% and 35%, or between 20% and 30% PD-L1). positive, such as 1% to 5%, 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40% , 40% to 45%, or 45% to 49% PD-L1 positive, such as less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15% , less than 10%, less than 9%, less than 8%, less than 7%, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than 1%, or about 0% PD-L1 positive) For example, in certain instances, a subject with lung cancer has been determined to have a TPS of 1% to 49% PD-L1 positive (eg, 1% to 5%, 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49% PD-L1 positive). In these cases, subjects with lung cancer were determined to have a TPS of less than 1% PD-L1 positive (eg, about 0%, or undetectable PD-L1 expression).
특정 구현예들에서, 상기 대상체는 PD-L1 발현으로부터 평가되지 않은 NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진다. 예를 들어, 일부 경우들에서, NSCLC를 가진 대상체는 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않았다(예컨대, 상기 대상체는 PD-L1 양성 종양 세포 분획이 45%, 40%, 35%, 또는 30% 이상인 것으로 결정되지 않았다). 예를 들어, 일부 경우들에서, 상기 대상체는, 예컨대 본원에 기재되거나 해당 기술 분야에 공지된 임의의 IHC 방법을 사용하여 평가된 바와 같이, TPS가 50% 이상 PD-L1 양성인 것으로 결정되지 않았다(예컨대, 상기 대상체는 TPS가 45% 이상 PD-L1 양성, 40% 이상 PD-L1 양성, 35% 이상 PD-L1 양성, 또는 30% 이상 PD-L1 양성인 것으로 결정되지 않았다).In certain embodiments, the subject has NSCLC that has not been assessed from PD-L1 expression (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)). For example, in some cases, the subject with NSCLC has not been determined to have a fraction of PD-L1 positive tumor cells greater than or equal to 50% (eg, the subject has a fraction of PD-L1 positive tumor cells of 45%, 40%, 35% , or 30% or higher).For example, in some cases, the subject has a TPS of 50, eg, as assessed using any IHC method described herein or known in the art. not determined to be at least % PD-L1 positive (e.g., the subject has a TPS of at least 45% PD-L1 positive, at least 40% PD-L1 positive, at least 35% PD-L1 positive, or at least 30% PD-L1 positive has not been determined).
일부 경우들에서, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체는 PD-L1 양성 종양 세포 분획이 50% 미만인 것으로 결정되었다(예컨대, 1% 내지 50%, 1% 내지 49%, 5% 내지 45%, 10% 내지 40%, 15% 내지 35%, 또는 20% 내지 30%, 예컨대 1% 내지 5 %, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40% , 40% 내지 45%, 또는 45% 내지 49%, 예컨대 49% 미만, 45% 미만, 40% 미만, 35% 미만, 30% 미만, 25% 미만, 20% 미만, 15% 미만, 10% 미만, 9% 미만, 8% 미만, 7% 미만, 6% 미만, 5% 미만, 4% 미만, 3% 미만, 2% 미만, 1% 미만, 또는 약 0%). 예를 들어, 특정 경우들에서, NSCLC를 가진 대상체는 PD-L1 양성 종양 세포 분획이 1% 내지 49% 미만인 것으로 결정되었다(예컨대, 1% 내지 5%, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40%, 40% 내지 45%, 또는 45% 내지 49%). 다른 경우들에서, NSCLC를 가진 대상체는 PD-L1 양성 종양 세포 분획이 1% 미만인 것으로 결정되었다(예컨대, 0%, 또는 검출 불가능한 PD-L1 발현).In some cases, a subject with NSCLC (e.g., nonsquamous NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)) has a fraction of PD-L1 positive tumor cells of less than 50%. has been determined (eg, between 1% and 50%, between 1% and 49%, between 5% and 45%, between 10% and 40%, between 15% and 35%, or between 20% and 30%, such as between 1% and 5%, 5 % to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49%, such as less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15%, less than 10%, less than 9%, less than 8%, 7 %, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than 1%, or about 0%).For example, in certain cases, a subject with NSCLC has PD-L1 It was determined that the fraction of benign tumor cells was between 1% and less than 49% (eg, between 1% and 5%, between 5% and 10%, between 10% and 15%, between 15% and 20%, between 20% and 25%, between 25% and 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49%) In other cases, the subject with NSCLC has a PD-L1 positive tumor cell fraction of less than 1% (eg, 0%, or undetectable PD-L1 expression).
예를 들어, 일부 경우들에서, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))를 가진 대상체는 TPS가 50%미만 PD-L1 양성인 것으로 결정되었다(예컨대, 1% 내지 50%, 1% 내지 49%, 5% 내지 45%, 10% 내지 40%, 15% 내지 35%, 또는 20% 내지 30% PD-L1 양성, 예컨대 1% 내지 5 %, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40% , 40% 내지 45%, 또는 45% 내지 49% PD-L1 양성, 예컨대 49% 미만, 45% 미만, 40% 미만, 35% 미만, 30% 미만, 25% 미만, 20% 미만, 15% 미만, 10% 미만, 9% 미만, 8% 미만, 7% 미만, 6% 미만, 5% 미만, 4% 미만, 3% 미만, 2% 미만, 1% 미만, 또는 약 0% PD-L1 양성). 예를 들어, 특정 경우들에서, NSCLC를 가진 대상체는 TPS가 1% 내지 49% PD-L1 양성인 것으로 결정되었다(예컨대, 1% 내지 5%, 5% 내지 10%, 10% 내지 15%, 15% 내지 20%, 20% 내지 25%, 25% 내지 30%, 30% 내지 35%, 35% 내지 40%, 40% 내지 45%, 또는 45% 내지 49% PD-L1 양성). 다른 경우들에서, NSCLC를 가진 대상체는 TPS가 1% 미만 PD-L1 양성인 것으로 결정되었다(예컨대, 약 0%, 또는 검출 불가능한 PD-L1 발현).For example, in some cases, a subject with NSCLC (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)) has a TPS of less than 50% PD-L1 determined to be positive (eg, 1%-50%, 1%-49%, 5%-45%, 10%-40%, 15%-35%, or 20%-30% PD-L1 positive, such as 1 % to 5%, 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49% PD-L1 positive, such as less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15%, less than 10% , less than 9%, less than 8%, less than 7%, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than 1%, or about 0% PD-L1 positive). , in certain instances, subjects with NSCLC have been determined to have a TPS of 1% to 49% PD-L1 positive (eg, 1% to 5%, 5% to 10%, 10% to 15%, 15% to 20 %, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45%, or 45% to 49% PD-L1 positive). subjects with TPS were determined to be less than 1% PD-L1 positive (eg, about 0%, or undetectable PD-L1 expression).
일부 경우들에서, 상기 개체로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 핵산 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플 및 혈장 샘플로 구성된 그룹에서 선택된다. 일부 경우들에서, 조직 샘플은 종양 샘플이다. 일부 경우들에서, 종양 샘플은 종양-침윤 면역 세포, 종양 세포, 간질 세포 및 이들의 임의의 조합을 포함한다. In some cases, a tumor sample obtained from the individual has a detectable nucleic acid expression level of PD-L1. In some cases, the detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. became In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample. In some cases, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
일부 경우들에서, 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체로부터 수득한 종양 샘플은 PD-L1의 핵산 발현 수준이 낮거나 검출 불가능하다. 일부 경우들에서, PD-L1의 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다. In some cases, a tumor sample obtained from a subject with lung cancer (eg, NSCLC (eg, nonsquamous NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)) is PD-L1 The nucleic acid expression level of PD-L1 is low or undetectable.In some cases, the nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technique. , ISH or combination thereof.In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample.In some cases, the tissue sample is a tumor sample In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
본원에 기재된 임의의 방법에 대한 일부 경우들에서, 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체는 상기 폐암에 대해 선행 전신 치료를 받은 적이 없다(예컨대, 치료 목적으로 선행 전신 치료를 받은 적이 없다). 특정 구현예들에서, 상기 대상체는 국소 진행성 폐암을 갖고, 상기 국소 진행성 폐암에 대한 선행 전신 치료를 받은 적이 없다. 일부 구현예들에서, 상기 대상체는 NSCLC(예컨대, 비편평 NSCLC, 예컨대 국소 진행성 절제불가능 또는 전이성 비편평 NSCLC)을 갖고, 상기 NSCLC(예컨대, 비편평 NSCLC, 예컨대 국소 진행성 절제불가능 또는 전이성 비편평 NSCLC)에 대한 선행 전신 치료를 받은 적이 없다. 선행 전신 치료는 비전이성 질병에 대한 치료 목적으로 선행 신보조, 보조 화학요법, 방사선 요법, 및 화학방사선 요법을 포함한다.In some cases for any of the methods described herein, the subject has lung cancer (eg, NSCLC (eg, squamous NSCLC (eg, locally advanced unresectable or metastatic squamous NSCLC (eg, stage IV nonsquamous NSCLC))) No prior systemic treatment for said lung cancer (e.g., no prior systemic treatment for therapeutic purposes) In certain embodiments, said subject has locally advanced lung cancer and prior systemic treatment for said locally advanced lung cancer In some embodiments, the subject has NSCLC (eg, nonsquamous NSCLC, such as locally advanced unresectable or metastatic nonsquamous NSCLC), and the NSCLC (eg, nonsquamous NSCLC, such as locally advanced unresectable NSCLC). or metastatic nonsquamous NSCLC).
다른 경우들에서, 폐암(예컨대, NSCLC(예컨대, 비편평 NSCLC(예컨대, 국소 진행성 절제불가능 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC))을 가진 대상체는 상기 폐암에 대해 선행 전신 치료를 받은 적이 없고, 본 발명의 임의의 방법에 따른 치료 전 적어도 12개월의 무치료 기간을 경험하였다. In other cases, a subject with lung cancer (e.g., NSCLC (e.g., nonsquamous NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)) receives prior systemic treatment for the lung cancer and have experienced a treatment-free period of at least 12 months prior to treatment according to any of the methods of the present invention.
iv. 절제불가능한 폐암을 치료하기 위한 방법 및 사용iv. Methods and uses for treating unresectable lung cancer
본원에서는 대상체에서 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))을 치료하는 방법 및 사용으로서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는 방법 및 사용이 제공된다. 일부 경우들에서, 적어도 1회의 투약 주기가 선행 보조 치료로서 투여된다. 일부 경우들에서, 상기 치료는 신보조 치료이다. 일부 경우들에서, 적어도 1회의 투약 주기가 보조 치료로서 투여된다. 일부 경우들에서, 상기 치료는 보조 치료이다. 일부 경우들에서, 상기 치료는 신보조 치료 및 보조 치료를 포함한다. 일부 경우들에서, 상기 폐암은 절제가능한 폐암이다. 일부 경우들에서, 상기 폐암은 초기 폐암(예컨대, II기, IIIA기, 또는 IIIB기 폐암)이다. 일부 경우들에서, 상기 폐암은 NSCLC(예컨대, 편평 또는 비편평 NSCLC)이다. 일부 경우들에서, 상기 폐암은 PD-L1 양성(예컨대, PD-L1 높음)이다. 일부 경우들에서, 상기 폐암은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 가지지 않는다. 일부 구현예들에서, 상기 대상체는 이전에 폐암 치료를 받은 적이 없다(예컨대, 선행 수술, 선행 면역요법, 선행 화학요법, 또는 선행 방사선요법). 일부 경우들에서, 상기 대상체는 백금계 화학요법에 적격이다. 일부 경우들에서, 상기 대상체는 치료 목적으로 R0 절제술에 적격이다. 상기 대상체는 바람직하게는 인간이다.Disclosed herein are methods and uses for treating lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)) in a subject, comprising an effective amount of an anti-TIGIT antagonist antibody (eg, disclosed herein) 1 of an anti-TIGIT antagonist antibody, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab), or an anti-PD-1 antagonist antibody, such as pembrolizumab) Provided are methods and uses comprising administering to the subject more than one dosing cycle.In some cases, at least one dosing cycle is administered as prior adjuvant treatment.In some cases, the treatment is neoadjuvant treatment. In some cases, at least one dosing cycle is administered as adjuvant treatment.In some cases, the treatment is adjuvant treatment.In some cases, the treatment comprises neoadjuvant treatment and adjuvant treatment. In some cases, the lung cancer is resectable lung cancer.In some cases, the lung cancer is early lung cancer (such as stage II, IIIA, or IIIB lung cancer).In some cases, the lung cancer is NSCLC (such as squamous or non-squamous NSCLC).In some cases, the lung cancer is PD-L1 positive (eg, PD-L1 high).In some cases, the lung cancer is epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) does not have a genomic tumor abnormality.In some embodiments, the subject has not previously received lung cancer treatment (eg, prior surgery, prior immunotherapy, prior chemotherapy, or prior radiotherapy). In , said subject is eligible for platinum-based chemotherapy.In some cases, said subject is eligible for R0 resection for therapeutic purposes.The subject is preferably human.
본 발명은 절제가능한 폐암(예컨대, 절제가능한 NSCLC(예컨대, 절제가능한 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용으로서, 상기 방법은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 30 mg 내지 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides methods and uses for treating a subject having resectable lung cancer (eg, resectable squamous or non-squamous NSCLC), wherein the method is administered every 3 weeks (eg, of each 21-day dosing cycle). on day 1) at a dose of about 30 mg to about 1200 mg (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), and every 3 weeks (eg, on
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이를 필요로 하는 대상체에게 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 투약 주기 중 적어도 1회는 3주마다(예컨대, 3주마다 600 mg의 용량) 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대 3주마다 약 1200 mg의 용량)(예컨대, 고정 용량) PD-1 축 결합 길항제를 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 투약 주기 중 적어도 1회는 3주마다(예컨대, 3주마다 600 mg의 용량) 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대 3주마다 약 1200 mg의 용량)(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 3주마다 600 mg의 용량)(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대 3주마다 1200 mg의 용량)(예컨대, 고정 용량) PD-1 축 결합 길항제를 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 3주마다 600 mg의 용량)(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대 3주마다 1200 mg의 용량)(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or methods and uses that involve administering an anti-PD-1 antagonist antibody, such as pembrolizumab) to a subject in need thereof every three weeks (eg, on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 투여받는 대상체는 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))에 대해 치료를 받고 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) A subject being administered is being treated for lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)).
상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 당해 기술 분야에서 공지된 임의의 적합한 방식으로 투여될 수 있다. 예를 들어, 상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 순차적으로(상이한 날에) 또는 동시에(동일한 날 또는 동일한 치료 주기 동안) 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체 및/또는 상기 PD-1 축 결합 길항제는 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 동일한 날에 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체 이전에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체 이후에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동시에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 투여되는 항 TIGIT 길항제 항체 이전에 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 투여되는 항 TIGIT 길항제 항체 이후에 투여될 수 있다. 또 다른 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동일한 시간에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 별개의 조성물로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동일한 조성물로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 환자에게 투여된 임의의 다른 치료제와 별개의 정맥내 라인을 통해 투여된다. 상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 동일한 투여 경로 또는 상이한 투여 경로에 의해 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제의 투여 후 제1 관찰 기간이 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제의 투여 후 제2 관찰 기간이 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간이 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체의 투여 후 제2 관찰 기간이 있다. 일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제는 정맥내 또는 피하 투여된다. 일부 경우들에는, 상기 정맥내 주입이 30 ± 10분 및/또는 60 ± 15분에 걸쳐 실시된다. 일례에서, 아테졸리주맙은 60분에 걸쳐 정맥내 투여될 수 있고; 제1 주입이 허용되면, 모든 후속 주입은 30분에 걸쳐 전달될 수 있다. 일부 예들에서, 상기 PD-1 축 결합 길항제는 정맥내 푸시(push) 또는 볼루스(bolus)로 투여되지 않는다. 일례에서, 티라골루맙은 60분에 걸쳐 정맥내 투여될 수 있고; 제1 주입이 허용되면, 모든 후속 주입은 30분에 걸쳐 전달될 수 있다. 일부 예들에서, 상기 항 TIGIT 길항제 항체는 정맥내 푸시(push) 또는 볼루스(bolus)로 투여되지 않는다.The PD-1 axis binding antagonist and anti-TIGIT antagonist antibodies may be administered in any suitable manner known in the art. For example, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody may be administered sequentially (on different days) or simultaneously (on the same day or during the same treatment cycle). In some cases, the anti-TIGIT antagonist antibody and/or the PD-1 axis binding antagonist is administered on about 1 day (eg, -3 days, -2 days, -1 days, 1 day, 2 days, or 3 days) of a dosing cycle. day) is administered. In some cases, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody may be administered on the same day. In some cases, the PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered after the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered concurrently with the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist may be administered prior to the anti-TIGIT antagonist antibody administered on the same day. In some cases, the PD-1 axis binding antagonist may be administered after the anti-TIGIT antagonist antibody administered on the same day. In still other instances, the PD-1 axis binding antagonist is administered at the same time as the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered in a separate composition from the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered in the same composition as the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered via a separate intravenous line from any other therapeutic agent administered to the patient on the same day. The PD-1 axis binding antagonist and anti-TIGIT antagonist antibody may be administered by the same route of administration or by different routes of administration. In some cases, the PD-1 axis binding antagonist is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly, or intranasally. In some cases, the PD-1 axis binding antagonist is administered intravenously. In some cases, the anti TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly or intranasally. In some cases, the anti-TIGIT antagonist antibody is administered intravenously. In some cases, there is a first observation period after administration of the PD-1 axis binding antagonist. In some cases, there is a second observation period following administration of the PD-1 axis binding antagonist. In some cases, there is a first observation period following administration of the anti-TIGIT antagonist antibody. In some cases, there is a second observation period following administration of the anti-TIGIT antagonist antibody. In some cases, the observation period is between about 30 minutes and about 60 minutes in length. In some cases, the anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist is administered intravenously or subcutaneously. In some cases, the intravenous infusion is administered over 30 ± 10 minutes and/or 60 ± 15 minutes. In one example, atezolizumab may be administered intravenously over 60 minutes; If the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some embodiments, the PD-1 axis binding antagonist is not administered as an intravenous push or bolus. In one example, tiragolumab may be administered intravenously over 60 minutes; If the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some embodiments, the anti-TIGIT antagonist antibody is not administered as an intravenous push or bolus.
선행하는 예들 중 임의의 것에서, 각각의 투여 주기는 임의의 적합한 길이, 예컨대 약 7일(약 5일, 6일, 7일, 8일, 또는 9일), 약 14일(예컨대, 약 12일, 13일, 14일, 15일, 16일), 약 21일(예컨대, 약 18일, 19일, 20일, 21일, 22일, 23일, 또는 24일), 약 28일(약 25일, 26일, 27일, 28일, 29일, 30일, 또는 31일), 또는 그 이상을 가질 수 있다. 일부 경우들에서, 각 투약 주기는 약 21일이다.In any of the preceding examples, each dosing cycle is of any suitable length, such as about 7 days (about 5 days, 6 days, 7 days, 8 days, or 9 days), about 14 days (eg, about 12 days). , 13 days, 14 days, 15 days, 16 days), about 21 days (eg, about 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, or 24 days), about 28 days (about 25 days) days, 26 days, 27 days, 28 days, 29 days, 30 days, or 31 days), or more. In some cases, each dosing cycle is about 21 days.
일부 경우들에서, 상기 대상체로부터 수득한 샘플(예컨대, 종양 샘플, 혈액 샘플(예컨대, 혈장 샘플), 또는 림프 샘플)의 PD-L1 발현 수준이 결정되었다. 일부 경우들에서, 상기 샘플은 PD-L1의 검출가능한 발현 수준(예컨대, PD-L1의 검출가능한 단백질 및/또는 핵산 발현 수준)을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 단백질 발현 수준이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 발현 수준은 PD-L1 양성 종양 세포 분획(예컨대, 50% 이상의 PD-L1 양성 종양 세포 분획)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체(예컨대, 항 PD-L1 항체 SP263)로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정되었다. 일부 경우들에서, 상기 IHC 분석은 벤타나 SP263 IHC 분석이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 핵산 발현 수준이다. 일부 경우들에서, 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK)의 돌연변이 상태가 결정된다. 일부 경우들에서, 상기 방법은 상기 대상체로부터 샘플을 수득하는 단계를 추가로 포함한다. 일부 경우들에서, 상기 방법은 PD-L1의 발현 수준을 결정하는 단계를 추가로 포함한다.In some cases, the PD-L1 expression level of a sample obtained from the subject (eg, a tumor sample, a blood sample (eg, a plasma sample), or a lymph sample) is determined. In some cases, the sample has been determined to have a detectable expression level of PD-L1 (eg, a detectable protein and/or nucleic acid expression level of PD-L1). In some cases, the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1. In some cases, the detectable expression level of PD-L1 is a fraction of PD-L1 positive tumor cells (eg, at least 50% of the fraction of PD-L1 positive tumor cells). In some cases, the detectable protein expression level of PD-L1 is determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody suitable for staining (eg, anti-PD-L1 antibody SP263). It was decided. In some cases, the IHC assay is a Ventana SP263 IHC assay. In some cases, the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1. In some cases, the mutation status of epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) is determined. In some cases, the method further comprises obtaining a sample from the subject. In some cases, the method further comprises determining the expression level of PD-L1.
일부 경우들에서, 상기 제1 투약 주기는 수술(예컨대, 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술) 이전에 개시된다. 일부 경우들에서, 1회 이상의 투약 주기는 수술 전에 완료된다. 일부 경우들에서, 적어도 1회, 2회, 3회, 또는 4회의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 또는 그 이상의 투약 주기)가 수술 전에 완료된다. 일부 경우들에서, 4회의 투약 주기는 수술 전에 완료된다. 일부 경우들에서, 1회 이상의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 20회 또는 그 이상의 투약 주기)는 수술 후 개시된다. 일부 경우들에서, 16회의 투약 주기는 수술 후 완료된다. 일부 경우들에서, 상기 치료는 수술을 포함한다. 일부 경우들에서, 상기 수술은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술이다. 일부 경우들에서, 상기 치료는 방사선 요법(예컨대, 수술 후 방사선 요법)을 포함한다.In some cases, the first dosing cycle is initiated prior to surgery (eg, lobectomy, lobectomy, bilobectomy, or pneumonectomy). In some cases, one or more dosing cycles are completed prior to surgery. In some cases, at least 1, 2, 3, or 4 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, or more dosing cycles) dosing cycle) is completed prior to surgery. In some cases, 4 dosing cycles are completed prior to surgery. In some cases, one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13) , 14, 15, 16, 17, 18, 19, 20 or more dosing cycles) are initiated post-operatively. In some cases, 16 dosing cycles are completed post surgery. In some cases, the treatment comprises surgery. In some cases, the surgery is lobectomy, lobectomy, bilobectomy, or pneumonectomy. In some cases, the treatment includes radiation therapy (eg, post-surgical radiation therapy).
일부 경우들에서, 상기 치료는 기준 MPR 비율과 비교하여 주요 병리학적 반응율(MPR)의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 병리학적 완전 반응(pCR) 및/또는 기준 pCR 비율과 비교하여 pCR 비율의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 기준 EFS 시간과 비교하여 무사건 생존(EFS)의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 기준 OS 시간과 비교하여 OS의 증가를 발생시킨다. 일부 경우들에서, 상기 기준 MPR 비율, 기준 pCR 비율, 및/또는 기준 EFS 시간은 하기의: (a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 MPR 비율, pCR 비율, 및/또는 EFS 시간이다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 MPR 비율의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 pCR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 EFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 OS의 증가를 발생시킨다. In some cases, the treatment results in an increase in the major pathological response rate (MPR) as compared to the baseline MPR rate. In some cases, the treatment results in a pathological complete response (pCR) and/or an increase in the pCR ratio compared to a baseline pCR ratio. In some cases, the treatment results in an increase in event-free survival (EFS) compared to baseline EFS time. In some cases, the treatment results in an increase in OS compared to baseline OS time. In some cases, the baseline MPR ratio, baseline pCR ratio, and/or baseline EFS time is determined by: (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or (b) the MPR rate, pCR rate, and/or EFS time of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in the MPR rate. In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab) results in pCR. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in EFS. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in OS.
일부 경우들에서, 상기 치료는 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈), 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)을 추가로 포함한다. 일부 경우들에서, 상기 신보조 및/또는 보조 치료는 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈), 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)을 추가로 포함한다. 일부 경우들에서, 상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제이다. 일부 경우들에서, 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이다. 일부 경우들에서, 상기 비백금계 화학요법제는 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)이다. 일부 경우들에서, 상기 하나 이상의 화학요법제는 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈), 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)이다. 일부 경우들에서, 적어도 하나 이상의 화학요법제는 하기의: (a) 카보플라틴 및 페메트렉시드; (b) 카보플라틴 및 파클리탁셀; (c) 시스플라틴 및 페메트렉시드; (d) 카보플라틴 및 젬시타빈; 또는 (e) 시스플라틴 및 젬시타빈이다. 일부 경우들에서, 비편평 NSCLC의 치료에 사용되는 하나 이상의 화학요법제는 (a) 카보플라틴 및 페메트렉시드, (b) 카보플라틴 및 파클리탁셀, 또는 (c) 시스플라틴 및 페메트렉시드이다. 일부 경우들에서, 편평 NSCLC의 치료에 사용되는 하나 이상의 화학요법제는 (a) 카보플라틴 및 젬시타빈, (b) 카보플라틴 및 파클리탁셀, 또는 (c) 시스플라틴 및 젬시타빈이다. 일부 경우들에서, 상기 치료는 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈), 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)을 투여하는 것을 추가로 포함한다. 일부 구현예들에서, 상기 하나 이상의 화학요법제는 3주마다 투여된다. 일부 경우들에서, 상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 투여된다. 일부 경우들에서, 상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일) 및 약 8일(예컨대, 5일, 6일, 7일, 8일, 9일, 10일, 또는 11일)에 투여된다. 일부 경우들에서, 상기 투약 주기는, 예컨대 약 7일(약 5일, 6일, 7일, 8일, 또는 9일), 약 14일(예컨대, 약 12일, 13일, 14일, 15일, 16일), 약 21일(예컨대, 약 18일, 19일, 20일, 21일, 22일, 23일, 또는 24일), 약 28일(약 25일, 26일, 27일, 28일, 29일, 30일, 또는 31일), 또는 그 이상이다. 일부 경우들에서, 각 투약 주기는 약 21일이다. 일부 경우들에서, 상기 1회 이상의 화학요법제는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제(예컨대, 아테졸리주맙) 및/또는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이후에 투여된다. 일부 경우들에서, 상기 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀))은 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 이전에 투여된다.In some cases, the treatment comprises one or more chemotherapeutic agents (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, antimetabolites (eg, peme)). Trexid or gemcitabine), and/or taxanes (such as paclitaxel, such as nap-paclitaxel) In some cases, the neoadjuvant and/or adjuvant treatment is one or more chemotherapeutic agents (such as platinum a chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an antimetabolite (eg, pemetrexed or gemcitabine), and/or a taxane (eg, paclitaxel, such as nap-paclitaxel).In some cases, the at least one chemotherapeutic agent is at least one platinum-based chemotherapeutic agent and/or at least one non-platinum-based chemotherapeutic agent.In some cases, the platinum-based chemotherapeutic agent The therapeutic agent is carboplatin or cisplatin In some cases, the non-platinum-based chemotherapeutic agent is an antimetabolite (such as pemetrexed or gemcitabine) and/or a taxane (such as paclitaxel, such as nap-paclitaxel) In some cases, the one or more chemotherapeutic agents are platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and non-platinum-based chemotherapeutic agents (eg, antimetabolites (eg, pemetrexed or gemcitabine); and/or a taxane (such as paclitaxel, such as nap-paclitaxel) In some cases, at least one chemotherapeutic agent is: (a) carboplatin and pemetrexed; (b) carboplatin and paclitaxel (c) cisplatin and pemetrexed; (d) carboplatin and gemcitabine; or (e) cisplatin and gemcitabine.In some cases, one or more chemotherapeutic agents used to treat nonsquamous NSCLC are ( a) carboplatin and pemetrexed, (b) carboplatin and paclitaxel, or (c) cisplatin and pemetrexed.In some cases, one or more chemotherapeutic agents used to treat squamous NSCLC are (a) ) carboplatin and gemcitabine, (b) carbo platin and paclitaxel, or (c) cisplatin and gemcitabine. In some cases, the treatment comprises one or more chemotherapeutic agents (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, antimetabolites (eg, peme)). Trexed or gemcitabine), and/or taxane (such as paclitaxel, such as nap-paclitaxel) In some embodiments, the one or more chemotherapeutic agents are administered every three weeks. In instances, the one or more chemotherapeutic agents are administered on about day 1 (eg, day -3, day -2, day -1,
본 발명은 절제가능한 폐암(예컨대, 초기 절제가능한 폐암(예컨대, 절제가능한 NSCLC(예컨대, 절제가능한 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용으로서, 상기 방법은 3주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법 및 사용을 포함한다. 일부 경우들에서, 상기 방법은 3주마다 30 mg 내지 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides methods and uses for treating a subject having resectable lung cancer (eg, early resectable lung cancer (eg, resectable NSCLC (eg, resectable squamous or non-squamous NSCLC)), the method comprising: about 30 every 3 weeks. mg to about 600 mg (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), and a dose of about 80 mg to about 1600 mg every 3 weeks ( eg, fixed dose) a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab), a platinum-based chemotherapeutic agent (eg, cisplatin or administering to the subject one or more dosing cycles of a carboplatin), and a non-platinum-based chemotherapeutic agent (eg, an antimetabolite (eg, pemetrexed or gemcitabine) or a taxane (eg, paclitaxel or nap-paclitaxel); In some cases, the method comprises a 30 mg to 600 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist as disclosed herein) every 3 weeks. antibody, such as tyragolumab), and a dose of 80 mg to 1600 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD- 1 Antagonist antibodies such as pembrolizumab), platinum-based chemotherapeutic agents (such as cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (such as antimetabolites (such as pemetrexed or gemcitabine) or taxanes (such as eg, administering to the subject one or more dosing cycles of paclitaxel or nap-paclitaxel.
본 발명은 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용으로서, 상기 방법은 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀))의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법 및 사용을 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제, 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀))을 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 600 mg 용량의(고정 용량) 상기 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) 상기 PD-1 축 결합 길항제, 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀))을 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides methods and uses for treating a subject having lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)), the method comprising an anti-TIGIT antagonist antibody (eg, An anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody such as atezolizumab, or an anti PD-1 antagonist antibody such as pembrolizumab) , platinum-based chemotherapeutic agents (such as cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (such as antimetabolites (such as pemetrexed or gemcitabine) or taxanes (such as paclitaxel or nap-paclitaxel)) methods and uses, comprising administering to the subject one or more dosing cycles of ) anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose), a platinum-based chemotherapeutic agent (eg, cisplatin or carboplatin), and a non-platinum-based chemistry administering to the subject a therapy (e.g., an antimetabolite (e.g., pemetrexed or gemcitabine) or a taxane (e.g., paclitaxel or nap-paclitaxel)) as neoadjuvant treatment. At least once of the dosing cycle is a dose of 30 mg to 600 mg (fixed dose) of the anti-TIGIT antagonist antibody every 3 weeks, a dose of 80 mg to 1600 mg every 3 weeks (eg, a fixed dose) of the PD-1 axis binding Antagonists, platinum-based chemotherapeutic agents (such as cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (such as antimetabolites (such as pemetrexed or gemcitabine) or taxanes (such as paclitaxel or nap-paclitaxel) ) as neoadjuvant treatment to the subject.
본 발명은 절제가능한 폐암(예컨대, 초기 절제가능한 폐암(예컨대, 절제가능한 NSCLC(예컨대, 절제가능한 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용으로서, 상기 방법은 3주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및: (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴); 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴); 및 (b) (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다 30 mg 내지 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 및: (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴); 또는 (ii) 3주마다 75 mg/m2 용량의 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴); 및 (b) (i) 3주마다 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 1000 mg/m2 또는 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 100 mg/m2, 175 mg/m2, 또는 200 mg/m2 용량의 탁산의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함한다.The present invention provides methods and uses for treating a subject with resectable lung cancer (eg, early resectable lung cancer (eg, resectable NSCLC (eg, resectable squamous or non-squamous NSCLC)), the method comprising: about 30 every 3 weeks. mg to about 600 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), and a dose of about 80 mg to about 1600 mg every 3 weeks ( eg, a fixed dose) a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab), and: (a) (i) 3 weeks Platinum-based chemotherapeutic agent (e.g., cisplatin or carboplatin) at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min, or (ii) about 75 mg every 3 weeks a platinum-based chemotherapeutic agent (eg, cisplatin or carboplatin) at a /m 2 dose, and (b) (i) about 500 mg/m 2 every 3 weeks or about 1000 on
본 발명은 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용으로서, 상기 방법은 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙), 백금계 화학요법제(예컨대, 시스플라틴 또는 카보플라틴), 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀))의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법 및 사용을 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 상기 대상체에게: (a) 3주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체; (b) 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산이며; 여기서 상기 치료는 신보조 치료이다. 일부 양태들에서, 상기 투약 주기 중 적어도 1회는 상기 대상체에게 하기의: (a) 3주마다 30 mg 내지 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체; (b) 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 1000 mg/m2 또는 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 100 mg/m2, 175 mg/m2, 또는 200 mg/m2 용량의 탁산이며; 여기서 상기 치료는 신보조 치료이다.The present invention provides methods and uses for treating a subject having lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)), the method comprising an anti-TIGIT antagonist antibody (eg, An anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody such as atezolizumab, or an anti PD-1 antagonist antibody such as pembrolizumab) , platinum-based chemotherapeutic agents (such as cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (such as antimetabolites (such as pemetrexed or gemcitabine) or taxanes (such as paclitaxel or nap-paclitaxel)) methods and uses, comprising administering to the subject one or more dosing cycles of a dose (eg, a fixed dose) of an anti TIGIT antagonist antibody; (b) a dose of from about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) of the PD-1 axis binding antagonist; at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m 2 every 3 weeks; and (d) administering a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) about 500 mg/m 2 every 3 weeks or about 1000 mg/m 2 on days 1 and 8 of each dosing cycle an antimetabolite at a dose of m 2 or about 1250 mg/m 2 ; or (ii) a taxane at a dose of about 100 mg/m 2 , about 175 mg/m 2 , or about 200 mg/m 2 every 3 weeks; The treatment is neoadjuvant treatment.In some embodiments, at least one dosing cycle is administered to the subject: (a) every 3 weeks at a dose of 30 mg to 600 mg (eg, a fixed dose) of an anti-TIGIT antagonist antibody; (b) every 3 weeks 8 a dose of 0 mg to 1600 mg (eg, a fixed dose) of a PD-1 axis binding antagonist; (c) at (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) a platinum-based chemotherapeutic agent at a dose of 75 mg/m 2 every 3 weeks; and (d) administering a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) 500 mg/m 2 every 3 weeks or 1000 on days 1 and 8 of each dosing cycle an antimetabolites at a dose of mg/m 2 or 1250 mg/m 2 ; or (ii) a taxane at a dose of 100 mg/m 2 , 175 mg/m 2 , or 200 mg/m 2 every 3 weeks; wherein the treatment is neoadjuvant treatment.
본 발명은 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용을 포함하고, 상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하며, 여기서: (a) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함하고; (b) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다. 일부 양태들에서, 상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함하고; (b) 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함한다.The present invention includes methods and uses for treating a subject having lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)), the method comprising an anti-TIGIT antagonist antibody and administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist, wherein: (a) at least one of said dosing cycles is from about 30 mg to about 1200 mg doses (e.g., every 3 weeks) , a fixed dose) of an anti-TIGIT antagonist antibody and a dose (eg, a fixed dose) of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist to the subject as neoadjuvant therapy; (b ) at least once in said dosing cycle, at a dose of about 30 mg to about 1200 mg (eg, a fixed dose) anti-TIGIT antagonist antibody every 3 weeks, and a dose of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) ) administering to the subject a PD-1 axis binding antagonist as adjuvant treatment In some aspects, the method administers to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist. administering: (a) a dose of 30 mg to 1200 mg (eg, a fixed dose) anti-TIGIT antagonist antibody every 3 weeks and a dose of 80 mg to 1600 mg every 3 weeks at least once in said dosing cycle (e.g., a fixed dose) of a PD-1 axis binding antagonist as neoadjuvant treatment to said subject; eg, a fixed dose) of an anti-TIGIT antagonist antibody, and an 80 mg to 1600 mg dose (eg, a fixed dose) of a PD-1 axis binding antagonist every 3 weeks as adjuvant treatment to the subject.
본 발명은 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))을 가진 대상체를 치료하는 방법 및 사용을 포함하고, 상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하며, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게: (a) 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체; (b) 신보조 치료로서 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산이며; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 투여하는 단계를 포함한다. 일부 양태들에서, 상기 방법은 상기 대상체에게: (a) 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체; (b) 신보조 치료로서 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 1000 mg/m2 또는 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 100 mg/m2, 175 mg/m2, 또는 200 mg/m2 용량의 탁산이며; (II) 상기 투약 주기 중 적어도 1회는 3주마다 30 mg 내지 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 80 mg 내지 1600 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제를 보조 치료로서 투여하는 단계를 포함한다.The present invention includes methods and uses for treating a subject having lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)), the method comprising an anti-TIGIT antagonist antibody and administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist, wherein: (I) at least one of said dosing cycles is neoadjuvant treatment and to the subject: (a) 3 weeks (e.g., a fixed dose) of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg per day (e.g., a fixed dose) (b) a dose of about 80 mg to about 1600 mg every 3 weeks as neoadjuvant treatment (e.g., a fixed dose) of the PD-1 axis (c) (i) at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks, or (ii) about 75 mg/m 2 every 3 weeks administering a dose of a platinum - based chemotherapeutic agent; on days 1 and 8 of about 1000 mg/m 2 or about 1250 mg/m 2 of the antimetabolite; or (ii) about 100 mg/m 2 , about 175 mg/m 2 , or about every 3 weeks a taxane at a dose of 200 mg/m 2 ; (II) at least one of said dosing cycles at a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody, and about 80 every 3 weeks Adjuvant treatment comprises the step of administering as adjuvant treatment a dose of from about 1600 mg to about 1600 mg of a PD-1 axis binding antagonist, (a) 30 mg every 3 weeks. (e.g., a fixed dose) of anti-TIGIT antagonist antibody at a dose of (e.g., a fixed dose) of from 80 mg to 1600 mg (e.g., a fixed dose) of the PD-1 axis binding antagonist every 3 weeks as neoadjuvant treatment; i) 5 mg/m every 3 weeks at a dose targeted to achieve an AUC of L/min or an AUC of 6 mg/mL/min; or (ii) a platinum-based chemotherapeutic agent at a dose of 75 mg/m 2 every 3 weeks; and (d) administering a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) 500 mg/m 2 every 3 weeks or 1000 on days 1 and 8 of each dosing cycle an antimetabolites at a dose of mg/m 2 or 1250 mg/m 2 ; or (ii) a taxane at a dose of 100 mg/m 2 , 175 mg/m 2 , or 200 mg/m 2 every 3 weeks; (II) at least one of said dosing cycles every 3 weeks at a dose of 30 mg to 1200 mg (eg, a fixed dose) anti-TIGIT antagonist antibody, and every 3 weeks at a dose of 80 mg to 1600 mg (eg, a fixed dose) PD - administering the -1 axis binding antagonist as adjuvant treatment.
일부 경우들에서, 상기 치료는 추가 요법을 더 포함할 수 있다. 당업계에 공지되어 있거나 본원에 기재된 임의의 적합한 추가 요법이 사용될 수 있다. 상기 추가 요법은 방사선 요법(예컨대, 수술 후 방사선 요법), 수술, 유전자 요법, DNA 요법, 바이러스 요법, RNA 요법, 면역요법, 골수 이식, 나노요법, 단일클론 항체 요법, 감마선 조사, 또는 전술한 것의 조합일 수 있다. In some cases, the treatment may further comprise an additional therapy. Any suitable additional therapy known in the art or described herein may be used. The additional therapy may include radiation therapy (eg, postoperative radiation therapy), surgery, gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, gamma irradiation, or any of the foregoing. It can be a combination.
일부 경우들에서, 상기 추가 요법은 부작용 제한 제제(예컨대, 치료의 부작용의 발생 및/또는 중증도를 줄이고자 하는 제제, 예컨대 항 메스꺼움 제제, 코르티코스테로이드(예컨대, 프레드니손 또는 등가물, 예컨대 1~2 mg/kg/일의 용량), 및 호르몬 대체 약물(들) 등)의 투여이다.In some cases, the additional therapy is a side-effect limiting agent (eg, an agent intended to reduce the incidence and/or severity of side effects of treatment, such as an anti-nausea agent, a corticosteroid (eg, prednisone or equivalent, such as 1-2 mg/ kg/day), and hormone replacement drug(s), etc.).
본원에서는 또한 대상체의 폐암을 치료하는 방법으로서, 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 및/또는 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀)) 및/또는 암 요법(예컨대, 수술 및/또는 방사선 요법)과 병용한 유효량의 PD-1 축 결합 길항제(예컨대, 아테졸리주맙) 및/또는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)을 포함한 치료 요법을 상기 대상체에게 투여하는 단계를 포함한 방법이 제공된다. 예를 들어, PD-1 축 결합 길항제는 추가 화학요법 또는 화학요법제(상기 정의를 참조); 표적 요법 또는 표적 치료제; 면역요법 또는 면역요법제, 예를 들어 단일클론 항체; 하나 이상의 세포독성제(상기 정의를 참조); 또는 이들의 조합과 병용하여 투여될 수 있다. Also disclosed herein is a method of treating lung cancer in a subject, comprising one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, antimetabolites) (eg, pemetrexed or gemcitabine) and/or taxanes (eg, paclitaxel, such as nap-paclitaxel) and/or an effective amount of PD-1 axis binding in combination with cancer therapy (eg, surgery and/or radiation therapy) Methods are provided comprising administering to the subject a treatment regimen comprising an antagonist (eg, atezolizumab) and/or an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) For example, a PD-1 axis binding antagonist may include additional chemotherapeutic or chemotherapeutic agents (see definition above); targeted therapy or targeted therapeutic agents; immunotherapeutic or immunotherapeutic agents, such as monoclonal antibodies; agent (see above definition); or a combination thereof.
제제의 투약dosing of the formulation
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 화학요법제의 투약은 섹션 III(K)에 기재되어 있다. Dosing of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, and chemotherapeutic agents is described in Section III(K).
암 특성화 및 선택Cancer characterization and selection
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 폐암(예컨대, 초기 폐암(예컨대, 절제가능한 폐암(예컨대, NSCLC(예컨대, 편평 또는 비편평 NSCLC))은 절제가능하다(예컨대, 치료 목적으로 R0 절제에 적격인). 일부 경우들에서, 상기 폐암은 NSCLC이다. 일부 경우들에서, 상기 NSCLC는 편평 또는 비편평 NSCLC이다. 일부 경우들에서, 상기폐암은 PD-L1 양성이다. 일부 경우들에서, 상기폐암은 PD-L1 높음이다. 일부 경우들에서, 상기 폐암은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 가지지 않는다. 일부 경우들에서, 상기 폐암은 II기, IIIA기, 또는 IIIB기 폐암이다. In some cases, in any method, use, or composition for use described herein, lung cancer (eg, early lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)) is resectable (e.g., eligible for R0 resection for therapeutic purposes.) In some cases, the lung cancer is NSCLC. In some cases, the NSCLC is squamous or non-squamous NSCLC. In some cases, the lung cancer is PD- L1 positive.In some cases, the lung cancer is PD-L1 high.In some cases, the lung cancer does not have epidermal growth factor receptor ( EGFR ) or anaplastic lymphoma kinase ( ALK ) genomic tumor abnormality.Some cases In these cases, the lung cancer is stage II, IIIA, or IIIB lung cancer.
일부 예들에서, 본원에 기재된 방법, 사용, 또는 사용를 위한 조성물들에서, 상기 대상체에는 백금계 화학요법에 적격이다. 일부 경우들에서, 상기 대상체는 0 또는 1의 이스턴 코퍼레이티브 종양학 그룹(ECOG) 전신 활동도(PS)를 가진다. 일부 경우들에서, 상기 대상체는 폐암에 대한 선행 요법(예컨대, 면역요법, 화학요법 또는 방사선요법)을 받지 않았다.In some embodiments, in a method, use, or compositions for use described herein, the subject is eligible for platinum-based chemotherapy. In some cases, the subject has an Eastern Corporate Oncology Group (ECOG) systemic activity (PS) of 0 or 1. In some cases, the subject has not received prior therapy (eg, immunotherapy, chemotherapy, or radiotherapy) for lung cancer.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 순환하는 종양 DNA(ctDNA)의 존재 또는 수준이 평가될 수 있다. 일부 경우들에서, ctDNA는 상기 대상체의 샘플(예컨대, 혈액 샘플(예컨대, 혈장 샘플))에서 평가된다. 일부 경우들에서, ctDNA는 제1 투약 주기(예컨대, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 제1 투약 주기)의 1일 전에 상기 대상체의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술 전에 상기 대상체의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술 후 상기 대상체의 샘플에서 평가된다.In some cases, in any method, use, or composition for use described herein, the presence or level of circulating tumor DNA (ctDNA) can be assessed. In some cases, ctDNA is evaluated in a sample of the subject (eg, a blood sample (eg, a plasma sample)). In some cases, ctDNA is assessed in a sample of the subject 1 day prior to a first dosing cycle (eg, a first dosing cycle of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist). In some cases, ctDNA is evaluated in a sample of the subject prior to surgery. In some cases, ctDNA is evaluated in a sample of the subject after surgery.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 면역 세포(예컨대, T 세포)의 존재 또는 수준이 평가될 수 있다. 일부 경우들에서, 면역 세포의 존재 또는 수준은 상기 대상체로부터의 샘플(예컨대, 혈액 샘플, 종양 조직 샘플, 또는 림프절 샘플)에서 평가된다. 일부 경우들에, 면역 세포의 존재 또는 수준은 수술 전에 상기 대상체의 샘플에서 평가된다. 일부 경우들에, 면역 세포의 존재 또는 수준은 수술 후에 상기 대상체의 샘플에서 평가된다.In some cases, in any of the methods, uses, or compositions for use described herein, the presence or level of immune cells (eg, T cells) can be assessed. In some cases, the presence or level of immune cells is assessed in a sample from the subject (eg, a blood sample, tumor tissue sample, or lymph node sample). In some cases, the presence or level of immune cells is assessed in a sample of the subject prior to surgery. In some cases, the presence or level of immune cells is assessed in a sample of the subject after surgery.
PD-L1 발현의 평가Assessment of PD-L1 expression
PD-L1의 발현은 섹션 III(L)에 기재된 바와 같이 평가할 수 있다. Expression of PD-L1 can be assessed as described in section III(L).
EGFR 및 ALK 이상의 평가Assessment of EGFR and ALK or higher
돌연변이 상태 EGFR 및 ALK를 검출하는 방법은 본원의 섹션 III(N)에 기재되어 있다. Methods for detecting the mutant state EGFR and ALK are described in Section III(N) herein.
치료에 대한 반응response to treatment
본원에 기재된 임의의 방법의 일부 구현예들에서, 요법에 대한 대상체의 반응은 하나 이상의 측정에 의해 특징지어질 수 있다. 일부 구현예들에서, 상기 치료는 주요 병리학적 반응율(MPR)의 증가를 발생시킨다. 일부 구현예들에서, 상기 치료는 pCR을 발생시킨다. 일부 구현예들에서, 상기 치료는 무사건 생존(EFS)의 증가를 발생시킨다. 일부 구현예들에서, 상기 치료는 환자 보고 결과를 개선시킨다. 일부 구현예들에서, 상기 치료는 EORTC-QLQ-C30으로 측정한 바와 같이 환자가 보고한 신체 기능, 역할 기능, 또는 GHS/QoL을 개선시킨다. 일부 구현예들에서, 상기 치료는 EORTC-QLQ-LC13의 사용을 통해 측정된 바와 같이 기침, 호흡곤란, 및 흉통에 대해 환자가 보고한 폐암 증상을 개선시킨다.In some embodiments of any of the methods described herein, the subject's response to therapy can be characterized by one or more measures. In some embodiments, the treatment results in an increase in the major pathological response rate (MPR). In some embodiments, the treatment results in pCR. In some embodiments, the treatment results in an increase in event-free survival (EFS). In some embodiments, the treatment improves patient-reported outcomes. In some embodiments, the treatment improves patient-reported bodily function, role function, or GHS/QoL as measured by EORTC-QLQ-C30. In some embodiments, the treatment improves lung cancer symptoms reported by the patient for cough, dyspnea, and chest pain as measured through use of EORTC-QLQ-LC13.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 MPR 비율의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는, 예컨대 화학요법(예컨대, 백금계 이중 화학요법(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)) 없이 상기 항 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 MPR 비율의 증가를 발생시킨다.In some cases, the treatment increases the MPR rate of the subject, e.g., as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. causes an increase. In some cases, the treatment includes, for example, chemotherapy (eg, platinum-based double chemotherapy (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (eg, antimetabolites ( e.g., pemetrexed or gemcitabine) or taxane (e.g., paclitaxel or nap-paclitaxel) resulting in an increase in the subject's MPR rate as compared to treatment with the anti-PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody make it
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 pCR의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는, 예컨대 화학요법(예컨대, 백금계 이중 화학요법(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)) 없이 상기 항 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 pCR의 증가를 발생시킨다.In some cases, the treatment increases the pCR of the subject, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. causes In some cases, the treatment includes, for example, chemotherapy (eg, platinum-based double chemotherapy (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (eg, antimetabolites ( e.g., pemetrexed or gemcitabine) or taxane (e.g., paclitaxel or nap-paclitaxel) results in an increase in pCR in a subject as compared to treatment with the anti-PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody .
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 OS를 연장시킨다. 일부 경우들에서, 상기 치료는, 예컨대 화학요법(예컨대, 백금계 이중 화학요법(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)) 없이 상기 항 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 OS를 연장시킨다.In some cases, the treatment prolongs the subject's OS, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. make it In some cases, the treatment includes, for example, chemotherapy (eg, platinum-based double chemotherapy (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (eg, antimetabolites ( Prolongs OS in a subject as compared to treatment with the anti-PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody without (eg, pemetrexed or gemcitabine) or a taxane (eg, paclitaxel or nap-paclitaxel).
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 EFS를 연장시킨다. 일부 경우들에서, 상기 치료는, 예컨대 화학요법(예컨대, 백금계 이중 화학요법(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈) 또는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀)) 없이 상기 항 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 EFS를 연장시킨다. In some cases, the treatment prolongs the subject's EFS, e.g., as compared to treatment with a PD-1 axis binding antagonist without an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody without a PD-1 axis binding antagonist. make it In some cases, the treatment includes, for example, chemotherapy (eg, platinum-based double chemotherapy (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (eg, antimetabolites ( Prolongs EFS in a subject compared to treatment with the anti-PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody without (eg, pemetrexed or gemcitabine) or a taxane (eg, paclitaxel or nap-paclitaxel).
일부 구현예들에서, 기재된 치료는 MPR 비율을 적어도 1% 만큼(예컨대, 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, 또는 100% 만큼) 증가시킨다.In some embodiments, the described treatment increases the MPR rate by at least 1% (eg, 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55 %, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100%).
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체의 pCR을 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월,3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 pCR을 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein lowers the subject's pCR by at least about 2 months (eg, by 2 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months, by 5.0 to by 48 months, by 6.0 to 36 months, by 8.0 to 24 months, or by 10 to 12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, by 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment lowers the subject's pCR by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months) by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체의 EFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월,3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 EFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein reduces the subject's EFS by at least about 2 months (eg, by 2 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months, by 5.0 to by 48 months, by 6.0 to 36 months, by 8.0 to 24 months, or by 10 to 12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, by 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's EFS by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months). by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 5.1개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some embodiments, OS is measured as the period from initiation of treatment to death. In some cases, the treatment reduces the subject's OS by at least about 2 months (eg, by 2-120 months, by 3-110 months, by 4-100 months, by 5-80 months, by 6-60 months) , by 7-48 months, by 8-36 months, by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months , 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the subject's OS by at least about 3.3 months (eg, by 3.3-120 months, by 4-100 months, by 5-80 months, by 6-60 months, by 7-48 months) , by 8-36 months, or by 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 5.1 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the subject's OS by at least about 5.3 months (eg, by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months). by, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months , by 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
A.A. 자궁경부암과 관련된 치료 및 진단 방법 및 사용Methods and uses for treatment and diagnosis related to cervical cancer
자궁경부암 cervical cancer
자궁경부암은 네 번째로 흔하게 진단되는 암이며 암 관련 사망의 네 번째 주요 원인이다. 매년 전 세계적으로 500,000명 이상의 여성이 자궁경부암 진단을 받고 300,000명 이상이 사망한다. 자궁경부암 사망의 거의 90%가 개발도상국에서 발생한다. 미국에서는, 매년 13,000명의 새로운 침습성 자궁경부암 사례가 발생하고 약 4000명의 암 관련 사망이 발생한다.Cervical cancer is the fourth most commonly diagnosed cancer and the fourth leading cause of cancer-related deaths. Each year, more than 500,000 women worldwide are diagnosed with cervical cancer and more than 300,000 die. Nearly 90% of cervical cancer deaths occur in developing countries. In the United States, there are 13,000 new cases of invasive cervical cancer each year and approximately 4000 cancer-related deaths.
조기 및 국소 진행성 자궁경부암의 치료는 각각 수술 및 최종 화학 방사선 요법으로 구성되며 관해를 이끌어내는 데 매우 효과적일 수 있다. 하지만, 암이 재발하거나 1차 치료로 소실되지 않으면, 5년 생존율이 약 15%로서, 새로운 전이성 질환 환자의 경우와 비슷하게 예후가 매우 좋지 않다. 몇 가지 예외를 제외하고, 재발성, 지속성, 또는 새로운 전이성 질환에 대한 치료 표준은 부인과 종양학 그룹(Gynecology Oncology Group) 240 시험에 기초한 베바시주맙을 포함한 화학요법이며, 화학요법에 추가된 베바시주맙은 화학요법 단독에 비해 OS 중앙값을 개선함을 보여주었다(각각 17개월 대 13.3개월).Treatment of early and locally advanced cervical cancer consists of surgery and definitive chemoradiation therapy, respectively, and can be very effective in eliciting remission. However, if the cancer does not recur or disappear with first-line treatment, the 5-year survival rate is about 15%, and the prognosis is very poor, similar to that of patients with new metastatic disease. With a few exceptions, the standard of care for recurrent, persistent, or new metastatic disease is chemotherapy, including bevacizumab, based on a Gynecology Oncology Group 240 trial, and bevacizumab added to chemotherapy. showed improvement in median OS compared to chemotherapy alone (17 months vs. 13.3 months, respectively).
현재, 베바시주맙을 포함한 화학요법에 대한 재발 또는 진행 후 세계적으로 인정되는 치료 표준은 존재하지 않다. 따라서, 이들 환자에 대한 치료 옵션은 단일 제제 또는 병용으로 투여되는 다양한 세포독성 화학요법제를 크게 포함한다. 하지만, 역사적으로 약 10%~15%의 낮은 반응률을 감안할 때 세포독성 화학요법은 환자의 삶의 질에 미치는 영향과 부담을 고려하여 최상의 지지 치료라기 보다는 수용 가능한 치료 표준을 나타내는지 여부에 점점 더 초점이 맞춰져 왔다.Currently, there is no globally accepted standard of care following relapse or progression for chemotherapy, including bevacizumab. Thus, treatment options for these patients largely include a variety of cytotoxic chemotherapeutic agents administered either as single agents or in combination. However, given historically low response rates of around 10% to 15%, it is increasingly questioned whether cytotoxic chemotherapy represents an acceptable standard of care rather than the best supportive care given the burden and impact on the patient's quality of life. focus has been
자궁경부 상피세포의 HPV 감염으로 인한 면역 반응의 개입과 결부되어 기존 치료법은 역사적으로 볼 때 효능 비율이 낮기 때문에, 자궁경부암은 새로운 면역 요법 기반 접근법을 시도하기에 특히 매력적인 기회로서 보인다.Because conventional therapies have historically low efficacy rates, coupled with the intervention of the immune response resulting from HPV infection of cervical epithelial cells, cervical cancer appears as a particularly attractive opportunity to try new immunotherapy-based approaches.
따라서, 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암의 치료를 위한 효과적인 면역요법 및 이를 투약하는 방법을 개발하는 분야에서 충족되지 않은 요구가 있다.Thus, effective immunotherapy for the treatment of cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer, and methods of administering the same) There are unmet needs in the field.
i. 자궁경부암 치료를 위한 방법 및 사용i. Methods and uses for the treatment of cervical cancer
본원에서는 대상체 또는 대상체 집단에서 PD-L1의 검출 가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 치료하는 방법 및 사용으로서, 상기 대상체 또는 대상체 집단에게 유효량의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 투여하는 단계를 포함한 방법 및 사용이 제공된다. Provided herein are cancers having a detectable expression level of PD-L1 in a subject or population of subjects (eg, cervical cancer, such as stage 4B, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) ), comprising administering to the subject or population of subjects an effective amount of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist). Methods and uses are provided comprising administering one or more dosing cycles of an antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)).
투약 요법 및 투여Dosage regimen and administration
일 양태에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 PD-L1의 검출 가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단에게 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 투여함으로써 상기 대상체 또는 대상체 집단을 치료하는 단계를 포함한다.In one aspect, the treatment methods and uses of the invention described herein can be used for cancers having a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or To a subject or population of subjects with recurrent PD-L1 positive cervical cancer) an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and an effective amount of a PD-1 axis binding antagonist ( For example, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) ) by administering one or more dosing cycles of said subject or population of subjects.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 600 mg(예컨대, 약 50 mg 내지 600 mg, 예컨대, 약 60 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 550 mg, 예컨대, 약 250 mg 내지 약 500 mg, 예컨대, 약 300 mg 내지 약 450 mg, 예컨대, 약 350 mg 내지 약 400 mg, 예컨대, 약 375 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 600 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 30 mg 내지 600 mg(예컨대, 50 mg 내지 600 mg, 예컨대, 60 mg 내지 600 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 200 mg 내지 600 mg, 예컨대, 200 mg 내지 550 mg, 예컨대, 250 mg 내지 500 mg, 예컨대, 300 mg 내지 450 mg, 예컨대, 350 mg 내지 400 mg, 예컨대, 375 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 600 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 600 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))와의 병용 치료)으로 투여되는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여되는 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about 1100) every 3 weeks. mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, For example, a dose (eg, a fixed dose) of 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 30 mg to about 600 mg (eg, from about 50 mg to 600 mg every 3 weeks). mg, such as about 60 mg to about 600 mg, such as about 100 mg to about 600 mg, such as about 200 mg to about 600 mg, such as about 200 mg to about 550 mg, such as about 250 mg to about 500 mg, such as from about 300 mg to about 450 mg, such as from about 350 mg to about 400 mg, such as about 375 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose (eg, a fixed dose) of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 30 mg to 1200 mg (eg, 30 mg to 1100 mg, eg, 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as , 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 30 mg to 600 mg (eg, 50 mg to 600 mg, such as every 3 weeks) , 60 mg to 600 mg, such as 100 mg to 600 mg, such as 200 mg to 600 mg, such as 200 mg to 550 mg, such as 250 mg to 500 mg, such as 300 mg to 450 mg, such as 350 mg to 400 mg, such as 375 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg (eg, a fixed dose) every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg (eg, a fixed dose) every 3 weeks. In some cases, combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or Dose of said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) administered in combination therapy with MK-3475 (pembrolizumab, formerly known as lambrolizumab) may be reduced compared to a standard dose of the anti-TIGIT antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 80 mg 내지 약 1950 mg, 예컨대, 약 80 mg 내지 약 1900 mg, 예컨대, 약 80 mg 내지 약 1800 mg, 예컨대, 약 100 mg 내지 약 1700 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1400 mg, 예컨대, 약 400 mg 내지 약 1300 mg, 예컨대, 약 500 mg 내지 약 1200 mg, 예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 700 mg 내지 약 1000 mg, 예컨대, 약 740 mg 내지 약 940 mg, 예컨대, 약 790 mg 내지 약 890 mg, 예컨대, 약 815 mg 내지 약 865 mg, 예컨대, 약 830 mg 내지 약 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 1900 mg, 예컨대, 약 300 mg 내지 약 1700 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 80 mg 내지 약 2000 mg(예컨대 약 100 mg 내지 약 2000 mg, 예컨대 약 200 mg 내지 약 2000 mg, 예컨대 약 300 mg 내지 약 2000 mg, 예컨대 약 400 mg 내지 약 2000 mg, 예컨대 약 500 mg 내지 약 2000 mg, 예컨대 약 600 mg 내지 약 1900 mg, 예컨대 약 700 mg 내지 약 1800 mg, 예컨대 약 800 mg 내지 약 1800 mg, 예컨대 약 900 mg 내지 약 1800 mg, 예컨대 약 1000 mg 내지 약 1800 mg, 예컨대 약 1100 mg 내지 약 1800 mg, 예컨대 약 1200 mg 내지 약 1800 mg, 예컨대 약 1300 mg 내지 약 1800 mg, 예컨대 약 1400 mg 내지 약 1800 mg, 예컨대 약 1500 mg 내지 약 1800 mg, 예컨대 약 1580 mg 내지 약 1780 mg, 예컨대 약 1630 mg 내지 약 1730 mg, 예컨대 약 1655 mg 내지 약 1705 mg, 예컨대 약 1670 mg 내지 약 1690 mg, 예컨대 1680 mg ± 5 mg, 예컨대 1680 ± 2.5 mg, 예컨대 1680 ± 1.0 mg, 예컨대 1680 ± 0.5 mg, 예컨대 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 약 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 80 mg 내지 2000 mg(예컨대, 80 mg 내지 1950 mg, 예컨대, 80 mg 내지 1900 mg, 예컨대, 80 mg 내지 1800 mg, 예컨대, 100 mg 내지 1700 mg, 예컨대, 200 mg 내지 1600 mg, 예컨대, 300 mg 내지 1400 mg, 예컨대, 400 mg 내지 1300 mg, 예컨대, 500 mg 내지 1200 mg, 예컨대, 600 mg 내지 1100 mg, 예컨대, 700 mg 내지 1000 mg, 예컨대, 740 mg 내지 940 mg, 예컨대, 790 mg 내지 890 mg, 예컨대, 815 mg 내지 865 mg, 예컨대, 830 mg 내지 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 1900 mg, 예컨대, 300 mg 내지 1700 mg, 예컨대, 400 mg 내지 1600 mg, 예컨대, 500 mg 내지 1600 mg, 예컨대, 600 mg 내지 1600 mg, 예컨대, 700 mg 내지 1600 mg, 예컨대, 800 mg 내지 1600 mg, 예컨대, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 2000 mg, 예컨대, 300 mg 내지 2000 mg, 예컨대, 400 mg 내지 2000 mg, 예컨대, 500 mg 내지 2000 mg, 예컨대, 600 mg 내지 1900 mg, 예컨대, 700 mg 내지 1800 mg, 예컨대, 800 mg 내지 1800 mg, 예컨대, 900 mg 내지 1800 mg, 예컨대, 1000 mg 내지 1800 mg, 예컨대 1100 mg 내지 1800 mg, 예컨대 1200 mg 내지 1800 mg, 예컨대 1300 mg 내지 1800 mg, 예컨대 1400 mg 내지 1800 mg, 예컨대 1500 mg 내지 1800 mg, 예컨대 1580 mg 내지 1780 mg, 예컨대 1630 mg 내지 1730 mg, 예컨대 1655 mg 내지 1705 mg, 예컨대 1670 mg 내지 1690 mg, 예컨대 1680 mg ± 5 mg, 예컨대 1680 ± 2.5 mg, 예컨대 1680 ± 1.0 mg, 예컨대 1680 ± 0.5 mg, 예컨대 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주 마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주 마다 약 1680 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주 마다 1680 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 80 mg to about) every two weeks. 1950 mg, such as about 80 mg to about 1900 mg, such as about 80 mg to about 1800 mg, such as about 100 mg to about 1700 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1400 mg, such as about 400 mg to about 1300 mg, such as about 500 mg to about 1200 mg, such as about 600 mg to about 1100 mg, such as about 700 mg to about 1000 mg, such as about 740 mg to about 940 mg, such as about 790 mg to about 890 mg, such as about 815 mg to about 865 mg, such as about 830 mg to about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as, a dose (eg, a fixed dose) of 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 3 weeks. 2000 mg, such as about 200 mg to about 1900 mg, such as about 300 mg to about 1700 mg, such as about 400 mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg , such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about 2000) every 3 weeks. mg, such as about 200 mg to about 2000 mg, such as about 300 mg to about 2000 mg, such as about 400 mg to about 2000 mg, such as about 500 mg to about 2000 mg, such as about 600 mg to about 1900 mg, such as about 700 mg to about 1800 mg, such as about 800 mg to about 1800 mg, such as about 900 mg to about 1800 mg, such as about 1000 mg to about 1800 mg, such as about 1100 mg to about 1800 mg, such as about 1200 mg to about 1800 mg , such as about 1300 mg to about 1800 mg, such as about 1400 mg to about 1800 mg, such as about 1500 mg to about 1800 mg, such as about 1580 mg to about 1780 mg, such as about 1630 mg to about 1730 mg, such as about 1655 mg to about 1705 mg, such as about 1670 mg to about 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 80 mg to 1950 mg, such as every two weeks) , 80 mg to 1900 mg, such as 80 mg to 1800 mg, such as 100 mg to 1700 mg, such as 200 mg to 1600 mg, such as 300 mg to 1400 mg, such as 400 mg to 1300 mg, such as 500 mg to 1200 mg, such as 600 mg to 1100 mg, such as 700 mg to 1000 mg, such as 740 mg to 940 mg, such as 790 mg to 890 mg, such as 815 mg to 865 mg, such as 830 mg to a dose (eg, a fixed dose) of 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 3 weeks) , 200 mg to 1900 mg, such as 300 mg to 1700 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 3 weeks) , 200 mg to 2000 mg, such as 300 mg to 2000 mg, such as 400 mg to 2000 mg, such as 500 mg to 2000 mg, such as 600 mg to 1900 mg, such as 700 mg to 1800 mg, such as 800 mg to 1800 mg, such as 900 mg to 1800 mg, such as 1000 mg to 1800 mg, such as 1100 mg to 1800 mg, such as 1200 mg to 1800 mg, such as 1300 mg to 1800 mg, such as 1400 mg to 1800 mg, such as 1500 mg to 1800 mg, such as 1580 mg to 1780 mg, such as 1630 mg to 1730 mg, such as 1655 mg to 1705 mg, such as 1670 mg to 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, anti-PD-) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of an L1 antagonist antibody (eg, atezolizumab) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대 약 1 mg/kg 내지 약 35 mg/kg, 예컨대 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대 약 5 mg/kg 내지 약 25 mg/kg, 예컨대 약 10 mg/kg 내지 약 20 mg/kg, 예컨대 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 투여되는 약 15 mg/kg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대 0.1 mg/kg 내지 40 mg/kg, 예컨대 1 mg/kg 내지 35 mg/kg, 예컨대 2.5 mg/kg 내지 30 mg/kg, 예컨대 5 mg/kg 내지 25 mg/kg, 예컨대 10 mg/kg 내지 20 mg/kg, 예컨대 12.5 mg/kg 내지 15 mg/kg, 예컨대 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대 0.5 mg/kg 내지 15 mg/kg, 예컨대 1 mg/kg 내지 15 mg/kg, 예컨대 2.5 mg/kg 내지 15 mg/kg, 예컨대 5 mg/kg 내지 15 mg/kg, 예컨대 7.5 mg/kg 내지 15 mg/kg, 예컨대 10 mg/kg 내지 15 mg/kg, 예컨대 12.5 mg/kg 내지 15 mg/kg, 예컨대 14 mg/kg 내지 15 mg/kg, 예컨대 15 ± 1 mg/kg, 예컨대 15 ± 0.5 mg/kg, 예컨대 15 ± 0.2 mg/kg, 예컨대 15 ± 0.1 mg/kg, 예컨대 15 mg/kg)의 용량이다. 일부 경우들에서, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주 마다 투여되는 15 mg/kg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일 요법으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 표준 용량에 비해 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 50 mg/kg of the subject's body weight every 3 weeks. kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg /kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 15 mg/kg of the subject's body weight every 3 weeks. (e.g., about 0.1 mg/kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, such as about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 10 mg/kg to about 15 mg/kg, such as , about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, such as about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, an effective amount of an anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg administered every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 50 mg/kg of body weight of the subject every 3 weeks ( For example, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 15 mg/kg of body weight of the subject every 3 weeks ( For example, 0.1 mg/kg to 15 mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 15 mg/kg, such as 10 mg/kg to 15 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 14 mg/kg to 15 mg/kg, for example 15 ± 1 mg/kg, such as 15 ± 0.5 mg/kg, such as 15 ± 0.2 mg/kg, such as 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, the effective amount of an anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of 15 mg/kg administered every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of the antibody (eg, atezolizumab) is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX) administered as a monotherapy. -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)).
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 180 mg 내지 약 250 mg, 예컨대, 약 180 mg 내지 약 220 mg, 예컨대, 약 190 mg 내지 약 210 mg, 예컨대, 200 mg ± 5 mg, 예컨대, 200 ± 2.5 mg, 예컨대, 200 ± 1.0 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주 마다 20 mg 내지 1000 mg(예컨대 40 mg 내지 900 mg, 예컨대 60 mg 내지 800 mg, 예컨대 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대 100 mg 내지 500 mg, 예컨대 120 mg 내지 400 mg, 예컨대 140 mg 내지 300 mg, 예컨대 160 mg 내지 350 mg, 예컨대 180 mg 내지 300 mg, 예컨대 180 mg 내지 250 mg, 예컨대 180 mg 내지 220 mg, 예컨대 190 mg 내지 210 mg, 예컨대 200 mg ± 5 mg, 예컨대 200 ± 2.5 mg, 예컨대 200 ± 1.0 mg, 예컨대 200 ± 0.5 mg, 예컨대 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주 마다 200 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제 (예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, pamprolizumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about) every 3 weeks. 900 mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 180 mg to about 250 mg, such as about 180 mg to about A dose of 220 mg, such as about 190 mg to about 210 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5 mg, such as 200 ± 1.0 mg, such as 200 ± 0.5 mg, such as 200 mg) For example, fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pamprolizumab)) is 20 mg to 1000 mg (eg 40 mg to 900 mg, such as 60) every 3 weeks. mg to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 160 mg to 350 mg, such as 180 mg to 300 mg, such as 180 mg to 250 mg, such as 180 mg to 220 mg, such as 190 mg to 210 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5 mg, such as 200 ± 1.0 mg, such as 200 ± 0.5 mg , eg 200 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, pamprolizumab)) is a dose (eg, a fixed dose) of 200 mg every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab). The dose of the antibody (eg, pembrolizumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 200 mg 내지 약 280 mg, 예컨대, 약 220 mg 내지 약 260 mg, 예컨대, 약 230 mg 내지 약 250 mg, 예컨대, 240 mg ± 5 mg, 예컨대, 240 ± 2.5 mg, 예컨대, 240 ± 1.0 mg, 예컨대, 240 ± 0.5 mg, 예컨대, 240 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주 마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 약 100 mg 내지 약 1000 mg(예컨대, 약 200 mg 내지 약 900 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 700 mg, 예컨대, 약 400 mg 내지 약 600 mg, 예컨대 약 400 mg 내지 약 550 mg, 예컨대, 약 420 mg 내지 약 540 mg, 예컨대, 약 440 mg 내지 약 520 mg, 예컨대, 약 460 mg 내지 약 500 mg, 예컨대, 약 470 mg 내지 약 490 mg, 예컨대, 480 mg ± 5 mg, 예컨대, 480 ± 2.5 mg, 예컨대, 480 ± 1.0 mg, 예컨대, 480 ± 0.5 mg, 예컨대, 480 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주 마다 20 mg 내지 1000 mg(예컨대 40 mg 내지 900 mg, 예컨대 60 mg 내지 800 mg, 예컨대 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대 100 mg 내지 500 mg, 예컨대 120 mg 내지 400 mg, 예컨대 140 mg 내지 300 mg, 예컨대 160 mg 내지 350 mg, 예컨대 180 mg 내지 300 mg, 예컨대 200 mg 내지 280 mg, 예컨대 220 mg 내지 260 mg, 예컨대 230 mg 내지 250 mg, 예컨대 240 mg ± 5 mg, 예컨대 240 ± 2.5 mg, 예컨대 240 ± 1.0 mg, 예컨대 240 ± 0.5 mg, 예컨대 240 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주 마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주 마다 100 mg 내지 1000 mg(예컨대 200 mg 내지 900 mg, 예컨대 300 mg 내지 800 mg, 예컨대 400 mg 내지 700 mg, 예컨대, 400 mg 내지 600 mg, 예컨대 400 mg 내지 550 mg, 예컨대 420 mg 내지 540 mg, 예컨대 440 mg 내지 520 mg, 예컨대 460 mg 내지 500 mg, 예컨대 470 mg 내지 490 mg, 예컨대 480 mg ± 5 mg, 예컨대 480 ± 2.5 mg, 예컨대 480 ± 1.0 mg, 예컨대 480 ± 0.5 mg, 예컨대 480 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주 마다 480 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제 (예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about 900) every two weeks. mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 200 mg to about 280 mg, such as about 220 mg to about 260 mg, such as from about 230 mg to about 250 mg, such as 240 mg ± 5 mg, such as 240 ± 2.5 mg, such as 240 ± 1.0 mg, such as 240 ± 0.5 mg, such as 240 mg). , fixed capacity). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is from about 100 mg to about 1000 mg (eg, from about 200 mg to about 900) every 4 weeks. mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 700 mg, such as about 400 mg to about 600 mg, such as about 400 mg to about 550 mg, such as about 420 mg to about 540 mg , such as from about 440 mg to about 520 mg, such as from about 460 mg to about 500 mg, such as from about 470 mg to about 490 mg, such as 480 mg ± 5 mg, such as 480 ± 2.5 mg, such as 480 ± 1.0 mg, such as 480 ± 0.5 mg, such as 480 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is 20 mg to 1000 mg (eg 40 mg to 900 mg, such as 60 mg) every two weeks. to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 160 mg to 350 mg, such as 180 mg. to 300 mg, such as 200 mg to 280 mg, such as 220 mg to 260 mg, such as 230 mg to 250 mg, such as 240 mg ± 5 mg, such as 240 ± 2.5 mg, such as 240 ± 1.0 mg, such as 240 ± 0.5 mg, eg 240 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is 100 mg to 1000 mg (eg 200 mg to 900 mg, such as 300 mg) every 4 weeks. to 800 mg, such as 400 mg to 700 mg, such as 400 mg to 600 mg, such as 400 mg to 550 mg, such as 420 mg to 540 mg, such as 440 mg to 520 mg, such as 460 mg to 500 mg, such as 470 mg to 490 mg, such as 480 mg ± 5 mg, such as 480 ± 2.5 mg, such as 480 ± 1.0 mg, such as 480 ± 0.5 mg, such as 480 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab). The dose of the antibody (eg, nivolumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
본 발명의 임의의 방법 및 사용에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 1회 이상의 투약 주기(예컨대, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 또는 50회 이상의 투약 주기)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체((예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망, 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일 내지 28일(예컨대, 14일, 15일, 16일, 17일, 18일, 19일, 20일, 21일, 22일, 23일, 24일, 25일, 26일, 27일, 또는 28일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 28일이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여된다. 유사하게, 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로 (즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여된다.In any of the methods and uses of the invention, said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered in one or more dosing cycles ( For example, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles. For example, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) )) continue until clinical benefit is lost (e.g., disease progression, drug resistance, death, or unacceptable toxicity is identified) In some cases, the length of each dosing cycle is about 14 days to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days, 27 days, or 28 days) days) In some cases, the length of each dosing cycle is about 21 days. In some cases, the length of each dosing cycle is about 14 days. In some cases, the length of each dosing cycle is about 28 days. In some cases, the anti-TIGIT antagonist antibody (eg, anti-TIGIT as disclosed herein) The antagonist antibody, such as tyragolumab) is administered on about day 1 (eg, day 1±3) of each dosing cycle. For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of about 600 mg (eg, a fixed dose) on Day 1 of each 21 day cycle (eg, a fixed dose) ( i.e., at a dose of about 600 mg every 3 weeks). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of 600 mg (eg, a fixed dose) on Day 1 of each 21-day cycle (eg, a fixed dose) i.e., at a dose of 600 mg every 3 weeks). Similarly, in some cases, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK) - 3475 (pembrolizumab, formerly known as lambrolizumab) is administered on about day 1 (e.g., day 1 ± 3) of each dosing cycle.For example, the PD-1 axis binding antagonist ( For example, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered intravenously at a dose of about 1200 mg (ie, at a dose of about 1200 mg every 3 weeks) on Day 1 of each 21 day cycle. For example, the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered at a dose of about 200 mg on Day 1 of each 21-day cycle (ie, every 3 weeks). In a dose of about 200 mg), for example, the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is administered on the first day of each 14-day cycle. Administer intravenously at a dose of 240 mg (i.e., at a dose of about 240 mg every 2 weeks), For example, the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., nivolumab)) is administered intravenously at a dose of about 480 mg (ie, at a dose of about 480 mg every 4 weeks) on Day 1 of each 28-day cycle In some cases, the PD-1 axis binding antagonist (eg, anti- PD-L1 antagonist antibody (eg, atezolizumab)) is administered intravenously at a dose of about 1200 mg (ie, at a dose of about 1200 mg every 3 weeks) on Day 1 of each 21 day cycle. , wherein the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered at a dose of about 200 mg on Day 1 of each 21 day cycle (ie, about 200 mg every 3 weeks). For example, the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is administered on day 1 of each 14-day cycle. It is administered intravenously at a dose of about 240 mg (ie, at a dose of about 240 mg every two weeks). For example, the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is administered at a dose of about 480 mg on Day 1 of each 28-day cycle (ie, about every 4 weeks). 480 mg) intravenously.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(고정 용량)(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여된다. 일부 예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(고정 용량)(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 200 mg의 용량으로(즉, 3주마다 200 mg의 용량으로) 정맥내 투여된다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) are all administered on about 1 day of each dosing cycle (e.g., Day 1 ± 3 days).For example, the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at about 600 mg on day 1 of each 21-day cycle. administered intravenously at a dose of (e.g., a fixed dose) (i.e., at a dose of about 600 mg every 3 weeks) and the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) ) is administered intravenously at a dose of about 1200 mg (fixed dose) (i.e., at a dose of about 1200 mg every 3 weeks) on Day 1 of each 21 day cycle.For example, the anti-TIGIT antagonist antibody (such as , an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered intravenously at a dose of about 600 mg (i.e., at a dose of about 600 mg every 3 weeks) on Day 1 of each 21 day cycle, The PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, pembrolizumab)) is administered at a dose of about 200 mg on Day 1 of each 21-day cycle (ie, about 200 mg every 3 weeks). In some embodiments, the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of 600 mg on day 1 of each 21-day cycle. administered intravenously (eg, a fixed dose) (ie, at a dose of 600 mg every 3 weeks), the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) each 21 At a dose of 1200 mg on day 1 of the cycle It is administered intravenously (fixed dose) (ie, at a dose of 1200 mg every 3 weeks). For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of 600 mg on Day 1 of each 21 day cycle (ie, 600 mg every 3 weeks). and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, pembrolizumab)) is administered at a dose of 200 mg on Day 1 of each 21-day cycle (i.e., , at a dose of 200 mg every 3 weeks).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 제1 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(고정 용량)(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여된다. 일부 예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 240 mg의 용량으로(고정 용량)(즉, 2주마다 240 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 480 mg의 용량으로(즉, 4주마다 480 mg의 용량으로) 정맥내 투여된다.In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) are all administered on about day 1 of the first dosing cycle (e.g. , day 1 ± 3 days).For example, the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered on day 1 of each 21-day cycle of about 600 Administered intravenously at a dose of mg (eg, a fixed dose) (ie, at a dose of about 600 mg every 3 weeks), the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, nivolumab)) ) is administered intravenously at a dose of about 240 mg (fixed dose) (ie, at a dose of about 240 mg every 2 weeks) on Day 1 of each 14-day cycle.For example, the anti-TIGIT antagonist antibody (such as , an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered intravenously at a dose of about 600 mg (i.e., at a dose of about 600 mg every 3 weeks) on Day 1 of each 21 day cycle, The PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, nivolumab)) is administered at a dose of about 480 mg on Day 1 of each 28-day cycle (ie, a dose of about 480 mg every 4 weeks). In some embodiments, the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of 600 mg on Day 1 of each 21-day cycle ( For example, a fixed dose) (ie, at a dose of 600 mg every 3 weeks) is administered intravenously, and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, nivolumab)) is administered on each 14-day cycle. at a dose of 240 mg (fixed dose) on day 1 of ( i.e., at a dose of 240 mg every 2 weeks). For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of 600 mg on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 60 ± 15분(예컨대, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 또는 약 70분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 60 ± 15 minutes (eg, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes , about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) in about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes) , about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes). administered to said subject or population of subjects by intravenous infusion.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 30 ± 10 분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 약 30 ± 10 분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 30 ± 10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes , about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) in about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes) , about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion to the subject or population of subjects.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 후에 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제2 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is combined with the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli). Zumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) to the subject or population of subjects prior to administration. In cases, e.g., after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, Prior to administration of MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab), the method comprises an interim first observation period. In some cases, the method comprises: The PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly) and further comprises a second observation period after administration of)))) In some cases, the method includes a first observation period after administration of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) )) after the second observation period.In some cases, the first and second observation period are each about 30 minutes to about 60 minutes in length.The first and second observation period are each about In cases that are 60 minutes in length, the method comprises the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab), respectively, during the first and second observation periods). or anti-PD- 1 Vital signs (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) of the subject or population of subjects at about 30 ± 10 minutes after administration for example, pulse rate, respiration rate, blood pressure and temperature). In cases where the first and second observation periods are each about 30 minutes in length, the method comprises the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD- After administration of an L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) recording vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects at 15±10 minutes.
다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 이후 및 상기 항 TIGIT 길항제 항체의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체 투여 이후 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제1 관찰 기간 및 상기 항 TIGIT 길항제 항체의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다.In other cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) is administered to said subject or population of subjects prior to said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab). In cases, for example, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK- After administration of 3475 (pembrolizumab, formerly known as lambrolizumab) and before administration of said anti-TIGIT antagonist antibody, said method comprises an interim first observation period. In some cases, said method comprises said and a second observation period following administration of anti-TIGIT antagonist antibody.In some cases, the method comprises said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 A first observation period following administration of an antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and a second observation following administration of said anti TIGIT antagonist antibody In some cases, the first and second observation period are each about 30 minutes to about 60 minutes in length.In cases where the first and second observation period are each about 60 minutes in length , the method comprises a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (eg, MDX-1106) nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) and the vital signs of the subject or population of subjects (e.g., pulse rate, respiration rate, blood pressure and temperature). In cases where the first and second observation periods are each about 30 minutes in length, the method comprises each of the first and second observation periods with a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and drug after administration of the anti-TIGIT antagonist antibody recording vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects at 15±10 minutes.
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 상기 대상체 또는 대상체 집단에 동시에 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후에, 상기 방법은 관찰 기간을 포함한다. 일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 중 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 관찰 기간이 약 30분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 중 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In other instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered to the subject or population of subjects simultaneously. In instances, for example, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106) After administration of (nivolumab) or MK-3475 (pembrolizumab, previously known as lambrolizumab), the method comprises an observation period.In some cases, the observation period is from about 30 minutes to about 60 minutes in length.In cases where the observation period is about 60 minutes in length, the method comprises administering a PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or about 30±10 minutes after administration of an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and the anti-TIGIT antagonist antibody and recording vital signs (e.g., pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects, In cases where the observation period is about 30 minutes in length, the method comprises the observation period either a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly (known as lambrolizumab)) and at about 15 ± 10 minutes after administration of the anti-TIGIT antagonist antibody, the vital signs (e.g., pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects are recorded. may include steps.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 4B기, 전이성, 재발성 또는 지속성 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재되는 바와 같이 서열번호 17 또는 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. In another embodiment, the present invention provides one or more dosing cycles of a 600 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks and a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks to the subject or There is provided a method of treating said subject or a population of subjects having stage 4B, metastatic, relapsed or persistent cervical cancer by administering to said subject population, wherein said anti-TIGIT antagonist antibody comprises SEQ ID NO: 17 or It has a VH domain having the amino acid sequence of 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 4B기, 전이성, 재발성 또는 지속성 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하는 방법을 제공한다.In another embodiment, the present invention provides a subject or subject with one or more dosing cycles of a 600 mg dose (eg, a fixed dose) tiragolumab every 3 weeks and a 1200 mg dose (eg, a fixed dose) atezolizumab every 3 weeks. Provided is a method of treating said subject or population of subjects having stage 4B, metastatic, relapsed or persistent cervical cancer by administering to the population.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 3주마다 200 mg 용량의(예컨대, 고정 용량) 펨브롤리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 4B기, 전이성, 재발성 또는 지속성 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하는 방법을 제공한다.In another aspect, the present invention provides a subject or subject with one or more dosing cycles of a 600 mg dose (eg, a fixed dose) tiragolumab every 3 weeks and a 200 mg dose (eg, a fixed dose) pembrolizumab every 3 weeks. Provided is a method of treating said subject or population of subjects having stage 4B, metastatic, relapsed or persistent cervical cancer by administering to the population.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 2주마다 240 mg 용량의(예컨대, 고정 용량) 니볼루맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 4B기, 전이성, 재발성 또는 지속성 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하는 방법을 제공한다. In another embodiment, the present invention provides one or more dosing cycles of a 600 mg dose (eg, a fixed dose) tiragolumab every 3 weeks and a 240 mg dose (eg, a fixed dose) nivolumab every 2 weeks to a subject or population of subjects. Provided is a method of treating said subject or population of subjects having stage 4B, metastatic, relapsed or persistent cervical cancer by administering to
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 4주마다 480 mg 용량의(예컨대, 고정 용량) 니볼루맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 4B기, 전이성, 재발성 또는 지속성 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하는 방법을 제공한다.In another embodiment, the present invention provides one or more dosing cycles of a 600 mg dose (eg, a fixed dose) tiragolumab every 3 weeks and a 480 mg dose (eg, a fixed dose) nivolumab every 4 weeks to a subject or population of subjects. Provided is a method of treating said subject or population of subjects having stage 4B, metastatic, relapsed or persistent cervical cancer by administering to
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))을 제공하고, 여기서 상기 방법은 유효량의 항 TIGIT 길항제 항체 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-L1) for use in a method of treating a subject or population of subjects having cervical cancer) An antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is provided, wherein The method comprises an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) ) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) to the subject or population of subjects.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 600 mg(예컨대, 약 50 mg 내지 600 mg, 예컨대, 약 60 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 550 mg, 예컨대, 약 250 mg 내지 약 500 mg, 예컨대, 약 300 mg 내지 약 450 mg, 예컨대, 약 350 mg 내지 약 400 mg, 예컨대, 약 375 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 30 mg 내지 600 mg(예컨대, 50 mg 내지 600 mg, 예컨대, 60 mg 내지 600 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 200 mg 내지 600 mg, 예컨대, 200 mg 내지 550 mg, 예컨대, 250 mg 내지 500 mg, 예컨대, 300 mg 내지 450 mg, 예컨대, 350 mg 내지 400 mg, 예컨대, 375 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 600 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))와의 병용 치료)으로 투여될 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여될 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about 1100) every 3 weeks. mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, For example, a dose (eg, a fixed dose) of 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 30 mg to about 600 mg (eg, from about 50 mg to 600 mg every 3 weeks). mg, such as about 60 mg to about 600 mg, such as about 100 mg to about 600 mg, such as about 200 mg to about 600 mg, such as about 200 mg to about 550 mg, such as about 250 mg to about 500 mg, such as from about 300 mg to about 450 mg, such as from about 350 mg to about 400 mg, such as about 375 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 30 mg to 1200 mg (eg, 30 mg to 1100 mg, eg, 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as , 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 30 mg to 600 mg (eg, 50 mg to 600 mg, such as every 3 weeks) , 60 mg to 600 mg, such as 100 mg to 600 mg, such as 200 mg to 600 mg, such as 200 mg to 550 mg, such as 250 mg to 500 mg, such as 300 mg to 450 mg, such as 350 mg to 400 mg, such as 375 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg every 3 weeks. In some cases, combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or Dose of said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to be administered in combination therapy with MK-3475 (pembrolizumab, formerly known as lambrolizumab) may be reduced compared to a standard dose of the anti-TIGIT antagonist antibody to be administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 80 mg 내지 약 1950 mg, 예컨대, 약 80 mg 내지 약 1900 mg, 예컨대, 약 80 mg 내지 약 1800 mg, 예컨대, 약 100 mg 내지 약 1700 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1400 mg, 예컨대, 약 400 mg 내지 약 1300 mg, 예컨대, 약 500 mg 내지 약 1200 mg, 예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 700 mg 내지 약 1000 mg, 예컨대, 약 740 mg 내지 약 940 mg, 예컨대, 약 790 mg 내지 약 890 mg, 예컨대, 약 815 mg 내지 약 865 mg, 예컨대, 약 830 mg 내지 약 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 1900 mg, 예컨대, 약 300 mg 내지 약 1700 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 2000 mg, 예컨대, 약 300 mg 내지 약 2000 mg, 예컨대, 약 400 mg 내지 약 2000 mg, 예컨대, 약 500 mg 내지 약 2000 mg, 예컨대, 약 600 mg 내지 약 1900 mg, 예컨대, 약 700 mg 내지 약 1800 mg, 예컨대, 약 800 mg 내지 약 1800 mg, 예컨대, 약 900 mg 내지 약 1800 mg, 예컨대, 약 1000 mg 내지 약 1800 mg, 예컨대, 약 1100 mg 내지 약 1800 mg, 예컨대, 약 1200 mg 내지 약 1800 mg, 예컨대, 약 1300 mg 내지 약 1800 mg, 예컨대, 약 1400 mg 내지 약 1800 mg, 예컨대, 약 1500 mg 내지 약 1800 mg, 예컨대, 약 1580 mg 내지 약 1780 mg, 예컨대, 약 1630 mg 내지 약 1730 mg, 예컨대, 약 1655 mg 내지 약 1705 mg, 예컨대, 약 1670 mg 내지 약 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대, 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 80 mg 내지 2000 mg(예컨대, 80 mg 내지 1950 mg, 예컨대, 80 mg 내지 1900 mg, 예컨대, 80 mg 내지 1800 mg, 예컨대, 100 mg 내지 1700 mg, 예컨대, 200 mg 내지 1600 mg, 예컨대, 300 mg 내지 1400 mg, 예컨대, 400 mg 내지 1300 mg, 예컨대, 500 mg 내지 1200 mg, 예컨대, 600 mg 내지 1100 mg, 예컨대, 700 mg 내지 1000 mg, 예컨대, 740 mg 내지 940 mg, 예컨대, 790 mg 내지 890 mg, 예컨대, 815 mg 내지 865 mg, 예컨대, 830 mg 내지 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 1900 mg, 예컨대, 300 mg 내지 1700 mg, 예컨대, 400 mg 내지 1600 mg, 예컨대, 500 mg 내지 1600 mg, 예컨대, 600 mg 내지 1600 mg, 예컨대, 700 mg 내지 1600 mg, 예컨대, 800 mg 내지 1600 mg, 예컨대, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 2000 mg, 예컨대, 300 mg 내지 2000 mg, 예컨대, 400 mg 내지 2000 mg, 예컨대, 500 mg 내지 2000 mg, 예컨대, 600 mg 내지 1900 mg, 예컨대, 700 mg 내지 1800 mg, 예컨대, 800 mg 내지 1800 mg, 예컨대, 900 mg 내지 1800 mg, 예컨대, 1000 mg 내지 1800 mg, 예컨대, 1100 mg 내지 1800 mg, 예컨대, 1200 mg 내지 1800 mg, 예컨대, 1300 mg 내지 1800 mg, 예컨대, 1400 mg 내지 1800 mg, 예컨대 1500 mg 내지 1800 mg, 예컨대, 1580 mg 내지 1780 mg, 예컨대 1630 mg 내지 1730 mg, 예컨대, 1655 mg 내지 1705 mg, 예컨대, 1670 mg 내지 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 1680 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 1680 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여될 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여될 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 80 mg to about) every two weeks. 1950 mg, such as about 80 mg to about 1900 mg, such as about 80 mg to about 1800 mg, such as about 100 mg to about 1700 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1400 mg, such as about 400 mg to about 1300 mg, such as about 500 mg to about 1200 mg, such as about 600 mg to about 1100 mg, such as about 700 mg to about 1000 mg, such as about 740 mg to about 940 mg, such as about 790 mg to about 890 mg, such as about 815 mg to about 865 mg, such as about 830 mg to about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as, a dose (eg, a fixed dose) of 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 3 weeks. 2000 mg, such as about 200 mg to about 1900 mg, such as about 300 mg to about 1700 mg, such as about 400 mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg , such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 4 weeks. 2000 mg, such as about 200 mg to about 2000 mg, such as about 300 mg to about 2000 mg, such as about 400 mg to about 2000 mg, such as about 500 mg to about 2000 mg, such as about 600 mg to about 1900 mg, such as about 700 mg to about 1800 mg, such as about 800 mg to about 1800 mg, such as about 900 mg to about 1800 mg, such as about 1000 mg to about 1800 mg, such as about 1100 mg to about 1800 mg, such as about 1200 mg to about 1800 mg, such as about 1300 mg to about 1800 mg, such as about 1400 mg to about 1800 mg, such as about 1500 mg to about 1800 mg, such as about 1580 mg to about 1780 mg, such as about 1630 mg to about 1730 mg, such as about 1655 mg to about 1705 mg, such as about 1670 mg to about 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as, 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 80 mg to 1950 mg, such as every two weeks) , 80 mg to 1900 mg, such as 80 mg to 1800 mg, such as 100 mg to 1700 mg, such as 200 mg to 1600 mg, such as 300 mg to 1400 mg, such as 400 mg to 1300 mg, such as 500 mg to 1200 mg, such as 600 mg to 1100 mg, such as 700 mg to 1000 mg, such as 740 mg to 940 mg, such as 790 mg to 890 mg, such as 815 mg to 865 mg, such as 830 mg to a dose (eg, a fixed dose) of 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 3 weeks) , 200 mg to 1900 mg, such as 300 mg to 1700 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 4 weeks) , 200 mg to 2000 mg, such as 300 mg to 2000 mg, such as 400 mg to 2000 mg, such as 500 mg to 2000 mg, such as 600 mg to 1900 mg, such as 700 mg to 1800 mg, such as 800 mg to 1800 mg, such as 900 mg to 1800 mg, such as 1000 mg to 1800 mg, such as 1100 mg to 1800 mg, such as 1200 mg to 1800 mg, such as 1300 mg to 1800 mg, such as 1400 mg to 1800 mg, such as 1500 mg to 1800 mg, such as 1580 mg to 1780 mg, such as 1630 mg to 1730 mg, such as 1655 mg to 1705 mg, such as 1670 mg to 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, anti-PD-) to be administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of an L1 antagonist antibody (eg, atezolizumab) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody to be administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 180 mg 내지 약 250 mg, 예컨대, 약 180 mg 내지 약 220 mg, 예컨대, 약 190 mg 내지 약 210 mg, 예컨대, 200 mg ± 5 mg, 예컨대, 200 ± 2.5 mg, 예컨대, 200 ± 1.0 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주 마다 20 mg 내지 1000 mg(예컨대, 40 mg 내지 900 mg, 예컨대, 60 mg 내지 800 mg, 예컨대, 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대, 100 mg 내지 500 mg, 예컨대, 120 mg 내지 400 mg, 예컨대, 140 mg 내지 300 mg, 예컨대, 160 mg 내지 350 mg, 예컨대, 180 mg 내지 300 mg, 예컨대, 180 mg 내지 250 mg, 예컨대, 180 mg 내지 220 mg, 예컨대, 190 mg 내지 210 mg, 예컨대, 200 mg ± 5 mg, 예컨대, 200 ± 2.5 mg, 예컨대, 200 ± 1.0 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 약 200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 200 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, pamprolizumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about) every 3 weeks. 900 mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 180 mg to about 250 mg, such as about 180 mg to about A dose of 220 mg, such as about 190 mg to about 210 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5 mg, such as 200 ± 1.0 mg, such as 200 ± 0.5 mg, such as 200 mg) For example, fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pamprolizumab)) is 20 mg to 1000 mg (eg, 40 mg to 900 mg, such as every 3 weeks) , 60 mg to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 160 mg to 350 mg, such as 180 mg to 300 mg, such as 180 mg to 250 mg, such as 180 mg to 220 mg, such as 190 mg to 210 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5 mg, eg, 200±1.0 mg, eg, 200±0.5 mg, eg, 200 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, pamprolizumab)) is a dose of about 200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pamprolizumab)) is a dose of 200 mg every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of the antibody (eg, pembrolizumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 200 mg 내지 약 280 mg, 예컨대, 약 220 mg 내지 약 260 mg, 예컨대, 약 230 mg 내지 약 250 mg, 예컨대, 240 mg ± 5 mg, 예컨대, 240 ± 2.5 mg, 예컨대, 240 ± 1.0 mg, 예컨대, 240 ± 0.5 mg, 예컨대, 240 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 약 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 약 100 mg 내지 약 1000 mg(예컨대, 약 200 mg 내지 약 900 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 700 mg, 예컨대, 약 400 mg 내지 약 600 mg, 예컨대 약 400 mg 내지 약 550 mg, 예컨대, 약 420 mg 내지 약 540 mg, 예컨대, 약 440 mg 내지 약 520 mg, 예컨대, 약 460 mg 내지 약 500 mg, 예컨대, 약 470 mg 내지 약 490 mg, 예컨대, 480 mg ± 5 mg, 예컨대, 480 ± 2.5 mg, 예컨대, 480 ± 1.0 mg, 예컨대, 480 ± 0.5 mg, 예컨대, 480 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 20 mg 내지 1000 mg(예컨대 40 mg 내지 900 mg, 예컨대 60 mg 내지 800 mg, 예컨대 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대 100 mg 내지 500 mg, 예컨대 120 mg 내지 400 mg, 예컨대 140 mg 내지 300 mg, 예컨대 160 mg 내지 350 mg, 예컨대 180 mg 내지 300 mg, 예컨대 200 mg 내지 280 mg, 예컨대 220 mg 내지 260 mg, 예컨대 230 mg 내지 250 mg, 예컨대 240 mg ± 5 mg, 예컨대 240 ± 2.5 mg, 예컨대 240 ± 1.0 mg, 예컨대 240 ± 0.5 mg, 예컨대 240 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 100 mg 내지 1000 mg(예컨대, 200 mg 내지 900 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 700 mg, 예컨대, 400 mg 내지 600 mg, 예컨대, 400 mg 내지 550 mg, 예컨대, 420 mg 내지 540 mg, 예컨대, 440 mg 내지 520 mg, 예컨대, 460 mg 내지 500 mg, 예컨대, 470 mg 내지 490 mg, 예컨대, 480 mg ± 5 mg, 예컨대, 480 ± 2.5 mg, 예컨대, 480 ± 1.0 mg, 예컨대, 480 ± 0.5 mg, 예컨대, 480 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 480 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 480 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제 (예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about 900) every two weeks. mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 200 mg to about 280 mg, such as about 220 mg to about 260 mg, such as from about 230 mg to about 250 mg, such as 240 mg ± 5 mg, such as 240 ± 2.5 mg, such as 240 ± 1.0 mg, such as 240 ± 0.5 mg, such as 240 mg). , fixed capacity). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is from about 100 mg to about 1000 mg (eg, from about 200 mg to about 900) every 4 weeks. mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 700 mg, such as about 400 mg to about 600 mg, such as about 400 mg to about 550 mg, such as about 420 mg to about 540 mg , such as from about 440 mg to about 520 mg, such as from about 460 mg to about 500 mg, such as from about 470 mg to about 490 mg, such as 480 mg ± 5 mg, such as 480 ± 2.5 mg, such as 480 ± 1.0 mg, such as 480 ± 0.5 mg, such as 480 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is 20 mg to 1000 mg (eg 40 mg to 900 mg, such as 60 mg) every two weeks. to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 160 mg to 350 mg, such as 180 mg. to 300 mg, such as 200 mg to 280 mg, such as 220 mg to 260 mg, such as 230 mg to 250 mg, such as 240 mg ± 5 mg, such as 240 ± 2.5 mg, such as 240 ± 1.0 mg, such as 240 ± 0.5 mg, eg 240 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is 100 mg to 1000 mg (eg, 200 mg to 900 mg, eg, every 4 weeks) 300 mg to 800 mg, such as 400 mg to 700 mg, such as 400 mg to 600 mg, such as 400 mg to 550 mg, such as 420 mg to 540 mg, such as 440 mg to 520 mg, such as 460 mg to 500 mg, such as 470 mg to 490 mg, such as 480 mg ± 5 mg, such as 480 ± 2.5 mg, such as 480 ± 1.0 mg, such as 480 ± 0.5 mg, such as 480 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab). The dose of the antibody (eg, nivolumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 투여될 약 15 mg/kg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대, 0.5 mg/kg 내지 15 mg/kg, 예컨대, 1 mg/kg 내지 15 mg/kg, 예컨대, 2.5 mg/kg 내지 15 mg/kg, 예컨대, 5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 15 mg/kg, 예컨대, 10 mg/kg 내지 15 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 14 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 1 mg/kg, 예컨대, 15 ± 0.5 mg/kg, 예컨대, 15 ± 0.2 mg/kg, 예컨대, 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 경우들에서, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 투여될 15 mg/kg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 용량은 단일 요법으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 표준 용량에 비해 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 50 mg/kg of the subject's body weight every 3 weeks. kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, For example, about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg ) is the capacity of In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 15 mg/kg of the subject's body weight every 3 weeks. (e.g., about 0.1 mg/kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, such as about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 10 mg/kg to about 15 mg/kg, such as , about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, such as about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, an effective amount of an anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg to be administered every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 50 mg/kg of body weight of the subject every 3 weeks ( For example, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as, 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some embodiments, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 15 mg/kg (eg, from 0.01 mg/kg to 15 mg/kg of body weight of the subject every 3 weeks) , 0.1 mg/kg to 15 mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 15 mg/kg, such as 10 mg/kg to 15 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 14 mg/kg kg to 15 mg/kg, such as 15 ± 1 mg/kg, such as 15 ± 0.5 mg/kg, such as 15 ± 0.2 mg/kg, such as 15 ± 0.1 mg/kg, such as 15 mg/kg) is the capacity of In some cases, the effective amount of an anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of 15 mg/kg to be administered every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). Doses of an antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) as monotherapy Administered PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab) previously known as lambrolizumab))).
상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 1회 이상의 투약 주기(예컨대, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 또는 50회 이상의 투약 주기)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체((예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망, 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 14 내지 28 일 (예를 들면, 14 일, 15일, 16 일, 17 일, 18 일, 19 일, 20 일, 21 일, 22 일, 23 일, 24 일, 25 일, 26 일, 27 일, 또는 28 일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 28일이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, 1일 ± 3 일)에 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 한다. 유사하게, 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여되어야 한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 제1 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여되어야 한다. 일부 예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(예컨대, 고정 용량)(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 각 21일 주기의 제 1일에 200 mg의 용량으로(즉, 3주마다 200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 240 mg의 용량으로(즉, 2주마다 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 480 mg의 용량으로(즉, 4주마다 480 mg의 용량으로) 정맥내 투여되어야 한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 각 투약 주기의 제 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 모두 제1 투약 주기의 제 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 14일 주기의 제 1일에 240 mg의 용량으로(즉, 2주마다 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 니볼루맙))는 각 28일 주기의 제 1일에 480 mg의 용량으로(즉, 4주마다 480 mg의 용량으로) 정맥내 투여되어야 한다.said anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD -1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered in one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles) In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (( Dosing cycles of, e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) lose clinical benefit (e.g., disease progression, drug resistance, death, or unacceptable toxicity is identified.) In some cases, the length of each dosing cycle is about 14 to 28 days (e.g., 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days, 27 days, or 28 days. The length of each dosing cycle is about 21 days. In some cases, the length of each dosing cycle is about 14 days. In some cases, the length of each dosing cycle is about 28 days. In some cases, the TIGIT antagonist antibodies (eg, anti-TIGIT antagonists as disclosed herein) The antibody, such as tyragolumab) should be administered on about day 1 (eg,
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 60 ± 15분(예컨대, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 또는 약 70분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 60 ± 15 minutes (eg, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes , about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) in about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes) , about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes). It should be administered to the subject or population of subjects by intravenous infusion.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 30 ± 10 분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 약 30 ± 10 분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 30 ± 10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes , about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) in about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes) , about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) to the subject or population of subjects by intravenous infusion.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 이전에 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 후에 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제2 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is combined with the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli). Zumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) to the subject or population of subjects prior to administration. In some cases, for example, after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, , MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), the method includes an interim first observation period. The PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab) )), formerly known as lambrolizumab, further comprises a second observation period after administration. In some cases, the method includes a first observation period after administration of said anti-TIGIT antagonist antibody and said PD-1 axis binding An antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) )) after administration of the second observation period.In some cases, the first and second observation period are each about 30 minutes to about 60 minutes in length.The first and second observation period are each In cases that are about 60 minutes in length, the method comprises the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab), respectively, during the first and second observation periods. ) or term vitality of the subject or population of subjects about 30 ± 10 minutes after administration of a PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) may include recording signs (eg, pulse rate, respiration rate, blood pressure and temperature). In cases where the first and second observation periods are each about 30 minutes in length, the method comprises the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD- After administration of an L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) recording vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects at 15±10 minutes.
다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 이후 및 상기 항 TIGIT 길항제 항체의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체 투여 이후 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후 제1 관찰 기간 및 상기 항 TIGIT 길항제 항체의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 중 각각 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다.In other cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab) should be administered to the subject or population of subjects prior to the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab). In some cases, for example, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or After administration of MK-3475 (pembrolizumab, formerly known as lambrolizumab) and before administration of said anti-TIGIT antagonist antibody, the method comprises an interim first observation period. comprises a second observation period after administration of said anti-TIGIT antagonist antibody In some cases, said method comprises said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD -1 first observation period after administration of antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and second after administration of said anti-TIGIT antagonist antibody includes both observation periods.In some cases, the first and second observation periods are each about 30 minutes to about 60 minutes in length, When the first and second observation periods are each about 60 minutes in length In some cases, the method comprises a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) and the vital signs of the subject or population of subjects about 30 ± 10 minutes after administration of the anti-TIGIT antagonist antibody may include recording the follow-up (eg, pulse rate, respiration rate, blood pressure and temperature). In cases where the first and second observation periods are each about 30 minutes in length, the method comprises each of the first and second observation periods with a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and drug after administration of the anti-TIGIT antagonist antibody recording vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) of the subject or population of subjects at 15±10 minutes.
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 상기 대상체 또는 대상체 집단에 동시에 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여 후에, 상기 방법은 관찰 기간을 포함한다. 일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 중 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 관찰 기간이 약 30분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 중 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 상기 항 TIGIT 길항제 항체의 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In other instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) should be administered to the subject or population of subjects simultaneously. In some cases, for example, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX- After administration of 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab), the method comprises an observation period.In some cases, the observation period is about 30 minutes to is about 60 minutes in length.In cases where the observation period is about 60 minutes in length, the method comprises a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) during the observation period) or about 30 ± 10 minutes after administration of an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and said anti-TIGIT antagonist antibody recording the subject's vital signs (e.g., pulse rate, respiration rate, blood pressure and temperature) in the case where the observation period is about 30 minutes in length, the method includes the PD during the observation period -1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly lamb (known as rolizumab)) and the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) about 15±10 minutes after administration of the anti-TIGIT antagonist antibody.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하며, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-L1) for use in a method of treating a subject or population of subjects having cervical cancer) An antagonist antibody (eg, atezolizumab) is provided, wherein the method comprises administering an anti-TIGIT antagonist antibody at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 1200 mg (eg, a fixed dose) every 3 weeks. administering to the subject or population of subjects one or more dosing cycles of atezolizumab, wherein the anti-TIGIT antagonist antibody is further described below: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 200 mg의 용량(예컨대, 고정 용량)의 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하며, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer An antagonist antibody (eg, pembrolizumab) is provided, wherein the method comprises administering an anti-TIGIT antagonist antibody at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 200 mg (eg, a fixed dose) every 3 weeks. administering to the subject or population of subjects one or more dosing cycles of pembrolizumab, wherein the anti-TIGIT antagonist antibody is further described below: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙)을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 240 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하며, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer Provided is an antagonist antibody (eg, nivolumab), wherein the method comprises a dose of 600 mg (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks and a dose of 240 mg (eg, a fixed dose) of nibol every 2 weeks administering to said subject or population of subjects one or more dosing cycles of lumab, wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a sequence as further described below: and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases In , the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙)을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 480 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하며, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer An antagonist antibody (eg, nivolumab) is provided, wherein the method comprises a dose of 600 mg (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks and a dose of 480 mg (eg, a fixed dose) of nibol every 4 weeks (eg, a fixed dose) administering to said subject or population of subjects one or more dosing cycles of lumab, wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a sequence as further described below: and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases In , the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-L1) for use in a method of treating a subject or population of subjects having cervical cancer) Provided is an antagonist antibody (eg, atezolizumab), wherein the method comprises a dose of 600 mg (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 1200 mg (eg, a fixed dose) of ate every 3 weeks (eg, a fixed dose) administering to the subject or population of subjects one or more dosing cycles of zolizumab.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 200 mg의 용량(예컨대, 고정 용량)의 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer An antagonist antibody (eg, MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is provided, wherein the method comprises a dose of 600 mg (eg, a fixed dose) of tiragolumab and 3 every 3 weeks administering to the subject or population of subjects one or more dosing cycles of pembrolizumab at a dose of 200 mg per week (eg, a fixed dose).
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙))을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 240 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer An antagonist antibody (eg, MDX-1106 (nivolumab)) is provided, wherein the method comprises a dose of 600 mg (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 240 mg (eg, a fixed dose) every 2 weeks dose) of at least one dosing cycle of nivolumab to said subject or population of subjects.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙))을 제공하고, 여기서 상기 방법은 3주마다 600 mg의 용량(예컨대, 고정 용량)의 티라골루맙 및 4주마다 480 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-1) for use in a method of treating a subject or population of subjects having cervical cancer An antagonist antibody (eg, MDX-1106 (nivolumab)) is provided, wherein the method comprises a dose of 600 mg (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 480 mg (eg, a fixed dose) every 4 weeks (eg, a fixed dose) dose) of at least one dosing cycle of nivolumab to said subject or population of subjects.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 유효량의 항 TIGIT 길항제 항체 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, , an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament comprises an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist. (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) ))).
다른 양태에서, 본 발명은 PD-L1의 검출 가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서 항 TIGIT 길항제 항체의 사용을 제공하고, 상기 방법은 상기 약제 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하며, 상기 약제는 유효량의 항 TIGIT 길항제 항체 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여를 위해 제형화된다.In another aspect, the present invention relates to a cancer having a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) ) provides the use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having one or more dosing cycles of (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) administering to the subject or population of subjects, wherein the medicament is an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD -1 is formulated for administration of an antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)).
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 투여될 상기 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), wherein said method comprises one or more of said medicament and an anti-TIGIT antagonist antibody. administering a dosing cycle to the subject or population of subjects, wherein the medicament is an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody) (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and the anti-TIGIT antagonist antibody to be administered.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 약 30 mg 내지 약 600 mg(예컨대, 약 50 mg 내지 600 mg, 예컨대, 약 60 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 550 mg, 예컨대, 약 250 mg 내지 약 500 mg, 예컨대, 약 300 mg 내지 약 450 mg, 예컨대, 약 350 mg 내지 약 400 mg, 예컨대, 약 375 mg) (예컨대, 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ±10 mg, 예컨대, 600 ± 6 mg, 예컨대 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다 30 mg 내지 600 mg(예컨대, 50 mg 내지 600 mg, 예컨대, 60 mg 내지 600 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 200 mg 내지 600 mg, 예컨대, 200 mg 내지 550 mg, 예컨대, 250 mg 내지 500 mg, 예컨대, 300 mg 내지 450 mg, 예컨대, 350 mg 내지 400 mg, 예컨대, 375 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주마다 600 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))와의 병용 치료)으로 투여될 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여될 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about 1100) every 3 weeks. mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, For example, a dose (eg, a fixed dose) of 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is about 30 mg to about 600 mg (eg, about 50 mg to 600 mg every 3 weeks). , such as about 60 mg to about 600 mg, such as about 100 mg to about 600 mg, such as about 200 mg to about 600 mg, such as about 200 mg to about 550 mg, such as about 250 mg to about 500 mg , such as about 300 mg to about 450 mg, such as about 350 mg to about 400 mg, such as about 375 mg) (eg, 30 mg to 1200 mg (eg, 30 mg to 1100 mg, such as 60 mg to 1000) mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, For example, 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg , such as 600 ± 0.5 mg, such as 600 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is 3 weeks. 30 mg to 600 mg (eg, 50 mg to 600 mg, such as 60 mg to 600 mg, such as 100 mg to 600 mg, such as 200 mg to 600 mg, such as 200 mg to 550 mg, such as 250 mg to 500 mg, such as 300 mg to 450 mg, such as 350 mg to 400 mg, such as 375 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is a dose of 600 mg every 3 weeks. In some cases, combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or Dose of said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to be administered in combination therapy with MK-3475 (pembrolizumab, formerly known as lambrolizumab) may be reduced compared to a standard dose of the anti-TIGIT antagonist antibody to be administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 80 mg 내지 약 1950 mg, 예컨대, 약 80 mg 내지 약 1900 mg, 예컨대, 약 80 mg 내지 약 1800 mg, 예컨대, 약 100 mg 내지 약 1700 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1400 mg, 예컨대, 약 400 mg 내지 약 1300 mg, 예컨대, 약 500 mg 내지 약 1200 mg, 예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 700 mg 내지 약 1000 mg, 예컨대, 약 740 mg 내지 약 940 mg, 예컨대, 약 790 mg 내지 약 890 mg, 예컨대, 약 815 mg 내지 약 865 mg, 예컨대, 약 830 mg 내지 약 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)(예컨대, 80 mg 내지 2000 mg(예컨대, 80 mg 내지 1950 mg, 예컨대, 80 mg 내지 1900 mg, 예컨대, 80 mg 내지 1800 mg, 예컨대, 100 mg 내지 1700 mg, 예컨대, 200 mg 내지 1600 mg, 예컨대, 300 mg 내지 1400 mg, 예컨대, 400 mg 내지 1300 mg, 예컨대, 500 mg 내지 1200 mg, 예컨대, 600 mg 내지 1100 mg, 예컨대, 700 mg 내지 1000 mg, 예컨대, 740 mg 내지 940 mg, 예컨대, 790 mg 내지 890 mg, 예컨대, 815 mg 내지 865 mg, 예컨대, 830 mg 내지 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg))의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 1900 mg, 예컨대, 약 300 mg 내지 약 1700 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 약 1225 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 1900 mg, 예컨대, 300 mg 내지 1700 mg, 예컨대, 400 mg 내지 1600 mg, 예컨대, 500 mg 내지 1600 mg, 예컨대 600 mg 내지 1600 mg, 예컨대, 700 mg 내지 1600 mg, 예컨대, 800 mg 내지 1600 mg, 예컨대, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대 1050 mg 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg), 예컨대, 약 1190 mg 내지 약 1210 mg (예컨대, 1190 mg 내지 1210 mg), 1200 mg ± 5 mg, 예컨대 1200 ± 2.5 mg, 예컨대 1200 ± 1.0 mg, 예컨대 1200 ± 0.5 mg, 예컨대 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 2000 mg, 예컨대, 약 300 mg 내지 약 2000 mg, 예컨대, 약 400 mg 내지 약 2000 mg, 예컨대, 약 500 mg 내지 약 2000 mg, 예컨대, 약 600 mg 내지 약 1900 mg, 예컨대, 약 700 mg 내지 약 1800 mg, 예컨대, 약 800 mg 내지 약 1800 mg, 예컨대, 약 900 mg 내지 약 1800 mg, 예컨대, 약 1000 mg 내지 약 1800 mg, 예컨대, 약 1100 mg 내지 약 1800 mg, 예컨대, 약 1200 mg 내지 약 1800 mg, 예컨대, 약 1300 mg 내지 약 1800 mg, 예컨대, 약 1400 mg 약 1800 mg, 예컨대, 약 1500 mg 내지 약 1800 mg, 예컨대, 약 1580 mg 내지 약 1780 mg, 예컨대, 약 1630 mg 내지 약 1730 mg, 예컨대, 약 1655 mg 내지 약 1705 mg, 약 1670 mg 내지 약 1690 mg (예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 2000 mg, 예컨대, 300 mg 내지 2000 mg, 예컨대, 400 mg 내지 2000 mg, 예컨대, 500 mg 내지 2000 mg, 예컨대, 600 mg 내지 1900 mg, 예컨대, 700 mg 내지 1800 mg, 예컨대, 800 mg 내지 1800 mg, 예컨대, 900 mg 내지 1800 mg, 예컨대 1000 mg 내지 1800 mg, 예컨대, 1100 mg 내지 1800 mg, 예컨대, 1200 mg 내지 1800 mg, 예컨대, 1300 mg 내지 1800 mg, 예컨대, 1400 mg 내지 1800 mg, 예컨대, 1500 mg 내지 1800 mg, 1580 mg 내지 1780 mg, 예컨대, 1630 mg 내지 1730 mg, 예컨대, 1655 mg 내지 1705 mg, 예컨대, 1670 mg 내지 1690 mg), 예컨대, 1680 mg ± 5 mg, 예컨대 1680 mg ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 1680 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 1680 mg의 용량이다. 일부 예들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여될 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 용량은 단일요법으로 투여될 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 80 mg to about) every two weeks. 1950 mg, such as about 80 mg to about 1900 mg, such as about 80 mg to about 1800 mg, such as about 100 mg to about 1700 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1400 mg, such as about 400 mg to about 1300 mg, such as about 500 mg to about 1200 mg, such as about 600 mg to about 1100 mg, such as about 700 mg to about 1000 mg, such as about 740 mg to about 940 mg, such as about 790 mg to about 890 mg, such as about 815 mg to about 865 mg, such as about 830 mg to about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as, 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg) (such as 80 mg to 2000 mg (such as 80 mg to 1950 mg, such as 80 mg to 1900 mg, such as 80 mg to 1800 mg, For example, 100 mg to 1700 mg, such as 200 mg to 1600 mg, such as 300 mg to 1400 mg, such as 400 mg to 1300 mg, such as 500 mg to 1200 mg, such as 600 mg to 1100 mg, such as, 700 mg to 1000 mg, such as 740 mg to 940 mg, such as 790 mg to 890 mg, such as 815 mg to 865 mg, such as 830 mg to 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as, 840 mg))). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 3 weeks. 2000 mg, such as about 200 mg to about 1900 mg, such as about 300 mg to about 1700 mg, such as about 400 mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 about 1225 mg (eg, 100 mg to 2000 mg, such as 200 mg to 1900 mg, such as 300 mg to 1700 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg), such as about 1190 mg to about 1210 mg (eg 1190 mg to 1210 mg), 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 4 weeks. 2000 mg, such as about 200 mg to about 2000 mg, such as about 300 mg to about 2000 mg, such as about 400 mg to about 2000 mg, such as about 500 mg to about 2000 mg, such as about 600 mg to about 1900 mg, such as about 700 mg to about 1800 mg, such as about 800 mg to about 1800 mg, such as about 900 mg to about 1800 mg, such as about 1000 mg to about 1800 mg, such as about 1100 mg to about 1800 mg, such as about 1200 mg to about 1800 mg, such as about 1300 mg to about 1800 mg, such as about 1400 mg, about 1800 mg, such as about 1500 mg to about 1800 mg, such as about 1580 mg to about 1780 mg, such as about 1630 mg to about 1730 mg, such as about 1655 mg to about 1705 mg, about 1670 mg to about 1690 mg (eg, 100 mg to 2000 mg, such as 200 mg to 2000 mg, such as 300 mg) to 2000 mg, such as 400 mg to 2000 mg, such as 500 mg to 2000 mg, such as 600 mg to 1900 mg, such as 700 mg to 1800 mg, such as 800 mg to 1800 mg, such as 900 mg to 1800 mg, such as 1000 mg to 1800 mg, such as 1100 mg to 1800 mg, such as 1200 mg to 1800 mg, such as 1300 mg to 1800 mg, such as 1400 mg to 1800 mg, such as 1500 mg to 1800 mg, 1580 mg to 1780 mg, such as 1630 mg to 1730 mg, such as 1655 mg to 1705 mg, such as 1670 mg to 1690 mg), such as 1680 mg ± 5 mg, such as 1680 mg ± 2.5 mg, such as 1680 ± 1.0 mg , eg 1680 ± 0.5 mg, eg 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some embodiments, a PD-1 axis binding antagonist (eg, anti-PD-L1) to be administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of an antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is monotherapy may be reduced compared to the standard dose of anti-PD-L1 antagonist antibody to be administered as a
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 180 mg 내지 약 250 mg, 예컨대, 약 180 mg 내지 약 220 mg, 예컨대, 약 190 mg 내지 약 210 mg(예컨대, 40 mg 내지 900 mg, 예컨대, 60 mg 내지 800 mg, 예컨대, 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대, 100 mg 내지 500 mg, 예컨대, 120 mg 내지 400 mg, 예컨대, 140 mg 내지 300 mg, 예컨대, 16 mg 내지 350 mg, 예컨대, 180 mg 내지 300 mg, 예컨대, 180 mg 내지 250 mg, 예컨대, 180 mg 내지 220 mg, 예컨대, 190 mg 내지 210 mg), 예컨대, 200 mg ± .5 mg, 예컨대, 200 ± 2.5 mg, 예컨대 200 ± 1.0 mg, 예컨대 200 ± 0.5 mg, 예컨대 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 약 200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 유효량은 3주마다 200 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨프롤리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pembrolizumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about) every 3 weeks. 900 mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 180 mg to about 250 mg, such as about 180 mg to about 220 mg, such as about 190 mg to about 210 mg (eg, 40 mg to 900 mg, such as 60 mg to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 16 mg to 350 mg, such as 180 mg to 300 mg, such as 180 mg to 250 mg, such as 180 mg to 220 mg , such as 190 mg to 210 mg), such as 200 mg ± 0.5 mg, such as 200 ± 2.5 mg, such as 200 ± 1.0 mg, such as 200 ± 0.5 mg, such as 200 mg) (eg, a fixed dose) to be. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, pamprolizumab)) is a dose of about 200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pamprolizumab)) is a dose of 200 mg every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of the antibody (eg, pembrolizumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 약 20 mg 내지 약 1000 mg(예컨대, 약 40 mg 내지 약 900 mg, 예컨대, 약 60 mg 내지 약 800 mg, 예컨대, 약 80 mg 내지 약 700 mg, 예컨대, 약 80 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 500 mg, 예컨대, 약 120 mg 내지 약 400 mg, 예컨대, 약 140 mg 내지 약 300 mg, 예컨대, 약 160 mg 내지 약 350 mg, 예컨대, 약 180 mg 내지 약 300 mg, 예컨대, 약 200 mg 내지 약 280 mg, 예컨대, 약 220 mg 내지 약 260 mg, 예컨대, 약 230 mg 내지 약 250 mg(예컨대, 40 mg 내지 900 mg, 예컨대, 60 mg 내지 800 mg, 예컨대, 80 mg 내지 700 mg, 예컨대, 80 mg 내지 600 mg, 예컨대, 100 mg 내지 500 mg, 예컨대, 120 mg 내지 400 mg, 예컨대, 140 mg 내지 300 mg, 예컨대, 16 내지 350 mg, 예컨대, 180 mg 내지 300 mg, 예컨대, 200 mg 내지 280 mg, 예컨대, 220 mg 내지 260 mg, 예컨대, 230 mg 내지 250 mg), 예컨대, 240 mg ± 5 mg, 예컨대 , 240 ± 2.5 mg, 예컨대 240 ± 1.0 mg, 예컨대 240 ± 0.5 mg, 예컨대 240 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 약 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 2주마다 240 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 약 100 mg 내지 약 1000 mg(예컨대, 100 mg 내지 1000 mg)(예컨대, 약 200 mg 내지 약 900 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 700 mg, 예컨대, 약 400 mg 내지 약 600 mg, 예컨대, 약 400 mg 내지 약 550 mg, 예컨대, 약 420 mg 내지 약 540 mg, 예컨대, 약 440 mg 내지 약 520 mg, 예컨대, 약 460 mg 내지 약 500 mg, 예컨대, 약 470 mg 내지 약 490 mg(예컨대, 200 mg 내지 900 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 700 mg, 예컨대, 400 mg 내지 600 mg, 예컨대, 400 mg 내지 550 mg, 예컨대, 420 mg 내지 540 mg, 예컨대, 440 mg 내지 520 mg, 예컨대, 460 mg 내지 500 mg, 예컨대, 470 mg 내지 490 mg), 예컨대, 480 mg ± 5 mg, 예컨대 , 480 ± 2.5 mg, 예컨대, 480 ± 1.0 mg, 예컨대, 480 ± 0.5 mg, 예컨대, 480 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 480 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 유효량은 4주마다 480 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제 (예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량에 비해 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is from about 20 mg to about 1000 mg (eg, from about 40 mg to about 900) every two weeks. mg, such as about 60 mg to about 800 mg, such as about 80 mg to about 700 mg, such as about 80 mg to about 600 mg, such as about 100 mg to about 500 mg, such as about 120 mg to about 400 mg, such as about 140 mg to about 300 mg, such as about 160 mg to about 350 mg, such as about 180 mg to about 300 mg, such as about 200 mg to about 280 mg, such as about 220 mg to about 260 mg, such as about 230 mg to about 250 mg (eg, 40 mg to 900 mg, such as 60 mg to 800 mg, such as 80 mg to 700 mg, such as 80 mg to 600 mg, such as 100 mg to 500 mg mg, such as 120 mg to 400 mg, such as 140 mg to 300 mg, such as 16 to 350 mg, such as 180 mg to 300 mg, such as 200 mg to 280 mg, such as 220 mg to 260 mg, such as , 230 mg to 250 mg), such as 240 mg ± 5 mg, such as 240 ± 2.5 mg, such as 240 ± 1.0 mg, such as 240 ± 0.5 mg, such as 240 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is about 100 mg to about 1000 mg (eg, 100 mg to 1000 mg) every 4 weeks. (e.g., about 200 mg to about 900 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 700 mg, such as about 400 mg to about 600 mg, such as about 400 mg to about 550 mg , such as about 420 mg to about 540 mg, such as about 440 mg to about 520 mg, such as about 460 mg to about 500 mg, such as about 470 mg to about 490 mg (eg, 200 mg to 900 mg, such as , 300 mg to 800 mg, such as 400 mg to 700 mg, such as 400 mg to 600 mg, such as 400 mg to 550 mg, such as 420 mg to 540 mg, such as 440 mg to 520 mg, such as 460 mg to 500 mg, such as 470 mg to 490 mg), such as 480 mg ± 5 mg, such as 480 ± 2.5 mg, such as 480 ± 1.0 mg, such as 480 ± 0.5 mg, such as 480 mg). to be. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab). The dose of the antibody (eg, nivolumab)) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 투여될 약 15 mg/kg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여된 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 용량은 단일요법으로 투여된 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 50 mg/kg of the subject's body weight every 3 weeks. kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, For example, about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg ) is the capacity of In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 15 mg/kg of the subject's body weight every 3 weeks. (e.g., about 0.1 mg/kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, such as about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 10 mg/kg to about 15 mg/kg, such as , about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, such as about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg to be administered every 3 weeks. In some cases, a PD-1 axis binding antagonist (eg, anti-PD-) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). A single dose of an L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is may be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as therapy.
본 발명의 임의의 사용에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 1회 이상의 투약 주기(예컨대, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 또는 50회 이상의 투약 주기)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체((예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망, 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일 내지 28일(예컨대, 14일, 15일, 16일, 17일, 18일, 19일, 20일, 21일, 22일, 23일, 24일, 25일, 26일, 27일, 또는 28일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)를 포함하는 약제는 각 투약 주기의 약 1일(예컨대, 1일 ± 3 일)에 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 한다. 유사하게, 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))를 포함하는 약제는 각 21일 주기의 제 1일 차에 약 1200 mg의 고정 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))를 포함하는 약제는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))를 포함하는 약제는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))를 포함하는 약제는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여되어야 한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 모두 포함하는 약제는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 하고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))를 포함하는 약제는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 하고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))를 포함하는 약제는 각 21일 주기의 제 1일에 약 200 mg의 용량으로(즉, 3주마다 약 200 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 하고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))를 포함하는 약제는 각 14일 주기의 제 1일에 약 240 mg의 용량으로(즉, 2주마다 약 240 mg의 용량으로) 정맥내 투여되어야 한다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되어야 하고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-1 길항제 항체(예컨대, 니볼루맙))를 포함하는 약제는 각 28일 주기의 제 1일에 약 480 mg의 용량으로(즉, 4주마다 약 480 mg의 용량으로) 정맥내 투여되어야 한다.
In any use of the present invention, said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, , atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) is administered in one or more doses. Period (e.g. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles.) In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding An antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly called lambrolizumab) known)), continue until clinical benefit is lost (e.g., disease progression, drug resistance, death, or unacceptable toxicity is identified) In some cases, each dosing cycle of about 14 to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days) , 27 days, or 28 days).In some cases, the length of each dosing cycle is about 21 days. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as , tiragolumab) about 1 day (eg, 1 day ± 3) should be administered. For example, a medicament comprising the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) may be administered at a dose of about 600 mg (eg, fixed) on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 약 60 ± 15분(예컨대, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 또는 약 70분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다.In some cases, the medicament comprising the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 60 ± 15 minutes (eg, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes , about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes). In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( pembrolizumab, formerly known as lambrolizumab) in about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes) , about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes. minutes) to the subject or population of subjects by intravenous infusion.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 약 30 ± 10분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 약 30 ± 10 분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여되어야 한다.In some cases, the medicament comprising the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 30 ± 10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes , about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( pembrolizumab, formerly known as lambrolizumab) in about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes) , about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion to the subject or population of subjects.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 포함하는 약제는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제 이전에 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 이후 상기 항 PD-L1 길항제 항체를 포함하는 약제의 투여 이전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 PD-L1 길항제 항체의 투여 이후에 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 포함하는 약제 투여 후 제1 관찰 기간 및 상기 항 PD-L1 길항제 항체를 포함하는 약제 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 동안 상기 항 TIGIT 길항제 항체를 포함하는 약제 및 상기 PD-L1 길항제 항체를 포함하는 약제의 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우, 상기 방법은 상기 제1 및 제2 관찰 기간 동안 상기 항 TIGIT 길항제 항체를 포함하는 약제 및 상기 PD-L1 길항제 항체를 포함하는 약제의 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the medicament comprising the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, anti-PD-L1 antagonist antibody) the subject prior to a medicament comprising, e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) or to the subject population.In some cases, for example, after the administration of the medicament comprising the anti-TIGIT antagonist antibody and prior to the administration of the medicament comprising the anti-PD-L1 antagonist antibody, the method comprises an intermediate agent 1 observation period.In some cases, the method comprises a second observation period after administration of the anti-PD-L1 antagonist antibody.In some cases, the method comprises the anti-TIGIT antagonist antibody includes both the first observation period after administration of the drug and the second observation period after administration of the drug comprising the anti-PD-L1 antagonist antibody, in some cases, the first and second observation period are each from about 30 minutes to about 60 minutes in length.In cases where the first and second observation periods are each about 60 minutes in length, the method comprises a medicament comprising the anti-TIGIT antagonist antibody and the PD during the first and second observation periods. - recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) about 30 ± 10 minutes after administration of the medicament comprising the L1 antagonist antibody. When the 2 observation periods are each about 30 minutes in length, the method comprises administering the medicament comprising the anti-TIGIT antagonist antibody and the medicament comprising the PD-L1 antagonist antibody during the first and second observation periods about 15 after administration. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at ±10 minutes.
다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체 집단에게 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 항 PD-L1 길항제 항체를 포함하는 약제의 투여 후 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 후 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 방법은 상기 항 PD-L1 길항제 항체를 포함하는 약제의 투여 후 제1 관찰 기간 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 및 제2 관찰 기간 동안 각각 상기 항 PD-L1 길항제 항체를 포함하는 약제 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 이후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우, 상기 방법은 상기 제1 및 제2 관찰 기간 동안 각각 상기 항 PD-L1 길항제 항체를 포함하는 약제 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 이후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. In other cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab, formerly known as lambrolizumab)) is administered to the subject or population of subjects prior to the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab). In some cases, for example, after administration of the medicament comprising the anti-PD-L1 antagonist antibody and prior to the administration of the medicament comprising the anti-TIGIT antagonist antibody, the method comprises an intervening first observation period. In some cases, the method comprises a second observation period after administration of the medicament comprising the anti-TIGIT antagonist antibody.In some cases, the method comprises the medicament comprising the anti-PD-L1 antagonist antibody. includes both the first observation period after administration of and the second observation period after administration of the medicament comprising the anti-TIGIT antagonist antibody In some cases, the first and second observation periods are each from about 30 minutes to about 60 minutes In cases where said first and second observation periods are each about 60 minutes in length, the method comprises a medicament comprising said anti-PD-L1 antagonist antibody during said first and second observation periods, respectively, and recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) about 30 ± 10 minutes after administration of the medicament comprising the anti-TIGIT antagonist antibody. When the second observation period is each about 30 minutes in length, the method comprises administering the medicament comprising the anti-PD-L1 antagonist antibody and the medicament comprising the anti-TIGIT antagonist antibody, respectively, during the first and second observation periods, respectively. then recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at about 15±10 minutes.
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 약제는 상기 대상체 또는 대상체 집단에 동시에 투여되어야 한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체를 포함하는 약제 및 상기 항 PD-L1 길항제 항체를 포함하는 약제의 투여 후, 상기 방법은 관찰 기간을 포함한다. 일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 상기 관찰 기간 동안 각각 상기 항 PD-L1 길항제 항체를 포함하는 약제 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 관찰 기간이 각각 약 30분의 길이인 경우, 상기 방법은 상기 관찰 기간 동안 각각 상기 항 PD-L1 길항제 항체를 포함하는 약제 및 상기 항 TIGIT 길항제 항체를 포함하는 약제의 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다.In other instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli medicaments comprising zumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) to the subject or population of subjects simultaneously In some cases, for example, after administration of the medicament comprising the anti-TIGIT antagonist antibody and the medicament comprising the anti-PD-L1 antagonist antibody, the method comprises an observation period. In , the observation period is from about 30 minutes to about 60 minutes in length.In cases where the observation period is about 60 minutes in length, the method comprises a medicament comprising the anti-PD-L1 antagonist antibody, respectively, during the observation period. and recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) about 30±10 minutes after administration of the medicament comprising the anti-TIGIT antagonist antibody. each of about 30 minutes in length, the method comprises administering to the subject about 15±10 minutes after administration of the medicament comprising the anti-PD-L1 antagonist antibody and the medicament comprising the anti-TIGIT antagonist antibody, respectively, during the observation period, respectively. recording vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) of
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and an anti-PD-L1 antagonist antibody (eg, , atezolizumab), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is from about 30 mg to about 1200 mg every 3 weeks. a (eg, 30 mg to 1200 mg) dose (eg, a fixed dose) of an anti TIGIT antagonist antibody, and a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) every 3 weeks A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))).
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and an anti-PD-L1 antagonist antibody (eg, , atezolizumab), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is from about 30 mg to about 1200 mg every 3 weeks. a (eg, 30 mg to 1200 mg) dose (eg, a fixed dose) of an anti TIGIT antagonist antibody, and a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) every two weeks A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))).
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 4주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and an anti-PD-L1 antagonist antibody (eg, , atezolizumab), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is from about 30 mg to about 1200 mg every 3 weeks. A dose (eg, a fixed dose) of an anti TIGIT antagonist antibody, and a dose (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) every 4 weeks of an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) formulated for administration.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), wherein said method comprises one or more of said medicament and an anti-TIGIT antagonist antibody. administering to the subject or population of subjects a dosing cycle, wherein the medicament is administered at a dose (eg, a fixed dose) of from about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) of the PD-1 axis every 3 weeks. A binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly called lambrolizumab) known)) and anti-TIGIT antagonist antibody to be administered at a dose (eg, a fixed dose) of about 30 mg to about 1200 mg (eg, 30 mg to 1200 mg) every 3 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 4주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), wherein said method comprises one or more of said medicament and an anti-TIGIT antagonist antibody. administering to the subject or population of subjects a dosing cycle, wherein the medicament is administered at a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) of the PD-1 axis every 4 weeks. A binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly called lambrolizumab) known)) and anti-TIGIT antagonist antibody to be administered at a dose (eg, a fixed dose) of about 30 mg to about 1200 mg (eg, 30 mg to 1200 mg) every 3 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg) 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), wherein said method comprises one or more of said medicament and an anti-TIGIT antagonist antibody. administering to the subject or population of subjects a dosing cycle, wherein the medicament is administered at a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) of the PD-1 axis every two weeks. A binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly called lambrolizumab) known)) and anti-TIGIT antagonist antibody to be administered at a dose (eg, a fixed dose) of about 30 mg to about 1200 mg (eg, 30 mg to 1200 mg) every 3 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 2000 mg)의 용량(예컨대, 고정 용량)의 항 PD-L1 길항제 항체의 투여를 위해 제형화된다.In another aspect, the present invention relates to a cancer having a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) Provided is the use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for use in a method of treating a subject or population of subjects having cervical cancer), wherein said method comprises said medicament and a PD-1 axis binding antagonist (eg, anti-PD- one or more doses of an L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) administering to the subject or population of subjects a dosing cycle, wherein the medicament is administered at a dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody from about 30 mg to about 1200 mg (eg, 30 mg to 1200 mg) every 3 weeks. and a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to 2000 mg) of the anti-PD-L1 antagonist antibody every 3 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament to said subject or population of subjects. administering, wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody every 3 weeks and a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks and wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 펨브롤리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 200 mg 용량(예컨대, 고정 용량)의 펨브롤리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody and pembrolizumab for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament to said subject or population of subjects. administering, wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody every 3 weeks and a 200 mg dose (eg, a fixed dose) of pembrolizumab every 3 weeks and wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 240 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody and nivolumab for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks and a dose of 240 mg (eg, a fixed dose) of nivolumab every 2 weeks wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 480 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody and nivolumab for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks and a dose of 480 mg (eg, a fixed dose) of nivolumab every 4 weeks wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament and atezolizumab to said subject or population of subjects. administering an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks (eg, a fixed dose) and atezolizumab to be administered at a dose of 1200 mg every 3 weeks (eg, a fixed dose) , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 200 mg의 용량(예컨대, 고정 용량)으로 투여할 펨브롤리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) provides the use of an anti-TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament and pembrolizumab to said subject or population of subjects. administering an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks (eg, a fixed dose) and pembrolizumab to be administered at a dose of 200 mg every 3 weeks (eg, a fixed dose) , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 240 mg의 용량(예컨대, 고정 용량)으로 투여할 니볼루맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 니볼루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 480 mg의 용량(예컨대, 고정 용량)으로 투여할 니볼루맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the present invention relates to a cancer having a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti-TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said agent and nivolumab. for administration of an anti-TIGIT antagonist antibody at a dose of 600 mg (eg, a fixed dose) every 3 weeks and nivolumab to be administered at a dose of 240 mg (eg, a fixed dose) every 2 weeks and wherein said anti-TIGIT antagonist antibody comprises: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In another aspect, the present invention relates to a cancer having a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti-TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said agent and nivolumab. for administration of an anti-TIGIT antagonist antibody at a dose of 600 mg (eg, a fixed dose) every 3 weeks and nivolumab to be administered at a dose of 480 mg (eg, a fixed dose) every 4 weeks and wherein said anti-TIGIT antagonist antibody comprises: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament and atezolizumab to said subject or population of subjects. administering an anti-TIGIT antagonist antibody at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab to be administered at a dose of 840 mg (eg, a fixed dose) every 2 weeks , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of an anti TIGIT antagonist antibody for use in a method of treating a subject or population of subjects, wherein said method administers one or more dosing cycles of said medicament and atezolizumab to said subject or population of subjects. administering an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks (eg, a fixed dose) and atezolizumab to be administered at a dose of 1680 mg every 4 weeks (eg, a fixed dose) , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein the method provides at least one dosing cycle of said medicament and an anti-TIGIT antagonist antibody to said subject or population of subjects. administering, wherein the medicament is atezolizumab at a dose of 1200 mg every 3 weeks (eg, a fixed dose) and an anti-TIGIT antagonist antibody to be administered at a dose of 600 mg every 3 weeks (eg, a fixed dose). , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 2주마다 840 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein the method provides at least one dosing cycle of said medicament and an anti-TIGIT antagonist antibody to said subject or population of subjects. administration of an anti-TIGIT antagonist antibody to be administered at a dose of 840 mg (eg, a fixed dose) of atezolizumab every two weeks and a dose of 600 mg (eg, a fixed dose) every three weeks; , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 펨브롤리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 200 mg 용량(예컨대, 고정 용량)의 펨브롤리주맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer), wherein the method provides the use of pembrolizumab for use in a method of treating a subject or population of subjects, wherein the method administers one or more dosing cycles of the medicament and an anti-TIGIT antagonist antibody to the subject or population of subjects. administering, wherein the medicament is pembrolizumab at a dose of 200 mg every 3 weeks (eg, a fixed dose) and an anti-TIGIT antagonist antibody to be administered at a dose of 600 mg every 3 weeks (eg, a fixed dose). , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 2주마다 240 mg 용량(예컨대, 고정 용량)의 니볼루맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer), wherein the method provides the use of nivolumab for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and an anti-TIGIT antagonist antibody. wherein the medicament is nivolumab at a dose of 240 mg every two weeks (eg, a fixed dose) and an anti-TIGIT antagonist antibody to be administered at a dose of 600 mg every three weeks (eg, a fixed dose). and wherein said anti-TIGIT antagonist antibody comprises: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 4주마다 480 mg 용량(예컨대, 고정 용량)의 니볼루맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer), wherein the method provides the use of nivolumab for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and an anti-TIGIT antagonist antibody. wherein the medicament is nivolumab at a dose of 480 mg every 4 weeks (eg, a fixed dose) and an anti-TIGIT antagonist antibody to be administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks. and wherein said anti-TIGIT antagonist antibody comprises: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 4주마다 1680 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 항 TIGIT 길항제 항체의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein the method provides at least one dosing cycle of said medicament and an anti-TIGIT antagonist antibody to said subject or population of subjects. administering, wherein the medicament is administered at a 1680 mg dose (eg, a fixed dose) of atezolizumab every 4 weeks and an anti-TIGIT antagonist antibody to be administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks (eg, a fixed dose) , wherein said anti TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 1200 mg (eg, a fixed dose) of atezolizumab every 3 weeks do.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 840 mg의 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 840 mg (eg, a fixed dose) of atezolizumab every 2 weeks do.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 840 mg의 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 840 mg (eg, a fixed dose) of atezolizumab every 2 weeks do.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 펨브롤리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 200 mg의 용량(예컨대, 고정 용량)의 펨브롤리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects one or more dosing cycles of said medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a 200 mg dose (eg, a fixed dose) of pembrolizumab every 3 weeks do.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 240 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of tiragolumab and nivolumab for use in a method of treating a subject or population of subjects, wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 240 mg (eg, a fixed dose) of nivolumab every 2 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 니볼루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 4주마다 480 mg의 용량(예컨대, 고정 용량)의 니볼루맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) cervical cancer) provides the use of tiragolumab and nivolumab for use in a method of treating a subject or population of subjects, wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament. wherein the medicament is formulated for administration of a 600 mg dose (eg, a fixed dose) of tiragolumab every 3 weeks and a dose of 480 mg (eg, a fixed dose) of nivolumab every 4 weeks.
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and atezolizumab. for administration of tiragolumab at a dose of 600 mg every 3 weeks (eg, a fixed dose) and atezolizumab to be administered at a dose of 1200 mg every 3 weeks (eg, a fixed dose) is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 840 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and atezolizumab. for administration of tiragolumab at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab to be administered at a dose of 840 mg (eg, a fixed dose) every 2 weeks is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 840 mg의 용량(예컨대, 고정 용량)으로 투여할 아테졸리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and atezolizumab. for administration of tiragolumab at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab to be administered at a dose of 840 mg (eg, a fixed dose) every 2 weeks is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 200 mg의 용량(예컨대, 고정 용량)으로 투여할 펨브롤리주맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and pembrolizumab. for administration of tiragolumab at a dose of 600 mg every 3 weeks (eg, a fixed dose) and pembrolizumab to be administered at a dose of 200 mg every 3 weeks (eg, a fixed dose) is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 2주마다 240 mg의 용량(예컨대, 고정 용량)으로 투여할 니볼루맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and pembrolizumab. wherein the medicament is formulated for administration of tiragolumab at a dose of 600 mg (eg, a fixed dose) every 3 weeks and nivolumab to be administered at a dose of 240 mg (eg, a fixed dose) every 2 weeks. get angry
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 펨브롤리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 4주마다 480 mg의 용량(예컨대, 고정 용량)으로 투여할 니볼루맙의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer) for use in a method of treating a subject or population of subjects, wherein said method administers to said subject or population of subjects at least one dosing cycle of said medicament and pembrolizumab. wherein the medicament is formulated for administration of tiragolumab at a dose of 600 mg every 3 weeks (eg, a fixed dose) and nivolumab to be administered at a dose of 480 mg (eg, a fixed dose) every 4 weeks. get angry
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 티라골루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여할 티라골루맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer), wherein the method provides the use of atezolizumab for use in a method of treating a subject or population of subjects, wherein the method administers to the subject or population of subjects one or more dosing cycles of the medicament and tiragolumab for administration of atezolizumab at a dose of 1200 mg (eg, a fixed dose) every 3 weeks and tiragolumab to be administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 티라골루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 2주마다 840 mg의 용량(예컨대, 고정 용량)으로 투여할 티라골루맙의 투여를 위해 제형화된다. In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer), wherein the method provides the use of atezolizumab for use in a method of treating a subject or population of subjects, wherein the method administers to the subject or population of subjects one or more dosing cycles of the medicament and tiragolumab for administration of atezolizumab at a dose of 1200 mg (eg, a fixed dose) every 3 weeks and tiragolumab to be administered at a dose of 840 mg (eg, a fixed dose) every 2 weeks is formulated
다른 양태에서, 본 발명은 PD-L1의 검출가능한 발현 수준을 갖는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 티라골루맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙 및 4주마다 1680 mg의 용량(예컨대, 고정 용량)으로 투여할 티라골루맙의 투여를 위해 제형화된다.In another aspect, the invention provides a cancer with a detectable expression level of PD-L1 (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive uterine cancer) and cervical cancer), wherein the method provides the use of atezolizumab for use in a method of treating a subject or population of subjects, wherein the method administers to the subject or population of subjects one or more dosing cycles of the medicament and tiragolumab for administration of atezolizumab at a dose of 1200 mg (eg, a fixed dose) every 3 weeks and tiragolumab to be administered at a dose of 1680 mg (eg, a fixed dose) every 4 weeks is formulated
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)), 또는 이의 약제는 하나 이상의 추가 항암 치료제(들)(예컨대, 화학요법제, 세포독성제, 성장 억제제, 방사선치료/방사선 요법, 및/또는 항호르몬제, 예컨대 상기 본원에 인용된 것들)와 병용으로(별로도 또는 함께) 투여할 수 있다.In any of the methods, uses, or compositions for use described herein, said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, anti A PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), or An agent thereof may be administered in combination with one or more additional anti-cancer therapeutic agent(s) (e.g., a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, radiotherapy/radiotherapy, and/or an anti-hormonal agent, such as those recited herein above) ( separately or together).
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)), 또는 이의 약제는 자궁경부암을 가진 상기 대상체 또는 대상체 집단을 치료하기 위한 것이다. 일부 경우들에서, 상기 자궁경부암은 4B기, 전이성, 재발성 또는 지속성 자궁경부암이다. 일부 경우들에서, 상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부암이다. 상기 암은 조기 또는 말기일 수 있다.In any of the methods, uses, or compositions for use described herein, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)); or medicament thereof is for treating said subject or subject population with cervical cancer.In some cases, said cervical cancer is stage 4B, metastatic, recurrent or persistent cervical cancer.In some cases, said cervical cancer is It is metastatic and/or recurrent PD-L1 positive cervical cancer.The cancer may be early or late stage.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 단백질 발현 수준이다. 일부 경우들에서, PD-L1의 검출 가능한 단백질 발현 수준은 면역조직화학적(IHC) 분석법에 의해 결정되었다. 일부 경우들에서, PD-L1의 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체를 사용하여 검출한다. 일부 경우들에서, 상기 종양 샘플은 포르말린 고정, 파라핀 포매(FFPE) 종양 샘플이다.In some cases, in a method, use, or compositions for use described herein, the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1. In some cases, detectable protein expression levels of PD-L1 were determined by immunohistochemical (IHC) assays. In some cases, the protein expression level of PD-L1 is detected using an anti-PD-L1 antibody suitable for staining. In some cases, the tumor sample is a formalin-fixed, paraffin-embedded (FFPE) tumor sample.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, PD-L1의 검출가능한 발현 수준은 PD-L1의 검출가능한 핵산 발현 수준이다. 일부 경우들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. In some cases, in a method, use, or compositions for use described herein, the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1. In some cases, the detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. became
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 자궁경부암은 편평세포 암종, 선편평 암종, 또는 선암종이다. 일부 경우들에서, 상기 자궁경부암은 4B기, 전이성, 재발성 또는 지속성이다. 일부 경우들에서, 상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부암이다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 적어도 한 라인의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 적어도 두 라인의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 이전에 전신 요법을 1회 이상 2회 이하로 받았고, 그리고/또는 이에 허용되는 치료 표준이 존재하지 않는다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 두 라인의 초과의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 선행 요법이 화학요법, 수술, 및/또는 방사선 요법이다. 일부 경우들에서, 상기 선행 요법은 면역 요법이다.In some cases, in any of the methods, uses, or compositions for use described herein, the cervical cancer is squamous cell carcinoma, adenosquamous carcinoma, or adenocarcinoma. In some cases, the cervical cancer is stage 4B, metastatic, recurrent, or persistent. In some cases, the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer. In some cases, the subject or population of subjects has not received prior therapy. In some cases, the subject or population of subjects has not received at least one line of prior therapy. In some cases, the subject or population of subjects has not received at least two lines of prior therapy. In some cases, the subject or population of subjects has previously received at least one or two or fewer systemic therapy, and/or there is no acceptable standard of care. In some cases, the subject or population of subjects has not received more than two lines of prior therapy. In some cases, the prior therapy is chemotherapy, surgery, and/or radiation therapy. In some cases, the prior therapy is immunotherapy.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여는 임상 반응을 유발한다. 일부 경우들에서, 상기 임상 반응은 기준 ORR과 비교하여 대상체 또는 대상체 집단의 객관적 반응률(ORR)의 증가이다. 일부 경우들에서, 상기 기준 ORR은 적어도 약 14.6% 내지 약 26%이다. 일부 경우들에서, 상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 ORR 중앙값이다. 일부 경우들에서, 상기 임상 반응은 기준 PFS와 비교하여 대상체 또는 대상체 집단에서의 PFS의 증가이다. 일부 경우들에서, 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이다. 일부 경우들에서, 상기 임상 반응은 기준 DOR 시간과 비교하여 대상체 또는 대상체 집단에서의 반응 지속 시간(DOR)의 증가이다. 일부 경우들에서, 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이다. 일부 경우들에서, 상기 임상 반응은 OS의 증가이다.In some cases, in any of the methods, uses, or compositions for use described herein, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or Administration of an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) elicits a clinical response. Clinical response is the increase in the objective response rate (ORR) of a subject or subject population compared to the reference ORR.In some cases, the reference ORR is at least about 14.6% to about 26%.In some cases, the reference ORR is PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (Pembb) without anti-TIGIT antagonist antibody) is the median ORR of a population of subjects receiving treatment with rolizumab (formerly known as lambrolizumab)) In some cases, the clinical response is an increase in PFS in a subject or population of subjects as compared to baseline PFS. In some cases, the baseline PFS time is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106) without an anti TIGIT antagonist antibody. (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) is the median PFS time in a population of subjects treated with. In some cases, the clinical response is compared with a baseline DOR time. to increase the duration of response (DOR) in a subject or population of subjects.In some cases, the reference DOR time is the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly is the median DOR time of a population of subjects receiving treatment including))), known as lambrolizumab. In some cases, the clinical response is an increase in OS.
자궁경부암과 관련된 진단 방법 및 사용Diagnostic methods and uses related to cervical cancer
본 발명은 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공하고, 여기서 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. The present invention provides a method for selecting a therapy for a subject or population of subjects having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer). Provided is a method, wherein the therapy is of one or more biomarkers (eg, PD-L1, TIGIT, activated T cells, or cytokines) in a sample (eg, a tumor sample or blood sample) obtained from the subject or population of subjects. Guided by a diagnostic method involving determining the presence and/or expression level/amount.
본원에서는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료로부터 이익을 얻을 수 있는, 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단를 확인하는 방법이 추가적으로 제공되고, 여기서 확인은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Disclosed herein are an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475) (pembrolizumab, formerly known as lambrolizumab)) cancers (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or or recurrent PD-L1 positive cervical cancer), wherein the identification is identified in a sample obtained from the subject or population of subjects (eg, a tumor sample or a blood sample) one or more biomarkers Guided by a diagnostic method involving determining the presence and/or expression level/amount of (eg, PD-L1, TIGIT, activated T cells, or cytokines).
본원에서는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법에 대한 반응성을 평가하는 방법이 추가적으로 제공되고, 여기서 추가적으로 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Disclosed herein is responsiveness to therapy for a subject or population of subjects having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer). Further provided is a method of assessing, wherein further therapy is administered from one or more biomarkers (eg, PD-L1, TIGIT, activated T cells, or cytokines) are present and/or expression levels/amounts are determined.
본원에서는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 최적화하는 방법이 추가적으로 제공되고, 여기서 추가적으로 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Disclosed herein are methods of optimizing therapy for a subject or population of subjects having cancer (eg, cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer). further provided, wherein additionally, the therapy is one or more biomarkers (eg, PD-L1, TIGIT, activated T cells, or cytokines) in a sample (eg, a tumor sample or blood sample) obtained from the subject or population of subjects. is guided by a diagnostic method involving determining the presence and/or expression level/amount of
본원에 기재된 방법에서 사용하기 위한 바이오마커는 종양 면역생물학(예컨대, TEFF), HPV 변경, 림프구 하위집단, T 세포 수용체 레퍼토리, T 세포 활성화와 관련된 사이토카인 및 혈장 유래 사이토카인과 관련된 유전자 또는 유전자 서명 분석(예컨대, CD274)인 WGS 및/또는 NGS를 통해 확인된 조직(예컨대, 종양 조직) 또는 혈액(예컨대, 전혈), 조직(예컨대, 종양 조직) 및/또는 혈액 내 순환 종양 DNA(돌연변이 로드, MSI 및 MMR 결함를 포함하지만 이에 제한되지는 않음)의 생식계열 및 체세포 돌연변이 상의 PD-L1 발현을 포함하지만, 이에 제한되지는 않는다. 일부 경우들에서, 상기 바이오마커는 PD-L1이다. 일부 경우들에서, 상기 샘플은 종양 샘플(예컨대, 포르말린 고정, 파라핀 포매(FFPE) 종양 샘플)이다.Biomarkers for use in the methods described herein include genes or gene signatures associated with tumor immunobiology (eg, TEFF), HPV alterations, lymphocyte subpopulations, T cell receptor repertoire, cytokines associated with T cell activation, and plasma-derived cytokines. Tissue (e.g., tumor tissue) or blood (e.g., whole blood), tissue (e.g., tumor tissue) and/or circulating tumor DNA (mutant load, PD-L1 expression on germline and somatic mutations including but not limited to MSI and MMR defects. In some cases, the biomarker is PD-L1. In some cases, the sample is a tumor sample (eg, a formalin fixed, paraffin embedded (FFPE) tumor sample).
일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 약 2000 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 2주마다 840 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 3주마다 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 4주마다 1680 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다.In some cases, the method comprises the presence of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects and/or or determining the expression level/amount and administering to the subject or population of subjects a dose (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, a fixed dose) of about 30 mg to about 1200 mg (eg, 30 mg to 1200 mg) every 3 weeks. One or more dosing cycles of an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab, and every 3 weeks PD- at a dose (eg, a fixed dose) of about 80 mg to about 2000 mg (eg, 80 mg to about 2000 mg) administering one or more dosing cycles of a uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some cases, the method comprises the presence of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects and/or or determining the expression level/amount and administering to the subject or population of subjects a dose (eg, a fixed dose) of about 600 mg (eg, 600 mg) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein) every 3 weeks. one or more dosing cycles of, e.g., tiragolumab) and an 840 mg dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) every two weeks) administering one or more dosing cycles. In some cases, the method comprises the presence of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects and/or or determining the expression level/amount and administering to the subject or population of subjects a dose (eg, a fixed dose) of about 600 mg (eg, 600 mg) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein) every 3 weeks. 1 or more dosing cycles of, e.g., tiragolumab) and a 1200 mg dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) every 3 weeks) administering one or more dosing cycles. In some cases, the method comprises the presence of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects and/or or determining the expression level/amount and administering to the subject or population of subjects a dose (eg, a fixed dose) of about 600 mg (eg, 600 mg) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein) every 3 weeks. one or more dosing cycles of, e.g., tiragolumab) and a 1680 mg dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) every 4 weeks) administering one or more dosing cycles.
바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양은 단백질, 단백질 단편, DNA, mRNA, cDNA, 및/또는 유전자 복제 수를 포함하지만 이에 제한되지는 않는 당해 분야에서 공지된 임의의 적합한 기준에 따라 정성적으로 및/또는 정량적으로 결정될 수 있다. The presence and/or expression level/amount of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) includes, but is not limited to, protein, protein fragment, DNA, mRNA, cDNA, and/or gene copy number. It may be determined qualitatively and/or quantitatively according to any suitable criteria known in the art without limitation.
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체 또는 대상체 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 단백질 발현 수준이다. 일부 경우들에서, PD-L1 단백질 발현 수준은 면역조직화학적(IHC) 분석에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of a biomarker is a detectable protein expression level of PD-L1 in a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects. In some cases, PD-L1 protein expression levels were determined by immunohistochemical (IHC) analysis. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects has been determined to have a detectable expression level of PD-L1. In some cases, a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects has been determined to have a detectable expression level of PD-L1 in tumor infiltrating immune cells. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체 또는 대상체 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 핵산 발현 수준이다. 일부 경우들에서, PD-L1의 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, 유전자 발현의 연속 분석(SAGE), MassARRAY® 기술, 조직내(in situ) 혼성화(ISH), 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of a biomarker is a detectable nucleic acid expression level of PD-L1 in a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects. In some cases, the nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY ® technology, in-tissue. (in situ) hybridization (ISH), or a combination thereof. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 이용한 요법에 적격인 것으로 상기 대상체 또는 대상체 집단을 선택하고, 예를 들어, 여기서 PD-L1의 검출가능한 발현 수준은 개체의 선택을 위한 바이오마커이다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플(예컨대, FFPE 종양 샘플)이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from a subject or population of subjects/ The amount is an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( selecting said subject or population of subjects as eligible for therapy with pembrolizumab, formerly known as lambrolizumab)), eg, wherein the detectable expression level of PD-L1 is marker.In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample.In some cases, the tissue sample is a tumor sample (eg, a FFPE tumor sample). In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof In some cases, the tumor sample is a FFPE tumor sample.
일 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다. In one aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and an anti-TIGIT antagonist administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. cancer (e.g., cervical cancer such as stage 4B, metastatic, recurrent) by identifying said subject and subject population as those who would benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as , or a method of selecting a therapy for a subject or population of subjects having a persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein the anti-TIGIT antagonist antibody is of SEQ ID NO: 17 or 18 It has a VH domain comprising an amino acid sequence and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. tiragoluumab administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on the detecting, and PD-L1 expression of the detected tumor sample. cancer (e.g., cervical cancer such as stage 4B, metastatic, recurrent) by identifying said subject and subject population as those who would benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as , or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer). In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and an anti-TIGIT antagonist administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. cancer (e.g., cervical cancer such as stage 4B, metastatic, recurrent) by identifying said subject and subject population as those who would benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as , or a method of selecting a therapy for a subject or population of subjects having a persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein the anti-TIGIT antagonist antibody is of SEQ ID NO: 17 or 18 It has a VH domain comprising an amino acid sequence and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. tiragoluumab administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on the detecting, and PD-L1 expression of the detected tumor sample. cancer (e.g., cervical cancer such as stage 4B, metastatic, recurrent) by identifying said subject and subject population as those who would benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as , or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer). In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 및 3주마다 1200의 mg 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg 용량으로 투여된 티라골루맙 및 3주마다 1200 mg 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks (eg, a fixed dose) and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. cancer (e.g., cervical cancer such as stage 4B, metastatic, recurrent) by identifying said subject and subject population as those who would benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as , or a method of selecting a therapy for a subject or population of subjects having a persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein the anti-TIGIT antagonist antibody is of SEQ ID NO: 17 or 18 It has a VH domain comprising an amino acid sequence and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and at least one dosing cycle of tiragolumab administered at a 600 mg dose every 3 weeks and atezolizumab administered at a 1200 mg dose every 3 weeks based on PD-L1 expression in the detected tumor sample. cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD, -L1-positive cervical cancer) provides a method of selecting a therapy for a subject or population of subjects. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. one or more doses of the anti-TIGIT antagonist administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, artezolith (zumab) or an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) that may benefit from therapy ( For example, provided is a method of identifying a subject or population of subjects having cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer, wherein the The TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 domain and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the regimen comprises one or more dosing cycles of anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. , the regimen is administered at a dose of 600 mg every 3 weeks. anti-TIGIT antagonist antibody administered and one or more dosing cycles of atezolizumab administered at a dose of 840 mg every two weeks. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancers that may benefit from therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) (e.g., cervical cancer, such as stage 4B, metastatic, relapsed) Provided is a method for identifying a subject or population of subjects with sexual or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method comprises an identified subject or population of subjects In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (e.g., an immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1) , PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody. (eg, ipilimumab ( YERVOY® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR) or an activating agent such as an OX-40 agonist such as an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above (separately or in combination).
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancers that may benefit from therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) (e.g., cervical cancer, such as stage 4B, metastatic, relapsed) Provided is a method of identifying a subject or population of subjects having sexual or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein said anti-TIGIT antagonist antibody comprises the amino acid sequence of SEQ ID NO: 17 or 18 has a VH domain comprising and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19 In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is 600 every 3 weeks. one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of mg and atezolizumab administered at a dose of 1680 mg every 4 weeks In some cases, the therapy is at a dose of 600 mg every 3 weeks. Anti-TIGIT antagonist antibody administered and 2 weeks one or more dosing cycles of atezolizumab administered at a dose of 840 mg per day. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancers that may benefit from therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) (e.g., cervical cancer, such as stage 4B, metastatic, relapsed) Provided is a method for identifying a subject or population of subjects with sexual or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method comprises an identified subject or population of subjects In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (e.g., an immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1) , PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody. (eg, ipilimumab ( YERVOY® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR) or an activating agent such as an OX-40 agonist such as an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above (separately or in combination).
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancers that may benefit from therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) (e.g., cervical cancer, such as stage 4B, metastatic, relapsed) Provided is a method of identifying a subject or population of subjects having sexual or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein said anti-TIGIT antagonist antibody comprises the amino acid sequence of SEQ ID NO: 17 or 18 has a VH domain comprising and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19 In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is 600 every 3 weeks. one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of mg and atezolizumab administered at a dose of 1680 mg every 4 weeks In some cases, the therapy is at a dose of 600 mg every 3 weeks. Anti-TIGIT antagonist antibody administered and 2 weeks one or more dosing cycles of atezolizumab administered at a dose of 840 mg per day. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancers that may benefit from therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) (e.g., cervical cancer, such as stage 4B, metastatic, relapsed) Provided is a method for identifying a subject or population of subjects with sexual or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method comprises an identified subject or population of subjects In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (e.g., an immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1) , PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody. (eg, ipilimumab ( YERVOY® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR) or an activating agent such as an OX-40 agonist such as an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above (separately or in combination).
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) A method is provided for assessing the reactivity of a subject or population of subjects having cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein said anti-TIGIT antagonist antibody comprises the amino acid sequence of SEQ ID NO: 17 or 18 has a VH domain and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19 In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at 600 mg every 3 weeks. one or more dosing cycles of anti-TIGIT antagonist antibody administered as a dose and atezolizumab administered at a dose of 1680 mg every 4 weeks In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. Anti-TIGIT antagonist antibody and 840 every 2 weeks one or more dosing cycles of atezolizumab administered in a mg dose. In some aspects, the present invention provides a method for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) Provided is a method for assessing the reactivity of a subject or a population of subjects with cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method provides an identified subject or population of Further comprising the step of administering therapy.In some cases, the therapy is one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1, PD) -1, an agent that reduces or inhibits one or more immune co-suppression receptors selected from -1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (such as , ipilimumab ( YERVOY® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR). agents, such as OX-40 agonists, such as OX-40 agonist antibodies), Therapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or together) may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) A method is provided for assessing the reactivity of a subject or population of subjects having cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein said anti-TIGIT antagonist antibody comprises the amino acid sequence of SEQ ID NO: 17 or 18 has a VH domain and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19 In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at 600 mg every 3 weeks. one or more dosing cycles of anti-TIGIT antagonist antibody administered as a dose and atezolizumab administered at a dose of 1680 mg every 4 weeks In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. Anti-TIGIT antagonist antibody and 840 every 2 weeks one or more dosing cycles of atezolizumab administered in a mg dose. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) Provided is a method for assessing the reactivity of a subject or a population of subjects with cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method provides an identified subject or population of Further comprising the step of administering therapy.In some cases, the therapy is one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1, PD) -1, an agent that reduces or inhibits one or more immune co-suppression receptors selected from -1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (such as , ipilimumab (YERVOY ® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR). agents, such as OX-40 agonists, such as OX-40 agonist antibodies), Therapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or together) may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대하여 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) A method is provided for assessing the reactivity of a subject or population of subjects having cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer, wherein said anti-TIGIT antagonist antibody comprises the amino acid sequence of SEQ ID NO: 17 or 18 has a VH domain and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19 In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at 600 mg every 3 weeks. one or more dosing cycles of anti-TIGIT antagonist antibody administered as a dose and atezolizumab administered at a dose of 1680 mg every 4 weeks In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. Anti-TIGIT antagonist antibody and 840 every 2 weeks one or more dosing cycles of atezolizumab administered in a mg dose. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. by identifying the subject and subject population as an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, Cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent) for therapy comprising MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) Provided is a method for assessing the reactivity of a subject or a population of subjects with cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer.In some cases, the method provides an identified subject or population of Further comprising the step of administering therapy.In some cases, the therapy is one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agent (e.g., one or more immune co-suppression receptors (e.g., TIGIT, PD-L1, PD) -1, an agent that reduces or inhibits one or more immune co-suppression receptors selected from -1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (such as , ipilimumab (YERVOY ® )) or one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR). agents, such as OX-40 agonists, such as OX-40 agonist antibodies), Therapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or together) may be administered.
일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab), wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and has a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab administered at a dose of 1680 mg every 4 weeks, in some cases, the therapy is an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks. Antibody and 840 mg every 2 weeks one or more dosing cycles of atezolizumab administered as a dose. In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab). In some cases, the method comprises administering the therapy to an identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppression receptors (eg, TIGIT, PD-L1, PD-1, Agents that decrease or inhibit one or more immune co-suppression receptors selected from CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimu) YERVOY® ) or an agent that increases or activates one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR); e.g., an OX-40 agonist such as an OX-40 agonist antibody), a chemotherapeutic agent, Cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or in combination).
일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab), wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and has a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab administered at a dose of 1680 mg every 4 weeks, in some cases, the therapy is an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks. 840 mg of antibody and every 2 weeks one or more dosing cycles of atezolizumab administered as a dose. In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab). In some cases, the method comprises administering the therapy to an identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppression receptors (eg, TIGIT, PD-L1, PD-1, Agents that decrease or inhibit one or more immune co-suppression receptors selected from CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimu). YERVOY® ) or an agent that increases or activates one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR); e.g., OX-40 agonists such as OX-40 agonist antibodies), chemotherapeutic agents, Cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or in combination).
일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 항 TIGIT 길항제 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 18의 아미노산 서열을 포함한 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 암(예컨대, 자궁경부암, 예컨대 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암)을 가진 대상체 또는 대상체 집단을 대상으로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다. In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab), wherein said anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and has a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the therapy is administered at a dose of 600 mg every 3 weeks. one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab administered at a dose of 1680 mg every 4 weeks, in some cases, the therapy is an anti-TIGIT antagonist administered at a dose of 600 mg every 3 weeks. 840 mg of antibody and every 2 weeks one or more dosing cycles of atezolizumab administered as a dose. In some cases, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining, the protein expression level of PD-L1 in the tumor sample. and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. a subject having cancer (e.g., cervical cancer, such as stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer) by identifying said subject and subject population as or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) in a population of subjects or MK-3475 (pembrolizumab, formerly known as lambrolizumab). In some cases, the method comprises administering the therapy to an identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppression receptors (eg, TIGIT, PD-L1, PD-1, Agents that decrease or inhibit one or more immune co-suppression receptors selected from CTLA-4, LAG3, TIM3, BTLA, and/or VISTA, such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimu) YERVOY® ) or an agent that increases or activates one or more immune co-stimulatory receptors (eg, one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR); e.g., OX-40 agonists such as OX-40 agonist antibodies), chemotherapeutic agents, Cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents such as the agents mentioned herein above) (separately or in combination).
일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; (e.g., OX-40 agonist antibody), chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents, such as the agents mentioned herein above (separately or in combination) may be administered.
일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; (e.g., OX-40 agonist antibody), chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents, such as the agents mentioned herein above (separately or in combination) may be administered.
일부 경우들에서, 본원에 기재된 임의의 진단 방법 또는 사용에서, 상기 자궁경부암은 4B기, 전이성, 재발성 또는 지속성 자궁경부암이다. 상기 암은 조기 또는 말기일 수 있다.In some cases, in any of the diagnostic methods or uses described herein, the cervical cancer is stage 4B, metastatic, recurrent, or persistent cervical cancer. The cancer may be early or late.
A.A. 유방암과 관련된 치료 방법 및 사용Treatment methods and uses associated with breast cancer
유방암 breast cancer
유방암은 여성에게 가장 빈번하게 진단되는 암으로서 2018년에 전 세계적으로 208만 건의 새로운 사례가 보고된 것으로 추산된다. 유방암은 전체 암 사망의 약 15%(약 626,700건)를 차지하며, 여성에게 암 관련 사망의 가장 흔한 원인이며, 전이 진단 후 5년 생존율은 약 15%이다. 대부분의 환자는 국소 유방암으로 진단되지만, 새로운 전이성 질환이 있는 환자의 약 6% 및 국소 유방암 환자의 10%~40%가 전신적으로 재발한다. 유방암의 초기 단계(1-3, 조기 유방암)에서는 대부분 무증상이며 일반적으로 수술이 가능하고 치유 목적으로 치료될 수 있다.Breast cancer is the most frequently diagnosed cancer in women, with an estimated 2.08 million new cases reported worldwide in 2018. Breast cancer accounts for about 15% of all cancer deaths (about 626,700 cases), and is the most common cause of cancer-related deaths in women, with a 5-year survival rate of about 15% after metastasis diagnosis. Although most patients are diagnosed with focal breast cancer, about 6% of patients with new metastatic disease and 10% to 40% of patients with focal breast cancer have systemic recurrence. In the early stages of breast cancer (1-3, early breast cancer), most are asymptomatic, usually surgical and curative.
유방암은 치료상의 이유로 에스트로겐 수용체(ER), 프로게스테론 수용체(PR) 및 인간 표피 성장 인자 수용체 2(HER2)의 상태에 따라 추가로 분류되는 약 15가지 상이한 유형의 암종을 수반하는 이질적인 질병이다. 상기 하위 군은 치료법 선택, 치료 결과, 재발률, 및 사망 위험도에 중요한 의미를 갖는다. 삼중 음성 유방암(TNBC)은 ER, PR 및 HER2의 발현 부족을 특징으로 한다. 전반적으로, 모든 유방암의 약 15%~20%가 TNBC로 분류된다. 대규모의 포괄적인 유전체 분석은 TNBC의 이질적 특성과 이의 다양한 유전자 발현 양상 및 기본적인 유전체 변화를 특성화했지만, 이러한 통찰력은 현재 실험실 단계 및 임상 조사 중인 임상적으로 효과적인 표적 요법의 식별을 위한 명확한 지침을 아직 제공하지 못하고 있다.Breast cancer is a heterogeneous disease involving about 15 different types of carcinoma further classified according to the status of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) for therapeutic reasons. This subgroup has important implications for treatment choice, treatment outcome, recurrence rate, and risk of death. Triple negative breast cancer (TNBC) is characterized by lack of expression of ER, PR and HER2. Overall, about 15% to 20% of all breast cancers are classified as TNBC. Although large-scale comprehensive genomic analyzes have characterized the heterogeneous nature of TNBC and its diverse gene expression patterns and underlying genomic changes, these insights still provide clear guidance for the identification of clinically effective targeted therapies that are currently under laboratory stage and clinical investigation. can't do it
TNBC는 높은 증식률과 같은 공격적인 특징을 가질 가능성이 더 크다. 전이성 TNBC를 가진 환자는 일반적으로 빠른 진행 및 약 16개월의 OS 비율의 중앙값이 특히 좋지 않은 임상 결과를 나타낸다. 최근의 치료 개선에도 불구하고, TNBC 환자의 예후는 최적과는 거리가 멀고 실제로 전이 진단 후 5년 생존율은 약 15%이다.TNBCs are more likely to have aggressive features such as high proliferation rates. Patients with metastatic TNBC generally show particularly poor clinical outcomes with rapid progression and a median OS rate of about 16 months. Despite recent treatment improvements, the prognosis for TNBC patients is far from optimal, and in fact, the 5-year survival rate after metastatic diagnosis is about 15%.
따라서, 조기 TNBC(eTNBC)를 포함하여 TNBC의 개선된 의학적 개입에 대한 충족되지 않은 요구가 높다.Therefore, there is a high unmet need for improved medical interventions in TNBC, including early TNBC (eTNBC).
유방암 치료를 위한 방법 및 사용Methods and uses for the treatment of breast cancer
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 및 화학요법(예컨대, 탁산(예컨대, 냅-파클리탁셀 또는 파클리탁셀))를 투여받은 대상체 또는 대상체 집단은 유방암(예컨대, HER2+ 유방암 및 TNBC)에 대해 치료를 받고 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 티라골루맙이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체이다. 일부 경우들에서, 상기 항 PD-L1 길항제 항체는 아테졸리주맙이다. 일부 경우들에서, 상기 화학요법은 탁산이다. 일부 경우들에서, 상기 탁산은 냅-파클리탁셀 또는 파클리탁셀이다. 일부 경우들에서, 상기 탁산은 냅-파클리탁셀이다. 일부 경우들에서, 상기 유방암은 TNBC이다. 일부 경우들에서, 상기 TNBC는 PD-L1 양성 TNBC이다. 일부 경우들에서, 상기 TNBC는 절제불가능한 국소 진행성 또는 전이성이다. 일부 경우들에서, 상기 PD-L1 양성 TNBC는 절제불가능한 국소 진행성 또는 전이성이다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 유방암에 대한 선행 전신 요법을 받지 않았다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 전이성 유방암에 대한 선행 전신 요법을 받지 않았다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) , and a subject or population of subjects who have received a taxane (eg, a taxane (eg, nap-paclitaxel or paclitaxel)) are being treated for breast cancer (eg, HER2+ breast cancer and TNBC). In some cases, the anti-TIGIT antagonist antibody is tyragolumab. In some cases, the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody. In some cases, the anti-PD-L1 antagonist antibody is atezolizumab. In some cases, the chemotherapy is a taxane. In some cases, the taxane is nap-paclitaxel or paclitaxel. In some cases, the taxane is nap-paclitaxel. In some cases, the breast cancer is TNBC. In some cases, the TNBC is a PD-L1 positive TNBC. In some cases, the TNBC is unresectable locally advanced or metastatic. In some cases, the PD-L1 positive TNBC is unresectable locally advanced or metastatic. In some embodiments, the subject or population of subjects has not received prior systemic therapy for breast cancer. In some embodiments, the subject or population of subjects has not received prior systemic therapy for metastatic breast cancer.
eTNBC 치료를 위한 방법 및 사용Methods and uses for the treatment of eTNBC
본원에서는 대상체 또는 대상체 집단에서 조기 TNBC(eTNBC)를 치료하는 방법 및 사용으로서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에는 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여함으로써 상기 대상체 또는 대상체 집단을 치료하는 단계를 포함하는 방법 및 사용이 제공된다Disclosed herein are methods and uses for treating early TNBC (eTNBC) in a subject or population of subjects, comprising an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and an effective amount of PD-1 An axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly lambrolizumab) Methods and uses are provided comprising treating said subject or subject population by administering to said subject or subject population a dosing regimen comprising one or more dosing cycles
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀), 예컨대, 냅-파클리탁셀) 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신))를 포함하거나 포함하지 않고 이를 필요로 하는 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 상기 방법은 하나 이상의 수술(예컨대, 유방절제술 및/또는 액와 림프절 수술)을 추가로 포함한다. 일부 경우들에서, 상기 수술은 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 하나 이상의 화학요법제, 및/또는 G-CSF 또는 GM-CSF를 포함하는 투약 요법을 투여한 후에 실시한다. 일부 경우들에서, 상기 수술은 유방절제술 및/또는 액와 림프절 수술이다. 일부 경우들에서, 상기 수술은 상기 투약 요법의 마지막 용량 후 2주 내지 6주(예컨대, 2주, 3주, 4주, 5주, 및 6주) 사이에 실시한다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab). methods and uses involving administration to a subject or population of subjects in need thereof. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) is one or more chemotherapeutic agents (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (eg, alkylating agents (eg, cyclophosphamide), taxanes (eg, paclitaxel)) ), eg, nap-paclitaxel) and/or a topoisomerase II inhibitor (eg, doxorubicin))). In some cases, the method further comprises one or more surgeries (eg, mastectomy and/or axillary lymph node surgery). In some cases, the surgery is performed after administering a dosing regimen comprising the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the one or more chemotherapeutic agents, and/or G-CSF or GM-CSF. . In some cases, the surgery is a mastectomy and/or axillary lymph node surgery. In some cases, the surgery is performed between 2 and 6 weeks (eg, 2 weeks, 3 weeks, 4 weeks, 5 weeks, and 6 weeks) after the last dose of the dosing regimen.
일부 경우들에서, 대상체 또는 대상체 집단에서 eTNBC를 치료하기 위한 임의의 방법 및 사용은 pCR을 발생시킬 수 있다. 일부 경우들에서, 대상체 또는 대상체 집단에서 eTNBC를 치료하기 위한 임의의 방법 및 사용은 OS 또는 무사건 생존(EFS)의 증가를 발생시킬 수 있다.In some cases, any method and use for treating eTNBC in a subject or population of subjects may result in pCR. In some cases, any method and use for treating eTNBC in a subject or population of subjects may result in an increase in OS or event-free survival (EFS).
투약 요법 및 투여 Dosage regimen and administration
일 양태에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475)(펨브롤리주맙(이전에 람브롤리주맙으로 공지됨)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 eTNBC를 가진 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)를 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀) 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 및/또는 G-CSF 또는 GM -CSF를 포함하거나 포함하지 않고 eTNBC를 가진 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다. 일부 양태들에서, 상기 토포이소머라제 II 억제제는 독소루비신이다. 일부 양태들에서, 독소루비신은 약 60 mg/m2의 용량으로 투여된다.In one aspect, the treatment methods and uses of the invention described herein comprise an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX) -1106 (nivolumab) or MK-3475) (pembrolizumab (formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody (eg, tyragolumab) in a subject or population of subjects with eTNBC In some cases, the treatment methods and uses of the invention described herein comprise an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti A PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab) are combined with one or more chemical agents. Therapeutic agents (eg, platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (eg, alkylating agents (eg, cyclophosphamide), taxanes (eg, paclitaxel, such as nap-paclitaxel)) ) and/or a topoisomerase II inhibitor (eg, doxorubicin)) and/or to a subject or population of subjects having eTNBC with or without G-CSF or GM-CSF. In , the topoisomerase II inhibitor is doxorubicin In some embodiments, doxorubicin is administered at a dose of about 60 mg/m 2 .
본원에 기재된 약학적 조성물은 섹션 III(K)에 기재된 바와 같이 투여용으로 제형화될 수 있다.The pharmaceutical compositions described herein may be formulated for administration as described in Section III(K).
화학요법제의 투약dosing of chemotherapeutic agents
다양한 화학요법제의 치료학적 유효량은 당업계에 공지되어 있고 본 발명에서 고려된다. 특정 경우들에서, 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대, 냅-파클리탁셀) 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신))는 본원의 섹션 III(K)에 언급된 용량에 따라 투여된다.Therapeutically effective amounts of various chemotherapeutic agents are known in the art and are contemplated by the present invention. In certain instances, one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide)); The taxane (eg, paclitaxel, eg, nap-paclitaxel) and/or topoisomerase II inhibitor (eg, doxorubicin)) is administered according to the doses mentioned in Section III(K) herein.
암 특성화 및 선택Cancer characterization and selection
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 암은 유방암일 수 있다. 일부 경우들에서, 상기 유방암은 TNBC이다. 일부 경우들에서, 상기 TNBC는 eTNBC이다. 일부 경우들에서, 상기 eTNBC는 T2-4d TNBC로 제시된다. 일부 경우들에서, 상기 eTNBC는 cT2-cT4, cN0-cN3, 및 cM0 TNBC로 제시된다. 일부 경우들에서, 상기 eTNBC는 PD-L1 양성이다. 일부 경우들에서, 상기 eTNBC는 PD-L1 음성이다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 eTNBC에 대해 이전에 치료를 받은 적이 없다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 유방암(예컨대, TNBC, 예컨대, eTNBC)에 대한 선행 전신 치료를 받지 않았다.In any of the methods, uses, or compositions for use described herein, the cancer can be breast cancer. In some cases, the breast cancer is TNBC. In some cases, the TNBC is an eTNBC. In some cases, the eTNBC is presented as a T2-4d TNBC. In some cases, the eTNBC is presented as cT2-cT4, cN0-cN3, and cM0 TNBC. In some cases, the eTNBC is PD-L1 positive. In some cases, the eTNBC is PD-L1 negative. In some cases, the subject or population of subjects has not been previously treated for eTNBC. In some cases, the subject or population of subjects has not received prior systemic treatment for breast cancer (eg, TNBC, eg, eTNBC).
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체 또는 대상체 집단은 PD-L1 선택된 종양을 갖는다(예컨대, PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 SP142 항체를 이용한 IHC에 의해 결정된 바와 같이 상기 종양 샘플에서 1% 이상이다). 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 발현 IC에 의해 차지하는 종양 면적의 비율이 면역조직화학적(IHC) 분석에 의해 1% 이상인 것으로 결정된 종양이다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142, SP263, 22C3, 또는 28-8을 사용한다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, 상기 IC는 1% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, PD-L1 발현 수준은 항 PD-L1 항체 22C3을 사용하여 검출한다. 일부 경우들에서, 상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 복합 양성 점수(CPS)가 1 이상이다. In some cases, in any of the methods, uses, or compositions for use described herein, the subject or population of subjects has a PD-L1-selected tumor (eg, occupied by PD-L1-expressing tumor infiltrating immune cells (IC)). proportion of tumor area is greater than or equal to 1% in said tumor sample as determined by IHC with SP142 antibody). In some cases, the PD-L1 selected tumor is a tumor in which the proportion of tumor area occupied by PD-L1 expressing IC is determined by immunohistochemical (IHC) analysis to be greater than or equal to 1%. In some cases, the IHC assay uses anti-PD-L1 antibodies SP142, SP263, 22C3, or 28-8. In some cases, the IHC assay uses anti-PD-L1 antibody SP142. In some cases, the IC was determined to be greater than or equal to 1% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, PD-L1 expression levels are detected using anti-PD-L1 antibody 22C3. In some cases, the detectable expression level of PD-L1 has a composite positive score (CPS) of 1 or greater in a sample from the subject.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 개체로부터 수득한 종양 샘플은 PD-L1의 검출가능한 핵산 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다.In some cases, in a method, use, or compositions for use described herein, a tumor sample obtained from an individual has a detectable nucleic acid expression level of PD-L1. In some cases, the detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. became In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample. In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플은 PD-L1 양성인 것으로 결정되었다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플은 PD-L1 음성인 것으로 결정되었다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 대부분 샘플은 PD-L1 음성인 것으로 결정되었다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 모든 샘플은 PD-L1 음성인 것으로 결정되었다. In some cases, a tumor sample from the subject or population of subjects has been determined to be PD-L1 positive. In some cases, the tumor sample from the subject or population of subjects has been determined to be PD-L1 negative. In some cases, the majority of samples from the subject or population of subjects have been determined to be PD-L1 negative. In some cases, all samples from the subject or population of subjects were determined to be PD-L1 negative.
치료에 대한 반응response to treatment
본원에 기재된 임의의 방법에 대한 일부 구현예들에서, 요법에 대한 대상체 또는 대상체 집단의 반응은 하나 이상의 측정에 의해 특징지어질 수 있다. 일부 구현예들에서, 상기 치료는 CR 또는 PR을 발생시킨다. In some embodiments of any of the methods described herein, the response of a subject or population of subjects to a therapy can be characterized by one or more measures. In some embodiments, the treatment results in CR or PR.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 무사건 생존의 증가를 발생시킨다. 예를 들어, 화학요법제가 투여되지 않는 구현예들에서(예컨대, PD-1 축 결합 길항제(예컨대, 아테졸리주맙)와 병용한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)만이 투여됨), 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 무사건 생존의 증가를 발생시킨다. 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀(예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 및/또는 G-CSF 또는 GM-CSF와 병용하여 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)가 투여된 구현예들에서, 상기 치료는 (i) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제 및 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF를 이용한 치료와 비교하거나; (ii) PD-1 축 결합 길항제가 없이 항 TIGIT 길항제 항체 및 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF를 이용한 치료와 비교하거나; 및/또는 (iii) 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF 없이 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 무사건 생존의 증가를 발생시킨다.In some cases, the treatment is compared to treatment with a PD-1 axis binding antagonist, eg, in the absence of an anti TIGIT antagonist antibody, or compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist, such as in the subject or population of subjects. increased event-free survival. For example, in embodiments where no chemotherapeutic agent is administered (eg, only an anti TIGIT antagonist antibody (eg, tyragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), the Treatment may include, for example, an increase in event-free survival of a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. generate one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide), a taxane (eg, paclitaxel)) (eg, nap-paclitaxel), and/or topoisomerase II inhibitors (eg, doxorubicin) and/or anti-TIGIT antagonist antibodies (eg, tyragolumab) and PD- in combination with G-CSF or GM-CSF In embodiments in which a uniaxial binding antagonist (eg, atezolizumab) is administered, the treatment comprises (i) a PD-1 axis binding antagonist and one or more chemotherapeutic agents and/or G-CSF or GM in the absence of an anti-TIGIT antagonist antibody. - compared to treatment with CSF; (ii) compared to treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents and/or G-CSF or GM-CSF in the absence of a PD-1 axis binding antagonist; and/or (iii) results in an increase in event-free survival in a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody without one or more chemotherapeutic agents and/or G-CSF or GM-CSF.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 OS를 연장시킨다. 예를 들어, 화학요법제가 투여되지 않는 구현예들에서(예컨대, PD-1 축 결합 길항제(예컨대, 아테졸리주맙)와 병용한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)만이 투여됨), 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 OS의 증가를 발생시킨다. 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀(예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 및/또는 G-CSF 또는 GM-CSF와 병용하여 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)가 투여된 구현예들에서, 상기 치료는 (i) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제 및 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF를 이용한 치료와 비교하거나; (ii) PD-1 축 결합 길항제가 없이 항 TIGIT 길항제 항체 및 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF를 이용한 치료와 비교하거나; 및/또는 (iii) 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF 없이 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 OS의 증가를 발생시킨다.In some cases, the treatment of the subject or population of subjects, eg, compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. Extend the OS. For example, in embodiments where no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tyragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), the Treatment results in an increase in OS of a subject or population of subjects, e.g., as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist . one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide), a taxane (eg, paclitaxel)) (eg, nap-paclitaxel), and/or topoisomerase II inhibitors (eg, doxorubicin) and/or anti-TIGIT antagonist antibodies (eg, tyragolumab) in combination with G-CSF or GM-CSF and PD- In embodiments in which a uniaxial binding antagonist (eg, atezolizumab) is administered, the treatment comprises (i) a PD-1 axis binding antagonist and one or more chemotherapeutic agents and/or G-CSF or GM in the absence of an anti-TIGIT antagonist antibody. - compared to treatment with CSF; (ii) compared to treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents and/or G-CSF or GM-CSF in the absence of a PD-1 axis binding antagonist; and/or (iii) results in an increase in OS in a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody without one or more chemotherapeutic agents and/or G-CSF or GM-CSF.
상기 대상체 또는 대상체 집단의 의 무사건 생존은 Eisenhauer et al., Eur. J. Cancer. 2009, 45:228-47에 기재된 바와 같이 RECIST v1.1 기준에 따른 측정한다. 일부 구현예들에서, EFS는 RECIST v1.1 기준에 의해 결정된 바와 같이 치료 시작부터 질병 진행의 최초 발생까지의 기간으로서 측정된다 일부 구현예들에서, EFS는 치료 시작부터 사망까지의 시간으로서 측정된다. The obligatory event-free survival of the subject or population of subjects is described in Eisenhauer et al., Eur. J. Cancer . 2009, 45:228-47 according to RECIST v1.1 criteria as described. In some embodiments, EFS is measured as the period from initiation of treatment to the first occurrence of disease progression as determined by RECIST v1.1 criteria. In some embodiments, EFS is measured as the time from initiation of treatment to death. .
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체 또는 대상체 집단의 EFS를 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월,3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 EFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 EFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein reduces the EFS of the subject or population of subjects by at least about 2.4 months (eg, by 2.4 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months). , by 5.0-48 months, by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the EFS of the subject or population of subjects by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 by -48 months, by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the EFS of the subject or population of subjects by at least about 2 months (eg, by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, 8 by -48 months, by 9-36 months, by 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months , 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 5.1개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 20개월(예컨대, 약 20개월 내지 약 36개월(예컨대, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월)의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 치료는 약 25.0개월의 대상체 집단의 OS 중앙값을 발생시킨다.In some embodiments, OS is measured as the period from initiation of treatment to death. In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 2 months (eg, by 2-120 months, by 3-110 months, by 4-100 months, by 5-80 months, by 6- by 60 months, by 7-48 months, by 8-36 months, by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months , 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 3.3 months (eg, by 3.3-120 months, by 4-100 months, by 5-80 months, by 6-60 months, by 7- by 48 months, by 8-36 months, or by 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 5.1 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months , 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 5.3 months (eg, by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 by -24 months, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months , 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment lasts for at least about 20 months (eg, from about 20 months to about 36 months (eg, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) of the subject population.In some embodiments, the treatment is about 25.0 months yields the median OS of the subject population of
일부 구현예들에서, 상기 치료는 적어도 약 53%(예컨대, 약 53% 내지 약 100%(예컨대, 약 53%, 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 75%, 80%, 85%, 90%, 95%, 또는 100%))의 대상체 집단의 ORR을 발생시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 53%(예컨대, 약 65% 내지 약 100%(예컨대, 65%, 65.5%, 66%, 66.5%, 67%, 67.5%, 68%, 68.5%, 69%, 69.5%, 70%, 71%, 72%, 73%, 74%, 75%, 76%, 77%, 78%, 79%, 80%, 85%, 90%, 95%, 또는 100%))의 대상체 집단의 ORR을 발생시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 53% 내지 적어도 약 67.5%(예컨대, 적어도 약 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 또는 67.5%)의 대상체 집단의 ORR을 발생시킨다. In some embodiments, the treatment is at least about 53% (eg, about 53% to about 100% (eg, about 53%, 54%, 55%, 56%, 57%, 58%, 59%, 60%) , 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 75%, 80%, 85%, 90%, 95%, or 100%) ) of the subject population. In some embodiments, the treatment is at least about 53% (eg, about 65% to about 100% (eg, 65%, 65.5%, 66%, 66.5%, 67%, 67.5%, 68%, 68.5%, 69%, 69.5%, 70%, 71%, 72%, 73%, 74%, 75%, 76%, 77%, 78%, 79%, 80%, 85%, 90%, 95%, or 100 %)) of the subject population. In some embodiments, the treatment is at least about 53% to at least about 67.5% (e.g., at least about 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, or 67.5%) of the subject population.
A.A. 두경부암과 관련된 치료 방법 및 진단 및 사용Treatment methods and diagnosis and use associated with head and neck cancer
두경부암head and neck cancer
두경부암은 2018년에 전 세계적으로 890,000 명의 새로운 사례 및 450,000명의 사망을 차지하는 심각한 이환률 및 사망률의 원인이다. 두경부암은 상부 호흡소화관의 점막 표면에서 시작하여 구강, 구강인두, 후두, 하인두 및 비인두에 영향을 미치는 암으로 구성된 이질적인 군이다. 지배적인 조직학적 유형은 편평세포 암종(SCC)이며 신체의 두경부 부위의 모든 악성 질환의 90% 이상을 차지한다.Head and neck cancer is a leading cause of serious morbidity and mortality, accounting for 890,000 new cases and 450,000 deaths worldwide in 2018. Head and neck cancer is a heterogeneous group consisting of cancers that originate on the mucosal surface of the upper aerodigestive tract and affect the oral cavity, oropharynx, larynx, hypopharynx, and nasopharynx. The dominant histological type is squamous cell carcinoma (SCC), accounting for more than 90% of all malignant diseases of the head and neck region of the body.
초기 단계 또는 국소 진행성 두경부 편평세포 암종(SCCHN)의 진단 및 치료의 발전에도 불구하고, 상기 환자의 65% 이상이 재발성 또는 전이성 질환으로 발전하게 된다. 또한, SCCHN 환자의 약 10%가 초기 진단 시 전이성 SCCHN을 가진 것으로 나타난다. 국소 재발성 질병을 가진 환자의 경우, 구제 수술은 절제가능한 국소 재발이 있는 일부 환자에 대해서만 치료가 가능하며, 방사선 재조사는 종종 선행 방사선 치료 이력 및 관련 독성 및 이환율에 의해 제한된다. 결과적으로, 재발성 또는 전이성 SCCHN 환자의 경우, 전신 요법은 표준(SOC) 요법이며 완화의 핵심이다. 상기 환자의 경우, 환자 및 질병 관련 요인에 따라 대부분의 임상 시험에서 평균 생존 기간이 6~15개월로 예후가 좋지 않다.Despite advances in the diagnosis and treatment of early stage or locally advanced head and neck squamous cell carcinoma (SCCHN), more than 65% of these patients will develop recurrent or metastatic disease. Additionally, approximately 10% of SCCHN patients appear to have metastatic SCCHN at initial diagnosis. For patients with locally recurrent disease, salvage surgery is only curative for some patients with resectable local recurrence, and re-irradiation is often limited by prior radiation therapy history and associated toxicity and morbidity. Consequently, for patients with relapsed or metastatic SCCHN, systemic therapy is the standard of care (SOC) therapy and is key to remission. In the case of the above patients, the prognosis is poor with an average survival period of 6 to 15 months in most clinical trials depending on the patient and disease-related factors.
따라서, 두경부암, 특히 SCCHN의 개선된 의학적 개입에 대한 충족되지 않은 요구가 높다.Therefore, there is a high unmet need for improved medical interventions in head and neck cancer, especially SCCHN.
두경부암 치료를 위한 방법 및 사용Methods and uses for the treatment of head and neck cancer
본원에서는 대상체 또는 대상체 집단에서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN(예컨대, PD-L1 양성 및/또는 HPV 양성 재발성 및/또는 전이성 SCCHN))을 치료하는 방법 및 사용으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX 1106(니볼루맙), MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨), MEDI-0680(AMP-514), PDR001(스파르탈리주맙), REGN2810(세미플리맙), BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙 또는 토리팔리맙)) 및 항 TIGIT 길항제(예컨대, 본워에 기재된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여함으로써 상기 대상체 또는 대상체 집단을 치료하는 단계를 포함하는 방법 및 사용이 제공된다. 또한, 본원에서는 PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서, 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법이 제공된다. 또한, 본원에서는 PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서, 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법이 제공된다. Disclosed herein are methods and uses for treating SCCHN (eg, relapsed and/or metastatic SCCHN (eg, PD-L1 positive and/or HPV positive relapsed and/or metastatic SCCHN)) in a subject or population of subjects, comprising an effective amount of PD -1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX 1106 (nivolumab)), MK-3475 (pembrolizumab, formerly lambrolizumab) known as zumab), MEDI-0680 (AMP-514), PDR001 (spartalizumab), REGN2810 (semipliumab), BGB-108, prolgolimab, camrelizumab, scintilimab, tislelizumab or torifalimab)) and an anti-TIGIT antagonist (eg, an anti-TIGIT antagonist antibody, such as tiragolumab, as described in Bonwoer), by administering to the subject or population of subjects a dosing regimen comprising one or more dosing cycles. Methods and uses are provided comprising treating a population. Also disclosed herein is a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and about 80 mg to about 1600 every 3 weeks. A method is provided comprising administering to the subject one or more dosing cycles of a mg dose of a PD-1 axis binding antagonist. Also disclosed herein is a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising a dose of about 600 mg tiragolumab every 3 weeks and a dose of about 1200 mg atezolizumab once every 3 weeks. A method is provided comprising administering to the subject at least one dosing cycle.
본 발명은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙) 및 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 본 발명은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙) 및 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 투여하는 것을 수반한 방법 및 사용을 포함한다.The present invention provides an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab) and an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab). methods and uses involving administration to a subject or population of subjects in need thereof. In some cases, the present invention provides an effective amount of a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) and an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) to a subject or population of subjects in need thereof.
일부 경우들에서, 대상체 또는 대상체 집단에서 SCCHN을 치료하기 위한 임의의 방법 및 사용은 CR 또는 PR을 발생시킬 수 있다. 일부 경우들에서, 대상체 또는 대상체 집단에서 SCCHN을 치료하기 위한 임의의 방법 및 사용은 상기 대상체 또는 대상체 집단의 객관적 반응률(ORR)의 증가를 발생시킬 수 있다. 일부 경우들에서, 대상체 또는 대상체 집단에서 SCCHN을 치료하기 위한 임의의 방법 및 사용은 상기 대상체 또는 대상체 집단의 PFS, 반응 지속 기간(DOR), 및/또는 OS의 증가를 발생시킬 수 있다. In some cases, any method and use for treating SCCHN in a subject or population of subjects may result in CR or PR. In some cases, any method and use for treating SCCHN in a subject or population of subjects may result in an increase in the objective response rate (ORR) of the subject or population of subjects. In some cases, any method and use for treating SCCHN in a subject or population of subjects may result in an increase in PFS, Duration of Response (DOR), and/or OS in the subject or population of subjects.
일부 경우들에서, 상기 SCCHN은 PD-L1의 검출가능한 발현 수준을 갖는 SCCHN이다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터 수득한 종양 샘플은 PD-L1의 검출가능한 발현 수준(예컨대, PD-L1의 검출가능한 단백질 및/또는 핵산 발현 수준(예컨대, 종양 관련 면역 세포(TIC)가 5% 이상))을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 5% 이상(예컨대, PD-L1 양성), 5% 이상 20% 미만(예컨대, PD-L1 낮음), 또는 20% 이상(예컨대, PD-L1 높음)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상, 10% 이상 50% 미만, 또는 50% 이상이다.In some cases, the SCCHN is a SCCHN having a detectable expression level of PD-L1. In some cases, a tumor sample obtained from the subject or population of subjects comprises a detectable expression level of PD-L1 (eg, a detectable protein and/or nucleic acid expression level of PD-L1 (eg, a tumor associated immune cell (TIC) ) was determined to have 5% or more)). In some cases, the detectable protein expression level of PD-L1 is a TIC in the tumor sample of at least 5% (eg, PD-L1 positive), at least 5% and less than 20% (eg, PD-L1 low), or greater than 20% (eg, high in PD-L1). In some cases, the detectable protein expression level of PD-L1 is at least 10%, at least 10% and less than 50%, or at least 50% of the TIC in the tumor sample.
일부 경우들에서, 상기 치료는 1차 치료이다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 재발성 및/또는 전이성 질병에 대한 선행 전신 요법을 받지 않았다.In some cases, the treatment is first-line treatment. In some cases, the subject or population of subjects has not received prior therapy. In some cases, the subject or population of subjects has not received prior systemic therapy for recurrent and/or metastatic disease.
투약 요법 및 투여 Dosage regimen and administration
일 양태에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475)(펨브롤리주맙(이전에 람브롤리주맙으로 공지됨))의 1회 이상의 투약 주기, 및 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기를 포함한 투약 요법을 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)를 가진 대상체 또는 대상체 집단에게 투여하는 단계를 포함한다.In one aspect, the treatment methods and uses of the invention described herein comprise an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX) one or more dosing cycles of -1106 (nivolumab) or MK-3475) (pembrolizumab (formerly known as lambrolizumab)), and an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT as disclosed herein). administering to the subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN) a dosing regimen comprising one or more dosing cycles of an antagonist antibody, such as tyragolumab.
본원에 기재된 약학적 조성물은 섹션 III(K)에 기재된 바와 같이 투여용으로 제형화될 수 있다.The pharmaceutical compositions described herein may be formulated for administration as described in Section III(K).
두경부암을 위한 진단 방법 및 사용Diagnostic methods and uses for head and neck cancer
본 발명은 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법(예컨대, 한 라인 요법)을 선택하는 방법을 제공하고, 여기서 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. The invention provides a method of selecting a therapy (eg, one line therapy) for a subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN), wherein the therapy is obtained from the subject or population of subjects. one or more biomarkers (eg, PD-L1 (eg, as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (eg, p16 IHC, ISH or is guided by a diagnostic method involving determining the presence and/or expression level/amount of )))) as determined by PCR.
본원에서는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨), MEDI-0680(AMP-514), PDR001(스파르탈리주맙), REGN2810(세미플리맙), BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙 또는 토리팔리맙))를 포함한 치료로부터 이익을 얻을 수 있는, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단를 확인하는 방법이 추가적으로 제공되고, 여기서 확인은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Disclosed herein are an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475) (pembrolizumab, formerly known as lambrolizumab), MEDI-0680 (AMP-514), PDR001 (spartalizumab), REGN2810 (semipliumab), BGB-108, prolgolimab, camrelizumab Further provided is a method of identifying a subject or population of subjects with SCCHN (e.g., recurrent and/or metastatic SCCHN) that may benefit from treatment including wherein the identification is one or more biomarkers (eg, PD-L1 (eg, as determined by PD-L1 protein and/or nucleic acid expression) in a sample (eg, a tumor sample or blood sample) obtained from the subject or population of subjects. or by a diagnostic method involving determining the presence and/or expression level/amount of HPV status (eg, as determined by p16 IHC, ISH or PCR).
본원에서는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법에 대한 반응성을 평가하는 방법이 추가적으로 제공되고, 여기서 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 추가적으로 안내된다. Further provided herein is a method of assessing responsiveness to therapy for a subject or population of subjects having SCCHN (eg, relapsed and/or metastatic SCCHN), wherein the therapy is a sample obtained from the subject or population of subjects (eg, one or more biomarkers (eg, PD-L1 (eg, as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (eg, determined by p16 IHC, ISH or PCR) in a tumor sample or blood sample) as))) and/or is further guided by a diagnostic method involving determining the level/amount of expression.
본원에서는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 최적화하는 방법이 추가적으로 제공되고, 여기서 요법은 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 추가적으로 안내된다. Further provided herein is a method of optimizing therapy for a subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN), wherein the therapy is a sample obtained from the subject or population of subjects (eg, a tumor sample or one or more biomarkers (e.g., as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (e.g., as determined by p16 IHC, ISH or PCR) in a blood sample) ) is further guided by a diagnostic method involving determining the presence and/or expression level/amount.
본원에 기재된 방법에서 사용하기 위한 바이오마커는 종양 면역생물학, HPV 변경, 림프구 하위집단, T 세포 수용체 레퍼토리, T 세포 활성화와 관련된 사이토카인 및 혈장 유래 사이토카인과 관련된 유전자 또는 유전자 서명 분석인 WGS 및/또는 NGS를 통해 확인된 조직(예컨대, 종양 조직) 또는 혈액(예컨대, 전혈), 조직(예컨대, 종양 조직) 및/또는 혈액 내 순환 종양 DNA(돌연변이 로드, MSI 및 MMR 결함를 포함하지만 이에 제한되지는 않음)의 생식계열 및 체세포 돌연변이 상의 PD-L1 발현을 포함하지만, 이에 제한되지는 않는다. 일부 경우들에서, 상기 바이오마커는 PD-L1이다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터 수득한 종양 샘플은 PD-L1의 검출가능한 발현 수준(예컨대, PD-L1의 검출가능한 단백질 및/또는 핵산 발현 수준(예컨대, 종양 관련 면역 세포(TIC)가 5% 이상))을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 상기 종양 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상(예컨대, PD-L1 양성), 5% 이상 20% 미만(예컨대, PD-L1 낮음), 또는 20% 이상(예컨대, PD-L1 높음)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상, 10% 이상 50% 미만, 또는 50% 이상이다. 일부 경우들에서, 상기 샘플은 종양 샘플(예컨대, 포르말린 고정, 파라핀 포매(FFPE) 종양 샘플)이다. 일부 경우들에서, 상기 종양 샘플은 종양 조직 샘플이다.Biomarkers for use in the methods described herein include WGS, a gene or gene signature analysis associated with tumor immunobiology, HPV alteration, lymphocyte subpopulations, T cell receptor repertoire, cytokines associated with T cell activation and plasma-derived cytokines and/or or circulating tumor DNA in tissue (e.g., tumor tissue) or blood (e.g., whole blood), tissue (e.g., tumor tissue) and/or blood identified via NGS (including, but not limited to, mutant load, MSI and MMR defects) PD-L1 expression on germline and somatic mutations of In some cases, the biomarker is PD-L1. In some cases, a tumor sample obtained from the subject or population of subjects comprises a detectable expression level of PD-L1 (eg, a detectable protein and/or nucleic acid expression level of PD-L1 (eg, a tumor associated immune cell (TIC) ) was determined to have 5% or more)). In some cases, the detectable protein expression level of PD-L1 is at least 5% (eg, PD-L1 positive), at least 5% and less than 20% (eg, PD) of tumor associated immune cells (TICs) in the tumor sample. -L1 low), or greater than 20% (eg, PD-L1 high). In some cases, the detectable protein expression level of PD-L1 is at least 10%, at least 10% and less than 50%, or at least 50% of the TIC in the tumor sample. In some cases, the sample is a tumor sample (eg, a formalin fixed, paraffin embedded (FFPE) tumor sample). In some cases, the tumor sample is a tumor tissue sample.
일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 (예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 30 mg 내지 1200 mg) 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 80 mg 내지 약 2000 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 (예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 2주마다 840 mg 용량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 (예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 3주마다 1200 mg 용량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 (예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체 또는 대상체 집단에게 3주마다 약 600 mg(예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 1회 이상의 투약 주기 및 4주마다 1680 mg 용량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 투여하는 단계를 포함한다.In some cases, the method comprises (eg, as determined by PD-L1 (eg, PD-L1 protein and/or nucleic acid expression) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects. or determining the presence and/or expression level/amount of HPV status (eg, as determined by p16 IHC, ISH or PCR) and administering to the subject or population of subjects from about 30 mg to about 1200 mg every 3 weeks ( For example, from 30 mg to 1200 mg) at a dose (eg, a fixed dose) of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) at one or more dosing cycles and about 80 mg to every 3 weeks One or more dosing cycles of about 2000 mg (eg, 80 mg to about 2000 mg) dose (eg, fixed dose) of a PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) It includes the step of administering. In some cases, the method comprises (eg, as determined by PD-L1 (eg, PD-L1 protein and/or nucleic acid expression) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects. or determining the presence and/or expression level/amount of HPV status (e.g., as determined by p16 IHC, ISH or PCR) and giving said subject or population of subjects about 600 mg (e.g., 600 mg every 3 weeks) ) at least one dosing cycle of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a dose of 840 mg every two weeks of a PD-1 axis binding antagonist (eg, anti-PD-L1) administering one or more dosing cycles of the antagonist antibody (eg, atezolizumab). In some cases, the method comprises (eg, as determined by PD-L1 (eg, PD-L1 protein and/or nucleic acid expression) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects. or determining the presence and/or expression level/amount of HPV status (e.g., as determined by p16 IHC, ISH or PCR) and giving said subject or population of subjects about 600 mg (e.g., 600 mg every 3 weeks) ) at least one dosing cycle of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) and a 1200 mg dose of a PD-1 axis binding antagonist (eg, anti-PD-L1 every 3 weeks) administering one or more dosing cycles of the antagonist antibody (eg, atezolizumab). In some cases, the method comprises (eg, as determined by PD-L1 (eg, PD-L1 protein and/or nucleic acid expression) in a sample (eg, a tumor sample or blood sample) from the subject or population of subjects. or determining the presence and/or expression level/amount of HPV status (e.g., as determined by p16 IHC, ISH or PCR) and giving said subject or population of subjects about 600 mg (e.g., 600 mg every 3 weeks) ) at least one dosing cycle of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) and a 1680 mg dose of a PD-1 axis binding antagonist (eg, anti-PD-L1 every 4 weeks) administering one or more dosing cycles of the antagonist antibody (eg, atezolizumab).
(예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양은 단백질, 단백질 단편, DNA, mRNA, cDNA, 및/또는 유전자 복제 수를 포함하지만 이에 제한되지는 않는 당해 분야에서 공지된 임의의 적합한 기준에 따라 정성적으로 및/또는 정량적으로 결정될 수 있다. Presence and/or expression level of (eg, PD-L1 (eg, as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (eg, as determined by p16 IHC, ISH or PCR)) The /amount can be determined qualitatively and/or quantitatively according to any suitable criterion known in the art, including, but not limited to, protein, protein fragment, DNA, mRNA, cDNA, and/or gene copy number.
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체 또는 대상체 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 단백질 발현 수준이다. 일부 경우들에서, 상기 PD-L1 단백질 발현 수준은 IHC 분석에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of a biomarker is a detectable protein expression level of PD-L1 in a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects. In some cases, the PD-L1 protein expression level was determined by IHC analysis. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects has been determined to have a detectable expression level of PD-L1. In some cases, a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects has been determined to have a detectable expression level of PD-L1 in tumor infiltrating immune cells. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체 또는 대상체 집단으로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 핵산 발현 수준이다. 일부 경우들에서, PD-L1의 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, 유전자 발현의 연속 분석(SAGE), MassARRAY® 기술, 조직내(in situ) 혼성화(ISH), 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of a biomarker is a detectable nucleic acid expression level of PD-L1 in a tumor sample (eg, a FFPE tumor sample) from the subject or population of subjects. In some cases, the nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY ® technology, in-tissue. (in situ) hybridization (ISH), or a combination thereof. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 대상체 또는 대상체 집단으로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 (예컨대, PD-L1(예컨대, PD-L1 단백질 및/또는 핵산 발현에 의해 결정된 바와 같이) 또는 HPV 상태(예컨대, p16 IHC, ISH 또는 PCR에 의해 결정된 바와 같이))의 존재 및/또는 발현 수준/양은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 이용한 요법에 적격인 것으로 상기 대상체 또는 대상체 집단을 선택하고, 예를 들어, 여기서 PD-L1의 검출가능한 발현 수준은 개체의 선택을 위한 바이오마커이다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플(예컨대, FFPE 종양 샘플)이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, in a sample (eg, a tumor sample or blood sample) from a subject or population of subjects (eg, as determined by PD-L1 (eg, PD-L1 protein and/or nucleic acid expression) or HPV status ( The presence and/or expression level/amount of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) ) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) as eligible for therapy with the subject or population of subjects. selecting, e.g., wherein the detectable expression level of PD-L1 is a biomarker for selection of an individual, in some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample In some cases, the tissue sample is a tumor sample (such as FFPE tumor sample).In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof. In some cases, the tumor sample is a FFPE tumor sample.
일 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다. In one aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks (eg, a fixed dose) and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as A method of selecting a therapy for a subject or population of subjects is provided. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression in the detected tumor sample. providing a method of selecting a therapy for a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising do. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks (eg, a fixed dose) and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as A method of selecting a therapy for a subject or population of subjects is provided. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression in the detected tumor sample. providing a method of selecting a therapy for a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising do. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 다른 양태에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 검출된 종양 샘플의 PD-L1 발현에 기초하여 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks (eg, a fixed dose) and a dose of 1200 mg every 3 weeks (eg, a fixed dose) based on PD-L1 expression in the detected tumor sample. with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as A method of selecting a therapy for a subject or population of subjects is provided. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1680 mg every 4 weeks. In some cases, the regimen comprises one or more dosing cycles of the anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 840 mg every 2 weeks. In another aspect, the invention provides a method for determining the protein expression level of PD-L1 in a tumor sample by obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, by IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting, and one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression in the detected tumor sample. providing a method of selecting a therapy for a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN) by identifying said subject and subject population as those who may benefit from a therapy comprising do. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN that may benefit from therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for identifying a subject or population of subjects with (eg, recurrent and/or metastatic SCCHN). In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of 1680 mg per day In some cases, the regimen includes an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 840 mg every 2 weeks. one or more dosing cycles of atezolizumab administered as a dose, in some aspects, the present invention provides an anti-PD-L1 antibody suitable for staining, comprising the steps of obtaining a tumor sample (eg, biopsy) from a subject or population of subjects. detecting the protein expression level of PD-L1 in the tumor sample by IHC analysis using the subject and population of subjects as those who may benefit from a therapy comprising one or more dosing cycles of by identifying an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) provide a way In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN that may benefit from therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for identifying a subject or population of subjects with (eg, recurrent and/or metastatic SCCHN). In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of 1680 mg per day In some cases, the regimen includes an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 840 mg every 2 weeks. one or more dosing cycles of atezolizumab administered as a dose, in some aspects, the present invention provides an anti-PD-L1 antibody suitable for staining, comprising the steps of obtaining a tumor sample (eg, biopsy) from a subject or population of subjects. detecting the protein expression level of PD-L1 in the tumor sample by IHC analysis using may benefit from a therapy comprising one or more dosing cycles of atezolizumab administered as a fixed dose (eg, a fixed dose). an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, SCCHN (e.g., recurrent and/or metastatic SCCHN) that may benefit from therapy comprising, e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) A method for identifying a subject or population of subjects with In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법으로부터 이익을 얻을 수 있는 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단을 확인하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN that may benefit from therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for identifying a subject or population of subjects with (eg, recurrent and/or metastatic SCCHN). In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of 1680 mg per day In some cases, the regimen includes an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 840 mg every 2 weeks. one or more dosing cycles of atezolizumab administered as a dose, in some aspects, the present invention provides an anti-PD-L1 antibody suitable for staining, comprising the steps of obtaining a tumor sample (eg, biopsy) from a subject or population of subjects. detecting the protein expression level of PD-L1 in the tumor sample by IHC analysis using the subject and population of subjects as those who may benefit from a therapy comprising one or more dosing cycles of by identifying an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) provide a way In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agent; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN (e.g., relapse) for therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for assessing the reactivity of a subject or population of subjects with sexual and/or metastatic SCCHN) In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 1680 every 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of mg.In some cases, the regimen comprises an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and a dose of 840 mg every 2 weeks. one or more dosing cycles of atezolizumab to be administered.In some aspects, the invention provides a method for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis, and 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. identifying said subject and subject population as those who would benefit from a therapy comprising more than one dosing cycle; By system, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK) Provided are methods for assessing the responsiveness of a subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN) to therapy comprising -3475 (pembrolizumab, formerly known as lambrolizumab)). . In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN (e.g., relapse) for therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for assessing the reactivity of a subject or population of subjects with sexual and/or metastatic SCCHN) In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 1680 every 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of mg.In some cases, the regimen comprises an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and a dose of 840 mg every 2 weeks. one or more dosing cycles of atezolizumab to be administered.In some aspects, the invention provides a method for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis, and 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. identifying said subject and subject population as those who would benefit from a therapy comprising more than one dosing cycle; By system, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK) Provided are methods for assessing the responsiveness of a subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN) to therapy comprising -3475 (pembrolizumab, formerly known as lambrolizumab)). . In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법에 대한 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단의 반응성을 평가하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, ate SCCHN (e.g., relapse) for therapy comprising zolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Provided is a method for assessing the reactivity of a subject or population of subjects with sexual and/or metastatic SCCHN) In some cases, the therapy comprises an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 1680 every 4 weeks. one or more dosing cycles of atezolizumab administered at a dose of mg.In some cases, the regimen comprises an anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and a dose of 840 mg every 2 weeks. one or more dosing cycles of atezolizumab to be administered.In some aspects, the invention provides a method for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis, and 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. identifying said subject and subject population as those who would benefit from a therapy comprising more than one dosing cycle; By system, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK) Provided are methods for assessing the responsiveness of a subject or population of subjects having SCCHN (eg, recurrent and/or metastatic SCCHN) to therapy comprising -3475 (pembrolizumab, formerly known as lambrolizumab)). . In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; (e.g., OX-40 agonist antibody), chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapeutic agents, and/or anti-hormonal agents, such as the agents mentioned herein above (separately or in combination) may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. an anti TIGIT antagonist antibody and in a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN), by identifying said subject and subject population as those who may benefit from a therapy comprising a dosing cycle; A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) In some cases, the therapy is an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and a dose of 1680 mg every 4 weeks. one or more dosing cycles of atezolizumab administered to one or more dosing cycles of zolizumab.In some aspects, the invention provides for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, for IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by means of one or more doses of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks identifying said subject and subject population as those who may benefit from a therapy comprising a cycle; , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD in a subject or population of subjects with SCCHN (eg, relapsed and/or metastatic SCCHN)) A method of optimizing therapy comprising a -1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is provided. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. an anti TIGIT antagonist antibody and in a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN), by identifying said subject and subject population as those who may benefit from a therapy comprising a dosing cycle; A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) In some cases, the therapy is an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and a dose of 1680 mg every 4 weeks. one or more dosing cycles of atezolizumab administered to one or more dosing cycles of zolizumab.In some aspects, the invention provides for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, for IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by means of one or more doses of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks identifying said subject and subject population as those who may benefit from a therapy comprising a cycle; , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD in a subject or population of subjects with SCCHN (eg, relapsed and/or metastatic SCCHN)) A method of optimizing therapy comprising a -1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is provided. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량(예컨대, 고정 용량)으로 투여된 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량(예컨대, 고정 용량)으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 4주마다 1680 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 요법은 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 2주마다 840 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한다. 일부 양태들에서, 본 발명은 대상체 또는 대상체 집단으로부터 종양 샘플(예컨대, 생검)을 수득하는 단계, 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계, 및 3주마다 600 mg의 용량으로 투여된 티라골루맙 및 3주마다 1200 mg의 용량으로 투여된 아테졸리주맙의 1회 이상의 투약 주기를 포함하는 요법으로부터 이익을 얻을 수 있는 자로서 상기 대상체 및 대상체 집단을 확인하는 단계에 의해서, SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)을 가진 대상체 또는 대상체 집단에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함하는 요법을 최적화하는 방법을 제공한다. 일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다. In some aspects, the invention provides a method for obtaining a tumor sample (eg, a biopsy) from a subject or population of subjects, the protein expression level of PD-L1 in the tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining. and one or more doses of anti-TIGIT antagonist antibody administered at a dose of 600 mg (eg, a fixed dose) every 3 weeks and atezolizumab administered at a dose of 1200 mg (eg, a fixed dose) every 3 weeks. an anti TIGIT antagonist antibody and in a subject or subject population having SCCHN (eg, recurrent and/or metastatic SCCHN), by identifying said subject and subject population as those who may benefit from a therapy comprising a dosing cycle; A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) In some cases, the therapy is an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and a dose of 1680 mg every 4 weeks. one or more dosing cycles of atezolizumab administered to one or more dosing cycles of zolizumab.In some aspects, the invention provides for obtaining a tumor sample (eg, biopsy) from a subject or population of subjects, for IHC analysis using an anti-PD-L1 antibody suitable for staining. detecting the protein expression level of PD-L1 in said tumor sample by means of one or more doses of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks identifying said subject and subject population as those who may benefit from a therapy comprising a cycle; , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD in a subject or population of subjects with SCCHN (eg, relapsed and/or metastatic SCCHN)) A method of optimizing therapy comprising a -1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is provided. In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 경우들에서, 상기 방법은 확인된 대상체 또는 대상체의 집단에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 항암 치료제(들)(예컨대, 면역조절제(예컨대, 하나 이상의 면역 공동억제 수용체(예컨대, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, 및/또는 VISTA로부터 선택된 하나 이상의 면역 공동억제 수용체)를 감소 또는 억제하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®)) 또는 하나 이상의 면역 공동 자극 수용체(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR로부터 선택된 하나 이상의 면역 공동 자극 수용체)를 증가 또는 활성화시키는 제제, 예컨대, OX-40 작용제, 예컨대, OX-40 작용제 항체), 화학요법제, 세포독성제, 성장 억제제, 방사선요법/방사선 치료제, 및/또는 항호르몬제, 예컨대, 상기 본원에 언급된 제제들)과 함께(별도로 또는 함께) 투여될 수 있다.In some cases, the method further comprises administering the therapy to the identified subject or population of subjects. In some cases, the therapy comprises one or more additional anti-cancer therapeutic agent(s) (eg, an immunomodulatory agent (eg, one or more immune co-suppressive receptors (eg, TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3) , BTLA, and/or one or more immune co-suppression receptors selected from VISTA), such as a CTLA-4 antagonist, such as an anti-CTLA-4 antagonist antibody (eg, ipilimumab ( YERVOY® )), or an agent that increases or activates one or more immune co-stimulatory receptors (e.g., one or more immune co-stimulatory receptors selected from CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR), such as an OX-40 agonist; In combination with (separately or in combination with, e.g., an OX-40 agonist antibody), a chemotherapeutic agent, a cytotoxic agent, a growth inhibitory agent, a radiotherapy/radiotherapeutic agent, and/or an anti-hormonal agent, such as the agents mentioned herein above). may be administered.
일부 경우들에서, 본원에 기재된 임의의 진단 방법 또는 사용에서, 상기 SCCHN은 재발성 및/또는 전이성 SCCHN이다. 상기 암은 조기 또는 말기일 수 있다. 일부 경우들에서, 상기 요법은 1라인 요법이다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 요법을 받지 않았다. 일부 경우들에서, 상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법이다.In some cases, in any of the diagnostic methods or uses described herein, the SCCHN is recurrent and/or metastatic SCCHN. The cancer may be early or late. In some cases, the therapy is a one-line therapy. In some cases, the subject or population of subjects has not received prior therapy. In some cases, the prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
암 특성화 및 선택Cancer characterization and selection
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 암은 SCCHN(예컨대, 재발성 및/또는 전이성 SCCHN)일 수 있다. 일부 경우들에서, 상기 SCCHN은 재발성 및/또는 전이성 SCCHN이다. 일부 경우들에서, 상기 SCCHN은 PD-L1 양성이다. 일부 경우들에서, 상기 SCCHN은 HPV 양성이다. 일부 경우들에서, 상기 SCCHN은 HPV 음성이다. 일부 경우들에서, 상기 SCCHN은 PD-L1 양성 및 HPV 양성이다. 일부 경우들에서, 상기 SCCHN은 PD-L1 양성 및 HPV 음성이다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 요법을 받지 않았다. 일부 경우들에서, 상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법이다.In any of the methods, uses, or compositions for use described herein, the cancer may be SCCHN (eg, recurrent and/or metastatic SCCHN). In some cases, the SCCHN is recurrent and/or metastatic SCCHN. In some cases, the SCCHN is PD-L1 positive. In some cases, the SCCHN is HPV positive. In some cases, the SCCHN is HPV negative. In some cases, the SCCHN is PD-L1 positive and HPV positive. In some cases, the SCCHN is PD-L1 positive and HPV negative. In some cases, the subject or population of subjects has not received prior therapy. In some cases, the prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체 또는 대상체의 집단은 PD-L1 선택된 종양(예컨대, PD-L1의 검출가능한 발현 수준을 갖는 종양(예컨대, PD-L1의 검출가능한 단백질 발현 수준(예컨대, 5% 이상의 종양 관련 면역 세포(TIC))을 가진다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단으로부터 수득한 샘플(예컨대, 종양 샘플(예컨대, 종양 조직 샘플))은 PD-L1의 검출가능한 단백질 발현 수준(예컨대, 5% 이상의 TIC)을 가진다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1의 검출가능한 발현 수준(예컨대, PD-L1의 검출가능한 단백질 발현 수준(예컨대, 5% 이상의 TIC))을 가진다. 일부 경우들에서, 상기 PD-L1 검출가능한 발현 수준은 PD-L1의 검출가능한 발현 수준(예컨대, 5% 이상의 TIC)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 5% 이상(예컨대, 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 70%, 75%, 80%, 90% 또는 그 이상)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 5% 이상 20% 미만(예컨대, 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 또는 20%)이다. 일부 경우들에서, 5% 이상 20% 미만의 TIC는 PD-L1 낮음으로 정의된다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 20% 이상(예컨대, 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, 99%, 또는 100%)이다. 일부 경우들에서, 20% 이상의 TIC는 PD-L1 높음으로 정의된다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 10% 이상(예컨대, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 70%, 75%, 80%, 90% 또는 그 이상)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 10% 이상 50% 미만(예컨대, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 46%, 47%, 48%, 49%, 49.5%, 49.9%, 또는 49.99%)이다. 일부 경우들에서, 상기 PD-L1의 검출가능한 단백질 발현 수준은 TIC가 약 50% 이상(예컨대, 50%, 51%, 52%, 53%, 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 71%, 72%, 73%, 74%, 75%, 76%, 77%, 78%, 79%, 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 95%, 99%, 또는 99.99%)이다.In some cases, in any method, use, or composition for use described herein, the subject or population of subjects is a PD-L1 selected tumor (eg, a tumor having a detectable expression level of PD-L1 (eg, has a detectable protein expression level of PD-L1 (eg, at least 5% tumor-associated immune cells (TIC)) In some cases, a sample obtained from the subject or population of subjects (eg, a tumor sample (eg, a tumor tissue sample)) has a detectable protein expression level (eg, a TIC of at least 5%) of PD-L1 In some cases, the PD-L1 selected tumor has a detectable expression level of PD-L1 (eg, PD- has a detectable protein expression level of L1 (eg, greater than or equal to 5% TIC) In some cases, the detectable expression level of PD-L1 is a detectable expression level of PD-L1 (eg, greater than or equal to 5% TIC) In some cases, the detectable protein expression level of PD-L1 has a TIC of at least about 5% (eg, 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 70%, 75% , 80%, 90% or greater) In some cases, the detectable protein expression level of PD-L1 has a TIC of about 5% to less than 20% (eg, 5%, 6%, 7%, 8 %, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, or 20%) In some cases, 5% or more 20 A TIC of less than % is defined as PD-L1 low In some cases, the detectable protein expression level of PD-L1 is a TIC of about 20% or greater (e.g., 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34%, 35%, 40%, 45%, 50%, 5 5%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, 99%, or 100%). In some cases, a TIC of 20% or more is defined as PD-L1 high. In some cases, the detectable protein expression level of PD-L1 has a TIC of at least about 10% (eg, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18 %, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 60%, 70%, 75%, 80%, 90% or more). In some cases, the detectable protein expression level of PD-L1 has a TIC of at least about 10% and less than 50% (eg, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17 %, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 46%, 47%, 48%, 49%, 49.5%, 49.9%, or 49.99%). In some cases, the detectable protein expression level of PD-L1 has a TIC of at least about 50% (eg, 50%, 51%, 52%, 53%, 54%, 55%, 56%, 57%, 58 %, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 71%, 72%, 73%, 74%, 75%, 76%, 77%, 78%, 79%, 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 95% , 99%, or 99.99%).
일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP263, SP142, 22C3, 또는 28-8을 사용한다. 일부 경우들에서, IHC 분석은 항 PD-L1 항체 SP263를 사용한다. 일부 경우들에서, 상기 TIC는 5% 이상인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. 일부 경우들에서, 상기 TIC는 5% 이상 20% 미만인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. 일부 경우들에서, 상기 TIC는 20% 이상인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. 일부 경우들에서, 상기 TIC는 10% 이상인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. 일부 경우들에서, 상기 TIC는 10% 이상 50% 미만인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. 일부 경우들에서, 상기 TIC는 50% 이상인 것으로(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여) 결정되었다. In some cases, the IHC assay uses anti-PD-L1 antibodies SP263, SP142, 22C3, or 28-8. In some cases, the IHC assay uses the anti-PD-L1 antibody SP263. In some cases, the TIC was determined to be greater than or equal to 5% (eg, using a Ventana (SP263) PD-L1 IHC assay). In some cases, the TIC was determined to be greater than or equal to 5% and less than 20% (eg, using a Ventana (SP263) PD-L1 IHC assay). In some cases, the TIC was determined to be greater than or equal to 20% (eg, using a Ventana (SP263) PD-L1 IHC assay). In some cases, the TIC was determined to be greater than or equal to 10% (eg, using a Ventana (SP263) PD-L1 IHC assay). In some cases, the TIC was determined to be greater than or equal to 10% and less than 50% (eg, using a Ventana (SP263) PD-L1 IHC assay). In some cases, the TIC was determined to be greater than or equal to 50% (eg, using a Ventana (SP263) PD-L1 IHC assay).
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체 또는 대상체 집단으로부터 수득한 샘플(예컨대, 종양 샘플)은 PD-L1의 검출가능한 핵산 발현 수준을 가진다. 일부 예들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다.In some cases, in a method, use, or composition for use described herein, a sample obtained from the subject or population of subjects (eg, a tumor sample) has a detectable nucleic acid expression level of PD-L1. In some instances, the detectable nucleic acid expression level of PD-L1 was determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. . In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample. In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체 또는 대상체의 집단은 검출가능한 HPV를 갖는 종양을 가진다. 일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체 또는 대상체의 집단은 검출가능한 HPV가 없는 종양을 가진다. 일부 경우들에서, 상기 HPV가 직접 또는 간접적으로 검출된다. 일부 경우들에서, 상기 HPV는 단백질 발현 수준(예컨대, p16 또는 HPV 바이러스 단백질)에 의해 검출된다. 일부 경우들에서, 상기 HPV는 핵산 발현 수준에 의해 검출된다. 일부 경우들에서, HPV 상태는 p16 IHC, 조직내(in situ) 또는 PCR에 의해 결정된다. 일부 경우들에서, 상기 HPV는 HPV16이다. 일부 경우들에서, 상기 HPV는 HPV18이다.In some cases, in any of the methods, uses, or compositions for use described herein, the subject or population of subjects has a tumor with detectable HPV. In some cases, in any of the methods, uses, or compositions for use described herein, the subject or population of subjects has a tumor free of detectable HPV. In some cases, the HPV is detected directly or indirectly. In some cases, the HPV is detected by protein expression level (eg, p16 or HPV viral protein). In some cases, the HPV is detected by the level of nucleic acid expression. In some cases, HPV status is determined by p16 IHC, in situ or PCR. In some cases, the HPV is HPV16. In some cases, the HPV is HPV18.
치료에 대한 반응response to treatment
본원에 기재된 임의의 방법에 대한 일부 구현예들에서, 요법에 대한 대상체 또는 대상체 집단의 반응은 하나 이상의 측정에 의해 특징지어질 수 있다. 일부 구현예들에서, 상기 치료는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 대상체 또는 대상체 집단에서 SCCHN을 치료하기 위한 임의의 방법 및 사용은 상기 대상체 또는 대상체 집단의 객관적 반응률(ORR)의 증가를 발생시킬 수 있다. 일부 경우들에서, 대상체 또는 대상체 집단에서 SCCHN을 치료하기 위한 임의의 방법 및 사용은 상기 대상체 또는 대상체 집단의 PFS, 반응 지속 기간(DOR), 및/또는 OS의 증가를 발생시킬 수 있다. In some embodiments of any of the methods described herein, the response of a subject or population of subjects to a therapy can be characterized by one or more measures. In some embodiments, the treatment results in CR or PR. In some cases, any method and use for treating SCCHN in a subject or population of subjects may result in an increase in the objective response rate (ORR) of the subject or population of subjects. In some cases, any method and use for treating SCCHN in a subject or population of subjects may result in an increase in PFS, Duration of Response (DOR), and/or OS in the subject or population of subjects.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))의 투여는 임상 반응을 유발한다. 일부 경우들에서, 상기 임상 반응은 기준 ORR과 비교하여 대상체 또는 대상체 집단에서의 ORR의 증가이다. 일부 경우들에서, 상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 ORR 중앙값이다. 일부 경우들에서, 상기 기준 ORR은 적어도 약 19%(예컨대, 약 19% 내지 약 80%, 예컨대 약 19% 내지 약 60%(예컨대, 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 또는 60%))이다. 일부 경우들에서, 상기 기준 ORR은 적어도 약 36%(예컨대, 약 36% 내지 약 80%, 예컨대 약 36% 내지 약 60%(예컨대, 36%, 37%, 38%, 39%, 40%, 45%, 50%, 55%, 또는 60%))이다. 일부 경우들에서, 상기 기준 ORR은 적어도 약 19% 내지 약 36%이다. 일부 경우들에서, 상기 임상 반응은 기준 PFS와 비교하여 대상체 또는 대상체 집단에서의 PFS의 증가이다. 일부 경우들에서, 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이다. 일부 경우들에서, 상기 임상 반응은 기준 DOR 시간과 비교하여 대상체 또는 대상체 집단에서의 DOR의 증가이다. 일부 경우들에서, 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이다. 일부 경우들에서, 상기 기준 DOR 시간은 적어도 약 4개월(예컨대, 약 4개월 내지 약 42개월(예컨대, 약 6개월 내지 약 30개월(예컨대, 6개월, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월 , 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월 또는 30개월))이다. 일부 경우들에서, 상기 기준 DOR 시간은 적어도 약 6.7개월(예컨대, 적어도 약 6.7개월, 6.8개월, 6.9개월, 7.0개월, 8.0개월, 9.0개월, 10.0개월, 11.0개월, 또는 12.0개월)이다. 일부 경우들에서, 상기 기준 DOR 시간은 적어도 약 6.7개월 내지 약 23.4개월이다. 일부 경우들에서, 상기 기준 DOR 시간은 적어도 약 23.4개월(예컨대, 적어도 약 23.4개월, 23.5개월, 23.6개월, 23.7개월, 23.8개월, 23.9개월, 24개월, 25개월, 26개월, 28개월, 30개월, 또는 32개월)이다. 일부 경우들에서, 상기 임상 반응은 OS의 증가이다.In some cases, in any of the methods, uses, or compositions for use described herein, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or Administration of an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) elicits a clinical response. The clinical response is an increase in ORR in a subject or a population of subjects compared to a reference ORR In some cases, the baseline ORR is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, an anti-PD-L1 antagonist antibody) without anti-TIGIT antagonist antibody. , atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) ORR in a Population of Subjects In some cases, the baseline ORR is at least about 19% (eg, between about 19% and about 80%, such as between about 19% and about 60% (eg, 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, or 60%) In some cases, the baseline ORR is at least about 36% (eg, about 36%). to about 80%, such as from about 36% to about 60% (eg, 36%, 37%, 38%, 39%, 40%, 45%, 50%, 55%, or 60%). In , the baseline ORR is at least about 19% to about 36%.In some cases, the clinical response is an increase in PFS in a subject or population compared to baseline PFS.In some cases, the baseline PFS time is a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (e.g., MDX-1106 (nivolumab) Pembrolizumab, formerly lambrolizumab is the median PFS time of a population of subjects receiving treatment including Zumab)). In some cases, the clinical response is an increase in DOR in a subject or population of subjects as compared to a baseline DOR time. In some cases, the baseline DOR time is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106) without an anti-TIGIT antagonist antibody. (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) is the median DOR time of a population of subjects receiving treatment. In some cases, the baseline DOR time is at least about 4 months. (e.g., from about 4 months to about 42 months (e.g., from about 6 months to about 30 months (e.g., 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months , 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months or 30 months)) In some cases, the baseline DOR time is at least about 6.7 months (eg, at least about 6.7 months, 6.8 months, 6.9 months, 7.0 months, 8.0 months, 9.0 months, 10.0 months, 11.0 months, or 12.0 months). In some cases, the reference DOR time is at least about 6.7 months to about 23.4 months In some cases, the reference DOR time is at least about 23.4 months (eg, at least about 23.4 months, 23.5 months, 23.6 months, 23.7 months) , 23.8 months, 23.9 months, 24 months, 25 months, 26 months, 28 months, 30 months, or 32 months) In some cases, the clinical response is an increase in OS.
일부 경우들에서, 상기 치료는 15% 초과(예컨대, 15%, 16%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34%, 35%, 36%, 37%, 38%, 39%, 40%, 41%, 42%, 43%, 44%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 90% 또는 그 이상)의 ORR을 발생시킨다. 일부 경우들에서, 상기 치료는 기준 ORR보다 큰 ORR을 발생시킨다. 일부 경우들에서, 상기 기준 ORR은 19%이다. 일부 경우들에서, 상기 기준 ORR은 24.4%이다. 일부 경우들에서, 상기 기준 ORR은 28.8%이다. 일부 경우들에서, 상기 기준 ORR은 35%이다.In some cases, the treatment is greater than 15% (eg, 15%, 16%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34%, 35%, 36%, 37%, 38%, 39%, 40%, 41%, 42%, 43% , 44%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 90% or more). In some cases, the treatment results in an ORR greater than the baseline ORR. In some cases, the baseline ORR is 19%. In some cases, the baseline ORR is 24.4%. In some cases, the baseline ORR is 28.8%. In some cases, the baseline ORR is 35%.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS, DOR, 또는 OS의 증가를 발생시킨다.In some cases, the treatment is compared to treatment with a PD-1 axis binding antagonist, eg, in the absence of an anti TIGIT antagonist antibody, or compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist, such as in the subject or population of subjects. causes an increase in PFS, DOR, or OS.
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 5.1개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 기준 OS 시간과 비교하여 OS의 증가를 발생시킨다. 일부 경우들에서, 상기 기준 OS 시간은 적어도 약 8개월(예컨대, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월 또는 18개월)이다. 일부 경우들에서, 상기 기준 OS 시간은 적어도 약 14.9개월(예컨대, 15개월, 16개월, 17개월, 18개월, 19개월 또는 20개월)이다. 일부 경우들에서, 상기 기준 OS 시간은 적어도 약 11.6개월 내지 약 14.9개월이다.In some embodiments, OS is measured as the period from initiation of treatment to death. In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 2 months (eg, by 2-120 months, by 3-110 months, by 4-100 months, by 5-80 months, by 6- by 60 months, by 7-48 months, by 8-36 months, by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months , 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 3.3 months (eg, by 3.3-120 months, by 4-100 months, by 5-80 months, by 6-60 months, by 7- by 48 months, by 8-36 months, or by 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 5.1 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months , 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment reduces the OS of the subject or population of subjects by at least about 5.3 months (eg, by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 by -24 months, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months , 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some cases, the treatment results in an increase in OS compared to baseline OS time. In some cases, the baseline OS time is at least about 8 months (eg, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, or 18 months) to be. In some cases, the baseline OS time is at least about 14.9 months (eg, 15 months, 16 months, 17 months, 18 months, 19 months, or 20 months). In some cases, the baseline OS time is at least about 11.6 months to about 14.9 months.
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월,3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some embodiments, the treatment described herein reduces the PFS of the subject or population of subjects by at least about 2.4 months (eg, by 2.4-120 months, by 2.5-100 months, by 3.0-80 months, by 4.0-60 months). , by 5.0-48 months, by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the PFS of the subject or population of subjects by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, 8 by -48 months, by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the PFS of the subject or population of subjects by at least about 2 months (eg, by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, 8 by -48 months, by 9-36 months, by 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months , 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체 또는 대상체 집단의 DOR을 적어도 약 2.4개월 만큼(예컨대, 2.4~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월,3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 DOR을 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체 또는 대상체 집단의 DOR을 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~100개월 만큼, 4~80개월 만큼, 6~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2.0개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein increases the DOR of the subject or population of subjects by at least about 2.4 months (eg, by 2.4 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months). , by 5.0-48 months, by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment increases the DOR of the subject or population of subjects by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, 8 by -48 months, by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment increases the DOR of the subject or population of subjects by at least about 2 months (eg, by 2 to 120 months, by 3 to 100 months, by 4 to 80 months, by 6 to 60 months, 8 by -48 months, by 9-36 months, by 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months , 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 경우들에서, 상기 치료는 환자 보고 결과 측정 정보 시스템®(PROMIS)® 아이템 뱅크(IItem Bank) v2.0-신체 기능에 관한 간편 양식(Physical Functioning-Short Form) 10b에 의해 측정된 바와 같이 환자가 보고한 신체 기능에서 확인된 악화까지의 경과 시간(TTCD)을 개선시킨다. 일부 경우들에서, 상기 치료는 PROMIS® 아이템 뱅크 v2.0-신체 기능에 관한 간편 양식 10b, PROMIS® 아이템 뱅크 v1.0-피로에 대한 간편 양식 4a, PROMIS® 아이템 뱅크 v1.0-통증 간섭에 관한 간편 양식(Pain Interference Short Form) 4a, 및 PROMIS® 수치 등급 척도(Numeric Rating Scale) v1.0-통증 강도(Pain Intensity) 1a에 의해 측정된 바와 같이 신체 기능, 피로 및/또는 통증의 기준선을 개선시킨다.In some cases, the treatment is administered to the patient as measured by the Patient Reported Outcomes Measurement Information System ® (PROMIS) ® IItem Bank v2.0-Physical Functioning-Short Form 10b. time to confirmed deterioration (TTCD) in bodily function reported by In some cases, the treatment is PROMIS ® Item Bank v2.0 - Quick Form 10b for Body Functions, PROMIS ® Item Bank v1.0 - Quick Form 4a for Fatigue, PROMIS ® Item Bank v1.0 - Quick Form for Fatigue Interference Baseline of body function, fatigue and/or pain as measured by the Pain Interference Short Form 4a, and the PROMIS ® Numeric Rating Scale v1.0-Pain Intensity 1a. improve
D.D. 간암과 관련된 치료 방법 및 사용Treatment methods and uses associated with liver cancer
간암liver cancer
간암은 연간 854,000건의 신규 사례 및 810,000건의 사망으로 전 세계적으로 다섯 번째로 가장 흔한 암이자 두 번째로 흔한 암 관련 사망의 원인이다. 진단 시, 대부분의 원발성 간암 환자는 완치 요법의 치료가 권장되지 않는 단계인 진행성 질환을 나타낸다. 세계보건기구(WHO)는 2030년에 100만 명이 넘는 사람들이 간암으로 사망할 것으로 추정하며, 이는 중대한 전 세계 공중 보건 문제를 제시한다. Liver cancer is the fifth most common cancer and the second most common cancer-related cause of death worldwide, with 854,000 new cases and 810,000 deaths annually. At diagnosis, most patients with primary liver cancer present with advanced disease, a stage at which curative treatment is not recommended. The World Health Organization (WHO) estimates that more than one million people will die of liver cancer by 2030, presenting a significant global public health problem.
간세포암종(HCC)은 원발성 간암의 가장 흔한 형태이며 모든 원발성 간암의 약 90%를 나타낸다. 간세포암종(HCC)은 임의의 고형 종양 중 사망률이 0.98로 가장 높은 치명적인 질병이다. 간세포암종(HCC)으로 처음 내원한 환자의 최대 80%는 증상의 늦은 출현으로 인해 절제 불가능한 또는 전이된 질병으로 진행되었다. 미국에서, 간세포암종(HCC) 환자의 5년 전체생존(OS) 비율은 17%이고 원격 전이가 있는 경우 3%로 상당히 떨어진다. Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer and accounts for approximately 90% of all primary liver cancers. Hepatocellular carcinoma (HCC) is the most lethal disease of any solid tumor with a mortality rate of 0.98. Up to 80% of patients initially presenting with hepatocellular carcinoma (HCC) have progressed to unresectable or metastatic disease due to the late onset of symptoms. In the United States, the 5-year overall survival (OS) rate of patients with hepatocellular carcinoma (HCC) is 17% and drops significantly to 3% with distant metastasis.
따라서, 간암, 예컨대, HCC, 예컨대, 국소 진행성 HCC, 전이성 HCC, 또는 절제불가능한 HCC의 치료를 위한 효과적인 면역요법의 개발 분야에서 충족되지 않은 요구가 있다. Accordingly, there is an unmet need in the field of development of effective immunotherapy for the treatment of liver cancer, such as HCC, such as locally advanced HCC, metastatic HCC, or unresectable HCC.
간암 치료를 위한 방법 및 사용Methods and uses for the treatment of liver cancer
본원에서는 대상체 또는 대상체 집단에서 간암, 예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 간세포암종(HCC)를 포함한 HCC를 치료하거나 이의 진행을 지연시키는 방법 및 사용으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는 방법 및 사용이 제공되고, 여기서 상기 대상체 또는 대상체의 집단은 이전에 간암(예컨대, HCC)에 대한 전신 치료를 받은 적이 없다. 또한, 본원에서는 대상체 또는 대상체 집단에서 간암, 예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 간세포암종(HCC)를 포함한 HCC를 치료하거나 이의 진행을 지연시키는 방법 및 사용으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는 방법 및 사용이 제공된다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다. 다른 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다. Disclosed herein are methods and uses for treating or delaying the progression of liver cancer, including locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC), in a subject or population of subjects, comprising: an effective amount of a PD-1 axis binding antagonist ( Methods and uses are provided comprising administering to the subject or population of subjects a treatment regimen comprising, e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab) wherein the subject or population of subjects has not previously received systemic treatment for liver cancer (eg, HCC). Also provided herein are methods and uses for treating or delaying the progression of liver cancer, including locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC), in a subject or population of subjects, comprising an effective amount of a PD-1 axis binding Treatments comprising an antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and an anti-TIGIT antagonist antibody (eg, tyragolumab) Methods and uses are provided comprising administering therapy to the subject or population of subjects. In some embodiments, the treatment regimen is one dose of an effective amount of a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, tyragolumab) more than one dosing cycle. In other embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) )), and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tyragolumab).
또한, 본원에서는 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)를 가진 대상체 또는 대상체 집단에서 면역 기능을 향상시키는 방법으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는 방법이 제공된다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다.Also disclosed herein is a method of enhancing immune function in a subject or population of subjects having liver cancer (eg, HCC including locally advanced or metastatic and/or unresectable HCC), comprising an effective amount of a PD-1 axis binding antagonist (eg, anti-PD). Methods are provided comprising administering to the subject or population of subjects a treatment regimen comprising an -L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, tiragolumab). In some embodiments, the treatment regimen is one dose of an effective amount of a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, tyragolumab) more than one dosing cycle.
예를 들어, 본원에서는 대상체 또는 대상체 집단에서 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)을 치료하거나 이의 진행을 지연시키는 방법 및 사용으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는 방법 및 사용이 제공된다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다.For example, disclosed herein are methods and uses for treating or delaying the progression of liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects, comprising an effective amount of a PD-1 axis binding antagonist Methods and uses comprising administering to the subject or population of subjects a treatment regimen comprising (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab) provided In some embodiments, the treatment regimen is one dose of an effective amount of a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, tyragolumab) more than one dosing cycle.
또한, 본원에서는 대상체 또는 대상체 집단에서 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)을 치료하는데 사용하기 위한 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))을 포함하는 약학적 조성물이 제공되며, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체(예컨대, 티라골루맙)와 병용한 상기 PD-1 축 결합 길항제의 투여를 포함한 치료 요법을 포함한다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다.Also disclosed herein is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, an anti-PD-L1 antagonist antibody) for use in treating liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects. , atezolizumab)), wherein said treatment comprises a treatment regimen comprising administration of said PD-1 axis binding antagonist in combination with said anti-TIGIT antagonist antibody (eg, tiragolumab). do. In some embodiments, the treatment regimen is one dose of an effective amount of a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, tyragolumab) more than one dosing cycle.
또한, 본원에서는 대상체 또는 대상체 집단에서 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)을 치료하는데 사용하기 위한 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))을 포함하는 약학적 조성물이 제공되며, 여기서 상기 치료는 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)와 병용한 상기 PD-1 축 결합 길항제의 투여를 포함한 치료 요법을 포함한다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다.Also disclosed herein is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, an anti-PD-L1 antagonist antibody) for use in treating liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects. , atezolizumab)), wherein the treatment is in combination with a VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) and an anti TIGIT antagonist antibody (eg, tiragolumab) treatment regimens comprising administration of one of said PD-1 axis binding antagonists. In some embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) )), and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tyragolumab).
다른 예에서, 본원에서는 대상체 또는 대상체 집단에서 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)을 치료하는데 사용하기 위한 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))를 포함하는 약학적 조성물이 제공되며, 여기서 상기 치료는 PD-1 축 결합 길항제(예: 항 PD-L1 길항제 항체(예: 아테졸리주맙)) 및 항 TIGIT 길항제 항체(예: 티라골루맙)와 병용한 상기 VEGF 길항제의 투여를 포함한 치료 요법을 포함한다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다.In another example, disclosed herein is a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) for use in treating liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects. ) is provided, wherein the treatment comprises a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tyragolumab) treatment regimens comprising administration of said VEGF antagonist in combination with In some embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) )), and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tyragolumab).
다른 예에서, 본원에서는 대상체 또는 대상체 집단에서 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC)을 치료하는데 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)를 포함하는 약학적 조성물이 제공되며, 여기서 상기 치료는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))와 병용한 상기 항 TIGIT 길항제 항체의 투여를 포함한 치료 요법을 포함한다. 일부 구현예들에서, 상기 치료 요법은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)의 1회 이상의 투약 주기를 포함한다. In another example, disclosed herein is a pharmaceutical comprising an anti-TIGIT antagonist antibody (eg, tyragolumab) for use in treating liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects. An antagonist composition is provided, wherein the treatment comprises a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab))) treatment regimens including administration of the anti-TIGIT antagonist antibody in combination with In some embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) )), and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tyragolumab).
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에 대한 일부 구현예들에서, 간암은 조기 또는 말기일 수 있다. 일부 구현예들에서, 상기 간암은 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)이다. 일부 경우들에서, 상기 간암은 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC이다. 일부 구현예들에서, 상기 간암은 고위험 간암(예컨대, 고위험 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)이다. 일부 구현예들에서, 상기 고위험 간암은 하기의 특징들: VP4 PVTT, 담관 침윤, 및/또는 간의 ≥ 50%의 종양 점유 중 하나 이상을 포함한다.In some embodiments of any method, use, or composition for use described herein, the liver cancer may be early or late. In some embodiments, the liver cancer is HCC (eg, locally advanced or metastatic and/or unresectable HCC). In some cases, the liver cancer is locally advanced or metastatic and/or unresectable HCC. In some embodiments, the liver cancer is high risk liver cancer (eg, high risk locally advanced or metastatic and/or unresectable HCC). In some embodiments, the high-risk liver cancer comprises one or more of the following characteristics: VP4 PVTT, bile duct infiltration, and/or tumor occupancy >50% of the liver.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 치료는 치료 후 상기 대상체 또는 대상체 집단에서 반응을 유발한다. 예를 들어, 일부 구현예들에서, 상기 치료는 기준 치료와 비교하여 상기 대상체 또는 대상체 집단이 객관적 반응을 가질 가능성을 증가시키고, 상기 대상체 또는 대상체 집단의 PFS를 연장시키고, 상기 대상체 또는 대상체의 OS를 연장시키고, 상기 대상체 또는 대상체 집단의 방사선 진행까지의 시간(TTRP)을 연장시키고, 상기 대상체 또는 대상체 집단의 반응 지속 기간(DOR)을 연장시키고, 그리고/또는, 사망 위험을 감소시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 5.6개월(예컨대, 5.6개월 내지 14개월(예컨대, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6개월, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 또는 14개월))의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 6.83개월(예컨대, 6.9개월, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 또는 14개월)의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 치료는 적어도 약 5.6개월 내지 적어도 약 6.83개월(예컨대, 적어도 약 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.1개월, 6.2개월, 6.3개월, 6.4개월, 6.5개월, 6.6개월, 6.7개월, 6.8개월, 또는 6.83개월)의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 구현예들에서, 상기 기준 치료는 현재의 치료 표준을 포함한다. 일부 구현예들에서, 상기 기준 치료는 항 TIGIT 길항제 항체 없는 PD-1 축 결합 길항제(예컨대, 아테졸리주맙) 및 VEGF 길항제(예컨대, 베바시주맙)를 포함한다. 일부 구현예들에서, 상기 기준 치료는 PD-1 축 결합 길항제 및 VEGF 길항제를 포함한다. 일부 구현예들에서, 상기 기준 치료는 VEGF 길항제 없이 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 포함한다. 일부 구현예들에서, 상기 기준 치료는 PD-1 축 결합 길항제 없이 VEGF 길항제 및 항 TIGIT 길항제 항체를 포함한다. 일부 구현예들에서, 상기 기준 치료는 VEGF 길항제 및 항 TIGIT 길항제 항체 없는 PD-1 축 결합 길항제를 포함한다. 일부 구현예들에서, 상기 기준 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제 없이 VEGF 길항제를 포함한다. 일부 구현예들에서, 상기 기준 치료는 VEGF 길항제 및 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한다. In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the treatment elicits a response in the subject or population of subjects following treatment. For example, in some embodiments, the treatment increases the likelihood that the subject or population of subjects will have an objective response, prolongs the PFS of the subject or population of subjects, and the OS of the subject or subject as compared to reference treatment prolongs the time to radiation progression (TTRP) of the subject or population of subjects, prolongs the duration of response (DOR) of the subject or population of subjects, and/or reduces the risk of death. In some embodiments, the treatment is at least about 5.6 months (eg, 5.6 to 14 months (eg, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6 months, 7 months, 8 months, 9 months, 10 months) , 11 months, 12 months, 13 months, or 14 months)))). In some embodiments, the treatment provides for a median PFS of a population of subjects of at least about 6.83 months (eg, 6.9 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months). causes In some embodiments, the treatment is at least about 5.6 months to at least about 6.83 months (e.g., at least about 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.1 months, 6.2 months, 6.3 months, 6.4 months, 6.5 months, 6.6 months, 6.7 months, 6.8 months, or 6.83 months). In some embodiments, the standard of care comprises current standard of care. In some embodiments, the standard of care comprises a PD-1 axis binding antagonist (eg, atezolizumab) and a VEGF antagonist (eg, bevacizumab) without an anti-TIGIT antagonist antibody. In some embodiments, the reference of treatment comprises a PD-1 axis binding antagonist and a VEGF antagonist. In some embodiments, the standard of care comprises a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody without a VEGF antagonist. In some embodiments, the standard of care comprises a VEGF antagonist and an anti TIGIT antagonist antibody without a PD-1 axis binding antagonist. In some embodiments, the reference of treatment comprises a PD-1 axis binding antagonist without a VEGF antagonist and an anti-TIGIT antagonist antibody. In some embodiments, the standard of care comprises an anti-TIGIT antagonist antibody and a VEGF antagonist without a PD-1 axis binding antagonist. In some embodiments, the standard of care comprises an anti-TIGIT antagonist antibody without a VEGF antagonist and a PD-1 axis binding antagonist.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 치료 반응(들)은 임의의 적합한 표준 암 치료 요법과 비교하여 개선될 수 있다. 일부 구현예들에서, 표준 암 치료 요법은 표준 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제 불가능한 HCC를 포함한 HCC) 치료 요법이다. 일부 구현예들에서, 상기 표준 간암(예컨대, HCC) 치료 요법은 티로신 키나아제 억제제를 포함한다. 일부 구현예들에서, 상기 티로신 키나아제 억제제는 다중 키나아제 억제제이다. 일부 구현예들에서, 상기 다중키나아제 억제제는 소라페닙 또는 렌바티닙이다. 일부 구현예들에서, 상기 다중키나아제 억제제는 소라페닙이다.In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the therapeutic response(s) may be improved as compared to any suitable standard cancer treatment regimen. In some embodiments, the standard of care cancer treatment regimen is standard liver cancer (eg, HCC including locally advanced or metastatic and/or unresectable HCC) treatment regimen. In some embodiments, the standard of care for liver cancer (eg, HCC) treatment regimen comprises a tyrosine kinase inhibitor. In some embodiments, the tyrosine kinase inhibitor is a multiple kinase inhibitor. In some embodiments, the multikinase inhibitor is sorafenib or lenvatinib. In some embodiments, the multikinase inhibitor is sorafenib.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 또는 이의 약제는 하나 이상의 추가 항암 치료제(들)(예컨대, 화학요법제, 세포독성제, 성장 억제제, 방사선치료/방사선 요법, 및/또는 항호르몬제, 예컨대 상기 본원에 인용된 것들)와 병용으로(별로도 또는 함께) 투여하거나, 약제의 제조에 사용하거나, 투여를 위해 제형화될 수 있다. In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab), PD- The uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), or an agent thereof, is one or more additional anti-cancer therapeutic agent(s) ) (e.g., chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapy, and/or anti-hormonal agents, such as those recited herein above) (separately or together), or It may be used in manufacture or formulated for administration.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 이전에 상기 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함한 HCC)에 대한 치료를 받은 적이 없다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 적어도 한 라인의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 적어도 두 라인의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 이전에 전신 요법을 1회 이상 2회 이하로 받았고, 그리고/또는 이에 허용되는 치료 표준이 존재하지 않는다. 일부 경우들에서, 상기 대상체 또는 대상체 집단은 두 라인의 초과의 선행 요법을 받지 않았다. 일부 경우들에서, 상기 선행 요법이 화학요법, 수술, 및/또는 방사선 요법이다. 일부 경우들에서, 상기 선행 요법은 면역 요법이다. 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 이전에 상기 간암(예컨대, HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC))에 대한 치료를 받은 적이 없다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 이전에 HCC에 대해 치료를 받는다. 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 이전에 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC에 대한 치료를 받지 않았다.In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the subject or population of subjects has previously had the liver cancer (e.g., locally advanced or metastatic and/or unresectable HCC comprising HCC) has never been treated. In some cases, the subject or population of subjects has not received prior therapy. In some cases, the subject or population of subjects has not received at least one line of prior therapy. In some cases, the subject or population of subjects has not received at least two lines of prior therapy. In some cases, the subject or population of subjects has previously received at least one or two or fewer systemic therapies, and/or there is no acceptable standard of care. In some cases, the subject or population of subjects has not received more than two lines of prior therapy. In some cases, the prior therapy is chemotherapy, surgery, and/or radiation therapy. In some cases, the prior therapy is immunotherapy. In some embodiments, the subject or population of subjects has not previously been treated for the liver cancer (eg, HCC (eg, locally advanced or metastatic and/or unresectable HCC)). In some embodiments, the subject or population of subjects has previously been treated for HCC. In some embodiments, the subject or population of subjects has not previously received treatment for locally advanced or metastatic and/or unresectable HCC.
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 대상체 또는 대상체의 집단은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함한 HCC)에 대한 선행 사전 요법을 받은 적이 없다. 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 간암(예컨대, HCC)에 대한 선행 전신 요법을 받은 적이 없다.In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the subject or population of subjects is suffering from liver cancer (eg, HCC including locally advanced or metastatic and/or unresectable HCC). No prior prior therapy for In some embodiments, the subject or population of subjects has not received prior systemic therapy for liver cancer (eg, HCC).
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 PD-1 축 결합 길항제, VEGF 길항제, 또는 항 TIGIT 길항제 항체를 이용한 선행 치료를 받은 적이 없다.In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the subject or population of subjects has received prior treatment with a PD-1 axis binding antagonist, VEGF antagonist, or anti-TIGIT antagonist antibody. never received
본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 약학적 조성물에 대한 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 임의의 적합한 차일드-퍼 간 기능을 가질 수 있다. 예를 들어, 일부 구현예들에서, 상기 대상체 또는 대상체 집단은 차일드-퍼 부류 A 간 기능을 가진다.In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the subject or population of subjects may have any suitable child-per-liver function. For example, in some embodiments, the subject or population of subjects has child-fur class A liver function.
임의의 적합한 PD-1 축 결합 길항제, VEGF 길항제, 또는 항 TIGIT 길항제 항체가 본원에 기재된 방법, 사용, 또는 사용을 위한 약학적 조성물에 사용될 수 있다. 예를 들어, 당해 분야에 공지되거나 본원에 기재된 임의의 PD-1 축 결합 길항제, VEGF 길항제, 또는 항 TIGIT 길항제 항체가 본원에 기재된 방법, 사용, 또는 사용을 위한 약학적 조성물에 사용될 수 있다. 일부 구현예들에서, 상기 PD-1 축 결합 길항제는 항 PD-L1 항체 또는 항 PD-1 항체이다. 일부 구현예들에서, 상기 항 PD-L1 항체는 아테졸리주맙이다. 일부 구현예들에서, 상기 VEGF 길항제는 항 VEGF 항체이다. 일부 구현예들에서, 상기 항 VEGF 항체는 베바시주맙이다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 티라골루맙이다.Any suitable PD-1 axis binding antagonist, VEGF antagonist, or anti-TIGIT antagonist antibody can be used in the methods, uses, or pharmaceutical compositions for use described herein. For example, any PD-1 axis binding antagonist, VEGF antagonist, or anti TIGIT antagonist antibody known in the art or described herein can be used in a method, use, or pharmaceutical composition for use described herein. In some embodiments, the PD-1 axis binding antagonist is an anti-PD-L1 antibody or an anti-PD-1 antibody. In some embodiments, the anti-PD-L1 antibody is atezolizumab. In some embodiments, the VEGF antagonist is an anti-VEGF antibody. In some embodiments, the anti-VEGF antibody is bevacizumab. In some embodiments, the anti-TIGIT antagonist antibody is tyragolumab.
예시적인 방법들Exemplary methods
일 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 대상체 또는 대상체 집단을 치료하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재되는 바와 같이 서열번호 17 또는 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 이전에 HCC, 예컨대 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC에 대한 치료를 받지 않았다.In one aspect, the invention provides a subject or one or more dosing cycles of a 600 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks and a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks. Provided is a method of treating a subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the subject population, wherein the anti-TIGIT antagonist antibody comprises a sequence as further described below a VH domain having the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the subject or population of subjects has not previously received treatment for HCC, such as locally advanced or metastatic and/or unresectable HCC.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙, 및 3주마다 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 대상체 또는 대상체 집단을 치료하는 방법을 제공하고, 여기서 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재되는 바와 같이 서열번호 17 또는 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another embodiment, the invention provides a 600 mg dose (eg, fixed dose) of anti-TIGIT antagonist antibody every 3 weeks, a 1200 mg dose (eg, fixed dose) of atezolizumab every 3 weeks, and 15 mg/kg every 3 weeks Provided is a method of treating a subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the subject or population of subjects one or more dosing cycles of a dose of bevacizumab, wherein The anti-TIGIT antagonist antibody comprises a VH domain having the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19 as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다. In another embodiment, the present invention provides a subject or subject with one or more dosing cycles of a 600 mg dose (eg, a fixed dose) tiragolumab every 3 weeks and a 1200 mg dose (eg, a fixed dose) atezolizumab every 3 weeks. Provided is a method of treating said subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the population.
다른 양태에서, 본 발명은 3주마다 600 mg 용량의(예컨대, 고정 용량) 티라골루맙, 3주마다 1200 mg 용량의(예컨대, 고정 용량) 아테졸리주맙, 및 3주마다 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다.In another embodiment, the present invention provides a dose of 600 mg (eg, a fixed dose) tiragolumab every 3 weeks, a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks, and a 15 mg/kg dose every 3 weeks. Provided is a method of treating a subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the subject or population of subjects one or more dosing cycles of bevacizumab of
다른 양태에서, 본 발명은 2주마다 420 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 2주마다 840 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다.In another embodiment, the invention provides a subject or subject one or more dosing cycles of a 420 mg dose (eg, a fixed dose) tiragolumab every 2 weeks and a 840 mg dose (eg, a fixed dose) atezolizumab every 2 weeks. Provided is a method of treating said subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the population.
다른 양태에서, 본 발명은 2주마다 420 mg 용량의(예컨대, 고정 용량) 티라골루맙, 2주마다 840 mg 용량의(예컨대, 고정 용량) 아테졸리주맙, 및 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다.In another embodiment, the present invention provides a dose of 420 mg (eg, a fixed dose) tiragolumab every 2 weeks, a 840 mg dose (eg, a fixed dose) of atezolizumab every 2 weeks, and 5 mg/kg every 2 weeks, The subject or subject having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the subject or population of subjects one or more dosing cycles of bevacizumab at a dose of 7.5 mg/kg, or 10 mg/kg. A method of treating a population of
다른 양태에서, 본 발명은 4주마다 840 mg 용량의(예컨대, 고정 용량) 티라골루맙 및 4주마다 1680 mg 용량의(예컨대, 고정 용량) 아테졸리주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다. In another embodiment, the invention provides a subject or subject one or more dosing cycles of an 840 mg dose (eg, a fixed dose) of tiragolumab every 4 weeks and a 1680 mg dose (eg, a fixed dose) of atezolizumab every 4 weeks. Provided is a method of treating said subject or population of subjects having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the population.
다른 양태에서, 본 발명은 4주마다 840 mg 용량의(예컨대, 고정 용량) 티라골루맙, 4주마다 1680 mg 용량의(예컨대, 고정 용량) 아테졸리주맙, 및 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 대상체 또는 대상체 집단에 투여함으로써 HCC(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC)를 가진 상기 대상체 또는 대상체의 집단을 치료하는 방법을 제공한다. In another embodiment, the present invention provides a dose of 840 mg (eg, a fixed dose) tiragolumab every 4 weeks, a 1680 mg dose (eg, a fixed dose) of atezolizumab every 4 weeks, and 5 mg/kg every 2 weeks, The subject or subject having HCC (eg, locally advanced or metastatic and/or unresectable HCC) by administering to the subject or population of subjects one or more dosing cycles of bevacizumab at a dose of 7.5 mg/kg, or 10 mg/kg. A method of treating a population of
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))을 제공하고, 여기서 상기 방법은 유효량의 항 TIGIT 길항제 항체 및 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에 투여하는 단계를 포함한다.In another aspect, the invention provides an anti-TIGIT antagonist antibody ( For example, provided are an anti TIGIT antagonist antibody, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) disclosed herein, wherein the method comprises an effective amount of an anti administering to the subject or population of subjects one or more dosing cycles of a TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에 사용하기 위한 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))을 제공하고, 여기서 상기 방법은 유효량의 항 TIGIT 길항제 항체, 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 유효량의 VEGF 길항제(예컨대, 항 VEGF 항체(예: 베바시주맙))의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에 투여하는 단계를 포함한다.In another aspect, the invention provides an anti-TIGIT antagonist antibody ( For example, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, , bevacizumab)), wherein the method comprises an effective amount of an anti TIGIT antagonist antibody, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an effective amount of VEGF administering to the subject or population of subjects one or more dosing cycles of an antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)).
예시적인 약제 및 이의 용도Exemplary medicaments and uses thereof
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 2000 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a dose (eg, a fixed dose) of about 30 mg to about 1200 mg (eg, a fixed dose) of anti-TIGIT every 3 weeks. Formulations for administration of an antagonist antibody, and a dose of about 80 mg to about 2000 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 3 weeks get angry In some embodiments, the medicament is a 30 mg to 1200 mg dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody every 3 weeks and a PD-1 axis binding at a 80 mg to 2000 mg dose (eg, a fixed dose) every 3 weeks It is formulated for administration of an antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 30 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 2000 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 3주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 3주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered for 3 weeks. at a dose of about 30 mg to about 1200 mg per (eg, fixed dose) anti-TIGIT antagonist antibody, every 3 weeks at a dose of about 80 mg to about 2000 mg (eg, fixed dose) of PD-1 axis binding antagonist (eg, anti-PD) -L1 antagonist antibody (eg, atezolizumab)), and formulations for administration of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) at a dose of about 0.1 mg/kg to 50 mg/kg every 3 weeks get angry In some aspects, the medicament is a 30 mg to 1200 mg dose (eg, fixed dose) of anti-TIGIT antagonist antibody every 3 weeks, a 80 mg to 2000 mg dose (eg, a fixed dose) of PD-1 axis binding every 3 weeks An antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) at a dose of about 0.1 mg/kg to 50 mg/kg every 3 weeks) ) is formulated for administration.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 2주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 2주마다 약 80 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 2주마다 30 mg 내지 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 80 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a dose (eg, a fixed dose) of about 30 mg to about 600 mg every two weeks (eg, a fixed dose) of anti-TIGIT. Formulations for administration of an antagonist antibody, and a dose of about 80 mg to about 1200 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every two weeks get angry In some embodiments, the medicament is a 30 mg to 600 mg dose (eg, a fixed dose) of anti-TIGIT antagonist antibody every 2 weeks and a PD-1 axis binding at a dose of 80 mg to 1200 mg (eg, a fixed dose) every 2 weeks. It is formulated for administration of an antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 2주마다 약 30 mg 내지 약 600 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 2주마다 약 80 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 2주마다 30 mg 내지 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 2주마다 80 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 2주마다 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered for 2 weeks. at a dose of about 30 mg to about 600 mg per (eg, fixed dose) anti-TIGIT antagonist antibody, every two weeks at a dose of about 80 mg to about 1200 mg (eg, fixed dose) of PD-1 axis binding antagonist (eg, anti-PD) -L1 antagonist antibody (eg, atezolizumab)), and formulations for administration of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) at a dose of about 0.1 mg/kg to 50 mg/kg every two weeks get angry In some embodiments, the medicament is a 30 mg to 600 mg dose (eg, fixed dose) of anti-TIGIT antagonist antibody every 2 weeks, a 80 mg to 1200 mg dose (eg, a fixed dose) of PD-1 axis binding every 2 weeks An antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), and a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab) at a dose of 0.1 mg/kg to 50 mg/kg every two weeks) formulated for administration.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 4주마다 약 600 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 및 4주마다 약 1200 mg 내지 약 2000 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 4주마다 600 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 1200 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a dose of about 600 mg to about 1200 mg (eg, a fixed dose) of anti-TIGIT every 4 weeks. Formulations for administration of an antagonist antibody, and a dose of about 1200 mg to about 2000 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 4 weeks get angry In some embodiments, the medicament is a 600 mg to 1200 mg dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody every 4 weeks and a 1200 mg to 2000 mg dose (eg, a fixed dose) of the PD-1 axis binding every 4 weeks It is formulated for administration of an antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 4주마다 약 600 mg 내지 약 1200 mg 용량의(예컨대, 고정 용량) 항 TIGIT 길항제 항체, 4주마다 약 1200 mg 내지 약 2000 mg 용량의(예컨대, 고정 용량) PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 4주마다 600 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 4주마다 1200 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 2주마다 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered for 4 weeks. at a dose of about 600 mg to about 1200 mg per (eg, fixed dose) anti-TIGIT antagonist antibody, every 4 weeks at a dose of about 1200 mg to about 2000 mg (eg, fixed dose) of PD-1 axis binding antagonist (eg, anti-PD) -L1 antagonist antibody (eg, atezolizumab)), and formulations for administration of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) at a dose of about 0.1 mg/kg to 50 mg/kg every two weeks get angry In some embodiments, the medicament is a 600 mg to 1200 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 4 weeks, a 1200 mg to 2000 mg dose (eg, a fixed dose) of the PD-1 axis binding every 4 weeks An antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) at a dose of 0.1 mg/kg to 50 mg/kg every 2 weeks) formulated for administration.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 80 mg 내지 약 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 3주마다 80 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the agent and an anti-TIGIT antagonist antibody, wherein the agent is administered at a dose of about 80 mg to about 2000 mg every 3 weeks (eg, a fixed dose). dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a dose of about 30 mg to about 1200 mg (e.g., a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks formulated for administration. In some aspects, the medicament is administered at a dose of 80 mg to 2000 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 3 weeks and 3 weeks It is formulated for administration of an anti TIGIT antagonist antibody to be administered in a 30 mg to 1200 mg dose (eg, a fixed dose) per hour.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 3주마다 약 80 mg 내지 약 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 및 3주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 3주마다 80 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체, 및 3주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the agent and an anti-TIGIT antagonist antibody, The agent is administered at a dose of about 80 mg to about 2000 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), about 30 every 3 weeks. Anti-TIGIT antagonist antibody at a dose of mg to about 1200 mg (eg, a fixed dose), and a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab) at a dose of about 0.1 mg/kg to 50 mg/kg every 3 weeks) formulated for administration. In some aspects, the medicament is administered at a dose of 80 mg to 2000 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 3 weeks, 3 weeks An anti-TIGIT antagonist antibody to be administered at a dose of 30 mg to 1200 mg per (eg, a fixed dose), and a dose of about 0.1 mg/kg to 50 mg/kg of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevaciz) every 3 weeks mob))).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 2주마다 약 80 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 2주마다 약 30 mg 내지 약 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 2주마다 80 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 2주마다 30 mg 내지 600 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects at least one dosing cycle of the agent and an anti-TIGIT antagonist antibody, wherein the agent is administered at a dose of about 80 mg to about 1200 mg every two weeks (e.g., a fixed dose) dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a dose of about 30 mg to about 600 mg (e.g., a fixed dose) of an anti TIGIT antagonist antibody every two weeks formulated for administration. In some aspects, the medicament is administered at a dose of 80 mg to 1200 mg (eg, a fixed dose) every 2 weeks of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and 2 weeks It is formulated for administration of an anti-TIGIT antagonist antibody to be administered in a 30 mg to 600 mg dose (eg, a fixed dose) per dose.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 2주마다 약 80 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 2주마다 약 30 mg 내지 약 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 2주마다 80 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 2주마다 30 mg 내지 600 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체, 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the agent and an anti-TIGIT antagonist antibody, The agent is administered at a dose of about 80 mg to about 1200 mg every two weeks (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), about 30 every two weeks. Anti-TIGIT antagonist antibody at a dose of mg to about 600 mg (eg, a fixed dose), and a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab) at a dose of about 0.1 mg/kg to 50 mg/kg every two weeks) formulated for administration. In some embodiments, the medicament is administered at a dose of 80 mg to 1200 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 2 weeks, 2 weeks An anti-TIGIT antagonist antibody to be administered at a dose of 30 mg to 600 mg per (eg, a fixed dose), and a dose of about 0.1 mg/kg to 50 mg/kg of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevaciz) every two weeks mob))).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 4주마다 약 1200 mg 내지 약 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 4주마다 약 600 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 4주마다 1200 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 및 4주마다 600 mg 내지 1200 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. providing the use of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein the method comprises administering to the subject or population of subjects at least one dosing cycle of the agent and an anti-TIGIT antagonist antibody, wherein the agent is administered at a dose of about 1200 mg to about 2000 mg every 4 weeks (e.g., a fixed dose) dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and a dose of about 600 mg to about 1200 mg every 4 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody formulated for administration. In some aspects, the medicament is administered at a dose of 1200 mg to 2000 mg (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 4 weeks and 4 weeks It is formulated for administration of an anti-TIGIT antagonist antibody to be administered in a 600 mg to 1200 mg dose (eg, a fixed dose) per dose.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 약제의 제조에서의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 사용을 제공하고, 여기서 상기 방법은 상기 약제 및 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 상기 약제는 4주마다 약 1200 mg 내지 약 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 4주마다 약 600 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다. 일부 양태들에서, 상기 약제는 4주마다 1200 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 4주마다 600 mg 내지 1200 mg 용량(예컨대, 고정 용량)으로 투여될 항 TIGIT 길항제 항체, 및 2주마다 약 0.1 mg/kg 내지 50 mg/kg 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 위해 제형화된다.In another aspect, the invention provides a medicament for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) in the manufacture of a medicament. anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, such as tyragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), and VEGF antagonists (eg, , an anti-VEGF antibody (eg, bevacizumab)), wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the agent and an anti-TIGIT antagonist antibody, The agent is administered at a dose of about 1200 mg to about 2000 mg every 4 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), about 600 every 4 weeks Anti-TIGIT antagonist antibody at a dose of mg to about 1200 mg (eg, a fixed dose), and a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab) at a dose of about 0.1 mg/kg to 50 mg/kg every two weeks) formulated for administration. In some aspects, the medicament is a 1200 mg to 2000 mg dose (eg, a fixed dose) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 4 weeks, 4 weeks An anti-TIGIT antagonist antibody to be administered at a dose of 600 mg to 1200 mg per day (eg, a fixed dose), and a dose of about 0.1 mg/kg to 50 mg/kg of a VEGF antagonist (eg, anti-VEGF antibody (eg, bevaciz) every two weeks mob))).
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the present invention provides an anti-TIGIT antagonist antibody and Provided is the use of atezolizumab, wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a 600 mg dose (e.g., fixed dose) of an anti TIGIT antagonist antibody and a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks, wherein the anti TIGIT antagonist antibody is further described in SEQ ID NO: 17 or a VH domain comprising the amino acid sequence of SEQ ID NO: 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체, 아테졸리주맙, 및 베바시주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 3주마다 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙, 3주마다 15 mg/kg 용량의 베바시주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides an anti-TIGIT antagonist antibody for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC); Provided is a use of atezolizumab, and bevacizumab, wherein the method comprises administering to the subject or population of subjects at least one dosing cycle of the medicament, wherein the medicament is 600 mg every 3 weeks. Formulated for administration of a dose (eg, a fixed dose) of an anti TIGIT antagonist antibody, a 1200 mg dose (eg, a fixed dose) of atezolizumab every 3 weeks, a 15 mg/kg dose of bevacizumab every 3 weeks, The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19, as further described below. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 2주마다 420 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 840 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides an anti-TIGIT antagonist antibody and Provided is the use of atezolizumab, wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a dose of 420 mg every two weeks (e.g., a fixed dose) of an anti TIGIT antagonist antibody and an 840 mg dose (eg, a fixed dose) of atezolizumab every two weeks, wherein the anti TIGIT antagonist antibody is further described in SEQ ID NO: 17 or a VH domain comprising the amino acid sequence of SEQ ID NO: 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체, 아테졸리주맙, 및 베바시주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 2주마다 420 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 2주마다 840 mg 용량(예컨대, 고정 용량)의 아테졸리주맙, 및 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg 용량의 베바시주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides an anti-TIGIT antagonist antibody for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC); Provided is a use of atezolizumab, and bevacizumab, wherein the method comprises administering to the subject or population of subjects at least one dosing cycle of the medicament, wherein the medicament is 420 mg every two weeks. A dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody, a dose of 840 mg (eg, a fixed dose) of atezolizumab every 2 weeks, and a dose of 5 mg/kg, 7.5 mg/kg, or 10 mg/kg every 2 weeks bevacizumab, wherein the anti-TIGIT antagonist antibody is further described below: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19 includes In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 4주마다 840 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 1680 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the present invention provides an anti-TIGIT antagonist antibody and Provided is the use of atezolizumab, wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of the medicament, wherein the medicament is administered at a dose of 840 mg every 4 weeks (e.g., a fixed dose) of an anti TIGIT antagonist antibody and a 1680 mg dose (eg, a fixed dose) of atezolizumab every 4 weeks, wherein the anti TIGIT antagonist antibody is further described in SEQ ID NO: 17 or a VH domain comprising the amino acid sequence of SEQ ID NO: 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
다른 양태에서, 본 발명은 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체, 아테졸리주맙, 및 베바시주맙의 사용을 제공하고, 여기서 상기 방법은 상기 약제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하며, 여기서 상기 약제는 4주마다 840 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 4주마다 1680 mg 용량(예컨대, 고정 용량)의 아테졸리주맙, 및 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg 용량의 베바시주맙의 투여를 위해 제형화되고, 상기 항 TIGIT 길항제 항체는 하기에 추가로 기재된 바와 같이: 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함한 VL 도메인을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 갖는 VH 도메인 및 서열번호 19의 아미노산 서열을 갖는 VL 도메인을 가진다.In another aspect, the invention provides an anti TIGIT antagonist antibody for use in a method of treating a subject or population of subjects having liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC); Provided is a use of atezolizumab, and bevacizumab, wherein the method comprises administering to the subject or population of subjects at least one dosing cycle of the medicament, wherein the medicament is 840 mg every 4 weeks. A dose (eg, a fixed dose) of the anti-TIGIT antagonist antibody, a 1680 mg dose (eg, a fixed dose) of atezolizumab every 4 weeks, and a 5 mg/kg, 7.5 mg/kg, or 10 mg/kg dose every 2 weeks bevacizumab, wherein the anti-TIGIT antagonist antibody is further described below: a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19 includes In some cases, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 17 and a VL domain having the amino acid sequence of SEQ ID NO: 19. In some cases, the anti TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO: 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19.
투약 요법 및 투여Dosage regimen and administration
일 양태에서, 본원에 기재된 본 발명의 치료 방법 및 사용은 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), VEGF 길항제(예컨대, 항 VEGF 길항제(예컨대, 베바시주맙)), 및 항 TIGIT 길항제 항체(예컨대, 티라골루맙)을 포함한 치료 요법을 간암(예컨대, 국소 진행성 또는 전이성 및/또는 절제불가능한 HCC를 포함하는 간세포 암종(HCC))을 가진 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다.In one aspect, the therapeutic methods and uses of the invention described herein comprise an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antagonist ( treatment regimens including bevacizumab), and an anti-TIGIT antagonist antibody (eg, tiragolumab) with liver cancer (eg, hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC). administering to a subject or population of subjects.
본원에 기재된 약학적 조성물은 하기 및 섹션 III(K)에 기재된 바와 같이 투여용으로 제형화될 수 있다.The pharmaceutical compositions described herein may be formulated for administration as described below and in Section III(K).
유효량effective amount
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 섹션 III(K)에 기재된 용량의 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))와의 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)와의 병용 치료)으로 투여되고, 상기 용량은 단일요법으로 투여되는 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 투약은 섹션 III(K)에 기재되어 있다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of the VEGF antagonist (eg, anti-VEGF antibody (eg, beva) described in Section III(K). shizumab))) (e.g., combination therapy with a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), wherein the dose is administered as a monotherapy. Can be reduced compared to standard dose of antagonist antibody Dosing of anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, and VEGF antagonist is described in section III(K).
투약 주기dosing cycle
본 발명의 임의의 방법 및 사용에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 1회 이상의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 20회, 21회, 22회, 23회, 24회, 25회, 26회, 27회, 28회, 29회, 30회, 31회, 32회, 33회, 34회, 35회, 36회, 37회, 38회, 39회, 40회, 41회, 42회, 43회, 44회, 45회, 46회, 47회, 48회, 49회, 또는 50회 이상의 투약 주기)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체((예컨대, 아테졸리주맙)), 및/또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망, 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일 내지 28일(예컨대, 14일, 15일, 16일, 17일, 18일, 19일, 20일, 21일, 22일, 23일, 24일, 25일, 26일, 27일, 또는 28일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 28일이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 21일 주기의 제 1일에 약 15 mg/kg의 용량으로(즉, 3주마다 약 15 mg/kg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 투약 주기의 제 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 투약 주기의 제 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 21일 주기의 제 1일에 15 mg/kg의 용량으로(즉, 3주마다 15 mg/kg의 용량으로) 정맥내 투여된다. In any of the methods and uses of the invention, said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) (eg, atezolizumab)), or the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered in one or more dosing cycles (eg, 1, 2, 3, 4, 5). , 6 times, 7 times, 8 times, 9 times, 10 times, 11 times, 12 times, 13 times, 14 times, 15 times, 16 times, 17 times, 18 times, 19 times, 20 times, 21 times, 22 times times, 23 times, 24 times, 25 times, 26 times, 27 times, 28 times, 29 times, 30 times, 31 times, 32 times, 33 times, 34 times, 35 times, 36 times, 37 times, 38 times, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, ate jolizumab)), and/or the dosing cycle of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) results in loss of clinical benefit (eg, disease progression, drug resistance, death, or unacceptable toxicity). In some cases, the length of each dosing cycle is between about 14 days and 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days, 27 days, or 28 days) In some cases, the length of each dosing cycle is about 21 days. In some cases, each dosing The length of the cycle is about 14 days.In some cases, the length of each dosing cycle is about 28 days. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as Tyra) Goluumab) is administered on about day 1 (eg,
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대 아테졸리주맙)), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) )), and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered on about 1 day (eg, 1 day±3 days) of each dosing cycle.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 21일 주기의 제 1일에 약 15 mg/kg의 용량으로(즉, 3주마다 약 15 mg/kg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 21일 주기의 제 1일에 15 mg/kg의 용량으로(즉, 3주마다 15 mg/kg의 용량으로) 정맥내 투여된다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 600 mg on
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 14일 주기의 제 1일에 약 420 mg의 용량으로(즉, 2주마다 약 420 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 14일 주기의 제 1일에 약 840 mg의 용량으로(즉, 2주마다 약 840 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 14일 주기의 제 1일에 약 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로(즉, 2주마다 약 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로) 정맥내 투여된다. 다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 14일 주기의 제 1일에 420 mg의 용량으로(즉, 2주마다 420 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 14일 주기의 제 1일에 840 mg의 용량으로(즉, 2주마다 840 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 14일 주기의 제 1일에 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로(즉, 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로) 정맥내 투여된다. In other cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 420 mg (ie, every 2 weeks) on
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 28일 주기의 제 1일에 약 840 mg의 용량으로(즉, 4주마다 약 840 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 28일 주기의 제 1일에 약 1680 mg의 용량으로(즉, 4주마다 약 1680 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 28일 주기의 제 1일 및 15일에 약 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로(즉, 2주마다 약 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로) 정맥내 투여된다. 다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 28일 주기의 제 1일에 840 mg의 용량으로(즉, 4주마다 840 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제(예컨대, 아테졸리주맙))는 각 28일 주기의 제 1일에 1680 mg의 용량으로(즉, 4주마다 1680 mg의 용량으로) 정맥내 투여되며, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 각 28일 주기의 제 1일 및 15일에 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로(즉, 2주마다 5 mg/kg, 7.5 mg/kg, 또는 10 mg/kg의 용량으로) 정맥내 투여된다.In other instances, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 840 mg on
투여 순서 및 관찰 기간Dosing sequence and observation period
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및/또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))은 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다.In some cases, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is combined with the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) and/or prior to said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to said subject or population of subjects. In some cases, for example, after administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and the VEGF antagonist (eg, an anti-VEGF antibody (eg, beva) shizumab)) or the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), the method includes an interim first observation period. In some cases, for example, after administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), the VEGF antagonist (eg, an anti-VEGF antibody (eg, beva) shizumab)) is administered to said subject or population of subjects prior to said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab). In other cases, following administration of the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)), the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein) , such as tiragolumab) is administered to the subject or population of subjects prior to the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)). In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is first administered to the subject or population of subjects, and the VEGF antagonist (eg, anti-VEGF antibody) (eg, bevacizumab)) is administered to said subject or population of subjects after administration of said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein said anti-TIGIT antagonist An antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tiragolumab) is administered to the subject or population of subjects after administration of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab). In some instances In , the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is first administered to the subject or population of subjects, and the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody (eg, an anti- A TIGIT antagonist antibody, such as tyragolumab) is administered to the subject or population of subjects following administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), wherein the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab) is administered to the subject or population of subjects following administration of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab).
일부 경우들에서, 상기 방법은 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제2 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제3 관찰 기간을 추가로 포함한다. In some cases, the method comprises administering the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) or the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab). Further comprising a second observation period after administration. In some cases, the method comprises the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab))) , and a third observation period after administration of said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody, such as tyragolumab as disclosed herein).
일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 제1 관찰 기간, 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제2 관찰 기간을 모두 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 제1 관찰 기간, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제2 관찰 기간, 및 상기 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제 및 상기 VEGF 길항제의 투여 후에 제3 관찰 기간을 포함한다. 일부 경우들에서, 상기 제1, 제2, 및/또는 제3 관찰 기간은 각각 약 30분 내지 약 120분 길이(예컨대, 약 30분 내지 60분의 길이, 60분 내지 90분의 길이, 및/또는 또는 90분 내지 120분의 길이)이다. 상기 제1, 제2, 및 제3 관찰 기간이 각각 약 60분인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 동안 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 약 30 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다. 상기 제1, 제2, 및 제3 관찰 기간이 각각 약 30분인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 동안 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 약 15 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다.In some cases, the method comprises a first observation period following administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), and the VEGF antagonist (eg, anti-VEGF antibody). (eg, bevacizumab)) or a second observation period after administration of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragolumab as disclosed herein). In some cases, the method comprises a first observation period following administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), the VEGF antagonist (eg, an anti-VEGF antibody ( eg bevacizumab)) or a second observation period following administration of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody, such as tiragolumab as disclosed herein), and the TIGIT antagonist antibody, the PD-1 axis a third observation period following administration of the binding antagonist and said VEGF antagonist. In some cases, the first, second, and/or third observation periods are each between about 30 minutes and about 120 minutes in length (eg, between about 30 minutes and 60 minutes in length, between 60 minutes and 90 minutes in length, and / or between 90 minutes and 120 minutes in length). In instances where the first, second, and third observation periods are each about 60 minutes, the method comprises administering the PD-1 axis binding antagonist (eg, anti-PD-) during the first, second, or third observation period. L1 antagonist antibody (eg, atezolizumab)), said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), or said VEGF antagonist (eg, anti-VEGF antibody (eg, beva) recording the subject's vital signs (eg, pulse, respiration rate, blood pressure, body temperature) at about 30 ± 10 minutes after administration of shizumab)). In cases where the first, second, and third observation periods are each about 30 minutes, the method comprises, during the first, second, or third observation period, the PD-1 axis binding antagonist (eg, anti-PD- L1 antagonist antibody (eg, atezolizumab)), said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), or said VEGF antagonist (eg, anti-VEGF antibody (eg, beva) recording the subject's vital signs (eg, pulse, respiration rate, blood pressure, body temperature) at about 15±10 minutes after administration of shizumab)).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is combined with the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli). zumab) or the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) to the subject or population of subjects prior to administration.
일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 후에 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 후에, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 다른 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 후에, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))가 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))가 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다. In some cases, for example, after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or the VEGF antagonist (eg, anti-VEGF) Prior to administration of the antibody (eg, bevacizumab)), the method includes an intermediate first observation period.In some cases, for example, after administration of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to said subject or population of subjects prior to said VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)). In, for example, after administration of the anti-TIGIT antagonist antibody, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is combined with the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody ( For example, atezolizumab)) is administered to said subject or population of subjects before.In some cases, said anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is first administered to said administered to a subject or population of subjects, wherein said PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist as disclosed herein) administered to the subject or population of subjects after an antibody, such as tyragolumab, wherein the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered to the PD-1 axis binding antagonist (eg, anti-PD- After administration of the L1 antagonist antibody (eg, atezolizumab) is administered to the subject or population of subjects, in some cases, the anti-TIGIT antagonist antibody (eg, the anti-TIGIT antagonist antibody as disclosed herein, such as tyragol) Luumab) is first administered to the subject or population of subjects, and the VEGF antagonist (eg, anti-V An EGF antibody (eg, bevacizumab)) is administered to the subject or population of subjects after the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), wherein the PD-1 An axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to the subject or population of subjects after administration of the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) .
일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 제2 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 제3 관찰 기간을 추가로 포함한다. In some cases, the method comprises the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) or the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab))) and a second observation period after administration of In some cases, the method comprises the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, , atezolizumab)), and a third observation period after administration of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)).
일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 또는 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체의 투여 후에 제1 관찰 기간, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 제2 관찰 기간, 및 상기 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 VEGF 길항제의 투여 후에 제3 관찰 기간을 포함한다. 일부 경우들에서, 상기 제1, 제2, 및 제3 관찰 기간은 각각 약 30 분 내지 약 60 분 길이이다. 상기 제1, 제2, 제3 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙), 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1, 제2, 제3 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 중 각각 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 또는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 약 15 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the method comprises a first observation period following administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) or VEGF antagonist (eg, , a second observation period after administration of an anti-VEGF antibody (eg, bevacizumab)). In some cases, the method comprises a first observation period following administration of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) or the VEGF antagonist ( For example, a second observation period following administration of an anti-VEGF antibody (eg, bevacizumab)) and a third observation period following administration of the TIGIT antagonist antibody, the PD-1 axis binding antagonist, and the VEGF antagonist. In some cases, the first, second, and third observation periods are each about 30 minutes to about 60 minutes in length. In cases where the first, second, and third observation periods each have a length of about 60 minutes, the method comprises the anti-TIGIT antagonist antibody, the PD-1 during each of the first, second, or third observation period About 30 ± 10 minutes after administration of an axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab), or the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) to the subject or recording vital signs (e.g., pulse rate, respiration rate, blood pressure and temperature) of the subject population, where the first, second, and third observation periods are each about 30 minutes in length; The method comprises, during the first, second, or third observation period, the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), or the recording the vital signs (e.g., pulse rate, respiratory rate, blood pressure and temperature) of the subject or population of subjects about 15 ± 10 minutes after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) may include
일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)이 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 다른 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))가 먼저 상기 대상체 또는 대상체의 집단에 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 이후에 상기 대상체 또는 대상체의 집단에 투여되며, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 상기 대상체 또는 대상체의 집단에 투여된다. In some cases, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) is the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) or the PD- A uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to the subject or population of subjects prior to. In some cases, for example, after administration of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) and the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyra Prior to administration of goluumab) or the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), the method includes an interim first observation period. In some cases, for example, after administration of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)), the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyra golumab) is administered to the subject or population of subjects prior to the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In other cases, for example, after administration of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)), the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, ate jolizumab)) is administered to said subject or population of subjects prior to said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab). In some cases, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) is first administered to the subject or population of subjects, and the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, For example, tiragolumab) is administered to the subject or population of subjects after administration of the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), and the PD-1 axis binding antagonist (eg, anti-PD-L1) The antagonist antibody (eg, atezolizumab)) is administered to the subject or population of subjects following administration of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, such as tyragolumab). In some cases, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) is first administered to the subject or population of subjects, and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody) (eg, atezolizumab)) is administered to said subject or population of subjects after said VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)), wherein said anti TIGIT antagonist antibody (eg, an anti A TIGIT antagonist antibody, such as tiragolumab) is administered to the subject or population of subjects following administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 제2 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 방법은 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 제3 관찰 기간을 추가로 포함한다. In some cases, the method comprises the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) or the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, , a second observation period after administration of atezolizumab)). In some cases, the method comprises the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab), and a third observation period following administration of said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)).
일부 경우들에서, 상기 방법은 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 제1 관찰 기간, 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 제2 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 방법은 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후에 제1 관찰 기간, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 제2 관찰 기간, 및 상기 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 VEGF 길항제의 투여 후에 제3 관찰 기간을 포함한다. 일부 경우들에서, 상기 제1, 제2, 및 제3 관찰 기간은 각각 약 30 분 내지 약 60 분 길이이다. 상기 제1, 제2, 및 제3 관찰 기간이 각각 약 60분인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 동안 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 약 30 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다. 상기 제1, 제2, 및 제3 관찰 기간이 각각 약 30분인 경우들에서, 상기 방법은 상기 제1, 제2, 또는 제3 관찰 기간 동안 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 약 15 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다.In some cases, the method comprises a first observation period after administration of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)), and the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist as disclosed herein). a second observation period following administration of the antibody (eg, tiragolumab) or the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some cases, the method comprises a first observation period after administration of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)), the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein). a second observation period following administration of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), and the TIGIT antagonist antibody, the PD-1 axis a third observation period following administration of the binding antagonist, and said VEGF antagonist. In some cases, the first, second, and third observation periods are each about 30 minutes to about 60 minutes in length. In cases where the first, second, and third observation periods are each about 60 minutes, the method comprises the VEGF antagonist (eg, anti-VEGF antibody (eg, Beva) during the first, second, or third observation period. shizumab)), the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), or the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, ate recording the subject's vital signs (eg, pulse, respiration rate, blood pressure, body temperature) at about 30 ± 10 minutes after administration of zolizumab). In cases where the first, second, and third observation periods are each about 30 minutes, the method comprises the VEGF antagonist (eg, anti-VEGF antibody (eg, Beva) during the first, second, or third observation period. shizumab)), the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab), or the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, ate recording the subject's vital signs (eg, pulse, respiration rate, blood pressure, body temperature) at about 15±10 minutes after administration of zolizumab).
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 대상체 또는 대상체 집단에게 동시에 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 이후, 상기 방법은 관찰 기간을 포함한다. In other instances, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) are administered to the subject or administered simultaneously to a population of subjects. In some cases, for example, following administration of the anti-TIGIT antagonist antibody and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)), the method comprises an observation period.
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 대상체 또는 대상체 집단에게 동시에 투여된다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 이후, 상기 방법은 관찰 기간을 포함한다. In other instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab)) is administered to said subject or population of subjects simultaneously. In some cases, e.g., after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), the method comprises a period of observation do.
다른 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 대상체 또는 대상체 집단에게 동시에 투여된다. 일부 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 이후, 상기 방법은 관찰 기간을 포함한다. In other instances, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) are administered to the subject or simultaneously administered to a population of subjects. In some cases, for example, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) ), the method includes an observation period.
일부 경우들에서, 상기 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 투여 후 약 30 ± 10분에 상기 대상체 또는 대상체 집단의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 관찰 기간이 약 30분의 길이인 경우들에서, 상기 방법은 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the observation period is between about 30 minutes and about 60 minutes in length. In cases where the observation period is about 60 minutes in length, the method comprises recording vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) of the subject or population of subjects at about 30 ± 10 minutes after administration. may include In cases where the observation period is about 30 minutes in length, the method may comprise recording the subject's vital signs (e.g., pulse rate, respiration rate, blood pressure, and temperature) at about 15 ± 10 minutes after administration. can
다른 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 동시 투여 후에 투여된다. In other instances, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as Tyra). golumab) and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) after simultaneous administration.
일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 동시 투여 후에 투여된다. In some cases, the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) comprises the anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD- Administered following concurrent administration of a uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 및 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 동시 투여 후에 투여된다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is combined with the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli). Zumab) and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) after simultaneous administration.
일부 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 이후에, 상기 방법은 제2 관찰 기간을 포함한다. 일부 경우들에서, 예를 들어, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙)) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 이후, 상기 방법은 제2 관찰 기간을 포함한다. 일부 경우들에서, 상기 제2 관찰 기간은 약 30분 내지 약 60분의 길이이다. 상기 제2 관찰 기간이 약 60분의 길이인 경우들에서, 상기 방법은 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제2 관찰 기간이 약 30분의 길이인 경우들에서, 상기 방법은 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압, 및 온도)를 기록하는 단계를 포함할 수 있다.In some cases, for example, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)), the anti-TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) , and after administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), the method includes a second observation period. In some cases, for example, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) ), the method includes a second observation period. In some cases, the second observation period is between about 30 minutes and about 60 minutes in length. In cases where the second observation period is about 60 minutes in length, the method comprises recording the subject's vital signs (e.g., pulse rate, respiration rate, blood pressure, and temperature) at about 30 ± 10 minutes after administration. may include In cases where the second observation period is about 30 minutes in length, the method comprises recording the subject's vital signs (e.g., pulse rate, respiration rate, blood pressure, and temperature) at about 15 ± 10 minutes after administration. may include
E.E. 요로 상피암과 관련된 치료 방법 및 사용 Treatment methods and uses associated with urothelial cancer
요로상피세포 암종urothelial cell carcinoma
요로 상피암(UC)은 전 세계적으로 가장 흔한 비뇨기계 암이다. 대부분의 사례는 방광에서 발생한다. UC는 비근육 침윤성, 근육 침윤성, 또는 전이성 질병으로 진단될 수 있으며, 신규 사례 3건 중 1건은 근육 침윤성 질환으로 진단된다(종양, 결절 및 전이(TNM) 분류에 따른 cT2-T4a Nx M0). 근육 침윤성 UC(MIUC)는 근육 침윤성 방광암(MIBC) 및 근육 침윤성 요로 상피암(UTUC)을 총칭한다. 2018년에는, 전 세계적으로 549,393명의 새로운 방광암 사례 및 199,922명의 사망자가 발생한 것으로 추산되었다. 유럽에서는, 197,110명의 새로운 방광암 사례 및 64,970명의 사망자가 발생한 것으로 추정되며, 여기에는 유럽 연합의 28개 회원국에서 164,450명의 새로운 사례 및 52,930명의 사망이 포함된다. 미국에서는, 2020년에 81,400명의 새로운 방광암 사례 및 17,980명의 사망자가 발생할 것으로 추정된다. 미국에서 UC로 진단된 환자의 연령 중앙값은 73세이며, 이는 모든 종양 유형 진단 시 가장 높은 연령이다.Urinary tract epithelial cancer (UC) is the most common urinary tract cancer worldwide. Most cases occur in the bladder. UC can be diagnosed as a non-muscle invasive, muscle invasive, or metastatic disease, with 1 in 3 new cases diagnosed as a muscle invasive disease (cT2-T4a Nx M0 according to tumor, nodule and metastasis (TNM) classification) . Muscle invasive UC (MIUC) is a generic term for muscle invasive bladder cancer (MIBC) and muscle invasive urothelial carcinoma (UTUC). In 2018, it was estimated that there were 549,393 new bladder cancer cases and 199,922 deaths worldwide. In Europe, it is estimated that there are 197,110 new bladder cancer cases and 64,970 deaths, including 164,450 new cases and 52,930 deaths in the 28 member states of the European Union. In the United States, it is estimated that there will be 81,400 new bladder cancer cases and 17,980 deaths in 2020. The median age of patients diagnosed with UC in the United States is 73 years, the highest age at diagnosis of any tumor type.
MIBC의 치료를 위한 치료적 접근이 특히 시급하게 요구된다. MIBC는 새로운 요로 상피암 사례의 약 30%를 나타낸다. MIBC의 5년 생존율은 25~50%(유럽 비뇨기과 협회 EAU 가이드라인 2013)로서 지난 30년간 개선이 거의 없었으며, 해당 질병 분야(감시, 역학, 최종 결과(SEER) 프로그램. 암 통계 정보: 방광암, 2020)에서 효과적인 새로운 치료법의 부재로 인해 지난 30년 동안 거의 개선되지 않았다. 따라서, 개선된 의학적 개입에 대한 충족되지 않은 요구가 높다.A therapeutic approach for the treatment of MIBC is particularly urgently needed. MIBC represents about 30% of new cases of urothelial cancer. The 5-year survival rate of MIBC is 25-50% (European Urology Association EAU Guideline 2013), with little improvement over the past 30 years, in the disease area (Surveillance, Epidemiology, and End Results (SEER) program. Cancer Statistical Information: Bladder Cancer, 2020) has seen little improvement over the past 30 years due to the lack of effective new therapies. Therefore, the unmet need for improved medical intervention is high.
요로 상피암의 치료를 위한 방법 및 사용Methods and uses for the treatment of urothelial cancer
본원에서는 대상체 또는 대상체의 집단에서 UC(예컨대, 방광암(예컨대, MIBC))을 치료하는 방법 및 사용으로서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하는 방법 및 사용이 제공된다. 상기 대상체는 바람직하게는 인간이다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 암 면역요법에 대해 이전에 치료를 받은 적이 없다.Disclosed herein are methods and uses for treating UC (eg, bladder cancer (eg, MIBC)) in a subject or population of subjects, comprising an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab). ) and one or more dosing cycles of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab) to the subject or population of subjects. Methods and uses comprising administering are provided. The subject is preferably a human. In some cases, the subject or population of subjects has not previously been treated for cancer immunotherapy.
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이를 필요로 하는 대상체 또는 대상체의 잡단에게 3주마다(예컨대, 각 21일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or including methods and uses involving administering an anti-PD-1 antagonist antibody, such as pembrolizumab), to a subject or group of subjects in need thereof every three weeks (eg, on
본 발명은 MIBC를 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체의 집단은 백금계 화학요법제(예컨대, 시스플라틴)를 이용한 치료에 부적격인, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체의 집단은 백금계 화학요법제(예컨대, 시스플라틴)를 이용한 치료에 부적격이다.The present invention provides a method of treating a subject or population of subjects having MIBC, the method comprising a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody and about 80 mg to about 80 mg every 3 weeks. administering to the subject or population of subjects at least one dosing cycle of an about 1600 mg dose (eg, a fixed dose) of a PD-1 axis binding antagonist, wherein the subject or population of subjects is subjected to platinum-based chemotherapy methods and uses that are ineligible for treatment with an agent (eg, cisplatin). In some aspects, the method comprises a 30 mg to 1200 mg dose (eg, a fixed dose) of anti-TIGIT antagonist antibody every 3 weeks and a PD-1 axis binding at a 80 mg to 1600 mg dose (eg, a fixed dose) every 3 weeks administering to the subject or population of subjects one or more dosing cycles of the antagonist, wherein the subject or population of subjects is ineligible for treatment with a platinum-based chemotherapeutic agent (eg, cisplatin).
본 발명은 MIBC를 가진 대상체 또는 대상체의 집단을 치료하는 방법 및 사용으로서, 상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체의 집단은 < 60 mL/분의 크레아티닌 제거율, 2 등급 이상의 청력 상실, 및/또는 2 등급 이상의 신경병증을 가지는, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체의 집단은 < 60 mL/분의 크레아티닌 제거율, 2 등급 이상의 청력 상실, 및/또는 2 등급 이상의 신경병증을 가진다.The present invention provides methods and uses for treating a subject or population of subjects with MIBC, the method comprising: a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody and about 80 every 3 weeks administering to the subject or population of subjects one or more dosing cycles of a mg to about 1600 mg dose (eg, a fixed dose) of a PD-1 axis binding antagonist, wherein the subject or population of subjects is <60 and methods and uses, having a creatinine clearance rate of mL/min, a
본 발명은 MIBC를 가진 대상체 또는 대상체의 집단을 치료하는 방법 및 사용으로서, 상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료이다.The present invention provides methods and uses for treating a subject or population of subjects with MIBC, the method comprising: a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody and about 80 every 3 weeks A method comprising administering to the subject or population of subjects one or more dosing cycles of a mg to about 1600 mg dose (eg, a fixed dose) of a PD-1 axis binding antagonist, wherein the treatment is perioperative treatment. and use. In some aspects, the method comprises a 30 mg to 1200 mg dose (eg, a fixed dose) of anti-TIGIT antagonist antibody every 3 weeks and a PD-1 axis binding at a 80 mg to 1600 mg dose (eg, a fixed dose) every 3 weeks administering to the subject or population of subjects one or more dosing cycles of the antagonist, wherein the treatment is perioperative treatment.
본 발명은 수술 가능한 MIBC를 가진 대상체 또는 대상체의 집단을 치료하는 방법 및 사용으로서, 상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하는, 방법 및 사용을 포함한다. 일부 양태들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다.The present invention provides methods and uses for treating a subject or a population of subjects with operable MIBC, the method comprising: a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody and every 3 weeks methods and uses comprising administering to said subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist at a dose (eg, a fixed dose) of about 80 mg to about 1600 mg. In some aspects, the method comprises a 30 mg to 1200 mg dose (eg, a fixed dose) of anti-TIGIT antagonist antibody every 3 weeks and a PD-1 axis binding at a 80 mg to 1600 mg dose (eg, a fixed dose) every 3 weeks administering to the subject or population of subjects one or more dosing cycles of the antagonist.
상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 당해 기술 분야에서 공지된 임의의 적합한 방식으로 투여될 수 있다. 예를 들어, 상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 순차적으로(상이한 날에) 또는 동시에(동일한 날 또는 동일한 치료 주기 동안) 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 동일한 날에 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체 이전에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체 이후에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동시에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 투여되는 항 TIGIT 길항제 항체 이전에 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 투여되는 항 TIGIT 길항제 항체 이후에 투여될 수 있다. 또 다른 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동일한 시간에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 별개의 조성물로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체와 동일한 조성물로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 동일한 날에 환자에게 투여된 임의의 다른 치료제와 별개의 정맥내 라인을 통해 투여된다. 상기 PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체는 동일한 투여 경로 또는 상이한 투여 경로에 의해 투여될 수 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 정맥내, 근육내, 피하, 국소, 경구, 경피, 복강내, 안와내, 이식, 흡입, 척수강내, 심실내 또는 비강내로 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제의 투여 후 제1 관찰 기간이 있다. 일부 경우들에서, 상기 PD-1 축 결합 길항제의 투여 후 제2 관찰 기간이 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간이 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체의 투여 후 제2 관찰 기간이 있다. 일부 예들에서, 관찰 기간은 약 30 분 내지 약 60 분 길이이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제는 정맥내 또는 피하 투여된다. 일부 경우들에는, 상기 정맥내 주입이 30 ± 10분 및/또는 60 ± 15분에 걸쳐 실시된다. 일례에서, 아테졸리주맙은 60분에 걸쳐 정맥내 투여될 수 있고; 제1 주입이 허용되면, 모든 후속 주입은 30분에 걸쳐 전달될 수 있다. 일부 예들에서, 상기 PD-1 축 결합 길항제는 정맥내 푸시(push) 또는 볼루스(bolus)로 투여되지 않는다. 일례에서, 티라골루맙은 60분에 걸쳐 정맥내 투여될 수 있고; 제1 주입이 허용되면, 모든 후속 주입은 30분에 걸쳐 전달될 수 있다. 일부 예들에서, 상기 항 TIGIT 길항제 항체는 정맥내 푸시(push) 또는 볼루스(bolus)로 투여되지 않는다.The PD-1 axis binding antagonist and anti-TIGIT antagonist antibodies may be administered in any suitable manner known in the art. For example, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody may be administered sequentially (on different days) or simultaneously (on the same day or during the same treatment cycle). In some cases, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody may be administered on the same day. In some cases, the PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered after the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered concurrently with the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist may be administered prior to the anti-TIGIT antagonist antibody administered on the same day. In some cases, the PD-1 axis binding antagonist may be administered after the anti-TIGIT antagonist antibody administered on the same day. In still other instances, the PD-1 axis binding antagonist is administered at the same time as the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered in a separate composition from the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered in the same composition as the anti-TIGIT antagonist antibody. In some cases, the PD-1 axis binding antagonist is administered via a separate intravenous line from any other therapeutic agent administered to the patient on the same day. The PD-1 axis binding antagonist and anti-TIGIT antagonist antibody may be administered by the same route of administration or by different routes of administration. In some cases, the PD-1 axis binding antagonist is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly, or intranasally. In some cases, the anti TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly or intranasally. In some cases, the anti TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly or intranasally. In some cases, the anti TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, implanted, inhaled, intrathecally, intraventricularly or intranasally. In some cases, there is a first observation period after administration of the PD-1 axis binding antagonist. In some cases, there is a second observation period following administration of the PD-1 axis binding antagonist. In some cases, there is a first observation period following administration of the anti-TIGIT antagonist antibody. In some cases, there is a second observation period following administration of the anti-TIGIT antagonist antibody. In some examples, the observation period is from about 30 minutes to about 60 minutes in length. In some cases, the anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist is administered intravenously or subcutaneously. In some cases, the intravenous infusion is administered over 30 ± 10 minutes and/or 60 ± 15 minutes. In one example, atezolizumab may be administered intravenously over 60 minutes; If the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some embodiments, the PD-1 axis binding antagonist is not administered as an intravenous push or bolus. In one example, tiragolumab may be administered intravenously over 60 minutes; If the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some embodiments, the anti-TIGIT antagonist antibody is not administered as an intravenous push or bolus.
일부 경우들에서, 제1 투약 주기는 수술 전에 개시된다. 일부 경우들에서, 1회 이상의 투약 주기는 수술 전에 완료된다. 일부 경우들에서, 적어도 1회, 2회 또는 3회의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 또는 그 이상의 투약 주기)가 수술 전에 완료된다. 일부 경우들에서, 1회 이상의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 20회 또는 그 이상의 투약 주기)는 수술 후 개시된다. 일부 경우들에서, 1회 내지 17회의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 또는 17회의 투약 주기)는 수술 후에 완료된다. 일부 경우들에서, 적어도 1회의 투약 주기는 수술 후 약 4 내지 6주(예컨대, 약 4주, 약 5주, 또는 약 6주) 사이에 개시된다. 일부 경우들에서, 상기 치료는 수술을 포함한다. 일부 경우들에서, 상기 수술은 방광 절제술 및/또는 액와 림프절 수술이다.In some cases, the first dosing cycle is initiated prior to surgery. In some cases, one or more dosing cycles are completed prior to surgery. In some cases, at least 1, 2, or 3 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, or more dosing cycles) completed before surgery. In some cases, one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13) , 14, 15, 16, 17, 18, 19, 20 or more dosing cycles) are initiated post-operatively. In some cases, 1 to 17 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12) , 13, 14, 15, 16, or 17 dosing cycles) are completed postoperatively. In some cases, at least one dosing cycle is initiated between about 4 to 6 weeks (eg, about 4 weeks, about 5 weeks, or about 6 weeks) post surgery. In some cases, the treatment comprises surgery. In some cases, the surgery is a cystectomy and/or axillary lymph node surgery.
일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 pCR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 무재발 생존(RFS), 예컨대 주요 RFS(예컨대, 12개월, 18개월, 또는 24개월에서 주요 RFS)의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 무사건 생존(EFS), 예컨대 주요 EFS(예컨대, 12개월, 18개월, 또는 24개월에서 주요 EFS)의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 OS, 예컨대 주요 OS(예컨대, 12개월, 18개월, 또는 24개월에서 주요 OS)의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 병리학적 병기하향 비율의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 pCR의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 EFS(예컨대, 주요 EFS)를 연장시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 RFS(예컨대, 주요 RFS)를 연장시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단의 OS(예컨대, 주요 OS)를 연장시킨다.In some cases, an effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as ate Zolizumab) results in pCR. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) results in an increase in relapse-free survival (RFS), such as major RFS (eg, major RFS at 12 months, 18 months, or 24 months). In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) results in an increase in event-free survival (EFS), such as major EFS (eg, major EFS at 12 months, 18 months, or 24 months). In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) results in an increase in OS, such as major OS (eg, major OS at 12 months, 18 months, or 24 months). In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) causes an increase in the pathological staging rate. In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) results in an increase in pCR in a subject or population of subjects, e.g., compared to treatment with a PD-1 axis binding antagonist without said anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without said PD-1 axis binding antagonist. make it In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) is, e.g., the EFS (e.g., major EFS) of a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist without the anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without the PD-1 axis binding antagonist. extend the In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) is, e.g., the RFS (e.g., major RFS) of a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist without the anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without the PD-1 axis binding antagonist. extend the In some cases, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ), e.g., the OS (e.g., major OS) of a subject or population of subjects as compared to treatment with a PD-1 axis binding antagonist without the anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without the PD-1 axis binding antagonist. extend the
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)은 4주마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대, 예를 들어 펨브롤리주맙)는 2주 마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에), 3주 마다(예컨대, 각 21일 투약 주기의 제 1일에), 또는 4주 마다(예컨대, 각 28일 투약 주기의 제 1일에) 투여된다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 CR 또는 PR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체 또는 대상체 집단에서 pCR의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 EFS 및/또는 RFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체 또는 대상체 집단에서 OR를 연장시킨다.The present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject or population of subjects in need thereof every 4 weeks (eg, the first of each 28-day dosing cycle). per day) and methods and uses involving administration. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered every 4 weeks (eg, on
본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이를 필요로 하는 대상체 또는 대상체의 집단에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 제공한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는 pCR을 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)의 투여는, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 EFS 및/또는 RFS의 증가를 발생시킨다. 일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)를 투여하는 것은, 예컨대 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료 또는 상기 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체 또는 대상체 집단에서 Os를 연장시킨다.The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab, or a method involving administering an anti-PD-1 antagonist antibody, such as pembrolizumab), to a subject or population of subjects in need thereof every two weeks (eg, on
특정 경우들에서, 본 발명은 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 이를 필요로 하는 대상체 또는 대상체 집단에게 2주마다(예컨대, 각 28일 투약 주기의 제 1일 및 15일에) 투여하는 것을 수반한 방법 및 사용을 포함한다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 pCR을 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 기준 PFS와 비교하여 대상체 또는 대상체 집단에서 EFS 및/또는 RFS 의 증가를 발생시킨다. 일부 경우들에서, 유효량의 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여는 대상체 또는 대상체 집단에서 OR를 연장시킨다. In certain instances, the present invention provides an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) to a subject or population of subjects in need thereof every two weeks (eg, each 28 on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)을 투여 받은 대상체 또는 대상체 집단은 MIBC에 대해 치료를 받고 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) ) is being treated for MIBC.
일부 경우들에서, 상기 치료는 추가 요법을 더 포함할 수 있다. 당업계에 공지되어 있거나 본원에 기재된 임의의 적합한 추가 요법이 사용될 수 있다. 부가적인 요법은 방사선 요법, 수술(예컨대, 방광 절제술), 유전자 요법, DNA 요법, 바이러스 요법, RNA 요법, 면역요법, 골수 이식, 나노요법, 단일클론 항체 요법, 감마선 조사, 또는 전술한 것의 조합일 수 있다. In some cases, the treatment may further comprise an additional therapy. Any suitable additional therapy known in the art or described herein may be used. The additional therapy may be radiation therapy, surgery (eg, cystectomy), gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, gamma irradiation, or a combination of the foregoing. can
일부 경우들에서, 상기 추가 요법은 부작용 제한 제제(예컨대, 치료의 부작용의 발생 및/또는 중증도를 줄이고자 하는 제제, 예컨대 항 메스꺼움 제제, 코르티코스테로이드(예컨대, 프레드니손 또는 등가물, 예컨대 1~2 mg/kg/일의 용량), 및 호르몬 대체 약물(들) 등)의 투여이다.In some cases, the additional therapy is a side-effect limiting agent (eg, an agent intended to reduce the incidence and/or severity of side effects of treatment, such as an anti-nausea agent, a corticosteroid (eg, prednisone or equivalent, such as 1-2 mg/ kg/day), and hormone replacement drug(s), etc.).
임의의 선행하는 예에서, 각각의 투약 주기는 임의의 적합한 길이, 예컨대, 약 7일, 약 14일, 약 21일, 약 28일 또는 그 이상일 수 있다. 일부 경우들에서, 각 투약 주기는 약 21일이다.In any preceding example, each dosing cycle can be of any suitable length, such as about 7 days, about 14 days, about 21 days, about 28 days or more. In some cases, each dosing cycle is about 21 days.
또한, 본원에서는 대상체 또는 대상체의 집단에서 MIBC를 치료하는 방법으로서, 유효량의 PD-1 축 결합 길항제(예컨대, 아테졸리주맙) 및/또는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)를 다른 항암제 또는 암 요법과 병용으로 투여하는 단계를 포함하는 방법이 제공된다. 예를 들어, PD-1 축 결합 길항제는 추가 화학요법 또는 화학요법제(상기 정의를 참조); 표적 요법 또는 표적 치료제; 면역요법 또는 면역요법제, 예를 들어 단일클론 항체; 하나 이상의 세포독성제(상기 정의를 참조); 또는 이들의 조합과 병용하여 투여될 수 있다. Also disclosed herein is a method of treating MIBC in a subject or population of subjects, comprising an effective amount of a PD-1 axis binding antagonist (eg, atezolizumab) and/or an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist as disclosed herein). Methods are provided comprising administering an antibody, such as tyragolumab) in combination with another anti-cancer agent or cancer therapy. For example, a PD-1 axis binding antagonist may include additional chemotherapy or chemotherapeutic agents (see definition above); targeted therapy or targeted therapeutics; immunotherapy or immunotherapeutic agents such as monoclonal antibodies; one or more cytotoxic agents (see definition above); Or it may be administered in combination with a combination thereof.
환자가 전이성 요로 상피암(mUC)이 있고 상기 mUC가 백금 함유 요법 중에 또는 이후에 진행된 일부 경우들에서, 본원에 제공된 방법은 상기 대상체 또는 대상체의 집단이 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체의 집단에 제2 투약 요법을 투여하는 단계를 추가로 포함한다. 일부 경우들에서, 상기 제2 투약 요법은 PD-1 축 결합 길항제 및 항체-약물 접합체(ADC)의 1회 이상의 투약 주기를 포함한다. 일부 경우들에서, 상기 ADC는 (a) 엔포르투맙 베도틴 또는 (b) 사시투주맙 고비테칸이다. In some cases where the patient has metastatic urothelial cancer (mUC) and the mUC has progressed during or after platinum-containing therapy, the methods provided herein can be performed after the subject or population of subjects experiences disease progression or unacceptable toxicity. and administering a second dosing regimen to the subject or population of subjects. In some cases, the second dosing regimen comprises one or more dosing cycles of the PD-1 axis binding antagonist and the antibody-drug conjugate (ADC). In some cases, the ADC is (a) enfortumab vedotin or (b) sacituzumab gobitecan.
또한, 본원에서는 mUC를 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체의 집단에 투여하는 단계를 포함하고, 여기서: (a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 약 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 방법이 제공된다. 일부 양태들에서, 본원에서는 mUC를 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체의 집단에 투여하는 단계를 포함하고, 여기서: (a) 상기 제1 투약 요법은 3주마다 600 mg 용량(예컨대, 고정 용량)의 티라골루맙 및 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (b) 상기 제2 투약 요법은 3주마다 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 방법이 제공된다.Also disclosed herein is a method of treating a subject or population of subjects having mUC, comprising administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein: (a) the agent one dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks (eg, a fixed dose) and atezolizumab at a dose of about 1200 mg every 3 weeks (eg, a fixed dose); and (b) said second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose of about 1200 mg (eg, a fixed dose) every 3 weeks, and (i) enfortumab vedotin is administered for 2 weeks. administered at a weekly dose of 1.25 mg/kg with a weekly break of one week, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/1 week off, wherein the second dosing regimen is A method is provided, wherein the subject or population of subjects is administered to the subject or population of subjects after experiencing disease progression or unacceptable toxicity during the first dosing regimen. In some aspects, disclosed herein is a method of treating a subject or population of subjects having mUC, comprising administering to the subject or population of subjects a first dosing regimen followed by a second dosing regimen, wherein: (a ) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a 600 mg dose (eg, a fixed dose) every 3 weeks and atezolizumab at a 1200 mg dose (eg, a fixed dose) every 3 weeks; and (b) said second dosing regimen comprises one or more dosing cycles of atezolizumab at a 1200 mg dose (eg, a fixed dose) every 3 weeks, and (i) enfortumab vedotin is administered for 2 weeks/ administered at a weekly dose of 1.25 mg/kg with a one-week break, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/week break, wherein the second dosing regimen is A method is provided, wherein the subject or population of subjects is administered to the subject or population of subjects after experiencing disease progression or unacceptable toxicity during the first dosing regimen.
일부 경우들에서, 상기 치료는 적어도 약 13.4% 내지 적어도 약 15%(예컨대, 적어도 약 13.5%, 14%, 14.5%, 또는 15%)의 대상체 집단의 ORR을 발생시킨다.In some cases, the treatment results in an ORR in the subject population of at least about 13.4% to at least about 15% (eg, at least about 13.5%, 14%, 14.5%, or 15%).
일부 구현예들에서, 상기 치료는 적어도 약 7.9개월(예컨대, 8.0개월, 8.1개월, 8.2개월, 8.3개월, 8.4개월, 8.5개월, 8.6개월, 8.7개월, 8.8개월, 8.9개월, 9개월, 9.5개월, 10개월, 11개월, 12개월, 13개월 또는 14개월)의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 8.6개월(예컨대, 8.6개월, 8.7개월, 8.8개월, 8.9개월, 9개월, 9.5개월, 10개월, 11개월, 12개월, 13개월, 14개월, 15개월 또는 16개월)의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 약 7.9개월 내지 약 8.6개월(예컨대, 약 8.0개월, 8.1개월, 8.2개월, 8.3개월, 8.4개월, 8.5개월, 또는 8.6개월)의 대상체 집단의 OS 중앙값을 발생시킨다.In some embodiments, the treatment is at least about 7.9 months (eg, 8.0 months, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8.5 months, 8.6 months, 8.7 months, 8.8 months, 8.9 months, 9 months, 9.5 months months, 10 months, 11 months, 12 months, 13 months, or 14 months). In some cases, the treatment lasts for at least about 8.6 months (eg, 8.6 months, 8.7 months, 8.8 months, 8.9 months, 9 months, 9.5 months, 10 months, 11 months, 12 months, 13 months, 14 months, 15 months) or 16 months) of the subject population. In some cases, the treatment results in a median OS of the subject population of about 7.9 months to about 8.6 months (eg, about 8.0 months, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8.5 months, or 8.6 months). .
일부 경우들에서, 상기 치료는 적어도 약 13.4% 내지 적어도 약 31%(예컨대, 적어도 약 13.5%, 14%, 15%, 18%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 또는 31%)의 대상체 집단의 ORR을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 31%(예컨대, 약 31% 내지 약 100%, 예컨대, 약 31% 내지 약 60%(예컨대, 35%, 40%, 45%, 50%, 55%, 또는 60%)의 대상체 집단의 ORR을 발생시킨다. In some cases, the treatment is at least about 13.4% to at least about 31% (eg, at least about 13.5%, 14%, 15%, 18%, 17%, 18%, 19%, 20%, 21%, 22 %, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, or 31%) of the subject population. In some cases, the treatment is at least about 31% (eg, about 31% to about 100%, such as about 31% to about 60% (eg, 35%, 40%, 45%, 50%, 55%, or 60%) of the subject population.
일부 경우들에서, 상기 치료는 적어도 약 7.9개월(예컨대, 약 7.9 내지 약 36개월(예컨대, 약 7.9 내지 약 24개월(예컨대, 8개월, 10개월, 12개월, 14개월, 16개월, 18개월, 20개월, 22개월, 또는 24개월))의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 16.3개월(예컨대, 약 16.3개월 내지 약 36개월(예컨대, 약 16.3개월 내지 약 24개월(예컨대, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 또는 24개월))의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 7.9개월 내지 약 16.3개월(예컨대, 8개월, 8.5개월, 9개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 12.5개월, 13개월, 13.5개월, 14개월, 14.5개월) , 15개월, 15.5개월, 16개월, 또는 16.3개월, 예컨대, 7.9~9개월, 9~10개월, 10~11개월, 11~12개월, 12~13개월, 13~14개월, 14~15개월 , 15~16개월, 또는 16개월 초과)의 대상체 집단의 OS 중앙값을 발생시킨다.In some cases, the treatment lasts for at least about 7.9 months (eg, between about 7.9 and about 36 months (eg, between about 7.9 and about 24 months (eg, 8 months, 10 months, 12 months, 14 months, 16 months, 18 months)). , 20 months, 22 months, or 24 months) in the subject population. to about 24 months (eg, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, or 24 months)). , said treatment is at least about 7.9 months to about 16.3 months (eg, 8 months, 8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 12.5 months, 13 months, 13.5 months , 14 months, 14.5 months), 15 months, 15.5 months, 16 months, or 16.3 months, such as 7.9-9 months, 9-10 months, 10-11 months, 11-12 months, 12-13 months, 13- 14 months, 14-15 months, 15-16 months, or greater than 16 months).
항 TIGIT 길항제 항체의 투약Dosing of Anti-TIGIT Antagonist Antibodies
항 TIGIT 길항제 항체의 투약은 섹션 III(K)에 기재되어 있다. Dosing of anti-TIGIT antagonist antibodies is described in Section III(K).
PD-1 축 결합 길항제의 투약Dosing of PD-1 axis binding antagonists
PD-1 축 결합 길항제의 투약은 섹션 III(K)에 기재되어 있다. Dosing of PD-1 axis binding antagonists is described in Section III(K).
암 특성화 및 선택Cancer characterization and selection
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, UC(예컨대, 방광암(예컨대, MIBC))는 외과적으로 수술가능하다(예컨대, 방광 절제술에 적합한 UC(예컨대, 방광암(예컨대, MIBC)). 일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 MIBC는 외과적으로 수술가능하다(예컨대, 방광 절제술에 적합한 MIBC).In some cases, in any method, use, or composition for use described herein, the UC (eg, bladder cancer (eg, MIBC)) is surgically operable (eg, a UC suitable for cystectomy (eg, Bladder cancer (eg, MIBC) In some cases, in any of the methods, uses, or compositions for use described herein, the MIBC is surgically operable (eg, a MIBC suitable for cystectomy).
일부 예들에서, 본원에 기재된 방법, 사용, 또는 사용를 위한 조성물들에서, 상기 대상체에는 백금계 화학요법에 부적격이다(예컨대, 시스플라틴에 적격임). 일부 경우들에서, 상기 대상체는 시스플라틴에 부적격이다. 일부 경우들에서, 상기 대상체는 크레아티닌 제거율이 60 mL/분 미만이다. 일부 경우들에서, 상기 대상체는 크레아티닌 제거율이 30 mL/분 이상이다. 일부 경우들에서, 상기 대상체는 2 등급 이상의 청력 손실을 가진다. 일부 경우들에서, 상기 대상체는 2 등급 이상의 신경병증을 가진다. 일부 경우들에서, 60 mL/분 미만의 크레아티닌 제거율, 2 등급 이상의 청력 손실, 및/또는 2 등급 이상의 신경병증을 갖는 대상체는 시스플라틴 부적격이다. 일부 경우들에서, 크레아티닌 제거율이 60 mL/분 미만인 대상체는 시스플라틴 부적격이다. 일부 경우들에서, 청력 손실이 2 등급 이상인 대상체는 시스플라틴 부적격이다. 일부 경우들에서, 신경병증이 2 등급 이상인 대상체는 시스플라틴 부적격이다. 일부 경우들에서, 시스플라틴 기반 화학요법을 거부하는 대상체는 시스플라틴 부적격이다. 일부 경우들에서, 상기 대상체는 0 또는 1의 이스턴 코퍼레이티브 종양학 그룹(ECOG) 전신 활동도(PS)를 가진다.In some embodiments, in a method, use, or compositions for use described herein, the subject is ineligible for platinum-based chemotherapy (eg, eligible for cisplatin). In some cases, the subject is ineligible for cisplatin. In some cases, the subject has a creatinine clearance of less than 60 mL/min. In some cases, the subject has a creatinine clearance of at least 30 mL/min. In some cases, the subject has a hearing loss of
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 순환하는 종양 DNA(ctDNA)의 존재 또는 수준이 평가될 수 있다. 일부 경우들에서, ctDNA는 상기 대상체로부터의 샘플(예컨대, 혈액 샘플에서 평가된다. 일부 경우들에서, ctDNA는 제1 투약 주기(예컨대, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 제1 투약 주기)의 1일 전에 상기 대상체로부터의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술(예컨대, 방광 절제술) 전에 상기 대상체의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술(예컨대, 방광 절제술) 후에 상기 대상체의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술(예컨대, 방광 절제술) 후 4~6주(예컨대, 4주, 5주, 또는 6주)에 상기 대상체로부터의 샘플에서 평가된다. 일부 경우들에서, ctDNA는 수술(예컨대, 방광 절제술) 후 6개월에 상기 대상체로부터의 샘플에서 평가된다.In some cases, in any method, use, or composition for use described herein, the presence or level of circulating tumor DNA (ctDNA) can be assessed. In some cases, the ctDNA is evaluated in a sample from the subject (eg, a blood sample. In some cases, the ctDNA is evaluated in a first dosing cycle (eg, a first dose of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist) in the sample from the subject before 1 day of cycle).In some cases, the ctDNA is evaluated in the sample of the subject before surgery (eg, cystectomy).In some cases, ctDNA is evaluated in the sample of the subject before surgery (eg, bladder resection). After surgery (eg, cystectomy), ctDNA is evaluated in the sample of the subject 4-6 weeks (eg, 4 weeks, 5 weeks, or 6 weeks) after surgery (eg, cystectomy) in the sample from the subject. In some cases, ctDNA is evaluated in a sample from the subject 6 months after surgery (eg, cystectomy).
PD-L1 발현의 평가Assessment of PD-L1 expression
PD-L1의 발현은 섹션 III(L)에 기재된 바와 같이 평가할 수 있다. Expression of PD-L1 can be assessed as described in section III(L).
치료에 대한 반응response to treatment
본원에 기재된 임의의 방법의 일부 구현예들에서, 요법에 대한 대상체의 반응은 하나 이상의 측정에 의해 특징지어질 수 있다. 일부 구현예들에서, 상기 치료는 pCR을 발생시킨다. 일부 구현예들에서, 상기 치료는 무재발 생존(RFS), 무사건 생존(EFS), 또는 OS의 증가를 발생시킨다. 일부 구현예들에서, 상기 치료는 주요 RFS, 주요 EFS, 또는 주요 OS의 증가를 발생시킨다. 일부 구현예들에서, 상기 치료는 주요 병리학적 병기하향 비율의 증가를 발생시킨다.In some embodiments of any of the methods described herein, the subject's response to therapy can be characterized by one or more measures. In some embodiments, the treatment results in pCR. In some embodiments, the treatment results in an increase in recurrence-free survival (RFS), event-free survival (EFS), or OS. In some embodiments, the treatment results in an increase in major RFS, major EFS, or major OS. In some embodiments, the treatment results in an increase in the rate of major pathological staging.
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 pCR의 증가를 발생시킨다.In some cases, the treatment increases the pCR of the subject, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. causes
일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 OS를 연장시킨다. 일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 EFS를 연장시킨다. 일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 RFS를 연장시킨다. 일부 경우들에서, 상기 치료는, 예컨대 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 이용한 치료와 비교하거나 또는 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 이용한 치료와 비교하여 대상체의 병리학적 병기하향 비율을 증가시킨다.In some cases, the treatment prolongs the subject's OS, eg, as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. make it In some cases, the treatment prolongs the subject's EFS, e.g., as compared to treatment with a PD-1 axis binding antagonist without an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody without a PD-1 axis binding antagonist. make it In some cases, the treatment prolongs the RFS of the subject, e.g., as compared to treatment with a PD-1 axis binding antagonist in the absence of an anti TIGIT antagonist antibody or as compared to treatment with an anti TIGIT antagonist antibody in the absence of a PD-1 axis binding antagonist. make it In some cases, the treatment is the pathological stage of the subject, eg, compared to treatment with a PD-1 axis binding antagonist without an anti TIGIT antagonist antibody or compared to treatment with an anti TIGIT antagonist antibody without a PD-1 axis binding antagonist. Increase the downward ratio.
일부 구현예들에서, 본원에 기재된 치료는 상기 대상체의 pCR을 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 pCR을 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, the treatment described herein lowers the subject's pCR by at least about 2 months (eg, by 2 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months, by 5.0 to by 48 months, by 6.0 to 36 months, by 8.0 to 24 months, or by 10 to 12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment lowers the subject's pCR by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months) by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, 치료는 상기 대상체의 EFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 EFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, treatment reduces the subject's EFS by at least about 2 months (eg, by 2 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months, by 5.0 to 48 months) , by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0, 5.1, 5.2, 5.3, 5.4, 5.5, 5.6, 5.7, 5.8, 5.9, 6.0, 6.5, 7.0, 7.5, 8.0, 8.5, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's EFS by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months). by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, 치료는 상기 대상체의 RFS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 2.5~100개월 만큼, 3.0~80개월 만큼, 4.0~60개월 만큼, 5.0~48개월 만큼, 6.0~36개월 만큼, 8.0~24개월 만큼, 또는 10~12개월 만큼, 예컨대 적어도 약 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 구현예들에서, 상기 치료는 상기 대상체의 RFS를 적어도 약 4개월 만큼(예컨대, 4~120개월 만큼, 5~100개월 만큼, 6~80개월 만큼, 7~60개월 만큼, 8~48개월 만큼, 9~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다.In some embodiments, treatment reduces the subject's RFS by at least about 2 months (eg, by 2 to 120 months, by 2.5 to 100 months, by 3.0 to 80 months, by 4.0 to 60 months, by 5.0 to 48 months) , by 6.0-36 months, by 8.0-24 months, or by 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months , 5.0, 5.1, 5.2, 5.3, 5.4, 5.5, 5.6, 5.7, 5.8, 5.9, 6.0, 6.5, 7.0, 7.5, 8.0, 8.5, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's RFS by at least about 4 months (eg, by 4 to 120 months, by 5 to 100 months, by 6 to 80 months, by 7 to 60 months, by 8 to 48 months) by 9-36 months, or by 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
일부 구현예들에서, OS은 치료 시작시부터 사망시까지의 기간으로서 측정된다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 2개월 만큼(예컨대, 2~120개월 만큼, 3~110개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 10~24개월 만큼, 예컨대 적어도 약 2개월, 2.1개월, 2.2개월, 2.3개월, 2.4개월, 2.5개월, 2.6개월, 2.7개월, 2.8개월, 2.9개월, 3.0개월, 3.1개월, 3.2개월, 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월, 4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 3.3개월 만큼(예컨대, 3.3~120개월 만큼, 4~100개월 만큼, 5~80개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 3.3개월, 3.4개월, 3.5개월, 3.6개월, 3.7개월, 3.8개월, 3.9개월,4.0개월, 4.1개월, 4.2개월, 4.3개월, 4.4개월, 4.5개월, 4.6개월, 4.7개월, 4.8개월, 4.9개월, 5.0개월, 5.1개월, 5.2개월, 5.3개월, 5.4개월, 5.5개월, 5.6개월, 5.7개월, 5.8개월, 5.9개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. 일부 경우들에서, 상기 치료는 상기 대상체의 OS를 적어도 약 5.3개월 만큼(예컨대, 5.3~120개월 만큼, 6~60개월 만큼, 7~48개월 만큼, 8~36개월 만큼, 또는 10~24개월 만큼, 예컨대 적어도 약 5.3개월, 5.5개월, 6.0개월, 6.5개월, 7.0개월, 7.5개월, 8.0개월, 8.5개월, 9.0개월, 9.5개월, 10개월, 10.5개월, 11개월, 11.5개월, 12개월, 13개월, 14개월, 15개월, 16개월, 17개월, 18개월, 19개월, 20개월, 21개월, 22개월, 23개월, 24개월, 25개월, 26개월, 27개월, 28개월, 29개월, 30개월, 31개월, 32개월, 33개월, 34개월, 35개월, 또는 36개월 만큼) 연장시킨다. In some embodiments, OS is measured as the period from initiation of treatment to death. In some cases, the treatment reduces the subject's OS by at least about 2 months (eg, by 2-120 months, by 3-110 months, by 4-100 months, by 5-80 months, by 6-60 months) , by 7-48 months, by 8-36 months, by 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months , 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 Months, 20 Months, 21 Months, 22 Months, 23 Months, 24 Months, 25 Months, 26 Months, 27 Months, 28 Months, 29 Months, 30 Months, 31 Months, 32 Months, 33 Months, 34 Months, 35 Months, or by 36 months). In some cases, the treatment reduces the subject's OS by at least about 3.3 months (eg, by 3.3-120 months, by 4-100 months, by 5-80 months, by 6-60 months, by 7-48 months) , by 8-36 months, or by 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months , 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, by 34 months, 35 months, or 36 months). In some cases, the treatment reduces the subject's OS by at least about 5.3 months (eg, by 5.3 to 120 months, by 6 to 60 months, by 7 to 48 months, by 8 to 36 months, or by 10 to 24 months). by, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months , by 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
F.F. 췌장암과 관련된 치료 방법 및 사용 Treatment methods and uses associated with pancreatic cancer
췌장암pancreatic cancer
췌장암 환자 중 80%는 초기 진단 시 진행성 질환으로 제시된다. 근치 수술을 받은 환자라도 질병이 재발하여, 췌십이지장절제술에서 결절 음성 및 결절 양성 질환 환자의 5년 생존율은 각각 25~30% 및 10%이다. 국소 진행성 및 절제불가능한 질병을 가진 환자는 종종 방사선화학요법을 받아 OS 중앙값이 9~13개월이지만, 장기 생존하는 경우는 드물다. 80% of pancreatic cancer patients present with advanced disease at initial diagnosis. Even in patients who underwent radical surgery, the disease recurs, and the 5-year survival rates of patients with nodular-negative and nodular-positive disease in pancreaticoduodenectomy are 25-30% and 10%, respectively. Patients with locally advanced and unresectable disease often receive radiochemotherapy with a median OS of 9 to 13 months, but long-term survival is rare.
따라서, 개선된 의학적 개입에 대한 충족되지 않은 요구가 높다.Therefore, the unmet need for improved medical intervention is high.
췌장암 치료를 위한 방법 및 사용Methods and uses for treating pancreatic cancer
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙), PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙), 항대사물질(예컨대, 젬시타빈), 및 탁산(예컨대, 파클리탁셀)를 투여받은 대상체 또는 대상체의 집단은 췌장암(예컨대, 췌장관 선암종(PDAC), 예컨대, 전이성 PDAC(mPDAC))에 대해 치료를 받고 있다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab), a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody, such as atezolizumab) , an antimetabolite (eg, gemcitabine), and a taxane (eg, paclitaxel), a subject or population of subjects receiving treatment for pancreatic cancer (eg, pancreatic ductal adenocarcinoma (PDAC), such as metastatic PDAC (mPDAC)). are receiving
본 발명은 췌장암을 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법을 포함한다. 일부 경우들에서, 상기 방법은 각 28일의 투약 주기의 제 1일 및 15일에 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 췌장암은 PDAC, 예컨대 mPDAC이다. 일부 양태들에서, 상기 대상체 또는 대상체들은 전이성 유방암에 대한 선행 전신 요법을 받지 않았다.The present invention provides a method of treating a subject or population of subjects having pancreatic cancer, comprising: tyragolumab at a dose of about 420 mg on
일부 경우들에서, 상기 치료는 적어도 약 41.7% 내지 적어도 약 46.7%(예컨대, 42%, 42.5%, 43%, 43.5%, 44%, 44.5%, 45%, 45.5%, 46%, 46.5%, 또는 46.7%(예컨대, 41.7%~43%, 43%~45%, 또는 45%~46.7%)의 대상체 집단의 ORR을 발생시킨다. 일부 경우들에서, 상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 없이 젬시타빈 및 냅-파클리탁셀을 포함한 치료와 비교하여 적어도 약 20%의 ORR의 증가를 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 5.5개월(예컨대, 약 5.5개월 내지 14개월(예컨대, 6개월, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 또는 14개월))의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 7개월(예컨대, 약 7개월 내지 14개월(예컨대, 7개월, 8개월, 9개월, 10개월, 11개월, 12개월, 13개월, 또는 14개월))의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 5.5개월 내지 약 7개월(예컨대, 6개월, 6.2개월, 6.4개월, 6.6개월, 6.8개월, 7개월, 또는 7개월 초과)의 대상체 집단의 PFS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 8.5개월(예컨대, 약 8.5개월 내지 16개월(8.5개월, 9개월, 9.5개월, 10개월, 10.5개월, 11개월, 12개월, 13개월, 14개월, 15개월, 또는 16개월))의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 10.6개월(예컨대, 약 10.6개월 내지 16개월(10.6개월, 11개월, 12개월, 13개월, 14개월, 15개월, 또는 16개월))의 대상체 집단의 OS 중앙값을 발생시킨다. 일부 경우들에서, 상기 치료는 적어도 약 8.5개월 내지 약 10.6개월(예컨대, 8.7개월, 9.0개월, 9.2개월, 9.4개월, 9.6개월, 9.8개월, 10개월, 10.2개월, 10.4개월, 10.6개월, 15개월 또는 10.6개월)의 대상체 집단의 OS 중앙값을 발생시킨다.In some cases, the treatment comprises at least about 41.7% to at least about 46.7% (e.g., 42%, 42.5%, 43%, 43.5%, 44%, 44.5%, 45%, 45.5%, 46%, 46.5%, or 46.7% (eg, 41.7%-43%, 43%-45%, or 45%-46.7%) of the subject population.In some cases, the treatment comprises an anti-TIGIT antagonist antibody and PD-1 Produces an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nap-paclitaxel without an axis binding antagonist In some cases, the treatment is at least about 5.5 months (e.g., between about 5.5 months and 14 months) (e.g., 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months)). develop a median PFS of a population of subjects of at least about 7 months (eg, between about 7 months and 14 months (eg, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months)) In some cases, the treatment is at least about 5.5 months to about 7 months (e.g., 6 months, 6.2 months, 6.4 months, 6.6 months, 6.8 months, 7 months, or greater than 7 months) of the median PFS of the subject population. In some cases, the treatment is at least about 8.5 months (eg, between about 8.5 months and 16 months (8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 12 months, 13 months, 14 months, 15 months, or 16 months) of the subject population) In some cases, the treatment produces at least about 10.6 months (eg, between about 10.6 months and 16 months (10.6 months, 11 months, 12 months) months, 13 months, 14 months, 15 months, or 16 months)) in the subject population, in some cases, the treatment is at least about 8.5 months to about 10.6 months (eg, 8.7 months, 9.0 months). , 9.2 months, 9.4 months, 9.6 months, 9.8 months, 10 months, 10.2 months, 10.4 months, 10.6 months, 15 months, or 10.6 months).
제제의 투약dosing of the formulation
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 항대사물질, 및 탁산의 투약은 섹션 III(K)에 기재되어 있다. Dosing of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, antimetabolites, and taxanes is described in Section III(K).
G.G. 식도암과 관련된 치료 방법 및 사용Treatment methods and uses associated with esophageal cancer
본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg(예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체, 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg(예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 mg ± 0.05 mg, 예컨대, 1200 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하는, 방법을 포함한다. 일부 경우들에서, 상기 방법은 각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg(예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체, 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg(예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 mg ± 0.05 mg, 예컨대, 1200 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 양태들에서, 상기 방법은 각 투약 주기의 제 1일에 500 mg 내지 700 mg(예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체, 및 각 투약 주기의 제 1일에 900 mg 내지 1500 mg(예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 mg ± 0.05 mg, 예컨대, 1200 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다.The present invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising about 30 mg to about 1200 mg (e.g., about 550 mg to about 650 mg, e.g., 600 mg) on
본 발명은 식도암을 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg(예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체, 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg(예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 mg ± 0.05 mg, 예컨대, 1200 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하고, 여기서 상기 대상체 또는 대상체의 집단은 이전에 백금계 화학요법제 및 비백금계 화학요법제로 치료받은 적이 있는, 단계를 포함한 방법을 포함한다. 일부 양태들에서, 상기 방법은 각 투약 주기의 제 1일에 500 mg 내지 700 mg(예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg) 용량의 항 TIGIT 길항제 항체, 및 각 투약 주기의 제 1일에 900 mg 내지 1500 mg(예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 mg ± 0.05 mg, 예컨대, 1200 mg) 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하고, 여기서 상기 대상체 또는 대상체의 집단은 이전에 백금계 화학요법제 및 비백금계 화학요법제로 치료받은 적이 있는, 단계를 포함한 방법을 포함한다.The present invention provides a method of treating a subject or population of subjects having esophageal cancer, wherein on
일부 경우들에서, 상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은 적이 있다. 일부 경우들에서, 상기 대상체 또는 대상체의 집단은 이전 치료 동안 질병 진행 또는 허용할 수 없는 독성을 경험하였다.In some instances, the subject or subjects have previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. In some cases, the subject or population of subjects experienced disease progression or unacceptable toxicity during a previous treatment.
일부 경우들에서, 상기 21일 투약 주기는 백금계 화학요법제 및 비백금계 화학요법제를 더 포함한다. 일부 경우들에서, 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략된다.In some cases, the 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. In some cases, the platinum-based chemotherapeutic agent is omitted from the dosing regimen after 6 doses.
일부 경우들에서, 상기 백금계 화학치료제는 시스플라틴이다. 일부 경우들에서, 시스플라틴은 각 투약 주기의 제 1일에 약 80 mg/m2의 용량으로 투여된다. 일부 경우들에서, 시스플라틴은 각 투약 주기의 제 1일에 80 mg/m2의 용량으로 투여된다.In some cases, the platinum-based chemotherapeutic agent is cisplatin. In some cases, cisplatin is administered at a dose of about 80 mg/m 2 on
일부 경우들에서, 상기 비백금계 화학치료제는 항대사물질이다. 일부 경우들에서, 상기 대사길항물질은 5-플루오로우라실이다. 일부 경우들에서, 5-플루오로우라실은 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간의 용량으로 투여된다.In some cases, the non-platinum-based chemotherapeutic agent is an antimetabolite. In some cases, the antagonist is 5-fluorouracil. In some cases, 5-fluorouracil is administered at a dose of about 800 mg/m 2 /24 hours on days 1-5 of each 21-day cycle.
일부 경우들에서, 상기 식도암은 진행성 또는 전이성 식도암이다. In some cases, the esophageal cancer is advanced or metastatic esophageal cancer.
일부 경우들에서, 상기 대상체 또는 대상체들은 전이성 식도암에 대한 선행 치료를 받은 적이 없다.In some cases, the subject or subjects have not received prior treatment for metastatic esophageal cancer.
본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 각 투약 주기의 제 1일에 약 600 mg 용량(예컨대, 고정 용량)의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 방법을 포함한다. 일부 경우들에서, 상기 방법은 각 투약 주기의 제 1일에 약 600 mg 용량(예컨대, 고정 용량)의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량(예컨대, 고정 용량)의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체의 집단에게 투여하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 단계를 포함한다.The present invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising: tyragolumab at a dose of about 600 mg (eg, a fixed dose) on
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 2주 마다(Q2W) 약 10 mg 내지 약 1000 mg(예컨대, 약 20 mg 내지 약 1000 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 850 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 600 mg, 예컨대, 약 400 mg 내지 약 500 mg, 예컨대, 약 405 mg 내지 약 450 mg, 예컨대, 약 410 mg 내지 약 430 mg, 예컨대, 약 420 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 2주 마다(Q2W) 10 mg 내지 1000 mg(예컨대, 20 mg 내지 1000 mg, 예컨대, 50 mg 내지 900 mg, 예컨대, 00 mg 내지 850 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 600 mg, 예컨대, 400 mg 내지 500 mg, 예컨대, 405 mg 내지 450 mg, 예컨대, 410 mg 내지 430 mg, 예컨대, 420 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 2주 마다 약 420 mg(예컨대, 2주 마다 420 mg ± 10 mg, 예컨대, 420 ± 6 mg, 예컨대, 420 ± 5 mg, 예컨대, 420 ± 3 mg, 예컨대, 420 ± 1 mg, 예컨대, 420 ± 0.5 mg, 예컨대, 420 mg)의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 10 mg to about 1000 mg (eg, about 20) every two weeks (Q2W). mg to about 1000 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 850 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 600 mg, such as about 400 mg to about 500 mg, such as about 405 mg to about 450 mg, such as about 410 mg to about 430 mg, such as about 420 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 10 mg to 1000 mg (eg, 20 mg to 1000) every two weeks (Q2W). mg, such as 50 mg to 900 mg, such as 00 mg to 850 mg, such as 200 mg to 800 mg, such as 300 mg to 600 mg, such as 400 mg to 500 mg, such as 405 mg to 450 mg, For example, a dose (eg, a fixed dose) of 410 mg to 430 mg, such as 420 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 420 mg every 2 weeks (eg, 420 mg ± 10 mg every 2 weeks, For example, a dose of 420 ± 6 mg, such as 420 ± 5 mg, such as 420 ± 3 mg, such as 420 ± 1 mg, such as 420 ± 0.5 mg, such as 420 mg).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주 마다(Q4W) 약 200 mg 내지 약 2000 mg(예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 250 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1600 mg, 예컨대, 약 400 mg 내지 약 1500 mg, 예컨대, 약 500 mg 내지 약 1400 mg, 예컨대, 약 600 mg 내지 약 1200 mg, 예컨대, 약 700 mg 내지 약 1100 mg, 예컨대, 약 800 mg 내지 약 1000 mg, 예컨대, 약 800 mg 내지 약 900 mg, 예컨대, 약 800, 약 810, 약 820, 약 830, 약 840, 약 850, 약 860, 약 870, 약 880, 약 890, 또는 약 900 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 4주 마다(Q4W) 200 mg 내지 2000 mg(예컨대, 200 mg 내지 1600 mg, 예컨대, 250 mg 내지 1600 mg, 예컨대, 300 mg 내지 1600 mg, 예컨대, 400 mg 내지 1500 mg, 예컨대, 500 mg 내지 1400 mg, 예컨대, 600 mg 내지 1200 mg mg, 예컨대, 700 mg 내지 1100 mg, 예컨대, 800 mg 내지 1000 mg, 예컨대, 800 mg 내지 900 mg, 예컨대, 800 mg, 810 mg, 820 mg, 830 mg, 840 mg, 850 mg, 860 mg, 870 mg, 880 mg, 890 mg, 또는 900 mg)의 용량이다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 200 mg to about 2000 mg (eg, about 200 mg) every 4 weeks (Q4W). to about 1600 mg, such as about 250 mg to about 1600 mg, such as about 300 mg to about 1600 mg, such as about 400 mg to about 1500 mg, such as about 500 mg to about 1400 mg, such as about 600 mg to about 1200 mg, such as about 700 mg to about 1100 mg, such as about 800 mg to about 1000 mg, such as about 800 mg to about 900 mg, such as about 800, about 810, about 820, about 830, about 840, about 850, about 860, about 870, about 880, about 890, or about 900 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 200 mg to 2000 mg (eg, 200 mg to 1600) every 4 weeks (Q4W). mg, such as 250 mg to 1600 mg, such as 300 mg to 1600 mg, such as 400 mg to 1500 mg, such as 500 mg to 1400 mg, such as 600 mg to 1200 mg mg, such as 700 mg to 1100 mg , such as 800 mg to 1000 mg, such as 800 mg to 900 mg, such as 800 mg, 810 mg, 820 mg, 830 mg, 840 mg, 850 mg, 860 mg, 870 mg, 880 mg, 890 mg, or 900 mg).
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 80 mg 내지 약 1950 mg, 예컨대, 약 80 mg 내지 약 1900 mg, 예컨대, 약 80 mg 내지 약 1800 mg, 예컨대, 약 100 mg 내지 약 1700 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1400 mg, 예컨대, 약 400 mg 내지 약 1300 mg, 예컨대, 약 500 mg 내지 약 1200 mg, 예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 700 mg 내지 약 1000 mg, 예컨대, 약 740 mg 내지 약 940 mg, 예컨대, 약 790 mg 내지 약 890 mg, 예컨대, 약 815 mg 내지 약 865 mg, 예컨대, 약 830 mg 내지 약 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 2000 mg, 예컨대, 약 300 mg 내지 약 2000 mg, 예컨대, 약 400 mg 내지 약 2000 mg, 예컨대, 약 500 mg 내지 약 2000 mg, 예컨대, 약 600 mg 내지 약 1900 mg, 예컨대, 약 700 mg 내지 약 1800 mg, 예컨대, 약 800 mg 내지 약 1800 mg, 예컨대, 약 900 mg 내지 약 1800 mg, 예컨대, 약 1000 mg 내지 약 1800 mg, 예컨대, 약 1100 mg 내지 약 1800 mg, 예컨대, 약 1200 mg 내지 약 1800 mg, 예컨대, 약 1300 mg 내지 약 1800 mg, 예컨대, 약 1400 mg 내지 약 1800 mg, 예컨대, 약 1500 mg 내지 약 1800 mg, 예컨대, 약 1580 mg 내지 약 1780 mg, 예컨대, 약 1630 mg 내지 약 1730 mg, 예컨대, 약 1655 mg 내지 약 1705 mg, 예컨대, 약 1670 mg 내지 약 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대, 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 80 mg 내지 2000 mg(예컨대, 80 mg 내지 1950 mg, 예컨대, 80 mg 내지 1900 mg, 예컨대, 80 mg 내지 1800 mg, 예컨대, 100 mg 내지 1700 mg, 예컨대, 200 mg 내지 1600 mg, 예컨대, 300 mg 내지 1400 mg, 예컨대, 400 mg 내지 1300 mg, 예컨대, 500 mg 내지 1200 mg, 예컨대, 600 mg 내지 1100 mg, 예컨대, 700 mg 내지 1000 mg, 예컨대, 740 mg 내지 940 mg, 예컨대, 790 mg 내지 890 mg, 예컨대, 815 mg 내지 865 mg, 예컨대, 830 mg 내지 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 2000 mg, 예컨대, 300 mg 내지 2000 mg, 예컨대, 400 mg 내지 2000 mg, 예컨대, 500 mg 내지 2000 mg, 예컨대, 600 mg 내지 1900 mg, 예컨대, 700 mg 내지 1800 mg, 예컨대, 800 mg 내지 1800 mg, 예컨대, 900 mg 내지 1800 mg, 예컨대, 1000 mg 내지 1800 mg, 예컨대, 1100 mg 내지 1800 mg, 예컨대, 1200 mg 내지 1800 mg, 예컨대, 1300 mg 내지 1800 mg, 예컨대, 1400 mg 내지 1800 mg, 예컨대 1500 mg 내지 1800 mg, 예컨대, 1580 mg 내지 1780 mg, 예컨대 1630 mg 내지 1730 mg, 예컨대, 1655 mg 내지 1705 mg, 예컨대, 1670 mg 내지 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 1680 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 1680 mg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체(예컨대, 티라골루맙)과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 80 mg to about) every two weeks. 1950 mg, such as about 80 mg to about 1900 mg, such as about 80 mg to about 1800 mg, such as about 100 mg to about 1700 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1400 mg, such as about 400 mg to about 1300 mg, such as about 500 mg to about 1200 mg, such as about 600 mg to about 1100 mg, such as about 700 mg to about 1000 mg, such as about 740 mg to about 940 mg, such as about 790 mg to about 890 mg, such as about 815 mg to about 865 mg, such as about 830 mg to about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as, 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 4 weeks. 2000 mg, such as about 200 mg to about 2000 mg, such as about 300 mg to about 2000 mg, such as about 400 mg to about 2000 mg, such as about 500 mg to about 2000 mg, such as about 600 mg to about 1900 mg, such as about 700 mg to about 1800 mg, such as about 800 mg to about 1800 mg, such as about 900 mg to about 1800 mg, such as about 1000 mg to about 1800 mg, such as about 1100 mg to about 1800 mg, such as about 1200 mg to about 1800 mg, such as about 1300 mg to about 1800 mg, such as about 1400 mg to about 1800 mg, such as about 1500 mg to about 1800 mg, such as about 1580 mg to about 1780 mg, such as about 1630 mg to about 1730 mg, such as about 1655 mg to about 1705 mg, such as about 1670 mg to about 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as, 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 80 mg to 1950 mg, such as every two weeks) , 80 mg to 1900 mg, such as 80 mg to 1800 mg, such as 100 mg to 1700 mg, such as 200 mg to 1600 mg, such as 300 mg to 1400 mg, such as 400 mg to 1300 mg, such as 500 mg to 1200 mg, such as 600 mg to 1100 mg, such as 700 mg to 1000 mg, such as 740 mg to 940 mg, such as 790 mg to 890 mg, such as 815 mg to 865 mg, such as 830 mg to 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 4 weeks) , 200 mg to 2000 mg, such as 300 mg to 2000 mg, such as 400 mg to 2000 mg, such as 500 mg to 2000 mg, such as 600 mg to 1900 mg, such as 700 mg to 1800 mg, such as 800 mg to 1800 mg, such as 900 mg to 1800 mg, such as 1000 mg to 1800 mg, such as 1100 mg to 1800 mg, such as 1200 mg to 1800 mg, such as 1300 mg to 1800 mg, such as 1400 mg to 1800 mg, such as 1500 mg to 1800 mg, such as 1580 mg to 1780 mg, such as 1630 mg to 1730 mg, such as 1655 mg to 1705 mg, such as 1670 mg to 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some cases, a PD-1 axis binding antagonist (eg, anti-PD) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody (eg, tyragolumab) disclosed herein). The dose of the -L1 antagonist antibody (eg, atezolizumab) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy.
본 발명은 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체의 집단을 치료하는 방법으로서, 제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: (a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함하는, 방법을 포함한다.The present invention provides a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, the method comprising administering to the subject or population a first dosage regimen and a second dosage regimen, wherein: (a) the agent One dosing regimen consisted of a dose of about 80 mg/m 2 of cisplatin on
상기 방법들 중 임의의 것에 대한 일부 양태들에서, 상기 치료는 적어도 약 14%의 대상체 집단의 ORR을 발생시킨다(예컨대, 적어도 약 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100%, e.g., 14%-16%, 16%-18%, 18%-20%, 20%-30%, 30%-40%, 40%-50%, 50%-60%, 60%-70%, 70%-80%, 80%-90%, 또는 90%~100%의 ORR을 발생시킨다).In some aspects of any of the above methods, the treatment results in an ORR of at least about 14% of a subject population (eg, at least about 14%, 15%, 16%, 17%, 18%, 19%). , 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100%, e.g., 14%-16%, 16%-18%, 18%-20%, 20%-30%, 30%-40%, 40%-50%, 50%-60%, 60%- 70%, 70%-80%, 80%-90%, or 90%-100% ORR).
H.H. 암과 관련된 진단 방법 및 사용 Diagnostic methods and uses related to cancer
본 발명은 암(예컨대, 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC))를 가진 대상체를 위한 요법을 선택하는 방법을 제공하고, 여기서 요법은 상기 대상체로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. The present invention relates to cancer (eg, lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), SCLC (eg, ES-SCLC), NSCLC (eg, squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB) NSCLC, relapsed or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., the subject has not been previously treated for stage IV NSCLC) if absent)); )) or HER2-positive breast cancer); , MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC ( Provided is a method of selecting a therapy for a subject having (eg, MSS or low MSI CRC)), wherein the therapy is one or more biomarkers (eg, PD) in a sample (eg, a tumor sample or a blood sample) obtained from the subject. -L1, TIGIT, activated T cells, or cytokines) are guided by a diagnostic method involving determining the presence and/or expression level/amount.
추가적으로, 본원에서는 암(예컨대, 조기 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, TNBC(예컨대, eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC)를 가지고, 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 포함한 치료로부터 이익을 얻을 수 있는 대상체를 확인하는 방법이 제공되고, 여기서 확인은 상기 대상체로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Additionally, disclosed herein is cancer (eg, early lung cancer (eg, resectable lung cancer), SCLC (eg ES-SCLC), NSCLC (eg, squamous or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent) or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., if the subject has not been previously treated for stage IV NSCLC)) cervical cancer (eg, stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (eg, TNBC (eg, TNBC (eg, eTNBC)); or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); liver cancer (eg, HCC, such as locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (eg, MIBC, locally advanced UC or mUC); or low MSI CRC), an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as ate Methods of identifying a subject that may benefit from treatment comprising zolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab, are provided, wherein the identifying comprises a sample obtained from the subject (e.g., a tumor sample or blood sample) is guided by a diagnostic method involving determining the presence and/or expression level/amount of one or more biomarkers (eg, PD-L1, TIGIT, activated T cells, or cytokines) in the sample.
추가적으로, 본원에서는 암(예컨대, 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC))를 가진 대상체를 위한 요법에 대한 반응성을 평가하는 방법이 제공하고, 여기서 추가적으로 요법은 상기 대상체로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Additionally, herein disclosed herein are cancers (eg, lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), SCLC (eg, ES-SCLC), NSCLC (eg, squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, IIIB) Stage NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously been treated for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (e.g., TNBC (e.g., early TNBC) eTNBC)) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); liver cancer (eg, HCC, such as locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer ( e.g., MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; A method of assessing responsiveness to therapy for a subject having (eg, MSS or low MSI CRC) is provided, wherein additionally the therapy is administered in a sample obtained from the subject (eg, a tumor sample or a blood sample) in one or more biologics. Guided by a diagnostic method involving determining the presence and/or expression level/amount of a marker (eg, PD-L1, TIGIT, activated T cells, or cytokines).
추가적으로, 본원에서는 암(예컨대, 폐암(예컨대, 초기 단계 폐암(예컨대, 절제 가능한 폐암), SCLC(예컨대, ES-SCLC), NSCLC(예컨대, 편평 NSCLC 또는 비편평 NSCLC, 국소 진행성 절제 불가능한 NSCLC, IIIB기 NSCLC, 재발성 또는 전이성 NSCLC(예컨대, 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC(예컨대, IV기 비편평 NSCLC)), 또는 IV기 NSCLC(예컨대, 대상체가 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는 경우)); 자궁경부암(예컨대, 4B기, 전이성, 재발성, 또는 지속성 자궁경부암, 예컨대 전이성 및/또는 재발성 PD-L1 양성 자궁경부암); 유방암(예컨대, TNBC(예컨대, 초기 TNBC(eTNBC)) 또는 HER2 양성 유방암); 두경부암(예컨대, SCCHN, 예컨대 재발성/전이성 PD-L1 양성 SCCHN); 간암(예컨대, HCC, 예컨대 국소 진행성 또는 전이성 HCC 및/또는 절제 불가능한 HCC); 방광암(예컨대, MIBC, 국소 진행성 UC 또는 mUC); 식도암; 췌장암(예컨대, PDAC, 예컨대 전이성 PDAC); 신장암(예컨대, RCC); 흑색종; 난소암; 위암(예컨대, 위식도 접합부 암); 또는 CRC(예컨대, MSS 또는 저 MSI CRC))를 가진 대상체를 위한 요법을 최적화하는 방법이 제공되고, 여기서 추가적으로 요법은 상기 대상체로부터 수득한 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 하나 이상의 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계를 수반한 진단 방법에 의해 안내된다. Additionally, herein disclosed herein are cancers (eg, lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), SCLC (eg, ES-SCLC), NSCLC (eg, squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, IIIB) Stage NSCLC, relapsed or metastatic NSCLC (eg, locally advanced unresectable or metastatic nonsquamous NSCLC (eg, stage IV nonsquamous NSCLC)), or stage IV NSCLC (eg, the subject has previously been treated for stage IV NSCLC) cervical cancer (e.g., stage 4B, metastatic, recurrent, or persistent cervical cancer, such as metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (e.g., TNBC (e.g., early TNBC) eTNBC)) or HER2 positive breast cancer); head and neck cancer (eg SCCHN, such as recurrent/metastatic PD-L1 positive SCCHN); liver cancer (eg, HCC, such as locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer ( e.g., MIBC, locally advanced UC or mUC); esophageal cancer; pancreatic cancer (eg, PDAC, such as metastatic PDAC); kidney cancer (eg, RCC); melanoma; A method of optimizing therapy for a subject with (eg, MSS or low MSI CRC) is provided, wherein the therapy additionally comprises one or more biomarkers (eg, a tumor sample or a blood sample) in a sample obtained from the subject (eg, a tumor sample or a blood sample). , PD-L1, TIGIT, activated T cells, or cytokines) are guided by a diagnostic method involving determining the presence and/or expression level/amount.
본원에 기재된 방법에서 사용하기 위한 바이오마커는 종양 면역생물학(예컨대, TEFF), 림프구 하위집단, T 세포 수용체 레퍼토리, T 세포 활성화와 관련된 사이토카인 및 혈장 유래 사이토카인과 관련된 유전자 또는 유전자 서명 분석(예컨대, CD274)인 WGS 및/또는 NGS를 통해 확인된 조직(예컨대, 종양 조직) 또는 혈액(예컨대, 전혈), 조직(예컨대, 종양 조직) 및/또는 혈액 내 순환 종양 DNA(돌연변이 로드, MSI 및 MMR 결함를 포함하지만 이에 제한되지는 않음)의 생식계열 및 체세포 돌연변이 상의 PD-L1 발현을 포함하지만, 이에 제한되지는 않는다. 일부 경우들에서, 상기 바이오마커는 PD-L1이다. 일부 경우들에서, 상기 샘플은 종양 샘플(예컨대, 포르말린 고정, 파라핀 포매(FFPE) 종양 샘플)이다.Biomarkers for use in the methods described herein may include tumor immunobiology (eg, TEFF), lymphocyte subpopulations, T cell receptor repertoire, cytokines associated with T cell activation, and gene or gene signature analysis (eg, associated with plasma-derived cytokines). , CD274) in tissues (eg, tumor tissue) or blood (eg, whole blood), tissue (eg, tumor tissue) and/or circulating tumor DNA (mutant load, MSI and MMR) in blood (eg, tumor tissue) identified via WGS and/or NGS PD-L1 expression on germline and somatic mutations (including but not limited to defects). In some cases, the biomarker is PD-L1. In some cases, the sample is a tumor sample (eg, a formalin fixed, paraffin embedded (FFPE) tumor sample).
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계, 및 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙, 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)의 1회 이상의 투약 주기를 상기 대상체에게 섹션 III(A)에 기재된 임의의 방법 또는 사용에 따라 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount, and an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as administering to the subject one or more dosing cycles of atezolizumab, or an anti-PD-1 antagonist antibody, such as pembrolizumab, according to any of the methods or uses described in Section III(A).
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 4주마다 약 700 mg 내지 약 1000 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 투약 요법은 4주마다 700 mg 내지 1000 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 4주마다 1400 mg 내지 2000 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and administering to the subject a dose of about 700 mg to about 1000 mg (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 4 weeks and a dose of about 1400 mg to about 2000 mg (eg, a fixed dose) every 4 weeks. administering a dosing regimen comprising one or more dosing cycles of the PD-1 axis binding antagonist. In some cases, the dosing regimen is a 700 mg to 1000 mg dose (eg, a fixed dose) of the anti TIGIT antagonist antibody every 4 weeks and a 1400 mg to 2000 mg dose (eg, a fixed dose) of the PD-1 axis every 4 weeks (eg, a fixed dose) one or more dosing cycles of the binding antagonist.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 2주마다 약 300 mg 내지 약 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체에게 2주마다 300 mg 내지 600 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체 및 2주마다 600 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and giving the subject a dose of about 300 mg to about 600 mg every two weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody and a dose of about 600 mg to about 1200 mg every two weeks (eg, a fixed dose) administering a dosing regimen comprising one or more dosing cycles of the PD-1 axis binding antagonist of In some cases, the method administers to the subject a 300 mg to 600 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every two weeks and a 600 mg to 1200 mg dose (eg, a fixed dose) of PD- every two weeks. administering a dosing regimen comprising one or more dosing cycles of the uniaxial binding antagonist.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학치료제, 및 3주마다 비백금계 화학치료제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and giving the subject a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody, a dose of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) administering a dosing regimen comprising at least one dosing cycle of a PD-1 axis binding antagonist of In some cases, the method comprises a 30 mg to 1200 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding at a 80 mg to 1600 mg dose (eg, a fixed dose) every 3 weeks administering to the subject a dosing regimen comprising at least one dosing cycle of the antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 200 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함하고, 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다. 일부 경우들에서, 상기 방법은 3주마다 30 mg 내지 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 200 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙이다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and dosing to the subject comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and an anti-PD-1 antagonist antibody at a dose of about 200 mg every 3 weeks administering therapy, wherein the anti-PD-1 antagonist antibody is pembrolizumab. In some cases, the method administers to the subject a dosing regimen comprising one or more dosing cycles of an anti TIGIT antagonist antibody at a dose of 30 mg to 1200 mg every 3 weeks and an anti-PD-1 antagonist antibody at a dose of 200 mg every 3 weeks. administering, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 티라골루맙과 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 100mg 내지 약 1000mg의 용량으로 투여된다. 일부 경우들에서, 상기 펨브롤리주맙은 6주 마다 약 400 mg의 용량으로 투여된다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and administering to the subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein said pembrolizumab is administered in an amount of from about 100 mg to about 1000 mg every 6 weeks. administered in dose. In some cases, the pembrolizumab is administered at a dose of about 400 mg every 6 weeks.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계, 및 상기 대상체에게 3주마다 약 30 mg 내지 약 1200 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량(예컨대, 고정 용량)의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체에게 3주마다 30 mg 내지 1200 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 10 mg/m2 내지 10000 mg/m2 용량(예컨대, 고정 용량)의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount, and giving the subject a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody, a dose of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist, and a dose (eg, a fixed dose) of about 10 mg/m 2 to about 10000 mg/m 2 orally twice daily every 3 weeks of a 2 week dosing/1 week washout. administering a dosing regimen comprising one or more dosing cycles of the antimetabolite. In some cases, the method administers to the subject a dose of 30 mg to 1200 mg (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks, a dose of 80 mg to 1600 mg (eg, a fixed dose) every 3 weeks. PD-1 axis binding antagonist, and 1 dose of 10 mg/m 2 to 10000 mg/m 2 dose (eg, fixed dose) of an antimetabolite orally twice daily for every 3 weeks of 2 weeks dosing/week rest administering a dosing regimen comprising more than one dosing cycle.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계 및 상기 대상체에게 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 젬시타빈 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체에게 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 젬시타빈 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount and administering to the subject a dose of about 30 mg to about 1200 mg (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks, a dose of about 80 mg to about 1600 mg (eg, a fixed dose) every 3 weeks. administering a dosing regimen comprising one or more dosing cycles of the PD-1 axis binding antagonist, gemcitabine, and nap-paclitaxel. In some cases, the method administers to the subject a 30 mg to 1200 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks, a PD- at a 80 mg to 1600 mg dose (eg, a fixed dose) every 3 weeks administering a dosing regimen comprising one or more dosing cycles of the uniaxial binding antagonist, gemcitabine, and nap-paclitaxel.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계, 및 상기 대상체에게 3주마다 약 30 mg 내지 약 1200 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg의 용량으로 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 대상체에게 3주마다 30 mg 내지 1200 mg의 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 및 3주마다 1mg/kg 내지 35mg/kg 용량의 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 투여하는 단계를 포함한다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount, and giving the subject a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti TIGIT antagonist antibody, a dose of about 80 mg to about 1600 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist, and administering a dosing regimen comprising one or more dosing cycles of the VEGF antagonist at a dose of about 1 mg/kg to about 35 mg/kg every 3 weeks. In some cases, the method administers to the subject a dose of 30 mg to 1200 mg (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks, a dose of 80 mg to 1600 mg (eg, a fixed dose) every 3 weeks. administering a dosing regimen comprising a PD-1 axis binding antagonist and one or more dosing cycles of a VEGF antagonist at a dose of 1 mg/kg to 35 mg/kg every 3 weeks.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계, 및 유도기 및 유지기를 포함하는 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학치료제, 및 3주마다 비백금계 화학치료제의 1회 이상의 투약 주기를 포함하고; (b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는다. 일부 경우들에서, (a) 상기 유도기는 3주마다 30 mg 내지 1200 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 80 mg 내지 1600 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학치료제, 및 3주마다 비백금계 화학치료제의 1회 이상의 투약 주기를 포함하고; (b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는다. In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount, and administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein: (a) the induction phase comprises a dose of about 30 mg to about 1200 mg every 3 weeks (eg, a fixed dose) of an anti-TIGIT antagonist antibody, a dose of about 80 mg to 1600 mg every 3 weeks (eg, a fixed dose) of a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks. comprising one or more dosing cycles; (b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said maintenance The phase does not include administration of said platinum-based chemotherapeutic agent. In some cases, (a) the induction phase is a 30 mg to 1200 mg dose (eg, a fixed dose) of an anti-TIGIT antagonist antibody every 3 weeks, a PD at a dose of 80 mg to 1600 mg every 3 weeks (eg, a fixed dose) - one or more dosing cycles of the axis binding antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks; (b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said maintenance The phase does not include administration of said platinum-based chemotherapeutic agent.
일부 경우들에서, 상기 방법은 상기 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양을 결정하는 단계, 및 유도기 및 유지기를 포함하는 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 상기 유도기는 3주마다 약 500 mg 내지 약 700 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학치료제, 및 3주마다 비백금계 화학치료제의 1회 이상의 투약 주기를 포함하고; (b) 상기 유지기는 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는다. 일부 경우들에서, (a) 상기 유도기는 3주마다 500 mg 내지 700 mg 용량(예컨대, 고정 용량)의 항 TIGIT 길항제 항체, 3주마다 900 mg 내지 1500 mg의 용량(예컨대, 고정 용량)의 PD-1 축 결합 길항제, 3주마다 백금계 화학치료제, 및 3주마다 비백금계 화학치료제의 1회 이상의 투약 주기를 포함하고; (b) 상기 유지기는 4주마다 700 mg 내지 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는다.In some cases, the method comprises the presence and/or expression level of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample (eg, a tumor sample or blood sample) from the subject. /determining the amount, and administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein: (a) the induction phase comprises a dose of about 500 mg to about 700 mg every 3 weeks (eg, a fixed dose) of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks (eg, a fixed dose), a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks one or more dosing cycles of (b) the maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks; , wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent. In some cases, (a) the induction phase is a 500 mg to 700 mg dose (eg, a fixed dose) of an anti TIGIT antagonist antibody every 3 weeks, PD at a dose of 900 mg to 1500 mg every 3 weeks (eg, a fixed dose) - one or more dosing cycles of the axis binding antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks; (b) said maintenance phase comprises one or more additional dosing cycles of anti-TIGIT antagonist antibody at a dose of 700 mg to 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of 1400 mg to 2000 mg every 4 weeks, wherein said The maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent.
바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양은 단백질, 단백질 단편, DNA, mRNA, cDNA, 및/또는 유전자 복제 수를 포함하지만 이에 제한되지는 않는 당해 분야에서 공지된 임의의 적합한 기준에 따라 정성적으로 및/또는 정량적으로 결정될 수 있다. 일부 경우들에서, 상기 바이오마커는 PD-L1이다. PD-L1의 발현은 섹션 III(L)에 기재된 바와 같이 평가할 수 있다. 일부 경우들에서, 상기 바이오마커는 TIGIT이다. TIGIT의 발현은 섹션 III(M)에 기재된 바와 같이 평가할 수 있다. 일부 경우들에서, 상기 바이오마커는 EGFR 및/또는 ALK 이상이다. EGFR 및/또는 ALK 이상은 섹션 III(N)에 기재된 바와 같이 평가할 수 있다.The presence and/or expression level/amount of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) includes, but is not limited to, protein, protein fragment, DNA, mRNA, cDNA, and/or gene copy number. It may be determined qualitatively and/or quantitatively according to any suitable criteria known in the art without limitation. In some cases, the biomarker is PD-L1. Expression of PD-L1 can be assessed as described in section III(L). In some cases, the biomarker is TIGIT. Expression of TIGIT can be assessed as described in section III(M). In some cases, the biomarker is above EGFR and/or ALK. EGFR and/or ALK abnormalities can be assessed as described in Section III(N).
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 단백질 발현 수준이다. 일부 경우들에서, 상기 PD-L1 단백질 발현 수준은 면역조직화학적(IHC) 분석에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of the biomarker is a detectable protein expression level of PD-L1 in a tumor sample from the subject (eg, a FFPE tumor sample). In some cases, the PD-L1 protein expression level was determined by immunohistochemical (IHC) analysis. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 상기 대상체로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 대상체로부터의 종양 샘플(예컨대, FFPE 종양 샘플)은 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, a tumor sample from the subject (eg, a FFPE tumor sample) has been determined to have a detectable expression level of PD-L1. In some cases, a tumor sample from the subject (eg, a FFPE tumor sample) has been determined to have a detectable expression level of PD-L1 in tumor infiltrating immune cells. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 바이오마커의 발현 수준 또는 양은 상기 대상체로부터의 종양 샘플(예컨대, FFPE 종양 샘플)에서 PD-L1의 검출가능한 핵산 발현 수준이다. 일부 경우들에서, PD-L1의 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, 유전자 발현의 연속 분석(SAGE), MassARRAY® 기술, 조직내(in situ) 혼성화(ISH), 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the expression level or amount of the biomarker is a detectable nucleic acid expression level of PD-L1 in a tumor sample (eg, FFPE tumor sample) from the subject. In some cases, the nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY ® technology, in-tissue. (in situ) hybridization (ISH), or a combination thereof. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 대상체로부터의 샘플(예컨대, 종양 샘플 또는 혈액 샘플)에서 바이오마커(예컨대, PD-L1, TIGIT, 활성화된 T 세포, 또는 사이토카인)의 존재 및/또는 발현 수준/양은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙 또는 항 PD-1 길항제 항체, 예컨대 펨브롤리주맙)를 이용한 요법에 적격인 것으로 상기 대상체를 선택하고, 예를 들어, 여기서 PD-L1의 검출가능한 발현 수준은 개체의 선택을 위한 바이오마커이다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플(예컨대, FFPE 종양 샘플)이다. 일부 예들에서, 종양 샘플은 종양-침윤 면역 세포, 종양 세포, 간질 세포 및 이들의 임의의 조합을 포함한다. 일부 경우들에서, 상기 종양 샘플은 FFPE 종양 샘플이다.In some cases, the presence and/or expression level/amount of a biomarker (eg, PD-L1, TIGIT, activated T cell, or cytokine) in a sample from the subject (eg, a tumor sample or blood sample) is anti-TIGIT selecting the subject as eligible for therapy with an antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody such as atezolizumab or an anti-PD-1 antagonist antibody such as pembrolizumab), e.g. For example, wherein the detectable expression level of PD-L1 is a biomarker for selection of an individual. In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample (eg, a FFPE tumor sample). In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof. In some cases, the tumor sample is a FFPE tumor sample.
일부 경우들에서, 상기 방법은 확인된 대상체에게 상기 요법을 투여하는 단계를 더 포함한다. 일부 경우들에서, 상기 요법은 하나 이상의 추가 치료제(들)(예컨대, 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 항체), VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀))를 추가로 포함하거나, 또는 병용으로(별로도 또는 함께) 투여할 수 있다.In some cases, the method further comprises administering the therapy to the identified subject. In some cases, the therapy comprises one or more additional therapeutic agent(s) (eg, anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (eg, anti-PD-L1 antibody), VEGF antagonist, chemotherapeutic agent (eg, platinum-based) chemotherapeutic or non-platinum chemotherapeutic agent), ADC (e.g. enfortumab vedotin or sacituzumab gobitecan), or CSF (e.g. pegfilgrastim, filgrastim or sagramostim) may be included or administered in combination (separately or together).
일부 경우들에서, 본원에 기재된 임의의 진단 방법 또는 사용에서, 상기 암은 고형 종양 및/또는 국소 진행성 또는 전이성 암이다.In some cases, in any of the diagnostic methods or uses described herein, the cancer is a solid tumor and/or a locally advanced or metastatic cancer.
I.I. 투약dosage
i.i. 항 TIGIT 길항제 항체의 투약Dosing of Anti-TIGIT Antagonist Antibodies
일반적인 제안으로서, 인간에게 투여되는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 치료적 유효량은 1회 또는 그 이상의 투여에 의한 것인지에 상관없이 환자 체중의 약 0.01 내지 약 50 mg/kg의 범위 안에 있을 것이다. 일부 구현예들에서, 인간에게 투여되는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 치료적 유효량은 1회 또는 그 이상의 투여에 의한 것인지에 상관없이 환자 체중의 0.01 내지 50 mg/kg의 범위 안에 있다.As a general suggestion, a therapeutically effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragolumab as disclosed herein) administered to a human, whether by one or more administrations, is approximately one dose of the patient's body weight. 0.01 to about 50 mg/kg. In some embodiments, a therapeutically effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragoluumab as disclosed herein) administered to a human is the weight of the patient, whether by one or more administrations. in the range of 0.01 to 50 mg/kg of
일부 예시적인 구현예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 예를 들어 매일, 매주, 2주마다, 3주마다, 또는 4주마다 약 0.01 내지 약 45 mg/kg, 약 0.01 내지 약 40 mg/kg, 약 0.01 내지 약 35 mg/kg, 약 0.01 내지 약 30 mg/kg, 약 0.01 내지 약 25 mg/kg, 약 0.01 내지 약 20 mg/kg, 약 0.01 내지 약 15 mg/kg, 약 0.01 내지 약 10 mg/kg, 약 0.01 내지 약 5 mg/kg, 또는 약 0.01 내지 약 1 mg/kg의 용량으로 투여된다. 예시적인 구현예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 예를 들어 매일, 매주, 2주마다, 3주마다, 또는 4주마다 0.01 내지 45 mg/kg, 0.01 내지 40 mg/kg, 0.01 내지 35 mg/kg, 0.01 내지 30 mg/kg, 0.01 내지 25 mg/kg, 0.01 내지 20 mg/kg, 0.01 내지 15 mg/kg, 0.01 내지 10 mg/kg, 0.01 내지 5 mg/kg, 또는 0.01 내지 1 mg/kg의 용량으로 투여된다. In some exemplary embodiments, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered, eg, daily, weekly, every 2 weeks, every 3 weeks, or every 4 weeks. about 0.01 to about 45 mg/kg, about 0.01 to about 40 mg/kg, about 0.01 to about 35 mg/kg, about 0.01 to about 30 mg/kg, about 0.01 to about 25 mg/kg, about 0.01 to about per 20 mg/kg, about 0.01 to about 15 mg/kg, about 0.01 to about 10 mg/kg, about 0.01 to about 5 mg/kg, or about 0.01 to about 1 mg/kg. In exemplary embodiments, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered, eg, daily, weekly, every 2 weeks, every 3 weeks, or every 4 weeks. 0.01 to 45 mg/kg, 0.01 to 40 mg/kg, 0.01 to 35 mg/kg, 0.01 to 30 mg/kg, 0.01 to 25 mg/kg, 0.01 to 20 mg/kg, 0.01 to 15 mg/kg, 0.01 to 10 mg/kg, 0.01 to 5 mg/kg, or 0.01 to 1 mg/kg.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about 1 day (eg, -3 days, -2 days, -1 days) of each dosing cycle. , day 1, 2, or 3).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 단계적 투약 요법(예컨대, 대상체의 체중(BW) 또는 체표면적(BSA)에 기초한 투약)으로 투여된다(예컨대, 3주마다). 상기 투약 요법은 비교적 낮은 체중(예컨대, 40kg 이하(예컨대, 5 kg 내지 40 kg, 15 kg 내지 40 kg, 또는 5 kg 내지 15 kg))을 갖는 대상체에 대한 치료에 활용될 수 있고, 성인 데이터에서 추정된 약동학적 매개변수의 외삽을 기반으로 한 생체 시뮬레이션 연구를 통해 개발되었다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in a step-by-step dosing regimen (eg, dosing based on the subject's body weight (BW) or body surface area (BSA)). ) (eg, every 3 weeks). The dosing regimen may be utilized to treat subjects with relatively low body weight (eg, 40 kg or less (eg, 5 kg to 40 kg, 15 kg to 40 kg, or 5 kg to 15 kg)), and in adult data It was developed through in vivo simulation studies based on extrapolation of estimated pharmacokinetic parameters.
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 250 mg 내지 약 350 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 350 mg 내지 약 450 mg(예컨대, 3주마다 약 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 550 mg 내지 약 650 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 250 mg 내지 350 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 350 mg 내지 450 mg(예컨대, 3주마다 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 550 mg 내지 650 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 600 mg의 용량으로 투여된다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) for treating a subject having cancer is a dose in steps based on the subject's body weight. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 250 mg to about 350 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 350 mg to about 450 mg every 3 weeks (eg, about 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of about 550 mg to about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 15 kg and no more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 250 mg to 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of 350 mg to 450 mg every 3 weeks (eg, 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of 550 mg to 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; (b) greater than 15 kg and not more than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (c) greater than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 40 kg을 초과하는 대상체의 경우(예컨대, 40.5 kg, 41 kg, 42 kg, 43 kg, 44 kg, 45 kg, 46 kg, 47 kg, 48 kg, 49 kg, 50 kg, 51 kg, 52 kg, 53 kg, 54 kg, 55 kg, 56 kg, 57 kg, 58 kg, 59 kg, 60 kg, 61 kg, 62 kg, 63 kg, 64 kg, 65 kg, 66 kg, 67 kg, 68 kg, 69 kg, 70 kg, 75 kg, 80 kg, 85 kg, 90 kg, 95 kg, 100 kg, 110 kg, 120 kg, 130 kg, 140 kg, 150 kg 또는 그 이상) 3주마다(Q3W) 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 40 kg을 초과하는 대상체의 경우 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 40 kg을 초과하는 대상체의 경우(예컨대, 40.5 kg, 41 kg, 42 kg, 43 kg, 44 kg, 45 kg, 46 kg, 47 kg, 48 kg, 49 kg, 50 kg, 51 kg, 52 kg, 53 kg, 54 kg, 55 kg, 56 kg, 57 kg, 58 kg, 59 kg, 60 kg, 61 kg, 62 kg, 63 kg, 64 kg, 65 kg, 66 kg, 67 kg, 68 kg, 69 kg, 70 kg, 75 kg, 80 kg, 85 kg, 90 kg, 95 kg, 100 kg, 110 kg, 120 kg, 130 kg, 140 kg, 150 kg 또는 그 이상) 3주마다(Q3W) 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 40 kg을 초과하는 대상체의 경우 3주마다 600 mg의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing more than 40 kg (eg, 40.5 kg, 41 kg, 42 kg, 43 kg, 44 kg, 45 kg, 46 kg, 47 kg, 48 kg, 49 kg, 50 kg, 51 kg, 52 kg, 53 kg, 54 kg, 55 kg, 56 kg, 57 kg, 58 kg , 59 kg, 60 kg, 61 kg, 62 kg, 63 kg, 64 kg, 65 kg, 66 kg, 67 kg, 68 kg, 69 kg, 70 kg, 75 kg, 80 kg, 85 kg, 90 kg, 95 kg, 100 kg, 110 kg, 120 kg, 130 kg, 140 kg, 150 kg or more) every 3 weeks (Q3W) about 30 mg to about 1200 mg (eg, about 30 mg to about 1100 mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 600 mg every 3 weeks for a subject weighing more than 40 kg . In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing more than 40 kg (eg, 40.5 kg, 41 kg, 42 kg, 43 kg, 44 kg, 45 kg, 46 kg, 47 kg, 48 kg, 49 kg, 50 kg, 51 kg, 52 kg, 53 kg, 54 kg, 55 kg, 56 kg, 57 kg, 58 kg , 59 kg, 60 kg, 61 kg, 62 kg, 63 kg, 64 kg, 65 kg, 66 kg, 67 kg, 68 kg, 69 kg, 70 kg, 75 kg, 80 kg, 85 kg, 90 kg, 95 kg, 100 kg, 110 kg, 120 kg, 130 kg, 140 kg, 150 kg or more) every 3 weeks (Q3W) 30 mg to 1200 mg (eg 30 mg to 1100 mg, eg 60 mg to 1000 mg) , such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as , 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg , eg 600±0.5 mg, eg 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg every 3 weeks for a subject weighing more than 40 kg.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 15 kg 초과 40 kg 이하인 대상체의 경우(예컨대, 15.1 kg, 15.2 kg, 15.3 kg, 15.4 kg, 15.5 kg, 16 kg, 17 kg, 18 kg, 19 kg, 20 kg, 21 kg, 22 kg, 23 kg, 24 kg, 25 kg, 26 kg, 27 kg, 28 kg, 29 kg, 30 kg, 31 kg, 32 kg, 33 kg, 34 kg, 35 kg, 36 kg, 37 kg, 38 kg, 39 kg, 또는 39.5 kg) 3주마다(Q3W) 약 10 mg 내지 약 1000 mg(예컨대, 약 20 mg 내지 약 1000 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 850 mg, 예컨대, 약 200 mg 내지 약 700 mg, 예컨대, 약 250 mg 내지 약 600 mg, 예컨대, 약 300 mg 내지 약 500 mg, 예컨대, 약 350 mg 내지 약 450 mg, 예컨대, 약 390 mg 내지 약 410 mg, 예컨대, 약 400 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체중이 15 kg 초과 40 kg 이하인 대상체의 경우 3주 마다 약 400 mg(예컨대, 3주 마다 400 mg ± 10 mg, 예컨대, 400 ± 6 mg, 예컨대, 400 ± 5 mg, 예컨대, 400 ± 3 mg, 예컨대, 400 ± 1 mg, 예컨대, 400 ± 0.5 mg, 예컨대, 400 mg )의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 15 kg 초과 40 kg 이하인 대상체의 경우(예컨대, 15.1 kg, 15.2 kg, 15.3 kg, 15.4 kg, 15.5 kg, 16 kg, 17 kg, 18 kg, 19 kg, 20 kg, 21 kg, 22 kg, 23 kg, 24 kg, 25 kg, 26 kg, 27 kg, 28 kg, 29 kg, 30 kg, 31 kg, 32 kg, 33 kg, 34 kg, 35 kg, 36 kg, 37 kg, 38 kg, 39 kg, 또는 39.5 kg) 3주마다(Q3W) 10 mg 내지 1000 mg(예컨대, 20 mg 내지 1000 mg, 예컨대, 50 mg 내지 900 mg, 예컨대, 100 mg 내지 850 mg, 예컨대, 200 mg 내지 700 mg, 예컨대, 250 mg 내지 600 mg, 예컨대, 300 mg 내지 500 mg, 예컨대, 350 mg 내지 450 mg, 예컨대, 390 mg 내지 410 mg, 예컨대, 400 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체중이 15 kg 초과 40 kg 이하인 대상체의 경우 3주마다 400 mg(예컨대, 3주마다 400 mg ± 10 mg, 예컨대, 400 ± 6 mg, 예컨대, 400 ± 5 mg, 예컨대, 400 ± 3 mg, 예컨대, 400 ± 1 mg, 예컨대, 400 ± 0.5 mg, 예컨대, 400 mg )의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing more than 15 kg and no more than 40 kg (eg, 15.1 kg, 15.2 kg). , 15.3 kg, 15.4 kg, 15.5 kg, 16 kg, 17 kg, 18 kg, 19 kg, 20 kg, 21 kg, 22 kg, 23 kg, 24 kg, 25 kg, 26 kg, 27 kg, 28 kg, 29 kg, 30 kg, 31 kg, 32 kg, 33 kg, 34 kg, 35 kg, 36 kg, 37 kg, 38 kg, 39 kg, or 39.5 kg) every 3 weeks (Q3W) from about 10 mg to about 1000 mg ( For example, about 20 mg to about 1000 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 850 mg, such as about 200 mg to about 700 mg, such as about 250 mg to about 600 mg, eg, from about 300 mg to about 500 mg, such as from about 350 mg to about 450 mg, such as from about 390 mg to about 410 mg, such as about 400 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (e.g., an anti TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is about 400 mg every 3 weeks for a subject weighing more than 15 kg and no more than 40 kg ( For example, every 3 weeks 400 mg ± 10 mg, such as 400 ± 6 mg, such as 400 ± 5 mg, such as 400 ± 3 mg, such as 400 ± 1 mg, such as 400 ± 0.5 mg, such as 400 mg ) is the capacity of In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing more than 15 kg and no more than 40 kg (eg, 15.1 kg, 15.2 kg). , 15.3 kg, 15.4 kg, 15.5 kg, 16 kg, 17 kg, 18 kg, 19 kg, 20 kg, 21 kg, 22 kg, 23 kg, 24 kg, 25 kg, 26 kg, 27 kg, 28 kg, 29 kg, 30 kg, 31 kg, 32 kg, 33 kg, 34 kg, 35 kg, 36 kg, 37 kg, 38 kg, 39 kg, or 39.5 kg) every 3 weeks (Q3W) 10 mg to 1000 mg (eg, 20 mg to 1000 mg, such as 50 mg to 900 mg, such as 100 mg to 850 mg, such as 200 mg to 700 mg, such as 250 mg to 600 mg, such as 300 mg to 500 mg, such as 350 mg to 450 mg, such as 390 mg to 410 mg, such as 400 mg). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 400 mg (eg, every 3 weeks) for a subject weighing more than 15 kg and not more than 40 kg. , 400 mg ± 10 mg, such as 400 ± 6 mg, such as 400 ± 5 mg, such as 400 ± 3 mg, such as 400 ± 1 mg, such as 400 ± 0.5 mg, such as 400 mg, every 3 weeks) is the capacity of
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 15 kg 이하인 대상체의 경우(예컨대, 0.5 kg, 1 kg, 1.5 kg, 2.0 kg, 2.5 kg, 3.0 kg, 3.5 kg, 4.0 kg, 4.5 kg, 5.0 kg, 5.5 kg, 6.0 kg, 6.5 kg, 7.0 kg, 7.5 kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14.0 kg, 14.5 kg, 또는 15.0 kg) 3주마다(Q3W) 약 10 mg 내지 약 1000 mg(예컨대, 약 10 mg 내지 약 900 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 750 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 150 mg 내지 약 500 mg, 예컨대, 약 200 mg 내지 약 400 mg, 예컨대, 약 250 mg 내지 약 350 mg, 예컨대, 약 290 mg 내지 약 310 mg, 예컨대, 약 300 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체중이 15 kg 이하인 대상체의 경우 3주마다 약 300 mg(예컨대, 3주마다 300 mg ± 10 mg, 예컨대, 300 ± 6 mg, 예컨대, 300 ± 5 mg, 예컨대, 300 ± 3 mg, 예컨대, 300 ± 1 mg, 예컨대, 300 ± 0.5 mg, 예컨대, 300 mg )의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체중이 15 kg 이하인 대상체의 경우(예컨대, 0.5 kg, 1 kg, 1.5 kg, 2.0 kg, 2.5 kg, 3.0 kg, 3.5 kg, 4.0 kg, 4.5 kg, 10 mg, 5.5 kg, 6.0 kg, 6.5 kg, 7.0 kg, 7.5 kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14.0 kg, 14.5 kg, 또는 15.0 kg) 3주마다(Q3W) 10 mg 내지 1000 mg(예컨대, 10 mg 내지 900 mg, 예컨대, 50 mg 내지 900 mg, 예컨대, 100 mg 내지 750 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 150 mg 내지 500 mg, 예컨대, 200 mg 내지 400 mg, 예컨대, 250 mg 내지 350 mg, 예컨대, 290 mg 내지 310 mg, 예컨대, 300 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체중이 15 kg 이하인 대상체의 경우 3주마다 300 mg(예컨대, 3주마다 300 mg ± 10 mg, 예컨대, 300 ± 6 mg, 예컨대, 300 ± 5 mg, 예컨대, 300 ± 3 mg, 예컨대, 300 ± 1 mg, 예컨대, 300 ± 0.5 mg, 예컨대, 300 mg )의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing 15 kg or less (eg, 0.5 kg, 1 kg, 1.5 kg). , 2.0 kg, 2.5 kg, 3.0 kg, 3.5 kg, 4.0 kg, 4.5 kg, 5.0 kg, 5.5 kg, 6.0 kg, 6.5 kg, 7.0 kg, 7.5 kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14.0 kg, 14.5 kg, or 15.0 kg) about 10 mg to about 1000 mg (e.g., about 10 mg to about 900 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 750 mg, such as about 100 mg to about 600 mg, such as about 150 mg to about 500 mg, such as about 200 mg to about 400 mg, such as about 250 mg to about 350 mg, such as about 290 mg to about 310 mg, such as about 300 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 300 mg (eg, 3 weeks) for a subject weighing 15 kg or less. a dose of 300 mg ± 10 mg, such as 300 ± 6 mg, such as 300 ± 5 mg, such as 300 ± 3 mg, such as 300 ± 1 mg, such as 300 ± 0.5 mg, such as 300 mg, weekly to be. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject weighing 15 kg or less (eg, 0.5 kg, 1 kg, 1.5 kg). , 2.0 kg, 2.5 kg, 3.0 kg, 3.5 kg, 4.0 kg, 4.5 kg, 10 mg, 5.5 kg, 6.0 kg, 6.5 kg, 7.0 kg, 7.5 kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14.0 kg, 14.5 kg, or 15.0 kg) every 3 weeks (Q3W) 10 mg to 1000 mg (e.g., 10 mg to 900 mg, such as 50 mg to 900 mg, such as 100 mg to 750 mg, such as 100 mg to 600 mg, such as 150 mg to 500 mg, such as 200 mg to 400 mg, such as 250 mg to 350 mg , such as 290 mg to 310 mg, such as 300 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 300 mg every 3 weeks (eg, 3 weeks) for a subject weighing 15 kg or less. 300 mg ± 10 mg, such as 300 ± 6 mg, such as 300 ± 5 mg, such as 300 ± 3 mg, such as 300 ± 1 mg, such as 300 ± 0.5 mg, such as 300 mg) .
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 250 mg 내지 약 350 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 400 mg(예컨대, 3주마다 약 350 mg)의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg 내지 약 500 mg(예컨대, 3주마다 약 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 550 mg 내지 약 650 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 450 mg의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 250 mg 내지 350 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg 내지 400 mg(예컨대, 3주마다 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg 내지 500 mg(예컨대, 3주마다 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 550 mg 내지 650 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 450 mg의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 600 mg의 용량으로 투여된다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) for treating a subject having cancer is a dose in steps based on the subject's body surface area. In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 250 mg to about 350 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg to about 400 mg every 3 weeks (eg, about 350 mg every 3 weeks); or (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg to about 500 mg every 3 weeks (eg, about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti TIGIT antagonist antibody is administered at a dose of about 550 mg to about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 0.75 m2 and less than or equal to 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 450 mg every 3 weeks; or (d) greater than 1.25 m 2 , wherein said anti TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) for treating a subject having cancer is a dose in steps based on the subject's body surface area. In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 250 mg to 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 300 mg to 400 mg every 3 weeks (eg, 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of 400 mg to 500 mg every 3 weeks (eg, 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein said anti TIGIT antagonist antibody is administered at a dose of 550 mg to 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; (b) greater than 0.5 m 2 and not more than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (c) greater than 0.75 m2 and less than or equal to 1.25 m2, wherein said anti-TIGIT antagonist antibody is administered at a dose of 450 mg every 3 weeks; or (d) greater than 1.25 m 2 , wherein said anti TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 1.25 m2를 초과하는 대상체의 경우(예컨대, 1.25 m2, 1.35 m2, 1.45 m2, 1.50 m2, 1.55 m2, 1.60 m2, 1.65 m2, 1.70 m2, 1.75 m2, 1.80 m2, 1.85 m2, 1.90 m2, 1.95 m2, 2.0 m2, 2.1 m2, 2.2 m2, 2.3 m2, 2.4 m2, 2.5 m2, 2.6 m2, 2.7 m2, 2.8 m2, 2.9 m2, 3.0 m2 또는 그 이상) 3주마다(Q3W) 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 1.25 m2를 초과하는 대상체의 경우 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 1.25 m2를 초과하는 대상체의 경우(예컨대, 1.25 m2, 1.35 m2, 1.45 m2, 1.50 m2, 1.55 m2, 1.60 m2, 1.65 m2, 1.70 m2, 1.75 m2, 1.80 m2, 1.85 m2, 1.90 m2, 1.95 m2, 2.0 m2, 2.1 m2, 2.2 m2, 2.3 m2, 2.4 m2, 2.5 m2, 2.6 m2, 2.7 m2, 2.8 m2, 2.9 m2, 3.0 m2 또는 그 이상) 3주마다(Q3W) 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 1.25 m2를 초과하는 대상체의 경우 3주마다 600 mg의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject with a body surface area greater than 1.25 m 2 (eg, 1.25 m 2 , 1.35 m 2 , 1.45 m 2 , 1.50 m 2 , 1.55 m 2 , 1.60 m 2 , 1.65 m 2 , 1.70 m 2 , 1.75 m 2 , 1.80 m 2 , 1.85 m 2 , 1.90 m 2 , 1.95 m 2 , 2.0 m 2 , 2.1 m 2 , 2.2 m 2 , 2.3 m 2 , 2.4 m 2 , 2.5 m 2 , 2.6 m 2 , 2.7 m 2 , 2.8 m 2 , 2.9 m 2 , 3.0 m 2 or more every 3 weeks (Q3W) ) about 30 mg to about 1200 mg (e.g., about 30 mg to about 1100 mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as , about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as , from about 550 mg to about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is about 600 mg every 3 weeks for a subject with a body surface area greater than 1.25 m 2 is the capacity. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject with a body surface area greater than 1.25 m 2 (eg, 1.25 m 2 , 1.35 m 2 , 1.45 m 2 , 1.50 m 2 , 1.55 m 2 , 1.60 m 2 , 1.65 m 2 , 1.70 m 2 , 1.75 m 2 , 1.80 m 2 , 1.85 m 2 , 1.90 m 2 , 1.95 m 2 , 2.0 m 2 , 2.1 m 2 , 2.2 m 2 , 2.3 m 2 , 2.4 m 2 , 2.5 m 2 , 2.6 m 2 , 2.7 m 2 , 2.8 m 2 , 2.9 m 2 , 3.0 m 2 or more every 3 weeks (Q3W) ) 30 mg to 1200 mg (eg 30 mg to 1100 mg, such as 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg every 3 weeks for a subject with a body surface area greater than 1.25 m 2 to be.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 0.75 m2 초과 1.25 m2 이하인 대상체의 경우(예컨대, 0.76 m2, 0.77 m2, 0.78 m2, 0.79 m2, 0.80 m2, 0.82 m2, 0.84 m2, 0.86 m2, 0.88 m2, 0.90 m2, 0.95 m2, 1.0 m2, 1.05 m2, 1.10 m2, 1.15 m2, 1.20 m2, 또는 1.25 m2) 3주마다(Q3W) 약 10 mg 내지 1000 mg(예컨대, 약 20 mg 내지 약 1000 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 850 mg, 예컨대, 약 200 mg 내지 약 700 mg, 예컨대, 약 250 mg 내지 약 600 mg, 예컨대, 약 300 mg 내지 약 500 mg, 예컨대, 약 400 mg 내지 약 500 mg, 예컨대, 약 440 mg 내지 약 460 mg, 예컨대, 약 450 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체표면적이 0.75 m2 초과 1.25 m2 이하인 대상체의 경우 3주 마다 약 450 mg(예컨대, 3주 마다 450 mg ± 10 mg, 예컨대, 450 ± 6 mg, 예컨대, 450 ± 5 mg, 예컨대, 450 ± 3 mg, 예컨대, 450 ± 1 mg, 예컨대, 450 ± 0.5 mg, 예컨대, 450 mg)의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject having a body surface area greater than 0.75 m 2 and less than or equal to 1.25 m 2 (eg, 0.76 m 2 ). 2 , 0.77 m 2 , 0.78 m 2 , 0.79 m 2 , 0.80 m 2 , 0.82 m 2 , 0.84 m 2 , 0.86 m 2 , 0.88 m 2 , 0.90 m 2 , 0.95 m 2 , 1.0 m 2 , 1.05 m 2 , 1.10 m 2 , 1.15 m 2 , 1.20 m 2 , or 1.25 m 2 ) every 3 weeks (Q3W) about 10 mg to 1000 mg (eg, about 20 mg to about 1000 mg, such as about 50 mg to about 900 mg, For example, about 100 mg to about 850 mg, such as about 200 mg to about 700 mg, such as about 250 mg to about 600 mg, such as about 300 mg to about 500 mg, such as about 400 mg to about 500 mg, eg, from about 440 mg to about 460 mg, such as about 450 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about every 3 weeks for a subject having a body surface area greater than 0.75 m 2 and less than or equal to 1.25 m 2 . 450 mg (e.g., every 3 weeks 450 mg ± 10 mg, such as 450 ± 6 mg, such as 450 ± 5 mg, such as 450 ± 3 mg, such as 450 ± 1 mg, such as 450 ± 0.5 mg, such as , 450 mg).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 0.5 m2 초과 0.75 m2 이하인 대상체의 경우(예컨대, 0.51 m2, 0.52 m2, 0.53 m2, 0.54 m2, 0.55 m2, 0.56 m2, 0.57 m2, 0.58 m2, 0.59 m2, 0.60 m2, 0.61 m2, 0.62 m2, 0.63 m2, 0.64 m2, 0.65 m2, 0.66 m2, 0.67 m2, 0.68 m2, 0.69 m2, 0.70 m2, 0.71 m2, 0.72 m2, 0.73 m2, 0.74 m2, 또는 0.75 m2) 3주마다(Q3W) 약 10 mg 내지 1000 mg(예컨대, 약 20 mg 내지 약 1000 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 850 mg, 예컨대, 약 200 mg 내지 약 700 mg, 예컨대, 약 250 mg 내지 약 600 mg, 예컨대, 약 300 mg 내지 약 500 mg, 예컨대, 약 300 mg 내지 약 400 mg, 예컨대, 약 340 mg 내지 약 360 mg, 예컨대, 약 350 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체표면적이 0.5 m2 초과 0.75 m2 이하인 대상체의 경우 3주 마다 약 350 mg(예컨대, 3주 마다 350 mg ± 10 mg, 예컨대, 350 ± 6 mg, 예컨대, 350 ± 5 mg, 예컨대, 350 ± 3 mg, 예컨대, 350 ± 1 mg, 예컨대, 350 ± 0.5 mg, 예컨대, 350 mg)의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is for a subject having a body surface area greater than 0.5 m 2 and no greater than 0.75 m 2 (eg, 0.51 m 2 ). 2 , 0.52 m 2 , 0.53 m 2 , 0.54 m 2 , 0.55 m 2 , 0.56 m 2 , 0.57 m 2 , 0.58 m 2 , 0.59 m 2 , 0.60 m 2 , 0.61 m 2 , 0.62 m 2 , 0.63 m 2 , 0.64 m 2 , 0.65 m 2 , 0.66 m 2 , 0.67 m 2 , 0.68 m 2 , 0.69 m 2 , 0.70 m 2 , 0.71 m 2 , 0.72 m 2 , 0.73 m 2 , 0.74 m 2 , or 0.75 m 2 ) 3 weekly (Q3W) about 10 mg to 1000 mg (eg, about 20 mg to about 1000 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 850 mg, such as about 200 mg to about 700 mg, such as about 250 mg to about 600 mg, such as about 300 mg to about 500 mg, such as about 300 mg to about 400 mg, such as about 340 mg to about 360 mg, such as about 350 mg). to be. In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about every 3 weeks for a subject with a body surface area greater than 0.5 m 2 and no greater than 0.75 m 2 . 350 mg (eg, every 3 weeks 350 mg ± 10 mg, such as 350 ± 6 mg, such as 350 ± 5 mg, such as 350 ± 3 mg, such as 350 ± 1 mg, such as 350 ± 0.5 mg, such as , 350 mg).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 체표면적이 0.5 m2 이하(예컨대, 0.02 m2, 0.04 m2, 0.06 m2, 0.08 m2, 0.1 m2, 0.15 m2, 0.20 m2, 0.25 m2, 0.30 m2, 0.35 m2, 0.40 m2, 0.45 m2, 또는 0.50 m2)인 대상체의 경우 약 10 mg 내지 약 1000 mg(예컨대, 약 10 mg 내지 약 900 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 750 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 150 mg 내지 약 500 mg, 예컨대, 약 200 mg 내지 약 400 mg, 예컨대, 약 250 mg 내지 약 350 mg, 예컨대, 약 290 mg 내지 약 310 mg, 예컨대, 약 300 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 체표면적이 0.5 m2 이하인 대상체의 경우 3주마다 약 300 mg(예컨대, 3주마다 300 mg ± 10 mg, 예컨대, 300 ± 6 mg, 예컨대, 300 ± 5 mg, 예컨대, 300 ± 3 mg, 예컨대, 300 ± 1 mg, 예컨대, 300 ± 0.5 mg, 예컨대, 300 mg)의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) has a body surface area of 0.5 m 2 or less (eg, 0.02 m 2 , 0.04 m 2 , 0.06 ). m 2 , 0.08 m 2 , 0.1 m 2 , 0.15 m 2 , 0.20 m 2 , 0.25 m 2 , 0.30 m 2 , 0.35 m 2 , 0.40 m 2 , 0.45 m 2 , or 0.50 m 2 ) about 10 mg to about 1000 mg (e.g., about 10 mg to about 900 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 750 mg, such as about 100 mg to about 600 mg, such as about 150 mg to about 500 mg, such as about 200 mg to about 400 mg, such as about 250 mg to about 350 mg, such as about 290 mg to about 310 mg, such as about 300 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 300 mg (eg, every 3 weeks) for a subject having a body surface area of 0.5 m 2 or less. , 300 mg ± 10 mg, such as 300 ± 6 mg, such as 300 ± 5 mg, such as 300 ± 3 mg, such as 300 ± 1 mg, such as 300 ± 0.5 mg, such as 300 mg, every 3 weeks) is the capacity of
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 2주 마다(Q2W) 약 10 mg 내지 약 1000 mg(예컨대, 약 20 mg 내지 약 1000 mg, 예컨대, 약 50 mg 내지 약 900 mg, 예컨대, 약 100 mg 내지 약 850 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 600 mg, 예컨대, 약 400 mg 내지 약 500 mg, 예컨대, 약 405 mg 내지 약 450 mg, 예컨대, 약 410 mg 내지 약 430 mg, 예컨대, 약 420 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 2주 마다 약 420 mg(예컨대, 2주 마다 420 mg ± 10 mg, 예컨대, 420 ± 6 mg, 예컨대, 420 ± 5 mg, 예컨대, 420 ± 3 mg, 예컨대, 420 ± 1 mg, 예컨대, 420 ± 0.5 mg, 예컨대, 420 mg)의 용량이다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 약 300 mg 내지 약 600 mg의 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 300 mg 내지 600 mg의 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 약 420 mg의 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 420 mg의 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체의 용량은 고정 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 10 mg to about 1000 mg (eg, about 20) every two weeks (Q2W). mg to about 1000 mg, such as about 50 mg to about 900 mg, such as about 100 mg to about 850 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 600 mg, such as about 400 mg to about 500 mg, such as about 405 mg to about 450 mg, such as about 410 mg to about 430 mg, such as about 420 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 420 mg every 2 weeks (eg, 420 mg ± 10 mg every 2 weeks, For example, a dose of 420 ± 6 mg, such as 420 ± 5 mg, such as 420 ± 3 mg, such as 420 ± 1 mg, such as 420 ± 0.5 mg, such as 420 mg). In some cases, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of about 300 mg to about 600 mg every two weeks. In some cases, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of 300 mg to 600 mg every two weeks. In some cases, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of about 420 mg every two weeks. In some cases, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of 420 mg every two weeks. In some cases, the dose of the anti-TIGIT antagonist antibody is a fixed dose.
일부 예들에서, 항 TIGIT 길항제 항체 (예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주 마다(Q3W) 약 30 mg 내지 약 1200 mg (예컨대어, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예를 들어, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다(Q3W) 약 200 mg 내지 약 2000 mg(예컨대, 약 200 mg 내지 약 2000 mg, 예컨대, 약 400 mg 내지 약 1900 mg, 예컨대, 약 500 mg 내지 약 1800 mg, 예컨대, 약 600 mg 내지 약 1700 mg, 예컨대, 약 700 mg 내지 약 1400 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg, 예컨대, 1200 mg ± 10 mg, 예컨대, 1200 ± 6 mg, 예컨대, 1200 ± 5 mg, 예컨대, 1200 ± 3 mg, 예컨대, 1200 ± 1 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 약 1200 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주 마다 1200 mg의 용량이다.In some embodiments, an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about) every 3 weeks (Q3W). 1100 mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 200 mg to about 2000 mg (eg, about 200 mg) every 3 weeks (Q3W). to about 2000 mg, such as about 400 mg to about 1900 mg, such as about 500 mg to about 1800 mg, such as about 600 mg to about 1700 mg, such as about 700 mg to about 1400 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg, such as 1200 mg ± 10 mg, such as 1200 ± 6 mg, such as 1200 ± 5 mg, eg, 1200±3 mg, eg, 1200±1 mg, eg, 1200±0.5 mg, eg, 1200 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 1200 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 1200 mg every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다(Q4W) 약 200 mg 내지 약 2000 mg(예컨대, 약 200~300 mg, 약 300~400 mg, 약 400~500 mg, 약 500~600 mg, 약 600~700 mg, 약 700~800 mg, 약 800~900 mg, 약 900~1000 mg, 약 1000~1100 mg, 약 1100~1200 mg, 약 1200~1300 mg, 약 1300~1400 mg, 약 1400~1500 mg, 약 1500~1600 mg, 약 1600~1700 mg, 약 1700~1800 mg, 약 1800~1900 mg, 또는 약 1900~2000 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 250 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1600 mg, 예컨대, 약 400 mg 내지 약1500 mg, 예컨대, 약 500 mg 내지 약1400 mg, 예컨대, 약 600 mg 내지 약 1200 mg, 예컨대, 약 700 mg 내지 약1100 mg, 예컨대, 약 800 mg 내지 약 1000 mg, 예컨대, 약 800 mg 내지 약 900 mg, 예컨대, 약 200 mg, 약 250 mg, 약 300 mg, 약 350 mg, 약 400 mg, 약 450 mg, 약 500 mg, 약 550 mg, 약 600 mg, 약 650 mg, 약 700 mg, 약 750 mg, 약 800 mg, 약 850 mg, 약 900 mg, 약 950 mg, 약 1000 mg, 약 1050 mg, 약 1100 mg, 약 1150 mg, 약 1200 mg, 약 1250 mg, 약 1300 mg, 약 1350 mg, 약 1400 mg, 약 1450 mg, 약 1500 mg, 약 1550 mg, 약 1600 mg, 약 1650 mg, 약 1700 mg, 약 1750 mg, 약 1800 mg, 약 1850 mg, 약 1900 mg, 약 1950 mg, 또는 약 2000 mg, 예컨대, 약 800 mg, 약 810 mg, 약 820 mg, 약 830 mg, 약 840 mg, 약 850 mg, 약 860 mg, 약 870 mg, 약 880 mg, 약 890, 또는 약 900 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 약 700 mg 내지 약 1000 mg이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 700 mg 내지 1000 mg이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 약 840 mg이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 840 mg이다. 840 mg Q4W 투약 요법은 PK 모델링 및 시뮬레이션 및 노출 안전성 분석의 결과에 의해 뒷받침된다. 간단히 말해서, 상기 840 mg Q4W 투약 요법 후의 평균 농도는 이전 연구에서 평가된 3주마다 600 mg 투약 요법의 농도와 유사하다. 840 mg Q4W 투약 요법의 Cmax는 3주마다 600 mg 투약 요법의 Cmax에 비해 정상 상태에서 28% 더 높은 것으로 시뮬레이션되었지만, 병원에서는 가장 높은 투여 용량의 관찰된 노출 범위 내에 속한다(3주마다 1200 mg). 이전 관찰(3주마다 단일 요법으로 또는 3주마다 아테졸리주맙 1200 mg과 병용으로 투여된 2-1200 mg의 티라골루맙 용량)을 기반으로 한 티라골루맙 노출-안전 관계에 대한 예비 분석은 티라골루맙이 균일한 노출-안전 관계를 나타냄을 시사한다. 요약하면, 상기 840 mg Q4W 투약 요법은 예측된 노출이 관찰된 유효 노출 범위 내에 있고 티라골루맙이 균일한 노출-안전 관계를 나타낸다는 점을 감안할 때 3주마다 600 mg 투약 요법과 유사한 안전성 및 유효성을 제공할 수 있다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 200 mg to about 2000 mg (eg, from about 200 to about 2000 mg every 4 weeks (Q4W) 300 mg, about 300-400 mg, about 400-500 mg, about 500-600 mg, about 600-700 mg, about 700-800 mg, about 800-900 mg, about 900-1000 mg, about 1000-1100 mg , about 1100 to 1200 mg, about 1200 to 1300 mg, about 1300 to 1400 mg, about 1400 to 1500 mg, about 1500 to 1600 mg, about 1600 to 1700 mg, about 1700 to 1800 mg, about 1800 to 1900 mg, or about 1900-2000 mg, such as about 200 mg to about 1600 mg, such as about 250 mg to about 1600 mg, such as about 300 mg to about 1600 mg, such as about 400 mg to about 1500 mg, such as about 500 mg to about 1400 mg, such as about 600 mg to about 1200 mg, such as about 700 mg to about 1100 mg, such as about 800 mg to about 1000 mg, such as about 800 mg to about 900 mg, such as about 200 mg, about 250 mg, about 300 mg, about 350 mg, about 400 mg, about 450 mg, about 500 mg, about 550 mg, about 600 mg, about 650 mg, about 700 mg, about 750 mg, about 800 mg, about 850 mg, about 900 mg, about 950 mg, about 1000 mg, about 1050 mg, about 1100 mg, about 1150 mg, about 1200 mg, about 1250 mg, about 1300 mg, about 1350 mg, about 1400 mg, about 1450 mg, about 1500 mg, about 1550 mg, about 1600 mg, about 1650 mg, about 1700 mg, about 1750 mg, about 1800 mg, about 1850 mg, about 1900 mg, about 1950 mg, or about 2000 mg, such as about 800 mg, about 810 mg, about 820 mg, about 830 mg, about 840 mg, about 850 mg, about 860 mg, about 870 mg, about 880 mg, about 890, or about 900 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 700 mg to about 1000 mg every 4 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 700 mg to 1000 mg every 4 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is about 840 mg every 4 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 840 mg every 4 weeks. The 840 mg Q4W dosing regimen is supported by the results of PK modeling and simulation and exposure safety analysis. Briefly, the mean concentrations after the 840 mg Q4W dosing regimen are similar to those of the 600 mg every 3 weeks dosing regimen evaluated in previous studies. The Cmax of the 840 mg Q4W dosing regimen was simulated to be 28% higher at steady state compared to the Cmax of the 600 mg dosing regimen every 3 weeks, but falls within the observed exposure range of the highest dosing dose in the hospital (1200 mg every 3 weeks). . A preliminary analysis of the tiragoluumab exposure-safety relationship based on previous observations (a dose of 2-1200 mg tiragoluumab administered as monotherapy every 3 weeks or in combination with atezolizumab 1200 mg every 3 weeks) was suggesting that golumab exhibits a uniform exposure-safety relationship. In summary, the 840 mg Q4W dosing regimen was similar in safety and efficacy to the 600 mg every 3 weeks dosing regimen given that the predicted exposure was within the observed effective exposure range and that tiragoluumab exhibited a uniform exposure-safety relationship. can provide
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 4주 마다 약 840 mg(예컨대, 4주 마다 840 mg ± 10 mg, 예컨대, 840 ± 6 mg, 예컨대, 840 ± 5 mg, 예컨대, 840 ± 3 mg, 예컨대, 840 ± 1 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 약 200 mg 내지 약 2000 mg(예컨대 , 약 200 mg 내지 약 2000 mg, 예컨대, 약 400 mg 내지 약 1900 mg, 예컨대, 약 500 mg 내지 약 1800 mg, 예컨대, 약 600 mg 내지 약 1700 mg, 예컨대, 약 700 mg 내지 약 1400 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg(예컨대, 200 mg 내지 2000 mg mg, 예컨대, 400 mg 내지 1900 mg, 예컨대, 500 mg 내지 1800 mg, 예컨대, 600 mg 내지 1700 mg, 예컨대, 700 mg 내지 1400 mg, 예컨대, 800 mg 내지 1600 mg, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대 1150 mg 내지 1250 mg, 예컨대 1175 mg 내지 1225 mg, 예컨대 1190 mg 내지 1210 mg), 예컨대, 약 1200 mg, 예컨대, 1200 mg ± 10 mg, 예컨대, 1200 ± 6 mg, 예컨대, 1200 ± 5 mg, 예컨대, 1200 ± 3 mg, 예컨대, 1200 ± 3 mg, 예컨대, 1200 ± 1 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주 마다 약 1200 mg의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 840 mg every 4 weeks (eg, 840 mg ± 10 mg every 4 weeks, For example, a dose of 840 ± 6 mg, such as 840 ± 5 mg, such as 840 ± 3 mg, such as 840 ± 1 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 200 mg to about 2000 mg (eg, from about 200 mg to about 2000) every 4 weeks. mg, such as about 400 mg to about 1900 mg, such as about 500 mg to about 1800 mg, such as about 600 mg to about 1700 mg, such as about 700 mg to about 1400 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg (eg, 200 mg to 2000 mg mg, such as 400 mg to 1900 mg, such as 500 mg to 1800 mg, such as 600 mg to 1700 mg, such as 700 mg to 1400 mg, such as 800 mg to 1600 mg, 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg , such as 1150 mg to 1250 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg), such as about 1200 mg, such as 1200 mg ± 10 mg, such as 1200 ± 6 mg, such as 1200 ± 5 mg, such as 1200 ± 3 mg, such as 1200 ± 3 mg, such as 1200 ± 1 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 1200 mg every 4 weeks.
일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)와의 병용 치료)으로 투여되는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여되는 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. In some cases, combination therapy (eg, combination therapy with a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab))) The dose of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragolumab as disclosed herein) administered as a monotherapy may be reduced compared to a standard dose of the anti-TIGIT antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 정맥내 투여된다. 대안적으로, 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 피하 투여된다. 일부 경우들에서, 티라골루맙은 2주마다 약 420 mg, 3주마다 약 1200 mg, 또는 4주마다 약 1200 mg의 용량으로 환자에게 정맥내 투여된다. 일부 경우들에서, 티라골루맙은 2주마다 420 mg, 3주마다 1200 mg, 또는 4주마다 1200 mg의 용량으로 상기 환자에게 정맥내 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered intravenously. Alternatively, in some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered subcutaneously. In some cases, tiragolumab is administered to the patient intravenously at a dose of about 420 mg every 2 weeks, about 1200 mg every 3 weeks, or about 1200 mg every 4 weeks. In some cases, tiragolumab is administered to the patient intravenously at a dose of 420 mg every 2 weeks, 1200 mg every 3 weeks, or 1200 mg every 4 weeks.
일부 경우들에서, 대상체는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 티라골루맙)의 총 1 내지 20회 용량, 예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 또는 20회 용량이 투여된다. 일부 경우들에서, 대상체는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 티라골루맙)의 총 1 내지 50회 용량, 예컨대, 1회 내지 50회 용량, 1회 내지 45회 용량, 1회 내지 40회 용량, 1회 내지 35회 용량, 1 내지 30회 용량, 1회 내지 25회 용량, 1회 내지 20회 용량, 1회 내지 15회 용량, 1회 내지 10회 용량, 1회 내지 5회 용량, 2회 내지 50회 용량, 2회 내지 45회 용량, 2회 내지 40회 용량, 2회 내지 35회 용량, 2회 내지 30회 용량, 2회 내지 25회 용량, 2회 내지 20회 용량, 2회 내지 15회 용량, 2회 내지 10회 용량, 2회 내지 5회 용량, 3회 내지 50회 용량, 3회 내지 45회 용량, 3회 내지 40회 용량, 3회 내지 35회 용량, 3회 내지 30회 용량, 3회 내지 25회 용량, 3회 내지 20회 용량, 3회 내지 15회 용량, 3회 내지 10회 용량, 3회 내지 5회 용량, 4회 내지 50회 용량, 4회 내지 45회 용량, 4회 내지 40회 용량, 4회 내지 35회 용량, 4회 내지 30회 용량, 4회 내지 25회 용량, 4회 내지 20회 용량, 4회 내지 15회 용량, 4회 내지 10회 용량, 4회 내지 5회 용량, 5회 내지 50회 용량, 5회 내지 45회 용량, 5회 내지 40회 용량, 5회 내지 35회 용량, 5회 내지 30회 용량 5회 내지 25회 용량, 5회 내지 20회 용량, 5회 내지 15회 용량, 5회 내지 10회 용량, 10회 내지 50회 용량, 10회 내지 45회 용량, 10회 내지 40회 용량, 10회 내지 35회 용량, 10회 내지 30회 용량, 10회 내지 25회 용량, 10회 내지 20회 용량, 10회 내지 15회 용량, 15회 내지 50회 용량, 15회 내지 45회 용량, 15회 내지 40회 용량, 15회 내지 35회 용량, 15회 내지 30회 용량, 15회 내지 25회 용량, 15회 내지 20회 용량, 20회 내지 50회 용량, 20회 내지 45회 용량, 20회 내지 40회 용량, 20회 내지 35회 용량, 20회 내지 30회 용량, 20회 내지 25회 용량, 25회 내지 50회 용량, 25회 내지 45회 용량, 25회 내지 40회 용량, 25회 내지 35회 용량, 25회 내지 30회 용량, 30회 내지 30회 용량, 30회 내지 45회 용량, 30회 내지 40회 용량, 30회 내지 35회 용량, 35회 내지 50회 용량, 35회 내지 45회 용량, 35회 내지 40회 용량, 40회 내지 50회 용량, 40회 내지 45회 용량, 또는 45회 내지 50회 용량이 투여된다. 특정 경우들에서, 상기 용량은 정맥내 투여될 수 있다.In some cases, the subject administers a total of 1 to 20 doses of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, tiragolumab), eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, or 20 doses is administered In some cases, the subject has a total of 1 to 50 doses, such as 1 to 50 doses, 1 to 45 doses, of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, tiragolumab). dose, 1 to 40 doses, 1 to 35 doses, 1 to 30 doses, 1 to 25 doses, 1 to 20 doses, 1 to 15 doses, 1 to 10 doses, 1 to 5 doses, 2 to 50 doses, 2 to 45 doses, 2 to 40 doses, 2 to 35 doses, 2 to 30 doses, 2 to 25 doses, 2 20 to 20 doses, 2 to 15 doses, 2 to 10 doses, 2 to 5 doses, 3 to 50 doses, 3 to 45 doses, 3 to 40 doses, 3 doses to 35 doses, 3 to 30 doses, 3 to 25 doses, 3 to 20 doses, 3 to 15 doses, 3 to 10 doses, 3 to 5 doses, 4 to 50 doses, 4 to 45 doses, 4 to 40 doses, 4 to 35 doses, 4 to 30 doses, 4 to 25 doses, 4 to 20 doses, 4 to 15 doses Dose, 4 to 10 doses, 4 to 5 doses, 5 to 50 doses, 5 to 45 doses, 5 to 40 doses, 5 to 35 doses, 5 to 30 doses 5 to 25 doses, 5 to 20 doses, 5 to 15 doses, 5 to 10 doses, 10 to 50 doses, 10 to 45 doses, 10 to 40 doses, 10 to 35 doses, 10 to 30 doses, 10 to 25 doses, 10 to 20 doses, 10 to 15 doses, 15 to 50 doses, 15 to 45 doses, 15 40 to 40 doses, 15 to 35 doses, 15 to 30 doses, 15 to 25 doses, 15 to 20 doses, 20 50 to 50 doses, 20 to 45 doses, 20 to 40 doses, 20 to 35 doses, 20 to 30 doses, 20 to 25 doses, 25 to 50 doses, 25 doses to 45 doses, 25 to 40 doses, 25 to 35 doses, 25 to 30 doses, 30 to 30 doses, 30 to 45 doses, 30 to 40 doses, 30 to 35 doses, 35 to 50 doses, 35 to 45 doses, 35 to 40 doses, 40 to 50 doses, 40 to 45 doses, or 45 to 50 doses are administered. In certain instances, the dose may be administered intravenously.
ii.ii. PD-1 축 결합 길항제의 투약Dosing of PD-1 axis binding antagonists
일반적의 제안으로서, 인간에게 투여된 PD-1 축 결합 길항제 항체(예컨대, 아테졸리주맙)의 치료적 유효량은, 1회 또는 그 이상의 투여에 의해 환자 체중당 약 0.01 내지 약 50 mg/kg의 범위일 것이다. As a general suggestion, a therapeutically effective amount of a PD-1 axis binding antagonist antibody (eg, atezolizumab) administered to a human is in the range of about 0.01 to about 50 mg/kg of body weight of the patient by one or more administrations. would.
일부 예시적인 구현예들에서, 상기 PD-1 축 결합 길항제 항체는, 예를 들어 매일, 매주, 2주마다, 3주마다, 또는 4주마다 약 0.01 내지 약 45 mg/kg, 약 0.01 내지 약 40 mg/kg, 약 0.01 내지 약 35 mg/kg, 약 0.01 내지 약 30 mg/kg, 약 0.01 내지 약 25 mg/kg, 약 0.01 내지 약 20 mg/kg, 약 0.01 내지 약 15 mg/kg, 약 0.01 내지 약 10 mg/kg, 약 0.01 내지 약 5 mg/kg, 또는 약 0.01 내지 약 1 mg/kg의 용량으로 투여된다. 일부 예시적인 구현예들에서, 상기 PD-1 축 결합 길항제 항체는, 예를 들어 매일, 매주, 2주마다, 3주마다, 또는 4주마다 0.01 내지 45 mg/kg, 0.01 내지 40 mg/kg, 0.01 내지 35 mg/kg, 0.01 내지 30 mg/kg, 0.01 내지 25 mg/kg, 0.01 내지 20 mg/kg, 0.01 내지 15 mg/kg, 0.01 내지 10 mg/kg, 0.01 내지 5 mg/kg, 또는 0.01 내지 1 mg/kg의 용량으로 투여된다. In some exemplary embodiments, the PD-1 axis binding antagonist antibody is, for example, from about 0.01 to about 45 mg/kg, from about 0.01 to about every day, weekly, every 2 weeks, every 3 weeks, or every 4 weeks. 40 mg/kg, about 0.01 to about 35 mg/kg, about 0.01 to about 30 mg/kg, about 0.01 to about 25 mg/kg, about 0.01 to about 20 mg/kg, about 0.01 to about 15 mg/kg, It is administered at a dose of about 0.01 to about 10 mg/kg, about 0.01 to about 5 mg/kg, or about 0.01 to about 1 mg/kg. In some exemplary embodiments, the PD-1 axis binding antagonist antibody is, for example, 0.01 to 45 mg/kg, 0.01 to 40 mg/kg every day, weekly, every 2 weeks, every 3 weeks, or every 4 weeks. , 0.01 to 35 mg/kg, 0.01 to 30 mg/kg, 0.01 to 25 mg/kg, 0.01 to 20 mg/kg, 0.01 to 15 mg/kg, 0.01 to 10 mg/kg, 0.01 to 5 mg/kg, or 0.01 to 1 mg/kg.
일부 경우들에서, 상기 PD-1 축 결합 길항제 항체는 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 투여된다.In some cases, the PD-1 axis binding antagonist antibody is administered on about day 1 (eg, day -3, day -2, day -1, day 1, day 2, or day 3) of a dosing cycle.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 2주 마다(Q2W) 약 20 mg 내지 약 1600 mg(예컨대, 약 40 mg 내지 약 1500 mg, 예컨대, 약 200 mg 내지 약 1400 mg, 예컨대, 약 300 mg 내지 약 1400 mg, 예컨대, 약 400 mg 내지 약 1400 mg, 예컨대, 약 500 mg 내지 약 1300 mg, 예컨대, 약 600 mg 내지 약 1200 mg, 예컨대, 약 700 mg 내지 약 1100 mg, 예컨대, 약 800 mg 내지 약 1000 mg, 예컨대, 약 800 mg 내지 약 900 mg, 예컨대, 약 800 mg, 약 810 mg, 약 820 mg, 약 830 mg, 약 840 mg, 약 850 mg, 약 860 mg, 약 870 mg, 약 880 mg, 약 890 mg, 또는 약 900 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 2주 마다(Q2W) 20 mg 내지 1600 mg(예컨대, 40 mg 내지 1500 mg, 예컨대, 200 mg 내지 1400 mg, 예컨대, 300 mg 내지 1400 mg, 예컨대, 400 mg 내지 1400 mg, 예컨대, 500 mg 내지 1300 mg, 예컨대, 600 mg 내지 1200 mg, 예컨대, 700 mg 내지 1100 mg, 예컨대, 800 mg 내지 1000 mg, 예컨대, 800 mg 내지 900 mg, 예컨대, 800 mg, 810 mg, 820 mg, 830 mg, 840 mg, 850 mg, 860 mg, 870 mg, 880 mg, 890 mg, 또는 900 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 2주 마다 약 840 mg의 용량(예컨대, 2주마다 840 mg ± 10 mg, 예컨대, 840 ± 6 mg, 예컨대, 840 ± 5 mg, 예컨대, 840 ± 3 mg, 예컨대, 840 ± 1 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 아테졸리주맙의 유효량은 2주마다 약 840 mg의 용량이다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every two weeks ( Q2W) about 20 mg to about 1600 mg (e.g., about 40 mg to about 1500 mg, such as about 200 mg to about 1400 mg, such as about 300 mg to about 1400 mg, such as about 400 mg to about 1400 mg, For example, about 500 mg to about 1300 mg, such as about 600 mg to about 1200 mg, such as about 700 mg to about 1100 mg, such as about 800 mg to about 1000 mg, such as about 800 mg to about 900 mg, For example, about 800 mg, about 810 mg, about 820 mg, about 830 mg, about 840 mg, about 850 mg, about 860 mg, about 870 mg, about 880 mg, about 890 mg, or about 900 mg) For example, fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every two weeks ( Q2W) 20 mg to 1600 mg (eg 40 mg to 1500 mg, such as 200 mg to 1400 mg, such as 300 mg to 1400 mg, such as 400 mg to 1400 mg, such as 500 mg to 1300 mg, such as, 600 mg to 1200 mg, such as 700 mg to 1100 mg, such as 800 mg to 1000 mg, such as 800 mg to 900 mg, such as 800 mg, 810 mg, 820 mg, 830 mg, 840 mg, 850 mg, 860 mg, 870 mg, 880 mg, 890 mg, or 900 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is about every two weeks. A dose of 840 mg (e.g., 840 mg ± 10 mg, e.g., 840 ± 6 mg, e.g., 840 ± 5 mg, e.g., 840 ± 3 mg, e.g., 840 ± 1 mg, e.g., 840 ± 0.5 mg, every two weeks , eg, 840 mg). In some cases, the effective amount of atezolizumab is a dose of about 840 mg every two weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙) 또는 항 PD-1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 12.5 mg/kg, 예컨대, 약 10 ± 2 mg/kg, 약 10 ± 1 mg/kg, 약 10 ± 0.5 mg/kg, 약 10 ± 0.2 mg/kg, 또는 약 10 ± 0.1 mg/kg, 예컨대, 약 10 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙) 또는 항 PD-1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 10 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 10 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 10 mg/kg, 예컨대, 약 1 mg/kg 내지 약 10 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 10 mg/kg, 예컨대, 약 5 mg/kg 내지 약 10 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 10 mg/kg, 예컨대, 약 8 mg/kg 내지 약 10 mg/kg, 예컨대, 약 9 mg/kg 내지 약 10 mg/kg, 예컨대, 약 9.5 mg/kg 내지 약 10 mg/kg, 예컨대, 약 10 ± 1 mg/kg, 예컨대, 약 10 ± 0.5 mg/kg, 예컨대, 약 10 ± 0.2 mg/kg, 예컨대, 약 10 ± 0.1 mg/kg, 예컨대, 약 10 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙) 또는 항 PD-1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 12.5 mg/kg, 예컨대, 10 ± 2 mg/kg, 10 ± 1 mg/kg, 10 ± 0.5 mg/kg, 10 ± 0.2 mg/kg, 또는 10 ± 0.1 mg/kg, 예컨대, 10 mg/kg)의 용량이다. 일부 예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙) 또는 항 PD-1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 10 mg/kg(예컨대, 0.1 mg/kg 내지 10 mg/kg, 예컨대, 0.5 mg/kg 내지 10 mg/kg, 예컨대, 1 mg/kg 내지 10 mg/kg, 예컨대, 2.5 mg/kg 내지 10 mg/kg, 예컨대, 5 mg/kg 내지 10 mg/kg, 예컨대, 7.5 mg/kg 내지 10 mg/kg, 예컨대, 8 mg/kg 내지 10 mg/kg, 예컨대, 9 mg/kg 내지 10 mg/kg, 예컨대, 9.5 mg/kg 내지 10 mg/kg, 예컨대, 10 ± 1 mg/kg, 예컨대, 10 ± 0.5 mg/kg, 예컨대, 10 ± 0.2 mg/kg, 예컨대, 10 ± 0.1 mg/kg, 예컨대, 10 mg/kg)의 용량이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 2주마다 약 10 mg/kg의 용량이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 2주마다 10 mg/kg의 용량이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, pembrolizumab) or an anti-PD-1 antagonist antibody (eg, atezolizumab)) is about 0.01 mg/kg to about 50 mg/kg (eg, about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg, of the subject's body weight) kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 5 mg/kg to about 15 mg/kg, For example, about 7.5 mg/kg to about 12.5 mg/kg, such as about 10 ± 2 mg/kg, about 10 ± 1 mg/kg, about 10 ± 0.5 mg/kg, about 10 ± 0.2 mg/kg, or about 10 ± 0.1 mg/kg, such as about 10 mg/kg). In some cases, an effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, pembrolizumab) or an anti-PD-1 antagonist antibody (eg, atezolizumab)) is administered to the subject every two weeks. about 0.01 mg/kg to about 10 mg/kg of body weight (eg, about 0.1 mg/kg to about 10 mg/kg, such as about 0.5 mg/kg to about 10 mg/kg, such as about 1 mg/kg to about 10 mg/kg, such as about 2.5 mg/kg to about 10 mg/kg, such as about 5 mg/kg to about 10 mg/kg, such as about 7.5 mg/kg to about 10 mg/kg, such as , about 8 mg/kg to about 10 mg/kg, such as about 9 mg/kg to about 10 mg/kg, such as about 9.5 mg/kg to about 10 mg/kg, such as about 10 ± 1 mg/kg , such as about 10 ± 0.5 mg/kg, such as about 10 ± 0.2 mg/kg, such as about 10 ± 0.1 mg/kg, such as about 10 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, pembrolizumab) or an anti-PD-1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, per body weight of the subject; For example, 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 12.5 mg/kg, such as, 10 ± 2 mg/kg, 10 ± 1 mg/kg, 10 ± 0.5 mg/kg, 10 ± 0.2 mg/kg, or 10 ± 0.1 mg/kg, such as 10 mg/kg). In some embodiments, an effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, pembrolizumab) or an anti-PD-1 antagonist antibody (eg, atezolizumab)) is administered to the subject every two weeks. 0.01 mg/kg to 10 mg/kg of body weight (eg, 0.1 mg/kg to 10 mg/kg, such as 0.5 mg/kg to 10 mg/kg, such as 1 mg/kg to 10 mg/kg, such as , 2.5 mg/kg to 10 mg/kg, such as 5 mg/kg to 10 mg/kg, such as 7.5 mg/kg to 10 mg/kg, such as 8 mg/kg to 10 mg/kg, such as 9 mg/kg to 10 mg/kg, such as 9.5 mg/kg to 10 mg/kg, such as 10 ± 1 mg/kg, such as 10 ± 0.5 mg/kg, such as 10 ± 0.2 mg/kg, such as, 10 ± 0.1 mg/kg, such as 10 mg/kg). In some cases, the effective amount of pembrolizumab is a dose of about 10 mg/kg every two weeks. In some cases, the effective amount of pembrolizumab is a dose of 10 mg/kg every two weeks.
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대, 0.5 mg/kg 내지 15 mg/kg, 예컨대, 1 mg/kg 내지 15 mg/kg, 예컨대, 2.5 mg/kg 내지 15 mg/kg, 예컨대, 5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 15 mg/kg, 예컨대, 10 mg/kg 내지 15 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 14 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 1 mg/kg, 예컨대, 15 ± 0.5 mg/kg, 예컨대, 15 ± 0.2 mg/kg, 예컨대, 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 투여되는 약 15 mg/kg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 1200 mg의 최대 용량으로 3주마다 투여되는 약 15 mg/kg의 용량이다. 일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다. 일부 구현예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 3주마다 1200 mg의 최대 용량으로 투여된다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) for treating a subject having cancer is about 0.01 per body weight of the subject every 3 weeks mg/kg to about 50 mg/kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg , eg, about 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 0.01 mg/kg to about 15 mg/kg of the subject's body weight every 3 weeks. (e.g., about 0.1 mg/kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, such as about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 10 mg/kg to about 15 mg/kg, such as , about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, such as about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) for treating a subject having cancer is 0.01 mg per body weight of the subject every 3 weeks /kg to 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg , 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some embodiments, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg to 15 mg/kg (eg, from 0.01 mg/kg to 15 mg/kg of body weight of the subject every 3 weeks) , 0.1 mg/kg to 15 mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 15 mg/kg, such as 10 mg/kg to 15 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 14 mg/kg kg to 15 mg/kg, such as 15 ± 1 mg/kg, such as 15 ± 0.5 mg/kg, such as 15 ± 0.2 mg/kg, such as 15 ± 0.1 mg/kg, such as 15 mg/kg) is the capacity of In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 15 mg/kg administered every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is about 15 mg/administered every 3 weeks with a maximum dose of 1200 mg every 3 weeks. capacity in kg. In some cases, a PD-1 axis binding antagonist (eg, anti-PD-) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of the L1 antagonist antibody (eg, atezolizumab) may be reduced compared to a standard dose of the PD-1 axis binding antagonist administered as monotherapy. In some embodiments, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a maximum dose of 1200 mg every 3 weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주마다(Q3W) 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 1600 mg, 예컨대, 약 200 mg 내지 약 1600 mg, 예컨대, 약 300 mg 내지 약 1600 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주 마다 약 1200 mg의 용량(예컨대, 3주마다 1200 mg ± 10 mg, 예컨대, 1200 ± 6 mg, 예컨대, 1200 ± 5 mg, 예컨대, 1200 ± 3 mg, 예컨대, 1200 ± 1 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 아테졸리주맙의 유효량은 3주마다 약 1200 mg의 용량이다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every 3 weeks ( Q3W) about 80 mg to about 2000 mg (e.g., about 100 mg to about 1600 mg, such as about 200 mg to about 1600 mg, such as about 300 mg to about 1600 mg, such as about 400 mg to about 1600 mg, For example, about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, For example, about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, For example, a dose of about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is about every 3 weeks. A dose of 1200 mg (e.g., 1200 mg ± 10 mg, e.g., 1200 ± 6 mg, e.g., 1200 ± 5 mg, e.g., 1200 ± 3 mg, e.g., 1200 ± 1 mg, e.g., 1200 ± 0.5 mg, every 3 weeks) , eg, 1200 mg). In some cases, the effective amount of atezolizumab is a dose of about 1200 mg every 3 weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주마다(Q3W) 약 10 mg 내지 약 800 mg(예컨대, 약 10 mg 내지 약 800 mg, 예컨대, 약 20 mg 내지 약 700 mg, 예컨대, 약 50 mg 내지 약 600 mg, 예컨대, 약 75 mg 내지 약 500 mg, 예컨대, 약 100 mg 내지 약 400 mg, 예컨대, 약 100 mg 내지 약 300 mg, 예컨대, 약 125 mg 내지 약 275 mg, 예컨대, 약 150 mg 내지 약 250 mg, 예컨대, 약 175 mg 내지 약 225 mg, 예컨대, 약 190 mg 내지 약 210 mg, 예컨대, 약 200 mg ± 10 mg, 예컨대, 200 mg ± 7.5 mg, 예컨대, 200 mg ± 5 mg, 예컨대, 200 ± 2.5 , 예컨대, 200 ± 1.0 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주 마다 약 200 mg의 용량(예컨대, 3주마다 200 mg ± 10 mg, 예컨대, 200 ± 6 mg, 예컨대, 200 ± 5 mg, 예컨대, 200 ± 3 mg, 예컨대, 200 ± 1 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량이다. 일부 경우들에서, 상기 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙)의 유효량은 3주 마다 약 200 mg의 용량(예컨대, 3주마다 200 mg ± 10 mg, 예컨대, 200 ± 6 mg, 예컨대, 200 ± 5 mg, 예컨대, 200 ± 3 mg, 예컨대, 200 ± 1 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주마다(Q3W) 10 mg 내지 800 mg(예컨대, 10 mg 내지 800 mg, 예컨대, 20 mg 내지 700 mg, 예컨대, 50 mg 내지 600 mg, 예컨대, 75 mg 내지 500 mg, 예컨대, 100 mg 내지 400 mg, 예컨대, 100 mg 내지 300 mg, 예컨대, 125 mg 내지 275 mg, 예컨대, 150 mg 내지 250 mg, 예컨대, 175 mg 내지 225 mg, 예컨대, 190 mg 내지 210 mg, 예컨대, 200 mg ± 10 mg, 예컨대, 200 mg ± 7.5 mg, 예컨대, 200 mg ± 5 mg, 예컨대, 200 ± 2.5 , 예컨대, 200 ± 1.0 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 3주 마다 200 mg의 용량(예컨대, 3주마다 200 mg ± 10 mg, 예컨대, 200 ± 6 mg, 예컨대, 200 ± 5 mg, 예컨대, 200 ± 3 mg, 예컨대, 200 ± 1 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량이다. 일부 경우들에서, 상기 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙)의 유효량은 3주 마다 200 mg의 용량(예컨대, 3주마다 200 mg ± 10 mg, 예컨대, 200 ± 6 mg, 예컨대, 200 ± 5 mg, 예컨대, 200 ± 3 mg, 예컨대, 200 ± 1 mg, 예컨대, 200 ± 0.5 mg, 예컨대, 200 mg)의 용량이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 3주마다 약 200 mg의 용량이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 3주마다 약 200 mg의 용량이다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every 3 weeks ( Q3W) about 10 mg to about 800 mg (e.g., about 10 mg to about 800 mg, such as about 20 mg to about 700 mg, such as about 50 mg to about 600 mg, such as about 75 mg to about 500 mg, For example, about 100 mg to about 400 mg, such as about 100 mg to about 300 mg, such as about 125 mg to about 275 mg, such as about 150 mg to about 250 mg, such as about 175 mg to about 225 mg, For example, from about 190 mg to about 210 mg, such as about 200 mg ± 10 mg, such as 200 mg ± 7.5 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5, such as 200 ± 1.0 mg, such as, 200 ± 0.5 mg, such as 200 mg) (eg, a fixed dose). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is about every 3 weeks. A dose of 200 mg (e.g., 200 mg ± 10 mg, e.g., 200 ± 6 mg, e.g., 200 ± 5 mg, e.g., 200 ± 3 mg, e.g., 200 ± 1 mg, e.g., 200 ± 0.5 mg, every 3 weeks) , eg 200 mg). In some cases, the effective amount of the anti-PD-L1 antagonist antibody (eg, pembrolizumab) is a dose of about 200 mg every 3 weeks (eg, 200 mg ± 10 mg, eg, 200 ± 6 mg, every 3 weeks, such as , 200 ± 5 mg, such as 200 ± 3 mg, such as 200 ± 1 mg, such as 200 ± 0.5 mg, such as 200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every 3 weeks ( Q3W) 10 mg to 800 mg (eg, 10 mg to 800 mg, such as 20 mg to 700 mg, such as 50 mg to 600 mg, such as 75 mg to 500 mg, such as 100 mg to 400 mg, such as, 100 mg to 300 mg, such as 125 mg to 275 mg, such as 150 mg to 250 mg, such as 175 mg to 225 mg, such as 190 mg to 210 mg, such as 200 mg ± 10 mg, such as 200 mg A dose (eg, a fixed dose) of ± 7.5 mg, such as 200 mg ± 5 mg, such as 200 ± 2.5 , such as 200 ± 1.0 mg, such as 200 ± 0.5 mg, such as 200 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is 200 every 3 weeks. a dose of mg (e.g., 200 mg ± 10 mg, e.g., 200 ± 6 mg, e.g., 200 ± 5 mg, e.g., 200 ± 3 mg, e.g., 200 ± 1 mg, e.g., 200 ± 0.5 mg, every 3 weeks; eg 200 mg). In some cases, the effective amount of the anti-PD-L1 antagonist antibody (eg, pembrolizumab) is a dose of 200 mg every 3 weeks (eg, 200 mg±10 mg every 3 weeks, eg 200±6 mg, eg, 200 ± 5 mg, such as 200 ± 3 mg, such as 200 ± 1 mg, such as 200 ± 0.5 mg, such as 200 mg). In some cases, the effective amount of pembrolizumab is a dose of about 200 mg every 3 weeks. In some cases, the effective amount of pembrolizumab is a dose of about 200 mg every 3 weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 4주마다(Q4W) 약 80 mg 내지 약 3000 mg(예컨대, 약 80~200 mg, 약 200~400 mg, 약400~600 mg, 약 600~800 mg, 약 800~1000 mg, 약 1000~1200 mg, 약 1200~1400 mg, 약 1400~1600 mg, 약 1600~1800 mg, 약 1800~2000 mg, 약 2200~2400 mg, 약 2400~2600 mg, 약 2600~2800 mg, 또는 약 2800~3000 mg, 예컨대, 약 100 mg 내지 약 3000 mg, 예컨대, 약 200 mg 내지 약 2900 mg, 예컨대, 약 500 mg 내지 약 2800 mg, 예컨대, 약 600 mg 내지 약 2700 mg, 예컨대, 약 650 mg 내지 약 2600 mg, 예컨대, 약 700 mg 내지 약 2500 mg, 예컨대, 약 1000 mg 내지 약 2400 mg, 예컨대, 약 1100 mg 내지 약 2300 mg, 예컨대, 약 1200 mg 내지 약 2200 mg, 예컨대, 약 1300 mg 내지 약 2100 mg, 예컨대, 약 1400 mg 내지 약 2000 mg, 예컨대, 약 1500 mg 내지 약 1900 mg, 예컨대, 약 1600 mg 내지 약 1800 mg, 예컨대, 약 1620 mg 내지 약 1700 mg, 예컨대, 약 1640 mg 내지 약 1690 mg, 예컨대, 약 1660 mg 내지 약 1680 mg, 약 1680 mg, 예컨대, 약 80 mg, 약 200 mg, 약 400 mg, 약 600 mg, 약 800 mg, 약 1000 mg, 약 1200 mg, 약 1400 mg, 약 1600 mg, 약 1800 mg, 약 2000 mg, 약 2200 mg, 약 2400 mg, 약 2600 mg, 약 2800 mg, 또는 약 3000 mg, 예컨대, 약 1600 mg, 약 1610 mg, 약 1620 mg, 약 1630 mg, 약 1640 mg, 약 1650 mg, 약 1660 mg, 약 1670 mg, 약 1680 mg, 약 1690 mg, 또는 약 1700 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 4주마다(Q4W) 500 mg 내지 3000 mg(예컨대, 500 mg 내지 2800 mg, 예컨대, 600 mg 내지 2700 mg, 예컨대, 650 mg 내지 2600 mg, 예컨대, 700 mg 내지 2500 mg, 예컨대, 1000 mg 내지 2400 mg, 예컨대 1100 mg 내지 2300 mg, 예컨대 1200 mg 내지 2200 mg, 예컨대 1300 mg 내지 2100 mg, 예컨대 1400 mg 내지 2000 mg, 예컨대 1500 mg 내지 1900 mg, 예컨대 1600 mg 내지 1800 mg, 예컨대 1620 mg 내지 1700 mg, 예컨대 1640 mg 내지 1690 mg, 예컨대 1660 mg 내지 1680 mg, 1680 mg, 예컨대, 1600 mg, 1610 mg, 1620 mg, 1630 mg, 1640 mg, 1650 mg, 1660 mg, 1670 mg, 1680 mg, 1690 mg, 또는 1700 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 유효량은 4주 마다 1680 mg의 용량(예컨대, 4주마다 1680 mg ± 10 mg, 예컨대, 1680 ± 6 mg, 예컨대, 1680 ± 5 mg, 예컨대, 1680 ± 3 mg, 예컨대, 1680 ± 1 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 아테졸리주맙의 유효량은 4주마다 약 1680 mg의 용량이다. 일부 경우들에서, 아테졸리주맙의 유효량은 4주마다 1680 mg의 용량이다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every 4 weeks ( Q4W) about 80 mg to about 3000 mg (eg, about 80-200 mg, about 200-400 mg, about 400-600 mg, about 600-800 mg, about 800-1000 mg, about 1000-1200 mg, about 1200) ~1400 mg, about 1400-1600 mg, about 1600-1800 mg, about 1800-2000 mg, about 2200-2400 mg, about 2400-2600 mg, about 2600-2800 mg, or about 2800-3000 mg, such as about 100 mg to about 3000 mg, such as about 200 mg to about 2900 mg, such as about 500 mg to about 2800 mg, such as about 600 mg to about 2700 mg, such as about 650 mg to about 2600 mg, such as about 700 mg to about 2500 mg, such as about 1000 mg to about 2400 mg, such as about 1100 mg to about 2300 mg, such as about 1200 mg to about 2200 mg, such as about 1300 mg to about 2100 mg, such as about 1400 mg to about 2000 mg, such as about 1500 mg to about 1900 mg, such as about 1600 mg to about 1800 mg, such as about 1620 mg to about 1700 mg, such as about 1640 mg to about 1690 mg, such as about 1660 mg to about 1680 mg, about 1680 mg, such as about 80 mg, about 200 mg, about 400 mg, about 600 mg, about 800 mg, about 1000 mg, about 1200 mg, about 1400 mg, about 1600 mg, about 1800 mg, about 2000 mg, about 2200 mg, about 2400 mg, about 2600 mg, about 2800 mg, or about 3000 mg, such as about 1600 mg, about 1610 mg, about 1620 mg, about 1630 mg, about 1640 mg, about 1650 mg, about 1660 mg, about 1670 mg, about 1680 mg, about 1690 mg, or about 1700 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) or anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered every 4 weeks. (Q4W) 500 mg to 3000 mg (such as 500 mg to 2800 mg, such as 600 mg to 2700 mg, such as 650 mg to 2600 mg, such as 700 mg to 2500 mg, such as 1000 mg to 2400 mg, such as 1100 mg to 2300 mg, such as 1200 mg to 2200 mg, such as 1300 mg to 2100 mg, such as 1400 mg to 2000 mg, such as 1500 mg to 1900 mg, such as 1600 mg to 1800 mg, such as 1620 mg to 1700 mg, such as 1640 mg to 1690 mg, such as 1660 mg to 1680 mg, 1680 mg, such as 1600 mg, 1610 mg, 1620 mg, 1630 mg, 1640 mg, 1650 mg, 1660 mg, 1670 mg, 1680 mg, 1690 mg, or 1700 mg ) is the capacity of In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is 1680 every 4 weeks. a dose of mg (e.g., 1680 mg ± 10 mg, e.g., 1680 ± 6 mg, e.g., 1680 ± 5 mg, e.g., 1680 ± 3 mg, e.g., 1680 ± 1 mg, e.g., 1680 ± 0.5 mg, every 4 weeks; eg 1680 mg). In some cases, the effective amount of atezolizumab is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of atezolizumab is a dose of 1680 mg every 4 weeks.
일부 경우들에서, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)의 유효량은 6주마다(Q6W) 약 50 mg 내지 약 2000 mg(예컨대, 약 50~100 mg, 약 100~250 mg, 약 250~500 mg, 약 500~750 mg, 약 750~1000 mg, 약 1000~1250 mg, 약 1250~1500 mg, 약 1500~1750 mg, 또는 약 1750~2000 mg, 예컨대, 약 100 mg 내지 약 1000 mg, 약 120 mg 내지 약 900 mg, 약 150 mg 내지 약 800 mg, 약 200 mg 내지 약 700 mg, 약 250 mg 내지 약 600 mg, 약 300 mg 내지 약 500 mg, 또는 약 350 mg 내지 약 450 mg, 예컨대, 약 50 mg 내지 약 100 mg, 약 100 mg 내지 약 200 mg, 약 200 mg 내지 약 300 mg, 약 300 mg 내지 약 400 mg, 약 400 mg 내지 약 500 mg, 약 500 mg 내지 약 600 mg, 약 600 mg 내지 약 700 mg, 약 700 mg 내지 약 800 mg, 또는 약 800 mg 내지 약 1000 mg, 예컨대, 약 50 mg, 약 100 mg, 약 250 mg, 약 500 mg, 약 750 mg, 약 1000 mg, 약 1250 mg, 약 1500 mg, 약 1750 mg, 또는 약 2000 mg, 예컨대, 약 300 mg, 약 310 mg, 약 320 mg, 약 330 mg, 약 340 mg, 약 350 mg, 약 360 mg, 약 370 mg, 약 380 mg, 약 390 mg, 약 400 mg, 약 410 mg, 약 420 mg, 약 430 mg, 약 440 mg, 약 450 mg, 약 460 mg, 약 470 mg, 약 480 mg, 약 490 mg, 또는 약 500 mg, 예컨대, 400 mg)의 용량이다. 일부 경우들에서, 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)의 유효량은 6주마다(Q6W) 50 mg 내지 2000 mg(예컨대 100 mg 내지 1000 mg, 120 mg 내지 900 mg, 150 mg 내지 800 mg, 200 mg 내지 700 mg, 250 mg 내지 600 mg, 300 mg 내지 500 mg, 또는 350 mg 내지 450 mg, 예컨대, 50 mg 내지 100 mg, 100 mg 내지 200 mg, 200 mg 내지 300 mg, 300 mg 내지 400 mg, 400 mg 내지 500 mg, 500 mg 내지 600 mg, 600 mg 내지 700 mg, 700 mg 내지 800 mg, 또는 800 mg 내지 1000 mg, 예컨대, 300 mg, 310 mg, 320 mg, 330 mg, 340 mg, 350 mg, 360 mg, 370 mg, 380 mg, 390 mg, 400 mg, 410 mg, 420 mg, 430 mg, 440 mg, 450 mg, 460 mg, 470 mg, 480 mg, 490 mg, 또는 500 mg, 예컨대, 400 mg)의 용량이다. 일부 경우들에서, 상기 항 PD-L1 길항제 항체(예컨대, 펨브롤리주맙)의 유효량은 6주 마다 약 400 mg의 용량(예컨대, 6주마다 400 mg ± 10 mg, 예컨대, 400 ± 6 mg, 예컨대, 400 ± 5 mg, 예컨대, 400 ± 3 mg, 예컨대, 400 ± 1 mg, 예컨대, 400 ± 0.5 mg, 예컨대, 400 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제의 용량은 고정 용량이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 6주마다 약 400 mg의 용량(예컨대, 고정 용량)이다. 일부 경우들에서, 펨브롤리주맙의 유효량은 6주마다 400 mg의 용량(예컨대, 고정 용량)이다. In some cases, an effective amount of an anti-PD-1 antagonist antibody (eg, pembrolizumab) is about 50 mg to about 2000 mg (eg, about 50-100 mg, about 100-250 mg, about every 6 weeks (Q6W) 250-500 mg, about 500-750 mg, about 750-1000 mg, about 1000-1250 mg, about 1250-1500 mg, about 1500-1750 mg, or about 1750-2000 mg, such as about 100 mg to about 1000 mg, about 120 mg to about 900 mg, about 150 mg to about 800 mg, about 200 mg to about 700 mg, about 250 mg to about 600 mg, about 300 mg to about 500 mg, or about 350 mg to about 450 mg , e.g., about 50 mg to about 100 mg, about 100 mg to about 200 mg, about 200 mg to about 300 mg, about 300 mg to about 400 mg, about 400 mg to about 500 mg, about 500 mg to about 600 mg , about 600 mg to about 700 mg, about 700 mg to about 800 mg, or about 800 mg to about 1000 mg, such as about 50 mg, about 100 mg, about 250 mg, about 500 mg, about 750 mg, about 1000 mg, about 1250 mg, about 1500 mg, about 1750 mg, or about 2000 mg, such as about 300 mg, about 310 mg, about 320 mg, about 330 mg, about 340 mg, about 350 mg, about 360 mg, about 370 mg, about 380 mg, about 390 mg, about 400 mg, about 410 mg, about 420 mg, about 430 mg, about 440 mg, about 450 mg, about 460 mg, about 470 mg, about 480 mg, about 490 mg , or about 500 mg, such as 400 mg). In some cases, an effective amount of an anti-PD-1 antagonist antibody (eg, pembrolizumab) is 50 mg to 2000 mg (eg, 100 mg to 1000 mg, 120 mg to 900 mg, 150 mg to 800 mg) every 6 weeks (Q6W). mg, 200 mg to 700 mg, 250 mg to 600 mg, 300 mg to 500 mg, or 350 mg to 450 mg, such as 50 mg to 100 mg, 100 mg to 200 mg, 200 mg to 300 mg, 300 mg to 400 mg, 400 mg to 500 mg, 500 mg to 600 mg, 600 mg to 700 mg, 700 mg to 800 mg, or 800 mg to 1000 mg, such as 300 mg, 310 mg, 320 mg, 330 mg, 340 mg , 350 mg, 360 mg, 370 mg, 380 mg, 390 mg, 400 mg, 410 mg, 420 mg, 430 mg, 440 mg, 450 mg, 460 mg, 470 mg, 480 mg, 490 mg, or 500 mg, eg 400 mg). In some cases, the effective amount of the anti-PD-L1 antagonist antibody (eg, pembrolizumab) is a dose of about 400 mg every 6 weeks (eg, 400 mg ± 10 mg, eg, 400 ± 6 mg, every 6 weeks, such as , 400 ± 5 mg, such as 400 ± 3 mg, such as 400 ± 1 mg, such as 400 ± 0.5 mg, such as 400 mg). In some cases, the dose of the PD-1 axis binding antagonist is a fixed dose. In some cases, an effective amount of pembrolizumab is a dose (eg, a fixed dose) of about 400 mg every 6 weeks. In some cases, the effective amount of pembrolizumab is a dose of 400 mg (eg, a fixed dose) every 6 weeks.
일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 용량은 단일요법으로 투여되는 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다. In some cases, a PD-1 axis binding antagonist (eg, anti-PD-) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab). The dose of an L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) may be reduced compared to a standard dose of a PD-1 axis binding antagonist administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 정맥내 투여된다. 대안적으로, 일부 구현예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 피하 투여된다. 일부 경우들에서, 아테졸리주맙은 2주마다 약 840 mg, 3주마다 약 1200 mg, 또는 4주마다 약 1680 mg의 용량으로 환자에게 정맥내 투여된다. 일부 경우들에서, 아테졸리주맙은 2주마다 840 mg, 3주마다 1200 mg, 또는 4주마다 1680 mg의 용량으로 상기 환자에게 정맥내 투여된다.In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered intravenously. Alternatively, in some embodiments, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered subcutaneously. is administered In some cases, atezolizumab is administered to the patient intravenously at a dose of about 840 mg every 2 weeks, about 1200 mg every 3 weeks, or about 1680 mg every 4 weeks. In some cases, atezolizumab is administered to the patient intravenously at a dose of 840 mg every 2 weeks, 1200 mg every 3 weeks, or 1680 mg every 4 weeks.
일부 경우들에서, 대상체는 PD-1 축 결합 길항제의 총 1 내지 20회 용량, 예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 또는 20회 용량이 투여된다. 일부 경우들에서, 대상체는 PD-1 축 결합 길항제의 총 1 내지 50회 용량, 예컨대, 1회 내지 50회 용량, 1회 내지 45회 용량, 1회 내지 40회 용량, 1회 내지 35회 용량, 1 내지 30회 용량, 1회 내지 25회 용량, 1회 내지 20회 용량, 1회 내지 15회 용량, 1회 내지 10회 용량, 1회 내지 5회 용량, 2회 내지 50회 용량, 2회 내지 45회 용량, 2회 내지 40회 용량, 2회 내지 35회 용량, 2회 내지 30회 용량, 2회 내지 25회 용량, 2회 내지 20회 용량, 2회 내지 15회 용량, 2회 내지 10회 용량, 2회 내지 5회 용량, 3회 내지 50회 용량, 3회 내지 45회 용량, 3회 내지 40회 용량, 3회 내지 35회 용량, 3회 내지 30회 용량, 3회 내지 25회 용량, 3회 내지 20회 용량, 3회 내지 15회 용량, 3회 내지 10회 용량, 3회 내지 5회 용량, 4회 내지 50회 용량, 4회 내지 45회 용량, 4회 내지 40회 용량, 4회 내지 35회 용량, 4회 내지 30회 용량, 4회 내지 25회 용량, 4회 내지 20회 용량, 4회 내지 15회 용량, 4회 내지 10회 용량, 4회 내지 5회 용량, 5회 내지 50회 용량, 5회 내지 45회 용량, 5회 내지 40회 용량, 5회 내지 35회 용량, 5회 내지 30회 용량 5회 내지 25회 용량, 5회 내지 20회 용량, 5회 내지 15회 용량, 5회 내지 10회 용량, 10회 내지 50회 용량, 10회 내지 45회 용량, 10회 내지 40회 용량, 10회 내지 35회 용량, 10회 내지 30회 용량, 10회 내지 25회 용량, 10회 내지 20회 용량, 10회 내지 15회 용량, 15회 내지 50회 용량, 15회 내지 45회 용량, 15회 내지 40회 용량, 15회 내지 35회 용량, 15회 내지 30회 용량, 15회 내지 25회 용량, 15회 내지 20회 용량, 20회 내지 50회 용량, 20회 내지 45회 용량, 20회 내지 40회 용량, 20회 내지 35회 용량, 20회 내지 30회 용량, 20회 내지 25회 용량, 25회 내지 50회 용량, 25회 내지 45회 용량, 25회 내지 40회 용량, 25회 내지 35회 용량, 25회 내지 30회 용량, 30회 내지 30회 용량, 30회 내지 45회 용량, 30회 내지 40회 용량, 30회 내지 35회 용량, 35회 내지 50회 용량, 35회 내지 45회 용량, 35회 내지 40회 용량, 40회 내지 50회 용량, 40회 내지 45회 용량, 또는 45회 내지 50회 용량이 투여된다. 특정 경우들에서, 상기 용량은 정맥내 투여될 수 있다.In some cases, the subject receives a total of 1 to 20 doses of the PD-1 axis binding antagonist, such as 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, or 20 doses are administered. In some cases, the subject has a total of 1 to 50 doses of the PD-1 axis binding antagonist, such as 1 to 50 doses, 1 to 45 doses, 1 to 40 doses, 1 to 35 doses of the PD-1 axis binding antagonist. , 1 to 30 doses, 1 to 25 doses, 1 to 20 doses, 1 to 15 doses, 1 to 10 doses, 1 to 5 doses, 2 to 50 doses, 2 From 2 to 45 doses, 2 to 40 doses, 2 to 35 doses, 2 to 30 doses, 2 to 25 doses, 2 to 20 doses, 2 to 15 doses, 2 doses to 10 doses, 2 to 5 doses, 3 to 50 doses, 3 to 45 doses, 3 to 40 doses, 3 to 35 doses, 3 to 30 doses, 3 to 25 doses, 3 to 20 doses, 3 to 15 doses, 3 to 10 doses, 3 to 5 doses, 4 to 50 doses, 4 to 45 doses, 4 to 40 doses Dose, 4 to 35 doses, 4 to 30 doses, 4 to 25 doses, 4 to 20 doses, 4 to 15 doses, 4 to 10 doses, 4 to 5 doses dose, 5 to 50 doses, 5 to 45 doses, 5 to 40 doses, 5 to 35 doses, 5 to 30 doses, 5 to 25 doses, 5 to 20 doses, 5 to 15 doses, 5 to 10 doses, 10 to 50 doses, 10 to 45 doses, 10 to 40 doses, 10 to 35 doses, 10 to 30 doses, 10 25 to 25 doses, 10 to 20 doses, 10 to 15 doses, 15 to 50 doses, 15 to 45 doses, 15 to 40 doses, 15 to 35 doses, 15 doses to 30 doses, 15 to 25 doses, 15 to 20 doses, 20 to 50 doses, 20 to 45 doses, 20 to 40 doses, 20 to 35 doses, 20 to 30 doses, 20 to 25 doses, 25 to 50 doses, 25 to 45 doses, 25 to 40 doses, 25 to 35 doses, 25 30 to 30 doses, 30 to 30 doses, 30 to 45 doses, 30 to 40 doses, 30 to 35 doses, 35 to 50 doses, 35 to 45 doses, 35 doses 40 to 40 doses, 40 to 50 doses, 40 to 45 doses, or 45 to 50 doses are administered. In certain instances, the dose may be administered intravenously.
i.i. 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 유효 투여량Effective dose of anti-TIGIT antagonist antibody and PD-1 axis binding antagonist
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 2주마다 약 30 mg 내지 약 600 mg(예컨대, 약 50 mg 내지 약 600 mg, 예컨대, 약 60 mg 내지 약 600 mg, 예컨대, 약 100 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 600 mg, 예컨대, 약 200 mg 내지 약 550 mg, 예컨대, 약 250 mg 내지 약 600 mg, 예컨대, 약 300 mg 내지 약 500 mg, 예컨대, 약 350 mg 내지 약 450 mg, 예컨대, 약 400 mg 내지 약 440 mg, 예컨대, 약 410 mg 내지 약 430 mg, 예컨대, 약 420 ± 10 mg, 예컨대, 420 ± 6 mg, 예컨대, 420 ± 5 mg, 예컨대, 420 ± 3 mg, 예컨대, 420 ± 1 mg, 예컨대, 420 ± 0.5 mg, 예컨대, 420 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 2주마다 30 mg 내지 600 mg(예컨대, 50 mg 내지 600 mg, 예컨대, 60 mg 내지 600 mg, 예컨대, 100 mg 내지 600 mg, 예컨대, 200 mg 내지 600 mg, 예컨대, 200 mg 내지 550 mg, 예컨대, 250 mg 내지 600 mg, 예컨대, 300 mg 내지 500 mg, 예컨대, 350 mg 내지 450 mg, 예컨대, 400 mg 내지 440 mg, 예컨대, 410 mg 내지 430 mg, 예컨대, 420 mg ± 10 mg, 예컨대, 420 ± 6 mg, 예컨대, 420 ± 5 mg, 예컨대, 420 ± 3 mg, 예컨대, 420 ± 1 mg, 예컨대, 420 ± 0.5 mg, 예컨대, 420 mg)의 용량(예컨대,고정 용량)이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 2주마다 약 420 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 2주마다 420 mg의 용량이다.In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 600 mg (eg, from about 50 mg to about 600) every two weeks. mg, such as about 60 mg to about 600 mg, such as about 100 mg to about 600 mg, such as about 200 mg to about 600 mg, such as about 200 mg to about 550 mg, such as about 250 mg to about 600 mg, such as about 300 mg to about 500 mg, such as about 350 mg to about 450 mg, such as about 400 mg to about 440 mg, such as about 410 mg to about 430 mg, such as about 420 ± 10 mg, For example, a dose (eg, a fixed dose) of 420 ± 6 mg, such as 420 ± 5 mg, such as 420 ± 3 mg, such as 420 ± 1 mg, such as 420 ± 0.5 mg, such as 420 mg. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 30 mg to 600 mg (eg, 50 mg to 600 mg, eg, 60 mg to 600 mg, such as 100 mg to 600 mg, such as 200 mg to 600 mg, such as 200 mg to 550 mg, such as 250 mg to 600 mg, such as 300 mg to 500 mg, such as 350 mg to 450 mg, such as 400 mg to 440 mg, such as 410 mg to 430 mg, such as 420 mg ± 10 mg, such as 420 ± 6 mg, such as 420 ± 5 mg, such as 420 ± 3 mg, such as , 420 ± 1 mg, such as 420 ± 0.5 mg, such as 420 mg) (eg, a fixed dose). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 420 mg every two weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 420 mg every two weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 약 30 mg 내지 약 1100 mg, 예컨대, 약 60 mg 내지 약 1000 mg, 예컨대, 약 100 mg 내지 약 900 mg, 예컨대, 약 200 mg 내지 약 800 mg, 예컨대, 약 300 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 800 mg, 예컨대, 약 400 mg 내지 약 750 mg, 예컨대, 약 450 mg 내지 약 750 mg, 예컨대, 약 500 mg 내지 약 700 mg, 예컨대, 약 550 mg 내지 약 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 30 mg 내지 1200 mg(예컨대, 30 mg 내지 1100 mg, 예컨대, 60 mg 내지 1000 mg, 예컨대, 100 mg 내지 900 mg, 예컨대, 200 mg 내지 800 mg, 예컨대, 300 mg 내지 800 mg, 예컨대, 400 mg 내지 800 mg, 예컨대, 400 mg 내지 750 mg, 예컨대, 450 mg 내지 750 mg, 예컨대, 500 mg 내지 700 mg, 예컨대, 550 mg 내지 650 mg, 예컨대, 600 mg ± 10 mg, 예컨대, 600 ± 6 mg, 예컨대, 600 ± 5 mg, 예컨대, 600 ± 3 mg, 예컨대, 600 ± 1 mg, 예컨대, 600 ± 0.5 mg, 예컨대, 600 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 3주마다 600 mg의 용량이다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is from about 30 mg to about 1200 mg (eg, from about 30 mg to about 1100) every 3 weeks. mg, such as about 60 mg to about 1000 mg, such as about 100 mg to about 900 mg, such as about 200 mg to about 800 mg, such as about 300 mg to about 800 mg, such as about 400 mg to about 800 mg, such as about 400 mg to about 750 mg, such as about 450 mg to about 750 mg, such as about 500 mg to about 700 mg, such as about 550 mg to about 650 mg, such as 600 mg ± 10 mg, For example, a dose of 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is 30 mg to 1200 mg (eg, 30 mg to 1100 mg, eg, 60 mg to 1000 mg, such as 100 mg to 900 mg, such as 200 mg to 800 mg, such as 300 mg to 800 mg, such as 400 mg to 800 mg, such as 400 mg to 750 mg, such as 450 mg to 750 mg, such as 500 mg to 700 mg, such as 550 mg to 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as , 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 600 mg every 3 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg every 3 weeks.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 4주마다 약 600 mg 내지 약 1200 mg(예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 600 mg 내지 약 1000 mg, 예컨대, 약 700 mg 내지 약 950 mg, 예컨대, 약 800 mg 내지 약 900 mg, 예컨대, 약 820 mg 내지 약 860 mg, 예컨대, 약 840 ± 10 mg, 예컨대, 840 ± 6 mg, 예컨대, 840 ± 5 mg, 예컨대, 840 ± 3 mg, 예컨대, 840 ± 1 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 유효량은 4주마다 600 mg 내지 1200 mg(예컨대, 600 mg 내지 1100 mg, 예컨대, 600 mg 내지 1000 mg, 예컨대, 700 mg 내지 950 mg, 예컨대, 800 mg 내지 900 mg, 예컨대, 820 mg 내지 860 mg, 예컨대, 840 ± 10 mg, 예컨대, 840 ± 6 mg, 예컨대, 840 ± 5 mg, 예컨대, 840 ± 3 mg, 예컨대, 840 ± 1 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 4주마다 840 mg의 용량이다. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is from about 600 mg to about 1200 mg (eg, from about 600 mg to about) every 4 weeks. 1100 mg, such as about 600 mg to about 1000 mg, such as about 700 mg to about 950 mg, such as about 800 mg to about 900 mg, such as about 820 mg to about 860 mg, such as about 840 ± 10 mg , such as 840 ± 6 mg, such as 840 ± 5 mg, such as 840 ± 3 mg, such as 840 ± 1 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 600 mg to 1200 mg (eg, 600 mg to 1100 mg, eg, every 4 weeks) , 600 mg to 1000 mg, such as 700 mg to 950 mg, such as 800 mg to 900 mg, such as 820 mg to 860 mg, such as 840 ± 10 mg, such as 840 ± 6 mg, such as 840 ± 5 mg, such as 840 ± 3 mg, such as 840 ± 1 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 840 mg every 4 weeks. In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 840 mg every 4 weeks.
일부 경우들에서, 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK-3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))와의 병용 치료)으로 투여되는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여되는 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. 일부 경우들에서, 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀) 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 및/또는 G-CSF 또는 GM -CSF를 포함하거나 포함하지 않고 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)와의 병용 치료)으로 투여되는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 단일요법으로 투여되는 상기 항 TIGIT 길항제 항체의 표준 용량과 비교하여 감소될 수 있다.In some cases, combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab)) or Dose of said anti TIGIT antagonist antibody (eg, anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) administered in combination therapy with MK-3475 (pembrolizumab, formerly known as lambrolizumab) can be reduced compared to the standard dose of the anti-TIGIT antagonist antibody administered as monotherapy In some cases, one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and / or non-platinum-based chemotherapeutic agents (eg, alkylating agents (eg, cyclophosphamide), taxanes (eg, paclitaxel, such as nap-paclitaxel) and/or topoisomerase II inhibitors (eg, doxorubicin)) and/or G -CSF or GM-CSF, said anti-TIGIT antagonist administered in combination therapy (eg, combination therapy with a PD-1 axis binding antagonist (eg, combination therapy with an anti-PD-L1 antagonist antibody (eg, atezolizumab)) with or without -CSF The dose of an antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) may be reduced compared to a standard dose of said anti TIGIT antagonist antibody administered as monotherapy.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 20 mg 내지 약 1600 mg(예컨대, 약 20~100 mg, 약 100~200 mg, 약 200~400 mg, 약 400~600 mg, 약 600~800 mg, 약 800~1000 mg, 약 1000~1200 mg, 약 1200~1400 mg, 또는 약 1400~1600 mg, 예컨대, 약 80 mg 내지 약 1200 mg, 예컨대, 약 100 mg 내지 약 1200 mg, 예컨대, 약 200 mg 내지 약 1200 mg, 예컨대, 약 300 mg 내지 약 1200 mg, 예컨대, 약 400 mg 내지 약 1200 mg, 예컨대, 약 500 mg 내지 약 1200 mg, 예컨대, 약 600 mg 내지 약 1100 mg, 예컨대, 약 700 mg 내지 약 1000 mg, 예컨대, 약 740 mg 내지 약 940 mg, 예컨대, 약 790 mg 내지 약 890 mg, 예컨대, 약 815 mg 내지 약 865 mg, 예컨대, 약 830 mg 내지 약 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 80 mg 내지 1200 mg(예컨대, 80 mg 내지 1200 mg, 예컨대, 100 mg 내지 1200 mg, 예컨대, 200 mg 내지 1200 mg, 예컨대, 300 mg 내지 1200 mg, 예컨대, 400 mg 내지 1200 mg, 예컨대, 500 mg 내지 1200 mg, 예컨대 600, mg 내지 1100 mg, 예컨대, 700 mg 내지 1000 mg, 예컨대, 740 mg 내지 940 mg, 예컨대, 790 mg 내지 890 mg, 예컨대, 815 mg 내지 865 mg, 예컨대, 830 mg 내지 850 mg, 예컨대, 840 mg ± 5 mg, 예컨대, 840 ± 2.5 mg, 예컨대, 840 ± 1.0 mg, 예컨대, 840 ± 0.5 mg, 예컨대, 840 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 20 mg, 100 mg, 200 mg, 300 mg, 400 mg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, 1000 mg, 1200 mg, 1400 mg, 또는 1600 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 약 840 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 2주마다 840 mg의 용량이다.In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is about 20 mg to about 1600 mg (eg, about 20-100 mg) every two weeks. , about 100-200 mg, about 200-400 mg, about 400-600 mg, about 600-800 mg, about 800-1000 mg, about 1000-1200 mg, about 1200-1400 mg, or about 1400-1600 mg, For example, about 80 mg to about 1200 mg, such as about 100 mg to about 1200 mg, such as about 200 mg to about 1200 mg, such as about 300 mg to about 1200 mg, such as about 400 mg to about 1200 mg, For example, about 500 mg to about 1200 mg, such as about 600 mg to about 1100 mg, such as about 700 mg to about 1000 mg, such as about 740 mg to about 940 mg, such as about 790 mg to about 890 mg, For example, about 815 mg to about 865 mg, such as about 830 mg to about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as , 840 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 1200 mg (eg, 80 mg to 1200 mg, eg, every 2 weeks) , 100 mg to 1200 mg, such as 200 mg to 1200 mg, such as 300 mg to 1200 mg, such as 400 mg to 1200 mg, such as 500 mg to 1200 mg, such as 600, mg to 1100 mg, such as 700 mg to 1000 mg, such as 740 mg to 940 mg, such as 790 mg to 890 mg, such as 815 mg to 865 mg, such as 830 mg to 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is about 20 mg, 100 mg, 200 mg, 300 mg, 400 mg every two weeks. , 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, 1000 mg, 1200 mg, 1400 mg, or 1600 mg. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 80 mg 내지 약 2000 mg(예컨대, 약 100 mg 내지 약 2000 mg, 예컨대, 약 200 mg 내지 약 1900 mg, 예컨대, 약 300 mg 내지 약 1700 mg, 예컨대, 약 400 mg 내지 약 1600 mg, 예컨대, 약 500 mg 내지 약 1600 mg, 예컨대, 약 600 mg 내지 약 1600 mg, 예컨대, 약 700 mg 내지 약 1600 mg, 예컨대, 약 800 mg 내지 약 1600 mg, 예컨대, 약 900 mg 내지 약 1500 mg, 예컨대, 약 1000 mg 내지 약 1400 mg, 예컨대, 약 1050 mg 내지 약 1350 mg, 예컨대, 약 1100 mg 내지 약 1300 mg, 예컨대, 약 1150 mg 내지 약 1250 mg, 예컨대, 약 1175 mg 내지 약 1225 mg, 예컨대, 약 1190 mg 내지 약 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 80 mg 내지 2000 mg(예컨대, 100 mg 내지 2000 mg, 예컨대, 200 mg 내지 1900 mg, 예컨대, 300 mg 내지 1700 mg, 예컨대, 400 mg 내지 1600 mg, 예컨대, 500 mg 내지 1600 mg, 예컨대, 600 mg 내지 1600 mg, 예컨대, 700 mg 내지 1600 mg, 예컨대, 800 mg 내지 1600 mg, 예컨대, 900 mg 내지 1500 mg, 예컨대, 1000 mg 내지 1400 mg, 예컨대, 1050 mg 내지 1350 mg, 예컨대, 1100 mg 내지 1300 mg, 예컨대, 1150 mg 내지 1250 mg, 예컨대, 1175 mg 내지 1225 mg, 예컨대, 1190 mg 내지 1210 mg, 예컨대, 1200 mg ± 5 mg, 예컨대, 1200 ± 2.5 mg, 예컨대, 1200 ± 1.0 mg, 예컨대, 1200 ± 0.5 mg, 예컨대, 1200 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 약 1200 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 3주마다 1200 mg의 용량이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 80 mg to about 2000 mg (eg, from about 100 mg to about) every 3 weeks. 2000 mg, such as about 200 mg to about 1900 mg, such as about 300 mg to about 1700 mg, such as about 400 mg to about 1600 mg, such as about 500 mg to about 1600 mg, such as about 600 mg to about 1600 mg, such as about 700 mg to about 1600 mg, such as about 800 mg to about 1600 mg, such as about 900 mg to about 1500 mg, such as about 1000 mg to about 1400 mg, such as about 1050 mg to about 1350 mg, such as about 1100 mg to about 1300 mg, such as about 1150 mg to about 1250 mg, such as about 1175 mg to about 1225 mg, such as about 1190 mg to about 1210 mg, such as 1200 mg ± 5 mg , such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 80 mg to 2000 mg (eg, 100 mg to 2000 mg, such as every 3 weeks) , 200 mg to 1900 mg, such as 300 mg to 1700 mg, such as 400 mg to 1600 mg, such as 500 mg to 1600 mg, such as 600 mg to 1600 mg, such as 700 mg to 1600 mg, such as 800 mg to 1600 mg, such as 900 mg to 1500 mg, such as 1000 mg to 1400 mg, such as 1050 mg to 1350 mg, such as 1100 mg to 1300 mg, such as 1150 mg to 1250 mg, such as 1175 mg to 1225 mg, such as 1190 mg to 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0.5 mg, such as 1200 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1200 mg every 3 weeks.
일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 1200 mg 내지 약 2000 mg(예컨대, 약 1200 mg 내지 약 1900 mg, 예컨대, 약 1200 mg 내지 약 1800 mg, 예컨대, 약 1300 mg 내지 약 1800 mg, 예컨대, 약 1400 mg 내지 약 1800 mg, 예컨대 약 1500 mg 내지 약 1800 mg, 예컨대, 약 1580 mg 내지 약 1780 mg, 예컨대, 약 1630 mg 내지 약 1730 mg, 예컨대, 약 1655 mg 내지 약 1705 mg, 예컨대, 약 1670 mg 내지 약 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대, 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 1200 mg 내지 2000 mg(예컨대, 1200 mg 내지 1900 mg, 예컨대, 1200 mg 내지 1800 mg, 예컨대, 1300 mg 내지 1800 mg, 예컨대, 1400 mg 내지 1800 mg, 예컨대, 1500 mg 내지 1800 mg, 예컨대, 1580 mg 내지 1780 mg, 예컨대, 1630 mg 내지 1730 mg, 예컨대, 1655 mg 내지 1705 mg, 예컨대, 1670 mg 내지 1690 mg, 예컨대, 1680 mg ± 5 mg, 예컨대, 1680 ± 2.5 mg, 예컨대, 1680 ± 1.0 mg, 예컨대, 1680 ± 0.5 mg, 예컨대, 1680 mg)의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 약 1680 mg의 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 유효량은 4주마다 1680 mg의 용량이다. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is from about 1200 mg to about 2000 mg (eg, from about 1200 mg to about) every 4 weeks. 1900 mg, such as about 1200 mg to about 1800 mg, such as about 1300 mg to about 1800 mg, such as about 1400 mg to about 1800 mg, such as about 1500 mg to about 1800 mg, such as about 1580 mg to about 1780 mg, such as about 1630 mg to about 1730 mg, such as about 1655 mg to about 1705 mg, such as about 1670 mg to about 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). In some cases, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 1200 mg to 2000 mg (eg, 1200 mg to 1900 mg, such as every 4 weeks) , 1200 mg to 1800 mg, such as 1300 mg to 1800 mg, such as 1400 mg to 1800 mg, such as 1500 mg to 1800 mg, such as 1580 mg to 1780 mg, such as 1630 mg to 1730 mg, such as 1655 mg to 1705 mg, such as 1670 mg to 1690 mg, such as 1680 mg ± 5 mg, such as 1680 ± 2.5 mg, such as 1680 ± 1.0 mg, such as 1680 ± 0.5 mg, such as 1680 mg). . In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some cases, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks.
일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체(예컨대, 티라골루맙)과의 병용 치료)으로 투여되는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 항 PD-L1 길항제 항체의 표준 용량과 비교하여 감소될 수 있다. 일부 경우들에서, 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)) 및/또는 G-CSF 또는 GM -CSF를 포함하거나 포함하지 않고 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙과의 병용 치료)으로 투여된 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 단일요법으로 투여되는 상기 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다. In some cases, a PD-1 axis binding antagonist (eg, anti-PD) administered in combination therapy (eg, combination therapy with an anti TIGIT antagonist antibody, eg, an anti TIGIT antagonist antibody (eg, tyragolumab) disclosed herein). The dose of the -L1 antagonist antibody (eg, atezolizumab) may be reduced compared to a standard dose of an anti-PD-L1 antagonist antibody administered as monotherapy. In some cases, one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or a non-platinum-based chemotherapeutic agent (eg, an alkylating agent (eg, cyclophosphamide), a taxane) Combination therapy (eg, anti-TIGIT antagonist antibody, eg, with or without paclitaxel, eg, nap-paclitaxel), and/or a topoisomerase II inhibitor (eg, doxorubicin) and/or G-CSF or GM-CSF For example, the dose of said PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) administered with an anti-TIGIT antagonist antibody disclosed herein, e.g., in combination treatment with tiragolumab, is compared to the standard dose of the PD-1 axis binding antagonist administered as monotherapy.
ii.ii. 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 투약 주기Dosing Cycles of Anti-TIGIT Antagonist Antibodies and PD-1 Axis Binding Antagonists
본 발명의 임의의 방법 및 사용에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 1회 이상의 투약 주기(예컨대, 1회, 2회, 3회, 4회, 5회, 6회, 7회, 8회, 9회, 10회, 11회, 12회, 13회, 14회, 15회, 16회, 17회, 18회, 19회, 20회, 21회, 22회, 23회, 24회, 25회, 26회, 27회, 28회, 29회, 30회, 31회, 32회, 33회, 34회, 35회, 36회, 37회, 38회, 39회, 40회, 41회, 42회, 43회, 44회, 45회, 46회, 47회, 48회, 49회, 또는 50회 이상의 투약 주기)로 투여될 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투약 주기는 임상 이익이 상실(예컨대, 질병 진행, 약물 내성, 사망 또는 허용할 수 없는 독성이 확인)될 때까지 계속된다. 일부 경우들에서, 각 투약 주기의 길이는 약 7 내지 42일(예컨대, 7일, 8일, 9일, 10일, 11일, 12일, 13일, 14일, 15일, 16일, 17일)이다. 일, 18일, 19일, 20일, 21일, 22일, 23일, 24일, 25일, 26일, 27일, 28일, 29일, 30일, 31일, 32일, 33일, 34일, 35일, 36일, 37일, 38일, 39일, 41일, 42일)이다. 일부 경우들에서, 각 투약 주기의 길이는 약 14일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 21일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 28일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 42일이다. 일부 경우들에서, 각 투약 주기의 길이는 약 7일이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 15일(예컨대, 15일 ± 3일)에 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 22일(예컨대, 22일 ± 3일)에 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 투약 주기의 약 29일(예컨대, 29일 ± 3일)에 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 28일 주기의 제 1일 및 15일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 2주마다 약 420 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 42일 주기의 제 1일, 15일, 및 29일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 2주마다 약 420 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 42일 주기의 제 1일 및 22일에 약 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 각 투약 주기의 약 15일(예컨대, 15일 ± 3일)에 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 28일 주기의 제 1일 및 15일에 약 1200 mg의 용량으로(즉, 2주마다 약 840 mg의 용량으로) 정맥내 투여된다. 일부 예들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량(예컨대, 고정 용량)으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, MDX-1106(니볼루맙) 또는 MK- 3475(펨브롤리주맙, 이전에 람브롤리주맙으로 공지됨))는 각 투약 주기의 제 1일(예컨대, 1일 ± 3일)에 투여된다. 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여된다.In any of the methods and uses of the invention, said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tiragolumab) and/or said PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist) The antibody (eg, atezolizumab) may be administered in one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11). , 12 times, 13 times, 14 times, 15 times, 16 times, 17 times, 18 times, 19 times, 20 times, 21 times, 22 times, 23 times, 24 times, 25 times, 26 times, 27 times, 28 times times, 29 times, 30 times, 31 times, 32 times, 33 times, 34 times, 35 times, 36 times, 37 times, 38 times, 39 times, 40 times, 41 times, 42 times, 43 times, 44 times, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, ate Zolizumab)), the dosing cycle is continued until clinical benefit is lost (eg, disease progression, drug resistance, death, or unacceptable toxicity is identified). In some cases, the length of each dosing cycle is between about 7 and 42 days (eg, 7 days, 8 days, 9 days, 10 days, 11 days, 12 days, 13 days, 14 days, 15 days, 16 days, 17 days). work) is Days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days, 27 days, 28 days, 29 days, 30 days, 31 days, 32 days, 33 days, 34 days, 35 days, 36 days, 37 days, 38 days, 39 days, 41 days, 42 days). In some cases, the length of each dosing cycle is about 14 days. In some cases, the length of each dosing cycle is about 21 days. In some cases, the length of each dosing cycle is about 28 days. In some cases, the length of each dosing cycle is about 42 days. In some cases, the length of each dosing cycle is about 7 days. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about day 1 (eg, day 1 ± 3 days) of each dosing cycle. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about 15 days (eg, 15 days ± 3 days) of each dosing cycle. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about 22 days (eg, 22 days ± 3 days) of each dosing cycle. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered on about 29 days (eg, 29 days ± 3 days) of each dosing cycle. For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of about 600 mg (eg, a fixed dose) on Day 1 of each 21 day cycle (eg, a fixed dose) ( i.e., at a dose of about 600 mg every 3 weeks). For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) may be administered at a dose of about 600 mg (eg, a fixed dose) on days 1 and 15 of each 28-day cycle. ) (ie, at a dose of about 420 mg every 2 weeks). For example, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) may be administered at a dose of about 600 mg on days 1, 15, and 29 of each 42-day cycle ( eg, as a fixed dose) (ie, at a dose of about 420 mg every two weeks). For example, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tyragolumab) may be administered at a dose of about 600 mg (eg, a fixed dose) on days 1 and 22 of each 42 day cycle. ) (ie, at a dose of about 600 mg every 3 weeks). In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 ( Pembrolizumab (previously known as lambrolizumab)) is administered on about day 1 of each dosing cycle (e.g., day 1 ± 3 days) In some cases, the PD-1 axis binding antagonist (e.g., An anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) Administer on about 15 days (eg, 15 days ± 3 days) of each dosing cycle.For example, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered on each Administer intravenously at a dose of about 1200 mg (ie, at a dose of about 1200 mg every 3 weeks) on Day 1 of a 21-day cycle, For example, the PD-1 axis binding antagonist (eg, anti-PD-L1 The antagonist antibody (eg, atezolizumab)) is administered intravenously at a dose of about 1200 mg (ie, at a dose of about 840 mg every two weeks) on days 1 and 15 of each 28-day cycle. , the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) is administered at a dose of 600 mg (eg, a fixed dose) on Day 1 of each 21-day cycle (ie, 3 weeks). In some cases, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered on Day 1 (e.g., Day 1 ± 3) of each dosing cycle. , wherein the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) It is administered intravenously at a dose of 1200 mg per day (ie at a dose of 1200 mg every 3 weeks).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 투약 주기의 약 1일(예컨대, 1일 ± 3일)에 투여된다. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli Zumab)) is administered on about day 1 (eg, day 1 ± 3 days) of each dosing cycle.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 약 600 mg의 용량으로(즉, 3주마다 약 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 약 1200 mg의 용량으로(즉, 3주마다 약 1200 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 21일 주기의 제 1일에 600 mg의 용량으로(즉, 3주마다 600 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 21일 주기의 제 1일에 1200 mg의 용량으로(즉, 3주마다 1200 mg의 용량으로) 정맥내 투여된다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 600 mg on Day 1 of each 21-day cycle (ie, every 3 weeks). at a dose of about 600 mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at about 1200 mg on Day 1 of each 21-day cycle. It is administered intravenously as a dose (ie, at a dose of about 1200 mg every 3 weeks). In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of 600 mg on Day 1 of each 21-day cycle (ie, 600 every 3 weeks). mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a dose of 1200 mg on Day 1 of each 21-day cycle ( i.e., administered intravenously (in a dose of 1200 mg every 3 weeks).
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 14일 주기의 제 1일에 약 420 mg의 용량으로(즉, 2주마다 약 420 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 14일 주기의 제 1일에 약 840 mg의 용량으로(즉, 2주마다 약 840 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 14일 주기의 제 1일에 420 mg의 용량으로(즉, 2주마다 약 420 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 14일 주기의 제 1일에 840 mg의 용량으로(즉, 2주마다 840 mg의 용량으로) 정맥내 투여된다. In other instances, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 420 mg (ie, every two weeks) on Day 1 of each 14-day cycle. at a dose of about 420 mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at about 840 mg on Day 1 of each 14-day cycle. It is administered intravenously as a dose (ie, at a dose of about 840 mg every two weeks). In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of 420 mg on Day 1 of each 14-day cycle (ie, about every two weeks). 420 mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a dose of 840 mg on Day 1 of each 14-day cycle. It is administered intravenously (ie, at a dose of 840 mg every 2 weeks).
다른 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 28일 주기의 제 1일에 약 840 mg의 용량으로(즉, 4주마다 약 840 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 28일 주기의 제 1일에 약 1680 mg의 용량으로(즉, 4주마다 약 1680 mg의 용량으로) 정맥내 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 각 28일 주기의 제 1일에 840 mg의 용량으로(즉, 4주마다 840 mg의 용량으로) 정맥내 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 각 28일 주기의 제 1일에 1680 mg의 용량으로(즉, 4주마다 1680 mg의 용량으로) 정맥내 투여된다.In other cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of about 840 mg on Day 1 of each 28-day cycle (ie, every 4 weeks). at a dose of about 840 mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at about 1680 mg on Day 1 of each 28-day cycle. It is administered intravenously as a dose (ie, at a dose of about 1680 mg every 4 weeks). In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered at a dose of 840 mg on Day 1 of each 28-day cycle (ie, 840 every 4 weeks). mg), and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a dose of 1680 mg on Day 1 of each 28-day cycle ( i.e., at a dose of 1680 mg every 4 weeks) intravenously.
iii.iii. 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 정맥내 주입 및 피하 투여Intravenous infusion and subcutaneous administration of anti-TIGIT antagonist antibody and PD-1 axis binding antagonist
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 정맥내 투여된다. 대안적으로, 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 피하 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 정맥내 투여된다. 대안적으로, 일부 구현예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 피하 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered intravenously. Alternatively, in some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered subcutaneously. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered intravenously. Alternatively, in some embodiments, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered subcutaneously.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)는 약 60 ± 10 분(예컨대, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 또는 약 70분)에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)는 약 60 ± 15분(예컨대, 약 45분, 약 46분, 약 47분, 약 48분, 약 49분, 약 50분, 약 51분, 약 52분, 약 53분, 약 54분, 약 55분, 약 56분, 약 57분, 약 58분, 약 59분, 약 60분, 약 61분, 약 62분, 약 63분, 약 64분, 약 65분, 약 66분, 약 67분, 약 68분, 약 69분, 약 70분, 약 71분, 약 72분, 약 73분, 약 74분, 또는 약 75분)에 걸쳐 정맥내 주입으로 상기 대상체에게 투여된다. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is administered in about 60 ± 15 minutes (eg, about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes). minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, About 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered in about 60 ± 10 minutes (eg, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes , about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) by intravenous infusion to the subject or population of subjects. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) is administered in about 60±15 minutes (eg, about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes , about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes) by intravenous infusion to the subject.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)는 약 30 ± 10분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체에게 투여된다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 약 30 ± 10분(예컨대, 약 20분, 약 21분, 약 22분, 약 23분, 약 24분, 약 25분, 약 26분, 약 27분, 약 28분, 약 29분, 약 30분, 약 31분, 약 32분, 약 33분, 약 34분, 약 35분, 약 36분, 약 37분, 약 38분, 약 39분, 또는 약 40분)에 걸쳐 정맥내 주입으로 상기 대상체에게 투여된다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered in about 30±10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, About 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion. In some cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered in about 30 ± 10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, About 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) by intravenous infusion.
iv.iv. 투여 순서 및 관찰 기간Dosing sequence and observation period
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제 둘 모두가 대상체 또는 대상체의 집단에 투여되는 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)) 전에 상기 대상체에게 투여된다. In some cases where both an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist are administered to a subject or population of subjects, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) ) is administered to the subject prior to the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)).
일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체 투여 이후 및 상기 PD-1 축 결합 길항제 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. 일부 경우들에서, 예를 들어, 상기 항 TIGIT 길항제 항체의 투여 이후에, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))가 상기 대상체에게 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)가 먼저 대상체에게 투여되고, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 투여 이후에 상기 대상체에게 투여된다. In some cases, for example, after administration of the anti-TIGIT antagonist antibody and prior to administration of the PD-1 axis binding antagonist, the method comprises an intermediate first observation period. In some cases, eg, following administration of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to the subject. In some cases, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is first administered to the subject, and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist) The antibody (eg, atezolizumab)) is administered to the subject following administration of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab).
일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 2차 관찰 기간을 추가로 포함한다.In some cases, the method further comprises a second observation period following administration of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체 투여 후 1차 관찰 기간 및 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 2차 관찰 기간을 모두 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분의 길이인 경우들에서, 상기 방법은 상기 제1 또는 제2 관찰 기간 중 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 약 30 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분의 길이인 경우들에서, 상기 방법은 상기 제1 또는 제2 관찰 기간 중 상기 항 TIGIT 길항제 항체 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 약 15 ± 10분에 상기 대상체의 활력 징후(예컨대, 맥박수, 호흡수, 혈압 및 온도)를 기록하는 단계를 포함할 수 있다. In some cases, the method comprises a first observation period after administration of the anti-TIGIT antagonist antibody and a second observation after administration of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) includes all periods. In some cases, the first and second observation periods are each between about 30 minutes and about 60 minutes in length. In instances where the first and second observation periods are each about 60 minutes in length, the method comprises the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist (eg, anti-PD) during the first or second observation period. - recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) about 30 ± 10 minutes after administration of the -L1 antagonist antibody (eg, atezolizumab). In instances where the first and second observation periods are each about 30 minutes in length, the method comprises the anti-TIGIT antagonist antibody or the PD-1 axis binding antagonist (eg, anti-PD) during the first or second observation period. - recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure and temperature) about 15±10 minutes after administration of the -L1 antagonist antibody (eg, atezolizumab).
일반 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 이전에 상기 대상체 또는 대상체 집단에게 투여된다. 일부 경우들에서, 예를 들어, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 투여 전에, 상기 방법은 중간 제1 관찰 기간을 포함한다. In general cases, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is the anti-TIGIT antagonist antibody ( eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is administered to said subject or population of subjects prior to. In some cases, e.g., after administration of said PD-1 axis binding antagonist (eg, anti PD-L1 antagonist antibody (eg, atezolizumab)) and said anti TIGIT antagonist antibody (eg, as disclosed herein) Prior to administration of an anti-TIGIT antagonist antibody (eg, tyragolumab), the method includes an interim first observation period.
일부 경우들에서, 상기 방법은 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제2 관찰 기간을 추가로 포함한다. In some cases, the method further comprises a second observation period following administration of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab).
일부 경우들에서, 상기 방법은 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 투여 후에 제1 관찰 기간, 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 제2 관찰 기간을 모두 추가로 포함한다. 일부 경우들에서, 상기 제1 및 제2 관찰 기간은 각각 약 30분 내지 약 60분의 길이이다. 상기 제1 및 제2 관찰 기간이 각각 약 60분인 경우들에서, 상기 방법은 상기 제1 또는 제2 관찰 기간 동안 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)) 또는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 약 30 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다. 상기 제1 및 제2 관찰 기간이 각각 약 30분인 경우들에서, 상기 방법은 상기 제1 또는 제2 관찰 기간 동안 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)), 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 투여 후에 약 15 ± 10분에서 상기 대상체의 활력 징후(예컨대, 맥박, 호흡수, 혈압, 체온)를 기록하는 단계를 포함할 수 있다.In some cases, the method comprises a first observation period following administration of the PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)), and the anti TIGIT antagonist antibody (eg, herein a second observation period all after administration of an anti-TIGIT antagonist antibody, such as tyragolumab, as disclosed in In some cases, the first and second observation periods are each between about 30 minutes and about 60 minutes in length. In instances where the first and second observation periods are each about 60 minutes, the method comprises, during the first or second observation period, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, artezoli). Zumab)) or the subject's vital signs (e.g., pulse, respiratory rate, blood pressure) at about 30±10 minutes after administration of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragolumab as disclosed herein). , body temperature). In cases where the first and second observation periods are each about 30 minutes, the method comprises, during the first or second observation period, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezoli zumab)), the subject's vital signs (eg, pulse, respiratory rate, blood pressure , body temperature).
일부 경우들에서, 상기 방법은 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여를 추가로 포함한다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙)) 및 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 이후에 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙) 또는 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))의 투여 후 상기 제2 관찰 기간 후에 투여된다.In some cases, the method further comprises administration of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)). In some cases, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD- 1 antagonist antibody (eg, pembrolizumab)) and the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some cases, the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) is the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) or the PD- Administration of the uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is followed by the second observation period.
일부 경우들에서, 상기 방법은 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 투여 후 제3 관찰 기간을 추가로 포함한다. 일부 경우들에서, 상기 제3 관찰 기간은 약 30분 내지 약 120분의 길이이다. 일부 경우들에서, 상기 제1 관찰 기간, 상기 제2 관찰 기간, 및 상기 제3 관찰 기간은 각각 약 30분 내지 약 120분의 길이이다.In some cases, the method further comprises a third observation period following administration of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)). In some cases, the third observation period is between about 30 minutes and about 120 minutes in length. In some cases, the first observation period, the second observation period, and the third observation period are each between about 30 minutes and about 120 minutes in length.
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 병용 투약Co-administration of anti-TIGIT antagonist antibody and PD-1 axis binding antagonist
일부 경우들에서, 유효량의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 용량은 In some cases, the dose of an effective amount of an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab) is
예컨대, 암을 가진 대상체의 치료를 위한 병용 요법(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)과 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 병용 치료)으로 유효량의 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량과 함께 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 2주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 2주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 2주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 3주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 2주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 4주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 2주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 6주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 3주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 2주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 3주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 3주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 3주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 4주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 3주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 6주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 4주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 2주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 4주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 3주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 4주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 4주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 4주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 6주마다 투여된다. 일부 경우들에서, 항 TIGIT 길항제 항체는 본원의 섹션 III(K)(i)에 기재된 바와 같이 2주, 3주, 또는 4주마다 투여되고, PD-1 축 결합 길항제는 본원의 섹션 III(K)(ii)에 기재된 바와 같이 2주, 3주, 4주, 또는 6주마다 투여된다. Combination therapy (eg, a PD-1 axis binding antagonist (eg, an anti PD-L1 antagonist antibody (eg, atezolizumab)) and an anti TIGIT antagonist antibody (eg, as disclosed herein) for the treatment of a subject having cancer combination therapy with an anti-TIGIT antagonist antibody, such as tyragolumab), with a dose of an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, such as atezolizumab). In these cases, the anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered 2 weeks as described in Section III(K)(ii) herein. In some cases, the anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein ( ii) is administered every 3 weeks as described in. In some cases, the anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered herein is administered every 4 weeks as described in Section III(K)(ii) of the In some cases, the anti-TIGIT antagonist antibody is administered every 2 weeks, as described in Section III(K)(i) herein, and The -1 axis binding antagonist is administered every 6 weeks as described in Section III(K)(ii) herein In some cases, the anti-TIGIT antagonist antibody is administered as described in Section III(K)(i) herein Administer every 3 weeks, and the PD-1 axis binding antagonist is administered every 2 weeks as described in Section III(K)(ii) herein In some cases, the anti-TIGIT antagonist antibody is administered in Section III(K) herein Administer every 3 weeks as described in (i), and the PD-1 axis binding antagonist is administered every 3 weeks as described in Section III(K)(ii) herein In some cases, the anti-TIGIT antagonist antibody is As described in Section III(K)(i) herein This is administered every 3 weeks, and the PD-1 axis binding antagonist is administered every 4 weeks as described in Section III(K)(ii) herein. In some cases, the anti-TIGIT antagonist antibody is administered every 3 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. administered together every 6 weeks. In some cases, the anti TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. administered together every 2 weeks. In some cases, the anti TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. administered every 3 weeks. In some cases, the anti TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. administered together every 4 weeks. In some cases, the anti TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. administered together every 6 weeks. In some cases, the anti-TIGIT antagonist antibody is administered every 2 weeks, 3 weeks, or 4 weeks as described in Section III(K)(i) herein, and the PD-1 axis binding antagonist is administered in Section III (K)(K) herein. ) every 2 weeks, 3 weeks, 4 weeks, or 6 weeks as described in (ii).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 3주마다 약 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 3주마다 600 mg의 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)는 단계적 투약 요법(예컨대, 대상체의 체중(BW) 또는 체표면적(BSA)에 기초한 투약) 및, 예컨대 3주마다 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 15 mg/kg) 내지 최대 1200 mg의 용량으로 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)로, 예컨대 3주마다 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)는 단계적 투약 요법(예컨대, 대상체의 체중(BW) 또는 체표면적(BSA)에 기초한 투약) 및, 예컨대 3주마다 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 15 mg/kg) 내지 최대 1200 mg의 용량으로 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대 아테졸리주맙)로 투여된다. 상기 투약 요법은 비교적 낮은 체중(예컨대, 40kg 이하(예컨대, 5 kg 내지 40 kg, 15 kg 내지 40 kg, 또는 5 kg 내지 15 kg))을 갖는 대상체에 대한 치료에 활용될 수 있고, 성인 데이터에서 추정된 약동학적 매개변수의 외삽을 기반으로 한 생체 시뮬레이션 연구를 통해 개발되었다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 용량은 대상체의 체중(예컨대, 체중(BW) > 40 kg: 600 mg, BW > 15 kg 및 ≤ 40 kg: 400 mg, 및 BW ≤ 15 kg: 300 mg))을 기준으로 한 단계적 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 대상체의 체중(예컨대, 15 mg/kg)을 기준으로 한 용량이다. 일부 경우들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량은 대상체의 체표면적(예컨대, 체표면적(BSA) > 1.25 m2: 600 mg, BSA > 0.75 m2 및 ≤ 1.25 m2: 450 mg, BSA > 0.5 m2 및 ≤ 0.75 m2: 350 mg, 및 BSA ≤ 0.5 m2: 300 mg)을 기준으로 한 단계적 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 용량(예컨대, 약 600 mg)은 3주마다 대상체의 체중(예컨대, 15 mg/kg)을 기준으로 한 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량과 병용으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량(예컨대, 체중(BW) > 40 kg: 600 mg, BW > 15 kg 및 ≤ 40 kg: 400 mg, 및 BW ≤ 15 kg: 300 mg)은 3주마다 대상체의 체중(예컨대, 15 mg/kg)을 기준으로 한 상기 항 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량과 병용으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량(예컨대, 체중(BW) > 40 kg: 600 mg, BW > 15 kg 및 ≤ 40 kg: 400 mg, 및 BW ≤ 15 kg: 300 mg)은 3주마다 대상체의 체표면적(예컨대, BSA > 1.25 m2 600 mg, BSA > 0.75 m2 및 ≤ 1.25 m2: 450 mg, BSA > 0.5 m2 및 ≤ 0.75 m2: 350 mg, 및 BSA ≤ 0.5 m2: 300 mg)을 기준으로 한 상기 항 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))의 용량과 병용으로 투여된다. 일부 구현예들에서, 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))는 3주마다 1200 mg의 최대 용량으로 투여된다. 일부 경우들에서, 상기 병용 요법은 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 비백금계 화학요법제(예컨대, 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)와 함께 투여된다.In some cases, the dose of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of about 600 mg every 3 weeks. In some cases, the dose of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose of 600 mg every 3 weeks. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered on a step-by-step dosing regimen (eg, based on the subject's body weight (BW) or body surface area (BSA)). dosing) and a PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody) at a dose of from about 0.01 mg/kg to about 50 mg/kg (eg, about 15 mg/kg) to up to 1200 mg, eg, every 3 weeks , such as atezolizumab), such as every 3 weeks. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered on a step-by-step dosing regimen (eg, based on the subject's body weight (BW) or body surface area (BSA)). dosing) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, such as atezolizumab). The dosing regimen can be utilized to treat subjects with relatively low body weight (eg, 40 kg or less (eg, 5 kg to 40 kg, 15 kg to 40 kg, or 5 kg to 15 kg)), and in adult data It was developed through in vivo simulation studies based on extrapolation of estimated pharmacokinetic parameters. In some cases, the dose of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a subject's body weight (eg, body weight (BW) > 40 kg: 600 mg, BW > 15 kg and ≤ 40 kg: 400 mg, and BW ≤ 15 kg: 300 mg))). In some cases, the dose of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose based on the subject's body weight (eg, 15 mg/kg). In some cases, the dose of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a body surface area (eg, body surface area (BSA) > 1.25 m 2 :600 of the subject) mg, BSA > 0.75 m 2 and ≤ 1.25 m 2 : 450 mg, BSA > 0.5 m 2 and ≤ 0.75 m 2 : 350 mg, and BSA ≤ 0.5 m 2 : 300 mg). In some cases, the dose (eg, about 600 mg) of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is administered at a dose (eg, about 600 mg) of the subject's body weight (eg, 15 mg/kg) every 3 weeks. ) in combination with a dose of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some cases, step-wise doses (eg, body weight (BW) > 40 kg: 600 mg, BW > 15 kg) of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and ≤ 40 kg: 400 mg, and BW ≤ 15 kg: 300 mg) of the anti-PD-1 axis binding antagonist (eg, anti-PD-) based on the subject's body weight (eg, 15 mg/kg) every 3 weeks. It is administered in combination with a dose of an L1 antagonist antibody (eg, atezolizumab). In some cases, step-wise doses (eg, body weight (BW) > 40 kg: 600 mg, BW > 15 kg) of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and ≤ 40 kg: 400 mg, and BW ≤ 15 kg: 300 mg) is the subject's body surface area (eg, BSA > 1.25 m 2 600 mg, BSA > 0.75 m 2 and ≤ 1.25 m 2 : 450 mg, The anti-PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, artezoli) based on BSA > 0.5 m 2 and ≤ 0.75 m 2 :350 mg, and BSA ≤ 0.5 m 2 :300 mg). It is administered in combination with a dose of Zumab)). In some embodiments, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a maximum dose of 1200 mg every 3 weeks. In some cases, the combination therapy comprises one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or a non-platinum-based chemotherapeutic agent (eg, an antimetabolites (eg, pemetrec)). Syd or gemcitabine).
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 250 mg 내지 약 350 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 350 mg 내지 약 450 mg(예컨대, 3주마다 약 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 550 mg 내지 약 650 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 대상체 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량은 대상체의 체중을 기준으로 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량과 병용으로 투여되고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg의 용량으로 투여되거나(예컨대, 3주마다 약 400 mg); 또는 (c) 40kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여된다(예컨대, 3주마다 약 600 mg). 일부 경우들에서, 체중이 15 kg 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 10 mg 내지 약 1000 mg의 용량(예컨대, 3주마다 약 300 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체중이 15 kg 초과 40 kg 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 10 mg 내지 약 1000 mg의 용량(예컨대, 3주마다 약 400 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체중이 40 kg 초과인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 30 mg 내지 약 1200 mg의 용량(예컨대, 3주마다 약 600 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) for treating a subject having cancer is a tiered dose based on the subject's body weight, wherein said the subject's body weight is (a) 15 kg or less, and the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 250 mg to about 350 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 350 mg to about 450 mg every 3 weeks (eg, about 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of about 550 mg to about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks. In some cases, about 0.01 mg/kg to about 50 mg/kg of the subject's body weight (eg, about 0.01 mg/kg of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, For example, about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg) Administered in combination with step-dose doses of said anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody, eg, tiragolumab as disclosed herein) as a reference, wherein said subject weighs (a) no more than 15 kg; the anti TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 15 kg and no more than 40 kg, wherein the anti TIGIT antagonist antibody is administered every 3 weeks administered at a dose of about 10 mg to about 1000 mg (eg, about 400 mg every 3 weeks); or (c) greater than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. (e.g., about 600 mg every 3 weeks) In some cases, the subject weighing 15 kg or less is administered with the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tyragolumab). a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks) and every 3 weeks for the PD - about 0.01 mg/kg to about 50 mg/kg of the subject's body weight (eg, about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, a subject weighing more than 15 kg and no more than 40 kg has from about 10 mg to about 1000 every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). about 0.01 of the subject's body weight for a dose of mg (eg, about 400 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) mg/kg to about 50 mg/kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg , eg, about 15 mg/kg). In some cases, the subject weighing more than 40 kg receives from about 30 mg to about 1200 mg every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). About 0.01 mg/m of the subject's body weight for a dose (eg, about 600 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) kg to about 50 mg/kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, For example, from about 2.5 mg/kg to about 30 mg/kg, such as from about 5 mg/kg to about 25 mg/kg, such as from about 10 mg/kg to about 20 mg/kg, such as from about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as , about 15 mg/kg).
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 250 mg 내지 350 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 350 mg 내지 450 mg(예컨대, 3주마다 400 mg)의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 550 mg 내지 650 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체중에 기초한 단계적 용량이고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg의 용량으로 투여되거나; 또는 (c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 600 mg의 용량으로 투여된다. 일부 경우들에서, 상기 대상체 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량은 대상체의 체중을 기준으로 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량과 병용으로 투여되고, 여기서 상기 대상체의 체중은 (a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 15 kg 초과 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg의 용량으로 투여되거나(예컨대, 3주마다 400 mg); 또는 (c) 40kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg의 용량으로 투여된다(예컨대, 3주마다 600 mg). 일부 경우들에서, 체중이 15 kg 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 10 mg 내지 1000 mg의 용량(예컨대, 3주마다 300 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체중이 15 kg 초과 40 kg 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 10 mg 내지 1000 mg의 용량(예컨대, 3주마다 400 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체중이 40 kg 초과인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 30 mg 내지 1200 mg의 용량(예컨대, 3주마다 600 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tyragolumab as disclosed herein) for treating a subject having cancer is a tiered dose based on the subject's body weight, wherein said the subject's body weight is (a) 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 15 kg and no more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 250 mg to 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 15 kg and not more than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of 350 mg to 450 mg every 3 weeks (eg, 400 mg every 3 weeks); or (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is administered at a dose of 550 mg to 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on a subject's body weight, wherein the subject's body weight is (a) 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; (b) greater than 15 kg and not more than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (c) greater than 40 kg, wherein said anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks. In some cases, 0.01 mg/kg to 50 mg/kg of the subject's body weight (eg, 0.01 mg/kg to 45 mg/kg of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 A dose of ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, e.g., 15 mg/kg) of said anti TIGIT antagonist antibody (e.g., an anti TIGIT antagonist antibody as disclosed herein, e.g., tyragolumab), wherein the subject's body weight is (a) 15 kg or less, and wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 300 mg every 3 weeks). (b) greater than 15 kg and up to 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg 400 mg every 3 weeks); or (c) 40 kg and the anti-TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (e.g., 600 mg every 3 weeks) In some cases, the subject weighing 15 kg or less is administered with the anti-TIGIT antagonist antibody ( For example, a dose of 10 mg to 1000 mg every 3 weeks (eg 300 mg every 3 weeks) and every 3 weeks for an anti TIGIT antagonist antibody, such as tiragolumab, as disclosed herein and the PD-1 axis binding antagonist every 3 weeks 0.01 of the subject's body weight for (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) mg/kg to 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, a subject weighing more than 15 kg and no more than 40 kg is administered 10 mg to 1000 mg every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). 0.01 mg/kg to the subject's body weight for a dose (eg, 400 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg /kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, the subject weighing more than 40 kg is administered at a dose of 30 mg to 1200 mg every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab) ( 0.01 mg/kg to 50 mg of the subject's body weight for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 3 weeks) and every 3 weeks /kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg , such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg /kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg).
일부 경우들에서, 암을 가진 대상체를 치료하기 위한 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 3주마다 약 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 250 mg 내지 약 350 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 400 mg(예컨대, 3주마다 약 350 mg)의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg 내지 약 500 mg(예컨대, 3주마다 약 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 550 mg 내지 약 650 mg(예컨대, 3주마다 약 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 450 mg의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여된다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tyragolumab) for treating a subject having cancer is a dose in steps based on the subject's body surface area. In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 250 mg to about 350 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg to about 400 mg every 3 weeks (eg, about 350 mg every 3 weeks); or (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg to about 500 mg every 3 weeks (eg, about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti TIGIT antagonist antibody is administered at a dose of about 550 mg to about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) greater than 0.5 m 2 and less than or equal to 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 0.75 m2 and less than or equal to 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 450 mg every 3 weeks; or (d) greater than 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
일부 경우들에서, 상기 대상체 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량은 대상체의 체표면적을 기준으로 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량과 병용으로 투여되고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10mg 내지 약 1000 mg(예컨대, 3주마다 약 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg(예컨대, 약 3주마다 약 350 mg)의 용량으로 투여되고; (c) 0.75 m2 초과 1.25 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 10 mg 내지 약 1000 mg의 용량으로 투여되거나(예컨대, 3주마다 약 450 mg); 또는 (d) 1.25 m2 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여된다(예컨대, 3주마다 약 600 mg). 일부 경우들에서, 체표면적이 0.5 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 10 mg 내지 약 1000 mg의 용량(예컨대, 3주마다 약 300 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 0.5 m2 초과 0.75 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 10 mg 내지 약 1000 mg의 용량(예컨대, 3주마다 약 350 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 0.75 m2 초과 1.25 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 10 mg 내지 약 1000 mg의 용량(예컨대, 3주마다 약 450 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 1.25 m2 초과인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 약 30 mg 내지 약 1200 mg의 용량(예컨대, 3주마다 약 600 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량을 투여받는다.In some cases, about 0.01 mg/kg to about 50 mg/kg of the subject's body weight (eg, about 0.01 mg/kg of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, For example, about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg) of the body surface area of the subject is administered in combination with a step-by-step dose of said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody, such as tiragolumab as disclosed herein) on the basis of, wherein the subject's body surface area is (a) 0.5 m 2 or less wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 and not more than 0.75 m 2 , wherein the anti-TIGIT antagonist the antibody is administered at a dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 350 mg every 3 weeks); (c) greater than 0.75 m 2 and no more than 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg per week (eg, about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is from about 30 mg to about 1200 mg every 3 weeks. (e.g., about 600 mg every 3 weeks) In some cases, a subject having a body surface area of 0.5 m 2 or less A dose of about 10 mg to about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks) and every 3 weeks for a TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) about 0.01 mg/kg to about 50 mg/kg (eg, about 0.01 mg/kg) of the subject's body weight for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as , about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg , about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, a subject having a body surface area greater than 0.5 m 2 and less than or equal to 0.75 m 2 receives about 10 mg every 3 weeks for said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). body weight of the subject for a dose of from about 1000 mg (eg, about 350 mg every 3 weeks) and every 3 weeks to the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) from about 0.01 mg/kg to about 50 mg/kg (e.g., from about 0.01 mg/kg to about 45 mg/kg, such as from about 0.1 mg/kg to about 40 mg/kg, such as from about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, a subject having a body surface area greater than 0.75 m 2 and less than or equal to 1.25 m 2 receives about 10 mg every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). body weight of the subject for a dose of from to about 1000 mg (eg, about 450 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) from about 0.01 mg/kg to about 50 mg/kg (e.g., from about 0.01 mg/kg to about 45 mg/kg, such as from about 0.1 mg/kg to about 40 mg/kg, such as from about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the subject having a body surface area greater than 1.25 m 2 has a dose of from about 30 mg to about 1200 every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). about 0.01 of the subject's body weight for a dose of mg (eg, about 600 mg every 3 weeks) and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) every 3 weeks mg/kg to about 50 mg/kg (e.g., about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg, such as about 12.5 mg/kg kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg , eg, about 15 mg/kg).
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 250 mg 내지 350 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg 내지 400 mg(예컨대, 3주마다 350 mg)의 용량으로 투여되고; (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg 내지 500 mg(예컨대, 3주마다 450 mg)의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 550 mg 내지 650 mg(예컨대, 3주마다 600 mg)의 용량으로 투여된다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대 티라골루맙)의 유효량은 대상체의 체표면적에 기초한 단계적 용량이고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 300 mg의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 400 mg의 용량으로 투여되거나; 또는 (c) 0.75㎡ 초과 1.25㎡ 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 450 mg의 용량으로 투여되거나; 또는 (d) 1.25㎡ 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 600 mg의 용량으로 투여된다.In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein the anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of 250 mg to 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m 2 and no greater than 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 300 mg to 400 mg every 3 weeks (eg, 350 mg every 3 weeks); (c) greater than 0.75 m2 and no greater than 1.25 m2, wherein the anti-TIGIT antagonist antibody is administered at a dose of 400 mg to 500 mg every 3 weeks (eg, 450 mg every 3 weeks); or (d) greater than 1.25 m 2 , wherein said anti TIGIT antagonist antibody is administered at a dose of 550 mg to 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some cases, the effective amount of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) is a dose in steps based on the subject's body surface area, wherein the subject's body surface area is (a ) 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; (b) greater than 0.5 m 2 and less than or equal to 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (c) greater than 0.75 m2 and less than or equal to 1.25 m2, wherein said anti-TIGIT antagonist antibody is administered at a dose of 450 mg every 3 weeks; or (d) greater than 1.25 m 2 , wherein said anti TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
일부 경우들에서, 상기 대상체 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)의 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량은 대상체의 체표면적을 기준으로 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)의 단계적 용량과 병용으로 투여되고, 여기서 상기 대상체의 체표면적은 (a) 0.5 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10mg 내지 1000 mg(예컨대, 3주마다 300 mg)의 용량으로 투여되고; (b) 0.5 m2 초과 0.75 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg(예컨대, 3주마다 350 mg)의 용량으로 투여되고; (c) 0.75 m2 초과 1.25 m2 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 10 mg 내지 1000 mg의 용량으로 투여되거나(예컨대, 3주마다 450 mg); 또는 (d) 1.25 m2 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 30 mg 내지 1200 mg의 용량으로 투여된다(예컨대, 3주마다 600 mg). 일부 경우들에서, 체표면적이 0.5 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 10 mg 내지 1000 mg의 용량(예컨대, 3주마다 300 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 0.5 m2 초과 0.75 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 10 mg 내지 1000 mg의 용량(예컨대, 3주마다 350 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 0.75 m2 초과 1.25 m2 이하인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 10 mg 내지 1000 mg의 용량(예컨대, 3주마다 450 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다. 일부 경우들에서, 체표면적이 1.25 m2 초과인 대상체는 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙)에 대하여 3주마다 30 mg 내지 1000 mg의 용량(예컨대, 3주마다 600 mg) 및 3주마다 상기 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙))에 대하여 상기 대상체의 체중의 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량을 투여받는다.In some cases, 0.01 mg/kg to 50 mg/kg of the subject's body weight (eg, 0.01 mg/kg to 45 mg/kg of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 A dose of ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, e.g., 15 mg/kg) of the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, such as , tiragolumab), wherein the subject's body surface area is (a) 0.5 m 2 or less, and wherein the anti-TIGIT antagonist antibody is 10 mg to 1000 mg every 3 weeks (eg, 300 every 3 weeks). mg), (b) greater than 0.5 m 2 and up to 0.75 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 350 mg every 3 weeks); (c) greater than 0.75 m 2 and less than or equal to 1.25 m 2 , wherein the anti-TIGIT antagonist antibody is administered at a dose of 10 mg to 1000 mg every 3 weeks (eg, 450 mg every 3 weeks); or (d) greater than 1.25 m 2 and the anti TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg every 3 weeks (eg, 600 mg every 3 weeks) In some cases, the subject with a body surface area of 0.5 m 2 or less is the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, such as tiragolumab) every 3 weeks body weight of the subject at a dose of 10 mg to 1000 mg (eg, 300 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) 0.01 mg/kg to 50 mg/kg of (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, a subject having a body surface area greater than 0.5 m 2 and less than or equal to 0.75 m 2 is administered from 10 mg to every 3 weeks for said anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). 0.01 mg of the subject's body weight for a dose of 1000 mg (eg, 350 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) /kg to 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg , 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, a subject having a body surface area greater than 0.75 m 2 and less than or equal to 1.25 m 2 is administered from 10 mg every 3 weeks to 0.01 mg of the subject's body weight for a dose of 1000 mg (eg, 450 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) /kg to 50 mg/kg (eg 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg , 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some cases, a subject with a body surface area greater than 1.25 m 2 is administered 30 mg to 1000 mg every 3 weeks for said anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody as disclosed herein, eg, tyragolumab). 0.01 mg/kg to the subject's body weight for a dose (eg, 600 mg every 3 weeks) and every 3 weeks for the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) 50 mg/kg (eg, 0.01 mg/kg to 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg /kg, such as 5 mg/kg to 25 mg/kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg).
화학요법제의 투약administration of chemotherapeutic agents
다양한 화학요법제의 치료학적 유효량은 당업계에 공지되어 있고 본 발명에서 고려된다. 특정 경우들에서, 하나 이상의 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및/또는 하나 이상의 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대, 냅-파클리탁셀) 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신))는 본원에 언급된 용량에 따라 투여된다.Therapeutically effective amounts of various chemotherapeutic agents are known in the art and are contemplated herein. In certain instances, one or more chemotherapeutic agents (eg, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (eg, an alkylating agent (eg, cyclophosphamide)); The taxane (eg, paclitaxel, eg, nap-paclitaxel) and/or topoisomerase II inhibitor (eg, doxorubicin)) is administered according to the doses recited herein.
백금계 화학요법제Platinum-based chemotherapeutic agents
일부 경우들에서, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 1~50 mg/ml/분(예컨대, 2~25 mg/ml/분, 3~15 mg/ml/분, 4~10 mg/ml/분, 또는 5 mg/ml/분, 예컨대 2 mg/ml/분, 3 mg/ml/분, 4 mg/ml/분, 5 mg/ml/분, 6 mg/ml/분, 7 mg/ml/분, 8 mg/ml/분, 9 mg/ml/분, 10 mg/ml/분, 11 mg/ml/분, 12 mg/ml/분, 13 mg/ml/분, 14 mg/ml/분, 15 mg/ml/분, 20 mg/ml/분, 25 mg/ml/분, 30 mg/ml/분, 35 mg/ml/분, 40 mg/ml/분, 45 mg/ml/분, 50 mg/ml/분)의 AUC를 달성하기에 충분한 용량이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 AUC = 5 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 AUC = 6 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 AUC = 5 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 AUC = 6 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 21일 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 21일 투약 주기의 제 1일에 AUC = 6 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 페메트렉시드 또는 젬시타빈 이후에 투여 시 AUC = 5 mg/ml/분을 달성하기에 충분한 용량이다. 일부 경우들에서, 카보플라틴의 유효량은 파클리탁셀 이후에 투여 시 AUC = 6 mg/ml/분을 달성하기에 충분한 용량이다. In some cases, an effective amount of a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 1-50 mg/ml/min (eg, 2-25 mg/ml/min, 3-15 mg/ml/min) , 4-10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml/min, 6 mg/min ml/min, 7 mg/ml/min, 8 mg/ml/min, 9 mg/ml/min, 10 mg/ml/min, 11 mg/ml/min, 12 mg/ml/min, 13 mg/ml /min, 14 mg/ml/min, 15 mg/ml/min, 20 mg/ml/min, 25 mg/ml/min, 30 mg/ml/min, 35 mg/ml/min, 40 mg/ml/ min, 45 mg/ml/min, 50 mg/ml/min). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is a dose sufficient to achieve AUC=5 mg/ml/min. In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is a dose sufficient to achieve AUC=6 mg/ml/min. In some cases, an effective amount of carboplatin is a dose sufficient to achieve AUC=5 mg/ml/min. In some cases, an effective amount of carboplatin is a dose sufficient to achieve AUC=6 mg/ml/min. In some cases, the effective amount of carboplatin is a dose sufficient to achieve AUC=5 mg/ml/min on Day 1 of a 21-day dosing cycle. In some cases, the effective amount of carboplatin is a dose sufficient to achieve AUC=6 mg/ml/min on Day 1 of a 21-day dosing cycle. In some cases, the effective amount of carboplatin is a dose sufficient to achieve AUC=5 mg/ml/min when administered after pemetrexed or gemcitabine. In some cases, the effective amount of carboplatin is a dose sufficient to achieve AUC=6 mg/ml/min when administered after paclitaxel.
AUC는 칼버트(Calvert) 공식을 사용하여 계산할 수 있다(Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):AUC can be calculated using the Calvert formula (Calvert et al., J. Clin. Oncol . 1989, 7:1748-56):
총 용량(mg) (목표 AUC) (사구체 여과율[GFR] 25)Total dose (mg) (target AUC) (glomerular filtration rate [GFR] 25)
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 200 mg~1500 mg(예컨대, 300 mg~1200 mg, 400 mg~1100 mg, 또는 500 mg~1000 mg, 예컨대 300 mg~400 mg, 400 mg~500 mg, 500 mg~600 mg, 600 mg~700 mg, 700 mg~750 mg, 750 mg~800 mg, 800 mg~900 mg, 900 mg~1000 mg, 1000 mg~1100 mg, 또는 1100 mg~1200 mg, 예컨대 약 200 mg, 약 300 mg, 약 400 mg, 약 500 mg, 약 600 mg, 약 700 mg, 약 800 mg, 약 900 mg, 약 1000 mg, 약 1100 mg, 약 1200 mg, 약 1300 mg, 약 1400 mg, 또는 약 1500 mg)이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 약 500 mg~1000 mg(예컨대, 약 500 mg, 약 600 mg, 약 700 mg, 약 800 mg, 약 900 mg, 또는 약 1000 mg)이다.In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, For example 300 mg-400 mg, 400 mg-500 mg, 500 mg-600 mg, 600 mg-700 mg, 700 mg-750 mg, 750 mg-800 mg, 800 mg-900 mg, 900 mg-1000 mg, 1000 mg-1100 mg, or 1100 mg-1200 mg, such as about 200 mg, about 300 mg, about 400 mg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, about 1000 mg, about 1100 mg, about 1200 mg, about 1300 mg, about 1400 mg, or about 1500 mg). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is between about 500 mg and 1000 mg (eg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg). mg, or about 1000 mg).
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 약 20 mg/m2 내지 약 200 mg/m2(예컨대, 약 20 mg/m2 내지 약 150 mg/m2, 예컨대, 약 30 mg/m2 내지 약 125 mg/m2, 예컨대, 약 40 mg/m2 내지 약 110 mg/m2, 예컨대, 약 50 mg/m2 내지 약 100 mg/m2, 예컨대, 약 60 mg/m2 내지 약 90 mg/m2, 예컨대, 약 70 mg/m2 내지 약 80 mg/m2, 예컨대, 약 75 mg/m2, 예컨대, 75 mg/m2)이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 약 75 mg/m2이다. 일부 경우들에서, 시스플라틴의 유효량은 약 75 mg/m2이다. 일부 경우들에서, 시스플라틴의 유효량은 3주마다 약 75 mg/m2이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 20 mg/m2 내지 200 mg/m2(예컨대, 20 mg/m2 내지 150 mg/m2, 예컨대, 30 mg/m2 내지 125 mg/m2, 예컨대, 40 mg/m2 내지 110 mg/m2, 예컨대, 50 mg/m2 내지 100 mg/m2, 예컨대, 60 mg/m2 내지 90 mg/m2, 예컨대, 70 mg/m2 내지 80 mg/m2, 예컨대, 75 mg/m2, 예컨대, 75 mg/m2)이다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)의 유효량은 75 mg/m2이다. 일부 경우들에서, 시스플라틴의 유효량은 75 mg/m2이다. 일부 경우들에서, 시스플라틴의 유효량은 3주마다 75 mg/m2이다.In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is from about 20 mg/m 2 to about 200 mg/m 2 (eg, from about 20 mg/m 2 to about 150 mg/m 2 ) m 2 , such as from about 30 mg/m 2 to about 125 mg/m 2 , such as from about 40 mg/m 2 to about 110 mg/m 2 , such as from about 50 mg/m 2 to about 100 mg/m 2 . , such as about 60 mg/m 2 to about 90 mg/m 2 , such as about 70 mg/m 2 to about 80 mg/m 2 , such as about 75 mg/m 2 , such as 75 mg/m 2 ) to be. In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is about 75 mg/m 2 . In some cases, the effective amount of cisplatin is about 75 mg/m 2 . In some cases, the effective amount of cisplatin is about 75 mg/m 2 every 3 weeks. In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 20 mg/m 2 to 200 mg/m 2 (eg, 20 mg/m 2 to 150 mg/m 2 , such as , 30 mg/m 2 to 125 mg/m 2 , such as 40 mg/m 2 to 110 mg/m 2 , such as 50 mg/m 2 to 100 mg/m 2 , such as 60 mg/m 2 to 90 mg/m 2 , such as 70 mg/m 2 to 80 mg/m 2 , such as 75 mg/m 2 , such as 75 mg/m 2 ). In some cases, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 75 mg/m 2 . In some cases, the effective amount of cisplatin is 75 mg/m 2 . In some cases, the effective amount of cisplatin is 75 mg/m 2 every 3 weeks.
일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 상기 대상체 또는 대상체의 집단에게 정맥내(예컨대, 30~120분 주입에 걸쳐) 투여된다. 일부 경우들에서, 카보플라틴을 30~60분 주입에 걸쳐 정맥내 투여된다. 일부 경우들에서, 시스플라틴을 60~120분 주입에 걸쳐 정맥내 투여된다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 상기 대상체 또는 대상체의 집단에게 3주마다 투여된다. 일부 경우들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 21일 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 상기 대상체 또는 대상체의 집단에게 투여된다. In some cases, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered to the subject or population of subjects intravenously (eg, over a 30-120 minute infusion). In some cases, carboplatin is administered intravenously over a 30-60 minute infusion. In some cases, cisplatin is administered intravenously over a 60-120 minute infusion. In some cases, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered to the subject or population of subjects every three weeks. In some cases, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered on about 1 day (eg, -3 days, -2 days, -1 days, 1 day, 2 days, or day 3) to said subject or population of subjects.
탁산taxane
인간에게 투여되는 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀(ABRAXANE®))의 치료적 유효량은 1회 또는 그 이상의 투여에 의해 약 25 내지 약 300 mg/m2(예컨대, 약 25 mg/m2, 약 50 mg/m2, 약 75 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 125 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 175 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 225 mg/m2, 약 250 mg/m2, 약 275 mg/m2, 또는 약 300 mg/m2 (예컨대, 25 mg/m2, 50 mg/m2, 75 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 125 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 175 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 225 mg/m2, 250 mg/m2, 275 mg/m2, 또는 300 mg/m2))의 범위일 것이다. 예를 들어, 일부 구현예들에서, 약 175 mg/m2의 파클리탁셀이 투여된다. 일부 구현예들에서, 약 175 mg/m2의 파클리탁셀이 투여된다. 일부 구현예들에서, 파클리탁셀은 3주마다 약 175 mg/m2 내지 약 200 mg/m2 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주 마다 약 175 mg/m2의 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주 마다 약 200 mg/m2의 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주마다 175 mg/m2 내지 200 mg/m2 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주 마다 175 mg/m2의 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주 마다 200 mg/m2의 용량으로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주마다 175 mg/m2 IV로 투여된다. 일부 구현예들에서, 파클리탁셀은 아시안 인종/민족의 대상체에게 3주마다 175 mg/m2 IV로 투여된다. 일부 구현예들에서, 파클리탁셀은 3주마다 200 mg/m2 IV로 투여된다. 일부 구현예들에서, 파클리탁셀은 비아시안 인종/민족의 대상체에게 3주마다 200 mg/m2 IV로 투여된다. 일부 구현예들에서, 약 100 mg/m2 의 냅-파클리탁셀(ABRAXANE®)이 투여된다. 일부 구현예들에서, 100 mg/m2 의 냅-파클리탁셀(ABRAXANE®)이 투여된다. 일부 구현예들에서, 냅-파클리탁셀(ABRAXANE®)은 매주 100 mg/m2 IV로 투여된다. 일부 구현예들에서, 냅-파클리탁셀(ABRAXANE®)은 4주마다 3회(예컨대, 각 28일 투약 주기의 제 1일, 8일, 및 15일에) 100 mg/m2 IV로 투여된다. 일부 구현예들에서, 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀(ABRAXANE®))은 매주, 2주마다, 3주마다, 4주마다, 각 21일 주기의 제 1일, 8일 및 15일에, 또는 각 28일 주기의 제 1일, 8일 및 15일에 투여될 수 있다.A therapeutically effective amount of a taxane (eg, paclitaxel or nap-paclitaxel (ABRAXANE®)) administered to a human is from about 25 to about 300 mg/m 2 (eg, about 25 mg/m 2 , in one or more administrations). about 50 mg/m 2 , about 75 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 125 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 175 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 225 mg/m 2 , about 250 mg/m 2 , about 275 mg/m 2 , or about 300 mg/m 2 (eg, 25 mg/m 2 , 50 mg/m 2 , 75 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg/m 2 , 125 mg /m 2 , 130 mg/m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 175 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 225 mg/m 2 , 250 mg/m 2 , 275 mg/m 2 , or 300 mg/m 2 )). For example, in some embodiments, about 175 mg/m 2 of paclitaxel is administered. In some embodiments, about 175 mg/m 2 of paclitaxel is administered. In some embodiments, paclitaxel is administered at a dose of about 175 mg/m 2 to about 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of about 175 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of about 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of 175 mg/m 2 to 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of 175 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at 175 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered to a subject of Asian race/ethnicity at 175 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered at 200 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered to a subject of non-Asian race/ethnicity at 200 mg/m 2 IV every 3 weeks. In some embodiments, about 100 mg/m 2 of nap-paclitaxel (ABRAXANE®) is administered. In some embodiments, 100 mg/m 2 of nap-paclitaxel (ABRAXANE®) is administered. In some embodiments, nap-paclitaxel (ABRAXANE®) is administered at 100 mg/m 2 IV weekly. In some embodiments, nap-paclitaxel (ABRAXANE®) is administered at 100 mg/m 2 IV three times every 4 weeks (eg, on days 1, 8, and 15 of each 28-day dosing cycle). In some embodiments, the taxane (eg, paclitaxel or nap-paclitaxel (ABRAXANE®)) is administered weekly, every 2 weeks, every 3 weeks, every 4 weeks, days 1, 8 and 15 of each 21 day cycle. , or on days 1, 8 and 15 of each 28-day cycle.
일부 구현예들에서, 상기 탁산(예컨대, 파클리탁셀 또는 냅-파클리탁셀(ABRAXANE®))은 상기 대상체 또는 대상체의 집단에게 정맥내로(예컨대, 3시간 주입에 걸쳐) 투여된다. 일부 구현예들에서, 상기 탁산은 3주마다 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 구현예들에서, 상기 탁산은 21일 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 구현예들에서, 파클리탁셀은 3주마다 상기 대상체에게 투여된다. 일부 구현예들에서, 파클리탁셀은 21일 투약 주기의 약 1일에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 구현예들에서, 냅-파클리탁셀(ABRAXANE®)은 3주마다 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 구현예들에서, 냅-파클리탁셀(ABRAXANE®)은 1일 투약 주기의 약 1일에 상기 대상체 또는 대상체의 집단에게 투여된다.In some embodiments, the taxane (eg, paclitaxel or nap-paclitaxel (ABRAXANE®)) is administered to the subject or population of subjects intravenously (eg, over a 3-hour infusion). In some embodiments, the taxane is administered to the subject or population of subjects every three weeks. In some embodiments, the taxane is administered to the subject or population of subjects on about day 1 (eg, day -3, day -2, day -1, day 1, day 2, or day 3) of a 21 day dosing cycle. is administered In some embodiments, paclitaxel is administered to the subject every 3 weeks. In some embodiments, paclitaxel is administered to the subject or population of subjects on about day 1 of a 21 day dosing cycle. In some embodiments, nap-paclitaxel (ABRAXANE®) is administered to the subject or population of subjects every 3 weeks. In some embodiments, nap-paclitaxel (ABRAXANE®) is administered to the subject or population of subjects on about day 1 of a daily dosing cycle.
항대사물질antimetabolites
일부 경우들에서, 본원에 기재된 방법의 일부로서 투여되는 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 10~0000 mg/m2(예컨대, 20~8000 mg/m2, 30~5000 mg/m2, 40~2500 mg/m2, 50~2000 mg/m2, 100~1500 mg/m2, 또는 400~1200 mg/m2, 예컨대, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 약 1000 mg/m2, 약 1100 mg/m2, 약 1200 mg/m2, 약 1250 mg/m2, 약 1300 mg/m2, 약 1400 mg/m2, 약 1500 mg/m2, 약 1750 mg/m2, 약 2000 mg/m2, 약 3000 mg/m2, 약 4000 mg/m2, 약 5000 mg/m2, 약 6000 mg/m2, 약 7000 mg/m2, 약 8000 mg/m2, 약 9000 mg/m2, 또는 약 10000 mg/m2)이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 약 500 mg/m2 내지 약 1250 mg/m2(예컨대, 20 mg/m2, 30 mg/m2, 40 mg/m2, 50 mg/m2, 60 mg/m2, 70 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 250 mg/m2, 300 mg/m2, 400 mg/m2, 500 mg/m2, 600 mg/m2, 700 mg/m2, 800 mg/m2, 900 mg/m2, 1000 mg/m2, 1100 mg/m2, 1200 mg/m2, 1250 mg/m2, 1300 mg/m2, 1400 mg/m2, 1500 mg/m2, 1750 mg/m2, 2000 mg/m2, 3000 mg/m2, 4000 mg/m2, 5000 mg/m2, 6000 mg/m2, 7000 mg/m2, 8000 mg/m2, 9000 mg/m2, 또는 10000 mg/m2)이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 약 500 mg/m2이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 약 1000 mg/m2이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 약 1250 mg/m2이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 500 mg/m2이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 1000 mg/m2이다. 일부 경우들에서, 상기 항대사물질(예컨대, 페메트렉시드 또는 젬시타빈)의 유효량은 1250 mg/m2이다.In some cases, the effective amount of an antimetabolite (eg, pemetrexed or gemcitabine) administered as part of a method described herein is 10-0000 mg/m 2 (eg, 20-8000 mg/m 2 , 30- 5000 mg/m 2 , 40-2500 mg/m 2 , 50-2000 mg/m 2 , 100-1500 mg/m 2 , or 400-1200 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg /m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/ m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , about 1000 mg/m 2 , about 1100 mg/m 2 , about 1200 mg/m 2 , about 1250 mg/m 2 , about 1300 mg/m 2 , about 1400 mg/m 2 , about 1500 mg/m 2 , about 1750 mg/m 2 , about 2000 mg/m 2 , about 3000 mg/m 2 , about 4000 mg/m 2 , about 5000 mg/m 2 , about 6000 mg/m 2 , about 7000 mg/m 2 , about 8000 mg/m 2 , about 9000 mg/m 2 , or about 10000 mg/m 2 ) to be. In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is from about 500 mg/m 2 to about 1250 mg/m 2 (eg, 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg /m 2 , 130 mg/m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , 1000 mg/m 2 , 1100 mg/m 2 , 1200 mg/m 2 , 1250 mg/m 2 , 1300 mg/m 2 , 1400 mg/m 2 , 1500 mg/m 2 , 1750 mg/m 2 , 2000 mg /m 2 , 3000 mg/m 2 , 4000 mg/m 2 , 5000 mg/m 2 , 6000 mg/m 2 , 7000 mg/m 2 , 8000 mg/m 2 , 9000 mg/m 2 , or 10000 mg/ m 2 ). In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 500 mg/m 2 . In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 1000 mg/m 2 . In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 1250 mg/m 2 . In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 500 mg/m 2 . In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 1000 mg/m 2 . In some cases, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 1250 mg/m 2 .
일부 경우들에서, 본원에 기재된 방법의 일부로서 투여되는 페메트렉시드의 유효량은 10~1000 mg/m2(예컨대, 20~900 mg/m2, 30~800 mg/m2, 40~700 mg/m2, 50~650 mg/m2, 100~600 mg/m2, 또는 200~550 mg/m2, 예컨대, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 또는 약 1000 mg/m2)이다. 일부 경우들에서, 페메트렉시드의 유효량은 약 500 mg/m2이다. 일부 경우들에서, 페메트렉시드의 유효량은 3주마다 약 500 mg/m2이다. 일부 경우들에서, 페메트렉시드의 유효량은 500 mg/m2이다. 일부 경우들에서, 페메트렉시드의 유효량은 3주마다 500 mg/m2이다.In some cases, an effective amount of pemetrexed administered as part of a method described herein is 10-1000 mg/m 2 (eg, 20-900 mg/m 2 , 30-800 mg/m 2 , 40-700 mg /m 2 , 50-650 mg/m 2 , 100-600 mg/m 2 , or 200-550 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 ). In some cases, the effective amount of pemetrexed is about 500 mg/m 2 . In some cases, the effective amount of pemetrexed is about 500 mg/m 2 every 3 weeks. In some cases, the effective amount of pemetrexed is 500 mg/m 2 . In some cases, the effective amount of pemetrexed is 500 mg/m 2 every 3 weeks.
일부 구현예들에서, 상기 페메트렉시드는 상기 대상체 또는 대상체의 집단에게 정맥내로(예컨대, 10분의 주입에 걸쳐) 투여된다. 일부 구현예들에서, 상기 페메트렉시드는 3주마다 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 구현예들에서, 상기 페메트렉시드는 21일 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 상기 대상체 또는 대상체의 집단에게 투여된다. In some embodiments, the pemetrexed is administered to the subject or population of subjects intravenously (eg, over a 10-minute infusion). In some embodiments, the pemetrexed is administered to the subject or population of subjects every 3 weeks. In some embodiments, the pemetrexed is administered to the subject or population of subjects on about 1 day (eg, -3 days, -2 days, -1 days, 1 day, 2 days, or 3 days) of a 21 day dosing cycle. is administered to
일부 경우들에서, 본원에 기재된 방법의 일부로서 투여되는 젬시타빈의 유효량은 10~10000 mg/m2(예컨대, 20~8000 mg/m2, 30~5000 mg/m2, 40~2500 mg/m2, 50~2000 mg/m2, 100~1500 mg/m2, 또는 400~1250 mg/m2, 예컨댜, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 약 1000 mg/m2, 약 1100 mg/m2, 약 1200 mg/m2, 약 1250 mg/m2, 약 1300 mg/m2, 약 1400 mg/m2, 약 1500 mg/m2, 약 1750 mg/m2, 약 2000 mg/m2, 약 3000 mg/m2, 약 4000 mg/m2, 약 5000 mg/m2, 약 6000 mg/m2, 약 7000 mg/m2, 약 8000 mg/m2, 약 9000 mg/m2, 또는 약 10000 mg/m2(예컨대, 20 mg/m2, 30 mg/m2, 40 mg/m2, 50 mg/m2, 60 mg/m2, 70 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 250 mg/m2, 300 mg/m2, 400 mg/m2, 500 mg/m2, 600 mg/m2, 700 mg/m2, 800 mg/m2, 900 mg/m2, 1000 mg/m2, 1100 mg/m2, 1200 mg/m2, 1250 mg/m2, 1300 mg/m2, 1400 mg/m2, 1500 mg/m2, 1750 mg/m2, 2000 mg/m2, 3000 mg/m2, 4000 mg/m2, 5000 mg/m2, 6000 mg/m2, 7000 mg/m2, 8000 mg/m2, 9000 mg/m2, 또는 10000 mg/m2))이다. 일부 경우들에서, 젬시타빈의 유효량은 약 500 mg/m2이 내지 약 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 약 500 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 약 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 카보플라틴 이전에 투여 시 약 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 약 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 시스플라틴 이전에 투여 시 약 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 21일 투약 주기의 제 1일 및 8일에 약 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 21일 투약 주기의 제 1일 및 8일에 약 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 카보플라틴 이전에 투여 시 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 시스플라틴 이전에 투여 시 1250 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 21일 투약 주기의 제 1일 및 8일에 1000 mg/m2이다. 일부 경우들에서, 젬시타빈의 유효량은 21일 투약 주기의 제 1일 및 8일에 1250 mg/m2이다.In some cases, the effective amount of gemcitabine administered as part of the methods described herein is 10-10000 mg/m 2 (eg, 20-8000 mg/m 2 , 30-5000 mg/m 2 , 40-2500 mg/m 2 ) m 2 , 50-2000 mg/m 2 , 100-1500 mg/m 2 , or 400-1250 mg/m 2 , for example, about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , about 1000 mg/m 2 , about 1100 mg/m 2 , about 1200 mg/m 2 , about 1250 mg/m 2 , about 1300 mg/m 2 , about 1400 mg/m 2 , about 1500 mg/m 2 , about 1750 mg/m 2 , about 2000 mg/m 2 , about 3000 mg/m 2 , about 4000 mg/m 2 , about 5000 mg /m 2 , about 6000 mg/m 2 , about 7000 mg/m 2 , about 8000 mg/m 2 , about 9000 mg/m 2 , or about 10000 mg/m 2 (eg, 20 mg/m 2 , 30 mg /m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg/m 2 , 130 mg/m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , 1000 mg/m 2 , 1100 mg/ m 2 , 1200 mg/m 2 , 1250 mg/m 2 , 1300 mg/m 2 , 1400 mg/m 2 , 1500 mg/m 2 , 1750 mg/m 2 , 2000 mg/m 2 , 3000 mg/m 2 , 4000 mg/m 2 , 5000 mg/m 2 , 6000 mg/m 2 , 7000 mg/m 2 , 8000 mg/m 2 , 9000 mg/m 2 , or 10000 mg/m 2 )). In some cases, the effective amount of gemcitabine is from about 500 mg/m 2 to about 1250 mg/m 2 . In some cases, the effective amount of gemcitabine is about 500 mg/m 2 . In some cases, the effective amount of gemcitabine is about 1000 mg/m 2 . In some cases, the effective amount of gemcitabine when administered prior to carboplatin is about 1000 mg/m 2 . In some cases, the effective amount of gemcitabine is about 1250 mg/m 2 . In some cases, the effective amount of gemcitabine is about 1250 mg/m 2 when administered prior to cisplatin. In some cases, the effective amount of gemcitabine is about 1000 mg/m 2 on days 1 and 8 of a 21 day dosing cycle. In some cases, the effective amount of gemcitabine is about 1250 mg/m 2 on days 1 and 8 of a 21 day dosing cycle. In some cases, the effective amount of gemcitabine is 1000 mg/m 2 . In some cases, the effective amount of gemcitabine is 1000 mg/m 2 when administered prior to carboplatin. In some cases, the effective amount of gemcitabine is 1250 mg/m 2 . In some cases, the effective amount of gemcitabine is 1250 mg/m 2 when administered prior to cisplatin. In some cases, the effective amount of gemcitabine is 1000 mg/m 2 on days 1 and 8 of a 21 day dosing cycle. In some cases, the effective amount of gemcitabine is 1250 mg/m 2 on days 1 and 8 of a 21 day dosing cycle.
일부 구현예들에서, 상기 젬시타빈은 상기 대상체 또는 대상체의 집단에게 정맥내로(예컨대, 30분의 주입에 걸쳐) 투여된다. 일부 경우들에서, 상기 젬시타빈은 21일 투약 주기의 약 1일(예컨대, -3일, -2일, -1일, 1일, 2일, 또는 3일)에 상기 대상체 또는 대상체의 집단에게 투여된다. 일부 경우들에서, 상기 젬시타빈은 21일 투약 주기의 약 1일 및 약 8일(예컨대, 5일, 6일, 7일, 8일, 9일, 10일, 또는 11일)에 상기 대상체 또는 대상체의 집단에게 투여된다.In some embodiments, the gemcitabine is administered to the subject or population of subjects intravenously (eg, over a 30 minute infusion). In some cases, the gemcitabine is administered to the subject or population of subjects on about day 1 (eg, day -3, day -2, day -1, day 1, day 2, or day 3) of a 21 day dosing cycle. is administered In some cases, the gemcitabine is administered to the subject or on about days 1 and about 8 (eg, 5, 6, 7, 8, 9, 10, or 11 days) of a 21 day dosing cycle. administered to a population of subjects.
토포이소머라제 II 억제제Topoisomerase II inhibitors
일부 경우들에서, 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 10~1000 mg/m2(예컨대, 20~800 mg/m2, 30~700 mg/m2, 40~500 mg/m2, 50~300 mg/m2, 75~200 mg/m2, 또는 80~150 mg/m2, 예컨대, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 또는 약 1000 mg/m2(예컨대, 20 mg/m2, 30 mg/m2, 40 mg/m2, 50 mg/m2, 60 mg/m2, 70 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 250 mg/m2, 300 mg/m2, 400 mg/m2, 500 mg/m2, 600 mg/m2, 700 mg/m2, 800 mg/m2, 900 mg/m2, 또는 1000 mg/m2))이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 약 100 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 3주마다 1일 내지 3일에 약 100 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)의 유효량은 3주마다 1일 내지 3일에 100 mg/m2이다.In some cases, an effective amount of a topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 (eg, 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg/m 2 , 130 mg/ m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , or 1000 mg/m 2 ) )to be. In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 . In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 on days 1 to 3 every 3 weeks. In some cases, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is 100 mg/m 2 on days 1 to 3 every 3 weeks.
일부 구현예들에서, 상기 토포이소머라제 II 억제제(예컨대, 에토포시드)는 상기 대상체에게 정맥내로(예컨대, 60분의 주입에 걸쳐) 투여된다.In some embodiments, the topoisomerase II inhibitor (eg, etoposide) is administered to the subject intravenously (eg, over a 60 minute infusion).
일부 경우들에서, 토포이소머라제 II 억제제(예컨대, 독소루비신)의 유효량은 10~1000 mg/m2(예컨대, 20~800 mg/m2, 30~700 mg/m2, 40~500 mg/m2, 50~300 mg/m2, 75~200 mg/m2, 또는 80~150 mg/m2, 예컨대, 약 20 mg/m2, 약 30 mg/m2, 약 40 mg/m2, 약 50 mg/m2, 약 60 mg/m2, 약 70 mg/m2, 약 80 mg/m2, 약 90 mg/m2, 약 100 mg/m2, 약 110 mg/m2, 약 120 mg/m2, 약 130 mg/m2, 약 140 mg/m2, 약 150 mg/m2, 약 160 mg/m2, 약 170 mg/m2, 약 180 mg/m2, 약 190 mg/m2, 약 200 mg/m2, 약 250 mg/m2, 약 300 mg/m2, 약 400 mg/m2, 약 500 mg/m2, 약 600 mg/m2, 약 700 mg/m2, 약 800 mg/m2, 약 900 mg/m2, 또는 약 1000 mg/m2(예컨대, 20 mg/m2, 30 mg/m2, 40 mg/m2, 50 mg/m2, 60 mg/m2, 70 mg/m2, 80 mg/m2, 90 mg/m2, 100 mg/m2, 110 mg/m2, 120 mg/m2, 130 mg/m2, 140 mg/m2, 150 mg/m2, 160 mg/m2, 170 mg/m2, 180 mg/m2, 190 mg/m2, 200 mg/m2, 250 mg/m2, 300 mg/m2, 400 mg/m2, 500 mg/m2, 600 mg/m2, 700 mg/m2, 800 mg/m2, 900 mg/m2, 또는 1000 mg/m2))이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)의 유효량은 약 60 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)의 유효량은 60 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)의 유효량은 약 100 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)의 유효량은 100 mg/m2이다. 일부 경우들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)의 용량은 독성을 피하기 위해 감소되거나 지연된다.In some cases, an effective amount of a topoisomerase II inhibitor (eg, doxorubicin) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 ) m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 . , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 (eg, 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 ) m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 , 120 mg/m 2 , 130 mg/m 2 , 140 mg/m 2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , or 1000 mg/m 2 )) . In some cases, the effective amount of the topoisomerase II inhibitor (eg, doxorubicin) is about 60 mg/m 2 . In some cases, the effective amount of the topoisomerase II inhibitor (eg, doxorubicin) is 60 mg/m 2 . In some cases, the effective amount of the topoisomerase II inhibitor (eg, doxorubicin) is about 100 mg/m 2 . In some cases, the effective amount of the topoisomerase II inhibitor (eg, doxorubicin) is 100 mg/m 2 . In some cases, the dose of the topoisomerase II inhibitor (eg, doxorubicin) is reduced or delayed to avoid toxicity.
일부 구현예들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)는 매주, 2주마다, 3주마다, 4주마다, 각 21일 주기의 제 1일, 8일 및 15일에, 또는 각 28일 주기의 제 1일, 8일 및 15일에 투여될 수 있다. 일부 구현예들에서, 상기 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴)는 2주마다 투여될 수 있다.In some embodiments, the topoisomerase II inhibitor (eg, doxorubicin) is administered weekly, every 2 weeks, every 3 weeks, every 4 weeks, on days 1, 8 and 15 of each 21 day cycle, or It may be administered on days 1, 8 and 15 of each 28-day cycle. In some embodiments, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) may be administered every two weeks.
일부 구현예들에서, 알킬화제(예컨대, 시클로포스파미드)는 상기 대상체에게 3~5분에 걸쳐 IV 볼루스로 투여된다. 일부 구현예들에서, 상기 알킬화제(예컨대, 시클로포스파미드)는 상기 대상체에게 15~30분에 걸쳐 IV 주입으로 투여된다. 일부 구현예들에서, 상기 토포이소머라제 II 억제제(예컨대, 독소루비신)는 상기 대상체에게 정맥내로(예컨대, 60분의 주입에 걸쳐) 투여된다.In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject as an IV bolus over 3-5 minutes. In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject by IV infusion over 15-30 minutes. In some embodiments, the topoisomerase II inhibitor (eg, doxorubicin) is administered to the subject intravenously (eg, over a 60 minute infusion).
알킬화제alkylating agent
인간에게 투여되는 알킬화제(예컨대, 시클로포스파미드)의 치료적 유효량은 1회 또는 그 이상의 투여에 의해 약 400 to 약 800 mg/m2(예컨대, 약 400 mg/m2, 약 425 mg/m2, 약 450 mg/m2, 약 475 mg/m2, 약 500 mg/m2, 약 525 mg/m2, 약 550 mg/m2, 약 575 mg/m2, 약 600 mg/m2, 약 625 mg/m2, 약 650 mg/m2, 약 675 mg/m2, 약 700 mg/m2, 약 725 mg/m2, 약 750 mg/m2, 약 775 mg/m2, 또는 약 800 mg/m2(예컨대, 400 mg/m2, 425 mg/m2, 450 mg/m2, 475 mg/m2, 500 mg/m2, 525 mg/m2, 550 mg/m2, 575 mg/m2, 600 mg/m2, 625 mg/m2, 650 mg/m2, 675 mg/m2, 700 mg/m2, 725 mg/m2, 750 mg/m2, 775 mg/m2, 또는 800 mg/m2)의 범위일 것이다. 예를 들어, 일부 구현예들에서, 약 600 mg/m2의 알킬화제(예컨대, 시클로포스파미드)가 투여된다. 일부 구현예들에서, 약 600 mg/m2의 알킬화제(예컨대, 시클로포스파미드)는 2주마다 투여된다. 일부 구현예들에서, 약 600 mg/m2의 시클로포스파미드이 투여된다. 일부 구현예들에서, 약 600 mg/m2의 시클로포스파미드가 2주마다 투여된다. 일부 구현예들에서, 600 mg/m2의 알킬화제(예컨대, 시클로포스파미드)는 2주마다 투여된다. 일부 구현예들에서, 상기 알킬화제(예컨대, 시클로포스파미드)는 매주, 2주마다, 3주마다, 4주마다, 각 21일 주기의 제 1일, 8일 및 15일에, 각 28일 주기의 제 1일 및 22일에, 또는 각 28일 주기의 제 1일, 8일 및 15일에 투여될 수 있다. A therapeutically effective amount of an alkylating agent (eg, cyclophosphamide) administered to a human can be from about 400 to about 800 mg/m 2 (eg, about 400 mg/m 2 , about 425 mg/m 2 , in one or more administrations). 2 , about 450 mg/m 2 , about 475 mg/m 2 , about 500 mg/m 2 , about 525 mg/m 2 , about 550 mg/m 2 , about 575 mg/m 2 , about 600 mg/m 2 , about 625 mg/m 2 , about 650 mg/m 2 , about 675 mg/m 2 , about 700 mg/m 2 , about 725 mg/m 2 , about 750 mg/m 2 , about 775 mg/m 2 , or about 800 mg/m 2 (eg, 400 mg/m 2 , 425 mg/m 2 , 450 mg/m 2 , 475 mg/m 2 , 500 mg/m 2 , 525 mg/m 2 , 550 mg/m 2 , 575 mg/m 2 , 600 mg/m 2 , 625 mg/m 2 , 650 mg/m 2 , 675 mg/m 2 , 700 mg/m 2 , 725 mg/m 2 , 750 mg/m 2 , 775 mg/m 2 , or 800 mg/m 2 ) For example, in some embodiments, about 600 mg/m 2 of an alkylating agent (eg, cyclophosphamide) is administered. In embodiments, about 600 mg/m 2 of alkylating agent (eg, cyclophosphamide) is administered every two weeks.In some embodiments, about 600 mg/m 2 of cyclophosphamide is administered. In some cases, about 600 mg/m 2 of cyclophosphamide is administered every two weeks, in some embodiments, 600 mg/m 2 of an alkylating agent (eg, cyclophosphamide) is administered every two weeks. In embodiments, the alkylating agent (eg, cyclophosphamide) is administered weekly, every 2 weeks, every 3 weeks, every 4 weeks, on days 1, 8 and 15 of each 21 day cycle, each 28 day cycle on days 1 and 22, or on days 1, 8 and 15 of each 28-day cycle.
일부 구현예들에서, 알킬화제(예컨대, 시클로포스파미드)는 상기 대상체에게 3~5분에 걸쳐 IV 볼루스로 투여된다. 일부 구현예들에서, 상기 알킬화제(예컨대, 시클로포스파미드)는 상기 대상체에게 IV 주입으로 투여된다.In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject as an IV bolus over 3-5 minutes. In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject by IV infusion.
집락 자극 인자의 투약Dosing of colony stimulating factors
인간에게 투여되는 집락 자극 인자(CSF(예컨대, G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예컨대, 사그라모스팀))의 치료적 유효량은 약 1 내지 약 100 mg(예컨대, 약 1 mg, 약 2 mg, 약 3 mg, 약 4 mg, 약 5 mg, 약 6 mg, 약 7 mg, 약 8 mg, 약 9 mg, 약 10 mg, 약 15 mg, 약 20 mg, 약 25 mg, 약 30 mg, 약 45 mg, 약 50 mg, 약 60 mg, 약 70 mg, 약 80 mg, 약 90 mg, 또는 약 100 mg)의 범위일 것이다. 예를 들어, 일부 구현예들에서, 약 6 mg이 투여된다. 인간에게 투여되는 집락 자극 인자(CSF)(예컨대, G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예컨대, 사그라모스팀))의 치료적 유효량은 약 1 내지 약 100 mg(예컨대, 1 mg, 2 mg, 3 mg, 4 mg, 5 mg, 6 mg, 7 mg, 8 mg, 9 mg, 10 mg, 15 mg, 20 mg, 25 mg, 30 mg, 45 mg, 50 mg, 60 mg, 70 mg, 80 mg, 90 mg, 또는 100 mg)의 범위일 것이다. 일부 구현예들에서, 6 mg의 페그필그라스팀이 투여된다. 일부 구현예들에서, 상기 집락 자극 인자는 페그필그라스팀이다. 일부 구현예들에서, 상기 집락 자극 인자는 필그라스팀이다. 일부 구현예들에서, 약 6 mg의 페그필그라스팀이 투여된다. A therapeutically effective amount of a colony stimulating factor (CSF (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sagramostim)) administered to a human is from about 1 to about 100 mg. (e.g., about 1 mg, about 2 mg, about 3 mg, about 4 mg, about 5 mg, about 6 mg, about 7 mg, about 8 mg, about 9 mg, about 10 mg, about 15 mg, about 20 mg , about 25 mg, about 30 mg, about 45 mg, about 50 mg, about 60 mg, about 70 mg, about 80 mg, about 90 mg, or about 100 mg).For example, in some embodiments In the field, about 6 mg is administered Colony stimulating factor (CSF) administered to humans (eg G-CSF (eg pegfilgrastim or filgrastim) and GM-CSF (eg sagramostim)) A therapeutically effective amount of about 1 to about 100 mg (eg, 1 mg, 2 mg, 3 mg, 4 mg, 5 mg, 6 mg, 7 mg, 8 mg, 9 mg, 10 mg, 15 mg, 20 mg, 25 mg, 30 mg, 45 mg, 50 mg, 60 mg, 70 mg, 80 mg, 90 mg, or 100 mg) In some embodiments, 6 mg of pegfilgrastim is administered. In some embodiments, the colony stimulating factor is pegfilgrastim.In some embodiments, the colony stimulating factor is filgrastim.In some embodiments, about 6 mg of pegfilgrastim is administered. .
인간에게 투여되는 집락 자극 인자(예컨대, G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예컨대, 사그라모스팀))의 치료적 유효량은 약 1 내지 약 400 mcg/kg/일(예컨대, 약 1 mcg/kg/일, 약 2 mcg/kg/일, 약 3 mcg/kg/일, 약 4 mcg/kg/일, 약 5 mcg/kg/일, 약 6 mcg/kg/일, 약 7 mcg/kg/일, 약 8 mcg/kg/일, 약 9 mcg/kg/일, 약 10 mcg/kg/day, 약 15 mcg/kg/일, 약 20 mcg/kg/일, 약 25 mcg/kg/일, 약 50 mcg/kg/일, 약 75 mcg/kg/일, 약 100 mcg/kg/일, 약 125 mcg/kg/일, 약 150 mcg/kg/일, 약 175 mcg/kg/일, 약 200 mcg/kg/일, 약 225 mcg/kg/일, 약 250 mcg/kg/일, 약 275 mcg/kg/일, 약 300 mcg/kg/일, 약 325 mcg/kg/일, 약 350 mcg/kg/일, 약 375 mcg/kg/일, 또는 약 400 mcg/kg/일)의 범위일 것이다. 예를 들어, 일부 구현예들에서, 약 250 mcg/m2/일이 투여된다. 일부 구현예들에서, 인간에게 투여되는 집락 자극 인자(예컨대, G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예컨대, 사그라모스팀))의 치료적 유효량은 1 내지 400 mcg/kg/일(예컨대, 1 mcg/kg/일, 2 mcg/kg/일, 3 mcg/kg/일, 4 mcg/kg/일, 5 mcg/kg/일, 6 mcg/kg/일, 7 mcg/kg/일, 8 mcg/kg/일, 9 mcg/kg/일, 10 mcg/kg/day, 15 mcg/kg/일, 20 mcg/kg/일, 25 mcg/kg/일, 50 mcg/kg/일, 75 mcg/kg/일, 100 mcg/kg/일, 125 mcg/kg/일, 150 mcg/kg/일, 175 mcg/kg/일, 200 mcg/kg/일, 225 mcg/kg/일, 250 mcg/kg/일, 275 mcg/kg/일, 300 mcg/kg/일, 325 mcg/kg/일, 약 350 mcg/kg/일, 375 mcg/kg/일, 또는 400 mcg/kg/일)의 범위일 것이다. 예를 들어, 일부 구현예들에서, 약 250 mcg/m2/일이 투여된다. 일부 구현예들에서, 상기 집락 자극 인자(예컨대, G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예컨대, 사그라모스팀))는 피하 주사로 투여된다. 일부 구현예들에서, 상기 집락 자극 인자는 사그라모스팀이다. 일부 구현예들에서, 사그라모스팀은 약 250 mcg/m2/일의 용량으로 상기 인간에게 투여된다. 일부 구현예들에서, 사그라모스팀은 250 mcg/m2/일의 용량으로 상기 인간에게 투여된다. A therapeutically effective amount of a colony stimulating factor (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sagrammostim)) administered to a human is from about 1 to about 400 mcg/kg per day (eg, about 1 mcg/kg/day, about 2 mcg/kg/day, about 3 mcg/kg/day, about 4 mcg/kg/day, about 5 mcg/kg/day, about 6 mcg/kg /day, about 7 mcg/kg/day, about 8 mcg/kg/day, about 9 mcg/kg/day, about 10 mcg/kg/day, about 15 mcg/kg/day, about 20 mcg/kg/day , about 25 mcg/kg/day, about 50 mcg/kg/day, about 75 mcg/kg/day, about 100 mcg/kg/day, about 125 mcg/kg/day, about 150 mcg/kg/day, about 175 mcg/kg/day, about 200 mcg/kg/day, about 225 mcg/kg/day, about 250 mcg/kg/day, about 275 mcg/kg/day, about 300 mcg/kg/day, about 325 mcg /kg/day, about 350 mcg/kg/day, about 375 mcg/kg/day, or about 400 mcg/kg/day). For example, in some embodiments, about 250 mcg/m 2 /day is administered. In some embodiments, a therapeutically effective amount of a colony stimulating factor (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sagramostim)) administered to a human is 1 to 400 mcg/kg/day (eg, 1 mcg/kg/day, 2 mcg/kg/day, 3 mcg/kg/day, 4 mcg/kg/day, 5 mcg/kg/day, 6 mcg/kg/day , 7 mcg/kg/day, 8 mcg/kg/day, 9 mcg/kg/day, 10 mcg/kg/day, 15 mcg/kg/day, 20 mcg/kg/day, 25 mcg/kg/day, 50 mcg/kg/day, 75 mcg/kg/day, 100 mcg/kg/day, 125 mcg/kg/day, 150 mcg/kg/day, 175 mcg/kg/day, 200 mcg/kg/day, 225 mcg/kg/day, 250 mcg/kg/day, 275 mcg/kg/day, 300 mcg/kg/day, 325 mcg/kg/day, about 350 mcg/kg/day, 375 mcg/kg/day, or 400 mcg/kg/day). For example, in some embodiments, about 250 mcg/m 2 /day is administered. In some embodiments, the colony stimulating factor (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sagramostim)) is administered by subcutaneous injection. In some embodiments, the colony stimulating factor is sagramostim. In some embodiments, sagramostim is administered to the human at a dose of about 250 mcg/m2/day. In some embodiments, sagramostim is administered to the human at a dose of 250 mcg/m2/day.
VEGF 길항제의 투약Dosing of VEGF antagonists
일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다(예컨대, 각 21일 투약 주기의 제 1일(예컨대, 1일 ± 3일)) 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 10 mg/kg 내지 약 20 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 2 mg/kg, 약 15 ± 1 mg/kg, 약 15 ± 0.5 mg/kg, 약 15 ± 0.2 mg/kg, 또는 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 10 mg/kg 내지 약 15 mg/kg, 예컨대, 약 12.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 14 mg/kg 내지 약 15 mg/kg, 예컨대, 약 15 ± 1 mg/kg, 예컨대, 약 15 ± 0.5 mg/kg, 예컨대, 약 15 ± 0.2 mg/kg, 예컨대, 약 15 ± 0.1 mg/kg, 예컨대, 약 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다 투여되는 약 15 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다(예컨대, 각 14일 투약 주기의 제 1일(예컨대, 1일 ± 3일) 또는 각 28일 투약 주기의 제 1일(예컨대, 1일 ± 3일) 및 15일(예컨대, 15일 ± 3일)) 상기 대상체의 체중 당 약 0.01 mg/kg 내지 약 50 mg/kg(예컨대, 약 0.01 mg/kg 내지 약 45 mg/kg, 예컨대, 약 0.1 mg/kg 내지 약 40 mg/kg, 예컨대, 약 1 mg/kg 내지 약 35 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 30 mg/kg, 예컨대, 약 5 mg/kg 내지 약 25 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 20 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 12.5 mg/kg, 예컨대, 약 10 ± 2 mg/kg, 약 10 ± 1 mg/kg, 약 10 ± 0.5 mg/kg, 약 10 ± 0.2 mg/kg, 또는 약 10 ± 0.1 mg/kg, 예컨대, 약 10 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 대상체의 체중 당 약 0.01 mg/kg 내지 약 15 mg/kg(예컨대, 약 0.1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 0.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 1 mg/kg 내지 약 15 mg/kg, 예컨대, 약 2.5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 5 mg/kg 내지 약 15 mg/kg, 예컨대, 약 7.5 mg/kg 내지 약 12.5 mg/kg, 예컨대, 약 8 mg/kg 내지 약 12 In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered every 3 weeks (eg, on Day 1 (eg, 1 day ± 3 days) of each 21-day dosing cycle)) about 0.01 mg/kg to about 50 mg/kg (eg, about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg, of the subject's body weight) /kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 10 mg/kg to about 20 mg/kg , such as from about 12.5 mg/kg to about 15 mg/kg, such as about 15 ± 2 mg/kg, about 15 ± 1 mg/kg, about 15 ± 0.5 mg/kg, about 15 ± 0.2 mg/kg, or about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, an anti VEGF antibody (eg, bevacizumab)) is from about 0.01 mg/kg to about 15 mg/kg (eg, about 0.1 mg/kg) of the subject's body weight every 3 weeks. kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, For example, from about 5 mg/kg to about 15 mg/kg, such as from about 7.5 mg/kg to about 15 mg/kg, such as from about 10 mg/kg to about 15 mg/kg, such as from about 12.5 mg/kg to about 15 mg/kg, such as about 14 mg/kg to about 15 mg/kg, such as about 15 ± 1 mg/kg, such as about 15 ± 0.5 mg/kg, such as about 15 ± 0.2 mg/kg, For example, a dose of about 15 ± 0.1 mg/kg, such as about 15 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) is a dose of about 15 mg/kg administered every 3 weeks. In some cases, the effective amount of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) is administered every 2 weeks (eg, on Day 1 (eg, 1 day±3 days) of each 14-day dosing cycle) or from about 0.01 mg/kg to about 50 mg/kg (eg, from about 0.01 mg/kg to about 50 mg/kg of body weight of the subject on days 1 (eg, day 1±3) and day 15 (eg, day 15±3)) of each 28-day dosing cycle about 0.01 mg/kg to about 45 mg/kg, such as about 0.1 mg/kg to about 40 mg/kg, such as about 1 mg/kg to about 35 mg/kg, such as about 2.5 mg/kg to about 30 mg/kg, such as about 5 mg/kg to about 25 mg/kg, such as about 7.5 mg/kg to about 20 mg/kg, such as about 7.5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 12.5 mg/kg, such as about 10 ± 2 mg/kg, about 10 ± 1 mg/kg, about 10 ± 0.5 mg/kg, about 10 ± 0.2 mg/kg, or about 10 ± 0.1 mg /kg, such as about 10 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is from about 0.01 mg/kg to about 15 mg/kg (eg, about 0.1 mg/kg) of the subject's body weight every two weeks. kg to about 15 mg/kg, such as about 0.5 mg/kg to about 15 mg/kg, such as about 1 mg/kg to about 15 mg/kg, such as about 2.5 mg/kg to about 15 mg/kg, For example, about 5 mg/kg to about 15 mg/kg, such as about 7.5 mg/kg to about 12.5 mg/kg, such as about 8 mg/kg to about 12
mg/kg, 예컨대, 약 9 mg/kg 내지 약 11 mg/kg, 예컨대, 약 9.5 mg/kg 내지 약 10.5 mg/kg, 예컨대, 약 10 ± 1 mg/kg, 예컨대, 약 10 ± 0.5 mg/kg, 예컨대, 약 10 ± 0.2 mg/kg, 예컨대, 약 10 ± 0.1 mg/kg, 예컨대, 약 10 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 약 10 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 약 5 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 약 7.5 mg/kg의 용량이다. mg/kg, such as about 9 mg/kg to about 11 mg/kg, such as about 9.5 mg/kg to about 10.5 mg/kg, such as about 10 ± 1 mg/kg, such as about 10 ± 0.5 mg/kg kg, such as about 10 ± 0.2 mg/kg, such as about 10 ± 0.1 mg/kg, such as about 10 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is a dose of about 10 mg/kg administered every two weeks. In some cases, the effective amount of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) is a dose of about 5 mg/kg administered every two weeks. In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is a dose of about 7.5 mg/kg administered every two weeks.
일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 10 mg/kg 내지 20 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, 또는 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 예들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대, 0.5 mg/kg 내지 15 mg/kg, 예컨대, 1 mg/kg 내지 15 mg/kg, 예컨대, 2.5 mg/kg 내지 15 mg/kg, 예컨대, 5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 15 mg/kg, 예컨대, 10 mg/kg 내지 15 mg/kg, 예컨대, 12.5 mg/kg 내지 15 mg/kg, 예컨대, 14 mg/kg 내지 15 mg/kg, 예컨대, 15 ± 1 mg/kg, 예컨대, 15 ± 0.5 mg/kg, 예컨대, 15 ± 0.2 mg/kg, 예컨대, 15 ± 0.1 mg/kg, 예컨대, 15 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 3주마다 투여되는 15 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 50 mg/kg(예컨대, 0.01 mg/kg 내지 45 mg/kg, 예컨대, 0.1 mg/kg 내지 40 mg/kg, 예컨대, 1 mg/kg 내지 35 mg/kg, 예컨대, 2.5 mg/kg 내지 30 mg/kg, 예컨대, 5 mg/kg 내지 25 mg/kg, 예컨대, 7.5 mg/kg 내지 20 mg/kg, 예컨대, 7.5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 12.5 mg/kg, 예컨대 10 ± 2 mg/kg, 10 ± 1 mg/kg, 10 ± 0.5 mg/kg, 10 ± 0.2 mg/kg, 또는 10 ± 0.1 mg/kg, 예컨대, 10 mg/kg)의 용량이다. 일부 예들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 상기 대상체의 체중 당 0.01 mg/kg 내지 15 mg/kg(예컨대, 0.1 mg/kg 내지 15 mg/kg, 예컨대, 0.5 mg/kg 내지 15 mg/kg, 예컨대, 1 mg/kg 내지 15 mg/kg, 예컨대, 2.5 mg/kg 내지 15 mg/kg, 예컨대, 5 mg/kg 내지 15 mg/kg, 예컨대, 7.5 mg/kg 내지 12.5 mg/kg, 예컨대, 8 mg/kg 내지 12 mg/kg, 예컨대, 9 mg/kg 내지 11 mg/kg, 예컨대, 9.5 mg/kg 내지 10.5 mg/kg, 예컨대, 10 ± 1 mg/kg, 예컨대, 10 ± 0.5 mg/kg, 예컨대, 10 ± 0.2 mg/kg, 예컨대, 10 ± 0.1 mg/kg, 예컨대, 10 mg/kg)의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 10 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 5 mg/kg의 용량이다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 유효량은 2주마다 투여되는 7.5 mg/kg의 용량이다. In some cases, the effective amount of the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is 0.01 mg/kg to 50 mg/kg (eg, 0.01 mg/kg to) of the subject's body weight every 3 weeks. 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg /kg, such as 10 mg/kg to 20 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± 0.1 mg/kg, such as 15 mg/kg). In some embodiments, the effective amount of the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is 0.01 mg/kg to 15 mg/kg (eg, 0.1 mg/kg to 15) of the subject's body weight every 3 weeks. mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg kg, such as 7.5 mg/kg to 15 mg/kg, such as 10 mg/kg to 15 mg/kg, such as 12.5 mg/kg to 15 mg/kg, such as 14 mg/kg to 15 mg/kg, eg 15±1 mg/kg, eg 15±0.5 mg/kg, eg 15±0.2 mg/kg, eg 15±0.1 mg/kg, eg 15 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is a dose of 15 mg/kg administered every 3 weeks. In some cases, the effective amount of the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is 0.01 mg/kg to 50 mg/kg (eg, 0.01 mg/kg to) of the subject's body weight every two weeks. 45 mg/kg, such as 0.1 mg/kg to 40 mg/kg, such as 1 mg/kg to 35 mg/kg, such as 2.5 mg/kg to 30 mg/kg, such as 5 mg/kg to 25 mg /kg, such as 7.5 mg/kg to 20 mg/kg, such as 7.5 mg/kg to 15 mg/kg, such as 7.5 mg/kg to 12.5 mg/kg, such as 10 ± 2 mg/kg, 10 ± 1 mg/kg, 10±0.5 mg/kg, 10±0.2 mg/kg, or 10±0.1 mg/kg, such as 10 mg/kg). In some embodiments, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is 0.01 mg/kg to 15 mg/kg (eg, 0.1 mg/kg to 15) of the subject's body weight every two weeks. mg/kg, such as 0.5 mg/kg to 15 mg/kg, such as 1 mg/kg to 15 mg/kg, such as 2.5 mg/kg to 15 mg/kg, such as 5 mg/kg to 15 mg/kg kg, such as 7.5 mg/kg to 12.5 mg/kg, such as 8 mg/kg to 12 mg/kg, such as 9 mg/kg to 11 mg/kg, such as 9.5 mg/kg to 10.5 mg/kg, For example, a dose of 10 ± 1 mg/kg, such as 10 ± 0.5 mg/kg, such as 10 ± 0.2 mg/kg, such as 10 ± 0.1 mg/kg, such as 10 mg/kg). In some cases, the effective amount of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) is a dose of 10 mg/kg administered every two weeks. In some cases, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is a dose of 5 mg/kg administered every two weeks. In some cases, the effective amount of the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) is a dose of 7.5 mg/kg administered every two weeks.
일부 경우들에서, 병용 요법(예컨대, 항 TIGIT 길항제 항체, 예컨대, 본원에 개시된 항 TIGIT 길항제 항체(예컨대, 티라골루맙) 및/또는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체(예컨대, 펨브롤리주맙))으로 투여되는 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))의 용량은 단일요법으로 투여되는 상기 PD-1 축 결합 길항제의 표준 용량과 비교하여 감소될 수 있다. In some cases, combination therapy (eg, an anti TIGIT antagonist antibody, such as an anti TIGIT antagonist antibody disclosed herein (eg, tiragolumab) and/or a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody) The dose of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) administered as an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is the PD administered as a monotherapy. -1 may be reduced compared to the standard dose of an axis binding antagonist.
일부 경우들에서, 상기VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 정맥내 투여된다. 일부 경우들에서, 상기 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 90 ± 15분(예컨대, 약 75분, 약 76분, 약 77분, 약 78분, 약 79분, 약 80분, 약 81분, 약 82분, 약 83분, 약 84분, 약 85분, 약 86분, 약 87분, 약 88분, 약 89분, 약 90분, 약 91분, 약 92분, 약 93분, 약 94분, 약 95분, 약 96분, 약 97분, 약 98분, 약 99분, 약 100분, 약 101분, 약 102분, 약 103분, 약 104분, 또는 약 105분)에 걸쳐 정맥내 투여된다. 대안적으로, 일부 구현예들에서, 상기VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 피하 투여된다.In some cases, the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is administered intravenously. In some cases, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered in 90±15 minutes (eg, about 75 minutes, about 76 minutes, about 77 minutes, about 78 minutes, about 79 minutes, About 80 minutes, about 81 minutes, about 82 minutes, about 83 minutes, about 84 minutes, about 85 minutes, about 86 minutes, about 87 minutes, about 88 minutes, about 89 minutes, about 90 minutes, about 91 minutes, about 92 minutes, about 93 minutes, about 94 minutes, about 95 minutes, about 96 minutes, about 97 minutes, about 98 minutes, about 99 minutes, about 100 minutes, about 101 minutes, about 102 minutes, about 103 minutes, about 104 minutes, or about 105 minutes). Alternatively, in some embodiments, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered subcutaneously.
J.J. PD-L1 발현의 평가Assessment of PD-L1 expression
PD-L1의 발현은 본원에 기재된 임의의 방법, 사용, 및 사용을 위한 조성물에 따라 치료되는 대상체에서 평가될 수 있다. 상기 방법, 사용, 및 사용을 위한 조성물은 상기 대상체로부터 수득한 생물학적 샘플(예컨대, 종양 샘플)에서 PD-L1의 발현 수준을 결정하는 단계를 포함할 수 있다. 일부 경우들에서, 환자는 방광암을 가지고, 상기 샘플은 방광 종양의 경요도 절제술(TURBT) 샘플이다. 일부 경우들에서, 상기 샘플은 방광 절제술 또는 신장 절제술 샘플이다. 일부 경우들에서, 상기 샘플은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술 샘플이다. 일부 경우들에서, 상기 샘플은 방광 절제술 또는 림프절 절제술 샘플이다. 다른 예들에서, 상기 대상체로부터 수득한 생물학적 샘플(예컨대, 종양 샘플)에서 PD-L1의 발현 수준은 치료 개시 전 또는 치료 개시 후에 결정되었다. PD-L1 발현은 임의의 적합한 접근법을 사용하여 결정할 수 있다. 예를 들어, PD-L1 발현은 미국 특허 출원 제US20180030138A1호 및 US20180037655A1호에 기재된 바와 같이 결정할 수 있다. 임의의 적합한 종양 샘플은 포르말린 고정 및 파라핀 포매(FFPE) 종양 샘플, 보관 종양 샘플, 냉장 종양 샘플, 또는 냉동 종양 샘플일 수 있다.Expression of PD-L1 can be assessed in a subject being treated according to any of the methods, uses, and compositions for use described herein. The methods, uses, and compositions for use may comprise determining the expression level of PD-L1 in a biological sample (eg, a tumor sample) obtained from the subject. In some cases, the patient has bladder cancer, and the sample is a transurethral resection (TURBT) sample of a bladder tumor. In some cases, the sample is a cystectomy or nephrectomy sample. In some cases, the sample is a lobectomy, lobectomy, bilobectomy, or pneumonectomy sample. In some cases, the sample is a cystectomy or lymphadenectomy sample. In other instances, the expression level of PD-L1 in a biological sample obtained from the subject (eg, a tumor sample) is determined prior to or after initiation of treatment. PD-L1 expression can be determined using any suitable approach. For example, PD-L1 expression can be determined as described in US Patent Application Nos. US20180030138A1 and US20180037655A1. Any suitable tumor sample may be a formalin-fixed and paraffin-embedded (FFPE) tumor sample, a storage tumor sample, a refrigerated tumor sample, or a frozen tumor sample.
예를 들어, PD-L1 발현은 종양 샘플 내에서 PD-L1의 검출가능한 발현 수준을 발현하는 종양 침윤성 면역 세포가 차지하는 백분율의 관점에서 PD-L1의 검출가능한 발현 수준을 발현하는 종양 샘플에서 종양 침윤성 면역 세포의 백분율로서, 및/또는 PD-L1의 검출가능한 발현 수준을 발현하는 종양 샘플 내 종양 세포의 백분율로서 결정될 수 있다. 임의의 선행하는 예들에서, 종양 샘플 내에서 종양 침윤성 면역 세포가 차지하는 백분율은, 예를 들어 항 PD-L1 항체(예컨대, SP142 항체)를 이용한 IHC로 평가할 때, 대상체로부터 수득한 샘플의 절편에서 종양 침윤성 면역 세포에 의해 커버되는 종양 구역의 백분율의 관점에서일 수 있는 것으로 이해되어야 한다. 임의의 적합한 항 PD-L1 항체가, 예컨대 SP142(벤타나), SP263(벤타나), 22C3(다코(Dako)), 28-8(다코), E1L3N(셀 시그널링 테크놀로지(Cell Signaling Technology)), 4059(ProSci, Inc. .), h5H1(어드반스드 셀 다이아그노스틱스(Advanced Cell Diagnostics) 및 9A11를 포함하여 사용될 수 있다. 일부 예들에서, 상기 항 PD-L1 항체는 SP142이다. 일부 예들에서, 상기 항 PD-L1 항체는 SP263이다. 일부 예들에서, 상기 항 PD-L1 항체는 22C3이다. 일부 예들에서, 상기 항 PD-L1 항체는 28-8이다.For example, PD-L1 expression is dependent on tumor invasiveness in a tumor sample expressing a detectable expression level of PD-L1 in terms of the percentage of tumor infiltrating immune cells expressing a detectable expression level of PD-L1 in the tumor sample. as a percentage of immune cells and/or as a percentage of tumor cells in a tumor sample that express a detectable expression level of PD-L1. In any of the preceding examples, the percentage of tumor-infiltrating immune cells in the tumor sample is, for example, as assessed by IHC with an anti-PD-L1 antibody (eg, SP142 antibody), tumor in a section of a sample obtained from the subject. It should be understood that it may be in terms of the percentage of tumor area covered by infiltrating immune cells. Any suitable anti-PD-L1 antibody is, for example, SP142 (Ventana), SP263 (Ventana), 22C3 (Dako), 28-8 (Dako), E1L3N (Cell Signaling Technology), 4059 (ProSci, Inc.), h5H1 (Advanced Cell Diagnostics) and 9A11. In some embodiments, the anti-PD-L1 antibody is SP142. In some embodiments, The anti-PD-L1 antibody is SP263 In some embodiments, the anti-PD-L1 antibody is 22C3 In some embodiments, the anti-PD-L1 antibody is 28-8.
일부 예들에서, 상기 대상체로부터 수득한 종양 샘플은 PD-L1의 검출가능한 발현 수준이 상기 종양 샘플 내 종양 세포의 1% 미만, 상기 종양 샘플 내 종양 세포의 1% 이상, 상기 종양 샘플 내 종양 세포의 1% 내지 5% 미만, 상기 종양 샘플 내 종양 세포의 5% 이상, 상기 종양 샘플 내 종양 세포의 5% 내지 50% 미만, 또는 상기 종양 샘플에서 종양 세포의 50% 이상이다.In some embodiments, the tumor sample obtained from the subject has a detectable expression level of PD-L1 of less than 1% of tumor cells in the tumor sample, greater than or equal to 1% of tumor cells in the tumor sample, of tumor cells in the tumor sample. between 1% and less than 5%, at least 5% of the tumor cells in the tumor sample, between 5% and less than 50% of the tumor cells in the tumor sample, or at least 50% of the tumor cells in the tumor sample.
일부 예들에서, 상기 대상체로부터 수득한 종양 샘플은 종양 침윤성 면역 세포 내 PD-L1의 검출가능한 발현 수준이 상기 종양 샘플의 1% 미만, 상기 종양 샘플의 1% 초과, 상기 종양 샘플의 1% 내지 5% 미만, 상기 종양 샘플의 5% 초과, 상기 종양 샘플의 5% 내지 10% 미만, 또는 상기 종양 샘플의 10% 초과를 포함한다.In some embodiments, the tumor sample obtained from the subject has a detectable expression level of PD-L1 in tumor infiltrating immune cells of less than 1% of the tumor sample, greater than 1% of the tumor sample, between 1% and 5% of the tumor sample. %, greater than 5% of the tumor sample, between 5% and less than 10% of the tumor sample, or greater than 10% of the tumor sample.
일부 양태들에서, 상기 대상체로부터 수득한 종양 샘플은 종양 침윤성 면역 세포 내 PD-L1의 검출가능한 발현 수준이 상기 종양 샘플의 5%~19%(예컨대, TIC 5%~19%)를 포함하고; 예컨대, PD-L1이 낮은 PD-L1 발현 수준을 가진다. 일부 양태들에서, 상기 대상체로부터 수득한 종양 샘플은 종양 침윤성 면역 세포 내 PD-L1의 검출가능한 발현 수준이 상기 종양 샘플의 20% 이상(예컨대, TIC 20% 이상)을 포함하고; 예컨대, PD-L1이 높은 PD-L1 발현 수준을 가진다. 일부 구현예들에서, TIC가 5% 이상인 것으로 결정된 종양 샘플은 1 이상의 CPS와 유사하다.In some aspects, the tumor sample obtained from the subject has a detectable expression level of PD-L1 in tumor infiltrating immune cells of 5%-19% (eg, 5%-19% TIC) of the tumor sample; For example, PD-L1 has a low PD-L1 expression level. In some aspects, the tumor sample obtained from the subject has a detectable expression level of PD-L1 in tumor infiltrating immune cells of at least 20% (eg, at least 20% TIC) of the tumor sample; For example, PD-L1 has a high level of PD-L1 expression. In some embodiments, a tumor sample determined to have a TIC of at least 5% is comparable to at least 1 CPS.
일부 예들에서, 종양 샘플은 각각 표 1 및/또는 표 2에 제시된 진단 평가 기준에 따라 종양 침윤설 면역 세포 및/또는 종양 세포에서 PD-L1 양성에 대해 점수를 매길 수 있다. In some examples, the tumor sample may be scored for PD-L1 positivity in tumor infiltrating immune cells and/or tumor cells according to the diagnostic evaluation criteria set forth in Table 1 and/or Table 2, respectively.
종양 세포, 관련 종양내 기질, 및 인접한 종양 주변 결합조직형성 기질이 차지하는 종양 영역의 <1%를 차지하는 종양 침윤성 면역 세포에서 임의의 강도의 식별가능한 PD-L1 염색의 존재No discernable PD-L1 staining OR
Presence of identifiable PD-L1 staining of any intensity in tumor-infiltrating immune cells occupying <1% of the tumor area occupied by tumor cells, associated intratumoral stroma, and adjacent peritumoral connective tissue forming stroma
종양 침윤설 면역 세포(IC)의 IHC 진단 기준IHC Diagnostic Criteria for Tumor Infiltrating Immune Cells (IC)
종양 세포의 <1%에서 임의의 강도의 식별 가능한 PD-L1 염색의 존재 No discernable PD-L1 staining OR
Presence of identifiable PD-L1 staining of any intensity in <1% of tumor cells
종양 세포(TC)의 IHC 진단 기준IHC diagnostic criteria for tumor cells (TC)
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체는 PD-L1 선택된 종양을 갖는다(예컨대, PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 SP142 항체를 이용한 IHC에 의해 결정된 바와 같이 상기 종양 샘플에서 5% 이상이다). 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 발현 면역 세포(IC)에 의해 차지하는 종양 면적의 비율이 면역조직화학적(IHC) 분석법에 의해 5% 이상인 것으로 결정된 종양이다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142, SP263, 22C3, 또는 28-8을 사용한다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, IHC IHC 분석은 항 PD-L1 항체 SP263을 사용한다. 일부 경우들에서, IHC 분석은 항 PD-L1 항체 22C3을 사용한다. 일부 경우들에서, IHC 분석은 항 PD-L1 항체 22C3을 사용한다. 일부 경우들에서, IHC 분석은 항 PD-L1 항체 28-8을 사용한다.In some cases, in any of the methods, uses, or compositions for use described herein, the subject has a PD-L1-selected tumor (eg, the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC)) ratio is greater than or equal to 5% in the tumor sample as determined by IHC with SP142 antibody). In some cases, the PD-L1-selected tumor is a tumor in which the proportion of tumor area occupied by PD-L1-expressing immune cells (IC) is determined to be greater than or equal to 5% by immunohistochemical (IHC) analysis. In some cases, the IHC assay uses anti-PD-L1 antibodies SP142, SP263, 22C3, or 28-8. In some cases, the IHC assay uses anti-PD-L1 antibody SP142. In some cases, the IHC IHC assay uses the anti-PD-L1 antibody SP263. In some cases, the IHC assay uses anti-PD-L1 antibody 22C3. In some cases, the IHC assay uses anti-PD-L1 antibody 22C3. In some cases, the IHC assay uses anti-PD-L1 antibody 28-8.
일부 경우들에서, 상기 IC는 5% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC 점수는 2 또는 3인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 10% 이상인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 50% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 IC는 1% 이상 30% 미만인 것으로 결정되었다(예컨대, 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이).In some cases, the IC was determined to be greater than or equal to 5% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC score was determined to be 2 or 3 (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 10% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 50% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay). In some cases, the IC was determined to be greater than or equal to 1% and less than 30% (eg, as determined using a Ventana (SP142) PD-L1 IHC assay).
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물에서, 개체로부터 수득한 종양 샘플은 PD-L1의 검출가능한 단백질 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 단백질 발현 수준은 IHC 분석에 의해 결정되었다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플의 5% 이상을 포함하는 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플의 1% 이상을 포함하는 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플의 1% 이상 5% 미만을 포함하는 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플의 5% 이상 10% 미만을 포함하는 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플의 10% 이상을 포함하는 종양 침윤성 면역 세포에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플 내 종양 세포의 1% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플 내 종양 세포의 1% 이상 5% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플 내 종양 세포의 5% 이상 50% 미만에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 상기 종양 샘플 내 종양 세포의 50% 이상에서 PD-L1의 검출가능한 발현 수준을 갖는 것으로 결정되었다. In some cases, in a method, use, or composition for use described herein, a tumor sample obtained from an individual has a detectable protein expression level of PD-L1. In some cases, detectable protein expression levels of PD-L1 were determined by IHC analysis. In some cases, the IHC assay uses anti-PD-L1 antibody SP142. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor infiltrating immune cells comprising at least 5% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 1% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor infiltrating immune cells comprising at least 1% and less than 5% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 5% and less than 10% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in tumor-infiltrating immune cells comprising at least 10% of the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 1% and less than 5% of tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 5% and less than 50% of the tumor cells in the tumor sample. In some cases, the tumor sample has been determined to have a detectable expression level of PD-L1 in at least 50% of the tumor cells in the tumor sample.
일부 경우들에서, 본원에 기재된 임의의 방법, 사용, 또는 사용을 위한 조성물에서, 상기 대상체는 PD-L1 선택된 종양을 갖는다(예컨대, PD-L1 높음(예컨대, SP263 항체를 갖는 IHC에 의해 결정된 바와 같이 종양 샘플에서 50% 이상의 PD-L1 종양 비율 점수(TPS)). 일부 경우들에서, 상기 PD-L1 선택된 종양은 PD-L1 높음으로 선택된 종양이다. 일부 경우들에서, 상기 PD-L1 선택된 종양은 TPS가 면역조직화학적(IHC) 분석에 의해 50% 이상인 것으로 결정된 종양이다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP263, SP142, 22C3, 또는 28-8을 사용한다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP263을 사용한다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP142를 사용한다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 22C3을 사용한다. 일부 경우들에서, 상기 TPS는 50% 이상인 것으로 결정되었다(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 TPS는 50% 미만인 것으로 결정되었다(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 TPS는 1% 이상인 것으로 결정되었다(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). 일부 경우들에서, 상기 TPS는 1% 이상 50% 미만인 것으로 결정되었다(예컨대, 벤타나(SP263) PD-L1 IHC 분석을 사용하여 결정된 바와 같이). In some cases, in any method, use, or composition for use described herein, the subject has a PD-L1 selected tumor (eg, as determined by IHC with PD-L1 high (eg, IHC with SP263 antibody). (PD-L1 tumor rate score (TPS) greater than 50% in the same tumor sample. In some cases, the PD-L1 selected tumor is the selected PD-L1 high. In some cases, the PD-L1 selected tumor is the tumor determined by immunohistochemical (IHC) analysis to be greater than or equal to 50% TPS.In some cases, the IHC analysis uses anti-PD-L1 antibody SP263, SP142, 22C3, or 28-8. In some cases, said IHC assay uses anti-PD-L1 antibody SP263.In some cases, said IHC assay uses anti-PD-L1 antibody SP142.In some cases, said IHC assay uses anti-PD-L1 antibody 22C3 is used.In some cases, the TPS is determined to be greater than or equal to 50% (eg, as determined using Ventana (SP263) PD-L1 IHC analysis).In some cases, the TPS is determined to be greater than 50%. was determined to be less than (eg, as determined using Ventana (SP263) PD-L1 IHC analysis) In some cases, the TPS was determined to be greater than or equal to 1% (eg, Ventana (SP263) PD-L1). As determined using an IHC assay) In some cases, the TPS was determined to be greater than or equal to 1% and less than 50% (eg, as determined using a Ventana (SP263) PD-L1 IHC assay).
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물에서, 개체로부터 수득한 종양 샘플은 PD-L1의 검출가능한 단백질 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 단백질 발현 수준은 IHC 분석에 의해 결정되었다. 일부 경우들에서, 상기 IHC 분석은 항 PD-L1 항체 SP263을 사용한다. 일부 경우들에서, 상기 종양 샘플은 PD-L1 양성 종양 세포 분획이 상기 종양 샘플의 50% 이상인 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 PD-L1 양성 종양 세포 분획이 상기 종양 샘플의 50% 미만인 것으로 결정되었다. 일부 경우들에서, 상기 종양 샘플은 PD-L1 양성 종양 세포 분획이 상기 종양 샘플의 1% 이상 50% 미만인 것으로 결정되었다. In some cases, in a method, use, or composition for use described herein, a tumor sample obtained from an individual has a detectable protein expression level of PD-L1. In some cases, detectable protein expression levels of PD-L1 were determined by IHC analysis. In some cases, the IHC assay uses the anti-PD-L1 antibody SP263. In some cases, the tumor sample has been determined to have a fraction of PD-L1 positive tumor cells greater than or equal to 50% of the tumor sample. In some cases, the tumor sample has been determined to have a fraction of PD-L1 positive tumor cells less than 50% of the tumor sample. In some cases, the tumor sample has been determined to have a fraction of PD-L1 positive tumor cells that is greater than or equal to 1% and less than 50% of the tumor sample.
일부 경우들에서, 상기 IHC 분석은 상기 항 PD-L1 항체 22C3을 사용한다. 일부 경우들에서, 상기 IHC 분석은 팜(pharm)Dx 22C3 IHC 분석이다. 일부 경우들에서, 상기 PD-L1 양성 종양 세포 분획은 상기 항 PD-L1 항체 22C3를 사용한 양성 염색에 의해 결정된 바와 같이 50% 이상이다. 일부 구현예들에서, 상기 종양 샘플은, 예컨대 팜Dx 22C3 IHC 분석의 일부로서 항 PD-L1 항체 22C3을 사용하여 결정된 바와 같이 상기 종양 샘플에서 복합 양성 점수(CPS)가 10 이상이고 종양 비율 점수(TPS)가 1% 이상인 것으로 결정되었다. 일부 구현예들에서, 상기 종양 샘플은, 예컨대 팜Dx 22C3 IHC 분석의 일부로서 항 PD-L1 항체 22C3을 사용하여 결정된 바와 같이 상기 종양 샘플에서 CPS가 10 이상이고 TPS가 1% 이상 50% 미만인 것으로 결정되었다. 일부 구현예들에서, 상기 종양 샘플은, 예컨대 팜Dx 22C3 IHC 분석의 일부로서 항 PD-L1 항체 22C3을 사용하여 결정된 바와 같이 상기 종양 샘플에서 CPS가 20 이상이고 TPS가 50% 이상인 것으로 결정되었다. 일부 구현예들에서, CPS가 1 이상인 것으로 결정된 종양 샘플은 5% 이상인 CPS와 유사하다. In some cases, the IHC assay uses the anti-PD-L1 antibody 22C3. In some cases, the IHC assay is a pharmDx 22C3 IHC assay. In some cases, the PD-L1 positive tumor cell fraction is greater than or equal to 50% as determined by positive staining with the anti-PD-L1 antibody 22C3. In some embodiments, the tumor sample has a composite positive score (CPS) of at least 10 and a tumor rate score in the tumor sample, e.g., as determined using anti-PD-L1 antibody 22C3 as part of a PalmDx 22C3 IHC assay TPS) was determined to be greater than or equal to 1%. In some embodiments, the tumor sample has a CPS of 10 or greater and a TPS of greater than or equal to 1% and less than 50% in the tumor sample, e.g., as determined using anti-PD-L1 antibody 22C3 as part of a PalmDx 22C3 IHC assay. It was decided. In some embodiments, the tumor sample has a CPS of 20 or greater and a TPS of 50% or greater in the tumor sample, eg, as determined using anti-PD-L1 antibody 22C3 as part of a PalmDx 22C3 IHC assay. In some embodiments, a tumor sample determined to have a CPS of 1 or greater is similar to a CPS of 5% or greater.
일부 경우들에서, 상기 IHC 분석은 상기 항 PD-L1 항체 28-8을 사용한다. 일부 경우들에서, 상기 IHC 분석은 팜Dx 28-8 IHC 분석이다. 일부 경우들에서, 상기 PD-L1 양성 종양 세포 분획은 항 PD-L1 항체 28-8을 사용한 양성 염색에 의해 결정 시 50% 이상이다.In some cases, the IHC assay uses the anti-PD-L1 antibody 28-8. In some cases, the IHC assay is a PalmDx 28-8 IHC assay. In some cases, the PD-L1 positive tumor cell fraction is greater than or equal to 50% as determined by positive staining with anti-PD-L1 antibody 28-8.
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물에서, 개체로부터 수득한 종양 샘플은 PD-L1의 검출가능한 핵산 발현 수준을 갖는다. 일부 경우들에서, PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되었다. 일부 경우들에서, 상기 샘플은 조직 샘플, 전혈 샘플, 혈청 샘플, 및 혈장 샘플로 이루어진 군으로부터 선택된다. 일부 경우들에서, 상기 조직 샘플은 종양 샘플이다. 일부 경우들에서, 상기 종양 샘플은 종양 침윤성 면역 세포, 종양 세포, 간질 세포, 및 이들의 임의의 조합을 포함한다. In some cases, in a method, use, or composition for use described herein, a tumor sample obtained from an individual has a detectable nucleic acid expression level of PD-L1. In some cases, the detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. became In some cases, the sample is selected from the group consisting of a tissue sample, a whole blood sample, a serum sample, and a plasma sample. In some cases, the tissue sample is a tumor sample. In some cases, the tumor sample comprises tumor infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
K.K. TIGIT 발현의 평가Assessment of TIGIT expression
TIGIT의 발현은 본원에 기재된 임의의 방법, 사용, 및 사용을 위한 조성물에 따라 치료되는 대상체에서 평가될 수 있다. 상기 방법, 사용, 및 사용을 위한 조성물은 상기 대상체로부터 수득한 생물학적 샘플(예컨대, 종양 샘플)에서 TIGIT의 발현 수준을 결정하는 단계를 포함할 수 있다. 다른 예들에서, 상기 대상체로부터 수득한 생물학적 샘플(예컨대, 종양 샘플)에서 TIGIT의 발현 수준은 치료 개시 전 또는 치료 개시 후에 결정되었다. TIGIT 발현은 임의의 적합한 접근법을 사용하여 결정할 수 있다. 임의의 적합한 종양 샘플은 포르말린 고정 및 파라핀 포매(FFPE) 종양 샘플, 보관 종양 샘플, 냉장 종양 샘플, 또는 냉동 종양 샘플일 수 있다.Expression of TIGIT can be assessed in a subject being treated according to any of the methods, uses, and compositions for use described herein. The methods, uses, and compositions for use may comprise determining the expression level of TIGIT in a biological sample (eg, a tumor sample) obtained from the subject. In other examples, the expression level of TIGIT in a biological sample obtained from the subject (eg, a tumor sample) is determined prior to or after initiation of treatment. TIGIT expression can be determined using any suitable approach. Any suitable tumor sample may be a formalin-fixed and paraffin-embedded (FFPE) tumor sample, a storage tumor sample, a refrigerated tumor sample, or a frozen tumor sample.
예를 들어, TIGIT 발현은 종양 샘플 내에서 TIGIT의 검출가능한 발현 수준을 발현하는 종양 침윤성 면역 세포가 차지하는 백분율의 관점에서 TIGIT의 검출가능한 발현 수준을 발현하는 종양 샘플에서 종양 침윤성 면역 세포의 백분율로서, 및/또는 TIGIT의 검출가능한 발현 수준을 발현하는 종양 샘플 내 종양 세포의 백분율로서 결정될 수 있다. 임의의 선행하는 예들에서, 종양 샘플 내에서 종양 침윤성 면역 세포가 차지하는 백분율은, 예를 들어 항 TIGIT 길항제 항체를 이용한 IHC로 평가할 때, 대상체로부터 수득한 샘플의 절편에서 종양 침윤성 면역 세포에 의해 커버되는 종양 구역의 백분율의 관점에서일 수 있는 것으로 이해되어야 한다. 임의의 적합한 항 TIGIT 길항제 항체가 사용될 수 있다. 일부 예들에서, 상기 항 TIGIT 길항제 항체는 10A7(WO 2009/126688A3; 미국 특허 제 9,499,596)이다.For example, TIGIT expression is defined as the percentage of tumor infiltrating immune cells in a tumor sample expressing a detectable expression level of TIGIT in terms of the percentage of tumor infiltrating immune cells expressing a detectable expression level of TIGIT in the tumor sample, and/or as the percentage of tumor cells in the tumor sample that express a detectable expression level of TIGIT. In any of the preceding examples, the percentage of tumor-infiltrating immune cells in the tumor sample that is covered by tumor-infiltrating immune cells in a section of the sample obtained from the subject, e.g., as assessed by IHC using an anti-TIGIT antagonist antibody. It should be understood that it may be in terms of a percentage of tumor area. Any suitable anti-TIGIT antagonist antibody may be used. In some embodiments, the anti-TIGIT antagonist antibody is 10A7 (WO 2009/126688A3; US Pat. No. 9,499,596).
L.L. EGFR 및 ALK 이상의 평가Assessment of EGFR and ALK or higher
일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는다. 일부 경우들에서, 본원에 기재된 방법, 사용, 또는 사용을 위한 조성물들에서, 상기 대상체는 EGFR 유전자 돌연변이(예컨대, 감작성 또는 활성화 EGFR 유전자 돌연변이) 또는 ALK 유전자 재배열(예컨대, ALK 융합 종양유전자)을 갖지 않는다. 일부 경우들에서, 상기 대상체는 0 또는 1의 이스턴 코퍼레이티브 종양학 그룹(ECOG) 전신 활동도(PS)를 가진다. In some cases, in a method, use, or compositions for use described herein, the subject does not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality. In some cases, in a method, use, or compositions for use described herein, the subject has an EGFR gene mutation (eg, a sensitizing or activating EGFR gene mutation) or an ALK gene rearrangement (eg, an ALK fusion oncogene) do not have In some cases, the subject has an Eastern Corporate Oncology Group (ECOG) systemic activity (PS) of 0 or 1.
돌연변이 상태 EGFR 및 ALK를 검출하는 방법은 당업계에 일반적으로 공지되어 있으며, 임상 샘플(예컨대, 종양 생검 또는 혈액 샘플(예컨대, 혈액 중 순환 종양 DNA)로부터의 DNA를 차세대 서열분석 방법을 사용하여, 예컨대 본원에 그 전체가 원용된 Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013)에 기재된 표적화된 유전자 풀다운 및 서열분석 방법을 사용하여 서열분석하는 것을 포함하지만 이에 제한되지는 않는다. 이러한 서열분석 방법은 다양한 돌연변이(예컨대, 삽입, 결실, 염기 치환, 국소 유전자 증폭 및/또는 동형 접합 유전자 결실)를 검출하기 위해 본원에 개시된 임의의 방법과 함께 사용될 수 있으며, 동시에 소형 샘플들(예컨대, 작은 코어 바늘 생검, 미세 바늘 흡인 및/또는 세포 블록들) 또는 고정된 샘플들(예컨대, 포르말린 고정 및 파라핀 포매(FFPE) 샘플)을 사용할 수 있게 한다. EGFR 및 ALK의 돌연변이 상태를 검출하기 위한 다른 방법에는 형광 인시튜 혼성화(FISH) 및 면역조직화학(IHC) 방법이 포함된다. ALK의 돌연변이 상태의 검출을 위한 예시적인 방법은 미국 특허 제 9,651,555에 개시되며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, VENTANA® 항 ALK (D5F3) IHC 분석은 ALK 유전자의 돌연변이 상태를 결정하기 위해 사용한다.Methods for detecting the mutant state EGFR and ALK are generally known in the art, and DNA from a clinical sample (e.g., a tumor biopsy or a blood sample (e.g., circulating tumor DNA in blood)) can be analyzed using next-generation sequencing methods; including, but not limited to, sequencing using, for example, targeted gene pulldown and sequencing methods described in Frampton et al. ( Nature Biotechnology . 31(11): 1023-1033, 2013), which is incorporated herein in its entirety. This sequencing method can be used in conjunction with any of the methods disclosed herein to detect a variety of mutations (eg, insertions, deletions, base substitutions, local gene amplifications and/or homozygous gene deletions), while simultaneously extracting small samples. (e.g. small core needle biopsy, fine needle aspiration and/or cell blocks) or fixed samples (e.g., formalin fixed and paraffin embedded (FFPE) samples).Detect mutation status of EGFR and ALK Other methods include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods.Exemplary methods for detection of mutant state of ALK are disclosed in US Pat. No. 9,651,555, which is herein incorporated by reference in its entirety. In some cases, the VENTANA® anti- ALK (D5F3) IHC assay is used to determine the mutation status of the ALK gene.
본원에 기재된 임의의 방법의 일부 경우들에서, 상기 돌연변이는 감작성 EGFR 돌연변이이다. 감작성 EGFR 돌연변이는 당업계에 일반적으로 공지되어 있으며 미국 특허 공보 제 US 2018/0235968 및 in Juan et al. (Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18-21 중 어느 하나에서의 돌연변이(예컨대, 엑손 18, 엑손 19, 엑손 20, 및/또는 엑손 21에서의 돌연변이)이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 19에서의 결실(del19)이다. 다른 예들에서, 상기 감작성 EGFR 돌연변이는 엑손 21에서의 L858R 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 C, A, 또는 S이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 엑손 18의 G719S 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 G719A 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 18에서의 S720F 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861Q 점 돌연변이이다. 일부 경우들에서, 감작성 EGFR 돌연변이는 엑손 21에서의 L861R 점 돌연변이이다. 다른 경우들에서, 감작성 EGFR 돌연변이는 T790M 점 돌연변이이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 E709X 점 돌연변이이며, 여기서 "X"는 가장 일반적으로 K, A, 또는 H이다. 일부 경우들에서, 상기 감작성 EGFR 돌연변이는 S768I 점 돌연변이이다.In some cases of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are generally known in the art and described in US Patent Publication Nos. US 2018/0235968 and in Juan et al. ( Therapeutic Advances in Medical Oncology. 9(3): 201-216, 2017), which is incorporated herein by reference in its entirety. In some cases, the sensitizing EGFR mutation is a mutation in any one of exon 18-21 (eg, a mutation in exon 18, exon 19, exon 20, and/or exon 21). In some cases, the sensitizing EGFR mutation is a deletion in exon 19 (del19). In other examples, the sensitizing EGFR mutation is an L858R point mutation in exon 21. In some cases, the sensitizing EGFR mutation is a G719X point mutation of exon 18, wherein "X" is most commonly C, A, or S. In some cases, the sensitizing EGFR mutation is a G719S point mutation of exon 18. In some cases, the sensitizing EGFR mutation is a G719A point mutation in exon 18. In some cases, the sensitizing EGFR mutation is an S720F point mutation in exon 18. In some cases, the sensitizing EGFR mutation is an L861Q point mutation in exon 21. In some cases, the sensitizing EGFR mutation is an L861R point mutation in exon 21. In other cases, the sensitizing EGFR mutation is the T790M point mutation. In some cases, the sensitizing EGFR mutation is an E709X point mutation, wherein “X” is most commonly K, A, or H. In some cases, the sensitizing EGFR mutation is an S768I point mutation.
본원에 기재된 방법들 중 임의의 것의 일부 경우들에서, 상기 돌연변이는 ALK 유전자 재배열이다. ALK 유전자 재배열은 당업계에 일반적으로 공지되어 있으며 미국 특허 제 9,651,555 및 in Du et al. (Thoracic Cancer. 9: 423-430, 2018)에 기재되어 있으며, 이는 본원에 그 전체가 원용된다. 일부 경우들에서, ALK 유전자 재배열은 하류 신호전달 경로를 활성화하여 세포 증식 및 생존을 증가시키는 발암성 ALK 티로신 키나제의 생성을 초래한다. 일부 경우들에서, ALK 유전자 재배열은 EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC, TMP4, 및 MSN로 구성된 그룹에서 선택된 유전자와의 ALK 재배열이며, 융합 종양유전자를 형성시킨다. 일부 경우들에서, ALK 유전자 재배열은 ALK 와의 EML4 재배열이며 융합 종양유전자 EML4-ALK를 형성한다.In some cases of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are generally known in the art and described in US Pat. Nos. 9,651,555 and in Du et al. ( Thoracic Cancer. 9: 423-430, 2018), which is incorporated herein by reference in its entirety. In some cases, ALK gene rearrangement results in the production of oncogenic ALK tyrosine kinases that activate downstream signaling pathways to increase cell proliferation and survival. In some cases, the ALK gene rearrangement is a gene selected from the group consisting of EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A , BIRC6, RANBP2, ATIC, CLTC, TMP4, and MSN . ALK rearrangement with and forms a fusion oncogene. In some cases, the ALK gene rearrangement is an EML4 rearrangement with ALK and forms the fusion oncogene EML4-ALK .
IV. 예시적인 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 기타 제제IV. Exemplary Anti-TIGIT Antagonist Antibodies, PD-1 Axis Binding Antagonists, and Other Agents
본 발명의 방법, 사용, 및 사용을 위한 방법에 따라 암을 가진 대상체(예컨대, 인간)를 치료하는데 유용한 예시적인 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 화학요법제, 집락 자극 인자, 및 VEGF 길항제가 본원에 기재되어 있다.Exemplary anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, chemotherapeutic agents, colony stimulating factors, and VEGF antagonists are described herein.
A. 예시적인 항 TIGIT 길항제 항체 A. Exemplary Anti-TIGIT Antagonist Antibodies
본 발명은 대상체(예컨대, 인간)에서 암을 치료하는데 유용한 항 TIGIT 길항제 항체를 제공한다.The present invention provides anti-TIGIT antagonist antibodies useful for treating cancer in a subject (eg, a human).
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 티라골루맙(CAS 등록 번호: 1918185-84-8)이다. 티라골루맙(제넨텍(Genentech))은 MTIG7192A로도 공지되어 있다.In some cases, the anti-TIGIT antagonist antibody is tiragolumab (CAS Accession Number: 1918185-84-8). Tiragolumab (Genentech) is also known as MTIG7192A.
특정 경우들에서, 상기 항 TIGIT 길항제 항체는 하기의: (a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1; (b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2; (c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3; (d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1; (e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2; 및/또는 (f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3, 또는 상기 HVR 중 하나 이상 및 서열번호 1 내지 서열번호 6 중 어느 하나와 적어도 약 90% 서열 동일성(예컨대, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 또는 99% 동일성)을 갖는 이의 하나 이상의 변이체의 조합으로부터 선택된 적어도 1개, 2개, 3개, 4개, 5개 또는 6개의 HVR을 포함한다. In certain instances, the anti-TIGIT antagonist antibody comprises: (a) HVR-H1 comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1); (b) HVR-H2 comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2); (c) HVR-H3 comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3); (d) HVR-L1 comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4); (e) HVR-L2 comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and/or (f) an HVR-L3 comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6), or at least about 90% sequence identity to one or more of said HVRs and any one of SEQ ID NO: 1 to SEQ ID NO: 6 (e.g., 90% %, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, or 99% identity). , 4, 5 or 6 HVRs.
일부 경우들에서, 항 TIGIT 길항제 항체는 SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1; (b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2; (c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3; (d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1; (e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2; 및/또는 (f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함할 수 있다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(서열번호 17) 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열 또는 QVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(서열번호 18) 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VH 도메인; 및/또는 DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIK(서열번호 19) 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VH 도메인, 및/또는 서열번호 19 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 17의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VH 도메인, 및/또는 서열번호 19 또는 이의 서열과 적어도 90%의 서열 동일성(예컨대, 적어도 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% 또는 99% 서열 동일성)을 갖는 아미노산 서열을 포함하는 VL 도메인을 가진다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 서열번호 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 가진다. In some cases, the anti-TIGIT antagonist antibody comprises HVR-H1 comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1); (b) HVR-H2 comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2); (c) HVR-H3 comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3); (d) HVR-L1 comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4); (e) HVR-L2 comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and/or (f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6). In some cases, the anti-TIGIT antagonist antibody is EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS, such as at least 90%, 91%, 94%, (such as at least 90%, 91%, 94%, SEQ ID NO: %, 98% or 99% sequence identity) or QVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS (at least 95% sequence identity), such as at least 95% sequence identity, or 92% identity, such as at least 90% sequence identity a VH domain comprising an amino acid sequence having 96%, 97%, 98% or 99% sequence identity; and/or DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIK (SEQ ID NO:19) or a sequence thereof with at least 90% sequence identity (such as at least 90% 99%, 91% 91%, such as a VL domain comprising an amino acid sequence with the same identity). In some cases, the anti-TIGIT antagonist antibody has at least 90% sequence identity to SEQ ID NO:17 or a sequence thereof (eg, at least 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98 A VH domain comprising an amino acid sequence having % or 99% sequence identity, and/or at least 90% sequence identity (eg, at least 91%, 92%, 93%, 94%, 95 %, 96%, 97%, 98% or 99% sequence identity). In some cases, the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19. In some cases, the anti-TIGIT antagonist antibody has at least 90% sequence identity to SEQ ID NO:18 or a sequence thereof (eg, at least 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98 A VH domain comprising an amino acid sequence having % or 99% sequence identity, and/or at least 90% sequence identity (eg, at least 91%, 92%, 93%, 94%, 95 %, 96%, 97%, 98% or 99% sequence identity). In some cases, the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19.
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 중쇄 및 경쇄 서열을 포함하고, 여기서: (a) 상기 중쇄는 하기의 아미노산 서열: EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK(서열번호 33)를 포함하고; (b) 상기 경쇄는 하기의 아미노산 서열: DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(서열번호 34)를 포함한다.일부 경우들에서, 상기 항 TIGIT 길항제 항체는 중쇄 및 경쇄 서열을 포함하고, 여기서: (a) 상기 중쇄는 하기의 아미노산 서열: EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK(서열번호 33)를 포함하고; (b) 상기 경쇄는 하기의 아미노산 서열: DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(서열번호 34)를 포함한다.
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역(FR): DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1; WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2; GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및/또는 FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4, 또는 상기 FR 중 하나 이상 및 서열번호 7 내지 서열번호 10 중 어느 하나와 적어도 약 90% 서열 동일성(예컨대, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 또는 99% 동일성)을 갖는 이의 하나 이상의 변이체의 조합으로부터 선택된 적어도 1개, 2개, 3개, 또는 4개를 더 포함한다. 일부 경우들에서, 예를 들어, 상기 항체는 DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1; WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2; GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및 FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4를 더 포함한다.In some cases, the anti-TIGIT antagonist antibody comprises a light chain variable region framework region (FR): FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7); FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8); FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and/or a FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), or at least about 90% sequence identity (e.g., 90%, 91 %, 92%, 93%, 94%, 95%, 96%, 97%, 98%, or 99% identity). more dogs. In some cases, for example, the antibody comprises FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7); FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8); FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR들: X1은 E 또는 Q인 X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1; WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2; RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및/또는 WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4, 또는 상기 FR 중 하나 이상 및 서열번호 11 내지 서열번호 14 중 어느 하나와 적어도 약 90% 서열 동일성(예컨대, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 또는 99% 동일성)을 갖는 이의 하나 이상의 변이체의 조합으로부터 선택된 적어도 1개, 2개, 3개, 또는 4개를 더 포함한다. 상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR들: EVQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 15)의 아미노산 서열을 포함하는 FR-H1; WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2; RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및/또는 WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4, 또는 상기 FR 중 하나 이상 및 서열번호 12 내지 서열번호 15 중 어느 하나와 적어도 약 90% 서열 동일성(예컨대, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 또는 99% 동일성)을 갖는 이의 하나 이상의 변이체의 조합으로부터 선택된 적어도 1개, 2개, 3개, 또는 4개를 더 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 EVQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 15)의 아미노산 서열을 포함하는 FR-H1; WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2; RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및 WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 포함한다. 다른 경우에서, 예를 들어, 상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR들: QVQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 16)의 아미노산 서열을 포함하는 FR-H1; WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2; RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및/또는 WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4, 또는 상기 FR 중 하나 이상 및 서열번호 12 내지 서열번호 14 및 서열번호 16 중 어느 하나와 적어도 약 90% 서열 동일성(예컨대, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 또는 99% 동일성)을 갖는 이의 하나 이상의 변이체의 조합으로부터 선택된 적어도 1개, 2개, 3개, 또는 4개를 더 포함한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 QVQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 16)의 아미노산 서열을 포함하는 FR-H1; WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2; RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및 WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 포함한다. In some cases, the anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs: FR-H1 comprising the amino acid sequence of X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X 1 is E or Q; FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14), or at least about 90% sequence identity (e.g., 90%, 91 %, 92%, 93%, 94%, 95%, 96%, 97%, 98%, or 99% identity). more dogs. The anti-TIGIT antagonist antibody comprises FR-H1 comprising the amino acid sequence of the following heavy chain variable region FRs: EVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 15); FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14), or at least about 90% sequence identity (e.g., 90%, 91 %, 92%, 93%, 94%, 95%, 96%, 97%, 98%, or 99% identity). more dogs. In some cases, the anti-TIGIT antagonist antibody comprises FR-H1 comprising the amino acid sequence of EVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 15); FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14). In other instances, for example, the anti-TIGIT antagonist antibody comprises FR-H1 comprising the amino acid sequence of the following heavy chain variable region FRs: QVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 16); FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14), or at least about 90% sequence identity with one or more of said FRs and any one of SEQ ID NO: 12 to SEQ ID NO: 14 and SEQ ID NO: 16 (e.g., at least 1, 2, 3 selected from combinations of one or more variants thereof having 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, or 99% identity). dogs, or 4 more. In some cases, the anti-TIGIT antagonist antibody comprises FR-H1 comprising the amino acid sequence of QVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 16); FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
또 다른 양태에서, 항 TIGIT 길항제 항체가 제공되고, 여기서 상기 항체는 상기 제공된 임의의 경우에서와 같은 VH 및 상기 제공된 임의의 경우에서와 같은 VL을 포함하고, 여기서 상기 가변 도메인 서열들 중 하나 또는 둘 모두는 번역후 변형을 포함한다.In another aspect, an anti TIGIT antagonist antibody is provided, wherein said antibody comprises a VH as in any of the instances provided above and a VL as in any of the instances provided above, wherein one or both of said variable domain sequences are provided. All include post-translational modifications.
일부 경우들에서, 상기 항 TIGIT 길항제 항체들 중 임의의 것은 인간 TIGIT 외에도 토끼 TIGIT에 결합할 수 있다. 일부 경우들에서, 상기 기재된 항 TIGIT 길항제 항체들 중 임의의 것은 인간 TIGIT 및 시노몰구스 원숭이(시노) TIGIT 모두에 결합할 수 있다. 일부 경우들에서, 상기 기재된 항 TIGIT 길항제 항체들 중 임의의 것은 인간 TIGIT, 시노 TIGIT, 및 토끼 TIGIT에 결합할 수 있다. 일부 경우들에서, 상기 기재된 항 TIGIT 길항제 항체들 중 임의의 것은 인간 TIGIT, 시노 TIGIT, 및 토끼 TIGIT에 결합할 수 있으나, 쥐과 TIGIT에는 그렇지 않다.In some cases, any of the anti-TIGIT antagonist antibodies are capable of binding rabbit TIGIT in addition to human TIGIT. In some cases, any of the anti-TIGIT antagonist antibodies described above can bind to both human TIGIT and cynomolgus monkey (cyno) TIGIT. In some cases, any of the anti-TIGIT antagonist antibodies described above are capable of binding to human TIGIT, cyno TIGIT, and rabbit TIGIT. In some cases, any of the anti-TIGIT antagonist antibodies described above can bind human TIGIT, cyno TIGIT, and rabbit TIGIT, but not murine TIGIT.
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 인간 TIGIT에 약 10 nM 이하의 KD로 및 시노 TIGIT에 약 10 nM 이하의 KD로 결합한다(예컨대, 인간 TIGIT에 약 0.1 nM 내지 약 1 nM의 KD로 및 시노 TIGIT에 약 0.5 nM 내지 약 1 nM의 KD로 결합하고, 예컨대 인간 TIGIT에 약 0.1 nM 이하의 KD로 및 시노 TIGIT에 약 0.5 nM 이하의 KD로 결합한다). In some cases, the anti TIGIT antagonist antibody binds human TIGIT with a K D of about 10 nM or less and cyno TIGIT with a K D of about 10 nM or less (eg, between about 0.1 nM and about 1 nM of human TIGIT). binds to cyno TIGIT with a K D of about 0.5 nM to about 1 nM, such as to human TIGIT with a K D of about 0.1 nM or less and to cyno TIGIT with a K D of about 0.5 nM or less).
일부 경우들에서, 상기 항 TIGIT 길항제 항체는 TIGIT에 특이적으로 결합하고 폴리오바이러스 수용체(PVR)와의 TIGIT 상호작용을 억제하거나 차단한다(예컨대, 상기 길항제 항체는 PVR에 대한 TIGIT 결합에 의해 매개되는 세포내 신호전달을 억제한다). 일부 경우들에서, 상기 길항제 항체는 10 nM 이하(예컨대, 1 nM 내지 약 10 nM)의 IC50 값으로 인간 PVR에 대한 인간 TIGIT의 결합을 억제 또는 차단한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 TIGIT에 특이적으로 결합하고 PVR-CD226 상호작용에 영향을 주지 않고 PVR와의 TIGIT 상호작용을 억제하거나 차단한다. 일부 경우들에서, 상기 길항제 항체는 50 nM 이하(예컨대, 1 nM 내지 약 50 nM, 예컨대, 1 nM 내지 약 5 nM)의 IC50 값으로 시노 PVR에 대한 시노 TIGIT의 결합을 억제 또는 차단한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는TIGIT와의 CD226의 상호작용을 억제 및/또는 차단한다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체는 CD226 동종이량체화를 방해하는 TIGIT의 능력을 억제 및/또는 차단한다.In some cases, the anti-TIGIT antagonist antibody specifically binds TIGIT and inhibits or blocks TIGIT interaction with a poliovirus receptor (PVR) (eg, the antagonist antibody binds to a cell mediated by TIGIT binding to PVR). inhibit my signaling). In some cases, the antagonist antibody inhibits or blocks binding of human TIGIT to human PVR with an IC50 value of 10 nM or less (eg, 1 nM to about 10 nM). In some cases, the anti-TIGIT antagonist antibody specifically binds TIGIT and inhibits or blocks TIGIT interaction with PVR without affecting PVR-CD226 interaction. In some cases, the antagonist antibody inhibits or blocks binding of cyno TIGIT to cyno PVR with an IC50 value of 50 nM or less (eg, 1 nM to about 50 nM, eg, 1 nM to about 5 nM). In some cases, the anti-TIGIT antagonist antibody inhibits and/or blocks the interaction of CD226 with TIGIT. In some cases, the anti-TIGIT antagonist antibody inhibits and/or blocks the ability of TIGIT to interfere with CD226 homodimerization.
일부 경우들에서, 본원에 기재된 방법 또는 사용은 TIGIT에 대한 결합에 대해 상기 기재된 임의의 항 TIGIT 길항제 항체와 경쟁하는 단리된 항 TIGIT 길항제 항체를 사용하거나 투여하는 것을 포함할 수 있다. 예를 들어, 상기 방법은 TIGIT에 대한 결합에 대해 하기 6개의 HVR: (a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1; (b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2; (c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3; (d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1; (e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2; 및/또는 (f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3을 갖는 항 TIGIT 길항제 항체 경쟁하는 단리된 항 TIGIT 길항제 항체를 투여하는 단계를 포함할 수 있다. 본원에 기재된 방법은 또한 상기 기재된 항 TIGIT 길항제 항체와 동일한 에피토프에 결합하는 단리된 항 TIGIT 길항제 항체를 투여하는 단계를 포함할 수 있다.In some cases, a method or use described herein may comprise using or administering an isolated anti TIGIT antagonist antibody that competes with any of the anti TIGIT antagonist antibodies described above for binding to TIGIT. For example, the method comprises the following six HVRs for binding to TIGIT: (a) HVR-H1 comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1); (b) HVR-H2 comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2); (c) HVR-H3 comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3); (d) HVR-L1 comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4); (e) HVR-L2 comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and/or (f) administering an isolated anti-TIGIT antagonist antibody that competes with the anti-TIGIT antagonist antibody having HVR-L3 comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO:6). The methods described herein may also comprise administering an isolated anti TIGIT antagonist antibody that binds to the same epitope as the anti TIGIT antagonist antibody described above.
일부 양태들에서, 상기 항 TIGIT 길항제 항체는 원형 Fc 매개 작동체 기능(예컨대, 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448 또는 TJ-T6) 또는 향상된 작동체 기능(예컨대, SGN-TGT)을 갖는 항체이다. In some aspects, the anti-TIGIT antagonist antibody is a prototypical Fc mediated effector function (eg, tiragolumab, bivostolimab, ethigilumab, EOS084448 or TJ-T6) or enhanced effector function (eg, SGN-TGT). an antibody with
다른 양태들에서, 상기 항 TIGIT 길항제 항체는 Fc 매개 작동체 기능이 결여된 항체(예를 들어, 돔바날리맙, BMS-986207, ASP8374, 또는 COM902)이다. In other aspects, the anti-TIGIT antagonist antibody is an antibody that lacks Fc-mediated effector function (eg, dombanalimab, BMS-986207, ASP8374, or COM902).
일부 양태들에서, 상기 항 TIGIT 길항제 항체는 IgG1 부류 항체, 예컨대 티라골루맙, 비보스톨리맙, 돔바날리맙, BMS-986207, 에티길리맙, BGB-A1217, SGN-TGT, EOS084448(EOS-448), TJ-T6, 또는 AB308이다.In some aspects, the anti-TIGIT antagonist antibody is an IgG1 class antibody, such as tiragolumab, bivostolimab, dombanalimab, BMS-986207, ethigilumab, BGB-A1217, SGN-TGT, EOS084448 (EOS-448) , TJ-T6, or AB308.
일부 양태들에서, 상기 항 TIGIT 길항제 항체는 IgG 부류 항체, 예컨대, ASP8374 또는 COM902이다. In some aspects, the anti-TIGIT antagonist antibody is an IgG class antibody, such as ASP8374 or COM902.
상기 항체를 함유하는 조성물을 포함하여 본 발명에 유용한 항 TIGIT 길항제 항체(예컨대, 티라골루맙)는 PD-1 축 결합 길항제(예컨대, PD-L1 결합 길항제(예컨대, 항 PD-L1 길항제 항체, 예컨대, 아테졸리주맙), PD-1 결합 길항제(예컨대, 항 PD-1 길항제 항체, 예컨대, 펨브롤리주맙), 및 PD-L2 결합 길항제(예컨대, 항 PD-L2 길항제 항체))와 병용으로 사용할 수 있다. Anti-TIGIT antagonist antibodies (eg, tyragolumab) useful in the present invention, including compositions containing such antibodies, include PD-1 axis binding antagonists (eg, PD-L1 binding antagonists (eg, anti-PD-L1 antagonist antibodies, such as , atezolizumab), a PD-1 binding antagonist (eg, an anti-PD-1 antagonist antibody, such as pembrolizumab), and a PD-L2 binding antagonist (eg, an anti-PD-L2 antagonist antibody)). have.
일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 TIGIT 신호전달을 억제하는 기능을 한다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 TIGIT가 이의 결합 짝들에 결합하는 것을 억제한다. 예시적인 TIGIT 결합 짝은 CD155(PVR), CD112(PVRL2 또는 넥틴-2), 및 CD113(PVRL3 또는 넥틴-3)을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 TIGIT 및 CD155 사이의 결합을 억제할 수 있다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 TIGIT 및 CD112 사이의 결합을 억제할 수 있다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 TIGIT 및 CD113 사이의 결합을 억제할 수 있다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 면역 세포에서 TIGIT 매개 세포 신호전달을 억제한다. 일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 조절 T 세포를 고갈시킴으로써(예컨대, FcγR와 맞물릴 때) TIGIT를 억제한다.In some embodiments, the anti-TIGIT antagonist antibody functions to inhibit TIGIT signaling. In some embodiments, the anti TIGIT antagonist antibody inhibits binding of TIGIT to its binding partners. Exemplary TIGIT binding partners include CD155 (PVR), CD112 (PVRL2 or Nectin-2), and CD113 (PVRL3 or Nectin-3). In some embodiments, the anti-TIGIT antagonist antibody is capable of inhibiting binding between TIGIT and CD155. In some embodiments, the anti-TIGIT antagonist antibody is capable of inhibiting binding between TIGIT and CD112. In some embodiments, the anti-TIGIT antagonist antibody is capable of inhibiting binding between TIGIT and CD113. In some embodiments, the anti-TIGIT antagonist antibody inhibits TIGIT-mediated cellular signaling in immune cells. In some embodiments, the anti TIGIT antagonist antibody inhibits TIGIT by depleting regulatory T cells (eg, when engaged with FcγRs).
일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 단일클론 항체이다. 일부 구현예들에서, 상기 항 TIGIT 1 항체는 Fab, Fab’-SH, Fv, scFv 및 (Fab’)2 단편으로 이루어진 군으로부터 선택되는 항체 단편이다. 일부 구현예들에서, 상기 항 TIGIT 항체는 인간화 항체이다. 일부 구현예들에서, 상기 항 TIGIT 항체는 인간 항체이다. 일부 구현예들에서, 본원에 기재된 항 PD-L1 항체는 인간 TIGIT에 결합한다. 일부 구현예들에서, 상기 항 TIGIT 항체는 Fc 융합 단백질이다. In some embodiments, the anti-TIGIT antagonist antibody is a monoclonal antibody. In some embodiments, the anti-TIGIT 1 antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv and (Fab') 2 fragments. In some embodiments, the anti-TIGIT antibody is a humanized antibody. In some embodiments, the anti-TIGIT antibody is a human antibody. In some embodiments, an anti-PD-L1 antibody described herein binds to human TIGIT. In some embodiments, the anti-TIGIT antibody is an Fc fusion protein.
일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙(MTIG7192A, RG6058 or RO7092284), 비보스톨리맙(MK-7684), ASP8374 (PTZ-201), EOS884448 (EOS-448), SEA-TGT (SGN-TGT)), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), IBI939, 돔바날리맙(AB154), M6223, AB308, AB154, TJ-T6, MG1131, NB6253, HLX301, HLX53, SL-9258(TIGIT-Fc-LIGHT), STW264, 및 YBL-012로 이루어진 군으로부터 선택된다. 일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙(MTIG7192A, RG6058 or RO7092284), 비보스톨리맙(MK-7684), ASP8374 (PTZ-201), EOS-448, 및 SEA-TGT(SGN-TGT)로 이루어진 군으로부터 선택된다. 상기 항 TIGIT 항체는 티라골루맙(MTIG7192A, RG6058 또는 RO7092284)일 수 있다.In some embodiments, the anti-TIGIT antibody is tyragolumab (MTIG7192A, RG6058 or RO7092284), vivostolimab (MK-7684), ASP8374 (PTZ-201), EOS884448 (EOS-448), SEA-TGT (SGN) -TGT)), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), IBI939, dombanalimab (AB154), M6223, AB308, AB154, TJ-T6, MG1131, NB6253, HLX301, HLX53, SL-9258 (TIGIT-Fc-LIGHT), STW264, and YBL-012. In some embodiments, the anti-TIGIT antibody is tyragolumab (MTIG7192A, RG6058 or RO7092284), vivostolimab (MK-7684), ASP8374 (PTZ-201), EOS-448, and SEA-TGT (SGN-TGT). ) is selected from the group consisting of The anti-TIGIT antibody may be tiragolumab (MTIG7192A, RG6058 or RO7092284).
본원에 개시된 방법 및 이의 제조 방법에 유용한 항 TIGIT 항체의 비제한적 예는 PCT 공보 제WO2018183889A1호, WO2019129261A1호, WO2016106302A9호, WO2018033798A1호, WO2020020281A1호, WO2019023504A1호, WO2017152088A1호, WO2016028656A1호, WO2017030823A2호, WO2018204405A1호, WO2019152574A1호, 및 WO2020041541A2; 미국 특허 제US 10,189,902호, US 10,213,505호, US 10,124,061호, US 10,537,633호, 및 US 10,618,958호; 및 미국 특허 공보 제2020/0095324호, 2019/0112375호, 2018/0371083호, 및 2020/0062859호에 기재되어 있으며, 이는 그 전체가 본원에 원용된다. 본원에 개시된 방법에 유용한 항 TIGIT 항체 및 이의 제조 방법에 관한 추가적인 비제한적 예는 PCT 공보 제WO2018204363A1호, WO2018047139A1호, WO2019175799A2호, WO2018022946A1호, WO2015143343A2호, WO2018218056A1호, WO2019232484A1호, WO2019079777A1호, WO2018128939A1호, WO2017196867A1호, WO2019154415A1호, WO2019062832A1호, WO2018234793A3호, WO2018102536A1호, WO2019137548A1호, WO2019129221A1호, WO2018102746A1호, WO2018160704A9호, WO2020041541A2호, WO2019094637A9호, WO2017037707A1호, WO2019168382A1호, WO2006124667A3호, WO2017021526A1호, WO2017184619A2호, WO2017048824A1호, WO2019032619A9호, WO2018157162A1호, WO2020176718A1호, WO2020047329A1호, WO2020047329A1호, WO2018220446A9호; 미국 특허 제US 9,617,338호, US 9,567,399호, US 10,604,576호, 및 US 9,994,637호; 및 특허 공보 제US 2018/0355040호, US 2019/0175654호, US 2019/0040154호, US 2019/0382477호, US 2019/0010246호, US 2020/0164071호, US 2020/0131267호, US 2019/0338032호, US 2019/0330351호, US 2019/0202917호, US 2019/0284269호, US 2018/0155422호, US 2020/0040082호, US 2019/0263909호, US 2018/0185480호, US 2019/0375843호, US 2017/0037133호, US 2019/0077869호, US 2019/0367579호, US 2020/0222503호, US 2020/0283496호, CN109734806A호, 및 CN110818795A호에 기재되어 있으며, 이는 그 전체가 본원에 원용된다.Non-limiting examples of anti-TIGIT antibodies useful in the methods disclosed herein and methods of making them include PCT Publication Nos. WO2018183889A1, WO2019129261A1, WO2016106302A9, WO2018033798A1, WO2020020281A1, WO2019023504A1, WO2017152088A1, WO2018405030856A1, WO2016402860823A , WO2019152574A1, and WO2020041541A2; US Pat. Nos. 10,189,902, US 10,213,505, US 10,124,061, US 10,537,633, and US 10,618,958; and US Patent Publication Nos. 2020/0095324, 2019/0112375, 2018/0371083, and 2020/0062859, which are incorporated herein by reference in their entirety. Additional non-limiting examples of anti-TIGIT antibodies useful in the methods disclosed herein and methods of making them are described in PCT Publication Nos. WO2018204363A1, WO2018047139A1, WO2019175799A2, WO2018022946A1, WO2015143343A2, WO2018218056A1, WO2019232484A1, WO2019079777 WO2017196867A1, WO2019154415A1, WO2019062832A1, WO2018234793A3, WO2018102536A1, WO2019137548A1, WO2019129221A1, WO2018102746A1, WO2018160704A9, WO2020041541A2, WO1824A No. , WO2019032619A9, WO2018157162A1, WO2020176718A1, WO2020047329A1, WO2020047329A1, WO2018220446A9; US Pat. Nos. 9,617,338, US 9,567,399, US 10,604,576, and US 9,994,637; and Patent Publication Nos. US 2018/0355040, US 2019/0175654, US 2019/0040154, US 2019/0382477, US 2019/0010246, US 2020/0164071, US 2020/0131267, US 2019/0338032 Nos., US 2019/0330351, US 2019/0202917, US 2019/0284269, US 2018/0155422, US 2020/0040082, US 2019/0263909, US 2018/0185480, US 2019/0375843, US 2017/0037133, US 2019/0077869, US 2019/0367579, US 2020/0222503, US 2020/0283496, CN109734806A, and CN110818795A, which are incorporated herein by reference in their entirety.
본원에 개시된 방법에 유용한 항 TIGIT 항체는 ASP8374(PTZ-201), BGB-A1217, BMS-986207(ONO-4686), COM902(CGEN-15137), M6223, IBI939, EOS-448, 돔바날리맙(AB154), 비보스톨리맙(MK-7684), 및 SEA-TGT(SGN-TGT)를 포함한다. 본원에 개시된 방법에 유용한 추가적인 항 TIGIT 항체는 하기를 포함한다: AGEN1307; AGEN1777; 항체 클론 pab2197 및 pab2196(아게누스(Agenus Inc.)); 항체 클론 TBB8, TDC8, 3TB3, 5TB10, 및 D1Y1A(안후이 안케 생명 공학 그룹(Anhui Anke Biotechnology Group Co. Ltd.)), 항체 클론 MAB1, MAB2, MAB3, MAB4, MAB5, MAB6, MAB 7, MAB8, MAB9, MAB 10, MAB 11, MAB 12, MAB13, MAB 14, MAB 15, MAB 16, MAB 17, MAB 18, MAB19, MAB20, MAB21(아스텔라스 제약(Astellas Pharma)/포텐자 테라퓨틱스(Potenza Therapeutics)), 항체 클론 hu1217-1-1 및 hu1217-2-2 (베이진(BeiGene)), 항체 클론 4D4 및 19G(브리검 & 여성 병원(Brigham & Women’s Hospital)), 항체 클론 11G11, 10D7, 15A6, 22G2, TIGIT G2a, 및 TIGIT G1 D265A - 변형된 중쇄 불변 영역(브리스톨-마이어스 스큅(Bristol-Myers Squibb))을 갖는 상기 항체를 포함함; 항체 클론 10A7, CPA.9.086, CPA.9.083.H4(S241P), CPA.9.086.H4(S241P), CHA.9.547.7.H4(S241P) 및 CHA.9.547.13.H4(S241P)(컴퓨젠(Compugen)); 항 PVRIG/항 TIGIT 이중특이적 항체(컴퓨젠), 항체 클론 315293, 328189, 350426, 326504, 및 331672(프레드 허친슨 암 연구 센터(Fred Hutchinson Cancer Research Center)); 항체 클론 T-01, T-02, T-03, T-04, T-05, T-06, T-07, T-08, T-09, 및 T-10(젠선 바이오파마(Gensun BioPharma Inc.)); 항체 클론 1H6, 2B11, 3A10, 4A5, 4A9, 4H5, 6A2, 6B7, 7F4, 8E1, 8G3, 9F4, 9G6, 10C1, 10F10, 11G4, 12B7, 12C8, 15E9, 16C11, 16D6, and 16E10 (허페이 루이다 면역약물 연구소(Hefei Ruida Immunological Drugs Research Institute Co. Ltd.)); 항체 클론 h3C5H1, h3C5H2, h3C5H3, h3C5H4, h3C5H3-1, h3C5H3-2, h3C5H3-3, h3C5L1, 및 h3C5L2(IGM 생명과학(IGM Biosciences Inc.)); 항체 클론 90D9, 101E1, 116H8, 118A12, 131A12, 143B6, 167F7, 221F11, 222H4, 327C9, 342A9, 344F2, 349H6, 및 350D10(아이-맙 바이오파마(I-Mab Biopharma)); 항체 클론 ADI-27238, ADI-30263, ADI-30267, ADI-30268, ADI-27243, ADI-30302, ADI-30336, ADI-27278, ADI-30193, ADI-30296, ADI-27291, ADI-30283, ADI-30286, ADI-30288, ADI27297, ADI-30272, ADI-30278, ADI-27301, ADI-30306, 및 ADI-30311(이노벤트 바이오로직스(Innovent Biologics, Inc.)); 항체 클론 26518, 29478, 26452, 29487, 29489, 31282, 26486, 29494, 29499, 26521, 29513, 26493, 29520, 29523, 29527, 31288, 32919, 32931, 26432, 및 32959(아이테오스 테라퓨틱스(iTeos Therapeutics)); 항체 클론 m1707, m1708, m1709, m1710, m1711, h1707, h1708, h1709, h1710, 및 h1711(강소 헹루이 메디슨(Jiangsu Hengrui Medicine Co. Ltd.)); 항체 클론 TIG1, TIG2, 및 TIG3(JN 생명과학(JN Biosciences LLC)); 항체 클론(예컨대, KY01, KY02, KY03, KY04, KY05, KY06, KY07, KY08, KY09, KY10, K11, K12, K13, K14, K15, K16, K17, K18, K19, K20, K21, K22, K23 Kymab TIGIT(항체 2), 및 툴(Tool) TIGIT(항체 4)(키맙 리미티드(Kymab Limited)); 이중특이적 항체 1D05/인하우스 항 TIGIT + 1D05 (항 PD-L1) 천연 가변 도메인 및 키맙 TIGIT 항원 결합 부위(ABS) 도메인(이중특이적 1), 인하우스 항 TIGIT/1D05 + 키맙 TIGIT 천연 가변 도메인 및 1D05 ABS 도메인(이중특이적 2), 툴 항 TIGIT/툴 항 PD-L1 + 툴 항 TIGIT 천연 가변 도메인 및 툴 항 PD-L1 ABS 도메인(이중특이적 3), 툴 항 PD-L1/툴 항 TIGIT + 툴 항 PD-L1 천연 가변 도메인 및 툴 항 TIGIT ABS 도메인(이중특이적 4)(키맙 리미티드); 항체 클론 및 항체 변이체 14D7, 26B10, Hu14D7, Hu26B10, 14A6, Hu14A6, 28H5, 31C6, Hu31C6, 25G10, MBS43, 37D10, 18G10, 11A11, c18G10, 및 LB155.14A6.G2.A8(머크(Merck)); 에티길리맙(OMP-313M32)(메레오바이오파마(Mereo BioPharma)); 항체 클론 64G1E9B4, 100C4E7D11, 83G5H11C12, 92E9D4B4, 104G12E12G2, 121C2F10B5, 128E3F10F3F2, 70A11A8E6, 11D8E124A, 16F10H12C11, 8F2D8E7, 48B5G4E12, 139E2C2D2, 128E3G7F5, AS19584, AS19852, AS19858, AS19886, AS19887, AS19888, AS20160, AS19584VH26, AS19584VH29, AS19584VH30, AS19584VH31, AS19886VH5, AS19886VH8, AS19886VH9, AS19886VH10, AS19886VH19, AS19886VH20, AS19584VH28-Fc, AS19886VH5-Fc, AS19886VH8-Fc, AS19584-Fc, and AS19886-Fc(난징 레전드 바이오테크놀로지(Nanjing Legend Biotechnology Co. Ltd.)); 항체 클론 ARE 클론: Ab58, Ab69, Ab75, Ab133, Ab177, Ab122, Ab86, Ab180, Ab83, Ab26, Ab20, Ab147, Ab12, Ab66, Ab176, Ab96, Ab123, Ab109, Ab149, Ab34, Ab61, Ab64, Ab105, Ab108, Ab178, Ab166, Ab29, Ab135, Ab171, Ab194, Ab184, Ab164, Ab183, Ab158, Ab55, Ab136, Ab39, Ab159, Ab151, Ab139, Ab107, Ab36, Ab193, Ab115, Ab106, Ab13f8, Ab127, Ab165, Ab155, Ab19, Ab6, Ab187, Ab179, Ab65, Ab114, Ab102, Ab94, Ab163, Ab110, Ab80, Ab92, Ab117, Ab162, Ab121, Ab195, Ab84, Ab161, Ab198, Ab24, Ab98, Ab116, Ab174, Ab196, Ab51, Ab91, Ab185, Ab23, Ab7, Ab95, Ab100, Ab140, Ab145, Ab150, Ab168, Ab54, Ab77, Ab43, Ab160, Ab82, Ab189, Ab17, Ab103, Ab18, Ab130, Ab132, Ab134, Ab144; ARG 클론: Ab2, Ab47, Ab49, Ab31, Ab53, Ab40, Ab5, Ab9, Ab48, Ab4, Ab10, Ab37, Ab33, Ab42, Ab45; ARV 클론: Ab44, Ab97, Ab81, Ab188, Ab186, Ab62, Ab57, Ab192, Ab73, Ab60, Ab28, Ab32, Ab78, Ab14, Ab152, Ab72, Ab137, Ab128, Ab169, Ab87, Ab74, Ab172, Ab153, Ab120, Ab13, Ab113, Ab16, Ab56, Ab129, Ab50, Ab90, Ab99, Ab3, Ab148, Ab124, Ab22, Ab41, Ab119, Ab157, Ab27, Ab15, Ab191, Ab190, Ab79, Ab181, Ab146, Ab167, Ab88, Ab199, Ab71, Ab85, Ab59, Ab141, Ab68, Ab143, Ab46, Ab197, Ab175, Ab156, Ab63, Ab11, Ab182, Ab89, Ab8, Ab101, Ab25, Ab154, Ab21, Ab111, Ab118, Ab173, Ab38, Ab76, Ab131, Ab1, Ab67, Ab70, Ab170, Ab30, Ab93, Ab142, Ab104, Ab112, Ab35, Ab126, 및 Ab125(리겔 제약(Rigel Pharmaceuticals, Inc.)); CASC-674(시애틀 제네틱스(Seattle Genetics)); 항체 클론 2, 2C, 3, 5, 13, 13A, 13B, 13C, 13D, 14, 16, 16C, 16D, 16E, 18, 21, 22, 25, 25A, 25B, 25C, 25D, 25E, 27, 54, 13 IgG2a 푸코실화, 13 hIgG1 야생형, 및 13 LALA-PG(시애틀 제네틱스); JS006(상하이 준시 바이오사이언스(Shanghai Junshi Biosciences Ltd.)); 항 TIGIT Fc 항체 및 이중특이적 항체 PD1 x TIGIT(젠코(Xencor)), 항체 클론 VSIG9#1(Vsig9.01) 및 258-CS1#4 (#4)(예루살렘 히브리 대학교 이섬 연구 개발 회사(Yissum Research Development Company of The Hebrew University Of Jerusalem Ltd.)); YH29143(유한(Yuhan Co, Ltd.)); 항체 클론 S02, S03, S04, S05, S06, S11, S12, S14, S19, S32, S39, S43, S62, S64, F01, F02, F03, F04, 32D7, 101H3, 10A7, 및 1F4(유한); 항 zB7R1 클론 318.4.1.1(E9310), 318.28.2.1(E9296), 318.39.1.1(E9311), 318.59.3.1(E9400), 및 318.77.1.10(자이모 제테틱스(ZymoGenetics, Inc)). Anti-TIGIT antibodies useful in the methods disclosed herein include ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS-448, dombanalimab (AB154). ), vivostolimab (MK-7684), and SEA-TGT (SGN-TGT). Additional anti-TIGIT antibodies useful in the methods disclosed herein include: AGEN1307; AGEN1777; antibody clones pab2197 and pab2196 (Agenus Inc.); Antibody clones TBB8, TDC8, 3TB3, 5TB10, and D1Y1A (Anhui Anke Biotechnology Group Co. Ltd.), antibody clones MAB1, MAB2, MAB3, MAB4, MAB5, MAB6, MAB 7, MAB8, MAB9 , MAB 10, MAB 11, MAB 12, MAB13, MAB 14, MAB 15, MAB 16, MAB 17, MAB 18, MAB19, MAB20, MAB21 (Astellas Pharma/Potenza Therapeutics )), antibody clones hu1217-1-1 and hu1217-2-2 (BeiGene), antibody clones 4D4 and 19G (Brigham & Women's Hospital), antibody clones 11G11, 10D7, 15A6, 22G2, TIGIT G2a, and TIGIT G1 D265A—including these antibodies with modified heavy chain constant regions (Bristol-Myers Squibb); Antibody clones 10A7, CPA.9.086, CPA.9.083.H4 (S241P), CPA.9.086.H4 (S241P), CHA.9.547.7.H4 (S241P) and CHA.9.547.13.H4 (S241P) (Compugen (Compugen)); anti PVRIG/anti TIGIT bispecific antibody (Compugen), antibody clones 315293, 328189, 350426, 326504, and 331672 (Fred Hutchinson Cancer Research Center); Antibody clones T-01, T-02, T-03, T-04, T-05, T-06, T-07, T-08, T-09, and T-10 (Gensun BioPharma Inc.) .)); Antibody clones 1H6, 2B11, 3A10, 4A5, 4A9, 4H5, 6A2, 6B7, 7F4, 8E1, 8G3, 9F4, 9G6, 10C1, 10F10, 11G4, 12B7, 12C8, 15E9, 16C11, 16D6, and 16E10 (Hefei Ruida) Hefei Ruida Immunological Drugs Research Institute Co. Ltd.); antibody clones h3C5H1, h3C5H2, h3C5H3, h3C5H4, h3C5H3-1, h3C5H3-2, h3C5H3-3, h3C5L1, and h3C5L2 (IGM Biosciences Inc.); antibody clones 90D9, 101E1, 116H8, 118A12, 131A12, 143B6, 167F7, 221F11, 222H4, 327C9, 342A9, 344F2, 349H6, and 350D10 (I-Mab Biopharma); Antibody clones ADI-27238, ADI-30263, ADI-30267, ADI-30268, ADI-27243, ADI-30302, ADI-30336, ADI-27278, ADI-30193, ADI-30296, ADI-27291, ADI-30283, ADI-30286, ADI-30288, ADI27297, ADI-30272, ADI-30278, ADI-27301, ADI-30306, and ADI-30311 (Innovent Biologics, Inc.); Antibody clones 26518, 29478, 26452, 29487, 29489, 31282, 26486, 29494, 29499, 26521, 29513, 26493, 29520, 29523, 29527, 31288, 32919, 32931, 26432, and 32959 (Aiteos Therapeutics ( iTeos Therapeutics)); antibody clones m1707, m1708, m1709, m1710, m1711, h1707, h1708, h1709, h1710, and h1711 (Jiangsu Hengrui Medicine Co. Ltd.); antibody clones TIG1, TIG2, and TIG3 (JN Biosciences LLC); Antibody clones (eg, KY01, KY02, KY03, KY04, KY05, KY06, KY07, KY08, KY09, KY10, K11, K12, K13, K14, K15, K16, K17, K18, K19, K20, K21, K22, K23 Kymab TIGIT (antibody 2), and Tool TIGIT (antibody 4) (Kymab Limited); bispecific antibody 1D05/in-house anti TIGIT + 1D05 (anti-PD-L1) native variable domain and kymab TIGIT Antigen binding site (ABS) domain (bispecific 1), in house anti TIGIT/1D05 + chimap TIGIT native variable domain and 1D05 ABS domain (bispecific 2), tool anti TIGIT/tool anti PD-L1 + tool anti TIGIT Native variable domain and tool anti PD-L1 ABS domain (bispecific 3), tool anti PD-L1/tool anti TIGIT + tool anti PD-L1 native variable domain and tool anti TIGIT ABS domain (bispecific 4) (Kimab) Ltd): antibody clones and antibody variants 14D7, 26B10, Hu14D7, Hu26B10, 14A6, Hu14A6, 28H5, 31C6, Hu31C6, 25G10, MBS43, 37D10, 18G10, 11A11, c18G10, and LB155.14A6.G2.A8 (Merck (Merck) )); Etigilimab (OMP-313M32) (Mereo BioPharma); Antibody clones 64G1E9B4, 100C4E7D11, 83G5H11C12, 92E9D4B4, 104G12E12G2, 121C2F102F2, 82D2, 121C2F10B5, 16F2, 703F11A, 48G1E9B4, 100C4E7D11F3 128E3G7F5, AS19584, AS19852, AS19858, AS19886, AS19887, AS19888, AS20160, AS19584VH26, AS19584VH29, AS19584VH30, AS19584VH31, AS19886VH 5, AS19886VH8, AS19886VH9, AS19886VH10, AS19886VH19, AS19886VH20, AS19584VH28-Fc, AS19886VH5-Fc, AS19886VH8-Fc, AS19584-Fc, and AS19886-Fc (Nanjing Legend Biotechnology Co. Ltd.)); Antibody clones ARE clones: Ab58, Ab69, Ab75, Ab133, Ab177, Ab122, Ab86, Ab180, Ab83, Ab26, Ab20, Ab147, Ab12, Ab66, Ab176, Ab96, Ab123, Ab109, Ab149, Ab34, Ab61, Ab64, Ab105 , Ab108, Ab178, Ab166, Ab29, Ab135, Ab171, Ab194, Ab184, Ab164, Ab183, Ab158, Ab55, Ab136, Ab39, Ab159, Ab151, Ab139, Ab107, Ab36, Ab193, Ab115, Ab106, Ab13f8, Ab127, Ab165 , Ab155, Ab19, Ab6, Ab187, Ab179, Ab65, Ab114, Ab102, Ab94, Ab163, Ab110, Ab80, Ab92, Ab117, Ab162, Ab121, Ab195, Ab84, Ab161, Ab198, Ab24, Ab98, Ab116, Ab174, Ab196 , Ab51, Ab91, Ab185, Ab23, Ab7, Ab95, Ab100, Ab140, Ab145, Ab150, Ab168, Ab54, Ab77, Ab43, Ab160, Ab82, Ab189, Ab17, Ab103, Ab18, Ab130, Ab132, Ab134, Ab144; ARG clones: Ab2, Ab47, Ab49, Ab31, Ab53, Ab40, Ab5, Ab9, Ab48, Ab4, Ab10, Ab37, Ab33, Ab42, Ab45; ARV clones: Ab44, Ab97, Ab81, Ab188, Ab186, Ab62, Ab57, Ab192, Ab73, Ab60, Ab28, Ab32, Ab78, Ab14, Ab152, Ab72, Ab137, Ab128, Ab169, Ab87, Ab74, Ab172, Ab153, Ab120 , Ab13, Ab113, Ab16, Ab56, Ab129, Ab50, Ab90, Ab99, Ab3, Ab148, Ab124, Ab22, Ab41, Ab119, Ab157, Ab27, Ab15, Ab191, Ab190, Ab79, Ab181, Ab146, Ab167, Ab88, Ab199 , Ab71, Ab85, Ab59, Ab141, Ab68, Ab143, Ab46, Ab197, Ab175, Ab156, Ab63, Ab11, Ab182, Ab89, Ab8, Ab101, Ab25, Ab154, Ab21, Ab111, Ab118, Ab173, Ab38, Ab76, Ab131 , Ab1, Ab67, Ab70, Ab170, Ab30, Ab93, Ab142, Ab104, Ab112, Ab35, Ab126, and Ab125 (Rigel Pharmaceuticals, Inc.); CASC-674 (Seattle Genetics); Antibody clones 2, 2C, 3, 5, 13, 13A, 13B, 13C, 13D, 14, 16, 16C, 16D, 16E, 18, 21, 22, 25, 25A, 25B, 25C, 25D, 25E, 27, 54, 13 IgG2a fucosylation, 13 hIgG1 wild-type, and 13 LALA-PG (Seattle Genetics); JS006 (Shanghai Junshi Biosciences Ltd.); Anti-TIGIT Fc antibody and bispecific antibody PD1 x TIGIT (Xencor), antibody clones VSIG9#1 (Vsig9.01) and 258-CS1#4 (#4) (Yissum Research, Hebrew University, Jerusalem) Development Company of The Hebrew University Of Jerusalem Ltd.)); YH29143 (Yuhan Co, Ltd.); antibody clones S02, S03, S04, S05, S06, S11, S12, S14, S19, S32, S39, S43, S62, S64, F01, F02, F03, F04, 32D7, 101H3, 10A7, and 1F4 (limited); Anti zB7R1 clones 318.4.1.1 (E9310), 318.28.2.1 (E9296), 318.39.1.1 (E9311), 318.59.3.1 (E9400), and 318.77.1.10 (ZymoGenetics, Inc).
일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙, ASP8374(PTZ-201), BGB-A1217, BMS-986207(ONO-4686), COM902(CGEN-15137), M6223, IBI939, EOS884448(EOS-448), 돔바날리맙(AB154), 비보스톨리맙(MK-7684), 및 SEA-TGT(SGN-TGT)로 이루어진 군으로부터 선택된다. ASP874(PTZ-201)는 PCT 공보 제WO2018183889A1호 및 미국 특허 공보 제2020/0095324호에 기재된 항 TIGIT 단일클론 항체이다. BGB-A1217은 PCT 공보 제WO2019129261A1호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. BMS-986207(ONO-4686)은 PCT 공보 제WO2016106302A9호, 미국 특허 제10,189,902호 및 미국 특허 공보 제2019/0112375호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. COM902(CGEN-15137)는 PCT 공보 제WO2018033798A1호 및 미국 특허 제10,213,505호 및 제10,124,061호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. IBI939는 PCT 공보 제WO2020020281A1호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. EOS884448(EOS-448)은 PCT 공보 제WO2019023504A1호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. 돔바날리맙(AB154)은 PCT 공보 제WO2017152088A1호 및 미국 특허 제10,537,633호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. 비보스톨리맙(MK-7684)은 PCT 공보 제WO2016028656A1호, WO2017030823A2호, WO2018204405A1호, 및/또는 WO2019152574A1호, 미국 특허 제10,618,958호 및 미국 특허 공보 제2018/0371083호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. SEA-TGT(SGN-TGT)는 PCT 공보 제WO2020041541A2호 및 미국 특허 공보 제2020/0062859호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. In some embodiments, the anti-TIGIT antibody is tyragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS- 448), dombanalimab (AB154), bivostolimab (MK-7684), and SEA-TGT (SGN-TGT). ASP874 (PTZ-201) is an anti-TIGIT monoclonal antibody described in PCT Publication No. WO2018183889A1 and US Patent Publication No. 2020/0095324. BGB-A1217 is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2019129261A1. BMS-986207 (ONO-4686) is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2016106302A9, U.S. Patent No. 10,189,902, and U.S. Patent Publication No. 2019/0112375. COM902 (CGEN-15137) is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2018033798A1 and US Patent Nos. 10,213,505 and 10,124,061. IBI939 is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2020020281A1. EOS884448 (EOS-448) is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2019023504A1. Dombanalimab (AB154) is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2017152088A1 and US Patent No. 10,537,633. Vivostolimab (MK-7684) is an anti-TIGIT monoclonal antibody as described in PCT Publication Nos. WO2016028656A1, WO2017030823A2, WO2018204405A1, and/or WO2019152574A1, U.S. Patent No. 10,618,958, and U.S. Patent Publication No. 2018/0371083 to be. SEA-TGT (SGN-TGT) is an anti-TIGIT monoclonal antibody as described in PCT Publication No. WO2020041541A2 and US Patent Publication No. 2020/0062859.
일부 구현예들에서, 상기 항 TIGIT 길항제 항체는 티라골루맙(CAS 등록 번호: 1918185-84-8)이다. 티라골루맙(제넨텍)은 MTIG7192A, RG6058 또는 RO7092284로도 공지되어 있다. 티라골루맙은 PCT 공보 제WO2003072305A8호, WO2004024068A3호, WO2004024072A3호, WO2009126688A2호, WO2015009856A2호, WO2016011264A1호, WO2016109546A2호, WO2017053748A2호, 및 WO2019165434A1호, 및 미국 특허 공보 제2017/0044256호, 2017/0037127호, 2017/0145093호, 2017/260594호, 2017/0088613호, 2018/0186875호, 2019/0119376호 및 미국 특허 제US9873740B2호, US10626174B2호, US10611836B2호, US9499596B2호, US8431350B2호, US10047158B2호, 및 US10017572B2호에 기재된 바와 같은 항 TIGIT 단일클론 항체이다. In some embodiments, the anti-TIGIT antagonist antibody is tiragolumab (CAS Accession Number: 1918185-84-8). Tiragolumab (Genentech) is also known as MTIG7192A, RG6058 or RO7092284. Tiragolumab is disclosed in PCT Publication Nos. WO2003072305A8, WO2004024068A3, WO2004024072A3, WO2009126688A2, WO2015009856A2, WO2016011264A1, WO2016109546A2, WO2017053748A2, and WO2019165434A1, and US Patent Publication Nos. 2017/0044 2017/0145093, 2017/260594, 2017/0088613, 2018/0186875, 2019/0119376 and US Patents US9873740B2, US10626174B2, US10611836B2, US9499596B2, US8431350B2, US10047158B2, and US10017572B2 Anti-TIGIT monoclonal antibody as described.
일부 구현예들에서, 상기 항 TIGIT 항체는 본원에 개시된 항 TIGIT 항체들 중 임의의 것의 적어도 1개, 2개, 3개, 4개, 5개, 또는 6개의 상보성 결정 영역(CDR)을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 항체는 본원에 개시된 항 TIGIT 항체들 중 임의의 것의 6개의 CDR을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙, ASP8374(PTZ-201), BGB-A1217, BMS-986207(ONO-4686), COM902(CGEN-15137), M6223, IBI939, EOS884448(EOS-448), 돔바날리맙(AB154), 비보스톨리맙(MK-7684), 및 SEA-TGT(SGN-TGT)로 이루어진 군으로부터 선택된 항체들 중 어느 하나의 6개의 CDR을 포함한다. In some embodiments, the anti-TIGIT antibody comprises at least one, two, three, four, five, or six complementarity determining regions (CDRs) of any of the anti-TIGIT antibodies disclosed herein. . In some embodiments, the anti-TIGIT antibody comprises 6 CDRs of any of the anti-TIGIT antibodies disclosed herein. In some embodiments, the anti-TIGIT antibody is tyragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS- 448), dombanalimab (AB154), bivostolimab (MK-7684), and SEA-TGT (SGN-TGT).
일부 구현예들에서, 상기 항 TIGIT 항체는 중쇄 및 경쇄를 포함하고, 여기서 상기 중쇄는 본원에 개시된 항 TIGIT 항체들 중 어느 하나의 중쇄 가변 영역(VH) 서열을 포함하고 상기 경쇄는 동일한 항체의 경쇄 가변 영역(VL)을 포함한다. 일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙, ASP8374(PTZ-201), BGB-A1217, BMS-986207(ONO-4686), COM902(CGEN-15137), M6223, IBI939, EOS884448(EOS-448), 돔바날리맙(AB154), 비보스톨리맙(MK-7684), 및 SEA-TGT(SGN-TGT)로 이루어진 군으로부터 항 TIGIT 항체의 VH 및 VL을 포함한다. In some embodiments, the anti-TIGIT antibody comprises a heavy chain and a light chain, wherein the heavy chain comprises a heavy chain variable region (VH) sequence of any one of the anti-TIGIT antibodies disclosed herein and the light chain is a light chain of the same antibody. variable region (VL). In some embodiments, the anti-TIGIT antibody is tyragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS- 448), dombanalimab (AB154), vivostolimab (MK-7684), and SEA-TGT (SGN-TGT).
일부 구현예들에서, 상기 항 TIGIT 항체는 본원에 개시된 항 TIGIT 항체들 중 임의의 것의 중쇄 및 경쇄를 포함한다. 일부 구현예들에서, 상기 항 TIGIT 항체는 티라골루맙, ASP8374(PTZ-201), BGB-A1217, BMS-986207(ONO-4686), COM902(CGEN-15137), M6223, IBI939, EOS884448(EOS-448), 돔바날리맙(AB154), 비보스톨리맙(MK-7684), 및 SEA-TGT(SGN-TGT)로 이루어진 군으로부터 항 TIGIT 항체의 중쇄 및 경쇄를 포함한다. In some embodiments, the anti-TIGIT antibody comprises the heavy and light chains of any of the anti-TIGIT antibodies disclosed herein. In some embodiments, the anti-TIGIT antibody is tyragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS- 448), dombanalimab (AB154), bivostolimab (MK-7684), and SEA-TGT (SGN-TGT).
일부 구현예들에서, 본원에 기재된 구현예들 중 임의의 것에 따른 항 TIGIT 길항제 항체는 하기의 섹션 C에 기재된 바와 같이 단독으로 또는 병용으로 상기 특징들 중 임의의 것을 수반할 수 있다. In some embodiments, an anti TIGIT antagonist antibody according to any of the embodiments described herein may carry any of the above features, alone or in combination, as described in Section C below.
B. PD-1 축 결합 길항제B. PD-1 axis binding antagonists
본원에서는 유효량의 PD-1 축 결합 길항제를 대상체에게 투여하는 단계를 포함하는, 상기 대상체(예컨대, 인간)에서 암을 치료하는 방법이 제공된다. PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제, 및 PD-L2 결합 길항제를 포함할 수 있다. 임의의 적합한 PD-1 축 결합 길항제가 사용될 수 있다.Provided herein are methods of treating cancer in a subject (eg, a human) comprising administering to the subject an effective amount of a PD-1 axis binding antagonist. The PD-1 axis binding antagonist may include a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist. Any suitable PD-1 axis binding antagonist may be used.
1. PD-L1 결합 길항제1. PD-L1 Binding Antagonists
일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1이 하나 이상의 이의 리간드 결합 짝에 결합하는 것을 억제한다. 다른 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1이 PD-1에 결합하는 것을 억제한다. 또 다른 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1이 B7-1에 결합하는 것을 억제한다. 일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1이 PD-1 및 B7-1 모두에 결합하는 것을 억제한다. 상기 PD-L1 결합 길항제는 제한 없이 항체, 이의 항원 결합 단편, 면역접합체, 융합 단백질, 올리고펩티드, 또는 소분자일 수 있다. 일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1(예컨대, GS-4224, INCB086550, MAX-10181, INCB090244, CA-170, 또는 ABSK041)을 억제하는 소분자이다. 일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1 및 VISTA를 억제하는 소분자이다. 일부 경우들에서, 상기 PD-L1 결합 길항제는 CA-170(AUPM-170으로도 공지된)이다. 일부 경우들에서, 상기 PD-L1 결합 길항제는 PD-L1 및 TIM3을 억제하는 소분자이다. 일부 경우들에서, 상기 소분자는 WO 2015/033301 및/또는 WO 2015/033299에 기재된 화합물이다. In some cases, the PD-L1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners. In other cases, the PD-L1 binding antagonist inhibits PD-L1 binding to PD-1. In still other cases, the PD-L1 binding antagonist inhibits PD-L1 binding to B7-1. In some cases, the PD-L1 binding antagonist inhibits the binding of PD-L1 to both PD-1 and B7-1. The PD-L1 binding antagonist may be, without limitation, an antibody, antigen-binding fragment thereof, immunoconjugate, fusion protein, oligopeptide, or small molecule. In some cases, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 (eg, GS-4224, INCB086550, MAX-10181, INCB090244, CA-170, or ABSK041). In some cases, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 and VISTA. In some cases, the PD-L1 binding antagonist is CA-170 (also known as AUPM-170). In some cases, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 and TIM3. In some cases, the small molecule is a compound described in WO 2015/033301 and/or WO 2015/033299.
일부 경우들에서, 상기 PD-L1 결합 길항제는 항 PD-L1 항체이다. 다양한 항 PD-L1 항체가 본원에서 고려되고 설명된다. 본원의 경우들 중 임의의 것에서, 단리된 항 PD-L1 항체는 인간 PD-L1, 예를 들어 유니프롯(UniProt)KB/스위스-프롯(Swiss-Prot) 수탁 번호 Q9NZQ7-1에서 도시된 바와 같은 인간 PD-L1, 또는 이의 변이체에 결합할 수 있다. 일부 경우들에서, 상기 항 PD-L1 항체는 PD-L1 및 PD-1 사이, 및/또는 PD-L1 및 B7-1 사이의 결합을 억제할 수 있다. 일부 경우들에서, 상기 항 PD-L1 항체는 단일클론 항체이다. 일부 경우들에서, 상기 항 PD-L1 항체는 Fab, Fab’-SH, Fv, scFv, 및 F(ab’)2 단편으로 이루어진 군으로부터 선택된 항체 단편이다. 일부 경우들에서, 상기 항 PD-L1 항체는 인간화 항체이다. 일부 경우들에서, 상기 항 PD-L1 항체는 인간 항체이다. 예시적인 항 PD-L1 항체는 아테졸리주맙, MDX-1105, MEDI4736(더발루맙), MSB0010718C(아벨루맙), SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 및 Hs-636을 포함한다. 본 발명의 방법에 유용한 항 PD-L1 항체의 예 및 이의 제조 방법은 국제 특허 출원 공보 제WO 2010/077634호 및 미국 특허 제8,217,149호에 기재되어 있으며, 이는 그 전체가 본원에 원용된다. In some cases, the PD-L1 binding antagonist is an anti-PD-L1 antibody. A variety of anti-PD-L1 antibodies are contemplated and described herein. In any of the cases herein, the isolated anti-PD-L1 antibody is human PD-L1, eg, as shown in UniProt KB/Swiss-Prot Accession No. Q9NZQ7-1. It is capable of binding to human PD-L1, or a variant thereof. In some cases, the anti-PD-L1 antibody may inhibit binding between PD-L1 and PD-1 and/or between PD-L1 and B7-1. In some cases, the anti-PD-L1 antibody is a monoclonal antibody. In some cases, the anti-PD-L1 antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv, and F(ab') 2 fragments. In some cases, the anti-PD-L1 antibody is a humanized antibody. In some cases, the anti-PD-L1 antibody is a human antibody. Exemplary anti-PD-L1 antibodies are atezolizumab, MDX-1105, MEDI4736 (durvalumab), MSB0010718C (avelumab), SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072 , IMC-001, KL-A167, APL-502, Cosibelimab, Rhodapoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL -GEX, KD036, KY1003, YBL-007, and Hs-636. Examples of anti-PD-L1 antibodies useful in the methods of the present invention and methods of making them are described in International Patent Application Publication No. WO 2010/077634 and US Patent No. 8,217,149, which are incorporated herein by reference in their entirety.
일부 경우들에서, 상기 항 PD-L1 항체(예컨대, 아테졸리주맙)는 하기의: (a) GFTFSDSWIH(서열번호 20)의 HVR-H1 서열; (b) AWISPYGGSTYYADSVKG(서열번호 21)의 HVR-H2 서열; (c) RHWPGGFDY(서열번호 22)의 HVR-H3 서열; (d) RASQDVSTAVA(서열번호 23)의 HVR-L1 서열; (e) SASFLYS(서열번호 24)의 HVR-L2 서열; 및 (f) QQYLYHPAT(서열번호 25)의 HVR-L3 서열로부터 선택된 적어도 1개, 2개, 3개, 4개, 5개, 또는 6개의 HVR을 포함한다. In some cases, the anti-PD-L1 antibody (eg, atezolizumab) comprises: (a) the HVR-H1 sequence of GFTFSDSWIH (SEQ ID NO: 20); (b) the HVR-H2 sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21); (c) the HVR-H3 sequence of RHWPGGFDY (SEQ ID NO: 22); (d) the HVR-L1 sequence of RASQDVSTAVA (SEQ ID NO: 23); (e) the HVR-L2 sequence of SASFLYS (SEQ ID NO: 24); and (f) at least 1, 2, 3, 4, 5, or 6 HVRs selected from the HVR-L3 sequence of QQYLYHPAT (SEQ ID NO: 25).
일부 경우들에서, 상기 항 PD-L1 항체는:In some cases, the anti-PD-L1 antibody comprises:
(a) 서열번호 20, 서열번호 21 및 서열번호 22의 HVR-H1, HVR-H2, 및 HVR-H3 서열을 각각 포함하고,(a) comprising the sequences HVR-H1, HVR-H2, and HVR-H3 of SEQ ID NO: 20, SEQ ID NO: 21 and SEQ ID NO: 22, respectively;
(b) 서열번호 23, 서열번호 24 및 서열번호 25의 HVR-L1, HVR-L2, 및 HVR-L3 서열을 각각 포함한다. (b) HVR-L1, HVR-L2, and HVR-L3 sequences of SEQ ID NO: 23, SEQ ID NO: 24 and SEQ ID NO: 25, respectively.
일부 경우들에서, 상기 항 PD-L1 항체(예컨대, 아테졸리주맙)는 중쇄 및 경쇄 서열을 포함하고, 여기서: (a) 중쇄 가변(VH) 영역 서열은 하기의 아미노산 서열: EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSS(서열번호 26)를 포함하고; (b) 경쇄 가변(VL) 영역 서열은 하기의 아미노산 서열: DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKR(서열번호 27)을 포함한다.In some cases, the anti-PD-L1 antibody (eg, atezolizumab) comprises a heavy chain and a light chain sequence, wherein: (a) the heavy chain variable (VH) region sequence has the following amino acid sequence: EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGTGAVYYWVAWISPYGGSTYYADSVKGRFTMSLRGTFDYSKNTAYCARWISPYGGSTISADTWGGTAYCARWISPYGGSTISADT. ); (b) the light chain variable (VL) region sequence comprises the following amino acid sequence: DIQMTQSPSSLSSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKR (SEQ ID NO: 27).
일부 경우들에서, 상기 항 PD-L1 항체(예컨대, 아테졸리주맙)는 중쇄 및 경쇄 서열을 포함하고, 여기서: (a) 상기 중쇄는 다음 아미노산 서열: EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYASTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPG(서열번호 28)를 포함하고; (b) 상기 경쇄는 하기의 아미노산 서열: DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(서열번호 29)를 포함한다.일부 경우들에서, 상기 항 PD-L1 항체(예컨대, 아테졸리주맙)는 중쇄 및 경쇄 서열을 포함하고, 여기서: (a) 상기 중쇄는 다음 아미노산 서열: EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYASTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPG(서열번호 28)를 포함하고; (b) 상기 경쇄는 하기의 아미노산 서열: DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(서열번호 29)를 포함한다.
일부 경우들에서, 상기 항 PD-L1 항체는 (a) (서열번호 26) 또는 이의 서열과 적어도 95%의 서열 동일성(예컨대, 적어도 95%, 96%, 97%, 98%, 또는 99% 서열 동일성)을 포함한 아미노산 서열을 포함하는 VH 도메인; (b) (서열번호 27) 또는 이의 서열과 적어도 95%의 서열 동일성(예컨대, 적어도 95%, 96%, 97%, 98%, 또는 99% 서열 동일성)을 포함한 아미노산 서열을 포함하는 VL 도메인; 또는 (c) (a)에서와 같은 VH 도메인 및 (b)에서와 같은 VL 도메인을 포함한다. 일 구현예에서, 상기 항 PD-L1 항체는 하기의: (a) 서열 번호 28의 중쇄 아미노산 서열, 및 (b) 서열 번호 29의 경쇄 아미노산 서열을 포함하는, 아테졸리주맙을 포함한다.In some cases, the anti-PD-L1 antibody comprises (a) (SEQ ID NO: 26) or a sequence thereof with at least 95% sequence identity (eg, at least 95%, 96%, 97%, 98%, or 99% sequence identity). a VH domain comprising an amino acid sequence comprising identity); (b) a VL domain comprising an amino acid sequence comprising (SEQ ID NO: 27) or a sequence thereof and at least 95% sequence identity (eg, at least 95%, 96%, 97%, 98%, or 99% sequence identity); or (c) a VH domain as in (a) and a VL domain as in (b). In one embodiment, the anti-PD-L1 antibody comprises atezolizumab, comprising (a) a heavy chain amino acid sequence of SEQ ID NO: 28, and (b) a light chain amino acid sequence of SEQ ID NO: 29.
일부 경우들에서, 상기 항 PD-L1 항체는 아벨루맙(CAS 등록 번호: 1537032-82-8)이다. MSB0010718C로도 공지된 아벨루맙은 인간 단일클론 IgG1 항 PD-L1 항체(머크 KGaA, 화이자)이다. In some cases, the anti-PD-L1 antibody is avelumab (CAS Accession Number: 1537032-82-8). Abelumab, also known as MSB0010718C, is a human monoclonal IgG1 anti-PD-L1 antibody (Merck KGaA, Pfizer).
일부 경우들에서, 상기 항 PD-L1 항체는 더발루맙(CAS 등록 번호: 1428935-60-7)이다. MEDI4736으로도 공지된 더발루맙은 WO2011/066389 및 US2013/034559에 기재된 Fc 최적화 인간 단일클론 IgG1 카파 항 PD-L1 항체(메드이뮨, 아스트라제네카)이다. In some cases, the anti-PD-L1 antibody is durvalumab (CAS Accession Number: 1428935-60-7). Durvalumab, also known as MEDI4736, is an Fc optimized human monoclonal IgG1 kappa anti PD-L1 antibody (MedImmune, AstraZeneca) described in WO2011/066389 and US2013/034559.
일부 경우들에서, 상기 항 PD-L1 항체는 MDX-1105(브리스톨 마이어스 스퀴브)이다. BMS-936559로도 공지된 MDX-1105는 WO2007/005874에 기재된 항 PD-L1 항체이다. In some cases, the anti-PD-L1 antibody is MDX-1105 (Bristol Myers Squibb). MDX-1105, also known as BMS-936559, is an anti-PD-L1 antibody described in WO2007/005874.
일부 경우들에서, 상기 항 PD-L1 항체는 LY3300054(엘리 릴리(Eli Lilly))이다. In some cases, the anti-PD-L1 antibody is LY3300054 (Eli Lilly).
일부 경우들에서, 상기 항 PD-L1 항체는 STI-A1014(소렌토(Sorrento))이다. STI-A1014는 인간 항 PD-L1 항체이다.In some cases, the anti-PD-L1 antibody is STI-A1014 (Sorrento). STI-A1014 is a human anti-PD-L1 antibody.
일부 경우들에서, 상기 항 PD-L1 항체는 KN035(쑤저우 알파맙(Suzhou Alphamab))이다. KN035는 낙타 파지 디스플레이 라이브러리로부터 생성된 단일 도메인 항체(dAB)이다.In some cases, the anti-PD-L1 antibody is KN035 (Suzhou Alphamab). KN035 is a single domain antibody (dAB) generated from a camel phage display library.
일부 경우들에서, 상기 항 PD-L1 항체는 절단될 때(예컨대, 종양 미세 환경에서 프로테아제에 의해) 항체 항원 결합 도메인을 활성화하여, 예컨대 비 결합 입체 모이어티를 제거함으로써 이의 항원에 결합하도록 하는 절단성 모이어티 또는 링커를 포함한다. 일부 경우들에서, 상기 항 PD-L1 항체는 CX-072(사이톰엑스 테라퓨틱스(CytomX Therapeutics))이다.In some cases, the anti-PD-L1 antibody is cleaved such that when cleaved (eg, by a protease in the tumor microenvironment) the antibody antigen binding domain is activated to bind its antigen, eg, by removing a non-binding steric moiety. sex moieties or linkers. In some cases, the anti-PD-L1 antibody is CX-072 (CytomX Therapeutics).
일부 경우들에서, 상기 항 PD-L1 항체는 US 20160108123호, WO 제9,205,148호, WO 2013/181634호, 또는 WO 2016/061142호에 기재된 항 PD-L1 항체로부터의 6개의 HVR 서열(예컨대, 3개의 중쇄 HVR 및 3개의 경쇄 HVR) 및/또는 중쇄 가변 도메인 및 경쇄 가변 도메인을 포함한다. In some cases, the anti-PD-L1 antibody comprises six HVR sequences from an anti-PD-L1 antibody described in US 20160108123, WO 9,205,148, WO 2013/181634, or WO 2016/061142 (eg 3 two heavy chain HVRs and three light chain HVRs) and/or a heavy chain variable domain and a light chain variable domain.
다른 추가의 특정 양태에서, 상기 항 PD-L1 항체는 감소된 또는 최소의 작동체 기능을 갖는다. 다른 추가의 특정 양태에서, 상기 최소의 작동체 기능은 "작동체 없는 Fc 돌연변이” 또는 비당화 돌연변이로부터 발생한다. 다른 추가의 경우에서, 상기 작동체 없는 Fc 돌연변이는 불변 영역에서 N297A 또는 D265A/N297A 치환이다. 다른 추가의 경우에서, 상기 작동체 없는 Fc 돌연변이는 불변 영역에서 N297A 치환이다. 일부 경우들에서, 상기 단리된 항 PD-L1 항체는 탈글리코실화된다. 항체들의 당화는 전형적으로 N 연결 또는 O 연결된다. N 연결은 탄수화물 모이어티가 아스파라긴 잔기의 측쇄에 부착되는 것을 의미한다. 트리펩티드 서열 아스파라긴-X-세린 및 아스파라긴-X-트레오닌(여기서 X는 프롤린을 제외한 임의의 아미노산임)은 탄수화물 모이어티를 아스파라긴 측쇄에 효소적으로 부착하기 위한 인식 서열이다. 따라서, 폴리펩티드에 상기 트리펩티드 서열들 중 어느 하나의 존재는 가능한 당화 부위를 생성한다. O 연결된 당화는 히드록시아미노산, 가장 일반적으로는 세린 또는 트레오닌으로의 당 N 아세틸갈락토사민, 갈락토오스 또는 자일로스의 부착을 의미하지만, 5-히드록시프롤린 또는 5-히드록시리신이 또한 사용될 수 있다. 항체의 당화부위의 제거는 전술된 트리펩티드 서열들(N 연결 당화 부위의 경우) 중 하나가 제거되도록 아미노산 서열을 변경함으로써 용이하게 달성된다. 상기 변경은 당화 부위 내의 아스파라긴, 세린 또는 트레오닌 잔기를 다른 아미노산 잔기로 치환(예컨대, 글리신, 알라닌 또는 보존적 치환)함으로써 이루어질 수 있다.In yet further specific embodiments, said anti-PD-L1 antibody has reduced or minimal effector function. In yet further specific embodiments, said minimal effector function results from an “effector-free Fc mutation” or aglycosylation mutation. In still further cases, said effector-free Fc mutation is N297A or D265A/N297A in the constant region. Substitution.In yet further cases, the Fc mutation without effector is N297A substitution in the constant region.In some cases, the isolated anti-PD-L1 antibody is deglycosylated.The glycosylation of antibodies is typically N-linked or O linkage.N linkage means that the carbohydrate moiety is attached to the side chain of the asparagine residue.The tripeptide sequences asparagine-X-serine and asparagine-X-threonine, where X is any amino acid except proline Recognition sequence for enzymatic attachment of carbohydrate moiety to asparagine side chain.Therefore, the presence of any of the above tripeptide sequences in the polypeptide creates a possible glycosylation site.O-linked glycosylation is hydroxyamino acid, most commonly refers to the attachment of the sugar N acetylgalactosamine, galactose or xylose to serine or threonine, but 5-hydroxyproline or 5-hydroxylysine can also be used. This is easily accomplished by altering the amino acid sequence so that one of the peptide sequences (for N-linked glycosylation sites) is removed.The alteration is to replace an asparagine, serine or threonine residue in the glycosylation site with another amino acid residue (e.g., glycine, alanine) or conservative substitution).
2. PD-1 결합 길항제2. PD-1 binding antagonists
일부 경우들에서, 상기 PD-1 축 결합 길항제는 PD-1 결합 길항제이다. 예를 들어, 상기 PD-1 결합 길항제는 PD-1이 하나 또는 그 이상의 이의 리간드 결합 짝에 결합하는 것을 억제한다. 일부 경우들에서, 상기 PD-1 결합 길항제는 PD-1이 PD-L1에 결합하는 것을 억제한다. 다른 경우들에서, 상기 PD-1 결합 길항제는 PD-1이 PD-L2에 결합하는 것을 억제한다. 또 다른 경우들에서, 상기 PD-1 결합 길항제는 PD-1이 PD-L1 및 PD-L2 모두에 결합하는 것을 억제한다. 상기 PD-1 결합 길항제는 제한 없이 항체, 이의 항원 결합 단편, 면역접합체, 융합 단백질, 올리고펩티드, 또는 소분자일 수 있다. 일부 경우들에서, 상기 PD-1 결합 길항제는 면역접합체(예컨대, 불변 영역(예컨대, 면역글로불린 서열의 Fc 영역)에 융합된 PD-L1 또는 PD-L2의 세포외 또는 PD-1 결합 부위를 포함하는 면역접합체)이다. 예를 들어, 일부 경우들에서, 상기 PD-1 결합 길항제는 Fc-융합 단백질이다. 일부 경우들에서, 상기 PD-1 결합 길항제는 AMP-224이다. B7-DCIg로도 공지된 AMP-224는 WO 2010/027827 및 WO 2011/066342에 기재된 PD-L2-Fc 융합 가용성 수용체이다. 일부 경우들에서, 상기 PD-1 결합 길항제는 펩티드 또는 소분자 화합물이다. 일부 경우들에서, 상기 PD-1 결합 길항제는 AUNP-12(피에르파브르(PierreFabre)/오리진(Aurigene))이다. 예컨대, WO 2012/168944, WO 2015/036927, WO 2015/044900, WO 2015/033303, WO 2013/144704, WO 2013/132317, 및 WO 2011/161699를 참조한다. 일부 경우들에서, 상기 PD-1 결합 길항제는 PD-1을 억제하는 소분자이다. In some cases, the PD-1 axis binding antagonist is a PD-1 binding antagonist. For example, the PD-1 binding antagonist inhibits the binding of PD-1 to one or more ligand binding partners thereof. In some cases, the PD-1 binding antagonist inhibits PD-1 binding to PD-L1. In other instances, the PD-1 binding antagonist inhibits PD-1 binding to PD-L2. In still other cases, the PD-1 binding antagonist inhibits PD-1 from binding to both PD-L1 and PD-L2. The PD-1 binding antagonist may be, without limitation, an antibody, antigen-binding fragment thereof, immunoconjugate, fusion protein, oligopeptide, or small molecule. In some cases, the PD-1 binding antagonist comprises an extracellular or PD-1 binding site of PD-L1 or PD-L2 fused to an immunoconjugate (eg, a constant region (eg, an Fc region of an immunoglobulin sequence)). immunoconjugate). For example, in some cases, the PD-1 binding antagonist is an Fc-fusion protein. In some cases, the PD-1 binding antagonist is AMP-224. AMP-224, also known as B7-DCIg, is a PD-L2-Fc fusion soluble receptor described in WO 2010/027827 and WO 2011/066342. In some cases, the PD-1 binding antagonist is a peptide or small molecule compound. In some cases, the PD-1 binding antagonist is AUNP-12 (PierreFabre/Aurigene). See, eg, WO 2012/168944, WO 2015/036927, WO 2015/044900, WO 2015/033303, WO 2013/144704, WO 2013/132317, and WO 2011/161699. In some cases, the PD-1 binding antagonist is a small molecule that inhibits PD-1.
일부 경우들에서, 상기 PD-1 결합 길항제는 항 PD-1 항체이다. 다양한 항 PD-1 항체가 본원에 개시된 방법 및 사용에서 활용될 수 있다. 본원의 경우들 중 임의의 것에서, 상기 PD-1 항체는 인간 PD-1 또는 이의 변이체에 결합할 수 있다. 일부 경우들에서, 상기 항 PD-1 항체는 단일클론 항체이다. 일부 경우들에서, 상기 항 PD-1 항체는 Fab, Fab’-SH, Fv, scFv, 및 F(ab’)2 단편으로 이루어진 군으로부터 선택된 항체 단편이다. 일부 경우들에서, 상기 항 PD-1 항체는 인간화 항체이다. 다른 경우들에서, 상기 항 PD-1 항체는 인간 항체이다. 예시적인 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, PDR001(스파르탈리주맙), REGN2810(세미플리맙), BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 및 hAb21을 포함한다. In some cases, the PD-1 binding antagonist is an anti-PD-1 antibody. A variety of anti-PD-1 antibodies can be utilized in the methods and uses disclosed herein. In any of the cases herein, the PD-1 antibody is capable of binding to human PD-1 or a variant thereof. In some cases, the anti-PD-1 antibody is a monoclonal antibody. In some cases, the anti-PD-1 antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv, and F(ab') 2 fragments. In some cases, the anti-PD-1 antibody is a humanized antibody. In other instances, the anti-PD-1 antibody is a human antibody. Exemplary anti-PD-L1 antagonist antibodies are nivolumab, pembrolizumab, MEDI-0680, PDR001 (spartalizumab), REGN2810 (semipliumab), BGB-108, prolgolimab, camrelizumab, scintilimab , tislelizumab, torifalimab, dostalimab, retipanrimab, sasanrimab, fenpulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab , YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, and hAb21.
일부 경우들에서, 상기 항 PD-1 항체는 니볼루맙(CAS 등록 번호: 946414-94-4)이다. MDX-1106-04, MDX-1106, ONO-4538, BMS-936558, 및 OPDIVO®로도 공지된 니볼루맙(브리스톨-마이어스-스퀴브(Bristol-Myers Squibb)/오노(Ono))은 WO2006/121168에 기재된 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is nivolumab (CAS Accession Number: 946414-94-4). Nivolumab (Bristol-Myers Squibb/Ono), also known as MDX-1106-04, MDX-1106, ONO-4538, BMS-936558, and OPDIVO® , is disclosed in WO2006/121168. described anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 펨브로리주맙(CAS 등록 번호: 1374853-91-4)이다. MK-3475, 머크(Merck) 3475, 람브롤리주맙, SCH-900475 및 KEYTRUDA®로도 공지되어 있는 펨브롤리주맙(머크)은 WO2009/114335에 기재되어 있는 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is pembrolizumab (CAS Accession Number: 1374853-91-4). Pembrolizumab (Merck), also known as MK-3475, Merck 3475, lambrolizumab, SCH-900475 and KEYTRUDA®, is an anti-PD-1 antibody described in WO2009/114335.
일부 경우들에서, 상기 항 PD-1 항체는 MEDI-0680(AMP-514; 아스트라제네카(AstraZeneca))이다. MEDI-0680은 인간화 IgG4 항 PD-1 항체이다.In some cases, the anti-PD-1 antibody is MEDI-0680 (AMP-514; AstraZeneca). MEDI-0680 is a humanized IgG4 anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 PDR001(CAS 등록 번호 1859072-53-9; 노바르티스)이다. PDR001은 PD-1에 대한 PD-L1 및 PD-L2의 결합을 차단하는 인간화 IgG4 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is PDR001 (CAS Accession No. 1859072-53-9; Novartis). PDR001 is a humanized IgG4 anti-PD-1 antibody that blocks the binding of PD-L1 and PD-L2 to PD-1.
일부 경우들에서, 상기 항 PD-1 항체는 REGN2810(리제네론(Regeneron))이다. REGN2810는 인간 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is REGN2810 (Regeneron). REGN2810 is a human anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 BGB-108(베이진(BeiGene)이다. In some cases, the anti-PD-1 antibody is BGB-108 (BeiGene).
일부 경우들에서, 상기 항 PD-1 항체는 BGB-A317(베이진(BeiGene)이다. In some cases, the anti-PD-1 antibody is BGB-A317 (BeiGene).
일부 경우들에서, 상기 항 PD-1 항체는 JS-001(상하이 준시(Shanghai Junshi))이다. JS-001은 인간화 항 PD-1 항체이다.In some cases, the anti-PD-1 antibody is JS-001 (Shanghai Junshi). JS-001 is a humanized anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 STI-A1110(소렌토(Sorrento))이다. STI-A1110는 인간 항 PD-1 항체이다.In some cases, the anti-PD-1 antibody is STI-A1110 (Sorrento). STI-A1110 is a human anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 INCSHR-1210(인사이트(Incyte))이다. INCSHR-1210은 인간 IgG4 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is INCSHR-1210 (Incyte). INCSHR-1210 is a human IgG4 anti-PD-1 antibody.
일부 경우들에서, 상기 항 PD-1 항체는 PF-06801591(화이자(Pfizer))이다. In some cases, the anti-PD-1 antibody is PF-06801591 (Pfizer).
일부 경우들에서, 상기 항 PD-1 항체는 TSR-042(ANB011; 테사로/아납티스바이오(Tesaro/AnaptysBio)로도 공지됨)이다.In some cases, the anti-PD-1 antibody is TSR-042 (ANB011; also known as Tesaro/AnaptysBio).
일부 경우들에서, 상기 항 PD-1 항체는 AM0001(ARMO 바이오사이언스(Biosciences))이다.In some cases, the anti-PD-1 antibody is AM0001 (ARMO Biosciences).
일부 경우들에서, 상기 항 PD-1 항체는 ENUM 244C8(이뉴머럴 바이오메디컬 홀딩스)이다. ENUM 244C8은 PD-1에 대한 PD-L1의 결합을 차단하지 않고 PD-1 기능을 억제하는 항 PD-1 항체이다. In some cases, the anti-PD-1 antibody is ENUM 244C8 (Enumeral Biomedical Holdings). ENUM 244C8 is an anti-PD-1 antibody that inhibits PD-1 function without blocking the binding of PD-L1 to PD-1.
일부 경우들에서, 상기 항 PD-1 항체는 ENUM 388D4(이뉴머럴 바이오메디컬 홀딩스)이다. ENUM 388D4는 PD-1에 대한 PD-L1의 결합을 경쟁적으로 억제하는 항 PD-1 항체이다.In some cases, the anti-PD-1 antibody is ENUM 388D4 (Enumeral Biomedical Holdings). ENUM 388D4 is an anti-PD-1 antibody that competitively inhibits the binding of PD-L1 to PD-1.
일부 경우들에서, 상기 항 PD-L1 항체는 WO 2015/112800, WO 2015/112805, WO 2015/112900, US 20150210769, WO2016/089873, WO 2015/035606, WO 2015/085847, WO 2014/206107, WO 2012/145493, US 9,205,148, WO 2015/119930, WO 2015/119923, WO 2016/032927, WO 2014/179664, WO 2016/106160, 및 WO 2014/194302에 기재된 항 PD-1 항체로부터의 6개의 HVR 서열(예컨대, 3개의 중쇄 HVR 및 3개의 경쇄 HVR) 및/또는 중쇄 가변 도메인 및 경쇄 가변 도메인을 포함한다. In some cases, the anti-PD-L1 antibody is WO 2015/112800, WO 2015/112805, WO 2015/112900, US 20150210769, WO2016/089873, WO 2015/035606, WO 2015/085847, WO 2014/206107, WO 6 HVR sequences from anti-PD-1 antibodies described in 2012/145493, US 9,205,148, WO 2015/119930, WO 2015/119923, WO 2016/032927, WO 2014/179664, WO 2016/106160, and WO 2014/194302 (eg, three heavy chain HVRs and three light chain HVRs) and/or a heavy chain variable domain and a light chain variable domain.
다른 추가의 특정 양태에서, 상기 항 PD-1 항체는 감소된 또는 최소의 Fc 매개 작동체 기능을 갖는다. 다른 추가의 특정 양태에서, 상기 최소의 Fc 매개 작동체 기능은 "작동체 없는 Fc 돌연변이” 또는 비당화 돌연변이로부터 발생한다. 다른 추가의 경우에서, 상기 작동체 없는 Fc 돌연변이는 불변 영역에서 N297A 또는 D265A/N297A 치환이다. 일부 경우들에서, 상기 단리된 항 PD-1 항체는 탈글리코실화된다. In still further specific embodiments, said anti-PD-1 antibody has reduced or minimal Fc-mediated effector function. In yet further specific embodiments, said minimal Fc mediated effector function results from an "effector-free Fc mutation" or aglycosylation mutation. In still further specific cases, said effector-free Fc mutation is N297A or D265A in the constant region. /N297A substitution In some cases, the isolated anti-PD-1 antibody is deglycosylated.
3. PD-L2 결합 길항제3. PD-L2 binding antagonists
일부 경우들에서, 상기 PD-1 축 결합 길항제는 PD-L2 결합 길항제이다. 일부 경우들에서, 상기 PD-L2 결합 길항제는 이의 리간드 결합 짝으로의 PD-L2 결합을 억제하는 분자이다. 특정 양태에서, 상기 PD-L2 결합 리간드 짝은 PD-1이다. 상기 PD-L2 결합 길항제는 제한 없이 항체, 이의 항원 결합 단편, 면역접합체, 융합 단백질, 올리고펩티드, 또는 소분자일 수 있다. In some cases, the PD-1 axis binding antagonist is a PD-L2 binding antagonist. In some cases, the PD-L2 binding antagonist is a molecule that inhibits PD-L2 binding to its ligand binding partner. In certain embodiments, the PD-L2 binding ligand partner is PD-1. The PD-L2 binding antagonist may be, without limitation, an antibody, antigen-binding fragment thereof, immunoconjugate, fusion protein, oligopeptide, or small molecule.
일부 경우들에서, 상기 PD-L2 결합 길항제는 항 PD-L2 항체이다. 본원의 경우들 중 임의의 것에서, 상기 항 PD-L2 항체는 인간 PD-L2 또는 이의 변이체에 결합할 수 있다. 일부 경우들에서, 상기 항 PD-L2 항체는 단일클론 항체이다. 일부 경우들에서, 상기 항 PD-L2 항체는 Fab, Fab’-SH, Fv, scFv, 및 F(ab’)2 단편으로 이루어진 군으로부터 선택된 항체 단편이다. 일부 경우들에서, 상기 항 PD-L2 항체는 인간화 항체이다. 다른 경우들에서, 상기 항 PD-L2 항체는 인간 항체이다. 다른 추가의 특정 양태에서, 상기 항 PD-L2 항체는 감소된 또는 최소의 작동체 기능을 갖는다. 다른 추가의 특정 양태에서, 상기 최소의 작동체 기능은 "작동체 없는 Fc 돌연변이” 또는 비당화 돌연변이로부터 발생한다. 다른 추가의 경우에서, 상기 작동체 없는 Fc 돌연변이는 불변 영역에서 N297A 또는 D265A/N297A 치환이다. 일부 경우들에서, 상기 단리된 항 PD-L2 항체는 탈글리코실화된다.In some cases, the PD-L2 binding antagonist is an anti-PD-L2 antibody. In any of the cases herein, the anti-PD-L2 antibody is capable of binding to human PD-L2 or a variant thereof. In some cases, the anti-PD-L2 antibody is a monoclonal antibody. In some cases, the anti-PD-L2 antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv, and F(ab') 2 fragments. In some cases, the anti-PD-L2 antibody is a humanized antibody. In other instances, the anti-PD-L2 antibody is a human antibody. In still further specific embodiments, said anti-PD-L2 antibody has reduced or minimal effector function. In yet further specific embodiments, said minimal effector function results from an “effector-free Fc mutation” or aglycosylation mutation. In yet further cases, said effector-free Fc mutation is N297A or D265A/N297A in the constant region. In some cases, the isolated anti-PD-L2 antibody is deglycosylated.
상기 분자를 함유하는 조성물을 포함하여 본 발명에 유용한 PD-1 축 결합 길항제(예컨대, 아테졸리주맙)는 항 TIGIT 길항제 항체와 병용으로 사용될 수 있다.PD-1 axis binding antagonists (eg, atezolizumab) useful in the present invention, including compositions containing such molecules, may be used in combination with anti-TIGIT antagonist antibodies.
추가의 양태에서, PD-1 축 결합 길항제는 상기 경우들 중 임의의 것에 따른 PD-1 축 결합 길항제 항체이고, 이는 하기의 섹션 C에 기재된 바와 같이 단독으로 또는 병용으로 상기 특징들 중 임의의 것을 통합할 수 있다.In a further aspect, the PD-1 axis binding antagonist is a PD-1 axis binding antagonist antibody according to any of the preceding instances, wherein any of the above features, alone or in combination, are described in Section C below. can be integrated
C. 항체 형식 및 속성C. Antibody Format and Properties
1. 항체 친화성1. Antibody Affinity
특정 경우들에서, 본원에 제공된 항 TIGIT 길항제 항체, PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체), 항 VEGF 항체, 및/또는 항 IL-6R 항체)는 ≤ 1μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, 또는 ≤ 0.001 nM(예컨대, 10-8 M 이하, 예컨대, 10-8 M 내지 10-13 M, 예컨대, 10-9 M 내지 10-13 M)의 해리 상수(KD)를 가진다. In certain instances, an anti TIGIT antagonist antibody, a PD-1 axis binding antagonist antibody (eg, an anti PD-L1 antagonist antibody or an anti PD-1 antagonist antibody), an anti VEGF antibody, and/or an anti IL-6R antibody provided herein ) is ≤ 1 μM, ≤ 100 nM, ≤ 10 nM, ≤ 1 nM, ≤ 0.1 nM, ≤ 0.01 nM, or ≤ 0.001 nM (e.g., 10 -8 M or less, such as 10 -8 M to 10 -13 M, For example, it has a dissociation constant (K D ) of 10 -9 M to 10 -13 M).
한 경우에서, KD는 방사표지된 항원 결합 분석(RIA)에 의해 측정된다. 한 경우에서, RIA는 관심 항체의 Fab 형태 및 이의 항원을 이용하여 실시된다. 예를 들어, 항원에 대한 Fab의 용해 결합 친화성은 표지화되지 않은 항원의 적정 연속의 존재하에 Fab를 최소 농도의 (125I) 표지된 항원과 평형시키고, 이후 결합된 항원을 항 Fab 항체 코팅된 플레이트로 포획함으로써 측정된다 (예컨대, Chen et al., J. Mol. Biol. 293:865-881(1999)을 참조). 분석을 위한 조건을 확립하기 위해, MICROTITER® 다중웰 평판 (Thermo Scientific)이 50 mM 탄산나트륨 (pH 9.6)에서 5 μg/ml의 포획 항 Fab 항체 (Cappel Labs)로 하룻밤 동안 코팅되고, 그리고 차후에, 실온 (대략 23℃)에서 2 내지 5 시간 동안 PBS에서 2% (w/v) 소 혈청 알부민으로 차단된다. 비흡착제 플레이트(눙크(Nunc) #269620)에서, 100 pM 또는 26 pM[125I] 항원은 관심이 되는 Fab의 연속 희석으로 혼합한다(예컨대, Presta et al., Cancer Res. 57:4593-4599 (1997)의 Fab-12인 항 VEGF 항체의 평과와 일치하게). 관심 Fab는 그 다음 하룻밤 동안 배양되고; 그러나, 평형에 확실하게 이를 수 있도록 더 오랜 기간(예로써, 약 65 시간) 동안 배양이 지속될 수 있다. 그 이후, 상기 혼합물은 실온 배양 (예로써, 1 시간 동안)을 위하여 포획 플레이트로 이전된다. 그런 다음 용액을 제거하고 플레이트를 PBS 중 0.1% 폴리소르베이트 20 (트윈(TWEEN)-20®) 으로 8회 세척한다. 플레이트가 건조되었을 때, 150 μl/웰의 섬광기(MICROSCINT-20 TM; 패커드(Packard))가 첨가되고, 플레이트는 TOPCOUNT TM 감마 계수기(패커드) 상에서 10분 동안 계수된다. 경쟁적 결합 분석에 사용하기 위하여 최대 결합의 20% 이하를 제공하는 각 Fab 농도가 선택된다. In one case, K D is determined by radiolabeled antigen binding assay (RIA). In one case, RIA is performed using the Fab form of the antibody of interest and its antigen. For example, the lytic binding affinity of a Fab for antigen is determined by equilibrating the Fab with a minimal concentration of ( 125 I) labeled antigen in the presence of a titer sequencing of unlabeled antigen, and then transferring the bound antigen to an anti Fab antibody coated plate. (see, eg, Chen et al., J. Mol. Biol. 293:865-881 (1999)). To establish the conditions for the assay, MICROTITER ® multiwell plates (Thermo Scientific) were coated overnight with 5 μg/ml of capture anti-Fab antibody (Cappel Labs) in 50 mM sodium carbonate, pH 9.6, and subsequently, at room temperature. Blocked with 2% (w/v) bovine serum albumin in PBS for 2-5 hours at (approx. 23° C.). In non-adsorbent plates (Nunc #269620), 100 pM or 26 pM [ 125 I] antigens are mixed in serial dilutions of the Fab of interest (e.g., Presta et al., Cancer Res. 57:4593-4599). (1997) Fab-12 anti-VEGF antibody). The Fabs of interest are then incubated overnight; However, the incubation may be continued for a longer period (eg, about 65 hours) to ensure equilibrium is reached. Thereafter, the mixture is transferred to the capture plate for room temperature incubation (eg, for 1 hour). The solution is then removed and the plate washed 8 times with 0.1% polysorbate 20 (TWEEN-20 ® ) in PBS. When the plates are dry, 150 μl/well of a scintillator (MICROSCINT-20™; Packard) is added and the plates are counted on a TOPCOUNT™ gamma counter (Packard) for 10 minutes. Each Fab concentration that provides 20% or less of maximal binding is selected for use in competitive binding assays.
또 다른 경우에 따르면, KD는 비아코어(BIACORE)® 표면 플라스몬 공명 분석을 사용하여 측정된다. 예를 들면, 비아코어®-2000 또는 비아코어 ®-3000 (비아코어(BIAcore, Inc.), 뉴저지주의 피스카타웨이 소재)을 이용한 분석이 ~10 반응 단위 (RU)에서 고정된 항원 CM5 칩으로 25℃에서 실시된다. 한 경우에서, 카르복시메틸화된 덱스트란 바이오센서 칩(CM5, 비아코어)은 공급업체의 지침에 따라 N-에틸-N'-(3-디메틸아미노프로필)-카르보디이미드 하이드로클로라이드 (EDC) 및 N-하이드록시숙신이미드(NHS)로 활성화된다. 항원은 10 mM 소듐 아세테이트, pH 4.8을 이용하여 5 μg/ml(~0.2 μM)으로 희석시킨 후, 5 μl/분의 유속으로 주사하여 결합된 단백질의 대략 10 반응 단위(RU)를 얻는다. 항원 주사 후, 1 M 에탄올아민을 주사하여 반응하지 않은 군을 차단한다. 동역학 측정을 위해, Fab의 2배 연속 희석액(0.78 nM 내지 500 nM)을 약 25 μl/분의 유속으로 25℃에서 0.05% 폴리소르베이트 20(트윈-20™) 계면활성제(PBST)를 포함하는 PBS 내에 주입한다. 결합율(kon) 및 해리율(koff)은 결합 및 해리 센서그램을 동시에 피팅함에 의해 단순한 1 대 1 랑무이르 결합 모델(비아코어® 평가 소프트웨어 버젼 3.2)을 사용하여 산출한다. 평형 해리 상수(KD)는 비율 koff/kon로 산출된다. 예를 들어, 문헌[Chen et al., Biol. 293:865-881(1999)을 참조한다. 온 레이트가 상기 표면 플라스몬 공명 분석에 의해 106 M1 s1를 초과하면, 온 레이트는 분광계, 예컨대 정지-유동 구비된 분광광도계 (Aviv Instruments) 또는 교반 큐벳이 달린 8000-시리즈 SLM-AMINCO TM 분광광도계 (ThermoSpectronic)에서 계측될 때 증가하는 농도의 항원의 존재에서 PBS, pH 7.2에서, 20 nM 항 항원 항체 (Fab 형태)의 25℃에서 형광 방출 강도 (여기 = 295 nm; 방출 = 340 nm, 16 nm 대역)의 증가 또는 감소를 계측하는 형광 퀀칭 기술을 이용함으로써 결정될 수 있다.According to another case, K D is determined using BIACORE® surface plasmon resonance analysis. For example, assays using Biacore ® -2000 or Biacore ® -3000 (BIAcore, Inc., Piscataway, NJ) can be performed with immobilized antigen CM5 chips at ~10 response units (RU). carried out at 25°C. In one case, a carboxymethylated dextran biosensor chip (CM5, Biacore) was prepared with N-ethyl-N'-(3-dimethylaminopropyl)-carbodiimide hydrochloride (EDC) and N -Activated with hydroxysuccinimide (NHS). Antigen is diluted to 5 μg/ml (~0.2 μM) with 10 mM sodium acetate, pH 4.8 and then injected at a flow rate of 5 μl/min to yield approximately 10 response units (RU) of bound protein. After antigen injection, 1 M ethanolamine is injected to block the unreacted group. For kinetics measurements, two-fold serial dilutions of Fab (0.78 nM to 500 nM) were mixed with 0.05% polysorbate 20 (Tween-20™) surfactant (PBST) at 25° C. at a flow rate of about 25 μl/min. Inject into PBS. Association rates (k on ) and dissociation rates (k off ) are calculated using a simple one-to-one Langmuir binding model ( BIACORE® evaluation software version 3.2) by simultaneously fitting association and dissociation sensorgrams. The equilibrium dissociation constant (K D ) is calculated as the ratio k off /k on . See, eg, Chen et al., Biol. 293:865-881 (1999). If the on-rate exceeds 10 6 M 1 s 1 by the surface plasmon resonance analysis, the on-rate is measured by a spectrometer, such as a spectrophotometer equipped with a stationary-flow (Aviv Instruments) or an 8000-series SLM-AMINCO ™ with stirring cuvette. Fluorescence emission intensity at 25° C. of 20 nM anti-antigen antibody (Fab form) in PBS, pH 7.2 in the presence of increasing concentrations of antigen as measured on a spectrophotometer (ThermoSpectronic) (excitation = 295 nm; emission = 340 nm, 16 nm band) can be determined by using a fluorescence quenching technique that measures the increase or decrease.
2. 항체 단편2. Antibody fragments
특정 경우들에서, 본원에 제공된 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)는 항체 단편이다. 항체 단편은, Fab, Fab’, Fab’-SH, F(ab’)2, Fv, 및 scFv 단편, 및 하기에 기재된 기타 단편들을 포함하지만 이에 제한되지는 않는다. 특정 항체 단편을 검토하려면, Hudson et al. Nat. Med. 9:129-134 (2003)을 참조한다. scFv 단편들의 검토는, 예컨대, Pluckth![]()
![]()
이중체는 2가 또는 이중특이적일 수 있는 2개의 항원 결합 부위를 갖는 항체 단편이다. 예를 들어, EP 404,097; WO 1993/01161; Hudson et al. Nat. Med. 9:129-134 (2003); 및 Hollinger et al. Proc. Natl. Acad. Sci. USA 90: 6444-6448 (1993)을 참조한다. 삼중체 및 사중체는 또한 Hudson et al. Nat. Med. 9:129-134 (2003)을 참조한다.A duplex is an antibody fragment having two antigen binding sites, which may be bivalent or bispecific. See, for example, EP 404,097; WO 1993/01161; Hudson et al. Nat. Med. 9:129-134 (2003); and Hollinger et al. Proc. Natl. Acad. Sci. USA 90: 6444-6448 (1993). Triplets and quadrules are also described by Hudson et al. Nat. Med. 9:129-134 (2003).
단일 도메인 항체는 항체의 중쇄 가변 도메인의 전부 또는 일부 또는 경쇄 가변 도메인의 전부 또는 일부를 포함하는 항체 단편이다. 특정 경우들에서, 단일 도메인 항체는 인간 단일 도메인 항체이다(도만티스(Domantis, Inc.), 매사추세츠 월섬 소재; 예컨대, 미국 특허 제6,248,516 B1호를 참조). Single domain antibodies are antibody fragments comprising all or part of the heavy chain variable domain or all or part of the light chain variable domain of an antibody. In certain instances, the single domain antibody is a human single domain antibody (Domantis, Inc., Waltham, MA; see, eg, US Pat. No. 6,248,516 B1).
항체 단편은 다양한 기술에 의해 제조될 수 있으며, 이에는 원형 항체의 단백질분해 절단뿐만 아니라, 본원에 기재된 바와 같이, 재조합 숙주 세포(예컨대, 대장균 (E. coli) 또는 파지)에 의해 생산된 항체를 포함하지만, 이에 제한되지 않는다.Antibody fragments can be prepared by a variety of techniques, including proteolytic cleavage of the original antibody, as well as antibodies produced by recombinant host cells (eg, E. coli or phage), as described herein. including, but not limited to.
3. 키메라 및 인간화 항체3. Chimeric and Humanized Antibodies
특정 경우들에서, 본원에 제공된 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)는 키메라 항체이다. 특정 키메라 항체는, 예컨대, 미국 특허 제4,816,567호; 및 Morrison et al., Proc. Proc. Natl. Acad. Sci. USA, 81:6851-6855 (1984))에 기재되어 있다. 일례에서, 키메라 항체는 비인간 가변 영역(예컨대, 마우스, 랫트, 햄스터, 토끼, 또는 비인간 영장류, 예컨대, 원숭이로부터 유래된 가변 영역) 및 인간 불변 영역을 포함한다. 추가의 예에서, 키메라 항체는 부류 또는 하위부류가 모 항체의 부류로부터 변화된 “부류 전환된” 항체이다. 키메라 항체는 이의 항원 결합 단편을 포함한다.In certain instances, an anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody) provided herein is a chimeric antibody. Certain chimeric antibodies are described, eg, in US Pat. Nos. 4,816,567; and Morrison et al., Proc. Proc. Natl. Acad. Sci. USA , 81:6851-6855 (1984)). In one example, a chimeric antibody comprises a non-human variable region (eg, a variable region derived from a mouse, rat, hamster, rabbit, or non-human primate, eg, monkey) and a human constant region. In a further example, a chimeric antibody is a “class switched” antibody in which the class or subclass has been changed from that of the parent antibody. A chimeric antibody comprises an antigen-binding fragment thereof.
특정 예들에서, 키메라 항체는 인간화 항체이다. 전형적으로, 비인간 항체는 부모 비인간 항체의 특이성 및 친화성을 유지하면서, 인간에 대한 면역원성을 감소시키기 위해 인간화된다. 일반적으로, 인간화된 항체는 하나 또는 그 이상의 가변적 도메인을 포함하는데, HVR들, 예로써, CDR들, (또는 이의 부분들)는 비-인간 항체로부터 유도되고, FRs (또는 이의 부분들)은 인간 항체 서열로부터 유도된다. 인간화 항체는 임의적으로, 인간 불변 영역의 적어도 일부를 또한 포함할 것이다. 일부 예들에 있어서, 인간화된 항체에서 일부 FR 잔기는 비-인간 항체 (예로써, HVR 잔기가 유도된 항체)의 대응 잔기로 대체되어, 예로써, 항체 특이성 또는 친화도가 복원 또는 개선된다. In certain embodiments, the chimeric antibody is a humanized antibody. Typically, non-human antibodies are humanized to reduce immunogenicity to humans, while maintaining the specificity and affinity of the parental non-human antibodies. Generally, a humanized antibody comprises one or more variable domains, wherein the HVRs, e.g., CDRs, (or portions thereof) are derived from a non-human antibody, and the FRs (or portions thereof) are human derived from antibody sequences. The humanized antibody will optionally also comprise at least a portion of a human constant region. In some embodiments, some FR residues in a humanized antibody are replaced with corresponding residues of a non-human antibody (eg, an antibody from which HVR residues are derived), eg, antibody specificity or affinity is restored or improved.
인간화 항체 및 이의 제조 방법은, 예컨대 Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008)에서 검토되고, 예컨대 Riechmann et al., Nature 332:323-329 (1988); Queen et al., Proc. Nat'l Acad. Sci. USA 86:10029-10033 (1989); 미국 특허 제 5,821,337호, 7,527,791호, 6,982,321호, 및 7,087,409호; Kashmiri et al., Methods 36:25-34 (2005) (특이성 결정 영역(SDR) 이식을 기재함); Padlan, Mol. Immunol. 28:489-498 (1991)(“표면 노출 잔기 변형(resurfacing)”을 기재함); Dall’Acqua et al., Methods 36:43-60 (2005)(“FR 셔플링(shuffling)”을 기재함); 및 Osbourn et al., Methods 36:61-68 (2005) 및 Klimka et al., Br. J. Cancer, 83:252-260 (2000)(FR 셔플링에 대한 “유도된 선택” 접근법을 기재함)에 추가로 기재되어 있다. Humanized antibodies and methods of making them are described, for example, in Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008), see eg Riechmann et al. , Nature 332:323-329 (1988); Queen et al., Proc. Nat'l Acad. Sci. USA 86:10029-10033 (1989); US Pat. Nos. 5,821,337, 7,527,791, 6,982,321, and 7,087,409; Kashmiri et al ., Methods 36:25-34 (2005) (describing specificity determining region (SDR) transplantation); Padlan, Mol. Immunol. 28:489-498 (1991) (describing “resurfacing”); Dall'Acqua et al., Methods 36:43-60 (2005) (describing “FR shuffling”); and Osbourn et al., Methods 36:61-68 (2005) and Klimka et al., Br. J. Cancer , 83:252-260 (2000) (describing a “guided selection” approach to FR shuffling).
인간화에 사용할 수 있는 인간 프레임워크 영역은: “최적의” 방법을 사용하여 선택된 프레임워크 영역(예컨대, Sims et al. J. Immunol. J. Immunol. 151:2296 (1993)을 참조); 특정 하위군의 경쇄 또는 중쇄 가변 영역의 인간 항체의 공통 서열로부터 유래된 프레임워크 영역(예컨대, Carter et al. Proc. Natl. Acad. Sci. USA, 89:4285 (1992); 및 Presta et al. J. Immunol., 151:2623 (1993)을 참조); 인간 성숙(체세포적으로 돌연변이된) 프레임워크 영역 또는 인간 생식계열 프레임워크 영역(예컨대, Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008)을 참조); 및 FR 라이브러리 선별로부터 유래된 프레임워크 영역(예컨대, J. Biol. Chem. 272:10678-10684 (1997) 및 Rosok et al., J. Biol. Chem. 271:22611-22618 (1996)).Human framework regions that can be used for humanization include: framework regions selected using “optimal” methods (see, eg, Sims et al. J. Immunol. J. Immunol. 151:2296 (1993)); Framework regions derived from the consensus sequence of human antibodies of specific subgroups of light or heavy chain variable regions (eg, Carter et al. Proc. Natl. Acad. Sci. USA , 89:4285 (1992); and Presta et al. J. Immunol. , 151:2623 (1993); human mature (somatically mutated) framework regions or human germline framework regions (see, eg, Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008)); and framework regions derived from FR library selection (eg, J. Biol. Chem. 272:10678-10684 (1997) and Rosok et al., J. Biol. Chem. 271:22611-22618 (1996)).
4. 4. 인간 항체 4. 4. Human Antibodies
특정 경우들에서, 본원에 제공된 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)는 인간 항체이다. 인간 항체는 당해 분야에서 공지된 다양한 기술을 이용하여 생산될 수 있다. 인간 항체는 van Dijk and van de Winkel, Curr. Opin. Pharmacol. 5: 368-74 (2001) 및 Lonberg, Curr. Opin. Immunol. 20:450-459 (2008)를 참조한다. In certain instances, an anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody) provided herein is a human antibody. Human antibodies can be produced using a variety of techniques known in the art. Human antibodies are described in van Dijk and van de Winkel, Curr. Opin. Pharmacol. 5: 368-74 (2001) and Lonberg, Curr. Opin. Immunol. 20:450-459 (2008).
인간 항체는 항원 공격에 대한 응답으로 무손상 인간 항체 또는 인간 가변 영역을 포함하는 무손상 항체를 생산하도록 변형된 유전자도입 동물에 면역원을 투여함으로써 제조될 수 있다. 이런 동물은 전형적으로, 내인성 면역글로불린 좌위를 대체하거나, 또는 염색체외로 존재하거나 또는 동물의 염색체 내로 무작위로 통합되는 인간 면역글로불린 좌위 중에서 전부 또는 일부를 내포한다. 상기 형질전환 마우스에서, 상기 내인성 면역글로불린 좌위는 일반적으로 비활성화되어 있다. 형질전환 동물로부터 인간 항체를 수득하는 방법을 검토하려면, LLonberg, Nat. Biotech. 23:1117-1125 (2005)를 참조한다. 또한, 예를 들어, XENOMOUSETM 기술을 기재하는 미국 특허 제 6,075,181 및 6,150,584; HuMab® 기술을 기재하는 미국 특허 제 5,770,429; K-M MOUSE® 기술을 기재하는 미국 특허 제 7,041,870, 그리고 VelociMouse® 기술을 기재하는 미국 특허출원 공개공보 US 2007/0061900)를 참조하라. 이런 동물에 의해 산출된 무손상 항체로부터 인간 가변 영역은 예를 들면, 상이한 인간 불변 영역과 조합함으로써 더욱 변형될 수 있다.Human antibodies can be prepared by administering an immunogen to a transgenic animal that has been modified to produce an intact human antibody or an intact antibody comprising a human variable region in response to an antigen challenge. Such animals typically contain all or some of the human immunoglobulin loci that replace endogenous immunoglobulin loci, or which exist extrachromosomally or integrate randomly into the animal's chromosomes. In the transgenic mice, the endogenous immunoglobulin locus is generally inactivated. For a review of methods for obtaining human antibodies from transgenic animals, see LLonberg, Nat. Biotech. 23:1117-1125 (2005). See also, for example, US Pat. Nos. 6,075,181 and 6,150,584, which describe XENOMOUSE ™ technology; US Pat. No. 5,770,429 describing HuMab ® technology; See US Pat. No. 7,041,870, which describes KM MOUSE® technology, and US Patent Application Publication No. US 2007/0061900, which describes VelociMouse® technology. Human variable regions from intact antibodies generated by such animals can be further modified, for example, by combining with different human constant regions.
인간 항체는 또한, 하이브리도마-기초된 방법에 의해 만들어질 수 있다. 인간 단일클론 항체의 생산을 위한 인간 골수종 및 생쥐-인간 헤테로골수종 세포주가 설명되었다. (예컨대, Kozbor J. Immunol., 133: 3001 (1984); Brodeur et al., Monoclonal Antibody Production Techniques and Applications, pp. 51-63 (Marcel Dekker, Inc., New York, 1987); and Boerner et al., J. Immunol., 147: 86 (1991)을 참조한다.) 인간 B 세포 하이브리도마 기술을 통해 생성된 인간 항체가 또한 Li et al., Proc. Natl. Acad. Sci. USA, 103:3557-3562 (2006)에 더 상세히 기재된다. 추가적인 방법들은, 예를 들어, 미국 특허 제 7,189,826호(하이브리도마 세포주로부터 단클론 인간 IgM 항체의 생산을 기재) 및 Ni, Xiandai Mianyixue, 26(4):265-268 (2006)(인간-인간 하이브리도마를 기재)에서 기재된 방법들을 포함한다. 인간 하이브리도마 기술 (Trioma technology)은 Vollmers and Brandlein, Histology and Histopathology, 20(3):927-937 (2005) 및 Vollmers and Brandlein, Methods and Findings in Experimental and Clinical Pharmacology, 27(3):185-91 (2005)에서 또한 설명된다.Human antibodies can also be made by hybridoma-based methods. Human myeloma and mouse-human heteromyeloma cell lines for the production of human monoclonal antibodies have been described. (e.g., Kozbor J. Immunol. , 133: 3001 (1984); Brodeur et al., Monoclonal Antibody Production Techniques and Applications , pp. 51-63 (Marcel Dekker, Inc., New York, 1987); and Boerner et al. ., J. Immunol ., 147: 86 (1991).) Human antibodies generated via human B cell hybridoma technology have also been described in Li et al. , Proc. Natl. Acad. Sci. USA , 103:3557-3562 (2006). Additional methods are described, for example, in US Pat. No. 7,189,826 (describing production of monoclonal human IgM antibodies from hybridoma cell lines) and Ni, Xiandai Mianyixue , 26(4):265-268 (2006) (human-human high described in Bridomas). Human hybridoma technology (Trioma technology) is described in Vollmers and Brandlein, Histology and Histopathology , 20(3):927-937 (2005) and Vollmers and Brandlein, Methods and Findings in Experimental and Clinical Pharmacology , 27(3):185- 91 (2005).
인간 항체는 또한 인간 유래된 파지 디스플레이 라이브러리로부터 선택되는 Fv 클론 가변 도메인 서열을 단리함으로써 생성될 수 있다. 이런 가변 도메인 서열은 이후, 원하는 인간 불변 도메인과 조합될 수 있다. 항체 라이브러리로부터 인간 항체를 선택하기 위한 기술은 아래에 설명된다.Human antibodies can also be generated by isolating Fv clone variable domain sequences selected from human derived phage display libraries. Such variable domain sequences can then be combined with the desired human constant domains. Techniques for selecting human antibodies from antibody libraries are described below.
5. 라이브러리 유래 항체5. Library Derived Antibodies
본 발명의 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)는 바람직한 활성 또는 활성들을 가진 항체에 대한 복합 라이브러리를 스크리닝함으로써 단리될 수 있다. 예를 들어, 파지 전시 라이브러리를 산출하고, 원하는 결합 특징을 소유하는 항체에 대해 상기 라이브러리를 선별검사하기 위한 다양한 방법이 당해 분야에서 공지된다. 이러한 방법은, 예컨대 Hoogenboom et al. in Methods in Molecular Biology 178:1-37 (O’Brien et al., ed., Human Press, Totowa, NJ, 2001)에서 검토되고, 예컨대, McCafferty et al., Nature 348:552-554; Clackson et al., Nature 352: 624-628 (1991); Marks et al., J. Mol. Biol. 222: 581-597 (1992); Marks and Bradbury, in Methods in Molecular Biology 248:161-175 (Lo, ed., Human Press, Totowa, NJ, 2003); Sidhu et al., J. Mol. Biol. 338(2): 299-310 (2004); Lee et al., J. Mol. Biol. 340(5): 1073-1093 (2004); Fellouse, Proc. Natl. Acad. Sci. USA 101(34): 12467-12472 (2004); and Lee et al., J. Immunol. Methods 284(1-2): 119-132(2004)에 추가로 기재되어 있다. An anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody) of the present invention is isolated by screening a complex library for antibodies with the desired activity or activities. can be For example, a variety of methods are known in the art for generating phage display libraries and screening such libraries for antibodies possessing the desired binding characteristics. Such methods are described, for example, in Hoogenboom et al. in Methods in Molecular Biology 178:1-37 (O'Brien et al., ed., Human Press, Totowa, NJ, 2001), eg, McCafferty et al., Nature 348:552-554; Clackson et al., Nature 352: 624-628 (1991); Marks et al., J. Mol. Biol. 222: 581-597 (1992); Marks and Bradbury, in Methods in Molecular Biology 248:161-175 (Lo, ed., Human Press, Totowa, NJ, 2003); Sidhu et al., J. Mol. Biol. 338(2): 299-310 (2004); Lee et al., J. Mol. Biol. 340(5): 1073-1093 (2004); Fellouse, Proc. Natl. Acad. Sci. USA 101(34): 12467-12472 (2004); and Lee et al., J. Immunol. Methods 284(1-2): 119-132 (2004).
특정 파아지 디스플레이 방법에서, VH 및 VL 유전자 레퍼토리는 중합효소 연쇄 반응(PCR)에 의해 별도로 클로닝되고 파아지 라이브러리에서 무작위로 재조합되며, Winter et al., Ann. Rev. Immunol., 12: 433-455 (1994)를 참조한다. 파지는 전형적으로, 단일 사슬 Fv (scFv) 단편으로서 또는 Fab 단편으로서 항체 단편을 전시한다. 면역화된 공급원으로부터 라이브러리는 하이브리도마를 구축하는 요건 없이 면역원에 대한 높은 친화성 항체를 제공한다. 대안적으로, 원형 레퍼토리는 Griffiths et al., EMBO J, 12: 725-734 (1993)를 참조한다. 최종적으로, 원형 라이브러리는 또한 Hoogenboom and Winter, J. Mol. Biol., 227: 381:-388 (1992)에 기재된 바와 같이 줄기 세포로부터 재배열되지 않은 V 유전자 절편을 복제하고 무작위 서열을 함유하는 PCR 프라이머를 사용하여 고도로 가변적인 CDR3 영역을 부호화하고 시험관 내 재배열을 달성함으로써 합성적으로 제조할 수 있다. 인간 항체 파지 라이브러리를 기재하는 특허 공보는, 예를 들어: 미국 특허 제 5,750,373호, 및 미국 특허 공보 제2005/0079574호, 제2005/0119455호, 제2005/0266000호, 제2007/0117126호, 제2007/0160598호, 제2007/0237764호, 제2007/0292936호, 및 제2009/0002360호를 포함한다.In certain phage display methods, the VH and VL gene repertoires are cloned separately by polymerase chain reaction (PCR) and recombined randomly in phage libraries, Winter et al., Ann. Rev. Immunol. , 12: 433-455 (1994). Phages typically display antibody fragments either as single chain Fv (scFv) fragments or as Fab fragments. Libraries from immunized sources provide high affinity antibodies to the immunogen without the requirement to construct hybridomas. Alternatively, see Griffiths et al., EMBO J, 12: 725-734 (1993) for a prototype repertoire. Finally, the prototype library is also described in Hoogenboom and Winter, J. Mol. Biol. , 227: 381:-388 (1992) cloned unrearranged V gene segments from stem cells and using PCR primers containing random sequences to encode highly variable CDR3 regions and to undergo in vitro rearrangement. By achieving it, it can be prepared synthetically. Patent publications describing human antibody phage libraries include, for example: U.S. Patent No. 5,750,373, and U.S. Patent Publication Nos. 2005/0079574, 2005/0119455, 2005/0266000, 2007/0117126, 2007/0160598, 2007/0237764, 2007/0292936, and 2009/0002360.
인간 항체 라이브러리들로부터 단리된 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체) 또는 항체 단편은 본원에서 인간 항체 또는 인간 항체 단편으로 간주된다.Anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies) or antibody fragments isolated from human antibody libraries are considered human antibodies or human antibody fragments herein.
6. 항체 변이체6. Antibody variants
특정 경우들에서, 본 발명의 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)의 아미노산 서열 변이체가 고려된다. 본원에 상세히 기재된 바와 같이, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제 항체 (예를 들어, 항 PD-L1 길항제 항체)는 원하는 구조적 및 기능적 특성들에 기반하여 최적화될 수 있다. 예를 들면, 항체의 상기 결합 친화도 및/또는 다른 생물학적 성질들을 개선하는 것이 바람직할 수 있다. 항체의 아미노산 서열 변이체들은 상기 항체를 인코드하는 뉴클레오티드 서열 내부에 적절한 변형을 도입시킴으로써, 또는 펩티드 합성에 의해 만들어질 수 있다. 이러한 변형은, 예를 들면, 항체의 아미노산 서열 내의 잔기의 결실, 및/또는 삽입 및/또는 치환을 포함한다. 만일 최종 구조체가 바람직한 특징, 예를 들어, 항원-결합을 보유한다면, 최종 구조체에 도달하기 위한 임의의 결실, 삽입, 및 치환의 조합이 이루어질 수 있다.In certain instances, amino acid sequence variants of an anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody) of the invention are contemplated. As detailed herein, anti-TIGIT antagonist antibodies and PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies) can be optimized based on desired structural and functional properties. For example, it may be desirable to improve the binding affinity and/or other biological properties of an antibody. Amino acid sequence variants of an antibody can be made by introducing appropriate modifications into the nucleotide sequence encoding the antibody, or by peptide synthesis. Such modifications include, for example, deletions, and/or insertions and/or substitutions of residues within the amino acid sequence of the antibody. Any combination of deletions, insertions, and substitutions can be made to arrive at the final construct if the final construct possesses desirable characteristics, eg, antigen-binding.
I. 치환, 삽입, 및 결실 변이체 I. Substitution, insertion, and deletion variants
특정 경우들에서, 하나 이상의 아미노산 치환을 가지는 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체) 변이체가 제공된다. 치환 돌연변이유발에 대한 관심 부위는 HVR 및 FR을 포함한다. 보존적 치환들을 표 3에서 “바람직한 치환”이라는 제목으로 나타낸다. 더 많은 실질적인 변화가 표 3의 “예시적 치환"이라는 제목하에 제시되며, 이는 아미노산 측쇄 클래스를 참조하여 이하에서 추가로 설명된다. 아미노산 치환들은 바람직한 활성, 예를 들면, 유지된/개선된 항원 결합, 감소된 면역원성, 또는 개선된 ADCC 또는 CDC에 대하여 스크리닝된 관심대상 항체 및 산물 안으로 도입될 수 있다.In certain instances, anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody) variants are provided having one or more amino acid substitutions. Sites of interest for substitutional mutagenesis include HVRs and FRs. Conservative substitutions are shown in Table 3 under the heading “preferred substitutions”. More substantial changes are presented in Table 3 under the heading of “Exemplary Substitutions”, which are further described below with reference to amino acid side chain classes. Amino acid substitutions are indicated for the desired activity, e.g., retained/improved antigen binding. , antibodies of interest and products screened for reduced immunogenicity, or improved ADCC or CDC.
잔기residue
치환substitution
치환substitution
예시적이고 바람직한 아미노산 치환Exemplary and Preferred Amino Acid Substitutions
아미노산은 공통 측쇄 특성에 따라 군화될 수 있다:Amino acids can be grouped according to common side chain properties:
(1) 소수성: 노르류신, Met, Ala, Val, Leu, Ile;(1) hydrophobic: norleucine, Met, Ala, Val, Leu, Ile;
(2) 중성 친수성: Cys, Ser, Thr, Asn, Gln;(2) neutral hydrophilicity: Cys, Ser, Thr, Asn, Gin;
(3) 산성: Asp, Glu;(3) acidic: Asp, Glu;
(4) 염기성: His, Lys, Arg;(4) basic: His, Lys, Arg;
(5) 측쇄 방향에 영향을 주는 잔기: Gly, Pro;(5) residues that affect side chain orientation: Gly, Pro;
(6) 방향족: Trp, Tyr, Phe.(6) Aromatics: Trp, Tyr, Phe.
비-보존성 치환들은 이들 분류 중 하나의 구성원을 또 다른 분류로 교환하게 할 것이다. Non-conservative substitutions will cause an exchange of a member of one of these classes for another class.
치환성 변이체의 한 가지 유형은 모 항체의 하나 또는 그 이상의 초가변적 영역 잔기의 치환 (예컨대, 인간화된 또는 인간 항체)과 연관된다. 일반적으로, 추가 연구를 위해 선택된 생성된 변이체(들)는 모 항체에 비해 특정 생물학적 특성(예를 들어, 증가된 친화도, 감소된 면역원성)에서 변형 (예를 들어, 개선)을 가질 것이고 및/또는 모 항체의 특정 생물학적 특성을 실질적으로 보유할 것이다. 예시적인 치환 변이체는 친화도 성숙 항체이며, 이는 예를 들어 본원에 기재된 것과 같은 파지 디스플레이 기반 친화도 성숙 기술을 사용하여 편리하게 생성될 수 있다. 간략하게 설명하자면, 하나 또는 그 이상의 HVR 잔기가 돌연변이되고, 변이체 항체는 파지 상에서 디스플레이되며, 그리고 특정 생물학적 활성 (예컨대, 결합 친화도)에 대하여 스크리닝된다. One type of substitutional variant involves the substitution of one or more hypervariable region residues of a parent antibody (eg, a humanized or human antibody). In general, the resulting variant(s) selected for further study will have modifications (eg, improvements) in certain biological properties (eg, increased affinity, decreased immunogenicity) relative to the parent antibody and /or will retain substantially certain biological properties of the parent antibody. Exemplary substitutional variants are affinity matured antibodies, which can be conveniently generated using, for example, phage display based affinity maturation techniques such as those described herein. Briefly, one or more HVR residues are mutated, the variant antibodies displayed on phage, and screened for a particular biological activity (eg, binding affinity).
변경 (예컨대, 치환들)은 예컨대, 항체 친화도를 개선하기 위해 HVR들에서 이루어질 수 있다. 상기 변경은 HVR "핫스팟," 즉, 체세포 성숙 과정 동안 높은 빈도로 돌연변이하는 코돈에 의해 부호화된 잔기(예컨대, Chowdhury, Methods Mol. Biol. 207:179-196 (2008)), 및/또는 항원과 접촉하는 잔기에서 이루어질 수 있으며, 이때 생성된 변이체 VH 또는 VL가 결합 친화도에 대하여 시험된다. 제 2 라이브러리를 구축하고, 재선별함에 의한 친화도 성숙은 예컨대, Hoogenboom 외. in Methods in Molecular Biology 178:1-37 (O’Brien 외, ed., Human Press, Totowa, NJ, (2001))에서 설명되어 있다. 친화도 성숙의 일부 예들에 있어서, 다양성은 다양한 방법들 중 임의의 방법에 의해 성숙을 위해 선택된 가변 유전자들에 도입된다(예컨대, 오류-발생(error-prone) PCR, 사슬 셔플링, 또는 올리고뉴클레오티드-지시된 돌연변이생성). 이어서 제 2 라이브러리가 생성된다. 이어서, 이 라이브러리를 스크리닝하여, 원하는 친화도를 갖는 임의의 항체 변이체를 식별한다. 다양성을 도입시키는 또 다른 방법은 HVR-지시된 방법을 포함하는데, 이때 몇 개의 HVR 잔기 (가령, 한번에 4-6개 잔기)가 무작위 배정된다. 항원 결합에 관여하는 HVR 잔기는 예컨대, 알라닌 스캐닝 돌연변이유발 또는 모델링을 이용하여 특이적으로 동정될 수 있다. 특히 CDR-H3 및 CDR-L3이 표적이 되는 경우가 많다.Alterations (eg, substitutions) can be made in the HVRs, eg, to improve antibody affinity. Such alterations are HVR "hotspots," ie residues encoded by codons that mutate with high frequency during somatic maturation (eg, Chowdhury, Methods Mol. Biol. 207:179-196 (2008)), and/or antigens and contacting residues, wherein the resulting variant VH or VL is tested for binding affinity. Affinity maturation by constructing a second library and reselecting is described, for example , in Hoogenboom et al. in Methods in Molecular Biology 178:1-37 (O'Brien et al., ed., Human Press, Totowa, NJ, (2001)). In some examples of affinity maturation, diversity is introduced into variable genes selected for maturation by any of a variety of methods (eg, error-prone PCR, chain shuffling, or oligonucleotides). -directed mutagenesis). A second library is then created. This library is then screened to identify any antibody variants with the desired affinity. Another method of introducing diversity involves HVR-directed methods, in which several HVR residues (eg, 4-6 residues at a time) are randomized. HVR residues involved in antigen binding can be specifically identified using, for example, alanine scanning mutagenesis or modeling. In particular, CDR-H3 and CDR-L3 are often targeted.
특정 예들에 있어서, 치환, 삽입, 또는 결손은 이러한 변경으로 이 항체가 항원에 결합하는 능력이 실질적으로 감소되지 않는 한, 하나 또는 그 이상의 HVR들에 발생될 수 있다. 예를 들면, 결합 친화도를 실질적으로 감소시키지 않는 보존적 변경 (예컨대, 본원에서 제공된 보존적 치환)이 HVR들에 이루어질 수 있다. 이러한 변경은 예를 들어, HVR의 항원 접촉 잔기의 외부에 있을 수 있다. 상기에서 제시된 변이체 VH 및 VL의 특정 예들에 있어서, 각 HVR은 변경되지 않거나, 또는 1, 2 또는 3개 이상의 아미노산 치환을 포함한다. In certain instances, substitutions, insertions, or deletions may be made in one or more HVRs so long as the alteration does not substantially reduce the ability of the antibody to bind antigen. For example, conservative alterations (eg, conservative substitutions provided herein) can be made to HVRs that do not substantially reduce binding affinity. Such alterations may be, for example, outside the antigen contacting residues of the HVRs. In certain examples of variants VH and VL set forth above, each HVR is either unaltered or comprises 1, 2, 3 or more amino acid substitutions.
돌연변이유발을 위해 표적화될 수 있는 항체의 잔기 또는 영역의 확인을 위한 유용한 방법은 Cunningham and Wells (1989) Science, 244:1081-1085에 의해 설명된 바와 같이 “알라닌 스캐닝 돌연변이유발”로 불린다. 이 방법에서, 표적 잔기 또는 표적 잔기들의 그룹 (예컨대, 하전된 잔기, 가령 Arg, Asp, His, Lys, 및 Glu)이 식별되고, 중성 또는 음으로 하전된 아미노산 (예컨대, 알라닌 또는 폴리알라닌)으로 대체되어, 항원과 항체의 상호작용이 영향을 받았는지를 판단한다. 초기 치환에 대한 기능적 민감성을 나타내는 아미노산 위치에 추가 치환이 도입될 수 있다. 대안으로, 또는 추가로, 항원-항체 복합체의 결정 구조를 이용하여 항체와 항원 간의 접촉점을 식별한다. 이러한 접촉 잔기와 이웃 잔기는 치환의 후보로서 표적되거나, 또는 제거될 수 있다. 변이체들이 원하는 성질을 포함하는지 여부를 결정하기 위해 이들을 스크리닝할 수 있다.A useful method for identification of residues or regions of an antibody that can be targeted for mutagenesis is called “alanine scanning mutagenesis” as described by Cunningham and Wells (1989) Science , 244:1081-1085. In this method, a target moiety or group of target moieties (eg, charged residues such as Arg, Asp, His, Lys, and Glu) is identified and converted to a neutral or negatively charged amino acid (eg, alanine or polyalanine). In turn, it is determined whether the interaction of the antigen with the antibody is affected. Additional substitutions may be introduced at amino acid positions that exhibit functional sensitivity to the initial substitution. Alternatively, or in addition, the crystal structure of the antigen-antibody complex is used to identify contact points between the antibody and antigen. Such contact residues and neighboring residues can be targeted as candidates for substitution, or eliminated. Variants can be screened to determine whether they contain a desired property.
아미노산 서열 삽입은 1개 잔기로부터 100개 이상의 잔기를 함유하는 폴리펩티드까지의 길이의 범위를 갖는 아미노 및/또는 카르복실 말단 융합뿐만 아니라 단일 또는 복수 아미노산 잔기의 서열내 삽입을 포함한다. 말단 삽입의 예는 N-말단 메티오닐 잔기를 갖는 항체를 포함한다. 항체 분자의 다른 삽입 변이체는 항체의 혈청 반감기를 증가시키는 효소 (예를 들면, ADEPT의 경우) 또는 폴리펩티드에 대한 항체의 N 또는 C 말단에 융합을 포함한다.Amino acid sequence insertions include amino and/or carboxyl terminus fusions ranging in length from one residue to polypeptides containing 100 or more residues, as well as intrasequence insertions of single or multiple amino acid residues. Examples of terminal insertions include antibodies having an N-terminal methionyl residue. Other insertional variants of the antibody molecule include a fusion to the N or C terminus of the antibody to an enzyme (eg, in the case of ADEPT) or polypeptide that increases the serum half-life of the antibody.
II. 글리코실화 변이체II. glycosylation variants
특정 경우들에서, 본 발명의 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)는 항체가 당화되는 정도를 증가 또는 감소시키도록 변경될 수 있다. 본 발명의 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체 (예를 들어, 항 PD-L1 길항제 항체)의 당화 부위의 추가 또는 결실은 하나 또는 그 이상의 당화 부위가 만들어지거나 또는 제거되도록 아미노산 서열을 변경시킴으로써 편의상 실행될 수 있다. In certain instances, an anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody) of the invention increases or decreases the extent to which the antibody is glycosylated. may be changed. The addition or deletion of glycosylation sites in the anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody) of the present invention is amino acid such that one or more glycosylation sites are created or removed. This can be done for convenience by altering the sequence.
항체가 Fc 영역을 포함할 때, 이에 부착된 탄수화물은 변경될 수 있다. 포유류 세포들에 의해 만들어지는 고유 항체는 Fc 영역의 CH2 도메인의 Asn297에 N 연결부에 의해 일반적으로 부착된 분지화된, 이촉각성(biantennary) 올리고당을 전형적으로 포함한다. 예컨대, Wright et al. TIBTECH 15:26-32 (1997). 올리고당류는 다양한 탄수화물, 예를 들면, 만노오스, N-아세틸 글루코사민(GlcNAc), 갈락토오스 및 시알산뿐만 아니라 바이안테나리 올리고당류 구조의 “줄기”에서 GlcNAc에 부착된 푸코오스를 포함할 수 있다. 일부 경우들에서, 특정한 개선된 특성을 갖는 항체 변이체를 생성하기 위해 본 발명의 항체의 올리고당의 변형이 이루어진다. When the antibody comprises an Fc region, the carbohydrate attached thereto may be altered. Native antibodies made by mammalian cells typically comprise a branched, biantennary oligosaccharide attached generally by an N linkage to Asn297 of the CH2 domain of the Fc region. See, eg, Wright et al. TIBTECH 15:26-32 (1997). Oligosaccharides can include a variety of carbohydrates, such as mannose, N-acetyl glucosamine (GlcNAc), galactose and sialic acid, as well as fucose attached to GlcNAc in the “stem” of the biantennary oligosaccharide structure. In some cases, modifications of the oligosaccharides of the antibodies of the invention are made to generate antibody variants with certain improved properties.
한 경우에서, Fc 영역에 부착된(직접 또는 간접적으로) 푸코스가 없는 탄수화물 구조를 가진 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체) 변이체들이 제공된다. 예를 들어, 이러한 항체에서 푸코스의 양은 1% 내지 80%, 1% 내지 65%, 5% 내지 65% 또는 20% 내지 40%가 될 수 있다. 푸코오스의 양은, 예를 들어 WO 2008/077546에서 기재된 바와 같이, MALDI-TOF 질량 분광분석법에 의해 측정될 때, Asn 297에 부착된 모든 당구조의 총합(예컨대, 복합체, 하이브리드 및 높은 만노오스 구조)에 비하여, 상대적으로 Asn297에서 당쇄 내에 푸코오스의 평균량을 계산함으로써 결정된다. Asn297은 Fc 영역 내에 대략 위치 297 (Fc 영역 잔기의 EU 넘버링)에서 위치된 아스파라긴 잔기를 지칭한다; 하지만, Asn297은 또한, 항체에서 경미한 서열 변이로 인해, 위치 297의 대략 ± 3개 아미노산 상류 또는 하류에, 다시 말하면, 위치 294 및 300 사이에 위치될 수 있다. 이러한 푸코실화는 개선된 ADCC 기능을 보유할 수 있다. 예컨대, 미국 특허 공보 제2003/0157108호(Presta, L.); US 2004/0093621(쿄와 하꼬 코교(Kyowa Hakko Kogyo Co., Ltd))을 참조한다. “탈푸코실화” 또는 “푸코스 결핍” 항체 변이체들과 관련된 문헌들의 예는 다음을 포함한다: US 2003/0157108; WO 2000/61739; WO 2001/29246; US 2003/0115614; US 2002/0164328; US 2004/0093621; US 2004/0132140; US 2004/0110704; US 2004/0110282; US 2004/0109865; WO 2003/085119; WO 2003/084570; WO 2005/035586; WO 2005/035778; WO2005/053742; WO2002/031140; Okazaki et al. J. Mol. Biol. 336:1239-1249 (2004); Yamane-Ohnuki et al. Biotech. Bioeng. 87: 614 (2004)에서 기재된 바와 같은 삼중특이적 항체를 제조하여 만들 수 있다. 탈푸코실화된 항체를 생성할 수 있는 세포주의 예는 단백질 푸코실화가 결핍된 Lec13 CHO 세포(Ripka et al. Arch. Biochem. Biophys. 249:533-545 (1986); 미국 특허 출원 제 US 2003/0157108 A1호, Presta, L; 및 WO 2004/056312 A1, Adams et al., 특히 실시예 11), 및 녹아웃 세포주, 예컨대 알파-1,6-푸코실전달효소 유전자, FUT8, 녹아웃 CHO 세포(예컨대, Yamane-Ohnuki et al. Biotech. Bioeng. 87: 614 (2004); Kanda, Y. et al., Biotechnol. Bioeng., 94(4):680-688 (2006); 및 WO2003/085107)를 포함한다.In one case, anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody) variants are provided having a carbohydrate structure that lacks fucose attached (directly or indirectly) to the Fc region. do. For example, the amount of fucose in such an antibody may be between 1% and 80%, between 1% and 65%, between 5% and 65% or between 20% and 40%. The amount of fucose is the sum of all sugar structures attached to Asn 297 (e.g. complex, hybrid and high mannose structures) as measured by MALDI-TOF mass spectrometry, as described, for example, in WO 2008/077546. In comparison, it is relatively determined by calculating the average amount of fucose in the sugar chain at Asn297. Asn297 refers to an asparagine residue located in the Fc region at approximately position 297 (EU numbering of Fc region residues); However, Asn297 may also be located approximately ± 3 amino acids upstream or downstream of position 297, ie between positions 294 and 300, due to minor sequence variations in the antibody. Such fucosylation may have improved ADCC function. See, eg, US Patent Publication Nos. 2003/0157108 (Presta, L.); See US 2004/0093621 (Kyowa Hakko Kogyo Co., Ltd). Examples of documents relating to “defucosylated” or “fucose deficient” antibody variants include: US 2003/0157108; WO 2000/61739; WO 2001/29246; US 2003/0115614; US 2002/0164328; US 2004/0093621; US 2004/0132140; US 2004/0110704; US 2004/0110282; US 2004/0109865; WO 2003/085119; WO 2003/084570; WO 2005/035586; WO 2005/035778; WO2005/053742; WO2002/031140; Okazaki et al. J. Mol. Biol. 336:1239-1249 (2004); Yamane-Ohnuki et al. Biotech. Bioeng. 87: 614 (2004). Examples of cell lines capable of producing afucosylated antibodies include Lec13 CHO cells deficient in protein fucosylation (Ripka et al. Arch. Biochem. Biophys. 249:533-545 (1986); US Patent Application No. US 2003/ 0157108 A1, Presta, L; and WO 2004/056312 A1, Adams et al ., especially Example 11), and knockout cell lines such as alpha-1,6-fucosyltransferase gene, FUT8 , knockout CHO cells (such as , Yamane-Ohnuki et al. Biotech. Bioeng. 87: 614 (2004); Kanda, Y. et al. , Biotechnol. Bioeng ., 94(4): 680-688 (2006); and WO2003/085107). do.
상기 내용을 고려할 때, 일부 예들에서, 본 발명의 방법은 비당화 부위 돌연변이를 포함하는 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체) 변이체를 분획화된 용량 증량 투약 요법과 관련하여 대상체에게 투여하는 것을 포함한다. 일부 경우들에서, 비당화 부위 돌연변이는 항체의 효과기 기능을 감소시킨다. 일부 경우들에서, 비당화 부위 돌연변이는 치환 돌연변이이다. 일부 경우들에서, 항체는 작동체 기능을 감소시키는, Fc 영역의 치환 돌연변이를 포함한다. 일부 경우들에서, 치환 돌연변이는 아미노산 잔기 N297, L234, L235, 및/또는 D265 (EU 넘버링)에 존재한다. 일부 경우들에서, 치환 돌연변이는 N297G, N297A, L234A, L235A, D265A, 및 P329G로 구성된 그룹에서 선택된다. 일부 경우들에서, 치환 돌연변이는 아미노산 잔기 N297에 존재한다. 바람직한 경우에서, 치환 돌연변이는 N297A이다.In view of the above, in some embodiments, the methods of the present invention comprise an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tyragolumab) comprising an aglycosylation site mutation and/or the PD-1 axis administering a binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody) variant to a subject in connection with a fractionated dose escalation dosing regimen. In some cases, aglycosylation site mutations reduce effector function of the antibody. In some cases, the aglycosylation site mutation is a substitution mutation. In some cases, the antibody comprises a substitution mutation in the Fc region that reduces effector function. In some cases, the substitution mutation is at amino acid residues N297, L234, L235, and/or D265 (EU numbering). In some cases, the substitution mutation is selected from the group consisting of N297G, N297A, L234A, L235A, D265A, and P329G. In some cases, the substitution mutation is at amino acid residue N297. In a preferred case, the substitution mutation is N297A.
항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-L1 길항제 항체)의 Fc 영역의 이촉각성 올리고당이 GlcNAc에 의해 양분되어 있는, 양분된 올리고당을 가진 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체변이체들이 추가로 제공된다. 이러한 항체 변이체는 감소된 푸코실화 및/또는 개선된 ADCC 기능을 가질 수 있다. 이러한 변이체들의 예들은 예로써, WO 2003/011878 (Jean-Mairet 외.); 미국 특허 제 6,602,684 (Umana et al.); 및 미국 2005/0123546(Umana et al.)에 기재되어 있다. Fc 영역에 부착된 올리고당에 최소한 한 개의 갈락토스 잔기를 가진 항체 변이체들이 또한 제공된다. 이러한 항체 변이체들은 개선된 CDC 기능을 보유할 수 있다. 이러한 항체 변이체들은 예로써, WO 1997/30087 (Patel 외.); WO 1998/58964 (Raju, S.); 그리고 WO 1999/22764 (Raju, S.)에서 기재되어 있다.Antitactile oligosaccharides in the Fc region of an anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody (eg, anti-PD-L1 antagonist antibody or anti-PD-L1 antagonist antibody) are bisected by GlcNAc, bisected oligosaccharides Anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist antibody variants are further provided. Such antibody variants may have reduced fucosylation and/or improved ADCC function. Examples of such variants are eg in WO 2003/011878 (Jean-Mairet et al.); US Pat. No. 6,602,684 to Umana et al.; and US 2005/0123546 (Umana et al .). Antibody variants having at least one galactose residue in the oligosaccharide attached to the Fc region are also provided. Such antibody variants may possess improved CDC function. Such antibody variants are described, for example, in WO 1997/30087 (Patel et al.); WO 1998/58964 (Raju, S.); and in WO 1999/22764 (Raju, S.).
III. Fc 영역 변이체 III. Fc region variants
특정 경우들에서, 하나 또는 그 이상의 아미노산 변형이 본 발명의 항 TIGIT 길항제(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체)의 Fc 영역 안으로 도입되고, 이로 인하여 Fc 영역 변이체가 생성된다(예컨대, US 2012/0251531을 참조). 상기 Fc 영역 변이체는 하나 또는 그 이상의 아미노산 위치에서 아미노산 변형(예컨대, 치환)을 포함하는 인간 Fc 영역 서열 (예컨대, 인간 IgG1, IgG2, IgG3 또는 IgG4 Fc 영역)를 포함할 수 있다.In certain instances, one or more amino acid modifications are altered by an anti TIGIT antagonist (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tyragolumab) antibody and/or a PD-1 axis binding antagonist antibody (eg, anti introduced into the Fc region of a PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody), resulting in Fc region variants (see, eg, US 2012/0251531). The Fc region variant may comprise a human Fc region sequence (eg, a human IgG1, IgG2, IgG3 or IgG4 Fc region) comprising amino acid modifications (eg substitutions) at one or more amino acid positions.
특정 경우들에서, 본 발명은 모든 효과기 기능은 아니지만 일부를 효과기 기능을 보유하는 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체 (예를 들어, 항 PD-L1 길항제 항체 변이체)를 고려하는데, 이는 생체내에서 항체의 반감기가 중요하지만 또한 특정 효과기 기능 (가령, 보체 및 ADCC)이 불필요하거나 유해한 응용분야에 있어서 바람직한 후보가 되게 한다. 시험관내 및/또는 생체내 세포독성 분석을 실행하여 CDC 및/또는 ADCC 활성의 감소/고갈을 확인할 수 있다. 예를 들면, Fc 수용체 (FcR) 결합 분석을 수행하여 상기 항체가 FcgR 결합은 없으나 (그리하여 ADCC 활성이 없을 수 있음), FcRn 결합 능력은 유지함을 확인할 수 있다. ADCC를 조정하는 주요 세포, NK 세포들은 오직 Fc(RIII만을 발현시키지만, 단핵구는 Fc(RI, Fc(RII 및 Fc(RIII를 발현시킨다. 조혈 세포상의 Fc 발현은: Ravetch and Kinet, Annu. Rev. Immunol. 9:457-492 (1991)의 464 페이지, 표 3을 참조한다. 관심이 되는 분자의 ADCC 활성을 평가하기 위한 시험관내 분석의 비제한적인 예는 미국 특허 제5,500,362(예컨대, Hellstrom, I. et al. Proc. Nat'l Acad. Sci. USA 83:7059-7063 (1986)) 및 Hellstrom, I et al., Proc. Nat'l Acad. Sci. USA 82:1499-1502 (1985); 5,821,337 (Bruggemann, M. et al., J. Exp. Med. 166:1351-1361 (1987)을 참조). 대안으로, 비방사능활성 분석 방법들이 이용될 수 있다(예를 들어, 유동 세포측정을 위한 ACTI™ 비방사능활성 세포독성 분석(셀 테크놀로지(CellTechnology, Inc.), 캘리포니아 주의 마운틴 뷰 소재); 및 사이토톡스(CytoTox) 96® 비방사능활성 세포독성 분석(프로메가(Promega), 위스콘신주의 매디슨 소재)을 참조). 이런 분석을 위한 유용한 작동체 세포는 말초혈 단핵 세포(PBMC) 및 자연 킬러(NK) 세포를 포함한다. 대안적으로 또는 추가로, 관심이 되는 분자의 ADCC 활성은 생체내, 예컨대 동물 모델에서, 예컨대 Clynes et al. Proc. Nat'l Acad. Sci. USA 95:652-656 (1998)에 개시된 바와 같이 평가될 수 있다. 상기 항체가 C1q에 결합할 수 없고, 이로 인하여 CDC 활성이 결여된다는 것을 확인하기 위하여 C1q 결합 분석이 또한 실행될 수 있다. 예컨대, WO 2006/029879와 WO 2005/100402에서 C1q 및 C3c 결합 ELISA 참조한다. 보체 활성화를 평가하기 위해, CDC 분석이 수행될 수 있다(예를 들어, Gazzano-Santoro et al. J. Immunol. Methods 202:163 (1996); Cragg, M.S. et al. Blood. 101:1045-1052 (2003); 및 Cragg, M.S. and M.J. Glennie Blood. 103:2738-2743 (2004)을 참조). FcRn 결합 및 생체내 청소율/반감기 측정은 또한 당업계에 공지된 방법을 사용하여 실시될 수 있다(예컨대, Petkova, S.B. et al. Int’l. Immunol. 18(12):1759-1769 (2006)를 참조).In certain instances, the present invention contemplates anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibody variants) that retain some but not all effector functions. , this makes it a desirable candidate for applications where the half-life of an antibody in vivo is important, but also where certain effector functions (eg, complement and ADCC) are unnecessary or detrimental. In vitro and/or in vivo cytotoxicity assays may be performed to confirm reduction/depletion of CDC and/or ADCC activity. For example, Fc receptor (FcR) binding assays can be performed to confirm that the antibody lacks FcgR binding (and thus may not have ADCC activity), but retains FcRn binding ability. The main cells that modulate ADCC, NK cells, express only Fc (RIII), whereas monocytes express Fc (RI, Fc (RII and Fc (RIII). Fc expression on hematopoietic cells is: Ravetch and Kinet, Annu. Rev. See Immunol. 9:457-492 (1991), page 464, Table 3. A non-limiting example of an in vitro assay for assessing ADCC activity of a molecule of interest is US Pat. et al. Proc. Nat'l Acad. Sci. USA 83:7059-7063 (1986)) and Hellstrom, I et al., Proc. Nat'l Acad. Sci. USA 82:1499-1502 (1985); 5,821,337 (see Bruggemann, M. et al., J. Exp. Med. 166:1351-1361 (1987)) Alternatively, non-radioactivity assay methods can be used (e.g., flow cytometry ACTI™ non-radioactive cytotoxicity assay (CellTechnology, Inc., Mountain View, CA); and CytoTox 96 ® non-radioactive cytotoxicity assay (Promega, Madison, Wis.) location).Useful effector cells for this assay include peripheral blood mononuclear cells (PBMC) and natural killer (NK) cells.Alternatively or additionally, ADCC activity of the molecule of interest can be determined in vivo , such as in animal models, such as as disclosed in Clynes et al. Proc. Nat'l Acad. Sci. USA 95:652-656 (1998). Clq binding assay can also be carried out to confirm lack of CDC activity.See, for example, Clq and C3c binding ELISA in WO 2006/029879 and WO 2005/100402. Assess complement activation To do this, a CDC analysis can be performed (eg, Gazzano-Santoro et al. J. Immunol. Methods 202:163 (1996); Cragg, MS et al. Blood. 101:1045-1052 (2003); and Cragg, MS and MJ Glennie Blood. 103:2738-2743 (2004)). FcRn binding and in vivo clearance/half-life measurements can also be performed using methods known in the art (eg, Petkova, SB et al. Int'l. Immunol. 18(12):1759-1769 (2006)) see).
감소된 효과기 기능를 가진 항체들은 Fc 영역 잔기 238, 265, 269, 270, 297, 327 및 329 중 하나 또는 그 이상의 치환을 가진 것들을 포함한다 (미국 특허 제 6,737,056 및 8,219,149). 이러한 Fc 돌연변이체들은 잔기 265 및 297의 잔기가 알라닌으로 치환된 소위 "DANA" Fc 돌연변이체를 비롯하여, 아미노산 위치 265, 269, 270, 297 및 327 중 2개 또는 그 이상에서 치환을 가진 Fc 돌연변이체들을 포함한다 (미국 특허 제 7,332,581 및 8,219,149 참조). Antibodies with reduced effector function include those with substitutions of one or more of Fc region residues 238, 265, 269, 270, 297, 327 and 329 (U.S. Pat. Nos. 6,737,056 and 8,219,149). Such Fc mutants include Fc mutants having substitutions at two or more of amino acid positions 265, 269, 270, 297 and 327, including the so-called "DANA" Fc mutants in which residues 265 and 297 are substituted with alanine. (see US Pat. Nos. 7,332,581 and 8,219,149).
특정 경우들에서, 항체에서 야생형 인간 Fc 영역의 위치 329의 프롤린은 글리신 또는 아르기닌 또는 Fc의 프롤린 329와 FcgRIII의 트립토판 잔기 Trp 87 및 Trp 110 사이에서 형성되는 Fc/Fcγ 수용체 경계면 내부의 프롤린 샌드위치를 파괴하기에 충분히 큰 아미노산 잔기로 치환된다 (Sondermann et al.: Nature 406, 267-273 (20 Jul. 2000)). 특정 경우들에서, 상기 항체는 적어도 하나의 추가 아미노산 치환을 포함한다. 한 경우에서, 추가 아미노산 치환은 S228P, E233P, L234A, L235A, L235E, N297A, N297D, 또는 P331S이고, 그리고 또한 또 다른 예에서 적어도 하나의 추가 아미노산 치환은 인간 IgG1 Fc 영역의 L234A 및 L235A 또는 S228P 및 인간 IgG4 Fc 영역의 L235E이고(예컨대, US 2012/0251531을 참조), 그리고 또한 또 다른 예에서 적어도 하나의 추가 아미노산 치환은 인간 IgG1 Fc 영역의 L234A 및 L235A 및 P329G이다.In certain instances, proline at position 329 of the wild-type human Fc region in the antibody disrupts the proline sandwich inside the Fc/Fcγ receptor interface formed between glycine or arginine or proline 329 of Fc and tryptophan residues Trp 87 and Trp 110 of FcgRIII Amino acid residues large enough to be substituted (Sondermann et al.: Nature 406, 267-273 (20 Jul. 2000)). In certain instances, the antibody comprises at least one additional amino acid substitution. In one case, the additional amino acid substitution is S228P, E233P, L234A, L235A, L235E, N297A, N297D, or P331S, and in yet another example the at least one additional amino acid substitution is L234A and L235A or S228P of a human IgG1 Fc region and L235E of the human IgG4 Fc region (see eg US 2012/0251531), and in yet another example the at least one further amino acid substitution is L234A and L235A and P329G of the human IgG1 Fc region.
FcR에 대한 결합이 개선 또는 감소된 특정 항체 변이체가 기재된다. (예컨대, 미국 특허 제6,737,056호; WO 2004/056312호, 및 Shields et al., J. Biol. Chem. 9(2): 6591-6604 (2001)를 참조). Certain antibody variants with improved or reduced binding to FcRs are described. (See, eg, US Pat. No. 6,737,056; WO 2004/056312, and Shields et al. , J. Biol. Chem. 9(2): 6591-6604 (2001)).
특정 경우들에서, 항체 변이체는 ADCC를 개선시키는 하나 이상의 아미노산 치환, 예컨대 Fc 영역의 위치 298, 333 및/또는 334(잔기의 EU 넘버링)에서 치환을 갖는 Fc 영역을 포함한다. In certain cases, the antibody variant comprises an Fc region having one or more amino acid substitutions that improve ADCC, such as substitutions at positions 298, 333 and/or 334 (EU numbering of residues) of the Fc region.
일부 경우들에서, 변경은, 예컨대 미국 특허 제6,194,551호, WO 99/51642호, 및 Idusogie et al. J. Immunol. 164: 4178-4184 (2000)에 기재된 바와 같이 변경된(즉, 개선되거나 감소된) C1q 결합 및/또는 보체 의존성 세포독성(CDC)을 초래하는 Fc 영역에서 이루어진다. In some cases, modifications are described, for example, in US Pat. Nos. 6,194,551, WO 99/51642, and Idusogie et al. J. Immunol. 164: 4178-4184 (2000), resulting in altered (ie, improved or reduced) Clq binding and/or complement dependent cytotoxicity (CDC) in the Fc region.
반감기가 증가되고, 태아로의 모체 IgG의 이동에 원인으로 작용하는 신생아 Fc 수용체(FcRn)로의 결합이 개선된 항체(Guyer et al., J. Immunol. 117:587 (1976) and Kim et al., J. Immunol. 24:249 (1994))가 US2005/0014934A1(Hinton et al.)에 기재되어 있다. 이들 항체는 FcRn에 대한 Fc 영역의 결합을 개선시키는 하나 또는 그 이상의 치환들을 가진 Fc 영역을 내부에 포함한다. 상기 Fc 변이체들은 Fc 영역 잔기들: 238, 256, 265, 272, 286, 303, 305, 307, 311, 312, 317, 340, 356, 360, 362, 376, 378, 380, 382, 413, 424 또는 434의 하나 이상에서 치환, 예컨대 Fc 영역 잔기 434의 치환 (US 특허 제7,371,826호).Antibodies with increased half-life and improved binding to neonatal Fc receptor (FcRn), which act as a causative agent for the transfer of maternal IgG to the fetus (Guyer et al., J. Immunol. 117:587 (1976) and Kim et al. , J. Immunol. 24:249 (1994)) are described in US2005/0014934A1 (Hinton et al.). These antibodies contain an Fc region therein with one or more substitutions that improve binding of the Fc region to FcRn. The Fc variants have Fc region residues: 238, 256, 265, 272, 286, 303, 305, 307, 311, 312, 317, 340, 356, 360, 362, 376, 378, 380, 382, 413, 424 or a substitution at one or more of 434, such as a substitution of Fc region residue 434 (US Pat. No. 7,371,826).
Fc 영역 변이체들의 다른 예들에 관련된 Duncan & Winter, Nature 322:738-40 (1988); U.S. 특허 제 5,648,260; U.S.특허 제 5,624,821; 그리고 WO 94/29351을 참조한다. Duncan & Winter, Nature 322:738-40 (1988) relating to other examples of Fc region variants; US Patent No. 5,648,260; US Patent No. 5,624,821; and WO 94/29351.
일부 양태들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)는 N297G 돌연변이를 포함하는 Fc 영역을 포함한다. In some aspects, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) and/or an anti-PD-L1 antagonist antibody (eg, atezolizumab) is an Fc comprising an N297G mutation includes area.
일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙) 또는 항 PD-1 길항제 항체)는 하나 이상의 중쇄 불변 도메인을 포함하고, 여기서 상기 하나 이상의 중쇄 불변 도메인은 제1 CH1(CH11) 도메인, 제1 CH2(CH21) 도메인, 제1 CH3(CH31) 도메인, 제2 CH1(CH12) 도메인, 제2 CH2(CH22) 도메인, 및 제2 CH3(CH32) 도메인으로부터 선택된다. 일부 예들에서, 하나 이상의 중쇄 불변 도메인 중 적어도 하나는 또 다른 중쇄 불변 도메인과 페어링된다. 일부 구현예에서, CH3 1 및 CH3 2 도메인 각각은 돌출부 또는 공동을 포함하고, 여기서 CH3 1 도메인에서 돌출부 또는 공동은 각각 CH3 2 도메인에서 공동 또는 돌출부에 위치할 수 있다. 일부 경우들에서, 상기 CH3 1 및 CH3 2 도메인은 상기 돌출부 및 공동 사이 계면에서 만난다. 일부 경우들에서, CH2 1 및 CH2 2 도메인 각각은 돌출부 또는 공동을 포함하고, 여기서 CH2 1 도메인에서 돌출부 또는 공동은 각각 CH2 2 도메인에서 공동 또는 돌출부에 위치할 수 있다. 일부 경우들에서, 상기 CH21 및 CH22 도메인은 상기 돌기 또는 공동 사이의 경계면에서 만난다. 일부 경우들에서, 상기 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 항 PD-L1 길항제 항체(예컨대, 아테졸리주맙)는 IgG1 항체이다.In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody (eg, ate zolizumab) or anti-PD-1 antagonist antibody) comprises one or more heavy chain constant domains, wherein said one or more heavy chain constant domains comprise a first CH1 (CH11) domain, a first CH2 (CH21) domain, a first CH3 (CH31) ) domain, a second CH1 (CH12) domain, a second CH2 (CH22) domain, and a second CH3 (CH32) domain. In some examples, at least one of the one or more heavy chain constant domains is paired with another heavy chain constant domain. In some embodiments, each of the CH3 1 and CH3 2 domains comprises an overhang or cavity, wherein the overhang or cavity in the CH3 1 domain may be located in the cavity or overhang in the CH3 2 domain, respectively. In some cases, the CH3 1 and CH3 2 domains meet at the interface between the protrusion and the cavity. In some cases, each of the CH2 1 and CH2 2 domains comprises an overhang or cavity, wherein the overhang or cavity in the CH2 1 domain may be located in the cavity or overhang in the CH2 2 domain, respectively. In some cases, the CH21 and CH22 domains meet at the interface between the protrusion or cavity. In some cases, the anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody disclosed herein, eg, tiragolumab) and/or an anti-PD-L1 antagonist antibody (eg, atezolizumab) is an IgG1 antibody.
IV. 시스테인 가공된 항체 변이체IV. Cysteine engineered antibody variants
특정 경우들에서, 항체의 하나 또는 그 이상의 잔기가 시스테인 잔기로 대체된, 항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체), 예컨대, "thioMAbs"를 만드는 것이 바람직할 수 있다. 특정 경우들에서, 상기 치환된 잔기는 항체의 접근가능한 부위에서 나타난다. 이들 잔기를 시스테인으로 치환함으로써, 반응성 티올 기는 따라서, 항체의 접근 가능한 부위에서 위치되고, 그리고 항체를 다른 모이어티, 예컨대 약물 모이어티 또는 링커-약물 모이어티에 접합하여 본원에서 더욱 설명된 바와 같은 면역접합체를 창출하는 데 이용될 수 있다. 특정 경우들에서, 다음과 같은 임의의 하나 또는 그 이상의 잔기는 시스테인으로 치환된다: 경쇄의 V205(카바트 넘버링); 중쇄의 A118(EU 넘버링); 및 중쇄 Fc 영역의 S400 (EU 넘버링). 시스테인 조작된 항체는 예를 들면, 미국 특허 제 7,521,541에서 설명된 것과 같이 생성될 수 있다. In certain instances, an anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody), wherein one or more residues of the antibody are replaced with cysteine residues. For example, it may be desirable to make "thioMAbs". In certain instances, the substituted residue appears at an accessible site of the antibody. By substituting these residues with cysteines, reactive thiol groups are thus positioned at accessible sites of the antibody, and the antibody is conjugated to other moieties, such as drug moieties or linker-drug moieties, to immunoconjugates as further described herein. can be used to create In certain instances, any one or more of the following residues are substituted with cysteine: V205 of the light chain (Kabat numbering); A118 (EU numbering) of the heavy chain; and S400 (EU numbering) of the heavy chain Fc region. Cysteine engineered antibodies can be generated as described, for example, in US Pat. No. 7,521,541.
V. 항체 유도체V. Antibody Derivatives
특정 경우들에서, 본원에 제공되는 본 발명의 항 TIGIT 길항제 항체 (예를 들어, 항 TIGIT 길항제 항체 (예를 들어, 티라골루맙) 또는 이의 변이체) 및/또는 PD-1 축 결합 길항제 항체 (예를 들어, 본 발명의 항 PD-L1 길항제 항체 (예를 들어, 아테졸리주맙 또는 이의 변이체))는 해당 분야에 공지되어 있고 쉽게 입수할 수 있는 추가의 비단백질성 모이어티를 함유하도록 추가로 변형된다. 항체의 유도체화에 적합한 모이어티는 수용성 중합체를 포함하지만 이들에 한정되지 않는다. 수용성 중합체의 무제한적 실례는 폴리에틸렌 글리콜 (PEG), 에틸렌 글리콜/프로필렌 글리콜의 공중합체, 카르복시메틸셀룰로오스, 덱스트란, 폴리비닐 알코올, 폴리비닐 피롤리돈, 폴리-1, 3-디옥솔란, 폴리-1,3,6-트리옥산, 에틸렌/말레산 무수물 공중합체, 폴리아미노산 (동종중합체 또는 무작위 공중합체), 그리고 덱스트란 또는 폴리(n-비닐 피롤리돈)폴리에틸렌 글리콜, 프로프로필렌 글리콜 동종중합체, 프롤릴프로필렌 산화물/에틸렌 산화물 공중합체, 폴리옥시에틸화된 폴리올 (예를 들면, 글리세롤), 폴리비닐 알코올, 그리고 이들의 혼합물을 포함하지만 이들에 한정되지 않는다. 폴리에틸렌 글리콜 프로피온알데히드는 물에서 안정성으로 인해, 제조 시에 이점을 가질 수 있다. 중합체는 임의의 분자량일 수 있고, 분지형 또는 비분지형일 수 있다. 상기 항체에 부착된 중합체의 수는 가변적일 수 있고, 만약 하나를 초과한 중합체가 부착된 경우, 중합체들은 동일하거나 상이한 분자일 수 있다. 일반적으로, 유도체화에 이용되는 중합체의 숫자 및/또는 유형은 향상되는 항체의 특정 특성 또는 기능, 항체 유도체가 규정된 조건하에 요법에서 이용될 것인지의 여부 등을 포함하지만 이들에 한정되지 않는 고려 사항에 근거하여 결정될 수 있다.In certain instances, an anti TIGIT antagonist antibody (eg, an anti TIGIT antagonist antibody (eg, tyragolumab) or variant thereof) of the invention provided herein and/or a PD-1 axis binding antagonist antibody (eg, For example, an anti-PD-L1 antagonist antibody of the invention (eg, atezolizumab or a variant thereof) is further modified to contain additional nonproteinaceous moieties known in the art and readily available. do. Suitable moieties for derivatization of antibodies include, but are not limited to, water-soluble polymers. Non-limiting examples of water-soluble polymers include polyethylene glycol (PEG), copolymers of ethylene glycol/propylene glycol, carboxymethylcellulose, dextran, polyvinyl alcohol, polyvinyl pyrrolidone, poly-1, 3-dioxolane, poly- 1,3,6-trioxane, ethylene/maleic anhydride copolymer, polyamino acid (homopolymer or random copolymer), and dextran or poly(n-vinyl pyrrolidone) polyethylene glycol, propropylene glycol homopolymer; prolylpropylene oxide/ethylene oxide copolymers, polyoxyethylated polyols (eg, glycerol), polyvinyl alcohol, and mixtures thereof. Polyethylene glycol propionaldehyde may have advantages in manufacturing due to its stability in water. The polymer may be of any molecular weight and may be branched or unbranched. The number of polymers attached to the antibody may vary, and if more than one polymer is attached, the polymers may be the same or different molecules. In general, the number and/or type of polymer used for derivatization will depend on considerations including, but not limited to, the particular property or function of the antibody being improved, whether the antibody derivative will be used in therapy under defined conditions, and the like. can be determined based on
또 다른 경우에서, 방사선에 노출에 의해 임의로 가열될 수 있는 비단백질성 모이어티 및 항체의 콘주게이트가 제공된다. 한 경우에서, 비단백질성 모이어티는 탄소 나노튜브이다(Kam et al., Proc. Natl. Acad. Sci. USA 102: 11600-11605 (2005)). 방사능은 임의의 파장일 수 있으며, 정상 세포들에게 해를 주지 않지만, 그러나 상기 항체-비단백질성 모이어티에 근접한 세포들은 사멸되는 온도에서 비단백질성 모이어티에 열을 가하는 파장이 포함되나, 이에 제한되는 것은 아니다.In another instance, a conjugate of an antibody and a nonproteinaceous moiety that can optionally be heated by exposure to radiation is provided. In one case, the nonproteinaceous moiety is a carbon nanotube (Kam et al., Proc. Natl. Acad. Sci. USA 102: 11600-11605 (2005)). Radioactivity can be of any wavelength and does not harm normal cells, but includes, but is not limited to, a wavelength that heats the nonproteinaceous moiety at a temperature at which cells in proximity to the antibody-nonproteinaceous moiety are killed. it is not
재조합 생산 방법Recombinant production methods
본 발명의 항 TIGIT 길항제 항체(예컨대, 본원에 개시된 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 PD-1 축 결합 길항제 항체(예컨대, 항 PD-L1 길항제 항체(예컨대,아테졸리주맙) 또는 항 PD-1 길항제 항체)는 예컨대, 미국 특허 제4,816,567호에 기재된 바와 같은 재조합 방법 및 조성물을 사용하여 제조 될 수 있으며, 이는 그 전체가 본원에 원용된다. An anti-TIGIT antagonist antibody of the invention (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tyragolumab) and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) or anti-PD-1 antagonist antibodies) can be prepared using recombinant methods and compositions, eg, as described in US Pat. No. 4,816,567, which is incorporated herein in its entirety.
항 TIGIT 길항제 항체 및/또는 PD-1 축 결합 길항제 항체 (예를 들어, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체)의 재조합 생산을 위해, 항체를 인코딩하는 핵산이 단리되고 숙주 세포에서의 추가 클로닝 및/또는 발현을 위해 하나 이상의 벡터 내로 삽입된다. 이러한 핵산은 통상적인 과정에 의해 용이하게 단리되고, 시퀀싱된다 (가령, 항체의 중쇄 및 경쇄를 인코드하는 유전자에 특이적으로 결합할 수 있는 올리고뉴클레오티드 프로브를 사용함으로써). For recombinant production of an anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (eg, an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody), a nucleic acid encoding the antibody is isolated and in a host cell. is inserted into one or more vectors for further cloning and/or expression of Such nucleic acids are readily isolated and sequenced by conventional procedures (eg, by using oligonucleotide probes capable of binding specifically to genes encoding the heavy and light chains of the antibody).
항체 부호화 벡터의 클로닝 또는 발현에 적합한 숙주 세포는 본원에 기재된 원핵 또는 진핵 세포를 포함한다. 예를 들어, 항체는 특히 당화 및 Fc 작동체 기능이 요구되지 않는 경우 박테리아에서 생성될 수 있다. 박테리아에서 항체 단편들 및 폴리펩티드 발현과 관련하여 예컨대, 미국 특허 제 5,648,237, 5,789,199, 및 5,840,523호를 참고하라. (또한, 대장균 내 항체 단편의 발현을 설명하는 Charlton, Methods in Molecular Biology, Vol. 248 (B.K.C. Lo, ed., Humana Press, Totowa, NJ, 2003), pp. 245-254를 참조한다.) 발현 후, 항체는 가용성 분획 중의 박테리아 세포 페이스트로부터 단리될 수 있으며 추가로 정제될 수 있다.Suitable host cells for cloning or expression of antibody encoding vectors include prokaryotic or eukaryotic cells described herein. For example, antibodies may be produced in bacteria, particularly when glycosylation and Fc effector function are not required. See, eg, US Pat. Nos. 5,648,237, 5,789,199, and 5,840,523 for antibody fragments and polypeptide expression in bacteria. (See also Charlton, Methods in Molecular Biology, Vol. 248 (BKC Lo, ed., Humana Press, Totowa, NJ, 2003), pp. 245-254, which describes the expression of antibody fragments in E. coli.) Expression Thereafter, the antibody can be isolated from the bacterial cell paste in the soluble fraction and can be further purified.
원핵생물에 더하여, 진핵 미생물, 예컨대 글리코실화 경로가 “인간화”되어, 부분적 또는 완전한 인간 글리코실화 패턴을 갖는 항체의 생성을 유발하는 균류 및 효모 균주를 포함한 실모양 균류 또는 효모는 항체 부호화 벡터에 적합한 클로닝 또는 발현 숙주이다. Gerngross, Nat. Biotech. 22:1409-1414 (2004), 및 Li et al., Nat. Biotech. 24:210-215 (2006)를 참조한다.In addition to prokaryotes, eukaryotic microorganisms such as filamentous fungi or yeast, including strains of fungi and yeast, in which the glycosylation pathway has been "humanized", resulting in the production of antibodies with a partially or fully human glycosylation pattern, are suitable for antibody encoding vectors. a cloning or expression host. Gerngross, Nat. Biotech. 22:1409-1414 (2004), and Li et al., Nat. Biotech. 24:210-215 (2006).
글리코실화된 항체의 발현에 적합한 숙주 세포는 또한 다세포 생물체(무척추동물 및 척추동물)로부터 유래된다. 무척추동물 세포의 실례는 식물과 곤충 세포를 포함한다. 특히, 스포도프테라 프루기페르다 (Spodoptera frugiperda) 세포의 형질감염을 위해, 곤충 세포와 함께 이용될 수 있는 다양한 바쿨로바이러스 계통이 확인되었다. Suitable host cells for expression of glycosylated antibodies are also derived from multicellular organisms (invertebrates and vertebrates). Examples of invertebrate cells include plant and insect cells. In particular, for transfection of Spodoptera frugiperda cells, various baculovirus strains that can be used with insect cells have been identified.
식물 세포 배양액 또한, 숙주로서 활용될 수 있다. 참조: 예를 들면, US 특허 번호 5,959,177, 6,040,498, 6,420,548, 7,125,978 및 6,417,429 (유전자도입 식물에서 항체를 생산하기 위한 PLANTIBODIESTM 기술을 설명).Plant cell cultures can also be utilized as hosts. See, for example, US Pat. Nos. 5,959,177, 6,040,498, 6,420,548, 7,125,978 and 6,417,429 (describing PLANTIBODIES ™ technology for producing antibodies in transgenic plants).
척추동물 세포 또한, 숙주로서 이용될 수 있다. 예를 들면, 현탁 상태에서 성장하도록 적응되는 포유류 세포주가 유용할 수 있다. 유용한 포유동물 숙주 세포주의 다른 예는 SV40(COS-7)에 의해 형질전환된 원숭이 신장 CV1 세포주; 인간 배아 신장 세포주(예컨대, Graham et al., J. Gen Virol. 36:59 (1977)에 기재된 바와 같은 293 또는 293 세포); 어린 햄스터 신장 세포(BHK); 마우스 세르톨리 세포(예컨대, Mather, Biol. Reprod. 23:243-251 (1980)에 기재된 바와 같은 TM4 세포); 원숭이 신장 세포(CV1); 아프리카 녹색 원숭이 신장 세포(VERO-76); 인간 자궁경부 암종 세포(HELA); 갯과 신장 세포(MDCK; 버팔로 랫트 간 세포(BRL 3A); 인간 폐 세포(W138); 인간 간 세포(Hep G2); 마우스 유선 종양(MMT 060562); 예컨대 Mather et al., Annals N.Y. Acad. Sci. 383:44-68 (1982)에 기재된 바와 같이 TRI 세포); MRC 5 세포; 및 FS4 세포. 다른 유용한 포유동물 숙주 세포주는 DHFR- CHO 세포(Urlaub et al., Proc. Natl. Acad. Sci. USA 77:4216 (1980))를 포함하는 중국 햄스터 난소(CHO) 세포; 및 골수종 세포주, 예컨대 Y0, NS0 및 Sp2/0을 포함한다. 항체 생성에 적합한 특정 포유류 숙주 세포주를 검토하려면, 예컨대 Yazaki and Wu, Methods in Molecular Biology, Vol. 248 (B.K.C. Lo, ed., Humana Press, Totowa, NJ), pp. 255-268 (2003)를 참조한다.Vertebrate cells can also be used as hosts. For example, mammalian cell lines adapted to grow in suspension may be useful. Other examples of useful mammalian host cell lines include the monkey kidney CV1 cell line transformed with SV40 (COS-7); human embryonic kidney cell lines (eg, 293 or 293 cells as described in Graham et al. , J. Gen Virol. 36:59 (1977)); young hamster kidney cells (BHK); mouse Sertoli cells (eg, TM4 cells as described in Mather, Biol. Reprod. 23:243-251 (1980)); monkey kidney cells (CV1); African green monkey kidney cells (VERO-76); human cervical carcinoma cells (HELA); canine kidney cells (MDCK; buffalo rat liver cells (BRL 3A); human lung cells (W138); human liver cells (Hep G2); mouse mammary gland tumors (MMT 060562); e.g. Mather et al. , Annals NY Acad. Sci TRI cells as described in 383:44-68 (1982); MRC 5 cells; and FS4 cells. Other useful mammalian host cell lines include Chinese hamster ovary (CHO) cells, including DHFR - CHO cells (Urlaub et al. , Proc. Natl. Acad. Sci. USA 77:4216 (1980)); and myeloma cell lines such as Y0, NS0 and Sp2/0. For a review of specific mammalian host cell lines suitable for antibody production, see, eg, Yazaki and Wu, Methods in Molecular Biology, Vol. 248 (BKC Lo, ed., Humana Press, Totowa, NJ), pp. 255-268 (2003).
면역접합체 immunoconjugate
본 발명은 또한 본원에 기재된 방법 또는 사용에 사용하기 위한 화학요법제 또는 약물과 같은 하나 이상의 세포독성제에 접합된 본 발명의 항 TIGIT 길항제(예컨대, 본원에 개시된 바와 같은 항 TIGIT 길항제 항체, 예컨대, 티라골루맙) 및/또는 PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체(예컨대, 펨블로리주맙)), 성장 억제제, 독소(예컨대, 단백질 독소, 박테리아, 진균, 식물 또는 동물 기원의 효소 활성 독소, 또는 이의 단편), 또는 방사성 동위 원소를 포함하는 면역 접합체를 제공한다. The invention also provides an anti-TIGIT antagonist of the invention conjugated to one or more cytotoxic agents such as chemotherapeutic agents or drugs for use in the methods or uses described herein (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and/or PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, pemblorizumab)), growth inhibitory agents, toxins (eg, protein toxins, bacterial, fungal, plant or animal origin) of an enzyme-active toxin, or fragment thereof), or an immunoconjugate comprising a radioactive isotope.
일부 경우들에서, 면역접합체는 항체가 메이탄시노이드(미국 특허 제5,208,020호, 제5,416,064호 및 유럽 특허 EP 0 425 235 B1호를 참조); 모노메틸아우리스타틴 약물 모이어티 DE 및 DF와 같은 아우리스타틴(MMAE 및 MMAF)(미국 특허 제5,635,483호 및 제5,780,588호 및 제7,498,298호를 참조); 돌라스타틴; 칼리케아미신 또는 이의 유도체(미국 특허 제5,712,374호, 제5,714,586호, 제5,739,116호, 제5,767,285호, 제5,770,701호, 제5,770,710호, 제5,773,001호, 및 제5,877,296호를 참조; Hinman et al., Cancer Res. 53:3336-3342 (1993); 및 Lode et al., Cancer Res. 58:2925-2928 (1998)); 안트라사이클린, 예컨대 다우노마이신 또는 독소루비신(Kratz et al., Current Med. Chem. 13:477-523 (2006); Jeffrey et al., Bioorganic & Med. Chem. Letters 16:358-362 (2006); Torgov et al., Bioconj. Chem. 16:717-721 (2005); Nagy et al., Proc. Natl. Acad. Sci. USA 97:829-834 (2000); Dubowchik et al., Bioorg. & Med. Chem. Letters 12:1529-1532 (2002); King et al., J. Med. Chem. 45:4336-4343 (2002); 및 미국 특허 제6,630,579호를 참조); 메토트렉세이트; 빈데신; 탁산, 예컨대 도세탁셀, 파클리탁셀, 라로탁셀, 테세탁셀, 및 오르타탁셀; 트리코테센; 및 CC1065를 포함하지만 이에 제한되지는 않는 하나 이상의 약물에 접합된 항체-약물 접합체(ADC)이다. In some cases, the immunoconjugate is an antibody to a maytansinoid (see US Pat. Nos. 5,208,020, 5,416,064 and European Patent EP 0 425 235 B1); auristatins (MMAE and MMAF), such as monomethylauristatin drug moieties DE and DF (see US Pat. Nos. 5,635,483 and 5,780,588 and 7,498,298); dolastatin; calicheamicin or a derivative thereof (see U.S. Patent Nos. 5,712,374, 5,714,586, 5,739,116, 5,767,285, 5,770,701, 5,770,710, 5,773,001, and 5,877,296; Hinman et al., Cancer Res. 53:3336-3342 (1993) and Lode et al., Cancer Res. 58:2925-2928 (1998)); anthracyclines such as daunomycin or doxorubicin (Kratz et al., Current Med. Chem. 13:477-523 (2006); Jeffrey et al., Bioorganic & Med. Chem. Letters 16:358-362 (2006); Torgov et al., Bioconj. Chem. 16:717-721 (2005); Nagy et al., Proc. Natl. Acad. Sci. USA 97:829-834 (2000); Dubowchik et al., Bioorg. & Med See Chem. Letters 12:1529-1532 (2002); King et al., J. Med. Chem. 45:4336-4343 (2002); and US Pat. No. 6,630,579); methotrexate; vindesine; taxanes such as docetaxel, paclitaxel, larotaxel, tecetaxel, and ortataxel; tricotecene; and an antibody-drug conjugate (ADC) conjugated to one or more drugs including, but not limited to, CC1065.
또 다른 예들에서, 면역접합체는 디프테리아 A 쇄, 디프테리아 독소의 비결합 활성 단편, (슈도모나스 에루기노사(Pseudomonas aeruginosa) 유래) 외독소 A 쇄, 리신 A 쇄, 아브린 A 쇄, 모덱신 A 쇄, 알파-사르신, 유동(Aleurites fordii) 단백질, 디안틴 단백질, 미국 자리공(Phytolaca americana) 단백질(PAPI, PAPII, 및 PAP-S), 모모르디카 카란티아(momordica charantia) 억제제, 쿠르신, 크로틴, 사파오나리아 오피시날리스(sapaonaria officinalis) 억제제, 젤로닌, 미토젤린, 레스트릭토신, 페노마이신, 에노마이신, 및 트리코테센을 포함하지만 이에 제한되지 않는 효소 활성 독소 또는 이의 단편에 접합된 본원에 기재된 바와 같은 항 TIGIT 길항제 항체 (예를 들어, 티라골루맙) 또는 PD-1 축 결합 길항제 (예를 들어, 항 PD-L1 길항제 항체 (예를 들어, 아테졸리주맙))를 포함한다. In still other examples, the immunoconjugate comprises diphtheria A chain, a nonbinding active fragment of diphtheria toxin, exotoxin A chain (from Pseudomonas aeruginosa), ricin A chain, abrin A chain, modexin A chain, alpha -Sarsine, Aleurites fordii protein, Dianthin protein, Phytolaca americana protein (PAPI, PAPII, and PAP-S), Momordica charantia inhibitor, Cursine, Crotin, herein conjugated to an enzymatically active toxin or fragment thereof, including but not limited to, sapaonaria officinalis inhibitors, gelonin, mitozellin, restrictocin, phenomycin, enomycin, and trichothecene anti-TIGIT antagonist antibody (eg, tiragolumab) or a PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) as described in
또 다른 예들에서, 면역접합체는 방사성 원자에 접합되어 방사성접합체를 형성하는 본원에 기재된 바와 같은 항 TIGIT 길항제 항체 (예를 들어, 티라골루맙) 및/또는 본원에 기재된 바와 같은 PD-1 축 결합 길항제 (예를 들어, 항 PD-L1 길항제 항체) (예를 들어, 아테졸리주맙)를 포함한다. 다양한 방사성 동위원소가 방사접합체의 생산에 가용하다. 실례는 At211, I131, I125, Y90, Re186, Re188, Sm153, Bi212, P32, Pb212 및 Lu의 방사성 동위원소를 포함한다. 상기 방사성접합체가 검출용으로 이용될 때, 이는 신티그래피 연구를 위한 방사성 원자, 예를 들어, tc99m 또는 I123, 또는 핵자기 공명(NMR) 영상화(또는 자기 공명 영상화, MRI로도 공지됨)를 위한 회전 표지, 예컨대, 요오드-123 다시, 요오드-131, 인듐-111, 불소-19, 탄소-13, 질소-15, 산소-17, 가돌리늄, 망간 또는 철을 포함할 수 있다. In still other examples, the immunoconjugate is an anti-TIGIT antagonist antibody (eg, tyragolumab) as described herein that is conjugated to a radioactive atom to form a radioconjugate and/or a PD-1 axis binding antagonist as described herein. (eg, anti-PD-L1 antagonist antibody) (eg, atezolizumab). A variety of radioactive isotopes are available for the production of radioconjugates. Examples include At 211 , I 131 , I 125 , Y 90 , Re 186 , Re 188 , Sm 153 , Bi 212 , P 32 , Pb 212 and radioactive isotopes of Lu. When the radioconjugate is used for detection, it is a radioactive atom for scintigraphic studies, such as tc99m or I123, or rotation for nuclear magnetic resonance (NMR) imaging (also known as magnetic resonance imaging, MRI). labels such as iodine-123 again, iodine-131, indium-111, fluorine-19, carbon-13, nitrogen-15, oxygen-17, gadolinium, manganese or iron.
항체 및 세포독성 작용제의 접합체는 다양한 이중기능성 단백질 연계 작용제, 예컨대 N-숙신이미딜-3-(2-피리딜디티오) 프로피온산염 (SPDP), 숙신이미딜-4-(N-말레이미도메틸) 시클로헥산-1-카르복실산염 (SMCC), 이미노티올란 (IT), 이미도에스테르의 이중기능성 유도체 (예를 들면, 디메틸 아디피미데이트 HCl), 활성 에스테르 (예를 들면, 디숙신이미딜 수베르산염), 알데히드 (예를 들면, 글루타르알데히드), 비스-아지도 화합물 (예를 들면, 비스 (p-아지도벤조일) 헥산디아민), 비스-디아조늄 유도체 (예를 들면, 비스-(p-디아조늄벤조일)-에틸렌디아민), 디이소시아네이트 (예를 들면, 톨루엔 2,6-디이소시아네이트) 및 비스-활성 플루오르 화합물 (예를 들면, 1,5-디플루오로-2,4-디니트로벤젠)을 이용하여 만들어질 수 있다. 예를 들면, 리신 면역독소는 Vitetta et al., Science 238:1098 (1987)에서 설명된 바와 같이 제조될 수 있다. 탄소-14-표지화된 1-이소티오시아나토벤질-3-메틸디에틸렌 트리아민펜타아세트산 (MX-DTPA)은 항체에 방사성뉴클레오티드의 접합을 위한 예시적인 킬레이트화제이다. WO94/11026 참조. 링커는 세포에서 세포독성 약물의 방출을 용이하게 하는 “개열 가능한 링커”일 수 있다. 예를 들어, 산 불안정 링커, 펩티다아제 민감성 링커, 광불안정 링커, 디메틸 링커 또는 이황화물 함유 링커(Chari et al., Cancer Res. 52:127-131 (1992); 미국 특허 제5,208,020호)가 이용될 수 있다.Conjugates of an antibody and a cytotoxic agent can be used with a variety of bifunctional protein-linked agents, such as N-succinimidyl-3-(2-pyridyldithio) propionate (SPDP), succinimidyl-4-(N-maleimidomethyl). ) cyclohexane-1-carboxylate (SMCC), iminothiolane (IT), bifunctional derivatives of imidoesters (eg dimethyl adipimidate HCl), active esters (eg disuccinimidyl water berate), aldehydes (eg glutaraldehyde), bis-azido compounds (eg bis (p-azidobenzoyl) hexanediamine), bis-diazonium derivatives (eg bis-( p-diazoniumbenzoyl)-ethylenediamine), diisocyanates (eg toluene 2,6-diisocyanate) and bis-active fluorine compounds (eg 1,5-difluoro-2,4-di nitrobenzene) can be used. For example, a ricin immunotoxin can be prepared as described in Vitetta et al., Science 238:1098 (1987). Carbon-14-labeled 1-isothiocyanatobenzyl-3-methyldiethylene triaminepentaacetic acid (MX-DTPA) is an exemplary chelating agent for conjugation of radionucleotides to antibodies. See WO94/11026. The linker may be a “cleavable linker” that facilitates release of the cytotoxic drug from the cell. For example, acid labile linkers, peptidase sensitive linkers, photolabile linkers, dimethyl linkers or disulfide containing linkers (Chari et al., Cancer Res. 52:127-131 (1992); U.S. Pat. No. 5,208,020) may be employed. can
본원에서 면역접합체 또는 ADCs는 상업적으로 가용한 (예를 들면, Pierce Biotechnology, Inc., Rockford, IL., U.S.A로부터) BMPS, EMCS, GMBS, HBVS, LC-SMCC, MBS, MPBH, SBAP, SIA, SIAB, SMCC, SMPB, SMPH, 술포-EMCS, 술포-GMBS, 술포-KMUS, 술포-MBS, 술포-SIAB, 술포-SMCC 및 술포-SMPB, 그리고 SVSB (숙신이미딜-(4-비닐술폰)벤조에이트)를 포함하지만 이들에 한정되지 않는 교차연결제 시약으로 제조된 이와 같은 접합체를 명시적으로 예기하지만, 이들에 한정되지 않는다.The immunoconjugates or ADCs herein are commercially available (eg, from Pierce Biotechnology, Inc., Rockford, IL., U.S.A.) BMPS, EMCS, GMBS, HBVS, LC-SMCC, MBS, MPBH, SBAP, SIA, SIAB, SMCC, SMPB, SMPH, sulfo-EMCS, sulfo-GMBS, sulfo-KMUS, sulfo-MBS, sulfo-SIAB, sulfo-SMCC and sulfo-SMPB, and SVSB (succinimidyl-(4-vinylsulfone)benzo 8) are expressly contemplated, but are not limited to, those conjugates prepared with crosslinker reagents, including but not limited to.
항 TIGIT 길항제 항체 또는 PD-1 축 결합 길항제를 포함하지 않는 ADC가 또한 본원에 기재된 방법에서 사용될 수 있다. 일부 경우들에서, 상기 ADC는 엔포르투맙 베도틴 또는 사시투주맙 고비테칸이다.ADCs that do not include anti-TIGIT antagonist antibodies or PD-1 axis binding antagonists may also be used in the methods described herein. In some cases, the ADC is enfortumab vedotin or sacituzumab gobitecan.
D. 화학요법제D. Chemotherapeutic Agents
1. 백금계 화학요법제1. Platinum-based chemotherapeutic agents
백금계 화학요법제는 백금을 분자의 필수적인 부분으로 함유하는 유기 화합물을 포함한다. 전형적으로 백금계 화학요법는 백금의 배위 착물이다. 이는 카보플라틴, 시스플라틴 및 옥살리플라틴을 포함하지만 이에 제한되지는 않는다. Platinum-based chemotherapeutic agents include organic compounds containing platinum as an integral part of the molecule. Typically platinum-based chemotherapy is a coordination complex of platinum. These include, but are not limited to, carboplatin, cisplatin and oxaliplatin.
백금계 화학요법제들(예컨대, 시스플라틴, 카보플라틴, 옥살리플라틴, 및 사트라플라틴)은 단일부가물의 가교, 사슬간 교차결합, 사슬간 교차결합 또는 DNA 단백질 교차결합으로서 DNA의 가교를 유발하는데 널리 쓰이는 항종양 약물들이다. 백금계 화학요법제는 전형적으로 구아닌의 인접한 N-7 위치에 작용하여, 1, 2 사슬내 교차연결을 형성한다(Poklar et al. (1996). Proc. Natl. Acad. Sci. U.S.A. 93 (15): 7606-11; Rudd et al. (1995). Cancer Chemother. Pharmacol. 35 (4): 323-6). 결과로서 생성된 교차연결은 암 세포에서 DNA 수복 및/또는 DNA 합성을 억제한다.Platinum-based chemotherapeutic agents (eg, cisplatin, carboplatin, oxaliplatin, and satraplatin) are widely used to cause crosslinking of DNA as single adduct crosslinking, interchain crosslinking, interchain crosslinking, or DNA protein crosslinking. antitumor drugs used. Platinum-based chemotherapeutic agents typically act on the adjacent N-7 position of guanine, forming one or two intrachain crosslinks (Poklar et al. (1996). Proc. Natl. Acad. Sci. USA 93 (15). ): 7606-11;Rudd et al. (1995) Cancer Chemother. Pharmacol . 35 (4): 323-6). The resulting crosslinking inhibits DNA repair and/or DNA synthesis in cancer cells.
카보플라틴은 본원에 기재된 방법에서 이용되는 예시적인 백금 배위 화합물이다. 카보플라틴에 대한 화학 명칭은 백금, 디암민[l, l-시클로부탄디카르복실락토(2-)- 0,0']-, (SP42)이고, 카보플라틴은 하기의 구조식을 갖는다:Carboplatin is an exemplary platinum coordination compound used in the methods described herein. The chemical name for carboplatin is platinum, diammine[l,l-cyclobutanedicarboxylacto(2-)-0,0']-, (SP42), carboplatin has the structural formula:

카플라틴은 분자식이 C6H12N204Pt이고 분자량이 371.25인 결정 분말이다. 약 14 mg/mL의 속도로 물에 용해되며, 1% 용액의 pH는 5 내지 7이다. 이는 에탄올, 아세톤, 및 디메틸아세트아미드에서 사실상 불용성이다. 카보플라틴은 지배적으로 사슬간 DNA 교차연결을 발생시키고, 이러한 효과는 세포 주기 비특이적이다. 카보플라틴은 PARAPLATIN®, BIOCARN, BLASTOCARB, BLASTOPLATIN, CARBOKEM, CARBOMAX, CARBOPA, CARBOPLAN, CARBOTEEN, CARBOTINAL, CYTOCARB, DUCARB, KARPLAT, KEMOCARB, NAPROPLAT, NEOPLATIN, NISCARBO, ONCOCARBIN, TEVACARB, WOMASTIN 등으로서 상업적으로 입수 가능하다.Caplatin is a crystalline powder with a molecular formula of C6H12N204Pt and a molecular weight of 371.25. It dissolves in water at a rate of about 14 mg/mL, and the pH of a 1% solution is 5-7. It is virtually insoluble in ethanol, acetone, and dimethylacetamide. Carboplatin predominantly causes interchain DNA crosslinking, and this effect is cell cycle non-specific. Carboplatin is available commercially as PARAPLATIN®, BIOCARN, BLASTOCARB, BLASTOPLATIN, CARBOKEM, CARBOMAX, CARBOPA, CARBOPLAN, CARBOTEEN, CARBOTINAL, CYTOCARB, DUCARB, KARPLAT, RBKEMOCARB, NAPROPLAT, NEOPLATIN, WOMASTSCINARBOARBO, ONCOIN, do.
본 발명의 방법에 유용한 다른 예시적인 백금계 화학요법제는 하기의 구조를 갖는 시스플라틴이다:Another exemplary platinum-based chemotherapeutic agent useful in the methods of the present invention is cisplatin having the structure:

2. 비백금계 화학요법제2. Non-platinum-based chemotherapeutic agents
비백금계 화학요법제는 본원에 기재된 방법, 사용 및 사용을 위한 조성물의 일부로서 유용한 화학요법제의 또 다른 부류이다. 예시적인 비백금계 화학요법제는 항대사물질(예컨대, 페메트렉시드 및 젬시타빈), 토포이소머라제 II 억제제(예컨대, 독소루비신, 에토포시드, 테니포시드, 다우노루비신, 미톡산트론, 암사크린, 카르복실산, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331), 알킬화제(예컨대, 시클로포스파미드) 및 탁산(예컨대, 파클리탁셀(예컨대, 나노입자-알부민 결합(냅)-파클리탁셀), 도세탁셀, 라로탁셀, 카바지탁셀, 밀라탁셀, 및/또는 오라탁셀)을 포함한다.Non-platinum-based chemotherapeutic agents are another class of chemotherapeutic agents useful as part of the methods, uses, and compositions for use described herein. Exemplary non-platinum-based chemotherapeutic agents include antimetabolites (eg, pemetrexed and gemcitabine), topoisomerase II inhibitors (eg, doxorubicin, etoposide, teniposide, daunorubicin, mitoxantrone, amsa krine, carboxylic acid, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331), alkylating agents (eg, cyclophosphamide) and taxanes (eg, paclitaxel (eg, nanoparticle- albumin binding (nap)-paclitaxel), docetaxel, larotaxel, cabazitaxel, milataxel, and/or orataxel).
3. 항대사물질3. Antimetabolites
항대사물질은 세포(예컨대, 암세포) 내의 내인성(정상) 대사 과정을 (전체적으로 또는 부분적으로)방해하고 억제한다. 항대사물질은 젬시타빈, 페메트렉시드, 카페시타빈, 히드록시우레아, 메토트렉세이트, 플루오로우라실, 클라드리빈, 머캅토퓨린 및 프랄라트렉세이트를 포함한다. Antimetabolites interfere (in whole or in part) and inhibit endogenous (normal) metabolic processes within cells (eg, cancer cells). Antimetabolites include gemcitabine, pemetrexed, capecitabine, hydroxyurea, methotrexate, fluorouracil, cladribine, mercaptopurine and pralatrexate.
젬시타빈은 본원에 기재된 방법에 사용되는 예시적인 항대사물질이며 하기의 구조를 가진다. Gemcitabine is an exemplary antimetabolite for use in the methods described herein and has the structure

일부 경우들에서, 페메트렉시드는 본 발명의 방법의 일부로 투여될 수 있다. 페메트렉시드는 하기의 구조는 가진다:In some cases, pemetrexed may be administered as part of a method of the invention. Pemetrexed has the following structure:

4. 토포이소머라제 II 억제제4. Topoisomerase II Inhibitors
토포이소머라제 II의 억저제(예컨대, 에토포시드(VP-16), 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산 및 HU-331)는 또한 효소 매개된 DNA 절단의 형성 이후에, 토포이소머라제 IEDNA 공유 복합체(즉, “개열 복합체”)를 안정시키는 폭넓게 이용되는 항암제이다. 이런 개열 복합체의 축적은 세포 사멸 경로를 유도한다.Inhibitors of topoisomerase II (such as etoposide (VP-16), teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid and HU-331 ) is also a widely used anticancer agent that stabilizes the topoisomerase IEDNA covalent complex (ie, the “cleavage complex”) following the formation of enzyme-mediated DNA cleavage. Accumulation of these cleavage complexes induces the apoptosis pathway.
안트라사이클린은 스트렙토마이세스 박테리아에서 추출되는 일종의 토포이소머라제 II 억제제이다. 이의 예는 독소루비신(아드리아마이신), 다우노루비신(다우노마이신), 에피루비신, 이다루비신, 로도마이신, 피라루비신, 발루비신, N-트리플루오로-아세틸 독소루비신-14-발레레이트, 아클라시노마이신, (모르폴리노-DOX), 시아노모르폴리노-독소루비신(시아노모르폴리노-DOX), 2-피롤리노-독소루비신(2-PDOX), 5-이미노다우노마이신, 미톡산트론 및 아클라시노마이신 A(아클라루비신)를 포함한다. 일부 구현예들에서, 안트라사이클린은 알킬화제, 예컨대 시클로포스파미드와 조합된 독소루비신(AC를 사용한 치료)과 병용으로 투여된다.Anthracyclines are a type of topoisomerase II inhibitor extracted from Streptomyces bacteria. Examples thereof include doxorubicin (adriamycin), daunorubicin (daunomycin), epirubicin, idarubicin, rhodomycin, pyrarubicin, valrubicin, N-trifluoro-acetyl doxorubicin-14-valerate, Aclasinomycin, (morpholino-DOX), cyanomorpholino-doxorubicin (cyanomorpholino-DOX), 2-pyrrolino-doxorubicin (2-PDOX), 5-iminodaunomycin, mitoxantrone and aclasinomycin A (aclarubicin). In some embodiments, the anthracycline is administered in combination with doxorubicin (treatment with AC) in combination with an alkylating agent, such as cyclophosphamide.
독소루비신(아드리아마이신®)은 본원에 기재된 방법에서 이용되는 예시적인 토포이소머라제 II 억제제이다. 이의 화학명은 10-[(3-아미노-2,3,6-트리데옥시-α-L-릭소-헥소피라노실)옥시]-7,8,9,10-테트라히드로-6,8,11-트리히드록시-8-(2-히드록시아세틸)-1-메톡시-(8S,10S)-5,12-나프타센디온이다. 독소루비신은 하기의 구조는 가진다:Doxorubicin (Adriamycin®) is an exemplary topoisomerase II inhibitor used in the methods described herein. Its chemical name is 10-[(3-amino-2,3,6-trideoxy-α-L-lyxo-hexopyranosyl)oxy]-7,8,9,10-tetrahydro-6,8, 11-trihydroxy-8-(2-hydroxyacetyl)-1-methoxy-(8S,10S)-5,12-naphthacenedione. Doxorubicin has the following structure:

에토포시드는 본원에 기재된 방법에서 이용되는 예시적인 토포이소머라제 II 억제제이다. 에토포시드는 일반적으로 전구약물 에포토시드 인산염으로서 투여되며, 이의 화학명은 4'-데메틸에피포도필로톡신 9-[4,6-0-(R)-에틸리덴- -D글루코피라노시드], 4'(인산이수소)이다.Etoposide is an exemplary topoisomerase II inhibitor used in the methods described herein. Etoposide is generally administered as the prodrug epotoside phosphate, whose chemical name is 4'-demethylepipodophyllotoxin 9-[4,6-0-(R)-ethylidene--Dglucopyranoside] , 4' (dihydrogen phosphate).
에토포시드 인산염은 하기 구조를 갖는다:Etoposide phosphate has the structure:

에토포시드의 인산염 에스테르인 에토포시드 인산염은 포도필로톡신의 반합성 유도체이고, 탈인산화에 의해 에토포시드로 전환된다. 에토포시드는 DNA-토포이소머라제 II와의 상호작용 또는 자유 라디칼의 형성에 의해 DNA 가닥 절단의 유도를 유발하여, 세포 주기 정지(세포 주기의 G2 기에서 일차적으로) 및 세포 사멸을 야기한다. 에토포시드는 ETOPOPHOS®, TOPOSAR™, VP-16, VEPESID®, ACTITOP, ASIDE, BIOPOSIDE, CTOP, CYTOP, EPOSED, ESIDE, ETHOPUL, ETOLON, ETONIS, ETOPLAST, ETOSID, ETOVEL, FYTOP, FYTOSID, LASTET, NZYTOP, ONCOSIDE, PLACID, POSID, RETOPSON, TEVASIDE, TOPOK, TOPOSIDE 등으로서 상업적으로 입수 가능하다.Etoposide phosphate, a phosphate ester of etoposide, is a semisynthetic derivative of podophyllotoxin and is converted to etoposide by dephosphorylation. Etoposide induces induction of DNA strand breaks by interaction with DNA-topoisomerase II or formation of free radicals, leading to cell cycle arrest (primarily in the G2 phase of the cell cycle) and cell death. Etoposide is ETOPOPHOS®, TOPOSAR™, VP-16, VEPESID®, ACTITOP, ASIDE, BIOPOSIDE, CTOP, CYTOP, EPOSED, ESIDE, ETHOPUL, ETOLON, ETONIS, ETOPLAST, ETOSID, ETOVEL, FYTOP, FYTO SID, LASTET, FYTO SID It is commercially available as ONCOSIDE, PLACID, POSID, RETOPSON, TEVASIDE, TOPOK, TOPOSIDE, and the like.
5. 탁산5. Taxanes
탁산은 미세소관 조립 및 안정화를 촉진하는 튜불린에 결합할 수 있고, 그리고/또는 미세소관 탈중합을 예방할 수 있는 화학요법제이다. 본원에 포함된 탁산은 탁소이드 10-데아세틸바카틴 III 및/또는 이의 유도체를 포함한다. 예시적인 탁산은 파클리탁셀(즉, 탁솔(TAXOL)®, CAS # 33069-62-4), 도세탁셀(즉, 탁소테레(TAXOTERE)®, CAS # 114977-28-5), 라로탁셀, 카바지탁셀, 밀라탁셀, 테세트탁셀 및/또는 오라탁셀을 포함하지만, 이에 제한되지는 않는다. 일부 구현예들에서, 상기 탁산은 알부민 코팅된 나노입자(예컨대, 나노-알부민 결합된 (냅)-파클리탁셀, 즉 아브락산(ABRAXANE)® 및/또는 냅-도세탁셀, ABI-008)이다. 일부 구현예들에서, 상기 탁산은 냅-파클리탁셀(아브락산®)이다. 일부 구현예들에서, 상기 탁산은 크레모포어(CREMAPHOR)®(예컨대, 탁솔(TAXOL)®) 및/또는 트윈(Tween), 예컨대, 폴리소르베이트 80(예컨대, 탁소테레®)으로 제형화된다. 일부 구현예들에서, 상기 탁산은 리포좀 캡슐화된 탁산이다. 일부 구현예들에서, 상기 탁산은 탁산의 전구약물 형태 및/또는 접합된 형태(예컨대, 파클리탁셀, 파클리탁셀 폴리글루멕스, 및/또는 리놀레일 카보네이트-파클리탁셀에 공유적으로 접합된 DHA)이다. 일부 구현예들에서, 상기 파클리탁셀은 실질적으로 계면활성제 없이(예컨대, 크레모포어 및/또는 트위-예컨대 토코솔(TOCOSOL)® 파클리탁셀의 부재하에서) 제형화된다.Taxanes are chemotherapeutic agents that can bind tubulin to promote microtubule assembly and stabilization, and/or prevent microtubule depolymerization. Taxanes included herein include the taxoid 10-deacetylbaccatin III and/or derivatives thereof. Exemplary taxanes are paclitaxel (ie, TAXOL ® , CAS # 33069-62-4), docetaxel (ie, TAXOTERE ® , CAS # 114977-28-5), larotaxel, cabazitaxel, mila taxel, tessetaxel and/or orataxel. In some embodiments, the taxane is an albumin-coated nanoparticle (eg, nano-albumin bound (NAP)-paclitaxel, ie, ABRAXANE® and/or Nap-docetaxel, ABI-008). In some embodiments, the taxane is nap-paclitaxel (Abraxane ® ). In some embodiments, the taxane is formulated with CREMAPHOR ® (eg, TAXOL ® ) and/or Tween, such as polysorbate 80 (eg, Taxotere ® ). . In some embodiments, the taxane is a liposomal encapsulated taxane. In some embodiments, the taxane is a prodrug form and/or a conjugated form of the taxane (eg, paclitaxel, paclitaxel polyglomex, and/or DHA covalently conjugated to linoleyl carbonate-paclitaxel). In some embodiments, the paclitaxel is formulated substantially free of surfactants (eg, in the absence of cremophor and/or twee-such as TOCOSOL® paclitaxel).
일부 경우들에서, 파클리탁셀은 본 발명의 방법의 일부로 투여된다. 파클리탁셀은 하기의 구조를 가질 수 있다:In some cases, paclitaxel is administered as part of a method of the invention. Paclitaxel may have the structure:

일부 경우들에서, 상기 방법 또는 사용은 나노-알부민 결합(냅)-파클리탁셀의 투여를 포함한다.In some cases, the method or use comprises administering nano-albumin binding (NAP)-paclitaxel.
6. 알킬화제6. Alkylating agent
알킬화제는 DNA 손상을 일으키는 화학요법제이다. 알킬화제에는 질소 머스타드, 니트로소우레아, 및 알킬 설포네이트가 포함된다. 예시적인 알킬화제는 시클로포스파미드, 1,3-비스(2-클로로에틸)-1-니트로소우레아, 1,4-부탄디올 디메탄술포네이트, (2S)-2-아미노-3-{4-[비스(2-클로로에틸)아미노]페닐}프로판산, 3-(2-클로로에틸)-2-[(2-클로로에틸)아미노]테트라히드로-2H-1,3,2-옥사자포스포린 2-옥사이드, 및 1-(2-클로로에틸)-3-사이클로헥실-1-니트로소우레아를 포함하지만, 이에 제한되지는 않는다. 일부 구현예들에서, 상기 알킬화제는 시클로포스파미드이다. 시클로포스파미드는 하기의 구조를 가질 수 있다:Alkylating agents are chemotherapeutic agents that cause DNA damage. Alkylating agents include nitrogen mustards, nitrosoureas, and alkyl sulfonates. Exemplary alkylating agents include cyclophosphamide, 1,3-bis(2-chloroethyl)-1-nitrosourea, 1,4-butanediol dimethanesulfonate, (2S)-2-amino-3-{4- [bis(2-chloroethyl)amino]phenyl}propanoic acid, 3-(2-chloroethyl)-2-[(2-chloroethyl)amino]tetrahydro-2H-1,3,2-oxazaphosphorine 2 -oxide, and 1-(2-chloroethyl)-3-cyclohexyl-1-nitrosourea. In some embodiments, the alkylating agent is cyclophosphamide. Cyclophosphamide can have the structure:

당업자는 전술한 화학요법제 중 임의의 것이 본 발명의 일부로서 고려되는 염 형태와 같은 다양한 형태로 투여될 수 있음을 이해할 것이다.One of ordinary skill in the art will appreciate that any of the aforementioned chemotherapeutic agents may be administered in a variety of forms, such as salt forms contemplated as part of the present invention.
E. 예시적인 집락 자극 인자E. Exemplary Colony Stimulating Factors
집락 자극 인자는 세포의 증식을 자극하는 단백질이다. 집락 자극 인자에는 G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀) 및 GM-CSF(예: 사그라모스팀)가 포함된다. 일부 구현예들에서, 상기 집락 자극 인자는 G-CSF(예컨대, 페그필그라스팀 또는 필그라스팀)이다. 일부 구현예들에서, 상기 G-CSF는 페그필그라스팀이다. 일부 구현예들에서, 상기 G-CSF는 필그라스팀이다. 일부 구현예들에서, 상기 집락 자극 인자는 GM-CSF(예컨대, 사그라모스팀)이다. 일부 구현예들에서, 상기 G-CSF는 사그라모스팀이다.Colony stimulating factors are proteins that stimulate the proliferation of cells. Colony stimulating factors include G-CSF (eg pegfilgrastim or filgrastim) and GM-CSF (eg sagramostim). In some embodiments, the colony stimulating factor is G-CSF (eg, pegfilgrastim or filgrastim). In some embodiments, the G-CSF is pegfilgrastim. In some embodiments, the G-CSF is filgrastim. In some embodiments, the colony stimulating factor is GM-CSF (eg, sagramostim). In some embodiments, the G-CSF is sagrammostim.
F. 예시적인 VEGF 길항제F. Exemplary VEGF antagonists
본 발명은 대상체(예컨대, 인간)에서 암을 치료하는데 유용한 VEGF 길항제를 제공한다. 본 발명의 VEGF 길항제는 VEGF에 결합하거나, VEGF 발현 수준을 감소시키거나, 또는 VEGF 생물학적 활성을 중화, 차단, 억제, 제거, 감소 또는 방해할 수 있는 임의의 분자를 포함한다. 예시적인 인간 VEGF는 유니프롯KB/스위스-프롯 수탁 번호 P15692, 유전자 ID (NCBI): 7422 하에 도시된다. The present invention provides VEGF antagonists useful for treating cancer in a subject (eg, a human). The VEGF antagonist of the present invention includes any molecule capable of binding to VEGF, reducing VEGF expression levels, or neutralizing, blocking, inhibiting, eliminating, reducing or interfering with VEGF biological activity. Exemplary human VEGF is shown under UniprotKB/Swiss-Prot Accession No. P15692, Gene ID (NCBI): 7422.
일부 경우들에서, 상기 VEGF 길항제는 항 VEGF 항체이다. 일부 구현예들에서, 상기 항 VEGF 항체는 “rhuMab VEGF” 또는 “아바스틴(AVASTIN)®”으로서 또한 공지된 베바시주맙이다. 베바시주맙은 Presta et al. (Cancer Res. 57:4593-4599, 1997)에 따라서 생성된 재조합 인간화 항 VEGF 단일클론 항체이다. 이는 돌연변이된 인간 IgG1 프레임워크 영역, 및 인간 VEGF의 이의 수용체에 대한 결합을 차단하는 뮤린 항 hVEGF 단일클론 항체 A.4.6.1로부터 항원 결합 상보성 결정 영역을 포함한다. 프레임워크 영역의 대부분을 포함하는, 베바시주맙의 아미노산 서열 중 대략 93%는 인간 IgG1로부터 유래되고, 상기 서열의 약 7%는 뮤린 항체 A4.6.1로부터 유래된다. 베바시주맙은 약 149,000 달톤의 분자량을 가지며 글리코실화된다. 베바시주맙 및 기타 인간화된 항 VEGF 항체는 2005년 2월 26일에 발행된 미국 특허 제6,884,879호에 추가로 기재되었으며, 이는 그 전체가 본원에 원용된다. 일부 경우들에서, 상기 항 VEGF 항체는 베바시주맙의 중쇄 가변(VH) 영역 서열 및 경쇄 가변(VL) 영역 서열을 포함한다.In some cases, the VEGF antagonist is an anti-VEGF antibody. In some embodiments, the anti-VEGF antibody is bevacizumab, also known as “rhuMab VEGF” or “AVASTIN®”. Bevacizumab is described by Presta et al. ( Cancer Res . 57:4593-4599, 1997) is a recombinant humanized anti-VEGF monoclonal antibody. It contains a mutated human IgG1 framework region and an antigen binding complementarity determining region from the murine anti-hVEGF monoclonal antibody A.4.6.1 that blocks binding of human VEGF to its receptor. Approximately 93% of the amino acid sequence of bevacizumab, including most of the framework region, is derived from human IgG1, and about 7% of the sequence is derived from the murine antibody A4.6.1. Bevacizumab has a molecular weight of about 149,000 Daltons and is glycosylated. Bevacizumab and other humanized anti-VEGF antibodies are further described in US Pat. No. 6,884,879, issued Feb. 26, 2005, which is incorporated herein by reference in its entirety. In some cases, the anti-VEGF antibody comprises a heavy chain variable (VH) region sequence and a light chain variable (VL) region sequence of bevacizumab.
추가의 바람직한 항체는 PCT 출원 공개 제WO 2005/012359호에 기재된 바와 같은 G6 또는 B20 계열 항체(예컨대, G6-31, B20-4.1)를 포함한다. 추가의 바람직한 항체에 대하여, 미국 특허 제7,060,269, 6,582,959호, 6,703,020호; 6,054,297호; WO98/45332호; WO 96/30046호; WO94/10202호; EP 0666868B1호; 미국 특허 출원 공보 제2006009360호, 20050186208호, 20030206899호, 20030190317호, 20030203409호 및 20050112126호; 그리고 Popkov et al. (Journal of Immunological Methods 288:149-164, 2004)를 참조한다. 다른 바람직한 항체는 잔기 F17, M18, D19, Y21, Y25, Q89, 191, K101, E103 및 C104를 포함하는, 또는 대안적으로, 잔기 F17, Y21, Q22, Y25, D63, 183 및 Q89를 포함하는 인간 VEGF 상에서 기능적 에피토프에 결합하는 것들을 포함한다.Further preferred antibodies include G6 or B20 family antibodies (eg G6-31, B20-4.1) as described in PCT Application Publication No. WO 2005/012359. For further preferred antibodies, see US Pat. Nos. 7,060,269, 6,582,959, 6,703,020; 6,054,297; WO98/45332; WO 96/30046; WO94/10202; EP 0666868B1; US Patent Application Publication Nos. 2006009360, 20050186208, 20030206899, 20030190317, 20030203409 and 20050112126; and Popkov et al. ( Journal of Immunological Methods 288:149-164, 2004). Other preferred antibodies comprise residues F17, M18, D19, Y21, Y25, Q89, 191, K101, E103 and C104, or alternatively comprise residues F17, Y21, Q22, Y25, D63, 183 and Q89 include those that bind to functional epitopes on human VEGF.
기타 경우들에서, 상기 VEGF 길항제는 항 VEGFR2 항체 또는 관련 분자(예컨대, 라무시루맙, 타니비루맙, 아플리베르셉트), 항 VEGFR1 항체 및 관련된 분자(예컨대, 이크루쿠맙, 아플리베르셉트(VEGF 트랩-아이(Trap-Eye); EYLEA®), 및 지브-아플리베르셉트(VEGF 트랩; ZALTRAP®)), 이중특이적 VEGF 항체(예컨대, MP-0250, 바누시주맙(VEGF-ANG2), 또는 US 2001/0236388에 개시된 이중특이적 항체), 항 VEGF, 항 VEGFR1, 및 항 VEGFR2 아암 중 둘의 조합을 포함하는 이중특이적 항체, 항 VEGFA 항체(예컨대, 베바시주맙, 세바시주맙), 항 VEGFB 항체, 항 VEGFC 항체(예컨대, VGX-100), 항 VEGFD 항체, 및 비펩티드 소분자 VEGF 길항제(예컨대, 파조파닙, 악시티닙, 반데타닙, 스티바가, 카보잔티닙, 렌바티닙, 닌테다닙, 오란티닙, 텔라티닙, 도비티니그, 세디라닙, 모테사닙, 설파티닙, 아파티닙, 포레티닙, 파미티닙, 또는 티보자닙)이다. In other cases, the VEGF antagonist is an anti-VEGFR2 antibody or related molecule (eg, ramucirumab, tanivirumab, aflibercept), an anti-VEGFR1 antibody and related molecule (eg, icrucumab, aflibercept (VEGF trap) -Eye (Trap-Eye; EYLEA®), and Ziv-aflibercept (VEGF Trap; ZALTRAP®)), bispecific VEGF antibodies (eg, MP-0250, vanucizumab (VEGF-ANG2), or US 2001/0236388), a bispecific antibody comprising a combination of two of anti-VEGF, anti-VEGFR1, and anti-VEGFR2 arms, an anti-VEGFA antibody (eg, bevacizumab, sebacizumab), anti-VEGFB Antibodies, anti-VEGFC antibodies (eg, VGX-100), anti-VEGFD antibodies, and non-peptide small molecule VEGF antagonists (eg, pazopanib, axitinib, vandetanib, stivaga, caboxantinib, lenvatinib, nintedanib , orantinib, telatinib, dovitinig, cediranib, motesanib, sulfatinib, afatinib, foretinib, pamitinib, or tivozanib).
추가의 양태에서, 상기 경우들 중 임의의 것에 따른 VEGF 길항제(예컨대, 항 VEGF 항체(예컨대, 베바시주맙))는 상기의 섹션 C에 기재된 바와 같이 단독으로 또는 병용으로 상기 특징들 중 임의의 것을 통합할 수 있다.In a further aspect, the VEGF antagonist (eg, anti VEGF antibody (eg, bevacizumab)) according to any of the preceding cases, alone or in combination, as described in Section C above, any of the above features can be integrated
G. 추가 치료제 G. Additional Therapeutics
본 발명에서 사용될 수 있는 추가 치료제(예컨대, 항 TIGIT 길항제 항체와 병용으로 사용됨)는 항체, 예컨대 알렘투주맙(캠패스(Campath)), 베바시주맙(아바스틴(AVASTIN)®, 제넨텍); 세툭시맙(어비툭스(ERBITUX)®, 임클론(Imclone)); 파니투무맙(벡티빅스(VECTIBIX)®, 암젠(Amgen)), 리툭시맙 (리툭산(RITUXAN)®, 제넨텍/바이오젠(Biogen Idec)), 페르투주맙(옴니타그(OMNITARG)®, 2C4, 제넨텍), 트라스투주맙(허셉틴(HERCEPTIN)®, 제넨텍), 토시투모맙(벡사르, 코릭사(Corixia)), 및 항체 약물 접합체, 겜투주맙 오조가마이신(마일로타그(MYLOTARG)®, 와이어스(Wyeth))를 포함한다. 기재된 화합물과 병용되는 작용제로서 치료 잠재력을 갖는 추가의 인간화 단일클론 항체는: 아폴리주맙, 아셀리주맙, 아틀리주맙, 바피네우주맙, 비바투주맙 메르탄신, 칸투주맙 메르탄신, 세델리주맙, 세르톨리주맙 페골, 시드푸시투주맙, 시드투주맙, 다클리주맙, 에쿨리주맙, 에팔리주맙, 에프라투주맙, 에를리주맙, 펠비주맙, 폰톨리주맙, 겜투주맙 오조가마이신, 이노투주맙 오조가마이신, 이플리무맙, 라베투주맙, 린투주맙, 마투주맙, 메폴리주맙, 모타비주맙, 모토비주맙, 나탈리주맙, 니모투주맙, 놀로비주맙, 누마비주맙, 오크렐리주맙, 오말리주맙, 팔리비주맙, 파스콜리주맙, 펙푸시투주맙, 펙투주맙, 펙셀리주맙, 랄리비주맙, 라니비주맙, 레슬리비주맙, 레슬리주맙, 레시비주맙, 로벨리주맙, 루플리주맙, 시브로투주맙, 시플리주맙, 손투주맙, 타카투주맙 테트라제탄, 타도시주맙, 탈리주맙, 테피바주맙, 토실리주맙, 토랄리주맙, 투코투주맙 셀모루킨, 투쿠시투주맙, 우마비주맙, 우르톡사주맙, 우스테키누맙, 비실리주맙, 그리고 인터류킨-12 p40 단백질을 인식하도록 유전적으로 변형된 재조합 배타적으로 인간-서열, 전장 IgG1 λ 항체인 항 인터류킨-12 (ABT-874/J695, 와이어스 리서치(Wyeth Research) 및 애보트 연구소(Abbott Laboratories))를 포함한다.Additional therapeutic agents that may be used in the present invention (eg, used in combination with an anti-TIGIT antagonist antibody) include antibodies such as alemtuzumab (Campath), bevacizumab ( AVASTIN® , Genentech); cetuximab (ERBITUX ® , Imclone); Panitumumab (VECTIBIX ® , Amgen), Rituximab (RITUXAN ® , Genentech/Biogen Idec), Pertuzumab (OMNITARG ® , 2C4, Genentech ), trastuzumab (HERCEPTIN ® , Genentech), tositumomab (bexar, Corixia), and antibody drug conjugate, gemtuzumab ozogamicin (MYLOTARG ® , Wyeth )) is included. Additional humanized monoclonal antibodies with therapeutic potential as agents in combination with the disclosed compounds are: apolizumab, acelizumab, atlizumab, bapineuzumab, vibatuzumab mertansine, cantuzumab mertansine, sedelizumab , Sertolizumab Pegol, Sidfucituzumab, Sidtuzumab, Daclizumab, Eculizumab, Efalizumab, Epratuzumab, Erlizumab, Felbizumab, Fontolizumab, Gemtuzumab Ozogamicin, Ino tuzumab ozogamicin, iplimumab, rabetuzumab, lintuzumab, matuzumab, mepolizumab, motavizumab, motobizumab, natalizumab, nimotuzumab, nolovizumab, numizumab, okrelizumab , omalizumab, palivizumab, pascolizumab, pekfucituzumab, pectuzumab, pexelizumab, ralivizumab, ranibizumab, reslibizumab, reslizumab, recibizumab, lobelizumab, luplizumab , cibrotuzumab, ciplizumab, sontuzumab, tacatuzumab tetrajetan, tadozumab, talizumab, tefivazumab, tocilizumab, toralizumab, tucotuzumab selmorukin, tucusituzumab, Umaizumab, urtoxazumab, ustekinumab, vicilizumab, and anti-interleukin-12 (ABT- 874/J695, Wyeth Research and Abbott Laboratories).
치료 항체는 또한 EGFR에 결합하는 항체를 포함한다. EGFR에 결합하는 항체들의 예는 MAb 579(ATCC CRL HB 8506), MAb 455(ATCC CRL HB8507), Mab 225(ATCC CRL 8508), MAb 528(ATCC CRL 8509)(미국 특허 제4,943,533호, Mendelsohn et al. 참조) 및 이의 변이체, 예컨대, 키메라화 225(C225 또는 세툭시맙; 어비툭스®) 및 재성형된 인간 225(H225)(WO 96/40210, 임클론 시스템즈(Imclone Systems Inc.) 참조); 완전한 인간 EGFR 표적 항체인 IMC-11F8(임클론); II형 돌연변이 EGFR에 결합하는 항체(미국 특허 제5,212,290호); 미국 특허 제5,891,996호에 기재된 바와 같이 EGFR에 결합하는 인간화 및 키메라 항체; 및 EGFR에 결합하는 인간 항체, 예컨대, ABX-EGF 또는 파니투무맙(WO98/50433, 어브제닉스(Abgenix)/암젠을 참조); EMD 55900(Stragliotto et al. EurCancer 32A:636-640 (1996)); EMD7200(마투주맙) EGFR 결합(EMD/머크)을 위하여 EGF 및 TGF-알파 둘 모두와 경쟁하는 EGFR에 대하여 지향된, 인간화된 EGFR 항체; 및 인간 EGFR 항체, HuMax-EGFR (GenMab); 완전 인간 항체(하기에 공지되고: E1.1, E2.4, E2.5, E6.2, E6.4, E2.11, E6 3 및 E7.6. 3 및 US 6,235,883; MDX-447(메다렉스(Medarex Inc))에 기재된; 및 mAb 806 또는 인간화 mAb 806(Johns et al., J. Biol. Chem. 279(29):30375-30384 (2004))를 포함한다. 상기 항 EGFR 항체는 세포독성제와 접합되어, 면역접합체를 생성할 수 있다(예컨대, EP659,439A2, Merck Patent GmbH를 참조). Therapeutic antibodies also include antibodies that bind EGFR. Examples of antibodies that bind EGFR include MAb 579 (ATCC CRL HB 8506), MAb 455 (ATCC CRL HB8507), Mab 225 (ATCC CRL 8508), MAb 528 (ATCC CRL 8509) (US Pat. No. 4,943,533, Mendelsohn et al . . IMC-11F8 (Imclone), a fully human EGFR targeting antibody; antibodies that bind to type II mutant EGFR (US Pat. No. 5,212,290); humanized and chimeric antibodies that bind EGFR as described in US Pat. No. 5,891,996; and human antibodies that bind EGFR, such as ABX-EGF or panitumumab (see WO98/50433, Abgenix/Amgen); EMD 55900 (Stragliotto et al. Eur Cancer 32A:636-640 (1996)); EMD7200 (matuzumab) a humanized EGFR antibody directed against EGFR that competes with both EGF and TGF-alpha for EGFR binding (EMD/Merck); and a human EGFR antibody, HuMax-EGFR (GenMab); fully human antibodies (known as: E1.1, E2.4, E2.5, E6.2, E6.4, E2.11, E6 3 and E7.6. 3 and US 6,235,883; MDX-447 (meda Medarex Inc.) and mAb 806 or humanized mAb 806 (Johns et al., J. Biol. Chem. 279(29):30375-30384 (2004)). It can be conjugated with a toxic agent to generate an immunoconjugate (see eg EP659,439A2, Merck Patent GmbH).
본원에 제공된 방법, 조성물 및 사용에 이용될 수 있는 추가 치료제는 공동 억제 표적(예컨대, CTLA-4, LAG3, TIM3, BTLA 및/또는 VISTA)을 표적으로 하는 제제, 예컨대, CTLA-4 길항제, 예컨대, 항 CTLA-4 길항제 항체(예컨대, 이필리무맙(YERVOY®) )); 공동 자극 표적(예컨대, CD226, OX-40, CD28, CD27, CD137, HVEM, 및/또는 GITR)을 표적으로 하는 제제; 방사선 요법; 항혈관신생제; 아폽토시스제; 및 항튜불린제를 포함한다. Additional therapeutic agents that may be employed in the methods, compositions and uses provided herein include agents that target co-inhibitory targets (eg, CTLA-4, LAG3, TIM3, BTLA and/or VISTA), such as CTLA-4 antagonists, such as , an anti-CTLA-4 antagonist antibody (eg, ipilimumab (YERVOY®)); agents that target co-stimulatory targets (eg, CD226, OX-40, CD28, CD27, CD137, HVEM, and/or GITR); radiotherapeutics; antiangiogenic agents; apoptotic agents; and antitubulin agents.
V. 약학적 조성물, 제형 및 키트V. Pharmaceutical Compositions, Formulations and Kits
본원에 기재된 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체), VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제(예컨대, 카보플라틴 또는 시스플라틴) 및 비백금계 화학요법제(예컨대, 알킬화제(예컨대, 시클로포스파미드), 탁산(예컨대, 파클리탁셀, 예컨대, 냅-파클리탁셀), 및/또는 토포이소머라제 II 억제제(예컨대, 독소루비신)), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/또는 CSF(예컨대, 페그필그라스팀, 필그라스팀, 또는 사그라모스팀) 중 임의의 것이 약학적 조성물 및 제형에 사용될 수 있다. 항 TIGIT 길항제 항체, PD-1 축 결합 길항제(예컨대, 항 PD-L1 길항제 항체), VEGF 길항제, 하나 이상의 화학요법제, ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/ 또는 CSF(예컨대, 페그필그라스팀, 필그라스팀, 또는 사그라모스팀)의 약학적 조성물 및 제형은 원하는 정도의 순도를 갖는 1개, 2개, 3개, 4개, 또는 4개 초과의 제제를 하나 이상의 임의의 약학적으로 허용가능한 담체(Remington’s Pharmaceutical Sciences 16th edition, Osol, A. Ed. (1980))와 혼합함으로써 동결건조 제제 또는 수용액 형태로 제조된다. 약학적으로 허용가능한 담체는 이용되는 투여량 및 농도에서 수용자에 비독성이며, 다음을 포함하나, 이에 제한되지 않는다: 완충액, 가령, 포스페이트, 시트레이트 및 다른 유기산; 아스코르브산 및 메티오닌을 포함하는 항산화제; 보존제(예컨대, 옥타데실디메틸벤질 암모늄 클로라이드; 헥사메토니움 클로라이드; 벤잘코니움 클로라이드; 벤제토늄 클로라이드; 페놀, 부탈 또는 벤질 알코올; 알킬 파라벤 가령, 메틸 또는 프로필 파라벤; 카테콜; 레소르치놀; 시클로헥사놀; 3-펜타놀; 그리고 m-크레졸); 낮은 분자량의(약 10개 잔기 미만) 폴리펩티드; 단백질, 가령, 혈청 알부민, 젤라틴, 또는 면역글로블린; 친수성 중합체 가령, 폴리비닐피롤리돈; 아미노산 가령, 글리신, 글루타민, 아스파라긴, 히스티딘, 아르기닌, 또는 리신; 모노사카라이드, 디사카라이드, 그리고 글루코스, 만노스, 또는 덱스트린을 포함하는 기타 탄수화물; 킬레이트 물질 가령, EDTA; 당, 예컨대, 슈크로스, 만니톨, 트레할로스 또는 소르비톨; 염 형성 카운터 이온, 가령, 나트륨; 금속 복합체(예컨대 Zn 단백질 복합체); 및/또는 비이온성 계면활성제 가령, 폴리에틸렌 글리콜 (PEG). 본원에서 예시적인 제약학적으로 허용되는 운반체는 세포간 약물 분산 작용제, 예컨대 가용성 중성 활성 히알루론산분해효소 당단백질(sHASEGP), 예컨대, 인간 가용성 PH-20 히알루론산분해효소 당단백질, 예컨대 rHuPH20(하이레넥스(HYLENEX)®, 박스터 인터내셔널(Baxter International, Inc.))을 추가로 포함한다. rHuPH20를 포함하는 특정 예시적인 sHASEGPs 및 이를 이용하는 방법은 미국 특허 공보 제2005/0260186호 및 2006/0104968호에 기재되어 있다. 일 양태에서, sHASEGP는 하나 이상의 추가 글리코사미노글리카나제, 예컨대 콘드로이티나제와 조합된다. An anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody) described herein, a VEGF antagonist, a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent (eg, carbo Platin or cisplatin) and non-platinum-based chemotherapeutic agents (eg, alkylating agents (eg, cyclophosphamide), taxanes (eg, paclitaxel, eg, nap-paclitaxel), and/or topoisomerase II inhibitors (eg, doxorubicin) . Anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (eg anti-PD-L1 antagonist antibody), VEGF antagonist, one or more chemotherapeutic agents, ADC (eg enfortumab vedotin or sassitu) Pharmaceutical compositions and formulations of zumab gobitecan), and/or CSF (eg, pegfilgrastim, filgrastim, or sagramostim) are prepared in one, two, three, four , or more than four agents are prepared in the form of a lyophilized formulation or aqueous solution by mixing with one or more optional pharmaceutically acceptable carriers ( Remington's Pharmaceutical Sciences 16th edition, Osol, A. Ed. (1980)). Acceptable carriers are nontoxic to recipients at the dosages and concentrations employed, and include, but are not limited to: buffers such as phosphate, citrate and other organic acids, antioxidants including ascorbic acid and methionine; preservatives (such as octadecyldimethylbenzyl ammonium chloride; hexamethonium chloride; benzalkonium chloride; benzethonium chloride; phenol, butal or benzyl alcohol; alkyl parabens such as methyl or propyl paraben; catechol; resorcinol; cyclo hexanol; 3-pentanol; and m-cresol); low molecular weight (less than about 10 residues) polypeptides; proteins such as blood blue albumin, gelatin, or immunoglobulin; hydrophilic polymers such as polyvinylpyrrolidone; amino acids such as glycine, glutamine, asparagine, histidine, arginine, or lysine; monosaccharides, disaccharides, and other carbohydrates including glucose, mannose, or dextrins; chelating agents such as EDTA; sugars such as sucrose, mannitol, trehalose or sorbitol; salt forming counterions such as sodium; metal complexes (such as Zn protein complexes); and/or nonionic surfactants such as polyethylene glycol (PEG). Exemplary pharmaceutically acceptable carriers herein are intercellular drug dispersing agents, such as soluble neutral active hyaluronase glycoprotein (sHASEGP), such as human soluble PH-20 hyaluronate glycoprotein, such as rHuPH20 (Hire HYLENEX® , Baxter International, Inc.). Certain exemplary sHASEGPs, including rHuPH20, and methods of using them are described in US Patent Publication Nos. 2005/0260186 and 2006/0104968. In one aspect, the sHASEGP is combined with one or more additional glycosaminoglycanases, such as chondroitinases.
예시적인 동결건조된 항체 제제는 미국 특허 제6,267,958호에서 기재된다. 수용액 항체 제제는 미국 특허 제 6,171,586로 및 WO 2006/044908호에서 기재된 것들을 포함하며, 후자 제제는 히스티딘-아세테이트 완충액을 포함한다.Exemplary lyophilized antibody formulations are described in US Pat. No. 6,267,958. Aqueous antibody formulations include those described in US Pat. No. 6,171,586 and WO 2006/044908, the latter formulations comprising a histidine-acetate buffer.
예시적인 아테졸리주맙 제형은 5.8의 pH를 갖는 아세트산, L-히스티딘, 폴리소르베이트 20 및 수크로스를 포함한다. 예를 들어, 아테졸리주맙은 5.8의 pH를 갖는 아세트산(16.5 mg), L-히스티딘(62 mg), 폴리소르베이트 20(8 mg), 및 자당(821.6 mg)으로 제형화된 1200 mg의 아테졸리주맙을 함유하는 20 mL 바이알에 제공될 수 있다. 다른 예에서, 아테졸리주맙은 5.8의 pH를 갖는 아세트산(11.5 mg), L-히스티딘(43.4 mg), 폴리소르베이트 20(5.6 mg), 및 자당(575.1 mg)으로 제형화된 840 mg의 아테졸리주맙을 함유하는 14 mL 바이알에 제공될 수 있다.An exemplary atezolizumab formulation comprises acetic acid, L-histidine, polysorbate 20 and sucrose having a pH of 5.8. For example, atezolizumab is administered in 1200 mg of atezolizumab formulated with acetic acid (16.5 mg), L-histidine (62 mg), polysorbate 20 (8 mg), and sucrose (821.6 mg) having a pH of 5.8. may be provided in a 20 mL vial containing zolizumab. In another example, atezolizumab is administered at 840 mg of atezolizumab formulated with acetic acid (11.5 mg), L-histidine (43.4 mg), polysorbate 20 (5.6 mg), and sucrose (575.1 mg) having a pH of 5.8. may be provided in a 14 mL vial containing zolizumab.
예시적인 티라골루맙 제형은 폴리소르베이트 20, 수크로스, L-메티오닌 및 WFI를 함유하는 히스티딘 용액을 포함한다. 티라골루맙은 60 mg/mL의 대략적인 티라골루맙 항체 농도에서 10 mL의 티라골루맙 의약품을 함유하는 15 mL 바이알에 제공될 수 있다.An exemplary tyragolumab formulation comprises a histidine solution containing polysorbate 20, sucrose, L-methionine and WFI. Tiragolumab may be presented in a 15 mL vial containing 10 mL of the tiragolumab drug product at an approximate concentration of tyragolumab antibody at 60 mg/mL.
본원에서 제제는 또한 치료되는 특정 징후에 대해 필요에 따라 하나 초과의 활성 성분, 바람직하게는 서로에 부정적으로 영향을 주지 않는 상보적 활성을 갖는 것들을 함유할 수 있다. 예를 들어, 추가 치료제를 추가로 제공하는 것이 바람직할 수 있다. 이러한 활성 성분들은 의도한 목적에 효과적인 양으로 복합물 내에 적합하게 존재한다.The formulations herein may also contain more than one active ingredient as needed for the particular indication being treated, preferably those with complementary activities that do not adversely affect each other. For example, it may be desirable to further provide an additional therapeutic agent. These active ingredients are suitably present in the complex in amounts effective for their intended purpose.
활성 성분은, 예를 들어 액적형성 기술에 의해 또는 계면 중합화에 의해 제조된 마이크로캡슐, 예를 들어 각각, 콜로이드성 약물 전달 시스템(예를 들어, 리포솜, 알부민 마이크로스피어, 마이크로유제, 나노입자 및 나노캡슐)에서 또는 마크로유제에서 히드록시메틸셀룰로오스 또는 젤라틴-마이크로캡슐 및 폴리-(메틸메타크릴레이트) 마이크로캡슐 내에 포획될 수 있다. 상기 기술은 Remington’s Pharmaceutical Sciences 16th edition, Osol, A. Ed. (1980)에 개시되어 있다.The active ingredient may be administered in microcapsules prepared, for example, by droplet formation techniques or by interfacial polymerization, such as, respectively, in colloidal drug delivery systems (eg, liposomes, albumin microspheres, microemulsions, nanoparticles and nanocapsules) or in macroemulsions, hydroxymethylcellulose or gelatin-microcapsules and poly-(methylmethacrylate) microcapsules. This technique is described in Remington's Pharmaceutical Sciences 16th edition, Osol, A. Ed. (1980).
서방형 제제가 제조될 수 있다. 서방형 제재의 적합한 예들에는 상기 항체를 함유하는 고체 소수성 중합체의 반투과성 매트릭스가 포함되며, 이러한 매트릭스는 성형된 제품 형태, 예를 들어, 필름, 또는 마이크로캡슐 형태로 존재한다. 생체내 투여에 사용되는 제제는 일반적으로 무균이다. 무균은, 예컨대 무균 여과막을 통한 여과에 의해 용이하게 구현될 수 있다.Sustained release formulations can be prepared. Suitable examples of sustained release formulations include semipermeable matrices of solid hydrophobic polymers containing the antibody, which matrices are in the form of a shaped article, eg, a film, or microcapsules. Formulations used for in vivo administration are generally sterile. Sterility can be readily achieved, for example, by filtration through a sterile filtration membrane.
본 발명은 본원에 제공된 방법들 중 임의의 것에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한, 예컨대 항 TIGIT 길항제 항체를 포함하는, 키트를 제공한다. The present invention provides a kit, eg, comprising an anti TIGIT antagonist antibody, for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to any of the methods provided herein.
본 발명의 다른 구현예에서, 본원에 제공된 방법들 중 임의의 것에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한 항 TIGIT 길항제 항체를 포함하는, 키트가 제공된다. 일부 경우들에서, 상기 키트는 상기 PD-1 축 결합 길항제를 추가로 포함한다. 일부 경우들에서, 제조품 또는 키트는 암(예컨대, 환자에게서)을 치료하거나 이의 진행을 지연시키기 위해 상기 PD-1 축 결합 길항제와 병용으로 항 TIGIT 길항제 항체를 사용하기 위한 지침서를 포함하는 패키지 삽입물을 추가로 포함한다.In another embodiment of the invention, there is provided a kit comprising an anti TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to any of the methods provided herein. . In some cases, the kit further comprises the PD-1 axis binding antagonist. In some cases, the article of manufacture or kit comprises a package insert comprising instructions for using an anti-TIGIT antagonist antibody in combination with the PD-1 axis binding antagonist to treat or delay the progression of cancer (eg, in a patient). additionally include
본 발명의 다른 구현예에서, 본원에 제공된 방법들 중 임의의 것에 따라 암을 가진 대상체를 치료하기 위해 항 TIGIT 길항제 항체와 병용으로 사용하기 위한 PD-1 축 결합 길항제를 포함하는, 키트가 제공된다. 일부 경우들에서, 상기 키트는 항 TIGIT 길항제 항체를 추가로 포함한다. 일부 경우들에서, 제조품 또는 키트는 환자에게서 암을 치료하거나 이의 진행을 지연시키기 위해 항 TIGIT 길항제 항체와 병용으로 상기 PD-1 축 결합 길항제를 사용하기 위한 지침서를 포함하는 패키지 삽입물을 추가로 포함한다.In another embodiment of the invention, there is provided a kit comprising a PD-1 axis binding antagonist for use in combination with an anti TIGIT antagonist antibody to treat a subject having cancer according to any of the methods provided herein. . In some cases, the kit further comprises an anti-TIGIT antagonist antibody. In some cases, the article of manufacture or kit further comprises a package insert comprising instructions for using the PD-1 axis binding antagonist in combination with an anti-TIGIT antagonist antibody to treat or delay the progression of cancer in a patient. .
다른 구현예에서, 키트는 본원에 기재된 방법등 중 임의의 것에 따라 암을 가진 대상체를 치료하기 위해 아테졸리주맙과 병용으로 사용하기 위한 티라골루맙을 포함한다. 일부 구현예들에서, 상기 키트는 아테졸리주맙을 더 포함한다. 일부 경우들에서, 제조품 또는 키트는 환자에게서 암을 치료하거나 이의 진행을 지연시키기 위해 아테졸리주맙과 병용으로 티라골루맙을 사용하기 위한 지침서를 포함하는 패키지 삽입물을 추가로 포함한다.In another embodiment, the kit comprises tiragolumab for use in combination with atezolizumab to treat a subject having cancer according to any of the methods and the like described herein. In some embodiments, the kit further comprises atezolizumab. In some cases, the article of manufacture or kit further comprises a package insert comprising instructions for using tiragolumab in combination with atezolizumab to treat or delay the progression of cancer in a patient.
다른 구현예에서, 키트는 본원에 기재된 방법등 중 임의의 것에 따라 암을 가진 대상체를 치료하기 위해 티라골루맙과 병용으로 사용하기 위한 아테졸리주맙을 포함한다. 일부 구현예들에서, 상기 키트는 티라골루맙을 더 포함한다. 일부 경우들에서, 제조품 또는 키트는 환자에게서 암을 치료하거나 이의 진행을 지연시키기 위해 티라골루맙과 병용으로 아테졸리주맙을 사용하기 위한 지침서를 포함하는 패키지 삽입물을 추가로 포함한다. In another embodiment, the kit comprises atezolizumab for use in combination with tiragolumab to treat a subject having cancer according to any of the methods and the like described herein. In some embodiments, the kit further comprises tiragolumab. In some cases, the article of manufacture or kit further comprises a package insert comprising instructions for using atezolizumab in combination with tiragolumab to treat or delay the progression of cancer in a patient.
일부 경우들에서, 상기 PD-1 축 결합 길항제 및 상기 항 TIGIT 길항제 항체는 동일한 용기 또는 별도의 용기에 존재한다. 적합한 용기들은, 예를 들어, 병, 바이알, 봉투 및 주사기를 포함한다. 상기 용기는 다양한 물질, 예컨대, 유리, 플라스틱(예컨대, 폴리비닐 클로라이드 또는 폴리올레핀), 또는 금속 합금(예컨대, 스테인레스강 또는 하스텔로이)로부터 형성될 수 있다. 일부 경우들에서, 상기 용기는 제제를 보유하며 용기 위의 라벨 또는 용기와 관련된 라벨은 사용지침을 표시할 수 있다. 상기 제조품 또는 키트는 다른 완충제, 희석제, 필터, 바늘, 주사기, 및 사용 설명서가 있는 패키지 삽입물을 포함하는, 상업적 및 사용자 관점에서 바람직한 다른 재료들을 추가로 포함할 수 있다. 일부 경우들에서, 상기 제조품은 다른 작용제(예컨대, 화학요법제 및 항신생물제) 중에서 한 가지 이상을 더 포함한다. 상기 하나 이상의 제제에 적합한 용기는, 예를 들어 병, 바이알, 봉투 및 주사기를 포함한다.In some cases, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are in the same container or in separate containers. Suitable containers include, for example, bottles, vials, envelopes and syringes. The container may be formed from a variety of materials, such as glass, plastic (eg, polyvinyl chloride or polyolefin), or metal alloy (eg, stainless steel or hastelloy). In some cases, the container holds the formulation and a label on the container or a label associated with the container may indicate instructions for use. The article of manufacture or kit may further include other materials desirable from a commercial and user standpoint, including other buffers, diluents, filters, needles, syringes, and package inserts with instructions for use. In some cases, the article of manufacture further comprises one or more of other agents (eg, chemotherapeutic agents and anti-neoplastic agents). Suitable containers for the one or more formulations include, for example, bottles, vials, envelopes and syringes.
일부 실시양태에서, PD-1 축 결합 길항제 및 항 TIGIT 길항제 항체를 포함하는 키트는 VEGF 길항제, 화학요법제(예컨대, 백금계 화학요법제 또는 비백금계 화학요법제), ADC(예컨대, 엔포르투맙 베도틴 또는 사시투주맙 고비테칸), 및/또는 CSF(예컨대, 페그필그라스팀, 필그라스팀 또는 사그라모스팀)를 더 포함한다. In some embodiments, a kit comprising a PD-1 axis binding antagonist and an anti TIGIT antagonist antibody comprises a VEGF antagonist, a chemotherapeutic agent (eg, a platinum-based chemotherapeutic agent or a non-platinum-based chemotherapeutic agent), an ADC (eg, enfortumab) vedotin or sacituzumab govitecan), and/or CSF (eg, pegfilgrastim, filgrastim or sagramostim).
본원에 기재된 PD-1 축 결합 길항제 및/또는 항 TIGIT 길항제 항체 중 임의의 것이 상기 제조품 또는 키트에 포함될 수 있다. 상기 제조품 또는 키트 중 임의의 것은 본원에 기재된 임의의 방법에 따라 대상체에게 PD-1 축 결합 길항제 및/또는 항 TIGIT 길항제 항체를 투여하기 위한 지침서를 포함할 수 있다. Any of the PD-1 axis binding antagonist and/or anti TIGIT antagonist antibodies described herein may be included in the article of manufacture or kit. Any of the above articles of manufacture or kits may comprise instructions for administering a PD-1 axis binding antagonist and/or anti TIGIT antagonist antibody to a subject according to any of the methods described herein.
VI. 실시예VI. Example
실시예의 목차Table of Contents of Examples
다음은 본 발명의 방법들에 관한 실시예이다. 다양한 다른 실시예가 전술한 일반적인 설명에 따라 실시될 수 있는 것으로 이해된다.The following are examples of the methods of the present invention. It is understood that various other embodiments may be practiced in accordance with the general description set forth above.
실시예 1. 국소 진행성 또는 전이성 종양을 가진 환자를 대상으로 단일 제제로서 및 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용 투여한 티라골루맙의 안전성 및 약동학에 관한 제Ia/Ib상, 공개 라벨, 용량 증량 연구Example 1. Phase Ia/Ib, Publication of the Safety and Pharmacokinetics of Tiragolumab as a Single Agent and Co-administered with Atezolizumab in Patients with Locally Advanced or Metastatic Tumors with or without Chemotherapy Label, dose escalation studies
상기 연구는 국소 진행성 또는 전이성 종양을 가진 환자에게 단일 제제(Ia상)로서 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용 투여할 때의(Ib상) 티라골루맙(MTIG7192A)의 안전성, PK, 약력학, 및 예비 항종양 활성을 평가한다. 구체적인 연구 목적 및 해당 평가변수는 표 5에 요약되어 있다.This study investigated the safety of tiragolumab (MTIG7192A) as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) in patients with locally advanced or metastatic tumors; PK, pharmacodynamics, and preliminary anti-tumor activity are assessed. The specific study objectives and corresponding endpoints are summarized in Table 5.
아테졸리주맙 및 화학요법(Ib상 화학요법 확장 코호트)과 병용한 티라골루맙의 안전성 및 내약성을 평가하기.When administered as a single agent (Phase Ia) or in combination with atezolizumab (Phase Ib), including estimation of the maximum tolerated dose (MTD) and recommended Phase II dose (RP2D) and characterization of dose limiting toxicity (DLT) To evaluate the safety and tolerability of tiragolumab.
To evaluate the safety and tolerability of tiragolumab in combination with atezolizumab and chemotherapy (Phase Ib Chemotherapy Expansion Cohort).
NCI CTCAE v4.0에 따라 등급이 매겨진 이상 반응의 발생률, 특성, 및 중증도
표적 활력 징후에서 기준선으로부터 변화
심전도(ECG)를 포함한 표적 임상 실험실 검사 결과에서 기준선으로부터 변화
투여받은 주기의 횟수 및 용량 강도
항 티라골루맙 항체(Ia상 또는 Ib상) 및/또는 항 아테졸리주맙 항체(Ib상)의 발생률 및 PK, 약력학, 안전성, 및 예비 유효성 매개변수와의 잠재적 상관관계Incidence and characteristics of DLT
Incidence, nature, and severity of adverse events graded according to NCI CTCAE v4.0
Changes from baseline in target vital signs
Changes from baseline in targeted clinical laboratory test results, including electrocardiogram (ECG)
Number of cycles received and dose intensity
Incidence of anti-tyragolumab antibody (Phase Ia or Ib) and/or anti-Atesolizumab antibody (Phase Ib) and potential correlation with PK, pharmacodynamics, safety, and preliminary efficacy parameters
화학요법을 포함하거나 포함하지 않고 티라골루맙과 병용 투여한(Ib상 단독) 아테졸리주맙의 PK 곡선을 특성화하기.
아테졸리주맙 및 티라골루맙과 병용으로 투여할 때의(Ib상 화학요법 확장 코호트) 시스플라틴, 카보플라틴, 페메트렉시드, 파클리탁셀, 및 에토포시드의 PK 곡선을 특성화하기.To characterize the pharmacokinetic (PK) curves of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib).
To characterize the PK curve of atezolizumab with or without chemotherapy in combination with tiragolumab (Phase Ib alone).
To characterize the PK curves of cisplatin, carboplatin, pemetrexed, paclitaxel, and etoposide when administered in combination with atezolizumab and tiragolumab (Phase Ib Chemotherapy Expansion Cohort).
- 농도-시간 곡선하 면적(AUC)
(AUC)
- 최대 혈청 농도(Cmax)
- 최소 혈청 농도(Cmin)
- 제거율(CL)
- 정상 상태의 분포 용적
(Vss)
다른 파라미터들, 예컨대 축적비, 반감기, 및 용량 비례가 또한 산출될 수 있다.
아테졸리주맙의 혈청 Cmax 및 Cmin
특정 시점에서의 시스플라틴, 카보플라틴, 페메트렉시드, 파클리탁셀, 및 에토포시드의 혈장 농도Serum concentrations of tiragolumab administered as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) at specific time points for the following parameters:
- Area under the concentration-time curve (AUC)
(AUC)
- Maximum serum concentration (Cmax)
- Minimum Serum Concentration (Cmin)
- Removal rate (CL)
- volume of distribution in steady state
(Vss)
Other parameters such as accumulation ratio, half-life, and dose proportionality can also be calculated.
Serum Cmax and Cmin of Atezolizumab
Plasma concentrations of cisplatin, carboplatin, pemetrexed, paclitaxel, and etoposide at specific time points
객관적 반응 지속 기간(DoR) - 시험자가 결정한 RECIST v1.1에 따라 문서화된 객관적 반응의 첫 번째 발생부터 문서화된 질병 진행 또는 임의의 원인으로 인한 사망에 이르기까지의 시간 중 먼저 발생한 시간으로 정의됨.
PFS - 시험자가 결정한 RECIST v.1.1에 따라 제1 연구 치료제로부터 진행의 발생 또는 임의의 원인으로 인한 사망에 이르기까지의 시간 중 먼저 발생한 시간으로 정의됨.
(e) 전체 생존(OS) - 제1 연구 치료제로부터 임의의 원인으로 인한 사망에 이르기까지의 시간으로 정의됨.
Objective Response - Defined as complete response (CR) or partial response (PR) according to the Solid Tumor Response Evaluation Criteria (RECIST) v.1.1, determined by the investigator and confirmed by a repeat assessment at least 4 weeks after initial documentation.
Duration of Objective Response (DoR) - defined as the time from the first occurrence of a documented objective response to documented disease progression or death from any cause, whichever occurs first, according to RECIST v1.1 as determined by the investigator.
PFS - defined as the time from the first study treatment to the onset of progression or death from any cause, whichever occurs first, per RECIST v.1.1 as determined by the investigator.
(e) Overall survival (OS)—defined as time from first study treatment to death from any cause.
다른 결과 측정(Ib상)과 이의 관계를 평가함으로써 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용으로 항 티라골루맙 항체를 측정하고 다른 결과 측정(Ia상)과 이의 관계를 평가함으로써
단일 제제로서 투여된 티라골루맙의 면역원성 잠재력을 특성화하기.measuring anti-tiragolumab and/or anti-atezolizumab antibodies, and
By measuring its relationship to other outcome measures (Phase Ib) and by evaluating its relationship to other outcome measures (Phase Ia) and anti-tyragolumab antibodies in combination with atezolizumab with or without chemotherapy
To characterize the immunogenic potential of tiragolumab administered as a single agent.
목적 및 평가변수Purpose and endpoints
A.A. 연구 설계study design
이는 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나, 또는 이에 대해 임상 시험용 제제의 임상 시험이 인정된 치료 표준인, 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자에게서 단일 제제로서 티라골루맙의 안전성, 내약성, 및 약동학을 평가하도록 설계된 인간을 대상으로 한 최초의 1상, 공개 라벨, 다기관, 글로벌, 용량 증량 연구이다. 본 연구는 또한 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나, 또는 이에 대해 임상시험용 제제의 임상 시험이 인정된 치료의 표준이건, 또는 이에 대해 항 PD-L1 항체를 병용한 임상 시험용 제제의 임상 시험이 허용가능한 치료 선택사항으로 간주되는, 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자를 대상으로 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 함께 투여될 때 티라골루맙의 안전성, 내약성, 및 Pk에 대한 평가를 가능하게 하도록 설계되었다. It is locally advanced, relapsing, or metastatic refractory for which standard therapy does not exist, has proven ineffective or intolerable, is deemed inappropriate, or for which clinical trials of investigational agents are the accepted standard of care. This is the first phase 1, open-label, multicenter, global, dose-escalation study in humans designed to evaluate the safety, tolerability, and pharmacokinetics of tiragolumab as a single agent in patients with tumors. The study also indicated that there is no standard therapy for this, has been demonstrated to be ineffective or intolerable, is considered inappropriate, or for which clinical trials of an investigational agent are the accepted standard of care for, or against, anti-PD. -Atezolizumab with or without chemotherapy in patients with locally advanced, relapsed, or metastatic refractory tumors for which clinical trials of investigational agents using L1 antibodies are considered acceptable treatment options. Designed to enable evaluation of the safety, tolerability, and Pk of tiragolumab when administered together.
도 1은 Ib상 화학요법 확장 및 Ib상 Q4W 투약 확장을 도시한 흐름도이다. 용량 증량 단계 동안, 각각 약 3~6명의 환자로 이루어진 코호트를 증량 용량 수준에서 평가하여 단일 제제로서 또는 아테졸리주맙과 병용한 티라골루맙에 대한 MTD 또는 최대 투여 용량(MAD)을 결정한다. 1 is a flow chart depicting Phase Ib Chemotherapy Expansion and Phase Ib Q4W Dosing Expansion. During the dose escalation phase, cohorts of approximately 3 to 6 patients each are evaluated at the escalating dose level to determine the MTD or maximum administered dose (MAD) for tiragolumab as a single agent or in combination with atezolizumab.
용량 확장 단계에서, 환자는 단일 제제로서(Ia상), 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용으로(Ib상) 한 티라골루맙의 MTD 또는 MAD 이하로 등록 및 치료된다. 단일 제제로서의 티라골루맙(Ia상) 또는 티라골루맙 및 아테졸리주맙의 조합(화학요법이 없는 Ib상 코호트)은 각 21일 주기의 제 1일 또는 각 28일 주기의 제 1일(Ib상 Q4W 용량 확장)에 IV 주입에 의해 투여되며, 티라골루맙은 화학요법이 없는 Ib상 코호트에서 아테졸리주맙 이전에 투여된다. 허용할 수 없는 독성이 없거나 질병 진행에 대한 임상적으로 강력한 증거가 없는 경우, 시험자의 이익 및 위험에 대한 유리한 평가에 기초하여 티라골루맙(Ia상) 또는 아테졸리주맙과 병용한 티라골루맙(Ib상)을 이용한 치료는 주기 1 이후에도 계속된다.In the dose expansion phase, patients are enrolled and treated below the MTD or MAD of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib). Tiragolumab as a single agent (Phase Ia) or the combination of tiragolumab and atezolizumab (Phase Ib cohort without chemotherapy) was administered on Day 1 of each 21-day cycle or Day 1 of each 28-day cycle (Phase Ib). Q4W dose expansion) by IV infusion, and tiragolumab is administered prior to atezolizumab in the Phase Ib cohort without chemotherapy. In the absence of unacceptable toxicity or clinically strong evidence of disease progression, tiragolumab (Phase Ia) or tiragolumab in combination with atezolizumab (Phase Ia) or Treatment with phase Ib) is continued after cycle 1.
상기 Ib상 화학요법 확장 코호트 및 Ib상 Q4W 투여 확장 코호트(도 1)에서, 3명의 환자에 대한 안전성 탐색이 완료되었다. 안전성 탐색의 모든 관련 안전 데이터는 등록을 계속하기 전에 IMC 및 조사관이 철저히 검토해야 한다.In the Phase Ib chemotherapy expansion cohort and Phase Ib Q4W dosing expansion cohort ( FIG. 1 ), a safety search for 3 patients was completed. All relevant safety data from the safety search must be thoroughly reviewed by the IMC and investigators before registration continues.
화학요법 확장 코호트에서, 티라골루맙 및 아테졸리주맙은 3개의 코호트 각각에서 특정 화학요법과 하기와 같이 병용된다: 코호트 A에서 카보플라틴 또는 시스플라틴 및 페메트렉시드, 코호트 B에서 카보플라틴 및 파클리탁셀, 및 코호트 C에서 카보플라틴 또는 시스플라틴 및 에토포시드(도 1을 참조). 각 코호트에서, 치료에는 유도기 및 유지기를 포함한다. 상기 유도기에서, 티라골루맙 및 아테졸리주맙의 화학요법과의 조합은 코호트 A 및 B에 대해 4회 내지 6회 주기 동안 및 코호트 C에 대해 4회 주기 동안 21일 주기로 IV 주입으로 투여된다. 코호토 A 및 코호트 B에 대한 유도 치료 주기의 횟수는 시험자의 재량에 따라 결정된다.In the chemotherapy expansion cohort, tiragolumab and atezolizumab were combined with specific chemotherapy in each of the three cohorts as follows: carboplatin or cisplatin and pemetrexed in cohort A, carboplatin and paclitaxel in cohort B , and carboplatin or cisplatin and etoposide in cohort C (see Figure 1). In each cohort, treatment includes an induction phase and a maintenance phase. In this induction phase, the combination of tiragolumab and atezolizumab with chemotherapy is administered as an IV infusion on a 21-day cycle for 4 to 6 cycles for Cohorts A and B and 4 cycles for Cohort C. The number of induction treatment cycles for Cohort A and Cohort B is at the discretion of the investigator.
상기 유도기 후에, 질병 진행이나 허용할 수 없는 독성을 경험하지 않은 환자는 유지 요법으로 치료를 계속한다. 상기 유지기 동안, 코호트 B 및 코호트 C의 환자는 티라골루맙 및 아테졸리주맙만 계속 투여받는 반면, 코호트 A의 환자는 페메트렉시드와 함께 티라골루맙 및 아테졸리주맙을 계속 투여한다. 모든 화학요법 확장 코호트에서, 아테졸리주맙은 티라골루맙보다 먼저 투여된다. 화학요법이 주어질 때, 이는 아테졸리주맙 및 티라골루맙 이후에 투여된다.After the induction phase, patients who have not experienced disease progression or unacceptable toxicity continue treatment with maintenance therapy. During this maintenance phase, patients in Cohort B and Cohort C continue to receive tiragolumab and atezolizumab alone, while patients in Cohort A continue to receive tiragolumab and atezolizumab in combination with pemetrexed. In all chemotherapy expansion cohorts, atezolizumab is administered before tiragolumab. When given chemotherapy, it is administered after atezolizumab and tiragolumab.
모든 환자는 연구 내내, 및 연구 치료제의 최종 용량 투여 후 적어도 90 일 동안, 또는 다른 항암 전신 요법의 개시 때까지(어느 것이든 먼저 발생하는 시기까지) 유해 사례에 대해 면밀하게 모니터링된다. 유해 사례는 NCI CTCAE v4.0에 따라 등급화한다.All patients are closely monitored for adverse events throughout the study and for at least 90 days after administration of the last dose of study treatment, or until initiation of other anti-cancer systemic therapy, whichever occurs first. Adverse events are graded according to NCI CTCAE v4.0.
단일 제제로서(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용으로(Ib상) 티라골루맙의 PK 특성, 면역원성 반응, 및 약력학적 효과를 특성화하기 위해, 투약 전후 다양한 시점에서 혈액 샘플을 채취한다. 중간 PK 분석의 결과에 따라, PK 샘플링의 빈도는 연구 후반부에 줄어들 수 있다.To characterize the PK properties, immunogenic response, and pharmacodynamic effects of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) at various time points before and after dosing a blood sample is taken from Depending on the results of the interim PK analysis, the frequency of PK sampling may be reduced later in the study.
환자는 스크리닝 및 연구 동안에 종양 평가를 받고, 이는 표준 고형 종양의 반응 평가 기준(RECIST) v1.1 기준에 의해 측정한다. 환자는, 계속된 치료에 대한 기준을 충족하는 경우, 연구의 Ia상 또는 Ib상 부분에서 질병 진행에 대한 표준 RECIST v1.1 기준이 충족되더라도 연구 치료제를 계속 받을 수 있다. 연구의 Ia상 부분을 중단한 환자는, 교차 기준을 충족하고 접근 가능한 병변에 대한 생검에 동의하는 경우, 연구의 Ib상 부분으로 전환되어 아테졸리주맙과 병용한 티라골루맙을 이용한 치료를 받을 수 있다.Patients receive tumor assessments during screening and study, as measured by the Standard Response Evaluation Criteria for Solid Tumors (RECIST) v1.1 criteria. Patients may continue to receive study treatment even if the standard RECIST v1.1 criteria for disease progression in the Phase Ia or Ib portion of the study are met, provided they meet the criteria for continued treatment. Patients who withdraw from the Phase Ia portion of the study may be transferred to the Phase Ib portion of the study and receive treatment with tiragolumab in combination with atezolizumab, provided they meet the crossover criteria and consent to a biopsy of an accessible lesion. have.
입수 가능한 표준 요법 후 진행된 국소 진행성, 재발성 또는 전이성 난치성 악성 종양을 가지거나; 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나; 또는 이에 대해 임상 시험용 제제의 임상 시험이 인정된 치료의 표준인 약 60~320명의 환자가 연구의 확장 코호트에 등록된다. 연구의 Ib상 부분의 경우, 화학요법을 포함하거나 포함하지 않고 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 환자가 확장 코호트에 등록될 수 있다.have locally advanced, recurrent, or metastatic refractory malignancies that have progressed following available standard therapy; for which standard therapies do not exist, have proven ineffective or intolerable, or have been deemed inadequate; Alternatively, approximately 60 to 320 patients for which clinical trials of the investigational product are the accepted standard of care are enrolled in the study's expansion cohort. For the Phase Ib portion of the study, patients with or without chemotherapy for an investigational product in combination with an anti-PD-L1 antibody may be enrolled in the expansion cohort if they are considered an acceptable treatment option.
상기 확장 단계는 특정 암 환경에서 단일 제제로서(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용으로(Ib상) 티라골루맙의 안전성, 내약성, PK 변동성, 약력학적 활성, 및 예비 항종양 활성을 보다 잘 특성화하기 위해 소정의 환자 코호트를 포함한다. 상기 확장 코호트의 등록은 축적된 안전성, 내약성, PK, 약력학, 및 항종양 활성 데이터의 평가를 기반으로 연구 시험자가 결정한 단일 제제로서의 티라골루맙(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용한 티라골루맙(Ib상)의 MAD 또는 MTD 이하의 선택된 용량 수준에서 개시된다.The expansion phase includes the safety, tolerability, PK variability, pharmacodynamic activity of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) in certain cancer settings, and In order to better characterize preliminary anti-tumor activity, we included a cohort of patients. Enrollment in the expansion cohort includes tyragolumab as a single agent (Phase Ia) or with or without chemotherapy as determined by the study investigator based on assessment of accumulated safety, tolerability, PK, pharmacodynamics, and antitumor activity data. It is initiated at a selected dose level below the MAD or MTD of tiragolumab (Phase Ib) in combination with zolizumab.
연구의 Ia상 부분에서, 최대 약 40명의 환자가 NSCLC, RCC, TNBC, 흑색종, HNSCC, OC, GEJ 암을 포함한 GC, UBC, 및 CRC(MSS 또는 MSI이 낮은 CRC 포함)를 포함하여 PD-L1 선택된 및/또는 TIGIT 선택된 다중 종양 적응증의 계획된 확장 코호트에 등록된다.In the Phase Ia portion of the study, up to about 40 patients were diagnosed with PD-, including NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC, UBC, and CRC (including CRCs with low MSS or MSI) GEJ cancers. Enroll in a planned expansion cohort of L1 selected and/or TIGIT selected multiple tumor indications.
연구의 Ib상 부분(화학요법 없음)에서, 약 20~40명의 환자가 하기의 계획된 적응증별 확장 코호트 각각에 등록된다: NSCLC: 암 면역요법(CIT) 경험이 없음(예컨대, 항 PD-L1/PD-1의 선행 치료를 받지 않았음); NSCLC: CIT 치료됨(예컨대, 항 PD-L1/PD-1의 선행 치료를 포함); RCC; TNBC; 흑색종; HNSCC; OC; GC, GEJ 암을 포함; UBC; CRC(MSS 또는 MSI이 낮은 CRC 포함); 흑색종, OC, RCC 및 UBC를 포함한 특정 종양 징후의 생검 코호트.In the Phase Ib portion of the study (no chemotherapy), approximately 20-40 patients are enrolled in each of the following planned indication-specific expansion cohorts: NSCLC: no cancer immunotherapy (CIT) experience (e.g., anti-PD-L1/ no prior treatment for PD-1); NSCLC: CIT treated (eg, including prior treatment with anti-PD-L1/PD-1); RCC; TNBC; melanoma; HNSCC; OC; including GC and GEJ cancers; UBC; CRC (including MSS or CRC with low MSI); Biopsy cohort of specific tumor indications including melanoma, OC, RCC and UBC.
연구의 Ib상 화학요법 확장 부분에서, 약 20~40명의 환자가 하기의 계획된 화학요법 확장 코호트 각각에 등록된다(도 1을 참조):In the Phase Ib chemotherapy expansion portion of the study, approximately 20-40 patients are enrolled in each of the following planned chemotherapy expansion cohorts (see Figure 1):
코호트 A:Cohort A:
- 유도기 - 아테졸리주맙 및 티라골루맙 - - Induction phase - Atezolizumab and Tiragolumab -
시스플라틴 또는 카보플라틴 및 페메트렉시드와 병용In combination with cisplatin or carboplatin and pemetrexed
- 유지기 - 아테졸리주맙 및 티라골루맙 - - Maintenance phase - Atezolizumab and Tiragolumab -
페메트렉시드와 병용In combination with pemetrexed
코호트 B:Cohort B:
- 유도기 - 아테졸리주맙 및 티라골루맙 - - Induction phase - Atezolizumab and Tiragolumab -
카보플라틴과 파클리탁셀Carboplatin and Paclitaxel
- 유지기 - 아테졸리주맙 및 티라골루맙 - Maintenance phase - Atezolizumab and Tiragolumab
코호트 C:Cohort C:
- 유도기 - 아테졸리주맙 및 티라골루맙 - - Induction phase - Atezolizumab and Tiragolumab -
시스플라틴 또는 카보플라틴 및 에토포시드와 병용In combination with cisplatin or carboplatin and etoposide
- 유지기 - 아테졸리주맙 및 티라골루맙 - Maintenance phase - Atezolizumab and Tiragolumab
각 코호트의 치료 조합은 표 6에 나타내었다.Treatment combinations for each cohort are shown in Table 6.
(21일 주기의 4회 또는 6회)induction period
(4 or 6 times in a 21-day cycle)
(21일 주기)retainer
(21 day cycle)
시스플라틴 또는 카보플라틴 + 페메트렉시드Atezolizumab + Tiragolumab +
Cisplatin or Carboplatin + Pemetrexed
페메트렉시드Atezolizumab + Tiragolumab +
Pemetrexed
카보플라틴 + 파클리탁셀Atezolizumab + Tiragolumab +
Carboplatin + Paclitaxel
티라골루맙Atezolizumab +
Tiragolumab
시스플라틴 또는 카보플라틴 + 에토포시드Atezolizumab + Tiragolumab +
Cisplatin or Carboplatin + Etoposide
티라골루맙Atezolizumab +
Tiragolumab
화학요법 확장 코호트의 치료 요법Treatment regimens in the chemotherapy expansion cohort
B.B. Ib상 화학요법 확장 코호트: 용량 및 투여Phase Ib Chemotherapy Expansion Cohort: Dose and Dosing
상기 유도기에서, 특정 화학요법 확장 코호트의 환자는 하기의 용량 및 투여를 받는다:In the induction phase, patients in certain chemotherapy expansion cohorts receive the following doses and administrations:
코호트 A는 21일 주기의 제 1일마다 아테졸리주맙 1200 mg IV, 티라골루맙 600 mg IV에 이어서 시스플라틴 75 mg/m2 IV 또는 카보플라틴 AUC 6 mg/mL·min IV 및 페메트렉시드 500 mg/m2 IV의 조합을 투여 받는다. 질병 진행이나 허용할 수 없는 독성이 없는 경우, 4 내지 6회 주기의 유도기 치료가 실시된다.Cohort A was atezolizumab 1200 mg IV, tiragolumab 600 mg IV, followed by cisplatin 75 mg/m 2 IV or carboplatin AUC 6 mg/mL min IV and pemetrexed 500 every day 1 of a 21-day cycle. A combination of mg/m 2 IV is administered. In the absence of disease progression or unacceptable toxicity, 4 to 6 cycles of induction phase treatment are administered.
코호트 B는 21일 주기의 제 1일마다 아테졸리주맙 1200 mg IV, 티라골루맙 600 mg IV에 이어서 카보플라틴 AUC 6 mg/mL·min IV 및 파클리탁셀 200 mg/m2 IV의 조합을 투여 받는다. 질병 진행이나 허용할 수 없는 독성이 없는 경우, 4 내지 6회 주기의 유도기 치료가 실시된다.Cohort B receives atezolizumab 1200 mg IV, tiragolumab 600 mg IV, followed by a combination of carboplatin AUC 6 mg/mL min IV and paclitaxel 200 mg/m 2 IV on Day 1 of a 21-day cycle . In the absence of disease progression or unacceptable toxicity, 4 to 6 cycles of induction phase treatment are administered.
코호트 C는 매 21일 주기의 제 1일에 아테졸리주맙 1200 mg IV, 티라골루맙 600 mg IV에 이어서 시스플라틴 75 mg/m2 IV 또는 카보플라틴 AUC 5 mg/mL·min IV 다음으로 매 21일 주기의 제 1일 내지 3일에 에토포시드 100 mg/m2 IV를 투여 받는다. 질병 진행이나 허용할 수 없는 독성이 없는 경우, 4회 주기의 유도기 치료가 실시된다.Cohort C is atezolizumab 1200 mg IV, tiragolumab 600 mg IV, then cisplatin 75 mg/m2 IV or carboplatin AUC 5 mg/mL min IV on day 1 of every 21-day cycle, then every 21 days Receive etoposide 100 mg/m 2 IV on days 1 to 3 of the cycle. In the absence of disease progression or unacceptable toxicity, 4 cycles of induction treatment are administered.
상기 유도기 후, 환자와 잠재적 위험 및 이점에 대한 신중한 평가 및 철저한 논의 후 시험자의 재량에 따라 허용할 수 없는 독성, 임상적으로 심각한 질병 진행, 및/또는 임상 이익의 손실이 없는 경우, 상기 유지기에서 치료를 계속한다. 상기 유지기에서, 특정 화학요법 확장 코호트의 환자는 하기의 용량 및 투여를 받는다:After the induction phase, if there is no unacceptable toxicity, clinically serious disease progression, and/or loss of clinical benefit, at the discretion of the investigator after careful evaluation and thorough discussion of potential risks and benefits with the patient, the maintenance phase continue treatment at In the maintenance phase, patients in certain chemotherapy expansion cohorts receive the following doses and administrations:
코호트 A는 매 21일 주기의 제 1일에 아테졸리주맙 1200 mg IV, 티라골루맙 600 mg IV에 이어서 페메트렉시드 500 mg/m2 IV를 투여 받고; 코호트 B는 매 21일 주기의 제 1일에 아테졸리주맙 1200 mg IV 후에 티라골루맙 600 mg IV를 투여 받으며; 코호트 C는 매 21일 주기의 일에 아테졸리주맙 1200 mg IV 다음으로 티라골루맙 600 mg IV를 투여 받는다.Cohort A received atezolizumab 1200 mg IV, tiragolumab 600 mg IV, followed by pemetrexed 500 mg/m 2 IV on day 1 of every 21-day cycle; Cohort B receives atezolizumab 1200 mg IV followed by tiragolumab 600 mg IV on Day 1 of every 21-day cycle; Cohort C receives atezolizumab 1200 mg IV followed by tyragolumab 600 mg IV on the day of every 21-day cycle.
독성이 있고 질병 진행이 없는 경우, 개별 화학요법 또는 면역요법 제제는 독립적으로 중단된다. In the case of toxicity and no disease progression, individual chemotherapy or immunotherapy agents are independently discontinued.
C.C. Ib상 Q4W 투약 확장 코호트Phase Ib Q4W Dosing Expansion Cohort
Ib상 Q4W 투약 확장 코호트의 목적은 매 4주(28일)의 투약 일정으로 아테졸리주맙 1680 mg IV와 병용으로 티라골루맙 840 mg IV로 치료받은 환자를 대상으로 안전성, 내약성, PK, 및 예비 유효성 데이터를 더 잘 특성화하고 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다.The purpose of the Phase Ib Q4W Dosing Expansion Cohort was to evaluate safety, tolerability, PK, and prospects in patients treated with tiragolumab 840 mg IV in combination with atezolizumab 1680 mg IV on a dosing schedule of every 4 weeks (28 days). To better characterize efficacy data and to explore potential tumor biomarkers of pharmacodynamic activity.
상기 Ib상 Q4W 코호트는 스크리닝 또는 재스크리닝 동안 종양 조직의 전향적 테스트를 기반으로 PD-L1 선택 및/또는 TIGIT 선택될 수 있는 종양을 가진 약 20~40명의 환자를 포함한다. 보관 조직이 불충분하거나 입수 불가능한 환자는 시험자의 논의를 바탕으로 의료 모니터(Medical Monitor)가 허용하는 경우 상기 코호트 등록에 적격일 수 있다. 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 종양 유형을 가진 환자가 상기 확장 코호트에 등록될 수 있다. The Phase Ib Q4W cohort includes about 20-40 patients with tumors that can be selected for PD-L1 and/or TIGIT based on prospective testing of tumor tissue during screening or re-screening. Patients with insufficient or unavailable archival tissue may be eligible for enrollment in this cohort if permitted by the Medical Monitor based on the investigator's discussion. Patients with tumor types for which clinical trials of investigational agents in combination with anti-PD-L1 antibodies are considered acceptable treatment options may be enrolled in this expansion cohort.
D.D. Ib상의 각 적응증별 확장 코호트에서의 환자에 대한 추가 포함 기준Additional inclusion criteria for patients in the expanded cohort for each indication in Phase Ib
NSCLC 코호트(CIT 미경험)는, CIT(항 PD-L1/PD-1 제제를 포함)가 현지 규제 당국에 의해 NSCLC 치료제로 승인된 경우, 항 PD-L1/PD-1 및/또는 항 CTLA-4를 포함하여 이전에 CIT(조사 또는 승인)로 치료한 적이 없는 조직학적으로 확인된 난치성, 진행성 NSCLC를 가지고, 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 환자를 포함한다. 종양이 공지된 감작성 표피 성장 인자 수용체(EGFR) 돌연변이 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 EGFR 티로신 키나아제 억제제(들)를 이용한 치료에 불내성을 경험했어야 한다. 종양이 공지된 역형성 림프종 키나아제(ALK) 재배열을 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 ALK 티로신 키나아제 억제제(들)을 이용한 치료에 불내성을 경험했어야 한다. 종양이 공지된 ROS1 재배열을 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 ROS1 티로신 키나아제 억제제(들)을 이용한 치료에 불내성을 경험했어야 한다. 종양이 BRAFV600E 돌연변이를 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 트라메티닙과 병용한 다브라페닙을 이용한 치료에 불내성을 경험했어야 한다.The NSCLC cohort (CIT naive) is considered anti-PD-L1/PD-1 and/or anti-CTLA-4 when CIT (including anti-PD-L1/PD-1 agents) has been approved as a treatment for NSCLC by local regulatory authorities. With histologically confirmed refractory, advanced NSCLC not previously treated with CIT (investigation or approval), including patients considered. Patients whose tumors have known sensitizing epidermal growth factor receptor (EGFR) mutations must also have experienced disease progression (during or after treatment) or intolerance to treatment with the EGFR tyrosine kinase inhibitor(s). Patients whose tumors have known anaplastic lymphoma kinase (ALK) rearrangements must also have experienced disease progression (during or after treatment) or intolerance to treatment with the ALK tyrosine kinase inhibitor(s). Patients whose tumors have known ROS1 rearrangements must also have experienced disease progression (during or after treatment) or intolerance to treatment with the ROS1 tyrosine kinase inhibitor(s). Patients whose tumors have the BRAFV600E mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with dabrafenib in combination with trametinib.
NSCLC 코호트(CIT 치료됨)는 항 PD-L1/PD-1을 포함하여 이전에 CIT(조사 또는 승인)로 치료된 적이 있는 조직학적으로 확인된 난치성, 진행성 NSCLC를 가진 환자를 포함한다. 종양이 공지된 감작성 EGFR 돌연변이 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 EGFR 티로신 키나아제 억제제(들)를 이용한 치료에 불내성을 경험했어야 한다. 종양이 공지된 ALK 재배열을 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 ALK 티로신 키나아제 억제제(들)을 이용한 치료에 불내성을 경험했어야 한다. 종양이 공지된 ROS1 재배열을 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 ROS1 티로신 키나아제 억제제(들)을 이용한 치료에 불내성을 경험했어야 한다. 종양이 BRAFV600E 돌연변이를 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 트라메티닙과 병용한 다브라페닙을 이용한 치료에 불내성을 경험했어야 한다. 환자는 이전에 항 PD-L1/PD-1을 포함해야 하는 CIT 단독요법 및/또는 병용요법(조사 또는 승인)에서 문서화된 질병 진행을 경험했어야 한다.The NSCLC cohort (CIT treated) includes patients with histologically confirmed refractory, advanced NSCLC who have previously been treated with CIT (investigation or approval), including anti-PD-L1/PD-1. Patients whose tumors have a known sensitizing EGFR mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with the EGFR tyrosine kinase inhibitor(s). Patients whose tumors have known ALK rearrangements must also have experienced disease progression (during or after treatment) or intolerance to treatment with the ALK tyrosine kinase inhibitor(s). Patients whose tumors have known ROS1 rearrangements must also have experienced disease progression (during or after treatment) or intolerance to treatment with the ROS1 tyrosine kinase inhibitor(s). Patients whose tumors have the BRAFV600E mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with dabrafenib in combination with trametinib. The patient must have previously experienced documented disease progression on CIT monotherapy and/or combination therapy (research or approval) that should include anti-PD-L1/PD-1.
단독요법 또는 병용요법으로 이전의 항 PD-L1/PD-1을 투여받는 동안 임의의 시간에 RECIST v1.1에 따라 시험자가 평가한 확인된 PR 또는 CR에 대한 문서화된 최상의 반응을 경험한 약 10명 이상의 환자가 등록될 수 있다. 단독요법 및/또는 병용요법으로 이전의 항 PD-L1/PD-1을 투여받는 동안 임의의 시간에 RECIST v1.1에 따라 시험자가 평가한 SD에 대한 문서화된 최상의 반응을 경험한 약 10명 이상의 환자가 등록될 수 있다. 단독요법 및/또는 병용요법으로 이전의 항 PD-L1/PD-1을 투여받는 동안 임의의 시간에 RECIST v1.1에 따라 시험자가 평가한 진행성 질병(PD)에 대한 문서화된 최상의 반응을 경험한 약 10명 이상의 환자가 등록될 수 있다. 단독요법 및/또는 병용요법으로서의 이전의 항 PD-L1/PD-1은 상기 확장 코호트에 등록하기 전에 투여된 가장 최근의 전신 항암 요법을 나타내야 한다. 주로 독성 또는 불내성을 이유로 이전의 항 PD-L1/PD-1 단일요법 및/또는 병용요법을 중단한 환자는 상기 확장 코호트 등록에 적격이지 않다.Approximately 10 experienced the best documented response for an identified PR or CR assessed by the investigator according to RECIST v1.1 at any time while receiving prior anti-PD-L1/PD-1 as monotherapy or combination therapy More than one patient may be enrolled. At any time while receiving prior anti-PD-L1/PD-1 as monotherapy and/or combination therapy, at least about 10 subjects experienced a documented best response to investigator-assessed SD according to RECIST v1.1 A patient may be enrolled. Experienced best documented response to investigator-assessed progressive disease (PD) according to RECIST v1.1 at any time while receiving prior anti-PD-L1/PD-1 as monotherapy and/or combination therapy More than about 10 patients may be enrolled. Previous anti-PD-L1/PD-1 as monotherapy and/or combination therapy should represent the most recent systemic anticancer therapy administered prior to enrollment in the expansion cohort. Patients who discontinue previous anti-PD-L1/PD-1 monotherapy and/or combination therapy, primarily for toxicity or intolerance, are not eligible for this expansion cohort enrollment.
TNBC 코호트는 조직학적으로 확인된 난치성, 진행성 에스트로겐 수용체(ER) 음성, 프로게스테론 수용체(PgR) 음성, 및 인간 EGFR 2(HER2) 음성 유방 선암종(삼중 음성)을 가진 환자를 포함한다. 삼중 음성 상태는 미국임상종양학회 미국병리학회(ASCO-CAP) 지침에 정의된 바와 같이 문서화해야 한다. 종양 세포 핵의 1% 미만이 ER에 대해 면역반응을 일으키고, 종양 세포 핵의 1% 미만이 프로게스테론 수용체에 대해 면역반응을 일으키며, HER2 검사에서 IHC 1+, IHC 0 또는 ISH(조직내 혼성화) 음성이 나타낸다. The TNBC cohort includes patients with histologically confirmed refractory, advanced estrogen receptor (ER) negative, progesterone receptor (PgR) negative, and human EGFR 2 (HER2) negative breast adenocarcinoma (triple negative). Triple negative status should be documented as defined in the American Society of Clinical Oncology (ASCO-CAP) guidelines. Less than 1% of tumor cell nuclei are immune to ER, less than 1% of tumor cell nuclei are immune to progesterone receptor, and HER2 test is negative for IHC 1+, IHC 0 or ISH (intra-tissue hybridization). This indicates
CRC 코호트는 조직학적으로 확인된The CRC cohort was histologically confirmed
결장 또는 직장의 난치성, 진행성 선암종을 가진 환자를 포함한다. 맹장 기원의 종양을 가진 환자는 적격이지 않다.patients with refractory, advanced adenocarcinoma of the colon or rectum. Patients with tumors of cecal origin are not eligible.
GC 코호트는 조직학적으로 확인된 수술이 불가능한, 국소 진행성 또는 전이성 또는 재발성 위 또는 GEJ 선암종(완치 요법에 적합하지 않음)을 가진 환자를 포함한다. R![]()
![]()
HNSCC 코호트는 조직학적으로 확인된 수술 불가능한, 국소 진행성 또는 전이성, 재발성, 또는 지속성 두경부 편평세포 암종(구강, 구인두, 하인두, 또는 후두)(근치 요법이 적합하지 않음)을 가진 환자를 포함한다. 머리 및 목의 다른 원발성 해부학적 위치에 HNSCC를 가진 환자, 원발성이 알려지지 않은 HNSCC를 가진 환자, 또는 비편평 조직학적 종양을 가진 환자는 적격이지 않다. 비인두의 HNSCC를 가진 환자는 적격일 수 있다. HNSCC에 대한 HPV 상태는 공지되어 있어야 한다.The HNSCC cohort includes patients with histologically confirmed inoperable, locally advanced or metastatic, recurrent, or persistent squamous cell carcinoma of the head and neck (oral, oropharyngeal, hypopharyngeal, or larynx) for which curative therapy is not suitable. Patients with HNSCC in other primary anatomical locations of the head and neck, patients with HNSCC of unknown primary, or patients with nonsquamous histological tumors are not eligible. Patients with HNSCC of the nasopharynx may be eligible. The HPV status for HNSCC should be known.
UBC 코호트는 조직학적으로 확인된 요로상피(신우, 요관, 방광, 및 요도를 포함)의 난치성 진행성 이행 세포 암종을 가진 환자를 포함한다. 혼합 조직을 가진 환자는 지배적인 이행 세포 패턴을 가져야 한다.The UBC cohort includes patients with histologically confirmed refractory advanced transitional cell carcinoma of the urothelium (including the renal pelvis, ureter, bladder, and urethra). Patients with mixed tissue should have a dominant transitional cell pattern.
흑색종 코호트는 조직학적으로 확인된 난치성, 진행성 전이성 흑색종을 가진 환자를 포함한다. CIT(항 PD-L1/PD-1 제제 및/또는 항 CTLA-4 제제를 포함)가 현지 규제 당국에 의해 흑색종 치료제로 승인된 경우, 이의 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 흑생종을 가진 환자를 포함한다. 종양이 공지된 BRAFV600 돌연변이를 갖는 환자는 또한 (치료 동안 또는 이후) 질병 진행 또는 BRAF 억제제(들) 및/또는 MEK 억제제(들)에 대한 불내성을 경험했어야 한다. 상기 코호트의 환자 중 약 20% 이하가 안구(포도막) 흑색종을 가진 환자가 되도록 등록을 관리한다.The melanoma cohort includes patients with histologically confirmed refractory, advanced metastatic melanoma. When CIT (including anti-PD-L1/PD-1 agents and/or anti-CTLA-4 agents) has been approved for the treatment of melanoma by local regulatory authorities, for investigational agents in combination with its anti-PD-L1 antibody Clinical trials include patients with melanoma who are considered an acceptable treatment option. Patients with a BRAFV600 mutation whose tumor is known must also have experienced disease progression (during or after treatment) or intolerance to the BRAF inhibitor(s) and/or MEK inhibitor(s). Enrollment is managed so that no more than about 20% of patients in this cohort have ocular (uveal) melanoma.
OC 코호트는 조직학적으로 확인된 난치성, 진행성 상피성 난소암, 나팔관암 또는 원발성 복막암을 가진 환자를 포함한다. 경계성 난소 상피 신생물(예컨대, 악성 가능성이 낮은 종양, 비정형 증식성 종양)은 제외한다.The OC cohort includes patients with histologically confirmed refractory, advanced epithelial ovarian cancer, fallopian tube cancer, or primary peritoneal cancer. Borderline ovarian epithelial neoplasms (eg, low malignant tumors, atypical proliferative tumors) are excluded.
RCC 코호트는 투명 세포 조직학의 성분 및/또는 육종양 조직학의 성분을 가진 조직학적으로 확인된 난치성, 진행성 RCC를 가진 환자를 포함한다. CIT(항 PD-L1/PD-1 제제를 포함)가 현지 규제 당국에 의해 RCC 치료제로 승인된 경우, 이의 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 RCC를 가진 환자를 포함한다.The RCC cohort includes patients with histologically confirmed refractory, advanced RCC with a component of clear cell histology and/or a component of sarcoma histology. When CITs (including anti-PD-L1/PD-1 agents) have been approved by local regulatory authorities for the treatment of RCC, clinical trials of their investigational agents in combination with their anti-PD-L1 antibodies are considered acceptable treatment options. Include patients with RCC considered.
E.E. 용량 및 투여Dosage and administration
상기 연구의 Ib상 부분에서 티라골루맙과 병용으로 투여한 아테졸리주맙의 용량은 아테졸리주맙 1680 mg IV Q4W가 투여되는 Ib상 Q4W 투약 코호트에서의 경우를 제외하고 3주마다 1200 mg IV이다. 상기 용량은 고정되고 체중에 의존하지 않는다. 화학요법을 포함하지 않은 모든 Ib상 코호트에서, 아테졸리주맙은 티라골루맙 주입 및 후속 관찰 기간 후에 투여된다. Ib상 화학요법 확장 코호트에서, 아테졸리주맙은 티라골루맙 이전에 투여된다.The dose of atezolizumab administered in combination with tiragolumab in the Phase Ib portion of the study was 1200 mg IV every 3 weeks, except in the Phase Ib Q4W dosing cohort where atezolizumab 1680 mg IV Q4W was administered. The dose is fixed and does not depend on body weight. In all Phase Ib cohorts that did not include chemotherapy, atezolizumab is administered after the tiragolumab infusion and subsequent observation period. In the Phase Ib chemotherapy expansion cohort, atezolizumab is administered prior to tiragolumab.
아테졸리주맙의 초기 용량은 60(±10) 분에 걸쳐 전달된다. 제1 주입이 주입 관련 유해 사례 없이 내약성이면, 제2 주입은 30(± 10)분에 걸쳐 전달될 수 있다. 30분 주입이 양호하게 용인되면, 후속하는 모든 주입은 30(±10)분에 걸쳐 전달될 수 있다. 주기 1의 경우, 아테졸리주맙 투약 후 90분의 관찰 기간이 이어진다. 이후의 모든 아테졸리주맙 주입 후에는 30분의 관찰 기간이 이어질 수 있다. 이전에 다른 임상 시험에서 아테졸리주맙을 투여받은 환자는 이전에 허용되었던 가장 빠른 속도로 초기 용량을 투여받을 수 있다. The initial dose of atezolizumab is delivered over 60 (±10) minutes. If the first infusion is well tolerated without infusion-related adverse events, the second infusion may be delivered over 30 (± 10) minutes. If a 30 minute infusion is well tolerated, all subsequent infusions can be delivered over 30 (±10) minutes. For Cycle 1, atezolizumab dosing is followed by a 90-minute observation period. A 30-minute observation period may follow after all subsequent atezolizumab infusions. Patients who have previously received atezolizumab in other clinical trials may receive the initial dose at the fastest rate previously permitted.
Ib상 확장 코호트에서의 화학요법Chemotherapy in the Phase Ib Expansion Cohort
화학요법은 아테졸리주맙 및 티라골루맙 주입에 이어서 후속하는 관찰 기간 후에 투여된다. 유도기 동안, 화학요법 주기는, 21일 주기 동안 적어도 하나의 화학요법 성분이 적어도 1회 투여되는 경우, 미리 정해진 유도 화학요법 주기의 수에 포함된다. 화학요법 성분이 제공되지 않은 주기는 총 유도 화학요법 주기의 수에 포함되지 않는다. Chemotherapy is administered following an infusion of atezolizumab and tiragolumab followed by an observation period. During the induction phase, chemotherapy cycles are included in the predetermined number of induction chemotherapy cycles when at least one chemotherapy component is administered at least once during a 21-day cycle. Cycles for which no chemotherapy component was given are not included in the total number of induction chemotherapy cycles.
환자는 현지 치료 표준 및 제조업체의 지침에 따라 화학요법제에 대한 항구토제 및 IV 수분 공급을 투여 받는다. 하지만, 스테로이드의 면역조절 효과로 인하여, 스테로이드 예비 투약은 임상적으로 가능한 범위 내에서 최소화해야 한다.Patients receive antiemetics and IV hydration for chemotherapeutic agents according to local standards of care and manufacturer's guidelines. However, due to the immunomodulatory effect of steroids, steroid premedication should be minimized to the extent clinically feasible.
코호트 A - 아테졸리주맙 + 티라골루맙 + 카보플라틴/시스플라틴 + 페메트렉시드Cohort A - atezolizumab + tyragolumab + carboplatin/cisplatin + pemetrexed
각 21일 주기의 제 1일에, 모든 적격 환자들은 약물 주입을 하기의 순서대로 투여받을 것이다:On Day 1 of each 21-day cycle, all eligible patients will receive drug infusions in the following order:
유도: 아테졸리주맙 > 티라골루맙 > 페메트렉시드 > 카보플라틴 또는 시스플라틴 Induction: atezolizumab > tyragolumab > pemetrexed > carboplatin or cisplatin
유도기에서 4회 내지 6회 주기 후, 환자는 하기의 투여 순서대로 유지 요법을 개시한다:After 4 to 6 cycles in the induction phase, the patient initiates maintenance therapy in the following order of administration:
유지: 아테졸리주맙 > 티라골루맙 > 페메트렉시드 Maintenance: atezolizumab > tyragolumab > pemetrexed
페메트렉시드 및 카보플라틴 또는 시스플라틴에 대한 치료 요법Treatment regimens for pemetrexed and carboplatin or cisplatin
AUC = 농도-시간 곡선하 면적; IV = 정맥 주사; Q3W = 3주마다.AUC = area under the concentration-time curve; IV = intravenous; Q3W = Every 3 weeks.
표 8은 유도기 동안 페메트렉시드 및 카보플라틴 또는 시스플라틴 및 유지기 동안 페메트렉시드의 치료 투여에 대한 권장 주입 시간을 나열한다.Table 8 lists the recommended infusion times for therapeutic administration of pemetrexed and carboplatin or cisplatin and pemetrexed during the maintenance phase during the induction phase.
파클리탁셀의 예비 투약Pre-administration of paclitaxel
IV = 정맥내; PO= 경구IV = intravenous; PO = oral
코호트 B - 아테졸리주맙 + 티라골루맙 + 카보플라틴 + 파클리탁셀Cohort B - Atezolizumab + Tiragolumab + Carboplatin + Paclitaxel
각 21일 주기의 제 1일에, 모든 적격 환자들은 약물 주입을On Day 1 of each 21-day cycle, all eligible patients received drug infusion.
하기의 순서대로 투여받는다.It is administered in the following order.
유도: 아테졸리주맙 > 티라골루맙 > 파클리탁셀 > 카보플라틴 Induction: atezolizumab > tyragolumab > paclitaxel > carboplatin
표 8은 코호트 B의 환자에 대한 유도 치료를 위해 제안된 예비 투약을 나열한다. 표 9는 유도기 동안 파클리탁셀 및 카보플라틴의 치료 투여를 위한 제안된 주입 시간을 나열한다.Table 8 lists the proposed pre-dosing for induction treatment for patients in Cohort B. Table 9 lists the suggested infusion times for therapeutic administration of paclitaxel and carboplatin during the induction phase.
(4회 내지 6회 주기)induction period
(4 to 6 cycles)
파클리탁셀 및 카보플라틴에 대한 치료 요법Treatment regimens for paclitaxel and carboplatin
AUC = 농도-시간 곡선하 면적; IV = 정맥 주사; Q3W = 3주마다.AUC = area under the concentration-time curve; IV = intravenous; Q3W = Every 3 weeks.
코호트 C - 아테졸리주맙 + 티라골루맙 + 카보플라틴 또는 시스플라틴 + 에토포시드Cohort C - atezolizumab + tyragolumab + carboplatin or cisplatin + etoposide
각 21일 주기의 제 1일에 모든 적격 환자에게 하기의 순서대로 연구 약물을 주입한다:On Day 1 of each 21-day cycle, all eligible patients are infused with study drug in the following order:
유도: 아테졸리주맙 > 티라골루맙 > 시스플라틴 또는 카보플라틴 > 에토포시드 Induction: atezolizumab > tyragolumab > cisplatin or carboplatin > etoposide
유도기 이후에, 환자는 하기의 투여 순서대로 유지 요법을 개시한다:After the induction phase, the patient initiates maintenance therapy in the following order of administration:
유지: 아테졸리주맙 > 티라골루맙 Maintenance: Atezolizumab > Tiragolumab
표 10은 유도기 동안 카보플라틴 또는 시스플라틴 및 에토포시드의 치료 투여에 대해 제안된 주입 시간을 나열한다.Table 10 lists the suggested infusion times for therapeutic administration of carboplatin or cisplatin and etoposide during the induction phase.
카보플라틴 또는 시스플라틴 및 에토포시드에 대한 치료 요법Treatment regimens for carboplatin or cisplatin and etoposide
IV = 정맥내; Q3W = 3주마다.IV = intravenous; Q3W = Every 3 weeks.
시스플라틴cisplatin
다양한 코호트에서의 시스플라틴 투여에 대한 지침이 표 11에 제시되어 있다.Guidance for cisplatin administration in various cohorts is presented in Table 11.
시스플라틴 투여 시간 및 지침Cisplatin Administration Times and Instructions
IV = 정맥내IV = intravenous
비고: 환자는 시스플라틴 투여 전후에 적절한 항구토 치료와 적절한 수분 공급을 받아야 한다. 자세한 내용은 현지 임상 진료 지침을 참조한다.Remarks: Patients should receive appropriate antiemetic therapy and adequate hydration before and after cisplatin administration. Refer to local clinical practice guidelines for details.
카보플라틴carboplatin
다양한 코호트에서의 시스플라틴 투여에 대한 지침이 표 12에 제시되어 있다.Guidelines for cisplatin administration in various cohorts are presented in Table 12.
카보플라틴 투여 시간 및 지침Carboplatin Administration Times and Instructions
AUC = 시간 농도 곡선하 면적; IV = 정맥내AUC = area under the time concentration curve; IV = intravenous
비고: 표준 항구토제는 현지 진료 지침에 따라 카보플라틴 투여와 함께 제공되어야 하며, AUC 5 또는 AUC 6의 카보플라틴 용량은 칼버트 공식을 사용하여 계산한다(Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):NOTE: Standard antiemetics should be given with carboplatin administration according to local practice guidelines, and the carboplatin dose of AUC 5 or AUC 6 is calculated using the Calvert formula (Calvert et al., J. Clin. Oncol . 1989, 7:1748-56):

여기서: CrCl = 크레아티닌 청소율, mL/분 here: CrCl = Creatinine clearance, mL/min
연령 = 환자의 연령 Age = Age of the patient
wt = 환자의 체중, kg wt = Patient's weight, kg
Scr = 혈청 크레아티닌, mg/dL Scr = serum creatinine, mg/dL
혈청 크레아티닌 수치가 비정상적으로 낮은 환자의 경우, 최소 크레아티닌 수치 0.8 mg/dL를 사용하여 상기 GFR을 추정하거나 추정된 GFR을 125 mL/분으로 그 상한치를 제한한다.For patients with abnormally low serum creatinine levels, estimate the GFR using a minimum creatinine level of 0.8 mg/dL or limit the upper limit of the estimated GFR to 125 mL/min.
환자의 GFR이 동위원소 희석 질량 분광법에 의한 혈청 크레아티닌 측정을 기반으로 추정되는 경우, 미국 FDA는 의사에게 과다 투약으로 인한 잠재적 독성을 피하기 위해 원하는 노출(AUC)에 대한 카보플라틴의 용량 제한을 고려할 것을 권장한다. 카보플라틴 라벨에 기재된 칼버트 공식을 기반으로 최대 용량은 하기와 같이 계산할 수 있다:If a patient's GFR is estimated based on serum creatinine measurements by isotopic dilution mass spectrometry, the FDA will advise physicians to consider limiting the dose of carboplatin for the desired exposure (AUC) to avoid potential toxicity from overdose. recommend that Based on the Calvert formula listed on the carboplatin label, the maximum dose can be calculated as follows:
최대 카보플라틴 용량(mg) = 목표 AUC(mg ![]()
![]()
상기 최대 용량은 정상 신장 기능을 가진 환자에게 150 mL/분으로 그 상한치가 제한된 GFR 추정치를 기반으로 한다. 이보다 높은 GFR 추정치는 사용하지 않는다.This maximum dose is based on an estimate of GFR with an upper limit of 150 mL/min in patients with normal renal function. GFR estimates higher than this are not used.
목표 AUC = 6의 경우, 최대 용량은 6 × 150 = 900 mg이다.For a target AUC = 6, the maximum dose is 6 x 150 = 900 mg.
목표 AUC = 5의 경우, 최대 용량은 5 × 150 = 750 mg이다.For a target AUC = 5, the maximum dose is 5 x 150 = 750 mg.
목표 AUC = 4의 경우, 최대 용량은 4 × 150 = 600 mg이다.For a target AUC = 4, the maximum dose is 4 x 150 = 600 mg.
페메트렉시드Pemetrexed
코호트 A에서의 페메트렉시드 투여에 대한 지침이 표 13에 제시되어 있다.Guidelines for administration of pemetrexed in Cohort A are presented in Table 13.
페메트렉시드 투여 시간 및 지침Pemetrexed dosing times and instructions
IV = 정맥내IV = intravenous
투여된 예비 투약 용량은 처방 정보를 따른다. 페메트렉시드 요법에 적격인 모든 환자는 페메트렉시드 투여 전 적어도 5일 동안, 투여 당일, 및 투여 후 적어도 2일 동안 소실 반감기가 긴 비스테로이드성 항염증제 복용을 피해야 한다.The pre-dosage dose administered is in accordance with the prescribing information. All patients eligible for pemetrexed therapy should avoid taking nonsteroidal anti-inflammatory drugs with a long elimination half-life for at least 5 days prior to, the day of, and at least 2 days post-administration of pemetrexed.
파클리탁셀paclitaxel
코호트 B에서의 파클리탁셀 투여에 대한 지침이 표 14에 제시되어 있다.Guidelines for administration of paclitaxel in Cohort B are presented in Table 14.
파클리탁셀 투여 시간 및 지침Paclitaxel Administration Times and Instructions
IV = 정맥내IV = intravenous
아시아 인종/민족의 환자는 3시간에 걸친 175 mg/m2 IV의 파클리탁셀 시작 용량이 더 낮다. 파클리탁셀의 시작 용량이 더 낮은 것은 폐암 임상 시험의 내부 안전성 검토에서 관찰된 바와 같이 비아시아 국가의 환자에 비해 아시아 국가의 환자에게서 전체 혈액학적 독성 발생률이 더 높은 것을 기반으로 한다. 상기 연구에서 사용된 바와 같이, 아시아 인종/민족은 동아시아, 동남아시아, 또는 남아시아에 거주하거나 조상 기원을 가진 다양한 인구 집단을 포함하는 범민족/인종 군을 나타낸다. 특정 환자에 대한 상기 용어의 적용 여부는 치료하는 시험자의 재량에 따르며, 환자의 임상적 특성 및 출신 국가를 기반으로 해야 한다.Patients of Asian ethnicity/ethnicity have a lower starting dose of paclitaxel at 175 mg/m2 IV over 3 hours. The lower starting dose of paclitaxel is based on the higher incidence of overall hematological toxicity in patients from Asian countries compared to patients from non-Asian countries, as observed in an internal safety review of lung cancer clinical trials. As used in this study, Asian race/ethnic refers to a pan-ethnic/ethnic group that includes diverse population groups of ancestral origin or residing in East Asia, Southeast Asia, or South Asia. The application of the above term to a particular patient is at the discretion of the treating investigator and should be based on the patient's clinical characteristics and country of origin.
에토포시드etoposide
코호트 C에서의 에토포시드 투여에 대한 지침이 표 15에 제시되어 있다.Guidelines for administration of etoposide in Cohort C are presented in Table 15.
에토포시드 투여 시간 및 지침Etoposide Administration Times and Instructions
IV = 정맥내IV = intravenous
실시예 2. 티라골루맙과 병용한 아테졸리주맙 및 화학요법에 관한 제Ib/II상, 공개 라벨, 무작위 연구 Example 2. A Phase Ib/II, Open Label, Randomized Study of Atezolizumab and Chemotherapy in Combination with Tiragolumab
본 연구는 전이성 췌장관 선암종(PDAC)에 대해 선행 전신 요법을 받은 적이 없는 환자를 대상으로 티라골루맙과 병용한 아테졸리주맙 및 화학요법(나노입자 알부민 결합 파클리탁셀(냅-파클리탁셀) 및 젬시타빈)의 유효성, 안전성, 및 약동학을 평가한다. 본 연구는 전이성 PDAC 환자에게서 면역요법 기반 치료 조합의 유효성, 안전성, 및 약동학을 평가한다.This study included atezolizumab and chemotherapy (nanoparticle albumin-bound paclitaxel (nap-paclitaxel) and gemcitabine) in combination with tiragolumab in patients who had never received prior systemic therapy for metastatic pancreatic ductal adenocarcinoma (PDAC). to evaluate the efficacy, safety, and pharmacokinetics of This study evaluates the efficacy, safety, and pharmacokinetics of an immunotherapy-based treatment combination in patients with metastatic PDAC.
A. 연구 설계A. Study Design
코호트 1의 환자는 대조군(화학요법) 또는 티라골루맙과 병용한 아테졸리주맙 및 화학요법으로 구성된 실험군에 무작위로 할당된다. 실험군 내 등록은 예비 단계에 이어 확장 단계의 두 단계로 진행된다. 약 20명의 환자가 예비 단계에서 등록된다. 무작위 배정은 최소 6명의 환자에 대한 안전성 평가를 위해 중단한다. 안전성 평가는 적어도 1회 용량의 치료(즉, 주어진 조합에 대해 각 제제의 1회 용량)를 받고 적어도 1회의 전체 치료 주기 동안 안전성 추적 평가를 완료한 최소 6명의 환자로부터 얻은 안전성 데이터를 기반으로 한다. 상기 조합이 충분히 안전한 것으로 결정되면, 해당 군의 등록을 재개한다. 예비 단계 동안 실험군에서 임상 활동이 관찰되면, 확장 단계 동안 약 25명의 추가 환자가 해당 군에 등록될 수 있다. 잠재적인 예측 바이오마커를 포함하여 인구 통계학적 및 기준선 특성과 관련하여 치료군들 간의 균형을 보장하기 위해 추가 환자를 등록함으로써 추가적인 하위군 분석이 가능할 수 있다.Patients in Cohort 1 are randomly assigned to either a control group (chemotherapy) or an experimental group consisting of atezolizumab in combination with tiragolumab and chemotherapy. Enrollment in the experimental group proceeds in two stages: the preliminary stage and the expansion stage. About 20 patients are enrolled in the preliminary phase. Randomization will be discontinued for safety evaluation in at least 6 patients. The safety assessment is based on safety data obtained from at least 6 patients who received at least one dose of treatment (i.e., one dose of each agent for a given combination) and completed a safety follow-up evaluation for at least one full treatment cycle. . If the combination is determined to be sufficiently safe, registration of the group is resumed. If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients can be enrolled in that group during the expansion phase. Additional subgroup analyzes may be possible by enrolling additional patients to ensure a balance between treatment groups with respect to demographic and baseline characteristics, including potential predictive biomarkers.
환자는 치료군에 무작위로 할당되고, 무작위 배정 비율은 등록을 위해 개방된 실험군의 수에 따라 달라진다(예컨대, 군이 추가되거나 예비 단계의 결과 분석이 보류되는 동안 군의 등록이 중단되는 경우). 단, 대조군에 할당될 가능성이 35% 이하여야 한다.Patients are randomly assigned to treatment groups, and the rate of randomization depends on the number of groups open for enrollment (e.g., if a group is discontinued while a group is added or a preliminary analysis of results is pending). However, the probability of being assigned to the control group must be less than or equal to 35%.
본 연구의 종료는 전화 또는 병원에서 실시한 생존 추적 방문을 포함하여 마지막 환자가 마지막 방문(LPLV)을 완료한 날짜로 정의한다. 제1 환자의 스크리닝부터 연구 종료까지의 총 연구 기간은 약 3~5년이다.End of the study is defined as the date the last patient completed the last visit (LPLV), including survival follow-up visits conducted by phone or hospital. The total study duration from screening of the first patient to study termination is approximately 3-5 years.
활동 일정은 표 16에 요약되어 있다.The activity schedule is summarized in Table 16.
활동 일정activity schedule
ADA = 항 약물 항체; 아테조 + 화학 + 티라 = 아테졸리주맙 + 화학요법(냅-파클리탁셀 및 젬시타빈) + 티라골루맙; CIT = 암 면역요법; CT = 컴퓨터 단층 촬영; Discon. = 중단; ECOG = 이스턴 코퍼레이티브 종양학 그룹; eCRF = 전자 사례 보고서 양식; HBV = B형 간염 바이러스; 냅-파클리탁셀 = 나노입자 알부민 결합된 파클리탁셀; PK = 약동학; RBR = 연구 바이오샘플 저장소; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1; T3 = 트리요오드티로닌; T4 = 티록신; Treat. = 치료; TSH = 갑상선 자극 호르몬.ADA = anti-drug antibody; atezo + chem + tyra = atezolizumab + chemotherapy (nap-paclitaxel and gemcitabine) + tyragolumab; CIT = cancer immunotherapy; CT = computed tomography; Discon. = abort; ECOG = Eastern Corporate Oncology Group; eCRF = electronic case report form; HBV = hepatitis B virus; nap-paclitaxel = nanoparticle albumin bound paclitaxel; PK = pharmacokinetics; RBR = study biosample repository; RECIST v1.1 = Response Evaluation Criteria for Solid Tumors, version 1.1; T3 = triiodothyronine; T4 = thyroxine; Treat. = treatment; TSH = thyroid stimulating hormone.
달리 명시되지 않는 한, 치료일에 모든 평가는 투약 전에 실시해야 한다.Unless otherwise specified, on the day of treatment, all assessments must be performed prior to dosing.
a 공휴일, 휴가, 또는 기타 상황으로 인해 방문이 불가한 경우, 의료 모니터의 동의가 있는 경우 지정된 기간 외 방문이 가능하다. a If visitation is not possible due to public holidays, vacations, or other circumstances, visits outside the designated period are possible with the consent of the medical monitor.
b 무작위 배정 후 7일 이내에 치료를 개시할 것을 권장한다. b It is recommended to start treatment within 7 days of randomization.
c 환자는 연구 치료제의 마지막 용량 투여 후 30일 이내에 치료 중단 방문을 위해 병원으로 다시 방문해야 한다. 질병 진행이 확인된 경우, 해당 방문은 치료 중단 방문으로 사용할 수 있다. 그런 다음, 환자는 후속 평가를 받는다. c The patient must return to the hospital for a treatment discontinuation visit within 30 days of administration of the last dose of study treatment. If disease progression is confirmed, the visit may be used as a treatment discontinuation visit. Then, the patient undergoes a follow-up evaluation.
d 활력 징후에는 호흡수, 맥박수, 환자가 앉은 자세에서 수축기 및 이완기 혈압, 맥박 산소 측정, 및 체온이 포함된다. 이상반응 eCRF에 새롭거나 악화된 임상적으로 유의한 이상을 기록한다. 아테졸리주맙의 제1 주입의 경우, 활력 징후는 해당 주입 전 60분 이내에 측정해야 하며, 임상적으로 지시된 경우 해당 주입 중 15(±5)분마다 및 주입 후 30(±10)분에 측정해야 한다. 후속 주입의 경우, 활력 징후는 해당 주입 전 60분 이내에 측정해야 하며, 임상적으로 지시되거나 이전 주입 중에 증상이 발생한 경우, 해당 주입 중 및 주입 후 30(±10)분에 측정해야 한다. 티라골루맙의 제1 주입의 경우, 활력 징후는 해당 주입 전 60분 이내에 측정해야 하며, 해당 주입 중 15(±5)분마다 및 주입 후 30(±10)분에 측정해야 한다. 티라골루맙의 후속 주입의 경우, 활력 징후는 해당 주입 전 60분 이내에 측정해야 하며, 임상적으로 지시되거나 이전 주입 중에 증상이 발생한 경우, 해당 주입 중 및 주입 후 15(±10)분에 측정해야 한다. d Vital signs include respiratory rate, pulse rate, systolic and diastolic blood pressure in the patient's sitting position, pulse oximetry, and body temperature. Adverse events Record new or worsening clinically significant abnormalities on the eCRF. For the first infusion of atezolizumab, vital signs should be measured within 60 minutes prior to that infusion and, if clinically indicated, every 15 (±5) minutes during that infusion and 30 (±10) minutes after that infusion. Should be. For subsequent infusions, vital signs should be measured within 60 minutes prior to the infusion and, if clinically indicated or if symptoms occurred during the previous infusion, during and 30 (±10) minutes after the infusion. For the first infusion of tiragolumab, vital signs should be measured within 60 minutes prior to the infusion, every 15 (±5) minutes during the infusion and at 30 (±10) minutes after the infusion. For subsequent infusions of tiragolumab, vital signs should be measured within 60 minutes prior to the infusion and, if clinically indicated or if symptoms occurred during the previous infusion, during and 15 (±10) minutes after the infusion. do.
e 전체 신체 검사는 머리, 눈, 귀, 코, 및 목, 및 심혈관, 피부, 근골격, 호흡, 위장, 비뇨생식, 및 신경계의 평가를 포함해야 한다. 이상반응 eCRF에 새롭거나 악화된 임상적으로 유의한 이상을 기록한다. e A full physical examination should include evaluation of the head, eyes, ears, nose, and throat, and cardiovascular, skin, musculoskeletal, respiratory, gastrointestinal, urogenital, and nervous system. Adverse events Record new or worsening clinically significant abnormalities on the eCRF.
f 지정된 시점 및 다른 시점에서 임상적으로 지시된 대로 제한된 증상 지향적 검사를 실시한다. 이상반응 eCRF에 새롭거나 악화된 임상적으로 유의한 이상을 기록한다. f Conduct limited symptom-directed testing as clinically indicated at designated time points and at other time points. Adverse events Record new or worsening clinically significant abnormalities on the eCRF.
g ECG 기록 전에 환자는 최소 10분 동안 바로 누운 자세로 쉬는 것을 권고한다. g It is recommended that the patient rest in the supine position for at least 10 minutes prior to recording the ECG.
h 혈액학은 WBC 수, RBC 수, 헤모글로빈, 헤마토크릿, 혈소판 수, 및 감별 계산(호중구, 호산구, 호염기구, 단핵구, 림프구, 기타 세포)을 포함한다. h Hematology includes WBC count, RBC count, hemoglobin, hematocrit, platelet count, and differential counts (neutrophils, eosinophils, basophils, monocytes, lymphocytes, other cells).
i 실험실 시험은 주기 1의 1일 이전 96시간 이내에 및 치료 기간 동안 지정된 후속 방문 이전 24시간 이내에 실시해야 한다. i Laboratory studies must be conducted within 96 hours prior to Day 1 of Cycle 1 and within 24 hours prior to the designated follow-up visit during the treatment period.
j 선별 검사실 평가가 주기 1의 1일 전 96시간 이내에 실시된 경우, 반복할 필요가 없다. j If the screening laboratory evaluation was performed within 96 hours prior to Day 1 of Cycle 1, no repeat is necessary.
k 화학 패널(혈청 또는 혈장)은 중탄산염 또는 총 이산화탄소(해당 지역의 치료 표준으로 고려되는 경우), 나트륨, 칼륨, 마그네슘, 염화물, 포도당, BUN 또는 요소, 크레아티닌, 총 단백질, 알부민, 인, 칼슘, 총 빌리루빈, ALP, ALT, 및 AST를 포함한다. k Chemistry panel (serum or plasma) contains bicarbonate or total carbon dioxide (if considered as the local standard of care), sodium, potassium, magnesium, chloride, glucose, BUN or urea, creatinine, total protein, albumin, phosphorus, calcium, total bilirubin, ALP, ALT, and AST.
l TSH, 유리 T3(또는 유리 T3이 실시되지 않는 부위의 경우 총 T3), 및 유리 T4는 선별 검사시 및 주기 1의 1일 및 이후 세번 째 주기마다(즉, 주기 4, 주기 7, 주기 10 등)에 평가한다. l TSH, free T3 (or total T3 for sites not subjected to free T3), and free T4 at screening and on day 1 of cycle 1 and every third cycle thereafter (i.e., cycle 4, cycle 7, cycle 10) etc) are evaluated.
m 선별 검사 시 양적 HBV DNA가 양성인 환자(적격 기준에 따라 < 500 IU/mL이어야 함)는 각 세번 째 주기(즉, 주기 3, 주기 6, 주기 9, 등)의 1일에, 치료 중단시(±7일), 및 치료 중단 후 3개월, 6개월, 9개월, 및 12개월에(각 시점에서 ±14일)에 추가 HBV DNA 검사를 받는다. 연구 치료 및 절차는 HBV DNA가 처리되는 동안 진행될 수 있지만, 결과는 입수 가능한 즉시 시험자가 검토해야 한다. HBV DNA가 < 500 IU/mL로 증가하는 경우, 연구 치료를 계속하기 전에 의료 모니터와 상의해야 하며, B형 간염에 대한 전문 지식을 갖춘 간장병 전문의 또는 위장병 전문의와 상의할 것을 권장한다. m Patients with positive quantitative HBV DNA at screening (must be < 500 IU/mL according to eligibility criteria) on Day 1 of each 3rd cycle (i.e., Cycle 3, Cycle 6, Cycle 9, etc.), upon discontinuation of treatment (±7 days), and additional HBV DNA testing at 3, 6, 9, and 12 months (±14 days at each time point) after discontinuation of treatment. Study treatments and procedures may proceed while HBV DNA is being processed, but results should be reviewed by investigators as soon as they are available. If HBV DNA increases to < 500 IU/mL, a medical monitor should be consulted before continuing study treatment, and it is recommended that a hepatologist or gastroenterologist with expertise in hepatitis B be consulted.
n 가임기의 모든 여성은 치료 중 지정된 방문 및 연구 치료제의 마지막 용량 투여 후 3개월 및 6개월에 소변 또는 혈청 임신 검사를 실시한다. 소변 임신 검사가 양성이면, 혈청 임신 검사로 확인해야 한다. n All women of childbearing age have a urine or serum pregnancy test at the designated on-treatment visit and 3 and 6 months after administration of the last dose of study treatment. If the urine pregnancy test is positive, it should be confirmed with a serum pregnancy test.
o pH, 비중, 포도당, 단백질, 케톤 및 혈액을 포함하고; 계량봉을 허용한다. o including pH, specific gravity, glucose, protein, ketones and blood; Allow the dipstick.
p 자가항체 분석은 항핵항체, 항이중나선 DNA, 순환 항호중구 세포질 항체, 및 핵주위 항호중구 세포질 항체를 포함한다. p autoantibody assays include antinuclear antibodies, anti-double-stranded DNA, circulating anti-neutrophil cytoplasmic antibodies, and perinuclear anti-neutrophil cytoplasmic antibodies.
q 자가면역 질환(예컨대, 홍반성 루푸스)을 암시하는 징후 또는 증상이 나타나는 환자의 경우, 자가항체 분석을 반복해야 한다. q For patients presenting with signs or symptoms suggestive of an autoimmune disease (eg, lupus erythematosus), the autoantibody assay should be repeated.
r RBR 샘플링에 대해 승인되지 않은 경우에는, 적용하지 않는다. 참여 장소에서 고지에 입각한 참여 서면 동의서를 제공한 환자에게만 실시한다. r If not approved for RBR sampling, it does not apply. Only patients who have provided informed written consent to participate at the location of participation.
s 시험자가 임상적으로 가능하다고 판단하면, 환자는 시험자에 의해 허용할 수 없는 독성 또는 임상 이익의 손실이 있다고 결정된 시점에 종양 생검 샘플 수집을 받는다. 생검은 허용할 수 없는 독성 또는 임상적 이익의 손실이 확인된 후 40일 이내에 또는 다음 항암 요법 이전 중 더 빠른 시점에 실시해야 한다. 또한, 치료 중 조직 샘플이 동일한 CIT 조합으로 치료된 최소 15명의 환자로부터 이미 수집되고 측정 가능하다고 판단되지 않는 한, 확장 단계 동안 등록한 환자는 치료 개시 후 4주(±7일) 후에 종양 생검 샘플 수집을 받는다(임상적으로 가능한 것으로 판단된 경우). s If the investigator determines that it is clinically feasible, the patient will receive a tumor biopsy sample collection at the time determined by the investigator that there is unacceptable toxicity or loss of clinical benefit. Biopsies should be performed within 40 days of confirmation of unacceptable toxicity or loss of clinical benefit or prior to the next anticancer therapy, whichever is earlier. In addition, patients enrolled during the expansion phase will receive tumor biopsy samples 4 weeks (±7 days) after initiation of treatment, unless on-treatment tissue samples have already been collected from at least 15 patients treated with the same CIT combination and are determined to be measurable. (if determined clinically feasible).
t 선택적 생검에 동의한 환자는 치료 개시 후 4주(±7일)에 종양 생검 샘플 수집을 받고, 만약 임상적으로 가능하다고 판단된 경우(확장 단계 중에 등록한 환자 중 이미 치료 중 생검을 받고 있는 환자에게는 적용되지 않음), 시험자의 재량에 따라 다른 시간에 추가적인 치료 중 생검을 받을 수 있다. t Patients who consent to elective biopsy will receive tumor biopsy sample collection 4 weeks (± 7 days) after initiation of treatment and, if deemed clinically feasible (patients enrolled during the expansion phase, who are already undergoing in-treatment biopsy) does not apply to patients), additional in-treatment biopsies may be taken at other times at the discretion of the investigator.
u 환자는 방사선 검사상 질병 진행 후에도 치료를 계속하는 환자의 경우를 제외하고 RECIST v1.1에 따른 방사선 검사상 질병 진행까지 용량 지연에 관계없이 기준선에서, 치료 개시 후 처음 48주 동안 매 6주(±1주)마다, 그 이후에는 매 12주(±2주)마다 종양 평가를 받고, 이러한 환자는 시험자에 의해 결정된 바와 같이 임상적 이익이 상실될 때까지 6주마다(±1주) 종양 평가를 받는다. 따라서, 질병 진행 이외의 이유로 치료를 중단한 환자의 경우, 프로토콜 상 지정되지 않은 새로운 항암 치료를 시작하더라도, 일정에 따라 종양 평가를 계속해야 한다. u Patients should be treated at baseline, regardless of dose delay, until radiological disease progression according to RECIST v1.1, every 6 weeks for the first 48 weeks after initiation of treatment, except in patients who continue treatment after radiological disease progression. ± 1 week), thereafter every 12 weeks (± 2 weeks), and these patients receive tumor assessments every 6 weeks (± 1 week) until loss of clinical benefit as determined by the investigator receive Therefore, for patients who discontinue treatment for reasons other than disease progression, tumor evaluation should continue according to schedule, even if new chemotherapy not specified in the protocol is started.
v 기준선에서 확인된 모든 측정 가능 및/또는 평가 가능한 병변은 상기에서 기재된 종양 평가 일정에 따라 각 후속 종양 평가에서 재평가해야 한다(각주 "t"를 참조). 선별 검사 시, 질병 부위를 평가하기 위해 사용된 것과 동일한 방사선학적 절차를 이후의 종양 평가에 사용해야 한다(예컨대, CT 스캔시 동일한 조영제 프로토콜). v All measurable and/or evaluable lesions identified at baseline should be re-evaluated at each subsequent tumor assessment according to the tumor assessment schedule described above (see footnote “t”). At the time of screening, the same radiological procedure used to evaluate the site of disease should be used for subsequent tumor evaluation (eg, the same contrast agent protocol for CT scans).
w 연구 치료제 개시 10일 전부터 치료 중단 방문시까지 프로토콜 필수 연구 치료제 외에 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)을 포함한다. w Includes any medications (eg, prescription drugs, over-the-counter medications, vaccines, herbal or homeopathic remedies, nutritional supplements) taken by the patient in addition to protocol essential study treatments from 10 days prior to study treatment initiation until the treatment discontinuation visit.
x 연구 치료제 개시 후, 모든 이상 반응은 최종 연구 치료제 용량 투여 후 30일 또는 새로운 전신 항암 요법의 시작 중 먼저 발생하는 시점까지 기록하며, 중증 이상 반응 및 특별히 관심이 되는 이상 반응은 최종 연구 치료제 용량 투여 후 135일 또는 새로운 전신 항암 요법의 시작 중 먼저 발생하는 시점까지 계속 기록한다. 상기 기간이 지나면, 원인에 관계없이 모든 사망이 보고되어야 한다. 시험자는 각 이상 반응이 기준선 등급 또는 그 보다 우수한 등급으로 해결되거나, 이상 반응이 시험자에 의해 안정한 것으로 평가되거나, 환자가 추적관찰에서 누락되거나, 환자가 동의를 철회할 때까지 각 이상 반응을 추적관찰해야 한다. 최종 결과가 보고될 수 있을 때까지 연구 치료 또는 시험 관련 절차와 관련된 것으로 간주되는 모든 중증 이상 반응들을 추적관찰하기 위해 모든 노력을 기울여야 한다. x After initiation of study treatment, all adverse events are recorded until 30 days after administration of the last study treatment dose or until initiation of new systemic anticancer therapy, whichever occurs first Continue to record until day 135 after or until initiation of new systemic chemotherapy, whichever occurs first. After this period, all deaths, regardless of cause, must be reported. The investigator will follow-up each adverse event until each adverse event has resolved to a baseline grade or better, the adverse event has been assessed as stable by the investigator, the patient is missed from follow-up, or the patient withdraws consent. Should be. Every effort should be made to follow-up all serious adverse events considered to be related to the study treatment or trial-related procedures until final results can be reported.
y 아테졸리주맙은 각 28일 주기의 제 1일 및 15일에 840 mg의 고정 용량으로 IV 주입으로 투여한다. 아테졸리주맙의 초기 용량은 60(±15) 분에 걸쳐 전달된다. 후속 주입은 이전 주입이 주입 관련 이상 반응 없이 내약성이었던 경우 30(±10)분에 걸쳐 전달되고, 환자가 이전 주입에서 주입 관련 이상 반응을 경험한 경우 60(±15)분에 걸쳐 전달된다. y Atezolizumab is administered as an IV infusion at a fixed dose of 840 mg on days 1 and 15 of each 28-day cycle. The initial dose of atezolizumab is delivered over 60 (±15) minutes. Subsequent infusions are delivered over 30 (±10) minutes if the previous infusion was well tolerated without infusion-related adverse events, and over 60 (±15) minutes if the patient experienced infusion-related adverse events from the previous infusion.
z 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 치료를 계속한다. z Continue treatment until there is unacceptable toxicity or loss of clinical benefit as determined by the investigator.
aa 티라골루맙은 각 28일 주기의 제 1일 및 15일에 420 mg의 고정 용량으로 IV 주입으로 투여한다. 티라골루맙의 초기 용량은 60(±10) 분에 걸쳐 전달된다. 후속 주입은 이전 주입이 주입 관련 이상 반응 없이 내약성이었던 경우 30(±10)분에 걸쳐 전달되고, 환자가 이전 주입에서 주입 관련 이상 반응을 경험한 경우 60(±10)분에 걸쳐 전달된다. 주기 1의 1일에, 티라골루맙은 아테졸리주맙 주입 완료 후 60분에 투여한다. 이후 주입들 간의 간격은 이전의 아테졸리주맙 주입이 IRR 없이 내약성이었던 경우는 30분이고, 또는 환자가 이전의 아테졸리주맙 주입으로 IRR을 경험한 경우, 60분이다. aa Tiragolumab is administered as an IV infusion at a fixed dose of 420 mg on days 1 and 15 of each 28-day cycle. The initial dose of tiragolumab is delivered over 60 (±10) minutes. Subsequent infusions are delivered over 30 (±10) minutes if the previous infusion was well tolerated without infusion-related adverse events, and over 60 (±10) minutes if the patient experienced infusion-related adverse events from the previous infusion. On Day 1 of Cycle 1, tiragolumab is administered 60 minutes after completion of the atezolizumab infusion. The interval between subsequent infusions is 30 minutes if the previous infusion of atezolizumab was well tolerated without an IRR, or 60 minutes if the patient experienced an IRR with a previous infusion of atezolizumab.
bb 1일, 8일 및 15일에 환자는 냅-파클리탁셀 125 mg/m2를 30(±5)분에 걸쳐 IV 주입으로 투여한 다음, 젬시타빈 1000 mg/m2를 30(±5)분에 걸쳐 IV 주입으로 투여받는다. 주기 1의 1일에, 티라골루맙 투여 후 관찰이 가능하도록 티라골루맙 주입 완료 후 60분에 냅-파클리탁셀을 투여한다. 이후 주입들 간의 간격은 이전의 티라골루맙 주입이 IRR 없이 내약성이었던 경우는 30분이고, 또는 환자가 이전의 티라골루맙 주입으로 IRR을 경험한 경우, 60분이다. bb On days 1, 8, and 15, patients were administered nap-paclitaxel 125 mg/m 2 as an IV infusion over 30 (±5) minutes followed by gemcitabine 1000 mg/m 2 for 30 (±5) minutes. administered by IV infusion. On Day 1 of Cycle 1, nap-paclitaxel is administered 60 minutes after completion of the tiragolumab infusion to allow observation after the tiragolumab administration. The interval between subsequent infusions is 30 minutes if the previous infusion of tiragolumab was well tolerated without an IRR, or 60 minutes if the patient experienced an IRR with a previous infusion of tiragolumab.
cc 치료 중단 후(환자가 동의를 철회하거나 연구가 종료되지 않는 한), 사망할 때까지 약 3개월마다 전화, 환자 진료 기록, 및/또는 병원 방문을 통해 생존 추적 및 새로운 항암 요법(표적요법 및 면역요법을 포함)에 대한 정보를 수집한다. 환자가 추적 조사에서 철회를 요청하는 경우, 상기 요청은 원본 문서 내에 문서화하고 시험자가 서명해야 한다. 환자가 연구에서 철회하는 경우, 연구 직원은 공개 정보 출처(예컨대, 지역 기록)를 사용하여 생존 상태에 대한 정보만 수득할 수 있다. cc After discontinuation of treatment (unless patient withdraws consent or study ends), survival follow-up and new chemotherapy (targeted and information on immunotherapy). If the patient requests withdrawal from follow-up, the request must be documented in the original document and signed by the investigator. If a patient withdraws from the study, study staff may use public information sources (eg, local records) to obtain information on survival status only.
평가 및 모니터링Assessment and monitoring
모든 환자는 연구 전반에 걸쳐 이상 반응에 대해 면밀히 모니터링되며, 이상 반응은 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0(NCI CTCAE v4.0)에 따라 등급이 매겨진다. 환자는 처음 48주 동안은 6주마다(주기 1의 1일부터) 종양 평가를 받고, 이후에는 6주 또는 12주마다 종양 평가를 받는다. 반응은 RECIST v1.1을 사용하여 시험자가 평가한다. 면역 기반 치료제(iRECIST)에 대한 수정된 RECIST v1.1에 따른 반응은 시험자가 평가한 개별 병변 데이터를 기반으로 프로그래밍 방식으로 결정한다. 임상 활동이 실험군에서 입증되면, 해당 군에 대한 종양 평가 스캔이 독립 검토 시설의 평가를 위해 제출될 수 있다.All patients are closely monitored for adverse events throughout the study, and adverse events are graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). Patients receive tumor assessments every 6 weeks (from Day 1 of Cycle 1) for the first 48 weeks, and then every 6 or 12 weeks thereafter. Response is assessed by the investigator using RECIST v1.1. Responses according to modified RECIST v1.1 to immune-based therapeutics (iRECIST) are determined programmatically based on investigator-assessed individual lesion data. Once clinical activity is demonstrated in an experimental arm, a tumor assessment scan for that arm may be submitted for evaluation by an independent review facility.
기준선 종양 조직 샘플은, 예를 들어 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 시험자가 생검을 실시할 수 없다고 판단한 경우, 등록 전 3개월 이내에 조직을 수득하고 해당 생검 이후로 환자가 임의의 항암 요법을 받은 적이 없는 경우, 보관된 종양 조직은 의료 모니터 승인을 받은 후 제출할 수 있다. 시험자가 임상적으로 가능하다고 판단한 경우, 종양 조직은 허용할 수 없는 독성, RECIST v1.1에 따른 질병 진행, 또는 시험자가 결정한 임상 이익의 손실로 인해 1단계를 중단한 환자에 대해 수집한다. 확장 단계에서 실험군에 등록한 환자의 경우, 치료 중 조직 샘플이 동일한 CIT 조합으로 치료된 최소 15명의 환자로부터 이미 수집되고 측정 가능하다고 판단되지 않는 한, 1 단계 치료의 개시 후 4주에 치료 중 종양 조직 샘플을 수집한다(임상적으로 가능한 것으로 판단된 경우). 상기 샘플은 바이오마커 연구에 활용한다(바이오마커 평가에 대한 근거를 참조).Baseline tumor tissue samples are collected from all patients, eg, via biopsies performed at the start of the study. If the investigator determines that a biopsy cannot be performed, if the tissue is obtained within 3 months prior to enrollment and the patient has not received any chemotherapy since the biopsy, the archived tumor tissue may be submitted after obtaining medical monitor approval. . If the investigator determines that it is clinically feasible, tumor tissue is collected from patients who discontinued Phase 1 due to unacceptable toxicity, disease progression according to RECIST v1.1, or loss of clinical benefit as determined by the investigator. For patients enrolled in the experimental arm in the expansion phase, tumor tissue during treatment 4 weeks after initiation of phase 1 therapy, unless tissue samples have already been collected from at least 15 patients treated with the same CIT combination and are determined to be measurable. Collect samples (if determined clinically feasible). The sample is utilized for biomarker studies (see Evidence for Biomarker Evaluation).
아테졸리주맙 및 기타 치료제의 약동학적(PK) 특성 및/또는 면역원성을 특성화하기 위해, 연구 치료제 투여 전 및 동안 다양한 시점에서 혈액 샘플을 채취한다(표 17). 실시간 안전성 데이터 및 입수 가능한 PK 데이터의 검토를 기반으로, 치료 요법을 수정할 수 있다.To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are taken at various time points prior to and during study therapy administration (Table 17). Based on review of real-time safety data and available PK data, treatment regimens can be modified.
아테졸리주맙 ADA(혈청)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)
바이오마커(혈장, 혈청, PBMC)Atezolizumab PK (serum)
Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
Biomarkers (plasma, serum, PBMC)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)
바이오마커(혈장, 혈청, PBMC)Atezolizumab PK (serum) Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
Biomarkers (plasma, serum, PBMC)
아테졸리주맙 ADA(혈청)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)Atezolizumab PK (serum)
Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
아테졸리주맙 ADA(혈청)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)
바이오마커(혈장, 혈청)Atezolizumab PK (serum)
Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
Biomarkers (plasma, serum)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)
바이오마커(혈장, 혈청)Atezolizumab PK (serum) Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
Biomarkers (plasma, serum)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)Atezolizumab PK (serum) Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
티라골루맙 PK(혈청)
티라골루맙 ADA(혈청)
바이오마커(혈장, 혈청)Atezolizumab PK (serum) Atezolizumab ADA (serum)
Tiragolumab PK (serum)
Tiragolumab ADA (serum)
Biomarkers (plasma, serum)
약동학, 면역원성 및 바이오마커 샘플의 일정Pharmacokinetic, immunogenicity and schedule of biomarker samples
ADA = 항 약물 항체; 아테조 + 화학 + 티라 = 아테졸리주맙 + 화학요법(냅-파클리탁셀 및 젬시타빈) + 티라골루맙; 냅-파클리탁셀 = 나노입자 알부민 결합 파클리탁셀; PBMC = 말초 혈액 단핵 세포; PK = 약동학.ADA = anti-drug antibody; atezo + chem + tyra = atezolizumab + chemotherapy (nap-paclitaxel and gemcitabine) + tyragolumab; nap-paclitaxel = nanoparticle albumin-bound paclitaxel; PBMC = peripheral blood mononuclear cells; PK = Pharmacokinetics.
비고: 새로운 안전성 또는 유효성 데이터를 기반으로, PK 및 ADA 샘플의 수가 감소하거나 샘플 수집이 모두 함께 중단될 수 있다. 또한, 수집한 샘플은 보증되지 않는 경우 분석하지 않을 수 있다. 새로운 바이오마커 데이터를 기반으로, 바이오마커 샘플의 수가 감소하거나 샘플 수집이 모두 함께 중단될 수 있다.NOTE: Based on new safety or efficacy data, the number of PK and ADA samples may be reduced or sample collection may be stopped altogether. In addition, collected samples may not be analyzed unless warranted. Based on the new biomarker data, the number of biomarker samples may be reduced or sample collection may be stopped altogether.
실험실, 바이오마커, 및 다른 생물학적 샘플laboratory, biomarkers, and other biological samples
탐색적 바이오마커 연구는 종양 면역생물학과 관련된 유전자 또는 유전자 특징, PD-L1, T 세포 활성화와 관련된 사이토카인, T 세포 수용체 레퍼토리, 암배아 항원, 또는 밀도, 국소화, 및 면역 세포 및 이의 하위집합의 활성화 상태에 대한 분석을 포함하지만, 이에 제한되지 않으며, DNA 또는 RNA 추출, 체세포 돌연변이의 분석, 및 NGS(WES 포함)의 사용을 수반할 수 있다.Exploratory biomarker studies include genes or genetic features associated with tumor immunobiology, PD-L1, cytokines associated with T cell activation, T cell receptor repertoire, carcinoembryonic antigens, or density, localization, and activation of immune cells and subsets thereof. analysis for status, but may involve DNA or RNA extraction, analysis of somatic mutations, and the use of NGS (including WES).
하기의 실험실 시험용 샘플들은 분석을 위해 연구 장소의 지역 실험실로 보내진다:The following laboratory test samples are sent to the local laboratory at the study site for analysis:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
환자가 스크리닝시 HBsAg 검사 음성이고 총 HBcAb 검사 양성인 경우, 환자의 HBV 감염 여부를 결정하기 위해 HBV DNA 검사도 실시해야 한다.If a patient is HBsAg test negative at screening and a total HBcAb test is positive, HBV DNA testing should also be performed to determine whether the patient has HBV infection.
HCV 혈청학: HCV 항체 및 (HCV 항체 검사가 양성인 경우) HCV RNA HCV serology: HCV antibody and (if HCV antibody test is positive) HCV RNA
환자가 스크리닝시 HCV 항체 검사 양성인 경우, 환자의 활성 HCV 감염 여부를 결정하기 위해 HCV RNA 검사도 실시해야 한다.If a patient is HCV antibody positive at screening, HCV RNA testing should also be performed to determine whether the patient has active HCV infection.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- EBV VCA IgM- EBV VCA IgM
- EBV VCA IgG 또는 EBNA IgG- EBV VCA IgG or EBNA IgG
- EBV PCR(임상적으로 지시된 경우에만)- EBV PCR (only if clinically indicated)
![]()
![]()
가임기 여성은 모두 단계 1의 스크리닝시 혈청 임신 검사를 받는다. 소변 또는 혈청 임신 검사는 지정된 후속 방문에서 실시한다. 소변 임신 검사가 양성이면 혈청 임신 검사로 확인해야 한다.All women of childbearing potential receive a serum pregnancy test at screening in Stage 1. Urine or serum pregnancy tests are performed at designated follow-up visits. If the urine pregnancy test is positive, it should be confirmed with a serum pregnancy test.
여성은 만약 비월경이고, 폐경후 상태(폐경 이외에 확인된 원인이 없는 ≥ 12개월 연속 무월경)에 도달하지 못하였고, 그리고 외과적 불임 수술(난소 및/또는 자궁의 제거)을 받지 않았다면 임신 가능성이 있는 것으로 간주한다.A woman has no chance of becoming pregnant if she is non-menstrual, has not reached postmenopausal status (≥ 12 consecutive months of amenorrhea with no identified cause other than menopause), and has not undergone surgical sterilization (removal of the ovaries and/or uterus). considered to be
![]()
![]()
계량봉 소변검사가 허용된다. 하지만, 선별 검사 시 계량봉 소변 검사에서 단백질이 2+ 이상인 환자는 베바시주맙 함유 군이 등록에 개방된 경우 단백질에 대한 24시간 소변 수집을 받아야 한다.Dipstick urinalysis is permitted. However, patients with a protein 2+ or higher in a dipstick urine test at screening should have a 24-hour urine collection for protein if the bevacizumab-containing arm is open to enrollment.
하기의 실험실 시험용 샘플들은 분석을 위해 중앙 실험실 또는 연구 장소의 지역 실험실로 보내진다:The following laboratory test samples are sent to a central laboratory or regional laboratory at the study site for analysis:
![]()
![]()
하기의 샘플들은 분석을 위해 하나 또는 여러 곳의 중앙 실험실 또는 임상시험 의뢰자에게 보내진다:The following samples are sent to one or more central laboratories or sponsors for analysis:
자가항체 분석을 위한 혈청 샘플: 항핵항체, 항이중나선 DNA, 순환 항호중구 세포질 항체, 및 핵주위 항호중구 세포질 항체 Serum samples for autoantibody analysis: antinuclear antibody, anti-double-stranded DNA, circulating anti-neutrophil cytoplasmic antibody, and perinuclear anti-neutrophil cytoplasmic antibody
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
1차 병변 또는 전이성 병변의 기준선 종양 조직 샘플은, 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 시험자가 생검을 실시할 수 없다고 판단한 경우, 등록 전 3개월 이내에 실시한 생검으로부터 조직을 수득하고 해당 생검 이후로 환자가 임의의 항암 요법을 받은 적이 없는 경우, 보관된 종양 조직은 의료 모니터 승인을 받은 후 제출할 수 있다.Baseline tumor tissue samples of primary lesions or metastatic lesions are collected from all patients, preferably via biopsies performed at the start of the study. If the investigator determines that a biopsy cannot be performed, if tissue is obtained from a biopsy performed within 3 months prior to enrollment and the patient has not received any chemotherapy since that biopsy, the stored tumor tissue will be removed after obtaining medical monitor approval. can be submitted
파라핀 블록(바람직한)의 대표적인 FFPE 종양 표본 또는 염색되지 않은 갓 절단된 연속 절편을 포함하는 최소 16개의 슬라이드를 관련 병리학 보고서와 함께 제출해야 한다. 10~15개의 슬라이드만 입수 가능한 경우, 의료 모니터의 승인을 받은 후에도 환자는 여전히 해당 연구에 적격일 수 있다.A minimum of 16 slides containing representative FFPE tumor specimens in paraffin blocks (preferred) or unstained, freshly excised serial sections should be submitted along with the relevant pathology report. If only 10 to 15 slides are available, the patient may still be eligible for the study after obtaining approval from the medical monitor.
종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 양호해야 한다. 샘플은 바늘 게이지 또는 검색 방법에 관계없이 세포 환경(context) 및 조직 구조를 보존하는 최소 50개의 생존 가능한 종양 세포를 함유해야 한다. 절제, 코어 바늘 생검(최소 3개의 코어, 18 게이지 이상의 바늘[16 게이지 바늘 선호], 단일 파라핀 블록에 포매) 또는 절제, 절개, 펀치 또는 겸자 생검을 통해 수집한 샘플이 허용 가능하다. 미세 바늘 흡인(조직 구조를 보존하지 않고 세포 현탁액 및/또는 도말을 생성하지 않는 샘플로 정의됨), 칫솔질, 흉막 삼출액의 세포 펠렛, 및 세척 샘플은 허용하지 않는다. 석회화가 제거된 뼈 전이로부터의 종양 조직은 허용하지 않는다.Tumor tissue should be of good quality based on total and viable tumor content. Samples should contain at least 50 viable tumor cells that preserve cellular context and tissue structure, regardless of needle gauge or retrieval method. Samples collected via excision, core needle biopsy (minimum 3 cores, 18 gauge or larger needles [16 gauge needles preferred], embedded in a single paraffin block) or via excision, incision, punch or forceps biopsy are acceptable. Fine needle aspiration (defined as a sample that does not preserve tissue structure and does not produce a cell suspension and/or smear), brushing, cell pellets of pleural effusion, and wash samples are not permitted. Tumor tissue from calcified bone metastases is not acceptable.
남아 있는 보관 종양 조직 블록은 요청 시 또는 연구 데이터베이스의 최종 폐쇄 후 18개월 중 먼저 발생하는 시점에 해당 장소로 반환된다.Remaining archived tumor tissue blocks will be returned to the site upon request or 18 months after final closure of the study database, whichever occurs first.
![]()
![]()
동일한 CIT 조합으로 치료된 최소 15명의 환자로부터 치료 중 조직 샘플이 이미 수집되고 평가 가능한 것으로 결정된 경우, 샘플은 수집되지 않는다.If an on-treatment tissue sample has already been collected from at least 15 patients treated with the same CIT combination and is determined to be evaluable, no sample is collected.
절제, 코어-바늘 생검(최소 3개의 코어 선호), 또는 절제, 절개, 펀치 또는 겸자 생검을 통해 수집된 샘플이 바람직하다.Samples collected via excision, core-needle biopsy (preferably at least 3 cores), or via excision, incision, punch or forceps biopsy are preferred.
![]()
![]()
생검은 허용할 수 없는 독성, 질병 진행, 또는 임상적 이익의 손실이 확인된 후 40일 이내에 또는 다음 항암 요법 이전 중 더 빠른 시점에 실시해야 한다. 절제, 코어-바늘 생검(최소 3개의 코어 선호), 또는 절제, 절개, 펀치 또는 겸자 생검을 통해 수집된 샘플이 바람직하다.Biopsies should be performed within 40 days of confirmation of unacceptable toxicity, disease progression, or loss of clinical benefit, or prior to the next anticancer therapy, whichever is earlier. Samples collected via excision, core-needle biopsy (preferably at least 3 cores), or via excision, incision, punch or forceps biopsy are preferred.
아테졸리주맙 용량 및 일정Atezolizumab Dosage and Schedule
아테졸리주맙은 2주마다(Q2W) 840 mg의 공정 용량으로(각 28일 주기의 제 1일 및 15일에 840 mg) 투여한다.Atezolizumab is administered at a fair dose of 840 mg every two weeks (Q2W) (840 mg on Days 1 and 15 of each 28-day cycle).
티라골루맙 용량 및 일정Tiragolumab Dosage and Schedule
티라골루맙은 Q2W 420 mg의 공정 용량으로(각 28일 주기의 제 1일 및 15일에 420 mg) 투여한다. 420 mg Q2W 용량 후 평균 농도는 3주마다(Q3W) 600 mg의 농도와 동일할 것으로 예상된다. 600 mg IV Q3W의 고정 티라골루맙 용량은 환자가 단일 제제 티라골루맙 또는 티라골루맙 및 아테졸리주맙을 병용하여 투여 받은 연구 GO30103으로부터 입수 가능한 약동학(PK), 유효성 및 안전성 데이터를 기반으로 선택하였다. MTD에 도달하지 않았으며, 티라골루맙 단일요법 또는 아테졸리주맙 1200 mg Q3W와 병용한 2-1200 mg Q3W 용량의 티라골루맙에서 DLT가 관찰되지 않았다. 또한, 티라골루맙(2-600 mg Q3W 용량)을 아테졸리주맙과 병용하여 투여받은 평가 가능한 환자 145명 중 3명에서 티라골루맙에 대한 항약물 항체(ADA)의 발생이 관찰되었다. CD4+, CD8+ 및 NK 세포에서 말초 TIGIT 수용체의 완전한 점유는 티라골루맙의 30 mg Q3W 용량에서 시작하는 것으로 관찰되었으며 더 높은 용량 모두에서 유지되었다. 항종양 활성(방사선 촬영 시 부분 반응)은 아테졸리주맙 1200 mg Q3W와 병용으로 투여할 때 30~600 mg Q3W의 티라골루맙 용량에서 관찰되었다.Tiragolumab is administered at a fair dose of 420 mg Q2W (420 mg on days 1 and 15 of each 28-day cycle). The mean concentration after the 420 mg Q2W dose is expected to be equal to the concentration of 600 mg every 3 weeks (Q3W). A fixed tiragolumab dose of 600 mg IV Q3W was selected based on pharmacokinetic (PK), efficacy, and safety data available from study GO30103 in which patients were administered either single agent tiragolumab or in combination tiragolumab and atezolizumab. . No MTD was reached and no DLTs were observed with tiragolumab monotherapy or tiragolumab at the 2-1200 mg Q3W dose in combination with atezolizumab 1200 mg Q3W. In addition, the development of anti-drug antibodies (ADA) to tiragolumab was observed in 3 of 145 evaluable patients who received tiragolumab (2-600 mg Q3W dose) in combination with atezolizumab. Complete occupancy of peripheral TIGIT receptors on CD4 + , CD8 + and NK cells was observed starting at the 30 mg Q3W dose of tiragolumab and maintained at all higher doses. Antitumor activity (partial response on radiography) was observed at doses of 30 to 600 mg Q3W of tyragolumab when co-administered with atezolizumab 1200 mg Q3W.
투여량 및 투여Dosage and administration
환자는 방사선 및 생화학적 데이터, 국소 생검 결과(입수 가능한 경우), 및 임상 상태(예컨대, 질병에 이차적인 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 대로 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 약술된 바와 같이 치료를 받는다. Patients should be assessed for unacceptable toxicity or clinical benefit as determined by the investigator after an integrated assessment of radiological and biochemical data, local biopsy results (if available), and clinical condition (e.g., worsening of symptoms such as pain secondary to disease). Treat as outlined until loss of
참가자는 표 18에 요약된 지침에 따라 각 28일 주기의 제 1일 및 15일에 아테졸리주맙 840 mg IV 주입을 받는다. Participants will receive an atezolizumab 840 mg IV infusion on days 1 and 15 of each 28-day cycle according to the guidelines outlined in Table 18.
참가자는 표 19에 요약된 지침에 따라 각 28일 주기의 제 1일 및 15일에 티라골루맙 420 mg IV 주입을 받는다. 주기 1의 1일에, 티라골루맙은 아테졸리주맙 주입 완료 후 60분에 투여한다. 이후 주입들 간의 간격은 이전의 아테졸리주맙 주입이 예비 투약없이 제공되고 주입 관련 반응(IRR) 없이 내약성이었던 경우는 30분이고, 또는 환자가 이전의 아테졸리주맙 주입으로 IRR을 경험한 경우, 60분이다. Participants will receive a tyragolumab 420 mg IV infusion on days 1 and 15 of each 28-day cycle according to the guidelines outlined in Table 19. On Day 1 of Cycle 1, tiragolumab is administered 60 minutes after completion of the atezolizumab infusion. The interval between subsequent infusions is 30 minutes if the previous atezolizumab infusion was given without a premedication and was well tolerated without an infusion-related reaction (IRR), or 60 minutes if the patient experienced an IRR with a previous atezolizumab infusion. to be.
참가자는 각 28일 주기의 제 1일, 8일 및 15일에 냅-파클리탁셀 125 mg/m2 IV 주입을 받고, 30(5)분에 걸쳐 IV 주입으로 투여받은 다음, 젬시타빈 1000 mg/m2를 30(10)분에 걸쳐 IV 주입으로 투여받는다. 주기 1의 1일에, 냅-파클리탁셀은 티라골루맙 주입 완료 후 60분에 투여한다. 이후 주입들 간의 간격은 이전의 티라골루맙 주입이 IRR 없이 내약성이었던 경우는 30분이고, 또는 환자가 이전의 티라골루맙 주입으로 IRR을 경험한 경우, 60분이다.Participants received a nap-paclitaxel 125 mg/m 2 IV infusion on days 1, 8 and 15 of each 28-day cycle, followed by an IV infusion over 30 (5) minutes, followed by gemcitabine 1000 mg/m 2 is administered as an IV infusion over 30 (10) minutes. On Day 1 of Cycle 1, nap-paclitaxel is administered 60 minutes after completion of the tyragolumab infusion. The interval between subsequent infusions is 30 minutes if the previous infusion of tiragolumab was well tolerated without an IRR, or 60 minutes if the patient experienced an IRR with a previous infusion of tiragolumab.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
제1 및 이후의 아테졸리주맙 주입 투여First and subsequent atezolizumab infusion administration
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
제1 및 이후의 티라골루맙 주입의 투여Administration of First and Subsequent Tiragolumab Infusions
용량 변경capacity change
본 연구에서 아테졸리주맙 또는 티라골루맙에 대한 용량 변경은 없다. 약물 관련 독성의 관리를 위해, 냅-파클리탁셀의 용량은 25 mg/m2(1회 용량 수준) 만큼 최대 2배까지 감소할 수 있으며, 젬시타빈의 용량은 표 20에 개략된 바와 같이 200 mg/m2(1회 용량 수준) 만큼 최대 2배까지 감소할 수 있다.There were no dose changes for atezolizumab or tiragolumab in this study. For the management of drug-related toxicity, the dose of nap-paclitaxel can be reduced by up to 2-fold by 25 mg/m 2 (single dose level), and the dose of gemcitabine is 200 mg/m 2 as outlined in Table 20. It can be reduced up to a factor of 2 by m 2 (one dose level).
2회 용량 감소 후 냅-파클리탁셀 및/또는 젬시타빈에 대해 추가 용량 감소가 지시된 경우, 해당 약물(또는 해당하는 경우 두 약물)을 중단하지만, 환자는 시험자의 재량에 따라 다른 연구 치료를 계속할 수 있다. 용량 감소 후, 시험자의 재량에 따라 후속 투여 동안 용량을 증량할 수 있다.If a further dose reduction is indicated for nap-paclitaxel and/or gemcitabine after 2 dose reductions, the drug (or both drugs, if applicable) will be discontinued, but the patient may continue on other study treatment at the investigator's discretion have. After the dose reduction, the dose may be increased during subsequent administration at the discretion of the investigator.
냅-파클리탁셀 및 젬시타빈에 대한 권장 용량 감소Reducing the recommended dose for nap-paclitaxel and gemcitabine
병용 요법combination therapy
병용 요법은 연구 치료제 개사 10일 전부터 치료 중단 방문시까지 프로토콜 필수 연구 치료제 외에 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)을 포함한다.Combination therapy includes any drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, nutritional supplements) taken by the patient in addition to protocol essential study remedies from 10 days prior to initiation of study treatment until the discontinuation visit.
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
매주 화학요법(즉, 냅-파클리탁셀)을 받는 환자에게서 지속형(PEG화된) G-CSF 형태의 사용을 뒷받침하는 증거는 제한적이다. 따라서, 시험자는 기존의 G-CSF 제형을 우선으로 하는 것을 고려해야 한다.There is limited evidence supporting the use of a long-acting (PEGylated) form of G-CSF in patients receiving weekly chemotherapy (ie, nap-paclitaxel). Therefore, the investigator should consider giving preference to the existing G-CSF formulation.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
완화 방사선 요법은 종양 표적 병변의 평가를 방해하지 않는 한 허용한다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 냅-파클리탁셀l 및 젬시타빈을 이용한 치료는 완화 방사선 요법 동안 보류되어야 한다. 아테졸리주맙 및 티라골루맙을 이용한 치료는 완화 방사선 요법 동안 계속될 수 있다.Palliative radiation therapy is acceptable as long as it does not interfere with the evaluation of tumor target lesions (eg, the lesion to be investigated should not be the only site of measurable disease). Treatment with nap-paclitaxel and gemcitabine should be withheld during palliative radiation therapy. Treatment with atezolizumab and tiragolumab may be continued during palliative radiation therapy.
![]()
![]()
두개외 종양 부담이 안정적이거나 연구 치료제에 반응하고 이후에 3개 이하의 뇌 전이가 있는 것으로 밝혀진 환자는 하기의 기준이 모두 충족되는 경우 뇌에 대한 방사선 요법(정위적 방사선 수술 또는 전뇌 방사선 요법)을 받을 수 있다:Patients with stable extracranial tumor burden or responsive to study treatment and subsequently found to have 3 or fewer brain metastases should receive radiation therapy to the brain (stereotactic radiosurgery or whole brain radiation therapy) if all of the following criteria are met: You can get:
- 상기 환자는 CNS 지향적 요법의 완료 후 진행이나 출혈의 증거가 없다.- The patient has no evidence of progression or bleeding after completion of CNS directed therapy.
- 상기 환자는 CNS 질병에 대한 요법으로서 지속적인 코르티코스테로이드를 필요로 하지 않는다.- The patient does not require continuous corticosteroids as therapy for CNS disease.
방사선 요법의 완료 후 7일을 초과하여 코르티코스테로이드 요법이 필요한 환자는 연구 치료제를 중단해야 한다.Patients requiring corticosteroid therapy for more than 7 days after completion of radiation therapy should discontinue study treatment.
- 필요한 경우, 항경련제를 안정적인 용량으로 투여한다.- If necessary, administer anticonvulsants at a stable dose.
항히스타민제, 해열제, 및/또는 진통제의 예비투약은 시험자의 재량에 따라 두 번째 및 이후의 아테졸리주맙 및 티라골루맙 주입에 대해서만 투여할 수 있다. Premedication of antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab and tiragolumab at the discretion of the investigator.
일반적으로, 시험자는 지역의 표준 관행에 따라 임상적으로 지시되는 바와 같은 보조 요법으로 환자의 치료를 관리해야 한다. 주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 보조 요법(예컨대, 보조 산소 및 β2 아드레날린 작용제)으로 관리해야 한다.In general, the investigator should administer the patient's treatment with adjuvant therapy as clinically indicated in accordance with local standard practice. Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related reactions presenting with dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea should be managed with adjuvant therapy as clinically indicated (e.g., adjuvant oxygen and β 2 adrenergic agonists). .
선정 기준Selection Criteria
환자는 하기의 기준을 충족한다:The patient meets the following criteria:
![]()
![]()
![]()
![]()
![]()
![]()
전이성 PDAC의 최종 진단은 임상 및 방사선 데이터의 맥락 내에서 조직병리학적 데이터를 평가함으로써 이루어진다.The definitive diagnosis of metastatic PDAC is made by evaluating histopathological data within the context of clinical and radiological data.
내분비 또는 췌장의 선방 세포암(acinar pancreatic carcinoma)을 가진 환자는 연구에 적격이 아니다.Patients with endocrine or acinar pancreatic carcinoma of the pancreas are not eligible for the study.
![]()
![]()
![]()
![]()
![]()
![]()
기준선 종양 조직 샘플은 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 시험자가 생검을 실시할 수 없다고 판단한 경우, 등록 전 3개월 이내에 실시한 생검으로부터 조직을 수득하고 해당 생검 이후로 환자가 임의의 항암 요법을 받은 적이 없는 경우, 보관된 종양 조직은 의료 모니터 승인을 받은 후 제출할 수 있다.Baseline tumor tissue samples are preferably collected from all patients via biopsies performed at the start of the study. If the investigator determines that a biopsy cannot be performed, if tissue is obtained from a biopsy performed within 3 months prior to enrollment and the patient has not received any chemotherapy since that biopsy, the stored tumor tissue will be removed after obtaining medical monitor approval. can be submitted
파라핀 블록(바람직한)의 포르말린 고정, 파라핀 포매 종양 표본 또는 염색되지 않은, 갓 절단된 연속 절편을 함유하는 최소 16개의 슬라이드를 관련 병리학 보고서와 함께 연구 등록 전에 제출해야 한다. 10~15개의 슬라이드만 입수 가능한 경우, 의료 모니터의 승인을 받은 후에도 환자는 여전히 해당 연구에 적격일 수 있다.A minimum of 16 slides containing either formalin-fixed, paraffin-embedded tumor specimens in paraffin blocks (preferred) or unstained, freshly cut serial sections, along with the relevant pathology report, should be submitted prior to study enrollment. If only 10 to 15 slides are available, the patient may still be eligible for the study after obtaining approval from the medical monitor.
![]()
![]()
![]()
![]()
![]()
![]()
이전에 방사선 조사된 병변은 방사선 조사 이후 해당 부위에서 진행성 질환이 명백하게 기록된 경우에만 측정 가능한 질환으로 간주할 수 있다.Previously irradiated lesions can be considered measurable disease only if progressive disease is clearly documented at the site after irradiation.
![]()
![]()
- ANC ≥ 1.5 x 109/L(1500/μL), 스크리닝 실험실 검사 전 14일 이내에 과립구 집락 자극 인자의 지원 없음- ANC ≥ 1.5 x 10 9 /L (1500/μL), no support of granulocyte colony stimulating factor within 14 days prior to screening laboratory test
- WBC 수 ≥ 2.5 x 109/L(2500/μL)- Number of WBCs ≥ 2.5 x 10 9 /L (2500/μL)
- 림프구 수 ≥ 0.5 x 109/L(500/μL)- Lymphocyte count ≥ 0.5 x 10 9 /L (500/μL)
- 혈소판 수 ≥ 100 x 109/L(100,000/μL), 스크리닝 실험실 검사 전 7일 이내 수혈 없음- Platelet count ≥ 100 x 10 9 /L (100,000/μL), no transfusion within 7 days before screening laboratory test
- 헤모글로빈 ≥ 90 g/L(9.0 g/dL)- Hemoglobin ≥ 90 g/L (9.0 g/dL)
환자는 의료 모니터와 논의한 후 상기 기준을 충족하기 위해 수혈될 수 있다.The patient may be transfused to meet the above criteria after discussion with the medical monitor.
AST, ALT 및 ALP ≤ 2.5 x 정상 상한치(ULN), 하기의 경우는 제외함: AST, ALT and ALP ≤ 2.5 x upper limit of normal (ULN), except for:
간 전이가 기록된 환자: AST 및 ALT ≤ 5 ULNPatients with documented liver metastases: AST and ALT ≤ 5 ULN
문서로 기록된 간 또는 골 전이를 가진 환자: ALP ≤ 5 x ULNPatients with documented liver or bone metastases: ALP ≤ 5 x ULN
- 혈청 빌리루빈 ≤ 1.5 x ULN, 하기의 경우는 제외함:- Serum bilirubin ≤ 1.5 x ULN, except for:
공지된 길버트병 환자: 혈청 빌리루빈 수준 ≤ 3 x ULNKnown Gilbert's Disease Patients: Serum Bilirubin Levels ≤ 3 x ULN
- 크레아티닌 청소율 ≥ 50 mL/분(콕크로프트-가울트 공식을 사용하여 계산)- Creatinine clearance ≥ 50 mL/min (calculated using the Cockcroft-Gault formula)
- 혈청 알부민 ≥ 25 g/L(2.5 g/dL)- Serum albumin ≥ 25 g/L (2.5 g/dL)
- 항응고제를 투여받지 않는 환자의 경우: INR 또는 aPTT ≤ 1.5 x ULN- For patients not receiving anticoagulants: INR or aPTT ≤ 1.5 x ULN
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
안전성safety
엄격한 선정 및 배제 기준을 사용하고 연구 기간 동안 환자를 면밀히 모니터링하는 것을 포함하고, 본 연구에 참여하는 환자의 안전을 보장하기 위한 조치를 취한다. 연구 치료제의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 실시한다. 이상 반응은 기재된 대로 보고한다.Measures are taken to ensure the safety of patients participating in this study, including using strict selection and exclusion criteria and closely monitoring patients during the study period. Administration of study treatment is conducted in a monitoring environment with immediate access to trained staff and appropriate equipment and medications to manage potentially severe reactions. Adverse events are reported as described.
이상 반응의 축어적 용어는 규제 활동을 위한 의학 사전(Medical Dictionary for Regulatory Activities)의 유의어 용어에 대응되며, 이상 반응의 증증도는 NCI CTCAE v4.0에 따라 등급이 매겨진다.Verbose terms of adverse events correspond to synonym terms in the Medical Dictionary for Regulatory Activities, and severity of adverse events is graded according to NCI CTCAE v4.0.
안전성은 이상 반응에 대한 요약, 실험실 검사 결과의 변화, 활력 징후 및 ECG의 변화, 연구 약물에 대한 노출을 통해 평가한다. 병용 치료에 대한 노출 및 안전성 추적 기간은 각 단계 내 치료군 별로 요약되어 있다.Safety is assessed through a summary of adverse events, changes in laboratory test results, changes in vital signs and ECGs, and exposure to study drug. Exposure and safety follow-up periods for combination therapy are summarized for each treatment group within each phase.
치료 개시 후 발생하는 치료 관련 이상 반응이 요약되어 있다. 각 환자에 대해, 각 이상 반응에 대해 보고된 최대 증증도는 증증도 등급별 요약에 사용된다. 모든 치료 관련 이상 반응, 중증 이상 반응, 연구 치료제 중단으로 이어지는 이상 반응, 3등급 이상 반응, 사망 및 사망 원인은 매핑된 용어, 적절한 유의어 수준, 및 NCI CTCAE 증증도 등급으로 나열 및 요약된다. 관련 실험실, 활력징후(맥박수, 호흡수, 혈압, 맥박 산소 측정, 및 체온) 및 ECG 데이터가 시간별로 표시되며, 적절한 경우 등급으로 식별된다. 또한, 선택된 실험실 시험의 변화표(shift table)는 기준선 및 기준선 이후 최대 중증도 등급을 요약하는 데 사용한다. 활력 징후 및 ECG의 변화가 요약되어 있다.Treatment-related adverse events occurring after initiation of treatment are summarized. For each patient, the maximum severity reported for each adverse event is used for the summary by severity grade. All treatment-related adverse events, serious adverse events, adverse events leading to discontinuation of study treatment,
아테졸리주맙은 하기와 같은 위험과 관련이 있다: IRR 및 면역 매개 간염, 폐렴, 대장염, 췌장염, 당뇨병, 갑상선 기능 저하증, 갑상선 기능 항진증, 부신 기능 부전증, 뇌하수체염, 길랭-바레 증후군, 근무력 증후군 또는 중증 근무력증, 수막뇌염, 심근염, 신장염 및 근염. 면역 매개 반응은 임의의 기관계와 관련될 수 있으며, 혈구탐식성 림프조직구증가증 및 대식세포 활성화 증후군(아테졸리주맙의 잠재적 위험으로 간주됨)을 유발할 수 있다.Atezolizumab is associated with the following risks: IRR and immune-mediated hepatitis, pneumonia, colitis, pancreatitis, diabetes, hypothyroidism, hyperthyroidism, adrenal insufficiency, pituitary gland, Guillain-Barré syndrome, myasthenia gravis or myasthenia gravis, meningoencephalitis, myocarditis, nephritis and myositis. Immune-mediated responses may involve any organ system and may lead to hemophagocytic lymphohistiocytosis and macrophage activation syndrome (considered a potential risk for atezolizumab).
하기는 PDAC 환자에게서 냅-파클리탁셀과 관련하여 관찰된 가장 흔한 이상반응이다: 호중구감소증, 피로, 말초 신경병증, 구역, 탈모, 말초 부종, 설사, 발열, 구토, 식욕 감소, 발진 및 탈수. 하기와 같은 이상 반응이 또한 관찰되었: 골수 억제(주로 호중구 감소증, 빈혈, 혈소판 감소증), 뇌신경 마비, 과민 반응, 폐렴, 근육통, 관절통, 심장 독성(심근 장애, 심부전, 협심증, 빈맥, 심실성 부정맥), 부종, 낭포황반부종, 스티븐스-존슨 증후군/독성표피괴사, 패혈증, 주입부위 반응/혈관외유출, 간독성(약물 유발 간 손상), 급성 신부전, 용혈성 요독 증후군, 및 약물 유발 홍반성 루푸스.The following are the most common adverse reactions observed with nap-paclitaxel in patients with PDAC: neutropenia, fatigue, peripheral neuropathy, nausea, hair loss, peripheral edema, diarrhea, fever, vomiting, decreased appetite, rash and dehydration. The following adverse events were also observed: myelosuppression (mainly neutropenia, anemia, thrombocytopenia), cranial nerve palsy, hypersensitivity reactions, pneumonia, myalgia, arthralgia, cardiac toxicity (myocardial disorders, heart failure, angina pectoris, tachycardia, ventricular arrhythmias) ), edema, cystic macular edema, Stevens-Johnson syndrome/toxic epidermal necrosis, sepsis, injection site reaction/extravascularization, hepatotoxicity (drug-induced liver injury), acute renal failure, hemolytic uremic syndrome, and drug-induced lupus erythematosus.
젬시타빈에서 관찰된 가장 흔한 이상반응은 메스꺼움/구토, 빈혈, 간 아미노전이염, 호중구감소증, ALP 증가, 단백뇨, 발열, 혈뇨, 발진, 혈소판 감소증, 호흡곤란 및 말초 부종이다.The most common adverse reactions observed with gemcitabine were nausea/vomiting, anemia, hepatic transaminaemia, neutropenia, increased ALP, proteinuria, fever, hematuria, rash, thrombocytopenia, dyspnea and peripheral edema.
IRR은 티라골루맙의 확인된 위험이다. 티라골루맙의 임상 평가는 제한적이고 모든 위험이 공지된 것은 아니지만, TIGIT의 길항제로서 티라골루맙은 T 세포 및 NK 세포 증식, 생존 및 기능을 향상시킬 것으로 예상된다. 따라서, 티라골루맙은 자가면역 염증(면역 매개 이상 반응이라고도 함)의 위험을 증가시킬 수 있다. 또한, 티라골루맙의 온전한 Fc 작동체 기능으로 인해 항체 의존성 세포 독성(ADCC)을 통한 림프구감소증이 이론적 위험이다.IRR is the identified risk of tiragolumab. Although the clinical evaluation of tiragolumab is limited and not all risks are known, as an antagonist of TIGIT, tiragolumab is expected to improve T cell and NK cell proliferation, survival and function. Thus, tiragolumab may increase the risk of autoimmune inflammation (also called immune-mediated adverse reaction). In addition, lymphopenia via antibody dependent cytotoxicity (ADCC) is a theoretical risk due to the intact Fc effector function of tiragolumab.
티라골루맙은 치료적 단일클론 항체이고 면역 세포를 표적으로 하기 때문에, 과민 반응, 표적 매개 사이토카인 방출, 및/또는 새로운 ADA와 관련된 IRR이 발생할 수 있다. 이러한 반응의 임상 징후 및 증상에는 경직, 오한, 천명, 가려움증, 홍조, 발진, 저혈압, 저산소혈증 및 발열이 포함될 수 있다. IRR은 단독으로 또는 아테졸리주맙과 병용으로 티라골루맙으로 치료받은 환자에서 보고되었다. 대부분의 반응들은 경증 내지 중등도였으며 관리가능하였다.Because tyragolumab is a therapeutic monoclonal antibody and targets immune cells, hypersensitivity reactions, target-mediated cytokine release, and/or IRRs associated with novel ADA may occur. Clinical signs and symptoms of these reactions may include stiffness, chills, wheezing, itching, flushing, rash, hypotension, hypoxemia and fever. IRR has been reported in patients treated with tiragolumab alone or in combination with atezolizumab. Most reactions were mild to moderate and manageable.
IRR의 위험 및 후유증을 최소화하기 위해, 티라골루맙의 초기 용량을 60분에 걸쳐 투여한 후 60분의 관찰 기간을 둔다. 선행 주입이 양호하게 내약성이 되면, 후속 주입 및 관찰 시간을 단축할 수 있다. 티라골루맙의 모든 주입은 적절한 의료 환경에서 투여한다.To minimize the risk of IRR and its sequelae, an initial dose of tiragolumab is administered over 60 minutes followed by an observation period of 60 minutes. If the preceding infusion is well tolerated, subsequent infusion and observation times can be shortened. All infusions of tiragolumab are administered in an appropriate medical setting.
비임상 모델은 자가면역에서 TIGIT 신호 전달 중단의 역할을 제시하였다. 녹아웃 모델(TIGIT -/-)에서, TIGIT 신호전달의 소실은 과증식성 T 세포 반응 및 실험적 자가면역 뇌염(EAE)의 악화를 초래하였다. TIGIT -/- 및 야생형 B6 마우스를 최적이 아닌 용량의 미엘린 희소돌기아교세포 당단백질 펩티드로 면역화하여 EAE를 유도하였다. 야생형 B6 마우스와 대조적으로, TIGIT-/- 마우스의 대다수는 중(Joller et al. 2011).Nonclinical models have suggested a role for disruption of TIGIT signaling in autoimmunity. In the knockout model (TIGIT −/−), loss of TIGIT signaling resulted in exacerbation of hyperproliferative T cell responses and experimental autoimmune encephalitis (EAE). EAE was induced by immunization of TIGIT −/− and wild-type B6 mice with suboptimal doses of myelin oligodendrocyte glycoprotein peptide. In contrast to wild-type B6 mice, the majority of TIGIT-/- mice are medium (Joller et al. 2011).
항종양 T 세포 반응을 향상시키기 위한 치료법에 대한 임상 경험에 따르면, 자가면역 염증 상태의 발병은 일반적인 위험이며, 따라서 티라골루맙의 잠재적 위험으로 간주될 수 있다. 이러한 면역 매개 이상 반응은 사실상 모든 기관계에서 설명된 바 있으며 대장염, 간염, 폐렴, 내분비병증, 안구 독성, 췌장 독성, 신경학적 독성, 심근염, 신염, 근염 및 발진을 포함하지만 이에 제한되지는 않는다.According to clinical experience with therapies to enhance anti-tumor T cell responses, the development of an autoimmune inflammatory condition is a common risk and can therefore be considered a potential risk for tyragolumab. These immune-mediated adverse events have been described in virtually all organ systems and include, but are not limited to, colitis, hepatitis, pneumonia, endocrinopathy, ocular toxicity, pancreatic toxicity, neurological toxicity, myocarditis, nephritis, myositis, and rash.
자가면역질병 이력이 있는 환자는 본 연구에서 제외한다. 또한, 선행 면역 요법과 관련된 심각한 면역 매개 이상 반응의 병력이 있거나 선행 면역 요법의 중단 후 기준선으로 해결되지 않은 이상 반응이 있는 환자는 본 연구에서 제외한다. Patients with a history of autoimmune diseases were excluded from this study. In addition, patients with a history of serious immune-mediated adverse events related to prior immunotherapy or unresolved adverse events at baseline after discontinuation of prior immunotherapy were excluded from this study.
본 연구에서, 특정 면역 매개 이상 반응은 특별한 관심의 이상 반응으로 간주되고 이에 따라 포착된다.In this study, certain immune-mediated adverse events are considered adverse events of special interest and captured accordingly.
Fc 작동체 기능이 온전한 티라골루맙의 IgG1 백본을 고려할 때, ADCC 매개 림프구 수 감소는 잠재적인 위험이다. 하지만, 시노몰구스 원숭이에 대한 반복 투여 독성 연구에서, 전체 림프구 수에서 티라골루맙과 관련된 감소는 없었다.Given the IgG1 backbone of tyragolumab with intact Fc effector function, ADCC-mediated lymphocyte count reduction is a potential risk. However, in a repeat-dose toxicity study in cynomolgus monkeys, there was no tyragolumab-related decrease in total lymphocyte count.
고형 종양에 대한 1상 연구(연구 GO30103)에서 티라골루맙 단독 또는 아테졸리주맙과 병용하여 치료받은 환자에게서 임상적 후유증 없이 일시적인 림프구 수 감소가 관찰되었다. 티라골루맙이 림프구감소증을 유발할 가능성이 있기 때문에, 림프구 수가 0.5 x 109/L(500/μL) 미만인 환자는 연구에서 제외한다. 전체 혈구 수는 연구 전반에 걸쳐 모니터링된다.In a
하기의 이상 반응은 아테졸리주맙, 냅-파클리탁셀, 젬시타빈, 및 티라골루맙의 병용과 관련된 잠재적인 중복 독성이다: 혈구탐식성 림프조직구증식증, 대식세포 활성화 증후군 등을 포함한 면역 매개 독성, 위장 독성, 혈액 독성 및 피부 독성.The following adverse events are potential overlapping toxicities associated with the concomitant use of atezolizumab, nap-paclitaxel, gemcitabine, and tiragolumab: immune-mediated toxicity including hemophagocytic lymphohistiocytosis, macrophage activation syndrome, etc., gastrointestinal Toxicity, blood toxicity and skin toxicity.
각 주기의 제 1일에 환자는 냅-파클리탁셀 및 젬시타빈을 이용한 치료를 받기 위해서, ANC가 1.5× 109/L(1500/μL)이고 혈소판 수는 100× 109/L(100,000/μL) 이상이여야 한다.On
독성으로 인한 치료 중단Discontinuation of treatment due to toxicity
아테졸리주맙 및/또는 티라골루맙은 연구 치료제와 관련된 것으로 간주되는 독성을 경험한 환자에게서 일시적으로 중단될 수 있다. 독성의 치료를 위해 코르티코스테로이드를 개시하는 경우, 약물을 재개하기 전에 1개월 이상에 걸쳐 10 mg/일 이하의 경구 프레드니손 또는 이에 상응하는 양으로 서서히 감량해야 한다. 아테졸리주맙 또는 티라골루맙을 12주를 초과하여 중단하는 경우, 환자는 해당 약물을 중단해야 한다. 하지만, 환자가 치료를 재개하기 전에 코르티코스테로이드를 서서히 줄일 수 있도록 상기 약물을 12주를 초과하여 보류할 수 있다. 아테졸리주맙 또는 티라골루맙은 의료 모니터가 환자가 임상적 이득을 얻을 가능성이 있다고 동의하는 경우 12주를 초과하여 보류 후 재개할 수 있다.Atezolizumab and/or tiragolumab may be temporarily discontinued in patients who experience toxicity considered to be related to the study treatment. When corticosteroids are initiated for the treatment of toxicity, oral prednisone or equivalent should be gradually reduced over a period of at least 1 month to 10 mg/day or less or equivalent before resumption of the drug. If atezolizumab or tiragolumab is discontinued for more than 12 weeks, the patient should discontinue the drug. However, the drug may be withheld for more than 12 weeks so that the patient can gradually reduce the corticosteroid before resuming treatment. Atezolizumab or tiragolumab may be resumed after withholding for more than 12 weeks if the medical monitor agrees that the patient has a potential for clinical benefit.
작용기전의 입수 가능한 특성화에 기초하여, 티라골루맙은 아테졸리주맙과 유사하지만 이와 독립적인 이상반응을 유발할 수 있다. 티라골루맙은 또한 아테졸리주맙과 관련된 이상반응의 빈도 또는 중증도를 악화시키거나 아테졸리주맙과 겹치지 않는 독성을 가질 수 있다. 이러한 시나리오는 임상 환경에서 서로 구별 가능하지 않을 수 있으므로, 면역 매개 이상 반응은 일반적으로 두 약물에 기인한 것이어야 하며, 면역 매개 이상 반응으로 인한 치료 중단은 티라골루맙 및 아테졸리주맙 둘 모두에 적용되어야 한다.Based on the available characterization of the mechanism of action, tiragolumab may induce adverse reactions similar to but independent of atezolizumab. Tiragolumab may also aggravate the frequency or severity of adverse events associated with atezolizumab or have toxicity that does not overlap with atezolizumab. As these scenarios may not be distinguishable from each other in the clinical setting, immune-mediated adverse events should generally be attributable to both drugs, and treatment discontinuation due to immune-mediated adverse events applies to both tiragolumab and atezolizumab. should be
냅-파클리탁셀 및/또는 젬시타빈은 연구 치료제와 관련된 것으로 간주되는 독성을 경험한 환자에게서 일시적으로 중단될 수 있다. 냅-파클리탁셀 또는 젬시타빈이 독성 때문에 56일을 초과하여 보류된 경우, 환자는 두 화학요법제를 모두 중단해야 한다. 하지만, 냅-파클리탁셀 또는 젬시타빈은 의료 모니터가 환자가 임상적 이득을 얻을 가능성이 있다고 동의하는 경우 56일을 초과하여 보류 후 재개할 수 있다.Nap-paclitaxel and/or gemcitabine may be temporarily discontinued in patients experiencing toxicity considered to be related to the study treatment. If nap-paclitaxel or gemcitabine is withheld for more than 56 days due to toxicity, the patient should discontinue both chemotherapeutic agents. However, nap-paclitaxel or gemcitabine may be resumed after withholding beyond 56 days if the medical monitor agrees that the patient is likely to benefit clinically.
아테졸리주맙을 중단하는 경우, 티라골루맙 또한 중단해야 하지만, 시험자가 결정한 대로 환자가 임상적 이득을 얻을 가능성이 있는 경우 냅-파클리탁셀 및 젬시타빈을 계속할 수 있다. 냅-파클리탁셀, 젬시타빈, 또는 티라골루맙을 중단한 경우, 시험자가 결정한 대로 환자가 임상적 이득을 얻을 가능성이 있는 경우 다른 약물을 계속 사용할 수 있다.If atezolizumab is discontinued, tiragolumab should also be discontinued, but nap-paclitaxel and gemcitabine may be continued if the patient is likely to achieve clinical benefit as determined by the investigator. If nap-paclitaxel, gemcitabine, or tiragolumab is discontinued, other drugs may be continued as determined by the investigator if the patient is likely to achieve clinical benefit.
통계statistics
최종 연구 분석은 연구 중단을 통해 수집한 환자 데이터를 기반으로 한다. 달리 명시되지 않은 경우, 유효성 분석은 할당된 치료 요법에 대해 각 약물의 적어도 1회 용량을 투여받는 모든 환자로 정의되는 유효성 평가 가능 모집단을 기초로 하고, 안전성 분석은 임의의 양의 연구 치료제를 투여 받은 모든 환자로 정의되는 안전성 평가 가능 모집단을 기초로 한다.The final study analysis is based on patient data collected through study discontinuation. Unless otherwise specified, efficacy analyzes are based on an efficacy evaluable population defined as all patients receiving at least one dose of each drug for their assigned treatment regimen, and safety analyzes are based on administration of any amount of study treatment. It is based on a safety evaluable population defined as all patients received.
데이터는 표본 크기에 따라 설명되고 요약된다. 연속 변수는 평균, 표준 편차, 중앙값, 및 범위를 사용하여 요약된다. 범주형 변수는 개수 및 백분율을 사용하여 요약된다. 표본 크기가 작은 경우에는 표 대신 목록을 사용한다.Data are described and summarized according to sample size. Continuous variables are summarized using mean, standard deviation, median, and range. Categorical variables are summarized using counts and percentages. For small sample sizes, a list is used instead of a table.
본 연구는 가설 분석을 위해 명시적 분석력 및 제1종 오류를 고려하도록 설계되지 않았다. 대신, 본 연구는 전이성 PDAC 환자에게 투여할 때 면역요법 기반 치료 조합에 대한 예비 유효성, 안전성, 및 PK 데이터를 수득하기 위해 설계되었다.This study was not designed to consider explicit analytical power and Type I error for hypothesis analysis. Instead, this study was designed to obtain preliminary efficacy, safety, and PK data for an immunotherapy-based treatment combination when administered to patients with metastatic PDAC.
표 21은 실험군 및 대조군 사이의 추정된 ORR 차이를 90% 신뢰 구간과 함께 나타내고, 표본 크기는 예비 단계에서 각각 15명의 환자를 대상으로 하며, 점근적 정규성을 가정한다.Table 21 shows the estimated ORR differences between the experimental and control groups with 90% confidence intervals, the sample size is 15 patients each in the preliminary phase, and asymptotic normality is assumed.
a 점근적 신뢰 한계(표본 크기가 매우 작기 때문에 연속성에 대해 수정되지 않음).CI = confidence interval.
a Asymptotic confidence limits (not corrected for continuity due to very small sample size).
각각 15명 환자의 실험군 및 대조군 간의 추정된 객관적 반응률의 차이(예비 단계)Differences in estimated objective response rates between experimental and control groups of 15 patients each (preliminary phase)
표 22은 실험군 및 대조군 사이의 추정된 ORR 차이를 90% 신뢰 구간과 함께 나타내고, 표본 크기는 예비 단계 및 확장 단계에서 각각 40명의 환자를 대상으로 하며, 점근적 정규성을 가정한다.Table 22 shows the estimated ORR differences between the experimental and control groups with 90% confidence intervals, the sample size covers 40 patients each in the preliminary phase and the expansion phase, and asymptotic normality is assumed.
a 점근적 신뢰 한계(표본 크기가 매우 작기 때문에 연속성에 대해 수정되지 않음).CI = confidence interval.
a Asymptotic confidence limits (not corrected for continuity due to very small sample size).
각각 15명 환자의 실험군 및 대조군 간의 추정된 객관적 반응률의 차이(예비 단계)Differences in estimated objective response rates between experimental and control groups of 15 patients each (preliminary phase)
목적 및 평가변수Purpose and endpoints
연구에 대한 목적 및 해당 평가 변수의 요약은 표 23에서 찾을 수 있다.A summary of the study objectives and corresponding endpoints can be found in Table 23.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
DOR, iRECIST에 따라 시험자가 결정함
![]()
![]()
![]()
![]()
DOR, determined by the examiner according to iRECIST
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
목적 및 해당 평가변수Purpose and corresponding endpoints
ADA = 항 약물 항체; DOR = 반응 지속 기간; iRECIST = 면역기반 치료제를 위한 수정된 RECIST v1.1; OS = 전체 생존; PFS = 무진행 생존; PK = 약동학; RECIST = 고형 종양의 반응 평가 기준.ADA = anti-drug antibody; DOR = duration of response; iRECIST = modified RECIST v1.1 for immune-based therapeutics; OS = overall survival; PFS = progression-free survival; PK = pharmacokinetics; RECIST = Criteria for evaluating the response of solid tumors.
단일 시점에서의 객관적 반응은 RECIST v1.1을 이용하여 시험자가 결정한다. iRECIST 따른 전체 반응은 eCRF에서 포착되지 않지만, eCRF에 기록된 시험자 평가 개별 병변 데이터를 기반으로 프로그래밍 방식으로 계산한다.The objective response at a single time point is determined by the investigator using RECIST v1.1. The overall response following iRECIST is not captured in the eCRF, but is calculated programmatically based on investigator-assessed individual lesion data recorded in the eCRF.
유효성 분석Validity analysis
1차 유효성 평가변수는 객관적 반응이다. 완전 또는 부분 반응을 보이는 환자의 비율인 ORR은 90% 신뢰 구간(클로퍼-피어슨(Clopper-Pearson) 방법)으로 각 군별로 계산한다. 실험군 및 대조군 사이의 ORR 차이는 90% 신뢰 구간으로 계산한다. 신뢰 구간은 표본 크기에 따라 점근적 정규성 방법으로 추정한다.The primary efficacy endpoint is objective response. ORR, the proportion of patients with a complete or partial response, is calculated for each group with a 90% confidence interval (Clopper-Pearson method). ORR differences between experimental and control groups are calculated as 90% confidence intervals. Confidence intervals are estimated by the asymptotic normality method according to the sample size.
2차 유효성 평가변수는 특정 시점(예컨대, 6개월)에서의 PFS, OS, OS, 반응 지속 기간(DOR)이며 질병 통제 PFS, DOR 및 질병 통제는 RECIST v1.1에 따라 시험자가 결정한다. DOR은 완전 또는 부분 반응이 있는 유효성 평가변수에 대해 파생된다. 연구 단계에서 기록된 질병 진행 또는 사망이 없는 환자의 경우, PFS 및 DOR은 마지막 종양 평가 당일에 검열 및 삭제된다. OS 분석 시점에서 계속 살아 있는 환자는 생존이 공지된 마지막 날짜에 중도 절단된다.Secondary efficacy endpoints are PFS, OS, OS, duration of response (DOR) at a specific time point (eg, 6 months), and disease control PFS, DOR, and disease control are determined by the investigator according to RECIST v1.1. DOR is derived for efficacy endpoints with full or partial responses. For patients with no documented disease progression or death during the study phase, PFS and DOR are censored and cleared on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day survival is known.
카플란-마이어(Kaplan-Meier) 방법은 브룩마이어와 크롤리(Brookmeyer and Crowley) 방법을 사용하여 구성된 90% 신뢰 구간으로 PFS, OS 및 DOR의 중앙값을 추정하는 데 사용한다. 특정 시점의 OS 비율은 분산에 대한 그린우드(Greenwood)의 추정치를 기반으로 계산된 90% 신뢰 구간과 함께 카플란-마이어 방법을 사용하여 추정한다. 12주 이상 동안 질병이 안정하고 부분 반응 또는 완전 반응을 보인 환자의 비율인 질병 통제율은 클로퍼-피어슨의 정확한 방법을 사용하여 추정한 90% 신뢰 구간으로 각 치료군에 대해 계산한다.The Kaplan-Meier method is used to estimate the median of PFS, OS, and DOR with 90% confidence intervals constructed using the Brookmeyer and Crowley method. The OS ratio at any point in time is estimated using the Kaplan-Meier method with a 90% confidence interval calculated based on Greenwood's estimate of variance. Disease control rate, which is the proportion of patients with stable disease and partial or complete response for at least 12 weeks, is calculated for each treatment arm with a 90% confidence interval estimated using Klopper-Pearson's exact method.
탐색적 유효성 평가변수는 iRECIST에 따라 시험자가 결정한 객관적 반응, PFS, DOR 및 질병 통제이고; 두 단계 동안의 후속 시점에서 CA19-9의 기준선으로부터의 변화이다. DOR은 완전 또는 부분 반응이 있는 유효성 평가변수에 대해 파생된다. 시간 경과에 따른 기준선으로부터의 CA19-9 변화가 요약되어 있다. 또한, CA19-9의 기준선에서 최대 감소가 50% 이상인 환자의 비율 또는 기타 임계값은 클로퍼-피어슨의 정확한 방법을 사용하여 추정한 90% 신뢰 구간으로 각 치료군에 대해 계산할 수 있다.Exploratory efficacy endpoints were investigator-determined objective response, PFS, DOR, and disease control according to iRECIST; Changes from baseline in CA19-9 at subsequent time points during the two phases. DOR is derived for efficacy endpoints with full or partial responses. CA19-9 changes from baseline over time are summarized. In addition, the proportion of patients with a CA19-9 maximal reduction greater than or equal to 50% from baseline, or other thresholds, can be calculated for each treatment arm with a 90% confidence interval estimated using the Klopper-Pearson's exact method.
약동학 분석Pharmacokinetic analysis
아테졸리주맙(적어도 1회 용량의 아테졸리주맙을 투여받는 환자) 및 아테졸리주맙과 병용으로 제공된 특정 약물(적어도 1회 용량의 약물을 투여받는 환자)의 잠재적 PK 분석을 위해 희소 샘플을 수집할 수 있다. 다양한 연구 약물의 혈청 또는 혈장 농도는 개별 값으로 보고할 수 있고, 적절하고 데이터가 허용하는 한 치료군, 주기 및 날짜별로 요약(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균, 및 기하 평균 변동 계수)할 수 있다. 다양한 연구 약물의 혈청 또는 혈장 농도의 개별 및 중앙값은 치료군 및 주기 및 일별로 플롯(plot)될 수 있다. 복합 약물에 대한 PK 데이터는 내부 및 공개된 이전 연구로부터 입수 가능한 과거 데이터와 비교할 수 있다. 아테졸리주맙 농도 데이터는 청소율, 분포 용적, 곡선하 면적과 같은 PK 매개변수를 도출하기 위해 확립된 모집단 PK 모델을 사용하는 다른 연구로부터의 데이터와 통합할 수 있다.Rare samples may be collected for potential PK analysis of atezolizumab (patients receiving at least one dose of atezolizumab) and certain drugs given in combination with atezolizumab (patients receiving at least one dose of the drug). can Serum or plasma concentrations of various study drugs can be reported as individual values and summarized by treatment group, cycle, and date (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean) as appropriate and data permitting. coefficient of variation) can be Individual and median serum or plasma concentrations of various study drugs can be plotted by treatment group and cycle and day. PK data for combination drugs can be compared with historical data available from internal and published previous studies. Atezolizumab concentration data can be integrated with data from other studies that use established population PK models to derive PK parameters such as clearance, volume of distribution, and area under the curve.
면역원성 분석Immunogenicity assay
면역원성은 적절한 경우 아테졸리주맙 및 기타 연구 치료제에 대해 평가할 수 있다(자세한 내용은 군별 부록을 참조). 면역원성 분석은 적어도 1회의 항약물 항체(ADA) 평가를 받은 모든 환자를 포함한다. 환자는 받은 치료에 따라, 또는 연구 중단 전에 치료를 받지 않은 경우 할당된 치료에 따라 그룹화된다.Immunogenicity may be assessed for atezolizumab and other study therapies, where appropriate (see the group-specific appendix for details). Immunogenicity assays included all patients who underwent at least one antidrug antibody (ADA) assessment. Patients are grouped according to treatment received, or according to assigned treatment if no treatment was received prior to study discontinuation.
아테졸리주맙의 경우, 기준선에서(기준선 유병률) 및 기준선 이후에서(기준선 이후 발생율) ADA 양성 및 ADA 음성 환자의 수 및 비율을 치료군별로 요약한다. 기준선 이후 발생율을 결정할 때, 환자가 기준선에서 ADA 음성이거나 데이터가 누락되었지만 연구 약물 노출 후 ADA 반응을 보인 경우(치료 유도 ADA 반응), 또는 기준선에서 ADA 양성이고 하나 이상의 기준선 이후 샘플의 역가가 기준선 샘플의 역가보다 0.60 역가 단위 이상 큰 경우(치료 강화 ADA 반응), 환자는 ADA 양성인 것으로 간주한다. 환자가 기준선에서 ADA 음성이거나 데이터가 누락되었고 기준선 이후의 모든 샘플들이 음성인 경우, 또는 기준선에서 ADA 양성이지만 역가가 기준선 샘플의 역가보다 0.60 역가 단위 이상 큰 기준선 이후 샘플들을 가지지 않는 경우(치료에 영향받지 않음), 환자는 ADA 음성으로 간주한다.For atezolizumab, the number and proportion of ADA-positive and ADA-negative patients at baseline (baseline prevalence) and post-baseline (post-baseline incidence) are summarized by treatment group. When determining post-baseline incidence rates, if a patient is ADA-negative at baseline or has missing data but has an ADA response following study drug exposure (treatment-induced ADA response), or is ADA positive at baseline and the titer of one or more post-baseline samples is equal to the baseline sample. A patient is considered ADA positive if it is at least 0.60 titer units greater than the titer of (treatment-enhanced ADA response). The patient is ADA negative at baseline or data is missing and all samples after baseline are negative, or if the patient is ADA positive at baseline but has no post-baseline samples whose titers are greater than or equal to 0.60 titer units greater than those of the baseline samples (treatment impacts). not received), the patient is considered ADA negative.
ADA가 시험되는 다른 연구 치료제의 경우, ADA 양성은 이러한 약물의 이전 연구에 대해 설정된 표준 방법에 따라 결정한다. ADA 상태와, 안전성, 유효성, PK 및 바이오마커 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고할 수 있다.For other study treatments for which ADA is tested, ADA positivity is determined according to standard methods established for previous studies of these drugs. The relationship between ADA status and safety, efficacy, PK and biomarker endpoints can be analyzed and reported through descriptive statistics.
실시예 3. 삼중 음성 유방암 환자를 대상으로 아테졸리주맙 및 화학요법과 병용한 티라골루맙의 안전성, 유효성 및 약동학에 관한 Ib상, 공개 라벨, 다중 코호트 연구 Example 3. A Phase Ib, Open Label, Multiple Cohort Study of the Safety, Efficacy and Pharmacokinetics of Tiragolumab in Combination with Atezolizumab and Chemotherapy in Patients with Triple Negative Breast Cancer
본 실시예는 전이성 삼중 음성 유방암(TNBC) 환자를 대상으로 아테졸리주맙 및 화학요법과 병용한 티라골루맙의 안전성, 유효성 및 약동학을 평가하기 위해 설계된 Ib상, 공개 라벨, 다중 코호트 연구를 설명한다. 본 연구는 하기의 코호트로 구성된다:This example describes a Phase Ib, open-label, multi-cohort study designed to evaluate the safety, efficacy, and pharmacokinetics of tiragolumab in combination with atezolizumab and chemotherapy in patients with metastatic triple negative breast cancer (TNBC). . This study consists of the following cohorts:
·코호트 A는 전이성 유방암에 대한 선행 전신 요법을 받은 적이 없는 절제 불가능한 국소 진행성 또는 전이성 예정된 세포 사멸 리간드 1(PD-L1) 양성 TNBC(1차 전이성 TNBC)를 가진 환자를 등록한다. 환자는 아테졸리주맙 및 냅-파클리탁셀과 병용으로 티라골루맙을 투여받는다.Cohort A enrolls patients with unresectable locally advanced or metastatic programmed cell death ligand 1 (PD-L1) positive TNBC (primary metastatic TNBC) who have not received prior systemic therapy for metastatic breast cancer. Patients receive tiragolumab in combination with atezolizumab and nap-paclitaxel.
A.A. 연구 설계study design
본 Ib상, 다중 코호트, 공개 라벨, 다기관, 글로벌 연구는 전이성 유방암에 대한 선행 전신 요법을 받은 적이 없는 절제 불가능한 국소 진행성 또는 전이성 PD-L1 양성 TNBC(코호트 A, 전이성 TNBC라고 함)를 가진 환자를 대상으로 아테졸루주맙 및 냅-파클리탁셀을 병용한 티라골루맙의 안전성 및 내약성, 예비 유효성, 및 약동학을 조사하기 위해 설계되었다. PD-L1 양성은 SP142 PD-L1 IHC 분석을 사용하여 평가한다. 도 2는 코호트 A에 대한 연구 설계를 도시한다.This Phase Ib, multi-cohort, open-label, multicenter, global study included patients with unresectable locally advanced or metastatic PD-L1-positive TNBC (Cohort A, termed metastatic TNBC) who had not received prior systemic therapy for metastatic breast cancer. It was designed to investigate the safety and tolerability, preliminary efficacy, and pharmacokinetics of tiragolumab in combination with atezoluzumab and nap-paclitaxel in subjects. PD-L1 positivity is assessed using the SP142 PD-L1 IHC assay. 2 depicts the study design for Cohort A.
적격 환자(즉, PD-L1 양성 환자)는 28일 주기의 제 1일에 IV 주입에 의해 티라골루맙(840 mg) 및 아테졸리주맙(1680 mg)을 투여 받고, 여기에 더하여 28일 주기의 제 1일, 8일, 15일에 IV 주입에 의해 냅-파클리탁셀(100 mg/m2) 투여 받기 위해 등록된다.Eligible patients (i.e., PD-L1-positive patients) will receive tiragolumab (840 mg) and atezolizumab (1680 mg) by IV infusion on
질병 진행 또는 허용할 수 없는 독성이 없는 경우, 냅-파클리탁셀은 최대값 없이 적어도 6회 주기를 목표로 투여된다.In the absence of disease progression or unacceptable toxicity, nap-paclitaxel is administered with a target of at least 6 cycles without a maximum.
종양 미세환경에서 약물 조합의 작용 기전 및 가능한 내성 기전을 평가하기 위해, 종양 조직은 선택적으로 주기 2의 1일에 투여 전에 수집할 수 있다.To evaluate the mechanism of action and possible resistance mechanisms of drug combinations in the tumor microenvironment, tumor tissues can optionally be collected prior to dosing on
종양 미세 환경에서 약물 조합에 대한 내성 기전을 시험하기 위해, 모든 환자는 RECIST v1.1에 따라 시험자가 평가한 대로 질병 진행의 첫 번째 증거에서 의무적인 종양 생검 수집(임상적으로 가능한 경우)을 (새로운 항암제의 개시 전에) 받는다.To test the mechanisms of resistance to drug combinations in the tumor microenvironment, all patients underwent mandatory tumor biopsy collection (if clinically feasible) at first evidence of disease progression as assessed by the investigator according to RECIST v1.1 ( before initiation of a new anticancer drug).
환자는 치료 지연에 관계없이 기준선에서 및 주기 1의 1일 이후 처음 48주 동안 8주(±7일)마다 종양 평가를 받는다. 48주차 종양 평가가 완료된 후, 종양 평가는 치료 지연에 관계없이 RECIST v1.1에 따라 시험자가 결정한 대로 질병 진행, 동의 철회, 사망 또는 연구 종료 중 먼저 발생하는 시점까지 12주(±7일) 마다 실시해야 한다.Patients receive tumor assessments every 8 weeks (± 7 days) at baseline and for the first 48 weeks after
연구 치료제는 RECIST v1.1에 따라 시험자가 결정한 대로 질병 진행 시 중단된다. 진행에 대한 모호한 발견(예컨대, 매우 작거나 불확실한 새로운 병변 또는 림프절; 기존 병변의 낭성 변화 또는 괴사)의 경우, 시험자가 평가한 RECIST v1.1에 따라 다음 예정된 평가까지 치료를 계속할 수 있다. 다음 예정된 평가에서 진행이 확인되면, 진행 날짜는 진행이 의심되었던 더 빠른 날짜여야 한다.Study treatment is discontinued upon disease progression as determined by the investigator per RECIST v1.1. In the case of ambiguous findings of progression (e.g., very small or uncertain new lesions or lymph nodes; cystic changes or necrosis of existing lesions), treatment may be continued until the next scheduled evaluation according to RECIST v1.1 assessed by the investigator. If progress is confirmed at the next scheduled evaluation, the date of progress should be the earlier date when progress was suspected.
B.B. 용량 및 투여Dosage and administration
치료 요법은 도 2에 요약되어 있다. The treatment regimen is summarized in FIG. 2 .
아테졸리주맙, 티라골루맙, 및 화학요법의 예정된 주입일에는, 아테졸리주맙 및 티라골루맙을 주입한 후 화학요법을 투여한다.On the scheduled infusion days of atezolizumab, tiragolumab, and chemotherapy, the atezolizumab and tiragolumab infusion are followed by chemotherapy.
아테졸리주맙 주입(1680 mg) 후, 환자는 840 mg의 티라골루맙을 투여 받는다. After atezolizumab infusion (1680 mg), patients receive 840 mg of tiragolumab.
아테졸리주맙, 티라골루맙, 및 화학요법의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 실시한다.Administration of atezolizumab, tiragolumab, and chemotherapy is performed in a monitored environment with immediate access to trained personnel and appropriate equipment and medications to manage potentially severe reactions.
약물 준비, 보관 및 투여에 대한 자세한 지침은 약국 설명서를 참조한다.For detailed instructions on drug preparation, storage, and administration, see the pharmacy instructions.
티라골루맙과 아테졸리주맙Tiragolumab and Atezolizumab
코호트 A에서, 환자들은 1680 mg 고정 용량의 아테졸리주맙을 각 28일 주기의 제 1일에 Q4W IV 주입으로 투여받으며, 그 후 840 mg 고정 용량의 티라골루맙이 환자들에게 각 28일 주기의 제 1일에 Q4W IV 주입으로 투여된다. 티라골루맙 용량은 고정이며 체중에 따라 달라지지 않는다. 티라골루맙 및 아테졸리주맙 주입(관찰 기간을 포함)은 표 24에 요약된 지침에 따라 투여된다.In Cohort A, patients receive a 1680 mg fixed dose of atezolizumab as a Q4W IV infusion on
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
제1 및 후속 티라골루맙 주입 및 아테졸리주맙 주입의 투여Administration of first and subsequent tiragolumab infusions and atezolizumab infusions
냅-파클리탁셀Nap-paclitaxel
냅-파클리탁셀은 지역 처방 정보에 따라 투여된다. 본 연구에서 냅-파클리탁셀의 시작 용량 수준은 각 28일 주기의 제 1일, 8일 및 15일에(3주 투약/1주 휴약 일정) 30분에 걸쳐 환자에게 정맥내 투여되는 100 mg/m2이다. 냅-파클리탁셀은 아테졸리주맙 및 티라골루맙 후에 투여해야 한다. 냅-파클리탁셀은 매 주기의 8일 및 15일에 단독으로 투여한다. 냅-파클리탁셀의 용량은 매 7일보다 더 자주 투여해서는 안 된다.Nap-paclitaxel is administered according to local prescribing information. The starting dose level of nap-paclitaxel in this study was 100 mg/m administered intravenously to patients over 30 minutes on
기관은 비만 환자를 위한 냅-파클리탁셀 용량을 결정하고 환자 체중 변화 시 용량 조정을 위해 해당 기관의 치료의 표준을 따라야 한다. 약물 투여 중 침윤 가능성에 대해 주입 부위를 면밀히 모니터링해야 한다.Institutions should follow the institution's standard of care to determine nap-paclitaxel doses for obese patients and adjust the dose for changes in patient body weight. The injection site should be closely monitored for possible infiltration during drug administration.
질병 진행 또는 허용할 수 없는 독성이 없는 경우, 냅-파클리탁셀은 최대값 없이 적어도 6회 주기를 목표로 투여된다.In the absence of disease progression or unacceptable toxicity, nap-paclitaxel is administered with a target of at least 6 cycles without a maximum.
냅-파클리탁셀의 준비 및 투여에 대한 자세한 내용은 현지 처방 정보를 참조한다.For more information on the preparation and administration of nap-paclitaxel, see local prescribing information.
용량 변경capacity change
본 연구에서 아테졸리주맙 또는 티라골루맙에 대한 용량 변경은 없다. 냅-파클리탁셀의 관리(즉, 용량 조절 및 치료 중단 규칙)는 표 25를 참조한다.There were no dose changes for atezolizumab or tiragolumab in this study. See Table 25 for administration of nap-paclitaxel (ie, dose adjustment and treatment discontinuation rules).
냅-파클리탁셀에 대한 권장 용량 감소Reducing the Recommended Dose for Nap-Paclitaxel
C.C. 병용 요법combination therapy
병용 요법은 연구 약물 개시 7일 전부터 치료 중단 방문시까지 프로토콜 필수 치료 외에 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)을 포함한다.Combination therapy includes any drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, nutritional supplements) used by the patient in addition to protocol essential treatment from 7 days prior to study drug initiation until the treatment discontinuation visit.
허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
완화 방사선 요법은 종양 표적 병변의 평가를 방해하지 않는 한 허용한다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 티라골루맙 및 아테졸리주맙을 이용한 치료는 완화 방사선 요법 동안 계속될 수 있다. 냅-파클리탁셀을 이용한 치료는 기관의 치표의 표준에 따라 중단되어야 한다.Palliative radiation therapy is acceptable as long as it does not interfere with the evaluation of tumor target lesions (eg, the lesion to be investigated should not be the only site of measurable disease). Treatment with tiragolumab and atezolizumab may be continued during palliative radiation therapy. Treatment with nap-paclitaxel should be discontinued according to institutional standards.
항히스타민제, 해열제, 및/또는 진통제의 예비투약은 시험자의 재량에 따라 두 번째 및 이후의 아테졸리주맙 및 티라골루맙 주입에 대해서만 투여할 수 있다.Premedication of antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab and tiragolumab at the discretion of the investigator.
주의 요법care
전신 코르티코스테로이드 및 TNF-α 억제제는 아테졸리주맙을 이용한 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여해야 하는 상황에서는, 항히스타민제를 포함한 대안을 고려해야 한다. 대안이 가능하지 않은 경우, 시험자의 재량에 따라 전신 코르티코스테로이드 및 TNF-α 억제제를 투여할 수 있다.Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines should be considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the investigator's discretion.
아테졸리주맙 요법과 관련된 특정 이상 반응을 치료하기 위해, 시험자의 재량에 따라 전신 코르티코스테로이드가 권장된다.For the treatment of certain adverse events associated with atezolizumab therapy, systemic corticosteroids are recommended at the discretion of the investigator.
금지된 요법forbidden therapy
다음과 같은 병용 요법의 사용은 하기와 같이 금지된다:The use of the following combination therapies is contraindicated as follows:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
연구 치료 중 전신 면역억제제(아자티오프린, 메토트렉세이트 및 탈리도마이드를 포함) - 상기 제제는 아테졸리주맙 및 티라골루맙의 유효성 및 안전성을 변경할 가능성이 있기 때문임.Systemic immunosuppressive agents (including azathioprine, methotrexate, and thalidomide) during study treatment, as these agents have the potential to alter the efficacy and safety of atezolizumab and tiragoluumab.
![]()
![]()
D.D. 선정 기준Selection Criteria
환자는 연구 등록을 위해 하기의 일반 기준에 부합해야 한다:Patients must meet the following general criteria for study enrollment:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
14일 이내에 수득한 하기와 같은 실험실 결과로 정의되는 적절한 혈액 및 말단 기관 기능(주기 1의Adequate blood and end organ function (of Cycle 1) defined by the following laboratory results obtained within 14 days.
1일):1 day):
- ANC ³ 1.5 ´ 109/L(1500/νL) - -
주기 1의 1일 전 2주 내에 G-CSF 지원 없음No G-CSF support within 2 weeks before 1 day of
- 림프구 수 ³ 0.5 ´ 109/L(³ 500/νL)-
- 혈소판 수 ³ 100 ´ 109/L(³ 100,000/νL) - -
주기 1의 1일 전 2주 내에 수혈 없음No transfusions within 2 weeks before
- 헤모글로빈 ³ 90 g/L(³ 9 g/dL)-
상기 기준을 충족하기 위해 환자는 수혈을 받거나 적혈구 생성 치료를To meet the above criteria, the patient will receive a blood transfusion or receive erythropoietic therapy.
받을 수 있다.can receive
- AST, ALT, 및 ALP £ 2.5 ´ 정상 상한치(ULN) - AST, ALT, and ALP £ 2.5 ´ Upper limit of normal (ULN)
- 혈청 빌리루빈 £ 1.5 ´ U, 하기의 경우는 제외함:- Serum bilirubin £ 1.5 ´ U, except for:
혈청 빌리루빈 수치가 £ 3 lULN인 것으로 공지된 길버트 병 환자가 등록할 수 있다.Gilbert's disease patients known to have serum bilirubin levels of £ 3 lULN can enroll.
- INR 및 aPTT £ 1.5 ´ ULN - INR and aPTT £ 1.5 ´ ULN
이는 치료적 항응고를 받지 않은 환자에게만 적용되었고; 항응고 치료를 받은 환자는 안정된 용량을 사용해야 한다.This only applied to patients who did not receive therapeutic anticoagulation; Patients on anticoagulant therapy should use a stable dose.
- 크레아티닌 청소율 ³ 30 mL/분(콕크로프트-가울트 공식을 사용하여 계산)-
- 혈청 알부민 ³ 25 g/L(³ 2.5 g/dL)-
![]()
![]()
![]()
![]()
![]()
![]()
하기의 경우 중 하나를 동반한 선별 검사시 HBsAb 음성HBsAb negative at screening with one of the following
- 총 B형 간염 코어 항체(HBcAb) 음성- Total hepatitis B core antibody (HBcAb) negative
- 총 HBcAb 검사 양성 후 정량적 B형 간염 바이러스(HBV) DNA- Quantitative hepatitis B virus (HBV) DNA after positive total HBcAb test
< 500 IU/mL< 500 IU/mL
HBV DNA 검사는 HBsAg 검사 음성, HBsAb 검사 음성, 총 HBcAb 검사 양성인 환자에게만 실시한다.The HBV DNA test is only performed on patients who have a negative HBsAg test, a negative HBsAb test, and a positive total HBcAb test.
![]()
![]()
HCV RNA 검사는 HCV 항체 검사 양성인 환자에게만 시행된다.The HCV RNA test is only performed on patients with a positive HCV antibody test.
![]()
![]()
여성은 치료 기간 동안 및 아테졸리주맙의 최종 투여 후 적어도 5개월, 티라골루맙의 최종 투여 후 90일, 냅-파클리탁셀의 최종 투여 후 1개월, 카보플라틴 또는 독소루비신의 최종 투여 후 6개월, 또는 시클로포스파미드의 최종 투여 후 12개월 중 더 늦은 날짜까지 금욕을 유지하거나 연 < 1%의 실패율을 갖는 피임 방법을 사용해야 한다. 여성은 상기 동일한 기간 동안 난자 기증을 자제해야 한다.Women during the treatment period and at least 5 months after the last dose of atezolizumab, 90 days after the last dose of tiragolumab, 1 month after the last dose of nap-paclitaxel, 6 months after the last dose of carboplatin or doxorubicin, or Abstinence should be maintained until the later of 12 months after the last dose of cyclophosphamide or a contraceptive method with a failure rate of <1% per year should be used. Women should refrain from donating eggs during the same period as above.
여성은 만약 비월경이고, 폐경후 상태(폐경 이외에 확인된 원인이 없는 (³ 12개월 연속 무월경)에 도달하지 못하였고, 외과적 불임 수술(난소 및/또는 자궁의 제거)을 받지 않았다면 임신 가능성이 있는 것으로 간주한다.A woman has no chance of becoming pregnant if she is non-menstrual, has not reached postmenopausal status (without confirmed cause (³ 12 consecutive months of amenorrhea) other than menopause, and has not undergone surgical sterilization (removal of the ovaries and/or uterus). considered to exist
지속적으로 정확하게 사용했을 때 매년 < 1%의 실패율을 보이는 피임법의 예는 배란 억제와 관련된 복합(에스트로겐 및 프로게스테론 함유) 호르몬 피임, 배란 억제와 관련된 프로게스테론 단독 호르몬 피임, 양측 난관 폐쇄; 남성 불임; 자궁 내 장치; 자궁내Examples of contraceptive methods that, when used correctly and consistently, have a failure rate of < 1% per year include combined (estrogen and progesterone-containing) hormonal contraception associated with ovulation inhibition, progesterone-only hormonal contraception associated with ovulation inhibition, bilateral tubal occlusion; male infertility; intrauterine device; intrauterine
호르몬 방출 시스템; 및 성적 금욕을 포함한다.hormone release system; and sexual abstinence.
성적 금욕의 신뢰성은 임상 연구의 지속기간 및 환자의 바람직한 및 일반 생활방식에 관련하여 평가해야 한다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical study and the desired and general lifestyle of the patient.
주기적 금욕(예컨대, 달력, 배란, 증상체온, 또는 배란후 방법) 및 회수는 피임의 허용가능한 방법이 아니다.Periodic abstinence (eg, calendar, ovulation, symptomatic body temperature, or postovulatory methods) and withdrawal are not acceptable methods of contraception.
연구 치료제 중단 후 임신을 원하는 여성은 화학요법 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료제를 개시하기 전에 난모세포 보존에 대한 조언을 구해야 한다.Women wishing to become pregnant after discontinuation of study treatment should seek advice on oocyte preservation prior to initiation of study treatment due to the potential for irreversible infertility due to chemotherapy treatment.
· 남성의 경우: 하기에 규정된 바와 같이, 금욕을 유지하거나(이성간 성교를 자제하거나) 또는 피임법을 이용하는 데 동의, 및 정자 기증의 자제하는 데 동의:For Men: Consent to maintain abstinence (abstain from heterosexual intercourse) or use contraceptive methods, and to refrain from donating sperm, as provided below:
가임기 여성 파트너 또는 임신한 여성 파트너와 함께, 치료 기간 동안 및 티라골루맙의 최종 투여 후 90일 동안, 또는 냅-파클리탁셀, 카보플라틴, 독소루비신, 또는 시클로포스파미드의 최종 투여 후 6개월 중 더 늦은 날짜 까지, 남성은 금욕을 유지하거나, 또는 실패율이 연간 < 1%인 추가적인 피임법을 사용해야 한다. 남성은 상기 동일한 기간 동안 정자 기증을 삼가야 한다.With a female partner of childbearing potential or a pregnant female partner, during treatment and for 90 days after the last dose of tiragolumab, or 6 months after the last dose of nap-paclitaxel, carboplatin, doxorubicin, or cyclophosphamide, whichever is more Until a later date, men must either maintain abstinence or use an additional method of contraception with a failure rate of < 1% per year. Men should refrain from donating sperm during the same period.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가되어야 한다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical trial and the patient's preferred daily lifestyle.
주기적 금욕(예컨대, 달력, 배란, 증상체온, 또는 배란후 방법) 및 회수는 피임의 허용가능한 방법이 아니다.Periodic abstinence (eg, calendar, ovulation, symptomatic body temperature, or postovulatory methods) and withdrawal are not acceptable methods of contraception.
연구 치료제 개시 후 아이를 갖기를 원하는 남성은 화학요법 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료제를 시작하기 전에 정자 보존에 대한 조언을 구해야 한다.Men wishing to have children after initiation of study treatment should seek advice on sperm conservation prior to initiating study treatment due to the potential for irreversible infertility due to chemotherapy treatment.
![]()
![]()
![]()
![]()
코호트 A의 환자는 연구 등록을 위해 하기의 암별 기준에 부합해야 한다:Patients in Cohort A must meet the following cancer-specific criteria for study enrollment:
![]()
![]()
![]()
![]()
HER2 음성은 지역 실험실 평가에 의해 하기 중 하나로 정의된다(Wolff et al. 2018): HER2 negative is defined as one of the following by local laboratory assessment (Wolff et al. 2018):
조직내 혼성화(ISH) 비증폭(HER2 대 CEP17의 비율 < 2.0 또는 단일 프로브 평균 HER2 유전자 복제 수 < 4 신호/세포), 또는 IHC 0 또는 IHC 1 +.Intra-tissue hybridization (ISH) unamplified (ratio of HER2 to CEP17 < 2.0 or single probe average number of HER2 gene copies < 4 signals/cell), or
ER 및 PgR 음성은 IHC 분석에 의해 결정된 바와 같이 호르몬 수용체를 발현하는 세포의 < 1%로 정의된다.ER and PgR negatives are defined as <1% of cells expressing hormone receptors as determined by IHC analysis.
![]()
![]()
재발되는 전이성 또는 국소 진행성 질병(해당되는 경우)에서 수득한 종양 샘플은 임상적으로 가능한 경우 제출해야 한다.Tumor samples obtained from recurrent metastatic or locally advanced disease (if applicable) should be submitted when clinically feasible.
파라핀 블록(바람직한) 또는 적어도 20개의 비염색 슬라이드의 대표적인 FFPE 종양 표본(보관 표본 또는 재발된 질병의 새로운 전처리 조직)Representative FFPE tumor specimens from paraffin blocks (preferred) or at least 20 unstained slides (archival specimens or fresh pretreated tissue from relapsed disease)
종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 우수해야 하며, 등록 전에 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이 PD-L1 발현에 대해 평가해야 하며, 양성은 중앙 실험실에서 측정한 임의의 강도의 PD-L1 발현 종양 침윤성 면역 세포가 차지하는 종양 면적의 ≥1%로 정의된다. 종양 조직이 PD-L1 발현에 대해 평가할 수 없는 환자는 적격이 아니다.Tumor tissue should be of good quality based on total and viable tumor content, and should be assessed for PD-L1 expression as determined using the Ventana (SP142) PD-L1 IHC assay prior to enrollment, with positivity being a central It is defined as ≧1% of the tumor area occupied by infiltrating immune cells expressing PD-L1-expressing tumors of any intensity measured in the laboratory. Patients whose tumor tissue cannot be assessed for PD-L1 expression are not eligible.
여러 종양 표본이 제출된 경우, 환자는 적어도 하나의 표본이 평가 가능하고 PD-L1 발현에 대해 양성인 경우 적격일 수 있다(조직이 보관 표본에서 유래했는지 또는 재발된 질병에서 유래했는지에 관계없이).If multiple tumor specimens are submitted, a patient may be eligible if at least one specimen is evaluable and positive for PD-L1 expression (regardless of whether the tissue is from archival specimens or from recurrent disease).
허용되는 샘플에는 심부 종양 조직에 대한 코어-바늘 생검(최소 3개 코어) 또는, 피부, 피하 또는 점막 병변에 대한 절제, 절개, 펀치 또는 겸자 생검이 포함된다.Acceptable samples include core-needle biopsies (minimum 3 cores) for deep tumor tissue, or excision, incision, punch or forceps biopsies for skin, subcutaneous or mucosal lesions.
파라핀 블록의 FFPE 종양 표본이 바람직하다.FFPE tumor specimens in paraffin blocks are preferred.
미세 바늘 흡입, 칫솔질, 흉막 삼출액의 세포 펠렛, 골 전이, 및 세척 샘플은 허용하지 않는다. 골 전이로부터의 종양 조직은 PD-L1 발현에 대해 평가할 수 없으므로 허용하지 않는다.Fine needle aspiration, brushing, cell pellets in pleural effusion, bone metastases, and wash samples are not permitted. Tumor tissue from bone metastases cannot be evaluated for PD-L1 expression and is therefore not acceptable.
![]()
![]()
전이성 질병에 대한 선행 방사선 요법은 허용하지 않는다. 방사선 요법에 필요한 최소 휴약 기간은 없다. 환자는 방사선의 영향에서 회복되어야 한다.Prior radiation therapy for metastatic disease is not permitted. There is no minimum washout period required for radiation therapy. The patient must recover from the effects of radiation.
신보조 또는 보조 치료 환경에서 선행 화학요법(탁산을 포함) 및/또는 CIT(항 PD-L1 또는 항 PD-1 제제만)는 연구 치료제 개시 전 ³ 12개월에 치료가 완료된 경우 허용한다.Prior chemotherapy (including taxanes) and/or CIT (anti-PD-L1 or anti-PD-1 agents only) in neoadjuvant or adjuvant treatment settings is permitted if treatment is completed ³ 12 months prior to initiation of study therapy.
![]()
![]()
이전에 방사선 조사된 병변은 방사선 조사 이후 해당 부위에서 질병 진행이 명백하게 기록된 경우에만 측정 가능한 질병으로 간주할 수 있다.Previously irradiated lesions can be considered measurable disease only if disease progression is clearly documented at the site after irradiation.
E.E. 배제 기준Exclusion Criteria
하기의 기준 중 임의의 것에 부합하는 환자는 연구 등록으로부터 배제한다:Patients meeting any of the following criteria are excluded from study enrollment:
![]()
![]()
가임 여성은 연구 치료제 개시 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다.Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
![]()
![]()
![]()
![]()
LVEF가 < 53%로 공지된 환자는 배제한다.Patients with known LVEF <53% are excluded.
상기 기준을 충족하지 않는 것으로 공지된 관상동맥 질환 또는 울혈성 심부전 환자.Patients with known coronary artery disease or congestive heart failure who do not meet the above criteria.
![]()
![]()
![]()
![]()
정기적인 항생제 예방(예컨대, 만성 폐쇄성 폐질환 악화 방지 또는 발치를 위해)을 받고 있는 환자가 적격이다.Patients receiving regular antibiotic prophylaxis (eg, to prevent exacerbation of chronic obstructive pulmonary disease or for tooth extraction) are eligible.
![]()
![]()
중심 정맥 접근 카테터(예컨대, 포트 또는 이와 유사한 것)의 배치는 주요 수술 절차로 간주되지 않으므로 허용한다.The placement of a central venous access catheter (eg, port or the like) is acceptable as it is not considered a major surgical procedure.
![]()
![]()
![]()
![]()
![]()
![]()
안정적인 용량의 갑상선 대체 호르몬에 대한 자가면역 매개 갑상선기능저하증의 병력이 있는 환자는 본 연구에 적격일 수 있다.Patients with a history of autoimmune-mediated hypothyroidism on stable doses of thyroid replacement hormone may be eligible for this study.
안정적인 인슐린 투약 요법으로 제1형 당뇨병이 조절된 환자는 본 연구에 적격이다.Patients with
습진, 건선, 만성 단순 태선 또는 피부과 증상만 있는 백반증(예컨대, 건선성 관절염 없음)이 있는 환자는 하기의 조건을 충족하는 경우 허용한다:Patients with eczema, psoriasis, chronic lichen simplex or vitiligo with only dermatological symptoms (eg, no psoriatic arthritis) are allowed if the following conditions are met:
- 발진이 체표면적의 < 10%를 차지함 - The rash occupies < 10% of the body surface area
- 질병이 기준선에서 잘 통제되고 낮은 역가의 국소 스테로이드만 필요함 - Disease is well controlled at baseline and requires only low titer topical steroids
- 지난 12개월 이내에 소랄렌에 더하여 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고효능 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았음- No acute exacerbation of an underlying condition requiring ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids in addition to psoralen within the past 12 months
- 이전에 다른 면역자극 항암제를 투여받는 동안 중증 또는 생명을 위협하는 피부 이상반응을 경험한 환자에게 아테졸리주맙을 고려할 때는 주의가 필요하다.- Caution should be exercised when considering atezolizumab in patients who have previously experienced severe or life-threatening skin adverse reactions while receiving other immunostimulatory anticancer drugs.
![]()
![]()
![]()
![]()
방사선 분야에서 방사선 폐렴(섬유증) 병력은 허용한다.A history of radiation pneumonitis (fibrosis) in the field of radiation is acceptable.
![]()
![]()
EBV 중합효소연쇄반응(PCR) 검사는 활동성 감염 또는 의심되는 만성 활동성 감염을 선별하기 위해 임상적으로 지시된 대로 실시해야 한다.EBV polymerase chain reaction (PCR) testing should be performed as clinically indicated to screen for active or suspected chronic active infection.
EBV PCR 검사가 양성인 환자는 제외한다.Patients with a positive EBV PCR test are excluded.
![]()
![]()
![]()
![]()
환자는 연구 치료제의 개시 전 28일 이내에, 치료 동안, 또는 연구 치료제의 최종 용량 투여 후 5개월 이내에 독성 약화 생백신(예컨대, 플루미스트®)을 제공받지 않는 데에 동의해야 한다.Patients must agree not to receive a live, attenuated vaccine (eg, Flumist ® ) within 28 days prior to initiation of study treatment, during treatment, or within 5 months after administration of the last dose of study treatment.
![]()
![]()
![]()
![]()
![]()
![]()
덱사메타손, 아자티오프린, 메토트렉세이트, 탈리도마이드 및 항종양 괴사 인자[항 TNF] 제제를 포함하지만 이에 제한되지는 않음)를 이용한 치료, 또는 연구 중 전신 면역억제제가 필요할 것으로 예상되는 경우treatment with, but not limited to, dexamethasone, azathioprine, methotrexate, thalidomide, and anti-tumor necrosis factor [anti-TNF] agents, or when systemic immunosuppressants are expected to be required during the study
급성, 저용량, 전신 면역억제제(예컨대, 메스꺼움으로 덱사메타손 1회 용량)를 받은 환자는 본 연구에 등록할 수 있다.Patients receiving acute, low-dose, systemic immunosuppressants (eg, single dose of dexamethasone for nausea) can be enrolled in this study.
스테로이드 전처리가 필요한 IV 조영제에 알레르기 반응의 병력이 있는 환자는 자기공명영상(MRI)을 사용하여 기준선 및 후속 종양 평가를 실시해야 한다.Patients with a history of allergic reactions to IV contrast media requiring steroid pretreatment should have baseline and follow-up tumor assessments using magnetic resonance imaging (MRI).
만성 폐쇄성 폐질환에 흡입 코르티코스테로이드, 기립성 저혈압 환자에 미네랄 코르티코이드(예컨대, 플루드로코르티손), 부신피질 기능 부전에 저용량 보조 코르티코스테로이드를 사용할 수 있다.Inhaled corticosteroids for chronic obstructive pulmonary disease, mineralocorticoids (eg, fludrocortisone) for patients with orthostatic hypotension, and low-dose adjuvant corticosteroids for adrenal insufficiency may be used.
하기의 배제 기준 중 임의의 것에 부합하는 코호트 A의 환자는 연구 등록에서 배제한다:Patients in Cohort A who meet any of the following exclusion criteria are excluded from study enrollment:
![]()
![]()
![]()
![]()
![]()
![]()
- 천막상 및 소뇌 전이만 허용됨(즉, 중뇌, 교뇌, 수질 또는 척수로의 전이 없음) -Only supratentorial and cerebellar metastases are allowed (i.e. no metastases to the midbrain, pons, medulla or spinal cord)
- CNS 질병에 대한 요법으로서 지속적인 코르티코스테로이드 필요성 없음 - No need for continuous corticosteroids as therapy for CNS disease
- 연구 치료제 개시 전 7일 이내에 정위적 방사선 조사 또는 14일 이내에 전뇌 방사선 조사 없음- No stereotactic irradiation within 7 days or whole brain irradiation within 14 days prior to initiation of study treatment
- CNS 지시 요법의 완료시 및 선별 검사 방사선촬영 연구 사이의 중간 진행에 대한 증거 없음 - No evidence of intermediate progression between completion of CNS-directed therapy and screening radiographic studies
비고: 선별검사 스캔에서 새로운 무증상 CNS 전이가 검출된 환자는 CNS 전이에 대한 방사선요법 및/또는 수술을 받아야 한다. 치료 후, 상기 환자는 다른 모든 기준이 충족되는 경우, 등록 전 추가 뇌 스캔의 필요없이 적격일 수 있다.Note: Patients with new asymptomatic CNS metastases detected on screening scans should receive radiotherapy and/or surgery for CNS metastases. After treatment, the patient may be eligible without the need for an additional brain scan prior to enrollment if all other criteria are met.
![]()
![]()
![]()
![]()
유치 카테터(예컨대, PLEURX®)를 장착한 환자는 허용한다.Patients with indwelling catheters (eg PLEURX ® ) are permitted.
![]()
![]()
마약성 진통제가 필요한 환자는 연구 시작시 안정 요법 중에 있어야 한다.Patients requiring opioid analgesia should be on stable therapy at the start of the study.
완화 방사선 요법으로 치료할 수 있는 증상이 있는 병변(예컨대, 골 전이 또는 신경 충돌을 유발하는 전이)은 등록 전에 치료해야 한다. 환자는 방사선의 영향에서 회복되어야 함. 환자는 방사선의 영향에서 회복되어야 함.Symptomatic lesions that can be treated with palliative radiation therapy (eg, bone metastases or metastases causing nerve impingement) should be treated prior to enrollment. The patient must recover from the effects of radiation. The patient must recover from the effects of radiation.
추가 성장이 기능성 결손 또는 난치성 통증(예컨대, 척수 압축과 현재 관련되지 않은 경막외 전이)을 유발할 수 있는 무증상 전이성 병변은 등록 전에 적절한 경우 국소 영역 요법에 대해 고려해야 한다.Asymptomatic metastatic lesions where further growth may result in functional deficits or refractory pain (eg, epidural metastases not currently associated with spinal cord compression) should be considered for local area therapy where appropriate prior to enrollment.
제어되지않는 고칼슘혈증(>1.5 mmol/L의 이온화 칼슘 또는 Ca+2 >12 mg/dL 또는 ULN 초과의 교정된 혈청 칼슘) 또는 지속적 비스포스포네이트 요법 사용을 요하는 증상이 있는 고칼슘혈증Uncontrolled hypercalcemia (>1.5 mmol/L ionized calcium or Ca+2 >12 mg/dL or corrected serum calcium >ULN) or symptomatic hypercalcemia requiring the use of continuous bisphosphonate therapy
특히 골격 사건을 예방하기 위해 비스포스포네이트 요법을 받고 있고 임상적으로 유의한 고칼슘혈증의 이력이 없는 환자가 적격이다.In particular, patients receiving bisphosphonate therapy to prevent skeletal events and without a history of clinically significant hypercalcemia are eligible.
![]()
![]()
![]()
![]()
F.F. 분석analysis
안전성 분석은 모든 환자에게서 실시한다.A safety analysis is performed in all patients.
유효성 분석은 코호트 A 및 코호트 B에 대해 ITT 접근 방식을 사용하며, 여기서 환자가 할당된 연구 약물을 투여 받는지 여부에 관계없이 등록된 모든 환자가 분석에 포함된다. ITT 모집단의 하위 집합을 기반으로 한 분석도 실시할 수 있다.The efficacy analysis uses an ITT approach for Cohort A and Cohort B, where all enrolled patients are included in the analysis, regardless of whether the patient is receiving the assigned study drug. Analyzes based on subsets of the ITT population may also be performed.
가설 분석은 달리 명시되지 않는 한 양측이다. Hypothesis analysis is two-sided unless otherwise specified.
표본 크기sample size
코호트 A의 목적은 객관적 반응으로 정의되는 1차 유효성 평가변수에 대하여 아테졸리주맙 및 냅-파클리탁셀과 병용한 티라골루맙의 효과를 추정하는 것이다. 과거 데이터와 비교할 때, 반응 비율은 향후 개발에 대해 유망하거나 유망하지 않은 것으로 간주된다. 공식적인 가설 분석은 없다. 통계는 양측 90% CI로 표시된다. 개발을 계속하거나 중단하도록 권고할 때, PFS, OS 및 하위군에 대한 분석 결과를 포함하지만 이에 제한되지는 않는 2차 유효성 평가변수에 대한 결과를 포함하여 데이터의 전체를 고려한다.The objective of Cohort A is to estimate the effect of tiragolumab in combination with atezolizumab and nap-paclitaxel on the primary efficacy endpoint defined as objective response. Compared with historical data, response rates are considered promising or not promising for future development. There is no formal hypothesis analysis. Statistics are presented as two-sided 90% CI. When making recommendations to continue or discontinue development, consider the entirety of the data, including results for secondary efficacy endpoints, including, but not limited to, analysis results for PFS, OS, and subgroups.
1차 유효성 분석은 CR 또는 PR(즉, ORR)을 수득할 것으로 예상되는 환자의 실제 비율을 추정하는 것이다. 유사한 질병 환경에서 완료되고 진행 중인 연구로부터의 데이터를 비교를 위한 과거 대조군으로서 사용할 수 있다. 현재 입수 가능한 데이터에 따르면, 국소 진행성 절제 불가능 또는 전이성 PD-L1 양성 TNBC에서 확인된 과거 반응률은 약 53%(티센트릭(TECENTRIQ)® 미국 패키지 인서트(U.S. Package Insert))이다.The primary efficacy analysis is to estimate the actual proportion of patients expected to obtain a CR or PR (ie, ORR). Data from completed and ongoing studies in similar disease settings can be used as historical controls for comparison. Based on currently available data, the confirmed historical response rate in locally advanced unresectable or metastatic PD-L1-positive TNBC is approximately 53% ( TECENTRIQ® US Package Insert).
40명의 환자 표본 크기는 양측 90% CI의 하한치 및 점 추정치에 대한 적절한 정밀도를 제공하여, 67.5%의 관찰된 반응률을 가정할 때 < 53%의 임상적으로 관심대상이 아닌 반응 확률을 배제하기에 충분한 것으로 간주한다. 구체적으로, 40명의 환자 중 적어도 27명이 반응을 보인다면, 상기 반응률이 53% 초과라고 결론지을 수 있다. 반응을 달성할 것으로 예상되는 환자 비율의 갱시된 추정치는 유효성 분석 시점까지 진행 중인 연구로부터 입수 가능할 것으로 예상되며 참조 데이터로 사용한다.The 40 patient sample size provides adequate precision for the lower bound and point estimates of the two-sided 90% CI, to rule out a probability of a response that is not clinically of interest of <53%, assuming an observed response rate of 67.5%. considered sufficient. Specifically, if at least 27 out of 40 patients respond, it can be concluded that the response rate is greater than 53%. Updated estimates of the proportion of patients expected to achieve a response are expected to be available from ongoing studies up to the time of efficacy analysis and serve as reference data.
표 26은 40명의 환자 표본을 기반으로 하여 관찰된 비율 범위에 대해 반응을 달성할 실제 확률에 대한 양측 90% 클로퍼-피어슨의 정확한 CI를 나열한다. 다양한 임계값에서 관찰된 ORR의 점 추정치 및 기본적인 실제 ORR을 기반으로 하는 양성 및 음성 신호를 검출할 확률이 표 27 및 표 28에 제시되어 있다.Table 26 lists the two-tailed 90% Klopper-Pearson's exact CIs for the true probability of achieving a response for the observed range of rates, based on a sample of 40 patients. The probabilities of detecting positive and negative signals based on point estimates of the observed ORR at various thresholds and the underlying true ORR are presented in Tables 27 and 28.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
반응을 달성할 실제 확률에 대한 양측 클로퍼-피어슨 정확한 신뢰 구간Two-tailed Clopper-Pearson exact confidence intervals for the true probability of achieving a response
양성 신호를 나타낼 확률(선택한 임계값 이상의 관찰된 ORR)Probability of showing a positive signal (observed ORR above the selected threshold)
음성 신호를 나타낼 확률(선택한 임계값 미만의 관찰된 ORR)Probability of presenting a negative signal (observed ORR below the selected threshold)
안전성 분석Safety analysis
안전성 평가에는 연구의 안전성 평가에 중요하다고 간주되는 이상 반응의 발생률, 특성 및 중증도, 프로토콜-필수 활력 징후, 실험실 이상 및 기타 프로토콜 지정 검사가 포함된다. 이상 반응은 NCI CTCAE v5.0에 따라 등급화된다.Safety assessments include the incidence, nature and severity of adverse events, protocol-essential vital signs, laboratory abnormalities, and other protocol-specific tests considered important for the safety assessment of the study. Adverse events are graded according to NCI CTCAE v5.0.
안전성은 ADA에 의해 측정된 이상 반응, 실험실 시험 결과의 변화, 활력 징후의 변화, 연구 치료제 노출, 면역원성의 요약을 통해 평가하고 치료군에서 제시된다.Safety is assessed by ADA-measured adverse events, changes in laboratory test results, changes in vital signs, exposure to study treatment, and summary of immunogenicity and presented in treatment groups.
이상 반응에 대한 축어적 설명은 MedDRA 용어에 매핑된다.Verbose descriptions of adverse events are mapped to MedDRA terminology.
치료 응급 반응(연구 치료제의 제1 용량 또는 이후에 발생하는 반응으로 정의됨)은 시험자가 평가한 연구 약물과의 관계에 상관없이 MedDRA 용어, 적절한 MedDRA 수준 및 NCI CTCAE v5.0 등급으로 요약된다. 각 환자에 대해 동일한 이상 반응이 여러 번 발생하는 경우, 보고된 최대 중증도가 요약에 사용된다.Treatment emergency response (defined as a response that occurs at or after the first dose of study treatment) is summarized in MedDRA terminology, appropriate MedDRA level, and NCI CTCAE v5.0 grade, regardless of relationship to investigator-assessed study drug. If the same adverse event occurs multiple times for each patient, the maximum reported severity is used for the summary.
하기와 치료 관련 이상 반응은 별도로 요약된다: 연구 약물 중단으로 이어지는 이상 반응, 용량 감소 또는 중단으로 이어지는 이상 반응, 등급 3의 이상 반응, 등급 5의 이상 반응, 심각한 이상 반응, 및 특별한 관심의 이상 반응.The following and treatment-related adverse events are summarized separately: Adverse Events Leading to Study Drug Discontinuation, Adverse Events Leading to Dose Reduction or Discontinuation,
모든 사망 및 사망 원인이 요약되어 있다.All deaths and causes of death are summarized.
관련 실험실 값은 적절한 경우 식별된 NCI CTCAE 등급 3 및 등급 4 값과 함께 시점별로 요약된다. NCI CTCAE 등급 변화를 치료군 별로 표로 작성한다.Relevant laboratory values are summarized by time point, along with identified
노출, 이상반응, 실험실 및 활력징후 데이터 분석Analysis of exposure, adverse events, laboratory and vital signs data
안전성은 연구 치료제에 대한 노출, 이상 반응, 실험실 시험 결과의 변화, 및 활력 징후 및 ECG의 변화에 Safety depends on exposure to study treatment, adverse events, changes in laboratory test results, and changes in vital signs and ECGs.
대한 요약을 통해 평가한다.Evaluate through a summary.
연구 치료제 노출(예컨대, 치료 기간, 투여 받은 총 용량, 및 주기 및 용량 변경의 횟수)은 기술적 통계와 함께 요약된다.Study treatment exposures (eg, duration of treatment, total dose administered, and number of cycles and dose changes) are summarized along with descriptive statistics.
이상 반응의 축어적 용어는MedDRA의 유의어 용어에 대응되며, 이상 반응의 중증도는 NCI CTCAE v5.0에 따라 등급이 매겨진다. 모든 이상 반응, 중증 이상 반응, 사망으로 이어지는 이상 반응, 특별한 관심의 이상 반응, 및 연구 치료제의 제1 용량 투여 시 또는 그 이후에 발생하는 연구 치료제 중단으로 이어지는 이상 반응(즉, 치료 관련 이상 반응)이 매핑된 용어, 적절한 유의어 수준 및 중증도 등급에 따라 요약된다. 가변적인 중증도를 가진 반응의 경우, 해당 요약에서 가장 높은 등급이 사용된다. 사망 및 사망 원인이 요약되어 있다.Verbose terms of adverse events correspond to synonymous terms in MedDRA, and the severity of adverse events is graded according to NCI CTCAE v5.0. All adverse events, serious adverse events, adverse events leading to death, adverse events of particular interest, and adverse events leading to discontinuation of study treatment (i.e., treatment-related adverse events) occurring at or after administration of the first dose of study treatment These are summarized according to the mapped terms, appropriate synonym levels, and severity ratings. For reactions of variable severity, the highest rating in that summary is used. Deaths and causes of death are summarized.
관련 실험실, 활력징후(맥박수, 호흡수, 혈압, 맥박 산소 측정, 및 체온) 및 ECG 데이터가 시간별로 표시되며, 적절한 경우 등급으로 식별된다. 또한, 선택된 실험실 시험의 변화표는 기준선 및 기준선 이후 최대 중증도 등급을 요약하는 데 사용한다. 활력 징후 및 ECG의 변화가 요약되어 있다.Relevant laboratory, vital signs (pulse rate, respiration rate, blood pressure, pulse oximetry, and body temperature) and ECG data are displayed hourly and identified by grade, where appropriate. In addition, tables of changes from selected laboratory tests are used to summarize baseline and post-baseline maximum severity ratings. Changes in vital signs and ECG are summarized.
유효성 분석Validity analysis
1차 유효성 목표Primary effectiveness goal
코호트 A에 대한 1차 유효성 목표는 하기의 평가변수를 기반으로 아테졸리주맙 및 냅-파클리탁셀과 병용한 티라골루맙의 유효성을 평가하는 것이다.The primary efficacy objective for Cohort A is to evaluate the efficacy of tiragolumab in combination with atezolizumab and nap-paclitaxel based on the following endpoints.
![]()
![]()
PR 또는 CR에 대한 확인이 필요하다. 기준선 이후 종양 평가가 없는 환자를 포함하여 상기 기준을 충족하지 않는 환자는 무반응자로 간주한다. ORR은 객관적인 반응을 보이는 환자의 비율로 정의한다.Confirmation of PR or CR is required. Patients who do not meet the above criteria, including those without a post-baseline tumor assessment, are considered non-responders. ORR is defined as the proportion of patients with an objective response.
일단 모든 환자가 적어도 2회의 종양 평가를 받은 후, 유효성 데이터를 가장 먼저 검토한다.Once all patients have undergone at least two tumor assessments, efficacy data are reviewed first.
2차 유효성 목표secondary effectiveness goal
코호트 A에 대한 2차 유효성 목표는 하기의 평가변수를 기반으로 아테졸리주맙 및 냅-파클리탁셀과 병용한 티라골루맙의 유효성에 대한 사전 데이터를 수득하는 것이다.The secondary efficacy goal for Cohort A is to obtain prior data on the efficacy of tiragolumab in combination with atezolizumab and nap-paclitaxel based on the following endpoints.
![]()
![]()
질병 진행을 경험하지 않았거나 사망한 환자에 대한 데이터는 해당 각각의 분석에 대한 임상 마감일 이전 또는 당일에 생존 및 무진행인 것으로 최종 공지된 일자에 중도절단된다. 기준선 이후 정보가 없는 환자는 등록 일자에 중도절단된다.Data for patients who did not experience disease progression or who died are censored on the last known date of survival and progression-free before or on the same day as the clinical deadline for that respective analysis. Patients without post-baseline information are censored on the enrollment date.
![]()
![]()
질병 진행을 경험하지 않았거나 사망한 환자에 대한 데이터는 마지막 종양 평가 일자에 중도절단된다. CR 또는 PR이 처음 발생한 일자 이후에 종양 평가가 실시되지 않으면, DOR에 대한 데이타는 CR 또는 PR이 처음 발생한 일자에 중도절단된다.Data for patients who have not experienced disease progression or who have died are censored on the date of last tumor evaluation. If no tumor evaluation is performed after the date of first occurrence of CR or PR, data for DOR is censored on the date of first occurrence of CR or PR.
![]()
![]()
분석시 사망한 것으로 보고되지 않은 환자는 마지막으로 생존이 확인된 일자에 중도절단된다. 기준선 이후 정보가 없는 환자는 등록 일자에 중도절단된다.Patients not reported to have died at the time of analysis are censored on the date of the last known survival. Patients without post-baseline information are censored on the enrollment date.
약동학 분석Pharmacokinetic analysis
PK 분석을 위해 샘플을 수집하고 본 연구의 노출을 이전 연구에서 수득한 노출과 비교한다. 티라골루맙 및 아테졸리주맙의 혈청 농도 및 냅-파클리탁셀, 카보플라틴, 독소루비신 및 시클로포스파미드의 혈장 농도는 개별 값으로 보고하고, 적절하고 데이터가 허용하는 한 치료군 및 주기별로 요약(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균, 및 기하 평균 변동 계수)할 수 있다.Samples are collected for PK analysis and exposures in this study are compared with exposures obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab and plasma concentrations of nap-paclitaxel, carboplatin, doxorubicin and cyclophosphamide are reported as individual values and summarized by treatment group and cycle (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean coefficient of variation).
개별 및 중앙값 혈청 티라골루맙 및 아테졸리주맙 농도는 치료군 및 일별로 플롯팅된다. 티라골루맙 및 아테졸리주맙 농도 데이터는 데이타에 의해 보장되는 바와 같이 청소율, 분포 용적, 및 AUC와 같은 PK 매개변수를 도출하기 위해 확립된 모집단 PK 모델을 사용하는 다른 연구로부터의 데이터와 통합할 수 있다. 용량, 안전성, 유효성 또는 바이오마커 결과와 관련된 PK 매개변수의 잠재적 상관관계를 조사할 수 있다.Individual and median serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be integrated with data from other studies that use established population PK models to derive PK parameters such as clearance, volume of distribution, and AUC as warranted by the data. have. Potential correlations of PK parameters with dose, safety, efficacy, or biomarker outcomes can be investigated.
면역원성 분석Immunogenicity assay
면역원성 분석에는 임의의 ADA 평가를 받은 환자가 포함되며, 환자는 투여받은 치료에 따라 분류한다. 치료 및 추적 기간 동안 치료 응급 ADA 양성 환자 및 ADA 음성 환자의 수 및 비율은 치료군별로 요약한다.Immunogenicity assays include patients undergoing any ADA assessment, and patients are classified according to treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients during the treatment and follow-up period will be summarized by treatment group.
ADA 상태와, 안전성, 유효성, 및 PK 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고할 수 있다.The relationship between ADA status and safety, efficacy, and PK endpoints can be analyzed and reported through descriptive statistics.
바이오마커 분석Biomarker analysis
탐색적 바이오마커에 대한 공식적인 통계 분석은 실시되지 않지만, 데이터는 본 연구의 맥락에서 그리고 다른 연구의 데이터와 통합하여 분석될 수 있다.Although no formal statistical analysis of exploratory biomarkers is performed, the data can be analyzed in the context of this study and in conjunction with data from other studies.
실시예 4. 국소 진행성 또는 전이성 종양을 가진 환자를 대상으로 단일 제제로서 및 아테졸리주맙 및/또는 기타 항암 요법과 병용한 티라골루맙의 안전성 및 약동학에 관한 제Ia/Ib상, 공개 라벨, 용량 증량 연구Example 4. Phase Ia/Ib, Open Label, Dosage Regarding the Safety and Pharmacokinetics of Tiragolumab as a Single Agent and in Combination with Atezolizumab and/or Other Anticancer Therapies in Patients with Locally Advanced or Metastatic Tumors incremental study
본 실시예는 하기를 평가하도록 설계된 인간을 대상으로 한 최초의 1상, 공개 라벨, 다기관, 글로벌, 용량 증량 연구를 설명한다:This example describes the
(Ia상) 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나, 또는 이에 대해 임상 시험용 제제의 임상 시험이 인정된 치료의 표준인, 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자에게서 단일 제제로서 티라골루맙의 안전성, 내약성, 및 PK; 및(Phase Ia) Locally progressive, recurrent, for which no standard therapy exists, has proven ineffective or intolerable, or has been deemed inappropriate, or for which clinical trials of investigational agents are the accepted standard of care. , or the safety, tolerability, and PK of tiragolumab as a single agent in patients with metastatic refractory tumors; and
(Ib상) 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되는 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자; 또는 이에 대한 임상 시험용 제제의 임상 시험이 인정된 치료의 표준이거나 이에 대해 항 PD-L1 항체를 병용한 임상 시험용 제제의 임상 시험이 허용가능한 치료 선택사항으로 간주되는 환자를 대상으로 치료 표준 요법과 병용으로 투여될 때 티라골루맙의 안전성, 내약성, 및 PK.(Phase Ib) patients with locally advanced, recurrent, or metastatic refractory tumors for which standard therapy has not been available, has proven ineffective, intolerable, or deemed inappropriate; or in combination with standard of care in patients for whom clinical trials of an investigational product are considered the accepted standard of care, or for which clinical trials of an investigational product using anti-PD-L1 antibodies are considered an acceptable treatment option. Safety, tolerability, and PK of tiragolumab when administered as
A. 연구 설계A. Study Design
이는 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나, 또는 이에 대해 임상 시험용 제제의 임상 시험이 인정된 치료 표준인, 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자에게서 단일 제제로서 티라골루맙의 안전성, 내약성, 및 약동학을 평가하도록 설계된 인간을 대상으로 한 최초의 1상, 공개 라벨, 다기관, 글로벌, 용량 증량 연구이다. 이는 연구의 Ia상 부분에서 평가한다.It is locally advanced, relapsing, or metastatic refractory for which standard therapy does not exist, has proven ineffective or intolerable, is deemed inappropriate, or for which clinical trials of investigational agents are the accepted standard of care. This is the
본 연구는 또한 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되는 국소 진행성, 재발성, 또는 전이성 난치성 종양을 가진 환자; 또는 이에 대한 임상 시험용 제제의 임상 시험이 인정된 치료의 표준이거나 이에 대해 항 PD-L1 항체를 병용한 임상 시험용 제제의 임상 시험이 허용가능한 치료 선택사항으로 간주되는 환자를 대상으로 치료 표준 요법과 병용으로 투여될 때 티라골루맙의 안전성, 내약성, 및 PK에 대한 평가를 가능하게 하도록 설계되었다. 이는 연구의 Ib상 부분의 다중 코호트에서 연구한다.This study also included patients with locally advanced, recurrent, or metastatic refractory tumors for which standard therapy did not exist, demonstrated ineffective or intolerable, or considered inappropriate; or in combination with standard of care in patients for whom clinical trials of an investigational product are considered the accepted standard of care, or for which clinical trials of an investigational product using anti-PD-L1 antibodies are considered an acceptable treatment option. designed to enable evaluation of the safety, tolerability, and PK of tiragolumab when administered as It is studied in multiple cohorts of the Phase Ib portion of the study.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
본 연구의 Ib상 부분은 단일 제제 티라골루맙의 적어도 2회 용량 수준에 대한 DLT 평가가 완료되고 모든 관련 단일 제제 안전성 데이터가 시험자 및 IMC와 함께 철저히 검토된 후 활성화된다. 적절하다고 판단되는 경우, Ib상 부분은 Ia상 부분에서와 동일한 용량 증량 계획 및 포괄적인 안전성 모니터링 계획을 사용하여 초기 티라골루맙 용량 수준 이하의 용량 수준에서 시작한다. 또한, 단일 제제 티라골루맙으로 연구의 Ia상 부분을 진행하는 환자는 연구의 Ib상 부분으로 전환될 수 있는 선택사항이 제공될 수 있다.The Phase Ib portion of this study will be activated after DLT assessments for at least two dose levels of single agent tyragolumab have been completed and all relevant single agent safety data have been thoroughly reviewed with the investigator and IMC. When deemed appropriate, the Phase Ib portion will be initiated at a dose level below the initial tiragolumab dose level using the same dose escalation plan and comprehensive safety monitoring plan as in the Phase Ia portion. In addition, patients undergoing the Phase Ia portion of the study with single agent tiragolumab may be offered the option to transition to the Phase Ib portion of the study.
연구의 Ia상 및 Ib상 부분은 모두 선별검사 기간, 치료 기간 및 치료 후 추적 기간으로 구성된다. 환자는 2가지 단계인 용량 증량 단계 및 용량 확장 단계에서 등록한다; Ia상 및 Ib상에 대하여 도 3 및 도 4를 참조한다. 도 4는 연속 생검 및 Q4W 코호트를 추가로 도시하는 반면, 도 5는 Ib상 화학요법 확장 코호트를 도시하고, 도 6은 Ib상 비화학요법 확장 코호트를 도시한다. 용량 증량 단계 동안, 각각 약 3~6명의 환자로 이루어진 코호트를 증량 용량 수준에서 평가하여 단일 제제로서 또는 아테졸리주맙과 병용한 티라골루맙에 대한 MTD 또는 최대 투여 용량(MAD)을 결정한다. 확장 코호트에 대한 용량 선택을 보다 충분히 알리도록 추가 안전성 및 약력학 데이터를 획득하기 위해, 하기에 기재된 용량 증량 기준에 따라 관련 MTD를 초과하지 않는 것으로 나타난 용량 수준에서 추가 환자를 코호트 보충을 위해 등록할 수 있다. 용량 증량 결정의 목적으로, 상기 환자는 DLT 평가가능 모집단의 일부로서 포함되지 않는다.Both the Phase Ia and Ib portions of the study consist of a screening period, a treatment period, and a post-treatment follow-up period. Patients are enrolled in two phases, a dose escalation phase and a dose expansion phase; See Figures 3 and 4 for phase Ia and Ib. Figure 4 further depicts serial biopsies and Q4W cohorts, while Figure 5 depicts the Phase Ib chemotherapy expansion cohort and Figure 6 depicts the Phase Ib non-chemotherapy expansion cohort. During the dose escalation phase, cohorts of approximately 3 to 6 patients each are evaluated at the escalating dose level to determine the MTD or maximum administered dose (MAD) for tiragolumab as a single agent or in combination with atezolizumab. To obtain additional safety and pharmacodynamic data to more fully inform dose selection for the expansion cohort, additional patients may be enrolled for cohort replenishment at dose levels shown not to exceed the relevant MTD according to the dose escalation criteria described below. have. For purposes of dose escalation decisions, the patient is not included as part of the DLT evaluable population.
용량 확장 단계에서, 환자는 단일 제제로서(Ia상), 또는 아테졸리주맙 및/또는 다른 항암 요법과 병용한(Ib상) 티라골루맙의 MTD 또는 MAD 이하로 등록 및 치료한다.In the dose expansion phase, patients are enrolled and treated below the MTD or MAD of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab and/or other anticancer therapies (Phase Ib).
단일 제제로서의 티라골루맙(Ia상), 또는 티라골루맙 및 아테졸리주맙, 티라골루맙 및 아테졸리주맙과 베바시주맙의 조합, 또는 티라골루맙과 펨브롤리주맙(화학요법이 없는 Ib상 코호트)은 각 21일 주기의 제 1일에 및 각 28일 주기의 제 1일에(Ib상 Q4W 투여 확장) IV 주입으로 투여한다. 티라골루맙은 화학요법 없이 Ib상 코호트에서 아테졸리주맙, 베바시주맙 또는 펨브롤리주맙보다 먼저 투여한다. 허용할 수 없는 독성이 없거나 질병 진행에 대한 임상적으로 강력한 증거가 없는 경우, 시험자의 이익 및 위험에 대한 유리한 평가에 기초하여 티라골루맙(Ia상) 또는 아테졸리주맙 및/또는 다른 항암 요법과 병용한 티라골루맙(Ib상)을 이용한 치료는 주기 1 이후에도 계속할 수 있다.Tiragolumab as a single agent (Phase Ia), or a combination of Tiragolumab and Atezolizumab, Tiragolumab and Atezolizumab and Bevacizumab, or Tiragolumab and Pembrolizumab (Phase Ib cohort without chemotherapy) ) are administered by IV infusion on
Ib상 화학요법 및 비화학요법 확장 코호트와 Ib상 Q4W 투약 확장 코호트에서 3명의 환자에 대한 안전성 탐색이 완료되었다. 안전성 탐색의 모든 관련 안전 데이터는 등록을 계속하기 전에 IMC 및 시험자가 철저히 검토한다.A safety investigation of 3 patients was completed in the Phase Ib chemotherapy and non-chemotherapy expansion cohorts and in the Phase Ib Q4W dosing expansion cohort. All relevant safety data from the safety search will be thoroughly reviewed by the IMC and investigators prior to continuing registration.
티라골루맙 및 아테졸리주맙은 4가지 화학요법 확장 코호트 각각에서 특정 화학요법과 병용된다: 코호트 A에서 카보플라틴 또는 시스플라틴 및 페메트렉시드, 코호트 B에서 카보플라틴 및 파클리탁셀, 코호트 C에서 카보플라틴 또는 시스플라틴 및 에토포시드, 코호트 D에서 카페시타빈. 코호트 A, B, 및 C에서, 치료는 유도기 및 유지기로 구성된다. 상기 유도기에서, 화학요법을 병용한 티라골루맙 및 아테졸리주맙의 조합은 코호트 A 및 코호트 B에 대해 4회 내지 6회 주기 동안 및 코호트 C에 대해 4회 주기 동안 21일 주기로 IV 주입을 통해 투여한다. 코호토 A 및 코호트 B에 대한 유도 치료 주기의 횟수는 시험자의 재량에 따라 결정된다. Tiragolumab and atezolizumab in combination with specific chemotherapy in each of the four chemotherapy expansion cohorts: carboplatin or cisplatin and pemetrexed in Cohort A, carboplatin and paclitaxel in Cohort B, and carbople in Cohort C Latin or cisplatin and etoposide, capecitabine in cohort D. In cohorts A, B, and C, treatment consists of an induction phase and a maintenance phase. In the induction phase, the combination of tiragolumab and atezolizumab in combination with chemotherapy is administered via IV infusion at 21 day cycles for 4 to 6 cycles for Cohort A and B and 4 cycles for Cohort C. do. The number of induction treatment cycles for Cohort A and Cohort B is at the discretion of the investigator.
상기 유도기 후에, 질병 진행이나 허용할 수 없는 독성을 경험하지 않은 환자는 유지 요법으로 치료를 계속한다. 상기 유지기 동안, 코호트 B 및 코호트 C의 환자는 티라골루맙 및 아테졸리주맙만 계속 투여받는 반면, 코호트 A의 환자는 페메트렉시드와 함께 티라골루맙 및 아테졸리주맙을 계속 투여한다. After the induction phase, patients who have not experienced disease progression or unacceptable toxicity continue treatment with maintenance therapy. During this maintenance phase, patients in Cohort B and Cohort C continue to receive tiragolumab and atezolizumab alone, while patients in Cohort A continue to receive tiragolumab and atezolizumab in combination with pemetrexed.
상기 유지기에서, 코호트 A는 아테졸리주맙, 티라골루맙 및 페메트렉시드를 사용하여 21일 주기로 계속한다. 코호트 B에서, 프로토콜 GO30103 버전 4에 등록한 환자는 아테졸리주맙 및 티라골루맙으로 21일 주기를 계속한다. 코호트 B에서, 프로토콜 GO30103 버전 5 이상에 등록한 환자는 아테졸리주맙 및 티라골루맙으로 28일 주기를 시작한다. 코호트 C는 아테졸리주맙과 티라골루맙으로 28일 주기를 시작한다.In this maintenance phase, Cohort A continues with a 21-day cycle with atezolizumab, tiragolumab and pemetrexed. In Cohort B, patients enrolled in
코호트 D에서, 환자는 시험자가 결정한 대로 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 티라골루맙, 아테졸리주맙 및 카페시타빈으로 치료를 받는다. 환자는 각 21일 주기의 제 1일부터 14일까지 1일 2회(BID) 1250 mg/m2의 용량으로 카페시타빈을 경구 투여받는다. 주기 1의 1일에 카페시타빈의 제1 용량은 아테졸리주맙 및 티라골루맙 주입 전에 병원에서 투여한다. 티라골루맙 및 아테졸리주맙의 조합은 21일 주기로 IV 주입으로 투여한다. In Cohort D, patients are treated with tiragolumab, atezolizumab and capecitabine until unacceptable toxicity or loss of clinical benefit as determined by the investigator. Patients are orally administered capecitabine at a dose of 1250 mg/m 2 twice daily (BID) from
모든 화학요법 확장 코호트에서, 아테졸리주맙은 티라골루맙보다 먼저 투여한다.In all chemotherapy expansion cohorts, atezolizumab is administered before tiragolumab.
연구 전반에 걸쳐 이상 반응에 대해 모든 환자들을 면밀히 모니터링한다. 이상 반응은 NCI CTCAE v4.0에 따라 등급이 매겨진다.All patients are closely monitored for adverse events throughout the study. Adverse events are graded according to NCI CTCAE v4.0.
단일 제제로서(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용으로(Ib상) 티라골루맙의 PK 특성, 면역원성 반응, 및 약력학적 효과를 특성화하기 위해, 투약 전후 다양한 시점에서 혈액 샘플을 채취한다. 중간 PK 분석의 결과에 따라, PK 샘플링의 빈도는 연구 후반부에 줄어들 수 있다.To characterize the PK properties, immunogenic response, and pharmacodynamic effects of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) at various time points before and after dosing a blood sample is taken from Depending on the results of the interim PK analysis, the frequency of PK sampling may be reduced later in the study.
환자는 스크리닝 및 연구 동안에 종양 평가를 받고, 이는 표준 고형 종양의 반응 평가 기준(RECIST) v1.1 기준에 의해 측정한다.Patients receive tumor assessments during screening and study, as measured by the Standard Response Evaluation Criteria for Solid Tumors (RECIST) v1.1 criteria.
환자는, 계속된 치료에 대한 기준을 충족하는 경우, 연구의 Ia상 또는 Ib상 부분에서 질병 진행에 대한 표준 RECIST v1.1 기준이 충족되더라도 연구 치료제를 계속 받을 수 있다(도 7). 연구의 Ia상 부분을 중단한 환자는, 교차 기준을 충족하고 접근 가능한 병변에 대한 생검에 동의하는 경우, 연구의 Ib상 부분으로 전환되어 아테졸리주맙과 병용한 티라골루맙을 이용한 치료를 받을 수 있다(도 8).Patients may continue to receive study treatment even if the standard RECIST v1.1 criteria for disease progression in the Phase Ia or Ib portion of the study are met, provided they meet the criteria for continued treatment ( FIG. 7 ). Patients who withdraw from the Phase Ia portion of the study may be transferred to the Phase Ib portion of the study and receive treatment with tiragolumab in combination with atezolizumab, provided they meet the crossover criteria and consent to a biopsy of an accessible lesion. There is (Fig. 8).
티라골루맙(Ia상) 또는 티라골루맙 및 아테졸리주맙, 티라골루맙 및 아테졸리주맙에 더한 화학요법, 티라골루맙 및 아테졸리주맙에 더한 베바시주맙, 또는 티라골루맙 및 펨브롤리주맙(Ib상)을 영구적으로 중단한 환자는 연구 치료제의 마지막 용량 투여 후 30일 이내에 치료 중단 방문을 위해 병원으로 다시 방문해야 한다. 다른 전신 항암 요법의 개시와 관계없이 연구 치료제의 마지막 용량 투여 후 최대 90일 동안 특별한 관심의 이상 반응에 대한 추가 모니터링 및 기록을 실시한다. 다른 모든 이상 반응에 대한 모니터링 및 기록은 연구 치료제의 최종 용량 투여 후 최대 90 일 동안, 또는 다른 항암 전신 요법의 개시 때까지(어느 것이든 먼저 발생하는 시점까지) 실시한다. 연구의 전체 환자는, 환자가 추적조사로부터의 철회를 요청하지 않는 한, 사망, 추적조사의 손실, 또는 연구 종료시까지 대략 3개월마다 생존 및 후속 항암 요법 정보에 대하여 추적한다. Tiragolumab (Phase Ia) or tiragolumab and atezolizumab, chemotherapy in addition to tiragolumab and atezolizumab, bevacizumab in addition to tiragolumab and atezolizumab, or tiragolumab and pembrolizumab ( Patients who permanently discontinue phase Ib) must return to the hospital for a treatment discontinuation visit within 30 days of administration of the last dose of study treatment. Additional monitoring and documentation of adverse events of particular interest should be performed for up to 90 days after administration of the last dose of study treatment, irrespective of initiation of other systemic anticancer therapies. Monitoring and documentation of all other adverse events will occur for up to 90 days after administration of the last dose of study treatment, or until initiation of other anticancer systemic therapy, whichever occurs first. All patients in the study are followed for survival and follow-up anti-cancer therapy information approximately every 3 months until death, loss of follow-up, or study termination, unless the patient requests withdrawal from follow-up.
IMC는 본 연구에서 치료된 모든 환자의 누적 안전성 데이터를 주기적으로 평가한다. 안전성 요약 데이터는 연구의 Ia상(단일제제 티라골루맙) 부분에서 처음 2개의 용량 코호트에 대한 DLT 평가가 완료된 후 IMC에 의해 평가된다. 상기 IMC는 안전성 데이터를 검토하여 Ia상에서 프로토콜 변경 없이 등록을 계속하여 아테졸리주맙과 병용한 티라골루맙으로 연구의 Ib상 부분에 등록을 시작하여 안전성 탐색 코호트의 안전성 데이터를 검토할지 여부를 권고하고, Ib상 화학요법 확장 코호트, 비화학요법 확장 코호트 및 Q4W 투약 확장 코호트에 등록을 계속하여, 안전성 모니터링 및/또는 적격성 기준을 수정하여 새로운 안전성 문제를 해결하기 위한 추가 안전성 검토를 추가하거나, 연구를 종료할지 여부를 권고한다. 이를 배제할 안전성 문제가 없는 경우, 안전 분석이 진행되는 동안 연구의 Ia상 부분에서의 연구 대상체 발생을 계속 진행한다. The IMC periodically evaluates the cumulative safety data of all patients treated in this study. Safety summary data will be assessed by IMC after completion of DLT assessments for the first two dose cohorts in the Phase Ia (single-agent tyragolumab) portion of the study. The IMC reviewed safety data and recommended whether to continue enrollment without protocol change in Phase Ia and begin enrollment in the Phase Ib portion of the study with tiragolumab in combination with atezolizumab to review safety data in the safety exploratory cohort; , continue enrollment in the Phase Ib chemotherapy expansion cohort, non-chemotherapy expansion cohort, and Q4W dosing expansion cohort, modifying safety monitoring and/or eligibility criteria to add additional safety reviews to address new safety issues, or end the study recommend whether to If there are no safety issues to rule out, proceed with study subject development in the Phase Ia portion of the study while the safety analysis proceeds.
잠재적인 예상치 못한 이상 반응의 더 완화하기 위해, 상기 IMC는 또한 정기적으로 연구의 Ia상 및 Ib상 부분의 확장 코호트에 입력된 환자의 안전성 데이터를 검토하여, 특히 새로운 시험 안전성 데이터에 기초하여 연구 수행에 관한 권고 사항을 제공함으로써 연구 치료제를 투여 받는 동안 환자의 안전을 보장한다. 상기 IMC에 의한 무익성에 대한 중간 분석은 Ia상 및 Ib상의 확장 코호트에서도 발생한다. 또한, 의료 모니터는 추가 안전성 보고서를 요청할 수 있으며 위험-이득 균형에 대한 진행 중인 안전성 데이터를 검토하기 위해 연구 중 언제든지 IMC의 임시 회의를 요청할 수 있다.To further mitigate potential unexpected adverse events, the IMC also periodically reviews the safety data of patients entered into the expansion cohorts of the Phase Ia and Phase Ib portions of the study, particularly based on new trial safety data, to conduct studies. Ensure patient safety while receiving study treatment by providing recommendations on The interim analysis of futility by the IMC also occurs in the phase Ia and phase Ib expansion cohorts. In addition, the Medical Monitor may request additional safety reports and may request an ad hoc meeting of the IMC at any time during the study to review ongoing safety data on risk-benefit balances.
용량 증량 단계 동안, 단일 제제로서 또는 아테졸리주맙과 병용으로 티라골루맙의 MTD 또는 MAD를 결정하기 위해 하기에 설명된 용량 증량 규칙에 따라 각 티라골루맙 용량 수준에서 적어도 3명의 환자가 치료된다. Ia상 또는 Ib상에서 티라골루맙의 새로운 용량 수준을 조사하는 각각의 새로운 용량 증량 코호트에 처음 3명의 환자를 시차를 두고 등록함으로써, 각각의 주기 1, 1일의 치료가 ₃7일 간격으로 투여되도록 한다. 모든 환자는 21일(주기 1의 1-21일)로 정의되는 DLT 평가 기간 동안 이상 반응에 대해 면밀히 모니터링한다.During the dose escalation phase, at least 3 patients at each tiragoluumab dose level are treated according to the dose escalation rules described below to determine the MTD or MAD of tiragolumab as a single agent or in combination with atezolizumab. Staggered enrollment of the first 3 patients into each new dose escalation cohort investigating a new dose level of tyragolumab in Phase Ia or Ib ensures that each
DLT 이외의 이유로 DLT 평가 기간을 완료하지 않은 임의의 용량 증량 환자는 용량 증량 결정 및 MTD 평가에 대하여 평가가 가능하지 않은 것으로 간주하고 그 동일한 용량 수준에서 추가의 환자에 의해 대체할 수 있다. (하기에 기재된 지지적 치료를 포함하지 않는)DLT의 평가를 혼동하는 DLT 평가 기간 동안 지지적 치료를 받은 환자는 의료 모니터의 재량에 따라 대체될 수 있다. 다음 계획된 용량의 투여가 7 일을 초과한 만큼 지연되는 정도로 DLT 이외의 이유로 DLT 평가 기간 동안 유지된 연구 치료제의 임의의 성분을 갖는 환자는 용량 증량 결정 및 MTD 또는 MAD 평가에 대하여 평가 가능하지 않은 것으로 간주하고 그 동일한 용량 수준에서 추가의 환자에 의해 대체될 수 있다.Any dose escalation patient who does not complete the DLT assessment period for reasons other than DLT will be considered not eligible for assessment for dose escalation decisions and MTD assessments and may be replaced by an additional patient at that same dose level. Patients receiving supportive care during the DLT assessment period that would confound the assessment of DLT (not including supportive care as described below) may be substituted at the discretion of the Medical Monitor. A patient with any component of the study treatment maintained during the DLT evaluation period for reasons other than DLT to the extent that administration of the next scheduled dose is delayed by more than 7 days is considered not evaluable for dose escalation decisions and MTD or MAD evaluation. considered and may be replaced by additional patients at that same dose level.
연구의 Ia상 부분에서 치료를 받고 티라골루맙 단독으로 질병 진행이 발생한 환자는 연구의 Ib상 부분에서 치료를 받기에 적격일 수 있다(도 8). 단, 이 경우에 전환에 대한 특정 자격 기준이 충족되어야 한다.Patients receiving treatment in the Phase Ia portion of the study and developing disease progression with tyragolumab alone may be eligible for treatment in the Phase Ib portion of the study ( FIG. 8 ). However, in this case, certain qualification criteria for conversion must be met.
용량 제한 독성의 정의Definition of dose limiting toxicity
연구의 Ia상 및 Ib상 부분 모두에서, DLT 평가 기간 동안 발생하고 연구 치료제와 관련된 것으로 시험자가 평가하는 경우 하기의 반응들 중 임의의 하나가 DLT로 간주된다:In both the Phase Ia and Phase Ib portions of the study, any one of the following reactions is considered a DLT if it occurs during the DLT assessment period and is assessed by the investigator as related to the study treatment:
![]()
![]()
![]()
![]()
-
≤ 3일 이내에 치료 표준의 요법으로 ≤3일에 ≤2 등급으로 회복되는 3 등급의 메스꺼움, 구토 또는 설사 -
-
≤ 3일에 ≤ 2 등급으로 회복되는 3 등급의 피로 -
≤ 3 등급의 발열(≤ 24시간 동안 〉40°C 만큼으로 정의됨)
≤
-
≤ 7일 이내에 ≤2 등급으로 회복되는 종양 발적의 등급 3 이상 반응(공지되거나 의심되는 종양 부위에 국한된 국소 통증, 자극, 또는 발진으로 정의됨) -
-
무증상이고 임상적으로 유의적이지 않은 것으로 시험자가 고려하는 등급 3의 실험실 검사수치 이상 -
-
프레드니손 10 mg/일 이하와 동등한 요법으로 ≤ 7 일 내에 ≤ 2 등급으로 회복되는 등급 3의 발진 -
-
지지적 치료로 적절하게 관리할 수 있거나 ≤7일 이내에 ≤2등급으로 회복되는 3 등급의 관절통 -
-
전신 코르티코스테로이드의 개시를 필요로 하지 않은 내분비 요법으로 관리할 수 있는 3 등급의 자가면역 갑상선염 또는 기타 내분비 이상(부신 기능 부전에 대한 대체 스테로이드 제외) -
≥ 4 등급의 호중구 감소증(> 7일 지속되는 절대 호중구 수(ANC) 500/μL) ≥
≥ 3 등급의 열성 호중구감소증 <≥
≥ 4 등급의 빈혈≥
≥ 4 등급의 혈소판감소증 또는 임상적으로 유의한 출혈과 관련된 3 등급의 혈소판감소증≥
〉7일 동안 지속되는 혈청 간 아미노전이효소(ALT 또는 AST)의 ≥ 3 등급의 상승>
간 전이로 인해 기준선에서 등급 1 ALT 또는 AST 상승이 있는 환자에게서, > 7일간 지속되는 ≥ 3 x 기준선인 ≥ 3 등급 상승만이 DLT로 간주됨 In patients with a
≥ 3 등급의 혈청 총빌리루빈 상승 ≥
ALT 또는 AST > 3 × 정상 상한치(ULN) 및 총 빌리루빈 > 2 × ULNALT or AST > 3 × upper limit of normal (ULN) and total bilirubin > 2 × ULN
용량 증량 규칙Capacity escalation rules
등록은 연구의 Ia상 부분에서 먼저 시작한다. 티라골루맙의 시작 용량은 2 mg이며 21일마다 IV로 투여한다. 티라골루맙의 용량은 연속적인 용량 수준 사이에서 4배 증가하며, 티라골루맙에 대한 평가를 위해 제안된 대략적인 용량 수준은 2 mg, 8 mg, 30 mg, 100 mg, 400 mg 및 1200 mg이다. 연속 용량 수준 사이의 최대 용량 증가는 감소될 수 있다. 새로운 비임상 유효성, 임상 안전성, 및/또는 임상 PK 데이터를 기반으로, 티라골루맙의 추가 중간 용량 수준을 평가할 수 있다. Enrollment begins first in the Phase Ia portion of the study. The starting dose of tiragolumab is 2 mg, administered IV every 21 days. The dose of tiragolumab is increased by a factor of 4 between successive dose levels, and the suggested approximate dose levels for evaluation for tiragolumab are 2 mg, 8 mg, 30 mg, 100 mg, 400 mg and 1200 mg. . The maximum dose increment between successive dose levels may be reduced. Based on new nonclinical efficacy, clinical safety, and/or clinical PK data, additional intermediate dose levels of tiragoluumab may be evaluated.
임의의 DLT에 더하여, 다른 입수 가능한 관련 인구통계학적, 이상 반응, 실험실, 용량 투여, PK(입수 가능한 경우) 및 약력학(입수 가능한 경우) 데이터는 용량 증량 결정 전에 검토하고, 이는 의학 모니터 요원이 안전성 전문 과학자, 통계학자, PK 과학자, 및/또는 임상 시험 관리자로 구성되지만 이에 제한되지는 않는 위원회 및 시험자 책임자와 협의하여 실시한다.In addition to any DLTs, other available relevant demographic, adverse event, laboratory, dose administration, PK (if available), and pharmacodynamic (if available) data are reviewed prior to dose escalation decisions, which are reviewed by medical monitor personnel to ensure safety Conducted in consultation with a committee and investigator head comprising, but not limited to, professional scientists, statisticians, PK scientists, and/or clinical trial administrators.
용량 증량은 하기의 나열된 규칙에 따라 실시한다.Dose escalation is done according to the rules listed below.
최소 3명의 환자가 각 용량 수준(코호트)에 등록된다.A minimum of 3 patients are enrolled at each dose level (cohort).
처음 3명의 DLT 평가 가능한 환자 중 그 누구도 DLT 평가 기간 동안 DLT를 경험하지 않은 경우, 상기에서 설명한 대로 결정된 증가된 용량 수준에서 다음 코호트의 등록이 진행될 수 있다.If none of the first 3 DLT evaluable patients experienced a DLT during the DLT evaluation period, enrollment into the next cohort may proceed at the escalated dose level determined as described above.
주어진 코호트에서 처음 3명의 DLT 평가 가능한 환자 중 1명이 DLT를 경험하면, 동일한 용량 수준에서 적어도 3명의 추가 환자가 등록된다(예컨대, 코호트가 6명의 환자로 확장됨). 평가 가능한 환자의 1/3 미만이 DLT를 경험하는 경우(예컨대, 환자 6명 중 2명 미만), 용량 증량을 계속하고, 증가된 용량 수준에서 다음 코호트의 등록이 진행될 수 있다.If 1 of the first 3 DLT evaluable patients in a given cohort experiences a DLT, at least 3 additional patients at the same dose level are enrolled (eg, the cohort is expanded to 6 patients). If less than one-third of evaluable patients experience a DLT (eg, less than two out of six patients), the dose escalation may continue and enrollment into the next cohort may proceed at the increased dose level.
코호트(예컨대, 환자 6명 중 2명 이상)의 용량 수준 당 DLT 평가 가능한 환자의 최소 1/3에서 DLT가 관찰되면, MTD가 초과되고 용량 증량이 중단된다. 6명의 환자가 해당 수준에서 이미 평가되지 않은 한, 이전 코호트는 최소 6명의 환자로 확장된다. 하지만, MTD가 초과되는 용량 수준이 이전의 용량 수준보다 2배 이상 더 높으면, 6면의 환자는 중간 용량 수준에서 평가될 수 있다.DLT per dose level in a cohort (eg, 2 or more of 6 patients) If a DLT is observed in at least 1/3 of evaluable patients, the MTD is exceeded and dose escalation is discontinued. The previous cohort is expanded to a minimum of 6 patients unless 6 patients have already been assessed at that level. However, if the dose level at which the MTD is exceeded is at least 2-fold higher than the previous dose level, patients on
임의의 용량 수준에서 MTD가 초과되면, DLT 평가 가능한 환자의 1/3 미만(즉, 6명의 환자 중 2명 미만)이 DLT를 경험하는 최고 용량이 MTD로 선언된다.If the MTD is exceeded at any dose level, the highest dose at which less than one third of DLT evaluable patients (ie, less than 2 out of 6 patients) experience a DLT is declared MTD.
MTD가 임의의 용량 수준에서 초과되지 않으면, 본 연구에서 투여된 최고 용량은 MAD로 선언된다.If the MTD is not exceeded at any dose level, the highest dose administered in this study is declared MAD.
주기 1 이후에 발생하는 반응 및 확장 코호트에서 관찰된 반응을 포함하는, 비 DLT 이상 반응의 대한 시험자의 평가에 기반하여 보증된 경우, MTD를 초과하지 않은 것으로 보이는 임의의 용량 수준이 확장될 수 있다.Any dose level that does not appear to exceed the MTD may be extended if warranted based on the investigator's assessment of non-DLT adverse events, including those occurring after
입수 가능한 예비 실시간 안전성 데이터 및 입수 가능한 예비 PK 데이터(Ia상 및/또는 Ib상 연구에서 수집됨)의 검토에 기초하여, Ia상 및/또는 Ib상의 용량 증량은 중단되거나, 제한되거나, 또는 적절한 것으로 간주될 수 있다. Based on a review of available preliminary real-time safety data and available preliminary PK data (collected in Phase Ia and/or Ib studies), dose escalation in Phase Ia and/or Ib may be discontinued, limited, or appropriate. can be considered
연구의 Ia상 부분에서 처음 2개의 투약 코호트에 대한 DLT 평가가 완료된 후, 시험자 및 IMC가 안전성 데이터를 검토하고, 연구의 Ib상 부분을 활성화할지 여부를 권고한다. Ib상을 활성화하는 것이 적절하다고 판단되는 경우, 연구의 두 부분에서 동시에 등록을 진행할 수 있다. 아테졸리주맙과 병용한 티라골루맙의 시작 용량은 2 mg이며, 아테졸리주맙은 고정 용량 1200 mg IV로 투여하며 두 약물은 21일마다 투여한다. 연구의 Ib상 부분에서 티라골루맙의 용량은 연구의 Ia상 부분에서 MTD를 초과하지 않는 것으로 나타난 최고 용량을 결코 초과하지 않는다. 연구의 Ib상 부분의 코호트 1에서 조합 MTD를 초과하는 경우, 더 낮은 용량의 티라골루맙을 아테졸리주맙과 병용하는 것을 고려할 수 있다.After the DLT evaluation for the first two dosing cohorts in the Phase Ia portion of the study is completed, the Investigator and IMC review the safety data and recommend whether to activate the Phase Ib portion of the study. If it is deemed appropriate to activate phase Ib, registration may proceed simultaneously in both parts of the study. The starting dose of tiragolumab in combination with atezolizumab is 2 mg, and atezolizumab is administered as a fixed dose of 1200 mg IV, with both drugs administered every 21 days. The dose of tiragolumab in the Phase Ib portion of the study never exceeds the highest dose shown not to exceed the MTD in the Phase Ia portion of the study. If the combination MTD is exceeded in
확장 코호트에 대한 용량 선택을 보다 충분히 알리도록 추가 안전성 및 약력학 데이터를 획득하기 위해, 상기에서 설명한 용량 증량 기준에 기초하여 MTD 또는 MAD 를 초과하지 않는 것으로 나타난 연구의 Ia상 및/또는 Ib상 부분의 용량 수준에 추가 환자를 등록할 수 있다. 용량 증량 결정의 목적으로, 상기 환자는 DLT 평가가능 모집단의 일부로서 고려되지 않는다. 상기 환자는 안전하게 접근할 수 있는 종양이 있어야 하며 생검에 동의해야 한다. 약력학의 평가를 알리기 위해, 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD-L1 및/또는 TIGIT를 발현하는 종양을 가진 환자가 등록된다. 또한, 용량 확장 단계를 시작하기 전에 추가 안전성 데이터를 제공하기 위해, 최대 약 12명의 추가 환자를 MTD 또는 MAD 또는 그 이하에서 Ia상 또는 Ib상 연구에서 선택된 용량 수준으로 등록할 수 있다. To obtain additional safety and pharmacodynamic data to more fully inform dose selection for the expansion cohort, the Phase Ia and/or Ib portion of the study that was shown not to exceed the MTD or MAD based on the dose escalation criteria described above. Additional patients may be enrolled at the dose level. For the purposes of dose escalation decisions, the patient is not considered part of the DLT evaluable population. The patient must have a safely accessible tumor and consent to a biopsy. To inform evaluation of pharmacodynamics, patients with tumors expressing PD-L1 and/or TIGIT based on prospective examination of tumor tissue during screening or prescreening are enrolled. In addition, up to about 12 additional patients may be enrolled at the selected dose level in the Phase Ia or Ib study at MTD or MAD or below to provide additional safety data prior to initiating the dose expansion phase.
연구의 Ia상 부분에서만 방사선 촬영상 질병 진행이 발생했거나 단일 제제 티라골루맙으로부터 임상적 이익을 더 이상 유도하지 못하는 환자는 안전하게 접근 가능한 종양을 가지고, 생검에 동의하고 전환에 대한 지정된 기준을 충족한 경우 연구의 Ib상 부분의 치료를 받는 것에 적격일 수 있다. Patients who have developed radiographic disease progression only in the Phase Ia portion of the study or who no longer derive clinical benefit from the single agent tyragolumab have safely accessible tumors, consent to biopsy, and meet the specified criteria for conversion. may be eligible for treatment in the Phase Ib portion of the study.
Ia상 및 Ib상 확장 단계Phase Ia and Phase Ib expansion phase
입수 가능한 표준 요법 후 진행된 국소 진행성, 재발성 또는 전이성 난치성 악성 종양을 가지거나; 이에 대해 표준 요법이 존재하지 않거나, 비효과적이거나 견딜 수 없는 것으로 입증되었거나, 부적절하다고 간주되거나; 또는 이에 대해 임상 시험용 제제의 임상 시험이 인정된 치료의 표준인 환자는 연구의 확장 코호트에 등록된다. 연구의 Ib상 부분에서만, 화학요법을 포함하거나 포함하지 않고 항 PD-L1/PD-1 항체 또는 항 VEGF 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 환자가 확장 코호트에 등록될 수 있다.have locally advanced, recurrent, or metastatic refractory malignancies that have progressed following available standard therapy; for which standard therapies do not exist, have proven ineffective or intolerable, or have been deemed inadequate; Alternatively, patients for whom a clinical trial of an investigational product is the accepted standard of care will be enrolled in the study's expansion cohort. In only the Phase Ib portion of the study, patients with or without chemotherapy for which clinical trials of investigational agents in combination with anti-PD-L1/PD-1 antibodies or anti-VEGF antibodies are considered acceptable treatment options are expanded. may be enrolled in a cohort.
상기 확장 단계는 특정 암 환경에서 단일 제제로서(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 하기의: 아테졸리주맙, 화학요법을 동반한 아테졸리주맙, 베바시주맙을 동반한 아테졸리주맙, 또는 펨브롤리주맙과 병용으로(Ib상) 티라골루맙의 안전성, 내약성, PK 변동성, 약력학적 활성, 및 예비 항종양 활성을 보다 잘 특성화하기 위해 소정의 환자 코호트로 구성된다. 상기 확장 코호트의 등록은 축적된 안전성, 내약성, PK, 약력학, 및 항종양 활성 데이터의 평가를 기반으로 단일 제제로서(Ia상) 또는 하기의: 아테졸리주맙, 화학요법을 동반한 아테졸리주맙, 베바시주맙을 동반한 아테졸리주맙, 또는 펨브롤리주맙과 병용한(Ib상) 티라골루맙의 MAD 또는 MTD 이하의 선택된 용량 수준에서 개시된다. The expansion phase may include: atezolizumab, atezolizumab with chemotherapy, atezolizumab with bevacizumab, with or without chemotherapy, either as a single agent (Phase Ia) or with or without chemotherapy in certain cancer settings; or in combination with pembrolizumab (Phase Ib) to better characterize the safety, tolerability, PK variability, pharmacodynamic activity, and prospective anti-tumor activity of tiragolumab. Enrollment of the expansion cohort was based on assessment of accumulated safety, tolerability, PK, pharmacodynamics, and antitumor activity data as a single agent (Phase Ia) or as: atezolizumab, atezolizumab with chemotherapy; At a selected dose level below the MAD or MTD of atezolizumab with bevacizumab, or tiragolumab in combination with pembrolizumab (Phase Ib).
연구의 Ia상 부분에서, 최대 약 40명의 환자가 NSCLC, RCC, TNBC, 흑색종, HNSCC, OC, GEJ 암을 포함한 GC, UBC, 및 CRC(MSS 또는 MSI이 낮은 CRC 포함)를 포함하여 PD-L1 선택된 및/또는 TIGIT 선택된 다중 종양 적응증의 계획된 확장 코호트에 등록된다.In the Phase Ia portion of the study, up to about 40 patients were diagnosed with PD-, including NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC, UBC, and CRC (including CRCs with low MSS or MSI) GEJ cancers. Enroll in the planned expansion cohort of L1 selected and/or TIGIT selected multiple tumor indications.
연구의 Ib상 부분(화학요법 없음)에서, 약 20~40명의 환자가 하기의 계획된 적응증별 확장 코호트를 포함하여 다중 종양 적응증에 등록될 수 있다:In the Phase Ib portion of the study (no chemotherapy), approximately 20-40 patients may be enrolled in multiple tumor indications, including the following planned indication-specific expansion cohorts:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
연구의 Ib상 화학요법 확장 부분에서, 약 20~40명의 환자가 하기의 계획된 화학요법 확장 코호트의 각각에 등록될 수 있다(도 5);In the Phase Ib chemotherapy expansion portion of the study, approximately 20-40 patients may be enrolled in each of the following planned chemotherapy expansion cohorts ( FIG. 5 );
![]()
![]()
- 유도기 - 시스플라틴 또는 카보플라틴 및 페메트렉시드와 병용한 아테졸리주맙 및 티라골루맙 - induction phase - atezolizumab and tiragolumab in combination with cisplatin or carboplatin and pemetrexed
- 유지기 - 페메트렉시드와 병용한 아테졸리주맙 및 티라골루맙 - Maintenance phase - Atezolizumab and Tiragolumab in combination with pemetrexed
![]()
![]()
- 유도기 - 카보플라틴 또는 파클리탁셀과 병용한 아테졸리주맙 및 티라골루맙 - Induction phase - Atezolizumab and Tiragolumab in combination with carboplatin or paclitaxel
- 유지기 - 아테졸리주맙 및 티라골루맙 - Maintenance phase - Atezolizumab and Tiragolumab
![]()
![]()
- 유도기 - 시스플라틴 또는 카보플라틴 및 에토포시드와 병용한 아테졸리주맙 및 티라골루맙 - induction phase - atezolizumab and tiragolumab in combination with cisplatin or carboplatin and etoposide
- 유지기 - 아테졸리주맙 및 티라골루맙 - Maintenance phase - Atezolizumab and Tiragolumab
![]()
![]()
- 카페시타빈과 병용한 아테졸리주맙 및 티라골루맙- Atezolizumab and Tiragolumab in combination with Capecitabine
연구의 Ib상 Q4W 확장 부분에서, 약 20~40명의 환자가 계획된 코호트에 등록될 수 있다(도 4).In the Phase Ib Q4W expansion portion of the study, approximately 20-40 patients can be enrolled in the planned cohort (Figure 4).
연구의 Ib상 비화학요법 확장 부분에서, 약 20~40명의 환자가 하기의 계획된 비화학요법 확장 코호트의 각각에 등록될 수 있다(도 6).In the Phase Ib non-chemotherapy expansion portion of the study, approximately 20-40 patients may be enrolled in each of the following planned non-chemotherapy expansion cohorts (Figure 6).
![]()
![]()
- 베바시주맙을 병용한 티라골루맙 및 아테졸리주맙 - Tiragolumab and atezolizumab in combination with bevacizumab
![]()
![]()
- 티라골루맙 및 펨브롤리주맙 - Tiragolumab and Pembrolizumab
이의 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 CIT 미경험 환자만이 연구의 Ib상 부분의 관련 확장 코호트 등록에 적격인 것으로 간주된다. 그렇지 않으면, 환자는 시험자의 재량에 따라 연구의 Ia상 또는 Ib상 부분에서 입수 가능한 확장 슬롯에 할당된다Only CIT-naive patients for whom clinical trials of an investigational agent in combination with its anti-PD-L1 antibody are considered an acceptable treatment option are considered eligible for enrollment in the relevant expansion cohort of the Phase Ib portion of the study. Otherwise, the patient will be assigned an available expansion slot in either the Phase Ia or Phase Ib portion of the study at the discretion of the Investigator.
단일 제제(Ia상)로서의 티라골루맙 또는 아테졸리주맙과 병용한 티라골루맙(Ib상)의 안전성 프로파일은 용량 증량 단계에서의 환자 평가 후 완전히 특성화되지 않을 수 있다는 점을 감안할 때, 확장 코호트 등록시 모든 잠재적 이상 반응 또는 이의 발생 가능성을 알 수 있는 것은 아니다. 입수 가능한 모든 안전성 데이터는 연구된 용량 수준의 내약성을 평가하기 위해 지속적으로 평가된다. 잠재적인 예상치 못한 이상 반응의 더 완화하기 위해, 상기 IMC는 또한 정기적으로 연구의 Ia상 및 Ib상 부분의 확장 코호트에 입력된 모든 환자의 안전성 데이터를 검토하고 환자 안정성과 관련된 연구 행위에 관한 권고 사항을 제공한다. 확장 단계 코호트에서 관찰된 3 등급 또는 4 등급의 독성 또는 기타 허용할 수 없는 독성의 빈도가 MTD가 Ia상 또는 Ib상에서 해당 용량 수준에서 초과되었음을 암시하는 경우, 해당 용량 수준에서 연구 대상체 발생을 중단한다. 그런 다음, 더 낮은 용량 수준의 확장 단계에 등록 재개가 고려된다. 또한, 축적된 안전성, 내약성, PK 또는 약력학 데이터가 확장 코호트의 용량 수준이 단일 제제(Ia상)로서의 티라골루맙 또는 아테졸리주맙과 병용한(Ib상) 티라골루맙의 예비 항종양 활성 평가에 대해 최적이 아님을 암시하는 차선책임을 시사하는 경우, 해당 코호트에 새로운 환자를 다른 용량 수준으로 등록하는 것이 고려된다. Ia상 또는 Ib상의 확장 단계에서 연구된 용량 수준은 Ia상 또는 Ib상의 각 용량 증량 단계에서 MTD를 초과하지 않는 것으로 나타난 최고 용량 수준을 결코 초과하지 않는다. Given that the safety profile of tiragolumab as a single agent (Phase Ia) or tiragolumab in combination with atezolizumab (Phase Ib) may not be fully characterized after patient evaluation in the dose escalation phase, upon enrollment in the expansion cohort Not all potential adverse events or their likelihood of occurrence are known. All available safety data are continuously evaluated to assess tolerability of the dose level studied. To further mitigate potential unexpected adverse events, the IMC also periodically reviews the safety data of all patients entered into the expansion cohorts of the Phase Ia and Ib portions of the study and makes recommendations regarding study conduct related to patient safety. provides If the frequency of
Ib상 화학요법 확장 코호트, Ib상 Q4W 투약 확장 코호트, 및 Ib상 비화학요법 확장 코호트에서, IMC는 또한 각 코호트의 처음 3명의 환자가 모두 안전성 탐색 동안 연구 치료제의 주기 1을 완료한 후 초기 안전성을 모니터링한다(도 7을 참조). IMC는 연구 치료제가 용인되는지 여부를 결정하기 위해 해당 코호트에 대한 처음 3명의 환자의 모든 안전성 데이터를 검토하며, 여기서 IMC 및 시험자는 환자에게 투약을 계속할 수 있도록 허용 가능한 위험 평가를 실시한다. 상기 연구 치료제가 각 코호트의 안전성 탐색에서 용인 가능한 것으로 간주되는 경우, 안전성에 대한 중간 분석까지 각 코호트에서 동일한 용량의 티라골루맙으로 등록을 계속할 수 있다. 이는 안전성 탐색에 참여하는 환자를 포함하여 약 20명의 환자가 등록된 후에 실시한다. In the Phase Ib Chemotherapy Expansion Cohort, the Phase Ib Q4W Dosing Expansion Cohort, and the Phase Ib Non-chemotherapy Expansion Cohort, the IMC also assessed initial safety after all the first 3 patients in each cohort completed
IMC는 또한 각 코호트에서 약 20명의 환자가 제1 종양 평가를 완료한 후 중간 분석을 실시하여 연구의 Ia상 및 Ib상 부분에서 확장 코호트의 유효성을 모니터링한다. 시험자에 따른 항종양 활성 및/또는 임상적 이득이 해당 확장 코호트에서 검출되지 않는 경우, 연구 시험자와 협의하여 IMC가 결정한 대로 등록이 중단될 수 있다. 시험자에 따른 항종양 활성 및/또는 임상적 이득이 해당 확장 코호트의 환자에게서 검출되는 경우, IMC는 약 40명의 환자를 계속 등록하도록 허용할 수 있다. 40명의 평가 가능한 환자를 초과하는 임의의 확장 코호트의 샘플 크기는 증가하지 않는다. 연속 생검에 동의했지만 평가 가능한 샘플이 없는 환자는 각 확장 코호트에 등록할 최대 40명의 평가 가능한 환자의 일부로 교체될 수 있다.The IMC also monitors the effectiveness of the expansion cohort in the Phase Ia and Phase Ib portions of the study by conducting an interim analysis after approximately 20 patients in each cohort have completed their first tumor assessment. If no investigator-dependent antitumor activity and/or clinical benefit is detected in that expansion cohort, enrollment may be discontinued as determined by the IMC in consultation with the study investigator. If an investigator-dependent antitumor activity and/or clinical benefit is detected in patients in that expansion cohort, the IMC may continue to enroll approximately 40 patients. The sample size of any expansion cohort beyond 40 evaluable patients does not increase. Patients who have consented to serial biopsies but do not have evaluable samples may be replaced with a subset of up to 40 evaluable patients to be enrolled in each expansion cohort.
Ia상 확장 코호트Phase Ia Expansion Cohort
Ia상 확장 코호트의 목표는 안전성, 내약성, PK 및 예비 유효성 데이터를 더 잘 특성화하고 단일 제제 MTD 또는 MAD 이하의 용량 수준에서 티라골루맙으로 치료받은 환자에게서 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다. 상기 코호트는 PD-L1선택 및/또는 TIGIT선택된 종양을 가진 약 20~40명의 환자로 구성된다. 등록은 처음에는 하기의 종양 유형을 가진 환자로 제한한다: NSCLC, RCC, TNBC, 흑색종, HNSCC, OC, GEJ 암을 포함한 GC, UBC 및 MSS 및 MSI 낮음을 포함한 CRC. 상기 연구에서 다른 종양 유형을 가진 환자에게서 시험자에 따른 항종양 활성 및/또는 임상적 이득이 관찰되는 경우, 등록을 확장 및/또는 수정하여 다른 적응증을 포함할 수 있다.The goals of the Phase Ia expansion cohort were to better characterize safety, tolerability, PK and preliminary efficacy data and to explore potential tumor biomarkers of pharmacodynamic activity in patients treated with tiragolumab at dose levels below the single agent MTD or MAD. will do The cohort consists of approximately 20-40 patients with PD-L1-selected and/or TIGIT-selected tumors. Enrollment is initially limited to patients with the following tumor types: NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC including GEJ cancer, UBC and CRC including low MSS and MSI. If investigator-dependent antitumor activity and/or clinical benefit is observed in the study in patients with other tumor types, the enrollment may be expanded and/or modified to include other indications.
Ia상의 상기 코호트에 등록된 환자의 최대 약 절반은 안전하게 접근 가능한 종양 병변이 있어야 하고 치료 전 및 치료 중 생검(코어 바늘, 펀치, 겸자 또는 절제/절단)에 동의해야 한다. 상기 코호트에 있는 환자의 약 절반이 생존 가능한 종양 함량이 충분한 평가 가능한 연속 생검을 받을 수 있도록 추가 환자를 등록할 수 있다. Up to about half of patients enrolled in this cohort on Phase Ia must have safely accessible tumor lesions and consent to pre- and intra-treatment biopsies (core needle, punch, forceps, or excision/amputation). Additional patients may be enrolled so that approximately half of the patients in this cohort receive evaluable serial biopsies with sufficient viable tumor content.
상기 Ia상 확장 코호트에서 방사선 촬영상 질병 진행이 발생했거나 단일 제제 티라골루맙로부터 임상적 이익을 더 이상 유도하지 못하는 환자는 연구의 Ib상 부분에 대한 전환 및 치료에 적격일 수 있다(도 8). 단, 이 경우에 환자는 안전하게 접근 가능한 종양이 있고, 생검에 동의하고, 전환에 대한 지정된 기준을 충족해야 한다. Patients who have developed radiographic disease progression in the Phase Ia expansion cohort or who no longer derive clinical benefit from the single agent tyragolumab may be eligible for transition and treatment to the Phase Ib portion of the study ( FIG. 8 ). . However, in this case, the patient must have a safely accessible tumor, consent to a biopsy, and meet the specified criteria for conversion.
Ib상 적응증별 확장 코호트Expansion Cohort by Phase Ib Indication
Ib상 적응증별 확장 코호트의 목표는 안전성, 내약성, PK 및 예비 유효성 데이터를 더 잘 특성화하고 아테졸리주맙과 병용한 이의 MTD 또는 MAD 이하의 용량 수준에서 티라골루맙으로 치료한 특정 암 유형을 가진 환자에게서 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다. 각 적응증별 확장 코호트는 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD-L1 선택 및/또는 TIGIT 선택되고, 하기의 종양 유형을 포함하여 여러 종양 적응증을 포함하는 종양을 가진 최대 약 20명의 환자를 우선 등록한다.The goal of the Phase Ib indication-specific expansion cohort is to better characterize safety, tolerability, PK, and preliminary efficacy data, and patients with specific cancer types treated with tyragolumab at dose levels below its MTD or MAD in combination with atezolizumab. to explore potential tumor biomarkers of pharmacodynamic activity in Expansion cohorts for each indication were selected for PD-L1 and/or TIGIT based on prospective examination of tumor tissue during screening or prescreening, and the maximum with tumors covering multiple tumor indications, including the following tumor types: About 20 patients are first enrolled.
![]()
![]()
![]()
![]()
![]()
![]()
상기 환자들은 항 PD-L1/PD-1을 포함하여 선행 CIT(조사 또는 승인)를 받은 적이 있다.These patients have had prior CIT (investigation or approval) with anti-PD-L1/PD-1.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
20명의 환자를 등록한 후, IMC는 약 40명의 환자를 계속 등록하기 위해 시험자가 평가한 항종양 활성 및/또는 임상적 이득의 증거가 있는지 확인하기 위해 중간 분석을 함께 실시한다. After enrolling 20 patients, the IMC will also conduct an interim analysis to determine if there is evidence of investigator-assessed antitumor activity and/or clinical benefit to continue enrolling approximately 40 patients.
Ib상의 상기 적응증별 확장 코호트에 등록된 환자의 최대 약 절반은 안전하게 접근 가능한 종양 병변이 있어야 하고 치료 전 및 치료 중 생검(예를 들어, 코어 바늘, 펀치, 겸자 또는 절제/절단 생검)에 동의해야 한다. 상기 코호트에 있는 환자의 약 절반이 생존 가능한 종양 함량이 충분한 평가 가능한 연속 생검을 받을 수 있도록 추가 환자를 등록할 수 있다. Up to about half of patients enrolled in the above indication-specific expansion cohort on phase Ib must have safely accessible tumor lesions and consent to pre- and intra-treatment biopsies (e.g., core needle, punch, forceps, or excision/amputation biopsies) do. Additional patients may be enrolled so that approximately half of the patients in this cohort receive evaluable serial biopsies with sufficient viable tumor content.
Ib상 연속 생검 확장 코호트Phase Ib Serial Biopsy Expansion Cohort
Ib상 연속 생검 확장 코호트의 목적은 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하고 아테졸리주맙과 병용으로 MTD 또는 MAD 이하의 용량 수준의 티라골루맙으로 치료한 특정 암 유형을 가진 환자에게서 안전성, 내약성, PK 및 예비 유효성 데이터를 더 잘 특성화하는 것이다. 상기 코호트는 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD-L1 선택 및/또는 TIGIT 선택되고, 하기의 종양 유형을 포함할 수 있는 약 20~40명의 환자로 구성된다.The purpose of the Phase Ib serial biopsy expansion cohort was to explore potential tumor biomarkers of pharmacodynamic activity and safety, safety, and safety in patients with certain cancer types treated with tyragolumab at dose levels below the MTD or MAD in combination with atezolizumab; To better characterize tolerability, PK and preliminary efficacy data. The cohort consists of approximately 20-40 patients selected for PD-L1 and/or TIGIT based on prospective examination of tumor tissue during screening or prescreening, and may include the following tumor types.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
상기 연속 생검 확장 코호트에 등록된 환자는 두 가지 종양 생검을 받아야 하므로 안전하게 접근 가능한 종양 병변이 있어야 한다: 1) 치료 전 생검: 모든 적격 기준(입수 가능한 보관 조직에 대한 요구 사항 제외)이 충족된 후 및 연구 약물의 투약 전 기준선에서, 및 2) 치료 중 생검: 아테졸립주맙과 병용한 티라골루맙의 제1 투여 후 약 2주에(주기 1의 15일-21일 또는 그 사이). RECIST 표적 병변은 생검하지 않는다.Patients enrolled in the continuous biopsy expansion cohort must have two tumor biopsies and therefore must have safely accessible tumor lesions: 1) Pre-treatment biopsy: After all eligibility criteria (except the requirement for available storage tissue) have been met and at baseline prior to dosing of study drug, and 2) on-treatment biopsy: approximately 2 weeks after the first dose of tiragoluumab in combination with atezolipzumab (days 15-21 of
조직 생검 방법에는 코어 바늘, 펀치, 겸자 또는 절제/절개 생검이 포함될 수 있다. 필요한 신선한 생검을 제공하는 환자는 입수 가능한 경우 보관 종양 표본도 제출해야 한다.Tissue biopsy methods may include core needle, punch, forceps, or excision/incision biopsy. Patients providing the necessary fresh biopsies should also submit archival tumor specimens, if available.
상기 연속 생검 코호트에서, 하기의 상황에서는 최신 기준선 생검 대신 최근 보관 표본을 사용할 수 있다:In this serial biopsy cohort, a recent archived specimen may be used instead of an up-to-date baseline biopsy in the following circumstances:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
이의 기준선 생검이 평가 가능하지 않은 것으로 밝혀진 환자(즉, 샘플에 물질이 불충분하거나 종양 세포가 부족하여)는 여전히 연구 치료제를 투여 받고 치료 중 생검을 고려한다. 상기 환자, 및 치료 중 생검이 평가 가능하지 않은 것으로 밝혀진 환자, 또는 생존 가능한 종양 함량이 충분하지 않은 생검을 가진 환자는 연속 생검 평가의 목적으로 대체될 수 있다. 추가의 선택적인 생검은 시험자의 재량에 따라, 바람직하게는 방사선 반응 또는 진행시에 수집될 수 있다.Patients whose baseline biopsy has been found not to be evaluable (ie, due to insufficient material or insufficient tumor cells in the sample) will still receive study treatment and be considered for an on-treatment biopsy. Such patients, and those whose biopsies have been found not to be evaluable on treatment, or those whose biopsies do not have sufficient viable tumor content, may be replaced for purposes of continuous biopsy evaluation. Additional optional biopsies may be collected at the discretion of the investigator, preferably at the time of the radiation response or progression.
확장 코호트의 선택적 생검Selective biopsy of expansion cohorts
확장 코호트에 등록된 환자는 단일 제제로서 또는 아테졸리주맙과 병용으로 티라골루맙의 활성과 관련된 약력학적 변화를 탐색하기 위해 선택적 생검(예컨대, 코어 바늘, 펀치, 겸자 또는 절제/절개 생검)을 고려하도록 요청받는다. 각 확장 코호트의 등록은 연구 대상체로서 발생한 환자의 최대 약 절반이 안전하게 접근 가능한 종양 병변이 있고 이러한 선택적 생검을 받는 데 동의하도록 관리한다. 이러한 시나리오에서 권고되는 생검 시점은 상기에서 설명한 것과 동일하다: 모든 적격 기준(입수 가능한 보관 조직에 대한 요구 사항을 제외)이 충족된 후 기준선에서, 및 티라골루맙의 제1 용량 후 약 2주에(주기 1의 15일-21일 및 그 사이).Patients enrolled in the expansion cohort should consider elective biopsies (e.g., core needle, punch, forceps, or excision/incision biopsy) to explore pharmacodynamic changes associated with the activity of tiragolumab as a single agent or in combination with atezolizumab. are asked to do Enrollment in each expansion cohort is administered so that up to about half of the patients who develop as study subjects have safely accessible tumor lesions and agree to undergo such elective biopsies. The recommended biopsy time point in this scenario is the same as described above: at baseline after all eligibility criteria (except for the requirement for available storage tissue) have been met, and at approximately 2 weeks after the first dose of tiragolumab. (Day 15-21 of
기준선 샘플이 평가 가능하지 않고 비교할 수 있는 최근 보관 표본이 없는 경우, 치료 중 생검이 필요하지 않다. 평가 가능하지 않은 기준선 또는 치료 중 생검(즉, 생검에 생존 가능한 종양 함량이 충분하지 않음)을 가진 환자는 연속 생검 평가의 목적으로 대체될 수 있다.If baseline samples are not evaluable and no comparable recent archival specimens are available, an on-treatment biopsy is not required. Patients with non-evaluable baseline or on-treatment biopsies (ie, biopsies that do not have sufficient viable tumor content) may be replaced for purposes of continuous biopsy evaluation.
선택적 생검을 제공하는 환자는 입수 가능한 경우 보관 종양 표본도 제출해야 한다.Patients offering elective biopsies should also submit archival tumor specimens, if available.
Ib상 화학요법 확장 코호트Phase Ib Chemotherapy Expansion Cohort
Ib상 화학요법 확장 코호트의 목적은 아테졸리주맙 및 화학요법과 병용으로 티라골루맙으로 치료를 받은 환자를 대상으로 안전성, 내약성, 약동학, 및 예비 유효성 데이터를 더 잘 특성화하고 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다. The purpose of the Phase Ib chemotherapy expansion cohort is to better characterize safety, tolerability, pharmacokinetics, and preliminary efficacy data in patients treated with atezolizumab and tiragolumab in combination with chemotherapy, and to better characterize potential pharmacodynamic activity Searching for tumor biomarkers.
각각의 코호트는 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD L1 선택 및/또는 TIGIT 선택될 수 있는 종양을 가진 약 20~40명의 환자로 구성된다. 보관 조직이 불충분하거나 입수 불가능한 환자는 시험자와의 논의를 바탕으로 의료 모니터(Medical Monitor)가 허용하는 경우 상기 코호트 등록에 적격일 수 있다. 화학요법 및 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 종양 유형을 가진 환자가 상기 확장 코호트에 등록될 수 있다. 특정 종양 유형(예컨대, NSCLC, SCLC, TNBC)을 가진 환자 또는 특정 치료 이력(예컨대, CIT 미경험)을 가진 환자의 수는 각 연구 코호트에서 제한될 수 있다. Each cohort consists of approximately 20-40 patients with tumors capable of PD L1 selection and/or TIGIT selection based on prospective examination of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archival tissue may be eligible for enrollment in this cohort if permitted by the Medical Monitor based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational agents in combination with chemotherapy and anti-PD-L1 antibodies are considered acceptable treatment options may be enrolled in this expansion cohort. The number of patients with a specific tumor type (eg, NSCLC, SCLC, TNBC) or with a specific treatment history (eg, CIT naive) may be limited in each study cohort.
각 코호트의 치료 조합은 표 29에 나타내었다. Treatment combinations for each cohort are shown in Table 29.
(21일 주기의 4회 또는 6회)induction period
(4 or 6 times in a 21-day cycle)
(21일 주기a 또는 28일 주기b)retainer
(21-day cycle a or 28-day cycle b )
티라골루맙 + 페메트렉시드Atezolizumab +
Tiragolumab + Pemetrexed
티라골루맙Atezolizumab +
Tiragolumab
티라골루맙
Atezolizumab +
Tiragolumab
a
Q4W 유지기가 있는 코호트 B(프로토콜 GO30103 버전 5 이상에 따라 등록됨) 및 코호트 C의 환자의 경우. a For patients in cohort A, cohort B (enrolled according to protocol GO30103 version 4) and cohort D with Q3W maintenance period.
a For patients in cohort B (enrolled according to
화학요법 확장 코호트의 치료 요법Treatment regimens in the chemotherapy expansion cohort
각 코호트에는 3명의 환자에 대한 초기 안전성 탐색이 있다(도 5를 참조). 코호트의 처음 3명의 환자가 21일의 연구 치료를 완료한 후(즉, 주기 1의 1일~21일), IMC는 연구 치료제가 용인되는지 여부를 결정하기 위해 해당 코호트에 대한 처음 3명의 환자의 모든 안전성 데이터를 검토하며, 여기서 IMC 및 시험자는 환자에게 아테졸리주맙 및 티라골루맙의 투약을 계속할 수 있도록 허용 가능한 위험 평가를 실시한다. 치료 관련 독성 이외의 이유로 처음 21일 간의 치료를 완료하지 않은 환자는 동일한 용량 수준의 추가 환자로 대체될 수 있다. 최소 3명의 환자가 등록하고 21일 간의 연구 치료를 완료한 후 IMC에 의해 코호트에 대한 안전성 탐색에서 연구 치료제가 용인 가능한 것으로 판단된 경우, 총 약 20명의 환자가 등록될 때까지 해당 코호트에 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 약 20명의 환자에 대한 유효성 데이터를 검토한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 총 약 40명의 환자가 될 때까지 계속할 수 있다.Each cohort has an initial safety search for 3 patients (see Figure 5). After the first 3 patients in a cohort have completed 21 days of study treatment (i.e.,
600 mg 용량의 티라골루맙이 그 어떤 코호트에서도 안전성 탐색 중에 용인되지 않는 경우, 해당 코호트에 등록된 3명의 추가 환자에 대해 더 낮은 용량의 티라골루맙에서 안전성 탐색을 개시할 수 있다. 상기 저용량 군에 대한 안전성 데이터는 해당 코호트의 처음 3명의 환자가 21일 간의 연구 치료를 완료한 후 평가한다(주기 1의 1일~21일). 그런 다음, 안전성 탐색에서 약 3명의 추가 환자를 등록하여 상기 더 낮은 용량에서 티라골루맙의 안전성 및 내약성을 추가로 평가할 것이다. 티라골루맙의 용량만을 감량할 수 있고; 아테졸리주맙의 용량은 변하지 않는다. 필요한 경우, 화학요법의 용량 조정은 하기의 지침을 따른다. 상기 더 낮은 용량의 연구 치료제가 내약성인 경우, 상기 더 낮은 용량의 안전성 탐색 중인 환자를 포함하여 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 더 낮은 용량으로 등록을 계속한다. IMC는 각 코호트의 20명의 환자에 대한 데이터를 검토하여 안전성과 유효성을 평가한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 상기 더 낮은 용량에서 총 약 40명의 환자가 될 때까지 계속할 수 있다.If the 600 mg dose of tiragolumab is not tolerated during the safety investigation in any cohort, the safety investigation may be initiated at the lower dose of tiragoluumab for 3 additional patients enrolled in that cohort. Safety data for the low-dose group will be assessed after the first 3 patients in this cohort have completed 21 days of study treatment (Days 1-21 of Cycle 1). About 3 additional patients will then be enrolled in the safety expedition to further evaluate the safety and tolerability of tiragolumab at this lower dose. Only the dose of tiragolumab can be reduced; The dose of atezolizumab does not change. Dosage adjustment of chemotherapy, if necessary, follows the guidelines below. If the lower dose of the study treatment is well tolerated, continue enrollment at the lower dose until a total of about 20 patients have been enrolled in each cohort, including those undergoing safety exploration of the lower dose. The IMC evaluates safety and efficacy by reviewing data from 20 patients in each cohort. If the IMC determines that there is a favorable benefit-risk, then enrollment in that cohort may continue until a total of about 40 patients at the lower dose.
600 mg 용량의 티라골루맙이 안전성 탐색 기간 동안 내약성이 양호하고 새로운 임상 PK 데이터(예컨대, PK 데이터는 화학요법과 상이함) 및/또는 약력학적 데이터(예컨대, 수용체 점유)가 더 높은 용량의 티라골루맙을 사용할 것을 암시하는 경우, 각 코호트에 등록된 다음 3명의 환자에 대해 더 높은 용량의 티라골루맙에서 안전성 탐색을 개시한다. 상기 더 높은 용량은 3주마다 1200 mg을 초과하지 않으며, 이는 본 연구의 Ia상 및 Ib상 부분 모두에서 MTG7192A에 대한 최대 평가 용량이며, 3주마다 1200 mg 용량 수준에서 관찰된 것보다 더 크게 관찰된 최대 농도(Cmax)는 없다. 상기 고용량의 티라골루맙에서 연구 치료제가 내약성인 경우, 최소 6명의 환자가 등록하고 21일 간의 연구 치료를 완료할 때까지 상기 고용량의 안전성 탐색에서 등록을 계속한다. 상기 고용량의 연구 치료제가 IMC에 의한 안전성 탐색에서 내약성인 것으로 판단된 경우, 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 고용량의 티라골루맙으로 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 20명의 환자에 데이터를 검토한다. IMC가 유리한 이익-위험 프로필이 있다고 결정하면, 해당 코호트의 등록을 상기 더 높은 용량에서 총 약 40명의 환자가 될 때까지 계속할 수 있다.Tiragolumab at a dose of 600 mg is well tolerated during the safety exploration period and new clinical PK data (e.g., PK data differs from chemotherapy) and/or pharmacodynamic data (e.g., receptor occupancy) at higher doses of tyra If the use of golumab is implied, a safety investigation is initiated at the higher dose of tiragolumab for the next three patients enrolled in each cohort. This higher dose does not exceed 1200 mg every 3 weeks, which is the highest evaluated dose for MTG7192A in both the Phase Ia and Ib portions of this study, observed to be greater than that observed at the 1200 mg dose level every 3 weeks. There is no maximum concentration (C max ). If the study treatment at the high-dose tiragolumab is well tolerated, enrollment continues in the high-dose safety expedition until a minimum of 6 patients have been enrolled and complete 21 days of study treatment. If the high-dose study treatment is judged to be well tolerated in a safety investigation by the IMC, enrollment with the high-dose tiragolumab may continue until a total of approximately 20 patients have been enrolled in each cohort. The IMC reviews data from the first 20 patients in each cohort to evaluate safety and efficacy. If the IMC determines that there is a favorable benefit-risk profile, then enrollment in that cohort may continue until a total of about 40 patients at that higher dose.
Ib상 화학요법 확장 코호트: 용량 및 투여Phase Ib Chemotherapy Expansion Cohort: Dose and Dosing
코호트 A, 코호트 B, 및 코호트 C의 환자는 유도기 및 유지기의 2단계로 치료를 받을 수 있다. 상기 유도기에서, 특정 화학요법 확장 코호트의 환자는 하기의 용량 및 투여를 받는다: Patients in Cohort A, Cohort B, and Cohort C may receive treatment in two phases: the induction phase and the maintenance phase. In the induction phase, patients in certain chemotherapy expansion cohorts receive the following doses and administrations:
![]()
![]()
![]()
![]()
![]()
![]()
코호트 A 및 코호트 C의 경우, 특정 백금계 화학요법제를 투여받는 환자의 수가 제한될 수 있지만, 시스플라틴 또는 카보플라틴의 선택은 시험자의 결정에 따른다. 코호트 A 및 코호트 B의 경우, 유도기(4회 내지 6회)에서 투여되는 주기의 수는 시험자의 결정에 따른다. For Cohort A and Cohort C, the choice of cisplatin or carboplatin is at the discretion of the investigator, although the number of patients receiving certain platinum-based chemotherapeutic agents may be limited. For Cohort A and Cohort B, the number of cycles administered in the induction phase (4-6) is at the discretion of the investigator.
상기 유도기 후, 환자와 잠재적 위험 및 이점에 대한 신중한 평가 및 철저한 논의 후 시험자의 재량에 따라 허용할 수 없는 독성, 임상적으로 심각한 질병 진행, 및/또는 임상 이익의 손실이 없는 경우, 상기 유지기에서 치료를 계속한다. After the induction phase, if there is no unacceptable toxicity, clinically serious disease progression, and/or loss of clinical benefit, at the discretion of the investigator after careful evaluation and thorough discussion of potential risks and benefits with the patient, the maintenance phase continue treatment at
상기 유지기에서, 연구 치료는 코호트 A, 프로토콜 버전 4에 따라 등록된 코호트 B, 및 코호트 D에 대해 Q3W마다 계속하거나, 프로토콜 버전 5 이상 및 코호트 C에 따라 등록된 코호트 B에 대해 Q4W마다 계속한다.In the maintenance phase, study treatment continues every Q3W for Cohort A, Cohort B enrolled according to
상기 유지기에서, 특정 화학요법 확장 코호트의 환자는 하기의 용량 및 투여를 받는다:In the maintenance phase, patients in certain chemotherapy expansion cohorts receive the following doses and administrations:
![]()
![]()
![]()
![]()
![]()
![]()
코호트 D의 환자는 시험자가 결정한 대로 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 카페시타빈, 아테졸리주맙 및 티라골루맙으로 치료를 받는다. 환자는 각 21일 주기의 제 1일부터 14일까지 1250 mg/m2 BID의 용량으로 카페시타빈을 경구 투여받는다. 주기 1의 1일에 카페시타빈의 제1 용량은 아테졸리주맙 및 티라골루맙 주입 전에 병원에서 투여한다. 아테졸리주맙 및 티라골루맙의 조합은 21일 주기로 IV 주입으로 투여한다.Patients in Cohort D are treated with capecitabine, atezolizumab, and tiragolumab until unacceptable toxicity or loss of clinical benefit as determined by the investigator. Patients receive orally capecitabine at a dose of 1250 mg/m 2 BID from
독성이 있고 질병 진행 또는 임상적 이득의 손실이 없는 경우, 개별 화학요법 또는 면역요법 제제는 독립적으로 중단될 수 있다. 하지만, 금기 사항이 없고 의료 모니터 요원과 논의한 후에만 아테졸리주맙 단독 또는 티라골루맙 단독(화학요법 유무에 관계없이) 치료를 고려할 수 있다.Individual chemotherapy or immunotherapeutic agents may be independently discontinued if toxic and without disease progression or loss of clinical benefit. However, treatment with atezolizumab alone or tiragolumab alone (with or without chemotherapy) may be considered with no contraindications and only after discussion with a medical monitor.
Ib상 Q4W 투약 확장 코호트Phase Ib Q4W Dosing Expansion Cohort
Ib상 Q4W 투약 확장 코호트의 목적은 매 4주(28일; Q4W)의 투약 일정으로 아테졸리주맙 1680 mg IV와 병용으로 티라골루맙 840 mg IV로 치료받은 환자를 대상으로 안전성, 내약성, PK, 및 예비 유효성 데이터를 더 잘 특성화하고 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다.The objective of the Phase Ib Q4W Dosing Expansion Cohort was to evaluate safety, tolerability, PK, and to better characterize preliminary efficacy data and to explore potential tumor biomarkers of pharmacodynamic activity.
상기 Ib상 Q4W 코호트는 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD L1 선택 및/또는 TIGIT 선택될 수 있는 종양을 가진 약 20~40명의 환자로 구성된다. 보관 조직이 불충분하거나 입수 불가능한 환자는 시험자와의 논의를 바탕으로 의료 모니터(Medical Monitor)가 허용하는 경우 상기 코호트 등록에 적격일 수 있다. 항 PD-L1 항체와 병용한 임상 시험용 제제에 대한 임상 시험이 허용 가능한 치료 선택 사항으로 간주되는 종양 유형을 가진 환자가 상기 확장 코호트에 등록될 수 있다. 특정 종양 유형(예컨대, NSCLC, SCLC)을 가진 환자 또는 특정 치료 이력(예컨대, CIT 미경험)을 가진 환자의 수는 각 연구 코호트에서 제한될 수 있다.The Phase Ib Q4W cohort consists of approximately 20-40 patients with tumors capable of PD L1 selection and/or TIGIT selection based on prospective examination of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archival tissue may be eligible for enrollment in this cohort if permitted by the Medical Monitor based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational agents in combination with anti-PD-L1 antibodies are considered acceptable treatment options may be enrolled in this expansion cohort. The number of patients with a specific tumor type (eg, NSCLC, SCLC) or with a specific treatment history (eg, CIT naive) may be limited in each study cohort.
각 코호트에는 3명의 환자에 대한 초기 안전성 탐색이 있다(도 4를 참조). 코호트의 처음 3명의 환자가 28일의 연구 치료를 완료한 후(즉, 주기 1의 1일~28일), IMC는 연구 치료제가 용인되는지 여부를 결정하기 위해 해당 코호트에 대한 처음 3명의 환자의 모든 안전성 데이터를 검토하며, 여기서 IMC 및 시험자는 환자에게 아테졸리주맙을 병용한 티라골루맙의 투약을 계속할 수 있도록 허용 가능한 위험 평가를 실시한다. 치료 관련 독성 이외의 이유로 처음 28일 간의 치료를 완료하지 않은 환자는 동일한 용량 수준의 추가 환자로 대체될 수 있다. 최소 3명의 환자가 등록하고 28일 간의 연구 치료를 완료한 후 IMC에 의해 코호트에 대한 안전성 탐색에서 연구 치료제가 용인 가능한 것으로 판단된 경우, 총 약 20명의 환자가 등록될 때까지 해당 코호트에 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 약 20명의 환자에 대한 유효성 데이터를 검토한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 총 약 40명의 환자가 될 때까지 계속할 수 있다.In each cohort there is an initial safety exploration of 3 patients (see Figure 4). After the first 3 patients in a cohort have completed 28 days of study treatment (i.e., Days 1-28 of Cycle 1), the IMC will review the first 3 patients in that cohort to determine whether the study treatment is tolerated. All safety data are reviewed, where the IMC and investigators conduct an acceptable risk assessment to allow the patient to continue treatment with tiragolumab in combination with atezolizumab. Patients who do not complete the first 28 days of treatment for reasons other than treatment-related toxicity may be replaced with additional patients at the same dose level. If, after at least 3 patients have enrolled and the study treatment has been completed for 28 days, if the study treatment is deemed acceptable in a safety investigation for a cohort by the IMC, then enrollment in that cohort will continue until a total of approximately 20 patients have been enrolled. can continue The IMC reviews efficacy data for the first approximately 20 patients in each cohort to evaluate safety and efficacy. If the IMC determines that there is a favorable benefit-risk, enrollment in that cohort may continue until a total of approximately 40 patients.
840 mg 용량의 티라골루맙이 그 어떤 코호트에서도 안전성 탐색 중에 용인되지 않는 경우, 해당 코호트에 등록된 3명의 추가 환자에 대해 더 낮은 용량의 티라골루맙에서 안전성 탐색을 개시할 수 있다. 상기 저용량 군에 대한 안전성 데이터는 해당 코호트의 처음 3명의 환자가 28일 간의 연구 치료를 완료한 후 평가한다(주기 1의 1일~28일). 안전성 탐색에서 약 3명의 추가 환자를 등록하여 상기 더 낮은 용량에서 티라골루맙의 안전성 및 내약성을 추가로 평가할 것이다. 티라골루맙의 용량만을 감량할 수 있고; 아테졸리주맙의 용량은 변하지 않는다. 상기 더 낮은 용량의 연구 치료제가 내약성인 경우, 상기 더 낮은 용량의 안전성 탐색 중인 환자를 포함하여 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 더 낮은 용량으로 등록을 계속한다. IMC는 각 코호트의 20명의 환자에 대한 데이터를 검토하여 안전성과 유효성을 평가한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 상기 더 낮은 용량에서 총 약 40명의 환자가 될 때까지 계속할 수 있다.If the 840 mg dose of tiragolumab is not tolerated during the safety investigation in any cohort, the safety investigation may be initiated at the lower dose of tiragoluumab for 3 additional patients enrolled in that cohort. Safety data for the low-dose group will be assessed after the first 3 patients in this cohort have completed 28 days of study treatment (Days 1-28 of Cycle 1). About 3 additional patients will be enrolled in the safety expedition to further evaluate the safety and tolerability of tiragolumab at this lower dose. Only the dose of tiragolumab can be reduced; The dose of atezolizumab does not change. If the lower dose of the study treatment is well tolerated, continue enrollment at the lower dose until a total of about 20 patients have been enrolled in each cohort, including those undergoing safety exploration of the lower dose. The IMC evaluates safety and efficacy by reviewing data from 20 patients in each cohort. If the IMC determines that there is a favorable benefit-risk, then enrollment in that cohort may continue until a total of about 40 patients at the lower dose.
840 mg 용량의 티라골루맙이 안전성 탐색 기간 동안 내약성이 양호하고 새로운 임상 PK 데이터 및/또는 약력학적 데이터(예컨대, 수용체 점유)가 더 높은 용량의 티라골루맙을 사용할 것을 암시하는 경우, 각 코호트에 등록된 다음 3명의 환자에 대해 더 높은 용량의 티라골루맙에서 안전성 탐색을 개시한다. 상기 더 높은 용량은 1200 mg을 초과하지 않으며, 이는 본 연구의 Ia상 및 Ib상 부분 모두에서 MTG7192A에 대한 최대 평가 용량이며, 3주마다 1200 mg 용량 수준에서 관찰된 것보다 더 크게 관찰된 최대 농도(Cmax)는 없다. 상기 고용량의 티라골루맙에서 연구 치료제가 내약성인 경우, 최소 6명의 환자가 등록하고 28일 간의 연구 치료를 완료할 때까지 상기 고용량의 안전 탐색에서 등록을 계속한다. 상기 고용량의 연구 치료제가 IMC에 의한 안전성 탐색에서 내약성인 것으로 판단된 경우, 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 고용량의 티라골루맙으로 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 20명의 환자에 데이터를 검토한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 상기 더 높은 용량에서 총 약 40명의 환자가 될 때까지 계속한다.If the 840 mg dose of tiragolumab is well tolerated during the safety exploration period, and new clinical PK data and/or pharmacodynamic data (e.g., receptor occupancy) suggest the use of a higher dose of tiragolumab, each cohort Initiate a safety investigation at higher doses of tiragolumab in the next three patients enrolled. This higher dose does not exceed 1200 mg, which is the maximum evaluated dose for MTG7192A in both the Phase Ia and Ib portions of this study, and the maximum observed concentration greater than that observed at the 1200 mg dose level every 3 weeks. (C max ) is absent. If the study treatment at the high-dose tiragolumab is well tolerated, enrollment continues in the high-dose safety expedition until a minimum of 6 patients have been enrolled and complete 28 days of study treatment. If the high-dose study treatment is judged to be well tolerated in a safety investigation by the IMC, enrollment with the high-dose tiragolumab may continue until a total of approximately 20 patients have been enrolled in each cohort. The IMC reviews data from the first 20 patients in each cohort to evaluate safety and efficacy. If the IMC determines that there is a beneficial benefit-risk, then enrollment in that cohort continues until a total of about 40 patients at the higher dose.
Ib상 비화학요법 확장 코호트Phase Ib Non-chemotherapy Expansion Cohort
Ib상 비화학요법 확장 코호트의 목적은 베바시주맙과 함께 티라골루맙 및 아테졸리주맙, 및 펨브롤리주맙과 병용한 티라골루맙으로 치료를 받은 환자를 대상으로 안전성, 내약성, 및 예비 유효성 데이터를 더 잘 특성화하고 약력학적 활성의 잠재적인 종양 바이오마커를 탐색하는 것이다.The purpose of the Phase Ib non-chemotherapy expansion cohort was to provide further safety, tolerability, and preliminary efficacy data in patients treated with tiragolumab and atezolizumab in combination with bevacizumab and tiragolumab in combination with pembrolizumab. The goal is to explore well-characterized and potential tumor biomarkers of pharmacodynamic activity.
각각의 코호트는 선별검사 또는 사전 선별검사 동안 종양 조직의 전향적 시험을 기반으로 PD-L1 선택 및/또는 TIGIT 선택될 수 있는 종양을 가진 약 20~40명의 환자로 구성된다. 보관 조직이 불충분하거나 입수 불가능한 환자는 시험자와의 논의를 바탕으로 의료 모니터(Medical Monitor)가 허용하는 경우 상기 코호트 등록에 적격일 수 있다. 베바시주맙을 포함하거나 포함하지 않고 항 PD-L1/PD-1과 병용한 임상 시험용 제제에 대한 임상 시험이 시험자의 재량에 따라 허용 가능한 치료 선택 사항으로 간주되는 종양 유형을 가진 환자가 상기 확장 코호트에 등록될 수 있다. 특정 종양 유형(예컨대, HCC, 흑색종)을 가진 환자 또는 특정 치료 이력(예컨대, CIT 미경험)을 가진 환자의 수는 각 연구 코호트에서 제한될 수 있다. Each cohort consists of approximately 20-40 patients with tumors that can be selected for PD-L1 and/or TIGIT based on prospective examination of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archival tissue may be eligible for enrollment in this cohort if permitted by the Medical Monitor based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational agents with or without bevacizumab in combination with anti-PD-L1/PD-1 are considered acceptable treatment options at the discretion of the investigator are included in the expansion cohort. can be registered in The number of patients with a specific tumor type (eg, HCC, melanoma) or with a specific treatment history (eg, CIT naive) may be limited in each study cohort.
각 코호트의 치료 조합은 표 30에 나타내었다. Treatment combinations for each cohort are shown in Table 30.
(21일 주기)treatment regimen a
(21 day cycle)
코호트별 치료 조합Treatment Combinations by Cohort
각 코호트에는 약 3명의 환자에 대한 초기 안전성 탐색이 있다(도 6). 코호트의 처음 3명의 환자가 3주 간(21일)의 연구 치료를 완료한 후(즉, 주기 1의 1일~21일), IMC는 연구 치료제가 용인되는지 여부를 결정하기 위해 해당 코호트에 대한 처음 3명의 환자의 모든 안전성 데이터를 검토하며, 여기서 IMC 및 시험자는 환자에게 베바시주맙과 함께 티라골루맙 및 아테졸리주맙(코호트 NC1) 또는 티라골루맙 및 펨브롤리주맙(코호트 NC2)의 투약을 계속할 수 있도록 허용 가능한 위험 평가를 실시한다. 치료 관련 독성 이외의 이유로 처음 3주 간의 치료를 완료하지 않은 환자는 동일한 용량 수준의 추가 환자로 대체될 수 있다. 최소 3명의 환자가 등록하고 3주 간의 연구 치료를 완료한 후 IMC에 의해 코호트에 대한 안전성 탐색에서 연구 치료제가 용인 가능한 것으로 판단된 경우, 총 약 20명의 환자가 등록될 때까지 해당 코호트에 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 약 20명의 환자에 대한 유효성 데이터를 검토한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 총 약 40명의 환자가 될 때까지 계속할 수 있다.There is an initial safety search for approximately 3 patients in each cohort ( FIG. 6 ). After the first 3 patients in a cohort have completed 3 weeks (Day 21) of study treatment (i.e.,
600 mg 용량의 티라골루맙이 그 어떤 코호트에서도 안전성 탐색 중에 용인되지 않는 경우, 해당 코호트에 등록된 약 3명의 추가 환자에 대해 더 낮은 용량의 티라골루맙에서 안전성 탐색을 개시할 수 있다. 상기 저용량 군에 대한 안전성 데이터는 해당 코호트의 처음 3명의 환자가 3주 간의 연구 치료를 완료한 후 평가한다(주기 1의 1일~21일). 그런 다음, 안전성 탐색에서 약 3명의 추가 환자를 등록하여 상기 더 낮은 용량에서 티라골루맙의 안전성 및 내약성을 추가로 평가할 것이다. 티라골루맙의 용량만을 감량할 수 있고; 베바시주맙과 함께 펨브롤리주맙 또는 아테졸리주맙의 용량은 변하지 않는다. 상기 더 낮은 용량의 연구 치료제가 내약성인 경우, 상기 더 낮은 용량의 안전성 탐색 중인 환자를 포함하여 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 더 낮은 용량으로 등록을 계속한다. IMC는 각 코호트의 20명의 환자에 대한 데이터를 검토하여 안전성과 유효성을 평가한다. IMC가 유리한 이익-위험이 있다고 결정하면, 해당 코호트의 등록을 상기 더 낮은 용량에서 총 약 40명의 환자가 될 때까지 계속할 수 있다.If a 600 mg dose of tiragolumab is not tolerated during a safety investigation in any cohort, a safety investigation at a lower dose of tiragoluumab may be initiated for approximately 3 additional patients enrolled in that cohort. Safety data for the low-dose group will be assessed after the first 3 patients in this cohort have completed 3 weeks of study treatment (Days 1-21 of Cycle 1). About 3 additional patients will then be enrolled in the safety expedition to further evaluate the safety and tolerability of tiragolumab at this lower dose. Only the dose of tiragolumab can be reduced; The dose of pembrolizumab or atezolizumab with bevacizumab does not change. If the lower dose of the study treatment is well tolerated, continue enrollment at the lower dose until a total of about 20 patients have been enrolled in each cohort, including those undergoing safety exploration of the lower dose. The IMC evaluates safety and efficacy by reviewing data from 20 patients in each cohort. If the IMC determines that there is a favorable benefit-risk, then enrollment in that cohort may continue until a total of about 40 patients at the lower dose.
600 mg 용량의 티라골루맙이 안전성 탐색 중에 용인되지 않는 경우, 각 코호트에 등록된 약 3명의 다음 환자에 대해 더 높은 용량의 티라골루맙에서 안전성 탐색을 개시할 수 있다. 상기 더 높은 용량은 3주마다 1200 mg을 초과하지 않으며, 이는 본 연구의 Ia상 및 Ib상 부분 모두에서 티라골루맙에 대한 최대 평가 용량이며, 관찰된 최대 농도(Cmax)는 3주마다 1200 mg 용량 수준에서 관찰된 것보다 더 크지 않다. 상기 고용량의 티라골루맙에서 연구 치료제가 내약성인 경우, 최소 6명의 환자가 등록하고 3주 간의 연구 치료를 완료할 때까지 상기 고용량의 안전성 탐색에서 등록을 계속한다. 상기 고용량의 연구 치료제가 IMC에 의한 안전성 탐색에서 내약성인 것으로 판단된 경우, 각 코호트에 총 약 20명의 환자가 등록될 때까지 상기 고용량의 티라골루맙으로 등록을 계속할 수 있다. IMC는 안전성 및 유효성을 평가하기 위해 각 코호트에서 처음 20명의 환자에 데이터를 검토한다. IMC가 유리한 이익-위험 프로필이 있다고 결정하면, 해당 코호트의 등록을 상기 더 높은 용량에서 총 약 40명의 환자가 될 때까지 계속할 수 있다.If the 600 mg dose of tiragolumab is not tolerated during the safety investigation, a safety investigation may be initiated at the higher dose of tiragolumab for the next approximately 3 patients enrolled in each cohort. This higher dose does not exceed 1200 mg every 3 weeks, which is the maximum evaluated dose for tiragolumab in both the Phase Ia and Ib portions of this study, and the maximum concentration observed (C max ) is 1200 every 3 weeks no greater than that observed at the mg dose level. If the study treatment at the high-dose tiragolumab is well tolerated, enrollment continues in the high-dose safety expedition until a minimum of 6 patients have been enrolled and have completed 3 weeks of study treatment. If the high-dose study treatment is judged to be well tolerated in a safety investigation by the IMC, enrollment with the high-dose tiragolumab may continue until a total of approximately 20 patients have been enrolled in each cohort. The IMC reviews data from the first 20 patients in each cohort to evaluate safety and efficacy. If the IMC determines that there is a favorable benefit-risk profile, then enrollment in that cohort may continue until a total of about 40 patients at that higher dose.
티라골루맙 및 아테졸리주맙 및 기타 비화학요법제의 용량 감소Decrease the dose of tiragolumab and atezolizumab and other non-chemotherapeutic agents
일반적으로, 본 연구에서 티라골루맙의 용량 감소는 없다. 하지만, 입수 가능한 누적 안전성 데이터에 따르면, 초기에 단일 제제(Ia상) 또는 아테졸리주맙과 병용으로(Ib상)으로 선택된 티라골루맙의 용량 수준이 MTD 또는 MAD를 초과하는 경우 해당 용량 수준에서의 연구 대상체 발생이 중단될 수 있으며, 적용 가능한 경우, 추가 용량 증량이 중단된다. In general, there is no dose reduction of tiragolumab in this study. However, based on available cumulative safety data, if the dose level of tiragolumab initially selected as a single agent (Phase Ia) or in combination with atezolizumab (Phase Ib) exceeds the MTD or MAD, the dose level at that dose level Study subject development may be discontinued and further dose escalation will be discontinued, if applicable.
이러한 상황에서, 개별 환자는 하기의 기준이 충족되는 경우 티라골루맙의 새로운 용량 수준으로 용량을 감량할 수 있다: In this situation, the individual patient may reduce the dose to a new dose level of tiragoluumab if the following criteria are met:
![]()
![]()
![]()
![]()
아테졸리주맙의 경우, 환자 내 용량 감소가 없고; 아테졸리주맙의 경우, 21일마다 1200 mg 또는 28일마다 1680mg의 고정 용량으로 투여된다(Q4W 용량 확장 코호트).For atezolizumab, there is no intra-patient dose reduction; For atezolizumab, it is administered as a fixed dose of 1200 mg every 21 days or 1680 mg every 28 days (Q4W dose expansion cohort).
베바시주맙의 경우, 환자 내 용량 감소가 없고; 베바시주맙은 3주마다 15 mg/kg의 고정 용량으로 투여된다.For bevacizumab, there is no intra-patient dose reduction; Bevacizumab is administered at a fixed dose of 15 mg/kg every 3 weeks.
펨브롤리주맙의 경우, 환자 내 용량 감소가 없고; 펨브롤리주맙은 3주마다 200 mg의 고정 용량으로 투여된다.For pembrolizumab, there is no intra-patient dose reduction; Pembrolizumab is administered as a fixed dose of 200 mg every 3 weeks.
질병 진행 이후 치료Treatment after disease progression
환자는 진행성 질병에 대한 표준 RECIST v1.1 기준이 의료 모니터 요원과 논의한 후 시험자의 재량에 따라 충족된 후에 그리고 환자가 하기의 기준을 모두 충족하는 경우 연구의 Ia상 또는 Ib상 부분에서 연구 치료를 계속할 수 있다(도 7):Patients may receive study treatment in the Phase Ia or Ib portion of the study after standard RECIST v1.1 criteria for advanced disease have been met at the investigator's discretion after discussion with the medical monitor and if the patient meets all of the following criteria: We can continue (Fig. 7):
![]()
![]()
![]()
![]()
![]()
![]()
환자는 방사선학적 진행을 넘어 연구 치료를 계속하는 것의 이익-위험 균형에 대한 치료 중 시험자와 논의를 수용하는데 동의해야 한다.Patients must agree to accept on-treatment investigator discussions about the benefit-risk balance of continuing study treatment beyond radiological progression.
방사선학적 질병 진행이 Ia상 또는 Ib상의 후속 종양 평가에서 확인되면, 환자는, 이들이 상기 기준을 계속 충족하고 하기의 적어도 하나에 의해 입증된 바와 같이 임상 이익이 계속되는 경우, 의료 모니터 요원과 논의 이후 시험자의 재량에 따라 계속된 연구 치료에 대하여 고려될 수 있다:If radiological disease progression is confirmed at subsequent tumor assessments in Phase Ia or Ib, patients, after discussion with medical monitor personnel, if they continue to meet the above criteria and continue clinical benefit as evidenced by at least one of the following: may be considered for continued study treatment at the discretion of:
![]()
![]()
![]()
![]()
연구의 Ia상 부분에서만, 단일 제제 티라골루맙으로 치료를 받고, 진행성 질병이 발병하고, 그리고/또는 상기에 개략된 바와 같이 임상적 이익을 더 이상 유도 못하는 환자는 안전하게 접근 가능한 종양을 가지고, 생검에 동의하고 전환에 대한 지정된 기준을 충족한 경우 아테졸리주맙과 병용한 티라골루맙에 대한 연구의 Ib상 부분에서 치료를 받는 것에 적격일 수 있다.Only in the Phase Ia portion of the study, patients treated with single agent tyragolumab, developing progressive disease, and/or no longer eliciting clinical benefit as outlined above, have safely accessible tumors, biopsy may be eligible to receive treatment in the Phase Ib portion of the study for tiragolumab in combination with atezolizumab if they consent to and meet the specified criteria for conversion.
화학요법 확장 코호트 A, B, C 및 D에서, 질병 진행 후 치료는 화학요법을 포함하거나 포함하지 않는 면역요법(아테졸리주맙 및/또는 티라골루맙)을 포함해야 하고, 화학요법 단독으로는 불가능하다. In chemotherapy expansion cohorts A, B, C and D, treatment after disease progression must include immunotherapy with or without chemotherapy (atezolizumab and/or tiragolumab) and not chemotherapy alone do.
진행 시 단일제제 티라골루맙 치료에서 아테졸리주맙과 병용한 티라골루맙으로의 전환Conversion from single agent tiragolumab treatment to tiragolumab in combination with atezolizumab during progression
연구의 Ia상 부분에서 단일 제제로서 티라골루맙으로 치료를 받고, 진행성 질병이 발병하고, 그리고/또는 더 이상 임상적 이득을 유도하지 못하는 환자는 연구의 Ib상 부분에서 아테졸리주맙과 병용한 티라골루맙으로의 치료를 받은 데에 적격일 수 있다(도 8). 단, 하기의 조건들을 충족해야 한다:Patients who were treated with tyragolumab as a single agent in the Phase Ia portion of the study, develop progressive disease, and/or no longer induce clinical benefit, were treated with Tyra in combination with Atezolizumab in the Phase Ib portion of the study. may be eligible for treatment with goluumab ( FIG. 8 ). However, the following conditions must be met:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
안전하게 접근 가능한 질병 부위(들)가 있는 환자의 경우, 종양 생검이 필요하다. 상기 생검은 Ib상 연구에서 티라골루맙 및 아테졸리주맙을 투약하기 전에 언제든지 실시할 수 있다. 선택적인 치료 중 생검은 또한 티라골루맙 및 아테졸리주맙을 투약한 후 주기 1의 15일~21일 또는 그 사이에 수집할 수 있다. RECIST 표적 병변은 생검하지 않는다.For patients with safely accessible disease site(s), a tumor biopsy is required. The biopsy may be performed at any time prior to dosing of tiragolumab and atezolizumab in a phase Ib study. Optional on-treatment biopsies may also be collected on or between days 15-21 of
Ib상 연구에서 아테졸리주맙과 병용한 티라골루맙의 치료 전환을 위한 용량 및 일정은 의료 모니터 요원의 승인을 필요로 한다. 일반적으로, 연구의 Ib상 부분으로 전환되는 환자는 아테졸리주맙과 병용하여 이의 MTD를 초과하지 않는 것으로 이미 밝혀진 최고 용량의 티라골루맙을 투여받는다(도 7). 따라서, Ib상 연구에서 평가된 티라골루맙의 용량 수준은 Ia상 연구의 동일한 환자에서 평가된 용량 수준과 상이할 수 있다. Ia상 연구에서 단일 제제로서 티라골루맙의 용량 및/또는 일정을 수정한 환자는, 티라골루맙의 해당 용량이 아테졸리주맙과 병용한 티라골루맙에 대한 MTD를 초과하지 않는 것으로 이전에 밝혀진 한, Ib상에서 동일한 용량 및/또는 일정으로 티라골루맙을 계속 투여받는다.Doses and schedules for treatment conversion of tiragolumab in combination with atezolizumab in phase Ib studies require approval from medical monitor personnel. In general, patients transitioning to the Phase Ib portion of the study receive the highest dose of tyragolumab that has already been shown not to exceed its MTD in combination with atezolizumab ( FIG. 7 ). Thus, the dose level of tiragolumab evaluated in the Phase Ib study may be different from the dose level evaluated in the same patient in the Phase Ia study. Patients who have modified their dose and/or schedule of tiragolumab as a single agent in a Phase Ia study, unless previously shown that the corresponding dose of tiragolumab does not exceed the MTD for tiragolumab in combination with atezolizumab , continue to receive tiragolumab at the same dose and/or schedule in phase Ib.
연구의 Ia상 부분에서 연구의 Ib상 부분으로 전환되는 환자는 하기와 같이 치료된다:Patients transitioning from the Phase Ia portion of the study to the Phase Ib portion of the study are treated as follows:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Ia상에서 Ib상으로의 전환 치료 이전에 수득한 종양 생검으로부터 파생된 임상 데이터 및 탐색 데이터를 지속적으로 모니터링한다. Clinical and exploratory data derived from tumor biopsies obtained prior to phase Ia transition treatment to phase Ib are continuously monitored.
Ia상 부분에서 Ib상 연구로의 전환 등록은 언제든지 제한되거나 중단될 수 있다. 그 이유에는 안전, 불만족스러운 환자 등록 및/또는 불완전한 데이터 기록이 포함될 수 있다.Enrollment for transition from the Phase Ia portion to the Phase Ib study may be restricted or discontinued at any time. Reasons may include safety, unsatisfactory patient enrollment, and/or incomplete data records.
C.C. 연구 치료research treatment
용량 및 투여Dosage and administration
단일 제제(Ia상)로서의 티라골루맙 또는 아테졸리주맙과 병용한 티라골루맙(Ib상)의 투여는 중환자실에 접근할 수 있는 응급 의료 시설과 의료 응급 상황을 모니터링하고 대응하도록 훈련된 직원이 있는 환경에서 실시한다. Administration of tiragolumab as a single agent (Phase Ia) or tiragolumab in combination with atezolizumab (Phase Ib) should be administered by emergency medical facilities with access to the intensive care unit and staff trained to monitor and respond to medical emergencies. carried out in an environment where
연구의 Ib상 부분(화학요법이 없는 코호트)에서의 치료의 경우, 예정된 연구 치료제 주입일에 티라골루맙은 중간 관찰 기간을 사이에 두고 아테졸리주맙 이전에 투여한다. For treatment in the Phase Ib portion of the study (cohort without chemotherapy), tiragolumab is administered prior to atezolizumab on the day of the scheduled study treatment infusion with an interim observation period.
Ib상 화학요법 확장 코호트에서의 치료의 경우, 예정된 연구 치료제 주입일에 아테졸리주맙은 중간 관찰 기간을 사이에 두고 티라골루맙 이전에 투여한다. 화학요법은 아테졸리주맙 및 티라골루맙 후에 투여하고, 티라골루맙에 대해서는 중간 관찰 기간을 둔다.For treatment in the Phase Ib chemotherapy expansion cohort, on the scheduled study treatment infusion day, atezolizumab is administered prior to tiragolumab with an intervening observation period. Chemotherapy is administered after atezolizumab and tiragolumab, with an interim observation period for tiragolumab.
Ib상 비화학요법 확장 코호트에서의 치료의 경우, 예정된 연구 치료제 주입일에 티라골루맙은 베바시주맙(코호트 NC1) 또는 펨브롤리주맙(코호트 Nc2)과 병용한 아테졸리주맙 이전에 중간 관찰 기간을 사이에 두고 투여한다. 베바시주맙은 티라골루맙 및 아테졸리주맙 후에 투여하고, 베바시주맙에 대해서는 중간 관찰 기간을 둔다. For treatment in the Phase Ib non-chemotherapy expansion cohort, on the day of the scheduled study treatment infusion, tiragolumab was administered between bevacizumab (Cohort NC1) or interim observation period prior to atezolizumab in combination with pembrolizumab (Cohort Nc2). placed in and administered Bevacizumab is administered after tiragolumab and atezolizumab, with an interim observation period for bevacizumab.
티라골루맙, 아테졸리주맙 또는 베바시주맙에 대한 용량 준비 및 투여 지침에 대한 자세한 내용은 각각의 시험자의 안내 책자 및 GO30103 약국 매뉴얼을 참조한다. For details on dosage preparation and administration instructions for tiragolumab, atezolizumab or bevacizumab, refer to the respective investigator's brochure and GO30103 Pharmacy Manual.
시스플라틴, 카보플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈, 에토포사이드 및 펨브롤리주맙의 용량 준비 및 투여 지침에 대한 자세한 내용은 패키지 삽입물 또는 SmPC를 참조한다.See the package insert or SmPC for details on dosage preparation and administration instructions for cisplatin, carboplatin, pemetrexed, paclitaxel, capecitabine, etoposide and pembrolizumab.
Ia상 및 Ib상의 티라골루맙Tiragolumab in Phase Ia and Ib
본 연구의 Ia상 및 Ib상 부분에서 평가할 티라골루맙의 대략적인 용량 수준은 IV 주입에 의해 3주마다 투여되는 2 mg, 8 mg, 30 mg, 100 mg, 400 mg 및 1200 mg이다. Ia상 또는 Ib상에서 MTD를 초과하지 않는 기타 용량 수준 또는 Ia상 및/또는 Ib상에서 티라골루맙의 새로운 투약 일정은 참여한 시험자와 협의한 후 새로운 비임상 유효성, 임상 안전성 및 임상 PK 데이터를 기초로 평가할 수 있다. 티라골루맙 1200 mg를 초과하는 용량 수준의 평가는 뒷받침하는 근거와 함께 프로토콜 수정이 필요할 것이다. Ib상 화학요법 및 비화학요법 확장 코호트의 경우, 티라골루맙 600 mg이 IV 주입에 의해 3주마다 투여되는 초기 용량이다. Q4W 유지가 포함된 Ib상 화학요법 코호트 B 및 코호트 C의 경우, 티라골루맙 용량은 유지 시 840 mg으로 변경된다. Ib상 Q4W 투약 코호트의 경우, 840 mg 티라골루맙이 IV 주입에 의해 Q4W으로 투여되는 초기 용량이다. 용량은 체중에 따라 달라지지 않는다. Approximate dose levels of tiragolumab to be evaluated in the Phase Ia and Phase Ib portions of this study are 2 mg, 8 mg, 30 mg, 100 mg, 400 mg and 1200 mg administered every 3 weeks by IV infusion. Other dose levels not exceeding the MTD in phase Ia or Ib, or new dosing schedules for tiragolumab in phases Ia and/or Ib will be evaluated based on new nonclinical efficacy, clinical safety, and clinical PK data after consultation with the participating investigators. can Evaluation of dose levels above tiragoluumab 1200 mg will require protocol modifications with supporting evidence. For the Phase Ib chemotherapy and non-chemotherapy expansion cohorts, tiragolumab 600 mg is the initial dose administered every 3 weeks by IV infusion. For Phase Ib chemotherapy cohorts B and C with Q4W maintenance, the tiragolumab dose is changed to 840 mg on maintenance. For the Phase Ib Q4W dosing cohort, 840 mg tyragolumab is the initial dose administered as Q4W by IV infusion. Dosage does not depend on body weight.
840 mg Q4W 투약 요법은 PK 모델링 및 시뮬레이션 및 노출 안전성 분석의 결과에 의해 뒷받침된다. 상기 840 mg Q4W 투약 요법 후의 평균 농도는 연구 GO30103 및 GO40290 연구에서 평가되었던 3주마다 600 mg 투약 요법의 농도와 유사하다. 840 mg Q4W 투약 요법의 Cmax는 3주마다 600 mg 투약 요법의 Cmax에 비해 정상 상태에서 28% 더 높지만, 병원에서는 가장 높은 투여 용량의 관찰된 노출 범위 내에 속한다(연구 GO30103에서 3주마다 1200 mg). 연구 GO30103의 데이터(3주마다 단일 요법으로 또는 3주마다 아테졸리주맙 1200 mg과 병용으로 투여된 2-1200 mg의 티라골루맙 용량)을 기반으로 한 티라골루맙 노출-안전 관계에 대한 예비 분석은 티라골루맙이 균일한 노출-안전 관계를 나타냄을 시사한다. 요약하면, 상기 840 mg Q4W 투약 요법은 노출이 관찰된 유효 노출 범위 내에 있고 티라골루맙이 균일한 노출-안전 관계를 갖는 것으로 보인다는 점을 감안할 때 3주마다 600 mg 투약 요법과 유사한 안전성 및 유효성을 제공할 수 있다.The 840 mg Q4W dosing regimen is supported by the results of PK modeling and simulation and exposure safety analysis. The mean concentrations after the 840 mg Q4W dosing regimen are similar to those of the 600 mg every 3 weeks dosing regimen evaluated in studies GO30103 and GO40290 studies. The Cmax of the 840 mg Q4W dosing regimen is 28% higher at steady state compared to the Cmax of the 600 mg every 3 weeks, but falls within the observed exposure range of the highest administered dose in the hospital (1200 mg every 3 weeks in study GO30103). . Preliminary analysis of tiragoluumab exposure-safety relationship based on data from study GO30103 (tiragoluumab dose of 2-1200 mg administered as monotherapy every 3 weeks or in combination with atezolizumab 1200 mg every 3 weeks) suggest that tiragolumab exhibits a uniform exposure-safety relationship. In summary, the 840 mg Q4W dosing regimen was similar in safety and efficacy to the 600 mg every 3 weeks dosing regimen given that exposures were within the observed effective exposure range and tiragoluumab appeared to have a uniform exposure-safety relationship. can provide
연구의 Ia상에서 티라골루맙의 초기 용량은 (주입이 주입 관련 증상을 경험한 환자의 경우 둔화 또는 방해될 수 있어도) 90(±10분) 동안 전달될 수 있고, 240분 관찰 기간이 이어진다. 연구의 Ib 단계에서 티라골루맙의 초기 용량은 60분(10분)에 걸쳐 전달되고, 60분의 관찰 기간이 이어진다. 초기 주입이 주입 관련 부작용 없이 내약성이 있는 경우, Ia상의 제2 주입은 60(10)분에 걸쳐 전달될 수 있고, 60분의 관찰 기간이 이어지며, Ib상의 제2 주입은 30(10)분에 걸쳐 전달될 수 있고, 30분의 관찰 시간이 이어진다. 60분 주입이 양호하게 용인되면, Ia상의 제3 주입이 30(±10)분 동안 전달될 수 있고, 30분 관찰 기간이 이어진다. Ia상의 제3 주입 또는 Ib상의 제2 주입이 양호하게 용인되면, Ia상의 모든 후속 주입이 30(±10)분 동안 전달될 수 있고, 30분 관찰 기간이 이어진다. 이전에 Ia상에서 단일 제제 티라골루맙을 투여받았고 현재 Ib상에서 아테졸리주맙과 병용한 티라골루맙을 투여 중인 환자는 환자가 이전에 내약했던 가장 빠른 속도로 Ib상의 초기 용량을 투여받을 수 있다.The initial dose of tiragolumab in Phase Ia of the study can be delivered for 90 (±10 minutes), followed by a 240 minute observation period (although the infusion may be blunted or obstructed for patients experiencing infusion-related symptoms). In Phase Ib of the study, an initial dose of tiragolumab is delivered over 60 minutes (10 minutes) followed by a 60 minute observation period. If the initial infusion is well tolerated without infusion-related side effects, the second infusion in Phase Ia can be delivered over 60 (10) minutes followed by a 60 minute observation period, and the second infusion in Phase Ib is 30 (10) minutes. can be delivered over a period of time, followed by an observation time of 30 min. If the 60 min infusion is well tolerated, a third infusion on Phase Ia can be delivered for 30 (±10) min followed by a 30 min observation period. If the third infusion in Phase Ia or the second infusion in Phase Ib is well tolerated, all subsequent infusions in Phase Ia can be delivered for 30 (±10) minutes, followed by a 30 minute observation period. Patients previously receiving single agent tiragolumab in phase Ia and currently receiving tiragolumab in combination with atezolizumab in phase Ib may receive the initial dose in phase Ib at the fastest rate the patient has previously tolerated.
명시된 경우를 제외하고 본 연구(Ia상 또는 Ib상)에서 티라골루맙에 대한 용량 감소는 없다. 티라골루맙의 용량 변경 및 치료 중단 또는 중단에 대한 지침이 제공된다. 특정 이상 반응 관리의 맥락에서 연구 약물 투여에 대한 지침이 제공된다. There are no dose reductions for tiragolumab in this study (Phase Ia or Phase Ib) except as noted. Guidance is provided for dose changes and discontinuation or discontinuation of treatment for tiragolumab. Guidance for study drug administration in the context of managing specific adverse events is provided.
연구 약물의 과다 복용 또는 부정확한 투여와 관련된 이상 반응이 기록된다. Adverse events related to overdose or incorrect administration of study drug are recorded.
Ib상 아테졸리주맙Phase Ib Atezolizumab
본 연구의 Ib상 부분에서 티라골루맙과 병용으로 투여되는 아테졸리주맙의 용량은 3주마다 1200 mg IV이다. Q4W 유지가 포함된 Ib상 화학요법 코호트 B 및 코호트 C의 경우, 아테졸리주맙 용량은 유지 시 1680 mg으로 변경된다. Ib상 Q4W 투약 코호트에서는 아테졸리주맙 1680 mg IV Q4W가 투여된다. 상기 용량은 고정되고 체중에 의존하지 않는다.The dose of atezolizumab administered in combination with tiragolumab in the Phase Ib portion of this study is 1200 mg IV every 3 weeks. For Phase Ib chemotherapy cohorts B and C with Q4W maintenance, the atezolizumab dose is changed to 1680 mg on maintenance. The Phase Ib Q4W dosing cohort is administered atezolizumab 1680 mg IV Q4W. The dose is fixed and does not depend on body weight.
화학요법을 포함하지 않은 모든 Ib상 코호트에서, 아테졸리주맙은 티라골루맙 주입 및 후속 관찰 기간 후에 투여된다. Ib상 화학요법 확장 코호트에서, 아테졸리주맙은 티라골루맙 이전에 투여된다.In all Phase Ib cohorts that did not include chemotherapy, atezolizumab is administered after the tiragolumab infusion and subsequent observation period. In the Phase Ib chemotherapy expansion cohort, atezolizumab is administered prior to tiragolumab.
아테졸리주맙의 초기 용량은 60(±10)분에 걸쳐 전달된다. 제1 주입이 주입 관련 유해 사례 없이 내약성이면, 제2 주입은 30 (±10)분에 걸쳐 전달될 수 있다. 30분 주입이 양호하게 용인되면, 후속하는 모든 주입은 30(±10)분에 걸쳐 전달될 수 있다. 주기 1의 경우, 아테졸리주맙 투약 후 60분의 관찰 기간이 이어진다. 이후의 모든 아테졸리주맙 주입 후에는 30분의 관찰 기간이 이어질 수 있다. 이전에 다른 임상 시험에서 아테졸리주맙을 투여받은 환자는 이전에 허용되었던 가장 빠른 속도로 초기 용량을 투여받을 수 있다. The initial dose of atezolizumab is delivered over 60 (±10) minutes. If the first infusion is well tolerated without infusion-related adverse events, the second infusion may be delivered over 30 (±10) minutes. If a 30 minute infusion is well tolerated, all subsequent infusions can be delivered over 30 (±10) minutes. For
본 연구에서 아테졸리주맙에 대한 용량 감소는 없다. 용량 변경 및 치료 중단 또는 중단에 대한 지침이 제공된다. 특정 이상 반응 관리의 맥락에서 연구 약물 투여에 대한 지침이 제공된다. There is no dose reduction for atezolizumab in this study. Guidance for dose changes and treatment discontinuation or discontinuation is provided. Guidance for study drug administration in the context of managing specific adverse events is provided.
연구 약물 EW의 과다 복용 또는 부정확한 투여와 관련된 이상 반응이 기록된다.Adverse events related to overdose or incorrect administration of study drug EW are recorded.
Ib상 확장 코호트에서의 비화학요법 코호트Non-chemotherapy cohort in phase lb expansion cohort
코호트 NC1: 베바시주맙을 병용한 티라골루맙 및 아테졸리주맙Cohort NC1: Tiragolumab and Atezolizumab with Bevacizumab
티라골루맙 및 아테졸리주맙 및 베바시주맙 코호트의 환자는 통합 평가 후 시험자가 결정한 바와 같이 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 표 31에 개략된 바와 같은 치료를 받는다. 등록 후 7일 이내에 치료를 개시하는 것을 권고한다. 하지만, 제1 용량 투여는 핵심 생검 또는 기타 수술 절차 후 7일 이내에 실시해서는 안 된다.Patients in the tiragolumab and atezolizumab and bevacizumab cohorts receive treatment as outlined in Table 31 after pooled evaluation until there is unacceptable toxicity or loss of clinical benefit as determined by the investigator. It is recommended to start treatment within 7 days of enrollment. However, the first dose should not be administered within 7 days of a core biopsy or other surgical procedure.
2. 아테졸리주맙: 1일에 1200 mg IV 주입
3. 베바시주맙: 1일에 15 mg/kg IV 주입b 1. Tiragolumab: 600 mg IV infusion per day
2. Atezolizumab: 1200 mg IV infusion per day
3. Bevacizumab: 15 mg/kg IV infusion per day b
a
투여 순서로 나열된 약물. 모든 약물은 각 21일 주기의 제 1일에 IV 주입으로 투여한다.
b
주기 1의 1일에, 베바시주맙은 아테졸리주맙 주입 완료 후 60분에 투여한다. 환자가 이전 약물 주입 중에 주입 관련 반응을 경험했다면, 후속 주입 사이의 간격은 60분이다. 이전 약물 주입이 주입 관련 반응 없이 내약성이었다면, 상기 간격을 30분으로 줄일 수 있다.IV = intravenous
a Drugs listed in order of administration. All drugs are administered by IV infusion on
b On
코호트 NC1에 대한 치료 요법Treatment regimen for cohort NC1
코호트 NC2: 티라골루맙 및 펨브롤리주맙Cohort NC2: Tiragolumab and Pembrolizumab
티라골루맙 및 펨브롤리주맙 코호트의 환자는 통합 평가 후 시험자가 결정한 바와 같이 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 표 32에 개략된 바와 같은 치료를 받는다. 등록 후 7일 이내에 치료를 개시하는 것을 권고한다. 하지만, 제1 용량 투여는 핵심 생검 또는 기타 수술 절차 후 7일 이내에 실시해서는 안 된다.Patients in the tiragolumab and pembrolizumab cohorts receive treatment as outlined in Table 32 after pooled evaluation until there is unacceptable toxicity or loss of clinical benefit as determined by the investigator. It is recommended to start treatment within 7 days of enrollment. However, the first dose should not be administered within 7 days of a core biopsy or other surgical procedure.
2. 펨브롤리주맙 1일에 200 mg IV 주입b 1. Tiragolumab: 600 mg IV infusion per day b
2.
a
투여 순서로 나열된 약물. 모든 약물은 각 21일 주기의 제 1일에 IV 주입으로 투여한다.
b
주기 1의 1일에, 펨브롤리주맙은 티라골루맙 주입 완료 후 60분에 투여한다. 환자가 이전의 티라골루맙 주입 중에 주입 관련 반응을 경험했다면, 후속 주입 사이의 간격은 60분이다. 이전의 티라골루맙 주입이 예비 투약 없이 투여되고 주입 관련 반응 없이 내약성이었다면, 상기 간격을 30분으로 줄일 수 있다.IV = intravenous
a Drugs listed in order of administration. All drugs are administered by IV infusion on
b On
코호트 NC2에 대한 치료 요법Treatment regimen for cohort NC2
Ib상 비화학요법 확장 코호트: 용량 및 투여Phase Ib Non-chemotherapy Expansion Cohort: Dose and Dosing
코호트 NC1의 환자는 매 3주 주기의 제 1일에 티라골루맙 600 mg IV 후, 아테졸리주맙 1200 mg IV 후, 베바시주맙 15 mg/kg IV를 투여 받는다. 시험자가 결정한 바와 같이 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 치료를 실시한다.Patients in cohort NC1 receive tiragolumab 600 mg IV followed by atezolizumab 1200 mg IV followed by bevacizumab 15 mg/kg IV on
코호트 NC2의 환자는 매 3주 주기의 제 1일에 티라골루맙 600 mg IV 후, 펨브롤리주맙 200 mg IV를 투여 받는다. 시험자가 결정한 바와 같이 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 치료를 실시한다.Patients in cohort NC2 receive tiragolumab 600 mg IV followed by
독성 및 임상적 이익의 손실이 있는 경우, 개별 면역요법 제제는 독립적으로 중단될 수 있다. 하지만, 금기 사항이 없고 의료 모니터 요원과 논의한 후에만 펨브롤리주맙 또는 베바시주맙 또는 아테졸리주맙 또는 티라골루주맙 단독의 치료를 고려할 수 있다.In the event of toxicity and loss of clinical benefit, individual immunotherapeutic agents may be independently discontinued. However, treatment with pembrolizumab or bevacizumab or atezolizumab or tiragoluzumab alone may be considered with no contraindications and only after discussion with a medical monitor.
Ib상 확장 코호트에서의 베바시주맙Bevacizumab in Phase Ib Expansion Cohort
베바시주맙은 각 21일 주기의 제 1일에 15 mg/kg의 고정 용량으로 IV 주입으로 투여한다. 베바시주맙의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 실시한다. 용량 변경 및 치료 중단 또는 중단에 대한 지침이 제공된다.Bevacizumab is administered as an IV infusion at a fixed dose of 15 mg/kg on
제1 베바시주맙 주입 이전에 사전투약은 허용되지 않는다. 환자가 이전에 약물 주입으로 IRR을 경험한 경우, 시험자의 재량에 따라 항히스타민제, 해열제 및/또는 진통제를 사전 투여할 수 있다. 상기 주입 전 60분 이내에 활력 징후(맥박수, 호흡수, 혈압, 및 체온)를 측정한다. 베바시주맙의 초기 용량은 90(±10)분에 걸쳐 전달된다. 제1 주입이 주입 관련 이상 반응 없이 내약성이면, 제2 주입은 60 (±10)분에 걸쳐 전달될 수 있다. 60분 주입이 양호하게 내약성이면, 후속하는 모든 주입은 30(±10)분에 걸쳐 전달될 수 있다. 주기 1의 경우, 베바시주맙 투약 후 60분의 관찰 기간이 이어진다. 이후의 모든 베바시주맙 주입 후에는 30분의 관찰 기간이 이어질 수 있다. 이전에 베바시주맙을 투여받은 환자는 이전에 내약성이었던 가장 빠른 속도로 초기 용량을 투여받을 수 있다. 환자에게 주입후 증상 지연 가능성에 관하여 알려주고 이러한 증상이 발생하는 경우 연구 담당의에게 연락하도록 지시한다. 활력징후 측정에 대한 지침이 제공된다. Premedication prior to the first infusion of bevacizumab is not permitted. If the patient has previously experienced an IRR with drug infusion, an antihistamine, antipyretic and/or analgesic may be pre-administered at the investigator's discretion. Vital signs (pulse rate, respiration rate, blood pressure, and body temperature) are measured within 60 minutes prior to the infusion. The initial dose of bevacizumab is delivered over 90 (±10) minutes. If the first infusion is well tolerated without infusion-related adverse events, the second infusion may be delivered over 60 (±10) minutes. If a 60 minute infusion is well tolerated, all subsequent infusions can be delivered over 30 (±10) minutes. For
Ib상 확장 코호트에서의 펨브롤리주맙Pembrolizumab in Phase Ib Expansion Cohort
본 연구의 Ib상 비화학요법 확장 코호트에서 티라골루맙과 병용으로 투여되는 펨브롤리주맙의 용량은 3주마다 200 mg IV이다. 상기 용량은 고정되고 체중에 의존하지 않는다.The dose of pembrolizumab administered in combination with tiragolumab in the Phase Ib non-chemotherapy expansion cohort of this study is 200 mg IV every 3 weeks. The dose is fixed and does not depend on body weight.
펨브롤리주맙의 용량 준비, 보관, 투여 및 치료 중단 또는 중단 지침에 대한 안내는 펨브롤리주맙 처방 정보를 참조한다.See Pembrolizumab Prescribing Information for guidance on dose preparation, storage, administration, and instructions for discontinuing or discontinuing treatment for pembrolizumab.
Ib상 확장 코호트에서의 화학요법Chemotherapy in the Phase Ib Expansion Cohort
화학요법(카페시타빈 제외)은 아테졸리주맙 및 티라골루맙 주입에 이어서 후속하는 관찰 기간 후에 투여된다.Chemotherapy (except capecitabine) is administered following an infusion of atezolizumab and tiragolumab followed by an observation period.
유도기 동안, 화학요법 주기는, 21일 주기 동안 적어도 하나의 화학요법 성분이 적어도 1회 투여되는 경우, 미리 정해진 유도 화학요법 주기의 수에 포함된다. 화학요법 성분이 제공되지 않은 주기는 총 유도 화학요법 주기의 수에 포함되지 않는다. During the induction phase, chemotherapy cycles are included in the predetermined number of induction chemotherapy cycles when at least one chemotherapy component is administered at least once during a 21-day cycle. Cycles for which no chemotherapy component was given are not included in the total number of induction chemotherapy cycles.
치료(유도 또는 유지) 동안 임상적 이익의 증거를 나타내는 환자는 PD에 대한 RECIST v1.1 기준이 충족된 후 치료를 계속할 수 있다.Patients presenting evidence of clinical benefit during treatment (induction or maintenance) may continue treatment after the RECIST v1.1 criteria for PD have been met.
환자는 현지 치료 표준 및 제조업체의 지침에 따라 화학요법제에 대한 항구토제 및 IV 수분 공급을 투여 받는다. 하지만, 스테로이드의 면역조절 효과로 인하여, 스테로이드 예비 투약은 임상적으로 가능한 범위 내에서 최소화한다. Patients receive antiemetics and IV hydration for chemotherapeutic agents according to local standards of care and manufacturer's guidelines. However, due to the immunomodulatory effect of steroids, steroid premedication is minimized to the extent clinically feasible.
화학요법의 용량 변경 및 치료 중단 또는 중지에 대한 지침이 제공된다.Guidance is provided for changing the dose of chemotherapy and stopping or discontinuing treatment.
코호트 A: 아테졸리주맙 + 티라골루맙 + 카보플라틴/시스플라틴 + 페메트렉시드Cohort A: atezolizumab + tiragolumab + carboplatin/cisplatin + pemetrexed
각 21일 주기의 제 1일에, 모든 적격 환자들은 약물 주입을 하기의 순서대로 투여받을 것이다:On
유도: 아테졸리주맙 ® 티라골루맙 ®페메트렉시드 ® 카보플라틴 또는 시스플라틴Induction: atezolizumab ® tyragolumab ® pemetrexed ® carboplatin or cisplatin
유도기에서 4회 내지 6회 주기 후, 환자는 하기의 투여 순서대로 유지 요법을 개시한다: After 4 to 6 cycles in the induction phase, the patient initiates maintenance therapy in the following order of administration:
유지: 아테졸리주맙 ® 티라골루맙 ®페메트렉시드Maintenance: Atezolizumab ® Tiragolumab ® Pemetrexed
표 33은 페메트렉시드에 대해 제안된 예비 투약을 나열한다. 표 7은 유도기 동안 페메트렉시드 및 카보플라틴 또는 시스플라틴 및 유지기 동안 페메트렉시드의 치료 투여에 대한 권장 주입 시간을 나열한다.Table 33 lists the proposed premedication for pemetrexed. Table 7 lists the recommended infusion times for therapeutic administration of pemetrexed and carboplatin or cisplatin and pemetrexed during the maintenance phase during the induction phase.
페메트렉시드의 예비 투약Premedication of pemetrexed
코호트 B: 아테졸리주맙 + 티라골루맙 + 카보플라틴 + 파클리탁셀Cohort B: Atezolizumab + Tiragolumab + Carboplatin + Paclitaxel
각 21일 주기의 제 1일에, 모든 적격 환자들은 약물 주입을 하기의 순서대로 투여받을 것이다:On
유도: 아테졸리주맙 ® 티라골루맙®파클리탁셀®카보플라틴Induction: Atezolizumab ® Tiragolumab® Paclitaxel® Carboplatin
유도기에서 4회 내지 6회 주기 후, 환자는 프로토콜 버전 4에 따라 등록된 경우 각 21일 주기의 제 1일에, 프로토콜 버전 5 이상에 등록된 경우 각 28일 주기의 제 1일에 유지 요법을 시작한다. 모든 적격 환자는 하기의 투여 순서대로 약물 주입을 받는다: After 4 to 6 cycles in the induction phase, patients receive maintenance therapy on
유지: 아테졸리주맙 ® 티라골루맙Maintenance: Atezolizumab ® Tiragolumab
표 8은 코호트 B의 환자에 대한 유도 치료를 위해 제안된 예비 투약을 나열한다. 표 9는 유도기 동안 파클리탁셀 및 카보플라틴의 치료 투여를 위한 제안된 주입 시간을 나열한다.Table 8 lists the proposed pre-dosing for induction treatment for patients in Cohort B. Table 9 lists the suggested infusion times for therapeutic administration of paclitaxel and carboplatin during the induction phase.
코호트 C: 아테졸리주맙 + 티라골루맙 + 카보플라틴 + 시스플라틴Cohort C: Atezolizumab + Tiragolumab + Carboplatin + Cisplatin
각 21일 주기의 제 1일에 모든 적격 환자에게 하기의 순서대로 연구 약물을 주입한다:On
유도: 아테졸리주맙 →티라골루맙 → 시스플라틴 또는 카보플라틴 → 에토포시드 Induction: atezolizumab → tyragolumab → cisplatin or carboplatin → etoposide
유도기 이후에, 환자는 하기의 투여 순서대로 각 28일 주기의 제 1일에 유지 요법을 시작한다:Following the induction phase, patients begin maintenance therapy on
유지: 아테졸리주맙 → 티라골루맙Maintenance: Atezolizumab → Tiragolumab
표 10은 유도기 동안 카보플라틴 또는 시스플라틴 및 에토포시드의 치료 투여에 대해 제안된 주입 시간을 나열한다.Table 10 lists the suggested infusion times for therapeutic administration of carboplatin or cisplatin and etoposide during the induction phase.
코호트 D: 카페시타빈 + 아테졸리주맙 + 티라골루맙Cohort D: Capecitabine + Atezolizumab + Tiragolumab
각 21일 주기의 제 1일에, 모든 적격 환자에게 하기의 순서대로 연구 약물을 투여하였다:On
카페시타빈 → 아테졸리주맙 → 티라골루맙 Capecitabine → Atezolizumab → Tiragolumab
표 34는 카페시타빈의 치료 투여에 대해 제안된 기간, 용량 경로, 및 요법을 나열한다. Table 34 lists the suggested duration, dose route, and regimen for therapeutic administration of capecitabine.
2. 아테졸리주맙: 1일에 1200 mg IV 주입
3. 티라골루맙: 1일에 600 mg IV 주입1. Capecitamine: 1250 mg/m 2 PO BID on days 1-14 followed by a 7-day resting period
2. Atezolizumab: 1200 mg IV infusion per day
3. Tiragolumab: 600 mg IV infusion per day
a
투여 순서로 나열된 약물. BID = twice a day; PO = oral.
a Drugs listed in order of administration.
카페시타빈 및 티라골루맙 및 아테졸리주맙을 이용한 코호트에 대한 치료 요법Treatment regimens for cohorts with capecitabine and tiragolumab and atezolizumab
시스플라틴cisplatin
상이한 코호트에서의 시스플라틴 투여에 대한 지침이 표 11에 제시되어 있다.Guidance for cisplatin administration in different cohorts is presented in Table 11.
카보플라틴carboplatin
상이한 코호트에서의 카보플라틴 투여에 대한 지침이 표 12에 제시되어 있다.Guidelines for carboplatin administration in different cohorts are presented in Table 12.
페메트렉시드Pemetrexed
코호트 A에서의 페메트렉시드 투여에 대한 지침이 표 13에 제시되어 있다.Guidelines for administration of pemetrexed in Cohort A are presented in Table 13.
파클리탁셀paclitaxel
코호트 B에서의 파클리탁셀 투여에 대한 지침이 표 14에 제시되어 있다.Guidelines for administration of paclitaxel in Cohort B are presented in Table 14.
에토포시드etoposide
코호트 C에서의 에토포시드 투여에 대한 지침이 표 15에 제시되어 있다.Guidelines for administration of etoposide in Cohort C are presented in Table 15.
카페시타민cape citamine
카페시타빈은 150 mg 및 500 mg 정제로 제공된다. 환자는 시험자가 결정한 대로 허용할 수 없는 독성 또는 임상적 이익의 손실이 있을 때까지 표 35에 개략된 치료를 받는다.Capecitabine is available in 150 mg and 500 mg tablets. Patients receive the treatment outlined in Table 35 until there is unacceptable toxicity or loss of clinical benefit as determined by the investigator.
카페시타빈은 물과 함께 식사 후 30분 이내에 복용한다. 환자는 사용한 약물과 사용하지 않은 약물을 연구 기관으로 반환하도록 지시한다. Capecitabine should be taken within 30 minutes after a meal with water. Patients are instructed to return used and unused medications to the study site.
D.D. 병용 요법combination therapy
병용 요법은 선별검사 이전에 7일부터 치료 중단 방문시까지 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 약초의 또는 동종 요법 치료제, 및/또는 영양 보조제)을 포함한다.Combination therapy includes any medications (eg, prescription drugs, over-the-counter medications, herbal or homeopathic remedies, and/or nutritional supplements) used by the patient from
허용된 요법accepted therapy
본 연구에서(Ia상 또는 Ib상) 주입 관련 증상을 경험하는 환자는 표준 관행에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 라니티딘 또는 다른 H2 수용체 길항제를 이용하여 징후에 의하여 치료될 수 있다(미국 외부의 기관에서는, 등가 약물이 지역 관행에 따라 대체될 수 있다). 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 지지 요법(예컨대, 산소 보충 및 β2 아드레날린 작용제)으로 관리한다. 항히스타민제 예비 투약을 치료 의사의 재량에 따라 Ia상 또는 Ib상에서 주기 2에 대해 투여할 수 있다.Patients experiencing infusion-related symptoms in this study (Phase Ia or Ib) may be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or ranitidine or other H2 receptor antagonists according to standard practice. (In institutions outside the United States, equivalent drugs may be substituted according to local practice). Severe infusion-related reactions, such as dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea, are managed with supportive care as clinically indicated (e.g., oxygen supplementation and β2 adrenergic agonists). An antihistamine premedication may be administered for
전신성 코르티코스테로이드, 면역억제 약물 및 TNFα 길항제는 단독 제제로서 티라골루맙 또는 항 PD-L1/PD-1와 병용한 티라골루맙을 이용한 치료의 잠재적으로 이로운 면역학적 효과를 감쇠시킬 수 있으나, 응급시 치료 담당의의 재량에 따라 또는 의료 모니터 요원과의 자문 후 투여할 수 있다. 가능하다면, 코르티코스테로이드, 면역억제제 또는 TNF- 길항제에 대한 대안이 고려된다. 티라골루맙, 아테졸리주맙, 베바시주맙, 및 펨브롤리주맙의 예비 투약은 주기 2 이상에서 의료 모니터 요원과의 협의 후 치료 담당의의 재량에 따라 투여할 수 있다. 흡입 코르티코스테로이드 및 미네랄코르티코스테로이드(예컨대, 기립성 저혈압 또는 부신피질 부전을 갖는 환자에 대해 플루드로코티손)의 사용은 허용된다. 부신기능부전용 코르티코스테로이드의 생리적 용량은 허용된다. 식욕 자극제로서 투여된 메게스트롤은 또한 허용된다. 다른 약물의 사용 계획은 의료 모니터 요원과 상의한다.Systemic corticosteroids, immunosuppressive drugs, and TNFα antagonists may attenuate the potentially beneficial immunological effects of treatment with tiragolumab alone or in combination with anti-PD-L1/PD-1. It may be administered at the discretion of the treating physician or after consultation with a medical monitor. If possible, alternatives to corticosteroids, immunosuppressants or TNF-antagonists are considered. Premedication of tiragolumab, atezolizumab, bevacizumab, and pembrolizumab may be administered at the discretion of the treating physician after consultation with a medical monitor in
Ib상 화학요법 확장 코호트의 환자의 경우, 항구토제 및 전신 스테로이드가 또한 하기의 상황에서 제공될 수 있다:For patients in the Phase Ib chemotherapy expansion cohort, antiemetics and systemic steroids may also be given in the following circumstances:
![]()
![]()
![]()
![]()
![]()
![]()
예방적 항생제의 계획된 사용(예컨대, 외과적 개입 후)은 의료 모니터 요원과 논의한다. 연구 약물 치료는 항생제 과정이 끝날 때까지 유지한다.The planned use of prophylactic antibiotics (eg, after surgical intervention) is discussed with the medical monitor. Study medication is maintained until the end of the antibiotic course.
경구 피임약, 호르몬 대체 요법, 예방적 또는 치료적 항응고 요법(예컨대, 안정적인 용량 수준의 저분자량 헤파린 또는 와파린) 또는 비악성 적응증에 대한 기타 유지 요법을 사용한 환자는 이의 사용을 계속해야 한다. 생식 잠재력을 가진 남성 및 여성은 고도로 효과적인 피임 수단을 이용해야 한다.Patients using oral contraceptives, hormone replacement therapy, prophylactic or therapeutic anticoagulant therapy (eg, stable dose levels of low molecular weight heparin or warfarin) or other maintenance therapy for non-malignant indications should continue their use. Men and women of reproductive potential should use highly effective contraceptives.
화학요법 확장 코호트에 속한 환자의 경우, 하기의 약물들을 사용할 때 주의해야 한다:For patients in the chemotherapy expansion cohort, caution should be exercised when using the following drugs:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
비화학요법 확장 코호트에 속한 환자의 경우, 하기의 약물들을 사용할 때 주의해야 한다:For patients in the non-chemotherapy expansion cohort, caution should be exercised when using the following drugs:
![]()
![]()
금지된 요법forbidden therapy
하기의 요법의 사용은 연구 기간 동안 금지된다: The use of the following therapies is contraindicated during the study period:
![]()
![]()
방사선요법은 환자가 달리 이익을 얻고 있다면 통증의 일시적 완화(예컨대, 공지된 뼈 전이의 치료)를 위해 고려될 수 있다. Ia상 또는 Ib상의 용량 증량 코호트 환자의 경우, 완화 방사선 요법은 DLT 평가 기간이 완료될 때까지 연기된다. 연구 치료제 투여는 의료 모니터 요원으로부터 동의를 받아 방사선요법 동안 유예될 수 있다. Radiation therapy may be considered for temporary relief of pain (eg, treatment of known bone metastases) if the patient is otherwise benefiting. For patients in the Phase Ia or Phase Ib dose escalation cohort, palliative radiation therapy is deferred until the completion of the DLT evaluation period. Administration of study treatment may be deferred during radiotherapy with consent from the medical monitor.
혼합된 반응을 경험하는 환자는 의료 모니터 요원의 승인시 3개 이하의 병변을 통제하기 위해 국부 요법(예컨대, 수술, 정위적 방사선수술, 방사선요법, 고주파 절제)을 받을 수 있다.Patients experiencing mixed reactions may receive local therapy (eg, surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) to
표적 병변에 대한 방사선 요법 또는 절제를 받은 환자는 이후에 RECIST v1.1에 따른 반응 결정을 위한 해당 표적 병변을 평가할 수 없게 된다. Patients who have undergone radiation therapy or resection for a target lesion will not be able to subsequently evaluate that target lesion for response determination according to RECIST v1.1.
![]()
![]()
![]()
![]()
![]()
![]()
코호트 NC1에 대해 고려되는 HCC 환자에게 특이적으로 금지된 요법:Contraindicated regimens specifically for HCC patients considered for cohort NC1:
· 전체 용량의 항응고제, 치료 용량의 혈전 용해 요법, 및 항혈소판 요법의 사용이 현재 금지되어 있다. · The use of full dose anticoagulants, therapeutic doses of thrombolytic therapy, and antiplatelet therapy is currently contraindicated.
항응고제 또는 혈전용해 요법의 예방적 사용을 위한 현지 라벨 권장 용량이 허용된다.Local label recommended doses for prophylactic use of anticoagulants or thrombolytic therapy are acceptable.
저용량 아스피린(325 mg 미만/일)은 허용된다. 잠재적인 위장 손상을 줄이기 위해 양성자 펌프 억제제의 병용 투여가 강력히 권장된다.Low-dose aspirin (less than 325 mg/day) is acceptable. Co-administration of proton pump inhibitors is strongly recommended to reduce potential gastrointestinal damage.
환자가 연구 약물 치료를 받는 동안 정맥 혈전색전증을 경험하는 경우, 항응고 치료에도 불구하고 환자가 연구 약물을 계속 복용하는 것이 여전히 가능할 수 있다.If a patient experiences a venous thromboembolism while receiving study drug treatment, it may still be possible for the patient to continue taking the study drug despite anticoagulant treatment.
![]()
![]()
저용량 항응고제, 미분획 헤파린 또는 LMWH의 예방적 사용은 허용된다. 항응고 치료에 대한 바람직한 선택은 ASCO 지침에 따른 LMWH이다(Lyman GH et al. J Clin Oncol 2015;33:654-6).The prophylactic use of low-dose anticoagulants, unfractionated heparin or LMWH is permitted. The preferred choice for anticoagulant treatment is LMWH according to ASCO guidelines (Lyman GH et al. J Clin Oncol 2015;33:654-6).
만성적인 저용량 아스피린(325 mg 미만/일)의 사용을 제외하고, 연구 약물을 받는 동안 NSAID의 만성적인 병용은 금지된다. 하지만, 의학적 상태(예컨대, 두통, 발열)의 증상 완화를 위해, 잠재적인 위장 손상을 줄이기 위해 양성자 펌프 억제제와 병용 투여하는 경우 경구 NSAID의 간헐적 또는 단기 섭취가 허용된다.With the exception of chronic low-dose aspirin (<325 mg/day) use, chronic concomitant use of NSAIDs while receiving study drug is contraindicated. However, intermittent or short-term ingestion of oral NSAIDs is permitted when co-administered with proton pump inhibitors to reduce potential gastrointestinal damage for symptom relief of medical conditions (eg headache, fever).
D. 선정 기준D. Selection Criteria
환자는 연구 참가를 위해 하기의 기준을 충족해야 한다:Patients must meet the following criteria for study entry:
일반 기준general standard
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
이는 치료적 항응고제를 투여받지 않는 환자에게만 적용된다.This applies only to patients not receiving therapeutic anticoagulants.
치료용 항응고제를 투여받는 환자는 안정적인 용량을 유지하고 있다. Patients receiving therapeutic anticoagulants are maintained at stable doses.
![]()
![]()
(140 연령) (체중 kg) (0.85, 여성의 경우)(140 years old) (weight kg) (0.85 for women)
72 (혈청 크레아티닌 mg/dL)72 (serum creatinine mg/dL)
시스플라틴을 투여받는 환자(코호트 A 또는 코호트 C)는 콕크로프트-가울트 추정치를 기반으로 하여 크레아티닌 청소율 ≥ 60 mL/분을 측정하거나 계산했어야 한다.Patients receiving cisplatin (Cohort A or Cohort C) should have measured or calculated a creatinine clearance ≥ 60 mL/min based on the Cockcroft-Gault estimate.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
가임기 여성 파트너와 함께, 남성은 배아 노출을 피하기 위해 치료 기간 중 및 티라골루맙의 최종 투여 후 90일 동안, 카페시타빈의 최종 투여 후 3개월, 화학요법의 최종 투여 후 6개월 동안 금욕을 유지하거나 콘돔을 사용해야 한다.With female partners of childbearing potential, males maintain abstinence during treatment and for 90 days after the last dose of tiragolumab, 3 months after the last dose of capecitabine, and 6 months after the last dose of chemotherapy to avoid embryo exposure or use a condom.
![]()
![]()
E.E. 암별 선정 기준Criteria for selection by cancer
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
F.F. Ia상 및 Ib상의 코호트 보충을 취소한 환자에 대한 추가 선정 기준Additional Inclusion Criteria for Patients Withdrawal of Phase Ia and Ib Cohort Replenishment
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
G.G. 확장 코호트에서의 환자에 대한 추가 선정 기준 Additional Inclusion Criteria for Patients in the Expansion Cohort
![]()
![]()
![]()
![]()
![]()
![]()
H.H. Ia상의 확장 코호트에서의 환자에 대한 추가 선정 기준 Additional Inclusion Criteria for Patients in the Phase Ia Expansion Cohort
![]()
![]()
I.I. Ib상의 각 적응증별 확장 코호트에서의 환자에 대한 추가 포함 기준 Additional inclusion criteria for patients in the expanded cohort for each indication in Phase Ib
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
그리고 and
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
J.J. Ib상의 연속 생검 확장 코호트에서의 환자에 대한 추가 선정 기준 Additional Inclusion Criteria for Patients in the Phase Ib Serial Biopsy Expansion Cohort
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
여러 병변이 있는 경우, 종양 또는 전이 부위와 관련된 이질성의 도입을 피하기 위해 가능한 경우 모든 시점에서 동일한 종양 병변을 생검해야 한다.In the presence of multiple lesions, the same tumor lesion should be biopsied at all time points whenever possible to avoid the introduction of heterogeneity associated with tumor or metastasis sites.
K.K. 배제 기준 Exclusion Criteria
하기의 기준 중 임의의 것에 부합하는 환자는 연구 등록으로부터 배제한다:Patients meeting any of the following criteria are excluded from study enrollment:
일반적인 배제 기준 General exclusion criteria
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
L. 암별 배제 기준L. Criteria for exclusion by cancer
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Ia상 및 Ib상의 모든 코호트(용량 증량, 보충 및 확장): All cohorts in Phase Ia and Ib (Dose Escalation, Supplementation, and Expansion) :
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Ia상 및 Ib상의 용량 증량 및 보충 코호트(용량 증량 중 등록): Phase Ia and Ib Dose Escalation and Supplemental Cohorts (Enrollment During Dose Escalation):
![]()
![]()
![]()
![]()
Ia상 및 Ib상의 용량 확장 및 보충 코호트(용량 확장 중 등록): Capacity Expansion and Supplemental Cohorts in Phase Ia and Ib (Enrollment During Dose Expansion):
![]()
![]()
선행 항 PD-L1/PD-1은 적어도 3주 간의 휴약 기간을 거쳐야 함The preceding anti-PD-L1/PD-1 must undergo a washout period of at least 3 weeks
선행 항 CTLA-4는 6주 간의 휴약 기간을 거쳐야 함Antecedent CTLA-4 must undergo a 6-week washout period
![]()
![]()
![]()
![]()
TLR 작용제, IDO/TDO 억제제, 또는 OX40 작용제를 포함한 면역조절제를 이용한 선행 치료는, 하기의 경우를 제외하고, 선행 치료의 마지막 용량 투여 내지 제안된 주기 1의 1일 사이에 약물의 적어도 5회 반감기 또는 최소 3주가 결과한 경우 허용된다:Prior treatment with an immunomodulatory agent, including a TLR agonist, IDO/TDO inhibitor, or OX40 agonist, includes at least 5 half-lives of the drug between administration of the last dose of the prior treatment and
Ib상의 NSCLC CIT 미경험 확장 코호트에서, 다른 면역조절제를 이용한 선행 치료는 허용되지 않는다.In the NSCLC CIT-naive Expansion Cohort on Phase Ib, prior treatment with other immunomodulatory agents is not permitted.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
치료된 CNS 전이의 이력을 갖는 환자는 하기의 기준 모두를 충족할 경우 적격이다:Patients with a history of treated CNS metastases are eligible if they meet all of the following criteria:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
특히 골격 사건을 예방하기 위해 비스포스포네이트 요법 또는 데노수맙을 받고 있고 임상적으로 유의한 고칼슘혈증의 이력이 없는 환자가 적격이다. 하지만, 데노수맙을 투여받는 환자는 연구 기간 동안 데노수맙 대신 비스포스포네이트를 투여받을 의향이 있거나 이에 적격이어야 한다.In particular, patients receiving bisphosphonate therapy or denosumab to prevent skeletal events and without a history of clinically significant hypercalcemia are eligible. However, patients receiving denosumab must be willing or eligible to receive bisphosphonates instead of denosumab for the duration of the study.
![]()
![]()
M.M. 치료별 배제 기준 Treatment-specific exclusion criteria
![]()
![]()
안정적인 용량의 갑상선 대체 호르몬에 대한 자가면역 갑상선기능저하증의 병력이 있는 환자는 적격일 수 있다.Patients with a history of autoimmune hypothyroidism on stable doses of thyroid replacement hormone may be eligible.
습진, 건선, 만성 단순 태선 또는 피부과 증상만 있는 백반증(예컨대, 건선성 관절염 없음)이 있는 환자는 하기의 조건을 충족하는 경우 적격일 수 있다:Patients with eczema, psoriasis, chronic lichen simplex or vitiligo with only dermatological symptoms (eg, no psoriatic arthritis) may be eligible if the following conditions are met:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
급성, 저용량, 전신 면역억제제(예컨대, 메스꺼움으로 덱사메타손 1회 용량)를 받은 환자는 의료 모니터 요원과 논의하고 승인받은 후 연구에 등록할 수 있다.Patients receiving acute, low-dose, systemic immunosuppressants (eg, a single dose of dexamethasone for nausea) may be enrolled in the study after discussion and approval with a medical monitor.
흡입용 코르티코스테로이드(예컨대, 만성 폐쇄성 폐질환용 플루티카손)의 사용은 허용된다.The use of inhaled corticosteroids (eg, fluticasone for chronic obstructive pulmonary disease) is permitted.
경구 미네랄 코르티코이드(예컨대, 기립성 저혈압 환자의 경우 플루드로코르티손)의 사용은 허용된다.The use of oral mineralocorticoids (eg, fludrocortisone in patients with orthostatic hypotension) is permitted.
부신기능부전용 코르티코스테로이드의 생리적 용량은 허용된다.Physiological doses of corticosteroids for adrenal insufficiency are acceptable.
![]()
![]()
방사선 분야에서 방사선 폐렴 (섬유증) 병력은 허용된다.A history of radiation pneumonitis (fibrosis) in the field of radiation is acceptable.
![]()
![]()
![]()
![]()
과거의 또는 회복된 B형 간염 감염이 있는 환자(HBsAg 검사가 음성이고 B형 간염 핵심 항원[항 HBc]에 대한 IgG 항체가 양성인 것으로 정의됨)는 적격이다. B형 간염 바이러스(HBV) DNA는 주기 1의 1일 이전에 상기 환자들에게서 수득해야 하며 활동성 감염을 나타내지 않아야 한다.Patients with previous or reversible hepatitis B infection (defined as negative HBsAg test and positive IgG antibody to the hepatitis B core antigen [anti-HBc]) are eligible. Hepatitis B virus (HBV) DNA should be obtained from these patients prior to
![]()
![]()
C형 간염 바이러스(HCV) 항체 양성 환자는 중합효소 연쇄 반응(PCR)이 HCV RNA에 대해 음성인 경우에만 적격이다. Hepatitis C virus (HCV) antibody positive patients are eligible only if the polymerase chain reaction (PCR) is negative for HCV RNA.
![]()
![]()
EBV IgG 및/또는 EBNA에 양성인 환자는 EBV IgM 및/또는 EBV PCR이 음성인 경우에만 적격이다.Patients positive for EBV IgG and/or EBNA are eligible only if EBV IgM and/or EBV PCR is negative.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
N.N. 화학요법 확장 코호트에 특정한 배제 기준 Exclusion Criteria Specific to the Chemotherapy Expansion Cohort
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
(140 - 연령) x (체중 kg) x (0.85, 여성의 경우) (140 - age) x (weight kg) x (0.85 for women)
72 x (혈청 크레아티딘 mg/dL)72 x (serum creatidine mg/dL)
O.O. 코호트 A에 특정한 배제 기준 Exclusion Criteria Specific to Cohort A
![]()
![]()
P.P. 코호트 B에 특정한 배제 기준 Exclusion Criteria Specific to Cohort B
![]()
![]()
![]()
![]()
Q.Q. 코호트 C에 특정한 배제 기준 Exclusion Criteria Specific to Cohort C
![]()
![]()
R.R. 코호트 D에 특정한 배제 기준 Exclusion Criteria Specific to Cohort D
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
S.S. 코호트 NC1에 특정한 배제 기준 Exclusion criteria specific to cohort NC1
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
T.T. 평가 evaluation
단일 제제(Ia상)로서 티라골루맙 또는 하기의: 아테졸리주맙, 화학요법과 아테졸리주맙, 베바시주맙과 아테졸리주맙, 또는 펨브롤리주맙과 병용으로(Ib상) 티라골루맙을 각각 투여하기 전에 환자의 안전성 및 내약성을 면밀히 모니터링하고 독성을 평가한다. 투약은 임상 평가 및 현지 실험실 검사 결과가 허용되는 경우에만 실시한다.Tiragolumab as a single agent (Phase Ia) or: Atezolizumab, chemotherapy and atezolizumab, bevacizumab and atezolizumab, or tiragolumab in combination with pembrolizumab (Phase Ib), respectively Closely monitor patient safety and tolerability and evaluate toxicity prior to initiation. Dosing should be done only when clinical evaluation and local laboratory test results allow.
기간이 지정되지 않는 한, 모든 평가는 예정된 방문 날짜에 실시한다. 연구 치료일에 예정된 평가는 달리 명시되지 않는 한 연구 약물(들)의 주입 전에 실시한다.Unless a time period is specified, all assessments will be conducted on the scheduled visit date. Assessments scheduled on study treatment days will be conducted prior to infusion of study drug(s) unless otherwise specified.
병력, 기준선 조건, 병용 약물, 및 인구 통계 데이터Medical history, baseline conditions, concomitant medications, and demographic data
병력에는 암 병력(선행 암 요법 및/또는 선행 CIT 및 절차, 및 호르몬 수용체 상태 또는 돌연변이 상태와 같은 종양 특성을 포함하지만, 이에 제한되지는 않음), 기타 임상적으로 유의한 질병, 수술, 흡연 이력, 알코올 사용 및/또는 남용 약물, 생식 상태 및 선별검사 방문 전 7일 이내에 상기 환자가 사용한 모든 약물(예컨대, 처방약, 일반의약품, 한약 또는 동종 요법 치료제, 영양 보조제)이 포함된다.Medical history includes, but is not limited to, history of cancer (including, but not limited to, prior cancer therapy and/or prior CITs and procedures, and tumor characteristics such as hormone receptor status or mutation status), other clinically significant disease, surgery, smoking history , alcohol use and/or abuse, reproductive status, and any medications (eg, prescription, over-the-counter, herbal or homeopathic remedies, nutritional supplements) used by the patient within 7 days prior to the screening visit.
연구의 Ia상에서 Ib상 부분으로 전환되는 환자의 경우, 질병 진행 시 치료 재개의 시점에 재선별검사 병력에는 프로토콜에 명시된 후속 조치 동안 포착되지 않은 초기 치료 중단 후 발생한 임의의 암 관련 절차 또는 연구 치료제와 관련된 임의의 이상 반응이 포함된다.For patients transitioning to the Phase Ia portion of the study, the history of rescreening at the time of resumption of treatment at disease progression includes any cancer-related procedures or study treatment that occurred after initial discontinuation of treatment not captured during follow-up as specified in the protocol. Any adverse events involved are included.
인구학적 데이터는 연령, 성별, 및 자가 보고한 인종/민족을 포함한다. 인종/민족은 상기 변수가 관찰된 PK, 약력학, 독성, 및/또는 치료 반응의 차이에 잠재적으로 기여하기 때문에 기록한다. Demographic data include age, gender, and self-reported race/ethnicity. Race/ethnicity is recorded as this variable potentially contributes to differences in observed PK, pharmacodynamics, toxicity, and/or treatment response.
활력 징후vital signs
활력징후에는 환자가 앉은 자세에서의 체온, 호흡수, 맥박수, 수축기 및 이완기 혈압 측정이 포함된다.Vital signs include measurements of body temperature, respiration rate, pulse rate, and systolic and diastolic blood pressure when the patient is seated.
연구 치료일에, 활력 징후는 당일의 제1 연구 약물 주입 전 60분 이내에 측정한다. On study treatment days, vital signs are measured within 60 minutes prior to the first study drug infusion of the day.
Ia상에서 티라골루맙의 제1 주입의 경우, 상기 주입 중 매 15(±5)분, 주입 종료시(±5분), 및 주입 종료 후 30(±10)분, 120(±15)분, 및 240(±15)분에 측정한다.For the first infusion of tiragolumab in phase la, every 15 (±5) minutes during the infusion, at the end of the infusion (±5 minutes), and at 30 (±10) minutes, 120 (±15) minutes after the end of the infusion, and Measure at 240 (±15) minutes.
Ib상에서 티라골루맙의 제1 주입의 경우, 상기 주입 중 매 15분(±5분), 주입 종료 시(±5분), 주입 종료 후 30분(±10분)에 활력 징후를 측정한다. 화학요법이 없는 모든 Ib상 코호트의 경우, 티라골루맙 주입 완료 후 60분 후에 아테졸리주맙 또는 펨브롤리주맙의 제1 주입이 투여되고; 베바시주맙의 제1 주입은 아테졸리주맙의 주입 완료 후 60분에 투여된다.For the first infusion of tiragolumab in Phase Ib, vital signs are measured every 15 min (±5 min) during the infusion, at the end of the infusion (±5 min), and at 30 min (±10 min) after the end of the infusion. For all Phase Ib cohorts without chemotherapy, the first infusion of atezolizumab or pembrolizumab is administered 60 minutes after completion of the tiragolumab infusion; The first infusion of bevacizumab is administered 60 minutes after completion of the infusion of atezolizumab.
화학요법을 포함한 Ib상 코호트의 경우, 티라골루맙의 제1 주입은 아테졸리주맙의 주입 완료 후 60분에 투여된다. For the Phase Ib cohort with chemotherapy, the first infusion of tiragolumab is administered 60 minutes after completion of the infusion of atezolizumab.
아테졸리주맙 및 펨브롤리주맙의 제1 주입 및 후속 주입, 그리고 티라골루맙의 후속 주입의 경우, 임상적으로 지시되거나 이전 주입에서 증상이 발생한 경우 상기 주입 중 및 주입 후 30(±10)분에 활력 징후를 측정한다. For the first and subsequent infusions of atezolizumab and pembrolizumab, and for subsequent infusions of tiragolumab, during and 30 (±10) minutes after the infusion, if clinically indicated or if symptoms occurred with the previous infusion Measure vital signs.
베바시주맙의 제1 주입의 경우, 임상적으로 지시되거나 이전 주입에서 증상이 발생한 경우 상기 주입 중, 주입 종료(±5분), 및 주입 후 30(±10)분에 활력 징후를 측정한다. For the first infusion of bevacizumab, vital signs are measured during the infusion, at the end of the infusion (±5 min), and at 30 (±10) minutes post-infusion if clinically indicated or if symptoms occurred from a previous infusion.
티라골루맙 및 아테졸리주맙 또는 펨브롤리주맙 사이, 또는 아테졸리주맙 및 베바시주맙 사이(화학요법을 포함하지 않는 모든 Ib상 코호트의 경우), 또는 아테졸리주맙 및 티라골루맙 사이(화학요법을 포함한 Ib상 코호트의 경우)의 후속 주입 간격은 이전 티라골루맙 또는 아테졸리주맙 주입이 IRR 없이 내약된 경우 30분이고, 또는 환자가 이전에 티라골루맙 또는 아테졸리주맙 주입으로 IRR을 경험한 경우 60분이다.Between tiragolumab and atezolizumab or pembrolizumab, or between atezolizumab and bevacizumab (for all Phase Ib cohorts not including chemotherapy), or between atezolizumab and tiragolumab (with chemotherapy) for the phase Ib cohort that included), the interval between subsequent infusions is 30 minutes if the previous infusion of tiragolumab or atezolizumab was tolerated without an IRR, or 60 if the patient previously experienced an IRR with a previous infusion of tiragolumab or atezolizumab is a minute
화학요법 확장 A, B 및 C 코호트에서, 마지막 화학요법 주입의 완료 후 30(10)분 이내에 주기 1에서 추가적인 활력 징후를 측정하고 기록한다(예컨대, 코호트 A: 카보플라틴 또는 시스플라틴 투여 후, 코호트 B: 투여 후 카보플라틴, 코호트 C: 에토포시드 후). 후속 주기에서, 임상적으로 지시된 경우 화학요법 주입 후 추가적인 활력 징후를 측정하고 기록한다.In chemotherapy expansion A, B, and C cohorts, additional vital signs are measured and recorded in
선별검사 방문에서, 수집된 활력 징후를 기록한다. 그 후 방문할 때마다, 당일의 제1 연구 약물 주입 이전에 수득하거나 이상 반응(예컨대, 발열 발생 시 체온) 또는 이상 반응의 주요 징후(예컨대, 주입 관련 반응과 관련된 혈압 또는 부정맥과 관련된 심박수)를 구성하는 활력 징후만 기록한다. 프로토콜에 따라 수집된 모든 활력 징후는 환자의 의료 기록에 문서화한다.At the screening visit, the collected vital signs are recorded. At each subsequent visit, either obtained prior to the first study drug infusion of the day or an adverse event (e.g., body temperature in case of fever) or major signs of an adverse event (e.g., blood pressure associated with infusion-related reactions or heart rate associated with arrhythmias) Record only constitutive vital signs. All vital signs collected according to the protocol are documented in the patient's medical record.
혈액 산소 포화도는 맥박 산소 측정법에 의해 기준선에서 측정한다.Blood oxygen saturation is measured at baseline by pulse oximetry.
신체 검사Physical examination
선별검사에서 실시된 전체 신체 검사는 머리, 눈, 귀, 코, 및 목, 및 심혈관, 피부과, 근골격, 호흡, 위장, 비뇨생식, 및 신경계의 평가를 포함한다. Full physical examinations performed at screening included assessments of the head, eyes, ears, nose, and throat, and cardiovascular, dermatological, musculoskeletal, respiratory, gastrointestinal, urogenital, and nervous system.
ECOG 전신 활동도를 평가한다.ECOG systemic activity is assessed.
후속 방문에서(또는 임상적으로 지시된 바와 같이), 제한된, 증상 지향된 신체 검사를 실시한다. 기준선 이상으로부터의 변화를 환자의 의료 기록에 기록한다. 새로운 또는 악화된 임상적으로 유의한 이상은 이상 반응으로서 기록한다.At follow-up visits (or as clinically indicated), a limited, symptom-directed physical examination is performed. Changes from baseline abnormalities are recorded in the patient's medical record. New or worsening clinically significant abnormalities are recorded as adverse events.
종양 평가의 일부로서, 신체 검사는 또한 림프절병증, 비장비대증, 간비대, 및 피부 신생물 또는 전이에 대한 평가를 포함한다. 모든 환자는 CNS 전이의 증상에 대하여 모니터링해야 하고 상기 보고된 증상은 전체 신경 검사가 뒤따라야 한다. 뇌 자기공명영상(MRI) 또는 조영제 증강 머리 CT는 신규한 또는 악화되는 뇌 관여를 확인 또는 반박하기 위해 임상적으로 지시된 바와 같이 실시한다.As part of the tumor evaluation, the physical examination also includes evaluation for lymphadenopathy, splenomegaly, hepatomegaly, and skin neoplasms or metastases. All patients should be monitored for symptoms of CNS metastasis and any symptoms reported above should be followed by a full neurological examination. Brain magnetic resonance imaging (MRI) or contrast-enhanced CT of the head is performed as clinically indicated to confirm or refute new or worsening brain involvement.
종양 및 반응 평가Tumor and Response Assessment
선별검사 screening test
질병의 모든 공지된 부위는 선별검사에서 문서화하고 각각의 후속 종양 평가에서 재평가해야 한다. All known sites of disease should be documented at screening and re-evaluated at each subsequent tumor assessment.
선별검사 및 후속 종양 평가는 (사용이 금지되지 않는다면 IV 조영제 및 기관 표준에 따라 적절한 경우 경구 조영제로)CT 스캔 또는 흉부, 복부, 및 골반의 MRI 스캔을 포함해야 한다. 종양 평가를 위한 CT 스캔이 양전자 방출 단층촬영(PET)/CT 스캐너에서 실시되면, CT 취득은 전체 조영 CT 스캔을 위한 표준과 일치되어야 한다. Screening and subsequent tumor evaluation should include CT scans or MRI scans of the chest, abdomen, and pelvis (with IV contrast media and oral contrast where appropriate according to institutional standards unless use is prohibited). If CT scans for tumor evaluation are performed on a positron emission tomography (PET)/CT scanner, the CT acquisition should be consistent with the standard for full-contrast CT scans.
뇌 이미지 촬영(MRI 또는 조영제 증강 CT)은 뇌 전이가 치료된 환자를 위한 선별검사에서 및 신규한 또는 악화되는 CNS 전이를 시사하는 증상 또는 징후에 기반하여 임상적으로 지시된 바와 같이 요구된다. 모호한 머리 CT의 사례에서, 뇌 MRI는 의심되는 뇌 전이의 존재 또는 정도를 명확화하기 위해 요구된다. Brain imaging (MRI or contrast-enhanced CT) is required at screening for patients with treated brain metastases and as clinically indicated based on symptoms or signs suggestive of new or worsening CNS metastases. In cases of ambiguous head CT, brain MRI is required to clarify the presence or extent of suspected brain metastases.
목의 뼈 스캔 및 CT 스캔과 같은 추가 조사가 또한 기저 질환에 따라 지시된 바와 같이 그리고 상기 나열된 최소 평가 일정에 의해 입증되지 않을 수 있는 임의의 부위에서 질병에 관한 임의의 임상적 의심이 있는 경우 실시된다(예컨대, 두경부 CT 스캔은 HNSCC 환자에게 지시됨). 시험자의 재량에 따라, RECIST v1.1에 따라 측정가능한 질환의 다른 평가 방법은 사용될 수 있다. Additional investigations, such as bone scans and CT scans of the neck, are also conducted if there is any clinical suspicion of disease at any site that may not be substantiated by the minimum evaluation schedule listed above and as indicated by the underlying disease. (eg, head and neck CT scans indicated for HNSCC patients). At the discretion of the investigator, other methods of assessment of measurable disease according to RECIST v1.1 may be used.
선별검사 시 질병 부위를 평가하는데 사용된 동일한 방사선 절차를 연구 내내 사용한다(예컨대, CT 스캔을 위한 동일한 조영제 프로토콜). 안정적인 뇌 전이는 기준선 연구와 동일한 방사선촬영 절차를 사용하여 각 종양 평가와 함께 평가해야 한다. 뇌 전이가 없는 환자는 임상적으로 보증되지 않는 한 종양 평가를 위한 뇌 스캔이 필요하지 않는다. 반응은 RECIST v1.1을 이용하여 상기 상세한 이미지 촬영 양식 및 신체 검사를 기준으로 시험자가 평가한다. 모든 시점에서 전체 종양 반응에 대한 시험자의 평가는 RECIST v1.1만을 기반으로 한다. 방문 전체에 걸쳐 내부 일관성을 보장하기 위해 가능한 경우 동일한 평가자가 평가를 실시한다.The same radiological procedures used to evaluate diseased sites at screening are used throughout the study (eg, same contrast agent protocol for CT scans). Stable brain metastases should be assessed with each tumor assessment using the same radiographic procedures as the baseline study. Patients without brain metastases do not require brain scans for tumor evaluation unless clinically warranted. Response is assessed by the investigator based on the detailed imaging modality and physical examination above using RECIST v1.1. Investigator's assessment of overall tumor response at all time points is based solely on RECIST v1.1. Assessments are conducted by the same evaluator whenever possible to ensure internal consistency throughout the visit.
종양 평가를 실시한다. PD가 의심되는 경우, 시험자의 재량에 따라 언제든지 스캔을 실시할 수 있다. A tumor assessment is performed. If PD is suspected, a scan may be performed at any time at the discretion of the investigator.
초기 연구 치료 중단 이후(중단이 질병 진행 이외의 이유인 경우), 추적 종양 평가는 사망, 질병 진행, 다른 전신 항암 요법의 개시, 추적 관찰의 상실, 동의 철회, 또는 연구 종료 중 먼저 발생하는 때까지 실시한다. After cessation of initial study treatment (if discontinuation is for reasons other than disease progression), follow-up tumor evaluations will occur until death, disease progression, initiation of other systemic chemotherapy, loss of follow-up, withdrawal of consent, or termination of study, whichever occurs first Conduct.
RECIST v1.1에 따라 방사선 촬영 질병 진행을 넘어 치료를 계속하는 환자는 6(±2)주에(즉, 스캔 빈도가 매 2주기인 경우 다음 계획된 종양 평가에서 또는 스캔 빈도가 매 4주기인 경우 미계획된 종양 평가로서) 추적조사 스캔으로, 또는 임상적으로 지시되면 더 빨리 모니터링될 수 있다. 종양 평가는 2회의 연속적인 스캔이 방사선 촬영 상의 질병 진행을 보여준 제1 스캔에 비해 안정성 또는 개선됨을 보여줄 때까지 그 후에 2주기마다 계속하고, 이 시점에서 스캔 빈도는 가능한 경우 매 4주기로 복귀 또는 전환되어야 한다. 모든 시점에서 전체 종양 반응에 대한 시험자 평가는 RECIST v1.1에만 기반한다.Patients continuing treatment beyond radiographic disease progression according to RECIST v1.1 should be considered at 6 (±2) weeks (i.e., at the next planned tumor assessment if the scan frequency is every 2 cycles, or if the scan frequency is every 4 cycles). as an unplanned tumor assessment) as a follow-up scan, or sooner if clinically indicated. Tumor evaluation continues every 2 cycles thereafter until 2 consecutive scans show stability or improvement compared to the first scan showing disease progression on radiography, at which point scan frequency returns or switches to every 4 cycles if possible should be Investigator assessments of overall tumor response at all time points are based solely on RECIST v1.1.
실험실, 바이오마커, 및 다른 생물학적 샘플laboratory, biomarkers, and other biological samples
Ia상 및 Ib상의 지역 실험실 시험Regional laboratory tests for Phase Ia and Ib
하기의 실험실 시험은 연구 기관의 지역 실험실에서 실시한다:The following laboratory tests are conducted in the local laboratory of the research institution:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
EBV IgM 검사 및/또는 EBV PCR 검사는 환자가 EBV IgG 및/또는 EBNA에 대한 혈청학 양성인 경우 적격성을 고려하기 위해 주기 1의 1일 전에 필요하다.An EBV IgM test and/or an EBV PCR test is required prior to
![]()
![]()
![]()
![]()
HBV DNA 검사는 환자가 항 HBc에 대한 혈청학적 검사에서 양성인 경우 주기 1의 1일 전에 수득해야 한다.An HBV DNA test should be obtained 1 day prior to
![]()
![]()
HCV RNA 검사는 환자가 항 HCV 혈청 검사에서 양성인 경우 적격성을 고려하기 위해 1주기의 제 1일 전에 필요하다.HCV RNA testing is required before
![]()
![]()
![]()
![]()
Ia상 및 Ib상 중앙 실험실 시험Phase Ia and Ib Central Laboratory Testing
하기에 나열된 시험은 중앙 실험실에서 실시한다. PK 또는 ADA 분석을 위해 수집된 샘플은 추가 면역원성 특성화, PK, 바이오마커 및/또는 면역원성 분석 개발 및 검증에 필요할 수 있다. 따라서, 해당 샘플은 최종 임상 연구 보고서가 완료된 후 5년 이내에 또는 현지 규정에 따라 더 일찍 폐기된다.The tests listed below are conducted in a central laboratory. Samples collected for PK or ADA assays may be required for further immunogenicity characterization, PK, biomarker and/or immunogenicity assay development and validation. Therefore, such samples are discarded within 5 years of completion of the final clinical study report or earlier according to local regulations.
혈액 샘플에서 수행된 평가Assessments performed on blood samples
![]()
![]()
검증된 분석을 사용하여 티라골루맙에 대한 ADA 측정을 위해 혈청 샘플을 수득한다(Ia상 및 Ib상).A validated assay is used to obtain serum samples for ADA determination for tiragolumab (Phases Ia and Ib).
검증된 분석을 사용하여 아테졸리주맙에 대한 ADA 측정을 위해 혈청 샘플을 수득한다(Ib상에만 해당).A validated assay is used to obtain serum samples for ADA determination for atezolizumab (Phase Ib only).
![]()
![]()
검증된 분석법을 사용하여 티라골루맙 농도 측정을 위해 혈청 샘플을 수득한다(Ia상 및 Ib상).Serum samples are obtained for determination of tyragolumab concentrations using validated assays (Phases Ia and Ib).
검증된 분석법을 사용하여 아테졸리주맙 농도 측정을 위해 혈청 샘플을 수득한다(Ib상에만 해당).Obtain serum samples for determination of atezolizumab concentrations using validated assays (phase Ib only).
검증된 분석법을 사용하요 시스플라틴, 카보플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈 및 에토포시드의 농도 측정을 위해 혈장 샘플을 수득한다(Ib상 화학요법 확장 코호트에만 해당).Plasma samples are obtained for determination of concentrations of cisplatin, carboplatin, pemetrexed, paclitaxel, capecitabine, and etoposide using validated assays (phase Ib chemotherapy expansion cohort only).
![]()
![]()
개별 환자 또는 연구 모집단 전체에 걸쳐 항핵항체, 항이중가닥 DNA, 항호중구 세포질 항체 및 갑상선 과산화효소 항체를 포함하지만 이에 제한되지는 않는 자가항체 검사를 위해 혈청 샘플을 수득하여 연구 기간 동안의 임상 사건에 근거하여 실시한다.Serum samples were obtained for autoantibody testing, including, but not limited to, antinuclear antibodies, anti-double-stranded DNA, anti-neutrophil cytoplasmic antibodies, and thyroid peroxidase antibodies, to clinical events during the study period, either for individual patients or across the study population. based on it.
![]()
![]()
선별검사 방문 및 치료 시 모든 적격 환자로부터 바이오마커 평가를 위해 혈액 샘플을 수득한다.Blood samples are obtained for biomarker evaluation from all eligible patients at screening visits and treatment.
![]()
![]()
WGS를 위해 단일 혈액 샘플을 수집하고 분석을 위해 하나 이상의 실험실로 보낼 수 있다. WGS 데이터 및 관련 임상 데이터는 인간의 건강 및 질병에 대한 연구를 실시하기 위해 다른 연구자와 광범위하게 공유할 수 있도록 연구에 참여하지 않는 연구자와 공유하거나 정부 또는 기타 건강 연구 데이터베이스에 제출할 수 있다. 연구 참가자는 이름이나 기타 개인 식별 정보로 확인되지 않는다.A single blood sample may be collected for WGS and sent to one or more laboratories for analysis. WGS data and related clinical data may be shared with non-researchers or submitted to government or other health research databases for broad sharing with other researchers to conduct research on human health and disease. Study participants are not identified by name or other personally identifiable information.
WGS는 각 기관의 IRB/EC 및 해당하는 경우 적절한 규제 기관의 검토 및 승인에 따라 결정된다. 기관이 WGS에 대한 승인을 받지 못한 경우, 상기 평가는 해당 기관에 적용되지 않는다. The WGS is subject to review and approval by the respective institutional IRB/EC and, where applicable, the appropriate regulatory body. If an institution is not accredited for WGS, the above assessment does not apply to that institution.
본 연구와 관련하여 WGS 데이터가 분석될 수 있으며 질병 병리생물학을 더 잘 이해하고 새로운 치료 접근법의 개발을 안내하기 위해 다른 연구들와 함께 통합하여 탐색될 수 있다. 이러한 분석의 복잡성과 탐색적 특성을 감안할 때, WGS 데이터 및 분석은 연구 목적으로만 사용되며 시험자 또는 연구 참가자와 공유되지 않는다.WGS data can be analyzed in the context of this study and explored in conjunction with other studies to better understand disease pathobiology and guide the development of new therapeutic approaches. Given the complexity and exploratory nature of these analyzes, WGS data and analyzes are used for research purposes only and are not shared with investigators or study participants.
상기 샘플은 고갈될 때까지 또는 환자가 샘플을 폐기할 것을 요청할 때까지 무기한 저장된다.The sample is stored indefinitely until depleted or until the patient requests that the sample be discarded.
종양 샘플에서 실시된 평가Assessments conducted on tumor samples
면역 관련 및 종양 관련 바이오마커의 상태(특정 세포 유형에 대한 PD-L1, TIGIT, PVR, 및/또는 CD226의 발현; 및 침윤 T 세포의 유병률 및/또는 활성화를 포함하지만 이에 제한되지는 않음)는 보관 및 신선한 종양 샘플 모두에서 IHC, IF 및 qRT-PCR을 포함하지만 이에 제한되지는 않는 방법을 사용하여 평가할 수 있다. 종양 RNA 및/또는 DNA는 정제되고 RNA 서열분석 및 WGS에 의해 특성화될 수 있다. 임상 및 비임상 데이터가 안내하는 경우, 추가적인 탐색적 바이오마커를 평가할 수도 있다. The status of immune-related and tumor-associated biomarkers (including but not limited to, expression of PD-L1, TIGIT, PVR, and/or CD226 on specific cell types; and prevalence and/or activation of infiltrating T cells) Both archived and fresh tumor samples can be evaluated using methods including, but not limited to, IHC, IF, and qRT-PCR. Tumor RNA and/or DNA can be purified and characterized by RNA sequencing and WGS. Additional exploratory biomarkers may also be evaluated if clinical and non-clinical data guides them.
![]()
![]()
입수 가능한 경우, 다른 목적을 위해 본 연구의 외부에서 수득한 보관 종양 조직 샘플들은 모든 환자로부터 수집한다(파라핀 블록이 바람직함; 적어도 15개의 염색되지 않은 연속 슬라이드가 허용 가능함). Ia상 또는 Ib상의 모든 환자의 경우, 연구 참가 전에 보관 종양 조직의 입수 가능성을 확인해야 한다. 미세 바늘 흡인물, 삼출물 또는 복수의 세포 펠릿, 세척 샘플 및 뼈 생검은 보관 조직에 대한 요건을 충족하지 않는다.If available, archival tumor tissue samples obtained outside of this study for other purposes are collected from all patients (paraffin blocks are preferred; at least 15 unstained serial slides are acceptable). For all patients with phase Ia or Ib, availability of archived tumor tissue should be confirmed prior to study entry. Fine needle aspirates, exudates or multiple cell pellets, wash samples and bone biopsies do not meet the requirements for storage tissue.
별개의 시점(예컨대, 초기 진단 시점 및 질병 재발 시점)에서 수득한 적절한 조직 및/또는 다중 전이성 종양이 입수 가능할 경우, 가장 최근에 수집된(이상적으로는 가장 최근의 전신 보조 요법 이후) 조직에 우선순위를 부여해야 한다. If appropriate tissue and/or multiple metastatic tumors obtained at separate time points (e.g., time of initial diagnosis and time of disease recurrence) are available, preference is given to the most recently collected (ideally after the most recent systemic adjuvant therapy). should be ranked.
보관 조직이 충분하지 않거나 입수 가능하지 않은 환자는 여전히 적격일 수 있다.Patients with insufficient or not available storage tissue may still be eligible.
보관 종양 조직은 단백질, RNA 및 DNA 분석을 위한 특성화된 분석을 사용하여 잠재적인 예측 바이오마커를 평가하는 데 사용한다.Archival tumor tissues are used to evaluate potential predictive biomarkers using specialized assays for protein, RNA and DNA analysis.
![]()
![]()
시점: 연속 생검은 하기의 두 시점에서 수득한다: 1) 모든 적격성 기준이 충족된 후 기준선에서 치료 전 생검을 수득하고, 2) 티라골루맙 및 아테졸리주맙 둘 모두의 제1 투여 후 약 2주(즉, 주기 1의 15일 내지 21일 또는 그 사이)에 치료 중 생검을 수득한다. Time points: Serial biopsies are obtained at two time points: 1) pre-treatment biopsies are obtained at baseline after all eligibility criteria have been met, and 2) approximately 2 weeks after the first administration of both tiragolumab and atezolizumab. An on-treatment biopsy is obtained (ie, on or between
추가적인 선택적 생검은 시험자의 재량에 따라, 바람직하게는 방사선학적 진행 시점(특히 가진행이 의심되는 경우) 또는 반응 시점에 수집할 수 있다.Additional selective biopsies may be collected at the discretion of the investigator, preferably at the time of radiological progression (especially when excitation is suspected) or at the time of response.
일련의 종양 생검은 단백질, RNA 및 DNA 분석을 위한 특성화된 분석을 사용하여 종양 약력학적 바이오마커 및 잠재적인 예측 바이오마커를 평가하는 데 사용한다.Serial tumor biopsies are used to evaluate tumor pharmacodynamic biomarkers and potential predictive biomarkers using specialized assays for protein, RNA and DNA analysis.
![]()
![]()
시험자가 샘플 수집을 임상적으로 가능한 것으로 간주하고 환자가 서면 동의서를 제공한 경우 진행 중 생검이 필요하다. 깊은 종양 조직 또는 림프절용 코어 바늘 생검 또는 피부, 피하, 또는 점막 병변용 절제, 절개, 펀치, 또는 겸자 생검으로 구성된 종양 조직 샘플을 수득한다. An in-progress biopsy is required if the investigator considers sample collection clinically feasible and the patient has provided written informed consent. A tumor tissue sample is obtained consisting of a core needle biopsy for deep tumor tissue or lymph nodes or an excision, incision, punch, or forceps biopsy for skin, subcutaneous, or mucosal lesions.
진행 중 생검은 단백질, RNA 및 DNA 분석을 위한 특성화된 분석을 사용하여 종양 약력학적 바이오마커 및 잠재적인 예측 바이오마커를 평가하는 데 사용한다.On-going biopsies are used to evaluate tumor pharmacodynamic biomarkers and potential predictive biomarkers using specialized assays for protein, RNA and DNA analysis.
![]()
![]()
선택적 생검에 동의한 환자는 모든 적격성 기준이 충족된 후 기준선에서, 및 단일 제제로서 티라골루맙의 제1 투여(Ia상) 후 약 2주에, 또는 티라골루맙 및 아테졸리주맙의 제1 투여(Ib상) 후 약 2주에(즉, 주기 1의 15일 내지 21일 또는 그 사이) 종양 생검을 제공한다.Patients who consented to elective biopsy were enrolled at baseline after all eligibility criteria have been met, and at about 2 weeks after the first dose of tiragolumab as a single agent (Phase Ia), or first dose of tiragolumab and atezolizumab Tumor biopsies are given about 2 weeks after (Phase Ib) (ie, days 15-21 of
접근가능한 잔여 종괴가 있고 연장된 CR 및/또는 PR(예컨대, 기간에서 대략 1년의)이 확인된 환자의 경우, 해당 잔여 종괴의 생검을 실시하여 생존 가능한 종양 세포(vs. 섬유성 또는 괴사성 조직)를 평가하도록 권장한다.For patients with an accessible residual mass and with confirmed prolonged CR and/or PR (eg, approximately 1 year in duration), a biopsy of that residual mass is performed to obtain viable tumor cells (vs. fibrous or necrotic) organization) is recommended.
종양 조직 샘플은 코어 바늘, 펀치, 절제 생검(상기에 명시된 대로) 또는 겸자 생검을 사용하여 수집할 수 있다. 선택한 생검 기술과 관련된 추가 지침에 대해서는 필수 종양 생검에 대해 상기에서 설명한 샘플 사양을 참조한다. Tumor tissue samples can be collected using a core needle, punch, excision biopsy (as specified above) or forceps biopsy. For additional guidance related to the selected biopsy technique, see the sample specifications described above for essential tumor biopsy.
선택적 종양 생검은 단백질, RNA 및 DNA 분석을 위한 특성화된 분석을 사용하여 종양 약력학적 바이오마커 및 잠재적인 예측 바이오마커를 평가하는 데 사용한다.Selective tumor biopsies are used to evaluate tumor pharmacodynamic biomarkers and potential predictive biomarkers using specialized assays for protein, RNA and DNA analysis.
![]()
![]()
깊은 종양 조직 또는 림프절의 코어 바늘 생검 또는 피부, 피하, 또는 점막 병변용 절제, 절개, 펀치, 또는 겸자 생검으로 구성된 종양 조직 샘플을 수득한다. 미세 바늘 흡인물, 삼출물 또는 복수의 세포 펠릿, 세척 샘플 및 뼈 생검은 허용하지 않는다. 코어 바늘 생검을 위해 고려되는 표적 병변은 주어진 시점(최소 직경 18 게이지)에서 적어도 3개의 코어를 탐색하는 데 적합한 것으로 간주된다. 가능한 경우, 동일한 병변을 연속적으로 통과할 때는 1 cm 이상 이격시켜야 한다.A tumor tissue sample is obtained consisting of a core needle biopsy of deep tumor tissue or lymph nodes or an excision, incision, punch, or forceps biopsy for skin, subcutaneous, or mucosal lesions. Fine needle aspirates, exudates or ascites cell pellets, wash samples and bone biopsies are not permitted. A target lesion considered for a core needle biopsy is considered suitable for exploring at least three cores at a given time point (
여러 병변이 입수 가능한 경우, 전이 부위와 관련된 이질성의 도입을 피하기 위해 가능한 경우 치료 전 생검과 동일한 병변(또는 장기)에서 치료 중 생검을 수득하는 것이 바람직하다.When multiple lesions are available, it is desirable to obtain an on-treatment biopsy from the same lesion (or organ) as the pre-treatment biopsy, if possible, to avoid the introduction of heterogeneity associated with the site of metastasis.
RECIST 표적 병변은 생검하지 않는다.RECIST target lesions are not biopsied.
조직 샘플 및 이의 파생물(예컨대, DNA 및 RNA)은 무기한 또는 다 사용되거나 환자가 샘플의 폐기를 요청할 때까지 보관한다. Tissue samples and their derivatives (eg, DNA and RNA) are stored indefinitely or until used up or until the patient requests disposal of the sample.
![]()
![]()
환자가 단일 제제(Ia상)로서의 티라골루맙 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용한(Ib상) 티라골루맙의 활성(항종양 또는 자가면역 여부)을 알릴 수 있는 종양 조직 또는 기타 조직을 산출하는 연구 과정 중 언제든지 의학적으로 지시된 절차(즉, 기관지 내시경, 식도위십이지장 내시경, 대장 내시경 등)를 받는 경우, 임의의 나머지 샘플 또는 의학적 진단에 필요하지 않은 샘플의 일부(체액 샘플 또는 남은 종양 조직)는 탐색적 분석을 위해 수득될 수 있다. 환자는 상기 샘플을 수집하고 평가하기 위해 특정 정보에 입각한 동의서를 제공해야 한다.Tumor tissue that may signal the patient's activity (anti-tumor or autoimmune) of tiragolumab as a single agent (phase Ia) or in combination with atezolizumab (phase Ib) with or without chemotherapy or any remaining sample or portion of a sample not necessary for a medical diagnosis (body fluids), if at any time during the course of a study that yields other tissue, a medically directed procedure (i.e., bronchoscopy, esophageal gastroduodenoscopy, colonoscopy, etc.) sample or remaining tumor tissue) can be obtained for exploratory analysis. Patients must provide informed consent to collect and evaluate the sample.
상기 나머지 종양 샘플은 단백질, RNA 및 DNA 분석을 위한 특성화된 분석을 사용하여 종양 약력학적 바이오마커 및 잠재적인 예측 바이오마커를 평가하는 데 사용한다.The remaining tumor samples are used to evaluate tumor pharmacodynamic biomarkers and potential predictive biomarkers using specialized assays for protein, RNA and DNA analysis.
심전도electrocardiogram
3중 ECG 기록은 티라골루맙 단독(Ia상)의 용량 증량 코호트 및 보충 코호트에 대해 지정된 시점에서, 단일 ECG 기록은 다른 모든 환자에 대해 수득한다. 상이한 요일에 수득한 ECG는 가능한 한 시간을 일치시킨다. 각 시점(5분)에서 3개의 해석 가능한 ECG 기록(예컨대, 인공물 제외)을 수득해야 한다. 상기 3개의 판독값의 평균은 ECG 간격(예컨대, PR, QRS, QT)을 결정하는 데 사용한다. 임상적으로 지시된 바와 같이 예정되지 않은 시점에 추가 ECG를 수득할 수 있다.Triple ECG records are obtained for all other patients at the time points designated for the dose escalation cohort and the supplemental cohort of tiragolumab alone (Phase Ia). ECGs obtained on different days of the week are as time-matched as possible. Three interpretable ECG records (eg, excluding artifacts) should be obtained at each time point (5 min). The average of the three readings is used to determine the ECG interval (eg, PR, QRS, QT). Additional ECGs may be obtained at unscheduled time points as clinically indicated.
모든 ECG 기록은 컴퓨터 기반 간격 측정이 장착된 표준 고품질, 고충실 디지털 심전도 기계를 사용하여 실시해야 한다. 리드(lead) 배치는 가능한 한 일관된다. ECG 기록은 환자가 적어도 10분 동안 바로 누운 자세를 취한 후에 실시해야 한다. 모든 ECG는 같은 시간에 예정된 다른 절차(예컨대, 활력징후 측정, 채혈) 이전에 수득하고 임의의 식사 후 3시간 이내에는 수득해서는 안 된다. 상기 지침을 따르는 것이 환자에게 어려울 수 있는 경우, 식사 섭취와 ECG 기록 사이의 시간은 모든 시점에서 동일한 최소 시간이 유지되는 한 2.5시간 또는 기관 표준으로 단축될 수 있다. 환경적 방해 요소(예컨대, 텔레비전, 라디오, 대화)를 포함하여 심박수의 변화를 유발할 수 있는 상황은 ECG 이전의 휴식 기간 및 ECG 기록 중에 피해야 한다. All ECG recordings should be performed using a standard high-quality, high-fidelity digital electrocardiogram machine equipped with computer-based interval measurement. Lead placement is as consistent as possible. ECG recordings should be performed after the patient has been in the supine position for at least 10 minutes. All ECGs should be obtained prior to other procedures scheduled at the same time (eg, vital signs measurement, blood collection) and should not be obtained within 3 hours after any meal. In cases where it may be difficult for the patient to follow the above guidelines, the time between meal intake and ECG recording may be shortened to 2.5 hours or to institutional standards as long as the same minimum time is maintained at all time points. Circumstances that may induce changes in heart rate, including environmental disturbances (eg television, radio, conversation), should be avoided during the rest period prior to ECG and during ECG recording.
안전 모니터링 목적을 위해, 시험자는 모든 ECG 추적을 검토하고 서명하고 날짜를 기입해야 한다. 임상적 의미가 있거나 없는 정상 또는 비정상인 ECG의 전반적인 평가가 기록된다. ECG 추적의 종이 또는 전자 사본은 기관에서 환자의 영구 연구 파일의 일부로서 보관된다. For safety monitoring purposes, the investigator must review, sign and date all ECG traces. An overall assessment of the ECG, normal or abnormal, with or without clinical significance is recorded. A paper or electronic copy of the ECG trace is maintained at the institution as part of the patient's permanent study file.
특정 투여 후 시점에서, 프리데리시아 (Fridericia) 공식(QTcF)을 통해 수정된 평균 QT 간격이 기준선 값보다 500 ms를 초과하여 및/또는 60 ms를 초과하여 더 길 경우, 다른 ECG를 이상적으로는 다음 5분 이내에 기록해야 하며, 2회의 연속 ECG에서 QTcF가 안정화될 때까지 ECG 모니터링을 계속한다. 치표의 표준에 따른 치료는 시험자의 재량에 따라 실시될 수 있다. PK 샘플이 해당 시점에 예약되지 않을 지라도, 예약되지 않은 PK 샘플을 획득한다. 시험자는 잠재적인 동시 위험 요소(예컨대, 전해질 이상, QT 간격을 연장하는 것으로 공지된 공동 약물, 심각한 서맥)에 대해 환자를 평가한다.If, at a specific post-dose time point, the mean QT interval, corrected via the Fredericia formula (QTcF), is >500 ms and/or >60 ms longer than the baseline value, then another ECG would ideally be Records should be made within the next 5 min, and on 2 consecutive ECGs, ECG monitoring is continued until QTcF has stabilized. Treatment according to the standard of the table may be performed at the discretion of the investigator. Even if a PK sample is not reserved at that time, an unreserved PK sample is obtained. The investigator evaluates the patient for potential concomitant risk factors (eg, electrolyte abnormalities, concomitant medications known to prolong the QT interval, severe bradycardia).
암 관련 절차Cancer-related procedures
암 관련 의료, 외과 및 방사선 절차의 수집은 1일에 시작하여 연구의 Ia상 및 Ib상 부분 모두에서 치료 기간과 생존 추적 기간 동안 실시한다.Collection of cancer-related medical, surgical, and radiological procedures begins on
항 약물 항체 검사Anti-drug antibody test
티라골루맙 및/또는 아테졸리주맙은 자체에 대한 면역 반응을 유발할 수 있다. 검증된 선별검사, 확인 및 역가 분석은 Ia상에서 단일 제제로서 티라골루맙을 이용한 치료 전, 치료 중 및 치료 후에 또는 Ib상에서 화학요법을 포함하거나 포함하지 않고 티라골루맙 및 아테졸리주맙의 조합으로 치료한 후 여러 시점에서 ADA를 검출하기 위해 사용된다. ADA 반응은 임상적 중요성을 이해하기 위해 관련 임상 종점과 상관관계가 있다. 추가적인 ADA 분석(예컨대, 중화 항체 분석)을 사용하여 ADA 반응을 추가로 특성화할 수 있다.Tiragolumab and/or atezolizumab may elicit an immune response against itself. Validated screening tests, confirmations, and assays of potency include pre-, during and post-treatment with tiragolumab as a single agent in phase Ia or treatment with a combination of tiragolumab and atezolizumab with or without chemotherapy in phase Ib. It is then used to detect ADA at multiple time points. ADA response correlates with relevant clinical endpoints to understand clinical significance. Additional ADA assays (eg, neutralizing antibody assays) can be used to further characterize the ADA response.
U.U. 환자 및 연구 치료 중단 Discontinuation of patient and study treatment
환자 중단patient discontinuation
연구에서 환자의 중단은 연구 치료 중단과 구별되며, 환자가 사망하거나 추적 관찰을 하지 못하거나 추적 동의를 철회할 때 발생한다. Discontinuation of a patient from a study is distinct from discontinuation of study treatment and occurs when the patient dies, fails to follow-up, or withdraws consent to follow-up.
환자는 이유를 불문하고 언제든지 연구를 자발적으로 철회할 권리가 있다. 또한, 시험자는 언제든지 연구에서 환자를 철회할 권리가 있다. 연구 철회 사유는 하기를 포함할 수 있지만 이에 제한되지는 않는다:Patients have the right to voluntarily withdraw from the study at any time for any reason. In addition, the investigator has the right to withdraw a patient from the study at any time. Reasons for study withdrawal may include, but are not limited to:
![]()
![]()
![]()
![]()
![]()
![]()
연구로부터 철회한 환자에 대한 정보를 수득하기 위해 모든 노력을 기울인다. 연구 또는 추적 조사에서 철회하는 주요 이유가 문서화된다. 단, 동의 철회 이후에는 어떠한 이유로든 환자를 추적하지 않는다. 연구에서 철회한 환자는 대체되지 않는다.Every effort is made to obtain information about patients withdrawn from the study. The main reasons for withdrawal from the study or follow-up are documented. However, after the withdrawal of consent, the patient will not be followed for any reason. Patients who withdraw from the study are not replaced.
연구 치료 중단study treatment discontinuation
환자는 하기 중 임의의 것을 경험하는 경우 연구 치료제를 중단해야 한다.Patients should discontinue study treatment if they experience any of the following:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
환자는 이유를 불문하고 언제든지 연구 치료를 자발적으로 철회할 권리가 있다. 또한, 시험자는 언제든지 연구 치료에서 환자를 철회할 권리가 있다. 연구 치료로부터의 철회 사유는 하기를 포함할 수 있지만 이에 제한되지는 않는다:Patients have the right to voluntarily withdraw from study treatment at any time for any reason. In addition, the investigator has the right to withdraw a patient from study treatment at any time. Reasons for withdrawal from study treatment may include, but are not limited to:
![]()
![]()
![]()
![]()
주로 질병 진행 이외의 이유로 연구 치료를 중단한 환자는 종양 평가를 계속하고, 연구 치료를 중단한 모든 환자는 동의를 철회하지 않는 한 3개월마다 생존을 위한 추적을 계속 한다.Patients who discontinue study treatment primarily for reasons other than disease progression continue tumor evaluation, and all patients who discontinue study treatment continue follow-up for survival every 3 months unless consent is withdrawn.
연구 치료를 중단한 환자는 연구 치료제의 마지막 투여 후 30일 이내에 치료 중단 방문을 위해 병원을 다시 방문해야 한다.Patients who discontinue study treatment must return to the hospital for a treatment discontinuation visit within 30 days of the last dose of study treatment.
이의 반응 평가에서 티라골루맙의 중단(Ia상) 또는 티라골루맙 및 아테졸리주맙, 티라골루맙 및 아테졸리주맙에 더한 베바시주맙, 또는 티라골루맙 및 펨브롤리주맙(Ib상)의 병용 중단을 초래하는 PD를 나타내는 방문은 해당하는 경우 치료 중단 방문으로 사용될 수 있으며, 이 경우 치료 중단 방문과 관련된 모든 평가가 해당 시점에 실시된다.Discontinuation of tiragolumab (Phase Ia) or concomitant discontinuation of tiragolumab and atezolizumab, tiragolumab and atezolizumab plus bevacizumab, or tiragolumab and pembrolizumab (Phase Ib) in the evaluation of its response A visit presenting PD that causes
연구 치료 중단 후, 모든 환자는 생존 및 후속 항암 요법을 추적한다. 생존 및 후속 항암 치료 추적 정보는 환자가 추적 중단을 요청하지 않는 한 사망, 추적 상실 또는 연구 종료까지 약 3개월마다 전화 통화, 환자 의료 기록, 및/또는 병원 방문을 통해 수집한다. 후속 항암 요법에 대한 정보에는 전신 요법(예컨대, 화학요법, 표적요법, 호르몬 요법 또는 CIT), 수술(예컨대, 전이성 질병의 절제), 및 방사선 절차(예컨대, 종양 병변에 대한 방사선 요법)가 포함된다.After discontinuation of study treatment, all patients are followed for survival and subsequent anticancer therapy. Survival and follow-up chemotherapy follow-up information is collected through phone calls, patient medical records, and/or hospital visits approximately every 3 months until death, loss of follow-up, or study termination, unless the patient requests discontinuation of follow-up. Information on subsequent anti-cancer therapy includes systemic therapy (eg, chemotherapy, targeted therapy, hormone therapy, or CIT), surgery (eg, resection of metastatic disease), and radiation procedures (eg, radiation therapy for tumor lesions). .
환자가 연구에서 철회하는 경우, 기관의 직원은 공개 정보 출처(예컨대, 지역 기록)를 사용하여 생존 상태에 대한 정보만 수득할 수 있다.If a patient withdraws from the study, the institution's staff may use public information sources (eg, local records) to obtain information on survival status only.
V.V. 분석 analysis
목적 및 평가변수Purpose and endpoints
본 연구는 국소 진행성 또는 전이성 종양을 가진 환자에게 단일 제제(Ia상)로서 또는 아테졸리주맙 또는 다른 항암 요법과 병용 투여할 때의(Ib상) 티라골루맙의 안전성, PK, 약력학, 및 예비 항종양 활성을 평가한다. 구체적인 연구 목적 및 해당 평가변수를 표 36에 요약한다. The present study investigated the safety, PK, pharmacodynamics, and prospective antibiotics of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab or other anticancer therapies (Phase Ib) in patients with locally advanced or metastatic tumors. Assess tumor activity. The specific study objectives and corresponding endpoints are summarized in Table 36.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
-
농도-시간 곡선하 면적(AUC)
-
최대 혈장 농도(C최대)
-
최소 혈장 농도(C최소)
-
청소율(CL)
-
정상 상태의 분포 용적(Vss)
![]()
![]()
![]()
![]()
- Area under the concentration-time curve (AUC)
- Maximum plasma concentration (C max )
- Minimum plasma concentration (C minimum )
- Cleaning rate (CL)
- volume of distribution in steady state (V ss )
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
RNA 서열분석 및 전체 유전체 서열분석(WGS)에 의한 바이오마커 측정 ![]()
Biomarker determination by RNA sequencing and whole genome sequencing (WGS)
Ia상 및 Ib상의 목적 및 및 해당 평가변수Phase Ia and Ib objectives and their endpoints
활동 분석activity analysis
하기에 기재되는 분석은 RECIST v1.1에 따른 객관적 반응의 정의를 기반으로 한다.The analysis described below is based on the definition of objective response according to RECIST v1.1.
반응 평가 데이터, 객관적 반응 지속 기간, PFS 및 OS는 적절한 경우 용량 수준 또는 종양 유형별로 치료된 모든 환자에 대해 나열된다.Response assessment data, objective duration of response, PFS and OS are listed for all treated patients by dose level or tumor type, where appropriate.
객관적 반응율objective response rate
ORR의 분석은 임의의 양의 연구 치료제를 투여받고 기준선에서 측정 가능한 질병을 가진 Ia상 또는 Ib상 연구의 환자가 포함한다. 객관적인 반응은 시험자 평가에 의해 결정되고 초기 문서화 후 4주 이상 반복 평가에 의해 확인된 CR 또는 PR로 정의된다. 기준선이 누락되었거나 반응 평가가 없는 환자는 무반응자로 분류된다. 객관적인 반응률은 종양 유형 및 해당되는 경우 용량별로 추정하고 요약된다.Analysis of ORR includes patients in Phase Ia or Ib studies who have received any amount of study treatment and have measurable disease at baseline. Objective response is defined as a CR or PR determined by investigator assessment and confirmed by repeated assessments at least 4 weeks after initial documentation. Patients with missing baseline or no response assessment are classified as non-responders. Objective response rates are estimated and summarized by tumor type and, if applicable, dose.
반응 지속기간duration of response
객관적 반응을 보인 환자 중, 객관적 반응의 지속기간은 초기의 완전 또는 부분 반응부터 질병 진행 또는 사망까지의 시간 중 먼저 발생하는 시간으로 정의된다. 연구 종료 전에 사망하지 않았거나 질병 진행을 경험하지 않았거나 추적 관찰에 실패한 환자의 경우, 객관적 반응 지속기간은 마지막 종양 평가일에 중도절단된다.Among patients with an objective response, the duration of the objective response is defined as the time from the initial complete or partial response to disease progression or death, whichever occurs first. For patients who did not die, did not experience disease progression, or failed follow-up prior to study termination, the duration of objective response is censored on the date of last tumor assessment.
무진행 생존progression-free survival
PFS 분석은 임의의 양의 연구 치료제를 투여받은 환자를 포함한다. PFS는 연구 치료제의 제1일부터 문서화된 질병 진행 또는 사망 중 먼저 발생하는 시점까지의 시간으로 정의된다. 연구 종료 전에 PD 또는 사망을 기록하지 않았거나 추적 관찰에 실패한 환자의 경우, PFS는 마지막 종양 평가 당일에 중도절단된다. 기준선 이후 종양 평가가 없는 환자의 경우, PFS는 연구 치료제의 제1일에 중도절단된다.The PFS analysis includes patients receiving any amount of study treatment. PFS is defined as the time from
전체 생존overall survival
OS 분석은 임의의 양의 연구 치료제를 투여받은 환자를 포함한다. OS는 연구 치료제의 제1 용량 투여로부터 연구 중 임의의 원인으로 인한 사망까지의 시간으로 정의된다. 연구가 종료되기 전에 사망하지 않았거나 추적 관찰에 실패한 환자의 경우, 생존이 마지막으로 공지된 날짜에 OS가 중도절단된다.OS analysis included patients who received any amount of study treatment. OS is defined as the time from administration of the first dose of study treatment to death from any cause during the study. For patients who do not die before study termination or fail to follow-up, OS is censored on the last known date of survival.
안전성 분석Safety analysis
안전성은 DLT, 이상 반응, 실험실 검사 결과의 변화, 활력 징후 및 ECG의 변화, 임의의 연구 치료제(티라골루맙, 아테졸리주맙, 베바시주맙, 펨브롤리주맙, 카보플라틴, 시스플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈, 에토포시드)에 대한 노출을 요약하여 평가한다. 임의의 양의 연구 치료제를 제공받은 모든 환자는 안전성 분석 내에 포함된다.Safety includes DLT, adverse events, changes in laboratory test results, changes in vital signs and ECG, and any study treatment (tiragolumab, atezolizumab, bevacizumab, pembrolizumab, carboplatin, cisplatin, pemetrexed). , paclitaxel, capecitabine, and etoposide). All patients who received any amount of study treatment are included in the safety analysis.
이상 반응에 대한 축어적 설명은 유의어 용어에 매핑된다. 이상 반응 데이터는 연구 기관, 용량 코호트 또는 적절한 종양 유형, 환자 번호, 및 연구 날짜별로 나열된다. 1일에 치료 중 또는 치료 후 발생하는 모든 반응은 매핑된 기간, 적합한 유의어 수준, 및 NCI CTCAE v4.0 등급에 의해 요약된다. 이에 더하여, 사망을 포함한 심각한 이상 반응은 별개로 나열되고 요약된다.Verbose descriptions of adverse events are mapped to synonym terms. Adverse event data are listed by study site, dose cohort or appropriate tumor type, patient number, and study date. All responses that occur during or after treatment on
치료 중단으로 이어지는 이상 반응이 나열된다. DLT 이외의 이유로 DLT 평가 기간을 완료하기 전에 연구를 철회한 환자는 DLT 및 MTD 평가에 대해 평가할 수 없는 것으로 간주된다.Adverse events leading to discontinuation of treatment are listed. Patients who withdraw from the study prior to completion of the DLT evaluation period for reasons other than DLT will be considered ineligible for DLT and MTD evaluation.
관련 실험실 값, 활력 징후, 및 ECG 데이터는 적절한 경우 식별된 NCI CTCAE 등급 3 및 등급 4 값과 함께 시점별로 제시된다. ADA 반응의 발생률(혈청 항 티라골루맙 또는 항 아테졸리주맙의 존재) 및 PK, 약력학 및 안전성 매개변수와의 잠재적인 상관관계를 평가할 수 있다.Relevant laboratory values, vital signs, and ECG data are presented by time point, along with identified
약동학 분석Pharmacokinetic analysis
Ia상 연구에서, 개별 및 평균 혈청 티라골루맙 농도 대 시간 데이터가 표로 작성되고 용량 수준에 의해 플롯팅된다. 티라골루맙의 약동학은 총 AUC, Cmax, Cmin, 총 CL, Vss, 및 최종 반감기(수집된 데이터에 적합)를 추정하여 요약된다. 이러한 매개변수에 대한 추정치는 표로 작성되고 요약된다(평균, 표준 편차 및 변동 계수). 환자 간 변동성 및 약물 축적이 평가된다.In the Phase Ia study, individual and mean serum tyragolumab concentration versus time data are tabulated and plotted by dose level. The pharmacokinetics of tiragolumab are summarized by estimating total AUC, C max , C min , total CL , V ss , and terminal half-life (fitted to collected data). Estimates for these parameters are tabulated and summarized (mean, standard deviation, and coefficient of variation). Inter-patient variability and drug accumulation are assessed.
Ib상 연구에서, 혈청 티라골루맙 및 아테졸리주맙 농도 데이터(Cmax 및 Cmin)가 표로 작성되고 수집된 각 주기별 용량 수준으로 요약된다. 기술 통계는 평균, 중앙값, 표준 편차 및 범위를 적절하게 포함한다. 다른 PK 매개변수는 데이터 보증으로 결정되고 요약될 수 있다. 이러한 결과는 티라골루맙 또는 아테졸리주맙 Pk가 다른 제제의 병용 투여에 의해 변경되는지 여부에 대한 예비 정보를 제공하기 때문에, 데이터를 과거 데이터와 비교할 수 있다. In the Phase Ib study, serum tyragolumab and atezolizumab concentration data (C max and C min ) were tabulated and summarized with each cycle dose level collected. Descriptive statistics include mean, median, standard deviation and range as appropriate. Other PK parameters can be determined and summarized as data assurance. Because these results provide preliminary information on whether tiragolumab or atezolizumab Pk is altered by concomitant administration of other agents, the data can be compared with historical data.
Ib상 화학요법 확장 코호트에서, 티라골루맙 및 아테졸리주맙의 혈청 농도 및 카보플라틴, 시스플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈 및 에토포시드의 혈장 농도가 수집된다. 티라골루맙, 아테졸리주맙, 카보플라틴, 시스플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈 및 에토포시드의 농도는 상기에서 설명한 기술 통계를 사용하여 요약된다. 이러한 결과는 티라골루맙, 아테졸리주맙, 카보플라틴, 시스플라틴, 페메트렉시드, 파클리탁셀, 카페시타빈 및 에토포시드 PK가 다른 제제의 동시 투여에 의해 변경되는지 여부에 대한 예비 정보를 제공하기 때문에 데이터를 과거 데이터와 비교한다. In the Phase Ib chemotherapy expansion cohort, serum concentrations of tiragolumab and atezolizumab and plasma concentrations of carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide are collected. Concentrations of tiragolumab, atezolizumab, carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide are summarized using the descriptive statistics described above. Because these results provide preliminary information on whether tiragolumab, atezolizumab, carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide PK are altered by the simultaneous administration of other agents. Compare the data with historical data.
약력학적 분석은 가능한 경우 종양 조직과 혈액 모두의 약력학적 바이오마커에 대한 평가를 포함한다. 추가 PK 및 약력학 분석이 적절하게 수행된다. 필요한 경우, 초기 환자에서 관찰된 바이오마커 반응을 기반으로 바이오마커 샘플링 시간의 잠재적 조정이 적용될 수 있다.Pharmacodynamic analyzes include evaluation of pharmacodynamic biomarkers in both tumor tissue and blood, where possible. Additional PK and pharmacodynamic analyzes are performed as appropriate. If necessary, a potential adjustment of the biomarker sampling time may be applied based on the observed biomarker response in the initial patient.
면역원성 분석Immunogenicity assay
환자가 기준선에서 ADA 음성이고 이후 연구 약물 투여 후 ADA 반응이 발생인 경우, 치료 유발 ADA 반응을 갖는 것으로 간주한다. 환자가 기준선에서 ADA 양성이고 하나 이상의 기준선 이후 샘플의 역가가 기준선 샘플의 역가보다 4배 이상(즉, 0.60 이상의 역가 단위) 더 큰 경우, 환자는 치료 강화 ADA 반응을 갖는 것으로 간주한다. 환자가 모든 시점에서 ADA 음성인 경우, 환자는 ADA에 대해 음성인 것으로 간주한다. 환자가 기준선에서 ADA 양성이지만 기준선 샘플의 역가보다 적어도 4배 이상 더 큰 역가를 갖는 기준선 이후 샘플이 없는 경우, 환자는 치료에 영향을 받지 않은 것으로 간주한다.A patient is considered to have a treatment-evoked ADA response if it is ADA negative at baseline and an ADA response occurs following study drug administration. A patient is considered to have a treatment-enhancing ADA response if the patient is ADA positive at baseline and the titer of one or more post-baseline samples is greater than or equal to 4 times the titer of the baseline sample (i.e., greater than or equal to 0.60 titer units). A patient is considered negative for ADA if it is ADA negative at all time points. A patient is considered unaffected by treatment if a patient is ADA positive at baseline but has no post-baseline sample with a titer at least 4 times greater than that of the baseline sample.
티라골루맙 및 아테졸리주맙에 대한 ADA 결과는 연구의 Ia상 및 Ib상 부분에 대해 환자 및 주기별로 요약 및 나열된다.ADA outcomes for tiragolumab and atezolizumab are summarized and listed by patient and cycle for the Phase Ia and Phase Ib portions of the study.
Ia상 및 Ib상 확장 코호트의 중간 분석Interim Analysis of Phase Ia and Phase Ib Expansion Cohorts
IMC는 활동의 증거가 없을 때 등록의 조기 중단 가능성을 안내할 수 있도록 Ia상 및 Ib상의 각 확장 코호트별로 중간 분석을 실시한다. 확장 코호트에 등록된 약 20명의 환자가 1~2개의 종양 평가를 완료한 후, IMC는 중간 분석을 실시하기 위해 만난다. 중간 분석에서 티라골루맙(Ia상) 또는 화학요법을 포함하거나 포함하지 않고 아테졸리주맙과 병용한 티라골루맙, 또는 아테졸리주맙 및 베바시주맙과 병용한 티라골루맙, 또는 펨브롤리주맙과 병용한 티라골루맙(Ib상)에 대한 객관적 종양 반응에 의해 제시된 활성이 해당 환자 군에 대한 관심 임계값 미만인 경우(예컨대, 처음 20명의 환자에서 반응이 관찰되지 않은 경우), IMC는 확장 코호트에 대한 등록을 중단할 것을 권고할 수 있다. The IMC will conduct an interim analysis for each expansion cohort in Phases Ia and Ib to guide the possibility of early termination of enrollment in the absence of evidence of activity. After approximately 20 patients enrolled in the expansion cohort have completed one or two tumor assessments, the IMC meets to conduct interim analyses. Tiragolumab in combination with atezolizumab (Phase Ia) or with or without chemotherapy in interim analysis, or tiragolumab in combination with atezolizumab and bevacizumab, or in combination with pembrolizumab If the activity presented by the objective tumor response to one tiragolumab (Phase Ib) is below the threshold of interest for that patient group (e.g., no response was observed in the first 20 patients), the IMC will be evaluated for the expansion cohort. You may be advised to discontinue registration.
예를 들어, 실제 ORR이 5%인 경우, 처음 20명의 환자에게서 반응이 관찰되지 않을 확률이 대략 35%이고, 실제 ORR이 10%인 경우, 처음 20명의 환자에게서 반응이 관찰되지 않을 확률이 대략 12%이다. For example, if the actual ORR is 5%, the probability that no response will be observed in the first 20 patients is approximately 35%, and if the true ORR is 10%, the probability that no response will be observed in the first 20 patients is approximately 12%.
IMC는 또한 활동의 The IMC is also responsible for
증거가 있거나 적절한 평가를 허용하기에 충분한 특정 환자가 등록되지 않은 경우(예컨대, 특정 종양 유형, 특정 종양 PD-L1 및/또는 TIGIT 발현 상태, 및/또는 특정 CIT 기록이 있는 환자) 해당 확장 코호트에 등록을 계속하도록 권고할 수 있다. If there is evidence or sufficient specific patients are not enrolled to permit an appropriate assessment (e.g., patients with specific tumor types, specific tumor PD-L1 and/or TIGIT expression status, and/or specific CIT history), You may be advised to continue your registration.
모든 경우에, 연구 시험자와 상의하여 의료 모니터 요원은 IMC 권고에 따라 무익성을 기반으로 확장 코호트 등록을 중단하는 결정이 내린다. 의료 모니터 요원은 Ia상 또는 Ib상의 각 확장 코호트에서 진행 중인 데이터를 검토하기 위해 IMC의 추가 임시 회의를 요청할 수도 있다.In all cases, in consultation with the study investigator, the medical monitor staff makes a decision to discontinue expansion cohort enrollment based on futility in accordance with IMC recommendations. Medical monitor personnel may request additional ad hoc meetings of the IMC to review ongoing data from each expansion cohort in Phase Ia or Phase Ib.
W.W. 티라골루맙에 대한 임상 연구 요약 Summary of Clinical Studies for Tiragolumab
국소 진행성 또는 전이성 종양이 있는 환자에게서 티라골루맙을 평가하는 상기 진행 중인 연구(GO30103)로부터 예비 임상 데이터를 입수할 수 있다. 2019년 12월 2일의 임상 마감일 기준으로, 연구 GO30103에는 190명의 환자가 등록되었으며, 이 중 42명의 환자는 Ia상 부분에, 171명의 환자는 Ib상 부분에 등록되었으며, 여기에는 질병 후 Ia상으로부터 전환된 23명의 환자가 포함된다.Preliminary clinical data are available from this ongoing study (GO30103) evaluating tiragolumab in patients with locally advanced or metastatic tumors. As of the clinical deadline of December 2, 2019, study GO30103 enrolled 190 patients, of which 42 patients were enrolled in the Phase Ia portion and 171 patients in the Phase Ib portion, which included post-disease Phase Ia. 23 patients converted from
진행 중인 II상 연구(GO40290, CITYSCAPE라고도 함)는 감작성 표피 성장 인자 수용체의 (EGFR) 돌연변이 또는 ALK 전위가 있는 환자를 제외한 국소 진행성 절제불가능 또는 전이성 PD-L1 선택된 NSCLC를 가진 화학요법 경험이 없는 환자를 대상으로 위약 + 아테졸리주맙과 비교하여 티라골루맙 및 아테졸리주맙의 유효성 및 안전성을 평가한다. An ongoing phase II study (GO40290, also known as CITYSCAPE) is a chemotherapy-naïve study with locally advanced unresectable or metastatic PD-L1 selected NSCLC, except in patients with sensitizing epidermal growth factor receptor (EGFR) mutations or ALK translocations. To evaluate the efficacy and safety of tiragolumab and atezolizumab compared to placebo plus atezolizumab in patients.
임상 약동학 및 면역원성Clinical Pharmacokinetics and Immunogenicity
2019년 12월 2일의 데이터 마감일을 기준으로, 입수 가능한 데이터(연구 GO30103의 Ia상 부분에서 3주마다 투여된 2~1200 mg의 티라골루맙 및 Ib상 부분에서 3주마다 투여된 1200 mg의 아테졸리주맙과 병용하여 3주마다 투여된 2~1200 mg의 티라골루맙)를 기반으로 예비 PK 분석이 표준 비구획 PK 방법을 사용하여 실시되었다. 아테졸리주맙과 병용한 티라골루맙의 약동학은 단일 제제로서 투여된 티라골루맙의 약동학과 일치하는 것으로 나타났다. 예비 집단-PK 분석에 따르면, 티라골루맙 노출은 100 mg 내지 1200 mg 범위의 용량으로 3주마다 단독 요법으로서 또는 3주마다 1200 mg의 아테졸리주맙과 병용으로 IV 투여한 후 용량에 비례하여 대략적으로 증가하였다. 예비 모집단 PK 분석에서는 약 15일의 선형 약물 제거 반감기로 0.28 L/일의 티라골루맙 청소율을 추정하였다. 연구 GO30103의 Ib상 부분에서 평가 가능한 환자 154명 중 3명(1.9%)에서 티라골루맙에 대한 항약물 항체(ADA)의 발달이 관찰되었다. 예비 데이터는 PK에 대한 티라골루맙 ADA의 명백한 영향이 없음을 시사한다. 하지만, 소수의 양성 ADA 환자는 티라골루맙의 약동학에 대한 ADA의 영향을 평가하기에 적절하지 않았다.As of the data deadline of December 2, 2019, available data (2-1200 mg tiragolumab administered every 3 weeks in the phase Ia portion of study GO30103 and 1200 mg administered every 3 weeks in the phase Ib portion of study GO30103) A preliminary PK analysis based on 2-1200 mg tyragolumab administered every 3 weeks in combination with atezolizumab) was performed using standard noncompartmental PK methods. The pharmacokinetics of tiragolumab in combination with atezolizumab were shown to be consistent with those of tiragoluumab administered as a single agent. According to a preliminary population-PK analysis, tiragolumab exposure was approximately dose-proportional after IV administration at doses ranging from 100 mg to 1200 mg as monotherapy every 3 weeks or in combination with 1200 mg atezolizumab every 3 weeks. increased to Pre-population PK analysis estimated a tyragolumab clearance of 0.28 L/day with a linear drug elimination half-life of approximately 15 days. Development of an antidrug antibody (ADA) to tiragolumab was observed in 3 of 154 (1.9%) evaluable patients in the Phase Ib portion of study GO30103. Preliminary data suggest no apparent effect of tiragolumab ADA on PK. However, a small number of patients with positive ADA were not adequate to assess the effect of ADA on the pharmacokinetics of tiragolumab.
임상 안전성clinical safety
2019년 12월 2일 데이터 마감일 기준으로, 연구 GO30103의 Ia상 부분에서 42명의 환자에 대한 안전성 데이터가 입수 가능하였다. 티라골루맙과의 관계와 상관없이 Ia상에서 일반적으로 보고된 이상 반응(모든 환자의 10% 이상에서 보고됨)은 피로, 변비, 구토, 식욕 감소, 빈혈, 기침, 호흡곤란, 두통, 주입 관련 반응(IRR), 악성 신생물, 메스꺼움 및 가려움증을 포함하였다. 티라골루맙과 관련하여 일반적으로 보고된 이상 반응(환자의 10% 이상에서 보고됨)에는 피로 및 IRR이 포함되었다. As of the December 2, 2019 data deadline, safety data were available for 42 patients in the Phase Ia portion of study GO30103. Adverse events commonly reported in phase Ia (reported in ≥10% of all patients) regardless of relationship to tiragolumab were fatigue, constipation, vomiting, decreased appetite, anemia, cough, dyspnea, headache, and infusion-related reactions. (IRR), malignant neoplasms, nausea and pruritus. Adverse events commonly reported with tiragolumab (reported in >10% of patients) included fatigue and IRR.
3등급 이상의 이상 반응(국립 암 연구소의 이상 반응에 대한 공통 용어 기준(National Cancer Institute Common Terminology Criteria for Adverse Events), 버전 4.0[NCI CTCAE v4.0]에 근거함)은 연구 약물로 인한 원인과 상관없이 연구 GO30103의 Ia상 부분의 16명의 환자(38.1%)에게서 보고되었고, 3명의 환자(7.1%)가 치료 관련 3등급 이상의 이상 반응을 경험하였다. 시험자가 티라골루맙과 관련하여 고려한 3등급 이상의 이상반응에는 아밀라아제 증가, 혈액 크레아티닌 증가, 간부전(하기에 설명), IRR 및 발진이 포함되었디.
2019년 12월 2일의 데이터 마감 날짜를 기준으로, 질병 진행 후 Ia상으로부터 전환된 23명의 환자를 포함하여 171명의 환자가 연구 GO30103의 Ib상 부분에 등록되었다. Ib상에서 치료받은 171명의 환자 중, 163명의 환자(95.9%)가 적어도 하나의 이상 반응을 경험했으며, 그중 110명의 환자(64.7%)는 치료와 관련된 이상 반응을 경험하였다. 티라골루맙과의 관계와 상관없이 Ib상에서 일반적으로 보고된 이상반응(모든 환자의 10% 이상에서 보고됨)에는 가려움증, 발열, 빈혈, 발진, 악성 신생물 진행, 변비, 식욕 감소, 설사, 기침, 무력증, 구토 및 피로가 포함되었다. 티라골루맙 및/또는 아테졸리주맙과 관련하여 일반적으로 보고된 이상 반응(환자의 10% 이상에서 보고됨)에는 가려움증 및 발진이 포함되었다.As of the data cut-off date of December 2, 2019, 171 patients were enrolled in the Phase Ib portion of study GO30103, including 23 patients who converted from Phase Ia after disease progression. Of the 171 patients treated in phase Ib, 163 patients (95.9%) experienced at least one adverse event, of which 110 patients (64.7%) experienced treatment-related adverse events. Adverse events commonly reported in phase Ib (reported in ≥10% of all patients) regardless of relationship to tiragolumab include pruritus, fever, anemia, rash, progression of malignant neoplasm, constipation, decreased appetite, diarrhea, and cough. , asthenia, vomiting and fatigue were included. Adverse reactions commonly reported with tiragolumab and/or atezolizumab (reported in more than 10% of patients) included itching and rash.
3등급 이상의 이상 반응(NCI CTCAE v4.0에 근거함)은 연구 약물로 인한 원인과 상관없이 연구 GO30103의 Ib상 부분의 91명의 환자(53.5%)에게서 보고되었고, 21명의 환자(12.4%)가 치료 관련 3등급 이상의 이상 반응을 경험하였다. 시험자가 티라골루맙 및/또는 아테졸리주맙과 관련하여 고려한 3등급 이상의 이상반응에는 림프구 수 감소, 리파아제 증가, 림프구감소증, 아밀라아제 증가, 부신 기능 부전, 무력증, 심장 눌림증, 두통, 고혈당증, 지방분해 혈증, 과단식 과잉증, 폐렴, 발진 소양증, 횡문근막염당뇨병, 당뇨병성 케톤산증, 및 리파아제가 포함되었다.
연구 GO30103의 Ia상 단일요법 확장 코호트에 등록된 환자에서 전격 간부전으로 정점에 이르는 간독성의 치명적인 사례가 발생하였다. 선별검사 시, 환자의 아미노전이효소는 정상 범위 내에 있었다. 투약 전 C1D1 시, AST 및 ALT가 1등급으로 상승하였다. C1D1에 대해 티라골루맙을 투여하는 동안, 환자는 투여 중단 및 차료 표준에 반응하는 주입 반응을 나타내었고, 환자는 목표로 한 1200 mg 용량의 약 733 mg의 티라골루맙을 투여받았다. 연구 8일에, ALT/AST가 3등급 발진과 관련된 3등급으로 상승하였고, 환자는 매일 프레드니손 60 mg으로 치료를 받았다. 연구 12일까지, 상기 발진은 개선되었지만 AST 및 ALT는 4등급(정상 빌리루빈 및 PT 국제 정상화 비율(INR)을 포함)이었고 제2 면역억제제(아자티오프린)가 추가되었다. 환자는 두 가지 면역억제제 사용에도 불구하고 점진적으로 악화되었고 빌리루빈 상승 및 진행성 간성뇌증과 함께 명백한 간부전이 발생하여 연구 30일에 사망하였다. 간염의 여러 대체 병인은 바이러스(HBV, HCV), 병용 약물 또는 해부학적 이상을 포함하여 제외되었다. 연구 16일에 실시된 간 생검은 독성 간염으로 해석되는 염증성 침윤이 거의 없는 융합성 아대량 괴사를 보여주었다. A fatal event of hepatotoxicity culminating in fulminant liver failure occurred in patients enrolled in the Phase Ia monotherapy expansion cohort of study GO30103. At screening, the patient's transaminases were within the normal range. At pre-dose C1D1, AST and ALT were elevated to
상기 사건 이후, 안전성 데이터 분석은 이상 반응 발견에 대한 유의미한 변화가 없음을 나타내었고 연구 GO30103의 Ia상 및 Ib상 부분에서 투여된 피험자에게서 새로운 유의미한 이상 반응이 관찰되지 않았다.After this event, analysis of safety data showed no significant change in the detection of adverse events and no new significant adverse events were observed in subjects administered in the Phase Ia and Ib portions of study GO30103.
2019년 6월 30일의 데이터 마감일을 기준으로, II상 맹검 연구 GO40290에서 135명의 안전성 평가 가능한 환자에게 아테졸리주맙을 병용한 티라골루맙(3주마다 600 mg) 또는 아테졸리주맙을 병용한 위약을 투여하였다. 티라골루맙 및 아테졸리주맙의 안전성 프로필은 모든 등급의 이상 반응(98.5% 대 95.6%), 3등급 이상의 AE(41.8% 대 44.1%), 심각한 AE(34.3% 대 35.3%) 및 치료 중단으로 이어지는 AE(7.5% 대 10.3%)에 대해 위약 및 아테졸리주맙과 유사하였다. 특별한 관심의 이상 반응은 티라골루맙 및 아테졸리주맙군 환자의 47.8%, 위약군 + 아테졸리주맙군 환자의 32.4%에서 보고되었다. 2019년 12월의 업데이트된 데이터는 유사한 안전성 프로필을 보여주었다.As of the data deadline of 30 June 2019, tiragolumab plus atezolizumab (600 mg every 3 weeks) or placebo plus atezolizumab in 135 safety evaluable patients in phase II blinded study GO40290 was administered. The safety profile of tiragolumab and atezolizumab included adverse events of all grades (98.5% vs. 95.6%), AEs ≥ Grade 3 (41.8% vs. 44.1%), serious AEs (34.3% vs. 35.3%), and leading to treatment discontinuation. Similar to placebo and atezolizumab for AEs (7.5% vs. 10.3%). Adverse events of particular interest were reported in 47.8% of patients in the tiragolumab and atezolizumab groups and 32.4% of patients in the placebo plus atezolizumab group. Updated data for December 2019 showed a similar safety profile.
NSCLC의 전이성 림프상피종 유사 암종 아형(PD-L1 양성)이 있는 대만의 69세 남성에게서 EBV 재활성화 및 가능한 이차성 혈구탐식성 림프조직구증(HLH)의 치명적인 사례 1건이 보고되었으며, 이는 아시아 환자의 EBV 감염과 관련될 수 있다. 선별심사에서, 상기 환자는 양성 혈청 엡스타인-바 핵항원(EBNA) 항체 검사를 받았지만, 치료 담당 시험자가 확인한 활성 EBV 감염의 임상적 징후는 없었다. 주기 1의 1일에, 상기 환자는 연구 약물인 아테졸리주맙 및 티라골루맙을 모두 투여받았고 치료를 잘 견뎠다. 10일에, 상기 환자는 상기도 감염으로 의심되는 열이 발생했으며 항생제로 치료를 받았다. 주기 2의 1일에, 상기 환자는 아테졸리주맙을 투여받았고 주입 후 20분에 2등급의 열이 발생하였다. 발열이 아테졸리주맙 IRR로 추정되었기 때문에, 2주기에는 티라골루맙을 투여하지 않았다. 상기 환자는 발열로 입원했으나, 감염원인에 대한 정밀검사는 음성이었다. 열이 해소되자, 상기 환자는 주기 2의 8일에 퇴원하였다. 주기 2의 15일에, 상기 환자는 간헐적 발열로 다시 입원했으며 저혈압, 대사성 산증, 급성 신장 손상, 범혈구감소증, 응고병증, 출혈, 정신 상태 변화, 아미노전이염, 고빌리루빈혈증, 및 호흡 부전을 동반한 쇼크가 발생하여 중환자실로 이송되었다. 상기 환자는 혈액 내 EBV 역가가 높았고 골수 생검은 HLH와 일치하였다. 다른 감염병인에 대한 배양은 음성이었다. 스테로이드 및 다중 면역억제제(토실리주맙, 히드록시클로로퀸 및 에타너셉트)로 치료했음에도 불구하고, 상기 환자는 주기 2의 31일에 악화되어 사망하였다. 전체적으로, 상기 환자는 1회 용량의 티라골루맙(주기 1) 및 2회 용량의 아테졸리주맙(주기 1 및 주기 2)을 투여 받았다. 본 개정 당시 사건의 정확한 원인은 공지되지 않고 조사가 진행 중이지만, 입수 가능한 정보에 따르면 상기 환자는 조직학적으로 드문 NSCLC 아형이 있었고, 티라골루맙 및 아테졸리주맙의 투여로 재활성화되었던 만성 활동성 EBV 감염이 의심되었다. 연구 약물 노출과 환자의 임상 경과 사이의 시간적 관계를 고려할 때, 상기 환자는 2차 HLH가 발생한 것으로 보인다. 폐림프상피종 유사 암종 환자에서 EBV 재활성화의 이러한 지표 사례 이후, 안전성 데이터를 주의 깊게 검토했으며, II상 연구(GO40290) 또는 현재 1상 연구(GO30103)에서 다른 바이러스 재활성화 사례가 관찰되지 않았다.One fatal case of EBV reactivation and possible secondary hemophagocytic lymphohistiocytosis (HLH) was reported in a 69-year-old male from Taiwan with a metastatic lymphothelioma-like carcinoma subtype (PD-L1-positive) of NSCLC, which was reported in an Asian patient. It may be associated with EBV infection. At screening, the patient had a positive serum Epstein-Barr nuclear antigen (EBNA) antibody test, but had no clinical signs of active EBV infection identified by the treating investigator. On
2019년 12월 2일 데이터 마감일 기준으로, 42명의 환자가 티라골루맙 단일 제제로 치료를 받았다. 단일제제 티라골루맙을 투여받는 환자는 IRR을 경험하였다. Ia상에서, 5명의 환자(12%)가 IRR을 경험하였다. IRR과 관련된 징후 및 증상은 일반적으로 경미했으며, 발열, 오한, 안면 홍조, 고혈압, 림프절병증, 메스꺼움, 근육통 및 피부 병변을 포함하였다. 모든 IRR 사례는 지원 조치로 성공적으로 처리되었다. 환자의 12%에서 단일제제 티라골루맙 주입 중 및 주입 후에 IRR이 발생했기 때문에, IRR이 잠재적 위험에서 확인된 위험으로 이동되었다. 티라골루맙에 대해 추가로 확인된 위험은 없지만, 티라골루맙이 단일 제제로 투여될 때 TIGIT 공동 억제 경로의 관여는 자가면역 염증의 위험을 증가시킬 수 있다. 따라서, 단일 제제로서 티라골루맙은 아테졸리주맙과 유사한 이상 반응을 유발할 수 있다. 이러한 면역 매개 부작용은 항 CTLA-4 및 항 PD-L1/PD-1과 같은 다른 면역 관문 억제제에 대해 잘 특성화되었다. As of the December 2, 2019 data deadline, 42 patients were treated with tiragolumab as a single agent. Patients receiving single agent tiragolumab experienced an IRR. In phase la, 5 patients (12%) experienced IRR. Signs and symptoms associated with IRR were generally mild and included fever, chills, hot flashes, hypertension, lymphadenopathy, nausea, myalgia, and skin lesions. All IRR cases were successfully dealt with as supportive actions. As IRR occurred during and after infusion of single agent tyragolumab in 12% of patients, the IRR was shifted from potential risk to identified risk. Although there is no additional identified risk for tiragolumab, involvement of the TIGIT co-inhibitory pathway may increase the risk of autoimmune inflammation when tiragolumab is administered as a single agent. Therefore, tiragolumab as a single agent may induce adverse reactions similar to those of atezolizumab. These immune-mediated adverse events have been well characterized for other immune checkpoint inhibitors such as anti-CTLA-4 and anti-PD-L1/PD-1.
이는 항 PD-L1/PD-1 제제와 병용한 티라골루맙의 첫 번째 임상 평가이다. 아테졸리주맙과 병용한 티라골루맙에 대한 임상 평가는 제한적이며 모든 위험이 공지된 것은 아니지만, 2019년 12월 2일을 기준으로 200명 이상의 환자가 아테졸리주맙을 병용한 티라골루맙으로 치료를 받았다. 현재 아테졸리주맙과 병용으로 투여된 티라골루맙에 대해 식별된 고유한 위험은 없지만, 티라골루맙이 아테졸리주맙과 병용으로 투여될 때 TIGIT 공동 억제 경로의 관여는 HLH 및 MAS를 포함한 일부 면역 반응의 위험을 증가시킬 수 있다. 따라서, 아테졸리주맙과 함께 투여하는 경우, 티라골루맙은 아테졸리주맙과 관련된 이상반응을 악화시키거나, 또는 아테졸리주맙과 중복되지 않는 독성을 가질 수 있다.This is the first clinical evaluation of tiragolumab in combination with an anti-PD-L1/PD-1 agent. Although clinical evaluation of tiragolumab in combination with atezolizumab is limited and not all risks are known, as of December 2, 2019, more than 200 patients were treated with tiragolumab in combination with atezolizumab. received. Although there are currently no identified inherent risks for tiragolumab administered in combination with atezolizumab, the involvement of the TIGIT co-inhibitory pathway when tiragolumab is administered in combination with atezolizumab is implicated in some immune responses, including HLH and MAS. may increase the risk of Therefore, when co-administered with atezolizumab, tiragolumab may exacerbate atezolizumab-related adverse events or may have toxicity that does not overlap with atezolizumab.
적응 면역의 상호 보완적 조절제들의 조합에 대한 현재까지 가장 큰 임상 경험은 니볼루맙과 병용된 이필리무맙의 시험에서 유래된다. 다른 항 TIGIT 항체 MK-7684(비보스톨리맙)는 펨브롤리주맙과 병용할 때 진행성 종양 환자에서 허용 가능한 안전성 프로필 및 유망한 항종양 활성을 보였다. 이러한 데이터에 기초하여, 면역 매개 이상 반응의 빈도 및 중증도는 단일 약제 억제제와 비교했을 때 병용 시 증가할 수 있지만, 복합 면역 매개 이상 반응은 임상 환경에서 모니터링하고 관리할 수 있을 것으로 예상된다. The greatest clinical experience to date with combinations of complementary modulators of adaptive immunity comes from trials of ipilimumab in combination with nivolumab. Another anti-TIGIT antibody MK-7684 (vivostolimab) showed an acceptable safety profile and promising antitumor activity in patients with advanced tumors when combined with pembrolizumab. Based on these data, it is expected that the frequency and severity of immune-mediated adverse events may increase with combination compared to single agent inhibitors, but complex immune-mediated adverse events can be monitored and managed in a clinical setting.
임상 유효성clinical effectiveness
2019년 12월 2일 데이터 마감일을 기준으로, 연구 GO30103의 Ia상 부분에 등록된 환자에 대해 객관적인 반응이 보고되지 않았고, 연구 중 종양 평가를 받은 환자 42명 중 8명의 가장 좋은 반응은 안정한 질환(SD)이었다. 연구의 Ib상 부분에서, 171명의 환자 중 4명의 환자에게서 완전 반응(CR) 및 171명의 환자 중 23명의 환자에게서 부분 반응(PR)을 포함한 객관적인 반응이 NSCLC, HNSCC 및 삼중 음성 유방암을 포함한 여러 종양 유형을 가진 암 면역요법(CIT)을 경험하지 않은 환자에게서 관찰되었다.As of the December 2, 2019 data cut-off date, no objective responses were reported for patients enrolled in the Phase Ia portion of study GO30103, and the best response in 8 of 42 patients who received oncological evaluation during the study was stable disease ( SD). In the Phase Ib portion of the study, objective responses, including complete response (CR) in 4 of 171 patients and partial response (PR) in 23 of 171 patients, were assessed for multiple tumors, including NSCLC, HNSCC, and triple negative breast cancer. It has been observed in patients who have not experienced cancer immunotherapy (CIT) of the same type.
2019년 6월 30일 데이터 마감일 기준으로, 맹검, 무작위, II상 연구 GO40290의 데이터에 따르면, 티라골루맙 및 아테졸리주맙의 조합은 ITT 모집단에서 위약 및 아테졸리주맙에 비해 ORR 및 PFS를 개선하였다. 티라골루맙 및 아테졸리주맙의 ORR은 16.2%(95% CI: 6.7~25.7)인 위약 및 아테졸리주맙에 비교하여 31.3%(95% CI: 19.5~43.2)이었다. 시험자가 평가한 티라골루맙 및 아테졸리주맙의 PFS는 HR 0.57(95% CI: 0.37~0.90)으로 3.6개월(95% CI: 2.7~4.4)인 위약 및 아테졸리주맙의 PFS와 비교하여 5.4개월(95% CI: 4.2, 미달)이었다. As of the June 30, 2019 data deadline, data from blinded, randomized, phase II study GO40290 showed that the combination of tiragolumab and atezolizumab improved ORR and PFS compared to placebo and atezolizumab in the ITT population. . The ORR of tiragolumab and atezolizumab was 31.3% (95% CI: 19.5-43.2) compared to placebo and atezolizumab, which was 16.2% (95% CI: 6.7-25.7). The investigator-evaluated PFS of tiragolumab and atezolizumab was HR 0.57 (95% CI: 0.37 to 0.90) = 5.4 months compared to the PFS of placebo and atezolizumab of 3.6 months (95% CI: 2.7 to 4.4) (95% CI: 4.2, below).
화학요법을 포함한 티라골루맙 및 아테졸리주맙의 Ib상Phase Ib of tiragolumab and atezolizumab including chemotherapy
진행성 고형 종양에 대한 다수의, 대규모, 무작위, 3상 시험에서, 표준 화학요법에 항 PD-L1/PD1을 추가하면 화학요법 단독과 비교하여 환자의 OS 및 PFS이 개선되었다. 상기 시험에서는 비편평 NSCLC에서 항 PD-1을 페메트렉시드 및 백금계 화학요법에 추가하고(Gandhi et al. N Engl J Med 2018; 378:2078-92) 및 편평 NSCLC에서 카보플라틴 및 파클리탁셀 또는 냅-파클리탁셀에 추가하는 것을 연구하였다(Paz-Ares et al. N Engl J Med 2018; 379:204051. 상기 시험은 또한 항PD-L1을 확장 병기 SCLC에서 카보플라틴 및 에토포시드에 추가하고(Horn et al. N Engl J Med 2018; 379:2220-9), TNBC에서 냅-파클리탁셀에 추가하는 것을 조사하였다(Schmid et al. N Engl J Med 2018; 379:2108-21). 상기 시험의 결과로, 화학요법과 병용한 항 PD-L1/PD-1은 진행성 암 환자에 대해 FDA 및 EMA의 승인을 받았다. 비임상 데이터에 따르면, 항 TIGIT 및 항 PD-L1/PD-1의 병용이 단일 제제인 항 PD-L1/PD-1 단독보다 항종양 면역 반응을 더 향상시킨다는 것을 시사하므로, 화학요법과 병용한 항 PD-L1/PD-1에 항 TIGIT를 추가하는 것이 화학요법에 항 PD-L1/PD-1을 추가하는 것보다 더 효과적일 수 있음을 가정한다. In multiple, large-scale, randomized,
항 PD-L1/PD-1과 화학요법의 병용으로 인한 안전성 프로필은 일반적으로 진행성 고형 종양에 대한 여러 임상 시험에서 관찰된 바와 같이 각 제제의 공지된 독성 효과와 일치하였다(Gandhi et al. N Engl J Med 2018; 378:2078-92; Horn et al. N Engl J Med 2018; 379:2220-9; Paz-Ares et al. N Engl J Med 2018; 379:2040-51; Schmid et al. N Engl J Med 2018; 379:2108-21). 티라골루맙 및 아테졸리주맙 간의 작용 기전의 유사성을 고려할 때, 아테졸리주맙 및 화학요법과 병용 투여되는 티라골루맙의 안전성 프로필일은 병용된 항 TIGIT 및 항 PD-L1의 면역 관련 독성 및 개별 화학요법제의 독성과 일치할 수 있을 것으로 예상된다. 따라서, Ib상 화학요법 확장 코호트에 대한 설계 및 안전 관리 계획에는 화학요법에 대한 광범위한 임상 경험 뿐만 아니라 참여 환자에 대한 잠재적 위험을 줄이기 위해 항 TIGIT와 항 PD-L1을 조합하는 것에 대해 설명된 고려사항이 포함된다. The safety profile of the combination of anti-PD-L1/PD-1 and chemotherapy was generally consistent with the known toxic effects of each agent as observed in several clinical trials for advanced solid tumors (Gandhi et al. N Engl). J Med 2018; 378:2078-92; Horn et al. N Engl J Med 2018; 379:2220-9; Paz-Ares et al. N Engl J Med 2018; 379:2040-51; Schmid et al. N Engl J Med 2018; 379:2108-21). Given the similarity of the mechanism of action between tiragolumab and atezolizumab, the safety profile of tiragolumab co-administered with atezolizumab and chemotherapy may be related to the immune-related toxicity of combined anti-TIGIT and anti-PD-L1 and individual chemotherapy. It is expected to be consistent with the toxicity of the drug. Therefore, the design and safety management plan for the Phase Ib chemotherapy expansion cohort includes the considerations outlined for combining anti-TIGIT with anti-PD-L1 to reduce potential risks to participating patients as well as extensive clinical experience with chemotherapy. This is included.
베바시주맙을 포함한 티라골루맙 및 아테졸리주맙의 Ib상Phase Ib of tiragolumab and atezolizumab, including bevacizumab
강력한 과학적 근거 및 새로운 임상 데이터는 결합된 PD-L1, VEGF 및 TIGIT 억제가 여러 종양 유형에서 임상적으로 유익할 수 있음을 시사한다.Strong scientific evidence and new clinical data suggest that combined PD-L1, VEGF and TIGIT inhibition may be of clinical benefit in several tumor types.
IV기 NSCLC를 가진 화학요법 경험이 없는 환자에게서, 연구 GO29436(IMpower150)의 결과에 따르면, 아테졸리주맙에 더한 베바시주맙 및 화학요법은 베바시주맙 및 화학요법 단독과 비교하여 OS가 유의하게 더 긴 것으로 나타났다(Socinski et al. N Engl J Med 2018; 378:2288-301). 수술이 불가능한, 국소 진행성, 또는 전이성 RCC 환자의 경우, 연구 WO29637(IMmotion151)의 결과는 치료 경험이 없는 환자 집단에서 아테졸리주맙 및 베바시주맙의 조합으로 치료한 후 수니티닙과 비교하여 개선된 PFS를 보였다(Motzer et al. J Clin Oncol 2018; 36(6_suppl):578, Rini et al. Lancet 2019; 393:2404-15). 1차 HCC에 대한 Ib상 연구 GO30140은 병인학, 지리학, 기준선 알파 태아단백질 수준, 및 간외 확산에 걸쳐 23명의 평가 가능한 환자에게서 ORR이 65%임을 밝혀내었다(Stein et al. J Clin Oncol 2018; 36(Suppl 15):4074, Lee et al. Lancet Oncol. 2020 Jun; 21(6):808-820). 이러한 결과를 바탕으로, 상기 치료제는 새로운 해결책으로 인정되었으며, 그 결과는 무작위 배정 임상 3상 연구인 YO40245(IMbrave150) 연구에서 확인되었다. 연구 YO40245(IMbrave150)는 이전에 전신 치료를 받은 적이 없는 진행성 또는 전이성 간세포암종 환자에게서 아테졸리주맙 및 베바시주맙 대 소라페닙의 유효성 및 안전성을 평가하기 위해 설계되었다. 상기 연구에는 2:1 비율로 무작위 배정된 501명의 환자가 등록되었다. 가장 최근의 연구 결과는 PFS 및 OS에서 통계적으로 유의하고 임상적으로 의미 있는 개선을 보여주었다. 사망 위험은 소라페닙군에 비해 아테졸리주맙 + 베바시주맙 군에서 42% 감소하였다(계층화된 HR 0.58(95% CI: 0.42~0.79), OS 중앙값, NE 대 13.24개월). 고형 종양의 반응 평가 기준(RECIST) v1.1에 따라 독립 검토 시설에서 평가한 PFS는 병용 치료를 선호하는 개선을 보여주었다(계층화된 HR 0.59(95% CI: 0.47~0.76); PFS 중앙값, 6.83 vs. 4.27개월)(Cheng et al. Ann Oncol 2019; 30:ix186-ix187, Finn et al. N Engl J Med 2020; 382:1894-1905). In chemotherapy-naïve patients with stage IV NSCLC, results from study GO29436 (IMpower150) showed that atezolizumab plus bevacizumab plus chemotherapy resulted in a significantly greater OS compared to bevacizumab and chemotherapy alone. long (Socinski et al. N Engl J Med 2018; 378:2288-301). For patients with inoperable, locally advanced, or metastatic RCC, the results of study WO29637 (IMmotion151) were improved compared to sunitinib after treatment with the combination of atezolizumab and bevacizumab in a treatment-naive patient population. showed PFS (Motzer et al. J Clin Oncol 2018; 36(6_suppl):578, Rini et al. Lancet 2019; 393:2404-15). A Phase Ib study of primary HCC, GO30140, revealed an ORR of 65% in 23 evaluable patients across etiology, geography, baseline alpha fetoprotein levels, and extrahepatic spread (Stein et al. J Clin Oncol 2018; 36 (Stein et al. J Clin Oncol 2018; 36) Suppl 15):4074, Lee et al. Lancet Oncol. 2020 Jun; 21(6):808-820). Based on these results, the treatment was recognized as a novel solution, and the results were confirmed in the YO40245 (IMbrave150) study, a
이는 다양한 종양 유형에서 아테졸리주맙 및 베바시주맙 간의 잠재적 시너지 효과의 예이며, 티라골루맙과의 조합에 대한 추가 탐색을 지지한다.This is an example of a potential synergistic effect between atezolizumab and bevacizumab in various tumor types and supports further exploration of combinations with tiragolumab.
실시예 5. 진행성 고형 종양을 가진 환자를 대상으로 단일 제제로서 및 아테졸리주맙과 병용한 항 TIGIT 항체 티라골루맙의 Ia/Ib상 용량 증량 연구에서의 약동학, 약력학, 안전성 및 유효성Example 5. Pharmacokinetics, Pharmacodynamics, Safety and Efficacy in Phase Ia/Ib Dose Escalation Study of Anti-TIGIT Antibody Tiragolumab as Single Agent and in Combination with Atezolizumab in Patients with Advanced Solid Tumors
A.A. 환자 특성Patient characteristics
연구의 Ia상 및 Ib상 부분에 있는 환자의 기준선 특성은 표 37에 나타내었다. Ia상 및 Ib상 모두의 환자는 사전 치료를 많이 받은 집단을 포함하며, Ia상 환자의 42% 및 Ib상 환자의 37%가 이전에 4가지 이상의 암 요법을 받았다. Ia상 및 Ib상 환자는 유사한 기준선 특성을 공유한다. The baseline characteristics of patients in the Phase Ia and Phase Ib portions of the study are shown in Table 37. Patients in both Phase Ia and Ib include a highly prior-treated population, with 42% of Phase Ia patients and 37% of Phase Ib patients receiving 4 or more prior cancer therapies. Phase Ia and Ib patients share similar baseline characteristics.
아테졸리주맙(n=49)Atezolizumab (n=49)
![]()
![]()
*기타는 하기를 포함한다:
Ia상: 자궁내막(n=2), 흑색종(n=2); 및 충수, 방광, 자궁경부, 담관암, 신장, 신경내분비, 복막, 육종 및 위(각각 n=1)
Ib상: 육종(n=4), 위(n=2), 흑색종(n=2); 및 항문, 맹장, 방광, 식도, GE 접합부, 메르켈 세포 및 복막(각각 n=1) ECOG = Eastern Corporate Oncology Group; PS = whole body activity
*Others include:
Phase Ia: endometrial (n=2), melanoma (n=2); and appendix, bladder, cervix, cholangiocarcinoma, kidney, neuroendocrine, peritoneum, sarcoma and stomach (n=1 each)
Phase Ib: sarcoma (n=4), gastric (n=2), melanoma (n=2); and anus, cecum, bladder, esophagus, GE junction, Merkel cells and peritoneum (n=1 each)
기준선 특성Baseline Characteristics
연구의 Ia상 및 Ib상 부분에 있는 대부분의 환자는 질병 진행을 위한 치료를 중단하였다(Ia상의 42% 및 Ib상의 76%). Ib상 전환 환자 중 그 누구도 반응을 보이지 않았다. 환자 성향은 표 38에서 나타내었다.Most patients in the Phase Ia and Phase Ib portions of the study discontinued treatment for disease progression (42% in Phase Ia and 76% in Phase Ib). None of the patients with phase Ib transition showed a response. Patient propensity is shown in Table 38.
환자 성향patient disposition
B. 티라골루맙의 약동학 및 약력학B. Pharmacokinetics and Pharmacodynamics of Tiragolumab
단일 제제(Ia상)로서 및 아테졸리주맙과 병용한(Ib상) 티라골루맙의 약동학을 측정하였다. 티라골루맙의 노출은 단일 제제로서 및 아테졸리주맙과의 병용한 용량 투여에 따라 증가하였다(도 9). 티라골루맙의 약동학은 아테졸리주맙과 병용 시 변경되지 않는다. The pharmacokinetics of tyragolumab as a single agent (Phase Ia) and in combination with atezolizumab (Phase Ib) were determined. The exposure of tiragolumab increased with dose administration as a single agent and in combination with atezolizumab ( FIG. 9 ). The pharmacokinetics of tiragolumab are not altered when co-administered with atezolizumab.
단일 제제(Ia상)로서의 티라골루맙의 약력학을 측정하였다(도 10). CD8+ T 세포 및 NK 세포에서 말초 TIGIT 수용체의 점유를 3주마다 2 mg, 8 mg, 30 mg, 100 mg, 400 mg, 600 mg 및 1200 mg의 용량으로 측정하였다. 30 mg 이상의 티라골루맙 용량에서 2일(C1D2) 후 말초 TIGIT 수용체의 완전하고 지속적인 점유가 관찰되었다.The pharmacodynamics of tiragolumab as a single agent (phase Ia) were measured ( FIG. 10 ). Occupancy of peripheral TIGIT receptors on CD8 + T cells and NK cells was measured at doses of 2 mg, 8 mg, 30 mg, 100 mg, 400 mg, 600 mg and 1200 mg every 3 weeks. Complete and persistent occupancy of peripheral TIGIT receptors was observed after 2 days (C1D2) at doses of tyragolumab above 30 mg.
C.C. 안전성safety
이상 반응의 요약은 표 39에 나타내었다. 3~5등급 이상 반응의 전체 비율은 Ia상 및 Ib상 부분에서 낮았고 그 어느 쪽도 5등급의 이상 반응은 없었다. 단일 제제로서 또는 아테졸리주맙과 병용한 티라골루맙의 용량 제한 독성은 관찰되지 않았다. Ia상 및 Ib상 환자의 10% 이상에 존재하는 모든 이상 반응은 도 11 및 도 12에 각각 나타내었다. 모든 면역 매개 이상 반응은 표 40에 나타내었다. 티라골루맙은 단일 제제로서 및 아테졸리주맙과 병용으로 내약성이 우수하였다.A summary of adverse events is presented in Table 39. The overall rate of
Ib상의 관련 AE는 3등급의 고지방혈증(n=1) 및 3등급의 림프구 수 감소(n=1)였다. 5등급의 AE는 티라골루맙 및/또는 아테졸리주맙과 관련이 없었다.
**한 환자는 임상 진행과 관련된 위장 장애에 대한 Ib상 연구에서 철회하였다. * Relevant AE on phase Ia was a
Relevant AEs in phase Ib were
** One patient withdrew from a Phase Ib study of gastrointestinal disorders related to clinical progression.
이상 반응의 안전성 요약Summary of Safety of Adverse Events
모든 면역 매개 이상 반응Any immune-mediated adverse reaction
D.D. 유효성effectiveness
Ia상 및 Ib상 용량 증량 연구에서 예비 유효성 분석을 실시하였다. Ia상 부분에서, 신경내분비암, 난소암 및 직장암에서 종양 크기의 감소가 관찰되었다(도 13). 연구의 Ia상 부분에서 객관적인 반응은 없었지만, 대부분의 환자는 암 면역요법(CIT)에 일반적으로 반응하지 않는 종양 유형을 가졌거나, PD-L1 발현이 낮은 종양을 가졌거나, 과도하게 사전 치료를 받았다. NSCLC, TNBC, HNSCC 및 식도암 유형에 대한 연구의 Ib상 부분에서 객관적인 반응이 관찰되었다(도 14). A preliminary efficacy analysis was performed in phase Ia and phase Ib dose escalation studies. In the phase la portion, a reduction in tumor size was observed in neuroendocrine cancer, ovarian cancer and rectal cancer ( FIG. 13 ). Although there was no objective response in the Phase Ia portion of the study, most patients had tumor types that did not normally respond to cancer immunotherapy (CIT), had tumors with low PD-L1 expression, or received excessive prior treatment. . Objective responses were observed in the Phase Ib portion of the study for NSCLC, TNBC, HNSCC and esophageal cancer types ( FIG. 14 ).
아테졸리주맙과 병용한 티라골루맙으로 치료받은 환자에게서 CIT 미경험 종양을 포함한 PD-L1 양성 NSCLC 종양의 크기가 크게 감소하였다(도 14). 아테졸리주맙과 병용한 티라골루맙으로 치료한 CIT 경험이 없는 PD-L1 양성 NSCLC는 46%의 전체 반응률을 보였고, 여기에는 2개의 완전한 반응 및 지속성을 나타내는 여러 반응이 포함되었다(도 15 및 도 16). In patients treated with tiragolumab in combination with atezolizumab, the size of PD-L1-positive NSCLC tumors including CIT-naive tumors was significantly reduced ( FIG. 14 ). CIT-naive PD-L1-positive NSCLC treated with tiragolumab in combination with atezolizumab had an overall response rate of 46%, including two complete responses and multiple responses with persistence (Figs. 16).
실시예 6: 진행성 간암에 대한 티라골루맙 및 베바시주맙과 병용한 아테졸리주맙 Example 6: Atezolizumab in combination with tiragolumab and bevacizumab for advanced liver cancer
간암은 연간 854,000건의 신규 사례 및 810,000건의 사망으로 전 세계적으로 다섯 번째로 가장 흔한 암이자 두 번째로 흔한 암 관련 사망의 원인이다. 간세포암종(HCC)은 원발성 간암의 가장 흔한 형태이며 모든 원발성 간암의 약 90%를 나타낸다. 덜 확산된 원발성 간암에는 간내 담관암(iCCA), 혈관육종 및 간모세포종이 포함된다. Liver cancer is the fifth most common cancer and the second most common cancer-related cause of death worldwide, with 854,000 new cases and 810,000 deaths annually. Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer and accounts for approximately 90% of all primary liver cancers. Less diffuse primary liver cancers include intrahepatic cholangiocarcinoma (iCCA), angiosarcoma, and hepatoblastoma.
연구 YO40245(IMbrave150)는 진행성 또는 전이성 HCC 환자의 1차 치료제로서 아테졸리주맙 + 베바시주맙 대 소라페닙을 평가하는 진행 중인 무작위 3상 연구이다. 상기 연구는 소라페닙과의 일대일 비교에서 새로운 치료 조합에 대해 OS 및 무진행 생존(PFS)에서 통계적으로 유의하고 임상적으로 의미 있는 개선을 입증한 최초의 연구이다. 1차 분석 당시, 아테졸리주맙+베바시주맙 군은 소라페닙군에 비해 사망 위험이 42% 감소하였다(계층화된 위험비[HR] 0.58[95% CI: 0.42~0.79]; p = 0.0006; OS 중앙값, 추정 불가[NE] vs. 13.24개월). RECIST v1.1에 따라 독립 검토 시설에서 평가한 PFS 또한 병용 치료를 선호하는 통계적으로 유의하고 임상적으로 의미 있는 개선을 보여주었다 (계층화된 HR = 0.59 [95% CI: 0.47~0.76]; p < 0.0001; PFS 중앙값, 6.83 vs. 4.27개월). 전반적으로, HCC에서 아테졸리주맙 + 베바시주맙은 관리 가능한 독성으로 일반적으로 내약성이 우수했으며 안전성 프로필일은 개별 연구 치료제 및 기저 질환의 공지된 위험과 일치하였다(Cheng et al. IMbrave150: 절제 불가능한 간세포 암종(HCC) 환자(pts)의 제1 치료법(tx)으로서 아테졸리주맙(아테조) 베바시주맙(베브) 대 소라페닙(소르)을 평가한 Ph 3 연구의 유효성 및 안전성 결과. ESMO 아시아 2019의 절차: 22-24, 2019년 11월[인용: 2019년 11월 27일]; 싱가로프. Study YO40245 (IMbrave150) is an ongoing, randomized,
이는 질병에 대한 선행 전신 요법을 받은 적이 없는 국소 진행성 또는 전이성 간세포 암종(HCC) 환자를 대상으로 하는 Ib/II상, 공개 라벨, 다기관, 무작위 포괄적 연구이다. This is a Phase Ib/II, open-label, multicenter, randomized, comprehensive study in patients with locally advanced or metastatic hepatocellular carcinoma (HCC) who have not received prior systemic therapy for the disease.
환자는 대조군(아테졸리주맙 + 베바시주맙[아테조 + 베브]) 또는 티라골루맙과 병용한 아테졸리주맙 및 베바시주맙으로 구성된 치료군(아테조 + 베브 + 티라)에 무작위로 할당된다. Patients are randomly assigned to a control group (atezolizumab + bevacizumab [atezo + bev]) or a treatment group consisting of atezolizumab and bevacizumab in combination with tiragolumab (atezo + bev + tyra).
대조군(아테조 + 베브) Control (Atezo + Bev)
아테졸리주맙 + 베바시주맙(아테조 + 베즈)군의 환자는 하기의 표에 요약된 대로 치료를 받는다.Patients in the atezolizumab + bevacizumab (atezo + bez) group receive treatment as summarized in the table below.
(투여 순서대로 나열된 약물)Dose, route, and regimen
(Drugs listed in order of administration)
1일에 베바시주맙 1200 mg IV 주입Atezolizumab 1200 mg IV infusion per day
아테조 + 베브 군의 치료 요법Therapeutic regimen of the Artezo + Bev group
아테조 + 베브 + 티라Artezo + Bev + Tyra
아테졸리주맙 + 베바시주맙 + 티라골루맙(아테조 + 베브 + 티라)군의 환자는 하기의 표에 요약된 대로 치료를 받는다. Patients in the Atezolizumab + Bevacizumab + Tiragolumab (Atezo + Bev + Tira) group receive treatment as summarized in the table below.
(투여 순서대로 나열된 약물)Dose, route, and regimen
(Drugs listed in order of administration)
1일에 베바시주맙 15 mg IV 주입
1일에 티라골루맙 600 mg IV 주입a Atezolizumab 1200 mg IV infusion per day
15 mg IV infusion of bevacizumab on
a 주기 1의 1일에 티라골루맙은 베바시주맙 주입 완료 후 60분에 투여한다. 이후 주입들 간의 간격은 이전의 베바시주맙 주입이 예비 투약없이 제공되고 주입 관련 반응(IRR) 없이 내약성이었던 경우는 30분이고, 또는 환자가 이전의 베바시주맙 주입으로 IRR을 경험한 경우, 60분일 것이다.atezo + bev + tyra = atezolumab + bevacizumab + tyragolumab; IRR = infusion-related reaction
a On
아테조 + 베브 + 티라 군의 치료 요법Artezo + Bev + Tyra-kun’s treatment regimen
B. 선정 기준B. Selection Criteria
환자는 하기의 기준을 모두 충족해야 한다: Patients must meet all of the following criteria:
![]()
![]()
![]()
![]()
![]()
![]()
진단의 조직학적 확인이 없는 간경변 환자의 경우, AASLD 기준에 따라 임상 확인이 필요하다.For cirrhosis patients without histological confirmation of diagnosis, clinical confirmation is required according to AASLD criteria.
![]()
![]()
![]()
![]()
수술 및/또는 국소 요법 후 진행성 질환이 있는 환자가 적격이다.Patients with progressive disease following surgery and/or topical therapy are eligible.
![]()
![]()
한약을 포함하여 라벨에 항암 활성이 표시된 한약 요법을 이용한 선행 치료는 이러한 약물이 무작위 배정 이전에 중단된 경우 허용된다.Prior treatment with herbal remedies with labeled anticancer activity, including herbal remedies, are permitted if these medications are discontinued prior to randomization.
![]()
![]()
유효성 및 안전성 목적 및 평가변수는 하기의 표에 기재되어 있다. 본원에서 아테조+베브+티라의 3중 조합으로 치료받은 환자는 허용 가능한 독성을 가지지만 위약 아테조+베브(즉, 티라 없이)와 비교하여 유효성 평가변수(ORR, PFS, OS, DOR 및/또는 질병 통제) 중 하나 이상을 달성할 것으로 예상된다.Efficacy and safety objectives and endpoints are listed in the table below. Here, patients treated with the triple combination of atezo+bev+tyra had acceptable toxicity but compared efficacy endpoints (ORR, PFS, OS, DOR, and/or) compared to placebo atezo+bev (i.e. without tyra). or disease control).


ADA = 항 약물 항체; DOR = 반응 지속 기간; HCC = 간세포 암종; HCC mRECIST = HCC별 수정된 RECIST; iRECIST = 면역 매개 치료제를 위한 수정된 RECIST v1.1; NCI CTCAE v5.0 = 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 5.0; ORR = 객관적 반응율; OS = overall survival; PFS = 무진행 생존; PK = 약동학; RECIST = 고형 종양의 반응 평가 기준.ADA = anti-drug antibody; DOR = duration of response; HCC = Hepatocellular Carcinoma; HCC mRECIST = HCC modified RECIST; iRECIST = modified RECIST v1.1 for immune-mediated therapeutics; NCI CTCAE v5.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0; ORR = objective response rate; OS = overall survival; PFS = Progression-free survival; PK = pharmacokinetics; RECIST = Criteria for evaluating the response of solid tumors.

ADA = 항 약물 항체; DOR = 반응 지속 기간; HCC = 간세포 암종; HCC mRECIST = HCC별 수정된 RECIST; iRECIST = 면역 매개 치료제를 위한 수정된 RECIST v1.1; NCI CTCAE v5.0 = 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 5.0; ORR = 객관적 반응율; OS = overall survival; PFS = 무진행 생존; PK = 약동학; RECIST = 고형 종양의 반응 평가 기준.ADA = anti-drug antibody; DOR = duration of response; HCC = Hepatocellular Carcinoma; HCC mRECIST = HCC modified RECIST; iRECIST = modified RECIST v1.1 for immune-mediated therapeutics; NCI CTCAE v5.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0; ORR = objective response rate; OS = overall survival; PFS = Progression-free survival; PK = pharmacokinetics; RECIST = Criteria for evaluating the response of solid tumors.
실시예 7. 치료받지 않은 확장기 소세포 폐암을 가진 환자를 대상으로 티라골루맙을 포함하거나 포함하지 않는 아테졸리주맙 + 카보플라틴 및 에토포시드에 관한 3상, 무작위, 이중 맹검, 위약 대조 연구Example 7. A
본 실시예는 OS, PFS, ORR 및 DOR로 측정한 바와 같은 아테졸리주맙 + 화학요법의 항종양 효과가 ES-SCLC 환자에게서 아테졸리주맙 및 화학요법에 항 TIGIT 항체 티라골루맙을 추가함으로써 개선될 수 있는지 여부를 평가하기 위해 설계된 무작위, 3상, 글로벌, 다기관, 이중 맹검, 위약 대조 연구를 설명한다. ES-SCLC를 갖고 확장 병기 질병에 대한 화학요법 경험이 없는 환자를 대상으로 아테졸리주맙 및 CE와 병용한 티라골루맙의 안전성 및 유효성을 아테졸리주맙과 병용한 위약을 이용한 치료와 비교한다.This example shows that the antitumor effect of atezolizumab plus chemotherapy, as measured by OS, PFS, ORR and DOR, could be improved by adding the anti-TIGIT antibody tyragolumab to atezolizumab and chemotherapy in patients with ES-SCLC. Describe a randomized,
A. 연구 설계A. Study Design
ES-SCLC를 갖고 있지만 이의 확장 병기 질병에 대한 화학요법 경험이 없는 환자를 대상으로 아테졸리주맙 및 CE와 병용한 위약을 이용한 치료와 비교하여 아테졸리주맙 및 CE와 병용한 티라골루맙의 안전성 및 유효성을 평가하기 위한 무작위, 3상, 다기관, 이중 맹검, 위약 대조 연구의 세부 사항이 하기와 같이 기재된다. 도 17은 연구 설계를 도시한다. Safety and efficacy of atezolizumab and tiragolumab in combination with CE compared to treatment with atezolizumab and placebo in combination with CE in patients with ES-SCLC but no chemotherapy experience for their advanced stage disease Details of a randomized,
적격 환자는 ECOG 전신 활동도(0 대 1), LDH(≤ 정상 상한치(ULN) 대 > ULN), 뇌 전이의 존재 또는 이력(예 대 아니오)으로 계층화되고, 표 46에 나타낸 바와 같이 하기의 치료 요법 중 하나를 받기 위해 1:1 비율로 무작위 배정되었다. ECOG 전신 활동도에 관한 추가적인 세부 사항은 Oken et al., Am. J. Clin Oncol. 1982, 5: 649-655에 제공된다.Eligible patients were stratified by ECOG systemic activity (0 vs. 1), LDH (≤ upper limit of normal (ULN) vs. >ULN), presence or history of brain metastases (yes vs. no), and treated with the following treatment as shown in Table 46. They were randomized in a 1:1 ratio to receive one of the regimens. Additional details on ECOG systemic activity can be found in Oken et al., Am. J. Clin Oncol. 1982, 5: 649-655.
총 약 470명의 환자가 연구에서 무작위로 배정되었다. 1차 모집단(PP)에는 기준선에서 뇌 전이의 존재 또는 이력의 15% 유병률을 가정하는 약 400명의 환자가 포함된다. ITT(치료 의향) 모집단은 모든 환자를 포함한다. A total of approximately 470 patients were randomly assigned to the study. The primary population (PP) includes approximately 400 patients assuming a 15% prevalence of the presence or history of brain metastases at baseline. The intent-to-treat (ITT) population includes all patients.

유도 치료는 4주기 동안 21일 주기로 실시된다. 유도기 이후, 환자들은 아테졸리주맙 + 티라골루맙(A군) 또는 아테졸리주맙 + 위약(B군)으로 유지 요법을 계속하였다. 상기 유지기 중에, 예방적 두개골 조사(PCI)는 현지 치료 표준에 따라 허용되며 상기 예방적 두개골 조사 전자 사례 보고서 양식(eCRF)에 따라 보고된다. 증상 관리를 위한 완화 방사선이 허용된다. 표 46의 용량 및 투약 일정은 하기의 표 47에 제공된다.Induction treatment is given in 21-day cycles for 4 cycles. After the induction phase, patients continued maintenance therapy with atezolizumab plus tiragolumab (group A) or atezolizumab plus placebo (group B). During the maintenance phase, prophylactic cranial examination (PCI) is permitted according to local standards of care and is reported according to the preventive cranial examination electronic case report form (eCRF). Palliative radiation for symptom management is permitted. The doses and dosing schedules in Table 46 are provided in Table 47 below.

각 주기의 제 1일에 모든 적격 환자는 연구 약물을On
하기의 순서대로 투여받는다.It is administered in the following order.
A군: 아테졸리주맙, 티라골루맙, 카보플라틴 및 에토포시드 Group A: atezolizumab, tiragolumab, carboplatin and etoposide
B군: 아테졸리주맙, 위약, 카보플라틴 및 에토포시드 Group B: atezolizumab, placebo, carboplatin and etoposide
환자는 현지 치료 표준 및 제조업체의 지침에 따라 카보플라틴 및 에토포시드에 대한 항구토제 및 IV 수분 공급을 투여 받을 수 있다. 코르티코스테로이드를 이용한 예비투약은 임상적으로 가능한 정도까지 최소화한다. 모든 약물은 적절한 병용 약물 eCRF에 기록한다.Patients may receive antiemetics and IV hydration for carboplatin and etoposide according to local standards of care and manufacturer's guidelines. Premedication with corticosteroids should be minimized to the extent clinically feasible. All drugs should be recorded on the appropriate concomitant drug eCRF.
유도기 동안, 연구 치료제는During the induction phase, the study treatment is
1일에 하기와 같은 방식으로 투여해야 한다”It should be administered in the following manner per day”
1. 아테졸리주맙 1200 mg을 60(±15)분에 걸쳐 정맥내 투여한 후(제1 주입의 경우 및 후속 주입의 경우 30[±10]분으로 단축)(표 48 참조),One. After intravenous administration of atezolizumab 1200 mg over 60 (±15) minutes (reduced to 30 [±10] minutes for the first infusion and subsequent infusions) (see Table 48),
2.
티라골루맙/위약 600 mg을 60(±15)분에 걸쳐 정맥내 투여한 후(제1 주입의 경우 및 후속 주입의 경우 30[±10]분으로 단축)(표 48 참조),2.
After intravenous administration of tiragolumab/
3. 카보플라틴을 5 mg/mL/분의 농도-시간 곡선(AUC) 하에서 초기 표적 영역을 달성하기 위해 30-60 분에 걸쳐 정맥 내로 투여(캘버트 공식 투여)한 후,3. After carboplatin was administered intravenously (Calbert formula administration) over 30-60 min to achieve the initial target area under a concentration-time curve (AUC) of 5 mg/mL/min,
4.
에토포시드(100 mg/m2)를 60분에 걸쳐 정맥내 투여한다. 유도기 동안, 에토포시드(100 mg/m2)를 또한 2일 및 3일에 60분에 걸쳐 정맥내 투여한다.4. Etoposide (100 mg/m 2 ) is administered intravenously over 60 minutes. During the induction phase, etoposide (100 mg/m 2 ) is also administered intravenously over 60 minutes on
화학요법이 제공되지 않은 주기는 총 유도 화학요법 주기의 수에 포함되지 않는다. 유도기 후, 환자는 아테졸리주맙 + 티라골루맙/위약으로 유지 요법을 시작한다. 카보플라틴 및 에토포시드의 권장 주입 시간은 현지 치료 표준에 따라 조정한다. 아테졸리주맙 및 티라골루맙/위약의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 실시한다. Cycles for which no chemotherapy was given are not included in the total number of induction chemotherapy cycles. After the induction phase, patients begin maintenance therapy with atezolizumab plus tiragolumab/placebo. The recommended infusion times for carboplatin and etoposide should be adjusted according to local standards of care. Administration of atezolizumab and tiragolumab/placebo is performed in a monitoring environment with trained staff and immediate access to appropriate equipment and medications to manage potentially severe reactions.
치료는 RECIST v1.1에 따른 방사선학적 질환 진행까지 또는 방사선사진 데이터, 생검 결과 (가능한 경우), 및 임상 상태를 통합 평가한 후 질병 진행으로 인한 허용할 수 없는 독성 또는 증상 악화가 없는 상태에서 시험자가 평가하여 환자들이 임상 이점을 경험하는 한 계속한다. RECIST v1.1에 따른 질병 진행 기준을 충족하는 환자는 모든 선정 기준을 충족하는 경우 연구 치료를 계속할 수 있다 (티라골루맙 + 아테졸리주맙 또는 위약 + 아테졸리주맙).Treatment was tested in the absence of unacceptable toxicity or worsening of symptoms due to disease progression until radiological disease progression according to RECIST v1.1 or after an integrated evaluation of radiographic data, biopsy results (if available), and clinical status. Continue self-evaluation as long as patients experience clinical benefit. Patients who meet the disease progression criteria per RECIST v1.1 may continue on study treatment if all inclusion criteria are met (tiragolumab + atezolizumab or placebo + atezolizumab).
아테졸리주맙atezolizumab
환자들은 각 21일 주기의 제 1일에 IV 주입으로 1200 mg 아테졸리주맙을 투여받는다. 아테졸리주맙 용량은 고정이며 체중에 따라 달라지지 않는다. 아테졸리주맙 주입은 표 48에 요약된 지침에 따라 투여된다. 아테졸리주맙 용량은 변경되지 않는다. 아테졸리주맙의 용량 준비, 보관 및 투여 지침에 대한 자세한 내용은 약국 매뉴얼 및/또는 아테졸리주맙 시험자의 안내 책자에서 찾을 수 있다.Patients receive 1200 mg atezolizumab as an IV infusion on
티라골루맙/위약Tiragolumab/placebo
아테졸리주맙 투여 및 관찰 기간 이후(표 48 참조), 환자는 각 21일 주기의 제 1일에 IV 주입으로 600 mg 티라골루맙/위약을 투여 받는다. 티라골루맙/위약 용량은 고정이며 체중에 따라 달라지지 않는다. 티라골루맙/위약 주입은 표 48에 요약된 지침에 따라 투여된다. 티라골루맙/위약 용량은 변경되지 않는다. 티라골루맙/위약의 용량 준비, 보관 및 투여 지침에 대한 자세한 내용은 약국 매뉴얼 및/또는 티라골루맙 시험자의 안내 책자에서 찾을 수 있다.Following atezolizumab administration and the observation period (see Table 48), patients receive 600 mg tyragolumab/placebo as an IV infusion on





카보플라틴carboplatin
유도기 동안, 카보플라틴은 지역 진료 지침에 따라 표준 항구토제를 사용하여 5 mg/mL/분(캘버트 공식 투약)의 초기 목표 AUC를 달성하기 위해 30-60분에 걸쳐 IV 주입으로 티라골루맙/위약을 완료한 후 투여된다. 코르티코스테로이드를 이용한 예비투약은 임상적으로 가능한 정도까지 최소화할 수 있다. 카보플라틴 주입 시간은 현지 치료 표준에 따라 조정한다.During the induction phase, carboplatin is administered as an IV infusion over 30-60 minutes to achieve an initial target AUC of 5 mg/mL/min (Calvert Official Dosing) using standard antiemetics according to local practice guidelines. /administered after completion of placebo. Premedication with corticosteroids can be minimized to the extent clinically feasible. Carboplatin infusion times are adjusted according to local standards of care.
AUC 5의 카보플라틴 용량은 캘버트 공식(Calvert et al. (1989) J Clin Oncol 7:174856)을 사용하여 계산한다(Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):The carboplatin dose of
캘버트 공식:Calvert's formula:
총 용량(mg) =(목표 AUC) ´(사구체 여과율[GFR] +25)Total dose (mg) =(target AUC) ´(glomerular filtration rate [GFR] +25)
비고: AUC 기반 용량을 계산하기 위해 상기 캘버트 공식에서 사용된 GFR은 125 mL/분을 초과하지 않아야 한다.Note: The GFR used in the Calvert formula above to calculate the AUC-based dose should not exceed 125 mL/min.
본원에 사용된 바와 같이, GFR은 크레아티닌 청소율(CRCL)과 동등한 것으로 간주된다. 상기CRCL 은 기관의 지침 또는 콕크로프트 및 가울트, Nephron 1976, 16:31-41의 방법에 따라 하기의 공식을 사용하여 계산한다:As used herein, GFR is considered equivalent to creatinine clearance (CRCL). The CRCL is calculated using the following formula according to institutional guidelines or the method of Cockcroft and Gault, Nephron 1976, 16:31-41:
CRCL = (140 - 연령) x (wt)CRCL = (140 - age) x (wt)
(x 0.85, 여성의 경우)(x 0.85, for women)
72 x Scr72 x Scr
여기서: CRCL = 크레아티닌 청소율, mL/분where: CRCL = creatinine clearance, mL/min
연령 = 환자의 연령Age = patient's age
wt = 환자의 체중, kgwt = patient's weight, kg
Scr = 혈청 크레아티닌, mg/dLScr = serum creatinine, mg/dL
비고: 혈청 크레아티닌 수치가 비정상적으로 낮은 환자의 경우, 최소 크레아티닌 수치 0.8 mg/dL를 사용하여 GFR을 추정하거나 추정된 GFR을 125 mL/분으로 그 상한치가 제한된다.Note: For patients with abnormally low serum creatinine levels, the GFR is estimated using a minimum creatinine level of 0.8 mg/dL, or the upper limit of the estimated GFR is 125 mL/min.
환자의 GFR이 동위원소 희석 질량 분광법에 의한 혈청 크레아티닌 측정을 기반으로 추정되는 경우, 의사는 과다 투약으로 인한 잠재적 독성을 피하기 위해 원하는 노출(AUC)에 대한 카보플라틴의 용량 제한을 고려한다. 카보플라틴 라벨에 기재된 칼베트 공식을 기반으로, 최대 용량은 하기와 같이 계산할 수 있다:When a patient's GFR is estimated based on serum creatinine measurements by isotopic dilution mass spectrometry, physicians consider limiting the dose of carboplatin for the desired exposure (AUC) to avoid potential toxicity due to overdose. Based on the Calvet formula described on the carboplatin label, the maximum dose can be calculated as follows:
최대 카보플라틴 용량(mg) = 목표 AUC(mg x min/분) x (GFR + 25 mL/분)Maximum carboplatin dose (mg) = target AUC (mg x min/min) x (GFR + 25 mL/min)
상기 최대 용량은 정상 신장 기능을 가진 환자에게 125 mL/분으로 그 상한치가 제한된 GFR 추정치를 기반으로 한다. 이보다 높은 GFR 추정치는 사용하지 않는다.This maximum dose is based on an estimate of GFR with an upper limit of 125 mL/min in patients with normal renal function. GFR estimates higher than this are not used.
목표 AUC = 5의 경우, 최대 용량은 5 x (125 + 25) = 5 x 150 = 750 mg이다.For a target AUC = 5, the maximum dose is 5 x (125 + 25) = 5 x 150 = 750 mg.
목표 AUC = 4의 경우, 최대 용량은 4 x (125 + 25) = 4 x 150 = 600 mg이다.For a target AUC = 4, the maximum dose is 4 x (125 + 25) = 4 x 150 = 600 mg.
에토포시드etoposide
유도기 동안, 각 주기의 제 1일에 에토포시드(100 mg/m2)를 카보플라틴 투여 후 60분에 걸쳐 IV 주입으로 투여한다. 각 주기의 2일 및 3일에, 에토포시드(100 mg/m2)를 60분에 걸쳐 IV 주입으로 투여한다. 예비투약은 현지 치료 표준에 따라 실시한다. 코르티코스테로이드를 이용한 예비투약은 임상적으로 가능한 정도까지 최소화할 수 있다. 에토포시드 주입 시간은 현지 치료 표준에 따라 조정할 수 있다.During the induction phase, etoposide (100 mg/m 2 ) is administered as an IV infusion over 60 minutes following administration of carboplatin on
기준선에서 뇌 전이가 없는 환자의 평가에 대한 근거(통계 분석을 위한 1차 모집단)Evidence for evaluation of patients without brain metastases at baseline (primary population for statistical analysis)
뇌는 ES-SCLC 환자의 일반적인 전이 부위이며, 일부 연구에서는 진단 시 최대 18%의 환자에게서 뇌 전이가 있고, 진단 후 처음 2년 동안 최대 80%가 뇌 질환 관여를 가질 것으로 예상된다(Seute et al., Cancer, 100: 801-806, 2004; Pacheco and Bunn, Clin Lung Cancer, 20: 148-160, 2019). 일반적으로, 면역요법과 화학요법 조합의 이점은 ES-SCLC 환자에서 나타났다. 하지만, 이러한 이점은 IMpower133 시험에서 볼 수 있듯이 기준선에서 뇌 전이가 있는 환자에게서 약화될 수 있고, 여기서 뇌 전이가 없는 환자의 위험 비율(HR)이 0.68인 것과 비교하여 상기 환자 하위군의 HR은 1.07이다(Horn et al., New Engl J Med, 379: 2220-2229, 2018).The brain is a common site of metastasis in patients with ES-SCLC, and in some studies, up to 18% of patients have brain metastases at diagnosis, and up to 80% are expected to have brain disease involvement during the first 2 years after diagnosis (Seute et al. ., Cancer , 100: 801-806, 2004; Pacheco and Bunn, Clin Lung Cancer , 20: 148-160, 2019). In general, the benefit of combining immunotherapy and chemotherapy has been shown in patients with ES-SCLC. However, this benefit may be attenuated in patients with brain metastases at baseline, as shown in the IMpower133 trial, where the HR of this patient subgroup was 1.07 compared to 0.68 in patients without brain metastases. (Horn et al., New Engl J Med , 379: 2220-2229, 2018).
KEYNOTE-604는 진단 시 뇌 전이가 있는 ES-SCLC 환자가 그렇지 않은 환자와 비교하여 1차 면역요법에 더한 화학요법에 대해 전체 생존 이점이 더 적거나 전혀 없을 수 있음을 시사하는 또 다른 3상 시험이다. 실제로, 뇌 전이가 있는 환자의 OS HR은 1.32이고 뇌 전이가 없는 환자의 OS HR은 0.75이다(Rudin et al., J Clin Oncology, 38: 2369-2379, 2020). CASPIAN 연구에서는 처음에 뇌 전이가 있는 환자에게서 OS HR이 0.69라고 보고했지만, 갱신된 분석에서 HR은 0.79가 되었다. 초기 및 갱신된 보고서에서 뇌 전이가 없는 환자의 OS HR은 각각 0.74 및 0.76이었다(Paz-Ares et al., N Engl J Med, 379: 2040-2051, 2018; Paz-Ares et al., Am Soc Clin Oncol 2020, abstract 9002, 2020).KEYNOTE-604 is another
두 환자 하위군 모두에서 연구 요법의 이점을 이해하는 것이 중요하다. 따라서, 시험 통계 계층 구조는 PP를 먼저 시험한 다음, ITT를 시험하기 위해 구현되었다.It is important to understand the benefits of the study regimen in both patient subgroups. Therefore, a test statistics hierarchy was implemented to test the PP first and then the ITT.
B.B. 평가evaluation
환자는 기준선에서 및 주기 1의 1일 이후 48주 동안 6주(±7일)마다 종양 평가를 받는다. 전처리 종양 조직(보관 또는 새로 수득한) 샘플은 무작위 배정 전 또는 후 4주 이내에 제출한다. 상기 표본에는 관련 병리학 보고서가 함께 동반된다. 입수 가능한 모든 종양 조직 샘플을 제출할 수 있지만, 바이오마커 분석(예컨대, PD-L1 상태, 면역 또는 SCLC 생물학과 관련된 마커, 예컨대, 추출된 DNA, RNA 또는 기타 생물학적 분자에서 NGS를 통해 식별된 T 세포 마커 또는 비유전 바이오마커)을 위해 파라핀 블록(바람직한) 또는 10개(또는 그 이상)의 연속적인 신선하고 염색되지 않은 슬라이드의 대표적인 종양 표본을 제출하는 것이 좋다. 예시적인 샘플 유형은 절제, 코어 바늘, 절제, 절개, 펀치, 겸자 생검, 미세 바늘 흡인 및 세포 펠릿 표본(예컨대, 흉막 삼출액 및 세척 샘플)으로부터 제조된 포르말린 고정 파라핀 포매(FFPE) 샘플을 포함한다. 종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 양호해야 한다. 탈석회화의 대상이 되는 뼈 전이의 종양 조직은 권장되지 않는다.Patients receive tumor assessments at baseline and every 6 weeks (± 7 days) for 48 weeks after
48주 종양 평가를 완료한 후, 이후 9주(77일)마다 종양 평가를 실시한다. RECIST v1.1에 따라 질병 진행 이상으로 치료된 환자는 치료가 중단될 때까지 종양 평가를 받는다. RECIST v1.1에 따른 방사선학적 질병 진행 이외의 이유로 치료를 중단한 환자(예컨대, 독성, 증상 악화)는 환자가 새로운 항암 요법을 시작하는지 여부와 관계없이 주기 1의 1일 후 48주 동안 6주(±7일)마다 및 그 후 9주(±7일)마다 예정된 종양 평가를 계속한다. After completing the 48-week tumor assessment, tumor assessments are performed every 9 weeks (77 days) thereafter. Patients treated for disease progression abnormality according to RECIST v1.1 receive tumor evaluation until treatment is discontinued. Patients who discontinued treatment for reasons other than radiological disease progression according to RECIST v1.1 (e.g., toxicity, worsening symptoms), regardless of whether the patient starts new chemotherapy or not, 6 weeks for 48 weeks after
혈청 샘플을 수집하여 티라골루맙 및 아테졸리주맙 약동학을 모니터링한다. 선택된 환자에게서, 화학요법 약동학을 위해 혈장 샘플을 수집한다. 안전성 평가는 이상 반응의 발생률, 특성 및 중증도, 프로토콜 필수 활력 징후, 및 실험실 이상을 포함한다.Serum samples are collected to monitor tiragolumab and atezolizumab pharmacokinetics. In selected patients, plasma samples are collected for chemotherapy pharmacokinetics. Safety assessments include the incidence, nature and severity of adverse events, protocol essential vital signs, and laboratory abnormalities.
종양 생검은 방사선 촬영 진행 시 실시한다. 예시적인 샘플 유형은 절제, 코어 바늘, 절제, 절개, 펀치, 겸자 생검, 미세 바늘 흡인 및 세포 펠릿 표본(예컨대, 흉막 삼출액 및 세척 샘플)으로부터 제조된 FFPE 샘플을 포함한다. 조직에서 DNA 및/또는 RNA 추출이 실시될 수 있다.Tumor biopsy is performed during radiographic progression. Exemplary sample types include FFPE samples prepared from ablation, core needle, ablation, incision, punch, forceps biopsy, fine needle aspiration, and cell pellet specimens (eg, pleural effusion and lavage samples). DNA and/or RNA extraction may be performed from the tissue.
C.C. 환자 보고 결과Patient Reported Results
환자 보고 결과(PRO) 데이터는 치료 이점을 기록하고 티라골루맙 + 아테졸리주맙의 임상 프로필을 보다 완전히 특성화하기 위해 수집된다. PRO 데이터는 하기의 도구들을 사용하여 수집된다: EORTC QLQ-C30, 단일 항목 EORTC IL46, PRO-CTCAE의 선택 항목, 및 EQ-5D-5L.Patient Reported Outcome (PRO) data is collected to document treatment benefit and more fully characterize the clinical profile of tiragolumab plus atezolizumab. PRO data was collected using the following tools: EORTC QLQ-C30, single item EORTC IL46, selection of PRO-CTCAE, and EQ-5D-5L.
EORTC QLQ-C30은 환자 기능의 5가지 측면(신체적, 정서적, 역할, 인지적, 사회적), 3가지 증상 척도(피로, 메스꺼움 및 구토, 통증), 전반적인 건강/삶의 질, 6가지 단일 항목(호흡곤란, 불면증, 식욕부진, 변비, 설사, 경제적 어려움)을 평가하는 30가지 질문으로 구성된 검증되고 신뢰할 수 있는 자체 보고 방식이다(Aaronson et al., J. Natl. Cancer Inst. 1993, 85:365-76; Fitzsimmons et al., Eur. J. Cancer 1999, 35:939-41). 다중 항목 척도에 대한 척도 점수를 수득할 수 있다.The EORTC QLQ-C30 measures five aspects of patient functioning (physical, emotional, role, cognitive, social), three symptom scales (fatigue, nausea and vomiting, pain), overall health/quality of life, six single items ( Dyspnea, insomnia, anorexia, constipation, diarrhea, economic hardship) is a validated and reliable self-report method consisting of 30 questions (Aaronson et al., J. Natl. Cancer Inst . 1993, 85:365). -76; Fitzsimmons et al., Eur. J. Cancer 1999, 35:939-41). Scale scores can be obtained for multi-item scales.
EORTC QLQ-C30 모듈을 완료하는 데 약 15분이 걸린다. 또한, 단일 항목 EORTC IL46을 수집한다. 상기 검증된 단일 항목 질문은 전반적인 부작용 영향을 평가한다.The EORTC QLQ-C30 module takes about 15 minutes to complete. Also collect the single entry EORTC IL46. The validated single-item question assesses the overall adverse effect.
PRO-CTCAE는 환자가 보고할 수 있는 78가지 증상 치료 독성의 존재, 빈도, 중증도 및 일상 기능 방해를 특성화하는 데 사용되는 검증된 문항 은행이다(Basch et al., J. Natl Cancer Inst. 2014, 106:1-11; Dueck et al., JAMA Oncol. 2015, 1:1051-52). PROCTCAE에는 5점 리커트(Likert) 척도(빈도, 중증도 및 간섭) 또는 이분법(존재/부재)으로 평가되는 124개의 질문이 포함되어 있다. 포함된 치료 독성 용어는 관찰 가능한 구성 요소(예컨대, 각각 구토 및 메스꺼움)가 있거나 없는 주관적이거나 주관적인 구성 요소(예컨대, 발진)와 함께 주로 관찰할 수 있다. 표준 PRO-CTCAE 리콜 기간은 “지난 7 일”이다. 현재 치료에 가장 적합하다고 여겨지는 세 가지 증상들의 하위집합이 본 연구를 위해 선택되었다.PRO-CTCAE is a validated question bank used to characterize the presence, frequency, severity, and disturbance of daily functioning of 78 patient-reportable symptomatic treatment toxicities (Basch et al., J. Natl Cancer Inst. 2014, 106:1-11; Dueck et al., JAMA Oncol . 2015, 1:1051-52). PROCTCAE contains 124 questions rated on a 5-point Likert scale (frequency, severity, and interference) or dichotomous (presence/absence). The therapeutic toxicity terms included are predominantly observable with or without an observable component (eg, vomiting and nausea, respectively) or with a subjective or subjective component (eg, rash). The standard PRO-CTCAE recall period is “last 7 days”. A subset of the three symptoms currently considered most suitable for treatment was selected for this study.
EQ-5D-5L은 환자의 건강 상태를 종합적으로 구축하는 데 사용되는 이동성, 자가 관리, 일상 활동, 통증/불편, 불안/우울에 대한 질문이 포함된 일반적인 선호도 기반 건강 효용 측정이다. EQ-5D-5L을 완료하는 데 약 2분이 걸린다. EQ-5D-5L은 경제 모델링을 위해 본 연구에서 활용될 것이다.EQ-5D-5L is a general preference-based health utility measure that includes questions about mobility, self-management, daily activities, pain/discomfort, and anxiety/depression used to comprehensively build a patient's health status. EQ-5D-5L takes about 2 minutes to complete. EQ-5D-5L will be utilized in this study for economic modeling.
PRO 도구의 종이 버전은 치료 방문 중에는 자가 관리되며, 후속 방문 중에는 현장 직원이 환자에게 전화로 면접관이 관리하므로, 환자가 임상 기곤으로 이동하지 않고도 데이터를 수집할 수 있다. PRO 데이터는 현장 직원이 연구 데이터베이스에 입력합니다. The paper version of the PRO tool is self-administered during treatment visits and interviewed by field staff calling patients during follow-up visits, allowing patients to collect data without having to travel to clinical hunger. PRO data is entered into the research database by field staff.
도구의 유효성을 보장하고 데이터 표준이 보건 당국의 요구 사항을 충족하도록 하기 위해, 진료소 방문 중 투여를 위해 예정된 설문지는 달리 명시되지 않는 한 질병 상태에 대한 임의의 정보를 받기 전, 환자의 답변에 편향을 줄 수 있는 비 PRO 평가를 실시하기 전, 및 연구 치료제를 투여하기 전 환자가 완전히 완료한다.To ensure the validity of the tool and to ensure that data standards meet the requirements of health authorities, questionnaires scheduled for administration during clinic visits are biased toward patient responses prior to receiving any information about disease status, unless otherwise specified. Patients complete complete prior to conducting non-PRO evaluations that may give
설문지(EORTC QLQ-C30, EORTC IL46, PRO-CTCAE(선택 항목) 및 EQ-5D-5L)는 연구 약물의 투여 전 주기 1의 1일(기준선)에서 유도기 동안; 연구 약물의 투여 전 모든 연구 치료 주기에서(즉, 주기 2의 1일; 주기 3의 1일; 및 주기 4의 1일)에 완료한다. 유지기 동안, 상기 설문지는 연구 약물 투여 전 연구 치료 주기를 하나 걸러서(즉, 주기 5의 1일; 주기 7의 1일; 주기 9의 1일 등) 및 연구 치료 중단 방문 시 완료한다. 생존 추적 중, PRO는 3개월(±30일)에 제1 생존 추적에서 수집되고 6개월(±30일)에 제2 생존 추적에서 수집된다. RECIST v1.1에 따른 방사선학적 질환 진행 이외의 다른 이유로 연구 치료를 중단한 환자(예컨대, 독성, 증상 악화)는 RECIST v1.1에 따른 방사선학적 질병 진행, 사망, 추적 관찰 상실, 동의 철회 또는 시험 의뢰자의 연구 종료 중 먼저 발생하는 시점까지 종양 평가 방문 시마다 각각 EORTC QLQ-C30, PRO-CTCAE(선택 항목) 및 EQ-5D-5L을 완료한다. 설문지에서 모국어를 사용할 수 없는 환자는 모든 PRO 평가를 완료하는 것이 면제된다.Questionnaires (EORTC QLQ-C30, EORTC IL46, PRO-CTCAE (optional) and EQ-5D-5L) were administered during the induction phase on Day 1 (baseline) of
이상 반응 보고서는 PRO 데이터에서 유래한 것이 아니다.Adverse event reports are not derived from PRO data.
D.D. 평가변수evaluation variable
시험자가 평가한 PFS(RECIST v1.1에 따라 발명자가 평가한 바와 같음) 및 PP의 OS는 본 연구의 공동 1차 평가변수이다. PP 및 ITT 모집단의 객관적 반응률, PP 및 ITT 모집단의 반응 지속 기간, ITT 모집단의 PFS 및 OS는 2차 평가변수이다.Investigator-assessed PFS (as assessed by inventor according to RECIST v1.1) and OS of PP were the joint primary endpoints of this study. Objective response rates in PP and ITT populations, duration of response in PP and ITT populations, and PFS and OS in ITT populations are secondary endpoints.
무진행 생존progression-free survival
PFS는 무작위배정 일자와 (RECIST v1.1에 따라 시험자가 평가한 바와 같은)최초로 기록된 질병 진행 또는 사망 일자 중 먼저 발생하는 것 사이의 시간이다. 질병 진행을 경험하지 않았거나 데이타 마감일까지 사망하지 않은 환자는 최종 종양 평가 시 중도절단된다. 기준선 이후 종양 평가가 없는 환자는 무작위배정 일자에 중도절단된다.PFS is the time between the date of randomization and the first recorded date of disease progression or death (as assessed by the investigator according to RECIST v1.1), whichever occurs first. Patients who have not experienced disease progression or have not died by the data deadline will be censored at the final tumor evaluation. Patients without post-baseline tumor evaluation are censored on the date of randomization.
평가변수로서의 PFS는 종양 성장을 반영할 수 있으며, 생존 이점을 결정하기 전에 평가할 수 있다. 또한, 이러한 결정은 일반적으로 후속 요법에 의해 혼동되지 않는다. PFS의 개선이 직접적인 임상적 이익을 나타내는지 아니면 임상적 이익의 대리물을 나타내는지 여부는 입수 가능한 요법과 비교되는 새로운 치료의 효과 및 이익-위험의 규모에 따라 달라진다(U.S. Food and Drug Administration (2007) Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics). PFS as an endpoint can reflect tumor growth and can be evaluated before determining survival benefits. In addition, these decisions are generally not confounded by subsequent therapy. Whether an improvement in PFS represents a direct clinical benefit or a surrogate of clinical benefit depends on the effect and benefit-risk magnitude of the new treatment compared to available therapies (US Food and Drug Administration (2007) ) Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics ).
시험자가 평가한 PFS의 유효성을 1차 평가변수로 보장하기 위해, 여러 가지 조치가 실시되었다: 이득-위험에 대한 강력한 평가를 가능하게 할 이득 및 연구 평가의 실질적인 목표 규모(두 치료군에서 동일한 고정된 평가 간격으로 방사선학적 질병 진행을 정의하기 위한 기존의 RECIST v1.1 기준, 및 민감도 분석을 포함하여 PFS를 평가, 정량화 및 분석하기 위한 PFS의 강력한 정의 및 전향적으로 정의된 방법).To ensure investigator-assessed efficacy of PFS as the primary endpoint, several measures were implemented: a practical target scale of benefit and study evaluations that would enable a robust benefit-risk assessment (the same fixed fixed size in both treatment groups). Existing RECIST v1.1 criteria for defining radiological disease progression as an evaluation interval, and robust definitions and prospectively defined methods of PFS for assessing, quantifying, and analyzing PFS, including sensitivity analysis).
PFS의 공동 일차 평가변수에 대한 일차 분석은 PPP에서 약 300건의 PFS 사례(400명의 환자 중 75%)가 관찰되었을 때 이루어진다. 이는 하기를 기반으로 양측 유의 수준 0.001에서 PFS에 대한 목표 HR 0.56을 검출하는 96% 분석력을 제공한다: 지수 분포를 따르는 PFS 곡선; 위약 + 아테졸리주맙 + EC 군에서 5.2개월 및 티라골루맙 + 아테졸리주맙 + EC 군에서 9.2개월의 PFS 중앙값(목표 HR 0.56에 해당); PFS의 경우 12개월 동안 중도 탈락률 5%; 및 PFS에 대한 중간 분석이 없다.A primary analysis of the co-primary endpoint of PFS is made when approximately 300 cases of PFS (75% of 400 patients) are observed in PPP. This gives 96% power to detect a target HR of 0.56 for PFS at a two-sided significance level of 0.001 based on: PFS curve following exponential distribution; median PFS of 5.2 months in the placebo + atezolizumab + EC group and 9.2 months in the tiragolumab + atezolizumab + EC group (corresponding to a target HR of 0.56); dropout rate of 5% over 12 months for PFS; and no interim analysis for PFS.
PFS에서 0.68 이상의 관찰된 HR은 치료군들 간에 통계적으로 유의한 차이에 해당한다. 즉, 0.68의 HR은 본 분석에서 최소한으로 검출할 수 있는 차이이며; 이는 위약 + 아테졸리주맙군 + CE군에서 5.2개월로부터 티라골루맙 + 아테졸리주맙 + CE군에서 7.6 개월까지의 PFS 중앙값이 2.4개월 개선된 것에 해당한다.An observed HR of 0.68 or greater in PFS corresponds to a statistically significant difference between treatment groups. That is, an HR of 0.68 is the minimally detectable difference in this assay; This corresponds to a 2.4-month improvement in median PFS from 5.2 months in the placebo + atezolizumab + CE group to 7.6 months in the tiragolumab + atezolizumab + CE group.
카플란-마이어 방법은 각 치료군의 PFS 중앙값을 추정하는 데 사용되며 카플란-마이어 곡선은 치료군 간의 차이를 시각적으로 설명하기 위해 작성된다. 브룩마이어와 크롤리(Brookmeyer-Crowley) 방법은 각 치료군의 PFS 중앙값에 대한 95% CI를 작성하는 데 사용된다(Brookmeyer and Crowley, Biometrics 1982, 38: 29-41).The Kaplan-Meier method is used to estimate the median PFS for each treatment group, and a Kaplan-Meier curve is created to visually account for differences between treatment groups. The Brookmeyer-Crowley method was used to generate a 95% CI for the median PFS for each treatment group (Brookmeyer and Crowley, Biometrics 1982, 38: 29-41).
무작위 배정 후 6개월 및 1년 후 PFS 비율은 그린우드(Greenwood) 공식에서 파생된 표준 오차를 사용하여 계산된 95% CI와 함께 각 치료군에 대해 카플란-마이어 방법을 사용하여 추정한다. 두 치료군 간의 PFS 비율 차이에 대한 95% CI는 정규 근사법을 사용하여 추정한다.PFS rates at 6 months and 1 year after randomization were estimated using the Kaplan-Meier method for each treatment group with a 95% CI calculated using standard errors derived from Greenwood's formula. A 95% CI for the difference in PFS rates between the two treatment groups was estimated using a normal approximation.
전체 생존overall survival
OS는 본 연구에서 공동 1차 평가변수이다. OS는 무작위 배정 날짜와 임의의 원인으로 인한 사망 사이의 시간이다. OS의 개선은 일반적으로 진행성/절제 불가능 또는 전이성 폐암 환자에 대한 임상적 이점의 최선의 척도로 받아들여진다. OS is the co-primary endpoint in this study. OS is the time between the date of randomization and death from any cause. Improvement in OS is generally accepted as the best measure of clinical benefit for patients with advanced/resectable or metastatic lung cancer.
층화된 로그-순위 분석법을 사용하여 치료군들 간 PFS 및 OS를 비교한다. PFS 및 OS에 대한 HR을 층화된 Cox 비례 위험 모델을 사용하여 추정한다. HR에 95% CI가 제공된다. 계층화 요소는 IxRS(즉, ECOG 전신 활동도 및 젖산 탈수소효소(LDH))에서 무작위 배정에 사용되는 요소이다. 과도한 계층화 위험이 있는 경우 계층화 요소(들)은 계층화 분석으로부터 제거될 수 있다. IxRS 기록과 eCRF 간에 상당한 불일치가 관찰되는 경우, 전자 사례 보고 양식(eCRF)에 기록된 계층화 요소를 기반으로 한 분석도 제공될 것이다. 계층화되지 않은 분석 결과도 제공된다.A stratified log-rank analysis is used to compare PFS and OS between treatment groups. HR for PFS and OS are estimated using a stratified Cox proportional hazards model. 95% CI is given to HR. Stratification factors are factors used for randomization in IxRS (ie ECOG systemic activity and lactate dehydrogenase (LDH)). The stratification element(s) may be removed from the stratification analysis if there is an excessive risk of stratification. If significant discrepancies are observed between IxRS records and eCRFs, an analysis based on the stratification factors recorded on the Electronic Case Reporting Form (eCRF) will also be provided. Non-stratified analysis results are also provided.
OS의 공동 일차 평가변수에 대한 최종 분석은 PP 집단에서 약 288명의 사망(400명 중 72%)이 관찰되었을 때 발생한다. 이는 하기를 기반으로 양측 유의 수준 0.049에서 OS에 대한 목표 HR 0.70을 검출하는 85% 분석력을 제공한다: 지수 분포를 따르는 OS 곡선; 위약 + 아테졸리주맙 + EC 군에서 12.3개월의 OS 중앙값 및 티라골루맙+ 아테졸리주맙 + EC 군에서 17.6개월(목표 HR 0.70에 해당); OS의 경우 24개월 동안 5%의 탈락률; 오브라이언-플레밍(O'Brien-Fleming) 함수의 Lan-DeMets 근사치를 기반으로 결정된 통계적 유의성에 대한 중간 경계를 사용한 정보 부분의 약 70%에서 OS에 대한 계획된 중간 분석 1개.The final analysis of the co-primary endpoint of OS occurs when approximately 288 deaths (72% of 400) are observed in the PP cohort. This provides 85% analytical power to detect a target HR 0.70 for OS at a two-sided significance level of 0.049 based on: OS curve following exponential distribution; median OS of 12.3 months in the placebo + atezolizumab + EC group and 17.6 months in the tiragolumab + atezolizumab + EC group (corresponding to a target HR of 0.70); 5% dropout rate over 24 months for OS; One planned interim analysis for OS in approximately 70% of the pieces of information with median bounds for statistical significance determined based on the Lan-DeMets approximation of the O'Brien-Fleming function.
PP에서 Os에 대한 0.789 이상의 관찰된 HR은 치료군들 간에 통계적으로 유의한 차이에 해당한다. 즉, 0.789의 HR은 본 분석에서 최소한으로 검출할 수 있는 차이이며; 이는 위약 + 아테졸리주맙군 + CE군에서 12.3개월로부터 티라골루맙 + 아테졸리주맙 + CE군에서 15.6 개월까지의 OS 중앙값이 3.3개월 개선된 것에 해당한다.An observed HR of 0.789 or greater for Os in PP corresponds to a statistically significant difference between treatment groups. That is, an HR of 0.789 is the minimally detectable difference in this assay; This corresponds to a 3.3-month improvement in the median OS from 12.3 months in the placebo + atezolizumab + CE group to 15.6 months in the tiragolumab + atezolizumab + CE group.
OS에 대한 중간 분석 및 최종 분석 시기는 표 49에 요약되어 있으며, 연구대상체 발생이 추가로 가정된다.Interim and final analysis times for OS are summarized in Table 49, and subject incidence is further assumed.

FPI = 첫 환자 투여; IA = 중간 분석; PP = 치료 모집단; OS = 전체 생존FPI = first patient dose; IA = interim analysis; PP = treatment population; OS = overall survival
a 분석력은 0.049의 양측 α를 사용하여 계산됨 a The analytical power is calculated using a two-sided α of 0.049
OS 중간 분석은 최종 PFS 분석시에 실시된다. 카플란-마이어 방법론은 각 치료군의 OS 중앙값을 추정하는 데 사용되며 카플란-마이어 곡선은 치료군 간의 차이를 시각적으로 설명하기 위해 작성된다. 브룩마이어-크롤리 방법론은 각 치료군의 OS 중앙값에 대한 95% CI를 작성하는 데 사용된다(Brookmeyer and Crowley, Biometrics 1982, 38: 29-41).The OS interim analysis is performed at the time of the final PFS analysis. The Kaplan-Meier methodology is used to estimate the median OS for each treatment group, and a Kaplan-Meier curve is created to visually account for differences between treatment groups. The Brookmeyer-Crowley methodology was used to generate a 95% CI for the median OS for each treatment group (Brookmeyer and Crowley, Biometrics 1982, 38: 29-41).
무작위 배정 후 1년 및 2년 후 OS 비율은 그린우드(Greenwood) 공식에서 파생된 표준 오차를 사용하여 계산된 95% CI와 함께 각 치료군에 대해 카플란-마이어 방법을 사용하여 추정한다. 두 치료군 간의 OS 비율 차이에 대한 95% CI는 정규 근사법을 사용하여 추정한다.OS rates at 1 and 2 years after randomization were estimated using the Kaplan-Meier method for each treatment group, with a 95% CI calculated using standard errors derived from the Greenwood formula. A 95% CI for the difference in OS ratio between the two treatment groups was estimated using a normal approximation.
이차 유효성 평가변수secondary efficacy endpoint
치료 의향 모집단의 무진행 생존 및 전체 생존Progression-Free Survival and Overall Survival in the Intent-to-Treat Population
PP의 OS 차이가 통계적으로 유의한 경우, 상기 기재된 공동 1차 유효성 평가변수 분석을 위한 동일한 α-할당 비율(1:49) 및 α-재활용 전략에 따라 PFS 및 OS를 ITT 모집단에서 시험한다. ITT 모집단의 PFS 및 OS는If the OS difference in PP is statistically significant, PFS and OS are tested in the ITT population according to the same α-assignment ratio (1:49) and α-recycling strategy for co-primary endpoint analysis described above. The PFS and OS of the ITT population were
IxRS(즉, ECOG 전신 활동도, LDH, 및 뇌 전이의 존재 또는 이력)로부터 무작위 배정에 사용된 세 가지 계층화 요소 모두가 ITT 모집단에 대한 계층화된 분석에 포함되는 점을 제외하고 상기 기재된 바와 동일한 방법을 사용하여 PP와 동시에 분석할 것이다. 과도한 계층화 위험이 있는 경우 층화 요인(들)은 층화 분석으로부터 제거될 수 있다.The same method as described above, except that all three stratification factors used for randomization from IxRS (i.e., ECOG systemic activity, LDH, and presence or history of brain metastases) were included in the stratified analysis for the ITT population. will be analyzed simultaneously with the PP. Stratification factor(s) may be removed from the stratification analysis if there is an excessive risk of stratification.
확인된 객관적 반응율Confirmed objective response rate
확인된 객관적 반응은 RECIST v1.1에 따라 시험자가 결정한 바와 같이 4주 이상의 간격으로 2회 연속 사건에서 확인된 CR 또는 PR일 수 있다. 기준선 이후 종양 평가가 없는 환자를 포함하여 이들 기준을 충족하지 않는 환자는 무반응자로 간주된다.An identified objective response may be a confirmed CR or PR in two consecutive events with an interval of at least 4 weeks as determined by the investigator according to RECIST v1.1. Patients who do not meet these criteria, including those without a post-baseline tumor assessment, are considered non-responders.
확인된 ORR은 확인된 객관적인 반응을 갖는 환자의 비율로 정의된다. 확인된 ORR에 대한 분석 모집단은 기준선에서 측정 가능한 질병이 있는 PP 및 ITT 모집단이다.Confirmed ORR is defined as the proportion of patients with an identified objective response. Analysis populations for identified ORRs are PP and ITT populations with measurable disease at baseline.
확인된 ORR의 추정치 및 이의 95% CI는 각 치료군에 대해 클로퍼-피어슨 방법을 사용하여 계산한다. 두 치료군 간의 확인된 ORR 차이에 대한 CI는 이항 분포에 대한 정규 근사치를 사용하여 결정된다. An estimate of the identified ORR and its 95% CI are calculated using the Klopper-Pearson method for each treatment group. The CI for the identified ORR differences between the two treatment groups is determined using a normal approximation to the binomial distribution.
반응 지속기간duration of response
확인된 반응의 DOR은 PP 및 ITT 모집단에서 RECIST v1.1을 사용하여 시험자가 결정한 객관적인 반응이 확인된 환자에게서 평가한다. 확인된 반응의 DOR은 확인된 객관적 반응의 최초 발생 일자로부터 RECIST v1.1에 따라 시험자가 결정한 진행성 진행의 최초 날짜 또는 사망이 기록될 때까지 중 먼저 발생하는 것까지의 시간으로 정의된다. 분석시 질병 진행이 없었고 사망하지 않은 환자는 마지막 종양 평가일에 중도절단된다. DOR은 환자들의 무작위배정 되지 않은 하위집합(특히, 확인된 객관적 반응을 달성한 환자)에 기반하므로; 이 평가변수에 대한 공식적인 가설 검사는 실시되지 않는다. 설명의 목적으로 치료군들을 비교한다. PFS 분석에 대해 자세히 설명된 방법론은 DOR 분석에 사용된다.The DOR of confirmed response is assessed in patients with confirmed objective responses as determined by the investigator using RECIST v1.1 in the PP and ITT populations. The DOR of a confirmed reaction is defined as the time from the date of the first occurrence of the identified objective reaction to the first date of progressive progression as determined by the investigator in accordance with RECIST v1.1 or until death is recorded, whichever occurs first. Patients with no disease progression and no death at the time of analysis are censored on the last tumor assessment date. Because the DOR is based on a non-randomized subset of patients (particularly those who achieved an identified objective response); No formal hypothesis testing is conducted for this endpoint. Treatment groups are compared for illustrative purposes. The methodology detailed for the PFS analysis is used for the DOR analysis.
계층화 요소layered elements
계층화 요소는 IxRS에서 무작위 배정에 사용되는 요소이다(즉, ECOG 전신 활동도, LDH, 뇌 전이의 존재 또는 이력). 적어도 하나의 계층(즉, ECOG 전신 활동도[0 대 1], LDH[≤ULN 대 >ULN], 및 IxRS에 따른 뇌 전이의 존재 또는 이력[예 대 아니오]에 걸친 계층화 요소 수준의 조합)이 10개 미만의 사건(PFS 또는 OS 사건)을 갖는 경우, 환자 수가 가장 적은 수준을 포함하는 계층화 요소(3개의 계층화 요소 중 하나: ECOG 수행 상태, LDH 및 IxRS에 따른 뇌 전이의 존재 또는 이력)는 계층화된 분석에서 제거된다. 계층화 요소의 제거는 10개 미만의 사건(PFS 또는 OS 사건)이 있는 계층이 없을 때까지 계속된다. 계층화 분석에 사용되는 최종 계층화 요소 세트는 계층화 분석이 계획된 모든 평가변수에 적용된다. IxRS 기록과 eCRF 간에 상당한 불일치가 관찰되는 경우, 전자 사례 보고 양식(eCRF)에 기록된 계층화 요소를 기반으로 한 분석도 제공된다.Stratification factors are factors used for randomization in IxRS (ie ECOG systemic activity, LDH, presence or history of brain metastases). At least one stratum (i.e., ECOG systemic activity [0 vs. 1], LDH [≤ULN vs. >ULN], and a combination of stratification factor levels across the presence or history of brain metastases according to IxRS [yes vs. no]) For those with fewer than 10 events (PFS or OS events), the stratification factor containing the lowest number of patients (one of the three stratification factors: ECOG performance status, presence or history of brain metastases according to LDH and IxRS) was removed from the stratified analysis. Removal of stratification elements continues until there are no tiers with less than 10 events (PFS or OS events). The final set of stratification elements used for stratification analysis is applied to all endpoints for which stratification analysis is planned. Where significant discrepancies are observed between IxRS records and eCRFs, an analysis based on the stratification factors recorded on the Electronic Case Reporting Form (eCRF) is also provided.
E.E. 적격성eligibility
환자는 이의 ES-SCLC에 대해 화학요법을 받은 적이 없고 하기의 적격 기준을 충족하는 경우 적격이다: 18세 이상; 시험자의 판단에 따라 연구 프로토콜을 준수하는 능력; 0 또는 1의 ECOG 전신 활동도; 조직학적 또는 세포학적으로 확인된 ES-SCLC(수정된 VALG(미국보훈부폐연구그룹) 병기 결정 시스템에 따름(Micke et al., Lung Cancer 2002, 37: 271-6)); ES-SCLC에 대한 선행 전신 치료 없음; 제한된 병기 SCLC에 대해 선행 화학방사선요법을 받은 환자는 완치 목적으로 치료를 받았어야 하며 화학요법, 흉부 방사선요법 또는 화학방사선요법의 마지막 용량/주기와 ES-SCLC 진단 사이에 최소 6개월의 무치료 간격이 있어야 함; RECIST v1.1에 정의된 측정 가능한 질병(이전에 조사된 병변은 (1) 방사선 요법 이후 해당 부위에서 질병 진행이 명백하게 기록되고, (2) 이전에 조사된 병변이 측정 가능한 질병의 유일한 부위가 아닌 경우에만 측정 가능한 질병으로 간주될 수 있음); 치료 전 종양 조직 샘플의 제출; 치료적 항응고 요법을 받는 환자의 경우: 안정적인 항응고 요법; 선별검사 시 음성 HIV 검사; 선별검사 시 음성 B형 간염 표면 항원(HBsAg) 검사; 연구 치료제 개시(주기 1의 1일) 전 14일 이내에 수득한 하기의 실험실 검사 결과에 의해 정의된 적절한 혈액학적 및 말단 기관 기능: 과립구 집락 자극 인자 지원 없이 절대 호중구 수(ANC) ≥ 1.5 × 109/L(1500/μL); 림프구 수 ≥ 0.5 × 109/L(500/μL); 수혈 없이 혈소판 수 ≥ 100 × 109/L(100,000/μL); 헤모글로빈 ≥ 90 g/L(9 g/dL)(환자는 상기 기준을 충족하기 위해 지역 치료 표준에 따라 수혈을 받거나 적혈구 생성 치료를 받을 수 있음); INR 또는 aPTT ≤ 1.5 x ULN(치료적 항응고제, INR 또는 aPTT ≤ 1.5 x ULN을 받지 않는 환자의 경우); AST, ALT 및 ALP ≤ 2.5 × ULN, 하기의 예외를 가짐: (간 전이가 기록된 환자: AST 및/또는 ALT ≤ 5 × ULN; 간 또는 뼈 전이가 기록된 환자: ALP ≤ 5 × ULN); 빌리루빈 ≤ 1.5 × ULN(하기의 예외를 가짐: 공지된 길버트병 환자: 빌리루빈 ≤ 3 × ULN); 크레아티닌 ≤ 1.5 × ULN; 알부민 ≥ 25 g/L(2.5 g/dL). Patients are eligible if they have never received chemotherapy for their ES-SCLC and meet the following eligibility criteria: 18 years of age or older; ability to comply with study protocols at the discretion of the investigator; ECOG systemic activity of 0 or 1; Histologically or cytologically confirmed ES-SCLC (according to the modified VALG (US Department of Veterans Affairs Research Group) staging system (Micke et al., Lung Cancer 2002, 37: 271-6)); No prior systemic treatment for ES-SCLC; Patients who received prior chemoradiation for limited-stage SCLC must have been treated for a curative purpose and a treatment-free interval of at least 6 months between the last dose/cycle of chemotherapy, chest radiotherapy, or chemoradiation and the diagnosis of ES-SCLC must have; Measurable disease as defined in RECIST v1.1 (a previously irradiated lesion is (1) an unambiguous documented disease progression at that site following radiation therapy, and (2) a previously irradiated lesion is not the only site of measurable disease. can only be considered a measurable disease); submission of tumor tissue samples prior to treatment; For patients receiving therapeutic anticoagulant therapy: stable anticoagulant therapy; negative HIV test at screening; negative hepatitis B surface antigen (HBsAg) test at screening; Adequate hematological and end organ function as defined by the following laboratory test results obtained within 14 days prior to study treatment initiation (Day 1 of Cycle 1): Absolute neutrophil count (ANC) ≥ 1.5 × 10 9 without granulocyte colony stimulating factor support /L (1500/μL); Lymphocyte count ≥ 0.5 × 10 9 /L (500/μL); platelet count ≥ 100 × 10 9 /L (100,000/μL) without transfusion; hemoglobin ≥ 90 g/L (9 g/dL) (patient may receive transfusion or erythropoietic therapy according to local standards of care to meet the above criteria); INR or aPTT ≤ 1.5 x ULN (for patients not receiving therapeutic anticoagulant, INR or aPTT ≤ 1.5 x ULN); AST, ALT, and ALP ≤ 2.5 × ULN, with the following exceptions: (Patients with documented liver metastases: AST and/or ALT ≤ 5 × ULN; Patients with documented liver or bone metastases: ALP ≤ 5 × ULN); bilirubin ≤ 1.5 x ULN (with the following exceptions: patients with known Gilbert's disease: bilirubin ≤ 3 x ULN); creatinine ≤ 1.5 x ULN; Albumin ≥ 25 g/L (2.5 g/dL).
배제 기준은 하기를 포함한다: 증상이 있거나 활동적으로 진행 중인 CNS 전이(참고: 치료(즉, 국소 CNS 지향 요법) 또는 치료되지 않은 CNS 병변이 있는 무증상 환자는 하기의 기준이 모두 충족되는 경우 적격이다: RECIST v1.1에 따른 측정 가능한 질병이 외부에 존재해야 하고; 환자가 CNS 질환으로 인한 두개내 출혈 또는 척수 출혈의 병력이 없어야 하고; 전이가 소뇌 또는 천막상 영역으로 제한되고(즉, 중뇌, 교뇌, 수질 또는 척수로 전이되지 않음); 환자는 CNS 질병으로 인한 증상이 없고(즉, 두통, 메스꺼움, 구토, 경련, 마비 등은 없음); 환자는 CNS 질병에 대한 항경련제에 대한 지속적인 요구 사항이 없고; 환자는 CNS 질병에 대한 덱사메타손/코르티코스테로이드에 대한 지속적인 요구 사항이 없고 (이전에 치료를 받지 않은 환자는 또한 CNS 질환에 대해 덱사메타손/코르티코스테로이드를 필요로 하거나 투여 받은 이력이 없어야 함); 이전에 치료를 받은 CNS 전이가 있는 환자의 경우, CNS 지향 요법의 완료와 무작위 배정 사이에 중간 CNS 진행의 증거가 없고; 이전에 치료를 받은 적이 없는 환자의 경우, CNS 질병과 관련된 뇌 부종의 증거가 없고(예컨대, 혈관성 부종); 이전에 치료를 받은 적이 없는 환자의 경우, 선별검사 시 조영제를 사용한 뇌 자기공명영상(MRI) 스캔이 필요하며, 그 후 예약된 모든 후속 종양 평가에 선호되는 방식이고(참고: 조영제를 사용한 컴퓨터 단층촬영(CT) 스캔은 하기의 기준이 충족되는 경우 모든 환자에게 허용될 수 있고: 치료되지 않은 CNS 질병을 평가하기 위해 선별검사 시 뇌 MRI 및 조영제를 사용한 CT 스캔을 모두 실시해야 하고; 조영제를 사용한 CT 스캔은 조영제가 포함된 선별검사 MRI에서 확인된 병변을 안정적으로 평가하는 데 사용할 수 있고; 조영제를 사용한 CT 스캔을 사용하여 조영제가 포함된 선별검사 MRI에서 확인된 병변을 안정적으로 평가할 수 없는 경우, 이후의 모든 예정된 후속 종양 평가에서 조영제를 사용한 MRI 스캔을 사용해야 하며; 모든 종양 평가에서 동일한 방식이 사용되는 경우, 수술 및/또는 방사선으로 확정적으로 치료되지 않은 척수 압박, 또는 무작위 배정 전 1주 이상 동안 질병이 임상적으로 안정하다는 증거 없이 이전에 진단 및 치료된 척수 압박; 연수막 질환; 조절되지 않는 흉막 삼출, 심낭 삼출 또는 반복적인 배액 절차가 필요한 복수(한 달에 한 번 또는 더 자주); 유치 카테터(예컨대, PLEURX®)를 장착한 환자는 배액 빈도에 관계없이 허용되고; 조절되지 않거나 증상이 있는 고칼슘혈증(이온화 칼슘 > 1.5 mmol/L, 총 혈청 칼슘 > 12 mg/dL, 또는 교정된 칼슘 > ULN); 활동성 바이러스성, 알코올성 또는 기타 간염, 간경변, 유전성 간 질환 또는 현재 알코올 남용을 포함한 공지된 임상적으로 유의한 간 질환; 무작위 배정 전 5년 이내에 SCLC 이외의 악성 종양 - 단, 예상되는 치료 결과(예컨대, 적절하게 치료된 자궁경부의 상피내 암종, 기저 또는 편평세포 피부암, 치료 의도가 있는 외과적 수술로 치료된 국소 전립선암, 치료 의도가 있는 외과적으로 치료된 제자리 유관 유방암)로 치료된 전이 또는 사망 위험이 무시할 수 있는 수준(예컨대, 예상 5년 OS > 90%)인 경우를 예외로 함; 다음 예외를 제외한 자가면역 질환 또는 면역 결핍의 활성 또는 병력: (갑상선 대체 호르몬 요법을 받고 있는 자가면역 관련 갑상선 기능 저하증의 병력이 있는 환자가 연구에 적격이고; 인슐린 요법을 받고 있는 조절된 제1형 진성 당뇨병 환자가 연구에 적격이며; 습진, 건선, 만성 단순 태선 또는 피부과적 징후만 보이는 백반증이 있는 환자(예컨대, 건선성 관절염 환자는 제외)는 하기의 조건이 모두 충족되는 경우 연구에 적격이고; 발진은 체표면적의 < 10%를 덮고 있어야 하고; 질병은 기준선에서 잘 통제되어야 하고 저역가 국소 코르티코스테로이드만 필요하고; 지난 12개월 이내에 소랄렌에 더하여 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제 또는 고역가 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았고; 특발성 폐 섬유증, 조직화 폐렴(예컨대, 폐쇄성 세기관지염), 약물 유발성 폐렴 또는 특발성 폐렴의 병력, 또는 선별검사 흉부 CT 스캔에서 활동성 폐렴의 증거가 있고; 방사선 분야(섬유증)에서 방사선 폐렴의 병력이 허용되고; 활동성 EBV 감염 또는 선별검사 시 만성 활동성 EBV 감염이 공지되거나 의심되고; EBV IgG 및/또는 EBV 핵 항원(EBNA)에 양성인 환자는 EBV IgM 및/또는 EBV 중합효소 연쇄 반응(PCR)이 음성인 경우에만 적격이고; 활동성 결핵; 감염, 균혈증 또는 중증 폐렴의 합병증으로 인한 입원을 포함하지만 이에 제한되지 않는 무작위 배정 시점의 중증 감염; 무작위 배정 전 3개월 이내의 뉴욕심장협회 심장 질환(부류 II 이상), 심근 경색 또는 뇌혈관 사고, 불안정성 부정맥 또는 불안정 협심증과 같은 심각한 심혈관 질환; 공지된 관상 동맥 질환, 상기 기준을 충족하지 않는 울혈성 심부전, 또는 좌심실 박출률 < 50%를 가진 환자는 적절한 경우 심장 전문의와 상의하여 치료 담당의의 의견에 최적화된 안정적인 의료 요법을 받아야 하고; 무작위 배정 전 28일 이내의 진단 이외의 목적을 가진 주요 수술 절차 또는 연구 과정 동안 주요 수술 절차의 필요성 예상; 이전의 동종 골수 이식 또는 고형 장기 이식; 기타 질병, 대사 기능 장애, 신체 검사 소견 또는 임상 실험실 소견에서 임상시험용 약물의 사용을 금하거나 결과 해석에 영향을 미치거나 환자를 치료 합병증의 위험이 높은 상태로 만들 수 있을 것으로 질병 또는 상태를 합리적으로 의심하는 경우; 연구 절차를 이해, 준수 및/또는 따르는 능력을 방해하는 질병 또는 상태를 가진 환자; 연구 치료제를 개시하기 전 28일 이내에 임의의 다른 임상시험용 약제를 사용한 치료; HBV 또는 HCV에 대한 항바이러스 요법을 통한 현재 치료; 무작위 배정 전 4주 이내에 독성약화 생백신을 투여하거나 연구 동안 독성약화 생백신이 필요할 것으로 예상하는 경우; 환자는 무작위 배정 전 4주 이내에, 치료 중, 및 연구 치료제의 마지막 용량 투여 후 5개월 동안 독성약화 인플루엔자 생백신(예컨대, 플루미스트®)을 투여받아서는 안 되고; CD137 작용제 또는 면역 관문 차단 요법, 항 CTLA-4, 항 TIGIT, 항 PD-1 및 항 PD-L1 치료 항체를 사용한 선행 치료; 무작위 배정 전 4주 이내에 전신 면역자극제(인터페론 및 인터루킨 2(IL-2)를 포함하지만 이에 제한되지 않음) 또는 5회의 약물 제거 반감기(둘 중 더 긴 것)로의 치료; 무작위 배정 전 1주 이내에 전신 면역억제제(코르티코스테로이드, 시클로포스파미드, 아자티오프린, 메토트렉세이트, 탈리도마이드 및 항종양 괴사 인자(항TNF) 제제를 포함하지만 이에 제한되지는 않음)로 치료하거나 기간 동안 전신 면역억제제의 필요성이 예상되는 경우, 단, 하기의 경우를 제외함: 급성, 저용량 전신 면역억제제 또는 1회 펄스 용량의 전신 면역억제제(예컨대, 조영제 알레르기를 위한 코르티코스테로이드 48시간)를 투여받은 환자는 의료 모니터 요원의 확인을 받은 후 연구에 적격이고; 미네랄 코르티코이드(예컨대, 플루드로코르티손), 만성 폐쇄성 폐질환(COPD) 또는 천식에 대한 코르티코스테로이드, 또는 기립성 저혈압에 대한 저용량 미네랄 코르티코이드 또는 부신 기능 부전에 대한 저용량 미네랄 코르티코이드 및 코르티코스테로이드를 투여받은 환자는 연구에 적합하고; 키메라 또는 인간화 항체 또는 융합 단백질에 대한 중증 알레르기 아나필락시스 반응의 병력; 차이니즈 햄스터 난소 세포 제품 또는 티라골루맙 또는 아테졸리주맙 제제의 성분에 대해 알려진 과민증; 카보플라틴 또는 에토포사이드에 대한 알레르기 반응의 병력; 연구 치료 중 또는 티라골루맙 또는 위약의 최종 투여 후 90일 이내, 아테졸리주맙의 최종 투여 후 5개월, 또는 카보플라틴 또는 에토포시드의 최종 투여 후 6개월 동안 임신 또는 모유 수유, 또는 임신 의도; 가임 여성은 연구 치료제 개시 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다.Exclusion criteria included: Asymptomatic patients with symptomatic or actively progressing CNS metastases (note: treated (i.e., local CNS directed therapy) or untreated CNS lesions are eligible if all of the following criteria are met) : Existing measurable disease according to RECIST v1.1; patient has no history of intracranial or spinal cord hemorrhage due to CNS disease; metastasis is limited to the cerebellar or supranial region (i.e., midbrain, midbrain, does not metastasize to the pons, medulla or spinal cord); patient has no symptoms due to CNS disease (i.e., no headache, nausea, vomiting, convulsions, paralysis, etc.); patient has ongoing requirements for anticonvulsant medications for CNS disease patient does not have an ongoing requirement for dexamethasone/corticosteroids for CNS disease (previously untreated patients must also have no history of needing or receiving dexamethasone/corticosteroids for CNS disease); In patients with previously treated CNS metastases, there is no evidence of intermediate CNS progression between completion of CNS-directed therapy and randomization; in previously untreated patients, evidence of cerebral edema associated with CNS disease In patients without prior treatment (e.g., angioedema); a brain magnetic resonance imaging (MRI) scan with a contrast medium is required at screening, which is the preferred method for all subsequent tumor evaluations scheduled thereafter (Note: Computed tomography (CT) scans with contrast media are acceptable for all patients if the following criteria are met: brain MRI and CT scans with contrast media at screening to evaluate untreated CNS disease. CT scan with contrast agent can be used to reliably evaluate lesions identified on screening MRI with contrast agent; CT scan with contrast agent confirmed on screening MRI with contrast agent If the lesion cannot be reliably evaluated, all subsequent planned follow-up MRI scans with contrast media should be used in both assessments; Compression that has not been definitively treated with surgery and/or radiation, or previously diagnosed and treated without evidence of clinical stability of disease for at least 1 week prior to randomization, if the same approach is used in all tumor evaluations ; leptomeningeal disease; uncontrolled pleural effusion, pericardial effusion, or ascites requiring repeated drainage procedures (once a month or more often); Patients with indwelling catheters (eg, PLEURX®) are admitted regardless of the frequency of drainage; uncontrolled or symptomatic hypercalcemia (ionized calcium > 1.5 mmol/L, total serum calcium > 12 mg/dL, or corrected calcium > ULN); known clinically significant liver disease, including active viral, alcoholic or other hepatitis, cirrhosis, hereditary liver disease or current alcohol abuse; Malignant tumors other than SCLC within 5 years prior to randomization, with the proviso that expected treatment outcomes (e.g., appropriately treated intraepithelial carcinoma of the cervix, basal or squamous cell skin cancer, localized prostate cancer treated with an intent-to-treat surgical procedure) , with negligible risk of metastasis or death treated with surgically treated ductal in situ breast cancer with an intended treatment (eg, predicted 5-year OS > 90%); Activity or history of autoimmune disease or immunodeficiency, with the following exceptions: (patients with a history of autoimmune-associated hypothyroidism receiving thyroid replacement hormone therapy are eligible for study; controlled type 1 receiving insulin therapy Patients with diabetes mellitus are eligible for the study; patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with only dermatological signs (e.g., excluding patients with psoriatic arthritis) are eligible for the study if all of the following conditions are met; The rash must cover <10% of the body surface area; disease must be well controlled at baseline and require only low titer topical corticosteroids; UV A radiation, methotrexate, retinoids, biologics, oral calci in addition to psoralen within the past 12 months No acute exacerbation of underlying conditions requiring neuroin inhibitor or high titer or oral corticosteroids; history of idiopathic pulmonary fibrosis, organized pneumonia (eg, bronchiolitis obliterans), drug-induced pneumonia or idiopathic pneumonia, or screening chest CT There is evidence of active pneumonia on the scan; a history of radiation pneumonia in the radiation field (fibrosis) is accepted; active EBV infection or known or suspected chronic active EBV infection at screening; EBV IgG and/or EBV nuclear antigen (EBNA) ) are eligible only if they are negative for EBV IgM and/or EBV polymerase chain reaction (PCR); active tuberculosis; at randomization time points including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia. Severe infection of; New York Heart Association heart disease (Class II or greater) within 3 months prior to randomization, serious cardiovascular disease such as myocardial infarction or cerebrovascular accident, unstable arrhythmia or unstable angina; Known coronary artery disease, meeting the above criteria Patients with congestive heart failure, or left ventricular ejection fraction < 50%, should receive stable medical therapy optimized in the opinion of the treating physician in consultation with a cardiologist as appropriate; within 28 days prior to randomization a major surgical procedure for purposes other than diagnosis within the hospital or anticipation of the need for a major surgical procedure during the course of the study; previous allogeneic bone marrow transplant or solid organ transplant; Other diseases, metabolic dysfunctions, physical examination findings, or clinical laboratory findings that reasonably constitute a disease or condition that would contraindicate the use of the investigational drug, influence the interpretation of results, or place the patient at a high risk of complications of treatment in case of doubt; patients with diseases or conditions that interfere with their ability to understand, comply with, and/or follow research procedures; treatment with any other investigational drug within 28 days prior to initiation of study treatment; Current treatment with antiviral therapy for HBV or HCV; Administered live attenuated vaccine within 4 weeks prior to randomization or expected to require live attenuated vaccine during the study; Patients should not receive live attenuated influenza vaccine (eg, Flumist®) within 4 weeks prior to randomization, on treatment, and for 5 months after administration of the last dose of study treatment; prior treatment with CD137 agonists or immune checkpoint blockade therapy, anti-CTLA-4, anti-TIGIT, anti-PD-1 and anti-PD-L1 therapeutic antibodies; treatment with systemic immunostimulants (including but not limited to interferon and interleukin 2 (IL-2)) or drug elimination half-lives of 5 (whichever is longer) within 4 weeks prior to randomization; Treatment with systemic immunosuppressants (including, but not limited to, corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide, and anti-tumor necrosis factor (anti-TNF) agents) within 1 week prior to randomization or systemic during the period Patients receiving an acute, low-dose systemic immunosuppressant or a single pulse dose of a systemic immunosuppressant (e.g., 48 hours of corticosteroids for contrast allergy) are eligible for study after confirmation by a medical monitor; Patients receiving mineralocorticoids (e.g., fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose mineralocorticoids for orthostatic hypotension or low-dose mineralocorticoids and corticosteroids for adrenal insufficiency suitable for research; history of severe allergic anaphylactic reactions to chimeric or humanized antibodies or fusion proteins; known hypersensitivity to any component of the Chinese Hamster Ovary Cell Products or tiragolumab or atezolizumab formulations; history of allergic reactions to carboplatin or etoposide; Pregnant or breastfeeding during study treatment or within 90 days of the last dose of tiragolumab or placebo, 5 months after the last dose of atezolizumab, or 6 months after the last dose of carboplatin or etoposide, or intention to become pregnant ; Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
F.F. 사이토카인 방출 증후군 cytokine release syndrome
티라골루맙/위약 또는 아테졸리주맙의 주기 1 투여에 대한 예비투약은 지시되지 않는다. 하지만, 티라골루맙/위약 또는 아테졸리주맙과 함께 사이토카인 방출 증후군(CRS)을 경험한 환자는 후속 주입을 위해 항히스타민제, 해열제 및/또는 진통제(예컨대, 아세트아미노펜)로 예비투약을 받을 수 있다. CRS는 내인성 또는 주입된 T 세포 및/또는 기타 면역 작동체 세포의 활성화 또는 결합을 유발하는 임의의 면역요법의 투여 후 초생리학적 반응으로 정의된다. 증상은 진행성일 수 있고, 항상 발병 시 발열을 포함하며, 저혈압, 모세혈관 누출(저산소증) 및 말단 기관 기능 장애를 포함할 수 있다 (Lee et al., Biol Blood Marrow Transplant, 25(4): 625-638, 2019). CRS는 키메라 항원 수용체 T 세포 요법 및 이중특이적 T 세포 관여 항체 요법으로 잘 문서화되었지만, 아테졸리주맙을 포함하여 PD-1 또는 PD-L1을 표적으로 하는 면역 요법에서도 보고되었다(Rotz et al., Pediatr Blood Cancer, 64: e26642, 2017; Adashek and Feldman, J Oncol Practice, 15: 502-504, 2019). No premedication is indicated for Cycle 1 administration of tiragolumab/placebo or atezolizumab. However, patients experiencing cytokine release syndrome (CRS) with tiragolumab/placebo or atezolizumab may be premedicated with an antihistamine, antipyretic and/or analgesic (e.g., acetaminophen) for subsequent infusions. . CRS is defined as a superphysiological response following administration of any immunotherapy that results in activation or binding of endogenous or infused T cells and/or other immune effector cells. Symptoms can be progressive and always include fever at onset, and can include hypotension, capillary leakage (hypoxia), and end-organ dysfunction (Lee et al., Biol Blood Marrow Transplant , 25(4): 625). -638, 2019). CRS is well documented as a chimeric antigen receptor T cell therapy and as a bispecific T cell engaging antibody therapy, but has also been reported in immunotherapy targeting PD-1 or PD-L1, including atezolizumab (Rotz et al., Pediatr Blood Cancer , 64: e26642, 2017; Adashek and Feldman, J Oncol Practice , 15: 502-504, 2019).
실시예 8. 이전에 치료받지 않은 진행성 비편평 비소세포 폐암을 가진 환자를 대상으로 티라골루맙과 아테졸리주맙 + 페메트렉시드 및 카보플라틴/시스플라틴 대 펨브롤리주맙 + 페메트렉시드 및 카보플라틴/시스플라틴의 병용에 관한 II상, 무작위, 이중 맹검, 위약 대조 연구Example 8. Tiragolumab plus atezolizumab plus pemetrexed and carboplatin/cisplatin vs pembrolizumab plus pemetrexed and carboplatin in patients with previously untreated advanced non-squamous non-small cell lung cancer /Phase II, randomized, double-blind, placebo-controlled study of concomitant use of cisplatin
본 실시예는 이전에 치료를 받은 적이 없는 국소 진행성 절제 불가능 또는 전이성 비편평 비소세포폐암(NSCLC) 환자를 대상으로 펨브롤리주맙 + 페메트렉시드 및 카보플라틴/시스플라틴과 병용한 위약과 비교하여 아테졸리주맙 + 페메트렉시드 및 카보플라틴/시스플라틴과 병용한 티라골루맙의 유효성 및 안전성을 평가하기 위해 설계된 무작위, II상, 글로벌, 다기관, 이중 맹검 연구를 기재한다. This example demonstrates Ate versus placebo in combination with pembrolizumab plus pemetrexed and carboplatin/cisplatin in previously untreated patients with locally advanced unresectable or metastatic non-squamous non-small cell lung cancer (NSCLC). Describe a randomized, phase II, global, multicenter, double-blind study designed to evaluate the efficacy and safety of tiragoluumab in combination with zolizumab plus pemetrexed and carboplatin/cisplatin.
A.A. 연구 설계study design
본 연구의 적격 환자에는 EGFR 또는 ALK 유전체 이상이 없는 국소 진행성 절제 불가능 또는 전이성 비편평 NSCLC를 가지고, ECOG 전신 활동도(0 대 1)를 보이는 치료를 받지 않은 18세 이상의 남성 및 여성 환자가 포함된다.Eligible patients for this study included untreated male and female patients 18 years of age or older with locally advanced unresectable or metastatic nonsquamous NSCLC without EGFR or ALK genomic abnormalities, and ECOG systemic activity (0 to 1). .
공지된 EGFR 또는 ALK 재배열이 있는 종양을 가진 환자들은 본Patients with tumors with known EGFR or ALK rearrangements
연구에서 배제된다. EGFR 또는 ALK 돌연변이 상태가 공지되지 않은 종양을 가진 환자는 등록 전에 검사를 받아야 한다. 적격 환자는 PD-L1 발현(지역 또는 중앙 분석에 의한 종양 비율 점수(TPS)/종양 세포(TC) < 1% 대 1%-49% vs. ³ 50%), 지리학적 지역(아시아 대 비아시아), 및 ECOG 전신 활동도(0 대 1)로 계층화되고, 하기의 치료 요법을 받기 위해 1:1로 무작위 배정된다:excluded from the study. Patients with tumors of unknown EGFR or ALK mutation status should be screened prior to enrollment. Eligible patients included PD-L1 expression (tumor percentage score (TPS)/tumor cells (TC) < 1% vs. 1%-49% vs. ³ 50% by regional or central analysis), geographic region (Asian vs. non-Asian). ), and ECOG systemic activity (0 versus 1), and randomized 1:1 to receive the following treatment regimens:
A군: 아테졸리주맙 + 페메트렉시드 및 시스플라틴/카보플라틴과 병용한 티라골루맙; Group A: atezolizumab plus pemetrexed and tiragolumab in combination with cisplatin/carboplatin;
B군: 펨브롤리주맙 + 페메트렉시드 및 시스플라틴/카보플라틴과 병용한 위약.Group B: Pembrolizumab plus pemetrexed and placebo in combination with cisplatin/carboplatin.
카보플라틴 또는 시스플라틴의 선택은 시험자의 선택에 따른다. 카보플라틴 또는 시스플라틴의 선택은 무작위 배정 이전에 이루어지며 주기 1의 1일 후에 변경할 수 없다.The choice of carboplatin or cisplatin is at the discretion of the investigator. The selection of carboplatin or cisplatin is made prior to randomization and cannot be changed after Day 1 of Cycle 1.
무작위 배정 계획은 모든 PD-L1 발현 하위군(TPS/TC < 1%, 1%-49%, 및 ³ 50%)을 적절히 대표하는 거의 동일한 수의 환자가 등록되도록 설계된다. 1차 NSCLC 환자에게서 관찰되는 PD-L1 발현의 자연스러운 분포를 반영하기 위해, 각 PD-L1 하위군에 등록된 환자의 비율은 임상시험용 벤타나(VENTANA) PD-L1(SP263) 동반 진단(CDx) 분석을 이용한 중앙 시험별로 약 80명의 환자(총 계획된 등록의 약 40%)로 제한된다. 지역 및 중앙 결과의 차이를 설명하기 위해, 중앙 결과에 의해 정의된 하위군 등록이 상한치를 초과하는 궤적에 있는 경우, 지역 PD-L1 상태를 기반으로 한 선택적 등록이 실시된다.The randomization scheme is designed to enroll an approximately equal number of patients adequately representing all PD-L1-expressing subgroups (TPS/TC < 1%, 1%-49%, and ³ 50%). To reflect the natural distribution of PD-L1 expression observed in patients with primary NSCLC, the proportion of patients enrolled in each PD-L1 subgroup was calculated as: Investigational VENTANA (VENTANA) PD-L1 (SP263) Companion Diagnostics (CDx) Limited to approximately 80 patients (approximately 40% of total planned enrollment) per central trial using the analysis. To account for differences in regional and median outcomes, selective enrollment based on regional PD-L1 status is enforced when the subgroup enrollment defined by the median outcome is on a trajectory that exceeds the upper limit.
A군 및 B군에 대한 유도 치료는 4회 주기 동안 21일 주기로 투여된다. 유도기 후에, 환자는 하기에 요약된 유지 요법을 계속할 것이다.Induction treatment for Groups A and B is administered in 21-day cycles for 4 cycles. After the induction phase, the patient will continue on the maintenance regimen outlined below.
![]()
![]()
![]()
![]()
환자들은 치료 용량 지연에 관계없이 1주기의 제 1일 후 48주 동안 기준선에서 및 6주(± 7일)마다 종양 평가를 받는다. 48주차 종양 평가가 완료된 후, 종양 평가는 RECIST v1.1에 따른 방사선학적 질병 진행, 동의 철회, 연구 종료, 또는 사망 중 먼저 발생하는 시점까지 용량 지연에 관계없이 그후로 9주마다(± 7일)마다 요구된다. RECIST v1.1에 따라 질병 진행 이후에도 치료받은 환자는 연구 치료가 중단될 때까지 상기 빈도로 종양 평가를 받게 될 것이다. RECIST v1.1에 따른 방사선학적 질병 진행(예컨대, 독성, 증상 악화) 이외의 이유로 치료를 중단한 환자는, 환자가 새로운 항암 치료를 시작했는지의 여부와 상관없이, 상기 환자가 연구 치료를 계속 받았다면 뒤이어 진행되었을 것과 동일한 빈도로 예정된 종양 평가를 계속할 것이다(즉, 주기 1의 1일 후 48주 동안 6주[± 7일]마다, 및 그 후로 RECIST v1.1에 따라 방사선학적 질병 진행, 동의 철회, 연구 종료 또는 사망 중 어느 것이든 먼저 발생한 시점까지 9주[± 7일]마다).Patients receive tumor assessments at baseline and every 6 weeks (± 7 days) for 48 weeks after Day 1 of Cycle 1, regardless of treatment dose delay. After completion of the oncology assessment at Week 48, tumor assessments are performed every 9 weeks thereafter (± 7 days) thereafter, regardless of dose delay, until radiological disease progression, withdrawal of consent, study termination, or death according to RECIST v1.1, whichever occurs first is required every Patients treated after disease progression according to RECIST v1.1 will receive tumor assessments at this frequency until study treatment is discontinued. Patients who discontinued treatment for reasons other than radiological disease progression (e.g., toxicity, worsening symptoms) according to RECIST v1.1 continued on study treatment, regardless of whether or not the patient started new chemotherapy. will continue with scheduled tumor evaluations at the same frequency as they would have subsequently progressed (i.e., every 6 weeks [± 7 days] for 48 weeks after day 1 of cycle 1, and thereafter radiological disease progression according to RECIST v1.1, consent every 9 weeks [± 7 days] until withdrawal, study termination, or death, whichever occurs first).
환자는 치료 중, 연구 치료 중단 시, 및 연구 치료 중단 방문 시 환자 보고 결과 설문지(EORTC QLQ-C30, EORTC QLQ-LC13 및 EORTC IL46)를 작성하도록 요청받는다.Patients are asked to complete a Patient Reported Outcome Questionnaire (EORTC QLQ-C30, EORTC QLQ-LC13 and EORTC IL46) on treatment, at study treatment discontinuation, and at study treatment discontinuation visits.
연구 방문 시 안전성 평가에는 연구의 안전성 평가에 중요하다고 간주되는 이상 반응의 발생률, 특성 및 중증도, 프로토콜-필수 활력 징후, 실험실 이상 및 기타 프로토콜 지정 검사가 포함된다.Safety assessments at study visits include the incidence, nature and severity of adverse events, protocol-essential vital signs, laboratory abnormalities, and other protocol-specific tests considered important for the safety assessment of the study.
연구 동안 혈청 샘플을 수집하여 티라골루맙 및 아테졸리주맙 약동학을 모니터링하고 티라골루맙 및 아테졸리주맙에 대한 항체의 존재를 검출한다.Serum samples are collected during the study to monitor tiragolumab and atezolizumab pharmacokinetics and detect the presence of antibodies to tiragolumab and atezolizumab.
탐색적 바이오마커 평가를 위해 보관 및 새로 얻은 종양 조직, 혈청, 혈장 및 혈액 샘플을 포함한 환자 샘플들 또한 수집한다.Patient samples, including archived and freshly obtained tumor tissue, serum, plasma and blood samples, are also collected for exploratory biomarker evaluation.
연구 동안, RECIST v1.1에 따른 질병 진행 기준을 충족하고 임상적 이점의 증거를 보이는 환자는 하기의 기준을 모두 충족하는 경우 시험자의 재량에 따라 티라골루맙/위약 및 아테졸리주맙/펨브롤리주맙을 이용한 치료를 계속할 수 있다.During the study, patients who met the disease progression criteria according to RECIST v1.1 and showed evidence of clinical benefit were tiragolumab/placebo and atezolizumab/pembrolizumab at the investigator's discretion if all of the following criteria were met: treatment can be continued with
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
모든 시점에서 전체 종양 반응에 대한 시험자 평가는 RECIST v1.1에만 기반한다. iRECIST에 따른 객관적 반응은 각 지정된 시점에서 개별 병변에 대한 시험자의 평가에 기반하여 프로그램 상에서 계산된다.Investigator assessments of overall tumor response at all time points are based solely on RECIST v1.1. Objective responses according to iRECIST are calculated on the program based on the investigator's assessment of individual lesions at each designated time point.
B.B. 용량 및 투여Dosage and administration
치료 요법은 도 18에 요약되어 있다.The treatment regimen is summarized in FIG. 18 .
아테졸리주맙 및 펨브롤리주맙Atezolizumab and Pembrolizumab
환자는 각 21일 주기의 제 1일에 A군에서 고정 용량 20 mL(1200 mg)의 아테졸리주맙 또는 B군에서 8 mL(200 mg)의 펨브롤리주맙을 투여 받는다. 아테졸리주맙/펨브롤리주맙의 주입은 표 50에 요약된 지침에 따라 투여된다. Patients receive a fixed dose of 20 mL (1200 mg) atezolizumab in group A or 8 mL (200 mg) pembrolizumab in group B on Day 1 of each 21-day cycle. Infusions of atezolizumab/pembrolizumab are administered according to the guidelines summarized in Table 50.




티라골루맙 및 위약Tiragolumab and placebo
환자는 각 21일 주기의 제 1일에 A군에서 고정 용량 10 mL(600 mg)의 티라골루맙 또는 B군에서 10 mL의 위약을 투여 받는다. 티라골루맙/위약 주입은 표 50에 요약된 지침에 따라 투여된다.Patients receive a fixed dose of 10 mL (600 mg) tiragolumab in group A or 10 mL placebo in group B on Day 1 of each 21-day cycle. Tiragolumab/placebo infusion is administered according to the guidelines summarized in Table 50.
페메트렉시드, 시스플라틴 및 카보플라틴Pemetrexed, cisplatin and carboplatin
표 51은 페메트렉시드, 카보플라틴 또는 시스플라틴의 치료 투여에 대한 용량 및 권장 주입 시간을 나열한다.Table 51 lists the doses and recommended infusion times for therapeutic administration of pemetrexed, carboplatin or cisplatin.

환자는 현지 치료 표준 및 제조업체의 지침에 따라 백금계 치료제에 대한 항구토제 및 IV 수분 공급을 투여 받는다. 하지만, 면역 조절 효과로 인해 임상적으로 가능한 경우 스테로이드의 예비투약이 제한된다. 또한, 페메트렉시드와 관련된 피부 발진의 경우, 임상적으로 가능할 때마다 제1선 치료로 국소 스테로이드 사용이 권장된다. Patients receive antiemetics and IV hydration for platinum-based therapies according to local standards of care and manufacturer's guidelines. However, the premedication of steroids is limited when clinically feasible due to the immunomodulatory effect. In addition, for skin rashes associated with pemetrexed, topical steroids are recommended as first-line treatment whenever clinically feasible.
표 52는 페메트렉시드에 대해 제안된 예비 투약을 나열한다.Table 52 lists the proposed premedication for pemetrexed.

유도기 동안, 화학요법 주기는, 21일 주기 동안 적어도 하나의 백금계 화학요법 성분이 적어도 1회 투여되는 경우, 유도 화학요법의 4회 주기의 수에 포함된다. 화학요법이 제공되지 않은 주기는 총 유도 화학요법 주기의 수에 포함되지 않는다.During the induction phase, chemotherapy cycles are included in the number of 4 cycles of induction chemotherapy if at least one platinum-based chemotherapy component is administered at least once for a 21-day cycle. Cycles for which no chemotherapy was given are not included in the total number of induction chemotherapy cycles.
용량 변경capacity change
페메트렉시드 및 시스플라틴/카보플라틴의 용량 변경은 처방 정보 및 현지 치료 표준에 따라 독성에 대해 허용된다.Dose changes of pemetrexed and cisplatin/carboplatin are permitted for toxicity according to prescribing information and local standards of care.
용량 변경 지침은 하기에 제공된다. 한번 감량하면, 용량은 100%로 다시 증량할 수 없다.Dosage change instructions are provided below. Once reduced, the dose cannot be increased back to 100%.
환자가 2회 용량 감량 후 임의의 혈액학적 또는 비혈액학적 3등급 또는 4등급의 독성을 경험하거나 독성으로 인해 치료가 63일 넘게 지연되는 경우 페메트렉시드 또는 시스플라틴/카보플라틴을 이용한 치료를 중단한다.Discontinue treatment with pemetrexed or cisplatin/carboplatin if the patient experiences any hematologic or non-hematologic Grade 3 or 4 toxicity after 2 dose reductions or if toxicity delays treatment for more than 63 days do.
혈액 독성blood toxicity
각 주기의 시작 시, ANC는 ³ 1500/νL 이고 혈소판 수는 ³ 100,000/νL이다. 회복을 위한 충분한 시간을 허용하기 위해 치료는 최대 63일 동안 지연될 수 있다. 성장인자는 미국임상종양학회(ASCO) 및 NCCN 지침(Smith et al. 2015; NCCN 2019)에 따라 사용된다. 회복 시, 이전 주기의 최저 혈소판 및 호중구 값을 기반으로 후속 주기의 시작 시 용량 조절이 이루어진다(표 53). ANC 및 혈소판 모두에 대해 용량 조절이 필요한 경우, 환자는 더 낮은 용량을 투여받아야 한다.At the beginning of each cycle, the ANC is ³ 1500/νL and the platelet count is ³ 100,000/νL. Treatment may be delayed for up to 63 days to allow sufficient time for recovery. Growth factors are used according to the American Society of Clinical Oncology (ASCO) and NCCN guidelines (Smith et al. 2015; NCCN 2019). Upon recovery, dose adjustments are made at the start of subsequent cycles based on trough platelet and neutrophil values from the previous cycle (Table 53). If a dose adjustment is required for both ANC and platelets, the patient should receive the lower dose.

시험자는 이러한 합병증이 신속하고 적절하게 관리될 수 있도록 골수억제, 감염 또는 열성 호중구감소증의 초기 및 명백한 징후에 경계한다. 환자는 이러한 징후를 인지하고 가능한 한 빨리 의료 조치를 취하도록 권장된다.Investigators are vigilant for early and obvious signs of myelosuppression, infection, or febrile neutropenia so that these complications can be managed promptly and appropriately. Patients are encouraged to recognize these signs and seek medical attention as soon as possible.
혈액학적 독성으로 인해 화학요법이 보류되는 경우, 전체 혈구 수(차등 WBC 포함)는 개수가 요약된 치료 하한선에 도달할 때까지 매주 수득한다. 그런 다음, 치료가 재개된다.If chemotherapy is withheld due to hematologic toxicity, a complete blood count (including differential WBC) is obtained weekly until the count reaches the summarized lower limit of treatment. Then, treatment is resumed.
빈혈에 대한 용량 감량은 권장되지 않는다. 환자는 시험자의 지침에 따라 지원된다.Dose reduction is not recommended for anemia. Patients are supported according to the investigator's instructions.
비혈액학적 독성non-hematologic toxicity
비혈액학적 독성(표 54)의 경우, 환자의 기준선 값(또는 환자가 기준선에서 독성이 없는 경우 1 등급 이하) 이하로 회복될 때까지 치료가 최대 63일 동안 지연된다. 후속 주기 시작 시 용량 감소는 이전 주기에서 투여된 용량의 비혈액학적 독성을 기반으로 실시한다. 표 54는 비혈액학적 독성에 대한 권장 용량 변경을 제공한다.For non-hematologic toxicity (Table 54), treatment is delayed for up to 63 days until recovery below the patient's baseline value (or grade 1 or lower if the patient is nontoxic at baseline). Dose reduction at the start of a subsequent cycle is based on the non-hematologic toxicity of the dose administered in the previous cycle. Table 54 provides recommended dose modifications for non-hematologic toxicity.

설사는 적절한 설사약으로 조절한다. 메스꺼움 및/또는 구토는 적절한 항구토제로 조절할 수 있다. 3 등급 또는 4 등급 신경독성의 경우, 화학요법은 개선 시 이전 용량의 50%로 재개하거나 즉시 중단한다(시험자의 임상 판단에 따름).Diarrhea is controlled with appropriate laxatives. Nausea and/or vomiting can be controlled with appropriate antiemetics. In case of grade 3 or 4 neurotoxicity, chemotherapy is resumed at 50% of the previous dose or stopped immediately upon improvement (according to the investigator's clinical judgment).
C.C. 병용 요법combination therapy
병용 요법은 연구 약물 개시 7일 전부터 연구 중단 방문시까지 프로토콜 필수 치료 외에 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)을 포함한다. 상기 전체 약물은 시험자에게 보고되고 기록된다.Combination therapy includes any drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, nutritional supplements) used by the patient in addition to protocol essential treatment from 7 days prior to study drug initiation until the study discontinuation visit. The total drug is reported and recorded to the investigator.
허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
방사선학적 질병 진행에 대한 문서화가 없는 환자의 경우, 증상 관리를 위한 지지적 치료를 최대화하고 종양 표적 병변의 평가를 방해할 방사선 요법을 피하는 것을 강력히 권장한다. 티라골루맙/위약 및 아테졸리주맙/펨브롤리주맙을 이용한 치료는 완화 방사선 요법 동안 계속될 수 있다.For patients with no documented radiologic disease progression, it is strongly recommended to maximize supportive treatment for symptom management and to avoid radiation therapy, which will interfere with the evaluation of tumor-targeted lesions. Treatment with tiragolumab/placebo and atezolizumab/pembrolizumab may be continued during palliative radiation therapy.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
일반적으로, 시험자는 지역 표준 관행에 따라 임상적으로 지시된 주의 또는 금지된 요법으로 정의된 것In general, the investigator is defined as a clinically directed caution or contraindicated therapy in accordance with local standard practice.
이외의 지지 요법으로 환자의 치료를 관리한다. 주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 지지 요법(예컨대, 산소 보충 및 β2 아드레날린 작용제)으로 관리한다. Manage patient care with other supportive care. Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related reactions, such as dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea, are managed with supportive care as clinically indicated (e.g., oxygen supplementation and β2 adrenergic agonists).
주의 요법care
전신 코르티코스테로이드 및 TNF-α 억제제는 티라골루맙 및/또는 아테졸리주맙을 이용한 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여해야 하는 상황에서는, 항히스타민제를 포함한 대안을 고려한다. 대안이 가능하지 않은 경우, 시험자의 재량에 따라 전신 코르티코스테로이드 및 TNF-α 억제제를 투여할 수 있다. Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with tiragolumab and/or atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines are considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the investigator's discretion.
티라골루맙 및/또는 아테졸리주맙 요법과 관련된 특정 이상 반응을 치료하기 위해, 시험자의 재량에 따라 전신 코르티코스테로이드가 권장된다.For the treatment of certain adverse events associated with tiragolumab and/or atezolizumab therapy, systemic corticosteroids are recommended at the discretion of the investigator.
금지된 요법forbidden therapy
다음과 같은 병용 요법의 사용은 하기와 같이 금지된다:The use of the following combination therapies is contraindicated as follows:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
D.D. 선정 기준Selection Criteria
환자는 연구 참가를 위해 하기의 기준을 충족해야 한다:Patients must meet the following criteria for study entry:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
전이성 비편평 NSCLCMetastatic nonsquamous NSCLC
혼합 NSCLC 조직학의 종양이 있는 환자는 주요 조직학적 성분에 기반하여 비편평으로 분류되어야 한다. 혼합 NSCLC 및 소세포 폐암이 있는 환자는 본 연구에 적격이 아니다.Patients with tumors of mixed NSCLC histology should be classified as nonsquamous based on their major histological components. Patients with mixed NSCLC and small cell lung cancer are not eligible for this study.
![]()
![]()
비전이성 질병에 대한 치료 목적으로 신보조, 보조 화학요법, 방사선요법 또는 화학방사선요법을 받은 환자는 화학요법 및/또는 방사선요법의 마지막 용량 투여 후 무작위 배정으로부터 적어도 12개월의 무치료 간격을 경험했어야 한다.Patients receiving neoadjuvant, adjuvant chemotherapy, radiotherapy, or chemoradiation therapy for non-metastatic disease must have experienced a treatment-free interval of at least 12 months from randomization after administration of the last dose of chemotherapy and/or radiotherapy do.
![]()
![]()
관련 병리 보고서와 함께 포르말린 고정, 파라핀 포매(FFPE) 블록(바람직한) 또는 15~20개의 비염색 연속 슬라이드에서 대표적인 종양 표본의 확인된 입수 가능성. EGFR 돌연변이 및/또는 ALK 전좌에 대한 중앙 검사가 필요한 경우, 추가로 5개의 염색되지 않은 슬라이드를 제공해야 한다.Confirmed availability of representative tumor specimens in formalin-fixed, paraffin-embedded (FFPE) blocks (preferred) or 15-20 unstained serial slides with relevant pathology reports. If central screening for EGFR mutations and/or ALK translocation is required, an additional 5 unstained slides should be provided.
종양 조직은 전체 및 생존 가능한 종양 함량(즉, 세포 환경 및 조직 구조가 보존된 최소 100개의 생존 가능한 종양 세포)을 기반으로 하여 품질이 양호하다. 허용되는 샘플에는 절제하여 얻은 샘플, 심부 종양 조직에 대한 코어-바늘 생검(새로 수집한 생검에 대해 최소 3개의 코어 포함) 또는 피부, 피하 또는 점막 병변에 대한 절제, 절개, 펀치 또는 겸자 생검, 또는 기관지내 초음파(EBUS) 코어 바늘 생검이 포함된다.Tumor tissue is of good quality based on total and viable tumor content (ie, at least 100 viable tumor cells with preserved cellular environment and tissue structure). Acceptable samples include excisional samples, core-needle biopsies of deep tumor tissue (with a minimum of 3 cores for freshly collected biopsies), or excisional, incisional, punch or forceps biopsies of skin, subcutaneous or mucosal lesions, or Endobronchial ultrasound (EBUS) core needle biopsy is included.
때때로 미세 바늘 흡인이라고도 하는 기관지내 초음파-경기관지 바늘 흡인(EBUS-TBNA)은, 상기에 기재된 바와 같이 조직이 품질이 양호하다면(즉, 세포 환경 및 조직 구조가 보존된 최소 00개의 생존 가능한 종양 세포), 허용 가능하다. 바늘 흡인의 경우, 18 게이지 이상의 바늘이 권장된다.Endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA), sometimes also referred to as fine needle aspiration, is performed, as described above, if the tissue is of good quality (i.e., at least 00 viable tumor cells with a preserved cellular environment and tissue structure). ), which is acceptable. For needle aspiration, an 18 gauge needle or larger is recommended.
조직 구조를 보존하지 않고 세포 현탁액 및/또는 도말을 생성하지 않는 미세 바늘 흡인, 칫솔질, 흉막 삼출액의 세포 펠렛, 및 세척 샘플은 허용 가능하지 않다.Fine needle aspiration, brushing, cell pellets in pleural effusion, and wash samples that do not preserve tissue structure and do not produce cell suspensions and/or smears are not acceptable.
골 전이로부터의 종양 조직은 IHC에 의한 종양 PD-L1 발현에 대해 평가할 수 없으므로 허용 가능하지 않다.Tumor tissue from bone metastases is not acceptable as it cannot be evaluated for tumor PD-L1 expression by IHC.
보관 조직이 불충분하거나 입수 가능하지 않은 경우, 생검 부위가 안전하게 접근 가능한 경우 환자는 선별검사 시 생검을 받을 수 있다. 생검을 제공할 수 없다면, 염색되지 않은 10개 이상의 연속 슬라이드를 제공할 수 있는 경우, 의료 모니터 요원과 논의 하에 환자는 여전히 적격이 될 수 있다.If storage tissue is insufficient or not available, patients may be biopsied at screening if the biopsy site is safely accessible. If biopsies cannot be provided, patients may still be eligible, in discussion with medical monitor personnel, if 10 or more consecutive unstained slides can be provided.
![]()
![]()
이전에 조사된 병변은 방사선 이후 해당 부위에서 질병 진행이 명백하게 기록되었고 이전에 조사된 병변이 측정 가능한 질병의 유일한 부위가 아닌 경우에만 측정 가능한 질병으로 간주될 수 있다.A previously irradiated lesion can be considered measurable disease only if, after radiation, disease progression at that site has been clearly documented and the previously irradiated lesion is not the only site of measurable disease.
![]()
![]()
· 연구 치료제 개시(주기 1의 1일) 전 14일 이내에 수득한, 하기와 같은 실험실 시험 결과로 정의되는 적절한 혈액학적 및 말단 장기 기능:Adequate hematological and terminal organ function, as defined by the following laboratory test results, obtained within 14 days prior to study treatment initiation (Day 1 of Cycle 1):
- ANC ³ 1.5 ´ 109/L (³ 1500/νL), 과립구 집락 자극 인자 보조 없음- ANC ³ 1.5 ´ 109/L (³ 1500/νL), without granulocyte colony stimulating factor adjuvant
- 림프구 수 ³ 0.5 ´ 109/L(³ 500/νL)- Lymphocyte count ³ 0.5 ´ 109/L (³ 500/νL)
- 혈소판 수 ³ 100 ´ 109/L (³ 100,000/νL), 수혈 없음- platelet count ³ 100 ´ 109/L (³ 100,000/νL), no transfusion
- 헤모글로빈 ³ 90 g/L(³ 9 g/dL)- Hemoglobin ³ 90 g/L (³ 9 g/dL)
환자는 이 기준을 충족하기 위해 지역 치료 표준에 따라 수혈을 받거나 적혈구 생성 치료를 받을 수 있다.Patients may receive transfusions or receive erythropoiesis according to local standards of care to meet these criteria.
- AST, ALT, 및 ALT £ 2.5 ´ 정상의 상한치(ULN), 하기를 예외로 함:- AST, ALT, and ALT £ 2.5 ´ Upper limit of normal (ULN), with the following exceptions:
간 전이가 기록된 환자: AST 및 ALT £ 5 ´ ULNPatients with documented liver metastases: AST and ALT £ 5 ´ ULN
문서로 기록된 간 또는 골 전이를 가진 환자: ALP £ 5 ´ ULNPatients with documented liver or bone metastases: ALP £ 5 ´ ULN
- 총 빌리루빈 £ 1.5 ´ ULN, 하기를 예외로 함: - Total Bilirubin £ 1.5 ´ ULN, with the following exceptions:
공지의 길버트병 환자: 빌리루빈 수준 £ 3 ´ ULNKnown Gilbert's Disease Patients: Bilirubin Levels £ 3 ´ ULN
- 크레아티닌 청소율(CrCl) ³ 40 mL/분(³ 60 mL/분, 시스플라틴에 요구됨), 콕크로프트-가울트 식(1976)을 사용하거나 CrCl 결정을 위해 24시간 소변 수집에 의해 계산됨 - Creatinine clearance (CrCl) ³ 40 mL/min (³ 60 mL/min, required for cisplatin), calculated using the Cockcroft-Gault equation (1976) or by 24-hour urine collection for CrCl determination
- 알부민 ³ 25 g/L (³ 2.5 g/dL)- albumin ³ 25 g/L (³ 2.5 g/dL)
· 치료적 항응고제를 투여받지 않는 환자의 경우: INR 및 aPTT £ 1.5 ´ ULNFor patients not receiving therapeutic anticoagulants: INR and aPTT £ 1.5 ´ ULN
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- 총 B형 간염 코어 항체(HBcAb) 음성- Total hepatitis B core antibody (HBcAb) negative
- 총 HBcAb 검사 양성, 이후 B형 간염 바이러스(HBV) DNA 검사 음성(지역 실험실 정의에 따름)- Total HBcAb test positive, then hepatitis B virus (HBV) DNA test negative (according to local laboratory definition)
![]()
![]()
![]()
![]()
여성은 치료 기간 동안 그리고 티라골루맙 또는 위약의 최종 용량 투여 후 90일, 아테졸리주맙 또는 펨브롤리주맙의 최종 용량 투여 후 5개월 동안, 페메트렉시드 및 카보플라틴 또는 시스플라틴의 최종 용량 투여 후 6개월 동안 금욕을 유지하거나 또는 연간 실패율이 < 1%인 피임법을 사용하여야 한다. 여성은 상기 동일한 기간 동안 난자 기증을 자제해야 한다.Women during the treatment period and 90 days after the last dose of tiragolumab or placebo, 5 months after the last dose of atezolizumab or pembrolizumab, and 6 after the last dose of pemetrexed and carboplatin or cisplatin Either abstinence for months or use of contraception with an annual failure rate of <1% should be used. Women should refrain from donating eggs during the same period as above.
여성이 초경 이후이고, 폐경 후 상태(³ 폐경 이외의 확인된 원인 없이 계속해서 12개월 동안 무월경이 지속됨)에 도달하지 않았으며, 수술(즉, 난소, 나팔관 및/또는 자궁 제거) 또는 시험자가 결정한 다른 원인(예컨대, 뮐러관 무발생)으로 인한 영구적인 불임이 아닌 경우, 가임기인 것으로 간주된다. 가임기의 정의는 지역 지침 또는 규정에 맞게 조정될 수 있다.The woman is post-menopausal, has not reached post-menopausal status (3 continued amenorrhea for 12 consecutive months without an identified cause other than menopause), and has not undergone surgery (i.e., removal of the ovaries, fallopian tubes and/or uterus) or as determined by the investigator. If it is not permanent infertility due to other causes (eg, absence of Muller's canal), it is considered to be of childbearing age. The definition of childbearing age may be adapted to local guidelines or regulations.
연간 실패율이 < 1%인 피임법의 예로는 양측 난관 결찰, 남성 불임술, 배란을 억제하는 호르몬 피임약, 호르몬 방출 자궁 내 장치 및 구리 자궁 내 장치가 있다.Examples of contraceptive methods with an annual failure rate of < 1% include bilateral tubal ligation, male sterilization, hormonal contraceptives that suppress ovulation, hormone-releasing intrauterine devices, and copper intrauterine devices.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가한다.The reliability of sexual abstinence is assessed with respect to the duration of the clinical trial and the patient's preferred daily lifestyle.
주기적 금욕(예컨대, 달력, 배란, 증상온, 배란 후 방법) 및 체외사정은 적절한 피임 방법이 아니다. Periodic abstinence (eg calendar, ovulation, symptom temperature, post-ovulation method) and extracorporeal ejaculation are not suitable methods of contraception.
연구 치료제 중단 후 임신을 원하는 여성은 카보플라틴 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료를 시작하기 전에 난모세포 보존에 대한 조언을 구해야 한다.Women wishing to become pregnant after discontinuation of study treatment should seek advice on oocyte preservation prior to initiating study treatment due to the potential for irreversible infertility with carboplatin treatment.
![]()
![]()
임신하지 않은 가임기 여성 파트너와 함께, 수술로 인한 불임이 아닌 남성은 치료 기간 동안 그리고 티라골루맙 또는 위약의 마지막 용량 투여 후 90일 동안, 아테졸리주맙 또는 펨브롤리주맙의 마지막 용량 투여 후 4개월, 페메트렉시드 및 카보플라틴 또는 시스플라틴의 마지막 용량 투여 후 6개월 동안 금욕을 유지하거나, 또는 콘돔에 더하여 실패율이 연간 1% 미만인 추가적인 피임법을 사용하여 배아 및/또는 유전독성 노출을 방지한다. 남성은 상기 동일한 기간 동안 정자 기증을 삼가야 한다.With a non-pregnant female partner of childbearing potential, men who are not surgically infertile during treatment and for 90 days after the last dose of tiragolumab or placebo, 4 months after the last dose of atezolizumab or pembrolizumab; Prevent embryonic and/or genotoxic exposure by maintaining abstinence for 6 months after administration of the last dose of pemetrexed and carboplatin or cisplatin, or by using condoms plus an additional method of contraception with a failure rate of less than 1% per year. Men should refrain from donating sperm during the same period.
가임기 여성 파트너와 함께, 남성은 배아 노출을 피하기 위해 치료 기간 중 및 티라골루맙 또는 위약의 최종 용량 투여 후 90일 동안, 아테졸리주맙 또는 펨브롤리주맙의 최종 용량 투여 후 4개월, 카보플라틴 및 파클리탁셀 또는 냅-파클리탁셀의 최종 용량 투여 후 6개월 동안 금욕을 유지하거나 콘돔을 사용해야 한다.With a female partner of childbearing potential, males should receive carboplatin and carboplatin during treatment and for 90 days after administration of the last dose of tiragolumab or placebo, 4 months after administration of the last dose of atezolizumab or pembrolizumab, to avoid embryo exposure. Abstinence or use of a condom should be maintained for 6 months after administration of the last dose of paclitaxel or nap-paclitaxel.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가한다.The reliability of sexual abstinence is assessed with respect to the duration of the clinical trial and the patient's preferred daily lifestyle.
주기적 금욕(예컨대, 달력, 배란, 증상온, 배란 후 방법) 및 체외사정은 적절한 피임 방법이 아니다.Periodic abstinence (eg calendar, ovulation, symptom temperature, post-ovulation method) and extracorporeal ejaculation are not suitable methods of contraception.
연구 치료제 개시 후 아이를 갖기를 원하는 남성은 화학요법 페메트렉시드, 시스플라틴, 또는 카보플라틴을 이용한 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료를 시작하기 전에 정자 보존에 대한 조언을 구해야 한다.Men wishing to have children after initiation of study treatment should seek advice on sperm conservation before beginning study treatment due to the potential for irreversible infertility due to treatment with chemotherapy pemetrexed, cisplatin, or carboplatin.
E.E. 배제 기준Exclusion Criteria
EGFR 유전자 또는 ALK 융합 종양유전자에 돌연변이가 있는 것으로 공지된 NSCLC를 가진 경우 환자는 연구 참가에서 배제된다. EGFR 또는 ALK 상태가 공지되지 않은 비편평 NSCLC를 가진 환자는 사전 선별 검사 또는 선별 검사에서 검사를 받는다. EGFR 및/또는 ALK 상태는 국부적으로 또는 중앙 실험실에서 평가된다. 국부적으로 평가된 EGFR 상태는 엑손 1821에서 돌연변이를 검출하는 검증된 보건 당국 승인 시험을 사용하여 조직 또는 세포학에서 실시한다. 중앙 EGFR 및/또는 ALK 검사를 위해 샘플을 제출하는 경우, 추가 슬라이드가 제공된다.Patients with NSCLC known to have a mutation in the EGFR gene or ALK fusion oncogene are excluded from study participation. Patients with nonsquamous NSCLC of unknown EGFR or ALK status are screened at prescreening or screening. EGFR and/or ALK status is assessed locally or in a central laboratory. Locally assessed EGFR status is performed in tissue or cytology using validated health authority approved tests that detect mutations in exon 1821. Additional slides are provided when samples are submitted for central EGFR and/or ALK testing.
F.F. 평가evaluation
연구 전반에 걸쳐 안전성 및 내약성에 대해 환자를 면밀히 모니터링한다. 각 용량 투여 전에 독성에 대해 환자들을 평가하고; 임상 평가 및 현지 실험실 검사 값이 허용 가능한 경우에만 투약을 실시한다.Patients are closely monitored for safety and tolerability throughout the study. Evaluate patients for toxicity prior to each dose administration; Dosing should be performed only when clinical evaluation and local laboratory test values are acceptable.
병력, 기준선 조건, 병용 약물, 및 인구 통계 데이터Medical history, baseline conditions, concomitant medications, and demographic data
임상적으로 유의적인 질병, 수술, 암 이력(선행 암 요법 및 절차 포함) 및 폐암 돌연변이 상태(예컨대, EGFR 및 ALK), 생식 상태, 흡연 이력, 알코올 및 남용 약물 사용을 포함한 병력이 기준선에서 기록된다. 또한, 연구 치료제 개시 전 7일 이내에 환자가 사용한 모든 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)가 기록된다. 각 후속 신체 검사 시, 구간 의료 기록을 수득하고 약물 및 알레르기의 모든 변화를 기록한다.Clinically significant disease, surgery, history of cancer (including prior cancer therapies and procedures) and lung cancer mutation status (e.g., EGFR and ALK ), reproductive status, history of smoking, history of alcohol and drugs of abuse are recorded at baseline. . In addition, all medications (eg, prescription medications, over-the-counter medications, vaccines, herbal or homeopathic remedies, nutritional supplements) taken by patients within 7 days prior to initiation of study treatment are recorded. At each subsequent physical examination, an interval medical record is obtained and any changes in medications and allergies are recorded.
인구학적 데이터는 연령, 성별, 및 자가 보고한 인종/민족을 포함한다.Demographic data include age, gender, and self-reported race/ethnicity.
신체 검사Physical examination
전체 신체 검사가 선별 검사에서 실시되고 머리, 눈, 귀, 코, 및 목, 및 심혈관, 피부과, 근골격, 호흡, 위장, 비뇨생식, 및 신경계의 평가를 포함한다. 기준선에서 확인된 이상을 기록한다.A full physical examination is performed at screening and includes evaluation of the head, eyes, ears, nose, and throat, and cardiovascular, dermatological, musculoskeletal, respiratory, gastrointestinal, urogenital, and nervous system. Any abnormalities identified at baseline are recorded.
제한된, 증상 지향적 신체 검사는 지정된 기준선 이후 방문 시 및 임상적으로 지시된 대로 실시한다. 기준선 이상으로부터의 변화를 환자의 환자 메모에 기록한다. 새로운 또는 악화된 임상적으로 유의한 이상을 기록한다.A limited, symptom-oriented physical examination is performed at designated post-baseline visits and as clinically indicated. Changes from baseline abnormalities are recorded in the patient's patient note. Record new or worsening clinically significant abnormalities.
활력 징후vital signs
활력징후에는 환자가 앉은 자세에서의 호흡수, 맥박수, 수축기 및 이완기 혈압, 및 체온을 포함한다. Vital signs include respiratory rate, pulse rate, systolic and diastolic blood pressure, and body temperature when the patient is seated.
일반 병력 및 기준선 상태 eCRF에 기준선에서 관찰된 이상을 기록한다. 후속 방문에서 새로운 또는 악화된 임상적으로 유의한 이상을 기록한다.General History and Baseline Status Document abnormalities observed at baseline in the eCRF. New or worsening clinically significant abnormalities are recorded at follow-up visits.
ECOG 전신 활동도ECOG whole body activity
수행 상태는 기준선에서 ECOG 전신 활동도를 사용하여 측정하며 연구 전반에 걸쳐 정기적으로 평가한다.Performance status is measured using ECOG systemic activity at baseline and is assessed regularly throughout the study.
종양 및 반응 평가Tumor and Response Assessment
선별 검사 및 후속 종양 평가는 (사용금지되지 않는 한 IV 조영제 및 기관 표준에 따라 적절한 경우 경구 조영제를 이용한) 복부 및 가슴의 CT 스캔을 포함한다. 골반의 조영제를 이용한 CT 스캔은 선별 검사 시 그리고 임상적으로 지시된 바와 같이 또는 후속 반응 평가에서 지역 치료 표준에 따라서 요구된다. 흉부의 비조영 CT 스캔과 함께 흉부, 복부 및 골반의 조영제를 이용한 MRI 스캔은 조영제를 사용한 CT 스캔이 금기인 환자(즉, 요오드 기반 조영제 알레르기 또는 신장 청소율 장애가 있는 환자)에서 사용할 수 있다.Screening and subsequent tumor evaluation include CT scans of the abdomen and chest (with IV contrast media and oral contrast media where appropriate according to institutional standards unless contraindicated). Contrast CT scans of the pelvis are required at screening and as clinically indicated or according to local standards of care in subsequent response assessments. Contrast-based MRI scans of the chest, abdomen, and pelvis in combination with non-contrast CT scans of the chest may be used in patients for whom CT scans with contrast agents are contraindicated (ie, patients with iodine-based contrast agent allergy or impaired renal clearance).
모든 환자의 CNS 전이를 평가하기 위해 선별 검사 시 머리의 조영제를 이용한 CT 스캔(조영제) 또는 MRI 스캔(CT 조영제가 금기인 경우)을 실시해야 한다. 조영제를 사용한 CT 스캔이 실시되고 뇌 전이의 존재가 불확실한 것으로 간주되는 경우, 기준선에서 CNS 전이 진단을 확인하거나 반박하기 위해 머리의 MRI 스캔이 필요하다.To evaluate CNS metastases in all patients, a CT scan of the head (contrast medium) or an MRI scan (if CT contrast medium is contraindicated) should be performed at screening. If a CT scan with a contrast agent is performed and the presence of brain metastases is considered uncertain, an MRI scan of the head is needed to confirm or refute the diagnosis of CNS metastases at baseline.
종양 평가를 위한 CT 스캔이 양전자 방출 단층촬영(PET)/CT 스캐너에서 실시되는 경우, CT 획득은 전체 조영제 진단 CT 스캔의 표준과 일치해야 한다.If CT scans for tumor evaluation are performed on a positron emission tomography (PET)/CT scanner, the CT acquisition should be consistent with the standard for full contrast diagnostic CT scans.
임상적으로 지시된 경우, 목의 뼈 스캔 및 CT 스캔과 같은 추가적인 조사도 실시되어야 한다. 시험자의 재량에 따라, RECIST v1.1에 따라 측정가능한 질환의 다른 평가 방법이 사용될 수 있다.If clinically indicated, additional investigations such as neck bone scans and CT scans should also be performed. At the discretion of the investigator, other methods of assessment of measurable disease according to RECIST v1.1 may be used.
검사를 반복하는 대신, 사전 동의를 수득하기 전 그리고 주기 1의 1일의 28일 이내에 치료 표준으로 실시된 종양 평가가 사용될 수 있다. 측정가능한 및/또는 측정 불가능한 질병을 포함하여 공지된 모든 질병 부위는 선별 검사 시 기록되고 각 후속 종양 평가에서 재평가된다. Instead of repeating the test, a tumor assessment conducted as a standard of care prior to obtaining informed consent and within 28 days of Day 1 of Cycle 1 may be used. All known disease sites, including measurable and/or non-measurable disease, are recorded at screening and re-evaluated at each subsequent tumor assessment.
환자는 치료 지연에 관계없이 기준선에서 및 주기 1의 1일 이후 48주 동안 6주(±7 일)마다 종양 평가를 받는다. 48주차 종양 평가가 완료된 후, 종양 평가는, 치료 지연과 관계없이, RECIST v1.1에 따른 방사선학적 질병 진행(또는 RECIST v1.1에 따른 질병 진행 후 연구 치료를 계속하는 환자들의 경우 임상적 이점 상실), 동의 철회, 사망 또는 연구 종료 중 먼저 발생하는 시점까지 9주(±7일)마다 실시한다. 진행성 질병 또는 임상적 이점의 소실이 예상되는 경우 시험자의 재량에 따라 언제든지 스캔이 실시될 수 있다.Patients receive tumor assessments at baseline and every 6 weeks (± 7 days) for 48 weeks after Day 1 of Cycle 1, regardless of treatment delay. After completion of the oncology evaluation at Week 48, the tumor evaluation, regardless of treatment delay, will result in radiological disease progression according to RECIST v1.1 (or clinical benefit for patients continuing study treatment following disease progression according to RECIST v1.1). loss), withdrawal of consent, death, or study termination, whichever occurs first, every 9 weeks (± 7 days). Scans may be performed at any time at the discretion of the investigator if progressive disease or loss of clinical benefit is anticipated.
반응은 RECIST v1.1을 사용하여 상기 자세히 설명한 이미징 방식으로 시험자가 평가한다. 모든 시점에서 전체 종양 반응에 대한 시험자의 평가는 RECIST v1.1 만을 기초로 한다. 방문 전체에 걸쳐 내부 일관성을 보장하기 위해 가능한 경우 동일한 평가자가 평가를 실시한다. 다음 주기에 투약 전에 시험자가 결과를 검토해야 한다.Response is assessed by the investigator using the imaging modality detailed above using RECIST v1.1. Investigator's assessment of overall tumor response at all time points is based on RECIST v1.1 only. Assessments are conducted by the same evaluator whenever possible to ensure internal consistency throughout the visit. Results should be reviewed by the investigator prior to dosing in the next cycle.
티라골루맙/위약 및 아테졸리주맙/펨브롤리주맙을 이용한 연구 치료제는 방사선사진 데이터, 생검 결과(가능한 경우), 및 임상 상태를 통합 평가한 후 질병 진행으로 인한 허용할 수 없는 독성 또는 증상 악화가 없는 상태에서 시험자가 평가한 바와 같이 환자들이 임상 이점을 경험하는 한 계속된다. RECIST v1.1에 따른 질병 진행 기준을 충족하는 환자는 지정된 모든 기준을 충족하고 서면 동의를 제공하는 경우 연구 치료를 계속할 수 있다.Study treatments with tiragolumab/placebo and atezolizumab/pembrolizumab showed unacceptable toxicity or worsening of symptoms due to disease progression after an integrated evaluation of radiographic data, biopsy results (if available), and clinical status. Continued as long as patients experience clinical benefit, as assessed by the investigator in the absence. Patients who meet disease progression criteria per RECIST v1.1 may continue on study treatment provided they meet all specified criteria and provide written consent.
RECIST v1.1에 따른 방사선학적 질환 진행 이외의 이유로(예컨대, 독성, 증상 악화) 치료를 중단한 환자는 RECIST v1.1에 따른 방사선학적 질환 진행, 동의 철회, 사망, 또는 연구 종료 중 먼저 발생하는 시점까지 상기에 기재된 빈도로 예정된 종양 평가를 계속할 것이다. RECIST v1.1에 따른 방사선학적 질환 진행 없이 새로운 항암 요법을 시작하는 환자는 RECIST v1.1에 따른 방사선학적 질병 진행, 동의 철회, 사망 또는 연구 종료 중 먼저 발생하는 시점까지 상기에 기재된 빈도로 종양 계속할 것이다.Patients who discontinued treatment for reasons other than radiological disease progression according to RECIST v1.1 (e.g., toxicity, worsening of symptoms) were treated according to RECIST v1.1 radiological disease progression, withdrawal of consent, death, or study termination, whichever occurs first. Tumor assessments scheduled at the frequency described above will continue until the time point. Patients starting new chemotherapy without radiologic disease progression according to RECIST v1.1 may continue tumors at the frequencies described above until radiological disease progression, withdrawal of consent, death, or study termination, whichever occurs first, according to RECIST v1.1. will be.
모든 시점에서 전체 종양 반응에 대한 시험자의 평가는 RECIST v1.1 만을 기초로 한다. 전체 종양 평가는 모든 표적 병변, 비표적 병변 및 새로운 병변에 대한 항목을 기반으로 하는 iRECIST에 따른다. iRECIST에 따른 반응 평가를 용이하게 하기 위해, 질병 진행 이후에도 연구 치료를 받는 환자의 경우 RECIST v1.1에 따른 진행 이후 종양 평가를 계속하여야 한다. 이러한 평가에는 표적 병변의 지속적인 측정, 비표적 병변의 평가(분명한 진행을 보인 비표적 병변의 추가 악화에 대한 모니터링 포함), 및 모든 후속 평가에서 새로 확인된 병변의 평가(병변이 측정 가능한 경우 측정 포함)가 포함된다.Investigator's assessment of overall tumor response at all time points is based on RECIST v1.1 only. Overall tumor assessment is according to iRECIST, which is based on items for all target lesions, non-target lesions, and new lesions. To facilitate response evaluation according to iRECIST, tumor evaluation should continue after progression according to RECIST v1.1 for patients receiving study treatment after disease progression. These assessments include continuous measurement of target lesions, assessment of non-target lesions (including monitoring for further deterioration of non-target lesions with clear progression), and evaluation of newly identified lesions at all subsequent assessments (including measurements if lesions are measurable). ) is included.
심전도electrocardiogram
ECG는 선별 검사 시 및 임상적으로 지시된 때에 필요하다. 각 환자의 ECG는 가능한 한 동일한 장치에서 수득한다. 리드(lead) 배치는 가능한 한 일관된다. ECG 기록은 환자가 적어도 10분 동안 바로 누운 자세를 취한 후에 실시해야 한다.ECG is required at screening and when clinically indicated. ECGs for each patient are obtained on the same device as far as possible. Lead placement is as consistent as possible. ECG recordings should be performed after the patient has been in the supine position for at least 10 minutes.
안전 모니터링 목적을 위해, 시험자는 모든 ECG 추적을 검토한다. ECG 추적의 사본은 기관에서 환자의 영구 연구 파일의 일부로서 보관된다. 형태학적 파형 변화 또는 기타 ECG 이상을 문서화해야 한다.For safety monitoring purposes, the investigator reviews all ECG traces. Copies of ECG traces are kept at the institution as part of the patient's permanent study file. Morphological waveform changes or other ECG abnormalities should be documented.
임상 결과 평가Clinical Outcome Evaluation
PRO 기기는 치료 이점을 문서화하고 파클리탁셀/냅-파클리탁셀과 함께 티라골루맙 및 아테졸리주맙 + 카보플라틴의 임상 프로파일을 보다 충분히 특성화하기 위해 완성된다. PRO 데이터는 하기의 도구들을 사용하여 수집된다: EORTC QLQ-C30, EORTC QLQ-LC13 및 EORTC IL46의 단일 항목.The PRO device is complete to document the therapeutic benefit and more fully characterize the clinical profile of tiragolumab and atezolizumab plus carboplatin in combination with paclitaxel/nap-paclitaxel. PRO data was collected using the following tools: single entry of EORTC QLQ-C30, EORTC QLQ-LC13 and EORTC IL46.
설문지(EORTC QLQ-C30, EORTC QLQ-LC13 및 EORTC IL46)는 연구 약물 투여 전 주기 1의 1일(기준선); 그런 다음 주기 4를 통한 연구 약물의 투여 전 1일의 모든 치료 주기에서(즉, 주기 2의 1일, 주기 3의 1일, 및 주기 4의 1일) 완료된다,The questionnaires (EORTC QLQ-C30, EORTC QLQ-LC13 and EORTC IL46) were administered on Day 1 of Cycle 1 (baseline) prior to study drug administration; then complete all treatment cycles of Day 1 prior to administration of study drug through Cycle 4 (i.e., Day 1 of Cycle 2, Day 1 of Cycle 3, and Day 1 of Cycle 4);
주기 5에서, 상기 설문지는 연구 치료 중지 방문 때까지 연구 약물 투여 전 1일의 연구 치료 주기를 하나 걸러서(즉, 주기 5의 1일; 주기 7의 1일; 주기 9의 1일 등) 및 연구 치료 중단 방문 시에 완료한다.In Cycle 5, the questionnaire was completed on every other study treatment cycle of 1 day prior to study drug administration (i.e., Day 1 of Cycle 5; Day 1 of Cycle 7; Day 1 of Cycle 9, etc.) and study until the Study Treatment Discontinuation visit. Complete at the treatment discontinuation visit.
전체 게놈 시퀀싱 또는 전체 엑솜 시퀀싱을 위한 혈액 샘플Blood samples for whole genome sequencing or whole exome sequencing
참여 기관에서, 연구 약물에 대한 반응을 예측하거나, 더 심각한 질병 상태로의 진행과 관련되거나, 연구 약물에 대한 후천적 내성과 관련되거나, 부작용 발생에 대한 민감성과 관련되거나, 개선된 이상 반응 모니터링 또는 조사를 유도하거나, 질병 생물학 및 약물 안전에 대한 지식과 이해를 향상시킬 수 있는 변이체를 WGS 또는 WES가 식별할 수 있도록 DNA 추출을 위해 혈액 샘플을 수집한다. 혈액에서 추출한 DNA를 조직에서 추출한 DNA와 비교하여 생식계열 변이체와 체세포 변이체를 구별하여 체세포 변이체를 식별할 수 있다. 샘플은 분석을 위해 하나 이상의 실험실로 보낼 수 있다.At participating institutions, monitoring or investigation of adverse events that are predictive of response to study drug, associated with progression to a more serious disease state, associated with acquired resistance to study drug, associated with susceptibility to adverse events, or improved Collect blood samples for DNA extraction so that WGS or WES can identify variants that can induce cancer or improve knowledge and understanding of disease biology and drug safety. By comparing DNA extracted from blood with DNA extracted from tissues, germline variants and somatic variants can be distinguished to identify somatic variants. The sample may be sent to one or more laboratories for analysis.
WGS 또는 WES를 위한 혈액 샘플의 수집 및 제출은 각 기관의 IRB/EC 및 해당하는 경우 적절한 규제 기관의 탐색적 연구 검토 및 승인에 달려 있다.The collection and submission of blood samples for WGS or WES is subject to exploratory study review and approval by each institution's IRB/EC and, where applicable, the appropriate regulatory body.
유전체학은 질병 병리생물학에 대한 연구원의 이해를 더욱 증진시킨다. WGS 및 WES는 각각 게놈 및 엑솜의 포괄적인 특성을 제공하며, 이 연구에서 수집된 임상 데이터와 함께, 유효성 및 안전성을 모니터링하거나 어떤 환자가 약물에 반응하거나 이상 반응이 발생할 가능성이 더 높은지 예측하기 위한 새로운 치료 접근법 또는 새로운 방법을 개발할 기회를 증가시킬 수 있다. 데이터는 이 연구의 맥락에서 분석되지만 다른 연구의 데이터와 통합하여 탐색할 수도 있다. 더 큰 데이터 세트의 가용성은 미래의 약물 개발을 지원하기 위한 중요한 바이오마커 및 경로의 식별 및 특성화에 도움이 될 것이다.Genomics further enhances researchers' understanding of disease pathology. WGS and WES provide comprehensive characterization of the genome and exome, respectively, and, together with the clinical data collected in this study, can be used to monitor efficacy and safety or predict which patients are more likely to respond to drugs or develop adverse events. It can increase the chances of developing new therapeutic approaches or new methods. The data are analyzed in the context of this study, but can also be explored in conjunction with data from other studies. The availability of larger data sets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
WGS 또는 WES를 위해 수집된 혈액 샘플은 더 이상 필요하지 않거나 소진될 때까지 보관해야 한다. Blood samples collected for WGS or WES should be stored until they are no longer needed or are depleted.
연구용 바이오샘플 저장소용 샘플Samples for Research Biosample Repository
연구용 바이오샘플 저장소(Research Biosample Repository)는 체액, 고형 조직 및 그 파생물(예: DNA, RNA, 단백질, 펩타이드)을 포함한 인간 생물학적 표본의 장기 보관에 사용되는 중앙 관리 시설 그룹이다. RBR 샘플의 수집, 저장 및 분석은 새로운 약제의 합리적인 설계와 진단 테스트의 개발을 용이하게 하여 향후 환자를 위한 개별화된 약물 요법을 가능하게 할 수 있다.The Research Biosample Repository is a group of centrally managed facilities used for long-term storage of human biological samples, including body fluids, solid tissues and their derivatives (eg DNA, RNA, proteins, peptides). The collection, storage, and analysis of RBR samples could facilitate the rational design of new drugs and the development of diagnostic tests, enabling individualized drug therapy for future patients.
RBR에 대한 샘플은 이 선택적 연구에 참여하는 데 구체적으로 동의한 환자로부터 수집된다. RBR 샘플은 다음 목표 중 하나 이상을 달성하기 위해 분석된다.Samples for RBR are collected from patients who specifically consented to participate in this elective study. RBR samples are analyzed to achieve one or more of the following goals:
· 유효성 또는 질병 진행에 대한 바이오마커의 연관성 연구Study of the association of biomarkers to efficacy or disease progression
· 부작용 발생을 발전시키는 민감성과 관련되거나 개선된 부작용 발생 모니터링 또는 조사로 이어질 수 있는 안전 바이오마커의 식별Identification of safety biomarkers that may lead to susceptibility to developing adverse events or to monitor or investigate the occurrence of ameliorated adverse events.
· 질병 생물학 및 약물 안전성에 대한 지식과 이해 향상Improve knowledge and understanding of disease biology and drug safety
· 약물 효과 및 약물 흡수 및 처리 과정을 포함한 약물 반응 연구Study drug response, including drug effects and drug absorption and processing processes
· 바이오마커 또는 진단 분석의 개발 및 이러한 분석의 성능 특성 확립Developing biomarkers or diagnostic assays and establishing performance characteristics of these assays
샘플 수집sample collection
다음 샘플은 RBR에 저장되고, 티라골루맙, 아테졸리주맙, 비편평 NSCLC 또는 약물 안전성과 관련된 바이오마커에 대한 연구를 포함하되, 이에 국한되지 않는 연구 목적으로 사용된다:The following samples are stored in RBR and used for research purposes, including, but not limited to, studies for tyragolumab, atezolizumab, nonsquamous NSCLC, or biomarkers related to drug safety:
![]()
![]()
![]()
![]()
상기 샘플들은 WGS, WES 또는 기타 게놈 분석 방법을 통해 생식선 또는 체세포 변이체의 분석을 위해 하나 이상의 실험실로 보낼 수 있다. 유전체학은 질병 병리생물학에 대한 연구원의 이해를 더욱 증진시킨다. WGS 및 WES는 각각 게놈 및 엑솜의 포괄적인 특성을 제공하며, 이 연구에서 수집된 임상 데이터와 함께, 유효성 및 안전성을 모니터링하거나 어떤 환자가 약물에 반응하거나 부작용이 발생할 가능성이 더 높은지 예측하기 위한 새로운 치료 접근법 또는 새로운 방법을 개발할 기회를 증가시킬 수 있다.The samples may be sent to one or more laboratories for analysis of germline or somatic variants via WGS, WES or other genomic analysis methods. Genomics further enhances researchers' understanding of disease pathology. WGS and WES provide comprehensive characterization of the genome and exome, respectively, and, together with the clinical data collected in this study, new novel approaches for monitoring efficacy and safety or predicting which patients are more likely to respond to drugs or develop adverse events. It can increase the chances of developing therapeutic approaches or new methods.
RBR 샘플에서 생성된 데이터는 이 연구의 맥락에서 분석되지만, 다른 연구의 데이터와 통합하여 탐색할 수도 있다. 더 큰 데이터 세트의 가용성은 미래의 약물 개발을 지원하기 위한 중요한 바이오마커 및 경로의 식별 및 특성화에 도움이 될 것이다.Data generated from the RBR sample are analyzed in the context of this study, but may be explored in conjunction with data from other studies. The availability of larger data sets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
G.G. 치료 및 환자 중단Treatment and patient discontinuation
치료 중단cessation of treatment
환자는 다음 중 하나를 경험하는 경우 연구 치료제를 영구적으로 중단해야 한다:Patients should permanently discontinue study treatment if they experience any of the following:
· 개별 환자의 치료에 대한 잠재적 반응 및 상태의 중증도를 고려할 때, 시험자가 허용할 수 없는 것으로 결정한 면역-관련 이상 반응의 발생을 포함하여 연구 치료와 관련된 허용할 수 없는 독성Unacceptable toxicities associated with the study treatment, including the occurrence of immune-related adverse events determined by the investigator to be unacceptable, given the individual patient's potential response to treatment and the severity of the condition.
· 조사관에 의해, 만약 개체가 연구 치료를 계속 제공받으면 환자의 안전이 위험해질 수 있는 것으로 결정된 임의의 의학적 상태Any medical condition determined by the investigator that the patient's safety may be at risk if the subject continues to receive study treatment
· 치료 중단이 환자에게 최선의 이익이라는 조사관의 결정Investigator's decision that discontinuation of treatment is in the patient's best interest
· 임신· Pregnant
· -비-프로토콜 지정 항암 요법의 사용- Use of non-protocol-specific anticancer therapies
· RECIST v1.1에 따른 방사선학적 질환 진행(연구 치료가 방사선학적 진행 그 이상으로 계속되지 않는 경우)Radiologic disease progression according to RECIST v1.1 (if study treatment does not continue beyond radiological progression)
· 방사선학적 질환 진행 그 이상으로 치료받은 환자의 경우, 방사선학적 및 생화학적 데이터의 통합 평가 후 시험자가 결정한 임상 이익의 상실(티라골루맙/위약 및 아테졸리주맙/펨브롤리주맙 치료가 방사선학적 질환 진행 이후에도 지속되는 경우), 국소 생검 결과(가능한 경우) 및 임상 상태(예: 증상 악화 For patients treated beyond radiological disease progression, loss of investigator-determined clinical benefit after integrated evaluation of radiological and biochemical data (tiragolumab/placebo and atezolizumab/pembrolizumab treatment is radiological disease) If it persists beyond progression), local biopsy results (if available), and clinical status (e.g. worsening of symptoms)
연구 치료제 중단의 주요 이유는 해당 eCRF에 문서화되어 있다. 연구 치료를 조기에 중단한 환자는 대체되지 않을 것이다.The main reasons for discontinuation of study treatment are documented in the appropriate eCRF. Patients who prematurely discontinue study treatment will not be replaced.
환자는 연구 약물의 최종 투여 후 30일이 지나기 전에 치료 중단 방문을 위해 클리닉으로 돌아간다. 반응 평가가 진행성 질환을 나타내는 방문의 경우 치료 중단 방문으로 사용할 수 있다. 진행성 질환 또는 임상적 이익의 상실 이외의 다른 이유로 연구 치료를 중단한 환자(방사선 질환 진행 그 이상으로 치료를 계속하는 환자의 경우)는 계속해서 종양 반응 평가 및 PRO 평가를 받을 것이다.Patients return to the clinic for a treatment discontinuation visit before 30 days have elapsed after the last dose of study drug. Visits where response assessments indicate progressive disease may be used as discontinuation visits. Patients who discontinue study treatment for reasons other than progressive disease or loss of clinical benefit (for patients continuing treatment beyond radiation disease progression) will continue to receive tumor response assessments and PRO assessments.
RECIST v1.1에 따른 연구 치료 중단 및 질병 진행 후, 전화 통화, 환자 의료 기록 및/또는 진료소 방문을 통해 생존 추적 및 새로운 항암 요법에 대한 정보가 사망할 때까지 약 3개월마다 수집된다(환자가 동의를 철회하지 않는 경우)Following study treatment discontinuation and disease progression according to RECIST v1.1, information on survival follow-up and new chemotherapy via phone calls, patient medical records and/or clinic visits is collected approximately every 3 months until death (if the patient If consent is not withdrawn)
H.H. 분석analysis
유효성 분석Validity analysis
유효성 분석은 무작위 치료에 따라 그룹화된 환자를 대상으로 ITT 집단에서 수행된다. 두 치료 부문과 PFS HRs 간의 ORR 차이 추정치는 95% CIs와 함께 계산된다.Efficacy analyzes are performed in the ITT population with patients grouped according to randomization treatment. An estimate of ORR difference between the two treatment arms and PFS HRs is calculated with 95% CIs.
공동 일차 유효성 평가변수에 대한 가설 테스트도 ITT 집단에서 수행될 것이다.Hypothesis testing for joint primary efficacy endpoints will also be performed in the ITT population.
질병 진행 및 객관적 반응에 대한 모든 공동 일차 분석은 RECIST v1.1을 사용한 종양 평가의 조사관 검토를 기반으로 한다.All joint primary analyzes of disease progression and objective response are based on investigator reviews of tumor assessments using RECIST v1.1.
일차 유효성 평가변수Primary efficacy endpoint
공동 일차 유효성 평가변수는 확인된 ORR 및 PFS이다.The joint primary endpoints are confirmed ORR and PFS.
확인된 ORR은 4주 이하의 간격으로 연속 2번의 CR 또는 PR을 특징으로 하는 객관적인 반응을 달성한 환자의 비율로 정의된다.Confirmed ORR is defined as the proportion of patients who achieved an objective response characterized by two consecutive CRs or PRs spaced no more than 4 weeks apart.
객관적 반응은 치료 부문에 의해 평가되고, 기준선 이후 전체 반응 평가가 없는 환자는 무반응자로 계산된다.Objective response is assessed by treatment arm, and patients without an overall response assessment after baseline are counted as non-responders.
두 부문의 ORR 차이 추정치는 95% CI과 함께 계산된다. Mantel-Haenszel 테스트는 프로토콜-정의된 계층화 요인으로 계층화된 5%의 양측 유의 수준에서 두 치료 부문 간의 ORR을 비교하는 데 사용된다.An estimate of the ORR difference between the two sectors is calculated with a 95% CI. The Mantel-Haenszel test is used to compare the ORR between two treatment arms at a two-sided significance level of 5% stratified with protocol-defined stratification factors.
PFS는, 무작위배정 일자와 최초로 기록된 질병 진행 또는 사망 일자 중 먼저 발생하는 것 사이의 시간으로 정의된다. 질병 진행을 경험하지 않았거나 분석시 사망하지 않은 환자는 최종 종양 평가 시 검열된다. 기준선 이후 종양 평가가 없는 환자는 무작위배정 일자에 중도절단된다.PFS is defined as the time between the date of randomization and the first recorded date of disease progression or death, whichever occurs first. Patients who have not experienced disease progression or who have not died at the time of analysis are censored at the final tumor evaluation. Patients without post-baseline tumor evaluation are censored on the date of randomization.
계층화된 로그-순위 분석법을 사용하여 치료 부문들 간의 PFS를 비교한다. A stratified log-rank analysis is used to compare PFS between treatment arms.
PFS에 대한 HR 및 95% CI을 계층화된 Cox 비례-위험 모델을 사용하여 추정한다.HR and 95% CI for PFS are estimated using a stratified Cox proportional-hazard model.
Kaplan-Meier 방법론은 각 치료군의 PFS 중앙값을 추정하는 데 사용되며 Kaplan-Meier 곡선은 치료군의 차이를 시각적으로 설명하기 위해 작성된다.The Kaplan-Meier methodology is used to estimate the median PFS for each treatment group, and a Kaplan-Meier curve is created to visually explain the difference between the treatment groups.
이차 유효성 평가변수secondary efficacy endpoint
전체 생존overall survival
OS는 무작위배정시부터 임의의 원인으로 인한 사망시까지의 시간으로 정의된다. 데이터 차단 시점에 생존한 환자에 대한 데이터는 생존이 확인된 마지막 날짜에 삭제된다. 기준선 이후 정보가 없는 환자에 대한 데이터는 무작위배정 일자에 삭제된다. 계층화된 Cox 비례-위험 모델을 사용하여 OS HR 및 95% CI를 추정했다. Kaplan-Meier 방법론을 사용하여 각 치료 부문에 대한 OS 곡선 및 OS 중앙값을 추정했다.OS is defined as the time from randomization to death from any cause. Data for patients surviving at the time of data blockade will be deleted on the last date survival was confirmed. Data for patients with no post-baseline information will be deleted on the randomization date. OS HR and 95% CI were estimated using a stratified Cox proportional-hazard model. The Kaplan-Meier methodology was used to estimate OS curves and median OS for each treatment arm.
확인된 반응 기간Confirmed response period
DOR은 문서화된 객관적 반응이 처음 발생한 시점부터 질병 진행 또는 여타의 원인으로 인한 사망 중 먼저 발생한 것 사이의 시간으로 정의된다. DOR 분석에는 연구 치료에 대해 객관적 반응을 달성한 환자만 포함된다. DOR은 Kaplan-Meier 방법론을 사용하여 추정된다. DOR은 환자의 비무작위 하위 집합을 기반으로 결정되므로, 공식적인 가설 테스트는 수행되지 않는다.DOR is defined as the time between the first occurrence of a documented objective response and death from disease progression or other cause, whichever occurs first. The DOR analysis included only patients who achieved an objective response to study treatment. The DOR is estimated using the Kaplan-Meier methodology. Since the DOR is determined based on a non-random subset of patients, no formal hypothesis testing is performed.
환자 보고 결과Patient Reported Results
EORTC QLQ-LC13, GHS/QoL을 사용한 기침, 호흡곤란 및 흉통 증상에 대한 TTCD와 EORTC QLQ-C30을 사용한 신체 기능에 대한 TTCD는 무작위 배정일로부터 임상적으로 의미 있는 악화가 처음 확인될 때까지의 시간으로 정의된다. 확인된 임상적으로 의미 있는 증상 악화는 최소 2회의 연속 평가 동안 유지해야 하는 증상 점수의 기준선에서 10점 이하의 점수 증가 또는 기준선에서 10점 이하의 초기 증가로 정의되며, 사망으로 이어진다. GHS/QoL 및 신체 기능에 대해 확인된 임상적으로 의미 있는 증상 악화는 GHS/QoL 또는 최소 2회의 연속 평가 동안 유지해야 하는 신체 기능 스케일 점수의 기준선에서 10점 이하의 감소 또는 10점 이하의 감소로 정의되며, 사망으로 이어진다.EORTC QLQ-LC13, TTCD for symptoms of cough, dyspnea and chest pain using GHS/QoL, and TTCD for physical function using EORTC QLQ-C30 were the time from randomization to first clinically significant deterioration. is defined as Identified clinically significant worsening of symptoms is defined as a score increase of 10 points or less from baseline or an initial increase of 10 points or less from baseline in symptom scores that must be maintained for at least two consecutive assessments, leading to death. A clinically significant worsening of symptoms identified for GHS/QoL and body function is defined as a decrease of 10 points or less or a decrease of 10 points or less from baseline in GHS/QoL or a body function scale score that must be maintained for at least two consecutive assessments. defined, leading to death.
TCD의 경우, 환자에 대한 데이터는 임상 마감일에 확인된 임상적으로 의미 있는 악화를 경험하지 않은 경우 평가를 완료한 마지막 시점에 삭제된다. 기준선 또는 기준선 이후 평가가 수행되지 않은 경우, 환자는 무작위 날짜에 삭제된다.In the case of TCD, data on patients are deleted at the last point of completion of the evaluation if they did not experience a clinically significant deterioration identified by the clinical deadline. If no baseline or post-baseline evaluation is performed, patients are withdrawn on the randomization date.
EORTC 스케일을 사용하는 TTCD는 PFS와 동일한 방법을 사용하여 분석된다.TTCD using the EORTC scale is analyzed using the same method as PFS.
요약 통계 및 선형-변환 점수의 기준선으로부터의 평균 변화는 EORTC 점수 매뉴얼 지침에 따른 EORTC QLQ-C30, EORTC QLQ-LC13, 및 EORTC IL46(부작용으로 인한 통증에 대한 항목) 설문지의 모든 항목 및 하위 스케일에 대해 보고된다.The mean change from baseline in summary statistics and linear-transformation scores was calculated on all items and subscales of the EORTC QLQ-C30, EORTC QLQ-LC13, and EORTC IL46 (item for pain due to adverse reactions) questionnaires according to the EORTC score manual guidelines. is reported about
안전성 분석Safety analysis
안전성 분석에는 임의의 양의 연구 치료를 받은 모든 치료 받은 환자가 포함된다.The safety analysis includes all treated patients who received any amount of study treatment.
안전성 분석은 치료 부문에서 수행되며 실제 받은 치료를 기반으로 한다. 구체적으로, 환자가 티라골루맙 또는 아테졸리주맙을 임의의 양으로 투여받는 경우, 무작위로 초기 치료 배정을 받은 것과 관계없이 환자는 안전성 분석에서 부문 A에 포함된다.Safety analyzes are performed in the treatment sector and are based on actual treatment received. Specifically, if a patient receives any amount of tiragolumab or atezolizumab, the patient is included in Arm A in the safety analysis, regardless of randomized initial treatment assignment.
기간, 복용량 및 복용량 강도를 포함하여 약물 노출이 요약된다. 이상 반응에 대한 축어적 설명은 MedDRA 동의어 사전 용어에 따른다.Drug exposure is summarized, including duration, dose, and dose intensity. Verbose descriptions of adverse events follow MedDRA Thesaurus Terminology.
모든 이상 반응에 대한 중증도는 NCI CTCAE v5.0에 따라 시험자가 등급을 매기고, CRS에 대한 중증도는 ASTCT 합의 등급 스케일에 따라 시험자가 등급을 매긴다. 모든 이상 반응은 치료 부문 및 NCI CTCAE 등급으로 요약된다. CRS는 또한 치료 부문 및 ASTCT 합의 등급으로 요약될 것이다. 또한, 연구 치료 중단 또는 중지로 이어지는 심각한 이상 반응들 및 이상 반응들이 그에 따라 요약된다. 동일한 이벤트가 여러 번 발생하면 최대 중증도에서 한 번만 계산된다. 정상 범위를 벗어난 값을 가진 실험실 데이터가 식별된다. 또한, ADA 결과를 포함하여 선택된 실험실 데이터가 치료 부문별로 요약된다. 사망 및 사망 원인들이 요약되어 있다.The severity of all adverse events is rated by the investigator according to the NCI CTCAE v5.0, and the severity for CRS is graded by the investigator according to the ASTCT consensus rating scale. All adverse events are summarized by treatment arm and NCI CTCAE grade. CRS will also be summarized by treatment arm and ASTCT consensus grade. In addition, serious adverse events and adverse events leading to discontinuation or discontinuation of study treatment are summarized accordingly. Multiple occurrences of the same event are counted only once at maximum severity. Laboratory data with values outside the normal range are identified. In addition, selected laboratory data, including ADA results, are summarized by treatment arm. Deaths and causes of death are summarized.
약동학 분석Pharmacokinetic analysis
약동학 샘플은 약동학 분석을 위해 그리고 이 연구의 성과를 이전 연구에서 얻은 성과와 비교하기 위해 수집한다. 티라골루맙 및 아테졸리주맙의 혈청 농도는 개별 값으로 보고되고 적절한 경우 데이터가 허용하는 대로 치료 부문 및 주기별로 요약(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균 및 기하 평균 변동 계수)된다.Pharmacokinetic samples are collected for pharmacokinetic analysis and to compare the performance of this study with those obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab are reported as individual values and, where appropriate, summarized by treatment arm and cycle as data permits (mean, standard deviation, coefficient of variation, median, range, geometric mean and geometric mean coefficient of variation) do.
개별 및 중앙값 혈청 티라골루맙 및 아테졸리주맙 농도는 치료군 및 일별로 플롯팅된다. 티라골루맙 및 아테졸리주맙 농도 데이터는, 데이터에 의해 보증된 대로 청소율, 분포 용적 및 AUC와 같은 PK 매개변수를 유도하기 위해, 확립된 모집단 PK 모델을 사용하는 다른 연구의 데이터와 통합될 수 있다. 관련 PK 매개변수와 안전성, 유효성 또는 바이오마커 결과의 잠재적 상관관계를 조사할 수 있다.Individual and median serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be integrated with data from other studies using established population PK models to derive PK parameters such as clearance, volume of distribution and AUC as warranted by the data. . Potential correlations between relevant PK parameters and safety, efficacy, or biomarker outcomes can be investigated.
면역원성 분석Immunogenicity assay
면역원성 분석에는 ADA 평가를 받은 환자가 포함되며, 환자는 받은 치료에 따라 분류된다. 티라골루맙과 아테졸리주맙 모두에 대한 치료-응급 ADA-양성 환자 및 ADA-음성 환자의 수와 비율은 치료 부문별로 요약되어 있다. ADA 상태와 안전성, 유효성 및 PK 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고될 수 있다.Immunogenicity assays include patients who have undergone an ADA assessment, and patients are classified according to treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients for both tiragolumab and atezolizumab are summarized by treatment arm. The relationship between ADA status and safety, efficacy, and PK endpoints can be analyzed and reported through descriptive statistics.
바이오마커 분석Biomarker analysis
바이오마커 분석은 적절한 마커(예를 들어, TIGIT)와 연구 치료 유효성의 연관성을 이해하기 위해 수행할 수 있다. 이러한 유효성 결과는 IHC 및/또는 RNA 분석으로 결정하여 종양에 높은 바이오마커 발현이 있는 환자 집단에서 탐색될 수 있다. 본 연구와 관련하여 WGS 데이터의 탐색적 분석이 수행될 수 있으며 이는 질병 병리생물학에 대한 연구원의 이해를 높이고 새로운 치료 접근법의 개발을 안내하기 위해 다른 연구들의 데이터와 통합하여 탐색될 수 있다. WGS 샘플링에 대한 규제 승인을 받지 않은 기관에는 WGS가 적용되지 않는다.Biomarker analysis can be performed to understand the association of an appropriate marker (eg, TIGIT) with the efficacy of the study treatment. These efficacy outcomes can be explored in patient populations with high biomarker expression in tumors as determined by IHC and/or RNA analysis. Exploratory analysis of WGS data can be performed in connection with this study, which can be explored in conjunction with data from other studies to improve researchers' understanding of disease pathobiology and guide the development of new therapeutic approaches. WGS does not apply to organizations that do not have regulatory approval for WGS sampling.
탐색적 분석exploratory analysis
인구통계학적(예: 연령, 성별, 인종/민족) 및 기준선 예후 특성(예: 중앙 실험실 테스트, 지정학적 지역 및 ECOG에 의한 PD-L1 발현)으로 정의된 하위 그룹에서 연구 결과의 일관성을 평가하기 위해, 이들 하위 그룹에서 확인된 ORR 및 PFS의 공동 일차 유효성 평가변수를 검토한다. 확인된 ORR 및 PFS의 요약은 두 치료 부문 간의 비교를 위해 범주형 변수의 각 수준에 대해 별도로 생성된다.To assess the consistency of study outcomes in subgroups defined by demographic (e.g., age, sex, race/ethnicity) and baseline prognostic characteristics (e.g., central laboratory testing, geographic region, and PD-L1 expression by ECOG) For this purpose, we review the joint primary efficacy endpoints of ORR and PFS identified in these subgroups. A summary of the identified ORRs and PFSs is generated separately for each level of the categorical variable for comparison between the two treatment arms.
중간 분석Interim analysis
이 연구를 위해 누적 안전성 데이터의 주기적 분석이 계획되어 있다. PFS의 유효성 중간 분석은 ITT 집단에서 대략 86개의 PFS 사건이 관찰되었을 때 수행된다. 이는 첫 번째 환자가 무작위 배정된 후 약 19개월 후에 발생할 것으로 예상된다. ORR의 초기 분석은 약 120명의 환자가 최소 2회의 종양 평가를 받은 경우에도 수행된다. 이는 첫 번째 환자가 무작위 배정된 후 약 14개월 후에 발생할 것으로 예상된다.Periodic analyzes of cumulative safety data are planned for this study. Interim analysis of effectiveness of PFS was performed when approximately 86 PFS events were observed in the ITT population. This is expected to occur approximately 19 months after the first patient is randomized. An initial analysis of ORR is performed even when approximately 120 patients have undergone at least two tumor evaluations. This is expected to occur approximately 14 months after the first patient is randomized.
실시예 9. 이전에 치료받지 않은 국소 진행성 절제가능한 II기, IIIA기 또는 일부 IIIB기 비소세포 폐암을 가진 환자를 대상으로 백금계 화학요법을 포함하거나 포함하지 않는 신보조 및 보조 티라골루맙 + 아테졸리주맙의 안전성 및 유효성을 평가하는 II상, 공개 라벨, 다기관 연구 Example 9. Neoadjuvant and adjuvant tyragolumab + ate with or without platinum-based chemotherapy in patients with previously untreated locally advanced resectable stage II, IIIA, or some stage IIIB non-small cell lung cancer A Phase II, Open Label, Multicenter Study Evaluating the Safety and Efficacy of Zolizumab
A.A. 연구 설계의 개요Overview of Study Design
GO42501은 이전에 치료받지 않았거나, 조직학적으로 또는 세포학적으로 확인된 절제가능한 II기, IIIA기 또는 일부 IIIB기(T3N2만) NSCLC을 가진 환자를 대상으로 백금계 화학요법(화학)을 포함하거나 포함하지 않는 신보조 및 보조 아테졸리주맙(아테조) + 티라골루맙(티라)의 안전성 및 유효성을 평가하는 글로벌 II상, 공개 라벨, 다기관 연구이다. 이 연구는 아테조 + 티라 또는 아테조 + 티라 + 화학을 사용한 신보조 치료가 안전하고 내약성이 있으며, 초기 단계의 절제 가능한 NSCLC 환자의 수술 결과에 임상적으로 유의한 부정적인 영향을 미치지 않는다는 개념 증명 임상 데이터를 확립하기 위해 설계되었다. 이 연구는 또한 주요 병리학적 반응(MPR)에 의해 측정된 신보조 아테조 + 티라 또는 아테조 + 티라 + 화학의 잠재적인 항종양 효과를 평가하도록 설계되었다. 이 연구는 새로운 치료 조합을 사용할 수 있게 되면 새로운 코호트를 열 수 있는 유연성을 갖도록 설계되었다.GO42501 includes platinum-based chemotherapy (chemo) or This is a global Phase II, open-label, multicenter study evaluating the safety and efficacy of non-neoadjuvant and adjuvant atezolizumab (Atezo) + tiragolumab (Tira). This study is a proof-of-concept clinical trial that neoadjuvant treatment with atezo + tyra or atezo + tyra + chemistry is safe, tolerable, and has no clinically significant adverse effects on surgical outcomes in patients with early-stage resectable NSCLC. It is designed to establish data. This study was also designed to evaluate the potential antitumor effect of neoadjuvant atezo + tyra or atezo + tyra + chemistry as measured by major pathological response (MPR). The study is designed to have the flexibility to open new cohorts as new treatment combinations become available.
투여된 연구 치료제는 표 55에 제공된다. 이 프로토콜에서, "연구 치료"는 이 연구의 일부로 환자에게 할당된 치료의 조합을 나타낸다(즉, 아테조 + 티라, 아테조 + 티라 + 화학, 또는 화학요법).Study treatments administered are provided in Table 55. In this protocol, "study treatment" refers to the combination of treatment assigned to a patient as part of this study (ie, atezo + tyra, atezo + tyra + chemo, or chemotherapy).

아테조 = 아테졸리주맙; 화학 = 백금계 화학요법; PD-L1 = 프로그램된 데스-리간드 1; 티라 = 티라골루맙.atezo = atezolizumab; Chemistry = platinum-based chemotherapy; PD-L1 = programmed death-ligand 1; Tira = tiragolumap.
a 보조 치료제로서 화학요법을 투여하기 위한 시험자의 선택. a Investigator's choice to administer chemotherapy as an adjuvant treatment.
도 19는 연구 설계의 개요를 나타낸다. 환자는 PD-L1 상태에 따라 코호트에 할당되고 다음과 같이 치료를 받는다:19 shows an outline of the study design. Patients are assigned to cohorts according to PD-L1 status and are treated as follows:
코호트 A(PD-L1 높음): 4주기 동안 신보조제 아테조 + 티라, 이어서 외과적 절제 및 16주기 동안 보조제 아테조 + 티라 또는 4주기 동안 보조 화학요법 중 하나. Cohort A (PD-L1 high) : neoadjuvant atezo + tyra for 4 cycles followed by surgical resection and either adjuvant atezo + tyra for 16 cycles or adjuvant chemotherapy for 4 cycles.
코호트 B(PD-L1 모든 진입자): 4주기 동안 신보조제 아테조 + 티라 + 화학, 이어서 16주기 동안 외과적 절제 및 보조제 아테조 + 티라Cohort B (PD-L1 all entrants): neoadjuvant atezo + tyra + chemistry for 4 cycles followed by surgical excision and adjuvant atezo + tyra for 16 cycles
백금계 화학요법의 선택은, 조직학 하위유형을 기반으로 하고, 개시 시점에 문서화된 시험자의 재량에 따른다. 이 연구에는 다음과 같은 백금계 화학요법 옵션이 허용된다.The choice of platinum-based chemotherapy is based on histological subtype and is at the discretion of the investigator documented at the time of initiation. The following platinum-based chemotherapy options are permitted in this study:
![]()
![]()
- 시스플라틴 + 페메트렉시드 - Cisplatin + Pemetrexed
- 카보플라틴 + 페메트렉시드 - Carboplatin + Pemetrexed
- 카보플라틴 + 파클리탁셀 - Carboplatin + Paclitaxel
· 편평 NSCLC의 경우:· For squamous NSCLC:
- 시스플라틴 + 젬시타빈 - Cisplatin + Gemcitabine
- 카보플라틴 + 젬시타빈 - Carboplatin + Gemcitabine
- 카보플라틴 + 파클리탁셀 - Carboplatin + Paclitaxel
외과적 표본은 독립적인 중앙 병리학 실험실과 시험자의 현장 병리학 실험실에서 병리학적 반응(MPR 및 병리학적 완전 반응(pCR))에 대해 평가된다. 또한, 탐색적 바이오마커 분석은 남은 수술 표본(일차 종양 조직 및 절개된 림프절)에 대해 수행될 수 있다.Surgical specimens are evaluated for pathologic response (MPR and complete pathological response (pCR)) at the independent central pathology laboratory and the investigator's on-site pathology laboratory. In addition, exploratory biomarker analysis can be performed on remaining surgical specimens (primary tumor tissue and dissected lymph nodes).
수술 후 방사선 요법(PORT)은 외과적 절제(ypN2 및/또는 R1/R2) 당시 확인된 병리학적 N2 + 질환 또는 양성 종양 마진이 있는 환자에게 허용되며, 보조 아테조 + 티라 치료 전 또는 보조 백금계 화학요법 후에 투여해야 한다.Postoperative radiotherapy (PORT) is permitted in patients with confirmed pathological N2 + disease or benign tumor margin at the time of surgical resection (ypN2 and/or R1/R2), prior to adjuvant atezo plus tyra therapy or adjuvant platinum-based It should be administered after chemotherapy.
모든 환자는 선별검사 시 컴퓨터 단층촬영(CT) 및 양전자 방출 단층촬영(PET) 모두에 의해 그리고 신보조 치료의 주기 2 및 4 후에만 CT에 의해 흉부 및 복부의 예정된 종양 평가를 완료한다. 종양 평가는 수술 후 재발할 때까지 계속된다. 질병 추적 평가에서 질병의 재발의 증거가 나타나는 경우, 이는 병리학적으로 및/또는 스캔으로부터 명백한 방사선학적 증거에 의해 확인되어야 한다. 스캔에서 불분명한 소견이 나타나면(예를 들어, 단축에 있어서 종격동 결절 측정값 < 1.5 cm, 최장 직경에 있어서 폐 실질 병변 또는 내장 병변 측정값 < 1 cm), 생검이 수행되어야 한다. 생검은 다음 항암 요법을 시작하기 전에 수행되어야 한다. 질병 재발 확인을 위한 생검을 수행하는 경우, 남은 생검 조직은 탐색적 바이오마커 연구를 위해 제출할 것이 강력히 권장된다. 생검이 가능하지 않거나 안전하지 않은 경우, 4~8주 이내에 확인 스캔을 다시 수행해야 한다.All patients complete scheduled tumor evaluation of the chest and abdomen by both computed tomography (CT) and positron emission tomography (PET) at screening and by CT only after cycles 2 and 4 of neoadjuvant treatment. Tumor evaluation continues after surgery until recurrence. If disease follow-up evaluation shows evidence of disease recurrence, this should be confirmed pathologically and/or by clear radiological evidence from the scan. If the scan reveals equivocal findings (eg, mediastinal nodule measurements < 1.5 cm for short axis, lung parenchymal lesions or visceral lesion measurements < 1 cm for longest diameter), a biopsy should be performed. A biopsy should be performed prior to initiating the next chemotherapy. If biopsies are performed to confirm disease recurrence, it is strongly recommended that the remaining biopsy tissue be submitted for exploratory biomarker studies. If a biopsy is not possible or unsafe, a confirmatory scan should be performed again within 4 to 8 weeks.
생검에서 질병 재발의 증거(예를 들어, 비악성 침윤)가 나타나지 않으면, 환자는 예정된 연구 치료, 평가 및/또는 추적관찰을 계속할 수 있다. 질병 재발이 없는 경우, 질병 추적 평가는 질병 재발, 동의 철회, 사망, 추적 관찰 상실 또는 시험의뢰자의 연구 종료 중 어느 것이든 먼저 발생하는 시점까지 계속되어야 한다.If the biopsy does not show evidence of disease recurrence (eg, non-malignant infiltrates), the patient may continue with the scheduled study treatment, evaluation, and/or follow-up. In the absence of disease recurrence, disease follow-up evaluation should continue until disease recurrence, withdrawal of consent, death, loss of follow-up, or end of study by the sponsor, whichever occurs first.
모든 환자는 신보조 치료 단계(코호트) 및 보조 치료 단계에서 각 주기의 제 1일차에 안전성, 내약성 및 탐색적 평가를 받는다. 치료 중단 후, 환자의 생존 상태 및 추가 항암 치료에 대해 주기적으로 추적 관찰한다. 안전성 평가에는 연구의 안전성 평가에 중요하다고 간주되는 이상 반응의 발생률, 특성 및 중증도, 프로토콜-필수 활력 징후, 실험실 이상 및 기타 프로토콜 지정 검사가 포함된다. 시험자는 이상 반응에 대해 NCI(National Cancer Institute)의 CTCAE(Common Terminology Criteria for Adverse Events) 버전 5.0(v 5.0)에 따라 등급을 매긴다.All patients undergo safety, tolerability, and exploratory evaluations on Day 1 of each cycle in the neoadjuvant treatment phase (cohort) and the adjuvant treatment phase. After discontinuation of treatment, follow-up periodically for patient survival and additional anticancer treatment. Safety assessments include the incidence, nature and severity of adverse events, protocol-essential vital signs, laboratory abnormalities, and other protocol-specific tests considered important for the safety assessment of the study. Investigators rate adverse events according to the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 (v 5.0).
보관 및 신선한 종양 및/또는 림프절 조직뿐만 아니라As well as stored and fresh tumor and/or lymph node tissue
혈청, 혈장 및 혈액을 포함하는 환자 샘플은 향후 탐색적 바이오마커 평가를 위해 수집된다. 또한, 환자에게 탐색적 미생물군집 연구를 위한 선택적 대변 수집에 동의할 기회가 제공된다.Patient samples, including serum, plasma and blood, are collected for future exploratory biomarker evaluation. In addition, patients are given the opportunity to consent to selective stool collection for exploratory microbiome studies.
구체적인 연구 목적 및 해당 평가변수를 표 56에 요약한다.The specific study objectives and corresponding endpoints are summarized in Table 56.




ADA = 항 약물 항체; ASTCT = 미국 이식 및 세포 치료 학회; 아테조 + 티라 = 아테졸리주맙 + 티라골루맙; 아테조 + 티라 + 화학 = 아테졸리주맙 + 티라골루맙 + 백금계 화학요법; CRS = 사이토카인 방출 증후군; ctDNA = 순환 종양 DNA; EFS = 무사건 생존; EORTCE = 유럽 암 연구 및 치료 기구; GHS/QoL = 글로벌 건강 상태 및 삶의 질; IL = 아이템 목록; MPR = 주요 병리학적 반응; NCI CTCAE v5.0 = 국립 암 연구소 이상 반응에 대한 공통 용어 기준, 버전 5.0; NSCLC = 비소세포폐암; PBMC = 말초혈액 단핵세포; pCR = 병리학적 완전 반응; PK = 약동학; PRO = 환자 중심 결과; QLQ-C30 = 암에 대한 삶의 질 설문지; QLQLC13 = 삶의 질 설문지 폐암 모듈; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1.ADA = anti-drug antibody; ASTCT = American Society for Transplantation and Cell Therapy; atezo + tyra = atezolizumab + tyragolumab; atezo + tyra + chemo = atezolizumab + tyragolumab + platinum-based chemotherapy; CRS = cytokine release syndrome; ctDNA = circulating tumor DNA; EFS = event-free survival; EORTCE = European Agency for Research and Treatment of Cancer; GHS/QoL = global health status and quality of life; IL = list of items; MPR = major pathological response; NCI CTCAE v5.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0; NSCLC = non-small cell lung cancer; PBMC = peripheral blood mononuclear cells; pCR = pathological complete response; PK = pharmacokinetics; PRO = patient-centric outcome; QLQ-C30 = Quality of Life Questionnaire for Cancer; QLQLC13 = Quality of Life Questionnaire Lung Cancer Module; RECIST v1.1 = Criteria for Response Evaluation of Solid Tumors, Version 1.1.
B.B. 치료 배정 및 안전성 도입Treatment assignment and safety introduction
환자는 선별 치료 시 치료 의도가 있는 R0 절제에 적합해야 하며 본원에 명시된 모든 적격 기준을 충족해야 한다. 이러한 연구 참여 기준을 충족하지 않는 환자는(선별 실패) 시험자의 재량에 따라 2회의 재선별 기회(참가자당 총 3회의 선별)에 대한 자격이 있을 수 있다. Patients must be eligible for an intended R0 resection on screening treatment and meet all eligibility criteria set forth herein. Patients who do not meet these study entry criteria (screening failure) may be eligible for two rescreening opportunities (3 total screenings per participant) at the investigator's discretion.
종양 PD-L1 상태에 따른 치료 배정 및 안전성 도입Treatment assignment and safety introduction according to tumor PD-L1 status
통보를 통해 동의를 제공한 후, 환자는 SP263 면역조직화학(IHC)(종양 세포(TC) 기반 분석)에 의한 PD-L1 상태의 중앙 평가를 포함한 선별치료 절차를 거친다. After giving informed consent, the patient undergoes a screening procedure including a central assessment of PD-L1 status by SP263 immunohistochemistry (IHC) (tumor cell (TC) based assay).
등록은 다음과 같이 단계적으로 완료되며(도 20 참조), 각 코호트에 약 41명의 환자가 등록되었다.Enrollment is completed in phases as follows (see Figure 20), with approximately 41 patients enrolled in each cohort.
1. 처음에는 안전성 도입이 있다:1. Initially there is a safety introduction:
- 선별치료 시 PD-L1 종양 비율 점수(TPS)가 ≥50%인 종양이 있는 6명의 환자가 코호트 A(PD-L1 높은 코호트)에 등록된다.- Six patients with tumors with a PD-L1 Tumor Rate Score (TPS) ≥50% at screening treatment are enrolled in Cohort A (PD-L1 High Cohort).
- 코호트 B(PD-L1 모든 진입자 코호트)는 PD-L1 TPS가 <50%인 종양 환자 6명의 등록으로 시작된다.- Cohort B (PD-L1 all entrant cohort) begins with enrollment of 6 tumor patients with PD-L1 TPS <50%.
2. 각 코호트의 안전성을 평가하고, 안전하다고 판단되는 경우:2. Assess the safety of each cohort, and if deemed safe:
- PD-L1 TPS가 ≥50%인 종양이 있는 환자를 포함하여 PD-L1 TPS가 ≥50%인 종양이 있는 8명의 환자가 해당 코호트에 등록될 때까지 환자는 코호트 B(PD-L1 모든 진입자)에만 등록된다.- Patients are enrolled in cohort B (PD-L1 all entrants) until 8 patients with tumors with PD-L1 TPS ≥50%, including those with tumors with PD-L1 TPS ≥50%, are enrolled in that cohort. ) is registered only.
- 나머지 코호트 B 환자는 PD-L1 TPS가 <50%인 종양 환자로 구성된다.- The remaining cohort B patients consist of tumor patients with PD-L1 TPS <50%.
3. PD-L1 TPS가 ≥50%인 종양이 있는 총 8명의 환자가 코호트 B(PD-L1 모든 진입자)에 등록된 후, 코호트 A(PD-L1 높음)에 대한 등록이 재개되고, PD-L1 TPS ≥50%을 가진 종양이 있는 모든 후속 환자가 해당 코호트에 등록된다.3. After a total of 8 patients with tumors with PD-L1 TPS ≥50% were enrolled in Cohort B (PD-L1 all entrants), enrollment into Cohort A (PD-L1 high) resumed, and PD-L1 All subsequent patients with tumors with L1 TPS ≥50% are enrolled in this cohort.
안전성 도입Safety introduction
연구 치료와 관련된 잠재적인 수술 지연, 취소 또는 합병증을 설명하기 위해, 약 6명의 환자가 신보조 치료를 완료하고 수술을 완료하거나 수술 계획이 변경된 후, 안전성 평가를 위해 각 코호트 내 등록이 중단된다. 코호트들은 동일한 속도로 등록할 수 없으며, 각 코호트는 개별적으로, 독립적으로 평가된다.To account for potential surgical delays, cancellations, or complications associated with study treatment, enrollment within each cohort is discontinued for safety assessment after approximately 6 patients have completed neoadjuvant treatment and completed surgery or surgical plan change. Cohorts cannot be enrolled at the same rate, and each cohort is evaluated individually and independently.
안전성 평가는 안전성 및 수술 데이터를 기반으로 한다. 데이터 검토를 기반으로, 해당 코호트에 대한 등록을 계속하거나, 코호트를 종료하는 것이 권장된다. 안전성 도입 기간 동안, 특별한 관심의 이상 반응 또는 질병 진행 이외의 이유로 수술을 진행하지 않는 환자는 교체될 수 있다.The safety assessment is based on safety and surgical data. Based on data review, it is recommended to either continue enrollment in the cohort or terminate the cohort. During the safety introduction period, patients who do not proceed with surgery for reasons other than adverse events of particular interest or disease progression may be replaced.
수술 및 보조 치료Surgery and adjuvant treatment
환자는 4주기의 신보조 요법이 완료되면, 종양의 외과적 절제를 받는다. 수술에 앞서, 담당 외과의와 종양 전문의가 환자를 재평가한다.The patient undergoes surgical resection of the tumor upon completion of 4 cycles of neoadjuvant therapy. Prior to surgery, the patient is reevaluated by the attending surgeon and oncologist.
수술 전 방문은 신보조 치료제의 마지막 투여 후 30일 이내에 이루어져야 한다: 반복 폐 기능 검사(PFT)(임상적으로 지시된 경우) 및 관련 평가는 현지 기관 관행에 따라 수행해야 한다. 주치의와 의료 종양 전문의 양자가 임상적으로 가능하다고 판단하는 경우, 수술 전 방문 후 30일 이내에 Preoperative visits should be made within 30 days of the last dose of neoadjuvant therapy: Repeat Pulmonary Function Test (PFT) (if clinically indicated) and related evaluations should be performed in accordance with local institutional practice. Within 30 days of the preoperative visit, if both the attending physician and the medical oncologist determine that it is clinically feasible
수술 절차를 수행해야 한다. A surgical procedure must be performed.
예정된 종양 평가(주기 2 및 주기 4 이후) 또는 신보조제 치료 중 어느 때라도 질병 진행이 있는 것으로 확인되고, 여전히 절제 가능하고 비전이성으로 간주되는 환자는, 모든 연구 치료 및 평가에 대해 순응하고 적격성을 유지하는 경우 수술을 진행한다.Patients who are confirmed to have disease progression at any time during scheduled tumor evaluation (cycle 2 and after cycle 4) or neoadjuvant therapy, and still considered resectable and non-metastatic, remain compliant and eligible for all study treatments and evaluations. If so, proceed with surgery.
시험자가 네 번의 신보조 치료를 모두 완료하기 전에 질병 진행 없이 환자가 수술을 진행하도록 계획하는 경우, 의학 모니터 요원과 상의해야 한다.If the investigator plans to allow the patient to proceed with surgery without disease progression prior to completing all four neoadjuvant treatments, the medical monitor should be consulted.
질병 진행으로 인해 신보조제 치료를 조기에 중단하고 수술을 진행하지 않는 환자는 추가 임상 연구 절차에서 중단되고, 시험자가 결정한 대로 다른 치료를 계속 받는다. 이러한 환자는 생존 추적 관찰을 위한 연구 대상이다. 신보조제 요법에 반응이 있지만 Patients who prematurely discontinue neoadjuvant treatment due to disease progression and do not proceed with surgery will be discontinued from further clinical study procedures and continue receiving other treatments as determined by the investigator. These patients are the subject of study for survival follow-up. responsive to neoadjuvant therapy
예상치 못한 의학적 문제(예: 폐색전증 또는 심근경색증)로 인해 수술을 진행할 수 없는 환자의 경우, 환자는 화학요법(코호트 A[PD-L1 높음]) 또는 아테조 티라(코호트 A 또는 B) 및 방사선 요법과 같은 프로토콜 지정 치료를 계속할 수 있다.For patients unable to proceed with surgery due to unforeseen medical problems (e.g., pulmonary embolism or myocardial infarction), patients receive chemotherapy (cohort A [PD-L1 high]) or atezotira (cohort A or B) and radiation therapy. You can continue with protocol-directed treatment, such as
외과적 절제 후, 환자는 다음 중 하나가 발생할 때까지 보조 아테조 + 티라 또는 보조 화학요법(코호트 A[PD-L1 높음]만 해당)을 계속 받는다: 16주기의 보조제 아테조 + 티라, 허용할 수 없는 독성, 질병 재발, 사망, 또는 연구 치료를 중단하기로 한 환자 및/또는 의사의 결정.After surgical resection, patients continue to receive adjuvant atezo + tyra or adjuvant chemotherapy (cohort A [PD-L1 high] only) until one of the following occurs: 16 cycles of adjuvant atezo + tyra, acceptable unavoidable toxicity, disease recurrence, death, or decision of the patient and/or physician to discontinue study treatment.
연구 종료 및 연구 기간Study End and Study Duration
이 연구의 종료는 마지막 환자의 마지막 방문이 발생한 날짜로 정의되며, 이는 마지막 환자가 수술 후 연구 약물의 최종 투여를 받은 후 약 3년 후에 발생한다.End of this study is defined as the date on which the last patient's last visit occurred, approximately 3 years after the last patient received the last dose of study drug after surgery.
첫 번째 환자의 선별검사부터 연구 종료시까지의 총 연구 기간은 약 56년일 수 있다. The total duration of the study from screening the first patient to the end of the study may be approximately 56 years.
C.C. 연구 설계에 대한 이론적 근거Rationale for Study Design
이 연구는 이전에 치료를 받은 적이 없는 국소 진행성 NSCLC 환자에 대한 신보조 치료로서 아테조 + 티라 또는 아테조 + 화학의 수술 안전성과 실행 가능성을 평가한다. 이 연구는 또한 보조제 아테조 또는 아테조 이어 보조제 아테조 또는 보조 화학요법의 유효성, 약동학, 면역원성 및 안전성을 평가한다.This study evaluates the surgical safety and feasibility of atezo + tyra or atezo + chemo as neoadjuvant treatment for previously untreated locally advanced NSCLC patients. This study also evaluates the efficacy, pharmacokinetics, immunogenicity and safety of adjuvant atezo or atezo followed by adjuvant atezo or adjuvant chemotherapy.
아테졸리주맙 + 티라골루맙 용량과 일정에 대한 이론적 근거Rationale for Atezolizumab + Tiragolumab Dosage and Schedule
아테졸리주맙은 처방 정보에 요약된 대로 아테졸리주맙에 대해 승인된 용량인 1200mg Q3W(각 21일 주기의 제 1일차에 1200mg)의 고정 용량으로 투여된다. 항종양 활성은 1 mg/kg 내지 20 mg/kg Q3W 범위의 용량에서 관찰되었다. I연구 GO27381(PCD4989g)에서, 아테졸리주맙의 최대 허용 용량에 도달하지 않았으며, 모든 용량에서 용량 제한 독성(DLT)이 관찰되지 않았다. 1200 mg Q3W의 고정 용량(15 mg/kg Q3W의 평균 체중 용량에 해당)은 두 비임상 연구(Deng et al., MAbs, 8: 593-603, 2016), 이용 가능한 임상 약동학(PK), 유효성 및 안전성 데이터를 기반으로 선택되었다.Atezolizumab is administered as a fixed dose of 1200 mg Q3W (1200 mg on Day 1 of each 21-day cycle), the approved dose for atezolizumab as outlined in the prescribing information. Antitumor activity was observed at doses ranging from 1 mg/kg to 20 mg/kg Q3W. In Study I GO27381 (PCD4989g), the maximally tolerated dose of atezolizumab was not reached and no dose limiting toxicity (DLT) was observed at any dose. A fixed dose of 1200 mg Q3W (corresponding to a mean body weight dose of 15 mg/kg Q3W) was obtained from two nonclinical studies (Deng et al., MAbs, 8: 593-603, 2016), available clinical pharmacokinetics (PK), and efficacy. and safety data.
티라골루맙은 실험군의 모든 환자에게 600 mg 고정 용량으로 각 21일 사이클의 1일차에 정맥 주사로 Q3W 투여된다. 고정 용량의 티라골루맙 600 mg IV Q3W는, 환자가 단일 제제 티라골루맙 또는 티라골루맙과 아테졸리주맙을 병용한 연구 GO30103의 이용 가능한 임상 약동학, 유효성 및 안전성 데이터를 기반으로 선택되었다. 연구 GO30103에서, 최대 허용 용량에 도달하지 않았으며, 티라골루맙 단독요법 또는 아테졸리주맙 1200 mg Q3W(티라골루맙 용량 범위 2-1200 mg Q3W)와 병용한 경우 DLT가 관찰되지 않았다. CD4+, CD8+ 및 NK 세포에서 말초 TIGIT 수용체의 완전한 점유는 30 mg Q3W의 티라골루맙 용량 수준에서 시작하여 관찰되었으며, 모든 더 높은 용량에서 유지되었다. 항종양 활성(방사선 사진 부분 반응(PR)으로 평가된)은 아테졸리주맙 1200 mg Q3W와 병용하여 제공될 때, 30600 mg Q3W의 용량 범위에서 티라골루맙에 대해 관찰되었다.Tiragolumab was administered by intravenous injection of Q3W on Day 1 of each 21-day cycle at a fixed dose of 600 mg to all patients in the experimental group. The fixed-dose tiragolumab 600 mg IV Q3W was selected based on available clinical pharmacokinetic, efficacy, and safety data from study GO30103, in which patients were either single agent tiragolumab or tiragolumab plus atezolizumab. In study GO30103, the maximum tolerated dose was not reached and no DLTs were observed with tiragolumab monotherapy or in combination with atezolizumab 1200 mg Q3W (tiragolumab dose range 2-1200 mg Q3W). Complete occupancy of peripheral TIGIT receptors on CD4+, CD8+ and NK cells was observed starting at the tyragolumab dose level of 30 mg Q3W and maintained at all higher doses. Anti-tumor activity (as assessed by radiographic partial response (PR)) was observed for tiragolumab in the dose range of 30600 mg Q3W when given in combination with atezolizumab 1200 mg Q3W.
II상 연구 GO40290에서, 아테졸리주맙 + 티라골루맙군에 등록된 모든 환자는 600 mg의 티라골루맙을 투여받았다. 이 용량에서, 티라골루맙은 내약성을 가졌으며, 아테졸리주맙 + 티라골루맙 병용은 위약과 아테졸리주맙의 병용에 비해 임상적으로 유의미한 PFS 개선 및 보다 높은 ORR을 가져왔다. 600 mg에서 관찰된 유리한 이익 감안하여, 이와 동일한 용량의 티라골루맙을 본 연구에서 사용한다.In phase II study GO40290, all patients enrolled in the atezolizumab plus tiragolumab group received 600 mg of tiragolumab. At this dose, tiragolumab was well tolerated, and the combination of atezolizumab plus tiragolumab resulted in clinically significant improvement in PFS and higher ORR compared to the combination of placebo and atezolizumab. Given the beneficial benefits observed at 600 mg, this same dose of tiragolumab is used in this study.
환자 모집단의 근거Evidence of Patient Population
이 연구는 선별 진료 시 결정된 절제 가능한 II기, IIIA기 및 일부 IIIB기(T3N2만) NSCLC 환자를 등록한다. PD-L1 발현이 높은 종양(TPS ≥50%, 중앙 실험실에서 SP263에 의해 면역조직화학[IHC]에 의해 결정됨)이 있는 환자는 코호트 A(PD-L1 높음)에 등록되며, 모든 진입자(PD-L1 발현에 관계 없음)는 코호트 B(PD-L1 모든 진입자)에 등록된다.This study enrolls patients with resectable stage II, IIIA, and some stage IIIB (T3N2 only) NSCLC determined at screening practice. Patients with tumors with high PD-L1 expression (TPS ≥50%, determined by immunohistochemistry [IHC] by SP263 in the central laboratory) are enrolled in cohort A (PD-L1 high), and all entrants (PD-L1 high) regardless of L1 expression) are enrolled in Cohort B (PD-L1 all entrants).
신보조 및 보조 화학요법은 초기 단계의 절제 가능한 NSCLC 환자에게 유의미하지만 보통의 이점을 보여주었고, 이 치료 환경에서 결과 개선에 대해 상당한 충족되지 않은 요구가 여전히 있다.Neoadjuvant and adjuvant chemotherapy have shown significant but modest benefits in patients with early-stage resectable NSCLC, and there is still a significant unmet need to improve outcomes in this treatment setting.
세포독성 화학요법에 의한 종양 세포 사멸은 면역 체계를 높은 수준의 종양 항원에 노출시킬 수 있다. PD-L1 및 TIGIT 경로를 차단하여 이 환경에서 종양 특이적 T 세포 면역을 강화하면, 표준 화학요법 단독으로 관찰된 것보다 더 깊고 더 지속적인 반응을 초래할 수 있으며(Merritt et al., J Thorac Cardiovasc Surg, 126: 1609-1617, 2003; Apetoh et al., Nat Med, 13: 1050-1059, 2007), 이는 PD-L1 발현에 관계없이 종양에서 합리적으로 발생할 수 있다.Tumor cell death by cytotoxic chemotherapy can expose the immune system to high levels of tumor antigens. Enhancing tumor-specific T-cell immunity in this setting by blocking the PD-L1 and TIGIT pathways may result in deeper and more sustained responses than observed with standard chemotherapy alone (Merritt et al., J Thorac Cardiovasc Surg). , 126: 1609-1617, 2003; Apetoh et al., Nat Med, 13: 1050-1059, 2007), which can reasonably occur in tumors regardless of PD-L1 expression.
PD-L1 TPS ≥50% 모집단의 혜택 규모와 절제 가능한 초기 NSCLC 환자의 생존율 향상 및 재발률 감소의 필요성을 보여주는 CITSCAPE의 강력한 데이터를 감안할 때, 이 연구는 무화학요법 옵션으로서 아테조 + 티라 조합의 유효성을 검토한다. 절제 가능한 비소세포폐암 환자를 위한 무화학요법 옵션은 환자에게 획기적인 개선이 될 것이며 환자에게 백금계 화학요법과 관련된 초기 및 후기 독성을 예방할 수 있다.Given the magnitude of benefit in the PD-L1 TPS ≥50% population and the robust data from CITSCAPE demonstrating the need to improve survival and reduce recurrence rates in patients with resectable early-stage NSCLC, this study demonstrates the efficacy of a atezo + Tyra combination as a chemo-free option. review A chemotherapy-free option for patients with resectable non-small cell lung cancer would be a significant improvement in patients and could prevent the early and late toxicity associated with platinum-based chemotherapy in patients.
일차 평가변수로서 주요 병리학적 반응에 대한 근거Evidence for Major Pathological Responses as Primary Endpoints
본 연구의 주요 유효성 목표는 중앙 병리학 실험실 평가 주요 병리학적 반응 (MPR)으로 측정한 절제 가능한 II기, IIIA기 또는 일부 IIIB기(T3N2만) NSCLC 환자에서 아테조 + 티라 또는 아테조 + 티라 + 화학을 사용한 신보조 치료의 효능을 평가하는 것이다.The main efficacy goal of this study was to achieve atezo + tyra or atezo + tyra + chemotherapy in patients with resectable stage II, IIIA, or some stage IIIB (T3N2 only) NSCLC, as measured by the Central Pathology Laboratory-Assessed Major Pathological Response (MPR). To evaluate the efficacy of neoadjuvant treatment using
전체 생존(OS)은 보조 및 신보조 NSCLC 시험에서 임상적 이점을 평가하는 표준이지만, OS 판독은 특히 초기 단계 질병에서 종종 수년이 걸린다. 따라서, 의미 있는 대리 평가변수를 채택하면 새로운 치료법의 평가를 촉진하고 NSCLC 환자에게 더 빨리 새로운 치료법을 제공할 수 있다. NSCLC의 외과적 절제 후 병리학적 반응은 OS에 대한 대리 평가변수로 제안되었다(Hellmann et al., Lancet Oncol, 15: e42-50, 2014). Hellmann et al. (2014)은 미국 식품의약국(FDA)의 대리 평가변수 정의를 인용했는데, 여기서 평가변수는 "임상적 이점을 합리적으로 예측할 가능성"이 있어야 한다. 그들은 세 가지 발견을 기반으로 신보강제 환경에서 병리학적 반응을 사용하는 것이 이 정의를 충족한다고 주장한다: 1) 병리학적 반응은 OS와 강한 상관관계가 있다; 2) 병리학적 반응은 신보조 화학요법을 반영한다; 및 3) 병리학적 반응의 정도는 OS 이익의 정도와 상관관계가 있다.Although overall survival (OS) is the standard for evaluating clinical benefit in adjuvant and neoadjuvant NSCLC trials, OS readouts often take years, especially in early-stage disease. Therefore, the adoption of meaningful surrogate endpoints may facilitate the evaluation of new therapies and provide new therapies to NSCLC patients more quickly. Pathological response after surgical resection of NSCLC has been proposed as a surrogate endpoint for OS (Hellmann et al., Lancet Oncol, 15: e42-50, 2014). Hellmann et al. (2014) cited the U.S. Food and Drug Administration's (FDA) definition of a surrogate endpoint, where the endpoint must be "possible to reasonably predict clinical benefit". They argue that the use of pathologic responses in neoadjuvant settings meets this definition based on three findings: 1) pathological responses are strongly correlated with OS; 2) pathological response reflects neoadjuvant chemotherapy; and 3) the degree of pathological response correlates with the degree of OS benefit.
대리 평가변수로 병리학적 반응을 사용하는 것은 전례가 없는 것은 아니다. 유방암에 대한 시험은 신보조 치료의 효능을 평가하기 위해 병리학적 완전 반응(pCR)을 사용했다. 그러나, 신보조 NSCLC 연구에서 pCR 비율은 다양했다. 또한, NSCLC에서 보고된 상대적으로 낮은 pCR 비율은 임상적으로 유의한 전체생존(OS) 이점으로 해석되지 않을 수 있으며, 따라서 NSCLC 시험에서 대리 생존 평가변수으로서 pCR의 유용성을 제한한다. 사실, 낮은 pCR 비율(중간 비율 4%) 때문에 NSCLC에서 pCR에 대한 필연적인 생존 데이터를 보고한 시험은 거의 없다(Hellmann et al., Lancet Oncol, 15: e42-50, 2014).The use of pathological response as a surrogate endpoint is not without precedent. The trial for breast cancer used pathological complete response (pCR) to evaluate the efficacy of neoadjuvant treatment. However, pCR ratios varied in neoadjuvant NSCLC studies. In addition, the relatively low pCR rates reported in NSCLC may not be interpreted as clinically significant overall survival (OS) benefits, thus limiting the utility of pCR as a surrogate survival endpoint in NSCLC trials. In fact, few trials have reported compelling survival data for pCR in NSCLC because of the low pCR rate (median rate 4%) (Hellmann et al., Lancet Oncol, 15: e42-50, 2014).
pCR 대신, Hellman et al. 은 신보조 화학요법 치료를 받는 절제 가능한 NSCLC 환자의 생존 대리용으로 10%의 잔여 생존 종양 조직으로 정의되는 MPR의 사용을 제안했다(Hellmann et al., Lancet Oncol, 15: e42-50, 2014). 이는 NSCLC에서 pCR의 희소성을 인정하면서 시험자들이 대리 생존 평가변수으로서 잔여 생존 종양을 포함하여 병리학적 반응의 다른 정의를 고려한 연구를 기반으로 한다. Junker et al. (J Cancer Res Clin Oncol, 123: 469-477,1997)은 순차적인 신보조 항암화학요법, 화학방사선요법 및 외과적 절제술을 받은 IIIA기 및 IIIB기 환자의 종양 40개에 대한 병리학적 분석을 수행했다. 이 그룹에서 잔존 종양이 ≤10%인 환자의 생존 기간 중간값은 36개월인 반면, 생존 가능한 종양 조직이 >10%인 환자의 생존 기간 중간값은 14개월이었다.Instead of pCR, Hellman et al. proposed the use of MPR, defined as 10% residual viable tumor tissue, as a surrogate for survival in patients with resectable NSCLC receiving neoadjuvant chemotherapy (Hellmann et al., Lancet Oncol, 15: e42-50, 2014). . It is based on a study where, while acknowledging the rarity of pCR in NSCLC, investigators considered other definitions of pathologic responses, including residual survival tumors as surrogate survival endpoints. Junker et al. ( J Cancer Res Clin Oncol, 123: 469-477,1997) performed a pathological analysis of 40 tumors from stage IIIA and IIIB patients who underwent sequential neoadjuvant chemotherapy, chemoradiation, and surgical resection. did. In this group, patients with ≤10% residual tumors had a median survival of 36 months, while those with viable tumor tissue >10% had a median survival of 14 months.
2건의 전향적 시험에서, NSCLC에서 신보조 화학요법의 MPR 비율은 약 22%라고 보고되었다. 첫 번째 연구에서는, 신보조 화학요법(시스플라틴 + 도세탁셀)을 받은 IIIA기 질환 환자 90명 중 병리학적 반응 중간값(종양 괴사와 섬유증의 양)이 60%였으며, 병리학적 반응이 ≤60%인 환자의 22개월과 비교할 때 전체 생존 기간(OS) 중간값은 61개월이었다(Betticher et al., Br J Cancer, 94(8): 1099-1106, 2006). 또 다른 연구에서는 베바시주맙과 병용하여 신보조 화학요법(시스플라틴 + 도세탁셀)을 받은 50명의 환자 중 MPR을 받은 환자가 MPR을 달성하지 못한 환자(각각 61개월 대 22개월)에 비해 3년 생존율이 유의하게 더 긴 것으로 나타났다(Chaft et al., J Thorac Oncol, 8: 1084-1090, 2013). William과 동료들의 MD Anderson Cancer Center의 후향적 연구(William et al., J Thorac Oncol, 8: 222-228, 2013)는 신보조 백금계 화학요법을 받은 160명의 환자에서 MPR이 고형 종양의 임상 반응 평가 기준(RECIST) 반응보다 OS의 더 강력한 예측인자임을 보여주었다.In two prospective trials, the MPR rate of neoadjuvant chemotherapy in NSCLC was reported to be approximately 22%. In the first study, among 90 patients with stage IIIA disease who received neoadjuvant chemotherapy (cisplatin + docetaxel), the median pathological response (amount of tumor necrosis and fibrosis) was 60% and the pathological response was ≤60%. The median overall survival (OS) was 61 months when compared to 22 months in Betticher et al., Br J Cancer, 94(8): 1099-1106, 2006). In another study, among 50 patients who received neoadjuvant chemotherapy (cisplatin + docetaxel) in combination with bevacizumab, those who received MPR had a 3-year survival rate compared to those who did not achieve MPR (61 months versus 22 months, respectively). significantly longer (Chaft et al., J Thorac Oncol , 8: 1084-1090, 2013). A retrospective study of William and colleagues at the MD Anderson Cancer Center (William et al., J Thorac Oncol, 8: 222-228, 2013) found that MPR was the clinical response of solid tumors in 160 patients receiving neoadjuvant platinum-based chemotherapy. It has been shown to be a stronger predictor of OS than RECIST response.
시험의뢰자는 OS의 개선 정도와의 상관관계에 근거하여 MPR을 대리 평가변수로 사용하는 데 상당한 근거가 있다고 믿는다. 현재, 1차 또는 2차 목표로서 MPR을 평가하는 화학요법 + PD-L1/PD-1 억제제 대 화학요법 단독에 대한 글로벌 III상 신보조 등록 시험이 진행 중이다. MPR을 대리 평가변수로 사용하면 임상 연구의 효과를 높이고 NSCLC 환자를 위한 새로운 치료법을 가속화할 수 있다.The sponsor believes that there is considerable evidence to use MPR as a surrogate endpoint based on its correlation with the degree of improvement in OS. A global phase III neoadjuvant enrollment trial of chemotherapy plus PD-L1/PD-1 inhibitors versus chemotherapy alone evaluating MPR as a primary or secondary goal is currently underway. The use of MPR as a surrogate endpoint could increase the effectiveness of clinical studies and accelerate new therapies for patients with NSCLC.
실시예 10. GO42501 연구를 위한 재료 및 방법Example 10. Materials and Methods for Studying GO42501
II기, IIIA기 또는 일부 IIIB기(T3N2만 해당)의 약 82명의 환자가 GO42501 연구에 등록되었다.Approximately 82 patients with stage II, IIIA, or some stage IIIB (T3N2 only) were enrolled in study GO42501.
A.A. 선정 기준Selection Criteria
환자는 연구 참가 자격을 얻기 위해 아래 나열된 선정 기준을 충족해야 한다.Patients must meet the selection criteria listed below to be eligible for study participation.
![]()
![]()
![]()
![]()
![]()
![]()
- T4 원발성 비소세포폐암 환자는 크기(종양 >7cm) 기준으로만 자격이 있다. 횡격막, 종격동, 심장, 대혈관, 기관, 재발성 후두신경, 식도, 척추체, 융기부 및 다른 동측엽의 개별 종양 결절이 침범된 환자는 자격이 없다.- Patients with T4 primary non-small cell lung cancer are eligible only on the basis of size (tumor >7 cm). Patients with involvement of the diaphragm, mediastinum, heart, great blood vessels, trachea, recurrent laryngeal nerve, esophagus, vertebral body, ridge, and other individual tumor nodules of the ipsilateral lobe are not eligible.
- 혼합 조직학(편평 및 비편평)의 NSCLC 환자에게 자격이 주어지며 주요 조직학적 구성요소(비편평 또는 편평)를 기준으로 분류되어야 한다.- NSCLC patients with mixed histology (squamous and nonsquamous) are eligible and must be classified based on their major histologic component (nonsquamous or squamous).
환자는 임상 단계에 따라 선별될 수 있지만, PET 양성 N2 결절의 경우 침습성 종격동 병기(예: CT 유도 생검, 기관지 초음파, 종격경 검사)에 의한 N2 결절 침범에 대한 필수 수술 전 문서화가 필요한다. 레벨 5 및 레벨 6 노드의 수술 전 병기는 선택 사항이다.Patients can be screened according to clinical stage, but for PET-positive N2 nodules, mandatory preoperative documentation of N2 nodule involvement by invasive mediastinal stage (e.g. CT-guided biopsy, bronchial ultrasound, mediastinoscopy) is required. Preoperative staging of level 5 and level 6 nodes is optional.
연마 유리 불투명도(GGO)가 나타나지 않고, CT 스캔에서 NSCLC의 고형 또는 아고형. 아고형 병변의 경우, 종양 크기(즉, 임상 T 병기)는 GGO 성분을 제외하고 고형 성분만을 기준으로 측정해야 한다. No abrasive glass opacity (GGO) is shown, solid or subsolid of NSCLC on CT scan. For subsolid lesions, tumor size (i.e., clinical stage T) should be determined based on the solid component only, excluding the GGO component.
![]()
![]()
![]()
![]()
- 수술 후(ppo) 예상되는 1초 동안의 강제 호기량(FEV1) 및 일산화탄소(DLCO)에 대한 폐의 ppo 확산 용량 ≥40%.≥40% of the lung's ppo diffusion capacity relative to the expected postoperative (ppo) forced expiratory volume (FEV1) and carbon monoxide (DLCO) for 1 second.
- 최대 산소 소비량(VO2max) ≥15 mL/kg/min.- Maximum oxygen consumption (VO 2 max) ≥15 mL/kg/min.
o ppoFEV1 또는 ppoDLCO 중 하나가 <40%이거나 폐절제술을 계획하는 경우, 심폐 운동 검사 수행, VO2max ≥15 mL/kg/min.o If either ppoFEV 1 or ppoDL CO is <40% or if pneumonectomy is planned, perform cardiopulmonary exercise test, VO 2 max ≥15 mL/kg/min.
o 계획된 절제 6개월 이전에 PFTs를 수행했거나 이전에 수행한 적이 없는 경우, 선별 치료 기간 동안 PFTs 수행.o PFTs performed during the screening treatment period if PFTs were or have not been performed before 6 months of planned resection.
백금계 화학요법을 받을 자격. 환자에 대해 의도된 요법에서 각 개별 화학요법 치료(즉, 카보플라틴, 시스플라틴, 페메트렉시드, 파클리탁셀 또는 젬시타빈)의 처방 정보에 있는 경고 및 주의 섹션은 적격성을 결정하는 데 사용된다.Eligibility for platinum-based chemotherapy. The Warnings and Cautions section in the prescribing information for each individual chemotherapy treatment (ie, carboplatin, cisplatin, pemetrexed, paclitaxel, or gemcitabine) in the regimen intended for the patient is used to determine eligibility.
o RECIST v1.1에 따라 시험자가 평가한 측정 가능한 질병.o Measurable disease assessed by the investigator per RECIST v1.1.
o 중앙 테스트를 통한 PD-L1 상태 및 기타 탐색적 바이오마커의 결정에 적합한 대표적인 종양 표본의 가용성.o Availability of representative tumor specimens suitable for determination of PD-L1 status and other exploratory biomarkers via central testing.
o 동부 종양학 협력 그룹 (ECOG) 수행 상태 0 또는 1o Eastern Oncology Collaborating Group (ECOG) Performance Status 0 or 1
o 폐암 사망 위험을 제외한 정상 기대 수명.o Normal life expectancy, excluding the risk of lung cancer death.
o 연구 치료 시작 전 14일 이내에 수득한, 다음과 같은 실험실 결과로 정의되는 적절한 혈액 및 말단 장기 기능:o Adequate blood and terminal organ function, as defined by the following laboratory results, obtained within 14 days prior to initiation of study treatment:
- 절대 호중구 수(ANC) ≥ 1.5 x 109/L(1500/μL), 과립구 집락 자극 인자 0지원 없음.- Absolute neutrophil count (ANC) ≥ 1.5 x 10 9 /L (1500/μL), no granulocyte colony stimulating factor 0 support.
- 림프구 수 ≥0.5 x 109/L(500/μL).- Lymphocyte count ≥0.5 x 10 9 /L (500/μL).
- 수혈 없이 혈소판 수 ≥100 x 109/L(100,000/μL).- Platelet count ≥100 x 10 9 /L (100,000/μL) without transfusion.
- 헤모글로빈 ≥90 g/L (9 g/dL). 환자들은 상기 기준을 충족하기 위해 수혈이 허용되었다.- Hemoglobin ≥90 g/L (9 g/dL). Patients were accepted for transfusions to meet the above criteria.
- 아스파르테이트 트랜스아미나제(AST), 알라닌 트랜스아미나제(ALT) 및 알칼리 포스파타제(ALP) ≤2.5 x 정상 상한(ULN).-aspartate transaminase (AST), alanine transaminase (ALT) and alkaline phosphatase (ALP) ≤2.5 x upper limit of normal (ULN).
총 빌리루빈 ≤ 1.5 x ULN, 다음은 예외: 공지의 길버트병 환자: 총 빌리루빈 ≤3 x ULN.Total bilirubin ≤ 1.5 x ULN, with the following exceptions: Patients with known Gilbert's disease: Total bilirubin ≤3 x ULN.
- 크레아티닌 청소율 45 mL/min(Cockcroft-Gault 공식을 사용하여 계산됨). 시스플라틴을 투여받는 환자: 크레아티닌 청소율 ≥60mL/min.- Creatinine clearance 45 mL/min (calculated using the Cockcroft-Gault formula). Patients receiving cisplatin: creatinine clearance ≥60 mL/min.
![]()
![]()
- 치료적 항응고제를 투여받지 않는 환자의 경우: INR 또는 aPTT ≤1.5 x ULN- For patients not receiving therapeutic anticoagulants: INR or aPTT ≤1.5 x ULN
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- 총 B형 간염 코어 항체 (HBcAb) 음성- Total hepatitis B core antibody (HBcAb) negative
- 총 HBcAb 검사 양성 후 정량적 B형 간염 바이러스(HBV) DNA <500 IU/mL. HBV DNA 검사는 HBsAg 검사 음성, HBsAb 검사 음성, 총 HBcAb 검사 양성인 환자에게만 시행된다.- Quantitative hepatitis B virus (HBV) DNA <500 IU/mL after positive total HBcAb test. The HBV DNA test is only performed on patients who have a negative HBsAg test, a negative HBsAb test, and a positive total HBcAb test.
![]()
![]()
가임 여성의 경우: 금욕 유지 (이성간 성교 금지) 또는 피임 방법 사용에 대한 동의 및 난자 기증 자제에 대한 동의.For women of childbearing potential: Consent to maintain abstinence (no intercourse) or to use contraceptive methods and to refrain from egg donation.
![]()
![]()
B.B. 배제 기준 Exclusion Criteria
하기 기준 중 어느 것에 부합하는 환자는 연구 엔트리로부터 배제된다.Patients meeting any of the following criteria are excluded from study entry.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
습진, 건선, 만성 단순 태선 또는 피부과적 징후만 있는 백반증이 있는 환자(예: 건선성 관절염 환자는 제외)는 다음 조건이 모두 충족되는 경우 연구에 적합하다:Patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with dermatological signs only (e.g., excluding patients with psoriatic arthritis) are eligible for study if all of the following conditions are met:
- 발진은 체표면적의 <10%를 차지해야 한다.- The rash should occupy <10% of the body surface area.
질병은 기준선에서 잘 제어되며, 낮은 역가의 국소 코르티코스테로이드만 필요하다.Disease is well controlled at baseline and only low titer topical corticosteroids are required.
- 지난 12개월 이내에 소랄렌과 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제 또는 고효능 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았다.- No acute exacerbation of an underlying condition requiring psoralen plus ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids within the past 12 months.
![]()
![]()
![]()
![]()
![]()
![]()
연구 치료 시작 전 4주 이내의 주요 수술 절차, 또는 연구 과정 중 주요 수술 절차의 필요성이 예상되는 경우.A major surgical procedure within 4 weeks prior to initiation of study treatment, or if a major surgical procedure is expected during the course of the study.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
선별 치료 시 양성 엡스타인-바 바이러스(EBV) 바이럴 캡시드 항원 면역글로불린 M(IgM) 테스트. 급성 감염 또는 의심되는 만성 활동성 감염을 선별하기 위해 임상적으로 지시된 대로 EBV PCR 검사를 수행해야 한다. EBV PCR 검사가 양성인 환자는 제외된다.Positive Epstein-Barr Virus (EBV) Viral Capsid Antigen Immunoglobulin M (IgM) Test in Selective Treatment. EBV PCR testing should be performed as clinically indicated to screen for acute infection or suspected chronic active infection. Patients with a positive EBV PCR test are excluded.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- 급성, 저용량 전신 면역억제제 또는 1회 펄스 용량의 전신 면역억제제(예: 조영제 알레르기를 위한 코르티코스테로이드 48시간)를 받은 환자는 연구에 적합하다.- Patients receiving acute, low-dose systemic immunosuppressants or single pulse doses of systemic immunosuppressants (eg, corticosteroids for contrast allergy 48 hours) are eligible for study.
- 무기질 코르티코이드(예: 플루드로코르티손), 만성 폐쇄성 폐질환(COPD) 또는 천식에 대한 코르티코스테로이드, 기립성 저혈압 또는 부신 기능 부전에 대한 저용량 코르티코이드를 투여받은 환자는 연구에 적합하다.- Patients receiving mineralocorticoids (eg fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose corticoids for orthostatic hypotension or adrenal insufficiency are eligible for study.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
가임 여성은 연구 치료 시작 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
C.C. 치료 배정treatment assignment
본 연구는 공개 연구이다. This study is a public study.
PD-L1 발현이 높은 환자(TPS 50%, 중앙 실험실에서 SP263 IHC에 의해 결정됨)는 코호트 A(PD-L1 높음)에 등록되는 반면 모든 신규 진입자(PD-L1 발현 수준에 관계 없음)는 코호트B(PD-L1 모든 진입자)에 등록된다. 등록은 다음과 같이 단계적으로 완료되며(도 20 참조), 각 코호트에 약 41명의 환자가 등록되었다. 등록은 다음과 같이 단계적으로 완료되며(도 20 참조), 각 코호트에 약 41명의 환자가 등록되었다.Patients with high PD-L1 expression (TPS 50%, determined by SP263 IHC in the central laboratory) were enrolled in Cohort A (PD-L1 high), while all new entrants (regardless of PD-L1 expression level) were enrolled in Cohort B (PD-L1 all entrants) is registered. Enrollment is completed in phases as follows (see Figure 20), with approximately 41 patients enrolled in each cohort. Enrollment is completed in phases as follows (see Figure 20), with approximately 41 patients enrolled in each cohort.
1. 처음에는 안전성 도입이 있다:One. First there is a safety introduction:
- 선별치료 시 PD-L1 TPS가 ≥50%인 종양이 있는 6명의 환자가 코호트 A(PD-L1 높은 코호트)에 등록된다.- Six patients with tumors with a PD-L1 TPS ≥50% on screening are enrolled in cohort A (PD-L1 high cohort).
- 코호트 B(PD-L1 모든 진입자 코호트)는 PD-L1 TPS가 <50%인 종양 환자 6명의 등록으로 시작된다.- Cohort B (PD-L1 all entrant cohort) begins with enrollment of 6 tumor patients with PD-L1 TPS <50%.
2. 각 코호트의 안전성을 평가하고, 안전하다고 판단되는 경우:2. Assess the safety of each cohort, and if deemed safe:
2. 각 코호트의 안전성을 평가하고, 안전하다고 판단되는 경우:2. Assess the safety of each cohort, and if deemed safe:
- PD-L1 TPS가 ≥50%인 종양이 있는 환자를 포함하여 PD-L1 TPS가 <50%인 종양이 있는 8명의 환자가 해당 코호트에 등록될 때까지 환자는 코호트 B(PD-L1 모든 진입자)에만 등록된다.- Patients are enrolled in cohort B (PD-L1 all entrants) until 8 patients with tumors with PD-L1 TPS <50%, including those with tumors with PD-L1 TPS ≥50%, are enrolled in that cohort. ) is registered only.
- 나머지 코호트 B 환자는 PD-L1 TPS가 <50%인 종양 환자로 구성된다.- The remaining cohort B patients consist of tumor patients with PD-L1 TPS <50%.
3. 3. PD-L1 TPS가 ≥50%인 종양이 있는 총 8명의 환자가 코호트 B(PD-L1 모든 진입자)에 등록된 후, 코호트 A(PD-L1 높음)에 대한 등록이 재개되고, PD-L1 TPS ≥50%을 가진 종양이 있는 모든 후속 환자가 해당 코호트에 등록된다.3. 3. After a total of 8 patients with tumors with PD-L1 TPS ≥50% were enrolled in Cohort B (PD-L1 all entrants), then enrollment into Cohort A (PD-L1 High) resumed; All subsequent patients with tumors with PD-L1 TPS ≥50% are enrolled in this cohort.
D.D. 연구 치료 용량, 투여 및 준수Study Treatment Dosage, Administration and Compliance
각 연구 치료제 성분은 표 57에 명시된 용량 및 빈도로 투여된다.Each study treatment component is administered at the dose and frequency specified in Table 57.

AUC = 농도-시간 곡선 아래 영역; IV = 정맥 주사.AUC = area under the concentration-time curve; IV = intravenous.
a. 카보플라틴은 페메트렉시드 또는 젬시타빈 투여 후 초기 목표 AUC 5 mg/mL/분으로 투여해야 하며, 파클리탁셀 투여 후 투여 시 초기 목표 AUC 6 mg/mL/분으로 투여해야 한다. a. Carboplatin should be administered at an initial target AUC of 5 mg/mL/min after administration of pemetrexed or gemcitabine, and should be administered at an initial target AUC of 6 mg/mL/min after administration of paclitaxel.
b. 젬시타빈은 카보플라틴 투여 전 1000 mg/m2, 시스플라틴 투여 전 1250 mg/m2로 투여해야 한다. b. Gemcitabine should be administered at 1000 mg/m 2 before carboplatin and 1250 mg/m 2 before cisplatin.
c. 파클리탁셀은 아시아인 인종/민족 환자의 경우 175 mg/m2, 비아시아인 인종/민족 환자의 경우 200 mg/m2로 투여해야 한다. c. Paclitaxel should be administered at 175 mg/m 2 in patients of Asian race/ethnicity and 200 mg/m 2 in patients of non-Asian race/ethnicity.
신보조제 치료 단계는 아테조 + 티라 또는 아테조 + 티라 + 화학의 4주기로 구성된다. 각 주기의 기간은 21일이다. 각 주기의 제 1일차에 모든 적격 환자에게 하기의 순서로 연구 약물을 주입하였다.The neoadjuvant treatment phase consists of 4 cycles of atezo + tyra or atezo + tyra + chemistry. The duration of each cycle is 21 days. On Day 1 of each cycle, all eligible patients were infused with study drug in the following order.
코호트 A(PD-L1 높음): (1) 아테졸리주맙, (2) 티라골루맙. Cohort A (PD-L1 high): (1) atezolizumab, (2) tiragolumab.
코호트 B(PD-L1 모든 진입자): 시험자는 조직학 하위유형 및 국소 SOC에 기초하여 나열된 요법 중 하나를 투여한다. Cohort B (PD-L1 all entrants): Investigators will receive one of the listed regimens based on histological subtype and local SOC.
- (1) 아테졸리주맙, (2) 티라골루맙, (3) 파클리탁셀, (4)카보플라틴- (1) atezolizumab, (2) tiragolumab, (3) paclitaxel, (4) carboplatin
- (1) 아테졸리주맙, (2) 티라골루맙, (3)페메트렉시드, (4)(카보플라틴 또는 시스플라틴)- (1) atezolizumab, (2) tiragolumab, (3) pemetrexed, (4) (carboplatin or cisplatin)
- (1) 아테졸리주맙, (2) 티라골루맙, (3) 젬시타빈, (4) (카보플라틴 또는 시스플라틴)- (1) atezolizumab, (2) tiragolumab, (3) gemcitabine, (4) (carboplatin or cisplatin)
아테졸리주맙(1200 mg)과 티라골루맙(600 mg)은 고정 용량으로 투여된다. 환자들은 가능한 경우 등록일에 연구 치료의 첫 용량을 투여 받았다. 등록 당일 치료가 불가능한 경우, 등록 후 5일 이내에 첫 번째 접종이 이루어진다.Atezolizumab (1200 mg) and tiragolumab (600 mg) are administered as fixed doses. Patients received their first dose of study treatment on the day of enrollment, if available. If treatment is not possible on the day of registration, the first dose is administered within 5 days of registration.
주기 1의 경우, 아테졸리주맙 및 티라골루맙의 1차 예방(항히스타민제, 해열제 및/또는 진통제)을 위한 예비투약은 허용되지 않는다. 환자는 지역 SOC 및 제조업체의 지침에 따라 선택된 화학치료 백본 요법에 대해 항구토제 및 IV 수화를 받아야 한다. 그러나, 코르티코스테로이드의 면역조절 효과 때문에 코르티코스테로이드의 사전투약은 임상적으로 가능한 범위 내에서 최소화해야 한다. For Cycle 1, premedication for primary prophylaxis (antihistamines, antipyretics and/or analgesics) of atezolizumab and tiragolumab is not permitted. Patients should receive antiemetics and IV hydration for the chemotherapeutic backbone regimen selected according to local SOC and manufacturer's guidelines. However, due to the immunomodulatory effect of corticosteroids, pre-administration of corticosteroids should be minimized to the extent clinically feasible.
아테조 + 티라의 보조 치료는 수술 후 14~60일 이내에 또는 마지막 PORT 치료 후 7~42일 이내에 시작된다. 보조 화학요법을 시행해야 하는 경우, 수술 후 28-72일 이내에 치료를 시작한 다음 보조 화학요법 후 21-60일 이내에 PORT(선택한 경우)를 시작한다. 수술 후 보조제 치료 동안, 주입은 다음 순서로 투여된다(환자당 하나의 요법). 코호트 A(PD-L1 높음) 요법의 선택은 각 환자에 대한 시험자의 재량에 따른다.Adjuvant treatment with Artezo + Tyra is started within 14 to 60 days after surgery or 7 to 42 days after the last PORT treatment. If adjuvant chemotherapy is required, start treatment within 28-72 days of surgery and then PORT (if selected) within 21-60 days of adjuvant chemotherapy. During postoperative adjuvant treatment, infusions are administered in the following order (one regimen per patient). The choice of cohort A (PD-L1 high) regimen is at the discretion of the investigator for each patient.
코호트 A(PD-L1 높음): 시험자는 아래 나열된 요법 중 하나를 투여한다. Cohort A (PD-L1 high): Investigators will receive one of the regimens listed below.
- (1) 아테졸리주맙, (2) 티라골루맙- (1) atezolizumab, (2) tiragolumab
- (1) 파클리탁셀, (2) 카보플라틴- (1) paclitaxel, (2) carboplatin
- (1) 페메트렉시드, (2) (카보플라틴 또는 시스플라틴)- (1) pemetrexed, (2) (carboplatin or cisplatin)
- (1) 젬시타빈, (2) (카보플라틴 또는 시스플라틴)- (1) gemcitabine, (2) (carboplatin or cisplatin)
코호트 B(PD-L1 모든 진입자): (1) 아테졸리주맙, (2) 티라골루맙 Cohort B (PD-L1 all entrants): (1) atezolizumab, (2) tiragolumab
아테졸리주맙 및 티라골루맙Atezolizumab and Tiragolumab
아테졸리주맙은 각 21일 주기의 제 1일째에 1200 mg의 고정 용량으로 IV 주입으로 투여된다. 아테졸리주맙 용량은 고정이며 체중에 따라 달라지지 않는다. 용량 감소는 허용되지 않는다.Atezolizumab is administered as an IV infusion at a fixed dose of 1200 mg on Day 1 of each 21-day cycle. Atezolizumab dose is fixed and does not vary with body weight. No dose reduction is permitted.
아테졸리주맙 투여 및 관찰 기간 이후, 환자는 각 21일 주기의 제 1일차에 IV 주입으로 투여되는 600 mg의 티라골루맙을 받는다. 티라골루맙 용량은 고정이며 체중에 따라 달라지지 않는다. 용량 감소는 허용되지 않는다.Following the atezolizumab administration and observation period, patients receive 600 mg of tyragolumab administered as an IV infusion on Day 1 of each 21-day cycle. The tiragolumab dose is fixed and does not vary with body weight. No dose reduction is permitted.
연구 치료제의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 수행된다. 아테졸리주맙 및 티라골루맙 주입은 Administration of study therapeutics is performed in a monitoring environment with immediate access to trained staff and appropriate equipment and medications to manage potentially severe reactions. Atezolizumab and tiragolumab injections
표 58에 요약된 지침에 따라 투여된다.Administer according to the guidelines summarized in Table 58.




IRR= 주입 관련 반응IRR = infusion-related reactions
아테졸리주맙 및 티라골루맙 투약 지연Delayed dosing of atezolizumab and tiragolumab
아테졸리주맙이나 티라골루맙이 영구적으로 중단되지 않는 한 다음 규칙이 적용된다:The following rules apply unless atezolizumab or tiragolumab is permanently discontinued:
![]()
![]()
![]()
![]()
화학요법chemotherapy
기관은 아래 정보와 현지 처방 정보를 준수해야 한다. 일반적으로, 기관은 또한 환자 체중 변화의 경우에 용량 조정을 결정하기 위해 기관 및 지역 SOC를 따라야 한다. 화학요법의 구성 요소 중 하나에서 발생하는 독성으로 인해 치료 주기가 지연되거나 중단된 경우, 두 화학요법 구성 요소를 모두 유지해야 하며, 재개되는 경우 동기화 상태를 유지하기 위해 둘 다 재개해야 한다.Agencies must adhere to the information below and local prescribing information. In general, institutions should also follow institutional and regional SOCs to determine dose adjustments in case of changes in patient weight. If a treatment cycle is delayed or interrupted due to toxicity arising from one of the components of the chemotherapy, both components of the chemotherapy should be maintained and, if resumed, both should be resumed to maintain synchronization.
파클리탁셀paclitaxel
아시아인 인종/민족의 환자는 3시간에 걸쳐 175 mg/m2 IV의 더 낮은 시작 용량의 파클리탁셀을 받는다. 독립적인 데이터 모니터링 위원회의 IMpower150 및 IMpower131 연구의 안전성 검토에서 관찰된 바에 따르면, 아시아인 인종/민족 환자에 대한 더 낮은 시작 용량의 파클리탁셀은, 비아시아 국가 환자에 비해 아시아 국가 환자의 전반적인 혈액 독성 발생률이 더 높다는 것에 기반한다. "아시아인 인종/민족"이라는 용어는 동아시아, 동남아시아 또는 남아시아에 거주하거나 조상 기원을 가진 다양한 인구를 포함하는 범민족/인종 그룹을 나타낸다. 특정 환자에 대한 이 용어의 적용은 치료하는 시험자의 재량이며, 환자의 임상적 특성과 출신 국가를 기반으로 해야 한다.Patients of Asian ethnicity/ethnicity receive a lower starting dose of paclitaxel at 175 mg/m 2 IV over 3 hours. An independent data monitoring committee's safety review of the IMpower150 and IMpower131 studies observed that lower starting doses of paclitaxel in patients of Asian ethnicity/ethnicity reduced the overall incidence of hematological toxicity in patients from Asian countries compared to patients from non-Asian countries. based on higher The term "Asian race/ethnicity" refers to a pan-ethnic/ethnic group comprising a diverse population of ancestral origin or residing in East Asia, Southeast Asia or South Asia. The application of this term to a particular patient is at the discretion of the treating investigator and should be based on the patient's clinical characteristics and country of origin.
파클리탁셀 주사제는 주입 전에 희석해야 한다. 파클리탁셀은, 0.9% 염화나트륨 USP; 5% 포도당 주사제, USP; 5% 포도당 및 0.9% 염화나트륨 주사제, USP; 또는 링거 주사제 내의 5% 포도당에 희석하여 최종 농도 0.3 ~ 1.2 mg/mL로 만들어야한다. 약물 투여 중 침윤 가능성에 대해 주입 부위를 면밀히 모니터링해야 한다.Paclitaxel injections should be diluted prior to infusion. Paclitaxel, 0.9% sodium chloride USP; 5% Glucose Injection, USP; 5% Glucose and 0.9% Sodium Chloride Injection, USP; Alternatively, it should be diluted in 5% glucose in Ringer's injection to a final concentration of 0.3 to 1.2 mg/mL. The injection site should be closely monitored for possible infiltration during drug administration.
희석하지 않은 농축액을 가소화된 폴리염화비닐(PVC) 장비 또는 주입용 용액을 준비하는 데 사용하는 장치와 접촉하는 것은 권장하지 않는다. 파클리탁셀은 0.22 m 이하의 미세다공성 멤브레인을 갖는 인라인 필터를 통해 투여해야 한다. 짧은 입구 및 출구 PVC 튜빙을 통합한 IVEX-2® 필터와 같은 필터 장치의 사용은 비스(2-에틸헥실)프탈레이트의 상당한 침출을 초래하지 않았다.Contact of undiluted concentrates with plasticized polyvinyl chloride (PVC) equipment or devices used to prepare solutions for injection is not recommended. Paclitaxel should be administered through an in-line filter with a microporous membrane of 0.22 m or less. The use of filter devices such as IVEX-2® filters incorporating short inlet and outlet PVC tubing did not result in significant leaching of bis(2-ethylhexyl)phthalate.
기관은 환자 체중 변화 시 파클리탁셀 용량 조정을 결정하기 위해 기관의 SOC 지침을 따라야 한다. 파클리탁셀 주입의 경우, 파클리탁셀을 더 빨리(90분 이상) 주입하거나, 더 느리게(첫 주입의 경우 최대 4시간) 주입하는 제도적 정책이 있는 기관의 경우 3시간의 주입 시간에 대한 예외가 허용된다.Institutions should follow their SOC guidelines to determine paclitaxel dose adjustments for changes in patient body weight. For paclitaxel infusions, an exception to the 3 hour infusion time is permitted for institutions with institutional policies to inject paclitaxel either faster (>90 minutes) or slower (up to 4 hours for the first infusion).
페메트렉시드Pemetrexed
기관은 페메트렉시드에 대한 표준 투여 절차를 따라야 한다. 페메트렉시드의 투여는 최소 10분에 걸쳐 IV 주입으로 투여해야 한다. 투여되는 사전 투약 용량은 처방 정보에 따라야 한다. 페메트렉시드 요법을 받을 자격이 있는 모든 환자는 페메트렉시드 투여 전 적어도 5일, 투여 당일 및 투여 후 최소 2일 동안 약물 제거 반감기가 긴 비스테로이드성 항염증제 복용을 피해야 한다.Institutions should follow standard dosing procedures for pemetrexed. Pemetrexed should be administered as an IV infusion over at least 10 minutes. Pre-dosage doses administered should be in accordance with the prescribing information. All patients eligible for pemetrexed therapy should avoid taking nonsteroidal anti-inflammatory drugs with long drug elimination half-lives for at least 5 days before, on the same day, and for at least 2 days after administration of pemetrexed.
젬시타빈Gemcitabine
젬시타빈은 카보플라틴 또는 시스플라틴 투여 30분 전에 IV 주입으로 투여해야 한다. 젬시타빈의 용량은 카보플라틴 전에 투여했을 때와 시스플라틴 전에 투여했을 때가 다르다는 것에 유의해야 한다(표 57). 젬시타빈은 주입 전에 희석해야 한다. 젬시타빈의Gemcitabine should be administered as an IV infusion 30 minutes prior to administration of carboplatin or cisplatin. It should be noted that the dose of gemcitabine was different when administered before carboplatin and before cisplatin (Table 57). Gemcitabine should be diluted prior to infusion. of gemcitabine
재구성에 권장되는 희석제는 방부제가 없는 0.9% 염화나트륨 주사제, USP이다. 젬시타빈의 투여는 현지 관행 및 처방 정보에 따라 수행되어야 한다.The recommended diluent for reconstitution is Preservative-Free 0.9% Sodium Chloride Injection, USP. Administration of gemcitabine should be done in accordance with local practice and prescribing information.
카보플라틴carboplatin
카보플라틴은 파클리탁셀 또는 페메트렉시드 투여 완료 직후 15-30분에 걸쳐 IV 주입으로 투여하여 농도-시간 곡선(AUC)에서 6 mg/mL/min(칼버트 공식 용량)의 초기 목표 면적을 달성해야 하며, 지역 진료 지침에 따라 표준 구토 방지제를 사용한다.Carboplatin should be administered as an IV infusion over 15-30 minutes immediately after completion of dosing with paclitaxel or pemetrexed to achieve an initial target area of 6 mg/mL/min (Calbert's official dose) on the concentration-time curve (AUC). and use standard antiemetics according to local practice guidelines.
AUC 6 mg/mL/min의 카보플라틴 용량은 칼버트 공식을 사용하여 계산된다The carboplatin dose of AUC 6 mg/mL/min is calculated using the Calvert formula
(Calvert et al., J Clin Oncol, 7: 1748-1756, 1989):(Calvert et al., J Clin Oncol , 7: 1748-1756, 1989):
총 용량(mg) = (목표 AUC) (사구체 여과율[GFR]+25)Total dose (mg) = (target AUC) (glomerular filtration rate [GFR]+25)
AUC 기반 투여량을 계산하기 위해 칼버트 공식에 사용된 GFR은 The GFR used in the Calvert formula to calculate the AUC-based dose is
125 mL/min을 초과하지 않아야 한다. 본 연구의 목적상 상기 GFR은 크레아티닌 청소율(CrCl)과 동등한 것으로 간주되었다. CrCl은 기관 지침에 따라 또는 It should not exceed 125 mL/min. For the purposes of this study, the GFR was considered equivalent to creatinine clearance (CrCl). CrCl according to institutional guidelines or
Cockcroft and Gault (Nephron, 16: 다음 공식을 사용한 콕크로프트와 골트(Nephron, 16: 31-41, (1976))의 방법을 사용하여 계산한다.It is calculated using the method of Cockcroft and Gault ( Nephron , 16: Nephron, 16: 31-41, (1976)) using the following formula.
CrCl = ((140 - 나이) (wt) / (72 x Scr)) 0.85, 여성의 경우CrCl = ((140 - age) (wt) / (72 x Scr)) 0.85 for women
여기서: CrCl = 크레아티닌 청소율(mL/min); 나이 = 환자의 나이(년); wt = 환자의 체중(kg);where: CrCl = creatinine clearance (mL/min); age = patient's age in years; wt = patient's weight (kg);
Scr = 혈청 크레아티닌(mg/dL)Scr = serum creatinine (mg/dL)
혈청 크레아티닌 수치가 비정상적으로 낮은 환자의 경우, 최소 크레아티닌 수치 0.8 mg/dL를 사용하여 상기 GFR을 추정하거나, 추정된 GFR을 125 mL/min으로 그 상한치를 제한하였다. 환자의 GFR이 동위원소 희석 질량 분광법에 의한 혈청 크레아티닌 측정을 기반으로 추정되는 경우, FDA는 의사가 과다 투여로 인한 잠재적 독성을 피하기 위해 원하는 노출(AUC)에 대한 카보플라틴의 용량 제한을 고려할 것을 권장한다. 카보플라틴 라벨에 기재된 칼버트 공식을 기반으로 최대 용량은 하기와 같이 계산할 수 있다:For patients with abnormally low serum creatinine levels, the GFR was estimated using a minimum creatinine level of 0.8 mg/dL, or the upper limit of the estimated GFR was limited to 125 mL/min. If a patient's GFR is estimated based on serum creatinine measurements by isotopic dilution mass spectrometry, FDA recommends that physicians consider limiting the dose of carboplatin for the desired exposure (AUC) to avoid potential toxicity from overdose. Recommended. Based on the Calvert formula listed on the carboplatin label, the maximum dose can be calculated as follows:
최대 카보플라틴 용량(mg) = 목표 AUC (mg ![]()
![]()
상기 최대 용량은 정상 신장 기능을 가진 환자에게 125 mL/분으로 그 상한치가 제한된 GFR 추정치를 기반으로 한다. 이보다 높은 GFR 추정치는 사용하지 않는다. 목표 AUC = 6의 경우, 최대 용량은 6 x (125 + 25) = 900 mg이다. 목표 AUC = 5의 경우, 최대 용량은 5x (125 + 25) = 750 mg이다. 목표 AUC = 4의 경우, 최대 용량은 4 x (125 + 25) = 600 mg이다.This maximum dose is based on an estimate of GFR with an upper limit of 125 mL/min in patients with normal renal function. GFR estimates higher than this are not used. For a target AUC = 6, the maximum dose is 6 x (125 + 25) = 900 mg. For a target AUC = 5, the maximum dose is 5x (125 + 25) = 750 mg. For a target AUC = 4, the maximum dose is 4 x (125 + 25) = 600 mg.
시스플라틴cisplatin
시스플라틴은 페메트렉시드 또는 젬시타빈 주입 완료 후 약 30분 후에 1-2시간에 걸쳐 또는 기관의 SOC에 따라 75 mg/m²의 용량으로 IV 주입으로 투여된다. 환자는 시스플라틴 투여 전후에 적절한 항구토 치료와 적절한 수분 공급을 받아야 한다.Cisplatin is administered as an IV infusion at a dose of 75 mg/m² over 1-2 hours approximately 30 minutes after completion of the pemetrexed or gemcitabine infusion or depending on the SOC of the institution. Patients should receive adequate antiemetic treatment and adequate hydration before and after cisplatin administration.
E.E. 수술적 치료 계획 surgical treatment plan
초기 단계의 절제 가능한 NSCLC 경험이 있는 담당 흉부 외과의가 선별 치료 시 환자를 평가하여 외과적 적합성과 외과적 절제에 대한 적격성을 결정한다. 환자는 선별 치료 시점에 치료 의도가 있는 R0 절제술을 받을 자격이 있어야 한다. 환자를 수술할 수 있게 하기 위해 병기하향(downstage)하려는 의도는 허용되지 않는다.A attending thoracic surgeon with experience with early-stage resectable NSCLC will evaluate the patient during screening to determine surgical suitability and eligibility for surgical resection. Patients must be eligible for an intended R0 resection at the time of screening treatment. The intent to downstage a patient to be able to operate is not permitted.
선별 치료 시 환자는 선정 기준에 설명된 대로 폐 기능 검사(PFT)를 기반으로 수술 적합성을 확인해야 한다. ppoFEV1 및 ppoDLCO는 다음 방법론을 사용하여 계산된다(Brunelli et al., Chest, 143(5 Suppl): e166S-e190S, 2013):In screening treatment, patients should confirm their suitability for surgery based on pulmonary function tests (PFT) as described in the selection criteria. ppoFEV 1 and ppoDL CO are calculated using the following methodology (Brunelli et al., Chest , 143(5 Suppl): e166S-e190S, 2013):
관류 방법(폐 환기/관류 스캔(VQ 스캔)이 수행 되는 경우:Perfusion method (if lung ventilation/perfusion scan (VQ scan) is performed:
ppoFEV1 또는 ppoDLCO = 수술 전 FEV1 또는 DLCO x (1 -x)ppoFEV 1 or ppoDL CO = preoperative FEV 1 or DL CO x (1 -x)
여기서: x 폐에 대한 총 관류의 분율where: x fraction of total perfusion for lungs
해부학적 방법:Anatomical method:
ppoFEV1 또는 ppoDLCO =수술 전 FEV1 또는 DLCOCO x (1 -(y/z))ppoFEV 1 or ppoDL CO = preoperative FEV 1 or DLCO CO x (1 -(y/z))
여기서: y = 제거할 기능적 또는 방해받지 않는 폐 분절; z = 19, 기능적 폐 세그먼트의 총 수.where: y = functional or undisturbed lung segment to be removed; z = 19, total number of functional lung segments.
기능적 폐 세그먼트(19)의 총 수는 The total number of functional lung segments 19 is
오른쪽 폐에 10개 분절(상엽에 3개, 중엽에 2개, 하엽에 5개) 및 왼쪽 폐에 9개 분절(상엽에 5개, 하엽에 4개)로 나타난다.It appears as 10 segments in the right lung (3 in the upper lobe, 2 in the middle, 5 in the lower lobe) and 9 segments in the left lung (5 in the upper lobe, 4 in the lower lobe).
환자는 신보조제 치료 완료 후 그리고 수술 전에 담당 외과의와 종양 전문의에 의해 재평가된다. 혈액 검사, 응고, 심장 검사 또는 PFTs(필요한 경우), 마취 평가 및 기타 평가 절차를 포함하되 이에 국한되지 않는 수술 전 평가는 지역 SOC에 따라 수행해야 한다.Patients are reevaluated by the attending surgeon and oncologist after completion of neoadjuvant treatment and prior to surgery. Preoperative assessments, including but not limited to blood tests, coagulation, cardiac tests or PFTs (if necessary), anesthesia assessments, and other assessment procedures should be performed in accordance with the local SOC.
수술 절차는 가능한 한 수술 전 방문 후 30일 이내에 수행되야 한다. 이 기간 내에 수술을 수행할 수 없는 경우(예: 장기간의 이상 반응으로 인해), 의료 요원과 상의해야 한다. 수술 전 방문 후 30일 이후에 수술을 계획하는 경우, 계획된 수술 전에 CT 스캔을 다시 받아야 한다.Surgical procedures should be performed as far as possible within 30 days of the preoperative visit. If surgery cannot be performed within this period (eg due to long-term adverse events), medical personnel should be consulted. If surgery is planned more than 30 days after the preoperative visit, a CT scan must be retaken before the planned surgery.
절제는 개방적이거나, 최소 침습적 절차(예: 개흉술, 흉골절개술, 클램쉘 또는 반클램쉘 절개, 비디오 보조 흉부 수술[VATS] 또는 로봇 보조 VATS)를 통해 수행해야 한다. Resection should be performed through an open or minimally invasive procedure (eg, thoracotomy, sternotomy, clamshell or semi-clamshell incision, video-assisted thoracic surgery [VATS], or robot-assisted VATS).
원발성 종양 및 관련 림프절의 병리학적 완전 절제(R0)를 수행해야 한다. 분절 절제술, 폐엽 절제술, 이중엽 절제술 또는 폐절제술을 통한 해부학적 절제가 필요한다. 모든 절제에는 모든 해부학적 구조(예: 동맥, 기관지, 정맥)의 분할이 포함되어야 한다. 쐐기 절제술은 허용되지 않는다. 앞서 언급한 해부학적 세부 사항을 제공하지 않는 분절(예: 정점 또는 상부 분절 쐐기 절제술)을 포함하는 깊은 쐐기 절제술은 분절 절제술로 고려되지 않는다.Pathological complete resection (R0) of the primary tumor and associated lymph nodes should be performed. Anatomical resection through segmental resection, lobectomy, double lobectomy, or pneumonectomy is required. All resections should include segmentation of all anatomical structures (eg arteries, bronchi, veins). Wedge resection is not permitted. Deep wedge resections involving segments that do not provide the aforementioned anatomical details (eg, apical or superior segmental wedge resections) are not considered segmental resections.
힐라르(Hilar) 및 종격동 림프절 절개 또는 샘플링은 필수이다. 우측 절제술의 경우, 최소한 4R, 7, 10R 및 11R 수준의 림프절이 포함된다.Hilar and mediastinal lymph node dissection or sampling is mandatory. For right resection, at least 4R, 7, 10R and 11R level lymph nodes are included.
레벨 2R 노드를 포함하는 것을 권장한다. 좌측 절제술의 경우, 최소한 5/6, 7, 10L 및 11L 수준의 림프절이 포함된다. 수준 8 또는 9를 포함한 하엽 절제술이 권장된다.It is recommended to include level 2R nodes. For left resection, at least 5/6, 7, 10L and 11L level lymph nodes are included. Lower lobectomy with level 8 or 9 is recommended.
F.F. 수술 후 방사선 요법Radiation therapy after surgery
수술 후 방사선 요법(PORT)은 외과적 절제 시점에 확인된 병리학적 N2+ 질환(ypN2) 또는 양성 종양 변연(R1 또는 R2)이 있는 환자에게 허용되며, 보조제 아테조 + 티라 치료 전 또는 보조 백금계 화학요법 후에 투여해야 한다.Postoperative radiation therapy (PORT) is permitted in patients with confirmed pathological N2+ disease (ypN2) or benign tumor margin (R1 or R2) at the time of surgical resection, prior to adjuvant atezo plus tyra therapy or adjuvant platinum-based chemotherapy. It should be administered after therapy.
1.8~2 Gy 분수에서, 50~66 그레이(Gy)의 권장 선량에 대한 등각 3차원 또는 강도-변조 방사선 요법은 기관 및/또는 국제 지침에 따라 시행되어야 한다. 강력하게 권장되는 제약 조건에는 폐엽절제술 후 31%을 넘지 않는 평균 폐선량 ≤20Gy 및 V20(20Gy 이상의 방사선량을 받는 폐 용적의 백분율)이 포함되며, 폐절제술 후 평균 폐선량 8Gy 및 V20 ≤5%가 포함된다.At a fraction of 1.8 to 2 Gy, conformal three-dimensional or intensity-modulated radiation therapy for a recommended dose of 50 to 66 gray (Gy) should be administered in accordance with institutional and/or international guidelines. Strongly recommended constraints include an average lung dose ≤20 Gy and V20 (percentage of lung volume receiving radiation dose greater than 20 Gy) not to exceed 31% after lobectomy, with an average lung dose after lobectomy of 8 Gy and V20 ≤5% is included
G.G. 병용 요법: Combination therapy:
병용 요법은 연구 약물 시작 7일 전부터 치료 중단 방문시까지 프로토콜-필수 치료 외에 환자가 사용한 모든 약물(예를 들어, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)로 구성된다. Combination therapy consists of all drugs used by the patient (e.g., prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, nutritional supplements) in addition to protocol-essential treatment from 7 days prior to study drug initiation until the treatment discontinuation visit.
허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
연간 실패율이 <1%인 경구 피임약.Oral contraceptives with an annual failure rate of <1%.
호르몬 대체 요법hormone replacement therapy
예방적 또는 치료적 항응고 요법(예: 안정적인 용량의 와파린 또는 저분자량 헤파린).Prophylactic or therapeutic anticoagulant therapy (eg, stable doses of warfarin or low molecular weight heparin).
비활성화된 인플루엔자 예방 접종.Inactivated influenza vaccination.
식욕 자극제로 투여되는 메게스트롤 아세테이트.Megestrol acetate administered as an appetite stimulant.
미네랄로코르티코이드(예: 플루드로코르티손).Mineralocorticoids, such as fludrocortisone.
COPD 또는 천식에 투여되는 코르티코스테로이드.Corticosteroids administered for COPD or asthma.
기립성 저혈압 또는 부신피질 기능 부전에 투여되는 저용량 코르티코스테로이드.Low-dose corticosteroids administered for orthostatic hypotension or adrenocortical insufficiency.
항히스타민제, 해열제 및/또는 진통제를 사용한 예비투약은 시험자의 재량에 따라 이차 및 후속 아테졸리주맙 주입에 대해서만 투여될 수 있다.Premedication with antihistamines, antipyretics and/or analgesics may be administered only for secondary and subsequent infusions of atezolizumab at the discretion of the investigator.
일반적으로, 시험자는 지역 표준 관행에 따라 임상적으로 표시된 주의 또는 금지된 요법으로 정의된 것 이외의 보조 요법으로 환자의 치료(기존 상태 포함)를 관리해야 한다.In general, investigators should manage the patient's treatment (including pre-existing conditions) with adjuvant therapies other than those defined as clinically indicated cautions or contraindications according to local standard practice.
주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡곤란, 저혈압, 쌕쌕거림, 기관지경련, 빈맥, 감소된 산소 포화, 또는 호흡 곤란에 의해 명시된 심각한 주입관련된 사례는 임상적으로 표시된 대로 지지 요법 (예를 들면, 보충의 산소 및 β2-아드레날린 작용제)로 관리되어야 한다.Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related events indicated by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation, or dyspnea are supported by supportive care (e.g., supplemental oxygen and β2-adrenergic agonists) as clinically indicated. should be managed as
아테졸리주맙 및 티라골루맙 치료 환자에 대한 주의 요법Caution for patients treated with atezolizumab and tiragolumab
코르티코스테로이드 및 TNF-α억제제Corticosteroids and TNF-α inhibitors
전신 코르티코스테로이드 및 TNF-α 억제제는 아테졸리주맙 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여해야 하는 상황에서는 항히스타민제를 포함한 대안을 고려해야 한다. 대안이 가능하지 않은 경우, 시험자의 재량에 따라 전신 코르티코스테로이드 및 TNF-α 억제제를 투여할 수 있다.Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of atezolizumab treatment. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines should be considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the investigator's discretion.
아테졸리주맙 및/또는 티라골루맙 요법과 관련된 특정 이상 반응의 치료를 위해 시험자의 재량에 따라 전신 코르티코스테로이드가 권장된다.Systemic corticosteroids are recommended at the discretion of the investigator for the treatment of certain adverse events associated with atezolizumab and/or tiragolumab therapy.
금지된 요법forbidden therapy
다음과 같은 병용 요법의 사용은 하기와 같이 금지된다:The use of the following combination therapies is contraindicated as follows:
-암 치료를 위한 병용 요법(화학요법, 호르몬 요법, 면역요법, 방사선 요법 및 한약 요법을 포함하되 이에 국한되지 않음)은 보건 당국이 승인했든 실험적이었든 연구 치료를 시작하기 전 다양한 기간 동안 제제에 따라 그리고 연구 치료 동안, 질병 진행이 문서화되고 환자가 연구 치료를 중단할 때까지 금지된다.-Combination therapy (including, but not limited to, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy) for the treatment of cancer, whether approved by health authorities or experimental, is And during study treatment, it is prohibited until disease progression is documented and the patient discontinues study treatment.
-연구 치료 시작 전 42일 이내 및 연구 치료 중 임상시험 요법.Investigation therapy within 42 days prior to initiation of study treatment and during study treatment.
-약독화 생백신(예: FLUMIST)은 연구 치료 시작 전 4주 이내, 연구 치료 중, 티라골루맙의 최종 투여 후 90일 동안 및 아테졸리주맙의 최종 투여 후 5개월 동안 금지된다. 화학요법(즉, 카보플라틴, 시스플라틴,- Live attenuated vaccines (eg, FLUMIST) are contraindicated within 4 weeks prior to the start of study treatment, during study treatment, for 90 days after the last dose of tiragolumab and for 5 months after the last dose of atezolizumab. Chemotherapy (i.e., carboplatin, cisplatin,
백신.페메트렉시드, 파클리탁셀 또는 젬시타빈)으로 치료받는 중인 환자는 생백신을 접종하면 안된다.Vaccines. Patients being treated with pemetrexed, paclitaxel or gemcitabine) should not receive live vaccines.
-전신 면역자극제(인터페론 및 IL-2를 포함하나 이에 국한되지 않음)는 연구 치료 시작 전 및 연구 치료 동안 4주 또는 5 약물-제거 반감기(둘 중 더 긴 것) 이내에 금지되는데, 이러한 제제는 아테졸리주맙 및 티라골루맙과 병용 투여 시 자가면역 질환의 위험을 잠재적으로 증가시킬 수 있기 때문이다.-Systemic immunostimulants (including but not limited to interferon and IL-2) are contraindicated within 4 weeks or 5 drug-elimination half-lives (whichever is longer) prior to initiation of study treatment and during study treatment, whichever is longer This is because co-administration with zolizumab and tiragolumab may potentially increase the risk of autoimmune diseases.
-연구 치료 중 전신 면역억제제(사이클로포스파미드, 아자티오프린, 메토트렉세이트 및 탈리도마이드를 포함하지만 이에 국한되지 않음)는 이러한 제제가 연구 치료의 유효성 및 안전성을 잠재적으로 변경할 수 있기 때문에 금지된다.-Systemic immunosuppressants (including, but not limited to, cyclophosphamide, azathioprine, methotrexate and thalidomide) during study treatment are contraindicated because these agents may potentially alter the efficacy and safety of study treatment.
H.H. 연구 평가 study evaluation
연구 전반에 걸쳐 안전성 및 내약성에 대해 환자를 면밀히 모니터링한다. 각 투여 전에 독성에 대해 환자들을 평가해야 하며; 임상 평가 및 현지 실험실 테스트 값이 허용 가능한 경우에만 투여가 허용된다.Patients are closely monitored for safety and tolerability throughout the study. Patients should be evaluated for toxicity prior to each dose; Administration is permitted only when clinical evaluation and local laboratory test values are acceptable.
모든 치료 방문은, 달리 명시되지 않는 한 예정된 날짜로부터 ±3일 후에 이루어져야 한다. 기간을 지정하지 않는 한, 모든 평가는 지정된 방문 당일에 수행해야 한다. 각 투여 전에 독성에 대해 환자들을 평가해야 하며; 임상 평가 및 현지 실험실 테스트 값이 허용 가능한 경우에만 투여가 허용된다. 달리 명시되지 않는 한, 연구 치료제 투여일에 예정된 평가는 투여 전에 수행되어야 한다.All treatment visits must occur ±3 days after the scheduled date, unless otherwise specified. Unless a time period is specified, all assessments must be performed on the day of the designated visit. Patients should be evaluated for toxicity prior to each dose; Administration is permitted only when clinical evaluation and local laboratory test values are acceptable. Unless otherwise specified, assessments scheduled on the day of study treatment administration should be performed prior to dosing.
다음의 평가들은 각 주기의 제 1일차 전 4일에 수행할 수 있다:The following assessments may be performed 4 days before Day 1 of each cycle:
제한된 신체 검사limited physical examination
-현지 실험실 테스트- Local laboratory testing
종양 평가를 제외하고, 주기 1의 1일차 전 ≤4일에 수행된 선별 치료 평가는 주기 1의 1일차에 반복할 필요가 없다.With the exception of tumor assessments, screening treatment evaluations performed ≤4 days prior to Day 1 of Cycle 1 do not need to be repeated on Day 1 of Cycle 1.
휴일, 주말 또는 기타 이벤트로 인해 예정된 투여가 불가능한 경우, 투여는 가장 빠른 다음 날짜로 연기될 수 있으며, 후속 투여는 21일 일정에 따라 계속된다. 치료가 3일 미만으로 연기된 경우, 환자는 원래 일정을 재개할 수 있다.If a scheduled dosing is not possible due to a holiday, weekend or other event, dosing may be postponed to the next earliest date, and subsequent dosing will continue according to the 21-day schedule. If treatment is delayed by less than 3 days, the patient may resume the original schedule.
I.I. 종양 반응 및 질병 상태 추적 평가Tumor response and disease status follow-up evaluation
수술 후 및 보조 치료 단계 동안, 모든 환자(양 코호트)는, 1년간은 수술일로부터 4개월마다 그리고 두 번째 해에는 6개월마다 IV 조영제(간 및 부신 포함)를 이용하여 흉부 CT로 질병 상태 추적 평가를 받는다. 조영제를 사용한 CT 스캔이 금지인 경우(예: 신장 청소율 장애가 있는 환자), 흉부에 대해 비조영제 CT 스캔을 수행할 수 있다. 질병의 재발을 경험하지 않은 환자는After surgery and during the adjuvant treatment phase, all patients (both cohorts) were followed up for disease status by chest CT with IV contrast medium (including liver and adrenal glands) every 4 months from the date of surgery for 1 year and every 6 months for the 2nd year. get evaluated If CT scans with contrast media are contraindicated (eg patients with impaired renal clearance), a non-contrast CT scan of the chest may be performed. Patients who have not experienced a recurrence of the disease
수술 후 3-5년 동안 IV 조영제(간 및 부신 포함)를 사용한 흉부 CT 스캔에 의해 6개월마다 질병 상태 추적 평가를 받는다.Follow-up of disease status every 6 months by chest CT scan with IV contrast medium (including liver and adrenal) for 3-5 years after surgery.
질병 상태 후속 평가는 예정된 후속 평가의 허용된 기간 내에 이루어져야 한다. 질병 상태 후속 평가는 예정된 후속 평가의 허용된 기간 내에 이루어져야 한다. 질병 상태 추적 평가에 허용되는 기간은 1년차에는 ±7일, 2-3년차에는 ±14일, 그 이후에는 ±4주이다.Disease status follow-up assessments must be made within the permitted period of scheduled follow-up assessments. Disease status follow-up assessments must be made within the permitted period of scheduled follow-up assessments. The allowable period for disease status follow-up evaluation is ±7 days in Year 1, ±14 days in Years 2-3, and ±4 weeks thereafter.
수술 후 질병 재발은 병리학적 및/또는 명백한 방사선학적 증거에 의해 확인되어야 한다. 스캔에서 불분명한 소견이 나타나면(예를 들어, 단축에 있어서 종격동 결절 측정값 < 1.5 cm, 최장 직경에 있어서 폐 실질 병변 또는 내장 병변 측정값 < 1 cm), 생검이 수행되어야 한다. 생검이 가능하지 않거나 안전하지 않은 경우, 4~8주 이내에 확인 스캔을 다시 수행해야 한다. 확인 스캔에서 질병 재발이 확인되면, 해당 이벤트는 모호한 이벤트를 표시한 이전 확인 스캔 날짜에 문서화되어야 한다.Postoperative disease recurrence should be confirmed by pathological and/or clear radiological evidence. If the scan reveals equivocal findings (eg, mediastinal nodule measurements < 1.5 cm for short axis, lung parenchymal lesions or visceral lesion measurements < 1 cm for longest diameter), a biopsy should be performed. If a biopsy is not possible or unsafe, a confirmatory scan should be performed again within 4 to 8 weeks. If a confirmatory scan confirms disease recurrence, the event should be documented on the date of the previous confirmatory scan that marked an ambiguous event.
생검은 다음 항암 요법을 시작하기 전에 수행되어야 한다. 생검에서 질병 재발의 증거(예를 들어, 비악성 침윤)가 나타나지 않으면, 환자는 예정된 연구 치료, 평가 및/또는 추적관찰을 계속할 수 있다.A biopsy should be performed prior to initiating the next chemotherapy. If the biopsy does not show evidence of disease recurrence (eg, non-malignant infiltrates), the patient may continue with the scheduled study treatment, evaluation, and/or follow-up.
종양 또는 질병 상태 추적 평가는 질병 진행 또는 재발(예: 독성 때문에) 이외의 이유로 조기에 치료를 중단한 환자에 대해 지속해야 한다. 질병의 진행이나 재발이 없는 경우, 새로운 항암 요법을 시작하는지 여부에 관계없이 모든 환자에 대해 종양 또는 질병 상태 추적 평가가, 질병 진행 또는 재발, 동의 철회, 사망, 추적 관찰 소실, 스폰서에 의한 연구 종료 중 어느 하나가 발생될 때까지 계속되어야 한다.Tumor or disease status follow-up evaluation should be continued for patients with early discontinuation of treatment for reasons other than disease progression or recurrence (eg, due to toxicity). In the absence of disease progression or recurrence, tumor or disease status follow-up assessment for all patients, whether starting new chemotherapy or not, disease progression or recurrence, withdrawal of consent, death, loss of follow-up, termination of study by sponsor This should continue until either one of them occurs.
J.J. 연구 치료 중단study treatment discontinuation
환자는 다음 중 하나를 경험하는 경우 연구 치료제를 영구적으로 중단해야 한다:Patients should permanently discontinue study treatment if they experience any of the following:
개별 환자의 치료에 대한 잠재적 반응 및 상태의 중증도를 고려할 때, 시험자가 허용할 수 없는 것으로 결정한 면역-관련 이상 반응의 발생을 포함하여 아테졸리주맙 및 티라골루맙과 관련된 허용할 수 없는 독성. 신보조 치료 단계에서 아테졸리주맙과 티라골루맙이 중단된 경우, 화학요법을 계속할 수 있다.Unacceptable toxicity associated with atezolizumab and tiragolumab, including the occurrence of immune-related adverse events determined by the investigator to be unacceptable given the severity of the condition and the potential response to treatment of the individual patient. Chemotherapy may be continued if atezolizumab and tiragolumab are discontinued during the neoadjuvant treatment phase.
-연구 치료제의 다른 성분과 관련된 허용할 수 없는 독성. 신보조 치료 단계 동안 화학요법 관련 독성으로 인해 일부 또는 모든 화학요법제가 중단된 경우에도 아테조 계속 투여해야 한다.-Unacceptable toxicity associated with other components of the study treatment. During the neoadjuvant treatment phase, atezo should be continued even if some or all chemotherapeutic agents have been discontinued due to chemotherapy-related toxicity.
-환자가 연구 치료를 계속할 경우, 환자의 안전을 위협할 수 있는 모든 의학적 상태.- Any medical condition that could endanger the patient's safety if the patient continued study treatment.
-치료 중단이 환자에게 최선의 이익이라는 조사관 또는 스폰서의 결정.- Determination of the Investigator or Sponsor that discontinuation of treatment is in the patient's best interest.
-또 다른 비-프로토콜 지정 항암 요법의 사용.- Use of another non-protocol directed anticancer therapy.
-임신.-Pregnant.
-신보조 치료 단계 동안 RECIST v1.1에 따른 명백한 방사선학적 질환 진행.-Clear radiological disease progression according to RECIST v1.1 during the neoadjuvant treatment phase.
-보조 치료 단계 동안 질병 재발에 대한 병리학적으로 확인되거나 명백한 방사선학적 증거.Pathologically confirmed or unequivocal radiological evidence of disease recurrence during the adjuvant treatment phase.
최소 2주기의 신보조 치료를 받고 연구 치료를 조기에 중단한 환자는 대체되지 않는다. 조기 치료 중단의 이유가 특별한 관심 또는 질병 진행의 이상 반응이 아닌 경우 2주기 미만의 신보조 치료를 받은 환자를 교체할 수 있다.Patients who have received at least 2 cycles of neoadjuvant therapy and who have prematurely discontinued study treatment will not be replaced. Patients who received less than 2 cycles of neoadjuvant therapy may be replaced if the reason for early discontinuation of treatment is not of special interest or an adverse reaction to disease progression.
4주기를 받기 전에 비보조 연구 치료를 중단한 환자(예: 치료 불내성 또는 반응 부족으로 인해)는 외과적 절제 또는 비외과적 치료 표준 치료 조치(수술에 순응할 수 없는 경우)를 위해 치료하는 종양 전문의와 담당 외과의에 의해 평가된다. 계획된 프로토콜 지정 수술을 진행하는 환자는, 모든 수술 후 연구 치료 및 절차에 대한 자격을 유지한다.Patients who discontinue non-adjuvant study treatment prior to receiving 4 cycles (e.g., due to treatment intolerance or lack of response) are treated for surgical resection or non-surgical standard of care treatment (if surgery is not compliant). It is evaluated by a specialist and the attending surgeon. Patients undergoing planned protocol-directed surgery remain eligible for all postoperative study treatments and procedures.
환자는 연구 치료의 최종 투여 후 30일이 지나기 전에 치료 중단 방문을 위해 클리닉으로 돌아간다. 질병 평가가 진행성 질병을 나타내거나 질병 재발을 확인하는 방문은 치료 중단 방문으로 사용될 수 있다. 진행성 질환 또는 재발 이외의 다른 이유로 연구 치료를 중단한 환자는 계속해서 종양 또는 질환 상태 평가를 받는다.Patients return to the clinic for a treatment discontinuation visit no later than 30 days after the last dose of study treatment. A visit where the disease assessment indicates progressive disease or confirms disease recurrence may be used as a treatment discontinuation visit. Patients who discontinue study treatment for reasons other than progressive disease or recurrence continue to undergo tumor or disease status assessment.
실시예 11. GO42501 연구에 대한 안전성 평가Example 11. Safety Assessment for the GO42501 Study
A.A. 안전성 계획safety plan
이 연구에서 환자에 대한 안전성 계획은 예상되는 작용 기전, 비임상 연구 결과, 유사한 분자에 대한 발표된 데이터, 1상 및 2상 연구에서 티라골루맙 단독 및 아테졸리주맙을 병용한 임상 경험, 및 아테졸리주맙의 임상 안전성 프로파일에 근거하고 있다..The safety plan for patients in this study included the expected mechanism of action, results from nonclinical studies, published data for similar molecules, clinical experience with tiragolumab alone and atezolizumab in phase 1 and 2 studies, and ate It is based on the clinical safety profile of Zolizumab.
엄격한 선정 및 배제 기준을 사용하고 연구 기간 동안 환자를 면밀히 모니터링하는 것을 포함하고, 본 연구에 참여하는 환자의 안전을 보장하기 위한 조치를 취한다. 아테졸리주맙 및 더발루맙의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 수행된다.Measures are taken to ensure the safety of patients participating in this study, including using strict selection and exclusion criteria and closely monitoring patients during the study period. Administration of atezolizumab and durvalumab is performed in a monitoring environment with immediate access to trained personnel and appropriate equipment and medications to manage potentially severe reactions.
B.B. 이상 반응 관리Adverse Event Management
용량 수정capacity modification
이 연구에서 아테졸리주맙 또는 티라골루맙에 대한 용량 감소를 포함한 용량 변경은 없다.There were no dose changes, including dose reductions, for atezolizumab or tiragolumab in this study.
치료 중단cessation of treatment
독성 관리에 적절한 경우 연구 치료가 일시적으로 중단될 수 있다. 작용기전의 이용 가능한 특성화에 기초하여, 티라골루맙은 아테졸리주맙과 유사하지만 독립적인 이상 반응을 유발할 수 있고, 아테졸리주맙 관련 이상반응의 빈도 또는 중증도를 악화시킬 수 있거나, 아테졸리주맙과 중복되지 않는 독성을 가질 수 있다. 이러한 시나리오는 임상 환경에서 서로 구별되지 않을 수 있으므로 면역-매개 이상 반응은 일반적으로 두 연구 약물 모두에 기인한 것이어야 하며, 면역-매개 이상 반응에 대한 투약 중단 또는 치료 중단은 아테졸리주맙 및 티라골루맙에 적용되어야 한다.Study treatment may be temporarily discontinued if appropriate for toxicity management. Based on the available characterization of the mechanism of action, tiragolumab may induce adverse events similar to but independent of atezolizumab and may exacerbate the frequency or severity of atezolizumab-related adverse events, or overlap with atezolizumab. may have non-toxic properties. Because these scenarios may not be distinct from each other in the clinical setting, immune-mediated adverse events should generally be attributable to both study drugs, and dosing or discontinuation of treatment for immune-mediated adverse events should be attributed to atezolizumab and tyragol It should be applied to lumab.
보조제 설정에서, 아테졸리주맙과 티라골루맙은 최대 12주 동안 유지될 수 있다. 어떤 이유로든 티라골루맙이 >12주 중단되면 환자는 티라골루맙 치료를 영구적으로 중단해야만 하지만, 금기가 없고 독성이 티라골루맙 및/또는 병용에 관련된 것으로 간주되는지 논의한 상태라면, 환자는 아테졸리주맙을 계속 투여할 수 있다. >12주의 보류 후 환자가 티라골루맙을 재개함으로써 임상적 이점을 얻을 가능성이 있다고 시험자가 판단한 경우 예외가 될 수 있다. 아테졸리주맙을 >12주 동안 중단하는 경우, 환자는 아테졸리주맙을 영구적으로 중단해야 한다. 그러나 시험자의 판단에 따라 환자가 >12주의 보류 후 아테졸리주맙의 임상적 이점을 얻을 가능성이 있는 경우에는 아테졸리주맙을 재개할 수 있다. In the adjuvant setting, atezolizumab and tiragolumab may be maintained for up to 12 weeks. If tiragolumab is discontinued for any reason >12 weeks, the patient must permanently discontinue tiragolumab treatment, but if there are no contraindications and if toxicity is considered to be related to tiragolumab and/or combination Zumab can be continued. Exceptions may be made if the investigator determines that the patient is likely to obtain clinical benefit by resuming tiragolumab after a hold of >12 weeks. If atezolizumab is discontinued for >12 weeks, the patient must permanently discontinue atezolizumab. However, atezolizumab may be resumed if, in the investigator's judgment, the patient is likely to obtain clinical benefit from atezolizumab after a hold of >12 weeks.
그러나 시험자의 판단에 따라 환자가 >12주의 보류 후 아테졸리주맙의 임상적 이점을 얻을 가능성이 있는 경우에는 아테졸리주맙을 재개할 수 있다. 단일 제제 아테졸리주맙을 환자에게 계속 투여하려면, 다른 모든 연구 적격성 기준이 계속 충족되어야 한다.However, atezolizumab may be resumed if, in the investigator's judgment, the patient is likely to obtain clinical benefit from atezolizumab after a hold of >12 weeks. To continue administering single agent atezolizumab to a patient, all other study eligibility criteria must continue to be met.
아테졸리주맙을 영구적으로 중단한 후 단일제제 티라골루맙을 계속 투여하는 것은Permanent discontinuation of atezolizumab and continued administration of single agent tiragolumab
허용되지 않는다.Not permitted.
환자가 이상 반응 치료에 사용되는 스테로이드를 감량해야 하는 경우, 스테로이드가 중단될 때까지 또는 스테로이드가 ≥10 mg/일 프레드니손 용량(또는 등가 용량)으로 감소될 때까지 아테졸리주맙 및/또는 티라골루맙은 최종 투약으로부터 ≥12주 이상의 추가 시간 동안 보류될 수 있고, 티라골루맙은 최종 투약으로부터 ≥12주 이상 추가 시간 동안 보류될 수 있다. 독성 이외의 이유(들)로 투여 중단이 허용될 수 있다. 두 연구 치료제가 모두 중단된 후, 환자는 안전성 및 유효성에 대해 모니터링된다. 두 연구 치료제가 모두 중단된 후, 환자는 안전성 및 유효성에 대해 모니터링된다.If the patient needs to reduce the steroid used to treat the adverse event, atezolizumab and/or tiragolumab until the steroid is discontinued or the steroid is reduced to a prednisone dose ≥10 mg/day (or equivalent dose) may be withheld for ≥12 weeks or more additional time from the last dose, and tiragolumab may be withheld for >12 weeks or more additional time from the last dose. Discontinuation of dosing may be tolerated for reasons other than toxicity(s). After both study treatments are discontinued, patients are monitored for safety and efficacy. After both study treatments are discontinued, patients are monitored for safety and efficacy.
C.C. 안전성 매개변수 및 정의Safety parameters and definitions
안전성 사정은 심각한 부작용 및 특히 관심되는 부작용을 비롯한 부작용을 모니터링하고 기록하며, 프로토콜-특정된 안전성 실험실 사정을 수행하고, 프로토콜-특정된 활력 징후를 계측하고, 그리고 연구의 안전성 평가에 결정적인 것으로 간주되는 다른 프로토콜-특정된 검사를 수행하는 것을 포함하였다.Safety assessments monitor and document adverse events, including serious adverse events and adverse events of particular interest, perform protocol-specific safety laboratory assessments, measure protocol-specific vital signs, and evaluate the safety of the study. Other protocol-specific tests were included.
이상 반응adverse reaction
의약품 임상시험 관리기준에 대한 ICH 지침에 따라서, 부작용은 인과 귀인과 상관없이, 제약학적 산물이 투여된 임상적 조사 개체에서 임의의 유해한 의학적 발생이다. 이상 반응은 이런 이유로, 다음 중 어느 것일 수 있다:According to the ICH guidelines for clinical trial practices for pharmaceuticals, an adverse event is any adverse medical occurrence in a clinically investigated subject administered a pharmaceutical product, regardless of causal attribution. Adverse events, for this reason, may be any of the following:
-의약품에 관련된 것으로 고려되는 지의 여부와 상관없이, 의약품의 이용과 일시적으로 연관된 임의의 불리하고 의도하지 않은 징후 (비정상적인 실험실 결과 포함), 증상 또는 질환-Any adverse and unintended sign (including abnormal laboratory results), symptom or disease temporarily associated with the use of a drug, whether or not considered to be drug-related;
-임의의 새로운 질환 또는 기존 질환의 악화 (공지된 장애의 특징, 빈도 또는 중증도에서 악화)-Any new disease or exacerbation of an existing disease (exacerbates in the nature, frequency, or severity of a known disorder)
-기준선에서 존재하지 않았던 간헐적 의학적 상태 (예를 들면, 두통)의 재발-recurrence of an intermittent medical condition (e.g., headache) that was not present at baseline
-증상과 연관되거나, 또는 연구 치료 또는 병행 치료에서 변화 또는 연구 치료제로부터 중단을 야기하는, 실험실 값 또는 다른 임상 시험 (예를 들면, ECG, 엑스선)에서 임의의 악화-Any exacerbation in laboratory values or other clinical trials (e.g. ECG, X-ray) that is associated with symptoms or that results in a change in study treatment or concomitant treatment or discontinuation from study treatment
-연구 치료의 배정에 앞서 일어난 것들을 비롯한, 프로토콜-강제된 개입 (예를 들면, 선별검사 침습성 절차 예컨대 생검)에 관련된 부작용- adverse events related to protocol-forced interventions (eg, screening invasive procedures such as biopsies), including those that occurred prior to assignment of study treatment
심각한 이상 반응serious adverse reactions
심각한 이상 반응은 다음 기준 중 하나를 충족하는 모든 이상 반응이다:A serious adverse event is any adverse event that meets one of the following criteria:
-(즉, 이상 반응이 실제로 사망을 유발하거나 사망에 이르게 함).- (i.e., the adverse event actually causes or causes death).
-생명을 위협한다(즉, 시험자의 관점에서 이상 반응은 환자를 즉각적인 사망 위험에 처하게 함). 여기에는 더 심각한 형태로 발생했거나 계속되도록 허용된 경우 사망을 초래할 수 있는 이상 반응은 포함되지 않는다.- life-threatening (ie, from the investigator's point of view, an adverse event puts the patient at risk of immediate death); This does not include adverse events that have occurred in a more serious form or could result in death if allowed to continue.
-환자의 입원이 필요하거나 연장된다.-The patient's hospitalization is necessary or prolonged.
-지속적이거나 심각한 장애/무능력을 초래한다(즉, 부작용으로 인해 정상적인 생활 기능을 수행하는 환자의 능력이 실질적으로 중단됨).-results in persistent or severe disability/incapacity (ie, the adverse effect substantially interrupts the patient's ability to perform normal life functions).
-연구 치료에 노출된 산모에게서 태어난 신생아/유아의 선천적 기형/선천적 결함이다.-Congenital malformations/birth defects in newborns/infants born to mothers exposed to study treatment.
-시험자의 판단에 따른 중대한 의학적 사건이다(예: 환자를 위험에 빠뜨릴 수 있거나, 위에 나열된 결과 중 하나를 방지하기 위해 의료/외과적 개입이 필요할 수 있음).- a serious medical event at the discretion of the investigator (e.g. may put the patient at risk or may require medical/surgical intervention to prevent one of the outcomes listed above);
용어 “중증” 및 “심각한”은 동의어가 아니다. 중증도는 이상 반응의 강도를 나타내며(예: 경증, 중등도 또는 중증으로 평가되거나 NCI CTCAE에 따라 평가됨): 반응 자체는 상대적으로 경미한 의학적 유의성(예: 더 이상의 소견이 없는 중증 두통)일 수 있다.The terms “severe” and “severe” are not synonymous. Severity indicates the strength of an adverse event (e.g., rated as mild, moderate or severe, or assessed according to the NCI CTCAE): the response itself may be of relatively mild medical significance (e.g., severe headache with no further findings).
특히 관심대상이 되는 이상 반응Adverse reactions of particular interest
본 연구에서 특정 관심 대상의 이상 반응은 다음과 같다:Adverse events of specific interest in this study were:
-Hy의 법칙에 의해 정의된, 빌리루빈 상승 또는 임상 황달과 함께 ALT 또는 AST 상승을 포함하는, 잠재적인 약물-유발 간 손상 사례.-Potential drug-induced liver injury events, including elevated ALT or AST with elevated bilirubin or clinical jaundice, as defined by Hy's Law.
-하기에 정의된 바와 같이 연구 치료제에 의한 감염원의 의심되는 전파:- Suspected transmission of an infectious agent by the study treatment as defined below:
병원성이든 비병원성이든 모든 유기체, 바이러스 또는 감염성 입자(예: 전염성 해면상뇌증을 전파하는 프리온 단백질)는 감염원으로 간주된다. 감염원의 전파는 의약품에 노출된 환자의 감염을 나타내는 임상 증상이나 검사실 소견에서 의심될 수 있다. 이 용어는 연구 치료제의 오염이 의심되는 경우에만 적용된다.Any organism, virus, or infectious particle, whether pathogenic or non-pathogenic (eg, a prion protein that transmits infectious spongiform encephalopathy), is considered an infectious agent. Transmission of an infectious agent may be suspected from clinical symptoms or laboratory findings indicative of infection in a patient exposed to the drug. This term applies only when contamination of the study product is suspected.
-폐렴.-Pneumonia.
-대장염.-colitis.
-내분비병증: 당뇨병, 췌장염, 부신 기능 부전, 갑상선 기능 항진증 및 뇌하수체염.-Endocrinopathy: diabetes, pancreatitis, adrenal insufficiency, hyperthyroidism and pituitary insufficiency.
-AST 또는 ALT 10 ULN을 포함한 간염.-Hepatitis including AST or ALT 10 ULN.
-전신성 홍반성 루푸스.-Systemic lupus erythematosus.
-신경학적 장애. 길랭-바레 증후군, 근무력 증후군 또는 중증 근무력증, 수막뇌염.- Neurological disorders. Guillain-Barré syndrome, myasthenia gravis or myasthenia gravis, meningoencephalitis.
-과민증, 주입 관련 반응, 사이토카인 방출 증후군, 혈구포식성 림프조직구증가증 및 대식세포 활성화 증후군을 암시하는 반응.-Reactions suggestive of hypersensitivity, infusion-related reactions, cytokine release syndrome, hemophagocytic lymphohistiocytosis and macrophage activation syndrome.
-신장증.-nephritis.
-안구 독성(예: 포도막염, 망막염, 시신경염).-ocular toxicity (eg uveitis, retinitis, optic neuritis).
-근염.- Myositis.
-횡문근 융해증을 포함한 근병증.-myopathy, including rhabdomyolysis.
-2등급 심장 장애(예: 심방세동, 심근염, 심낭염).-2 grade heart disorders (eg, atrial fibrillation, myocarditis, pericarditis).
-혈관염.- Vasculitis.
-자가 면역 용혈성 빈혈.- Autoimmune hemolytic anemia.
-심한 피부 반응(예: 스티븐스-존슨 증후군, 수포성 피부염, 독성 표피 괴사).-Severe skin reactions (eg Stevens-Johnson syndrome, bullous dermatitis, toxic epidermal necrosis).
이상 반응의 중증도 평가Assess the severity of adverse events
NCI CTCAE(v5.0)에 대한 이상 반응 중증도 등급 스케일은 이상 반응 중증도를 평가하는 데 사용된다. CRS의 중증도를 보고할 때, NCI CTCAE v5.0과 함께 ASTCT(American Society for Transplantation and Cellular Therapy) CRS 합의 등급 스케일을 사용해야 한다.The Adverse Event Severity Rating Scale for NCI CTCAE (v5.0) is used to assess adverse event severity. When reporting the severity of CRS, the American Society for Transplantation and Cellular Therapy (ASTCT) CRS consensus rating scale with NCI CTCAE v5.0 should be used.
실시예 12. GO42501 연구에 대한 통계적 고려 사항 및 분석 계획Example 12. Statistical Considerations and Analysis Plan for the GO42501 Study
유효성 및 안전성 분석은 각 코호트에 대해 연구 약물의 적어도 1회 용량을 받은 GO42501 연구에 등록된 모든 환자에 대해 수행된다.Efficacy and safety analyzes are performed for all patients enrolled in the GO42501 study who received at least one dose of study drug for each cohort.
샘플 크기 결정Determining sample size
본 연구의 일차 유효성 목표는 주요 병리학적 반응(MPR) 비율을 평가하는 것이다. 약 41명의 환자가 연구의 각 코호트에 등록된다. 약 41명의 환자가 연구의 각 코호트에 등록된다.The primary efficacy objective of this study was to evaluate the rate of major pathologic response (MPR). Approximately 41 patients are enrolled in each cohort of the study. Approximately 41 patients are enrolled in each cohort of the study.
61%로 가정하면, 이 표본 크기는 양측 95% CI의 하한이 46%를 초과하는 각 코호트의 MPR 비율에 대한 점 추정에 적절한 정밀도를 제공하며, 이 비율은 이 설정에서 병용 요법에 대한 추가 조사를 보증한다. .Assuming 61%, this sample size provides adequate precision in estimating the point for the MPR rate for each cohort where the lower bound of the two-sided 95% CI is greater than 46%, which in this setting is a factor for further investigation into combination therapy. to guarantee .
연구 수행 요약Summary of Study Conduct
연구를 등록, 중단 또는 완료한 환자의 수가 요약된다. 조기 연구 철회 이유가 나열되고 요약된다. 등록 및 주요 프로토콜 편차는 각 치료 코호트에 대해 나열된다.The number of patients who enrolled, discontinued, or completed the study is summarized. Reasons for early study withdrawal are listed and summarized. Enrollment and major protocol deviations are listed for each treatment cohort.
A.A. 인구통계 및 기준선 특성 요약Summary of Demographic and Baseline Characteristics
연령 및 인종과 같은 인구 통계 정보가 표로 작성된다. 연속 매개변수에 대한 평균, 표준 편차, 범위, 범주 매개변수에 대한 백분율 및 빈도를 포함한 기술 통계가 제공된다. 전체 인구 및 각 치료 집단에 대한 요약이 제시된다. 기준 측정은, 달리 명시되지 않는 한, 환자가 연구 약물 성분의 첫 번째 용량을 받기 전에 얻은 마지막 이용 가능한 데이터이다.Demographic information such as age and race is tabulated. Descriptive statistics are provided, including mean, standard deviation, range for continuous parameters, percentages and frequencies for categorical parameters. A summary of the total population and each treatment cohort is presented. Baseline measures, unless otherwise specified, are the last available data obtained before the patient received the first dose of the study drug component.
B.B. 안전성 분석Safety analysis
각 코호트에 있어서, 안전성 분석은 연구 치료제를 1회 이상 투여받은 등록된 모든 환자가 포함된다.For each cohort, the safety analysis included all enrolled patients who received at least one dose of study treatment.
연구 치료 노출은 치료 기간, 투여량 및 투여 강도를 포함하여 요약된다.Study treatment exposures are summarized including treatment duration, dosage, and dosing intensity.
수술 지연의 발생률 및 기간, 수술 및 수술 후 합병증의 발생률 및/또는 연구 치료와 관련된 수술 취소 횟수가 각 코호트에 대해 평가된다.The incidence and duration of surgical delay, the incidence of surgery and postoperative complications, and/or the number of surgical cancellations associated with study treatment are assessed for each cohort.
이상 반응에 대한 축어적 설명은 MedDRA 동의어 사전 용어에 따른다. 모든 이상 반응에 대한 중증도는 NCI CTCAE v5.0에 따라 시험자가 등급을 매기고, CRS에 대한 중증도는 ASTCT 합의 등급 스케일에 따라 시험자가 등급을 매긴다. 이 요약은 치료 부문에서 제공된다. 모든 이상 반응은 치료 부문 및 NCI CTCAE 등급으로 요약된다. CRS는 또한 치료 부문과 ASTCT 합의 등급으로 요약된다. 또한, 연구 치료제와 관련하여 용량 감소 또는 중단으로 이어지는 연구 치료의 취소를 야기하는 치료제-발생 이상 반응, 중증(즉, 등급 3 이상 반응), 치명적인 이상 반응(즉, 등급 5) 및 심각한 이상 반응, 그리고 특히 관심이 있는 이상 반응도 요약되어 있다. 동일한 반응이 여러 번 발생하면 최대 중증도에서 한 번 계산된다. 정상 범위를 벗어난 값을 가진 실험실 데이터가 식별된다. 또한 ADA 결과 및 활력 징후의 변화를 포함한 선택된 실험실 데이터가 치료 부문별로 요약된다. 사망 및 사망 원인들이 요약되어 있다.Verbose descriptions of adverse events follow MedDRA Thesaurus Terminology. The severity of all adverse events is rated by the investigator according to the NCI CTCAE v5.0, and the severity for CRS is graded by the investigator according to the ASTCT consensus rating scale. This summary is provided in the Therapeutic section. All adverse events are summarized by treatment arm and NCI CTCAE grade. CRS is also summarized by treatment arm and ASTCT consensus grade. In addition, with respect to the study treatment, treatment-occurring adverse events, severe (i.e., Grade 3 adverse events), fatal (i.e., Grade 5), and serious adverse events resulting in cancellation of study treatment leading to dose reduction or discontinuation, Adverse events of particular interest are also summarized. Multiple occurrences of the same reaction are counted once at maximum severity. Laboratory data with values outside the normal range are identified. In addition, selected laboratory data, including changes in ADA outcomes and vital signs, are summarized by treatment arm. Deaths and causes of death are summarized.
C.C. 유효성 분석Validity analysis
유효성 분석 모집단에는 연구 치료제의 최소 1회 용량을 받은 등록된 모든 환자가 포함된다.The efficacy analysis population included all enrolled patients who received at least one dose of study treatment.
일차 유효성 평가변수Primary efficacy endpoint
MPR 비율은 MPR을 달성한 환자의 비율로 정의되며, 유효성 분석 모집단의 각 치료 코호트에 대해 추정된다. MPR은 중앙 병리학 실험실에서 평가한 원발성 종양의 외과적 절제 시점에 ≤10%의 생존 가능한 종양으로 정의된다. 수술을 진행하지 않는 환자는 MPR에 대한 무반응자로 간주된다. Clopper-Pearson 방법을 사용하여 계산된 MPR 비율에 대한 양측 95% CI가 보고된다.The MPR rate is defined as the proportion of patients who achieved MPR and is estimated for each treatment cohort in the efficacy analysis population. MPR is defined as ≤10% viable tumors at the time of surgical resection of primary tumors evaluated by the Central Pathology Laboratory. Patients not undergoing surgery are considered non-responders to MPR. A two-sided 95% CI for the MPR ratio calculated using the Clopper-Pearson method is reported.
이차 유효성 평가변수secondary efficacy endpoint
병리학적 완전 반응(pCR) 비율은 pCR을 달성한 환자의 비율로 정의된다. pCR은 중앙 병리학 실험실에서 평가한 바와 같이 외과적 절제 시점에 생존 가능한 원발성 종양의 부재로 정의된다. pCR 비율은 유효성 분석 모집단에 대한 각 치료 코호트에 대한 MPR 비율과 동일한 통계적 방법을 사용하여 분석된다.The pathological complete response (pCR) rate is defined as the proportion of patients who achieved pCR. pCR is defined as the absence of viable primary tumors at the time of surgical resection, as assessed by the Central Pathology Laboratory. The pCR ratios are analyzed using the same statistical methods as the MPR ratios for each treatment cohort for the efficacy analysis population.
무사건 생존(EFS)은 연구 약물의 첫 번째 투여부터 다음 사건들 중 먼저 발생한 사건까지의 시간으로 정의된다: RECIST v1.1에 따라 시험자가 평가한 바와 같이, 수술이 불가능한 질병 진행; 국소 또는 원거리 질병 재발(새로운 원발성 NSCLC의 발생 포함); 또는 어떤 원인으로 인한 사망. 수술이 불가능한 질병 진행, 국소 또는 원격 질병 재발을 경험하지 않았거나 분석 당시 사망한 환자는Event-free survival (EFS) is defined as the time from the first administration of study drug to the first of the following events: inoperable disease progression, as assessed by the investigator according to RECIST v1.1; local or distant disease recurrence (including the occurrence of new primary NSCLC); or death from any cause. Patients who have not experienced inoperable disease progression, local or distant disease recurrence, or who died at the time of analysis
마지막 종양 또는 질병 추적 평가 시점에서 검열 및 삭제된다. 기준선 이후 종양 평가가 없는 환자는 연구 약물의 1차 투여 일자에 검열 및 삭제된다. EFS는 유효성 분석 모집단에 대한 각 치료 코호트에 대해 Kaplan-Meier 방법을 사용하여 평가된다.Censored and deleted at the time of the last tumor or disease follow-up assessment. Patients with no post-baseline tumor assessment will be screened and deleted on the first dose of study drug. EFS is assessed using the Kaplan-Meier method for each treatment cohort for the efficacy analysis population.
D.D. 약동학 분석Pharmacokinetic analysis
샘플은 약동학 분석을 위해 그리고 이 연구의 성과를 이전 연구에서 얻은 성과와 비교하기 위해 수집된다. 아테졸리주맙 및 티라골루맙의 혈청 농도는 개별 값으로 보고되고, 적절한 경우 데이터가 허용하는 대로 코호트 및 주기별로 요약(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균 및 기하 평균 변동 계수)된다.Samples are collected for pharmacokinetic analysis and to compare the performance of this study with those obtained in previous studies. Serum concentrations of atezolizumab and tiragolumab are reported as individual values and, where appropriate, summarized by cohort and period as data permits (mean, standard deviation, coefficient of variation, median, range, geometric mean and geometric mean coefficient of variation) do.
아테졸리주맙 및 티라골루맙의 개별 및 중앙 혈청 농도는 코호트 및 일별로 요약된다. 아테졸리주맙 및 티라골루맙 농도 데이터는, 데이터에 의해 보증된 대로 청소율, 분포 용적 및 AUC와 같은 - PK 매개변수를 유도하기 위해, 확립된 모집단 PK 모델을 사용하는 다른 연구의 데이터와 통합될 수 있다. 관련 PK 매개변수와 안전성, 유효성 또는 바이오마커 결과의 잠재적 상관관계를 조사할 수 있다.Individual and median serum concentrations of atezolizumab and tiragolumab are summarized by cohort and by day. Atezolizumab and tiragolumab concentration data can be combined with data from other studies using established population PK models to derive PK parameters - such as clearance, volume of distribution and AUC, as warranted by the data. have. Potential correlations between relevant PK parameters and safety, efficacy, or biomarker outcomes can be investigated.
E.E. 면역원성 분석Immunogenicity assay
면역원성 분석에는 항약물 항체(ADA) 평가를 받은 환자가 포함되며, 환자는 받은 치료에 따라 분류된다. 아테졸리주맙 및 티라골루맙 모두에 대한 치료-응급 ADA-양성 환자 및 ADA-음성 환자의 수 및 비율이 코호트별로 요약된다. ADA 상태와 안전성, 유효성 및 PK 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고될 수 있다.Immunogenicity assays include patients who have undergone an antidrug antibody (ADA) assessment, and patients are classified according to the treatment they receive. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients for both atezolizumab and tiragolumab are summarized by cohort. The relationship between ADA status and safety, efficacy, and PK endpoints can be analyzed and reported through descriptive statistics.
F.F. 바이오마커 분석Biomarker analysis
탐색적 바이오마커 분석은 암의 여러 병리학적, 면역학적 및 게놈 특성과 이들 환자의 임상 결과 사이의 관계를 탐색하기 위해 수행된다. 이러한 분석에는 종양 미세 환경 및/또는 주변부에서 면역 세포 및 ctDNA의 특성 분석이 포함되지만, 이에 국한되지 않는다. MPR, pCR 및 EFS를 포함한 임상 효능 결과는 가능한 경우 치료 이점을 평가하기 위해 바이오마커 하위 그룹(예: PD-L1 및 TIGIT 상태를 기반으로 함)에서 분석된다.Exploratory biomarker analysis is performed to explore the relationship between several pathological, immunological and genomic characteristics of cancer and the clinical outcome of these patients. Such assays include, but are not limited to, characterization of immune cells and ctDNA in and/or in the tumor microenvironment. Clinical efficacy outcomes, including MPR, pCR, and EFS, are analyzed in biomarker subgroups (eg, based on PD-L1 and TIGIT status) to evaluate treatment benefit, if possible.
실시예 13. 자궁경부암 환자를 대상으로 PD-1 축 결합 길항제와 병용한 항 TIGIT 길항제 항체의 유효성 Example 13. Efficacy of anti-TIGIT antagonist antibody in combination with PD-1 axis binding antagonist for cervical cancer patients
적어도 하나의 그러나 두 개 이하의 백금계 전신 요법에서 진행 또는 재발한 후, 전이성 및/또는 재발성 PD-L1 -양성(종양 세포 및 종양 관련 면역 세포[TICs] ≥5%) 자궁경부암 환자에 대해 PD-1 축 결합 길항제(예를 들어, 항 PD-L1 길항제 항체(예를 들어, 아테졸리주맙))와 병용하여 항 TIGIT 길항제(예를 들어, 본원에 개시된 항 TIGIT 항체, 예를 들어, 티라골루맙)를 사용한 치료 및 아테졸리주맙 단독 요법에 의한 치료의 효능 및 안전성이 평가된다 자격을 갖추려면, 환자는 ECOG(Eastern Cooperative Oncology Group) 수행 상태가 0 또는 1이고, 전이성 및/또는 재발성 PD-L1 양성 자궁경부암이 있어야 한다. For patients with metastatic and/or recurrent PD-L1-positive (tumor cells and tumor-associated immune cells [TICs] ≥5%) cervical cancer following progression or relapse on at least one but no more than two platinum-based systemic therapies An anti TIGIT antagonist (e.g., an anti-TIGIT antibody disclosed herein, e.g., Tyra in combination with a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) Efficacy and safety of treatment with gorumab) and with atezolizumab monotherapy are evaluated. You must have PD-L1-positive cervical cancer.
임상 시험은 하기 상세히 설명되고 도 21에 도시된 바와 같이, 단일 단계로 구성되었다.The clinical trial consisted of a single phase, as detailed below and shown in FIG. 21 .
무작위배정 randomization
이 연구에서는, 약 160명의 환자가 등록되었고, 아테졸리주맙과 병용하는 티라골루맙 또는 아테졸리주맙 단독 요법의 두 가지 치료 부문 중 하나에 배정되었다. 무작위 배정은 각 치료 부문에 균형 잡힌 배정을 보장하기 위해 순열 블록 무작위 배정 방법을 사용하여 3:1 비율로 발생한다. 무작위 배정은 ECOG 수행 상태(0 대 1), 화학방사선 요법 또는 방사선 요법의 이전 사용(예 대 아니오), 치료 이력(지속성 대 재발성 질환)에 따라 계층화된다.In this study, approximately 160 patients were enrolled and assigned to one of two treatment arms: tiragolumab in combination with atezolizumab or atezolizumab monotherapy. Randomization occurs in a 3:1 ratio using a permutation block randomization method to ensure a balanced assignment to each treatment arm. Randomization is stratified according to ECOG performance status (0 versus 1), previous use of chemoradiation or radiotherapy (yes versus no), and treatment history (persistent versus recurrent disease).
적격성eligibility
이 연구는 다음의 선정 기준에 따라 최소 연령이 18세인 여성 환자를 등록한다:This study enrolled female patients with a minimum age of 18 years according to the following inclusion criteria:
- 전신 화학요법, 수술, 및/또는 방사선 요법으로 근치적 치료를 받을 수 없는 이전 전신 화학요법의 1-두 라인 후, 조직학적으로 확인된 재발성 또는 지속성 편평세포암종, 선편평세포암종 또는 자궁경부 선암종(신경내분비계, 투명세포, 육종 조직학은 허용되지 않음).- Histologically confirmed recurrent or persistent squamous cell carcinoma, adenosquamous cell carcinoma, or uterine after 1 or 2 lines of previous systemic chemotherapy incapable of curative treatment with systemic chemotherapy, surgery, and/or radiation therapy Adenocarcinoma of the neck (neuroendocrine system, clear cell, sarcoma histology not allowed).
백금계 전신 화학요법의 적어도 하나의 이전 라인. 방사선 요법과 함께 제공되는 방사선 과민성 시스플라틴은 전신 화학요법의 계열로 간주되지 않는다.At least one previous line of platinum-based systemic chemotherapy. Radiation-sensitive cisplatin given with radiation therapy is not considered a class of systemic chemotherapy.
- 방사선학적으로 측정 가능한 질병- Radiologically measurable disease
- 0 또는 1의 동부 종양학 협력 그룹 (ECOG) 수행 상태- Eastern Oncology Collaborative Group (ECOG) performance status of 0 or 1
- 연구 분석을 위한 자궁경부암 조직(보관 또는 신선한 생검 표본)- Cervical cancer tissue (archived or fresh biopsy specimens) for research analysis
- ≥ 12 주의 기대 수명- Life expectancy of ≥ 12 weeks
- 적절한 혈액 및 장기 기능- Proper blood and organ function
- 가임기 여성은 적절한 피임법을 기꺼이 준수해야 한다.- Women of childbearing age should be willing to adhere to appropriate contraceptive practices.
환자는 다음 기준에 따라 등록에서 제외된다:Patients are excluded from enrollment based on the following criteria:
- 무작위 배정 전 28일 이내 및 연구 치료 중 치료 의도가 있는 임상시험 요법으로 치료 - Treatment with an intended clinical trial regimen within 28 days prior to randomization and during study treatment
- 모든 중추신경계(CNS) 또는 뇌 전이- Any central nervous system (CNS) or brain metastases
- 자가면역 질환 또는 면역 결핍의 활성 또는 병력- active or history of autoimmune disease or immunodeficiency
- 활성 결핵;- active tuberculosis;
- 알려진 임상적으로 유의한 간 질환- Known clinically significant liver disease
- 무작위 배정 시 시험자 판단에 따른 중증 감염- Severe infection according to the investigator's judgment at randomization
- CD137 작용제 또는 면역 관문 차단 요법, 항 CTLA-4, 항 TIGIT, 항 PD-1 및 항 PD-L1 치료 항체를 사용한 선행 치료 - Prior treatment with CD137 agonists or immune checkpoint blockade therapy, anti-CTLA-4, anti-TIGIT, anti-PD-1 and anti-PD-L1 therapeutic antibodies
- 무작위 배정 전 4주 이내 또는 5회 약물 제거 반감기(둘 중 더 긴 것) 이내에 전신 면역자극제로 치료- Treatment with systemic immunostimulants within 4 weeks prior to randomization or within 5 drug elimination half-lives (whichever is longer)
- 무작위 배정 전 1주 이내에 전신 면역억제제를 사용한 치료 또는 연구 중 전신 면역억제제의 필요성이 예상되는 경우- Treatment with systemic immunosuppressants within 1 week prior to randomization or if the need for systemic immunosuppressants is expected during the study
- 임신 또는 모유 영양 여성.- Pregnant or breastfeeding women.
- 티라골루맙 또는 아테졸리주맙 제제의 성분에 대해 알려진 과민증- Known hypersensitivity to any component of the formulation of tiragolumab or atezolizumab
A.A. 연구 치료 투여량 및 투여Study Treatment Dosage and Administration
치료 기간 동안, 환자는 고정 용량의 아테졸리주맙 1200 mg 또는 고정 용량의 아테졸리주맙 1200 mg과 고정 용량의 티라골루맙 600 mg을 받는다. 아테졸리주맙은 1200 mg Q3W(각 21일 주기의 제 1일째에 1200 mg)의 고정 용량으로 투여된다. 아테졸리주맙과 병용하는 티라골루맙은 실험군의 모든 환자에게 600 mg 고정 용량으로 각 21일 사이클의 1일 차에 IV로 Q3W 투여된다. During the treatment period, patients receive a fixed dose of atezolizumab 1200 mg or a fixed dose of atezolizumab 1200 mg and a fixed dose of tiragoluumab 600 mg. Atezolizumab is administered as a fixed dose of 1200 mg Q3W (1200 mg on Day 1 of each 21-day cycle). Tiragolumab in combination with atezolizumab is administered IV Q3W on Day 1 of each 21-day cycle at a fixed dose of 600 mg to all patients in the experimental group.
대체 시험에서는, 투여 당일에 아테졸리주맙을 표 59에 요약된 지침에 따라 단독요법으로 투여한다. 1차 주입 이전에, 주입 시작 전 60분 이내에 환자의 활력 징후 (예를 들어, 맥박수, 호흡수, 혈압, 체온)를 기록한다. 아테졸리주맙의 첫 번째 주입은 60(±15)분에 걸쳐 투여되며, 환자의 활력징후는 주입 중 매 15(±5)분 및 주입 후 30(10)분에 기록된다. 첫 번째 주입 동안 주입 관련 이상 반응이 발생하지 않은 경우, 후속 주입은 30분(±10)분에 걸쳐 투여할 수 있다. 활력 징후의 주입 전 기록은 아테졸리주맙 주입 시작 전 60분 이내에 계속 기록되었다.In an alternative trial, on the day of dosing, atezolizumab is administered as monotherapy according to the guidelines summarized in Table 59. Prior to the first infusion, the patient's vital signs (e.g., pulse rate, respiration rate, blood pressure, body temperature) are recorded within 60 minutes prior to initiation of the infusion. The first infusion of atezolizumab is administered over 60 (± 15) minutes, and the patient's vital signs are recorded every 15 (± 5) minutes during the infusion and 30 (10) minutes after the infusion. Subsequent infusions may be administered over 30 minutes (±10) minutes if no infusion-related adverse events occurred during the first infusion. Pre-infusion recordings of vital signs continued to be recorded within 60 minutes prior to initiation of atezolizumab infusion.

1차 주입 이전에, 주입 시작 전 60분 이내에 환자의 활력 징후 (예를 들어, 맥박수, 호흡수, 혈압, 체온)를 기록한다. 1차 주입 이전에, 주입 시작 전 60분 이내에 환자의 활력 징후 (예를 들어, 맥박수, 호흡수, 혈압, 체온)를 기록한다. 아테졸리주맙의 첫 번째 주입은 60(±15)분에 걸쳐 투여되며, 환자의 활력징후는 주입 중 매 15(±5)분 및 주입 후 30(±10)분에 기록된다. 항 TIGIT 항체(예를 들어, 본원에 개시된 항 TIGIT 항체, 예를 들어, 티라골루맙)의 첫 번째 주입은 60(±10)분에 걸쳐 투여되는 반면 환자의 활력 징후는 주입 동안 15(±5)분마다 기록되고 주입 후 30(±10)분에 기록된다. 첫 번째 주입 동안 주입 관련 이상 반응이 발생하지 않은 경우, 후속 주입은 30분(±10)분에 걸쳐 투여할 수 있다. 활력 징후의 주입 전 기록은 아테졸리주맙 주입 시작 전 60분 이내에 계속 기록되었다.Prior to the first infusion, the patient's vital signs (e.g., pulse rate, respiration rate, blood pressure, body temperature) are recorded within 60 minutes prior to initiation of the infusion. Prior to the first infusion, the patient's vital signs (e.g., pulse rate, respiration rate, blood pressure, body temperature) are recorded within 60 minutes prior to initiation of the infusion. The first infusion of atezolizumab is administered over 60 (±15) minutes, and the patient's vital signs are recorded every 15 (±5) minutes during the infusion and 30 (±10) minutes after the infusion. The first infusion of an anti-TIGIT antibody (eg, an anti-TIGIT antibody disclosed herein, eg, tiragolumab) is administered over 60 (±10) minutes while the patient's vital signs are 15 (±5) during the infusion. ) minutes and 30 (±10) minutes after injection. Subsequent infusions may be administered over 30 minutes (±10) minutes if no infusion-related adverse events occurred during the first infusion. Pre-infusion recordings of vital signs continued to be recorded within 60 minutes prior to initiation of atezolizumab infusion.
방사선 사진 데이터, 생검 결과 및 임상 상태의 통합 평가한 후, 질병 진행으로 인한 허용할 수 없는 독성 또는 증상 악화가 없는 환자가 임상적 이점을 경험하는 한 치료를 계속할 수 있다. IRC(Independent Review Committee)에서 결정한 RECIST v1.1에 따른 모호한 질병 진행 기준을 충족하는 환자는 지정된 기준을 모두 충족하는 경우 치료를 계속할 수 있다(티라골루맙과 아테졸리주맙 병용 또는 아테졸리주맙 단독). After an integrated evaluation of radiographic data, biopsy results, and clinical status, treatment can be continued as long as patients experience clinical benefit without unacceptable toxicity or worsening of symptoms due to disease progression. Patients who meet the criteria for ambiguous disease progression according to RECIST v1.1 as determined by the Independent Review Committee (IRC) may continue treatment (tiragolumab plus atezolizumab or atezolizumab alone) if all specified criteria are met. .



B.B. 병용 요법combination therapy
특정 병용 요법이 허용되었다. 병용 요법에는 연구 치료 시작 7일 전부터 치료 중단 방문시까지 프로토콜-필수 연구 치료 외에 환자가 사용한 모든 약물(예를 들어, 경구 피임약, 호르몬 대체 요법, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)이 포함된다. 환자는 연구 기간 동안 다음과 같은 병용 요법을 사용하는 것이 허용된다. Certain combination therapies were permitted. Combination therapy includes any medications used by the patient other than protocol-essential study treatment (e.g., oral contraceptives, hormone replacement therapy, prescription drugs, over the counter, vaccines, herbal or homeopathic remedies; nutritional supplements). Patients are permitted to use the following combination therapies for the duration of the study.
전신 코르티코스테로이드 및 TNF-α 억제제는 아테졸리주맙 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여해야 하는 상황에서는 항히스타민제를 포함한 대안을 고려해야 한다. 대안이 가능하지 않은 경우, 전신 코르티코스테로이드 및 TNF-α 억제제를 시험자의 재량에 따라 투여할 수 있다.Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of atezolizumab treatment. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines should be considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the discretion of the investigator.
항히스타민제, 해열제 및/또는 진통제를 사용한 예비투약은 시험자의 재량에 따라 이차 및 후속 연구 주입에 대해서만 투여될 수 있다. Premedication with antihistamines, antipyretics and/or analgesics may be administered only for secondary and subsequent study infusions at the discretion of the investigator.
C.C. 유효성 평가변수Efficacy endpoint
아테졸리주맙 단독 요법과 비교하여 티라골루맙과 아테졸리주맙 병용 요법의 유효성을 평가하기 위해, 4주 이상의 간격(RECIST v1.1에 따라 조사관에 의해 결정됨)으로 2회 연속 완전 반응(CR) 또는 부분 반응(PR)을 경험한 환자의 백분율로 정의된 객관적 반응률(ORR)을 1차 평가변수로서 측정하였다. 1차 유효성 분석은 모든 환자가 등록되고, ORR 평가를 위한 추적 관찰에 남아 있는 환자들 사이에서 최소 약 6개월의 추적 관찰이 달성되면 수행된다. 1차 분석에서, ORR 평가가 누락된 환자는 반응을 달성하지 못한 것으로 간주된다. 비율에 대한 1-샘플 z-분석은 아테졸리주맙군과 티라골루맙 병용요법의 ORR을 과거 기준과 비교하는 데 사용된다. ORR의 추정치와 95% CI(Clopper-Pearson; Clopper and Pearson 1934)은 각 치료 부문에 대해 계산된다. 병용군에서 ORR의 95% CI의 하한값(표 61) 및 단독요법군에서 관찰된 ORR(표 62)은 기준점을 제외해야 할 것으로 예상된다.To evaluate the effectiveness of tiragolumab plus atezolizumab compared to atezolizumab monotherapy, two consecutive complete responses (CR) or The objective response rate (ORR), defined as the percentage of patients experiencing a partial response (PR), was measured as the primary endpoint. A primary efficacy analysis is performed when all patients are enrolled and a minimum of approximately 6 months of follow-up is achieved among patients remaining on follow-up for ORR evaluation. In the primary analysis, patients who miss an ORR assessment are considered to have failed to achieve a response. A 1-sample z-analysis of ratios is used to compare the ORR of the atezolizumab arm with tiragolumab combination to historical baselines. Estimates of ORR and 95% CI (Clopper-Pearson; Clopper and Pearson 1934) are calculated for each treatment arm. The lower limit of 95% CI of ORR in the combination arm (Table 61) and ORR observed in the monotherapy arm (Table 62) are expected to exclude baseline.

MDO = 최소 검출 가능 관찰; ORR = 전체 응답률.MDO = minimum detectable observation; ORR = overall response rate.
a 자원: Chung et al. 2019.a Resource: Chung et al. 2019.
b MDO는 최종 분석에서 통계적 유의성을 나타내는 가장 작게 관찰된 ORR로 정의된다.b MDO is defined as the smallest observed ORR showing statistical significance in the final analysis.

ORR = 전체 응답률.ORR = overall response rate.
이 연구의 2차 유효성 목표는 반응 지속 기간(DOR), 질병 통제율(DCR), 최상의 임상 반응(BCR), 무진행 생존(PFS), 및 전체 생존(OS)을 기반으로 아테졸리주맙과 아테졸리주맙 병용 티라골루맙 및 아테졸리주맙 단독 요법의 유효성을 평가하는 것이다. DOR은 RECIST v1.1에 따라 IRC에서 결정한 바와 같이, 객관적인 반응을 보인 환자에 대해 문서화된 객관적 반응(CR 또는 PR)이 처음 발생한 날부터 질병 진행 날짜 또는 모든 원인으로 인한 사망 날짜(둘 중 먼저 발생하는 날짜)까지의 시간으로 정의된다. DCR은 RECIST v1.1에 따라 IRC에서 결정한 바와 같이, CR, PR 또는 SD가 있는 환자의 비율로 정의된다. BCR은 시험자가 결정한 바와 같이, CR, PR 또는 SD가 있는 환자의 비율로 정의된다. 무진행생존(PFS)은 RECIST v1.1에 따라 IRC에서 결정한 바와 같이, 무작위 배정부터 질병 진행 또는 모든 원인으로 인한 사망(둘 중 먼저 발생하는 것)이 처음 발생하기까지의 시간으로 정의된다. OS는 무작위배정시부터 임의의 원인으로 인한 사망시까지의 시간으로 정의된다.The secondary efficacy goals of this study were based on duration of response (DOR), disease control rate (DCR), best clinical response (BCR), progression-free survival (PFS), and overall survival (OS). To evaluate the efficacy of tiragolumab and atezolizumab monotherapy in combination with zolizumab. DOR is the date of disease progression or death from any cause (whichever occurs first) from the first occurrence of a documented objective response (CR or PR) for a patient with an objective response, as determined by the IRC per RECIST v1.1. is defined as the time until the date). DCR is defined as the proportion of patients with CR, PR, or SD as determined by the IRC per RECIST v1.1. BCR is defined as the proportion of patients with CR, PR, or SD, as determined by the investigator. Progression-free survival (PFS) is defined as the time from randomization to the first occurrence of disease progression or death from any cause, whichever occurs first, as determined by the IRC per RECIST v1.1. OS is defined as the time from randomization to death from any cause.
추가 탐색적 유효성 평가변수는 RECIST v1.1에 따라 시험자가 결정한 바와 같이, 질병 통제(≥6주 동안 SD 또는 CR 또는 PR로 정의)를 추가로 포함할 수 있다.Additional exploratory efficacy endpoints may additionally include disease control (defined as SD or CR or PR for ≥6 weeks), as determined by the investigator per RECIST v1.1.
아테졸리주맙 단독 요법과 비교하여 아테졸리주맙과 병용한 티라골루맙의 안전성 및 내약성을 평가하기 위해, 이상 반응(AE)의 발생률, 특성 및 중증도(예: 국립 암 연구소(National Cancer Institute) 이상 반응에 대한 공통 용어 기준 버전 5.0(NCI)에 따라 등급이 매겨진 AE CTCAE v5.0))가 측정된다(NCI CTCAE에 구체적으로 나열되지 않은 이상 반응은 표 63에 따라 측정됨). 사이토카인 방출 증후군(CRS)의 중증도는 미국 이식 세포 치료 학회 CRS 합의 등급 스케일에 따라 결정된다. 또한, 아테졸리주맙 단독 요법과 비교하여 티라골루맙과 아테졸리주맙을 병용 투여하는 동안 및 투여 후 기준선으로부터의 활력 징후, 신체 소견 및 임상 실험실 결과의 임상적으로 유의한 변화도 측정된다.To evaluate the safety and tolerability of tiragolumab in combination with atezolizumab compared to atezolizumab alone, the incidence, nature, and severity of adverse events (AEs) (e.g., National Cancer Institute adverse events) (AE CTCAE v5.0) graded according to Common Terminology Criteria Version 5.0 (NCI) for CTCAE (adverse events not specifically listed in NCI CTCAE are measured according to Table 63). The severity of cytokine release syndrome (CRS) is determined according to the American Society for Transplantation Cell Therapy CRS Consensus Rating Scale. In addition, clinically significant changes from baseline in vital signs, physical findings and clinical laboratory results during and after tiragolumab plus atezolizumab compared to atezolizumab alone are also measured from baseline.

a 일상 생활의 도구적 활동은 식사 준비, 식료품이나 옷 쇼핑, 전화 사용, 돈 관리 등을 의미한다. a Instrumental activities of daily life include preparing meals, shopping for groceries or clothes, using the phone, and managing money.
b 일상 생활의 자가 관리 활동의 예로는 침대에 누워 있지 않은 환자가 수행하는 목욕, 옷 입기 및 옷 벗기기, 스스로 식사하기, 화장실 사용하기, 약물 복용 등이 있다. b Examples of self-management activities of daily living include bathing, dressing and undressing, eating on their own, using the bathroom, and taking medications by a patient not lying in bed.
결과 측정 기간Result measurement period
1차 결과 측정 기간인 객관적 반응률(ORR)은 질병 진행 날짜 또는 모든 원인으로 인한 사망 날짜 중 먼저 발생한 날짜(최대 36개월)까지 문서화된 객관적 반응의 첫 번째 발생이 될 것이다. 2차 결과 측정 기간은 표 64에서 확인할 수 있다.The primary outcome measure, the objective response rate (ORR), will be the first occurrence of a documented objective response up to the date of disease progression or the date of all-cause death, whichever occurs first (up to 36 months). The secondary result measurement period can be found in Table 64.



바이오마커 biomarker
본 무작위 연구의 모든 환자에 대한 탐색적 바이오마커 평가를 위해, 보관 종양 조직, 뿐만 아니라 혈청, 혈장, 전혈 및 대변을 포함한 환자 샘플을 수집한다. PD-L1 상태를 평가하는 것 외에도, 내성, 질병 진행 및 티라골루맙 및/또는 아테졸리주맙의 임상적 이점과 관련된 바이오마커를 분석한다. 예를 들어, 티라골루맙 및/또는 아테졸리주맙의 임상적 이점 및 안전성과 관련된 잠재적 예측 및 예후 바이오마커가 분석된다. For exploratory biomarker evaluation for all patients in this randomized study, patient samples including archival tumor tissue, as well as serum, plasma, whole blood, and feces are collected. In addition to assessing PD-L1 status, biomarkers associated with resistance, disease progression and clinical benefit of tiragolumab and/or atezolizumab are analyzed. For example, potential predictive and prognostic biomarkers related to the clinical benefit and safety of tiragolumab and/or atezolizumab are analyzed.
기준선에서 수집된 종양 조직 및 혈액 샘플 (및 시험자가 임상적으로 가능한 것으로 간주하는 경우 질병 진행 시점에 수집된 종양 조직)로 전체 엑솜 시퀀싱(WES) 및/또는 차세대 시퀀싱(NGS)하여 연구 치료제에 대한 반응을 예측할 수 있는, 더 중증 질병 상태로의 진행과 관련되는, 연구 치료제에 대한 후천적 내성과 관련되는, 이상 반응 발병에 대한 민감성과 관련되는, 또는 질병 생물학에 대한 지식 및 이해를 증가시킬 수 있는 체세포 돌연변이를 식별할 수 있다.Whole exome sequencing (WES) and/or next-generation sequencing (NGS) of tumor tissue and blood samples collected at baseline (and tumor tissue collected at the time of disease progression if deemed clinically feasible by the investigator) for study therapeutics that may be predictive of a response, associated with progression to a more severe disease state, associated with acquired resistance to a study treatment, associated with susceptibility to the development of an adverse event, or that may increase knowledge and understanding of disease biology Somatic mutations can be identified.
바이오마커는, 종양 조직 상의 PD-L1 및/또는 TIGIT 발현, 종양 조직 및/또는 혈액 내 순환 종양 DNA로부터의 생식계열 및 체세포 돌연변이(돌연변이 로드, MSI, 및 MMR 결함을 포함하지만 이에 국한되지 않음), WGS 및/또는 NGS를 통한 식별, 유전자 분석(예: CD274) 또는 종양 면역생물학과 관련된 유전자 서명, 예를 들어 Teffector 유전자, PD-L1, TIGIT, HPV 변경, 림프구 하위집단, T 세포-수용체 레퍼토리, T-세포 및 NK-세포 활성화와 관련된 사이토카인, 및 혈장 유래 사이토카인을 포함하지만 이에 국한되지는 않는다. Biomarkers include, but are not limited to, PD-L1 and/or TIGIT expression on tumor tissue, germline and somatic mutations from circulating tumor DNA in tumor tissue and/or blood, including, but not limited to, mutation load, MSI, and MMR defects. , identification via WGS and/or NGS, genetic analysis (e.g. CD274) or genetic signatures relevant to tumor immunobiology, e.g. T effector genes, PD-L1, TIGIT, HPV alterations, lymphocyte subpopulations, T cell-receptor repertoire , cytokines involved in T-cell and NK-cell activation, and plasma-derived cytokines.
PD-L1/PD-1 경로가 1차 환자 집단에서 ORR, PFS, DOR 및/또는 OS에 미치는 영향을 평가하기 위해, 유효성, 안전성, PK, 면역원성 및 환자 중심 결과 (PRO)에 대한 종양 조직 및/또는 혈액에서 단백질, RNA, DNA, 종양 돌연변이 부담, 및 기타 탐색적 바이오마커 간의 관계를 평가할 수 있다. 추가로, 일차 집단에서 ORR, PFS, DOR 및/또는 OS에 대한 TIGIT 경로의 효과를 평가하기 위해, 단백질 및/또는 RNA 발현으로 정의되는, 종양에 TIGIT 발현이 있는 환자 집단에서 ORR, DOR, PFS 및 OS를 평가할 수 있다.To evaluate the effect of the PD-L1/PD-1 pathway on ORR, PFS, DOR and/or OS in the primary patient population, tumor tissue for efficacy, safety, PK, immunogenicity and patient-centred outcome (PRO). and/or assess relationships between proteins, RNA, DNA, tumor mutation burden, and other exploratory biomarkers in blood. Further, to evaluate the effect of the TIGIT pathway on ORR, PFS, DOR and/or OS in the primary population, ORR, DOR, PFS in a patient population with TIGIT expression in the tumor, defined as protein and/or RNA expression and OS.
탐색적 바이오마커 분석은 이러한 마커(예를 들어, TIGIT IHC 상태)와 연구 치료 효능의 연관성을 이해하기 위해 수행할 수 있다. 이러한 유효성 결과는 IHC 및/또는 RNA 분석으로 결정하여 종양에 높은 TIGIT 발현이 있는 환자 집단에서 탐색될 수 있다. 본 연구와 관련하여 WGS 데이터의 탐색적 분석이 수행될 수 있으며 이는 질병 병리생물학에 대한 연구원의 이해를 높이고 새로운 치료 접근법의 개발을 안내하기 위해 다른 연구들의 데이터와 통합하여 탐색될 수 있다.Exploratory biomarker analysis can be performed to understand the association of these markers (eg, TIGIT IHC status) with study treatment efficacy. These efficacy outcomes can be explored in patient populations with high TIGIT expression in their tumors as determined by IHC and/or RNA analysis. Exploratory analysis of WGS data can be performed in connection with this study, which can be explored in conjunction with data from other studies to improve researchers' understanding of disease pathobiology and guide the development of new therapeutic approaches.
면역원성 분석Immunogenicity assay
티라골루맙 및 아테졸리주맙에 대한 면역 반응을 평가하기 위해, 치료-응급 항 약물 항체(ADA)의 발생률과 안전성, 유효성 및 약동학(PK)에 대한 잠재적 영향을 평가한다.To evaluate the immune response to tiragolumab and atezolizumab, the incidence and potential impact on safety, efficacy, and pharmacokinetics (PK) of treatment-emergent anti-drug antibodies (ADA) are evaluated.
2019년 12월, 연구 GO30103의 Ia상 부분에서 티라골루맙에 대한 치료 응급 항약물 항체(ADA)가 검출되지 않았다. 연구 GO30103의 Ib상 부분에서, 평가 가능한 환자 154명 중 3명(1.9%)이 티라골루맙에 대한 치료 응급 ADA에 대해 양성이었다. 2019년 10월, 연구 GO40290에서 평가된 환자 66명 중 1명(1.5%)이 티라골루맙에 대한 치료 응급 ADA에 대해 양성이었다. 2019년 10월, 연구 GO40290에서 평가된 환자 66명 중 1명(1.5%)이 티라골루맙에 대한 치료 응급 ADA에 대해 양성이었고 환자는 한 시점에서만 양성이었다.In December 2019, no therapeutic rescue antidrug antibodies (ADA) were detected against tyragolumab in the Phase Ia portion of study GO30103. In the Phase Ib portion of study GO30103, 3 of 154 evaluable patients (1.9%) were positive for treatment-emergent ADA to tiragolumab. In October 2019, 1 in 66 patients (1.5%) evaluated in study GO40290 was positive for treatment-emergent ADA to tiragolumab. In October 2019, 1 out of 66 patients (1.5%) evaluated in study GO40290 were positive for therapeutic emergency ADA to tiragolumab and the patient was positive at only one time point.
F. 약동학 분석F. Pharmacokinetic Analysis
아테졸리주맙과 병용하여 투여할 때 티라골루맙의 약동학을 특성화하기 위해, 티라골루맙의 혈청 농도는 상이한 시점의 피험자로부터 결정된다. 또한, 아테졸리주맙을 티라골루맙과 병용하여 투여하거나 단독 요법으로 투여할 때, 아테졸리주맙의 약동학을 특성화하기 위해 연구 중 상이한 시점에서 대상체로부터 아테졸리주맙의 혈장 농도를 수득한다.To characterize the pharmacokinetics of tiragolumab when administered in combination with atezolizumab, serum concentrations of tiragolumab are determined from subjects at different time points. In addition, plasma concentrations of atezolizumab are obtained from subjects at different time points during the study to characterize the pharmacokinetics of atezolizumab when administered in combination with tiragolumab or as monotherapy.
실시예 14. 삼중 음성 유방암 환자를 대상으로 아테졸리주맙 및 화학요법과 병용한 티라골루맙의 안전성, 유효성 및 약동학에 관한 Ib상, 공개 라벨, 다중 코호트 연구Example 14. A Phase Ib, Open Label, Multiple Cohort Study of the Safety, Efficacy and Pharmacokinetics of Tiragolumab in Combination with Atezolizumab and Chemotherapy in Patients with Triple Negative Breast Cancer
본 실시예는 조기 삼중 음성 유방암(eTNBC) 환자에서 아테졸리주맙 및 화학요법과 병용되는 티라골루맙의 안전성, 유효성 및 약동학을 평가하기 위해 설계된 Ib상, 공개 라벨, 다중 코호트 연구를 설명한다. 본 연구는 하기의 코호트로 구성된다:This example describes a Phase Ib, open label, multi-cohort study designed to evaluate the safety, efficacy and pharmacokinetics of tiragolumab in combination with atezolizumab and chemotherapy in patients with early triple negative breast cancer (eTNBC). This study consists of the following cohorts:
![]()
![]()
- A군: 아테졸리주맙과 병용되는 티라골루맙, 독소루비신, 및 시클로포스파미드로 이어지는, 티라골루맙과 병용되는 아테졸리주맙, 냅-파클리탁셀, 및 카보플라틴(티라골루맙 및 아테졸리주맙 + nab-pac-carbo-AC로 지칭됨)- Group A: tiragolumab in combination with atezolizumab, doxorubicin, and cyclophosphamide followed by atezolizumab in combination with tiragolumab, nap-paclitaxel, and carboplatin (tiragolumab and atezolizumab + referred to as nab-pac-carbo-AC)
- B군: 아테졸리주맙과 병용되는 티라골루맙, 독소루비신 및 시클로포스파미드로 이어지는, 티라골루맙과 병용되는 아테졸리주맙, 냅-파클리탁셀(티라골루맙 및 아테졸리주맙 + nab-pac-AC로 지칭됨)- Group B: tiragolumab in combination with atezolizumab, followed by doxorubicin and cyclophosphamide, atezolizumab in combination with tiragolumab, nap-paclitaxel (with tiragolumab and atezolizumab + nab-pac-AC) referred to)
추가로, AC 및 G-CSF(예: 필그라스팀 또는 페그필그라스팀) 또는 GM-CSF가 코호트 B의 환자에게 냅-파클리탁셀 후 배경 치료로 투여된다.Additionally, AC and G-CSF (eg, filgrastim or pegfilgrastim) or GM-CSF are administered to patients in Cohort B as background treatment following nap-paclitaxel.
본 연구는 초기에 임상적으로 평가된 T2-4d TNBC로 수술하기 적격한 환자에서, AC로 이어지는, 아테졸리주맙과 병용되는 신보조제 티라골루맙, 냅-파클리탁셀, 및 카보플라틴 또는 AC로 이어지는, 아테졸리주맙과 병용되는 신보조 티라골루맙, 냅-파클리탁셀의 안전성 및 내약성, 예비 유효성 및 약동학을 평가할 수 있도록 설계되었다. This study was conducted in patients eligible for surgery with initially clinically evaluated T2-4d TNBC, leading to AC, neoadjuvant tyragolumab in combination with atezolizumab, nap-paclitaxel, and carboplatin or leading to AC , designed to evaluate the safety and tolerability, preliminary efficacy and pharmacokinetics of neoadjuvant tiragolumab and nap-paclitaxel in combination with atezolizumab.
A.A. 연구 설계study design
이러한 Ib상, 다중 코호트, 공개 라벨, 다중 센터, 글로벌 연구는 초기에 임상적으로 평가된 T2-4d TNBC(PD-L1 모든 진입자 집단)로 수술하기 적격한 환자에서, 독소루비신 및 시클로포스파미드(AC)로 이어지는, 아테졸리주맙과 병용되는 신보조제 티라골루맙 및 카보플라틴 또는 AC로 이어지는, 아테졸리주맙과 병용되는 신보조 티라골루맙, 냅-파클리탁셀의 안전성 및 내약성, 예비 유효성 및 약동학을 조사할 수 있도록 설계되었다. 도 22는 코토트 B에 대한 연구 설계를 예시한다.This Phase Ib, multi-cohort, open-label, multi-center, global study initially demonstrated that doxorubicin and cyclophosphamide ( The safety and tolerability, preliminary efficacy and pharmacokinetics of neoadjuvant tiragolumab in combination with atezolizumab leading to AC) and carboplatin or neoadjuvant tiragolumab in combination with atezolizumab leading to AC), nap-paclitaxel designed to be investigated. 22 illustrates the study design for Cotote B.
동의하고 적격성을 갖춘 환자는 다음 두 치료군 중 하나에 1:1 비율로 무작위 배정된다:Consent and eligible patients will be randomized in a 1:1 ratio to one of two treatment groups:
![]()
![]()
![]()
![]()
탐색적 평가변수(병리학적 완전 반응(pCR): 유방 및 림프절의 침습성 종양 근절(ypT0/is ypN0))은 신보조 요법 및 수술 완료 후 현지 검토에 의해 설정된다. 수술은 신보조 요법의 최종 투여 후 14일 이내에 수행되어야 하고, 늦어도 6주 이후에는 수행되어야 한다. 혈소판 수는 수술 전에 확인해야 하며, ≥ 75,000 cells/μL이어야 한다.Exploratory endpoints (pathological complete response (pCR): eradication of invasive tumors of the breast and lymph nodes (ypT0/is ypN0)) are established by local review after completion of neoadjuvant therapy and surgery. Surgery should be performed within 14 days after the last administration of neoadjuvant therapy, and at the latest 6 weeks later. The platelet count should be checked prior to surgery and should be ≥ 75,000 cells/μL.
수술 후 환자 관리에는 임상적으로 지시된 대로 방사선 요법이 포함될 수 있으며, pCR에 도달하지 못한 환자 관리는 현재 표준 치료 지침을 따라야 한다.Postoperative patient management may include radiation therapy as clinically indicated, and management of patients who do not achieve pCR should follow current standard of care guidelines.
신체 검사 또는 기준선에서의 방사선 영상 촬영에 의해 평가된 임상적으로 양성인 겨드랑이 결절이 있는 환자는 무작위 배정 전에 미세-바늘 흡인 또는 코어-바늘 생검을 받는 것이 권장되고, 액와 림프절 절제술(ALND) 또는 최소 감시 림프절 생검(SLNB)이 최종 수술 시에 수행되는 것이 권장된다. 기준선 미세-바늘 흡인 또는 코어-바늘 생검의 결과는 결절 병기 결정에 사용되어(국제 암 통제 연합/미국 암 공동 위원회[UICC/AJCC], 8판에 따른 해부학적 병기 그룹에 따름), 생검 결과가 양성인 환자는 림프절 양성(N1-N3c)으로 병기결정해야 하는 반면, 생검 결과가 음성이거나 모호한 환자는 다른 임상 측정과 상관없이 림프절 음성(N0)으로 병기결정해야 한다.It is recommended that patients with clinically benign axillary nodules assessed by physical examination or radiographic imaging at baseline undergo micro-needle aspiration or core-needle biopsy prior to randomization, axillary lymph node dissection (ALND) or minimal surveillance It is recommended that a lymph node biopsy (SLNB) be performed at the final surgery. Results from baseline fine-needle aspiration or core-needle biopsy were used for nodular staging (according to the International Coalition for Control/American Cancer Joint Committee [UICC/AJCC], anatomical staging group according to 8th ed.), so that the biopsy results were Patients who are positive should be staged as lymph node positive (N1-N3c), whereas patients with negative or ambiguous biopsy results should be staged as lymph node negative (N0) regardless of other clinical measurements.
기준선에서 임상적으로 또는 미세-바늘 생검 또는 코어-바늘 생검으로 입증된 음성 겨드랑이 결절이 있는 환자의 경우, 신보조 요법 완료 후 겨드랑이 수술 관리에는 SLNB 또는 ALND가 포함될 수 있다. SLNB가 수행되는 경우, 하나 이상의 림프절(최소 2~3개)을 제거하고 감시 림프절에 양성 거대 전이가 있는 모든 환자는 양성 림프절 수에 관계없이 ALND를 받아야 한다.For patients with negative axillary nodules at baseline, clinically or evidenced by micro-needle biopsy or core-needle biopsy, management of axillary surgery after completion of neoadjuvant therapy may include SLNB or ALND. If SLNB is performed, all patients with one or more lymph nodes (at least 2-3) removed and with benign large metastases to the sentinel lymph nodes should receive an ALND, regardless of the number of benign lymph nodes.
환자는 연구 동안 예정된 간격으로 임상 및 방사선 종양 평가를 모두 받는다.Patients receive both clinical and radiation oncology assessments at scheduled intervals during the study.
종양 미세 환경에서 약물 조합의 작용 기전 및 가능한 내성 기전을 평가하기 위해, 종양 조직은 주기 2의 1일차에 투여 전에 수집될 수 있다.To evaluate the mechanism of action and possible resistance mechanisms of drug combinations in the tumor microenvironment, tumor tissues can be collected prior to dosing on Day 1 of Cycle 2.
종양 조직은 시험자가 평가하고 문서화한 대로, 그리고 질병 진행의 첫 번째 증거가 있을 때(새로운 항암 치료를 시작하기 전) 임상적으로 가능하지 않은 경우를 제외하고는 생검에 의해 수집된다. 샘플은 아테졸리주맙과 병용하는 티라골루맙의 내성 또는 질병 진행 및 임상적 이점과 관련된 종양 조직 바이오마커의 분석을 가능하게 하기 위해 사용된다.Tumor tissue is collected by biopsy, as assessed and documented by the investigator, and when there is first evidence of disease progression (before starting new chemotherapy), unless clinically feasible. The samples are used to enable analysis of tumor tissue biomarkers related to resistance or disease progression and clinical benefit of tiragolumab in combination with atezolizumab.
B.B. 용량 및 투여Dosage and administration
치료 요법은 도 도 22에 요약되어 있다.The treatment regimen is summarized in FIG. 22 .
아테졸리주맙, 티라골루맙, 및 화학요법의 예정된 주입일에는, 아테졸리주맙 및 티라골루맙을 주입한 후 화학요법을 투여한다.On the scheduled infusion days of atezolizumab, tiragolumab, and chemotherapy, the atezolizumab and tiragolumab infusion are followed by chemotherapy.
아테졸리주맙(840 mg)을 주입한 후, 환자는 티라골루맙 420 mg을 투여 받는다.After infusion of atezolizumab (840 mg), the patient receives tiragolumab 420 mg.
아테졸리주맙, 티라골루맙, 및 화학요법의 투여는 훈련된 직원과 잠재적인 중증 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 환경에서 실시한다.Administration of atezolizumab, tiragolumab, and chemotherapy is performed in a monitored environment with immediate access to trained personnel and appropriate equipment and medications to manage potentially severe reactions.
약물 준비, 보관 및 투여에 대한 자세한 지침은 약국 매뉴얼을 참조한다.Refer to the pharmacy manual for detailed instructions on drug preparation, storage and administration.
티라골루맙과 아테졸리주맙Tiragolumab and Atezolizumab
코호트 B에서, 환자들은 840 mg 고정 용량의 아테졸리주맙을 각 28일 주기의 제 1일 및 15일 차에 IV 주입 Q2W로 투여받으며, 그 후 420 mg 고정 용량의 티라골루맙이 환자들에게 각 28일 주기의 제 1일 및 15일 차에 IV 주입 Q2W로 투여된다( 도 22 참조). 티라골루맙 및 아테졸리주맙 용량은 고정이며, 체중에 따라 달라지지 않는다. 티라골루맙 및 아테졸리주맙 주입(관찰 기간을 포함)은 표 65에 요약된 지침에 따라 투여된다.In Cohort B, patients receive a fixed dose of 840 mg of atezolizumab as IV infusion Q2W on days 1 and 15 of each 28-day cycle, after which 420 mg of fixed dose tyragolumab is administered to patients each Administered as IV infusion Q2W on Days 1 and 15 of a 28-day cycle (see Figure 22). Tiragolumab and atezolizumab doses are fixed and do not vary with body weight. Tiragolumab and atezolizumab infusions (including observation period) are administered according to the guidelines summarized in Table 65.




냅-파클리탁셀Nap-paclitaxel
냅-파클리탁셀은 30분에 걸쳐 IV 주입으로 환자에게 투여된다.Nap-paclitaxel is administered to the patient as an IV infusion over 30 minutes.
냅-파클리탁셀은 아테졸리주맙 및 티라골루맙 후에 투여해야 한다. 냅-파클리탁셀의 용량은 12주 동안 IV 주입 QW에 의해 환자에게 투여되는 125 mg/m2이다. 냅-파클리탁셀의 용량은 매 7일보다 더 자주 투여해서는 안 된다.Nap-paclitaxel should be administered after atezolizumab and tiragolumab. The dose of nap-paclitaxel is 125 mg/m 2 administered to patients by IV infusion QW for 12 weeks. Doses of nap-paclitaxel should not be administered more frequently than every 7 days.
기관은 환자 체중 변화의 경우에 냅-파클리탁셀의 용량 조정을 결정하기 위해 기관의 관리 표준을 따라야 한다. 주입 부위는 연구 약물 투여 중 침윤 가능성으로 인해 면밀히 모니터링해야 한다.Institutions should follow institutional standards of care to determine dose adjustments of nap-paclitaxel in case of changes in patient weight. The injection site should be closely monitored due to possible infiltration during study drug administration.
냅-파클리탁셀의 준비 및 투여에 대한 자세한 내용은 현지 처방 정보를 참조한다.For more information on the preparation and administration of nap-paclitaxel, see local prescribing information.
카보플라틴carboplatin
카보플라틴은 4회 용량에 대해 3주마다 5mg/mL/min의 AUC를 목표로 15-60분에 걸쳐 단기 IV 주입에 의해 nab-파클리탁셀 투여 완료 후 투여된다.Carboplatin is administered after completion of nab-paclitaxel dosing by short IV infusion over 15-60 minutes with an AUC of 5 mg/mL/min every 3 weeks for 4 doses.
카보플라틴 과다 복용에 대한 공지된 해독제는 없다. 필요한 경우, 환자는 골수 억제 및 신장, 간 및 청각 기능 장애와 관련된 지지 치료가 필요할 수 있다. 최대 1600 mg/m2의 용량은 설사 및 탈모증의 발병과 함께 극도로 통증을 느끼는 환자와 관련이 있었다. 권장량을 초과하는 양의 카보플라틴을 사용하는 것은 시력 상실과도 관련이 있었다. 자세한 내용은 카보플라틴에 대한 현지 처방 정보를 참조한다.There is no known antidote for carboplatin overdose. If necessary, patients may require bone marrow suppression and supportive care related to renal, hepatic and auditory dysfunction. Doses of up to 1600 mg/m2 have been associated with patients experiencing extreme pain with onset of diarrhea and alopecia. The use of carboplatin in excess of the recommended dose was also associated with vision loss. See your local prescribing information for carboplatin for more information.
시클로포스파미드cyclophosphamide
시클로포스파미드는 3-5분에 걸쳐 IV 볼루스로 또는 현지 주의 기준에 따른 IV 주입으로 제공되어야 한다. AC는 아테졸리주맙과 티라골루맙 이후에 투여해야 한다. 사이클로포스파미드의 용량은 600mg/m2로 정맥내 투여한다. 독성에 대한 용량 지연 및 용량 감소는 허용된다. 시클로포스파미드는 G-CSF 또는 GM-CSF 지원과 함께 4회 용량(용량 밀도 AC) 동안 Q2W로 투여된다. 비고: 경구 시클로포스파미드는 허용되지 않는다.Cyclophosphamide should be given as an IV bolus over 3-5 minutes or as an IV infusion according to local state standards. AC should be administered after atezolizumab and tiragolumab. The dose of cyclophosphamide is administered intravenously at 600 mg/m 2 . Dose delays and dose reductions for toxicity are acceptable. Cyclophosphamide is administered as Q2W for 4 doses (dose density AC) with G-CSF or GM-CSF support. Note: Oral cyclophosphamide is not allowed.
화학요법 유도된 메스꺼움 및 구토 예방 및 치료는 임상적으로 지시된 대로 시행되어야 한다. 전신성 코르티코스테로이드는 아테졸리주맙 및 티라골루맙 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있으므로, 임상적으로 가능하다면 대체 약제를 고려해야 한다.Prevention and treatment of chemotherapy-induced nausea and vomiting should be administered as clinically indicated. Because systemic corticosteroids may attenuate the potentially beneficial immunological effects of atezolizumab and tiragolumab treatment, alternative agents should be considered when clinically feasible.
사이클로포스파미드의 조제 및 투여에 관한 세부 사항은 지역 처방 정보를 참조한다.Refer to local prescribing information for details regarding the preparation and administration of cyclophosphamide.
독소루비신doxorubicin
독소루비신은 현지 주의 기준에 따라, 3-5분에 걸쳐 IV 볼루스로 투여하거나 15-30분에 걸쳐 IV 주입으로 투여해야 한다. AC는 아테졸리주맙과 티라골루맙 이후에 투여해야 한다. IV 주입에 의해 환자에게 투여되는 독소루비신의 용량은 60 mg/m2이다. 독성에 대한 용량 지연 및 감소는 허용된다. 독소루비신은 G-CSF 또는 GM-CSF 지원과 함께 4회 용량(용량 밀도 AC) 동안 Q2W로 투여된다.Doxorubicin should be administered as an IV bolus over 3-5 minutes or as an IV infusion over 15-30 minutes, depending on local state standards. AC should be administered after atezolizumab and tiragolumab. The dose of doxorubicin administered to a patient by IV infusion is 60 mg/m 2 . Dose delays and reductions for toxicity are acceptable. Doxorubicin is administered as Q2W for 4 doses (dose density AC) with G-CSF or GM-CSF support.
독소루비신의 조제 및 투여에 관한 세부 사항은 지역 처방 정보를 참조한다For details on the preparation and administration of doxorubicin, see local prescribing information.
사전 투약 및 지지 요법Pre-medication and supportive care
일반적으로, 화학요법 지지 요법은 미국임상종양학회(American Society of Clinical Oncology; ASCO), 유럽암연구및치료기구(European Organization for Research and Treatment of Cancer; EORTC) 또는 ESMO 지침 또는 현지 주의 기준에 따라 투여되어야 한다.In general, chemotherapy supportive therapy is administered according to the American Society of Clinical Oncology (ASCO), European Organization for Research and Treatment of Cancer (EORTC), or ESMO guidelines or local state standards. should be
화학요법 유도된 메스꺼움 및 구토 예방 및 치료는 임상적으로 지시된 대로 시행되어야 한다. 전신 코르티코스테로이드는 아테졸리주맙 및 티라골루맙 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있으므로, 임상적으로 가능하다면 프로토콜에 제공된 지침 외에는 대체 약제를 고려해야 한다. Prevention and treatment of chemotherapy-induced nausea and vomiting should be administered as clinically indicated. Because systemic corticosteroids may attenuate the potentially beneficial immunological effects of atezolizumab and tyragolumab treatment, alternative agents should be considered, if clinically feasible, outside the guidelines provided in the protocol.
예방적 G-CSF 또는 GM-CSF는 지역 정책에 따라 혈액학적 독성의 위험을 완화하기 위해 사용될 수 있으며 화학요법의 AC 부분 중에 요구된다. G-CSF 또는 GM-CSF를 사용한 호중구감소증 치료는 현지 정책에 따라 허용된다.Prophylactic G-CSF or GM-CSF may be used to mitigate the risk of hematologic toxicity according to local policy and is required during the AC portion of chemotherapy. Treatment of neutropenia with G-CSF or GM-CSF is permitted in accordance with local policy.
용량 변경capacity change
본 연구에서 아테졸리주맙 또는 티라골루맙에 대한 용량 변경은 없다. 냅-파클리탁셀의 관리(즉, 용량 조절 및 치료 중단 규칙)는 표 25를 참조한다. 카보플라틴, 독소루비신 또는 시클로포스파미드 관련 독성의 관리에 관한 지침(즉, 용량 조절 및 치료 중단 규칙)은 각 제제에 대한 해당 지역 처방 정보를 참조한다.There were no dose changes for atezolizumab or tiragolumab in this study. See Table 25 for administration of nap-paclitaxel (ie, dose adjustment and treatment discontinuation rules). For guidance on the management of carboplatin, doxorubicin, or cyclophosphamide-related toxicity (i.e., dosing adjustment and treatment discontinuation rules), refer to your local prescribing information for each agent.
C.C. 병용 요법combination therapy
병용 요법은 연구 약물 개시 7일 전부터 치료 중단 방문시까지 프로토콜 필수 치료 외에 환자가 사용한 임의의 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)을 포함한다.Combination therapy includes any drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, nutritional supplements) used by the patient in addition to protocol essential treatment from 7 days prior to study drug initiation until the treatment discontinuation visit.
허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
완화 방사선 요법은 종양 표적 병변의 평가를 방해하지 않는 한 허용한다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 티라골루맙 및 아테졸리주맙을 이용한 치료는 완화 방사선 요법 동안 계속될 수 있다. 냅-파클리탁셀을 이용한 치료는 기관의 치표의 표준에 따라 중단되어야 한다.Palliative radiation therapy is acceptable as long as it does not interfere with the evaluation of tumor target lesions (eg, the lesion to be investigated should not be the only site of measurable disease). Treatment with tiragolumab and atezolizumab may be continued during palliative radiation therapy. Treatment with nap-paclitaxel should be discontinued according to institutional standards.
![]()
![]()
1차 예방은 ASCO, EORTC 또는 ESMO 지침에 따라 또는 지역 표준 관행에 따라 환자, 즉, ≥ 60세 이상 및/또는 동반 질환이 있는 환자에게 투여되야 한다(Smith et al. 2006; Crawford et al. 2010; Aapro et al. 2011).Primary prophylaxis should be administered to patients ≥ 60 years of age and/or with comorbidities according to ASCO, EORTC or ESMO guidelines or according to local standard practice (Smith et al. 2006; Crawford et al. 2010) ; Aapro et al. 2011).
매주 nab-파클리탁셀을 투여받는 환자에 있어서 지속형(페길화된) G-CSF 형태의 사용을 뒷받침하는 증거는 제한되며, 시험자들은 기존의 G-CSF 제형을 우선적으로 고려해야 한다.Evidence supporting the use of a long-acting (pegylated) form of G-CSF in patients receiving weekly nab-paclitaxel is limited, and investigators should give preference to conventional G-CSF formulations.
항히스타민제, 해열제, 및/또는 진통제의 예비투약은 시험자의 재량에 따라 두 번째 및 이후의 아테졸리주맙 및 티라골루맙 주입에 대해서만 투여할 수 있다.Premedication of antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab and tiragolumab at the discretion of the investigator.
주의 요법attention therapy
전신 코르티코스테로이드 및 TNF-α 억제제는 아테졸리주맙을 이용한 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여해야 하는 상황에서는, 항히스타민제를 포함한 대안을 고려해야 한다. 대안이 가능하지 않은 경우, 시험자의 재량에 따라 전신 코르티코스테로이드 및 TNF-α 억제제를 투여할 수 있다.Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines should be considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the investigator's discretion.
아테졸리주맙 요법과 관련된 특정 이상 반응을 치료하기 위해, 시험자의 재량에 따라 전신 코르티코스테로이드가 권장된다.For the treatment of certain adverse events associated with atezolizumab therapy, systemic corticosteroids are recommended at the discretion of the investigator.
금지된 요법forbidden therapy
다음과 같은 병용 요법의 사용은 하기와 같이 금지된다:The use of the following combination therapies is contraindicated as follows:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
카보플라틴 화학요법 관련 추가 제한Additional limitations related to carboplatin chemotherapy
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
D.D. 선정 기준Selection Criteria
환자는 연구 등록을 위해 하기의 일반 기준에 부합해야 한다:Patients must meet the following general criteria for study enrollment:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
연구 치료 시작 전 14일 이내에 얻은 결과들(1일차 Results obtained within 14 days prior to initiation of study treatment (Day 1)
사이클 1):Cycle 1):
- ANC ![]()
![]()
사이클 1 중 1일차Day 1 of Cycle 1
- 림프구 수 ![]()
![]()
![]()
![]()
- 혈소판 수 ![]()
![]()
![]()
![]()
주기 1의 1일 전 2주 내에 수혈 없음No transfusions within 2 weeks before Day 1 of Cycle 1
- 헤모글로빈 ![]()
![]()
![]()
![]()
상기 기준을 충족하기 위해 환자는 수혈을 받거나 적혈구 생성 치료를To meet the above criteria, the patient will receive a blood transfusion or receive erythropoietic therapy.
받을 수 있다.can receive
- AST, ALT, 및 ALP ![]()
![]()
- 혈청 빌리루빈 ![]()
![]()
혈청 빌리루빈 수치가 ![]()
![]()
- INR 및 aPTT 1.5 ULN- INR and aPTT 1.5 ULN
이는 치료적 항응고를 받지 않은 환자에게만 적용되었고; 항응고 치료를 받은 환자는 안정된 용량을 사용해야 한다.This only applied to patients who did not receive therapeutic anticoagulation; Patients on anticoagulant therapy should use a stable dose.
- 크레아티닌 청소율 ![]()
![]()
- 혈청 알부민 ![]()
![]()
![]()
![]()
· 선별 검사시 HIV 검사 음성・Negative HIV test at screening
· 선별 검사 시 B형 간염 표면 항원(HBsAg) 검사 음성Hepatitis B surface antigen (HBsAg) test negative during screening
· 선별 검사시 B형 간염 표면 항체(HBsAb) 검사 양성, 또는A positive hepatitis B surface antibody (HBsAb) test at screening, or
하기의 경우 중 하나를 동반한 선별 검사시 HBsAb 음성HBsAb negative at screening with one of the following
- 총 B형 간염 코어 항체(HBcAb) 음성- Total hepatitis B core antibody (HBcAb) negative
- 총 HBcAb 검사 양성 후 정량적 B형 간염 바이러스(HBV) DNA- Quantitative hepatitis B virus (HBV) DNA after positive total HBcAb test
< 500 IU/mL< 500 IU/mL
HBV DNA 검사는 HBsAg 검사 음성, HBsAb 검사 음성, 총 HBcAb 검사 양성인 환자에게만 실시한다.The HBV DNA test is only performed on patients who have a negative HBsAg test, a negative HBsAb test, and a positive total HBcAb test.
· 선별 검사시 C형 간염 바이러스(HCV) 항체 검사 음성, 또는 선별 검사시 HCV 항체 검사 양성 후 HCV RNA 검사 음성. · Hepatitis C virus (HCV) antibody test negative at screening test, or HCV RNA test negative after HCV antibody test positive at screening test.
HCV RNA 검사는 HCV 항체 검사 양성인 환자에게만 시행된다.The HCV RNA test is only performed on patients with a positive HCV antibody test.
· 가임 여성의 경우: 금욕 유지(이성간 성교 금지) 또는 하기에 정의된 바와 같이 피임 방법 사용에 대한 동의 및 난자 기증 자제에 대한 동의For women of childbearing potential: Consent to maintain abstinence (no intercourse) or to use contraceptive methods as defined below and to refrain from egg donation
여성은 치료 기간 동안 및 아테졸리주맙의 최종 투여 후 적어도 5개월, 티라골루맙의 최종 투여 후 90일, 냅-파클리탁셀의 최종 투여 후 1개월, 카보플라틴 또는 독소루비신의 최종 투여 후 6개월, 또는 시클로포스파미드의 최종 투여 후 12개월 중 더 늦은 날짜까지 금욕을 유지하거나 연 < 1%의 실패율을 갖는 피임 방법을 사용해야 한다. 여성은 상기 동일한 기간 동안 난자 기증을 자제해야 한다.Women during the treatment period and at least 5 months after the last dose of atezolizumab, 90 days after the last dose of tiragolumab, 1 month after the last dose of nap-paclitaxel, 6 months after the last dose of carboplatin or doxorubicin, or Abstinence should be maintained until the later of 12 months after the last dose of cyclophosphamide or a contraceptive method with a failure rate of <1% per year should be used. Women should refrain from donating eggs during the same period as above.
여성은 만약 비월경이고, 폐경후 상태(폐경 이외에 확인된 원인이 없는 (³ 12개월 연속 무월경)에 도달하지 못하였고, 외과적 불임 수술(난소 및/또는 자궁의 제거)을 받지 않았다면 임신 가능성이 있는 것으로 간주한다.A woman has no chance of becoming pregnant if she is non-menstrual, has not reached postmenopausal status (without confirmed cause (³ 12 consecutive months of amenorrhea) other than menopause, and has not undergone surgical sterilization (removal of the ovaries and/or uterus). considered to exist
지속적으로 정확하게 사용했을 때 매년 < 1%의 실패율을 보이는 피임법의 예는 배란 억제와 관련된 복합(에스트로겐 및 프로게스테론 함유) 호르몬 피임, 배란 억제와 관련된 프로게스테론 단독 호르몬 피임, 양측 난관 폐쇄; 남성 불임; 자궁 내 장치; 자궁내Examples of contraceptive methods that, when used correctly and consistently, have a failure rate of < 1% per year include combined (estrogen and progesterone-containing) hormonal contraception associated with ovulation inhibition, progesterone-only hormonal contraception associated with ovulation inhibition, bilateral tubal occlusion; male infertility; intrauterine device; intrauterine
호르몬 방출 시스템; 및 성적 금욕을 포함한다.hormone release system; and sexual abstinence.
성적 금욕의 신뢰성은 임상 연구의 지속기간 및 환자의 바람직한 및 일반 생활방식에 관련하여 평가해야 한다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical study and the desired and general lifestyle of the patient.
주기적 금욕(예컨대, 달력, 배란, 증상체온, 또는 배란후 방법) 및 회수는 피임의 허용가능한 방법이 아니다.Periodic abstinence (eg, calendar, ovulation, symptomatic body temperature, or postovulatory methods) and withdrawal are not acceptable methods of contraception.
연구 치료 중단 후 임신을 원하는 여성은 화학요법 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료를 시작하기 전에 난모세포 보존에 대한 조언을 구해야 한다.Women wishing to become pregnant after discontinuation of study treatment should seek advice on oocyte preservation prior to initiation of study treatment due to the potential for irreversible infertility due to chemotherapy treatment.
· 남성의 경우: 하기에 규정된 바와 같이, 금욕을 유지하거나(이성간 성교를 자제하거나) 또는 피임법을 이용하는 데 동의, 및 정자 기증의 자제하는 데 동의:For Men: Consent to maintain abstinence (abstain from heterosexual intercourse) or use contraceptive methods, and to refrain from donating sperm, as provided below:
가임기 여성 파트너 또는 임신한 여성 파트너와 함께, 치료 기간 동안 및 티라골루맙의 최종 투여 후 90일 동안, 또는 냅-파클리탁셀, 카보플라틴, 독소루비신, 또는 시클로포스파미드의 최종 투여 후 6개월 중 더 늦은 날짜까지, 남성은 금욕을 유지하거나, 또는 실패율이 연간 < 1%인 추가적인 피임법을 사용해야 한다. 남성은 상기 동일한 기간 동안 정자 기증을 삼가야 한다.With a female partner of childbearing potential or a pregnant female partner, during treatment and for 90 days after the last dose of tiragolumab, or 6 months after the last dose of nap-paclitaxel, carboplatin, doxorubicin, or cyclophosphamide, whichever is more Until a later date, men must either maintain abstinence or use an additional method of contraception with a failure rate of < 1% per year. Men should refrain from donating sperm during the same period.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가되어야 한다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical trial and the patient's preferred daily lifestyle.
주기적 금욕(예컨대, 달력, 배란, 증상체온, 또는 배란후 방법) 및 회수는 피임의 허용가능한 방법이 아니다.Periodic abstinence (eg, calendar, ovulation, symptomatic body temperature, or postovulatory methods) and withdrawal are not acceptable methods of contraception.
연구 치료 개시 후 아이를 갖기를 원하는 남성은 화학요법 치료로 인한 비가역적 불임의 가능성 때문에 연구 치료를 시작하기 전에 정자 보존에 대한 조언을 구해야 한다.Men wishing to have children after initiation of study treatment should seek advice on sperm conservation prior to beginning study treatment due to the potential for irreversible infertility due to chemotherapy treatment.
· 폐경 후가 아닌 여성(비치료 유발 무월경 ³ 12개월) 또는 불임 시술을 받은 여성의 경우, 연구 치료제 개시 전 14일 이내에 음성 혈청 임신 검사 결과가 필요하다.· For non-postmenopausal women (non-treatment-induced amenorrhea ³ 12 months) or women who have undergone sterilization, a negative serum pregnancy test result is required within 14 days prior to initiation of study treatment.
· 예정된 방문, 치료 계획, 실험실 검사, 및 기타 연구 절차를 준수하려는 의지 및 능력Willingness and ability to comply with scheduled visits, treatment plans, laboratory tests, and other research procedures;
환자는 다음과 같은 암 관련 자격 기준을 충족해야 한다.Patients must meet the following cancer-related eligibility criteria:
· 조직학적으로 문서화된 TNBC(국부 테스트에 의해 평가된 음성 HER2, ER 및 PR 상태)Histologically documented TNBC (negative HER2, ER and PR status assessed by local testing)
HER2 음성은 지역 실험실 평가에 의해 하기 중 하나로 정의된다(Wolff et al. 2018): HER2 negative is defined as one of the following by local laboratory assessment (Wolff et al. 2018):
ISH 비증폭(HER2 대 CEP17 비율 <2.0 또는 단일 프로브 평균 HER2 유전자 카피 수 <4 신호/세포 또는 IHC 0 또는 IHC 1 +ER 및 PgR 음성은 IHC 분석에서 호르몬 수용체를 발현하는 세포들의 <1%로 정의된다.ISH unamplified (HER2 to CEP17 ratio <2.0 or single probe average HER2 gene copy number <4 signal/cell or IHC 0 or IHC 1 + ER and PgR negative defined as <1% of cells expressing hormone receptors in IHC assay do.
다초점 종양(원발성 종양과 동일한 사분면에 국한된 하나 이상의 개별 종양)을 갖는 환자는, 하나 이상의 초점이 샘플링되고, 국소적으로 확인되고, TNBC로 문서화되는 경우 자격이 있다.Patients with multifocal tumors (one or more individual tumors confined to the same quadrant as the primary tumor) are eligible if one or more foci are sampled, locally identified, and documented as TNBC.
다심성 종양(하나 이상의 개별 사분면을 포함하는 다중 종양)을 갖는 환자는, 모든 개별 병변이 샘플링되고, 국소적으로 확인되고, TNBC로 문서화되는 경우 자격이 있다.Patients with multiple tumors (multiple tumors comprising one or more separate quadrants) are eligible if all individual lesions are sampled, locally identified, and documented as TNBC.
· 파라핀 블록(선호) 또는 최소 20개의 염색되지 않은 슬라이드에서 대표적인 FFPE 종양 조직 표본의 중앙 테스트를 통해 문서화된 확인된 종양 PD-L1 평가Documented identifiable tumor PD-L1 assessment via central testing of representative FFPE tumor tissue specimens on paraffin blocks (preferred) or at least 20 unstained slides
종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 우수해야 하며, 등록 전에 벤타나(SP142) PD-L1 IHC 분석을 사용하여 결정된 바와 같이 PD-L1 발현에 대해 평가해야 하며, 양성은 중앙 실험실에서 측정한 임의의 강도의 PD-L1 발현 종양 침윤성 면역 세포가 차지하는 종양 면적의 ≥1%로 정의된다. 종양 조직이 PD-L1 발현에 대해 평가할 수 없는 환자는 적격이 아니다.Tumor tissue should be of good quality based on total and viable tumor content, and should be assessed for PD-L1 expression as determined using the Ventana (SP142) PD-L1 IHC assay prior to enrollment, with positivity being a central It is defined as ≧1% of the tumor area occupied by infiltrating immune cells expressing PD-L1-expressing tumors of any intensity measured in the laboratory. Patients whose tumor tissue cannot be assessed for PD-L1 expression are not eligible.
여러 개의 종양 표본이 제출된 경우 환자는 PD-L1에 대해 평가할 수 있는 표본이 하나 이상 있다면 자격이 있을 수 있다. 허용되는 샘플에는 심부 종양 조직에 대한 코어-바늘 생검(최소 3개 코어) 또는, 피부, 피하 또는 점막 병변에 대한 절제, 절개, 펀치 또는 겸자 생검이 포함된다.If multiple tumor specimens are submitted, patients may be eligible if they have more than one specimen that can be evaluated for PD-L1. Acceptable samples include core-needle biopsies (minimum 3 cores) for deep tumor tissue, or excision, incision, punch or forceps biopsies for skin, subcutaneous or mucosal lesions.
파라핀 블록의 FFPE 종양 표본이 바람직하다.FFPE tumor specimens in paraffin blocks are preferred.
미세 바늘 흡입, 칫솔질, 흉막 삼출액의 세포 펠렛, 골 전이, 및 세척 샘플은 허용하지 않는다.Fine needle aspiration, brushing, cell pellets in pleural effusion, bone metastases, and wash samples are not permitted.
· 적어도 하나의 방사선 또는 임상 측정에서 >2cm의 원발성 유방 종양 크기Primary breast tumor size >2 cm in at least one radiographic or clinical measurement
· 발표 시 단계: cT2-cT4, cN0-cN3 및 cM0Stage at the time of presentation: cT2-cT4, cN0-cN3 and cM0
· 신보조제 치료 완료 후 적절한 수술 관리(예: 액와 림프절 수술 및 부분적 또는 전체적 유방 절제술 포함)를 받기로 한 환자의 동의Consent of the patient to undergo appropriate surgical management (e.g., including axillary lymph node surgery and partial or total mastectomy) after completion of neoadjuvant therapy
· 심초음파(ECHO) 또는 다중 게이트 획득(MUGA) 스캔에서 측정한 기준선 좌심실 구혈률(LVEF) ≥53%Baseline left ventricular ejection fraction (LVEF) ≥53% measured on echocardiography (ECHO) or multiple gate acquisition (MUGA) scans
E.E. 배제 기준Exclusion Criteria
하기의 기준 중 임의의 것에 부합하는 환자는 연구 등록으로부터 배제한다:Patients meeting any of the following criteria are excluded from study enrollment:
-연구 치료 중, 티라골루맙 치료 후 90일 이내, 아테졸리주맙 치료 후 5개월 이내, 냅-파클리탁셀, 카보플라틴 또는 독소루비신 치료 후 6개월 이내, 또는 시클로포스파미드 치료 후 12개월 이내 중 더 늦은 날짜까지 임신 또는 수유 중인 경우-During study treatment, within 90 days of treatment with tiragolumab, within 5 months of treatment with atezolizumab, within 6 months of treatment with nap-paclitaxel, carboplatin or doxorubicin, or within 12 months of treatment with cyclophosphamide, whichever is more If you are pregnant or lactating until late
가임 여성은 연구 치료 시작 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다.Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
-유의미한 간 질환(예컨대, 간경변, 조절되지 않는 주요 발작 장애, 또는 상대정맥 증후군)을 포함하여 프로토콜 준수 또는 결과 해석에 영향을 미칠 수 있는 유의미한 조절되지 않는 동시 질병의 증거- Evidence of significant concurrent uncontrolled disease that could affect protocol compliance or interpretation of results, including significant liver disease (e.g., cirrhosis, uncontrolled major seizure disorder, or superior venous syndrome)
- 상당한 심혈관 질환, 예컨대 뉴욕 심장 협회 심장 질환(부류 II 이상), 연구 치료제 개시 전 3 개월 이내 심근경색증, 불안정 부정맥, 또는 불안정 협심증 - Significant cardiovascular disease, such as New York Heart Association heart disease (Class II or higher), myocardial infarction within 3 months prior to initiation of study treatment, unstable arrhythmia, or unstable angina
LVEF가 53%로 공지된 환자는 배제한다.Patients with known LVEF of 53% are excluded.
상기 기준을 충족하지 않는 것으로 공지된 관상동맥 질환 또는 울혈성 심부전 환자.Patients with known coronary artery disease or congestive heart failure who do not meet the above criteria.
-감염 합병증, 세균혈증 또는 중증 폐렴으로 인한 입원을 포함하지만, 이에 제한되지는 않는 연구 치료제 개시 전 4주 이내의 중증 감염-Severe infection within 4 weeks prior to initiation of study treatment, including, but not limited to, hospitalization for infectious complications, bacteremia, or severe pneumonia
-연구 치료제 개시 전 2주 이내에 경구 또는 IV 항생제를 이용한 치료-Treatment with oral or IV antibiotics within 2 weeks prior to initiation of study treatment
정기적인 항생제 예방(예컨대, 만성 폐쇄성 폐질환 악화 방지 또는 발치를 위해)을 받고 있는 환자가 적격이다.Patients receiving regular antibiotic prophylaxis (eg, to prevent exacerbation of chronic obstructive pulmonary disease or for tooth extraction) are eligible.
-연구 치료제 개시 전 28일 이내의 주요 수술 또는 진단 이외의 연구 동안 주요 수술 절차의 필요성 예상되는 경우- Major surgery within 28 days prior to initiation of study treatment or the need for major surgical procedures during non-diagnostic studies
중심 정맥 접근 카테터(예컨대, 포트 또는 이와 유사한 것)의 배치는 주요 수술 절차로 간주되지 않으므로 허용한다.The placement of a central venous access catheter (eg, port or the like) is acceptable as it is not considered a major surgical procedure.
- 키메라성 또는 인간화 항체 또는 융합 단백질에 중증 알러지성, 과민성, 또는 다른 과민증 반응의 병력- History of severe allergic, hypersensitivity, or other hypersensitivity reactions to chimeric or humanized antibodies or fusion proteins
-CHO 세포 또는 티라골루맙 또는 아테졸리주맙 제제의 임의의 성분에서 생성된 생물의약품에 대한 알려진 과민성 또는 알레르기- Known hypersensitivity or allergy to biologics produced from CHO cells or any component of the tiragolumab or atezolizumab formulations
-중증 근무력증, 근염, 자가면역 간염, 전신성 홍반 루푸스, 류마티스 관절염, 염증성 장 질환, 항인지질 증후군과 관련된 혈관 혈전증, 베게너 육아종증, 쇼그렌 증후군, 길랭-바레 증후군, 다발성 경화증, 혈관염 또는 사구체신염을 포함하지만 이에 제한되지는 않는 자가면역 질환의 활성 또는 병력-Including myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, vascular thrombosis associated with antiphospholipid syndrome, Wegener's granulomatosis, Sjogren's syndrome, Guillain-Barré syndrome, multiple sclerosis, vasculitis or glomerulonephritis but not limited to, activity or history of autoimmune disease
안정적인 용량의 갑상선 대체 호르몬에 대한 자가면역 매개 갑상선기능저하증의 병력이 있는 환자는 본 연구에 적격일 수 있다.Patients with a history of autoimmune-mediated hypothyroidism on stable doses of thyroid replacement hormone may be eligible for this study.
안정적인 인슐린 투약 요법으로 제1형 당뇨병이 조절된 환자는 본 연구에 적격이다.Patients with type 1 diabetes mellitus controlled with a stable insulin dosing regimen are eligible for this study.
습진, 건선, 만성 단순 태선 또는 피부과 증상만 있는 백반증(예컨대, 건선성 관절염 없음)이 있는 환자는 하기의 조건을 충족하는 경우 허용한다:Patients with eczema, psoriasis, chronic lichen simplex or vitiligo with only dermatological symptoms (eg, no psoriatic arthritis) are allowed if the following conditions are met:
- 발진이 체표면적의 <10%를 차지함 - The rash occupies <10% of the body surface area
- 질병이 기준선에서 잘 통제되고 낮은 역가의 국소 스테로이드만 필요함 - Disease is well controlled at baseline and requires only low titer topical steroids
- 지난 12개월 이내에 소랄렌에 더하여 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고효능 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았음- No acute exacerbation of an underlying condition requiring ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids in addition to psoralen within the past 12 months
-선행 동종이계 줄기 세포 이식 또는 고형 장기 이식-Prior allogeneic stem cell transplantation or solid organ transplantation
-특발성 폐 섬유증(폐렴을 포함), 약물 유발 폐렴, 조직성 폐렴(즉, 폐쇄성 세기관지염, 잠복성 조직성 폐렴)의 병력, 또는 선별 검사시 흉부 컴퓨터 단층촬영(CT) 스캔에서 활동성 폐렴의 증거- History of idiopathic pulmonary fibrosis (including pneumonia), drug-induced pneumonia, systemic pneumonia (i.e. bronchiolitis obliterans, latent systemic pneumonia), or evidence of active pneumonia on chest computed tomography (CT) scan at screening
방사선 분야에서 방사선 폐렴 (섬유증) 병력은 허용됨A history of radiation pneumonitis (fibrosis) in the field of radiation is acceptable
-선별 검사시 EBV 바이러스 캡시드 항원(VCA) IgM 검사 양성- EBV virus capsid antigen (VCA) IgM test positive during screening test
EBV 중합효소연쇄반응(PCR) 검사는 활동성 감염 또는 의심되는 만성 활동성 감염을 선별하기 위해 임상적으로 지시된 대로 실시해야 한다.EBV polymerase chain reaction (PCR) testing should be performed as clinically indicated to screen for active or suspected chronic active infection.
EBV PCR 검사가 양성인 환자는 제외한다.Patients with a positive EBV PCR test are excluded.
활동성 결핵active tuberculosis
-연구 치료제의 개시 전 4주 이내에 독성 약화 생백신을 투여 또는 연구 중에 독성 약화 생백신이 필요할 것으로 예상되는 경우- If the live attenuated vaccine is administered within 4 weeks prior to initiation of the study treatment, or if it is expected that the attenuated live vaccine will be required during the study
환자는 연구 치료제의 개시 전 28일 이내에, 치료 동안, 또는 연구 치료제의 최종 용량 투여 후 5개월 이내에 독성 약화 생백신(예컨대, 플루미스트®)을 제공받지 않는 데에 동의해야 한다.Patients must agree not to receive a live, attenuated vaccine (eg, Flumist ® ) within 28 days prior to initiation of study treatment, during treatment, or within 5 months after administration of the last dose of study treatment.
-항 PD-1 또는 항 PD-L1 치료 항체를 제외하고 항 CTLA-4를 포함한 CD137 작용제 또는 면역 관문 차단 요법을 이용한 선행 치료- Prior treatment with CD137 agonists including anti-CTLA-4 or immune checkpoint blockade, except for anti-PD-1 or anti-PD-L1 therapeutic antibodies
-연구 치료제 개시 전 4주 이내 또는 약물의 5회 약물 제거 반감기(둘 중 더 늦은 날짜) 이내에 전신 면역자극제(인터페론 또는 IL-2를 포함하지만 이제 제한되지는 않음)를 이용한 치료-Treatment with systemic immunostimulants (including but not limited to interferon or IL-2) within 4 weeks prior to initiation of study therapy or within 5 drug elimination half-lives of the drug (whichever is later)
-연구 치료제 개시 전 2주 이내에 전신 면역억제제(프레드니손,-Systemic immunosuppressants (prednisone,
덱사메타손, 아자티오프린, 메토트렉세이트, 탈리도마이드 및 항종양 괴사 인자[항 TNF] 제제를 포함하지만 이에 제한되지는 않음)를 이용한 치료, 또는 연구 중 전신 면역억제제가 필요할 것으로 예상되는 경우treatment with, but not limited to, dexamethasone, azathioprine, methotrexate, thalidomide, and anti-tumor necrosis factor [anti-TNF] agents, or when systemic immunosuppressants are expected to be required during the study
급성, 저용량, 전신 면역억제제(예컨대, 메스꺼움으로 덱사메타손 1회 용량)를 받은 환자는 본 연구에 등록할 수 있다.Patients receiving acute, low-dose, systemic immunosuppressants (eg, single dose of dexamethasone for nausea) can be enrolled in this study.
만성 폐쇄성 폐질환에 흡입 코르티코스테로이드, 기립성 저혈압 환자에 미네랄 코르티코이드(예컨대, 플루드로코르티손), 부신피질 기능 부전에 저용량 보조 코르티코스테로이드를 사용할 수 있다.Inhaled corticosteroids for chronic obstructive pulmonary disease, mineralocorticoids (eg, fludrocortisone) for patients with orthostatic hypotension, and low-dose adjuvant corticosteroids for adrenal insufficiency may be used.
-침윤성 유방암의 병력- History of invasive breast cancer
-IV 기(전이성) 유방암- Stage IV (metastatic) breast cancer
-유방암의 치료 및 예방을 위한 사전 전신 요법-Pre-systemic therapy for the treatment and prevention of breast cancer
-모든 악성 종양에 대한 안트라사이클린, 백금 또는 탁산을 이용한 이전의 요법-Previous therapy with anthracyclines, platinum or taxanes for all malignancies
비고: 비-다형성 LCIS(치료를 받지 않았거나 수술로 치료)가 있는 환자는 자격이 있다.Remarks: Patients with non-polymorphic LCIS (untreated or treated surgically) are eligible.
-동시성, 양측 침윤성 유방암-Simultaneous, bilateral invasive breast cancer
-원발성 종양 및/또는 액와 림프절의 이전의 절개 및/또는 절제 생검-Previous incision and/or excisional biopsy of the primary tumor and/or axillary lymph nodes
-신보조제 요법 시작 전 액와 림프절 절단-Axillary lymph node amputation prior to initiation of neoadjuvant therapy
-적절하게 치료된 자궁경부의 상피암종, 비흑색종 피부암종, 국소 전립선암 또는 I기 자궁암과 같은 전이 또는 사망의 무시가 가능한 위험(예: 5년 전체생존(OS) >90%)이 있는 경우는 제외한, 선별검사 전 5년 이내에 다른 악성 종양의 병력-with a negligible risk of metastasis or death (e.g., 5-year overall survival (OS) >90%) History of other malignancies within 5 years prior to screening
-연구 치료 시작 전 12개월 이내에 뇌혈관 사고의 병력- History of cerebrovascular events within 12 months prior to initiation of study treatment
-NCI CTCAE v5.0 3등급 증상성 울혈성 심부전 또는 뉴욕심장협회 클래스 II 이상의 심장 질환의 병력- NCI CTCAE v5.0 Grade 3 Symptomatic Congestive Heart Failure or History of New York Heart Association Class II or greater heart disease
- NCI CTCAE v5.0 3등급 증상성 울혈성 심부전 또는 뉴욕심장협회 클래스 II 이상의 심장 질환의 병력- NCI CTCAE v5.0 Grade 3 Symptomatic Congestive Heart Failure or History of New York Heart Association Class II or higher heart disease
- 항협심증 약제를 필요로 하는 협심증, 적절한 약제에 의해 통제되지 않는 심각한 심장 부정맥, 중증 전도 이상, 또는 임상적으로 유의미한 판막증. - Angina requiring antianginal medications, severe cardiac arrhythmias not controlled by appropriate medications, severe conduction abnormalities, or clinically significant valvular disease.
- 고위험 통제되지 않는 부정맥(즉, 안정 시 심박수가 100회/분인 심방 빈맥, 유의한 심실 미부정맥[심실 빈맥], 고급 방실[AV] 차단[2도 방실 차단 유형 2[Mobitz 2], 또는 3도 AV 차단])- high-risk uncontrolled arrhythmias (i.e., atrial tachycardia with resting heart rate of 100 beats/min, significant ventricular tail arrhythmias [ventricular tachycardia], advanced atrioventricular [AV] block [2nd degree atrioventricular block type 2 [Mobitz 2], or 3 also AV blocking])
- 좌심실 기능장애, 부정맥 또는 심장허혈과 관련된 유의미한 증상(Grade -2)- Significant symptoms related to left ventricular dysfunction, arrhythmia, or cardiac ischemia (Grade -2)
- 연구 치료 시작 전 12개월 이내에 심근경색증- Myocardial infarction within 12 months prior to initiation of study treatment
- 통제되지 않는 고혈압(수축기 혈압 >180 mmHg 및/또는 확장기 혈압 >100 mmHg)- uncontrolled hypertension (systolic blood pressure >180 mmHg and/or diastolic blood pressure >100 mmHg)
- ECG에 대한 경벽 경색의 증거- Evidence of transmural infarction on ECG
- 산소 요법에 대한 요구 사항- Requirements for oxygen therapy
-nab-파클리탁셀, 사이클로포스파미드, 독소루비신 또는 카보플라틴 제형의 성분에 대한 알려진 알레르기 또는 과민증-A known allergy or hypersensitivity to a component of the formulation -nab-paclitaxel, cyclophosphamide, doxorubicin or carboplatin
-G-CSF 또는 GM-CSF 제형에 대한 알려진 알레르기 또는 과민증- Known allergy or hypersensitivity to G-CSF or GM-CSF formulations
F.F. 분석analysis
안전성 분석Safety analysis
티라골루맙 및 아테졸리주맙+nab-pac+AC에 대한 아테졸리주맙+nab-pac-carbo+AC의 안전성 프로파일을 평가하기 위해 환자를 코호트 B의 두 군 중 하나에 1:1 비율로 무작위 배정한다. 1차 안전성 종단에 대한 공식적인 통계적 비교는 수행되지 않으며 안전성 분석은 서술적이다. 따라서, 공신력 계산은 수행되지 않았다. 샘플 크기는 티라골루맙 및 아테졸리주맙+nab-pac-AC에 대해 아테졸리주맙 + nab-pac-carbo-AC의 내약성을 평가하기 위한 서술적 안전성 분석을 제공하기에 충분한 것으로 간주된다. 계획된 샘플 크기를 통해, 각 치료 부문과 두 조합된 부문에 걸쳐 허용 가능한 확률을 갖는 ≥10%의 실제 발생률로 이상 반응을 관찰할 수 있다(표 66 참조).To evaluate the safety profile of atezolizumab + nab-pac-carbo + AC versus tiragolumab and atezolizumab + nab-pac + AC, patients were randomized in a 1:1 ratio to one of two groups in Cohort B. do. Formal statistical comparisons of the primary safety endpoints are not performed and safety analyzes are descriptive. Therefore, the credibility calculation was not performed. The sample size is considered sufficient to provide a descriptive safety analysis to evaluate the tolerability of atezolizumab plus nab-pac-carbo-AC to tiragolumab and atezolizumab plus nab-pac-AC. The planned sample size allows to observe adverse events with an actual incidence ≥10% with an acceptable probability across each treatment arm and both combined arms (see Table 66).

안전성 평가에는 연구의 안전성 평가에 중요하다고 간주되는 이상 반응의 발생률, 특성 및 중증도, 프로토콜-필수 활력 징후, 실험실 이상 및 기타 프로토콜 지정 검사가 포함된다. 이상 반응은 NCI CTCAE v5.0에 따라 등급화된다.Safety assessments include the incidence, nature and severity of adverse events, protocol-essential vital signs, laboratory abnormalities, and other protocol-specific tests considered important for the safety assessment of the study. Adverse events are graded according to NCI CTCAE v5.0.
안전성은 ADA에 의해 측정된 이상 반응, 실험실 시험 결과의 변화, 활력 징후의 변화, 연구 치료제 노출, 면역원성의 요약을 통해 평가하고 치료군에서 제시된다.Safety is assessed by ADA-measured adverse events, changes in laboratory test results, changes in vital signs, exposure to study treatment, and summary of immunogenicity and presented in treatment groups.
유해 반응에 대한 축어적 설명은 MedDRA 용어에 대응된다.Verbose descriptions of adverse reactions correspond to MedDRA terms.
치료 응급 반응(연구 치료제의 제1 용량 또는 이후에 발생하는 반응으로 정의됨)은 시험자가 평가한 연구 약물과의 관계에 상관없이 MedDRA 용어, 적절한 MedDRA 수준 및 NCI CTCAE v5.0 등급으로 요약된다. 각 환자에 대해 동일한 이상 반응이 여러 번 발생하는 경우 보고된 최대 중증도가 요약에 사용된다.Treatment emergency response (defined as a response that occurs at or after the first dose of study treatment) is summarized in MedDRA terminology, appropriate MedDRA level, and NCI CTCAE v5.0 grade, regardless of relationship to investigator-assessed study drug. If the same adverse event occurs multiple times for each patient, the maximum reported severity is used for the summary.
하기와 치료 관련 이상 반응은 별도로 요약된다: 연구 약물 중단으로 이어지는 이상 반응, 용량 감소 또는 중단으로 이어지는 이상 반응, 등급 3의 이상 반응, 등급 5의 이상 반응, 심각한 이상 반응, 및 특별한 관심의 이상 반응.The following and treatment-related adverse events are summarized separately: Adverse Events Leading to Study Drug Discontinuation, Adverse Events Leading to Dose Reduction or Discontinuation, Grade 3 Adverse Events, Grade 5 Adverse Events, Serious Adverse Events, and Adverse Events of Special Interest .
모든 사망 및 사망 원인이 요약되어 있다.All deaths and causes of death are summarized.
관련 실험실 값은 적절한 경우 식별된 NCI CTCAE 등급 3 및 등급 4 값과 함께 시점별로 요약된다. NCI CTCAE 등급 변화를 치료 군 별로 표로 작성한다.Relevant laboratory values are summarized by time point, along with identified NCI CTCAE Grade 3 and Grade 4 values where appropriate. NCI CTCAE grade changes are tabulated by treatment group.
노출, 이상반응, 실험실 및 활력징후 데이터 분석Analysis of exposure, adverse events, laboratory and vital signs data
안전성은 연구 치료제에 대한 노출, 이상 반응, 실험실 시험 결과의 변화, 및 활력 징후 및 ECG의 변화에 Safety depends on exposure to study treatment, adverse events, changes in laboratory test results, and changes in vital signs and ECGs.
대한 요약을 통해 평가한다.Evaluate through a summary of
연구 치료제 노출(예컨대, 치료 기간, 투여 받은 총 용량, 및 주기 및 용량 변경의 횟수)은 기술적 통계와 함께 요약된다.Study treatment exposures (eg, duration of treatment, total dose administered, and number of cycles and dose changes) are summarized along with descriptive statistics.
이상 반응의 축어적 용어는MedDRA의 유의어 용어에 대응되며, 이상 반응의 증증도는 NCI CTCAE v5.0에 따라 등급이 매겨진다. 모든 이상 반응, 중증 이상 반응, 사망으로 이어지는 이상 반응, 특별한 관심의 이상 반응, 및 연구 치료제의 제1 용량 투여 시 또는 그 이후에 발생하는 연구 치료 중단으로 이어지는 이상 반응(즉, 치료 관련 이상 반응)이 매핑된 용어, 적절한 유의어 수준 및 증증도 등급에 따라 요약된다. 가변적인 증증도를 가진 반응의 경우, 해당 요약에서 가장 높은 등급이 사용된다. 사망 및 사망 원인이 요약되어 있다.Verbose terms of adverse events correspond to synonymous terms in MedDRA, and the severity of adverse events is graded according to NCI CTCAE v5.0. All adverse events, serious adverse events, adverse events leading to death, adverse events of particular interest, and adverse events leading to study treatment discontinuation (i.e., treatment-related adverse events) occurring at or after administration of the first dose of study treatment These are summarized according to the mapped terms, appropriate synonym levels, and severity ratings. For reactions with variable severity, the highest rating in that summary is used. Deaths and causes of death are summarized.
관련 실험실, 활력징후(맥박수, 호흡수, 혈압, 맥박 산소 측정, 및 체온) 및 ECG 데이터가 시간별로 표시되며, 적절한 경우 등급으로 식별된다. 또한, 선택된 실험실 시험의 변화표는 기준선 및 기준선 이후 최대 증증도 등급을 요약하는 데 사용한다. 활력 징후 및 ECG의 변화가 요약되어 있다.Relevant laboratory, vital signs (pulse rate, respiration rate, blood pressure, pulse oximetry, and body temperature) and ECG data are displayed hourly and identified by grade, where appropriate. In addition, tables of changes from selected laboratory tests are used to summarize baseline and post-baseline maximum severity grades. Changes in vital signs and ECG are summarized.
유효성 분석Validity analysis
유효성 분석은 ITT 접근법을 사용하며, 여기서 환자가 어떠한 할당된 연구 약물을 받는지 여부에 관계없이 모든 등록된 환자는 분석에 포함되며, 코호트 B의 환자는 1:1 비율로 무작위 배정된 치료에 따라 그룹화된다. ITT 모집단의 하위 집합을 기반으로 한 분석도 실시할 수 있다. 가설 분석은 달리 명시되지 않는 한 양측이다.Efficacy analysis uses an ITT approach, where all enrolled patients, regardless of whether the patient receives any assigned study drug, are included in the analysis, and patients in Cohort B are grouped according to treatment randomized in a 1:1 ratio. do. Analyzes based on subsets of the ITT population may also be performed. Hypothesis analysis is two-sided unless otherwise specified.
코호트 B에 대한 탐색적 유효성 목표는 하기의 종점에 기초하여 티라골루맙 및 아테졸리주맙 + nab-pac-AC에 대한 티라골루맙 및 아테졸리주맙 + nab-pac-carbo-AC의 유효성을 조사하는 것이다.The exploratory efficacy goal for Cohort B was to investigate the effectiveness of tiragolumab and atezolizumab plus nab-pac-carbo-AC against tiragolumab and atezolizumab plus nab-pac-AC based on the following endpoints. will be.
-유방 및 림프절 모두에서 종양의 근절로 정의되는, pCR(ypT0/is ypN0)-pCR (ypT0/is ypN0), defined as eradication of tumors in both breast and lymph nodes
이러한 유효성 종점은 신보조제 요법 및 수술의 완료 후에 설정된다. pCR 평가가 누락된 환자는 pCR을 달성하지 않은 것으로 간주된다.These efficacy endpoints are established after completion of neoadjuvant therapy and surgery. Patients who miss a pCR assessment are considered not to have achieved pCR.
-무작위 배정부터 임의의 원인으로 인한 문서화된 질병 재발, 진행 또는 사망까지의 시간으로 정의되는, EFS-EFS, defined as the time from randomization to documented disease recurrence, progression, or death from any cause
분석 시점에 사건이 없는 환자는 사건 없이 생존한 것으로 마지막에 알려진 일자에 중도절단된다.Event-free patients at the time of analysis are censored on the last known event-free survival.
기준선 정보가 없는 환자는 무작위배정 일자에 중도절단된다.Patients without baseline information are censored on the date of randomization.
-무작위 배정에서부터 임의의 원인으로 인한 사망일까지의 시간으로 정의되는 OS OS defined as the time from randomization to the date of death from any cause
분석시 사망한 것으로 보고되지 않은 환자는 마지막으로 생존이 확인된 일자에 중도절단된다. 기준선 이후 정보가 없는 환자는 무작위배정 일자에 중도절단된다.Patients not reported to have died at the time of analysis are censored on the date of the last known survival. Patients with no post-baseline information are censored on the date of randomization.
약동학 분석Pharmacokinetic analysis
PK 분석을 위해 샘플을 수집하고 본 연구의 노출을 이전 연구에서 수득한 노출과 비교한다. 티라골루맙 및 아테졸리주맙의 혈청 농도 및 냅-파클리탁셀, 카보플라틴, 독소루비신 및 시클로포스파미드의 혈장 농도는 개별 값으로 보고하고, 적절하고 데이터가 허용하는 한 치료군 및 주기별로 요약(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균, 및 기하 평균 변동 계수)할 수 있다.Samples are collected for PK analysis and exposures in this study are compared with exposures obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab and plasma concentrations of nap-paclitaxel, carboplatin, doxorubicin and cyclophosphamide are reported as individual values and summarized by treatment group and cycle (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean coefficient of variation).
개별 및 중앙값 혈청 티라골루맙 및 아테졸리주맙 농도는 치료군 및 일별로 플롯팅된다. 티라골루맙 및 아테졸리주맙 농도 데이터는 데이타에 의해 보장되는 바와 같이 청소율, 분포 용적, 및 AUC와 같은 PK 매개변수를 도출하기 위해 확립된 모집단 PK 모델을 사용하는 다른 연구로부터의 데이터와 통합할 수 있다. 용량, 안전성, 유효성 또는 바이오마커 결과와 관련된 PK 매개변수의 잠재적 상관관계를 조사할 수 있다.Individual and median serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be integrated with data from other studies that use established population PK models to derive PK parameters such as clearance, volume of distribution, and AUC as warranted by the data. have. Potential correlations of PK parameters with dose, safety, efficacy, or biomarker outcomes can be investigated.
면역원성 분석Immunogenicity assay
면역원성 분석에는 ADA 평가를 받은 환자, 받은 치료에 따라 그룹화된 환자를 포함한다. 치료 및 추적 기간 동안 치료 응급 ADA 양성 환자 및 ADA 음성 환자의 수 및 비율은 치료군별로 요약한다.Immunogenicity assays included patients with ADA assessments, grouped according to treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients during the treatment and follow-up period will be summarized by treatment group.
ADA 상태와, 안전성, 유효성, 및 PK 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고할 수 있다.The relationship between ADA status and safety, efficacy, and PK endpoints can be analyzed and reported through descriptive statistics.
바이오마커 분석Biomarker analysis
탐색적 바이오마커에 대한 공식적인 통계 분석은 실시되지 않지만, 데이터는 본 연구의 맥락에서 그리고 다른 연구의 데이터와 통합하여 분석될 수 있다.Although no formal statistical analysis of exploratory biomarkers is performed, the data can be analyzed in the context of this study and in conjunction with data from other studies.
실시예 15. 두경부의 재발성/전이성 PD-L1 양성 편평세포암을 가진 환자를 대상으로 1차 치료로서의 아테졸리주맙 + 티라골루맙 및 아테졸리주맙 + 위약에 관한 II상, 무작위, 이중 맹검 연구Example 15. A Phase II, Randomized, Double-Blind Study of Atezolizumab + Tiragolumab and Atezolizumab + Placebo as First-Line Treatment in Patients with Recurrent/Metastatic PD-L1-positive Squamous Cell Carcinoma of the Head and Neck
본 실시예는 두경부의 재발성/전이성 PD-L1 양성 편평 세포암(SCCHN)에서 1차(1L) 치료로서 아테졸리주맙 + 티라골루맙 및 아테졸리주맙 플러스 위약의 유효성 및 안전성을 평가하기 위해 설계된 II상, 무작위, 이중 맹검, 글로벌 연구를 설명한다. 연구는 하기의 부문으로 구성된다:This example was designed to evaluate the efficacy and safety of atezolizumab plus tiragolumab and atezolizumab plus placebo as first-line (1L) treatment in relapsed/metastatic PD-L1-positive squamous cell carcinoma (SCCHN) of the head and neck. A phase II, randomized, double-blind, global study is described. The study consists of the following sections:
부문 A: 환자들은 각 21일 주기의 제 1일차에 IV 주입으로 3주마다(Q3W) 투여된 1200 mg 고정 용량의 아테졸리주맙을 받으며, 이후 600 mg 고정 용량의 티라골루맙이 환자들에게 각 21일 사이클의 1일차에 IV 주입으로 Q3W 투여된다.Arm A: Patients receive a 1200 mg fixed dose of atezolizumab administered as an IV infusion every 3 weeks (Q3W) on Day 1 of each 21-day cycle, followed by a 600 mg fixed dose of tiragoluumab administered to patients each Q3W is administered as an IV infusion on Day 1 of the 21-day cycle.
부문 B: 환자들은 1200 mg 고정 용량의 아테졸리주맙을 각 21일 주기의 제 1일차에 IV 주입으로 Q3W 투여받으며, 이후 위약이 각 21일 주기의 제 1일차에 IV 주입으로 Q3W 투여된다.Arm B: Patients will receive a 1200 mg fixed dose of atezolizumab Q3W as an IV infusion on Day 1 of each 21-day cycle followed by placebo Q3W as an IV infusion on Day 1 of each 21-day cycle.
A.A. 연구 설계study design
이러한 II상, 무작위, 이중 맹검, 글로벌 연구는 재발성/전이성 PD-L1 양성 SCCHN에서 1L 치료로서 아테졸리주맙 플러스 티라골루맙 및 아테졸리주맙 플러스 위약의 유효성과 안전성을 평가하도록 설계되었다. 적격 환자는 치유 의도 및/또는 전이성 PD-L1 양성 SCCHN(종양 관련 면역 세포(TIC) ≥ 5%)을 갖는 국소 요법에 적합하지 않은 재발성 질환이 있고 재발성/전이성 질환에 대해 이전에 전신 요법을 받은 적이 없는 동부협력종양학회(ECOG) 수행 상태가 0 또는 1인 ≥18세의 남성 및 여성 환자이다.This Phase II, randomized, double-blind, global study was designed to evaluate the efficacy and safety of atezolizumab plus tiragolumab and atezolizumab plus placebo as 1L treatment in relapsed/metastatic PD-L1-positive SCCHN. Eligible patients have recurrent disease unsuitable for topical therapy with curative intent and/or metastatic PD-L1-positive SCCHN (tumor-associated immune cells (TIC) ≥ 5%) and have previously received systemic therapy for relapsed/metastatic disease Male and female patients ≥18 years of age with an Eastern Cooperative Oncology (ECOG) performance status of 0 or 1.
선별검사 동안, 잠재적으로 적격한 각 환자로부의 종양 표본은 연구용 VENTANA PD-L1(SP263) 동반 진단(CDx) 분석을 사용하여 중앙 실험실에서 평가한 대로 PD-L1 발현에 대해 전향적으로 테스트된다. 중앙에서 평가된 TIC ≥ 5%인 PD-L1 양성인 환자만 적격성을 갖는다. PD-L1 발현은 TIC가 5%-19%로 PD-L1이 낮고 TIC가 ≥20%로 PD-L1이 높은 것으로 정의된다.During screening, tumor specimens from each potentially eligible patient are prospectively tested for PD-L1 expression as assessed by a central laboratory using the investigative VENTANA PD-L1 (SP263) companion diagnostic (CDx) assay. Only PD-L1-positive patients with a centrally assessed TIC ≥ 5% are eligible. PD-L1 expression is defined as a low PD-L1 with a TIC of 5%-19% and a high PD-L1 with a TIC ≥20%.
적격 환자는 구인두암에 대한 인유두종바이러스(HPV) 상태(HPV 양성 구인두암: 예 대 아니오) 및 PD-L1 상태(PD-L1: 낮음 대 높음)로 계층화된다. 각 PD-L1 하위 그룹(PD-L1 낮음[TIC 5%-19%] 및 PD-L1 높음[TIC ≥ 20%])에 대한 등록은 총 계획 등록의 약 55%로 제한된다(즉, 약 66명의 환자).Eligible patients are stratified into human papillomavirus (HPV) status for oropharyngeal cancer (HPV positive oropharyngeal cancer: yes vs. no) and PD-L1 status (PD-L1: low vs. high). Enrollment for each PD-L1 subgroup (PD-L1 low [TIC 5%-19%] and PD-L1 high [TIC ≥ 20%]) is limited to approximately 55% of total planned enrollment (i.e., approximately 66%). patients).
적격 환자는 2:1 비율로 무작위 배정되어 아테졸리주맙 + 티라골루맙(부문 A) 또는 아테졸리주맙 + 위약(부문 B)을 받는다.Eligible patients will be randomized in a 2:1 ratio to receive either atezolizumab plus tiragolumab (Arm A) or atezolizumab plus placebo (Arm B).
부문 A: 환자들은 각 21일 주기의 제 1일차에 IV 주입으로 3주마다(Q3W) 투여된 1200 mg 고정 용량의 아테졸리주맙을 받으며, 이후 600 mg 고정 용량의 티라골루맙이 환자들에게 각 21일 사이클의 1일차에 IV 주입으로 Q3W 투여된다.Arm A: Patients receive a 1200 mg fixed dose of atezolizumab administered as an IV infusion every 3 weeks (Q3W) on Day 1 of each 21-day cycle, followed by a 600 mg fixed dose of tiragoluumab administered to patients each Q3W is administered as an IV infusion on Day 1 of the 21-day cycle.
부문 B: 환자들은 1200 mg 고정 용량의 아테졸리주맙을 각 21일 주기의 제 1일차에 IV 주입으로 Q3W 투여받으며, 이후 위약이 각 21일 주기의 제 1일차에 IV 주입으로 Q3W 투여된다.Arm B: Patients will receive a 1200 mg fixed dose of atezolizumab Q3W as an IV infusion on Day 1 of each 21-day cycle followed by placebo Q3W as an IV infusion on Day 1 of each 21-day cycle.
환자는 기준선에서, 주기 1의 1일차 이후 처음 30주 동안은 6주마다(± 7일), 30주차 종양 평가 완료 후 9주마다(± 7일) 종양 평가를 받는다. 종양 평가는 RECIST v1.1에 따른 방사선학적 질환 진행 또는 RECIST v1.1에 따른 방사선학적 질환 진행 후 연구 치료를 계속하는 환자에 대한 임상적 이익 상실, 동의 철회, 사망 또는 스폰서에 의한 연구 종료 중 먼저 발생하는 때까지의 치료 지연에 관계없이 일정에 따라 계속된다. 진행성 질병 또는 임상적 이익의 손실이 의심되면 시험자의 재량에 따라 언제든지 스캔을 수행해야 한다.Patients receive tumor assessments at baseline, every 6 weeks (± 7 days) for the first 30 weeks after Day 1 of Cycle 1, and every 9 weeks (± 7 days) after completion of tumor assessments at Week 30. Tumor evaluation is based on loss of clinical benefit, withdrawal of consent, death, or termination of study by sponsor for patients continuing on study treatment after radiological disease progression according to RECIST v1.1 or radiological disease progression according to RECIST v1.1, whichever occurs first. Continue on schedule regardless of treatment delay until it occurs. If progressive disease or loss of clinical benefit is suspected, a scan should be performed at any time at the discretion of the investigator.
RECIST v1.1에 따른 방사선학적 질환 진행이 없는 상태에서 (임상 저하 또는 독성을 포함하되 이에 국한되지 않는 이유로) 연구 치료를 중단한 환자는 예정된 종양 평가를 RECIST v1에 따른 방사선학적 질환 진행, 동의 철회, 사망 또는 스폰서에 의한 연구 종료 중 먼저 발생하는 때까지 전술한 빈도로 계속한다. RECIST v1.1에 따른 방사선학적 질병 진행이 없는 경우, 환자가 새로운 항암 요법을 시작하는지 여부에 관계없이 종양 평가를 계속해야 한다. 단일 시점에서의 객관적인 반응은 RECIST v1.1에 따라 시험자가 판단한다.Patients who discontinue study treatment (including, but not limited to, clinical decline or toxicity) in the absence of radiologic disease progression per RECIST v1.1 will have their scheduled tumor evaluation scheduled for radiologic disease progression per RECIST v1, withdraw consent Continue at the above-mentioned frequency until death, or end of study by the sponsor, whichever occurs first. In the absence of radiologic disease progression according to RECIST v1.1, tumor evaluation should continue regardless of whether the patient is starting new chemotherapy. The objective response at a single time point is judged by the investigator according to RECIST v1.1.
혈청 샘플을 수집하여 아테졸리주맙 및 티라골루맙 PK를 모니터링하고 아테졸리주맙 및 티라골루맙에 대한 항체의 존재를 검출한다. 보관 및 새로 얻은 종양 조직, 혈장 및 혈액 샘플을 포함한 환자 샘플들을 탐색적 바이오마커 평가를 위해 수집한다.Serum samples are collected to monitor atezolizumab and tiragolumab PK and detect the presence of antibodies to atezolizumab and tiragolumab. Patient samples, including archival and freshly obtained tumor tissue, plasma and blood samples, are collected for exploratory biomarker evaluation.
안전성 평가에는 연구의 안전성 평가에 중요한 것으로 간주되는 이상 반응의 발생률, 특성 및 증증도 및 기타 프로토콜별 테스트(예: 실험실 이상)가 포함된다.Safety assessments include the incidence, nature, and severity of adverse events considered important for the safety assessment of the study, and other protocol-specific tests (eg, laboratory abnormalities).
연구 치료 중단 이후 생존 추적 정보는 사망, 추적 실패 또는 시험의뢰자에 의한 연구 종료 중 먼저 발생하는 때까지 약 3개월마다 전화 통화, 환자 의료 기록 및/또는 진료소 방문을 통해 수집된다. 환자가 생존 추적 조사에서 철회를 요청하지 않는 한 모든 환자는 생존 및 새로운 항암 요법 정보를 위해 주기적으로 연락해야 한다(이러한 요청은 원본 문서에 문서화되고 시험자가 서명해야 한다). 환자가 생존 추적 조사를 철회하는 경우 연구 직원은 공개 정보 출처(예: 카운티 기록)를 사용하여 생존 상태에 대한 정보를 얻을 수 있다.Survival follow-up information after study treatment discontinuation is collected via phone calls, patient medical records, and/or clinic visits approximately every 3 months until death, follow-up failure, or end of study by the sponsor, whichever occurs first. All patients should be contacted periodically for survival and new anticancer therapy information unless the patient requests withdrawal from survival follow-up (these requests must be documented in the original document and signed by the investigator). If a patient withdraws from survival follow-up, research staff may use public information sources (eg, county records) to obtain information about their survival status.
방사선사진 데이터, 생검 결과(가능한 경우), 및 임상 상태를 통합 평가한 후 질병 진행으로 인한 허용 불가성 독성 또는 증상 악화가 없는 상태에서 시험자가 평가하여 환자들이 임상 이익을 경험하는 한 치료는 계속될 수 있다. RECIST v1.1에 따른 질병 진행 기준을 충족하지만 계속해서 임상적 이익을 갖는 환자는 설명된 기준을 모두 충족하고 서면 동의를 제공하는 경우 치료를 계속할 수 있다(아테졸리주맙 + 티라골루맙 또는 아테졸리주맙 + 위약).After an integrated assessment of radiographic data, biopsy results (if available), and clinical status, treatment will continue as long as patients experience clinical benefit as assessed by the investigator in the absence of unacceptable toxicity or worsening of symptoms due to disease progression. can Patients who meet the criteria for disease progression according to RECIST v1.1 but continue to have clinical benefit may continue treatment provided they meet all of the described criteria and provide written informed consent (atezolizumab + tyragolumab or atezoli Zumab + placebo).
B.B. 용량 및 투여Dosage and administration
치료 요법은 도 23에 요약되어 있다.The treatment regimen is summarized in FIG. 23 .
아테졸리주맙atezolizumab
모든 환자는 각 21일 주기의 제 1일째에 IV 주입으로 1200mg의 아테졸리주맙을 투여받는다. 아테졸리주맙 용량은 고정이며 체중에 따라 달라지지 않는다. 아테졸리주맙 주입은 표 67에 요약된 지침에 따라 투여된다.All patients receive 1200 mg of atezolizumab by IV infusion on Day 1 of each 21-day cycle. Atezolizumab dose is fixed and does not vary with body weight. Atezolizumab infusion is administered according to the guidelines summarized in Table 67.


티라골루맙 및 위약Tiragolumab and placebo
아테졸리주맙 투여 및 관찰 기간 이후(표 67 참조), 환자는 각 21일 주기의 제 1일에 IV 주입으로 600 mg 티라골루맙/위약을 투여 받는다. 티라골루맙/위약 용량은 고정이며 체중에 따라 달라지지 않는다. 티라골루맙/위약 주입은 표 68에 요약된 지침에 따라 투여된다.Following atezolizumab administration and the observation period (see Table 67), patients receive 600 mg tyragolumab/placebo as an IV infusion on Day 1 of each 21-day cycle. The tiragolumab/placebo dose is fixed and does not vary with body weight. Tiragolumab/placebo infusion is administered according to the guidelines summarized in Table 68.


아테졸리주맙 및 티라골루맙/위약Atezolizumab and Tiragolumab/Placebo
아테졸리주맙이나 티라골루맙/위약이 영구적으로 중단되지 않는 한 다음 규칙이 적용된다:The following rules apply unless atezolizumab or tiragolumab/placebo is permanently discontinued:
-치료 사이클은 각 21일 사이클의 1일차에 아테졸리주맙 및 티라골루맙/위약 투약으로 시작한다. 약물 관련 독성으로 인해 연구 약물 중 하나가 지연되면, 아테졸리주맙과 티라골루맙에 대한 안전성 프로파일이 유사하기 때문에 그 외 다른 연구 약물도 지연되는 것이 권장된다; 그러나 시험자의 재량에 따라 적절하다고 판단되는 경우 그 외 다른 연구 약물을 투여하면서 사이클이 시작될 수 있다.-Treatment cycle begins with atezolizumab and tiragolumab/placebo dosing on Day 1 of each 21-day cycle. If one of the study drugs is delayed due to drug-related toxicity, it is recommended that the other study drugs be delayed because the safety profiles for atezolizumab and tiragolumab are similar; However, if deemed appropriate at the investigator's discretion, the cycle may be initiated with the administration of other study drugs.
-약물 관련 독성으로 인해 한 연구 약물의 투여가 지연되는 반면 다른 연구 약물은 계획대로 투여되는 경우, 지연되는 연구 약물은 다음 예정된 주입시(즉, 다음 예정된 21일 사이클)에 투여되는 것이 권장된다.-If administration of one study drug is delayed due to drug-related toxicity while the other study drug is administered as scheduled, it is recommended that the delayed study drug be administered at the next scheduled infusion (i.e., the next scheduled 21-day cycle).
용량 변경capacity change
본 연구에서 아테졸리주맙 또는 티라골루맙/위약에 대해, 용량 감소를 포함한, 용량 조절은 없다. There is no dose adjustment, including dose reduction, for atezolizumab or tiragolumab/placebo in this study.
C.C. 병용 요법combination therapy
병용 요법은 연구 치료 시작 7일 전부터 치료 중단 방문시까지 프로토콜-필수 치료 외에 환자가 사용한 모든 약물(예를 들어, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)로 구성된다.Combination therapy consists of all medications (e.g., prescription drugs, over-the-counter medications, vaccines, herbal or homeopathic remedies, nutritional supplements) taken by the patient in addition to protocol-essential treatment from 7 days before study treatment start to the treatment discontinuation visit.
허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
-예방적 또는 치료적 항응고 요법(예컨대, 안정된 용량의 와파린 또는 저분자량 헤파린)-prophylactic or therapeutic anticoagulant therapy (eg, stable doses of warfarin or low molecular weight heparin)
-비활성화 인플루엔자 예방 접종- Inactivated influenza vaccination
-식욕 자극제로 투여되는 메게스트롤 아세테이트 - Megestrol acetate administered as an appetite stimulant
-미네랄로코르티코이드(예컨대, 플루드로코르티손)-mineralocorticoids (eg, fludrocortisone)
-COPD 또는 천식용으로 투여되는 흡입 또는 저용량 코르티코스테로이드- Inhaled or low-dose corticosteroids administered for COPD or asthma
-기립성 저혈압 또는 부신피질 기능부전에 투여된 저용량 코르티코스테로이드-Low-dose corticosteroids administered for orthostatic hypotension or adrenocortical insufficiency
-하기에 개략된 바와 같은 완화 방사선 요법(예컨대, 공지된 골 전이의 치료 또는 통증의 증상 완화):Palliative radiation therapy (eg, treatment of known bone metastases or relief of symptoms of pain) as outlined below:
RECIST v1.1에 따라 방사선학적 질병 진행에 대한 문서가 없는 환자의 경우, 증상 관리를 위한 지지 치료를 최대화하고 종양 표적 병변의 평가를 방해하는 방사선 요법을 회피하는 것이 강력히 권장된다.For patients with no documented radiologic disease progression per RECIST v1.1, it is strongly recommended to maximize supportive care for symptom management and to avoid radiation therapy that impedes evaluation of tumor-targeted lesions.
완화 방사선 요법 중에는 아테졸리주맙 및 티라골루맙/위약으로 치료를 계속할 수 있다.Treatment may be continued with atezolizumab and tiragolumab/placebo during palliative radiation therapy.
항히스타민제, 해열제 및/또는 진통제를 사용한 예비약물은, 시험자의 재량에 따라, 2번째 이후의 아테졸리주맙 및 티라골루맙/위약 주입에 대해서만 투여될 수 있다.Premedication with antihistamines, antipyretics and/or analgesics may be administered only for the second subsequent infusion of atezolizumab and tiragolumab/placebo, at the discretion of the investigator.
일반적으로, 시험자는 지역 표준 관행에 따라, 임상적으로 표시된 주의 또는 금지된 요법으로 정의된 것 이외의 보조 요법으로 환자의 치료(기존 상태 포함)를 관리해야 한다. 주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡곤란, 저혈압, 쌕쌕거림, 기관지경련, 빈맥, 감소된 산소 포화, 또는 호흡 곤란에 의해 명시된 심각한 주입-관련된 사례는 임상적으로 표시된 대로 지지 요법 (예를 들면, 보충의 산소 및 2-아드레날린 작용제)로 관리되어야 한다.In general, the investigator should manage the patient's treatment (including pre-existing conditions) with adjuvant therapies other than those defined as clinically indicated cautions or contraindicated therapies, in accordance with local standard practice. Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related events indicated by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation, or dyspnea, as clinically indicated, support supportive care (e.g., supplemental oxygen and 2-adrenergic agonists) ) should be managed.
주의 요법care
전신 코르티코스테로이드 및 TNF-α 억제제는 아테졸리주맙 및/또는 티라골루맙 치료의 잠재적인 유익한 면역학적 효과를 약화시킬 수 있다. 따라서, 전신 코르티코스테로이드 또는 TNF-α 억제제를 일상적으로 투여하는 상황에서는 항히스타민제를 포함한 대안을 고려해야 한다. 대안이 가능하지 않은 경우, 시험자의 재량에 따라 전신 코르티코스테로이드 및 TNF-α 억제제를 투여할 수 있다.Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of atezolizumab and/or tiragolumab treatment. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines should be considered. If no alternative is possible, systemic corticosteroids and TNF-α inhibitors may be administered at the investigator's discretion.
아테졸리주맙 및/또는 티라골루맙 요법과 관련된 경우의 특정 이상 반응의 치료를 위해서는, 시험자의 재량에 따라, 전신 코르티코스테로이드가 권장된다.For the treatment of certain adverse events when associated with atezolizumab and/or tiragolumab therapy, systemic corticosteroids are recommended, at the investigator's discretion.
금지된 요법forbidden therapy
다음과 같은 병용 요법의 사용은 하기와 같이 금지된다:The use of the following combination therapies is contraindicated as follows:
보건 당국이 승인했든 실험적이든, 암 치료에 의도된 병용 요법(수술, 화학요법, 호르몬 요법, 면역 요법, 방사선 요법 및 약초 요법을 포함하지만 이에 한정되지 않음)은, 연구 치료를 시작하기 전 다양한 기간 동안, 제제에 따라, 그리고 연구 치료 동안, 질병 진행이 문서화되고 환자가 완화적 방사선 요법 및 특정 환경에서의 국부 요법을 제외한 연구 치료를 중단할 때까지 금지된다.Combination therapies (including, but not limited to, surgery, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy) intended for the treatment of cancer, whether approved by health authorities or experimental, may vary for various periods of time prior to initiation of study treatment. During, depending on the agent, and during study treatment, disease progression is documented and the patient discontinues study treatment except for palliative radiation therapy and topical therapy in certain circumstances.
연구 치료 개시 전 28일 이내 및 연구 치료 중에 임상시험 요법은 금지된다.Investigational therapy is contraindicated within 28 days prior to initiation of study treatment and during study treatment.
-약독화 생 백신(예: 플루미스트®)은 연구 치료 시작 전 4주 이내, 연구 치료 중, 아테졸리주맙의 최종 투여 후 5개월 및 티라골루맙/위약의 최종 투여 후 90일 동안 금지된다.- Live attenuated vaccines (eg Flumist ® ) are contraindicated within 4 weeks prior to initiation of study treatment, during study treatment, 5 months after the last dose of atezolizumab and 90 days after the last dose of tiragolumab/placebo.
-전신 면역자극제(인터페론 및 IL-2 포함하지만, 이에 제한되지 않음)는, 이들 제제가 연구 치료와 병용하여 제공되면 자가면역 질환의 위험을 잠재적으로 증가시킬 수 있으므로 연구 치료 시작 전 및 연구 치료 동안 4주 또는 5회의 약물 제거 반감기(둘 중 더 긴 경우) 이내에는 금지된다.-Systemic immunostimulants (including, but not limited to, interferon and IL-2) prior to initiation of study treatment and during study treatment as these agents may potentially increase the risk of autoimmune disease if given in combination with study treatment Contraindicated within 4 weeks or 5 drug elimination half-lives, whichever is longer.
-전신 면역억제제(시클로포스파미드, 아자티오프린, 메토트렉세이트 및 탈리도마이드를 포함하지만 이에 국한되지 않음)는, 이들 제제가 연구 치료의 유효성 및 안전성을 잠재적으로 변경할 수 있으므로 연구 치료 중에는 금지된다.-Systemic immunosuppressants (including, but not limited to, cyclophosphamide, azathioprine, methotrexate and thalidomide) are contraindicated during study treatment as these agents may potentially alter the efficacy and safety of study treatment.
D.D. 선정 기준Selection Criteria
환자는 연구 참가를 위해 하기의 기준을 충족해야 한다:Patients must meet the following criteria for study entry:
-서명한 사전 동의서- signed informed consent
-사전 동의서에 서명할 당시의 연령 ≤ 18세-Age at the time of signing the informed consent ≤ 18
-연구 프로토콜을 준수할 능력- Ability to comply with research protocols
-조직학적으로 또는 세포학적으로 확인된 재발성/전이성 SCCHN(구인두, 구강, 후두 또는 하인두를 포함하며, 국소 요법으로 치료할 수 없는 것으로 간주됨)-histologic or cytologically confirmed recurrent/metastatic SCCHN (including oropharyngeal, buccal, larynx or hypopharyngeal, considered incurable with topical therapy)
어떠한 조직학이든 비인두 또는 이하선에 원발성 부위의 종양을 갖는 환자는 자격이 없다.Patients with tumors of primary sites in the nasopharynx or parotid gland, of any histology, are not eligible.
-p16 면역조직화학(IHC), 제자리 교잡 또는 중합효소 사슬 기반 분석에 의해 국소적으로 판단된 구인두암에 대한 HPV 상태 테스트로부터 공지된 결과Known results from HPV status testing for oropharyngeal cancer locally judged by -p16 immunohistochemistry (IHC), in situ hybridization or polymerase chain based assays
비고: 구강암, 후두암, 하인두암에 대한 HPV 검사는 필요하지 않다.Note: HPV testing is not required for oral cancer, laryngeal cancer, and hypopharyngeal cancer.
-전이성 및/또는 재발성 SCCHN에 대한 이전의 전신 요법 없음-No previous systemic therapy for metastatic and/or recurrent SCCHN
국소 진행성 질환에 대한 다중 모드 치료(예: 동시 화학방사선)의 일부로 제공된 전신 요법을 받았고 전신 요법의 마지막 용량이 무작위화 전 6개월이었던 환자는 허용된다.Patients who have received systemic therapy given as part of a multimodal treatment (eg, concurrent chemoradiation) for locally advanced disease and whose last dose of systemic therapy was 6 months prior to randomization are admitted.
-Measurable disease per RECIST v1.1-Measurable disease per RECIST v1.1
이전에 방사선 조사된 병변은 방사선 조사 이후 해당 부위에서 진행성 질환이 명백하게 기록된 경우에만 측정 가능한 질환으로 간주할 수 있다.Previously irradiated lesions can be considered measurable disease only if progressive disease is clearly documented at the site after irradiation.
-이전에 얻은 보관 종양 조직 또는 사전 선별/선별시 생검에서 얻은 조직 내의, 연구용 VENTANA PD-L1(SP263) CDx 분석에 의해 판단되고 대표적인 종양 조직 표본의 중앙 테스트를 통해 문서화된 TIC 5%의 종양 PD-L1 발현. 약 66명의 환자(총 계획 등록의 55%)가 PD-L1 하위 그룹(PD-L1 낮음(TIC 5%-19%) 및 PD-L1 높음(TIC ≥20%))에 등록된 후, 해당 PD- L1 하위 그룹에서의 추가적인 환자는 등록되지 않는다.- Tumor PD with a TIC of 5%, judged by investigational VENTANA PD-L1 (SP263) CDx analysis and documented through central testing of representative tumor tissue specimens, within previously obtained archival tumor tissue or tissue obtained from biopsies at pre-screening/screening -L1 expression. After approximately 66 patients (55% of total plan enrollment) were enrolled in the PD-L1 subgroups (PD-L1 low (TIC 5%-19%) and PD-L1 high (TIC ≥20%)), their PD - Additional patients in the L1 subgroup are not enrolled.
포르말린 고정 파라핀 포매(FFPE) 블록(선호) 또는 관련 병리 보고서와 함께 염색되지 않은 갓 절단된 연속 섹션을 함유하는 최소 20개의 슬라이드에서의 대표적인 종양 표본의 확인된 가용성. 15-19개의 슬라이드만 사용할 수 있다면 Medical Monitor 확인을 받은 후에 환자는 여전히 연구에 적격일 수 있다.Confirmed availability of representative tumor specimens on at least 20 slides containing either formalin-fixed paraffin-embedded (FFPE) blocks (preferred) or unstained, freshly excised continuous sections with relevant pathology reports. If only 15-19 slides are available, the patient may still be eligible for the study after receiving Medical Monitor confirmation.
보관 종양 조직을 사용할 수 없거나 필요 검사에 부적합한 것으로 판단되는 경우 종양 조직은 사전 선별/선별시 수행된 생검으로부터 얻어야 한다. 환자의 보관 조직 검사 결과가 적격 기준을 충족하지 않는 경우 생검은 사전 선별/선별시에 수행할 수도 있다.If archival tumor tissue is not available or is judged unsuitable for the required testing, tumor tissue should be obtained from a biopsy performed at the time of pre-screening/screening. A biopsy may be performed at prescreening/screening if the patient's archived biopsy results do not meet the eligibility criteria.
-0 또는 1의 ECOG 전신 활동도ECOG systemic activity of -0 or 1
-기대 수명 ≥12주-Life expectancy ≥12 weeks
-무작위화 전 14일 이내에 얻은, 다음과 같은 실험실 결과로 정의되는 적절한 혈액 및 말단 장기 기능:- Adequate blood and terminal organ function, as defined by the following laboratory results, obtained within 14 days prior to randomization:
- ANC ≥1.5 x 109/L (1500/μL), 과립구 집락 자극 인자 보조 없음- ANC ≥1.5 x 10 9 /L (1500/μL), no granulocyte colony stimulating factor adjuvant
- 림프구 수 ≥0.5 x109/L(500/μL)- Lymphocyte count ≥ 0.5 x10 9 /L (500/μL)
- 혈소판 수 ≥100 x109/L (100,000/μL), 수혈 없음- Platelet count ≥ 100 x10 9 /L (100,000/μL), no transfusion
- 헤모글로빈 ≥90 g/L(9 g/dL)- Hemoglobin ≥90 g/L (9 g/dL)
환자는 이 기준을 충족하기 위해 지역 SOC에 따라 수혈을 받거나 적혈구 생성 치료를 받을 수 있다.Patients may receive transfusions or receive erythropoietic therapy according to their local SOC to meet this criterion.
- AST, ALT, 및 ALP ≤2.5 x 정상의 상한 (ULN), 다음은 예외임:- AST, ALT, and ALP ≤ 2.5 x upper limit of normal (ULN), with the following exceptions:
간 전이가 기록된 환자: AST 및 ALT ≤ 5 x ULNPatients with documented liver metastases: AST and ALT ≤5 x ULN
문서로 기록된 간 또는 골 전이를 가진 환자: ALP ≤5 x ULNPatients with documented liver or bone metastases: ALP ≤5 x ULN
- 총 빌리루빈 ≤1.5 x ULN, 하기를 예외로 함: - Total bilirubin ≤1.5 x ULN, with the following exceptions:
공지의 길버트병 환자: 총 빌리루빈 ≤3 xULNKnown Gilbert's Disease Patients: Total Bilirubin ≤3 xULN
- 크레아티닌 ≤1.5 xULN - Creatinine ≤1.5 xULN
- 알부민 ≥25 g/L (2.5 g/dL)- Albumin ≥ 25 g/L (2.5 g/dL)
- 치료적 항응고제를 투여받지 않는 환자의 경우: INR 및 aPTT ≤1.5 x ULN - For patients not receiving therapeutic anticoagulants: INR and aPTT ≤1.5 x ULN
-치료적 항응고 요법을 투여 받은 환자의 경우: 안정적인 항응제-For patients receiving therapeutic anticoagulant therapy: stable anticoagulant
-선별 검사시 HIV 검사 음성-Negative HIV test at screening test
-선별 검사시 B형 간염 표면 항원 (HBsAg) 검사 음성-Negative hepatitis B surface antigen (HBsAg) test during screening
-선별검사 시 B형 간염 표면 항체(HBsAb) 검사 양성 또는 하기 중 하나를 동반한 선별검사 시 HBsAb 음성:-Hepatitis B surface antibody (HBsAb) positive at screening or HBsAb negative at screening with one of the following:
- 총 B형 간염 코어 항체(HBcAb) 음성- Total hepatitis B core antibody (HBcAb) negative
- 총 HBcAb 검사 양성 후 정량적 B형 간염 바이러스(HBV) DNA <500 IU/mL- Quantitative hepatitis B virus (HBV) DNA <500 IU/mL after total HBcAb test positive
HBV DNA 검사는 HBsAg 검사 음성, HBsAb 검사 음성, 총 HBcAb 검사 양성인 환자에게만 실시해야 한다.HBV DNA testing should only be performed on patients who have a negative HBsAg test, a negative HBsAb test, and a positive total HBcAb test.
-선별 검사시 C형 간염 바이러스(HCV) 항체 검사 음성, 또는 선별 검사시 HCV 항체 검사 양성 후 HCV RNA 검사 음성.-Negative hepatitis C virus (HCV) antibody test at screening test, or negative HCV RNA test after positive HCV antibody test at screening test.
HCV RNA 검사는 HCV 항체 검사 양성인 환자에게만 실시해야 한다.HCV RNA testing should only be performed on patients with a positive HCV antibody test.
-가임기 여성의 경우: 하기에 정의된 바와 같은 금욕 유지 (이성간 성교 금지) 또는 피임 사용에 동의:-For women of childbearing age: Consent to maintain abstinence (no intercourse) or use contraception as defined below:
여성은 치료 기간 동안, 아테졸리주맙의 최종 투여 후 5개월 동안 및 티라골루맙/위약의 최종 투여 후 90일 동안 금욕을 유지하거나 또는 연간 실패율이 1% 미만인 피임법을 사용하여야 한다.Women should maintain abstinence for the duration of treatment, for 5 months after the last dose of atezolizumab and for 90 days after the last dose of tiragolumab/placebo, or use contraception with an annual failure rate of less than 1%.
여성이 초경 이후이고, 폐경 후 상태(폐경 이외의 확인된 원인 없이 계속해서 12개월 동안 무월경이 지속됨)에 도달하지 않았으며, 수술(즉, 난소, 나팔관 및/또는 자궁 제거) 또는 시험자가 결정한 다른 원인(예컨대, 뮐러관 무발생)으로 인한 영구적인 불임이 아닌 경우, 가임기인 것으로 간주된다. 가임기의 정의는 지역 지침 또는 규정에 맞게 조정될 수 있다.The woman is post-menopausal, has not reached post-menopausal status (amenorrhea continues for 12 consecutive months without an identified cause other than menopause), and has not undergone surgery (i.e., removal of the ovaries, fallopian tubes, and/or uterus) or another as determined by the investigator A woman of childbearing age is considered to be of childbearing age unless it is permanent infertility due to cause (eg, absence of Muller's canal). The definition of childbearing age may be adapted to local guidelines or regulations.
연간 실패율이 <1%인 피임법의 예로는 양측 난관 결찰, 남성 불임술, 배란을 억제하는 호르몬 피임약, 호르몬 방출 자궁 내 장치 및 구리 자궁 내 장치가 있다.Examples of contraceptive methods with an annual failure rate of <1% include bilateral tubal ligation, male sterilization, hormonal contraceptives to suppress ovulation, hormone-releasing intrauterine devices, and copper intrauterine devices.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가되어야 한다. 주기적 금욕 (예를 들어, 달력, 배란, 증상온, 배란 후 방법) 및 체외사정은 적절한 피임 방법이 아니다. 로컬 가이드라인 또는 규정에 따라 필요한 경우 로컬에서 인정하는 적절한 피임법과 금욕의 신뢰성에 대한 정보가 로컬 사전 동의서에 설명되어 있다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical trial and the patient's preferred daily lifestyle. Periodic abstinence (eg calendar, ovulation, symptom temperature, post-ovulation method) and extracorporeal ejaculation are not suitable methods of contraception. Information on the reliability of appropriate locally accepted methods of contraception and abstinence as required by local guidelines or regulations is described in the local informed consent form.
-남성의 경우: 하기에 정의된 바와 같은 금욕 유지 (이성간 성교 금지) 또는 콘돔 사용에 대한 동의 및 정자 기증 자제에 대한 동의:-For men: Consent to maintain abstinence (no intercourse) or to use condoms and to refrain from donating sperm, as defined below:
가임기 여성 파트너 또는 임신한 여성 파트너와 함께 남성은 배아 노출을 피하기 위해 티라골루맙/위약 치료 동안 및 티라골루맙/위약 최종 투여 후 90일 동안 금욕을 유지하거나 콘돔을 사용해야 한다. 남성은 상기 동일한 기간 동안 정자 기증을 삼가야 한다.Men with a female partner of childbearing potential or with a pregnant female partner should maintain abstinence or use condoms during tiragolumab/placebo treatment and for 90 days after the last dose of tiragolumab/placebo to avoid embryo exposure. Men should refrain from donating sperm during the same period.
성적 금욕의 신뢰성은 임상 시험 기간 및 환자가 선호하는 일상적인 생활 방식과 관련하여 평가되어야 한다. 주기적 금욕 (예를 들어, 달력, 배란, 증상온, 배란 후 방법) 및 체외사정은 적절한 약물 노출 방지 방법이 아니다. 로컬 가이드라인 또는 규정에 따라 필요한 경우 금욕의 신뢰성에 대한 정보가 로컬 사전 동의서에 설명되어 있다.The reliability of sexual abstinence should be evaluated with respect to the duration of the clinical trial and the patient's preferred daily lifestyle. Periodic abstinence (eg, calendar, ovulation, symptom temperature, postovulation method) and extracorporeal ejaculation are not adequate methods of preventing drug exposure. Information on the credibility of abstinence when required by local guidelines or regulations is described in the local informed consent form.
E.E. 배제 기준Exclusion Criteria
하기의 기준 중 임의의 것에 부합하는 환자는 연구 등록으로부터 배제한다:Patients meeting any of the following criteria are excluded from study enrollment:
-치료 의도를 갖는 국소 치료에 적합한 질병-diseases suitable for topical treatment with therapeutic intent
-국소 진행성 SCCHN에 대한 근치적 전신 치료의 마지막 투여 후 6개월 이내의 진행성 또는 재발성 질환-Progressive or recurrent disease within 6 months of last administration of curative systemic therapy for locally advanced SCCHN
-수술 또는 이전의 기타 요법과 관련된 ≤2 등급 미해결 독성- Grade ≤2 unresolved toxicity related to surgery or other previous therapy
-2등급 탈모증 또는 신경병증이 있는 환자는 허용된다.-Patients with grade-2 alopecia or neuropathy are allowed.
대수술을 받은 환자는 중재술과 관련된 합병증으로부터의 회복을 포함하여 충분히 회복되었어야 한다.Patients who underwent major surgery should have recovered sufficiently, including recovery from complications related to interventions.
연구 약물 치료로 악화되지 않을 것으로 예상되고 관리되는 비가역적 독성을 갖는 환자는 Medical Monitor와 상의 후에 포함될 수 있다.Patients with managed irreversible toxicity that are not expected to worsen with study drug treatment and may be included after consultation with the Medical Monitor.
-증상이 있거나 치료되지 않았거나 활발히 진행 중인 중추신경계(CNS) 전이-symptomatic, untreated, or active central nervous system (CNS) metastases
치료된 CNS 병변이 있는 무증상 환자는 다음 기준이 모두 충족되는 경우 자격이 있다:Asymptomatic patients with treated CNS lesions are eligible if all of the following criteria are met:
- RECIST v1.1에 따라 측정가능한 질병은 CNS 외부에 있어야 한다. - According to RECIST v1.1, measurable disease must be outside the CNS.
- 환자는 두개내 출혈 또는 척수 출혈의 병력이 없다.- The patient has no history of intracranial hemorrhage or spinal cord hemorrhage.
- 환자는 무작위화 전 7일 이내에 정위 방사선 요법, 무작위화 전 14일 이내에 전뇌 방사선 요법, 또는 무작위화 전 28일 이내에 신경외과적 절제술을 받지 않았다.- The patient had not received stereotactic radiotherapy within 7 days prior to randomization, whole brain radiotherapy within 14 days prior to randomization, or neurosurgical resection within 28 days prior to randomization.
- 환자는 CNS 질환에 대한 요법으로서 코르티코스테로이드에 대한 지속적인 요구 사항이 없다. 안정적인 용량의 항경련제 요법이 허용된다.- The patient has no ongoing requirement for corticosteroids as therapy for CNS disease. Stable dose anticonvulsant therapy is permitted.
-연수막 질환의 병력- History of meningeal disease
-통제되지 않는 종양 관련 통증-Uncontrolled tumor-related pain
통증 약제를 필요로 하는 환자는 연구 엔트리에서 안정된 섭생 중에 있어야 한다.Patients requiring pain medication must be on a stable regimen at study entry.
고식적 방사선요법으로 치료할 수 있는 증상이 있는 병변(예를 들어, 골 전이 또는 신경 충돌 유발 전이)은 등록 전에 치료해야 한다.Symptomatic lesions that can be treated with palliative radiotherapy (eg, bone metastases or nerve impingement-induced metastases) should be treated prior to enrollment.
환자는 방사선의 영향에서 회복되어야 함. 환자는 방사선의 영향에서 회복되어야 함.The patient must recover from the effects of radiation. The patient must recover from the effects of radiation.
추가 성장시 기능적 결함이나 난치성 통증을 유발할 가능성이 있는 무증상 전이성 병변 (예를 들어, 현재 척수 압박과 관련이 없는 경막외 전이)은 등록 전에 적절한 경우 국소 치료를 고려해야 함.Asymptomatic metastatic lesions (e.g., epidural metastases not currently associated with spinal cord compression) that have the potential to cause functional defects or refractory pain upon further growth should be considered for local treatment if appropriate prior to enrollment.
-통제되지 않거나 증상이 있는 고칼슘혈증-Uncontrolled or symptomatic hypercalcemia
-중증 근무력증, 근염, 자가면역 간염, 전신성 홍반 루푸스, 류마티스 관절염, 염증성 장 질환, 항인지질항체증후군, 베게너 육아종증, 쇼그렌 증후군, 길랭-바레 증후군, 또는 하기의 예외를 갖는 다발성 경화증을 포함하나 이에 국한되지 않는 자가면역 질환 또는 면역 결핍의 활성 또는 병력:-myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjogren's syndrome, Guillain-Barré syndrome, or multiple sclerosis with the exception of Activity or history of autoimmune disease or immunodeficiency, but not limited to:
자가면역 관련 갑상선기능저하증의 병력이 있고 갑상선 대체 호르몬을 투여받고 있는 환자는 본 연구에 적격이다.Patients with a history of autoimmune-related hypothyroidism and taking thyroid replacement hormone are eligible for this study.
인슐린 요법을 받고 있는 조절된 제1형 진성 당뇨병 환자는 연구에 적격이다.Patients with controlled type 1 diabetes mellitus receiving insulin therapy are eligible for the study.
습진, 건선, 만성 단순 태선 또는 피부과적 징후만 있는 백반증의 환자(예: 건선성 관절염 환자는 제외)는 다음 조건이 모두 충족되는 경우 본 연구에 적격이다.Patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with only dermatological signs (eg, excluding patients with psoriatic arthritis) are eligible for this study if all of the following conditions are met:
- 발진이 체표면적의 <10%를 차지함 - The rash occupies <10% of the body surface area
- 질병이 기준선에서 잘 통제되고 낮은 역가의 국소 스테로이드만 필요함 - Disease is well controlled at baseline and requires only low titer topical steroids
- 지난 12개월 이내에 소랄렌에 더하여 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고효능 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았음- No acute exacerbation of an underlying condition requiring ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids in addition to psoralen within the past 12 months
-특발성 폐섬유증, 기질화 폐렴(예: 폐쇄성 세기관지염), 약물 유발성 폐렴 또는 간질성 폐렴의 병력, 또는 선별 흉부 컴퓨터 단층촬영(CT) 스캔 상의 활동성 폐렴의 증거- History of idiopathic pulmonary fibrosis, organic pneumonia (eg, bronchiolitis obliterans), drug-induced pneumonia or interstitial pneumonia, or evidence of active pneumonia on a screening chest computed tomography (CT) scan
방사선 분야에서 방사선 폐렴 (섬유증) 병력은 허용됨A history of radiation pneumonitis (fibrosis) in the field of radiation is acceptable
-활동성 결핵-active tuberculosis
연구 치료 시작 전 3개월 이내에 유의미한 심혈관 질환(예: 뉴욕심장협회 클래스 II 이상의 심장 질환, 심근경색증 또는 뇌혈관 사고), 불안정성 부정맥 또는 불안정형 협심증Significant cardiovascular disease (e.g., New York Heart Association Class II or higher heart disease, myocardial infarction or cerebrovascular accident), unstable arrhythmia, or unstable angina within 3 months prior to study treatment initiation
-연구 치료 시작 전 4주 이내에 진단을 제외한 주요 수술 절차, 연구 동안 주요 수술 절차에 대한 계획되거나 예상된 필요-Major surgical procedures excluding diagnosis within 4 weeks prior to initiation of study treatment, planned or anticipated need for major surgical procedures during the study
-적절하게 치료된 자궁경부의 상피암종, 비흑색종 피부암종, 국소 전립선암 또는 I기 자궁암과 같은, 전이 또는 사망의 무시가 가능한 위험(예: 5년 OS 비율 90%)을 갖는 악성 종양을 제외한, 무작위화 전 5년 이내에 SCCHN 이외의 추가적인 악성 종양의 병력-Malignant tumors with a negligible risk of metastasis or death (e.g., a 5-year OS rate of 90%), such as appropriately treated epithelial carcinoma of the cervix, non-melanoma skin carcinoma, focal prostate cancer, or stage I uterine cancer excluding, history of additional malignancies other than SCCHN within 5 years prior to randomization
-감염, 세균혈증 또는 중증 폐렴의 합병증으로 인한 입원을 포함하나 이에 국한되지 않는 연구 치료 시작 전 4주 이내의 중증 감염-Severe infection within 4 weeks prior to initiation of study treatment, including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia
-연구 치료 시작 전 2주 이내에 치료적 경구 또는 IV 항생제 치료-therapeutic oral or IV antibiotic treatment within 2 weeks prior to initiation of study treatment
예방적 항생제를 투여받는 환자(예를 들어, 요로 감염 또는 만성 폐쇄성 폐질환 악화의 예방)는 본 연구에 적격이다.Patients receiving prophylactic antibiotics (eg, prophylaxis of urinary tract infections or exacerbations of chronic obstructive pulmonary disease) are eligible for this study.
-선행 동종이계 줄기 세포 이식 또는 고형 장기 이식-Prior allogeneic stem cell transplantation or solid organ transplantation
-연구용 약물의 사용을 금하거나, 결과 해석에 영향을 미칠 수 있거나 환자를 치료 합병증으로 인한 고위험에 빠뜨릴 수 있는 기타 질병, 대사 기능장애, 신체 검사 소견 또는 임상 실험실 소견-Other diseases, metabolic dysfunctions, physical examination findings or clinical laboratory findings that may contraindicate the use of research drugs, may affect the interpretation of results, or put the patient at high risk for complications of treatment
-연구 치료 시작 전 4주 이내의 약독화 생백신 치료, 또는 연구 치료 중에, 아테졸리주맙의 최종 투여 후 5개월 이내, 또는 티라골루맙/위약의 최종 투여 후 90일 이내에 이러한 백신의 필요성에 대한 예상.- Expectations of the need for live attenuated vaccine treatment within 4 weeks prior to initiation of study treatment, or during study treatment, within 5 months of the last dose of atezolizumab, or within 90 days of the last dose of tiragolumab/placebo .
-HBV 또는 HCV에 대한 항바이러스 요법의 현재 치료-Current treatment of antiviral therapy for HBV or HCV
-선별검사시 Epstein-Barr 바이러스(EBV) 바이러스 캡시드 항원(VCA) IgM 검사 양성- Positive Epstein-Barr virus (EBV) virus capsid antigen (VCA) IgM test during screening
EEBV 중합효소연쇄반응(PCR) 검사는 급성 감염 또는 의심되는 만성 활성 감염을 선별하기 위해 임상적으로 지시된 대로 수행되어야 한다. EBV PCR 검사가 양성인 환자는 제외한다.EEBV polymerase chain reaction (PCR) testing should be performed as clinically indicated to screen for acute infection or suspected chronic active infection. Patients with a positive EBV PCR test are excluded.
-연구 치료 시작 전 28주 이내에 임상시험 요법으로 치료-Treatment with investigational therapy within 28 weeks prior to initiation of study treatment
-항 CTLA-4, 항 TIGIT, 항 PD-L1 및 항 PD-1 치료 항체를 포함한 CD137 작용제 또는 면역 관문 차단 요법을 이용한 이전의 치료-Previous treatment with CD137 agonists or immune checkpoint blockade therapy, including anti-CTLA-4, anti-TIGIT, anti-PD-L1 and anti-PD-1 therapeutic antibodies
-연구 치료 시작 전 4주 이내 또는 5회 약물 제거 반감기(둘 중 더 긴 기간) 이내에 전신 면역자극제(인터페론 또는 인터류킨 2[IL-2]를 포함하나 이에 국한되지 않음)를 사용한 치료-Treatment with systemic immunostimulants (including but not limited to interferon or interleukin 2 [IL-2]) within 4 weeks prior to initiation of study treatment or within 5 drug elimination half-lives (whichever is longer)
-연구 치료 시작 전 2주 이내에 전신 면역억제(코르티코스테로이드, 사이클로포스파미드, 아자티오프린, 메토트렉세이트, 탈리도마이드 및 항 TNF- 제제를 포함하나 이에 제한되지 않음)을 사용한 치료, 또는 연구 치료 동안 전신 면역억제제의 필요성에 대한 예상으로서, 다음 예외를 제외:-treatment with systemic immunosuppression (including, but not limited to, corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide and anti-TNF- agents) within 2 weeks prior to initiation of study treatment, or systemic immunity during study treatment Anticipation of the need for inhibitors, with the following exceptions:
- 급성, 저용량 전신 면역억제제 또는 1회 펄스 용량의 전신 면역억제제(예: 조영제 알레르기용 코르티코스테로이드 48시간)를 투여받은 환자는 Medical Monitor 확인을 얻은 후에 본 연구에 자격이 있다.- Patients receiving acute, low-dose systemic immunosuppressants or single pulse doses of systemic immunosuppressants (eg, corticosteroids for contrast allergy 48 hours) are eligible for this study after obtaining Medical Monitor confirmation.
- 무기질 코르티코이드(예: 플루드로코르티손), 만성 폐쇄성 폐질환 또는 천식용 흡입 또는 저용량 전신 코르티코스테로이드, 기립성 저혈압 또는 부신 기능 부전용 저용량 코르티코스테로이드를 투여받는 환자는 본 연구에 자격이 있다.- Patients receiving mineralocorticoids (e.g., fludrocortisone), inhaled or low-dose systemic corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency are eligible for this study.
-키메라 또는 인간화 항체 또는 융합 단백질에 대한 심각한 알레르기 아나필락시스 반응의 병력- History of severe allergic anaphylactic reaction to chimeric or humanized antibodies or fusion proteins
중국 햄스터 난소 세포 생성물에 대해 또는 아테졸리주맙 또는 티라골루맙 제형의 성분에 대해 알려진 과민증Known hypersensitivity to Chinese hamster ovary cell products or to any component of the atezolizumab or tiragolumab formulation
-연구 치료 중, 아테졸리주맙의 최종 투여 후 5개월 이내, 또는 티라골루맙/위약의 최종 투여 후 90일 이내의 임신 또는 모유 수유 또는 임신 의도.- Pregnancy or breastfeeding or intention to become pregnant during study treatment, within 5 months of the last dose of atezolizumab, or within 90 days of the last dose of tiragolumab/placebo.
가임 여성은 연구 치료 시작 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다.Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
F.F. 평가evaluation
연구 전반에 걸쳐 안전성 및 내약성에 대해 환자를 면밀히 모니터링한다. 각 용량 투여 전에 독성에 대해 환자들을 평가하고; 임상 평가 및 현지 실험실 검사 값이 허용 가능한 경우에만 투약을 실시한다.Patients are closely monitored for safety and tolerability throughout the study. Evaluate patients for toxicity prior to each dose administration; Dosing should be performed only when clinical evaluation and local laboratory test values are acceptable.
병력, 기준선 조건, 병용 약물, 및 인구 통계 데이터Medical history, baseline conditions, concomitant medications, and demographic data
임상적으로 유의미한 질병, 수술, 암 이력(이전의 암 요법 및 시술 포함), 생식 상태, 흡연 이력, 알코올 및 약물의 남용을 포함한 병력이 기준선에 기록된다. 또한, 연구 치료제 개시 전 7일 이내에 환자가 사용한 모든 약물(예컨대, 처방약, 일반의약품, 백신, 약초 또는 동종 요법 치료제, 영양 보조제)가 기록된다. 각 후속 신체 검사 시, 구간 의료 기록을 수득하고 약물 및 알레르기의 모든 변화를 기록한다.Medical history including clinically significant disease, surgery, history of cancer (including previous cancer therapies and procedures), reproductive status, history of smoking, and abuse of alcohol and drugs is recorded at baseline. In addition, all medications (eg, prescription medications, over-the-counter medications, vaccines, herbal or homeopathic remedies, nutritional supplements) taken by the patient within 7 days prior to initiation of study treatment are recorded. At each subsequent physical examination, an interval medical record is obtained and any changes in medications and allergies are recorded.
인구학적 데이터는 연령, 성별, 및 자가 보고한 인종/민족을 포함한다.Demographic data include age, gender, and self-reported race/ethnicity.
ECOG 전신 활동도ECOG whole body activity
성능 상태는 ECOG 성능 상태 척도를 사용하여 측정된다.Performance status is measured using the ECOG Performance Status Scale.
신체 검사Physical examination
완전한 신체 검사는 선별시 수행되어야 하며, 머리, 눈, 귀, 코, 및 목, 및 심혈관, 피부, 근골격, 호흡, 위장, 비뇨생식, 및 신경 시스템의 평가를 포함해야 한다. 기준선에서 확인된 어떠한 비정상이든지 기록되어야 한다.A complete physical examination should be performed at screening and should include evaluation of the head, eyes, ears, nose, and throat, and cardiovascular, skin, musculoskeletal, respiratory, gastrointestinal, urogenital, and nervous systems. Any abnormalities identified at baseline should be recorded.
제한된, 증상 지향적 신체 검사는 특정 기준선 이후 방문 시 임상적으로 지시된 대로 수행되어야 한다. 기준선 비정상으로부터 변화는 환자 노트에 기록되어야 한다. 신규한 또는 악화된 임상적으로 유의미한 비정상은 유해 사례로서 기록되어야 한다.A limited, symptom-oriented physical examination should be performed as clinically indicated at specific post-baseline visits. Changes from baseline abnormalities should be recorded in the patient note. New or worsening clinically significant abnormalities should be recorded as adverse events.
신체 검사Physical examination
활력 징후에는 호흡수, 맥박수, 수축기 및 이완기 혈압, 및 체온의 측정이 포함된다. 기준선에서 관찰된 이상 및 후속 방문에서 새로 또는 악화된 임상적으로 유의한 이상이 기록된다.Vital signs include measurements of respiratory rate, pulse rate, systolic and diastolic blood pressure, and body temperature. Abnormalities observed at baseline and new or worsening clinically significant abnormalities at follow-up visits are recorded.
종양 및 반응 평가Tumor and Response Assessment
선별 평가 및 후속 종양 평가에는 흉부 및 복부의 CT 스캔(구강 또는 IV 조영제 사용) 및 CT 스캔(구강 또는 IV 조영제 사용) 또는 머리와 목(두개골에서 쇄골 기저부)의 자기공명영상(MRI)(조영제 사용)을 포함하여야 한다. 골반의 조영제를 사용한 CT 스캔은 임상적으로 지시된 대로 또는 선별검사 및 후속 반응 평가 시 현지 SOC에 따라 수행해야 한다. 조영제를 사용한 CT 스캔이 금지된다면(예: 신장 청소율 장애가 있는 환자의 경우), 흉부의 비조영제 CT 스캔을 수행할 수 있고 머리와 목, 복부 및 골반의 조영제를 사용한 MRI 스캔(해당되는 경우)을 수행해야 한다. 기준선 및 후속 반응 평가에서 임상적으로 지시된 경우 뼈 스캔과 같은 추가 조사도 수행해야 한다.Screening evaluation and subsequent tumor evaluation include CT scans of the chest and abdomen (with oral or IV contrast) and CT scans (with oral or IV contrast) or magnetic resonance imaging (MRI) of the head and neck (skull to base of the clavicle) (with contrast). ) should be included. Contrast CT scans of the pelvis should be performed as clinically indicated or according to local SOC for screening and subsequent response evaluation. If CT scans with contrast media are prohibited (for example, in patients with impaired renal clearance), non-contrast CT scans of the chest may be performed and MRI scans with contrast media (if applicable) of the head and neck, abdomen and pelvis should be done Additional investigations, such as bone scans, should also be performed if clinically indicated at baseline and subsequent response assessments.
뇌에 대한 조영제를 사용한 CT 스캔 또는 조영제를 사용한 MRI 스캔(조영제를 사용한 CT가 금기인 경우)은 선별검사 및 후속 반응 평가에서 CNS 전이를 평가하기 위해 임상적으로 지시된 대로 수행해야 한다. 조영제를 사용한 CT 스캔이 수행되고 뇌 전이의 존재가 모호한 것으로 간주되는 경우, 기준선에서 CNS 전이의 진단을 확인하거나 반박하기 위해 머리에 대한 MRI 스캔이 요구된다. 활성 또는 치료되지 않은 CNS 전이가 있는 환자는 본 연구에 적합하지 않다. 선별검사시 방사선 조사된 뇌 전이의 병력이 있는 환자는 임상적으로 지시되지 않는 한 후속 반응 평가에서 뇌 스캔을 받을 필요가 없다.Contrast CT scans of the brain or MRI scans with contrast media (if contrast-medium CT is contraindicated) should be performed as clinically indicated to evaluate CNS metastases at screening and subsequent response evaluation. If a CT scan with a contrast agent is performed and the presence of brain metastases is considered ambiguous, an MRI scan of the head is required to confirm or refute the diagnosis of CNS metastases at baseline. Patients with active or untreated CNS metastases are not eligible for this study. Patients with a history of irradiated brain metastases at screening do not need a brain scan at subsequent response assessment unless clinically indicated.
종양 평가를 위한 CT 스캔이 양전자 방출 단층촬영 (PET)/CT 스캐너에서 수행되는 경우 CT 획득은 전체 조영제 진단 CT 스캔의 표준과 일치해야 한다.If CT scans for tumor evaluation are performed on a positron emission tomography (PET)/CT scanner, the CT acquisition should be consistent with the standard for full contrast diagnostic CT scans.
사전 동의를 얻기 전에 SOC로 수행된 종양 평가는, 스캔이 진단 품질이고 무작위 배정 후 28일 이내에 수행되는 조건으로, 검사를 반복하는 대신에 사용할 수 있다.Tumor evaluation performed with SOC prior to obtaining informed consent may be used as an alternative to repeating the examination, provided that the scan is of diagnostic quality and performed within 28 days of randomization.
선별검사시 사용된 동일한 방사선 촬영 방식(예: 조영제를 사용한 CT 스캔) 및 절차(예: CT 스캔에 대한 동일한 조영제 프로토콜)는 모든 후속 종양 평가에 사용되어야 한다. 측정가능한 및/또는 측정 불가능한 질병을 포함하여 공지된 모든 질병 부위는 선별 검사 시 기록되고 각 후속 종양 평가에서 재평가된다.The same radiographic modality (eg, CT scan with contrast medium) and procedure (eg, same contrast medium protocol for CT scan) used during screening should be used for all subsequent tumor evaluations. All known disease sites, including measurable and/or non-measurable disease, are recorded at screening and re-evaluated at each subsequent tumor assessment.
환자는 기준선에서, 주기 1의 1일차 이후 처음 30주 동안은 6주마다(± 7일), 30주차 종양 평가 완료 후 9주마다(± 7일) 종양 평가를 받는다. 종양 평가는 RECIST v1.1에 따른 방사선학적 질환 진행 또는 RECIST v1.1에 따른 방사선학적 질환 진행 후 연구 치료를 계속하는 환자에 대한 임상적 이익 상실, 동의 철회, 사망 또는 스폰서에 의한 연구 종료 중 먼저 발생하는 때까지의 치료 지연에 관계없이 일정에 따라 계속된다. 또한, 진행성 질병 또는 임상적 이익의 손실이 의심되면 시험자의 재량에 따라 언제든지 스캔을 수행해야 한다.Patients receive tumor assessments at baseline, every 6 weeks (± 7 days) for the first 30 weeks after Day 1 of Cycle 1, and every 9 weeks (± 7 days) after completion of tumor assessments at Week 30. Tumor evaluation is based on loss of clinical benefit, withdrawal of consent, death, or termination of study by sponsor for patients continuing on study treatment after radiological disease progression according to RECIST v1.1 or radiological disease progression according to RECIST v1.1, whichever occurs first. Continue on schedule regardless of treatment delay until it occurs. In addition, if progressive disease or loss of clinical benefit is suspected, a scan should be performed at any time at the discretion of the investigator.
RECIST v.1.1에 따른 방사선학적 질환 진행이 없는 상태에서 연구 치료를 중단한 환자(임상 저하 또는 독성을 포함하되 이에 국한되지 않음)는 새로운 항암 요법의 시작 여부에 관계없이 전술한 일정에 따라 종양 반응 평가를 계속한다. 종양 평가는 RECIST v1.1에 따른 방사선학적 질병 진행, 동의 철회, 사망 또는 시험의뢰자에 의한 연구 종료 중 먼저 발생하는 시점까지 계속된다. 응답은 RECIST v1.1을 사용하여 자세히 전술한 영상기법에 대해 시험자에 의해 평가된다. 모든 시점에서 전체 종양 반응에 대한 시험자의 평가는 RECIST v1.1만을 기반으로 하여야 한다. 평가는 방문을 통해 내부 일관성을 확보하는 것이 가능하다면 동일한 평가자에 의해 수행되어야 한다.Patients who discontinue study treatment in the absence of radiologic disease progression according to RECIST v.1.1 (including, but not limited to, clinical decline or toxicity) will receive tumor response according to the above schedule, regardless of whether new anticancer therapy is initiated or not. Continue the evaluation. Tumor evaluation continues until radiological disease progression, withdrawal of consent, death, or end of study by the sponsor, whichever occurs first according to RECIST v1.1. Responses are assessed by the investigator for the imaging techniques detailed above using RECIST v1.1. The investigator's assessment of overall tumor response at all time points should be based solely on RECIST v1.1. Assessments should be conducted by the same evaluator if possible to ensure internal consistency throughout the visit.
모든 시점에서 전체 종양 반응에 대한 시험자의 평가는 RECIST v1.1 만을 기초로 한다. 질병 진행 이후에도 연구 치료를 받는 환자의 경우 RECIST v1.1에 따른 진행 이후 종양 평가를 계속하여야 한다. 여기에는 표적 병변의 지속적인 측정, 비표적 병변의 평가, 모든 후속 평가에서 새로 식별된 병변의 평가가 포함된다.Investigator's assessment of overall tumor response at all time points is based on RECIST v1.1 only. For patients receiving study treatment after disease progression, tumor evaluation should continue following progression according to RECIST v1.1. This includes ongoing measurement of target lesions, evaluation of non-target lesions, and evaluation of newly identified lesions at all subsequent evaluations.
실험실, 바이오마커, 및 다른 생물학적 샘플laboratory, biomarkers, and other biological samples
하기의 실험실 시험용 샘플들은 분석을 위해 연구 장소의 지역 실험실로 보내진다:The following laboratory test samples are sent to the local laboratory at the study site for analysis:
o 혈액학적: 백혈구 수, 적혈구 수, 헤모글로빈, 헤마토크릿, 혈소판 수 및 감별 수 (호중구, 호산구, 호염기구, 단핵구 및 림프구).o Hematology: white blood cell count, red blood cell count, hemoglobin, hematocrit, platelet count and differential count (neutrophils, eosinophils, basophils, monocytes and lymphocytes).
o 화학 패널(혈청 또는 혈장): 중탄산염 또는 총 이산화탄소(해당 지역의 SOC로 고려되는 경우), 나트륨, 칼륨, 마그네슘, 염화물, 포도당, BUN 또는 요소, 크레아티닌, 총 단백질, 알부민, 인산염, 칼슘, 총 빌리루빈, ALP, ALT, AST 및 LDH.o Chemical panel (serum or plasma): bicarbonate or total carbon dioxide (if considered local SOC), sodium, potassium, magnesium, chloride, glucose, BUN or urea, creatinine, total protein, albumin, phosphate, calcium, total Bilirubin, ALP, ALT, AST and LDH.
o 응집: INR 및 aPTTo Aggregation: INR and aPTT
o 갑상선 기능 검사: 갑상선 자극 호르몬, 유리 트리아이오도티로닌(T3)(또는 유리 T3가 실시되지 않은 부위의 경우 총 T3), 및 유리 티록신(T4로도 공지됨)o Thyroid function tests: thyroid stimulating hormone, free triiodothyronine (T3) (or total T3 for sites where free T3 has not been administered), and free thyroxine (also known as T4)
- 다음을 포함하는 EBV 혈청학- EBV serology, including
o EBV VCA IgMo EBV VCA IgM
o EBV VCA IgG 또는 Epstein-Barr 바이러스 핵 항원(EBNA) IgGo EBV VCA IgG or Epstein-Barr Virus Nuclear Antigen (EBNA) IgG
o 임상적으로 지시된 경우: EBV PCRo If clinically indicated: EBV PCR
o HIV 혈청학o HIV serology
- 다음으로 구성된 HBV 혈청학:- HBV serology consisting of:
o 모든 환자에 대한 HBsAg, HBsAb 및 총 HBcAbo HBsAg, HBsAb and total HBcAb for all patients
o HBsAg 및 HBsAb 검사가 음성이고 총 HBcAb 검사가 양성인 환자의 HBV DNAo HBV DNA from patients with negative HBsAg and HBsAb tests and positive total HBcAb tests
선별검사시 정량적 HBV DNA가 양성인 환자(적격 기준에 따라 ≥500IU/mL이어야 함)는 활동 일정에 요약된 대로 추가적인 HBV DNA 검사를 받는다.Patients with positive quantitative HBV DNA at screening (must be ≥500 IU/mL according to eligibility criteria) receive additional HBV DNA testing as outlined in the activity schedule.
o HCV 혈청학: HCV 항체 및 (HCV 항체 검사가 양성인 경우) HCV RNAo HCV serology: HCV antibody and (if HCV antibody test is positive) HCV RNA
o 구인두와 관련된 SCCHN 환자의 경우: p16 IHC, 제자리 교잡 또는 PCR 기반 분석에 의해 결정된 종양 조직의 HPV 상태o For SCCHN patients with oropharyngeal involvement: HPV status of tumor tissue as determined by p16 IHC, in situ hybridization or PCR-based analysis
o o
임신 검사.pregnancy test.
가임기 여성은 모두 스크리닝시 혈청 임신 검사를 받는다. 연구 치료 동안 소변 임신 테스트는 각각의 주기의 제 1일차에 수행된다. 소변 임신 검사는 치료 중단 방문 시에도 수행된다. 소변 임신 검사가 양성이면 혈청 임신 검사로 확인해야 한다.All women of childbearing potential are tested for serum pregnancy at screening. During study treatment, a urine pregnancy test is performed on Day 1 of each cycle. A urine pregnancy test is also performed at the treatment discontinuation visit. If the urine pregnancy test is positive, it should be confirmed with a serum pregnancy test.
여성이 초경 이후이고, 폐경 후 상태(폐경 이외의 확인된 원인 없이 계속해서 12개월 동안 무월경이 지속됨)에 도달하지 않았으며, 수술(즉, 난소, 나팔관 및/또는 자궁 제거) 또는 시험자가 결정한 다른 원인(예컨대, 뮐러관 무발생)으로 인한 영구적인 불임이 아닌 경우, 가임기인 것으로 간주된다.The woman is post-menopausal, has not reached post-menopausal status (amenorrhea continues for 12 consecutive months without an identified cause other than menopause), and has not undergone surgery (i.e., removal of the ovaries, fallopian tubes, and/or uterus) or another as determined by the investigator A woman of childbearing age is considered to be of childbearing age unless it is permanent infertility due to cause (eg, absence of Muller's canal).
o 소변 검사(pH, 비중, 포도당, 단백질, 케톤 및 혈액); 계량봉 허용o Urinalysis (pH, specific gravity, glucose, protein, ketones and blood); Dipstick Allowed
하기의 샘플들은 분석을 위해 하나 또는 여러 중앙 실험실이나 시험의뢰자 또는 피지명인에게 보낸다:The following samples are sent for analysis to one or several central laboratories or to the sponsor or designee:
o 자가항체 분석을 위한 혈청 샘플: 항핵항체, 항이중나선 DNA, 순환 항호중구 세포질 항체, 및 핵주위 항호중구 세포질 항체o Serum samples for autoantibody analysis: antinuclear antibody, anti-double-stranded DNA, circulating anti-neutrophil cytoplasmic antibody, and perinuclear anti-neutrophil cytoplasmic antibody
o C-반응성 단백질에 대한 혈청 샘플o Serum samples for C-reactive protein
o 검증된 분석을 통한 아테졸리주맙 및 티라골루맙 PK 분석을 위한 혈청 샘플o Serum samples for atezolizumab and tiragolumab PK assays with validated assays
o 검증된 분석을 통한 아테졸리주맙 및 티라골루맙에 대한 ADA 평가를 위한 혈청 샘플o Serum samples for ADA evaluation for atezolizumab and tiragolumab with validated assays
o 바이오마커에 대한 예비 연구를 위한 혈액 및 혈장 샘플 o Blood and plasma samples for preliminary research on biomarkers
혈액 샘플은 말초 혈액 단핵 세포(PBMC) 및 기타 유도체(예: RNA, DNA 등)를 얻기 위해 처리될 수 있다.Blood samples can be processed to obtain peripheral blood mononuclear cells (PBMCs) and other derivatives (eg, RNA, DNA, etc.).
o PD-L1 발현의 판단 및 바이오마커에 대한 탐색 연구를 위한 기준선에서 얻은 보관 또는 새로 수집된 종양 조직 샘플o Archived or freshly collected tumor tissue samples from baseline for evaluation of PD-L1 expression and exploratory studies for biomarkers
파라핀 블록(선호)의 대표적인 FFPE 종양 표본 또는 염색되지 않은 갓 절단된 연속 섹션을 포함하는 최소 20개의 슬라이드를 연구 등록 전에 관련 병리학 보고서와 함께 제출해야 한다. 15~19개의 슬라이드만 입수 가능한 경우, 의료 모니터의 승인을 받은 후에도 환자는 여전히 해당 연구에 적격일 수 있다.A minimum of 20 slides containing representative FFPE tumor specimens in paraffin blocks (preferred) or unstained, freshly excised continuous sections should be submitted along with the relevant pathology report prior to study enrollment. If only 15 to 19 slides are available, the patient may still be eligible for the study after approval by the medical monitor.
종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 양호해야 한다. Tumor tissue should be of good quality based on total and viable tumor content.
샘플은 바늘 게이지 또는 검색 방법에 관계없이 세포 맥락 및 조직 구조를 보존하는 최소 50개의 생존 가능한 TC를 함유하여야 한다.Samples should contain at least 50 viable TCs that preserve cellular context and tissue structure, regardless of needle gauge or retrieval method.
절제(resection), 코어-바늘 생검(최소 3개의 코어이고, 단일 파라핀 블록에 내장) 또는 절제, 절개, 펀치 또는 겸자 생검을 통해 수집된 샘플은 허용된다. 미세 바늘 흡인(조직 구조를 보존하지 않고 세포 현탁액 및/또는 도말을 생성하지 않는 샘플로 정의됨), 칫솔질, 흉막 삼출액의 세포 펠렛, 및 세척 샘플은 허용하지 않는다. 석회화가 제거된 뼈 전이로부터의 종양 조직은 허용하지 않는다.Samples collected via resection, core-needle biopsy (minimum of three cores, embedded in a single paraffin block) or via resection, incision, punch or forceps biopsy are acceptable. Fine needle aspiration (defined as a sample that does not preserve tissue structure and does not produce a cell suspension and/or smear), brushing, cell pellets in pleural effusion, and wash samples are not permitted. Tumor tissue from calcified bone metastases is not acceptable.
보관 종양 조직을 사용할 수 없거나 필요 검사에 부적합하다고 판단되면 치료 전 종양 생검이 요굳된다. 환자의 보관 조직 검사 결과가 적격 기준을 충족하지 않는 경우 치료 전 종양 생검을 수행할 수도 있다.A pre-treatment tumor biopsy is recommended if archived tumor tissue is not available or is judged unsuitable for the required testing. A pre-treatment tumor biopsy may be performed if the patient's archival biopsy results do not meet the eligibility criteria.
바이오마커에 대한 예비 연구를 위해, 임상적으로 가능하다고 판단되는 경우, 진행 시점에 얻은 종양 조직 샘플For preliminary studies of biomarkers, tumor tissue samples obtained at the time of progression, if considered clinically feasible.
진행 시점의 생검은 진행 후 40일 이내에 또는 다음 항암 요법 이전 중 더 빠른 시점에 수행해야 한다.A biopsy at the time of progression should be performed within 40 days of progression or before the next chemotherapy, whichever is earlier.
절제, 코어-바늘 생검(최소 3개의 코어 선호), 또는 절제, 절개, 펀치 또는 겸자 생검을 통해 수집된 샘플이 바람직하다.Samples collected via excision, core-needle biopsy (preferably at least 3 cores), or via excision, incision, punch or forceps biopsy are preferred.
NGS는 Foundation Medicine에 의해 수행될 수 있다. Foundation Medicine에 의해 수행되는 경우, 시험자는 Foundation Medicine의 웹 포털을 통해 NGS 보고서를 얻을 수 있다. 현지 법률에서 허용하는 경우, 환자가 달리 선택하지 않는 한, 시험자는 환자와 결과를 공유하고 논의할 수 있다. NGS 보고서는 연구 목적으로 생성되며 향후 치료 결정을 안내할 목적으로 제공되지 않는다. 테스트 기준을 충족하지 않는 샘플에 대해서는 결과가 제공되지 않는다.NGS may be performed by Foundation Medicine. If conducted by Foundation Medicine, investigators can obtain NGS reports through Foundation Medicine's web portal. Where permitted by local law, investigators may share and discuss results with patients, unless the patient chooses otherwise. NGS reports are generated for research purposes and are not intended to guide future treatment decisions. Results are not provided for samples that do not meet the test criteria.
탐색적 바이오마커 연구에는 종양 유전자 변경, HPV 상태 또는 종양 면역생물학 관련 유전자 서명, PD-L1, TIGIT, 림프구 하위집단 및 T 세포 수용체 레퍼토리가 포함될 수 있지만 이에 국한되지 않는다. 연구는 DNA, 무세포 DNA 또는 RNA의 추출; 돌연변이 및 기타 종양 특이적 게놈 변이체 분석; 및 포괄적인 유전자 패널의 NGS 사용을 통한 게놈 프로파일링과 관련될 수 있다. 혈액에서 추출한 DNA는 조직에서 추출한 DNA와 비교하여, 생식계열 변이체와 체세포 변이체를 구별함으로써 체세포 변이체를 식별할 수 있다. NGS 방법에는 조직 및 혈액 샘플의 WGS 또는 WES가 포함될 수 있지만 혈액 샘플의 WGS 또는 WES는 참여 기관은에서만 수행된다.Exploratory biomarker studies may include, but are not limited to, oncogene alterations, HPV status or gene signatures associated with tumor immunobiology, PD-L1, TIGIT, lymphocyte subpopulations, and T cell receptor repertoire. Studies include extraction of DNA, cell-free DNA or RNA; analysis of mutations and other tumor-specific genomic variants; and genomic profiling through the use of NGS in a comprehensive panel of genes. DNA extracted from blood can be compared to DNA extracted from tissues, and somatic variants can be identified by distinguishing germline variants from somatic variants. NGS methods may include WGS or WES of tissue and blood samples, but WGS or WES of blood samples is only performed by participating institutions.
샘플링 절차, 보관 조건 및 배송 지침은 실험실 설명서를 참조한다.Refer to the laboratory manual for sampling procedures, storage conditions, and shipping instructions.
환자가 선택적인 예비 연구를 위해 자신의 남은 샘플을 저장하는 것에 대해 구체적인 동의를 하지 않는 한, 생물학적 샘플은 다음 예외를 제외하고 최종 임상 연구 보고서가 완성되는 시점까지 파기된다:Unless the patient specifically consents to the storage of his or her remaining samples for an optional preliminary study, biological samples will be destroyed until the completion of the final clinical study report with the following exceptions:
·PK 또는 면역원성 분석을 위해 수집된 혈청 샘플은 추가 면역원성 특성화 및 PK 또는 면역원성 분석 개발 및 검증에 필요할 수 있다; 따라서 이러한 샘플은 최종 임상 연구 보고서가 완료된 후 5년 이내에 폐기된다.Serum samples collected for PK or immunogenicity assays may be needed for further immunogenicity characterization and development and validation of PK or immunogenicity assays; Therefore, these samples are discarded within 5 years of completion of the final clinical study report.
·바이오마커 연구를 위해 수집된 혈액, 혈장 및 PBMC 샘플은 최종 임상 연구 보고서가 완료된 후 5년 이내에 파기된다. 단, WGS 또는 WES를 거치는 조직 샘플은 예외로 하며 더 이상 필요하지 않거나 소진될 때까지 보관된다. 다만, 보관 기간은 IRB/EC가 승인한 사전 동의 양식 및 적용가능한 법률(예: 보건 당국 요구 사항)을 따른다.· Blood, plasma and PBMC samples collected for biomarker studies will be destroyed within 5 years of completion of the final clinical study report. With the exception of tissue samples that have undergone WGS or WES, they are no longer needed or stored until depleted. However, the storage period is subject to the informed consent form approved by the IRB/EC and applicable laws (eg health authority requirements).
·등록된 환자의 경우, 요청 시 또는 최종 임상 연구 보고서 후 18개월 이내 중 먼저 발생하는 시점에 나머지 보관 조직 블록은 기관으로 반환된다. 등록되지 않은 환자의 경우, 남아 있는 보관 조직 블록은 적격성 판단 후 6주 이내에 기관으로 반환된다.·For enrolled patients, the remaining archived tissue blocks will be returned to the institution upon request or within 18 months of the final clinical study report, whichever occurs first. For unenrolled patients, the remaining archived tissue blocks will be returned to the institution within six weeks of eligibility determination.
환자가 연구에서 철회하는 경우, 환자가 샘플의 폐기를 특별히 요청하거나 현지 법률이 샘플의 폐기를 요구하지 않는 한, 철회 날짜 이전에 수집된 샘플은 계속 분석될 수 있다. 다만, 철회 전에 샘플을 테스트한 경우 해당 테스트로부터의 결과는 전체 연구 데이터의 일부로 남는다.If a patient withdraws from the study, samples collected prior to the withdrawal date may continue to be analyzed, unless the patient specifically requests the destruction of the sample or local law requires that the sample be discarded. However, if a sample is tested prior to withdrawal, the results from that test remain part of the overall study data.
탐색적 바이오마커 분석의 복잡성과 탐색적 특성을 감안할 때, 이러한 분석에서 도출된 데이터는 법에서 요구하지 않는 한 일반적으로 연구 시험자 또는 환자에게 제공되지 않는다(질병 진행 시 얻은 생검에만 적용되는 Foundation Medicine의 보고서는 제외). 수행된 연구의 집계 결과는 연구 데이터 출판에 대한 효과적인 후원 정책에 따라 제공 가능하다.Given the complexity and exploratory nature of exploratory biomarker assays, data derived from these assays are generally not made available to study investigators or patients unless required by law (see Foundation Medicine's guideline, which applies only to biopsies obtained at the time of disease progression). excluding reports). The aggregated results of the conducted research can be provided according to the effective sponsorship policy for the publication of research data.
심전도electrocardiogram
ECG는 선별검사시 그리고 연구 중 다른 시점에서 임상적으로 지시된 대로 요구된다. 각 환자에 대한 ECG는 가능한 동일한 기계에서 얻어야 한다. 리드 배치는 가능한 일관되어야 한다. ECG 기록은 환자가 적어도 10분 동안 바로 누운 자세를 취한 후에 실시해야 한다.ECG is required at screening and as clinically indicated at other time points during the study. ECGs for each patient should be obtained from the same machine whenever possible. Lead placement should be as consistent as possible. ECG recordings should be performed after the patient has been in the supine position for at least 10 minutes.
안전 모니터링 목적을 위해, 시험자는 모든 ECG 추적을 검토하고 서명하고 날짜를 기입해야 한다. ECG 추적의 사본은 기관에서 환자의 영구 연구 파일의 일부로서 보관된다. 모든 형태학적 파형 변화 또는 기타 ECG 이상은 eCRF에 문서화해야 한다.For safety monitoring purposes, the investigator must review, sign and date all ECG traces. Copies of ECG traces are kept at the institution as part of the patient's permanent study file. Any morphological waveform changes or other ECG abnormalities should be documented in the eCRF.
임상 결과 평가Clinical Outcome Evaluation
PRO 기구는 아테졸리주맙 + 티라골루맙 및 아테졸리주맙 + 위약의 임상 프로파일을 더 온전히 특성화하도록 완성된다. 또한, PRO 기구를 통해 아테졸리주맙+티라골루맙 및 아테졸리주맙+위약에 대한 각 환자의 직접적인 경험을 갈무리할 수 있다.The PRO instrument is completed to more fully characterize the clinical profile of atezolizumab + tiragolumab and atezolizumab + placebo. In addition, the PRO instrumentation allows us to capture each patient's first-hand experience with atezolizumab + tyragolumab and atezolizumab + placebo.
PRO 데이터는 하기의 기구들을 사용하여 수집된다:PRO data is collected using the following instruments:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
대한 환자의 전체적 인상(PGI-S) Patient's overall impression of Korea (PGI-S)
![]()
![]()
![]()
![]()
![]()
![]()
PRO 질문지(즉, PROMIS®, PGI-S/PGI-CI, MIS 및 PRO-CTCAE)는 치료 중 및 치료 중단 방문시 완료된다.PRO questionnaires (ie, PROMIS ® , PGI-S/PGI-CI, MIS and PRO-CTCAE) are completed at the on-treatment and discontinuation visits.
임상 결과 평가를 위한 데이터 수집 방법Data Collection Methods for Evaluation of Clinical Outcomes
아테졸리주맙 + 티라골루맙 및 아테졸리주맙 + 위약의 임상 프로필을 특성화하도록 사용되는 PRO 기구는 연구 중 특정 시점에 클리닉에서 자가투여되거나 면접관에 의해 (적절한 경우) 투여된다. PROMIS®, PGI-S/PGI-CI, MIS 및 PRO-CTCAE 설문지를 사용하여 얻은 PRO 데이터.The PRO instruments used to characterize the clinical profile of atezolizumab + tiragolumab and atezolizumab + placebo are self-administered in the clinic or administered by an interviewer (if appropriate) at specific time points during the study. PRO data obtained using the PROMIS ® , PGI-S/PGI-CI, MIS and PRO-CTCAE questionnaires.
클리닉에서, 기구는 달리 명시되지 않는 한 환자가 질병 상태에 대한 정보를 받기 전, 비-PRO 평가를 수행하기 전, 연구 치료제를 투여하기 전에 투입된다.In the clinic, the device is put in before the patient is informed of the disease status, prior to performing a non-PRO assessment, and prior to administering the study treatment, unless otherwise specified.
클리닉 방문 중에 투여 예정된 적절한 지역 언어로 번역된 종이 PRO 설문지는 평가 편향을 가능한 방지하기 위해 다른 연구 평가 이전 및 연구 치료의 투여 전에 클리닉 방문 시작 시 연구 현장에서 환자가 작성해야 한다. 환자는 현장 스태프가 제공한 종이 버전의 설문지를 완료한다. 면접관 평가는 허용되지만 스스로 측정을 완료할 수 없는 환자의 경우에는 진료소 스태프에 의해서만 수행될 수 있다.Translated paper PRO questionnaires into the appropriate local language scheduled for administration during the clinic visit should be completed by the patient at the study site prior to other study evaluations and at the beginning of the clinic visit prior to administration of study treatment to avoid possible evaluation bias. The patient completes a paper version of the questionnaire provided by the field staff. Interviewer assessments are permitted but may only be performed by clinic staff for patients unable to complete measurements on their own.
연구 직원은 환자가 연구 현장을 떠나기 전에 완전성을 위해 모든 설문지를 검토해야 한다.The study staff should review all questionnaires for completeness before the patient leaves the study site.
클리닉 방문 중, PRO 기구는 하기의 개요와 같이 관리되어야 한다:During clinic visits, PRO instruments should be administered as outlined below:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
임상 결과 평가 도구에 대한 설명Description of Clinical Outcome Assessment Tools
PROMISPROMIS ®® 아이템 뱅크 v2.0-신체 기능-간편 양식 10b Item Bank v2.0 - Body Functions - Quick Form 10b
PROMIS® 아이템 뱅크 v2.0-신체 기능-간편 양식 10b는, 일상 생활의 도구적 활동뿐만 아니라, 상지(손놀림), 하지(걷기 또는 이동성) 및 중앙 부위(목, 등)의 기능을 포함한 신체 활동의 자가 보고 능력을 측정하도록 설계된 10개의 질문으로 구성된다. 모든 질문은 1-5점 척도로 채점되며, 5점은 환자의 가장 높은 기능 능력에 해당하고 1점은 환자의 가장 낮은 기능 능력에 해당한다. 리콜 기간은 7일이다.PROMIS ® Item Bank v2.0-Body Functions-Simple Form 10b, includes not only instrumental activities of daily life, but also physical activities including functions of the upper extremities (hand movements), lower extremities (walking or mobility) and central regions (neck, back). It consists of 10 questions designed to measure a person's self-reporting ability. All questions are scored on a 1-5 point scale, where 5 corresponds to the patient's highest functional ability and 1 corresponds to the patient's lowest functional ability. The recall period is 7 days.
PROMISPROMIS ® ® 아이템 뱅크 v1.0-피로도-간편 양식 4aItem Bank v1.0 - Fatigue - Quick Form 4a
PROMIS® 아이템 뱅크 v1.0-피로도-간편 양식 4a는 자가 보고된 피로 증상의 범위와 환자의 일상 활동 수행 능력을 평가하도록 설계된 4개 항목으로 구성된다. 설문지의 항목은 환자가 지난 7일 동안 경험한 피로의 정도를 묻는다. 항목은 1-5점 척도로 되어 있으며, 5점은 환자가 경험한 가장 높은 피로도에 해당하고, 1점은 환자가 경험한 가장 낮은 피로도에 해당한다. 리콜 기간은 7일이다.The PROMIS ® Item Bank v1.0-Fatigue-Simple Form 4a consists of four items designed to assess the range of self-reported fatigue symptoms and the patient's ability to perform daily activities. The items on the questionnaire asked the degree of fatigue experienced by the patient in the past 7 days. Items are on a scale of 1-5, with 5 representing the highest degree of fatigue experienced by the patient, and 1 representing the lowest level of fatigue experienced by the patient. The recall period is 7 days.
PROMISPROMIS ®® 아이템 뱅크 v1.1-통증 간섭-간편 양식 4aItem Bank v1.1 - Pain Interference - Quick Form 4a
PROMIS® 아이템 뱅크 v1.1-통증 간섭-간편 양식 4a는 환자 인생의 관련 측면에 대한 통증의 결과/간섭을 평가하도록 설계된 자가 보고 척도의 4개 질문으로 구성된다. 모든 질문은 1-5점 척도로 채점되며, 5점은 환자가 경험하는 가장 높은 통증 간섭 수준에 해당하고, 1점은 가장 낮은 통증 간섭 수준에 해당한다. 리콜 기간은 7일이다.The PROMIS ® Item Bank v1.1-Pain Intervention-Simple Form 4a consists of 4 questions on a self-reported scale designed to assess the outcome/interference of pain on relevant aspects of a patient's life. All questions are scored on a 1-5 point scale, where 5 corresponds to the highest level of pain interference experienced by the patient, and 1 corresponds to the lowest level of pain interference. The recall period is 7 days.
PROMISPROMIS ® ® 숫자 등급 척도-v1.0-통증 강도 1aNumeric Rating Scale - v1.0 - Pain Intensity 1a
PROMIS® 숫자 등급 척도-v1.0-통증 강도 1a는 환자의 평균 통증 수준을 평가하도록 설계된 자가 보고 척도의 1개 질문으로 구성된다.The PROMIS ® Numeric Rating Scale-v1.0-Pain Intensity 1a consists of one question on a self-reported scale designed to assess a patient's average pain level.
질문은 1-10 척도로 채점되며, 10점은 "상상가능한 최악의 통증"에 해당하고, 1점은 "통증 없음"에 해당한다. 리콜 기간은 7일이다. Questions are scored on a scale of 1-10, where 10 corresponds to “worst pain imaginable” and 1 corresponds to “no pain”. The recall period is 7 days.
중증도에 대한 환자의 전체적 인상(PGI-S)Patient's overall impression of severity (PGI-S)
중증도에 대한 환자의 전체적 인상(PGI-S)은 지난 7일 동안의 전반적인 상태의 증증도에 대한 환자의 인상을 평가하도록 사용되는 단일 항목, 자가 보고 척도이다. PGI-S는 5점 응답 척도를 사용하며 5점은 "매우 심함"에 해당하고 1점은 "없음"에 해당한다(도입자 Guy et al. 1976).Patient's Global Impression of Severity (PGI-S) is a single-item, self-reported scale used to evaluate a patient's impression of the severity of the overall condition over the past 7 days. The PGI-S uses a 5-point response scale, with 5 being “very severe” and 1 being “none” (introducer Guy et al. 1976).
변화와 그 중요성에 대한 환자의 전체적 인상(PGI-CI)Patient's overall impression of change and its importance (PGI-CI)
환자의 변화에 대한 전체적인 인상은 본 연구를 시작할 때와 비교하여 환자 상태의 변화에 관한 환자의 인상을 평가하도록 사용되는 단일 항목의 자가 보고 측정이다. 이는 7점 응답 척도를 사용하며, 7점은 "매우 나쁨"에 해당하고 1점은 "매우 개선됨"에 해당한다(도입자 Guy et al. 1976). 변화에 대한 환자의 전체적 인상에 관한 후속 질문에서, 환자는 경험한 변화가 자신에게 중요한지 여부를 표시하도록 요청받되, 응답 선택지는 "예" 또는 "아니오"이다. 또는 환자가 어떠한 경험을 하지 않았다면 "해당 없음"이다.A patient's overall impression of change is a single-item self-reported measure used to evaluate a patient's impression of a change in the patient's condition compared to at the beginning of the study. It uses a 7-point response scale, where 7 corresponds to “very poor” and 1 corresponds to “very improved” (Introducer Guy et al. 1976). In a follow-up question regarding the patient's overall impression of the change, the patient is asked to indicate whether the change experienced is important to him or her, with the answer option being "yes" or "no". or “N/A” if the patient has not experienced any.
가장 중요한 증상(MIS)Most important symptom (MIS)
가장 중요한 증상이라는 설문의 목적은 지난 7일 동안 환자에게 가장 문제가 된 증상을 식별하는 것이다. MIS는 질병 및/또는 치료와 관련된 여러 증상이 추가된, 워싱턴 대학 삶의 질 설문지 척도 2.0 이상의 중요도 등급 척도를 기반으로 한다(Rogers et al. 2002). 환자들은 지난 주에 가장 골치 아픈 증상을 4개까지 선택하도록 요청받는다.The purpose of the Most Significant Symptom questionnaire was to identify the most problematic symptom for the patient in the past 7 days. MIS is based on a severity rating scale of 2.0 or higher on the University of Washington Quality of Life Questionnaire Scale, plus several symptoms related to disease and/or treatment (Rogers et al. 2002). Patients are asked to select up to four of the most troublesome symptoms of the past week.
PRO-CTCAEPRO-CTCAE
PRO-CTCAE는 환자가 보고할 수 있는 78가지 증상 치료 독성의 존재, 발생 빈도, 중증도 및/또는 일상 기능 방해 정도를 특성화하는 데 사용되는 검증된 문항 은행이다(Basch et al. 2014; Dueck et al. 2015). PRO-CTCAE에는 이분법적으로(존재 vs. 부재 결정용) 또는 5점 척도(발생 빈도, 중증도 및 일상 기능 방해 결정용)로 평가되는 124개의 설문이 포함되어 있다. 치료 독성은 다음과 같이 나타날 수 있다: 관찰가능한 징후(예를 들어, 구토) 또는 관찰할 수 없는 증상PRO-CTCAE is a validated question bank used to characterize the presence, frequency, severity, and/or extent of disturbance of daily functioning of 78 patient-reportable symptomatic treatment toxicities (Basch et al. 2014; Dueck et al. 2015). The PRO-CTCAE included 124 questionnaires rated either dichotomously (to determine presence vs. absence) or on a 5-point scale (to determine frequency, severity, and disturbance of daily functioning). Therapeutic toxicity may be as follows: observable signs (eg, vomiting) or unobservable symptoms.
(예를 들어, 메스꺼움). 표준 PRO-CTCAE 리콜 기간은 지난 7일이다.(eg, nausea). The standard PRO-CTCAE recall period is 7 days.
현재 치료에 가장 적합하다고 여겨지는 11가지 증상들의 하위세트가 본 연구를 위해 선택되었다. 증상은 하기의 이전 연구들을 기반으로 선택되었다: 아테졸리주맙 + 티라골루맙을 사용(Rodriguez-Abreu et al. 2020), 환자 및 임상의가 보고한 면역요법과 관련된 증상 치료 독성(Hansen et al. 2020), 두경부암에서 측정해야 할 증상에 대한 권장 사항(Cella et al. 2011; Chera et la. 2014)A subset of the 11 symptoms currently considered most suitable for treatment was selected for this study. Symptoms were selected based on the following previous studies: with atezolizumab + tiragolumab (Rodriguez-Abreu et al. 2020), patient and clinician-reported symptomatic therapeutic toxicity (Hansen et al. 2020), recommendations for symptoms to be measured in head and neck cancer (Cella et al. 2011; Chera et la. 2014)
전체 게놈 서열 또는 전체 엑솜 서열을 위한 혈액 샘플Blood sample for whole genome sequence or whole exome sequence
참여 현장에서, DNA 추출을 위해 혈액 샘플을 수집하여, 연구 약물에 대한 반응이 예측되는, 더 심각한 질병 상태로의 진행과 관련 있는 종양에서 특이적으로 발생한 변이체를 WGS 또는 WES가 식별할 수 있도록 한다. 혈액에서 추출한 DNA는 조직에서 추출한 DNA와 비교하여, 생식계열 변이체와 체세포 변이체를 구별함으로써 체세포 변이체를 식별할 수 있다. 샘플은 분석을 위해 하나 이상의 실험실로 보낼 수 있다.At participating sites, blood samples are collected for DNA extraction so that WGS or WES can identify variants that occur specifically in tumors associated with progression to more severe disease states that are predictive of response to study drug. . DNA extracted from blood can be compared to DNA extracted from tissues, and somatic variants can be identified by distinguishing germline variants from somatic variants. The sample may be sent to one or more laboratories for analysis.
WGS 또는 WES를 위한 혈액 샘플의 수집 및 제출은 각 기관의 IRB/EC 및, 해당되는 경우, 적절한 규제 기관에 의한 예비 연구의 검토 및 승인에 달려 있다. 기관이 WGS 또는 WES에 대한 승인을 부여받지 않은 경우 프로토콜의 이러한 섹션은 해당 기관에 적용되지 않는다.The collection and submission of blood samples for WGS or WES is subject to the review and approval of preliminary studies by the respective institutional IRB/EC and, where applicable, the appropriate regulatory body. If an institution has not been granted accreditation for WGS or WES, then these sections of the protocol do not apply to that institution.
유전체학은 연구원에게 질병 병리생물학에 대한 정보를 점점 더 많이 제공하고 있다. WGS 및 WES는 각각 게놈 및 엑솜의 종합적인 특성화를 제공하며, 본 연구에서 수집된 임상 데이터를 통해, 유효성 및 안전성을 모니터링하거나 어떤 환자가 약물에 반응하거나 부작용이 발현할 가능성이 더 있는지 예측하기 위한 새로운 치료 접근법 또는 새로운 방법을 개발할 기회를 증가시킬 수 있다. 데이터는 본 연구의 맥락에서 분석되지만 다른 연구의 데이터와 통합하여 탐색될 수도 있다. 더 큰 데이터 세트의 가용성은 미래의 약물 개발을 지원하기 위한 중요한 바이오마커 및 경로의 식별 및 특성화에 도움이 된다.Genomics is increasingly providing researchers with information about disease pathobiology. WGS and WES provide comprehensive characterization of the genome and exome, respectively, and use the clinical data collected in this study to monitor efficacy and safety or predict which patients are more likely to respond to drugs or develop adverse events. It can increase the chances of developing new therapeutic approaches or new methods. The data are analyzed in the context of this study, but may also be explored in conjunction with data from other studies. The availability of larger data sets aids in the identification and characterization of important biomarkers and pathways to support future drug development.
샘플링 절차, 보관 조건 및 배송 지침은 실험실 설명서를 참조한다.Refer to the laboratory manual for sampling procedures, storage conditions, and shipping instructions.
WGS 또는 WES를 위해 수집된 혈액 샘플은 더 이상 필요하지 않거나 소진될 때까지 보관해야 한다. 다만, 보관 기간은 IRB/EC가 승인한 사전 동의 양식 및 적용가능한 법률(예: 보건 당국 요구 사항)을 따른다.Blood samples collected for WGS or WES should be stored until they are no longer needed or are depleted. However, the storage period is subject to the informed consent form approved by the IRB/EC and applicable laws (eg health authority requirements).
연구용 바이오샘플 저장소를 위한 샘플Samples for Research Biosample Repository
연구용 바이오샘플 저장소(RBR)는 체액, 고형 조직 및 그 파생물(예: DNA, RNA, 단백질, 펩타이드)을 포함한 인간 생물학적 표본의 장기 보관에 사용되는 중앙 관리 시설 그룹이다. RBR 샘플의 수집, 저장 및 분석은 새로운 약제의 합리적인 설계와 진단 테스트의 개발을 용이하게 하여 향후 환자를 위한 개별화된 약물 요법을 가능하게 할 수 있다.A Research Biosample Repository (RBR) is a group of centrally managed facilities used for long-term storage of human biological specimens, including body fluids, solid tissues and their derivatives (eg, DNA, RNA, proteins, peptides). The collection, storage, and analysis of RBR samples could facilitate the rational design of new drugs and the development of diagnostic tests, enabling individualized drug therapy for future patients.
RBR에 대한 샘플은 이러한 선택적 연구에 참여하는 것에 특정한 동의를 제공한 환자로부터 수집된다. RBR 샘플은 다음 목표 중 하나 이상을 달성하기 위해 분석된다:Samples for RBR are collected from patients who have given specific consent to participate in this elective study. RBR samples are analyzed to achieve one or more of the following goals:
·유효성 또는 질병 진행과 바이오마커의 연관성 연구Research on the association of biomarkers with efficacy or disease progression
·부작용 발현에 대한 민감성과 관련되거나 개선된 부작용 모니터링 또는 조사로 이어질 수 있는 안전성 바이오마커 식별Identification of safety biomarkers associated with susceptibility to adverse events or that may lead to improved monitoring or investigation of adverse events
·질병 생물학 및 약물 안전성에 대한 지식과 이해 증진Promote knowledge and understanding of disease biology and drug safety
·약물 효과 및 약물 흡수 및 처리 과정을 포함한 약물 반응 연구Study drug response, including drug effects and drug absorption and treatment processes
·바이오마커 또는 진단 분석의 개발 및 이러한 분석의 성능 특성 확립Development of biomarkers or diagnostic assays and establishment of performance characteristics of these assays
샘플 수집sample collection
하기의 샘플은 RBR에 저장되며, 아테졸리주맙, 티라골루맙, 두경부암 또는 약물 안전성과 관련된 바이오마커에 대한 연구를 포함하되 이에 국한되지 않는 연구 목적으로 사용된다.The following samples are stored in RBR and used for research purposes including, but not limited to, studies on atezolizumab, tiragolumab, head and neck cancer or biomarkers related to drug safety.
·잔류 혈액, 혈장, PBMC 및 종양 조직 샘플(현장으로 반환되는 나머지 보관 조직 블록 제외) 및 의학적으로 지시되어 연구 과정 동안 시험자의 재량에 따라 수행된 절차(예: 기관지경검사, 식도위십이지장경검사, 대장내시경 검사)로부터의 잔류 조직 샘플을 포함한 상기 샘플의 파생물(예: DNA, RNA, 단백질, 펩티드)Residual blood, plasma, PBMC and tumor tissue samples (excluding the remaining stored tissue blocks returned to the site) and procedures medically ordered and performed at the investigator's discretion during the course of the study (e.g., bronchoscopy, esophageal gastroduodenoscopy) Derivatives (e.g., DNA, RNA, proteins, peptides), including residual tissue samples from colonoscopy)
·연구 중 언제든지 수집된 DNA 추출을 위한 선택적 혈액 샘플Optional blood samples for DNA extraction collected at any time during the study
·사이클 1, 1일째의 투여 전에 그리고 사이클 2, 15일째와 사이클 3, 1일째 투여 전 사이에 수집된 선택적 대변 샘플 이들 샘플은 집에서 수집될 수 있다.Optional stool samples collected prior to dosing on Cycle 1, Day 1 and between Cycle 2, Day 15 and before dosing on Cycle 3, Day 1 These samples may be collected at home.
상기 샘플은 WGS, WES 또는 기타 게놈 분석 방법을 통한 전체 메타게놈 시퀀싱, 미생물 배양, 생식계열 또는 체세포 변이체를 통한 미생물 군집 분석을 위해 하나 이상의 실험실로 보낼 수 있다. 유전체학은 연구원에게 질병 병리생물학에 대한 정보를 점점 더 많이 제공하고 있다. WGS 및 WES는 각각 게놈 및 엑솜의 종합적인 특성화를 제공하며, 본 연구에서 수집된 임상 데이터를 통해, 유효성 및 안전성을 모니터링하거나 어떤 환자가 약물에 반응하거나 부작용이 발현할 가능성이 더 있는지 예측하기 위한 새로운 치료 접근법 또는 새로운 방법을 개발할 기회를 증가시킬 수 있다.The sample may be sent to one or more laboratories for whole metagenomic sequencing via WGS, WES or other genomic analysis methods, microbial culture, and microbial community analysis via germline or somatic variants. Genomics is increasingly providing researchers with information about disease pathobiology. WGS and WES provide comprehensive characterization of the genome and exome, respectively, and use the clinical data collected in this study to monitor efficacy and safety or predict which patients are more likely to respond to drugs or develop adverse events. It can increase the chances of developing new therapeutic approaches or new methods.
RBR로부터 생성된 데이터는 본 연구의 맥락에서 분석되지만 다른 연구의 데이터와 통합하여 탐색될 수도 있다. 더 큰 데이터 세트의 가용성은 미래의 약물 개발을 지원하기 위한 중요한 바이오마커 및 경로의 식별 및 특성화에 도움이 된다.Data generated from RBR are analyzed in the context of this study, but can also be explored by integrating with data from other studies. The availability of larger data sets aids in the identification and characterization of important biomarkers and pathways to support future drug development.
RBR 샘플은 더 이상 필요하지 않거나 소진될 때까지 보관해야 한다. 다만, RBR 보관 기간은 IRB/EC가 승인한 사전 동의 양식 및 적용가능한 법률(예: 보건 당국 요구 사항)을 따른다.RBR samples should be stored until they are no longer needed or are depleted. However, the retention period of the RBR is subject to the informed consent form approved by the IRB/EC and applicable laws (eg health authorities requirements).
G.G. 치료 및 환자 중단Treatment and patient discontinuation
치료 중단cessation of treatment
환자는 다음 중 하나를 경험하는 경우에는 연구 치료제를 영구적으로 중단해야 한다:Patients should permanently discontinue study treatment if they experience any of the following:
·치료에 대한 개별 환자의 잠재적 반응 및 사건의 중증도를 고려할 때 시험자가 허용할 수 없는 것으로 판단한 면역 매개 부작용의 발현을 포함하여 연구 치료와 관련된 용인 불가능한 독성Unacceptable toxicity associated with the study treatment, including the development of immune-mediated adverse events that the investigator deems unacceptable given the severity of the event and the potential response of the individual patient to treatment.
·환자가 연구 치료를 계속할 경우 환자의 안전을 위협할 수 있는 모든 의학적 상태Any medical condition that could endanger the patient's safety if the patient continues research treatment
·치료 중단이 환자에게 최선의 이익이라는 조사관 또는 시험의뢰자의 판단Judgment by the investigator or sponsor that discontinuation of treatment is in the best interest of the patient
·또 다른 비-프로토콜 항암 요법의 사용Use of another non-protocol anticancer therapy
·임신·Pregnant
·RECIST v1.1에 따른 방사선학적 질환 진행Radiological disease progression according to RECIST v1.1
예외: 방사선학적 진행을 넘어서는 치료에 대해 요약된 모든 기준을 충족하는 경우에는 환자는 진행성 질환에 대한 RECIST v1.1 기준이 충족된 후에 연구 치료를 계속하는 것이 허용된다.Exception: Patients are permitted to continue study treatment after the RECIST v1.1 criteria for advanced disease have been met if all criteria outlined for treatment beyond radiological progression are met.
·RECIST v1.1에 따라 방사선학적 진행을 넘어서는 치료받은 환자의 경우: 방사선학적 데이터, 생검 결과(가능한 경우) 및 임상 상태의 통합 평가 후에 시험자가 판단한 임상 이익의 손실For patients treated beyond radiological progression in accordance with RECIST v1.1: loss of clinical benefit as determined by the investigator after integrated evaluation of radiological data, biopsy results (if available) and clinical status
연구 치료제 중단의 주된 이유는 적절한 eCRF에 문서화되어야 한다. 연구 치료를 조기에 중단한 환자는 대체되지 않는다.The primary reason for discontinuation of study treatment should be documented in the appropriate eCRF. Patients who prematurely discontinue study treatment are not replaced.
환자는 연구 치료의 마지막 투여 후 ≤30일에 치료 중단 방문을 위해 클리닉으로 복귀한다. 반응 평가가 질병 진행을 나타내는 방문은 치료 중단 방문으로 사용될 수 있으며, 이 경우 치료 중단 방문과 관련된 모든 평가는 그 시점에 수행되어야 한다.Patients return to the clinic for a treatment discontinuation visit ≤30 days after the last dose of study treatment. A visit where the response assessment indicates disease progression may be used as a discontinuation visit, in which case all assessments related to the discontinuation visit must be performed at that time.
환자가 연구 치료제와 관련된 것으로 간주되는 이상 반응(특별 관심 이상반응 포함)으로 인해 연구 치료를 중단하고 해당 반응이 연구 치료제의 마지막 투여 후 30일 동안 지속되는 경우, 해당 반응이 사건이 안정되거나 되돌릴 수 없게 되었다는 시험자의 해결 또는 판단 시까지 해당 반응을 추적해야 한다.If a patient discontinues study treatment for an adverse event considered to be related to the study treatment (including an adverse event of special interest) and the reaction persists for 30 days after the last dose of study treatment, the reaction may cause the event to stabilize or be reversible. The response should be followed until resolution or judgment by the investigator that the absence has occurred.
추적 평가follow-up evaluation
종양 평가Tumor Assessment
RECIST v.1.1에 따라 방사선학적 질병 진행이 없는 상태에서 연구 치료를 중단하는 환자(임상 감소 또는 독성을 포함하되 이에 국한되지 않음)는, 환자가 새로운 항암 치료를 시작하는지 여부와 상관없이, RECIST v1.1에 따른 방사선학적 질환 진행, 동의 철회, 사망 또는 시험의뢰자에 의한 연구 종료 중 먼저 발생하는 때까지 활동 일정에 요약된 대로 종양 반응 평가를 계속 받아야 한다. 진행성 질병이 의심되는 경우 시험자의 재량에 따라 언제든지 스캔을 수행해야 한다.Patients who discontinue study treatment (including, but not limited to, clinical decline or toxicity) in the absence of radiological disease progression in accordance with RECIST v.1.1, regardless of whether the patient is starting new chemotherapy, are treated with RECIST v1 Tumor response assessments as outlined in the activity schedule should continue until radiological disease progression, withdrawal of consent, death, or termination of the study by the sponsor according to .1, whichever occurs first. If progressive disease is suspected, a scan should be performed at any time at the discretion of the investigator.
생존 및 후속 요법Survival and follow-up therapy
치료 중단 후, (환자가 생존 추적에 대한 동의를 철회하거나 시험의뢰자가 연구를 종료하지 않는 한) 환자가 사망할 때까지 약 3개월마다 전화, 환자 진료기록 및/또는 클리닉 방문을 통해 생존 추적 및 새로운 항암 요법에 대한 정보를 수집한다.After discontinuation of treatment (unless the patient withdraws consent to follow-up or the sponsor terminates the study), follow-up and follow-up of survival via phone, patient records and/or clinic visit approximately every 3 months until patient death Gather information on new anticancer therapies.
후속 항암 요법에 대한 정보에는 전신 요법(예: 화학요법, 표적 요법, 면역 요법), 수술(예: 국소 및/또는 전이성 질환의 절제) 및 방사선 시술(예: 종양 병변에 대한 방사선 요법)이 포함된다.Information on follow-up chemotherapy includes systemic therapy (e.g., chemotherapy, targeted therapy, immunotherapy), surgery (e.g., resection of local and/or metastatic disease), and radiation procedures (e.g., radiation therapy for tumor lesions) do.
환자 중단patient discontinuation
환자는 이유를 불문하고 언제든지 연구를 자발적으로 철회할 권리가 있다. 또한, 시험자는 언제든지 연구에서 환자를 철회할 권리가 있다.Patients have the right to voluntarily withdraw from the study at any time for any reason. In addition, the investigator has the right to withdraw a patient from the study at any time.
환자가 해당 연구를 중단하는 이유에는 다음이 포함될 수 있지만 이에 국한되지는 않는다:Reasons for a patient to discontinue the study may include, but are not limited to:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
환자가 연구를 중단한 이유를 얻기 위해 모든 노력을 기울여야 한다. 연구 중단의 주요 이유는 적절한 eCRF에 문서화되어야 한다. 환자가 연구로부터의 철회를 요청(즉, 모든 생존 추적 조사에서 철회를 요청)하는 경우, 상기 요청은 원본 문서에 문서화하고 시험자가 서명해야 한다. 연구에서 철회한 환자(즉, 생존 추적)는 대체되지 않는다.Every effort should be made to obtain a reason for the patient to discontinue the study. The main reason for study discontinuation should be documented in the appropriate eCRF. If a patient requests withdrawal from the study (i.e., request withdrawal from any survival follow-up), the request must be documented in the original document and signed by the investigator. Patients who withdraw from the study (ie, follow-up survival) are not replaced.
환자가 연구에서 철회하는 경우(즉, 생존 추적), 연구 직원은 공개 정보 출처(예: 카운티 기록)를 사용하여 생존 상태에 대한 정보를 얻을 수 있다.If a patient withdraws from the study (ie, survival follow-up), research staff may use publicly available sources of information (eg, county records) to obtain information about their survival status.
H.H. 분석analysis
유효성 분석Validity analysis
일차 유효성 평가변수Primary efficacy endpoint
1차 유효성 평가변수는 확인된 ORR이다. 확인된 객관적 반응은 RECIST v1.1에 따라 시험자가 판단하여, 4주 간격으로 2회 연속 CR 또는 PR 발생으로 정의된다. 기준선 이후 종양 평가가 없는 환자를 포함하여 이러한 기준들을 충족하지 않는 환자는 무반응자로 간주된다. 확인된 ORR은 확인된 객관적인 반응을 갖는 환자의 비율로 정의된다.The primary efficacy endpoint is the confirmed ORR. A confirmed objective response is defined as two consecutive CR or PR occurrences at 4-week intervals, as judged by the investigator according to RECIST v1.1. Patients who do not meet these criteria, including those without post-baseline tumor assessment, are considered non-responders. Confirmed ORR is defined as the proportion of patients with an identified objective response.
모든 환자가 등록되고 ORR 평가를 위해 추적 관찰 중인 환자들 사이에서 최소 약 5개월의 추적 관찰이 달성되면 1차 유효성 분석이 이루어진다.A primary efficacy analysis occurs when all patients are enrolled and a follow-up of at least approximately 5 months is achieved among patients being followed for ORR evaluation.
1차 유효성 분석 모집단은 할당된 치료에 따라 그룹화된 모든 무작위 환자로 구성된다. ORR의 추정치와 95% CI는 각 치료군에 대해 Cloper-Pearson 방법을 사용하여 계산된다.The primary efficacy analysis population consists of all randomized patients grouped according to their assigned treatment. Estimates of ORR and 95% CI were calculated using the Cloper-Pearson method for each treatment group.
이차 유효성 평가변수secondary efficacy endpoint
반응 지속기간duration of response
DOR은 RECIST v1.1에 따라 시험자가 판단하여 확인된 객관적 반응을 달성한 환자에서 평가된다. DOR은 확인된 객관적 반응의 최초 발생 일자로부터 RECIST v1.1에 따라 시험자가 판단한 최초 질병 진행 또는 임의의 원인으로 인한 사망 일자(둘 중 먼저 발생하는 것)까지의 시간으로 정의된다. 분석시 질환진행이 없었고 사망하지 않은 환자는 해당 마지막 종양 평가일에 중도절단된다. 카플란-마이어 방법론을 사용하여 각 치료 부문의 DOR 중앙값을 추정하고 카플란-마이어 곡선을 생성한다. Brookmeyer-Crowley 방법론은 각 치료군의 DOR 중앙값에 대한 95% CI를 구성하는 데 사용된다.DOR is assessed in patients who have achieved an identified objective response as judged by the investigator according to RECIST v1.1. DOR is defined as the time from the first occurrence of an identified objective response to the date of first disease progression or death from any cause, whichever occurs first, as determined by the investigator in accordance with RECIST v1.1. Patients with no progression and no death at the time of analysis are censored on the date of their last tumor assessment. The Kaplan-Meier methodology is used to estimate the median DOR for each treatment arm and generate a Kaplan-Meier curve. The Brookmeyer-Crowley methodology is used to construct a 95% CI for the median DOR for each treatment group.
6개월 무진행 생존율을 포함한 무진행 생존Progression-free survival, including 6-month progression-free survival
PFS는, 무작위배정 일자와 RECIST v1.1에 따라 시험자가 평가한, 최초로 기록된 질병 진행 또는 사망 일자(둘 중 먼저 발생하는 것) 사이의 시간으로 정의된다. 질병 진행을 경험하지 않았거나 데이타 마감일까지 사망하지 않은 환자는 최종 종양 평가 시 중도절단된다. 기준선 이후 종양 평가가 없는 환자는 무작위배정 일자에 중도절단된다.PFS is defined as the time between the date of randomization and the first documented date of disease progression or death, whichever occurs first, as assessed by the investigator according to RECIST v1.1. Patients who have not experienced disease progression or have not died by the data deadline will be censored at the final tumor evaluation. Patients without post-baseline tumor evaluation are censored on the date of randomization.
카플란-마이어 방법론을 사용하여 각 치료 부문의 PFS 중앙값을 추정하고 카플란-마이어 곡선을 생성한다. Brookmeyer-Crowley 방법론은 각 치료군의 PFS 중앙값에 대한 95% CI를 구성하는 데 사용된다. 무작위 배정 후 6개월의 PFS 비율은 그린우드 공식에서 도출된 표준 오차를 사용하여 계산된 95% CI와 함께 각 치료 부문에 대해 Kaplan-Meier 방법론을 사용하여 추정된다.The Kaplan-Meier methodology is used to estimate the median PFS for each treatment arm and generate a Kaplan-Meier curve. The Brookmeyer-Crowley methodology is used to construct a 95% CI for the median PFS for each treatment group. The PFS rate at 6 months after randomization was estimated using the Kaplan-Meier methodology for each treatment arm with a 95% CI calculated using the standard error derived from the Greenwood formula.
6개월 및 12개월의 전체 생존율을 포함한 전체 생존율Overall survival including 6-month and 12-month overall survival rates
OS는 무작위화 날짜와 임의의 원인으로 인한 사망 사이의 시간으로 정의된다. 데이터 마감일까지 사망한 것으로 보고되지 않은 환자에 대한 데이터는 마지막으로 생존이 확인된 날짜에 중도절단된다. 기준선 이후 정보가 없는 환자에 대한 데이터는 무작위화 날짜에 중도절단된다. 6개월 및 12개월에서의 OS 및 OS 비율은 PFS에 대해 설명한 것과 동일한 방법을 사용하여 분석된다.OS is defined as the time between the date of randomization and death from any cause. Data for patients not reported as dead by the data deadline will be censored on the last confirmed survival date. Data for patients with no post-baseline information are censored on the date of randomization. OS and OS ratios at 6 and 12 months are analyzed using the same method described for PFS.
환자 보고 결과Patient Reported Results
PROMISPROMIS
아이템 뱅크 v2.0-신체 기능-숏 폼 10b를 사용한 신체 기능에 대한 TTCD는 무작위화 날짜부터 임상적으로 의미 있는 악화가 처음 확인된 시점까지의 시간으로 정의된다. 확인된 신체 기능의 임상적으로 의미 있는 악화는 최소 2회의 연속 평가 동안 유지되어야 하는 기준선으로부터의 임상적으로 의미 있는 감소 또는 기준선을 초과한 초기 임상적으로 의미 있는 증가 후 사망으로 정의된다. T-점수 변화 > 4점은 신체 기능 하위척도 점수에 대해 임상적으로 의미 있는 것으로 간주된다. TTCD for bodily function using Item Bank v2.0-Body Functions-Short Form 10b is defined as the time from the date of randomization to the first clinically significant deterioration. Clinically significant deterioration in identified bodily function is defined as death following an initial clinically meaningful increase above baseline or a clinically significant decrease from baseline that must be maintained for at least two consecutive evaluations. A T-score change >4 is considered clinically significant for a score on the Body Function subscale.
TTCD는 ITT 모집단에서 평가된다. 임상 마감일에 확인된 임상적으로 의미 있는 악화를 경험하지 않은 환자는 평가를 완료한 마지막 시간에 중도절단된다. 기준선 또는 기준선 이후 평가가 수행되지 않은 경우 환자는 무작위화 날짜에 중도절단된다. PROMIS 척도를 사용하는 TTCD는 PFS와 동일한 방법을 사용하여 분석된다.TTCD is assessed in the ITT population. Patients who have not experienced clinically significant deterioration identified by the clinical deadline are censored at the last hour of completing the evaluation. Patients are censored on the date of randomization if no baseline or post-baseline evaluation has been performed. TTCD using the PROMIS scale is analyzed using the same method as the PFS.
PROMIS![]()
![]()
개수 및 비율을 포함한 요약 통계는 PGI-CI, PGI-S 및 가장 중요한 증상에 대해 제시되며 탐색적이다.Summary statistics, including counts and proportions, are presented for PGI-CI, PGI-S and most important symptoms and are exploratory.
PRO-CTCAE의 분석은 본질적으로 탐색적이고 주로 서술적이며, 본 연구 중 질병 및 증상 치료 독성의 패턴을 특성화하는 데 중점을 둔다. 이러한 탐색적 분석의 결과는 다른 안전성 분석과 별도로 제시된다. PRO-CTCAE 데이터는 데이터 처리에 대한 현재의 NCI 권장 사항에 따라 항목 수준에서 분석된다. 각 치료 부문에 대해 "빈도", "증증도", "간섭" 및 "존재" 범주별로 증상을 보고하는 환자의 수(백분율)가 각 평가에서 보고된다.The analysis of PRO-CTCAE is exploratory in nature and mainly descriptive, focusing on characterizing the patterns of disease and symptomatic treatment toxicity during this study. The results of these exploratory analyzes are presented separately from other safety analyses. PRO-CTCAE data is analyzed at the item level in accordance with current NCI recommendations for data processing. For each treatment arm, the number (percent) of patients reporting symptoms by category "frequency", "severity", "interference" and "presence" is reported at each assessment.
또한, 증상의 빈도를 증상의 증증도와 교차 도표화하여 증상이 발생했을 때의 영향을 탐색한다. 치료 부문에서 연구 중에 "심각한" 또는 "매우 심각한" 증상의 중증도를 보고한 환자의 백분율에 대한 요약 표도 제공된다.In addition, the frequency of symptoms is cross-plotted with the severity of symptoms to explore the effects of symptoms when they occur. A summary table is also provided of the percentage of patients in the treatment arm who reported severity of "severe" or "very serious" symptoms during the study.
안전성 분석Safety analysis
안전성 분석 모집단은 아테졸리주맙 또는 티라골루맙/위약을 1회 이상 투여받은 모든 무작위 환자로 구성된다.The safety analysis population consisted of all randomized patients who received at least one dose of atezolizumab or tiragolumab/placebo.
안전성 분석은 치료 부문에서 수행되며 실제 받은 치료를 기반으로 한다. 구체적으로, 환자가 임의의 양의 티라골루맙을 투여받는 경우, 무작위 배정 시 초기 치료 할당과 상관없이 환자는 안전성 분석에서 아테졸리주맙 + 티라골루맙 군에 포함된다.Safety analyzes are performed in the treatment sector and are based on actual treatment received. Specifically, if a patient is receiving any amount of tyragolumab, at randomization, regardless of the initial treatment assignment, the patient is included in the atezolizumab + tiragolumab arm in the safety analysis.
기간, 복용량 및 복용량 강도를 포함하여 약물 노출이 요약된다.Drug exposure is summarized, including duration, dose, and dose intensity.
부작용에 대한 축어적 설명은 MedDRA 동의어 용어에 매핑되고 NCI CTCAE v5.0에 따라 등급이 매겨지며 CRS에 대한 증증도 또한 ASTCT 합의 등급 척도에 따라 시험자가 등급을 매긴다. 모든 유해 사례는 치료 부문 및 NCI CTCAE 등급으로 요약된다. 또한 CRS는 치료 부문 및 ASTCT 합의 등급별로 요약된다. 또한, 중대한 이상반응, 면역매개 이상반응 및 연구 치료제 중단 또는 방해를 초래하는 이상반응이 이에 따라 요약된다. 동일한 이벤트의 다중 발생은 최대 증증도에서 한 번 계산된다.Verbose descriptions of adverse events are mapped to MedDRA synonym terms and graded according to NCI CTCAE v5.0, and severity for CRS is also graded by investigators according to the ASTCT consensus grade scale. All adverse events are summarized by treatment arm and NCI CTCAE grade. CRS is also summarized by treatment category and ASTCT consensus grade. In addition, serious adverse events, immune-mediated adverse events, and adverse events that result in discontinuation or interference with the study treatment are summarized accordingly. Multiple occurrences of the same event are counted once at the maximum severity.
모든 사망 및 사망 원인이 치료 부문별로 요약되어 있다.All deaths and causes of death are summarized by treatment category.
정상 범위를 벗어난 값을 가진 실험실 데이터가 식별된다. 추가적으로, ADA 결과를 포함하여 선택된 실험실 데이터가 요약된다.Laboratory data with values outside the normal range are identified. Additionally, selected laboratory data, including ADA results, are summarized.
약동학 분석Pharmacokinetic analysis
본 연구에서 티라골루맙 및 아테졸리주맙의 PK 샘플이 수집된다. 티라골루맙 및 아테졸리주맙 혈청 농도 데이터(최소 혈청 농도 및 최대 혈청 농도)가 표로 작성되고 요약된다.PK samples of tiragolumab and atezolizumab are collected in this study. Tiragolumab and atezolizumab serum concentration data (minimum serum concentration and maximum serum concentration) are tabulated and summarized.
기술 통계에는, 적절한 경우, 평균, 중앙값, 범위 및 표준 편차가 포함된다.Descriptive statistics include mean, median, range and standard deviation, where appropriate.
추가적 PK 분석은 데이터의 가용성에 따라, 적절하게, 수행된다.Additional PK analyzes are performed, as appropriate, depending on the availability of data.
면역원성 분석Immunogenicity assay
면역원성 분석에는 ADA 평가를 받은 환자가 포함되며 환자는 받은 치료에 따라 분류된다. 치료-응급 ADA-양성 환자 및 ADA-음성 환자의 수 및 비율은 치료 부문별로 요약된다.Immunogenicity assays include patients who have undergone an ADA assessment, and patients are classified according to treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients are summarized by treatment arm.
ADA 상태와, 안전성, 유효성, 및 PK 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고할 수 있다.The relationship between ADA status and safety, efficacy, and PK endpoints can be analyzed and reported through descriptive statistics.
바이오마커 분석Biomarker analysis
바이오마커 분석은 설명적이다. 기술 통계는 유효성 종점에 대한 바이오마커 하위 그룹들 및 이들의 관계를 요약하는 데 사용되며; 데이터는 본 연구의 맥락에서 그리고 다른 연구의 데이터와 통합하여 분석될 수 있다.Biomarker analysis is descriptive. Descriptive statistics are used to summarize biomarker subgroups and their relationships to efficacy endpoints; Data can be analyzed in the context of this study and in conjunction with data from other studies.
중간 분석Interim analysis
약 60명의 환자가 등록되고 약 5개월 이상 추적 관찰할 기회가 있는 경우, 유효성 중간 분석이 계획되고 IMC에 의해 검토된다.When approximately 60 patients are enrolled and have the opportunity to follow up for approximately 5 months or longer, an interim analysis of efficacy is planned and reviewed by the IMC.
실시예 16. 근육 침윤성 방광암(MIBC)을 가진 환자를 대상으로 다중 면역요법 기반 치료 및 병용의 유효성과 안전성을 평가하는 Ib/II상, 공개 라벨, 다기관, 무작위 포괄적 연구Example 16. A Phase Ib/II, Open Label, Multicenter, Randomized Comprehensive Study Evaluating the Efficacy and Safety of Multiple Immunotherapy-Based Treatments and Combinations in Patients with Muscle Invasive Bladder Cancer (MIBC)
근육 침윤성 방광암(MIBC) 진단으로부터 방광 절제술까지의 시간은 일반적으로 4-8주이며, 재발률 및 OS를 개선하기 위한 신보조제 요법을 제공할 수 있는 기회가 환자에게 제공된다. 신보조제 화학요법의 이점은 방광 절제술과 단독 비교하여 신보조제 화학요법으로 치료받은 환자의 전체 생존(OS)이 5% 증가하여 보통 정도이다(Vale et al., Eur Urol, 48: 202-205, 2005). 병리학적 완전 반응(pCR)을 달성한 환자는 신보조제의 시스플라틴 기반 화학요법을 받았을 때 가장 큰 이점을 얻었으며 5년 추적 조사에서 80-90%가 생존했다; 그러나 환자의 최대 50%가 수술시 잔류 고위험 질환(pT2 이상)을 가질 수 있으며, 5년 생존율은 50% 미만이다(Rosenblatt et al., Eur Urol, 61: 1229-1238, 2011; Bhindi et al., Eur Urol, 72: 660-664, 2017). 따라서, pCR은 MIBC에 대한 신보조제 요법에서 유효성 및 생존 증가에 대한 대리 마커가 될 수 있다.The time from diagnosis of muscle invasive bladder cancer (MIBC) to cystectomy is typically 4-8 weeks, providing patients with the opportunity to provide neoadjuvant therapy to improve recurrence rates and OS. The benefit of neoadjuvant chemotherapy is moderate compared to cystectomy alone, with a 5% increase in overall survival (OS) in patients treated with neoadjuvant chemotherapy (Vale et al., Eur Urol , 48: 202-205, 2005). Patients who achieved a pathological complete response (pCR) achieved the greatest benefit when receiving neoadjuvant cisplatin-based chemotherapy, with 80-90% survival at 5-year follow-up; However, up to 50% of patients may have residual high-risk disease (pT2 or higher) at the time of surgery, and the 5-year survival rate is less than 50% (Rosenblatt et al., Eur Urol, 61: 1229-1238, 2011; Bhindi et al. , Eur Urol , 72: 660-664, 2017). Thus, pCR could be a surrogate marker for increased efficacy and survival in neoadjuvant therapy for MIBC.
WO39613은 시스플라틴 부적격 MIBC를 갖 환자에서 다중 면역요법 기반 치료 및 조합의 유효성과 안전성을 평가하는 Ib/II상, 개방표지, 다중심, 무작위화 포괄 연구이다. 본 연구는 새로운 치료법이 사용 가능하면 새로운 치료법을 개설하거나, 최소 임상 활성 또는 허용불가능한 독성을 나타내는 기존 치료 부문을 폐쇄하거나, 환자 모집단을 수정할 수 있는 유연성을 갖도록 설계된다(예: 이전의 항암 치료 또는 바이오마커 상태 관련). 환자는 대조군(아테졸리주맙(아테조)) 또는 티라골루맙과 조합된 아테졸리주맙(아테조 + 티라)으로 구성된 실험군에 무작위로 할당된다(도 24 및 표 69). WO39613 is a Phase Ib/II, open-label, multicenter, randomized, comprehensive study evaluating the efficacy and safety of multiple immunotherapy-based treatments and combinations in patients with cisplatin-incompetent MIBC. The study is designed to have the flexibility to open new therapies, close existing treatment segments that exhibit minimal clinical activity or unacceptable toxicity, or modify patient populations as new treatments become available (e.g., previous chemotherapy or related to biomarker status). Patients are randomly assigned to an experimental group consisting of a control group (atezolizumab (Atezo)) or atezolizumab in combination with tiragolumab (Atezo + Tyra) (Figure 24 and Table 69).

아테조: 아테졸리주맙; MIBC: 근육 침윤성 방광암; 티라: 티라골루맙. a시험의뢰자는 주어진 치료 부문 내에서 등록을 연기하거나 중단하기로 결정할 수 있다. 따라서 모든 실험 부문이 등록을 위해 동시에 개설되지 않을 수 있다. b예비 단계 동안 실험 부문에서 임상 활동이 관찰되면, 확장 단계 동안 약 25명의 추가 환자가 해당 부문에 등록된다. c무작위화 비율은 무작위화를 위해 개설되는 실험 부문의 수에 따라 다르며(예: 예비 단계로부터의 결과 분석이 보류되면서 부문이 추가되거나 부문에 무작위 배정이 중단되는 경우), 통제 부문에 배정될 가능성은 35%를 넘지 않는다는 조건을 따른다. atezo: atezolizumab; MIBC: muscle invasive bladder cancer; Tyra: Tiragolumab. a The sponsor may decide to postpone or discontinue enrollment within a given treatment area. Therefore, not all experimental divisions may be opened for registration at the same time. b If clinical activity is observed in the trial arm during the preliminary phase, approximately 25 additional patients will be enrolled in the arm during the expansion phase. c The rate of randomization depends on the number of experimental arms opened for randomization (e.g., if an arm is added or randomization to an arm is stopped while analysis of results from the preliminary phase is withheld) and the likelihood of being assigned to a control arm is subject to the condition that it does not exceed 35%.
아테졸리주맙과 티라골루맙에 대한 표적 및 제안된 작용기전 분류는 표 70에 요약되어 있다. The classification of targets and proposed mechanisms of action for atezolizumab and tiragolumab is summarized in Table 70.

PD-L1 = 프로그램된 사멸 리간드 1; Ig 및 ITIM 도메인을 갖는 TIGIT = T-세포 면역수용체PD-L1 = programmed death ligand 1; TIGIT = T-cell immunoreceptor with Ig and ITIM domains
구체적인 연구 목적 및 해당 평가변수를 표 71에 요약한다. The specific study objectives and corresponding endpoints are summarized in Table 71.



ADA = 항 약물 항체; CR = 완전한 반응; DOR = 반응 기간; EFS = 증상 없는ADA = anti-drug antibody; CR = complete response; DOR = duration of response; EFS = no symptoms
생존; iRECIST = 면역 RECIST; MIBC = 근육 침윤성 방광암; NCI CTCAE v4.0 = 국립 암 연구소의 유해 사례에 대한 공통 용어 기준, 버전 4.0; OS = 전체 생존; PK = 약동학; RFS = 무재발 생존.survival; iRECIST = immune RECIST; MIBC = muscle invasive bladder cancer; NCI CTCAE v4.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0; OS = overall survival; PK = pharmacokinetics; RFS = relapse-free survival.
단일 시점에서의 객관적 반응은 RECIST v1.1을 이용하여 시험자가 결정한다. iRECIST에 따른 전체 반응은 시험자가 평가한 개별 병변 데이터를 기반으로 시험의뢰자가 프로그래밍 방식으로 계산한다.The objective response at a single time point is determined by the investigator using RECIST v1.1. The overall response according to iRECIST is programmatically calculated by the sponsor based on individual lesion data evaluated by the investigator.
약 150-350명의 환자가 등록되며, MIBC 코호트 1(PD-L1+)과 MIBC 코호트 2(PD-L1-) 사이에서 나뉜다. 실험 부문 내 등록은 하기 2단계로 이루어진다: 예비 단계, 이후의 확장 단계. 모든 치료 군은 예비 단계에서 MIBC 코호트 1(PD-L1+) 및 MIBC 코호트 2(PD-L1-)에 대해 동일하다. 환자는 VENTANA PD-L1(SP142) 분석을 사용하여 방광 종양의 경요도 절제술(TURBT) 샘플에 대한 중앙 집중식 PD-L1 테스트 후 MIBC 코호트 1(PD-L1+) 또는 MIBC 코호트 2(PD-L1-)에 할당된다. PD-L1 면역 세포(IC) 점수가 2 또는 3(IC2/3)로서, 종양 세포, 관련 종양 내 및 인접 종양 주위 기질이 차지하는 종양 면적의 5% 이상을 덮는 종양 침윤 면역 세포에서 모든 강도의 식별 가능한 PD-L1 염색의 존재에 해당하는 환자는 MIBC 코호트 1(PD-L1+)에 할당된다. IC 점수가 0 또는 1(IC0/1, 종양 세포가 차지하는 종양 면적의 ≤5%를 덮는 종양 침윤 면역 세포에서 모든 강도의 식별 가능한 PD-L1 염색의 존재에 해당함, 관련 종양 내 및 인접 종양 주위 기질)인 환자는 MIBC 코호트 2(PD-L1-)에 할당된다.Approximately 150-350 patients are enrolled, divided between MIBC Cohort 1 (PD-L1+) and MIBC Cohort 2 (PD-L1-). Enrollment in the experimental section consists of two phases: a preliminary phase, followed by an expansion phase. All treatment groups are identical for MIBC Cohort 1 (PD-L1+) and MIBC Cohort 2 (PD-L1-) in the preliminary phase. Patients were tested in either MIBC Cohort 1 (PD-L1+) or MIBC Cohort 2 (PD-L1-) after centralized PD-L1 testing on transurethral resection (TURBT) samples of bladder tumors using the VENTANA PD-L1 (SP142) assay. is assigned to Identification of all intensities in tumor-infiltrating immune cells with a PD-L1 immune cell (IC) score of 2 or 3 (IC2/3), covering at least 5% of the tumor area occupied by tumor cells, the relevant intratumoral and adjacent peritumoral stroma Patients corresponding to the presence of possible PD-L1 staining are assigned to MIBC Cohort 1 (PD-L1+). An IC score of 0 or 1 (IC0/1, corresponding to the presence of identifiable PD-L1 staining of any intensity in tumor-infiltrating immune cells covering ≤5% of the tumor area occupied by tumor cells, the relevant intratumoral and adjacent peritumoral stroma ) are assigned to MIBC Cohort 2 (PD-L1-).
예비 단계에서, 최대 30명의 환자가 아테조 + 티라 군에 등록되고 약 15명의 환자가 각 MIBC PD-L1 코호트에 대해 다른 모든 군에 등록된다. 예비 단계 중에 실험 부문에서 임상 활동이 관찰되면, 확장 단계 중에 약 25명의 추가 환자가 해당 부문에 등록된다.In the preliminary phase, up to 30 patients are enrolled in the Artezo + Tyra group and approximately 15 patients are enrolled in all other groups for each MIBC PD-L1 cohort. If clinical activity is observed in the trial arm during the preliminary phase, approximately 25 additional patients will be enrolled in the arm during the expansion phase.
시험의뢰자는 주어진 치료 부문 내에서 등록을 연기하거나 중단하기로 결정할 수 있다. 임상 활동이 불충분하거나 독성이 허용되지 않는 실험군은 확장되지 않는다. 추가 하위 그룹 분석을 가능하게 하기 위해서는, 잠재적인 예측 바이오마커를 포함하는, 인구통계학적 및 기준선 특성과 관련하여 치료군 간의 균형을 보장하도록 추가 환자를 등록할 수 있다. The sponsor may decide to postpone or discontinue enrollment within a given treatment arm. Experimental groups with insufficient clinical activity or unacceptable toxicity will not be expanded. To enable further subgroup analysis, additional patients can be enrolled to ensure a balance between treatment groups with respect to demographic and baseline characteristics, including potential predictive biomarkers.
무작위 비율은 사용 가능한 실험 부문의 수에 따라 다르며(예: 예비 단계의 결과 분석이 보류되는 동안 부문이 추가되거나 부문 등록이 일시 중단된 경우), 통제 부문에 배정될 가능성은 35%를 넘지 않는다는 조건을 따른다. 무작위 배정은 부문별 제외 기준을 고려한다. 환자는 하기의 경우에 특정 부분에 대해 자격이 있다:The randomization rate depends on the number of available trial arms (e.g., if a segment is added or segment enrollment is suspended while the preliminary stage results analysis is pending), provided that the probability of being assigned to a controlled segment does not exceed 35%. follow Randomization takes into account divisional exclusion criteria. Patients are eligible for certain parts if:
해당 부문에 대해 설명된 제외 기준 중 하나라도 충족하는 경우.Meets any of the exclusion criteria described for that sector.
아테졸리주맙 대조군 및 실험군에 속한 환자는 허용할 수 없는 독성 또는 임상적 이점의 손실이 있을 때까지 치료되며, 이는 Patients in the atezolizumab control and experimental groups are treated until there is unacceptable toxicity or loss of clinical benefit, which
방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예: 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정에 따른다. 환자는 수술 후 최대 1년의 치료를 받은 후 2년의 3개월 추적 평가를 받는다. After an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical status (eg worsening of symptoms such as pain with disease), the investigator's decision is followed by the investigator's decision. Patients receive up to 1 year of treatment after surgery, followed by 2 years of 3-month follow-up evaluation.
A.A. 평가 및 모니터링Assessment and monitoring
모든 환자는 연구 전반에 걸쳐 이상 반응에 대해 면밀히 모니터링되며, 이상 반응은 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0(NCI CTCAE v4.0)에 따라 등급이 매겨진다. 환자는 처음 54주 동안은 9주마다(주기 1의 1일째에 시작), 그 후로는 12주마다 종양 평가를 받는다. 반응은 하기에 의해 평가된다:All patients are closely monitored for adverse events throughout the study, and adverse events are graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). Patients receive tumor assessments every 9 weeks (starting on Day 1 of Cycle 1) for the first 54 weeks and then every 12 weeks thereafter. The response is evaluated by:
RECIST v1.1을 사용하는 시험자(Eisenhauer et al., Eur J Cancer, 45: 228-247, 2009)). 임상 활동이 실험 부문에서 입증된 경우, 시험의뢰자는 중앙 판독 시설의 평가를 위해Investigators using RECIST v1.1 (Eisenhauer et al., Eur J Cancer, 45: 228-247, 2009). If clinical activity has been demonstrated in the trial sector, the sponsor will
해당 군에 대한 종양 평가 스캔을 제출하도록 요청할 수 있다.You may be asked to submit a tumor assessment scan for that group.
기준선 종양 조직 샘플은 모든 환자로부터, 바람직하게는 연구 시작 시에 수행된 생검에 의해 수집된다. 시험자가 생검을 실행할 수 없다고 간주하는 경우, 보관 종양 조직을 제출할 수 있다. 종양 조직은 시험자에 의해 결정된 바와 같이(시험자가 임상적으로 가능한 것으로 간주하는 경우) 허용 불가능한 독성 또는 임상적 이점의 손실로 인해 1단계를 중단한 환자로부터도 수집된다. 이러한 샘플 뿐만 아니라 연구 중에 수집된 혈액 샘플도 바이오마커 연구에 활용된다.Baseline tumor tissue samples are collected from all patients, preferably by biopsies performed at the start of the study. If the investigator considers that a biopsy cannot be performed, the archived tumor tissue may be submitted. Tumor tissue is also collected from patients who discontinue Phase 1 due to unacceptable toxicity or loss of clinical benefit, as determined by the investigator (if deemed clinically feasible) by the investigator. These samples as well as blood samples collected during the study are utilized for biomarker studies.
아테졸리주맙 및 기타 치료제의 약동학(PK) 특성 및/또는 면역원성을 특성화하기 위해, 연구 치료제 투여 전 및 동안 다양한 시점에서 혈액 샘플을 수득한다.To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points prior to and during study therapy administration.
B.B. 연구 종료 및 연구 기간Study End and Study Duration
연구 종료일은 전화 또는 현장 방문에 의한 생존 추적 방문을 포함하여 두 단계 모두에서 마지막 환자가 마지막 방문을 완료한 날짜로 정의된다.Study end date is defined as the date the last patient completed the last visit in both phases, including survival follow-up visits by phone or site visit.
제1 환자의 스크리닝부터 연구 종료까지의 총 연구 기간은 약 3~5년이다.The total study duration from screening of the first patient to study termination is approximately 3-5 years.
C.C. 연구 설계에 대한 이론적 근거Rationale for Study Design
연구 근거 및 유익성-위험 평가Research Evidence and Benefit-Risk Assessment
본 연구는 시스플라틴 부적격 MIBC 환자에서 초기 신호를 식별하고 개념 증명 임상 데이터를 확립함으로써 암 면역 요법(CIT) 조합의 발현을 가속화하도록 설계되었다. This study was designed to accelerate the expression of cancer immunotherapy (CIT) combinations by identifying early signals and establishing proof-of-concept clinical data in cisplatin-incompetent MIBC patients.
백금계 신보조제 화학요법은 OS 개선과 관련이 있지만 소수의 환자에게만 적합하다. 시스플라틴 부적격 MIBC 환자에 대한 상대적으로 제한된 치료 선택지와 추가로 국소 진행성 또는 전이성 UC에 대한 치료와 관련된 불량한 예후 및 잠재적 독성을 감안할 때, 이러한 모집단은 치료 선택지가 필요하고 따라서 새로운 치료 후보의 시험에 적합한 것으로 간주된다. 현재 널리 퍼져 있는 CIT 접근 방식은 PD-L1(프로그램된 사멸 리간드 1)/PD-1(프로그램된 사멸-1)과 같은 T-세포 억제 인자를 표적으로 하여 면역 회피 메커니즘을 우회하고 항종양 반응을 활성화하는 것이다.Platinum-based neoadjuvant chemotherapy has been associated with improved OS but is only suitable for a small number of patients. Given the relatively limited treatment options for patients with cisplatin ineligible MIBC and, in addition, the poor prognosis and potential toxicity associated with treatment for locally advanced or metastatic UC, this population appears to be in need of treatment options and therefore suitable for testing new treatment candidates. is considered The currently prevalent CIT approach targets T-cell inhibitory factors such as PD-L1 (programmed death ligand 1)/PD-1 (programmed death-1) to bypass immune evasion mechanisms and promote anti-tumor responses. it will activate
CIT는 여러 진행성 악성 종양에서 관찰된 유의미한 생존 이점과 함께 명백한 임상 유효성을 입증했으며, PD-1/PD-L1 체크포인트 차단은 UC 환자에서 pCR 및 지속적인 반응을 생성할 수 있다는 증거가 있다(Powles et al., Nat Med, 25: 1706-1714, 2019; Necchi et al., Int J Clin Oncol, 36: 3353-3360, 2018). 이러한 표적이 다양한 암 적응증에 대해 놀라운 임상적 치료 성공을 가져왔지만, 진행 중인 연구는 효과적인 항종양 면역 반응의 생성을 위해서는 일련의 단계적 이벤트가 필요하다는 것을 나타낸다(Chen and Mellman, Immunity, 39: 1-10, 2013). 각 이벤트는 효과적인 반응에 중요하며, 각각은 여러 종양 면역 회피 메커니즘에도 민감하다. 따라서, 암면역 확산과 CIT 분야의 발전을 위해서는, 효과적인 항암 면역 반응의 부재 또는 회피에 영향을 미치는 다양한 요인을 식별하고 우회할 필요성이 중요하게 된다. 상이한 면역 회피 기전 또는 신규한 2세대 CPI를 표적으로 하는 약제와 아테졸리주맙의 조합은 해당 모집단에서 반응률을 증가시키고 질병 재발률을 추가로 감소시킬 수 있다.CIT has demonstrated clear clinical efficacy with significant survival benefits observed in several advanced malignancies, and there is evidence that PD-1/PD-L1 checkpoint blockade can generate pCR and sustained responses in UC patients (Powles et al. al., Nat Med, 25: 1706-1714, 2019; Necchi et al., Int J Clin Oncol , 36: 3353-3360, 2018). Although these targets have resulted in surprising clinical therapeutic success for a variety of cancer indications, ongoing research indicates that a sequence of stepwise events is required for generation of an effective anti-tumor immune response (Chen and Mellman, Immunity, 39: 1- 10, 2013). Each event is critical for an effective response, and each is also sensitive to multiple tumor immune evasion mechanisms. Therefore, for the development of cancer immunity spread and CIT field, the need to identify and bypass various factors affecting the absence or avoidance of an effective anticancer immune response becomes important. Combination of atezolizumab with agents targeting different immune evasion mechanisms or novel second-generation CPIs may increase response rates and further reduce disease recurrence rates in this population.
MIBC 환자의 잠재적 위험은 연구 치료와 관련된 이상반응과 관련이 있다. 대부분의 국가에서 환자는 요로상피암 진단과 수술 사이에 평균 4-8주를 대기한다. 수술 전 치료가 포함된 본 시도에 참여하는 것이 참가자의 수술 지연과 관련있는 것으로 예상되지 않는다. 게다가, 아테졸리주맙은 ABACUS 연구에서 수술성에 영향을 미치거나 수술과 관련된 위험을 증가시키지 않았다(Powles et al., Nat Med, 25: 1706-1714, 2019).A potential risk in patients with MIBC is associated with adverse events related to study treatment. In most countries, patients wait an average of 4-8 weeks between diagnosis and surgery for urothelial cancer. Participation in this trial that includes preoperative care is not expected to be associated with a participant's surgical delay. Furthermore, atezolizumab did not affect operability or increase surgery-related risks in the ABACUS study (Powles et al., Nat Med, 25: 1706-1714, 2019).
근육 침윤성 방광암에서 수술 전후 치료에 대한 근거Evidence for perioperative treatment in muscle-invasive bladder cancer
신보조제 요법 및 수술 후 유지 요법의 치료적 기여는 공지되어 있지 않다. WO39613 연구는 치료 효능을 평가하고 순차적인 환자 조직에 대한 광범위한 바이오마커 분석을 수행하도록 설계된다. The therapeutic contribution of neoadjuvant therapy and postoperative maintenance therapy is unknown. The WO39613 study is designed to evaluate therapeutic efficacy and to perform extensive biomarker analysis on sequential patient tissues.
IMVigor010은 MIBC 환자가 외과적 절제 및 림프절 절제술 후 보조 요법으로 아테졸리주맙 대 관찰을 받도록 한 III상으로서 무작위화한 연구에 해당한다. 본 연구는 치료 의향이 있는 모집단에서 아테졸리주맙 보조 요법으로 무병 생존 이익을 보이는 해당 1차 평가변수를 충족하지 못했지만, T3 및 T4 환자의 하위 그룹 분석 및 비임상 데이터(Liu et al., Cancer Discov, 6: 1382-1399, 2016; Pai et al., Immunity, 50: 477-492, 2019; Hussain et al., J Clin Oncol, 38(15 Suppl.): 5000, 2020)는, 면역 요법은 체크포인트 면역 요법이 효과적이기 위해 환자에게 잔여 또는 활성 질환이 있어야 할 수 있음을 시사한다.IMVigor010 is a phase III randomized study in which patients with MIBC received atezolizumab versus observation as adjuvant therapy after surgical resection and lymphadenectomy. Although this study did not meet the corresponding primary endpoint of disease-free survival benefit with atezolizumab adjuvant therapy in the willing-to-treat population, subgroup analysis and nonclinical data of T3 and T4 patients (Liu et al., Cancer Discov ) , 6: 1382-1399, 2016; Pai et al., Immunity , 50: 477-492, 2019; Hussain et al., J Clin Oncol , 38(15 Suppl.): 5000, 2020), immunotherapy check This suggests that the patient may have to have residual or active disease for point immunotherapy to be effective.
D.D. 시스플라틴 기반 화학요법에 부적격한 근육 침윤성 방광암 환자의 면역 요법에 대한 증거Evidence for immunotherapy in patients with muscle-invasive bladder cancer ineligible for cisplatin-based chemotherapy
MIBC 환자의 약 50%는 시스플라틴 기반 신보조제 화학요법을 받을 자격이 없으며 현재 이러한 환자에게 권장되는 수술 전후 전신 치료는 존재하지 않는다; 양측 골반 림프절 절제술을 동반한 방광 절제술이 치료의 표준이다. 또한, 신보조제 화학요법을 받을 자격이 있는 MIBC 환자의 절반 미만이 개인 선호도 또는 기타 동반 질환으로 인해 이를 받게 된다. 따라서 MIBC 환자의 결과를 개선하려면 새로운 요법이 필요하다.Approximately 50% of patients with MIBC are not eligible for cisplatin-based neoadjuvant chemotherapy, and there is currently no perioperative systemic therapy recommended for these patients; Cystectomy with bilateral pelvic lymphadenectomy is the standard of care. In addition, less than half of MIBC patients eligible for neoadjuvant chemotherapy will receive it due to personal preference or other comorbidities. Therefore, new therapies are needed to improve outcomes in MIBC patients.
mUC에 대한 화학요법이 진행된 모든 환자 및 백금계 화학요법에 부적격하거나 종양이 PD-L1+인 경우 시스플라틴 기반 화학요법에 부적격한 1L mUC 환자에 대해, PD-1/PD-L1 체크포인트 면역요법이 승인된다. MIBC 환자에서 PD-1/PD-L1 체크포인트 신보조제 면역요법의 안전성과 유효성을 조사한 가장 큰 연구는 ABACUS 및 PURE-01 연구이다(Powles et al., Nat Med, 25: 1706-1714, 2019; Necchi et al., Int J Clin Oncol, 36: 3353-3360, 2018).PD-1/PD-L1 checkpoint immunotherapy is approved for all patients who have undergone chemotherapy for mUC and for 1L mUC patients ineligible for platinum-based chemotherapy or cisplatin-based chemotherapy if the tumor is PD-L1+ do. The largest studies investigating the safety and efficacy of PD-1/PD-L1 checkpoint neoadjuvant immunotherapy in patients with MIBC are the ABACUS and PURE-01 studies (Powles et al., Nat Med , 25: 1706-1714, 2019; Necchi et al., Int J Clin Oncol , 36: 3353-3360, 2018).
E.E. 1차 평가변수로서의 병리학적 완전 관해에 대한 근거Evidence for pathological complete remission as a primary endpoint
병리학적 완전 관해(pCR) 및 병리학적 단계하향(탐색 평가변수)은 지속적인 관해가 없는 생존과의 연관성으로 인해 본 설정에서 활성의 대리 마커로 검증되었다(Rosenblatt et al., Eur Urol, 61: 1229-1238, 2011; Bhindi et al., Eur Urol, 72: 660-664, 2017).Pathological complete remission (pCR) and pathological downgrade (exploratory endpoint) were validated as surrogate markers of activity in this setting due to their association with sustained remission-free survival (Rosenblatt et al., Eur Urol , 61: 1229). -1238, 2011; Bhindi et al., Eur Urol , 72: 660-664, 2017).
증가된 기준선 CD8 T 세포 침윤 및 PD-L1+ 질환은 신보조제 설정에서 면역 요법으로 pCR의 가능성을 증가시키는 것으로 나타났다(Powles et al., Nat Med, 25: 1706-1714, 2019).Increased baseline CD8 T cell infiltration and PD-L1+ disease have been shown to increase the potential of pCR as immunotherapy in the neoadjuvant setting (Powles et al., Nat Med , 25: 1706-1714, 2019).
F.F. 아테졸리주맙을 대조제로서 사용하는 근거 Evidence for using atezolizumab as a control
시스플라틴 기반 신보조제 화학요법이 거부되거나 부적격인 MIBC 환자에 대해 외과적 절제 전후에 전신 요법을 제공하기 위한 치료 표준은 존재하지 않는다.There is no standard of care to provide systemic therapy before or after surgical resection for MIBC patients who are rejected or ineligible for cisplatin-based neoadjuvant chemotherapy.
ABACUS 및 PURE-01 연구를 통해 PD-1/PD-L1 체크포인트 면역요법은 MIBC 환자에서 활동적이고 안전하며, 반응률은 시스플라틴 기반 화학요법에서 역사적으로 관찰된 것과 유사한 것으로 나타났기 때문에, 아테졸리주맙이 대조제로 선택됐다. ABACUS 및 PURE-01 데이터에 의하면, mUC에 비해 MIBC가 일반적으로 더 염증이 있고 따라서 PD-1/PD-L1 체크포인트 면역요법의 이점을 얻을 가능성이 더 높은데, 이는 IMVigor211 및 KN-045 연구에서 PD-L1 발현이 mUC 치료를 받은 환자의 25% 및 28.5%에서만 관찰되었기 때문이다.Because ABACUS and PURE-01 studies showed that PD-1/PD-L1 checkpoint immunotherapy is active and safe in patients with MIBC, and response rates are similar to those historically observed with cisplatin-based chemotherapy, atezolizumab zero was chosen. ABACUS and PURE-01 data show that compared to mUC, MIBCs are generally more inflamed and therefore more likely to benefit from PD-1/PD-L1 checkpoint immunotherapy, which indicates that PD in the IMVigor211 and KN-045 studies This is because -L1 expression was only observed in 25% and 28.5% of patients treated with mUC.
면역 요법 조합을 평가하는 무작위 연구를 통해 시스플라틴 기반 화학요법에 부적격한 MIBC 환자에 대한 안전하고 효과적인 치료법을 식별할 수 있으며, 또한 동시에 암 생물학에 대한 이해를 크게 높이고 모든 MIBC 환자를 위한 새로운 시도 및 치료법을 설계할 때의 반복 능력을 향상시킬 수 있다. 본 연구는 적절한 임상 안전성이 입증된 면역요법 조합을 사용하는 가능한 미래의 군 및 코호트가 포함될 수도 있다.Randomized studies evaluating immunotherapy combinations could identify safe and effective treatments for MIBC patients who are ineligible for cisplatin-based chemotherapy, while at the same time greatly enhancing our understanding of cancer biology and new trials and therapies for all MIBC patients. It can improve the repeatability when designing. This study may include possible future groups and cohorts using immunotherapy combinations for which adequate clinical safety has been demonstrated.
G.G. 별도의 PD-L1+ 및 PD-L1- 코호트에 대한 근거 Evidence for separate PD-L1+ and PD-L1- cohorts
2L mUC 및 시스플라틴 기반 화학요법을 받을 자격이 없는 PD-L1+ mUC 환자에 대해 PD-1/PD-L1 차단은 FDA의 승인을 받았지만 MIBC 환자에는 적용되지 않는다. ABACUS 연구에서 pCR 이익은 PD-L1-(24.5%, n = 12/49) 질환보다 아테졸리주맙 치료된 PD-L1+(37.1%, n = 13/35) 환자에서 더 높았지만 PD-L1-질병의 일부 환자는 여전히 아테졸리주맙 또는 면역요법 조합으로부터 이익을 받을 수 있다. 연구 설계를 통해 시험의뢰자는 이러한 환자 하위 집합에서 아테졸리주맙 및 기타 면역요법 조합의 유효성을 별도로 평가할 수 있고 다른 코호트에서의 조사에 영향을 미치지 않으면서 이익의 증거가 없는 각 코호트의 군에 등록을 마감할 수 있다.PD-1/PD-L1 blockade is FDA-approved for patients with PD-L1+ mUC ineligible for 2L mUC and cisplatin-based chemotherapy, but not for MIBC patients. In the ABACUS study, pCR benefit was higher in atezolizumab-treated PD-L1+ (37.1%, n = 13/35) patients than in PD-L1- (24.5%, n = 12/49) disease, although PD-L1-disease Some patients may still benefit from atezolizumab or an immunotherapy combination. The study design allows the sponsor to separately evaluate the effectiveness of atezolizumab and other immunotherapy combinations in these patient subsets and to enroll in groups in each cohort with no evidence of benefit without affecting investigations in other cohorts. can be finished
H.H. 근육 침윤성 방광암 코호트의 ctDNA에 있어서의 수술 전후 치료의 영향에 대한 조사의 근거Evidence of investigation into the effect of perioperative treatment on ctDNA in muscle-invasive bladder cancer cohort
시간 경과에 따른 순환 종양 DNA(ctDNA) 농도의 변화는 질병 재발을 감지하도록 사용될 가능성을 갖는다(Moding et al., Nat Cancer, 1: 176-183, 2020). 암세포에서 말초혈액으로 흘러내린 ctDNA는 비침습적으로 수집되어 종양 특이 돌연변이의 존재 여부를 테스트할 수 있다. UC의 몇 가지 특성은 ctDNA 검사를 사용하여 질병 재발을 예측하기 위한 강력한 후보에 해당한다.Changes in circulating tumor DNA (ctDNA) concentrations over time have the potential to be used to detect disease recurrence (Moding et al., Nat Cancer , 1: 176-183, 2020). ctDNA shed from cancer cells into peripheral blood can be collected non-invasively and tested for the presence of tumor-specific mutations. Several characteristics of UC make them strong candidates for predicting disease recurrence using ctDNA testing.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
이러한 데이터는 긴급 치료 선택지에 대한 충족되지 않은 요구가 높은 MIBC 환자의 바이오마커 선택된 하위 모집단을 나타낸다. 그러나, 현재로서는 다음에 관한 데이터가 존재하지 않는다: 1) 요로상피암 환자의 방광 절제술 전후 ctDNA에 대한 신보조제 면역 요법의 영향; 2) 신보조제 면역요법으로 치료받은 환자에서 유지 면역요법이 방광 절제술 후 요로상피암의 재발을 예방하는 데 도움이 될 수 있는 경우; 3) 유지 면역 요법이 질병 재발 위험을 감소시키는 경우로서,These data represent a biomarker selected subpopulation of MIBC patients with high unmet need for urgent treatment options. However, there are currently no data on: 1) the effect of neoadjuvant immunotherapy on ctDNA before and after cystectomy in patients with urothelial cancer; 2) In patients treated with neoadjuvant immunotherapy, maintenance immunotherapy may help prevent recurrence of urothelial cancer after cystectomy; 3) when maintenance immunotherapy reduces the risk of disease recurrence,
신보조제 면역요법으로 치료받은 환자가 방광 절제술 후 측정 가능한 ctDNA를 가지고 있는 경우.Patients treated with neoadjuvant immunotherapy have measurable ctDNA after cystectomy.
본 연구의 일환으로 ctDNA는 아테졸리주맙 및 아테졸리주맙 + 티라골루맙으로 치료받은 모든 PD-L1+ MIBC 환자에서 4가지 시점에서 후향적으로 측정된다. 1) 주기 1의 1일차 전; 2) 방광 절제술 전; 3) 방광 절제술 후 4-6주; 및 4) 방광 절제술 후 6개월. 무사건 생존(EFS) 및 OS와 이러한 시점에서의 ctDNA 결과 사이의 연관성이 조사된다. 이러한 결과를 통해, 체크포인트 면역 요법을 받는 환자에서 신보조제의 영향과As part of this study, ctDNA was measured retrospectively at four time points in all PD-L1+ MIBC patients treated with atezolizumab and atezolizumab plus tiragolumab. 1) before Day 1 of Cycle 1; 2) before cystectomy; 3) 4-6 weeks after cystectomy; and 4) 6 months after cystectomy. The association between event-free survival (EFS) and OS and ctDNA outcome at these time points is investigated. Through these results, the effect of neoadjuvant and the
유지 요법의 가치에 대한 향후 연구 설계를 알게 된다. 이러한 조사 결과를 기다리는 동안 연구의 다른 부문에서 이러한 시점에 조사된 ctDNA 및 다른 부문에서 관찰된 임상 활성.Know the design of future studies on the value of maintenance therapy. ctDNA investigated at these time points in different segments of the study and clinical activity observed in other segments of the study while awaiting the results of these studies.
본 설계 및 ctDNA의 사용을 통해 하기의 것들을 평가할 수 있다: 1) ctDNA 및 병리학적 반응에 대한 신보조제 요법의 영향; 2) 신보조제 면역요법 후 잔여 ctDNA에 대한 수술의 영향; 및 3) 유지 면역요법이 수술 후 MIBC 환자에서 ctDNA 및 질병 재발의 위험을 감소시키는지 여부.The use of this design and ctDNA allows the evaluation of: 1) the effect of neoadjuvant therapy on ctDNA and pathological response; 2) effect of surgery on residual ctDNA after neoadjuvant immunotherapy; and 3) whether maintenance immunotherapy reduces the risk of ctDNA and disease recurrence in postoperative MIBC patients.
실시예 17. WO39613 연구를 위한 재료 및 방법Example 17. Materials and Methods for Study WO39613
A.A. 선정 기준Selection Criteria
환자는 하기의 기준을 모두 충족해야 한다:Patients must meet all of the following criteria:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
o TURBT 후 잔류 질환(외과적 소견, 방광경검사/내시경검사 또는 방사선학적 존재).o Residual disease after TURBT (surgical findings, cystoscopy/endoscopy or radiologic presence).
o 혼합 조직을 가진 환자는 지배적인 이행 세포 패턴을 가져야 한다.o Patients with mixed tissue should have a dominant transitional cell pattern.
![]()
![]()
o TURBT 표본은 관련 병리 보고서와 함께 제출해야 한다. 종양 조직은 2가지 상이한 방법으로 처리된다(즉, 별도의 바이오마커 분석을 위해 파라핀 고정 조직과 신선한 조직이 필요). 방광 또는 상부 요로의 종양 조직은 전체 및 생존 가능한 종양 함량을 기준으로 품질이 좋아야 하며, 국소 병리학 검토에 의해 확인된 바와 같이 종양의 근육 침습성 성분(즉, T2 이상)을 함유해야 한다.o TURBT specimens must be submitted with the relevant pathology report. Tumor tissue is processed in two different ways (ie, paraffin-fixed tissue and fresh tissue are required for separate biomarker analysis). Tumor tissue of the bladder or upper urinary tract should be of good quality based on total and viable tumor content, and should contain a muscle-invasive component of the tumor (ie, T2 or greater) as confirmed by local pathology review.
o MIBC 과정에서 상이한 시간에 수행된 절차로부터 추가 조직 샘플(예: 이전 TURBT의 샘플)이 있는 환자는 중앙 테스트를 위해 이러한 샘플도 제출하도록 요청될 수 있다(필수는 아님).o Patients who have additional tissue samples from procedures performed at different times in the course of the MIBC (eg samples from the previous TURBT) may be asked (but not required) to also submit these samples for central testing.
![]()
![]()
![]()
![]()
- G-CSF 지원 없이 절대 호중구 수(ANC) ≥ 1.5 x 109/L (1500/μL)- Absolute neutrophil count (ANC) ≥ 1.5 x 10 9 /L (1500/μL) without G-CSF support
- 백혈구(WBC) 수 ≥ 2.5 x 109/L (2500/μL)- White blood cell (WBC) count ≥ 2.5 x 10 9 /L (2500/μL)
- 림프구 수 ≥ 0.5 x 109/L (500/μL)- Lymphocyte count ≥ 0.5 x 10 9 /L (500/μL)
- 수혈 없이 혈소판 수 ≥ 100 x 109/L (100,000/μL)- Platelet count ≥ 100 x 10 9 /L (100,000/μL) without transfusion
- 헤모글로빈 ≥ 90 g/L(9.0 g/dL)- Hemoglobin ≥ 90 g/L (9.0 g/dL)
환자는 수혈될 수 있다; 그러나 적격 여부에 대한 검사실 검사를 받은 후 2주 이내에는 수혈이 허용되지 않는다.The patient may be transfused; However, blood transfusions are not permitted within two weeks of being tested for eligibility.
에리스로포이에틴 생성이 낮은 단발성 신장 또는 만성 신장 질환이 있는 환자는 에리트로포이에틴 자극제를 사용할 수 있다.Erythropoietin stimulants may be used in patients with epilepsy or chronic kidney disease with low erythropoietin production.
- AST, ALT 및 알칼리성 인산분해효소(ALP) ≤ 2.5 x 정상 상한(ULN)- AST, ALT and alkaline phosphatase (ALP) ≤ 2.5 x upper limit of normal (ULN)
- 빌리루빈 ≤ 1.5 x ULN, 다음 예외:- Bilirubin ≤ 1.5 x ULN, with the following exceptions:
알려진 길버트병 환자: 빌리루빈 수준 ≤ 3 x ULNKnown Gilbert's disease patients: bilirubin levels ≤ 3 x ULN
- 알부민 ≥ 25 g/L (2.5 g/dL)- albumin ≥ 25 g/L (2.5 g/dL)
- 크레아티닌 청소율 ≥ 30mL/min(Cockcroft-Gault 공식을 사용하여 계산)- Creatinine clearance ≥ 30 mL/min (calculated using the Cockcroft-Gault formula)
- 치료적 항응고제를 투여받지 않는 환자의 경우:- For patients not receiving therapeutic anticoagulants:
부분 트롬보플라스틴 시간(PTT) 또는 aPTT ≤ 1.5 x ULNPartial thromboplastin time (PTT) or aPTT ≤ 1.5 x ULN
프로트롬빈 시간(PT) 또는 국제 표준화 비율(INR) ≤ 1.5 x ULNProthrombin time (PT) or International Normalized Ratio (INR) ≤ 1.5 x ULN
![]()
![]()
o 이전에 양성 HIV 검사 결과가 없는 환자는 지역 규정에 따라 허용되지 않는 한 선별시 HIV 검사를 받게 된다.o Patients without a prior positive HIV test result will be tested for HIV at screening unless permitted by local regulations.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
B.B. 배제 기준Exclusion Criteria
하기의 기준 중 임의의 것에 부합하는 환자는 연구 등록으로부터 배제한다: 제외 기준의 이벤트 등급은 NCI CTCAE v4.0을 기반으로 한다.Patients meeting any of the following criteria are excluded from study enrollment: Event grades for exclusion criteria are based on NCI CTCAE v4.0.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
급성, 저용량, 전신 면역억제제 또는 1회 펄스 용량의 전신 면역억제제(예: 조영제 알레르기용 코르티코스테로이드 48시간)를 투여받은 환자는 본 연구에 자격이 있다.Patients receiving acute, low-dose, systemic immunosuppressants or single pulse doses of systemic immunosuppressants (eg, corticosteroids for contrast allergy 48 hours) are eligible for this study.
무기질 코르티코이드(예: 플루드로코르티손), 만성 폐쇄성 폐질환 또는 천식용 코르티코스테로이드, 기립성 저혈압 또는 부신 기능 부전용 저용량 코르티코스테로이드를 투여받는 환자는 본 연구에 자격이 있다.Patients receiving mineralocorticoids (eg, fludrocortisone), corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency were eligible for this study.
![]()
![]()
![]()
![]()
![]()
![]()
자가면역 관련 갑상선기능저하증의 병력이 있고 갑상선 대체 호르몬을 투여받고 있는 환자는 본 연구에 적격이다.Patients with a history of autoimmune-related hypothyroidism and taking thyroid replacement hormone are eligible for this study.
안정적인 인슐린 요법을 받고 있는 조절된 제1형 진성 당뇨병 환자는 본 연구에 적격이다.Patients with controlled type 1 diabetes mellitus on stable insulin therapy are eligible for this study.
습진, 건선, 만성 단순 태선 또는 피부과적 징후만 있는 백반증의 환자(예: 건선성 관절염 환자는 제외)는 다음 조건이 모두 충족되는 경우 본 연구에 적격이다.Patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with only dermatological signs (eg, excluding patients with psoriatic arthritis) are eligible for this study if all of the following conditions are met:
- 발진은 체표면적의 <10%를 차지해야 한다.- The rash should occupy <10% of the body surface area.
- 질병은 기준선에서 잘 제어되며 저효능 국소 코르티코스테로이드만 필요로 한다. - Disease is well controlled at baseline and requires only low potency topical corticosteroids.
- 지난 12개월 이내에 소랄렌에 더하여 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고효능 또는 경구 코르티코스테로이드를 필요로 하는 기저 상태의 급성 악화가 발생하지 않았음- No acute exacerbation of an underlying condition requiring ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids in addition to psoralen within the past 12 months
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
아테졸리주맙 + 티라골루맙 군에 대한 추가 제외 기준 Additional exclusion criteria for the atezolizumab + tiragolumab group
다음 기준 중 어느 하나에 부합하는 환자는 아테졸리주맙 + 티라골루맙 군으로부터 제외된다:Patients meeting any of the following criteria are excluded from the atezolizumab + tiragolumab group:
![]()
![]()
선별검사 시 EBV 바이러스 캡시드 항원(VCA) IgM 검사가 양성인 환자는 이 군으로부터 제외된다. EBV 중합효소연쇄반응(PCR) 검사는 활동성 감염 또는 의심되는 만성 활동성 감염을 선별하기 위해 임상적으로 지시된 대로 실시해야 한다. EBV PCR 검사가 양성인 환자는 이 군으로부터 제외된다.Patients with a positive EBV virus capsid antigen (VCA) IgM test at screening are excluded from this group. EBV polymerase chain reaction (PCR) testing should be performed as clinically indicated to screen for active or suspected chronic active infection. Patients with a positive EBV PCR test are excluded from this group.
C.C. 허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
2 사이클의 치료 후, 종양 표적 병변의 평가를 방해하지 않는 한 고식적 방사선요법이 허용된다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 아테졸리주맙 치료는 고식적 방사선요법 동안 계속될 수 있다.After 2 cycles of treatment, palliative radiotherapy is allowed as long as it does not interfere with the evaluation of the tumor target lesion (eg, the lesion to be irradiated must not be the only site of measurable disease). Atezolizumab treatment may be continued during palliative radiotherapy.
![]()
![]()
3개 이하의 병변을 조절하기 위해 국소 요법이 필요한 혼합 반응을 경험하는 환자는 의학 모니터 요원의 승인을 받은 후에도 여전히 연구 치료를 계속하기에 적격일 수 있다. 표적 병변에 대한 국소 요법을 받는 환자는 더 이상 방사선학적 반응에 대해 평가할 수 없지만Patients experiencing mixed reactions requiring topical therapy to control 3 or fewer lesions may still be eligible to continue study treatment after approval from a medical monitor. Patients receiving topical therapy for the target lesion can no longer be evaluated for radiological response, but
진행에 대해서는 계속 평가할 수 있다.Progress can be evaluated continuously.
항히스타민제, 해열제 및/또는 진통제를 사용한 사전 투약은 시험자의 재량에 따라 2차 및 후속 아테졸리주맙 주입에 대해서만 투여될 수 있다. Prior dosing with antihistamines, antipyretics and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab at the discretion of the investigator.
주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 보조 요법(예컨대, 보조 산소 및 β2 아드레날린 작용제)으로 관리해야 한다.Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related reactions presenting with dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea should be managed with adjuvant therapy as clinically indicated (e.g., adjuvant oxygen and β 2 adrenergic agonists). .
D. 아테졸리주맙 군의 재료 및 방법D. Materials and Methods of the Atezolizumab Group
아테졸리주맙은 승인된 용량(TECENTRIQ® U.S. Package Insert; TECENTRIQ® SmPC)인 3주마다 1200 mg 고정 용량(Q3W)(각 21일 사이클의 1일차에 1200 mg)으로 투여된다(표 72). 항종양 활성은 1 내지 20 mg/kg Q3W 범위의 용량에 걸쳐 관찰되었다. 연구 PCD4989g에서, 아테졸리주맙의 최대 내약성 용량은 도달되지 않았으며, 어떤 용량에서도 용량 제한 독성이 관찰되지 않았다. 1200 mg Q3W의 고정 용량(15 mg/kg Q3W의 평균 체중 기반 용량에 해당)은 비임상 연구(Deng et al., MAbs, 8: 593-603, 2016)와 이용 가능한 임상 약동학, 유효성 및 안전성 데이터를 기반으로 선택되었다.Atezolizumab is administered at an approved dose (TECENTRIQ® US Package Insert; TECENTRIQ® SmPC), a 1200 mg fixed dose (Q3W) every 3 weeks (1200 mg on Day 1 of each 21-day cycle) (Table 72). Antitumor activity was observed over doses ranging from 1 to 20 mg/kg Q3W. In study PCD4989g, the maximally tolerated dose of atezolizumab was not reached and no dose limiting toxicity was observed at any dose. A fixed dose of 1200 mg Q3W (corresponding to a mean weight-based dose of 15 mg/kg Q3W) has been compared with nonclinical studies (Deng et al., MAbs , 8: 593-603, 2016) and available clinical pharmacokinetic, efficacy and safety data. was selected based on
아테졸리주맙 대조군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 치료를 받는다. 치료 배정 후 7일 이내에 치료를 개시해야 한다. 환자는 사이클 3 이후에 수술을 받는다; 사이클 4의 치료는 수술 후 4주 내지 6주에 다시 개시되어야 한다.Atezolizumab control patients had unacceptable toxicity or clinical findings as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical condition (e.g., worsening of symptoms such as disease-related pain). Treatment is continued until loss of benefit is achieved. Treatment must be initiated within 7 days of treatment assignment. Patients undergo surgery after cycle 3; Cycle 4 treatment should be resumed 4-6 weeks post surgery.

아테졸리주맙의 투여는 훈련된 직원과 잠재적인 심각한 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 설정에서 수행된다. Administration of atezolizumab is performed in a monitoring setting with trained staff and immediate access to appropriate equipment and medications to manage potentially serious reactions.
아테졸리주맙 주입은 표 73에 요약된 지침에 따라 투여된다.Atezolizumab infusion is administered according to the guidelines summarized in Table 73.

D.D. D.D. 아테졸리주맙 + 티라골루맙 암의 재료 및 방법Materials and methods of atezolizumab + tyragolumab cancer
아테졸리주맙은 전술한 바와 같이 투여된다(표 73 참조). Atezolizumab is administered as described above (see Table 73).
티라골루맙은 600 mg 고정 용량으로 IV로 Q3W(각 21일 사이클의 1일차에 600 mg) 투여된다. 600 mg 고정 용량으로 IV로 Q3W은 단일 제제 티라골루맙 또는 티라골루맙과 병용한 아테졸리주맙을 이용한 결합된 Ia상/Ib상 연구 GO30103의 이용 가능한 임상 PK, 유효성 및 안전성 데이터를 기반으로 선택되었다. 단일 제제로서 티라골루맙을 사용한 연구의 Ia상 부분에서, MTD에 도달하지 못했으며, 용량 증량에서 DLT가 관찰되지 않았다. 임상Tiragolumab is administered as a fixed dose of 600 mg IV Q3W (600 mg on Day 1 of each 21-day cycle). Q3W as a 600 mg fixed dose IV was selected based on available clinical PK, efficacy and safety data from the combined Phase Ia/Ib study GO30103 with either single agent tiragolumab or atezolizumab in combination with tiragolumab . In the Phase Ia portion of the study using tyragolumab as a single agent, MTD was not reached and no DLT was observed at dose escalation. clinical
마감일 현재, 티라골루맙에 대한 항약물 항체(ADA)는 모든 용량 수준에 걸쳐 Ia상 또는 Ib상 부분에서 드물었다. 400 mg에서 시작하는 티라골루맙 용량에서, 연구의 Ia상 부분에서 장기간 안정한 질병이 환자에게서 관찰되었다. 티라골루맙과 병용한 아테졸리주맙을 이용한 연구의 Ib상 부분에서, MTD에 도달하지 못했다. 방사선학적 부분 반응에 의해 측정된 항종양 활성은 1200 mg의 아테졸리주맙과 병용한 30 mg에서 시작하여 최대 600 mg 범위의 티라골루맙 용량에 걸쳐 관찰되었다.As of the deadline, antidrug antibodies (ADA) to tiragolumab were rare in the Phase Ia or Ib portion across all dose levels. At tiragolumab doses starting at 400 mg, long-term stable disease was observed in patients in the Phase Ia portion of the study. In the Phase Ib portion of the study with atezolizumab in combination with tiragolumab, MTD was not reached. Antitumor activity, as measured by radiological partial response, was observed over tiragoluumab doses ranging up to 600 mg starting at 30 mg in combination with 1200 mg atezolizumab.
아테졸리주맙 + 티라골루맙 군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 표 74에 요약된 치료를 받는다. 환자는 사이클 3 이후에 수술을 받는다; 사이클 4의 치료는 수술 후 4주 내지 6주에 다시 개시된다. Patients in the atezolizumab + tiragolumab arm were considered unacceptable as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as disease-related pain). Receive treatment summarized in Table 74 until loss of toxicity or clinical benefit. Patients undergo surgery after cycle 3; Cycle 4 treatment is resumed 4-6 weeks post surgery.

티라골루맙은 표 75에 기재된 바와 같이 각 21일 사이클의 1일차에 600 mg 고정 용량으로 IV 주입에 의해 투여되며, 주입 후 관찰 기간을 갖는다. 티라골루맙의 투여는 훈련된 직원과 잠재적인 심각한 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 설정에서 수행된다. Tiragolumab is administered by IV infusion at a fixed dose of 600 mg on Day 1 of each 21-day cycle, as described in Table 75, with a post-infusion observation period. Administration of tiragolumab is performed in a monitoring setting with trained staff and immediate access to appropriate equipment and medications to manage potentially serious reactions.

실시예 18. WO39613 연구에 대한 안전성 평가Example 18. Safety evaluation for study WO39613
A.A. 안전 매개변수 및 정의Safety parameters and definitions
안전성 평가는 심각한 이상 반응 및 특정 관심 대상의 이상 반응을 포함한 이상 반응의 모니터링 및 기록, 프로토콜-특정된 안전 실험실 평가의 수행, 프로토콜-특정된 활력 징후의 측정 및 연구의 안전성 평가에 중요하다고 간주되는 기타 프로토콜-특정된 검사의 수행으로 구성된다.Safety assessments are those considered important for monitoring and recording adverse events, including serious adverse events and adverse events of particular interest, performing protocol-specific safety laboratory assessments, measuring protocol-specific vital signs, and evaluating the safety of a study. Others consist of performing protocol-specific checks.
B.B. 이상 사례anomalies
의약품 임상시험 관리기준에 대한 국제의약품규제조화위원회(ICH) 지침에 따르면, 이상 반응은 인과 귀인과 상관없이, 제약학적 산물이 투여된 임상적 조사 개체에서의 임의의 유해한 의학적 발생이다. 따라서 이상 반응은According to the International Council for Harmonization of Drug Regulations (ICH) guidelines for clinical trial practices for pharmaceuticals, an adverse event is any adverse medical occurrence in a clinically investigated subject to whom a pharmaceutical product has been administered, regardless of causal attribution. Therefore, the adverse reaction is
다음 중 어느 하나일 수 있다:It can be any of the following:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
심각한 이상 반응serious adverse reactions
심각한 이상 반응은 다음의 기준 중 어느 하나를 충족하는 임의의 이상 반응이다:A serious adverse event is any adverse event that meets any of the following criteria:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
용어 “중증” 및 “심각한”은 동의어가 아니다. 중증도는 이상 반응의 강도를 나타낸다(예컨대, 경증, 중등증 또는 중증으로 평가되거나 NCI CTCAE에 따라 평가됨; 이상 반응 자체는 비교적 경미한 의학적 유의성(예컨대, 추가 소견이 없는 중증 두통)을 가질 수 있다).The terms “severe” and “severe” are not synonymous. Severity indicates the intensity of the adverse event (e.g., assessed as mild, moderate or severe, or assessed according to the NCI CTCAE; the adverse event itself may have relatively mild medical significance (e.g., severe headache without further findings)).
특정 관심 대상의 이상 반응 Adverse reactions of specific interest
아테졸리주맙 + 티라골루맙 군에 대한 특정 관심 대상의 이상 반응은 다음과 같다:Adverse events of particular interest to the atezolizumab plus tyragolumab group include:
![]()
![]()
![]()
![]()
임의의 병원성 또는 비병원성 유기체, 바이러스 또는 감염성 입자(예컨대, 전염성 해면상뇌증을 전파하는 프리온 단백질)가 감염원으로 간주된다. 감염원의 전파는 의약품에 노출된 환자의 감염을 나타내는 임상 증상 또는 실험실 소견으로부터 의심될 수 있다. 이 용어는 연구 치료의 오염이 의심되는 경우에만 적용된다.Any pathogenic or non-pathogenic organism, virus or infectious particle (eg, a prion protein that transmits infectious spongiform encephalopathy) is considered an infectious agent. Transmission of an infectious agent may be suspected from clinical symptoms or laboratory findings indicative of infection in a patient exposed to the drug. This term applies only when contamination of the study treatment is suspected.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
실시예 19. WO39613 연구에 대한 통계적 고려 사항 및 분석 계획Example 19. Statistical considerations and analysis plan for WO39613 study
WO39613 연구는 연구 중단을 통해 수집된 환자 데이터를 기반으로 분석된다. 달리 명시되지 않는 경우, 유효성 분석은 배정된 치료 요법에 대해 각 약물의 적어도 1회 용량이 투여된 모든 환자로 정의되는 유효성 평가 가능한 집단에 기반하며, 안전성 분석은 연구 치료를 받는 모든 환자로 정의되는 안전성 평가 가능한 집단에 기반한다.The WO39613 study is analyzed based on patient data collected through study discontinuation. Unless otherwise specified, efficacy analyzes are based on an efficacy evaluable population defined as all patients receiving at least one dose of each drug for the assigned treatment regimen, and safety analyzes are based on all patients receiving study treatment. It is based on a population that can be evaluated for safety.
분석 결과는 환자가 실제로 받는 치료로 요약된다. 데이터는 샘플 크기에 따라 설명되고 요약된다. 연속 변수는 평균, 표준 편차, 중앙값, 최소값 및 최대값을 사용하여 요약된다. 범주형 변수는 개수 및 백분율을 사용하여 요약된다. 목록은 표본 크기가 작은 경우 표 대신 사용된다.The results of the analysis are summarized in the treatment the patient actually receives. Data are described and summarized according to sample size. Continuous variables are summarized using mean, standard deviation, median, minimum and maximum values. Categorical variables are summarized using counts and percentages. Lists are used instead of tables when the sample size is small.
A.A. 샘플 크기의 결정Determination of sample size
WO39613 연구는 가설 분석을 위해 명백한 분석력 및 제1종 오류를 고려하도록 설계되지WO39613 study was not designed to account for apparent analytical power and type I error for hypothesis analysis.
않았다. 대신, 상기 연구는 시스플라틴 부적격 MIBC 환자에게 투여시 면역요법 기반 치료 조합에 대한 예비 유효성, 안전성 및 PK 데이터를 얻기 위해 설계되었다. 약 150명 내지 350명의 환자가 연구 기간 동안 대조군 및 실험군에 무작위로 배정된다.didn't Instead, this study was designed to obtain preliminary efficacy, safety, and PK data for an immunotherapy-based treatment combination when administered to patients with cisplatin ineligible MIBC. Approximately 150 to 350 patients are randomly assigned to control and experimental groups for the duration of the study.
B.B. 유효성 분석Validity analysis
일차 유효성 평가변수 Primary efficacy endpoint
일차 유효성 평가변수는 병리학적 완전 반응(pCR)으로, 완전 절제된 표본의 잔류 침습성 암이 존재하지 않는 환자의 비율로 정의된다. pCR 비율은 90% 신뢰 구간으로 각 군에 대해 계산된다. 또한, 실험군(들)과 대조군 사이의 pCR 차이가 90% 신뢰 구간으로 계산된다. 신뢰 구간은 표본 크기에 따라 직접 확률법 또는 왈드(Wald) 방법으로 추정된다. 반응 평가가 누락되거나 존재하지 않는 환자는 무반응자로 분류된다.The primary endpoint is pathological complete response (pCR), defined as the proportion of patients free of residual invasive cancer in completely resected specimens. pCR ratios are calculated for each group with 90% confidence intervals. In addition, the pCR difference between the experimental group(s) and the control group is calculated with a 90% confidence interval. Confidence intervals are estimated by direct probability method or Wald method according to the sample size. Patients with missing or non-existent response assessments are classified as non-responders.
이차 유효성 평가변수 secondary efficacy endpoint
이차 유효성 평가변수는 각각 특정 시점(예컨대, 12, 18, 24개월)에서의 랜드마크 무재발 생존(RFS), 랜드마크 무사건 생존(EFS) 및 랜드마크 전체 생존(OS)이다. 이러한 평가변수는 아래에 기재된다. 랜드마크 RFS 비율, 랜드마크 EFS 비율 및 랜드마크 OS 비율은 카플란-마이어(Kaplan-Meier) 방법을 사용하여 각 연구군에 대해 추정되며, 90% CI는 그린우드(Greenwood) 공식을 사용하여 계산된다.Secondary efficacy endpoints are landmark recurrence-free survival (RFS), landmark event-free survival (EFS), and landmark overall survival (OS) at specific time points (eg, 12, 18, 24 months), respectively. These endpoints are described below. Landmark RFS ratio, landmark EFS ratio, and landmark OS ratio are estimated for each study group using Kaplan-Meier method, and 90% CI is calculated using Greenwood formula .
탐색적 유효성 평가변수 Exploratory validity endpoints
탐색적 유효성 평가변수는 RFS, EFS, OS 및 병리학적 하향병기 비율이다.Exploratory efficacy endpoints were RFS, EFS, OS, and pathologic downstage ratio.
무재발 생존(RFS)은 수술 후 첫 번째 사이클의 1일차로부터 처음으로 보고된 질병의 재발 또는 임의의 원인으로 인한 사망시까지의 시간으로 정의된다. 질병의 재발 또는 사망이 보고되지 않은 환자의 경우 RFS는 수술 후 마지막 종양 평가 당일에 중도절단된다.Relapse-free survival (RFS) is defined as the time from Day 1 of the first postoperative cycle to the first reported disease recurrence or death from any cause. For patients with no reported disease recurrence or death, RFS is censored on the day of the last tumor evaluation after surgery.
무사건 생존(EFS)은 무작위 배정시부터 다음 사건(하기 중 먼저 발생하는 것)까지의 시간으로 정의된다: 시험자에 의해 평가된, 수술을 불가능하게 하는 질병 진행; 국소 또는 원격 질병 재발; 또는 임의의 원인으로 인한 사망. 이러한 사건을 경험하지 않은 환자는 마지막 종양 후 종양 평가 시점에 중도절단된다.Event-free survival (EFS) is defined as the time from randomization to the next event (whichever occurs first): inoperable disease progression, assessed by the investigator; local or distant disease recurrence; or death from any cause. Patients who do not experience these events are censored at the time of tumor assessment after the last tumor.
전체 생존(OS)은 무작위 배정시부터 임의의 원인으로 인한 사망시까지의 시간으로 정의된다. 사망하지 않은Overall survival (OS) is defined as the time from randomization to death from any cause. not dead
환자에 대한 데이터는 생존한 것으로 알려진 마지막 날짜에서 중도절단된다. Data for patients are censored from the last known surviving date.
병리학적 하향병기율은 방광 절제술 시 ≤ pT1pN0에 도달한 환자의 비율로 정의된다.Pathological downstaging is defined as the proportion of patients achieving ≤ pT1pN0 at cystectomy.
카플란-마이어(Kaplan-Meier) 방법은 각 연구군의 RFS, EFS 및 OS 중앙값을 추정하는 데 사용된다. 브룩마이어(Brookmeyer) 및 크라울리(Crowley) 방법은 각 연구군의 RFS, EFS 및 OS 중앙값에 대한 90% CI를 작성하는 데 사용된다.The Kaplan-Meier method is used to estimate the median RFS, EFS, and OS for each study group. The Brookmeyer and Crowley methods were used to generate 90% CIs for the median RFS, EFS, and OS for each study group.
C.C. 안전성 분석Safety analysis
축어적 이상 반응 용어는 규제 활동을 위한 의학 사전(Medical Dictionary for Regulatory Activities)의 시소러스 용어에 매핑되며, 이상 반응 중증도는 NCI CTCAE v4.0에 따라 등급이 나뉜다.Verbose adverse event terms are mapped to thesaurus terms in the Medical Dictionary for Regulatory Activities, and adverse event severity is graded according to NCI CTCAE v4.0.
안전성은 이상 반응의 요약, 실험실 검사 결과의 변화, 활력 징후 및 ECG의 변화, 및 연구 약물에 대한 노출을 통해 평가된다. 병용 치료에 대한 노출 및 안전성 추적 기간은 각 병기 내 치료군별로 요약된다.Safety is assessed through a summary of adverse events, changes in laboratory test results, changes in vital signs and ECGs, and exposure to study drug. Exposure and safety follow-up periods for combination therapy are summarized for each treatment group within each arm.
치료 개시 후 발생하는 치료 관련 이상 반응이 요약되어 있다. 각 환자에 대해, 각 이상 반응에 대해 보고된 최대 증증도는 증증도 등급별 요약에 사용된다. 모든 치료 유발 이상 반응, 심각한 이상 반응, 연구 치료의 중단을 초래하는 이상 반응, ≥ 3등급 이상 반응, 사망 및 사망 원인이Treatment-related adverse events occurring after initiation of treatment are summarized. For each patient, the maximum severity reported for each adverse event is used for the summary by severity grade. All treatment-induced adverse events, serious adverse events, adverse events leading to discontinuation of study treatment, ≥ Grade 3 adverse events, deaths and causes of death
매핑된 용어, 적절한 시소러스 수준 및 NCI CTCAE 중증도 등급으로 나열 및 요약된다.Listed and summarized by mapped term, appropriate thesaurus level, and NCI CTCAE severity rating.
관련 실험실, 활력징후(맥박수, 호흡수, 혈압, 맥박 산소 측정, 및 체온) 및 ECG 데이터가 시간별로 표시되며, 적절한 경우 등급으로 식별된다. 추가적으로, 선택된 실험실 시험 결과의 교대표를 사용하여 기준선 및 기준선 이후 최대 중증도 등급을 요약한다. 활력 징후의 변화가 요약된다.Relevant laboratory, vital signs (pulse rate, respiration rate, blood pressure, pulse oximetry, and body temperature) and ECG data are displayed hourly and identified by grade, where appropriate. Additionally, the baseline and post-baseline maximal severity ratings are summarized using alternate representations of selected laboratory test results. Changes in vital signs are summarized.
D.D. 약동학 분석Pharmacokinetic analysis
아테졸리주맙(적어도 1회 용량의 아테졸리주맙을 투여받는 환자) 및 아테졸리주맙과 병용하여 투여되는 약물(적어도 1회 용량의 약물을 투여받는 환자)의 PK 분석을 위해 희소 샘플을 수집한다. 다양한 연구 약물의 혈청 또는 혈장 농도는 개별 값으로 보고되고, 적절한 경우 데이터가 허용하는 한 치료군별 및 사이클 및 날짜별로 요약된다(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균 및 기하 평균 변동 계수). 다양한 연구 약물의 혈청 또는 혈장 농도의 개별 및 중앙값은 치료군별 및 사이클 및 날짜별로 표시된다. 복합 약물에 대한 PK 데이터는 내부 및 공개된 이전 연구로부터 입수 가능한 과거 데이터와 비교할 수 있다. 농도 데이터는 간격, 분포 용적, 곡선 아래 면적과 같은 PK 매개변수를 도출하기 위해 확립된 집단 PK 모델을 사용하는 다른 연구의 데이터와 통합될 수 있다.Rare samples are collected for PK analysis of atezolizumab (patients receiving at least one dose of atezolizumab) and drugs administered in combination with atezolizumab (patients receiving at least one dose of the drug). Serum or plasma concentrations of various study drugs are reported as individual values and, where appropriate, summarized by treatment group and by cycle and date as data permits (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean variation). Coefficient). Individual and median serum or plasma concentrations of various study drugs are presented by treatment group and by cycle and date. PK data for combination drugs can be compared with historical data available from internal and published previous studies. Concentration data can be integrated with data from other studies using established population PK models to derive PK parameters such as interval, volume of distribution, and area under the curve.
PK 매개변수와 안전성, 유효성, PK 및 바이오마커 평가변수 간의 관계는 기술 통계를 통해 분석 및 보고될 수 있다.Relationships between PK parameters and safety, efficacy, PK and biomarker endpoints can be analyzed and reported via descriptive statistics.
E.E. 면역원성 분석Immunogenicity assay
면역원성은 아테졸리주맙 및 기타 연구 치료에 대해 적절하게 평가된다. 면역원성 분석은 적어도 1회의 항약물 항체(ADA) 평가를 받은 모든 환자를 포함한다. 환자는 받은 치료에 따라, 또는 연구 중단 전에 치료를 받지 않은 경우 할당된 치료에 따라 그룹화된다.Immunogenicity is assessed as appropriate for atezolizumab and other study treatments. Immunogenicity assays included all patients who underwent at least one antidrug antibody (ADA) assessment. Patients are grouped according to treatment received, or according to assigned treatment if no treatment was received prior to study discontinuation.
아테졸리주맙의 경우, 기준선(기준선 유병률)에서 및 약물 투여 이후(기준선 이후 발생율)에서 ADA-양성 환자 및 ADA-음성 환자의 수 및 비율을 치료 그룹별로 요약한다. 기준선 이후 발생율을 결정할 때, 환자가 기준선에서 ADA 음성이거나 데이터가 누락되었지만 연구 약물 노출 후 ADA 반응이 발생하는 경우(치료 유도 ADA 반응), 또는 기준선에서 ADA 양성이고 하나 이상의 기준선 이후 샘플의 역가가 기준선 샘플의 역가보다 0.60-역가 단위 이상 큰 경우(치료 강화 ADA 반응), 환자는 ADA 양성으로 간주된다. 환자가 기준선에서 ADA 음성이거나 데이터가 누락되었고 기준선 이후의 모든 샘플들이 음성인 경우, 또는 기준선에서 ADA 양성이지만 역가가 기준선 샘플의 역가보다 0.60-역가 단위 이상 큰 기준선 이후 샘플들을 가지지 않는 경우(치료에 영향받지 않음), 환자는 ADA 음성으로 간주된다.For atezolizumab, the number and proportion of ADA-positive and ADA-negative patients at baseline (baseline prevalence) and after drug administration (post-baseline incidence) are summarized by treatment group. When determining post-baseline incidence rates, if a patient is ADA-negative at baseline or data is missing, but an ADA response occurs after study drug exposure (treatment-induced ADA response), or is ADA positive at baseline and the titer of one or more post-baseline samples is A patient is considered ADA positive if it is at least 0.60-titer units greater than the titer of the sample (treatment-enhanced ADA response). The patient is ADA negative at baseline or data is missing and all samples since baseline are negative, or if the patient is ADA positive at baseline but has no post-baseline samples whose titers are at least 0.60-titer units greater than the titers of the baseline samples ( unaffected), the patient is considered ADA negative.
ADA가 검사되는 다른 연구 치료의 경우, 해당 약물에 대한 이전 연구에서 확립된 표준 방법에 따라 양성이 결정된다.For other study treatments for which ADA is tested, a positive determination is made according to standard methods established in previous studies of the drug.
ADA 상태와 안전성, 유효성, PK 및 바이오마커 평가변수 간의 관계는The relationship between ADA status and safety, efficacy, PK, and biomarker endpoints was
기술 통계를 통해 분석 및 보고될 수 있다.It can be analyzed and reported through descriptive statistics.
F.F. 바이오마커 분석Biomarker analysis
탐색적 바이오마커 분석은 유효성, 안전성, PK, 면역원성 및 기타 바이오마커 평가변수를 고려하여 연구 약물에 대한 반응과 이러한 바이오마커의 연관성을 이해하기 위한 노력의 일환으로 수행된다.Exploratory biomarker analyzes are performed in an effort to understand the association of these biomarkers with response to study drug, taking into account efficacy, safety, PK, immunogenicity, and other biomarker endpoints.
G.G. 중간 분석Interim analysis
중간 분석은 연구 기간 동안 수행되며, 가장 빠른 중간 분석은 적어도 하나의 실험군이 예비 단계에서 등록을 완료하고 환자가 수술 후 pCR 평가를 완료한 경우 수행된다. 시험의뢰자가 적절하다고 판단하는 경우 추가 중간 분석을 수행할 수 있다. 사후 확률은 대조군과 비교한 실험군에서의 임상 활동성의 중간 분석을 기반으로 추가 등록을 안내하는 데 사용될 수 있다. 중간 분석에서 실험군의 활동성이 대조군의 활동성보다 높다고 시사되는 경우, 각 MIBC 코호트에 대해 실험군(확장 단계)에 25명의 추가 환자가 더 등록될 수 있다. 1b상 임상 시험의 확장 및 종료에 대한 최종 결정은 전반적인 유익성-위해성 균형과, 새로운 외부 정보뿐만 아니라 시간-대-사건 평가변수 및 안전성 데이터를 비롯한 데이터 전체를 고려하여 이루어진다.Interim analyzes are performed during the study period, and the earliest interim analyzes are performed when at least one experimental group has completed enrollment in the preliminary phase and the patient has completed postoperative pCR evaluation. Additional interim analyzes may be performed if the sponsor deems it appropriate. The posterior probability can be used to guide further enrollment based on an interim analysis of clinical activity in the experimental group compared to the control group. If the interim analysis suggests that the activity of the experimental group is higher than that of the control group, an additional 25 additional patients can be enrolled in the experimental group (expansion phase) for each MIBC cohort. Final decisions about expansion and termination of Phase 1b clinical trials are made taking into account the overall benefit-risk balance and data as a whole, including time-to-event endpoints and safety data, as well as new external information.
실시예 20. 전이성 요로상피세포 암종(mUC)을 가진 환자를 대상으로 아테졸리주맙과 병용한 티라골루맙의 유효성 및 안전성을 평가하는 Ib/II상, 공개 라벨, 다기관, 무작위 포괄적 연구Example 20. Phase Ib/II, open-label, multicenter, randomized comprehensive study evaluating the efficacy and safety of tiragolumab in combination with atezolizumab in patients with metastatic urothelial cell carcinoma (mUC)
WO39613은 백금 함유 요법 동안 또는 이후에 진행된 국소 진행성 또는 전이성 UC 환자에서 아테졸리주맙과 병용한 티라골루맙의 유효성 및 안전성을 평가하는 Ib/II상, 라벨 공개, 다기관, 무작위 우산형 연구이다. 이 연구는 새로운 치료법이 나오면 새로운 치료군을 개방하거나, 최소한의 임상 활동성 또는 허용할 수 없는 독성을 나타내는 기존 치료군을 폐쇄하거나, 환자 집단을 수정할 수 있는 유연성을 갖도록 설계되었다(예컨대, 이전 항암 치료 또는 바이오마커 상태와 관련하여). 적격 환자는 처음에 여러 치료군 중 하나에 배정된다(도 25 참조). 병기 1 동안 임상적 이점의 상실 또는 허용할 수 없는 독성을 경험한 환자는 병기 2에서 다른 치료 요법으로 치료를 계속하기에 적격일 수 있다(도 25 참조). WO39613 is a Phase Ib/II, open-label, multicenter, randomized umbrella study evaluating the efficacy and safety of tiragolumab in combination with atezolizumab in patients with locally advanced or metastatic UC who progressed during or after platinum-containing therapy. This study is designed to have the flexibility to open new treatment groups as new treatments become available, close existing treatments with minimal clinical activity or unacceptable toxicity, or modify patient populations (e.g., previous chemotherapy or biologic therapies). with respect to marker status). Eligible patients are initially assigned to one of several treatment groups (see FIG. 25 ). Patients who experience unacceptable toxicity or loss of clinical benefit during Stage 1 may be eligible to continue treatment with another treatment regimen in Stage 2 (see FIG. 25 ).
A.A. 병기 1weapon 1
병기 1 동안, 환자는 대조군(아테졸리주맙[아테조]) 또는 티라골루맙과 병용한 아테졸리주맙으로 구성된 실험군(아테조+티라)에 무작위로 배정된다(도 25 및 표 76 참조).During Stage 1, patients are randomly assigned to either a control group (atezolizumab [Atezo]) or an experimental group consisting of atezolizumab in combination with tyragolumab (Atezo+Tira) (see Figure 25 and Table 76).

아테조 = 아테졸리주맙; 티라 = 티라골루맙. a시험의뢰자는 주어진 치료군 내에서 등록을 연기하거나 보류하기로 결정할 수 있다. 따라서, 모든 실험군이 동시에 등록을 위해 개방되지 않을 수 있다. atezo = atezolizumab; Tira = tiragolumap. a The sponsor may decide to defer or withhold enrollment within a given treatment arm. Therefore, not all experimental groups may be open for enrollment at the same time.
b예비 단계 동안 실험군에서 임상 활동성이 관찰되면, 확장 단계 동안 약 25명의 추가 환자가 해당 군에 등록된다. c무작위 배정 비율은 무작위 배정을 위해 개방되어 있는 실험군의 수에 따라 달라지며(예컨대, 군이 추가되거나 b If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients will be enrolled in that group during the expansion phase. c The rate of randomization depends on the number of experimental groups open for randomization (e.g., if more groups are added or
군의 무작위 배정이 보류되는 경우, 예비 단계의 결과 분석이 보류됨), 대조군에 배정될 가능성은 35%를 넘지 않는다. If randomization of a group is withheld, preliminary analysis of the outcome is withheld), the probability of being assigned to a control group is no more than 35%.

PD-L1 프로그램된 사멸 리간드 1; Ig 및 ITIM 도메인이 있는 TIGIT T 세포 면역수용체.PD-L1 programmed death ligand 1; TIGIT T cell immunoreceptor with Ig and ITIM domains.
실험군 내 등록은 예비 단계에 이어 확장 단계의 두 단계로 진행된다. 약 15명의 환자가 예비 단계에서 등록된다. 예비 단계 동안 실험군에서 임상 활동이 관찰되면, 확장 단계 동안 약 25명의 추가 환자가 해당 군에 등록될 수 있다.Enrollment in the experimental group proceeds in two stages: the preliminary stage and the expansion stage. About 15 patients are enrolled in the preliminary phase. If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients can be enrolled in that group during the expansion phase.
시험의뢰자는 주어진 치료군 내에서 등록을 연기하거나 보류하기로 결정할 수 있다. 임상 활동성이 불충분하거나 허용할 수 없는 독성이 있는 실험군은 확장되지 않는다. 추가적인 하위군 분석을 가능하게 하기 위해, 잠재적인 예측적 바이오마커를 포함한 인구 통계학적 및 기준선 특성과 관련하여 치료군 간의 균형을 보장하기 위해 추가 환자를 등록할 수 있다. 프로토콜을 수정하여 연구 중에 새로운 실험군을 추가할 수 있다.The sponsor may decide to defer or withhold enrollment within a given treatment arm. Experimental groups with insufficient clinical activity or unacceptable toxicity are not expanded. To enable further subgroup analysis, additional patients may be enrolled to ensure balance between treatment groups with respect to demographic and baseline characteristics, including potential predictive biomarkers. The protocol can be modified to add new experimental groups during the study.
환자는 병기 2 치료군을 제외하고 치료군에 무작위로 배정된다. 또한, 무작위 배정 비율은 이용 가능한 실험군의 수에 따라서 달라지며(예컨대, 군이 추가되거나 군의 등록이 보류되는 경우, 예비 단계의 결과 분석이 보류됨), 대조군에 배정될 가능성은 35%를 넘지 않는다. 무작위 배정에는 군별 제외 기준이 고려된다. 환자가 특정군에 대해Patients are randomly assigned to treatment groups with the exception of the Stage 2 treatment group. In addition, the rate of randomization depends on the number of available experimental groups (e.g., if a group is added or enrollment of a group is withheld, preliminary analysis of results is withheld), and the probability of being assigned to a control group is not greater than 35%. does not Randomization takes into account group exclusion criteria. patient for a specific group
요약된 제외 기준 중 어느 하나라도 충족하는 경우, 환자는 해당 군에 대해 부적격이다(아래 참조).If any of the outlined exclusion criteria are met, the patient is ineligible for that group (see below).
아테졸리주맙 대조군 및 실험군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 치료를 받는다. 암 면역요법(CIT)(예컨대, 아테졸리주맙)을 사용한 T 세포 반응(가성 진행이라고 명명함) 설정에서 면역 세포 침윤으로 인한 종양 부담의 초기 증가 가능성으로 인해, 고형 종양의 반응 평가 기준, 버전 1.1(RECIST v1.1)에 따른 방사선학적 진행은 실제 질병 진행을 나타내지 않을 수 있다. 허용할 수 없는 독성이 없는 경우,Patients in the atezolizumab control and experimental groups had unacceptable toxicity or toxicity or Treatment is continued until loss of clinical benefit. Criteria for Assessing Response in Solid Tumors, Version 1.1, due to the potential for an initial increase in tumor burden due to immune cell infiltration in the setting of a T cell response (termed pseudoprogression) with cancer immunotherapy (CIT) (eg, atezolizumab). Radiological progression according to (RECIST v1.1) may not represent actual disease progression. In the absence of unacceptable toxicity,
CIT 약물로 치료를 받는 동안 RECIST v1.1에 따른 질병 진행 기준을 충족하는 환자는 다음 기준을 모두 충족하는 경우 연구 치료를 계속할 수 있다:Patients who meet the disease progression criteria per RECIST v1.1 while being treated with CIT drugs may continue on study treatment if all of the following criteria are met:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
B.B. 병기 2weapon 2
병기 1 동안, 시험자가 결정한 임상적 이점의 상실 또는 허용할 수 없는 독성을 경험한 환자는 적격 기준을 충족하는 경우 병기 2 동안 다른 치료 조합을 받기에 적격일 수 있다(도 25 참조). 하나 이상의 치료군에 적격인 병기 2의 환자에 대해 시험자가 치료군을 배정한다. Patients who experience unacceptable toxicity or loss of clinical benefit as determined by the investigator during Stage 1 may be eligible to receive another treatment combination during Stage 2 if they meet the eligibility criteria (see FIG. 25 ). Treatment groups are assigned by investigators to patients in Stage 2 who are eligible for one or more treatment groups.
병기 2 치료는 환자가 임상적 이점의 상실 또는 허용할 수 없는 독성을 경험한 후 3개월 이내에 시작되어야 하며, 시험자가 결정한 임상적 이점의 상실 또는 허용할 수 없는 독성이 있을 때까지 계속된다. 환자는 가능한 빨리 병기 2 치료를 시작하도록 권장된다.Stage 2 treatment should be initiated within 3 months of the patient experiencing loss of clinical benefit or unacceptable toxicity and continued until loss of clinical benefit or unacceptable toxicity as determined by the investigator. Patients are encouraged to begin stage 2 treatment as soon as possible.
시험의뢰자는 적절한 경우 안전성 데이터, 예비 유효성 데이터 및 지원 정보(예컨대, 바이오마커 연구 데이터)의 검토를 기반으로 병기 2 치료군의 등록을 보류하거나 중단하기로 결정할 수 있다.The sponsor may decide to withhold or discontinue enrollment in the Stage 2 treatment arm based on review of safety data, preliminary efficacy data, and supporting information (eg, biomarker study data) as appropriate.
C.C. 연구 설계에 대한 이론적 근거Rationale for Study Design
환자 집단 및 아테졸리주맙 대조군에 대한 이론적 근거Rationale for Patient Population and Atezolizumab Controls
이 연구는 백금 함유 요법 동안 또는 이후에 진행된 국소 진행성 또는 전이성 UC 환자를 등록한다.This study enrolls patients with locally advanced or metastatic UC who progressed during or after platinum-containing therapy.
아테졸리주맙(Tecentriq)은 백금 함유 요법, 비소세포폐암, 소세포폐암, 삼중 음성 유방암, 간세포암 및 흑색종 동안 또는 이후에 진행한 환자의 UC 치료에 승인되었다. 이전의 백금 함유 요법에 따라 진행된 UC 환자의 2치 치료에 대한 승인은 진행 중인 II상 연구 GO29293(IMvigor210)의 코호트 2의 데이터를 기반으로 했으며, 이후Atezolizumab (Tecentriq) is approved for the treatment of UC in patients who progressed during or after platinum-containing therapy, non-small cell lung cancer, small cell lung cancer, triple negative breast cancer, hepatocellular carcinoma, and melanoma. Approval for secondary treatment in patients with UC who progressed following a previous platinum-containing regimen was based on data from cohort 2 of the ongoing phase II study GO29293 (IMvigor210), followed by
IMvigor210과 III상 연구 GO29294(IMvigor211)의 결과를 기반으로 유럽에서 동일한 적응증에 대한 완전한 승인이 이루어졌다. IMvigor210 코호트 2에서, 2017년 7월 12일 현재 310명의 환자가 등록되었으며, 완전 반응(CR) 비율 7% 중 ORR이 16%(95% CI: 13, 21)이고 반응 기간(DOR) 중앙값은 24.8개월(95% CI: 13.8, 30.4)인 것으로 관찰되었다. 안전성 평가에 따르면, 환자의 8%는 치료 중단으로 이어진 이상 반응이 있었고, 환자의 16%는Based on the results of IMvigor210 and phase III study GO29294 (IMvigor211), full approval for the same indication was achieved in Europe. In IMvigor210 cohort 2, 310 patients were enrolled as of July 12, 2017, with an ORR of 16% (95% CI: 13, 21) of a 7% complete response (CR) rate and a median duration of response (DOR) of 24.8 months (95% CI: 13.8, 30.4). According to the safety assessment, 8% of patients had an adverse event that led to treatment discontinuation, and 16% of patients
치료와 관련된 3등급 또는 4등급 이상 반응을 경험했으며, 가장 흔한 이상 반응은 피로, 설사, 가려움증이었다. 면역 매개 이상 반응은 전체 환자의 12%에서 발생했으며, 환자의 7%는 3등급 또는 4등급 면역 매개 이상 반응을 경험했다(3등급 또는 4등급 발진[1%], ALT 증가[2%], 혈액 빌리루빈 증가[2%], 횡문근융해증[1%]). IMvigor211에서는 2017년 3월 13일 현재 치료 목적(ITT) 집단에서 OS 중앙값이 8.6개월, ORR이 13.4%(10.5, 16.9), 그리고 DOR 중앙값이 21.7개월인 것으로 관찰되었다.Treatment-related grade 3 or 4 adverse events were experienced, with the most common adverse events being fatigue, diarrhea, and pruritus. Immune-mediated adverse events occurred in 12% of all patients, and 7% of patients experienced a grade 3 or 4 immune-mediated adverse event (grade 3 or 4 rash [1%], increased ALT [2%], increased blood bilirubin [2%], rhabdomyolysis [1%]). In IMvigor211, as of March 13, 2017, a median OS of 8.6 months, an ORR of 13.4% (10.5, 16.9), and a median DOR of 21.7 months in the purpose of treatment (ITT) group were observed.
단일 제제 관문 억제제의 가능성에도 불구하고, 상대적으로 적은 비율의 환자만이 이점을 경험하므로, 면역요법 조합의 필요성이 강조된다. 아테졸리주맙의 이점을 보다 많은 수술이 불가능한 국소 진행성 및 전이성 UC 환자 집단으로 확대하기 위해, 이 연구의 여러 조합 짝은 다양한 기전을 통해 면역 체계를 자극할 것으로 예상된다.Despite the potential of single agent checkpoint inhibitors, only a relatively small proportion of patients experience benefit, highlighting the need for immunotherapeutic combinations. To extend the benefits of atezolizumab to a larger population of patients with inoperable locally advanced and metastatic UC, the multiple combinatorial partners in this study are expected to stimulate the immune system through a variety of mechanisms.
병기 2의 이론적 근거The rationale for stage 2
면역요법의 출현은 30년 만에 처음으로 mUC의 진정한 발전을 이루어냈다. 이러한 발전에도 불구하고, 더 많은 비율의 환자에게 이점을 확대하려면 실질적으로 더 많은 작업이 필요하다. 면역요법을 발전시키는 능력의 핵심은 근본적인 종양 면역 환경과 치료 순서가 반응에 어떻게 영향을 미치는지를 더 잘 이해하는 것에 있을 것이다.The advent of immunotherapy marked the first real advance in mUC in 30 years. Despite these advances, substantially more work is needed to extend the benefits to a larger proportion of patients. The key to the ability to advance immunotherapy will lie in a better understanding of the underlying tumor immune environment and how the treatment sequence influences response.
이 연구의 병기 2 부분을 통해 일부 환자는 질병 진행 후 후속 CIT 조합을 진행하여 CIT 요법에 반응하지 않거나 진행하는 환자의 면역 탈출 기전에 대한 과학적 이해를 높일 수 있다. 병기 2에 등록할 수 있는 환자의 능력에 중요한 것은 면역 환경과 병기 1 치료 동안 발생할 수 있는 모든 변화를 평가할 수 있도록 생검을 받을 수 있는 능력이다. 병기 2에 참여하면 환자와 제공자는 기존의 화학요법을 통해 얻을 수 없는 지속적인 반응과 개선된 독성 프로필의 잠재력을 가진 치료 옵션에 접근할 수 있다. 병기 2 치료는 다른 잠재적으로 더 표준적인 옵션을 제공하는 치료를 배제한다; 따라서, 환자는 병기 2에 등록함으로써 생존 이점이 있을 수 있는 요법을 포기하게 된다는 사실이 병기 2 동의 과정에서 통지된다.The Stage 2 part of this study may allow some patients to progress to subsequent CIT combinations after disease progression, increasing the scientific understanding of immune escape mechanisms in patients who do not respond or progress to CIT therapy. Critical to a patient's ability to be enrolled in Stage 2 is the ability to undergo a biopsy to assess the immune environment and any changes that may occur during Stage 1 treatment. Participation in Stage 2 gives patients and providers access to treatment options with the potential of a sustained response and improved toxicity profile not attainable with conventional chemotherapy. Stage 2 treatment precludes treatment providing other potentially more standard options; Thus, patients are informed during the Stage 2 consent process that by enrolling in Stage 2, they will forgo a therapy that may have a survival advantage.
병기 2에서 아테조 + EV 및 아테조 + SG 군의 이론적 근거 Rationale for Artezo + EV and Artezo + SG Groups in Stage 2
환자는 임상적 이점이 상실된 후 아테조 +EV 또는 아테조 +Sg로 병기 2 치료를 받을 기회가 주어질 수 있다.Patients may be given the opportunity to receive stage 2 treatment with atezo + EV or atezo + Sg after loss of clinical benefit.
이전에 CPI 치료를 받은, 단일 제제 엔포르투맙 베도틴을 투여받은 환자에서 보고된 강력한 치료 반응으로 인해, 아테조 + EV의 조합이 병기 2에 선택되었다. 특히, 엔포르투맙 베도틴의 I상 임상 시험에서, 권장 II상 엔포르투맙 베도틴 용량으로 치료받은 전이성 방광 환자 17명 중 8명(47%; 95% CI: 23, 72.2)이 PR을 획득했다(Petrylak et al., J Clin Oncol, 35(15 Suppl): 106, 2017). 이러한 발견은 엔포르투맙 베도틴이 CPI 이후 공간에서 이점을 제공할 수 있음을 시사한다. 엔포르투맙 베도틴에 아테졸리주맙을 추가하면 반응 지속성을 개선할 잠재력이 있다. 또한, 미세소관 교란 요법은 면역원성 세포 사멸을 유도하고 항종양 면역 반응을 개시할 잠재력이 있다.Because of the strong therapeutic response reported in patients previously treated with CPI, receiving single agent enfortumab vedotin, the combination of atezo plus EV was chosen for stage 2. In particular, in a phase I clinical trial of enfortumab vedotin, 8 of 17 patients with metastatic bladder (47%; 95% CI: 23, 72.2) treated with the recommended phase II enfortumab vedotin dose had PR was obtained (Petrylak et al., J Clin Oncol , 35(15 Suppl): 106, 2017). These findings suggest that enfortumab vedotin may provide an advantage in the post-CPI space. The addition of atezolizumab to enfortumab vedotin has the potential to improve response duration. In addition, microtubule perturbation therapy has the potential to induce immunogenic cell death and initiate an anti-tumor immune response.
백금계 요법 및 관문 억제제 요법을 진행한, 단일 제제 사시투주맙 고비테칸을 투여받은 mUC 환자에서 관찰된 강력한 치료 반응으로 인해, 아테조 +SG의 조합이 병기 2에 선택되었다. 특히, II상 TROPHY-U-01 연구에서, 사시투주맙 고비테칸은 간 전이 환자에서 25.0%의 ORR을 비롯하여 35명의 환자에서 29%의 ORR을 나타냈다(Tagawa et al., J Clin Oncol, 37(7 Suppl): 3199-3212, 2019). 이러한 발견은 사시투주맙 고비테칸이 CPI 이후 공간에서 이점을 제공할 수 있음을 시사한다. 화학요법 및 면역요법 후 진행된 환자에서 아테졸리주맙과 사시투주맙 고비테칸의 병용은, 아테졸리주맙이 사시투주맙 고비테칸의 항종양 활성에 의해 매개되는 염증으로부터 유도된 항종양 면역 반응을 강화할 수 있게 함으로써 시너지를 제공할 수 있다.Because of the strong therapeutic response observed in mUC patients receiving single agent sacituzumab gobitecan on platinum-based therapy and on checkpoint inhibitor therapy, the combination of atezo plus SG was selected for stage 2. In particular, in the Phase II TROPHY-U-01 study, sacituzumab gobitecan exhibited an ORR of 29% in 35 patients, including an ORR of 25.0% in patients with liver metastases (Tagawa et al., J Clin Oncol , 37 (Tagawa et al., J Clin Oncol, 37) 7 Suppl): 3199-3212, 2019). These findings suggest that sacituzumab gobitecan may provide an advantage in the post-CPI space. Combination of atezolizumab with sacituzumab gobitecan in patients who progressed after chemotherapy and immunotherapy may potentiate the antitumor immune response induced from inflammation where atezolizumab is mediated by the antitumor activity of sacituzumab gobitecan. This can provide synergy.
초기 방사선학적 진행 이후 면역요법 기반 치료의 이론적 근거Rationale for Immunotherapy-Based Treatment after Initial Radiological Progression
면역 치료제 연구에서, CR, 부분 반응(PR) 및 안정적인 질병은 각각 종양 부담의 명백한 증가에 대한 방사선학적 증거 이후에 발생하는 것으로 나타났다. T 세포 반응의 설정에서 면역 세포 침윤에 의해 야기된 이러한 종양 부담의 초기 증가는 가성 진행으로 명명되었다(Hales et al., Ann Oncol, 21: 1944-1951, 2010).In immunotherapeutic studies, CR, partial response (PR) and stable disease, respectively, have been shown to occur after radiological evidence of an apparent increase in tumor burden. This initial increase in tumor burden caused by immune cell infiltration in the setting of T cell responses has been termed pseudoprogression (Hales et al., Ann Oncol , 21: 1944-1951, 2010).
연구 PCD4989g에서, 종양 성장의 증거와 그에 따른 반응이 여러 종양 유형에서 관찰되었다. 또한, 방사선학적 진행의 증거가 있는 일부 반응 환자에서, 새로운 병변의 생검 또는 기존 병변의 새로운 성장 부위에는 면역 세포가 있고 생존 가능한 암세포가 없는 것으로 나타났다. 가성 진행 후 반응의 가능성으로 인해, 이 연구에서 면역요법 기반 치료군에 무작위로 배정된 환자는 유익성-위해성 비율이 시험자에 의해 유리한 것으로 판단되는 경우 RECIST v1.1에 따른 명백한 방사선학적 진행 이후에In study PCD4989g, evidence of tumor growth and consequent response was observed in several tumor types. In addition, in some responding patients with evidence of radiological progression, biopsies of new lesions or new growth sites of existing lesions showed immune cells and no viable cancer cells. Because of the potential for post-pseudo-progressive response, patients randomly assigned to the immunotherapy-based treatment arm in this study were treated after overt radiological progression according to RECIST v1.1 if the benefit-risk ratio was judged favorable by the investigator.
병용 치료를 계속할 수 있다. 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 경우 환자는 치료를 중단해야 한다.Combination therapy can be continued. Patients should discontinue treatment if there is unacceptable toxicity or loss of clinical benefit as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical status.
구체적인 연구 목적 및 해당 평가변수를 표 78 및 표 79에 요약한다. The specific study objectives and corresponding endpoints are summarized in Tables 78 and 79.




ADA = 항약물 항체; CR = 완전 반응; DOR = 반응 기간; iRECIST = 면역 RECIST; NCI CTCAE v4.0 = 미국 국립 암연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0; OS = 전체 생존; PFS = 무진행 생존; PK = 약동학; PR = 부분 반응; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1.ADA = anti-drug antibody; CR = complete response; DOR = duration of response; iRECIST = immune RECIST; NCI CTCAE v4.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0; OS = overall survival; PFS = progression-free survival; PK = pharmacokinetics; PR = partial response; RECIST v1.1 = Criteria for Response Evaluation of Solid Tumors, Version 1.1.



ADA = 항약물 항체; CR = 완전 반응; DOR = 반응 기간; iRECIST = 면역 RECIST; NCI CTCAE v4.0 = 미국 국립 암연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0; OS = 전체 생존; PFS = 무진행 생존; PK = 약동학; PR = 부분 반응; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1.ADA = anti-drug antibody; CR = complete response; DOR = duration of response; iRECIST = immune RECIST; NCI CTCAE v4.0 = National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0; OS = overall survival; PFS = progression-free survival; PK = pharmacokinetics; PR = partial response; RECIST v1.1 = Criteria for Response Evaluation of Solid Tumors, Version 1.1.
D.D. 평가 및 모니터링Assessment and monitoring
모든 환자는 연구 전반에 걸쳐 이상 반응에 대해 면밀히 모니터링되며, 이상 반응은 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0(NCI CTCAE v4.0)에 따라 등급이 매겨진다. 환자는 처음 54주 동안은 9주마다(사이클 1의 1일차에 시작함) 종양 평가를 받고, 그 후로는 12주마다 종양 평가를 받는다. 반응은All patients are closely monitored for adverse events throughout the study, and adverse events are graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). Patients receive tumor assessments every 9 weeks (starting on Day 1 of Cycle 1) for the first 54 weeks and then every 12 weeks thereafter. the reaction is
시험자가 RECIST v1.1(Eisenhauer et al., Eur J Cancer, 45: 228-247, 2009))을 사용하여 평가한다. 실험군에서 임상 활동성이 나타나면, 시험의뢰자는 중앙 판독 시설의 평가를 위해 해당 군에 대한 종양 평가 스캔을The investigator evaluates using RECIST v1.1 (Eisenhauer et al., Eur J Cancer, 45: 228-247, 2009). If clinical activity appears in the experimental group, the sponsor will conduct a tumor assessment scan for that group for evaluation by a central reading facility.
제출하도록 요청할 수 있다.You may request to submit.
기준선 종양 조직 샘플은 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 시험자가 생검을 시행할 수 없다고 판단하는 경우, 보관 종양 조직을 제출할 수 있다. 또한, (시험자가 임상적으로 가능하다고 판단하는 경우) 종양 조직은 시험자에 의해 결정된 허용할 수 없는 독성 또는 임상적 이점의 상실로 인해 병기 1을 중단한 환자로부터 수집된다. 이 샘플과 연구 기간 동안 수집된 혈액 샘플은 바이오마커 연구에 활용된다.Baseline tumor tissue samples are preferably collected from all patients via biopsies performed at the start of the study. If the investigator determines that a biopsy cannot be performed, the archived tumor tissue may be submitted. In addition, (if the investigator determines that it is clinically feasible), tumor tissue is collected from patients who have discontinued Stage 1 due to unacceptable toxicity or loss of clinical benefit as determined by the investigator. These samples and blood samples collected during the study period are used for biomarker studies.
아테졸리주맙 및 기타 치료제의 약동학(PK) 특성 및/또는 면역원성을 특성화하기 위해, 연구 치료의 투여 이전 및 동안의 다양한 시점에서 혈액 샘플을 획득한다.To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points prior to and during administration of study treatment.
E. 연구 종료 및 연구 기간E. Study End and Study Duration
연구 종료는 전화 또는 현장 방문에 의해 수행되는 생존 추적 방문을 포함하여 두 병기 모두에서 마지막 환자가 마지막 방문을 완료한 날짜로 정의된다.Study end is defined as the date the last patient completed the last visit in both arms, including survival follow-up visits performed by phone or site visit.
제1 환자의 스크리닝부터 연구 종료까지의 총 연구 기간은 약 3~5년이다.The total study duration from screening of the first patient to study termination is approximately 3-5 years.
실시예 21. WO39613 mUC 연구를 위한 재료 및 방법Example 21. WO39613 Materials and Methods for mUC Study
A.A. 병기 1의 포함 기준Inclusion criteria for stage 1
환자는 병기 1에 대한 자격을 갖추기 위해 아래에 요약된 기준을 모두 충족해야 한다.Patients must meet all of the criteria outlined below to be eligible for Stage 1.
·사전 동의서에 서명할 당시의 연령 18세 이상・Age 18 or older at the time of signing the informed consent form
·시험자가 결정한 기대 수명 ≥ 3개월.· Life expectancy ≥ 3 months as determined by the investigator.
·조직학적으로 보고된 국소 진행성(T4b, 임의의 N; 또는 임의의 T, N2-N3) 또는 전이성 UC(M1, 병기 IV)(신우, 요관, 방광 및 요도를 포함하는 요로의 TCC 또는 요로상피 세포 암종이라고도 명명함). 혼합 조직을 가진 환자는 지배적인 이행 세포 패턴을 가져야 한다. 국소 진행성 방광암은 골반 측벽 또는 인접한 내장의 침윤(임상 병기 T4b) 또는 부피가 큰Histologically reported locally advanced (T4b, any N; or any T, N2-N3) or metastatic UC (M1, stage IV) (TCC or urothelium of the urinary tract including the renal pelvis, ureter, bladder and urethra) Also called cell carcinoma). Patients with mixed tissue should have a dominant transitional cell pattern. Locally advanced bladder cancer is characterized by infiltration of the side walls of the pelvis or adjacent intestines (clinical stage T4b) or bulky
결절 전이(N2-N3)를 기준으로 수술이 불가능해야 한다.Surgery should not be possible based on nodular metastasis (N2-N3).
·중앙 검사를 통한 PD-L1 및/또는 추가 바이오마커 상태의 결정에 적합한 대표적인 종양 표본의 가용성. 기준선 종양 조직 샘플은 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. Availability of representative tumor specimens suitable for determination of PD-L1 and/or additional biomarker status via central examination. Baseline tumor tissue samples are preferably collected from all patients via biopsies performed at the start of the study.
파라핀 블록의 포르말린 고정 파라핀 포매(FFPE) 종양 표본(바람직함) 또는 염색되지 않은 갓 절단된 연속 절편을 포함하는 적어도 16개의 슬라이드를 관련 병리 보고서와 함께 제출해야 한다. 10-15개의 슬라이드만 사용할 수 있는 경우, 환자는 여전히 연구에 대해 적격일 수 있다. 종양 조직은 전체 및 생존 가능한 종양 함량을 기반으로 하여 품질이 양호해야 한다.At least 16 slides containing either formalin-fixed paraffin-embedded (FFPE) tumor specimens in paraffin blocks (preferred) or unstained, freshly excised serial sections should be submitted with relevant pathology reports. If only 10-15 slides are available, the patient may still be eligible for the study. Tumor tissue should be of good quality based on total and viable tumor content.
미세 바늘 흡입, 칫솔질, 흉막 삼출액의 세포 펠렛, 골 전이, 및 세척 샘플은 허용하지 않는다. 코어-바늘 생검 표본의 경우, 평가를 위해 최소 3개의 코어를 제출해야 한다. 사용 가능한 코어가 3개 미만인 환자는 여전히 적격일 수 있다. TURBT 표본은 국소 병리학적 검토에 의해 확인된 방광 종양의 근육 침습성 성분(즉, T2 이상)을 포함해야 한다. TURBT 표본에 근육 침습성 성분이 포함되어 있지 않은 경우, 방광 절제술/신장 절제술 또는 전이성 확산 시 획득한 표본(즉, 전이성 병변의 표본)이 무작위 배정 이전에 요구된다.Fine needle aspiration, brushing, cell pellets in pleural effusion, bone metastases, and wash samples are not permitted. For core-needle biopsy specimens, a minimum of three cores must be submitted for evaluation. Patients with less than 3 cores available may still be eligible. TURBT specimens should contain a muscle-invasive component (ie, T2 or greater) of bladder tumors confirmed by local pathological review. Specimens obtained during cystectomy/nephrectomy or metastatic spread (ie, specimens from metastatic lesions) are required prior to randomization, unless the TURBT specimen contains a muscle-invasive component.
·수술 불가능, 국소 진행성 또는 전이성 UC 또는 질병 재발에 대한 1개 이하의 백금 함유 요법(예컨대, GC, MVAC, CarboGem)을 통한 치료 동안 또는 이후의 질병 진행. 요법은 적어도 2 사이클의 백금 함유 요법을 받는Disease progression during or after treatment with 1 or less platinum-containing therapies (eg, GC, MVAC, CarboGem) for inoperable, locally advanced or metastatic UC or disease recurrence. The regimen includes at least 2 cycles of platinum-containing therapy.
환자로 정의된다. 이전에 보조/신보조 화학요법을 받고 백금 함유 보조/신보조 요법으로 치료 후 12개월 이내에 진행한 환자는 2라인 환자로 간주된다. 환자는 진행성 또는 전이성 UC에 대해 이전에 2개 이하의 치료 요법(필요한 백금계 요법 포함)을 받았을 수 있다. 환자는 모든 이전 요법(들) 동안 또는 이후에 질병 진행을 나타내야 한다. 화학방사선 요법 이후 질병 진행이 있는 환자는 이전 방사선요법 포트 외부에서 진행을 나타내야 한다.defined as a patient. Patients who have previously received adjuvant/neoadjuvant chemotherapy and progressed within 12 months of treatment with platinum-containing adjuvant/neoadjuvant therapy are considered line 2 patients. The patient may have previously received no more than 2 treatment regimens (including required platinum-based therapy) for advanced or metastatic UC. The patient must show disease progression during or after all previous therapy(s). Patients with disease progression following chemoradiation should show progression outside the previous radiotherapy port.
B.B. 병기 1 및 병기 2의 포함 기준Inclusion Criteria for Stage 1 and Stage 2
환자는 병기 1 또는 병기 2에 대한 자격을 갖추기 위해 아래에 요약된 기준을 모두 충족해야 한다.Patients must meet all of the criteria outlined below to be eligible for either Stage 1 or Stage 2.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
14일 이내에 획득한 적절한 혈액 및 종말 기관 기능:Adequate blood and terminal organ function achieved within 14 days:
- ANC ≥ 1.5 x 109/L(1500/μL), 과립구 집락 자극 인자(G-CSF) 지원 없음.- ANC ≥ 1.5 x 10 9 /L (1500/μL), no granulocyte colony stimulating factor (G-CSF) support.
- WBC 수 ≥2.5 x 109/L(2500/μL).- Number of WBCs ≥2.5 x 10 9 /L (2500/μL).
- 림프구 수 ≥0.5 x 109/L(500/μL).- Lymphocyte count ≥0.5 x 10 9 /L (500/μL).
- 혈소판 수 ≥100 x 109/L(100,000/μL), 수혈 없음.- Platelet count ≥100 x 10 9 /L (100,000/μL), no transfusion.
- 헤모글로빈 ≥90 g/L(9.0 g/dL).- Hemoglobin ≥90 g/L (9.0 g/dL).
환자는 수혈을 받을 수 있다; 그러나, 수혈은 적격성에 대한 선별 실험실 검사 후 2주 이내에 허용되지 않는다.The patient may receive a blood transfusion; However, transfusions are not permitted within 2 weeks of screening laboratory testing for eligibility.
에리트로포이에틴 생성이 낮은 단발성 신장 또는 만성 신장 질환이 있는 환자는 에리트로포이에틴 자극제를 사용할 수 있다.Erythropoietin stimulants may be used in patients with episodic or chronic kidney disease with low erythropoietin production.
- AST, ALT, 및 알칼리성 인산분해효소(ALP) ≤2.5 x 정상 상한치(ULN), 다음은 예외임:- AST, ALT, and alkaline phosphatase (ALP) ≤2.5 x upper limit of normal (ULN), with the following exceptions:
간 전이가 보고된 환자: AST 및/또는 ALT ≤ 5 x ULNPatients with reported liver metastases: AST and/or ALT ≤ 5 x ULN
문서로 기록된 간 또는 골 전이를 가진 환자: ALP ≤ 5 x ULN.Patients with documented liver or bone metastases: ALP ≤ 5 x ULN.
- 빌리루빈 ≤ 1.5 x ULN, 다음은 예외임:- Bilirubin ≤ 1.5 x ULN, with the following exceptions:
공지의 길버트병 환자: 빌리루빈 수준 ≤ 3 x ULN.Known Gilbert's disease patients: bilirubin levels ≤ 3 x ULN.
- 알부민 ≥25 g/L(2.5 g/dL).- Albumin ≥25 g/L (2.5 g/dL).
- 크레아티닌 청소율 ≥ 30 mL/분(콕크로프트-골트(Cockcroft-Gault) 공식을 사용하여 계산됨).- Creatinine clearance ≥ 30 mL/min (calculated using the Cockcroft-Gault formula).
- 치료적 항응고제를 투여받지 않는 환자의 경우:- For patients not receiving therapeutic anticoagulants:
PTT 또는 aPTT ≤1.5 x ULNPTT or aPTT ≤1.5 x ULN
PT 또는 INR < 1.5 x ULN.PT or INR < 1.5 x ULN.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
C.C. 병기 2의 선정 기준Selection criteria for stage 2
환자는 병기 2에 대한 자격을 갖추기 위해 다음 기준을 모두 충족해야 한다:Patients must meet all of the following criteria to be eligible for Stage 2:
·아테졸리주맙 대조군 환자: 대조군 치료를 받는 동안 시험자가 결정한 임상적 이점의 상실 후 3개월 이내에 병기 2 치료를 개시할 수 있는 능력.Atezolizumab control patients: ability to initiate Stage 2 treatment within 3 months of loss of investigator-determined clinical benefit while receiving control treatment.
·병기 1 동안 실험군에 속한 환자: 병기 1 치료를 받는 동안 시험자가 결정한 아테졸리주맙과 관련이 없는 허용할 수 없는 독성 또는 임상적 이점의 상실을 경험한 후 3개월 이내에 병기 2 치료를 개시할 수 있는 능력.Patients in the experimental arm during Stage 1: cannot initiate Stage 2 treatment within 3 months of experiencing an investigator-determined unacceptable toxicity or loss of clinical benefit unrelated to atezolizumab while receiving treatment at Stage 1. ability to have.
·병기 1 중단 시 수행된 생검에서 채취된 종양 표본의 가용성.Availability of tumor specimens from biopsies performed at stage 1 discontinuation.
D.D. 배제 기준Exclusion Criteria
다음 기준 중 어느 하나에 부합하는 환자는 병기 1 및 병기 2 동안 등록에서 제외된다. 제외 기준의 사건 등급은 NCI CTCAE v4.0을 기반으로 한다.Patients meeting any of the following criteria will be excluded from enrollment during Stages 1 and 2. Event ratings for exclusion criteria are based on NCI CTCAE v4.0.
병기 1의 제외 기준Stage 1 exclusion criteria
다음 기준 중 어느 하나에 부합하는 환자는 병기 1로부터 제외된다:Patients meeting any of the following criteria are excluded from Stage 1:
T 세포 공동 자극 요법 또는 항-TLA-4, 항-PD-1 및 항-PD-L1 치료 항체를 포함하는 CPI를 사용한 이전 치료.Previous treatment with T cell co-stimulation therapy or CPI comprising anti-TLA-4, anti-PD-1 and anti-PD-L1 therapeutic antibodies.
폴리(아데노신 디포스페이트[ADP]-리보스) 폴리머라제(PARP) 억제제, 넥틴-4 표적화제, 신호 조절 단백질 α-표적화제, TIGIT 표적화제, Trop-2 표적화제, FAP 지시 요법, 4-1BB(CD137) 지시 요법 또는 토포이소머라제 1 억제제를 사용한 치료를 포함하는 프로토콜 지정 연구 치료 중 어느 하나를 통한 이전 치료.Poly(adenosine diphosphate [ADP]-ribose) polymerase (PARP) inhibitor, nectin-4 targeting agent, signal regulatory protein α-targeting agent, TIGIT targeting agent, Trop-2 targeting agent, FAP directed therapy, 4-1BB ( CD137) prior treatment with either directed therapy or protocol directed study treatment including treatment with a topoisomerase 1 inhibitor.
![]()
![]()
![]()
![]()
- 골 전이 또는 연조직 병변에 대한 완화 방사선요법은 기준선 영상화 >14일 전에 완료해야 한다.- Palliative radiotherapy for bone metastases or soft tissue lesions should be completed >14 days prior to baseline imaging.
- 호르몬 대체 요법 또는 경구 피임약 - Hormone replacement therapy or oral contraceptives
![]()
![]()
병기 1 및 병기 2의 제외 기준Exclusion Criteria for Stage 1 and Stage 2
다음 기준 중 어느 하나에 부합하는 환자는 병기 1 및Patients meeting any of the following criteria are stage 1 and
병기 2로부터 제외된다:Excluded from Stage 2:
![]()
![]()
![]()
![]()
![]()
![]()
급성 저용량 전신 면역억제 약물 또는 1회 펄스 용량의 전신 면역억제 약물(예컨대, 조영제 알레르기에 대한 코르티코스테로이드 48시간)을 투여받은 환자는 연구에 적격이다.Patients receiving an acute low-dose systemic immunosuppressive drug or a single pulsed dose of a systemic immunosuppressive drug (eg, corticosteroids for contrast allergy 48 hours) are eligible for the study.
무기질 코르티코이드(예컨대, 플루드로코르티손), 만성 폐쇄성 폐질환 또는 천식에 대한 코르티코스테로이드, 또는 기립성 저혈압 또는 부신피질 기능부전에 대한 저용량 코르티코스테로이드를 투여받은 환자는 연구에 적격이다.Patients receiving mineralocorticoids (eg, fludrocortisone), corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenocortical insufficiency are eligible for study.
![]()
![]()
![]()
![]()
![]()
![]()
등록 전에 적절한 경우 국소 치료를 고려해야 한다.Topical treatment should be considered when appropriate prior to enrollment.
![]()
![]()
![]()
![]()
- RECIST v1.1에 따라 측정 가능한 질병은 CNS 외부에 있어야 한다.- According to RECIST v1.1, measurable diseases must be outside the CNS.
- 환자는 두개내 출혈 또는 척수 출혈의 병력이 없다.- The patient has no history of intracranial hemorrhage or spinal cord hemorrhage.
- 환자는 연구 치료 개시 전 7일 이내에 정위 방사선요법, 연구 치료 개시 전 14일 이내에 전뇌 방사선요법, 또는 연구 치료 개시 전 28일 이내에 신경외과적 절제술을 받지 않았다.-Patient had not undergone stereotactic radiotherapy within 7 days prior to study treatment initiation, whole brain radiotherapy within 14 days prior to study treatment initiation, or neurosurgical resection within 28 days prior to study treatment initiation.
- 환자는 CNS 질환에 대한 요법으로서 지속적인 코르티코스테로이드 필요성이 없다. 안정적인 용량의 항경련제 요법이 허용된다.- The patient has no need for ongoing corticosteroids as therapy for CNS disease. Stable dose anticonvulsant therapy is permitted.
![]()
![]()
![]()
![]()
자가면역 관련 갑상선 기능저하증의 병력이 있고 갑상선 대체 호르몬을 투여받고 있는 환자는 연구에 적격이다. 안정적인 인슐린 요법을 받고 있는 조절된 제1형 당뇨병 환자는 연구에 적격이다. 습진, 건선, 만성 단순 태선 또는 피부과적 징후만 있는 백반증이 있는 환자(예컨대, 건선성 관절염 환자는 제외됨)는 다음 조건이 모두 충족되는 경우 연구에 적격이다:Patients with a history of autoimmune-related hypothyroidism and taking thyroid replacement hormone are eligible for the study. Patients with controlled type 1 diabetes on stable insulin therapy are eligible for the study. Patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with dermatological signs only (e.g., excluding patients with psoriatic arthritis) are eligible for study if all of the following conditions are met:
- 발진은 체표면적의 10%를 차지해야 한다.- The rash should occupy 10% of the body surface area.
- 질병은 기준선에서 잘 조절되며, 저역가 국소 코르티코스테로이드만 필요하다.- Disease is well controlled at baseline and requires only low titer topical corticosteroids.
- 지난 12개월 이내에 소랄렌 + 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고역가 또는 경구 코르티코스테로이드를 필요로 하는 기저 조건의 급성 악화가 발생하지 않았다.- No acute exacerbation of underlying conditions requiring psoralen plus ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high titers or oral corticosteroids within the past 12 months.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
(예컨대, 요로 감염 또는 만성 폐쇄성 폐질환 악화를 예방하기 위해) 예방적 항생제를 투여받는 환자는 연구에 적격이다.Patients receiving prophylactic antibiotics (eg, to prevent exacerbation of urinary tract infection or chronic obstructive pulmonary disease) are eligible for study.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
병기 1 동안 아테조+티라 군에 대한 추가적인 제외 기준 Additional Exclusion Criteria for the Artezo + Tyra group during Stage 1
다음 기준 중 어느 하나를 충족하는 환자는 병기 1 동안 아테조+티라 군에서 제외된다.Patients who meet any of the following criteria are excluded from the atezo+tyra group for stage 1.
![]()
![]()
E.E. 허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
2 사이클의 치료 후, 종양 표적 병변의 평가를 방해하지 않는 한 고식적 방사선요법이 허용된다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 아테졸리주맙 치료는 고식적 방사선요법 동안 계속될 수 있다.After 2 cycles of treatment, palliative radiotherapy is allowed as long as it does not interfere with the evaluation of the tumor target lesion (eg, the lesion to be irradiated must not be the only site of measurable disease). Atezolizumab treatment may be continued during palliative radiotherapy.
![]()
![]()
3개 이하의 병변을 조절하기 위해 국소 요법이 필요한 혼합 반응을 경험하는 환자는 의학 모니터 요원의 승인을 받은 후에도 여전히 연구 치료를 계속하기에 적격일 수 있다. 표적 병변에 대한 국소 요법을 받는 환자는 더 이상 방사선학적 반응에 대해 평가할 수 없지만Patients experiencing mixed reactions requiring topical therapy to control 3 or fewer lesions may still be eligible to continue study treatment after approval from a medical monitor. Patients receiving topical therapy for the target lesion can no longer be evaluated for radiological response, but
진행에 대해서는 계속 평가할 수 있다.Progress can be evaluated continuously.
항히스타민제, 해열제 및/또는 진통제를 사용한 사전 투약은 시험자의 재량에 따라 2차 및 후속 아테졸리주맙 주입에 대해서만 투여될 수 있다. Prior dosing with antihistamines, antipyretics and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab at the discretion of the investigator.
주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 보조 요법(예컨대, 보조 산소 및 β2 아드레날린 작용제)으로 관리해야 한다.Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related reactions presenting with dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea should be managed with adjuvant therapy as clinically indicated (e.g., adjuvant oxygen and β 2 adrenergic agonists). .
D. 아테졸리주맙 군의 재료 및 방법D. Materials and Methods of the Atezolizumab Group
아테졸리주맙은 승인된 용량(TECENTRIQ® U.S. Package Insert; TECENTRIQ® SmPC)인 3주마다 1200 mg 고정 용량(Q3W)(각 21일 사이클의 1일차에 1200 mg)으로 투여된다(표 80). 항종양 활성은 1 내지 20 mg/kg Q3W 범위의 용량에 걸쳐 관찰되었다. 연구 PCD4989g에서, 아테졸리주맙의 최대 내약성 용량은 도달되지 않았으며, 어떤 용량에서도 용량 제한 독성이 관찰되지 않았다. 1200 mg Q3W의 고정 용량(15 mg/kg Q3W의 평균 체중 기반 용량에 해당)은 비임상 연구(Deng et al., MAbs, 8: 593-603, 2016)와 이용 가능한 임상 약동학, 유효성 및 안전성 데이터를 기반으로 선택되었다.Atezolizumab is administered at an approved dose (TECENTRIQ® U.S. Package Insert; TECENTRIQ® SmPC), a 1200 mg fixed dose (Q3W) every 3 weeks (1200 mg on Day 1 of each 21-day cycle) (Table 80). Antitumor activity was observed over doses ranging from 1 to 20 mg/kg Q3W. In study PCD4989g, the maximally tolerated dose of atezolizumab was not reached and no dose limiting toxicity was observed at any dose. A fixed dose of 1200 mg Q3W (corresponding to a mean weight-based dose of 15 mg/kg Q3W) has been compared with nonclinical studies (Deng et al., MAbs, 8: 593-603, 2016) and available clinical pharmacokinetic, efficacy and safety data. was selected based on
아테졸리주맙 대조군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 치료를 받는다. 치료 배정 후 7일 이내에 치료를 개시해야 한다. 환자는 사이클 3 이후에 수술을 받는다; 사이클 4의 치료는 수술 후 4주 내지 6주에 다시 개시되어야 한다.Atezolizumab control patients had unacceptable toxicity or clinical findings as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical condition (e.g., worsening of symptoms such as disease-related pain). Treatment is continued until loss of benefit is achieved. Treatment must be initiated within 7 days of treatment assignment. Patients undergo surgery after cycle 3; Cycle 4 treatment should be resumed 4 to 6 weeks after surgery.

아테졸리주맙의 투여는 훈련된 직원과 잠재적인 심각한 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 설정에서 수행된다. Administration of atezolizumab is performed in a monitoring setting with trained staff and immediate access to appropriate equipment and medications to manage potentially serious reactions.
아테졸리주맙 주입은 표 81에 요약된 지침에 따라 투여된다.Atezolizumab infusion is administered according to the guidelines summarized in Table 81.

F.F. 아테졸리주맙 + 티라골루맙 군의 재료 및 방법Materials and Methods of the Atezolizumab + Tiragolumab Group
아테졸리주맙은 전술한 바와 같이 투여된다(표 81 참조). Atezolizumab is administered as described above (see Table 81).
티라골루맙은 600 mg 고정 용량으로 IV로 Q3W(각 21일 사이클의 1일차에 600 mg) 투여된다. 600 mg 고정 용량으로 IV로 Q3W은 단일 제제 티라골루맙 또는 티라골루맙과 병용한 아테졸리주맙을 이용한 결합된 Ia상/Ib상 연구 GO30103의 이용 가능한 임상 PK, 유효성 및 안전성 데이터를 기반으로 선택되었다. 단일 제제로서 티라골루맙을 사용한 연구의 Ia상 부분에서, MTD에 도달하지 못했으며, 용량 증량에서 DLT가 관찰되지 않았다. 임상Tiragolumab is administered as a fixed dose of 600 mg IV Q3W (600 mg on Day 1 of each 21-day cycle). Q3W as a 600 mg fixed dose IV was selected based on available clinical PK, efficacy and safety data from the combined Phase Ia/Ib study GO30103 with either single agent tiragolumab or atezolizumab in combination with tiragolumab . In the Phase Ia portion of the study using tyragolumab as a single agent, MTD was not reached and no DLT was observed at dose escalation. clinical
마감일 현재, 티라골루맙에 대한 항약물 항체(ADA)는 모든 용량 수준에 걸쳐 Ia상 또는 Ib상 부분에서 드물었다. 400 mg에서 시작하는 티라골루맙 용량에서, 연구의 Ia상 부분에서 장기간 안정한 질병이 환자에게서As of the deadline, antidrug antibodies (ADA) to tiragolumab were rare in the Phase Ia or Ib portion across all dose levels. At tiragolumab doses starting at 400 mg, long-term stable disease was observed in patients in the Phase Ia portion of the study.
관찰되었다. 티라골루맙과 병용한 아테졸리주맙을 이용한 연구의 Ib상 부분에서, MTD에 도달하지 못했다. 방사선학적 부분 반응에 의해 측정된 항종양 활성은 1200 mg의 아테졸리주맙과 병용한 30 mg에서 시작하여 최대 600 mg 범위의 티라골루맙 용량에 걸쳐 관찰되었다.observed. In the Phase Ib portion of the study with atezolizumab in combination with tiragolumab, MTD was not reached. Antitumor activity, as measured by radiological partial response, was observed over tiragoluumab doses ranging up to 600 mg starting at 30 mg in combination with 1200 mg atezolizumab.
아테졸리주맙 + 티라골루맙 군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 표 82에 요약된 치료를 받는다. 환자는 사이클 3 이후에 수술을 받는다; 사이클 4의 치료는 수술 후 4주 내지 6주에 다시 개시된다. Patients in the atezolizumab + tiragolumab arm were considered unacceptable as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as disease-related pain). Receive treatment summarized in Table 82 until loss of toxicity or clinical benefit. Patients undergo surgery after cycle 3; Cycle 4 treatment is resumed 4-6 weeks post surgery.

티라골루맙은 표 83에 기재된 바와 같이 각 21일 사이클의 1일차에 600 mg 고정 용량으로 IV 주입에 의해 투여되며, 주입 후 관찰 기간을 갖는다. 티라골루맙의 투여는 훈련된 직원과 잠재적인 심각한 반응들을 관리하기에 적절한 장비 및 의약품에 즉시 접근할 수 있는 모니터링 설정에서 수행된다. Tiragolumab is administered by IV infusion at a fixed dose of 600 mg on Day 1 of each 21-day cycle, as described in Table 83, with a post-infusion observation period. Administration of tiragolumab is performed in a monitoring setting with trained staff and immediate access to appropriate equipment and medications to manage potentially serious reactions.

WO39613 mUC 연구에 대한 안전성 평가를 실시예 18에 기재된 바와 같이 수행하였다. A safety assessment for the WO39613 mUC study was performed as described in Example 18.
실시예 22. WO39613 mUC 연구에 대한 통계적 고려 사항 및 분석 계획Example 22. Statistical considerations and analysis plan for WO39613 mUC study
WO39613 분석은 연구 중단을 통해 수집한 환자 데이터를 기반으로 한다. 달리 명시되지 않는 경우, 유효성 분석은 배정된 치료 요법에 대해 각 약물의 적어도 1회 용량이 투여된 모든 환자로 정의되는 유효성 평가 가능한 집단에 기반하며, 안전성 분석은 연구 치료를 받는 모든 환자로 정의되는 안전성 평가 가능한 집단에 기반한다.WO39613 analysis is based on patient data collected through study discontinuation. Unless otherwise specified, efficacy analyzes are based on an efficacy evaluable population defined as all patients receiving at least one dose of each drug for the assigned treatment regimen, and safety analyzes are based on all patients receiving study treatment. It is based on a population that can be evaluated for safety.
분석 결과는 환자가 실제로 받는 치료와 해당되는 경우 병기(병기 1 또는 병기 2)별로 요약된다. 데이터는 샘플 크기에 따라 설명되고 요약된다. 연속 변수는 평균, 표준 편차, 중앙값, 최소값 및 최대값을 사용하여 요약된다. 범주형 변수는 개수 및 백분율을 사용하여 요약된다. 목록은 표본 크기가 작은 경우 표 대신 사용된다.The results of the analysis are summarized by the treatment actually received by the patient and, if applicable, by stage (Stage 1 or Stage 2). Data are described and summarized according to sample size. Continuous variables are summarized using mean, standard deviation, median, minimum and maximum values. Categorical variables are summarized using counts and percentages. Lists are used instead of tables when the sample size is small.
A.A. 샘플 크기의 결정Determination of sample size
WO39613 연구는 가설 분석을 위해 명백한 분석력 및 제1종 오류를 고려하도록 설계되지WO39613 study was not designed to account for apparent analytical power and type I error for hypothesis analysis.
않았다 대신, 상기 연구는 백금 함유 요법 동안 또는 이후에 진행된 국소 진행성 또는 전이성 UC 환자에게 투여시 면역요법 기반 치료 조합에 대한 예비 유효성, 안전성 및 PK 데이터를 얻기 위해 설계되었다. 약 160명 내지 385명의 환자가 연구 기간 동안 대조군 및 실험군에 무작위로 배정된다.Instead, this study was designed to obtain preliminary efficacy, safety, and PK data for an immunotherapy-based treatment combination when administered to patients with locally advanced or metastatic UC who progressed during or after platinum-containing therapy. Approximately 160 to 385 patients are randomly assigned to control and experimental groups for the duration of the study.
B.B. 유효성 분석Validity analysis
일차 유효성 평가변수 Primary efficacy endpoint
일차 유효성 평가변수는 RECIST v1.1에 따라 시험자가 결정하고 상기와 같이 정의되는 병기 1 동안의 객관적 반응률(ORR)이다(표 78 참조). 반응 평가가 누락되거나 존재하지 않는 환자는 무반응자로 분류된다.The primary endpoint is the objective response rate (ORR) during stage 1 as determined by the investigator according to RECIST v1.1 and defined as above (see Table 78). Patients with missing or non-existent response assessments are classified as non-responders.
CR 또는 PR을 보인 환자의 비율로 정의되는 ORR은 90% CI(클로퍼-피어슨(Clopper-Pearson) 직접 확률법)로 각 군에 대해 계산된다. 또한, 실험군과 대조군 사이의 ORR 차이가 90% CI로 계산된다. CI는 표본 크기에 따라 직접 확률법 또는 왈드(Wald) 방법으로 추정된다.ORR, defined as the proportion of patients with CR or PR, is calculated for each group with a 90% CI (Clopper-Pearson direct probability method). In addition, the ORR difference between the experimental group and the control group is calculated as 90% CI. CI is estimated by direct probability method or Wald method according to the sample size.
이차 유효성 평가변수 secondary efficacy endpoint
이차 유효성 평가변수는 상기에서 정의된 바와 같은 병기 1 동안의 무진행 생존(PFS), OS, 특정 시점(예컨대, 12개월)에서의 OS, DOR, 및 질병 통제이다(표 78 참조). PFS, DOR 및 질병 통제는 RECIST v1.1에 따라 시험자가 결정한다. Secondary efficacy endpoints are progression-free survival (PFS), OS, OS at a specific time point (eg, 12 months), DOR, and disease control during Stage 1 as defined above (see Table 78). PFS, DOR and disease control are determined by the investigator according to RECIST v1.1.
DOR은 CR 또는 PR을 보인 유효성 평가 가능한 환자에 대해 도출된다.A DOR is derived for evaluable patients with CR or PR.
연구 단계에서 기록된 질병 진행 또는 사망이 없는 환자의 경우, PFS 및 DOR은 마지막 종양 평가 당일에 검열 및 삭제된다. OS 분석 시점에서 계속 살아 있는 환자는 생존이 공지된 마지막 날짜에 중도 절단된다.For patients with no documented disease progression or death during the study phase, PFS and DOR are censored and cleared on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day survival is known.
카플란-마이어 방법은 브룩마이어 및 크라울리 방법을 사용하여 구성된 90% CI로 PFS, OS 및 DOR의 중앙값을 추정하는 데 사용된다. 또한, 특정 시점에서의 OS 비율이 분산의 그린우드 추정치에 기반하여 계산된 90% Ci로 카플란-마이어 방법을 사용하여 추정된다.The Kaplan-Meier method is used to estimate the median of PFS, OS, and DOR with 90% CI constructed using Brookmeier and Crowley methods. In addition, the OS ratio at any point in time is estimated using the Kaplan-Meier method with 90% Ci calculated based on Greenwood estimates of variance.
18주 동안의 안정적인 질병, PR 또는 CR을 보인 환자의 비율로 정의되는 질병 통제율은 클로퍼-피어슨 직접 확률법을 사용하여 추정된 90% CI로 각 치료군에 대해 계산된다Disease control rate, defined as the proportion of patients with stable disease, PR or CR for 18 weeks is calculated for each treatment arm with an estimated 90% CI using the Klopper-Pearson direct probability method.
탐색적 유효성 평가변수 Exploratory validity endpoints
탐색적 유효성 평가변수는 iRECIST에 따라 시험자가 결정한 병기 1 동안의 ORR, PFS, DOR 및 질병 통제; 및 RECIST v1.1 및 iRECIST에 따라 시험자가 결정한 병기 2 동안의 객관적 반응, PFS, DOR 및 질병 통제이다. ORR, PFS, DOR 및 질병 통제는 전술한 동일한 방법을 사용하여 분석된다 DOR은 CR 또는 PR을 보인 유효성 평가 가능한 환자에 대해 도출된다.Exploratory efficacy endpoints included ORR, PFS, DOR, and disease control during stage 1 as determined by investigators according to iRECIST; and Investigator-determined objective response, PFS, DOR, and disease control during Stage 2 according to RECIST v1.1 and iRECIST. ORR, PFS, DOR and disease control are analyzed using the same method described above. DOR is derived for evaluable patients with CR or PR.
C.C. 중간 분석Interim analysis
중간 분석은 연구 기간 동안 수행되며, 가장 빠른 중간 분석은 적어도 하나의 실험군이 병기 1 예비 단계에서 등록을 완료하고 환자를 최소 9주 동안 추적한 경우 수행된다. 적절하다고 판단되는 경우 추가 중간 분석을 수행할 수 있다. 사후 확률은 대조군과 비교한 실험군에서의 임상 활동성의 중간 분석을 기반으로 추가 등록을 안내하는 데 사용될 수 있다. 중간 분석에서 실험군의 활동성이 대조군의 활동성보다 높다고 시사되는 경우, 실험군(확장 단계)에 25명의 추가 환자가 더 등록될 수 있다. 이러한Interim analyzes are performed during the study period, and the earliest interim analyzes are performed when at least one experimental group has completed enrollment in the Stage 1 preliminary stage and patients have been followed for at least 9 weeks. Additional interim analyzes may be performed if deemed appropriate. The posterior probability can be used to guide further enrollment based on an interim analysis of clinical activity in the experimental group compared to the control group. If the interim analysis suggests that the activity of the experimental group is higher than that of the control group, 25 additional patients can be enrolled in the experimental group (expansion phase). Such
1b상 임상 시험의 확장 및 종료에 대한 최종 결정은 전반적인 유익성-위해성 균형과, 새로운 외부 정보뿐만 아니라 시간-대-사건 평가변수 및 안전성 데이터를 비롯한 데이터 전체를 고려하여 이루어진다.Final decisions about expansion and termination of Phase 1b clinical trials are made taking into account the overall benefit-risk balance and data as a whole, including time-to-event endpoints and safety data, as well as new external information.
또한, 분석은 약 15명의 환자가 병기 2 치료군에 등록되고 최소 9주 동안 추적된 후에 수행된다. 병기 2 치료군에서 임상 활동성이 관찰되지 않으면, 해당 군의 추가 등록이 중단된다.In addition, analysis is performed after approximately 15 patients have been enrolled in the Stage 2 treatment group and followed for at least 9 weeks. If clinical activity is not observed in the Stage 2 treatment arm, further enrollment in that arm will be discontinued.
D.D. 기타 분석Other analysis
안전성 분석, 약동학 분석, 면역원성 분석 및 바이오마커 분석을 실시예 19에 기재된 바와 같이 수행하였다. Safety analysis, pharmacokinetic analysis, immunogenicity analysis and biomarker analysis were performed as described in Example 19.
실시예 23. 국소 진행성 또는 전이성 식도암을 가진 환자를 대상으로 면역요법 기반 치료 조합의 유효성과 안전성을 평가하는 Ib/II상, 공개 라벨, 다기관, 무작위, 포괄적 연구Example 23. A Phase Ib/II, Open Label, Multicenter, Randomized, Comprehensive Study Evaluating the Efficacy and Safety of Immunotherapy-Based Treatment Combinations in Patients with Locally Advanced or Metastatic Esophageal Cancer
A.A. 연구 설계의 개요Overview of Study Design
YO39609는 식도암 환자에서 면역요법 기반 치료 조합의 유효성, 안전성 및 약동학을 평가하는 Ib/II상, 라벨 공개, 다기관, 무작위 우산형 연구이다. 이 연구는 식도암 환자에게 투여시 면역요법 기반 치료 조합에 대한 예비 유효성, 안전성 및 PK 데이터를 얻기 위해 설계되었다. 또한, 이 연구는 새로운 치료법이 나오면 새로운 치료군을 개방하거나, 최소한의 임상 활동성 또는 허용할 수 없는 독성을 나타내는 기존 치료군을 폐쇄하거나, 환자 집단을 수정할 수 있는 유연성을 갖도록 설계되었다(예컨대, 이전 항암 치료 또는 바이오마커 상태와 관련하여). YO39609 is a Phase Ib/II, open-label, multicenter, randomized umbrella study evaluating the efficacy, safety, and pharmacokinetics of an immunotherapy-based treatment combination in patients with esophageal cancer. This study was designed to obtain preliminary efficacy, safety, and PK data for an immunotherapy-based treatment combination when administered to patients with esophageal cancer. In addition, the study is designed to have the flexibility to open new treatment groups as new treatments become available, close existing treatments that exhibit minimal clinical activity or unacceptable toxicity, or modify patient populations (e.g., previous anticancer treatments). or with respect to biomarker status).
이전에 질병에 대한 전신 치료를 받은 적이 없는 식도암 환자가 이 연구에 등록된다. 적격 환자는 3개의 치료군 중 하나에 무작위 배정된다. 병기 1 동안 질병 진행 또는 허용할 수 없는 독성을 경험한 대조군의 환자는 병기 2에서 다른 치료 요법으로 치료를 계속하기에 적격일 수 있다.Esophageal cancer patients who have not previously received systemic treatment for the disease are enrolled in this study. Eligible patients will be randomized to one of three treatment groups. Control patients who experienced disease progression or unacceptable toxicity during Stage 1 may be eligible to continue treatment with another treatment regimen in Stage 2.
병기 1 치료Stage 1 treatment
병기 1 동안, 식도암 환자는 화학요법 대조군(시스플라틴 + 5-FU) 또는 2개의 실험군 중 하나에 무작위로 배정된다: 티라골루맙 및 화학요법과 병용한 아테졸리주맙(아테조 + 티라골루맙 + 시스플라틴 + 5-FU), 또는 화학요법과 병용한 아테졸리주맙(아테조 + 시스플라틴 + 5-FU). 병기 1의 치료 요법에 대한 세부사항은 표 84에 제공된다. 병기 1의 치료 요법에 대한 세부사항은 표 84에 제공된다.During Stage 1, patients with esophageal cancer are randomly assigned either to a chemotherapy control group (cisplatin + 5-FU) or to one of two experimental groups: tiragolumab and atezolizumab in combination with chemotherapy (atezo + tiragolumab + cisplatin). + 5-FU), or atezolizumab in combination with chemotherapy (Atezo + Cisplatin + 5-FU). Details of the treatment regimen for Stage 1 are provided in Table 84. Details of the treatment regimen for Stage 1 are provided in Table 84.

1L = 1라인; 5-FU = 5-플루오로우라실; 아테조 + 아테졸리주맙; 티라 + 티라골루맙. A 무작위 배정 a 무작위 배정 비율은 등록을 위해 개방되어 있는 실험군의 수에 따라 달라지며(예컨대, 군이 추가되거나 군의 등록이 보류되는 경우, 예비 단계의 결과 분석이 보류됨), 주어진 시간에 35% 이하의 환자가 대조군에 무작위로 배정된다. 무작위 배정 비율은 유망한 임상 활동성을 나타낸 실험군의 등록을 증가시키기 위해 변경될 수 있다. b 시험의뢰자는 주어진 치료군 내에서 등록을 연기하거나 보류하기로 결정할 수 있다. 최소 임상 활동성 또는 허용할 수 없는 독성이 있는 실험군은1L = 1 line; 5-FU = 5-fluorouracil; atezo + atezolizumab; Tira + Tiragolumap. A Randomization a The rate of randomization depends on the number of groups open for enrollment (e.g., if a group is added or enrollment of a group is withheld, preliminary analysis of results is withheld), and at any given time 35 % or fewer patients are randomly assigned to the control group. Randomization rates may be altered to increase enrollment in experimental groups exhibiting promising clinical activity. b The sponsor may decide to defer or withhold enrollment within a given treatment arm. The experimental group with minimal clinical activity or unacceptable toxicity
확장되지 않는다. c 예비 단계 동안 실험군에서 임상 활동성이 관찰되면,does not expand c If clinical activity is observed in the experimental group during the preliminary phase,
확장 단계 동안 약 25명의 추가 환자가 해당 군에 등록된다.About 25 additional patients are enrolled in the group during the expansion phase.
병기 1의 구체적인 연구 목적 및 해당 평가변수를 표 85에 요약한다.Table 85 summarizes the specific study objectives of stage 1 and corresponding endpoints.



ADA = 항약물 항체; DOR = 반응 기간; IC = 면역 세포; IHC = 면역조직화학; iRECIST = 면역 기반 치료제를 위한 수정 RECIST v1.1; PFS = 무진행 생존; PK = 약동학; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1; TC = 종양 세포; TIGIT = Ig 및 ITIM 도메인을 갖는 T 세포 면역수용체ADA = anti-drug antibody; DOR = duration of response; IC = immune cells; IHC = immunohistochemistry; iRECIST = modified RECIST v1.1 for immune-based therapeutics; PFS = progression-free survival; PK = pharmacokinetics; RECIST v1.1 = Response Evaluation Criteria for Solid Tumors, version 1.1; TC = tumor cells; TIGIT = T cell immunoreceptor with Ig and ITIM domains
비고: 한 시점에서의 전체 반응은 RECIST v1.1을 사용하여 시험자가 평가한다.Note: The overall response at one time point is assessed by the investigator using RECIST v1.1.
2개의 실험군의 등록은 예비 단계와 이후 확장 단계의The registration of the two experimental groups was performed in the preliminary phase and in the subsequent expansion phase.
두 단계로 진행된다.It proceeds in two steps.
약 100명 내지 165명의 환자가 병기 1 동안 등록된다. 최대 약 40명의 환자가 예비 단계 동안 2개의 실험군에 등록되어 TIGIT 및 PD-L1 발현이 높은 충분한 수의 환자를 확보하여 이 하위집단 내에서 이점 및 위험 평가를 용이하도록 한다. 예비 단계 동안 실험군에서 임상 활동이 관찰되면, 확장 단계 동안 약 25명의 추가 환자가 해당 군에 등록될 수 있다. 시험의뢰자는 주어진 치료군 내에서 등록을 연기하거나 보류하기로 결정할 수 있다.About 100 to 165 patients are enrolled during Stage 1. Up to approximately 40 patients will be enrolled in the two experimental groups during the preliminary phase to ensure a sufficient number of patients with high TIGIT and PD-L1 expression to facilitate benefit and risk assessment within this subpopulation. If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients can be enrolled in that group during the expansion phase. The sponsor may decide to defer or withhold enrollment within a given treatment arm.
최소 임상 활동성 또는 허용할 수 없는 독성이 있는 실험군은 확장되지 않는다. 프로토콜을 수정하여 연구 중에 새로운 실험군을 추가할 수 있다.Experimental groups with minimal clinical activity or unacceptable toxicity are not expanded. The protocol can be modified to add new experimental groups during the study.
병기 1의 환자는 치료군에 무작위로 배정되고, 무작위 배정 비율은 이용 가능한 실험군의 수에 따라서 달라지며(예컨대, 군이 추가되거나 군의 등록이 보류되는 경우, 예비 단계의 결과 분석이 보류됨), 대조군에 배정될 가능성은 35%를 넘지 않는다. 무작위 배정 비율은 유망한 임상 활동성을 나타낸 실험군의 등록을 증가시키기 위해 변경될 수 있다. 무작위 배정에는 군별 제외 기준이 고려된다. 환자가 특정군에 대해 요약된 제외 기준 중 어느 하나라도 충족하는 경우, 환자는 해당 군에 대해 부적격이다.Patients in Stage 1 are randomly assigned to treatment groups, and the randomization rate depends on the number of available experimental groups (e.g., if a group is added or enrollment in a group is withheld, preliminary analysis of results is withheld); The probability of being assigned to a control group does not exceed 35%. Randomization rates may be altered to increase enrollment in experimental groups exhibiting promising clinical activity. Randomization takes into account group exclusion criteria. If a patient meets any of the exclusion criteria outlined for a particular group, the patient is ineligible for that group.
대조군의 환자는 허용할 수 없는 독성 또는 RECIST v1.1에 따른 질병 진행이 있을 때까지 치료를 받는다. 대조군의 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 치료를 받는다. 암 면역요법(CIT)(예컨대, 아테졸리주맙)을 사용한 T 세포 반응(가성 진행이라고 명명함) 설정에서 면역 세포 침윤으로 인한 종양 부담의 초기 증가 가능성으로 인해, RECIST v1.1에 따른 방사선학적 진행은 실제 질병 진행을 나타내지 않을 수 있다. 허용할 수 없는 독성이 없는 경우, CIT 약물로 치료를 받는 동안 RECIST v1.1에 따른 질병 진행 기준을 충족하는 환자는 다음 기준을 모두 충족하는 경우 연구 치료를 계속할 수 있다:Control patients receive treatment until unacceptable toxicity or disease progression according to RECIST v1.1. Patients in the control group had unacceptable toxicity or clinical benefit as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical condition (e.g., worsening of symptoms such as disease-related pain). Treatment is continued until there is loss. Radiological progression according to RECIST v1.1, due to the potential for an initial increase in tumor burden due to immune cell infiltration in the setting of a T-cell response (termed pseudo-progression) with cancer immunotherapy (CIT) (eg, atezolizumab) may not represent actual disease progression. In the absence of unacceptable toxicity, patients who meet disease progression criteria according to RECIST v1.1 while being treated with CIT drugs may continue on study treatment if all of the following criteria are met:
- 사용 가능한 모든 데이터를 검토한 후 시험자가 결정한 임상적 이점의 증거. - Evidence of clinical benefit as determined by the investigator after reviewing all available data.
- 질병의 명백한 진행을 나타내는 증상 및 징후(새로운 또는 악화되는 고칼슘혈증과 같은 실험실 값을 포함함)의 부재. - Absence of symptoms and signs (including laboratory values such as new or worsening hypercalcemia) indicative of apparent progression of the disease.
- 질병 진행에 기인할 수 있는 ECOG 전신 활동도 감소의 부재. - Absence of reduced ECOG systemic activity that could be attributed to disease progression.
- 프로토콜이 허용하는 의료적 개입으로 관리할 수 없는 중요한 해부학적 부위(예컨대, 연수막 질환)에서 종양 진행의 부재. - Absence of tumor progression in critical anatomical sites (eg, leptomeningeal disease) that cannot be managed with medical interventions permitted by the protocol.
- 초기 질병 진행 시점에 연구 치료를 계속하기 위해 다른 치료 옵션을 연기하는 것을 인정하는 환자의 서면 동의. -Patient 's written consent to adjourn other treatment options to continue study treatment at the time of initial disease progression.
병기 2 치료Stage 2 treatment
RECIST v1.1에 따른 질병 진행을 경험한 대조군의 환자는 적격 기준을 충족하고 병기 2 군이 등록을 위해 개방되어 있는 경우 병기 2 동안 다른 치료 조합을 받는 옵션을 제공받는다. 병기 2 치료 요법은 아테졸리주맙 + 티라골루맙이다.Control patients who experience disease progression according to RECIST v1.1 will be offered the option to receive another treatment combination during Stage 2 if they meet eligibility criteria and Arm 2 is open for enrollment. The stage 2 treatment regimen is atezolizumab plus tiragolumab.
허용할 수 없는 독성을 경험한 대조군의 환자는 의학 모니터 요원의 승인을 받은 후 병기 2 치료에 대해 적격일 수 있다. 병기 2 치료는 환자가 RECIST v1.1에 따른 질병 진행 또는 병기 1에서 허용할 수 없는 독성을 경험한 후 3개월 이내에 시작되어야 하며, 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 계속된다.Control patients who experience unacceptable toxicity may be eligible for stage 2 treatment after approval by a medical monitor. Stage 2 treatment must be initiated within 3 months of the patient experiencing disease progression or stage 1 unacceptable toxicity according to RECIST v1.1, and there is no unacceptable toxicity or loss of clinical benefit as determined by the investigator. continues until
병기 2의 구체적인 연구 목적 및 해당 평가변수를 표 86에 요약한다.Table 86 summarizes the specific study objectives for stage 2 and corresponding endpoints.


ADA = 항약물 항체; DOR = 반응 기간; iRECIST = 면역 기반 치료제를 위한 수정 RECIST v1.1; OS = 전체 생존; PFS = 무진행 생존; PK = 약동학; RECIST v1.1 = 고형 종양의 반응 평가 기준, 버전 1.1.ADA = anti-drug antibody; DOR = duration of response; iRECIST = modified RECIST v1.1 for immune-based therapeutics; OS = overall survival; PFS = progression-free survival; PK = pharmacokinetics; RECIST v1.1 = Criteria for Response Evaluation of Solid Tumors, Version 1.1.
비고: 한 시점에서의 전체 반응은 RECIST v1.1을 사용하여 시험자가 평가한다.Note: The overall response at one time point is assessed by the investigator using RECIST v1.1.
병기 2 치료는 환자가 RECIST v1.1에 따른 질병 진행 또는 병기 1에서 허용할 수 없는 독성을 경험한 후 3개월 이내에 시작되어야 하며, 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 계속된다. 그러나, 환자는 가능한 빨리 병기 2 치료를 시작하도록 권장된다.Stage 2 treatment must be initiated within 3 months of the patient experiencing disease progression or stage 1 unacceptable toxicity according to RECIST v1.1, and there is no unacceptable toxicity or loss of clinical benefit as determined by the investigator. continues until However, patients are encouraged to start stage 2 treatment as soon as possible.
또한, 시험의뢰는 적절한 경우 안전성 데이터, 예비 유효성 데이터 및 지원 정보(예컨대, 바이오마커 연구 데이터)의 검토를 기반으로 병기 2 치료군의 등록을 중단하기로 결정할 수 있다.In addition, a referral may decide to discontinue enrollment in the Stage 2 treatment arm, if appropriate, based on review of safety data, preliminary efficacy data, and supporting information (eg, biomarker study data).
B.B. 연구 종료 및 연구 기간Study End and Study Duration
연구 종료는 전화 또는 현장 방문에 의해 수행되는 생존 추적 방문을 포함하여 마지막 환자가 마지막 방문을 완료한 날짜로 정의된다.Study end is defined as the date the last patient completed the last visit, including survival follow-up visits performed by phone or site visit.
첫 번째 환자의 선별검사 시부터 연구 종료시까지의 총 연구 기간은 약 3년 내지 6년이다.The total study duration from the first patient's screening to the end of the study is approximately 3 to 6 years.
C.C. 연구 설계 및 환자 집단의 이론적 근거Study Design and Patient Population Rationale
이 연구는 식도암 환자에서 초기 신호를 식별하고 개념 입증 임상 데이터를 확립함으로써 암 면역요법(CIT) 조합의 개발을 가속화하도록 설계되었다.This study is designed to accelerate the development of cancer immunotherapy (CIT) combinations by identifying early signs and establishing proof-of-concept clinical data in patients with esophageal cancer.
CIT는 여러 진행성 악성 종양에 걸쳐 관찰된 유의한 생존 이점과 함께 놀라운 성공을 나타냈다. 현재, 널리 퍼져 있는 CIT 접근 방식은 CTLA-4 및 PD-L1/PD-1과 같은 T 세포 공동 억제 표면 수용체를 식별하고 표적화하여 면역 회피 기전을 우회하고 항종양 반응을 활성화하는 것이다. 이러한 표적이 다양한 암 적응증에 대해 놀라운 임상적 치료 성공을 거두었지만, 진행 중인 연구는 지속적인 항종양 면역 반응의 생성에 필요한 일련의 단계적 사건을 나타낸다(Chen and Mellman, Immunity, 39: 1-10, 2013). 각 사건은 효과적인 반응을 위해 중요하며, 각각 여러 종양 면역 회피 기전에 대해 취약하다. 따라서, 종양 면역 회피와 관련된 다양한 요인의 식별 및 우회의 필요성은 항종양 면역 반응을 전파하고 CIT 분야를 발전시키기 위해 매우 중요하며, 이는 조합 요법을 통해 이루어질 가능성이 가장 높다.CIT has shown remarkable success with significant survival benefits observed across several advanced malignancies. Currently, the prevalent CIT approach is to identify and target T cell co-inhibitory surface receptors such as CTLA-4 and PD-L1/PD-1 to bypass immune evasion mechanisms and activate anti-tumor responses. Although these targets have achieved surprising clinical therapeutic success for a variety of cancer indications, ongoing research represents a series of cascading events necessary for the generation of a sustained anti-tumor immune response (Chen and Mellman, Immunity , 39:1-10, 2013). ). Each event is critical for an effective response, each vulnerable to multiple tumor immune evasion mechanisms. Therefore, the need to identify and bypass the various factors involved in tumor immune evasion is of great importance to propagate anti-tumor immune responses and advance the field of CIT, which is most likely achieved through combination therapy.
식도암은 5년 생존율이 전이성 질병 설정에서 5%, 국소 진행성 질병 설정에서 24%로, 높은 의학적 요구가 충족되지 않은 질병이다. 진행성 또는 전이성 식도암 환자에 대한 치료 옵션은 제한적이며, 전체 생존 이점이 최소인 불량한 예후를 보인다. 따라서, 이 환자 집단에 대해 더 효과적이고 더 양호한 내약성 치료에 대한 지속적인 요구가 있다.Esophageal cancer is an unmet disease with a high 5-year survival rate of 5% in the metastatic disease setting and 24% in the locally advanced disease setting. Treatment options for patients with advanced or metastatic esophageal cancer are limited and have a poor prognosis with minimal overall survival benefit. Therefore, there is an ongoing need for more effective and better tolerated treatments for this patient population.
실시예 24. YO39609 연구를 위한 재료 및 방법Example 24. Materials and Methods for Studying YO39609
이 설정에서 이전에 전신 요법을 받은 적이 없는 식도암 환자 약 100명 내지 165명을 YO39609 연구 기간 동안 대조군과 실험군으로 무작위 배정한다.In this setting, approximately 100 to 165 patients with esophageal cancer who have not previously received systemic therapy will be randomized into control and experimental groups for the duration of the YO39609 study.
A.A. 병기 1의 포함 기준Inclusion criteria for stage 1
환자는 병기 1에 대한 자격을 갖추기 위해 아래에 요약된 다음 기준을 모두 충족해야 한다.Patients must meet all of the following criteria summarized below to be eligible for Stage 1.
사전 동의서에 서명할 당시의 연령 ≥ 18세. Age ≥ 18 years at the time the informed consent was signed.
![]()
![]()
![]()
![]()
전이성 식도암의 최종 진단은 임상 및 방사선 사진 데이터의 맥락 내에서 조직병리학적 데이터를 평가하여 이루어진다.The definitive diagnosis of metastatic esophageal cancer is made by evaluating histopathological data within the context of clinical and radiographic data.
![]()
![]()
- 국소 진행성 설정에서 화학요법으로 치료받은 환자의 경우: 화학요법의 마지막 투여로부터 6개월 후 전이 발생.- For patients treated with chemotherapy in a locally progressive setting: metastasis occurred 6 months after the last dose of chemotherapy.
![]()
![]()
- HER2 음성 상태는 ISH 비증폭(CEP17에 대한 HER2의 비율 < 2.0, 또는 단일 프로브 평균 HER2 유전자 복사 수 < 4 신호/세포) IHC 0 또는 IHC 1+을 기준으로 결정된다(하나 이상의 검사 결과가 이용 가능하고 모든 결과가 포함 기준 정의를 충족하지는 않는 경우, 모든 결과는 환자의 적격성을 확립하기 위해 의학 모니터 요원과 논의해야 한다).- HER2 negative status is determined on the basis of no ISH amplification (ratio of HER2 to CEP17 < 2.0, or single probe average HER2 gene copy number < 4 signals/cell) IHC 0 or IHC 1 + (one or more test results are available) If possible and not all outcomes meet the inclusion criteria definition, all outcomes should be discussed with the medical monitor to establish the patient's eligibility).
![]()
![]()
![]()
![]()
![]()
![]()
- 기준선 종양 조직 샘플은 모든 환자로부터, 바람직하게는 연구 시작 시에 수행된 생검에 의해 수집된다. 시험자가 생검을 실행할 수 없다고 판단하는 경우, 보관 종양 조직이 등록 전 6개월 이내에 수행된 생검에서 얻은 조직이고 환자가 생검 시점 이후로 어떠한 항암 요법도 받지 않았다면, 보관 종양 조직을 의학 모니터 요원의 승인 후에 제출할 수 있다.- Baseline tumor tissue samples are collected from all patients, preferably by biopsy performed at the start of the study. If the investigator determines that a biopsy cannot be performed, if the archival tumor tissue is from a biopsy performed within 6 months prior to enrollment and the patient has not received any chemotherapy since the time of the biopsy, the archival tumor tissue will be removed after approval by the medical monitor. can be submitted
- 파라핀 블록의 FFPE 종양 표본(바람직함) 또는 염색되지 않은 갓 절단된 연속 절편을 포함하는 적어도 16개의 슬라이드를 관련 병리 보고서와 함께 제출해야 한다. 10 내지 15개의 슬라이드만 사용할 수 있는 경우, 의학 모니터 요원의 승인 이후, 환자는 여전히 연구에 대해 적격일 수 있다.- At least 16 slides containing FFPE tumor specimens in paraffin blocks (preferred) or unstained, freshly excised serial sections should be submitted with the relevant pathology report. If only 10 to 15 slides are available, after approval by the medical monitor, the patient may still be eligible for the study.
B.B. 병기 1 및 병기 2의 포함 기준 Inclusion Criteria for Stage 1 and Stage 2
환자는 병기 1 및 병기 2에 대한 자격을 갖추기 위해 아래에 요약된 다음 기준을 모두 충족해야 한다.Patients must meet all of the following criteria summarized below to be eligible for Stage 1 and Stage 2.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- ANC ≥ 1.5 ×109/L(1500/μL), 과립구 집락 자극 인자 지원 없음.- ANC ≥ 1.5 × 10 9 /L (1500/μL), no granulocyte colony stimulating factor support.
- 림프구 수 ≥ 0.5 × 109/L(500/μL).- Lymphocyte count ≥ 0.5 × 10 9 /L (500/μL).
- 혈소판 수 ≥ 100 × 109/L(100,000/μL), 수혈 없음.- Platelet count ≥ 100 × 10 9 /L (100,000/μL), no transfusion.
- 헤모글로빈 ≥ 90 g/L(9 g/dL). 환자는 이 기준을 충족하기 위해 수혈을 받을 수 있다.- Hemoglobin ≥ 90 g/L (9 g/dL). Patients may receive blood transfusions to meet these criteria.
- AST, ALT, 및 알칼리성 인산분해효소(ALP) ≤ 2.5 × 정상 상한치(ULN), 다음은 예외임:- AST, ALT, and alkaline phosphatase (ALP) ≤ 2.5 × upper limit of normal (ULN), with the following exceptions:
간 전이가 기록된 환자: AST 및 ALT ≤ 5 × ULN.Patients with documented liver metastases: AST and ALT ≤ 5 × ULN.
문서로 기록된 간 또는 골 전이를 가진 환자: ALP ≤ 5 × ULN.Patients with documented liver or bone metastases: ALP ≤ 5 × ULN.
- 빌리루빈 ≤ 1.5 × ULN, 다음은 예외임:- Bilirubin ≤ 1.5 × ULN, with the following exceptions:
공지의 길버트병 환자: 빌리루빈 수준 ≤ 3 × ULN.Known Gilbert's disease patients: bilirubin levels ≤ 3 x ULN.
- 알부민 ≥ 25 g/L(2.5 g/dL).- Albumin ≥ 25 g/L (2.5 g/dL).
- 치료적 항응고제를 투여받지 않는 환자의 경우: INR 또는 aPTT ≤ 1.5 × ULN.- For patients not receiving therapeutic anticoagulants: INR or aPTT ≤ 1.5 × ULN.
- 치료적 항응고제를 투여받는 환자의 경우: 안정적인 항응고 요법.- For patients receiving therapeutic anticoagulants: stable anticoagulant therapy.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
C.C. 병기 2의 포함 기준Inclusion criteria for stage 2
환자는 병기 2에 대한 자격을 갖추기 위해 아래에 요약된 다음 기준을 모두 충족해야 한다.Patients must meet all of the following criteria summarized below to be eligible for Stage 2.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
D.D. 배제 기준Exclusion Criteria
다음 기준 중 어느 하나에 부합하는 환자는 병기 1 및 병기 2 동안 등록에서 제외된다.Patients meeting any of the following criteria will be excluded from enrollment during Stages 1 and 2.
병기 1의 제외 기준Stage 1 exclusion criteria
다음 기준 중 어느 하나에 부합하는 환자는 병기 1로부터 제외된다:Patients meeting any of the following criteria are excluded from Stage 1:
·프로토콜 지정 연구 치료 중 어느 하나를 통한 이전 치료.·Previous treatment with any of the protocol-directed study treatments.
·공지된 청력 장애가 있는 환자.·Patients with known hearing impairment.
·NCI CTCAE v4.0 기준에 의해 정의된 ≥ 2등급 말초 신경병증.≥ Grade 2 peripheral neuropathy as defined by the NCI CTCAE v4.0 criteria.
·공지된 디히드로피리미딘 탈수소효소 결핍증, 또는 환자를 5-FU 독성에 취약하게 하는 티미딜레이트 합성효소 유전자 다형성.Known dihydropyrimidine dehydrogenase deficiency, or thymidylate synthase gene polymorphism that predisposes the patient to 5-FU toxicity.
병기 1 및 병기 2의 제외 기준Exclusion Criteria for Stage 1 and Stage 2
다음 기준 중 어느 하나에 부합하는 환자는 병기 1 및 병기 2로부터 제외된다:Patients meeting any of the following criteria are excluded from Stage 1 and Stage 2:
![]()
![]()
![]()
![]()
- RECIST v1.1에 따라 측정 가능한 질병은 CNS 외부에 있어야 한다.- According to RECIST v1.1, measurable diseases must be outside the CNS.
- 환자는 두개내 출혈 또는 척수 출혈의 병력이 없다.- The patient has no history of intracranial hemorrhage or spinal cord hemorrhage.
- 환자는 연구 치료 개시 전 7일 이내에 정위 방사선요법, 연구 치료 개시 전 14일 이내에 전뇌 방사선요법, 또는 연구 치료 개시 전 28일 이내에 신경외과적 절제술을 받지 않았다.-Patient had not undergone stereotactic radiotherapy within 7 days prior to study treatment initiation, whole brain radiotherapy within 14 days prior to study treatment initiation, or neurosurgical resection within 28 days prior to study treatment initiation.
- 상기 환자는 CNS 질병에 대한 요법으로서 지속적인 코르티코스테로이드를 필요로 하지 않는다. 안정적인 용량의 항경련제 요법이 허용된다.- The patient does not require continuous corticosteroids as therapy for CNS disease. Stable dose anticonvulsant therapy is permitted.
- 전이가 소뇌 또는 천막 상부 영역으로 한정된다(즉, 중뇌, 교뇌, 수질 또는 척수로 전이되지 않음).- Metastasis is limited to the cerebellum or supramial region (ie, no metastasis to the midbrain, pons, medulla or spinal cord).
- CNS 지시 요법의 완료와 연구 치료 개시 사이에 중간 진행의 증거가 없다.- There is no evidence of intermediate progression between completion of CNS-directed therapy and initiation of study treatment.
- 선별검사 시 새롭게 발견된 CNS 전이가 있는 무증상 환자는 선별 뇌 스캔을 반복할 필요 없이 방사선 치료 또는 수술을 받은 후 연구에 대해 적격이다.- Asymptomatic patients with newly discovered CNS metastases at screening are eligible for the study after undergoing radiotherapy or surgery without the need to repeat screening brain scans.
![]()
![]()
![]()
![]()
·통제되지 않는 종양 관련 통증. 통증 약제를 필요로 하는 환자는 연구 엔트리에서 안정된 섭생 중에 있어야 한다. 고식적 방사선요법으로 처리할 수 있는 증상이 있는 병변(예컨대, 골 전이 또는 신경 충돌을 유발하는 전이)은 등록 전에 치료해야 한다. 환자는 방사선의 영향에서 회복되어야 한다. 환자는 방사선의 영향에서 회복되어야 함. 추가 성장시 기능적 결함이나 난치성 통증을 유발할 가능성이 있는 무증상 전이성 병변 (예를 들어, 현재 척수 압박과 관련이 없는 경막외 전이)은 등록 전에 적절한 경우 국소 치료를 고려해야 함.Uncontrolled tumor-related pain. Patients requiring pain medication must be on a stable regimen at study entry. Symptomatic lesions that can be treated with palliative radiotherapy (eg, bone metastases or metastases causing nerve impingement) should be treated prior to enrollment. The patient must recover from the effects of radiation. The patient must recover from the effects of radiation. Asymptomatic metastatic lesions (e.g., epidural metastases not currently associated with spinal cord compression) that have the potential to cause functional defects or refractory pain upon further growth should be considered for local treatment if appropriate prior to enrollment.
![]()
![]()
![]()
![]()
![]()
![]()
자가면역 관련 갑상선 기능저하증의 병력이 있고 갑상선 대체 호르몬을 투여받고 있는 환자는 연구에 적격이다.Patients with a history of autoimmune-related hypothyroidism and taking thyroid replacement hormone are eligible for the study.
안정적인 인슐린 요법을 받고 있는 조절된 제1형 당뇨병 환자는 연구에 적격이다.Patients with controlled type 1 diabetes on stable insulin therapy are eligible for the study.
습진, 건선, 만성 단순 태선 또는 피부과적 징후만 있는 백반증이 있는 환자(예컨대, 건선성 관절염 환자는 제외됨)는 다음 조건이 모두 충족되는 경우 연구에 적격이다:Patients with eczema, psoriasis, chronic lichen simplex, or vitiligo with dermatological signs only (e.g., excluding patients with psoriatic arthritis) are eligible for study if all of the following conditions are met:
- 발진은 체표면적의 < 10%를 차지해야 한다.- The rash should occupy < 10% of the body surface area.
- 질병은 기준선에서 잘 조절되며, 저역가 국소 코르티코스테로이드만 필요하다.- Disease is well controlled at baseline and requires only low titer topical corticosteroids.
- 지난 12개월 이내에 소랄렌 + 자외선 A 방사선, 메토트렉세이트, 레티노이드, 생물학적 제제, 경구 칼시뉴린 억제제, 또는 고역가 또는 경구 코르티코스테로이드를 필요로 하는 기저 조건의 급성 악화가 발생하지 않았다.- No acute exacerbation of underlying conditions requiring psoralen plus ultraviolet A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high titers or oral corticosteroids within the past 12 months.
·특발성 폐섬유증, 폐색성 기관지염(예컨대, 폐쇄성 세기관지염), 약물 유발성 폐렴 또는 특발성 폐렴의 병력, 또는 선별 흉부 컴퓨터 단층촬영(CT) 스캔에서의 활동성 폐렴의 증거. 방사선 분야에서 방사선 폐렴 (섬유증) 병력은 허용됨History of idiopathic pulmonary fibrosis, obstructive bronchitis (eg, bronchiolitis obliterans), drug-induced pneumonia or idiopathic pneumonia, or evidence of active pneumonia on a screening chest computed tomography (CT) scan. A history of radiation pneumonitis (fibrosis) in the field of radiation is acceptable
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- 급성 저용량 전신 면역억제 약물 또는 1회 펄스 용량의 전신 면역억제 약물(예컨대, 조영제 알레르기에 대한 코르티코스테로이드 48시간)을 투여받은 환자는 의학 모니터 요원의 승인을 받은 후 연구에 적격이다.- Patients receiving acute low-dose systemic immunosuppressive drugs or single pulse doses of systemic immunosuppressive drugs (eg, corticosteroids for contrast allergy 48 hours) are eligible for study after obtaining approval from the medical monitor.
- 무기질 코르티코이드(예컨대, 플루드로코르티손), 만성 폐쇄성 폐질환(COPD) 또는 천식에 대한 코르티코스테로이드, 또는 기립성 저혈압 또는 부신피질 기능부전에 대한 저용량 코르티코스테로이드를 투여받은 환자는 연구에 적격이다.- Patients receiving mineralocorticoids (e.g., fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenocortical insufficiency are eligible for study.
![]()
![]()
![]()
![]()
·연구 치료 동안, 또는 아테졸리주맙의 최종 투여 후 5개월 이내 및 티라골루맙의 최종 투여 후 5개월 이내에 임신 또는 수유 중이거나, 임신할 의사가 있는 경우. 가임 여성은 연구 치료 시작 전 14일 이내에 혈청 임신 검사 결과가 음성이어야 한다.Pregnant, lactating, or intending to become pregnant during study treatment, or within 5 months of the last dose of atezolizumab and within 5 months of the last dose of tiragolumab. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
E.E. 허용된 요법accepted therapy
환자는 연구 기간 동안 하기의 요법을 사용하는 것이 허용된다:Patients are allowed to use the following regimens during the study period:
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
완화 방사선 요법은 종양 표적 병변의 평가를 방해하지 않는 한 허용한다(예컨대, 조사할 병변이 측정 가능한 질병의 유일한 부위가 아니어야 함). 아테졸리주맙 치료는 고식적 방사선요법 동안 계속될 수 있다.Palliative radiation therapy is acceptable as long as it does not interfere with the evaluation of tumor target lesions (eg, the lesion to be investigated should not be the only site of measurable disease). Atezolizumab treatment may be continued during palliative radiotherapy.
· 하기 요약된 국소 요법(예컨대, 수술, 정위 방사선 수술, 방사선요법, 고주파 절제):· Local therapies (e.g., surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) summarized below:
3개 이하의 병변을 조절하기 위해 국소 요법이 필요한 혼합 반응을 경험하는 환자는 의학 모니터 요원의 승인을 받은 후에도 여전히 연구 치료를 계속하기에 적격일 수 있다. 표적 병변에 대한 국소 요법을 받는 환자는 더 이상 방사선학적 반응에 대해 평가할 수 없지만Patients experiencing mixed reactions requiring topical therapy to control 3 or fewer lesions may still be eligible to continue study treatment after approval from a medical monitor. Patients receiving topical therapy for the target lesion can no longer be evaluated for radiological response, but
진행에 대해서는 계속 평가할 수 있다.Progress can be evaluated continuously.
항히스타민제, 해열제 및/또는 진통제를 사용한 사전 투약은 시험자의 재량에 따라 2차 및 후속 아테졸리주맙 주입에 대해서만 투여될 수 있다. Prior dosing with antihistamines, antipyretics and/or analgesics may be administered only for the second and subsequent infusions of atezolizumab at the discretion of the investigator.
주입 관련 증상을 경험한 환자는 증상에 따라 아세트아미노펜, 이부프로펜, 디펜히드라민, 및/또는 H2 수용체 길항제(예컨대, 파모티딘, 시메티딘), 또는 지역 표준 관행에 따른 등가의 약물로 치료를 받을 수 있다. 호흡 곤란, 저혈압, 쌕쌕 거림, 기관지경련, 빈맥, 산소 포화도 감소 또는 호흡 곤란으로 나타나는 중증 주입 관련 반응들은 임상적으로 지시된 바와 같은 보조 요법(예컨대, 보조 산소 및 β2 아드레날린 작용제)으로 관리해야 한다.Patients experiencing infusion-related symptoms may be treated with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice, depending on the symptoms. have. Severe infusion-related reactions presenting with dyspnea, hypotension, wheezing, bronchospasm, tachycardia, decreased oxygen saturation or dyspnea should be managed with adjuvant therapy as clinically indicated (e.g., adjuvant oxygen and β 2 adrenergic agonists). .
F.F. 용량 및 투여Dosage and administration
하기 치료군 환자는 방사선 사진 및 생화학적 데이터, 국소 생검 결과(가능한 경우) 및 임상 상태(예컨대, 질병에 따른 통증과 같은 증상 악화)의 통합 평가 후 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 요약된 치료를 받는다.Patients in the following treatment groups were evaluated for unacceptable toxicity or clinical benefit as determined by the investigator after an integrated evaluation of radiographic and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as disease-related pain). Receive summarized treatment until loss.
아테졸리주맙 + 티라골루맙 + 시스플라틴 + 5-플루우라실 군Atezolizumab + Tiragolumab + Cisplatin + 5-fluuracil group
아테졸리주맙 + 티라골루맙 + 시스플라틴 + 5-FU 군의 환자는 표 87에 요약된 치료를 받는다.Patients in the atezolizumab + tiragolumab + cisplatin + 5-FU group receive the treatment summarized in Table 87.

5-FU = 5-플루오로우라실; a 시스플라틴 치료는 6회 투여 후에 제한된다. b 시스플라틴 및 5-FU의 주입 시간은 현지 표준 관행에 따라 조정할 수 있다.5-FU = 5-fluorouracil; a Cisplatin treatment is limited after 6 doses. b Infusion times of cisplatin and 5-FU may be adjusted according to local standard practice.
아테졸리주맙 + 시스플라틴 + 5-플루우라실 군Atezolizumab + cisplatin + 5-fluuracil group
아테졸리주맙 + 시스플라틴 + 5-FU 군의 환자는 표 88에 요약된 치료를 받는다.Patients in the atezolizumab + cisplatin + 5-FU group receive the treatment summarized in Table 88.

5-FU = 5-플루오로우라실; a 시스플라틴 치료는 6회 투여 후에 제한된다. b 시스플라틴 및 5-FU의 주입 시간은 현지 표준 관행에 따라 조정할 수 있다.5-FU = 5-fluorouracil; a Cisplatin treatment is limited after 6 doses. b Infusion times of cisplatin and 5-FU may be adjusted according to local standard practice.
대조군(시스플라틴 + 5-FU)Control (cisplatin + 5-FU)
시스플라틴은 처음 6회의 21일 사이클 중 1일차에 80 mg/m2의 용량으로 120분에 걸쳐 IV 주입에 의해 투여된다. 5-FU는 각 21일 사이클의 1일차에 시작하여 800 mg/m2/24시간의 용량으로 1일 내지 5일(120시간)차에 걸쳐 연속적인 IV 주입에 의해 투여된다. 시스플라틴 치료는 허용할 수 없는 독성이 발생하거나 환자가 임의의 이유로 연구 치료를 중단하지 않는 한 총 6 사이클 동안 지속된다. 시스플라틴 + 5-FU 대조군의 환자는 허용할 수 없는 독성 또는 RECIST v1.1에 따른 질병 진행이 있을 때까지 치료를 받는다. Cisplatin is administered by IV infusion over 120 minutes at a dose of 80 mg/m2 on Day 1 of the first 6 21-day cycles. 5-FU is administered by continuous IV infusion over days 1 to 5 (120 hours) at a dose of 800 mg/m 2 /24 hours starting on Day 1 of each 21-day cycle. Cisplatin treatment is continued for a total of 6 cycles unless unacceptable toxicity develops or the patient discontinues study treatment for any reason. Patients in the cisplatin + 5-FU control group are treated until unacceptable toxicity or disease progression according to RECIST v1.1.
대조군에 대한 병기 2 치료(아테졸리주맙 + 티라골루맙) Stage 2 treatment versus control (atezolizumab + tyragolumab)
아테졸리주맙 + 티라골루맙 군의 환자는 표 89에 요약된 치료를 받는다.Patients in the atezolizumab + tyragolumab group receive the treatment summarized in Table 89.

RECIST v1.1에 따른 질병 진행을 경험한 환자는 적격 기준을 충족하고 병기 2 군이 등록을 위해 개방되어 있는 경우 연구의 병기 2 동안 다른 치료 조합을 받는 옵션을 제공받는다. Patients experiencing disease progression according to RECIST v1.1 will be offered the option to receive another treatment combination during Stage 2 of the study if they meet eligibility criteria and Arm 2 is open for enrollment.
또한, 허용할 수 없는 독성을 경험한 환자는 적격 기준을 충족하고 의학 모니터 요원의 승인을 받은 후 병기 2 동안 치료를 받기에 적격일 수 있다. 병기 2 치료는 환자가 질병 진행 또는 허용할 수 없는 독성을 경험한 후 3개월 이내에 시작되어야 한다. 병기 2 치료 개시(즉, 사이클 1의 1일차) 전 28일 이내에 종양 평가를 수행하는 경우, 병기 1동안 질병 진행 또는 허용할 수 없는 독성의 발생시 또는 발생 이전에 수행된 종양 평가는 병기 2의 기준선 평가의 역할을 할 수 있다. 병기 2 치료는 시험자가 결정한 허용할 수 없는 독성 또는 임상적 이점의 상실이 있을 때까지 지속된다.In addition, patients who experience unacceptable toxicity may be eligible for treatment during Stage 2 after meeting eligibility criteria and obtaining approval from a medical monitor. Stage 2 treatment should be initiated within 3 months of the patient experiencing disease progression or unacceptable toxicity. If tumor evaluations are performed within 28 days prior to initiation of Stage 2 treatment (i.e., Day 1 of Cycle 1), tumor evaluations performed at or prior to the onset of disease progression or unacceptable toxicity during Stage 1 are the baseline in Stage 2 It can play a role in evaluation. Stage 2 treatment is continued until there is unacceptable toxicity or loss of clinical benefit as determined by the investigator.
아테졸리주맙 주입은 표 90에 요약된 지침에 따라 투여된다.Atezolizumab infusion is administered according to the guidelines summarized in Table 90.

티라골루맙 주입은 표 91에 요약된 지침에 따라 투여된다.Tiragolumab infusions are administered according to the guidelines summarized in Table 91.

G.G. 안전성 평가 단계Safety Assessment Steps
아테졸리주맙 + 티라골루맙 + 시스플라틴 + 5-FU 군에서 잠재적인 중복 독성을 설명하기 위해, 안전성 평가를 위해 약 6명의 환자가 등록된 후 등록이 보류된다. 안전성 평가는 적어도 1회 용량의 치료(즉, 주어진 조합에 대해 각 제제의 1회 용량)를 받고 적어도 1회의 전체 치료 사이클 동안 안전성 추적을 완료한 최소 6명의 환자로부터 획득한 안전성 데이터를 기반으로 한다. 조합이 충분히 안전한 것으로 판단되면, 등록이 상기 군에서 재개된다. To account for potential overlapping toxicity in the atezolizumab + tiragolumab + cisplatin + 5-FU group, enrollment is withheld after approximately 6 patients have been enrolled for safety evaluation. The safety assessment is based on safety data obtained from at least 6 patients who received at least one dose of treatment (i.e., one dose of each agent for a given combination) and completed safety follow-up for at least one full treatment cycle. . If the combination is judged to be sufficiently safe, registration is resumed in that group.
H.H. 평가 및 모니터링Assessment and monitoring
모든 환자는 연구 전반에 걸쳐 이상 반응에 대해 면밀히 모니터링되며, 이상 반응은 국립 암 연구소의 이상 반응에 대한 공통 용어 기준, 버전 4.0(NCI CTCAE v4.0)에 따라 등급이 매겨진다. 환자는 처음 12개월 동안은 6주마다(사이클 1의 1일차에 시작함) 종양 평가를 받고, 그 후로는 6주 또는 12주마다 종양 평가를 받는다. 반응은 RECIST v1.1을 사용하여 시험자가 평가한다(Eisenhauer et al., Eur J Cancer, 45: 228-247, 2009). 면역 기반 치료제를 위한 수정 RECIST v1.1(iRECIST)에 대한 반응은 시험자가 평가한 개별 병변 데이터를 기반으로 시험의뢰자가 프로그래밍 방식으로 결정한다(Seymour et al., Lancet Oncol, 18: e143-152, 2017). 실험군에서 임상 활동성이 나타나면, 시험의뢰자는 중앙 판독 시설의 평가를 위해 해당 군에 대한 종양 평가 스캔을 제출하도록 요청할 수 있다.All patients are closely monitored for adverse events throughout the study, and adverse events are graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). Patients receive tumor evaluations every 6 weeks (starting on Day 1 of Cycle 1) for the first 12 months, and then every 6 or 12 weeks thereafter. Response is assessed by the investigator using RECIST v1.1 (Eisenhauer et al., Eur J Cancer , 45: 228-247, 2009). Response to modified RECIST v1.1 (iRECIST) for immune-based therapeutics is determined programmatically by the sponsor based on individual lesion data evaluated by the investigator (Seymour et al., Lancet Oncol , 18: e143-152, 2017). If clinical activity appears in the experimental group, the sponsor may request to submit a tumor assessment scan for that group for evaluation by a central reading facility.
기준선 종양 조직 샘플은 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 시험자가 생검을 시행할 수 없다고 판단하는 경우, 보관 종양 조직을 제출할 수 있다. 또한, 시험자가 임상적으로 가능하다고 판단하는 경우, 종양 조직은 시험자에 의해 결정된 허용할 수 없는 독성, RECIST v1.1에 따른 질병 진행(대조군) 또는 임상적 이점의 상실(실험군)로 인해 병기 1을 중단한 환자로부터 수집된다. 확장 단계에서 실험군에 등록한 환자의 경우, 치료 중 조직 샘플이 동일한 CIT 조합으로 치료된 최소 15명의 환자로부터 이미 수집되고 측정 가능하다고 판단되지 않는 한, 1 단계 치료의 개시 후 4주에 치료 중 종양 조직 샘플을 수집한다(임상적으로 가능한 것으로 판단된 경우). 이 샘플과 연구 기간 동안 수집된 혈액 샘플은 바이오마커 연구에 활용된다.Baseline tumor tissue samples are preferably collected from all patients via biopsies performed at the start of the study. If the investigator determines that a biopsy cannot be performed, the archived tumor tissue may be submitted. In addition, if the investigator determines that it is clinically feasible, the tumor tissue will be staged 1 due to unacceptable toxicity as determined by the investigator, disease progression (control group), or loss of clinical benefit (experimental group) according to RECIST v1.1. collected from patients who discontinued For patients enrolled in the experimental arm in the expansion phase, tumor tissue during treatment 4 weeks after initiation of phase 1 therapy, unless tissue samples have already been collected from at least 15 patients treated with the same CIT combination and are determined to be measurable. Collect samples (if determined clinically feasible). These samples and blood samples collected during the study period are used for biomarker studies.
아테졸리주맙 및 기타 치료제의 약동학(PK) 특성 및/또는 면역원성을 특성화하기 위해, 연구 치료의 투여 이전 및 동안의 다양한 시점에서 혈액 샘플을 획득한다.To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points prior to and during administration of study treatment.
종양 및 반응 평가Tumor and Response Assessment
환자는 방사선학적 질환 진행 후 치료를 계속하는 환자의 경우를 제외하고 RECIST v1.1에 따른 방사선학적 질환 진행 전까지 용량 지연에 관계없이 치료 개시 후 처음 12개월 동안은 6주(±1주)마다, 그 이후에는 12주(±2주)마다 기준선에서 종양 평가를 받는다; 이러한 환자는 시험자에 의해 결정된 임상적 이점이 상실될 때까지 8주(±1주)마다 종양 평가를 받는다.Every 6 weeks (± 1 week) for the first 12 months after initiation of treatment, regardless of dose delay, until radiological disease progression according to RECIST v1.1, except for patients who continue treatment after radiological disease progression; Thereafter, tumors are assessed at baseline every 12 weeks (±2 weeks); These patients receive tumor assessments every 8 weeks (±1 weeks) until loss of clinical benefit as determined by the investigator.
따라서, 프로토콜 지정되지 않은 새로운 항암 요법을 시작하더라도, 질병의 진행이나 임상적 이점 상실 이외의 이유로 치료를 중단한 환자에 대해서는 일정에 따라 종양 평가를 계속한다. 진행성 질환이 의심되는 경우, 시험자의 재량에 따라 종양 평가를 언제든지 반복할 수 있다.Therefore, even if new non-protocol therapy is initiated, tumor evaluation continues according to schedule for patients who discontinue treatment for reasons other than disease progression or loss of clinical benefit. If progressive disease is suspected, the tumor evaluation may be repeated at any time at the investigator's discretion.
병기 2에 대한 기준선 종양 평가는 병기 2 치료 개시 전(즉, 사이클 1의 1일차) 28일 이내에 수행해야 한다. 병기 2에 대해 적격인 환자의 경우, 병기 2 치료 개시 전 28일 이내에 종양 평가를 수행하면, 병기 1 동안 허용할 수 없는 독성 또는 RECIST v1.1에 따른 질병(대조군) 또는 임상적 이점의 상실(실험군)의 발생시 또는 발생 이전에 수행된 종양 평가는 병기 2의 기준선 평가의 역할을 할 수 있다.Baseline tumor assessment for Stage 2 must be performed within 28 days prior to initiation of Stage 2 treatment (ie, Day 1 of Cycle 1). For patients eligible for Stage 2, if tumor evaluation is performed within 28 days prior to initiation of Stage 2 treatment, unacceptable toxicity or disease (control) or loss of clinical benefit according to RECIST v1.1 during Stage 1 ( Tumor assessments performed at or before the onset of the experimental group) may serve as a baseline assessment of stage 2.
모든 측정 가능하고 평가 가능한 병변은 선별검사 시 평가되고 보고되어야 한다(병기 1 및 병기 2 모두). 방사선 요법이나 수술로 치료된 뇌 전이는 측정 가능하거나 평가할 수 있는 것으로 간주되지 않지만, 전이성 질환 부위로 보고된다. 사전 동의를 받기 이전 및 연구 치료 개시 전 28일 이내에 표준 치료로서 수행된 종양 평가는 선별검사 시 반복할 필요가 없다.All measurable and evaluable lesions should be evaluated and reported at screening (both Stage 1 and Stage 2). Brain metastases treated with radiation therapy or surgery are not considered measurable or evaluable, but are reported as sites of metastatic disease. Tumor assessments performed as standard of care prior to obtaining informed consent and within 28 days prior to initiation of study treatment do not need to be repeated at screening.
선별 평가에는 CT 스캔(구강 및/또는 IV 조영제 사용) 또는 흉부, 복부 및 골반의 자기공명영상(MRI) 스캔이 포함되어야 한다. 흉부의 나선형 CT 스캔을 획득할 수 있으나, 필수 사항은 아니다. 조영제를 사용한 CT 스캔이 금지되는 경우(즉, 조영제 알레르기 또는 신장 청소 장애가 있는 환자의 경우), 흉부의 비조영 CT 스캔을 수행할 수 있으며, 복부와 골반의 MRI 스캔(가능한 경우, IV 조영제 사용)을 수행해야 한다. 또한, 임상적으로 지시된 경우, 목의 뼈 스캔 및 CT 스캔을 수행해야 한다. 시험자의 재량에 따라 RECIST v1.1에 따라 측정가능한 질병을 평가하는 다른 방법이 사용될 수 있다.Screening assessments should include CT scans (using oral and/or IV contrast) or magnetic resonance imaging (MRI) scans of the chest, abdomen and pelvis. A spiral CT scan of the chest can be obtained, but is not required. If CT scans with contrast agents are contraindicated (i.e., in patients with contrast agent allergy or renal clearance impairment), non-contrast CT scans of the chest may be performed, and MRI scans of the abdomen and pelvis (using IV contrast, if possible) should be performed In addition, if clinically indicated, a bone scan of the neck and a CT scan should be performed. Other methods of assessing measurable disease according to RECIST v1.1 may be used at the discretion of the investigator.
종양 평가를 위한 CT 스캔이 양전자 방출 단층촬영/CT 스캐너에서 수행되는 경우, CT 획득은 전체 조영 진단 CT 스캔의 표준과 일치해야 한다.If CT scans for tumor evaluation are performed on a positron emission tomography/CT scanner, the CT acquisition should be consistent with the standard for full-contrast diagnostic CT scans.
기준선에서 식별된 모든 측정 가능 및/또는 평가 가능한 병변은 후속 종양 평가에서 재평가되어야 한다. 방사선 요법이나 수술로 치료된, 기준선에서 식별된 뇌 전이는 뇌에 질병 진행이 의심되는 경우(즉, 환자가 증상을 보이는 경우)가 아니면 측정 가능하거나 평가할 수 있는 것으로 간주되지 않는다. 따라서, 임상적으로 지시되지 않는 한 후속 두부 CT 스캔은 필요하지 않다. 선별검사 시 질병 부위를 평가하는 데 사용된 동일한 방사선 사진 절차는 후속 종양 평가에 사용되어야 한다(예컨대, CT 스캔을 위한 동일한 조영제 프로토콜). iRECIST에 따른 반응 평가를 용이하게 하기 위해, 질병 진행 이후에도 치료를 받는 환자의 경우 RECIST v1.1에 따른 질병 진행 이후 종양 평가를 계속하여야 한다. 이러한 평가에는 표적 병변의 지속적인 측정, 비표적 병변의 평가(분명한 진행을 보인 비표적 병변의 추가 악화에 대한 모니터링 포함), 및 모든 후속 평가에서 새로 확인된 병변의 평가(병변이 측정 가능한 경우 측정 포함)가 포함된다. 한 시점에서의 전체 반응은 RECIST v1.1을 사용하여 시험자가 평가한다.All measurable and/or evaluable lesions identified at baseline should be re-evaluated at subsequent tumor assessments. Brain metastases identified at baseline, treated with radiation therapy or surgery, are not considered measurable or evaluable unless disease progression in the brain is suspected (ie, the patient is symptomatic). Therefore, a subsequent CT scan of the head is not required unless clinically indicated. The same radiographic procedure used to evaluate the site of disease at screening should be used for subsequent tumor evaluation (eg, the same contrast agent protocol for CT scans). To facilitate response evaluation according to iRECIST, tumor evaluation should continue after disease progression according to RECIST v1.1 for patients receiving treatment after disease progression. These assessments include continuous measurement of target lesions, assessment of non-target lesions (including monitoring for further deterioration of non-target lesions with clear progression), and evaluation of newly identified lesions at all subsequent assessments (including measurements if lesions are measurable). ) is included. The overall response at one time point is assessed by the investigator using RECIST v1.1.
바이오마커 평가Biomarker evaluation
탐색적 바이오마커 연구에는 종양 분자 아형 및 종양 면역생물학과 관련된 유전자 또는 유전자 서명, PD-L1, 림프구 하위집단, T 세포 수용체 레퍼토리, T 세포 활성화와 관련된 사이토카인, 또는 IC의 밀도, 국소화 및 활성화 상태 및 그 하위집합의 분석이 포함될 수 있으나 이에 한정되지 않으며, DNA 또는 RNA 추출, 체세포 돌연변이 분석, 차세대 시퀀싱(NGS) 사용(전체 엑솜 시퀀싱((WES) 포함)이 포함될 수 있다. Exploratory biomarker studies include the density, localization and activation status of tumor molecular subtypes and genes or gene signatures associated with tumor immunobiology, PD-L1, lymphocyte subpopulations, T cell receptor repertoire, cytokines associated with T cell activation, or ICs; Analysis of that subset may include, but is not limited to, DNA or RNA extraction, analysis of somatic mutations, and use of next-generation sequencing (NGS) (including whole exome sequencing (WES)).
바이오마커 평가를 위한 혈액 샘플은 연구 기간 동안 기준선에서 수집된다. 혈액 내 바이오마커의 변화는 특정 치료 조합의 생물학적 활성의 증거를 제공할 수 있다. 혈액 내 대리 바이오마커(예컨대, 종양 부하 마커, 사이토카인, 케모카인, IC 하위집단, 유전자 발현 및 순환 종양 DNA)와 약물 용량, 유효성 및 안전성 평가변수 간의 상관관계를 통해, 어떤 환자가 특정 치료 조합으로부터 이점을 획득할 가능성이 더 높은지 예측할 수 있는 미래 치료를 정의하는 데 도움이 되는 혈액 기반 바이오마커를 개발할 수 있다.Blood samples for biomarker evaluation are collected at baseline during the study period. Changes in biomarkers in the blood can provide evidence of biological activity of a particular treatment combination. Correlation between surrogate biomarkers in blood (e.g., tumor burden markers, cytokines, chemokines, IC subpopulations, gene expression, and circulating tumor DNA) and drug dose, efficacy, and safety endpoints can help determine whether a patient is from a particular treatment combination. Blood-based biomarkers could be developed to help define future treatments that could predict whether they are more likely to achieve a benefit.
기준선 종양 조직 샘플은 바람직하게는 연구 시작 시 실시한 생검을 통해 모든 환자로부터 수집한다. 기준선에서 수집된 종양 조직 샘플은 PD-L1 및 TIGIT 발현의 결정 및 바이오마커에 대한 탐색 연구에 사용된다. 시험자가 임상적으로 가능하다고 판단하는 경우, 종양 조직은 시험자에 의해 결정된 허용할 수 없는 독성, RECIST v1.1에 따른 질병 진행 또는 임상적 이점의 상실로 인해 병기 1 동안 중단한 환자로부터 수집되어, 내성, 질병 진행 및 연구 치료의 임상적 이점과 관련된 종양 조직 바이오마커의 분석을 할 수 있다. Baseline tumor tissue samples are preferably collected from all patients via biopsies performed at the start of the study. Tumor tissue samples collected at baseline are used for determination of PD-L1 and TIGIT expression and for screening studies for biomarkers. If the investigator determines that it is clinically feasible, tumor tissue is collected from a patient who discontinued during Stage 1 due to unacceptable toxicity as determined by the investigator, disease progression according to RECIST v1.1, or loss of clinical benefit; Analysis of tumor tissue biomarkers associated with resistance, disease progression, and clinical benefit of the study treatment is possible.
시험자가 임상적으로 가능하다고 판단하는 경우, 동일한 CIT 조합으로 치료된 최소 15명의 환자로부터 치료 중 조직 샘플이 이미 수집되고 평가 가능한 것으로 결정되지 않는 한, 확장 단계 동안 실험군에 등록된 환자는 병기 1 치료 개시 후 4주(±7일)에 치료 중 생검을 받는다. CIT 조합(면역 탈출 포함)을 사용한 치료 동안 발생하는 잠재적인 생물학적 변화를 더 잘 이해하거나, 약력학적 효과의 증거를 제공하거나, 또는 가정된 작용 기전을 확인하기 위한 노력의 일환으로 치료 중 조직 샘플이 수집된다.If the investigator determines that it is clinically feasible, patients enrolled in the experimental arm during the expansion phase will be treated with Stage 1 unless tissue samples have already been collected during treatment from at least 15 patients treated with the same CIT combination and determined to be evaluable. On-treatment biopsies are taken 4 weeks (± 7 days) after initiation. In an effort to better understand the potential biological changes that occur during treatment with CIT combinations (including immune escape), to provide evidence of pharmacodynamic effects, or to identify a hypothesized mechanism of action, tissue samples are are collected
종양 샘플은 종양 침윤 IC, PD-L1, TIGIT 및 CD8과 같은 바이오마커에 대해 평가된다. 종양 침윤 IC의 개수 및 기능적 상태의 변화를 비롯한 각 군 내 치료에 대한 종양 미세 환경의 평가를 통해, 상정된 작용 기전을 검증하고 특정 치료 조합에 대한 적절한 용량 및 노출이 달성되었는지 확인할 수 있다.Tumor samples are evaluated for biomarkers such as tumor infiltrating IC, PD-L1, TIGIT and CD8. Assessment of the tumor microenvironment for treatments within each group, including changes in the number and functional status of tumor infiltrating ICs, can validate the postulated mechanism of action and ensure that appropriate doses and exposures for specific treatment combinations have been achieved.
종양 조직 및 혈액 샘플은 WES를 포함한 NGS를 사용하여 분석되어, 연구 약물에 대한 반응을 예측하거나, 더 중증의 질병 상태로의 진행과 연관되거나, 연구 약물에 대한 획득 내성과 연관되거나, 이상 반응 발생에 대한 민감성과 연관되거나, 또는 질병 생물학에 대한 지식과 이해를 높일 수 있는 체세포 돌연변이를 식별할 수 있다.Tumor tissue and blood samples are analyzed using NGS, including WES, to predict response to study drug, to be associated with progression to a more severe disease state, to be associated with acquired resistance to study drug, or to develop adverse events Identify somatic mutations that are associated with susceptibility to, or that may increase knowledge and understanding of disease biology.
실시예 25. YO39609 연구에 대한 통계적 고려 사항 및 분석 계획Example 25. Statistical Considerations and Analysis Plan for the YO39609 Study
최종 연구 분석은 연구 중단을 통해 수집한 환자 데이터를 기반으로 한다. 달리 명시되지 않은 경우, 유효성 분석은 할당된 치료 요법에 대해 각 약물의 적어도 1회 용량을 투여받는 모든 환자로 정의되는 유효성 평가 가능 모집단을 기초로 하고, 안전성 분석은 임의의 양의 연구 치료제를 투여 받은 모든 환자로 정의되는 안전성 평가 가능 모집단을 기초로 한다.The final study analysis is based on patient data collected through study discontinuation. Unless otherwise specified, efficacy analyzes are based on an efficacy evaluable population defined as all patients receiving at least one dose of each drug for their assigned treatment regimen, and safety analyzes are based on administration of any amount of study treatment. It is based on a safety evaluable population defined as all patients received.
또한, 결과는 병기 2 치료가 가능할 때마다 병기(병기 1 또는 병기 2)별로 요약된다. 또한, 결과는 병기 2 치료가 가능할 때마다 병기(병기 1 또는 병기 2)별로 요약된다. 데이터는 샘플 크기에 따라 설명되고 요약된다. 연속 변수는 평균, 표준 편차, 중앙값, 및 범위를 사용하여 요약된다. 범주형 변수는 개수 및 백분율을 사용하여 요약된다. 표본 크기가 작은 경우에는 표 대신 목록을 사용한다.In addition, results are summarized by stage (Stage 1 or Stage 2) whenever stage 2 treatment is available. In addition, results are summarized by stage (Stage 1 or Stage 2) whenever stage 2 treatment is available. Data are described and summarized according to sample size. Continuous variables are summarized using mean, standard deviation, median, and range. Categorical variables are summarized using counts and percentages. For small sample sizes, a list is used instead of a table.
병기 2 유효성 및 안전성 분석을 위해 새로운 기준선 값이 설정된다. 종양 반응의 평가를 위해, 새로운 기준선 종양 평가가 수립된다. 다른 평가변수(예컨대, 활력 징후 또는 실험실 검사 결과의 기준선으로부터의 변화)의 경우, 병기 2 동안 환자의 첫 번째 투여 이전의 누락되지 않은 마지막 값이 새로운 기준선의 역할을 한다.New baseline values are established for stage 2 efficacy and safety analyses. For assessment of tumor response, a new baseline tumor assessment is established. For other endpoints (eg, changes from baseline in vital signs or laboratory test results), the last unassigned value prior to the patient's first dose during Stage 2 serves as the new baseline.
샘플 크기의 결정Determination of sample size
이 연구는 가설 분석을 위해 명백한 분석력 및 제1종 오류를 고려하도록 설계되지 않았다. 대신, 이 연구는 식도암 환자에게 투여시 면역요법 기반 치료 조합에 대한 예비 유효성, 안전성 및 PK 데이터를 얻기 위해 설계되었다.This study was not designed to account for apparent analytical power and Type I error for hypothesis analysis. Instead, this study was designed to obtain preliminary efficacy, safety, and PK data for an immunotherapy-based treatment combination when administered to patients with esophageal cancer.
상기 연구는 이 설정에서 이전에 전신 요법을 받은 적이 없는 식도암 환자를 등록한다. 약 100명 내지 165명의 환자가 연구 기간 동안 대조군 및 실험군에 무작위로 배정된다.The study enrolls patients with esophageal cancer who have not previously received systemic therapy in this setting. Approximately 100 to 165 patients are randomly assigned to control and experimental groups for the duration of the study.
G.G. 유효성 분석Validity analysis
유효성 평가 가능한 집단은 배정된 치료 요법에 대해 각 약물의 적어도 1회 용량을 투여받은 모든 환자로 정의된다. 유효성 평가변수는 실제 치료군별로 요약된다.Efficacy evaluable population is defined as all patients who received at least one dose of each drug for their assigned treatment regimen. Efficacy endpoints are summarized by actual treatment group.
일차 유효성 평가변수Primary efficacy endpoint
일차 유효성 평가변수는 객관적 반응을 보인 환자의 비율로 정의되는 RECIST v1.1을 기반으로 한 병기 1 동안의 객관적 반응률(ORR)이다. 객관적 반응은 RECIST v1.1을 사용하여 시험자가 결정한 ≥ 4주 간격으로 연속 2회에 걸친 완전 반응 또는 부분 반응으로 정의된다. 기준선 이후 종양 평가가 없는 환자를 포함하여 이 기준을 충족하지 않는 환자는 무반응자로 간주된다. ORR과 그 95% Ci(클로퍼-피어슨 방법)가 요약된다. ORR에 대한 분석 집단은 유효성 평가 가능한 집단이다.The primary endpoint is the objective response rate (ORR) during stage 1 based on RECIST v1.1, defined as the proportion of patients with an objective response. Objective response is defined as a complete response or partial response in two consecutive ≥ 4 weeks intervals as determined by the investigator using RECIST v1.1. Patients who do not meet these criteria, including those without a post-baseline tumor assessment, are considered non-responders. ORR and its 95% Ci (Cloper-Pearson method) are summarized. The analysis population for ORR is a population that can be evaluated for effectiveness.
이차 유효성 평가변수secondary efficacy endpoint
이차 유효성 평가변수는 표 77에 정의된 PFS, OS, 특정 시점(예컨대, 6개월 및 12개월)에서의 OS, 반응 기간(DOR), 병기 1 동안 질병 통제, TIGIT 양성 종양 환자의 객관적 반응 및 PD-L1 양성 종양 환자의 객관적 반응이다. PFS, DOR 및 질병 통제는 RECIST v1.1에 따라 시험자가 결정한다.Secondary efficacy endpoints were PFS, OS, OS at specific time points (e.g., 6 and 12 months), duration of response (DOR), disease control during stage 1, objective response and PD in patients with TIGIT positive tumors as defined in Table 77. -The objective response of patients with L1-positive tumors. PFS, DOR and disease control are determined by the investigator according to RECIST v1.1.
DOR은 확인된 완전 또는 부분 반응을 보인 유효성 평가 가능한 환자에 대해 도출된다. 연구 단계에서 기록된 질병 진행 또는 사망이 없는 환자의 경우, PFS 및 DOR은 마지막 종양 평가 당일에 검열 및 삭제된다. OS 분석 시점에서 계속 살아 있는 환자는 생존이 공지된 마지막 날짜에 중도 절단된다.A DOR is derived for evaluable patients with a confirmed complete or partial response. For patients with no documented disease progression or death during the study phase, PFS and DOR are censored and cleared on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day survival is known.
카플란-마이어 방법은 브룩마이어 및 크라울리 방법을 사용하여 구성된 90% 신뢰 구간(CI)으로 PFS, OS 및 DOR의 중앙값을 추정하는 데 사용된다. 또한, 특정 시점에서의 OS 비율이 분산의 그린우드 추정치에 기반하여 계산된 90% Ci로 카플란-마이어 방법을 사용하여 추정된다.The Kaplan-Meier method is used to estimate the median of PFS, OS, and DOR with 90% confidence intervals (CI) constructed using Brookmeier and Crowley methods. In addition, the OS ratio at any point in time is estimated using the Kaplan-Meier method with 90% Ci calculated based on Greenwood estimates of variance.
≥ 16주 동안의 안정적인 질병, 부분 반응 또는 완전 반응을 보인 환자의 비율로 정의되는 질병 통제율은 클로퍼-피어슨 직접 확률법을 사용하여 추정된 90% CI로 각 치료군에 대해 계산된다.Disease control rate, defined as the proportion of patients with stable disease, partial response, or complete response for ≥ 16 weeks, is calculated for each treatment arm with an estimated 90% CI using the Klopper-Pearson direct probability method.
탐색적 유효성 평가변수Exploratory validity endpoints
탐색적 유효성 평가변수는 iRECIST에 따라 시험자가 결정한 병기 1 동안의 객관적 반응, PFS, DOR 및 질병 통제, 및 RECIST v1.1 및 iRECIST에 따라 시험자가 결정한 병기 2 동안의 객관적 반응, PFS, DOR 및 질병 통제이다.Exploratory efficacy endpoints were investigator-determined objective response during Stage 1, PFS, DOR, and disease control according to iRECIST, and investigator-determined objective response, PFS, DOR, and disease during stage 2 according to RECIST v1.1 and iRECIST. it is control
H.H. 안전성 분석Safety analysis
안전성 분석에는 연구 치료의 임의의 구성 요소의 적어도 1회 용량을 투여받은 모든 환자가 포함된다. 연구 치료에 대한 노출은 전반적으로 그리고 각 병기 내에서 실제 치료군별로 요약된다.The safety analysis includes all patients who received at least one dose of any component of the study treatment. Exposure to study treatment is summarized by actual treatment group, both overall and within each arm.
이상 반응의 축어적 용어는 규제 활동을 위한 의학 사전(Medical Dictionary for Regulatory Activities)의 유의어 용어에 대응되며, 이상 반응의 증증도는 NCI CTCAE v4.0에 따라 등급이 매겨진다.Verbose terms of adverse events correspond to synonym terms in the Medical Dictionary for Regulatory Activities, and severity of adverse events is graded according to NCI CTCAE v4.0.
안전성은 이상 반응에 대한 요약, 실험실 검사 결과의 변화, 활력 징후 및 ECG의 변화, 연구 약물에 대한 노출을 통해 평가한다. 병용 치료에 대한 노출 및 안전성 추적 기간은 각 단계 내 치료군 별로 요약되어 있다.Safety is assessed through a summary of adverse events, changes in laboratory test results, changes in vital signs and ECGs, and exposure to study drug. Exposure and safety follow-up periods for combination therapy are summarized for each treatment group within each phase.
치료 개시 후 발생하는 치료 관련 이상 반응이 요약되어 있다. 각 환자에 대해, 각 이상 반응에 대해 보고된 최대 증증도는 증증도 등급별 요약에 사용된다. 모든 치료 유발 이상 반응, 심각한 이상 반응, 연구 치료의 중단을 초래하는 이상 반응, ≥ 3등급 이상 반응, 사망 및 사망 원인이 매핑된 용어, 적절한 시소러스 수준 및 NCI CTCAE 중증도 등급으로 나열 및 요약된다.Treatment-related adverse events occurring after initiation of treatment are summarized. For each patient, the maximum severity reported for each adverse event is used for the summary by severity grade. All treatment-induced adverse events, serious adverse events, adverse events leading to discontinuation of study treatment, ≥ Grade 3 adverse events, death and cause of death are listed and summarized in terms of mapped, appropriate thesaurus level, and NCI CTCAE severity grade.
관련 실험실, 활력 징후(맥박수, 호흡수, 맥박 산소 측정, 혈압 및 체온) 및 ECG 데이터가 시간별로 표시되며, 적절한 경우 등급이 식별된다. 또한, 선택된 실험실 시험의 변화표(shift table)는 기준선 및 기준선 이후 최대 증증도 등급을 요약하는 데 사용한다. 활력 징후 및 ECG의 변화가 요약되어 있다.Relevant laboratories, vital signs (pulse rate, respiration rate, pulse oximetry, blood pressure and body temperature) and ECG data are displayed hourly and, where appropriate, grades identified. In addition, shift tables from selected laboratory tests are used to summarize baseline and post-baseline maximal severity grades. Changes in vital signs and ECG are summarized.
I.I. 약동학 분석Pharmacokinetic analysis
아테졸리주맙(적어도 1회 용량의 아테졸리주맙을 투여받는 환자) 및 아테졸리주맙과 병용하여 투여되는 특정 약물(적어도 1회 용량의 약물을 투여받는 환자)의 PK 분석을 위해 희소 샘플을 수집한다. 다양한 연구 약물의 혈청 또는 혈장 농도는 개별 값으로 보고되고, 적절한 경우 데이터가 허용하는 한 치료군별 및 사이클 및 날짜별로 요약된다(평균, 표준 편차, 변동 계수, 중앙값, 범위, 기하 평균 및 기하 평균 변동 계수). 다양한 연구 약물의 혈청 또는 혈장 농도의 개별 및 중앙값은 치료군별, 사이클별 및 날짜별로 표시된다. 복합 약물에 대한 PK 데이터는 내부 및 공개된 이전 연구로부터 입수 가능한 과거 데이터와 비교할 수 있다. 아테졸리주맙농도 데이터는 간격, 분포 용적, 농도-시간 곡선 아래 면적과 같은 PK 매개변수를 도출하기 위해 확립된 집단 PK 모델을 사용하는 다른 연구의 데이터와 통합될 수 있다.Rare samples are collected for PK analysis of atezolizumab (patients receiving at least one dose of atezolizumab) and certain drugs administered in combination with atezolizumab (patients receiving at least one dose of the drug) . Serum or plasma concentrations of various study drugs are reported as individual values and, where appropriate, summarized by treatment group and by cycle and date as data permits (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean variation). Coefficient). Individual and median serum or plasma concentrations of various study drugs are presented by treatment group, by cycle, and by date. PK data for combination drugs can be compared with historical data available from internal and published previous studies. Atezolizumab concentration data can be integrated with data from other studies using established population PK models to derive PK parameters such as interval, volume of distribution, and area under the concentration-time curve.
J.J. 면역원성 분석Immunogenicity assay
면역원성은 아테졸리주맙 및 기타 연구 치료에 대해 적절하게 평가된다. 아테졸리주맙의 면역원성 분석은 적어도 1회의 항약물 항체(ADA) 평가를 받은 모든 환자를 포함한다. 환자는 받은 치료에 따라, 또는 연구 중단 전에 치료를 받지 않은 경우 할당된 치료에 따라 그룹화된다. 아테졸리주맙의 경우, 기준선(기준선 유병률)에서 및 기준선 이후(기준선 이후 발생율)에서 ADA-양성 환자 및 ADA-음성 환자의 수 및 비율을 치료군별로 요약한다. ADA가 시험되는 다른 연구 치료제의 경우, ADA 양성은 이러한 약물의 이전 연구에 대해 설정된 표준 방법에 따라 결정한다. ADA 상태와 안전성, 유효성, PK 및 바이오마커 평가변수 간의 관계는 기술 통계를 사용하여 분석 및 보고될 수 있다.Immunogenicity is assessed as appropriate for atezolizumab and other study treatments. The immunogenicity assay of atezolizumab included all patients who received at least one antidrug antibody (ADA) evaluation. Patients are grouped according to treatment received, or according to assigned treatment if no treatment was received prior to study discontinuation. For atezolizumab, the number and proportion of ADA-positive and ADA-negative patients at baseline (baseline prevalence) and after baseline (post-baseline incidence) are summarized by treatment group. For other study treatments for which ADA is tested, ADA positivity is determined according to standard methods established for previous studies of these drugs. The relationship between ADA status and safety, efficacy, PK, and biomarker endpoints can be analyzed and reported using descriptive statistics.
K.K. 바이오마커 분석Biomarker analysis
탐색적 바이오마커 분석은 작용 및 안전성 평가변수를 고려하여 연구 약물에 대한 반응과 이러한 바이오마커의 연관성을 이해하기 위한 노력의 일환으로 수행된다.Exploratory biomarker analyzes are performed in an effort to understand the association of these biomarkers with response to study drug, taking into account action and safety endpoints.
L.L. 중간 분석Interim analysis
중간 분석은 연구 과정에 걸쳐 수행되며, 가장 빠른(병기 1) 중간 분석은 적어도 하나의 실험군이 예비 단계에서 등록을 완료하고 환자를 최소 6주 동안 추적한 경우 수행된다. 사후 확률은 대조군과 비교한 실험군에서의 임상 활동성의 중간 분석을 기반으로 치료군에 추가 등록을 안내하는 데 사용될 수 있다. 중간 분석에서 실험군의 활동성이 대조군의 활동성보다 높다고 시사되는 경우, 실험군에 25명의 추가 환자가 등록될 수 있다. 또한, 분석은 약 15명의 환자가 병기 2 치료군에 등록되고 최소 6주 동안 추적된 후에 수행된다. 병기 2 치료군에서 임상 활동성이 관찰되지 않으면, 해당 군의 추가 등록이 중단된다.Interim analyzes are performed throughout the course of the study, and the earliest (Stage 1) interim analyzes are performed when at least one experimental group has completed enrollment in the preliminary phase and patients have been followed for at least 6 weeks. The posterior probability can be used to guide further enrollment in the treatment group based on an interim analysis of clinical activity in the experimental group compared to the control group. If the interim analysis suggests that the activity of the experimental group is higher than that of the control group, 25 additional patients can be enrolled in the experimental group. In addition, the analysis is performed after approximately 15 patients have been enrolled in the Stage 2 treatment group and followed for at least 6 weeks. If clinical activity is not observed in the Stage 2 treatment arm, further enrollment in that arm will be discontinued.
실시예 26. 티라골루맙 + 아테졸리주맙 치료에 대한 예측적 바이오마커로서의 PD-L1Example 26. PD-L1 as a predictive biomarker for tiragolumab plus atezolizumab treatment
Ib상 연구(GO30103; NCT02794571)에서, 티라골루맙은 단일 요법으로, 그리고 여러 고형 종양 유형에서 아테졸리주맙과 병용되어 양호한 내약성을 나타냈다. 1L NSCLC의 무작위 II상 CITYSCAPE 연구(NCT03563716)에서, 치료 목적(ITT) 집단에서 티라골루맙 + 아테졸리주맙 대 위약 + 아테졸리주맙의 ORR 및 PFS가 임상적으로 의미있는 개선을 나타냈다. PD-L1 종양 비율 점수(TPS) ≥ 50% 하위그룹은 더 큰 개선을 나타냈다(PharmDx 22C3 IHC 분석을 사용하여 평가됨; 2019년 12월 데이터 절단; 추적 조사 중앙값 10.9개월). In a phase Ib study (GO30103; NCT02794571), tiragolumab was well tolerated as monotherapy and in combination with atezolizumab in several solid tumor types. In the randomized Phase II CITYSCAPE study of 1L NSCLC (NCT03563716), the ORR and PFS of tiragolumab plus atezolizumab versus placebo plus atezolizumab in the purpose-to-treat (ITT) population showed clinically meaningful improvements. PD-L1 Tumor Rate Score (TPS) ≥ 50% subgroups showed greater improvement (assessed using PharmDx 22C3 IHC analysis; data cutoff December 2019; median follow-up of 10.9 months).
티라골루맙 + 아테졸리주맙 치료에 대한 예측적 바이오마커로서의 PD-L1의 가치는 상이한 PD-L1 분석에서 일관된 것으로 밝혀졌다. IHC는 pharmDx 22C3 분석(ITT 집단) 및 유럽 적합성(Conformitι Europιenne) 체외 진단(CE-IVD0 VENTANA SP263 IHC 분석(바이오마커 평가 가능한 집단)을 사용하여 이용 가능한 모든 환자 샘플에 대한 PD-L1 단백질 발현을 평가하기 위해 수행되었다; PD-L1 발현 수준은 각 분석에 대해 확립된 알고리즘을 사용하여 점수를 매겼다. BEP 및 ITT 집단의 기준선 특성은 서로 유사했다(표 92).The value of PD-L1 as a predictive biomarker for tiragolumab plus atezolizumab treatment was found to be consistent across different PD-L1 assays. IHC assessed PD-L1 protein expression for all available patient samples using the pharmDx 22C3 assay (ITT population) and Conformitι Europιenne in vitro diagnostics (CE-IVD0 VENTANA SP263 IHC assay (biomarker evaluable population) The PD-L1 expression level was scored using an algorithm established for each analysis.The baseline characteristics of the BEP and ITT populations were similar to each other (Table 92).

*모든 환자가 SP263 IHC 분석으로 검사할 수 있는 이용 가능한 조직 샘플을 갖고 있지는 않았다. *Not all patients had available tissue samples that could be tested with the SP263 IHC assay.
PD-L1 하위그룹의 유병률은 2개의 IHC 분석 간에 비등했다(도 26). PD-L1 22C3 분석의 경우, 높은 TPS는 TPS ≥ 50%로 분류되었다; 낮은 TPS는 TPS 1 내지 49%로 분류되었다. SP263 IHC 분석의 경우, 높은 TC는 TC ≥ 50%로 분류되었다; 낮은 TC는 TC 1 내지 49%로 분류되었다. 티라골루맙 + 아테졸리주맙 대 아테졸리주맙 단독 요법의 비등한 ORR 및 PFS 개선이 SP263에 의해 정의된 PD-L1 양성(TC ≥ 1%) 하위그룹(PFS HR 0.56, 95% CI: 0.34-0.92)과 22C3에 의해 정의된 PD-L1-양성(TPS ≥ 1%) 하위그룹의 사이에서 나타났다(도 27a, 도 27b, 도 28a 및 도 28b). 또한, 티라골루맙 + 아테졸리주맙 대 아테졸리주맙 단독 요법의 비등한 ORR 및 PFS 개선이 SP263에 의해 정의된 고-PD-L1(TC ≥ 50%) 하위그룹(PFS HR 0.23, 95% CI: 0.10-0.53)과 22C3에 의해 정의된 고-PD-L1(TPS ≥ 50%) 하위그룹의 사이에서 나타났다 (도 29A, 29B, 30A 및 30B).The prevalence of PD-L1 subgroups was comparable between the two IHC analyzes ( FIG. 26 ). For the PD-L1 22C3 assay, high TPS was classified as TPS ≥ 50%; Low TPS was classified as TPS 1-49%. For the SP263 IHC analysis, high TC was classified as TC ≥ 50%; Low TC was classified as TC 1-49%. Equal ORR and PFS improvement of tiragolumab plus atezolizumab versus atezolizumab alone was in the PD-L1 positive (TC ≥ 1%) subgroup (PFS HR 0.56, 95% CI: 0.34-0.92) as defined by SP263 and PD-L1-positive (TPS ≥ 1%) subgroup defined by 22C3 (Fig. 27a, Fig. 27b, Fig. 28a and Fig. 28b). In addition, comparable ORR and PFS improvements of tiragolumab plus atezolizumab versus atezolizumab alone were in the high-PD-L1 (TC ≥ 50%) subgroup (PFS HR 0.23, 95% CI: 0.10) defined by SP263. −0.53) and high-PD-L1 (TPS > 50%) subgroups defined by 22C3 ( FIGS. 29A, 29B, 30A and 30B).
22C3 또는 SP263 IHC에 의해 평가되는 고 PD-L1 발현은 티라골루맙 + 아테졸리주맙 병용 요법에 대한 중요한 예측적 바이오마커일 수 있다.High PD-L1 expression as assessed by 22C3 or SP263 IHC may be an important predictive biomarker for tiragolumab plus atezolizumab combination therapy.
VII. 기타 구현예들VII. Other implementations
본원에 기재된 기술의 일부 구현예들은 구현예 세트 A, B 및 C의 번호가 부여된 구현예들 중 어느 하나에 따라 정의할 수 있다.Some implementations of the technology described herein may be defined according to any one of the numbered implementations of implementation sets A, B, and C.
구현예 세트 A:Embodiment Set A:
1. 암을 가진 대상체를 치료하는 방법으로서,1. A method of treating a subject having cancer, comprising:
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and an evacuation every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a gold-based chemotherapeutic agent.
2. 암을 가진 대상체를 치료하는 방법으로서,2. A method of treating a subject having cancer, comprising:
4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 1400 mg to 2000 mg every 4 weeks A method comprising steps.
3. 암을 가진 대상체를 치료하는 방법으로서,3. A method of treating a subject having cancer, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks A method comprising the step of
4. 구현예 2 또는 구현예 3에 있어서,4. according to embodiment 2 or embodiment 3,
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.The method further comprising administering to the subject one or more chemotherapeutic agents.
5. 구현예 1 내지 구현예 4 중 어느 한 구현예에 있어서,5. The method according to any one of embodiments 1 to 4,
상기 항 TIGIT 길항제 항체는 IgG 부류 항체, 특히 IgG1 하위부류 항체인, 방법.wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6. 구현예 1 내지 구현예 5 중 어느 한 구현예에 있어서,6. The method according to any one of embodiments 1 to 5,
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
(a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
(d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
(f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 방법.(f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
7. 구현예 1 내지 구현예 6 중 어느 한 구현예에 있어서,7. The method according to any one of embodiments 1 to 6,
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR): The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
(a) DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3 서열; 및(c) a FR-L3 sequence comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
(d) FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4, 그리고(d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and
하기의 중쇄 가변 영역 FR들:The following heavy chain variable region FRs:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
(b) WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
(d) WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 방법.(d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
8. 구현예 1 내지 구현예 7 중 어느 한 구현예에 있어서,8. The method according to any one of embodiments 1 to 7,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.(c) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19.
9. 구현예 1 내지 구현예 8 중 어느 한 구현예에 있어서,9. The method according to any one of embodiments 1 to 8,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
10. 구현예 1 내지 구현예 9 중 어느 한 구현예에 있어서,10. The method according to any one of embodiments 1 to 9,
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제 또는 PD-1 결합 길항제인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
11. 구현예 1 내지 구현예 10 중 어느 한 구현예에 있어서,11. The method according to any one of embodiments 1 to 10,
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
12. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,12. The method according to any one of embodiments 1 to 11,
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
13. 구현예 12에 있어서,13. The method of embodiment 12,
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 방법.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636.
14. 구현예 1 내지 구현예 13 중 어느 한 구현예에 있어서,14. The method according to any one of embodiments 1 to 13,
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is atezolizumab.
15. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,15. The method according to any one of embodiments 1 to 11,
상기 PD-1 축 결합 길항제는 항 PD-1 길항제 항체인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
16. 구현예 15에 있어서,16. The method of embodiment 15,
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 방법.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21.
17. 구현예 2 내지 구현예 16 중 어느 한 구현예에 있어서,17. The method according to any one of embodiments 2 to 16,
유효량의 백금계 화학요법제 및 비백금계 화학요법제를 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
18. 구현예 1 또는 구현예 17에 있어서,18. according to embodiment 1 or embodiment 17,
상기 비백금계 화학요법제는 토포이소머라제 II 억제제인, 방법.The method of claim 1, wherein the non-platinum-based chemotherapeutic agent is a topoisomerase II inhibitor.
19. 구현예 18에 있어서,19. The method of embodiment 18,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331, 특히 에토포시드인, 방법.wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331, in particular etoposide; Way.
20. 구현예 18 또는 구현예 19에 있어서,20. The method of embodiment 18 or embodiment 19,
상기 토포이소머라제 II 억제제는 100 mg/m2의 용량으로 투여되는, 방법.wherein the topoisomerase II inhibitor is administered at a dose of 100 mg/m2.
21. 구현예 17 내지 구현예 20 중 어느 한 구현예에 있어서,21. The method according to any one of embodiments 17 to 20,
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴, 특히 카보플라틴인, 방법.The method according to claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin.
22. 구현예 17 내지 구현예 21 중 어느 한 구현예에 있어서,22. The method according to any one of embodiments 17 to 21,
상기 백금계 화학요법제는 투여 당일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 방법.wherein the platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
23. 구현예 1 내지 구현예 22 중 어느 한 구현예에 있어서,23. The method according to any one of embodiments 1-22,
유도기 및 유지기를 포함한 투약 요법을 포함하는, 방법.A method comprising a dosing regimen comprising an induction phase and a maintenance phase.
24. 구현예 23에 있어서,24. The method of embodiment 23,
상기 유도기는 4회의 초기 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제가 4회의 초기 투약 주기의 각각에서 투여되는, 방법.wherein the induction phase comprises four initial dosing cycles and the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles.
25. 구현예 23 또는 구현예 24에 있어서,25. according to embodiment 23 or embodiment 24,
상기 유지기는 상기 백금계 화학요법제 및/또는 비백금계 화학요법제의 투여를 포함하지 않는, 방법.wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent and/or the non-platinum-based chemotherapeutic agent.
26. 구현예 1 내지 구현예 25 중 어느 한 구현예에 있어서,26. The method according to any one of embodiments 1 to 25,
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장하는, 방법.wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody.
27. 구현예 1 내지 구현예 26 중 어느 한 구현예에 있어서,27. The method according to any one of embodiments 1-26,
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 전체 생존을 연장하는, 방법.wherein said treatment prolongs overall survival of said subject compared to treatment without said anti-TIGIT antagonist antibody.
28. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,28. The method according to any one of embodiments 1 to 27,
상기 암은 폐암인, 방법.The method of claim 1, wherein the cancer is lung cancer.
29. 구현예 28에 있어서,29. The method of embodiment 28,
상기 폐암은 소세포 폐암(SCLC), 특히 확장기 SCLC(ES-SCLC)인, 방법.The method of claim 1, wherein the lung cancer is small cell lung cancer (SCLC), in particular expanded stage SCLC (ES-SCLC).
30. 구현예 28에 있어서,30. The method of embodiment 28,
상기 폐암은 소세포 폐암(SCLC), 특히 국소 진행성 절제 불가능한 NSCLC(IIIB기 NSCLC)인, 방법.wherein the lung cancer is small cell lung cancer (SCLC), in particular locally advanced unresectable NSCLC (stage IIIB NSCLC).
31. 구현예 28에 있어서,31. The method of embodiment 28,
상기 폐암은 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 방법.wherein the lung cancer is locally advanced unresectable or metastatic nonsquamous NSCLC.
32. 구현예 28에 있어서,32. The method of embodiment 28,
상기 폐암은 절제 가능한 폐암인, 방법.The method of claim 1, wherein the lung cancer is resectable lung cancer.
33. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,33. The method according to any one of embodiments 1 to 27,
상기 암은 자궁경부암인, 방법.The method of claim 1, wherein the cancer is cervical cancer.
34. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,34. The method according to any one of embodiments 1 to 27,
상기 암은 초기 삼중음성 유방암(eTNBC)인, 방법.wherein the cancer is early triple negative breast cancer (eTNBC).
35. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,35. The method according to any one of embodiments 1 to 27,
상기 암은 두경부암인, 방법.The method of claim 1, wherein the cancer is head and neck cancer.
36. 구현예 1 내지 구현예 27 중 어느 한 구현예있어서,36. The method of any of embodiments 1-27,
상기 암은 간암, 특히 간세포 암종(HCC)인, 방법.wherein the cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
37. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,37. The method according to any one of embodiments 1 to 27,
상기 암은 방광암인, 방법.wherein the cancer is bladder cancer.
38. 구현예 37에 있어서,38. The method of embodiment 37,
상기 암은 요로상피세포 암종(UC), 특히 전이성 요로상피세포 암종(mUC)인, 방법.wherein the cancer is urothelial cell carcinoma (UC), in particular metastatic urothelial cell carcinoma (mUC).
39. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,39. The method according to any one of embodiments 1 to 27,
상기 암은 췌장암, 특히 췌장 관세포암(PDAC)인, 방법.The method of claim 1, wherein the cancer is pancreatic cancer, particularly pancreatic ductal cell carcinoma (PDAC).
40. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,40. The method according to any one of embodiments 1 to 27,
상기 암은 식도암, 특히 진행성 또는 전이성 식도암인, 방법.The method of claim 1, wherein the cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
41. 구현예 1 내지 구현예 40 중 어느 한 구현예의 방법에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한 항 TIGIT 길항제 항체를 포함하는, 키트.41. A kit comprising an anti TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to the method of any one of embodiments 1-40.
42. 구현예 41에 있어서,42. The method of embodiment 41,
하나 이상의 화학요법제를 포함하는, 키트.A kit comprising one or more chemotherapeutic agents.
43. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,43. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 방법은 구현예 1 내지 구현예 40 중 어느 한 구현예에 따르는, 항 TIGIT 길항제 항체 및 항 PD-1 축 결합 길항제.The method comprises an anti-TIGIT antagonist antibody and an anti-PD-1 axis binding antagonist according to any one of embodiments 1 to 40.
44. 암을 가진 대상체를 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용되는 항 TIGIT 길항제 항체의 사용으로서,44. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, comprising:
상기 치료는 구현예 1 내지 구현예 40 중 어느 한 구현예의 방법에 따르는, 사용.Use, wherein said treatment is according to the method of any one of embodiments 1 to 40.
45. 구현예 44에 있어서,45. The method of embodiment 44,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
46. 구현예 44에 있어서,46. The method of embodiment 44,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
47. 암을 가진 대상체를 치료하는 방법으로서,47. A method of treating a subject having cancer, comprising:
4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks A method comprising steps.
48. 암을 가진 대상체를 치료하는 방법으로서,48. A method of treating a subject having cancer, comprising:
4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a dose of about 20 mg to about 1600 mg of a PD-1 axis binding antagonist every 2 weeks A method comprising steps.
49. 암을 가진 대상체를 치료하는 방법으로서,49. A method of treating a subject having cancer, comprising:
2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every 2 weeks and a dose of about 20 mg to about 1600 mg of a PD-1 axis binding antagonist every 2 weeks A method comprising the step of
50. 암을 가진 대상체를 치료하는 방법으로서,50. A method of treating a subject having cancer, comprising:
2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every 2 weeks and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks A method comprising steps.
51. 암을 가진 대상체를 치료하는 방법으로서,51. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 6주마다 약 100 mg 내지 약 1000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 100 mg to about 1000 mg every 6 weeks A method comprising steps.
52. 구현예 47 내지 구현예 51 중 어느 한 구현예에 있어서,52. The method according to any one of embodiments 47 to 51,
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.The method further comprising administering to the subject one or more chemotherapeutic agents.
53. 구현예 52에 있어서,53. The method of embodiment 52,
백금계 화학요법제 및 비백금계 화학요법제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent to the subject.
54. 암을 가진 대상체를 치료하는 방법으로서,54. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, platinum-based chemotherapeutic agent every 3 weeks, and non-vaccine every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a gold-based chemotherapeutic agent.
55. 구현예 53 또는 구현예 54에 있어서,55. according to embodiment 53 or embodiment 54,
유도기 및 유지기를 포함하는, 방법.A method comprising an induction phase and a maintenance phase.
56. 구현예 55에 있어서,56. of embodiment 55,
상기 유도기 및 유지기는 각각 1회 이상의 투약 주기를 포함하는, 방법.wherein the induction and maintenance phases each comprise one or more dosing cycles.
57. 구현예 55 또는 구현예 56에 있어서,57. according to embodiment 55 or embodiment 56,
상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent.
58. 구현예 55 내지 구현예 57 중 어느 한 구현예에 있어서,58. The method according to any one of embodiments 55 to 57,
상기 유지기는 상기 비백금계 화학요법제의 투여를 포함하지 않는, 방법.The method of claim 1, wherein the maintenance phase does not include administration of the non-platinum-based chemotherapeutic agent.
59. 구현예 58에 있어서,59. The method of embodiment 58,
상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하는, 방법.wherein said maintenance phase comprises one or more dosing cycles of anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks.
60. 암을 가진 대상체를 치료하는 방법으로서,60. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and an anti-PD-1 antagonist antibody at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the anti-PD-1 antagonist antibody is pembrolizumab.
61. 암을 가진 대상체를 치료하는 방법으로서,61. A method of treating a subject having cancer, comprising:
티라골루맙 및 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 100 mg 내지 약 1000 mg의 용량으로 투여되는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein the pembrolizumab is administered at a dose of about 100 mg to about 1000 mg every 6 weeks; Way.
62. 암을 가진 대상체를 치료하는 방법으로서,62. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and 1 day every 3 weeks of 2 weeks dosing/1 week washout A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of an antimetabolite at a dose of about 10 mg/m2 to about 10000 mg/m2 orally in two oral doses.
63. 암을 가진 대상체를 치료하는 방법으로서,63. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 젬시타빈, 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.one or more dosing cycles of anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, gemcitabine, and nap-paclitaxel A method comprising administering to the subject a dosing regimen comprising
64. 구현예 52에 있어서,64. The method of embodiment 52,
상기 하나 이상의 화학요법제는 젬시타빈 및 냅-파클리탁셀인, 방법.wherein the one or more chemotherapeutic agents are gemcitabine and nap-paclitaxel.
65. 암을 가진 대상체를 치료하는 방법으로서,65. A method of treating a subject having cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg 용량의 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and about 1 mg/kg to about 35 mg/kg every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a kg dose of a VEGF antagonist.
66. 암을 가진 대상체를 치료하는 방법으로서,66. A method of treating a subject having cancer, comprising:
유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.(b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said maintenance wherein the phase does not include administration of the platinum-based chemotherapeutic agent.
67. 암을 가진 대상체를 치료하는 방법으로서,67. A method of treating a subject having cancer, comprising:
유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는, 방법.(b) the maintenance phase comprises one or more additional dosing cycles of the anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks and wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent.
68. 구현예 56 내지 구현예 59, 구현예 66 및 구현예 67 중 어느 한 구현예에 있어서,68. The method of any one of embodiments 56-59, 66 and 67,
상기 유도기는 4 내지 6회의 투약 주기를 포함하는, 방법.wherein the induction phase comprises 4 to 6 dosing cycles.
69. 구현예 53 내지 구현예 59 및 구현예 66 내지 구현예 68 중 어느 한 구현예에 있어서,69. The method of any one of embodiments 53-59 and 66-68,
(a) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고;(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이거나; 또는(a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel; or
(c) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 에토포시드인, 방법.(c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is etoposide.
70. 구현예 47 내지 구현예 69 중 어느 한 구현예에 있어서,70. The method according to any one of embodiments 47 to 69,
상기 암은 고형 종양인, 방법. wherein the cancer is a solid tumor.
71. 구현예 47 내지 구현예 70 중 어느 한 구현예에 있어서,71. The method according to any one of embodiments 47 to 70,
상기 암은 국소 진행성 또는 전이성인, 방법.wherein the cancer is locally advanced or metastatic.
72. 구현예 47 내지 구현예 71 중 어느 한 구현예에 있어서,72. The method according to any one of embodiments 47 to 71,
상기 암은 폐암, 췌장암, 자궁경부암, 유방암, 두경부암, 간암, 방광암, 식도암, 위암, 결장직장암, 신장암, 신장암, 흑색종, 또는 난소암인, 방법.wherein the cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, kidney cancer, melanoma, or ovarian cancer.
73. 구현예 72에 있어서,73. The method of embodiment 72,
상기 암은 폐암인, 방법.The method of claim 1, wherein the cancer is lung cancer.
74. 구현예 73에 있어서,74. The method of embodiment 73,
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 NSCLC인, 방법.wherein the lung cancer is NSCLC, in particular locally advanced unresectable NSCLC.
75. 구현예 74에 있어서,75. The method of embodiment 74,
상기 NSCLC는 IIIB기 NSCLC인, 방법.wherein said NSCLC is stage IIIB NSCLC.
76. 구현예 73 내지 구현예 75 중 어느 한 구현예에 있어서,76. The method according to any one of embodiments 73 to 75,
상기 폐암은 재발성 또는 전이성 NSCLC인, 방법.wherein the lung cancer is relapsed or metastatic NSCLC.
77. 구현예 76에 있어서,77. The method of embodiment 76,
상기 NSCLC는 3기 NSCLC인, 방법.The method of claim 1, wherein the NSCLC is stage 3 NSCLC.
78. 구현예 77에 있어서,78. The method of embodiment 77,
상기 대상체는 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는, 방법.wherein the subject has not been previously treated for stage IV NSCLC.
79. 구현예 73에 있어서,79. The method of embodiment 73,
상기 폐암은 소세포 폐암(SCLC)인, 방법.wherein the lung cancer is small cell lung cancer (SCLC).
80. 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,80. A method of treating a subject or population of subjects having lung cancer, the method comprising:
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장시키는, 방법.administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody; Way.
81. 폐암을 가진 대상체 집단을 치료하는 방법으로서,81. A method of treating a population of subjects having lung cancer, comprising:
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 치료는 약 8.2개월 내지 약 9.2개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor, wherein wherein said treatment results in a median PFS of the subject population of from about 8.2 months to about 9.2 months.
82. 구현예 80 또는 구현예 81에 있어서,82. The method of embodiment 80 or embodiment 81,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)을 연장시키는, 방법.wherein said treatment prolongs overall survival (OS) of said subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody; Way.
83. 구현예 80 내지 구현예 82 중 어느 한 구현예에 있어서,83. The method according to any one of embodiments 80 to 82,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼 연장시키는, 방법.wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 2.4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , Way.
84. 구현예 83에 있어서,84. The method of embodiment 83,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3개월 내지 약 4개월 만큼 연장시키는, 방법.wherein said treatment reduces the PFS of said subject or population of subjects by at least about 3 months to about 4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. How to extend by months.
85. 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,85. A method of treating a subject or population of subjects having lung cancer, the method comprising:
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 OS를 연장시키는, 방법.administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; , wherein said treatment prolongs OS in said subject as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor without said anti-TIGIT antagonist antibody.
86. 폐암을 가진 대상체 집단을 치료하는 방법으로서,86. A method of treating a population of subjects having lung cancer, comprising:
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 치료는 약 15.3개월 내지 약 17.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor, wherein wherein said treatment results in a median OS in the subject population of about 15.3 months to about 17.6 months.
87. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,87. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼 연장시키는, 방법.wherein the treatment prolongs the OS of the subject or population of subjects by at least about 3.3 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , Way.
88. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,88. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3개월 내지 약 5.3개월 만큼 연장시키는, 방법.wherein said treatment reduces the OS of said subject or population of subjects by at least about 3 months to about 5.3 as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. How to extend by months.
89. 구현예 80 내지 구현예 88 중 어느 한 구현예에 있어서,89. The method according to any one of embodiments 80 to 88,
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각에서 투여되는, 방법.wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered in each of four initial dosing cycles.
90. 구현예 80 내지 구현예 89 중 어느 한 구현예에 있어서,90. The method according to any one of embodiments 80 to 89,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 제4 초기 투약 주기 이후에 1회 이상의 추가 주기로 더 투여되는, 방법.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are further administered in one or more additional cycles after the fourth initial dosing cycle.
91. 구현예 90에 있어서,91. The method of embodiment 90,
상기 백금계 화학요법제 및 상기 토포이소머라제 II 억제제가 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 방법.wherein said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are omitted from each of one or more additional dosing cycles.
92. 구현예 80 내지 구현예 91 중 어느 한 구현예에 있어서,92. The method according to any one of embodiments 80 to 91,
상기 백금계 화학요법제는 카보플라틴이고 상기 토포이소머라제 II 억제제는 에토포시드인, 방법.wherein the platinum-based chemotherapeutic agent is carboplatin and the topoisomerase II inhibitor is etoposide.
93. 구현예 80 내지 구현예 92 중 어느 한 구현예에 있어서,93. The method according to any one of embodiments 80 to 92,
상기 폐암은 소세포 폐암(SCLC)인, 방법.wherein the lung cancer is small cell lung cancer (SCLC).
94. 구현예 93에 있어서,94. The method of embodiment 93,
상기 SCLC는 확장 병기의 SCLC(ES-SCLC)인, 방법.wherein the SCLC is an expanded stage SCLC (ES-SCLC).
95. 구현예 94에 있어서,95. The method of embodiment 94,
상기 대상체 또는 대상체들은 ES-SCLC에 대한 치료 경험이 없는, 방법.The method of claim 1, wherein the subject or subjects is naive for treatment for ES-SCLC.
96. 구현예 80 내지 구현예 95 중 어느 한 구현예에 있어서,96. The method according to any one of embodiments 80 to 95,
상기 대상체 또는 대상체들은 뇌 전이의 존재 또는 병력이 없는, 방법.The method of claim 1, wherein the subject or subjects do not have the presence or history of brain metastases.
97. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,97. The method according to any one of embodiments 80 to 96,
상기 폐암은 PD-L1 발현에 대해 선택되지 않는, 방법.The method of claim 1, wherein the lung cancer is not selected for PD-L1 expression.
98. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,98. The method according to any one of embodiments 80 to 96,
상기 폐암은 PD-L1 발현에 대해 선택되는, 방법.wherein the lung cancer is selected for PD-L1 expression.
99. 구현예 98에 있어서,99. The method of embodiment 98,
상기 폐암은 PD-L1의 검출 가능한 발현 수준에 의해 PD-L1 발현에 대해 선택되는, 방법.wherein the lung cancer is selected for PD-L1 expression by a detectable expression level of PD-L1.
100. 구현예 80 내지 구현예 99 중 어느 한 구현예에 있어서,100. The method according to any one of embodiments 80 to 99,
상기 폐암은 전이성인, 방법.wherein the lung cancer is metastatic.
101. 구현예 100에 있어서,101. The method of embodiment 100,
상기 폐암은 뇌, 간, 림프절, 및/또는 부신으로 전이된, 방법.The method of claim 1, wherein the lung cancer has metastasized to the brain, liver, lymph nodes, and/or adrenal glands.
102. 구현예 100 또는 구현예 101에 있어서,102. The method of embodiment 100 or embodiment 101,
상기 폐암은 뇌로 전이되지 않는, 방법.The method of claim 1, wherein the lung cancer does not metastasize to the brain.
103. 구현예 100 내지 구현예 102 중 어느 한 구현예에 있어서,103. The method of any one of embodiments 100-102,
상기 치료는 완전 반응(CR) 또는 부분 반응(PR)을 유발하는, 방법.wherein the treatment results in a complete response (CR) or a partial response (PR).
104. 구현예 80 내지 구현예 103 중 어느 한 구현예에 있어서,104. The method according to any one of embodiments 80 to 103,
상기 항 TIGIT 길항제 항체는 2주마다, 3주마다, 또는 4주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 2 weeks, every 3 weeks, or every 4 weeks.
105. 구현예 80 내지 구현예 104 중 어느 한 구현예에 있어서,105. The method of any one of embodiments 80-104,
상기 PD-1 축 결합 길항제는 2주마다, 3주마다, 또는 4주마다 약 80 mg 내지 약 2000 mg의 용량으로 투여되는, 방법.wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 2 weeks, every 3 weeks, or every 4 weeks.
106. 구현예 80 내지 구현예 105 중 어느 한 구현예에 있어서,106. The method of any one of embodiments 80 to 105,
상기 PD-1 축 결합 길항제, 상기 항 TIGIT 길항제 항체, 상기 백금계 화학요법제, 및 상기 포토이소머라제 II 억제제는 순차적으로 투여되는, 방법.wherein the PD-1 axis binding antagonist, the anti-TIGIT antagonist antibody, the platinum-based chemotherapeutic agent, and the photoisomerase II inhibitor are administered sequentially.
107. 구현예 106에 있어서,107. The method of embodiment 106,
상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체보다 먼저 투여되고, 상기 항 TIGIT 길항제 항체는 상기 백금계 화학요법제보다 먼저 투여되며, 상기 백금제는 상기 토포이소머라제 II 억제제보다 먼저 투여되는, 방법.The PD-1 axis binding antagonist is administered before the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered before the platinum-based chemotherapeutic agent, and the platinum agent is administered before the topoisomerase II inhibitor. , Way.
108. 구현예 80 내지 구현예 107 중 어느 한 구현예에 있어서,108. The method according to any one of embodiments 80 to 107,
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제는 정맥내 투여되는, 방법.wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered intravenously.
109. 구현예 80 내지 구현예 108 중 어느 한 구현예에 있어서,109. The method according to any one of embodiments 80 to 108,
상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제는 피하 투여되는, 방법.wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered subcutaneously.
110. SCLC를 가진 대상체를 치료하는 방법으로서,110. A method of treating a subject having SCLC, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 방법.Anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle, Atezolizumab at a dose of about 80 mg to about 1600 mg on Day 1 of each dosing cycle, Day 1 of each dosing cycle Carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min, and one dose of etoposide at 100 mg/m2 on each of Days 1, 2, and 3 of each dosing cycle. administering to said subject at least a 21-day dosing cycle, wherein said treatment comprises the subject's PFS and/or compared to treatment with atezolizumab, carboplatin, and etoposide in the absence of said anti-TIGIT antagonist antibody. or extending the OS.
111. SCLC를 가진 대상체를 치료하는 방법으로서,111. A method of treating a subject having SCLC, comprising:
각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 방법.Anti TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg on day 1 of each dosing cycle, atezolizumab at a dose of about 900 mg to about 1500 mg on Day 1 of each dosing cycle, Day 1 of each dosing cycle Carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min, and one dose of etoposide at 100 mg/m2 on each of Days 1, 2, and 3 of each dosing cycle. administering to said subject at least a 21-day dosing cycle, wherein said treatment comprises the subject's PFS and/or compared to treatment with atezolizumab, carboplatin, and etoposide in the absence of said anti-TIGIT antagonist antibody. or extending the OS.
112. 구현예 110 또는 구현예 111에 있어서,112. The method of embodiment 110 or embodiment 111,
각 추가적인 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 추가적인 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 추가적인 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 카보플라틴 및 에토포시드는 상기 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 방법.One or more additional 21 doses of anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each additional dosing cycle and atezolizumab at a dose of about 80 mg to about 1600 mg on Day 1 of each additional dosing cycle administering one dosing cycle to the subject, wherein carboplatin and etoposide are omitted from each of the one or more additional dosing cycles.
113. ES-SCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,113. A method of treating a subject or population of subjects having ES-SCLC, comprising:
4회의 초기 투약 주기에 이어서 1회 이상의 추가적인 투약 주기를 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서:administering to the subject or population of subjects, four initial dosing cycles followed by one or more additional dosing cycles, wherein:
(a) 상기 4회의 초기 투약 주기는 각 초기 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 초기 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 초기 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 초기 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드를 투여하는 단계를 포함하고; 그리고(a) said four initial dosing cycles are tiragolumab at a dose of about 600 mg on day 1 of each initial dosing cycle, atezolizumab at a dose of about 1200 mg on day 1 of each initial dosing cycle, each initial dosing cycle Carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min on Day 1 of administering poside; and
(b) 상기 1회 이상의 추가적인 투약 주기는 각각의 추가적인 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각각의 추가적인 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙을 투여하는 단계를 포함하고,(b) said one or more additional dosing cycles administering about 600 mg of tiragolumab on day 1 of each additional dosing cycle and about 1200 mg of atezolizumab on day 1 of each additional dosing cycle comprising the steps of
여기서 상기 4회의 초기 투약 주기 및 상기 1회 이상의 추가적인 투약 주기는 각각의 21일 투약 주기이고, 여기서 상기 치료는 상기 티라골루맙 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 방법.wherein said four initial dosing cycles and said one or more additional dosing cycles are each 21 day dosing cycle, wherein said treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without said tiragolumab to prolong the PFS and/or OS of the subject or population of subjects.
114. 암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,114. A method of treating a subject or population of subjects having cancer, the method comprising:
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제인 제1 화학요법제, 및 비백금계 화학요법제인 제2 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하는, 방법.a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent, and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent; A method comprising administering to
115. 구현예 114에 있어서,115. The method of embodiment 114,
상기 폐암은 PD-L1 발현에 대해 평가되지 않는, 방법.wherein the lung cancer is not assessed for PD-L1 expression.
116. 구현예 114 또는 구현예 115에 있어서,116. The method of embodiment 114 or embodiment 115,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않는, 방법.The method of claim 1, wherein the subject or subjects is not determined to have a fraction of PD-L1 positive tumor cells greater than or equal to 50%.
117. 구현예 116에 있어서,117. The method of embodiment 116,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 미만인 것으로 결정되지 않는, 방법.The method of claim 1 , wherein the subject or subjects is not determined to have a fraction of PD-L1 positive tumor cells of less than 50%.
118. 구현예 116 또는 구현예 117에 있어서,118. The method of embodiment 116 or embodiment 117,
상기 PD-L1 양성 종양 세포 분획은 항 PD-L1 항체를 사용한 양성 염색에 의해 결정되고, 여기서 상기 항 PD-L1 항체는 SP263 또는 22C3인, 방법.wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, wherein said anti-PD-L1 antibody is SP263 or 22C3.
119. 구현예 114 내지 구현예 118 중 어느 한 구현예에 있어서,119. The method according to any one of embodiments 114 to 118,
상기 대상체 또는 대상체들은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 방법.The method of claim 1 , wherein the subject or subjects do not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality.
120. 구현예 114 내지 구현예 119항 중 어느 한 구현예에 있어서,120. The method according to any one of embodiments 114 to 119,
상기 대상체 또는 대상체들은 상기 폐암에 대해 선행 전신 요법을 받은 적이 없는, 방법.The method of claim 1, wherein said subject or subjects has not received prior systemic therapy for said lung cancer.
121. 구현예 114 내지 구현예 120 중 어느 한 구현예에 있어서,121. The method of any one of embodiments 114 to 120,
상기 폐암은 국소 진행성 폐암인, 방법.wherein the lung cancer is locally advanced lung cancer.
122. 구현예 114 내지 구현예 121 중 어느 한 구현예에 있어서,122. The method according to any one of embodiments 114 to 121,
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 방법.wherein the lung cancer is NSCLC, in particular locally advanced unresectable or metastatic nonsquamous NSCLC.
123. 구현예 122에 있어서,123. The method of embodiment 122,
상기 비편평 NSCLC는 IV기 비편평 NSCLC인, 방법.wherein said nonsquamous NSCLC is stage IV nonsquamous NSCLC.
124. 구현예 114 내지 구현예 123 중 어느 한 구현예에 있어서,124. The method according to any one of embodiments 114 to 123,
상기 투약 요법은 4회의 투약 주기를 포함한 유도기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 비백금계 화학요법제는 상기 유도기의 각 투약 주기의 제 1일에 투여되는, 방법.wherein the dosing regimen includes an induction phase comprising 4 dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent include each dosing cycle of the induction phase. administered on the first day of
125. 구현예 124에 있어서,125. The method of embodiment 124,
상기 투약 요법은 상기 유도기 이후에 유지기를 포함하고, 여기서 상기 유지기는 1회 이상의 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 비백금계 화학요법제는 상기 유지기의 각 투약 주기의 제 1일에 투여되는, 방법.wherein the dosing regimen comprises a maintenance phase after the induction phase, wherein the maintenance phase includes one or more dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and the non-platinum chemotherapeutic agent are the maintenance phases. administered on Day 1 of each dosing cycle of the phase.
126. 구현예 125에 있어서,126. The method of embodiment 125,
상기 유지기의 1회 이상의 투약 주기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.wherein the one or more dosing cycles of the maintenance phase do not include administration of the platinum-based chemotherapeutic agent.
127. 구현예 114 내지 구현예 126 중 어느 한 구현예에 있어서,127. The method according to any one of embodiments 114 to 126,
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드인, 방법.The method of claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed.
128. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,128. A method of treating a subject or population of subjects having advanced nonsquamous NSCLC, comprising:
티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg의 용량으로 투여되고, 상기 카보플라틴은 3주마다 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되거나, 또는 상기 시스플라틴은 3주마다 75 mg/m2의 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2의 용량으로 투여되는, 방법.administering to said subject or population of subjects a dosing regimen comprising four 21-day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed, wherein said tiragolumab comprises: Administered at a dose of about 600 mg every 3 weeks, the atezolizumab is administered at a dose of about 1200 mg every 3 weeks, and the carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min every 3 weeks. , or the cisplatin is administered at a dose of 75 mg/m2 every 3 weeks, and the pemetrexed is administered at a dose of about 500 mg/m2 every 3 weeks on each day of 4 21-day dosing cycles. , Way.
129. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,129. A method of treating a subject or population of subjects having advanced nonsquamous NSCLC, comprising:
상기 대상체 또는 대상체 집단에:To said subject or population of subjects:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m 2 every 3 weeks wherein the one or more 21-day dosing cycles of the maintenance phase do not include administration of the carboplatin,
여기서 상기 대상체 또는 대상체의 집단은 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법. wherein the subject or population of subjects has not received prior systemic therapy for advanced nonsquamous NSCLC.
130. 진행성 비편평 NSCLC를 가진 대상체를 치료하는 방법으로서,130. A method of treating a subject having advanced nonsquamous NSCLC, comprising:
상기 대상체에게:To the subject:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m2 every 3 weeks. administering, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
여기서 상기 대상체는 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법.wherein the subject has never received prior systemic therapy for advanced nonsquamous NSCLC.
131. 진행성 비편평 NSCLC를 가진 대상체를 치료하는 방법으로서,131. A method of treating a subject with advanced nonsquamous NSCLC, comprising:
티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg의 용량으로 투여되고, 상기 시스플라틴은 75 mg/m2의 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2의 용량으로 투여되는, 방법.administering to the subject a dosing regimen comprising four 21-day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed, wherein the tiragolumab is administered every three weeks is administered at a dose of about 600 mg, the atezolizumab is administered at a dose of about 1200 mg every 3 weeks, the cisplatin is administered at a dose of 75 mg/m2, and the pemetrexed is administered in each of 4 21 day dosing cycles. administered at a dose of about 500 mg/m 2 every 3 weeks on day 1 of the method.
132. 구현예 114 내지 구현예 131 중 어느 한 구현예에 있어서,132. The method according to any one of embodiments 114 to 131,
상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3.5개월 또는 약 4.7개월 만큼 연장시키는, 방법.wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 3.5 months or about 4.7 months.
133. 구현예 114 내지 구현예 132 중 어느 한 구현예에 있어서,133. The method according to any one of embodiments 114 to 132,
상기 치료는 약 12.5개월 내지 약 14.7개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.wherein said treatment results in a median PFS of a population of subjects from about 12.5 months to about 14.7 months.
134. 구현예 114 내지 구현예 133 중 어느 한 구현예에 있어서,134. The method according to any one of embodiments 114 to 133,
상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.5개월 또는 약 8.0개월 만큼 연장시키는, 방법.wherein the treatment prolongs the OS of the subject or population of subjects by at least about 5.5 months or about 8.0 months.
135. 구현예 114 내지 구현예 134 중 어느 한 구현예에 있어서,135. The method according to any one of embodiments 114 to 134,
상기 치료는 약 27.5개월 내지 약 32.0개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.wherein said treatment results in a median OS in the subject population of about 27.5 months to about 32.0 months.
136. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,136. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks How to.
137. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,137. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks How to.
138. 폐암을 가진 대상체를 치료하는 방법으로서,138. A method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of said dosing cycles is from about 30 mg to about 1200 mg every three weeks. A method comprising administering as neoadjuvant treatment a TIGIT antagonist antibody and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks.
139. 폐암을 가진 대상체를 치료하는 방법으로서,139. A method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of said dosing cycles is from about 300 mg to about 800 mg every 3 weeks. A method comprising administering as neoadjuvant treatment a TIGIT antagonist antibody and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks.
140. 구현예 138 또는 구현예 139에 있어서,140. The method of embodiment 138 or embodiment 139,
상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 용량의 PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.At least one of said dosing cycles is administered to said subject as adjuvant treatment with an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 every 3 weeks A method comprising the step of
141. 구현예 140에 있어서,141. The method of embodiment 140,
상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 용량의 PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.At least once in said dosing cycle administering to said subject as adjuvant treatment a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks and a dose of about 900 mg to about 1500 of a PD-1 axis binding antagonist every 3 weeks A method comprising the step of
142. 구현예 138 내지 구현예 141 중 어느 한 구현예에 있어서,142. The method according to any one of embodiments 138 to 141,
상기 폐암은 절제 가능한 폐암인, 방법.The method of claim 1, wherein the lung cancer is resectable lung cancer.
143. 구현예 136 내지 구현예 142 중 어느 한 구현예에 있어서,143. The method according to any one of embodiments 136 to 142,
상기 폐암은 초기 폐암인, 방법.The method of claim 1, wherein the lung cancer is early stage lung cancer.
144. 구현예 136 내지 구현예143 중 어느 한 구현예에 있어서,144. The method according to any one of embodiments 136 to 143,
상기 폐암은 II기, 2A기, 또는 IIIB기 폐암인, 방법.The method of claim 1, wherein the lung cancer is stage II, stage 2A, or stage IIIB lung cancer.
145. 구현예 136 내지 구현예 144 중 어느 한 구현예에 있어서,145. The method according to any one of embodiments 136 to 144,
상기 폐암은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 방법.wherein the lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormalities.
146. 구현예 136 내지 구현예 145 중 어느 한 구현예에 있어서,146. The method according to any one of embodiments 136 to 145,
상기 대상체는 치료 목적으로 R0 절제술에 적격인, 방법.wherein the subject is eligible for R0 resection for therapeutic purposes.
147. 구현예 136 내지 구현예 146 중 어느 한 구현예에 있어서,147. The method according to any one of embodiments 136 to 146,
상기 대상체는 폐암에 대해 선행 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject has never received prior therapy for lung cancer.
148. 구현예 147에 있어서,148. The method of embodiment 147,
상기 선행 요법은 면역요법, 화학요법, 또는 방사선요법인, 방법.wherein the prior therapy is immunotherapy, chemotherapy, or radiotherapy.
149. 구현예 136 내지 구현예 148 중 어느 한 구현예에 있어서,149. The method according to any one of embodiments 136 to 148,
상기 대상체는 백금계 화학요법에 적격인, 방법.wherein the subject is eligible for platinum-based chemotherapy.
150. 구현예 136 내지 구현예 149 중 어느 한 구현예에 있어서,150. The method of any one of embodiments 136 to 149,
상기 제1 투약 주기는 수술 전에 개시되는, 방법.wherein the first dosing cycle is initiated prior to surgery.
151. 구현예 150에 있어서,151. The method of embodiment 150,
적어도 1, 2, 3, 또는 4회의 투약 주기는 상기 수술 전에 완료되는, 방법.at least 1, 2, 3, or 4 dosing cycles are completed prior to the surgery.
152. 구현예 150 또는 구현예 151에 있어서,152. The method of embodiment 150 or embodiment 151,
4회의 투약 주기는 상기 수술 전에 완료되는, 방법.and 4 dosing cycles are completed prior to the surgery.
153. 구현예 136 내지 구현예 152 중 어느 한 구현예에 있어서,153. The method according to any one of embodiments 136 to 152,
적어도 1회의 투약 주기는 수술 후에 개시되는, 방법.at least one dosing cycle is initiated after surgery.
154. 구현예 153에 있어서,154. The method of embodiment 153,
16회의 투약 주기는 상기 수술 후에 완료되는, 방법.16 dosing cycles are completed after said surgery.
155. 구현예 150 내지 구현예 154 중 어느 한 구현예에 있어서,155. The method of any one of embodiments 150 to 154,
상기 수술은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술인, 방법.wherein the operation is lobectomy, lobectomy, bilobectomy, or pneumonectomy.
156. 구현예 136 내지 구현예 155 중 어느 한 구현예에 있어서,156. The method according to any one of embodiments 136 to 155,
방사선 요법을 더 포함하는, 방법.The method further comprising radiation therapy.
157. 구현예 156에 있어서, 157. The method of embodiment 156,
상기 방사선 요법은 수술 후 방사선 요법인, 방법.The method of claim 1, wherein the radiation therapy is post-surgery radiation therapy.
158. 구현예 136 내지 구현예 157 중 어느 한 구현예에 있어서,158. The method according to any one of embodiments 136 to 157,
하나 이상의 화학요법제를 투여하는 단계를 더 포함하는, 방법.The method further comprising administering one or more chemotherapeutic agents.
159. 구현예 158에 있어서,159. The method of embodiment 158,
상기 하나 이상의 화학요법제는 수술 후 투여되는, 방법.wherein the one or more chemotherapeutic agents are administered post-surgery.
160. 구현예 159에 있어서,160. The method of embodiment 159,
상기 하나 이상의 화학요법제는 상기 수술 후 4회 투약 주기로 투여되는, 방법.The method of claim 1, wherein the one or more chemotherapeutic agents are administered in 4 dosing cycles after the surgery.
161. 구현예 158 내지 구현예 160 중 어느 한 구현예에 있어서,161. The method according to any one of embodiments 158 to 160,
상기 하나 이상의 화학요법제는 백금계 화학요법제 및 비백금계 화학요법제인, 방법.wherein the at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
162. 구현예 161에 있어서:162. The method of embodiment 161:
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고; (a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 젬시타빈이고; (b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이고; (c) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이거나; 또는 (d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or
(e) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 젬시타빈인, 방법. (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine.
163. 구현예 136 내지 구현예 162 중 어느 한 구현예에 있어서,163. The method according to any one of embodiments 136 to 162,
상기 치료는 기준 MPR 비율과 비교하여 주요 병리학적 반응율(MPR)의 증가를 유발하는, 방법.wherein the treatment results in an increase in the major pathological response rate (MPR) compared to the baseline MPR rate.
164. 구현예 163에 있어서,164. The method of embodiment 163,
상기 기준 MPR 비율은:The reference MPR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 MPR 비율인, 방법. (b) the MPR ratio of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
165. 구현예 136 내지 구현예 164 중 어느 한 구현예에 있어서,165. The method of any one of embodiments 136 to 164,
상기 치료는 병리학적 완전 반응(pCR) 및/또는 기준 pCR 비율과 비교하여 pCR 비율의 증가를 유발하는, 방법.wherein the treatment results in an increase in the pathological complete response (pCR) and/or pCR ratio compared to a baseline pCR ratio.
166. 구현예 165에 있어서,166. The method of embodiment 165,
상기 기준 pCR 비율은:The reference pCR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 pCR 비율인, 방법. (b) the pCR ratio of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
167. 구현예 136 내지 구현예 166 중 어느 한 구현예에 있어서,167. The method according to any one of embodiments 136 to 166,
상기 치료는 기준 EFS 시간과 비교하여 무사건 생존(EFS)의 증가를 유발하는, 방법.wherein said treatment results in an increase in event-free survival (EFS) compared to baseline EFS time.
168. 구현예 167에 있어서,168. The method of embodiment 167,
상기 기준 EFS 시간은:The reference EFS time is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 EFS 시간인, 방법. (b) EFS time of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
169. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,169. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 600 mg every 3 weeks and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks How to.
170. 폐암을 가진 대상체를 치료하는 방법으로서,170. A method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of said dosing cycles is a dose of about 30 mg to about 600 mg every 3 weeks A method comprising administering as neoadjuvant treatment a TIGIT antagonist antibody and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks.
171. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,171. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.1 of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent A method comprising administering to the subject one or more dosing cycles.
172. 폐암을 가진 대상체를 치료하는 방법으로서,172. A method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제를 신보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one of the dosing cycles comprises: anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent A method comprising administering as an adjuvant treatment.
173. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,173. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및: (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금계 화학요법제; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (b) (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and: (a) (i) 5 mg/m every 3 weeks a platinum-based chemotherapeutic agent at a dose targeted to achieve an AUC of mL/min or an AUC of 6 mg/mL/min; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (b) (i) an antimetabolite at a dose of about 500 mg/m2 every 3 weeks or about 1000 mg/m2 or about 1250 mg/m2 on days 1 and 8 of each dosing cycle; or (ii) administering to the subject one or more dosing cycles of the taxane at a dose of about 100 mg/m2, about 175 mg/m2, or about 200 mg/m2 every three weeks.
174. 폐암을 가진 대상체를 치료하는 방법으로서,174. A method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 상기 대상체에게: (a) 3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체; (b) 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산이며; 여기서 상기 치료는 신보조 치료인, 방법.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one of the dosing cycles comprises: To the subject: (a) an anti TIGIT antagonist antibody at a dose of about 30 mg to about 600 mg every 3 weeks; (b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks; (c) at (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (d) administering a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) about 500 mg/m2 every 3 weeks or on days 1 and 8 of each dosing cycle. an antimetabolite at a dose of 1000 mg/m2 or about 1250 mg/m2; or (ii) a taxane at a dose of about 100 mg/m2, about 175 mg/m2, or about 200 mg/m2 every 3 weeks; wherein the treatment is neoadjuvant treatment.
175. 절제 가능한 폐암을 가진 대상체를 치료하는 방법으로서,175. A method of treating a subject having resectable lung cancer, comprising:
3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및: Tiragolumab at a dose of about 600 mg every 3 weeks, Atezolizumab at a dose of about 1200 mg every 3 weeks, and:
(a) (a)
(i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or
(ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및(ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and
(b) (b)
(i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on days 1 and 8 of each dosing cycle; or
(ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.(ii) administering to the subject one or more dosing cycles of paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every three weeks.
176. 폐암을 가진 대상체를 치료하는 방법으로서,176. A method of treating a subject having lung cancer, comprising:
티라골루맙, 아테졸리주맙, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 3주마다 약 1200 mg 용량의 아테졸리주맙; (c) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 백금계 화학요법제는: (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는 (ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및 (d) 비백금계 화학요법제이고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀이고; 여기서 상기 치료는 신보조 치료인, 방법.administering to the subject one or more dosing cycles of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one of the dosing cycles is administered to the subject: (a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks; (c) administering a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent: (i) achieves an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks a dose of carboplatin targeted to or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and (d) a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or about 1000 on days 1 and 8 of each dosing cycle gemcitabine at a dose of mg/m2 or about 1250 mg/m2; or (ii) paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; wherein the treatment is neoadjuvant treatment.
177. 비편평 NSCLC를 가진 대상체를 치료하는 방법으로서,177. A method of treating a subject having nonsquamous NSCLC, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 1200 mg의 용량으로 아테졸리주맙을 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함하고; (b) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (a) at least one dosing cycle is about a 600 mg dose of tiragolumab every 3 weeks and 3 weeks administering to the subject as neoadjuvant treatment atezolizumab at a dose of 1200 mg per time; (b) at least one dosing cycle comprising administering to the subject as adjuvant treatment a dose of about 600 mg of tiragolumab every 3 weeks and a dose of about 1200 mg of atezolizumab every 3 weeks.
178. 비편평 NSCLC를 가진 대상체를 치료하는 방법으로서,178. A method of treating a subject having nonsquamous NSCLC, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉시드; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉스를 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment and to the subject: (a) 3 weeks tiragolumab at a dose of about 600 mg each; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a targeted dose to achieve an AUC of 5 mg/mL/min every 3 weeks and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and pemetrex at a dose of about 500 mg/m2 every 3 weeks; (II) at least one of said dosing cycles is adjuvant treatment with an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising administering.
179. 폐암을 가진 대상체를 치료하는 방법으로서,179. A method of treating a subject having lung cancer, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment and to the subject: (a) 3 weeks tiragolumab at a dose of about 600 mg each; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles comprises administering as adjuvant treatment a dose of about 30 mg to about 1200 mg of tiragolumab every 3 weeks and a dose of about 80 mg to about 1600 mg of atezolizumab every 3 weeks Including method.
180. 폐암을 가진 대상체를 치료하는 방법으로서,180. A method of treating a subject having lung cancer, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein:
(I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게:(I) at least one of said dosing cycles is neoadjuvant treatment and to said subject:
(a) 3주마다 약 1200 mg 용량의 티라골루맙;(a) tyragolumab at a dose of about 1200 mg every 3 weeks;
(b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and
(c) (c)
(i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle;
(ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or
(iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 또는 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; 그리고 (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks or gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; and
(II) 상기 투약 주기 중 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 티라골루맙 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.(II) administering to the subject as adjuvant treatment at least one of said dosing cycles is tiragolumab at a dose of about 300 mg to about 800 mg every 3 weeks and atezolizumab at a dose of about 900 mg to about 1500 mg every 3 weeks A method comprising the step of:
181. 폐암을 가진 대상체를 치료하는 방법으로서,181. A method of treating a subject having lung cancer, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment and to the subject: (a) 3 weeks tiragolumab at a dose of about 600 mg each; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles comprises administering as adjuvant treatment a dose of about 600 mg of tiragolumab every 3 weeks and a dose of about 1200 mg of atezolizumab every 3 weeks.
182. 절제 가능한 편평 NSCLC를 가진 대상체를 치료하는 방법으로서,182. A method of treating a subject having resectable squamous NSCLC, comprising:
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment and to the subject: (a) 3 weeks tiragolumab at a dose of about 600 mg each; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles comprises administering as adjuvant treatment a dose of about 600 mg of tiragolumab every 3 weeks and a dose of about 1200 mg of atezolizumab every 3 weeks.
183. 구현예 136 내지 구현예 182 중 어느 한 구현예에 있어서,183. The method according to any one of embodiments 136 to 182,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.A method, wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
184. 구현예 183에 있어서,184. The method of embodiment 183,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 방법.The method, wherein the detectable protein expression level of PD-L1 is at least 50% of the PD-L1 positive tumor cell fraction.
185. 구현예 73, 구현예 114 내지 구현예 121, 및 구현예 136 내지 구현예 184 중 어느 한 구현예에 있어서,185. The method of any one of embodiments 73, 114 to 121, and embodiments 136 to 184,
상기 폐암은 NSCLC인, 방법.wherein the lung cancer is NSCLC.
186. 구현예 185에 있어서,186. The method of embodiment 185,
상기 NSCLC는 편평 NSCLC인, 방법.wherein the NSCLC is squamous NSCLC.
187. 구현예 185에 있어서,187. The method of embodiment 185,
상기 NSCLC는 비편평 NSCLC인, 방법.wherein the NSCLC is non-squamous NSCLC.
188. 구현예 72에 있어서,188. The method of embodiment 72,
상기 암은 자궁경부암인, 방법.The method of claim 1, wherein the cancer is cervical cancer.
189. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,189. A method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1, the method comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising steps.
190. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,190. A method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1, the method comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising steps.
191. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법으로서:191. A method of selecting a therapy for a subject having cervical cancer comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg의 용량으로 투여되는 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) an anti-TIGIT antagonist antibody administered at a dose of about 30 mg to about 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 and 3 selecting a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist administered at a dose of about 80 mg to about 1600 mg per week.
192. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,192. The method of any one of embodiments 189 to 191,
상기 자궁경부암은 편평세포 암종, 선편평세포 암종, 또는 선암종인, 방법.The method of claim 1, wherein the cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
193. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,193. The method according to any one of embodiments 189 to 191,
상기 자궁경부암은 IVB기, 전이성, 재발성, 또는 지속성인, 방법.wherein the cervical cancer is stage IVB, metastatic, recurrent, or persistent.
194. 구현예 189 내지 구현예 193 중 어느 한 구현예에 있어서,194. The method according to any one of embodiments 189 to 193,
상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부암인, 방법.The method of claim 1, wherein the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer.
195. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,195. The method of any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 적어군 한 라인의 선행 요법을 받은, 방법.The method of claim 1, wherein the subject or subjects have received at least one line of prior therapy.
196. 구현예 189 내지 구현예 195 중 어느 한 구현예에 있어서,196. The method according to any one of embodiments 189 to 195,
상기 대상체 또는 대상체들은 두 라인의 선행 요법을 받은, 방법.The subject or subjects have received two lines of prior therapy.
197. 구현예 189 내지 구현예 196 중 어느 한 구현예에 있어서,197. The method according to any one of embodiments 189 to 196,
상기 대상체 또는 대상체들은 2라인 초과의 선행 요법을 받은, 방법.The method of claim 1, wherein the subject or subjects have received more than two lines of prior therapy.
198. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,198. The method according to any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects have not received prior therapy.
199. 구현예 195 내지 구현예 198 중 어느 한 항에 있어서,199. The method according to any one of embodiments 195 to 198,
상기 선행 요법은 화학요법, 수술, 및/또는 방사선요법인, 방법.wherein the prior therapy is chemotherapy, surgery, and/or radiation therapy.
200. 구현예 189 및 구현예 192 내지 구현예 199 중 어느 한 구현예에 있어서,200. The method according to any one of embodiments 189 and 192 to 199,
상기 치료는 임상 반응을 유발하는, 방법.wherein said treatment elicits a clinical response.
201. 구현예 200에 있어서,201. The method of embodiment 200,
상기 임상 반응은 기준 ORR과 비교하여 대상체 집단의 객관적 반응률(ORR)의 증가인, 방법.wherein the clinical response is an increase in the objective response rate (ORR) of the subject population as compared to a baseline ORR.
202. 구현예 201에 있어서,202. The method of embodiment 201,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 방법.wherein said baseline ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
203. 구현예 200에 있어서,203. The method of embodiment 200,
상기 기준 ORR은 적어도 약 14.6% 내지 약 26%인, 방법.wherein the baseline ORR is at least about 14.6% to about 26%.
204. 구현예 200에 있어서,204. The method of embodiment 200,
상기 임상 반응은 CR 또는 PR인, 방법.wherein the clinical response is CR or PR.
205. 구현예 200 내지 구현예 204 중 어느 한 구현예에 있어서,205. The method of any one of embodiments 200 to 204,
상기 임상 반응은 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가인, 방법.The clinical response is an increase in progression-free survival (PFS) of the subject compared to a baseline PFS time, an increase in the duration of response (DOR) in the subject compared to a baseline DOR time, or an increase in the subject's progression-free survival (DOR) compared to a baseline OS time. An increase in overall survival (OS).
206. 구현예 205에 있어서:206. The method of embodiment 205:
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는(b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 방법.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
207. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법으로서,207. A method of treating a subject having cervical cancer having a detectable expression level of PD-L1, the method comprising:
3주마다 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject one or more dosing cycles of a 600 mg dose of anti-TIGIT antagonist antibody every 3 weeks and atezolizumab at a 1200 mg dose every 3 weeks.
208. 항 TIGIT 길항제 항체 및 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자궁경부암을 가진 대상체를 확인하는 방법으로서:208. A method of identifying a subject with cervical cancer who is likely to benefit from therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab, comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 식별하는 단계를 포함하는, 방법.(c) one or more dosing cycles of anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks, based on PD-L1 expression on detected tumor cells. identifying the subject as likely to benefit from a therapy comprising
209. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법으로서:209. A method of selecting a therapy for a subject having cervical cancer comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 A method comprising selecting a regimen comprising one or more dosing cycles of atezolizumab administered as a dose.
210. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법으로서,210. A method of treating a subject having cervical cancer having a detectable expression level of PD-L1, the method comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
211. 자궁경부암을 가진 대상체를 치료하는 방법으로서:211. A method of treating a subject having cervical cancer comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (a) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라졸루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 식별하는 단계; 및(c) one or more dosing cycles of tyrazolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression on detected tumor cells. identifying the subject as likely to benefit from therapy; and
(d) 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering the therapy to the identified subject.
212. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법으로서:212. A method of selecting a therapy for a subject having cervical cancer comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라골루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) tiragolumab administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 selecting a regimen comprising one or more dosing cycles of atezolizumab administered as
213. 전이성 및/또는 재발성 양성 자궁경부암을 가진 대상체를 치료하는 방법으로서:213. A method of treating a subject having metastatic and/or recurrent benign cervical cancer comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라졸루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 식별하는 단계; 및(c) one or more dosing cycles of tyrazolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression on detected tumor cells. identifying the subject as likely to benefit from therapy; and
(d) 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering the therapy to the identified subject.
214. 전이성 및/또는 재발성 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법으로서:214. A method of selecting therapy for a subject with metastatic and/or recurrent cervical cancer comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라골루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) tiragolumab administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 selecting a regimen comprising one or more dosing cycles of atezolizumab administered as
215. 구현예 189 내지 구현예 214 중 어느 한 구현예에 있어서,215. The method of any one of embodiments 189 to 214,
상기 대상체는 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 식별되는, 방법.wherein the subject is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
216. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,216. The method according to any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 SP263을 사용하여 검출되는, 방법.The method of claim 1, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
217. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,217. The method according to any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 방법.wherein the detectable expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the sample from the subject.
218. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,218. The method of any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 22C3을 사용하여 검출되는, 방법.The method of claim 1, wherein the PD-L1 expression level is detected using anti-PD-L1 antibody 22C3.
219. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,219. The method of any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 복합 양성 점수(CPS)가 1 이상인, 방법.wherein the detectable expression level of PD-L1 has a composite positive score (CPS) of 1 or greater in a sample from the subject.
220. 구현예 72에 있어서, 상기 암은 유방암인, 방법.220. The method of embodiment 72, wherein the cancer is breast cancer.
221. 유방암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,221. A method of treating a subject or population of subjects having breast cancer, comprising:
4주마다 약 840 mg 용량의 티라골루맙, 4주마다 약 1680 mg 용량의 아테졸리주맙, 및 3주 투약/1주 휴약의 약 100 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.One or more dosing cycles of tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and nap-paclitaxel at a dose of about 100 mg/m2 of 3 weeks on/1 week off A method comprising administering to the subject or population of subjects a dosing regimen comprising
222. 구현예 220 또는 구현예 221에 있어서,222. The method of embodiment 220 or embodiment 221,
상기 유방암은 삼중 음성 유방암(TNBC)인, 방법.The method of claim 1, wherein the breast cancer is triple negative breast cancer (TNBC).
223. 구현예 222에 있어서,223. The method of embodiment 222,
상기 TNBC는 절제 가능한 국소 진행성 또는 전이성 TNBC인, 방법.wherein the TNBC is resectable locally advanced or metastatic TNBC.
224. 구현예 220 내지 구현예 223 중 어느 한 구현예에 있어서,224. The method of any one of embodiments 220 to 223,
상기 대상체는 전이성 유방암에 대해 선행 전신 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject has not received prior systemic therapy for metastatic breast cancer.
225. 구현예 220 내지 구현예 224 중 어느 한 구현예에 있어서,225. The method of any one of embodiments 220-224,
상기 치료는 적어도 약 53% 내지 약 67.5%의 대상체 집단의 ORR을 유발하는, 방법.wherein said treatment results in an ORR in at least about 53% to about 67.5% of the subject population.
226. 구현예 222 내지 구현예 225 중 어느 한 구현예에 있어서,226. The method of any one of embodiments 222 to 225,
상기 치료는 약 25.0개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.wherein said treatment results in a median OS in the subject population of about 25.0 months.
227. 초기 삼중 음성 유방암(eTNBC)을 가진 대상체를 치료하는 방법으로서,227. A method of treating a subject having early stage triple negative breast cancer (eTNBC), comprising:
2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every two weeks A method comprising the step of
228. 구현예 227에 있어서,228. The method of embodiment 227,
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.The method further comprising administering to the subject one or more chemotherapeutic agents.
229. 구현예 228에 있어서,229. The method of embodiment 228,
상기 하나 이상의 화학요법제는 백금계 화학요법제, 탁산, 토포이소머라제 II 억제제, 또는 알킬화제인, 방법.The method of claim 1, wherein the at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
230. 구현예 227에 있어서,230. The method of embodiment 227,
(a) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 탁산 또는 탁산 및 백금계 화학요법제의 1회 이상의 투약 주기; 및 (b) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 토포이소머라제 II 억제제, 알킬화제, 및 과립구 집락 자극 인자(G-CSF) 또는 과립구-대식세포 집락 자극 인자(GM-CSF)의 1회 이상의 투약 주기를 투여하는 단계를 더 포함하는, 방법.(a) at least one dosing cycle of said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, and a taxane or a taxane and a platinum-based chemotherapeutic agent; and (b) said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony stimulating factor (G-CSF) or granulocyte-macrophage colony stimulating factor (GM-CSF) The method further comprising administering one or more dosing cycles of
231. 구현예 229 또는 구현예 230에 있어서,231. The method of embodiment 229 or embodiment 230,
상기 알킬화제는 시클로포스파미드인, 방법.wherein the alkylating agent is cyclophosphamide.
232. 구현예 231에 있어서,232. The method of embodiment 231,
상기 시클로포스파미드는 약 600 mg/m2의 용량으로 투여되는, 방법.wherein the cyclophosphamide is administered at a dose of about 600 mg/m2.
233. 구현예 227 내지 구현예 229, 구현예 231 및 구현예 232 중 어느 한 구현예에 있어서,233. The embodiment of any one of embodiments 227 to 229, embodiment 231 and embodiment 232,
G-CSF 또는 GM-CSF를 상기 대상체에게 더 투여하는 단계를 포함하는, 방법.further administering G-CSF or GM-CSF to the subject.
234. 구현예 230 또는 구현예 233에 있어서,234. The method of embodiment 230 or embodiment 233,
상기 G-CSF는 페그필그라스팀 또는 필그라스팀인, 방법.The G-CSF is pegfilgrastim or filgrastim, the method.
235. 구현예 234에 있어서,235. The method of embodiment 234,
상기 G-CSF는 페그필그라스팀인, 방법.The G-CSF is pegfilgrastim, the method.
236. 구현예 235에 있어서,236. The method of embodiment 235,
상기 페그필그라스팀은 약 6 mg의 용량으로 투여되는, 방법.The method of claim 1, wherein the pegfilgrastim is administered at a dose of about 6 mg.
237. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 236 중 어느 한 구현예에 있어서,237. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 236,
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF의 하나 이상의 후속 용량을 상기 대상체에게 더 투여하는 단계를 포함하는, 방법.further administering to the subject the one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF.
238. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 237 중 어느 한 구현예에 있어서,238. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 237,
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF는 각각 매주마다 1회, 2주마다 1회, 또는 3주마다 1회 투여되는, 방법.wherein the one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once every week, once every 2 weeks, or once every 3 weeks, respectively.
239. 구현예 229 내지 구현예 238 중 어느 한 구현예에 있어서,239. The method of any one of embodiments 229 to 238,
상기 백금계 화학요법제는 3주마다 투여되고, 상기 탁산은 매주 투여되고, 상기 토포이소머라제 II 억제제는 2주마다 투여되고, 상기 알킬화제는 2주마다 투여되며, 상기 G-CSF 또는 GM-CSF는 2주마다 투여되는, 방법.The platinum-based chemotherapeutic agent is administered every 3 weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every 2 weeks, the alkylating agent is administered every 2 weeks, and the G-CSF or GM- The CSF is administered every two weeks.
240. 구현예 229 내지 구현예 239 중 어느 한 구현예에 있어서,240. The method of any one of embodiments 229 to 239,
상기 탁산 또는 상기 탁산 및 상기 백금계 화학요법제는 상기 투약 요법의 처음 12주 동안 투여되는, 방법.wherein said taxane or said taxane and said platinum-based chemotherapeutic agent are administered during the first 12 weeks of said dosing regimen.
241. 구현예 229 내지 구현예 240 중 어느 한 구현예에 있어서,241. The method of any one of embodiments 229-240,
상기 토포이소머라제 II 억제제, 상기 알킬화제, 및 상기 G-CSF 또는 GM-CSF는 투약 요법의 13주 내지 19주 동안 투여되는, 방법.wherein the topoisomerase II inhibitor, the alkylating agent, and the G-CSF or GM-CSF are administered for 13 to 19 weeks of a dosing regimen.
242. 구현예 227 내지 구현예 241 중 어느 한 구현예에 있어서,242. The method according to any one of embodiments 227 to 241,
상기 투약 요법의 총 기간은 19주인, 방법.The total duration of said dosing regimen is 19 weeks.
243. 구현예 227 내지 구현예 242 중 어느 한 구현예에 있어서,243. The method of any one of embodiments 227 to 242,
신보조 치료인, 방법.Neoadjuvant therapy, method.
244. 구현예 227 내지 구현예 243 중 어느 한 구현예에 있어서,244. The method according to any one of embodiments 227 to 243,
상기 투약 요법 후에 수술이 실시되는, 방법.wherein surgery is performed after said dosing regimen.
245. 구현예 244에 있어서,245. The method of embodiment 244,
상기 수술은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 실시되는, 방법.wherein said surgery is performed between 2 and 6 weeks after the last dose of said dosing regimen.
246. 구현예 244 또는 구현예 245에 있어서,246. The method of embodiment 244 or embodiment 245,
상기 수술은 유방절제술을 포함하는, 방법.wherein the surgery comprises a mastectomy.
247. 구현예 244 내지 구현예 246 중 어느 한 구현예에 있어서,247. The method according to any one of embodiments 244 to 246,
상기 수술은 액와 림프절 수술을 포함하는, 방법.wherein the surgery comprises axillary lymph node surgery.
248. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,248. The method of any one of embodiments 229 to 247,
상기 토포이소머라제 II 억제제는 독소루비신인, 방법.wherein the topoisomerase II inhibitor is doxorubicin.
249. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,249. The method according to any one of embodiments 229 to 247,
상기 탁산은 냅-파클리탁셀이고, 상기 백금계 화학요법제는 카보플라틴이며, 상기 토포이소머라제 II 억제제는 독소루비신인, 방법.wherein the taxane is nap-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin.
250. 구현예 248 또는 구현예 249에 있어서,250. The method of embodiment 248 or embodiment 249,
독소루비신은 약 60 mg/m2의 용량으로 투여되는, 방법.The method of claim 1, wherein doxorubicin is administered at a dose of about 60 mg/m2.
251. eTNBC를 가진 대상체를 치료하는 방법으로서,251. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제, 및:Anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
252. eTNBC를 가진 대상체를 치료하는 방법으로서,252. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-L1 결합 길항제, 및:Anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and a PD-L1 binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
253. eTNBC를 가진 대상체를 치료하는 방법으로서,253. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 항 PD-L1 길항제 항체, 및:an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and an anti-PD-L1 antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
254. eTNBC를 가진 대상체를 치료하는 방법으로서,254. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 항 PD-L1 길항제 항체, 및:Thiragolumab at a dose of about 300 mg to about 600 mg every 2 weeks and an anti-PD-L1 antagonist antibody at a dose of about 600 mg to about 1200 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
255. eTNBC를 가진 대상체를 치료하는 방법으로서,255. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
256. eTNBC를 가진 대상체를 치료하는 방법으로서,256. A method of treating a subject having eTNBC, comprising:
2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:Tiragolumab at a dose of about 300 mg to about 600 mg every two weeks and atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen administering to the subject a dosing regimen comprising CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
257. eTNBC를 가진 대상체를 치료하는 방법으로서,257. A method of treating a subject having eTNBC, comprising:
2주마다 약 420 mg 용량의 티라골루맙, 2주마다 약 840 mg 용량의 아테졸리주맙, 및:Tiragolumab at a dose of about 420 mg every 2 weeks, Atezolizumab at a dose of about 840 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen administering to the subject a dosing regimen comprising CSF;
여기서 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
258. 구현예 220 내지 구현예 257 중 어느 한 구현예에 있어서,258. The method of any one of embodiments 220 to 257,
상기 대상체로부터의 종양 샘플에서 PD-L1의 검출 가능한 단백질 발현 수준은 항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정되는, 방법.wherein the detectable protein expression level of PD-L1 in a tumor sample from said subject is determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142.
259. 구현예 258에 있어서,259. The method of embodiment 258,
상기 종양 샘플에서 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율은 1% 이상인, 방법.The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (ICs) in the tumor sample is at least 1%.
260. 구현예 227 내지 구현예 259 중 어느 한 구현예있어서,260. The method of any one of embodiments 227 to 259,
상기 eTNBC는 T2-4d TNBC로 제시되는, 방법.wherein the eTNBC is presented as T2-4d TNBC.
261. 구현예 227 내지 구현예 260 중 어느 한 구현예에 있어서,261. The method according to any one of embodiments 227 to 260,
상기 eTNBC는 cT2-cT4, cN0-cN3, 및 cM0 TNBC로 제시되는, 방법.wherein the eTNBC is presented as cT2-cT4, cN0-cN3, and cM0 TNBC.
262. 구현예 227 내지 구현예 261 중 어느 한 구현예에 있어서,262. The method of any one of embodiments 227 to 261,
상기 대상체는 이전에 eTNBC에 대해 치료받은 적이 없는, 방법.wherein the subject has not been previously treated for eTNBC.
263. 구현예 227 내지 구현예 262 중 어느 한 구현예에 있어서,263. The method according to any one of embodiments 227 to 262,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 방법.wherein the treatment results in a pathological complete response (pCR).
264. 구현예 227 내지 구현예 263 중 어느 한 구현예에 있어서,264. The method of any one of embodiments 227 to 263,
상기 치료는 전체 생존(OS) 또는 무사건 생존(EFS)의 증가를 유발하는, 방법.wherein the treatment results in an increase in overall survival (OS) or event-free survival (EFS).
265. 구현예 72에 있어서,265. The method of embodiment 72,
상기 암은 두경부암인, 방법.The method of claim 1, wherein the cancer is head and neck cancer.
266. 구현예 265에 있어서,266. The method of embodiment 265,
상기 두경부암은 상기 두경부의 편평세포 암종(SCCHN)인, 방법.The method of claim 1, wherein the head and neck cancer is squamous cell carcinoma (SCCHN) of the head and neck.
267. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,267. A method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising steps.
268. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,268. A method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising steps.
269. SCCHN을 가진 대상체 또는 대상체 집단를 위한 요법을 선택하는 방법으로서:269. A method of selecting a therapy for a subject or population of subjects with SCCHN comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체 또는 대상체 집단에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and 3 weeks based on PD-L1 expression detected for said subject or population of subjects having a detectable expression level of PD-L1 selecting a regimen comprising at least one dosing cycle of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg per time.
270. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,270. A method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
271. 구현예 267 내지 구현예 270 중 어느 한 구현예에 있어서,271. The method according to any one of embodiments 267 to 270,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.wherein the subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
272. 구현예 266 내지 구현예 271 중 어느 한 구현예에 있어서,272. The method of any one of embodiments 266 to 271,
상기 SSCHN은 인간 유두종 바이러스(HPV) 양성인, 방법.wherein the SSCHN is human papillomavirus (HPV) positive.
273. 구현예 266 내지 구현예 272 중 어느 한 구현예에 있어서,273. The method according to any one of embodiments 266 to 272,
상기 SSCHN은 HPV 음성인, 방법.wherein the SSCHN is HPV negative.
274. 구현예 272 또는 구현예 273항에 있어서,274. The method of embodiment 272 or embodiment 273,
HPV 상태는 p16 IHC, 조직내(in situ) 혼성화, 또는 PCR에 의해 결정되는, 방법.HPV status is determined by p16 IHC, in situ hybridization, or PCR.
275. 구현예 266 내지 구현예 274 중 어느 한 구현예에 있어서,275. The method according to any one of embodiments 266 to 274,
상기 SCCHN은 재발성 및/또는 전이성 SCCHN인, 방법.wherein the SCCHN is recurrent and/or metastatic SCCHN.
276. 구현예 265 내지 구현예 275 중 어느 한 구현예에 있어서,276. The method according to any one of embodiments 265 to 275,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects have not received prior therapy.
277. 구현예 276에 있어서,277. The method of embodiment 276,
상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법인, 방법.wherein said prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
278. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,278. The embodiment of any one of embodiments 265-268 and embodiments 270-277,
상기 치료는 CR 또는 PR을 유발하는, 방법.wherein said treatment results in CR or PR.
279. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,279. The method according to any one of embodiments 265 to 268 and 270 to 277,
상기 치료는 기준 ORR과 비교하여 상기 대상체 집단의 객관적 반응률(ORR)의 증가를 유발하는, 방법.wherein the treatment results in an increase in the objective response rate (ORR) of the subject population as compared to a baseline ORR.
280. 구현예 279에 있어서,280. The method of embodiment 279,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 방법.wherein said baseline ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
281. 구현예 279 또는 구현예 280에 있어서,281. The method of embodiment 279 or embodiment 280,
상기 기준 ORR은 적어도 약 19% 내지 약 36%인, 방법.wherein the baseline ORR is at least about 19% to about 36%.
282. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 281 중 어느 한 구현예에 있어서,282. The method of any one of embodiments 265-268 and 270-281,
상기 치료는 기준 PFS 시간과 비교하여 상기 대상체 또는 대상체 집단의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체 또는 대상체 집단의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)의 증가를 유발하는, 방법.wherein the treatment is associated with an increase in progression-free survival (PFS) of the subject or subject population as compared to a baseline PFS time, an increase in the duration of response (DOR) of the subject or subject population compared to a baseline DOR time, or a baseline OS time and as compared to cause an increase in overall survival (OS) of the subject or population of subjects.
283. 구현예 282에 있어서:283. The method of embodiment 282:
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는 (b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 방법.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
284. 구현예 282에 있어서,284. The method of embodiment 282,
상기 기준 DOR 시간은 적어도 약 6.7개월 내지 약 23.4개월인, 방법.wherein the baseline DOR time is at least about 6.7 months to about 23.4 months.
285. 구현예 282에 있어서,285. The method of embodiment 282,
상기 기준 OS 시간은 적어도 약 11.6개월 내지 약 14.9개월인, 방법.wherein the baseline OS time is at least about 11.6 months to about 14.9 months.
286. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서,286. A method of treating a subject having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks How to.
287. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서,287. A method of treating a subject having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject one or more dosing cycles of a dose of about 1200 mg of the PD-1 axis binding antagonist every 3 weeks and a dose of about 600 mg of an anti TIGIT antagonist antibody every 3 weeks.
288. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서,288. A method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks , Way.
289. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서,289. A method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks.
290. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법으로서,290. A method of treating a subject having SCCHN having a detectable expression level of PD-L1, the method comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
291. SCCHN을 가진 대상체의 치료 방법으로서:291. A method of treating a subject with SCCHN comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 식별하는 단계; 및(c) administering the subject to one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks. identifying as a person likely to benefit from; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
292. SCCHN을 가진 대상체를 치료하는 방법으로서:292. A method of treating a subject having SCCHN comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 식별하는 단계; 및(c) administering the subject to a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks. identifying as and
(d) PD-L1의 검출가능한 발현 수준을 갖는 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
293. SCCHN을 가진 대상체를 치료하는 방법으로서:293. A method of treating a subject having SCCHN comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 식별하는 단계; 및 (c) subjecting the subject to one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks. identifying as a probable person; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
294. SCCHN을 가진 대상체를 치료하는 방법으로서:294. A method of treating a subject having SCCHN comprising:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 식별하는 단계; 및 (c) identifying the subject as likely to benefit from a therapy comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks. ; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
295. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법으로서:295. A method of selecting a therapy for a subject with SCCHN comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 selecting a regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of mg to about 1200 mg.
296. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법으로서:296. A method of selecting a therapy for a subject with SCCHN comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) a dose of about 1200 mg of a PD-1 axis binding antagonist every 3 weeks and a dose of about 600 mg of anti every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 A method comprising selecting a regimen comprising at least one dosing cycle of the TIGIT antagonist antibody.
297. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법으로서:297. A method of selecting a therapy for a subject with SCCHN comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 mg to about every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 A method comprising selecting a regimen comprising one or more dosing cycles of tiragolumab at a dose of 1200 mg.
298. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법으로서:298. A method of selecting a therapy for a subject with SCCHN comprising:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.(b) atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 A method comprising selecting a regimen comprising one or more dosing cycles.
299. 구현예 267 내지 구현예 298 중 어느 한 구현예에 있어서,299. The method according to any one of embodiments 267 to 298,
상기 PD-L1의 검출 가능한 발현 수준은 항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준인, 방법.wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1 determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody SP263.
300. 구현예 299에 있어서,300. The method of embodiment 299,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기의 종양 샘플에서:The detectable protein expression level of PD-L1 is in the tumor sample:
(a) 5% 이상; (a) at least 5%;
(b) 5% 이상 및 20% 미만; 또는 (b) at least 5% and less than 20%; or
(c) 20% 이상의 종양 관련 면역 세포(TIC)인, 방법.(c) at least 20% tumor-associated immune cells (TICs).
301. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법으로서,301. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks A method of identifying a subject having SCCHN as a probable person, comprising:
염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 방법.detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein expression level of PD-L1 with a TIC of at least 5% is and identifying the subject as likely to benefit from the therapy.
302. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법으로서,302. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks A method of identifying a subject having SCCHN as a probable person, comprising:
염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상이고 20% 미만인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 방법.detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the TIC of PD-L1 is greater than or equal to 5% and less than 20%. The method of claim 1, wherein the protein expression level identifies the subject as likely to benefit from the therapy.
303. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법으로서,303. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks A method of identifying a subject having SCCHN as a probable person, comprising:
염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 20% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 식별하는, 방법.detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein expression level of PD-L1 having a TIC of at least 20% is identifying the subject as likely to benefit from the therapy.
304. 구현예 301 내지 구현예 303 중 어느 한 구현예에 있어서,304. The method of any one of embodiments 301 to 303,
상기 대상체는 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로 확인되고 상기 방법은 상기 대상체에게 상기 요법을 투여하는 단계를 더 포함하는, 방법.wherein the subject is identified as likely to benefit from the therapy and the method further comprises administering the therapy to the subject.
305. 구현예 301 내지 구현예 304 중 어느 한 구현예에 있어서,305. The method of any one of embodiments 301 to 304,
상기 TIC는 벤타나 SP263 IHC 분석을 사용하여 결정되는, 방법.wherein the TIC is determined using a Ventana SP263 IHC assay.
306. 구현예 267 내지 구현예 305 중 어느 한 구현예에 있어서,306. The method of any one of embodiments 267 to 305,
상기 대상체 또는 대상체 집단은 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 확인되는, 방법.wherein the subject or population of subjects is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
307. 구현예 72에 있어서,307. The method of embodiment 72,
상기 암은 간암인, 방법.The method of claim 1, wherein the cancer is liver cancer.
308. 구현예 307에 있어서,308. The method of embodiment 307,
상기 간암은 간세포 암종(HCC)인, 방법. wherein the liver cancer is hepatocellular carcinoma (HCC).
309. 간세포 암종(HCC)을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,309. A method of treating a subject or population of subjects having hepatocellular carcinoma (HCC), comprising:
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체 집단은 HCC에 대해 선행 전신 요법을 받은 적이 없는, 방법.A method comprising administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the subject or population of subjects has not received prior systemic therapy for HCC. .
310. 구현예 309에 있어서,310. The method of embodiment 309,
VEGF 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 더 포함하는, 방법.The method of claim 1, further comprising administering a VEGF antagonist to the subject or population of subjects.
311. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,311. A method of treating a subject or population of subjects having HCC, comprising:
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject or population of subjects one or more dosing cycles of an anti TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist.
312. 구현예 310 및 구현예 311에 있어서,312. The method of embodiment 310 and embodiment 311,
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
313. 구현예 309 내지 구현예 312 중 어느 한 구현예에 있어서,313. The method of any one of embodiments 309 to 312,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks.
314. 구현예 313에 있어서,314. The method of embodiment 313,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 800 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 800 mg every 3 weeks.
315. 구현예 309 내지 구현예 314 중 어느 한 구현예에 있어서,315. The method of any one of embodiments 309 to 314,
상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
316. 구현예 309 내지 구현예 315 중 어느 한 구현예에 있어서,316. The method of any one of embodiments 309 to 315,
상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg의 용량으로 투여되는, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 1600 mg every 3 weeks.
317. 구현예 309 내지 구현예 316 중 어느 한 구현예에 있어서,317. The method of any one of embodiments 309 to 316,
상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 투여되는, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 900 mg to about 1500 mg every 3 weeks.
318. 구현예 310 또는 구현예 311에 있어서,318. The method of embodiment 310 or embodiment 311,
상기 VEGF 길항제는 2주마다 약 1 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
319. 구현예 318에 있어서,319. The method of embodiment 318,
상기 VEGF 길항제는 2주마다 약 5 mg/kg 내지 약 10 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
320. 구현예 319에 있어서,320. The method of embodiment 319,
상기 VEGF 길항제는 2주마다 약 5 mg/kg, 약 7.5 mg/kg, 또는 약 10 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10 mg/kg every two weeks.
321. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,321. The method of any one of embodiments 309 to 311 and 318 to 320,
상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks.
322. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 321 중 어느 한 구현예에 있어서, 상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg의 용량으로 투여되는, 방법.322. The method of any one of embodiments 309 to 311 and embodiments 318 to 321, wherein the PD-1 axis binding antagonist is administered at a dose of about 20 mg to about 1600 mg every two weeks. .
323. 구현예 309 내지 구현예 311에 있어서,323. according to embodiment 309 to embodiment 311,
상기 항 TIGIT 길항제 항체는 4주마다 약 200 mg 내지 약 2000 mg의 용량으로 투여되는, 방법.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks.
324. 구현예 309 내지 구현예 311 및 구현예 323 중 어느 한 구현예에 있어서,324. The method according to any one of embodiments 309 to 311 and 323,
상기 PD-1 축 결합 길항제는 4주마다 약 80 mg 내지 약 2000 mg의 용량으로 투여되는, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 4 weeks.
325. 구현예 309 내지 구현예 311, 구현예 323, 및 구현예 324 중 어느 한 구현예에 있어서,325. The embodiment of any one of embodiments 309 to 311, 323, and 324,
상기 PD-1 축 결합 길항제는 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 투여되는, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 1400 mg to about 2000 mg every 4 weeks.
326. 구현예 309 내지 구현예 325 중 어느 한 구현예에 있어서,326. The method of any one of embodiments 309 to 325,
상기 HCC는 국소 진행성 또는 전이성 HCC인, 방법.wherein the HCC is locally advanced or metastatic HCC.
327. 구현예 309 내지 구현예 326 중 어느 한 구현예에 있어서,327. The method of any one of embodiments 309 to 326,
상기 HCC는 절제 불가능한 HCC인, 방법.wherein the HCC is unresectable HCC.
328. 구현예 309 내지 구현예 327 중 어느 한 구현예에 있어서,328. The method of any one of embodiments 309 to 327,
상기 대상체 또는 대상체들은 적절한 간 기능을 갖는 것으로 결정되는, 방법.The subject or subjects are determined to have adequate liver function.
329. 구현예 328에 있어서,329. The method of embodiment 328,
상기 적절한 간 기능은 차일드-퍼(Child-Pugh) 분류 A로 특징지어지는, 방법.wherein said adequate liver function is characterized by Child-Pugh class A.
330. 구현예 309 내지 구현예 329 중 어느 한 구현예에 있어서,330. The method of any one of embodiments 309 to 329,
상기 대상체 또는 대상체들로부터 수득한 HCC 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.wherein the subject or HCC tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
331. 구현예 309 내지 구현예 330 중 어느 한 구현예에 있어서,331. The method of any one of embodiments 309 to 330,
상기 대상체 또는 대상체 집단에 적어도 4회의 투약 주기를 투여하는 단계를 포함하는, 방법.and administering to the subject or population of subjects at least four dosing cycles.
332. 구현예 331에 있어서,332. The method of embodiment 331,
상기 대상체 또는 대상체 집단에 적어도 16회의 투약 주기를 투여하는 단계를 포함하는, 방법.and administering to the subject or population of subjects at least 16 dosing cycles.
333. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,333. A method of treating a subject or population of subjects having HCC, comprising:
3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and bevacizumab at a dose of about 15 mg/kg every 3 weeks. A method comprising steps.
334. 구현예 311 내지 구현예 333 중 어느 한 구현예에 있어서,334. The method of any one of embodiments 311 to 333,
상기 대상체 또는 대상체들은 HCC에 대해 선행 전신 치료를 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects have not received prior systemic treatment for HCC.
335. 구현예 309 내지 구현예 334 중 어느 한 구현예에 있어서,335. The method of any one of embodiments 309 to 334,
상기 치료는 적어도 약 5.6개월 내지 적어도 약 6.83개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.wherein said treatment results in a median PFS in the subject population of at least about 5.6 months to at least about 6.83 months.
336. 구현예 72에 있어서,336. The method of embodiment 72,
상기 암은 방광암인, 방법.wherein the cancer is bladder cancer.
337. 구현예 336에 있어서,337. The method of embodiment 336,
상기 방광암은 근육 침윤성 방광암(MIBC)인, 방법.wherein the bladder cancer is muscle invasive bladder cancer (MIBC).
338. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,338. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising the steps of, wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
339. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,339. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising the steps of, wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
340. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,340. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising the steps of, wherein the treatment is perioperative treatment.
341. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,341. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising the steps of, wherein the treatment is perioperative treatment.
342. 구현예 338 내지 구현예 341 중 어느 한 구현예에 있어서,342. The method of any one of embodiments 338 to 341,
상기 대상체 또는 대상체들은 크레아티닌 청소율이 60 mL/분 미만인, 방법.The method of claim 1, wherein the subject or subjects have a creatinine clearance of less than 60 mL/min.
343. 구현예 338 내지 구현예 342 중 어느 한 구현예에 있어서,343. The method of any one of embodiments 338 to 342,
상기 대상체 또는 대상체들은 2등급 이상의 청력 상실을 갖는, 방법.The method of claim 1, wherein the subject or subjects have a hearing loss of grade 2 or greater.
344. 구현예 338 내지 구현예 343 중 어느 한 구현예에 있어서,344. The method of any one of embodiments 338 to 343,
상기 대상체 또는 대상체들은 2등급 이상의 신경병증을 갖는, 방법.The method of claim 1 , wherein the subject or subjects have grade 2 or greater neuropathy.
345. 구현예 338 내지 구현예 344 중 어느 한 구현예에 있어서,345. The method of any one of embodiments 338 to 344,
상기 대상체 또는 대상체들은 백금계 화학요법제를 이용한 치료를 거부한, 방법.The method of claim 1, wherein the subject or subjects refused treatment with a platinum-based chemotherapeutic agent.
346. 구현예 338 또는 구현예 342 내지 구현예 345 중 어느 한 구현예에 있어서,346. The method according to any one of embodiments 338 or 342 to 345,
상기 백금계 화학요법제는 시스플라틴인, 방법.The method of claim 1, wherein the platinum-based chemotherapeutic agent is cisplatin.
347. 구현예 338 내지 구현예 346 중 어느 한 구현예에 있어서,347. The method of any one of embodiments 338 to 346,
상기 MIBC는 외과 수술이 가능한, 방법.wherein the MIBC is surgically feasible.
348. 구현예 347에 있어서,348. The method of embodiment 347,
수술을 더 포함하는, 방법.The method further comprising surgery.
349. 구현예 348에 있어서,349. The method of embodiment 348,
적어도 1회의 투약 주기는 상기 수술 전에 개시되는, 방법.at least one dosing cycle is initiated prior to the surgery.
350. 구현예 348 또는 구현예 349에 있어서,350. The method of embodiment 348 or embodiment 349,
적어도 1, 2, 또는 3회의 투약 주기는 상기 수술 전에 완료되는, 방법.at least 1, 2, or 3 dosing cycles are completed prior to the surgery.
351. 구현예 348 내지 구현예 350 중 어느 한 구현예에 있어서,351. The method of any one of embodiments 348 to 350,
적어도 1회의 투약 주기는 상기 수술 후 4주 내지 6주 사이에 개시되는, 방법.at least one dosing cycle is initiated between 4 and 6 weeks post surgery.
352. 구현예 351에 있어서,352. The method of embodiment 351,
1 내지 17회의 투약 주기는 상기 수술 후에 완료되는, 방법.1 to 17 dosing cycles are completed after said surgery.
353. 구현예 348 내지 구현예 352 중 어느 한 구현예에 있어서,353. The method of any one of embodiments 348 to 352,
상기 수술은 방광 절제술 및/또는 림프절 절제술인, 방법.wherein the surgery is cystectomy and/or lymphadenectomy.
354. 구현예 338 내지 구현예 353 중 어느 한 구현예에 있어서,354. The method of any one of embodiments 338 to 353,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 방법.wherein the treatment results in a pathological complete response (pCR).
355. 구현예 338 내지 구현예 354 중 어느 한 구현예에 있어서,355. The method of any one of embodiments 338 to 354,
상기 치료는 기준 RFS 시간과 비교하여 상기 대상체 또는 대상체들의 무재발 생존(RFS)의 증가, 기준 EFS 시간과 비교하여 상기 대상체 또는 대상체들의 무사건 생존(EFS)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체들의 OS의 증가를 유발하는, 방법.wherein the treatment is an increase in relapse-free survival (RFS) of the subject or subjects as compared to a baseline RFS time, an increase in the event-free survival (EFS) of the subject or subjects compared to a baseline EFS time, or an increase in the event-free survival (EFS) of the subject or subjects as compared to a baseline OS time. causing an increase in OS of the subject or subjects.
356. 구현예 355에 있어서:356. The method of embodiment 355:
(a) 상기 기준 RFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 RFS 시간 중앙값이고;(a) said baseline RFS time is the median RFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 EFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 EFS 시간 중앙값이거나; 또는 (b) said baseline EFS time is the median EFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 방법.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
357. 구현예 338 내지 구현예 356 중 어느 한 구현예에 있어서,357. The method of any one of embodiments 338 to 356,
상기 치료는 병리학적 병기하향(downstaging)을 유발하는, 방법.wherein the treatment results in pathological downstaging.
358. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,358. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising the steps of, wherein the subject is cisplatin ineligible.
359. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,359. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising the steps of, wherein the treatment is perioperative treatment.
360. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,360. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the subject is cisplatin ineligible.
361. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,361. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the treatment is perioperative treatment.
362. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,362. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks; , wherein the subject is cisplatin ineligible.
363. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,363. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks; , wherein the treatment is perioperative treatment.
364. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,364. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체들은 시스플라틴 부적격인, 방법.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein the subject or subjects have cisplatin ineligible, method.
365. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,365. A method of treating a subject or population of subjects having MIBC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 방법.administering to said subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein said treatment comprises perioperative treatment In, way.
366. 구현예 338 내지 구현예 365 중 어느 한 구현예에 있어서,366. The method of any one of embodiments 338-365,
상기 치료는 적어도 약 13.4% 내지 약 15%의 대상체 집단의 ORR을 유발하는, 방법.wherein said treatment results in an ORR in at least about 13.4% to about 15% of the subject population.
367. 구현예 338 내지 구현예 366 중 어느 한 구현예에 있어서,367. The method of any one of embodiments 338 to 366,
상기 치료는 적어도 약 7.9개월 내지 약 8.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.wherein said treatment results in a median OS in the subject population of at least about 7.9 months to about 8.6 months.
368. 구현예 338 내지 구현예 367 중 어느 한 구현예에 있어서,368. The method of any one of embodiments 338 to 367,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
369. 구현예 368에 있어서,369. The method of embodiment 368,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 5% 이상인 PD-L1 양성 종양 세포 분획인, 방법.The method of claim 1, wherein the detectable protein expression level of PD-L1 is a PD-L1-positive tumor cell fraction in which the proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) is 5% or more.
370. 구현예 336에 있어서,370. The method of embodiment 336,
상기 방광암은 요로상피세포 암종 (UC)인, 방법.wherein the bladder cancer is urothelial cell carcinoma (UC).
371. 구현예 370에 있어서,371. The method of embodiment 370,
상기 UC는 전이성 요로상피세포 암종(mUC)인, 방법.wherein the UC is metastatic urothelial cell carcinoma (mUC).
372. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,372. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. A method comprising administering to a population.
373. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,373. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks to the subject or subject. A method comprising administering to a population.
374. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,374. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 선행 암 면역요법을 받은 적이 없는, 방법.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. A method comprising administering to a population, wherein the subject has not received prior cancer immunotherapy.
375. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,375. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 2차 치료인, 방법.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. A method comprising administering to a population, wherein the treatment is a second line treatment.
376. 구현예 372, 구현예 372, 및 구현예 375 중 어느 한 구현예에 있어서,376. The method of any one of embodiments 372, 372, and 375,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects have not received prior therapy.
377. 구현예 372 내지 구현예 374 중 어느 한 구현예에 있어서,377. The method according to any one of embodiments 372 to 374,
상기 치료는 2차 치료인, 방법.wherein the treatment is a second line treatment.
378. 구현예 372 내지 구현예 377 중 어느 한 구현예에 있어서,378. The method of any one of embodiments 372 to 377,
상기 mUC는 백금 함유 요법 중에 또는 이후에 진행하는, 방법.wherein the mUC progresses during or after platinum containing therapy.
379. 구현예 372 내지 구현예 378 중 어느 한 구현예에 있어서,379. The method according to any one of embodiments 372 to 378,
상기 방법은 상기 대상체 또는 대상체 집단이 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체들에게 제2 투약 요법을 투여하는 단계를 더 포함하는, 방법.The method further comprising administering a second dosing regimen to the subject or subjects after the subject or population of subjects has experienced disease progression or unacceptable toxicity.
380. 구현예 379에 있어서,380. The method of embodiment 379,
상기 제2 투약 요법은 PD-1 축 결합 길항제 및 항체-약물 접합체(ADC)의 1회 이상의 투약 주기를 포함하는, 방법.wherein the second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist and an antibody-drug conjugate (ADC).
381. 구현예 380에 있어서,381. The method of embodiment 380,
상기 ADC는 (a) 엔포르투맙 베도틴 또는 (b) 사시투주맙 고비테칸인, 방법.The method of claim 1, wherein the ADC is (a) enfortumab vedotin or (b) sacituzumab gobitecan.
382. 구현예 381에 있어서,382. The method of embodiment 381,
(a) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (b) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되는, 방법.(a) enfortumab vedotin is administered at a weekly dose of 1.25 mg/kg on a 2-week dosing/week break, or (b) sacituzumab gobitecan is administered at 10 mg/week on a 2-week dos/week break Administered in kg dose.
383. 구현예 381 또는 구현예 382에 있어서,383. The method of embodiment 381 or embodiment 382,
(a) 엔포르투맙 베도틴은 각 21일 주기의 제 1일 및 8일에 1.25 mg/kg의 용량으로 투여되거나, 또는 (b) 사시투주맙 고비테칸은 각 21일 주기의 제 1일 및 8일에 10 mg/kg의 용량으로 투여되는, 방법.(a) enfortumab vedotin is administered at a dose of 1.25 mg/kg on days 1 and 8 of each 21-day cycle, or (b) sacituzumab gobitecan is administered on day 1 of each 21-day cycle and at a dose of 10 mg/kg on day 8.
384. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,384. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks; A method comprising administering to
385. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,385. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects a dosing regimen comprising one or more dosing cycles of tyragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks A method comprising steps.
386. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,386. A method of treating a subject or population of subjects having mUC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
387. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,387. A method of treating a subject or population of subjects having mUC, comprising:
제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises at least one dosing cycle of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks comprising; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 방법.(b) said second dosing regimen comprises one or more dosing cycles of the PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and (i) Enfortumab vedotin is administered for 2 weeks. administered at a weekly dose of 1.25 mg/kg with a weekly break of one week, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/1 week off, wherein the second dosing regimen is wherein said subject or population of subjects is administered to said subject or population of subjects after experiencing disease progression or unacceptable toxicity during said first dosing regimen.
388. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,388. A method of treating a subject or population of subjects having mUC, comprising:
제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks including; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에 투여되는, 방법.(b) said second dosing regimen comprises one or more dosing cycles of the PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, (i) Enfortumab vedotin is administered for 2 weeks / administered at a weekly dose of 1.25 mg/kg with a one-week break, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/week break, wherein the second dosing regimen is The method of claim 1, wherein the method is administered to the subject after the subject experiences disease progression or unacceptable toxicity during the first dosing regimen.
389. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,389. A method of treating a subject or population of subjects having mUC, comprising:
제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and
(b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에 투여되는, 방법.(b) said second dosing regimen comprises at least one dosing cycle of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin is administered at 1.25 weekly doses of 2 weeks on/1 week off. is administered in a mg/kg dose, or (ii) sacituzumab gobitecan is administered at a weekly 10 mg/kg dose of 2 weeks dosing/1 week off, wherein the second dosing regimen is such that the subject administers the first dose The method is administered to the subject after experiencing disease progression or unacceptable toxicity during therapy.
390. 구현예 372 내지 구현예 389 중 어느 한 구현예에 있어서,390. The method of any one of embodiments 372 to 389,
상기 치료는 적어도 약 13.4% 내지 적어도 약 31%의 대상체 집단의 ORR을 유발하는, 방법.wherein said treatment results in an ORR in at least about 13.4% to at least about 31% of the subject population.
391. 구현예 372 내지 구현예 390 중 어느 한 구현예에 있어서,391. The method of any one of embodiments 372 to 390,
상기 치료는 약 7.9개월 내지 약 16.3개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.wherein said treatment results in a median OS of the subject population of about 7.9 months to about 16.3 months.
392. 구현예 72에 있어서,392. The method of embodiment 72,
상기 암은 췌장암인, 방법.The method of claim 1, wherein the cancer is pancreatic cancer.
393. 췌장암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,393. A method of treating a subject or population of subjects having pancreatic cancer, the method comprising:
각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.Tiragolumab at a dose of about 420 mg on days 1 and 15 of each 28-day dosing cycle, atezolizumab at a dose of about 840 mg on days 1 and 15 of each 28-day dosing cycle, each 28 days. Gemcitabine at a dose of about 1000 mg/m2 on days 1, 8, and 15 of the dosing cycle, and at a dose of about 125 mg/m2 on days 1, 8, and 15 of each 28-day dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising at least one 28-day dosing cycle of nap-paclitaxel.
394. 구현예 392 또는 구현예 393에 있어서,394. The method of embodiment 392 or embodiment 393,
상기 췌장암은 췌장관 선암(PDAC)인, 방법.The method of claim 1, wherein the pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395. 구현예 394에 있어서,395. The method of embodiment 394,
상기 PDAC는 전이성 PDAC인, 방법.wherein the PDAC is a metastatic PDAC.
396. 구현예 392 내지 구현예 395 중 어느 한 구현예에 있어서,396. The method of any one of embodiments 392 to 395,
상기 대상체 또는 대상체들은 전이성 PDAC에 대해 선행 전신 요법을 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects have not received prior systemic therapy for metastatic PDAC.
397. 구현예 392 내지 구현예 396 중 어느 한 구현예에 있어서,397. The method of any one of embodiments 392 to 396,
상기 치료는 적어도 약 41.7% 내지 약 46.7%의 대상체 집단의 ORR을 유발하는, 방법.wherein said treatment results in an ORR in at least about 41.7% to about 46.7% of the subject population.
398. 구현예 392 내지 구현예 397 중 어느 한 구현예에 있어서,398. The method of any one of embodiments 392 to 397,
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 없는 젬시타빈 및 냅-파클리탁셀을 포함한 치료와 비교하여 적어도 약 20%의 ORR의 증가를 유발하는, 방법.wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nap-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
399. 구현예 392 내지 구현예 398 중 어느 한 구현예에 있어서,399. The method of any one of embodiments 392 to 398,
상기 치료는 적어도 약 5.5개월 내지 약 7개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.wherein said treatment results in a median PFS in the subject population of at least about 5.5 months to about 7 months.
400. 구현예 392 내지 구현예 399 중 어느 한 구현예에 있어서,400. The method of any one of embodiments 392 to 399,
상기 치료는 적어도 약 8.5개월 내지 약 10.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.wherein said treatment results in a median OS in the subject population of at least about 8.5 months to about 10.6 months.
401. 구현예 72에 있어서,401. The method of embodiment 72,
상기 암은 식도암인, 방법.wherein the cancer is esophageal cancer.
402. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,402. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.One or more times 21 of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle.
403. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,403. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.One or more 21 doses of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle 21 A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle.
404. 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,404. A method of treating a subject or population of subjects having esophageal cancer, the method comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법.One or more times 21 of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle, wherein the subject has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
405. 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,405. A method of treating a subject or population of subjects having esophageal cancer, the method comprising:
각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법.One or more times 21 of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg on Day 1 of each dosing cycle and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle, wherein the subject has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
406. 구현예 402 또는 구현예 403에 있어서,406. The method of embodiment 402 or embodiment 403,
상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법.The method of claim 1, wherein the subject or subjects has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
407. 구현예 404 또는 구현예 406에 있어서,407. The method of embodiment 404 or embodiment 406,
상기 대상체 또는 대상체들은 상기 선행 치료 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한, 방법.wherein said subject or subjects experienced disease progression or unacceptable toxicity during said prior treatment.
408. 구현예 402 또는 구현예 403에 있어서,408. The method of embodiment 402 or embodiment 403,
상기 21일 투약 주기는 백금계 화학요법제 및 비백금계 화학요법제를 더 포함하는, 방법.The 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409. 구현예 408에 있어서,409. The method of embodiment 408,
상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
410. 구현예 404 내지 구현예 409 중 어느 한 구현예에 있어서,410. The method of any one of embodiments 404 to 409,
상기 백금계 화학요법제는 시스플라틴인, 방법.The method of claim 1, wherein the platinum-based chemotherapeutic agent is cisplatin.
411. 구현예 410에 있어서,411. The method of embodiment 410,
시스플라틴은 각 투약 주기의 제 1일에 약 80 mg/m2의 용량으로 투여되는, 방법.The method of claim 1 wherein cisplatin is administered at a dose of about 80 mg/m2 on Day 1 of each dosing cycle.
412. 구현예 404 내지 구현예 411 중 어느 한 구현예에 있어서,412. The method of any one of embodiments 404 to 411,
상기 비백금계 화학요법제는 항대사물질인, 방법.The method of claim 1, wherein the non-platinum-based chemotherapeutic agent is an antimetabolites.
413. 구현예 412에 있어서,413. The method of embodiment 412,
상기 항대사물질은 5-플루오로우라실인, 방법.wherein the antimetabolite is 5-fluorouracil.
414. 구현예 413에 있어서,414. The method of embodiment 413,
5-플루오로우라실은 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간의 용량으로 투여되는, 방법.5-fluorouracil is administered at a dose of about 800 mg/m2/24 hours on days 1-5 of each 21-day cycle.
415. 구현예 404 내지 구현예 414 중 어느 한 구현예에 있어서,415. The method of any one of embodiments 404 to 414,
상기 식도암은 진행성 또는 전이성 식도암인, 방법.The method of claim 1, wherein the esophageal cancer is advanced or metastatic esophageal cancer.
416. 구현예 402, 구현예 403, 구현예 408, 및 구현예 409 중 어느 한 구현예에 있어서,416. The embodiment of any one of embodiments 402, 403, 408, and 409,
상기 대상체 또는 대상체들은 전이성 식도암에 대해 선행 치료를 받은 적이 없는, 방법.The method of claim 1, wherein the subject or subjects has not received prior treatment for metastatic esophageal cancer.
417. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,417. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle, a dose of about 80 mg to about 1600 mg of PD-1 axis binding antagonist on Day 1 of each dosing cycle, One or more 21 doses of a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on Day 1, and a non-platinum-based chemotherapeutic agent at a dose of about 800 mg/m2/24 hours on days 1-5 of each 21-day cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle, wherein the platinum-based chemotherapeutic agent is omitted from the dosing regimen after six doses.
418. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,418. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 600 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 1200 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.Anti-TIGIT antagonist antibody at a dose of about 600 mg on day 1 of each dosing cycle, a dose of about 1200 mg of PD-1 axis binding antagonist on day 1 of each dosing cycle, about 80 mg/day on day 1 of each dosing cycle a dosing regimen comprising one or more 21-day dosing cycles of cisplatin at an m2 dose, and 5-fluorouracil at a dose of about 800 mg/m2/24 hour on days 1-5 of each 21-day cycle to the subject or subject administering to a population, wherein cisplatin is omitted from the dosing regimen after 6 doses.
419. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,419. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.Tiragolumab at a dose of about 600 mg on day 1 of each dosing cycle, atezolizumab at a dose of about 1200 mg on day 1 of each dosing cycle, cisplatin at a dose of about 80 mg/m2 on day 1 of each dosing cycle and administering to the subject or population of subjects a dosing regimen comprising one or more 21-day dosing cycles of 5-fluorouracil at a dose of about 800 mg/m2/24 hours on days 1-5 of each 21-day cycle. wherein cisplatin is omitted from the dosing regimen after 6 doses.
420. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,420. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 백금계 화학요법제 및 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises at least one 21-day dosing cycle of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses; ; and
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 방법.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle and PD- at a dose of about 80 mg to about 1600 mg on Day 1 of each dosing cycle. A method comprising at least one 21 day dosing cycle of a uniaxial binding antagonist.
421. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,421. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on Day 1 of each dosing cycle and 800 mg/m2/24 hour dose on Days 1-5 of each 21-day cycle. at least one 21-day dosing cycle of a non-platinum-based chemotherapeutic agent, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses; and
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 방법.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle and PD- at a dose of about 80 mg to about 1600 mg on Day 1 of each dosing cycle. A method comprising at least one 21 day dosing cycle of a uniaxial binding antagonist.
422. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법으로서,422. A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen is cisplatin at a dose of about 80 mg/m2 on day 1 of each dosing cycle and 5-fluoro at a dose of 800 mg/m2/24 hours on days 1-5 of each 21 day cycle one or more 21-day dosing cycles of lauracil, wherein cisplatin is omitted from said dosing regimen after 6 doses; and
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함하는, 방법.(b) said second dosing regimen is one or more 21 day dosing cycles of tiragolumab at a dose of about 600 mg on day 1 of each dosing cycle and atezolizumab at a dose of about 1200 mg on day 1 of each dosing cycle A method comprising
423. 구현예 402 내지 구현예 422 중 어느 한 구현예에 있어서,423. The method of any one of embodiments 402 to 422,
상기 치료는 적어도 약 14%의 대상체 집단의 ORR을 유발하는, 방법.wherein the treatment results in an ORR in at least about 14% of the subject population.
424. 구현예 47 내지 구현예 423 어느 한 구현예에 있어서,424. The method according to any one of embodiments 47 to 423,
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 방법.A method comprising an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
425. 구현예 424에 있어서,425. The method of embodiment 424,
항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR):Anti-TIGIT antagonist antibodies have the following light chain variable region framework regions (FR):
DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4를 더 포함하는, 방법.FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
426. 구현예 424에 있어서,426. The method of embodiment 424,
상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR:The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 방법.FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
427. 구현예 426에 있어서,427. The method of embodiment 426,
X1은 E인, 방법.X1 is E, the method.
428. 구현예 426에 있어서,428. The method of embodiment 426,
X1은 Q인, 방법.X1 is Q; the method.
429. 구현예 424 내지 구현예 428 중 어느 한 구현예에 있어서,429. The method of any one of embodiments 424 to 428,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 방법.(c) a VH domain as in case (a) and a VL domain as in case (b).
430. 구현예 424 내지 구현예 429 중 어느 한 구현예에 있어서,430. The method of any one of embodiments 424 to 429,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.(b) A method comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
431. 구현예 424 내지 구현예 427, 구현예 429, 및 구현예 430 중 어느 한 구현예에 있어서,431. The embodiment of any one of embodiments 424 to 427, 429, and 430,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.(b) A method comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
432. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 431 중 어느 한 구현예에 있어서,432. The method of any one of embodiments 424 to 427 and embodiments 429 to 431,
상기 항 TIGIT 길항제 항체는 하기의: The anti-TIGIT antagonist antibody is:
(a) 서열번호 33의 아미노산 서열을 포함하는 중쇄; 및 (a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 33; and
(b) 서열번호 34의 아미노산 서열을 포함하는 경쇄를 포함하는, 방법.(b) a light chain comprising the amino acid sequence of SEQ ID NO:34.
433. 구현예 424 내지 구현예 432 중 어느 한 구현예에 있어서,433. The method of any one of embodiments 424 to 432,
상기 항 TIGIT 길항제 항체는 단일클론 항체인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
434. 구현예 424 내지 구현예 433 중 어느 한 구현예에 있어서,434. The method of any one of embodiments 424 to 433,
상기 항 TIGIT 길항제 항체는 인간 항체인, 방법.wherein the anti-TIGIT antagonist antibody is a human antibody.
435. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,435. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 전장 항체인, 방법.wherein the anti-TIGIT antagonist antibody is a full length antibody.
436. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 436 중 어느 한 구현예에 있어서,436. The method of any one of embodiments 424 to 427 and embodiments 429 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법. The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
437. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 구현예 421, 및 구현예 424 내지 구현예 436 중 어느 한 구현예에 있어서,437. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, embodiment 421, and embodiment any one of embodiments 424 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT 또는 TJ-T6인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tiragolumab, bivostolimab, ethigilumab, EOS084448, SGN-TGT or TJ-T6.
438. 구현예 437에 있어서,438. The method of embodiment 437,
상기 항 TIGIT 길항제 항체는 원형 Fc 매개 작동체 기능을 갖는, 방법.wherein the anti-TIGIT antagonist antibody has prototypical Fc-mediated effector function.
439. 구현예 437 또는 구현예 438에 있어서,439. according to embodiment 437 or embodiment 438,
상기 항 TIGIT 길항제 항체는 강화된 Fc 매개 작동체 기능을 갖는, 방법.wherein the anti-TIGIT antagonist antibody has enhanced Fc-mediated effector function.
440. 구현예 437 내지 구현예 439 중 어느 한 구현예에 있어서,440. The method of any one of embodiments 437 to 439,
상기 항 TIGIT 길항제 항체는 SGN-TGT인, 방법.wherein the anti-TIGIT antagonist antibody is SGN-TGT.
441. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421 중 어느 한 구현예에 있어서,441. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421 according to any one of embodiments,
상기 항 TIGIT 길항제 항체는 돔바날리맙, BMS-986207, ASP8374 또는 COM902인, 방법.wherein the anti-TIGIT antagonist antibody is dombanalimab, BMS-986207, ASP8374 or COM902.
442. 구현예 424 내지 구현예 431, 및 구현예 441 중 어느 한 구현예에 있어서,442. The embodiment of any one of embodiments 424 to 431, and embodiment 441,
상기 항 TIGIT 길항제 항체는 Fc 매개 작동체 기능을 갖지 않는, 방법.wherein the anti-TIGIT antagonist antibody has no Fc mediated effector function.
443. 구현예 47 내지 구현예 442 중 어느 한 구현예에 있어서,443. The method according to any one of embodiments 47 to 442,
상기 항 TIGIT 길항제 항체는 IgG 부류 항체인, 방법.wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444. 구현예 443에 있어서,444. The method of embodiment 443,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 방법.wherein the IgG class antibody is an IgG1 subclass antibody.
445. 구현예 444에 있어서,445. of embodiment 444,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, 돔바날리맙 또는 BMS-986207인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tiragolumab, bivostolimab, etigilimab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, dombanalimab or BMS-986207.
446. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421에 있어서,446. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421,
상기 IgG 부류 항체는 IgG4 하위부류 항체인, 방법.wherein the IgG class antibody is an IgG4 subclass antibody.
447. 구현예 446에 있어서,447. The method of embodiment 446,
상기 항 TIGIT 길항제 항체는 ASP8374 또는 COM902인, 방법.wherein the anti-TIGIT antagonist antibody is ASP8374 or COM902.
448. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,448. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 Fab, 비스-Fab, Fab’, Fab’-SH, Fv, 단일 사슬 가변 단편(scFv), 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 TIGIT에 결합하는 항체 단편인, 방법.wherein the anti-TIGIT antagonist antibody is an antibody fragment that binds to TIGIT selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv), and (Fab')2 fragment, Way.
449. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,449. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 단일특이적 항체인, 방법. wherein the anti-TIGIT antagonist antibody is a monospecific antibody.
450. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,450. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 다중특이적 항체인, 방법.wherein the anti-TIGIT antagonist antibody is a multispecific antibody.
451. 구현예 450에 있어서,451. The method of embodiment 450,
상기 다중특이적 항체는 이중특이적 항체인, 방법.wherein the multispecific antibody is a bispecific antibody.
452. 구현예 424 내지 구현예 451 중 어느 한 구현예에 있어서452. The method of any one of embodiments 424 to 451
PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제, 및 PD-L2 결합 길항제로 이루어진 군으로부터 선택되는, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
453. 구현예 452에 있어서,453. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist.
454. 구현예 453에 있어서,454. The method of embodiment 453,
상기 PD-L1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 방법.wherein the PD-L1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners.
455. 구현예 454에 있어서,455. The method of embodiment 454,
상기 PD-L1 결합 길항제는 PD-L1이 PD-1, B7-1, 또는 PD-1 및 B7-1 둘 모두에 결합하는 것을 억제하는, 방법.wherein the PD-L1 binding antagonist inhibits PD-L1 from binding to PD-1, B7-1, or both PD-1 and B7-1.
456. 구현예 453 내지 구현예 455 중 어느 한 구현예에 있어서,456. The method according to any one of embodiments 453-455,
상기 PD-L1 결합 길항제는 항 PD-L1 길항제 항체인, 방법.The method of claim 1, wherein the PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457. 구현예 456에 있어서,457. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 방법.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636.
458. 구현예 457에 있어서,458. The method of embodiment 457,
상기 항 PD-L1 길항제 항체는 아테졸리주맙인, 방법.The method of claim 1, wherein the anti-PD-L1 antagonist antibody is atezolizumab.
459. 구현예 456에 있어서,459. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 하기의 HVR:The anti-PD-L1 antagonist antibody has the following HVRs:
GFTFSDSWIH(서열번호 20)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
AWISPYGGSTYYADSVKG(서열번호 21)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
RHWPGGFDY(서열번호 22)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
RASQDVSTAVA(서열번호 23)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
SASFLYS(서열번호 24)의 아미노산 서열을 포함하는 HVR-L2; 및HVR-L2 comprising the amino acid sequence of SASFLYS (SEQ ID NO: 24); and
QQYLYHPAT(서열번호 25)의 아미노산 서열을 포함하는 HVR-L3을 포함하는, 방법.A method comprising HVR-L3 comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
460. 구현예 459에 있어서,460. The method of embodiment 459,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) 서열번호 27의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 방법.(c) a VH domain as in case (a) and a VL domain as in case (b).
461. 구현예 460에 있어서,461. The method of embodiment 460,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and
(b) 서열번호 27의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.(b) A method comprising a VL domain comprising the amino acid sequence of SEQ ID NO:27.
462. 구현예 461에 있어서,462. The method of embodiment 461,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 28의 아미노산 서열을 포함하는 중쇄; 및(a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 28; and
(b) 서열번호 29의 아미노산 서열을 포함하는 경쇄를 포함하는, 방법.(b) A method comprising a light chain comprising the amino acid sequence of SEQ ID NO:29.
463. 구현예 459 내지 구현예 462 중 어느 한 구현예에 있어서,463. The method according to any one of embodiments 459 to 462,
상기 항 PD-L1 길항제 항체는 단일클론 항체인, 방법.The method of claim 1, wherein the anti-PD-L1 antagonist antibody is a monoclonal antibody.
464. 구현예 459 내지 구현예 463 중 어느 한 구현예에 있어서,464. The method of any one of embodiments 459 to 463,
상기 항 PD-L1 길항제 항체는 인간화 항체인, 방법.The method of claim 1, wherein the anti-PD-L1 antagonist antibody is a humanized antibody.
465. 구현예 463 또는 구현예 464에 있어서,465. The method of embodiment 463 or embodiment 464,
상기 항 PD-L1 길항제 항체는 전장 항체인, 방법.wherein the anti-PD-L1 antagonist antibody is a full length antibody.
466. 구현예 459 내지 구현예 464 중 어느 한 구현예에 있어서,466. The method according to any one of embodiments 459 to 464,
상기 항 PD-L1 길항제 항체는 Fab, Fab’, Fab’-SH, Fv, scFv, 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 PD-L1에 결합하는 항체 단편인, 방법.The method of claim 1, wherein the anti-PD-L1 antagonist antibody is an antibody fragment that binds to PD-L1 selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab')2 fragments.
467. 구현예 459 내지 구현예 465 중 어느 한 구현예에 있어서,467. The method according to any one of embodiments 459 to 465,
상기 항 PD-L1 길항제 항체는 IgG 부류 항체인, 방법.wherein the anti-PD-L1 antagonist antibody is an IgG class antibody.
468. 구현예 467에 있어서,468. The method of embodiment 467,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 방법.wherein the IgG class antibody is an IgG1 subclass antibody.
469. 구현예 452에 있어서,469. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-1 결합 길항제인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-1 binding antagonist.
470. 구현예 469에 있어서,470. The method of embodiment 469,
상기 PD-1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 방법.wherein the PD-1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners.
471. 구현예 470에 있어서,471. The method of embodiment 470,
상기 PD-1 결합 길항제는 PD-L1이 PD-L1, PD-L2, 또는 PD-L1 및 PD-L2 둘 모두에 결합하는 것을 억제하는, 방법.wherein the PD-1 binding antagonist inhibits PD-L1 from binding to PD-L1, PD-L2, or both PD-L1 and PD-L2.
472. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,472. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 항 PD-1 길항제 항체인, 방법.The method of claim 1, wherein the PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473. 구현예 472에 있어서,473. The method of embodiment 472,
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 방법.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21.
474. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,474. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 Fc 융합 단백질인, 방법.The method of claim 1, wherein the PD-1 binding antagonist is an Fc fusion protein.
475. 구현예 474에 있어서,475. The method of embodiment 474,
상기 Fc 융합 단백질은 AMP-224인, 방법.The Fc fusion protein is AMP-224, the method.
476. 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 및 구현예 309 내지 구현예 312 중 어느 한 구현예에 있어서,476. The embodiment of any one of embodiments 80-112, 114-127, and embodiments 309-312,
상기 항 TIGIT 길항제 항체를 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering said anti-TIGIT antagonist antibody to said subject or population of subjects at a dose of about 30 mg to about 1200 mg every three weeks.
477. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,477. Embodiment 51, Embodiment 54, Embodiment 60, Embodiment 62, Embodiment 63, Embodiment 65-67, Embodiment 80-112, Embodiment 114-127, Embodiment 136- Embodiment 140, embodiment 169-174, embodiment 189, embodiment 191, embodiment 267, embodiment 269, embodiment 286, embodiment 288, embodiment 291, embodiment 295, embodiment 301, embodiment 302, embodiment 303, embodiment 313, embodiment 315, embodiment 338, embodiment 340, embodiment 358 to embodiment 361, embodiment 372, embodiment 384, embodiment 387, embodiment 388, embodiment 402 to The embodiment of any one of embodiments 404, 417, 420, 421, and 476,
상기 항 TIGIT 길항제 항체를 3주마다 약 600 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering said anti-TIGIT antagonist antibody to said subject at a dose of about 600 mg every 3 weeks.
478. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 309, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,478. Embodiment 51, Embodiment 54, Embodiment 60, Embodiment 62, Embodiment 63, Embodiment 65-67, Embodiment 80-112, Embodiment 114-127, Embodiment 136- Embodiment 140, embodiment 169-174, embodiment 189, embodiment 191, embodiment 267, embodiment 269, embodiment 286, embodiment 288, embodiment 291, embodiment 295, embodiment 301, embodiment 302, Embodiment 303, Embodiment 309, Embodiment 313, Embodiment 315, Embodiment 338, Embodiment 340, Embodiment 358 to Embodiment 361, Embodiment 372, Embodiment 384, Embodiment 387, Embodiment 388, The embodiment of any one of Embodiments 402 to 404, Embodiment 417, Embodiment 420, Embodiment 421, and Embodiment 476,
상기 항 TIGIT 길항제 항체를 대상체의 체중에 기초한 단계적 용량으로 상기 대상체 또는 대상체의 집단에 투여하는 단계를 포함하고, 여기서 상기 대상체는 하기의 체중으로서: administering said anti-TIGIT antagonist antibody to said subject or population of subjects in stepwise doses based on the body weight of said subject, wherein said subject has a body weight of:
(a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (a) weighing 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks;
(b) 15 kg 초과 및 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (b) greater than 15 kg and less than or equal to 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or
(c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여되는, 방법. (c) greater than 40 kg, wherein the anti TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
479. 구현예 47, 구현예 48, 구현예 77, 구현예 78, 구현예 82, 및 구현예 83 중 어느 한 구현예에 있어서,479. The embodiment of any one of embodiments 47, 48, 77, 78, 82, and 83,
상기 항 TIGIT 길항제 항체를 4주마다 약 700 mg 내지 약 1000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering said anti TIGIT antagonist antibody to said subject or population of subjects at a dose of about 700 mg to about 1000 mg every 4 weeks.
480. 구현예 47, 구현예 48, 구현예 59, 구현예 67, 구현예 323, 및 구현예 479 중 어느 한 구현예에 있어서,480. The embodiment of any one of embodiments 47, 48, 59, 67, 323, and 479,
상기 항 TIGIT 길항제 항체를 4주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering the anti-TIGIT antagonist antibody to the subject at a dose of about 840 mg every 4 weeks.
481. 구현예 49, 구현예 50, 및 구현예 104 중 어느 한 구현예에 있어서,481. The embodiment of any one of embodiments 49, 50, and 104,
상기 항 TIGIT 길항제 항체를 2주마다 약 300 mg 내지 약 600 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of about 300 mg to about 600 mg every two weeks.
482. 구현예 49, 구현예 50, 구현예 227, 구현예 251 내지 구현예 253, 구현예 255, 및 구현예 481 중 어느 한 구현예에 있어서,482. The embodiment of any one of embodiments 49, 50, 227, 251 to 253, 255, and 481,
상기 항 TIGIT 길항제 항체를 2주마다 약 420 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering the anti-TIGIT antagonist antibody to the subject at a dose of about 420 mg every two weeks.
483. 구현예 47 내지 구현예 482 중 어느 한 구현예에 있어서,483. The method according to any one of embodiments 47 to 482,
상기 항 TIGIT 길항제 항체의 용량은 고정 용량인, 방법.wherein the dose of the anti-TIGIT antagonist antibody is a fixed dose.
484. 구현예 54, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 27 내지 구현예 2698 중 어느 한 구현예에 있어서,484. The embodiment of any one of embodiments 54, 62, 63, 65-67, 80-109, and 27-2698,
상기 PD-1 축 결합 길항제를 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 900 mg to about 1500 mg every three weeks.
485. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 172, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301 내지 구현예 303, 구현예 309, 구현예 311, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372 내지 구현예 375, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 405, 구현예 417, 구현예 420, 구현예 421, 및 구현예 484 중 어느 한 구현예에 있어서,485. embodiment 54, embodiment 60, embodiment 62, embodiment 63, embodiment 65-67, embodiment 80-112, embodiment 114-127, embodiment 136-140, Embodiment 169 to embodiment 172, embodiment 189, embodiment 191, embodiment 267, embodiment 269, embodiment 286, embodiment 288, embodiment 291, embodiment 295, embodiment 301 to embodiment 303, embodiment 309, embodiment 311, embodiment 313, embodiment 315, embodiment 338, embodiment 340, embodiment 358 to embodiment 361, embodiment 372 to embodiment 375, embodiment 384, embodiment 387, embodiment 388, The embodiment of any one of Embodiments 402 to 405, Embodiment 417, Embodiment 420, Embodiment 421, and Embodiment 484,
상기 PD-1 축 결합 길항제를 3주마다 약 1200 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering the PD-1 axis binding antagonist to the subject at a dose of about 1200 mg every 3 weeks.
486. 구현예 47, 구현예 50, 구현예 80 내지 구현예 109, 및 구현예 324 중 어느 한 구현예에 있어서,486. The embodiment of any one of embodiments 47, 50, 80-109, and embodiment 324,
상기 방법은 PD-1 축 결합 길항제를 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.The method comprises administering to the subject or population of subjects a PD-1 axis binding antagonist at a dose of about 1400 mg to about 2000 mg every 4 weeks.
487. 구현예 47, 구현예 50, 구현예 59, 구현예 67, 구현예 324, 및 구현예 479 중 어느 한 구현예에 있어서,487. The embodiment of any one of embodiments 47, 50, 59, 67, 324, and 479,
상기 PD-1 축 결합 길항제를 4주마다 약 1680 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering the PD-1 axis binding antagonist to the subject at a dose of about 1680 mg every 4 weeks.
488. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 481에 있어서,488. according to embodiment 48, embodiment 49, embodiment 80-109, and embodiment 481,
상기 PD-1 축 결합 길항제를 2주마다 약 600 mg 내지 약 1200 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 600 mg to about 1200 mg every two weeks.
489. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 구현예 227, 구현예 251 내지 구현예 253, 및 구현예 481 중 어느 한 구현예에 있어서,489. The embodiment of any one of embodiments 48, 49, 80 to 109, 227, 251 to 253, and 481,
상기 PD-1 축 결합 길항제를 2주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.administering the PD-1 axis binding antagonist to the subject at a dose of about 840 mg every two weeks.
490. 구현예 47 내지 구현예 489 중 어느 한 구현예에 있어서,490. The method according to any one of embodiments 47 to 489,
상기 PD-1 축 결합 길항제의 용량은 고정 용량인, 방법.The method of claim 1, wherein the dose of the PD-1 axis binding antagonist is a fixed dose.
491. 구현예 60 또는 구현예 61에 있어서,491. The method of embodiment 60 or embodiment 61,
펨브롤리주맙을 3주마다 약 200 mg 또는 6주마다 400 mg의 고정 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject pembrolizumab at a fixed dose of about 200 mg every 3 weeks or 400 mg every 6 weeks.
492. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65, 구현예 80 내지 구현예 109, 및 구현예 191 중 어느 한 구현예에 있어서,492. The embodiment of any one of embodiments 54, 60, 62, 63, 65, 80-109, and 191,
상기 1회 이상의 투약 주기의 각각의 길이는 21일인, 방법.The length of each of said one or more dosing cycles is 21 days.
493. 구현예 47, 구현예 59, 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,493. The embodiment of any one of embodiments 47, 59, 67, 80 to 109, and embodiments 309 to 311,
상기 1회 이상의 투약 주기의 각각의 길이는 28일인, 방법.The length of each of the one or more dosing cycles is 28 days.
494. 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,494. The embodiment of any one of embodiments 49, 80 to 109, and embodiments 309 to 311,
상기 1회 이상의 투약 주기의 각각의 길이는 14일인, 방법.The length of each of the one or more dosing cycles is 14 days.
495. 구현예 47 내지 구현예 494 중 어느 한 구현예에 있어서,495. The method according to any one of embodiments 47 to 494,
상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering said anti TIGIT antagonist antibody to said subject or population of subjects on about Day 1 of each of said one or more dosing cycles.
496. 구현예 47 내지 구현예 495 중 어느 한 구현예에 있어서,496. The method according to any one of embodiments 47 to 495,
상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering the PD-1 axis binding antagonist to the subject or population of subjects on about Day 1 of each of the one or more dosing cycles.
497. 구현예 321 또는 구현예 493에 있어서,497. according to embodiment 321 or embodiment 493,
상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering said anti-TIGIT antagonist antibody to said subject on about day 15 of each of said one or more dosing cycles.
498. 구현예 322 또는 구현예 493에 있어서,498. The method of embodiment 322 or embodiment 493,
상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering the PD-1 axis binding antagonist to the subject on about day 15 of each of the one or more dosing cycles.
499. 구현예 47 내지 구현예 498 중 어느 한 구현예에 있어서,499. The method according to any one of embodiments 47 to 498,
상기 항 TIGIT 길항제 항체 전에 상기 PD-1 축 결합 길항제를 또는 상기 PD-1 축 결합 길항제 전에 상기 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering to the subject or population of subjects the PD-1 axis binding antagonist prior to the anti TIGIT antagonist antibody or the anti TIGIT antagonist antibody prior to the PD-1 axis binding antagonist.
500. 구현예 499에 있어서,500. The method of embodiment 499,
상기 PD-1 축 결합 길항제 또는 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간을 포함하는, 방법.a first observation period following administration of said PD-1 axis binding antagonist or said anti-TIGIT antagonist antibody.
501. 구현예 500에 있어서,501. The method of embodiment 500,
상기 1차 관찰 기간은 약 30분 내지 약 60분의 길이인, 방법.The method of claim 1, wherein the first observation period is from about 30 minutes to about 60 minutes in length.
502. 구현예 500 또는 구현예 501에 있어서,502. The method of embodiment 500 or embodiment 501,
상기 항 TIGIT 길항제 항체 또는 상기 PD-1 축 결합 길항제의 투여 후 제2 관찰 기간을 포함하는, 방법.a second observation period following administration of said anti-TIGIT antagonist antibody or said PD-1 axis binding antagonist.
503. 구현예 502에 있어서,503. The method of embodiment 502,
상기 제2 관찰 기간은 약 30분 내지 약 60분의 길이인, 방법.and the second observation period is between about 30 minutes and about 60 minutes in length.
504. 구현예 47 내지 구현예 503 중 어느 한 구현예에 있어서,504. The method of any one of embodiments 47 to 503,
상기 항 TIGIT 길항제 항체와 동시에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering the PD-1 axis binding antagonist to the subject or population of subjects concurrently with the anti-TIGIT antagonist antibody.
505. 구현예 47 내지 구현예 504 중 어느 한 구현예에 있어서,505. The method of any one of embodiments 47 to 504,
상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 정맥내 투여하는 단계를 포함하는, 방법.and administering the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist intravenously to the subject or population of subjects.
506. 구현예 505에 있어서,506. The method of embodiment 505,
상기 PD-1 축 결합 길항제를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.administering the PD-1 axis binding antagonist to the subject or population of subjects as an intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
507. 구현예 505 또는 구현예 506에 있어서,507. The method of embodiment 505 or embodiment 506,
상기 항 TIGIT 길항제 항체를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.and administering said anti-TIGIT antagonist antibody to said subject or population of subjects by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
508. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 507 중 어느 한 구현예에 있어서,508. The method of any one of embodiments 47-114 and 116-507,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플의 PD-L1 발현 수준이 결정되는, 방법.A method, wherein the level of PD-L1 expression in the subject or a tumor sample obtained from subjects is determined.
509. 구현예 508에 있어서,509. The method of embodiment 508,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.wherein the subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
510. 구현예 509에 있어서,510. The method of embodiment 509,
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 단백질 발현 수준인, 방법.wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1.
511. 구현예 510에 있어서,511. The method of embodiment 510,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정되는, 방법.The method of claim 1, wherein the detectable protein expression level of PD-L1 is determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody suitable for staining.
512. 구현예 511에 있어서,512. The method of embodiment 511,
염색에 적합한 상기 항 PD-L1 항체는 상기 항 PD-L1 항체 SP263, SP142, 22C3 또는 28-8인, 방법.wherein said anti-PD-L1 antibody suitable for staining is said anti-PD-L1 antibody SP263, SP142, 22C3 or 28-8.
513. 구현예 511 또는 구현예 512에 있어서,513. The method of embodiment 511 or embodiment 512,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 벤타나(Ventana) SP263 IHC 분석, 팜(pharm)Dx 22C3 IHC 분석, 벤타나 SP142 IHC 분석, 또는 팜Dx 28-8 IHC 분석을 사용하여 결정되는, 방법.wherein the detectable protein expression level of PD-L1 is determined using a Ventana SP263 IHC assay, a pharmDx 22C3 IHC assay, a Ventana SP142 IHC assay, or a PalmDx 28-8 IHC assay. .
514. 구현예 47 내지 구현예 109, 구현예 188, 구현예 220 내지 구현예 265, 및 구현예 307 내지 구현예 423 중 어느 한 구현예에 있어서,514. The embodiment of any of embodiments 47 to 109, 188, 220 to 265, and embodiments 307 to 423,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.A method, wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
515. 구현예 47 내지 구현예 220, 구현예 265 내지 구현예 338, 및 구현예 370 내지 구현예 423 중 어느 한 구현예에 있어서,515. The embodiment of any one of embodiments 47 to 220, 265 to 338, and embodiments 370 to 423,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
516. 구현예 47 내지 구현예 113, 구현예 136 내지 구현예 187 및 구현예 220 내지 구현예 423 중 어느 한 구현예에 있어서,516. The embodiment of any one of embodiments 47 to 113, 136 to 187, and 220 to 423,
항 PD-L1 항체 22C3으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 22C3 is determined.
517. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 423 중 어느 한 구현예에 있어서,517. The method of any one of embodiments 47 to 114 and embodiments 116 to 423,
항 PD-L1 항체 28-8로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 28-8 is determined.
518. 구현예 514에 있어서,518. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 방법.wherein the detectable protein expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the tumor sample.
519. 구현예 514에 있어서,519. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 5% 이상 및 20% 미만인, 방법.wherein the detectable protein expression level of PD-L1 has a TIC of at least 5% and less than 20% in the tumor sample.
520. 구현예 514에 있어서,520. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상인, 방법.wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% in the tumor sample.
521. 구현예 514에 있어서,521. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 20% 이상인, 방법.wherein the detectable protein expression level of PD-L1 has a TIC of at least 20% in the tumor sample.
522. 구현예 514에 있어서,522. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상 및 50% 미만인, 방법.wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% and less than 50% in the tumor sample.
523. 구현예 514에 있어서,523. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 50% 이상인, 방법.wherein the detectable protein expression level of PD-L1 has a TIC of at least 50% in the tumor sample.
524. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,524. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 1% 이상인, 방법.The method of claim 1, wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% of the PD-L1 positive tumor cell fraction.
525. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,525. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 30% 이상인, 방법.The method of claim 1, wherein the detectable protein expression level of PD-L1 is greater than or equal to 30% in the fraction of PD-L1 positive tumor cells.
526. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,526. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 PD-L1 양성 종양 세포 분획이 1% 이상 및 50% 미만인, 방법.wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% and less than 50% of a fraction of PD-L1-positive tumor cells in the tumor sample.
527. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,527. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 방법.The method, wherein the detectable protein expression level of PD-L1 is at least 50% of the PD-L1 positive tumor cell fraction.
528. 구현예 515에 있어서,528. The method of embodiment 515,
상기 PD-L1 양성 종양 세포 분획은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율인, 방법.wherein the PD-L1-positive tumor cell fraction is a proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (ICs).
529. 구현예 515에 있어서,529. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 1% 이상인, 방법.The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 1%.
530. 구현예 515에 있어서,530. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 5% 이상인, 방법.The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 5%.
531. 구현예 516에 있어서,531. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 복합 양성 점수(CPS)가 1 이상인, 방법.The method of claim 1, wherein the detectable protein expression level of PD-L1 has a composite positive score (CPS) of 1 or more.
532. 구현예 516에 있어서,532. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 10 이상인, 방법.The method, wherein the detectable protein expression level of PD-L1 has a CPS of 10 or more.
533. 구현예 516에 있어서,533. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 20 이상인, 방법.The method, wherein the detectable protein expression level of PD-L1 has a CPS of 20 or more.
534. 구현예 528 내지 구현예 530 중 어느 한 구현예에 있어서,534. The method of any one of embodiments 528 to 530,
상기 IHC 분석은 벤타나 SP142 IHC 분석인, 방법.wherein the IHC assay is a Ventana SP142 IHC assay.
535. 구현예 509에 있어서,535. The method of embodiment 509,
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 핵산 발현 수준인, 방법.wherein the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1.
536. 구현예 535에 있어서,536. The method of embodiment 535,
PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되는, 방법.The detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH or a combination thereof.
537. 구현예 47 내지 구현예 423 중 어느 한 구현예에 있어서, 537. The method according to any one of embodiments 47 to 423,
상기 치료는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가 및/또는 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가를 유발하는, 방법.wherein the treatment results in an increase in overall survival (OS) of the subject compared to baseline OS time and/or an increase in progression free survival (PFS) in the subject compared to baseline PFS time.
538. 구현예 537에 있어서: 538. The method of embodiment 537:
(a) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값이고; 그리고/또는 (a) said baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist; and/or
(b) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값인, 방법.(b) the baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist.
539. 구현예 52, 구현예 158, 및 구현예 228 중 어느 한 구현예에 있어서,539. The embodiment of any one of embodiments 52, 158, and 228,
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 방법.The method of claim 1, wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
540. 구현예 539에 있어서,540. The method of embodiment 539,
상기 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 방법.The method of claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541. 구현예 69, 구현예 92, 구현예 127, 구현예 131, 구현예 249, 및 구현예 540에 있어서,541. The method of embodiment 69, embodiment 92, embodiment 127, embodiment 131, embodiment 249, and embodiment 540,
상기 카보플라틴은 AUC = 5 mg/ml/분 또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 방법.wherein the carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min or AUC=6 mg/ml/min.
542. 구현예 69, 구현예 127, 구현예 162, 구현예 164, 구현예 166, 구현예 168, 및 구현예 540에 있어서,542. The method of embodiment 69, embodiment 127, embodiment 162, embodiment 164, embodiment 166, embodiment 168, and embodiment 540,
상기 시스플라틴은 약 75 mg/m2 또는 80 mg/m2의 용량으로 투여되는, 방법.wherein the cisplatin is administered at a dose of about 75 mg/m2 or 80 mg/m2.
543. 구현예 539 내지 구현예 542 중 어느 한 구현예에 있어서,543. The method of any one of embodiments 539 to 542,
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 방법.The method of claim 1, wherein the one or more non-platinum-based chemotherapeutic agents are antimetabolites, taxanes, or topoisomerase II inhibitors.
544. 구현예 62, 구현예 173, 구현예 174, 및 구현예 543에 있어서,544. The method of embodiment 62, embodiment 173, embodiment 174, and embodiment 543,
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 방법.wherein the antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
545. 구현예 69, 구현예 127, 구현예 162, 및 구현예 544 중 어느 한 구현예에 있어서,545. The embodiment of any one of embodiments 69, 127, 162, and 544,
상기 페메트렉시드는 약 500 mg/m2의 용량으로 투여되는, 방법.The method of claim 1, wherein the pemetrexed is administered at a dose of about 500 mg/m2.
546. 구현예 63, 구현예 64, 구현예 162, 구현예 398, 및 구현예 544 중 어느 한 구현예에 있어서,546. The embodiment of any one of embodiments 63, 64, 162, 398, and 544,
상기 젬시타빈은 약 1000 mg/m2 또는 약 1250 mg/m2의 용량으로 투여되는, 방법.wherein the gemcitabine is administered at a dose of about 1000 mg/m2 or about 1250 mg/m2.
547. 구현예 544에 있어서,547. The method of embodiment 544,
상기 항대사물질은 카페시타빈인, 방법.The method of claim 1, wherein the antimetabolite is capecitabine.
548. 구현예 544 또는 구현예 547에 있어서,548. The method of embodiment 544 or embodiment 547,
상기 카페시타빈은 약 1250 mg/m2의 용량으로 투여되는, 방법.wherein the capecitabine is administered at a dose of about 1250 mg/m2.
549. 구현예 173, 구현예 174, 구현예 229, 구현예 230, 구현예 239, 구현예 240, 및 구현예 543 내지 구현예 548 중 어느 한 구현예에 있어서,549. The embodiment of any one of embodiments 173, 174, 229, 230, 239, 240, and 543 to 548,
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 방법.The method of claim 1, wherein the taxane is paclitaxel or nap-paclitaxel.
550. 구현예 69, 구현예 162, 및 구현예 549 중 어느 한 구현예에 있어서,550. The method of any one of embodiments 69, 162, and 549,
상기 파클리탁셀은 약 175 mg/m2 또는 약 200 mg/m2의 용량으로 투여되는, 방법.wherein the paclitaxel is administered at a dose of about 175 mg/m2 or about 200 mg/m2.
551. 구현예 63, 구현예 64, 구현예 249, 구현예 398, 및 구현예 549 중 어느 한 구현예에 있어서,551. The embodiment of any one of embodiments 63, 64, 249, 398, and 549,
상기 냅-파클리탁셀은 약 100 mg/m2의 용량으로 투여되는, 방법.wherein the nap-paclitaxel is administered at a dose of about 100 mg/m2.
552. 구현예 80 내지 구현예 91, 구현예 229, 구현예 230, 구현예 239, 구현예 241, 구현예 251 내지 구현예 255, 및 구현예 543항 내지 구현예 551 중 어느 한 구현예에 있어서,552. The embodiment of any one of embodiments 80-91, 229, 230, 239, 241, 251, 255, and 543-551. ,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 방법.wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331.
553. 구현예 69, 구현예 92, 및 구현예 552 중 어느 한 구현예에 있어서,553. The embodiment of any one of embodiments 69, 92, and 552,
상기 에토포시드는 약 100 mg/m2의 용량으로 투여되는, 방법.wherein the etoposide is administered at a dose of about 100 mg/m2.
554. 구현예 543 내지 구현예 553 중 어느 한 구현예에 있어서,554. The method of any one of embodiments 543 to 553,
상기 하나 이상의 화학요법제는 각각 매주 1회, 2주마다 1회, 3주마다 1회, 3주마다 2회, 4주마다 1회, 4주마다 2회, 또는 4주마다 3회 투여되는, 방법.The one or more chemotherapeutic agents are each administered once every week, once every 2 weeks, once every 3 weeks, twice every 3 weeks, once every 4 weeks, twice every 4 weeks, or 3 times every 4 weeks. , Way.
555. 구현예 543 내지 구현예 554 중 어느 한 구현예에 있어서,555. The method of any one of embodiments 543 to 554,
상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 제 1일에 투여되는, 방법.The method of claim 1, wherein the one or more chemotherapeutic agents are administered on Day 1 of one or more dosing cycles.
556. 구현예 544 내지 구현예 555 중 어느 한 구현예에 있어서,556. The method of any one of embodiments 544 to 555,
상기 젬시타빈은 4주마다 3회 투여되는, 방법.wherein the gemcitabine is administered three times every four weeks.
557. 구현예 544 내지 구현예 556항 중 어느 한 구현예에 있어서,557. The method according to any one of embodiments 544 to 556,
상기 젬시타빈은 1회 이상의 투약 주기의 제 1일, 8일, 및/또는 15일에 투여되는, 방법.wherein the gemcitabine is administered on days 1, 8, and/or 15 of one or more dosing cycles.
558. 구현예 544 내지 구현예 557 중 어느 한 구현예에 있어서,558. The method of any one of embodiments 544 to 557,
상기 카페시타빈은 2주 동안 매일 투여되는, 방법.wherein the capecitabine is administered daily for 2 weeks.
559. 구현예 544 내지 구현예 558 중 어느 한 구현예에 있어서,559. The method according to any one of embodiments 544 to 558,
상기 카페시타빈은 1회 이상의 투약 주기의 제 1일 내지 14일에 투여되는, 방법.wherein the capecitabine is administered on days 1 to 14 of one or more dosing cycles.
560. 구현예 549 내지 구현예 559 중 어느 한 구현예에 있어서,560. The method of any one of embodiments 549 to 559,
상기 냅-파클리탁셀은 4주마다 3회 투여되는, 방법.wherein the nap-paclitaxel is administered 3 times every 4 weeks.
561. 구현예 549 내지 구현예 560 중 어느 한 구현예에 있어서,561. The method of any one of embodiments 549 to 560,
상기 냅-파클리탁셀은 1회 이상의 투약 주기의 제 1일, 8일, 및 15일에 투여되는, 방법.wherein said nap-paclitaxel is administered on days 1, 8, and 15 of one or more dosing cycles.
562. 구현예 552 내지 구현예 561 중 어느 한 구현예에 있어서,562. The method of any one of embodiments 552 to 561,
상기 에토포시드는 3주마다 1일 내지 3일에 투여되는, 방법.The method of claim 1, wherein the etoposide is administered on days 1 to 3 every 3 weeks.
563. 구현예 552 내지 구현예 562 중 어느 한 구현예에 있어서,563. The method of any one of embodiments 552 to 562,
상기 에토포시드는 1회 이상의 투약 주기의 제 1일 내지 3일에 투여되는, 방법.wherein the etoposide is administered on days 1-3 of one or more dosing cycles.
564. 구현예 543 내지 구현예 563 중 어느 한 구현예에 있어서,564. The method of any one of embodiments 543 to 563,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이전에 투여되는, 방법.wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
565. 구현예 543 내지 구현예 564 중 어느 한 구현예에 있어서,565. The method of any one of embodiments 543 to 564,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이후에 투여되는, 방법.wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
566. 구현예 543 내지 구현예 565 중 어느 한 구현예에 있어서,566. The method of any one of embodiments 543 to 565,
상기 하나 이상의 화학요법제는 정맥내 또는 경구로 투여되는, 방법.The method of claim 1, wherein the one or more chemotherapeutic agents are administered intravenously or orally.
567. 구현예 65, 구현예 310, 및 구현예 311 중 어느 한 구현예에 있어서,567. The embodiment of any one of embodiments 65, 310, and 311,
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
568. 구현예 312 또는 구현예 567에 있어서,568. The method of embodiment 312 or embodiment 567,
상기 VEGF 길항제는 3주마다 약 10 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 10 mg/kg to about 20 mg/kg every 3 weeks.
569. 구현예 318 및 구현예 568에 있어서,569. according to embodiment 318 and embodiment 568,
상기 VEGF 길항제는 3주마다 약 15 mg/kg의 용량으로 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 15 mg/kg every 3 weeks.
570. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 569 중 어느 한 구현예에 있어서,570. The embodiment of any one of embodiments 65, 310 to 312, 318 to 320, and embodiments 567 to 569,
상기 VEGF 길항제는 항 VEGF 항체인, 방법.The method of claim 1, wherein the VEGF antagonist is an anti-VEGF antibody.
571. 구현예 570에 있어서,571. The method of embodiment 570,
상기 항 VEGF 항체는 베바시주맙의 VH 도메인 및 VL 도메인을 포함하는, 방법.The method of claim 1, wherein the anti-VEGF antibody comprises a VH domain and a VL domain of bevacizumab.
572. 구현예 570 또는 구현예 571에 있어서,572. The method of embodiment 570 or embodiment 571,
상기 항 VEGF 항체는 베바시주맙인, 방법.The anti-VEGF antibody is bevacizumab, the method.
573. 구현예 65, 구현예 310 내지 구현예 312, 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,573. The embodiment of any one of embodiments 65, 310 to 312, and embodiments 318 to 320,
상기 항 TIGIT 길항제 항체는 티라골루맙이고, 상기 PD-1 축 결합 길항제는 아테졸리주맙이며, 상기 VEGF 길항제는 베바시주맙인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tiragolumab, the PD-1 axis binding antagonist is atezolizumab, and the VEGF antagonist is bevacizumab.
574. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 573 중 어느 한 구현예에 있어서,574. The embodiment of any one of embodiments 65, 310 to 312, 318 to 320, and embodiments 567 to 573,
1회 이상의 투약 주기의 제 1일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering the VEGF antagonist to the subject on Day 1 of one or more dosing cycles.
575. 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,575. The method of any one of embodiments 318 to 320,
1회 이상의 투약 주기의 15일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.and administering the VEGF antagonist to the subject on day 15 of one or more dosing cycles.
576. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 575 중 어느 한 구현예에 있어서,576. The embodiment of any one of embodiments 65, 310 to 312, 318 to 320, and embodiments 567 to 575,
상기 VEGF 길항제는 정맥내 투여되는, 방법.The method of claim 1, wherein the VEGF antagonist is administered intravenously.
577. 구현예 576에 있어서,577. The method of embodiment 576,
상기 VEGF 길항제는 90 ± 15분에 걸쳐 정맥내 주입으로 상기 대상체에게 투여되는, 방법.wherein the VEGF antagonist is administered to the subject as an intravenous infusion over 90 ± 15 minutes.
578. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 577 중 어느 한 구현예에 있어서,578. The embodiment of any one of embodiments 65, 310 to 312, 318 to 320, and embodiments 567 to 577,
상기 VEGF 길항제 이전에 상기 PD-1 축 결합 길항제, 및 상기 항 TIGIT 길항제 항체 이전에 상기 VEGF 길항제를 상기 대상체에 투여하는 단계를 포함하는, 방법.A method comprising administering to the subject the PD-1 axis binding antagonist prior to the VEGF antagonist, and the VEGF antagonist prior to the anti-TIGIT antagonist antibody.
579. 구현예 578에 있어서,579. The method of embodiment 578,
상기 PD-1 축 결합 길항제 투여 후 제1 관찰 기간, 상기 VEGF 길항제 투여 후 제2 관찰 기간, 및 상기 항 TIGIT 길항제 항체 투여 후 제3 관찰 기간을 포함하는, 방법.A method comprising a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody.
580. 구현예 579에 있어서,580. The method of embodiment 579,
상기 제1 관찰 기간, 상기 제2 관찰 기간, 및 상기 제3 관찰 기간은 각각 약 30분 내지 약 120분의 길이인, 방법.wherein the first observation period, the second observation period, and the third observation period are each from about 30 minutes to about 120 minutes in length.
581. 구현예 113, 구현예 128, 구현예 129 내지 구현예 131, 구현예 175 내지 구현예 182, 구현예 210 내지 구현예 214, 구현예 221, 구현예 256, 구현예 257, 구현예 270, 구현예 289, 구현예 290, 구현예 293, 구현예 294, 구현예 297, 구현예 298, 구현예 333, 구현예 362 내지 구현예 365, 구현예 385, 구현예 386, 구현예 389, 구현예 393, 구현예 419, 및 구현예 422 중 어느 한 구현예에 있어서,581. Embodiment 113, Embodiment 128, Embodiment 129 to Embodiment 131, Embodiment 175 to Embodiment 182, Embodiment 210 to Embodiment 214, Embodiment 221, Embodiment 256, Embodiment 257, Embodiment 270, Embodiment 289, Embodiment 290, Embodiment 293, Embodiment 294, Embodiment 297, Embodiment 298, Embodiment 333, Embodiment 362 to Embodiment 365, Embodiment 385, Embodiment 386, Embodiment 389, Embodiment 393, embodiment 419, and embodiment 422 according to any one of embodiments,
티라골루맙 및 아테졸리주맙은 투여 이전에 IV 백(bag)에 결합되는, 방법.wherein tiragolumab and atezolizumab are bound to an IV bag prior to administration.
582. 구현예 47 내지 구현예 581 중 어느 한 구현예에 있어서, 상기 대상체는 인간인, 방법.582. The method of any one of embodiments 47-581, wherein the subject is a human.
583. 구현예 47 내지 구현예 190, 구현예 192 내지 구현예 208, 구현예 210 내지 구현예 211, 구현예 213, 구현예 215 내지 구현예 268, 구현예 270 내지 구현예 294, 및 구현예 299 내지 구현예 582 중 어느 한 구현예의 방법에 따라 암을 가진 대상체를 치료하기 위한 PD-1 축 결합 길항제 및/또는 항 TIGIT 길항제 항체를 포함하는, 키트.583. Embodiment 47-190, Embodiment 192-208, Embodiment 210-211, Embodiment 213, Embodiment 215-268, Embodiment 270-294, and Embodiment 299 A kit comprising a PD-1 axis binding antagonist and/or anti TIGIT antagonist antibody for treating a subject having cancer according to the method of any one of embodiments to embodiment 582.
584. 구현예 47 내지 구현예 190, 구현예 192 내지 구현예 208, 구현예 210 내지 구현예 211, 구현예 213, 구현예 215 내지 구현예 268, 구현예 270 내지 구현예 294, 및 구현예 299 내지 구현예 582 중 어느 한 구현예의 방법에 따라 암을 가진 대상체를 치료하기 위해 항 TIGIT 길항제 항체와 병용으로 사용하기 위한 PD-1 축 결합 길항제를 포함하는, 키트.584. Embodiment 47-190, Embodiment 192-208, Embodiment 210-211, Embodiment 213, Embodiment 215-268, Embodiment 270-294, and Embodiment 299 A kit comprising a PD-1 axis binding antagonist for use in combination with an anti TIGIT antagonist antibody to treat a subject having cancer according to the method of any one of embodiments to embodiment 582.
585. 구현예 584에 있어서,585. The method of embodiment 584,
항 TIGIT 길항제 항체를 더 포함하는, 키트.The kit further comprising an anti-TIGIT antagonist antibody.
586. 구현예 583 내지 구현예 585 중 어느 한 구현예에 있어서,586. The method of any one of embodiments 583 to 585,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
587. 구현예 583 내지 구현예 586 중 어느 한 구현예에 있어서,587. The method according to any one of embodiments 583 to 586,
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 방법.The method of claim 1, wherein the PD-1 axis binding antagonist is atezolizumab.
588. 구현예 47 내지 구현예 190, 구현예 192 내지 구현예 208, 구현예 210 내지 구현예 211, 구현예 213, 구현예 215 내지 구현예 268, 구현예 270 내지 구현예 294, 및 구현예 299 내지 구현예 582 중 어느 한 구현예의 방법에 따라 암을 가진 대상체를 치료하기 위해 PD-1 축 결합 길항제와 병용으로 사용하기 위한 항 TIGIT 길항제 항체를 포함하는, 키트.588. Embodiment 47 to embodiment 190, embodiment 192 to embodiment 208, embodiment 210 to embodiment 211, embodiment 213, embodiment 215 to embodiment 268, embodiment 270 to embodiment 294, and embodiment 299 A kit comprising an anti TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject having cancer according to the method of any one of embodiments to embodiment 582.
589. 구현예 588에 있어서,589. The method of embodiment 588,
PD-1 축 결합 길항제를 더 포함하는, 키트.A kit, further comprising a PD-1 axis binding antagonist.
590. 구현예 588 또는 구현예 589에 있어서,590. The method of embodiment 588 or embodiment 589,
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 키트.The kit, wherein the PD-1 axis binding antagonist is atezolizumab.
591. 구현예 588 내지 구현예 590 중 어느 한 구현예에 있어서,591. The method of any one of embodiments 588 to 590,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법.The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
592. 구현예 583 내지 구현예 591 중 어느 한 구현예에 있어서,592. The method according to any one of embodiments 583 to 591,
하나 이상의 화학요법제를 더 포함하는, 키트.A kit, further comprising one or more chemotherapeutic agents.
593. 구현예 592에 있어서,593. The method of embodiment 592,
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 키트.wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
594. 구현예 593에 있어서,594. The method of embodiment 593,
상기 하나 이상의 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 키트.wherein the at least one platinum-based chemotherapeutic agent is carboplatin or cisplatin.
595. 구현예 593 또는 구현예 594에 있어서,595. The method of embodiment 593 or embodiment 594,
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 키트.wherein the at least one non-platinum-based chemotherapeutic agent is an antimetabolite, a taxane, or a topoisomerase II inhibitor.
596. 구현예 595에 있어서,596. The method of embodiment 595,
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 키트.wherein the antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
597. 구현예 595 또는 구현예 596에 있어서,597. The method of embodiment 595 or embodiment 596,
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 키트.wherein the taxane is paclitaxel or nap-paclitaxel.
598. 구현예 595 내지 구현예 597 중 어느 한 구현예에 있어서,598. The method according to any one of embodiments 595 to 597,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 키트.wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331.
599. 구현예 583 내지 구현예 598 중 어느 한 구현예에 있어서,599. The method of any one of embodiments 583 to 598,
VEGF 길항제를 더 포함하는, 키트.A kit, further comprising a VEGF antagonist.
600. 구현예 599에 있어서,600. The method of embodiment 599,
상기 VEGF 길항제는 항 VEGF 항체인, 키트.The VEGF antagonist is an anti-VEGF antibody, kit.
601. 구현예 600에 있어서,601. The method of embodiment 600,
상기 항 VEGF 항체는 베바시주맙인, 키트.The anti-VEGF antibody is bevacizumab, the kit.
602. 암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,602. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cancer, comprising:
상기 방법은 구현예 47 내지 구현예 190, 구현예 192 내지 구현예 208, 구현예 210 내지 구현예 211, 구현예 213, 구현예 215 내지 구현예 268, 구현예 270 내지 구현예 294, 및 구현예 299 내지 구현예 582 중 어느 한 구현예에 따르는, 항 TIGIT 길항제 항체 및 항 PD-1 축 결합 길항제.The method includes embodiments 47 to 190, 192 to 208, 210 to 211, 213, 215 to 268, 270 to 294, and embodiments An anti TIGIT antagonist antibody and an anti PD-1 axis binding antagonist according to any one of 299 to embodiment 582.
603. 암을 가진 대상체 또는 대상체 집단을 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용되는 항 TIGIT 길항제 항체의 사용으로서,603. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or population of subjects having cancer, comprising:
구현예 47 내지 구현예 190, 구현예 192 내지 구현예 208, 구현예 210 내지 구현예 211, 구현예 213, 구현예 215 내지 구현예 268, 구현예 270 내지 구현예 294, 및 구현예 299 내지 구현예 582 중 어느 한 구현예의 방법에 따르는, 사용.Embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-implementation Use according to the method of any one of Example 582.
604. 구현예 603에 있어서,604. The method of embodiment 603,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
605. 구현예 603에 있어서,605. The method of embodiment 603,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
구현예 세트 B:Implementation Set B:
1. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,1. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 500 mg 내지 약 700 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화되고, 여기서 상기 치료는 3주마다 백금계 화학요법제 및 3주마다 비백금계 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 500 mg to about 700 mg every 3 weeks. and wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 900 mg to about 1500 mg every 3 weeks, wherein said treatment is a platinum-based chemotherapeutic agent every 3 weeks and a non-platinum-based chemotherapy every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, further comprising the use of an agent.
2. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,2. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 4주마다 약 700 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 4주마다 약 1400 mg 내지 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti TIGIT antagonist antibody is administered at a dose of about 700 mg to about 1000 mg every 4 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 1400 mg to 2000 mg every 4 weeks.
3. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,3. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 2주마다 약 600 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 300 mg to about 600 mg every two weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks.
4. 구현예 2 또는 구현예 3에 있어서,4. according to embodiment 2 or embodiment 3,
상기 치료는 하나 이상의 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of one or more chemotherapeutic agents.
5. 구현예 1 내지 구현예 4 중 어느 한 구현예에 있어서,5. The method according to any one of embodiments 1 to 4,
상기 항 TIGIT 길항제 항체는 IgG 부류 항체, 특히 IgG1 하위부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6. 구현예 1 내지 구현예 5 중 어느 한 구현예에 있어서,6. The method according to any one of embodiments 1 to 5,
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
(a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
(d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
(f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(f) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
7. 구현예 1 내지 구현예 6 중 어느 한 구현예에 있어서,7. The method according to any one of embodiments 1 to 6,
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR): The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
(a) DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
(d) FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4, 및(d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and
하기의 중쇄 가변 영역 FR들:The following heavy chain variable region FRs:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
(b) WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
(d) WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(d) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, further comprising FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
8. 구현예 1 내지 구현예 7 중 어느 한 구현예에 있어서,8. The method according to any one of embodiments 1 to 7,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19.
9. 구현예 1 내지 구현예 8 중 어느 한 구현예에 있어서,9. The method according to any one of embodiments 1 to 8,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody is tyragolumab; an anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
10. 구현예 1 내지 구현예 9 중 어느 한 구현예에 있어서,10. The method according to any one of embodiments 1 to 9,
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제 또는 PD-1 결합 길항제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
11. 구현예 1 내지 구현예 10 중 어느 한 구현예에 있어서,11. The method according to any one of embodiments 1 to 10,
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
12. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,12. The method according to any one of embodiments 1 to 11,
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
13. 구현예 12에 있어서,13. The method of embodiment 12,
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
14. 구현예 1 내지 구현예 13 중 어느 한 구현예에 있어서,14. The method according to any one of embodiments 1 to 13,
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is atezolizumab.
15. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,15. The method according to any one of embodiments 1 to 11,
상기 PD-1 축 결합 길항제는 항 PD-1 길항제 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
16. 구현예 15에 있어서,16. The method of embodiment 15,
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, For use which is HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21 Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists.
17. 구현예 2 내지 구현예 16 중 어느 한 구현예에 있어서,17. The method according to any one of embodiments 2 to 16,
상기 치료는 유효량의 백금계 화학요법제 및 비백금계 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
18. 구현예 1 또는 구현예 17에 있어서,18. according to embodiment 1 or embodiment 17,
상기 비백금계 화학요법제는 토포이소머라제 II 억제제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the non-platinum-based chemotherapeutic agent is a topoisomerase II inhibitor.
19. 구현예 18에 있어서,19. The method of embodiment 18,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331, 특히 에토포시드인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331, in particular etoposide; Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
20. 구현예 18 또는 구현예 19에 있어서,20. The method of embodiment 18 or embodiment 19,
상기 토포이소머라제 II 억제제는 100 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said topoisomerase II inhibitor is formulated for administration at a dose of 100 mg/m2.
21. 구현예 17 내지 구현예 20 중 어느 한 구현예에 있어서,21. The method according to any one of embodiments 17 to 20,
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴, 특히 카보플라틴인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
22. 구현예 17 내지 구현예 21 중 어느 한 구현예에 있어서,22. The method according to any one of embodiments 17 to 21,
상기 백금계 화학요법제는 투여 당일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
23. 구현예 1 내지 구현예 22 중 어느 한 구현예에 있어서,23. The method according to any one of embodiments 1-22,
상기 방법은 유도기 및 유지기를 포함한 투약 요법을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said method comprises a dosing regimen comprising an induction phase and a maintenance phase.
24. 구현예 23에 있어서,24. The method of embodiment 23,
상기 유도기는 4회의 초기 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제가 4회의 초기 투약 주기의 각각에서 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the induction phase comprises 4 initial dosing cycles and the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent, and non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for
25. 구현예 23 또는 구현예 24에 있어서,25. according to embodiment 23 or embodiment 24,
상기 유지기는 상기 백금계 화학요법제 및/또는 비백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said maintenance phase does not include administration of said platinum-based chemotherapeutic agent and/or non-platinum-based chemotherapeutic agent.
26. 구현예 1 내지 구현예 25 중 어느 한 구현예에 있어서,26. The method according to any one of embodiments 1 to 25,
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
27. 구현예 1 내지 구현예 26 중 어느 한 구현예에 있어서,27. The method according to any one of embodiments 1-26,
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 전체 생존을 연장하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment prolongs overall survival of said subject as compared to treatment without said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
28. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,28. The method according to any one of embodiments 1 to 27,
상기 암은 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is lung cancer.
29. 구현예 1 내지 구현예 28 중 어느 한 구현예에 있어서,29. The method according to any one of embodiments 1 to 28,
상기 폐암은 소세포 폐암(SCLC), 특히 확장기 SCLC(ES-SCLC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said lung cancer is small cell lung cancer (SCLC), in particular diastolic SCLC (ES-SCLC).
30. 구현예 28에 있어서,30. The method of embodiment 28,
상기 폐암은 소세포 폐암(SCLC), 특히 국소 진행성 절제 불가능한 NSCLC(IIIB기 NSCLC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said lung cancer is small cell lung cancer (SCLC), in particular locally advanced unresectable NSCLC (stage IIIB NSCLC).
31. 구현예 28에 있어서,31. The method of embodiment 28,
상기 폐암은 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is locally advanced unresectable or metastatic nonsquamous NSCLC.
32. 구현예 28에 있어서,32. The method of embodiment 28,
상기 폐암은 절제 가능한 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is resectable lung cancer.
33. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,33. The method according to any one of embodiments 1 to 27,
상기 암은 자궁경부암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is cervical cancer.
34. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,34. The method according to any one of embodiments 1 to 27,
상기 암은 초기 삼중음성 유방암(eTNBC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is early triple negative breast cancer (eTNBC).
35. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,35. The method according to any one of embodiments 1 to 27,
상기 암은 두경부암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is head and neck cancer.
36. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,36. The method according to any one of embodiments 1 to 27,
상기 암은 간암, 특히 간세포 암종(HCC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
37. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,37. The method according to any one of embodiments 1 to 27,
상기 암은 방광암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is bladder cancer.
38. 구현예 37에 있어서,38. The method of embodiment 37,
상기 암은 요로상피세포 암종(UC), 특히 전이성 요로상피세포 암종(mUC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cancer is urothelial cell carcinoma (UC), in particular metastatic urothelial cell carcinoma (mUC).
39. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,39. The method according to any one of embodiments 1 to 27,
상기 암은 췌장암, 특히 췌장 관세포암(PDAC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cancer is pancreatic cancer, in particular pancreatic ductal cell carcinoma (PDAC).
40. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,40. The method according to any one of embodiments 1 to 27,
상기 암은 식도암, 특히 진행성 또는 전이성 식도암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
41. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,41. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 500 mg 내지 약 700 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises an anti TIGIT antagonist antibody formulated for administration at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist formulated for administration of a dose of about 900 mg to about 1500 mg every 3 weeks. An anti TIGIT antagonist antibody and PD- for use comprising administering to the subject a dosing regimen comprising at least one dosing cycle of a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks uniaxial binding antagonists.
42. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,42. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist formulated for administration of a dose of about 1400 mg to about 2000 mg every 4 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising administering to the subject a dosing regimen comprising one or more dosing cycles.
43. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,43. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises an anti TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every two weeks and a PD-1 axis binding antagonist formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising administering to the subject a dosing regimen comprising one or more dosing cycles of
44. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서:44. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
(a) 상기 방법은 3주마다 약 500 mg 내지 약 700 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고; (b) 상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하거나; 또는 (c) 상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(a) the method comprises an anti TIGIT antagonist antibody formulated for administration at a dose of about 500 mg to about 700 mg every 3 weeks, PD-1 formulated for administration of a dose of about 900 mg to about 1500 mg every 3 weeks administering to the subject a dosing regimen comprising one or more dosing cycles of an axis-binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks; (b) the method comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis formulated for administration of a dose of about 1400 mg to about 2000 mg every 4 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the binding antagonist; or (c) the method comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every two weeks and a PD- formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the uniaxial binding antagonist.
45. 구현예 44에 있어서,45. The method of embodiment 44,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist.
46. 구현예 44에 있어서,46. The method of embodiment 44,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single formulation.
47. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,47. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 4주마다 약 200 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 4주마다 약 80 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is formulated for administration of a dose of about 80 mg to about 2000 mg every 4 weeks.
48. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,48. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 4주마다 약 200 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is formulated for administration of a dose of about 20 mg to about 1600 mg every two weeks.
49. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,49. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is formulated for administration of a dose of about 20 mg to about 1600 mg every two weeks.
50. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,50. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 4주마다 약 80 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is formulated for administration of a dose of about 80 mg to about 2000 mg every 4 weeks.
51. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,51. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 6주마다 약 100 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 axis binding antagonist is formulated for administration of a dose of about 100 mg to about 1000 mg every 6 weeks.
52. 구현예 47 내지 구현예 51 중 어느 한 구현예에 있어서,52. The method according to any one of embodiments 47 to 51,
상기 치료는 하나 이상의 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of one or more chemotherapeutic agents.
53. 구현예 52에 있어서,53. The method of embodiment 52,
상기 치료는 백금계 화학요법제 및 비백금계 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
54. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,54. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되고, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein the PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of a chemotherapeutic agent.
55. 구현예 53 또는 구현예 54에 있어서,55. according to embodiment 53 or embodiment 54,
상기 방법은 유도기 및 유지기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the method comprises an induced phase and a maintenance phase.
56. 구현예 55에 있어서,56. The method of embodiment 55,
상기 유도기 및 유지기는 각각 1회 이상의 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said induction phase and maintenance phase each comprise at least one dosing cycle.
57. 구현예 55 또는 구현예 56에 있어서,57. according to embodiment 55 or embodiment 56,
상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent.
58. 구현예 55 내지 구현예 57 중 어느 한 구현예에 있어서,58. The method according to any one of embodiments 55 to 57,
상기 유지기는 상기 비백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said maintenance phase does not include administration of said non-platinum-based chemotherapeutic agent.
59. 구현예 58에 있어서,59. The method of embodiment 58,
상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The maintenance phase is one or more dosing cycles of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks and a dose of about 80 mg to about 2000 mg of the PD-1 axis binding antagonist every 4 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising:
60. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,60. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고 항 PD-1 길항제 항체는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein the anti-PD-1 antagonist antibody is formulated for administration of a dose of about 80 mg to about 1600 mg every three weeks, wherein the anti-PD-1 antagonist antibody is pembrolizumab. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists.
61. 암을 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 펨브롤리주맙으로서,61. Tiragolumab and pembrolizumab for use in a method of treating a subject having cancer, comprising:
상기 치료는 티라골루맙 및 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법에서 티라골루맙 및 펨브롤리주맙의 사용을 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 100 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되는, 방법.wherein said treatment comprises the use of tiragolumab and pembrolizumab in a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein said pembrolizumab is about 100 mg to about 1000 mg every 6 weeks. A method formulated for administration of a dose.
62. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,62. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량의 항대사물질의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and orally about 10 mg/m2 twice daily every 3 weeks of dosing for 2 weeks/1 week off. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising the use of a dose of from to about 10000 mg/m2 of the antimetabolite.
63. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,63. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량, 젬시타빈, 및 냅-파클리탁셀의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. An anti-TIGIT antagonist antibody and PD for use, wherein the PD-1 axis binding antagonist comprises the use of a dose of about 80 mg to about 1600 mg every 3 weeks, gemcitabine, and nap-paclitaxel. -1 axis binding antagonists.
64. 구현예 52에 있어서,64. The method of embodiment 52,
상기 하나 이상의 화학요법제는 젬시타빈 및 냅-파클리탁셀인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said at least one chemotherapeutic agent is gemcitabine and nap-paclitaxel.
65. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,65. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg의 용량의 VEGF 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks. is formulated for administration of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and a dose of about 1 mg/kg to about 35 mg/kg of a VEGF antagonist every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
66. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,66. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 유도기 및 유지기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, 3 weeks comprising at least one dosing cycle of a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum chemotherapeutic agent every 3 weeks, wherein said maintenance An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein the group does not include administration of said platinum-based chemotherapeutic agent.
67. 암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,67. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
상기 치료는 유도기 및 유지기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, 3 weeks comprising at least one dosing cycle of a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) the maintenance phase is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks and PD-1 formulated for administration of a dose of about 80 mg to about 2000 mg every 4 weeks. an anti-TIGIT antagonist antibody and PD-1 axis binding for use comprising one or more additional dosing cycles of the axis binding antagonist, wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent antagonist.
68. 구현예 56 내지 구현예 59, 구현예 66, 및 구현예 67 중 어느 한 구현예에 있어서,68. The method of any one of embodiments 56 to 59, embodiment 66, and embodiment 67,
상기 유도기는 4회 내지 6회의 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said induction phase comprises 4 to 6 dosing cycles.
69. 구현예 53 내지 구현예 59 및 구현예 66 내지 구현예 68 중 어느 한 구현예에 있어서:69. The method of any one of embodiments 53-59 and 66-68:
(a) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고;(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이거나; 또는(a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel; or
(c) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 에토포시드인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) said platinum-based chemotherapeutic agent is carboplatin or cisplatin and said non-platinum-based chemotherapeutic agent is etoposide.
70. 구현예 47 내지 구현예 69 중 어느 한 구현예에 있어서,70. The method according to any one of embodiments 47 to 69,
상기 암은 고형 종양인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is a solid tumor.
71. 구현예 47 내지 구현예 70 중 어느 한 구현예에 있어서,71. The method according to any one of embodiments 47 to 70,
상기 암은 국소 진행성 또는 전이성인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the cancer is locally advanced or metastatic; an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
72. 구현예 47 내지 구현예 71 중 어느 한 구현예에 있어서,72. The method according to any one of embodiments 47 to 71,
상기 암은 폐암, 췌장암, 자궁경부암, 유방암, 두경부암, 간암, 방광암, 식도암, 위암, 결장직장암, 신장암, 신장암, 흑색종, 또는 난소암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, kidney cancer, melanoma, or ovarian cancer. uniaxial binding antagonists.
73. 구현예 72에 있어서,73. The method of embodiment 72,
상기 암은 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is lung cancer.
74. 구현예 73에 있어서,74. The method of embodiment 73,
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is NSCLC, in particular locally advanced unresectable NSCLC.
75. 구현예 74에 있어서,75. The method of embodiment 74,
상기 NSCLC는 IIIB기 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said NSCLC is stage IIIB NSCLC.
76. 구현예 73 내지 구현예 75 중 어느 한 구현예에 있어서,76. The method according to any one of embodiments 73 to 75,
상기 폐암인 재발성 또는 전이성 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is relapsed or metastatic NSCLC.
77. 구현예 76에 있어서,77. The method of embodiment 76,
상기 NSCLC는 IV기 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said NSCLC is stage IV NSCLC.
78. 구현예 77에 있어서,78. The method of embodiment 77,
상기 대상체는 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject has not previously been treated for stage IV NSCLC.
79. 구현예 73에 있어서,79. The method of embodiment 73,
상기 폐암은 소세포 폐암(SCLC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is small cell lung cancer (SCLC).
80. 폐암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,80. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer,
상기 치료는 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor, wherein the anti-TIGIT antagonist antibody and the PD- comprising the use of a uniaxial binding antagonist, wherein said treatment comprises the treatment of said subject without said anti-TIGIT antagonist antibody as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, prolonging progression survival (PFS).
81. 폐암을 가진 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,81. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a population of subjects with lung cancer,
상기 치료는 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 약 8.2개월 내지 약 9.2개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor, wherein the anti-TIGIT antagonist antibody and the PD- An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising the use of a uniaxial binding antagonist, wherein said treatment results in a median PFS in a population of subjects from about 8.2 months to about 9.2 months.
82. 구현예 80 또는 구현예 81에 있어서,82. The method of embodiment 80 or embodiment 81,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)을 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment prolongs overall survival (OS) of said subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody; Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
83. 구현예 80 내지 구현예 82 중 어느 한 구현예에 있어서,83. The method according to any one of embodiments 80 to 82,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 2.4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
84. 구현예 83에 있어서,84. The method of embodiment 83,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3개월 내지 약 4개월 만큼 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment reduces the PFS of said subject or population of subjects by at least about 3 months to about 4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use extending by months.
85. 폐암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,85. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer,
상기 치료는 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 OS를 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor, wherein the anti-TIGIT antagonist antibody and the PD- comprising the use of a uniaxial binding antagonist, wherein said treatment comprises the OS of said subject compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor without said anti-TIGIT antagonist antibody. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
86. 폐암을 가진 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,86. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a population of subjects with lung cancer,
상기 치료는 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 약 15.3개월 내지 약 17.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an effective amount of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist in one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in a median OS in a population of subjects from about 15.3 months to about 17.6 months.
87. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,87. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment prolongs the OS of the subject or population of subjects by at least about 3.3 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
88. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,88. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3개월 내지 약 5.3개월 만큼 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment reduces the OS of said subject or population of subjects by at least about 3 months to about 5.3 as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use extending by months.
89. 구현예 80 내지 구현예 88 중 어느 한 구현예에 있어서,89. The method according to any one of embodiments 80 to 88,
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각에서 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the anti TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered in each of 4 initial dosing cycles. binding antagonists.
90. 구현예 80 내지 구현예 89 중 어느 한 구현예에 있어서,90. The method according to any one of embodiments 80 to 89,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 제4 초기 투약 주기 이후에 1회 이상의 추가 주기로 더 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are further administered in one or more additional cycles after the fourth initial dosing cycle.
91. 구현예 90에 있어서,91. The method of embodiment 90,
상기 백금계 화학요법제 및 상기 토포이소머라제 II 억제제가 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are omitted from each of one or more additional dosing cycles.
92. 구현예 80 내지 구현예 91 중 어느 한 구현예에 있어서,92. The method according to any one of embodiments 80 to 91,
상기 백금계 화학요법제는 카보플라틴이고 상기 토포이소머라제 II 억제제는 에토포시드인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said platinum-based chemotherapeutic agent is carboplatin and said topoisomerase II inhibitor is etoposide.
93. 구현예 80 내지 구현예 92 중 어느 한 구현예에 있어서,93. The method according to any one of embodiments 80 to 92,
상기 폐암은 소세포 폐암 (SCLC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is small cell lung cancer (SCLC).
94. 구현예 93에 있어서,94. The method of embodiment 93,
상기 SCLC는 확장 병기의 SCLC(ES-SCLC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said SCLC is an expanded stage SCLC (ES-SCLC).
95. 구현예 94에 있어서,95. The method of embodiment 94,
상기 대상체 또는 대상체들은 ES-SCLC에 대한 치료 경험이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects is naive to treat ES-SCLC.
96. 구현예 80 내지 구현예 95 중 어느 한 구현예에 있어서,96. The method according to any one of embodiments 80 to 95,
상기 대상체 또는 대상체들은 뇌 전이의 존재 또는 병력이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject or subjects has no presence or history of brain metastases.
97. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,97. The method according to any one of embodiments 80 to 96,
상기 폐암은 PD-L1 발현에 대해 선택되지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said lung cancer is not selected for PD-L1 expression.
98. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,98. The method according to any one of embodiments 80 to 96,
상기 폐암은 PD-L1 발현에 대해 선택되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is selected for PD-L1 expression.
99. 구현예 98에 있어서,99. The method of embodiment 98,
상기 폐암은 PD-L1의 검출 가능한 발현 수준에 의해 PD-L1 발현에 대해 선택되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is selected for PD-L1 expression by a detectable expression level of PD-L1.
100. 구현예 80 내지 구현예 99 중 어느 한 구현예에 있어서,100. The method according to any one of embodiments 80 to 99,
상기 폐암은 전이성인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is metastatic.
101. 구현예 100에 있어서,101. The method of embodiment 100,
상기 폐암은 뇌, 간, 림프절, 및/또는 부신으로 전이된, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer has metastasized to the brain, liver, lymph node, and/or adrenal gland.
102. 구현예 100 또는 구현예 101에 있어서,102. The method of embodiment 100 or embodiment 101,
상기 폐암은 뇌로 전이되지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer does not metastasize to the brain.
103. 구현예 100 내지 구현예 102 중 어느 한 구현예에 있어서,103. The method of any one of embodiments 100-102,
상기 치료는 완전 반응(CR) 또는 부분 반응(PR)을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment elicits a complete response (CR) or a partial response (PR).
104. 구현예 80 내지 구현예 103 중 어느 한 구현예에 있어서,104. The method according to any one of embodiments 80 to 103,
상기 항 TIGIT 길항제 항체는 2주마다, 3주마다, 또는 4주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 2 weeks, every 3 weeks, or every 4 weeks.
105. 구현예 80 내지 구현예 104 중 어느 한 구현예에 있어서,105. The method of any one of embodiments 80-104,
상기 PD-1 축 결합 길항제는 2주마다, 3주마다, 또는 4주마다 약 80 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 2000 mg every 2 weeks, every 3 weeks, or every 4 weeks, an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use .
106. 구현예 80 내지 구현예 105 중 어느 한 구현예에 있어서,106. The method of any one of embodiments 80 to 105,
상기 PD-1 축 결합 길항제, 상기 항 TIGIT 길항제 항체, 상기 백금계 화학요법제, 및 상기 포토이소머라제 II 억제제는 순차적으로 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist, said anti-TIGIT antagonist antibody, said platinum-based chemotherapeutic agent, and said photoisomerase II inhibitor are administered sequentially.
107. 구현예 106에 있어서,107. The method of embodiment 106,
상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체보다 먼저 투여되고, 상기 항 TIGIT 길항제 항체는 상기 백금계 화학요법제보다 먼저 투여되며, 상기 백금제는 상기 토포이소머라제 II 억제제보다 먼저 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The PD-1 axis binding antagonist is administered before the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered before the platinum-based chemotherapeutic agent, and the platinum agent is administered before the topoisomerase II inhibitor. , anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
108. 구현예 80 내지 구현예 107 중 어느 한 구현예에 있어서,108. The method according to any one of embodiments 80 to 107,
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 정맥내 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent, and topoisomerase II inhibitor are administered intravenously.
109. 구현예 80 내지 구현예 108 중 어느 한 구현예에 있어서,109. The method according to any one of embodiments 80 to 108,
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제 중 하나 이상은 정맥내 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least one of said anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent, and topoisomerase II inhibitor is administered intravenously.
110. SCLC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,110. An anti TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with SCLC, comprising:
상기 치료는 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg on Day 1 of each dosing cycle, atezoli at a dose of about 80 mg to about 1600 mg on Day 1 of each dosing cycle. Zumab, carboplatin in a dose sufficient to achieve AUC=5 mg/ml/min on Day 1 of each dosing cycle, and 100 mg/day on each of Days 1, 2, and 3 of each dosing cycle comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more 21-day dosing cycles of an m2 dose of etoposide, wherein said treatment is atezolizumab, carbople without said anti-TIGIT antagonist antibody. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, prolonging PFS and/or OS in said subject compared to treatment with Latin, and etoposide.
111. SCLC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,111. An anti TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with SCLC,
상기 치료는 각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 800 mg on Day 1 of each dosing cycle, atezoli at a dose of about 900 mg to about 1500 mg on Day 1 of each dosing cycle. Zumab, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min on Day 1 of each dosing cycle, and 100 mg/day on each of Days 1, 2, and 3 of each dosing cycle comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in at least one 21-day dosing cycle of an m2 dose of etoposide, wherein said treatment is atezolizumab, carbople without said anti-TIGIT antagonist antibody. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, prolonging PFS and/or OS in said subject compared to treatment with Latin, and etoposide.
112. 구현예 110 또는 구현예 111에 있어서,112. The method of embodiment 110 or embodiment 111,
상기 치료는 각 추가적인 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 추가적인 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 추가적인 21일 투약 주기를 더 포함하고, 카보플라틴 및 에토포시드는 상기 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg on Day 1 of each additional dosing cycle and a dose of about 80 mg to about 1600 mg on Day 1 of each additional dosing cycle. Anti-TIGIT antagonist antibody and PD-1 axis binding for use further comprising one or more additional 21-day dosing cycles of atezolizumab, wherein carboplatin and etoposide are omitted from each of said one or more additional dosing cycles. antagonist.
113. ES-SCLC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,113. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with ES-SCLC,
상기 치료는 4회의 초기 투약 주기에 이어서 1회 이상의 추가적인 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고:wherein said treatment comprises the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in 4 initial dosing cycles followed by one or more additional dosing cycles:
(a) 상기 4회의 초기 투약 주기는 각 초기 투약 주기의 제 1일에 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙, 각 초기 투약 주기의 제 1일에 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙, 각 초기 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 초기 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드를 포함하고; 그리고(a) said four initial dosing cycles comprise administration of a tiragolumab formulated for administration of a dose of about 600 mg on Day 1 of each initial dosing cycle, administration of a dose of about 1200 mg on Day 1 of each initial dosing cycle. Atezolizumab formulated for this purpose, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min on Day 1 of each initial dosing cycle, and Days 1, 2, and 2 of each initial dosing cycle, and with etoposide at a dose of 100 mg/m2 on each of 3 days; and
(b) 상기 1회 이상의 추가적인 투약 주기는 각각의 추가적인 투약 주기의 제 1일에 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 각각의 추가적인 투약 주기의 제 1일에 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 포함하고,(b) said one or more additional dosing cycles comprise a tiragolumab formulated for administration of a dose of about 600 mg on Day 1 of each additional dosing cycle and a dose of about 1200 mg on Day 1 of each additional dosing cycle. Atezolizumab formulated for administration of
여기서 상기 4회의 초기 투약 주기 및 상기 1회 이상의 추가적인 투약 주기는 각각의 21일 투약 주기이고, 여기서 상기 치료는 상기 티라골루맙 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said four initial dosing cycles and said one or more additional dosing cycles are each 21 day dosing cycle, wherein said treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without said tiragolumab tiragolumab and atezolizumab for use, thereby prolonging PFS and/or OS of said subject or population of subjects.
114. 폐암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,114. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer,
상기 치료는 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제인 제1 화학요법제, 및 비백금계 화학요법제인 제2 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment comprises at least one dosing cycle of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent, and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of a TIGIT antagonist antibody and said PD-1 axis binding antagonist.
115. 구현예 114에 있어서,115. The method of embodiment 114,
상기 폐암은 PD-L1 발현에 대해 평가되지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said lung cancer is not evaluated for PD-L1 expression.
116. 구현예 114 또는 구현예 115에 있어서,116. The method of embodiment 114 or embodiment 115,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject or subjects has not been determined to have a PD-L1 positive tumor cell fraction greater than or equal to 50%.
117. 구현예 116에 있어서,117. The method of embodiment 116,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 미만인 것으로 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects is determined to have a fraction of PD-L1 positive tumor cells of less than 50%.
118. 구현예 116 또는 구현예 117에 있어서,118. The method of embodiment 116 or embodiment 117,
상기 PD-L1 양성 종양 세포 분획은 항 PD-L1 항체를 사용한 양성 염색에 의해 결정되고, 여기서 상기 항 PD-L1 항체는 SP263 또는 22C3인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, wherein said anti-PD-L1 antibody is SP263 or 22C3, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use .
119. 구현예 114 내지 구현예 118 중 어느 한 구현예에 있어서,119. The method according to any one of embodiments 114 to 118,
상기 대상체 또는 대상체들은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects does not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality.
120. 구현예 114 내지 구현예 119 중 어느 한 구현예에 있어서,120. The method according to any one of embodiments 114 to 119,
상기 대상체 또는 대상체들은 상기 폐암에 대해 선행 전신 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has not received prior systemic therapy for said lung cancer.
121. 구현예 114 내지 구현예 120 중 어느 한 구현예에 있어서,121. The method of any one of embodiments 114 to 120,
상기 폐암은 국소 진행성 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is locally advanced lung cancer.
122. 구현예 114 내지 구현예 121 중 어느 한 구현예에 있어서,122. The method according to any one of embodiments 114 to 121,
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is NSCLC, in particular locally advanced unresectable or metastatic nonsquamous NSCLC.
123. 구현예 122에 있어서,123. The method of embodiment 122,
상기 비편평 NSCLC는 IV기 비편평 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said nonsquamous NSCLC is stage IV nonsquamous NSCLC.
124. 구현예 114 내지 구현예 123 중 어느 한 구현예에 있어서,124. The method according to any one of embodiments 114 to 123,
상기 투약 요법은 4회의 투약 주기를 포함한 유도기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 비백금계 화학요법제는 상기 유도기의 각 투약 주기의 제 1일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the dosing regimen includes an induction phase comprising 4 dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent include each dosing cycle of the induction phase. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, administered on day 1 of
125. 구현예 124에 있어서,125. The method of embodiment 124,
상기 투약 요법은 상기 유도기 이후에 유지기를 포함하고, 여기서 상기 유지기는 1회 이상의 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 비백금계 화학요법제는 상기 유지기의 각 투약 주기의 제 1일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the dosing regimen comprises a maintenance phase after the induction phase, wherein the maintenance phase includes one or more dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and the non-platinum-based chemotherapeutic agent are the maintenance phases. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, administered on Day 1 of each dosing cycle of the phase.
126. 구현예 125에 있어서,126. The method of embodiment 125,
상기 유지기의 1회 이상의 투약 주기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said one or more dosing cycles of said maintenance phase do not comprise administration of said platinum-based chemotherapeutic agent.
127. 구현예 114 내지 구현예 126 중 어느 한 구현예에 있어서,127. The method according to any one of embodiments 114 to 126,
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin and said non-platinum-based chemotherapeutic agent is pemetrexed.
128. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,128. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with advanced nonsquamous NSCLC, comprising:
상기 치료는 티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 상기 아테졸리주맙은 3주마다 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 카보플라틴은 3주마다 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되거나, 또는 상기 시스플라틴은 3주마다 75 mg/m2 용량의 투여를 위해 제형화되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2 용량의 투여를 위해 제형화되는, 티라골루맙 및 아테졸리주맙wherein the treatment comprises the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising four 21-day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed; , wherein said tiragolumab is formulated for administration of a dose of about 600 mg every 3 weeks, said atezolizumab is formulated for administration of a dose of about 1200 mg every 3 weeks, and said carboplatin is formulated for administration of a dose of about every 3 weeks. Administered at a dose sufficient to achieve AUC=5 mg/ml/min, or the cisplatin is formulated for administration of a 75 mg/m2 dose every 3 weeks, and the pemetrexed is administered in each of 4 21 day dosing cycles. tiragolumab and atezolizumab, formulated for administration at a dose of about 500 mg/m2 every 3 weeks on day 1 of
129. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,129. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with advanced nonsquamous NSCLC,
상기 치료는:The treatment is:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) at one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m 2 every 3 weeks use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
여기서 상기 대상체 또는 대상체의 집단은 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법. wherein the subject or population of subjects has not received prior systemic therapy for advanced nonsquamous NSCLC.
130. 진행성 비편평 NSCLC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,130. Tiragolumab and atezolizumab for use in a method of treating a subject with advanced nonsquamous NSCLC,
상기 치료는:The treatment is:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) at one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m 2 every 3 weeks use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
여기서 상기 대상체는 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법.wherein the subject has never received prior systemic therapy for advanced nonsquamous NSCLC.
131. 진행성 비편평 NSCLC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,131. Tiragolumab and atezolizumab for use in a method of treating a subject with advanced nonsquamous NSCLC,
상기 치료는 티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 상기 아테졸리주맙은 3주마다 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 시스플라틴은 75 mg/m2 용량의 투여를 위해 제형화되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 약 500 mg/m2 용량의 투여를 위해 제형화되는, 티라골루맙 및 아테졸리주맙.wherein the treatment comprises the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising four 21-day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed; , wherein the tiragolumab is formulated for administration at a dose of about 600 mg every 3 weeks, the atezolizumab is formulated for administration at a dose of about 1200 mg every 3 weeks, and the cisplatin is at a dose of 75 mg/m2 tiragolumab and atezolizumab, wherein the pemetrexed is formulated for administration of a dose of about 500 mg/m2 on day 1 of each of four 21 day dosing cycles.
132. 구현예 114 내지 구현예 131 중 어느 한 구현예에 있어서,132. The method according to any one of embodiments 114 to 131,
상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3.5개월 또는 약 4.7개월 만큼 연장시키는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment prolongs PFS of said subject or population of subjects by at least about 3.5 months or about 4.7 months.
133. 구현예 114 내지 구현예 132 중 어느 한 구현예에 있어서,133. The method according to any one of embodiments 114 to 132,
상기 치료는 약 12.5개월 내지 약 14.7개월의 대상체 집단의 PFS 중앙값을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median PFS in a population of subjects from about 12.5 months to about 14.7 months.
134. 구현예 114 내지 구현예 133 중 어느 한 구현예에 있어서,134. The method according to any one of embodiments 114 to 133,
상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.5개월 또는 약 8.0개월 만큼 연장시키는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment prolongs the OS of said subject or population of subjects by at least about 5.5 months or about 8.0 months.
135. 구현예 114 내지 구현예 134 중 어느 한 구현예에 있어서,135. The method according to any one of embodiments 114 to 134,
상기 치료는 약 27.5개월 내지 약 32.0개월의 대상체 집단의 OS 중앙값을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median OS of a population of subjects from about 27.5 months to about 32.0 months.
136. 절제 가능한 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,136. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist on a cycle.
137. 절제 가능한 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,137. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment includes an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks, and one or more doses of a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist on a cycle.
138. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,138. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer, comprising:
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기의 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein at least one of said dosing cycles is 3 Neoadjuvant an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg per week, and a PD-1 axis binding antagonist formulated for administration of a dose of about 80 mg to about 1600 mg every 3 weeks. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, including as therapy.
139. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,139. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer, comprising:
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기의 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein at least one of said dosing cycles is 3 Neoadjuvant an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 800 mg per week, and a PD-1 axis binding antagonist formulated for administration of a dose of about 900 mg to about 1500 mg every 3 weeks. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, including as therapy.
140. 구현예 138 또는 구현예 139에 있어서,140. The method of embodiment 138 or embodiment 139,
상기 투약 주기의 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.At least one of said dosing cycles is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and an anti-TIGIT antagonist antibody formulated for administration of a dose of about 80 mg to about 1600 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the PD-1 axis binding antagonist as neoadjuvant therapy.
141. 구현예 140에 있어서,141. The method of embodiment 140,
상기 투약 주기의 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.At least one of said dosing cycles is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 500 mg to about 700 mg every 3 weeks, and an anti-TIGIT antagonist antibody formulated for administration of a dose of about 900 mg to about 1500 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the PD-1 axis binding antagonist as neoadjuvant therapy.
142. 구현예 138 내지 구현예 141 중 어느 한 구현예에 있어서,142. The method according to any one of embodiments 138 to 141,
상기 폐암은 절제 가능한 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is resectable lung cancer.
143. 구현예 136 내지 구현예 142 중 어느 한 구현예에 있어서,143. The method according to any one of embodiments 136 to 142,
상기 폐암은 초기 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is early lung cancer.
144. 구현예 136 내지 구현예 143 중 어느 한 구현예에 있어서,144. The method according to any one of embodiments 136 to 143,
상기 폐암은 II기, IIIA기, 또는 IIIB기 폐암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is stage II, IIIA, or IIIB lung cancer.
145. 구현예 136 내지 구현예 144 중 어느 한 구현예에 있어서,145. The method according to any one of embodiments 136 to 144,
상기 폐암은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer does not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality.
146. 구현예 136 내지 구현예 145 중 어느 한 구현예에 있어서,146. The method according to any one of embodiments 136 to 145,
상기 대상체는 치료 목적으로 R0 절제술에 적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject is eligible for R0 resection for therapeutic purposes.
147. 구현예 136 내지 구현예 146 중 어느 한 구현예에 있어서,147. The method according to any one of embodiments 136 to 146,
상기 대상체는 폐암에 대해 선행 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject has never received prior therapy for lung cancer.
148. 구현예 147에 있어서,148. The method of embodiment 147,
상기 선행 요법은 면역요법, 화학요법, 또는 방사선요법인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said prior therapy is immunotherapy, chemotherapy, or radiotherapy.
149. 구현예 136 내지 구현예 148 중 어느 한 구현예에 있어서,149. The method according to any one of embodiments 136 to 148,
상기 대상체는 백금계 화학요법에 적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said subject is eligible for platinum-based chemotherapy. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
150. 구현예 136 내지 구현예 149 중 어느 한 구현예에 있어서,150. The method of any one of embodiments 136 to 149,
상기 제1 투약 주기는 수술 전에 개시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said first dosing cycle is initiated prior to surgery.
151. 구현예 150에 있어서,151. The method of embodiment 150,
적어도 1, 2, 3, 또는 4회의 투약 주기는 상기 수술 전에 완료되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least 1, 2, 3, or 4 dosing cycles are completed prior to said surgery.
152. 구현예 150 또는 구현예 151에 있어서,152. The method of embodiment 150 or embodiment 151,
4회의 투약 주기는 상기 수술 전에 완료되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein 4 dosing cycles are completed prior to said surgery.
153. 구현예 136 내지 구현예 152 중 어느 한 구현예에 있어서,153. The method according to any one of embodiments 136 to 152,
적어도 1회의 투약 주기는 수술 후에 개시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least one dosing cycle is initiated after surgery.
154. 구현예 153에 있어서,154. The method of embodiment 153,
16회의 투약 주기는 상기 수술 후에 완료되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein 16 dosing cycles are completed after said surgery.
155. 구현예 150 내지 구현예 154 중 어느 한 구현예에 있어서,155. The method of any one of embodiments 150 to 154,
상기 수술은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the operation is lobectomy, lobectomy, bilobectomy, or pneumonectomy.
156. 구현예 136 내지 구현예 155 중 어느 한 구현예에 있어서,156. The method according to any one of embodiments 136 to 155,
상기 방법은 방사선 요법을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the method further comprises radiation therapy.
157. 구현예 156에 있어서,157. The method of embodiment 156,
상기 방사선 요법은 수술 후 방사선 요법인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the radiation therapy is postoperative radiation therapy.
158. 구현예 136 내지 구현예 157 중 어느 한 구현예에 있어서,158. The method according to any one of embodiments 136 to 157,
상기 치료는 하나 이상의 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of one or more chemotherapeutic agents.
159. 구현예 158에 있어서,159. The method of embodiment 158,
상기 하나 이상의 화학요법제는 수술 후 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said one or more chemotherapeutic agents are administered post-surgery.
160. 구현예 159에 있어서,160. The method of embodiment 159,
상기 하나 이상의 화학요법제는 상기 수술 후 4회 투약 주기로 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is administered in 4 dosing cycles after said surgery.
161. 구현예 158 내지 구현예 160 중 어느 한 구현예에 있어서,161. The method according to any one of embodiments 158 to 160,
상기 하나 이상의 화학요법제는 백금계 화학요법제 및 비백금계 화학요법제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
162. 구현예 161에 있어서,162. The method of embodiment 161,
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고; (a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 젬시타빈이고; (b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이고; (c) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이거나; 또는 (d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or
(e) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 젬시타빈인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. (e) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said platinum-based chemotherapeutic agent is cisplatin and said non-platinum-based chemotherapeutic agent is gemcitabine.
163. 구현예 136 내지 구현예 162 중 어느 한 구현예에 있어서,163. The method according to any one of embodiments 136 to 162,
상기 치료는 기준 MPR 비율과 비교하여 주요 병리학적 반응율(MPR)의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in an increase in the major pathological response rate (MPR) compared to a baseline MPR rate.
164. 구현예 163에 있어서,164. The method of embodiment 163,
상기 기준 MPR 비율은:The reference MPR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 MPR 비율인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. (b) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, which is the MPR ratio of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
165. 구현예 136 내지 구현예 164 중 어느 한 구현예에 있어서,165. The method of any one of embodiments 136 to 164,
상기 치료는 병리학적 완전 반응(pCR) 및/또는 기준 pCR 비율과 비교하여 pCR 비율의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in a pathological complete response (pCR) and/or an increase in the pCR ratio compared to a reference pCR ratio.
166. 구현예 165에 있어서,166. The method of embodiment 165,
상기 기준 pCR 비율은:The reference pCR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 pCR 비율인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. (b) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, which is the pCR ratio of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
167. 구현예 136 내지 구현예 166 중 어느 한 구현예에 있어서,167. The method according to any one of embodiments 136 to 166,
상기 치료는 기준 EFS 시간과 비교하여 무사건 생존(EFS)의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in an increase in event-free survival (EFS) compared to baseline EFS time.
168. 구현예 167에 있어서,168. The method of embodiment 167,
상기 기준 EFS 시간은:The reference EFS time is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 EFS 시간인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. (b) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, which is the EFS time of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
169. 절제 가능한 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,169. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment includes one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 600 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist on a cycle.
170. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,170. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer, comprising:
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기의 적어도 1회는 3주마다 약 30 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein at least one of said dosing cycles is 3 Neoadjuvant an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 600 mg per week, and a PD-1 axis binding antagonist formulated for administration of a dose of about 80 mg to about 1600 mg every 3 weeks. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use, including as therapy.
171. 절제 가능한 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,171. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent. and the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist with at least one dosing cycle of a non-platinum based chemotherapeutic agent.
172. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,172. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer, comprising:
상기 치료는 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기의 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제를 신보조 치료로서 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises the use of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist in one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent. wherein at least one dosing cycle is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, for administration of a dose of about 80 mg to about 1600 mg every 3 weeks An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising a formulated PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent as neoadjuvant therapy.
173. 절제 가능한 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,173. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및: (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금계 화학요법제; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (b) (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and: (a) (i) a platinum-based chemotherapeutic agent at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (b) (i) an antimetabolite at a dose of about 500 mg/m2 every 3 weeks or about 1000 mg/m2 or about 1250 mg/m2 on days 1 and 8 of each dosing cycle; or (ii) one or more dosing cycles of the taxane at a dose of about 100 mg/m2, about 175 mg/m2, or about 200 mg/m2 every 3 weeks, using said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
174. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,174. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer,
상기 치료는 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기 중 적어도 1회는: (a) 3주마다 약 30 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체; (b) 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산이며; 여기서 상기 치료는 신보조 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist with one or more dosing cycles of anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent, and non-platinum-based chemotherapeutic agent wherein at least one of said dosing cycles comprises: (a) an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 600 mg every 3 weeks; (b) a PD-1 axis binding antagonist formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks; (c) at (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (d) a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) about 500 mg/m2 every 3 weeks or about 1000 mg/m2 on days 1 and 8 of each dosing cycle or an antimetabolite at a dose of about 1250 mg/m2; or (ii) a taxane at a dose of about 100 mg/m2, about 175 mg/m2, or about 200 mg/m2 every 3 weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment is neoadjuvant therapy.
175. 절제 가능한 폐암을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,175. Tiragolumab and atezolizumab for use in a method of treating a subject with resectable lung cancer, comprising:
상기 치료는 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및: The treatment includes tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and:
(a) (a)
(i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or
(ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및(ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and
(b) (b)
(i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on days 1 and 8 of each dosing cycle; or
(ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙(ii) one or more dosing cycles of paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist. Lumab and Atezolizumab
176. 폐암을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,176. Tiragolumab and atezolizumab for use in a method of treating a subject having lung cancer,
상기 치료는 티라골루맙, 아테졸리주맙, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 투약 주기 중 적어도 1회는: (a) 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙; (b) 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; (c) 비백금계 화학요법제를 포함하고, 여기서 상기 백금계 화학요법제는: (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는 (ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및 (d) 비백금계 화학요법제이고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀이고; 여기서 상기 치료는 신보조 치료인, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist with one or more dosing cycles of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein said At least one dosing cycle includes: (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks; (c) a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent is: (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks of carboplatin; or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and (d) a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or about 1000 on days 1 and 8 of each dosing cycle gemcitabine at a dose of mg/m2 or about 1250 mg/m2; or (ii) paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; Tiragolumab and atezolizumab for use, wherein said treatment is neoadjuvant treatment.
177. 비편평 NSCLC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,177. Tiragolumab and atezolizumab for use in a method of treating a subject with nonsquamous NSCLC,
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: (a) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 1200 mg의 용량의 투여를 위해 제형화된 아테졸리주맙을 신보조 치료로서 포함하고; (b) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab, wherein: (a) at least one dosing cycle is every 3 weeks tiragolumab formulated for administration of a dose of about 600 mg and atezolizumab formulated for administration of a dose of 1200 mg every 3 weeks as neoadjuvant treatment; (b) at least one dosing cycle comprising tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks and atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as adjuvant treatment tiragolumab and atezolizumab for use.
178. 비편평 NSCLC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 항체 및 아테졸리주맙으로서,178. A tiragolumab antibody and atezolizumab for use in a method of treating a subject with nonsquamous NSCLC, comprising:
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: (I) 투약 주기 중 적어도 1회는 신보조 치료이고: (a) 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉시드; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉스이고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 티라골루맙, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one dosing cycle is neoadjuvant treatment and: (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a targeted dose to achieve an AUC of 5 mg/mL/min every 3 weeks and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and pemetrex at a dose of about 500 mg/m2 every 3 weeks; (II) tiragolumab formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and for administration of a dose of about 80 mg to about 1600 mg every 3 weeks, at least once in said dosing cycle Tiragolumab and atezolizumab for use comprising atezolizumab formulated as adjuvant treatment.
179. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,179. Tiragolumab and atezolizumab for use in a method of treating a subject with lung cancer,
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: (I) 투약 주기 중 적어도 1회는 신보조 치료이고: (a) 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one dosing cycle is neoadjuvant treatment and: (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles is formulated for administration of a dose of about 30 mg to about 1200 mg every 3 weeks and a dose of about 80 mg to about 1600 mg every 3 weeks. tiragolumab and atezolizumab for use comprising as adjuvant treatment atezolizumab.
180. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,180. Tiragolumab and atezolizumab for use in a method of treating a subject with lung cancer,
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist with one or more dosing cycles of tiragolumab and atezolizumab, wherein:
(I) 투약 주기 중 적어도 1회는 신보조 치료이고:(I) at least one dosing cycle is neoadjuvant treatment:
(a) 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 티라골루맙; (a) tiragolumab formulated for administration at a dose of about 1200 mg every 3 weeks;
(b) 신보조 치료로서 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; 및 (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and
(c) (c)
(i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle;
(ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or
(iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 또는 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 포함하고; 그리고 (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks or gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; and
(II) 상기 투약 주기 중 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(II) at least one of said dosing cycles is formulated for administration of a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg every 3 weeks. tiragolumab and atezolizumab for use comprising as adjuvant treatment atezolizumab.
181. 폐암을 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,181. Tiragolumab and atezolizumab for use in a method of treating a subject with lung cancer,
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: (I) 투약 주기 중 적어도 1회는 신보조 치료이고: (a) 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one dosing cycle is neoadjuvant treatment and: (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles as adjuvant treatment with tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks and atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks. tiragolumab and atezolizumab for use.
182. 절제 가능한 편평 NSCLC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,182. Tiragolumab and atezolizumab for use in a method of treating a subject with resectable squamous NSCLC,
상기 치료는 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: (I) 투약 주기 중 적어도 1회는 신보조 치료이고: (a) 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 약 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙을 보조 치료로서 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one dosing cycle is neoadjuvant treatment and: (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; (b) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on days 1 and 8 of each dosing cycle; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/m2 on days 1 and 8 of each dosing cycle; (II) at least one of said dosing cycles as adjuvant treatment with tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks and atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks. tiragolumab and atezolizumab for use.
183. 구현예 136 내지 구현예 182 중 어느 한 구현예에 있어서,183. The method according to any one of embodiments 136 to 182,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 is determined by IHC analysis comprising staining with the anti-PD-L1 antibody SP263.
184. 구현예 183에 있어서,184. The method of embodiment 183,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is at least 50% of a fraction of PD-L1 positive tumor cells.
185. 구현예 73, 구현예 114 내지 구현예 121, 및 구현예 136 내지 구현예 184 중 어느 한 구현예에 있어서,185. The method of any one of embodiments 73, 114 to 121, and embodiments 136 to 184,
상기 폐암은 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the lung cancer is NSCLC.
186. 구현예 185에 있어서,186. The method of embodiment 185,
상기 NSCLC는 편평 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said NSCLC is squamous NSCLC.
187. 구현예 185에 있어서,187. The method of embodiment 185,
상기 NSCLC는 비편평 NSCLC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said NSCLC is non-squamous NSCLC.
188. 구현예 72에 있어서,188. The method of embodiment 72,
상기 암은 자궁경부암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is cervical cancer.
189. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,189. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1,
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist on a cycle.
190. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,190. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화되고, 상기 항 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg의 용량인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks. wherein said anti-PD-1 axis binding antagonist is in a dose of about 900 mg to about 1500 mg every 3 weeks.
191. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,191. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a therapy for a subject with cervical cancer, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) an anti-TIGIT antagonist formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 An anti TIGIT antagonist antibody for use, comprising selecting a regimen comprising one or more dosing cycles of the antibody and one or more dosing cycles of the PD-1 axis binding antagonist formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks. and PD-1 axis binding antagonists.
192. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,192. The method of any one of embodiments 189 to 191,
상기 자궁경부암은 편평세포 암종, 선편평세포 암종, 또는 선암종인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
193. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,193. The method according to any one of embodiments 189 to 191,
상기 자궁경부암은 4B기, 전이성, 재발성, 또는 지속성인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cervical cancer is stage 4B, metastatic, recurrent, or persistent.
194. 구현예 189 내지 구현예 193 중 어느 한 구현예에 있어서,194. The method according to any one of embodiments 189 to 193,
상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cervical cancer is metastatic and/or recurrent PD-L1-positive cervical cancer.
195. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,195. The method of any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 적어군 한 라인의 선행 요법을 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have received at least one line of prior therapy.
196. 구현예 189 내지 구현예 195 중 어느 한 구현예에 있어서,196. The method according to any one of embodiments 189 to 195,
상기 대상체 또는 대상체들은 두 라인의 선행 요법을 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject or subjects have received two lines of prior therapy.
197. 구현예 189 내지 구현예 196 중 어느 한 구현예에 있어서,197. The method according to any one of embodiments 189 to 196,
상기 대상체 또는 대상체들은 2라인 초과의 선행 요법을 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have received more than two lines of prior therapy.
198. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,198. The method according to any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have not received prior therapy.
199. 구현예 195 내지 구현예 198 중 어느 한 구현예에 있어서,199. The method according to any one of embodiments 195 to 198,
상기 선행 요법은 화학요법, 수술, 및/또는 방사선요법인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said prior therapy is chemotherapy, surgery, and/or radiotherapy.
200. 구현예 189 및 구현예 192 내지 구현예 199 중 어느 한 구현예에 있어서,200. The method according to any one of embodiments 189 and 192 to 199,
상기 치료는 임상 반응을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment elicits a clinical response, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
201. 구현예 200에 있어서,201. The method of embodiment 200,
상기 임상 반응은 기준 ORR과 비교하여 대상체 집단의 객관적 반응률(ORR)의 증가인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the clinical response is an increase in the objective response rate (ORR) of the subject population as compared to a baseline ORR.
202. 구현예 201에 있어서,202. The method of embodiment 201,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said reference ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody and an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
203. 구현예 200에 있어서,203. The method of embodiment 200,
상기 기준 ORR은 적어도 약 14.6% 내지 약 26%인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said reference ORR is at least about 14.6% to about 26%.
204. 구현예 200에 있어서,204. The method of embodiment 200,
상기 임상 반응은 CR 또는 PR인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the clinical response is CR or PR.
205. 구현예 200 내지 구현예 204 중 어느 한 구현예에 있어서,205. The method of any one of embodiments 200 to 204,
상기 임상 반응은 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The clinical response is an increase in progression-free survival (PFS) of the subject compared to a baseline PFS time, an increase in the duration of response (DOR) in the subject compared to a baseline DOR time, or an increase in the subject's progression-free survival (DOR) compared to a baseline OS time. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, which is an increase in overall survival (OS).
206. 구현예 205에 있어서,206. The method of embodiment 205,
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는(b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
207. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,207. An anti TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject having cervical cancer having a detectable expression level of PD-L1,
상기 치료는 3주마다 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 아테졸리주맙.The treatment includes an anti TIGIT antagonist antibody formulated for administration at a dose of 600 mg every 3 weeks, and at least one dosing cycle of atezolizumab at a dose of 1200 mg every 3 weeks, the anti TIGIT antagonist antibody and the PD-1 axis binding Anti-TIGIT antagonist antibodies and atezolizumab for use, including the use of antagonists.
208. 항 TIGIT 길항제 항체 및 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자궁경부암을 가진 대상체를 확인하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,208. An anti TIGIT antagonist antibody and atezolizumab for use in a method of identifying a subject with cervical cancer likely to benefit from a therapy comprising at least one dosing cycle of the anti TIGIT antagonist antibody and atezolizumab,
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 아테졸리주맙.(c) an anti-TIGIT antagonist antibody formulated for administration of a 600 mg dose every 3 weeks and atezolizumab formulated for administration of a 1200 mg dose every 3 weeks based on PD-L1 expression on detected tumor cells. An anti TIGIT antagonist antibody and atezolizumab for use, comprising identifying said subject as likely to benefit from a therapy comprising one or more dosing cycles.
209. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,209. An anti TIGIT antagonist antibody and atezolizumab for use in a method of selecting a therapy for a subject with cervical cancer, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여을 위해 제형화된 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 아테졸리주맙.(b) an anti TIGIT antagonist antibody formulated for administration at a dose of 600 mg every 3 weeks and 1200 every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 An anti TIGIT antagonist antibody and atezolizumab for use comprising selecting a regimen comprising one or more dosing cycles of atezolizumab formulated for administration of a mg dose.
210. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,210. Tiragolumab and atezolizumab for use in a method of treating a subject having cervical cancer having a detectable expression level of PD-L1,
상기 치료는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; Tiragolumab and atezolizumab for use.
211. 자궁경부암을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,211. Tiragolumab and atezolizumab for use in a method of treating a subject having cervical cancer,
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(c) 1 of tiragolumab formulated for administration of a 600 mg dose every 3 weeks and atezolizumab formulated for administration of a 1200 mg dose every 3 weeks based on PD-L1 expression on detected tumor cells Tiragolumab and atezolizumab for use, comprising identifying said subject as likely to benefit from a therapy comprising more than one dosing cycle.
(d) 식별된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 방법.(d) administering the therapy to the identified subject.
212. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,212. Tiragolumab and atezolizumab for use in a method of selecting a therapy for a subject with cervical cancer,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여을 위해 제형화된 티라골루맙 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) tiragolumab formulated for administration at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 Tiragolumab and atezolizumab for use, comprising selecting a regimen comprising one or more dosing cycles of atezolizumab formulated for administration of a dose.
213. 전이성 및/또는 재발성 자궁경부암을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,213. Tiragolumab and atezolizumab for use in a method of treating a subject having metastatic and/or recurrent cervical cancer,
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여를 위해 제형화된 티라골루맙 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계; 및(c) 1 of tiragolumab formulated for administration of a 600 mg dose every 3 weeks and atezolizumab formulated for administration of a 1200 mg dose every 3 weeks based on PD-L1 expression on detected tumor cells identifying the subject as likely to benefit from a therapy comprising more than one dosing cycle; and
(d) 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(d) tiragolumab and atezolizumab for use, comprising administering said therapy to the identified subject.
214. 전이성 및/또는 재발성 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,214. Tiragolumab and atezolizumab for use in a method of selecting a therapy for a subject with metastatic and/or recurrent cervical cancer,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg 용량의 투여을 위해 제형화된 티라골루맙 및 3주마다 1200 mg 용량의 투여를 위해 제형화된 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) tiragolumab formulated for administration at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 Tiragolumab and atezolizumab for use, comprising selecting a regimen comprising one or more dosing cycles of atezolizumab formulated for administration of a dose.
215. 구현예 189 내지 구현예 214 중 어느 한 구현예에 있어서,215. The method of any one of embodiments 189 to 214,
상기 대상체는 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 확인되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
216. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,216. The method according to any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 SP263을 사용하여 검출되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-L1 expression level is detected using an anti-PD-L1 antibody SP263.
217. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,217. The method according to any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable expression level of PD-L1 is at least 5% of tumor associated immune cells (TIC) in a sample from said subject.
218. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,218. The method of any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 22C3을 사용하여 검출되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-L1 expression level is detected using anti-PD-L1 antibody 22C3.
219. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,219. The method of any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 복합 양성 점수(CPS)가 1 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said detectable expression level of PD-L1 has a composite positive score (CPS) of 1 or greater in a sample from said subject.
220. 구현예 72에 있어서,220. The method of embodiment 72,
상기 암은 유방암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is breast cancer.
221. 유방암을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,221. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having breast cancer,
상기 치료는 4주마다 약 840 mg 용량의 티라골루맙, 4주마다 약 1680 mg 용량의 아테졸리주맙, 및 3주 투약/1주 휴약의 약 100 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment includes one or more doses of tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and nap-paclitaxel at a dose of about 100 mg/m2 of 3 weeks on/1 week off. Tiragolumab and atezolizumab for use comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising a dosing cycle.
222. 구현예 220 또는 구현예 221에 있어서,222. The method of embodiment 220 or embodiment 221,
상기 유방암은 삼중 음성 유방암(TNBC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the breast cancer is triple negative breast cancer (TNBC).
223. 구현예 222에 있어서,223. The method of embodiment 222,
상기 TNBC는 절제 가능한 국소 진행성 또는 전이성 TNBC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said TNBC is resectable locally advanced or metastatic TNBC.
224. 구현예 220 내지 구현예 223 중 어느 한 구현예에 있어서,224. The method of any one of embodiments 220 to 223,
상기 대상체는 전이성 유방암에 대해 선행 전신 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject has not received prior systemic therapy for metastatic breast cancer.
225. 구현예 220 내지 구현예 224 중 어느 한 구현예에 있어서,225. The method of any one of embodiments 220-224,
상기 치료는 적어도 약 53% 내지 약 67.5%의 대상체 집단의 ORR을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits an ORR in at least about 53% to about 67.5% of the subject population.
226. 구현예 222 내지 구현예 225 중 어느 한 구현예에 있어서,226. The method of any one of embodiments 222 to 225,
상기 치료는 약 25.0개월의 대상체 집단의 OS 중앙값을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits a median OS of a population of subjects of about 25.0 months of age.
227. 초기 삼중 음성 유방암(eTNBC)을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,227. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with early triple negative breast cancer (eTNBC), comprising:
상기 치료는 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg 용량이 되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising at least one dosing cycle, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use formulated for administration, wherein said PD-1 axis binding antagonist is in a dose of about 20 mg to about 1600 mg every two weeks.
228. 구현예 227에 있어서,228. The method of embodiment 227,
상기 치료는 하나 이상의 화학요법제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises the use of one or more chemotherapeutic agents.
229. 구현예 228에 있어서,229. The method of embodiment 228,
상기 하나 이상의 화학요법제는 백금계 화학요법제, 탁산, 토포이소머라제 II 억제제, 또는 알킬화제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
230. 구현예 227에 있어서,230. The method of embodiment 227,
상기 방법은 (a) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 탁산 또는 탁산 및 백금계 화학요법제의 1회 이상의 투약 주기; 및 (b) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 토포이소머라제 II 억제제, 알킬화제, 및 과립구 집락 자극 인자(G-CSF) 또는 과립구-대식세포 집락 자극 인자(GM-CSF)의 1회 이상의 투약 주기를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises (a) one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and a taxane or a taxane and a platinum-based chemotherapeutic agent; and (b) said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony stimulating factor (G-CSF) or granulocyte-macrophage colony stimulating factor (GM-CSF) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, further comprising one or more dosing cycles of
231. 구현예 229 또는 구현예 230에 있어서,231. The method of embodiment 229 or embodiment 230,
상기 알킬화제는 시클로포스파미드인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said alkylating agent is cyclophosphamide.
232. 구현예 231에 있어서,232. The method of embodiment 231,
상기 시클로포스파미드는 약 600 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cyclophosphamide is formulated for administration at a dose of about 600 mg/m2.
233. 구현예 227 내지 구현예 229, 구현예 231, 및 구현예 232 중 어느 한 구현예에 있어서,233. The embodiment of any of embodiments 227-229, embodiment 231, and embodiment 232,
상기 치료는 G-CSF 또는 GM-CSF의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment further comprises the use of G-CSF or GM-CSF.
234. 구현예 230 또는 구현예 233에 있어서,234. The method of embodiment 230 or embodiment 233,
상기 G-CSF는 페그필그라스팀 또는 필그라스팀인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said G-CSF is pegfilgrastim or filgrastim, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
235. 구현예 234에 있어서,235. The method of embodiment 234,
상기 G-CSF는 페그필그라스팀인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the G-CSF is pegfilgrastim, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
236. 구현예 235에 있어서,236. The method of embodiment 235,
상기 페그필그라스팀는 약 6 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said pegfilgrastim is formulated for administration in a dose of about 6 mg.
237. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 236 중 어느 한 구현예에 있어서,237. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 236,
상기 치료는 상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF의 하나 이상의 후속 용량의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment further comprises use of said one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF.
238. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 237 중 어느 한 구현예에 있어서,238. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 237,
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF는 각각 매주마다 1회, 2주마다 1회, 또는 3주마다 1회 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once weekly, once every two weeks, or once every three weeks, respectively. binding antagonists.
239. 구현예 229 내지 구현예 238 중 어느 한 구현예에 있어서,239. The method of any one of embodiments 229 to 238,
상기 백금계 화학요법제는 3주마다 투여되고, 상기 탁산은 매주 투여되고, 상기 토포이소머라제 II 억제제는 2주마다 투여되고, 상기 알킬화제는 2주마다 투여되며, 상기 G-CSF 또는 GM-CSF는 2주마다 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The platinum-based chemotherapeutic agent is administered every 3 weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every 2 weeks, the alkylating agent is administered every 2 weeks, and the G-CSF or GM- Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, CSF administered every two weeks.
240. 구현예 229 내지 구현예 239 중 어느 한 구현예에 있어서,240. The method of any one of embodiments 229 to 239,
상기 탁산 또는 상기 탁산 및 상기 백금계 화학요법제는 상기 투약 요법의 처음 12주 동안 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said taxane or said taxane and said platinum-based chemotherapeutic agent are administered during the first 12 weeks of said dosing regimen.
241. 구현예 229 내지 구현예 240 중 어느 한 구현예에 있어서,241. The method of any one of embodiments 229-240,
상기 토포이소머라제 II 억제제, 상기 알킬화제, 및 상기 G-CSF 또는 GM-CSF는 투약 요법의 13주 내지 19주 동안 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said topoisomerase II inhibitor, said alkylating agent, and said G-CSF or GM-CSF are administered for 13 to 19 weeks of a dosing regimen.
242. 구현예 227 내지 구현예 241 중 어느 한 구현예에 있어서,242. The method according to any one of embodiments 227 to 241,
상기 투약 요법의 총 기간은 19주인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, the total duration of the dosing regimen is 19 weeks.
243. 구현예 227 내지 구현예 242 중 어느 한 구현예에 있어서,243. The method of any one of embodiments 227 to 242,
상기 방법은 신보조 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the method is neoadjuvant therapy, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
244. 구현예 227 내지 구현예 243 중 어느 한 구현예에 있어서,244. The method according to any one of embodiments 227 to 243,
상기 투약 요법 후에 수술이 실시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein surgery is performed after said dosing regimen.
245. 구현예 244에 있어서,245. The method of embodiment 244,
상기 수술은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 실시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said surgery is performed between 2 and 6 weeks after the last dose of said dosing regimen.
246. 구현예 244 또는 구현예 245에 있어서,246. The method of embodiment 244 or embodiment 245,
상기 수술은 유방절제술을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the surgery comprises a mastectomy.
247. 구현예 244 내지 구현예 246 중 어느 한 구현예에 있어서,247. The method according to any one of embodiments 244 to 246,
상기 수술은 액와 림프절 수술을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said surgery comprises axillary lymph node surgery.
248. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,248. The method of any one of embodiments 229 to 247,
상기 토포이소머라제 II 억제제는 독소루비신인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the topoisomerase II inhibitor is doxorubicin, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
249. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,249. The method according to any one of embodiments 229 to 247,
상기 탁산은 냅-파클리탁셀이고, 상기 백금계 화학요법제는 카보플라틴이며, 상기 토포이소머라제 II 억제제는 독소루비신인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said taxane is nap-paclitaxel, said platinum-based chemotherapeutic agent is carboplatin, and said topoisomerase II inhibitor is doxorubicin.
250. 구현예 248 또는 구현예 249에 있어서,250. The method of embodiment 248 or embodiment 249,
상기 독소루비신은 약 60 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said doxorubicin is formulated for administration at a dose of about 60 mg/m2.
251. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,251. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with eTNBC, comprising:
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제, 및:The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every 2 weeks, a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising GM-CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
252. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,252. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with eTNBC, comprising:
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-L1 결합 길항제, 및:The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every 2 weeks, a PD-L1 binding antagonist at a dose of about 600 mg to about 1200 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising GM-CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
253. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 항 PD-L1 길항제 항체로서,253. An anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody for use in a method of treating a subject with eTNBC, comprising:
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량 투여를 위해 제형화된 항 PD-L1 길항제 항체, 및:The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every two weeks, an anti-PD-L1 antagonist antibody formulated for administration of a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 항 PD-L1 길항제 항체의 사용을 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or comprising the use of an anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody in a dosing regimen comprising GM-CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 항 PD-L1 길항제 항체.wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
254. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 항 PD-L1 길항제 항체로서,254. A tiragolumab and an anti-PD-L1 antagonist antibody for use in a method of treating a subject with eTNBC, comprising:
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙, 2주마다 약 600 mg 내지 약 1200 mg 용량 투여를 위해 제형화된 항 PD-L1 길항제 항체, 및:The treatment comprises tiragolumab at a dose of about 300 mg to about 600 mg every two weeks, an anti-PD-L1 antagonist antibody formulated for administration of a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 항 PD-L1 길항제 항체의 사용을 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or comprising the use of an anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody in a dosing regimen comprising GM-CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 티라골루맙 및 항 PD-L1 길항제 항체.wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
255. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 아테졸리주맙으로서,255. An anti TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with eTNBC,
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every 2 weeks, atezolizumab at a dose of about 600 mg to about 1200 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising GM-CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 아테졸리주맙.wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
256. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,256. Tiragolumab and atezolizumab for use in a method of treating a subject with eTNBC,
상기 치료는 2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙, 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:The treatment includes tiragolumab at a dose of about 300 mg to about 600 mg every 2 weeks, atezolizumab at a dose of about 600 mg to about 1200 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.tiragolumab and atezolizumab for use, wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
257. eTNBC를 가진 대상체의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,257. Tiragolumab and atezolizumab for use in a method of treating a subject with eTNBC,
상기 치료는 2주마다 약 420 mg 용량의 티라골루맙, 2주마다 약 840 mg 용량의 아테졸리주맙, 및:The treatment includes tiragolumab at a dose of about 420 mg every 2 weeks, atezolizumab at a dose of about 840 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for weeks 13 to 19 of the dosing regimen comprising the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a dosing regimen comprising CSF,
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.tiragolumab and atezolizumab for use, wherein said method further comprises surgery between 2 and 6 weeks after the last dose of said dosing regimen.
258. 구현예 220 내지 구현예 257 중 어느 한 구현예에 있어서,258. The method of any one of embodiments 220 to 257,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 상기 대상체로부터의 종양 샘플에서 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Anti-TIGIT antagonist antibody and PD-1 axis for use, wherein detectable protein expression level of PD-L1 is determined in a tumor sample from said subject determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 binding antagonists.
259. 구현예 258에 있어서,259. The method of embodiment 258,
상기 종양 샘플에서 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율은 1% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) in the tumor sample is at least 1%.
260. 구현예 227 내지 구현예 259 중 어느 한 구현예에 있어서,260. The method according to any one of embodiments 227 to 259,
상기 eTNBC는 T2-4d TNBC로 제시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said eTNBC is represented as T2-4d TNBC, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
261. 구현예 227 내지 구현예 260 중 어느 한 구현예에 있어서,261. The method according to any one of embodiments 227 to 260,
상기 eTNBC는 cT2-cT4, cN0-cN3, 및 cM0 TNBC로 제시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said eTNBC is presented as cT2-cT4, cN0-cN3, and cM0 TNBC.
262. 구현예 227 내지 구현예 261 중 어느 한 구현예에 있어서,262. The method of any one of embodiments 227 to 261,
상기 대상체는 eTNBC에 대해 이전에 치료받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the subject has not previously been treated for eTNBC, an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
263. 구현예 227 내지 구현예 262 중 어느 한 구현예에 있어서,263. The method according to any one of embodiments 227 to 262,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment elicits a pathological complete response (pCR).
264. 구현예 227 내지 구현예 263 중 어느 한 구현예에 있어서,264. The method of any one of embodiments 227 to 263,
상기 치료는 전체 생존(OS) 또는 무사건 생존(EFS)의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in an increase in overall survival (OS) or event-free survival (EFS).
265. 구현예 72에 있어서,265. The method of
상기 암은 두경부암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is head and neck cancer.
266. 구현예 265에 있어서,266. The method of embodiment 265,
상기 두경부암은 상기 두경부의 편평세포 암종(SCCHN)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said head and neck cancer is squamous cell carcinoma (SCCHN) of said head and neck.
267. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,267. Use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 항 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein said anti-PD-1 axis binding antagonist is in a dose of about 80 mg to about 1600 mg every 3 weeks.
268. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,268. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화되고, 상기 항 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg 용량인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks. wherein said anti-PD-1 axis binding antagonist is in a dose of about 900 mg to about 1500 mg every 3 weeks.
269. SCCHN을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,269. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a therapy for a subject or population of subjects with SCCHN,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체 또는 대상체 집단에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and 3 weeks based on PD-L1 expression detected for said subject or population of subjects having a detectable expression level of PD-L1 Anti-TIGIT antagonist antibody for use and PD-1 axis binding, comprising selecting a regimen comprising one or more dosing cycles of the anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg per time. antagonist.
270. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,270. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the method comprising:
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 1200 mg의 용량인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration at a dose of about 600 mg every 3 weeks and atezolizumab is 1200 mg every 3 weeks. tiragolumab and atezolizumab for use.
271. 구현예 267 내지 구현예 270 중 어느 한 구현예에 있어서,271. The method according to any one of embodiments 267 to 270,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
272. 구현예 266 내지 구현예 271 중 어느 한 구현예에 있어서,272. The method of any one of embodiments 266 to 271,
상기 SSCHN은 인간 유두종 바이러스(HPV) 양성인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said SSCHN is human papillomavirus (HPV) positive.
273. 구현예 266 내지 구현예 272 중 어느 한 구현예에 있어서,273. The method according to any one of embodiments 266 to 272,
상기 SSCHN은 HPV 음성인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the SSCHN is HPV negative, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
274. 구현예 272 또는 구현예 273에 있어서,274. The method of embodiment 272 or embodiment 273,
HPV 상태는 p16 IHC, 조직내(in situ) 혼성화, 또는 PCR에 의해 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein HPV status is determined by p16 IHC, in situ hybridization, or PCR.
275. 구현예 266 내지 구현예 274 중 어느 한 구현예에 있어서,275. The method according to any one of embodiments 266 to 274,
상기 SCCHN은 재발성 및/또는 전이성 SCCHN인, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said SCCHN is recurrent and/or metastatic SCCHN.
276. 구현예 265 내지 구현예 275 중 어느 한 구현예에 있어서,276. The method according to any one of embodiments 265 to 275,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have not received prior therapy.
277. 구현예 276에 있어서,277. The method of embodiment 276,
상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
278. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,278. The embodiment of any one of embodiments 265-268 and embodiments 270-277,
상기 치료는 CR 또는 PR을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in CR or PR.
279. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,279. The method according to any one of embodiments 265 to 268 and 270 to 277,
상기 치료는 기준 ORR과 비교하여 상기 대상체 집단의 객관적 반응률(ORR)의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in an increase in objective response rate (ORR) in said subject population compared to a baseline ORR.
280. 구현예 279에 있어서,280. The method of embodiment 279,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said reference ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody and an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
281. 구현예 279 또는 구현예 280에 있어서,281. The method of embodiment 279 or embodiment 280,
상기 기준 ORR은 적어도 약 19% 내지 약 36%인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said reference ORR is at least about 19% to about 36%.
282. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 281 중 어느 한 구현예에 있어서,282. The method of any one of embodiments 265-268 and 270-281,
상기 치료는 기준 PFS 시간과 비교하여 상기 대상체 또는 대상체 집단의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체 또는 대상체 집단의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment is associated with an increase in progression-free survival (PFS) of the subject or subject population as compared to a baseline PFS time, an increase in the duration of response (DOR) of the subject or subject population compared to a baseline DOR time, or a baseline OS time and An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, as compared to cause an increase in overall survival (OS) of said subject or population of subjects.
283. 구현예 282에 있어서,283. The method of embodiment 282,
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는 (b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
284. 구현예 282에 있어서,284. The method of embodiment 282,
상기 기준 DOR 시간은 적어도 약 6.7개월 내지 약 23.4개월인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said reference DOR time is at least about 6.7 months to about 23.4 months.
285. 구현예 282에 있어서,285. The method of embodiment 282,
상기 기준 OS 시간은 적어도 약 11.6개월 내지 약 14.9개월인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said baseline OS time is at least about 11.6 months to about 14.9 months.
286. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,286. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN having a detectable expression level of PD-L1, comprising:
상기 치료는 매 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist with one or more dosing cycles of said PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, said anti TIGIT An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks.
287. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,287. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN having a detectable expression level of PD-L1, comprising:
상기 치료는 매 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks, wherein said anti TIGIT antagonist antibody is 3 An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use formulated for administration of a dose of about 600 mg per week.
288. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,288. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN having a detectable expression level of PD-L1,
상기 치료는 매 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein said anti TIGIT antagonist An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks.
289. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,289. Tiragolumab and atezolizumab for use in a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
상기 치료는 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment includes an anti-TIGIT antagonist antibody and the PD-1 axis in one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks. Tiragolumab and atezolizumab for use, including the use of binding antagonists.
290. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,290. Tiragolumab and atezolizumab for use in a method of treating a subject having SCCHN having a detectable expression level of PD-L1,
상기 치료는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.wherein said treatment comprises the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; Tiragolumab and atezolizumab for use.
291. SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,291. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및(c) administering to the subject a dose of about 80 mg to about 1600 mg of the PD-1 axis binding antagonist every 3 weeks and a dose of about 30 mg to about 1200 mg of an anti TIGIT antagonist antibody formulated for administration every 3 weeks. identifying as a person likely to benefit from a therapy comprising more than one dosing cycle; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
292. SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,292. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및(c) administering the subject to a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks. confirming as; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
293. SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,293. Tiragolumab and atezolizumab for use in a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및 (c) subjecting the subject to one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks. identifying as a potential person; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(d) tiragolumab and atezolizumab for use, comprising administering said therapy to an identified subject having a detectable expression level of PD-L1.
294. SCCHN을 가진 대상체를 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,294. Tiragolumab and atezolizumab for use in a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및 (c) identifying the subject as likely to benefit from a therapy comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks. ; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(d) tiragolumab and atezolizumab for use, comprising administering said therapy to an identified subject having a detectable expression level of PD-L1.
295. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,295. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising selecting a regimen comprising one or more dosing cycles of the anti-TIGIT antagonist antibody formulated for administration of a dose of mg to about 1200 mg.
296. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,296. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) administering a dose of about 1200 mg of a PD-1 axis binding antagonist every 3 weeks and a dose of about 600 mg every 3 weeks based on detected PD-L1 expression for said subject having a detectable expression level of PD-L1 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising selecting a regimen comprising one or more dosing cycles of the anti-TIGIT antagonist antibody formulated for use.
297. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,297. Tiragolumab and atezolizumab for use in a method of selecting a therapy for a subject with SCCHN,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 mg to about every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 Tiragolumab and atezolizumab for use, comprising selecting a regimen comprising one or more dosing cycles of tiragolumab at a dose of 1200 mg.
298. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,298. Tiragolumab and atezolizumab for use in a method of selecting a therapy for a subject with SCCHN,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 Tiragolumab and atezolizumab for use, comprising selecting a regimen comprising one or more dosing cycles.
299. 구현예 267 내지 구현예 298 중 어느 한 구현예에 있어서,299. The method according to any one of embodiments 267 to 298,
상기 PD-L1의 검출 가능한 발현 수준은 항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1 determined by immunohistochemical (IHC) analysis comprising the step of staining with anti-PD-L1 antibody SP263, an anti-TIGIT antagonist for use Antibodies and PD-1 axis binding antagonists.
300. 구현예 299에 있어서,300. The method of embodiment 299,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기의 종양 샘플에서:The detectable protein expression level of PD-L1 is in the tumor sample:
(a) 5% 이상; (a) at least 5%;
(b) 5% 이상 및 20% 미만; 또는 (b) at least 5% and less than 20%; or
(c) 20% 이상의 종양 관련 면역 세포(TIC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least 20% tumor-associated immune cells (TIC).
301. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,301. One or more dosing cycles of the PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of identifying a subject having SCCHN as a person likely to benefit from a therapy comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein of PD-L1 has a TIC of at least 5%. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the expression level identifies the subject as likely to benefit from the therapy.
302. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,302. One or more dosing cycles of the PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of identifying a subject having SCCHN as a person likely to benefit from a therapy comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상 20% 미만인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from the subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the PD-L1 TIC is greater than or equal to 5% and less than 20%. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the protein expression level of L1 identifies the subject as likely to benefit from the therapy.
303. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,303. One or more dosing cycles of the PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of identifying a subject having SCCHN as a person likely to benefit from a therapy comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 20% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein of PD-L1 has a TIC of at least 20%. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the expression level identifies the subject as likely to benefit from the therapy.
304. 구현예 301 내지 구현예 303 중 어느 한 구현예에 있어서,304. The method of any one of embodiments 301 to 303,
상기 대상체는 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로 확인되고 상기 방법은 상기 대상체에게 상기 요법을 투여하는 단계를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said subject is identified as likely to benefit from said therapy and said method further comprises administering said therapy to said subject.
305. 구현예 301 내지 구현예 304 중 어느 한 구현예에 있어서,305. The method of any one of embodiments 301 to 304,
상기 TIC는 벤타나 SP263 IHC 분석을 사용하여 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said TIC is determined using a Ventana SP263 IHC assay.
306. 구현예 267 내지 구현예 305 중 어느 한 구현예에 있어서,306. The method of any one of embodiments 267 to 305,
상기 대상체 또는 대상체 집단은 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 확인되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or population of subjects is identified as likely to benefit from a treatment based on PD-L1 expression on a detected tumor cell.
307. 구현예 72에 있어서,307. The method of
상기 암은 간암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is liver cancer.
308. 구현예 307에 있어서,308. The method of embodiment 307,
상기 간암은 간세포 암종(HCC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the liver cancer is hepatocellular carcinoma (HCC).
309. 간세포 암종(HCC)을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,309. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having hepatocellular carcinoma (HCC), comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 투여를 위해 제형화되고 상기 PD-1 축 결합 길항제이며, 여기서 상기 대상체 또는 대상체 집단은 HCC에 대해 선행 전신 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti TIGIT antagonist antibody is formulated for administration and is said PD-1 axis binding antagonist, wherein An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or population of subjects has not received prior systemic therapy for HCC.
310. 구현예 309에 있어서,310. The method of embodiment 309,
상기 치료는 VEGF 길항제의 사용을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the treatment further comprises the use of a VEGF antagonist.
311. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,311. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having HCC, comprising:
상기 치료는 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist with one or more dosing cycles of anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, and VEGF antagonist, anti TIGIT antagonist antibody for use and PD-1 axis binding antagonists.
312. 구현예 310 및 구현예 311에 있어서,312. The method of embodiment 310 and embodiment 311,
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
313. 구현예 309 내지 구현예 312 중 어느 한 구현예에 있어서,313. The method of any one of embodiments 309 to 312,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks.
314. 구현예 313에 있어서,314. The method of embodiment 313,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 800 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 800 mg every 3 weeks.
315. 구현예 309 내지 구현예 314 중 어느 한 구현예에 있어서,315. The method of any one of embodiments 309 to 314,
상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 600 mg every 3 weeks.
316. 구현예 309 내지 구현예 315 중 어느 한 구현예에 있어서,316. The method of any one of embodiments 309 to 315,
상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks.
317. 구현예 309 내지 구현예 316 중 어느 한 구현예에 있어서,317. The method of any one of embodiments 309 to 316,
상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 900 mg to about 1500 mg every 3 weeks.
318. 구현예 310 또는 구현예 311에 있어서,318. The method of embodiment 310 or embodiment 311,
상기 VEGF 길항제는 2주마다 약 1 mg/kg 내지 약 20 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
319. 구현예 318에 있어서,319. The method of embodiment 318,
상기 VEGF 길항제는 2주마다 약 5 mg/kg 내지 약 10 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
320. 구현예 319에 있어서,320. The method of embodiment 319,
상기 VEGF 길항제는 2주마다 약 5 mg/kg, 약 7.5 mg/kg, 또는 약 10 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the VEGF antagonist is formulated for administration at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10 mg/kg every two weeks.
321. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,321. The embodiment of any one of embodiments 309 to 311 and embodiments 318 to 320,
상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 10 mg to about 1000 mg every two weeks.
322. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 321 중 어느 한 구현예에 있어서,322. The embodiment of any one of embodiments 309 to 311 and embodiments 318 to 321,
상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 20 mg to about 1600 mg every two weeks.
323. 구현예 309 내지 구현예 311에 있어서,323. according to embodiment 309 to embodiment 311,
상기 항 TIGIT 길항제 항체는 4주마다 약 200 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks.
324. 구현예 309 내지 구현예 311 및 구현예 323 중 어느 한 구현예에 있어서,324. The method according to any one of embodiments 309 to 311 and 323,
상기 PD-1 축 결합 길항제는 4주마다 약 80 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 2000 mg every 4 weeks.
325. 구현예 309 내지 구현예 311, 구현예 323, 및 구현예 324 중 어느 한 구현예에 있어서,325. The embodiment of any one of embodiments 309 to 311, 323, and 324,
상기 PD-1 축 결합 길항제는 4주마다 약 1400 mg 내지 약 2000 mg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 1400 mg to about 2000 mg every 4 weeks.
326. 구현예 309 내지 구현예 325 중 어느 한 구현예에 있어서,326. The method of any one of embodiments 309 to 325,
상기 HCC는 국소 진행성 또는 전이성 HCC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said HCC is locally advanced or metastatic HCC.
327. 구현예 309 내지 구현예 326 중 어느 한 구현예에 있어서,327. The method of any one of embodiments 309 to 326,
상기 HCC는 절제 불가능한 HCC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said HCC is unresectable HCC.
328. 구현예 309 내지 구현예 327 중 어느 한 구현예에 있어서,328. The method of any one of embodiments 309 to 327,
상기 대상체 또는 대상체들은 적절한 간 기능을 갖는 것으로 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects is determined to have adequate liver function.
329. 구현예 328에 있어서,329. The method of embodiment 328,
상기 적절한 간 기능은 차일드-퍼(Child-Pugh) 분류 A로 특징지어지는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said appropriate liver function is characterized as Child-Pugh class A.
330. 구현예 309 내지 구현예 329 중 어느 한 구현예에 있어서,330. The method of any one of embodiments 309 to 329,
상기 대상체 또는 대상체들로부터 수득한 HCC 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the subject or HCC tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
331. 구현예 309 내지 구현예 330 중 어느 한 구현예에 있어서,331. The method of any one of embodiments 309 to 330,
상기 방법은 상기 대상체 또는 대상체 집단에 적어도 4회의 투약 주기를 투여하는 단계를 포함하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the method comprises administering to the subject or population of subjects at least 4 dosing cycles.
332. 구현예 331에 있어서,332. The method of embodiment 331,
상기 방법은 상기 대상체 또는 대상체 집단에 적어도 16회의 투약 주기를 투여하는 단계를 포함하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the method comprises administering to the subject or population of subjects at least 16 dosing cycles.
333. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,333. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having HCC,
상기 치료는 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기로 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment includes one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and bevacizumab at a dose of about 15 mg/kg every 3 weeks with one or more dosing cycles of the anti-TIGIT antagonist. Tiragolumab and atezolizumab for use, comprising the use of antibodies and PD-1 axis binding antagonists.
334. 구현예 311 내지 구현예 333 중 어느 한 구현예에 있어서,334. The method of any one of embodiments 311 to 333,
상기 대상체 또는 대상체들은 HCC에 대해 선행 전신 치료를 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has not received prior systemic treatment for HCC.
335. 구현예 309 내지 구현예 334 중 어느 한 구현예에 있어서,335. The method of any one of embodiments 309 to 334,
상기 치료는 적어도 약 5.6개월 내지 적어도 약 6.83개월의 대상체 집단의 PFS 중앙값을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median PFS in the subject population of at least about 5.6 months to at least about 6.83 months.
336. 구현예 72에 있어서,336. The method of
상기 암은 방광암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is bladder cancer.
337. 구현예 336에 있어서,337. The method of embodiment 336,
상기 방광암은 근육 침윤성 방광암(MIBC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said bladder cancer is muscle invasive bladder cancer (MIBC).
338. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,338. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein the PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent. TIGIT antagonist antibodies and PD-1 axis binding antagonists.
339. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,339. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks. wherein the PD-1 axis binding antagonist is formulated for administration at a dose of about 900 mg to about 1500 mg every 3 weeks, wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent. TIGIT antagonist antibodies and PD-1 axis binding antagonists.
340. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,340. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC, comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment. Axial bond antagonists.
341. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,341. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC, comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg 용량이며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks. wherein said PD-1 axis binding antagonist is in a dose of about 900 mg to about 1500 mg every 3 weeks, wherein said treatment is perioperative treatment.
342. 구현예 338 내지 구현예 341 중 어느 한 구현예에 있어서,342. The method of any one of embodiments 338 to 341,
상기 대상체 또는 대상체들은 크레아티닌 청소율이 60 mL/분 미만인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has a creatinine clearance of less than 60 mL/min.
343. 구현예 338 내지 구현예 342 중 어느 한 구현예에 있어서,343. The method of any one of embodiments 338 to 342,
상기 대상체 또는 대상체들은 2등급 이상의 청력 상실을 갖는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has a hearing loss of
344. 구현예 338 내지 구현예 343 중 어느 한 구현예에 있어서,344. The method of any one of embodiments 338 to 343,
상기 대상체 또는 대상체들은 2등급 이상의 신경병증을 갖는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject or subjects has neuropathy of
345. 구현예 338 내지 구현예 344 중 어느 한 구현예에 있어서,345. The method of any one of embodiments 338 to 344,
상기 대상체 또는 대상체들은 백금계 화학요법제를 이용한 치료를 거부한, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have refused treatment with a platinum-based chemotherapeutic agent.
346. 구현예 338 또는 구현예 342 내지 구현예 345 중 어느 한 구현예에 있어서,346. The method according to any one of embodiments 338 or 342 to 345,
상기 백금계 화학요법제는 시스플라틴인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the platinum-based chemotherapeutic agent is cisplatin.
347. 구현예 338 내지 구현예 346 중 어느 한 구현예에 있어서,347. The method of any one of embodiments 338 to 346,
상기 MIBC는 외과 수술이 가능한, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The MIBC is an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, capable of surgery.
348. 구현예 347에 있어서,348. The method of embodiment 347,
상기 방법은 수술을 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the method further comprises surgery.
349. 구현예 348에 있어서,349. The method of embodiment 348,
적어도 1회의 투약 주기는 상기 수술 전에 개시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least one dosing cycle is initiated prior to said surgery.
350. 구현예 348 또는 구현예 349에 있어서,350. The method of embodiment 348 or embodiment 349,
적어도 1, 2, 또는 3회의 투약 주기는 상기 수술 전에 완료되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least one, two, or three dosing cycles are completed prior to said surgery.
351. 구현예 348 내지 구현예 350 중 어느 한 구현예에 있어서,351. The method of any one of embodiments 348 to 350,
적어도 1회의 투약 주기는 상기 수술 후 4주 내지 6주 사이에 개시되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein at least one dosing cycle is initiated between 4 and 6 weeks post-surgery.
352. 구현예 351에 있어서,352. The method of embodiment 351,
1 내지 17회의 투약 주기는 상기 수술 후에 완료되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein 1 to 17 dosing cycles are completed after said surgery.
353. 구현예 348 내지 구현예 352 중 어느 한 구현예에 있어서,353. The method of any one of embodiments 348 to 352,
상기 수술은 방광 절제술 및/또는 림프절 절제술인, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the surgery is cystectomy and/or lymphadenectomy.
354. 구현예 338 내지 구현예 353 중 어느 한 구현예에 있어서,354. The method of any one of embodiments 338 to 353,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment elicits a pathological complete response (pCR).
355. 구현예 338 내지 구현예 354 중 어느 한 구현예에 있어서,355. The method of any one of embodiments 338 to 354,
상기 치료는 기준 RFS 시간과 비교하여 상기 대상체 또는 대상체들의 무재발 생존(RFS)의 증가, 기준 EFS 시간과 비교하여 상기 대상체 또는 대상체들의 무사건 생존(EFS)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체들의 OS의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the treatment is an increase in relapse-free survival (RFS) of the subject or subjects as compared to a baseline RFS time, an increase in the event-free survival (EFS) of the subject or subjects compared to a baseline EFS time, or an increase in the event-free survival (EFS) of the subject or subjects as compared to a baseline OS time. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, which cause an increase in OS in the subject or subjects.
356. 구현예 355에 있어서,356. The method of embodiment 355,
(a) 상기 기준 RFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 RFS 시간 중앙값이고;(a) said baseline RFS time is the median RFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 EFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 EFS 시간 중앙값이거나; 또는 (b) said baseline EFS time is the median EFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said baseline OS time is the median OS time of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
357. 구현예 338 내지 구현예 356 중 어느 한 구현예에 있어서,357. The method of any one of embodiments 338 to 356,
상기 치료는 병리학적 병기하향(downstaging)을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment results in pathological downstaging.
358. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,358. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC,
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체는 시스플라틴 부적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein the PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein the subject is cisplatin ineligible, an anti TIGIT antagonist antibody for use and the PD-1 axis binding antagonists.
359. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,359. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC, comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment. Axial bond antagonists.
360. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,360. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC, comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-L1 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체는 시스플라틴 부적격인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein the PD-L1 binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein the subject is cisplatin ineligible, an anti TIGIT antagonist antibody for use and a PD-1 axis binding antagonist.
361. MIBC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,361. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with MIBC, comprising:
상기 치료는 1회 이상의 투약 주기로 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 상기 PD-L1 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment comprises the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. wherein said PD-L1 binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment. binding antagonists.
362. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,362. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with MIBC,
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체는 시스플라틴 부적격인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration in a dose of about 30 mg to about 1200 mg every 3 weeks, and atezolizumab is administered in 3 Tiragolumab and atezolizumab for use, wherein the subject is cisplatin ineligible, formulated for administration of a dose of about 80 mg to about 1600 mg per week.
363. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,363. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having MIBC,
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화되며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration in a dose of about 30 mg to about 1200 mg every 3 weeks, and atezolizumab is administered in 3 Tiragolumab and atezolizumab for use, wherein the treatment is perioperative treatment, wherein the treatment is formulated for administration of a dose of about 80 mg to about 1600 mg per week.
364. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,364. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with MIBC,
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 약 1200 mg 용량의 투여를 위해 제형화되며, 여기서 상기 대상체 또는 대상체들은 시스플라틴 부적격인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration of a dose of about 600 mg every 3 weeks and atezolizumab is about 1200 every 3 weeks. Tiragolumab and atezolizumab for use, formulated for administration of a mg dose, wherein the subject or subjects are cisplatin ineligible.
365. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,365. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having MIBC,
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 약 1200 mg 용량의 투여를 위해 제형화되며, 여기서 상기 치료는 수술 전후 치료인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration of a dose of about 600 mg every 3 weeks and atezolizumab is about 1200 every 3 weeks. Tiragolumab and atezolizumab for use, wherein the treatment is perioperative treatment.
366. 구현예 338 내지 구현예 365 중 어느 한 구현예에 있어서,366. The method of any one of embodiments 338-365,
상기 치료는 적어도 약 13.4% 내지 약 15%의 대상체 집단의 ORR을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits an ORR in at least about 13.4% to about 15% of a subject population.
367. 구현예 338 내지 구현예 366 중 어느 한 구현예에 있어서,367. The method of any one of embodiments 338 to 366,
상기 치료는 적어도 약 7.9개월 내지 약 8.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median OS in the subject population of at least about 7.9 months to about 8.6 months.
368. 구현예 338 내지 구현예 367 중 어느 한 구현예에 있어서,368. The method of any one of embodiments 338 to 367,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 is determined by IHC analysis comprising staining with the anti-PD-L1 antibody SP142.
369. 구현예 368에 있어서,369. The method of embodiment 368,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 5% 이상인 PD-L1 양성 종양 세포 분획인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable protein expression level of PD-L1 is a PD-L1-positive tumor cell fraction in which the proportion of tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) is 5% or more, anti-TIGIT antagonist antibody and PD for use -1 axis binding antagonists.
370. 구현예 336에 있어서,370. The method of embodiment 336,
상기 방광암은 요로상피세포 암종(UC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the bladder cancer is urothelial cell carcinoma (UC).
371. 구현예 370에 있어서,371. The method of embodiment 370,
상기 UC는 전이성 요로상피세포 암종(mUC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said UC is metastatic urothelial cell carcinoma (mUC).
372. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,372. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising a cycle.
373. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,373. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment includes an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 800 mg every 3 weeks, and one or more doses of a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising a cycle.
374. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,374. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 대상체는선행 암 면역요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. an anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist for use, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising a cycle, wherein said subject has not received prior cancer immunotherapy binding antagonists.
375. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,375. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 치료는 2차 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more administrations of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of a PD-1 axis binding antagonist every 3 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising a cycle, wherein said treatment is a second line treatment.
376. 구현예 372, 구현예 372, 및 구현예 375 중 어느 한 구현예에 있어서,376. The method of any one of embodiments 372, 372, and 375,
상기 대상체 또는 대상체들은 선행 암 면역요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has not received prior cancer immunotherapy.
377. 구현예 372 내지 구현예 374 중 어느 한 구현예에 있어서,377. The method according to any one of embodiments 372 to 374,
상기 치료는 2차 치료인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said treatment is second-line treatment.
378. 구현예 372 내지 구현예 377 중 어느 한 구현예에 있어서,378. The method of any one of embodiments 372 to 377,
상기 mUC는 백금 함유 요법 중에 또는 이후에 진행하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said mUC is during or after platinum containing therapy.
379. 구현예 372 내지 구현예 378 중 어느 한 구현예에 있어서,379. The method according to any one of embodiments 372 to 378,
상기 방법은 상기 대상체 또는 대상체 집단이 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체들에게 제2 투약 요법을 투여하는 단계를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method further comprises administering to the subject or subjects a second dosing regimen after the subject or population of subjects has experienced disease progression or unacceptable toxicity. uniaxial binding antagonists.
380. 구현예 379에 있어서,380. The method of embodiment 379,
상기 제2 투약 요법은 상기 PD-1 축 결합 길항제 및 항체-약물 접합체(ADC)의 1회 이상의 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said second dosing regimen comprises at least one dosing cycle of said PD-1 axis binding antagonist and an antibody-drug conjugate (ADC).
381. 구현예 380에 있어서,381. The method of embodiment 380,
상기 ADC는 (a) 엔포르투맙 베도틴 또는 (b) 사시투주맙 고비테칸인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said ADC is (a) enfortumab vedotin or (b) sacituzumab gobitecan.
382. 구현예 381에 있어서,382. The method of embodiment 381,
(a) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량의 투여를 위해 제형화되거나, 또는 (b) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(a) enfortumab vedotin is formulated for administration at a weekly dose of 1.25 mg/kg with a 2-week dosing/1 week off, or (b) sacituzumab gobitecan is administered at a 2-week dosing/1 week off An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use formulated for administration at a dose of 10 mg/kg weekly.
383. 구현예 381 또는 구현예 382에 있어서,383. The method of embodiment 381 or embodiment 382,
(a) 엔포르투맙 베도틴은 각 21일 주기의 제 1일 및 8일에 1.25 mg/kg 용량의 투여를 위해 제형화되거나, 또는 (b) 사시투주맙 고비테칸은 각 21일 주기의 제 1일 및 8일에 10 mg/kg 용량의 투여를 위해 제형화되는. 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(a) enfortumab vedotin is formulated for administration at a dose of 1.25 mg/kg on
384. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,384. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises one or more dosing cycles of an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and a dose of about 80 mg to about 1600 mg of PD-L1 binding antagonist every 3 weeks. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising use of said anti TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising
385. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,385. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골리주맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함한 투약 요법에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment includes an anti-TIGIT antagonist antibody and Tiragolumab and atezolizumab for use, comprising the use of a PD-1 axis binding antagonist.
386. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,386. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 1회 이상의 투약 주기로 티라골루맙 및 아테졸리주맙의 사용을 포함하고, 여기서 티라골루맙은 3주마다 약 600 mg 용량의 투여를 위해 제형화되고, 아테졸리주맙은 3주마다 1200 mg의 용량인, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is formulated for administration at a dose of about 600 mg every 3 weeks and atezolizumab is 1200 mg every 3 weeks. tiragolumab and atezolizumab for use.
387. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,387. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 제1 투약 요법에 이어서 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen followed by a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen is an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks and a dose of about 80 mg to about 1600 mg every 3 weeks. comprising one or more dosing cycles of a PD-1 axis binding antagonist; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 투여를 위해 제형화된 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량의 투여를 위해 제형화되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량의 투여를 위해 제형화되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) said second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist formulated for administration of a dose of about 80 mg to about 1600 mg every 3 weeks, and (i) Enfortumab Be Dotin is formulated for administration at a weekly dose of 1.25 mg/kg on a 2-week dosing/1 week off, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg on a 2-week dos/week off. formulated for administration, wherein said second dosing regimen is administered to said subject or subject population after said subject or subject population experiences disease progression or unacceptable toxicity during said first dosing regimen. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists.
388. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,388. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 제1 투약 요법에 이어서 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen followed by a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks and a dose of about 80 mg to about 1600 mg of a PD-L1 binding antagonist every 3 weeks. comprising one or more dosing cycles; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량의 투여를 위해 제형화되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량의 투여를 위해 제형화되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에게 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) said second dosing regimen comprises one or more dosing cycles of the PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, (i) Enfortumab vedotin is administered for 2 weeks / is formulated for administration of a weekly dose of 1.25 mg/kg of a week off, or (ii) sacituzumab gobitecan is formulated for administration of a weekly dose of 10 mg/kg of a dose of two weeks of dosing/week off; wherein said second dosing regimen is administered to said subject after said subject experiences disease progression or unacceptable toxicity during said first dosing regimen.
389. mUC를 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,389. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects with mUC, comprising:
상기 치료는 제1 투약 요법에 이어서 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen followed by a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and
(b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량의 투여를 위해 제형화되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량의 투여를 위해 제형화되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에게 투여되는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) said second dosing regimen comprises at least one dosing cycle of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin is administered at 1.25 weekly doses of 2 weeks on/1 week off. is formulated for administration of a mg/kg dose, or (ii) sacituzumab gobitecan is formulated for administration of a weekly 10 mg/kg dose of 2 weeks dosing/1 week off, wherein the second dosing regimen is administered to said subject after said subject experiences disease progression or unacceptable toxicity during said first dosing regimen.
390. 구현예 372 내지 구현예 389 중 어느 한 구현예에 있어서,390. The method of any one of embodiments 372 to 389,
상기 치료는 적어도 약 13.4% 내지 적어도 약 31%의 대상체 집단의 ORR을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits an ORR in at least about 13.4% to at least about 31% of the subject population.
391. 구현예 372 내지 구현예 390 중 어느 한 구현예에 있어서,391. The method of any one of embodiments 372 to 390,
상기 치료는 약 7.9개월 내지 약 16.3개월의 대상체 집단의 OS 중앙값을 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits a median OS of a population of subjects from about 7.9 months to about 16.3 months.
392. 구현예 72에 있어서,392. The method of
상기 암은 췌장암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is pancreatic cancer.
393. 췌장암을 가진 대상체 또는 대상체 집단을 치료하는 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,393. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having pancreatic cancer,
상기 치료는 각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법에서 상기 항 TGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment comprises tiragolumab at a dose of about 420 mg on
394. 구현예 392 또는 구현예 393에 있어서,394. The method of embodiment 392 or embodiment 393,
상기 췌장암은 췌장관 선암(PDAC)인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395. 구현예 394에 있어서,395. The method of embodiment 394,
상기 PDAC는 전이성 PDAC인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said PDAC is a metastatic PDAC.
396. 구현예 392 내지 구현예 395 중 어느 한 구현예에 있어서,396. The method of any one of embodiments 392 to 395,
상기 대상체 또는 대상체들은 전이성 PDAC에 대해 선행 전신 요법을 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects have not received prior systemic therapy for metastatic PDAC.
397. 구현예 392 내지 구현예 396 중 어느 한 구현예에 있어서,397. The method of any one of embodiments 392 to 396,
상기 치료는 적어도 약 41.7% 내지 약 46.7%의 대상체 집단의 ORR을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in an ORR in at least about 41.7% to about 46.7% of the subject population.
398. 구현예 392 내지 구현예 397 중 어느 한 구현예에 있어서,398. The method of any one of embodiments 392 to 397,
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 없이 젬시타빈 및 냅-파클리탁셀을 포함한 치료와 비교하여 적어도 약 20%의 ORR의 증가를 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in an increase in ORR of at least about 20% as compared to treatment comprising gemcitabine and nap-paclitaxel in the absence of anti-TIGIT antagonist antibody and PD-1 axis binding antagonist and anti-TIGIT antagonist antibody and PD- uniaxial binding antagonists.
399. 구현예 392 내지 구현예 398 중 어느 한 구현예에 있어서,399. The method of any one of embodiments 392 to 398,
상기 치료는 적어도 약 5.5개월 내지 약 7개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median PFS in a population of subjects of at least about 5.5 months to about 7 months.
400. 구현예 392 내지 구현예 399 중 어느 한 구현예에 있어서,400. The method of any one of embodiments 392 to 399,
상기 치료는 적어도 약 8.5개월 내지 약 10.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in a median OS in the subject population of at least about 8.5 months to about 10.6 months.
401. 구현예 72에 있어서,401. The method of
상기 암은 식도암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the cancer is esophageal cancer.
402. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,402. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
상기 치료는 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of about 30 mg to about 1200 mg on
403. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,403. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
상기 치료는 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of about 30 mg to about 1200 mg on
404. 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,404. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having esophageal cancer,
상기 치료는 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of about 30 mg to about 1200 mg on
405. 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,405. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having esophageal cancer,
상기 치료는 각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 800 mg on
406. 구현예 402 또는 구현예 403에 있어서,406. The method of embodiment 402 or embodiment 403,
상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject or subjects has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
407. 구현예 404 내지 구현예 406 중 어느 한 구현예에 있어서,407. The method of any one of embodiments 404 to 406,
상기 대상체 또는 대상체들은 상기 선행 치료 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects experienced disease progression or unacceptable toxicity during said prior treatment.
408. 구현예 402 또는 구현예 403에 있어서,408. The method of embodiment 402 or embodiment 403,
상기 21일 투약 주기는 백금계 화학요법제 및 비백금계 화학요법제를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409. 구현예 408에 있어서,409. The method of embodiment 408,
상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
410. 구현예 404 내지 구현예 409 중 어느 한 구현예에 있어서,410. The method of any one of embodiments 404 to 409,
상기 백금계 화학요법제는 시스플라틴인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the platinum-based chemotherapeutic agent is cisplatin.
411. 구현예 410에 있어서,411. The method of embodiment 410,
시스플라틴은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein cisplatin is formulated for administration at a dose of about 80 mg/m2 on
412. 구현예 404 내지 구현예 411 중 어느 한 구현예에 있어서,412. The method of any one of embodiments 404 to 411,
상기 비백금계 화학요법제는 항대사물질인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the non-platinum-based chemotherapeutic agent is an antimetabolites.
413. 구현예 412에 있어서,413. The method of embodiment 412,
상기 항대사물질은 5-플루오로우라실인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said antimetabolite is 5-fluorouracil. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
414. 구현예 413에 있어서,414. The method of embodiment 413,
5-플루오로우라실은 각 21일 주기의 제 1일 내지 5일에 800mg/m2/24시간 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein 5-fluorouracil is formulated for administration at a dose of 800 mg/
415. 구현예 404 내지 구현예 414 중 어느 한 구현예에 있어서,415. The method of any one of embodiments 404 to 414,
상기 식도암은 진행성 또는 전이성 식도암인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the esophageal cancer is advanced or metastatic esophageal cancer.
416. 구현예 402, 구현예 403, 구현예 408, 및 구현예 409 중 어느 한 구현예에 있어서,416. The embodiment of any one of embodiments 402, 403, 408, and 409,
상기 대상체 또는 대상체들은 전이성 식도암에 대해 선행 치료를 받은 적이 없는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or subjects has not received prior treatment for metastatic esophageal cancer.
417. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,417. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 치료는 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg on
418. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,418. An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 치료는 각 투약 주기의 제 1일에 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 1200 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 600 mg on
419. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,419. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 치료는 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 사용을 위한 티라골루맙 및 아테졸리주맙.The treatment is tiragolumab at a dose of about 600 mg on
420. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,420. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 치료는 제1 투약 요법 및 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen and a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 백금계 화학요법제 및 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises at least one 21-day dosing cycle of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses; ; and
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of from about 30 mg to about 1200 mg on
421. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제로서,421. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
상기 치료는 제1 투약 요법 및 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen and a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody formulated for administration of a dose of from about 30 mg to about 1200 mg on
422. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단의 치료 방법에서 사용하기 위한 티라골루맙 및 아테졸리주맙으로서,422. Tiragolumab and atezolizumab for use in a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 치료는 제1 투약 요법 및 제2 투약 요법에서 상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제의 사용을 포함하고, 여기서: wherein said treatment comprises use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a first dosing regimen and a second dosing regimen, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen is cisplatin at a dose of about 80 mg/m2 on
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함하는, 사용을 위한 티라골루맙 및 아테졸리주맙.(b) said second dosing regimen is one or more 21 day dosing cycles of tiragolumab at a dose of about 600 mg on
423. 구현예 402 내지 구현예 422 중 어느 한 구현예에 있어서,423. The method of any one of embodiments 402 to 422,
상기 치료는 적어도 약 14%의 대상체 집단의 ORR을 유발하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment elicits an ORR in at least about 14% of the subject population.
424. 구현예 47 내지 구현예 423 중 어느 한 구현예에 있어서,424. The method according to any one of embodiments 47 to 423,
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
425. 구현예 424에 있어서,425. The method of embodiment 424,
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR):The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, further comprising FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
426. 구현예 424에 있어서,426. The method of embodiment 424,
상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR:The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, further comprising FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
427. 구현예 426에 있어서,427. The method of embodiment 426,
X1은 E인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.X1 is E, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
428. 구현예 426에 있어서,428. The method of embodiment 426,
X1은 Q인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.X1 is Q; an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
429. 구현예 424 내지 구현예 428 중 어느 한 구현예에 있어서,429. The method of any one of embodiments 424 to 428,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a VH domain as in case (a) and a VL domain as in case (b).
430. 구현예 424 내지 구현예 429 중 어느 한 구현예에 있어서,430. The method of any one of embodiments 424 to 429,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
431. 구현예 424 내지 구현예 427, 구현예 429, 및 구현예 430 중 어느 한 구현예에 있어서,431. The embodiment of any one of embodiments 424 to 427, 429, and 430,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
432. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 431 중 어느 한 구현예에 있어서,432. The method of any one of embodiments 424 to 427 and embodiments 429 to 431,
상기 항 TIGIT 길항제 항체는 하기의: The anti-TIGIT antagonist antibody is:
(a) 서열번호 33의 아미노산 서열을 포함하는 중쇄; 및 (a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 33; and
(b) 서열번호 34의 아미노산 서열을 포함하는 경쇄를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use comprising a light chain comprising the amino acid sequence of SEQ ID NO:34.
433. 구현예 424 내지 구현예 432 중 어느 한 구현예에 있어서,433. The method of any one of embodiments 424 to 432,
상기 항 TIGIT 길항제 항체는 단일클론 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-TIGIT antagonist antibody is a monoclonal antibody, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
434. 구현예 424 내지 구현예 433 중 어느 한 구현예에 있어서,434. The method of any one of embodiments 424 to 433,
상기 항 TIGIT 길항제 항체는 인간 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is a human antibody.
435. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,435. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 전장 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is a full-length antibody.
436. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 436 중 어느 한 구현예에 있어서,436. The method of any one of embodiments 424 to 427 and embodiments 429 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. wherein said anti-TIGIT antagonist antibody is tyragolumab; an anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
437. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 구현예 421, 및 구현예 424 내지 구현예 436 중 어느 한 구현예에 있어서,437. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, embodiment 421, and embodiment any one of embodiments 424 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT 또는 TJ-T6인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is tiragolumab, bivostoliumab, etigilumab, EOS084448, SGN-TGT or TJ-T6.
438. 구현예 437에 있어서,438. The method of embodiment 437,
상기 항 TIGIT 길항제 항체는 원형 Fc 매개 작동체 기능을 갖는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody has a prototypical Fc-mediated effector function.
439. 구현예 437 또는 구현예 438에 있어서,439. according to embodiment 437 or embodiment 438,
상기 항 TIGIT 길항제 항체는 향상된 Fc 매개 작동체 기능을 갖는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody has enhanced Fc-mediated effector function.
440. 구현예 437 내지 구현예 439 중 어느 한 구현예에 있어서,440. The method of any one of embodiments 437 to 439,
상기 항 TIGIT 길항제 항체는 SGN-TGT인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody is SGN-TGT.
441. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421 중 어느 한 구현예에 있어서,441. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421 according to any one of embodiments,
상기 항 TIGIT 길항제 항체는 돔바날리맙, BMS-986207, ASP8374 또는 COM902인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제..wherein said anti-TIGIT antagonist antibody is dombanalimab, BMS-986207, ASP8374 or COM902, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
442. 구현예 424 내지 구현예 431 및 구현예 441 중 어느 한 구현예에 있어서,442. The method of any one of embodiments 424 to 431 and 441,
상기 항 TIGIT 길항제 항체는 Fc 매개 작동체 기능을 갖지 않는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody has no Fc-mediated effector function.
443. 구현예 47 내지 구현예 442 중 어느 한 구현예에 있어서,443. The method according to any one of embodiments 47 to 442,
상기 항 TIGIT 길항제 항체는 IgG 부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444. 구현예 443에 있어서,444. The method of embodiment 443,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said IgG class antibody is an IgG1 subclass antibody.
445. 구현예 444에 있어서,445. of embodiment 444,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, 돔바날리맙, 또는 BMS-986207인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody is tiragolumab, bivostolimab, etigilimab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, dombanalimab, or BMS-986207. Antibodies and PD-1 axis binding antagonists.
446. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421 중 어느 한 구현예에 있어서,446. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421 according to any one of embodiments,
상기 IgG 부류 항체는 IgG4 하위부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said IgG class antibody is an IgG4 subclass antibody.
447. 구현예 446에 있어서,447. The method of embodiment 446,
상기 항 TIGIT 길항제 항체는 ASP8374 또는 COM902인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody is ASP8374 or COM902.
448. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,448. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 Fab, bis-Fab, Fab’, Fab’-SH, Fv, 단일 사슬 가변 단편(scFv), 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 TIGIT에 결합하는 항체 단편인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the anti-TIGIT antagonist antibody is an antibody fragment that binds to TIGIT selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv), and (Fab')2 fragment, Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
449. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,449. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 단일특이적 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is a monospecific antibody.
450. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,450. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 다중특이적 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-TIGIT antagonist antibody is a multispecific antibody.
451. 구현예 450에 있어서,451. The method of embodiment 450,
상기 다중특이적 항체는 이중특이적 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said multispecific antibody is a bispecific antibody, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
452. 구현예 424 내지 구현예 451 중 어느 한 구현예에 있어서452. The method of any one of embodiments 424 to 451
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제, 및 PD-L2 결합 길항제로 이루어진 군으로부터 선택되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
453. 구현예 452에 있어서,453. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist.
454. 구현예 453에 있어서,454. The method of embodiment 453,
상기 PD-L1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-L1 binding antagonist inhibits binding of PD-L1 to one or more of its ligand binding partners.
455. 구현예 454에 있어서,455. The method of embodiment 454,
상기 PD-L1 결합 길항제는 PD-L1이 PD-1, B7-1, 또는 PD-1 및 B7-1 둘 모두에 결합하는 것을 억제하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said PD-L1 binding antagonist inhibits the binding of PD-L1 to PD-1, B7-1, or both PD-1 and B7-1, anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use .
456. 구현예 453 내지 구현예 455 중 어느 한 구현예에 있어서,456. The method according to any one of embodiments 453-455,
상기 PD-L1 결합 길항제는 항 PD-L1 길항제 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457. 구현예 456에 있어서,457. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
458. 구현예 457에 있어서,458. The method of embodiment 457,
상기 항 PD-L1 길항제 항체는 아테졸리주맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-PD-L1 antagonist antibody is atezolizumab.
459. 구현예 456에 있어서,459. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 하기의 HVR들:The anti-PD-L1 antagonist antibody has the following HVRs:
GFTFSDSWIH(서열번호 20)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
AWISPYGGSTYYADSVKG(서열번호 21)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
RHWPGGFDY(서열번호 22)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
RASQDVSTAVA(서열번호 23)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
SASFLYS(서열번호 24)의 아미노산 서열을 포함하는 HVR-L2; 및HVR-L2 comprising the amino acid sequence of SASFLYS (SEQ ID NO: 24); and
QQYLYHPAT(서열번호 25)의 아미노산 서열을 포함하는 HVR-L3을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising HVR-L3 comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
460. 구현예 459에 있어서,460. The method of embodiment 459,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) 서열번호 27의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(c) an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a VH domain as in case (a) and a VL domain as in case (b).
461. 구현예 460에 있어서,461. The method of embodiment 460,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and
(b) 서열번호 27의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a VL domain comprising the amino acid sequence of SEQ ID NO:27.
462. 구현예 461에 있어서,462. The method of embodiment 461,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 28의 아미노산 서열을 포함하는 중쇄; 및(a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 28; and
(b) 서열번호 29의 아미노산 서열을 포함하는 경쇄를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, comprising a light chain comprising the amino acid sequence of SEQ ID NO:29.
463. 구현예 459 내지 구현예 462 중 어느 한 구현예에 있어서,463. The method according to any one of embodiments 459 to 462,
상기 항 PD-L1 길항제 항체는 단일클론 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-PD-L1 antagonist antibody is a monoclonal antibody, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
464. 구현예 459 내지 구현예 463 중 어느 한 구현예에 있어서,464. The method of any one of embodiments 459 to 463,
상기 항 PD-L1 길항제 항체는 인간화 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-PD-L1 antagonist antibody is a humanized antibody.
465. 구현예 463 또는 구현예 464에 있어서,465. The method of embodiment 463 or embodiment 464,
상기 항 PD-L1 길항제 항체는 전장 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-PD-L1 antagonist antibody is a full-length antibody.
466. 구현예 459 내지 구현예 464 중 어느 한 구현예에 있어서,466. The method according to any one of embodiments 459 to 464,
상기 항 PD-L1 길항제 항체는 Fab, Fab’, Fab’-SH, Fv, scFv, 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 PD-L1에 결합하는 항체 단편인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the anti-PD-L1 antagonist antibody is an antibody fragment that binds to PD-L1 selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab')2 fragments. Antibodies and PD-1 axis binding antagonists.
467. 구현예 459 내지 구현예 465 중 어느 한 구현예에 있어서,467. The method according to any one of embodiments 459 to 465,
상기 항 PD-L1 길항제 항체는 IgG 부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said anti-PD-L1 antagonist antibody is an IgG class antibody.
468. 구현예 467에 있어서,468. The method of embodiment 467,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said IgG class antibody is an IgG1 subclass antibody.
469. 구현예 452에 있어서,469. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-1 결합 길항제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 axis binding antagonist is a PD-1 binding antagonist.
470. 구현예 469에 있어서,470. The method of embodiment 469,
상기 PD-1 결합 길항제는 PD-1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 binding antagonist inhibits binding of PD-1 to one or more of its ligand binding partners.
471. 구현예 470에 있어서,471. The method of embodiment 470,
상기 PD-1 결합 길항제는 PD-L1이 PD-L1, PD-L2, 또는 PD-L1 및 PD-L2 둘 모두에 결합하는 것을 억제하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said PD-1 binding antagonist inhibits PD-L1 from binding to PD-L1, PD-L2, or both PD-L1 and PD-L2. .
472. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,472. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 항 PD-1 길항제 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473. 구현예 472에 있어서,473. The method of embodiment 472,
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenpulimab, CS1003, HLX10, SCT-I10A, gimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, For use which is HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21 Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists.
474. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,474. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 Fc 융합 단백질인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the PD-1 binding antagonist is an Fc fusion protein.
475. 구현예 474에 있어서,475. The method of embodiment 474,
상기 Fc 융합 단백질은 AMP-224인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The Fc fusion protein is AMP-224, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
476. 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127 및 구현예 309 내지 구현예 312중 어느 한 구현예에 있어서,476. The method of any one of embodiments 80-112, 114-127 and 309-312,
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects an anti TIGIT antagonist antibody and PD-1 formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks. Axial binding antagonists.
477. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,477. Embodiment 51, Embodiment 54,
상기 방법은 3주마다 약 600 mg 용량의 투여를 위한 제형화된 항 TIGIT 길항제 항체를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject an anti TIGIT antagonist antibody formulated for administration at a dose of about 600 mg every three weeks.
478. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 309, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,478. Embodiment 51, Embodiment 54,
상기 방법은 상기 항 TIGIT 길항제 항체를 대상체의 체중에 기초한 단계적 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 하기의 체중으로서: The method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects in stepwise doses based on the body weight of said subject, wherein said subject has a body weight of:
(a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg 용량의 투여를 위해 제형화되고; (a) weighing no more than 15 kg, wherein the anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg every 3 weeks;
(b) 15 kg 초과 및 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg 용량의 투여를 위해 제형화되거나; 또는 (b) greater than 15 kg and less than or equal to 40 kg, wherein the anti-TIGIT antagonist antibody is formulated for administration at a dose of about 400 mg every 3 weeks; or
(c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg 용량의 투여를 위해 제형화되는. 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제. (c) greater than 40 kg, wherein said anti TIGIT antagonist antibody is formulated for administration at a dose of about 600 mg every 3 weeks. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
479. 구현예 47, 구현예 48, 구현예 77, 구현예 78, 구현예 82, 및 구현예 83 중 어느 한 구현예에 있어서,479. The embodiment of any one of
상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects an anti TIGIT antagonist antibody and PD-1 formulated for administration at a dose of about 700 mg to about 1000 mg every 4 weeks. Axial binding antagonists.
480. 구현예 47, 구현예 48, 구현예 59, 구현예 67, 구현예 323, 및 구현예 479 중 어느 한 구현예에 있어서,480. The embodiment of any one of
상기 방법은 4주마다 약 840 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject an anti TIGIT antagonist antibody formulated for administration at a dose of about 840 mg every 4 weeks.
481. 구현예 49, 구현예 50, 및 구현예 104 중 어느 한 구현예에 있어서,481. The embodiment of any one of
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects an anti TIGIT antagonist antibody and PD-1 formulated for administration at a dose of about 300 mg to about 600 mg every two weeks. Axial binding antagonists.
482. 구현예 49, 구현예 50, 구현예 227, 구현예 251 내지 구현예 253, 구현예 255, 및 구현예 481 중 어느 한 구현예에 있어서,482. The embodiment of any one of
상기 방법은 2주마다 약 420 mg 용량의 투여를 위해 제형화된 항 TIGIT 길항제 항체를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject an anti TIGIT antagonist antibody formulated for administration at a dose of about 420 mg every two weeks.
483. 구현예 47 내지 구현예 482 중 어느 한 구현예에 있어서,483. The method according to any one of embodiments 47 to 482,
상기 항 TIGIT 길항제 항체의 용량은 고정 용량인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the dose of said anti-TIGIT antagonist antibody is a fixed dose.
484. 구현예 54, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 27 내지 구현예 2698 중 어느 한 구현예에 있어서,484. The embodiment of any one of
상기 방법은 3주마다 약 900 mg 내지 약 1500 mg 용량의 투여를 위해 제형화된 Pd-1축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects a Pd-1 axis binding antagonist formulated for administration at a dose of about 900 mg to about 1500 mg every 3 weeks. -1 axis binding antagonists.
485. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 172, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301 내지 구현예 303, 구현예 309, 구현예 311, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372 내지 구현예 375, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 405, 구현예 417, 구현예 420, 구현예 421, 및 구현예 484 중 어느 한 구현예에 있어서,485. embodiment 54,
상기 방법은 3주마다 약 1200 mg 용량의 투여를 위한 제형화된 PD-1 축 결합 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject a PD-1 axis binding antagonist formulated for administration at a dose of about 1200 mg every 3 weeks.
486. 구현예 47, 구현예 50, 구현예 80 내지 구현예 109, 및 구현예 324 중 어느 한 구현예에 있어서,486. The embodiment of any one of
상기 방법은 4주마다 약 1400 mg 내지 약 2000 mg 용량의 투여를 위해 제형화된 PD-1축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects an anti-TIGIT antagonist antibody and PD formulated for administration at a dose of about 1400 mg to about 2000 mg every 4 weeks to the subject or population of subjects. -1 axis binding antagonists.
487. 구현예 47, 구현예 50, 구현예 59, 구현예 67, 구현예 324, 및 구현예 479 중 어느 한 구현예에 있어서,487. The embodiment of any one of
상기 방법은 4주마다 약 1680 mg 용량의 투여를 위해 제형화된 항 PD-1 축 결합 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject an anti-PD-1 axis binding antagonist formulated for administration at a dose of about 1680 mg every 4 weeks.
488. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 481 중 어느 한 구현예에 있어서,488. The method of any one of
상기 방법은 2주마다 약 600 mg 내지 약 1200 mg 용량의 투여를 위해 제형화된 PD-1축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises administering to the subject or population of subjects an anti-TIGIT antagonist antibody and PD formulated for administration of a dose of about 600 mg to about 1200 mg every two weeks to the subject or population of subjects. -1 axis binding antagonists.
489. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 구현예 227, 구현예 251 내지 구현예 253, 및 구현예 481 중 어느 한 구현예에 있어서,489. The embodiment of any one of
상기 방법은 2주마다 약 840 mg 용량의 투여를 위해 제형화된 항 PD-1 축 결합 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject an anti-PD-1 axis binding antagonist formulated for administration at a dose of about 840 mg every two weeks.
490. 구현예 47 내지 구현예 489 중 어느 한 구현예에 있어서,490. The method according to any one of embodiments 47 to 489,
상기 PD-1 축 결합 길항제의 용량은 고정 용량인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the dose of the PD-1 axis binding antagonist is a fixed dose.
491. 구현예 60 또는 구현예 61에 있어서,491. The method of
상기 방법은 펨브롤리주맙을 3주마다 약 200 mg 또는 6주마다 400 mg의 고정 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, the method comprising administering to the subject pembrolizumab at a fixed dose of about 200 mg every 3 weeks or 400 mg every 6 weeks.
492. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65, 구현예 80 내지 구현예 109, 및 구현예 191 중 어느 한 구현예에 있어서,492. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 21일인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein each of said one or more dosing cycles is 21 days in length.
493. 구현예 47, 구현예 59, 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,493. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 28일인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein each of said one or more dosing cycles is 28 days in length.
494. 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,494. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 14일인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein each of said one or more dosing cycles is 14 days in length.
495. 구현예 47 내지 구현예 494 중 어느 한 구현예에 있어서,495. The method according to any one of embodiments 47 to 494,
상기 방법은 상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said anti TIGIT antagonist antibody to said subject or population of subjects on about
496. 구현예 47 내지 구현예 495 중 어느 한 구현예에 있어서,496. The method according to any one of embodiments 47 to 495,
상기 방법은 상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects on about
497. 구현예 321 또는 구현예 493에 있어서,497. according to embodiment 321 or embodiment 493,
상기 방법은 상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said anti TIGIT antagonist antibody to said subject on about 15 days of each of said one or more dosing cycles.
498. 구현예 321 또는 구현예 493에 있어서,498. The method of embodiment 321 or embodiment 493,
상기 방법은 상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said PD-1 axis binding antagonist to said subject on about 15 days of each of said one or more dosing cycles.
499. 구현예 47 내지 구현예 498 중 어느 한 구현예에 있어서,499. The method according to any one of embodiments 47 to 498,
상기 방법은 상기 항 TIGIT 길항제 항체 전에 상기 PD-1 축 결합 길항제를 또는 상기 PD-1 축 결합 길항제 전에 상기 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering to said subject or population of subjects said anti-TIGIT antagonist antibody prior to said anti-TIGIT antagonist antibody or said anti-TIGIT antagonist antibody prior to said PD-1 axis binding antagonist or said PD-1 axis binding antagonist. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
500. 구현예 499에 있어서,500. The method of embodiment 499,
상기 방법은 상기 PD-1 축 결합 길항제 또는 상기 항 TIGIT 길항제 항체의 투여 후 제1 관찰 기간을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises a first observation period following administration of said PD-1 axis binding antagonist or said anti TIGIT antagonist antibody.
501. 구현예 500에 있어서,501. The method of
상기 제1 관찰 기간은 약 30분 내지 약 60분의 길이인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said first observation period is between about 30 minutes and about 60 minutes in length.
502. 구현예 500 또는 구현예 501에 있어서,502. The method of
상기 방법은 상기 항 TIGIT 길항제 항체 또는 상기 PD-1 축 결합 길항제의 투여 후 제2 관찰 기간을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises a second observation period following administration of said anti-TIGIT antagonist antibody or said PD-1 axis binding antagonist.
503. 구현예 502에 있어서,503. The method of embodiment 502,
상기 제2 관찰 기간은 약 30분 내지 약 60분의 길이인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said second observation period is between about 30 minutes and about 60 minutes in length.
504. 구현예 47 내지 구현예 503 중 어느 한 구현예에 있어서,504. The method of any one of embodiments 47 to 503,
상기 방법은 상기 항 TIGIT 길항제 항체와 동시에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects concurrently with said anti TIGIT antagonist antibody.
505. 구현예 47 내지 구현예 504 중 어느 한 구현예에 있어서,505. The method of any one of embodiments 47 to 504,
상기 방법은 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 정맥내 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said method comprises intravenously administering said anti TIGIT antagonist antibody and PD-1 axis binding antagonist to said subject or population of subjects.
506. 구현예 505에 있어서,506. The method of embodiment 505,
상기 방법은 상기 PD-1 축 결합 길항제를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes over an anti TIGIT antagonist antibody and PD -1 axis binding antagonists.
507. 구현예 505 또는 구현예 506에 있어서,507. The method of embodiment 505 or embodiment 506,
상기 방법은 상기 항 TIGIT 길항제 항체를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said anti TIGIT antagonist antibody to said subject or population of subjects by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes over an anti TIGIT antagonist antibody and PD-1 Axial binding antagonists.
508. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 507 중 어느 한 구현예에 있어서,508. The method of any one of embodiments 47-114 and 116-507,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플의 PD-L1 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the level of PD-L1 expression in said subject or a tumor sample obtained from said subjects is determined.
509. 구현예 508에 있어서,509. The method of embodiment 508,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
510. 구현예 509에 있어서,510. The method of embodiment 509,
상기 PD-L1의 검출 가능한 발현 수준은 PD-L1의 검출 가능한 단백질 발현 수준인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1.
511. 구현예 510에 있어서,511. The method of embodiment 510,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable protein expression level of PD-L1 is determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody suitable for staining, anti-TIGIT antagonist antibody for use and the PD-1 axis binding antagonists.
512. 구현예 511에 있어서,512. The method of embodiment 511,
염색에 적합한 상기 항 PD-L1 항체는 상기 항 PD-L1 항체 SP263, SP142, 22C3 또는 28-8인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-PD-L1 antibody suitable for staining is said anti-PD-L1 antibody SP263, SP142, 22C3 or 28-8, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
513. 구현예 511 또는 구현예 512에 있어서,513. The method of embodiment 511 or embodiment 512,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 벤타나(Ventana) SP263 IHC 분석, 팜(pharm)Dx 22C3 IHC 분석, 벤타나 SP142 IHC 분석, 또는 팜Dx 28-8 IHC 분석을 사용하여 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable protein expression level of PD-L1 is determined using a Ventana SP263 IHC assay, a pharmDx 22C3 IHC assay, a Ventana SP142 IHC assay, or a PalmDx 28-8 IHC assay. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for
514. 구현예 47 내지 구현예 109, 구현예 188, 구현예 220 내지 구현예 265, 및 구현예 307 내지 구현예 423 중 어느 한 구현예에 있어서,514. The embodiment of any of embodiments 47 to 109, 188, 220 to 265, and embodiments 307 to 423,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 is determined by IHC analysis comprising staining with the anti-PD-L1 antibody SP263.
515. 구현예 47 내지 구현예 220, 구현예 265 내지 구현예 338, 및 구현예 370 내지 구현예 423 중 어느 한 구현예에 있어서,515. The embodiment of any one of embodiments 47 to 220, 265 to 338, and embodiments 370 to 423,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 is determined by IHC analysis comprising staining with the anti-PD-L1 antibody SP142.
516. 구현예 47 내지 구현예 113, 구현예 136 내지 구현예 187, 및 구현예 220 내지 구현예 423 중 어느 한 구현예에 있어서,516. The embodiment of any of embodiments 47 to 113, 136 to 187, and any of embodiments 220 to 423,
항 PD-L1 항체 22C3으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 22C3 is determined.
517. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 423 중 어느 한 구현예에 있어서,517. The method of any one of embodiments 47 to 114 and embodiments 116 to 423,
항 PD-L1 항체 28-8로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 28-8 is determined.
518. 구현예 514에 있어서,518. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the tumor sample.
519. 구현예 514에 있어서,519. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 5% 이상 및 20% 미만인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a TIC of greater than or equal to 5% and less than 20% in the tumor sample.
520. 구현예 514에 있어서,520. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% in the tumor sample.
521. 구현예 514에 있어서,521. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 20% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a TIC of at least 20% in the tumor sample.
522. 구현예 514에 있어서,522. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상 및 50% 미만인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a TIC of greater than or equal to 10% and less than 50% in the tumor sample.
523. 구현예 514에 있어서,523. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 50% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a TIC of at least 50% in the tumor sample.
524. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,524. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 1% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is at least 1% of a fraction of PD-L1 positive tumor cells.
525. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,525. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 30% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is at least 30% of a fraction of PD-L1 positive tumor cells.
526. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,526. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 1% 이상 50% 미만인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% and less than 50% of a fraction of PD-L1 positive tumor cells.
527. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,527. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 is at least 50% of a fraction of PD-L1 positive tumor cells.
528. 구현예 515에 있어서,528. The method of embodiment 515,
상기 PD-L1 양성 종양 세포 분획은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the PD-L1-positive tumor cell fraction is a proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC).
529. 구현예 515에 있어서,529. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 1% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 1%.
530. 구현예 515에 있어서,530. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 5% 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 5%.
531. 구현예 516에 있어서,531. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 복합 양성 점수(CPS)가 1 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the detectable protein expression level of PD-L1 has a composite positive score (CPS) of 1 or greater.
532. 구현예 516에 있어서,532. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 10 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable protein expression level of PD-L1 is a CPS of 10 or more, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
533. 구현예 516에 있어서,533. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 20 이상인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable protein expression level of PD-L1 is a CPS of 20 or more, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
534. 구현예 528 내지 구현예 530 중 어느 한 구현예에 있어서,534. The method of any one of embodiments 528 to 530,
상기 IHC 분석은 벤타나 SP142 IHC 분석인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the IHC assay is a Ventana SP142 IHC assay.
535. 구현예 509에 있어서,535. The method of embodiment 509,
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 핵산 발현 수준인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1.
536. 구현예 535에 있어서,536. The method of embodiment 535,
상기 PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정된, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof. Antibodies and PD-1 axis binding antagonists.
537. 구현예 47 내지 구현예 423 중 어느 한 구현예에 있어서, 537. The method according to any one of embodiments 47 to 423,
상기 치료는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가 및/또는 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가를 유발하는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said treatment results in an increase in overall survival (OS) of said subject compared to baseline OS time and/or an increase in progression free survival (PFS) in said subject compared to baseline PFS time. uniaxial binding antagonists.
538. 구현예 537에 있어서, 538. The method of embodiment 537,
(a) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값이고; 그리고/또는 (a) said baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist; and/or
(b) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값인, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.(b) the baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
539. 구현예 52, 구현예 158, 및 구현예 228 중 어느 한 구현예에 있어서,539. The embodiment of any one of embodiments 52, 158, and 228,
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
540. 구현예 539에 있어서,540. The method of embodiment 539,
상기 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541. 구현예 69, 구현예 92, 구현예 127, 구현예 131, 구현예 249, 및 구현예 540에 있어서,541. The method of embodiment 69, embodiment 92, embodiment 127, embodiment 131, embodiment 249, and embodiment 540,
상기 카보플라틴은 AUC = 5 mg/ml/분 또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min or AUC=6 mg/ml/min.
542. 구현예 69, 구현예 127, 구현예 162, 구현예 164, 구현예 166, 구현예 168, 및 구현예 540에 있어서,542. The method of embodiment 69, embodiment 127, embodiment 162, embodiment 164, embodiment 166, embodiment 168, and embodiment 540,
상기 시스플라틴은 약 75 mg/m2 또는 80 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said cisplatin is formulated for administration at a dose of about 75 mg/m2 or 80 mg/m2.
543. 구현예 539 내지 구현예 542 중 어느 한 구현예에 있어서,543. The method of any one of embodiments 539 to 542,
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one non-platinum-based chemotherapeutic agent is an antimetabolite, a taxane, or a topoisomerase II inhibitor.
544. 구현예 62, 구현예 173, 구현예 174, 및 구현예 543 중 어느 한 구현예에 있어서,544. The embodiment of any one of embodiments 62, 173, 174, and 543,
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
545. 구현예 69, 구현예 127, 구현예 162, 및 구현예 544 중 어느 한 구현예에 있어서,545. The embodiment of any one of embodiments 69, 127, 162, and 544,
상기 페메트렉시드는 약 500 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein said pemetrexed is formulated for administration at a dose of about 500 mg/m2.
546. 구현예 63, 구현예 64, 구현예 162, 구현예 398, 및 구현예 544 중 어느 한 구현예에 있어서,546. The embodiment of any one of
상기 젬시타빈은 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use, wherein said gemcitabine is formulated for administration at a dose of about 1000 mg/m2 or about 1250 mg/m2.
547. 구현예 544에 있어서,547. The method of embodiment 544,
상기 항대사물질은 카페시타빈인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein the antimetabolite is capecitabine, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
548. 구현예 544 또는 구현예 547에 있어서,548. The method of embodiment 544 or embodiment 547,
상기 카페시타빈은 약 1250 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said capecitabine is formulated for administration at a dose of about 1250 mg/m2.
549. 구현예 173, 구현예 174, 구현예 229, 구현예 230, 구현예 239, 구현예 240, 및 구현예 543 내지 구현예 548 중 어느 한 구현예에 있어서,549. The embodiment of any one of embodiments 173, 174, 229, 230, 239, 240, and 543 to 548,
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said taxane is paclitaxel or nap-paclitaxel.
550. 구현예 69, 구현예 162, 및 구현예 549 중 어느 한 구현예에 있어서,550. The method of any one of embodiments 69, 162, and 549,
상기 파클리탁셀은 약 175 mg/m2 또는 약 200 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said paclitaxel is formulated for administration at a dose of about 175 mg/m2 or about 200 mg/m2.
551. 구현예 63, 구현예 64, 구현예 249, 구현예 398, 및 구현예 549 중 어느 한 구현예에 있어서,551. The embodiment of any one of
상기 냅-파클리탁셀은 약 100 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said nap-paclitaxel is formulated for administration at a dose of about 100 mg/m2.
552. 구현예 80 내지 구현예 91, 구현예 229, 구현예 230, 구현예 239, 구현예 241, 구현예 251 내지 구현예 255, 및 구현예 543항 내지 구현예 551 중 어느 한 구현예에 있어서,552. The embodiment of any one of embodiments 80-91, 229, 230, 239, 241, 251, 255, and 543-551. ,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
553. 구현예 69, 구현예 92, 및 구현예 552 중 어느 한 구현예에 있어서,553. The embodiment of any one of embodiments 69, 92, and 552,
상기 에토포시드는 약 100 mg/m2 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said etoposide is formulated for administration at a dose of about 100 mg/m2.
554. 구현예 543 내지 구현예 553 중 어느 한 구현예에 있어서,554. The method of any one of embodiments 543 to 553,
상기 하나 이상의 화학요법제는 각각 매주 1회, 2주마다 1회, 3주마다 1회, 3주마다 2회, 4주마다 1회, 4주마다 2회, 또는 4주마다 3회 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The one or more chemotherapeutic agents are each administered once every week, once every 2 weeks, once every 3 weeks, twice every 3 weeks, once every 4 weeks, twice every 4 weeks, or 3 times every 4 weeks. , anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
555. 구현예 543 내지 구현예 554 중 어느 한 구현예에 있어서,555. The method of any one of embodiments 543 to 554,
상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 제 1일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is administered on
556. 구현예 544 내지 구현예 555 중 어느 한 구현예에 있어서,556. The method of any one of embodiments 544 to 555,
상기 젬시타빈은 4주마다 3회 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the gemcitabine is administered 3 times every 4 weeks.
557. 구현예 544 내지 구현예 556 중 어느 한 구현예에 있어서,557. The method of any one of embodiments 544 to 556,
상기 젬시타빈은 1회 이상의 투약 주기의 제 1일, 8일, 및/또는 15일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said gemcitabine is administered on
558. 구현예 544 내지 구현예 557 중 어느 한 구현예에 있어서,558. The method of any one of embodiments 544 to 557,
상기 카페시타빈은 2주 동안 매일 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said capecitabine is administered daily for 2 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
559. 구현예 544 내지 구현예 558 중 어느 한 구현예에 있어서,559. The method according to any one of embodiments 544 to 558,
상기 카페시타빈은 1회 이상의 투약 주기의 제 1일 내지 14일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said capecitabine is administered on
560. 구현예 549 내지 구현예 559 중 어느 한 구현예에 있어서,560. The method of any one of embodiments 549 to 559,
상기 냅-파클리탁셀은 4주마다 3회 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said nap-paclitaxel is administered three times every four weeks.
561. 구현예 549 내지 구현예 560 중 어느 한 구현예에 있어서,561. The method of any one of embodiments 549 to 560,
상기 냅-파클리탁셀은 1회 이상의 투약 주기의 제 1일, 8일, 및 15일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said nap-paclitaxel is administered on
562. 구현예 552 내지 구현예 561 중 어느 한 구현예에 있어서,562. The method of any one of embodiments 552 to 561,
상기 에토포시드는 3주마다 1일 내지 3일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said etoposide is administered on
563. 구현예 552 내지 구현예 562 중 어느 한 구현예에 있어서,563. The method of any one of embodiments 552 to 562,
상기 에토포시드는 1회 이상의 투약 주기의 제 1일 내지 3일에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said etoposide is administered on days 1-3 of one or more dosing cycles.
564. 구현예 543 내지 구현예 563 중 어느 한 구현예에 있어서,564. The method of any one of embodiments 543 to 563,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이전에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is administered prior to said PD-1 axis binding antagonist and/or said anti TIGIT antagonist antibody.
565. 구현예 543 내지 구현예 564 중 어느 한 구현예에 있어서,565. The method of any one of embodiments 543 to 564,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이후에 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti TIGIT antagonist antibody.
566. 구현예 543 내지 구현예 565 중 어느 한 구현예에 있어서,566. The method of any one of embodiments 543 to 565,
상기 하나 이상의 화학요법제는 정맥내 또는 경구로 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said at least one chemotherapeutic agent is administered intravenously or orally.
567. 구현예 65, 구현예 310, 및 구현예 311 중 어느 한 구현예에 있어서,567. The embodiment of any one of
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
568. 구현예 312 또는 구현예 567에 있어서,568. The method of embodiment 312 or embodiment 567,
상기 VEGF 길항제는 3주마다 약 10 mg/kg 내지 약 20 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 10 mg/kg to about 20 mg/kg every 3 weeks.
569. 구현예 318 또는 구현예 568에 있어서,569. The method of embodiment 318 or embodiment 568,
상기 VEGF 길항제는 3주마다 약 15 mg/kg 용량의 투여를 위해 제형화되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is formulated for administration at a dose of about 15 mg/kg every 3 weeks.
570. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 569중 어느 한 구현예에 있어서,570. The embodiment of any one of
상기 VEGF 길항제는 항 VEGF 항체인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The VEGF antagonist is an anti-VEGF antibody, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
571. 구현예 570에 있어서,571. The method of embodiment 570,
상기 항 VEGF 항체는 베바시주맙의 VH 도메인 및 VL 도메인을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-VEGF antibody comprises a VH domain and a VL domain of bevacizumab, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use.
572. 구현예 570 또는 구현예 571에 있어서,572. The method of embodiment 570 or embodiment 571,
상기 항 VEGF 항체는 베바시주맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-VEGF antibody is bevacizumab, anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use.
573. 구현예 65, 구현예 310 내지 구현예 312, 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,573. The embodiment of any one of
상기 항 TIGIT 길항제 항체는 티라골루맙이고, 상기 PD-1 축 결합 길항제는 아테졸리주맙이며, 상기 VEGF 길항제는 베바시주맙인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The anti-TIGIT antagonist antibody is tiragolumab, the PD-1 axis binding antagonist is atezolizumab, and the VEGF antagonist is bevacizumab.
574. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 573 중 어느 한 구현예에 있어서,574. The embodiment of any one of
상기 방법은 1회 이상의 투약 주기의 제 1일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said method comprises administering said VEGF antagonist to said subject on
575. 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,575. The method of any one of embodiments 318 to 320,
상기 방법은 1회 이상의 투약 주기의 15일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein said method comprises administering said VEGF antagonist to said subject on
576. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 575 중 어느 한 구현예에 있어서,576. The embodiment of any one of
상기 VEGF 길항제는 정맥내 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the VEGF antagonist is administered intravenously.
577. 구현예 576에 있어서,577. The method of embodiment 576,
상기 VEGF 길항제는 90 ± 15분에 걸쳐 정맥내 주입으로 상기 대상체에게 투여되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said VEGF antagonist is administered to said subject by intravenous infusion over 90±15 minutes.
578. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 577 중 어느 한 구현예에 있어서,578. The embodiment of any one of
상기 방법은 상기 VEGF 길항제 이전에 상기 PD-1 축 결합 길항제, 및 상기 항 TIGIT 길항제 항체 이전에 상기 VEGF 길항제를 상기 대상체에 투여하는 단계를 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said method comprises administering said PD-1 axis binding antagonist prior to said VEGF antagonist, and said VEGF antagonist prior to said anti TIGIT antagonist antibody to said subject, anti TIGIT antagonist antibody and PD-1 axis for use binding antagonists.
579. 구현예 578에 있어서,579. The method of embodiment 578,
상기 방법은 상기 PD-1 축 결합 길항제 투여 후 제1 관찰 기간, 상기 VEGF 길항제 투여 후 제2 관찰 기간, 및 상기 항 TIGIT 길항제 항체 투여 후 제3 관찰 기간을 포함하는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.The method comprises a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody. and PD-1 axis binding antagonists.
580. 구현예 579에 있어서,580. The method of embodiment 579,
상기 제1 관찰 기간, 상기 제2 관찰 기간, 및 상기 제3 관찰 기간은 각각 약 30분 내지 약 120분의 길이인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said first observation period, said second observation period, and said third observation period are each about 30 minutes to about 120 minutes in length.
581. 구현예 113, 구현예 128, 구현예 129 내지 구현예 131, 구현예 175 내지 구현예 182, 구현예 210 내지 구현예 214, 구현예 221, 구현예 256, 구현예 257, 구현예 270, 구현예 289, 구현예 290, 구현예 293, 구현예 294, 구현예 297, 구현예 298, 구현예 333, 구현예 362 내지 구현예 365, 구현예 385, 구현예 386, 구현예 389, 구현예 393, 구현예 419, 및 구현예 422 중 어느 한 구현예에 있어서,581. Embodiment 113, Embodiment 128, Embodiment 129 to Embodiment 131, Embodiment 175 to Embodiment 182, Embodiment 210 to Embodiment 214, Embodiment 221, Embodiment 256, Embodiment 257, Embodiment 270, Embodiment 289, Embodiment 290, Embodiment 293, Embodiment 294, Embodiment 297, Embodiment 298, Embodiment 333, Embodiment 362 to Embodiment 365, Embodiment 385, Embodiment 386, Embodiment 389, Embodiment 393, embodiment 419, and embodiment 422 according to any one of embodiments,
티라골루맙 및 아테졸리주맙은 투여 이전에 IV 백(bag)에 결합되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein tiragolumab and atezolizumab are bound to an IV bag prior to administration.
582. 구현예 47 내지 구현예 581 중 어느 한 구현예에 있어서,582. The method according to any one of embodiments 47 to 581,
상기 대상체는 인간인, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use, wherein the subject is a human.
583. 구현예 47 내지 구현예 582 중 어느 한 구현예에 있어서,583. The method according to any one of embodiments 47 to 582,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in separate formulations.
584. 구현예 47 내지 구현예 582 중 어느 한 구현예에 있어서,584. The method according to any one of embodiments 47 to 582,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 사용을 위한 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in a single dosage form.
구현예 세트 C:Implementation Set C:
1. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,1. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks, a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and 3 A use comprising administering to the subject a dosing regimen comprising at least one dosing cycle of a non-platinum-based chemotherapeutic agent per week.
2. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,2. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체, 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks, and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. Use comprising administering to a subject.
3. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,3. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks. use comprising administering to the subject.
4. 구현예 2 또는 구현예 3에 있어서,4. according to
상기 방법은 하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 사용.The method further comprises administering to the subject one or more chemotherapeutic agents.
5. 구현예 1 내지 구현예 4 중 어느 한 구현예에 있어서,5. The method according to any one of
상기 항 TIGIT 길항제 항체는 IgG 부류 항체, 특히 IgG1 하위부류 항체인, 사용.wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6. 구현예 1 내지 구현예 5 중 어느 한 구현예에 있어서,6. The method according to any one of
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
(a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
(d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
(f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3을 포함하는, 사용.(f) use comprising HVR-L3 comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
7. 구현예 1 내지 구현예 6 중 어느 한 구현예에 있어서,7. The method according to any one of
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR): The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
(a) DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
(d) FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4, 및(d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and
하기의 중쇄 가변 영역 FR들:The following heavy chain variable region FRs:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
(b) WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
(d) WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 사용.(d) use, further comprising FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
8. 구현예 1 내지 구현예 7 중 어느 한 구현예에 있어서,8. The method according to any one of
상기 항 TIGIT 길항제 항체는:The anti-TIGIT antagonist antibody comprises:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용.(c) a use comprising a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19.
9. 구현예 1 내지 구현예 8 중 어느 한 구현예에 있어서,9. The method according to any one of
상기 항 TIGIT 길항제 항체는 티라골루맙인, 사용.wherein the anti-TIGIT antagonist antibody is tyragolumab.
10. 구현예 1 내지 구현예 9 중 어느 한 구현예에 있어서,10. The method according to any one of
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제 또는 PD-1 결합 길항제인, 사용.wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
11. 구현예 1 내지 구현예 10 중 어느 한 구현예에 있어서,11. The method according to any one of
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체인, 사용.The use wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
12. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,12. The method according to any one of
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체인, 사용.The use of
13. 구현예 12에 있어서,13. The method of
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 사용.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636, used.
14. 구현예 1 내지 구현예 13 중 어느 한 구현예에 있어서,14. The method according to any one of
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 사용.wherein the PD-1 axis binding antagonist is atezolizumab.
15. 구현예 1 내지 구현예 11 중 어느 한 구현예에 있어서,15. The method according to any one of
상기 PD-1 축 결합 길항제는 항 PD-1 길항제 항체인, 사용.The use of
16. 구현예 15에 있어서,16. The method of
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 사용.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21, for use.
17. 구현예 2 내지 구현예 16 중 어느 한 구현예에 있어서,17. The method according to any one of
상기 방법은 유효량의 백금계 화학요법제 및 비백금계 화학요법제를 대상체에게 투여하는 단계를 포함하는, 방법.The method comprises administering to the subject an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
18. 구현예 1 또는 구현예 17에 있어서,18. according to
상기 비백금계 화학요법제는 토포이소머라제 II 억제제인, 사용.The non-platinum-based chemotherapeutic agent is a topoisomerase II inhibitor.
19. 구현예 18에 있어서,19. The method of
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331, 특히 에토포시드인, 사용.wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331, in particular etoposide; use.
20. 구현예 18 또는 구현예 19에 있어서,20. The method of
상기 토포이소머라제 II 억제제는 100 mg/m2 용량으로 투여되는, 사용.wherein the topoisomerase II inhibitor is administered at a dose of 100 mg/m2.
21. 구현예 17 내지 구현예 20 중 어느 한 구현예에 있어서,21. The method according to any one of
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴, 특히 카보플라틴인, 사용.wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin.
22. 구현예 17 내지 구현예 21 중 어느 한 구현예에 있어서,22. The method according to any one of
상기 백금계 화학요법제는 투여 당일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 사용.wherein the platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
23. 구현예 1 내지 구현예 22 중 어느 한 구현예에 있어서,23. The method according to any one of embodiments 1-22,
상기 방법은 유도기 및 유지기를 포함한 투약 요법을 포함하는, 방법.The method comprises a dosing regimen comprising an induction phase and a maintenance phase.
24. 구현예 23에 있어서,24. The method of
상기 유도기는 4회의 초기 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제가 4회의 초기 투약 주기의 각각에서 투여되는, 사용.wherein the induction phase comprises 4 initial dosing cycles and the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles.
25. 구현예 23 또는 구현예 24에 있어서,25. according to
상기 유지기는 상기 백금계 화학요법제 및/또는 비백금계 화학요법제의 투여를 포함하지 않는, 사용.wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent and/or the non-platinum-based chemotherapeutic agent.
26. 구현예 1 내지 구현예 25 중 어느 한 구현예에 있어서,26. The method according to any one of
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장하는, 사용.wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody.
27. 구현예 1 내지 구현예 26 중 어느 한 구현예에 있어서,27. The method according to any one of embodiments 1-26,
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 전체 생존을 연장하는, 사용.wherein said treatment prolongs the overall survival of said subject as compared to treatment without said anti-TIGIT antagonist antibody.
28. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,28. The method according to any one of
상기 암은 폐암인, 사용.wherein the cancer is lung cancer.
29. 구현예 28에 있어서,29. The method of
상기 폐암은 소세포 폐암(SCLC), 특히 확장기 SCLC(ES-SCLC)인, 사용.wherein the lung cancer is small cell lung cancer (SCLC), in particular expanded stage SCLC (ES-SCLC).
30. 구현예 28에 있어서,30. The method of
상기 폐암은 소세포 폐암(SCLC), 특히 국소 진행성 절제 불가능한 NSCLC(IIIB기 NSCLC)인, 사용.wherein the lung cancer is small cell lung cancer (SCLC), in particular locally advanced unresectable NSCLC (stage IIIB NSCLC).
31. 구현예 28에 있어서,31. The method of
상기 폐암은 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 사용.wherein the lung cancer is locally advanced unresectable or metastatic nonsquamous NSCLC.
32. 구현예 28에 있어서,32. The method of
상기 폐암은 절제 가능한 폐암인, 사용.wherein the lung cancer is resectable lung cancer.
33. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,33. The method according to any one of
상기 암은 자궁경부암인, 사용.wherein the cancer is cervical cancer.
34. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,34. The method according to any one of
상기 암은 초기 삼중음성 유방암(eTNBC)인, 사용.wherein the cancer is early triple negative breast cancer (eTNBC).
35. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,35. The method according to any one of
상기 암은 두경부암인, 사용.wherein the cancer is head and neck cancer.
36. 구현예 1 내지 구현예 27 중 어느 한 구현예있어서,36. The method of any one of
상기 암은 간암, 특히 간세포 암종(HCC)인, 사용.wherein the cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
37. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,37. The method according to any one of
상기 암은 방광암인, 사용.wherein the cancer is bladder cancer.
38. 구현예 37에 있어서,38. The method of
상기 암은 요로상피세포 암종(UC), 특히 전이성 요로상피세포 암종(mUC)인, 사용.wherein the cancer is urothelial cell carcinoma (UC), in particular metastatic urothelial cell carcinoma (mUC).
39. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,39. The method according to any one of
상기 암은 췌장암, 특히 췌장 관세포암(PDAC)인, 사용.wherein the cancer is pancreatic cancer, in particular pancreatic ductal cell carcinoma (PDAC).
40. 구현예 1 내지 구현예 27 중 어느 한 구현예에 있어서,40. The method according to any one of
상기 암은 식도암, 특히 진행성 또는 전이성 식도암인, 사용.wherein said cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
41. 암을 가진 대상체를 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용한 항 TIGIT 길항제 항체의 사용으로서,41. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, comprising:
상기 방법은 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks, a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and 3 A use comprising administering to the subject a dosing regimen comprising at least one dosing cycle of a non-platinum-based chemotherapeutic agent per week.
42. 암을 가진 대상체를 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용한 항 TIGIT 길항제 항체의 사용으로서,42. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, comprising:
상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체, 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks, and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. Use comprising administering to a subject.
43. 암을 가진 대상체를 치료하기 위한 약제의 제조에서 PD-1 축 결합 길항제와 병용한 항 TIGIT 길항제 항체의 사용으로서,43. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks. use comprising administering to the subject.
44. 암을 가진 대상체를 치료하기 위한 약제의 제조에서 항 TIGIT 길항제 항체와 병용한 PD-1 축 결합 길항제의 사용으로서,44. Use of a PD-1 axis binding antagonist in combination with an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject having cancer, comprising:
(a) 상기 방법은 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고; (b) 상기 방법은 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하거나; 또는 (c) 상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.(a) the method comprises a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks, a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks and administering to the subject a dosing regimen comprising at least one dosing cycle of a non-platinum-based chemotherapeutic agent every three weeks; (b) the method comprises one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. or administering to the subject; or (c) the method comprises one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks. use comprising administering a dosing regimen to the subject.
45. 구현예 44에 있어서,45. The method of
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
46. 구현예 44에 있어서,46. The method of
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
47. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,47. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체, 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks, and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks. use comprising administering to the subject.
48. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,48. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체, 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks, and a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every 2 weeks. use comprising administering to the subject.
49. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,49. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체, 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks, and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every two weeks. use comprising administering to the subject.
50. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,50. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체, 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks, and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks. use comprising administering to the subject.
51. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,51. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 및 6주마다 약 100 mg 내지 약 1000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, and a PD-1 axis binding antagonist at a dose of about 100 mg to about 1000 mg every 6 weeks. use comprising administering to the subject.
52. 구현예 47 내지 구현예 51 중 어느 한 구현예에 있어서,52. The method according to any one of embodiments 47 to 51,
상기 방법은 하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 사용.The method further comprises administering to the subject one or more chemotherapeutic agents.
53. 구현예 52에 있어서,53. The method of embodiment 52,
상기 방법은 백금계 화학요법제 및 비백금계 화학요법제를 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering to said subject a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
54. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,54. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and 3 A use comprising administering to the subject a dosing regimen comprising at least one dosing cycle of a non-platinum-based chemotherapeutic agent per week.
55. 구현예 53 또는 구현예 54에 있어서,55. according to embodiment 53 or embodiment 54,
상기 방법은 유도기 및 유지기를 포함하는, 사용.wherein the method comprises an induction phase and a maintenance phase.
56. 구현예 55에 있어서,56. The method of embodiment 55,
상기 유도기 및 유지기는 각각 1회 이상의 투약 주기를 포함하는, 사용.wherein the induction phase and maintenance phase each comprise one or more dosing cycles.
57. 구현예 55 또는 구현예 56에 있어서,57. according to embodiment 55 or embodiment 56,
상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용.wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent.
58. 구현예 55 내지 구현예 57 중 어느 한 구현예에 있어서,58. The method according to any one of embodiments 55 to 57,
상기 유지기는 상기 비백금계 화학요법제의 투여를 포함하지 않는, 사용.wherein the maintenance phase does not include administration of the non-platinum-based chemotherapeutic agent.
59. 구현예 58에 있어서,59. The method of embodiment 58,
상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하는, 사용.wherein said maintenance phase comprises one or more dosing cycles of anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks.
60. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,60. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks. administering to the subject, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
61. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,61. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 티라골루맙 및 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 100 mg 내지 약 1000 mg의 용량으로 투여되는, 사용.The method comprises administering to the subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein the pembrolizumab is administered at a dose of about 100 mg to about 1000 mg every 6 weeks. administered, use.
62. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,62. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dose of about 30 mg to about 1200 mg of anti-TIGIT antagonist antibody every 3 weeks, a dose of about 80 mg to about 1600 mg of PD-1 axis binding antagonist every 3 weeks, and 3 weeks of 2 weeks dosing/ 1 week washout. Use, comprising administering to the subject a dosing regimen comprising one or more dosing cycles of an antimetabolite at a dose of about 10 mg/m2 to about 10000 mg/m2 orally twice daily every time.
63. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,63. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 젬시타빈, 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises one or more doses of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, gemcitabine, and nap-paclitaxel. Use comprising administering to the subject a dosing regimen comprising a dosing cycle.
64. 구현예 52에 있어서,64. The method of embodiment 52,
상기 하나 이상의 화학요법제는 젬시타빈 및 냅-파클리탁셀인, 사용.wherein said at least one chemotherapeutic agent is gemcitabine and nap-paclitaxel.
65. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,65. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg의 용량의 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and about 1 mg/kg to about every 3 weeks. Use comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a VEGF antagonist at a dose of 35 mg/kg.
66. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,66. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용.(b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said maintenance wherein the phase does not include administration of said platinum-based chemotherapeutic agent.
67. 암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,67. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having cancer, comprising:
상기 방법은 유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) 상기 유도기는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) 상기 유지기는 4주마다 약 200 mg 내지 약 2000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 80 mg 내지 약 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는, 사용.(b) the maintenance phase comprises one or more additional dosing cycles of the anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks and wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent.
68. 구현예 56 내지 구현예 59, 구현예 66 및 구현예 67 중 어느 한 구현예에 있어서,68. The method of any one of embodiments 56-59, 66 and 67,
상기 유도기는 4 내지 6회의 투약 주기를 포함하는, 사용.wherein the induction phase comprises 4 to 6 dosing cycles.
69. 구현예 53 내지 구현예 59 및 구현예 66 내지 구현예 68 중 어느 한 구현예에 있어서,69. The method of any one of embodiments 53-59 and 66-68,
(a) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고;(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이거나; 또는(a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel; or
(c) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 에토포시드인, 사용.(c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is etoposide.
70. 구현예 47 내지 구현예 69 중 어느 한 구현예에 있어서,70. The method according to any one of embodiments 47 to 69,
상기 암은 고형 종양인, 사용. wherein the cancer is a solid tumor.
71. 구현예 47 내지 구현예 70 중 어느 한 구현예에 있어서,71. The method according to any one of embodiments 47 to 70,
상기 암은 국소 진행성 또는 전이성인, 사용.wherein the cancer is locally advanced or metastatic.
72. 구현예 47 내지 구현예 71 중 어느 한 구현예에 있어서,72. The method according to any one of embodiments 47 to 71,
상기 암은 폐암, 췌장암, 자궁경부암, 유방암, 두경부암, 간암, 방광암, 식도암, 위암, 결장직장암, 신장암, 신장암, 흑색종, 또는 난소암인, 사용.wherein said cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, kidney cancer, melanoma, or ovarian cancer.
73. 구현예 72에 있어서,73. The method of
상기 암은 폐암인, 사용.wherein the cancer is lung cancer.
74. 구현예 73에 있어서,74. The method of
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 NSCLC인, 사용.wherein the lung cancer is NSCLC, in particular locally advanced unresectable NSCLC.
75. 구현예 74에 있어서,75. The method of embodiment 74,
상기 NSCLC는 IIIB기 NSCLC인, 사용.wherein said NSCLC is stage IIIB NSCLC.
76. 구현예 73 내지 구현예 75 중 어느 한 구현예에 있어서,76. The method according to any one of
상기 폐암은 재발성 또는 전이성 NSCLC인, 사용.wherein the lung cancer is relapsed or metastatic NSCLC.
77. 구현예 76에 있어서,77. The method of
상기 NSCLC는 IV기 NSCLC인, 사용.wherein said NSCLC is stage IV NSCLC.
78. 구현예 77에 있어서,78. The method of embodiment 77,
상기 대상체는 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는, 사용.The subject has not previously been treated for stage IV NSCLC.
79. 구현예 73에 있어서,79. The method of
상기 폐암은 소세포 폐암(SCLC)인, 사용.wherein the lung cancer is small cell lung cancer (SCLC).
80. 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,80. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having lung cancer,
상기 방법은 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장시키는, 사용.The method comprises administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. wherein said treatment improves progression-free survival (PFS) of said subject as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. prolonged use.
81. 폐암을 가진 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,81. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a population of subjects having lung cancer, comprising:
상기 방법은 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하고, 상기 치료는 약 8.2개월 내지 약 9.2개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용.The method comprises administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. and wherein the treatment results in a median PFS of the subject population of about 8.2 months to about 9.2 months.
82. 구현예 80 또는 구현예 81에 있어서,82. The method of
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)을 연장시키는, 사용.wherein said treatment prolongs overall survival (OS) of said subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody; use.
83. 구현예 80 내지 구현예 82 중 어느 한 구현예에 있어서,83. The method according to any one of
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼 연장시키는, 사용.wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 2.4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , use.
84. 구현예 83에 있어서,84. The method of embodiment 83,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3개월 내지 약 4개월 만큼 연장시키는, 사용.wherein said treatment reduces the PFS of said subject or population of subjects by at least about 3 months to about 4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. Extending by months, use.
85. 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,85. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having lung cancer,
상기 방법은 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 OS를 연장시키는, 사용.The method comprises administering to the subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. wherein the treatment prolongs the OS of the subject as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor without the anti-TIGIT antagonist antibody.
86. 폐암을 가진 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,86. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a population of subjects having lung cancer, comprising:
상기 방법은 유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에 투여하는 단계를 포함하고, 상기 치료는 약 15.3개월 내지 약 17.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.The method comprises administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. and wherein the treatment results in a median OS in the subject population of about 15.3 months to about 17.6 months.
87. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,87. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼 연장시키는, 사용.wherein the treatment prolongs the OS of the subject or population of subjects by at least about 3.3 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , use.
88. 구현예 82 내지 구현예 86 중 어느 한 구현예에 있어서,88. The method according to any one of embodiments 82 to 86,
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3개월 내지 약 5.3개월 만큼 연장시키는, 사용.wherein said treatment reduces the OS of said subject or population of subjects by at least about 3 months to about 5.3 as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. Extending by months, use.
89. 구현예 80 내지 구현예 88 중 어느 한 구현예에 있어서,89. The method according to any one of
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각에서 투여되는, 사용.wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered in each of four initial dosing cycles.
90. 구현예 80 내지 구현예 89 중 어느 한 구현예에 있어서,90. The method according to any one of
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 제4 초기 투약 주기 이후에 1회 이상의 추가 주기로 더 투여되는, 사용.wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are further administered in one or more additional cycles after the fourth initial dosing cycle.
91. 구현예 90에 있어서,91. The method of
상기 백금계 화학요법제 및 상기 토포이소머라제 II 억제제가 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 사용.wherein said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are omitted from each of one or more additional dosing cycles.
92. 구현예 80 내지 구현예 91 중 어느 한 구현예에 있어서,92. The method according to any one of
상기 백금계 화학요법제는 카보플라틴이고 상기 토포이소머라제 II 억제제는 에토포시드인, 사용.wherein the platinum-based chemotherapeutic agent is carboplatin and the topoisomerase II inhibitor is etoposide.
93. 구현예 80 내지 구현예 92 중 어느 한 구현예에 있어서,93. The method according to any one of
상기 폐암은 소세포 폐암(SCLC)인, 사용.wherein the lung cancer is small cell lung cancer (SCLC).
94. 구현예 93에 있어서,94. The method of embodiment 93,
상기 SCLC는 확장 병기의 SCLC(ES-SCLC)인, 사용.wherein the SCLC is an extended-stage SCLC (ES-SCLC).
95. 구현예 94에 있어서,95. The method of embodiment 94,
상기 대상체 또는 대상체들은 ES-SCLC에 대한 치료 경험이 없는, 사용.wherein the subject or subjects is naive to treat ES-SCLC.
96. 구현예 80 내지 구현예 95 중 어느 한 구현예에 있어서,96. The method according to any one of
상기 대상체 또는 대상체들은 뇌 전이의 존재 또는 병력이 없는, 사용.wherein the subject or subjects do not have the presence or history of brain metastases.
97. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,97. The method according to any one of
상기 폐암은 PD-L1 발현에 대해 선택되지 않는, 사용.wherein the lung cancer is not selected for PD-L1 expression.
98. 구현예 80 내지 구현예 96 중 어느 한 구현예에 있어서,98. The method according to any one of
상기 폐암은 PD-L1 발현에 대해 선택되는, 사용.wherein the lung cancer is selected for PD-L1 expression.
99. 구현예 98에 있어서,99. The method of embodiment 98,
상기 폐암은 PD-L1의 검출 가능한 발현 수준에 의해 PD-L1 발현에 대해 선택되는, 사용.wherein the lung cancer is selected for PD-L1 expression by a detectable expression level of PD-L1.
100. 구현예 80 내지 구현예 99 중 어느 한 구현예에 있어서,100. The method according to any one of
상기 폐암은 전이성인, 사용.wherein the lung cancer is metastatic.
101. 구현예 100에 있어서,101. The method of
상기 폐암은 뇌, 간, 림프절, 및/또는 부신으로 전이된, 사용.wherein the lung cancer has metastasized to the brain, liver, lymph nodes, and/or adrenal glands.
102. 구현예 100 또는 구현예 101에 있어서,102. The method of
상기 폐암은 뇌로 전이되지 않는, 사용.The lung cancer does not metastasize to the brain.
103. 구현예 100 내지 구현예 102 중 어느 한 구현예에 있어서,103. The method of any one of embodiments 100-102,
상기 치료는 완전 반응(CR) 또는 부분 반응(PR)을 유발하는, 사용.wherein the treatment elicits a complete response (CR) or a partial response (PR).
104. 구현예 80 내지 구현예 103 중 어느 한 구현예에 있어서,104. The method according to any one of
상기 항 TIGIT 길항제 항체는 2주마다, 3주마다, 또는 4주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 2 weeks, every 3 weeks, or every 4 weeks.
105. 구현예 80 내지 구현예 104 중 어느 한 구현예에 있어서,105. The method of any one of embodiments 80-104,
상기 PD-1 축 결합 길항제는 2주마다, 3주마다, 또는 4주마다 약 80 mg 내지 약 2000 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 2 weeks, every 3 weeks, or every 4 weeks.
106. 구현예 80 내지 구현예 105 중 어느 한 구현예에 있어서,106. The method of any one of
상기 PD-1 축 결합 길항제, 상기 항 TIGIT 길항제 항체, 상기 백금계 화학요법제, 및 상기 포토이소머라제 II 억제제는 순차적으로 투여되는, 사용.wherein the PD-1 axis binding antagonist, the anti-TIGIT antagonist antibody, the platinum-based chemotherapeutic agent, and the photoisomerase II inhibitor are sequentially administered.
107. 구현예 106에 있어서,107. The method of embodiment 106,
상기 PD-1 축 결합 길항제는 상기 항 TIGIT 길항제 항체보다 먼저 투여되고, 상기 항 TIGIT 길항제 항체는 상기 백금계 화학요법제보다 먼저 투여되며, 상기 백금제는 상기 토포이소머라제 II 억제제보다 먼저 투여되는, 사용.The PD-1 axis binding antagonist is administered before the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered before the platinum-based chemotherapeutic agent, and the platinum agent is administered before the topoisomerase II inhibitor. , use.
108. 구현예 80 내지 구현예 107 중 어느 한 구현예에 있어서,108. The method according to any one of
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제는 정맥내 투여되는, 사용.wherein said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent, and said topoisomerase II inhibitor are administered intravenously.
109. 구현예 80 내지 구현예 108 중 어느 한 구현예에 있어서,109. The method according to any one of
상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 토포이소머라제 II 억제제는 피하 투여되는, 사용.wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered subcutaneously.
110. SCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,110. The use of an anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCLC,
상기 방법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 사용.The method comprises a dose of about 30 mg to about 1200 mg of an anti-TIGIT antagonist antibody on
111. SCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,111. The use of an anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCLC, comprising:
각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체의 PFS 및/또는 OS를 연장시키는, 방법.Anti TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg on
112. 구현예 110 또는 구현예 111에 있어서,112. The method of embodiment 110 or embodiment 111,
각 추가적인 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 추가적인 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 추가적인 21일 투약 주기를 상기 대상체에 투여하는 단계를 포함하고, 카보플라틴 및 에토포시드는 상기 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 사용.One or more additional 21 doses of anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
113. ES-SCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,113. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with ES-SCLC,
상기 방법은 4회의 초기 투약 주기에 이어서 1회 이상의 추가적인 투약 주기를 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서:The method comprises administering to the subject or population of subjects four initial dosing cycles followed by one or more additional dosing cycles, wherein:
(a) 상기 4회의 초기 투약 주기는 각 초기 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 초기 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 초기 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 초기 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드를 투여하는 단계를 포함하고; 그리고(a) said four initial dosing cycles are tiragolumab at a dose of about 600 mg on
(b) 상기 1회 이상의 추가적인 투약 주기는 각각의 추가적인 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각각의 추가적인 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙을 투여하는 단계를 포함하고,(b) said one or more additional dosing cycles administering about 600 mg of tiragolumab on
여기서 상기 4회의 초기 투약 주기 및 상기 1회 이상의 추가적인 투약 주기는 각각의 21일 투약 주기이고, 여기서 상기 치료는 상기 티라골루맙 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 사용.wherein said four initial dosing cycles and said one or more additional dosing cycles are each 21 day dosing cycle, wherein said treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without said tiragolumab to prolong the PFS and/or OS of the subject or population of subjects.
114. 폐암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,114. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having lung cancer,
상기 방법은 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제인 제1 화학요법제, 및 비백금계 화학요법제인 제2 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent, and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent. or administering to a population of subjects.
115. 구현예 114에 있어서,115. The method of embodiment 114,
상기 폐암은 PD-L1 발현에 대해 평가되지 않는, 사용.wherein the lung cancer is not evaluated for PD-L1 expression.
116. 구현예 114 또는 구현예 115에 있어서,116. The method of embodiment 114 or embodiment 115,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않는, 사용.wherein the subject or subjects has not been determined to have a fraction of PD-L1 positive tumor cells greater than or equal to 50%.
117. 구현예 116에 있어서,117. The method of embodiment 116,
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 미만인 것으로 결정되지 않는, 사용.wherein the subject or subjects is not determined to have a fraction of PD-L1 positive tumor cells of less than 50%.
118. 구현예 116 또는 구현예 117에 있어서,118. The method of embodiment 116 or embodiment 117,
상기 PD-L1 양성 종양 세포 분획은 항 PD-L1 항체를 사용한 양성 염색에 의해 결정되고, 여기서 상기 항 PD-L1 항체는 SP263 또는 22C3인, 사용.wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, wherein said anti-PD-L1 antibody is SP263 or 22C3.
119. 구현예 114 내지 구현예 118 중 어느 한 구현예에 있어서,119. The method according to any one of embodiments 114 to 118,
상기 대상체 또는 대상체들은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 사용.wherein said subject or subjects do not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality.
120. 구현예 114 내지 구현예 119항 중 어느 한 구현예에 있어서,120. The method according to any one of embodiments 114 to 119,
상기 대상체 또는 대상체들은 상기 폐암에 대해 선행 전신 요법을 받은 적이 없는, 사용.wherein said subject or subjects have not received prior systemic therapy for said lung cancer.
121. 구현예 114 내지 구현예 120 중 어느 한 구현예에 있어서,121. The method of any one of embodiments 114 to 120,
상기 폐암은 국소 진행성 폐암인, 사용.wherein the lung cancer is locally advanced lung cancer.
122. 구현예 114 내지 구현예 121 중 어느 한 구현예에 있어서,122. The method according to any one of embodiments 114 to 121,
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 사용.wherein the lung cancer is NSCLC, in particular locally advanced unresectable or metastatic non-squamous NSCLC.
123. 구현예 122에 있어서,123. The method of embodiment 122,
상기 비편평 NSCLC는 IV기 비편평 NSCLC인, 사용.wherein said nonsquamous NSCLC is stage IV nonsquamous NSCLC.
124. 구현예 114 내지 구현예 123 중 어느 한 구현예에 있어서,124. The method according to any one of embodiments 114 to 123,
상기 투약 요법은 4회의 투약 주기를 포함한 유도기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 비백금계 화학요법제는 상기 유도기의 각 투약 주기의 제 1일에 투여되는, 사용.wherein the dosing regimen includes an induction phase comprising 4 dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent include each dosing cycle of the induction phase. Administered on the first day of the use.
125. 구현예 124에 있어서,125. The method of embodiment 124,
상기 투약 요법은 상기 유도기 이후에 유지기를 포함하고, 여기서 상기 유지기는 1회 이상의 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 비백금계 화학요법제는 상기 유지기의 각 투약 주기의 제 1일에 투여되는, 사용.wherein the dosing regimen comprises a maintenance phase after the induction phase, wherein the maintenance phase includes one or more dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and the non-platinum chemotherapeutic agent are the maintenance phases. Use, administered on
126. 구현예 125에 있어서,126. The method of embodiment 125,
상기 유지기의 1회 이상의 투약 주기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 사용.wherein one or more dosing cycles of the maintenance phase do not include administration of the platinum-based chemotherapeutic agent.
127. 구현예 114 내지 구현예 126 중 어느 한 구현예에 있어서,127. The method according to any one of embodiments 114 to 126,
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드인, 사용.wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed.
128. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,128. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with advanced nonsquamous NSCLC, comprising:
상기 방법은 티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg의 용량으로 투여되고, 상기 카보플라틴은 3주마다 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되거나, 또는 상기 시스플라틴은 3주마다 75 mg/m2의 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2의 용량으로 투여되는, 사용.The method comprises administering to the subject or population of subjects a dosing regimen comprising four 21 day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed, wherein the tyra Golumab is administered at a dose of about 600 mg every 3 weeks, the atezolizumab is administered at a dose of about 1200 mg every 3 weeks, and the carboplatin is administered at a dose of about 1200 mg every 3 weeks to achieve AUC=5 mg/ml/min every 3 weeks. or the cisplatin is administered at a dose of 75 mg/m2 every 3 weeks, and the pemetrexed at a dose of about 500 mg/m2 every 3 weeks on
129. 진행성 비편평 NSCLC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,129. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with advanced nonsquamous NSCLC, comprising:
상기 방법은 상기 대상체 또는 대상체 집단에:The method comprises administering to the subject or population of subjects:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m2 every 3 weeks. administering, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
여기서 상기 대상체 또는 대상체의 집단은 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 사용. wherein the subject or population of subjects has not received prior systemic therapy for advanced nonsquamous NSCLC.
130. 진행성 비편평 NSCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,130. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with advanced nonsquamous NSCLC, comprising:
상기 방법은 상기 대상체 또는 대상체 집단에:The method comprises administering to the subject or population of subjects:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m2 per week; and
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,(ii) one or more maintenance phase dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m2 every 3 weeks. administering, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
여기서 상기 대상체는 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 사용.wherein the subject has not received prior systemic therapy for advanced nonsquamous NSCLC.
131. 진행성 비편평 NSCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,131. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with advanced nonsquamous NSCLC, comprising:
상기 방법은 티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체에 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg의 용량으로 투여되고, 상기 시스플라틴은 75 mg/m2의 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 1일에 3주마다 약 500 mg/m2의 용량으로 투여되는, 사용.The method comprises administering to the subject a dosing regimen comprising four 21 day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed, wherein the tiragolumab is Administered at a dose of about 600 mg every 3 weeks, the atezolizumab is administered at a dose of about 1200 mg every 3 weeks, the cisplatin is administered at a dose of 75 mg/
132. 구현예 114 내지 구현예 131 중 어느 한 구현예에 있어서,132. The method according to any one of embodiments 114 to 131,
상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3.5개월 또는 약 4.7개월 만큼 연장시키는, 사용.wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 3.5 months or about 4.7 months.
133. 구현예 114 내지 구현예 132 중 어느 한 구현예에 있어서,133. The method according to any one of embodiments 114 to 132,
상기 치료는 약 12.5개월 내지 약 14.7개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용.wherein said treatment results in a median PFS of a population of subjects from about 12.5 months to about 14.7 months.
134. 구현예 114 내지 구현예 133 중 어느 한 구현예에 있어서,134. The method according to any one of embodiments 114 to 133,
상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.5개월 또는 약 8.0개월 만큼 연장시키는, 사용.wherein the treatment prolongs the OS of the subject or population of subjects by at least about 5.5 months or about 8.0 months.
135. 구현예 114 내지 구현예 134 중 어느 한 구현예에 있어서,135. The method according to any one of embodiments 114 to 134,
상기 치료는 약 27.5개월 내지 약 32.0개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.wherein said treatment results in a median OS in the subject population of about 27.5 months to about 32.0 months.
136. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,136. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks. Use, including steps.
137. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,137. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks. Use, including steps.
138. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,138. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of the dosing cycles is from about 30 mg to about 1200 mg every 3 weeks. Use comprising administering as neoadjuvant treatment a dose of anti-TIGIT antagonist antibody and a dose of about 80 mg to about 1600 mg of PD-1 axis binding antagonist every 3 weeks.
139. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,139. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of the dosing cycles is from about 300 mg to about 800 mg every 3 weeks. Use comprising administering as neoadjuvant treatment a dose of anti-TIGIT antagonist antibody and a dose of about 900 mg to about 1500 mg of PD-1 axis binding antagonist every 3 weeks.
140. 구현예 138 또는 구현예 139에 있어서,140. The method of embodiment 138 or embodiment 139,
상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 용량의 PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 사용.At least one of said dosing cycles is administered to said subject as adjuvant treatment with an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 every 3 weeks Use, comprising the step of:
141. 구현예 140에 있어서,141. The method of embodiment 140,
상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 용량의 PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 사용.At least once in said dosing cycle administering to said subject as adjuvant treatment a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks and a dose of about 900 mg to about 1500 of a PD-1 axis binding antagonist every 3 weeks Use, comprising the step of:
142. 구현예 138 내지 구현예 141 중 어느 한 구현예에 있어서,142. The method according to any one of embodiments 138 to 141,
상기 폐암은 절제 가능한 폐암인, 사용.wherein the lung cancer is resectable lung cancer.
143. 구현예 136 내지 구현예 142 중 어느 한 구현예에 있어서,143. The method according to any one of embodiments 136 to 142,
상기 폐암은 초기 폐암인, 사용.wherein the lung cancer is early lung cancer.
144. 구현예 136 내지 구현예143 중 어느 한 구현예에 있어서,144. The method according to any one of embodiments 136 to 143,
상기 폐암은 II기, IIIA기, 또는 IIIB기 폐암인, 사용.wherein the lung cancer is stage II, IIIA, or IIIB lung cancer.
145. 구현예 136 내지 구현예 144 중 어느 한 구현예에 있어서,145. The method according to any one of embodiments 136 to 144,
상기 폐암은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 사용.wherein the lung cancer does not have an epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor abnormality.
146. 구현예 136 내지 구현예 145 중 어느 한 구현예에 있어서,146. The method according to any one of embodiments 136 to 145,
상기 대상체는 치료 목적으로 R0 절제술에 적격인, 사용.wherein said subject is eligible for R0 resection for therapeutic purposes.
147. 구현예 136 내지 구현예 146 중 어느 한 구현예에 있어서,147. The method according to any one of embodiments 136 to 146,
상기 대상체는 폐암에 대해 선행 요법을 받은 적이 없는, 사용.wherein the subject has never received prior therapy for lung cancer.
148. 구현예 147에 있어서,148. The method of embodiment 147,
상기 선행 요법은 면역요법, 화학요법, 또는 방사선요법인, 사용.wherein said prior therapy is immunotherapy, chemotherapy, or radiotherapy.
149. 구현예 136 내지 구현예 148 중 어느 한 구현예에 있어서,149. The method according to any one of embodiments 136 to 148,
상기 대상체는 백금계 화학요법에 적격인, 사용.wherein the subject is eligible for platinum-based chemotherapy.
150. 구현예 136 내지 구현예 149 중 어느 한 구현예에 있어서,150. The method of any one of embodiments 136 to 149,
상기 제1 투약 주기는 수술 전에 개시되는, 사용.wherein the first dosing cycle is initiated prior to surgery.
151. 구현예 150에 있어서,151. The method of embodiment 150,
적어도 1, 2, 3, 또는 4회의 투약 주기는 상기 수술 전에 완료되는, 사용.wherein at least 1, 2, 3, or 4 dosing cycles are completed prior to said surgery.
152. 구현예 150 또는 구현예 151에 있어서,152. The method of embodiment 150 or embodiment 151,
4회의 투약 주기는 상기 수술 전에 완료되는, 사용.4 dosing cycles are completed prior to the surgery.
153. 구현예 136 내지 구현예 152 중 어느 한 구현예에 있어서,153. The method according to any one of embodiments 136 to 152,
적어도 1회의 투약 주기는 수술 후에 개시되는, 사용.wherein at least one dosing cycle is initiated after surgery.
154. 구현예 153에 있어서,154. The method of embodiment 153,
16회의 투약 주기는 상기 수술 후에 완료되는, 사용.16 dosing cycles completed after said surgery.
155. 구현예 150 내지 구현예 154 중 어느 한 구현예에 있어서,155. The method of any one of embodiments 150 to 154,
상기 수술은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술인, 사용.wherein the operation is lobectomy, lobectomy, bilobectomy, or pneumonectomy.
156. 구현예 136 내지 구현예 155 중 어느 한 구현예에 있어서,156. The method according to any one of embodiments 136 to 155,
상기 방법은 방사선 요법을 더 포함하는, 사용.The method further comprises radiation therapy.
157. 구현예 156에 있어서, 157. The method of embodiment 156,
상기 방사선 요법은 수술 후 방사선 요법인, 사용.wherein the radiation therapy is post-operative radiation therapy.
158. 구현예 136 내지 구현예 157 중 어느 한 구현예에 있어서,158. The method according to any one of embodiments 136 to 157,
상기 방법은 하나 이상의 화학요법제를 투여하는 단계를 더 포함하는, 사용.The method further comprises administering one or more chemotherapeutic agents.
159. 구현예 158에 있어서,159. The method of embodiment 158,
상기 하나 이상의 화학요법제는 수술 후 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered after surgery.
160. 구현예 159에 있어서,160. The method of embodiment 159,
상기 하나 이상의 화학요법제는 상기 수술 후 4회 투약 주기로 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered in 4 dosing cycles after said surgery.
161. 구현예 158 내지 구현예 160 중 어느 한 구현예에 있어서,161. The method according to any one of embodiments 158 to 160,
상기 하나 이상의 화학요법제는 백금계 화학요법제 및 비백금계 화학요법제인, 사용.wherein said at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
162. 구현예 161에 있어서:162. The method of embodiment 161:
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고; (a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 젬시타빈이고; (b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이고; (c) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이거나; 또는 (d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or
(e) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 젬시타빈인, 사용. (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine.
163. 구현예 136 내지 구현예 162 중 어느 한 구현예에 있어서,163. The method according to any one of embodiments 136 to 162,
상기 치료는 기준 MPR 비율과 비교하여 주요 병리학적 반응율(MPR)의 증가를 유발하는, 사용.wherein the treatment results in an increase in the major pathological response rate (MPR) compared to the baseline MPR rate.
164. 구현예 163에 있어서,164. The method of embodiment 163,
상기 기준 MPR 비율은:The reference MPR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 MPR 비율인, 사용. (b) use, which is the MPR rate of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
165. 구현예 136 내지 구현예 164 중 어느 한 구현예에 있어서,165. The method of any one of embodiments 136 to 164,
상기 치료는 병리학적 완전 반응(pCR) 및/또는 기준 pCR 비율과 비교하여 pCR 비율의 증가를 유발하는, 사용.wherein said treatment results in a pathological complete response (pCR) and/or an increase in the pCR ratio compared to a baseline pCR ratio.
166. 구현예 165에 있어서,166. The method of embodiment 165,
상기 기준 pCR 비율은:The reference pCR ratio is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 pCR 비율인, 방법. (b) the pCR ratio of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
167. 구현예 136 내지 구현예 166 중 어느 한 구현예에 있어서,167. The method according to any one of embodiments 136 to 166,
상기 치료는 기준 EFS 시간과 비교하여 무사건 생존(EFS)의 증가를 유발하는, 사용.wherein said treatment results in an increase in event-free survival (EFS) compared to baseline EFS time.
168. 구현예 167에 있어서,168. The method of embodiment 167,
상기 기준 EFS 시간은:The reference EFS time is:
(a) 항 TIGIT 길항제 항체를 포함하지 않는 PD-1 축 결합 길항제; 및/또는 (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 대상체 집단의 EFS 시간인, 사용. (b) use, which is the EFS time of a population of subjects receiving treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
169. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,169. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 600 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks. Use, including steps.
170. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,170. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 신보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of the dosing cycles is from about 30 mg to about 600 mg every 3 weeks. Use comprising administering as neoadjuvant treatment a dose of anti-TIGIT antagonist antibody and a dose of about 80 mg to about 1600 mg of PD-1 axis binding antagonist every 3 weeks.
171. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,171. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapy. use comprising administering to the subject one or more dosing cycles of the agent.
172. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,172. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제를 신보조 치료로서 투여하는 단계를 포함하는, 사용.administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one of the dosing cycles comprises: anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent Use, comprising administering as an adjuvant treatment.
173. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,173. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 및: (a) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금계 화학요법제; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (b) (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and: (a) (i) every 3 weeks a platinum-based chemotherapeutic agent at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (b) (i) an antimetabolite at a dose of about 500 mg/m2 every 3 weeks or about 1000 mg/m2 or about 1250 mg/m2 on
174. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,174. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 상기 대상체에게: (a) 3주마다 약 30 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체; (b) 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제; (c) (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의; 또는 (ii) 3주마다 약 75 mg/m2 용량의 백금계 화학요법제; 및 (d) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 항대사물질; 또는 (ii) 3주마다 약 100 mg/m2, 약 175 mg/m2, 또는 약 200 mg/m2 용량의 탁산이며; 여기서 상기 치료는 신보조 치료인, 사용.The method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one of the dosing cycles One dose is administered to the subject: (a) an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 600 mg every 3 weeks; (b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks; (c) at (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every 3 weeks; and (d) administering a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) about 500 mg/m2 every 3 weeks or on
175. 절제 가능한 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,175. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with resectable lung cancer, comprising:
상기 방법은 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및: The method comprises tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and:
(a) (a)
(i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or
(ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및(ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and
(b) (b)
(i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on
(ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.(ii) administering to the subject one or more dosing cycles of paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks.
176. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,176. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having lung cancer,
상기 방법은 티라골루맙, 아테졸리주맙, 백금계 화학요법제, 및 비백금계 화학요법제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 3주마다 약 1200 mg 용량의 아테졸리주맙; (c) 비백금계 화학요법제를 투여하는 단계를 포함하고, 여기서 상기 백금계 화학요법제는: (i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는 (ii) 3주마다 약 75 mg/m2 용량의 시스플라틴; 및 (d) 비백금계 화학요법제이고, 여기서 상기 비백금계 화학요법제는: (i) 3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는 (ii) 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀이고; 여기서 상기 치료는 신보조 치료인, 사용.The method comprises administering to the subject one or more dosing cycles of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent, wherein at least one dosing cycle comprises said To the subject: (a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks; (c) administering a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent: (i) achieves an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks a dose of carboplatin targeted to or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks; and (d) a non-platinum-based chemotherapeutic agent, wherein the non-platinum-based chemotherapeutic agent is: (i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks or about 1000 on
177. 비편평 NSCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,177. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with nonsquamous NSCLC, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (a) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 1200 mg의 용량으로 아테졸리주맙을 신보조 치료로서 상기 대상체에게 투여하는 단계를 포함하고; (b) 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (a) at least one of the dosing cycles is about a 600 mg dose of tiragolumab every 3 weeks and administering to the subject as neoadjuvant treatment atezolizumab at a dose of 1200 mg every 3 weeks; (b) use of at least one dosing cycle comprising administering to the subject as adjuvant treatment a dose of about 600 mg of tiragolumab every 3 weeks and a dose of about 1200 mg of atezolizumab every 3 weeks.
178. 비편평 NSCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,178. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with nonsquamous NSCLC, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉시드; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 3주마다 약 500 mg/m2 용량의 페메트렉스를 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제를 보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment, and to the subject: ( a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a targeted dose to achieve an AUC of 5 mg/mL/min every 3 weeks and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and pemetrex at a dose of about 500 mg/m2 every 3 weeks; (II) at least one of said dosing cycles is adjuvant treatment with an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks Use comprising administering.
179. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,179. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment, and to the subject: ( a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
180. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,180. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein:
(I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게:(I) at least one of said dosing cycles is neoadjuvant treatment, to said subject:
(a) 3주마다 약 1200 mg 용량의 티라골루맙; (a) tyragolumab at a dose of about 1200 mg every 3 weeks;
(b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and
(c) (c)
(i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈;
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
(ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks; or
(iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 또는 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; 그리고
(iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks or gemcitabine at a dose of about 1250 mg/m2 on
(II) 상기 투약 주기 중 적어도 1회는 3주마다 약 300 mg 내지 약 800 mg 용량의 티라골루맙 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 사용.(II) administering to the subject as adjuvant treatment at least one of said dosing cycles is tiragolumab at a dose of about 300 mg to about 800 mg every 3 weeks and atezolizumab at a dose of about 900 mg to about 1500 mg every 3 weeks Use, comprising the step of:
181. 폐암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,181. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having lung cancer, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment, and to the subject: ( a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
182. 절제 가능한 편평 NSCLC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,182. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with resectable squamous NSCLC, comprising:
상기 방법은 티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서: (I) 상기 투약 주기 중 적어도 1회는 신보조 치료이고, 상기 대상체에게: (a) 3주마다 약 600 mg 용량의 티라골루맙; (b) 신보조 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및 (c) (i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈; (ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는 (iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; (II) 상기 투약 주기 중 적어도 1회는 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙을 보조 치료로서 투여하는 단계를 포함하는, 사용The method comprises administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein: (I) at least one of the dosing cycles is neoadjuvant treatment, and to the subject: ( a) tyragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and (c) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
183. 구현예 136 내지 구현예 182 중 어느 한 구현예에 있어서,183. The method according to any one of embodiments 136 to 182,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
184. 구현예 183에 있어서,184. The method of embodiment 183,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 사용.The detectable protein expression level of PD-L1 is 50% or more in the fraction of PD-L1 positive tumor cells.
185. 구현예 73, 구현예 114 내지 구현예 121, 및 구현예 136 내지 구현예 184 중 어느 한 구현예에 있어서,185. The method of any one of
상기 폐암은 NSCLC인, 사용.wherein the lung cancer is NSCLC.
186. 구체예 185에 있어서,186. according to embodiment 185,
상기 NSCLC는 편평 NSCLC인, 사용.wherein said NSCLC is squamous NSCLC.
187. 구현예 185에 있어서,187. The method of embodiment 185,
상기 NSCLC는 비편평 NSCLC인, 사용.wherein said NSCLC is non-squamous NSCLC.
188. 구현예 72에 있어서,188. The method of
상기 암은 자궁경부암인, 사용.wherein the cancer is cervical cancer.
189. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,189. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1,
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.The method comprises administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or population of subjects. Use, comprising the step of administering to.
190. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,190. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1,
상기 방법은 3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.The method comprises administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks to the subject or population of subjects. Use, comprising the step of administering to.
191. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,191. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting a therapy for a subject with cervical cancer, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg의 용량으로 투여되는 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용(b) an anti-TIGIT antagonist antibody administered at a dose of about 30 mg to about 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 and 3 use comprising selecting a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist administered at a dose of about 80 mg to about 1600 mg per week
192. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,192. The method of any one of embodiments 189 to 191,
상기 자궁경부암은 편평세포 암종, 선편평세포 암종, 또는 선암종인, 사용.wherein the cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
193. 구현예 189 내지 구현예 191 중 어느 한 구현예에 있어서,193. The method according to any one of embodiments 189 to 191,
상기 자궁경부암은 4B기, 전이성, 재발성, 또는 지속성인, 사용.wherein the cervical cancer is stage 4B, metastatic, recurrent, or persistent.
194. 구현예 189 내지 구현예 193 중 어느 한 구현예에 있어서,194. The method according to any one of embodiments 189 to 193,
상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부암인, 사용.wherein the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer.
195. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,195. The method of any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 적어군 한 라인의 선행 요법을 받은, 사용.The subject or subjects have received at least one line of prior therapy.
196. 구현예 189 내지 구현예 195 중 어느 한 구현예에 있어서,196. The method according to any one of embodiments 189 to 195,
상기 대상체 또는 대상체들은 두 라인의 선행 요법을 받은, 사용.wherein the subject or subjects have received two lines of prior therapy.
197. 구현예 189 내지 구현예 196 중 어느 한 구현예에 있어서,197. The method according to any one of embodiments 189 to 196,
상기 대상체 또는 대상체들은 2라인 초과의 선행 요법을 받은, 사용.The subject or subjects received more than 2 lines of prior therapy.
198. 구현예 189 내지 구현예 194 중 어느 한 구현예에 있어서,198. The method according to any one of embodiments 189 to 194,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 사용.wherein said subject or subjects have not received prior therapy.
199. 구현예 195 내지 구현예 198 중 어느 한 항에 있어서,199. The method according to any one of embodiments 195 to 198,
상기 선행 요법은 화학요법, 수술, 및/또는 방사선요법인, 사용.wherein said prior therapy is chemotherapy, surgery, and/or radiation therapy.
200. 구현예 189 및 구현예 192 내지 구현예 199 중 어느 한 구현예에 있어서,200. The method according to any one of embodiments 189 and 192 to 199,
상기 치료는 임상 반응을 유발하는, 사용.wherein said treatment elicits a clinical response.
201. 구현예 200에 있어서,201. The method of
상기 임상 반응은 기준 ORR과 비교하여 대상체 집단의 객관적 반응률(ORR)의 증가인, 사용.wherein the clinical response is an increase in the objective response rate (ORR) of the subject population as compared to a baseline ORR.
202. 구현예 201에 있어서,202. The method of embodiment 201,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 사용.wherein the reference ORR is the median ORR of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
203. 구현예 200에 있어서,203. The method of
상기 기준 ORR은 적어도 약 14.6% 내지 약 26%인, 사용.wherein the reference ORR is at least about 14.6% to about 26%.
204. 구현예 200에 있어서,204. The method of
상기 임상 반응은 CR 또는 PR인, 사용.wherein the clinical response is CR or PR.
205. 구현예 200 내지 구현예 204 중 어느 한 구현예에 있어서,205. The method of any one of
상기 임상 반응은 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가인, 사용.The clinical response is an increase in progression-free survival (PFS) of the subject compared to a baseline PFS time, an increase in the duration of response (DOR) in the subject compared to a baseline DOR time, or an increase in the subject's progression-free survival (DOR) compared to a baseline OS time. Use, which is an increase in overall survival (OS).
206. 구현예 205에 있어서:206. The method of embodiment 205:
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는(b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
207. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,207. The use of an anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of treating a subject having cervical cancer having a detectable expression level of PD-L1,
3주마다 600 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.Use comprising administering to the subject one or more dosing cycles of a 600 mg dose of anti-TIGIT antagonist antibody every 3 weeks and atezolizumab at a 1200 mg dose every 3 weeks.
208. 항 TIGIT 길항제 항체 및 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자궁경부암을 가진 대상체를 확인하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,208. Anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of identifying a subject with cervical cancer likely to benefit from a therapy comprising one or more dosing cycles of anti TIGIT antagonist antibody and atezolizumab As the use of
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계를 포함하는, 사용.(c) one or more dosing cycles of anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks, based on PD-L1 expression on detected tumor cells. Use comprising identifying the subject as likely to benefit from a therapy comprising
209. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,209. The use of an anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of selecting a therapy for a subject with cervical cancer,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 Use comprising selecting a regimen comprising one or more dosing cycles of atezolizumab administered as a dose.
210. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,210. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having cervical cancer having a detectable expression level of PD-L1,
상기 방법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙에 대한1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
211. 자궁경부암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,211. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having cervical cancer, comprising:
상기 방법은:The method is:
(a) 대상체로부터 종양 샘플을 얻는 단계;(a) obtaining a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라졸루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계; 및(c) one or more dosing cycles of tyrazolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression on detected tumor cells. identifying the subject as likely to benefit from therapy; and
(d) 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to the identified subject.
212. 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,212. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting a therapy for a subject having cervical cancer, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라골루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) tiragolumab administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 Selecting a regimen comprising one or more dosing cycles of atezolizumab administered as
213. 전이성 및/또는 재발성 자궁경부암을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,213. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having metastatic and/or recurrent cervical cancer, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라졸루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 상기 대상체를 확인하는 단계; 및(c) one or more dosing cycles of tyrazolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on PD-L1 expression on detected tumor cells. identifying the subject as likely to benefit from therapy; and
(d) 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to the identified subject.
214. 전이성 및/또는 재발성 자궁경부암을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,214. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting a therapy for a subject with metastatic and/or recurrent cervical cancer, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기초로 3주마다 600 mg의 용량으로 투여되는 티라골루맙 및 3주마다 1200 mg의 용량으로 투여되는 아테졸리주맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) tiragolumab administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1 Selecting a regimen comprising one or more dosing cycles of atezolizumab administered as
215. 구현예 189 내지 구현예 214 중 어느 한 구현예에 있어서,215. The method of any one of embodiments 189 to 214,
상기 대상체는 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 확인되는, 사용.wherein the subject is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
216. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,216. The method according to any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 SP263을 사용하여 검출되는, 사용.Using, the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
217. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,217. The method according to any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 사용.wherein the detectable expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the sample from the subject.
218. 구현예 189 내지 구현예 215 중 어느 한 구현예에 있어서,218. The method of any one of embodiments 189 to 215,
PD-L1 발현 수준은 항 PD-L1 항체 22C3을 사용하여 검출되는, 사용.Using, PD-L1 expression levels are detected using anti-PD-L1 antibody 22C3.
219. 구현예 189 내지 구현예 216 중 어느 한 구현예에 있어서,219. The method of any one of embodiments 189 to 216,
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 복합 양성 점수(CPS)가 1 이상인, 사용.wherein the detectable expression level of PD-L1 has a composite positive score (CPS) of 1 or greater in a sample from the subject.
220. 구현예 72에 있어서, 상기 암은 유방암인, 사용.220. The use of
221. 유방암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,221. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having breast cancer,
상기 방법은 4주마다 약 840 mg 용량의 티라골루맙, 4주마다 약 1680 mg 용량의 아테졸리주맙, 및 3주 투약/1주 휴약의 약 100 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.The method comprises one or more doses of tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and nap-paclitaxel at a dose of about 100 mg/m2 of 3 weeks dosing/1 week holiday. A use comprising administering to the subject or population of subjects a dosing regimen comprising a dosing cycle.
222. 구현예 220 또는 구현예 221에 있어서,222. The method of embodiment 220 or embodiment 221,
상기 유방암은 삼중 음성 유방암(TNBC)인, 사용.wherein the breast cancer is triple negative breast cancer (TNBC).
223. 구현예 222에 있어서,223. The method of embodiment 222,
상기 TNBC는 절제 가능한 국소 진행성 또는 전이성 TNBC인, 사용.wherein said TNBC is resectable locally advanced or metastatic TNBC.
224. 구현예 220 내지 구현예 223 중 어느 한 구현예에 있어서,224. The method of any one of embodiments 220 to 223,
상기 대상체는 전이성 유방암에 대해 선행 전신 요법을 받은 적이 없는, 사용.wherein the subject has not received prior systemic therapy for metastatic breast cancer.
225. 구현예 220 내지 구현예 224 중 어느 한 구현예에 있어서,225. The method of any one of embodiments 220-224,
상기 치료는 적어도 약 53% 내지 약 67.5%의 대상체 집단의 ORR을 유발하는, 사용.wherein said treatment results in an ORR in at least about 53% to about 67.5% of the subject population.
226. 구현예 222 내지 구현예 225 중 어느 한 구현예에 있어서,226. The method of any one of embodiments 222 to 225,
상기 치료는 약 25.0개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.wherein said treatment results in a median OS of a subject population of about 25.0 months.
227. 초기 삼중 음성 유방암(eTNBC)을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,227. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with early stage triple negative breast cancer (eTNBC), comprising:
상기 방법은 2주마다 약 10 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체, 및 2주마다 약 20 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks, and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every two weeks. use comprising administering to the subject.
228. 구현예 227에 있어서,228. The method of embodiment 227,
상기 방법은 하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 사용.The method further comprises administering to the subject one or more chemotherapeutic agents.
229. 구현예 228에 있어서,229. The method of embodiment 228,
상기 하나 이상의 화학요법제는 백금계 화학요법제, 탁산, 토포이소머라제 II 억제제, 또는 알킬화제인, 사용.wherein said at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
230. 구현예 227에 있어서,230. The method of embodiment 227,
상기 방법은 (a) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 탁산 또는 탁산 및 백금계 화학요법제의 1회 이상의 투약 주기; 및 (b) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 토포이소머라제 II 억제제, 알킬화제, 및 과립구 집락 자극 인자(G-CSF) 또는 과립구-대식세포 집락 자극 인자(GM-CSF)의 1회 이상의 투약 주기를 투여하는 단계를 더 포함하는, 사용.The method comprises (a) one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and a taxane or a taxane and a platinum-based chemotherapeutic agent; and (b) said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, topoisomerase II inhibitor, alkylating agent, and granulocyte colony stimulating factor (G-CSF) or granulocyte-macrophage colony stimulating factor (GM-CSF) use, further comprising administering one or more dosing cycles of
231. 구현예 229 또는 구현예 230에 있어서,231. The method of embodiment 229 or embodiment 230,
상기 알킬화제는 시클로포스파미드인, 사용.wherein the alkylating agent is cyclophosphamide.
232. 구현예 231에 있어서,232. The method of embodiment 231,
상기 시클로포스파미드는 약 600 mg/m2의 용량으로 투여되는, 사용.wherein the cyclophosphamide is administered at a dose of about 600 mg/m2.
233. 구현예 227 내지 구현예 229, 구현예 231 및 구현예 232 중 어느 한 구현예에 있어서,233. The embodiment of any one of embodiments 227 to 229, embodiments 231 and 232,
G-CSF 또는 GM-CSF를 상기 대상체에게 더 투여하는 단계를 포함하는, 사용.Use, comprising further administering to the subject G-CSF or GM-CSF.
234. 구현예 230 또는 구현예 233에 있어서,234. The method of embodiment 230 or embodiment 233,
상기 G-CSF는 페그필그라스팀 또는 필그라스팀인, 사용.The G-CSF is pegfilgrastim or filgrastim, use.
235. 구현예 234에 있어서,235. The method of embodiment 234,
상기 G-CSF는 페그필그라스팀인, 사용.The G-CSF is pegfilgrastim, use.
236. 구현예 235에 있어서,236. The method of embodiment 235,
상기 페그필그라스팀은 약 6 mg의 용량으로 투여되는, 사용.wherein the pegfilgrastim is administered in a dose of about 6 mg.
237. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 236 중 어느 한 구현예에 있어서,237. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 236,
상기 방법은 상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF의 하나 이상의 후속 용량을 상기 대상체에게 더 투여하는 단계를 포함하는, 사용.wherein said method further comprises administering to said subject said one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF.
238. 구현예 228, 구현예 229, 및 구현예 231 내지 구현예 237 중 어느 한 구현예에 있어서,238. The embodiment of any one of embodiments 228, 229, and embodiments 231 to 237,
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF는 각각 매주마다 1회, 2주마다 1회, 또는 3주마다 1회 투여되는, 사용.wherein said one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once every week, once every 2 weeks, or once every 3 weeks, respectively.
239. 구현예 229 내지 구현예 238 중 어느 한 구현예에 있어서,239. The method of any one of embodiments 229 to 238,
상기 백금계 화학요법제는 3주마다 투여되고, 상기 탁산은 매주 투여되고, 상기 토포이소머라제 II 억제제는 2주마다 투여되고, 상기 알킬화제는 2주마다 투여되며, 상기 G-CSF 또는 GM-CSF는 2주마다 투여되는, 사용.The platinum-based chemotherapeutic agent is administered every 3 weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every 2 weeks, the alkylating agent is administered every 2 weeks, and the G-CSF or GM- CSF used, administered every two weeks.
240. 구현예 229 내지 구현예 239 중 어느 한 구현예에 있어서,240. The method of any one of embodiments 229 to 239,
상기 탁산 또는 상기 탁산 및 상기 백금계 화학요법제는 상기 투약 요법의 처음 12주 동안 투여되는, 사용.wherein said taxane or said taxane and said platinum-based chemotherapeutic agent are administered during the first 12 weeks of said dosing regimen.
241. 구현예 229 내지 구현예 240 중 어느 한 구현예에 있어서,241. The method of any one of embodiments 229-240,
상기 토포이소머라제 II 억제제, 상기 알킬화제, 및 상기 G-CSF 또는 GM-CSF는 투약 요법의 13주 내지 19주 동안 투여되는, 사용.wherein said topoisomerase II inhibitor, said alkylating agent, and said G-CSF or GM-CSF are administered for 13 to 19 weeks of a dosing regimen.
242. 구현예 227 내지 구현예 241 중 어느 한 구현예에 있어서,242. The method according to any one of embodiments 227 to 241,
상기 투약 요법의 총 기간은 19주인, 사용.The total duration of the dosing regimen was 19 weeks, use.
243. 구현예 227 내지 구현예 242 중 어느 한 구현예에 있어서,243. The method of any one of embodiments 227 to 242,
상기 방법은 신보조 치료인, 사용.The method is neoadjuvant treatment.
244. 구현예 227 내지 구현예 243 중 어느 한 구현예에 있어서,244. The method according to any one of embodiments 227 to 243,
상기 투약 요법 후에 수술이 실시되는, 사용.wherein surgery is performed after said dosing regimen.
245. 구현예 244에 있어서,245. The method of embodiment 244,
상기 수술은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 실시되는, 사용.wherein said surgery is performed between 2 and 6 weeks after the last dose of said dosing regimen.
246. 구현예 244 또는 구현예 245에 있어서,246. The method of embodiment 244 or embodiment 245,
상기 수술은 유방절제술을 포함하는, 사용.wherein said surgery comprises a mastectomy.
247. 구현예 244 내지 구현예 246 중 어느 한 구현예에 있어서,247. The method according to any one of embodiments 244 to 246,
상기 수술은 액와 림프절 수술을 포함하는, 사용.wherein said surgery comprises axillary lymph node surgery.
248. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,248. The method of any one of embodiments 229 to 247,
상기 토포이소머라제 II 억제제는 독소루비신인, 사용.wherein the topoisomerase II inhibitor is doxorubicin.
249. 구현예 229 내지 구현예 247 중 어느 한 구현예에 있어서,249. The method according to any one of embodiments 229 to 247,
상기 탁산은 냅-파클리탁셀이고, 상기 백금계 화학요법제는 카보플라틴이며, 상기 토포이소머라제 II 억제제는 독소루비신인, 사용.wherein the taxane is nap-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin.
250. 구현예 248 또는 구현예 249에 있어서,250. The method of embodiment 248 or embodiment 249,
독소루비신은 약 60 mg/m2의 용량으로 투여되는, 사용.Doxorubicin is administered at a dose of about 60 mg/m2.
251. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,251. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제, 및:The method comprises an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
252. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,252. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-L1 축 결합 길항제, 및:The method comprises an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, a PD-L1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
253. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,253. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 항 PD-L1 길항제 항체, 및:The method comprises an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, an anti-PD-L1 antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
254. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,254. Use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙, 2주마다 약 600 mg 내지 약 1200 mg 용량의 항 PD-L1 길항제 항체, 및:The method comprises tyragolumab at a dose of about 300 mg to about 600 mg every two weeks, an anti-PD-L1 antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
255. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 아테졸리주맙의 사용으로서,255. The use of an anti TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체, 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:The method comprises an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks, atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 백금제; 및(i) a dose of about 125 mg/m2 of taxane every week for the first 12 weeks of the dosing regimen and a dose of platinum agent targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 탁산; 및(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 토포이소머라제 II 억제제, 2주마다 약 600 mg/m2 용량의 알킬화제, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
256. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,256. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 300 mg 내지 약 600 mg 용량의 티라골루맙, 2주마다 약 600 mg 내지 약 1200 mg 용량의 아테졸리주맙, 및:The method comprises tiragolumab at a dose of about 300 mg to about 600 mg every two weeks, atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
257. eTNBC를 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,257. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, comprising:
상기 방법은 2주마다 약 420 mg 용량의 티라골루맙, 2주마다 약 840 mg 용량의 아테졸리주맙, 및:The method comprises tiragolumab at a dose of about 420 mg every 2 weeks, atezolizumab at a dose of about 840 mg every 2 weeks, and:
(a) (a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는(ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for
(b) (b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및(i) nap-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; and
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, (ii) doxorubicin at a dose of about 60 mg/m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m2 every 2 weeks, and G-CSF or GM- every 2 weeks for
여기서 상기 방법은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 사용.wherein the method further comprises surgery between 2 and 6 weeks after the last dose of the dosing regimen.
258. 구현예 220 내지 구현예 257 중 어느 한 구현예에 있어서,258. The method of any one of embodiments 220 to 257,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 상기 대상체로부터의 종양 샘플에서 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 is determined in a tumor sample from said subject determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142.
259. 구현예 258에 있어서,259. The method of embodiment 258,
상기 종양 샘플에서 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율은 1% 이상인, 사용.In the tumor sample, the proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) is 1% or more.
260. 구현예 227 내지 구현예 259 중 어느 한 구현예있어서,260. The method of any one of embodiments 227 to 259,
상기 eTNBC는 T2-4d TNBC로 제시되는, 사용.wherein said eTNBC is referred to as T2-4d TNBC.
261. 구현예 227 내지 구현예 260 중 어느 한 구현예에 있어서,261. The method according to any one of embodiments 227 to 260,
상기 eTNBC는 cT2-cT4, cN0-cN3, 및 cM0 TNBC로 제시되는, 사용.wherein the eTNBC is presented as cT2-cT4, cN0-cN3, and cM0 TNBC.
262. 구현예 227 내지 구현예 261 중 어느 한 구현예에 있어서,262. The method of any one of embodiments 227 to 261,
상기 대상체는 eTNBC에 대해 이전에 치료받은 적이 없는, 사용.wherein the subject has not been previously treated for eTNBC.
263. 구현예 227 내지 구현예 262 중 어느 한 구현예에 있어서,263. The method according to any one of embodiments 227 to 262,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 사용.wherein said treatment results in a pathological complete response (pCR).
264. 구현예 227 내지 구현예 263 중 어느 한 구현예에 있어서,264. The method of any one of embodiments 227 to 263,
상기 치료는 전체 생존(OS) 또는 무사건 생존(EFS)의 증가를 유발하는, 방법.wherein the treatment results in an increase in overall survival (OS) or event-free survival (EFS).
265. 구현예 72에 있어서,265. The method of
상기 암은 두경부암인, 사용.wherein the cancer is head and neck cancer.
266. 구현예 265에 있어서,266. The method of embodiment 265,
상기 두경부암은 상기 두경부의 편평세포 암종(SCCHN)인, 사용.wherein the head and neck cancer is squamous cell carcinoma (SCCHN) of the head and neck.
267. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,267. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the use of
상기 방법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.The method comprises administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or population of subjects. Use, comprising the step of administering to.
268. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,268. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1,
상기 방법은 3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.The method comprises administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks to the subject or population of subjects. Use, comprising the step of administering to.
269. SCCHN을 가진 대상체 또는 대상체 집단을 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,269. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting a therapy for a subject or population of subjects with SCCHN,
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체 또는 대상체 집단에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and 3 weeks based on PD-L1 expression detected for said subject or population of subjects having a detectable expression level of PD-L1 selecting a regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg per time.
270. PD-L1의 검출 가능한 발현 수준을 갖는 자궁경부암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,270. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1, the use of
상기 방법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙에 대한1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
271. 구현예 267 내지 구현예 270 중 어느 한 구현예에 있어서,271. The method according to any one of embodiments 267 to 270,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 사용.wherein said subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
272. 구현예 266 내지 구현예 271 중 어느 한 구현예에 있어서,272. The method of any one of embodiments 266 to 271,
상기 SSCHN은 인간 유두종 바이러스(HPV) 양성인, 사용.wherein the SSCHN is human papillomavirus (HPV) positive.
273. 구현예 266 내지 구현예 272 중 어느 한 구현예에 있어서,273. The method according to any one of embodiments 266 to 272,
상기 SSCHN은 HPV 음성인, 사용.wherein the SSCHN is HPV negative.
274. 구현예 272 또는 구현예 273항에 있어서,274. The method of embodiment 272 or embodiment 273,
HPV 상태는 p16 IHC, 제자리(in situ) 부합법, 또는 PCR에 의해 결정되는, 사용.HPV status is determined by p16 IHC, in situ hybridization, or PCR.
275. 구현예 266 내지 구현예 274 중 어느 한 구현예에 있어서,275. The method according to any one of embodiments 266 to 274,
상기 SCCHN은 재발성 및/또는 전이성 SCCHN인, 사용.wherein said SCCHN is recurrent and/or metastatic SCCHN.
276. 구현예 265 내지 구현예 275 중 어느 한 구현예에 있어서,276. The method according to any one of embodiments 265 to 275,
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 사용.wherein said subject or subjects have not received prior therapy.
277. 구현예 276에 있어서,277. The method of embodiment 276,
상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법인, 사용.wherein said prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
278. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,278. The embodiment of any one of embodiments 265-268 and embodiments 270-277,
상기 치료는 CR 또는 PR을 유발하는, 사용.wherein said treatment causes CR or PR.
279. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 277 중 어느 한 구현예에 있어서,279. The method according to any one of embodiments 265 to 268 and 270 to 277,
상기 치료는 기준 ORR과 비교하여 상기 대상체 집단의 객관적 반응률(ORR)의 증가를 유발하는, 사용.wherein said treatment results in an increase in objective response rate (ORR) in said subject population compared to a baseline ORR.
280. 구현예 279에 있어서,280. The method of embodiment 279,
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 사용.wherein the reference ORR is the median ORR of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
281. 구현예 279 또는 구현예 280에 있어서,281. The method of embodiment 279 or embodiment 280,
상기 기준 ORR은 적어도 약 19% 내지 약 36%인, 사용.wherein the reference ORR is at least about 19% to about 36%.
282. 구현예 265 내지 구현예 268 및 구현예 270 내지 구현예 281 중 어느 한 구현예에 있어서,282. The method of any one of embodiments 265-268 and 270-281,
상기 치료는 기준 PFS 시간과 비교하여 상기 대상체 또는 대상체 집단의 무진행 생존(PFS)의 증가, 기준 DOR 시간과 비교하여 상기 대상체 또는 대상체 집단의 반응 지속 기간(DOR)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)의 증가를 유발하는, 사용.wherein the treatment is associated with an increase in progression-free survival (PFS) of the subject or subject population as compared to a baseline PFS time, an increase in the duration of response (DOR) of the subject or subject population compared to a baseline DOR time, or a baseline OS time and as compared to cause an increase in overall survival (OS) of the subject or population of subjects.
283. 구현예 282에 있어서:283. The method of embodiment 282:
(a) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값이고;(a) said baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 DOR 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 시간 중앙값이거나; 또는 (b) said baseline DOR time is the median DOR time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
284. 구현예 282에 있어서,284. The method of embodiment 282,
상기 기준 DOR 시간은 적어도 약 6.7개월 내지 약 23.4개월인, 사용.wherein the baseline DOR time is at least about 6.7 months to about 23.4 months.
285. 구현예 282에 있어서,285. The method of embodiment 282,
상기 기준 OS 시간은 적어도 약 11.6개월 내지 약 14.9개월인, 사용.wherein the baseline OS time is at least about 11.6 months to about 14.9 months.
286. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,286. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
상기 방법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks. Use, including steps.
287. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,287. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
상기 방법은 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject one or more dosing cycles of an anti-TGIT antagonist antibody at a dose of about 1200 mg every 3 weeks and an anti-TGIT antagonist antibody at a dose of about 600 mg every 3 weeks.
288. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-L1 결합 길항제의 사용으로서,288. The use of an anti-TIGIT antagonist antibody and a PD-L1 binding antagonist in the manufacture of a medicament for a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
상기 방법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TGIT 길항제 항체의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.The method comprises administering to the subject one or more dosing cycles of a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks. including, use.
289. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,289. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.Use comprising administering to the subject one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks.
290. PD-L1의 검출 가능한 발현 수준을 갖는 SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,290. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject having SCCHN having a detectable expression level of PD-L1, comprising:
상기 방법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙에 대한1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
291. SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,291. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및(c) administering the subject to one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks. identifying as a person likely to benefit from; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
292. SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,292. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및(c) administering the subject to a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks. confirming as; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
293. SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,293. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및 (c) subjecting the subject to one or more dosing cycles of atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks. identifying as a potential person; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
294. SCCHN을 가진 대상체를 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,294. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 상기 대상체로부터의 종양 샘플을 제공하는 단계;(a) providing a tumor sample from the subject;
(b) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; (b) detecting the protein expression level of PD-L1 in said tumor sample by IHC analysis using an anti-PD-L1 antibody suitable for staining;
(c) 상기 대상체를 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 확인하는 단계; 및 (c) identifying the subject as likely to benefit from a therapy comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks. ; and
(d) PD-L1의 검출가능한 발현 수준을 갖는 확인된 대상체에게 상기 요법을 투여하는 단계를 포함하는, 사용.(d) administering said therapy to an identified subject having a detectable expression level of PD-L1.
295. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,295. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 selecting a regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of mg to about 1200 mg.
296. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,296. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 600 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) a dose of about 1200 mg of a PD-1 axis binding antagonist every 3 weeks and a dose of about 600 mg of anti every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 A use comprising selecting a regimen comprising one or more dosing cycles of the TIGIT antagonist antibody.
297. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,297. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks and about 30 mg to about every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 and selecting a regimen comprising one or more dosing cycles of tiragoluumab at a dose of 1200 mg.
298. SCCHN을 가진 대상체를 위한 요법을 선택하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,298. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting a therapy for a subject with SCCHN, comprising:
상기 방법은:The method is:
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 PD-L1 발현을 기초로 3주마다 약 1200 mg 용량의 아테졸리주맙 및 3주마다 약 600 mg 용량의 티라골루맙의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 사용.(b) atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on PD-L1 expression detected for said subject having a detectable expression level of PD-L1 Use, comprising selecting a regimen comprising one or more dosing cycles.
299. 구현예 267 내지 구현예 298 중 어느 한 구현예에 있어서,299. The method according to any one of embodiments 267 to 298,
상기 PD-L1의 검출 가능한 발현 수준은 항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준인, 사용.wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1 determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody SP263.
300. 구현예 299에 있어서,300. The method of embodiment 299,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기의 종양 샘플에서:The detectable protein expression level of PD-L1 is in the tumor sample:
(a) 5% 이상; (a) at least 5%;
(b) 5% 이상 및 20% 미만; 또는 (b) at least 5% and less than 20%; or
(c) 20% 이상의 종양 관련 면역 세포(TIC)인, 사용.(c) at least 20% tumor-associated immune cells (TICs).
301. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,301. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying a subject with SCCHN as a probable one, comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein of PD-L1 has a TIC of at least 5%. The expression level identifies the subject as likely to benefit from the therapy.
302. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,302. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying a subject with SCCHN as a probable one, comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 5% 이상 20% 미만인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from the subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the PD-L1 TIC is greater than or equal to 5% and less than 20%. wherein the protein expression level of L1 identifies the subject as likely to benefit from the therapy.
303. 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법으로부터 이익을 얻을 가능성이 있는 자로서 SCCHN을 가진 대상체를 확인하는 방법을 위한 약제의 제조에서의 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,303. would benefit from a therapy comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks and an anti TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying a subject with SCCHN as a probable one, comprising:
상기 방법은 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계를 포함하고, 여기서 TIC가 20% 이상인 PD-L1의 단백질 발현 수준은 상기 대상체를 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로서 확인하는, 사용.The method comprises detecting the protein expression level of PD-L1 in a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining, wherein the protein of PD-L1 has a TIC of at least 20%. The expression level identifies the subject as likely to benefit from the therapy.
304. 구현예 301 내지 구현예 303 중 어느 한 구현예에 있어서,304. The method of any one of embodiments 301 to 303,
상기 대상체는 상기 요법으로부터 이익을 얻을 가능성이 있는 것으로 확인되고 상기 방법은 상기 대상체에게 상기 요법을 투여하는 단계를 더 포함하는, 사용.wherein said subject is identified as likely to benefit from said therapy and said method further comprises administering said therapy to said subject.
305. 구현예 301 내지 구현예 304 중 어느 한 구현예에 있어서,305. The method of any one of embodiments 301 to 304,
상기 TIC는 벤타나 SP263 IHC 분석을 사용하여 결정되는, 사용.The TIC used, determined using the Ventana SP263 IHC assay.
306. 구현예 267 내지 구현예 305 중 어느 한 구현예에 있어서,306. The method of any one of embodiments 267 to 305,
상기 대상체 또는 대상체 집단은 검출된 종양 세포 상의 PD-L1 발현에 기초한 치료로부터 이익을 얻을 가능성이 있는 자로서 확인되는, 사용.wherein the subject or population of subjects is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
307. 구현예 72에 있어서,307. The method of
상기 암은 간암인, 사용.wherein the cancer is liver cancer.
308. 구현예 307에 있어서,308. The method of embodiment 307,
상기 간암은 간세포 암종(HCC)인, 사용. wherein the liver cancer is hepatocellular carcinoma (HCC).
309. 간세포 암종(HCC)을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,309. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having hepatocellular carcinoma (HCC), comprising:
상기 방법은 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체 집단은 HCC에 대해 선행 전신 요법을 받은 적이 없는, 사용.The method comprises administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the subject or population of subjects has not received prior systemic therapy for HCC. no, use.
310. 구현예 309에 있어서,310. The method of embodiment 309,
상기 방법은 VEGF 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 더 포함하는, 사용.The method further comprises administering to the subject or population of subjects a VEGF antagonist.
311. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,311. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having HCC, comprising:
상기 방법은 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist.
312. 구현예 310 및 구현예 311에 있어서,312. The method of embodiment 310 and embodiment 311,
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
313. 구현예 309 내지 구현예 312 중 어느 한 구현예에 있어서,313. The method of any one of embodiments 309 to 312,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 3 weeks.
314. 구현예 313에 있어서,314. The method of embodiment 313,
상기 항 TIGIT 길항제 항체는 3주마다 약 30 mg 내지 약 800 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 800 mg every 3 weeks.
315. 구현예 309 내지 구현예 314 중 어느 한 구현예에 있어서,315. The method of any one of embodiments 309 to 314,
상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
316. 구현예 309 내지 구현예 315 중 어느 한 구현예에 있어서,316. The method of any one of embodiments 309 to 315,
상기 PD-1 축 결합 길항제는 3주마다 약 80 mg 내지 약 1600 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 1600 mg every 3 weeks.
317. 구현예 309 내지 구현예 316 중 어느 한 구현예에 있어서,317. The method of any one of embodiments 309 to 316,
상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 900 mg to about 1500 mg every 3 weeks.
318. 구현예 310 또는 구현예 311에 있어서,318. The method of embodiment 310 or embodiment 311,
상기 VEGF 길항제는 2주마다 약 1 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
319. 구현예 318에 있어서,319. The method of embodiment 318,
상기 VEGF 길항제는 2주마다 약 5 mg/kg 내지 약 10 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
320. 구현예 319에 있어서,320. The method of embodiment 319,
상기 VEGF 길항제는 2주마다 약 5 mg/kg, 약 7.5 mg/kg, 또는 약 10 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10 mg/kg every two weeks.
321. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,321. The embodiment of any one of embodiments 309 to 311 and embodiments 318 to 320,
상기 항 TIGIT 길항제 항체는 2주마다 약 10 mg 내지 약 1000 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks.
322. 구현예 309 내지 구현예 311 및 구현예 318 내지 구현예 321 중 어느 한 구현예에 있어서,322. The embodiment of any one of embodiments 309 to 311 and embodiments 318 to 321,
상기 PD-1 축 결합 길항제는 2주마다 약 20 mg 내지 약 1600 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 20 mg to about 1600 mg every two weeks.
323. 구현예 309 내지 구현예 311에 있어서,323. according to embodiment 309 to embodiment 311,
상기 항 TIGIT 길항제 항체는 4주마다 약 200 mg 내지 약 2000 mg의 용량으로 투여되는, 사용.wherein the anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks.
324. 구현예 309 내지 구현예 311 및 구현예 323 중 어느 한 구현예에 있어서,324. The method according to any one of embodiments 309 to 311 and 323,
상기 PD-1 축 결합 길항제는 4주마다 약 80 mg 내지 약 2000 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 4 weeks.
325. 구현예 309 내지 구현예 311, 구현예 323, 및 구현예 324 중 어느 한 구현예에 있어서,325. The embodiment of any one of embodiments 309 to 311, 323, and 324,
상기 PD-1 축 결합 길항제는 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 투여되는, 사용.wherein the PD-1 axis binding antagonist is administered at a dose of about 1400 mg to about 2000 mg every 4 weeks.
326. 구현예 309 내지 구현예 325 중 어느 한 구현예에 있어서,326. The method of any one of embodiments 309 to 325,
상기 HCC는 국소 진행성 또는 전이성 HCC인, 사용.wherein the HCC is locally advanced or metastatic HCC.
327. 구현예 309 내지 구현예 326 중 어느 한 구현예에 있어서,327. The method of any one of embodiments 309 to 326,
상기 HCC는 절제 불가능한 HCC인, 사용.wherein the HCC is unresectable HCC.
328. 구현예 309 내지 구현예 327 중 어느 한 구현예에 있어서,328. The method of any one of embodiments 309 to 327,
상기 대상체 또는 대상체들은 적절한 간 기능을 갖는 것으로 결정되는, 사용.wherein the subject or subjects is determined to have adequate liver function.
329. 구현예 328에 있어서,329. The method of embodiment 328,
상기 적절한 간 기능은 차일드-퍼(Child-Pugh) 분류 A로 특징지어지는, 사용.wherein said adequate liver function is characterized by Child-Pugh class A.
330. 구현예 309 내지 구현예 329 중 어느 한 구현예에 있어서,330. The method of any one of embodiments 309 to 329,
상기 대상체 또는 대상체들로부터 수득한 HCC 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 사용.wherein the subject or HCC tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
331. 구현예 309 내지 구현예 330 중 어느 한 구현예에 있어서,331. The method of any one of embodiments 309 to 330,
상기 방법은 상기 대상체 또는 대상체 집단에 적어도 4회의 투약 주기를 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects at least 4 dosing cycles.
332. 구현예 331에 있어서,332. The method of embodiment 331,
상기 방법은 상기 대상체 또는 대상체 집단에 적어도 16회의 투약 주기를 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects at least 16 dosing cycles.
333. HCC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,333. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having HCC,
3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 사용.administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and bevacizumab at a dose of about 15 mg/kg every 3 weeks. Use, including steps.
334. 구현예 311 내지 구현예 333 중 어느 한 구현예에 있어서,334. The method of any one of embodiments 311 to 333,
상기 대상체 또는 대상체들은 HCC에 대해 선행 전신 치료를 받은 적이 없는, 사용.The subject or subjects have not received prior systemic treatment for HCC.
335. 구현예 309 내지 구현예 334 중 어느 한 구현예에 있어서,335. The method of any one of embodiments 309 to 334,
상기 치료는 적어도 약 5.6개월 내지 적어도 약 6.83개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용.wherein said treatment results in a median PFS in the subject population of at least about 5.6 months to at least about 6.83 months.
336. 구현예 72에 있어서,336. The method of
상기 암은 방광암인, 사용.wherein the cancer is bladder cancer.
337. 구현예 336에 있어서,337. The method of embodiment 336,
상기 방광암은 근육 침윤성 방광암(MIBC)인, 사용.wherein the bladder cancer is muscle invasive bladder cancer (MIBC).
338. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,338. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
339. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,339. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks wherein the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
340. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,340. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC,
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the treatment is perioperative treatment.
341. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,341. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks wherein the treatment is perioperative treatment.
342. 구현예 338 내지 구현예 341 중 어느 한 구현예에 있어서,342. The method of any one of embodiments 338 to 341,
상기 대상체 또는 대상체들은 크레아티닌 청소율이 60 mL/분 미만인, 사용.wherein the subject or subjects have a creatinine clearance of less than 60 mL/min.
343. 구현예 338 내지 구현예 342 중 어느 한 구현예에 있어서,343. The method of any one of embodiments 338 to 342,
상기 대상체 또는 대상체들은 2등급 이상의 청력 상실을 갖는, 사용.wherein the subject or subjects have a hearing loss of
344. 구현예 338 내지 구현예 343 중 어느 한 구현예에 있어서,344. The method of any one of embodiments 338 to 343,
상기 대상체 또는 대상체들은 2등급 이상의 신경병증을 갖는, 사용.wherein said subject or subjects have
345. 구현예 338 내지 구현예 344 중 어느 한 구현예에 있어서,345. The method of any one of embodiments 338 to 344,
상기 대상체 또는 대상체들은 백금계 화학요법제를 이용한 치료를 거부한, 사용.The subject or subjects refused treatment with a platinum-based chemotherapeutic agent.
346. 구현예 338 또는 구현예 342 내지 구현예 345 중 어느 한 구현예에 있어서,346. The method according to any one of embodiments 338 or 342 to 345,
상기 백금계 화학요법제는 시스플라틴인, 사용.The platinum-based chemotherapeutic agent is cisplatin.
347. 구현예 338 내지 구현예 346 중 어느 한 구현예에 있어서,347. The method of any one of embodiments 338 to 346,
상기 MIBC는 외과 수술이 가능한, 사용.The MIBC can be used, surgically.
348. 구현예 347에 있어서,348. The method of embodiment 347,
상기 방법은 수술을 더 포함하는, 사용.The method further comprises surgery.
349. 구현예 348에 있어서,349. The method of embodiment 348,
적어도 1회의 투약 주기는 상기 수술 전에 개시되는, 사용.at least one dosing cycle is initiated prior to the surgery.
350. 구현예 348 또는 구현예 349에 있어서,350. The method of embodiment 348 or embodiment 349,
적어도 1, 2, 또는 3회의 투약 주기는 상기 수술 전에 완료되는, 사용.wherein at least 1, 2, or 3 dosing cycles are completed prior to the surgery.
351. 구현예 348 내지 구현예 350 중 어느 한 구현예에 있어서,351. The method of any one of embodiments 348 to 350,
적어도 1회의 투약 주기는 상기 수술 후 4주 내지 6주 사이에 개시되는, 사용.wherein at least one dosing cycle is initiated between 4 and 6 weeks after said surgery.
352. 구현예 351에 있어서,352. The method of embodiment 351,
1 내지 17회의 투약 주기는 상기 수술 후에 완료되는, 사용.1 to 17 dosing cycles are completed after said surgery.
353. 구현예 348 내지 구현예 352 중 어느 한 구현예에 있어서,353. The method of any one of embodiments 348 to 352,
상기 수술은 방광 절제술 및/또는 림프절 절제술인, 사용.wherein the operation is cystectomy and/or lymphadenectomy.
354. 구현예 338 내지 구현예 353 중 어느 한 구현예에 있어서,354. The method of any one of embodiments 338 to 353,
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 사용.wherein said treatment results in a pathological complete response (pCR).
355. 구현예 338 내지 구현예 354 중 어느 한 구현예에 있어서,355. The method of any one of embodiments 338 to 354,
상기 치료는 기준 RFS 시간과 비교하여 상기 대상체 또는 대상체들의 무재발 생존(RFS)의 증가, 기준 EFS 시간과 비교하여 상기 대상체 또는 대상체들의 무사건 생존(EFS)의 증가, 또는 기준 OS 시간과 비교하여 상기 대상체 또는 대상체들의 OS의 증가를 유발하는, 사용.wherein the treatment is an increase in relapse-free survival (RFS) of the subject or subjects as compared to a baseline RFS time, an increase in the event-free survival (EFS) of the subject or subjects compared to a baseline EFS time, or an increase in the event-free survival (EFS) of the subject or subjects as compared to a baseline OS time. causing an increase in OS of the subject or subjects.
356. 구현예 355에 있어서:356. The method of embodiment 355:
(a) 상기 기준 RFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 RFS 시간 중앙값이고;(a) said baseline RFS time is the median RFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) 상기 기준 EFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 EFS 시간 중앙값이거나; 또는 (b) said baseline EFS time is the median EFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값인, 사용.(c) the baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
357. 구현예 338 내지 구현예 356 중 어느 한 구현예에 있어서,357. The method of any one of embodiments 338 to 356,
상기 치료는 병리학적 병기하향(downstaging)을 유발하는, 사용.wherein said treatment results in pathological downstaging.
358. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,358. Use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC,
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the subject is cisplatin ineligible.
359. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,359. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the treatment is perioperative treatment.
360. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,360. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the subject is cisplatin ineligible.
361. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,361. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks wherein the treatment is perioperative treatment.
362. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,362. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 시스플라틴 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks; , wherein the subject is cisplatin ineligible.
363. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,363. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks; , wherein said treatment is perioperative treatment.
364. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,364. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체들은 시스플라틴 부적격인, 사용.administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein the subject or subjects have cisplatin ineligible for use.
365. MIBC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,365. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with MIBC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 수술 전후 치료인, 사용.administering to said subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein said treatment comprises perioperative treatment In, use.
366. 구현예 338 내지 구현예 365 중 어느 한 구현예에 있어서,366. The method of any one of embodiments 338-365,
상기 치료는 적어도 약 13.4% 내지 약 15%의 대상체 집단의 ORR을 유발하는, 사용.wherein said treatment results in an ORR in at least about 13.4% to about 15% of the subject population.
367. 구현예 338 내지 구현예 366 중 어느 한 구현예에 있어서,367. The method of any one of embodiments 338 to 366,
상기 치료는 적어도 약 7.9개월 내지 약 8.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.wherein said treatment results in a median OS in the subject population of at least about 7.9 months to about 8.6 months.
368. 구현예 338 내지 구현예 367 중 어느 한 구현예에 있어서,368. The method of any one of embodiments 338 to 367,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
369. 구현예 368에 있어서,369. The method of embodiment 368,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 5% 이상인 PD-L1 양성 종양 세포 분획인, 사용.wherein the detectable protein expression level of PD-L1 is a fraction of PD-L1-positive tumor cells in which the proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) is 5% or more.
370. 구현예 336에 있어서,370. The method of embodiment 336,
상기 방광암은 요로상피세포 암종(UC)인, 사용.wherein the bladder cancer is urothelial cell carcinoma (UC).
371. 구현예 370에 있어서,371. The method of embodiment 370,
상기 UC는 전이성 요로상피세포 암종(mUC)인, 사용.wherein the UC is metastatic urothelial cell carcinoma (mUC).
372. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,372. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. Use comprising administering to a population.
373. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,373. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks to the subject or subject. Use comprising administering to a population.
374. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,374. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 선행 암 면역요법을 받은 적이 없는, 사용.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. administering to a population, wherein the subject has not received prior cancer immunotherapy.
375. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,375. Use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 2차 치료인, 사용.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks to the subject or subject. administering to a population, wherein said treatment is a second line treatment.
376. 구현예 372, 구현예 372, 및 구현예 375 중 어느 한 구현예에 있어서,376. The method of any one of embodiments 372, 372, and 375,
상기 대상체 또는 대상체들은 선행 암 면역요법을 받은 적이 없는, 사용.wherein said subject or subjects have not received prior cancer immunotherapy.
377. 구현예 372 내지 구현예 374 중 어느 한 구현예에 있어서,377. The method according to any one of embodiments 372 to 374,
상기 치료는 2차 치료인, 사용.wherein the treatment is a second line treatment.
378. 구현예 372 내지 구현예 377 중 어느 한 구현예에 있어서,378. The method of any one of embodiments 372 to 377,
상기 mUC는 백금 함유 요법 중에 또는 이후에 진행하는, 사용.wherein said mUC proceeds during or after platinum containing therapy.
379. 구현예 372 내지 구현예 378 중 어느 한 구현예에 있어서,379. The method according to any one of embodiments 372 to 378,
상기 방법은 상기 대상체 또는 대상체 집단이 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체들에게 제2 투약 요법을 투여하는 단계를 더 포함하는, 사용.The method further comprises administering a second dosing regimen to the subject or subjects after the subject or population of subjects has experienced disease progression or unacceptable toxicity.
380. 구현예 379에 있어서,380. The method of embodiment 379,
상기 제2 투약 요법은 PD-1 축 결합 길항제 및 항체-약물 접합체(ADC)의 1회 이상의 투약 주기를 포함하는, 사용.wherein the second dosing regimen comprises one or more dosing cycles of the PD-1 axis binding antagonist and the antibody-drug conjugate (ADC).
381. 구현예 380에 있어서,381. The method of embodiment 380,
상기 ADC는 (a) 엔포르투맙 베도틴 또는 (b) 사시투주맙 고비테칸인, 사용.wherein said ADC is (a) enfortumab vedotin or (b) sacituzumab gobitecan.
382. 구현예 381에 있어서,382. The method of embodiment 381,
(a) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (b) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되는, 사용.(a) enfortumab vedotin is administered at a weekly dose of 1.25 mg/kg on a 2-week dosing/week break, or (b) sacituzumab gobitecan is administered at 10 mg/week on a 2-week dos/week break Administered in kg dose, use.
383. 구현예 381 또는 구현예 382에 있어서,383. The method of embodiment 381 or embodiment 382,
(a) 엔포르투맙 베도틴은 각 21일 주기의 제 1일 및 8일에 1.25 mg/kg의 용량으로 투여되거나, 또는 (b) 사시투주맙 고비테칸은 각 21일 주기의 제 1일 및 8일에 10 mg/kg의 용량으로 투여되는, 사용.(a) enfortumab vedotin is administered at a dose of 1.25 mg/kg on
384. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,384. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks; Use, comprising the step of administering to.
385. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,385. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 30 mg 내지 약 1200 mg 용량의 티라골루맙 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.administering to the subject or population of subjects a dosing regimen comprising one or more dosing cycles of tyragolumab at a dose of about 30 mg to about 1200 mg every 3 weeks and atezolizumab at a dose of about 80 mg to about 1600 mg every 3 weeks Use, including steps.
386. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서의 티라골루맙 및 아테졸리주맙의 사용으로서,386. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.Use comprising administering to said subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
387. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,387. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
상기 방법은 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises at least one dosing cycle of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks comprising; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체 또는 대상체 집단에 투여되는, 사용.(b) said second dosing regimen comprises one or more dosing cycles of the PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, and (i) Enfortumab vedotin is administered for 2 weeks. administered at a weekly dose of 1.25 mg/kg with a weekly break of one week, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/1 week off, wherein the second dosing regimen is wherein said subject or population of subjects experiences disease progression or unacceptable toxicity during said first dosing regimen.
388. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,388. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
상기 방법은 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks including; and
(b) 상기 제2 투약 요법은 3주마다 약 80 mg 내지 약 1600 mg 용량의 PD-L1 결합 길항제의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에 투여되는, 사용.(b) said second dosing regimen comprises one or more dosing cycles of the PD-L1 binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, (i) Enfortumab vedotin is administered for 2 weeks / administered at a weekly dose of 1.25 mg/kg with a one-week break, or (ii) sacituzumab gobitecan is administered at a weekly dose of 10 mg/kg with a two-week dosing/week break, wherein the second dosing regimen is administered to the subject after the subject experiences disease progression or unacceptable toxicity during said first dosing regimen.
389. mUC를 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,389. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects with mUC, comprising:
상기 방법은 제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고 (a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and
(b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체가 상기 제1 투약 요법 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한 후 상기 대상체에 투여되는, 사용.(b) said second dosing regimen comprises at least one dosing cycle of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin is administered at 1.25 weekly doses of 2 weeks on/1 week off. is administered in a mg/kg dose, or (ii) sacituzumab gobitecan is administered at a weekly 10 mg/kg dose of 2 weeks dosing/1 week off, wherein the second dosing regimen is such that the subject administers the first dose The use of which is administered to a subject after experiencing disease progression or unacceptable toxicity during therapy.
390. 구현예 372 내지 구현예 389 중 어느 한 구현예에 있어서,390. The method of any one of embodiments 372 to 389,
상기 치료는 적어도 약 13.4% 내지 적어도 약 31%의 대상체 집단의 ORR을 유발하는, 사용.wherein said treatment results in an ORR in at least about 13.4% to at least about 31% of the subject population.
391. 구현예 372 내지 구현예 390 중 어느 한 구현예에 있어서,391. The method of any one of embodiments 372 to 390,
상기 치료는 약 7.9개월 내지 약 16.3개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.wherein said treatment results in a median OS in the subject population of about 7.9 months to about 16.3 months.
392. 구현예 72에 있어서,392. The method of
상기 암은 췌장암인, 사용.wherein the cancer is pancreatic cancer.
393. 췌장암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,393. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having pancreatic cancer,
각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.Tiragolumab at a dose of about 420 mg on
394. 구현예 392 또는 구현예 393에 있어서,394. The method of embodiment 392 or embodiment 393,
상기 췌장암은 췌장관 선암(PDAC)인, 사용.wherein the pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395. 구현예 394에 있어서,395. The method of embodiment 394,
상기 PDAC는 전이성 PDAC인, 사용.wherein the PDAC is a metastatic PDAC.
396. 구현예 392 내지 구현예 395 중 어느 한 구현예에 있어서,396. The method of any one of embodiments 392 to 395,
상기 대상체 또는 대상체들은 전이성 PDAC에 대해 선행 전신 요법을 받은 적이 없는, 사용.The subject or subjects have not received prior systemic therapy for metastatic PDAC.
397. 구현예 392 내지 구현예 396 중 어느 한 구현예에 있어서,397. The method of any one of embodiments 392 to 396,
상기 치료는 적어도 약 41.7% 내지 약 46.7%의 대상체 집단의 ORR을 유발하는, 사용.wherein said treatment results in an ORR in at least about 41.7% to about 46.7% of the subject population.
398. 구현예 392 내지 구현예 397 중 어느 한 구현예에 있어서,398. The method of any one of embodiments 392 to 397,
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 없이 젬시타빈 및 냅-파클리탁셀을 포함한 치료와 비교하여 적어도 약 20%의 ORR의 증가를 유발하는, 사용.wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nap-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
399. 구현예 392 내지 구현예 398 중 어느 한 구현예에 있어서,399. The method of any one of embodiments 392 to 398,
상기 치료는 적어도 약 5.5개월 내지 약 7개월의 대상체 집단의 PFS 중앙값을 유발하는, 사용.wherein said treatment results in a median PFS in the subject population of at least about 5.5 months to about 7 months.
400. 구현예 392 내지 구현예 399 중 어느 한 구현예에 있어서,400. The method of any one of embodiments 392 to 399,
상기 치료는 적어도 약 8.5개월 내지 약 10.6개월의 대상체 집단의 OS 중앙값을 유발하는, 사용.wherein said treatment results in a median OS in the subject population of at least about 8.5 months to about 10.6 months.
401. 구현예 72에 있어서,401. The method of
상기 암은 식도암인, 사용.wherein the cancer is esophageal cancer.
402. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,402. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.One or
403. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,403. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.One or more 21 doses of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
404. 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,404. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having esophageal cancer,
상기 방법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용.The method comprises one dose of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
405. 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,405. Use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having esophageal cancer,
상기 방법은 각 투약 주기의 제 1일에 약 300 mg 내지 약 800 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용.The method comprises one dose of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg on
406. 구현예 402 또는 구현예 403에 있어서,406. The method of embodiment 402 or embodiment 403,
상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 사용.wherein the subject or subjects has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
407. 구현예 404 또는 구현예 406에 있어서,407. The method of embodiment 404 or embodiment 406,
상기 대상체 또는 대상체들은 상기 선행 치료 동안에 질병 진행 또는 허용할 수 없는 독성을 경험한, 사용.wherein said subject or subjects experienced disease progression or unacceptable toxicity during said prior treatment.
408. 구현예 402 또는 구현예 403에 있어서,408. The method of embodiment 402 or embodiment 403,
상기 21일 투약 주기는 백금계 화학요법제 및 비백금계 화학요법제를 더 포함하는, 사용.The 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409. 구현예 408에 있어서,409. The method of embodiment 408,
상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
410. 구현예 404 내지 구현예 409 중 어느 한 구현예에 있어서,410. The method of any one of embodiments 404 to 409,
상기 백금계 화학요법제는 시스플라틴인, 사용.The platinum-based chemotherapeutic agent is cisplatin.
411. 구현예 410에 있어서,411. The method of embodiment 410,
시스플라틴은 각 투약 주기의 제 1일에 약 80 mg/m2의 용량으로 투여되는, 사용.Cisplatin is administered at a dose of about 80 mg/m2 on
412. 구현예 404 내지 구현예 411 중 어느 한 구현예에 있어서,412. The method of any one of embodiments 404 to 411,
상기 비백금계 화학요법제는 항대사물질인, 사용.The non-platinum-based chemotherapeutic agent is an antimetabolites.
413. 구현예 412에 있어서,413. The method of embodiment 412,
상기 항대사물질은 5-플루오로우라실인, 사용.wherein the antimetabolite is 5-fluorouracil.
414. 구현예 413에 있어서,414. The method of embodiment 413,
5-플루오로우라실은 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간의 용량으로 투여되는, 사용.5-fluorouracil is administered at a dose of about 800 mg/m2/24 hours on days 1-5 of each 21-day cycle.
415. 구현예 404 내지 구현예 414 중 어느 한 구현예에 있어서,415. The method of any one of embodiments 404 to 414,
상기 식도암은 진행성 또는 전이성 식도암인, 사용.wherein the esophageal cancer is advanced or metastatic esophageal cancer.
416. 구현예 402, 구현예 403, 구현예 408, 및 구현예 409 중 어느 한 구현예에 있어서,416. The embodiment of any one of embodiments 402, 403, 408, and 409,
상기 대상체 또는 대상체들은 전이성 식도암에 대해 선행 치료를 받은 적이 없는, 사용.wherein said subject or subjects have not received prior treatment for metastatic esophageal cancer.
417. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,417. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 사용.Anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
418. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,418. The use of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
각 투약 주기의 제 1일에 약 600 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 1200 mg 용량의 PD-1 축 결합 길항제, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 사용.Anti-TIGIT antagonist antibody at a dose of about 600 mg on
419. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,419. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 사용.Tiragolumab at a dose of about 600 mg on
420. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,420. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
상기 방법은 제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 백금계 화학요법제 및 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises at least one 21-day dosing cycle of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses; ; and
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 사용.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
421. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 사용으로서,421. The use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, comprising:
상기 방법은 제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 백금계 화학요법제 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 비백금계 화학요법제의 1회 이상의 21일 투약 주기를 포함하고, 여기서 상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 30 mg 내지 약 1200 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 80 mg 내지 약 1600 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함하는, 사용.(b) said second dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
422. 진행성 또는 전이성 식도암을 가진 대상체 또는 대상체 집단을 치료하는 방법을 위한 약제의 제조에서 티라골루맙 및 아테졸리주맙의 사용으로서,422. The use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or population of subjects having advanced or metastatic esophageal cancer,
상기 방법은 제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에 투여하는 단계를 포함하고, 여기서: The method comprises administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고 (a) said first dosing regimen is cisplatin at a dose of about 80 mg/m2 on
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함하는, 사용.(b) said second dosing regimen is one or more 21 day dosing cycles of tiragolumab at a dose of about 600 mg on
423. 구현예 402 내지 구현예 422 중 어느 한 구현예에 있어서,423. The method of any one of embodiments 402 to 422,
상기 치료는 적어도 약 14%의 대상체 집단의 ORR을 유발하는, 사용.wherein said treatment results in an ORR in at least about 14% of the subject population.
424. 구현예 47 내지 구현예 423 중 어느 한 구현예에 있어서,424. The method according to any one of embodiments 47 to 423,
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 사용.A use comprising an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
425. 구현예 424에 있어서,425. The method of embodiment 424,
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR):The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4를 더 포함하는, 사용.The use, further comprising FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
426. 구현예 424에 있어서,426. The method of embodiment 424,
상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR:The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X1 is E or Q;
WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 사용.The use, further comprising FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
427. 구현예 426에 있어서,427. The method of embodiment 426,
X1은 E인, 사용.X1 is E, use.
428. 구현예 426에 있어서,428. The method of embodiment 426,
X1은 Q인, 사용.X1 is Q, use.
429. 구현예 424 내지 구현예 428 중 어느 한 구현예에 있어서,429. The method of any one of embodiments 424 to 428,
상기 항 TIGIT 길항제 항체는:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 사용.(c) a use comprising a VH domain as in case (a) and a VL domain as in case (b).
430. 구현예 424 내지 구현예 429 중 어느 한 구현예에 있어서,430. The method of any one of embodiments 424 to 429,
상기 항 TIGIT 길항제 항체는:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용.(b) A use comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
431. 구현예 424 내지 구현예 427, 구현예 429, 및 구현예 430 중 어느 한 구현예에 있어서,431. The embodiment of any one of embodiments 424 to 427, 429, and 430,
상기 항 TIGIT 길항제 항체는 하기의:The anti-TIGIT antagonist antibody is:
(a) 서열번호 17의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17; and
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용.(b) A use comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
432. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 431 중 어느 한 구현예에 있어서,432. The method of any one of embodiments 424 to 427 and embodiments 429 to 431,
상기 항 TIGIT 길항제 항체는 하기의: The anti-TIGIT antagonist antibody is:
(a) 서열번호 33의 아미노산 서열을 포함하는 중쇄; 및 (a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 33; and
(b) 서열번호 34의 아미노산 서열을 포함하는 경쇄를 포함하는, 사용.(b) use comprising a light chain comprising the amino acid sequence of SEQ ID NO:34.
433. 구현예 424 내지 구현예 432 중 어느 한 구현예에 있어서,433. The method of any one of embodiments 424 to 432,
상기 항 TIGIT 길항제 항체는 단일클론 항체인, 사용.wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
434. 구현예 424 내지 구현예 433 중 어느 한 구현예에 있어서,434. The method of any one of embodiments 424 to 433,
상기 항 TIGIT 길항제 항체는 인간 항체인, 사용.wherein the anti-TIGIT antagonist antibody is a human antibody.
435. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,435. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 전장 항체인, 사용.wherein the anti-TIGIT antagonist antibody is a full-length antibody.
436. 구현예 424 내지 구현예 427 및 구현예 429 내지 구현예 436 중 어느 한 구현예에 있어서,436. The method of any one of embodiments 424 to 427 and embodiments 429 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙인, 사용. wherein the anti-TIGIT antagonist antibody is tyragolumab.
437. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 구현예 421, 및 구현예 424 내지 구현예 436 중 어느 한 구현예에 있어서,437. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, embodiment 421, and embodiment any one of embodiments 424 to 436,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT 또는 TJ-T6인, 사용.wherein said anti-TIGIT antagonist antibody is tiragolumab, bivostoliumab, ethigiliumab, EOS084448, SGN-TGT or TJ-T6.
438. 구현예 437에 있어서,438. The method of embodiment 437,
상기 항 TIGIT 길항제 항체는 원형 Fc 매개 작동체 기능을 갖는, 사용.wherein said anti-TIGIT antagonist antibody has prototypical Fc-mediated effector function.
439. 구현예 437 또는 구현예 438에 있어서,439. according to embodiment 437 or embodiment 438,
상기 항 TIGIT 길항제 항체는 강화된 Fc 매개 작동체 기능을 갖는, 사용.wherein said anti-TIGIT antagonist antibody has enhanced Fc-mediated effector function.
440. 구현예 437 내지 구현예 439 중 어느 한 구현예에 있어서,440. The method of any one of embodiments 437 to 439,
상기 항 TIGIT 길항제 항체는 SGN-TGT인, 사용.wherein the anti-TIGIT antagonist antibody is SGN-TGT.
441. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421 중 어느 한 구현예에 있어서,441. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421 according to any one of embodiments,
상기 항 TIGIT 길항제 항체는 돔바날리맙, BMS-986207, ASP8374 또는 COM902인, 사용.wherein the anti-TIGIT antagonist antibody is dombanalimab, BMS-986207, ASP8374 or COM902.
442. 구현예 424 내지 구현예 431, 및 구현예 441 중 어느 한 구현예에 있어서,442. The embodiment of any one of embodiments 424 to 431, and embodiment 441,
상기 항 TIGIT 길항제 항체는 Fc 매개 작동체 기능을 갖지 않는, 사용.wherein said anti-TIGIT antagonist antibody has no Fc-mediated effector function.
443. 구현예 47 내지 구현예 442 중 어느 한 구현예에 있어서,443. The method according to any one of embodiments 47 to 442,
상기 항 TIGIT 길항제 항체는 IgG 부류 항체인, 사용.wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444. 구현예 443에 있어서,444. The method of embodiment 443,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 사용.wherein said IgG class antibody is an IgG1 subclass antibody.
445. 구현예 444에 있어서,445. of embodiment 444,
상기 항 TIGIT 길항제 항체는 티라골루맙, 비보스톨리맙, 에티길리맙, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, 돔바날리맙, 또는 BMS-986207인, 사용.wherein said anti-TIGIT antagonist antibody is tiragolumab, bivostolimab, etigilumab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, dombanalimab, or BMS-986207.
446. 구현예 47 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 174, 구현예 188 내지 구현예 209, 구현예 227 내지 구현예 253, 구현예 255, 구현예 265 내지 구현예 269, 구현예 286 내지 구현예 288, 구현예 291, 구현예 292, 구현예 295, 구현예 296, 구현예 301 내지 구현예 332, 구현예 336 내지 구현예 361, 구현예 370 내지 구현예 384, 구현예 387, 구현예 388, 구현예 401 내지 구현예 418, 구현예 420, 및 구현예 421에 있어서,446. Embodiment 47 to embodiment 112, embodiment 114 to embodiment 127, embodiment 136 to embodiment 174, embodiment 188 to embodiment 209, embodiment 227 to embodiment 253, embodiment 255, embodiment 265 to Embodiment 269, Embodiment 286 to Embodiment 288, Embodiment 291, Embodiment 292, Embodiment 295, Embodiment 296, Embodiment 301 to Embodiment 332, Embodiment 336 to Embodiment 361, Embodiment 370 to Embodiment 384, embodiment 387, embodiment 388, embodiment 401 to embodiment 418, embodiment 420, and embodiment 421,
상기 IgG 부류 항체는 IgG4 하위부류 항체인, 사용.wherein said IgG class antibody is an IgG4 subclass antibody.
447. 구현예 446에 있어서,447. The method of embodiment 446,
상기 항 TIGIT 길항제 항체는 ASP8374 또는 COM902인, 사용.wherein the anti-TIGIT antagonist antibody is ASP8374 or COM902.
448. 구현예 424 내지 구현예 434 중 어느 한 구현예에 있어서,448. The method of any one of embodiments 424 to 434,
상기 항 TIGIT 길항제 항체는 Fab, 비스-Fab, Fab’, Fab’-SH, Fv, 단일 사슬 가변 단편(scFv), 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 TIGIT에 결합하는 항체 단편인, 사용.wherein the anti-TIGIT antagonist antibody is an antibody fragment that binds to TIGIT selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv), and (Fab')2 fragment, use.
449. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,449. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 단일특이적 항체인, 사용. wherein the anti-TIGIT antagonist antibody is a monospecific antibody.
450. 구현예 424 내지 구현예 448 중 어느 한 구현예에 있어서,450. The method of any one of embodiments 424 to 448,
상기 항 TIGIT 길항제 항체는 다중특이적 항체인, 사용.wherein the anti-TIGIT antagonist antibody is a multispecific antibody.
451. 구현예 450에 있어서,451. The method of embodiment 450,
상기 다중특이적 항체는 이중특이적 항체인, 사용.wherein said multispecific antibody is a bispecific antibody.
452. 구현예 424 내지 구현예 451 중 어느 한 구현예에 있어서452. The method of any one of embodiments 424 to 451
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제, 및 PD-L2 결합 길항제로 이루어진 군으로부터 선택되는, 사용.wherein the PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
453. 구현예 452에 있어서,453. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-1 결합 길항제인, 사용.wherein the PD-1 axis binding antagonist is a PD-1 binding antagonist.
454. 구현예 453에 있어서,454. The method of embodiment 453,
상기 PD-L1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 사용.wherein the PD-L1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners.
455. 구현예 454에 있어서,455. The method of embodiment 454,
상기 PD-L1 결합 길항제는 PD-L1이 PD-1, B7-1, 또는 PD-1 및 B7-1 둘 모두에 결합하는 것을 억제하는, 사용.wherein the PD-L1 binding antagonist inhibits the binding of PD-L1 to PD-1, B7-1, or both PD-1 and B7-1.
456. 구현예 453 내지 구현예 455 중 어느 한 구현예에 있어서,456. The method according to any one of embodiments 453-455,
상기 PD-L1 결합 길항제는 항 PD-L1 길항제 항체인, 사용.wherein the PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457. 구현예 456에 있어서,457. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 사용.The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636, used.
458. 구현예 457에 있어서,458. The method of embodiment 457,
상기 항 PD-L1 길항제 항체는 아테졸리주맙인, 사용.wherein the anti-PD-L1 antagonist antibody is atezolizumab.
459. 구현예 456에 있어서,459. The method of embodiment 456,
상기 항 PD-L1 길항제 항체는 하기의 HVR들:The anti-PD-L1 antagonist antibody has the following HVRs:
GFTFSDSWIH(서열번호 20)의 아미노산 서열을 포함하는 HVR-H1 서열;HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
AWISPYGGSTYYADSVKG(서열번호 21)의 아미노산 서열을 포함하는 HVR-H2 서열;HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
RHWPGGFDY(서열번호 22)의 아미노산 서열을 포함하는 HVR-H3 서열;HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
RASQDVSTAVA(서열번호 23)의 아미노산 서열을 포함하는 HVR-L1 서열;HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
SASFLYS(서열번호 24)의 아미노산 서열을 포함하는 HVR-L2; 및HVR-L2 comprising the amino acid sequence of SASFLYS (SEQ ID NO: 24); and
QQYLYHPAT(서열번호 25)의 아미노산 서열을 포함하는 HVR-L3을 포함하는, 사용.use comprising HVR-L3 comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
460. 구현예 459에 있어서,460. The method of embodiment 459,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인; (a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) 서열번호 27의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는 (b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 사용.(c) a use comprising a VH domain as in case (a) and a VL domain as in case (b).
461. 구현예 460에 있어서,461. The method of embodiment 460,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 26의 아미노산 서열을 포함하는 VH 도메인; 및(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and
(b) 서열번호 27의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 사용.(b) A use comprising a VL domain comprising the amino acid sequence of SEQ ID NO:27.
462. 구현예 461에 있어서,462. The method of embodiment 461,
상기 항 PD-L1 길항제 항체는 하기의:The anti-PD-L1 antagonist antibody comprises:
(a) 서열번호 28의 아미노산 서열을 포함하는 중쇄; 및(a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 28; and
(b) 서열번호 29의 아미노산 서열을 포함하는 경쇄를 포함하는, 사용.(b) A use comprising a light chain comprising the amino acid sequence of SEQ ID NO:29.
463. 구현예 459 내지 구현예 462 중 어느 한 구현예에 있어서,463. The method according to any one of embodiments 459 to 462,
상기 항 PD-L1 길항제 항체는 단일클론 항체인, 사용.wherein the anti-PD-L1 antagonist antibody is a monoclonal antibody.
464. 구현예 459 내지 구현예 463 중 어느 한 구현예에 있어서,464. The method of any one of embodiments 459 to 463,
상기 항 PD-L1 길항제 항체는 인간화 항체인, 사용.wherein the anti-PD-L1 antagonist antibody is a humanized antibody.
465. 구현예 463 또는 구현예 464에 있어서,465. The method of embodiment 463 or embodiment 464,
상기 항 PD-L1 길항제 항체는 전장 항체인, 사용.wherein the anti-PD-L1 antagonist antibody is a full-length antibody.
466. 구현예 459 내지 구현예 464 중 어느 한 구현예에 있어서,466. The method according to any one of embodiments 459 to 464,
상기 항 PD-L1 길항제 항체는 Fab, Fab’, Fab’-SH, Fv, scFv, 및 (Fab’)2 단편으로 이루어진 군으로부터 선택된 PD-L1에 결합하는 항체 단편인, 사용.wherein the anti-PD-L1 antagonist antibody is an antibody fragment that binds to PD-L1 selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab')2 fragments.
467. 구현예 459 내지 구현예 465 중 어느 한 구현예에 있어서,467. The method according to any one of embodiments 459 to 465,
상기 항 PD-L1 길항제 항체는 IgG 부류 항체인, 사용.wherein the anti-PD-L1 antagonist antibody is an IgG class antibody.
468. 구현예 467에 있어서,468. The method of embodiment 467,
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 사용.wherein said IgG class antibody is an IgG1 subclass antibody.
469. 구현예 452에 있어서,469. The method of embodiment 452,
상기 PD-1 축 결합 길항제는 PD-1 결합 길항제인, 사용.wherein the PD-1 axis binding antagonist is a PD-1 binding antagonist.
470. 구현예 469에 있어서,470. The method of embodiment 469,
상기 PD-1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 사용.wherein the PD-1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners.
471. 구현예 470에 있어서,471. The method of embodiment 470,
상기 PD-1 결합 길항제는 PD-L1이 PD-L1, PD-L2, 또는 PD-L1 및 PD-L2 둘 모두에 결합하는 것을 억제하는, 사용.wherein the PD-1 binding antagonist inhibits PD-L1 from binding to PD-L1, PD-L2, or both PD-L1 and PD-L2.
472. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,472. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 항 PD-1 길항제 항체인, 사용.wherein said PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473. 구현예 472에 있어서,473. The method of embodiment 472,
상기 항 PD-L1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 사용.Said anti-PD-L1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, progolimab, camrelizumab, scintilimab, tislelizumab, torifaliz Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21, for use.
474. 구현예 469 내지 구현예 471 중 어느 한 구현예에 있어서,474. The method according to any one of embodiments 469 to 471,
상기 PD-1 결합 길항제는 Fc 융합 단백질인, 사용.wherein the PD-1 binding antagonist is an Fc fusion protein.
475. 구현예 474에 있어서,475. The method of embodiment 474,
상기 Fc 융합 단백질은 AMP-224인, 사용.The Fc fusion protein is AMP-224, use.
476. 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 및 구현예 309 내지 구현예 312 중 어느 한 구현예에 있어서,476. The embodiment of any one of embodiments 80-112, 114-127, and embodiments 309-312,
상기 방법은 항 TIGIT 길항제 항체를 3주마다 약 30 mg 내지 약 1200 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks.
477. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,477. Embodiment 51, Embodiment 54,
상기 방법은 상기 항 TIGIT 길항제 항체를 3주마다 약 600 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject at a dose of about 600 mg every 3 weeks.
478. 구현예 51, 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 174, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301, 구현예 302, 구현예 303, 구현예 309, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 404, 구현예 417, 구현예 420, 구현예 421, 및 구현예 476 중 어느 한 구현예에 있어서,478. Embodiment 51, Embodiment 54,
상기 방법은 상기 항 TIGIT 길항제 항체를 대상체의 체중에 기초한 단계적 용량으로 상기 대상체 또는 대상체의 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체는 하기의 체중으로서: The method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects in stepwise doses based on the body weight of said subject, wherein said subject has a body weight of:
(a) 15 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 300 mg의 용량으로 투여되고; (a) weighing 15 kg or less, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks;
(b) 15 kg 초과 및 40 kg 이하이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 400 mg의 용량으로 투여되거나; 또는 (b) greater than 15 kg and less than or equal to 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or
(c) 40 kg 초과이고, 상기 항 TIGIT 길항제 항체는 3주마다 약 600 mg의 용량으로 투여되는, 사용. (c) greater than 40 kg, wherein the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
479. 구현예 47, 구현예 48, 구현예 77, 구현예 78, 구현예 82, 및 구현예 83 중 어느 한 구현예에 있어서,479. The embodiment of any one of
상기 방법은 상기 항 TIGIT 길항제 항체를 4주마다 약 700 mg 내지 약 1000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti TIGIT antagonist antibody to said subject or population of subjects at a dose of about 700 mg to about 1000 mg every 4 weeks.
480. 구현예 47, 구현예 48, 구현예 59, 구현예 67, 구현예 323, 및 구현예 479 중 어느 한 구현예에 있어서,480. The embodiment of any one of
상기 방법은 상기 항 TIGIT 길항제 항체를 4주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject at a dose of about 840 mg every 4 weeks.
481. 구현예 49, 구현예 50, 및 구현예 104 중 어느 한 구현예에 있어서,481. The embodiment of any one of
상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 약 300 mg 내지 약 600 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects at a dose of about 300 mg to about 600 mg every two weeks.
482. 구현예 49, 구현예 50, 구현예 227, 구현예 251 내지 구현예 253, 구현예 255, 및 구현예 481 중 어느 한 구현예에 있어서,482. The embodiment of any one of
상기 방법은 상기 항 TIGIT 길항제 항체를 2주마다 약 420 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject at a dose of about 420 mg every two weeks.
483. 구현예 47 내지 구현예 482 중 어느 한 구현예에 있어서,483. The method according to any one of embodiments 47 to 482,
상기 항 TIGIT 길항제 항체의 용량은 고정 용량인, 사용.wherein the dose of the anti-TIGIT antagonist antibody is a fixed dose.
484. 구현예 54, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 27 내지 구현예 2698 중 어느 한 구현예에 있어서,484. The embodiment of any one of
상기 방법은 상기 PD-1 축 결합 길항제를 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects at a dose of about 900 mg to about 1500 mg every 3 weeks.
485. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65 내지 구현예 67, 구현예 80 내지 구현예 112, 구현예 114 내지 구현예 127, 구현예 136 내지 구현예 140, 구현예 169 내지 구현예 172, 구현예 189, 구현예 191, 구현예 267, 구현예 269, 구현예 286, 구현예 288, 구현예 291, 구현예 295, 구현예 301 내지 구현예 303, 구현예 309, 구현예 311, 구현예 313, 구현예 315, 구현예 338, 구현예 340, 구현예 358 내지 구현예 361, 구현예 372 내지 구현예 375, 구현예 384, 구현예 387, 구현예 388, 구현예 402 내지 구현예 405, 구현예 417, 구현예 420, 구현예 421, 및 구현예 484 중 어느 한 구현예에 있어서,485. embodiment 54,
상기 방법은 상기 PD-1 축 결합 길항제를 3주마다 약 1200 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject the PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks.
486. 구현예 47, 구현예 50, 구현예 80 내지 구현예 109, 및 구현예 324 중 어느 한 구현예에 있어서,486. The embodiment of any one of
상기 방법은 PD-1 축 결합 길항제를 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects a PD-1 axis binding antagonist at a dose of about 1400 mg to about 2000 mg every 4 weeks.
487. 구현예 47, 구현예 50, 구현예 59, 구현예 67, 구현예 324, 및 구현예 479 중 어느 한 구현예에 있어서,487. The embodiment of any one of
상기 방법은 상기 PD-1 축 결합 길항제를 4주마다 약 1680 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said PD-1 axis binding antagonist to said subject at a dose of about 1680 mg every 4 weeks.
488. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 481에 있어서,488. according to
상기 방법은 상기 PD-1 축 결합 길항제를 2주마다 약 600 mg 내지 약 1200 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 600 mg to about 1200 mg every two weeks.
489. 구현예 48, 구현예 49, 구현예 80 내지 구현예 109, 구현예 227, 구현예 251 내지 구현예 253, 및 구현예 481 중 어느 한 구현예에 있어서,489. The embodiment of any one of
상기 방법은 상기 PD-1 축 결합 길항제를 2주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject the PD-1 axis binding antagonist at a dose of about 840 mg every two weeks.
490. 구현예 47 내지 구현예 489 중 어느 한 구현예에 있어서,490. The method according to any one of embodiments 47 to 489,
상기 PD-1 축 결합 길항제의 용량은 고정 용량인, 사용.wherein the dose of the PD-1 axis binding antagonist is a fixed dose.
491. 구현예 60 또는 구현예 61에 있어서,491. The method of
상기 방법은 펨브롤리주맙을 3주마다 약 200 mg 또는 6주마다 400 mg의 고정 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject pembrolizumab in a fixed dose of about 200 mg every 3 weeks or 400 mg every 6 weeks.
492. 구현예 54, 구현예 60, 구현예 62, 구현예 63, 구현예 65, 구현예 80 내지 구현예 109, 및 구현예 191 중 어느 한 구현예에 있어서,492. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 21일인, 사용.The length of each of said one or more dosing cycles is 21 days.
493. 구현예 47, 구현예 59, 구현예 67, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,493. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 28일인, 사용.The length of each of said one or more dosing cycles is 28 days.
494. 구현예 49, 구현예 80 내지 구현예 109, 및 구현예 309 내지 구현예 311 중 어느 한 구현예에 있어서,494. The embodiment of any one of
상기 1회 이상의 투약 주기의 각각의 길이는 14일인, 사용.The length of each of said one or more dosing cycles is 14 days.
495. 구현예 47 내지 구현예 494 중 어느 한 구현예에 있어서,495. The method according to any one of embodiments 47 to 494,
상기 방법은 상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects on about
496. 구현예 47 내지 구현예 495 중 어느 한 구현예에 있어서,496. The method according to any one of embodiments 47 to 495,
상기 방법은 상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 1일에 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering the PD-1 axis binding antagonist to the subject or population of subjects on about
497. 구현예 321 또는 구현예 493에 있어서,497. according to embodiment 321 or embodiment 493,
상기 방법은 상기 항 TIGIT 길항제 항체를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject on about
498. 구현예 321 또는 구현예 493에 있어서,498. The method of embodiment 321 or embodiment 493,
상기 방법은 상기 PD-1 축 결합 길항제를 상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 대상체에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering the PD-1 axis binding antagonist to the subject on about
499. 구현예 47 내지 구현예 498 중 어느 한 구현예에 있어서,499. The method according to any one of embodiments 47 to 498,
상기 방법은 상기 항 TIGIT 길항제 항체 전에 상기 PD-1 축 결합 길항제를 또는 상기 PD-1 축 결합 길항제 전에 상기 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering to the subject or population of subjects the PD-1 axis binding antagonist prior to the anti TIGIT antagonist antibody or the anti TIGIT antagonist antibody prior to the PD-1 axis binding antagonist.
500. 구현예 499에 있어서,500. The method of embodiment 499,
상기 PD-1 축 결합 길항제 또는 상기 항 TIGIT 길항제 항체의 투여 후 1차 관찰 기간을 포함하는, 방법.a first observation period following administration of the PD-1 axis binding antagonist or the anti-TIGIT antagonist antibody.
501. 구현예 500에 있어서,501. The method of
상기 제1 관찰 기간은 약 30분 내지 약 60분의 길이인, 사용.wherein said first observation period is between about 30 minutes and about 60 minutes in length.
502. 구현예 500 또는 구현예 501에 있어서,502. The method of
상기 방법은 상기 항 TIGIT 길항제 항체 또는 상기 PD-1 축 결합 길항제의 투여 후 제2 관찰 기간을 포함하는, 사용.wherein said method comprises a second observation period following administration of said anti-TIGIT antagonist antibody or said PD-1 axis binding antagonist.
503. 구현예 502에 있어서,503. The method of embodiment 502,
상기 제2 관찰 기간은 약 30분 내지 약 60분의 길이인, 사용.wherein the second observation period is between about 30 minutes and about 60 minutes in length.
504. 구현예 47 내지 구현예 503 중 어느 한 구현예에 있어서,504. The method of any one of embodiments 47 to 503,
상기 방법은 상기 항 TIGIT 길항제 항체와 동시에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects concurrently with said anti-TIGIT antagonist antibody.
505. 구현예 47 내지 구현예 504 중 어느 한 구현예에 있어서,505. The method of any one of embodiments 47 to 504,
상기 방법은 상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 정맥내 투여하는 단계를 포함하는, 사용.use, wherein said method comprises intravenously administering said anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist to said subject or population of subjects.
506. 구현예 505에 있어서,506. The method of embodiment 505,
상기 방법은 상기 PD-1 축 결합 길항제를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering the PD-1 axis binding antagonist to the subject or population of subjects as an intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
507. 구현예 505 또는 구현예 506에 있어서,507. The method of embodiment 505 or embodiment 506,
상기 방법은 상기 항 TIGIT 길항제 항체를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 사용.wherein the method comprises administering the anti TIGIT antagonist antibody to the subject or population of subjects as an intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
508. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 507 중 어느 한 구현예에 있어서,508. The method of any one of embodiments 47-114 and 116-507,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플의 PD-L1 발현 수준이 결정되는, 사용.A use, wherein the level of PD-L1 expression in the subject or a tumor sample obtained from subjects is determined.
509. 구현예 508에 있어서,509. The method of embodiment 508,
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 사용.wherein said subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
510. 구현예 509에 있어서,510. The method of embodiment 509,
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 단백질 발현 수준인, 사용.wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1.
511. 구현예 510에 있어서,511. The method of embodiment 510,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정되는, 사용.wherein the detectable protein expression level of PD-L1 is determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody suitable for staining.
512. 구현예 511에 있어서,512. The method of embodiment 511,
염색에 적합한 상기 항 PD-L1 항체는 상기 항 PD-L1 항체 SP263, SP142, 22C3 또는 28-8인, 사용.wherein said anti-PD-L1 antibody suitable for staining is said anti-PD-L1 antibody SP263, SP142, 22C3 or 28-8.
513. 구현예 511 또는 구현예 512에 있어서,513. The method of embodiment 511 or embodiment 512,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 벤타나(Ventana) SP263 IHC 분석, 팜(pharm)Dx 22C3 IHC 분석, 벤타나 SP142 IHC 분석, 또는 팜Dx 28-8 IHC 분석을 사용하여 결정되는, 사용.The detectable protein expression level of PD-L1 is determined using a Ventana SP263 IHC assay, a pharmDx 22C3 IHC assay, a Ventana SP142 IHC assay, or a PalmDx 28-8 IHC assay. .
514. 구현예 47 내지 구현예 109, 구현예 188, 구현예 220 내지 구현예 265, 및 구현예 307 내지 구현예 423 중 어느 한 구현예에 있어서,514. The embodiment of any of embodiments 47 to 109, 188, 220 to 265, and embodiments 307 to 423,
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
515. 구현예 47 내지 구현예 220, 구현예 265 내지 구현예 338, 및 구현예 370 내지 구현예 423 중 어느 한 구현예에 있어서,515. The embodiment of any one of embodiments 47 to 220, 265 to 338, and embodiments 370 to 423,
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
516. 구현예 47 내지 구현예 113, 구현예 136 내지 구현예 187 및 구현예 220 내지 구현예 423 중 어느 한 구현예에 있어서,516. The embodiment of any one of embodiments 47 to 113, 136 to 187, and 220 to 423,
항 PD-L1 항체 22C3으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 22C3 is determined.
517. 구현예 47 내지 구현예 114 및 구현예 116 내지 구현예 423 중 어느 한 구현예에 있어서,517. The method of any one of embodiments 47 to 114 and embodiments 116 to 423,
항 PD-L1 항체 28-8로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 사용.wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 28-8 is determined.
518. 구현예 514에 있어서,518. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 5% of tumor-associated immune cells (TICs) in the tumor sample.
519. 구현예 514에 있어서,519. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 5% 이상 및 20% 미만인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 5% and less than 20% of the TIC in the tumor sample.
520. 구현예 514에 있어서,520. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상인, 사용.wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% in the tumor sample.
521. 구현예 514에 있어서,521. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 20% 이상인, 사용.wherein the detectable protein expression level of PD-L1 has a TIC of at least 20% in the tumor sample.
522. 구현예 514에 있어서,522. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상 및 50% 미만인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 10% and less than 50% of the TIC in the tumor sample.
523. 구현예 514에 있어서,523. The method of embodiment 514,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 50% 이상인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 50% TIC in the tumor sample.
524. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,524. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 1% 이상인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% of the PD-L1 positive tumor cell fraction.
525. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,525. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 30% 이상인, 사용.wherein the detectable protein expression level of PD-L1 is 30% or more in a fraction of PD-L1 positive tumor cells.
526. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,526. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 PD-L1 양성 종양 세포 분획이 1% 이상 및 50% 미만인, 사용.wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% and less than 50% of a fraction of PD-L1-positive tumor cells in the tumor sample.
527. 구현예 514, 구현예 516, 및 구현예 517 중 어느 한 구현예에 있어서,527. The embodiment of any one of embodiments 514, 516, and 517,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 사용.The detectable protein expression level of PD-L1 is 50% or more in the fraction of PD-L1 positive tumor cells.
528. 구현예 515에 있어서,528. The method of embodiment 515,
상기 PD-L1 양성 종양 세포 분획은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율인, 사용.wherein the PD-L1-positive tumor cell fraction is a proportion of the tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (IC).
529. 구현예 515에 있어서,529. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 1% 이상인, 사용.Use, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is 1% or more.
530. 구현예 515에 있어서,530. The method of embodiment 515,
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 5% 이상인, 사용.Use, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is 5% or more.
531. 구현예 516에 있어서,531. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 복합 양성 점수(CPS)가 1 이상인, 사용.wherein the detectable protein expression level of PD-L1 has a composite positive score (CPS) of 1 or more.
532. 구현예 516에 있어서,532. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 10 이상인, 사용.The detectable protein expression level of PD-L1 is a CPS of 10 or more.
533. 구현예 516에 있어서,533. The method of embodiment 516,
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 20 이상인, 사용.The detectable protein expression level of PD-L1 is CPS of 20 or more.
534. 구현예 528 내지 구현예 530 중 어느 한 구현예에 있어서,534. The method of any one of embodiments 528 to 530,
상기 IHC 분석은 벤타나 SP142 IHC 분석인, 사용.wherein the IHC assay is a Ventana SP142 IHC assay.
535. 구현예 509에 있어서,535. The method of embodiment 509,
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 핵산 발현 수준인, 사용.wherein the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1.
536. 구현예 535에 있어서,536. The method of embodiment 535,
상기 PD-L1의 검출가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정된, 사용.The detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH or a combination thereof.
537. 구현예 47 내지 구현예 423 중 어느 한 구현예에 있어서, 537. The method according to any one of embodiments 47 to 423,
상기 치료는 기준 OS 시간과 비교하여 상기 대상체의 전체 생존(OS)의 증가 및/또는 기준 PFS 시간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가를 유발하는, 사용.wherein said treatment results in an increase in overall survival (OS) of said subject compared to baseline OS time and/or an increase in progression free survival (PFS) in said subject compared to baseline PFS time.
538. 구현예 537에 있어서: 538. The method of embodiment 537:
(a) 상기 기준 OS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 OS 시간 중앙값이고; 그리고/또는 (a) said baseline OS time is the median OS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist; and/or
(b) 상기 기준 PFS 시간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 PFS 시간 중앙값인, 사용.(b) the baseline PFS time is the median PFS time of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist.
539. 구현예 52, 구현예 158, 및 구현예 228 중 어느 한 구현예에 있어서,539. The embodiment of any one of embodiments 52, 158, and 228,
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 사용.wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
540. 구현예 539에 있어서,540. The method of embodiment 539,
상기 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 사용.The platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541. 구현예 69, 구현예 92, 구현예 127, 구현예 131, 구현예 249, 및 구현예 540에 있어서,541. The method of embodiment 69, embodiment 92, embodiment 127, embodiment 131, embodiment 249, and embodiment 540,
상기 카보플라틴은 AUC = 5 mg/ml/분 또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 사용.wherein the carboplatin is administered in a dose sufficient to achieve AUC=5 mg/ml/min or AUC=6 mg/ml/min.
542. 구현예 69, 구현예 127, 구현예 162, 구현예 164, 구현예 166, 구현예 168, 및 구현예 540에 있어서,542. The method of embodiment 69, embodiment 127, embodiment 162, embodiment 164, embodiment 166, embodiment 168, and embodiment 540,
상기 시스플라틴은 약 75 mg/m2 또는 80 mg/m2의 용량으로 투여되는, 사용.wherein the cisplatin is administered at a dose of about 75 mg/m2 or 80 mg/m2.
543. 구현예 539 내지 구현예 542 중 어느 한 구현예에 있어서,543. The method of any one of embodiments 539 to 542,
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 사용.wherein the at least one non-platinum-based chemotherapeutic agent is an antimetabolite, a taxane, or a topoisomerase II inhibitor.
544. 구현예 62, 구현예 173, 구현예 174, 및 구현예 543에 있어서,544. The method of embodiment 62, embodiment 173, embodiment 174, and embodiment 543,
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 사용.wherein the antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
545. 구현예 69, 구현예 127, 구현예 162, 및 구현예 544 중 어느 한 구현예에 있어서,545. The embodiment of any one of embodiments 69, 127, 162, and 544,
상기 페메트렉시드는 약 500 mg/m2의 용량으로 투여되는, 사용.wherein the pemetrexed is administered at a dose of about 500 mg/m2.
546. 구현예 63, 구현예 64, 구현예 162, 구현예 398, 및 구현예 544 중 어느 한 구현예에 있어서,546. The embodiment of any one of
상기 젬시타빈은 약 1000 mg/m2 또는 약 1250 mg/m2의 용량으로 투여되는, 사용.wherein the gemcitabine is administered at a dose of about 1000 mg/m2 or about 1250 mg/m2.
547. 구현예 544에 있어서,547. The method of embodiment 544,
상기 항대사물질은 카페시타빈인, 사용.The antimetabolite is capecitabine, use.
548. 구현예 544 또는 구현예 547에 있어서,548. The method of embodiment 544 or embodiment 547,
상기 카페시타빈은 약 1250 mg/m2의 용량으로 투여되는, 사용.wherein the capecitabine is administered at a dose of about 1250 mg/m2.
549. 구현예 173, 구현예 174, 구현예 229, 구현예 230, 구현예 239, 구현예 240, 및 구현예 543 내지 구현예 548 중 어느 한 구현예에 있어서,549. The embodiment of any one of embodiments 173, 174, 229, 230, 239, 240, and 543 to 548,
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 사용.wherein the taxane is paclitaxel or nap-paclitaxel.
550. 구현예 69, 구현예 162, 및 구현예 549 중 어느 한 구현예에 있어서,550. The method of any one of embodiments 69, 162, and 549,
상기 파클리탁셀은 약 175 mg/m2 또는 약 200 mg/m2의 용량으로 투여되는, 사용.wherein the paclitaxel is administered at a dose of about 175 mg/m2 or about 200 mg/m2.
551. 구현예 63, 구현예 64, 구현예 249, 구현예 398, 및 구현예 549 중 어느 한 구현예에 있어서,551. The embodiment of any one of
상기 냅-파클리탁셀은 약 100 mg/m2의 용량으로 투여되는, 사용.wherein the nap-paclitaxel is administered at a dose of about 100 mg/m2.
552. 구현예 80 내지 구현예 91, 구현예 229, 구현예 230, 구현예 239, 구현예 241, 구현예 251 내지 구현예 255, 및 구현예 543항 내지 구현예 551 중 어느 한 구현예에 있어서,552. The embodiment of any one of embodiments 80-91, 229, 230, 239, 241, 251, 255, and 543-551. ,
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 사용.wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331.
553. 구현예 69, 구현예 92, 및 구현예 552 중 어느 한 구현예에 있어서,553. The embodiment of any one of embodiments 69, 92, and 552,
상기 에토포시드는 약 100 mg/m2의 용량으로 투여되는, 사용.wherein the etoposide is administered at a dose of about 100 mg/m2.
554. 구현예 543 내지 구현예 553 중 어느 한 구현예에 있어서,554. The method of any one of embodiments 543 to 553,
상기 하나 이상의 화학요법제는 각각 매주 1회, 2주마다 1회, 3주마다 1회, 3주마다 2회, 4주마다 1회, 4주마다 2회, 또는 4주마다 3회 투여되는, 사용.The one or more chemotherapeutic agents are each administered once every week, once every 2 weeks, once every 3 weeks, twice every 3 weeks, once every 4 weeks, twice every 4 weeks, or 3 times every 4 weeks. , use.
555. 구현예 543 내지 구현예 554 중 어느 한 구현예에 있어서,555. The method of any one of embodiments 543 to 554,
상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 제 1일에 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered on
556. 구현예 544 내지 구현예 555 중 어느 한 구현예에 있어서,556. The method of any one of embodiments 544 to 555,
상기 젬시타빈은 4주마다 3회 투여되는, 사용.wherein the gemcitabine is administered 3 times every 4 weeks.
557. 구현예 544 내지 구현예 556항 중 어느 한 구현예에 있어서,557. The method according to any one of embodiments 544 to 556,
상기 젬시타빈은 1회 이상의 투약 주기의 제 1일, 8일, 및/또는 15일에 투여되는, 사용.wherein the gemcitabine is administered on
558. 구현예 544 내지 구현예 557 중 어느 한 구현예에 있어서,558. The method of any one of embodiments 544 to 557,
상기 카페시타빈은 2주 동안 매일 투여되는, 사용.wherein the capecitabine is administered daily for 2 weeks.
559. 구현예 544 내지 구현예 558 중 어느 한 구현예에 있어서,559. The method according to any one of embodiments 544 to 558,
상기 카페시타빈은 1회 이상의 투약 주기의 제 1일 내지 14일에 투여되는, 사용.wherein said capecitabine is administered on
560. 구현예 549 내지 구현예 559 중 어느 한 구현예에 있어서,560. The method of any one of embodiments 549 to 559,
상기 냅-파클리탁셀은 4주마다 3회 투여되는, 사용.wherein the nap-paclitaxel is administered 3 times every 4 weeks.
561. 구현예 549 내지 구현예 560 중 어느 한 구현예에 있어서,561. The method of any one of embodiments 549 to 560,
상기 냅-파클리탁셀은 1회 이상의 투약 주기의 제 1일, 8일, 및 15일에 투여되는, 사용.wherein said nap-paclitaxel is administered on
562. 구현예 552 내지 구현예 561 중 어느 한 구현예에 있어서,562. The method of any one of embodiments 552 to 561,
상기 에토포시드는 3주마다 1일 내지 3일에 투여되는, 사용.wherein said etoposide is administered on
563. 구현예 552 내지 구현예 562 중 어느 한 구현예에 있어서,563. The method of any one of embodiments 552 to 562,
상기 에토포시드는 1회 이상의 투약 주기의 제 1일 내지 3일에 투여되는, 사용.wherein said etoposide is administered on
564. 구현예 543 내지 구현예 563 중 어느 한 구현예에 있어서,564. The method of any one of embodiments 543 to 563,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이전에 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
565. 구현예 543 내지 구현예 564 중 어느 한 구현예에 있어서,565. The method of any one of embodiments 543 to 564,
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이후에 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
566. 구현예 543 내지 구현예 565 중 어느 한 구현예에 있어서,566. The method of any one of embodiments 543 to 565,
상기 하나 이상의 화학요법제는 정맥내 또는 경구로 투여되는, 사용.wherein said one or more chemotherapeutic agents are administered intravenously or orally.
567. 구현예 65, 구현예 310, 및 구현예 311 중 어느 한 구현예에 있어서,567. The embodiment of any one of
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
568. 구현예 312 또는 구현예 567에 있어서,568. The method of embodiment 312 or embodiment 567,
상기 VEGF 길항제는 3주마다 약 10 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 10 mg/kg to about 20 mg/kg every 3 weeks.
569. 구현예 318 및 구현예 568에 있어서,569. according to embodiment 318 and embodiment 568,
상기 VEGF 길항제는 3주마다 약 15 mg/kg의 용량으로 투여되는, 사용.wherein the VEGF antagonist is administered at a dose of about 15 mg/kg every 3 weeks.
570. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 569 중 어느 한 구현예에 있어서,570. The embodiment of any one of
상기 VEGF 길항제는 항 VEGF 항체인, 사용.The VEGF antagonist is an anti-VEGF antibody, use.
571. 구현예 570에 있어서,571. The method of embodiment 570,
상기 항 VEGF 항체는 베바시주맙의 VH 도메인 및 VL 도메인을 포함하는, 사용.The use of the anti-VEGF antibody comprising the VH domain and the VL domain of bevacizumab.
572. 구현예 570 또는 구현예 571에 있어서,572. The method of embodiment 570 or embodiment 571,
상기 항 VEGF 항체는 베바시주맙인, 사용.The anti-VEGF antibody is bevacizumab, use.
573. 구현예 65, 구현예 310 내지 구현예 312, 및 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,573. The embodiment of any one of
상기 항 TIGIT 길항제 항체는 티라골루맙이고, 상기 PD-1 축 결합 길항제는 아테졸리주맙이며, 상기 VEGF 길항제는 베바시주맙인, 사용.The anti-TIGIT antagonist antibody is tiragolumab, the PD-1 axis binding antagonist is atezolizumab, and the VEGF antagonist is bevacizumab.
574. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 573 중 어느 한 구현예에 있어서,574. The embodiment of any one of
1회 이상의 투약 주기의 제 1일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용.use, comprising administering said VEGF antagonist to said subject on
575. 구현예 318 내지 구현예 320 중 어느 한 구현예에 있어서,575. The method of any one of embodiments 318 to 320,
1회 이상의 투약 주기의 15일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 사용.use, comprising administering said VEGF antagonist to said subject on
576. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 575 중 어느 한 구현예에 있어서,576. The embodiment of any one of
상기 VEGF 길항제는 정맥내 투여되는, 사용.wherein the VEGF antagonist is administered intravenously.
577. 구현예 576에 있어서,577. The method of embodiment 576,
상기 VEGF 길항제는 90 ± 15분에 걸쳐 정맥내 주입으로 상기 대상체에게 투여되는, 사용.wherein said VEGF antagonist is administered to said subject by intravenous infusion over 90 ± 15 minutes.
578. 구현예 65, 구현예 310 내지 구현예 312, 구현예 318 내지 구현예 320, 및 구현예 567 내지 구현예 577 중 어느 한 구현예에 있어서,578. The embodiment of any one of
상기 VEGF 길항제 이전에 상기 PD-1 축 결합 길항제, 및 상기 항 TIGIT 길항제 항체 이전에 상기 VEGF 길항제를 상기 대상체에 투여하는 단계를 포함하는, 사용.Use comprising administering to the subject the PD-1 axis binding antagonist prior to the VEGF antagonist, and the VEGF antagonist prior to the anti-TIGIT antagonist antibody.
579. 구현예 578에 있어서,579. The method of embodiment 578,
상기 방법은 상기 PD-1 축 결합 길항제 투여 후 제1 관찰 기간, 상기 VEGF 길항제 투여 후 제2 관찰 기간, 및 상기 항 TIGIT 길항제 항체 투여 후 제3 관찰 기간을 포함하는, 사용.wherein the method comprises a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody.
580. 구현예 579에 있어서,580. The method of embodiment 579,
상기 제1 관찰 기간, 상기 제2 관찰 기간, 및 상기 제3 관찰 기간은 각각 약 30분 내지 약 120분의 길이인, 사용.wherein the first observation period, the second observation period, and the third observation period are each about 30 minutes to about 120 minutes in length.
581. 구현예 113, 구현예 128, 구현예 129 내지 구현예 131, 구현예 175 내지 구현예 182, 구현예 210 내지 구현예 214, 구현예 221, 구현예 256, 구현예 257, 구현예 270, 구현예 289, 구현예 290, 구현예 293, 구현예 294, 구현예 297, 구현예 298, 구현예 333, 구현예 362 내지 구현예 365, 구현예 385, 구현예 386, 구현예 389, 구현예 393, 구현예 419, 및 구현예 422 중 어느 한 구현예에 있어서,581. Embodiment 113, Embodiment 128, Embodiment 129 to Embodiment 131, Embodiment 175 to Embodiment 182, Embodiment 210 to Embodiment 214, Embodiment 221, Embodiment 256, Embodiment 257, Embodiment 270, Embodiment 289, Embodiment 290, Embodiment 293, Embodiment 294, Embodiment 297, Embodiment 298, Embodiment 333, Embodiment 362 to Embodiment 365, Embodiment 385, Embodiment 386, Embodiment 389, Embodiment 393, embodiment 419, and embodiment 422 according to any one of embodiments,
티라골루맙 및 아테졸리주맙은 투여 이전에 IV 백(bag)에 결합되는, 사용.Use, wherein tiragolumab and atezolizumab are bound to an IV bag prior to administration.
582. 구현예 47 내지 구현예 581 중 어느 한 구현예에 있어서,582. The method according to any one of embodiments 47 to 581,
상기 대상체는 인간인, 사용.wherein the subject is a human.
583. 구현예 47 내지 구현예 582 중 어느 한 구현예에 있어서,583. The method according to any one of embodiments 47 to 582,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
584. 구현예 47 내지 구현예 582 중 어느 한 구현예에 있어서,584. The method according to any one of embodiments 47 to 582,
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 사용.wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
비록 전술한 발명이 이해의 명료함을 위해 예시 및 실례로서 일부 상세하게 설명되긴 했지만, 이들 설명 및 실례는 발명의 범위를 제한하는 것으로 해석되지 않아야 한다. 본원에서 인용된 모든 특허 및 과학 문헌의 개시는 명시적으로 그 전체가 본원에 원용된다.Although the foregoing invention has been described in some detail by way of illustration and example for purposes of clarity of understanding, these descriptions and examples should not be construed as limiting the scope of the invention. The disclosures of all patents and scientific literature cited herein are expressly incorporated herein in their entirety.
SEQUENCE LISTING <110> Genentech, Inc. F. Hoffmann-La Roche AG Hoffmann-La Roche Inc. <120> METHODS FOR TREATMENT OF CANCER WITH AN ANTI-TIGIT ANTAGONIST ANTIBODY <130> 50474-206WO2 <150> US 63/127,109 <151> 2020-12-17 <150> US 63/124,693 <151> 2020-12-11 <150> US 63/114,517 <151> 2020-11-16 <150> US 63/105,198 <151> 2020-10-23 <150> US 63/085,890 <151> 2020-09-30 <150> PCT/US2020/049415 <151> 2020-09-04 <150> US 63/074,827 <151> 2020-09-04 <150> US 63/074,807 <151> 2020-09-04 <150> US 63/059,960 <151> 2020-07-31 <150> US 63/059,054 <151> 2020-07-30 <150> PCT/US2020/024526 <151> 2020-03-24 <150> US 62/994,272 <151> 2020-03-24 <150> US 62/985,822 <151> 2020-03-05 <150> US 62/966,448 <151> 2020-01-27 <160> 34 <170> PatentIn version 3.5 <210> 1 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 1 Ser Asn Ser Ala Ala Trp Asn 1 5 <210> 2 <211> 18 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 2 Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala Val Ser Val 1 5 10 15 Lys Gly <210> 3 <211> 14 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 3 Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro Phe Asp Tyr 1 5 10 <210> 4 <211> 17 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 4 Lys Ser Ser Gln Thr Val Leu Tyr Ser Ser Asn Asn Lys Lys Tyr Leu 1 5 10 15 Ala <210> 5 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 5 Trp Ala Ser Thr Arg Glu Ser 1 5 <210> 6 <211> 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 6 Gln Gln Tyr Tyr Ser Thr Pro Phe Thr 1 5 <210> 7 <211> 23 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 7 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys 20 <210> 8 <211> 15 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 8 Trp Tyr Gln Gln Lys Pro Gly Gln Pro Pro Asn Leu Leu Ile Tyr 1 5 10 15 <210> 9 <211> 32 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 9 Gly Val Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr 1 5 10 15 Leu Thr Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys 20 25 30 <210> 10 <211> 10 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 10 Phe Gly Pro Gly Thr Lys Val Glu Ile Lys 1 5 10 <210> 11 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <220> <221> MISC_FEATURE <222> (1)..(1) <223> Xaa is Gln or Glu <400> 11 Xaa Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 <210> 12 <211> 14 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 12 Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu Trp Leu Gly 1 5 10 <210> 13 <211> 32 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 13 Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn Gln Phe Ser Leu Gln 1 5 10 15 Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val Phe Tyr Cys Thr Arg 20 25 30 <210> 14 <211> 11 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 14 Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 1 5 10 <210> 15 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 15 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 <210> 16 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 16 Gln Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 <210> 17 <211> 126 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 17 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gly Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 115 120 125 <210> 18 <211> 126 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 18 Gln Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gly Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 115 120 125 <210> 19 <211> 113 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 19 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys Lys Ser Ser Gln Thr Val Leu Tyr Ser 20 25 30 Ser Asn Asn Lys Lys Tyr Leu Ala Trp Tyr Gln Gln Lys Pro Gly Gln 35 40 45 Pro Pro Asn Leu Leu Ile Tyr Trp Ala Ser Thr Arg Glu Ser Gly Val 50 55 60 Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr 65 70 75 80 Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys Gln Gln 85 90 95 Tyr Tyr Ser Thr Pro Phe Thr Phe Gly Pro Gly Thr Lys Val Glu Ile 100 105 110 Lys <210> 20 <211> 10 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 20 Gly Phe Thr Phe Ser Asp Ser Trp Ile His 1 5 10 <210> 21 <211> 18 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 21 Ala Trp Ile Ser Pro Tyr Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 1 5 10 15 Lys Gly <210> 22 <211> 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 22 Arg His Trp Pro Gly Gly Phe Asp Tyr 1 5 <210> 23 <211> 11 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 23 Arg Ala Ser Gln Asp Val Ser Thr Ala Val Ala 1 5 10 <210> 24 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 24 Ser Ala Ser Phe Leu Tyr Ser 1 5 <210> 25 <211> 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 25 Gln Gln Tyr Leu Tyr His Pro Ala Thr 1 5 <210> 26 <211> 118 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 26 Glu Val Gln Leu Val Glu Ser Gly Gly Gly Leu Val Gln Pro Gly Gly 1 5 10 15 Ser Leu Arg Leu Ser Cys Ala Ala Ser Gly Phe Thr Phe Ser Asp Ser 20 25 30 Trp Ile His Trp Val Arg Gln Ala Pro Gly Lys Gly Leu Glu Trp Val 35 40 45 Ala Trp Ile Ser Pro Tyr Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 50 55 60 Lys Gly Arg Phe Thr Ile Ser Ala Asp Thr Ser Lys Asn Thr Ala Tyr 65 70 75 80 Leu Gln Met Asn Ser Leu Arg Ala Glu Asp Thr Ala Val Tyr Tyr Cys 85 90 95 Ala Arg Arg His Trp Pro Gly Gly Phe Asp Tyr Trp Gly Gln Gly Thr 100 105 110 Leu Val Thr Val Ser Ser 115 <210> 27 <211> 108 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 27 Asp Ile Gln Met Thr Gln Ser Pro Ser Ser Leu Ser Ala Ser Val Gly 1 5 10 15 Asp Arg Val Thr Ile Thr Cys Arg Ala Ser Gln Asp Val Ser Thr Ala 20 25 30 Val Ala Trp Tyr Gln Gln Lys Pro Gly Lys Ala Pro Lys Leu Leu Ile 35 40 45 Tyr Ser Ala Ser Phe Leu Tyr Ser Gly Val Pro Ser Arg Phe Ser Gly 50 55 60 Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr Ile Ser Ser Leu Gln Pro 65 70 75 80 Glu Asp Phe Ala Thr Tyr Tyr Cys Gln Gln Tyr Leu Tyr His Pro Ala 85 90 95 Thr Phe Gly Gln Gly Thr Lys Val Glu Ile Lys Arg 100 105 <210> 28 <211> 447 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 28 Glu Val Gln Leu Val Glu Ser Gly Gly Gly Leu Val Gln Pro Gly Gly 1 5 10 15 Ser Leu Arg Leu Ser Cys Ala Ala Ser Gly Phe Thr Phe Ser Asp Ser 20 25 30 Trp Ile His Trp Val Arg Gln Ala Pro Gly Lys Gly Leu Glu Trp Val 35 40 45 Ala Trp Ile Ser Pro Tyr Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 50 55 60 Lys Gly Arg Phe Thr Ile Ser Ala Asp Thr Ser Lys Asn Thr Ala Tyr 65 70 75 80 Leu Gln Met Asn Ser Leu Arg Ala Glu Asp Thr Ala Val Tyr Tyr Cys 85 90 95 Ala Arg Arg His Trp Pro Gly Gly Phe Asp Tyr Trp Gly Gln Gly Thr 100 105 110 Leu Val Thr Val Ser Ser Ala Ser Thr Lys Gly Pro Ser Val Phe Pro 115 120 125 Leu Ala Pro Ser Ser Lys Ser Thr Ser Gly Gly Thr Ala Ala Leu Gly 130 135 140 Cys Leu Val Lys Asp Tyr Phe Pro Glu Pro Val Thr Val Ser Trp Asn 145 150 155 160 Ser Gly Ala Leu Thr Ser Gly Val His Thr Phe Pro Ala Val Leu Gln 165 170 175 Ser Ser Gly Leu Tyr Ser Leu Ser Ser Val Val Thr Val Pro Ser Ser 180 185 190 Ser Leu Gly Thr Gln Thr Tyr Ile Cys Asn Val Asn His Lys Pro Ser 195 200 205 Asn Thr Lys Val Asp Lys Lys Val Glu Pro Lys Ser Cys Asp Lys Thr 210 215 220 His Thr Cys Pro Pro Cys Pro Ala Pro Glu Leu Leu Gly Gly Pro Ser 225 230 235 240 Val Phe Leu Phe Pro Pro Lys Pro Lys Asp Thr Leu Met Ile Ser Arg 245 250 255 Thr Pro Glu Val Thr Cys Val Val Val Asp Val Ser His Glu Asp Pro 260 265 270 Glu Val Lys Phe Asn Trp Tyr Val Asp Gly Val Glu Val His Asn Ala 275 280 285 Lys Thr Lys Pro Arg Glu Glu Gln Tyr Ala Ser Thr Tyr Arg Val Val 290 295 300 Ser Val Leu Thr Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu Tyr 305 310 315 320 Lys Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu Lys Thr 325 330 335 Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln Val Tyr Thr Leu 340 345 350 Pro Pro Ser Arg Glu Glu Met Thr Lys Asn Gln Val Ser Leu Thr Cys 355 360 365 Leu Val Lys Gly Phe Tyr Pro Ser Asp Ile Ala Val Glu Trp Glu Ser 370 375 380 Asn Gly Gln Pro Glu Asn Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp 385 390 395 400 Ser Asp Gly Ser Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Lys Ser 405 410 415 Arg Trp Gln Gln Gly Asn Val Phe Ser Cys Ser Val Met His Glu Ala 420 425 430 Leu His Asn His Tyr Thr Gln Lys Ser Leu Ser Leu Ser Pro Gly 435 440 445 <210> 29 <211> 214 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 29 Asp Ile Gln Met Thr Gln Ser Pro Ser Ser Leu Ser Ala Ser Val Gly 1 5 10 15 Asp Arg Val Thr Ile Thr Cys Arg Ala Ser Gln Asp Val Ser Thr Ala 20 25 30 Val Ala Trp Tyr Gln Gln Lys Pro Gly Lys Ala Pro Lys Leu Leu Ile 35 40 45 Tyr Ser Ala Ser Phe Leu Tyr Ser Gly Val Pro Ser Arg Phe Ser Gly 50 55 60 Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr Ile Ser Ser Leu Gln Pro 65 70 75 80 Glu Asp Phe Ala Thr Tyr Tyr Cys Gln Gln Tyr Leu Tyr His Pro Ala 85 90 95 Thr Phe Gly Gln Gly Thr Lys Val Glu Ile Lys Arg Thr Val Ala Ala 100 105 110 Pro Ser Val Phe Ile Phe Pro Pro Ser Asp Glu Gln Leu Lys Ser Gly 115 120 125 Thr Ala Ser Val Val Cys Leu Leu Asn Asn Phe Tyr Pro Arg Glu Ala 130 135 140 Lys Val Gln Trp Lys Val Asp Asn Ala Leu Gln Ser Gly Asn Ser Gln 145 150 155 160 Glu Ser Val Thr Glu Gln Asp Ser Lys Asp Ser Thr Tyr Ser Leu Ser 165 170 175 Ser Thr Leu Thr Leu Ser Lys Ala Asp Tyr Glu Lys His Lys Val Tyr 180 185 190 Ala Cys Glu Val Thr His Gln Gly Leu Ser Ser Pro Val Thr Lys Ser 195 200 205 Phe Asn Arg Gly Glu Cys 210 <210> 30 <211> 244 <212> PRT <213> Homo sapiens <400> 30 Met Arg Trp Cys Leu Leu Leu Ile Trp Ala Gln Gly Leu Arg Gln Ala 1 5 10 15 Pro Leu Ala Ser Gly Met Met Thr Gly Thr Ile Glu Thr Thr Gly Asn 20 25 30 Ile Ser Ala Glu Lys Gly Gly Ser Ile Ile Leu Gln Cys His Leu Ser 35 40 45 Ser Thr Thr Ala Gln Val Thr Gln Val Asn Trp Glu Gln Gln Asp Gln 50 55 60 Leu Leu Ala Ile Cys Asn Ala Asp Leu Gly Trp His Ile Ser Pro Ser 65 70 75 80 Phe Lys Asp Arg Val Ala Pro Gly Pro Gly Leu Gly Leu Thr Leu Gln 85 90 95 Ser Leu Thr Val Asn Asp Thr Gly Glu Tyr Phe Cys Ile Tyr His Thr 100 105 110 Tyr Pro Asp Gly Thr Tyr Thr Gly Arg Ile Phe Leu Glu Val Leu Glu 115 120 125 Ser Ser Val Ala Glu His Gly Ala Arg Phe Gln Ile Pro Leu Leu Gly 130 135 140 Ala Met Ala Ala Thr Leu Val Val Ile Cys Thr Ala Val Ile Val Val 145 150 155 160 Val Ala Leu Thr Arg Lys Lys Lys Ala Leu Arg Ile His Ser Val Glu 165 170 175 Gly Asp Leu Arg Arg Lys Ser Ala Gly Gln Glu Glu Trp Ser Pro Ser 180 185 190 Ala Pro Ser Pro Pro Gly Ser Cys Val Gln Ala Glu Ala Ala Pro Ala 195 200 205 Gly Leu Cys Gly Glu Gln Arg Gly Glu Asp Cys Ala Glu Leu His Asp 210 215 220 Tyr Phe Asn Val Leu Ser Tyr Arg Ser Leu Gly Asn Cys Ser Phe Phe 225 230 235 240 Thr Glu Thr Gly <210> 31 <211> 223 <212> PRT <213> Homo sapiens <400> 31 Met Met Thr Gly Thr Ile Glu Thr Thr Gly Asn Ile Ser Ala Glu Lys 1 5 10 15 Gly Gly Ser Ile Ile Leu Gln Cys His Leu Ser Ser Thr Thr Ala Gln 20 25 30 Val Thr Gln Val Asn Trp Glu Gln Gln Asp Gln Leu Leu Ala Ile Cys 35 40 45 Asn Ala Asp Leu Gly Trp His Ile Ser Pro Ser Phe Lys Asp Arg Val 50 55 60 Ala Pro Gly Pro Gly Leu Gly Leu Thr Leu Gln Ser Leu Thr Val Asn 65 70 75 80 Asp Thr Gly Glu Tyr Phe Cys Ile Tyr His Thr Tyr Pro Asp Gly Thr 85 90 95 Tyr Thr Gly Arg Ile Phe Leu Glu Val Leu Glu Ser Ser Val Ala Glu 100 105 110 His Gly Ala Arg Phe Gln Ile Pro Leu Leu Gly Ala Met Ala Ala Thr 115 120 125 Leu Val Val Ile Cys Thr Ala Val Ile Val Val Val Ala Leu Thr Arg 130 135 140 Lys Lys Lys Ala Leu Arg Ile His Ser Val Glu Gly Asp Leu Arg Arg 145 150 155 160 Lys Ser Ala Gly Gln Glu Glu Trp Ser Pro Ser Ala Pro Ser Pro Pro 165 170 175 Gly Ser Cys Val Gln Ala Glu Ala Ala Pro Ala Gly Leu Cys Gly Glu 180 185 190 Gln Arg Gly Glu Asp Cys Ala Glu Leu His Asp Tyr Phe Asn Val Leu 195 200 205 Ser Tyr Arg Ser Leu Gly Asn Cys Ser Phe Phe Thr Glu Thr Gly 210 215 220 <210> 32 <211> 290 <212> PRT <213> Homo sapiens <400> 32 Met Arg Ile Phe Ala Val Phe Ile Phe Met Thr Tyr Trp His Leu Leu 1 5 10 15 Asn Ala Phe Thr Val Thr Val Pro Lys Asp Leu Tyr Val Val Glu Tyr 20 25 30 Gly Ser Asn Met Thr Ile Glu Cys Lys Phe Pro Val Glu Lys Gln Leu 35 40 45 Asp Leu Ala Ala Leu Ile Val Tyr Trp Glu Met Glu Asp Lys Asn Ile 50 55 60 Ile Gln Phe Val His Gly Glu Glu Asp Leu Lys Val Gln His Ser Ser 65 70 75 80 Tyr Arg Gln Arg Ala Arg Leu Leu Lys Asp Gln Leu Ser Leu Gly Asn 85 90 95 Ala Ala Leu Gln Ile Thr Asp Val Lys Leu Gln Asp Ala Gly Val Tyr 100 105 110 Arg Cys Met Ile Ser Tyr Gly Gly Ala Asp Tyr Lys Arg Ile Thr Val 115 120 125 Lys Val Asn Ala Pro Tyr Asn Lys Ile Asn Gln Arg Ile Leu Val Val 130 135 140 Asp Pro Val Thr Ser Glu His Glu Leu Thr Cys Gln Ala Glu Gly Tyr 145 150 155 160 Pro Lys Ala Glu Val Ile Trp Thr Ser Ser Asp His Gln Val Leu Ser 165 170 175 Gly Lys Thr Thr Thr Thr Asn Ser Lys Arg Glu Glu Lys Leu Phe Asn 180 185 190 Val Thr Ser Thr Leu Arg Ile Asn Thr Thr Thr Asn Glu Ile Phe Tyr 195 200 205 Cys Thr Phe Arg Arg Leu Asp Pro Glu Glu Asn His Thr Ala Glu Leu 210 215 220 Val Ile Pro Glu Leu Pro Leu Ala His Pro Pro Asn Glu Arg Thr His 225 230 235 240 Leu Val Ile Leu Gly Ala Ile Leu Leu Cys Leu Gly Val Ala Leu Thr 245 250 255 Phe Ile Phe Arg Leu Arg Lys Gly Arg Met Met Asp Val Lys Lys Cys 260 265 270 Gly Ile Gln Asp Thr Asn Ser Lys Lys Gln Ser Asp Thr His Leu Glu 275 280 285 Glu Thr 290 <210> 33 <211> 456 <212> PRT <213> Homo sapiens <400> 33 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gly Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser Ala Ser 115 120 125 Thr Lys Gly Pro Ser Val Phe Pro Leu Ala Pro Ser Ser Lys Ser Thr 130 135 140 Ser Gly Gly Thr Ala Ala Leu Gly Cys Leu Val Lys Asp Tyr Phe Pro 145 150 155 160 Glu Pro Val Thr Val Ser Trp Asn Ser Gly Ala Leu Thr Ser Gly Val 165 170 175 His Thr Phe Pro Ala Val Leu Gln Ser Ser Gly Leu Tyr Ser Leu Ser 180 185 190 Ser Val Val Thr Val Pro Ser Ser Ser Leu Gly Thr Gln Thr Tyr Ile 195 200 205 Cys Asn Val Asn His Lys Pro Ser Asn Thr Lys Val Asp Lys Lys Val 210 215 220 Glu Pro Lys Ser Cys Asp Lys Thr His Thr Cys Pro Pro Cys Pro Ala 225 230 235 240 Pro Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe Pro Pro Lys Pro 245 250 255 Lys Asp Thr Leu Met Ile Ser Arg Thr Pro Glu Val Thr Cys Val Val 260 265 270 Val Asp Val Ser His Glu Asp Pro Glu Val Lys Phe Asn Trp Tyr Val 275 280 285 Asp Gly Val Glu Val His Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln 290 295 300 Tyr Asn Ser Thr Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln 305 310 315 320 Asp Trp Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser Asn Lys Ala 325 330 335 Leu Pro Ala Pro Ile Glu Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro 340 345 350 Arg Glu Pro Gln Val Tyr Thr Leu Pro Pro Ser Arg Glu Glu Met Thr 355 360 365 Lys Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly Phe Tyr Pro Ser 370 375 380 Asp Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro Glu Asn Asn Tyr 385 390 395 400 Lys Thr Thr Pro Pro Val Leu Asp Ser Asp Gly Ser Phe Phe Leu Tyr 405 410 415 Ser Lys Leu Thr Val Asp Lys Ser Arg Trp Gln Gln Gly Asn Val Phe 420 425 430 Ser Cys Ser Val Met His Glu Ala Leu His Asn His Tyr Thr Gln Lys 435 440 445 Ser Leu Ser Leu Ser Pro Gly Lys 450 455 <210> 34 <211> 220 <212> PRT <213> Homo sapiens <400> 34 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys Lys Ser Ser Gln Thr Val Leu Tyr Ser 20 25 30 Ser Asn Asn Lys Lys Tyr Leu Ala Trp Tyr Gln Gln Lys Pro Gly Gln 35 40 45 Pro Pro Asn Leu Leu Ile Tyr Trp Ala Ser Thr Arg Glu Ser Gly Val 50 55 60 Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr 65 70 75 80 Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys Gln Gln 85 90 95 Tyr Tyr Ser Thr Pro Phe Thr Phe Gly Pro Gly Thr Lys Val Glu Ile 100 105 110 Lys Arg Thr Val Ala Ala Pro Ser Val Phe Ile Phe Pro Pro Ser Asp 115 120 125 Glu Gln Leu Lys Ser Gly Thr Ala Ser Val Val Cys Leu Leu Asn Asn 130 135 140 Phe Tyr Pro Arg Glu Ala Lys Val Gln Trp Lys Val Asp Asn Ala Leu 145 150 155 160 Gln Ser Gly Asn Ser Gln Glu Ser Val Thr Glu Gln Asp Ser Lys Asp 165 170 175 Ser Thr Tyr Ser Leu Ser Ser Thr Leu Thr Leu Ser Lys Ala Asp Tyr 180 185 190 Glu Lys His Lys Val Tyr Ala Cys Glu Val Thr His Gln Gly Leu Ser 195 200 205 Ser Pro Val Thr Lys Ser Phe Asn Arg Gly Glu Cys 210 215 220 SEQUENCE LISTING <110> Genentech, Inc. F. Hoffmann-La Roche AG Hoffmann-La Roche Inc. <120> METHODS FOR TREATMENT OF CANCER WITH AN ANTI-TIGIT ANTAGONIST ANTIBODY <130> 50474-206WO2 <150> US 63/127,109 <151> 2020-12-17 <150> US 63/124,693 <151> 2020-12- 11 <150> US 63/114,517 <151> 2020-11-16 <150> US 63/105,198 <151> 2020-10-23 <150> US 63/085,890 <151> 2020-09-30 <150> PCT /US2020/049415 <151> 2020-09-04 <150> US 63/074,827 <151> 2020-09-04 <150> US 63/074,807 <151> 2020-09-04 <150> US 63/059,960 < 151> 2020-07-31 <150> US 63/059,054 <151> 2020-07-30 <150> PCT/US2020/024526 <151> 2020-03-24 <150> US 62/994,272 <151> 2020- 03-24 <150> US 62/985,822 <151> 2020-03-05 <150> US 62/966,448 <151> 2020-01-27 <160> 34 <170> PatentIn version 3.5 <210> 1 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 1 Ser Asn Ser Ala Ala Trp Asn 1 5 <210> 2 <211> 18 <212> PRT <213> Artificial Sequence <220 > <223> Synthetic Construct <400> 2 Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala Val Ser Val 1 5 10 15 Lys Gly <210> 3 <211> 1 4 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 3 Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro Phe Asp Tyr 1 5 10 <210> 4 <211> 17 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 4 Lys Ser Ser Gln Thr Val Leu Tyr Ser Ser Asn Asn Lys Lys Tyr Leu 1 5 10 15 Ala <210> 5 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 5 Trp Ala Ser Thr Arg Glu Ser 1 5 <210> 6 <211> 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 6 Gln Gln Tyr Tyr Ser Thr Pro Phe Thr 1 5 <210> 7 <211> 23 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 7 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys 20 <210> 8 <211> 15 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct < 400> 8 Trp Tyr Gln Gln Lys Pro Gly Gln Pro Pro Asn Leu Leu Ile Tyr 1 5 10 15 <210> 9 <211> 32 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 9 Gly Val Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr 1 5 10 15 Leu Thr Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys 20 25 30 <210> 10 <211> 10 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 10 Phe Gly Pro Gly Thr Lys Val Glu Ile Lys 1 5 10 <210> 11 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <220> <221> MISC_FEATURE <222> (1 )..(1) <223> Xaa is Gln or Glu <400> 11 Xaa Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 <210> 12 <211> 14 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 12 Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu Trp Leu Gly 1 5 10 <210> 13 <211> 32 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 1 3 Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn Gln Phe Ser Leu Gln 1 5 10 15 Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val Phe Tyr Cys Thr Arg 20 25 30 <210> 14 <211> 11 <212 > PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 14 Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 1 5 10 <210> 15 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 15 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 < 210> 16 <211> 30 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 16 Gln Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser 20 25 30 <210> 17 <211> 126 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 17 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gly Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 115 120 125 <210> 18 <211> 126 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 18 Gln Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gl y Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser 115 120 125 <210> 19 <211> 113 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 19 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys Lys Ser Ser Gln Thr Val Leu Tyr Ser 20 25 30 Ser Asn Asn Lys Lys Tyr Leu Ala Trp Tyr Gln Gln Lys Pro Gly Gln 35 40 45 Pro Pro Asn Leu Leu Ile Tyr Trp Ala Ser Thr Arg Glu Ser Gly Val 50 55 60 Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr 65 70 75 80 Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys Gln Gln 85 90 95 Tyr Tyr Ser Thr Pro Phe Thr Phe Gly Pro Gly Thr Lys Val Glu Ile 100 105 110 L ys <210> 20 <211> 10 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 20 Gly Phe Thr Phe Ser Asp Ser Trp Ile His 1 5 10 <210> 21 <211> 18 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 21 Ala Trp Ile Ser Pro Tyr Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 1 5 10 15 Lys Gly <210> 22 <211 > 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 22 Arg His Trp Pro Gly Gly Phe Asp Tyr 1 5 <210> 23 <211> 11 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 23 Arg Ala Ser Gln Asp Val Ser Thr Ala Val Ala 1 5 10 <210> 24 <211> 7 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 24 Ser Ala Ser Phe Leu Tyr Ser 1 5 <210> 25 <211> 9 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 25 Gln Gln Tyr Leu Tyr His Pro Ala Thr 1 5 <210> 26 <211> 118 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 26 Glu Val Gln Leu Val Glu Ser Gly Gly Gly Leu Val Gln Pro Gly Gly 1 5 10 15 Ser Leu Arg Leu Ser Cys Ala Ala Ser Gly Phe Thr Phe Ser Asp Ser 20 25 30 Trp Ile His Trp Val Arg Gln Ala Pro Gly Lys Gly Leu Glu Trp Val 35 40 45 Ala Trp Ile Ser Pro Tyr Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 50 55 60 Lys Gly Arg Phe Thr Ile Ser Ala Asp Thr Ser Lys Asn Thr Ala Tyr 65 70 75 80 Leu Gln Met Asn Ser Leu Arg Ala Glu Asp Thr Ala Val Tyr Tyr Cys 85 90 95 Ala Arg Arg His Trp Pro Gly Gly Phe Asp Tyr Trp Gly Gln Gly Thr 100 105 110 Leu Val Thr Val Ser Ser 115 <210> 27 <211> 108 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 27 Asp Ile Gln Met Thr Gln Ser Pro Ser Ser Leu Ser Ala Ser Val Gly 1 5 10 15 Asp Arg Val Thr Ile Thr Cys Arg Ala Ser Gln Asp Val Ser Thr Ala 20 25 30 Val Ala Trp Tyr Gln Gln Lys Pro Gly Lys Ala Pro Lys Leu Leu Ile 35 40 45 Tyr Ser Ala Ser Phe Leu Tyr Ser GlyVal Pro Ser Arg Phe Ser Gly 50 55 60 Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr Ile Ser Ser Leu Gln Pro 65 70 75 80 Glu Asp Phe Ala Thr Tyr Tyr Cys Gln Gln Tyr Leu Tyr His Pro Ala 85 90 95 Thr Phe Gly Gln Gly Thr Lys Val Glu Ile Lys Arg 100 105 <210> 28 <211> 447 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 28 Glu Val Gln Leu Val Glu Ser Gly Gly Gly Leu Val Gln Pro Gly Gly 1 5 10 15 Ser Leu Arg Leu Ser Cys Ala Ala Ser Gly Phe Thr Phe Ser Asp Ser 20 25 30 Trp Ile His Trp Val Arg Gln Ala Pro Gly Lys Gly Leu Glu Trp Val 35 40 45 Ala Trp Ile Ser Pro Tyr Gly Gly Gly Ser Thr Tyr Tyr Ala Asp Ser Val 50 55 60 Lys Gly Arg Phe Thr Ile Ser Ala Asp Thr Ser Lys Asn Thr Ala Tyr 65 70 75 80 Leu Gln Met Asn Ser Leu Arg Ala Glu Asp Thr Ala Val Tyr Tyr Cys 85 90 95 Ala Arg Arg His Trp Pro Gly Gly Phe Asp Tyr Trp Gly Gln Gly Thr 100 105 110 Leu Val Thr Val Ser Ser Ala Ser Thr Lys Gly Pro Ser Val Phe Pro 115 120 125 Leu Ala Pro Ser Ser Lys Ser Thr Ser Gly Gly Thr Ala Ala Leu Gly 130 135 140 Cys Leu Val Lys Asp Tyr Phe Pro Glu Pro Val Thr Val Ser Trp Asn 145 150 155 160 Ser Gly Ala Leu Thr Ser Gly Val His Thr Phe Pro Ala Val Leu Gln 165 170 175 Ser Ser Gly Leu Tyr Ser Leu Ser Ser Val Val Thr Val Pro Ser Ser 180 185 190 Ser Leu Gly Thr Gln Thr Tyr Ile Cys Asn Val Asn His Lys Pro Ser 195 200 205 Asn Thr Lys Val Asp Lys Lys Val Glu Pro Lys Ser Cys Asp Lys Thr 210 215 220 His Thr Cys Pro Pro Cys Pro Ala Pro Glu Leu Leu Gly Gly Pro Ser 225 230 235 240 Val Phe Leu Phe Pro Lys Pro Lys Asp Thr Leu Met Ile Ser Arg 245 250 255 Thr Pro Glu Val Thr Cys Val Val Val Asp Val Ser His Glu Asp Pro 260 265 270 Glu Val Lys Phe Asn Trp Tyr Val Asp Gly Val Glu Val His Asn Ala 275 280 285 Lys Thr Lys Pro Arg Glu Glu Gln Tyr Ala Ser Thr Tyr Arg Val Val 290 295 300 Ser Val Leu Thr Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu Tyr 305 310 315 320 Lys Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu Lys Thr 325 330 335 Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln Val Tyr Thr Leu 340 345 350 Pro Pro Ser Arg Glu Glu Met Thr Lys Asn Gln Val Ser Leu Thr Cys 355 360 365 Leu Val Lys Gly Phe Tyr Pro Ser Asp Ile Ala Val Glu Trp Glu Ser 370 375 380 Asn Gly Gln Pro Glu Asn Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp 385 390 395 400 Ser Asp Gly Ser Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Ly s Ser 405 410 415 Arg Trp Gln Gln Gly Asn Val Phe Ser Cys Ser Val Met His Glu Ala 420 425 430 Leu His Asn His Tyr Thr Gln Lys Ser Leu Ser Leu Ser Pro Gly 435 440 445 <210> 29 <211> 214 <212> PRT <213> Artificial Sequence <220> <223> Synthetic Construct <400> 29 Asp Ile Gln Met Thr Gln Ser Pro Ser Ser Leu Ser Ala Ser Val Gly 1 5 10 15 Asp Arg Val Thr Ile Thr Cys Arg Ala Ser Gln Asp Val Ser Thr Ala 20 25 30 Val Ala Trp Tyr Gln Gln Lys Pro Gly Lys Ala Pro Lys Leu Leu Ile 35 40 45 Tyr Ser Ala Ser Phe Leu Tyr Ser Gly Val Pro Ser Arg Phe Ser Gly 50 55 60 Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr Ile Ser Ser Leu Gln Pro 65 70 75 80 Glu Asp Phe Ala Thr Tyr Tyr Cys Gln Gln Tyr Leu Tyr His Pro Ala 85 90 95 Thr Phe Gly Gln Gly Thr Lys Val Glu Ile Lys Arg Thr Val Ala Ala 100 105 110 Pro Ser Val Phe Ile Phe Pro Pro Ser Asp Glu Gln Leu Lys Ser Gly 115 120 125 Thr Ala Ser Val Val Cys Leu Leu Asn Asn Phe Tyr Pro Arg Glu Ala 130 135 140 Lys Val Gln Trp Lys Val Asp Asn Ala Leu Gln Ser Gly Asn Ser Gln 145 150 155 160 Glu Ser Val Thr Glu Gln Asp Ser Lys Asp Ser Thr Tyr Ser Leu Ser 165 170 175 Ser Thr Leu Thr Leu Ser Lys Ala Asp Tyr Glu Lys His Lys Val Tyr 180 185 190 Ala Cys Glu Val Thr His Gln Gly Leu Ser Ser Pro Val Thr Lys Ser 195 200 205 Phe Asn Arg Gly Glu Cys 210 <210> 30 <211> 244 <212> PRT <213> Homo sapiens <400> 30 Met Arg Trp Cys Leu Leu Leu Ile Trp Ala Gln Gly Leu Arg Gln Ala 1 5 10 15 Pro Leu Ala Ser Gly Met Met Thr Gly Thr Ile Glu Thr Thr Gly Asn 20 25 30 Ile Ser Ala Glu Lys Gly Gly Ser Ile Ile Leu Gln Cys His Leu Ser 35 40 45 Ser Thr Thr Ala Gln Val Thr Gln Val Asn Trp Glu Gln Gln Asp Gln 50 55 60 Leu Leu Ala Ile Cy s Asn Ala Asp Leu Gly Trp His Ile Ser Pro Ser 65 70 75 80 Phe Lys Asp Arg Val Ala Pro Gly Pro Gly Leu Gly Leu Thr Leu Gln 85 90 95 Ser Leu Thr Val Asn Asp Thr Gly Glu Tyr Phe Cys Ile Tyr His Thr 100 105 110 Tyr Pro Asp Gly Thr Tyr Thr Gly Arg Ile Phe Leu Glu Val Leu Glu 115 120 125 Ser Ser Val Ala Glu His Gly Ala Arg Phe Gln Ile Pro Leu Leu Gly 130 135 140 Ala Met Ala Ala Thr Leu Val Val Ile Cys Thr Ala Val Ile Val Val 145 150 155 160 Val Ala Leu Thr Arg Lys Lys Lys Ala Leu Arg Ile His Ser Val Glu 165 170 175 Gly Asp Leu Arg Arg Lys Ser Ala Gly Gin Glu Glu Trp Ser Pro Ser 180 185 190 Ala Pro Ser Pro Pro Gly Ser Cys Val Gln Ala Glu Ala Ala Pro Ala 195 200 205 Gly Leu Cys Gly Glu Gln Arg Gly Glu Asp Cys Ala Glu Leu His Asp 210 215 220 Tyr Phe Asn Val Leu Ser Tyr Arg Ser Leu Gly Asn Cys Ser Phe Phe 225 230 235 240 Thr Glu Thr Gly <210> 31 <211> 223 <212> PRT <213> Homo sapiens <400> 31 Met Met Thr Gly Thr Ile Glu Thr Thr Gly Asn Ile Ser Ala Glu Lys 1 5 10 15 Gly Gly Ser Ile Ile Leu Gln Cys His Leu Ser Ser Thr Thr Ala Gln 20 25 30 Val Thr Gln Val Asn Trp Glu Gln Gln Asp Gln Leu Leu Ala Ile Cys 35 40 45 Asn Ala Asp Leu Gly Trp His Ile Ser Pro Ser Phe Lys Asp Arg Val 50 55 60 Ala Pro Gly Pro Gly Leu Gly Leu Thr Leu Gln Ser Leu Thr Val Asn 65 70 75 80 Asp Thr Gly Glu Tyr Phe Cys Ile Tyr His Thr Tyr Pro Asp Gly Thr 85 90 95 Tyr Thr Gly Arg Ile Phe Leu Glu Val Leu Glu Ser Ser Val Ala Glu 100 105 110 His Gly Ala Arg Phe Gln Ile Pro Leu Leu Gly Ala Met Ala Ala Thr 115 120 125 Leu Val Val Ile Cys Thr Ala Val Ile Val Val Val Ala Leu Thr Arg 130 135 140 Lys Lys Lys Ala Leu Arg Ile His Ser Val Glu Gly Asp Leu Arg Arg 145 150 155 160 Lys Ser Ala Gly Gln Glu Glu Trp Ser Pro Ser Ala Pro Ser Pro Pro 165 170 175 Gly Ser Cys Val Gln Ala Glu Ala Ala Pro Ala Gly Leu Cys Gly Glu 180 185 190 Gln Arg Gly Glu Asp Cys Ala Glu Leu His Asp Tyr Phe Asn Val Leu 195 200 205 Ser Tyr Arg Ser Leu Gly Asn Cys Ser Phe Phe Thr Glu Thr Gly 210 215 220 <210> 32 <211 > 290 <212> PRT <213> Homo sapiens <400> 32 Met Arg Ile Phe Ala Val Phe Ile Phe Met Thr Tyr Trp His Leu Leu 1 5 10 15 Asn Ala Phe Thr Val Thr Val Pro Lys Asp Leu Tyr Val Val Glu Tyr 20 25 30 Gly Ser Asn Met Thr Ile Glu Cys Lys Phe Pro Val Glu Lys Gln Leu 35 40 45 Asp Leu Ala Ala Leu Ile Val Tyr Trp Glu Met Glu Asp Lys Asn Ile 50 55 60 Ile Gln Phe Val His Gly Glu Glu Asp Leu Lys Val Gln His Ser Ser 65 70 75 80 Tyr Arg Gln Arg Ala Arg Leu Leu Lys Asp Gln Leu Ser Leu Gly Asn 85 90 95 Ala Ala Leu Gln Ile Thr Asp Val Lys Leu Gln Asp Ala Gly Val Tyr 100 105 110 Arg Cys Met Ile Ser Tyr Gly Gly Ala Asp Tyr Lys Arg Ile Thr Val 115 120 125 Lys Val Asn Ala Pro Tyr Asn Lys Ile Asn Gln Arg Ile Leu Val Val 130 135 140 Asp Pro Val Thr Ser Glu His Glu Leu Thr Cys Gln Ala Glu Gly Tyr 145 150 155 160 Pro Lys Ala Glu Val Ile Trp Thr Ser Ser Asp His Gln Val Leu Ser 165 170 175 Gly Lys Thr Thr Thr Thr Asn Ser Lys Arg Glu Glu Lys Leu Phe Asn 180 185 190 Val Thr Ser Thr Leu Arg Ile Asn Thr Thr Thr Asn Glu Ile Phe Tyr 195 200 205 Cys Thr Phe Arg Arg Leu Asp Pro Glu Glu Asn His Thr Ala Glu Leu 210 215 220 Val Ile Pro Glu Leu Pro Leu Ala His Pro Asn Glu Arg Thr His 225 230 235 240 Leu Val Ile Leu Gly Ala Ile Leu Leu Cys Leu Gly Val Ala Leu Thr 245 250 255 Phe Ile Phe Arg Leu Arg Lys Gly Arg Met Met Asp Val Lys Lys Cys 260 265 270 Gly Ile Gln Asp Thr Asn Ser Lys Lys Gln Ser Asp Thr His Leu Glu 275 280 285 Glu Thr 290 <210> 33 <211> 456 <212> PRT <213> Homo sapiens <400> 33 Glu Val Gln Leu Gln Gln Ser Gly Pro Gly Leu Val Lys Pro Ser Gln 1 5 10 15 Thr Leu Ser Leu Thr Cys Ala Ile Ser Gly Asp Ser Val Ser Ser Asn 20 25 30 Ser Ala Ala Trp Asn Trp Ile Arg Gln Ser Pro Ser Arg Gly Leu Glu 35 40 45 Trp Leu Gly Lys Thr Tyr Tyr Arg Phe Lys Trp Tyr Ser Asp Tyr Ala 50 55 60 Val Ser Val Lys Gly Arg Ile Thr Ile Asn Pro Asp Thr Ser Lys Asn 65 70 75 80 Gln Phe Ser Leu Gln Leu Asn Ser Val Thr Pro Glu Asp Thr Ala Val 85 90 95 Phe Tyr Cys Thr Arg Glu Ser Thr Thr Tyr Asp Leu Leu Ala Gly Pro 100 105 110 Phe Asp Tyr Trp Gly Gln Gly Thr Leu Val Thr Val Ser Ser Ala Ser 115 120 125 Thr Lys Gly Pro Ser Val Phe Pro Leu Ala Pro Ser Ser Lys Ser Thr 130 135 140 Ser Gly Gly Thr Ala Ala Leu Gly Cys Leu Val Lys Asp Tyr Phe Pro 145 150 155 160 Glu Pro Val Thr Val Ser Trp Asn Ser Gly Ala Leu Thr Ser Gly Val 165 170 175 His Thr Phe Pro Ala Val Leu Gln Ser Ser Gly Leu Tyr Ser Leu Ser 180 185 190 Ser Val Val Thr Val Pro Ser Ser Ser Leu Gly Thr Gln Thr Tyr Ile 195 200 205 Cys Asn Val Asn His Lys Pro Ser Asn Thr Lys Val Asp Lys Lys Val 210 215 220 Glu Pro Lys Ser Cys Asp Lys Thr His Thr Cys Pro Cys Pro Ala 225 230 235 240 Pro Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe Pro Pro Lys Pro 245 250 255 Lys Asp Thr Leu Met Ile Ser Arg Thr Pro Glu Val Thr Cys Val Val 260 265 270 Val Asp Val Ser His Glu Asp Pro Glu Val Lys Phe Asn Trp Tyr Val 275 280 285 Asp Gly Val Glu Val His Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln 290 295 300 Tyr Asn Ser Thr Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln 305 310 315 320 Asp Trp Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser Asn Lys Ala 325 330 335 Leu Pro Ala Pro Ile Glu Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro 340 345 350 Arg Glu Pro Gln Val Tyr Thr Leu Pro Pro Ser Arg Glu Glu Met Thr 355 360 365 Lys Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly Phe Tyr Pro Ser 370 375 380 Asp Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro Glu Asn Asn Tyr 385 390 395 400 Lys Thr Thr Pro Pro Val Leu Asp Ser Asp Gly Ser Phe Phe Leu Tyr 405 410 415 Ser Lys Leu Thr Val Asp Lys Ser Arg Trp Gln Gln Gly Asn Val Phe 420 425 430 Ser Cys Ser Val Met His Glu Ala Leu His Asn His Tyr Thr Gln Lys 435 440 445 Ser Leu Ser Leu Ser Pro Gly Lys 450 455 <210> 34 <211> 220 <212> PRT <213> Homo sapiens <400> 34 Asp Ile Val Met Thr Gln Ser Pro Asp Ser Leu Ala Val Ser Leu Gly 1 5 10 15 Glu Arg Ala Thr Ile Asn Cys Lys Ser Ser Ser Gln Thr Val Leu Tyr Ser 20 25 30 Ser Asn Asn Lys Lys Tyr Leu Ala Trp Tyr Gln Gln Lys Pro Gly Gln 35 40 45 Pro Pro Asn Leu Leu Ile Tyr Trp Ala Ser Thr Arg Glu Ser Gly Val 50 55 60 Pro Asp Arg Phe Ser Gly Ser Gly Ser Gly Thr Asp Phe Thr Leu Thr 65 70 75 80 Ile Ser Ser Leu Gln Ala Glu Asp Val Ala Val Tyr Tyr Cys Gln Gln 85 90 95 Tyr Tyr Ser Thr Pro Phe Thr Phe Gly Pro Gly Thr Lys Val Glu Ile 100 105 110 Lys Arg Thr Val Ala Ala Pro Ser Val Phe Ile Phe Pro Pro Ser Asp 115 120 125 Glu Gl n Leu Lys Ser Gly Thr Ala Ser Val Val Cys Leu Leu Asn Asn 130 135 140 Phe Tyr Pro Arg Glu Ala Lys Val Gln Trp Lys Val Asp Asn Ala Leu 145 150 155 160 Gln Ser Gly Asn Ser Gln Glu Ser Val Thr Glu Gln Asp Ser Lys Asp 165 170 175 Ser Thr Tyr Ser Leu Ser Ser Thr Leu Thr Leu Ser Lys Ala Asp Tyr 180 185 190 Glu Lys His Lys Val Tyr Ala Cys Glu Val Thr His Gln Gly Leu Ser 195 200 205Ser Pro Val Thr Lys Ser Phe Asn Arg Gly Glu Cys 210 215 220
Claims (503)
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and an evacuation every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a gold-based chemotherapeutic agent.
4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 1400 mg to 2000 mg every 4 weeks A method comprising steps.
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks A method comprising the step of
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.4. The method of claim 2 or 3,
The method further comprising administering to the subject one or more chemotherapeutic agents.
상기 항 TIGIT 길항제 항체는 IgG 부류 항체, 특히 IgG1 하위부류 항체인, 방법.5. The method according to any one of claims 1 to 4,
wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):
(a) SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;
(b) KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;
(c) ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;
(d) KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;
(e) WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및
(f) QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 방법.6. The method according to any one of claims 1 to 5,
The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
(f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR):
(a) DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;
(b) WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;
(c) GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3 서열; 및
(d) FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4, 그리고
하기의 중쇄 가변 영역 FR들:
(a) X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;
(b) WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;
(c) RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및
(d) WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 방법.7. The method according to any one of claims 1 to 6,
The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) a FR-L3 sequence comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
(d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and
The following heavy chain variable region FRs:
(a) FR-H1 comprising the amino acid sequence of X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X 1 is E or Q;
(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
(d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
상기 항 TIGIT 길항제 항체는 하기의:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는
(c) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인 및 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.8. The method according to any one of claims 1 to 7,
The anti-TIGIT antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO: 19.
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법.9. The method according to any one of claims 1 to 8,
The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제 또는 PD-1 결합 길항제인, 방법.10. The method according to any one of claims 1 to 9,
The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체 또는 항 PD-1 길항제 항체인, 방법.11. The method according to any one of claims 1 to 10,
The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
상기 PD-1 축 결합 길항제는 항 PD-L1 길항제 항체인, 방법.12. The method according to any one of claims 1 to 11,
The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 방법.13. The method of claim 12,
The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636.
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 방법.14. The method according to any one of claims 1 to 13,
The method of claim 1, wherein the PD-1 axis binding antagonist is atezolizumab.
상기 PD-1 축 결합 길항제는 항 PD-1 길항제 항체인, 방법.12. The method according to any one of claims 1 to 11,
The method of claim 1, wherein the PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
상기 항 PD-1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 방법.16. The method of claim 15,
Said anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, prolgolimab, camrelizumab, scintilimab, tislelizumab, torifalizumab Mab, dostalimab, retipanrimab, sasanrimab, fenfulimab, CS1003, HLX10, SCT-I10A, zimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21.
유효량의 백금계 화학요법제 및 비백금계 화학요법제를 대상체에게 투여하는 단계를 포함하는, 방법.17. The method according to any one of claims 2 to 16,
A method comprising administering to the subject an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
상기 비백금계 화학요법제는 토포이소머라제 II 억제제인, 방법.18. The method of claim 1 or 17,
The method of claim 1, wherein the non-platinum-based chemotherapeutic agent is a topoisomerase II inhibitor.
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331, 특히 에토포시드인, 방법.19. The method of claim 18,
wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331, in particular etoposide; Way.
상기 토포이소머라제 II 억제제는 100 mg/m2 용량으로 투여되는, 방법.20. The method of claim 18 or 19,
wherein the topoisomerase II inhibitor is administered at a dose of 100 mg/m 2 .
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴, 특히 카보플라틴인, 방법.21. The method according to any one of claims 17 to 20,
The method according to claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin.
상기 백금계 화학요법제는 투여 당일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 방법.22. The method according to any one of claims 17 to 21,
wherein the platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
유도기 및 유지기를 포함한 투약 요법을 포함하는, 방법.23. The method of any one of claims 1-22,
A method comprising a dosing regimen comprising an induction phase and a maintenance phase.
상기 유도기는 4회의 초기 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 비백금계 화학요법제가 4회의 초기 투약 주기의 각각에서 투여되는, 방법.24. The method of claim 23,
wherein the induction phase comprises four initial dosing cycles and the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles.
상기 유지기는 상기 백금계 화학요법제 및/또는 비백금계 화학요법제의 투여를 포함하지 않는, 방법.25. The method of claim 23 or 24,
wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent and/or the non-platinum-based chemotherapeutic agent.
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장하는, 방법.26. The method according to any one of claims 1 to 25,
wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody.
상기 치료는 상기 항 TIGIT 길항제 항체를 이용하지 않는 치료와 비교하여 상기 대상체의 전체 생존을 연장하는, 방법.27. The method of any one of claims 1-26,
wherein said treatment prolongs overall survival of said subject compared to treatment without said anti-TIGIT antagonist antibody.
상기 암은 폐암인, 방법.28. The method according to any one of claims 1 to 27,
The method of claim 1, wherein the cancer is lung cancer.
상기 폐암은 소세포 폐암(SCLC), 특히 확장기 SCLC(ES-SCLC)인, 방법.29. The method of claim 28,
The method of claim 1, wherein the lung cancer is small cell lung cancer (SCLC), in particular expanded stage SCLC (ES-SCLC).
상기 폐암은 비소세포 폐암(NSCLC), 특히 국소 진행성 절제 불가능한 NSCLC(IIIB기 NSCLC)인, 방법.29. The method of claim 28,
wherein the lung cancer is non-small cell lung cancer (NSCLC), in particular locally advanced unresectable NSCLC (stage IIIB NSCLC).
상기 폐암은 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 방법.29. The method of claim 28,
wherein the lung cancer is locally advanced unresectable or metastatic nonsquamous NSCLC.
상기 폐암은 절제 가능한 폐암인, 방법.29. The method of claim 28,
The method of claim 1, wherein the lung cancer is resectable lung cancer.
상기 암은 자궁경부암인, 방법.28. The method according to any one of claims 1 to 27,
The method of claim 1, wherein the cancer is cervical cancer.
상기 암은 초기 삼중음성 유방암(eTNBC)인, 방법.
28. The method according to any one of claims 1 to 27,
wherein the cancer is early triple negative breast cancer (eTNBC).
상기 암은 두경부암인, 방법.28. The method according to any one of claims 1 to 27,
The method of claim 1, wherein the cancer is head and neck cancer.
상기 암은 간암, 특히 간세포 암종(HCC)인, 방법.28. The method according to any one of claims 1 to 27,
wherein the cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
상기 암은 방광암인, 방법.28. The method according to any one of claims 1 to 27,
The method of claim 1, wherein the cancer is bladder cancer.
상기 암은 요로상피세포 암종(UC), 특히 전이성 요로상피세포 암종(mUC)인, 방법.38. The method of claim 37,
wherein the cancer is urothelial cell carcinoma (UC), in particular metastatic urothelial cell carcinoma (mUC).
상기 암은 췌장암, 특히 췌장 도관 선암종(PDAC)인, 방법.28. The method according to any one of claims 1 to 27,
wherein said cancer is pancreatic cancer, in particular pancreatic ductal adenocarcinoma (PDAC).
상기 암은 식도암, 특히 진행성 또는 전이성 식도암인, 방법.28. The method according to any one of claims 1 to 27,
The method of claim 1, wherein the cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
하나 이상의 화학요법제를 더 포함하는, 키트.42. The method of claim 41,
A kit, further comprising one or more chemotherapeutic agents.
상기 방법은 제1항 내지 제40항 중 어느 한 항에 따르는, 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject having cancer, comprising:
41. The method according to any one of claims 1 to 40, wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist.
상기 치료는 제1항 내지 제40항 중 어느 한 항의 방법에 따르는, 용도.1. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having cancer, comprising:
41. Use according to the method of any one of claims 1-40.
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 용도.45. The method of claim 44,
The use of claim 1, wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 용도.45. The method of claim 44,
The use of claim 1, wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and at least one dosing cycle of a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks A method comprising
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks A method comprising the step of:
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.49. The method of claim 47 or 48,
The method further comprising administering to the subject one or more chemotherapeutic agents.
백금계 화학요법제 및 비백금계 화학요법제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.50. The method of claim 49,
A method comprising administering a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent to the subject.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and an evacuation every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a gold-based chemotherapeutic agent.
유도기 및 유지기를 포함하는, 방법.52. The method of claim 50 or 51,
A method comprising an induction phase and a maintenance phase.
상기 유도기 및 유지기는 각각 1회 이상의 투약 주기를 포함하는, 방법.53. The method of claim 52,
wherein the induction and maintenance phases each comprise one or more dosing cycles.
상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.54. The method of claim 52 or 53,
wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent.
상기 유지기는 상기 비백금계 화학요법제의 투여를 포함하지 않는, 방법.55. The method according to any one of claims 52 to 54,
The method of claim 1, wherein the maintenance phase does not include administration of the non-platinum-based chemotherapeutic agent.
상기 유지기는 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함하는, 방법.56. The method of claim 55,
wherein said maintenance phase comprises one or more dosing cycles of anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 100 mg 내지 약 300 mg 용량의 항 PD-1 길항제 항체의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 항 PD-1 길항제 항체는 펨브롤리주맙인, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and an anti-PD-1 antagonist antibody at a dose of about 100 mg to about 300 mg every 3 weeks wherein the anti-PD-1 antagonist antibody is pembrolizumab.
티라골루맙 및 펨브롤리주맙의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 펨브롤리주맙은 6주마다 약 300 mg 내지 약 500 mg의 용량으로 투여되는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising at least one dosing cycle of tiragolumab and pembrolizumab, wherein the pembrolizumab is administered at a dose of about 300 mg to about 500 mg every 6 weeks; Way.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 및 2주 투약/1주 휴약의 3주마다 1일 2회 경구로 약 10 mg/m2 내지 약 10000 mg/m2 용량의 항대사물질의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
Anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, and 1 day every 3 weeks of 2 weeks dosing/1 week washout A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of an antimetabolite at a dose of about 10 mg/m 2 to about 10000 mg/m 2 orally in two doses.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 젬시타빈, 및 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
one or more dosing cycles of anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, gemcitabine, and nap-paclitaxel A method comprising administering to the subject a dosing regimen comprising
상기 하나 이상의 화학요법제는 젬시타빈 및 냅-파클리탁셀인, 방법.50. The method of claim 49,
wherein the one or more chemotherapeutic agents are gemcitabine and nap-paclitaxel.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 및 3주마다 약 1 mg/kg 내지 약 35 mg/kg 용량의 VEGF 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cancer, comprising:
Anti TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, and about 1 mg/kg to about 35 mg/kg every 3 weeks A method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of a kg dose of a VEGF antagonist.
유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서:
(a) 상기 유도기는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고
(b) 상기 유지기는 3주마다 상기 항 TIGIT 길항제 항체, 3주마다 상기 PD-1 축 결합 길항제, 및 3주마다 상기 비백금계 화학요법제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) said maintenance phase comprises at least one additional dosing cycle of said anti-TIGIT antagonist antibody every 3 weeks, said PD-1 axis binding antagonist every 3 weeks, and said non-platinum-based chemotherapeutic agent every 3 weeks, wherein said maintenance wherein the phase does not include administration of the platinum-based chemotherapeutic agent.
유도기 및 유지기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고, 여기서:
(a) 상기 유도기는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제, 3주마다 백금계 화학요법제, 및 3주마다 비백금계 화학요법제의 1회 이상의 투약 주기를 포함하고; 그리고
(b) 상기 유지기는 4주마다 약 700 mg 내지 약 1000 mg 용량의 항 TIGIT 길항제 항체 및 4주마다 약 1400 mg 내지 2000 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 추가적인 투약 주기를 포함하고, 여기서 상기 유지기는 상기 백금계 화학요법제 또는 비백금계 화학요법제의 투여를 포함하지 않는, 방법.A method of treating a subject having cancer, comprising:
administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein:
(a) the induction phase is an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks , and at least one dosing cycle of a non-platinum-based chemotherapeutic agent every 3 weeks; and
(b) the maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks; , wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent.
상기 유도기는 4 내지 6회의 투약 주기를 포함하는, 방법.57. The method of any one of claims 53-56, 63 and 64,
wherein the induction phase comprises 4 to 6 dosing cycles.
(a) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드;
(b) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀; 또는
(c) 상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 에토포시드인, 방법.66. The method of any one of claims 50-56 and 63-65,
(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel; or
(c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is etoposide.
상기 암은 고형 종양인, 방법.67. The method according to any one of claims 47 to 66,
wherein the cancer is a solid tumor.
상기 암은 국소 진행성 또는 전이성인, 방법.68. The method according to any one of claims 47 to 67,
wherein the cancer is locally advanced or metastatic.
상기 암은 폐암, 췌장암, 자궁경부암, 유방암, 두경부암, 간암, 방광암, 식도암, 위암, 결장직장암, 신장암, 신장암, 흑색종, 또는 난소암인, 방법.69. The method according to any one of claims 47 to 68,
wherein the cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, kidney cancer, melanoma, or ovarian cancer.
제69항에 있어서,
상기 암은 폐암인, 방법.
70. The method of claim 69,
The method of claim 1, wherein the cancer is lung cancer.
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 NSCLC인, 방법.71. The method of claim 70,
wherein the lung cancer is NSCLC, in particular locally advanced unresectable NSCLC.
상기 NSCLC는 IIIB기 NSCLC인, 방법.72. The method of claim 71,
wherein said NSCLC is stage IIIB NSCLC.
상기 폐암은 재발성 또는 전이성 NSCLC인, 방법.73. The method of any one of claims 70-72,
wherein the lung cancer is relapsed or metastatic NSCLC.
상기 NSCLC는 IV기 NSCLC인, 방법.74. The method of claim 73,
wherein said NSCLC is stage IV NSCLC.
상기 대상체는 IV기 NSCLC에 대해 이전에 치료를 받은 적이 없는, 방법.75. The method of claim 74,
wherein the subject has not been previously treated for stage IV NSCLC.
상기 폐암은 소세포 폐암(SCLC)인, 방법.71. The method of claim 70,
wherein the lung cancer is small cell lung cancer (SCLC).
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 무진행 생존(PFS)을 연장시키는, 방법.A method of treating a subject or population of subjects having lung cancer, the method comprising:
administering to said subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; , wherein the treatment prolongs progression-free survival (PFS) of the subject compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor without the anti-TIGIT antagonist antibody .
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에게 투여하는 단계를 포함하고, 상기 치료는 약 8.2개월 내지 약 9.2개월의 대상체 집단의 PFS 중앙값을 발생시키는, 방법.A method of treating a population of subjects having lung cancer, the method comprising:
administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; wherein the treatment results in a median PFS of the subject population of from about 8.2 months to about 9.2 months.
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 전체 생존(OS)을 연장시키는, 방법.79. The method of claim 77 or 78,
wherein said treatment prolongs overall survival (OS) of said subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody; Way.
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 2.4개월 만큼 연장시키는, 방법.80. The method according to any one of claims 77 to 79,
wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 2.4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , Way.
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3개월 내지 약 4개월까지 연장시키는, 방법.81. The method of claim 80,
wherein said treatment reduces the PFS of said subject or population of subjects by at least about 3 months to about 4 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. How to extend by months.
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체의 OS를 연장시키는, 방법.A method of treating a subject or population of subjects having lung cancer, the method comprising:
administering to said subject or population of subjects a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; , wherein said treatment prolongs the OS of said subject compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody.
유효량의 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 집단에게 투여하는 단계를 포함하고, 상기 치료는 약 15.3개월 내지 약 17.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.A method of treating a population of subjects having lung cancer, the method comprising:
administering to said subject population a dosing regimen comprising at least one dosing cycle of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor; wherein the treatment results in a median OS of the subject population of from about 15.3 months to about 17.6 months.
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3.3개월 만큼 연장시키는, 방법.84. The method of any one of claims 79-83,
wherein the treatment prolongs the OS of the subject or population of subjects by at least about 3.3 months as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of the anti-TIGIT antagonist antibody. , Way.
상기 치료는 상기 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 OS를 적어도 약 3개월 내지 약 5.3개월 만큼 연장시키는, 방법.84. The method of any one of claims 79-83,
wherein said treatment reduces the OS of said subject or population of subjects by at least about 3 months to about 5.3 as compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor in the absence of said anti-TIGIT antagonist antibody. How to extend by months.
상기 항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제, 및 토포이소머라제 II 억제제는 4회의 초기 투약 주기의 각각에서 투여되는, 방법.86. The method of any one of claims 77-85, wherein
wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the topoisomerase II inhibitor are administered in each of four initial dosing cycles.
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 제4 초기 투약 주기 이후에 1회 이상의 추가 주기로 더 투여되는, 방법.87. The method of any one of claims 77-86,
wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are further administered in one or more additional cycles after the fourth initial dosing cycle.
상기 백금계 화학요법제 및 상기 토포이소머라제 II 억제제는 1회 이상의 추가적인 투약 주기의 각각으로부터 생략되는, 방법.88. The method of claim 87,
wherein said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are omitted from each of one or more additional dosing cycles.
상기 백금계 화학요법제는 카보플라틴이고 상기 토포이소머라제 II 억제제는 에토포시드인, 방법.89. The method according to any one of claims 77 to 88,
wherein the platinum-based chemotherapeutic agent is carboplatin and the topoisomerase II inhibitor is etoposide.
상기 폐암은 소세포 폐암(SCLC)인, 방법.90. The method according to any one of claims 77 to 89,
wherein the lung cancer is small cell lung cancer (SCLC).
상기 SCLC는 확장기 SCLC(ES-SCLC)인, 방법.91. The method of claim 90,
wherein the SCLC is extended SCLC (ES-SCLC).
상기 대상체 또는 대상체들은 ES-SCLC에 대한 치료 경험이 없는, 방법.92. The method of claim 91,
The method of claim 1, wherein the subject or subjects is naive for treatment for ES-SCLC.
상기 대상체 또는 대상체들은 뇌 전이의 존재 또는 병력이 없는, 방법.93. The method of any one of claims 77-92, wherein
The method of claim 1, wherein the subject or subjects do not have the presence or history of brain metastases.
상기 폐암은 PD-L1 발현에 대해 선택되지 않는, 방법.94. The method according to any one of claims 77 to 93,
The method of claim 1, wherein the lung cancer is not selected for PD-L1 expression.
상기 폐암은 PD-L1 발현에 대해 선택되는, 방법.94. The method according to any one of claims 77 to 93,
wherein the lung cancer is selected for PD-L1 expression.
상기 폐암은 PD-L1의 검출 가능한 발현 수준에 의해 PD-L1 발현에 대해 선택되는, 방법.96. The method of claim 95,
wherein the lung cancer is selected for PD-L1 expression by a detectable expression level of PD-L1.
상기 폐암은 전이성인, 방법.97. The method of any one of claims 77-96,
wherein the lung cancer is metastatic.
상기 폐암은 뇌, 간, 림프절, 및/또는 부신으로 전이된, 방법.98. The method of claim 97,
The method of claim 1, wherein the lung cancer has metastasized to the brain, liver, lymph nodes, and/or adrenal glands.
상기 폐암은 뇌로 전이되지 않은, 방법.99. The method of claim 97 or 98,
The method of claim 1, wherein the lung cancer has not metastasized to the brain.
상기 치료는 완전 반응(CR) 또는 부분 반응(PR)을 유발하는, 방법.101. The method of any one of claims 77-99,
wherein the treatment results in a complete response (CR) or a partial response (PR).
각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체, 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드의 1회 이상의 21일 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 치료는 상기 항 TIGIT 길항제 항체 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 방법.A method of treating a subject or population of subjects having SCLC comprising:
Anti TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg on day 1 of each dosing cycle, atezolizumab at a dose of about 900 mg to about 1500 mg on day 1 of each dosing cycle, Day 1 of each dosing cycle Carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min, and 1 of a 100 mg/m 2 dose of etoposide on each of Days 1, 2, and 3 of each dosing cycle. administering to said subject or population of subjects at least one 21 day dosing cycle, wherein said treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without said anti-TIGIT antagonist antibody to said subject or prolonging the PFS and/or OS of the subject population.
4회의 초기 투약 주기에 이어서 1회 이상의 추가적인 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서:
(a) 상기 4회의 초기 투약 주기는 각 초기 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 초기 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 초기 투약 주기의 제 1일에 AUC = 5 mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 각 초기 투약 주기의 제 1일, 2일, 및 3일의 각각에 100 mg/m2 용량의 에토포시드를 투여하는 단계를 포함하고; 그리고
(b) 상기 1회 이상의 추가적인 투약 주기는 각 추가적인 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 추가적인 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙을 투여하는 단계를 포함하고,
여기서 상기 4회의 초기 투약 주기 및 상기 1회 이상의 추가적인 투약 주기는 각각의 21일 투약 주기이고, 여기서 상기 치료는 상기 티라골루맙 없이 아테졸리주맙, 카보플라틴, 및 에토포시드를 이용한 치료와 비교하여 상기 대상체 또는 대상체 집단의 PFS 및/또는 OS를 연장시키는, 방법.A method of treating a subject or population of subjects having ES-SCLC comprising:
administering to the subject or population of subjects one or more additional dosing cycles following four initial dosing cycles, wherein:
(a) said four initial dosing cycles are tiragolumab at a dose of about 600 mg on day 1 of each initial dosing cycle, atezolizumab at a dose of about 1200 mg on day 1 of each initial dosing cycle, each initial dosing cycle Carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min on Day 1 of administering etoposide; and
(b) said one or more additional dosing cycles comprises administering a dose of about 600 mg of tiragolumab on Day 1 of each additional dosing cycle and a dose of about 1200 mg of Atezolizumab on Day 1 of each additional dosing cycle. including,
wherein said four initial dosing cycles and said one or more additional dosing cycles are each 21 day dosing cycle, wherein said treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without said tiragolumab to prolong the PFS and/or OS of the subject or population of subjects.
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 백금계 화학요법제인 제1 화학요법제, 및 비백금계 화학요법제인 제2 화학요법제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having lung cancer, the method comprising:
a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent, and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent; A method comprising administering to
상기 폐암은 PD-L1 발현에 대해 평가되지 않은, 방법.104. The method of claim 103,
The method of claim 1, wherein the lung cancer has not been assessed for PD-L1 expression.
상기 대상체 또는 대상체들은 PD-L1 양성 종양 세포 분획이 50% 이상인 것으로 결정되지 않는, 방법.105. The method of claim 103 or 104,
The method of claim 1, wherein the subject or subjects is not determined to have a fraction of PD-L1 positive tumor cells greater than or equal to 50%.
상기 대상체 또는 대상체들은 50% 미만의 PD-L1 양성 종양 세포 분획을 갖는 것으로 결정된, 방법.107. The method of claim 105,
The method of claim 1 , wherein the subject or subjects is determined to have a fraction of PD-L1 positive tumor cells of less than 50%.
상기 PD-L1 양성 종양 세포 분획은 항 PD-L1 항체를 사용한 양성 염색에 의해 결정되고, 여기서 상기 항 PD-L1 항체는 SP263 또는 22C3인, 방법.107. The method of claim 105 or 106,
wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, wherein said anti-PD-L1 antibody is SP263 or 22C3.
상기 대상체 또는 대상체들은 표피 성장 인자 수용체(EGFR) 또는 역형성 림프종 키나제(ALK) 게놈 종양 이상을 갖지 않는, 방법.108. The method of any one of claims 103-107,
The method of claim 1, wherein the subject or subjects do not have an epidermal growth factor receptor ( EGFR ) or anaplastic lymphoma kinase ( ALK ) genomic tumor abnormality.
상기 대상체 또는 대상체들은 상기 폐암에 대해 선행 전신 요법을 받은 적이 없는, 방법.109. The method of any one of claims 103-108,
The method of claim 1, wherein said subject or subjects has not received prior systemic therapy for said lung cancer.
상기 폐암은 국소 진행성 폐암인, 방법.110. The method of any one of claims 103-109,
wherein the lung cancer is locally advanced lung cancer.
상기 폐암은 NSCLC, 특히 국소 진행성 절제 불가능한 또는 전이성 비편평 NSCLC인, 방법.112. The method of any one of claims 103-110,
wherein the lung cancer is NSCLC, in particular locally advanced unresectable or metastatic nonsquamous NSCLC.
상기 비편평 NSCLC는 IV기 비편평 NSCLC인, 방법.112. The method of claim 111,
wherein said nonsquamous NSCLC is stage IV nonsquamous NSCLC.
상기 투약 요법은 4회의 투약 주기를 포함한 유도기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 상기 백금계 화학요법제, 및 상기 비백금계 화학요법제는 상기 유도기의 각 투약 주기의 제 1일에 투여되는, 방법.113. The method of any one of claims 103-112,
wherein the dosing regimen includes an induction phase comprising 4 dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent, and the non-platinum-based chemotherapeutic agent include each dosing cycle of the induction phase. administered on the first day of
상기 투약 요법은 상기 유도기 이후에 유지기를 포함하고, 여기서 상기 유지기는 1회 이상의 투약 주기를 포함하고, 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 상기 비백금계 화학요법제는 상기 유지기의 각 투약 주기의 제 1일에 투여되는, 방법.114. The method of claim 113,
wherein the dosing regimen comprises a maintenance phase after the induction phase, wherein the maintenance phase includes one or more dosing cycles, and wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, and the non-platinum chemotherapeutic agent are the maintenance phases. administered on Day 1 of each dosing cycle of the phase.
상기 유지기의 1회 이상의 투약 주기는 상기 백금계 화학요법제의 투여를 포함하지 않는, 방법.115. The method of claim 114,
wherein the one or more dosing cycles of the maintenance phase do not include administration of the platinum-based chemotherapeutic agent.
상기 백금계 화학요법제는 카보플라틴 또는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드인, 방법.116. The method of any one of claims 103-115,
The method of claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed.
티라골루맙, 아테졸리주맙, 카보플라틴 또는 시스플라틴, 및 페메트렉시드에 대한 4회의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 티라골루맙은 3주마다 약 600 mg 용량으로 투여되고, 상기 아테졸리주맙은 3주마다 약 1200 mg 용량으로 투여되고, 상기 카보플라틴은 3주마다 AUC = 5 mg/ml/분을 달성하기에 충분한 용량으로 투여되거나, 또는 상기 시스플라틴은 3주마다 75 mg/m2 용량으로 투여되며, 상기 페메트렉시드는 4회의 21일 투약 주기의 각각의 제 1일에 3주마다 약 500 mg/m2 용량으로 투여되는, 방법.A method of treating a subject or population of subjects having advanced nonsquamous NSCLC, comprising:
administering to said subject or population of subjects a dosing regimen comprising four 21-day dosing cycles for tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed, wherein said tiragolumab comprises: is administered at a dose of about 600 mg every 3 weeks, the atezolizumab is administered at a dose of about 1200 mg every 3 weeks, and the carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min every 3 weeks. or, the cisplatin is administered at a dose of 75 mg/m 2 every 3 weeks, and the pemetrexed is administered at a dose of about 500 mg/m 2 every 3 weeks on the first day of each of four 21-day dosing cycles. , Way.
상기 대상체 또는 대상체 집단에:
(i) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 3주마다 AUC = 5mg/ml/분을 달성하기에 충분한 용량의 카보플라틴, 및 3주마다 약 500 mg/m2 용량의 페메트렉시드에 대한 4회의 유도기 투약 주기; 및
(ii) 3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 500 mg/㎡ 용량의 페메트렉시드의 1회 이상의 유지기 투약 주기를 투여하는 단계를 포함하고, 여기서 상기 유지기의 1회 이상의 21일 투약 주기는 상기 카보플라틴의 투여를 포함하지 않고,
여기서 상기 대상체 또는 대상체의 집단은 진행성 비편평 NSCLC에 대해 선행 전신 요법을 받은 적이 없는, 방법.A method of treating a subject or population of subjects having advanced nonsquamous NSCLC, comprising:
To said subject or population of subjects:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin in a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 4 cycles of induction dosing for pemetrexed at a dose of about 500 mg/m 2 per week; and
(ii) one or more maintenance phase dosing cycles of tyragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/m 2 every 3 weeks. administering, wherein at least one 21-day dosing cycle of said maintenance phase does not comprise administration of said carboplatin;
wherein the subject or population of subjects has not received prior systemic therapy for advanced nonsquamous NSCLC.
상기 치료는 상기 대상체 또는 대상체 집단의 PFS를 적어도 약 3.5개월 또는 약 4.7개월 만큼 연장시키는, 방법.119. The method of any one of claims 103-118,
wherein the treatment prolongs the PFS of the subject or population of subjects by at least about 3.5 months or about 4.7 months.
상기 치료는 약 12.5개월 내지 약 14.7개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.119. The method of any one of claims 103-118,
wherein said treatment results in a median PFS of a population of subjects from about 12.5 months to about 14.7 months.
상기 치료는 상기 대상체 또는 대상체 집단의 OS를 적어도 약 5.5개월 또는 약 8.0개월 만큼 연장시키는, 방법.119. The method of any one of claims 103-118,
wherein the treatment prolongs the OS of the subject or population of subjects by at least about 5.5 months or about 8.0 months.
상기 치료는 약 27.5개월 내지 약 32.0개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.119. The method of any one of claims 103-118,
wherein said treatment results in a median OS in the subject population of about 27.5 months to about 32.0 months.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject with resectable lung cancer, comprising:
administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks How to.
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서 상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제를 신보조제 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having lung cancer, comprising:
administering to said subject one or more dosing cycles of an anti TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein at least one of said dosing cycles is from about 500 mg to about 700 mg of an antibiotic every 3 weeks. A method comprising administering to the subject as neoadjuvant treatment a TIGIT antagonist antibody and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks.
상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 용량의 PD-1 축 결합 길항제를 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.125. The method of claim 124,
At least once in said dosing cycle administering to said subject as adjuvant treatment a dose of about 500 mg to about 700 mg of an anti-TIGIT antagonist antibody every 3 weeks and a dose of about 900 mg to about 1500 of a PD-1 axis binding antagonist every 3 weeks A method comprising the step of:
상기 폐암은 절제 가능한 폐암인, 방법.127. The method of claim 124 or 125,
The method of claim 1, wherein the lung cancer is resectable lung cancer.
상기 폐암은 초기 폐암인, 방법.127. The method of any one of claims 123-126,
The method of claim 1, wherein the lung cancer is early stage lung cancer.
상기 폐암은 II기, IIIA기, 또는 IIIB기 폐암인, 방법.127. The method of any one of claims 123 to 127,
The method of claim 1, wherein the lung cancer is stage II, IIIA, or IIIB lung cancer.
상기 대상체는 근치적 목적의 R0 절제술에 적격인, 방법.129. The method according to any one of claims 123 to 128,
The method of claim 1, wherein the subject is eligible for a curative-purpose RO resection.
상기 대상체는 폐암에 대해 선행 요법을 받은 적이 없는, 방법.130. The method according to any one of claims 123 to 129,
The method of claim 1, wherein the subject has never received prior therapy for lung cancer.
상기 선행 요법은 면역요법, 화학요법, 또는 방사선요법인, 방법.130. The method of claim 130,
wherein the prior therapy is immunotherapy, chemotherapy, or radiotherapy.
상기 대상체는 백금계 화학요법에 적격인, 방법.132. The method of any one of claims 123-131,
wherein the subject is eligible for platinum-based chemotherapy.
상기 제1 투약 주기는 수술 전에 개시되는, 방법.134. The method according to any one of claims 123 to 132,
wherein the first dosing cycle is initiated prior to surgery.
적어도 1, 2, 3, 또는 4회의 투약 주기는 상기 수술 전에 완료되는, 방법.134. The method of claim 133,
at least 1, 2, 3, or 4 dosing cycles are completed prior to the surgery.
4회의 투약 주기는 상기 수술 전에 완료되는, 방법.134. The method of claim 133 or 134,
and 4 dosing cycles are completed prior to the surgery.
적어도 1회의 투약 주기는 수술 후에 개시되는, 방법.136. The method of any one of claims 123 to 135,
at least one dosing cycle is initiated after surgery.
16회의 투약 주기는 상기 수술 후에 완료되는, 방법.137. The method of claim 136,
16 dosing cycles are completed after said surgery.
상기 수술은 분엽 절제술, 폐엽 절제술, 양엽 절제술, 또는 폐절제술인, 방법.137. The method of any one of claims 133 to 137,
wherein the operation is lobectomy, lobectomy, bilobectomy, or pneumonectomy.
방사선 요법을 더 포함하는, 방법.139. The method of any one of claims 123 to 138,
The method further comprising radiation therapy.
상기 방사선 요법은 수술 후 방사선 요법인, 방법.140. The method of claim 139,
The method of claim 1, wherein the radiation therapy is post-surgery radiation therapy.
하나 이상의 화학요법제를 투여하는 단계를 더 포함하는, 방법.140. The method of any one of claims 123-140,
The method further comprising administering one or more chemotherapeutic agents.
상기 하나 이상의 화학요법제는 수술 후 투여되는, 방법.142. The method of claim 141,
wherein the one or more chemotherapeutic agents are administered post-surgery.
상기 하나 이상의 화학요법제는 상기 수술 후 4회 투약 주기로 투여되는, 방법.143. The method of claim 142,
The method of claim 1, wherein the one or more chemotherapeutic agents are administered in 4 dosing cycles after the surgery.
상기 하나 이상의 화학요법제는 백금계 화학요법제 및 비백금계 화학요법제인, 방법.144. The method of any one of claims 141 to 143,
wherein the at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
(a) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이고;
(b) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 젬시타빈이고;
(c) 상기 백금계 화학요법제는 카보플라틴이고 상기 비백금계 화학요법제는 파클리탁셀이고;
(d) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 페메트렉시드이거나; 또는
(e) 상기 백금계 화학요법제는 시스플라틴이고 상기 비백금계 화학요법제는 젬시타빈인, 방법.145. The method of claim 144,
(a) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or
(e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine.
상기 치료는 기준 주요 병리학적 반응률(MPR)과 비교하여 MPR 비율의 증가를 유발하는, 방법.145. The method of any one of claims 123-145,
wherein said treatment results in an increase in the MPR rate as compared to a baseline major pathological response rate (MPR).
상기 기준 MPR 비율은:
(a) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제; 및/또는
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 적이 있는 대상체 집단의 MPR 비율인, 방법.147. The method of claim 146,
The reference MPR ratio is:
(a) a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody; and/or
(b) the MPR rate of a population of subjects who have ever received treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
상기 치료는 병리학적 완전 반응(pCR) 및/또는 기준 pCR 비율과 비교하여 pCR 비율의 증가를 유발하는, 방법.147. The method according to any one of claims 123 to 147,
wherein the treatment results in an increase in the pathological complete response (pCR) and/or pCR ratio compared to a baseline pCR ratio.
상기 기준 pCR 비율은:
(a) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제; 및/또는
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 적이 있는 대상체 집단의 pCR 비율인, 방법.149. The method of claim 148,
The reference pCR ratio is:
(a) a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody; and/or
(b) cisplatin and docetaxel or the pCR ratio of a population of subjects that have ever received treatment comprising cisplatin, docetaxel, and bevacizumab.
상기 치료는 기준 무사건 생존(EFS) 기간과 비교하여 EFS의 증가를 유발하는, 방법.149. The method of any one of claims 123-149, wherein
wherein said treatment results in an increase in EFS compared to a baseline event-free survival (EFS) period.
상기 기준 EFS 기간은:
(a) 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제; 및/또는
(b) 시스플라틴 및 도세탁셀 또는 시스플라틴, 도세탁셀, 및 베바시주맙을 포함한 치료를 받은 적이 있는 대상체 집단의 EFS 기간인, 방법.150. The method of claim 150,
The reference EFS period is:
(a) a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody; and/or
(b) the duration of EFS in a population of subjects who have ever received treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab.
3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및:
(a)
(i) 3주마다 5 mg/mL/분의 AUC 또는 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 또는
(ii)3주마다 약 75 mg/m2 용량의 시스플라틴; 및
(b)
(i)3주마다 약 500 mg/m2 용량의 페메트렉시드 또는 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 또는 약 1250 mg/m2 용량의 젬시타빈; 또는
(ii)3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀에 대해 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject with resectable lung cancer, comprising:
Tiragolumab at a dose of about 600 mg every 3 weeks, Atezolizumab at a dose of about 1200 mg every 3 weeks, and:
(a)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or
(ii) cisplatin at a dose of about 75 mg/m 2 every 3 weeks; and
(b)
(i) pemetrexed at a dose of about 500 mg/m 2 every 3 weeks or gemcitabine at a dose of about 1000 mg/m 2 or about 1250 mg/m 2 on days 1 and 8 of each dosing cycle; or
(ii) administering to the subject one or more dosing cycles for paclitaxel at a dose of about 175 mg/m 2 or about 200 mg/m 2 every 3 weeks.
티라골루맙 및 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 여기서:
(I) 상기 투약 주기 중 적어도 1회는 신보조제 치료이고 상기 대상체에게:
(a) 3주마다 약 1200 mg 용량의 티라골루맙;
(b) 신보조제 치료로서 3주마다 약 1200 mg 용량의 아테졸리주맙; 및
(c)
(i) 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 각 투약 주기의 제 1일 및 8일에 약 1000 mg/m2 용량의 젬시타빈;
(ii) 3주마다 6 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴 및 3주마다 약 175 mg/m2 또는 약 200 mg/m2 용량의 파클리탁셀; 또는
(iii) 3주마다 약 75 mg/m2 용량의 시스플라틴 및 각 투약 주기의 제 1일 및 8일에 1250 mg/m2 용량의 젬시타빈을 투여하는 단계를 포함하고; 그리고
(II) 상기 투약 주기 중 적어도 1회는 3주마다 약 500 mg 내지 약 700 mg 용량의 티라골루맙 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 아테졸리주맙을 보조 치료로서 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having lung cancer, comprising:
administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein:
(I) at least one of said dosing cycles is neoadjuvant treatment and to said subject:
(a) tyragolumab at a dose of about 1200 mg every 3 weeks;
(b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; and
(c)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m 2 on days 1 and 8 of each dosing cycle;
(ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m 2 or about 200 mg/m 2 every 3 weeks; or
(iii) administering cisplatin at a dose of about 75 mg/m 2 every 3 weeks and gemcitabine at a dose of 1250 mg/m 2 on days 1 and 8 of each dosing cycle; and
(II) administering to the subject as adjuvant treatment at least one of said dosing cycles is tiragolumab at a dose of about 500 mg to about 700 mg every 3 weeks and atezolizumab at a dose of about 900 mg to about 1500 mg every 3 weeks A method comprising the step of
항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.154. The method according to any one of claims 123 to 153,
A method, wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 방법.154. The method of claim 154,
The method, wherein the detectable protein expression level of PD-L1 is at least 50% of the PD-L1 positive tumor cell fraction.
상기 폐암은 NSCLC인, 방법.107. The method of any one of claims 70, 103-110, and 123-155, wherein
The method of claim 1, wherein the lung cancer is NSCLC.
상기 NSCLC는 편평 NSCLC인, 방법.157. The method of claim 156,
wherein the NSCLC is squamous NSCLC.
상기 NSCLC는 비편평 NSCLC인, 방법.157. The method of claim 156,
wherein the NSCLC is non-squamous NSCLC.
상기 암은 자궁경부암인, 방법.70. The method of claim 69,
The method of claim 1, wherein the cancer is cervical cancer.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having cervical cancer having a detectable expression level of PD-L1, the method comprising:
administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising steps.
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체로부터의 종양 샘플로부터 종양 세포 상의 PD-L1의 단백질 발현 수준을 검출하는 단계; 및
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체에 대해 검출된 종양 세포 상의 PD-L1 발현을 기반으로 하여 3주마다 약 500 mg 내지 약 700 mg의 용량으로 투여되는 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 투여되는 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.A method of selecting therapy for a subject having cervical cancer comprising:
(a) detecting the protein expression level of PD-L1 on tumor cells from a tumor sample from said subject by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) an anti-TIGIT antagonist antibody administered at a dose of about 500 mg to about 700 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject having a detectable expression level of PD-L1, and selecting a regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist administered at a dose of about 900 mg to about 1500 mg every 3 weeks.
상기 자궁경부암은 편평세포 암종, 선편평세포 암종, 또는 선암종인, 방법.162. The method of claim 160 or 161,
The method of claim 1, wherein the cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
상기 자궁경부암은 IVB기, 전이성, 재발성, 또는 지속성인, 방법.163. The method of any one of claims 160 to 162,
wherein the cervical cancer is stage IVB, metastatic, recurrent, or persistent.
상기 자궁경부암은 전이성 및/또는 재발성 PD-L1 양성 자궁경부 암종인, 방법.164. The method of any one of claims 160 to 163,
The method of claim 1, wherein the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical carcinoma.
상기 대상체 또는 대상체들은 적어도 한 라인의 선행 요법을 받은, 방법.165. The method of any one of claims 160 to 164,
The subject or subjects have received at least one line of prior therapy.
상기 대상체 또는 대상체들은 두 라인의 선행 요법을 받은, 방법.167. The method of any one of claims 160 to 165,
The subject or subjects have received two lines of prior therapy.
상기 대상체 또는 대상체들은 두 라인 초과의 선행 요법을 받은, 방법.166. The method of any one of claims 160 to 166,
wherein the subject or subjects have received more than two lines of prior therapy.
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 방법.165. The method of any one of claims 160 to 164,
The method of claim 1, wherein the subject or subjects have not received prior therapy.
상기 선행 요법은 화학요법, 수술 및/또는 방사선요법인, 방법.169. The method of any one of claims 165-168,
wherein said prior therapy is chemotherapy, surgery and/or radiation therapy.
상기 치료는 임상 반응을 유발하는, 방법.169. The method of any one of claims 160 and 162-169,
wherein said treatment elicits a clinical response.
상기 임상 반응은 기준 ORR과 비교하여 대상체 집단의 객관적 반응률(ORR)의 증가인, 방법.170. The method of claim 170,
wherein the clinical response is an increase in the objective response rate (ORR) of the subject population as compared to a baseline ORR.
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 방법.172. The method of claim 171,
wherein said baseline ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
상기 기준 ORR은 적어도 약 14.6% 내지 약 26%인, 방법.170. The method of claim 170,
wherein the baseline ORR is at least about 14.6% to about 26%.
상기 임상 반응은 CR 또는 PR인, 방법.170. The method of claim 170,
wherein the clinical response is CR or PR.
상기 임상 반응은 기준 무진행 생존(PFS) 기간과 비교하여 상기 대상체의 PFS의 증가, 기준 반응 지속 (DOR) 기간과 비교하여 상기 대상체의 DOR의 증가, 또는 기준 전체 생존(OS) 기간과 비교하여 상기 대상체의 OS의 증가인, 방법.175. The method of any one of claims 170-174,
The clinical response is an increase in the subject's PFS compared to a baseline progression-free survival (PFS) period, an increase in the subject's DOR compared to a baseline duration of response (DOR) period, or an increase in the subject's DOR compared to a baseline overall survival (OS) period compared to a baseline overall survival (OS) period. an increase in the subject's OS.
(a) 상기 기준 PFS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 기간 중앙값이고;
(b) 상기 기준 DOR 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 기간 중앙값이거나; 또는
(c) 상기 기준 OS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 기간 중앙값인, 방법.175. The method of claim 175:
(a) said baseline PFS duration is the median duration of PFS in a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) said baseline DOR duration is the median DOR duration of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) the baseline OS duration is the median OS duration of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having cervical cancer having a detectable expression level of PD-L1, the method comprising:
A method comprising administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
상기 대상체는 검출된 종양 세포 상의 PD-L1 발현에 근거한 치료로부터 이익을 얻을 가능성이 있는 자로서 식별되는, 방법.178. The method of any one of claims 160-177,
wherein the subject is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
PD-L1 발현 수준은 항 PD-L1 항체 SP263을 사용하여 검출되는, 방법.178. The method of any one of claims 160-178,
The method of claim 1, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 방법.180. The method of any one of claims 160 to 179,
wherein the detectable expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the sample from the subject.
PD-L1 발현 수준은 항 PD-L1 항체 22C3을 사용하여 검출되는, 방법.178. The method of any one of claims 160-178,
The method of claim 1, wherein the PD-L1 expression level is detected using anti-PD-L1 antibody 22C3.
상기 PD-L1의 검출 가능한 발현 수준은 상기 대상체로부터의 샘플에서 복합 양성 점수(CPS)가 1 이상인, 방법.180. The method of any one of claims 160 to 179,
wherein the detectable expression level of PD-L1 has a composite positive score (CPS) of 1 or greater in a sample from the subject.
상기 암은 유방암인, 방법.70. The method of claim 69,
The method of claim 1, wherein the cancer is breast cancer.
4주마다 약 840 mg 용량의 티라골루맙, 4주마다 약 1680 mg 용량의 아테졸리주맙, 및 3주 투약/1주 휴약의 약 100 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having breast cancer, the method comprising:
One or more dosing cycles of tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and nap-paclitaxel at a dose of about 100 mg/m 2 of 3 weeks dosing/1 week off A method comprising administering to the subject or population of subjects a dosing regimen comprising
상기 유방암은 삼중 음성 유방암(TNBC)인, 방법.185. The method of claim 183 or 184,
The method of claim 1, wherein the breast cancer is triple negative breast cancer (TNBC).
상기 TNBC는 절제 불가능한 국소 진행성 또는 전이성 TNBC인, 방법.185. The method of claim 185,
wherein the TNBC is unresectable locally advanced or metastatic TNBC.
상기 대상체 또는 대상체들은 전이성 유방암에 대해 선행 전신 요법을 받은 적이 없는, 방법.189. The method of any one of claims 183 to 186,
The method of claim 1, wherein the subject or subjects has not received prior systemic therapy for metastatic breast cancer.
상기 치료는 적어도 약 53% 내지 적어도 약 67.5%의 대상체 집단의 ORR을 유발하는, 방법.189. The method of any one of claims 183 to 187,
wherein said treatment results in an ORR in at least about 53% to at least about 67.5% of the subject population.
상기 치료는 약 25.0개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.189. The method according to any one of claims 183 to 188,
wherein said treatment results in a median OS in the subject population of about 25.0 months.
2주마다 약 300 mg 내지 약 600 mg 용량의 항 TIGIT 길항제 항체 및 2주마다 약 600 mg 내지 약 1200 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having early triple negative breast cancer (eTNBC), comprising:
administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks A method comprising the step of
하나 이상의 화학요법제를 상기 대상체에게 투여하는 단계를 더 포함하는, 방법.190. The method of claim 190,
The method further comprising administering to the subject one or more chemotherapeutic agents.
상기 하나 이상의 화학요법제는 백금계 화학요법제, 탁산, 토포이소머라제 II 억제제, 또는 알킬화제인, 방법.192. The method of claim 191,
The method of claim 1, wherein the at least one chemotherapeutic agent is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
(a) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 및 탁산 또는 탁산 및 백금계 화학요법제의 1회 이상의 투약 주기; 및 (b) 상기 항 TIGIT 길항제 항체, 상기 PD-1 축 결합 길항제, 토포이소머라제 II 억제제, 알킬화제, 및 과립구 집락 자극 인자(G-CSF) 또는 과립구-대식세포 집락 자극 인자(GM-CSF)의 1회 이상의 투약 주기를 투여하는 단계를 더 포함하는, 방법.190. The method of claim 190,
(a) at least one dosing cycle of said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, and a taxane or a taxane and a platinum-based chemotherapeutic agent; and (b) said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony stimulating factor (G-CSF) or granulocyte-macrophage colony stimulating factor (GM-CSF) The method further comprising administering one or more dosing cycles of
상기 알킬화제는 시클로포스파미드인, 방법.194. The method of claim 192 or 193,
wherein the alkylating agent is cyclophosphamide.
상기 시클로포스파미드는 약 600 mg/m2의 용량으로 투여되는, 방법.194. The method of claim 194,
wherein the cyclophosphamide is administered at a dose of about 600 mg/m 2 .
G-CSF 또는 GM-CSF를 상기 대상체에게 더 투여하는 단계를 포함하는, 방법.194. The method of any one of claims 190-192, 194 and 195, wherein
further administering G-CSF or GM-CSF to the subject.
상기 G-CSF는 페그필그라스팀 또는 필그라스팀인, 방법.197. The method of claim 193 or 196,
The G-CSF is pegfilgrastim or filgrastim, the method.
상기 G-CSF는 페그필그라스팀인, 방법.197. The method of claim 197,
The G-CSF is pegfilgrastim, the method.
상기 페그필그라스팀은 약 6 mg의 용량으로 투여되는, 방법.199. The method of claim 198,
The method of claim 1, wherein the pegfilgrastim is administered at a dose of about 6 mg.
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF의 하나 이상의 후속 용량을 상기 대상체에게 더 투여하는 단계를 포함하는, 방법.199. The method of any one of claims 191, 192, and 194-199, wherein
further administering to the subject the one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF.
상기 하나 이상의 화학요법제 및/또는 G-CSF 또는 GM-CSF는 각각 매주마다 1회, 2주마다 1회, 또는 3주마다 1회 투여되는, 방법.201. The method of any one of claims 191, 192, and 194-200, wherein
wherein the one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once every week, once every 2 weeks, or once every 3 weeks, respectively.
상기 백금계 화학요법제는 3주마다 투여되고, 상기 탁산은 매주 투여되고, 상기 토포이소머라제 II 억제제는 2주마다 투여되고, 상기 알킬화제는 2주마다 투여되며, 상기 G-CSF 또는 GM-CSF는 2주마다 투여되는, 방법.202. The method of any one of claims 192-201, wherein
The platinum-based chemotherapeutic agent is administered every 3 weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every 2 weeks, the alkylating agent is administered every 2 weeks, and the G-CSF or GM- CSF is administered every two weeks.
상기 탁산 또는 상기 탁산 및 상기 백금계 화학요법제는 상기 투약 요법의 처음 12주 동안 투여되는, 방법.202. The method of any one of claims 192-202, wherein
wherein said taxane or said taxane and said platinum-based chemotherapeutic agent are administered during the first 12 weeks of said dosing regimen.
상기 토포이소머라제 II 억제제, 상기 알킬화제, 및 상기 G-CSF 또는 GM-CSF는 투약 요법의 13주 내지 19주 동안 투여되는, 방법.203. The method of any one of claims 192-203, wherein
wherein the topoisomerase II inhibitor, the alkylating agent, and the G-CSF or GM-CSF are administered for 13 to 19 weeks of a dosing regimen.
상기 투약 요법의 총 기간은 19주인, 방법.204. The method of any one of claims 190-204,
The total duration of said dosing regimen is 19 weeks.
신보조제 치료인, 방법.205. The method of any one of claims 190-205,
A neoadjuvant treatment, a method.
상기 투약 요법 후에 수술이 실시되는, 방법.206. The method of any one of claims 190-206, wherein
wherein surgery is performed after said dosing regimen.
상기 수술은 상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 실시되는, 방법.208. The method of claim 207,
wherein said surgery is performed between 2 and 6 weeks after the last dose of said dosing regimen.
상기 수술은 유방절제술을 포함하는, 방법.209. The method of claim 207 or 208,
wherein the surgery comprises a mastectomy.
상기 수술은 액와 림프절 수술을 포함하는, 방법.209. The method of any one of claims 207-209,
wherein the surgery comprises axillary lymph node surgery.
상기 토포이소머라제 II 억제제는 독소루비신인, 방법.212. The method of any one of claims 192-210, wherein
wherein the topoisomerase II inhibitor is doxorubicin.
상기 탁산은 냅-파클리탁셀이고, 상기 백금계 화학요법제는 카보플라틴이며, 상기 토포이소머라제 II 억제제는 독소루비신인, 방법.212. The method of any one of claims 192-210, wherein
wherein the taxane is nap-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin.
독소루비신은 약 60 mg/m2의 용량으로 투여되는, 방법.223. The method of claim 211 or 212,
The method of claim 1, wherein doxorubicin is administered at a dose of about 60 mg/m 2 .
2주마다 약 420 mg 용량의 티라골루맙, 2주마다 약 840 mg 용량의 아테졸리주맙, 및:
(a)
(i) 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀 및 3주마다 5 mg/mL/분의 AUC를 달성하도록 표적화된 용량의 카보플라틴; 및
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF; 또는
(b)
(i) 상기 투약 요법의 처음 12주 동안 매주마다 약 125 mg/m2 용량의 냅-파클리탁셀; 및
(ii) 상기 투약 요법의 13주 내지 19주 동안 2주마다 약 60 mg/m2 용량의 독소루비신, 2주마다 약 600 mg/m2 용량의 시클로포스파미드, 및 2주마다 G-CSF 또는 GM-CSF를 포함한 투약 요법을 상기 대상체에게 투여하는 단계를 포함하고,
상기 투약 요법의 마지막 용량 후 2주 내지 6주 사이에 수술을 더 포함하는, 방법.A method of treating a subject having eTNBC comprising:
Tiragolumab at a dose of about 420 mg every 2 weeks, Atezolizumab at a dose of about 840 mg every 2 weeks, and:
(a)
(i) nap-paclitaxel at a dose of about 125 mg/m 2 every week for the first 12 weeks of the dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; and
(ii) doxorubicin at a dose of about 60 mg/m 2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m 2 every 2 weeks, and G-CSF every 2 weeks or GM-CSF; or
(b)
(i) nap-paclitaxel at a dose of about 125 mg/m 2 weekly for the first 12 weeks of said dosing regimen; and
(ii) doxorubicin at a dose of about 60 mg/m 2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/m 2 every 2 weeks, and G-CSF every 2 weeks or administering to the subject a dosing regimen comprising GM-CSF;
and surgery between 2 and 6 weeks after the last dose of the dosing regimen.
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 상기 대상체로부터의 종양 샘플에서 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.214. The method of any one of claims 184-214,
wherein a detectable protein expression level of PD-L1 is determined in a tumor sample from said subject determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142.
상기 종양 샘플에서 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율은 1% 이상인, 방법.225. The method of claim 215,
The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (ICs) in the tumor sample is at least 1%.
상기 eTNBC는 T2-4d TNBC로 제시되는, 방법.217. The method of any one of claims 190-216,
wherein the eTNBC is presented as T2-4d TNBC.
상기 eTNBC는 cT2-cT4, cN0-cN3, 및 cM0 TNBC로 제시되는, 방법.218. The method of any one of claims 190-217,
wherein the eTNBC is presented as cT2-cT4, cN0-cN3, and cM0 TNBC.
상기 대상체는 이전에 eTNBC에 대해 치료받은 적이 없는, 방법.218. The method of any one of claims 190 to 218,
wherein the subject has not been previously treated for eTNBC.
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 방법.221. The method of any one of claims 190 to 219,
wherein the treatment results in a pathological complete response (pCR).
상기 치료는 전체 생존(OS) 또는 무사건 생존(EFS)의 증가를 유발하는, 방법.221. The method of any one of claims 190-220, wherein
wherein the treatment results in an increase in overall survival (OS) or event-free survival (EFS).
제69항에 있어서,
상기 암은 두경부암인, 방법.
70. The method of claim 69,
The method of claim 1, wherein the cancer is head and neck cancer.
상기 두경부암은 상기 두경부의 편평세포 암종(SCCHN)인, 방법.223. The method of claim 222,
The method of claim 1, wherein the head and neck cancer is squamous cell carcinoma (SCCHN) of the head and neck.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having SCCHN having a detectable expression level of PD-L1, the method comprising:
administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks A method comprising steps.
(a) 염색에 적합한 항 PD-L1 항체를 사용한 IHC 분석에 의해 상기 대상체 또는 대상체 집단으로부터의 종양 샘플에서 PD-L1의 단백질 발현 수준을 검출하는 단계; 및
(b) PD-L1의 검출 가능한 발현 수준을 갖는 상기 대상체 또는 대상체 집단에 대해 검출된 PD-L1 발현을 근거로 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제 및 3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체의 1회 이상의 투약 주기를 포함한 요법을 선택하는 단계를 포함하는, 방법.A method of selecting a therapy for a subject or population of subjects with SCCHN comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject or population of subjects by IHC analysis using an anti-PD-L1 antibody suitable for staining; and
(b) a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks and 3 weeks based on PD-L1 expression detected for said subject or population of subjects having a detectable expression level of PD-L1 selecting a regimen comprising at least one dosing cycle of an anti TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg per time.
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject having SCCHN having a detectable expression level of PD-L1 comprising:
A method comprising administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.227. The method of any one of claims 224 to 226,
wherein the subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
상기 SSCHN은 인간 유두종 바이러스(HPV) 양성인, 방법.227. The method according to any one of claims 223 to 227,
wherein the SSCHN is human papillomavirus (HPV) positive.
상기 SSCHN은 HPV 음성인, 방법.223. The method of any one of claims 223 to 228,
wherein the SSCHN is HPV negative.
HPV 상태는 p16 IHC, 제자리(in situ) 부합법, 또는 PCR에 의해 결정되는, 방법.229. The method of claim 228 or 229,
HPV status is determined by p16 IHC, in situ hybridization, or PCR.
상기 SCCHN은 재발성 및/또는 전이성 SCCHN인, 방법.234. The method of any one of claims 223 to 230,
wherein the SCCHN is recurrent and/or metastatic SCCHN.
상기 대상체 또는 대상체들은 선행 요법을 받은 적이 없는, 방법.232. The method according to any one of claims 222 to 231,
The method of claim 1, wherein the subject or subjects have not received prior therapy.
상기 선행 요법은 재발성 및/또는 전이성 질환에 대한 선행 전신 요법인, 방법.232. The method of claim 232,
wherein said prior therapy is prior systemic therapy for recurrent and/or metastatic disease.
상기 치료는 CR 또는 PR을 유발하는, 방법.224. The method of any one of claims 222-224 and 226-233,
wherein said treatment results in CR or PR.
상기 치료는 기준 객관적 반응률(ORR)과 비교하여 상기 대상체 집단의 ORR의 증가를 유발하는, 방법.224. The method of any one of claims 222-224 and 226-233,
wherein the treatment results in an increase in the ORR of the subject population as compared to a baseline objective response rate (ORR).
상기 기준 ORR은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 중앙값 ORR인, 방법.234. The method of claim 235,
wherein said baseline ORR is the median ORR of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody.
상기 기준 ORR은 적어도 약 19% 내지 약 36%인, 방법.237. The method of claim 235 or 236,
wherein the baseline ORR is at least about 19% to about 36%.
상기 치료는 기준 무진행 생존(PFS) 기간과 비교하여 상기 대상체 또는 대상체 집단의 PFS의 증가, 기준 반응 지속 기간(DOR)과 비교하여 상기 대상체 또는 대상체 집단의 DOR의 증가, 또는 기준 전체 생존(OS) 기간과 비교하여 상기 대상체 또는 대상체 집단의 OS의 증가를 유발하는, 방법.223. The method of any one of claims 222-224 and 226-237, wherein
The treatment comprises an increase in PFS of the subject or population of subjects as compared to a baseline progression-free survival (PFS) period, an increase in the DOR of the subject or population of subjects as compared to a baseline duration of response (DOR), or a baseline overall survival (OS) ) causes an increase in OS of the subject or population of subjects compared to a period of time.
(a) 상기 기준 PFS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 PFS 기간 중앙값이고;
(b) 상기 기준 DOR 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 DOR 기간 중앙값이거나; 또는
(c) 상기 기준 OS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 기간 중앙값인, 방법.238. The method of claim 238:
(a) said baseline PFS duration is the median duration of PFS in a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) said baseline DOR duration is the median DOR duration of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; or
(c) the baseline OS duration is the median OS duration of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
상기 기준 DOR 기간은 적어도 약 6.7개월 내지 약 23.4개월인, 방법.238. The method of claim 238,
wherein the baseline DOR period is at least about 6.7 months to about 23.4 months.
상기 기준 OS 기간은 적어도 약 11.6개월 내지 약 14.9개월인, 방법.238. The method of claim 238,
wherein the baseline OS duration is at least about 11.6 months to about 14.9 months.
상기 PD-L1의 검출 가능한 발현 수준은 항 PD-L1 항체 SP263으로 염색하는 단계를 포함하는 면역조직화학적(IHC) 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준인, 방법.25. The method of any one of claims 224 to 241,
wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1 determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody SP263.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기의 종양 샘플에서:
(a) 5% 이상;
(b) 5% 이상 및 20% 미만; 또는
(c) 20% 이상의 종양 관련 면역 세포(TIC)인, 방법.252. The method of claim 242,
The detectable protein expression level of PD-L1 is in the tumor sample:
(a) at least 5%;
(b) at least 5% and less than 20%; or
(c) at least 20% tumor associated immune cells (TICs).
상기 대상체 또는 대상체 집단은 검출된 종양 세포 상의 PD-L1 발현에 근거한 치료로부터 이익을 얻을 가능성이 있는 자로서 식별되는, 방법.24. The method of any one of claims 224 to 243,
wherein the subject or population of subjects is identified as likely to benefit from treatment based on PD-L1 expression on the detected tumor cells.
제69항에 있어서,
상기 암은 간암인, 방법.
70. The method of claim 69,
The method of claim 1, wherein the cancer is liver cancer.
상기 간암은 간세포 암종(HCC)인, 방법.245. The method of claim 245,
The method of claim 1, wherein the liver cancer is hepatocellular carcinoma (HCC).
항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서 상기 대상체 또는 대상체 집단은 HCC에 대해 선행 전신 요법을 받은 적이 없는, 방법.A method of treating a subject or population of subjects having hepatocellular carcinoma (HCC), the method comprising:
A method comprising administering to the subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the subject or population of subjects has not received prior systemic therapy for HCC. .
VEGF 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 더 포함하는, 방법.247. The method of claim 247,
The method of claim 1, further comprising administering a VEGF antagonist to the subject or population of subjects.
항 TIGIT 길항제 항체, PD-1 축 결합 길항제, 및 VEGF 길항제의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having HCC comprising:
A method comprising administering to the subject or population of subjects one or more dosing cycles of an anti TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist.
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 방법.249. The method of claims 248 and 249,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
상기 항 TIGIT 길항제 항체는 3주마다 약 500 mg 내지 약 700 mg의 용량으로 투여되는, 방법.250. The method of any one of claims 247-250, wherein
wherein the anti-TIGIT antagonist antibody is administered at a dose of about 500 mg to about 700 mg every 3 weeks.
상기 PD-1 축 결합 길항제는 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 투여되는, 방법.252. The method of any one of claims 247-251,
The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 900 mg to about 1500 mg every 3 weeks.
상기 VEGF 길항제는 2주마다 약 1 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 방법.252. The method of claim 248 or 249,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
상기 VEGF 길항제는 2주마다 약 5 mg/kg 내지 약 10 mg/kg의 용량으로 투여되는, 방법.252. The method of claim 253,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
상기 VEGF 길항제는 2주마다 약 5 mg/kg, 약 7.5 mg/kg, 또는 약 10 mg/kg의 용량으로 투여되는, 방법.254. The method of claim 254,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10 mg/kg every two weeks.
상기 항 TIGIT 길항제 항체는 2주마다 약 300 mg 내지 약 800 mg의 용량으로 투여되는, 방법.257. The method of any one of claims 247-249 and 253-255, wherein
wherein the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg to about 800 mg every two weeks.
상기 PD-1 축 결합 길항제는 2주마다 약 200 mg 내지 약 1200 mg의 용량으로 투여되는, 방법.257. The method of any one of claims 247-249 and 253-256, wherein
The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 200 mg to about 1200 mg every two weeks.
상기 항 TIGIT 길항제 항체는 4주마다 약 700 mg 내지 약 1000 mg의 용량으로 투여되는, 방법.252. The method of claims 247-249,
wherein the anti-TIGIT antagonist antibody is administered at a dose of about 700 mg to about 1000 mg every 4 weeks.
상기 PD-1 축 결합 길항제는 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 투여되는, 방법.258. The method of any one of claims 247-249 and 258,
The method of claim 1, wherein the PD-1 axis binding antagonist is administered at a dose of about 1400 mg to about 2000 mg every 4 weeks.
상기 HCC는 국소 진행성 또는 전이성 HCC인, 방법.262. The method of any one of claims 247 to 259,
wherein the HCC is locally advanced or metastatic HCC.
상기 HCC는 절제 불가능한 HCC인, 방법.260. The method of any one of claims 247 to 260,
wherein the HCC is unresectable HCC.
상기 대상체 또는 대상체들은 충분한 간 기능을 갖는 것으로 결정되는, 방법.27. The method of any one of claims 247 to 261,
wherein the subject or subjects is determined to have sufficient liver function.
상기 충분한 간 기능은 차일드-퍼(Child-Pugh) 분류 A로 특징지어지는, 방법.262. The method of claim 262,
wherein said sufficient liver function is characterized by Child-Pugh class A.
상기 대상체 또는 대상체들로부터 수득한 HCC 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.267. The method of any one of claims 247 to 263,
wherein the subject or HCC tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
상기 대상체 또는 대상체 집단에게 적어도 4회의 투약 주기를 투여하는 단계를 포함하는, 방법.267. The method of any one of claims 247 to 264,
A method comprising administering to the subject or population of subjects at least four dosing cycles.
상기 대상체 또는 대상체 집단에게 적어도 16회의 투약 주기를 투여하는 단계를 포함하는, 방법.261. The method of claim 261,
and administering to the subject or population of subjects at least 16 dosing cycles.
3주마다 약 600 mg 용량의 티라골루맙, 3주마다 약 1200 mg 용량의 아테졸리주맙, 및 3주마다 약 15 mg/kg 용량의 베바시주맙의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having HCC comprising:
administering to the subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and bevacizumab at a dose of about 15 mg/kg every 3 weeks. A method comprising steps.
상기 대상체 또는 대상체들은 HCC에 대해 선행 전신 치료를 받은 적이 없는, 방법.267. The method of any one of claims 249-267,
The method of claim 1, wherein the subject or subjects have not received prior systemic treatment for HCC.
상기 치료는 적어도 약 5.6개월 내지 적어도 약 6.83개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.269. The method of any one of claims 247 to 268,
wherein said treatment results in a median PFS in the subject population of at least about 5.6 months to at least about 6.83 months.
상기 암은 방광암인, 방법.70. The method of claim 69,
wherein the cancer is bladder cancer.
상기 방광암은 근육 침윤성 방광암(MIBC)인, 방법.270. The method of claim 270,
wherein the bladder cancer is muscle invasive bladder cancer (MIBC).
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 상기 대상체는 백금계 화학요법제를 이용한 치료에 부적격인, 방법.A method of treating a subject or population of subjects having MIBC comprising:
administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks and, the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 상기 대상체에게 투여하는 단계를 포함하고, 상기 치료는 수술 전후 치료인, 방법.A method of treating a subject or population of subjects having MIBC comprising:
administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist every 3 weeks And, the treatment is a treatment before and after surgery, the method.
상기 대상체 또는 대상체들은 크레아티닌 청소율이 60 mL/분 미만인, 방법.274. The method of claim 272 or 273,
The method of claim 1, wherein the subject or subjects have a creatinine clearance of less than 60 mL/min.
상기 대상체 또는 대상체들은 2등급 이상의 청력 상실을 갖는, 방법.275. The method of any one of claims 272-274,
The method of claim 1, wherein the subject or subjects have a hearing loss of grade 2 or greater.
상기 대상체 또는 대상체들은 2등급 이상의 신경병증을 갖는, 방법.275. The method of any one of claims 272-275,
The method of claim 1 , wherein the subject or subjects have grade 2 or greater neuropathy.
상기 대상체 또는 대상체들은 백금계 화학요법제를 이용한 치료를 거부한, 방법.279. The method of any one of claims 272-276,
The method of claim 1, wherein the subject or subjects refused treatment with a platinum-based chemotherapeutic agent.
상기 백금계 화학요법제는 시스플라틴인, 방법.277. The method of any one of claims 272 or 274-277,
The method of claim 1, wherein the platinum-based chemotherapeutic agent is cisplatin.
상기 MIBC는 외과 수술이 가능한, 방법.279. The method of any one of claims 272-278,
wherein the MIBC is surgically feasible.
수술을 더 포함하는, 방법.279. The method of claim 279,
The method further comprising surgery.
적어도 1회의 투약 주기는 상기 수술 전에 개시되는, 방법.280. The method of claim 280,
at least one dosing cycle is initiated prior to the surgery.
적어도 1, 2, 또는 3회의 투약 주기는 상기 수술 전에 완료되는, 방법.280. The method of claim 280,
at least 1, 2, or 3 dosing cycles are completed prior to the surgery.
적어도 1회의 투약 주기는 상기 수술 후 4주 내지 6주 사이에 개시되는, 방법.289. The method of any one of claims 280 to 282,
at least one dosing cycle is initiated between 4 and 6 weeks post surgery.
1회 내지 17회의 투약 주기는 상기 수술 후에 완료되는, 방법.283. The method of claim 283,
1 to 17 dosing cycles are completed after said surgery.
상기 수술은 방광 절제술 및/또는 림프절 절제술인, 방법.289. The method of any one of claims 280-284,
wherein the surgery is cystectomy and/or lymphadenectomy.
상기 치료는 병리학적 완전 반응(pCR)을 유발하는, 방법.289. The method of any one of claims 272-285,
wherein the treatment results in a pathological complete response (pCR).
상기 치료는 기준 RFS 기간과 비교하여 상기 대상체 또는 대상체들의 무재발 생존(RFS)의 증가, 기준 EFS 기간과 비교하여 상기 대상체 또는 대상체들의 무사건 생존(EFS)의 증가, 또는 기준 OS 기간과 비교하여 상기 대상체 또는 대상체들의 전체 생존(OS)의 증가를 유발하는, 방법.297. The method of any one of claims 272-286,
wherein the treatment is an increase in relapse-free survival (RFS) of the subject or subjects as compared to a baseline RFS duration, an increase in event-free survival (EFS) of the subject or subjects compared to a baseline EFS duration, or an increase in the event-free survival (EFS) of the subject or subjects compared to a baseline OS duration, or compared to a baseline OS duration. causing an increase in overall survival (OS) in the subject or subjects.
(a) 상기 기준 RFS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 RFS 기간 중앙값이고;
(b) 상기 기준 EFS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 EFS 기간 중앙값이거나; 또는
(c) 상기 기준 OS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료를 받은 대상체 집단의 OS 기간 중앙값인, 방법.289. The method of claim 287:
(a) said baseline RFS duration is the median RFS duration of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody;
(b) said baseline EFS duration is the median duration of EFS in a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody; or
(c) the baseline OS duration is the median OS duration of a population of subjects receiving treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
상기 치료는 병리학적 병기하향(downstaging)을 유발하는, 방법.289. The method of any one of claims 272-288,
wherein the treatment results in pathological downstaging.
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 대상체 또는 대상체들은 시스플라틴 부적격인, 방법.A method of treating a subject or population of subjects having MIBC comprising:
administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein the subject or subjects are cisplatin ineligible In, way.
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 치료는 수술 전후 치료인, 방법.A method of treating a subject or population of subjects having MIBC comprising:
administering to said subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks, wherein said treatment is perioperative treatment. , Way.
상기 치료는 적어도 약 13.4% 내지 적어도 약 15%의 대상체 집단의 ORR을 유발하는, 방법.302. The method of any one of claims 272-291,
wherein said treatment results in an ORR in at least about 13.4% to at least about 15% of the subject population.
상기 치료는 약 7.9개월 내지 약 8.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.302. The method of any one of claims 272-292,
wherein said treatment results in a median OS in the subject population of about 7.9 months to about 8.6 months.
항 PD-L1 항체 SP142로 염색하는 단계를 포함하는 IHC 분석에 의해 결정된 PD-L1의 검출 가능한 단백질 발현 수준이 결정되는, 방법.294. The method of any one of claims 272-293,
wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율이 5% 이상인 PD-L1 양성 종양 세포 분획인, 방법.295. The method of claim 294,
The method of claim 1, wherein the detectable protein expression level of PD-L1 is a PD-L1-positive tumor cell fraction in which the proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (IC) is 5% or more.
상기 방광암은 요로상피세포 암종(UC)인, 방법.270. The method of claim 270,
The method of claim 1, wherein the bladder cancer is urothelial cell carcinoma (UC).
상기 UC는 전이성 요로상피세포 암종(mUC)인, 방법.297. The method of claim 296,
wherein the UC is metastatic urothelial cell carcinoma (mUC).
3주마다 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 3주마다 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having mUC, comprising:
administering a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks to the subject or subject. A method comprising administering to a population.
상기 대상체 또는 대상체들은 선행 암 면역요법을 받은 적이 없는, 방법.298. The method of claim 298,
The method of claim 1, wherein the subject or subjects have not received prior cancer immunotherapy.
상기 치료는 2차 치료인, 방법.302. The method of claim 298 or 299,
wherein the treatment is a second line treatment.
상기 mUC는 백금 함유 요법 중에 또는 이후에 진행하는, 방법.300. The method of any one of claims 298-300,
wherein the mUC progresses during or after platinum containing therapy.
상기 대상체 또는 대상체 집단이 질병 진행 또는 허용 불가능한 독성을 경험한 후 상기 대상체 또는 대상체 집단에게 제2 투약 요법을 투여하는 단계를 더 포함하는, 방법.302. The method of any one of claims 298-301,
and administering a second dosing regimen to the subject or population of subjects after the subject or population of subjects has experienced disease progression or unacceptable toxicity.
상기 제2 투약 요법은 PD-1 축 결합 길항제 및 항체-약물 접합체(ADC)의 1회 이상의 투약 주기를 포함하는, 방법.302. The method of claim 302,
wherein the second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist and an antibody-drug conjugate (ADC).
상기 ADC는 (a) 엔포르투맙 베도틴 또는 (b) 사시투주맙 고비테칸인, 방법.303. The method of claim 303,
The method of claim 1, wherein the ADC is (a) enfortumab vedotin or (b) sacituzumab gobitecan.
(a) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (b) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되는, 방법.305. The method of claim 304,
(a) enfortumab vedotin is administered at a weekly dose of 1.25 mg/kg on a 2-week dosing/week break, or (b) sacituzumab gobitecan is administered at 10 mg/week on a 2-week dos/week break Administered in kg dose.
3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having mUC, comprising:
A method comprising administering to the subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
제1 투약 요법에 이어서 제2 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서:
(a) 상기 제1 투약 요법은 3주마다 약 600 mg 용량의 티라골루맙 및 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고; 그리고
(b) 상기 제2 투약 요법은 3주마다 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 투약 주기를 포함하고, (i) 엔포르투맙 베도틴은 2주 투약/1주 휴약의 매주 1.25 mg/kg 용량으로 투여되거나, 또는 (ii) 사시투주맙 고비테칸은 2주 투약/1주 휴약의 매주 10 mg/kg 용량으로 투여되고, 여기서 상기 제2 투약 요법은 상기 대상체 또는 대상체 집단이 상기 제1 투약 요법 동안에 질병 진행 또는 허용 불가능한 독성을 경험한 후 상기 대상체 또는 대상체 집단에게 투여되는, 방법.A method of treating a subject or population of subjects having mUC, comprising:
administering to the subject or population of subjects a first dosage regimen followed by a second dosage regimen, wherein:
(a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and
(b) said second dosing regimen comprises at least one dosing cycle of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin is administered at 1.25 weekly doses of 2 weeks on/1 week off. is administered at a mg/kg dose, or (ii) sacituzumab gobitecan is administered at a weekly 10 mg/kg dose of 2 weeks dosing/1 week off, wherein said second dosing regimen is wherein said subject or population of subjects The method is administered to the subject or population of subjects after experiencing disease progression or unacceptable toxicity during a first dosing regimen.
상기 치료는 적어도 약 13.4% 내지 적어도 약 31%의 대상체 집단의 ORR을 유발하는, 방법.312. The method of any one of claims 298-307,
wherein said treatment results in an ORR in at least about 13.4% to at least about 31% of the subject population.
상기 치료는 약 7.9개월 내지 약 16.3개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.309. The method of any one of claims 298-308,
wherein said treatment results in a median OS of the subject population of about 7.9 months to about 16.3 months.
상기 암은 췌장암인, 방법.70. The method of claim 69,
The method of claim 1, wherein the cancer is pancreatic cancer.
각 28일의 투약 주기의 제 1일 및 15일에 약 420 mg 용량의 티라골루맙, 각 28일의 투약 주기의 제 1일 및 15일에 약 840 mg 용량의 아테졸리주맙, 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 1000 mg/m2 용량의 젬시타빈, 및 각 28일의 투약 주기의 제 1일, 8일, 및 15일에 약 125 mg/m2 용량의 냅-파클리탁셀의 1회 이상의 28일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having pancreatic cancer, the method comprising:
Tiragolumab at a dose of about 420 mg on days 1 and 15 of each 28-day dosing cycle, atezolizumab at a dose of about 840 mg on days 1 and 15 of each 28-day dosing cycle, each 28 days. Gemcitabine at a dose of about 1000 mg/m 2 on days 1, 8, and 15 of the dosing cycle, and about 125 mg/m 2 on days 1, 8, and 15 of each 28-day dosing cycle A method comprising administering to the subject or population of subjects a dosing regimen comprising one or more 28-day dosing cycles of a dose of nap-paclitaxel.
상기 췌장암은 췌장 도관 선암종(PDAC)인, 방법.312. The method of claim 310 or 311,
wherein the pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
상기 PDAC는 전이성 PDAC인, 방법.312. The method of claim 312,
wherein the PDAC is a metastatic PDAC.
상기 대상체 또는 대상체들은 전이성 PDAC에 대해 선행 전신 요법을 받은 적이 없는, 방법.314. The method according to any one of claims 310 to 313,
The method of claim 1, wherein the subject or subjects have not received prior systemic therapy for metastatic PDAC.
상기 치료는 적어도 약 41.7% 내지 약 46.7%의 대상체 집단의 ORR을 유발하는, 방법.314. The method of any one of claims 310-314,
wherein said treatment results in an ORR in at least about 41.7% to about 46.7% of the subject population.
상기 치료는 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제가 없는 젬시타빈 및 냅-파클리탁셀을 포함한 치료와 비교하여 적어도 약 20%의 ORR의 증가를 유발하는, 방법.315. The method of any one of claims 310-315,
wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nap-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
상기 치료는 적어도 약 5.5개월 내지 약 7개월의 대상체 집단의 PFS 중앙값을 유발하는, 방법.316. The method of any one of claims 310-316,
wherein said treatment results in a median PFS in the subject population of at least about 5.5 months to about 7 months.
상기 치료는 적어도 약 8.5개월 내지 약 10.6개월의 대상체 집단의 OS 중앙값을 유발하는, 방법.312. The method of any one of claims 310 to 317, wherein
wherein said treatment results in a median OS in the subject population of at least about 8.5 months to about 10.6 months.
상기 암은 식도암인, 방법.70. The method of claim 69,
wherein the cancer is esophageal cancer.
각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, the method comprising:
One or more times 21 of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg on Day 1 of each dosing cycle and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle.
각 투약 주기의 제 1일에 약 500 mg 내지 약 700 mg 용량의 항 TIGIT 길항제 항체 및 각 투약 주기의 제 1일에 약 900 mg 내지 약 1500 mg 용량의 PD-1 축 결합 길항제의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법.A method of treating a subject or population of subjects having esophageal cancer, the method comprising:
One or more times 21 of an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg on Day 1 of each dosing cycle and a dose of about 900 mg to about 1500 mg of a PD-1 axis binding antagonist on Day 1 of each dosing cycle. A method comprising administering to the subject or population of subjects a dosing regimen comprising one dosing cycle, wherein the subject or subjects have previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
상기 대상체 또는 대상체들은 백금계 화학요법제 및 비백금계 화학요법제로 이전에 치료를 받은, 방법.320. The method of claim 320,
The method of claim 1, wherein the subject or subjects has previously been treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
상기 대상체 또는 대상체들은 상기 선행 치료 동안에 질병 진행 또는 허용 불가능한 독성을 경험한, 방법.323. The method of claim 321 or 322,
wherein said subject or subjects experienced disease progression or unacceptable toxicity during said prior treatment.
상기 21일 투약 주기는 백금계 화학요법제 및 비백금계 화학요법제를 더 포함하는, 방법.320. The method of claim 320,
The 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
상기 백금계 화학요법제는 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.325. The method of claim 324,
wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
상기 백금계 화학요법제는 시스플라틴인, 방법.325. The method of any one of claims 321 to 325,
The method of claim 1, wherein the platinum-based chemotherapeutic agent is cisplatin.
시스플라틴은 각 투약 주기의 제 1일에 약 80 mg/m2의 용량으로 투여되는, 방법.326. The method of claim 326,
The method of claim 1 wherein cisplatin is administered at a dose of about 80 mg/m 2 on Day 1 of each dosing cycle.
상기 비백금계 화학요법제는 항대사물질인, 방법.321. The method of any one of claims 321 to 327,
The method of claim 1, wherein the non-platinum-based chemotherapeutic agent is an antimetabolites.
상기 항대사물질은 5-플루오로우라실인, 방법.339. The method of claim 328,
wherein the antimetabolite is 5-fluorouracil.
5-플루오로우라실은 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간의 용량으로 투여되는, 방법.329. The method of claim 329,
5-fluorouracil is administered at a dose of about 800 mg/m 2 /24 hours on days 1-5 of each 21-day cycle.
상기 식도암은 진행성 또는 전이성 식도암인, 방법.335. The method of any one of claims 321 to 330,
The method of claim 1, wherein the esophageal cancer is advanced or metastatic esophageal cancer.
상기 대상체 또는 대상체들은 전이성 식도암에 대해 선행 치료를 받은 적이 없는, 방법.335. The method of claim 320 or 331,
The method of claim 1, wherein the subject or subjects has not received prior treatment for metastatic esophageal cancer.
각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙, 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙, 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴, 및 각 21일 주기의 제 1일 내지 5일에 약 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함한 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되는, 방법.A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, the method comprising:
Tiragolumab at a dose of about 600 mg on Day 1 of each dosing cycle, atezolizumab at a dose of about 1200 mg on Day 1 of each dosing cycle, at a dose of about 80 mg/m 2 on Day 1 of each dosing cycle administering to the subject or population of subjects a dosing regimen comprising one or more 21-day dosing cycles of cisplatin, and 5-fluorouracil at a dose of about 800 mg/m 2 /24 hours on days 1-5 of each 21-day cycle. administering, wherein cisplatin is omitted from the dosing regimen after 6 doses.
제1 투약 요법 및 제2 투약 요법을 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하고, 여기서:
(a) 상기 제1 투약 요법은 각 투약 주기의 제 1일에 약 80 mg/m2 용량의 시스플라틴 및 각 21일 주기의 제 1일 내지 5일에 800 mg/m2/24시간 용량의 5-플루오로우라실의 1회 이상의 21일 투약 주기를 포함하고, 여기서 시스플라틴은 6회 용량 후에 상기 투약 요법에서 생략되고; 그리고
(b) 상기 제2 투약 요법은 각 투약 주기의 제 1일에 약 600 mg 용량의 티라골루맙 및 각 투약 주기의 제 1일에 약 1200 mg 용량의 아테졸리주맙의 1회 이상의 21일 투약 주기를 포함하는, 방법.A method of treating a subject or population of subjects having advanced or metastatic esophageal cancer, the method comprising:
administering a first dosage regimen and a second dosage regimen to the subject or population of subjects, wherein:
(a) said first dosing regimen is cisplatin at a dose of about 80 mg/m 2 on day 1 of each dosing cycle and 5 at a dose of 800 mg/m 2 /24 hour on days 1-5 of each 21 day cycle. - one or more 21 day dosing cycles of fluorouracil, wherein cisplatin is omitted from said dosing regimen after 6 doses; and
(b) said second dosing regimen is one or more 21 day dosing cycles of tiragolumab at a dose of about 600 mg on day 1 of each dosing cycle and atezolizumab at a dose of about 1200 mg on day 1 of each dosing cycle A method comprising
상기 치료는 적어도 약 14%의 대상체 집단의 ORR을 유발하는, 방법.35. The method of any one of claims 321 to 334,
wherein the treatment results in an ORR in at least about 14% of the subject population.
상기 항 TIGIT 길항제 항체는 하기의 초가변 영역들(HVR):
SNSAAWN(서열번호 1)의 아미노산 서열을 포함하는 HVR-H1 서열;
KTYYRFKWYSDYAVSVKG(서열번호 2)의 아미노산 서열을 포함하는 HVR-H2 서열;
ESTTYDLLAGPFDY(서열번호 3)의 아미노산 서열을 포함하는 HVR-H3 서열;
KSSQTVLYSSNNKKYLA(서열번호 4)의 아미노산 서열을 포함하는 HVR-L1 서열;
WASTRES(서열번호 5)의 아미노산 서열을 포함하는 HVR-L2 서열; 및
QQYYSTPFT(서열번호 6)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 방법.335. The method of any one of claims 47 to 335,
The anti-TIGIT antagonist antibody has the following hypervariable regions (HVR):
HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and
A method comprising an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
상기 항 TIGIT 길항제 항체는 하기의 경쇄 가변 영역 프레임워크 영역들(FR):
DIVMTQSPDSLAVSLGERATINC(서열번호 7)의 아미노산 서열을 포함하는 FR-L1;
WYQQKPGQPPNLLIY(서열번호 8)의 아미노산 서열을 포함하는 FR-L2;
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(서열번호 9)의 아미노산 서열을 포함하는 FR-L3; 및
FGPGTKVEIK(서열번호 10)의 아미노산 서열을 포함하는 FR-L4를 더 포함하는, 방법.336. The method of claim 336,
The anti-TIGIT antagonist antibody has the following light chain variable region framework regions (FR):
FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and
FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
상기 항 TIGIT 길항제 항체는 하기의 중쇄 가변 영역 FR:
X1이 E 또는 Q인, X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(서열번호 11)의 아미노산 서열을 포함하는 FR-H1;
WIRQSPSRGLEWLG(서열번호 12)의 아미노산 서열을 포함하는 FR-H2;
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(서열번호 13)의 아미노산 서열을 포함하는 FR-H3; 및
WGQGTLVTVSS(서열번호 14)의 아미노산 서열을 포함하는 FR-H4를 더 포함하는, 방법.336. The method of claim 336,
The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
FR-H1 comprising the amino acid sequence of X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), wherein X 1 is E or Q;
FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and
FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
X1은 E인, 방법.339. The method of claim 338,
X 1 is E;
X1은 Q인, 방법.339. The method of claim 338,
X 1 is Q.
상기 항 TIGIT 길항제 항체는 하기의:
(a) 서열번호 17 또는 18의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인;
(b) 서열번호 19의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 방법.340. The method of any one of claims 336-340,
The anti-TIGIT antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or
(c) a VH domain as in case (a) and a VL domain as in case (b).
상기 항 TIGIT 길항제 항체는 하기의:
(a) 서열번호 17 또는 18의 아미노산 서열을 포함하는 VH 도메인; 및
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.34. The method of any one of claims 336 to 341,
The anti-TIGIT antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and
(b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
상기 항 TIGIT 길항제 항체는 하기의:
(a) 서열번호 17의 아미노산 서열을 포함하는 VH 도메인; 및
(b) 서열번호 19의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.The method of any one of claims 336-339, 341, and 342, wherein
The anti-TIGIT antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17; and
(b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
상기 항 TIGIT 길항제 항체는 하기의:
(a) 서열번호 33의 아미노산 서열을 포함하는 중쇄; 및
(b) 서열번호 34의 아미노산 서열을 포함하는 경쇄를 포함하는, 방법.34. The method of any one of claims 336-339 and 341-343, wherein
The anti-TIGIT antagonist antibody is:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO: 33; and
(b) a light chain comprising the amino acid sequence of SEQ ID NO:34.
항-TIGIT 길항제 항체는 단일클론 항체인, 방법.335. The method of any one of claims 336 to 344,
wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
상기 항 TIGIT 길항제 항체는 인간 항체인, 방법.345. The method of any one of claims 336-345,
wherein the anti-TIGIT antagonist antibody is a human antibody.
상기 항 TIGIT 길항제 항체는 전장 항체인, 방법.346. The method of any one of claims 336-346,
wherein the anti-TIGIT antagonist antibody is a full length antibody.
상기 항 TIGIT 길항제 항체는 원형 Fc 매개 작용기 기능을 갖는, 방법.347. The method of any one of claims 336-347,
wherein the anti-TIGIT antagonist antibody has a prototypical Fc-mediated agonist function.
상기 항 TIGIT 길항제 항체는 티라골루맙인, 방법.335. The method of any one of claims 336-339 and 341-348, wherein
The method of claim 1, wherein the anti-TIGIT antagonist antibody is tyragolumab.
상기 항 TIGIT 길항제 항체는 Fab, Fab’, Fab’-SH, Fv, 단일 사슬 가변 단편(scFv), 및 (Fab’)2 단편으로 이루어진 군으로부터 선택되는 TIGIT에 결합하는 항체 단편인, 방법.346. The method of any one of claims 336-346,
wherein the anti-TIGIT antagonist antibody is an antibody fragment that binds TIGIT selected from the group consisting of Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv), and (Fab') 2 fragment.
상기 항 TIGIT 길항제 항체는 IgG 부류 항체인, 방법.349. The method of any one of claims 336-349, wherein
wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 방법.351. The method of claim 351
wherein the IgG class antibody is an IgG1 subclass antibody.
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제, PD-1 결합 길항제, 및 PD-L2 결합 길항제로 이루어진 군으로부터 선택되는, 방법.335. The method of any one of claims 336 to 352,
wherein the PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
상기 PD-1 축 결합 길항제는 PD-L1 결합 길항제인, 방법.355. The method of claim 353,
The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist.
상기 PD-L1 결합 길항제는 PD-L1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 방법.355. The method of claim 354,
wherein the PD-L1 binding antagonist inhibits the binding of PD-L1 to one or more of its ligand binding partners.
상기 PD-L1 결합 길항제는 PD-L1이 PD-1, B7-1, 또는 PD-1 및 B7-1 둘 모두에 결합하는 것을 억제하는, 방법.355. The method of claim 355,
wherein the PD-L1 binding antagonist inhibits PD-L1 from binding to PD-1, B7-1, or both PD-1 and B7-1.
상기 PD-L1 결합 길항제는 항 PD-L1 길항제 항체인, 방법.356. The method of any one of claims 354 to 356,
The method of claim 1, wherein the PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
상기 항 PD-L1 길항제 항체는 아테졸리주맙, MDX-1105, 더발루맙, 아벨루맙, SHR-1316, CS1001, 엔바폴리맙, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502, 코시벨리맙, 로다폴리맙, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007, 또는 HS-636인, 방법.358. The method of claim 357,
The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, enbapoliumab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL -A167, APL-502, Cosibelimab, Rhodafoliumab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003 , YBL-007, or HS-636.
상기 항 PD-L1 길항제 항체는 아테졸리주맙인, 방법.358. The method of claim 358,
The method of claim 1, wherein the anti-PD-L1 antagonist antibody is atezolizumab.
상기 항 PD-L1 길항제 항체는 하기의 HVR:
GFTFSDSWIH(서열번호 20)의 아미노산 서열을 포함하는 HVR-H1 서열;
AWISPYGGSTYYADSVKG(서열번호 21)의 아미노산 서열을 포함하는 HVR-H2 서열;
RHWPGGFDY(서열번호 22)의 아미노산 서열을 포함하는 HVR-H3 서열;
RASQDVSTAVA(서열번호 23)의 아미노산 서열을 포함하는 HVR-L1 서열;
SASFLYS(서열번호 24)의 아미노산 서열을 포함하는 HVR-L2 서열; 및
QQYLYHPAT(서열번호 25)의 아미노산 서열을 포함하는 HVR-L3 서열을 포함하는, 방법.358. The method of claim 357,
The anti-PD-L1 antagonist antibody has the following HVRs:
HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
HVR-L2 sequence comprising the amino acid sequence of SASFLYS (SEQ ID NO: 24); and
A method comprising an HVR-L3 sequence comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
상기 항 PD-L1 길항제 항체는 하기의:
(a) 서열번호 26의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 중쇄 가변(VH) 도메인;
(b) 서열번호 27의 아미노산 서열과 적어도 95% 서열 동일성을 갖는 아미노산 서열을 포함하는 경쇄 가변(VL) 도메인; 또는
(c) (a)의 경우에서와 같은 VH 도메인 및 (b)의 경우에서와 같은 VL 도메인을 포함하는, 방법.360. The method of claim 360,
The anti-PD-L1 antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or
(c) a VH domain as in case (a) and a VL domain as in case (b).
상기 항 PD-L1 길항제 항체는 하기의:
(a) 서열번호 26의 아미노산 서열을 포함하는 VH 도메인; 및
(b) 서열번호 27의 아미노산 서열을 포함하는 VL 도메인을 포함하는, 방법.361. The method of claim 361,
The anti-PD-L1 antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and
(b) a VL domain comprising the amino acid sequence of SEQ ID NO:27.
상기 항 PD-L1 길항제 항체는 하기의:
(a) 서열번호 28의 아미노산 서열을 포함하는 중쇄; 및
(b) 서열번호 29의 아미노산 서열을 포함하는 경쇄를 포함하는, 방법.362. The method of claim 362,
The anti-PD-L1 antagonist antibody is:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:28; and
(b) a light chain comprising the amino acid sequence of SEQ ID NO:29.
상기 항 PD-L1 길항제 항체는 단일클론 항체인, 방법.37. The method of any one of claims 360 to 363,
The method of claim 1, wherein the anti-PD-L1 antagonist antibody is a monoclonal antibody.
상기 항 PD-L1 길항제 항체는 인간화 항체인, 방법.375. The method of any one of claims 360 to 364,
The method of claim 1, wherein the anti-PD-L1 antagonist antibody is a humanized antibody.
상기 항 PD-L1 길항제 항체는 전장 항체인, 방법.365. The method of claim 364 or 365,
wherein the anti-PD-L1 antagonist antibody is a full length antibody.
상기 항 PD-L1 길항제 항체는 Fab, Fab’, Fab’-SH, Fv, scFv, 및 (Fab’)2 단편으로 이루어진 군에서 선택된 PD-L1에 결합하는 항체 단편인, 방법.36. The method of any one of claims 360-365,
wherein the anti-PD-L1 antagonist antibody is an antibody fragment that binds to PD-L1 selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab') 2 fragments.
상기 항 PD-L1 길항제 항체는 IgG 부류 항체인, 방법.370. The method of any one of claims 360-366,
wherein the anti-PD-L1 antagonist antibody is an IgG class antibody.
상기 IgG 부류 항체는 IgG1 하위부류 항체인, 방법.368. The method of claim 368,
wherein the IgG class antibody is an IgG1 subclass antibody.
상기 PD-1 축 결합 길항제는 PD-1 결합 길항제인, 방법.355. The method of claim 353,
The method of claim 1, wherein the PD-1 axis binding antagonist is a PD-1 binding antagonist.
상기 PD-1 결합 길항제는 PD-1이 이의 리간드 결합 짝들 중 하나 이상에 결합하는 것을 억제하는, 방법.370. The method of claim 370,
wherein the PD-1 binding antagonist inhibits PD-1 from binding to one or more of its ligand binding partners.
상기 PD-1 결합 길항제는 PD-1이 PD-L1, PD-L2, 또는 PD-L1 및 PD-L2 둘 모두에 결합하는 것을 억제하는, 방법.371. The method of claim 371,
wherein the PD-1 binding antagonist inhibits PD-1 from binding to PD-L1, PD-L2, or both PD-L1 and PD-L2.
상기 PD-1 결합 길항제는 항 PD-1 길항제 항체인, 방법.373. The method of any one of claims 370 to 372,
The method of claim 1, wherein the PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
상기 항 PD-1 길항제 항체는 니볼루맙, 펨브롤리주맙, MEDI-0680, 스파르탈리주맙, 세미플리맙, BGB-108, 프롤골리맙, 캄렐리주맙, 신틸리맙, 티슬렐리주맙, 토리팔리맙, 도스탈리맙, 레티판리맙, 사산리맙, 펜풀리맙, CS1003, HLX10, SCT-I10A, 짐베렐리맙, 발스틸리맙, 제놀림주맙, BI 754091, 세트렐리맙, YBL-006, BAT1306, HX008, 부디갈리맙, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, 또는 hAb21인, 방법.373. The method of claim 373,
Said anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiflimab, BGB-108, prolgolimab, camrelizumab, scintilimab, tislelizumab, torifalizumab Mab, dostalimab, retipanrimab, sasanrimab, fenpulimab, CS1003, HLX10, SCT-I10A, gimberelimab, valstilimab, genolimzumab, BI 754091, cetrelimab, YBL-006, BAT1306, HX008, budigalimab, AMG 404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103, or hAb21.
상기 PD-1 결합 길항제는 Fc 융합 단백질인, 방법.373. The method of any one of claims 370 to 372,
The method of claim 1, wherein the PD-1 binding antagonist is an Fc fusion protein.
상기 Fc 융합 단백질은 AMP-224인, 방법.375. The method of claim 375,
The Fc fusion protein is AMP-224, the method.
상기 항 TIGIT 길항제 항체를 3주마다 약 500 mg 내지 약 700 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.107. The method of any one of claims 77-101, 103-116, 119-122, and 247-249, wherein
and administering said anti-TIGIT antagonist antibody to said subject or population of subjects at a dose of about 500 mg to about 700 mg every three weeks.
상기 항 TIGIT 길항제 항체를 3주마다 약 600 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.57, 59, 60, 62-64, 101, 123-151, 160, 161, 224, 225, 247 325. The method of any one of claims 255-255, 272-289, 298-305, 320-332, and 377, wherein
and administering the anti-TIGIT antagonist antibody to the subject at a dose of about 600 mg every 3 weeks.
상기 항 TIGIT 길항제 항체를 4주마다 약 700 mg 내지 약 1000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.84. The method of any one of claims 77, 78, 82, and 83, wherein
and administering said anti TIGIT antagonist antibody to said subject or population of subjects at a dose of about 700 mg to about 1000 mg every 4 weeks.
상기 항 TIGIT 길항제 항체를 4주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.58. The method of any one of claims 47, 56, 64, 258, and 379, wherein
and administering the anti-TIGIT antagonist antibody to the subject at a dose of about 840 mg every 4 weeks.
상기 항 TIGIT 길항제 항체를 2주마다 약 300 mg 내지 약 600 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.87. The method of any one of claims 77, 78, 82, 83, and 256, wherein
and administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of about 300 mg to about 600 mg every two weeks.
상기 항 TIGIT 길항제 항체를 2주마다 약 420 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.249. The method of any one of claims 48, 190-213, 215-221, 256, and 381, wherein
and administering the anti-TIGIT antagonist antibody to the subject at a dose of about 420 mg every two weeks.
상기 항 TIGIT 길항제 항체의 용량은 고정 용량인, 방법.339. The method according to any one of claims 47 to 382,
wherein the dose of the anti-TIGIT antagonist antibody is a fixed dose.
상기 PD-1 축 결합 길항제를 3주마다 약 900 mg 내지 약 1500 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법. 107. The method of any one of claims 77-100, 103-116, 119-122, and 243-245, wherein
and administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 900 mg to about 1500 mg every three weeks.
상기 PD-1 축 결합 길항제를 3주마다 약 1200 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.272 The method of any one of claims-289, 298-305, 320-332, and 384, wherein
administering the PD-1 axis binding antagonist to the subject at a dose of about 1200 mg every 3 weeks.
상기 PD-1 축 결합 길항제를 4주마다 약 1400 mg 내지 약 2000 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.84. The method of any one of claims 77, 78, 82, and 83, wherein
and administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 1400 mg to about 2000 mg every 4 weeks.
상기 PD-1 축 결합 길항제를 4주마다 약 1680 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.57. The method of any one of claims 47, 56, 64, 259, and 386,
administering the PD-1 axis binding antagonist to the subject at a dose of about 1680 mg every 4 weeks.
상기 PD-1 축 결합 길항제를 2주마다 약 600 mg 내지 약 1200 mg의 용량으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.78. The method of any one of claims 77, 78, 82, 83, and 257, wherein
and administering the PD-1 axis binding antagonist to the subject or population of subjects at a dose of about 600 mg to about 1200 mg every two weeks.
상기 PD-1 축 결합 길항제를 2주마다 약 840 mg의 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.249. The method of any one of claims 48, 190-213, 215-221, 257, and 388,
administering the PD-1 axis binding antagonist to the subject at a dose of about 840 mg every two weeks.
상기 PD-1 축 결합 길항제의 용량은 고정 용량인, 방법.389. The method of any one of claims 47-389,
The method of claim 1, wherein the dose of the PD-1 axis binding antagonist is a fixed dose.
펨브롤리주맙을 6주마다 약 400 mg의 고정 용량으로 상기 대상체에게 투여하는 단계를 포함하는, 방법.59. The method of claim 58,
A method comprising administering to the subject pembrolizumab at a fixed dose of about 400 mg every 6 weeks.
상기 1회 이상의 투약 주기의 각 기간은 21일인, 방법.163. The method of any one of claims 51, 57, 59, 60, 62, 77, 78, 82, 83, 103, and 161. ,
wherein each period of said one or more dosing cycles is 21 days.
상기 1회 이상의 투약 주기의 각 기간은 28일인, 방법.57. The method of any one of claims 47, 56, 64, 77, 184 to 189, and 253 to 259,
wherein each period of said one or more dosing cycles is 28 days.
상기 1회 이상의 투약 주기의 각각의 약 제 1일에 상기 항 TIGIT 길항제 항체를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.404. The method according to any one of claims 47 to 393,
administering said anti-TIGIT antagonist antibody to said subject or population of subjects on about Day 1 of each of said one or more dosing cycles.
상기 1회 이상의 투약 주기의 각각의 약 제 1일에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.395. The method of any one of claims 47-394,
administering the PD-1 axis binding antagonist to the subject or population of subjects on about Day 1 of each of the one or more dosing cycles.
상기 1회 이상의 투약 주기의 각각의 약 15일에 상기 항 TIGIT 길항제 항체를 상기 대상체에게 투여하는 단계를 포함하는, 방법.256. The method of claim 256,
administering said anti-TIGIT antagonist antibody to said subject on about 15 days of each of said one or more dosing cycles.
상기 1회 이상의 투약 주기의 각각의 약 제 15일에 상기 PD-1 축 결합 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.257. The method of claim 257,
administering the PD-1 axis binding antagonist to the subject on about day 15 of each of the one or more dosing cycles.
상기 항 TIGIT 길항제 항체 이전에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.399. The method according to any one of claims 47 to 397,
and administering the PD-1 axis binding antagonist to the subject or population of subjects prior to the anti TIGIT antagonist antibody.
상기 PD-1 축 결합 길항제의 투여 후 제1 관찰 기간을 포함하는, 방법.399. The method of claim 398,
a first observation period following administration of the PD-1 axis binding antagonist.
상기 1차 관찰 기간은 약 30분 내지 약 60분의 길이인, 방법.399. The method of claim 399,
The method of claim 1, wherein the first observation period is from about 30 minutes to about 60 minutes in length.
상기 항 TIGIT 길항제 항체의 투여 후 제2 관찰 기간을 포함하는, 방법.401. The method of claim 399 or 400,
a second observation period following administration of said anti-TIGIT antagonist antibody.
상기 제2 관찰 기간은 약 30분 내지 약 60분의 길이인, 방법.401. The method of claim 401,
and the second observation period is between about 30 minutes and about 60 minutes in length.
상기 항 TIGIT 길항제 항체와 동시에 상기 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법. 399. The method according to any one of claims 47 to 397,
administering the PD-1 axis binding antagonist to the subject or population of subjects concurrently with the anti-TIGIT antagonist antibody.
상기 항 TIGIT 길항제 항체 및 PD-1 축 결합 길항제를 상기 대상체 또는 대상체 집단에게 정맥내 투여하는 단계를 포함하는, 방법.404. The method of any one of claims 47 to 403,
and administering the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist intravenously to the subject or population of subjects.
상기 PD-1 축 결합 길항제를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.404. The method of claim 404,
administering the PD-1 axis binding antagonist to the subject or population of subjects as an intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
상기 항 TIGIT 길항제 항체를 30 ± 10분 및/또는 60 ± 10분에 걸쳐 정맥내 주입으로 상기 대상체 또는 대상체 집단에게 투여하는 단계를 포함하는, 방법.405. The method of claim 404 or 405,
and administering said anti-TIGIT antagonist antibody to said subject or population of subjects by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes.
상기 대상체 또는 대상체들로부터 수득한 종양 샘플의 PD-L1 발현 수준이 결정되는, 방법.104. The method of any one of claims 47-103 and 105-406, wherein
A method, wherein the level of PD-L1 expression in the subject or a tumor sample obtained from subjects is determined.
상기 대상체 또는 대상체들로부터 수득한 종양 샘플은 PD-L1의 검출 가능한 발현 수준을 갖는 것으로 결정되는, 방법.407. The method of claim 407,
wherein the subject or a tumor sample obtained from subjects is determined to have a detectable expression level of PD-L1.
상기 PD-L1의 검출 가능한 발현 수준은 PD-L1의 검출가능한 단백질 발현 수준인, 방법.408. The method of claim 408,
wherein the detectable expression level of PD-L1 is a detectable protein expression level of PD-L1.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 염색에 적합한 항 PD-L1 항체로 염색하는 단계를 포함한 면역조직화학적(IHC) 분석에 의해 결정되는, 방법.409. The method of claim 409,
The method of claim 1, wherein the detectable protein expression level of PD-L1 is determined by immunohistochemical (IHC) analysis comprising staining with an anti-PD-L1 antibody suitable for staining.
상기 염색에 적합한 항 PD-L1 항체는 항 PD-L1 항체 SP263, SP142, 22C3, 또는 28-8인, 방법.410. The method of claim 410,
An anti-PD-L1 antibody suitable for said staining is an anti-PD-L1 antibody SP263, SP142, 22C3, or 28-8.
상기 PD-L1의 검출가능한 단백질 발현 수준은 벤타나(Ventana) SP263 IHC 분석, 팜(pharm)Dx 22C3 IHC 분석, 벤타나 SP142 IHC 분석, 또는 팜Dx 28-8 IHC 분석을 사용하여 결정되는, 방법.420. The method of claim 410 or 411,
wherein the detectable protein expression level of PD-L1 is determined using a Ventana SP263 IHC assay, a pharmDx 22C3 IHC assay, a Ventana SP142 IHC assay, or a PalmDx 28-8 IHC assay. .
항 PD-L1 항체 SP263으로 염색하는 단계를 포함한 IHC 분석에 의해 결정된 PD-L1의 검출가능한 단백질 발현 수준이 결정되는, 방법.103. The method of any one of claims 47-102, 159, 181-223, and 245-335,
wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP263 is determined.
항 PD-L1 항체 SP142로 염색하는 단계를 포함한 IHC 분석에 의해 결정된 PD-L1의 검출가능한 단백질 발현 수준이 결정되는, 방법.189. The method of any one of claims 47-189, 222-269, and 296-335, wherein
wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody SP142 is determined.
항 PD-L1 항체 22C3으로 염색하는 단계를 포함한 IHC 분석에 의해 결정된 PD-L1의 검출가능한 단백질 발현 수준이 결정되는, 방법.189. The method of any one of claims 47-189, and 222-335, wherein
wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 22C3 is determined.
항 PD-L1 항체 28-8로 염색하는 단계를 포함한 IHC 분석에 의해 결정된 PD-L1의 검출가능한 단백질 발현 수준이 결정되는, 방법.104. The method of any one of claims 47-103 and 105-335, wherein
wherein the detectable protein expression level of PD-L1 determined by IHC analysis comprising staining with anti-PD-L1 antibody 28-8 is determined.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 종양 관련 면역 세포(TIC)가 5% 이상인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 is greater than or equal to 5% of tumor associated immune cells (TICs) in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 5% 이상 및 20% 미만인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 has a TIC of at least 5% and less than 20% in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 20% 이상인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 has a TIC of at least 20% in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 10% 이상 및 50% 미만인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 has a TIC of at least 10% and less than 50% in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 TIC가 50% 이상인, 방법.413. The method of claim 413,
wherein the detectable protein expression level of PD-L1 has a TIC of at least 50% in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 1% 이상인, 방법.416. The method of any one of claims 413, 415, and 416,
The method of claim 1, wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% of the PD-L1 positive tumor cell fraction.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 30% 이상인, 방법.416. The method of any one of claims 413, 415, and 416,
The method of claim 1, wherein the detectable protein expression level of PD-L1 is greater than or equal to 30% in the fraction of PD-L1 positive tumor cells.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 상기 종양 샘플에서 PD-L1 양성 종양 세포 분획이 1% 이상 및 50% 미만인, 방법.416. The method of any one of claims 413, 415, and 416,
wherein the detectable protein expression level of PD-L1 is greater than or equal to 1% and less than 50% of a fraction of PD-L1-positive tumor cells in the tumor sample.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 PD-L1 양성 종양 세포 분획이 50% 이상인, 방법.416. The method of any one of claims 413, 415, and 416,
The method, wherein the detectable protein expression level of PD-L1 is at least 50% of the PD-L1 positive tumor cell fraction.
상기 PD-L1 양성 종양 세포 분획은 PD-L1 발현 종양 침윤성 면역 세포(IC)가 차지하는 종양 면적의 비율인, 방법.414. The method of claim 414,
wherein the PD-L1-positive tumor cell fraction is a proportion of the tumor area occupied by PD-L1-expressing tumor infiltrating immune cells (ICs).
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 1% 이상인, 방법.414. The method of claim 414,
The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 1%.
PD-L1 발현 종양 침윤성 IC가 차지하는 종양 면적의 비율은 5% 이상인, 방법.414. The method of claim 414,
The method of claim 1, wherein the proportion of tumor area occupied by PD-L1-expressing tumor invasive IC is at least 5%.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 복합 양성 점수(CPS)가 1 이상인, 방법.415. The method of claim 415,
The method of claim 1, wherein the detectable protein expression level of PD-L1 has a composite positive score (CPS) of 1 or more.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 10 이상인, 방법.415. The method of claim 415,
The method, wherein the detectable protein expression level of PD-L1 has a CPS of 10 or more.
상기 PD-L1의 검출 가능한 단백질 발현 수준은 CPS가 20 이상인, 방법.415. The method of claim 415,
The method, wherein the detectable protein expression level of PD-L1 has a CPS of 20 or more.
상기 IHC 분석은 벤타나 SP142 IHC 분석인, 방법.427. The method of any one of claims 427 to 429,
wherein the IHC assay is a Ventana SP142 IHC assay.
상기 PD-L1의 검출가능한 발현 수준은 PD-L1의 검출 가능한 핵산 발현 수준인, 방법.408. The method of claim 408,
wherein the detectable expression level of PD-L1 is a detectable nucleic acid expression level of PD-L1.
상기 PD-L1의 검출 가능한 핵산 발현 수준은 RNA-seq, RT-qPCR, qPCR, 멀티플렉스 qPCR 또는 RT-qPCR, 마이크로어레이 분석, SAGE, MassARRAY 기술, ISH 또는 이들의 조합에 의해 결정되는, 방법.434. The method of claim 434,
The detectable nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof.
상기 치료는 기준 OS 기간과 비교하여 상기 대상체의 전체 생존(OS)의 증가 및/또는 기준 PFS 기간과 비교하여 상기 대상체의 무진행 생존(PFS)의 증가를 유발하는, 방법.335. The method of any one of claims 47 to 335,
wherein the treatment results in an increase in overall survival (OS) of the subject as compared to a baseline OS duration and/or an increase in progression-free survival (PFS) in the subject compared to a baseline PFS duration.
(a) 상기 기준 OS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 OS 기간 중앙값이고; 그리고/또는
(b) 상기 기준 PFS 기간은 항 TIGIT 길항제 항체 없이 PD-1 축 결합 길항제를 포함한 치료 또는 항 PD-1 축 결합 길항제 없이 항 TIGIT 길항제 항체를 포함한 치료를 받은 대상체 집단의 PFS 기간 중앙값인, 방법.436. The method of claim 436:
(a) said baseline OS duration is the median OS duration of a population of subjects receiving treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without an anti-PD-1 axis binding antagonist; and/or
(b) the baseline PFS duration is the median PFS duration of a population of subjects receiving treatment with a PD-1 axis binding antagonist without anti-TIGIT antagonist antibody or treatment with an anti-TIGIT antagonist antibody without anti-PD-1 axis binding antagonist.
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 방법.149. The method of any one of claims 49, 141, and 190, wherein
The method of claim 1, wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
상기 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 방법.438. The method of claim 438,
The method of claim 1, wherein the platinum-based chemotherapeutic agent is carboplatin or cisplatin.
상기 카보플라틴은 AUC = 5 mg/ml/분 또는 AUC = 6 mg/ml/분을 달성하기에 충분한 용량으로 투여되는, 방법.71. The method of claim 66, 89, 116, 145, 212, and 439,
wherein the carboplatin is administered at a dose sufficient to achieve AUC=5 mg/ml/min or AUC=6 mg/ml/min.
상기 시스플라틴은 약 75 mg/m2 또는 80 mg/m2의 용량으로 투여되는, 방법.173. The method of claim 66, 116, 145, 147, 149, 151, 278, and 326,
wherein the cisplatin is administered at a dose of about 75 mg/m 2 or 80 mg/m 2 .
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 방법. 438. The method of any one of claims 438 to 441,
The method of claim 1, wherein the one or more non-platinum-based chemotherapeutic agents are antimetabolites, taxanes, or topoisomerase II inhibitors.
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 방법.60. The method of claim 59 or 442,
wherein the antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
상기 페메트렉시드는 약 500 mg/m2의 용량으로 투여되는, 방법.147. The method of any one of claims 66, 116, 145, and 443,
The method of claim 1, wherein the pemetrexed is administered at a dose of about 500 mg/m 2 .
상기 젬시타빈은 약 1000 mg/m2 또는 약 1250 mg/m2의 용량으로 투여되는, 방법.64. The method of any one of claims 60, 61, 145, 316, and 443,
wherein the gemcitabine is administered at a dose of about 1000 mg/m 2 or about 1250 mg/m 2 .
상기 항대사물질은 카페시타빈인, 방법.443. The method of claim 59 or 443,
The method of claim 1, wherein the antimetabolite is capecitabine.
상기 카페시타빈은 약 1250 mg/m2의 용량으로 투여되는, 방법.447. The method of claim 443 or 446,
The method of claim 1, wherein the capecitabine is administered at a dose of about 1250 mg/m 2 .
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 방법.203. The method of any one of claims 193, 202, 203, and 442-447,
The method of claim 1, wherein the taxane is paclitaxel or nap-paclitaxel.
상기 파클리탁셀은 약 175 mg/m2 또는 약 200 mg/m2의 용량으로 투여되는, 방법.69. The method of any one of claims 66, 145, and 448, wherein
wherein the paclitaxel is administered at a dose of about 175 mg/m 2 or about 200 mg/m 2 .
상기 냅-파클리탁셀은 약 100 mg/m2의 용량으로 투여되는, 방법.62. The method of any one of claims 60, 61, 212, 316, and 448, wherein
wherein the nap-paclitaxel is administered at a dose of about 100 mg/m 2 .
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 방법.74. The method of any one of claims 77, 78, 82, 83, 192, 193, and 442 to 450,
wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331.
상기 에토포시드는 약 100 mg/m2의 용량으로 투여되는, 방법.69. The method of any one of claims 66, 89, and 451, wherein
wherein the etoposide is administered at a dose of about 100 mg/m 2 .
상기 하나 이상의 화학요법제는 각각 매주 1회, 2주마다 1회, 3주마다 1회, 3주마다 2회, 4주마다 1회, 4주마다 2회, 또는 4주마다 3회 투여되는, 방법.45. The method of any one of claims 438 to 452,
The one or more chemotherapeutic agents are each administered once every week, once every 2 weeks, once every 3 weeks, twice every 3 weeks, once every 4 weeks, twice every 4 weeks, or 3 times every 4 weeks. , Way.
상기 하나 이상의 화학요법제는 1회 이상의 투약 주기의 제 1일에 투여되는, 방법.45. The method of any one of claims 438 to 453,
The method of claim 1, wherein the one or more chemotherapeutic agents are administered on Day 1 of one or more dosing cycles.
상기 젬시타빈은 4주마다 3회 투여되는, 방법.45. The method of any one of claims 443-454,
wherein the gemcitabine is administered three times every four weeks.
상기 젬시타빈은 1회 이상의 투약 주기의 제 1일, 8일, 및/또는 15일에 투여되는, 방법.455. The method of any one of claims 443 to 455,
wherein the gemcitabine is administered on days 1, 8, and/or 15 of one or more dosing cycles.
상기 카페시타빈은 2주 동안 매일 투여되는, 방법.456. The method of any one of claims 443 to 456,
wherein the capecitabine is administered daily for 2 weeks.
상기 카페시타빈은 1회 이상의 투약 주기의 제 1일 내지 14일에 투여되는, 방법.45. The method of any one of claims 443 to 457,
wherein the capecitabine is administered on days 1 to 14 of one or more dosing cycles.
상기 냅-파클리탁셀은 4주마다 3회 투여되는, 방법.459. The method of any one of claims 448 to 458,
wherein the nap-paclitaxel is administered 3 times every 4 weeks.
상기 냅-파클리탁셀은 1회 이상의 투약 주기의 제 1일, 8일, 및 15일에 투여되는, 방법.459. The method of any one of claims 448 to 459,
wherein said nap-paclitaxel is administered on days 1, 8, and 15 of one or more dosing cycles.
상기 에토포시드는 3주마다 제 1일 내지 3일에 투여되는, 방법.460. The method of any one of claims 451-460,
wherein the etoposide is administered on days 1 to 3 every 3 weeks.
상기 에토포시드는 1회 이상의 투약 주기의 제 1일 내지 3일에 투여되는, 방법.47. The method of any one of claims 451 to 461,
wherein the etoposide is administered on days 1-3 of one or more dosing cycles.
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이전에 투여되는, 방법.47. The method of any one of claims 438 to 462,
wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
상기 하나 이상의 화학요법제는 상기 PD-1 축 결합 길항제 및/또는 상기 항 TIGIT 길항제 항체 이후에 투여되는, 방법.47. The method of any one of claims 438 to 463,
wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
상기 하나 이상의 화학요법제는 정맥내 또는 경구로 투여되는, 방법.475. The method of any one of claims 438 to 464,
The method of claim 1, wherein the one or more chemotherapeutic agents are administered intravenously or orally.
상기 VEGF 길항제는 3주마다 약 5 mg/kg 내지 약 25 mg/kg의 용량으로 투여되는, 방법.65. The method of any one of claims 62, 248, and 249, wherein
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks.
상기 VEGF 길항제는 3주마다 약 10 mg/kg 내지 약 20 mg/kg의 용량으로 투여되는, 방법.470. The method of claim 250 or 466,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 10 mg/kg to about 20 mg/kg every 3 weeks.
상기 VEGF 길항제는 3주마다 약 15 mg/kg의 용량으로 투여되는, 방법.467. The method of claim 467,
The method of claim 1, wherein the VEGF antagonist is administered at a dose of about 15 mg/kg every 3 weeks.
상기 VEGF 길항제는 항 VEGF 항체인, 방법.65. The method of any one of claims 62, 248 to 250, 253 to 255, and 466 to 468,
The method of claim 1, wherein the VEGF antagonist is an anti-VEGF antibody.
상기 항 VEGF 항체는 베바시주맙인, 방법.469. The method of claim 469,
The anti-VEGF antibody is bevacizumab, the method.
상기 항 TIGIT 길항제 항체는 티라골루맙이고, 상기 PD-1 축 결합 길항제는 아테졸리주맙이며, 상기 VEGF 길항제는 베바시주맙인, 방법.62. The method of any one of claims 62, 248-250, and 253-255, wherein
The method of claim 1, wherein the anti-TIGIT antagonist antibody is tiragolumab, the PD-1 axis binding antagonist is atezolizumab, and the VEGF antagonist is bevacizumab.
1회 이상의 투약 주기의 제 1일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.62. The method of any one of claims 62, 248 to 250, 253 to 255, and 466 to 471,
and administering the VEGF antagonist to the subject on Day 1 of one or more dosing cycles.
1회 이상의 투약 주기의 15일에 상기 VEGF 길항제를 상기 대상체에게 투여하는 단계를 포함하는, 방법.256. The method of any one of claims 253-255,
and administering the VEGF antagonist to the subject on day 15 of one or more dosing cycles.
상기 VEGF 길항제는 정맥내 투여되는, 방법.62. The method of any one of claims 62, 248 to 250, 253 to 255, and 466 to 471,
The method of claim 1, wherein the VEGF antagonist is administered intravenously.
상기 VEGF 길항제는 90 ± 15분에 걸쳐 정맥내 주입으로 상기 대상체에게 투여되는, 방법.474. The method of claim 474,
wherein the VEGF antagonist is administered to the subject as an intravenous infusion over 90 ± 15 minutes.
상기 VEGF 길항제 이전에 상기 PD-1 축 결합 길항제, 및 상기 항 TIGIT 길항제 항체 이전에 상기 VEGF 길항제를 상기 대상체에 투여하는 단계를 포함하는, 방법.62. The method of any one of claims 62, 248 to 250, 253 to 255, and 466 to 475,
A method comprising administering to the subject the PD-1 axis binding antagonist prior to the VEGF antagonist, and the VEGF antagonist prior to the anti-TIGIT antagonist antibody.
상기 PD-1 축 결합 길항제 투여 후 제1 관찰 기간, 상기 VEGF 길항제 투여 후 제2 관찰 기간, 및 상기 항 TIGIT 길항제 항체 투여 후 제3 관찰 기간을 포함하는, 방법.476. The method of claim 476,
A method comprising a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody.
상기 제1 관찰 기간, 상기 제2 관찰 기간, 및 상기 제3 관찰 기간은 각각 약 30분 내지 약 120분의 길이인, 방법.479. The method of claim 477,
wherein the first observation period, the second observation period, and the third observation period are each from about 30 minutes to about 120 minutes in length.
티라골루맙 및 아테졸리주맙은 투여 이전에 IV 백(bag)에서 합쳐지는, 방법.112, 117, 118, 152, 153, 177, 184, 214, 226, 267, 290, 291, 306 333. The method of any one of claims, 307, 311, 333, and 334, wherein
wherein tiragolumab and atezolizumab are combined in an IV bag prior to administration.
상기 대상체는 인간인, 방법.479. The method of any one of claims 47 to 479,
wherein the subject is a human.
항 TIGIT 길항제 항체를 더 포함하는, 키트.482. The method of claim 482,
The kit further comprising an anti-TIGIT antagonist antibody.
상기 항 TIGIT 길항제 항체는 티라골루맙인, 키트.49. The method of any one of claims 481 to 483,
The anti-TIGIT antagonist antibody is tyragolumab, the kit.
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 키트.49. The method of any one of claims 481 to 484,
The kit, wherein the PD-1 axis binding antagonist is atezolizumab.
PD-1 축 결합 길항제를 더 포함하는, 키트.486. The method of claim 486,
A kit, further comprising a PD-1 axis binding antagonist.
상기 PD-1 축 결합 길항제는 아테졸리주맙인, 키트.49. The method of claim 486 or 487,
The kit, wherein the PD-1 axis binding antagonist is atezolizumab.
상기 항 TIGIT 길항제 항체는 티라골루맙인, 키트.497. The method of any one of claims 486-488,
The anti-TIGIT antagonist antibody is tyragolumab, the kit.
하나 이상의 화학요법제를 더 포함하는, 키트.49. The method of any one of claims 486 to 489,
A kit, further comprising one or more chemotherapeutic agents.
상기 하나 이상의 화학요법제는 하나 이상의 백금계 화학요법제 및/또는 하나 이상의 비백금계 화학요법제인, 키트.490. The method of claim 490,
wherein the one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
상기 하나 이상의 백금계 화합요법제는 카보플라틴 또는 시스플라틴인, 키트.491. The method of claim 491,
wherein the at least one platinum-based chemotherapeutic agent is carboplatin or cisplatin.
상기 하나 이상의 비백금계 화학요법제는 항대사물질, 탁산, 또는 토포이소머라제 II 억제제인, 키트.495. The method of claim 491 or 492,
wherein the at least one non-platinum-based chemotherapeutic agent is an antimetabolite, a taxane, or a topoisomerase II inhibitor.
상기 항대사물질은 페메트렉시드, 젬시타빈, 카페시타빈, 또는 5-플루오로우라실인, 키트.493. The method of claim 493,
wherein the antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
상기 탁산은 파클리탁셀 또는 냅-파클리탁셀인, 키트.495. The method of claim 493 or 494,
wherein the taxane is paclitaxel or nap-paclitaxel.
상기 토포이소머라제 II 억제제는 에토포시드, 테니포시드, 독소루비신, 다우노루비신, 미톡산트론, 암사크린, 엘립티신, 아우린트리카르복실산, 또는 HU-331인, 키트.495. The method of any one of claims 493-495,
wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticin, aurintricarboxylic acid, or HU-331.
VEGF 길항제를 더 포함하는, 키트.497. The method of any one of claims 481-496,
A kit, further comprising a VEGF antagonist.
상기 VEGF 길항제는 항 VEGF 항체인, 키트.497. The method of claim 497,
The VEGF antagonist is an anti-VEGF antibody, kit.
상기 항 VEGF 항체는 베바시주맙인, 키트.497. The method of claim 498,
The anti-VEGF antibody is bevacizumab, the kit.
상기 방법은 제47항 내지 제160항, 제162항 내지 제224항, 및 제226항 내지 제480항 중 어느 한 항에 따르는, 항 TIGIT 길항제 항체 및 항 PD-1 축 결합 길항제.An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having cancer, comprising:
The method comprises an anti-TIGIT antagonist antibody and an anti-PD-1 axis binding antagonist according to any one of claims 47-160, 162-224, and 226-480.
상기 치료는 제47항 내지 제160항, 제162항 내지 제224항, 및 제226항 내지 제480항 중 어느 한 항의 방법에 따르는, 용도.1. Use of an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or population of subjects having cancer, comprising:
Use according to any one of claims 47 to 160, 162 to 224, and 226 to 480, wherein the treatment is according to the method.
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 별도의 제형으로 제공되는, 용도.501. The method of claim 501,
The use of claim 1, wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in separate formulations.
상기 항 TIGIT 길항제 항체 및 상기 PD-1 축 결합 길항제는 단일의 제형으로 제공되는, 용도.501. The method of claim 501,
The use of claim 1, wherein the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single dosage form.
Applications Claiming Priority (29)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202062966448P | 2020-01-27 | 2020-01-27 | |
| US62/966,448 | 2020-01-27 | ||
| US202062985822P | 2020-03-05 | 2020-03-05 | |
| US62/985,822 | 2020-03-05 | ||
| US202062994272P | 2020-03-24 | 2020-03-24 | |
| PCT/US2020/024526 WO2021194481A1 (en) | 2020-03-24 | 2020-03-24 | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies |
| US62/994,272 | 2020-03-24 | ||
| USPCT/US2020/024526 | 2020-03-24 | ||
| US202063059054P | 2020-07-30 | 2020-07-30 | |
| US63/059,054 | 2020-07-30 | ||
| US202063059960P | 2020-07-31 | 2020-07-31 | |
| US63/059,960 | 2020-07-31 | ||
| US202063074807P | 2020-09-04 | 2020-09-04 | |
| US202063074827P | 2020-09-04 | 2020-09-04 | |
| USPCT/US2020/049415 | 2020-09-04 | ||
| PCT/US2020/049415 WO2022050954A1 (en) | 2020-09-04 | 2020-09-04 | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies |
| US63/074,807 | 2020-09-04 | ||
| US63/074,827 | 2020-09-04 | ||
| US202063085890P | 2020-09-30 | 2020-09-30 | |
| US63/085,890 | 2020-09-30 | ||
| US202063105198P | 2020-10-23 | 2020-10-23 | |
| US63/105,198 | 2020-10-23 | ||
| US202063114517P | 2020-11-16 | 2020-11-16 | |
| US63/114,517 | 2020-11-16 | ||
| US202063124693P | 2020-12-11 | 2020-12-11 | |
| US63/124,693 | 2020-12-11 | ||
| US202063127109P | 2020-12-17 | 2020-12-17 | |
| US63/127,109 | 2020-12-17 | ||
| PCT/US2021/015143 WO2021154761A1 (en) | 2020-01-27 | 2021-01-26 | Methods for treatment of cancer with an anti-tigit antagonist antibody |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| KR20220133243A true KR20220133243A (en) | 2022-10-04 |
Family
ID=74626264
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| KR1020227029306A KR20220133243A (en) | 2020-01-27 | 2021-01-26 | Method of treating cancer using anti-TIGIT antagonist antibody |
Country Status (10)
| Country | Link |
|---|---|
| EP (1) | EP4096646A1 (en) |
| JP (1) | JP2023511595A (en) |
| KR (1) | KR20220133243A (en) |
| CN (1) | CN115315256A (en) |
| AU (1) | AU2021212662A1 (en) |
| CA (1) | CA3165187A1 (en) |
| IL (1) | IL294800A (en) |
| MX (1) | MX2022009170A (en) |
| TW (1) | TW202142230A (en) |
| WO (1) | WO2021154761A1 (en) |
Families Citing this family (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| AU2021293038A1 (en) * | 2020-06-16 | 2023-02-02 | F. Hoffmann-La Roche Ag | Methods and compositions for treating triple-negative breast cancer |
| BR112023026966A2 (en) * | 2021-07-02 | 2024-03-12 | Hoffmann La Roche | METHODS FOR TREATING AN INDIVIDUAL WITH MELANOMA, FOR ACHIEVING A CLINICAL RESPONSE, FOR TREATING AN INDIVIDUAL WITH NON-HODGKIN LYMPHOMA, FOR TREATING A POPULATION OF INDIVIDUALS WITH NON-HODGKIN LYMPHOMA, AND FOR TREATING AN INDIVIDUAL WITH METASTATIC COLORECTAL CANCER |
| TW202320848A (en) * | 2021-07-28 | 2023-06-01 | 美商建南德克公司 | Methods and compositions for treating cancer |
| WO2023018675A1 (en) * | 2021-08-10 | 2023-02-16 | Merck Sharp & Dohme Llc | A therapeutic combination comprising a tigit antagonist, a pd-1 antagonist, and lenvatinib |
| WO2023018677A1 (en) * | 2021-08-10 | 2023-02-16 | Merck Sharp & Dohme Llc | A therapeutic combination comprising a t1git antagonist, a pd-1 antagonist, and a chemotherapeutic agent(s) |
| WO2023040804A1 (en) * | 2021-09-14 | 2023-03-23 | 信达生物制药(苏州)有限公司 | Pharmaceutical composition of anti-pd-1 antibody and chemotherapy agent and method for using same |
| TW202328195A (en) * | 2021-09-15 | 2023-07-16 | 大陸商江蘇恆瑞醫藥股份有限公司 | Proteins that specifically bind to pd-1 and the pharmaceutical use thereof |
| WO2023122665A1 (en) * | 2021-12-22 | 2023-06-29 | Genentech, Inc. | Clinical formulations of anti-tigit antibodies |
| CN114181310B (en) * | 2022-02-14 | 2022-07-05 | 中山康方生物医药有限公司 | anti-TIGIT antibody, and pharmaceutical composition and use thereof |
Family Cites Families (38)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816567A (en) | 1983-04-08 | 1989-03-28 | Genentech, Inc. | Recombinant immunoglobin preparations |
| US6548640B1 (en) | 1986-03-27 | 2003-04-15 | Btg International Limited | Altered antibodies |
| DE3920358A1 (en) | 1989-06-22 | 1991-01-17 | Behringwerke Ag | BISPECIFIC AND OLIGO-SPECIFIC, MONO- AND OLIGOVALENT ANTI-BODY CONSTRUCTS, THEIR PRODUCTION AND USE |
| US6075181A (en) | 1990-01-12 | 2000-06-13 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| US6150584A (en) | 1990-01-12 | 2000-11-21 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| JPH07501451A (en) | 1991-11-25 | 1995-02-16 | エンゾン・インコーポレイテッド | Multivalent antigen binding protein |
| AU661533B2 (en) | 1992-01-20 | 1995-07-27 | Astrazeneca Ab | Quinazoline derivatives |
| GB9314893D0 (en) | 1993-07-19 | 1993-09-01 | Zeneca Ltd | Quinazoline derivatives |
| IL112249A (en) | 1994-01-25 | 2001-11-25 | Warner Lambert Co | Pharmaceutical compositions containing di and tricyclic pyrimidine derivatives for inhibiting tyrosine kinases of the epidermal growth factor receptor family and some new such compounds |
| US5679683A (en) | 1994-01-25 | 1997-10-21 | Warner-Lambert Company | Tricyclic compounds capable of inhibiting tyrosine kinases of the epidermal growth factor receptor family |
| IL112248A0 (en) | 1994-01-25 | 1995-03-30 | Warner Lambert Co | Tricyclic heteroaromatic compounds and pharmaceutical compositions containing them |
| WO1996003397A1 (en) | 1994-07-21 | 1996-02-08 | Akzo Nobel N.V. | Cyclic ketone peroxide formulations |
| US5804396A (en) | 1994-10-12 | 1998-09-08 | Sugen, Inc. | Assay for agents active in proliferative disorders |
| DK0817775T3 (en) | 1995-03-30 | 2001-11-19 | Pfizer | quinazoline |
| US5641870A (en) | 1995-04-20 | 1997-06-24 | Genentech, Inc. | Low pH hydrophobic interaction chromatography for antibody purification |
| GB9508538D0 (en) | 1995-04-27 | 1995-06-14 | Zeneca Ltd | Quinazoline derivatives |
| GB9508565D0 (en) | 1995-04-27 | 1995-06-14 | Zeneca Ltd | Quiazoline derivative |
| US5747498A (en) | 1996-05-28 | 1998-05-05 | Pfizer Inc. | Alkynyl and azido-substituted 4-anilinoquinazolines |
| IL122855A (en) | 1995-07-06 | 2004-08-31 | Novartis Ag | N-PHENYL (ALKYL)-7H-PYRROLO [2,3-d] PYRIMIDIN-4-AMINE DERIVATIVES, THEIR PREPARATION AND PHARMACEUTICAL COMPOSITIONS CONTAINING THEM |
| US5760041A (en) | 1996-02-05 | 1998-06-02 | American Cyanamid Company | 4-aminoquinazoline EGFR Inhibitors |
| GB9603095D0 (en) | 1996-02-14 | 1996-04-10 | Zeneca Ltd | Quinazoline derivatives |
| PT892789E (en) | 1996-04-12 | 2002-07-31 | Warner Lambert Co | IRREVERSIVE INHIBITORS OF TYROSINE KINASES |
| US6391874B1 (en) | 1996-07-13 | 2002-05-21 | Smithkline Beecham Corporation | Fused heterocyclic compounds as protein tyrosine kinase inhibitors |
| ID18494A (en) | 1996-10-02 | 1998-04-16 | Novartis Ag | PIRAZOLA DISTRIBUTION IN THE SEQUENCE AND THE PROCESS OF MAKING IT |
| US6002008A (en) | 1997-04-03 | 1999-12-14 | American Cyanamid Company | Substituted 3-cyano quinolines |
| UA73073C2 (en) | 1997-04-03 | 2005-06-15 | Уайт Холдінгз Корпорейшн | Substituted 3-cyan chinolines |
| DK0980244T3 (en) | 1997-05-06 | 2003-09-29 | Wyeth Corp | Use of quinazoline compounds to treat polycystic kidney disease |
| ZA986729B (en) | 1997-07-29 | 1999-02-02 | Warner Lambert Co | Irreversible inhibitors of tyrosine kinases |
| ZA986732B (en) | 1997-07-29 | 1999-02-02 | Warner Lambert Co | Irreversible inhibitiors of tyrosine kinases |
| TW436485B (en) | 1997-08-01 | 2001-05-28 | American Cyanamid Co | Substituted quinazoline derivatives |
| AU1308799A (en) | 1997-11-06 | 1999-05-31 | American Cyanamid Company | Use of quinazoline derivatives as tyrosine kinase inhibitors for treating colonic polyps |
| ES2375931T3 (en) | 1997-12-05 | 2012-03-07 | The Scripps Research Institute | HUMANIZATION OF ANTIBODY MURINO. |
| IL143089A0 (en) | 1998-11-19 | 2002-04-21 | Warner Lambert Co | N-[4-(3-chloro-4-fluoro-phenylamino)-7-(3-morpholin-4-yl-propoxy)-quinazolin-6-yl]-acrylamide, an irreversible inhibitor of tyrosine kinases |
| AU2005250484B2 (en) | 2004-06-04 | 2011-08-11 | Genentech, Inc. | EGFR mutations |
| AU2013318618B2 (en) | 2012-09-24 | 2017-04-06 | Ventana Medical Systems, Inc. | Method of identifying treatment responsive non-small cell lung cancer using anaplastic lymphoma kinase (ALK) as a marker |
| RS61152B1 (en) | 2015-05-12 | 2020-12-31 | Hoffmann La Roche | Therapeutic and diagnostic methods for cancer |
| IL255372B (en) | 2015-05-29 | 2022-07-01 | Genentech Inc | Therapeutic and diagnostic methods for cancer |
| MX2020008882A (en) * | 2018-02-26 | 2021-01-08 | Genentech Inc | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies. |
-
2021
- 2021-01-26 KR KR1020227029306A patent/KR20220133243A/en unknown
- 2021-01-26 MX MX2022009170A patent/MX2022009170A/en unknown
- 2021-01-26 JP JP2022545057A patent/JP2023511595A/en active Pending
- 2021-01-26 EP EP21705841.1A patent/EP4096646A1/en active Pending
- 2021-01-26 CN CN202180022830.2A patent/CN115315256A/en active Pending
- 2021-01-26 CA CA3165187A patent/CA3165187A1/en active Pending
- 2021-01-26 IL IL294800A patent/IL294800A/en unknown
- 2021-01-26 TW TW110102913A patent/TW202142230A/en unknown
- 2021-01-26 WO PCT/US2021/015143 patent/WO2021154761A1/en unknown
- 2021-01-26 AU AU2021212662A patent/AU2021212662A1/en active Pending
Also Published As
| Publication number | Publication date |
|---|---|
| AU2021212662A1 (en) | 2022-08-11 |
| TW202142230A (en) | 2021-11-16 |
| JP2023511595A (en) | 2023-03-20 |
| CA3165187A1 (en) | 2021-08-05 |
| MX2022009170A (en) | 2022-08-17 |
| WO2021154761A1 (en) | 2021-08-05 |
| CN115315256A (en) | 2022-11-08 |
| EP4096646A1 (en) | 2022-12-07 |
| IL294800A (en) | 2022-09-01 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| TWI775781B (en) | Therapeutic and diagnostic methods for cancer | |
| US20180346586A1 (en) | Methods of treating cancer using anti-ox40 antibodies | |
| KR20220133243A (en) | Method of treating cancer using anti-TIGIT antagonist antibody | |
| KR20180008449A (en) | Treatment and Diagnosis Methods for Cancer | |
| JP2018518483A (en) | Methods of treating cancer using anti-OX40 antibodies and PD-1 axis binding antagonists | |
| KR20210124535A (en) | Therapeutic and diagnostic methods for cancer | |
| KR20230082632A (en) | Dosing for Treatment with Anti-FCRH5/Anti-CD3 Bispecific Antibodies | |
| US20220016243A1 (en) | Methods for treatment of cancer with an anti-tigit antagonist antibody | |
| US20220098318A1 (en) | Dosing for treatment with anti-tigit and anti-cd20 or anti-cd38 antibodies | |
| US20200171146A1 (en) | Methods of treating lung cancer with a pd-1 axis binding antagonist, an antimetabolite, and a platinum agent | |
| KR20230024368A (en) | Treatment with anti-TIGIT antibodies and PD-1 axis binding antagonists | |
| KR20220070237A (en) | Dosing for treatment with anti-TIGIT and anti-PD-L1 antagonist antibodies | |
| TWI836278B (en) | Dosing for treatment with anti-fcrh5/anti-cd3 bispecific antibodies | |
| US20230312723A1 (en) | Methods and compositions for non-small cell lung cancer immunotherapy | |
| TW202320848A (en) | Methods and compositions for treating cancer | |
| KR20240028452A (en) | Methods and compositions for treating cancer | |
| CN117715936A (en) | Methods and compositions for treating cancer |