JP2023511595A - Methods for treating cancer using anti-TIGIT antagonist antibodies - Google Patents
Methods for treating cancer using anti-TIGIT antagonist antibodies Download PDFInfo
- Publication number
- JP2023511595A JP2023511595A JP2022545057A JP2022545057A JP2023511595A JP 2023511595 A JP2023511595 A JP 2023511595A JP 2022545057 A JP2022545057 A JP 2022545057A JP 2022545057 A JP2022545057 A JP 2022545057A JP 2023511595 A JP2023511595 A JP 2023511595A
- Authority
- JP
- Japan
- Prior art keywords
- subject
- dose
- weeks
- cancer
- antibody
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Pending
Links
- 239000005557 antagonist Substances 0.000 title claims abstract description 473
- 206010028980 Neoplasm Diseases 0.000 title claims abstract description 207
- 201000011510 cancer Diseases 0.000 title claims abstract description 120
- 238000000034 method Methods 0.000 title claims description 685
- 238000011282 treatment Methods 0.000 claims abstract description 180
- 206010058467 Lung neoplasm malignant Diseases 0.000 claims abstract description 58
- 201000005202 lung cancer Diseases 0.000 claims abstract description 58
- 208000020816 lung neoplasm Diseases 0.000 claims abstract description 58
- 206010008342 Cervix carcinoma Diseases 0.000 claims abstract description 26
- 208000006105 Uterine Cervical Neoplasms Diseases 0.000 claims abstract description 26
- 201000010881 cervical cancer Diseases 0.000 claims abstract description 26
- 208000000461 Esophageal Neoplasms Diseases 0.000 claims abstract description 18
- 206010030155 Oesophageal carcinoma Diseases 0.000 claims abstract description 18
- 201000004101 esophageal cancer Diseases 0.000 claims abstract description 18
- 206010005003 Bladder cancer Diseases 0.000 claims abstract description 17
- 206010006187 Breast cancer Diseases 0.000 claims abstract description 12
- 208000026310 Breast neoplasm Diseases 0.000 claims abstract description 12
- 206010009944 Colon cancer Diseases 0.000 claims abstract description 12
- 208000001333 Colorectal Neoplasms Diseases 0.000 claims abstract description 11
- 206010061902 Pancreatic neoplasm Diseases 0.000 claims abstract description 11
- 208000007097 Urinary Bladder Neoplasms Diseases 0.000 claims abstract description 11
- 208000015486 malignant pancreatic neoplasm Diseases 0.000 claims abstract description 11
- 201000002528 pancreatic cancer Diseases 0.000 claims abstract description 11
- 208000008443 pancreatic carcinoma Diseases 0.000 claims abstract description 11
- 201000005112 urinary bladder cancer Diseases 0.000 claims abstract description 11
- 201000010536 head and neck cancer Diseases 0.000 claims abstract description 10
- 208000014829 head and neck neoplasm Diseases 0.000 claims abstract description 10
- 206010033128 Ovarian cancer Diseases 0.000 claims abstract description 9
- 206010061535 Ovarian neoplasm Diseases 0.000 claims abstract description 9
- 208000005718 Stomach Neoplasms Diseases 0.000 claims abstract description 9
- 206010017758 gastric cancer Diseases 0.000 claims abstract description 9
- 201000011549 stomach cancer Diseases 0.000 claims abstract description 9
- 201000007270 liver cancer Diseases 0.000 claims abstract description 7
- 208000014018 liver neoplasm Diseases 0.000 claims abstract description 7
- 230000027455 binding Effects 0.000 claims description 288
- BASFCYQUMIYNBI-UHFFFAOYSA-N platinum Chemical compound [Pt] BASFCYQUMIYNBI-UHFFFAOYSA-N 0.000 claims description 285
- 229940127089 cytotoxic agent Drugs 0.000 claims description 180
- 239000002246 antineoplastic agent Substances 0.000 claims description 178
- 108010074708 B7-H1 Antigen Proteins 0.000 claims description 166
- 229910052697 platinum Inorganic materials 0.000 claims description 142
- 102100040678 Programmed cell death protein 1 Human genes 0.000 claims description 136
- 101710089372 Programmed cell death protein 1 Proteins 0.000 claims description 131
- 230000014509 gene expression Effects 0.000 claims description 90
- 229960003852 atezolizumab Drugs 0.000 claims description 88
- 229950007133 tiragolumab Drugs 0.000 claims description 79
- 125000003275 alpha amino acid group Chemical group 0.000 claims description 69
- 102000008096 B7-H1 Antigen Human genes 0.000 claims description 67
- 230000004044 response Effects 0.000 claims description 56
- 238000003364 immunohistochemistry Methods 0.000 claims description 52
- 229960001592 paclitaxel Drugs 0.000 claims description 48
- RCINICONZNJXQF-MZXODVADSA-N taxol Chemical compound O([C@@H]1[C@@]2(C[C@@H](C(C)=C(C2(C)C)[C@H](C([C@]2(C)[C@@H](O)C[C@H]3OC[C@]3([C@H]21)OC(C)=O)=O)OC(=O)C)OC(=O)[C@H](O)[C@@H](NC(=O)C=1C=CC=CC=1)C=1C=CC=CC=1)O)C(=O)C1=CC=CC=C1 RCINICONZNJXQF-MZXODVADSA-N 0.000 claims description 48
- 230000004083 survival effect Effects 0.000 claims description 47
- 229960004562 carboplatin Drugs 0.000 claims description 46
- 238000003556 assay Methods 0.000 claims description 44
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 claims description 44
- 208000002154 non-small cell lung carcinoma Diseases 0.000 claims description 44
- 208000029729 tumor suppressor gene on chromosome 11 Diseases 0.000 claims description 44
- 229960004316 cisplatin Drugs 0.000 claims description 42
- DQLATGHUWYMOKM-UHFFFAOYSA-L cisplatin Chemical compound N[Pt](N)(Cl)Cl DQLATGHUWYMOKM-UHFFFAOYSA-L 0.000 claims description 42
- 206010061289 metastatic neoplasm Diseases 0.000 claims description 42
- 230000001394 metastastic effect Effects 0.000 claims description 40
- AOJJSUZBOXZQNB-TZSSRYMLSA-N Doxorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 AOJJSUZBOXZQNB-TZSSRYMLSA-N 0.000 claims description 38
- 102100024213 Programmed cell death 1 ligand 2 Human genes 0.000 claims description 38
- 210000004881 tumor cell Anatomy 0.000 claims description 36
- 229940124087 DNA topoisomerase II inhibitor Drugs 0.000 claims description 34
- -1 HLX10 Chemical compound 0.000 claims description 34
- 239000000317 Topoisomerase II Inhibitor Substances 0.000 claims description 34
- 239000003814 drug Substances 0.000 claims description 34
- 206010073071 hepatocellular carcinoma Diseases 0.000 claims description 34
- 108700030875 Programmed Cell Death 1 Ligand 2 Proteins 0.000 claims description 31
- 108010019530 Vascular Endothelial Growth Factors Proteins 0.000 claims description 31
- 102000005789 Vascular Endothelial Growth Factors Human genes 0.000 claims description 31
- 231100000844 hepatocellular carcinoma Toxicity 0.000 claims description 31
- 101000831007 Homo sapiens T-cell immunoreceptor with Ig and ITIM domains Proteins 0.000 claims description 30
- 102100024834 T-cell immunoreceptor with Ig and ITIM domains Human genes 0.000 claims description 30
- 201000010099 disease Diseases 0.000 claims description 30
- 238000001356 surgical procedure Methods 0.000 claims description 30
- 238000012423 maintenance Methods 0.000 claims description 28
- SDUQYLNIPVEERB-QPPQHZFASA-N gemcitabine Chemical compound O=C1N=C(N)C=CN1[C@H]1C(F)(F)[C@H](O)[C@@H](CO)O1 SDUQYLNIPVEERB-QPPQHZFASA-N 0.000 claims description 27
- 229940123751 PD-L1 antagonist Drugs 0.000 claims description 26
- 229940123237 Taxane Drugs 0.000 claims description 26
- 108010058566 130-nm albumin-bound paclitaxel Proteins 0.000 claims description 25
- 229960005277 gemcitabine Drugs 0.000 claims description 23
- 108090000623 proteins and genes Proteins 0.000 claims description 23
- 229930012538 Paclitaxel Natural products 0.000 claims description 22
- 208000000102 Squamous Cell Carcinoma of Head and Neck Diseases 0.000 claims description 22
- 201000000459 head and neck squamous cell carcinoma Diseases 0.000 claims description 22
- 206010044412 transitional cell carcinoma Diseases 0.000 claims description 22
- 229940124060 PD-1 antagonist Drugs 0.000 claims description 20
- 206010041067 Small cell lung cancer Diseases 0.000 claims description 20
- 208000003721 Triple Negative Breast Neoplasms Diseases 0.000 claims description 20
- VJJPUSNTGOMMGY-MRVIYFEKSA-N etoposide Chemical group COC1=C(O)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@@H](O[C@H]3[C@@H]([C@@H](O)[C@@H]4O[C@H](C)OC[C@H]4O3)O)[C@@H]3[C@@H]2C(OC3)=O)=C1 VJJPUSNTGOMMGY-MRVIYFEKSA-N 0.000 claims description 20
- 208000000587 small cell lung carcinoma Diseases 0.000 claims description 20
- 238000010186 staining Methods 0.000 claims description 20
- 208000022679 triple-negative breast carcinoma Diseases 0.000 claims description 20
- 208000023747 urothelial carcinoma Diseases 0.000 claims description 20
- 229960005420 etoposide Drugs 0.000 claims description 19
- 210000002865 immune cell Anatomy 0.000 claims description 19
- 229960005079 pemetrexed Drugs 0.000 claims description 19
- QOFFJEBXNKRSPX-ZDUSSCGKSA-N pemetrexed Chemical group C1=N[C]2NC(N)=NC(=O)C2=C1CCC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 QOFFJEBXNKRSPX-ZDUSSCGKSA-N 0.000 claims description 19
- DKPFODGZWDEEBT-QFIAKTPHSA-N taxane Chemical class C([C@]1(C)CCC[C@@H](C)[C@H]1C1)C[C@H]2[C@H](C)CC[C@@H]1C2(C)C DKPFODGZWDEEBT-QFIAKTPHSA-N 0.000 claims description 19
- 229960004679 doxorubicin Drugs 0.000 claims description 17
- 201000008129 pancreatic ductal adenocarcinoma Diseases 0.000 claims description 17
- 229960002621 pembrolizumab Drugs 0.000 claims description 17
- 230000006698 induction Effects 0.000 claims description 16
- 230000009467 reduction Effects 0.000 claims description 16
- 108010017080 Granulocyte Colony-Stimulating Factor Proteins 0.000 claims description 15
- 239000002256 antimetabolite Substances 0.000 claims description 15
- 239000012634 fragment Substances 0.000 claims description 15
- 201000008443 lung non-squamous non-small cell carcinoma Diseases 0.000 claims description 15
- 230000002829 reductive effect Effects 0.000 claims description 15
- CMSMOCZEIVJLDB-UHFFFAOYSA-N Cyclophosphamide Chemical group ClCCN(CCCl)P1(=O)NCCCO1 CMSMOCZEIVJLDB-UHFFFAOYSA-N 0.000 claims description 14
- GHASVSINZRGABV-UHFFFAOYSA-N Fluorouracil Chemical compound FC1=CNC(=O)NC1=O GHASVSINZRGABV-UHFFFAOYSA-N 0.000 claims description 14
- 230000000340 anti-metabolite Effects 0.000 claims description 14
- 229940100197 antimetabolite Drugs 0.000 claims description 14
- 229960002949 fluorouracil Drugs 0.000 claims description 14
- 102000004169 proteins and genes Human genes 0.000 claims description 14
- 230000000306 recurrent effect Effects 0.000 claims description 14
- 208000024891 symptom Diseases 0.000 claims description 14
- 206010061818 Disease progression Diseases 0.000 claims description 13
- 108010017213 Granulocyte-Macrophage Colony-Stimulating Factor Proteins 0.000 claims description 13
- ZDZOTLJHXYCWBA-VCVYQWHSSA-N N-debenzoyl-N-(tert-butoxycarbonyl)-10-deacetyltaxol Chemical compound O([C@H]1[C@H]2[C@@](C([C@H](O)C3=C(C)[C@@H](OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=4C=CC=CC=4)C[C@]1(O)C3(C)C)=O)(C)[C@@H](O)C[C@H]1OC[C@]12OC(=O)C)C(=O)C1=CC=CC=C1 ZDZOTLJHXYCWBA-VCVYQWHSSA-N 0.000 claims description 13
- 239000003795 chemical substances by application Substances 0.000 claims description 13
- 229960004397 cyclophosphamide Drugs 0.000 claims description 13
- 230000005750 disease progression Effects 0.000 claims description 13
- 239000000203 mixture Substances 0.000 claims description 13
- 230000001575 pathological effect Effects 0.000 claims description 13
- 230000003442 weekly effect Effects 0.000 claims description 13
- 239000002253 acid Substances 0.000 claims description 12
- 229940100198 alkylating agent Drugs 0.000 claims description 12
- 239000002168 alkylating agent Substances 0.000 claims description 12
- 102100039619 Granulocyte colony-stimulating factor Human genes 0.000 claims description 11
- 229960000397 bevacizumab Drugs 0.000 claims description 11
- 229950004930 enfortumab vedotin Drugs 0.000 claims description 11
- 102000001301 EGF receptor Human genes 0.000 claims description 10
- 108060006698 EGF receptor Proteins 0.000 claims description 10
- 229960003668 docetaxel Drugs 0.000 claims description 10
- 238000002560 therapeutic procedure Methods 0.000 claims description 10
- GAGWJHPBXLXJQN-UORFTKCHSA-N Capecitabine Chemical compound C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1[C@H]1[C@H](O)[C@H](O)[C@@H](C)O1 GAGWJHPBXLXJQN-UORFTKCHSA-N 0.000 claims description 9
- 241000701806 Human papillomavirus Species 0.000 claims description 9
- 229940049595 antibody-drug conjugate Drugs 0.000 claims description 9
- 230000008901 benefit Effects 0.000 claims description 9
- 238000002512 chemotherapy Methods 0.000 claims description 9
- 230000006870 function Effects 0.000 claims description 9
- 238000001990 intravenous administration Methods 0.000 claims description 9
- 230000001404 mediated effect Effects 0.000 claims description 9
- 238000009099 neoadjuvant therapy Methods 0.000 claims description 9
- HQQSBEDKMRHYME-UHFFFAOYSA-N pefloxacin mesylate Chemical compound [H+].CS([O-])(=O)=O.C1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC(F)=C1N1CCN(C)CC1 HQQSBEDKMRHYME-UHFFFAOYSA-N 0.000 claims description 9
- 108010044644 pegfilgrastim Proteins 0.000 claims description 9
- 229960001373 pegfilgrastim Drugs 0.000 claims description 9
- GAGWJHPBXLXJQN-UHFFFAOYSA-N Capecitabine Natural products C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1C1C(O)C(O)C(C)O1 GAGWJHPBXLXJQN-UHFFFAOYSA-N 0.000 claims description 8
- 208000008839 Kidney Neoplasms Diseases 0.000 claims description 8
- 206010038389 Renal cancer Diseases 0.000 claims description 8
- 229960004117 capecitabine Drugs 0.000 claims description 8
- 229950009791 durvalumab Drugs 0.000 claims description 8
- 239000012636 effector Substances 0.000 claims description 8
- CTSPAMFJBXKSOY-UHFFFAOYSA-N ellipticine Chemical compound N1=CC=C2C(C)=C(NC=3C4=CC=CC=3)C4=C(C)C2=C1 CTSPAMFJBXKSOY-UHFFFAOYSA-N 0.000 claims description 8
- 230000001965 increasing effect Effects 0.000 claims description 8
- 201000010982 kidney cancer Diseases 0.000 claims description 8
- 229950000143 sacituzumab govitecan Drugs 0.000 claims description 8
- ULRUOUDIQPERIJ-PQURJYPBSA-N sacituzumab govitecan Chemical compound N([C@@H](CCCCN)C(=O)NC1=CC=C(C=C1)COC(=O)O[C@]1(CC)C(=O)OCC2=C1C=C1N(C2=O)CC2=C(C3=CC(O)=CC=C3N=C21)CC)C(=O)COCC(=O)NCCOCCOCCOCCOCCOCCOCCOCCOCCN(N=N1)C=C1CNC(=O)C(CC1)CCC1CN1C(=O)CC(SC[C@H](N)C(O)=O)C1=O ULRUOUDIQPERIJ-PQURJYPBSA-N 0.000 claims description 8
- 229940124597 therapeutic agent Drugs 0.000 claims description 8
- 108010029961 Filgrastim Proteins 0.000 claims description 7
- 238000009098 adjuvant therapy Methods 0.000 claims description 7
- 239000000611 antibody drug conjugate Substances 0.000 claims description 7
- 238000002619 cancer immunotherapy Methods 0.000 claims description 7
- STQGQHZAVUOBTE-VGBVRHCVSA-N daunorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(C)=O)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 STQGQHZAVUOBTE-VGBVRHCVSA-N 0.000 claims description 7
- 229960004177 filgrastim Drugs 0.000 claims description 7
- 238000001959 radiotherapy Methods 0.000 claims description 7
- 229950007213 spartalizumab Drugs 0.000 claims description 7
- 238000009121 systemic therapy Methods 0.000 claims description 7
- STQGQHZAVUOBTE-UHFFFAOYSA-N 7-Cyan-hept-2t-en-4,6-diinsaeure Natural products C1=2C(O)=C3C(=O)C=4C(OC)=CC=CC=4C(=O)C3=C(O)C=2CC(O)(C(C)=O)CC1OC1CC(N)C(O)C(C)O1 STQGQHZAVUOBTE-UHFFFAOYSA-N 0.000 claims description 6
- 238000011529 RT qPCR Methods 0.000 claims description 6
- 229960000975 daunorubicin Drugs 0.000 claims description 6
- 238000001802 infusion Methods 0.000 claims description 6
- 229960003301 nivolumab Drugs 0.000 claims description 6
- 102100033793 ALK tyrosine kinase receptor Human genes 0.000 claims description 5
- 101710168331 ALK tyrosine kinase receptor Proteins 0.000 claims description 5
- 238000009472 formulation Methods 0.000 claims description 5
- 238000007901 in situ hybridization Methods 0.000 claims description 5
- 238000004519 manufacturing process Methods 0.000 claims description 5
- KKZJGLLVHKMTCM-UHFFFAOYSA-N mitoxantrone Chemical compound O=C1C2=C(O)C=CC(O)=C2C(=O)C2=C1C(NCCNCCO)=CC=C2NCCNCCO KKZJGLLVHKMTCM-UHFFFAOYSA-N 0.000 claims description 5
- 229960001156 mitoxantrone Drugs 0.000 claims description 5
- 210000003205 muscle Anatomy 0.000 claims description 5
- 102000039446 nucleic acids Human genes 0.000 claims description 5
- 108020004707 nucleic acids Proteins 0.000 claims description 5
- 150000007523 nucleic acids Chemical class 0.000 claims description 5
- 230000036961 partial effect Effects 0.000 claims description 5
- NRUKOCRGYNPUPR-QBPJDGROSA-N teniposide Chemical compound COC1=C(O)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@@H](O[C@H]3[C@@H]([C@@H](O)[C@@H]4O[C@@H](OC[C@H]4O3)C=3SC=CC=3)O)[C@@H]3[C@@H]2C(OC3)=O)=C1 NRUKOCRGYNPUPR-QBPJDGROSA-N 0.000 claims description 5
- 231100000402 unacceptable toxicity Toxicity 0.000 claims description 5
- ZIXGXMMUKPLXBB-UHFFFAOYSA-N Guatambuinine Natural products N1C2=CC=CC=C2C2=C1C(C)=C1C=CN=C(C)C1=C2 ZIXGXMMUKPLXBB-UHFFFAOYSA-N 0.000 claims description 4
- 108010021625 Immunoglobulin Fragments Proteins 0.000 claims description 4
- 102000008394 Immunoglobulin Fragments Human genes 0.000 claims description 4
- 101100407308 Mus musculus Pdcd1lg2 gene Proteins 0.000 claims description 4
- SUYXJDLXGFPMCQ-INIZCTEOSA-N SJ000287331 Natural products CC1=c2cnccc2=C(C)C2=Nc3ccccc3[C@H]12 SUYXJDLXGFPMCQ-INIZCTEOSA-N 0.000 claims description 4
- 229960001220 amsacrine Drugs 0.000 claims description 4
- XCPGHVQEEXUHNC-UHFFFAOYSA-N amsacrine Chemical compound COC1=CC(NS(C)(=O)=O)=CC=C1NC1=C(C=CC=C2)C2=NC2=CC=CC=C12 XCPGHVQEEXUHNC-UHFFFAOYSA-N 0.000 claims description 4
- 229950002916 avelumab Drugs 0.000 claims description 4
- 229940067219 cetrelimab Drugs 0.000 claims description 4
- 229940011248 cosibelimab Drugs 0.000 claims description 4
- 238000009799 cystectomy Methods 0.000 claims description 4
- 210000001165 lymph node Anatomy 0.000 claims description 4
- 201000001441 melanoma Diseases 0.000 claims description 4
- 230000002085 persistent effect Effects 0.000 claims description 4
- 238000011518 platinum-based chemotherapy Methods 0.000 claims description 4
- 230000009885 systemic effect Effects 0.000 claims description 4
- 229960001278 teniposide Drugs 0.000 claims description 4
- 229950007123 tislelizumab Drugs 0.000 claims description 4
- 208000003174 Brain Neoplasms Diseases 0.000 claims description 3
- 108091006020 Fc-tagged proteins Proteins 0.000 claims description 3
- 241000282414 Homo sapiens Species 0.000 claims description 3
- 229950007712 camrelizumab Drugs 0.000 claims description 3
- 238000009169 immunotherapy Methods 0.000 claims description 3
- 230000002980 postoperative effect Effects 0.000 claims description 3
- 238000002271 resection Methods 0.000 claims description 3
- 229940018073 sasanlimab Drugs 0.000 claims description 3
- 206010041823 squamous cell carcinoma Diseases 0.000 claims description 3
- 210000004100 adrenal gland Anatomy 0.000 claims description 2
- 238000005516 engineering process Methods 0.000 claims description 2
- 210000004185 liver Anatomy 0.000 claims description 2
- 238000010208 microarray analysis Methods 0.000 claims description 2
- 238000011519 second-line treatment Methods 0.000 claims description 2
- 190000008236 carboplatin Chemical group 0.000 claims 26
- 102000004269 Granulocyte Colony-Stimulating Factor Human genes 0.000 claims 11
- 102000004457 Granulocyte-Macrophage Colony-Stimulating Factor Human genes 0.000 claims 9
- RZVAJINKPMORJF-UHFFFAOYSA-N Acetaminophen Chemical compound CC(=O)NC1=CC=C(O)C=C1 RZVAJINKPMORJF-UHFFFAOYSA-N 0.000 claims 3
- FWMNVWWHGCHHJJ-SKKKGAJSSA-N 4-amino-1-[(2r)-6-amino-2-[[(2r)-2-[[(2r)-2-[[(2r)-2-amino-3-phenylpropanoyl]amino]-3-phenylpropanoyl]amino]-4-methylpentanoyl]amino]hexanoyl]piperidine-4-carboxylic acid Chemical compound C([C@H](C(=O)N[C@H](CC(C)C)C(=O)N[C@H](CCCCN)C(=O)N1CCC(N)(CC1)C(O)=O)NC(=O)[C@H](N)CC=1C=CC=CC=1)C1=CC=CC=C1 FWMNVWWHGCHHJJ-SKKKGAJSSA-N 0.000 claims 2
- 102220517071 Transcriptional regulator PINT87aa_I10A_mutation Human genes 0.000 claims 2
- 210000004556 brain Anatomy 0.000 claims 2
- 239000002131 composite material Substances 0.000 claims 2
- DDRJAANPRJIHGJ-UHFFFAOYSA-N creatinine Chemical compound CN1CC(=O)NC1=N DDRJAANPRJIHGJ-UHFFFAOYSA-N 0.000 claims 2
- 229940121432 dostarlimab Drugs 0.000 claims 2
- 239000003446 ligand Substances 0.000 claims 2
- 230000003908 liver function Effects 0.000 claims 2
- 238000003762 quantitative reverse transcription PCR Methods 0.000 claims 2
- 206010055113 Breast cancer metastatic Diseases 0.000 claims 1
- 206010011878 Deafness Diseases 0.000 claims 1
- 206010059282 Metastases to central nervous system Diseases 0.000 claims 1
- 238000003559 RNA-seq method Methods 0.000 claims 1
- 238000007792 addition Methods 0.000 claims 1
- 208000009956 adenocarcinoma Diseases 0.000 claims 1
- 201000008395 adenosquamous carcinoma Diseases 0.000 claims 1
- 230000004075 alteration Effects 0.000 claims 1
- 208000019065 cervical carcinoma Diseases 0.000 claims 1
- 229940109239 creatinine Drugs 0.000 claims 1
- 230000010370 hearing loss Effects 0.000 claims 1
- 231100000888 hearing loss Toxicity 0.000 claims 1
- 208000016354 hearing loss disease Diseases 0.000 claims 1
- 238000007850 in situ PCR Methods 0.000 claims 1
- 201000001119 neuropathy Diseases 0.000 claims 1
- 230000007823 neuropathy Effects 0.000 claims 1
- 208000033808 peripheral neuropathy Diseases 0.000 claims 1
- 235000002020 sage Nutrition 0.000 claims 1
- 238000013538 segmental resection Methods 0.000 claims 1
- 238000002648 combination therapy Methods 0.000 abstract description 3
- 101100519207 Mus musculus Pdcd1 gene Proteins 0.000 description 117
- 102100024216 Programmed cell death 1 ligand 1 Human genes 0.000 description 102
- 210000004027 cell Anatomy 0.000 description 27
- 239000000090 biomarker Substances 0.000 description 26
- 102000004196 processed proteins & peptides Human genes 0.000 description 23
- 108090000765 processed proteins & peptides Proteins 0.000 description 23
- 239000003112 inhibitor Substances 0.000 description 22
- BHKICZDKIIDMNR-UHFFFAOYSA-L azane;cyclobutane-1,1-dicarboxylate;platinum(4+) Chemical compound N.N.[Pt+4].[O-]C(=O)C1(C([O-])=O)CCC1 BHKICZDKIIDMNR-UHFFFAOYSA-L 0.000 description 20
- 229940079593 drug Drugs 0.000 description 20
- 229920001184 polypeptide Polymers 0.000 description 20
- 102000036639 antigens Human genes 0.000 description 19
- 108091007433 antigens Proteins 0.000 description 19
- 239000000427 antigen Substances 0.000 description 18
- 230000000694 effects Effects 0.000 description 17
- 102100039620 Granulocyte-macrophage colony-stimulating factor Human genes 0.000 description 15
- 210000001744 T-lymphocyte Anatomy 0.000 description 15
- 230000003993 interaction Effects 0.000 description 15
- 208000035475 disorder Diseases 0.000 description 14
- 230000011664 signaling Effects 0.000 description 12
- 102100030086 Receptor tyrosine-protein kinase erbB-2 Human genes 0.000 description 11
- 102000040430 polynucleotide Human genes 0.000 description 11
- 108091033319 polynucleotide Proteins 0.000 description 11
- 239000002157 polynucleotide Substances 0.000 description 11
- 239000000523 sample Substances 0.000 description 11
- 101001012157 Homo sapiens Receptor tyrosine-protein kinase erbB-2 Proteins 0.000 description 10
- 108060003951 Immunoglobulin Proteins 0.000 description 10
- 238000004458 analytical method Methods 0.000 description 10
- 102000018358 immunoglobulin Human genes 0.000 description 10
- 208000037821 progressive disease Diseases 0.000 description 10
- 206010027476 Metastases Diseases 0.000 description 9
- 150000001875 compounds Chemical class 0.000 description 9
- AAKJLRGGTJKAMG-UHFFFAOYSA-N erlotinib Chemical compound C=12C=C(OCCOC)C(OCCOC)=CC2=NC=NC=1NC1=CC=CC(C#C)=C1 AAKJLRGGTJKAMG-UHFFFAOYSA-N 0.000 description 9
- 208000032818 Microsatellite Instability Diseases 0.000 description 8
- 208000006265 Renal cell carcinoma Diseases 0.000 description 8
- 238000013461 design Methods 0.000 description 8
- BCFGMOOMADDAQU-UHFFFAOYSA-N lapatinib Chemical compound O1C(CNCCS(=O)(=O)C)=CC=C1C1=CC=C(N=CN=C2NC=3C=C(Cl)C(OCC=4C=C(F)C=CC=4)=CC=3)C2=C1 BCFGMOOMADDAQU-UHFFFAOYSA-N 0.000 description 8
- 101001117312 Homo sapiens Programmed cell death 1 ligand 2 Proteins 0.000 description 7
- 101000611936 Homo sapiens Programmed cell death protein 1 Proteins 0.000 description 7
- 208000015914 Non-Hodgkin lymphomas Diseases 0.000 description 7
- 239000002254 cytotoxic agent Substances 0.000 description 7
- 231100000599 cytotoxic agent Toxicity 0.000 description 7
- 230000034994 death Effects 0.000 description 7
- 231100000517 death Toxicity 0.000 description 7
- 231100000371 dose-limiting toxicity Toxicity 0.000 description 7
- 239000000126 substance Substances 0.000 description 7
- 108020004414 DNA Proteins 0.000 description 6
- KDGFLJKFZUIJMX-UHFFFAOYSA-N alectinib Chemical compound CCC1=CC=2C(=O)C(C3=CC=C(C=C3N3)C#N)=C3C(C)(C)C=2C=C1N(CC1)CCC1N1CCOCC1 KDGFLJKFZUIJMX-UHFFFAOYSA-N 0.000 description 6
- 230000004071 biological effect Effects 0.000 description 6
- 238000001574 biopsy Methods 0.000 description 6
- 229950002826 canertinib Drugs 0.000 description 6
- 238000001514 detection method Methods 0.000 description 6
- XGALLCVXEZPNRQ-UHFFFAOYSA-N gefitinib Chemical compound C=12C=C(OCCCN3CCOCC3)C(OC)=CC2=NC=NC=1NC1=CC=C(F)C(Cl)=C1 XGALLCVXEZPNRQ-UHFFFAOYSA-N 0.000 description 6
- 229940072221 immunoglobulins Drugs 0.000 description 6
- 230000009401 metastasis Effects 0.000 description 6
- JZZFDCXSFTVOJY-UHFFFAOYSA-N n-[4-(3-chloro-4-fluoroanilino)-7-(3-morpholin-4-ylpropoxy)quinazolin-6-yl]prop-2-enamide;hydron;dichloride Chemical compound Cl.Cl.C1=C(Cl)C(F)=CC=C1NC1=NC=NC2=CC(OCCCN3CCOCC3)=C(NC(=O)C=C)C=C12 JZZFDCXSFTVOJY-UHFFFAOYSA-N 0.000 description 6
- 230000035755 proliferation Effects 0.000 description 6
- 238000003127 radioimmunoassay Methods 0.000 description 6
- 108010038379 sargramostim Proteins 0.000 description 6
- 229960002530 sargramostim Drugs 0.000 description 6
- QFJCIRLUMZQUOT-HPLJOQBZSA-N sirolimus Chemical compound C1C[C@@H](O)[C@H](OC)C[C@@H]1C[C@@H](C)[C@H]1OC(=O)[C@@H]2CCCCN2C(=O)C(=O)[C@](O)(O2)[C@H](C)CC[C@H]2C[C@H](OC)/C(C)=C/C=C/C=C/[C@@H](C)C[C@@H](C)C(=O)[C@H](OC)[C@H](O)/C(C)=C/[C@@H](C)C(=O)C1 QFJCIRLUMZQUOT-HPLJOQBZSA-N 0.000 description 6
- 230000001225 therapeutic effect Effects 0.000 description 6
- 210000001519 tissue Anatomy 0.000 description 6
- XRYJULCDUUATMC-CYBMUJFWSA-N 4-[4-[[(1r)-1-phenylethyl]amino]-7h-pyrrolo[2,3-d]pyrimidin-6-yl]phenol Chemical compound N([C@H](C)C=1C=CC=CC=1)C(C=1C=2)=NC=NC=1NC=2C1=CC=C(O)C=C1 XRYJULCDUUATMC-CYBMUJFWSA-N 0.000 description 5
- 108010071942 Colony-Stimulating Factors Proteins 0.000 description 5
- 101001117317 Homo sapiens Programmed cell death 1 ligand 1 Proteins 0.000 description 5
- FBOZXECLQNJBKD-ZDUSSCGKSA-N L-methotrexate Chemical compound C=1N=C2N=C(N)N=C(N)C2=NC=1CN(C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 FBOZXECLQNJBKD-ZDUSSCGKSA-N 0.000 description 5
- 239000005551 L01XE03 - Erlotinib Substances 0.000 description 5
- 239000002136 L01XE07 - Lapatinib Substances 0.000 description 5
- 108010029485 Protein Isoforms Proteins 0.000 description 5
- 102000001708 Protein Isoforms Human genes 0.000 description 5
- 102100033479 RAF proto-oncogene serine/threonine-protein kinase Human genes 0.000 description 5
- 238000011156 evaluation Methods 0.000 description 5
- 230000002401 inhibitory effect Effects 0.000 description 5
- 239000002050 international nonproprietary name Substances 0.000 description 5
- 230000003902 lesion Effects 0.000 description 5
- 229960000485 methotrexate Drugs 0.000 description 5
- 238000012986 modification Methods 0.000 description 5
- 239000008194 pharmaceutical composition Substances 0.000 description 5
- 238000003752 polymerase chain reaction Methods 0.000 description 5
- 235000018102 proteins Nutrition 0.000 description 5
- 150000003384 small molecules Chemical class 0.000 description 5
- WYWHKKSPHMUBEB-UHFFFAOYSA-N tioguanine Chemical compound N1C(N)=NC(=S)C2=C1N=CN2 WYWHKKSPHMUBEB-UHFFFAOYSA-N 0.000 description 5
- 229940121358 tyrosine kinase inhibitor Drugs 0.000 description 5
- XRASPMIURGNCCH-UHFFFAOYSA-N zoledronic acid Chemical compound OP(=O)(O)C(P(O)(O)=O)(O)CN1C=CN=C1 XRASPMIURGNCCH-UHFFFAOYSA-N 0.000 description 5
- IAKHMKGGTNLKSZ-INIZCTEOSA-N (S)-colchicine Chemical compound C1([C@@H](NC(C)=O)CC2)=CC(=O)C(OC)=CC=C1C1=C2C=C(OC)C(OC)=C1OC IAKHMKGGTNLKSZ-INIZCTEOSA-N 0.000 description 4
- 102000004127 Cytokines Human genes 0.000 description 4
- 108090000695 Cytokines Proteins 0.000 description 4
- 229940122558 EGFR antagonist Drugs 0.000 description 4
- 241000282412 Homo Species 0.000 description 4
- 239000002147 L01XE04 - Sunitinib Substances 0.000 description 4
- 241000124008 Mammalia Species 0.000 description 4
- 108091092878 Microsatellite Proteins 0.000 description 4
- NWIBSHFKIJFRCO-WUDYKRTCSA-N Mytomycin Chemical compound C1N2C(C(C(C)=C(N)C3=O)=O)=C3[C@@H](COC(N)=O)[C@@]2(OC)[C@@H]2[C@H]1N2 NWIBSHFKIJFRCO-WUDYKRTCSA-N 0.000 description 4
- 208000002193 Pain Diseases 0.000 description 4
- 241000700159 Rattus Species 0.000 description 4
- FOCVUCIESVLUNU-UHFFFAOYSA-N Thiotepa Chemical compound C1CN1P(N1CC1)(=S)N1CC1 FOCVUCIESVLUNU-UHFFFAOYSA-N 0.000 description 4
- 241000251539 Vertebrata <Metazoa> Species 0.000 description 4
- 125000000539 amino acid group Chemical group 0.000 description 4
- 230000009286 beneficial effect Effects 0.000 description 4
- 229960001433 erlotinib Drugs 0.000 description 4
- YLMAHDNUQAMNNX-UHFFFAOYSA-N imatinib methanesulfonate Chemical compound CS(O)(=O)=O.C1CN(C)CCN1CC1=CC=C(C(=O)NC=2C=C(NC=3N=C(C=CN=3)C=3C=NC=CC=3)C(C)=CC=2)C=C1 YLMAHDNUQAMNNX-UHFFFAOYSA-N 0.000 description 4
- 230000000977 initiatory effect Effects 0.000 description 4
- HPJKCIUCZWXJDR-UHFFFAOYSA-N letrozole Chemical compound C1=CC(C#N)=CC=C1C(N1N=CN=C1)C1=CC=C(C#N)C=C1 HPJKCIUCZWXJDR-UHFFFAOYSA-N 0.000 description 4
- GLVAUDGFNGKCSF-UHFFFAOYSA-N mercaptopurine Chemical compound S=C1NC=NC2=C1NC=N2 GLVAUDGFNGKCSF-UHFFFAOYSA-N 0.000 description 4
- 230000004048 modification Effects 0.000 description 4
- 229940021182 non-steroidal anti-inflammatory drug Drugs 0.000 description 4
- 229940127073 nucleoside analogue Drugs 0.000 description 4
- 238000011275 oncology therapy Methods 0.000 description 4
- 230000036407 pain Effects 0.000 description 4
- 229940068196 placebo Drugs 0.000 description 4
- 239000000902 placebo Substances 0.000 description 4
- ZAHRKKWIAAJSAO-UHFFFAOYSA-N rapamycin Natural products COCC(O)C(=C/C(C)C(=O)CC(OC(=O)C1CCCCN1C(=O)C(=O)C2(O)OC(CC(OC)C(=CC=CC=CC(C)CC(C)C(=O)C)C)CCC2C)C(C)CC3CCC(O)C(C3)OC)C ZAHRKKWIAAJSAO-UHFFFAOYSA-N 0.000 description 4
- 150000003839 salts Chemical class 0.000 description 4
- 230000019491 signal transduction Effects 0.000 description 4
- 229960002930 sirolimus Drugs 0.000 description 4
- 238000005549 size reduction Methods 0.000 description 4
- 239000005483 tyrosine kinase inhibitor Substances 0.000 description 4
- 229960005486 vaccine Drugs 0.000 description 4
- 229960004276 zoledronic acid Drugs 0.000 description 4
- INAUWOVKEZHHDM-PEDBPRJASA-N (7s,9s)-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-7-[(2r,4s,5s,6s)-5-hydroxy-6-methyl-4-morpholin-4-yloxan-2-yl]oxy-4-methoxy-8,10-dihydro-7h-tetracene-5,12-dione;hydrochloride Chemical compound Cl.N1([C@H]2C[C@@H](O[C@@H](C)[C@H]2O)O[C@H]2C[C@@](O)(CC=3C(O)=C4C(=O)C=5C=CC=C(C=5C(=O)C4=C(O)C=32)OC)C(=O)CO)CCOCC1 INAUWOVKEZHHDM-PEDBPRJASA-N 0.000 description 3
- PTOAARAWEBMLNO-KVQBGUIXSA-N Cladribine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@H]1C[C@H](O)[C@@H](CO)O1 PTOAARAWEBMLNO-KVQBGUIXSA-N 0.000 description 3
- 108010047041 Complementarity Determining Regions Proteins 0.000 description 3
- PMATZTZNYRCHOR-CGLBZJNRSA-N Cyclosporin A Chemical compound CC[C@@H]1NC(=O)[C@H]([C@H](O)[C@H](C)C\C=C\C)N(C)C(=O)[C@H](C(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@@H](C)NC(=O)[C@H](C)NC(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](C(C)C)NC(=O)[C@H](CC(C)C)N(C)C(=O)CN(C)C1=O PMATZTZNYRCHOR-CGLBZJNRSA-N 0.000 description 3
- 108010036949 Cyclosporine Proteins 0.000 description 3
- 238000002965 ELISA Methods 0.000 description 3
- 102100034671 L-lactate dehydrogenase A chain Human genes 0.000 description 3
- 108010088350 Lactate Dehydrogenase 5 Proteins 0.000 description 3
- 102000018697 Membrane Proteins Human genes 0.000 description 3
- 108010052285 Membrane Proteins Proteins 0.000 description 3
- 241000699670 Mus sp. Species 0.000 description 3
- 102000015636 Oligopeptides Human genes 0.000 description 3
- 108010038807 Oligopeptides Proteins 0.000 description 3
- 102100029740 Poliovirus receptor Human genes 0.000 description 3
- 241000288906 Primates Species 0.000 description 3
- 206010060862 Prostate cancer Diseases 0.000 description 3
- 208000000236 Prostatic Neoplasms Diseases 0.000 description 3
- IIDJRNMFWXDHID-UHFFFAOYSA-N Risedronic acid Chemical compound OP(=O)(O)C(P(O)(O)=O)(O)CC1=CC=CN=C1 IIDJRNMFWXDHID-UHFFFAOYSA-N 0.000 description 3
- 241000283984 Rodentia Species 0.000 description 3
- 101710090983 T-cell immunoreceptor with Ig and ITIM domains Proteins 0.000 description 3
- NAVMQTYZDKMPEU-UHFFFAOYSA-N Targretin Chemical compound CC1=CC(C(CCC2(C)C)(C)C)=C2C=C1C(=C)C1=CC=C(C(O)=O)C=C1 NAVMQTYZDKMPEU-UHFFFAOYSA-N 0.000 description 3
- 102000007537 Type II DNA Topoisomerases Human genes 0.000 description 3
- 108010046308 Type II DNA Topoisomerases Proteins 0.000 description 3
- IEDXPSOJFSVCKU-HOKPPMCLSA-N [4-[[(2S)-5-(carbamoylamino)-2-[[(2S)-2-[6-(2,5-dioxopyrrolidin-1-yl)hexanoylamino]-3-methylbutanoyl]amino]pentanoyl]amino]phenyl]methyl N-[(2S)-1-[[(2S)-1-[[(3R,4S,5S)-1-[(2S)-2-[(1R,2R)-3-[[(1S,2R)-1-hydroxy-1-phenylpropan-2-yl]amino]-1-methoxy-2-methyl-3-oxopropyl]pyrrolidin-1-yl]-3-methoxy-5-methyl-1-oxoheptan-4-yl]-methylamino]-3-methyl-1-oxobutan-2-yl]amino]-3-methyl-1-oxobutan-2-yl]-N-methylcarbamate Chemical compound CC[C@H](C)[C@@H]([C@@H](CC(=O)N1CCC[C@H]1[C@H](OC)[C@@H](C)C(=O)N[C@H](C)[C@@H](O)c1ccccc1)OC)N(C)C(=O)[C@@H](NC(=O)[C@H](C(C)C)N(C)C(=O)OCc1ccc(NC(=O)[C@H](CCCNC(N)=O)NC(=O)[C@@H](NC(=O)CCCCCN2C(=O)CCC2=O)C(C)C)cc1)C(C)C IEDXPSOJFSVCKU-HOKPPMCLSA-N 0.000 description 3
- 230000002159 abnormal effect Effects 0.000 description 3
- 229940028652 abraxane Drugs 0.000 description 3
- USZYSDMBJDPRIF-SVEJIMAYSA-N aclacinomycin A Chemical compound O([C@H]1[C@@H](O)C[C@@H](O[C@H]1C)O[C@H]1[C@H](C[C@@H](O[C@H]1C)O[C@H]1C[C@]([C@@H](C2=CC=3C(=O)C4=CC=CC(O)=C4C(=O)C=3C(O)=C21)C(=O)OC)(O)CC)N(C)C)[C@H]1CCC(=O)[C@H](C)O1 USZYSDMBJDPRIF-SVEJIMAYSA-N 0.000 description 3
- 229960004176 aclarubicin Drugs 0.000 description 3
- SHGAZHPCJJPHSC-YCNIQYBTSA-N all-trans-retinoic acid Chemical compound OC(=O)\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C SHGAZHPCJJPHSC-YCNIQYBTSA-N 0.000 description 3
- 239000003242 anti bacterial agent Substances 0.000 description 3
- 229940088710 antibiotic agent Drugs 0.000 description 3
- 238000013459 approach Methods 0.000 description 3
- 239000012472 biological sample Substances 0.000 description 3
- GXJABQQUPOEUTA-RDJZCZTQSA-N bortezomib Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)B(O)O)NC(=O)C=1N=CC=NC=1)C1=CC=CC=C1 GXJABQQUPOEUTA-RDJZCZTQSA-N 0.000 description 3
- 230000003915 cell function Effects 0.000 description 3
- 230000022534 cell killing Effects 0.000 description 3
- 230000004663 cell proliferation Effects 0.000 description 3
- VERWOWGGCGHDQE-UHFFFAOYSA-N ceritinib Chemical compound CC=1C=C(NC=2N=C(NC=3C(=CC=CC=3)S(=O)(=O)C(C)C)C(Cl)=CN=2)C(OC(C)C)=CC=1C1CCNCC1 VERWOWGGCGHDQE-UHFFFAOYSA-N 0.000 description 3
- 229960002436 cladribine Drugs 0.000 description 3
- ACSIXWWBWUQEHA-UHFFFAOYSA-N clodronic acid Chemical compound OP(O)(=O)C(Cl)(Cl)P(O)(O)=O ACSIXWWBWUQEHA-UHFFFAOYSA-N 0.000 description 3
- 230000016396 cytokine production Effects 0.000 description 3
- 230000002354 daily effect Effects 0.000 description 3
- CYQFCXCEBYINGO-IAGOWNOFSA-N delta1-THC Chemical compound C1=C(C)CC[C@H]2C(C)(C)OC3=CC(CCCCC)=CC(O)=C3[C@@H]21 CYQFCXCEBYINGO-IAGOWNOFSA-N 0.000 description 3
- 238000003745 diagnosis Methods 0.000 description 3
- 238000010494 dissociation reaction Methods 0.000 description 3
- 230000005593 dissociations Effects 0.000 description 3
- 210000003236 esophagogastric junction Anatomy 0.000 description 3
- 238000010195 expression analysis Methods 0.000 description 3
- 108020001507 fusion proteins Proteins 0.000 description 3
- 102000037865 fusion proteins Human genes 0.000 description 3
- 229960002584 gefitinib Drugs 0.000 description 3
- 229940088597 hormone Drugs 0.000 description 3
- 239000005556 hormone Substances 0.000 description 3
- 102000049823 human TIGIT Human genes 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- 229960004891 lapatinib Drugs 0.000 description 3
- 230000003211 malignant effect Effects 0.000 description 3
- 229960001428 mercaptopurine Drugs 0.000 description 3
- 208000037819 metastatic cancer Diseases 0.000 description 3
- 208000011575 metastatic malignant neoplasm Diseases 0.000 description 3
- 210000000056 organ Anatomy 0.000 description 3
- DWAFYCQODLXJNR-BNTLRKBRSA-L oxaliplatin Chemical compound O1C(=O)C(=O)O[Pt]11N[C@@H]2CCCC[C@H]2N1 DWAFYCQODLXJNR-BNTLRKBRSA-L 0.000 description 3
- 229960001756 oxaliplatin Drugs 0.000 description 3
- WRUUGTRCQOWXEG-UHFFFAOYSA-N pamidronate Chemical compound NCCC(O)(P(O)(O)=O)P(O)(O)=O WRUUGTRCQOWXEG-UHFFFAOYSA-N 0.000 description 3
- 230000007170 pathology Effects 0.000 description 3
- WVUNYSQLFKLYNI-AATRIKPKSA-N pelitinib Chemical compound C=12C=C(NC(=O)\C=C\CN(C)C)C(OCC)=CC2=NC=C(C#N)C=1NC1=CC=C(F)C(Cl)=C1 WVUNYSQLFKLYNI-AATRIKPKSA-N 0.000 description 3
- 108010048507 poliovirus receptor Proteins 0.000 description 3
- 230000008569 process Effects 0.000 description 3
- 230000002035 prolonged effect Effects 0.000 description 3
- 230000009257 reactivity Effects 0.000 description 3
- 241000894007 species Species 0.000 description 3
- RCINICONZNJXQF-XAZOAEDWSA-N taxol® Chemical compound O([C@@H]1[C@@]2(CC(C(C)=C(C2(C)C)[C@H](C([C@]2(C)[C@@H](O)C[C@H]3OC[C@]3(C21)OC(C)=O)=O)OC(=O)C)OC(=O)[C@H](O)[C@@H](NC(=O)C=1C=CC=CC=1)C=1C=CC=CC=1)O)C(=O)C1=CC=CC=C1 RCINICONZNJXQF-XAZOAEDWSA-N 0.000 description 3
- 229940063683 taxotere Drugs 0.000 description 3
- 229960003989 tocilizumab Drugs 0.000 description 3
- 239000003053 toxin Substances 0.000 description 3
- 231100000765 toxin Toxicity 0.000 description 3
- 108700012359 toxins Proteins 0.000 description 3
- 238000011277 treatment modality Methods 0.000 description 3
- 229960000653 valrubicin Drugs 0.000 description 3
- ZOCKGBMQLCSHFP-KQRAQHLDSA-N valrubicin Chemical compound O([C@H]1C[C@](CC2=C(O)C=3C(=O)C4=CC=CC(OC)=C4C(=O)C=3C(O)=C21)(O)C(=O)COC(=O)CCCC)[C@H]1C[C@H](NC(=O)C(F)(F)F)[C@H](O)[C@H](C)O1 ZOCKGBMQLCSHFP-KQRAQHLDSA-N 0.000 description 3
- 229950000578 vatalanib Drugs 0.000 description 3
- YCOYDOIWSSHVCK-UHFFFAOYSA-N vatalanib Chemical compound C1=CC(Cl)=CC=C1NC(C1=CC=CC=C11)=NN=C1CC1=CC=NC=C1 YCOYDOIWSSHVCK-UHFFFAOYSA-N 0.000 description 3
- QARLNMDDSQMINK-BVRKHOPBSA-N (3R)-1-[[7-cyano-2-[3-[3-[[3-[[(3R)-3-hydroxypyrrolidin-1-yl]methyl]-1,7-naphthyridin-8-yl]amino]-2-methylphenyl]-2-methylphenyl]-1,3-benzoxazol-5-yl]methyl]pyrrolidine-3-carboxylic acid Chemical compound C(#N)C1=CC(=CC=2N=C(OC=21)C=1C(=C(C=CC=1)C1=C(C(=CC=C1)NC=1N=CC=C2C=C(C=NC=12)CN1C[C@@H](CC1)O)C)C)CN1C[C@@H](CC1)C(=O)O QARLNMDDSQMINK-BVRKHOPBSA-N 0.000 description 2
- NOPNWHSMQOXAEI-PUCKCBAPSA-N (7s,9s)-7-[(2r,4s,5s,6s)-4-(2,3-dihydropyrrol-1-yl)-5-hydroxy-6-methyloxan-2-yl]oxy-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-4-methoxy-8,10-dihydro-7h-tetracene-5,12-dione Chemical compound N1([C@H]2C[C@@H](O[C@@H](C)[C@H]2O)O[C@H]2C[C@@](O)(CC=3C(O)=C4C(=O)C=5C=CC=C(C=5C(=O)C4=C(O)C=32)OC)C(=O)CO)CCC=C1 NOPNWHSMQOXAEI-PUCKCBAPSA-N 0.000 description 2
- 108091032973 (ribonucleotides)n+m Proteins 0.000 description 2
- YIMDLWDNDGKDTJ-QLKYHASDSA-N 3'-deamino-3'-(3-cyanomorpholin-4-yl)doxorubicin Chemical compound N1([C@H]2C[C@@H](O[C@@H](C)[C@H]2O)O[C@H]2C[C@@](O)(CC=3C(O)=C4C(=O)C=5C=CC=C(C=5C(=O)C4=C(O)C=32)OC)C(=O)CO)CCOCC1C#N YIMDLWDNDGKDTJ-QLKYHASDSA-N 0.000 description 2
- QGJZLNKBHJESQX-UHFFFAOYSA-N 3-Epi-Betulin-Saeure Natural products C1CC(O)C(C)(C)C2CCC3(C)C4(C)CCC5(C(O)=O)CCC(C(=C)C)C5C4CCC3C21C QGJZLNKBHJESQX-UHFFFAOYSA-N 0.000 description 2
- CLOUCVRNYSHRCF-UHFFFAOYSA-N 3beta-Hydroxy-20(29)-Lupen-3,27-oic acid Natural products C1CC(O)C(C)(C)C2CCC3(C)C4(C(O)=O)CCC5(C)CCC(C(=C)C)C5C4CCC3C21C CLOUCVRNYSHRCF-UHFFFAOYSA-N 0.000 description 2
- AOJJSUZBOXZQNB-VTZDEGQISA-N 4'-epidoxorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@@H](O)[C@H](C)O1 AOJJSUZBOXZQNB-VTZDEGQISA-N 0.000 description 2
- AKJHMTWEGVYYSE-AIRMAKDCSA-N 4-HPR Chemical compound C=1C=C(O)C=CC=1NC(=O)/C=C(\C)/C=C/C=C(C)C=CC1=C(C)CCCC1(C)C AKJHMTWEGVYYSE-AIRMAKDCSA-N 0.000 description 2
- YWLXLRUDGLRYDR-ZHPRIASZSA-N 5beta,20-epoxy-1,7beta,10beta,13alpha-tetrahydroxy-9-oxotax-11-ene-2alpha,4alpha-diyl 4-acetate 2-benzoate Chemical compound O([C@H]1[C@H]2[C@@](C([C@H](O)C3=C(C)[C@@H](O)C[C@]1(O)C3(C)C)=O)(C)[C@@H](O)C[C@H]1OC[C@]12OC(=O)C)C(=O)C1=CC=CC=C1 YWLXLRUDGLRYDR-ZHPRIASZSA-N 0.000 description 2
- VVIAGPKUTFNRDU-UHFFFAOYSA-N 6S-folinic acid Natural products C1NC=2NC(N)=NC(=O)C=2N(C=O)C1CNC1=CC=C(C(=O)NC(CCC(O)=O)C(O)=O)C=C1 VVIAGPKUTFNRDU-UHFFFAOYSA-N 0.000 description 2
- 229940125559 AB154 Drugs 0.000 description 2
- 229940125554 ASP-8374 Drugs 0.000 description 2
- QTBSBXVTEAMEQO-UHFFFAOYSA-M Acetate Chemical compound CC([O-])=O QTBSBXVTEAMEQO-UHFFFAOYSA-M 0.000 description 2
- OGSPWJRAVKPPFI-UHFFFAOYSA-N Alendronic Acid Chemical compound NCCCC(O)(P(O)(O)=O)P(O)(O)=O OGSPWJRAVKPPFI-UHFFFAOYSA-N 0.000 description 2
- 244000003377 Allium tuberosum Species 0.000 description 2
- 235000005338 Allium tuberosum Nutrition 0.000 description 2
- 108020000948 Antisense Oligonucleotides Proteins 0.000 description 2
- BFYIZQONLCFLEV-DAELLWKTSA-N Aromasine Chemical compound O=C1C=C[C@]2(C)[C@H]3CC[C@](C)(C(CC4)=O)[C@@H]4[C@@H]3CC(=C)C2=C1 BFYIZQONLCFLEV-DAELLWKTSA-N 0.000 description 2
- IJGRMHOSHXDMSA-UHFFFAOYSA-N Atomic nitrogen Chemical compound N#N IJGRMHOSHXDMSA-UHFFFAOYSA-N 0.000 description 2
- MLDQJTXFUGDVEO-UHFFFAOYSA-N BAY-43-9006 Chemical compound C1=NC(C(=O)NC)=CC(OC=2C=CC(NC(=O)NC=3C=C(C(Cl)=CC=3)C(F)(F)F)=CC=2)=C1 MLDQJTXFUGDVEO-UHFFFAOYSA-N 0.000 description 2
- 229940125557 BMS-986207 Drugs 0.000 description 2
- DIZWSDNSTNAYHK-XGWVBXMLSA-N Betulinic acid Natural products CC(=C)[C@@H]1C[C@H]([C@H]2CC[C@]3(C)[C@H](CC[C@@H]4[C@@]5(C)CC[C@H](O)C(C)(C)[C@@H]5CC[C@@]34C)[C@@H]12)C(=O)O DIZWSDNSTNAYHK-XGWVBXMLSA-N 0.000 description 2
- 229940122361 Bisphosphonate Drugs 0.000 description 2
- 206010058019 Cancer Pain Diseases 0.000 description 2
- 201000009030 Carcinoma Diseases 0.000 description 2
- 208000005443 Circulating Neoplastic Cells Diseases 0.000 description 2
- UHDGCWIWMRVCDJ-CCXZUQQUSA-N Cytarabine Chemical compound O=C1N=C(N)C=CN1[C@H]1[C@@H](O)[C@H](O)[C@@H](CO)O1 UHDGCWIWMRVCDJ-CCXZUQQUSA-N 0.000 description 2
- 108010092160 Dactinomycin Proteins 0.000 description 2
- 208000000059 Dyspnea Diseases 0.000 description 2
- 206010013975 Dyspnoeas Diseases 0.000 description 2
- 102000004190 Enzymes Human genes 0.000 description 2
- 108090000790 Enzymes Proteins 0.000 description 2
- HTIJFSOGRVMCQR-UHFFFAOYSA-N Epirubicin Natural products COc1cccc2C(=O)c3c(O)c4CC(O)(CC(OC5CC(N)C(=O)C(C)O5)c4c(O)c3C(=O)c12)C(=O)CO HTIJFSOGRVMCQR-UHFFFAOYSA-N 0.000 description 2
- 108700039887 Essential Genes Proteins 0.000 description 2
- 108010008165 Etanercept Proteins 0.000 description 2
- VWUXBMIQPBEWFH-WCCTWKNTSA-N Fulvestrant Chemical compound OC1=CC=C2[C@H]3CC[C@](C)([C@H](CC4)O)[C@@H]4[C@@H]3[C@H](CCCCCCCCCS(=O)CCCC(F)(F)C(F)(F)F)CC2=C1 VWUXBMIQPBEWFH-WCCTWKNTSA-N 0.000 description 2
- 229940126656 GS-4224 Drugs 0.000 description 2
- 101001023712 Homo sapiens Nectin-3 Proteins 0.000 description 2
- 101100407307 Homo sapiens PDCD1LG2 gene Proteins 0.000 description 2
- 229940126063 INCB086550 Drugs 0.000 description 2
- XDXDZDZNSLXDNA-TZNDIEGXSA-N Idarubicin Chemical compound C1[C@H](N)[C@H](O)[C@H](C)O[C@H]1O[C@@H]1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2C[C@@](O)(C(C)=O)C1 XDXDZDZNSLXDNA-TZNDIEGXSA-N 0.000 description 2
- XDXDZDZNSLXDNA-UHFFFAOYSA-N Idarubicin Natural products C1C(N)C(O)C(C)OC1OC1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2CC(O)(C(C)=O)C1 XDXDZDZNSLXDNA-UHFFFAOYSA-N 0.000 description 2
- 108010047761 Interferon-alpha Proteins 0.000 description 2
- 102000006992 Interferon-alpha Human genes 0.000 description 2
- 108010050904 Interferons Proteins 0.000 description 2
- 102000014150 Interferons Human genes 0.000 description 2
- 102000000589 Interleukin-1 Human genes 0.000 description 2
- 108010002352 Interleukin-1 Proteins 0.000 description 2
- 102000003816 Interleukin-13 Human genes 0.000 description 2
- 108090000176 Interleukin-13 Proteins 0.000 description 2
- 102000004889 Interleukin-6 Human genes 0.000 description 2
- 108090001005 Interleukin-6 Proteins 0.000 description 2
- 241000764238 Isis Species 0.000 description 2
- 239000005517 L01XE01 - Imatinib Substances 0.000 description 2
- 239000005411 L01XE02 - Gefitinib Substances 0.000 description 2
- 239000005511 L01XE05 - Sorafenib Substances 0.000 description 2
- 239000002146 L01XE16 - Crizotinib Substances 0.000 description 2
- JLERVPBPJHKRBJ-UHFFFAOYSA-N LY 117018 Chemical compound C1=CC(O)=CC=C1C1=C(C(=O)C=2C=CC(OCCN3CCCC3)=CC=2)C2=CC=C(O)C=C2S1 JLERVPBPJHKRBJ-UHFFFAOYSA-N 0.000 description 2
- BTYYWOYVBXILOJ-UHFFFAOYSA-N N-{4-[(3-bromophenyl)amino]quinazolin-6-yl}but-2-ynamide Chemical compound C12=CC(NC(=O)C#CC)=CC=C2N=CN=C1NC1=CC=CC(Br)=C1 BTYYWOYVBXILOJ-UHFFFAOYSA-N 0.000 description 2
- FTFRZXFNZVCRSK-UHFFFAOYSA-N N4-(3-chloro-4-fluorophenyl)-N6-(1-methyl-4-piperidinyl)pyrimido[5,4-d]pyrimidine-4,6-diamine Chemical compound C1CN(C)CCC1NC1=NC=C(N=CN=C2NC=3C=C(Cl)C(F)=CC=3)C2=N1 FTFRZXFNZVCRSK-UHFFFAOYSA-N 0.000 description 2
- 101150065403 NECTIN2 gene Proteins 0.000 description 2
- 108091007491 NSP3 Papain-like protease domains Proteins 0.000 description 2
- 102100035488 Nectin-2 Human genes 0.000 description 2
- 102100035487 Nectin-3 Human genes 0.000 description 2
- REFJWTPEDVJJIY-UHFFFAOYSA-N Quercetin Chemical compound C=1C(O)=CC(O)=C(C(C=2O)=O)C=1OC=2C1=CC=C(O)C(O)=C1 REFJWTPEDVJJIY-UHFFFAOYSA-N 0.000 description 2
- 101710141955 RAF proto-oncogene serine/threonine-protein kinase Proteins 0.000 description 2
- 230000006044 T cell activation Effects 0.000 description 2
- CYQFCXCEBYINGO-UHFFFAOYSA-N THC Natural products C1=C(C)CCC2C(C)(C)OC3=CC(CCCCC)=CC(O)=C3C21 CYQFCXCEBYINGO-UHFFFAOYSA-N 0.000 description 2
- NKANXQFJJICGDU-QPLCGJKRSA-N Tamoxifen Chemical compound C=1C=CC=CC=1C(/CC)=C(C=1C=CC(OCCN(C)C)=CC=1)/C1=CC=CC=C1 NKANXQFJJICGDU-QPLCGJKRSA-N 0.000 description 2
- DKJJVAGXPKPDRL-UHFFFAOYSA-N Tiludronic acid Chemical compound OP(O)(=O)C(P(O)(O)=O)SC1=CC=C(Cl)C=C1 DKJJVAGXPKPDRL-UHFFFAOYSA-N 0.000 description 2
- 208000006593 Urologic Neoplasms Diseases 0.000 description 2
- JXLYSJRDGCGARV-WWYNWVTFSA-N Vinblastine Natural products O=C(O[C@H]1[C@](O)(C(=O)OC)[C@@H]2N(C)c3c(cc(c(OC)c3)[C@]3(C(=O)OC)c4[nH]c5c(c4CCN4C[C@](O)(CC)C[C@H](C3)C4)cccc5)[C@@]32[C@H]2[C@@]1(CC)C=CCN2CC3)C JXLYSJRDGCGARV-WWYNWVTFSA-N 0.000 description 2
- IBXPAFBDJCXCDW-MHFPCNPESA-A [Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].Cc1cn([C@H]2C[C@H](O)[C@@H](COP([S-])(=O)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3CO)n3cc(C)c(=O)[nH]c3=O)n3ccc(N)nc3=O)n3cc(C)c(=O)[nH]c3=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3cnc4c3nc(N)[nH]c4=O)n3cc(C)c(=O)[nH]c3=O)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)O2)c(=O)[nH]c1=O Chemical compound [Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].Cc1cn([C@H]2C[C@H](O)[C@@H](COP([S-])(=O)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3COP([O-])(=S)O[C@H]3C[C@@H](O[C@@H]3CO)n3cc(C)c(=O)[nH]c3=O)n3ccc(N)nc3=O)n3cc(C)c(=O)[nH]c3=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3cnc4c3nc(N)[nH]c4=O)n3cc(C)c(=O)[nH]c3=O)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3cnc4c3nc(N)[nH]c4=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)O2)c(=O)[nH]c1=O IBXPAFBDJCXCDW-MHFPCNPESA-A 0.000 description 2
- 150000007513 acids Chemical class 0.000 description 2
- 229930188522 aclacinomycin Natural products 0.000 description 2
- RJURFGZVJUQBHK-UHFFFAOYSA-N actinomycin D Natural products CC1OC(=O)C(C(C)C)N(C)C(=O)CN(C)C(=O)C2CCCN2C(=O)C(C(C)C)NC(=O)C1NC(=O)C1=C(N)C(=O)C(C)=C2OC(C(C)=CC=C3C(=O)NC4C(=O)NC(C(N5CCCC5C(=O)N(C)CC(=O)N(C)C(C(C)C)C(=O)OC4C)=O)C(C)C)=C3N=C21 RJURFGZVJUQBHK-UHFFFAOYSA-N 0.000 description 2
- 230000001154 acute effect Effects 0.000 description 2
- 229940009456 adriamycin Drugs 0.000 description 2
- 230000002411 adverse Effects 0.000 description 2
- 108700025316 aldesleukin Proteins 0.000 description 2
- 229960001611 alectinib Drugs 0.000 description 2
- YBBLVLTVTVSKRW-UHFFFAOYSA-N anastrozole Chemical compound N#CC(C)(C)C1=CC(C(C)(C#N)C)=CC(CN2N=CN=C2)=C1 YBBLVLTVTVSKRW-UHFFFAOYSA-N 0.000 description 2
- 210000004102 animal cell Anatomy 0.000 description 2
- 229940045799 anthracyclines and related substance Drugs 0.000 description 2
- 230000002280 anti-androgenic effect Effects 0.000 description 2
- 230000003110 anti-inflammatory effect Effects 0.000 description 2
- 230000000692 anti-sense effect Effects 0.000 description 2
- 239000000051 antiandrogen Substances 0.000 description 2
- 229940030495 antiandrogen sex hormone and modulator of the genital system Drugs 0.000 description 2
- 239000000074 antisense oligonucleotide Substances 0.000 description 2
- 238000012230 antisense oligonucleotides Methods 0.000 description 2
- QZPQTZZNNJUOLS-UHFFFAOYSA-N beta-lapachone Chemical compound C12=CC=CC=C2C(=O)C(=O)C2=C1OC(C)(C)CC2 QZPQTZZNNJUOLS-UHFFFAOYSA-N 0.000 description 2
- QGJZLNKBHJESQX-FZFNOLFKSA-N betulinic acid Chemical compound C1C[C@H](O)C(C)(C)[C@@H]2CC[C@@]3(C)[C@]4(C)CC[C@@]5(C(O)=O)CC[C@@H](C(=C)C)[C@@H]5[C@H]4CC[C@@H]3[C@]21C QGJZLNKBHJESQX-FZFNOLFKSA-N 0.000 description 2
- 229960002938 bexarotene Drugs 0.000 description 2
- 150000004663 bisphosphonates Chemical class 0.000 description 2
- 229960001467 bortezomib Drugs 0.000 description 2
- BMQGVNUXMIRLCK-OAGWZNDDSA-N cabazitaxel Chemical compound O([C@H]1[C@@H]2[C@]3(OC(C)=O)CO[C@@H]3C[C@@H]([C@]2(C(=O)[C@H](OC)C2=C(C)[C@@H](OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=3C=CC=CC=3)C[C@]1(O)C2(C)C)C)OC)C(=O)C1=CC=CC=C1 BMQGVNUXMIRLCK-OAGWZNDDSA-N 0.000 description 2
- 229960001573 cabazitaxel Drugs 0.000 description 2
- OMZCMEYTWSXEPZ-UHFFFAOYSA-N canertinib Chemical compound C1=C(Cl)C(F)=CC=C1NC1=NC=NC2=CC(OCCCN3CCOCC3)=C(NC(=O)C=C)C=C12 OMZCMEYTWSXEPZ-UHFFFAOYSA-N 0.000 description 2
- 229960000590 celecoxib Drugs 0.000 description 2
- RZEKVGVHFLEQIL-UHFFFAOYSA-N celecoxib Chemical compound C1=CC(C)=CC=C1C1=CC(C(F)(F)F)=NN1C1=CC=C(S(N)(=O)=O)C=C1 RZEKVGVHFLEQIL-UHFFFAOYSA-N 0.000 description 2
- 238000004113 cell culture Methods 0.000 description 2
- 210000003169 central nervous system Anatomy 0.000 description 2
- 229960001602 ceritinib Drugs 0.000 description 2
- 229960004630 chlorambucil Drugs 0.000 description 2
- JCKYGMPEJWAADB-UHFFFAOYSA-N chlorambucil Chemical compound OC(=O)CCCC1=CC=C(N(CCCl)CCCl)C=C1 JCKYGMPEJWAADB-UHFFFAOYSA-N 0.000 description 2
- 229960001265 ciclosporin Drugs 0.000 description 2
- 229960002286 clodronic acid Drugs 0.000 description 2
- 229960001338 colchicine Drugs 0.000 description 2
- 238000002591 computed tomography Methods 0.000 description 2
- 229940111134 coxibs Drugs 0.000 description 2
- KTEIFNKAUNYNJU-GFCCVEGCSA-N crizotinib Chemical compound O([C@H](C)C=1C(=C(F)C=CC=1Cl)Cl)C(C(=NC=1)N)=CC=1C(=C1)C=NN1C1CCNCC1 KTEIFNKAUNYNJU-GFCCVEGCSA-N 0.000 description 2
- 239000003255 cyclooxygenase 2 inhibitor Substances 0.000 description 2
- 229930182912 cyclosporin Natural products 0.000 description 2
- 229960000684 cytarabine Drugs 0.000 description 2
- 238000012303 cytoplasmic staining Methods 0.000 description 2
- OPTASPLRGRRNAP-UHFFFAOYSA-N cytosine Chemical compound NC=1C=CNC(=O)N=1 OPTASPLRGRRNAP-UHFFFAOYSA-N 0.000 description 2
- 230000007423 decrease Effects 0.000 description 2
- 210000004443 dendritic cell Anatomy 0.000 description 2
- 230000001627 detrimental effect Effects 0.000 description 2
- 238000011161 development Methods 0.000 description 2
- 230000018109 developmental process Effects 0.000 description 2
- 229960003957 dexamethasone Drugs 0.000 description 2
- UREBDLICKHMUKA-CXSFZGCWSA-N dexamethasone Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)CO)(O)[C@@]1(C)C[C@@H]2O UREBDLICKHMUKA-CXSFZGCWSA-N 0.000 description 2
- PZXJOHSZQAEJFE-UHFFFAOYSA-N dihydrobetulinic acid Natural products C1CC(O)C(C)(C)C2CCC3(C)C4(C)CCC5(C(O)=O)CCC(C(C)C)C5C4CCC3C21C PZXJOHSZQAEJFE-UHFFFAOYSA-N 0.000 description 2
- AUZONCFQVSMFAP-UHFFFAOYSA-N disulfiram Chemical compound CCN(CC)C(=S)SSC(=S)N(CC)CC AUZONCFQVSMFAP-UHFFFAOYSA-N 0.000 description 2
- 230000009977 dual effect Effects 0.000 description 2
- 230000004064 dysfunction Effects 0.000 description 2
- 229940121647 egfr inhibitor Drugs 0.000 description 2
- 230000008030 elimination Effects 0.000 description 2
- 238000003379 elimination reaction Methods 0.000 description 2
- 230000002708 enhancing effect Effects 0.000 description 2
- 229940088598 enzyme Drugs 0.000 description 2
- 229960001904 epirubicin Drugs 0.000 description 2
- 102000015694 estrogen receptors Human genes 0.000 description 2
- 108010038795 estrogen receptors Proteins 0.000 description 2
- 229960004945 etoricoxib Drugs 0.000 description 2
- MNJVRJDLRVPLFE-UHFFFAOYSA-N etoricoxib Chemical compound C1=NC(C)=CC=C1C1=NC=C(Cl)C=C1C1=CC=C(S(C)(=O)=O)C=C1 MNJVRJDLRVPLFE-UHFFFAOYSA-N 0.000 description 2
- 229940087476 femara Drugs 0.000 description 2
- 238000001943 fluorescence-activated cell sorting Methods 0.000 description 2
- OVBPIULPVIDEAO-LBPRGKRZSA-N folic acid Chemical compound C=1N=C2NC(N)=NC(=O)C2=NC=1CNC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 OVBPIULPVIDEAO-LBPRGKRZSA-N 0.000 description 2
- 235000008191 folinic acid Nutrition 0.000 description 2
- 239000011672 folinic acid Substances 0.000 description 2
- VVIAGPKUTFNRDU-ABLWVSNPSA-N folinic acid Chemical compound C1NC=2NC(N)=NC(=O)C=2N(C=O)C1CNC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 VVIAGPKUTFNRDU-ABLWVSNPSA-N 0.000 description 2
- 230000004927 fusion Effects 0.000 description 2
- CHPZKNULDCNCBW-UHFFFAOYSA-N gallium nitrate Chemical compound [Ga+3].[O-][N+]([O-])=O.[O-][N+]([O-])=O.[O-][N+]([O-])=O CHPZKNULDCNCBW-UHFFFAOYSA-N 0.000 description 2
- 229940080856 gleevec Drugs 0.000 description 2
- 208000005017 glioblastoma Diseases 0.000 description 2
- 230000036541 health Effects 0.000 description 2
- 102000048362 human PDCD1 Human genes 0.000 description 2
- 102000048119 human PDCD1LG2 Human genes 0.000 description 2
- JYGXADMDTFJGBT-VWUMJDOOSA-N hydrocortisone Chemical compound O=C1CC[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 JYGXADMDTFJGBT-VWUMJDOOSA-N 0.000 description 2
- 229960000908 idarubicin Drugs 0.000 description 2
- 229960003685 imatinib mesylate Drugs 0.000 description 2
- 230000028993 immune response Effects 0.000 description 2
- 230000036039 immunity Effects 0.000 description 2
- CGIGDMFJXJATDK-UHFFFAOYSA-N indomethacin Chemical compound CC1=C(CC(O)=O)C2=CC(OC)=CC=C2N1C(=O)C1=CC=C(Cl)C=C1 CGIGDMFJXJATDK-UHFFFAOYSA-N 0.000 description 2
- 229940079322 interferon Drugs 0.000 description 2
- 229940100601 interleukin-6 Drugs 0.000 description 2
- 238000007912 intraperitoneal administration Methods 0.000 description 2
- 230000002601 intratumoral effect Effects 0.000 description 2
- 229940084651 iressa Drugs 0.000 description 2
- UWKQSNNFCGGAFS-XIFFEERXSA-N irinotecan Chemical compound C1=C2C(CC)=C3CN(C(C4=C([C@@](C(=O)OC4)(O)CC)C=4)=O)C=4C3=NC2=CC=C1OC(=O)N(CC1)CCC1N1CCCCC1 UWKQSNNFCGGAFS-XIFFEERXSA-N 0.000 description 2
- 229950005692 larotaxel Drugs 0.000 description 2
- SEFGUGYLLVNFIJ-QDRLFVHASA-N larotaxel dihydrate Chemical compound O.O.O([C@@H]1[C@@]2(C[C@@H](C(C)=C(C2(C)C)[C@H](C([C@@]23[C@H]1[C@@]1(CO[C@@H]1C[C@@H]2C3)OC(C)=O)=O)OC(=O)C)OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=1C=CC=CC=1)O)C(=O)C1=CC=CC=C1 SEFGUGYLLVNFIJ-QDRLFVHASA-N 0.000 description 2
- 229960003881 letrozole Drugs 0.000 description 2
- 229960001691 leucovorin Drugs 0.000 description 2
- 208000032839 leukemia Diseases 0.000 description 2
- 150000002632 lipids Chemical class 0.000 description 2
- 210000000207 lymphocyte subset Anatomy 0.000 description 2
- 231100000682 maximum tolerated dose Toxicity 0.000 description 2
- SGDBTWWWUNNDEQ-LBPRGKRZSA-N melphalan Chemical compound OC(=O)[C@@H](N)CC1=CC=C(N(CCCl)CCCl)C=C1 SGDBTWWWUNNDEQ-LBPRGKRZSA-N 0.000 description 2
- 229960001924 melphalan Drugs 0.000 description 2
- 239000012528 membrane Substances 0.000 description 2
- 229960004857 mitomycin Drugs 0.000 description 2
- 230000035772 mutation Effects 0.000 description 2
- LBWFXVZLPYTWQI-IPOVEDGCSA-N n-[2-(diethylamino)ethyl]-5-[(z)-(5-fluoro-2-oxo-1h-indol-3-ylidene)methyl]-2,4-dimethyl-1h-pyrrole-3-carboxamide;(2s)-2-hydroxybutanedioic acid Chemical compound OC(=O)[C@@H](O)CC(O)=O.CCN(CC)CCNC(=O)C1=C(C)NC(\C=C/2C3=CC(F)=CC=C3NC\2=O)=C1C LBWFXVZLPYTWQI-IPOVEDGCSA-N 0.000 description 2
- 239000002105 nanoparticle Substances 0.000 description 2
- 230000001613 neoplastic effect Effects 0.000 description 2
- MQYXUWHLBZFQQO-UHFFFAOYSA-N nepehinol Natural products C1CC(O)C(C)(C)C2CCC3(C)C4(C)CCC5(C)CCC(C(=C)C)C5C4CCC3C21C MQYXUWHLBZFQQO-UHFFFAOYSA-N 0.000 description 2
- 239000002777 nucleoside Substances 0.000 description 2
- 230000008520 organization Effects 0.000 description 2
- 229940046231 pamidronate Drugs 0.000 description 2
- 230000002093 peripheral effect Effects 0.000 description 2
- 201000002628 peritoneum cancer Diseases 0.000 description 2
- 239000008177 pharmaceutical agent Substances 0.000 description 2
- 238000009521 phase II clinical trial Methods 0.000 description 2
- IUGYQRQAERSCNH-UHFFFAOYSA-M pivalate Chemical compound CC(C)(C)C([O-])=O IUGYQRQAERSCNH-UHFFFAOYSA-M 0.000 description 2
- 229950010765 pivalate Drugs 0.000 description 2
- 230000004481 post-translational protein modification Effects 0.000 description 2
- 208000017805 post-transplant lymphoproliferative disease Diseases 0.000 description 2
- 229960005205 prednisolone Drugs 0.000 description 2
- OIGNJSKKLXVSLS-VWUMJDOOSA-N prednisolone Chemical compound O=C1C=C[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 OIGNJSKKLXVSLS-VWUMJDOOSA-N 0.000 description 2
- 238000012545 processing Methods 0.000 description 2
- 230000002062 proliferating effect Effects 0.000 description 2
- 230000000069 prophylactic effect Effects 0.000 description 2
- RXWNCPJZOCPEPQ-NVWDDTSBSA-N puromycin Chemical compound C1=CC(OC)=CC=C1C[C@H](N)C(=O)N[C@H]1[C@@H](O)[C@H](N2C3=NC=NC(=C3N=C2)N(C)C)O[C@@H]1CO RXWNCPJZOCPEPQ-NVWDDTSBSA-N 0.000 description 2
- 230000002285 radioactive effect Effects 0.000 description 2
- 229960004622 raloxifene Drugs 0.000 description 2
- GZUITABIAKMVPG-UHFFFAOYSA-N raloxifene Chemical compound C1=CC(O)=CC=C1C1=C(C(=O)C=2C=CC(OCCN3CCCCC3)=CC=2)C2=CC=C(O)C=C2S1 GZUITABIAKMVPG-UHFFFAOYSA-N 0.000 description 2
- 229940099538 rapamune Drugs 0.000 description 2
- 230000001105 regulatory effect Effects 0.000 description 2
- 230000004043 responsiveness Effects 0.000 description 2
- 238000012552 review Methods 0.000 description 2
- 231100000279 safety data Toxicity 0.000 description 2
- 238000012216 screening Methods 0.000 description 2
- 229940095743 selective estrogen receptor modulator Drugs 0.000 description 2
- 239000000333 selective estrogen receptor modulator Substances 0.000 description 2
- 210000002966 serum Anatomy 0.000 description 2
- 239000000243 solution Substances 0.000 description 2
- 230000004936 stimulating effect Effects 0.000 description 2
- 210000002536 stromal cell Anatomy 0.000 description 2
- 208000035458 subtype of a disease Diseases 0.000 description 2
- 229960001796 sunitinib Drugs 0.000 description 2
- WINHZLLDWRZWRT-ATVHPVEESA-N sunitinib Chemical compound CCN(CC)CCNC(=O)C1=C(C)NC(\C=C/2C3=CC(F)=CC=C3NC\2=O)=C1C WINHZLLDWRZWRT-ATVHPVEESA-N 0.000 description 2
- 230000002459 sustained effect Effects 0.000 description 2
- 229940034785 sutent Drugs 0.000 description 2
- FQZYTYWMLGAPFJ-OQKDUQJOSA-N tamoxifen citrate Chemical compound [H+].[H+].[H+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O.C=1C=CC=CC=1C(/CC)=C(C=1C=CC(OCCN(C)C)=CC=1)/C1=CC=CC=C1 FQZYTYWMLGAPFJ-OQKDUQJOSA-N 0.000 description 2
- 229940120982 tarceva Drugs 0.000 description 2
- MODVSQKJJIBWPZ-VLLPJHQWSA-N tesetaxel Chemical compound O([C@H]1[C@@H]2[C@]3(OC(C)=O)CO[C@@H]3CC[C@@]2(C)[C@H]2[C@@H](C3=C(C)[C@@H](OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=4C(=CC=CN=4)F)C[C@]1(O)C3(C)C)O[C@H](O2)CN(C)C)C(=O)C1=CC=CC=C1 MODVSQKJJIBWPZ-VLLPJHQWSA-N 0.000 description 2
- 229950009016 tesetaxel Drugs 0.000 description 2
- 238000011285 therapeutic regimen Methods 0.000 description 2
- 229960001196 thiotepa Drugs 0.000 description 2
- 229960003087 tioguanine Drugs 0.000 description 2
- PLHJCIYEEKOWNM-HHHXNRCGSA-N tipifarnib Chemical compound CN1C=NC=C1[C@](N)(C=1C=C2C(C=3C=C(Cl)C=CC=3)=CC(=O)N(C)C2=CC=1)C1=CC=C(Cl)C=C1 PLHJCIYEEKOWNM-HHHXNRCGSA-N 0.000 description 2
- 229960001727 tretinoin Drugs 0.000 description 2
- 230000004614 tumor growth Effects 0.000 description 2
- 230000005851 tumor immunogenicity Effects 0.000 description 2
- 229940094060 tykerb Drugs 0.000 description 2
- GFNNBHLJANVSQV-UHFFFAOYSA-N tyrphostin AG 1478 Chemical compound C=12C=C(OC)C(OC)=CC2=NC=NC=1NC1=CC=CC(Cl)=C1 GFNNBHLJANVSQV-UHFFFAOYSA-N 0.000 description 2
- 229960003048 vinblastine Drugs 0.000 description 2
- JXLYSJRDGCGARV-XQKSVPLYSA-N vincaleukoblastine Chemical compound C([C@@H](C[C@]1(C(=O)OC)C=2C(=CC3=C([C@]45[C@H]([C@@]([C@H](OC(C)=O)[C@]6(CC)C=CCN([C@H]56)CC4)(O)C(=O)OC)N3C)C=2)OC)C[C@@](C2)(O)CC)N2CCC2=C1NC1=CC=CC=C21 JXLYSJRDGCGARV-XQKSVPLYSA-N 0.000 description 2
- 229960004528 vincristine Drugs 0.000 description 2
- OGWKCGZFUXNPDA-XQKSVPLYSA-N vincristine Chemical compound C([N@]1C[C@@H](C[C@]2(C(=O)OC)C=3C(=CC4=C([C@]56[C@H]([C@@]([C@H](OC(C)=O)[C@]7(CC)C=CCN([C@H]67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)C[C@@](C1)(O)CC)CC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-XQKSVPLYSA-N 0.000 description 2
- OGWKCGZFUXNPDA-UHFFFAOYSA-N vincristine Natural products C1C(CC)(O)CC(CC2(C(=O)OC)C=3C(=CC4=C(C56C(C(C(OC(C)=O)C7(CC)C=CCN(C67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)CN1CCC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-UHFFFAOYSA-N 0.000 description 2
- LSHVYAFMTMFKBA-PZJWPPBQSA-N (+)-catechin-3-O-gallate Chemical compound O([C@H]1CC2=C(O)C=C(C=C2O[C@@H]1C=1C=C(O)C(O)=CC=1)O)C(=O)C1=CC(O)=C(O)C(O)=C1 LSHVYAFMTMFKBA-PZJWPPBQSA-N 0.000 description 1
- BMKDZUISNHGIBY-ZETCQYMHSA-N (+)-dexrazoxane Chemical compound C([C@H](C)N1CC(=O)NC(=O)C1)N1CC(=O)NC(=O)C1 BMKDZUISNHGIBY-ZETCQYMHSA-N 0.000 description 1
- DNXHEGUUPJUMQT-UHFFFAOYSA-N (+)-estrone Natural products OC1=CC=C2C3CCC(C)(C(CC4)=O)C4C3CCC2=C1 DNXHEGUUPJUMQT-UHFFFAOYSA-N 0.000 description 1
- WMBWREPUVVBILR-WIYYLYMNSA-N (-)-Epigallocatechin-3-o-gallate Chemical compound O([C@@H]1CC2=C(O)C=C(C=C2O[C@@H]1C=1C=C(O)C(O)=C(O)C=1)O)C(=O)C1=CC(O)=C(O)C(O)=C1 WMBWREPUVVBILR-WIYYLYMNSA-N 0.000 description 1
- ZIUSSTSXXLLKKK-KOBPDPAPSA-N (1e,4z,6e)-5-hydroxy-1,7-bis(4-hydroxy-3-methoxyphenyl)hepta-1,4,6-trien-3-one Chemical compound C1=C(O)C(OC)=CC(\C=C\C(\O)=C\C(=O)\C=C\C=2C=C(OC)C(O)=CC=2)=C1 ZIUSSTSXXLLKKK-KOBPDPAPSA-N 0.000 description 1
- RIWLPSIAFBLILR-WVNGMBSFSA-N (2s)-1-[(2s)-2-[[(2s,3s)-2-[[(2s)-2-[[(2s,3r)-2-[[(2r,3s)-2-[[(2s)-2-[[2-[[2-[acetyl(methyl)amino]acetyl]amino]acetyl]amino]-3-methylbutanoyl]amino]-3-methylpentanoyl]amino]-3-hydroxybutanoyl]amino]pentanoyl]amino]-3-methylpentanoyl]amino]-5-(diaminomethy Chemical compound CC(=O)N(C)CC(=O)NCC(=O)N[C@@H](C(C)C)C(=O)N[C@H]([C@@H](C)CC)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CCC)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H](CCCN=C(N)N)C(=O)N1CCC[C@H]1C(=O)NCC RIWLPSIAFBLILR-WVNGMBSFSA-N 0.000 description 1
- RDJGLLICXDHJDY-NSHDSACASA-N (2s)-2-(3-phenoxyphenyl)propanoic acid Chemical compound OC(=O)[C@@H](C)C1=CC=CC(OC=2C=CC=CC=2)=C1 RDJGLLICXDHJDY-NSHDSACASA-N 0.000 description 1
- YXTKHLHCVFUPPT-YYFJYKOTSA-N (2s)-2-[[4-[(2-amino-5-formyl-4-oxo-1,6,7,8-tetrahydropteridin-6-yl)methylamino]benzoyl]amino]pentanedioic acid;(1r,2r)-1,2-dimethanidylcyclohexane;5-fluoro-1h-pyrimidine-2,4-dione;oxalic acid;platinum(2+) Chemical compound [Pt+2].OC(=O)C(O)=O.[CH2-][C@@H]1CCCC[C@H]1[CH2-].FC1=CNC(=O)NC1=O.C1NC=2NC(N)=NC(=O)C=2N(C=O)C1CNC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 YXTKHLHCVFUPPT-YYFJYKOTSA-N 0.000 description 1
- FLWWDYNPWOSLEO-HQVZTVAUSA-N (2s)-2-[[4-[1-(2-amino-4-oxo-1h-pteridin-6-yl)ethyl-methylamino]benzoyl]amino]pentanedioic acid Chemical compound C=1N=C2NC(N)=NC(=O)C2=NC=1C(C)N(C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 FLWWDYNPWOSLEO-HQVZTVAUSA-N 0.000 description 1
- OQANPHBRHBJGNZ-FYJGNVAPSA-N (3e)-6-oxo-3-[[4-(pyridin-2-ylsulfamoyl)phenyl]hydrazinylidene]cyclohexa-1,4-diene-1-carboxylic acid Chemical compound C1=CC(=O)C(C(=O)O)=C\C1=N\NC1=CC=C(S(=O)(=O)NC=2N=CC=CC=2)C=C1 OQANPHBRHBJGNZ-FYJGNVAPSA-N 0.000 description 1
- TVIRNGFXQVMMGB-OFWIHYRESA-N (3s,6r,10r,13e,16s)-16-[(2r,3r,4s)-4-chloro-3-hydroxy-4-phenylbutan-2-yl]-10-[(3-chloro-4-methoxyphenyl)methyl]-6-methyl-3-(2-methylpropyl)-1,4-dioxa-8,11-diazacyclohexadec-13-ene-2,5,9,12-tetrone Chemical compound C1=C(Cl)C(OC)=CC=C1C[C@@H]1C(=O)NC[C@@H](C)C(=O)O[C@@H](CC(C)C)C(=O)O[C@H]([C@H](C)[C@@H](O)[C@@H](Cl)C=2C=CC=CC=2)C/C=C/C(=O)N1 TVIRNGFXQVMMGB-OFWIHYRESA-N 0.000 description 1
- HMLGSIZOMSVISS-ONJSNURVSA-N (7r)-7-[[(2z)-2-(2-amino-1,3-thiazol-4-yl)-2-(2,2-dimethylpropanoyloxymethoxyimino)acetyl]amino]-3-ethenyl-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound N([C@@H]1C(N2C(=C(C=C)CSC21)C(O)=O)=O)C(=O)\C(=N/OCOC(=O)C(C)(C)C)C1=CSC(N)=N1 HMLGSIZOMSVISS-ONJSNURVSA-N 0.000 description 1
- MWWSFMDVAYGXBV-MYPASOLCSA-N (7r,9s)-7-[(2r,4s,5s,6s)-4-amino-5-hydroxy-6-methyloxan-2-yl]oxy-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-4-methoxy-8,10-dihydro-7h-tetracene-5,12-dione;hydrochloride Chemical compound Cl.O([C@@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 MWWSFMDVAYGXBV-MYPASOLCSA-N 0.000 description 1
- RCFNNLSZHVHCEK-IMHLAKCZSA-N (7s,9s)-7-(4-amino-6-methyloxan-2-yl)oxy-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-4-methoxy-8,10-dihydro-7h-tetracene-5,12-dione;hydrochloride Chemical compound [Cl-].O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)C1CC([NH3+])CC(C)O1 RCFNNLSZHVHCEK-IMHLAKCZSA-N 0.000 description 1
- IEXUMDBQLIVNHZ-YOUGDJEHSA-N (8s,11r,13r,14s,17s)-11-[4-(dimethylamino)phenyl]-17-hydroxy-17-(3-hydroxypropyl)-13-methyl-1,2,6,7,8,11,12,14,15,16-decahydrocyclopenta[a]phenanthren-3-one Chemical compound C1=CC(N(C)C)=CC=C1[C@@H]1C2=C3CCC(=O)C=C3CC[C@H]2[C@H](CC[C@]2(O)CCCO)[C@@]2(C)C1 IEXUMDBQLIVNHZ-YOUGDJEHSA-N 0.000 description 1
- FDKXTQMXEQVLRF-ZHACJKMWSA-N (E)-dacarbazine Chemical compound CN(C)\N=N\c1[nH]cnc1C(N)=O FDKXTQMXEQVLRF-ZHACJKMWSA-N 0.000 description 1
- LKJPYSCBVHEWIU-KRWDZBQOSA-N (R)-bicalutamide Chemical compound C([C@@](O)(C)C(=O)NC=1C=C(C(C#N)=CC=1)C(F)(F)F)S(=O)(=O)C1=CC=C(F)C=C1 LKJPYSCBVHEWIU-KRWDZBQOSA-N 0.000 description 1
- MHFRGQHAERHWKZ-HHHXNRCGSA-N (R)-edelfosine Chemical compound CCCCCCCCCCCCCCCCCCOC[C@@H](OC)COP([O-])(=O)OCC[N+](C)(C)C MHFRGQHAERHWKZ-HHHXNRCGSA-N 0.000 description 1
- WHTVZRBIWZFKQO-AWEZNQCLSA-N (S)-chloroquine Chemical compound ClC1=CC=C2C(N[C@@H](C)CCCN(CC)CC)=CC=NC2=C1 WHTVZRBIWZFKQO-AWEZNQCLSA-N 0.000 description 1
- AGNGYMCLFWQVGX-AGFFZDDWSA-N (e)-1-[(2s)-2-amino-2-carboxyethoxy]-2-diazonioethenolate Chemical compound OC(=O)[C@@H](N)CO\C([O-])=C\[N+]#N AGNGYMCLFWQVGX-AGFFZDDWSA-N 0.000 description 1
- WNXJIVFYUVYPPR-UHFFFAOYSA-N 1,3-dioxolane Chemical compound C1COCO1 WNXJIVFYUVYPPR-UHFFFAOYSA-N 0.000 description 1
- HJTAZXHBEBIQQX-UHFFFAOYSA-N 1,5-bis(chloromethyl)naphthalene Chemical compound C1=CC=C2C(CCl)=CC=CC2=C1CCl HJTAZXHBEBIQQX-UHFFFAOYSA-N 0.000 description 1
- VSNHCAURESNICA-NJFSPNSNSA-N 1-oxidanylurea Chemical compound N[14C](=O)NO VSNHCAURESNICA-NJFSPNSNSA-N 0.000 description 1
- ABEXEQSGABRUHS-UHFFFAOYSA-N 16-methylheptadecyl 16-methylheptadecanoate Chemical compound CC(C)CCCCCCCCCCCCCCCOC(=O)CCCCCCCCCCCCCCC(C)C ABEXEQSGABRUHS-UHFFFAOYSA-N 0.000 description 1
- BTOTXLJHDSNXMW-POYBYMJQSA-N 2,3-dideoxyuridine Chemical compound O1[C@H](CO)CC[C@@H]1N1C(=O)NC(=O)C=C1 BTOTXLJHDSNXMW-POYBYMJQSA-N 0.000 description 1
- QCXJFISCRQIYID-IAEPZHFASA-N 2-amino-1-n-[(3s,6s,7r,10s,16s)-3-[(2s)-butan-2-yl]-7,11,14-trimethyl-2,5,9,12,15-pentaoxo-10-propan-2-yl-8-oxa-1,4,11,14-tetrazabicyclo[14.3.0]nonadecan-6-yl]-4,6-dimethyl-3-oxo-9-n-[(3s,6s,7r,10s,16s)-7,11,14-trimethyl-2,5,9,12,15-pentaoxo-3,10-di(propa Chemical compound C[C@H]1OC(=O)[C@H](C(C)C)N(C)C(=O)CN(C)C(=O)[C@@H]2CCCN2C(=O)[C@H](C(C)C)NC(=O)[C@H]1NC(=O)C1=C(N=C2C(C(=O)N[C@@H]3C(=O)N[C@H](C(N4CCC[C@H]4C(=O)N(C)CC(=O)N(C)[C@@H](C(C)C)C(=O)O[C@@H]3C)=O)[C@@H](C)CC)=C(N)C(=O)C(C)=C2O2)C2=C(C)C=C1 QCXJFISCRQIYID-IAEPZHFASA-N 0.000 description 1
- CPJAOFOWDGRJQD-NJVNFBHUSA-N 2-aminoacetic acid;(2s)-2-amino-3-phenylpropanoic acid;(2s)-2,5-diamino-5-oxopentanoic acid Chemical compound NCC(O)=O.OC(=O)[C@@H](N)CCC(N)=O.OC(=O)[C@@H](N)CC1=CC=CC=C1 CPJAOFOWDGRJQD-NJVNFBHUSA-N 0.000 description 1
- NDMPLJNOPCLANR-UHFFFAOYSA-N 3,4-dihydroxy-15-(4-hydroxy-18-methoxycarbonyl-5,18-seco-ibogamin-18-yl)-16-methoxy-1-methyl-6,7-didehydro-aspidospermidine-3-carboxylic acid methyl ester Natural products C1C(CC)(O)CC(CC2(C(=O)OC)C=3C(=CC4=C(C56C(C(C(O)C7(CC)C=CCN(C67)CC5)(O)C(=O)OC)N4C)C=3)OC)CN1CCC1=C2NC2=CC=CC=C12 NDMPLJNOPCLANR-UHFFFAOYSA-N 0.000 description 1
- UZFPOOOQHWICKY-UHFFFAOYSA-N 3-[13-[1-[1-[8,12-bis(2-carboxyethyl)-17-(1-hydroxyethyl)-3,7,13,18-tetramethyl-21,24-dihydroporphyrin-2-yl]ethoxy]ethyl]-18-(2-carboxyethyl)-8-(1-hydroxyethyl)-3,7,12,17-tetramethyl-22,23-dihydroporphyrin-2-yl]propanoic acid Chemical compound N1C(C=C2C(=C(CCC(O)=O)C(C=C3C(=C(C)C(C=C4N5)=N3)CCC(O)=O)=N2)C)=C(C)C(C(C)O)=C1C=C5C(C)=C4C(C)OC(C)C1=C(N2)C=C(N3)C(C)=C(C(O)C)C3=CC(C(C)=C3CCC(O)=O)=NC3=CC(C(CCC(O)=O)=C3C)=NC3=CC2=C1C UZFPOOOQHWICKY-UHFFFAOYSA-N 0.000 description 1
- HVCOBJNICQPDBP-UHFFFAOYSA-N 3-[3-[3,5-dihydroxy-6-methyl-4-(3,4,5-trihydroxy-6-methyloxan-2-yl)oxyoxan-2-yl]oxydecanoyloxy]decanoic acid;hydrate Chemical compound O.OC1C(OC(CC(=O)OC(CCCCCCC)CC(O)=O)CCCCCCC)OC(C)C(O)C1OC1C(O)C(O)C(O)C(C)O1 HVCOBJNICQPDBP-UHFFFAOYSA-N 0.000 description 1
- 125000004180 3-fluorophenyl group Chemical group [H]C1=C([H])C(*)=C([H])C(F)=C1[H] 0.000 description 1
- CLPFFLWZZBQMAO-UHFFFAOYSA-N 4-(5,6,7,8-tetrahydroimidazo[1,5-a]pyridin-5-yl)benzonitrile Chemical compound C1=CC(C#N)=CC=C1C1N2C=NC=C2CCC1 CLPFFLWZZBQMAO-UHFFFAOYSA-N 0.000 description 1
- DODQJNMQWMSYGS-QPLCGJKRSA-N 4-[(z)-1-[4-[2-(dimethylamino)ethoxy]phenyl]-1-phenylbut-1-en-2-yl]phenol Chemical compound C=1C=C(O)C=CC=1C(/CC)=C(C=1C=CC(OCCN(C)C)=CC=1)/C1=CC=CC=C1 DODQJNMQWMSYGS-QPLCGJKRSA-N 0.000 description 1
- NFBCSWGEYDCCDW-UHFFFAOYSA-N 4-n-(3-methylphenyl)quinazoline-4,6-diamine Chemical compound CC1=CC=CC(NC=2C3=CC(N)=CC=C3N=CN=2)=C1 NFBCSWGEYDCCDW-UHFFFAOYSA-N 0.000 description 1
- OBKXEAXTFZPCHS-UHFFFAOYSA-N 4-phenylbutyric acid Chemical compound OC(=O)CCCC1=CC=CC=C1 OBKXEAXTFZPCHS-UHFFFAOYSA-N 0.000 description 1
- RONQPWQYDRPRGG-UHFFFAOYSA-N 5,6-bis(4-fluoroanilino)isoindole-1,3-dione Chemical compound C1=CC(F)=CC=C1NC(C(=C1)NC=2C=CC(F)=CC=2)=CC2=C1C(=O)NC2=O RONQPWQYDRPRGG-UHFFFAOYSA-N 0.000 description 1
- IDPUKCWIGUEADI-UHFFFAOYSA-N 5-[bis(2-chloroethyl)amino]uracil Chemical compound ClCCN(CCCl)C1=CNC(=O)NC1=O IDPUKCWIGUEADI-UHFFFAOYSA-N 0.000 description 1
- NMUSYJAQQFHJEW-KVTDHHQDSA-N 5-azacytidine Chemical compound O=C1N=C(N)N=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](CO)O1 NMUSYJAQQFHJEW-KVTDHHQDSA-N 0.000 description 1
- GLYMPHUVMRFTFV-QLFBSQMISA-N 6-amino-5-[(1r)-1-(2,6-dichloro-3-fluorophenyl)ethoxy]-n-[4-[(3r,5s)-3,5-dimethylpiperazine-1-carbonyl]phenyl]pyridazine-3-carboxamide Chemical compound O([C@H](C)C=1C(=C(F)C=CC=1Cl)Cl)C(C(=NN=1)N)=CC=1C(=O)NC(C=C1)=CC=C1C(=O)N1C[C@H](C)N[C@H](C)C1 GLYMPHUVMRFTFV-QLFBSQMISA-N 0.000 description 1
- WYXSYVWAUAUWLD-SHUUEZRQSA-N 6-azauridine Chemical compound O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C=N1 WYXSYVWAUAUWLD-SHUUEZRQSA-N 0.000 description 1
- 229960005538 6-diazo-5-oxo-L-norleucine Drugs 0.000 description 1
- YCWQAMGASJSUIP-YFKPBYRVSA-N 6-diazo-5-oxo-L-norleucine Chemical compound OC(=O)[C@@H](N)CCC(=O)C=[N+]=[N-] YCWQAMGASJSUIP-YFKPBYRVSA-N 0.000 description 1
- ZGXJTSGNIOSYLO-UHFFFAOYSA-N 88755TAZ87 Chemical compound NCC(=O)CCC(O)=O ZGXJTSGNIOSYLO-UHFFFAOYSA-N 0.000 description 1
- SHGAZHPCJJPHSC-ZVCIMWCZSA-N 9-cis-retinoic acid Chemical compound OC(=O)/C=C(\C)/C=C/C=C(/C)\C=C\C1=C(C)CCCC1(C)C SHGAZHPCJJPHSC-ZVCIMWCZSA-N 0.000 description 1
- 208000002008 AIDS-Related Lymphoma Diseases 0.000 description 1
- MGGBYMDAPCCKCT-UHFFFAOYSA-N ASP-3026 Chemical compound COC1=CC(N2CCC(CC2)N2CCN(C)CC2)=CC=C1NC(N=1)=NC=NC=1NC1=CC=CC=C1S(=O)(=O)C(C)C MGGBYMDAPCCKCT-UHFFFAOYSA-N 0.000 description 1
- PITHJRRCEANNKJ-UHFFFAOYSA-N Aclacinomycin A Natural products C12=C(O)C=3C(=O)C4=CC=CC=C4C(=O)C=3C=C2C(C(=O)OC)C(CC)(O)CC1OC(OC1C)CC(N(C)C)C1OC(OC1C)CC(O)C1OC1CCC(=O)C(C)O1 PITHJRRCEANNKJ-UHFFFAOYSA-N 0.000 description 1
- 208000024893 Acute lymphoblastic leukemia Diseases 0.000 description 1
- 206010060933 Adverse event Diseases 0.000 description 1
- 108010012934 Albumin-Bound Paclitaxel Proteins 0.000 description 1
- 102000009027 Albumins Human genes 0.000 description 1
- 108010088751 Albumins Proteins 0.000 description 1
- 229930183010 Amphotericin Natural products 0.000 description 1
- QGGFZZLFKABGNL-UHFFFAOYSA-N Amphotericin A Natural products OC1C(N)C(O)C(C)OC1OC1C=CC=CC=CC=CCCC=CC=CC(C)C(O)C(C)C(C)OC(=O)CC(O)CC(O)CCC(O)C(O)CC(O)CC(O)(CC(O)C2C(O)=O)OC2C1 QGGFZZLFKABGNL-UHFFFAOYSA-N 0.000 description 1
- 206010061424 Anal cancer Diseases 0.000 description 1
- 108090000644 Angiozyme Proteins 0.000 description 1
- 108010078554 Aromatase Proteins 0.000 description 1
- 102000015790 Asparaginase Human genes 0.000 description 1
- 108010024976 Asparaginase Proteins 0.000 description 1
- DCXYFEDJOCDNAF-UHFFFAOYSA-N Asparagine Natural products OC(=O)C(N)CC(N)=O DCXYFEDJOCDNAF-UHFFFAOYSA-N 0.000 description 1
- BSYNRYMUTXBXSQ-UHFFFAOYSA-N Aspirin Chemical compound CC(=O)OC1=CC=CC=C1C(O)=O BSYNRYMUTXBXSQ-UHFFFAOYSA-N 0.000 description 1
- NOWKCMXCCJGMRR-UHFFFAOYSA-N Aziridine Chemical compound C1CN1 NOWKCMXCCJGMRR-UHFFFAOYSA-N 0.000 description 1
- 208000003950 B-cell lymphoma Diseases 0.000 description 1
- 239000012664 BCL-2-inhibitor Substances 0.000 description 1
- 229940125556 BGB-A1217 Drugs 0.000 description 1
- 229940123711 Bcl2 inhibitor Drugs 0.000 description 1
- VGGGPCQERPFHOB-MCIONIFRSA-N Bestatin Chemical compound CC(C)C[C@H](C(O)=O)NC(=O)[C@@H](O)[C@H](N)CC1=CC=CC=C1 VGGGPCQERPFHOB-MCIONIFRSA-N 0.000 description 1
- 102100026189 Beta-galactosidase Human genes 0.000 description 1
- 108010006654 Bleomycin Proteins 0.000 description 1
- VOVIALXJUBGFJZ-KWVAZRHASA-N Budesonide Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@@H]2[C@@H]1[C@@H]1C[C@H]3OC(CCC)O[C@@]3(C(=O)CO)[C@@]1(C)C[C@@H]2O VOVIALXJUBGFJZ-KWVAZRHASA-N 0.000 description 1
- 108010037003 Buserelin Proteins 0.000 description 1
- LLVZBTWPGQVVLW-SNAWJCMRSA-N CP-724714 Chemical compound C12=CC(/C=C/CNC(=O)COC)=CC=C2N=CN=C1NC(C=C1C)=CC=C1OC1=CC=C(C)N=C1 LLVZBTWPGQVVLW-SNAWJCMRSA-N 0.000 description 1
- 239000005461 Canertinib Substances 0.000 description 1
- SHHKQEUPHAENFK-UHFFFAOYSA-N Carboquone Chemical compound O=C1C(C)=C(N2CC2)C(=O)C(C(COC(N)=O)OC)=C1N1CC1 SHHKQEUPHAENFK-UHFFFAOYSA-N 0.000 description 1
- 208000010667 Carcinoma of liver and intrahepatic biliary tract Diseases 0.000 description 1
- AOCCBINRVIKJHY-UHFFFAOYSA-N Carmofur Chemical compound CCCCCCNC(=O)N1C=C(F)C(=O)NC1=O AOCCBINRVIKJHY-UHFFFAOYSA-N 0.000 description 1
- DLGOEMSEDOSKAD-UHFFFAOYSA-N Carmustine Chemical compound ClCCNC(=O)N(N=O)CCCl DLGOEMSEDOSKAD-UHFFFAOYSA-N 0.000 description 1
- 108090000994 Catalytic RNA Proteins 0.000 description 1
- 102000053642 Catalytic RNA Human genes 0.000 description 1
- 102000000844 Cell Surface Receptors Human genes 0.000 description 1
- 108010001857 Cell Surface Receptors Proteins 0.000 description 1
- 206010008479 Chest Pain Diseases 0.000 description 1
- MKQWTWSXVILIKJ-LXGUWJNJSA-N Chlorozotocin Chemical compound OC[C@@H](O)[C@@H](O)[C@H](O)[C@H](C=O)NC(=O)N(N=O)CCCl MKQWTWSXVILIKJ-LXGUWJNJSA-N 0.000 description 1
- 108010066551 Cholestenone 5 alpha-Reductase Proteins 0.000 description 1
- KRKNYBCHXYNGOX-UHFFFAOYSA-K Citrate Chemical compound [O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O KRKNYBCHXYNGOX-UHFFFAOYSA-K 0.000 description 1
- FBRAWBYQGRLCEK-AVVSTMBFSA-N Clobetasone butyrate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)CCl)(OC(=O)CCC)[C@@]1(C)CC2=O FBRAWBYQGRLCEK-AVVSTMBFSA-N 0.000 description 1
- 206010010774 Constipation Diseases 0.000 description 1
- ITRJWOMZKQRYTA-RFZYENFJSA-N Cortisone acetate Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)COC(=O)C)(O)[C@@]1(C)CC2=O ITRJWOMZKQRYTA-RFZYENFJSA-N 0.000 description 1
- 206010011224 Cough Diseases 0.000 description 1
- 229930188224 Cryptophycin Natural products 0.000 description 1
- XZMCDFZZKTWFGF-UHFFFAOYSA-N Cyanamide Chemical compound NC#N XZMCDFZZKTWFGF-UHFFFAOYSA-N 0.000 description 1
- 229930105110 Cyclosporin A Natural products 0.000 description 1
- VVNCNSJFMMFHPL-VKHMYHEASA-N D-penicillamine Chemical compound CC(C)(S)[C@@H](N)C(O)=O VVNCNSJFMMFHPL-VKHMYHEASA-N 0.000 description 1
- 230000005778 DNA damage Effects 0.000 description 1
- 231100000277 DNA damage Toxicity 0.000 description 1
- 238000012270 DNA recombination Methods 0.000 description 1
- 238000001712 DNA sequencing Methods 0.000 description 1
- 229940123780 DNA topoisomerase I inhibitor Drugs 0.000 description 1
- 108010019673 Darbepoetin alfa Proteins 0.000 description 1
- 101710088194 Dehydrogenase Proteins 0.000 description 1
- XXGMIHXASFDFSM-UHFFFAOYSA-N Delta9-tetrahydrocannabinol Natural products CCCCCc1cc2OC(C)(C)C3CCC(=CC3c2c(O)c1O)C XXGMIHXASFDFSM-UHFFFAOYSA-N 0.000 description 1
- 108010002156 Depsipeptides Proteins 0.000 description 1
- 206010012735 Diarrhoea Diseases 0.000 description 1
- 206010061819 Disease recurrence Diseases 0.000 description 1
- CYQFCXCEBYINGO-DLBZAZTESA-N Dronabinol Natural products C1=C(C)CC[C@H]2C(C)(C)OC3=CC(CCCCC)=CC(O)=C3[C@H]21 CYQFCXCEBYINGO-DLBZAZTESA-N 0.000 description 1
- 208000005171 Dysmenorrhea Diseases 0.000 description 1
- 206010013935 Dysmenorrhoea Diseases 0.000 description 1
- 229940125560 EOS-884448 Drugs 0.000 description 1
- 241000196324 Embryophyta Species 0.000 description 1
- SAMRUMKYXPVKPA-VFKOLLTISA-N Enocitabine Chemical compound O=C1N=C(NC(=O)CCCCCCCCCCCCCCCCCCCCC)C=CN1[C@H]1[C@@H](O)[C@H](O)[C@@H](CO)O1 SAMRUMKYXPVKPA-VFKOLLTISA-N 0.000 description 1
- OBMLHUPNRURLOK-XGRAFVIBSA-N Epitiostanol Chemical compound C1[C@@H]2S[C@@H]2C[C@]2(C)[C@H]3CC[C@](C)([C@H](CC4)O)[C@@H]4[C@@H]3CC[C@H]21 OBMLHUPNRURLOK-XGRAFVIBSA-N 0.000 description 1
- 108010074604 Epoetin Alfa Proteins 0.000 description 1
- LFQSCWFLJHTTHZ-UHFFFAOYSA-N Ethanol Chemical compound CCO LFQSCWFLJHTTHZ-UHFFFAOYSA-N 0.000 description 1
- DBVJJBKOTRCVKF-UHFFFAOYSA-N Etidronic acid Chemical compound OP(=O)(O)C(O)(C)P(O)(O)=O DBVJJBKOTRCVKF-UHFFFAOYSA-N 0.000 description 1
- 108010087819 Fc receptors Proteins 0.000 description 1
- 102000009109 Fc receptors Human genes 0.000 description 1
- CITFYDYEWQIEPX-UHFFFAOYSA-N Flavanol Natural products O1C2=CC(OCC=C(C)C)=CC(O)=C2C(=O)C(O)C1C1=CC=C(O)C=C1 CITFYDYEWQIEPX-UHFFFAOYSA-N 0.000 description 1
- WJOHZNCJWYWUJD-IUGZLZTKSA-N Fluocinonide Chemical compound C1([C@@H](F)C2)=CC(=O)C=C[C@]1(C)[C@]1(F)[C@@H]2[C@@H]2C[C@H]3OC(C)(C)O[C@@]3(C(=O)COC(=O)C)[C@@]2(C)C[C@@H]1O WJOHZNCJWYWUJD-IUGZLZTKSA-N 0.000 description 1
- WMBWREPUVVBILR-UHFFFAOYSA-N GCG Natural products C=1C(O)=C(O)C(O)=CC=1C1OC2=CC(O)=CC(O)=C2CC1OC(=O)C1=CC(O)=C(O)C(O)=C1 WMBWREPUVVBILR-UHFFFAOYSA-N 0.000 description 1
- 206010017993 Gastrointestinal neoplasms Diseases 0.000 description 1
- 208000031852 Gastrointestinal stromal cancer Diseases 0.000 description 1
- JRZJKWGQFNTSRN-UHFFFAOYSA-N Geldanamycin Natural products C1C(C)CC(OC)C(O)C(C)C=C(C)C(OC(N)=O)C(OC)CCC=C(C)C(=O)NC2=CC(=O)C(OC)=C1C2=O JRZJKWGQFNTSRN-UHFFFAOYSA-N 0.000 description 1
- 229930186217 Glycolipid Natural products 0.000 description 1
- 102000003886 Glycoproteins Human genes 0.000 description 1
- 108090000288 Glycoproteins Proteins 0.000 description 1
- 201000005569 Gout Diseases 0.000 description 1
- 208000017891 HER2 positive breast carcinoma Diseases 0.000 description 1
- 206010019233 Headaches Diseases 0.000 description 1
- 206010073069 Hepatic cancer Diseases 0.000 description 1
- 102100034458 Hepatitis A virus cellular receptor 2 Human genes 0.000 description 1
- 101710083479 Hepatitis A virus cellular receptor 2 homolog Proteins 0.000 description 1
- 101000840258 Homo sapiens Immunoglobulin J chain Proteins 0.000 description 1
- 101000984753 Homo sapiens Serine/threonine-protein kinase B-raf Proteins 0.000 description 1
- VEXZGXHMUGYJMC-UHFFFAOYSA-N Hydrochloric acid Chemical compound Cl VEXZGXHMUGYJMC-UHFFFAOYSA-N 0.000 description 1
- VSNHCAURESNICA-UHFFFAOYSA-N Hydroxyurea Chemical compound NC(=O)NO VSNHCAURESNICA-UHFFFAOYSA-N 0.000 description 1
- MPBVHIBUJCELCL-UHFFFAOYSA-N Ibandronate Chemical compound CCCCCN(C)CCC(O)(P(O)(O)=O)P(O)(O)=O MPBVHIBUJCELCL-UHFFFAOYSA-N 0.000 description 1
- HEFNNWSXXWATRW-UHFFFAOYSA-N Ibuprofen Chemical compound CC(C)CC1=CC=C(C(C)C(O)=O)C=C1 HEFNNWSXXWATRW-UHFFFAOYSA-N 0.000 description 1
- JJKOTMDDZAJTGQ-DQSJHHFOSA-N Idoxifene Chemical compound C=1C=CC=CC=1C(/CC)=C(C=1C=CC(OCCN2CCCC2)=CC=1)/C1=CC=C(I)C=C1 JJKOTMDDZAJTGQ-DQSJHHFOSA-N 0.000 description 1
- 102100029571 Immunoglobulin J chain Human genes 0.000 description 1
- 206010061218 Inflammation Diseases 0.000 description 1
- 102100040018 Interferon alpha-2 Human genes 0.000 description 1
- 108010079944 Interferon-alpha2b Proteins 0.000 description 1
- 108010074328 Interferon-gamma Proteins 0.000 description 1
- 102000008070 Interferon-gamma Human genes 0.000 description 1
- 102000051628 Interleukin-1 receptor antagonist Human genes 0.000 description 1
- 108700021006 Interleukin-1 receptor antagonist Proteins 0.000 description 1
- 102100030694 Interleukin-11 Human genes 0.000 description 1
- FHFHNVHRVKQQHN-UHFFFAOYSA-N Islandicin Chemical compound C1=CC=C2C(=O)C3=C(O)C(C)=CC(O)=C3C(=O)C2=C1O FHFHNVHRVKQQHN-UHFFFAOYSA-N 0.000 description 1
- IPMYMEWFZKHGAX-UHFFFAOYSA-N Isotheaflavin Natural products OC1CC2=C(O)C=C(O)C=C2OC1C(C1=C2)=CC(O)=C(O)C1=C(O)C(=O)C=C2C1C(O)CC2=C(O)C=C(O)C=C2O1 IPMYMEWFZKHGAX-UHFFFAOYSA-N 0.000 description 1
- UETNIIAIRMUTSM-UHFFFAOYSA-N Jacareubin Natural products CC1(C)OC2=CC3Oc4c(O)c(O)ccc4C(=O)C3C(=C2C=C1)O UETNIIAIRMUTSM-UHFFFAOYSA-N 0.000 description 1
- DCXYFEDJOCDNAF-REOHCLBHSA-N L-asparagine Chemical compound OC(=O)[C@@H](N)CC(N)=O DCXYFEDJOCDNAF-REOHCLBHSA-N 0.000 description 1
- ZDXPYRJPNDTMRX-VKHMYHEASA-N L-glutamine Chemical compound OC(=O)[C@@H](N)CCC(N)=O ZDXPYRJPNDTMRX-VKHMYHEASA-N 0.000 description 1
- 102000003855 L-lactate dehydrogenase Human genes 0.000 description 1
- 108700023483 L-lactate dehydrogenases Proteins 0.000 description 1
- 108010059881 Lactase Proteins 0.000 description 1
- 229920001491 Lentinan Polymers 0.000 description 1
- 108010000817 Leuprolide Proteins 0.000 description 1
- HLFSDGLLUJUHTE-SNVBAGLBSA-N Levamisole Chemical compound C1([C@H]2CN3CCSC3=N2)=CC=CC=C1 HLFSDGLLUJUHTE-SNVBAGLBSA-N 0.000 description 1
- MEPSBMMZQBMKHM-UHFFFAOYSA-N Lomatiol Natural products CC(=C/CC1=C(O)C(=O)c2ccccc2C1=O)CO MEPSBMMZQBMKHM-UHFFFAOYSA-N 0.000 description 1
- GQYIWUVLTXOXAJ-UHFFFAOYSA-N Lomustine Chemical compound ClCCN(N=O)C(=O)NC1CCCCC1 GQYIWUVLTXOXAJ-UHFFFAOYSA-N 0.000 description 1
- 206010025312 Lymphoma AIDS related Diseases 0.000 description 1
- 206010025323 Lymphomas Diseases 0.000 description 1
- 102000043136 MAP kinase family Human genes 0.000 description 1
- 108091054455 MAP kinase family Proteins 0.000 description 1
- 208000025205 Mantle-Cell Lymphoma Diseases 0.000 description 1
- SBDNJUWAMKYJOX-UHFFFAOYSA-N Meclofenamic Acid Chemical compound CC1=CC=C(Cl)C(NC=2C(=CC=CC=2)C(O)=O)=C1Cl SBDNJUWAMKYJOX-UHFFFAOYSA-N 0.000 description 1
- 206010027145 Melanocytic naevus Diseases 0.000 description 1
- ZRVUJXDFFKFLMG-UHFFFAOYSA-N Meloxicam Chemical compound OC=1C2=CC=CC=C2S(=O)(=O)N(C)C=1C(=O)NC1=NC=C(C)S1 ZRVUJXDFFKFLMG-UHFFFAOYSA-N 0.000 description 1
- XOGTZOOQQBDUSI-UHFFFAOYSA-M Mesna Chemical compound [Na+].[O-]S(=O)(=O)CCS XOGTZOOQQBDUSI-UHFFFAOYSA-M 0.000 description 1
- 208000036631 Metastatic pain Diseases 0.000 description 1
- 241001465754 Metazoa Species 0.000 description 1
- QXKHYNVANLEOEG-UHFFFAOYSA-N Methoxsalen Chemical compound C1=CC(=O)OC2=C1C=C1C=COC1=C2OC QXKHYNVANLEOEG-UHFFFAOYSA-N 0.000 description 1
- 108091022875 Microtubule Proteins 0.000 description 1
- 102000029749 Microtubule Human genes 0.000 description 1
- 208000019695 Migraine disease Diseases 0.000 description 1
- VFKZTMPDYBFSTM-KVTDHHQDSA-N Mitobronitol Chemical compound BrC[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)CBr VFKZTMPDYBFSTM-KVTDHHQDSA-N 0.000 description 1
- 229930192392 Mitomycin Natural products 0.000 description 1
- 208000034578 Multiple myelomas Diseases 0.000 description 1
- 101100523539 Mus musculus Raf1 gene Proteins 0.000 description 1
- OVBPIULPVIDEAO-UHFFFAOYSA-N N-Pteroyl-L-glutaminsaeure Natural products C=1N=C2NC(N)=NC(=O)C2=NC=1CNC1=CC=C(C(=O)NC(CCC(O)=O)C(O)=O)C=C1 OVBPIULPVIDEAO-UHFFFAOYSA-N 0.000 description 1
- 230000004988 N-glycosylation Effects 0.000 description 1
- 108010072915 NAc-Sar-Gly-Val-(d-allo-Ile)-Thr-Nva-Ile-Arg-ProNEt Proteins 0.000 description 1
- CMWTZPSULFXXJA-UHFFFAOYSA-N Naproxen Natural products C1=C(C(C)C(O)=O)C=CC2=CC(OC)=CC=C21 CMWTZPSULFXXJA-UHFFFAOYSA-N 0.000 description 1
- 206010028813 Nausea Diseases 0.000 description 1
- 208000007256 Nevus Diseases 0.000 description 1
- 238000000636 Northern blotting Methods 0.000 description 1
- 206010030113 Oedema Diseases 0.000 description 1
- 108700020796 Oncogene Proteins 0.000 description 1
- 238000010222 PCR analysis Methods 0.000 description 1
- 239000012828 PI3K inhibitor Substances 0.000 description 1
- VREZDOWOLGNDPW-ALTGWBOUSA-N Pancratistatin Chemical compound C1=C2[C@H]3[C@@H](O)[C@H](O)[C@@H](O)[C@@H](O)[C@@H]3NC(=O)C2=C(O)C2=C1OCO2 VREZDOWOLGNDPW-ALTGWBOUSA-N 0.000 description 1
- VREZDOWOLGNDPW-MYVCAWNPSA-N Pancratistatin Natural products O=C1N[C@H]2[C@H](O)[C@H](O)[C@H](O)[C@H](O)[C@@H]2c2c1c(O)c1OCOc1c2 VREZDOWOLGNDPW-MYVCAWNPSA-N 0.000 description 1
- 108091000080 Phosphotransferase Proteins 0.000 description 1
- IIXHQGSINFQLRR-UHFFFAOYSA-N Piceatannol Natural products Oc1ccc(C=Cc2c(O)c(O)c3CCCCc3c2O)cc1O IIXHQGSINFQLRR-UHFFFAOYSA-N 0.000 description 1
- KMSKQZKKOZQFFG-HSUXVGOQSA-N Pirarubicin Chemical compound O([C@H]1[C@@H](N)C[C@@H](O[C@H]1C)O[C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1CCCCO1 KMSKQZKKOZQFFG-HSUXVGOQSA-N 0.000 description 1
- 206010035226 Plasma cell myeloma Diseases 0.000 description 1
- HRHKSTOGXBBQCB-UHFFFAOYSA-N Porfiromycine Chemical compound O=C1C(N)=C(C)C(=O)C2=C1C(COC(N)=O)C1(OC)C3N(C)C3CN12 HRHKSTOGXBBQCB-UHFFFAOYSA-N 0.000 description 1
- 208000004550 Postoperative Pain Diseases 0.000 description 1
- HFVNWDWLWUCIHC-GUPDPFMOSA-N Prednimustine Chemical compound O=C([C@@]1(O)CC[C@H]2[C@H]3[C@@H]([C@]4(C=CC(=O)C=C4CC3)C)[C@@H](O)C[C@@]21C)COC(=O)CCCC1=CC=C(N(CCCl)CCCl)C=C1 HFVNWDWLWUCIHC-GUPDPFMOSA-N 0.000 description 1
- CWEZAWNPTYBADX-UHFFFAOYSA-N Procyanidin Natural products OC1C(OC2C(O)C(Oc3c2c(O)cc(O)c3C4C(O)C(Oc5cc(O)cc(O)c45)c6ccc(O)c(O)c6)c7ccc(O)c(O)c7)c8c(O)cc(O)cc8OC1c9ccc(O)c(O)c9 CWEZAWNPTYBADX-UHFFFAOYSA-N 0.000 description 1
- 108090000459 Prostaglandin-endoperoxide synthases Proteins 0.000 description 1
- 102000004005 Prostaglandin-endoperoxide synthases Human genes 0.000 description 1
- 229940079156 Proteasome inhibitor Drugs 0.000 description 1
- 108010076504 Protein Sorting Signals Proteins 0.000 description 1
- 102100024924 Protein kinase C alpha type Human genes 0.000 description 1
- 101710109947 Protein kinase C alpha type Proteins 0.000 description 1
- 102000004022 Protein-Tyrosine Kinases Human genes 0.000 description 1
- 108090000412 Protein-Tyrosine Kinases Proteins 0.000 description 1
- 201000001263 Psoriatic Arthritis Diseases 0.000 description 1
- 208000036824 Psoriatic arthropathy Diseases 0.000 description 1
- 208000010378 Pulmonary Embolism Diseases 0.000 description 1
- 206010037660 Pyrexia Diseases 0.000 description 1
- ZVOLCUVKHLEPEV-UHFFFAOYSA-N Quercetagetin Natural products C1=C(O)C(O)=CC=C1C1=C(O)C(=O)C2=C(O)C(O)=C(O)C=C2O1 ZVOLCUVKHLEPEV-UHFFFAOYSA-N 0.000 description 1
- AHHFEZNOXOZZQA-ZEBDFXRSSA-N Ranimustine Chemical compound CO[C@H]1O[C@H](CNC(=O)N(CCCl)N=O)[C@@H](O)[C@H](O)[C@H]1O AHHFEZNOXOZZQA-ZEBDFXRSSA-N 0.000 description 1
- 229940127361 Receptor Tyrosine Kinase Inhibitors Drugs 0.000 description 1
- 101710100968 Receptor tyrosine-protein kinase erbB-2 Proteins 0.000 description 1
- 208000015634 Rectal Neoplasms Diseases 0.000 description 1
- 208000033464 Reiter syndrome Diseases 0.000 description 1
- 206010038419 Renal colic Diseases 0.000 description 1
- QNVSXXGDAPORNA-UHFFFAOYSA-N Resveratrol Natural products OC1=CC=CC(C=CC=2C=C(O)C(O)=CC=2)=C1 QNVSXXGDAPORNA-UHFFFAOYSA-N 0.000 description 1
- 229930194692 Rhodomycin Natural products 0.000 description 1
- HWTZYBCRDDUBJY-UHFFFAOYSA-N Rhynchosin Natural products C1=C(O)C(O)=CC=C1C1=C(O)C(=O)C2=CC(O)=C(O)C=C2O1 HWTZYBCRDDUBJY-UHFFFAOYSA-N 0.000 description 1
- CIEYTVIYYGTCCI-UHFFFAOYSA-N SJ000286565 Natural products C1=CC=C2C(=O)C(CC=C(C)C)=C(O)C(=O)C2=C1 CIEYTVIYYGTCCI-UHFFFAOYSA-N 0.000 description 1
- 206010061934 Salivary gland cancer Diseases 0.000 description 1
- 206010039491 Sarcoma Diseases 0.000 description 1
- 229940124639 Selective inhibitor Drugs 0.000 description 1
- 102100027103 Serine/threonine-protein kinase B-raf Human genes 0.000 description 1
- 208000013738 Sleep Initiation and Maintenance disease Diseases 0.000 description 1
- 238000002105 Southern blotting Methods 0.000 description 1
- 206010041591 Spinal osteoarthritis Diseases 0.000 description 1
- 229940126547 T-cell immunoglobulin mucin-3 Drugs 0.000 description 1
- 210000000662 T-lymphocyte subset Anatomy 0.000 description 1
- WFWLQNSHRPWKFK-UHFFFAOYSA-N Tegafur Chemical compound O=C1NC(=O)C(F)=CN1C1OCCC1 WFWLQNSHRPWKFK-UHFFFAOYSA-N 0.000 description 1
- BPEGJWRSRHCHSN-UHFFFAOYSA-N Temozolomide Chemical compound O=C1N(C)N=NC2=C(C(N)=O)N=CN21 BPEGJWRSRHCHSN-UHFFFAOYSA-N 0.000 description 1
- UXRMWRBWCAGDQB-UHFFFAOYSA-N Theaflavin Natural products C1=CC(C2C(CC3=C(O)C=C(O)C=C3O2)O)=C(O)C(=O)C2=C1C(C1OC3=CC(O)=CC(O)=C3CC1O)=CC(O)=C2O UXRMWRBWCAGDQB-UHFFFAOYSA-N 0.000 description 1
- YTPLMLYBLZKORZ-UHFFFAOYSA-N Thiophene Chemical group C=1C=CSC=1 YTPLMLYBLZKORZ-UHFFFAOYSA-N 0.000 description 1
- 208000034841 Thrombotic Microangiopathies Diseases 0.000 description 1
- 208000024770 Thyroid neoplasm Diseases 0.000 description 1
- 101710183280 Topoisomerase Proteins 0.000 description 1
- 239000000365 Topoisomerase I Inhibitor Substances 0.000 description 1
- IWEQQRMGNVVKQW-OQKDUQJOSA-N Toremifene citrate Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O.C1=CC(OCCN(C)C)=CC=C1C(\C=1C=CC=CC=1)=C(\CCCl)C1=CC=CC=C1 IWEQQRMGNVVKQW-OQKDUQJOSA-N 0.000 description 1
- LUKBXSAWLPMMSZ-OWOJBTEDSA-N Trans-resveratrol Chemical compound C1=CC(O)=CC=C1\C=C\C1=CC(O)=CC(O)=C1 LUKBXSAWLPMMSZ-OWOJBTEDSA-N 0.000 description 1
- FYAMXEPQQLNQDM-UHFFFAOYSA-N Tris(1-aziridinyl)phosphine oxide Chemical compound C1CN1P(N1CC1)(=O)N1CC1 FYAMXEPQQLNQDM-UHFFFAOYSA-N 0.000 description 1
- 102000004243 Tubulin Human genes 0.000 description 1
- 108090000704 Tubulin Proteins 0.000 description 1
- 208000031128 Upper tract urothelial carcinoma Diseases 0.000 description 1
- 108091008605 VEGF receptors Proteins 0.000 description 1
- 102000009484 Vascular Endothelial Growth Factor Receptors Human genes 0.000 description 1
- 229940122803 Vinca alkaloid Drugs 0.000 description 1
- 206010047700 Vomiting Diseases 0.000 description 1
- 206010047741 Vulval cancer Diseases 0.000 description 1
- 208000004354 Vulvar Neoplasms Diseases 0.000 description 1
- PCWZKQSKUXXDDJ-UHFFFAOYSA-N Xanthotoxin Natural products COCc1c2OC(=O)C=Cc2cc3ccoc13 PCWZKQSKUXXDDJ-UHFFFAOYSA-N 0.000 description 1
- XZSRRNFBEIOBDA-CFNBKWCHSA-N [2-[(2s,4s)-4-[(2r,4s,5s,6s)-4-amino-5-hydroxy-6-methyloxan-2-yl]oxy-2,5,12-trihydroxy-7-methoxy-6,11-dioxo-3,4-dihydro-1h-tetracen-2-yl]-2-oxoethyl] 2,2-diethoxyacetate Chemical compound O([C@H]1C[C@](CC2=C(O)C=3C(=O)C4=CC=CC(OC)=C4C(=O)C=3C(O)=C21)(O)C(=O)COC(=O)C(OCC)OCC)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 XZSRRNFBEIOBDA-CFNBKWCHSA-N 0.000 description 1
- 108010023617 abarelix Proteins 0.000 description 1
- AIWRTTMUVOZGPW-HSPKUQOVSA-N abarelix Chemical compound C([C@@H](C(=O)N[C@H](CC(N)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCCNC(C)C)C(=O)N1[C@@H](CCC1)C(=O)N[C@H](C)C(N)=O)N(C)C(=O)[C@H](CO)NC(=O)[C@@H](CC=1C=NC=CC=1)NC(=O)[C@@H](CC=1C=CC(Cl)=CC=1)NC(=O)[C@@H](CC=1C=C2C=CC=CC2=CC=1)NC(C)=O)C1=CC=C(O)C=C1 AIWRTTMUVOZGPW-HSPKUQOVSA-N 0.000 description 1
- 229960002184 abarelix Drugs 0.000 description 1
- 229960003697 abatacept Drugs 0.000 description 1
- 230000001594 aberrant effect Effects 0.000 description 1
- 150000001242 acetic acid derivatives Chemical class 0.000 description 1
- 229960001138 acetylsalicylic acid Drugs 0.000 description 1
- 229930183665 actinomycin Natural products 0.000 description 1
- RJURFGZVJUQBHK-IIXSONLDSA-N actinomycin D Chemical compound C[C@H]1OC(=O)[C@H](C(C)C)N(C)C(=O)CN(C)C(=O)[C@@H]2CCCN2C(=O)[C@@H](C(C)C)NC(=O)[C@H]1NC(=O)C1=C(N)C(=O)C(C)=C2OC(C(C)=CC=C3C(=O)N[C@@H]4C(=O)N[C@@H](C(N5CCC[C@H]5C(=O)N(C)CC(=O)N(C)[C@@H](C(C)C)C(=O)O[C@@H]4C)=O)C(C)C)=C3N=C21 RJURFGZVJUQBHK-IIXSONLDSA-N 0.000 description 1
- 230000009471 action Effects 0.000 description 1
- 230000003213 activating effect Effects 0.000 description 1
- 229940037127 actonel Drugs 0.000 description 1
- 229960002964 adalimumab Drugs 0.000 description 1
- 239000002671 adjuvant Substances 0.000 description 1
- JZMHCANOTJFLQJ-IEQBYLOXSA-A affinitac Chemical compound [Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].[Na+].O=C1NC(=O)C(C)=CN1[C@@H]1O[C@H](COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP([O-])(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)CO)[C@@H](OP([S-])(=O)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=NC=NC(N)=C3N=C2)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(N=C(N)C=C2)=O)OP([O-])(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=NC=NC(N)=C3N=C2)O)C1 JZMHCANOTJFLQJ-IEQBYLOXSA-A 0.000 description 1
- 235000004279 alanine Nutrition 0.000 description 1
- 125000003295 alanine group Chemical group N[C@@H](C)C(=O)* 0.000 description 1
- 229960005310 aldesleukin Drugs 0.000 description 1
- 229960000548 alemtuzumab Drugs 0.000 description 1
- 229940062527 alendronate Drugs 0.000 description 1
- 229960001445 alitretinoin Drugs 0.000 description 1
- 125000000217 alkyl group Chemical group 0.000 description 1
- OFCNXPDARWKPPY-UHFFFAOYSA-N allopurinol Chemical compound OC1=NC=NC2=C1C=NN2 OFCNXPDARWKPPY-UHFFFAOYSA-N 0.000 description 1
- 229960003459 allopurinol Drugs 0.000 description 1
- 229960000473 altretamine Drugs 0.000 description 1
- ILKJAFIWWBXGDU-MOGDOJJUSA-N amcinonide Chemical compound O([C@@]1([C@H](O2)C[C@@H]3[C@@]1(C[C@H](O)[C@]1(F)[C@@]4(C)C=CC(=O)C=C4CC[C@H]13)C)C(=O)COC(=O)C)C12CCCC1 ILKJAFIWWBXGDU-MOGDOJJUSA-N 0.000 description 1
- 229960003099 amcinonide Drugs 0.000 description 1
- JKOQGQFVAUAYPM-UHFFFAOYSA-N amifostine Chemical compound NCCCNCCSP(O)(O)=O JKOQGQFVAUAYPM-UHFFFAOYSA-N 0.000 description 1
- 229960001097 amifostine Drugs 0.000 description 1
- 235000001014 amino acid Nutrition 0.000 description 1
- ROBVIMPUHSLWNV-UHFFFAOYSA-N aminoglutethimide Chemical compound C=1C=C(N)C=CC=1C1(CC)CCC(=O)NC1=O ROBVIMPUHSLWNV-UHFFFAOYSA-N 0.000 description 1
- 229960003437 aminoglutethimide Drugs 0.000 description 1
- 229960002749 aminolevulinic acid Drugs 0.000 description 1
- 229940009444 amphotericin Drugs 0.000 description 1
- APKFDSVGJQXUKY-INPOYWNPSA-N amphotericin B Chemical compound O[C@H]1[C@@H](N)[C@H](O)[C@@H](C)O[C@H]1O[C@H]1/C=C/C=C/C=C/C=C/C=C/C=C/C=C/[C@H](C)[C@@H](O)[C@@H](C)[C@H](C)OC(=O)C[C@H](O)C[C@H](O)CC[C@@H](O)[C@H](O)C[C@H](O)C[C@](O)(C[C@H](O)[C@H]2C(O)=O)O[C@H]2C1 APKFDSVGJQXUKY-INPOYWNPSA-N 0.000 description 1
- 230000003321 amplification Effects 0.000 description 1
- 229960004238 anakinra Drugs 0.000 description 1
- 201000007538 anal carcinoma Diseases 0.000 description 1
- 230000000202 analgesic effect Effects 0.000 description 1
- 229960002932 anastrozole Drugs 0.000 description 1
- BBDAGFIXKZCXAH-CCXZUQQUSA-N ancitabine Chemical compound N=C1C=CN2[C@@H]3O[C@H](CO)[C@@H](O)[C@@H]3OC2=N1 BBDAGFIXKZCXAH-CCXZUQQUSA-N 0.000 description 1
- 229950000242 ancitabine Drugs 0.000 description 1
- 239000003098 androgen Substances 0.000 description 1
- 229940030486 androgens Drugs 0.000 description 1
- 239000004037 angiogenesis inhibitor Substances 0.000 description 1
- 229940121369 angiogenesis inhibitor Drugs 0.000 description 1
- 208000022531 anorexia Diseases 0.000 description 1
- 229940046836 anti-estrogen Drugs 0.000 description 1
- 230000001833 anti-estrogenic effect Effects 0.000 description 1
- 229940044684 anti-microtubule agent Drugs 0.000 description 1
- 230000001754 anti-pyretic effect Effects 0.000 description 1
- 238000011319 anticancer therapy Methods 0.000 description 1
- 230000000890 antigenic effect Effects 0.000 description 1
- 230000007503 antigenic stimulation Effects 0.000 description 1
- 239000013059 antihormonal agent Substances 0.000 description 1
- 229940111131 antiinflammatory and antirheumatic product propionic acid derivative Drugs 0.000 description 1
- 229940045686 antimetabolites antineoplastic purine analogs Drugs 0.000 description 1
- 229940045687 antimetabolites folic acid analogs Drugs 0.000 description 1
- 229940045719 antineoplastic alkylating agent nitrosoureas Drugs 0.000 description 1
- 229940045688 antineoplastic antimetabolites pyrimidine analogues Drugs 0.000 description 1
- 229940045988 antineoplastic drug protein kinase inhibitors Drugs 0.000 description 1
- 239000002221 antipyretic Substances 0.000 description 1
- 239000003435 antirheumatic agent Substances 0.000 description 1
- OVDSPTSBIQCAIN-UHFFFAOYSA-N ap26113 Chemical compound COC1=CC(N2CCC(CC2)N(C)C)=CC=C1NC(N=1)=NC=C(Cl)C=1NC1=CC=CC=C1P(C)(C)=O OVDSPTSBIQCAIN-UHFFFAOYSA-N 0.000 description 1
- 230000006907 apoptotic process Effects 0.000 description 1
- NMYKBZSMOUFOJV-FJSWQEPZSA-N aprinocarsen Chemical compound O=C1NC(=O)C(C)=CN1[C@@H]1O[C@H](COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)O[C@@H]2[C@H](O[C@H](C2)N2C3=C(C(NC(N)=N3)=O)N=C2)CO)[C@@H](OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=NC=NC(N)=C3N=C2)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C(N=C(N)C=C2)=O)OP(O)(=S)OC[C@@H]2[C@H](C[C@@H](O2)N2C3=NC=NC(N)=C3N=C2)O)C1 NMYKBZSMOUFOJV-FJSWQEPZSA-N 0.000 description 1
- 229940078010 arimidex Drugs 0.000 description 1
- 229940087620 aromasin Drugs 0.000 description 1
- 239000003886 aromatase inhibitor Substances 0.000 description 1
- 229940046844 aromatase inhibitors Drugs 0.000 description 1
- GOLCXWYRSKYTSP-UHFFFAOYSA-N arsenic trioxide Inorganic materials O1[As]2O[As]1O2 GOLCXWYRSKYTSP-UHFFFAOYSA-N 0.000 description 1
- 229960002594 arsenic trioxide Drugs 0.000 description 1
- 206010003246 arthritis Diseases 0.000 description 1
- 229960003272 asparaginase Drugs 0.000 description 1
- DCXYFEDJOCDNAF-UHFFFAOYSA-M asparaginate Chemical compound [O-]C(=O)C(N)CC(N)=O DCXYFEDJOCDNAF-UHFFFAOYSA-M 0.000 description 1
- 229960001230 asparagine Drugs 0.000 description 1
- 235000009582 asparagine Nutrition 0.000 description 1
- 230000000712 assembly Effects 0.000 description 1
- 238000000429 assembly Methods 0.000 description 1
- 230000002238 attenuated effect Effects 0.000 description 1
- 239000012822 autophagy inhibitor Substances 0.000 description 1
- 229960002756 azacitidine Drugs 0.000 description 1
- GRHLMSBCOPRFNA-UHFFFAOYSA-M azanide 2-oxidoacetate platinum(4+) Chemical compound N[Pt]1(N)OCC(=O)O1 GRHLMSBCOPRFNA-UHFFFAOYSA-M 0.000 description 1
- 229950011321 azaserine Drugs 0.000 description 1
- 229960002170 azathioprine Drugs 0.000 description 1
- LMEKQMALGUDUQG-UHFFFAOYSA-N azathioprine Chemical compound CN1C=NC([N+]([O-])=O)=C1SC1=NC=NC2=C1NC=N2 LMEKQMALGUDUQG-UHFFFAOYSA-N 0.000 description 1
- 150000001541 aziridines Chemical class 0.000 description 1
- 210000003719 b-lymphocyte Anatomy 0.000 description 1
- 230000001580 bacterial effect Effects 0.000 description 1
- 210000003651 basophil Anatomy 0.000 description 1
- 230000006399 behavior Effects 0.000 description 1
- 230000003542 behavioural effect Effects 0.000 description 1
- 108010005774 beta-Galactosidase Proteins 0.000 description 1
- 229960002537 betamethasone Drugs 0.000 description 1
- UREBDLICKHMUKA-DVTGEIKXSA-N betamethasone Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)CO)(O)[C@@]1(C)C[C@@H]2O UREBDLICKHMUKA-DVTGEIKXSA-N 0.000 description 1
- 229960001102 betamethasone dipropionate Drugs 0.000 description 1
- CIWBQSYVNNPZIQ-XYWKZLDCSA-N betamethasone dipropionate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)COC(=O)CC)(OC(=O)CC)[C@@]1(C)C[C@@H]2O CIWBQSYVNNPZIQ-XYWKZLDCSA-N 0.000 description 1
- PLCQGRYPOISRTQ-LWCNAHDDSA-L betamethasone sodium phosphate Chemical compound [Na+].[Na+].C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)COP([O-])([O-])=O)(O)[C@@]1(C)C[C@@H]2O PLCQGRYPOISRTQ-LWCNAHDDSA-L 0.000 description 1
- 229960005354 betamethasone sodium phosphate Drugs 0.000 description 1
- 229960004311 betamethasone valerate Drugs 0.000 description 1
- SNHRLVCMMWUAJD-SUYDQAKGSA-N betamethasone valerate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)CO)(OC(=O)CCCC)[C@@]1(C)C[C@@H]2O SNHRLVCMMWUAJD-SUYDQAKGSA-N 0.000 description 1
- 229960000997 bicalutamide Drugs 0.000 description 1
- 230000003115 biocidal effect Effects 0.000 description 1
- 230000015572 biosynthetic process Effects 0.000 description 1
- 229940126587 biotherapeutics Drugs 0.000 description 1
- 201000000053 blastoma Diseases 0.000 description 1
- 229960001561 bleomycin Drugs 0.000 description 1
- OYVAGSVQBOHSSS-UAPAGMARSA-O bleomycin A2 Chemical compound N([C@H](C(=O)N[C@H](C)[C@@H](O)[C@H](C)C(=O)N[C@@H]([C@H](O)C)C(=O)NCCC=1SC=C(N=1)C=1SC=C(N=1)C(=O)NCCC[S+](C)C)[C@@H](O[C@H]1[C@H]([C@@H](O)[C@H](O)[C@H](CO)O1)O[C@@H]1[C@H]([C@@H](OC(N)=O)[C@H](O)[C@@H](CO)O1)O)C=1N=CNC=1)C(=O)C1=NC([C@H](CC(N)=O)NC[C@H](N)C(N)=O)=NC(N)=C1C OYVAGSVQBOHSSS-UAPAGMARSA-O 0.000 description 1
- 239000008280 blood Substances 0.000 description 1
- 210000004369 blood Anatomy 0.000 description 1
- 230000036770 blood supply Effects 0.000 description 1
- 210000004204 blood vessel Anatomy 0.000 description 1
- 229950004272 brigatinib Drugs 0.000 description 1
- 229960005520 bryostatin Drugs 0.000 description 1
- MJQUEDHRCUIRLF-TVIXENOKSA-N bryostatin 1 Chemical compound C([C@@H]1CC(/[C@@H]([C@@](C(C)(C)/C=C/2)(O)O1)OC(=O)/C=C/C=C/CCC)=C\C(=O)OC)[C@H]([C@@H](C)O)OC(=O)C[C@H](O)C[C@@H](O1)C[C@H](OC(C)=O)C(C)(C)[C@]1(O)C[C@@H]1C\C(=C\C(=O)OC)C[C@H]\2O1 MJQUEDHRCUIRLF-TVIXENOKSA-N 0.000 description 1
- MUIWQCKLQMOUAT-AKUNNTHJSA-N bryostatin 20 Natural products COC(=O)C=C1C[C@@]2(C)C[C@]3(O)O[C@](C)(C[C@@H](O)CC(=O)O[C@](C)(C[C@@]4(C)O[C@](O)(CC5=CC(=O)O[C@]45C)C(C)(C)C=C[C@@](C)(C1)O2)[C@@H](C)O)C[C@H](OC(=O)C(C)(C)C)C3(C)C MUIWQCKLQMOUAT-AKUNNTHJSA-N 0.000 description 1
- 229960004436 budesonide Drugs 0.000 description 1
- CUWODFFVMXJOKD-UVLQAERKSA-N buserelin Chemical compound CCNC(=O)[C@@H]1CCCN1C(=O)[C@H](CCCN=C(N)N)NC(=O)[C@H](CC(C)C)NC(=O)[C@@H](COC(C)(C)C)NC(=O)[C@@H](NC(=O)[C@H](CO)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CC=1NC=NC=1)NC(=O)[C@H]1NC(=O)CC1)CC1=CC=C(O)C=C1 CUWODFFVMXJOKD-UVLQAERKSA-N 0.000 description 1
- 229960002719 buserelin Drugs 0.000 description 1
- 108700002839 cactinomycin Proteins 0.000 description 1
- 229950009908 cactinomycin Drugs 0.000 description 1
- 150000001720 carbohydrates Chemical class 0.000 description 1
- 235000014633 carbohydrates Nutrition 0.000 description 1
- 229960002115 carboquone Drugs 0.000 description 1
- 229960002438 carfilzomib Drugs 0.000 description 1
- 108010021331 carfilzomib Proteins 0.000 description 1
- BLMPQMFVWMYDKT-NZTKNTHTSA-N carfilzomib Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(=O)N[C@@H](CC(C)C)C(=O)[C@]1(C)OC1)NC(=O)CN1CCOCC1)CC1=CC=CC=C1 BLMPQMFVWMYDKT-NZTKNTHTSA-N 0.000 description 1
- 229960003261 carmofur Drugs 0.000 description 1
- 229960005243 carmustine Drugs 0.000 description 1
- 230000022131 cell cycle Effects 0.000 description 1
- 230000030833 cell death Effects 0.000 description 1
- 230000010261 cell growth Effects 0.000 description 1
- 230000004709 cell invasion Effects 0.000 description 1
- 230000001413 cellular effect Effects 0.000 description 1
- 229960003115 certolizumab pegol Drugs 0.000 description 1
- 230000008859 change Effects 0.000 description 1
- BLLIIPIJZPKUEG-HPTNQIKVSA-N chembl3304020 Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=N)C3=C(O)C=21)OC)C(C)=O)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 BLLIIPIJZPKUEG-HPTNQIKVSA-N 0.000 description 1
- 229940044683 chemotherapy drug Drugs 0.000 description 1
- 210000000038 chest Anatomy 0.000 description 1
- 229960003677 chloroquine Drugs 0.000 description 1
- WHTVZRBIWZFKQO-UHFFFAOYSA-N chloroquine Natural products ClC1=CC=C2C(NC(C)CCCN(CC)CC)=CC=NC2=C1 WHTVZRBIWZFKQO-UHFFFAOYSA-N 0.000 description 1
- 229960001480 chlorozotocin Drugs 0.000 description 1
- ZYVSOIYQKUDENJ-WKSBCEQHSA-N chromomycin A3 Chemical compound O([C@@H]1C[C@@H](O[C@H](C)[C@@H]1OC(C)=O)OC=1C=C2C=C3C[C@H]([C@@H](C(=O)C3=C(O)C2=C(O)C=1C)O[C@@H]1O[C@H](C)[C@@H](O)[C@H](O[C@@H]2O[C@H](C)[C@@H](O)[C@H](O[C@@H]3O[C@@H](C)[C@H](OC(C)=O)[C@@](C)(O)C3)C2)C1)[C@H](OC)C(=O)[C@@H](O)[C@@H](C)O)[C@@H]1C[C@@H](O)[C@@H](OC)[C@@H](C)O1 ZYVSOIYQKUDENJ-WKSBCEQHSA-N 0.000 description 1
- 230000001684 chronic effect Effects 0.000 description 1
- 229960004703 clobetasol propionate Drugs 0.000 description 1
- CBGUOGMQLZIXBE-XGQKBEPLSA-N clobetasol propionate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H](C)[C@@](C(=O)CCl)(OC(=O)CC)[C@@]1(C)C[C@@H]2O CBGUOGMQLZIXBE-XGQKBEPLSA-N 0.000 description 1
- 229960005465 clobetasone butyrate Drugs 0.000 description 1
- HJKBJIYDJLVSAO-UHFFFAOYSA-L clodronic acid disodium salt Chemical compound [Na+].[Na+].OP([O-])(=O)C(Cl)(Cl)P(O)([O-])=O HJKBJIYDJLVSAO-UHFFFAOYSA-L 0.000 description 1
- 229960000928 clofarabine Drugs 0.000 description 1
- WDDPHFBMKLOVOX-AYQXTPAHSA-N clofarabine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1F WDDPHFBMKLOVOX-AYQXTPAHSA-N 0.000 description 1
- 230000001149 cognitive effect Effects 0.000 description 1
- 208000029742 colonic neoplasm Diseases 0.000 description 1
- 238000011284 combination treatment Methods 0.000 description 1
- 239000000562 conjugate Substances 0.000 description 1
- BMCQMVFGOVHVNG-TUFAYURCSA-N cortisol 17-butyrate Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)CO)(OC(=O)CCC)[C@@]1(C)C[C@@H]2O BMCQMVFGOVHVNG-TUFAYURCSA-N 0.000 description 1
- FZCHYNWYXKICIO-FZNHGJLXSA-N cortisol 17-valerate Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)CO)(OC(=O)CCCC)[C@@]1(C)C[C@@H]2O FZCHYNWYXKICIO-FZNHGJLXSA-N 0.000 description 1
- ALEXXDVDDISNDU-JZYPGELDSA-N cortisol 21-acetate Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)COC(=O)C)(O)[C@@]1(C)C[C@@H]2O ALEXXDVDDISNDU-JZYPGELDSA-N 0.000 description 1
- 229960003290 cortisone acetate Drugs 0.000 description 1
- 239000006071 cream Substances 0.000 description 1
- 229960005061 crizotinib Drugs 0.000 description 1
- 108010089438 cryptophycin 1 Proteins 0.000 description 1
- PSNOPSMXOBPNNV-VVCTWANISA-N cryptophycin 1 Chemical compound C1=C(Cl)C(OC)=CC=C1C[C@@H]1C(=O)NC[C@@H](C)C(=O)O[C@@H](CC(C)C)C(=O)O[C@H]([C@H](C)[C@@H]2[C@H](O2)C=2C=CC=CC=2)C/C=C/C(=O)N1 PSNOPSMXOBPNNV-VVCTWANISA-N 0.000 description 1
- 108010090203 cryptophycin 8 Proteins 0.000 description 1
- PSNOPSMXOBPNNV-UHFFFAOYSA-N cryptophycin-327 Natural products C1=C(Cl)C(OC)=CC=C1CC1C(=O)NCC(C)C(=O)OC(CC(C)C)C(=O)OC(C(C)C2C(O2)C=2C=CC=CC=2)CC=CC(=O)N1 PSNOPSMXOBPNNV-UHFFFAOYSA-N 0.000 description 1
- 235000012754 curcumin Nutrition 0.000 description 1
- 238000005520 cutting process Methods 0.000 description 1
- UWFYSQMTEOIJJG-FDTZYFLXSA-N cyproterone acetate Chemical compound C1=C(Cl)C2=CC(=O)[C@@H]3C[C@@H]3[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(C)=O)(OC(=O)C)[C@@]1(C)CC2 UWFYSQMTEOIJJG-FDTZYFLXSA-N 0.000 description 1
- 229960000978 cyproterone acetate Drugs 0.000 description 1
- 229940104302 cytosine Drugs 0.000 description 1
- 229960003901 dacarbazine Drugs 0.000 description 1
- 229960000640 dactinomycin Drugs 0.000 description 1
- 230000006378 damage Effects 0.000 description 1
- 229960005029 darbepoetin alfa Drugs 0.000 description 1
- 206010061428 decreased appetite Diseases 0.000 description 1
- 230000003111 delayed effect Effects 0.000 description 1
- WBGKWQHBNHJJPZ-LECWWXJVSA-N desonide Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@@H]2[C@@H]1[C@@H]1C[C@H]3OC(C)(C)O[C@@]3(C(=O)CO)[C@@]1(C)C[C@@H]2O WBGKWQHBNHJJPZ-LECWWXJVSA-N 0.000 description 1
- 229960003662 desonide Drugs 0.000 description 1
- 230000006866 deterioration Effects 0.000 description 1
- 229950003913 detorubicin Drugs 0.000 description 1
- 229960002344 dexamethasone sodium phosphate Drugs 0.000 description 1
- PLCQGRYPOISRTQ-FCJDYXGNSA-L dexamethasone sodium phosphate Chemical compound [Na+].[Na+].C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)COP([O-])([O-])=O)(O)[C@@]1(C)C[C@@H]2O PLCQGRYPOISRTQ-FCJDYXGNSA-L 0.000 description 1
- 229960000605 dexrazoxane Drugs 0.000 description 1
- NIJJYAXOARWZEE-UHFFFAOYSA-N di-n-propyl-acetic acid Natural products CCCC(C(O)=O)CCC NIJJYAXOARWZEE-UHFFFAOYSA-N 0.000 description 1
- 229960001259 diclofenac Drugs 0.000 description 1
- DCOPUUMXTXDBNB-UHFFFAOYSA-N diclofenac Chemical compound OC(=O)CC1=CC=CC=C1NC1=C(Cl)C=CC=C1Cl DCOPUUMXTXDBNB-UHFFFAOYSA-N 0.000 description 1
- 235000014113 dietary fatty acids Nutrition 0.000 description 1
- RGLYKWWBQGJZGM-ISLYRVAYSA-N diethylstilbestrol Chemical compound C=1C=C(O)C=CC=1C(/CC)=C(\CC)C1=CC=C(O)C=C1 RGLYKWWBQGJZGM-ISLYRVAYSA-N 0.000 description 1
- 229960000452 diethylstilbestrol Drugs 0.000 description 1
- VFLDPWHFBUODDF-UHFFFAOYSA-N diferuloylmethane Natural products C1=C(O)C(OC)=CC(C=CC(=O)CC(=O)C=CC=2C=C(OC)C(O)=CC=2)=C1 VFLDPWHFBUODDF-UHFFFAOYSA-N 0.000 description 1
- 230000008034 disappearance Effects 0.000 description 1
- NYDXNILOWQXUOF-UHFFFAOYSA-L disodium;2-[[4-[2-(2-amino-4-oxo-1,7-dihydropyrrolo[2,3-d]pyrimidin-5-yl)ethyl]benzoyl]amino]pentanedioate Chemical compound [Na+].[Na+].C=1NC=2NC(N)=NC(=O)C=2C=1CCC1=CC=C(C(=O)NC(CCC([O-])=O)C([O-])=O)C=C1 NYDXNILOWQXUOF-UHFFFAOYSA-L 0.000 description 1
- 229960002563 disulfiram Drugs 0.000 description 1
- 229930004069 diterpene Natural products 0.000 description 1
- 150000004141 diterpene derivatives Chemical class 0.000 description 1
- 239000003534 dna topoisomerase inhibitor Substances 0.000 description 1
- AMRJKAQTDDKMCE-UHFFFAOYSA-N dolastatin Chemical compound CC(C)C(N(C)C)C(=O)NC(C(C)C)C(=O)N(C)C(C(C)C)C(OC)CC(=O)N1CCCC1C(OC)C(C)C(=O)NC(C=1SC=CN=1)CC1=CC=CC=C1 AMRJKAQTDDKMCE-UHFFFAOYSA-N 0.000 description 1
- 229930188854 dolastatin Natural products 0.000 description 1
- ZWAOHEXOSAUJHY-ZIYNGMLESA-N doxifluridine Chemical compound O[C@@H]1[C@H](O)[C@@H](C)O[C@H]1N1C(=O)NC(=O)C(F)=C1 ZWAOHEXOSAUJHY-ZIYNGMLESA-N 0.000 description 1
- 229950005454 doxifluridine Drugs 0.000 description 1
- NOTIQUSPUUHHEH-UXOVVSIBSA-N dromostanolone propionate Chemical compound C([C@@H]1CC2)C(=O)[C@H](C)C[C@]1(C)[C@@H]1[C@@H]2[C@@H]2CC[C@H](OC(=O)CC)[C@@]2(C)CC1 NOTIQUSPUUHHEH-UXOVVSIBSA-N 0.000 description 1
- 229960004242 dronabinol Drugs 0.000 description 1
- 229950004683 drostanolone propionate Drugs 0.000 description 1
- 229960001850 droxicam Drugs 0.000 description 1
- OEHFRZLKGRKFAS-UHFFFAOYSA-N droxicam Chemical compound C12=CC=CC=C2S(=O)(=O)N(C)C(C2=O)=C1OC(=O)N2C1=CC=CC=N1 OEHFRZLKGRKFAS-UHFFFAOYSA-N 0.000 description 1
- 229940000406 drug candidate Drugs 0.000 description 1
- 229960005501 duocarmycin Drugs 0.000 description 1
- VQNATVDKACXKTF-XELLLNAOSA-N duocarmycin Chemical compound COC1=C(OC)C(OC)=C2NC(C(=O)N3C4=CC(=O)C5=C([C@@]64C[C@@H]6C3)C=C(N5)C(=O)OC)=CC2=C1 VQNATVDKACXKTF-XELLLNAOSA-N 0.000 description 1
- 229930184221 duocarmycin Natural products 0.000 description 1
- JWJOTENAMICLJG-QWBYCMEYSA-N dutasteride Chemical compound O=C([C@H]1CC[C@H]2[C@H]3[C@@H]([C@]4(C=CC(=O)N[C@@H]4CC3)C)CC[C@@]21C)NC1=CC(C(F)(F)F)=CC=C1C(F)(F)F JWJOTENAMICLJG-QWBYCMEYSA-N 0.000 description 1
- 229960004199 dutasteride Drugs 0.000 description 1
- VLCYCQAOQCDTCN-UHFFFAOYSA-N eflornithine Chemical compound NCCCC(N)(C(F)F)C(O)=O VLCYCQAOQCDTCN-UHFFFAOYSA-N 0.000 description 1
- 201000008184 embryoma Diseases 0.000 description 1
- 229940073621 enbrel Drugs 0.000 description 1
- 229950011487 enocitabine Drugs 0.000 description 1
- 230000002255 enzymatic effect Effects 0.000 description 1
- 210000003979 eosinophil Anatomy 0.000 description 1
- 229940030275 epigallocatechin gallate Drugs 0.000 description 1
- 230000001973 epigenetic effect Effects 0.000 description 1
- YJGVMLPVUAXIQN-UHFFFAOYSA-N epipodophyllotoxin Natural products COC1=C(OC)C(OC)=CC(C2C3=CC=4OCOC=4C=C3C(O)C3C2C(OC3)=O)=C1 YJGVMLPVUAXIQN-UHFFFAOYSA-N 0.000 description 1
- 229950002973 epitiostanol Drugs 0.000 description 1
- 229960003388 epoetin alfa Drugs 0.000 description 1
- 230000008029 eradication Effects 0.000 description 1
- 229960001842 estramustine Drugs 0.000 description 1
- FRPJXPJMRWBBIH-RBRWEJTLSA-N estramustine Chemical compound ClCCN(CCCl)C(=O)OC1=CC=C2[C@H]3CC[C@](C)([C@H](CC4)O)[C@@H]4[C@@H]3CCC2=C1 FRPJXPJMRWBBIH-RBRWEJTLSA-N 0.000 description 1
- 229940011871 estrogen Drugs 0.000 description 1
- 239000000262 estrogen Substances 0.000 description 1
- 239000000328 estrogen antagonist Substances 0.000 description 1
- JKKFKPJIXZFSSB-CBZIJGRNSA-N estrone 3-sulfate Chemical compound OS(=O)(=O)OC1=CC=C2[C@H]3CC[C@](C)(C(CC4)=O)[C@@H]4[C@@H]3CCC2=C1 JKKFKPJIXZFSSB-CBZIJGRNSA-N 0.000 description 1
- 229960000403 etanercept Drugs 0.000 description 1
- 125000001495 ethyl group Chemical group [H]C([H])([H])C([H])([H])* 0.000 description 1
- 229940009626 etidronate Drugs 0.000 description 1
- 229940115924 etigilimab Drugs 0.000 description 1
- 229960005293 etodolac Drugs 0.000 description 1
- XFBVBWWRPKNWHW-UHFFFAOYSA-N etodolac Chemical compound C1COC(CC)(CC(O)=O)C2=N[C]3C(CC)=CC=CC3=C21 XFBVBWWRPKNWHW-UHFFFAOYSA-N 0.000 description 1
- 229960000255 exemestane Drugs 0.000 description 1
- 229950011548 fadrozole Drugs 0.000 description 1
- 229940043168 fareston Drugs 0.000 description 1
- 229940087861 faslodex Drugs 0.000 description 1
- 206010016256 fatigue Diseases 0.000 description 1
- 229930195729 fatty acid Natural products 0.000 description 1
- 239000000194 fatty acid Substances 0.000 description 1
- 150000004665 fatty acids Chemical class 0.000 description 1
- ZWJINEZUASEZBH-UHFFFAOYSA-N fenamic acid Chemical class OC(=O)C1=CC=CC=C1NC1=CC=CC=C1 ZWJINEZUASEZBH-UHFFFAOYSA-N 0.000 description 1
- 229960001419 fenoprofen Drugs 0.000 description 1
- 229950003662 fenretinide Drugs 0.000 description 1
- 210000002950 fibroblast Anatomy 0.000 description 1
- 229960004039 finasteride Drugs 0.000 description 1
- DBEPLOCGEIEOCV-WSBQPABSSA-N finasteride Chemical compound N([C@@H]1CC2)C(=O)C=C[C@]1(C)[C@@H]1[C@@H]2[C@@H]2CC[C@H](C(=O)NC(C)(C)C)[C@@]2(C)CC1 DBEPLOCGEIEOCV-WSBQPABSSA-N 0.000 description 1
- 150000002206 flavan-3-ols Chemical class 0.000 description 1
- 235000011987 flavanols Nutrition 0.000 description 1
- 238000000684 flow cytometry Methods 0.000 description 1
- 229960000961 floxuridine Drugs 0.000 description 1
- ODKNJVUHOIMIIZ-RRKCRQDMSA-N floxuridine Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C(F)=C1 ODKNJVUHOIMIIZ-RRKCRQDMSA-N 0.000 description 1
- 229960000390 fludarabine Drugs 0.000 description 1
- GIUYCYHIANZCFB-FJFJXFQQSA-N fludarabine phosphate Chemical compound C1=NC=2C(N)=NC(F)=NC=2N1[C@@H]1O[C@H](COP(O)(O)=O)[C@@H](O)[C@@H]1O GIUYCYHIANZCFB-FJFJXFQQSA-N 0.000 description 1
- 229960004369 flufenamic acid Drugs 0.000 description 1
- LPEPZBJOKDYZAD-UHFFFAOYSA-N flufenamic acid Chemical compound OC(=O)C1=CC=CC=C1NC1=CC=CC(C(F)(F)F)=C1 LPEPZBJOKDYZAD-UHFFFAOYSA-N 0.000 description 1
- 229960001347 fluocinolone acetonide Drugs 0.000 description 1
- FEBLZLNTKCEFIT-VSXGLTOVSA-N fluocinolone acetonide Chemical compound C1([C@@H](F)C2)=CC(=O)C=C[C@]1(C)[C@]1(F)[C@@H]2[C@@H]2C[C@H]3OC(C)(C)O[C@@]3(C(=O)CO)[C@@]2(C)C[C@@H]1O FEBLZLNTKCEFIT-VSXGLTOVSA-N 0.000 description 1
- 229960000785 fluocinonide Drugs 0.000 description 1
- YLRFCQOZQXIBAB-RBZZARIASA-N fluoxymesterone Chemical compound C1CC2=CC(=O)CC[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1CC[C@](C)(O)[C@@]1(C)C[C@@H]2O YLRFCQOZQXIBAB-RBZZARIASA-N 0.000 description 1
- 229960001751 fluoxymesterone Drugs 0.000 description 1
- DEFOZIFYUBUHHU-IYQKUMFPSA-N fluprednidene acetate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1CC(=C)[C@@](C(=O)COC(=O)C)(O)[C@@]1(C)C[C@@H]2O DEFOZIFYUBUHHU-IYQKUMFPSA-N 0.000 description 1
- 229960002650 fluprednidene acetate Drugs 0.000 description 1
- 229960002390 flurbiprofen Drugs 0.000 description 1
- SYTBZMRGLBWNTM-UHFFFAOYSA-N flurbiprofen Chemical compound FC1=CC(C(C(O)=O)C)=CC=C1C1=CC=CC=C1 SYTBZMRGLBWNTM-UHFFFAOYSA-N 0.000 description 1
- 229960002074 flutamide Drugs 0.000 description 1
- MKXKFYHWDHIYRV-UHFFFAOYSA-N flutamide Chemical compound CC(C)C(=O)NC1=CC=C([N+]([O-])=O)C(C(F)(F)F)=C1 MKXKFYHWDHIYRV-UHFFFAOYSA-N 0.000 description 1
- 235000019152 folic acid Nutrition 0.000 description 1
- 239000011724 folic acid Substances 0.000 description 1
- 229960000304 folic acid Drugs 0.000 description 1
- 150000002224 folic acids Chemical class 0.000 description 1
- 230000003325 follicular Effects 0.000 description 1
- 229940001490 fosamax Drugs 0.000 description 1
- YAKWPXVTIGTRJH-UHFFFAOYSA-N fotemustine Chemical compound CCOP(=O)(OCC)C(C)NC(=O)N(CCCl)N=O YAKWPXVTIGTRJH-UHFFFAOYSA-N 0.000 description 1
- 229960004783 fotemustine Drugs 0.000 description 1
- 229960002258 fulvestrant Drugs 0.000 description 1
- 230000002538 fungal effect Effects 0.000 description 1
- 229940044658 gallium nitrate Drugs 0.000 description 1
- LVJJFMLUMNSUFN-UHFFFAOYSA-N gallocatechin gallate Natural products C1=C(O)C=C2OC(C=3C=C(O)C(O)=CC=3)C(O)CC2=C1OC(=O)C1=CC(O)=C(O)C(O)=C1 LVJJFMLUMNSUFN-UHFFFAOYSA-N 0.000 description 1
- 229940044627 gamma-interferon Drugs 0.000 description 1
- QTQAWLPCGQOSGP-GBTDJJJQSA-N geldanamycin Chemical compound N1C(=O)\C(C)=C/C=C\[C@@H](OC)[C@H](OC(N)=O)\C(C)=C/[C@@H](C)[C@@H](O)[C@H](OC)C[C@@H](C)CC2=C(OC)C(=O)C=C1C2=O QTQAWLPCGQOSGP-GBTDJJJQSA-N 0.000 description 1
- 229940020967 gemzar Drugs 0.000 description 1
- 238000011223 gene expression profiling Methods 0.000 description 1
- 238000001415 gene therapy Methods 0.000 description 1
- 230000002068 genetic effect Effects 0.000 description 1
- 150000004676 glycans Chemical class 0.000 description 1
- 229930182470 glycoside Natural products 0.000 description 1
- 150000002343 gold Chemical class 0.000 description 1
- 229960001743 golimumab Drugs 0.000 description 1
- 210000003714 granulocyte Anatomy 0.000 description 1
- 230000012010 growth Effects 0.000 description 1
- 239000003966 growth inhibitor Substances 0.000 description 1
- 201000009277 hairy cell leukemia Diseases 0.000 description 1
- 231100000869 headache Toxicity 0.000 description 1
- UUVWYPNAQBNQJQ-UHFFFAOYSA-N hexamethylmelamine Chemical compound CN(C)C1=NC(N(C)C)=NC(N(C)C)=N1 UUVWYPNAQBNQJQ-UHFFFAOYSA-N 0.000 description 1
- FUZZWVXGSFPDMH-UHFFFAOYSA-M hexanoate Chemical compound CCCCCC([O-])=O FUZZWVXGSFPDMH-UHFFFAOYSA-M 0.000 description 1
- 210000003701 histiocyte Anatomy 0.000 description 1
- 239000003276 histone deacetylase inhibitor Substances 0.000 description 1
- HHXHVIJIIXKSOE-QILQGKCVSA-N histrelin Chemical compound CCNC(=O)[C@@H]1CCCN1C(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CO)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CC=1N=CNC=1)NC(=O)[C@H]1NC(=O)CC1)CC(N=C1)=CN1CC1=CC=CC=C1 HHXHVIJIIXKSOE-QILQGKCVSA-N 0.000 description 1
- 229960003911 histrelin acetate Drugs 0.000 description 1
- 102000048776 human CD274 Human genes 0.000 description 1
- 210000005260 human cell Anatomy 0.000 description 1
- 229940048921 humira Drugs 0.000 description 1
- 229960000890 hydrocortisone Drugs 0.000 description 1
- 229960001067 hydrocortisone acetate Drugs 0.000 description 1
- 229960001524 hydrocortisone butyrate Drugs 0.000 description 1
- 229960001330 hydroxycarbamide Drugs 0.000 description 1
- XXSMGPRMXLTPCZ-UHFFFAOYSA-N hydroxychloroquine Chemical compound ClC1=CC=C2C(NC(C)CCCN(CCO)CC)=CC=NC2=C1 XXSMGPRMXLTPCZ-UHFFFAOYSA-N 0.000 description 1
- 229960004171 hydroxychloroquine Drugs 0.000 description 1
- KNOSIOWNDGUGFJ-UHFFFAOYSA-N hydroxysesamone Natural products C1=CC(O)=C2C(=O)C(CC=C(C)C)=C(O)C(=O)C2=C1O KNOSIOWNDGUGFJ-UHFFFAOYSA-N 0.000 description 1
- 210000003026 hypopharynx Anatomy 0.000 description 1
- 229940015872 ibandronate Drugs 0.000 description 1
- 229960001680 ibuprofen Drugs 0.000 description 1
- HOMGKSMUEGBAAB-UHFFFAOYSA-N ifosfamide Chemical compound ClCCNP1(=O)OCCCN1CCCl HOMGKSMUEGBAAB-UHFFFAOYSA-N 0.000 description 1
- 229960001101 ifosfamide Drugs 0.000 description 1
- 238000005417 image-selected in vivo spectroscopy Methods 0.000 description 1
- RAXXELZNTBOGNW-UHFFFAOYSA-N imidazole Substances C1=CNC=N1 RAXXELZNTBOGNW-UHFFFAOYSA-N 0.000 description 1
- 230000001900 immune effect Effects 0.000 description 1
- 230000008073 immune recognition Effects 0.000 description 1
- 210000000987 immune system Anatomy 0.000 description 1
- 208000026278 immune system disease Diseases 0.000 description 1
- 238000003119 immunoblot Methods 0.000 description 1
- 230000002163 immunogen Effects 0.000 description 1
- 230000005847 immunogenicity Effects 0.000 description 1
- 239000002955 immunomodulating agent Substances 0.000 description 1
- 238000001114 immunoprecipitation Methods 0.000 description 1
- 230000001771 impaired effect Effects 0.000 description 1
- 230000001976 improved effect Effects 0.000 description 1
- 229960000905 indomethacin Drugs 0.000 description 1
- 230000001939 inductive effect Effects 0.000 description 1
- 230000002757 inflammatory effect Effects 0.000 description 1
- 230000004054 inflammatory process Effects 0.000 description 1
- 229960000598 infliximab Drugs 0.000 description 1
- 238000011221 initial treatment Methods 0.000 description 1
- 239000007924 injection Substances 0.000 description 1
- 238000002347 injection Methods 0.000 description 1
- 206010022437 insomnia Diseases 0.000 description 1
- 108010042209 insulin receptor tyrosine kinase Proteins 0.000 description 1
- 238000012739 integrated shape imaging system Methods 0.000 description 1
- 108010021315 integrin beta7 Proteins 0.000 description 1
- 239000000138 intercalating agent Substances 0.000 description 1
- 208000003243 intestinal obstruction Diseases 0.000 description 1
- 238000001361 intraarterial administration Methods 0.000 description 1
- 238000007917 intracranial administration Methods 0.000 description 1
- 238000007918 intramuscular administration Methods 0.000 description 1
- 230000009545 invasion Effects 0.000 description 1
- 229960004768 irinotecan Drugs 0.000 description 1
- OMEUGRCNAZNQLN-UHFFFAOYSA-N isis 5132 Chemical compound O=C1NC(=O)C(C)=CN1C1OC(COP(O)(=S)OC2C(OC(C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=NC=NC(N)=C3N=C2)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)OC2C(OC(C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=NC=NC(N)=C3N=C2)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=NC=NC(N)=C3N=C2)COP(O)(=S)OC2C(OC(C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(S)(=O)OC2C(OC(C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)OC2C(OC(C2)N2C(NC(=O)C(C)=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C3=C(C(NC(N)=N3)=O)N=C2)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C(N=C(N)C=C2)=O)COP(O)(=S)OC2C(OC(C2)N2C(NC(=O)C(C)=C2)=O)CO)C(O)C1 OMEUGRCNAZNQLN-UHFFFAOYSA-N 0.000 description 1
- 229950002252 isoxicam Drugs 0.000 description 1
- YYUAYBYLJSNDCX-UHFFFAOYSA-N isoxicam Chemical compound OC=1C2=CC=CC=C2S(=O)(=O)N(C)C=1C(=O)NC=1C=C(C)ON=1 YYUAYBYLJSNDCX-UHFFFAOYSA-N 0.000 description 1
- MWDZOUNAPSSOEL-UHFFFAOYSA-N kaempferol Natural products OC1=C(C(=O)c2cc(O)cc(O)c2O1)c3ccc(O)cc3 MWDZOUNAPSSOEL-UHFFFAOYSA-N 0.000 description 1
- DKYWVDODHFEZIM-UHFFFAOYSA-N ketoprofen Chemical compound OC(=O)C(C)C1=CC=CC(C(=O)C=2C=CC=CC=2)=C1 DKYWVDODHFEZIM-UHFFFAOYSA-N 0.000 description 1
- 229960000991 ketoprofen Drugs 0.000 description 1
- 229940043355 kinase inhibitor Drugs 0.000 description 1
- 229940116108 lactase Drugs 0.000 description 1
- CWPGNVFCJOPXFB-UHFFFAOYSA-N lapachol Chemical compound C1=CC=C2C(=O)C(=O)C(CC=C(C)C)=C(O)C2=C1 CWPGNVFCJOPXFB-UHFFFAOYSA-N 0.000 description 1
- SIUGQQMOYSVTAT-UHFFFAOYSA-N lapachol Natural products CC(=CCC1C(O)C(=O)c2ccccc2C1=O)C SIUGQQMOYSVTAT-UHFFFAOYSA-N 0.000 description 1
- 210000000867 larynx Anatomy 0.000 description 1
- 229950002183 lebrikizumab Drugs 0.000 description 1
- 229960004942 lenalidomide Drugs 0.000 description 1
- GOTYRUGSSMKFNF-UHFFFAOYSA-N lenalidomide Chemical compound C1C=2C(N)=CC=CC=2C(=O)N1C1CCC(=O)NC1=O GOTYRUGSSMKFNF-UHFFFAOYSA-N 0.000 description 1
- 229940115286 lentinan Drugs 0.000 description 1
- GFIJNRVAKGFPGQ-LIJARHBVSA-N leuprolide Chemical compound CCNC(=O)[C@@H]1CCCN1C(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CC(C)C)NC(=O)[C@@H](CC(C)C)NC(=O)[C@@H](NC(=O)[C@H](CO)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CC=1N=CNC=1)NC(=O)[C@H]1NC(=O)CC1)CC1=CC=C(O)C=C1 GFIJNRVAKGFPGQ-LIJARHBVSA-N 0.000 description 1
- 229960004338 leuprorelin Drugs 0.000 description 1
- 229960001614 levamisole Drugs 0.000 description 1
- 125000005645 linoleyl group Chemical group 0.000 description 1
- 201000002250 liver carcinoma Diseases 0.000 description 1
- 229960002247 lomustine Drugs 0.000 description 1
- DHMTURDWPRKSOA-RUZDIDTESA-N lonafarnib Chemical compound C1CN(C(=O)N)CCC1CC(=O)N1CCC([C@@H]2C3=C(Br)C=C(Cl)C=C3CCC3=CC(Br)=CN=C32)CC1 DHMTURDWPRKSOA-RUZDIDTESA-N 0.000 description 1
- 229960000994 lumiracoxib Drugs 0.000 description 1
- KHPKQFYUPIUARC-UHFFFAOYSA-N lumiracoxib Chemical compound OC(=O)CC1=CC(C)=CC=C1NC1=C(F)C=CC=C1Cl KHPKQFYUPIUARC-UHFFFAOYSA-N 0.000 description 1
- 210000004072 lung Anatomy 0.000 description 1
- 201000005249 lung adenocarcinoma Diseases 0.000 description 1
- 201000005243 lung squamous cell carcinoma Diseases 0.000 description 1
- RVFGKBWWUQOIOU-NDEPHWFRSA-N lurtotecan Chemical compound O=C([C@]1(O)CC)OCC(C(N2CC3=4)=O)=C1C=C2C3=NC1=CC=2OCCOC=2C=C1C=4CN1CCN(C)CC1 RVFGKBWWUQOIOU-NDEPHWFRSA-N 0.000 description 1
- 229950002654 lurtotecan Drugs 0.000 description 1
- 230000000527 lymphocytic effect Effects 0.000 description 1
- 210000002540 macrophage Anatomy 0.000 description 1
- 230000036210 malignancy Effects 0.000 description 1
- 210000004962 mammalian cell Anatomy 0.000 description 1
- MQXVYODZCMMZEM-ZYUZMQFOSA-N mannomustine Chemical compound ClCCNC[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)CNCCCl MQXVYODZCMMZEM-ZYUZMQFOSA-N 0.000 description 1
- 229950008612 mannomustine Drugs 0.000 description 1
- 229940099262 marinol Drugs 0.000 description 1
- 229950002736 marizomib Drugs 0.000 description 1
- 238000005259 measurement Methods 0.000 description 1
- 229960003803 meclofenamic acid Drugs 0.000 description 1
- PSGAAPLEWMOORI-PEINSRQWSA-N medroxyprogesterone acetate Chemical compound C([C@@]12C)CC(=O)C=C1[C@@H](C)C[C@@H]1[C@@H]2CC[C@]2(C)[C@@](OC(C)=O)(C(C)=O)CC[C@H]21 PSGAAPLEWMOORI-PEINSRQWSA-N 0.000 description 1
- 229960002985 medroxyprogesterone acetate Drugs 0.000 description 1
- 229960003464 mefenamic acid Drugs 0.000 description 1
- HYYBABOKPJLUIN-UHFFFAOYSA-N mefenamic acid Chemical compound CC1=CC=CC(NC=2C(=CC=CC=2)C(O)=O)=C1C HYYBABOKPJLUIN-UHFFFAOYSA-N 0.000 description 1
- 229960001929 meloxicam Drugs 0.000 description 1
- 229960000901 mepacrine Drugs 0.000 description 1
- 229960004635 mesna Drugs 0.000 description 1
- 108020004999 messenger RNA Proteins 0.000 description 1
- 230000002503 metabolic effect Effects 0.000 description 1
- 230000004060 metabolic process Effects 0.000 description 1
- 229960004469 methoxsalen Drugs 0.000 description 1
- 125000000956 methoxy group Chemical group [H]C([H])([H])O* 0.000 description 1
- 125000002496 methyl group Chemical group [H]C([H])([H])* 0.000 description 1
- 230000011987 methylation Effects 0.000 description 1
- 238000007069 methylation reaction Methods 0.000 description 1
- VQJHOPSWBGJHQS-UHFFFAOYSA-N metoprine, methodichlorophen Chemical compound CC1=NC(N)=NC(N)=C1C1=CC=C(Cl)C(Cl)=C1 VQJHOPSWBGJHQS-UHFFFAOYSA-N 0.000 description 1
- VAOCPAMSLUNLGC-UHFFFAOYSA-N metronidazole Chemical compound CC1=NC=C([N+]([O-])=O)N1CCO VAOCPAMSLUNLGC-UHFFFAOYSA-N 0.000 description 1
- 229960000282 metronidazole Drugs 0.000 description 1
- HPNSFSBZBAHARI-UHFFFAOYSA-N micophenolic acid Natural products OC1=C(CC=C(C)CCC(O)=O)C(OC)=C(C)C2=C1C(=O)OC2 HPNSFSBZBAHARI-UHFFFAOYSA-N 0.000 description 1
- 210000004688 microtubule Anatomy 0.000 description 1
- 230000025090 microtubule depolymerization Effects 0.000 description 1
- 206010027599 migraine Diseases 0.000 description 1
- CFCUWKMKBJTWLW-BKHRDMLASA-N mithramycin Chemical compound O([C@@H]1C[C@@H](O[C@H](C)[C@H]1O)OC=1C=C2C=C3C[C@H]([C@@H](C(=O)C3=C(O)C2=C(O)C=1C)O[C@@H]1O[C@H](C)[C@@H](O)[C@H](O[C@@H]2O[C@H](C)[C@H](O)[C@H](O[C@@H]3O[C@H](C)[C@@H](O)[C@@](C)(O)C3)C2)C1)[C@H](OC)C(=O)[C@@H](O)[C@@H](C)O)[C@H]1C[C@@H](O)[C@H](O)[C@@H](C)O1 CFCUWKMKBJTWLW-BKHRDMLASA-N 0.000 description 1
- 229960005485 mitobronitol Drugs 0.000 description 1
- 230000009149 molecular binding Effects 0.000 description 1
- 238000010369 molecular cloning Methods 0.000 description 1
- 230000003990 molecular pathway Effects 0.000 description 1
- 229960001664 mometasone Drugs 0.000 description 1
- QLIIKPVHVRXHRI-CXSFZGCWSA-N mometasone Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(Cl)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)CCl)(O)[C@@]1(C)C[C@@H]2O QLIIKPVHVRXHRI-CXSFZGCWSA-N 0.000 description 1
- 210000001616 monocyte Anatomy 0.000 description 1
- 210000000214 mouth Anatomy 0.000 description 1
- 238000011512 multiplexed immunoassay Methods 0.000 description 1
- 229960000951 mycophenolic acid Drugs 0.000 description 1
- HPNSFSBZBAHARI-RUDMXATFSA-N mycophenolic acid Chemical compound OC1=C(C\C=C(/C)CCC(O)=O)C(OC)=C(C)C2=C1C(=O)OC2 HPNSFSBZBAHARI-RUDMXATFSA-N 0.000 description 1
- 210000000066 myeloid cell Anatomy 0.000 description 1
- 208000025113 myeloid leukemia Diseases 0.000 description 1
- 230000001114 myogenic effect Effects 0.000 description 1
- 229960004719 nandrolone Drugs 0.000 description 1
- NPAGDVCDWIYMMC-IZPLOLCNSA-N nandrolone Chemical compound O=C1CC[C@@H]2[C@H]3CC[C@](C)([C@H](CC4)O)[C@@H]4[C@@H]3CCC2=C1 NPAGDVCDWIYMMC-IZPLOLCNSA-N 0.000 description 1
- 229960002009 naproxen Drugs 0.000 description 1
- CMWTZPSULFXXJA-VIFPVBQESA-M naproxen(1-) Chemical compound C1=C([C@H](C)C([O-])=O)C=CC2=CC(OC)=CC=C21 CMWTZPSULFXXJA-VIFPVBQESA-M 0.000 description 1
- 210000001989 nasopharynx Anatomy 0.000 description 1
- 210000000822 natural killer cell Anatomy 0.000 description 1
- 229930014626 natural product Natural products 0.000 description 1
- 230000008693 nausea Effects 0.000 description 1
- 229950007221 nedaplatin Drugs 0.000 description 1
- 230000009826 neoplastic cell growth Effects 0.000 description 1
- 210000000440 neutrophil Anatomy 0.000 description 1
- 239000002547 new drug Substances 0.000 description 1
- 229940080607 nexavar Drugs 0.000 description 1
- 229960002653 nilutamide Drugs 0.000 description 1
- XWXYUMMDTVBTOU-UHFFFAOYSA-N nilutamide Chemical compound O=C1C(C)(C)NC(=O)N1C1=CC=C([N+]([O-])=O)C(C(F)(F)F)=C1 XWXYUMMDTVBTOU-UHFFFAOYSA-N 0.000 description 1
- VFEDRRNHLBGPNN-UHFFFAOYSA-N nimustine Chemical compound CC1=NC=C(CNC(=O)N(CCCl)N=O)C(N)=N1 VFEDRRNHLBGPNN-UHFFFAOYSA-N 0.000 description 1
- 229960001420 nimustine Drugs 0.000 description 1
- 229950011068 niraparib Drugs 0.000 description 1
- PCHKPVIQAHNQLW-CQSZACIVSA-N niraparib Chemical compound N1=C2C(C(=O)N)=CC=CC2=CN1C(C=C1)=CC=C1[C@@H]1CCCNC1 PCHKPVIQAHNQLW-CQSZACIVSA-N 0.000 description 1
- 125000000449 nitro group Chemical group [O-][N+](*)=O 0.000 description 1
- 229910052757 nitrogen Inorganic materials 0.000 description 1
- 229960005419 nitrogen Drugs 0.000 description 1
- 229940085033 nolvadex Drugs 0.000 description 1
- 239000012740 non-selective inhibitor Substances 0.000 description 1
- 230000000683 nonmetastatic effect Effects 0.000 description 1
- 238000003199 nucleic acid amplification method Methods 0.000 description 1
- 230000001293 nucleolytic effect Effects 0.000 description 1
- 150000003833 nucleoside derivatives Chemical class 0.000 description 1
- 229960000435 oblimersen Drugs 0.000 description 1
- 238000002515 oligonucleotide synthesis Methods 0.000 description 1
- 229950011093 onapristone Drugs 0.000 description 1
- 108010046821 oprelvekin Proteins 0.000 description 1
- 229960001840 oprelvekin Drugs 0.000 description 1
- 229940035567 orencia Drugs 0.000 description 1
- 150000002894 organic compounds Chemical class 0.000 description 1
- 210000003300 oropharynx Anatomy 0.000 description 1
- 201000008482 osteoarthritis Diseases 0.000 description 1
- 229960002739 oxaprozin Drugs 0.000 description 1
- OFPXSFXSNFPTHF-UHFFFAOYSA-N oxaprozin Chemical compound O1C(CCC(=O)O)=NC(C=2C=CC=CC=2)=C1C1=CC=CC=C1 OFPXSFXSNFPTHF-UHFFFAOYSA-N 0.000 description 1
- VREZDOWOLGNDPW-UHFFFAOYSA-N pancratistatine Natural products C1=C2C3C(O)C(O)C(O)C(O)C3NC(=O)C2=C(O)C2=C1OCO2 VREZDOWOLGNDPW-UHFFFAOYSA-N 0.000 description 1
- 229960004662 parecoxib Drugs 0.000 description 1
- TZRHLKRLEZJVIJ-UHFFFAOYSA-N parecoxib Chemical compound C1=CC(S(=O)(=O)NC(=O)CC)=CC=C1C1=C(C)ON=C1C1=CC=CC=C1 TZRHLKRLEZJVIJ-UHFFFAOYSA-N 0.000 description 1
- 230000007119 pathological manifestation Effects 0.000 description 1
- 230000037361 pathway Effects 0.000 description 1
- 229960001218 pegademase Drugs 0.000 description 1
- 108010027841 pegademase bovine Proteins 0.000 description 1
- 229960003349 pemetrexed disodium Drugs 0.000 description 1
- 229960001639 penicillamine Drugs 0.000 description 1
- 208000030940 penile carcinoma Diseases 0.000 description 1
- 201000008174 penis carcinoma Diseases 0.000 description 1
- 230000010412 perfusion Effects 0.000 description 1
- SZFPYBIJACMNJV-UHFFFAOYSA-N perifosine Chemical compound CCCCCCCCCCCCCCCCCCOP([O-])(=O)OC1CC[N+](C)(C)CC1 SZFPYBIJACMNJV-UHFFFAOYSA-N 0.000 description 1
- 229950010632 perifosine Drugs 0.000 description 1
- 230000003285 pharmacodynamic effect Effects 0.000 description 1
- 125000001997 phenyl group Chemical group [H]C1=C([H])C([H])=C(*)C([H])=C1[H] 0.000 description 1
- 229950009215 phenylbutanoic acid Drugs 0.000 description 1
- 229940043441 phosphoinositide 3-kinase inhibitor Drugs 0.000 description 1
- 102000020233 phosphotransferase Human genes 0.000 description 1
- 239000003757 phosphotransferase inhibitor Substances 0.000 description 1
- 230000004962 physiological condition Effects 0.000 description 1
- CDRPUGZCRXZLFL-OWOJBTEDSA-N piceatannol Chemical compound OC1=CC(O)=CC(\C=C\C=2C=C(O)C(O)=CC=2)=C1 CDRPUGZCRXZLFL-OWOJBTEDSA-N 0.000 description 1
- IIMIOEBMYPRQGU-UHFFFAOYSA-L picoplatin Chemical compound N.[Cl-].[Cl-].[Pt+2].CC1=CC=CC=N1 IIMIOEBMYPRQGU-UHFFFAOYSA-L 0.000 description 1
- 229950005566 picoplatin Drugs 0.000 description 1
- 229960000952 pipobroman Drugs 0.000 description 1
- NJBFOOCLYDNZJN-UHFFFAOYSA-N pipobroman Chemical compound BrCCC(=O)N1CCN(C(=O)CCBr)CC1 NJBFOOCLYDNZJN-UHFFFAOYSA-N 0.000 description 1
- 229960001221 pirarubicin Drugs 0.000 description 1
- 229960002702 piroxicam Drugs 0.000 description 1
- QYSPLQLAKJAUJT-UHFFFAOYSA-N piroxicam Chemical compound OC=1C2=CC=CC=C2S(=O)(=O)N(C)C=1C(=O)NC1=CC=CC=N1 QYSPLQLAKJAUJT-UHFFFAOYSA-N 0.000 description 1
- 229960004403 pixantrone Drugs 0.000 description 1
- PEZPMAYDXJQYRV-UHFFFAOYSA-N pixantrone Chemical compound O=C1C2=CN=CC=C2C(=O)C2=C1C(NCCN)=CC=C2NCCN PEZPMAYDXJQYRV-UHFFFAOYSA-N 0.000 description 1
- 210000002381 plasma Anatomy 0.000 description 1
- 150000003057 platinum Chemical class 0.000 description 1
- 229960003171 plicamycin Drugs 0.000 description 1
- 229960001237 podophyllotoxin Drugs 0.000 description 1
- YJGVMLPVUAXIQN-XVVDYKMHSA-N podophyllotoxin Chemical compound COC1=C(OC)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@H](O)[C@@H]3[C@@H]2C(OC3)=O)=C1 YJGVMLPVUAXIQN-XVVDYKMHSA-N 0.000 description 1
- YVCVYCSAAZQOJI-UHFFFAOYSA-N podophyllotoxin Natural products COC1=C(O)C(OC)=CC(C2C3=CC=4OCOC=4C=C3C(O)C3C2C(OC3)=O)=C1 YVCVYCSAAZQOJI-UHFFFAOYSA-N 0.000 description 1
- 239000000244 polyoxyethylene sorbitan monooleate Substances 0.000 description 1
- 235000010482 polyoxyethylene sorbitan monooleate Nutrition 0.000 description 1
- 229920001282 polysaccharide Polymers 0.000 description 1
- 239000005017 polysaccharide Substances 0.000 description 1
- 229920000136 polysorbate Polymers 0.000 description 1
- 229920000053 polysorbate 80 Polymers 0.000 description 1
- 229940068968 polysorbate 80 Drugs 0.000 description 1
- 229960004293 porfimer sodium Drugs 0.000 description 1
- 230000001323 posttranslational effect Effects 0.000 description 1
- 229960000214 pralatrexate Drugs 0.000 description 1
- OGSBUKJUDHAQEA-WMCAAGNKSA-N pralatrexate Chemical compound C1=NC2=NC(N)=NC(N)=C2N=C1CC(CC#C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 OGSBUKJUDHAQEA-WMCAAGNKSA-N 0.000 description 1
- 229960002794 prednicarbate Drugs 0.000 description 1
- FNPXMHRZILFCKX-KAJVQRHHSA-N prednicarbate Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@@](C(=O)COC(=O)CC)(OC(=O)OCC)[C@@]1(C)C[C@@H]2O FNPXMHRZILFCKX-KAJVQRHHSA-N 0.000 description 1
- 229960004694 prednimustine Drugs 0.000 description 1
- 229960004618 prednisone Drugs 0.000 description 1
- XOFYZVNMUHMLCC-ZPOLXVRWSA-N prednisone Chemical compound O=C1C=C[C@]2(C)[C@H]3C(=O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 XOFYZVNMUHMLCC-ZPOLXVRWSA-N 0.000 description 1
- 229940063238 premarin Drugs 0.000 description 1
- 125000002924 primary amino group Chemical group [H]N([H])* 0.000 description 1
- 230000000861 pro-apoptotic effect Effects 0.000 description 1
- CPTBDICYNRMXFX-UHFFFAOYSA-N procarbazine Chemical compound CNNCC1=CC=C(C(=O)NC(C)C)C=C1 CPTBDICYNRMXFX-UHFFFAOYSA-N 0.000 description 1
- 229960000624 procarbazine Drugs 0.000 description 1
- 229920002414 procyanidin Polymers 0.000 description 1
- 229940002612 prodrug Drugs 0.000 description 1
- 239000000651 prodrug Substances 0.000 description 1
- 239000000047 product Substances 0.000 description 1
- 102000003998 progesterone receptors Human genes 0.000 description 1
- 108090000468 progesterone receptors Proteins 0.000 description 1
- 238000004393 prognosis Methods 0.000 description 1
- 230000000750 progressive effect Effects 0.000 description 1
- 229940087463 proleukin Drugs 0.000 description 1
- 230000001737 promoting effect Effects 0.000 description 1
- 238000011321 prophylaxis Methods 0.000 description 1
- 150000005599 propionic acid derivatives Chemical class 0.000 description 1
- 239000003207 proteasome inhibitor Substances 0.000 description 1
- 238000000159 protein binding assay Methods 0.000 description 1
- 239000003909 protein kinase inhibitor Substances 0.000 description 1
- 230000017854 proteolysis Effects 0.000 description 1
- WOLQREOUPKZMEX-UHFFFAOYSA-N pteroyltriglutamic acid Chemical compound C=1N=C2NC(N)=NC(=O)C2=NC=1CNC1=CC=C(C(=O)NC(CCC(=O)NC(CCC(=O)NC(CCC(O)=O)C(O)=O)C(O)=O)C(O)=O)C=C1 WOLQREOUPKZMEX-UHFFFAOYSA-N 0.000 description 1
- 230000005180 public health Effects 0.000 description 1
- 150000003212 purines Chemical class 0.000 description 1
- 229950010131 puromycin Drugs 0.000 description 1
- 150000003230 pyrimidines Chemical class 0.000 description 1
- JOZPEVMCAKXSEY-UHFFFAOYSA-N pyrimido[5,4-d]pyrimidine Chemical class N1=CN=CC2=NC=NC=C21 JOZPEVMCAKXSEY-UHFFFAOYSA-N 0.000 description 1
- 150000004944 pyrrolopyrimidines Chemical class 0.000 description 1
- 229960001285 quercetin Drugs 0.000 description 1
- 235000005875 quercetin Nutrition 0.000 description 1
- GPKJTRJOBQGKQK-UHFFFAOYSA-N quinacrine Chemical compound C1=C(OC)C=C2C(NC(C)CCCN(CC)CC)=C(C=CC(Cl)=C3)C3=NC2=C1 GPKJTRJOBQGKQK-UHFFFAOYSA-N 0.000 description 1
- 150000003246 quinazolines Chemical class 0.000 description 1
- 150000003252 quinoxalines Chemical class 0.000 description 1
- 229960002185 ranimustine Drugs 0.000 description 1
- 229960000424 rasburicase Drugs 0.000 description 1
- 108010084837 rasburicase Proteins 0.000 description 1
- 208000002574 reactive arthritis Diseases 0.000 description 1
- 206010038038 rectal cancer Diseases 0.000 description 1
- 201000001275 rectum cancer Diseases 0.000 description 1
- 229940116176 remicade Drugs 0.000 description 1
- 238000011160 research Methods 0.000 description 1
- 235000021283 resveratrol Nutrition 0.000 description 1
- 229940016667 resveratrol Drugs 0.000 description 1
- 229940018007 retifanlimab Drugs 0.000 description 1
- 229930002330 retinoic acid Natural products 0.000 description 1
- 150000004492 retinoid derivatives Chemical class 0.000 description 1
- 206010039073 rheumatoid arthritis Diseases 0.000 description 1
- 108020004418 ribosomal RNA Proteins 0.000 description 1
- 108091092562 ribozyme Proteins 0.000 description 1
- 229940089617 risedronate Drugs 0.000 description 1
- 229960000371 rofecoxib Drugs 0.000 description 1
- RZJQGNCSTQAWON-UHFFFAOYSA-N rofecoxib Chemical compound C1=CC(S(=O)(=O)C)=CC=C1C1=C(C=2C=CC=CC=2)C(=O)OC1 RZJQGNCSTQAWON-UHFFFAOYSA-N 0.000 description 1
- 229960003452 romidepsin Drugs 0.000 description 1
- 108010091666 romidepsin Proteins 0.000 description 1
- OHRURASPPZQGQM-GCCNXGTGSA-N romidepsin Chemical compound O1C(=O)[C@H](C(C)C)NC(=O)C(=C/C)/NC(=O)[C@H]2CSSCC\C=C\[C@@H]1CC(=O)N[C@H](C(C)C)C(=O)N2 OHRURASPPZQGQM-GCCNXGTGSA-N 0.000 description 1
- OHRURASPPZQGQM-UHFFFAOYSA-N romidepsin Natural products O1C(=O)C(C(C)C)NC(=O)C(=CC)NC(=O)C2CSSCCC=CC1CC(=O)NC(C(C)C)C(=O)N2 OHRURASPPZQGQM-UHFFFAOYSA-N 0.000 description 1
- VHXNKPBCCMUMSW-FQEVSTJZSA-N rubitecan Chemical compound C1=CC([N+]([O-])=O)=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 VHXNKPBCCMUMSW-FQEVSTJZSA-N 0.000 description 1
- NGWSFRIPKNWYAO-SHTIJGAHSA-N salinosporamide A Chemical compound C([C@@H]1[C@H](O)[C@]23C(=O)O[C@]2([C@H](C(=O)N3)CCCl)C)CCC=C1 NGWSFRIPKNWYAO-SHTIJGAHSA-N 0.000 description 1
- NGWSFRIPKNWYAO-UHFFFAOYSA-N salinosporamide A Natural products N1C(=O)C(CCCl)C2(C)OC(=O)C21C(O)C1CCCC=C1 NGWSFRIPKNWYAO-UHFFFAOYSA-N 0.000 description 1
- 201000003804 salivary gland carcinoma Diseases 0.000 description 1
- 229960005399 satraplatin Drugs 0.000 description 1
- 190014017285 satraplatin Chemical compound 0.000 description 1
- WUWDLXZGHZSWQZ-WQLSENKSSA-N semaxanib Chemical compound N1C(C)=CC(C)=C1\C=C/1C2=CC=CC=C2NC\1=O WUWDLXZGHZSWQZ-WQLSENKSSA-N 0.000 description 1
- 230000035945 sensitivity Effects 0.000 description 1
- 238000012163 sequencing technique Methods 0.000 description 1
- 238000003196 serial analysis of gene expression Methods 0.000 description 1
- 230000007781 signaling event Effects 0.000 description 1
- 229940068638 simponi Drugs 0.000 description 1
- 238000009097 single-agent therapy Methods 0.000 description 1
- 229940112726 skelid Drugs 0.000 description 1
- 239000007787 solid Substances 0.000 description 1
- 230000000392 somatic effect Effects 0.000 description 1
- 229960003787 sorafenib Drugs 0.000 description 1
- 210000000952 spleen Anatomy 0.000 description 1
- 208000005801 spondylosis Diseases 0.000 description 1
- ICXJVZHDZFXYQC-UHFFFAOYSA-N spongistatin 1 Natural products OC1C(O2)(O)CC(O)C(C)C2CCCC=CC(O2)CC(O)CC2(O2)CC(OC)CC2CC(=O)C(C)C(OC(C)=O)C(C)C(=C)CC(O2)CC(C)(O)CC2(O2)CC(OC(C)=O)CC2CC(=O)OC2C(O)C(CC(=C)CC(O)C=CC(Cl)=C)OC1C2C ICXJVZHDZFXYQC-UHFFFAOYSA-N 0.000 description 1
- 230000006641 stabilisation Effects 0.000 description 1
- 238000011105 stabilization Methods 0.000 description 1
- 230000000087 stabilizing effect Effects 0.000 description 1
- 150000003431 steroids Chemical class 0.000 description 1
- 230000000638 stimulation Effects 0.000 description 1
- 238000013517 stratification Methods 0.000 description 1
- 229960001052 streptozocin Drugs 0.000 description 1
- ZSJLQEPLLKMAKR-GKHCUFPYSA-N streptozocin Chemical compound O=NN(C)C(=O)N[C@H]1[C@@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O ZSJLQEPLLKMAKR-GKHCUFPYSA-N 0.000 description 1
- 238000007920 subcutaneous administration Methods 0.000 description 1
- 238000006467 substitution reaction Methods 0.000 description 1
- 235000000346 sugar Nutrition 0.000 description 1
- NCEXYHBECQHGNR-UHFFFAOYSA-N sulfasalazine Natural products C1=C(O)C(C(=O)O)=CC(N=NC=2C=CC(=CC=2)S(=O)(=O)NC=2N=CC=CC=2)=C1 NCEXYHBECQHGNR-UHFFFAOYSA-N 0.000 description 1
- 229960001940 sulfasalazine Drugs 0.000 description 1
- 239000013589 supplement Substances 0.000 description 1
- 230000008093 supporting effect Effects 0.000 description 1
- 230000001629 suppression Effects 0.000 description 1
- 239000004094 surface-active agent Substances 0.000 description 1
- 208000034223 susceptibility to 2 systemic lupus erythematosus Diseases 0.000 description 1
- 208000011580 syndromic disease Diseases 0.000 description 1
- 239000000454 talc Substances 0.000 description 1
- 229910052623 talc Inorganic materials 0.000 description 1
- 229960001603 tamoxifen Drugs 0.000 description 1
- 229960003454 tamoxifen citrate Drugs 0.000 description 1
- 229950007866 tanespimycin Drugs 0.000 description 1
- AYUNIORJHRXIBJ-TXHRRWQRSA-N tanespimycin Chemical compound N1C(=O)\C(C)=C\C=C/[C@H](OC)[C@@H](OC(N)=O)\C(C)=C\[C@H](C)[C@@H](O)[C@@H](OC)C[C@H](C)CC2=C(NCC=C)C(=O)C=C1C2=O AYUNIORJHRXIBJ-TXHRRWQRSA-N 0.000 description 1
- 230000008685 targeting Effects 0.000 description 1
- 229940099419 targretin Drugs 0.000 description 1
- 229960001674 tegafur Drugs 0.000 description 1
- WFWLQNSHRPWKFK-ZCFIWIBFSA-N tegafur Chemical compound O=C1NC(=O)C(F)=CN1[C@@H]1OCCC1 WFWLQNSHRPWKFK-ZCFIWIBFSA-N 0.000 description 1
- 229960004964 temozolomide Drugs 0.000 description 1
- 229960002871 tenoxicam Drugs 0.000 description 1
- WZWYJBNHTWCXIM-UHFFFAOYSA-N tenoxicam Chemical compound O=C1C=2SC=CC=2S(=O)(=O)N(C)C1=C(O)NC1=CC=CC=N1 WZWYJBNHTWCXIM-UHFFFAOYSA-N 0.000 description 1
- 229960005353 testolactone Drugs 0.000 description 1
- BPEWUONYVDABNZ-DZBHQSCQSA-N testolactone Chemical compound O=C1C=C[C@]2(C)[C@H]3CC[C@](C)(OC(=O)CC4)[C@@H]4[C@@H]3CCC2=C1 BPEWUONYVDABNZ-DZBHQSCQSA-N 0.000 description 1
- IPMYMEWFZKHGAX-ZKSIBHASSA-N theaflavin Chemical compound C1=C2C([C@H]3OC4=CC(O)=CC(O)=C4C[C@H]3O)=CC(O)=C(O)C2=C(O)C(=O)C=C1[C@@H]1[C@H](O)CC2=C(O)C=C(O)C=C2O1 IPMYMEWFZKHGAX-ZKSIBHASSA-N 0.000 description 1
- 235000014620 theaflavin Nutrition 0.000 description 1
- 229940026509 theaflavin Drugs 0.000 description 1
- 210000000115 thoracic cavity Anatomy 0.000 description 1
- 201000002510 thyroid cancer Diseases 0.000 description 1
- RSAQARAFWMUYLL-UHFFFAOYSA-N tic-10 Chemical group CC1=CC=CC=C1CN1C(CCN(CC=2C=CC=CC=2)C2)=C2C(=O)N2CCN=C21 RSAQARAFWMUYLL-UHFFFAOYSA-N 0.000 description 1
- 229940019375 tiludronate Drugs 0.000 description 1
- 229950009158 tipifarnib Drugs 0.000 description 1
- 208000037816 tissue injury Diseases 0.000 description 1
- 229960002905 tolfenamic acid Drugs 0.000 description 1
- YEZNLOUZAIOMLT-UHFFFAOYSA-N tolfenamic acid Chemical compound CC1=C(Cl)C=CC=C1NC1=CC=CC=C1C(O)=O YEZNLOUZAIOMLT-UHFFFAOYSA-N 0.000 description 1
- 230000000699 topical effect Effects 0.000 description 1
- 229940044693 topoisomerase inhibitor Drugs 0.000 description 1
- 229960000303 topotecan Drugs 0.000 description 1
- UCFGDBYHRUNTLO-QHCPKHFHSA-N topotecan Chemical compound C1=C(O)C(CN(C)C)=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 UCFGDBYHRUNTLO-QHCPKHFHSA-N 0.000 description 1
- 229960005026 toremifene Drugs 0.000 description 1
- XFCLJVABOIYOMF-QPLCGJKRSA-N toremifene Chemical compound C1=CC(OCCN(C)C)=CC=C1C(\C=1C=CC=CC=1)=C(\CCCl)C1=CC=CC=C1 XFCLJVABOIYOMF-QPLCGJKRSA-N 0.000 description 1
- 231100000331 toxic Toxicity 0.000 description 1
- 230000002588 toxic effect Effects 0.000 description 1
- 238000013518 transcription Methods 0.000 description 1
- 230000035897 transcription Effects 0.000 description 1
- 238000012546 transfer Methods 0.000 description 1
- 238000013519 translation Methods 0.000 description 1
- 238000011269 treatment regimen Methods 0.000 description 1
- IUCJMVBFZDHPDX-UHFFFAOYSA-N tretamine Chemical compound C1CN1C1=NC(N2CC2)=NC(N2CC2)=N1 IUCJMVBFZDHPDX-UHFFFAOYSA-N 0.000 description 1
- 229950001353 tretamine Drugs 0.000 description 1
- 229960005294 triamcinolone Drugs 0.000 description 1
- GFNANZIMVAIWHM-OBYCQNJPSA-N triamcinolone Chemical compound O=C1C=C[C@]2(C)[C@@]3(F)[C@@H](O)C[C@](C)([C@@]([C@H](O)C4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 GFNANZIMVAIWHM-OBYCQNJPSA-N 0.000 description 1
- 229960002117 triamcinolone acetonide Drugs 0.000 description 1
- YNDXUCZADRHECN-JNQJZLCISA-N triamcinolone acetonide Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@H]3OC(C)(C)O[C@@]3(C(=O)CO)[C@@]1(C)C[C@@H]2O YNDXUCZADRHECN-JNQJZLCISA-N 0.000 description 1
- NOYPYLRCIDNJJB-UHFFFAOYSA-N trimetrexate Chemical compound COC1=C(OC)C(OC)=CC(NCC=2C(=C3C(N)=NC(N)=NC3=CC=2)C)=C1 NOYPYLRCIDNJJB-UHFFFAOYSA-N 0.000 description 1
- 229960001099 trimetrexate Drugs 0.000 description 1
- UMKFEPPTGMDVMI-UHFFFAOYSA-N trofosfamide Chemical compound ClCCN(CCCl)P1(=O)OCCCN1CCCl UMKFEPPTGMDVMI-UHFFFAOYSA-N 0.000 description 1
- 229960000875 trofosfamide Drugs 0.000 description 1
- 229950010147 troxacitabine Drugs 0.000 description 1
- RXRGZNYSEHTMHC-BQBZGAKWSA-N troxacitabine Chemical compound O=C1N=C(N)C=CN1[C@H]1O[C@@H](CO)OC1 RXRGZNYSEHTMHC-BQBZGAKWSA-N 0.000 description 1
- 229950009811 ubenimex Drugs 0.000 description 1
- 229960001055 uracil mustard Drugs 0.000 description 1
- 230000002485 urinary effect Effects 0.000 description 1
- 210000002700 urine Anatomy 0.000 description 1
- 206010046766 uterine cancer Diseases 0.000 description 1
- 208000012991 uterine carcinoma Diseases 0.000 description 1
- 229960002004 valdecoxib Drugs 0.000 description 1
- LNPDTQAFDNKSHK-UHFFFAOYSA-N valdecoxib Chemical compound CC=1ON=C(C=2C=CC=CC=2)C=1C1=CC=C(S(N)(=O)=O)C=C1 LNPDTQAFDNKSHK-UHFFFAOYSA-N 0.000 description 1
- MSRILKIQRXUYCT-UHFFFAOYSA-M valproate semisodium Chemical compound [Na+].CCCC(C(O)=O)CCC.CCCC(C([O-])=O)CCC MSRILKIQRXUYCT-UHFFFAOYSA-M 0.000 description 1
- 229960000604 valproic acid Drugs 0.000 description 1
- 230000002792 vascular Effects 0.000 description 1
- LLDWLPRYLVPDTG-UHFFFAOYSA-N vatalanib succinate Chemical compound OC(=O)CCC(O)=O.C1=CC(Cl)=CC=C1NC(C1=CC=CC=C11)=NN=C1CC1=CC=NC=C1 LLDWLPRYLVPDTG-UHFFFAOYSA-N 0.000 description 1
- 239000013598 vector Substances 0.000 description 1
- 229940099039 velcade Drugs 0.000 description 1
- 229960003862 vemurafenib Drugs 0.000 description 1
- GPXBXXGIAQBQNI-UHFFFAOYSA-N vemurafenib Chemical group CCCS(=O)(=O)NC1=CC=C(F)C(C(=O)C=2C3=CC(=CN=C3NC=2)C=2C=CC(Cl)=CC=2)=C1F GPXBXXGIAQBQNI-UHFFFAOYSA-N 0.000 description 1
- UGGWPQSBPIFKDZ-KOTLKJBCSA-N vindesine Chemical compound C([C@@H](C[C@]1(C(=O)OC)C=2C(=CC3=C([C@]45[C@H]([C@@]([C@H](O)[C@]6(CC)C=CCN([C@H]56)CC4)(O)C(N)=O)N3C)C=2)OC)C[C@@](C2)(O)CC)N2CCC2=C1N=C1[C]2C=CC=C1 UGGWPQSBPIFKDZ-KOTLKJBCSA-N 0.000 description 1
- 229960004355 vindesine Drugs 0.000 description 1
- 230000002747 voluntary effect Effects 0.000 description 1
- 230000008673 vomiting Effects 0.000 description 1
- WAEXFXRVDQXREF-UHFFFAOYSA-N vorinostat Chemical compound ONC(=O)CCCCCCC(=O)NC1=CC=CC=C1 WAEXFXRVDQXREF-UHFFFAOYSA-N 0.000 description 1
- 229960000237 vorinostat Drugs 0.000 description 1
- 201000005102 vulva cancer Diseases 0.000 description 1
- 238000001262 western blot Methods 0.000 description 1
- 238000012070 whole genome sequencing analysis Methods 0.000 description 1
- 229940049068 xalkori Drugs 0.000 description 1
- 229940053867 xeloda Drugs 0.000 description 1
- 229940002005 zometa Drugs 0.000 description 1
- 229960000641 zorubicin Drugs 0.000 description 1
- FBTUMDXHSRTGRV-ALTNURHMSA-N zorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(\C)=N\NC(=O)C=1C=CC=CC=1)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 FBTUMDXHSRTGRV-ALTNURHMSA-N 0.000 description 1
- 229940052129 zykadia Drugs 0.000 description 1
Images


































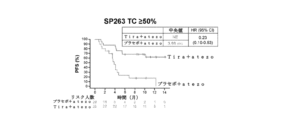
Classifications
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2827—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against B7 molecules, e.g. CD80, CD86
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/335—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin
- A61K31/337—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin having four-membered rings, e.g. taxol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/335—Heterocyclic compounds having oxygen as the only ring hetero atom, e.g. fungichromin
- A61K31/365—Lactones
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/555—Heterocyclic compounds containing heavy metals, e.g. hemin, hematin, melarsoprol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7042—Compounds having saccharide radicals and heterocyclic rings
- A61K31/7052—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides
- A61K31/706—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom
- A61K31/7064—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines
- A61K31/7068—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines having oxo groups directly attached to the pyrimidine ring, e.g. cytidine, cytidylic acid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K33/00—Medicinal preparations containing inorganic active ingredients
- A61K33/24—Heavy metals; Compounds thereof
- A61K33/243—Platinum; Compounds thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
- A61K2039/507—Comprising a combination of two or more separate antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/54—Medicinal preparations containing antigens or antibodies characterised by the route of administration
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/545—Medicinal preparations containing antigens or antibodies characterised by the dose, timing or administration schedule
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K2300/00—Mixtures or combinations of active ingredients, wherein at least one active ingredient is fully defined in groups A61K31/00 - A61K41/00
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/90—Immunoglobulins specific features characterized by (pharmaco)kinetic aspects or by stability of the immunoglobulin
Abstract
本発明は、がん(例えば、肺がん;子宮頸がん;乳がん;頭頸部がん;肝臓がん;膀胱がん;胃がん;食道がん;膵臓がん;腎臓がん又は腎がん;黒色腫;卵巣がん;又は結腸直腸がん)を処置するための方法、使用及び組成物に関する。より具体的には、本発明は、併用療法における抗TIGITアンタゴニスト抗体による処置を含む、抗TIGITアンタゴニスト抗体によるがんを有する患者の処置に関する。【選択図】なしCancer (e.g., lung cancer; cervical cancer; breast cancer; head and neck cancer; liver cancer; bladder cancer; stomach cancer; esophageal cancer; pancreatic cancer; cancer; ovarian cancer; or colorectal cancer). More specifically, the invention relates to treatment of patients with cancer with anti-TIGIT antagonist antibodies, including treatment with anti-TIGIT antagonist antibodies in combination therapy. [Selection figure] None
Description
この出願は、2020年1月27日に出願された米国特許出願第62/966,448号;2020年3月5日に出願された米国特許出願第62/985,822号;2020年3月24日に出願された米国特許出願第62/994,272号;2020年3月24日に出願された国際出願PCT/US2020/024526;2020年7月30日に出願された米国特許出願第63/059,054号;2020年7月31日に出願された米国特許出願第63/059,960号;2020年9月4日に出願された米国特許出願第63/074,807号;2020年9月4日に出願された米国特許出願第63/074,827号;2020年9月4日に出願された国際出願PCT/US2020/049415;2020年9月30日に出願された米国特許出願第63/085,890号;2020年10月23日に出願された米国特許出願第63/105,198号;2020年11月16日に出願された米国特許出願第63/114,517号;2020年12月11日に出願された米国特許出願第63/124,693号;及び2020年12月17日に出願された米国特許出願第63/127,109号の優先権を主張し、それぞれの内容全体が参照により本明細書に組み込まれる。 No. 62/966,448, filed Jan. 27, 2020; U.S. Patent Application No. 62/985,822, filed Mar. 5, 2020; U.S. patent application Ser. No. 62/994,272 filed on 24th March; U.S. Patent Application No. 63/059,960 filed July 31, 2020; U.S. Patent Application No. 63/074,807 filed September 4, 2020; U.S. Patent Application No. 63/074,827 filed September 4; International Application PCT/US2020/049415 filed September 4, 2020; No. 63/085,890; U.S. Patent Application No. 63/105,198 filed Oct. 23, 2020; U.S. Patent Application No. 63/114,517 filed Nov. 16, 2020; Claiming priority from U.S. Patent Application No. 63/124,693, filed December 11, 2020; and U.S. Patent Application No. 63/127,109, filed December 17, 2020; is incorporated herein by reference in its entirety.
配列表
本出願は、ASCII形式にて電子的に提出されており、その全体が参照により本明細書に組み込まれる配列表を含む。2021年1月25日に作成された上記ASCIIコピーの名称は50474-206WO2_Sequence_Listing_1_25_2021_ST25であり、サイズは30,641バイトである。
SEQUENCE LISTING This application has been submitted electronically in ASCII format and contains a Sequence Listing which is hereby incorporated by reference in its entirety. The name of the above ASCII copy created on January 25, 2021 is 50474-206WO2_Sequence_Listing_1_25_2021_ST25 and is 30,641 bytes in size.
発明の分野
本発明は、がんを処置するための方法、使用及び組成物に関する。より具体的には、本発明は、抗TIGITアンタゴニスト抗体(例えば、単剤療法又は併用療法としての抗TIGITアンタゴニスト抗体による処置)によるがんを有する患者の処置に関する。
FIELD OF THE INVENTION The present invention relates to methods, uses and compositions for treating cancer. More specifically, the invention relates to treatment of patients with cancer with anti-TIGIT antagonist antibodies (eg, treatment with anti-TIGIT antagonist antibodies as monotherapy or combination therapy).
発明の背景
がんは、細胞亜集団の制御されない増殖を特徴とする。がんは、先進国における主な死因であり、発展途上国における2番目に多い死因であり、1400万を超える新たながん症例が診断され、毎年800万を超えるがん死が発生している。したがって、がんのケアは、重大で増え続ける社会的負担となる。
BACKGROUND OF THE INVENTION Cancer is characterized by the uncontrolled proliferation of cell subpopulations. Cancer is the leading cause of death in developed countries and the second leading cause of death in developing countries, with over 14 million new cancer cases diagnosed and over 8 million cancer deaths occurring each year. there is Cancer care therefore represents a significant and growing social burden.
したがって、がんの処置のために有効な免疫療法及びそれを投与する方法を開発する分野における満たされていない必要性がある。 Accordingly, there is an unmet need in the area of developing effective immunotherapies and methods of administering them for the treatment of cancer.
発明の概要
一態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、対象に、3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。
SUMMARY OF THE INVENTION In one aspect, the invention provides a method of treating a subject with cancer, the method comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks; administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks including doing
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、対象に、4週間ごとに約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体及び4週間ごとに約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every four weeks and about administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of 1400 mg to 2000 mg.
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、2週間ごとに約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとに約600mg~約1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, the method comprising administering an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and about 600 mg to about 600 mg every two weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg.
別の態様では、本発明は、本明細書で提供される方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含むキットを提供する。 In another aspect, the invention provides a kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject with cancer according to the methods provided herein. do.
別の態様では、本発明は、がんを有する対象を処置する方法で使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを提供し、方法は本明細書で提供される方法によるものである。 In another aspect, the invention provides anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in methods of treating a subject with cancer, the methods according to the methods provided herein is.
別の態様では、本発明は、PD-1軸結合アンタゴニストと組み合わせてがんを有する対象を処置するための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、処置が本明細書で提供される方法によるものである使用を提供する。 In another aspect, the invention is the use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject with cancer in combination with a PD-1 axis binding antagonist, the treatment provided herein. to provide a use that is in accordance with the method of
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、対象に、4週間ごとに約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体及び4週間ごとに約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every four weeks and about administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of 1400 mg to 2000 mg.
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、対象に、2週間ごとに約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとに約600mg~1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, the method comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to 1200 mg.
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、対象に、3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every three weeks, about administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of 900 mg to about 1500 mg, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks. including.
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとに約100mg~約300mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含み、抗PD-1アンタゴニスト抗体がペンブロリズマブである。 In another aspect, the invention provides a method of treating a subject with cancer, the method comprising administering an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks and about 100 mg to about 100 mg every 3 weeks. comprising administering to the subject a dosing regimen comprising one or more dosing cycles of an anti-PD-1 antagonist antibody at a dose of about 300 mg, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は、チラゴルマブ及びペンブロリズマブの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含み、ペンブロリズマブが、6週間ごとの約300mgと約500mgの間の用量で投与される。 In another aspect, the invention provides a method of treating a subject with cancer, the method comprising administering to the subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein pembrolizumab is , at doses between about 300 mg and about 500 mg every 6 weeks.
別の態様では、本発明は、がんを有する対象を処置するための方法を提供し、方法は2週間の投薬/1週間の休薬の間、3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとに1日2回の経口の約10mg/m2と約10000mg/m2の間の用量の代謝拮抗剤の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In another aspect, the invention provides a method for treating a subject with cancer, the method comprising between about 500 mg and about 700 mg every 3 weeks for 2 weeks on/1 week off. PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every 3 weeks, and about 10 mg/m2 and about 10000 mg/ m2 orally twice daily every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the antimetabolite at a dose between m2 .
別の態様では、本発明は、がんを有する対象を処置する方法を提供し、方法は3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、ゲムシタビン及びnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In another aspect, the invention provides a method of treating a subject with cancer, comprising administering an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every three weeks, about 900 mg to about 1500 mg every three weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist, gemcitabine and nab-paclitaxel at doses of .
別の態様では、本発明は、がんを有する対象を処置するための方法を提供し、方法は3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約1mg/kgと約35mg/kgの間の用量のVEGFアンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In another aspect, the invention provides a method for treating a subject with cancer, the method comprising administering an anti-TIGIT antagonist antibody at a dose of between about 500 mg and about 700 mg every three weeks, about Subject to a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg and a VEGF antagonist at a dose between about 1 mg/kg and about 35 mg/kg every 3 weeks. including administering to
別の態様では、本発明は、がんを有する対象を処置する方法であって、導入期及び維持期を含む投薬レジメンを対象に投与することを含み、(a)導入期が、3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含み、(b)維持期が、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト、及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、維持期は白金系化学療法剤の投与を含まない方法を提供する。 In another aspect, the invention provides a method of treating a subject with cancer comprising administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein (a) the induction phase is every 3 weeks an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum every 3 weeks (b) the maintenance phase is an anti-TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding antagonist every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks. Methods are provided that include one or more additional dosing cycles of a therapeutic agent and the maintenance phase does not include administration of a platinum-based chemotherapeutic agent.
別の態様では、本発明は、がんを有する対象を処置する方法であって、導入期及び維持期を含む投薬レジメンを対象に投与することを含み、(a)導入期が、3週間ごとに約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含み、(b)維持期が、4週間ごとに約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとに約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、維持期は、白金系化学療法剤又は非白金系化学療法剤の投与を含まない方法を提供する。 In another aspect, the invention provides a method of treating a subject with cancer comprising administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein (a) the induction phase is every 3 weeks an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum every 3 weeks (b) a maintenance phase of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a dose of about 1400 mg to 2000 mg every 4 weeks; Methods are provided comprising one or more additional dosing cycles of a PD-1 axis binding antagonist, wherein the maintenance phase does not comprise administration of a platinum-based or non-platinum-based chemotherapeutic agent.
別の態様では、本発明は、肺がんを有する対象又は対象集団を処置する方法を提供し、方法は有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、処置が、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象の無増悪生存期間(PFS)を延長する。 In another aspect, the invention provides a method of treating a subject or population of subjects with lung cancer, comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. The treatment comprises administering to the subject or subject population a dosing regimen comprising one or more dosing cycles of the agent, wherein the treatment is a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and topoisomerase II without an anti-TIGIT antagonist antibody. Prolongs progression-free survival (PFS) in subjects compared to treatment with an inhibitor.
別の態様では、本発明は、肺がんを有する対象集団を処置する方法を提供し、方法は有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象集団に投与することを含み、処置が、約8.2ヶ月~約9.2ヶ月の対象集団のPFS中央値をもたらす。 In another aspect, the invention provides a method of treating a subject population having lung cancer, the method comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. The treatment comprises administering to the subject population a dosing regimen comprising one or more dosing cycles, wherein the treatment results in a median PFS for the subject population of from about 8.2 months to about 9.2 months.
別の態様では、本発明は、肺がんを有する対象又は対象集団を処置する方法を提供し、方法は有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、処置が、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象のOSを延長する。 In another aspect, the invention provides a method of treating a subject or population of subjects with lung cancer, comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. The treatment comprises administering to the subject or subject population a dosing regimen comprising one or more dosing cycles of the agent, wherein the treatment is a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and topoisomerase II without an anti-TIGIT antagonist antibody. Prolongs the subject's OS compared to treatment with the inhibitor.
別の態様では、本発明は、肺がんを有する対象集団を処置する方法を提供し、方法は有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象集団に投与することを含み、処置が、約15.3ヶ月~約17.6ヶ月の対象集団のOS中央値をもたらす。 In another aspect, the invention provides a method of treating a subject population having lung cancer, the method comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. The treatment comprises administering to the subject population a dosing regimen comprising one or more dosing cycles, wherein the treatment results in a median OS for the subject population of from about 15.3 months to about 17.6 months.
別の態様では、本発明は、SCLCを有する対象又は対象集団を処置するための方法を提供し、方法は各投薬サイクルの1日目に約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約900mg~約1500mgの用量のアテゾリズマブ、各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドの1回以上の21日間投薬サイクルを対象又は対象集団に投与することを含み、処置が、抗TIGITアンタゴニスト抗体を用いない、アテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、対象又は対象集団のPFS及び/又はOSを延長する。
In another aspect, the invention provides a method for treating a subject or subject population with SCLC, comprising administering an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg on
別の態様では、本発明は、ES-SCLCを有する対象又は対象集団を処置するための方法を提供し、方法は、対象又は対象集団に4回の初期投薬サイクルとそれに続く1回以上の追加の投薬サイクルとを投与することを含み、(a)4回の初期投薬サイクルが、各初期投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各初期投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各初期投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び各初期投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドを投与することを含み、(b)1回以上の追加の投薬サイクルが、各追加の投薬サイクルの1日目に約600mgの用量のチラゴルマブを投与すること、及び各追加の投薬サイクルの1日目に約1200mgの用量のアテゾリズマブを投与することを含み、4回の初期投薬サイクル及び1回以上の追加の投薬サイクルが、各21日間投薬サイクルであり、処置が、チラゴルマブを用いない、アテゾリズマブ、カルボプラチン、及びエトポシドによる処置と比較して、対象又は対象集団のPFS及び/又はOSを延長する。
In another aspect, the invention provides a method for treating a subject or population of subjects with ES-SCLC, wherein the method comprises administering to the subject or population of subjects four initial dosing cycles followed by one or more additional doses. (a) the four initial dosing cycles are tiragolumab at a dose of about 600 mg on
別の態様では、本発明は、肺がんを有する対象又は対象集団を処置する方法を提供し、方法は抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤である第1の化学療法剤、及び非白金系化学療法剤である第2の化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む。 In another aspect, the invention provides a method of treating a subject or population of subjects with lung cancer, wherein the method is an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent. and one or more dosing cycles of a second chemotherapeutic agent that is a non-platinum chemotherapeutic agent to the subject or population of subjects.
別の態様では、本発明は、進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法を提供し、方法は対象又は対象集団に、チラゴルマブ、アテゾリズマブ、カルボプラチン又はシスプラチン及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンを投与することを含み、4回の21日間投薬サイクルの各々の1日目に、チラゴルマブが3週間ごとに約600mgの用量で投与され、アテゾリズマブが3週間ごとに約1200mgの用量で投与され、カルボプラチンが3週間ごとにAUC=5mg/ml/分を達成するのに十分な用量で投与されるか又はシスプラチンが3週間ごとに75mg/m2の用量で投与され、ペメトレキセドが3週間ごとに約500mg/m2の用量で投与される。
In another aspect, the invention provides a method of treating a subject or subject population having advanced non-squamous NSCLC, wherein the subject or subject population is treated with four doses of tiragolumab, atezolizumab, carboplatin or cisplatin and pemetrexed. comprising administering a dosing regimen comprising 21-day dosing cycles, wherein tiragolumab is administered every 3 weeks at a dose of about 600 mg and atezolizumab is administered every 3 weeks on
別の態様では、本発明は、進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法を提供し、方法は、対象又は対象集団に、(i)3週間ごとに約600mgの用量のチラゴルマブ、3週間ごとに約1200mgの用量のアテゾリズマブ、AUC=5mg/ml/分を達成するのに十分な用量でカルボプラチン、及び3週間ごとに約500mg/m2の用量のペメトレキセドの4つの導入期投薬サイクル、並びに(ii)3週間ごとに約600mgの用量のチラゴルマブ、3週間ごとに約1200mgの用量のアテゾリズマブ、及び3週間ごとに約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルを投与することを含み、維持期の1回以上の21日間投薬サイクルはカルボプラチンの投与を含まず、対象又は対象集団は、進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない。 In another aspect, the invention provides a method of treating a subject or subject population having advanced non-squamous NSCLC, the method comprising administering to the subject or subject population: (i) a dose of about 600 mg every 3 weeks; Four run-in phases of tiragolumab, atezolizumab at a dose of approximately 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min, and pemetrexed at a dose of approximately 500 mg/m2 every 3 weeks. and (ii) one or more maintenance phases of tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and pemetrexed at a dose of about 500 mg/ m2 every 3 weeks. one or more 21-day dosing cycles in the maintenance phase does not include administration of carboplatin, and the subject or subject population has not received prior systemic therapy for advanced non-squamous NSCLC .
別の態様では、本発明は、切除可能な肺がんを有する対象を処置するための方法を提供し、方法は3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとに約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含む。 In another aspect, the invention provides a method for treating a subject with resectable lung cancer, the method comprising an anti-TIGIT antagonist antibody at a dose of between about 500 mg and about 700 mg every 3 weeks and administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg per dose.
別の態様では、本発明は、肺がんを有する対象を処置するための方法を提供し、方法は抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含み、投薬サイクルの少なくとも1つが、ネオアジュバント処置として、抗TIGITアンタゴニスト抗体を3週間ごとの約500mgと約700mgの間の用量で、及びPD-1軸結合アンタゴニストを3週間ごとの約900mgと約1500mgの間の用量で対象に投与することを含む。 In another aspect, the invention provides a method for treating a subject with lung cancer, the method comprising administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist. wherein at least one of the dosing cycles comprises an anti-TIGIT antagonist antibody at a dose between about 500 mg and about 700 mg every 3 weeks and a PD-1 axis binding antagonist at a dose between about 900 mg and about 700 mg every 3 weeks as a neoadjuvant treatment. including administering to the subject at a dose of between 1500 mg.
別の態様では、本発明は、切除可能な肺がんを有する対象を処置するための方法を提供し、方法は、3週間ごとに約600mgの用量のチラゴルマブ、3週間ごとに約1200mgの用量のアテゾリズマブ、及び(a)(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は(ii)3週間ごとに約75mg/m2の用量のシスプラチン;並びに(b)(i)3週間ごとに約500mg/m2の用量のペメトレキセド、又は各投薬サイクルの1日目及び8日目に約1000mg/m2若しくは約1250mg/m2の用量のゲムシタビン;又は(ii)3週間ごとに約175mg/m2若しくは約200mg/m2の用量のパクリタキセルの1回以上の投薬サイクルを対象に投与することを含む。 In another aspect, the invention provides a method for treating a subject with resectable lung cancer, the method comprising tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks and (a) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) about 75 mg/min every 3 weeks and (b)(i) pemetrexed at a dose of about 500 mg/ m2 every three weeks, or about 1000 mg/m2 or about 1250 mg/ m2 on days 1 and 8 of each dosing cycle. or (ii) one or more dosing cycles of paclitaxel at a dose of about 175 mg/m 2 or about 200 mg/ m 2 every three weeks.
別の態様では、本発明は、肺がんを有する対象を処置するための方法を提供し、方法は、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを対象に投与することを含み、(I)投薬サイクルの少なくとも1つはネオアジュバント処置であり、対象に(a)3週間ごとに約1200mgの用量のチラゴルマブ、(b)ネオアジュバント処置として3週間ごとに約1200mgの用量のアテゾリズマブ;(c)(i)各投薬サイクルの1日目及び8日目に、3週間ごとに5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び約1000mg/m2の用量のゲムシタビン;(ii)3週間ごとに6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン及び3週間ごとに約175mg/m2又は約200mg/m2の用量のパクリタキセル;又は(iii)3週間ごとに約75mg/m2の用量のシスプラチン及び各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)投薬サイクルの少なくとも1つは、アジュバント処置として、対象に、3週間ごとの約500mgと約700mgの間の用量のチラゴルマブ及び3週間ごとの約900mgと約1500mgの間の用量のアテゾリズマブを投与することを含む。
In another aspect, the invention provides a method for treating a subject with lung cancer, the method comprising administering to the subject one or more dosing cycles of tiragolumab and atezolizumab, wherein (I) the dosing cycle is a neoadjuvant treatment, wherein the subject is administered (a) tiragolumab at a dose of about 1200 mg every 3 weeks, (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; ) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of approximately 1000 mg/ m2 on
別の態様では、本発明は、検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法を提供し、方法は3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 In another aspect, the invention provides a method for treating a subject or subject population having cervical cancer with a detectable PD-L1 expression level, the method comprising about 500 mg and about 700 mg every 3 weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every three weeks to the subject or population of subjects.
別の態様において、本発明は、子宮頸がんを有する対象のための治療法を選択する方法を提供し、方法は、(a)対象からの腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを、染色に適した抗PD-L1抗体を使用するIHCアッセイによって検出すること、並びに(b)検出可能なPD-L1発現レベルを有する対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとの約500mgと約700mgの間の用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとの約900mgと約1500mgの間の用量で投与されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む治療法を選択すること、を含む。 In another aspect, the invention provides a method of selecting a therapy for a subject with cervical cancer, the method comprising the steps of: (a) PD-L1 on tumor cells from a tumor sample from the subject; detecting protein expression levels by an IHC assay using an anti-PD-L1 antibody suitable for staining, and (b) for subjects with detectable PD-L1 expression levels, PD-L1 on detected tumor cells; Based on L1 expression, an anti-TIGIT antagonist antibody administered at a dose of between about 500 mg and about 700 mg every 3 weeks and a PD-1 axis binding administered at a dose of between about 900 mg and about 1500 mg every 3 weeks. selecting a therapy that includes one or more dosing cycles of the antagonist.
別の態様では、本発明は、検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法を提供し、方法は対象に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む。 In another aspect, the invention provides a method for treating a subject with cervical cancer with a detectable level of PD-L1 expression, the method comprising administering to the subject a dose of about 600 mg every three weeks. administering one or more dosing cycles of tiragolumab and atezolizumab at a dose of about 1200 mg every 3 weeks.
別の態様では、本発明は、乳がんを有する対象又は対象集団を処置する方法であって、4週間ごとの約840mgの用量のチラゴルマブ、4週間ごとの約1680mgの用量のアテゾリズマブ、及び3週間の投薬/1週間の休薬の間で約100mg/m2の用量のnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む、方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population with breast cancer comprising tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and Methods are provided comprising administering to a subject or population of subjects a dosing regimen comprising one or more dosing cycles of nab-paclitaxel at a dose of about 100 mg/m 2 between on/one week off.
別の態様では、本発明は、初期トリプルネガティブ乳がん(eTNBC)を有する対象を処置する方法を提供し、方法は2週間ごとに約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとに約600mg~1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In another aspect, the invention provides a method of treating a subject with early triple-negative breast cancer (eTNBC), comprising an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and administering to the subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to 1200 mg.
別の態様では、本発明は、eTNBCを有する対象を処置する方法であって、2週間ごとに約420mgの用量のチラゴルマブ、2週間ごとに約840mgの用量のアテゾリズマブ、及び(a)(i)毎週約125mg/m2の用量のnab-パクリタキセル、及び投薬レジメンの最初の12週間について3週間ごとに5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとに約60mg/m2の用量のドキソルビシン、2週間ごとに約600mg/m2の用量のシクロホスファミド、及び2週間ごとにG-CSF又はGM-CSF;又は(b)(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル;(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとに約60mg/m2の用量のドキソルビシン、2週間ごとに約600mg/m2の用量のシクロホスファミド、及び2週間ごとにG-CSF又はGM-CSFを含む投薬レジメンを対象に投与するステップを含む方法を提供し、方法は、投薬レジメンの最後の投与の2週間後と6週間後の間の手術を更に含む。
In another aspect, the invention provides a method of treating a subject with eTNBC comprising tiragolumab at a dose of about 420 mg every two weeks, atezolizumab at a dose of about 840 mg every two weeks, and (a)(i) nab-paclitaxel at a dose of about 125 mg/ m2 weekly and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks for the first 12 weeks of the dosing regimen, (ii) a dosing regimen doxorubicin at a dose of about 60 mg/ m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/ m2 every 2 weeks, and G-CSF or GM-CSF; or (b) (i) nab-paclitaxel at a dose of about 125 mg/m 2 weekly for the first 12 weeks of the dosing regimen; (ii) every 2 weeks for
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するSCCHNを有する対象又は対象集団を処置するための方法を提供し、方法は3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 In another aspect, the invention provides a method for treating a subject or subject population having SCCHN with detectable levels of PD-L1 expression, wherein the method comprises between about 500 mg and about 700 mg every three weeks administering to the subject or population of subjects a dose of an anti-TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every three weeks.
別の態様では、本発明は、SCCHNを有する対象又は対象集団のための治療法を選択する方法を提供し、方法は、(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、対象又は対象集団からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、(b)検出可能なPD-L1発現レベルを有する対象又は対象集団について、検出されたPD-L1発現に基づいて、3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療法を選択すること、を含む。 In another aspect, the invention provides a method of selecting a therapy for a subject or subject population with SCCHN, comprising: (a) by an IHC assay using an anti-PD-L1 antibody suitable for staining; , detecting a protein expression level of PD-L1 in a tumor sample from a subject or population of subjects; (b) for a subject or population of subjects having a detectable PD-L1 expression level, One or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of between about 500 mg and about 700 mg every 3 weeks on a daily basis. selecting a therapy comprising
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するSCCHNを有する対象を処置するための方法を提供し、方法は対象に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む。 In another aspect, the invention provides a method for treating a subject having SCCHN with a detectable level of PD-L1 expression, the method comprising administering to the subject tiragolumab at a dose of about 600 mg every three weeks, and administering one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks.
別の態様では、本発明は、肝細胞癌腫(HCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、対象又は対象集団がHCCの事前全身治療を受けたことがない、方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having hepatocellular carcinoma (HCC), wherein the subject or subject population is treated with one or more anti-TIGIT antagonist antibodies and a PD-1 axis binding antagonist. A method is provided comprising administering a dosing cycle, wherein the subject or subject population has not received prior systemic treatment for HCC.
別の態様では、本発明は、HCCを有する対象又は対象集団を処置する方法であって、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、及びVEGFアンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含む、方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC, comprising one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist. A method is provided comprising administering to a population.
別の態様では、本発明は、HCCを有する対象又は対象集団を処置する方法を提供し、方法は3週間ごとに約600mgの用量のチラゴルマブ、3週間ごとに約1200mgの用量のアテゾリズマブ、及び3週間ごとに約15mg/kgの用量のベバシズマブの1回以上の投薬サイクルを対象に投与することを含む。 In another aspect, the invention provides a method of treating a subject or subject population with HCC, comprising tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and administering to the subject one or more dosing cycles of bevacizumab at a dose of about 15 mg/kg every week.
別の態様では、本発明は、MIBCを有する対象又は対象集団を処置するための方法を提供し、方法は対象に、3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、対象が白金系化学療法剤による処置に不適格である。 In another aspect, the invention provides a method for treating a subject or subject population with MIBC, the method comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of between about 500 mg and about 700 mg every three weeks; and administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every 3 weeks and the subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
別の態様では、本発明は、MIBCを有する対象又は対象集団を処置するための方法を提供し、方法は対象に、3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、処置が周術期処置である。 In another aspect, the invention provides a method for treating a subject or subject population with MIBC, the method comprising administering to the subject an anti-TIGIT antagonist antibody at a dose of between about 500 mg and about 700 mg every three weeks; and administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every three weeks, wherein the treatment is perioperative treatment.
別の態様では、本発明は、MIBCを有する対象又は対象集団を処置するための方法を提供し、方法は対象又は対象集団に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、1又は複数の対象がシスプラチン不適格である。 In another aspect, the invention provides a method for treating a subject or subject population having MIBC, wherein the subject or subject population is administered tiragolumab at a dose of about 600 mg every three weeks and One or more subjects are cisplatin ineligible, including administering one or more dosing cycles of atezolizumab at a dose of about 1200 mg.
別の態様では本発明は、MIBCを有する対象又は対象集団を処置するための方法を提供し、方法は対象又は対象集団に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、処置が周術期処置である。 In another aspect, the invention provides a method for treating a subject or subject population having MIBC, wherein the subject or subject population is administered tiragolumab at a dose of about 600 mg every three weeks and about The treatment is perioperative treatment, comprising administering one or more dosing cycles of atezolizumab at a dose of 1200 mg.
別の態様では、本発明は、mUCを有する対象又は対象集団を処置するための方法を提供し、方法は対象又は対象集団に、3週間ごとの約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。 In another aspect, the invention provides a method for treating a subject or subject population having mUC, wherein the subject or subject population is administered anti-TIGIT at a dose of between about 500 mg and about 700 mg every three weeks. administering a dosing regimen comprising one or more dosing cycles of an antagonist antibody and a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every three weeks.
別の態様では、本発明は、mUCを有する対象又は対象集団を処置するための方法を提供し、方法は対象又は対象集団に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む。 In another aspect, the invention provides a method for treating a subject or subject population having mUC, wherein the subject or subject population is administered tiragolumab at a dose of about 600 mg every three weeks and administering one or more dosing cycles of atezolizumab at a dose of about 1200 mg.
別の態様では、本発明は、mUCを有する対象又は対象集団を処置するための方法を提供し、方法は、対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、(a)第1の投薬レジメンが、3週間ごとに約600mgの用量のチラゴルマブと3週間ごとに約1200mgの用量のアテゾリズマブを含み、(b)第2の投薬レジメンは、3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンは、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与され、又は(ii)サクツズマブゴビテカンは、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、第2の投薬レジメンは、第1の投薬レジメン中に対象又は対象集団が疾患進行又は許容できない毒性を経験した後に対象又は対象集団に投与される。 In another aspect, the invention provides a method for treating a subject or population of subjects with mUC, the method comprising administering to the subject or population of subjects a first dosing regimen followed by a second dosing regimen (a) the first dosing regimen comprises tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks; and (b) the second dosing regimen is (i) enfortumab vedotin at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off or (ii) suctuzumab govitecan administered at a dose of 10 mg/kg weekly for 2 weeks on/1 week off, the second dosing regimen being the first dosing regimen It is administered to a subject or subject population during which the subject or subject population experiences disease progression or unacceptable toxicity.
別の態様では、本発明は、膵臓がんを有する対象又は対象集団を処置する方法を提供し、方法は対象又は対象集団に、各28日間投薬サイクルの1日目及び15日目に約420mgの用量のチラゴルマブ、各28日間投薬サイクルの第1及び15日目に約840mgの用量のアテゾリズマブ、各28日間投薬サイクルの第1、8及び15日目に約1000mg/m2の用量のゲムシタビン、並びに各28日間投薬サイクルの第1、8及び15日目に約125mg/m2の用量のnab-パクリタキセルの1回以上の28日間投薬サイクルを含む投薬レジメンを投与することを含む。
In another aspect, the invention provides a method of treating a subject or subject population having pancreatic cancer, wherein the subject or subject population is administered about 420 mg on
別の態様では、本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を提供し、方法は各投薬サイクルの1日目に約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む。
In another aspect, the invention provides a method for treating a subject or subject population with advanced or metastatic esophageal cancer, wherein the method comprises between about 500 mg and about 700 mg on
別の態様では、本発明は、食道がんを有する対象又は対象集団を処置するための方法を提供し、方法は各投薬サイクルの1日目に約500mgと約700mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、一又は複数の対象が白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある。
In another aspect, the invention provides a method for treating a subject or subject population having esophageal cancer, comprising administering anti-TIGIT at a dose of between about 500 mg and about 700 mg on
別の態様では、本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を提供し、方法は対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に投薬レジメンからシスプラチンが省略される。
In another aspect, the invention provides a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein the method comprises administering to the subject or population of subjects about Tiragolumab at a dose of 600 mg, Atezolizumab at a dose of approximately 1200 mg on
別の態様では、本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を提供し、方法は、対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、(a)第1の投薬レジメンが、各投薬サイクルの第1日目に約80mg/m 2の用量のシスプラチンと、各21日サイクルの第1~5日目に800mg/m2/24時間の用量の5-フルオロウラシルとの1回以上の21日間投薬サイクルを含み、シスプラチンが6回投与後に投薬レジメンから省略され(b)第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量での1回以上の21日間投薬サイクルのチラゴルマブと、各投薬サイクルの1日目に約1200mgの用量でのアテゾリズマブとを含む。
In another aspect, the invention provides a method for treating a subject or subject population with advanced or metastatic esophageal cancer, the method comprising administering to the subject or subject population a first dosing regimen and a second (a) the first dosing regimen comprises cisplatin at a dose of about 80 mg/ m2 on
別の態様では、本発明は、本明細書で提供される方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニスト及び/又は抗TIGITアンタゴニスト抗体を含むキットを提供する。 In another aspect, the invention provides kits comprising PD-1 axis binding antagonists and/or anti-TIGIT antagonist antibodies for treating a subject with cancer according to the methods provided herein.
別の態様では、本発明は、本明細書で提供される方法に従ってがんを有する対象を処置するための抗TIGITアンタゴニスト抗体と組み合わせて使用するためのPD-1軸結合アンタゴニストを含むキットを提供する。 In another aspect, the invention provides a kit comprising a PD-1 axis binding antagonist for use in combination with an anti-TIGIT antagonist antibody to treat a subject with cancer according to the methods provided herein. do.
別の態様では、本発明は、本明細書で提供される方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含むキットを提供する。 In another aspect, the invention provides a kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject with cancer according to the methods provided herein. do.
別の態様では、本発明は、がんを有する対象又は対象集団を処置するための方法で使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを提供し、方法は本明細書で提供される方法によるものである。 In another aspect, the invention provides an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with cancer, the method provided herein It is due to the method used.
別の態様では、本発明は、PD-1軸結合アンタゴニストと組み合わせてがんを有する対象又は対象集団を処置するための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、処置が本明細書で提供される方法によるものである使用を提供する。 In another aspect, the invention is the use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject or subject population with cancer in combination with a PD-1 axis binding antagonist, wherein treatment is as described herein. provides a use that is by the method provided in
発明の詳細な説明
本発明は、がん(例えば、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、初期TNBC(eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC))の処置のための治療方法及び組成物を提供する。本発明は、PD-1軸結合アンタゴニスト、VEGFアンタゴニスト及び/又は化学療法剤と組み合わせた抗TIGIT抗体(例えば、抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む免疫療法ががんの処置に有用であり得るという発見に少なくとも部分的に基づく。そのような組み合わせ及び/又は投薬レジメンを含む組成物、使用及びキットも本明細書で提供される。
Detailed Description of the Invention The present invention is directed to cancer (e.g., lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer)), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC). locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., , subject has not been previously treated for stage IV NSCLC))): cervical cancer (e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent breast cancer (e.g. TNBC (e.g. early TNBC (eTNBC))) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD- L1 positive SCCHN); liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer pancreatic cancer (e.g. PDAC, e.g. metastatic PDAC); renal cancer or renal cancer (e.g. RCC); melanoma; ovarian cancer; gastric cancer (e.g. gastroesophageal junction cancer); For example, therapeutic methods and compositions for the treatment of MSS or MSI-Low CRC) are provided. The present invention provides that immunotherapy comprising anti-TIGIT antibodies (e.g. anti-TIGIT antagonist antibodies such as tiragolumab) in combination with PD-1 axis binding antagonists, VEGF antagonists and/or chemotherapeutic agents are useful for treating cancer. Based at least in part on the discovery of obtaining Compositions, uses and kits comprising such combinations and/or dosing regimens are also provided herein.
I.一般的技術
本明細書に記載又は参照される技術及び手順は、一般によく理解されており、例えば、Sambrook et al.,Molecular Cloning:A Laboratory Manual 3d edition(2001)Cold Spring Harbor Laboratory Press,Cold Spring Harbor,N.Y.;Current Protocols in Molecular Biology(F.M.Ausubel,et al.eds.,(2003));Methods in Enzymologyのシリーズ(Academic Press,Inc.):PCR 2:A Practical Approach(M.J.MacPherson,B.D.Hames and G.R.Taylor eds.(1995)),Harlow and Lane,eds.(1988)Antibodies,A Laboratory Manual,and Animal Cell Culture(R.I.Freshney,ed.(1987));Oligonucleotide Synthesis(M.J.Gait,ed.,1984);Methods in Molecular Biology,Humana Press;Cell Biology:A Laboratory Notebook(J.E.Cellis,ed.,1998)Academic Press;Animal Cell Culture(R.I.Freshney),ed.,1987);Introduction to Cell and Tissue Culture(J.P.Mather and P.E.Roberts,1998)Plenum Press;Cell and Tissue Culture:Laboratory Procedures(A.Doyle,J.B.Griffiths,and D.G.Newell,eds.,1993-8)J.Wiley and Sons;Handbook of Experimental Immunology(D.M.Weir and C.C.Blackwell,eds.);Gene Transfer Vectors for Mammalian Cells(J.M.Miller and M.P.Calos,eds.,1987);PCR:The Polymerase Chain Reaction,(Mullis et al.,eds.,1994);Current Protocols in Immunology(J.E.Coligan et al.,eds.,1991);Short Protocols in Molecular Biology(Wiley and Sons,1999);Immunobiology(C.A.Janeway and P.Travers,1997);Antibodies(P.Finch,1997);Antibodies:A Practical Approach(D.Catty.,ed.,IRL Press,1988-1989);Monoclonal Antibodies:A Practical Approach(P.Shepherd and C.Dean,eds.,Oxford University Press,2000);Using Antibodies:A Laboratory Manual(E.Harlow and D.Lane(Cold Spring Harbor Laboratory Press,1999);The Antibodies(M.Zanetti and J.D.Capra,eds.,Harwood Academic Publishers,1995);及びCancer:Principles and Practice of Oncology(V.T.DeVita et al.,eds.,J.B.Lippincott Company,1993)に記載される広く利用されている方法論等の従来の方法論を使用して当業者によって一般的に用いられる。
I. General Techniques The techniques and procedures described or referenced herein are generally well understood and can be found, for example, in Sambrook et al. , Molecular Cloning: A Laboratory Manual 3d edition (2001) Cold Spring Harbor Laboratory Press, Cold Spring Harbor, N.J. Y. Current Protocols in Molecular Biology (FM Ausubel, et al. eds., (2003)); Methods in Enzymology series (Academic Press, Inc.): PCR 2: A Practical Approach (MJ MacPherson BD Hames and GR Taylor eds.(1995)), Harlow and Lane, eds. (1988) Antibodies, A Laboratory Manual, and Animal Cell Culture (RI Freshney, ed. (1987)); Oligonucleotide Synthesis (MJ Gait, ed., 1984); Cell Biology: A Laboratory Notebook (JE Cellis, ed., 1998) Academic Press; Animal Cell Culture (RI Freshney), ed. , 1987); Introduction to Cell and Tissue Culture (JP Mather and PE Roberts, 1998) Plenum Press; Cell and Tissue Culture: Laboratory Procedures (A. Doyle, Jf. Newell, eds., 1993-8) J. Am. Wiley and Sons; Handbook of Experimental Immunology (DM Weir and CC Blackwell, eds.); Gene Transfer Vectors for Mammalian Cells (JM Miller and MP Calos, 8, eds.); PCR: The Polymerase Chain Reaction, (Mullis et al., eds., 1994); Current Protocols in Immunology (JE Coligan et al., eds., 1991); ); Immunobiology (CA Janeway and P. Travers, 1997); Antibodies (P. Finch, 1997); Antibodies: A Practical Approach (D. Catty., ed., IRL Press, 1988-1989); :A Practical Approach(P.Shepherd and C.Dean,eds.,Oxford University Press,2000);Using Antibodies:A Laboratory Manual(E.Harlow and D.Lane(Cold Spring Harbor Laboratory Press,1999);The Antibodies( M. Zanetti and JD Capra, eds., Harwood Academic Publishers, 1995); commonly employed by those skilled in the art using conventional methodologies such as the widely used methodology described in .
II.定義
本明細書に記載の本発明の態様及び実施形態は、態様及び実施形態「を含む」、「からなる」、及び「から本質的になる」を含むことが理解される。本明細書で使用される場合、単数形「a」、「an」、及び「the」は、別途示されない限り、複数のものを含む。
II. DEFINITIONS Aspects and embodiments of the invention described herein are understood to include “comprising,” “consisting of,” and “consisting essentially of” aspects and embodiments. As used herein, the singular forms "a,""an," and "the" include plural unless otherwise indicated.
本明細書で使用される「約」という用語は、この技術分野の当業者であれば容易に理解する、それぞれの値の通常の誤差範囲を指す。本明細書において、値又はパラメーターについての「約」の参照は、それ自体がその値又はパラメーターに向けられた態様を含む(及び説明する)。例えば、「約X」について言及する記述は、「X」の記述を含む。 As used herein, the term "about" refers to the normal error range for the respective value, readily understood by those skilled in the art. As used herein, reference to "about" a value or parameter includes (and describes) aspects that are directed to that value or parameter per se. For example, description referring to "about X" includes description of "X."
「発現のレベル」又は「発現レベル」という用語は、一般に、同義に使用され、一般に、生物学的試料中のバイオマーカーの量を指す。「発現」は、一般に、情報(例えば、遺伝子コード及び/又はエピジェネティック情報)が、細胞中に存在し、機能する構造に変換されるプロセスを指す。したがって、本明細書で使用される場合、「発現」とは、ポリヌクレオチドへの転写、ポリペプチドへの翻訳、又は更にポリヌクレオチド及び/若しくはポリペプチド修飾(例えば、ポリペプチドの翻訳後修飾)を指す場合がある。転写されたポリヌクレオチド、翻訳されたポリペプチド、又はポリヌクレオチド及び/若しくはポリペプチド修飾(例えば、ポリペプチドの翻訳後修飾)のフラグメントも、それらが選択的スプライシングによって生成された転写物若しくは分解された転写物に由来するか又は例えばタンパク質分解によるポリペプチドの翻訳後プロセシングに由来するかどうかにかかわらず、発現されたものとみなされるべきである。「発現した遺伝子」とは、mRNAとしてポリヌクレオチドに転写され、その後、ポリペプチドに翻訳されるもの、及びまたRNAに転写されるが、ポリペプチドに翻訳されないもの(例えば、転移及びリボソームRNA)を含む。バイオマーカーの「量」又は「レベル」(例えば、発現レベル)は、当業者に公知の方法によって測定することができ、本明細書にも開示される。個体に対する臨床的利益の増加に関連するバイオマーカーの「量」又は「レベル」は、例えば、生物学的試料中で検出可能なレベルであり得る。いくつかの態様では、バイオマーカーの発現レベル又は量を使用して、特定の治療(例えば、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療、又は抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療)に応答するか又はそれから利益を得る可能性があるがんを有する対象を同定/特徴付けることができる。 The terms "level of expression" or "expression level" are generally used interchangeably and generally refer to the amount of a biomarker in a biological sample. "Expression" generally refers to the process by which information (eg, genetic code and/or epigenetic information) is converted into structures present and functional in a cell. Thus, as used herein, "expression" refers to transcription into a polynucleotide, translation into a polypeptide, or further polynucleotide and/or polypeptide modification (e.g., post-translational modification of a polypeptide). may point. Transcribed polynucleotides, translated polypeptides, or fragments of polynucleotide and/or polypeptide modifications (e.g., post-translational modifications of polypeptides) may also be transcripts they are produced by alternative splicing or degraded Expressed is to be considered whether derived from transcript or from post-translational processing of the polypeptide, eg, by proteolysis. "Expressed genes" include those that are transcribed as mRNA into polynucleotides that are subsequently translated into polypeptides, and those that are also transcribed into RNA but not translated into polypeptides (e.g., transposed and ribosomal RNA). include. The "amount" or "level" (eg, expression level) of a biomarker can be measured by methods known to those of skill in the art and are also disclosed herein. An "amount" or "level" of a biomarker associated with increased clinical benefit to an individual can be, for example, a detectable level in a biological sample. In some aspects, the biomarker expression level or amount is used to determine a particular treatment (e.g., a treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody, or an anti-TIGIT antagonist Subjects with cancer who are likely to respond to or benefit from a treatment comprising one or more dosing cycles of an antibody) can be identified/characterized.
「増加した発現」、「増加した発現レベル」、「増加したレベル」、「上昇した発現」、「上昇した発現レベル」、又は「上昇したレベル」とは、疾患若しくは障害(例えば、がん)に罹患していない一又は複数の個体又は内部対照(例えば、ハウスキーピングバイオマーカ)等の対照と比較した個体におけるバイオマーカーの発現の増加又はそのレベルの増加を指す。 "Increased expression", "increased expression level", "increased level", "elevated expression", "elevated expression level" or "elevated level" refers to a disease or disorder (e.g., cancer) Refers to an increase in the expression of a biomarker or an increase in its level in an individual compared to one or more individuals who are not afflicted with HIV or a control, such as an internal control (eg, a housekeeping biomarker).
「減少した発現」、「減少した発現レベル」、「減少したレベル」、「低減した発現」、「低減した発現レベル」、又は「低減したレベル」とは、疾患若しくは障害(例えば、がん)に罹患していない一又は複数の個体又は内部対照(例えば、ハウスキーピングバイオマーカー)等の対照と比較した個体におけるバイオマーカーの低減した発現又は低減したレベルを指す。いくつかの態様では、低減した発現とは、発現がほとんど又はまったくないことである。 "Reduced expression," "reduced expression level," "reduced level," "reduced expression," "reduced expression level," or "reduced level" refers to a disease or disorder (e.g., cancer) Refers to reduced expression or reduced levels of a biomarker in an individual compared to one or more individuals not suffering from HIV or a control, such as an internal control (eg, a housekeeping biomarker). In some aspects, reduced expression is little or no expression.
試料における本明細書に記載の様々なバイオマーカーの存在及び/又は発現レベル/量は、いくつかの方法論によって分析され得、これらの多くは、当該技術分野で知られ、当業者に理解されており、免疫組織化学(「IHC」)、ウェスタンブロット分析、免疫沈降、分子結合アッセイ、ELISA、ELIFA、フローサイトメトリー、蛍光活性化細胞選別(「FACS」)、MassARRAY、プロテオミクス、定量的血液ベースアッセイ(例えば、血清ELISA)、生化学的酵素活性アッセイ、インサイチュハイブリダイゼーション(ISH)、蛍光インサイチュハイブリダイゼーション(FISH)、サザン分析、ノーザン分析、全ゲノム配列決定、大規模並列DNA配列決定(例えば、次世代配列決定)、NANOSTRING(登録商標)、例えば、分岐状DNA、SISBA、TMA等の、定量的リアルタイムPCR(qRT-PCR)及び他の増幅型検出方法を含むポリメラーゼ連鎖反応(PCR)、RNA-Seq、マイクロアレイ分析、遺伝子発現プロファイリング、及び/又は遺伝子発現連続分析(「SAGE」)、並びにタンパク質、遺伝子、及び/又は組織アレイ分析によって行われ得る多種多様なアッセイのうちのいずれか1つを含むが、これらに限定されない。遺伝子及び遺伝子生成物の状態を評価するための典型的なプロトコルは、例えば、Ausubel et al.,eds.,1995,Current Protocols In Molecular Biologyの第2部(ノーザンブロット法)、第4部(サザンブロット法)、第15部(免疫ブロット法)、及び第18部(PCR分析)において見出される。Rules Based Medicine又はMeso Scale Discovery(「MSD」)から入手可能なアッセイ等の多重化免疫アッセイも使用され得る。 The presence and/or expression level/amount of various biomarkers described herein in a sample can be analyzed by several methodologies, many of which are known in the art and understood by those of ordinary skill in the art. Cages, Immunohistochemistry (“IHC”), Western Blot Analysis, Immunoprecipitation, Molecular Binding Assays, ELISA, ELISA, Flow Cytometry, Fluorescence Activated Cell Sorting (“FACS”), MassARRAY, Proteomics, Quantitative Blood-Based Assays (e.g. serum ELISA), biochemical enzymatic activity assays, in situ hybridization (ISH), fluorescence in situ hybridization (FISH), Southern analysis, Northern analysis, whole genome sequencing, massively parallel DNA sequencing (e.g. generational sequencing), NANOSTRING®, polymerase chain reaction (PCR) including quantitative real-time PCR (qRT-PCR) and other amplification-type detection methods such as branched-DNA, SISBA, TMA, RNA- Seq, microarray analysis, gene expression profiling, and/or serial gene expression analysis (“SAGE”), and any one of a wide variety of assays that can be performed by protein, gene, and/or tissue array analysis. but not limited to these. Exemplary protocols for assessing gene and gene product status are described, for example, in Ausubel et al. , eds. , 1995, Current Protocols In Molecular Biology, Part 2 (Northern blotting), Part 4 (Southern blotting), Part 15 (Immunoblotting), and Part 18 (PCR analysis). Multiplexed immunoassays, such as those available from Rules Based Medicine or Meso Scale Discovery (“MSD”), may also be used.
「相関する」又は「相関すること」とは、任意の方法で、第1の解析又はプロトコルの性能及び/又は結果を第2の解析又はプロトコルの性能及び/又は結果と比較することを意味する。例えば、第1の分析若しくはプロトコルの結果を、第2のプロトコルを行う際に使用してもよく、及び/又は第1の分析若しくはプロトコルの結果を使用して、第2の分析若しくはプロトコルを行うべきかどうかを決定してもよい。ポリペプチド解析又はプロトコルの態様関して、ポリペプチド発現解析又はプロトコルの結果を使用して、特定の治療レジメンを行うべきかどうかを判定することができる。ポリヌクレオチド解析又はプロトコルの態様に関して、ポリヌクレオチド発現解析又はプロトコルの結果を使用して、特定の治療レジメンを行うべきかどうかを判定することができる。 "Correlate" or "correlating" means comparing the performance and/or results of a first analysis or protocol to the performance and/or results of a second analysis or protocol in any manner . For example, the results of a first analysis or protocol may be used in performing a second protocol and/or the results of the first analysis or protocol are used to perform the second analysis or protocol. may decide whether to With respect to aspects of the polypeptide analysis or protocol, the results of the polypeptide expression analysis or protocol can be used to determine whether a particular therapeutic regimen should be administered. With respect to the polynucleotide analysis or protocol aspect, the results of the polynucleotide expression analysis or protocol can be used to determine whether a particular therapeutic regimen should be administered.
「実質的に低減された」又は「実質的に異なる」という表現は、本明細書で使用される場合、2つの数値(一般に、一方がある分子と関連付けられており、他方が参照/比較分子と関連付けられている)の間の十分に高い相違を表し、結果として、当業者であれば、これら2つの値の間の相違が、そのような値(例えば、KD値)によって測定される生物学的特徴に関して、統計学的に有意なものであると見なすであろう。そのような2つの値の間の相違は、例えば、参照/比較分子の値の関数として、約10%超、約20%超、約30%超、約40%超、及び/又は約50%超である。 The terms "substantially reduced" or "substantially different" as used herein refer to two numerical values (generally one associated with a molecule and the other a reference/comparison molecule). ), such that the difference between these two values is measured by such values (e.g., K D values) to those skilled in the art. With respect to biological characteristics, it will be considered statistically significant. The difference between two such values is, for example, greater than about 10%, greater than about 20%, greater than about 30%, greater than about 40%, and/or about 50% as a function of the value of the reference/comparison molecule. Super.
「実質的に同様の」又は「実質的に同じ」という用語は、本明細書で使用される場合、2つの数値(一般に、一方が分子と関連付けられており、他方が基準/比較分子と関連付けられている)の間の十分に高い類似性を示し、結果として、当業者であれば、これら2つの値の間の相違が、そのような値(例えば、KD値)によって測定される生物学的特徴に関して、生物学的及び/又は統計的有意性がほとんどない、又は全くないと見なすであろう。そのような2つの値の間の相違は、例えば、基準/比較対象の値の関数として、約50%未満、約40%未満、約30%未満、約20%未満、及び/又は約10%である。 The terms "substantially similar" or "substantially the same" as used herein refer to two numerical values, generally one associated with the molecule and the other with the reference/comparison molecule. ), such that the difference between these two values is determined by such values (e.g., K D values). With respect to scientific characteristics, one would assume little or no biological and/or statistical significance. The difference between two such values is, for example, less than about 50%, less than about 40%, less than about 30%, less than about 20%, and/or about 10% as a function of the reference/comparison value. is.
「に基づく」という語句は、本明細書で使用される場合、1つ以上のバイオマーカーについての情報が、処置の決定、添付文書に提供される情報、又はマーケティング/宣伝指針等を伝えるために使用されることを意味する。 The phrase "based on," as used herein, means that information about one or more biomarkers is used to inform treatment decisions, information provided in package inserts, marketing/promotional guidance, or the like. meant to be used.
本明細書に使用される「TIGIT」又は「Ig及びITIMドメインを有するT細胞免疫受容体(T-cell immunoreceptor with Ig and ITIM domains)」は、別途示されない限り、霊長類(例えば、ヒト)及び齧歯類(例えば、マウス及びラット)等の哺乳動物を含む、任意の脊椎動物源由来の任意の天然のTIGITを指す。TIGITはまた、当該技術分野において、DKFZp667A205、FLJ39873、Vセット及び免疫グロブリンドメイン含有タンパク質9、Vセット及び膜貫通ドメイン含有タンパク質3、VSIG9、VSTM3、及びWUCAMとしても知られている。この用語は、「完全長」の未処理のTIGIT(例えば、配列番号30のアミノ酸配列を有する完全長ヒトTIGIT)、並びに細胞内での処理から生じる任意の形態のTIGIT(例えば、配列番号31のアミノ酸配列を有する、シグナル配列を有しないプロセシングされたヒトTIGIT)を包含する。この用語は、TIGITの天然に存在するバリアント、例えば、スプライスバリアント、又は対立遺伝子バリアントも包含する。例示的なヒトTIGITのアミノ酸配列は、例えば、UniProt受託番号Q495A1に見出すことができる。
As used herein, "TIGIT" or "T-cell immunoreceptor with Ig and ITIM domains" refers to primates (e.g., humans) and Refers to any naturally occurring TIGIT from any vertebrate source, including mammals such as rodents (eg, mice and rats). TIGIT is also known in the art as DKFZp667A205, FLJ39873, V-set and immunoglobulin domain-containing
「プログラム死リガンド1」及び「PD-L1」という用語は、本明細書では、天然配列のヒトPD-L1ポリペプチドを指す。天然配列PD-L1ポリペプチドは、Uniprot受託番号Q9NZQ7(配列番号32)で提供される。例えば、天然配列PD-L1は、Uniprot受託番号Q9NZQ7-1(アイソフォーム1)に記載のアミノ酸配列を有し得る。別の例において、天然配列PD-L1は、Uniprot受託番号Q9NZQ7-2(アイソフォーム2)に記載のアミノ酸配列を有し得る。更に別の例において、天然配列PD-L1は、Uniprot受託番号Q9NZQ7-3(アイソフォーム3)に記載のアミノ酸配列を有し得る。この用語は、天然に存在するPD-L1のバリアント、例えば、スプライスバリアント又は対立遺伝子バリアントも包含する。PD-L1はまた、当該技術分野において「プログラム細胞死1リガンド1」、「PDCD1LG1」、「CD274」、「B7-H」、及び「PDL1」としても言及される。
The terms "programmed
「PD-1」又は「プログラム細胞死タンパク質1」という用語は、本明細書では、特に示されていない限り、哺乳動物、例えば、霊長類(例えばヒト)及びげっ歯類(例えば、マウス及びラット)を含め、任意の脊椎動物源由来の任意の天然PD-1を指す。PD-1は、CD279、PDCD1、及びプログラム細胞死1としても当該技術分野で公知である。この用語は、天然に存在するPD-1のバリアント、例えば、スプライスバリアント又は対立遺伝子バリアントも包含する。例示的なヒトPD-1酸配列は、例えば、UniProt受託番号Q15116に見出すことができる。
The terms "PD-1" or "programmed
「PD-L2」又は「プログラム細胞死1リガンド2」という用語は、本明細書では、特に示されていない限り、哺乳動物、例えば、霊長類(例えばヒト)及びげっ歯類(例えば、マウス及びラット)を含め、任意の脊椎動物源由来の任意の天然PD-L2を指す。PD-L2は、CD273分子、B7DC、及びPDCD1L2としても当該技術分野で公知である。この用語は、天然に存在するPD-L2のバリアント、例えば、スプライスバリアント又は対立遺伝子バリアントも包含する。例示的なヒトPD-L2酸配列は、例えば、UniProt受託番号Q9BQ51に見出すことができる。
The terms "PD-L2" or "
「アンタゴニスト」という用語は、最も広義に使用され、本明細書に開示される天然ポリペプチドの生物活性を部分的又は完全に遮断、阻害、又は中和する任意の分子を含む。適切なアンタゴニスト分子としては、具体的には、アンタゴニスト抗体又は抗体フラグメント(例えば、抗原結合フラグメント)、天然ポリペプチドのフラグメント又はアミノ酸配列バリアント、ペプチド、アンチセンスオリゴヌクレオチド、有機小分子等が挙げられる。ポリペプチドのアンタゴニストを同定するための方法は、ポリペプチドを候補アンタゴニスト分子と接触させること、及びポリペプチドに通常関連する1つ以上の生物学的活性の検出可能な変化を測定することを含み得る。 The term "antagonist" is used in its broadest sense and includes any molecule that partially or fully blocks, inhibits, or neutralizes the biological activity of the native polypeptides disclosed herein. Suitable antagonist molecules specifically include antagonist antibodies or antibody fragments (eg, antigen-binding fragments), fragments or amino acid sequence variants of naturally occurring polypeptides, peptides, antisense oligonucleotides, small organic molecules, and the like. Methods for identifying antagonists of a polypeptide can comprise contacting the polypeptide with a candidate antagonist molecule and measuring a detectable change in one or more biological activities normally associated with the polypeptide. .
「PD-1軸結合アンタゴニスト」という用語は、PD-1シグナル伝達軸上のシグナル伝達に起因するT細胞機能障害を除去するようにPD-1軸結合パートナーとその結合パートナーのうちのいずれか1つ以上との相互作用を阻害し、結果として、T細胞機能(例えば、増殖、サイトカイン産生、及び/又は標的細胞死滅)を復元又は増強する分子を指す。本明細書で使用される場合、PD-1軸結合アンタゴニストは、PD-L1結合拮抗剤、PD-1結合拮抗剤、及びPD-L2結合拮抗剤を含む。いくつかの例では、PD-1軸結合アンタゴニストは、PD-L1結合アンタゴニスト又はPD-1結合アンタゴニストを含む いくつかの態様では、PD-1軸結合アンタゴニストは、PD-L1結合アンタゴニストである。別の態様では、PD-1軸結合アンタゴニストは、PD-1結合アンタゴニストである。別の態様では、PD-1軸結合アンタゴニストは、PD-L2結合アンタゴニストである。 The term "PD-1 axis binding antagonist" refers to a PD-1 axis binding partner and any one of its binding partners so as to eliminate T cell dysfunction resulting from signaling on the PD-1 signaling axis. Refers to a molecule that inhibits interaction with one or more and, as a result, restores or enhances T cell function (eg, proliferation, cytokine production, and/or target cell killing). As used herein, PD-1 axis binding antagonists include PD-L1 binding antagonists, PD-1 binding antagonists, and PD-L2 binding antagonists. In some examples, the PD-1 axis binding antagonist comprises a PD-L1 binding antagonist or PD-1 binding antagonist In some embodiments, the PD-1 axis binding antagonist is a PD-L1 binding antagonist. In another aspect, the PD-1 axis binding antagonist is a PD-1 binding antagonist. In another aspect, the PD-1 axis binding antagonist is a PD-L2 binding antagonist.
「PD-1結合アンタゴニスト」という用語は、PD-1とその結合パートナーのうちの1つ以上、例えば、PD-L1及び/又はPD-L2との相互作用に起因するシグナル伝達を減少させる、遮断する、阻害する、抑止する、又は妨害する分子を指す。PD-1(プログラム死1)はまた、当該技術分野において「プログラム細胞死1」、「PDCD1」、「CD279」、及び「SLEB2」としても言及される。例示的なヒトPD-1は、UniProtKB/Swiss-Prot受入番号Q15116に示されている。いくつかの例では、PD-1結合アンタゴニストは、PD-1の、その結合パートナー農地の1つ以上に対する結合を阻害する分子である。特定の態様では、PD-1結合アンタゴニストは、PD-1のPD-L1及び/又はPD-L2への結合を阻害する。例えば、PD-1結合アンタゴニストは、抗PD-1抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド、並びにPD-1とPD-L1及び/又はPD-L2との相互作用に起因するシグナル伝達を減少させる、遮断する、阻害する、抑止する、又は妨害する他の分子を含む。一例では、PD-1結合アンタゴニストは、機能不全のT細胞を機能不全にしないようにする(例えば、抗原認識に対するエフェクター応答を増強する)ように、PD-1を介するシグナル伝達を介してTリンパ球上で発現される細胞表面タンパク質によって又はそれを介して媒介される負の共刺激シグナルを低減する。いくつかの例では、PD-1結合アンタゴニストはPD-1に結合する。いくつかの例では、PD-1結合アンタゴニストは、抗PD-1抗体(例えば、抗PD-1アンタゴニスト抗体)である。例示的な抗PD-1アンタゴニスト抗体としては、ニボルマブ、ペンブロリズマブ、MEDI-0680(AMP 514)、PDR001(スパルタリズマブ)、REGN2810(セミプリマブ)、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG 404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103及びhAb21が挙げられる。特定の態様では、PD-1結合アンタゴニストはMDX-1106(ニボルマブ)である。別の特定の態様では、PD-1結合アンタゴニストは、MK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)である。別の特定の態様では、PD-1結合アンタゴニストは、PD-L2 Fc融合タンパク質、例えばAMP-224である。別の特定の態様では、PD-1結合アンタゴニストはMEDI-0680である。別の特定の態様では、PD-1結合アンタゴニストはPDR001(スパルタリズマブ)である。別の特定の態様では、PD-1結合アンタゴニストはREGN2810(セミプリマブ)である。別の特定の態様では、PD-1結合アンタゴニストはBGB-108である。別の特定の態様では、PD-1結合アンタゴニストはプロゴリマブである。別の特定の態様では、PD-1結合アンタゴニストはカンレリズマブである。別の具体的な態様において、PD-1結合アンタゴニストはシンチリマブである。別の特定の態様では、PD-1結合アンタゴニストはチセレリズマブである。別の具体的な態様において、PD-1結合アンタゴニストはトリパリマブである。他の更なる例示的なPD-1結合アンタゴニストとしては、BION-004、CB201、AUNP-012、ADG104及びLBL-006が挙げられる。
The term "PD-1 binding antagonist" refers to a blockade that reduces signaling due to interaction of PD-1 with one or more of its binding partners, e.g. Refers to a molecule that acts, inhibits, abrogates, or interferes. PD-1 (programmed death 1) is also referred to in the art as "
「抗PD-1アンタゴニスト抗体」という用語は、PD-1の生物学的活性を実質的に又は完全に阻害するように十分な親和性でPD-1に結合することができる抗体又はその抗原結合フラグメント若しくはバリアントを指す。例えば、抗PD-1アンタゴニスト抗体は、PD-1とその結合パートナー(PD-L1及び/又はPD-L2等)のいずれか1つ以上との相互作用から生じるシグナル伝達を減少、遮断、阻害、抑止又は干渉し得る。いくつかの例では、抗PD-1アンタゴニスト抗体は、別のPD-1活性に影響を及ぼすことなく1つのPD-1活性に拮抗し得ることが当業者によって理解されるであろう。例えば、本明細書に記載される特定の方法又は使用において使用されるための抗PD-1アンタゴニスト抗体は、他のPD-1相互作用のいずれかに影響を及ぼすことなく、又はその影響を最小限に抑えることなく、その結合パートナー(例えば、PD-L1又はPD-L2)の1つに応答してPD-1活性に拮抗する抗PD-1アンタゴニスト抗体である。一態様では、非関連非PD-1タンパク質への抗PD-1アンタゴニスト抗体の結合の程度は、例えばラジオイムノアッセイ(RIA)によって測定した場合に、PD-1への抗体の結合の約10%未満である。特定の態様では、抗PD-1アンタゴニスト抗体に結合すPD-1は、≦1μM、≦100nM、≦10nM、≦1nM、≦0.1nM、≦0.01nM又は≦0.001nM(例えば、10-8M以下、例えば10-8M~10-13M、例えば10-9M~10--13M)の解離定数(KD)を有する。特定の態様では、抗PD-1アンタゴニスト抗体は、異なる種からのPD-1の間で保存されているPD-1のエピトープ、又は交差種反応性を可能にするPD-1上のエピトープに結合する。一態様では、抗PD-1アンタゴニスト抗体はペンブロリズマブ(以前はラムブロリズマブとして知られていた)である。一態様では、抗PD-1アンタゴニスト抗体はニボルマブである。 The term "anti-PD-1 antagonist antibody" refers to an antibody or antigen-binding antibody capable of binding PD-1 with sufficient affinity to substantially or completely inhibit the biological activity of PD-1. Refers to a fragment or variant. For example, an anti-PD-1 antagonist antibody may reduce, block, inhibit, can deter or interfere; It will be appreciated by those skilled in the art that, in some instances, an anti-PD-1 antagonist antibody may antagonize one PD-1 activity without affecting another PD-1 activity. For example, an anti-PD-1 antagonist antibody for use in certain methods or uses described herein may have no effect or minimal effect on any other PD-1 interactions. Without limitation, anti-PD-1 antagonist antibodies that antagonize PD-1 activity in response to one of its binding partners (eg, PD-L1 or PD-L2). In one aspect, the extent of binding of the anti-PD-1 antagonist antibody to unrelated non-PD-1 protein is less than about 10% of the binding of the antibody to PD-1, eg, as measured by radioimmunoassay (RIA). is. In certain aspects, the PD-1 binding to the anti-PD-1 antagonist antibody is ≤1 μM, ≤100 nM, ≤10 nM, ≤1 nM, ≤0.1 nM, ≤0.01 nM or ≤0.001 nM (e.g., 10- It has a dissociation constant (K D ) of 8 M or less, such as from 10 −8 M to 10 −13 M, such as from 10 −9 M to 10− −13 M). In certain aspects, the anti-PD-1 antagonist antibody binds to an epitope on PD-1 that is conserved among PD-1 from different species or to an epitope on PD-1 that allows for cross-species reactivity. do. In one aspect, the anti-PD-1 antagonist antibody is pembrolizumab (previously known as lambrolizumab). In one aspect, the anti-PD-1 antagonist antibody is nivolumab.
「PD-L1結合アンタゴニスト」という用語は、PD-L1とその結合パートナーのうちのいずれか1つ以上、例えば、PD-1及び/又はB7-1との相互作用に起因するシグナル伝達を低減する、遮断する、阻害する、消失させる、又は妨害する分子を指す。いくつかの例では、PD-L1結合アンタゴニストは、PD-L1のその結合パートナーへの結合を阻害する分子である。具体的な態様では、PD-L1結合アンタゴニストは、PD-L1のPD-1及び/又はB7-1への結合を阻害する。いくつかの例では、PD-L1結合アンタゴニストは、抗PD-L1抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド、並びにPD-L1とその結合パートナーのうちの1つ以上、例えば、PD-1及び/又はB7-1との相互作用に起因するシグナル伝達を減少させる、遮断する、阻害する、抑止する、又は妨害する他の分子を含む。一例では、PD-L1結合アンタゴニストは、機能不全のT細胞を機能不全にしないようにする(例えば、抗原認識に対するエフェクター応答を増強する)ように、PD-L1を介するシグナル伝達を介してTリンパ球上で発現される細胞表面タンパク質によって又はそれを介して媒介される負の共刺激性シグナルを低減する。いくつかの例では、PD-L1結合アンタゴニストはPD-L1に結合する。いくつかの例では、PD-L1結合アンタゴニストは、抗PD-L1抗体(例えば、抗PD-L1アンタゴニスト抗体)である。例示的な抗PD-L1アンタゴニスト抗体としては、アテゾリズマブ、MDX-1105、MEDI4736(デュルバルマブ)、MSB0010718C(アベルマブ)、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007及びHS-636が挙げられる。いくつかの態様では、抗PD-L1抗体は、アテゾリズマブ、MDX-1105、MEDI4736(デュルバルマブ)、又はMSB0010718C(アベルマブ)である。特定の一態様では、PD-L1結合アンタゴニストはMDX-1105である。別の特定の態様では、PD-L1結合アンタゴニストはMEDI4736(デュルバルマブ)である。別の特定の態様では、PD-L1結合アンタゴニストはMSB0010718C(セミプリマブ)である。他の態様では、PD-L1結合アンタゴニストは、小分子、例えばGS-4224、INCB086550、MAX-10181、INCB090244、CA-170又はABSK041であり得、いくつかの例では経口投与され得る。他の例示的なPD-L1結合アンタゴニストとしては、AVA-004、MT-6035、VXM10、LYN192、GB7003及びJS-003が挙げられる。好ましい態様では、PD-L1結合アンタゴニストは、TECENTRIQ(商標)として市販されているアテゾリズマブである。アテゾリズマブは、2015年1月16日に発行されたWHO Drug Information(International Nonproprietary Names for Pharmaceutical Substances),Proposed INN:List 112,Vol.28,No.4に記載されている(485頁を参照)。別の特定の態様では、抗PD-L1 抗体はMSB0015718Cである。 The term "PD-L1 binding antagonist" reduces signaling due to the interaction of PD-L1 with any one or more of its binding partners, e.g. PD-1 and/or B7-1 , refers to a molecule that blocks, inhibits, abolishes, or interferes. In some examples, a PD-L1 binding antagonist is a molecule that inhibits the binding of PD-L1 to its binding partner. In a specific aspect, the PD-L1 binding antagonist inhibits binding of PD-L1 to PD-1 and/or B7-1. In some examples, the PD-L1 binding antagonist is one or more of an anti-PD-L1 antibody, an antigen-binding fragment thereof, an immunoadhesin, a fusion protein, an oligopeptide, and PD-L1 and its binding partner, such as , PD-1 and/or other molecules that reduce, block, inhibit, abrogate or interfere with signaling due to interaction with B7-1. In one example, a PD-L1 binding antagonist can bind T lymphocytes through PD-L1-mediated signaling so as to render dysfunctional T cells non-dysfunctional (eg, enhance effector responses to antigen recognition). Reduce negative co-stimulatory signals mediated by or through cell surface proteins expressed on the sphere. In some examples, the PD-L1 binding antagonist binds to PD-L1. In some examples, the PD-L1 binding antagonist is an anti-PD-L1 antibody (eg, an anti-PD-L1 antagonist antibody). Exemplary anti-PD-L1 antagonist antibodies include atezolizumab, MDX-1105, MEDI4736 (durvalumab), MSB0010718C (avelumab), SHR-1316, CS1001, embafolimab, TQB2450, ZKAB001, LP-002, CX-072, IMC- 001, KL-A167, APL-502, cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 and HS-636. In some aspects, the anti-PD-L1 antibody is atezolizumab, MDX-1105, MEDI4736 (durvalumab), or MSB0010718C (avelumab). In one particular aspect, the PD-L1 binding antagonist is MDX-1105. In another specific aspect, the PD-L1 binding antagonist is MEDI4736 (durvalumab). In another specific aspect, the PD-L1 binding antagonist is MSB0010718C (semiplimab). In other aspects, the PD-L1 binding antagonist can be a small molecule such as GS-4224, INCB086550, MAX-10181, INCB090244, CA-170 or ABSK041, and in some instances can be administered orally. Other exemplary PD-L1 binding antagonists include AVA-004, MT-6035, VXM10, LYN192, GB7003 and JS-003. In a preferred embodiment, the PD-L1 binding antagonist is atezolizumab, marketed as TECENTRIQ™. Atezolizumab is listed in WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN: List 112, Vol. 28, No. 4 (see page 485). In another specific aspect, the anti-PD-L1 antibody is MSB0015718C.
「抗PD-L1アンタゴニスト抗体」という用語は、PD-1Lの生物学的活性を実質的に又は完全に阻害するように十分な親和性でPD-L1に結合することができる抗体又はその抗原結合フラグメント若しくはバリアントを指す。例えば、抗PD-L1アンタゴニスト抗体は、PD-L1とその結合パートナー(PD-1及び/又はB7-1等)のいずれか1つ以上との相互作用から生じるシグナル伝達を減少、遮断、阻害、抑止又は干渉し得る。いくつかの例では、抗PD-L1アンタゴニスト抗体は、別のPD-L1活性に影響を及ぼすことなく1つのPD-L1活性に拮抗し得ることが当業者によって理解されるであろう。例えば、本明細書に記載される特定の方法又は使用において使用されるための抗PD-L1アンタゴニスト抗体は、他のPD-L1相互作用のいずれかに影響を及ぼすことなく、又はその影響を最小限に抑えることなく、その結合パートナー(例えば、PD-1又はB7-1)の1つに応答してPD-L1活性に拮抗する抗PD-L1アンタゴニスト抗体である。一態様では、非関連非PD-L1タンパク質への抗PD-L1アンタゴニスト抗体の結合の程度は、例えばラジオイムノアッセイ(RIA)によって測定した場合に、PD-L1への抗体の結合の約10%未満である。特定の態様では、抗PD-L1アンタゴニスト抗体に結合すPD-L1は、≦1μM、≦100nM、≦10nM、≦1nM、≦0.1nM、≦0.01nM又は≦0.001nM(例えば、10-8M以下、例えば10-8M~10-13M、例えば10-9M~10--13M)の解離定数(KD)を有する。特定の態様では、抗PD-L1アンタゴニスト抗体は、異なる種からのPD-L1の間で保存されているPD-L1のエピトープ、又は交差種反応性を可能にするPD-L1上のエピトープに結合する。一態様では、抗PD-L1アンタゴニスト抗体はアテゾリズマブである。 The term "anti-PD-L1 antagonist antibody" refers to an antibody or antigen-binding antibody capable of binding PD-L1 with sufficient affinity to substantially or completely inhibit the biological activity of PD-1L. Refers to a fragment or variant. For example, an anti-PD-L1 antagonist antibody may reduce, block, inhibit, can deter or interfere; It will be appreciated by those skilled in the art that, in some instances, an anti-PD-L1 antagonist antibody may antagonize one PD-L1 activity without affecting another PD-L1 activity. For example, anti-PD-L1 antagonist antibodies for use in certain methods or uses described herein do not affect, or minimally affect, any other PD-L1 interactions. Without limitation, anti-PD-L1 antagonist antibodies that antagonize PD-L1 activity in response to one of its binding partners (eg, PD-1 or B7-1). In one aspect, the extent of binding of the anti-PD-L1 antagonist antibody to unrelated non-PD-L1 protein is less than about 10% of the binding of the antibody to PD-L1, eg, as measured by radioimmunoassay (RIA). is. In certain aspects, the PD-L1 that binds to the anti-PD-L1 antagonist antibody is ≦1 μM, ≦100 nM, ≦10 nM, ≦1 nM, ≦0.1 nM, ≦0.01 nM, or ≦0.001 nM (eg, 10 − It has a dissociation constant (K D ) of 8 M or less, such as from 10 −8 M to 10 −13 M, such as from 10 −9 M to 10− −13 M). In certain aspects, the anti-PD-L1 antagonist antibody binds to an epitope on PD-L1 that is conserved among PD-L1 from different species or to an epitope on PD-L1 that allows for cross-species reactivity. do. In one aspect, the anti-PD-L1 antagonist antibody is atezolizumab.
「PD-L2結合拮抗剤」という用語は、PD-L2とPD-1等の1つ以上の結合パートナーのいずれかとの相互作用の結果として生じるシグナル伝達を減少させたり、遮断したり、阻害したり、妨害したりする分子を指す。PD-L2(プログラム死リガンド2)はまた、当該技術分野において「プログラム細胞死1リガンド2」、「PDCD1LG2」、「CD273」、「B7-DC」、「Btdc」、及び「PDL2」としても言及される。例示的なヒトPD-L2は、UniProtKB/Swiss-Prot Accession No.Q9BQ51に示されている。いくつかの例では、PD-L2結合アンタゴニストは、PD-L2のその結合パートナーの1つ以上への結合を阻害する分子である。具体的な一態様では、PD-L2結合アンタゴニストは、PD-L2のPD-1への結合を阻害する。例示的なPD-L2アンタゴニストとしては、抗PD-L2抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド、及びPD-L2と、PD-1といったその結合パートナーのいずれか1つ以上との相互作用に起因するシグナル伝達を低減、遮断、阻害、抑止、又は妨害する他の分子が挙げられる。一つの態様において、PD-L2結合拮抗剤は、機能不全T細胞をより機能不全に陥らせないように(例えば、抗原認識に対するエフェクター応答を増強するように)、PD-L2を介してシグナル伝達を媒介するTリンパ球上に発現された細胞表面タンパク質によって媒介される、又はそれを介して媒介される負の共刺激シグナルを減少させる。いくつかの態様では、PD-L2結合アンタゴニストはPD-L2に結合する。いくつかの態様では、PD-L2結合アンタゴニストはイムノアドヘシンである。
The term "PD-L2 binding antagonist" reduces, blocks or inhibits signaling resulting from the interaction of PD-L2 with one or more of its binding partners, such as PD-1. It refers to molecules that interact with or interfere with PD-L2 (programmed death ligand 2) is also referred to in the art as "
PD-1軸結合アンタゴニストの更なる例としては、セミプリマブ、プロルゴリマブ、カムレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、スパルタリズマブ、サザンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、CX-072、IMC-001、KL-A167、ブジカリマブ、AMG 404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、APL-502、コシベリマブ、ロダポリマブ、GS-4224、INCB086550、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、MAX-10181、RC98、BION-004、AM0001、CB201、ENUM 244C8、ENUM 388D4、AUNP-012、STI-1110、ADG104、AK-103、LBL-006、hAb21、AVA-004、PDL-GEX、INCB090244、KD036、KY1003、LYN192、MT-6035、VXM10、YBL-007、ABSK041、GB7003、JS-003、及びHS-636が挙げられる。 Further examples of PD-1 axis binding antagonists include semiplimab, prorgolimab, camrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, spartalizumab, southernlimab, penplimab, CS1003, HLX10, SCT-I10A, SHR-1316, CS1001 , embafolimab, TQB2450, ZKAB001, LP-002, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, CX-072, IMC-001, KL-A167, budicarimab, AMG 404, CX-18 JTX-4014, 609A, Sym021, LZM009, F520, SG001, APL-502, cosibelimab, rhodapolimab, GS-4224, INCB086550, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, MAX-10181, RC98, BION-004, AM0001, CB201, ENUM 244C8, ENUM 388D4, AUNP-012, STI-1110, ADG104, AK-103, LBL-006, hAb21, AVA-004, PDL- GEX, INCB090244, KD036, KY1003, LYN192, MT-6035, VXM10, YBL-007, ABSK041, GB7003, JS-003, and HS-636.
本明細書の目的では、「アテゾリズマブ」は、PD-L1に結合し、配列番号28の重鎖配列及び配列番号29の軽鎖配列を含むFc操作ヒト化非グリコシル化IgG1カッパ免疫グロブリンである。アテゾリズマブは、Fc領域アミノ酸残基のEUナンバリングを使用して重鎖(N297A)の297位に単一アミノ酸置換(アスパラギンからアラニンへ)を含み、Fc受容体への結合が最小限の非グリコシル化抗体をもたらす。アテゾリズマブは、2015年1月16日に発行されたWHO Drug Information(International Nonproprietary Names for Pharmaceutical Substances),Proposed INN:List 112,Vol.28,No.4にも記載されている(485頁を参照)。 For purposes herein, "atezolizumab" is an Fc engineered humanized non-glycosylated IgG1 kappa immunoglobulin that binds PD-L1 and comprises the heavy chain sequence of SEQ ID NO:28 and the light chain sequence of SEQ ID NO:29. Atezolizumab contains a single amino acid substitution (asparagine to alanine) at position 297 of the heavy chain (N297A) using EU numbering of Fc region amino acid residues and is non-glycosylated with minimal binding to Fc receptors. produce antibodies. Atezolizumab is listed in WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN: List 112, Vol. 28, No. 4 (see page 485).
本明細書で使用される場合、「ペンブロリズマブ」は、ヒト細胞表面受容体PD-1に対する組換えヒト化モノクローナルIgG 4抗体である。ペンブロリズマブは、2014年に発行されたWHO Drug Information(International Nonproprietary Names for Pharmaceutical Substances),Proposed INN:List 72,Vol.28,No.3(407頁を参照)にも記載されている。
As used herein, "pembrolizumab" is a recombinant humanized monoclonal IgG4 antibody directed against the human cell surface receptor PD-1. Pembrolizumab is listed in the 2014 WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN:
本明細書で使用される場合、「チラゴルマブ」は、TIGITに結合し、配列番号33の重鎖配列及び配列番号34の軽鎖配列を含む、Open Monoclonal Technology(OMT)ラットに由来する完全ヒトIgG1/カッパMAbである。チラゴルマブは、Fcドメインに2つのN結合型グリコシル化部位(N306)を含む。チラゴルマブはまた、2017年7月7日に発行されたWHO Drug Information(International Nonproprietary Names for Pharmaceutical Substances),Proposed INN:List 117,Vol.31,No.2(343頁を参照)に記載されている。 As used herein, "tiragolumab" is a fully human IgG1 derived from Open Monoclonal Technology (OMT) rats that binds to TIGIT and comprises the heavy chain sequence of SEQ ID NO:33 and the light chain sequence of SEQ ID NO:34. /kappa MAb. Tiragolumab contains two N-linked glycosylation sites (N306) in the Fc domain. Tiragolumab is also listed in WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN: List 117, Vol. 31, No. 2 (see page 343).
本明細書で使用される場合、「ベバシズマブ」は、2000年に発行されたWHO Drug Information(International Nonproprietary Names for Pharmaceutical Substances),Proposed INN:List 83,Vol.14,No.2(107頁を参照)に記載されているVEGFの全てのアイソフォームを認識する組換えヒト化モノクローナル抗体である。ベバシズマブは、配列番号:Xの重鎖可変領域配列及び配列番号:Xの軽鎖可変領域配列を含む。 As used herein, "bevacizumab" is defined in WHO Drug Information (International Nonproprietary Names for Pharmaceutical Substances), Proposed INN: List 83, Vol. 14, No. 2 (see page 107), a recombinant humanized monoclonal antibody that recognizes all isoforms of VEGF. Bevacizumab comprises a heavy chain variable region sequence of SEQ ID NO:X and a light chain variable region sequence of SEQ ID NO:X.
「抗TIGITアンタゴニスト抗体」という用語は、TIGITの生物学的活性を実質的に又は完全に阻害するように十分な親和性でTIGITに結合することができる抗体又はその抗原結合フラグメント若しくはバリアントを指す。例えば、抗TIGITアンタゴニスト抗体は、T細胞による機能不全状態(例えば、増殖、サイトカイン産生、標的細胞殺傷)から抗原刺激への機能的応答を回復させるために、PVR、PVRL2、及び/又はPVRL3を介したシグナル伝達を遮断し得る。例えば、抗TIGITアンタゴニスト抗体は、PVR-CD 226相互作用に影響を与えることなく、PVRを介したシグナル伝達を遮断し得る。いくつかの例では、抗TIGITアンタゴニスト抗体は、別のTIGIT活性に影響を及ぼすことなく、1つのTIGIT活性に拮抗し得ることが当業者によって理解されるであろう。例えば、本明細書に記載される特定の方法又は使用において使用するための抗TIGITアンタゴニスト抗体は、例えば、他のTIGIT相互作用のいずれかに影響を及ぼすことなく、又は最小限に影響を及ぼす、PVR相互作用、PVRL3相互作用又はPVRL2相互作用の1つに応答してTIGIT活性に拮抗する抗TIGITアンタゴニスト抗体である。一態様では、非関連非TIGITタンパク質への抗TIGITアンタゴニスト抗体の結合の程度は、例えばラジオイムノアッセイ(RIA)によって測定した場合に、TIGITへの抗体の結合の約10%未満である。特定の態様では、抗TIGITアンタゴニスト抗体に結合するTIGITは、≦1μM、≦100nM、≦10nM、≦1nM、≦0.1nM、≦0.01nM又は≦0.001nM(例えば、10-8M以下、例えば10-8M~10-13M、例えば10-9M~10--13M)の解離定数(KD)を有する。特定の態様では、抗TIGITアンタゴニスト抗体は、異なる種からのTIGITの間で保存されているTIGITのエピトープ、又は交差種反応性を可能にするTIGIT上のエピトープに結合する。いくつかの態様では、抗TIGIT結合抗体は、インタクトなFc媒介エフェクター機能を有する(例えば、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS084448又はTJ-T6)。いくつかの態様では、抗TIGIT結合抗体は、Fc媒介エフェクター機能を増強している(例えば、SGN-TGT)。他の態様では、抗TIGIT結合抗体は、Fc媒介エフェクター機能を欠く(例えば、ドムバナリマブ(domvanalimab)、BMS-986207、ASP 8374、又はCOM902)。いくつかの態様では、抗TIGIT結合抗体はIgG 1クラスの抗体(例えば、チラゴルマブ、ビボストリマブ、ドムバナリマブ、BMS-986207、エチギリマブ、BGB-A1217、SGN-TGT、EOS084448(EOS-448)、TJ-T6、又はAB308)である。いくつかの態様では、抗TIGITアンタゴニスト抗体は、IgG4クラス抗体(例えば、ASP8374又はCOM902)である。一態様では、抗TIGITアンタゴニスト抗体は、チラゴルマブである。
The term "anti-TIGIT antagonist antibody" refers to an antibody, or antigen-binding fragment or variant thereof, capable of binding TIGIT with sufficient affinity to substantially or completely inhibit the biological activity of TIGIT. For example, an anti-TIGIT antagonist antibody may mediate PVR, PVRL2, and/or PVRL3 to restore functional responses to antigen stimulation from dysfunctional states (e.g., proliferation, cytokine production, target cell killing) by T cells. can block signal transduction. For example, an anti-TIGIT antagonist antibody can block signaling through PVR without affecting the PVR-CD226 interaction. It will be appreciated by those skilled in the art that in some instances, an anti-TIGIT antagonist antibody may antagonize one TIGIT activity without affecting another TIGIT activity. For example, an anti-TIGIT antagonist antibody for use in certain methods or uses described herein will, for example, not affect, or minimally affect, any other TIGIT interactions, An anti-TIGIT antagonist antibody that antagonizes TIGIT activity in response to one of a PVR interaction, a PVRL3 interaction or a PVRL2 interaction. In one aspect, the extent of binding of the anti-TIGIT antagonist antibody to an unrelated non-TIGIT protein is less than about 10% of the binding of the antibody to TIGIT, eg, as measured by radioimmunoassay (RIA). In certain aspects, the TIGIT that binds to the anti-TIGIT antagonist antibody is ≦1 μM, ≦100 nM, ≦10 nM, ≦1 nM, ≦0.1 nM, ≦0.01 nM, or ≦0.001 nM (e.g., 10 −8 M or less, It has a dissociation constant (K D ) of eg 10 −8 M to 10 −13 M, eg 10 −9 M to 10− −13 M). In certain aspects, the anti-TIGIT antagonist antibody binds to an epitope on TIGIT that is conserved among TIGIT from different species or to an epitope on TIGIT that allows for cross-species reactivity. In some aspects, the anti-TIGIT binding antibody has intact Fc-mediated effector functions (eg, tiragolumab, vivostolimab, etiglimab, EOS084448 or TJ-T6). In some aspects, the anti-TIGIT binding antibody has enhanced Fc-mediated effector function (eg, SGN-TGT). In other aspects, the anti-TIGIT binding antibody lacks Fc-mediated effector functions (eg, domvanalimab, BMS-986207, ASP 8374, or COM902). In some aspects, the anti-TIGIT binding antibody is an
本明細書で使用される場合、「投与する」は、化合物(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体)、VEGFアンタゴニスト若しくは化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))、又は組成物(例えば、医薬組成物、例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体)を含む医薬組成物、化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン))、抗体-薬物コンジュゲート(ADC)(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)及び/又はコロニー刺激因子(CSF)(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム))の投与量を対象に与える方法を意味する。本明細書に記載される方法に用いられる化合物及び/又は組成物は、例えば、静脈内(例えば、静脈内注入による)、皮下、筋肉内、皮内、経皮的、動脈内、腹腔内、病巣内、頭蓋内、関節内、前立腺内、胸膜内、気管内、鼻腔内、硝子体内、膣内、直腸内、局所的(topically)、腫瘍内、腹膜内、結膜下、小胞内、経粘膜、心膜内、臍帯内、眼球内、経口、局所的(topically)、局所的(locally)、吸入、注射、注入、持続注入、標的細胞に直接的に流す局所灌流、カテーテル、洗浄、クリーム、又は脂質組成物で投与することができる。投与方法は、様々な因子(例えば、投与される化合物又は組成物、及び処置される状態、疾患、又は障害の重症度)に応じて変化し得る。 As used herein, "administering" refers to a compound (e.g., anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (e.g., anti-PD-L1 antibody), VEGF antagonist or chemotherapeutic agent (e.g., platinum chemotherapeutic agents (e.g. carboplatin or cisplatin) and/or one or more non-platinum chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and /or a topoisomerase II inhibitor (e.g., doxorubicin))), or a pharmaceutical composition comprising a composition (e.g., a pharmaceutical composition, e.g., an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antibody) chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclophosphamide), taxanes ( paclitaxel, eg nab-paclitaxel) and/or topoisomerase II inhibitors (eg doxorubicin)), antibody-drug conjugates (ADC) (eg enfortumab vedotin or sacituzumab govitecan) and/or colonies A method of providing a dose of a stimulating factor (CSF) (e.g., pegfilgrastim, filgrastim, or sargramostim) to a subject Compounds and/or compositions used in the methods described herein is, for example, intravenous (e.g. by intravenous infusion), subcutaneous, intramuscular, intradermal, percutaneous, intraarterial, intraperitoneal, intralesional, intracranial, intraarticular, intraprostatic, intrapleural, intratracheal , intranasal, intravitreal, intravaginal, intrarectal, topically, intratumoral, intraperitoneal, subconjunctival, intravesicular, transmucosal, intrapericardial, intraumbilical, intraocular, oral, topical ( Administration can be topically, locally, inhalation, injection, infusion, continuous infusion, local perfusion that flows directly into the target cells, catheters, lavages, creams, or lipid compositions. may vary depending on various factors such as the compound or composition administered and the severity of the condition, disease or disorder being treated.
治療剤(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体)、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム))の「固定」又は「フラット」用量は、患者の体重又は体表面積(BSA)に関係なく患者に投与される用量を指す。したがって、固定用量又はフラット用量は、mg/kg用量又はmg/m2用量としてではなく、治療剤の絶対量(例えば、治療剤の絶対量(mg))として提供される。 therapeutic agent (e.g., anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (e.g., anti-PD-L1 antibody), VEGF antagonist, chemotherapeutic agent (e.g., platinum-based or non-platinum-based chemotherapeutic agent), ADC (e.g., enfortuzumab vedotin or sacituzumab govitecan) or CSF (e.g., pegfilgrastim, filgrastim, or sargramostim). It refers to the dose administered to a patient regardless of surface area (BSA). Thus, a fixed or flat dose is provided as an absolute amount of therapeutic agent (eg, absolute amount (mg) of therapeutic agent) rather than as a mg/kg or mg/m 2 dose.
本明細書で使用される場合、「処置(treatment)」又は「処置すること(treating)」という用語は、臨床的病変の経過中に処置される個体又は細胞の自然経過を変化させるように設計された臨床的介入を指す。処置の望ましい効果としては、疾患進行速度の遅延又は低減、疾患状態の回復又は緩和、及び予後の寛解又は改善が挙げられる。例えば、個体は、がん性細胞の増殖の低減(若しくはその破壊)、疾患から生じる症状の減少、疾患を患うものの生活の質の向上、疾患を処置するのに必要な他の医薬品の用量の減少、疾患の進行の遅延、及び/又は個体の生存期間の延長を含むがこれらに限定されない、がんと関連する1つ以上の症状が軽減又は排除された場合に、「処置」が成功したことになる。例えば、処置は、有効量の治療剤(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)及び/又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム))又は治療剤の組み合わせによる有効ながんの処置を含む。本明細書における処置には、とりわけ、アジュバント療法、ネオアジュバント療法、非転移性がん療法(例えば、局所進行性がん治療)及び転移性がん療法が含まれる。処置は、第一選択処置(例えば、患者は以前に処置されていない可能性がある、又は事前全身治療を受けたことがない)又は第二選択処置若しくはそれ以降の処置であり得る。 As used herein, the term "treatment" or "treating" is designed to alter the natural course of the individual or cells being treated during the course of a clinical pathology. Refers to clinical interventions that have been Desirable effects of treatment include slowing or reducing the rate of disease progression, ameliorating or alleviating the disease state, and ameliorating or improving prognosis. For example, an individual may reduce the growth of (or destroy) cancerous cells, reduce the symptoms resulting from the disease, improve the quality of life of those with the disease, reduce the dose of other pharmaceutical agents needed to treat the disease. "Treatment" is successful if one or more symptoms associated with cancer are reduced or eliminated, including, but not limited to, reduction, slowing disease progression, and/or prolonging survival of the individual. It will be. For example, treatment may include an effective amount of a therapeutic agent (e.g., an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a VEGF antagonist, a chemotherapeutic agent (e.g., a platinum-based chemotherapeutic agent or a non-platinum-based chemotherapeutic agent), an ADC ( e.g., enfortuzumab vedotin or sacituzumab govitecan) and/or CSF (e.g., pegfilgrastim, filgrastim, or sargramostim)) or effective cancer treatment with a combination of therapeutic agents. Treatment herein includes, inter alia, adjuvant therapy, neoadjuvant therapy, non-metastatic cancer therapy (eg, locally advanced cancer therapy) and metastatic cancer therapy. Treatment may be first-line treatment (eg, the patient may have been previously untreated or has not received prior systemic therapy) or second-line treatment or subsequent treatment.
本明細書で使用される場合、「と組み合わせて」又は「と組み合わせて」は、別の処置様式に加えて1つの治療処置、例えば、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)、及び/又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム)及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与を含む処置レジメンの投与を指す。したがって、「と組み合わせて」とは、患者への他の処置様式の投与前、投与中、又は投与後の1つの処置様式の投与を指す。 As used herein, "in combination with" or "in combination with" means one therapeutic treatment in addition to another treatment modality, e.g., PD-1 axis binding antagonists (e.g., atezolizumab), VEGF antagonists , chemotherapeutic agents (e.g., platinum-based or non-platinum-based chemotherapeutic agents), ADCs (e.g., enfortumab vedotin or sacituzumab govitecan), and/or CSF (e.g., pegfilgrastim) , filgrastim, or sargramostim) and an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). Thus, “in combination with” refers to administration of one treatment modality before, during, or after administration of another treatment modality to a patient.
1つ以上の他の薬物と「同時に」投与される薬物は、同一処置サイクル中、1つ以上の他の薬物と同じ処置日に、また必要に応じて1つ以上の他の薬物と同じ時間に投与される。例えば、3週間ごとに付与されるがん療法の場合、同時に投与される薬物はそれぞれ、3週間のサイクルの1日目に投与される。
Drugs that are administered "concurrently" with one or more other drugs are administered during the same treatment cycle, on the same treatment days as the one or more other drugs, and optionally at the same time as the one or more other drugs. administered to For example, for cancer therapy given every 3 weeks, each co-administered drug is administered on
本明細書で使用される場合、「周術期処置」という用語は、手術の前後に投与される処置を指す。周術期処置は、手術前のネオアジュバント療法(例えば、膀胱切除術)及び手術後の療法(例えば、補助療法)の投与を含み得る。例えば、周術期処置には、診断後かつ手術(例えば、膀胱切除術)前(例えば、約1、2、3、4、5、6、7、8、9、12、13、14、15週間又はそれ以上前)に投与されるネオアジュバント療法(例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストのネオアジュバント療法)、及び手術後(例えば、手術後約1、2、3、4、5、6、7、8、9、12、13、14、15週間以上)の治療(例えば、アジュバント療法(例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストアジュバント療法))が含まれ得る。 As used herein, the term "perioperative treatment" refers to treatment administered before or after surgery. Perioperative treatment may include the administration of pre-operative neoadjuvant therapy (eg, cystectomy) and post-operative therapy (eg, adjuvant therapy). For example, for perioperative treatment, post-diagnosis and prior to surgery (e.g., cystectomy) (e.g., about 1, 2, 3, 4, 5, 6, 7, 8, 9, 12, 13, 14, 15) a week or more before) and after surgery (e.g., about 1, 2, 3, 4, 1, 2, 3, 4, 4, 5, 6, 7, 9, 10 or 12 after surgery). 5, 6, 7, 8, 9, 12, 13, 14, 15 weeks or more) treatment (eg, adjuvant therapy, such as anti-TIGIT antagonist antibody and PD-1 axis binding antagonist adjuvant therapy).
「障害」又は「疾患」は、ある程度の異常な細胞増殖、例えばがんに関連する障害を含むがこれらに限定されない処置から利益を得る任意の状態である。 A "disorder" or "disease" is any condition that would benefit from treatment, including but not limited to disorders associated with some degree of abnormal cell proliferation, such as cancer.
免疫機能障害に関して「機能障害」という用語は、抗原刺激に対する免疫応答性が低下した状態を指す。 The term "dysfunction" with respect to immune dysfunction refers to a state of reduced immune responsiveness to antigenic stimulation.
本明細書で使用される場合、「機能不全性」という用語にはまた、抗原認識に対する不応性又は無応答性、特に、抗原認識を下流T細胞エフェクター機能、例えば増殖、サイトカイン産生(例えばガンマインターフェロン)、及び/又は標的細胞殺滅に変換する能力の障害も含まれる。 As used herein, the term "dysfunctional" also includes refractory or unresponsiveness to antigen recognition, in particular antigen recognition to downstream T cell effector functions such as proliferation, cytokine production (e.g. gamma interferon) ), and/or impaired ability to convert to target cell killing.
「がん」及び「がん性」という用語は、制御されていない細胞成長を典型的に特徴とする哺乳動物における生理学的状態を指すか又は説明する。がんには、固形腫瘍がん及び非固形腫瘍がん並びに局所進行性がん又は転移性がん(例えば、局所進行性又は転移性腫瘍)が含まれる。がんの例としては、癌腫、リンパ腫、芽細胞腫、肉腫、及び白血病又はリンパ性悪性腫瘍が挙げられるが、これらに限定されない。そのようながんのより具体的な例としては、限定されないが、局所進行性及び転移性UC(mUC)、膀胱がん(例えば、筋肉浸潤性膀胱がん(MIBC)及び非筋肉浸潤性膀胱がん(NMIBC)、例えば、BCG不応性NMIBC)、MIBC尿路上皮膀胱がん(UBC)を含む尿路上皮癌腫(UC);腎臓がん又は腎がん(例えば、腎細胞癌腫(RCC));尿路がん;小細胞肺がん(SCLC)等の肺がん(進展型SCLC(ES-SCLC)を含む);非小細胞肺がん(NSCLC)(局所進行性切除不能NSCLC(例えば、IIIB NSCLC)、又は再発若しくは転移性NSCLC(例えば、IV期のNSCLC)を含む)、肺の腺癌、又は扁平上皮がん(例えば、扁平上皮がん(例えば、肺の扁平上皮癌腫));膵臓がん(例えば、膵管腺癌(PDAC)、例えば、転移性PDAC));頭頸部がん(例えば、SCCHN、例えば、再発/転移性PD-L1陽性SCCHN、頭頸部扁平上皮がん(HNSCC);卵巣がん(OC);食道がん;腹膜がん;肝細胞がん;胃がん(GC)(例えば、胃食道接合部(GEJ)がん)又は胃腸がん及び胃腸間質がんを含む胃がん;神経膠芽腫;尿路がん;肝腫;乳がん(例えば、HER2+乳がん及びトリプルネガティブ乳がん(TNBC(例えば、早期TNBC(eTNBC))、エストロゲン受容体(ER-)、プロゲステロン受容体(PgR-)、及びHER2(HER2-)陰性);去勢抵抗性前立腺がん(CRPC)等の前立腺がん、腹膜がん、肝細胞がん、胃がん又は胃がん(胃腸がん及び胃腸間質がんを含む)膵がん(例えば、膵管腺癌(PDAC));神経膠芽腫;子宮頸がん(例えば、IVB期、転移性、再発、又は持続性の子宮頸がん、例えば、転移性及び/又は再発PD-L1陽性子宮頸がん);卵巣がん;肝臓がん(例えば、肝細胞がん(HCC)、例えば、局所進行性又は転移性のHCC及び/又は切除不能HCC);肝腫;結腸がん;直腸がん;結腸直腸がん(CRC;例えば、マイクロサテライト安定(MSS)及びマイクロサテライト不安定性(MSI)低い(MSI-Low)を伴うCRC)、;子宮内又は子宮癌腫;唾液腺癌腫;前立腺がん;外陰がん;甲状腺がん;肝癌腫;肛門癌腫;陰茎癌腫;黒色腫(表在性転移性黒色腫、黒色腫悪性黒色腫、先端黒色腫、結節性黒色腫を含む);多発性骨髄腫及びB細胞リンパ腫(低悪性度/濾胞性非ホジキンリンパ腫(NHL)含む));小リンパ球(SL)NHL;中悪性度/濾胞性NHL;中間悪性度びまん性NHL;高悪性度免疫芽球性NHL;高悪性度リンパ芽球性NHL;高悪性度非切断細胞NHL;巨大腫瘤性疾患NHL;マントル細胞リンパ腫;AIDS関連リンパ腫;及びWaldenstromのマクログロブリン血症);慢性リンパ球性白血病(CLL);急性リンパ芽球性白血病(ALL);急性筋原性白血病(AML);有毛細胞白血病;慢性骨髄芽球性白血病(CML);移植後リンパ増殖性障害(PTLD);及び骨髄異形成症候群(MDS)、並びに母斑症、浮腫(脳腫瘍に関連するもの等)、メグズ症候群、脳がん、頭頸部がん、及び関連する転移に関連する異常な血管増殖が挙げられる。 The terms "cancer" and "cancerous" refer to or describe the physiological condition in mammals that is typically characterized by uncontrolled cell growth. Cancer includes solid and non-solid tumor cancers and locally advanced or metastatic cancers (eg, locally advanced or metastatic tumors). Examples of cancer include, but are not limited to, carcinoma, lymphoma, blastoma, sarcoma, and leukemia or lymphoid malignancies. More specific examples of such cancers include, but are not limited to, locally advanced and metastatic UC (mUC), bladder cancer (e.g., muscle invasive bladder cancer (MIBC) and non-muscle invasive bladder cancer). urothelial carcinoma (UC), including carcinoma (NMIBC), e.g. BCG refractory NMIBC), MIBC urothelial bladder cancer (UBC); kidney cancer or kidney cancer (e.g. renal cell carcinoma (RCC) ); urinary tract cancer; lung cancer such as small cell lung cancer (SCLC) (including extensive-stage SCLC (ES-SCLC)); non-small cell lung cancer (NSCLC) (locally advanced unresectable NSCLC (eg, IIIB NSCLC), or recurrent or metastatic NSCLC (e.g., stage IV NSCLC), adenocarcinoma of the lung, or squamous cell carcinoma (e.g., squamous cell carcinoma (e.g., squamous cell carcinoma of the lung)); pancreatic cancer ( e.g., pancreatic ductal adenocarcinoma (PDAC), e.g., metastatic PDAC); head and neck cancers (e.g., SCCHN, e.g., recurrent/metastatic PD-L1 positive SCCHN, head and neck squamous cell carcinoma (HNSCC); cancer (OC); esophageal cancer; peritoneal cancer; hepatocellular carcinoma; Glioblastoma; urinary tract cancer; hepatoma; and HER2 (HER2-) negative); prostate cancer such as castration-resistant prostate cancer (CRPC), peritoneal cancer, hepatocellular carcinoma, gastric cancer or gastric cancer (including gastrointestinal cancer and gastrointestinal stromal cancer) pancreatic cancer (e.g. pancreatic ductal adenocarcinoma (PDAC)); glioblastoma; cervical cancer (e.g. stage IVB, metastatic, recurrent, or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive cervical cancer); ovarian cancer; liver cancer (e.g. hepatocellular carcinoma (HCC), e.g. locally advanced or metastatic HCC and/or unresectable HCC); hepatoma; colon Cancer; rectal cancer; colorectal cancer (CRC; e.g., CRC with microsatellite stable (MSS) and microsatellite instability (MSI) low (MSI-Low); intrauterine or uterine carcinoma; salivary gland carcinoma) ;prostate cancer; vulvar cancer; thyroid cancer; liver carcinoma; anal carcinoma; penile carcinoma; multiple myeloma and B-cell lymphoma; Small lymphocytic (SL) NHL; Intermediate-grade/follicular NHL; Intermediate-grade diffuse NHL; High-grade immunoblastic NHL high-grade lymphoblastic NHL; high-grade non-cutting cell NHL; bulky mass disease NHL; mantle cell lymphoma; AIDS-related lymphoma; acute lymphoblastic leukemia (ALL); acute myogenic leukemia (AML); hairy cell leukemia; chronic myeloblastic leukemia (CML); post-transplant lymphoproliferative disorder (PTLD); MDS), as well as nevus, edema (such as those associated with brain tumors), Megs syndrome, brain cancer, head and neck cancer, and associated metastasis-related abnormal vascular proliferation.
本明細書で使用される場合、「持続性子宮頸がん」という用語は、以前の治療後に検出不能又は良性になっていない子宮頸がんを指す。 As used herein, the term "persistent cervical cancer" refers to cervical cancer that has not become undetectable or benign after previous treatment.
本明細書で使用される場合、「IVB期子宮頸がん」は、子宮頸がん病期分類システム(例えば、International Federation of Gynecology and Obstetrics(FIGO)病期分類システム)を使用してそのように分類される子宮頸がんを指す。いくつかの態様では、子宮頸がんが遠隔器官(脾臓又は肝臓の実質を含む)又は鼠径リンパ節及び腹部外リンパ節に転移したことがある場合、ステージIVBとして分類される。 As used herein, “Stage IVB cervical cancer” is defined as such using the cervical cancer staging system (e.g., the International Federation of Gynecology and Obstetrics (FIGO) staging system). Refers to cervical cancer classified as In some aspects, cervical cancer is classified as stage IVB if it has metastasized to distant organs (including the parenchyma of the spleen or liver) or inguinal and extra-abdominal lymph nodes.
本明細書で使用される場合、「再発性子宮頸がん」という用語は、手術、放射線療法、及び/又は化学療法による初期の処置後に検出された又は戻ってきた子宮頸がんを指す。 As used herein, the term "recurrent cervical cancer" refers to cervical cancer that is detected or has returned after initial treatment with surgery, radiation therapy, and/or chemotherapy.
「TNBC」という用語は、ER、PR及びHER 2の発現を欠く乳がんを指す。「eTNBC」という用語は、T2-4d TNBC(例えば、cT2-cT4、cN0-cN3、及びcM0)を指す。 The term "TNBC" refers to breast cancer that lacks expression of ER, PR and HER2. The term "eTNBC" refers to T2-4d TNBC (eg, cT2-cT4, cN0-cN3, and cM0).
頭頸部がんには、上部気道消化管の粘膜表面で始まり、口腔、中咽頭、喉頭、下咽頭、及び鼻咽頭に影響を及ぼすがんが含まれる。 Head and neck cancers include cancers that begin in the mucosal surfaces of the upper aerodigestive tract and affect the oral cavity, oropharynx, larynx, hypopharynx, and nasopharynx.
本明細書で使用される場合、「尿路上皮癌腫」及び「UC」は、典型的には泌尿器系で発生するがんの種類を指し、筋肉浸潤性膀胱がん(MIBC)及び筋肉浸潤性尿路上皮がん(UTUC)を含む。UCは、当該技術分野では移行細胞癌腫(TCC)とも呼ばれる。 As used herein, "urothelial carcinoma" and "UC" refer to types of cancer that typically arise in the urinary system, including muscle invasive bladder cancer (MIBC) and muscle invasive bladder cancer (MIBC). Includes urothelial carcinoma (UTUC). UC is also called transitional cell carcinoma (TCC) in the art.
「腫瘍」という用語は、悪性又は良性にかかわらず、全ての腫瘍性細胞の成長及び増殖、並びに全ての前がん性及びがん性の細胞及び組織を指す。「がん」、「がん性」、「細胞増殖性障害」、「増殖性障害」、及び「腫瘍」という用語は、本明細書で言及される場合、相互排他的ではない。 The term "tumor" refers to all neoplastic cell growth and proliferation, whether malignant or benign, and all precancerous and cancerous cells and tissues. The terms "cancer", "cancerous", "cell proliferative disorder", "proliferative disorder" and "tumor" are not mutually exclusive when referred to herein.
本明細書で使用される場合、「腫瘍細胞」とは、腫瘍又はその試料中に存在する任意の腫瘍細胞を指す。腫瘍細胞を、当該技術分野で公知であり、かつ/又は本明細書に記載される方法を使用して、腫瘍試料中に存在し得る他の細胞、例えば、間質細胞及び腫瘍浸潤免疫細胞と区別することができる。 As used herein, "tumor cell" refers to any tumor cell present in a tumor or sample thereof. Tumor cells are combined with other cells that may be present in the tumor sample, such as stromal cells and tumor-infiltrating immune cells, using methods known in the art and/or described herein. can be distinguished.
「腫瘍免疫」とは、腫瘍が免疫認識及び排除を回避する過程を指す。したがって、治療的概念として、腫瘍免疫は、そのような回避が減弱し、腫瘍が免疫系によって認識かつ攻撃されるときに「処置される」。腫瘍認識の例としては、腫瘍結合、腫瘍収縮、及び腫瘍クリアランスが挙げられる。 "Tumor immunity" refers to the process by which tumors evade immune recognition and elimination. Thus, as a therapeutic concept, tumor immunity is "treated" when such evasion is attenuated and the tumor is recognized and attacked by the immune system. Examples of tumor recognition include tumor binding, tumor shrinkage, and tumor clearance.
本明細書で使用される場合、「転移」は、その原発部位から体内の他の場所へのがんの拡がりを意味する。がん細胞は、原発腫瘍から離脱し、リンパ管及び血管に浸透し、血流を通じて循環し、体内の他の場所の正常組織内の遠位焦点で成長する(転移する)場合がある。転移は、局所的又は遠位であり得る。転移は、腫瘍細胞が原発腫瘍から離脱し、血流を通じて移動し、遠位部位で停止することを条件とする逐次プロセスである。新たな部位で、細胞は、血液供給を確立し、成長して、生命を脅かす塊を形成し得る。腫瘍細胞内の刺激性と阻害性との両方の分子経路がこの挙動を制御し、遠隔部位における腫瘍細胞と宿主細胞との間の相互作用もまた重要である。 As used herein, "metastasis" means the spread of cancer from its primary site to other locations in the body. Cancer cells may break away from a primary tumor, penetrate lymphatics and blood vessels, circulate through the bloodstream, and grow (metastasize) in distant foci in normal tissue elsewhere in the body. Metastases can be local or distant. Metastasis is a sequential process that requires tumor cells to break away from the primary tumor, migrate through the bloodstream, and arrest at distant sites. At the new site, the cells establish a blood supply and can grow to form life-threatening masses. Both stimulatory and inhibitory molecular pathways within tumor cells control this behavior, and interactions between tumor cells and host cells at distant sites are also important.
本明細書で使用される場合、「細胞傷害剤」という用語は、細胞に有害な任意の薬剤(例えば、細胞死若しくは細胞破壊を引き起こし、増殖を阻害し、又はそうでなければ細胞機能を阻害若しくは防止する)を指す。細胞毒性剤としては、放射性同位体(例えば、At211、I131、I125、Y90、Re186、Re188、Sm153、Bi212、P32、Pb212、及びLuの放射性同位体);化学療法剤又は薬物(例えば、メトトレキサート、アドリアマイシン、ビンカアルカロイド(ビンクリスチン、ビンブラスチン、エトポシド)、ドキソルビシン、メルファラン、マイトマイシンC、クロラムブシル、ダウノルビシン又は他の挿入剤);成長阻害剤;酵素及びそのフラグメント、例えば核分解酵素;抗生物質;及び細菌、真菌、植物又は動物由来の低分子毒素又は酵素的活性毒素等の毒素(そのフラグメント及び/又はバリアントを含む);並びに下記に開示される様々な抗腫瘍剤又は抗がん剤が挙げられるが、これらに限定されない。例示的な細胞傷害剤は、抗微小管薬、白金配位錯体、アルキル化剤、トポイソメラーゼII阻害剤、代謝拮抗剤、トポイソメラーゼI阻害剤、ホルモン及びホルモン類似体、シグナル伝達経路阻害剤、非受容体チロシンキナーゼ血管新生阻害剤、免疫療法薬、アポトーシス促進剤、LDH-A阻害剤、脂肪酸生合成阻害剤、細胞周期シグナル伝達阻害剤、HDAC阻害剤、プロテアソーム阻害剤、並びに代謝阻害剤から選択され得る。一例では、細胞傷害剤は白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)である。一例では、細胞毒性剤は、EGFRのアンタゴニスト、例えば、N-(3-エチニルフェニル)-6,7-ビス(2-メトキシエトキシ)キナゾリン-4-アミン(例えば、エルロチニブ)である。一例では、細胞傷害剤は、RAF阻害剤、例えばBRAF及び/又はCRAF阻害剤である。一例では、RAF阻害剤はベムラフェニブである。一例では、細胞傷害剤はPI3K阻害剤である。 As used herein, the term "cytotoxic agent" refers to any agent that is detrimental to cells (e.g., causes cell death or destruction, inhibits proliferation, or otherwise inhibits cell function). or prevent). Cytotoxic agents include radioactive isotopes (e.g., radioactive isotopes of At211 , I131 , I125 , Y90 , Re186 , Re188 , Sm153 , Bi212 , P32 , Pb212 , and Lu); Chemotherapeutic agents or drugs (e.g., methotrexate, adriamycin, vinca alkaloids (vincristine, vinblastine, etoposide), doxorubicin, melphalan, mitomycin C, chlorambucil, daunorubicin, or other intercalating agents); growth inhibitors; enzymes and fragments thereof, such as nucleolytic enzymes; antibiotics; and toxins such as small molecule toxins or enzymatically active toxins of bacterial, fungal, plant or animal origin (including fragments and/or variants thereof); and various antitumor agents disclosed below. or anticancer agents, but are not limited to these. Exemplary cytotoxic agents include antimicrotubule agents, platinum coordination complexes, alkylating agents, topoisomerase II inhibitors, antimetabolites, topoisomerase I inhibitors, hormones and hormone analogues, signal transduction pathway inhibitors, non-receptive selected from somatic tyrosine kinase angiogenesis inhibitors, immunotherapeutic agents, proapoptotic agents, LDH-A inhibitors, fatty acid biosynthesis inhibitors, cell cycle signaling inhibitors, HDAC inhibitors, proteasome inhibitors, and metabolic inhibitors. obtain. In one example, the cytotoxic agent is a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin). In one example, the cytotoxic agent is an EGFR antagonist, such as N-(3-ethynylphenyl)-6,7-bis(2-methoxyethoxy)quinazolin-4-amine (eg, erlotinib). In one example, the cytotoxic agent is a RAF inhibitor, such as a BRAF and/or CRAF inhibitor. In one example, the RAF inhibitor is vemurafenib. In one example, the cytotoxic agent is a PI3K inhibitor.
「化学療法剤」は、がんの処置に有用な化学化合物を含む。化学療法剤及びその誘導体の例としては、以下のものが挙げられる:エルロチニブ(TARCEVA(登録商標)、Genentech/OSI Pharm.)、ボルテゾミブ(VELCADE(登録商標)、Millennium Pharm.)、ジスルフィラム、エピガロカテキンガレート、サリノスポラミドA、カーフィルゾミブ、17-AAG(ゲルダナマイシン)、ラジコール、乳酸脱水素酵素A(LDH-A)、フルベストラント(FASLODEX(登録商標)、AstraZeneca)、スニチニブ(SUTENT(登録商標)、Pfizer/Sugen)、レトロゾール(FEMARA(登録商標)、Novartis)、メシル酸イマチニブ(GLEEVEC(登録商標)、Novartis)、フィナサン酸塩(VATALANIB(登録商標)、Novartis)、オキサリプラチン((登録商標)、Sanofi)、5-FU(5-フルオロウラシル)、ロイコボリン、ラパマイシン(シロリムス、RAPAMUNE(登録商標)、Wyeth)、ラパチニブ(TYKERB(登録商標)、GSK572016、Glaxo Smith Kline)、ロナファミブ(SCH66336)、ソラフェニブ(NEXAVAR(登録商標)、Bayer Labs)、ゲフィチニブ(IRESSA(登録商標))、AstraZeneca)、AG1478、チオテパ、CYTOXAN(登録商標)シクロホスファミド等のアルキル化剤;ブスルファン、インプロスルファン及びピポスルファン等のアルキルスルホネート;ベンゾドーパ、カルボクオン、メチュレドーパ、ウレドパ等のアジリジン;アルトレタミン、トリエチレンメラミン、トリエチレンホスホルアミド、トリエチレンチオホスホルアミド及びトリメチロメラミンを含むエチレンイミン及びメチルアメラミン;アセトゲニン(特にブラタシンとブラタシノン);カンプトテシン(トポテカンとイリノテカンを含む);ブリオスタチン;カリスタチン;CC-1065(アドゼレシン、カルゼレシン、ビゼレシン合成類似体を含む);クリプトフィシン(特にクリプトフィシン1及びクリプトフィシン8);アドレノコルチコステロイド(プレドニゾン及びプレドニゾロンを含む);酢酸シプロテロン;フィナステリド及びデュタステリドを含む5α-レダクターゼ);ボリノスタット、ロミデプシン、パノビノスタット、バルプロ酸、モセチノスタットドラスタチン;アルデスロイキン、タルクデュオカルマイシン(合成類似体、KW-2189及びCB1-TM1を含む);エレタロビン;パンクラチスタチン;サルコジクチン;スポンギスタチン;クロラムブシル、クロマファジン、クロロホスファミド、エストラムスチン、イホスファミド、メクロレスタミン、メクロレスタミンオキシド塩酸塩、メルファラン、ノベンビチン、フェネステリン、プレドニムスチン、トロホスファミド、ウラシルマスタード等の窒素マスタード、カルムスチン、クロロゾトシン、フォテムスチン、ロムスチン、ニムスチン、及びラニムスチンのようなニトロソウレア;エニジン系抗生物質のような抗生物質(例えば、カリチェマイシン、特にカリチェマイシンγ1I及びカリチェマイシンω1I(Angew Chem.Intl.Ed.Engl.1994 33:183-186);ダイネマイシンAを含むダイネマイシン;クロドロネート等のビスホスホネート;エスペラマイシンと同様に、ネオカルジノスタチン発色団及び関連する発色団エンジイン抗生物質発色団)、アクラシノマイシン、アクチノマイシン、オートラマイシン、アザセリン、ブレオマイシン、カクチノマイシン、カラビシン、カミノマイシン、カルジノフィリン、クロモマイシン、ダクチノマイシン、ダウノルビシン、デトルビシン、6-ジアゾ-5-オキソ-L-ノルロイシン、ADRIAMYCIN(登録商標)(ドキソルビシン)、モルホリノドキソルビシン、シアノモルホリノドキソルビシン、2-ピロリノドキソルビシン、デオキシドキソルビシン)、エピルビシン、エソルビシン、イダルビシン、マルセロマイシン、マイトマイシンC等のマイトマイシン、マイコフェノール酸、ノガラマイシン、オリボマイシン、ペプロマイシン、ポルフィロマイシン、ピュロマイシン、ケラマイシン、ロドルビシン、ストレプトゾシン、ツベルクリジン、ウベニメックス、ジノスタチン、ゾルビシン メトトレキサート及び5-フルオロウラシル(5-FU)等の抗メタボローム剤;デノプテリン、メトトレキサート、プテロプテリン、トリメトレキサート等の葉酸アナログ;フルダラビン、6-メルカプトプリン、チアミプリン、チオグアニン等のプリンアナログ。アンシタビン、アザシチジン、6-アザウリジン、カルモフール、シタラビン、ジデオキシウリジン、ドキシフルリジン、エノシタビン、フロクスリジン等のピリミジン類縁体、カルステロン、プロピオン酸ドロモスタノロン、エピチオスタノール、メピチオステイン、テストラクトン等のアンドロゲン;アミノグルテチミド、ミトタン、トリロステイン等の抗アドレナール;フロリン酸等の葉酸補充剤;エースグラトン;アルドホスファミド配糖体;アミノレブリン酸;エニルラシル;アムサクリン;ベストラブシル;ビサントレン;エダトラキサート;デフォファミン;デメコルシン;ジアジキオン;エルフォミチン;酢酸エリプチン;アンエポチロン;エトグルシド;硝酸ガリウム;ヒドロキシウレア;レンティナン;ロニダイニン;メイタンシン、アンサミトシン等のメイタンシノイド類 ミトグアゾン;マイトキサントロン;モピダムノール;ニトラエリン;ペントスタチン;フェナメット;ピラルビシン;ロソキサントロン;ポドフィリン酸;2-エチルヒドラジド;プロカルバジン;PSK(登録商標)多糖複合体(JHS Natural Products,Eugene,Oreg.);ラゾキサン;リゾキシン;シゾフラン;スピロゲルマニウム;テヌアゾン酸;トリアジキオン;2,2’,2’’-トリクロロトリエチルアミン;トリコテセン(特にT-2毒素、ベラキュリンA、ロリジンA及びアングイジン);ウレタン;ビンデシン;ダカルバジン;マンノムスチン;マイトブロニトール;マイトラクトール;ピポブロマン;ガシトシン;アラビノシド(「Ara-C」);シクロホスファミド;チオテパ;タキサン(タキソイド)、例えば、TAXOL(登録商標)(パクリタキセル;Bristol-Myers Squibb Oncology、ニュージャージー州プリンストン)、ABRAXANE(登録商標)(クレモフォフリー)、パクリタキセルのアルブミン設計ナノ粒子製剤(例えば、ナノ粒子アルブミン操作パクリタキセル(nab-パクリタキセル))(American Pharmaceutical Partners、イリノイ州シャウンバーグ)、及びTAXOTERE(登録商標)(ドセタキセル、ドクセタキセル(doxetaxel);Sanofi-Aventis)、クロランブシル、GEMZAR(登録商標)(ゲムシタビン)、6-チオグアニン、メルカプトプリン、メトトレキサート;シスプラチン及びカルボプラチン等の白金アナログ;ビンブラスチン;エトポシド(VP-16);イボスファミド;マイトキサントロン;ビンクリスチン;NAVELBINE(登録商標)(vinorelbine);ノバンドロン;テニポシド;エダトレキサート;ダウノマイシン;アミノプテリン;カペシタビン(XELODA(登録商標));イバンドロネート;CPT-11;トポイソメラーゼ阻害剤RFS2000;ジフルオロメチルオルニチン(DMFO);レチノイン酸等のレチノイド;並びに上記のいずれかの薬学的に許容され得る塩、酸、及び誘導体。 A "chemotherapeutic agent" includes chemical compounds useful in the treatment of cancer. Examples of chemotherapeutic agents and their derivatives include: Erlotinib (TARCEVA®, Genentech/OSI Pharm.), Bortezomib (VELCADE®, Millennium Pharm.), Disulfiram, Epigaro Catechin Gallate, Salinosporamide A, Carfilzomib, 17-AAG (Geldanamycin), Radicol, Lactate Dehydrogenase A (LDH-A), Fulvestrant (FASLODEX®, AstraZeneca), Sunitinib (SUTENT®) , Pfizer/Sugen), Letrozole (FEMARA®, Novartis), Imatinib Mesylate (GLEEVEC®, Novartis), Finasanate (VATALANIB®, Novartis), Oxaliplatin (® ), Sanofi), 5-FU (5-fluorouracil), leucovorin, rapamycin (sirolimus, RAPAMUNE®, Wyeth), lapatinib (TYKERB®, GSK572016, Glaxo Smith Kline), lonafamib (SCH66336), sorafenib (NEXAVAR®, Bayer Labs), gefitinib (IRESSA®), AstraZeneca), AG1478, thiotepa, CYTOXAN® cyclophosphamide; aziridines such as benzodopa, carboquone, metuledopa, uredopa; ethyleneimine and methylamelamine, including altretamine, triethylenemelamine, triethylenephosphoramide, triethylenethiophosphoramide and trimethylomelamin; camptothecins (including topotecan and irinotecan); bryostatin; callistatin; CC-1065 (including adzelesin, calzelesin, vizelesin synthetic analogues); cryptophycins (particularly cryptophycin 1 and cryptophycin 8); Steroids (including prednisone and prednisolone); cyproterone acetate; 5α-reductase, including finasteride and dutasteride); vorinostat, romidepsin, panovy nostat, valproic acid, mosetinostat dolastatin; aldesleukin, talc duocarmycin (including synthetic analogues, KW-2189 and CB1-TM1); eletharobin; pancratistatin; sarcodictin; spongistatin; , chlorophosphamide, estramustine, ifosfamide, mechlorestamine, mechlorestamine oxide hydrochloride, melphalan, novenvitine, phenesterin, prednimustine, trophosphamide, nitrogen mustards such as uracil mustard, carmustine, chlorozotocin, fotemustine, lomustine, nimustine , and nitrosoureas such as ranimustine; antibiotics such as enidine antibiotics (eg calichemycins, particularly calichemycin γ1I and calichemycin ω1I (Angew Chem. Intl. Ed. Engl. 1994 33:183-186); dynemycins, including dynemycin A; bisphosphonates such as clodronate; neocardinostatin chromophore and related chromophores, endiyne antibiotic chromophores, as well as esperamycin), aclacinomycin, actinomycin. , autoramycin, azaserine, bleomycin, cactinomycin, carabicin, caminomycin, cardinophylline, chromomycin, dactinomycin, daunorubicin, detorubicin, 6-diazo-5-oxo-L-norleucine, ADRIAMYCIN® (doxorubicin), morpholinodoxorubicin, cyanomorpholinodoxorubicin, 2-pyrrolinotoxorubicin, deoxydoxorubicin), epirubicin, ethorubicin, idarubicin, marceromycin, mitomycins such as mitomycin C, mycophenolic acid, nogaramycin, olibomycin, pepromycin, porphyromycin , puromycin, keramycin, rhodorubicin, streptozocin, tuberculidine, ubenimex, dinostatin, zorubicin methotrexate and 5-fluorouracil (5-FU); folic acid analogues such as denopterin, methotrexate, pteropterin, trimetrexate; Purine analogues such as 6-mercaptopurine, thiamipurine, thioguanine. pyrimidine analogues such as ancitabine, azacitidine, 6-azauridine, carmofur, cytarabine, dideoxyuridine, doxifluridine, enocitabine, floxuridine; androgens such as carsterone, dromostanolone propionate, epithiostanol, mepithiosteine, testolactone; , anti-adrenals such as trilosteine; folic acid supplements such as floric acid; ace gratone; aldophosphamide glycoside; aminolevulinic acid; eriptine acetate; anepothilone; etogluside; gallium nitrate; hydroxyurea; lentinan; 2-ethylhydrazide; procarbazine; PSK® polysaccharide complex (JHS Natural Products, Eugene, Oreg.); lazoxane; vindesine; dacarbazine; mannomustine; mitobronitol; mitractol; pipobroman; gacytosine; thiotepa; taxanes (taxoids) such as TAXOL® (paclitaxel; Bristol-Myers Squibb Oncology, Princeton, NJ), ABRAXANE® (cremopho-free), albumin-engineered nanoparticulate formulations of paclitaxel ( For example, nanoparticulate albumin-engineered paclitaxel (nab-paclitaxel) (American Pharmaceutical Partners, Schaumburg, Ill.), and TAXOTERE® (docetaxel, doxetaxel; Sanofi-Aventis), chlorambucil, GEMZAR® (gemcitabine) , 6-thioguanine, mercaptopurine, methotrexate; platinum analogues such as cisplatin and carboplatin; vinblastine; etoposide (VP-16); capecitabine (XELODA®); ibandronate; CPT-11; topoisomerase inhibitor RFS2000; difluoromethylornithine (DMFO); a retinoid such as retinoic acid; salts, acids, and derivatives that can be
また、化学療法剤としては、以下が挙げられる:(i)抗エストロゲン及び選択的エストロゲン受容体モジュレーター(SERM)等、腫瘍に対するホルモン作用を調節又は阻害するように作用する抗ホルモン剤、例えば、タモキシフェン(NOLVADEX(登録商標)を含む;クエン酸タモキシフェン)、ラロキシフェン、ドロキシフェン、ヨードキシフェン、4-ヒドロキシタモキシフェン、トリオキシフェン、ケオキシフェン、LY117018、オナプリストン、及びFARESTON(登録商標)(クエン酸トレミフィン);(ii)副腎においてエストロゲン産生を調節する酵素アロマターゼを阻害するアロマターゼ阻害剤、例えば、4(5)-イミダゾール、アミノグルテチミド、MEGASE(登録商標)(酢酸メグストロール)、AROMASIN(登録商標)(エキセメスタン;Pfizer)、フォルメスタニー、ファドロゾール、RIVISOR(登録商標)(ボルゾール)、FEMARA(登録商標)(レトロゾール;Novartis)、ARIMIDEX(登録商標)(アナストロゾール;AstraZeneca)等の抗アンドロゲン剤、(iii)フルタミド、ニルタミド、ビカルタミド、リュープロライド、及びゴセレレリン等の抗アンドロゲン剤;ブセレリン、トリプレリン、メドロキシプロゲステロンアセテート、ジエチルスチルベストロール、プレマリン、フルオキシメステロン、全てのトランスレチオン酸、フェンレチニドと並んでトロキサシタビン(1,3-ジオキソランヌクレオシドシトシン類縁体);(iv)プロテインキナーゼ阻害剤(例えば、未分化リンパ腫キナーゼ(Alk)阻害剤、例えばAF-802(CH-5424802又はアレクチニブとしても知られる);(v)脂質キナーゼ阻害剤;(vi)アンチセンスオリゴヌクレオチド、特に異常細胞増殖に関与するシグナル伝達経路の遺伝子の発現を阻害するもの、例えばPKC-α、Ralf及びH-Ras;;(vii)VEGF発現阻害剤(例えば、ANGIOZYME(登録商標))及びHER2発現阻害剤等のリボザイム;(viii)遺伝子治療ワクチン、例えば、ALLOVECTIN(登録商標)、LEUVECTIN(登録商標)及びVAXID(登録商標)等のワクチン;PROLEUKIN(登録商標)、rIL-2;LURTOTECAN(登録商標)等のトポイソメラーゼ1阻害剤;ABARELIX(登録商標)rmRH;並びに(ix)上記のいずれかの薬学的に許容され得る塩、酸及び誘導体。 Chemotherapeutic agents also include: (i) antihormonal agents that act to modulate or inhibit hormone action on tumors, such as antiestrogens and selective estrogen receptor modulators (SERMs), e.g., tamoxifen; (including NOLVADEX®; tamoxifen citrate), raloxifene, droxifene, iodoxifene, 4-hydroxy tamoxifen, trioxyfen, keoxifene, LY117018, onapristone, and FARESTON® (toremifine citrate); (ii) aromatase inhibitors that inhibit the enzyme aromatase that regulates estrogen production in the adrenal glands, such as 4(5)-imidazole, aminoglutethimide, MEGASE® (megstrol acetate), AROMASIN® ( exemestane; Pfizer), formestani, fadrozole, RIVISOR® (borzole), FEMARA® (letrozole; Novartis), ARIMIDEX® (anastrozole; AstraZeneca), antiandrogens such as (iii) antiandrogens such as flutamide, nilutamide, bicalutamide, leuprolide, and gosererelin; buserelin, triprelin, medroxyprogesterone acetate, diethylstilbestrol, premarin, fluoxymesterone, all trans-rethioic acid, fenretinide (iv) protein kinase inhibitors (e.g. anaplastic lymphoma kinase (Alk) inhibitors such as AF-802 (CH-5424802, also known as alectinib), along with troxacitabine (a 1,3-dioxolane nucleoside cytosine analog); (v) lipid kinase inhibitors; (vi) antisense oligonucleotides, particularly those that inhibit the expression of genes in signaling pathways involved in abnormal cell proliferation, such as PKC-α, Ralf and H-Ras; vii) ribozymes such as VEGF expression inhibitors (e.g. ANGIOZYME®) and HER2 expression inhibitors; (viii) gene therapy vaccines such as ALLOVECTIN®, LEUVECTIN® and VAXID® vaccines such as PROLEUKIN®, rIL-2; topoisomerases such as LURTOTECAN® ABARELIX® rmRH; and (ix) pharmaceutically acceptable salts, acids and derivatives of any of the above.
化学療法剤には、分子の不可欠な部分として白金を含有する有機化合物を含む、本明細書では「白金剤」とも呼ばれる「白金系」化学療法剤も含まれる。典型的には、白金系化学療法剤は、白金の配位錯体である。白金系化学療法剤は、当該技術分野において「プラチン」と呼ばれることもある。白金系化学療法剤の例としては、シスプラチン、カルボプラチン、オキサリプラチン、ネダプラチン、トリプラチンテトラニトレート、フェナントリプラチン、ピコプラチン、リポプラチン及びサトラプラチンが挙げられるが、これらに限定されない。白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)は、1つ以上の追加の化学療法剤、例えば、ヌクレオシド類似体(例えば、ゲムシタビン)、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル)と組み合わせて投与され得る。 Chemotherapeutic agents also include "platinum-based" chemotherapeutic agents, also referred to herein as "platinum agents," which contain organic compounds containing platinum as an integral part of the molecule. Typically, platinum-based chemotherapeutic agents are coordination complexes of platinum. Platinum-based chemotherapeutic agents are sometimes referred to as "platin" in the art. Examples of platinum-based chemotherapeutic agents include, but are not limited to, cisplatin, carboplatin, oxaliplatin, nedaplatin, tripplatin tetranitrate, phenanthriplatin, picoplatin, lipoplatin, and satraplatin. A platinum-based chemotherapeutic agent (e.g., cisplatin or carboplatin) may be combined with one or more additional chemotherapeutic agents, such as a nucleoside analogue (e.g., gemcitabine), an antimetabolite (e.g., pemetrexed or gemcitabine) or a taxane (e.g., paclitaxel or nab-paclitaxel).
「白金系化学療法による処置に適格である」という用語は、対象が、主治医の判断で、又は当該技術分野で公知の白金系化学療法の適格性についての標準化された基準に従って、白金系化学療法による処置に適格であることを意味する。 The term "eligible for treatment with platinum-based chemotherapy" means that a subject is eligible for platinum-based chemotherapy, either at the discretion of the attending physician or according to standardized criteria for platinum-based chemotherapy eligibility known in the art. means eligible for treatment by
化学療法剤には、本明細書で使用される場合、「白金系ではない」化学療法剤を指す「非白金系化学療法剤」も含まれる。本明細書で使用される場合、「非白金系化学療法剤」及び「非白金剤」という用語は互換的に使用される。例示的な非白金系化学療法剤としては、代謝拮抗剤(例えば、ペメトレキセド及びゲムシタビン)、トポイソメラーゼII阻害剤(例えば、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331)、タキサン(例えば、パクリタキセル(例えば、ナノ粒子アルブミン結合パクリタキセル(nab-パクリタキセル)とも呼ばれるアルブミン操作パクリタキセル)、ドセタキセル、ラロタキセル、カバジタキセル、ミラタキセル、テセタキセル、及び/又はオラタキセル)が挙げられる。例示的な非白金系化学療法剤には、アルキル化剤(例えば、シクロホスファミド)も含まれる。 Chemotherapeutic agents, as used herein, also include "non-platinum-based chemotherapeutic agents," which refer to chemotherapeutic agents that are "non-platinum-based." As used herein, the terms "non-platinum chemotherapeutic agent" and "non-platinum agent" are used interchangeably. Exemplary non-platinum chemotherapeutic agents include antimetabolites (e.g., pemetrexed and gemcitabine), topoisomerase II inhibitors (e.g., etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticine, orintricarboxylic acid, or HU-331), taxanes (eg, paclitaxel (eg, albumin-engineered paclitaxel, also called nanoparticle albumin-bound paclitaxel (nab-paclitaxel)), docetaxel, larotaxel, cabazitaxel, mirataxel, tesetaxel, and/or orataxel). Exemplary non-platinum chemotherapeutic agents also include alkylating agents (eg, cyclophosphamide).
本明細書で使用される場合、「ヌクレオシド類似体」は、核酸類縁体及び糖を含むヌクレオシドを指す。ヌクレオシド類縁体は、代謝拮抗剤として機能し得る。例示的なヌクレオシド類縁体には、ゲムシタビン、シタラビン、フルダラビン及びクラドリビンが含まれるが、これらに限定されない。 As used herein, "nucleoside analogue" refers to a nucleoside containing a nucleic acid analogue and a sugar. Nucleoside analogues can function as antimetabolites. Exemplary nucleoside analogues include, but are not limited to gemcitabine, cytarabine, fludarabine and cladribine.
本明細書で使用される場合、「タキサン」は、微小管アセンブリ及び安定化を促進し、かつ/又は微小管脱重合を阻止するチューブリンに結合し得るジテルペンである。本明細書に含まれるタキサンは、タキソイド10-デアセチルバッカチンIII及び/又はその誘導体を含む。例示的なタキサンとしては、パクリタキセル(すなわち、TAXOL(登録商標)、CAS#33069-62-4)、ドセタキセル(すなわち、TAXOTERE(登録商標)、CAS#114977-28-5)、ラロタキセル、カバジタキセル、ミラタキセル、テセタキセル、及び/又はオルタタキセル(orataxel)が挙げられるが、これらに限定されない。いくつかの態様では、タキサンはアルブミン被覆ナノ粒子(例えば、nab-パクリタキセル、すなわち、ABRAXANE(登録商標)及び/又はnab-ドセタキセル、ABI-008)である。いくつかの態様では、タキサンはnab-パクリタキセル(ABRAXANE(登録商標))である。いくつかの態様では、タキサンは、CREMAPHOR(登録商標)(例えば、TAXOL(登録商標))及び/又はTween、例えばポリソルベート80(例えば、TAXOTERE(登録商標))に製剤化される。いくつかの態様では、タキサンはリポソーム封入タキサンである。いくつかの態様では、タキサンは、プロドラッグの形態及び/又はタキサンのコンジュゲート形態(例えば、パクリタキセル、パクリタキセルポリグルメクス、及び/又は炭酸リノレイル-パクリタキセルに共有結合的にコンジュゲートしたDHA)である。いくつかの態様では、パクリタキセルは、実質的に界面活性剤なしで(例えば、CREMAPHOR及び/又はTweenの不在下で-TOCOSOL(登録商標)パクリタキセル等)製剤化される。 As used herein, a "taxane" is a diterpene that can bind to tubulin to promote microtubule assembly and stabilization and/or prevent microtubule depolymerization. Taxanes included herein include taxoid 10-deacetylbaccatin III and/or derivatives thereof. Exemplary taxanes include paclitaxel (ie, TAXOL®, CAS#33069-62-4), docetaxel (ie, TAXOTERE®, CAS#114977-28-5), larotaxel, cabazitaxel, mirataxel. , tesetaxel, and/or orataxel. In some aspects, the taxane is an albumin-coated nanoparticle (eg, nab-paclitaxel, ie ABRAXANE®, and/or nab-docetaxel, ABI-008). In some aspects, the taxane is nab-paclitaxel (ABRAXANE®). In some aspects, the taxane is formulated in a CREMAPHOR® (eg, TAXOL®) and/or a Tween, such as polysorbate 80 (eg, TAXOTERE®). In some aspects, the taxane is a liposome-encapsulated taxane. In some aspects, the taxane is in the form of a prodrug and/or a conjugate form of the taxane (e.g., DHA covalently conjugated to paclitaxel, paclitaxel polygourmex, and/or linoleyl carbonate-paclitaxel). . In some aspects, paclitaxel is formulated substantially without surfactants (eg, in the absence of CREMAPHOR and/or Tween—TOCOSOL® paclitaxel, etc.).
本明細書で使用される「代謝拮抗剤」は、細胞(例えば、がん細胞)内の内因性(正常)代謝過程を干渉し、(全体的又は部分的に)阻害する化学療法剤である。代謝拮抗剤としては、ゲムシタビン、ペメトレキセド、カペシタビン、ヒドロキシ尿素、メトトレキサート、フルオロウラシル、クラドリビン、メルカプトプリン及びプララトレキセートが挙げられる。 As used herein, an "antimetabolic agent" is a chemotherapeutic agent that interferes with and inhibits (totally or partially) endogenous (normal) metabolic processes within cells (e.g., cancer cells). . Antimetabolites include gemcitabine, pemetrexed, capecitabine, hydroxyurea, methotrexate, fluorouracil, cladribine, mercaptopurine and pralatrexate.
化学療法剤としてはまた、デキサメタゾン、インターフェロン、コルヒチン、メトプリン、シクロスポリン、アンホテリシン、メトロニダゾール、アレムツズマブ、アリトレチノイン、アロプリノール、アミホスチン、三酸化ヒ素、アスパラギナーゼ、生BCG、ベバシズマブ、ベキサロテン、クラドリビン、クロファラビン、ダルベポエチンアルファ、デニロイキン、デクスラゾキサン、エポエチンアルファ、エロチニブ、フィルグラスチム、酢酸ヒストレリン、イブリツモマブ、インターフェロンアルファ-2a、インターフェロンアルファ-2b、レナリドミド、レバミゾール、メスナ、メトキサレン、ナンドロロン、ネララビン、ノフェツモマブ、オプレルベキン、パリフェルミン、パミドロネート、ペガデマーゼ、ペグアスパラガーゼ、ペグフィルグラスチム、ペメトレキセド二ナトリウム、プリカマイシン、ポルフィマーナトリウム、キナクリン、ラスブリカーゼ、サルグラモスチム、テモゾロミド、VM-26、6-TG、トレミフェン、トレチノイン、ATRA、バルルビシン、ゾレドロネート、及びゾレドロン酸、ならにそれらの薬学的に許容され得る塩も挙げられる。 Chemotherapeutic agents also include dexamethasone, interferon, colchicine, metoprine, cyclosporine, amphotericin, metronidazole, alemtuzumab, alitretinoin, allopurinol, amifostine, arsenic trioxide, asparaginase, live BCG, bevacizumab, bexarotene, cladribine, clofarabine, darbepoetin alfa, Denileukin, dexrazoxane, epoetin alfa, erotinib, filgrastim, histrelin acetate, ibritumomab, interferon alpha-2a, interferon alpha-2b, lenalidomide, levamisole, mesna, methoxsalen, nandrolone, nerarabine, nofetumomab, oprelvekin, palyfermin, pamidronate, pegademase , pegasparagase, pegfilgrastim, pemetrexed disodium, plicamycin, porfimer sodium, quinacrine, rasburicase, sargramostim, temozolomide, VM-26, 6-TG, toremifene, tretinoin, ATRA, valrubicin, zoledronate, and zoledronic acid , as well as pharmaceutically acceptable salts thereof.
また、化学療法剤としては、以下が挙げられる:ヒドロコルチゾン、酢酸ヒドロコルチゾン、酢酸コルチゾン、ピバル酸チクソコルトール、トリアムシノロンアセトニド、トリアムシノロンアルコール、モメタゾン、アムシノニド、ブデソニド、デソニド、フルオシノニド、フルオシノロンアセトニド、ベタメタゾン、ベタメタゾンナトリウムリン酸塩、デキサメタゾン、デキサメタゾンナトリウムリン酸塩、フルオコルトン、ヒドロコルチゾン-17-ブチレート、ヒドロコルチゾン-17-バレレート、アクロメタゾンジプロピオン酸塩、ベタメタゾンバレレート、ベタメタゾンジプロピオン酸塩、プレドニカルベート、クロベタゾン-17-ブチレート、クロベタゾール-17-プロピオン酸塩、フルオコルトンカプロエート、フルオコルトンピバル酸塩及びフルプレドニデンアセテート、フェニルアラニン-グルタミン-グリシン(FEG)及びそのD異性体形態(feG)等の免疫選択的抗炎症ペプチド(ImSAID)(IMULAN BioTherapeutics,LLC);アザチオプリン、シクロスポリン(シクロスポリンA)、D-ペニシラミン、金塩、ヒドロキシクロロキン、レフルノミデミノサイクリン、スルファサラジン等の抗リウマチ薬;エタネルセプト(エンブレル)、インフリキシマブ(レミケード)、アダリムマブ(ヒュミラ)、セルトリズマブペゴール(チムジア)、ゴリムマブ(シンポニ)、アナキンラ(キネレ)等のインターロイキン1(IL-1)遮断薬、アバタセプト(オレンシア)等のT細胞共刺激ブロッカー、トシリズマブ(ACTEMERA(登録商標))等のインターロイキン6(IL-6)ブロッカー、レブリキズマブ等のインターロイキン13(IL-13)遮断薬;ロンタリズマブ等のインターフェロンアルファ(IFN)ブロッカー;rhuMAb Beta7等のBeta7インテグリンブロッカー;抗M1 prime等のIgE経路ブロッカー、分泌されたホモ三量体LTa3及び抗リンホトキシンアルファ(LTa)等の膜結合ヘテロ三量体LTa1 /β2ブロッカー;放射性同位元素(例えば、At211、I131、I125、Y90、Re186、Re188、Sm153、Bi212、P32、Pb212及びLuの放射性同位体);チオプラチン、PS-341、フェニルブチレート、ET-18-OCH3、又はファルネシルトランスフェラーゼ阻害剤(L-739749、L-744832)等のその他の治験薬;ケルセチン、レスベラトロール、ピセアタンノール、没食子酸エピガロカテキン、テアフラビン、フラバノール、プロシアニジン、ベツリン酸及びそれらの誘導体等のポリフェノール;クロロキン等のオートファジー阻害剤;デルタ-9-テトラヒドロカンナビノール(ドロナビノール、MARINOL(登録商標));ベータラパコン;ラパコール;コルヒチン;ベツリン酸及びその誘導体;アセチルカンプトテシン、スコポレクチン、及び9-アミノカンプトテシン);ポドフィロトキシン;テガフール(UFTORAL(登録商標));ベキサロテン(TARGRETIN(登録商標));クロドロネート(例えば、BONEFOS(登録商標)又はOSTAC(登録商標))、エチドロネート(DIDROCAL(登録商標))、NE-58095、ゾレドロン酸/ゾレドロネート(ZOMETA(登録商標))、アレンドロネート(FOSAMAX(登録商標))、パミドロネート(AREDIA(登録商標))、チルドロネート(SKELID(登録商標))等のビスホスホネート)、又はリセドロネート(ACTONEL(登録商標));並びに上皮成長因子受容体(EGF-R);THERATOPE(登録商標)ワクチン等のワクチン;ペリホシン、COX-2阻害剤(例えば、セレコキシブ又はエトリコキシブ)、プロテオソーム阻害剤(例えば、PS341);CCI-779;ティピファルニブ(R11577);オラフェニブ、ABT510;オブリメルセンナトリウム(GENASENSE(登録商標))等のBcl-2阻害剤:ピキサントロン;ロナファルニブ(SCH 6636、SARASAR(商標))等のファルネシルトランスフェラーゼ阻害剤;及び上記のいずれかの薬学的に許容され得る塩、酸又は誘導体;並びにシクロホスファミド、ドキソルビシン、ビンクリスチン、プレドニゾロンの併用療法の略であるCHOP、及び5-FUとロイコボリンを組み合わせたオキサリプラチン(ELOXATIN(商標))の処置レジメンの略であるFOLFOXのような上記の2つ以上の組合せ。 Chemotherapeutic agents also include: hydrocortisone, hydrocortisone acetate, cortisone acetate, thixocortol pivalate, triamcinolone acetonide, triamcinolone alcohol, mometasone, amcinonide, budesonide, desonide, fluocinonide, fluocinolone acetonide, betamethasone, betamethasone sodium phosphate, dexamethasone, dexamethasone sodium phosphate, fluocortone, hydrocortisone-17-butyrate, hydrocortisone-17-valerate, acrometasone dipropionate, betamethasone valerate, betamethasone dipropionate, pred Nicarbate, clobetasone-17-butyrate, clobetasol-17-propionate, fluocortone caproate, fluocortone pivalate and fluprednidene acetate, phenylalanine-glutamine-glycine (FEG) and its D isomeric forms ( feG) and other immunoselective anti-inflammatory peptides (ImSAIDs) (IMULAN BioTherapeutics, LLC); antirheumatic drugs such as azathioprine, cyclosporine (cyclosporine A), D-penicillamine, gold salts, hydroxychloroquine, leflunomideminocycline, sulfasalazine, etc. interleukin-1 (IL-1) blockers such as etanercept (Enbrel), infliximab (Remicade), adalimumab (Humira), certolizumab pegol (Timzia), golimumab (Simponi), anakinra (Kinele), abatacept (Orencia) ), interleukin 6 (IL-6) blockers such as tocilizumab (ACTEMERA®), interleukin 13 (IL-13) blockers such as lebrikizumab; interferon alpha (IFN) such as lontarizumab Beta7 integrin blockers such as rhuMAb Beta7; IgE pathway blockers such as anti-M1 prime, secreted homotrimeric LTa3 and membrane bound heterotrimeric LTa1/β2 blockers such as anti-lymphotoxin alpha (LTa); radioisotopes (such as radioisotopes of At211, I131, I125, Y90, Re186, Re188, Sm153, Bi212, P32, Pb212 and Lu); thioplatin, PS-341, phenylbutyrate, ET-18-OCH3, or fal Other investigational drugs such as Nesyltransferase inhibitors (L-739749, L-744832); quercetin, resveratrol, piceatannol, epigallocatechin gallate, theaflavin, flavanols, procyanidins, betulinic acid and their derivatives, etc. autophagy inhibitors such as chloroquine; delta-9-tetrahydrocannabinol (dronabinol, MARINOL®); beta-lapachone; lapachol; colchicine; betulinic acid and its derivatives; ); podophyllotoxin; tegafur (UFTORAL®); bexarotene (TARGRETIN®); clodronate (e.g. BONEFOS® or OSTAC®), etidronate (DIDROCAL®) , NE-58095, bisphosphonates such as zoledronic acid/zoledronate (ZOMETA®), alendronate (FOSAMAX®), pamidronate (AREDIA®), tiludronate (SKELID®)), or risedronate (ACTONEL®); and epidermal growth factor receptor (EGF-R); vaccines such as THERATOPE® vaccine; perifosine, COX-2 inhibitors (eg celecoxib or etoricoxib), proteosome inhibitors tipifarnib (R11577); olafenib, ABT510; Bcl-2 inhibitors such as oblimersen sodium (GENASENSE®): pixantrone; and a pharmaceutically acceptable salt, acid or derivative of any of the above; and CHOP, which stands for combination therapy of cyclophosphamide, doxorubicin, vincristine, prednisolone, and 5-FU and leucovorin. A combination of two or more of the above, such as FOLFOX, which stands for oxaliplatin (ELOXATIN™) treatment regimen combined with
化学療法剤としてはまた、鎮痛効果、解熱効果、及び抗炎症効果を有する非ステロイド抗炎症薬が挙げられ得る。NSAIDは、酵素シクロオキシゲナーゼの非選択的阻害剤を含む。非ステロイド性抗炎症薬の具体例としては、アスピリン、イブプロフェン、フェノプロフェン、ケトプロフェン、フルルビプロフェン、オキサプロジン、ナプロキセン等のプロピオン酸誘導体、インドメタシン、スルリンダック、エトドラック、ジクロフェナク等の酢酸誘導体、ピロキシカム、メロキシカム等のエノリック酸誘導体。テノキシカム、ドロキシカム、ローノキシカム、イソキシカム、メフェナム酸、メクロフェナム酸、フルフェナム酸、トルフェナム酸等のフェナム酸誘導体、セレコキシブ、エトリコキシブ、ルミラコキシブ、パレコキシブ、ロフェコキシブ、バルデコキシブ等のCOX-2阻害剤が挙げられる。NSAIDは、リウマチ性関節炎、変形性関節炎、炎症性関節症、強直性脊椎症、乾癬性関節炎、ライター症候群、急性痛風、月経困難症、転移性骨痛、頭痛、及び片頭痛、術後痛、炎症及び組織傷害に起因する軽度から中度の疼痛、発熱、腸閉塞、及び腎疝痛等の病態の症状緩和のために示され得る。 Chemotherapeutic agents can also include non-steroidal anti-inflammatory drugs that have analgesic, antipyretic, and anti-inflammatory effects. NSAIDs include non-selective inhibitors of the enzyme cyclooxygenase. Specific examples of non-steroidal anti-inflammatory drugs include propionic acid derivatives such as aspirin, ibuprofen, fenoprofen, ketoprofen, flurbiprofen, oxaprozin and naproxen, acetic acid derivatives such as indomethacin, sullindac, etodolac and diclofenac, piroxicam, Enolic acid derivatives such as meloxicam. Fenamic acid derivatives such as tenoxicam, droxicam, ronoxicam, isoxicam, mefenamic acid, meclofenamic acid, flufenamic acid and tolfenamic acid, and COX-2 inhibitors such as celecoxib, etoricoxib, lumiracoxib, parecoxib, rofecoxib and valdecoxib. NSAIDs are used to treat rheumatoid arthritis, osteoarthritis, inflammatory arthritis, ankylosing spondylosis, psoriatic arthritis, Reiter's syndrome, acute gout, dysmenorrhea, metastatic bone pain, headache and migraine, postoperative pain, It may be indicated for symptomatic relief of conditions such as mild to moderate pain, fever, intestinal obstruction, and renal colic resulting from inflammation and tissue injury.
化学療法剤には、EGFRに結合するか又はさもなければそれと直接相互作用し、そのシグナル伝達活性を妨害又は低減する化合物を指す「EGFR阻害剤」も含まれ、代わりに「EGFRアンタゴニスト」とも称される。そのような薬剤の例としては、EGFRに結合する小分子が挙げられる。EGFRアンタゴニストは、米国特許第5,616,582号、同第5,457,105号、同第5,475,001号、同第5,654,307号、同第5,679,683号、同第6,084,095号、同第6,265,410号、同第6,455,534号、同第6,521,620号、同第6,596,726号、同第6,713,484号、同第5,770,599号、同第6,140,332号、同第5,866,572号、同第6,399,602号、同第6,344,459号、同第6,602,863号、同第6,391,874号、同第6,344,455号、同第5,760,041号、同第6,002,008号、及び同第5,747,498号、並びに以下のPCT公報:国際公開第98/14451号、同第98/50038号、同第99/09016号、及び同第99/24037号に記載の化合物等の小分子を含む。特定の低分子EGFRアンタゴニストとしては、OSI-774(CP-358774、エルロチニブ、TARCEVA(登録商標)、Genentech/OSI Pharmaceuticals)、PD183805(CI1033、2-プロペンアミド、N-[4-[(3-クロロ-4-フルオロフェニル)アミノ]-7-[3-(4-モルホリニル)プロポキシ]-6-キナゾリニル]-、ジヒドロクロリド、Pfizer Inc.)、ZD1839、ゲフィチニブ(IRESSA(登録商標))4-(3’-クロロ-4’-フルオロアニリノ)-7-メトキシ-6-(3-モルホリノプロポキシ)キナゾリン、AstraZeneca)、ZM105180((6-アミノ-4-(3-メチルフェニル-アミノ)-キナゾリン、Zeneca)、BIBX-1382(N8-(3-クロロ-4-フルオロ-フェニル)-N2-(1-メチル-ピペリジン-4-イル)-ピリミド[5,4-d]ピリミジン-2,8-ジアミン、Boehringer Ingelheim)、PKI-166((R)-4-[4-[(1-フェニルエチル)アミノ]-1H-ピロロ[2,3-d]ピリミジン-6-イル]-フェノール)、(R)-6-(4-ヒドロキシフェニル)-4-[(1-フェニルエチル)アミノ]-7H-ピロロ[2,3-d]ピリミジン)、CL-387785(N-[4-[(3-ブロモフェニル)アミノ]-6-キナゾリニル]-2-ブチンアミド)、EKB-569(N-[4-[(3-クロロ-4-フルオロフェニル)アミノ]-3-シアノ-7-エトキシ-6-キノリニル]-4-(ジメチルアミノ)-2-ブチンアミド)(Wyeth)、AG1478(Pfizer)、AG1571(SU5271、Pfizer)、及び二重EGFR/HER2チロシンキナーゼ阻害剤、例えば、ラパチニブ(TYKERB(登録商標)、GSK572016又はN-[3-クロロ-4-[(3-フルオロフェニル)メトキシ]フェニル]-6[5[[[2メチルスルホニル)エチル]アミノ]メチル]-2-フラニル]-4-キナゾリンアミン)が挙げられる。 Chemotherapeutic agents also include "EGFR inhibitors," which refer to compounds that bind to or otherwise interact directly with EGFR and block or reduce its signaling activity, alternatively referred to as "EGFR antagonists." be done. Examples of such agents include small molecules that bind to EGFR. EGFR antagonists are disclosed in U.S. Pat. Nos. 6,084,095, 6,265,410, 6,455,534, 6,521,620, 6,596,726, 6,713 , 484, 5,770,599, 6,140,332, 5,866,572, 6,399,602, 6,344,459, 6,602,863, 6,391,874, 6,344,455, 5,760,041, 6,002,008, and 5,747 , 498, and the following PCT publications: WO 98/14451, WO 98/50038, WO 99/09016, and WO 99/24037. Specific small molecule EGFR antagonists include OSI-774 (CP-358774, erlotinib, TARCEVA®, Genentech/OSI Pharmaceuticals), PD183805 (CI1033, 2-propenamide, N-[4-[(3-chloro -4-fluorophenyl)amino]-7-[3-(4-morpholinyl)propoxy]-6-quinazolinyl]-, dihydrochloride, Pfizer Inc.), ZD1839, gefitinib (IRESSA®) 4-(3 '-chloro-4'-fluoroanilino)-7-methoxy-6-(3-morpholinopropoxy)quinazoline, AstraZeneca), ZM105180 ((6-amino-4-(3-methylphenyl-amino)-quinazoline, Zeneca ), BIBX-1382 (N8-(3-chloro-4-fluoro-phenyl)-N2-(1-methyl-piperidin-4-yl)-pyrimido[5,4-d]pyrimidine-2,8-diamine, Boehringer Ingelheim), PKI-166 ((R)-4-[4-[(1-phenylethyl)amino]-1H-pyrrolo[2,3-d]pyrimidin-6-yl]-phenol), (R) -6-(4-hydroxyphenyl)-4-[(1-phenylethyl)amino]-7H-pyrrolo[2,3-d]pyrimidine), CL-387785 (N-[4-[(3-bromophenyl ) amino]-6-quinazolinyl]-2-butynamide), EKB-569 (N-[4-[(3-chloro-4-fluorophenyl)amino]-3-cyano-7-ethoxy-6-quinolinyl]- 4-(dimethylamino)-2-butynamide) (Wyeth), AG1478 (Pfizer), AG1571 (SU5271, Pfizer), and dual EGFR/HER2 tyrosine kinase inhibitors such as lapatinib (TYKERB®, GSK572016 or N-[3-chloro-4-[(3-fluorophenyl)methoxy]phenyl]-6[5[[[2methylsulfonyl)ethyl]amino]methyl]-2-furanyl]-4-quinazolinamine); be done.
化学療法剤としては、「チロシンキナーゼ阻害剤」、例えば、前段落に記載のEGFR標的薬物;インスリン受容体チロシンキナーゼの阻害剤、例えば、未分化リンパ腫キナーゼ(Alk)阻害剤、例えば、AF-802(CH-5424802又はアレクチニブとしても知られる)、ASP3026、X396、LDK378、AP26113、クリゾチニブ(XALKORI(登録商標))及びセリチニブ(ZYKADIA(登録商標))等;小分子HER2チロシンキナーゼ阻害剤、例えば、Takedaから入手可能なTAK165;ErbB2受容体チロシンキナーゼの経口選択的阻害剤であるCP-724,714(Pfizer及びOSI);二重HER阻害剤、例えば、EGFRに優先的に結合するが、HER2及びEGFR過剰発現細胞の両方を阻害するEKB-569(Wyethから入手可能);ラパチニブ(GSK572016、Glaxo-SmithKlineから入手可能);経口HER2及びEGFRチロシンキナーゼ阻害剤;PKI-166(Novartisから入手可能);pan-HER阻害剤、例えば、カネルチニブ(CI-1033、Pharmacia);Raf-1阻害剤、例えば、Raf-1シグナル伝達を阻害するISIS Pharmaceuticalsから入手可能なアンチセンス薬剤ISIS-5132;非HER標的TK阻害剤、例えば、メシル酸イマチニブ(GLEEVEC(登録商標)、Glaxo SmithKlineから入手可能);多標的チロシンキナーゼ阻害剤、例えば、スニチニブ(SUTENT(登録商標)、Pfizerから入手可能);VEGF受容体チロシンキナーゼ阻害剤、例えば、バタラニブ(PTK787/ZK222584、Novartis/Schering AGから入手可能);MAPK細胞外制御キナーゼI阻害剤CI-1040(Pharmaciaから入手可能);キナゾリン、例えば、PD 153035,4-(3-クロロアニリノ)キナゾリン;ピリドピリミジン;ピリミドピリミジン;ピロロピリミジン、例えば、CGP 59326、CGP 60261、及びCGP 62706;ピラゾロピリミジン、4-(フェニルアミノ)-7H-ピロロ[2,3-d]ピリミジン;クルクミン(ジフェルロイルメタン、4,5-ビス(4-フルオロアニリノ)フタルイミド);ニトロチオフェン部分を含有するチルホスチン;PD-0183805(Warner-Lamber);アンチセンス分子(例えば、HERコード核酸に結合するもの);キノキサリン(米国特許第5,804,396号);トリホスチン(tryphostin)(米国特許第5,804,396号);ZD6474(Astra Zeneca);PTK-787(Novartis/Schering AG);pan-HER阻害剤、例えば、CI-1033(Pfizer);Affinitac(ISIS 3521;Isis/Lilly);メシル酸イマチニブ(GLEEVEC(登録商標));PKI 166(Novartis);GW2016(Glaxo SmithKline);CI-1033(Pfizer);EKB-569(Wyeth);セマキシニブ(Pfizer);ZD6474(AstraZeneca);PTK-787(Novartis/Schering AG);INC-1C11(Imclone)、ラパマイシン(シロリムス、RAPAMUNE(登録商標);又は以下の特許公報:米国特許第5,804,396号;国際公開第1999/09016号(American Cyanamid);国際公開第1998/43960号(American Cyanamid);国際公開第1997/38983号(Warner Lambert);国際公開第1999/06378号(Warner Lambert);国際公開第1999/06396号(Warner Lambert);国際公開第1996/30347号(Pfizer,Inc);国際公開第1996/33978号(Zeneca);国際公開第1996/3397号(Zeneca);及び国際公開第1996/33980号(Zeneca)のうちのいずれかに記載のものも挙げられる。 Chemotherapeutic agents include "tyrosine kinase inhibitors", such as the EGFR-targeted drugs described in the preceding paragraph; inhibitors of insulin receptor tyrosine kinases, such as anaplastic lymphoma kinase (Alk) inhibitors, such as AF-802. (also known as CH-5424802 or alectinib), ASP3026, X396, LDK378, AP26113, crizotinib (XALKORI®) and ceritinib (ZYKADIA®); small molecule HER2 tyrosine kinase inhibitors such as Takeda CP-724,714 (Pfizer and OSI), an oral selective inhibitor of the ErbB2 receptor tyrosine kinase; a dual HER inhibitor, such as binding preferentially to EGFR, but HER2 and EGFR EKB-569, which inhibits both overexpressing cells (available from Wyeth); lapatinib (GSK572016, available from Glaxo-SmithKline); oral HER2 and EGFR tyrosine kinase inhibitor; PKI-166 (available from Novartis); - HER inhibitors such as canertinib (CI-1033, Pharmacia); Raf-1 inhibitors such as the antisense drug ISIS-5132 available from ISIS Pharmaceuticals that inhibits Raf-1 signaling; non-HER targeted TK inhibition agents such as imatinib mesylate (GLEEVEC®, available from Glaxo SmithKline); multitargeted tyrosine kinase inhibitors, such as sunitinib (SUTENT®, available from Pfizer); VEGF receptor tyrosine kinase inhibitors agents such as vatalanib (PTK787/ZK222584, available from Novartis/Schering AG); MAPK extracellular-regulated kinase I inhibitor CI-1040 (available from Pharmacia); quinazolines, such as PD 153035,4-(3-chloroanilino pyridopyrimidines; pyrimidopyrimidines; pyrrolopyrimidines such as CGP 59326, CGP 60261, and CGP 62706; (diferuloylmethane, 4,5-bis(4-fluoroanilino)phthalimide); nitro tyrphostins containing a thiophene moiety; PD-0183805 (Warner-Lamber); antisense molecules (eg, those that bind to HER-encoding nucleic acids); quinoxalines (US Pat. No. 5,804,396); PTK-787 (Novartis/Schering AG); pan-HER inhibitors such as CI-1033 (Pfizer); Affinitac (ISIS 3521; Isis/Lilly). PKI 166 (Novartis); GW2016 (Glaxo SmithKline); CI-1033 (Pfizer); EKB-569 (Wyeth); Semaxinib (Pfizer); 787 (Novartis/Schering AG); INC-1C11 (Imclone), rapamycin (sirolimus, RAPAMUNE®); or the following patent publications: US Patent No. 5,804,396; WO 1998/43960 (American Cyanamid); WO 1997/38983 (Warner Lambert); WO 1999/06378 (Warner Lambert); WO 1999/06396 (Warner Lambert) WO 1996/30347 (Pfizer, Inc); WO 1996/33978 (Zeneca); WO 1996/3397 (Zeneca); and WO 1996/33980 (Zeneca) The thing of description in either is also mentioned.
「アントラサイクリン」という用語は、化学療法剤、好ましくはトポイソメラーゼIIにおけるDNAの再結合を阻害することによってアポトーシスを誘導するための抗がん剤に関する。例としては、ドキソルビシン(アドリアマイシン)、ダウノルビシン(ダウノマイシン)、エピルビシン、イダルビシン、ロドマイシン、ピラルビシン、バルルビシン、N-トリフルオロ-アセチルドキソルビシン-14-バレレート、アクラシノマイシン、モルホリノドキソルビシン(モルホリノ-DOX)、シアノモルホリノ-ドキソルビシン(シアノモルホリノ-DOX)、2-ピロリノドキソルビシン(2-PDOX)、5-イミノダウノマイシン、ミトキサントロン及びアクラシノマイシンA(アクラルビシン)が挙げられる。いくつかの態様では、アントラサイクリンはアルキル化剤、例えばシクロホスファミドと組み合わせたドキソルビシン(ACによる処置)と組み合わせて投与される。 The term "anthracycline" relates to chemotherapeutic agents, preferably anticancer agents for inducing apoptosis by inhibiting DNA recombination in topoisomerase II. Examples include doxorubicin (adriamycin), daunorubicin (daunomycin), epirubicin, idarubicin, rhodomycin, pirarubicin, valrubicin, N-trifluoro-acetyldoxorubicin-14-valerate, aclacinomycin, morpholinodoxorubicin (morpholino-DOX), cyanomorpholino -doxorubicin (cyanomorpholino-DOX), 2-pyrrolinodoxorubicin (2-PDOX), 5-iminodaunomycin, mitoxantrone and aclacinomycin A (acrubicin). In some aspects, an anthracycline is administered in combination with an alkylating agent, such as doxorubicin in combination with cyclophosphamide (treatment with AC).
本明細書で使用される「アルキル化剤」は、アルキル基をDNAに結合することによってDNA損傷を引き起こす化学療法剤である。アルキル化剤としては、シクロホスファミド及びN,N’,N’’-トリエチレンチオホスホラミドが挙げられる。 As used herein, an "alkylating agent" is a chemotherapeutic agent that causes DNA damage by attaching alkyl groups to DNA. Alkylating agents include cyclophosphamide and N,N',N''-triethylenethiophosphoramide.
化合物、例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体)、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)、又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム)の「有効量」は、少なくとも、所望の治療結果、例えば、特定の疾患又は障害(例えば、がん)の全生存又は無増悪生存の測定可能な増加を達成するために必要な最小量である。本明細書における有効量は、患者の疾患状態、年齢、性別、及び体重、並びに対象における所望の応答を誘発する抗体の能力等の要因に応じて異なり得る。有効量は、処置上有益な作用が処置の任意の毒性作用又は有害作用を上回るものでもある。予防的使用のための有益な又は所望の結果には、疾患の生化学的、組織学的及び/又は行動学的症状、その合併症、及び疾患の発症中に現れる中間的な病理学的表現型を含む、リスクの除去又は軽減、重症度の軽減、又は疾患の発症の遅延等の結果が含まれる。治療的な使用のために、有益な又は所望の結果には、疾患に起因する1つ以上の症状の減少(例えば、がん関連疼痛、症候性骨格関連事象(SSE)の減少又は遅延、European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire(EORTC QLQ-C30、例えば、疲労、悪心、嘔吐、疼痛、呼吸困難、不眠症、食欲不振、便秘、下痢、又は身体的感情、認知、若しくは社会的機能の一般的レベル)による症状の減少、例えば、10ポイントの疼痛重症度(最悪の場合に測定)の数値評価尺度(NRS)によって測定される疼痛の減少、疾患に罹患している人の生活の質の増加、疾患を処置するために必要な他の薬物の用量の減少、標的化等による別の薬物の効果の増強、疾患の進行の遅延(例えば、無増悪生存期間又は放射線無増悪生存期間(rPFS);明確な臨床的進行(例えば、がん関連疼痛の進行、症候性の骨格関連事象、米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)の低下(例えば、疾患が患者の日常生活能力にどのように影響するか)、及び/又は次の全身性抗がん療法の開始)の遅延、及び/又は生存期間の延長が含まれる。がん又は腫瘍の場合、有効量の薬物は、がん細胞の数を減少させ、腫瘍サイズを低減させ、がん細胞の末梢器官への浸潤を阻害し(すなわち、ある程度遅らせるか又は望ましくは停止し)、腫瘍転移を阻害し(すなわち、ある程度遅らせるか又は望ましくは停止し)、腫瘍成長をある程度阻害し、かつ/又は障害に関連する症状のうちの1つ以上をある程度軽減する効果を有し得る。有効量は、1回又は複数回の投与でもよい。本発明の目的のために、薬物、化合物、又は医薬組成物の有効量は、予防的治療又は治療的処置を直接又は間接的に達成するのに十分な量である。臨床分野において理解されるように、薬物、化合物、又は医薬組成物の有効量は、別の薬物、化合物、又は医薬組成物と併せて達成されてもされなくてもよい。したがって、「有効量」は、1つ以上の治療剤の投与との関連で考慮することができ、単剤は、1つ以上の他の薬剤と併せて、望ましい結果が達成され得るか又は達成される場合、有効量で与えられると見ることができる。いくつかの態様では、有益な又は所望の結果は、肺がん(SILC)スケールの症状(例えば、咳呼吸困難及び胸痛における悪化までの時間(TTD))及び/又は肺特異的抗原進行までの時間の遅延によって評定される健康関連生活の質(HRQoL)アンケートによる肺がんに関連する症状の減少である。 Compounds such as anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists (e.g., anti-PD-L1 antibodies), VEGF antagonists, chemotherapeutic agents (e.g., platinum-based or non-platinum-based chemotherapeutic agents), ADCs ( e.g., enfortuzumab vedotin or sacituzumab govitecan) or CSF (e.g., pegfilgrastim, filgrastim, or sargramostim) is at least the desired therapeutic result, e.g. is the minimum amount required to achieve a measurable increase in overall survival or progression-free survival for a disease or disorder (eg, cancer) of Effective amounts herein may vary depending on factors such as the disease state, age, sex, and weight of the patient, and the ability of the antibody to elicit the desired response in the subject. An effective amount is also one in which any toxic or detrimental effects of the treatment are outweighed by the beneficial effects of the treatment. Beneficial or desired results for prophylactic use include biochemical, histological and/or behavioral manifestations of the disease, its complications, and intermediate pathological manifestations during the development of the disease. Outcomes such as elimination or reduction of risk, reduction in severity, or delay in onset of disease, including type. For therapeutic use, beneficial or desired results include reduction of one or more symptoms attributable to the disease (e.g., cancer-related pain, reduction or delay of symptomatic skeletal-related events (SSE), European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire (EORTC QLQ-C30, including fatigue, nausea, vomiting, pain, dyspnea, insomnia, anorexia, constipation, diarrhea, or physical, cognitive, or reduction in symptoms according to the general level of social functioning), e.g., reduction in pain as measured by a Numerical Rating Scale (NRS) of 10-point pain severity (measured at worst), those with the disease decrease the dose of other drugs needed to treat the disease; enhance the effect of another drug, such as by targeting; delay disease progression (e.g., progression-free survival or radiation-free progression survival (rPFS); definite clinical progression (e.g. cancer-related pain progression, symptomatic skeletal-related events, US East Coast Cancer Clinical Trials Group (ECOG) performance (PS) decline impact on the patient's ability to perform daily activities), and/or delaying initiation of subsequent systemic anticancer therapy), and/or prolonging survival. Effective amounts of the drug reduce the number of cancer cells, reduce tumor size, inhibit (i.e., slow or desirably stop to some extent) invasion of cancer cells into peripheral organs, and inhibit tumor metastasis. may have the effect of slowing (i.e., slowing or desirably halting to some extent), inhibiting to some degree tumor growth, and/or alleviating one or more of the symptoms associated with the disorder. Administration may be in single or multiple doses.For the purposes of this invention, an effective amount of a drug, compound, or pharmaceutical composition is an amount sufficient to achieve, directly or indirectly, prophylactic or therapeutic treatment. As understood in the clinical arts, an effective amount of a drug, compound or pharmaceutical composition may or may not be achieved in conjunction with another drug, compound or pharmaceutical composition. An "effective amount" can be considered in the context of administration of one or more therapeutic agents, which alone can or are capable of achieving a desired result in combination with one or more other agents. In some embodiments, beneficial or local Desirable outcomes are assessed by symptoms of the lung cancer (SILC) scale (e.g., time to deterioration (TTD) in cough dyspnea and chest pain) and/or delay in time to lung-specific antigen progression in health-related living. Reduction in lung cancer-related symptoms by quality (HRQoL) questionnaire.
「免疫原性」とは、免疫応答を誘発する特定の物質の能力を指す。腫瘍は、免疫原性であり、腫瘍免疫原性を増強させることは、免疫応答による腫瘍細胞の排除を助ける。腫瘍免疫原性を増強する例としては、限定されるものではないが、TIGIT及び/又はPD-L1アンタゴニスト(例えば、抗TIGITアンタゴニスト抗体及び/又は抗PD-L1抗体)による処置が挙げられる。 "Immunogenicity" refers to the ability of a particular substance to elicit an immune response. Tumors are immunogenic, and enhancing tumor immunogenicity helps the immune response eliminate tumor cells. Examples of enhancing tumor immunogenicity include, but are not limited to, treatment with TIGIT and/or PD-L1 antagonists (eg, anti-TIGIT antagonist antibodies and/or anti-PD-L1 antibodies).
「個々の応答」又は「応答」は、限定されないが、(1)疾患の進行(がんの進行、例えば、肺がん(例えば、小細胞肺がん(例えば、進展型SCLC(ES-SCLC)を含む小細胞肺がん(SCLC)、非小細胞肺がん(NSCLC)(平上皮性NSCLC又は非扁平上皮性NSCLCを含む(局所進行性切除不能NSCLC(例えば、IIIB期のNSCLC)を含む))、又は再発若しくは転移性NSCLC(例えば、IV期のNSCLC)、肺の腺癌)、UC、例えば、膀胱がん(例えば、MIBC)、尿路上皮膀胱がん(UBC)、膵臓がん(例えば、膵管腺癌(PDAC)、例えば、転移性PDAC))、腎臓がん又は腎がん(例えば、腎細胞癌腫(RCC))、黒色腫、頭頸部がん(例えば、頭頸部扁平上皮がん(HNSCC))、卵巣がん(OC)、胃がん(GC)(例えば、胃食道接合部(GEJ)がん)、肝細胞癌腫(HCC)、結腸直腸がん(CRC;例えば、マイクロサテライト安定(MSS)及びマイクロサテライト不安定性(MSI)低(MSI-低)のCRC)、又は乳がん(例えば、HER2+乳がん及びトリプルネガティブ乳がん(TNBC)(エストロゲン受容体(ER-)、プロゲステロン受容体(PgR-)、及びHER2(HER2-)陰性))をある程度まで阻害し、減速及び完全停止を含む;(2)腫瘍サイズの縮小;(3)隣接する末梢臓器及び/又は組織へのがん細胞浸潤の抑制(すなわち、減少、減速又は完全停止);(4)転移の阻害(すなわち、減少、減速又は完全停止);(5)疾患又は障害に関連する1つ以上の症状(例えば、がん)のある程度の軽減;(6)全生存及び無増悪生存を含む生存期間の延長又は延長;及び/又は(9)処置後の所与の時点で死亡率の低下、を含む対象に対する利益を示す任意のエンドポイントを使用して評定することができる。 "Individual response" or "response" includes, but is not limited to: (1) disease progression (cancer progression, e.g., lung cancer (e.g., small cell lung cancer, including small cell lung cancer [e.g., extensive-stage SCLC (ES-SCLC)); Cell lung cancer (SCLC), non-small cell lung cancer (NSCLC), including squamous NSCLC or non-squamous NSCLC (including locally advanced unresectable NSCLC (e.g., stage IIIB NSCLC)), or recurrence or metastasis UC, such as bladder cancer (eg, MIBC), urothelial bladder cancer (UBC), pancreatic cancer (eg, pancreatic ductal adenocarcinoma ( PDAC), e.g. metastatic PDAC)), renal cancer or kidney cancer (e.g. renal cell carcinoma (RCC)), melanoma, head and neck cancer (e.g. head and neck squamous cell carcinoma (HNSCC)), Ovarian cancer (OC), gastric cancer (GC) (e.g. gastroesophageal junction (GEJ) cancer), hepatocellular carcinoma (HCC), colorectal cancer (CRC; e.g. microsatellite stable (MSS) and microsatellite instability (MSI) low (MSI-low) CRC), or breast cancer (e.g., HER2+ breast cancer and triple negative breast cancer (TNBC) (estrogen receptor (ER-), progesterone receptor (PgR-), and HER2 (HER2 (2) reduction in tumor size; (3) suppression of cancer cell invasion into adjacent peripheral organs and/or tissues (i.e., reduction, (4) inhibition of metastasis (i.e., reduction, slowing or complete arrest); (5) some relief of one or more symptoms associated with the disease or disorder (e.g., cancer); (6) and/or (9) reduced mortality at a given time point after treatment using any endpoint that indicates benefit to the subject. can be graded.
本明細書で使用される場合、「病理学的完全奏効」(pCR)は、完全に切除された検体の残存浸潤がんがない患者の割合として定義される。乳がんとの関連において、「病理学的完全奏効」又は「pCR」は、乳がん及びリンパ節の両方からの腫瘍の根絶を指す(ypT0/はypN0である)。 As used herein, "pathologic complete response" (pCR) is defined as the percentage of patients with completely resected specimens with no residual invasive cancer. In the context of breast cancer, "pathologic complete response" or "pCR" refers to eradication of tumor from both breast cancer and lymph nodes (ypT0/ is ypN0).
尿路上皮癌腫(UC)に関して本明細書で使用される場合、「病理的進展度の低下率」は、膀胱切除術時に≦pT1pN0に達する患者の割合として定義される。 As used herein with respect to urothelial carcinoma (UC), "rate of reduction in pathologic extent" is defined as the proportion of patients reaching ≤pT1pN0 at cystectomy.
本明細書で使用される場合、「完全奏功」又は「CR」は、全標的病巣の消滅を指す。 As used herein, "complete response" or "CR" refers to the disappearance of all target lesions.
本明細書で使用される場合、「部分奏功」又は「PR」は、ベースラインSLDを参照として、標的病巣の最長径の合計(SLD)における少なくとも30%の低下を指す。 As used herein, "partial response" or "PR" refers to at least a 30% reduction in the sum of the longest diameters (SLD) of the target lesions relative to the baseline SLD.
本明細書で使用される場合、「客観的奏効率」(ORR)とは、完全奏功(CR)率と、部分奏功(PR)率との和を意味する。 As used herein, "objective response rate" (ORR) means the sum of the complete response (CR) rate and the partial response (PR) rate.
本明細書で使用される場合、「客観的応答期間」(DOR)は、疾患進行に対する実証された客観的応答の最初の発生からの時間、又は処置の最後の用量の30日間以内の任意の原因による死のうち、いずれか早く発生する時間として定義される。 As used herein, "period of objective response" (DOR) is the time from the first onset of a documented objective response to disease progression or any It is defined as the time of death from any cause, whichever occurs first.
「持続的応答」とは、処置の休止後に腫瘍成長を低減させることに対する持続的効果を指す。例えば、腫瘍サイズは、投与期の開始時のサイズと比較して同じままであるか又はより小さくなり得る。いくつかの態様では、持続性応答は、処置期間と少なくとも同じ期間、処置期間の少なくとも1.5倍、2.0倍、2.5倍、又は3.0倍の期間を有する。 "Durable response" refers to a sustained effect on reducing tumor growth after cessation of treatment. For example, tumor size may remain the same or become smaller compared to the size at the start of the dosing phase. In some aspects, the sustained response has a duration that is at least as long as the treatment period, at least 1.5, 2.0, 2.5, or 3.0 times the treatment period.
医薬を用いた処置に対する対象の「有効な応答」又は対象の「応答性」及び類似の単語は、がん等の疾患若しくは障害の危険性があるか又はそれを患う対象に付与される臨床的又は治療的有益性を指す。一態様では、そのような利益は、生存期間の延長(全生存期間及び無増悪生存期間を含む);客観的応答(CR又はPRを含む)をもたらす;又はがんの徴候若しくは症状を改善する、のいずれか1つ以上を含む。 A subject's "effective response" or a subject's "responsiveness" to treatment with a pharmaceutical agent and similar terms refer to a clinical term given to a subject at risk for or suffering from a disease or disorder, such as cancer. or refers to therapeutic benefit. In one aspect, such benefit is prolonged survival (including overall survival and progression-free survival); results in an objective response (including CR or PR); or ameliorates cancer signs or symptoms , any one or more of
処置に対して「有効な応答を有しない」対象とは、生存期間の延長(全生存期間及び無増悪生存期間を含む);客観的応答(CR又はPRを含む)をもたらす;又はがんの徴候若しくは症状を改善する、のいずれも有しない対象を指す。 A subject "no effective response" to treatment results in prolonged survival (including overall survival and progression-free survival); results in an objective response (including CR or PR); Refers to a subject who has neither improved signs nor symptoms.
本明細書で使用される場合、「生存」という用語は、患者が生存していることを指し、全生存、及び無増悪生存を含む。 As used herein, the term "survival" refers to patient survival and includes overall survival and progression-free survival.
本明細書で使用される場合、「全生存」及び「OS」は、患者がまだ生存している疾患(例えば、がん)の診断日又は処置開始日のいずれかからの時間の長さを指す。例えば、OSは、ランダム化から任意の原因による死亡までの時間として定義され得る。 As used herein, “overall survival” and “OS” refer to the length of time from either the date of diagnosis of the disease (e.g., cancer) or the date of initiation of treatment that the patient is still alive. Point. For example, OS can be defined as the time from randomization to death from any cause.
本明細書で使用される場合、「全生存率」は、特定の期間、例えば診断又は処置の時点から6ヵ月、1年又は5年後に生存している群の対象の割合を指す。 As used herein, "overall survival" refers to the proportion of subjects in a group who are alive after a specified period of time, eg, 6 months, 1 year or 5 years from the time of diagnosis or treatment.
本明細書で使用される場合、「無再発生存期間」(RFS)は、手術後の最初のサイクルにおける1日目から、疾患の最初に実証された再発までの時間又は任意の原因による死亡までの時間として定義される。
As used herein, "recurrence-free survival" (RFS) is the time from
本明細書で使用される場合、「無症候生存期間」(EFS)は、ランダム化から、疾患進行(例えば、治験責任医師によって評定される手術を妨げる進行);局所又は遠隔疾患再発;又は何らかの原因による死亡の事象のいずれか(いずれか最初に起こる)までの時間として定義される。 As used herein, "symptom-free survival" (EFS) is defined as from randomization to disease progression (e.g., progression precluding surgery as assessed by the investigator); local or distant disease recurrence; Defined as the time to either (whichever occurs first) event of death from any cause.
本明細書で使用される場合、「無増悪生存」(PFS)は、処置されている疾患(例えば、がん)が悪化しない、処置中及び処置後の時間の長さを指す。無増悪生存は、患者がCR又はPRを経験した時間量、並びに患者が安定な疾患を経験した時間量を含み得る。 As used herein, “progression-free survival” (PFS) refers to the length of time during and after treatment that the disease (eg, cancer) being treated does not get worse. Progression-free survival can include the amount of time a patient experiences a CR or PR, as well as the amount of time a patient experiences stable disease.
本明細書で使用される場合、「安定疾患」又は「SD」は、処置開始以降の最小SLDを基準として、CR又はPRと言えるほどの十分な標的病変の収縮も、PDと言えるほどの十分な増加もないことを指す。 As used herein, "stable disease" or "SD" is based on minimal SLD since treatment initiation, with target lesion shrinkage sufficient to qualify as CR or PR, or sufficient to qualify as PD. It means that there is no significant increase.
本明細書で使用される場合、「進行性疾患」又は「PD」とは、処置開始以降、又は1つ以上の新たな病変の存在以降、記録された最小SLDを基準として、標的病変の最長直径(SLD)の少なくとも20%の増加を指す。 As used herein, “progressive disease” or “PD” refers to the longest disease of a target lesion relative to the smallest SLD recorded since treatment initiation or since the presence of one or more new lesions. Refers to an increase in diameter (SLD) of at least 20%.
本明細書で使用される場合、「病理学的著効」(MPR)は、原発腫瘍の外科的切除時に10%以下の残存生存腫瘍として定義される。 As used herein, "pathologic response" (MPR) is defined as 10% or less residual viable tumor upon surgical resection of the primary tumor.
本明細書で使用される場合、疾患又は障害の「進行を遅らせる」とは、疾患又は障害(例えば、がん)の発生を延期する、妨げる、遅らせる、遅らせる、安定化させる、及び/又は延期することを指す。この遅延は、病歴及び/又は処置されている対象に応じて様々な期間のものであり得る。当業者に明らかであるように、十分又は著しい遅延は、対象が疾患を発症しないという点で、予防を事実上包含し得る。例えば、後期がんでは、中枢神経系(CNS)転移の発生が遅延し得る。 As used herein, "slowing progression" of a disease or disorder means postponing, preventing, delaying, delaying, stabilizing, and/or postponing the onset of a disease or disorder (e.g., cancer). refers to doing This delay can be of varying duration depending on the medical history and/or subject being treated. As will be apparent to one skilled in the art, a sufficient or significant delay can in effect encompass prophylaxis, in that the subject will not develop the disease. For example, in late-stage cancer, the development of central nervous system (CNS) metastases may be delayed.
本明細書で使用される場合、「がん再発を低減又は阻害する」という用語は、腫瘍若しくはがんの再発、又は腫瘍若しくはがんの進行を低減又は阻害することを意味する。 As used herein, the term "reducing or inhibiting cancer recurrence" means reducing or inhibiting tumor or cancer recurrence or tumor or cancer progression.
「低減又は阻害する」とは、20%、30%、40%、50%、60%、70%、75%、80%、85%、90%、95%、又はそれ以上の全体的な減少をもたらす能力を意味する。低減又は阻害は、処置されている障害(例えば、がん)の症状、転移の存在若しくはサイズ、又は原発腫瘍のサイズに対して言及する場合がある。 "Reduce or inhibit" means an overall reduction of 20%, 30%, 40%, 50%, 60%, 70%, 75%, 80%, 85%, 90%, 95% or more means the ability to bring about Reduction or inhibition may refer to the symptoms of the disorder (eg, cancer) being treated, the presence or size of metastases, or the size of the primary tumor.
「生存延長」による意味は、処置されていない患者に対して(例えば、医薬で処置されていない患者に対して)、又は指定されたレベルでバイオマーカーを発現しない患者に対して、かつ/又は承認済み抗腫瘍剤で処置された患者に対して、処置された患者における全生存期間又は無増悪生存期間が増加することである。客観的応答とは、CR又はPRを含む測定可能な応答を指す。 By "prolonged survival" is meant relative to untreated patients (e.g., untreated patients) or to patients who do not express the biomarker at a specified level, and/or An increase in overall survival or progression-free survival in treated patients relative to patients treated with approved anti-tumor agents. Objective response refers to a measurable response, including CR or PR.
「検出する」及び「検出」という用語は、標的分子の質的測定及び量的測定の両方を含むために本明細書で最も広義に使用される。検出は、単に試料中の標的分子の存在を特定すること、並びに標的分子が検出可能なレベルで試料中に存在するかを決定することを含む。検出は、直接的であっても間接的であってもよい。 The terms "detect" and "detection" are used most broadly herein to include both qualitative and quantitative measurement of target molecules. Detection involves simply identifying the presence of the target molecule in the sample as well as determining whether the target molecule is present in the sample at detectable levels. Detection may be direct or indirect.
本明細書で使用される場合、「PD-L1陽性腫瘍細胞分率」は、免疫組織化学(IHC)アッセイ、例えば抗体SP263、SP142、22C3、又は28-8を使用してPD-L1を染色するためのIHCアッセイに関して試料の染色後に、試料中に存在する全ての生存腫瘍細胞に対して任意の強度で部分的又は完全な膜染色(細胞質染色を除く)を示す生存腫瘍細胞のパーセンテージである。したがって、PD-L1陽性腫瘍細胞分率は、PD-L1 IHC SP263(Ventana)アッセイを使用して、例えば、式:PD-L1陽性腫瘍細胞分率=(PD-L1陽性腫瘍細胞の数)/(PD-L1陽性及びPD-L1陰性腫瘍細胞の総数)によって計算することができ、腫瘍細胞及び全ての非腫瘍細胞(例えば、腫瘍浸潤免疫細胞、正常細胞、壊死細胞及び残屑)のPD-L1細胞質染色は、評価及びスコアリングから除外される。任意の所与の診断PD-L1抗体は、PD-L1陽性腫瘍細胞分率を得るために使用することのできる特定のIHCアッセイプロトコル及び/又はスコアリング用語に対応し得ることが理解されるであろう。例えば、PD-L1陽性腫瘍細胞分率は、それぞれBenchmark ULTRAでのOPTIVIEW(登録商標)検出、AutostainerLink 48でのEnVision Flex、Benchmark ULTRAでのOPTIVIEW(登録商標)検出及び増幅、又はAutostainerLink 48でのEnVision Flexを使用して、SP263、22C3、SP142、又は28-8で染色した腫瘍細胞試料から得ることができる。別の例では、PD-L1 IHC 22C3 pharmDxアッセイ(Dako)を上記の式に従って使用して、PD-L1陽性腫瘍細胞分率を計算することができる。当業者は、IHCアッセイで使用される異なるPD-L1抗体間で感度が変動し得ることを理解するであろう。例えば、28-8又は22C3及びSP263で染色することによってそれぞれ定義される1% TC又は25% TC閾値を満たす試料の約64%のみが、SP142を使用して染色した場合に閾値を満たす。Hirsch et al.,Journal of Thoracic Oncology 2016,12(2):208-222.本明細書で使用される場合、PD-L1陽性腫瘍細胞分率及び「腫瘍割合スコア」(TPS)という用語は互換的に使用される。 As used herein, a “PD-L1 positive tumor cell fraction” is an immunohistochemistry (IHC) assay, such as those staining for PD-L1 using antibodies SP263, SP142, 22C3, or 28-8. Percentage of viable tumor cells showing partial or complete membrane staining (excluding cytoplasmic staining) of any intensity relative to all viable tumor cells present in the sample after staining of the sample for an IHC assay for . Therefore, the PD-L1 positive tumor cell fraction can be determined using the PD-L1 IHC SP263 (Ventana) assay, eg, with the formula: PD-L1 positive tumor cell fraction = (number of PD-L1 positive tumor cells)/ (total number of PD-L1-positive and PD-L1-negative tumor cells), the PD- L1 cytoplasmic staining is excluded from evaluation and scoring. It will be appreciated that any given diagnostic PD-L1 antibody may correspond to a particular IHC assay protocol and/or scoring term that can be used to obtain a PD-L1 positive tumor cell fraction. be. For example, the PD-L1 positive tumor cell fraction can be determined by OPTVIEW® detection on Benchmark ULTRA, EnVision Flex on AutostainerLink 48, OPTVIEW® detection and amplification on Benchmark ULTRA, or EnVision on AutostainerLink 48, respectively. Flex can be used from tumor cell samples stained with SP263, 22C3, SP142, or 28-8. In another example, the PD-L1 IHC 22C3 pharmDx assay (Dako) can be used according to the formula above to calculate the PD-L1 positive tumor cell fraction. One skilled in the art will appreciate that sensitivity may vary between different PD-L1 antibodies used in IHC assays. For example, only about 64% of the samples meeting the 1% TC or 25% TC threshold defined by staining with 28-8 or 22C3 and SP263, respectively, meet the threshold when stained using SP142. Hirsch et al. , Journal of Thoracic Oncology 2016, 12(2): 208-222. As used herein, the terms PD-L1 positive tumor cell fraction and "tumor percentage score" (TPS) are used interchangeably.
本明細書で使用される場合、「Ventana SP142 IHCアッセイ」は、参照によりその全体が本明細書に組み込まれるVentana PD-L1(SP142)Assay添付文書(アリゾナ州ツーソン:Ventana Medical Systems,Inc.)に従って行われる。 As used herein, "Ventana SP142 IHC assay" refers to the Ventana PD-L1 (SP142) Assay package insert (Tucson, AZ: Ventana Medical Systems, Inc.), which is incorporated herein by reference in its entirety. carried out according to
本明細書で使用される場合、「Ventana SP263 IHCアッセイ」は、Ventana PD-L1(SP263)アッセイ添付文書(アリゾナ州ツーソン:Ventana Medical Systems,Inc.)に記載され、参照によりその全体が本明細書に組み込まれる。 As used herein, the "Ventana SP263 IHC assay" is described in the Ventana PD-L1 (SP263) assay package insert (Tucson, Ariz.: Ventana Medical Systems, Inc.), which is incorporated herein by reference in its entirety. incorporated into the book.
本明細書で使用される場合、「pharmDx 22C3 IHCアッセイ」は、その全体が参照により本明細書に組み込まれるPD-L1 IHC 22C3 pharmDx添付文書(カリフォルニア州カーピンテリア:Dako,Agilent Pathology Solutions)に従って行われる。 As used herein, the "pharmDx 22C3 IHC assay" is according to the PD-L1 IHC 22C3 pharmDx package insert (Carpinteria, Calif.: Dako, Agilent Pathology Solutions), which is incorporated herein by reference in its entirety. done.
本明細書で使用される場合、「pharmDx 28-8 IHCアッセイ」は、その全体が参照により本明細書に組み込まれるPD-L1 IHC 28-8 pharmDx添付文書(カリフォルニア州カーピンテリア:Dako,Agilent Pathology Solutions)に従って行われる。 As used herein, "pharmDx 28-8 IHC assay" refers to the PD-L1 IHC 28-8 pharmDx package insert (Carpinteria, CA: Dako, Agilent), which is incorporated herein by reference in its entirety. Pathology Solutions).
「腫瘍浸潤免疫細胞」とは、本明細書で使用される場合、腫瘍又はその試料中に存在する任意の免疫細胞を指す。腫瘍浸潤免疫細胞としては、腫瘍内免疫細胞、腫瘍周辺免疫細胞、他の腫瘍間質細胞(例えば、線維芽細胞)、又はこれらの任意の組合せが挙げられるが、これらに限定されない。そのような腫瘍浸潤免疫細胞は、例えばTリンパ球(CD8+Tリンパ球及び/又はCD4+Tリンパ球等)、Bリンパ球、又は顆粒球(例えば、好中球、好酸球、及び好塩基球)、単球、マクロファージ、樹状細胞(例えば、互いに組み合う樹状細胞)、組織球、及びナチュラルキラー細胞を含む他の骨髄系細胞であり得る。 A "tumor-infiltrating immune cell" as used herein refers to any immune cell present in a tumor or sample thereof. Tumor-infiltrating immune cells include, but are not limited to, intratumoral immune cells, peritumoral immune cells, other tumor stromal cells (eg, fibroblasts), or any combination thereof. Such tumor-infiltrating immune cells are, for example, T lymphocytes (such as CD8+ T lymphocytes and/or CD4+ T lymphocytes), B lymphocytes, or granulocytes (e.g., neutrophils, eosinophils, and basophils), It can be monocytes, macrophages, dendritic cells (eg, dendritic cells that assemble with each other), histiocytes, and other myeloid cells, including natural killer cells.
本明細書で使用される場合、「バイオマーカー」という用語は、試料、例えばPD-L1、ctDNA、又はサイトカイン(例えば、T細胞活性化及び/又はリンパ球亜集団に関連するサイトカイン)で検出することができる指標、例えば予測、診断、及び/又は予後を指す。バイオマーカーは、ある特定の分子的、病理学的、組織学的、及び/又は臨床的特徴によって特徴付けられる疾患又は障害(例えば、がん)の特定のサブタイプの指標としての機能を果たし得る。いくつかの態様では、バイオマーカーは遺伝子である。バイオマーカーとしては、ポリペプチド、ポリヌクレオチド(例えば、DNA(例えば、ctDNA)、及び/又はRNA)、ポリヌクレオチドコピー数の変化(例えば、DNAコピー数)、ポリペプチド及びポリヌクレオチド修飾(例えば、翻訳後修飾)、炭水化物、及び/又は糖脂質ベースの分子マーカーが挙げられるが、これらに限定されない。いくつかの態様では、バイオマーカーはPD-L1である。いくつかの態様では、バイオマーカーはctDNAである。いくつかの態様では、バイオマーカーは、1つ以上のサイトカイン(例えば、T細胞活性化及び/又はリンパ球亜集団に関連する1つ以上のサイトカイン)である。いくつかの態様では、バイオマーカーは細胞(例えば免疫細胞、例えばT細胞、例えばT細胞サブセット、例えば活性化T細胞)である。いくつかの態様では、バイオマーカーは、ヒトパピローマウイルス(HPV)状態の直接的又は間接的な指標である。いくつかの態様では、バイオマーカーはp 16である。いくつかの態様では、バイオマーカーはHPVタンパク質又は核酸である。 As used herein, the term "biomarker" is detected in a sample, such as PD-L1, ctDNA, or cytokines (eg, cytokines associated with T cell activation and/or lymphocyte subpopulations) It refers to a predictable, diagnostic, and/or prognostic indicator. A biomarker can serve as an indicator of a particular subtype of a disease or disorder (e.g., cancer) characterized by certain molecular, pathological, histological, and/or clinical features. . In some embodiments, biomarkers are genes. Biomarkers include polypeptides, polynucleotides (e.g., DNA (e.g., ctDNA), and/or RNA), polynucleotide copy number changes (e.g., DNA copy number), polypeptide and polynucleotide modifications (e.g., translational post-modification), carbohydrate, and/or glycolipid-based molecular markers. In some aspects, the biomarker is PD-L1. In some aspects, the biomarker is ctDNA. In some aspects, the biomarkers are one or more cytokines (eg, one or more cytokines associated with T cell activation and/or lymphocyte subpopulations). In some aspects, the biomarkers are cells (eg, immune cells, eg, T cells, eg, T cell subsets, eg, activated T cells). In some aspects, a biomarker is a direct or indirect indicator of human papillomavirus (HPV) status. In some aspects, the biomarker is p16. In some aspects, the biomarkers are HPV proteins or nucleic acids.
「ハウスキーピングバイオマーカー」という用語は、通常、全ての細胞型に同様に存在する、バイオマーカー又はバイオマーカー(例えば、ポリヌクレオチド及び/又はポリペプチド)の群を指す。いくつかの態様では、ハウスキーピングバイオマーカーは「ハウスキーピング遺伝子」である。「ハウスキーピング遺伝子」は、本明細書において、その活性が細胞機能の維持に必須であるタンパク質をコードし、通常、全ての細胞型に同様に存在する遺伝子又は遺伝子の群を指す。 The term "housekeeping biomarker" generally refers to a biomarker or group of biomarkers (eg, polynucleotides and/or polypeptides) that are similarly present in all cell types. In some aspects, the housekeeping biomarker is a "housekeeping gene." A "housekeeping gene", as used herein, refers to a gene or group of genes that encode proteins whose activity is essential for the maintenance of cellular function and are generally similarly present in all cell types.
本明細書で使用される場合、「循環腫瘍DNA」及び「ctDNA」は、細胞に関連しない循環系の腫瘍由来DNAを指す。ctDNAは、腫瘍細胞又は循環腫瘍細胞(CTC)に由来し得る無細胞DNA(cfDNA)の一種である。ctDNAは、例えば、患者の血流中、又は患者から得られた生物学的試料(例えば、血液、血清、血漿又は尿)中に見出され得る。いくつかの態様では、ctDNAは、異常突然変異(例えば、患者特異的バリアント)及び/又はメチル化パターンを含み得る。 As used herein, "circulating tumor DNA" and "ctDNA" refer to tumor-derived DNA in the circulating system that is not associated with cells. ctDNA is a type of cell-free DNA (cfDNA) that can be derived from tumor cells or circulating tumor cells (CTCs). ctDNA can be found, for example, in a patient's bloodstream or in a biological sample obtained from a patient (eg, blood, serum, plasma, or urine). In some aspects, the ctDNA may contain aberrant mutations (eg, patient-specific variants) and/or methylation patterns.
「抗体」という用語は、モノクローナル抗体(免疫グロブリンFc領域を有する完全長抗体を含む)、ポリクローナル抗体、ポリエピトープ特異性を有する抗体組成物、多重特異性抗体(例えば、二重特異性抗体)、ダイアボディ、及び単鎖分子、並びに所望の生物学的活性を示す限り、Fab、F(ab’)2、及びFv等の抗原結合フラグメントを含む抗体フラグメントを含む。「免疫グロブリン」(Ig)という用語は、本明細書において「抗体」と互換的に使用される。一例では、抗体は完全長モノクローナル抗体である。 The term "antibody" includes monoclonal antibodies (including full-length antibodies having an immunoglobulin Fc region), polyclonal antibodies, antibody compositions with polyepitopic specificity, multispecific antibodies (e.g., bispecific antibodies), Included are diabodies and single chain molecules, as well as antibody fragments, including antigen binding fragments such as Fab, F(ab') 2 and Fv, so long as they exhibit the desired biological activity. The term "immunoglobulin" (Ig) is used interchangeably with "antibody" herein. In one example, the antibody is a full-length monoclonal antibody.
本明細書で使用されるIgG「アイソタイプ」又は「サブクラス」という用語は、それらの定常領域の化学的及び抗原的特性によって定義される免疫グロブリンのサブクラスのうちのいずれかを意味する。 The terms IgG "isotype" or "subclass" as used herein refer to any of the immunoglobulin subclasses defined by the chemical and antigenic properties of their constant regions.
それらの重鎖の定常ドメインのアミノ酸配列に応じて、抗体(免疫グロブリン)は、異なるクラスに割り当てられ得る。免疫グロブリンには5つの主なクラス:IgA、IgD、IgE、IgG、及びIgMがあり、これらのいくつかは、サブクラス(アイソタイプ)、例えば、IgG1、IgG2、IgG3、IgG4、IgA1、及びIgA2に更に分類することができる。免疫グロブリンの異なるクラスに対応する重鎖定常ドメインは、それぞれ、α、γ、ε、γ、及びμと呼ばれる。異なるクラスの免疫グロブリンのサブユニット構造及び三次元構成は周知であり、例えば、Abbas et al.Cellular and Mol.Immunology,4th ed.(W.B.Saunders,Co.,2000)に一般に記載されている。抗体は、抗体と1つ以上の他のタンパク質又はペプチドとの共有又は非共有会合によって形成されるより大きい融合分子の一部であり得る。 Depending on the amino acid sequences of the constant domain of their heavy chains, antibodies (immunoglobulins) can be assigned to different classes. There are five main classes of immunoglobulins: IgA, IgD, IgE, IgG and IgM, some of which are further subclassed (isotypes), e.g. can be classified. The heavy-chain constant domains that correspond to the different classes of immunoglobulins are called α, γ, ε, γ, and μ, respectively. The subunit structures and three-dimensional organization of different classes of immunoglobulins are well known, see, for example, Abbas et al. Cellular and Mol. Immunology, 4th ed. (WB Saunders, Co., 2000). An antibody can be part of a larger fusion molecule formed by covalent or non-covalent association of the antibody with one or more other proteins or peptides.
基本的な4本の鎖の抗体ユニットは、2本の同一な軽鎖(L)と2本の同一な重鎖(H)とから構成されるヘテロ四量体糖タンパク質である。IgM抗体は、5つの基本的なヘテロ四量体ユニットと併せて、J鎖と呼ばれる追加のポリペプチドからなり、10個の抗原結合部位を含有しているが、一方でIgA抗体は、2~5個の基本的な4本鎖ユニットから構成されており、このユニットは、重合してJ鎖と組み合わさった多価集合体を形成することができる。IgGの場合、4本鎖ユニットは、一般に、約150,000ダルトンである。各L鎖は、1つのジスルフィド共有結合によってH鎖に連結されているが、一方で2本のH鎖は、H鎖アイソタイプに応じて1つ以上のジスルフィド結合によって互いに連結されている。H鎖及びL鎖はそれぞれ、規則的に離間した鎖間ジスルフィド架橋も有する。各H鎖は、N末端に可変ドメイン(VH)を有し、続いてα鎖及びγ鎖のそれぞれについては3つの定常ドメイン(CH)、並びにμ及びεアイソタイプについては4つのCHドメインを有する。各L鎖は、N末端に可変ドメイン(VL)を有し、続いてその反対側の端部に定常ドメインを有する。VLは、VHと整列しており、CLは、重鎖の第1の定常ドメイン(CH1)と整列している。特定のアミノ酸残基は、軽鎖可変ドメインと重鎖可変ドメインとの間に界面を形成すると考えられている。VHとVLとが一緒に対合することにより、単一の抗原結合部位を形成する。様々なクラスの抗体の構造及び特性については、例えば、Basic and Clinical Immunology,8th Edition,Daniel P.Sties,Abba I.Terr and Tristram G.Parsolw(eds),Appleton&Lange,Norwalk,CT,1994の71頁及び第 6章を参照されたい。任意の脊椎動物種に由来するL鎖は、それらの定常ドメインのアミノ酸配列に基づいて、カッパ及びラムダと呼ばれる2つの明確に異なる種類のうちの1つに割り当てられ得る。それらの重鎖(CH)の定常ドメインのアミノ酸配列に応じて、免疫グロブリンは、異なるクラス又はアイソタイプに割り当てることができる。免疫グロブリンには、IgA、IgD、IgE、IgG、及びIgMの5つのクラスがあり、それぞれ、α、δ、ε、γ、及びμと表記される重鎖を有する。γ及びαクラスは、更に、CH配列及び機能における比較的わずかな相違に基づいて更にサブクラスに分類され、例えば、ヒトは、以下のサブクラス:IgG1、IgG2A、IgG2B、IgG3、IgG4、IgA1、及びIgA2を発現する。
The basic four-chain antibody unit is a heterotetrameric glycoprotein composed of two identical light (L) chains and two identical heavy (H) chains. IgM antibodies consist of five basic heterotetrameric units, plus an additional polypeptide called the J chain, which contains ten antigen-binding sites, whereas IgA antibodies consist of two to It is composed of five basic four-stranded units, which can polymerize to form multivalent assemblies that combine with J chains. For IgG, a four-stranded unit is generally about 150,000 daltons. Each L chain is linked to an H chain by one covalent disulfide bond, while the two H chains are linked to each other by one or more disulfide bonds depending on the H chain isotype. Each H and L chain also has regularly spaced intrachain disulfide bridges. Each H chain has at its N-terminus a variable domain (V H ) followed by three constant domains (C H ) for each of the α and γ chains and four C H domains for the μ and ε isotypes. have Each L chain has at its N-terminus a variable domain (V L ) followed by a constant domain at its opposite end. The V L is aligned with the V H and the C L is aligned with the first constant domain (C H 1) of the heavy chain. Particular amino acid residues are believed to form an interface between the light and heavy chain variable domains. The VH and VL pair together to form a single antigen-binding site. For the structure and properties of various classes of antibodies, see, eg, Basic and Clinical Immunology, 8th Edition, Daniel P.; Sties, Abba I.; Terr and TristramG. See page 71 and
本明細書で使用される、「超可変領域」又は「HVR」という用語は、配列において超可変性であり、抗原結合特異性を決定する、抗体可変ドメインの領域、例えば「相補性決定領域」(CDR)のそれぞれを指す。
一般に、抗体は6つのCDRを含み、3つがVH中にあり(CDR-H1、CDR-H2、CDR-H3)、3つがVL中にある(CDR-L1、CDR-L2、CDR-L3)。本明細書における例示的なCDRとしては、
(a)アミノ酸残基26-32(L1)、50-52(L2)、91-96(L3)、26-32(H1)、53-55(H2)及び96-101(H3)で生じる超可変ループ(Chothia and Lesk,J.Mol.Biol.196:901-917(1987));
As used herein, the term "hypervariable region" or "HVR" refers to regions of antibody variable domains that are hypervariable in sequence and determine antigen-binding specificity, e.g., "complementarity determining regions" (CDR).
In general, antibodies contain 6 CDRs, 3 in VH (CDR-H1, CDR-H2, CDR-H3) and 3 in VL (CDR-L1, CDR-L2, CDR-L3). Exemplary CDRs herein include:
(a) excesses occurring at amino acid residues 26-32 (L1), 50-52 (L2), 91-96 (L3), 26-32 (H1), 53-55 (H2) and 96-101 (H3); variable loops (Chothia and Lesk, J. Mol. Biol. 196:901-917 (1987));
(b)アミノ酸残基24-34(L1)、50-56(L2)、89-97(L3)、31-35b(H1)、50-65(H2)及び95-102(H3)に存在するCDR(Kabat et al.,Sequences of Proteins of Immunological Interest,5th Ed.Public Health Service,National Institutes of Health,Bethesda,MD(1991));並びに (b) at amino acid residues 24-34 (L1), 50-56 (L2), 89-97 (L3), 31-35b (H1), 50-65 (H2) and 95-102 (H3); CDR (Kabat et al., Sequences of Proteins of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, Md. (1991));
(c)アミノ酸残基27c-36(L1)、46-55(L2)、89-96(L3)、30-35b(H1)、47-58(H2)及び93-101(H3)で生じる抗原接触(MacCallum et al.J.Mol.Biol.262:732-745(1996))が挙げられる。 (c) antigens occurring at amino acid residues 27c-36 (L1), 46-55 (L2), 89-96 (L3), 30-35b (H1), 47-58 (H2) and 93-101 (H3) contact (MacCallum et al. J. Mol. Biol. 262:732-745 (1996)).
特に断りのない限り、CDRは、上記のKabat et al.に従い決定される。当業者は、CDRの表記は、上記Chothia、上記McCallum、又は、任意の他の、科学的に認可された命名システムに従い決定することができることを理解するであろう。 Unless otherwise noted, CDRs are according to Kabat et al., supra. determined according to Those skilled in the art will appreciate that CDR designations may be determined according to Chothia, supra, McCallum, supra, or any other scientifically accepted nomenclature system.
「フレームワーク」又は「FR」は、相補性決定領域(CDR)以外の可変ドメイン残基を指す。可変ドメインのFRは、一般的に、FR1、FR2、FR3及びFR4の4つのFRドメインからなる。したがって、CDR及びFR配列は、一般に、VH(又はVL)において次の配列:FR1-CDR-H1(CDR-L1)-FR2-CDR-H2(CDR-L2)-FR3-CDR-H3(CDR-L3)-FR4。 "Framework" or "FR" refers to variable domain residues other than the complementarity determining regions (CDRs). The FRs of a variable domain generally consist of four FR domains, FR1, FR2, FR3 and FR4. Thus, the CDR and FR sequences are generally arranged in the VH (or VL) in the following sequence: FR1-CDR-H1 (CDR-L1)-FR2-CDR-H2 (CDR-L2)-FR3-CDR-H3 (CDR- L3)-FR4.
「Kabatにおけるような可変ドメイン残基ナンバリング」又は「Kabatにおけるようなアミノ酸位置ナンバリング」という用語、及びそれらの変形は、上記のKabat et al.における抗体の編集物の重鎖可変ドメイン又は軽鎖可変ドメインに使用されるナンバリングシステムを指す。このナンバリングシステムを使用して、実際の直鎖状アミノ酸配列は、可変ドメインのFR若しくはHVRの短縮、又はそれへの挿入に対応する、より少ないアミノ酸又は追加のアミノ酸を含み得る。例えば、重鎖可変ドメインは、H2の残基52の後に単一のアミノ酸挿入(例えば、Kabatに従った残基52a)を含み、重鎖FR残基82の後に挿入された残基(例えば、Kabatに従った残基82a、82b、及び82c等)を含み得る。残基のKabatナンバリングは、所与の抗体に対して、抗体の配列と「標準の」Kabatによってナンバリングされた配列との相同領域での整列によって決定され得る。 The terms "variable domain residue numbering as in Kabat" or "amino acid position numbering as in Kabat" and variations thereof are described in Kabat et al. refers to the numbering system used for the heavy or light chain variable domains of antibody compilations in . Using this numbering system, the actual linear amino acid sequence may contain fewer or additional amino acids corresponding to truncations or insertions into the FRs or HVRs of the variable domain. For example, the heavy chain variable domain contains a single amino acid insertion after residue 52 of H2 (e.g. residue 52a according to Kabat) and the inserted residue after heavy chain FR residue 82 (e.g. residues 82a, 82b, and 82c, etc.) according to Kabat). The Kabat numbering of residues can be determined for a given antibody by aligning the regions of homology between the antibody's sequence and the "standard" Kabat numbered sequences.
Kabatナンバリングシステムは、一般に、可変ドメイン中の残基(およそ軽鎖の残基1~107及び重鎖の残基1~113)を指す場合に使用される(例えば、Kabat et al.,Sequences of Immunological Interest.5th Ed.Public Health Service,National Institutes of Health,Bethesda,Md.(1991))。「EUナンバリングシステム」又は「EU指標」は、一般に、免疫グロブリン重鎖定常領域における残基について言及する際に使用される(例えば、上記のKabat et al.で報告されるEU指標)。「KabatにおけるようなEUインデックス」は、ヒトIgG1 EU抗体の残基ナンバリングを指す。 The Kabat numbering system is generally used when referring to residues in variable domains, approximately residues 1-107 of the light chain and 1-113 of the heavy chain (see, eg, Kabat et al., Sequences of Immunological Interest, 5th Ed. Public Health Service, National Institutes of Health, Bethesda, Md. (1991)). The "EU numbering system" or "EU index" is commonly used when referring to residues in immunoglobulin heavy chain constant regions (eg, the EU index reported in Kabat et al., supra). The "EU index as in Kabat" refers to the residue numbering of the human IgG1 EU antibody.
「可変」という用語は、可変ドメインの特定のセグメントが、配列において抗体間で広範囲にわたって異なるという事実を指す。Vドメインは、抗原結合を媒介し、特定の抗体の、その特定の抗原に対する特異性を定義する。しかしながら、可変性は、可変ドメイン全体に均等に分布しているわけではない。むしろ、それは、軽鎖及び重鎖の両方の可変ドメインにおいて、超可変領域(HVR)と呼ばれる3つのセグメントに集中している。可変ドメインのより高度に保存された部分は、フレームワーク領域(FR)と呼ばれる。天然の重鎖及び軽鎖の可変ドメインはそれぞれ、ベータ-シート構造を接続し、かついくつかの場合では、ベータ-シート構造の一部を形成するループを形成する3つのHVRによって接続されたベータシート立体配置を大いに採用する4つのFR領域を含む。各鎖内のHVRは、FR領域によって近接して互いに結び付いており、他方の鎖のHVRと共に、抗体の抗原結合部位の形成に寄与する(Kabat et al.,Sequences of Immunological Interest,Fifth Edition,National Institute of Health,Bethesda,MD(1991)を参照されたい)。定常ドメインは、抗原への抗体の結合に直接関与しないが、抗体依存性細胞毒性における抗体の関与等、様々なエフェクター機能を示す。 The term "variable" refers to the fact that certain segments of the variable domains differ extensively in sequence among antibodies. The V domain mediates antigen binding and defines the specificity of a particular antibody for its particular antigen. However, the variability is not evenly distributed throughout the variable domains. Rather, it is concentrated in three segments called hypervariable regions (HVRs) in both the light and heavy chain variable domains. The more highly conserved portions of variable domains are called the framework regions (FR). The variable domains of the naturally occurring heavy and light chains each connect a beta-sheet structure and, in some cases, a beta connected by three HVRs forming a loop forming part of the beta-sheet structure. It contains four FR regions that heavily adopt the seat configuration. The HVRs within each chain are closely linked to each other by the FR regions and, together with the HVRs of the other chain, contribute to the formation of the antibody's antigen-binding site (Kabat et al., Sequences of Immunological Interest, Fifth Edition, National Institute of Health, Bethesda, Md. (1991)). The constant domains are not directly involved in binding an antibody to an antigen, but exhibit various effector functions, such as participation of the antibody in antibody-dependent cellular cytotoxicity.
抗体の「可変領域」又は「可変ドメイン」とは、抗体の重鎖又は軽鎖のアミノ末端ドメインを指す。重鎖及び軽鎖の可変ドメインは、それぞれ、「VH」及び「VL」と称されてもよい。これらのドメインは、一般に、抗体の最も可変性の高い部分であり(同じクラスの他の抗体と比べて)、抗原結合部位を含有する。 An antibody "variable region" or "variable domain" refers to the amino-terminal domain of the heavy or light chain of an antibody. The heavy and light chain variable domains may also be referred to as "VH" and "VL", respectively. These domains are generally the most variable parts of an antibody (relative to other antibodies of the same class) and contain the antigen binding sites.
「フレームワーク」又は「FR」は、超可変領域(hypervariable region:HVR)残基以外の可変ドメイン残基を指す。可変ドメインのFRは、概して、FR1、FR2、FR3及びFR4の4つのFRドメインからなる。したがって、HVR及びFR配列は、一般的に、VH(又はVL)中において以下の配列で現れる:FR1-H1(L1)-FR2-H2(L2)-FR3-H3(L3)-FR4。 "Framework" or "FR" refers to variable domain residues other than hypervariable region (HVR) residues. The FRs of a variable domain generally consist of four FR domains: FR1, FR2, FR3 and FR4. Thus, HVR and FR sequences generally appear in VH (or VL) in the following sequence: FR1-H1 (L1)-FR2-H2 (L2)-FR3-H3 (L3)-FR4.
「完全長抗体」、「インタクトな抗体」、及び「全抗体」という用語は、抗体フラグメントとは対照的に、その実質的にインタクトな形態にある抗体を指して互換的に使用される。具体的には、全抗体は、Fc領域を含む重鎖及び軽鎖を有するものを含む。定常ドメインは、天然配列の定常ドメイン(例えば、ヒト天然配列の定常ドメイン)又はそのアミノ酸配列バリアントであり得る。一部の場合では、インタクトな抗体は、1つ以上のエフェクター機能を有し得る。 The terms "full-length antibody," "intact antibody," and "whole antibody" are used interchangeably to refer to an antibody in its substantially intact form, as opposed to antibody fragments. Specifically, whole antibodies include those having heavy and light chains, including an Fc region. The constant domains may be native sequence constant domains (eg, human native sequence constant domains) or amino acid sequence variant thereof. In some cases, an intact antibody may possess one or more effector functions.
「裸の抗体」は、異種性部分(例えば、細胞傷害性部分)又は放射標識にコンジュゲートされていない抗体を指す。ネイキッド抗体は、医薬組成物中に存在していてもよい。
「抗体フラグメント」は、インタクトな抗体の一部分、好ましくは、インタクトな抗体の抗原結合領域及び/又は可変領域を含む。抗体フラグメントの例として、Fab、Fab’、F(ab’)2;ダイアボディ;線状抗体(米国特許第5,641,870号の実施例2;Zapata et al.,Protein Eng.8(10):1057-1062[1995]
A "naked antibody" refers to an antibody that is not conjugated to a heterologous moiety (eg, a cytotoxic moiety) or radiolabel. A naked antibody may be present in a pharmaceutical composition.
An "antibody fragment" comprises a portion of an intact antibody, preferably the antigen-binding region and/or variable region of the intact antibody. Examples of antibody fragments include Fab, Fab', F(ab') 2 ; diabodies; linear antibodies (Example 2 of US Pat. No. 5,641,870; Zapata et al., Protein Eng. 8 (10 ): 1057-1062 [1995]
を参照されたい);一本鎖抗体分子;及び抗体フラグメントから形成される多重特異性抗体が挙げられるが、これらに限定されない。抗体のパパイン消化により、「Fab」フラグメントと呼ばれる2つの同一な抗原結合フラグメントと、容易に結晶化する能力を反映して表記される残りの「Fc」フラグメントとが得られた。Fabフラグメントは、L鎖全体と共にH鎖の可変領域ドメイン(VH)、並びに1つの重鎖の第1の定常ドメイン(CH1)からなる。各Fabフラグメントは、抗原結合に関しては一価である、すなわち、単一の抗原結合部位を有する。抗体のペプシン処置により、単一の大きなF(ab’)2フラグメントが得られ、これは、異なる抗原結合活性を有する2つのFabフラグメントがジスルフィド結合したものにほぼ相当し、依然として抗原に架橋することが可能である。Fab’フラグメントは、抗体のヒンジ領域由来の1つ以上のシステインを含め、CH1ドメインのカルボキシ末端に数個の追加の残基を有することが、Fabフラグメントとは異なる。Fab’-SHは、定常ドメインのシステイン残基(複数可)が、遊離チオール基を持つFab’の本明細書での呼称である。F(ab’)2抗体フラグメントは、元来、間にヒンジシステインを有するFab’フラグメントの対として産生されたものであった。抗体フラグメントの他の化学的カップリングも公知である。
single-chain antibody molecules; and multispecific antibodies formed from antibody fragments. Papain digestion of antibodies yields two identical antigen-binding fragments, called "Fab" fragments, and a residual "Fc" fragment, designated to reflect its ability to crystallize readily. A Fab fragment consists of the variable region domain of the H chain (V H ) along with the entire L chain, as well as the first constant domain of one heavy chain (C H 1). Each Fab fragment is monovalent with respect to antigen binding, ie, has a single antigen binding site. Pepsin treatment of the antibody yields a single large F(ab') 2 fragment that roughly corresponds to a disulfide-linked disulfide-bonded Fab fragment with different antigen-binding activities, yet capable of cross-linking antigen. is possible. Fab' fragments differ from Fab fragments by having a few additional residues at the carboxy terminus of the
Fcフラグメントは、ジスルフィドによって一緒に保持された両方のH鎖のカルボキシ末端を含む。抗体のエフェクター機能は、Fc領域における配列によって決定され、この領域はまた、ある特定の細胞型に見られるFc受容体(FcR)によって認識される。 The Fc fragment contains the carboxy termini of both heavy chains held together by a disulfide. The effector functions of antibodies are determined by sequences in the Fc region, which region is also recognized by Fc receptors (FcR) found on certain cell types.
本発明の抗体の「機能性フラグメント」は、インタクトな抗体の一部分を含み、これには、概して、インタクトな抗体の抗原結合領域若しくは可変領域、又はFcR結合能力を保持するか若しくは修飾されたFcR結合能力を有する抗体のFc領域が含まれる。抗体フラグメントの例としては、線形抗体、一本鎖抗体分子、及び抗体フラグメントから形成された多重特異性抗体が挙げられる。 A "functional fragment" of an antibody of the invention comprises a portion of an intact antibody, generally including the antigen-binding or variable region of an intact antibody, or an FcR that retains FcR-binding ability or has been modified. Included are Fc regions of antibodies capable of binding. Examples of antibody fragments include linear antibodies, single chain antibody molecules, and multispecific antibodies formed from antibody fragments.
「Fv」とは、完全な抗原認識及び抗原結合部位を含む最小抗体フラグメントである。このフラグメントは1つの重鎖可変領域ドメインと1つの軽鎖可変領域ドメインが、非共有結合で緊密に結合した二量体からなる。これらの2つのドメインの折り畳みにより、抗原結合のためのアミノ酸残基を提供し、かつ抗原結合特異性を抗体に与える6つの超可変ループ(H鎖及びL鎖から各3つループ)が生じる。しかし、単一の可変ドメイン(又は抗原に特異的なHVRを3つしか含まないFvの半分)であっても、全結合部位よりも低い親和性であるが、抗原を認識し、それに結合する能力を有する。 "Fv" is the minimum antibody fragment which contains a complete antigen-recognition and -binding site. This fragment consists of a dimer of one heavy and one light chain variable region domain in tight, non-covalent association. Folding of these two domains creates six hypervariable loops (three loops each from the H and L chains) that provide the amino acid residues for antigen binding and confer antigen-binding specificity to the antibody. However, even a single variable domain (or half of an Fv containing only three antigen-specific HVRs) recognizes and binds antigen, albeit with lower affinity than the entire binding site. have the ability.
「sFv」又は「scFv」とも略される「一本鎖Fv」は、接続されて単一のポリペプチド鎖となったVH及びVL抗体ドメインを含む抗体フラグメントである。好ましくは、sFvポリペプチドは、VHドメインとVLドメインとの間にポリペプチドリンカーを更に含んでおり、このリンカーにより、sFvが抗原結合に望ましい構造を成すことが可能となっている。sFvの概説については、PluckthunのThe Pharmacology of Monoclonal Antibodies,vol.113,Rosenburg and Moore eds.,Springer-Verlag,New York,pp.269-315(1994)を参照されたい。 "Single-chain Fv" also abbreviated as "sFv" or "scFv" are antibody fragments that comprise the VH and VL antibody domains connected into a single polypeptide chain. Preferably, the sFv polypeptide further comprises a polypeptide linker between the VH and VL domains, which linker enables the sFv to form the desired structure for antigen binding. For a review of sFvs, see Pluckthun, The Pharmacology of Monoclonal Antibodies, vol. 113, Rosenburg and Moore eds. , Springer-Verlag, New York, pp. 269-315 (1994).
「Fc領域」という用語は、本明細書では定常領域の少なくとも一部分を含有する免疫グロブリン重鎖のC末端領域を定義するために使用される。本用語は、天然配列Fc領域とバリアントFc領域とを含む。一態様では、ヒトIgG重鎖Fc領域は、Cys226から、又はPro230から、重鎖のカルボキシル末端までに及ぶ。しかし、宿主細胞によって産生される抗体は、重鎖のC末端から1つ以上、特に1つ又は2つのアミノ酸の翻訳後開裂を受けてもよい。したがって、完全長重鎖をコードする特定の核酸分子の発現によって、宿主細胞によって産生する抗体は、完全長重鎖を含んでいてもよく、又は完全長重鎖の開裂したバリアントを含んでいてもよい。これは、重鎖の最後の2つのC末端アミノ酸がグリシン(G446)及びリジン(K447)である場合にあり得る。したがって、Fc領域のC末端リジン(Lys447)、又はC末端グリシン(Gly446)及びリジン(Lys447)が存在してもよく、又は存在していなくてもよい。Fc領域を含む重鎖のアミノ酸配列は、別途示されない限り、本明細書ではC末端リジン(Lys 447)なしで示される。一態様では、本明細書に開示される抗体に含まれる、本明細書で明記したFc領域を含む重鎖は、更なるC末端グリシン-リジンジペプチド(G446及びK447)を含む。一態様では、本明細書に開示される抗体に含まれる、本明細書で明記したFc領域を含む重鎖は、更なるC末端グリシン残基(G446)を含む。一態様では、本明細書に開示される抗体に含まれる、本明細書で明記したFc領域を含む重鎖は、更なるC末端リジン残基(K447)を含む。一態様では、Fc領域は、重鎖の単一アミノ酸置換N297Aを含む。本明細書で特に指示がない限り、Fc領域又は定常領域のアミノ酸残基のナンバリングは、Kabat et al.,Sequences of Proteins of Immunological Interest,5th Ed.Public Health Service,National Institutes of Health,Bethesda,MD,1991に記載されている、EUインデックスとも呼ばれるEUナンバリングシステムに従う。 The term "Fc region" is used herein to define a C-terminal region of an immunoglobulin heavy chain containing at least a portion of a constant region. The term includes native sequence Fc regions and variant Fc regions. In one aspect, the human IgG heavy chain Fc region extends from Cys226 or from Pro230 to the carboxyl terminus of the heavy chain. However, antibodies produced by host cells may undergo post-translational cleavage of one or more, particularly one or two, amino acids from the C-terminus of the heavy chain. Thus, by expression of a particular nucleic acid molecule encoding a full-length heavy chain, the antibody produced by the host cell may contain the full-length heavy chain or may contain cleaved variants of the full-length heavy chain. good. This can be the case when the last two C-terminal amino acids of the heavy chain are glycine (G446) and lysine (K447). Thus, the C-terminal lysine (Lys447) or the C-terminal glycine (Gly446) and lysine (Lys447) of the Fc region may or may not be present. Amino acid sequences of heavy chains, including the Fc region, are shown herein without the C-terminal lysine (Lys 447) unless otherwise indicated. In one aspect, the heavy chains comprising the Fc regions specified herein included in the antibodies disclosed herein comprise additional C-terminal glycine-lysine dipeptides (G446 and K447). In one aspect, the heavy chains comprising the Fc regions specified herein included in the antibodies disclosed herein comprise an additional C-terminal glycine residue (G446). In one aspect, the heavy chains comprising the Fc regions specified herein included in the antibodies disclosed herein comprise an additional C-terminal lysine residue (K447). In one aspect, the Fc region comprises the heavy chain single amino acid substitution N297A. Unless otherwise indicated herein, amino acid residue numbering in the Fc region or constant region is that of Kabat et al. , Sequences of Proteins of Immunological Interest, 5th Ed. It follows the EU numbering system, also called the EU index, as described in Public Health Service, National Institutes of Health, Bethesda, MD, 1991.
「Fc受容体」又は「FcR」は、抗体のFc領域に結合する受容体を表す。好ましいFcRは、天然配列ヒトFcRである。更に、好ましいFcRは、IgG抗体(ガンマ受容体)に結合するものであり、これには、FcγRI、FcγRII、及びFcγRIIIサブクラスの受容体(これらの受容体のアレルバリアント及び代替的にはスプライス型を含む)が含まれ、FcγRII受容体には、FcγRIIA(「活性化受容体」)及びFcγRIIB(「阻害受容体」)が含まれ、これらは、主にそれらの細胞質ドメインが異なる、同様のアミノ酸配列を有する。活性化受容体FcγRIIAは、その細胞質ドメイン内に免疫受容体チロシンベース活性化モチーフ(ITAM)を含有する。抑制受容体FcγRIIBは、その細胞質ドメイン中に免疫受容抑制性チロシンモチーフ(ITIM)を含有する(M.Daeron,Annu.Rev.Immunol.15:203-234(1997)を参照)。FcRは、Ravetch and Kinet,Annu.Rev.Immunol.9:457-92(1991);Capel et al.,Immunomethods 4:25-34(1994);及び、de Haas et al.,J.Lab.Clin.Med.126:330-41(1995)に総説されている。今後特定されるものを含む他のFcRは、本明細書において「FcR」という用語により包含されている。 "Fc receptor" or "FcR" refers to a receptor that binds to the Fc region of an antibody. A preferred FcR is a native sequence human FcR. Further preferred FcRs are those that bind IgG antibodies (gamma receptors), including receptors of the FcγRI, FcγRII, and FcγRIII subclasses (allelic variants and alternatively splice forms of these receptors). ), and FcγRII receptors include FcγRIIA (an “activating receptor”) and FcγRIIB (an “inhibiting receptor”), which have similar amino acid sequences that differ primarily in their cytoplasmic domains. have Activating receptor FcγRIIA contains an immunoreceptor tyrosine-based activation motif (ITAM) within its cytoplasmic domain. Inhibitory receptor FcγRIIB contains an immunoreceptor tyrosine inhibitory motif (ITIM) in its cytoplasmic domain (see M. Daeron, Annu. Rev. Immunol. 15:203-234 (1997)). FcRs are reviewed in Ravetch and Kinet, Annu. Rev. Immunol. 9:457-92 (1991); Capel et al. , Immunomethods 4:25-34 (1994); and de Haas et al. , J. Lab. Clin. Med. 126:330-41 (1995). Other FcRs, including those hereafter identified, are encompassed by the term "FcR" herein.
「ダイアボディ」という用語は、鎖内ではなく鎖間のVドメイン対合を達成し、それによって二価フラグメント、すなわち、2つの抗原結合部位を有するフラグメントが得られるように、VHドメインとVLドメインとの間に短いリンカー(約5~10個の残基)を用いてsFvフラグメント(前の段落を参照されたい)を構築することによって調製された小さな抗体フラグメントを指す。二重特異性ダイアボディは、2つの抗体のVHドメイン及びVLドメインが異なるポリペプチド鎖に存在している、2つの「交差」sFvフラグメントのヘテロ二量体である。ダイアボディは、例えば、欧州特許第404,097号、国際公開第93/11161号;Hollinger et al.,Proc.Natl.Acad.Sci.USA 90:6444-6448(1993)により詳細に記載されている。 The term "diabody" refers to the combination of a VH domain and a V domain to achieve interchain, but not intrachain V domain pairing, thereby resulting in a bivalent fragment, i.e., a fragment with two antigen-binding sites. Refers to a small antibody fragment prepared by constructing an sFv fragment (see previous paragraph) with a short linker (about 5-10 residues) between it and the L domain. Bispecific diabodies are heterodimers of two "crossed" sFv fragments in which the VH and VL domains of the two antibodies are present in different polypeptide chains. Diabodies are described, for example, in EP 404,097, WO 93/11161; Hollinger et al. , Proc. Natl. Acad. Sci. USA 90:6444-6448 (1993).
本明細書におけるモノクローナル抗体には、具体的には、重鎖及び/又は軽鎖の一部分が、特定の種に由来するか又は特定の抗体クラス若しくはサブクラスに属する抗体内の対応する配列と同一又は相同である一方で、鎖(複数可)の残りの部分が、別の種に由来するか又は別の抗体クラス若しくはサブクラスに属する抗体内の対応する配列と同一又は相同である「キメラ」抗体(免疫グロブリン)、並びに所望の生物学的活性を呈する限り、そのような抗体のフラグメントが含まれる(米国特許第4,816,567号;Morrisonら、Proc.Natl.Acad.Sci.USA、81:6851~6855(1984))。本明細書における目的のキメラ抗体としては、PRIMATIZED(登録商標)抗体が含まれ、ここで、この抗体の抗原結合領域は、例えば、マカクザルに目的の抗原で免疫付与を行うことによって産生される抗体に由来する。本明細書で使用される場合、「ヒト化抗体」は、「キメラ抗体」のサブセットとして使用される。 Monoclonal antibodies herein specifically include a portion of the heavy and/or light chain identical to or corresponding sequences in an antibody from a particular species or belonging to a particular antibody class or subclass. "Chimeric" antibodies that are homologous, while the remainder of the chain(s) are identical or homologous to corresponding sequences in an antibody from another species or belonging to another antibody class or subclass ( immunoglobulins), and fragments of such antibodies are included so long as they exhibit the desired biological activity (U.S. Pat. No. 4,816,567; Morrison et al., Proc. Natl. Acad. Sci. USA, 81: 6851-6855 (1984)). Chimeric antibodies of interest herein include PRIMATIZED® antibodies, wherein the antigen-binding region of the antibody is, for example, an antibody produced by immunizing macaque monkeys with an antigen of interest derived from As used herein, "humanized antibody" is used as a subset of "chimeric antibody."
抗体の「クラス」は、その重鎖によって保有される定常ドメイン又は定常領域の型を指す。抗体の5つの主要なクラスがあり、すなわち、IgA、IgD、IgE、IgG、及びIgMがあり、これらのいくつかは、更にサブクラス(アイソタイプ)、例えば、IgG1、IgG2、IgG3、IgG4、IgA1、及びIgA2に分けることができる。免疫グロブリンの異なるクラスに対応する重鎖定常ドメインは、それぞれ、α、δ、ε、γ、及びμと呼ばれる。 The "class" of an antibody refers to the type of constant domain or region carried by its heavy chains. There are five major classes of antibodies, namely IgA, IgD, IgE, IgG, and IgM, some of which have further subclasses (isotypes), e.g., IgG1 , IgG2 , IgG3 , IgG4 . , IgA 1 , and IgA 2 . The heavy-chain constant domains that correspond to the different classes of immunoglobulins are called α, δ, ε, γ, and μ, respectively.
「親和性」は、分子(例えば、抗体)の単一の結合部位とその結合相手(例えば、抗原、例えば、TIGIT、PD-L1又はVEGF)との間の、合計の非共有性相互作用の強度を指す。別途示されない限り、本明細書で使用される場合、「結合親和性」は、結合対のメンバー(例えば、抗体及び抗原)間の1:1の相互作用を反映する固有の結合親和性を指す。分子Xの、そのパートナーYに対する親和性は一般に、解離定数(KD)によって表し得る。親和性は、本明細書に記載するものを含め、当該技術分野で一般的な方法によって測定することができる。結合親和性を測定するための特定の説明的かつ例示的な態様は、以下に記載される。 "Affinity" is the total non-covalent interaction between a single binding site of a molecule (eg, an antibody) and its binding partner (eg, an antigen, such as TIGIT, PD-L1 or VEGF). refers to strength. Unless otherwise indicated, "binding affinity" as used herein refers to the intrinsic binding affinity that reflects a 1:1 interaction between members of a binding pair (e.g., antibody and antigen). . The affinity of molecule X for its partner Y can generally be expressed by the dissociation constant (K D ). Affinity can be measured by methods common in the art, including those described herein. Certain illustrative and exemplary aspects for measuring binding affinity are described below.
「ヒト抗体」は、ヒトによって産生された抗体のアミノ酸配列に対応するアミノ酸配列を有する抗体、及び/又は本明細書に開示されるヒト抗体を作製する技法の内の任意のものを用いて作製された抗体である。このヒト抗体の定義は、非ヒト抗原結合残基を含むヒト化抗体を明確に除外する。ヒト抗体は、ファージディスプレイライブラリ等の当該技術分野で既知の様々な技法を使用して産生され得る。Hoogenboom and Winter,J.Mol.Biol.,227:381(1991);Marks et al.,J.Mol.Biol.,222:581(1991)。Cole et al.,Monoclonal antibodies and Cancer Therapy,Alan R.Liss,p.77(1985);Boerner et al.,J.Immunol.,147(1):86-95(1991)に記載されている方法も、ヒトモノクローナル抗体の調製に利用可能である。van Dijk and van de Winkel,Curr.Opin.Pharmacol.,5:368-74(2001).もまた参照されたい。ヒト抗体は、抗原投与に応答してこのような抗体を産生するよう改変されているが、その内在性遺伝子座は無能になっているトランスジェニック動物、例えば免疫化ゼノマウスに抗原を投与することによって調製することが可能である(例えば、XENOMOUSE(商標)技術に関する米国特許第6,075,181号及び同第6,150,584号を参照)。また、ヒトB細胞ハイブリドーマ技術により産生されるヒト抗体については、例えば、Li et al.,Proc.Natl.Acad.Sci.USA,103:3557-3562(2006)を参照されたい。 A "human antibody" is an antibody that has an amino acid sequence corresponding to that of an antibody produced by a human and/or produced using any of the techniques for producing human antibodies disclosed herein. It is an antibody that has been This definition of human antibody specifically excludes humanized antibodies that contain non-human antigen-binding residues. Human antibodies can be produced using various techniques known in the art, such as phage display libraries. Hoogenboom and Winter, J.; Mol. Biol. , 227:381 (1991); Marks et al. , J. Mol. Biol. , 222:581 (1991). Cole et al. , Monoclonal antibodies and Cancer Therapy, Alan R.; Liss, p. 77 (1985); Boerner et al. , J. Immunol. , 147(1):86-95 (1991) are also available for the preparation of human monoclonal antibodies. van Dijk and van de Winkel, Curr. Opin. Pharmacol. , 5:368-74 (2001). See also Human antibodies are modified to produce such antibodies in response to antigenic challenge, but by administering the antigen to a transgenic animal in which its endogenous locus has been disabled, e.g., an immunized xeno-mouse. (See, eg, US Pat. Nos. 6,075,181 and 6,150,584 for XENOMOUSE™ technology). Also, for human antibodies produced by human B-cell hybridoma technology, see, for example, Li et al. , Proc. Natl. Acad. Sci. USA, 103:3557-3562 (2006).
「ヒト化」型の非ヒト(例えば、マウス)抗体は、非ヒト免疫グロブリンに由来する最小の配列を含有するキメラ抗体である。一態様では、ヒト化抗体は、レシピエントのHVR(以下に定義される)からの残基が、所望される特異性、親和性、及び/又は能力を有するマウス、ラット、ウサギ、又は非ヒト霊長類等の非ヒト種(ドナー抗体)のHVRからの残基で置き換えられている、ヒト免疫グロブリン(レシピエント抗体)である。いくつかの例では、ヒト免疫グロブリンのフレームワーク(「FR」)残基は、対応する非ヒト残基で置き換えられている。更に、ヒト化抗体は、レシピエント抗体にもドナー抗体にも見られない残基を含んでもよい。これらの修飾は、結合親和性等、抗体の性能を更に改良するために行われ得る。一般に、ヒト化抗体は、少なくとも1つ、典型的には2つの可変ドメインの実質的に全てを含むものとし、超可変ループの全て又は実質的に全てが、非ヒト免疫グロブリン配列のものに対応し、FR領域の全て又は実質的に全てが、ヒト免疫グロブリン配列のものに対応するが、FR領域には、結合親和性、異性体化、免疫原性等の抗体の性能を向上させる1つ以上の個々のFR残基置換が含まれてもよい。FRにおけるこれらのアミノ酸置換の数は、典型的には、H鎖では6以下であり、L鎖では3以下である。ヒト化抗体は、任意に、免疫グロブリン定常領域(Fc)、典型的には、ヒト免疫グロブリンのFcの少なくとも一部も含む。更なる詳細については、例えば、Jones et al.,Nature 321:522-525(1986);Riechmann et al.,Nature 332:323-329(1988);及びPresta,Curr.Op.Struct.Biol.2:593-596(1992)を参照されたい。例えば、Vaswani and Hamilton,Ann.Allergy,Asthma&Immunol.1:105-115(1998);Harris,Biochem.Soc.Transactions 23:1035-1038(1995);Hurle and Gross,Curr.Op.Biotech.5:428-433(1994);並びに米国特許第6,982,321号及び同第7,087,409号を参照されたい。 “Humanized” forms of non-human (eg, murine) antibodies are chimeric antibodies that contain minimal sequence derived from non-human immunoglobulin. In one aspect, a humanized antibody is a murine, rat, rabbit, or non-human antibody in which residues from the recipient's HVR (defined below) have the desired specificity, affinity, and/or ability. A human immunoglobulin (recipient antibody) that has been replaced with residues from the HVR of a non-human species such as a primate (donor antibody). In some instances, framework (“FR”) residues of the human immunoglobulin are replaced by corresponding non-human residues. Furthermore, humanized antibodies may comprise residues that are found neither in the recipient antibody nor in the donor antibody. These modifications can be made to further refine antibody performance, such as binding affinity. In general, a humanized antibody will comprise substantially all of at least one, typically two, variable domains, wherein all or substantially all of the hypervariable loops correspond to those of non-human immunoglobulin sequences. , all or substantially all of the FR regions correspond to those of a human immunoglobulin sequence, but the FR regions contain one or more that improve antibody performance, such as binding affinity, isomerization, immunogenicity, etc. individual FR residue substitutions may be included. The number of these amino acid substitutions in the FRs is typically 6 or less for H chains and 3 or less for L chains. The humanized antibody optionally also will comprise at least a portion of an immunoglobulin constant region (Fc), typically that of a human immunoglobulin. For further details see, for example, Jones et al. , Nature 321:522-525 (1986); Riechmann et al. , Nature 332:323-329 (1988); and Presta, Curr. Op. Struct. Biol. 2:593-596 (1992). For example, Vaswani and Hamilton, Ann. Allergy, Asthma & Immunol. 1:105-115 (1998); Harris, Biochem. Soc. Transactions 23:1035-1038 (1995); Hurle and Gross, Curr. Op. Biotech. 5:428-433 (1994); and US Pat. Nos. 6,982,321 and 7,087,409.
「単離された抗体」という用語は、本明細書に開示される様々な抗体を説明するために使用されるとき、抗体が発現された細胞又は細胞培養物から特定され、分離及び/又は回収された抗体を意味する。その天然環境の混入成分は、典型的にはポリペプチドの診断的又は治療的使用を妨害する材料であり、酵素、ホルモン、及び他のタンパク質性又は非タンパク質性溶質を含み得る。いくつかの態様では、抗体は、例えば、電気泳動(例えば、SDS-PAGE、等電点電気泳動(IEF)、キャピラリー電気泳動)又はクロマトグラフ(例えば、イオン交換又は逆相HPLC)によって決定される、95%超又は99%超の純度まで精製される。抗体純度の評定のための方法の総説については、例えば、Flatman et al.,J.Chromatogr.B 848:79-87(2007)を参照されたい。好ましい態様では、抗体は、(1)スピニングカップシークエネーター(spinning cup sequenator)を使用してN末端若しくは内部アミノ酸配列の少なくとも15個の残基を得るのに十分な程度まで、又は(2)クマシーブルー若しくは好ましくは銀染色を使用して非還元条件又は還元条件下でSDS-PAGEによって均質になるまで精製される。単離された抗体としては、組換え細胞内のin situの抗体が挙げられるが、これは、ポリペプチド天然環境の少なくとも1つの成分が存在しないためである。しかしながら、通常、単離されたポリペプチドは、少なくとも1つの精製ステップにより調製される。 The term "isolated antibody" when used to describe the various antibodies disclosed herein has been identified, separated and/or recovered from a cell or cell culture in which the antibody was expressed. means an antibody that has been Contaminant components of its natural environment are materials that would typically interfere with diagnostic or therapeutic uses for the polypeptide, and may include enzymes, hormones, and other proteinaceous or nonproteinaceous solutes. In some aspects, antibodies are determined, for example, by electrophoresis (eg, SDS-PAGE, isoelectric focusing (IEF), capillary electrophoresis) or chromatography (eg, ion-exchange or reverse-phase HPLC). , purified to greater than 95% or greater than 99% purity. For a review of methods for assessment of antibody purity, see, eg, Flatman et al. , J. Chromatogr. B 848:79-87 (2007). In a preferred embodiment, the antibody is (1) sufficient to obtain at least 15 residues of N-terminal or internal amino acid sequence using a spinning cup sequenator, or (2) a Coomassie Purify to homogeneity by SDS-PAGE under non-reducing or reducing conditions using blue or preferably silver staining. Isolated antibody includes the antibody in situ within recombinant cells since at least one component of the polypeptide's natural environment will not be present. Ordinarily, however, isolated polypeptide will be prepared by at least one purification step.
「モノクローナル抗体」という用語は、本明細書で使用される場合、実質的に均一な抗体の集合から得られる抗体を指す。すなわち、例えば、天然に存在する変異又はモノクローナル抗体調製物の製造中に生じる変異を含む、一般的に、少量存在する可能なバリアント抗体を除いて、集合を構成する個々の抗体は同一である及び/又は同じエピトープを結合する。様々な決定基(エピトープ)に対する様々な抗体を通常含むポリクローナル抗体調製物とは対照的に、モノクローナル抗体調製物の各モノクローナル抗体は、抗原上の単一の決定基に対するものである。したがって、修飾語「モノクローナル」は、抗体の実質的に均一な集合から得られる抗体の特徴を示し、任意の特定の方法による抗体の産生を必要とするように解釈すべきではない。例えば、本発明に従って使用されるモノクローナル抗体は、ハイブリドーマ法、組換えDNA法、ファージディスプレイ法、及びヒト免疫グロブリン遺伝子座の全部又は一部を含むトランスジェニック動物を利用する方法を含むがこれらに限定されない種々の技術によって作製されてもよい。 The term "monoclonal antibody," as used herein, refers to an antibody obtained from a substantially homogeneous population of antibodies. That is, the individual antibodies that make up the population are identical, except for possible variant antibodies that are generally present in minor amounts, including, for example, naturally-occurring mutations or mutations that arise during the manufacture of a monoclonal antibody preparation, and /or bind the same epitope. In contrast to polyclonal antibody preparations, which usually include different antibodies directed against different determinants (epitopes), each monoclonal antibody of a monoclonal antibody preparation is directed against a single determinant on the antigen. Thus, the modifier "monoclonal" indicates the characteristics of antibodies obtained from a substantially homogeneous population of antibodies and should not be construed as requiring production of the antibody by any particular method. For example, monoclonal antibodies for use in accordance with the present invention include, but are not limited to, hybridoma methods, recombinant DNA methods, phage display methods, and methods utilizing transgenic animals containing all or part of the human immunoglobulin loci. may be made by a variety of techniques that are not
本明細書で使用される場合、「結合する」、「~に特異的に結合する」、又は「~に特異的である」という用語は、標的と抗体との間の結合等、測定可能かつ再生可能な相互作用を指し、これは、生体分子を含む分子の異種集団の存在下において、標的の存在を決定づけるものである。例えば、標的(これはエピトープであり得る)に特異的に結合する抗体は、他の標的に結合するよりも高い親和性、結合力で、より容易に、及び/又はより長い持続時間でこの標的に結合する、抗体である。一態様では、抗体が無関係の標的に結合する程度は、放射免疫測定法(RIA)によって測定した場合に、標的に対する抗体の結合の約10%未満である。特定の態様では、標的に特異的に結合する抗体は、1μM以下、100nM以下、10nM以下、1nM以下、又は0.1nM以下の解離定数(KD)を有する。特定の態様では、抗体は、異なる種由来のタンパク質間で保存されるタンパク質上のエピトープに特異的に結合する。別の態様では、特異的結合は、排他的結合を含み得るが、それを必要としない。本明細書で使用される用語は、例えば、標的に対して10-4 M以下、あるいは10-5 M以下、あるいは10-6M以下、あるいは10-7M以下、あるいは10-8M以下、あるいは10-9M以下、あるいは10-10M以下、あるいは10-11M以下、あるいは10-12M以下のKD、又は10-4M~10-6M、若しくは10-6M~10-10M、若しくは10-7M~10-9Mの範囲KDを有する分子によって示され得る。当業者によって理解されるように、親和性とKD値は逆相関する。抗原に対する高い親和性は、低いKD値により測定される。一態様では、「特異的結合」という用語は、分子が、いずれの他のポリペプチド又はポリペプチドエピトープにも実質的に結合することなく、特定のポリペプチド上の特定のポリペプチド又はエピトープに結合する場合の結合を指す。 As used herein, the terms “binds,” “binds specifically to,” or “is specific to” refer to a measurable and Refers to reproducible interactions, which dictate the presence of a target in the presence of a heterogeneous population of molecules, including biomolecules. For example, an antibody that specifically binds a target, which may be an epitope, binds to this target with higher affinity, avidity, more readily, and/or for a longer duration than it binds to other targets. It is an antibody that binds to In one aspect, the extent to which the antibody binds to an irrelevant target is less than about 10% of the antibody's binding to the target as measured by radioimmunoassay (RIA). In certain aspects, an antibody that specifically binds to a target has a dissociation constant (K D ) of 1 μM or less, 100 nM or less, 10 nM or less, 1 nM or less, or 0.1 nM or less. In certain aspects, the antibody specifically binds to an epitope on the protein that is conserved among proteins from different species. In another aspect, specific binding may, but does not require, exclusive binding. The term as used herein means, for example, 10 −4 M or less, alternatively 10 −5 M or less, alternatively 10 −6 M or less, alternatively 10 −7 M or less, alternatively 10 −8 M or less, to the target, alternatively a K D of 10 −9 M or less, alternatively 10 −10 M or less, alternatively 10 −11 M or less, alternatively 10 −12 M or less, or 10 −4 M to 10 −6 M, or 10 −6 M to 10 − It can be demonstrated by molecules with a K D of 10 M, or in the range of 10 −7 M to 10 −9 M. As will be appreciated by those skilled in the art, affinity and KD values are inversely correlated. A high affinity for an antigen is measured by a low KD value. In one aspect, the term "specific binding" refers to the molecule binding to a particular polypeptide or epitope on a particular polypeptide without substantially binding to any other polypeptide or polypeptide epitope. Refers to the combination when
参照ポリペプチド配列に関する「アミノ酸配列同一性パーセント(%)」は、配列を整列させ、最大のパーセント配列同一性を得るために必要ならば間隙を導入した後、いかなる保存的置換も配列同一性の一部と考えないとした場合の、参照ポリペプチドのアミノ酸残基と同一である候補配列中のアミノ酸残基のパーセンテージとして定義される。アミノ酸配列同一性パーセントを決定する目的のための整列は、当該技術分野における技術の範囲内にある種々の方法において、例えば、BLAST、BLAST-2、ALIGN、又はMegalign(DNASTAR)ソフトウェア等の公的に入手可能なコンピュータソフトウェアを用いて達成され得る。当業者であれば、比較される配列の全長にわたって最大のアラインメントを達成するために必要な任意のアルゴリズムを含む、配列のアラインメントのための適切なパラメーターを決定することができる。しかしながら、本明細書での目的のために、アミノ酸配列同一性%値は、配列比較コンピュータプログラムALIGN-2を用いて生成している。ALIGN-2配列比較コンピュータプログラムは、Genentech,Inc.が作成したものであり、ソースコードは、使用者用書類と共に、米国著作権局、Washington D.C.、20559に提出され、ここで、米国著作権登録番号TXU510087として登録されている。ALIGN-2プログラムは、Genentech,Inc.(South San Francisco,California)から公的に入手可能であり、又はそのソースコードからコンパイルし得る。ALIGN-2プログラムは、デジタルUNIX V4.0Dを含め、UNIXオペレーティングシステムで使用するためにコンパイルされるべきである。全ての配列比較パラメーターは、ALIGN-2プログラムによって設定されており、変わらない。 A "percent (%) amino acid sequence identity" with respect to a reference polypeptide sequence is obtained after aligning the sequences and introducing gaps, if necessary, to obtain the maximum percent sequence identity, after which any conservative substitutions are considered It is defined as the percentage of amino acid residues in a candidate sequence that are identical to amino acid residues in a reference polypeptide, if not considered a fraction. Alignment for purposes of determining percent amino acid sequence identity may be performed in a variety of ways within the skill in the art, for example, by BLAST, BLAST-2, ALIGN, or Megalign (DNASTAR) software. can be accomplished using computer software available at Those skilled in the art can determine appropriate parameters for alignment of sequences, including any algorithms needed to achieve maximal alignment over the entire length of the sequences being compared. For purposes herein, however, % amino acid sequence identity values are generated using the sequence comparison computer program ALIGN-2. The ALIGN-2 sequence comparison computer program is available from Genentech, Inc.; and the source code, together with user documentation, is available from the United States Copyright Office, Washington, D.C. C. , 20559, where it is registered under US Copyright Registration Number TXU510087. The ALIGN-2 program is available from Genentech, Inc. (South San Francisco, California) or may be compiled from its source code. ALIGN-2 programs should be compiled for use on UNIX operating systems, including digital UNIX V4.0D. All sequence comparison parameters were set by the ALIGN-2 program and remain unchanged.
ALIGN-2がアミノ酸配列比較に用いられる状況では、所与のアミノ酸配列Bへの、アミノ酸配列Bとの、又はアミノ酸配列Bに対する、所与のアミノ酸配列Aのアミノ酸配列同一性%(或いは、所与のアミノ酸配列Bへの、アミノ酸配列Bとの、又はアミノ酸配列Bに対する、ある特定のアミノ酸配列同一性%を有する又は含む、所与のアミノ酸配列Aとして記述され得る)は、以下のように計算される:
100×分数X/Y
式中、Xは、配列アラインメントプログラムALIGN-2によって、そのプログラムのAとBのアラインメントにおいて同一のマッチとしてスコア付けされたアミノ酸残基の数であり、Yは、B中のアミノ酸残基の総数である。アミノ酸配列Aの長さがアミノ酸配列Bの長さに等しくない場合、A対Bのアミノ酸配列同一性%は、B対Aのアミノ酸配列同一性%に等しくないことが理解されよう。特に明記しない限り、本明細書で使用される全ての%アミノ酸配列同一性値は、ALIGN-2コンピュータプログラムを使用して直前の段落に記載されているように得られる。
In situations where ALIGN-2 is used for amino acid sequence comparison, the % amino acid sequence identity of a given amino acid sequence A to, with, or against a given amino acid sequence B (or A given amino acid sequence A having or including a certain % amino acid sequence identity to, with, or to a given amino acid sequence B) can be described as: Computed:
100 x Fractional X/Y
where X is the number of amino acid residues scored as identical matches in the alignment of A and B by the sequence alignment program ALIGN-2, and Y is the total number of amino acid residues in B is. It will be understood that the % amino acid sequence identity of A to B is not equal to the % amino acid sequence identity of B to A if the length of amino acid sequence A is not equal to the length of amino acid sequence B. Unless otherwise stated, all % amino acid sequence identity values used herein are obtained using the ALIGN-2 computer program as described in the immediately preceding paragraph.
本明細書で使用される場合、「対象」又は「個体」は、ヒト又は非ヒト哺乳動物、例えば、ウシ、ウマ、イヌ、ヒツジ、又はネコ等を含むがこれらに限定されない、哺乳動物を意味する。いくつかの態様では、対象はヒトである。患者もまた、本明細書における対象である。 As used herein, "subject" or "individual" means a mammal, including, but not limited to, a human or non-human mammal, such as a bovine, equine, canine, ovine, or feline. do. In some embodiments, the subject is human. Patients are also a subject herein.
「患者」という用語は、ヒト患者を指す。例えば、患者は成人であってもよい。 The term "patient" refers to a human patient. For example, the patient may be an adult.
「診断」という用語は、分子的又は病理学的状態、疾患、又は病態(例えば、がん)の特定又は分類を指すために本明細書で使用される。例えば、「診断」とは、特定のタイプのがんの同定を指し得る。「診断」はまた、例えば組織病理学的基準によるか又は分子的特徴による、がんの特定のサブタイプ(例えば、バイオマーカー(例えば、特定の遺伝子、又は遺伝子によりコードされるタンパク質)のうちの1つ又はその組合せの発現によって特徴付けられるサブタイプ)の分類を指す場合もある。 The term "diagnosis" is used herein to refer to the identification or classification of a molecular or pathological condition, disease, or condition (eg, cancer). For example, "diagnosis" can refer to identification of a particular type of cancer. "Diagnosis" may also include detection of a particular subtype of cancer (e.g., biomarkers (e.g., particular genes, or proteins encoded by genes), e.g., by histopathological criteria or by molecular characteristics. It may also refer to a classification of subtypes characterized by the expression of one or a combination thereof.
本明細書で使用される場合、「試料」という用語は、例えば、物理的、生化学的、化学的及び/又は生理学的特性に基づいて特徴づけられる及び/又は同定される細胞実体及び/又は他の分子実体を含有する、目的の対象及び/又は個体から得られるか又は由来する組成物を指す。例えば、「腫瘍試料」、「疾患試料」という語句及びその変化形は、特徴づけられる細胞及び/又は分子実体を含有することが予期されるか又は含有することが既知である、目的の対象から得られた任意の試料を指す。試料としては、組織試料、初代若しくは培養細胞又は細胞株、細胞上清、細胞溶解物、血小板、血清、血漿、硝子体液、リンパ液、滑液、卵胞液、精液、羊水、乳、全血、血液由来の細胞、尿、脳脊髄液、唾液、痰、涙、汗、粘液、便、腫瘍溶解物、及び組織培養培地、組織抽出物、例えば、ホモジナイズされた組織、腫瘍組織、細胞抽出物、並びにそれらの組合せが挙げられるが、これらに限定されない。 As used herein, the term "sample" refers to cellular entities and/or Refers to a composition obtained or derived from a subject and/or individual of interest that contains other molecular entities. For example, the phrases “tumor sample,” “disease sample,” and variations thereof are used from a subject of interest that is expected or known to contain the cellular and/or molecular entity to be characterized. Refers to any sample obtained. Samples include tissue samples, primary or cultured cells or cell lines, cell supernatants, cell lysates, platelets, serum, plasma, vitreous humor, lymph, synovial fluid, follicular fluid, semen, amniotic fluid, milk, whole blood, blood derived cells, urine, cerebrospinal fluid, saliva, sputum, tears, sweat, mucus, stool, tumor lysates, and tissue culture media, tissue extracts such as homogenized tissue, tumor tissue, cell extracts, and Combinations thereof include, but are not limited to.
「組織試料」又は「細胞試料」は、対象又は個体の組織から得られた同様の細胞の集合を意味する。組織又は細胞試料の供給源は、新鮮な、凍結した、及び/又は保存された器官、組織試料、生検、及び/又は吸引液から等の固形組織;血漿等の血液又は任意の血液構成物;脳脊髄液、羊水、腹水、又は間質液等の体液;対象の妊娠又は発育における任意の時期の細胞であってもよい。組織試料は、初代又は培養細胞又は細胞株であってもよい。任意に、組織又は細胞試料は、疾患組織/器官から得られる。例えば、「腫瘍試料」は、腫瘍又は他のがん組織から得られた組織試料である。組織試料は、細胞型(例えば、腫瘍細胞及び非腫瘍細胞、がん性細胞及び非がん性細胞)の混合集団を含有し得る。組織試料は、保存剤、抗凝固剤、緩衝液、固定剤、ワックス、栄養剤、又は抗生物質等の天然の組織と天然では混合しない化合物を含有し得る。いくつかの態様では、組織試料は、腫瘍組織試料である。いくつかの態様では、腫瘍組織試料はUC腫瘍組織試料(例えば、膀胱がん腫瘍組織試料(例えば、MIBC腫瘍組織試料))である。いくつかの態様において、試料は、膀胱腫瘍の経尿道切除術(TURBT)試料である。いくつかの態様では、試料は膀胱切除術又は腎尿管切除術の試料である。他の態様では、腫瘍組織試料は肺がん腫瘍組織試料(例えば、初期肺がん組織試料(例えば、NSCLC腫瘍組織試料(例えば、ステージII、IIIA又はIIIB NSCLC腫瘍組織試料)、例えば、扁平上皮又は非扁平上皮NSCLC腫瘍組織試料、例えば、切除可能なNSCLC腫瘍組織試料))である。いくつかの態様において、試料は、局所進行性切除不能NSCLC腫瘍組織試料(例えば、ステージIIIB NSCLC腫瘍組織試料)、又は再発性若しくは転移性NSCLC腫瘍組織試料(例えば、ステージIV NSCLC腫瘍組織試料))、膵臓がん腫瘍組織試料(例えば、PDAC腫瘍組織試料)、例えば転移性PDAC腫瘍組織試料)、又は乳がん腫瘍組織試料(例えば、HER 2+乳がん腫瘍組織試料又はTNBC腫瘍組織試料)である。 A "tissue sample" or "cell sample" refers to a similar collection of cells obtained from tissue of a subject or individual. Sources of tissue or cell samples may be solid tissues such as from fresh, frozen and/or preserved organs, tissue samples, biopsies, and/or aspirates; blood such as plasma or any blood constituent. body fluids such as cerebrospinal fluid, amniotic fluid, ascites, or interstitial fluid; cells at any stage in the subject's pregnancy or development. A tissue sample may be a primary or cultured cell or cell line. Optionally, tissue or cell samples are obtained from diseased tissues/organs. For example, a "tumor sample" is a tissue sample obtained from a tumor or other cancerous tissue. A tissue sample may contain a mixed population of cell types (eg, tumor and non-tumor cells, cancerous and non-cancerous cells). Tissue samples may contain compounds that are not naturally mixed with native tissue, such as preservatives, anticoagulants, buffers, fixatives, waxes, nutrients, or antibiotics. In some aspects, the tissue sample is a tumor tissue sample. In some aspects, the tumor tissue sample is a UC tumor tissue sample (eg, a bladder cancer tumor tissue sample (eg, an MIBC tumor tissue sample)). In some embodiments, the sample is a bladder tumor transurethral resection (TURBT) sample. In some aspects, the sample is a cystectomy or nephroureterectomy sample. In other aspects, the tumor tissue sample is a lung cancer tumor tissue sample (e.g., early stage lung cancer tissue sample (e.g., NSCLC tumor tissue sample (e.g., stage II, IIIA or IIIB NSCLC tumor tissue sample)), e.g., squamous or non-squamous NSCLC tumor tissue sample, eg resectable NSCLC tumor tissue sample)). In some embodiments, the sample is a locally advanced unresectable NSCLC tumor tissue sample (eg, stage IIIB NSCLC tumor tissue sample), or a recurrent or metastatic NSCLC tumor tissue sample (eg, stage IV NSCLC tumor tissue sample)). , pancreatic cancer tumor tissue sample (eg, PDAC tumor tissue sample), eg metastatic PDAC tumor tissue sample), or breast cancer tumor tissue sample (eg, HER2+ breast cancer tumor tissue sample or TNBC tumor tissue sample).
本明細書における目的では、組織試料の「切片」は、組織試料の単一の部分又は小片、例えば、組織試料(例えば、腫瘍試料)から切り取られた組織又は細胞の薄切片を意味する。組織試料の複数の切片を、採取し、分析に供することができることが理解され、但し、組織試料の同じ切片を、形態学的レベル及び分子レベルの両方で分析することができ、あるいはポリペプチド(例えば、免疫組織化学によって)及び/又はポリヌクレオチド(例えば、原位置ハイブリダイゼーションによって)に関して分析することができることが理解されるものとする。 For purposes herein, a "section" of a tissue sample means a single portion or piece of tissue sample, eg, a thin section of tissue or cells cut from a tissue sample (eg, a tumor sample). It is understood that multiple sections of the tissue sample can be taken and subjected to analysis, provided that the same section of the tissue sample can be analyzed at both the morphological and molecular level, or the polypeptide ( for example, by immunohistochemistry) and/or for polynucleotides (eg, by in situ hybridization).
本明細書で使用される場合、「参照試料」、「参照細胞」、「参照組織」、「対照試料」、「対照細胞」、又は「対照組織」は、比較目的のために使用される試料、細胞、組織、標準物、又はレベルを指す。一態様では、参照試料、参照細胞、参照組織、対照試料、対照細胞、又は対照組織は、同じ対象又は個体の身体の健常な及び/又は罹患していない部分(例えば、組織又は細胞)から得られる。例えば、参照試料、参照細胞、参照組織、対照試料、対照細胞、又は対照組織は、疾患細胞又は組織に隣接する健康及び/又は非疾患細胞又は組織(例えば、腫瘍に隣接する細胞又は組織)であり得る。別の態様では、参照試料は、同じ対象又は個体の身体の未処置な組織及び/又は細胞から得られる。更に別の態様では、参照試料、参照細胞、参照組織、対照試料、対照細胞、又は対照組織は、対象又は個体ではない個体の身体の健常な及び/又は罹患していない部分(例えば、組織又は細胞)から得られる。更に別の態様では、参照試料、参照細胞、参照組織、対照試料、対照細胞、又は対照組織は、対象又は個体ではない個体の身体の未処置な組織及び/又は細胞から得られる。 As used herein, a "reference sample," "reference cell," "reference tissue," "control sample," "control cell," or "control tissue" refers to a sample used for comparison purposes. , refers to a cell, tissue, standard, or level. In one aspect, the reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is obtained from a healthy and/or unaffected portion (e.g., tissue or cell) of the body of the same subject or individual. be done. For example, a reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is healthy and/or non-disease cells or tissue adjacent to a diseased cell or tissue (e.g., cells or tissue adjacent to a tumor). could be. In another aspect, the reference sample is obtained from untreated tissue and/or cells of the same subject's or individual's body. In yet another aspect, the reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is a healthy and/or unaffected portion of the body of an individual that is not the subject or individual (e.g., tissue or cells). In yet another aspect, the reference sample, reference cell, reference tissue, control sample, control cell, or control tissue is obtained from untreated tissue and/or cells of the body of an individual that is not the subject or individual.
本明細書で使用される場合、「タンパク質」という用語は、別段の指示がない限り、霊長類(例えば、ヒト)並びにげっ歯類(例えば、マウス及びラット)等の哺乳類を含む、任意の脊椎動物源からの任意の天然タンパク質を指す。この用語は、「完全長」、未処理のタンパク質及び細胞内での処理から生じるタンパク質の任意の形態も含む。この用語は、タンパク質の天然に存在するバリアント、例えば、スプライスバリアント又は対立遺伝子バリアントも包含する。 As used herein, the term "protein" refers to any vertebral protein, including mammals such as primates (e.g., humans) and rodents (e.g., mice and rats), unless otherwise indicated. It refers to any naturally occurring protein from an animal source. The term also includes "full-length," unprocessed protein and any form of protein resulting from processing within a cell. The term also includes naturally occurring variants of proteins, eg, splice or allelic variants.
本明細書で同義に使用される「ポリヌクレオチド」又は「核酸」とは、任意の長さのヌクレオチドのポリマーを指し、DNA及びRNAを含む。ヌクレオチドは、デオキシリボヌクレオチド、リボヌクレオチド、修飾ヌクレオチド若しくは塩基、及び/若しくはそれらの類似体であっても、又はDNA若しくはRNAポリメラーゼによって若しくは合成反応によってポリマーに組み込まれ得る任意の基質であってもよい。したがって、例えば、本明細書で定義されるポリヌクレオチドとしては、一本鎖及び二本鎖DNA、一本鎖及び二本鎖領域を含むDNA、一本鎖及び二本鎖RNA、並びに一本鎖及び二本鎖領域を含むRNA、一本鎖若しくはより典型的には二本鎖を含むか又は一本鎖及び二本鎖領域を含み得るDNA及びRNAを含むハイブリッド分子が挙げられるが、これらに限定されない。加えて、本明細書で使用される「ポリヌクレオチド」という用語は、RNA若しくはDNA、又はRNA及びDNAの両方を含む三本鎖領域を指す。このような領域内の鎖は、同じ分子由来であっても、又は異なる分子由来であってもよい。これらの領域は、これらの分子のうちの1つ以上の全てを含み得るが、より典型的には、これらの分子のうちのいくつかの領域のみを含む。三重らせん領域の分子のうちの1つは、多くの場合、オリゴヌクレオチドである。「ポリヌクレオチド」及び「核酸」という用語は、具体的にはmRNA及びcDNAを含む。 "Polynucleotide," or "nucleic acid," as used interchangeably herein, refer to polymers of nucleotides of any length, and include DNA and RNA. Nucleotides can be deoxyribonucleotides, ribonucleotides, modified nucleotides or bases, and/or analogs thereof, or any substrate that can be incorporated into a polymer by a DNA or RNA polymerase or by a synthetic reaction. Thus, for example, polynucleotides as defined herein include single- and double-stranded DNA, DNA containing single- and double-stranded regions, single- and double-stranded RNA, and single-stranded and RNA containing double-stranded regions, hybrid molecules comprising DNA and RNA which may contain single-stranded or more typically double-stranded or may contain single- and double-stranded regions, including but not limited to: Not limited. In addition, the term "polynucleotide" as used herein refers to triple-stranded regions comprising RNA or DNA or both RNA and DNA. The strands within such regions may be from the same molecule or from different molecules. These regions may include all of one or more of these molecules, but more typically include only regions of some of these molecules. One of the molecules in the triple helix region is often an oligonucleotide. The terms "polynucleotide" and "nucleic acid" specifically include mRNA and cDNA.
ポリヌクレオチドは、メチル化ヌクレオチド及びそれらの類似体等の修飾されたヌクレオチドを含んでもよい。存在する場合には、ヌクレオチド構造に対する修飾は、ポリマーのアセンブリの前に付与されても、又は後に付与されてもよい。ヌクレオチドの配列は、非ヌクレオチド成分によって遮られ得る。ポリヌクレオチドは、標識との複合等によって、合成後に更に修飾されてもよい。修飾の他の種類としては、天然に存在するヌクレオチドのうちの1つ以上の類似体での置換、ヌクレオチド間修飾、例えば、非電荷性結合(例えば、メチルホスホン酸塩、ホスホトリエステル、ホスホアミデート、カルバメート等)によるもの、及び電荷性結合(例えば、ホスホロチオエート、ホスホロジチオエート等)によるもの、懸垂部分、例えばタンパク質(例えば、ヌクレアーゼ、毒素、抗体、シグナルペプチド、ポリ-L-リシン等)等を含むもの、挿入剤(例えば、アクリジン、ソラーレン等)によるもの、キレート剤(例えば、金属、放射活性金属、ホウ素、酸化金属等)を含むもの、アルキル化剤を含むもの、修飾結合(例えば、アルファアノマー核酸等)によるもの、並びにポリヌクレオチド(複数可)の未修飾形態等が挙げられる。更に、糖内に通常存在するヒドロキシル基のうちのいずれかは、例えば、ホスホン酸基、リン酸基により代置されるか、標準的な保護基により保護されるか、若しくは活性化されて追加のヌクレオチドへの追加の結合を準備してもよく、又は固体若しくは半固体支持体にコンジュゲートされてもよい。5’及び3’末端OHは、リン酸化され得るか又はアミン若しくは1~20個の炭素原子の有機キャッピング基部分で置換され得る。他のヒドロキシルもまた、標準的な保護基に誘導体化されてもよい。ポリヌクレオチドは、例えば、2’-O-メチル-、2’-O-アリル-、2’-フルオロ-、又は2’-アジド-リボース、炭素環糖の類似体、α-アノマ-糖、エピマー糖、例えば、アラビノース、キシロース、又はリキソース、ピラノース糖、フラノース糖、セドヘプツロース、アクリル酸類似体、及び脱塩基ヌクレオシド類似体、例えば、メチルリボシドを含む、当該技術分野で一般的に知られているリボース糖又はデオキシリボース糖の類似形態も含み得る。1つ以上のホスホジエステル結合は、代替的な連結基によって代置されてもよい。これらの代替的な連結基には、限定されないが、リン酸塩がP(O)S(「チオエート」)、P(S)S(「ジチオエート」)、「(O)NR2(「アミデート」)、P(O)R、P(O)OR’、CO又はCH2(「ホルムアセタール」)に置き換えられる態様が含まれ、各R又はR’は、独立してHであるか又は置換若しくは非置換アルキル(1~20C)(任意にエーテル(-O-)結合を含む)、アリール、アルケニル、シクロアルキル、シクロアルケニル、又はアラルジルである。ポリヌクレオチドにおける結合全てが同一である必要はない。前述の説明は、RNA及びDNAを含む本明細書で言及される全てのポリヌクレオチドに適用される。 A polynucleotide may comprise modified nucleotides, such as methylated nucleotides and their analogs. Modifications to the nucleotide structure, if present, may be imparted before or after assembly of the polymer. A sequence of nucleotides may be interrupted by non-nucleotide components. A polynucleotide may be further modified after synthesis, such as by conjugation with a label. Other types of modifications include substitutions of one or more analogs of naturally occurring nucleotides, internucleotide modifications, e.g., uncharged bonds (e.g., methylphosphonates, phosphotriesters, phosphoamidates, , carbamates, etc.), and by charged bonds (e.g., phosphorothioates, phosphorodithioates, etc.), pendent moieties, such as proteins (e.g., nucleases, toxins, antibodies, signal peptides, poly-L-lysine, etc.), etc. by intercalating agents (e.g., acridine, psoralen, etc.), chelating agents (e.g., metals, radioactive metals, boron, metal oxides, etc.), alkylating agents, modified linkages (e.g., alpha anomeric nucleic acids), as well as unmodified forms of the polynucleotide(s). Furthermore, any of the hydroxyl groups normally present in sugars may be replaced by, for example, a phosphonate group, a phosphate group, protected by standard protecting groups, or activated and added. may be provided with additional attachments to nucleotides of or may be conjugated to a solid or semi-solid support. The 5' and 3' terminal OH can be phosphorylated or substituted with amines or organic capping group moieties of 1-20 carbon atoms. Other hydroxyls may also be derivatized to standard protecting groups. Polynucleotides may include, for example, 2′-O-methyl-, 2′-O-allyl-, 2′-fluoro-, or 2′-azido-ribose, carbocyclic sugar analogs, α-anomeric sugars, epimeric Ribose sugars commonly known in the art, including sugars such as arabinose, xylose, or lyxose, pyranose sugars, furanose sugars, sedoheptulose, acrylic acid analogues, and abasic nucleoside analogues such as methylriboside or analogous forms of deoxyribose sugars. One or more phosphodiester bonds may be replaced by alternative linking groups. These alternative linking groups include, but are not limited to, phosphates P(O)S (“thioates”), P(S)S (“dithioates”), “(O)NR 2 (“amidates” ), P(O)R, P(O)OR′, CO or CH 2 (“formacetal”), wherein each R or R′ is independently H or substituted or unsubstituted alkyl (1-20C) (optionally containing an ether (--O--) bond), aryl, alkenyl, cycloalkyl, cycloalkenyl, or araldyl; Not all bonds in a polynucleotide need be identical. The foregoing description applies to all polynucleotides referred to herein, including RNA and DNA.
本明細書で使用される「担体」には、用いられる投与量及び濃度でそれに曝露されている細胞又は哺乳動物にとって無毒である、薬学的に許容可能な担体、賦形剤、又は安定剤が含まれる。多くの場合、生理学的に許容可能な担体はpH緩衝水溶液である。生理学的に許容可能な担体の例としては、リン酸、クエン酸、及び他の有機酸等の緩衝液;アスコルビン酸を含む抗酸化剤;低分子量(約10残基未満)ポリペプチド;血清アルブミン、ゼラチン、若しくは免疫グロブリン等のタンパク質;ポリビニルピロリドン等の親水性ポリマー;グリシン、グルタミン、アスパラギン、アルギニン、若しくはリジン等のアミノ酸;グルコース、マンノース、若しくはデキストリンを含む、単糖類、二糖類、及び他の炭水化物;EDTA等のキレート剤;マンニトール若しくはソルビトール等の糖アルコール;ナトリウム等の塩形成対イオン;並びに/又はTWEEN(商標)、ポリエチレングリコール(PEG)、及びPLURONICS(商標)等の非イオン性界面活性剤が挙げられる。 A "carrier" as used herein is a pharmaceutically acceptable carrier, excipient, or stabilizer that is non-toxic to cells or mammals to which it is exposed at the dosages and concentrations employed. included. Often the physiologically acceptable carrier is an aqueous pH buffered solution. Examples of physiologically acceptable carriers include buffers such as phosphate, citrate, and other organic acids; antioxidants, including ascorbic acid; low molecular weight (less than about 10 residues) polypeptides; serum albumin. hydrophilic polymers such as polyvinylpyrrolidone; amino acids such as glycine, glutamine, asparagine, arginine, or lysine; monosaccharides, disaccharides, and other sugars, including glucose, mannose, or dextrins; carbohydrates; chelating agents such as EDTA; sugar alcohols such as mannitol or sorbitol; salt-forming counterions such as sodium; agents.
「薬学的に許容され得る」という語句は、物質又は組成物が、製剤を構成する他の成分及び/又はそれを用いて処置されている哺乳動物と、化学的及び/又は毒物学的に適合しなければならないことを示す。 The phrase "pharmaceutically acceptable" means that a substance or composition is chemically and/or toxicologically compatible with the other ingredients that make up the formulation and/or the mammal being treated therewith. Indicates what must be done.
「薬学的製剤」又は「薬学的組成物」という用語は、内部に含まれる活性成分の生物学的活性が有効になるような形態であり、かつ製剤が投与される対象が受け入れられない程度に毒性のいかなる成分も含まない調製物を指す。 The term "pharmaceutical formulation" or "pharmaceutical composition" means a form in which the biological activity of the active ingredients contained therein is effective and to an extent unacceptable to the subject to whom the formulation is administered. It refers to preparations that do not contain any toxic ingredients.
「添付文書」という用語は、適応症、用法、用量、投与、併用療法、包装された製品と組み合わせる他の医薬、及び/又はそのような治療用製品若しくは医薬品の使用に関する禁忌及び/又は警告に関する情報を含む治療用製品又は医薬の市販包装に通例含まれる説明書を指すために使用される。 The term "package insert" refers to indications, usage, dosage, administration, concomitant therapy, other medicines in combination with the packaged product, and/or contraindications and/or warnings regarding the use of such therapeutic products or medicines. Used to refer to instructions that are commonly included in the commercial packaging of therapeutic products or pharmaceuticals that contain information.
本明細書で使用される場合、「導入期」という用語は、対象に投与される1つ以上の治療剤(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及び/又は化学療法剤)の一連の1回以上の投薬サイクル(例えば、約4~6サイクル)のことを指し、その1回以上の投薬サイクルの後には、必要に応じて、維持期が続く。 As used herein, the term “introduction phase” refers to the period of one or more therapeutic agents (e.g., anti-TIGIT antagonist antibody, PD-1 axis binding antagonist and/or chemotherapeutic agent) administered to the subject. Refers to a series of one or more dosing cycles (eg, about 4-6 cycles), optionally followed by a maintenance phase.
本明細書で使用される場合、「維持期」という用語は、導入期に続いて対象に投与される1つ以上の治療剤(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及び/又は化学療法剤)の一連の1回以上の投薬サイクルを指す。いくつかの例では、維持期は、対象が導入期の間に疾患進行又は許容できない毒性を経験しなかった場合にのみ開始される。導入期及び維持期は、同じ治療剤の使用を含んでも含まなくてもよい。例えば、いくつかの例では、導入期は、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤の使用を含み、維持期は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含む。 As used herein, the term "maintenance phase" refers to one or more therapeutic agents (e.g., anti-TIGIT antagonist antibody, PD-1 axis binding antagonist and/or A series of one or more dosing cycles of a chemotherapeutic agent). In some instances, the Maintenance Phase is initiated only if the subject did not experience disease progression or unacceptable toxicity during the Run-in Phase. The induction phase and maintenance phase may or may not involve the use of the same therapeutic agent. For example, in some instances, the induction phase includes the use of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents, and the maintenance phase includes anti-TIGIT antagonist antibodies and Including the use of PD-1 axis binding antagonists.
膀胱がんに関連して、「白金系化学療法による処置に不適格である」又は「白金系化学療法による処置に不適格である」という用語は、対象が、主治医の判断において、又は当該技術分野で公知の白金系化学療法に適格であるための標準化された基準に従って、白金系化学療法による処置に不適格又は不適格であることを意味する。例えば、その全体が参照により本明細書に組み込まれるGalsky et al.Lancet Oncol.12(3):211-4,2011に記載される基準は、対象がシスプラチンに基づく化学療法に適格であるかどうかを判定するために使用され得る。Galsky et al.は、以下の少なくとも1つを満たす患者がシスプラチンに基づく化学療法に適さないと考えられる転移性UC(mUC)を有する患者のコンセンサス定義を記載している:(i)世界保健協会(WHO)若しくは米国東海岸がん臨床試験グループ(ECOG)のパフォーマンスステータス2、又はカルノフスキー(Karnofsky)パフォーマンスステータス60~70%;(ii)クレアチニンクリアランス(計算値又は測定値)が1mL/s未満;(iii)国立がん研究所(NCI)有害事象共通用語規準(CTCAE)v 4.0グレード≧2聴力損失;(iv)CTCAE v.4.0グレード≧2末梢神経障害;及び/又はニューヨーク心臓病学会(NYHA)クラスIII心不全。一例では、以下の1つ以上有する場合、患者はシスプラチンに基づく化学療法に不適であると考えられる:腎機能障害(例えば、糸球体濾過量(GFR)>30であるが<60mL/分);GFRは、直接測定(すなわち、クレアチニンクリアランス又はエチルジアミンテトラアセテート)によって、又は利用可能でない場合、血清/血漿クレアチニンからの計算(Cockcroft-Gault式)によって評定され得る;聴力損失(例えば、NCI CTCAE v 4.0グレード≧2、2つの連続周波数で25デシベルの聴力損失);末梢神経障害(例えば、NCI CTCAE v4.0グレード≧2末梢神経障害(すなわち、刺痛を含む感覚変化又は知覚異常));及び/又はECOGパフォーマンスステータス評価(Oken et al.Am.J.Clin.Oncol.5:649-655,1982、その全体が参照により本明細書に組み込まれる)(例えば、ECOGパフォーマンスステータスが2)。いくつかの態様では、以下のうちの1つを有する対象がカルボプラチンに基づく化学療法に適格であり得る:腎機能障害(例えば、GFR>30であるが<60mL/分);GFRは、直接測定(すなわち、クレアチニンクリアランス又はエチルジアミンテトラアセテート)によって、又は利用可能でない場合、血清/血漿クレアチニンからの計算(Cockcroft-Gault式)によって評定され得る;聴力損失(例えば、2つの連続周波数で25デシベルのCTCAE v 4.0グレード≧2聴力損失);末梢神経障害(例えば、NCI CTCAE v 4.0グレード≧2末梢神経障害(すなわち、刺痛を含む感覚変化又は知覚異常));及び/又はECOGパフォーマンスステータス評定(例えば、ECOGパフォーマンスステータスが2)。例えば、シスプラチンの不適格性は、以下の基準のいずれか1つによって定義され得る:(i)腎機能障害(GFR<60mL/分);GFRは、直接測定(すなわち、クレアチニンクリアランス又はエチルジアミンテトラアセテート)によって、又は利用可能でない場合、血清/血漿クレアチニンからの計算(Cockcroft Gault式)によって評定され得る;(ii)隣接する二つの周波数で25 dBの難聴(聴力検査によって測定);(iii)グレード2以上の末梢神経障害(すなわち、刺痛を含む感覚変化又は知覚異常(parasthesis));及び(iv)ECOGパフォーマンスステータス2。
In the context of bladder cancer, the term "ineligible for treatment with platinum-based chemotherapy" or "ineligible for treatment with platinum-based chemotherapy" means that the subject, in the judgment of the attending physician or in the art Means ineligible or ineligible for treatment with platinum-based chemotherapy according to standardized criteria for platinum-based chemotherapy eligibility known in the art. See, for example, Galsky et al. Lancet Oncol. 12(3):211-4, 2011 can be used to determine whether a subject is eligible for cisplatin-based chemotherapy. Galsky et al. describes a consensus definition of patients with metastatic UC (mUC) who are considered ineligible for cisplatin-based chemotherapy if they meet at least one of the following: (i) World Health Association (WHO) or US East Coast Cancer Clinical Trials Group (ECOG)
III.治療及び診断方法並びに使用
A.がんに関する治療方法及び使用
治療方法及び組成物
本明細書では、有効量の抗TIGITアンタゴニスト抗体(例えば、抗TIGITアンタゴニスト抗体、例えばチラゴルマブ)、又は抗TIGITアンタゴニスト抗体とPD-1軸結合アンタゴニストの両方の組み合わせ(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は抗PD-1アンタゴニスト抗体(ペムブロリズマブ等)の1回以上の投薬サイクルを対象に投与することを含む、がん(例えば、固形腫瘍、及び/又は局所進行性又は転移性のがん、例えば、肺がん(例えば、早期肺がん(例えば、切除可能な肺がん)、小細胞肺がん(SCLC)(例えば、進展型(ES)-SCLC)、非小細胞肺がん(NSCLC)(例えば、扁平上皮性NSCLC又は非扁平上皮性NSCLC、局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発又は転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮性 NSCLC(例えば、ステージIV以外扁平上皮NSCLC))、又はIV期のNSCLC(例えば、対象が以前にIV期のNSCLCの処置を受けたことがない)));子宮頸がん(例えば、IVB期、転移性、再発、又は持続性の子宮頸がん、例えば、転移性及び/又は再発したPD-L1陽性子宮頸がん);乳がん(例えば、トリプルネガティブ乳がん(TNBC)(例えば、エストロゲン受容体陰性(ER-)、プロゲステロン受容体陰性(PR-)、及びHER2陰性(HER2-)乳がん、例えば、早期TNBC(eTNBC))又はHER2陽性乳がん);頭頸部がん(例えば、頭頸部扁平上皮癌腫(SCCHN)、例えば、再発/転移性PD-L1陽性SCCHN);肝臓がん(例えば、肝細胞癌腫(HCC)、例えば、局所進行性又は転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、筋浸潤性膀胱がん(MIBC)又は局所進行性又は転移性尿路上皮癌腫(mUC));食道がん;膵がん(例えば、膵管腺癌(PDAC)、例えば、転移性PDAC);腎臓がん又は腎がん(例えば、腎細胞がん(RCC));黒色腫、卵巣がん、胃がん(例えば、胃食道接合部がん)、又は結腸直腸がん(CRC;例えば、マイクロサテライト安定(MSS)又はマイクロサテライト不安定(MSI)低(MSI-Low)を伴うCRC)を処置するための方法及び使用が提供される。
III. THERAPEUTIC AND DIAGNOSTIC METHODS AND USES A. Treatment Methods and Uses for Cancer Treatment Methods and Compositions As used herein, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody, such as tiragolumab), or both an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or an anti-PD-1 antagonist antibody (e.g., pembrolizumab) in a combination of cancers (e.g., solid tumors, and/or locally advanced or metastatic cancer, such as lung cancer (eg, early stage lung cancer (eg, resectable lung cancer), small cell lung cancer (SCLC) (eg, extensive stage (ES)-SCLC), non-small Cell lung cancer (NSCLC) (e.g. squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g. locally advanced unresectable or metastatic non-squamous NSCLC (e.g., non-stage IV squamous NSCLC)), or stage IV NSCLC (e.g., subject has not been previously treated for stage IV NSCLC)); cervical cancer (e.g., stage IVB) , metastatic, recurrent, or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (e.g. triple negative breast cancer (TNBC) (e.g. estrogen receptor negative (ER-), progesterone receptor-negative (PR-), and HER2-negative (HER2-) breast cancer, e.g. early TNBC (eTNBC) or HER2-positive breast cancer); head and neck cancers (e.g. head and neck squamous cell carcinoma) (SCCHN), e.g., recurrent/metastatic PD-L1 positive SCCHN); liver cancer (e.g., hepatocellular carcinoma (HCC), e.g., locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. muscle invasive bladder cancer (MIBC) or locally advanced or metastatic urothelial carcinoma (mUC)); esophageal cancer; pancreatic cancer (e.g. pancreatic ductal adenocarcinoma (PDAC), e.g. metastatic PDAC) ); renal cancer or kidney cancer (e.g., renal cell carcinoma (RCC)); melanoma, ovarian cancer, gastric cancer (e.g., gastroesophageal junction cancer), or colorectal cancer (CRC; Methods and uses are provided for treating CRC with Microsatellite Stable (MSS) or Microsatellite Instable (MSI) Low (MSI-Low).
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)を、それを必要とする対象に4週間(例えば、各28日間投薬サイクルの1日目に)毎に投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、完全奏効(CR)又は部分奏効(PR)をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、無増悪生存期間(PFS)又は客観的応答期間(DOR)の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、全生存期間(OS)の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). (e.g., an anti-PD-1 antagonist antibody, such as pembrolizumab) to a subject in need thereof every four weeks (e.g., on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象に4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ、又は抗PD-1アンタゴニスト抗体、例えば、ペンブロリズマブ)を2週間(例えば、各28日間投薬サイクルの1及び15日目に)ごと、3週間(例えば、各21日間投薬サイクルの1日目に)ごと、又は4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与する。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、DORの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject in need thereof for four weeks (e.g., 28 days each dosing). on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象に2週間(例えば、各28日間投薬サイクルの1日目及び15日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を2週間(例えば、各28日間投薬サイクルの1日目及び15日目に)ごとに投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ、又は抗PD-1アンタゴニスト抗体、例えば、ペンブロリズマブ)を2週間(例えば、各28日間投薬サイクルの1及び15日目に)ごと、3週間(例えば、各21日間投薬サイクルの1日目に)ごと、又は4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与する。本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)を、それを必要とする対象に2週間(例えば、各28日間投薬サイクルの1日目及び15日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject in need thereof for two weeks (e.g., 28 days each dosing). on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象に3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を3週間(例えば、各21日間投薬サイクルの1日目に)ごとに投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ、又は抗PD-1アンタゴニスト抗体、例えば、ペンブロリズマブ)を2週間(例えば、各28日間投薬サイクルの1及び15日目に)ごと、3週間(例えば、各21日間投薬サイクルの1日目に)ごと、又は4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与する。特定の例では、本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象に3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象のOSを延長する。いくつかの例では、本発明は、がんを有する対象を処置する方法であって、対象に、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法を含む。いくつかの例では、方法は、対象に、3週間ごとの500mg~700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの900mg~1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを投与することを含む。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject in need thereof every three weeks (e.g., each 21 doses). on
特定の例では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、化学療法剤なしで投与される(例えば、化学療法剤なしでは、例えば、投薬レジメン全体が対象への化学療法剤の投与を欠いている)。 In certain examples, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered without a chemotherapeutic agent (e.g., without a chemotherapeutic agent, e.g., if the overall dosing regimen requires administration of a chemotherapeutic agent to the subject). missing).
いくつかの実施形態では、対象は、がんの治療法(例えば、がん免疫療法及び/又は化学療法剤)で以前に処置されたことがない。いくつかの実施形態では、対象は、がんの治療(例えば、がん免疫療法及び/又は化学療法剤)による事前の処置を受けている。いくつかの例では、対象は、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を投与する少なくとも1ヶ月以内(例えば、PD-1軸結合アンタゴニストと抗TIGITアンタゴニスト抗体との投与の2ヶ月前以内、3ヶ月前以内、4ヶ月前以内、6ヶ月前以内、1年前、2年前、3年前、4年前、5年前、又は10年前)に事前全身治療(例えば、治癒目的の事前全身治療、例えば化学療法)を受けたことがない。いくつかの例では、対象は化学療法未経験である。 In some embodiments, the subject has not been previously treated with cancer therapies (eg, cancer immunotherapy and/or chemotherapeutic agents). In some embodiments, the subject has undergone prior treatment with cancer therapy (eg, cancer immunotherapy and/or chemotherapeutic agents). In some examples, the subject is within at least 1 month of administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (e.g., within 2 months prior to administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody, Prior systemic treatment (e.g., curative intent) within 3 months, 4 months, 6 months, 1 year, 2 years, 3 years, 4 years, 5 years, or 10 years No previous systemic therapy (e.g., chemotherapy). In some examples, the subject is chemotherapy naive.
いくつかの実施形態では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、化学療法と組み合わせて投与される。例えば、PD-1軸結合アンタゴニスト及び/又は抗TIGITアンタゴニスト抗体の2週間に1回(Q2W)、3週間に1回(Q3W)又は4週間に1回(Q4W)の投薬レジメンを、1つ以上の化学療法剤と併せて投与することができる。1つ以上の化学療法剤は、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の投与頻度と同じ頻度(Q2W、Q3W、又はQ4W)又は異なる頻度(例えば、3週間の投薬/1週間の休薬のスケジュール(例えば、28日周期ごとの第1、8、及び15日目))で投与することができる。例えば、いくつかの実施形態では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を2週間ごとに投与し、1つ以上の化学療法剤を毎週、3週間の投薬/1週間の休薬、2週間ごと、3週間ごと、又は4週間ごとに投与する。あるいは、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を3週間ごとに投与し、1つ以上の化学療法剤を1週間ごと、2週間ごと、3週間ごと、又は4週間ごとに投与する。あるいは、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を4週間ごとに投与し、1つ以上の化学療法剤を毎週、3週間の投薬/1週間の休薬、2週間ごと、3週間ごと、又は4週間ごとに投与する。ある特定の例では、化学療法剤は、週に複数回(例えば、週に2、3、4、5、6又は7回(例えば、投薬サイクルの1日目、2日目及び3日目に)投与される。
In some embodiments, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody are administered in combination with chemotherapy. For example, one or more PD-1 axis binding antagonist and/or anti-TIGIT antagonist antibody once every two weeks (Q2W), once every three weeks (Q3W) or once every four weeks (Q4W) dosing regimens can be administered in combination with a chemotherapeutic agent. The one or more chemotherapeutic agents are administered at the same frequency (Q2W, Q3W, or Q4W) or at a different frequency (e.g., 3 weeks on/1 week off) than the dosing frequency of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody. schedule (eg,
いくつかの実施形態では、化学療法剤の用量は、1回以上の初期用量(例えば、1回、2回、3回、4回、又はそれ以上の初期投与後)の後に減少する。例えば、化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))のその後の用量は、初期用量の約95%、90%、85%、80%、75%、70%、65%、60%、55%、50%、45%、40%、35%、30%、25%、20%、15%、10%又は5%で投与することができる。例えば、125mg/m2のnab-パクリタキセルの初期用量を、その後の用量のために、例えば100mg/m2又は75mg/m2に減少させることができる;100mg/m2のnab-パクリタキセルの初期用量を、その後の用量のために、例えば75mg/m2に減少させることができる;約175mg/m2のパクリタキセルの初期用量を、その後の用量のために、例えば、150mg/m2、125mg/m2、100mg/m2、又は75mg/m2に減少させることができる;約200mg/m2のパクリタキセルの初期用量を、その後の用量のために、例えば、175mg/m2、150mg/m2、125mg/m2、100mg/m2、又は75mg/m2に減少させることができる;約1000mg/m2のゲムシタビンの初期用量を、その後の用量のために、例えば、900mg/m2、800mg/m2、750mg/m2、700mg/m2、600mg/m2、又は500mg/m2に減少させることができる;約75mg/m2のシスプラチンの初期用量を、その後の用量のために、例えば、70mg/m2、65mg/m2、60mg/m2、55mg/m2、50mg/m2、又は45mg/m2に減少させることができる;約500mg/m2のペメトレキセドの初期用量を、その後の用量のために、例えば、450mg/m2、400mg/m2、350mg/m2、300mg/m2、250mg/m2、又は200mg/m2に減少させることができる;及び/又はAUC=6mg/ml/分を達成するのに十分な用量のカルボプラチンの初期用量は、その後の用量、例えばAUC=5.5.mg/ml/分、5.0mg/ml/分、4.5mg/ml/分、又は4.0mg/ml/分を達成するのに十分な用量まで減少させることができる。いくつかの例では、125mg/m2のnab-パクリタキセルの初期用量を、その後の用量のために、例えば100mg/m2又は75mg/m2に減少させることができる;100mg/m2のnab-パクリタキセルの初期用量を、その後の用量のために、例えば75mg/m2に減少させることができる;175mg/m2のパクリタキセルの初期用量を、その後の用量のために、例えば、150mg/m2、125mg/m2、100mg/m2、又は75mg/m2に減少させることができる;200mg/m2のパクリタキセルの初期用量を、その後の用量のために、例えば、175mg/m2、150mg/m2、125mg/m2、100mg/m2、又は75mg/m2に減少させることができる;1000mg/m2のゲムシタビンの初期用量を、その後の用量のために、例えば、900mg/m2、800mg/m2、750mg/m2、700mg/m2、600mg/m2、又は500mg/m2に減少させることができる;75mg/m2のシスプラチンの初期用量を、その後の用量のために、例えば、70mg/m2、65mg/m2、60mg/m2、55mg/m2、50mg/m2、又は45mg/m2に減少させることができる;500mg/m2のペメトレキセドの初期用量を、その後の用量のために、例えば、450mg/m2、400mg/m2、350mg/m2、300mg/m2、250mg/m2、又は200mg/m2に減少させることができる;及び/又はAUC=6mg/ml/分を達成するのに十分な用量のカルボプラチンの初期用量は、その後の用量、例えばAUC=5.5.mg/ml/分、5.0mg/ml/分、4.5mg/ml/分、又は4.0mg/ml/分を達成するのに十分な用量まで減少させることができる。 In some embodiments, the dose of the chemotherapeutic agent is decreased after one or more initial doses (eg, after 1, 2, 3, 4, or more initial doses). For example, chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclophosphamide), taxanes ( For example, subsequent doses of paclitaxel, eg nab-paclitaxel) and/or topoisomerase II inhibitors (eg, doxorubicin))) are about 95%, 90%, 85%, 80%, 75%, 70% of the initial dose, It can be dosed at 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25%, 20%, 15%, 10% or 5%. For example, an initial dose of 125 mg/m 2 nab-paclitaxel can be reduced for subsequent doses, eg, to 100 mg/m 2 or 75 mg/m 2 ; an initial dose of 100 mg/m 2 nab-paclitaxel. can be reduced for subsequent doses , e.g. 2 , 100 mg/m 2 , or 75 mg/m 2 ; an initial dose of paclitaxel of about 200 mg/m 2 for subsequent doses such as 175 mg/m 2 , 150 mg/m 2 , initial doses of gemcitabine of about 1000 mg/m 2 may be reduced to 125 mg/m 2 , 100 mg/m 2 , or 75 mg / m 2 ; m 2 , 750 mg/m 2 , 700 mg/m 2 , 600 mg/m 2 , or 500 mg/m 2 ; , 70 mg/m 2 , 65 mg/m 2 , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 , or 45 mg/m 2 ; and / or AUC for subsequent doses , e.g. An initial dose of carboplatin sufficient to achieve AUC = 5.5. The dose may be reduced enough to achieve mg/ml/min, 5.0 mg/ml/min, 4.5 mg/ml/min, or 4.0 mg/ml/min. In some examples, an initial dose of 125 mg/m 2 nab-paclitaxel can be reduced for subsequent doses, eg , 100 mg/m 2 or 75 mg/m 2 ; The initial dose of paclitaxel can be reduced to, for example, 75 mg/m 2 for subsequent doses; initial dose of paclitaxel of 200 mg/m 2 may be reduced to 125 mg/m 2 , 100 mg/m 2 , or 75 mg/m 2 ; 2 , 125 mg/m 2 , 100 mg/m 2 , or 75 mg/ m 2 ; /m 2 , 750 mg/m 2 , 700 mg/m 2 , 600 mg/m 2 , or 500 mg/m 2 ; , 70 mg/m 2 , 65 mg/m 2 , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 , or 45 mg/m 2 ; and / or AUC = _ An initial dose of carboplatin sufficient to achieve 6 mg/ml/min was followed by subsequent doses, eg, AUC=5.5. The dose may be reduced enough to achieve mg/ml/min, 5.0 mg/ml/min, 4.5 mg/ml/min, or 4.0 mg/ml/min.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法の組み合わせを、それを必要とする対象に投与することを含む方法及び使用を含む。いくつかの実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、2週間ごと(例えば、各28日間投薬サイクルの1日目及び15日目)、3週間ごと(例えば、各21日間投薬サイクルの1日目)、又は4週間ごと(例えば、各28日間投薬サイクルの1日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)を2週間(例えば、各28日間投薬サイクルの1及び15日目に)ごと、3週間(例えば、各21日間投薬サイクルの1日目に)ごと、又は4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与する。いくつかの例では、化学療法の組み合わせは、有効量の第1の非白金系化学療法剤及び有効量の第2の非白金系化学療法剤を含む。いくつかの例では、第1の非白金系化学療法剤は代謝拮抗剤であり、第2の非白金系化学療法剤はタキサンである。いくつかの実施形態では、化学療法併用(例えば、代謝拮抗剤(例えば、ゲムシタビン、ペメトレキセド又はカペシタビン)及びタキサン(例えば、nab-パクリタキセル及びパクリタキセル))は、毎週、隔週又は4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)投与される。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). antibodies, or anti-PD-1 antagonist antibodies such as pembrolizumab) and chemotherapy in combination to a subject in need thereof. In some embodiments, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg, , atezolizumab) every 2 weeks (e.g., on
特定の実施形態では、本方法は、それを必要とする対象に有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、ゲムシタビン及びパクリタキセルを投与することを含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は2週間ごとに(例えば、各28日間投薬サイクルの1及び15日目に)投与され、化学療法の組み合わせ(例えば、代謝拮抗剤及びタキサン(例えば、ゲムシタビン及びパクリタキセル))はより頻繁に(例えば、4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に))投与される。
In certain embodiments, the method comprises administering to a subject in need thereof an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), PD-1 axis administration of a binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab), gemcitabine and paclitaxel; tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) are administered biweekly (e.g., on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、代謝拮抗剤(例えば、ゲムシタビン)及びタキサン(例えば、パクリタキセル)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、代謝拮抗剤(例えば、ゲムシタビン)及びタキサン(例えば、パクリタキセル)の投与は、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、代謝拮抗剤(例えば、ゲムシタビン)及びタキサン(例えば、パクリタキセル)の投与は、対象のOSを延長させる。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), antimetabolites (eg gemcitabine) and taxanes (eg paclitaxel) result in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), antimetabolites (eg gemcitabine) and taxanes (eg paclitaxel) result in increased PFS in subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), antimetabolites (eg gemcitabine) and taxanes (eg paclitaxel) prolong OS in subjects.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、及び化学療法の組み合わせを、それを必要とする対象に投与することを含む方法及び使用を含み、化学療法の組み合わせは、有効量の白金系化学療法剤及び有効量の非白金系化学療法剤を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、2週間ごと(例えば、各28日間投薬サイクルの1日目及び15日目)、3週間ごと(例えば、各21日間投薬サイクルの1日目)、又は4週間ごと(例えば、各28日間投薬サイクルの1日目)に投与される。いくつかの例では、白金系化学療法剤はカルボプラチン又はシスプラチンであり、非白金系化学療法剤は代謝拮抗剤(例えば、ペメトレキセド)である。いくつかの実施形態では、化学療法併用(例えば、白金系化学療法剤及び代謝拮抗剤(例えば、ペメトレキセド))は、毎週、2週間ごと、4週間ごと、又は4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)投与される。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). or an anti-PD-1 antagonist antibody, such as pembrolizumab), and a chemotherapeutic combination, wherein the chemotherapeutic combination comprises an effective amount of a platinum-based A chemotherapeutic agent and an effective amount of a non-platinum chemotherapeutic agent. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 2 weeks (e.g., on
特定の実施形態では、本方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及び代謝拮抗剤(例えば、ペメトレキセド)を、それを必要とする対象に投与することを含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与され、化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)は同じ頻度で(例えば、3週間ごとに、例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの例では、投薬は、4~6回の導入投薬サイクルにわたって継続する(例えば、4回の導入投薬サイクル、5回の導入投薬サイクル、又は6回の導入投薬サイクル)。導入投薬サイクルの後、維持療法は、1回以上のその後の(維持)投薬サイクルで投与することができる。特定の実施形態では、1回以上の維持投薬サイクルは、白金系化学療法剤を含まない。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD - an anti-TIGIT antagonist, including administering an L1 antagonist antibody (e.g., atezolizumab), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and an antimetabolite (e.g., pemetrexed) to a subject in need thereof Antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies, e.g., atezolizumab) every 3 weeks (e.g. , on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、対象のOSを延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and antimetabolites (eg pemetrexed) result in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and antimetabolite agents (eg, pemetrexed) result in increased PFS in subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and antimetabolite agents (eg, pemetrexed) prolong OS in subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)を投与されている対象は、固形腫瘍又は局所進行性がん若しくは転移性がんの処置を受けている。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、初期TNBC(eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab). ), platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin), and subjects receiving antimetabolite agents (e.g., pemetrexed) undergoing treatment for solid tumors or locally advanced or metastatic cancer . Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. early TNBC (eTNBC))) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN) liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g., PDAC, e.g., metastatic PDAC); renal cancer or renal cancer (e.g., RCC); melanoma; ovarian cancer; gastric cancer (e.g., gastroesophageal junction cancer); MSI-Low CRC).
本発明はまた、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、パクリタキセル又はnab-パクリタキセル))を、それを必要とする対象に投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、2週間ごと(例えば、各28日間投薬サイクルの1日目及び15日目)、3週間ごと(例えば、各21日間投薬サイクルの1日目)、又は4週間ごと(例えば、各28日間投薬サイクルの1日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)を4週間ごとに(例えば、各28日間投薬サイクルの1日目に)投与する。いくつかの実施形態では、化学療法は、毎週、2週間ごと、4週間ごと、又は4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)投与される。いくつかの実施形態では、化学療法は毎週投与される。
The present invention also provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD-L1, such as atezolizumab). antagonist antibodies, or anti-PD-1 antagonist antibodies such as pembrolizumab) and chemotherapy (e.g., taxanes (e.g., paclitaxel or nab-paclitaxel)) to a subject in need thereof. . In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 2 weeks (e.g., on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、パクリタキセル又はnab-パクリタキセル))の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、パクリタキセル又はnab-パクリタキセル))の投与は、参照と比較して対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、パクリタキセル又はnab-パクリタキセル))の投与は、DORの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、パクリタキセル又はnab-パクリタキセル))の投与は、対象のOSを延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies, or anti-PD-1 antagonist antibodies such as pembrolizumab) and chemotherapy (eg, taxanes (eg, paclitaxel or nab-paclitaxel)) results in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of an L1 antagonist antibody, or an anti-PD-1 antagonist antibody such as pembrolizumab) and chemotherapy (eg, a taxane (eg, paclitaxel or nab-paclitaxel)) results in an increase in the subject's PFS compared to the reference. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies, or anti-PD-1 antagonist antibodies such as pembrolizumab) and chemotherapy (eg, taxanes (eg, paclitaxel or nab-paclitaxel)) results in an increase in DOR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of an L1 antagonist antibody, or an anti-PD-1 antagonist antibody such as pembrolizumab) and chemotherapy (eg, taxanes (eg, paclitaxel or nab-paclitaxel)) prolongs OS in subjects.
本発明はまた、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、及び化学療法の組み合わせを、それを必要とする対象に投与することを含む方法及び使用を含み、化学療法の組み合わせは、有効量の白金系化学療法剤及び有効量の非白金系化学療法剤を含み、非白金系化学療法剤はタキサン(例えば、パクリタキセル又はnab-パクリタキセル)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、2週間ごと(例えば、各28日間投薬サイクルの1日目及び15日目)、3週間ごと(例えば、各21日間投薬サイクルの1日目)、又は4週間ごと(例えば、各28日間投薬サイクルの1日目)に投与される。いくつかの実施形態では、化学療法併用(例えば、白金系化学療法剤及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル))は、毎週、2週間ごと、4週間ごと、又は4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)投与される。
The present invention also provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD-L1, such as atezolizumab). antagonist antibody, or an anti-PD-1 antagonist antibody such as pembrolizumab), and a chemotherapeutic combination comprising administering to a subject in need thereof, the chemotherapeutic combination comprising an effective amount of platinum A chemotherapeutic agent and an effective amount of a non-platinum chemotherapeutic agent, wherein the non-platinum chemotherapeutic agent is a taxane (eg, paclitaxel or nab-paclitaxel). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 2 weeks (e.g., on
特定の実施形態では、方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)を、それを必要とする対象に投与することを含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与され、化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)は同じ頻度で(例えば、3週間ごとに、例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの例では、投薬は、4~6回の導入投薬サイクルにわたって継続する(例えば、4回の導入投薬サイクル、5回の導入投薬サイクル、又は6回の導入投薬サイクル)。導入投薬サイクルの後、維持療法は、1回以上のその後の(維持)投薬サイクルで投与することができる。特定の実施形態では、1回以上の維持投薬サイクルは、白金系化学療法剤を含まない。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD- anti-TIGIT, including administering an L1 antagonist antibody (e.g., atezolizumab), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and a taxane (e.g., paclitaxel or nab-paclitaxel) to a subject in need thereof; Antagonist antibody (e.g., anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 3 weeks ( for example, on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)の投与は、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)の投与は、対象のOSを延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and taxanes (eg paclitaxel or nab-paclitaxel) result in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and taxanes (eg, paclitaxel or nab-paclitaxel) result in increased PFS in subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and taxanes (eg paclitaxel or nab-paclitaxel) prolong OS in subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びタキサン(例えば、パクリタキセル又はnab-パクリタキセル)を投与されている対象は、固形腫瘍又は局所進行性がん若しくは転移性がんの処置を受けている。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、初期TNBC(eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab). ), platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and taxanes (e.g., paclitaxel or nab-paclitaxel) undergoing treatment for solid tumors or locally advanced or metastatic cancer. ing. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. early TNBC (eTNBC))) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN) liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer renal or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI- Low CRC).
有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、及び化学療法の組み合わせを、それを必要とする対象に投与することを含む方法及び使用も本明細書で提供され、化学療法の組み合わせは、有効量の白金系化学療法剤及び有効量の非白金系化学療法剤を含み、非白金系化学療法剤はトポイソメラーゼII阻害剤(例えば、エトポシド)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、2週間ごと(例えば、各28日間投薬サイクルの1日目及び15日目)、3週間ごと(例えば、各21日間投薬サイクルの1日目)、又は4週間ごと(例えば、各28日間投薬サイクルの1日目)に投与される。いくつかの実施形態では、化学療法併用(例えば、白金系化学療法剤及びトポイソメラーゼII阻害剤(例えば、エトポシド))は、毎週、2週間ごと、4週間ごと、又は4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)投与される。いくつかの実施形態では、トポイソメラーゼII阻害剤(例えば、エトポシド)は、白金系化学療法剤(例えば、週に3回、例えば、各投薬サイクルの1日目、2日目及び3日目に)よりも頻繁に投与される。
an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or pembrolizumab) Also provided herein are methods and uses comprising administering to a subject in need thereof a combination of an anti-PD-1 antagonist antibody, such as an anti-PD-1 antagonist antibody), and a chemotherapy, wherein the chemotherapy combination comprises an effective amount of platinum A chemotherapeutic agent and an effective amount of a non-platinum chemotherapeutic agent, wherein the non-platinum chemotherapeutic agent is a topoisomerase II inhibitor (eg, etoposide). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 2 weeks (e.g., on
特定の実施形態では、方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及びトポイソメラーゼII阻害剤(例えば、エトポシド)を、それを必要とする対象に投与することを含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与され、化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)は同じ頻度で(例えば、3週間ごとに、例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの例では、投薬は、4~6回の導入投薬サイクルにわたって継続する(例えば、4回の導入投薬サイクル、5回の導入投薬サイクル、又は6回の導入投薬サイクル)。導入投薬サイクルの後、維持療法は、1回以上のその後の(維持)投薬サイクルで投与することができる。特定の実施形態では、1回以上の維持投薬サイクルは、白金系化学療法剤又はトポイソメラーゼII阻害剤(例えば、エトポシド)を含まない。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD- an anti-TIGIT antagonist, including administering an L1 antagonist antibody (e.g., atezolizumab), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and a topoisomerase II inhibitor (e.g., etoposide) to a subject in need thereof; Antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies, e.g., atezolizumab) every 3 weeks (e.g. , on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)は、(a)CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)は、対象のPFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)は、対象のOSを延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and topoisomerase II inhibitors (eg etoposide) lead to (a) CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and topoisomerase II inhibitors (eg etoposide) result in increased PFS in subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and topoisomerase II inhibitors (eg etoposide) prolong OS in subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)を投与されている対象は、固形腫瘍又は局所進行性がん若しくは転移性がんの処置を受けている。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、初期TNBC(eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab). ), platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin), and subjects receiving topoisomerase II inhibitors (e.g., etoposide) undergoing treatment for solid tumors or locally advanced or metastatic cancer there is Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. early TNBC (eTNBC))) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN) liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer renal or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI- Low CRC).
有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、それを必要とする対象に投与することを含む方法及び使用も本明細書で提供される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与する。
an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or pembrolizumab) Also provided herein are methods and uses comprising administering an anti-PD-1 antagonist antibody (such as an anti-PD-1 antagonist antibody) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) to a subject in need thereof. In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies, e.g., atezolizumab) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) are administered every 3 weeks (eg, on
特定の実施形態では、本方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の、それを必要とする対象への投与を含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、対象のOSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、対象のPFSの増加をもたらす。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD - an L1 antagonist antibody (e.g., atezolizumab) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) to a subject in need thereof, including an anti-TIGIT antagonist antibody (e.g., disclosed herein) anti-TIGIT antagonist antibodies, such as tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies, such as atezolizumab) and VEGF antagonists (e.g., anti-VEGF antibodies (e.g., bevacizumab)) , administered every 3 weeks (eg, on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与されている対象は、固形腫瘍又は局所進行性若しくは転移性がんについて処置されている。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えばeTNBC))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab). ) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is being treated for solid tumors or locally advanced or metastatic cancer. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. eTNBC)) or HER2 positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer ( bladder cancer (e.g., MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g., PDAC, renal cancer or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI-Low CRC) may be
本発明は、がん患者のがんを処置する方法であって、がんを処置するのに有効な量のアテゾリズマブ、ベバシズマブ、及びチラゴルマブの組み合わせを患者に投与することを含む方法を含む。 The present invention includes a method of treating cancer in a cancer patient comprising administering to the patient a cancer-treating effective amount of a combination of atezolizumab, bevacizumab, and tiragolumab.
有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の、それを必要とする対象への投与を含む方法及び使用も本明細書で提供され、抗PD-1アンタゴニスト抗体はペンブロリズマブである。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与し、抗PD-1アンタゴニスト抗体はペンブロリズマブである。
an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), an anti-PD-1 antagonist antibody and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) Also provided herein are methods and uses comprising administering to a subject in need thereof, the anti-PD-1 antagonist antibody is pembrolizumab. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), an anti-PD-1 antagonist antibody and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is administered every 3 weeks (eg, on
特定の実施形態では、本方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体、及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の、それを必要とする対象への投与を含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体、及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与され、抗PD-1アンタゴニスト抗体は、ペンブロリズマブである。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、対象のOSの増加をもたらし、抗PD-1アンタゴニスト抗体はペンブロリズマブである。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、対象のPFSの増加をもたらし、抗PD-1アンタゴニスト抗体はペンブロリズマブである。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), an anti-PD-1 antagonist antibody, and a VEGF antagonist ( anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject in need thereof; , an anti-PD-1 antagonist antibody, and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) are administered every three weeks (e.g., on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、抗PD-1アンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を受けている対象は、固形腫瘍又は局所進行性若しくは転移性がんについて処置されており、抗PD-1アンタゴニスト抗体はペンブロリズマブである。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えばeTNBC))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), an anti-PD-1 antagonist antibody and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., Subjects receiving bevacizumab)) are being treated for solid tumors or locally advanced or metastatic cancer, and the anti-PD-1 antagonist antibody is pembrolizumab. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. eTNBC)) or HER2 positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer ( bladder cancer (e.g., MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g., PDAC, renal or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI-Low CRC). may
有効量のチラゴルマブ及びペンブロリズマブをそれを必要とする対象に投与することを含む方法及び使用も本明細書で提供される。いくつかの例では、チラゴルマブは3週間ごとに(例えば、各42日間の投薬サイクルの1日目及び22日目に)投与され、ペンブロリズマブは6週間ごとに(例えば、各42日間の投薬サイクルの1日目に)投与される。
Also provided herein are methods and uses comprising administering an effective amount of tiragolumab and pembrolizumab to a subject in need thereof. In some examples, tiragolumab is administered every 3 weeks (e.g., on
特定の実施形態では、方法は、有効量のチラゴルマブ及びペンブロリズマブをそれを必要とする対象に投与することを含み、チラゴルマブは3週間ごとに投与され(例えば、各42日間の投薬サイクルの1日目及び22日目に)、ペンブロリズマブは6週間ごとに投与される(例えば、各42日間の投薬サイクルの1日目に)。いくつかの例では、有効量のチラゴルマブ及びペンブロリズマブは、対象のOSの増加をもたらし、抗PD-1アンタゴニスト抗体はペンブロリズマブである。いくつかの例では、有効量のチラゴルマブ及びペンブロリズマブは、対象のPFSの増加をもたらし、抗PD-1アンタゴニスト抗体はペンブロリズマブである。
In certain embodiments, the method comprises administering to a subject in need thereof an effective amount of tiragolumab and pembrolizumab, wherein tiragolumab is administered every three weeks (e.g., on
いくつかの例では、チラゴルマブ及びペンブロリズマブを受けている対象は、固形腫瘍又は局所進行性若しくは転移性がんについて処置されており、抗PD-1アンタゴニスト抗体はペンブロリズマブである。追加的又は代替的に、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えばeTNBC))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)であってもよい。 In some examples, the subject receiving tiragolumab and pembrolizumab is being treated for a solid tumor or locally advanced or metastatic cancer and the anti-PD-1 antagonist antibody is pembrolizumab. Additionally or alternatively, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced resection). Inoperable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic nonsquamous NSCLC (e.g., stage IV nonsquamous NSCLC)), or stage IV NSCLC (e.g., subject is at stage IV NSCLC never previously treated))): Cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 breast cancer (e.g. TNBC (e.g. eTNBC)) or HER2 positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer ( bladder cancer (e.g., MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g., PDAC, renal or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI-Low CRC). may
また、がんを有する対象を処置する方法であって、対象に、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法が本明細書で提供される。いくつかの例では、方法は、導入期及び維持期を含む。いくつかの例では、導入期及び維持期がそれぞれ、1回以上の投薬サイクルを含む。いくつかの例では、維持期は、白金系化学療法剤の投与を含まない。いくつかの例では、維持期は、非白金系化学療法剤の投与を含まない。いくつかの例では、維持期は、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む。 Also, a method of treating a subject with cancer, wherein the subject is administered an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every three weeks, PD-1 at a dose of about 900 mg to about 1500 mg every three weeks. Provided herein are methods comprising administering a dosing regimen comprising one or more dosing cycles of an axially bound antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks. be done. In some examples, the method includes an induction phase and a maintenance phase. In some examples, the induction phase and the maintenance phase each include one or more dosing cycles. In some examples, the maintenance phase does not include administration of a platinum-based chemotherapeutic agent. In some examples, the maintenance phase does not include administration of non-platinum chemotherapeutic agents. In some examples, the maintenance phase comprises one or more administrations of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks. Including dosing cycles.
また、がんを有する対象を処置する方法であって、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約100mg~約300mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含み、抗PD-1アンタゴニスト抗体がペンブロリズマブである方法も本明細書で提供される。 Also, a method of treating a subject with cancer comprising an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every three weeks and an anti-PD-1 antagonist at a dose of about 100 mg to about 300 mg every three weeks Also provided herein are methods comprising administering to the subject a dosing regimen comprising one or more dosing cycles of the antibody, wherein the anti-PD-1 antagonist antibody is pembrolizumab.
がんを有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストも本明細書で提供され、方法は本明細書で提供される方法によるものである。 Also provided herein are anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in methods of treating a subject or population of subjects having cancer, the methods according to the methods provided herein. .
PD-1軸結合アンタゴニストと組み合わせてがんを有する対象又は対象集団を処置するための医薬品の製造における抗TIGITアンタゴニスト抗体の使用も本明細書で提供され、処置は本明細書で提供される方法によるものである。いくつかの態様では、PD-1軸結合アンタゴニストは、別個の製剤で提供される。他の態様では、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストは、単一製剤で提供される。いくつかの態様では、チラゴルマブ及びアテゾリズマブは、投与前にIVバッグにおいて組み合わされる。 Also provided herein is the use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject or subject population with cancer in combination with a PD-1 axis binding antagonist, the treatment methods provided herein. It is due to In some aspects, the PD-1 axis binding antagonist is provided in a separate formulation. In other aspects, the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist are provided in a single formulation. In some aspects, tiragolumab and atezolizumab are combined in an IV bag prior to administration.
薬剤の投薬
抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、VEGFアンタゴニスト及び化学療法剤の投与は、セクションIII(K)に記載されている。
Drug Administration Administration of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, VEGF antagonists and chemotherapeutic agents is described in Section III(K).
がんの特性評価及び選択
本明細書に記載の方法、使用又は使用のための組成物のいずれにおいても、がんは、固形腫瘍又は局所進行性若しくは転移性のがんであり得る。いくつかの例では、がんは肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLC若しくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性若しくは転移性NSCLC(例えば、局所進行切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、初期TNBC(eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性若しくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC)である。対象が乳がんを有するいくつかの例では、対象は転移性乳がんの事前全身治療を受けたことがない。
Characterization and Selection of Cancer In any of the methods, uses or compositions for use described herein, the cancer can be a solid tumor or a locally advanced or metastatic cancer. In some examples, the cancer is lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)), or stage IV NSCLC (e.g., if the subject has stage IV never previously treated for NSCLC))): cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive child cervical cancer); breast cancer (e.g. TNBC (e.g. early TNBC (eTNBC))) or HER2 positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g. , PDAC, such as metastatic PDAC); renal or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); ). In some instances the subject has breast cancer, the subject has no prior systemic treatment for metastatic breast cancer.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、上皮成長因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない。いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、感作EGFR遺伝子変異又はALK遺伝子再編成を有しない。いくつかの例では、対象は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)を有する。 In some examples, in any of the methods, uses or compositions for use described herein, the subject has epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumors. No abnormalities. In some examples, the subject does not have a sensitizing EGFR gene mutation or ALK gene rearrangement in any of the methods, uses or compositions for use described herein. In some examples, the subject has a US East Coast Clinical Trials Group (ECOG) Performance (PS) of 0 or 1.
突然変異状態EGFR及びALKを検出するための方法は当該技術分野で周知であり、それだけに限らないが、参照によりその全体が本明細書に組み込まれるFrampton et al.(Nature Biotechnology.31(11):1023-1033,2013)に記載されている標的遺伝子プルダウン及び配列決定法等の次世代配列決定法を使用して、臨床試料(例えば、腫瘍生検又は血液試料(例えば、血液中の循環腫瘍DNA))からのDNAを配列決定することが挙げられる。このような次世代配列決定方法は、小試料(例えば、小コア針生検、細針吸引、及び/又はセルブロック由来)又は固定試料(例えば、ホルマリン固定パラフィン包埋(FFPE)試料)の使用を可能にしながら、様々な突然変異(例えば、挿入、欠失、塩基置換、焦点遺伝子増幅、及び/又はホモ接合性遺伝子欠失)を検出する本明細書に開示される方法のいずれかと共に使用することができる。EGFR及びALKの突然変異状態を検出するための他の方法としては、蛍光インサイチュハイブリダイゼーション(FISH)法及び免疫組織化学(IHC)法が挙げられる。ALKの突然変異状態を検出するための例示的な方法は、参照によりその全体が本明細書に組み込まれる米国特許第9,651,555号に開示されている。いくつかの例では、VENTANA(登録商標)抗ALK(D5F3)IHCアッセイを使用して、ALK遺伝子の変異状態を決定する。 Methods for detecting mutational status EGFR and ALK are well known in the art and include, but are not limited to, Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013) using next-generation sequencing methods such as targeted gene pull-down and sequencing methods described in Clinical samples (e.g., tumor biopsies or blood samples). (eg, circulating tumor DNA in blood)). Such next-generation sequencing methods employ the use of small samples (e.g., from small core needle biopsies, fine needle aspirates, and/or cell blocks) or fixed samples (e.g., formalin-fixed paraffin-embedded (FFPE) samples). use with any of the methods disclosed herein to detect various mutations (e.g., insertions, deletions, base substitutions, focal gene amplifications, and/or homozygous gene deletions) while allowing be able to. Other methods for detecting EGFR and ALK mutational status include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods. An exemplary method for detecting the mutational status of ALK is disclosed in US Pat. No. 9,651,555, which is incorporated herein by reference in its entirety. In some examples, the VENTANA® Anti-ALK (D5F3) IHC assay is used to determine the mutational status of the ALK gene.
本明細書に記載される方法のいずれかのいくつかの例では、突然変異は感作EGFR突然変異である。感作EGFR突然変異は当該技術分野で周知であり、米国特許出願公開第2018/0235968号及びJuan et al.(Therapeutic Advances in Medical Oncology.9(3):201-216,2017)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、感作EGFR突然変異は、エクソン18~21(例えば、エクソン18、エクソン19、エクソン20及び/又はエクソン21における突然変異)のいずれか一つにおける突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン19の欠失(del19)である。他の例では、感作EGFR突然変異は、エクソン21中のL858R点突然変異である。いくつかの例では、感作EGFR変異は、エクソン18におけるG719X点変異であり、「X」は、最も一般的には、C、A又はSである。いくつかの例では、感作EGFR突然変異は、エクソン18におけるG719S点突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン18におけるG719A点突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン18におけるS720F点突然変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861Q点変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861R点変異である。他の例では、感作EGFR突然変異はT790M点突然変異である。いくつかの例では、感作EGFR突然変異はE709X点突然変異であり、「X」は最も一般的にはK、A、又はHである。いくつかの例では、感作EGFR変異は、S768I点変異である。
In some examples of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are well known in the art and are described in US Patent Application Publication No. 2018/0235968 and Juan et al. (Therapeutic Advances in Medical Oncology. 9(3):201-216, 2017), which are incorporated herein by reference in their entireties. In some examples, the sensitizing EGFR mutation is a mutation in any one of exons 18-21 (eg, mutations in
本明細書に記載される方法のいずれかのいくつかの例では、突然変異はALK遺伝子再編成である。ALK遺伝子再編成は当該技術分野で周知であり、米国特許第9,651,555号及びDu et al.(Thoracic Cancer.9:423-430,2018)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、ALK遺伝子再構成は、下流のシグナル伝達経路を活性化して細胞増殖及び生存を増加させる発がん性ALKチロシンキナーゼの作製をもたらす。いくつかの例では、ALK遺伝子再編成は、融合がん遺伝子の形成をもたらす、EML4、KIF5B、KLC1、TFG、TPR、HIP1、STRN、DCTN1、SQSTM1、NPM1、BCL11A、BIRC6、RANBP2、ATIC、CLTC、TMP4、及びMSNからなる群から選択される遺伝子によるALK再編成である。いくつかの例では、ALK遺伝子再編成は、ALKとのEML4再編成であり、融合がん遺伝子EML4-ALKの形成をもたらす。 In some examples of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are well known in the art and are described in US Pat. No. 9,651,555 and Du et al. (Thoracic Cancer. 9:423-430, 2018), which are incorporated herein by reference in their entireties. In some instances, ALK gene rearrangement results in the creation of an oncogenic ALK tyrosine kinase that activates downstream signaling pathways to increase cell proliferation and survival. In some instances, the ALK gene rearrangement results in the formation of a fusion oncogene, EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC , TMP4, and MSN. In some instances, the ALK gene rearrangement is an EML4 rearrangement with ALK, resulting in the formation of the fusion oncogene EML4-ALK.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、NSCLCの肺リンパ上皮腫様癌腫サブタイプを有しない。NSCLCのサブタイプを検出するための方法は当該技術分野で周知であり、限定されないが、組織病理学的基準又は分子的特徴(例えば、バイオマーカー(例えば、特定の遺伝子又は該遺伝子によってコードされるタンパク質)の1つ又は組み合わせの発現を特徴とするサブタイプ)による決定方法を含む。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, in any of the methods, uses or compositions for use described herein, the subject does not have pulmonary lymphoepithelioma-like carcinoma subtype of NSCLC. Methods for detecting subtypes of NSCLC are well known in the art and include, but are not limited to, histopathological criteria or molecular characteristics (e.g., biomarkers (e.g., specific genes or (subtype) characterized by expression of one or a combination of proteins). In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample.
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、対象は、活動性エプスタイン・バー・ウイルス(EBV)感染を有していない、又は既知の慢性活動性EBV感染を有していない、若しくはその疑いがない。本明細書に記載の方法で使用するための活動性又は慢性活動性EBV感染の指標としては、限定されないが、EBV IgM、EBV IgG、Epstein-Barr核抗原(EBNA)、及び対象由来の試料(例えば、血液又は血清試料)中に検出されたEpstein-Barrウイルス粒子を挙げることができる。対象由来の試料中のEBV IgM、EBV IgG、Epstein-Barr核抗原(EBNA)、及びEpstein-Barrウイルス粒子を含む、活動性又は慢性活動性EBV感染の1つ以上の指標の存在を検出するための方法は、当該技術分野で周知であり、血清学的診断(例えば、EBV DNAの検出(例えば、EBVウイルス粒子を検出するための血液試料のPCR分析による)又はEBV抗原又は抗EBV抗体の検出(例えば、異種親和性抗体を用いたEBNA、EBV IgM又はEBV IgGの検出)を含む方法を含むが、これらに限定されない。いくつかの例では、試料は、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、対象はEBV IgMについて陰性であり、及び/又はEBV PCRによって陰性である。いくつかの例では、対象は、EBV IgMについて陰性であり、及び/又はEBV PCRについて陰性であり、かつEBV IgGについて陽性であり、及び/又はエプスタイン・バー核抗原(EBNA)について陽性である。他の例では、対象はEBV IgGについて陰性であり、及び/又はEBNAについて陰性である。 In some examples, in any of the methods, uses, or compositions for use described herein, the subject does not have an active Epstein-Barr virus (EBV) infection; or no known or suspected chronic active EBV infection. Indicators of active or chronically active EBV infection for use in the methods described herein include, but are not limited to, EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and subject-derived samples ( Examples include Epstein-Barr virus particles detected in blood or serum samples). To detect the presence of one or more indicators of active or chronically active EBV infection, including EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein-Barr virus particles in a sample from a subject are well known in the art and include serological diagnostics (e.g. detection of EBV DNA (e.g. by PCR analysis of blood samples to detect EBV virions) or detection of EBV antigens or anti-EBV antibodies (e.g., detection of EBNA, EBV IgM or EBV IgG using heterophilic antibodies) In some examples, the sample is a whole blood sample, a serum sample and a plasma sample. is selected from the group consisting of: In some examples, the subject is EBV IgM negative and/or is negative by EBV PCR, In some examples, the subject is EBV IgM negative and /or negative for EBV PCR and positive for EBV IgG and/or positive for Epstein-Barr nuclear antigen (EBNA) In other examples, the subject is negative for EBV IgG and/or Negative for EBNA.
いくつかの例では、本明細書に記載される方法、使用又は使用のための組成物のいずれかにおいて、対象はPD-L1選択腫瘍(例えば、SP 263若しくは22C3抗体を用いたIHCによって決定される最小PD-L1陽性腫瘍細胞分率又はTPS≧30%(例えば、50%以上)を有する腫瘍PD-L1発現、又はSP 142抗体を用いたIHCによって決定される腫瘍試料中のPD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合が1%以上である)を有する。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって30%以上(例えば、50%以上)のPD-L1陽性腫瘍細胞分率又はPD-L1 TPSを有すると判定された腫瘍である。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって、PD-L1発現免疫細胞(IC)が占める腫瘍面積の割合が1%以上であると判定された腫瘍である。いくつかの例では、IHCアッセイは、抗PD-L1抗体SP263、22C3、SP142又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、腫瘍試料は、50%以上のTPSを有すること判定されている。いくつかの例では、PD-L1陽性腫瘍細胞分率は、50%以上である(例えば、抗PD-L1抗体SP263による陽性染色によって決定される場合(例えば、Ventana assayを使用)、抗PD-L1抗体22C3による陽性染色によって決定される場合(例えば、pharmDxアッセイの使用)、又は抗PD-L1抗体28-8による陽性染色によって決定される場合)。いくつかの実施形態では、PD-L1陽性腫瘍細胞分率は、抗PD-L1抗体SP142を用いる陽性染色によって判定される場合、30%以上である。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)5%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)10%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上50%未満であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上30%未満であると判定されている。
In some examples, in any of the methods, uses or compositions for use described herein, the subject has a PD-L1 selected tumor (e.g., as determined by IHC using the
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1タンパク質発現レベルを有する。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、IHCアッセイによって決定されたものである。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上5%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の5%以上50%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の50%以上において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上5%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の5%以上10%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の10%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 protein expression level. In some examples, the detectable PD-L1 protein expression level was determined by an IHC assay. In some examples, the IHC assay uses the anti-PD-L1 antibody SP142. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more and less than 5% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 5% or more and less than 50% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in 50% or more of the tumor cells in the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more and less than 5% of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 5% or more and less than 10% of the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 10% or more of the tumor sample.
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
処置に対する応答
本明細書に記載される方法のいずれかのいくつかの実施形態では、治療に対する対象の応答は、1つ以上の尺度によって特徴付けることができる。いくつかの実施形態において、処置はCR又はPRをもたらす。いくつかの実施形態では、処置はPFS又はDORの増加をもたらす。
Response to Treatment In some embodiments of any of the methods described herein, a subject's response to treatment can be characterized by one or more measures. In some embodiments, treatment results in CR or PR. In some embodiments, treatment results in an increase in PFS or DOR.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のPFSの増加をもたらす。例えば、化学療法剤が投与されない(例えば、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)と組み合わせた抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)のみを投与する)実施形態では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のPFSの増加をもたらし得る。抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)が1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン))と組み合わせて投与される実施形態では、処置は、例えば、(i)抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト及び1つ以上の化学療法剤による治療と比較して;(ii)PD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体及び1つ以上の化学療法剤による処置と比較して;並びに/又は(iii)1つ以上の化学療法剤を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体での処置と比較して、対象又は対象集団のPFSの増加をもたらし得る。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. In comparison, it results in an increase in the subject's PFS. For example, in embodiments in which no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tiragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), treatment may include, for example, anti-TIGIT Compared to treatment with a PD-1 axis binding antagonist without an antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist, it may result in an increase in PFS in a subject. an anti-TIGIT antagonist antibody (e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., atezolizumab) with one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more of non-platinum chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin)) In embodiments, the treatment is, for example, (i) compared to treatment with a PD-1 axis binding antagonist and one or more chemotherapeutic agents without an anti-TIGIT antagonist antibody; (ii) PD-1 axis binding compared to treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents without an antagonist; and/or (iii) a PD-1 axis binding antagonist and anti-TIGIT without one or more chemotherapeutic agents. It may result in an increase in PFS of the subject or population of subjects compared to treatment with the antagonist antibody.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSを延長する。例えば、化学療法剤が投与されない(例えば、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)と組み合わせた抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)のみを投与する)実施形態では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSの増加をもたらし得る。抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)が1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド、ゲムシタビン又はカペシタビン)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、エトポシド)))と組み合わせて投与される実施形態では、処置は、例えば、(i)抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト及び1つ以上の化学療法剤による治療と比較して;(ii)PD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体及び1つ以上の化学療法剤による処置と比較して;並びに/又は(iii)1つ以上の化学療法剤を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体での処置と比較して、対象又は対象集団のOSの増加をもたらし得る。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Compare and extend the target OS. For example, in embodiments in which no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tiragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), treatment may include, for example, anti-TIGIT Compared to treatment with a PD-1 axis binding antagonist without an antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist, it may result in increased OS in the subject. an anti-TIGIT antagonist antibody (e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., atezolizumab) with one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more of non-platinum chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed, gemcitabine or capecitabine), taxanes (e.g., paclitaxel, such as nab-paclitaxel) and/or topoisomerase II inhibitors (e.g., etoposide))) In administered embodiments, the treatment is, for example, (i) compared to treatment with a PD-1 axis binding antagonist and one or more chemotherapeutic agents without an anti-TIGIT antagonist antibody; (ii) PD-1 compared to treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents without an axis binding antagonist; and/or (iii) a PD-1 axis binding antagonist and without one or more chemotherapeutic agents. It may result in an increase in OS of the subject or population of subjects compared to treatment with an anti-TIGIT antagonist antibody.
対象の無増悪生存期間は、Eisenhauer et al.,Eur.J.Cancer.2009,45:228-47に記載されるRECIST v1.1基準に従って測定され得る。いくつかの実施形態では、PFSは、処置の開始から、RECIST第1.1版の基準によって決定される疾患進行の初回発生までの期間として測定される。いくつかの実施形態では、PFSは、処置の開始から死亡時までの期間として測定される。 Subject progression-free survival was determined according to Eisenhauer et al. , Eur. J. Cancer. 2009, 45:228-47, according to the RECIST v1.1 standard. In some embodiments, PFS is measured as the time from initiation of treatment to the first occurrence of disease progression as determined by the criteria of RECIST version 1.1. In some embodiments, PFS is measured as the time from initiation of treatment to death.
いくつかの実施形態では、本明細書に記載される処置は、対象のPFSを少なくとも約2.4ヵ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月又は10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のPFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のPFSを少なくとも約2ヵ月(例えば、2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment described herein reduces the subject's PFS by at least about 2.4 months (eg, 2.4-120 months, 2.5-100 months, 3.0-80 months). , 4.0-60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months or 10-12 months, such as at least about 2.4 months, 2.5 months,2. 6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3. 6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4. 6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5. 6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9. 0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months , 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) Extend. In some embodiments, treatment reduces a subject's PFS by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment reduces a subject's PFS by at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months , 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months , 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、本明細書に記載される処置は、対象のDORを少なくとも約2.4ヵ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月又は10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のDORを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のDORを少なくとも約2ヵ月(例えば、2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment described herein reduces the subject's DOR by at least about 2.4 months (eg, 2.4-120 months, 2.5-100 months, 3.0-80 months). , 4.0-60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months or 10-12 months, such as at least about 2.4 months, 2.5 months,2. 6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3. 6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4. 6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5. 6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9. 0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months , 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) Extend. In some embodiments, treatment reduces the subject's DOR by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment reduces the subject's DOR by at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months , 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months , 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、対象のOSを少なくとも約2ヵ月(例えば、2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば、少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約3.3ヵ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヶ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約5.3ヶ月(例えば5.3~120、6~60ヵ月、7~48ヵ月、8~36 ヵ月、又は10~24ヵ月、例えば、少なくとも約5.3ヵ月、5.5ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, the treatment reduces the subject's OS by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months,2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months; 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5. 7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9. 5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-3 months). 36 months, or 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11 months. 5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months , 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 5.3 months (eg, 5.3-120, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months , 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
B.肺がんに関する処置方法及び使用
肺がんは依然として世界中でがん死の主な原因である。米国では、それは男性及び女性の両方において最も一般的ながんであり、全ての新規がん症例の12%~14%を占める。2020年には、推定228,820人の新たな肺がん症例があり、米国では135,720人が死亡する(Siegel et al.CA Cancer J Clin.70:7-30(2020))。
B. Treatment Methods and Uses for Lung Cancer Lung cancer remains the leading cause of cancer death worldwide. In the United States, it is the most common cancer in both men and women, accounting for 12%-14% of all new cancer cases. There will be an estimated 228,820 new lung cancer cases and 135,720 deaths in the United States in 2020 (Siegel et al. CA Cancer J Clin. 70:7-30 (2020)).
非小細胞肺がん
非小細胞肺がん(NSCLC)は、肺がんの主要なサブタイプであり、全症例の約85%を占める。
Non-Small Cell Lung Cancer Non-small cell lung cancer (NSCLC) is the major subtype of lung cancer, accounting for approximately 85% of all cases.
非小細胞肺がん(NSCLC)は、肺がんの主要なサブタイプであり、全症例の約80%~85%を占める(Osmani et al.Semin Cancer Biol.52(Pt 1):103-9(2018))。NSCLCは、2つの主要な組織型:腺癌及び扁平上皮癌腫に分けることができる(Travis et al.2011)。腺癌組織像は全NSCLCの約40%~50%を占め、扁平上皮組織像はNSCLCの約20%~30%を占める(Osmani et al.Semin Cancer Biol.52(Pt 1):103-9(2018))。NSCLCの残りの症例は、大細胞癌腫、神経内分泌腫瘍、肉腫様癌腫、及び低分化組織学に代表される。 Non-small cell lung cancer (NSCLC) is the major subtype of lung cancer, accounting for about 80%-85% of all cases (Osmani et al. Semin Cancer Biol. 52(Pt 1):103-9 (2018) ). NSCLC can be divided into two major histologic types: adenocarcinoma and squamous cell carcinoma (Travis et al. 2011). Adenocarcinoma histology accounts for approximately 40%-50% of all NSCLCs, and squamous histology accounts for approximately 20%-30% of NSCLCs (Osmani et al. Semin Cancer Biol. 52(Pt 1):103-9). (2018)). The remaining cases of NSCLC are represented by large cell carcinoma, neuroendocrine tumors, sarcomatoid carcinoma, and poorly differentiated histology.
初期段階では、NSCLCは治癒目的で外科的に処置される。しかしながら、切除を受けている患者の30%-70%が再発を発症し、疾患進行の結果として死亡する(Siegel et al.Cancer Statistics.CA Cancer J Clin.70:7-30(2020))。したがって、初期段階のNSCLCに対する改善された医学的介入に対する満たされていないニーズが高い。 In the early stages, NSCLC is treated surgically with curative intent. However, 30%-70% of patients undergoing resection develop recurrence and die as a result of disease progression (Siegel et al. Cancer Statistics. CA Cancer J Clin. 70:7-30 (2020)). Therefore, there is a high unmet need for improved medical interventions for early stage NSCLC.
進行性疾患の場合、全5年生存率は2%-4%である。NSCLC患者の生存に関する予後不良因子としては、初期診断時の疾患の進行期、パフォーマンスステータス不良、及び意図しない体重減少の病歴が挙げられる。NSCLC患者の半数超が遠隔疾患と診断されており、これは生存見込みの低さに直接寄与する。 For progressive disease, the overall 5-year survival rate is 2%-4%. Poor prognostic factors for survival of NSCLC patients include advanced stage of the disease at initial diagnosis, poor performance status, and a history of unintended weight loss. More than half of NSCLC patients are diagnosed with distant disease, which directly contributes to their poor survival prospects.
より長い生存期間及び疾患関連症状の減少をもたらした、NSCLCが進行した患者の第一選択処置の改善にもかかわらず、ほぼ全ての患者が疾患進行を経験する。がん免疫療法は、特に、長期疾患制御の可能性を提供する。転移性NSCLCの状況において、PD-L1/PD-1遮断抗体(例えば、アテゾリズマブ、ニボルマブ、及びペムブロリズマブ)は、非選択又はPD-L1-選択の進行したNSCLC患者のいずれかにおいて臨床的に意味のある利益をもたらした。しかしながら、かなりの割合の患者が依然として抗PD-L1/PD-1処置に対して無応答又は進行したままであり、そのような処置に対する逃避機構はほとんど理解されていない。 Despite improvements in first-line treatment of patients with advanced NSCLC that have resulted in longer survival and fewer disease-related symptoms, nearly all patients experience disease progression. Cancer immunotherapy, in particular, offers the potential for long-term disease control. In the setting of metastatic NSCLC, PD-L1/PD-1 blocking antibodies (eg, atezolizumab, nivolumab, and pembrolizumab) are clinically relevant in either unselected or PD-L1-selected advanced NSCLC patients. brought some benefit. However, a significant proportion of patients remain unresponsive or progressing to anti-PD-L1/PD-1 treatment, and the escape mechanisms for such treatment are poorly understood.
したがって、より良好なベネフィット-リスクプロファイルを達成する肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))の処置(例えば、第一選択治療)のための有効な免疫療法及びそれを投与する方法の開発に対する当分野での満たされていない必要性がある。 Therefore, lung cancers (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)) that achieve a better benefit-risk profile. There is an unmet need in the art for the development of effective immunotherapies and methods of administering them for the treatment (eg, first-line therapy) of )).
小細胞肺がん
小細胞肺がん(SCLC)は、肺がんの全症例の約15%を占める。SCLC患者の大部分(約70%)は、進行期疾患(ES-SCLC)と診断され、これは生存見込みが乏しい(OS中央値約10~12ヶ月)。化学療法単独では、ES-SCLC患者の症状を緩和し、生存期間を延ばすことができるが、長期生存はまれである。I期SCLCの人々の5年相対生存率は約31%である。ステージIVでは、5年相対生存率は約2%に低下する。
Small Cell Lung Cancer Small cell lung cancer (SCLC) accounts for approximately 15% of all cases of lung cancer. The majority of SCLC patients (approximately 70%) are diagnosed with advanced-stage disease (ES-SCLC), which has a poor survival prospect (median OS approximately 10-12 months). Chemotherapy alone can relieve symptoms and prolong survival in ES-SCLC patients, but long-term survival is rare. The 5-year relative survival rate for people with stage I SCLC is about 31%. In Stage IV, the 5-year relative survival rate drops to approximately 2%.
したがって、肺がん(例えば、SCLC、例えば、ES-SCLC)のための改善された処置が当該分野で必要とされている。 Therefore, there is a need in the art for improved treatments for lung cancer (eg, SCLC, eg, ES-SCLC).
i.肺がんを処置するための方法及び使用
肺がんを有する対象集団を処置する方法であって、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象集団に投与することを含み、処置が、少なくとも約6ヵ月(例えば、少なくとも約6ヵ月(例えば、6ヵ月と24ヵ月の間(例えば、約6ヵ月と約15ヵ月の間(例えば、6ヵ月、7ヵ月、8ヵ月、9ヵ月、10ヵ月、11ヵ月、12ヵ月、13ヵ月、14ヵ月、又は15ヵ月)、例えば、約6ヵ月と約13ヵ月の間(例えば、6ヵ月、6.5ヵ月、7ヵ月、7.5ヵ月、8ヵ月、8.5ヵ月、9ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、12.5ヵ月、13ヵ月))、例えば、約8ヵ月と約10ヵ月の間(例えば、8.1ヵ月、8.2ヵ月、8.3ヵ月、8.4ヵ月、8.5ヵ月、8.6ヵ月、8.7ヵ月、8.8ヵ月、8.9ヵ月、9.0ヵ月、9.1ヵ月、9.2ヵ月、9.3ヵ月、9.4ヵ月、9.5ヵ月、9.6ヵ月、9.7ヵ月、9.8ヵ月、9.9ヵ月、10.0ヵ月))の対象集団のPFS中央値をもたらす方法が本明細書で提供される。いくつかの例では、処置は、約8.2ヶ月~約9.2ヶ月(例えば、約8.2、8.4、8.6、8.8、9.0、又は9.2ヶ月、例えば、8.2~8.4、8.4~8.6、8.6~8.8、8.8~9.0、又は9.0~9.2ヶ月)の対象集団のPFS中央値をもたらす。
i. Methods and Uses for Treating Lung Cancer United States Patent Application 20070010000 Kind Code: A1 A method of treating a subject population with lung cancer comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. wherein the treatment is at least about 6 months (e.g., at least about 6 months (e.g., between 6 months and 24 months (e.g., about 6 months and about for 15 months (eg, 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months, or 15 months), such as between about 6 months and about 13 months (For example, 6 months, 6.5 months, 7 months, 7.5 months, 8 months, 8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months , 12 months, 12.5 months, 13 months)), for example, between about 8 months and about 10 months (eg, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8.1 months, 8.2 months, 8.3 months, 8.4 months; 5 months, 8.6 months, 8.7 months, 8.8 months, 8.9 months, 9.0 months, 9.1 months, 9.2 months, 9.3 months, 9.4 months, 9. Provided herein are methods that yield a median PFS for a subject population of 5 months, 9.6 months, 9.7 months, 9.8 months, 9.9 months, 10.0 months)). In an example of, the treatment is for about 8.2 months to about 9.2 months (eg, about 8.2, 8.4, 8.6, 8.8, 9.0, or 9.2 months, such as 8.2-8.4, 8.4-8.6, 8.6-8.8, 8.8-9.0, or 9.0-9.2 months) median PFS of the target population Bring.
肺がんを有する対象集団を処置する方法であって、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを対象集団に投与することを含み、処置が少なくとも約12ヶ月(例えば、約12ヶ月と約40ヶ月の間(例えば、約12ヶ月と約30ヶ月の間(例えば、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、又は30ヶ月)、例えば、約12ヶ月と約20ヶ月の間(例えば、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、又は20ヶ月)))の対象集団のOS中央値をもたらす方法も本明細書で提供される。いくつかの例では、処置は、約15.3ヶ月~約17.6ヶ月(例えば、約15.5、16、16.5、17、17.5、又は17.6ヶ月、例えば、15.3~16ヶ月、16~17ヶ月、又は17~17.6ヶ月)の対象集団のOS中央値をもたらす。 A method of treating a subject population having lung cancer, comprising a dosing regimen comprising one or more dosing cycles of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a topoisomerase II inhibitor. administering to a subject population, wherein the treatment is at least about 12 months (e.g., between about 12 months and about 40 months (e.g., between about 12 months and about 30 months (e.g., 12 months, 13 months, 14 months) , 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, or 30 months) , e.g., between about 12 months and about 20 months (e.g., 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, or 20 months))) of the subject population Also provided herein is a method for generating the median value. In some examples, the treatment is for about 15.3 months to about 17.6 months (eg, about 15.5, 16, 16.5, 17, 17.5, or 17.6 months, eg, 15.6 months). 3-16 months, 16-17 months, or 17-17.6 months).
ii.小細胞肺がんを処置するための方法及び使用
対象又は対象集団における肺がん(例えば、小細胞肺がん(SCLC)、例えば、進展型SCLC(ES-SCLC))を処置するための方法及び使用であって、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)の1回以上の投薬サイクルを対象又は対象集団に投与することを含む方法及び使用が本明細書で提供される。
ii. Methods and uses for treating small cell lung cancer an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab), platinum Provided herein are methods and uses comprising administering to a subject or population of subjects one or more dosing cycles of a systemic chemotherapeutic agent (e.g., carboplatin or cisplatin) and a topoisomerase II inhibitor (e.g., etoposide). .
投薬レジメン、投与及び処置に対する応答
本明細書に記載の本発明の処置方法及び使用は、一態様では、肺がん(例えば、SCLC、例えば、ES-SCLC)を有する対象又は対象集団に有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、白金系化学療法剤及びトポイソメラーゼII阻害剤を投与することを含み、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団の無増悪生存期間(PFS)を延長し、それによって対象又は対象集団を処置する。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを延長する。
Dosing Regimens, Administration, and Response to Treatment The treatment methods and uses of the invention described herein, in one aspect, provide a subject or subject population with lung cancer (eg, SCLC, eg, ES-SCLC) with an effective amount of an antimicrobial agent. TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies as disclosed herein, eg, tiragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)), platinum-based chemistries comprising administering a therapeutic agent and a topoisomerase II inhibitor, wherein the treatment compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody or prolong the progression-free survival (PFS) of a subject population, thereby treating the subject or subject population. In some examples, the treatment prolongs OS of a subject or population of subjects compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody. .
いくつかの実施形態では、個体のPFSは、RECIST v1.1 criteria,as described in Eisenhauer et al.,Eur.J.Cancer.2009,45:228-47に従って測定される。いくつかの実施形態では、PFSは、処置の開始から、RECIST第1.1版の基準によって決定される疾患進行の初回発生までの期間として測定される。いくつかの実施形態では、PFSは、処置の開始から死亡時までの期間として測定される。 In some embodiments, an individual's PFS is determined according to RECIST v1.1 criteria, as described in Eisenhauer et al. , Eur. J. Cancer. 2009, 45:228-47. In some embodiments, PFS is measured as the time from initiation of treatment to the first occurrence of disease progression as determined by the criteria of RECIST version 1.1. In some embodiments, PFS is measured as the time from initiation of treatment to death.
いくつかの実施形態では、処置は、抗TIGITアンタゴニスト抗体を含まないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のPFSを少なくとも約2.4ヶ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月、or10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による治療と比較して、対象又は対象集団のPFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、or10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のPFSを少なくとも約2ヶ月(例えば、2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、or10~24ヵ月、例えば少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの態様では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のPFSを少なくとも約3ヶ月~約4ヶ月延長する。 In some embodiments, the treatment reduces the subject's or subject population's PFS by at least about 2.4 months (e.g., 2.4-120 months, 2.5-100 months, 3.0-80 months, 4.0-60 months, 5.0-48 months, 6.0-36 months, 8 .0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10 months. 5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's or population of subjects' PFS to at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months, or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10 months. 5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's or population of subjects' PFS to at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-36 months, or 10-24 months, such as at least about 2.0 months, 2 .1 month, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3 months .1 month, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4 months .1 month, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5 months .5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some aspects, the treatment reduces the subject's or population of subjects' PFS by at least about Extend for 3 to 4 months.
いくつかの例では、肺がん(例えば、SCLC、例えば、ES-SCLC)を有する対象又は対象集団を処置する方法及び使用は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)を対象又は対象集団に投与することを含み、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを延長する。 In some examples, methods and uses of treating a subject or subject population with lung cancer (eg, SCLC, eg, ES-SCLC) include an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antibody disclosed herein). TIGIT antagonist antibodies (eg, tiragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies such as atezolizumab), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and topoisomerase II inhibitors (eg, etoposide). ) to a subject or population of subjects, wherein the treatment is compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody, in the subject or Extend OS in the subject population.
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを少なくとも約2ヶ月(例えば、2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを少なくとも少なくとも約3.3ヵ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長させる。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを少なくとも約5.3ヶ月(例えば5.3~120ヵ月、6~60ヵ月7~48ヵ月8~36ヵ月or10~24ヵ月例えば少なくとも約5.3ヵ月5.5ヵ月6.0ヵ月6.5ヵ月7.0ヵ月7.5ヵ月8.0ヵ月8.5ヵ月9.0ヵ月9.5ヵ月10ヵ月10.5ヵ月11ヵ月11.5ヵ月12ヵ月13ヵ月14ヵ月15ヵ月16ヵ月17ヵ月18ヵ月19ヵ月20ヵ月21ヵ月22ヵ月23ヵ月24ヵ月25ヵ月26ヵ月27ヵ月28ヵ月29ヵ月30ヵ月31ヵ月32ヵ月33ヵ月34ヵ月35ヵ月又はr36ヵ月)延長させる。
In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, treatment reduces the OS of a subject or population of subjects by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11 months. 5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months , 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, treatment reduces OS of a subject or population of subjects by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, eg, at least about 3.3 months; 3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4. 3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6. 5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, treatment reduces the OS of a subject or population of subjects by at least about 5.3 months (eg 5.3 to 120 months, 6 to 60 months 7 to 48
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約600mgの間(例えば、約50mgと600mgの間、例えば、約60mgと約600mgの間、例えば、約100mgと約600mgの間、例えば、約200mgと約600mgの間、例えば、約200mgと約550mgの間、例えば、約250mgと約500mgの間、例えば、約300mgと約450mgの間、例えば、約350mgと約400mgの間、例えば、約375mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量(例えば、固定用量)である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg (e.g., about 30 mg) every three weeks. and about 1100 mg, for example between about 60 mg and about 1000 mg, for example between about 100 mg and about 900 mg, for example between about 200 mg and about 800 mg, between about 300 mg and about 800 mg, for example between about 400 mg and about between 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg; For example, a dose (eg, fixed dose) of 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 600 mg (e.g., about 50 mg) every three weeks. and 600 mg, for example between about 60 mg and about 600 mg, for example between about 100 mg and about 600 mg, for example between about 200 mg and about 600 mg, for example between about 200 mg and about 550 mg, for example about 250 mg between about 500 mg, eg between about 300 mg and about 450 mg, eg between about 350 mg and about 400 mg, eg about 375 mg) (eg a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is a dose (e.g., fixed dose) of about 600 mg every 3 weeks .
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ))の有効量は、3週間ごとに30mgと1200mgの間(例えば、30mgと1100mgの間、例えば、60mgと1000mgの間、例えば、100mgと900mgの間、例えば、200mgと800mgの間、例えば、300mgと800mgの間、例えば、400mgと800mgの間、例えば、400mgと750mgの間、例えば、450mgと750mgの間、例えば、500mgと700mgの間、例えば、550mgと650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに30mgと600mgの間(例えば、50mgと600mgの間、例えば、60mgと600mgの間、例えば、100mgと600mgの間、例えば、200mgと600mgの間、例えば、200mgと550mgの間、例えば、250mgと500mgの間、例えば、300mgと450mgの間、例えば、350mgと400mgの間、例えば、375mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量(例えば、固定用量)用量である。 In some examples, the effective amount of the anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody (e.g., tiragolumab)) is between 30 mg and 1200 mg (e.g., between 30 mg and 1100 mg, e.g., 60 mg) every three weeks. between 1000 mg, such as between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg, such as between 450 mg and 750 mg between, such as between 500 mg and 700 mg, such as between 550 mg and 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600±0.5 mg, eg, 600 mg) dose (eg, fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between 30 mg and 600 mg (e.g., 50 mg and 600 mg) every three weeks. between 60 mg and 600 mg, such as between 100 mg and 600 mg, such as between 200 mg and 600 mg, such as between 200 mg and 550 mg, such as between 250 mg and 500 mg, such as between 300 mg and 450 mg; For example, a dose (eg, fixed dose) between 350 mg and 400 mg, eg, 375 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is a dose (e.g., fixed dose) dose of 600 mg every 3 weeks .
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量(例えば、固定用量)である。いくつかの例では、併用療法(例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)との併用処置)、トポイソメラーゼII阻害剤(例えば、エトポシド)、及び/又は白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)で投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量(例えば、固定用量)は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg (eg, fixed dose) every three weeks. In some examples, combination therapy (e.g., combination treatment with a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody, e.g., atezolizumab)), a topoisomerase II inhibitor (e.g., etoposide), and/or A dose (e.g., fixed dose) of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) administered with a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) can be It may be reduced compared to standard doses of anti-TIGIT antagonist antibody administered as drug therapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約80mgと約2000mgの間(例えば、約100mgと約1600mgの間、例えば、約200mgと約1600mgの間、例えば、約300mgと約1600mgの間、例えば、約400mgと約1600mgの間、例えば、約500mgと約1600mgの間、例えば、約600mgと約1600mgの間、例えば、約700mgと約1600mgの間、例えば、約800mgと約1600mgの間、例えば、約900mgと約1500mgの間、例えば、約1000mgと約1400mgの間、例えば、約1050mgと約1350mgの間、例えば、約1100mgと約1300mgの間、例えば、約1150mgと約1250mgの間、例えば、約1175mgと約1225mgの間、例えば、約1190mgと約1210mgの間、例えば、1200mg±5mg、例えば、1200±2.5mg、例えば、1200±1.0mg、例えば、1200±0.5mg、例えば、1200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約1200mgの用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに80mgと2000mgの間(例えば100mgと1600mgの間、例えば200mgと1600mgの間、例えば300mgと1600mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量(例えば、固定用量)である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about between about 200 mg and about 1600 mg, such as between about 300 mg and about 1600 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg, such as between about 600 mg and about Between 1600 mg, such as between about 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about between 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as 1200 mg±5 mg; 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg) (eg, fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, fixed dose) of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, fixed dose) of about 1200 mg every three weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 1600 mg) every three weeks, e.g. between 200 mg and 1600 mg, such as between 300 mg and 1600 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg, such as between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg, such as between 1190 mg and 1210 mg, such as 1200 mg ± 5 mg, such as 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg) (eg a fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg (eg, fixed dose) every two weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1400mg~2000mgの用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1400mg~2000mgの用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量(例えば、固定用量)である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置。)、トポイソメラーゼII阻害剤(例えば、エトポシド)及び/又は白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量(例えば、固定用量)は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して減少され得る。 In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is a dose (e.g., fixed dose) of about 1400 mg to 2000 mg every 4 weeks. . In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, fixed dose) of 1400 mg to 2000 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose (eg, fixed dose) of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg (eg, fixed dose) every 4 weeks. In some examples, combination therapy (e.g., combination treatment with an anti-TIGIT antagonist antibody, e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab), a topoisomerase II inhibitor (e.g., etoposide), and / or a dose (e.g., fixed dose) of a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) administered with a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) It may be reduced compared to standard doses of PD-1 axis binding antagonists administered as drug therapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば、約0.1mg/kgと約40mg/kgの間、例えば、約1mg/kgと約35mg/kgの間、例えば、約2.5mg/kgと約30mg/kgの間、例えば、約5mg/kgと約25mg/kgの間、例えば、約10mg/kgと約20mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約15mg/kgの間、例えば、約10mg/kgと約15mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約14mg/kgと約15mg/kgの間、例えば、約15±1mg/kg、例えば、約15±0.5mg/kg、例えば、約15±0.2mg/kg、例えば、約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに投与される約15mg/kgの用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg, e.g., between about 1 mg/kg and about 35 mg/kg) such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as about 12 mg/kg. between 5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0 .1 mg/kg, eg about 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 15 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.1 mg/kg and about 15 mg/kg, e.g., between about 0.5 mg/kg and about 15 mg/kg, e.g., between about 1 mg/kg and about 15 mg/kg) between about 2.5 mg/kg and about 15 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 15 mg/kg, such as about between 10 mg/kg and about 15 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as between about 14 mg/kg and about 15 mg/kg, such as about 15±1 mg/kg; For example, about 15±0.5 mg/kg, such as about 15±0.2 mg/kg, such as about 15±0.1 mg/kg, such as about 15 mg/kg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 15 mg/kg administered every 3 weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば、0.1mg/kgと40mg/kgの間、例えば、1mg/kgと35mg/kgの間、例えば、2.5mg/kgと30mg/kgの間、例えば、5mg/kgと25mg/kgの間、例えば、10mg/kgと20mg/kgの間、例えば、12.5mg/kgと15mg/kgの間、例えば、15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば、15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに対象の体重の0.01mg/kgと15mg/kgの間(例えば0.1mg/kgと15mg/kgの間、例えば0.5mg/kgと15mg/kgの間、例えば1mg/kgと15mg/kgの間、例えば2.5mg/kgと15mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば10mg/kgと15mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば14mg/kgと15mg/kgの間、例えば15±1mg/kg、例えば15±0.5mg/kg、例えば15±0.2mg/kg、例えば15±0.1mg/kg、例えば15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに投与される15mg/kgの用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 50 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.01 mg/kg and 45 mg/kg, e.g. between 0.1 mg/kg and 40 mg/kg, e.g. between 1 mg/kg and 35 mg/kg, e.g. 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg /kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0.1 mg/kg, such as 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 15 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.1 mg/kg and 15 mg/kg, such as between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 10 mg/kg and 15 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, between 14 mg/kg and 15 mg/kg, such as 15±1 mg/kg, such as 15±0.5 mg/kg, such as 15±0.2 mg/kg, such as 15±0.1 mg/kg, such as 15 mg/kg) is the dose of In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 15 mg/kg administered every 3 weeks.
いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置。)、トポイソメラーゼII阻害剤(例えば、エトポシド)及び/又は白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して減少され得る。 In some examples, combination therapy (e.g., combination treatment with an anti-TIGIT antagonist antibody, e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab), a topoisomerase II inhibitor (e.g., etoposide), and /or a dose of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) administered with a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) is administered as monotherapy It may be reduced compared to standard doses of PD-1 axis binding antagonists.
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、1~50mg/ml/分(例えば、2~25mg/ml/分、3~15mg/ml/分、4~10mg/ml/分、又は5mg/ml/分、例えば、2mg/ml/分、3mg/ml/分、4mg/ml/分、5mg/ml/分、6mg/ml/分、7mg/ml/分、8mg/ml/分、9mg/ml/分、10mg/ml/分、11mg/ml/分、12mg/ml/分、13mg/ml/分、14mg/ml/分、15mg/ml/分、20mg/ml/分、25mg/ml/分、30mg/ml/分、35mg/ml/分、40mg/ml/分、45mg/ml/分、50mg/ml/分)のAUCを達成するのに十分な用量である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、AUC=5mg/ml/分を達成するのに十分な用量である。
In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 1-50 mg/ml/min (eg, 2-25 mg/ml/min, 3-15 mg/ml/min, 4 ~10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml/min, 6 mg/ml/min, 7 mg/ml/
AUCは、カルバート式(Calvert et al.,J.Clin.Oncol.1989,7:1748-56)を使用して計算することができる:
総投与量(mg)=(目標AUC)X(糸球体濾過率[GFR]+25)
AUC can be calculated using the Calvert formula (Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):
Total Dose (mg) = (Target AUC) X (Glomerular Filtration Rate [GFR] + 25)
いくつかの例では、例えば、アテゾリズマブ1200mgは、平均体重ベースの用量15m/kgに相当する。 In some instances, for example, 1200 mg of atezolizumab corresponds to an average weight-based dose of 15 m/kg.
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、200mg~1500mg(例えば、300mg~1200mg、400mg~1100mg又は500mg~1000mg、例えば、300mg~400mg、400mg~500mg、500mg~600mg、600mg~700mg、700mg~750mg、750mg~800mg、800mg~900mg、900mg~1000mg、1000mg~1100mg又は1100mg~1200mg、例えば、約200mg、約300mg、約400mg、約500mg、約600mg、約700mg、約800mg、約900mg、約1000mg、約1100mg、約1200mg、約1300mg、1400mg又は約1500mg)である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、500mg~1000mg(例えば、約500mg、約600mg、約700mg、約800mg、約900mg、又は約1000mg)である。 In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, such as 300 mg to 400 mg, 400 mg to 500 mg). , 500 mg to 600 mg, 600 mg to 700 mg, 700 mg to 750 mg, 750 mg to 800 mg, 800 mg to 900 mg, 900 mg to 1000 mg, 1000 mg to 1100 mg or 1100 mg to 1200 mg, such as about 200 mg, about 300 mg, about 400 mg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, about 1000 mg, about 1100 mg, about 1200 mg, about 1300 mg, 1400 mg or about 1500 mg). In some examples, the effective amount of the platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) is 500 mg to 1000 mg (e.g., about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, or about 1000 mg) .
いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、10~1000mg/m2(例えば、20~800mg/m2、30~700mg/m2、40~500mg/m2、50~300mg/m2、75~200mg/m2、又は80~150mg/m2、例えば、約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、又は約1000mg/m2)である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、約100mg/m2である。 In some examples, the effective amount of topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg / m2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/ m2 , about 100 mg/m2, about 110 mg/ m2 , about 120 mg/ m2 , about 130 mg/m2 , about 140 mg/m 2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/m2, about 180 mg /m2, about 190 mg/m2, about 200 mg/m2, about 250 mg/m2 , about 300 mg / m2 , about 400 mg/ m2 , about 500 mg/ m2 , about 600 mg/ m2 , about 700 mg/ m2 , about 800 mg/ m2 , about 900 mg/ m2 , or about 1000 mg/ m2 ). In some examples, an effective amount of topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 .
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、200mg~1500mg(例えば、300mg~1200mg、400mg~1100mg又は500mg~1000mg、例えば、300mg~400mg、400mg~500mg、500mg~600mg、600mg~700mg、700mg~750mg、750mg~800mg、800mg~900mg、900mg~1000mg、1000mg~1100mg又は1100mg~1200mg、例えば、200mg、300mg、400mg、500mg、600mg、700mg、800mg、900mg、1000mg、1100mg、1200mg、1300mg、1400mg又は1500mg)である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、500mg~1000mg(例えば、500mg、600mg、700mg、800mg、900mg、又は1000mg)である。 In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, such as 300 mg to 400 mg, 400 mg to 500 mg). , 500 mg to 600 mg, 600 mg to 700 mg, 700 mg to 750 mg, 750 mg to 800 mg, 800 mg to 900 mg, 900 mg to 1000 mg, 1000 mg to 1100 mg or 1100 mg to 1200 mg, such as 200 mg, 300 mg, 400 mg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg , 1000 mg, 1100 mg, 1200 mg, 1300 mg, 1400 mg or 1500 mg). In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 500 mg to 1000 mg (eg, 500 mg, 600 mg, 700 mg, 800 mg, 900 mg, or 1000 mg).
いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、10~1000mg/m2(例えば、20~800mg/m2、30~700mg/m2、40~500mg/m2、50~300mg/m2、75~200mg/m2、又は80~150mg/m2、例えば、20mg/m2、30mg/m2、40mg/m2、50mg/m2、60mg/m2、70mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、180mg/m2、190mg/m2、200mg/m2、250mg/m2、300mg/m2、400mg/m2、500mg/m2、600mg/m2、700mg/m2、800mg/m2、900mg/m2、又は1000mg/m2)である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は100mg/m2である。 In some examples, the effective amount of topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 , 50-300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg / m2 , 80 mg/ m2 , 90 mg/ m2 , 100 mg/m2 , 110 mg/ m2 , 120 mg/ m2 , 130 mg/ m2 , 140 mg/ m2 , 150 mg/ m2 , 160 mg/ m2 , 170 mg / m2 , 180 mg/ m2 , 190 mg/ m2 , 200 mg/m2, 250 mg/ m2 , 300 mg/ m2 , 400 mg/ m2 , 500 mg/ m2 , 600 mg/ m2 , 700 mg/ m2 , 800 mg /m 2 , 900 mg/m 2 , or 1000 mg/m 2 ). In some examples, the effective amount of topoisomerase II inhibitor (eg, etoposide) is 100 mg/m 2 .
本発明の方法及び使用のいずれかにおいて、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド))は、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))(白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又はトポイソメラーゼII阻害剤(例えば、エトポシド)の有無にかかわらず、)の投薬サイクルは、臨床的利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約18日~24日(例えば、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間又は24日間)である。いくつかの例では、投薬サイクルの長さは、約21日間である。他の例では、投薬サイクルの長さは、約14日間である。他の例では、投薬サイクルの長さは、約28日間である。 In any of the methods and uses of the invention, anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies as disclosed herein, eg, tiragolumab), PD-1 axis binding antagonists (eg, anti-PD-L1 Antagonist antibodies (e.g., atezolizumab)), platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin), and topoisomerase II inhibitors (e.g., etoposide)) may be administered for one or more dosing cycles (e.g., 1, 2, 3, 4). , 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29 , 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles) can be administered at In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) (with or without platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or topoisomerase II inhibitors (e.g., etoposide)) to clinical benefit (e.g., confirmed disease progression, drug resistance, death, or unacceptable toxicity). In some examples, the length of each dosing cycle is about 18 days to 24 days (e.g., 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days or 24 days). In some examples, the dosing cycle length is about 21 days. In another example, the dosing cycle length is about 14 days. In another example, the dosing cycle length is about 28 days.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクル、例えば各21日間サイクルの1日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクル、例えば各21日間サイクルの1日目に600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに600mgの用量で)静脈内投与される。同様に、いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、各投薬サイクルの約1日目(例えば、1±3日目)に投与する。例えば、いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。他の例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、1200mgの用量で各21日間サイクルの1日目に(すなわち、1200mgの用量で3週間ごとに)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の両方を、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与する。いくつかの例では、白金系化学療法剤は、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。いくつかの例では、トポイソメラーゼII阻害剤は、各投薬サイクルの約1日目(例えば、1日目±3日目)に存在する。例えば、いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、21日間の各サイクルの1日目(すなわち、3週間ごとに約600mgの用量で)に約600mgの用量で静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、21日間の各サイクルの1日目(すなわち、3週間ごとに約1200mgの用量で)に約1200mgの用量で静脈内投与し、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)を、4回の初期投薬サイクルのそれぞれの1日目にAUC=5mg/ml/分を達成するのに十分な用量で投与し、トポイソメラーゼII阻害剤(例えば、エトポシド)を、4回の初期投薬サイクルのそれぞれの1日目、2日目、及び3日目のそれぞれに100mg/m2 の用量で投与する。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、21日間の各サイクルの1日目(すなわち、3週間ごとに600mgの用量で)に約600mgの用量で静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、21日間の各サイクルの1日目(すなわち、3週間ごとに1200mgの用量で)に1200mgの用量で静脈内投与し、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)を、4回の初期投薬サイクルのそれぞれの1日目にAUC=5mg/ml/分を達成するのに十分な用量で投与し、トポイソメラーゼII阻害剤(例えば、エトポシド)を、4回の初期投薬サイクルのそれぞれの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量で投与する。
In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered on about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が、4回の初期投薬サイクルの各々で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、4回の初期投薬サイクルのそれぞれの1日目に約30mg~約1200mgの用量で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、4回の初期投薬サイクルのそれぞれの1日目に約30mg~約600mgの用量で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、4回の初期投薬サイクルのそれぞれの1日目に約600mgの用量で投与される。いくつかの例では、PD-1軸結合アンタゴニストは、4回の初期投薬サイクルの各々の1日目に約80mg~約1600mgの用量で、(例えば、4回の初期投薬サイクルのそれぞれの1日目に約1200mgの用量で)投与される。いくつかの例では、抗TIGITアンタゴニスト抗体を、4回の初期投薬サイクルのそれぞれの1日目に30mg~1200mgの用量で投与する。いくつかの例では、抗TIGITアンタゴニスト抗体を、4回の初期投薬サイクルのそれぞれの1日目に30mg~600mgの用量で投与する。いくつかの例では、抗TIGITアンタゴニスト抗体は、4回の初期投薬サイクルのそれぞれの1日目に600mgの用量で投与される。いくつかの例では、PD-1軸結合アンタゴニストは、4回の初期投薬サイクルの各々の1日目に80mg~1600mgの用量で、(例えば、4回の初期投薬サイクルのそれぞれの1日目に1200mgの用量で)投与される。いくつかの例では、白金系化学療法剤は、4回の初期投薬サイクルのそれぞれの1日目にAUC=5mg/ml/分を達成するのに十分な用量で投与され、及び/又はトポイソメラーゼII阻害剤は、4回の初期投薬サイクルのそれぞれの1日目、2日目、及び3日目のそれぞれに100mg/m 2 の用量で投与される。
In some examples, an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor are administered in each of four initial dosing cycles. In some examples, the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg on
いくつかの例では、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストが、第4の初期投薬サイクルに続いて1回以上の追加のサイクルで更に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、1回以上の追加の投薬サイクルのそれぞれの1日目に約30mg~約1200mgの用量で(例えば、1回以上の追加の投薬サイクルのそれぞれの1日目に約30mg~約600mgの用量で)投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、1回以上の追加の投薬サイクルのそれぞれの1日目に約600mgの用量で投与される。いくつかの例では、PD-1軸結合アンタゴニストは、1回以上の追加の投薬サイクルのそれぞれの1日目に約80mg~約2000mgの用量で(例えば、1回以上の追加の投薬サイクルのそれぞれの1日目に約840mg、1200mg又は1680mgの用量で)投与される。いくつかの例では、追加の投薬サイクルには、2週間ごとに約840mg、3週間ごとに約1200mg又は4週間ごとに約1680mgの用量でのPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)の投与が含まれる。例えば、いくつかの例では、1回以上の追加の投薬サイクルの各々は約14日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に約840mgの用量で投与される。いくつかの例では、1回以上の追加の投薬サイクルの各々は約21日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に約1200mgの用量で投与される。いくつかの例では、1回以上の投薬サイクルの各々は約28日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に約1680mgの用量で投与される。
In some examples, the anti-TIGIT antagonist antibody and PD-1 axis binding antagonist are further administered in one or more additional cycles following the fourth initial dosing cycle. In some examples, the anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg on
いくつかの例では、抗TIGITアンタゴニスト抗体は、1回以上の追加の投薬サイクルのそれぞれの1日目に30mg~1200mgの用量で(例えば、1回以上の追加の投薬サイクルのそれぞれの1日目に30mg~600mgの用量で)投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、1回以上の追加の投薬サイクルのそれぞれの1日目に600mgの用量で投与される。いくつかの例では、PD-1軸結合アンタゴニストは、1回以上の追加の投薬サイクルのそれぞれの1日目に80mg~2000mgの用量で(例えば、1回以上の追加の投薬サイクルのそれぞれの1日目に840mg、1200mg又は1680mgの用量で)投与される。いくつかの例では、追加の投薬サイクルには、2週間ごとに840mg、3週間ごとに1200mg又は4週間ごとに1680mgの用量でのPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)の投与が含まれる。例えば、いくつかの例では、1回以上の追加の投薬サイクルの各々は14日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に840mgの用量で投与される。いくつかの例では、1回以上の投薬サイクルの各々は21日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に1200mgの用量で投与される。いくつかの例では、1回以上の投薬サイクルの各々は28日間であり、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の追加の投薬サイクルの各々の1日目に1680mgの用量で投与される。
In some examples, the anti-TIGIT antagonist antibody is administered at a dose of 30 mg to 1200 mg on
いくつかの例では、肺がんを有する対象又は対象集団(例えばSCLC、例えばES-SCLC)は、各投薬サイクルの1日目に、約30mgと約1200mgの間(例えば約30mgと約1100mgの間、例えば約60mgと約1000mgの間、例えば約100mgと約900mgの間、例えば約200mgと約800mgの間、例えば約300mgと約800mgの間、例えば約400mgと約800mgの間、例えば約400mgと約750mgの間、例えば約450mgと約750mgの間、例えば約500mgと約700mgの間、例えば約550mgと約650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えばチラゴルマブ)、投薬サイクルの1日目に約80mgと約2000mgの間(例えば約100mgと約1600mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1600mgの間、例えば約400mgと約1600mgの間、例えば約500mgと約1600mgの間、例えば約600mgと約1600mgの間、例えば約700mgと約1600mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)(例えば約30mgと1200mgの間(例えば30mgと1100mgの間、例えば60mgと1000mgの間、例えば100mgと900mgの間、例えば200mgと800mgの間、例えば300mgと800mgの間、例えば400mgと800mgの間、例えば400mgと750mgの間、例えば450mgと750mgの間、例えば500mgと700mgの間、例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量のPD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))、各投薬サイクルの1日目に80mgと2000mgの間(例えば100mgと1600mgの間、例えば200mgと1600mgの間、例えば300mgと1600mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量のPD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))、各投薬サイクルの1日目に、1~50mg/ml/分(例えば2~25mg/ml/分、3~15mg/ml/分、4~10mg/ml/分、又は5mg/ml/分、例えば2mg/ml/分、3mg/ml/分、4mg/ml/分、5mg/ml/分、6mg/ml/分、7mg/ml/分、8mg/ml/分、9mg/ml/分、10mg/ml/分、11mg/ml/分、12mg/ml/分、13mg/ml/分、14mg/ml/分、15mg/ml/分、20mg/ml/分、25mg/ml/分、30mg/ml/分、35mg/ml/分、40mg/ml/分、45mg/ml/分、50mg/ml/分、例えば5mg/ml/分)のAUCを達成するのに十分な用量の白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及び各投薬サイクルの1日目、2日目、3日目に100mg/m2の用量トポイソメラーゼII阻害剤(例えば、エトポシド)の1回以上の投薬サイクル(例えば21日間投薬サイクル)を対象又は対象集団に投与することによって処置され、この処置は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及びトポイソメラーゼII阻害剤(例えば、エトポシド)を含む処置と比較して、対象又は対象集団のPFS及び/又はOSを延長する。
In some examples, a subject or subject population with lung cancer (eg, SCLC, eg, ES-SCLC) is administered between about 30 mg and about 1200 mg (eg, between about 30 mg and about 1100 mg, for example between about 60 mg and about 1000 mg, such as between about 100 mg and about 900 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 800 mg, such as between about 400 mg and about 800 mg, such as between about 400 mg and about between 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg±10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg , e.g., 600±1 mg, e.g., 600±0.5 mg, e.g., 600 mg) of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) on Day 1 of the dosing cycle of about between 80 mg and about 2000 mg, such as between about 100 mg and about 1600 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1600 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg between about 600 mg and about 1600 mg, such as between about 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg) (eg between about 30 mg and 1200 mg (eg between 30 mg and 1100 mg, such as between 60 mg and 1000 mg, such as between 100 mg and 900 mg) between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg, such as between 450 mg and 750 mg, such as between 500 mg and 700 mg, such as between 550 mg and 650 mg, For example 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) PD-1 axis binding antagonist (eg anti-PD-L1 antagonist) antibody (e.g., atezolizumab)), between 80 mg and 2000 mg on day 1 of each dosing cycle (e.g., between 100 mg and 1600 mg, such as between 200 mg and 1600 mg, such as between 300 mg and 1600 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg, such as between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as between 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg, such as between 1190 mg and 1210 mg, such as 1200 mg±5 mg, such as 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0. PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) at a dose of 1-50 mg/ml/min (eg, 2-25 mg/min) on
いくつかの例では、肺がんを有する対象又は対象集団(例えばSCLC、例えばES-SCLC)は、各投薬サイクルの1日目に、約30mg~1200mg(例えば30mgと1100mgの間、例えば60mgと1000mgの間、例えば100mgと900mgの間、例えば200mgと800mgの間、例えば300mgと800mgの間、例えば400mgと800mgの間、例えば400mgと750mgの間、例えば450mgと750mgの間、例えば500mgと700mgの間、例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えばチラゴルマブ)、各投薬サイクルの1日目に80mg~2000mg(例えば100mgと1600mgの間、例えば200mgと1600mgの間、例えば300mgと1600mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量のPD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))、各投薬サイクルの1日目に、1~50mg/ml/分(例えば2~25mg/ml/分、3~15mg/ml/分、4~10mg/ml/分、又は5mg/ml/分、例えば2mg/ml/分、3mg/ml/分、4mg/ml/分、5mg/ml/分、6mg/ml/分、7mg/ml/分、8mg/ml/分、9mg/ml/分、10mg/ml/分、11mg/ml/分、12mg/ml/分、13mg/ml/分、14mg/ml/分、15mg/ml/分、20mg/ml/分、25mg/ml/分、30mg/ml/分、35mg/ml/分、40mg/ml/分、45mg/ml/分、50mg/ml/分、例えば5mg/ml/分)のAUCを達成するのに十分な用量の白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及び各投薬サイクルの1日目、2日目、3日目に100mg/m2の用量トポイソメラーゼII阻害剤(例えば、エトポシド)の1回以上の投薬サイクル(例えば21日間投薬サイクル)を対象又は対象集団に投与することによって処置され、この処置は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及びトポイソメラーゼII阻害剤(例えば、エトポシド)を含む処置と比較して、対象又は対象集団のPFS及び/又はOSを延長する。
In some examples, a subject or subject population (eg, SCLC, eg, ES-SCLC) with lung cancer is administered about 30 mg to 1200 mg (eg, between 30 mg and 1100 mg, such as 60 mg and 1000 mg) on
いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを少なくとも少なくとも約3.3ヵ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長させる。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のOSを少なくとも約5.3ヶ月(例えば5.3~120ヵ月、6~60ヵ月7~48ヵ月8~36ヵ月or10~24ヵ月例えば少なくとも約5.3ヵ月5.5ヵ月6.0ヵ月6.5ヵ月7.0ヵ月7.5ヵ月8.0ヵ月8.5ヵ月9.0ヵ月9.5ヵ月10ヵ月10.5ヵ月11ヵ月11.5ヵ月12ヵ月13ヵ月14ヵ月15ヵ月16ヵ月17ヵ月18ヵ月19ヵ月20ヵ月21ヵ月22ヵ月23ヵ月24ヵ月25ヵ月26ヵ月27ヵ月28ヵ月29ヵ月30ヵ月31ヵ月32ヵ月33ヵ月34ヵ月35ヵ月又はr36ヵ月)延長させる。
In some examples, treatment reduces OS of a subject or population of subjects by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, eg, at least about 3.3 months; 3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4. 3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6. 5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, treatment reduces the OS of a subject or population of subjects by at least about 5.3 months (eg 5.3 to 120 months, 6 to 60 months 7 to 48
いくつかの実施形態では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のPFSを少なくとも約2.4ヶ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月、or10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、対象又は対象集団のPFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, the treatment reduces the subject's or population of subjects' PFS to at least about 2.4 months (e.g., 2.4-120 months, 2.5-100 months, 3.0-80 months, 4.0-60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months , 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months , 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10 months .5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months , 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's or population of subjects' PFS to at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months, or 10-24 months, eg, at least about 4.0 months , 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months , 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10 months .5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months , 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、対象又は対象集団は、各追加投薬サイクルの1日目に約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体及び各追加の投薬サイクルの1日目に約80mg~約2000mgの用量のアテゾリズマブの1回以上の追加の投薬サイクル(例えば、21日間投薬サイクル)を受け、カルボプラチン及びエトポシドは1回以上の追加の投薬サイクルのそれぞれから省略される。
In some embodiments, the subject or subject population is administered an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約60±15分(例えば約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、又は約70分)わたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 60 ± 15 minutes (e.g., about 50 minutes, about 51 minutes, about 52 minutes, About 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) to the subject or population of subjects. In some examples, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered for about 60±15 minutes (eg, about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes , about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about administered to a subject or population of subjects by intravenous infusion over a period of 73 minutes, about 74 minutes, or about 75 minutes).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の前に対象又は対象集団に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後及びPD-1軸結合アンタゴニストの投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、PD-1軸結合アンタゴニストの投与後の第2の観察期間を更に含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間及びPD-1軸結合アンタゴニストの投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分である例では、方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分である例では、方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab)) to the subject or subject population. In some examples, the method includes an intervening first observation period, eg, after administration of the anti-TIGIT antagonist antibody and before administration of the PD-1 axis binding antagonist. In some examples, the method further comprises a second observation period after administration of the PD-1 axis binding antagonist. In some examples, the method includes both a first observation period after administration of the anti-TIGIT antagonist antibody and a second observation period after administration of the PD-1 axis binding antagonist. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. In examples in which the first and second observation periods are each about 60 minutes, the method comprises administering the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist during the first and second observation periods about 30±10 minutes. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at . In examples where the first and second observation periods are each about 30 minutes, the method includes administering the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist during the first and second observation periods about 15±10 minutes. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at .
他の例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、PD-1軸結合アンタゴニストの投与後及び抗TIGITアンタゴニスト抗体の投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間を含む。いくつかの例では、方法は、PD-1軸結合アンタゴニストの投与後の第1の観察期間及び抗TIGITアンタゴニスト抗体の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分である例では、方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分である例では、方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。 In other examples, the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is combined with an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, such as tiragolumab). ) to a subject or population of subjects. In some examples, the method includes an intervening first observation period, eg, after administration of the PD-1 axis binding antagonist and before administration of the anti-TIGIT antagonist antibody. In some examples, the method includes a second observation period after administration of the anti-TIGIT antagonist antibody. In some examples, the method includes both a first observation period following administration of the PD-1 axis binding antagonist and a second observation period following administration of the anti-TIGIT antagonist antibody. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. In examples in which the first and second observation periods are each about 60 minutes, the method includes administering the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody during the first and second observation periods about 30±10 minutes. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at . In examples in which the first and second observation periods are about 30 minutes each, the method comprises administering the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody during the first and second observation periods about 15±10 minutes. recording the subject's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) at .
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1(アテゾリズマブ)アンタゴニスト抗体)は、対象又は対象集団に同時に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体)の投与後に、方法は観察期間を含む。いくつかの例では、観察期間は、約30分と約60分の間の長さである。観察期間が約60分の長さである場合、方法は、観察期間中、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体)及び抗TIGITアンタゴニスト抗体の投与後約30±10分に、対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。観察期間が約30分の長さである場合、方法は、観察期間中、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体)及び抗TIGITアンタゴニスト抗体の投与後約15±10分に、対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 (atezolizumab) antagonist antibody) are The subjects or populations of subjects are administered simultaneously. In some examples, the method includes an observation period, eg, after administration of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody). In some examples, the observation period is between about 30 minutes and about 60 minutes long. If the observation period is about 60 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody) and an anti-TIGIT antagonist antibody during the observation period at about 30±10 minutes. , may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature). If the observation period is about 30 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody) and an anti-TIGIT antagonist antibody during the observation period about 15±10 minutes. , may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature).
本明細書に記載される使用のための任意の方法、使用又は組成物において、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体(例えば、アテゾリズマブ))、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド))又はその医薬は、1つ以上の追加の抗がん治療剤(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又はOX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法/放射線療法、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)と併せて(別々に又は一緒に)投与される場合がある。 In any method, use or composition for use described herein, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), PD-1 axial binding antagonists (e.g., anti-PD-L1 antibodies (e.g., atezolizumab)), platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and topoisomerase II inhibitors (e.g., etoposide)) or pharmaceutical agents thereof One or more immune co-inhibitory receptors such as additional anti-cancer therapeutic agents (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab (YERVOY®))) (e.g., one or more immune co-inhibitory receptors selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA), or one or more immune co-stimulatory receptors (e.g. one or more selected from CD226, OX-40, CD28, CD27, CD137, HVEM and/or GITR) such as OX-40 agonists, e.g. chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapy, and/or anti-hormonal agents such as those listed hereinabove. ) in conjunction with (separately or together).
いくつかの例では、肺がんは、小細胞肺がん(SCLC)、例えば、進展型SCLC(ES-SCLC)である。いくつかの例では、対象又は対象集団は、ES-SCLC(例えば、ES-SCLCのための化学療法未経験)に対して処置未経験である。 In some examples, the lung cancer is small cell lung cancer (SCLC), eg, extensive-stage SCLC (ES-SCLC). In some examples, the subject or subject population is treatment naive for ES-SCLC (eg, chemotherapy naive for ES-SCLC).
いくつかの例では、肺がんはPD-L1発現について選択されない。他の例では、肺がんをPD-L1発現について選択する。いくつかの例では、肺がんは、SP 263、22C3、SP 142、又は28-8等の抗PD-L1抗体で染色することを含む免疫組織化学(IHC)アッセイによってPD-L1発現について選択される。いくつかの例では、抗PD-L1抗体はSP 263であり、IHCアッセイはVentana SP 263 IHCアッセイである。抗PD-L1抗体は22C3であり、IHCアッセイはpharmDx 22C3 IHCアッセイであり、抗PD-L1抗体がSP 142であり、IHCアッセイがVentana SP 142 IHCアッセイであるか、又は抗PD-L1抗体が28-8であり、IHCアッセイがpharmDx 28-8 IHCアッセイである。
In some examples, lung cancers are not selected for PD-L1 expression. In another example, lung cancers are selected for PD-L1 expression. In some examples, lung cancers are selected for PD-L1 expression by an immunohistochemistry (IHC) assay comprising staining with an anti-PD-L1 antibody such as
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
いくつかの実施形態では、肺がんは小細胞肺がん(SCLC)である。いくつかの実施形態では、SCLCは、ステージ4(IV)SCLCとも呼ばれる進行期小細胞肺がん(ES-SCLC)である。いくつかの実施形態では、SCLCは、Veterans Administration Lung Study Group(VALG)病期分類システム(例えば、Micke et al.Lung Cancer 2002,37:271-6を参照)による、又はそれによって定義されるように、組織学的又は細胞学的に確認されるES-SCLCである。いくつかの実施形態では、SCLCは、個体が手術不能であり、限定的又は限定的なステージのSCLC(L-SCLC又はLS-SCLC)を有するものとして分類することができない場合、ES-SCLCとして分類される。いくつかの実施形態では、ES-SCLCは検出可能であり、及び/又は元々患っていた肺の外に広がっている。いくつかの実施形態では、ESSCLCは、肝臓、副腎、リンパ節及び/又は脳等の他の(例えば、遠隔の)器官に検出可能であり、及び/又は更に広がっている。いくつかの実施形態では、ESSCLCは処置が困難である。 In some embodiments, the lung cancer is small cell lung cancer (SCLC). In some embodiments, the SCLC is advanced small cell lung cancer (ES-SCLC), also called stage 4 (IV) SCLC. In some embodiments, SCLC is according to or as defined by the Veterans Administration Lung Study Group (VALG) staging system (see, e.g., Micke et al. Lung Cancer 2002, 37:271-6). In addition, ES-SCLC confirmed histologically or cytologically. In some embodiments, SCLC is classified as ES-SCLC if the individual is inoperable and cannot be classified as having limited or limited stage SCLC (L-SCLC or LS-SCLC). being classified. In some embodiments, ES-SCLC is detectable and/or has spread outside the originally affected lung. In some embodiments, ESSCLC is detectable and/or has spread further to other (eg, remote) organs such as the liver, adrenal glands, lymph nodes and/or brain. In some embodiments, ESSCLC is difficult to treat.
いくつかの実施形態において、対象又は対象集団は予後不良を有する。いくつかの実施形態では、対象又は対象集団は、処置未経験の対象又は対象集団(例えば、化学療法未経験の対象又は対象集団)である。いくつかの実施形態では、治療未経験の対象は、例えば、がん、SCLC又はES-SCLCに対する事前処置を受けたことがない対象である。いくつかの実施形態では、治療未経験の対象は、ES-SCLCの事前処置を受けたことがない対象である。いくつかの実施形態において、処置未経験の対象は、化学療法未経験であり、例えば、がん、SCLC及び/又はES-SCLC等の処置のための事前の化学療法を受けたことがない対象である。いくつかの実施形態において、対象又は対象集団はES-SCLCのための処置を受けたことがない。いくつかの実施形態において、対象又は対象集団はES-SCLCのための事前の全身処置を受けたことがない。いくつかの実施形態において、対象又は対象集団は、治癒を意図して、限局型SCLC(LS-SCLC)に対する事前の化学放射線療法を受けており、ES-SCLCの診断からの最後の化学療法、放射線療法又は化学放射線療法サイクルから少なくとも6ヶ月の無処置サイクルを経験したことがある。いくつかの実施形態において、対象又は対象集団は無症候性のテント上又は小脳中枢神経系(CNS)転移を有する。いくつかの実施形態において、対象又は対象集団は、中脳、橋、延髄又は脊髄への転移を有しない。いくつかの実施形態において、対象又は対象集団はCNS疾患を有し、CNS疾患のためのコルチコステロイド処置を必要としない。いくつかの実施形態では、対象又は対象集団は、新しい無症候性転移を有し、CNS転移に対する放射線療法及び/又は手術を受けている。いくつかの実施形態において、対象又は対象集団は、RECIST v1.1基準(例えば、Eisenhauer et al.,Eur.J.Cancer 2009,45:228-247)に従って/によって定義されるように、測定可能な疾患を有する。いくつかの実施形態では、対象又は対象集団は、CD 137アゴニスト又は免疫チェックポイント遮断療法による事前の処置を受けたことがない。 In some embodiments, the subject or subject population has a poor prognosis. In some embodiments, the subject or subject population is a treatment-naive subject or subject population (eg, a chemotherapy-naive subject or subject population). In some embodiments, a treatment-naive subject is, for example, a subject who has had no prior treatment for cancer, SCLC, or ES-SCLC. In some embodiments, a treatment-naive subject is a subject who has never had prior treatment for ES-SCLC. In some embodiments, the treatment-naive subject is chemotherapy-naive, e.g., a subject who has not received prior chemotherapy for treatment of cancer, SCLC and/or ES-SCLC. . In some embodiments, the subject or subject population is treatment naïve for ES-SCLC. In some embodiments, the subject or subject population has no prior systemic treatment for ES-SCLC. In some embodiments, the subject or subject population has received prior chemoradiation therapy for limited-stage SCLC (LS-SCLC) with curative intent, and the last chemotherapy since the diagnosis of ES-SCLC; Have undergone at least 6 months of treatment-free cycle from a radiotherapy or chemoradiation cycle. In some embodiments, the subject or subject population has an asymptomatic supratentorial or cerebellar central nervous system (CNS) metastasis. In some embodiments, the subject or subject population does not have metastasis to the midbrain, pons, medulla oblongata, or spinal cord. In some embodiments, the subject or subject population has CNS disease and does not require corticosteroid treatment for CNS disease. In some embodiments, the subject or subject population has new asymptomatic metastases and has undergone radiation therapy and/or surgery for CNS metastases. In some embodiments, the subject or subject population is a measurable disease. In some embodiments, the subject or subject population has no prior treatment with a CD 137 agonist or immune checkpoint blockade therapy.
いくつかの例では、処置はCR又はPRをもたらす。いくつかの例では、対象又は対象集団のPFSは、基準PFS時間と比較して増加する。いくつかの例では、基準PFS時間が、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)なしで(例えば、抗PD-L1抗体(例えば、アテゾリズマブ))、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及びトポイソメラーゼII阻害剤(例えば、エトポシド)による処置を受けたことがある対象集団のPFS時間中央値である。 In some instances, treatment results in CR or PR. In some examples, the subject or subject population's PFS is increased compared to the baseline PFS time. In some examples, the baseline PFS time is without an anti-TIGIT antagonist antibody (e.g., tiragolumab) (e.g., an anti-PD-L1 antibody (e.g., atezolizumab)), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) and Median PFS time in a subject population that has received treatment with a topoisomerase II inhibitor (eg, etoposide).
いくつかの例では、本方法は、更なる治療を更に含む。更なる治療法は、放射線療法、手術(例えば、腫瘍摘出手術及び乳房切除)、化学療法、遺伝子療法、DNA療法、ウイルス療法、RNA療法、免疫療法、骨髄移植術、ナノ療法、モノクローナル抗体療法、又は前述の組み合わせであり得る。追加の治療は、アジュバント療法又はネオアジュバント療法の形態であり得る。いくつかの実施形態では、追加の治療は、小分子酵素阻害剤又は抗転移薬の投与である。いくつかの実施形態では、更なる治療法は、副作用制限剤(例えば、処置の副作用の発生及び/又は重症度を軽減するよう意図された薬剤、例えば、制嘔吐剤等)の投与である。いくつかの実施形態では、追加の治療は放射線療法である。いくつかの実施形態では、追加の治療は手術である。いくつかの実施形態では、追加の治療は放射線療法と手術の組合せである。いくつかの実施形態では、追加の治療はγ線照射である。 In some examples, the method further comprises an additional treatment. Further treatments include radiotherapy, surgery (e.g. lumpectomy and mastectomy), chemotherapy, gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, or a combination of the foregoing. Additional treatment may be in the form of adjuvant or neoadjuvant therapy. In some embodiments, the additional therapy is administration of small molecule enzyme inhibitors or antimetastatic agents. In some embodiments, the additional therapy is administration of side effect limiting agents (eg, agents intended to reduce the incidence and/or severity of side effects of treatment, such as antiemetic agents, etc.). In some embodiments, the additional therapy is radiation therapy. In some embodiments, the additional treatment is surgery. In some embodiments, the additional treatment is a combination of radiation therapy and surgery. In some embodiments, the additional treatment is gamma irradiation.
本明細書で使用が意図される追加の治療用抗体としては、限定されないが、アレムツズマブ(Campath)、ベバシズマブ(AVASTIN(登録商標)、Genentech)、セツキシマブ(ERBITUX(登録商標)、Imclone)、パニツムマブ(VECTIBIX(登録商標)、Amgen)、リツキシマブ(RITUXAN(登録商標)、Genentech/Biogen Idec)、ペルツズマブ(OMNITARG(登録商標)、2C4、Genentech)、トラスツズマブ(HERCEPTIN(登録商標)、Genentech)、トシツモマブ(Bexxar、Corixia)、抗体薬物コンジュゲートゲムツズマブオゾガマイシン(マイロターク(登録商標)、Wyeth)、アポリズマブ、アセリズマブ、アトリズマブ、バピヌズマブ、ビバツズマブメルタンシン、カンツズマブメルタンシン、セデリズマブ、セロリズマブペゴール、シドフシツズマブ、シドツズマブ、ダクリズマブ、エクリズマブ、エファリズマブ、エプラツズマブ、エルリズマブ、フェルビズマブ、フォントリズマブ、ゲムツズマブオゾガマイシン、イノツズマブオゾガマイシン、イピリムマブ、ラベツズマブ、リンツズマブ、マッツズマブ、メポリズマブ、モタビズマブ、モトビズマブ、ナタリズマブ、ニモツズマブ、ノロビズマブ、ヌマビズマブ、オクレリズマブ、オマリズマブ、パリビズマブ、パスコリズマブ、ペクフシツズマブ、ペクセリズマブ、ペクセリズマブ、ラリビズマブ、ラニビズマブ、レスリビズマブ、レスリズマブ、レスリビズマブ、ロベリズマブ、ルピズマブ、シブロツズマブ、シプリズマブ、ソンツズマブ、タカタツズマブテトラキセタン、タドキシズマブ、タリズマブ、テフィバズマブ、トシリズマブ、トラリズマブ、ツコツズマブセルモレウキン、ツクシツズマブ、ウマビズマブ、ウルトキサズマブ、ウステキヌマブ、ビジリズマブ、及びインターロイキン-12(ABT-874/J695、Wyeth Research and Abbott Laboratories)が挙げられる。 Additional therapeutic antibodies contemplated for use herein include, but are not limited to, alemtuzumab (Campath), bevacizumab (AVASTIN®, Genentech), cetuximab (ERBITUX®, Imclone), panitumumab ( VECTIBIX®, Amgen), rituximab (RITUXAN®, Genentech/Biogen Idec), pertuzumab (OMNITARG®, 2C4, Genentech), trastuzumab (HERCEPTIN®, Genentech), tositumomab (Bexxar , Corixia), antibody-drug conjugate gemtuzumab ozogamicin (Myrotak®, Wyeth), apolizumab, acelizumab, atolizumab, bapinuzumab, vivatuzumab mertansine, cantuzumab mertansine, cedelizumab, celolizumab mabpegor, sidovucituzumab, sidutuzumab, daclizumab, eculizumab, efalizumab, epratuzumab, erulizumab, felubizumab, vontolizumab, gemtuzumab ozogamicin, inotuzumab ozogamicin, ipilimumab, labetuzumab, lintuzumab, mattuzumab, mepolizumab,モタビズマブ、モトビズマブ、ナタリズマブ、ニモツズマブ、ノロビズマブ、ヌマビズマブ、オクレリズマブ、オマリズマブ、パリビズマブ、パスコリズマブ、ペクフシツズマブ、ペクセリズマブ、ペクセリズマブ、ラリビズマブ、ラニビズマブ、レスリビズマブ、レスリズマブ、レスリビズマブ、ロベリズマブ、ルピズマブ、シブロツズマブ、シプリズマブ、ソンツズマブ、タカタツズマブTetraxetane, tadoxizumab, talizumab, tefibazumab, tocilizumab, tralizumab, tucuzumab cermoreukin, tuxituzumab, umabizumab, ultoxazumab, ustekinumab, vigilizumab, and interleukin-12 (ABT-874/J695, Wyeth Research and Abbott) mentioned.
いくつかの実施形態では、追加の治療は、PI3K/AKT/mTOR経路、HSP 90阻害剤、チューブリン阻害剤、アポトーシス阻害剤、及び/又は化学予防剤を標的とする治療である。いくつかの実施形態では、追加療法は、CTLA-4(CD152としても知られている)、例えば、ブロッキング抗体、イピリムマブ(MDX-010、MDX-101、又はYervoy(登録商標)としても知られる)、トレメリムマブ(チシリムマブ又はCP-675、206としても知られる)であり、B7-H3(CD276としても知られる)に対するアンタゴニスト、例えば、ブロッキング抗体、MGA271、TGFベータに対するアンタゴニスト、例えば、メテリムマブ(CAT-192としても知られている)、フレゾリムマブ(GC1008としても知られる)、又はLY2157299、キメラ抗原受容体(CAR)を発現するT細胞(例えば、細胞傷害性T細胞又はCTL)の養子導入を含む処置、ドミナントネガティブTGFベータ受容体、例えば、ドミナントネガティブTGFベータタイプII受容体を含むT細胞の養子移入を含む処置、HERCREEMプロトコルを含む処置(例えば、ClinicalTrials.GOV Identifier NCT00889954を参照)、CD137(TNFRSF9、4-1BB、又はILAとしても知られる)に対するアゴニスト、例えば、活性化抗体、ウレルマブ(BMS-663513としても知られている)CD40に対するアゴニスト、例えば、活性化抗体、CP-870893、OX40(CD134としても知られる)に対するアゴニスト、例えば、活性化抗体、異なる抗OX40抗体(例えば、AgonOx)と併せて投与される活性化抗体、CD27に対するアゴニスト、例えば、活性化抗体、CDX-1127、インドールアミン-2,3-ジオキシゲナーゼ(IDO)、1-メチル-D-トリプトファン(1-D-MTとしても知られる)、抗体薬物コンジュゲート(一部の実施形態では、メルタンシン又はモノメチルアウリスタチンE(MMAE)を含む)、抗NAPI2B抗体-MMAEコンジュゲート(DNIB0600A又はRG7599としても知られる)、トラスツズマブエムタンシン(TDM1、アドトラスツズマブエムタンシン、又はKADCYLA(登録商標)、Genentechとしても知られる)、DMUC5754A、エンドセリンB受容体(EDNBR)を標的とする抗体薬物コンジュゲート、例えば、MMAEとコンジュゲートされたEDNBRに対する抗体、血管新生阻害剤、VEGFに対する抗体、例えば、VEGF-A、ベバシズマブ(AVASTIN(登録商標)、Genentechとしても知られる)、アンジオポエチン2(Ang2としても知られる)に対する抗体、MEDI3617、抗腫瘍剤、CSF-1R(M-CSFR又はCD115としても知られている)を標的とする薬剤、抗CSF-1R(IMCCS4としても知られている)、インターフェロン、例えばインターフェロンアルファ又はインターフェロンガンマ、ロフェロンA、GM-CSF(組換えヒト顆粒球マクロファージコロニー刺激因子、rhu GMCSF、サルグラモスチム、又はロイキン(登録商標)としても知られる)、IL-2(アルデスロイキン又はプロロイキン(登録商標)としても知られる)、IL-12、CD20を標的とする抗体(いくつかの実施形態では、CD20を標的とする抗体はオビヌツズマブ(GA101又はGazyva(登録商標)としても知られている)又はリツキシマブである)、GITRを標的とする抗体(いくつかの実施形態では、GITRを標的とする抗体はTRX518である)がんワクチンと併用して(いくつかの実施形態では、がんワクチンはペプチドがんワクチンであり、いくつかの実施形態では個別化ペプチドワクチンである;いくつかの実施形態では、ペプチドがんワクチンは、多価長鎖ペプチド、マルチペプチド、ペプチドカクテル、ハイブリッドペプチド、又はペプチドパルス化樹状細胞ワクチンである(例えば、Yamada et al.,Cancer Sci,104:14-21,2013を参照))、アジュバント、TLRアゴニスト、例えば、ポリiCLC(ヒルトノール(登録商標)としても知られる)、LPS、MPL、又はCpG ODNと組み合わせて、腫瘍壊死因子(TNF)α、IL-1、HMGB1、IL-10アンタゴニスト、IL-4アンタゴニスト、IL-13アンタゴニスト、HVEMアンタゴニスト、ICOSアゴニスト、例えばICOS-Lの投与によるICOSアゴニスト、又はICOSに対して指向されるアゴニスト抗体、CX3CL1を標的とする処置、CXCL10を標的とする処置、CCL5を標的とする処置、LFA-1又はICAM1アゴニスト、セレクチンアゴニスト、標的療法、B-Rafの阻害剤、ベムラフェニブ(ゼルボラフ(登録商標)としても知られる)、ダブラフェニブ(Tafinlar(登録商標)としても知られる)、エルロチニブ(タルセバ(登録商標)としても知られる)、MEK1(MAP2K1としても知られている)又はMEK2(MAP2K2としても知られている)等のMEKの阻害剤。コビメチニブ(GDC-0973又はXL-518としても知られている)、トラメチニブ(Mekinist(登録商標)としても知られている)、K-Rasの阻害剤、c-Met、オナルツズマブ(MetMABとしても知られている)の阻害剤、Alkの阻害剤、AF802(CH5424802又はアレクチニブとしても知られている)、ホスファチジルイノシトール3-キナーゼ(PI3K)、BKM120、イデラリシブ(GS-1101又はCAL 101としても知られている)、ペリホシン(KRX-0401としても知られている)、Akt、MK2206、GSKK690693、GDC-0941、mTOR、シロリムス(ラパマイシンとしても知られている)の阻害剤、テムシロリムス(CCI-779又はTorisel(登録商標)としても知られる)、エベロリムス(RAD001としても知られている)、リダフォロリムス(AP-23573、MK-8669、又はデフォロリムスとしても知られている)、OSI-027、AZD8055、INK128、デュアルPI3K/mTOR阻害剤、XL765、GDC-0980、BEZ235(NVP-BEZ235としても知られている)、GT226、GSK2126458、PF-04691502、PF-05212384(PKI-587としても知られている)である。追加の治療は、本明細書に記載の1つ以上の化学療法剤であり得る。
In some embodiments, the additional therapy is a therapy targeting the PI3K/AKT/mTOR pathway,
iii.局所進行性切除不能又は転移性肺がんを処置するための方法及び使用
対象又は対象集団における肺がん(例えば、扁平上皮NSCLC又は非扁平上皮NSCLC(局所進行性切除不能NSCLCを含む(例えば、ステージIIIB NSCLC))を含む非小細胞肺がん(NSCLC)、又は再発性若しくは転移性NSCLC(例えば、ステージIV NSCLC)、進展型SCLC(ES-SCLC)を含む小細胞肺がん(SCLC)、及び肺の腺癌)を処置するための方法及び使用であって、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)並びに第1及び第2の化学療法剤(例えば、白金系化学療法剤及び非白金系化学療法剤)の1回以上の投薬サイクルを対象又は対象集団に投与することを含む方法及び使用が本明細書で提供される。
iii. Methods and uses for treating locally advanced unresectable or metastatic lung cancer Lung cancer (e.g., squamous NSCLC or non-squamous NSCLC, including locally advanced unresectable NSCLC (e.g., stage IIIB NSCLC) in a subject or population of subjects ), or recurrent or metastatic NSCLC (e.g., stage IV NSCLC), small cell lung cancer (SCLC), including extensive-stage SCLC (ES-SCLC), and adenocarcinoma of the lung). Methods and uses for treatment, comprising an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., atezolizumab) anti-PD-L1 antagonist antibody, etc.) and one or more dosing cycles of the first and second chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents) are administered to the subject or population of subjects Provided herein are methods and uses comprising:
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法の組み合わせを、それを必要とする対象又は対象集団に投与することを含む方法及び使用を含む。いくつかの実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は、3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの態様では、本発明は、3週間ごと(例えば、各21日間投薬サイクルの1日目に)の対象又は対象集団の体重(BW)又は体表面積(BSA)に基づいて有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与を含む方法及び使用を含む。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). antibodies), and chemotherapeutic combinations to a subject or population in need thereof. In some embodiments, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody, eg, , atezolizumab) is administered every 3 weeks (eg, on
いくつかの態様では、本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法の組み合わせを、それを必要とする対象又は対象集団に投与することを含む方法及び使用を含み、化学療法の組み合わせは、有効量の白金系化学療法剤及び有効量の非白金系化学療法剤を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)を3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与する。いくつかの例では、白金系化学療法剤はカルボプラチン又はシスプラチンであり、非白金系化学療法剤は代謝拮抗剤(例えば、ペメトレキセド)である。
In some aspects, the invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, atezolizumab, etc.). anti-PD-L1 antagonist antibody), and a chemotherapeutic combination comprising administering to a subject or subject population in need thereof, wherein the chemotherapeutic combination comprises an effective amount of platinum-based chemotherapy and an effective amount of a non-platinum chemotherapeutic agent. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 3 weeks (eg, on
特定の実施形態では、本方法は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)、及び代謝拮抗剤(例えば、ペメトレキセド)を、それを必要とする対象又は対象集団に投与することを含み、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)は3週間ごとに(例えば、各21日間投薬サイクルの1日目に)投与され、化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)は同じ頻度で(例えば、3週間ごとに、例えば、各21日間投薬サイクルの1日目に)投与される。いくつかの例では、投薬は、4~6回の導入投薬サイクルにわたって継続する(例えば、4回の導入投薬サイクル、5回の導入投薬サイクル、又は6回の導入投薬サイクル)。導入投薬サイクルの後、維持療法は、1回以上のその後の(維持)投薬サイクルで投与することができる。特定の実施形態では、1回以上の維持投薬サイクルは、白金系化学療法剤を含まない。
In certain embodiments, the method comprises an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD - administering an L1 antagonistic antibody (e.g., atezolizumab), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and an antimetabolite (e.g., pemetrexed) to a subject or population of subjects in need thereof; Anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody, e.g., atezolizumab) every 3 weeks (e.g., on
いくつかの例では、本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を、それを必要とする対象又は対象集団に4週間ごとに(例えば、各28日間投薬サイクルの1日目に)投与することを含む方法及び使用を含む。
In some examples, the present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, atezolizumab, etc.). anti-PD-L1 antagonist antibody) to a subject or population in need thereof every four weeks (eg, on
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、PFS又はDORの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、OSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団の無増悪生存期間の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOSを延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in an increase in PFS or DOR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of L1 antagonist antibody) results in increased OS. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. resulting in increased progression-free survival in a subject or subject population. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. , to prolong the OS of a subject or subject population.
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及び化学療法の組み合わせの、それを必要とする対象又は対象集団(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペメトレキセド)との組み合わせ)への投与は、ペンブロリズマブ及び化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド)及び白金系化学療法剤(例えば、カルボプラチン又はシスプラチン))の組み合わせによる処置と比較して、対象又は対象集団のPFS中央値の増加をもたらす。いくつかの例では、処置は、対象また対象集団のPFSを少なくとも約3.5ヶ月又は約4.7ヶ月(例えば、少なくとも約3.5、3.6、3.7、3.8、3.9、4.0、4.1、4.2、4.3、4.4、4.5、4.6、又は4.7ヶ月、例えば、少なくとも約3.5~3.7ヶ月、3.7~3.9ヶ月、3.9~4.1ヶ月、4.1~4.3ヶ月、4.3~4.5ヶ月、又は4.5~4.7ヶ月)延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody) and a combination of chemotherapy to a subject or population in need thereof (e.g., a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) in combination with an antimetabolite agent (e.g., pemetrexed)) Dosing improved the median PFS of the subject or subject population compared to treatment with a combination of pembrolizumab and a chemotherapeutic agent (e.g., an antimetabolite (e.g., pemetrexed) and a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin)) resulting in an increase in In some examples, the treatment reduces the subject's or subject population's PFS by at least about 3.5 months or about 4.7 months (e.g., at least about 3.5, 3.6, 3.7, 3.8, 3 .9, 4.0, 4.1, 4.2, 4.3, 4.4, 4.5, 4.6, or 4.7 months, such as at least about 3.5-3.7 months, 3.7-3.9 months, 3.9-4.1 months, 4.1-4.3 months, 4.3-4.5 months, or 4.5-4.7 months).
いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、8.8ヶ月を超える(例えば、少なくとも8.9ヵ月、少なくとも9.0ヵ月、少なくとも9.2ヵ月、少なくとも9.5ヵ月、少なくとも10ヵ月、少なくとも11ヵ月、少なくとも12ヵ月、少なくとも13ヵ月、少なくとも14ヵ月、少なくとも15ヵ月、少なくとも16ヵ月、少なくとも17ヵ月、少なくとも18ヵ月、少なくとも20ヵ月、少なくとも24ヵ月、少なくとも30ヵ月、少なくとも36ヵ月、少なくとも42ヵ月、少なくとも48ヵ月、少なくとも54ヵ月、又は例えば約8.9ヵ月、約9.0ヵ月、約9.2ヵ月、約9.5ヵ月、約10ヵ月、約11ヵ月、約12ヵ月、約13ヵ月、約14ヵ月、約15ヵ月、約16ヵ月、約17ヵ月、約18ヵ月、約20ヵ月、約24ヵ月、約30ヵ月、約36ヵ月、約42ヵ月、約48ヵ月、約54ヵ月、又はそれ以上)PFS中央値をもたらす。いくつかの例では、処置は、少なくとも約8ヶ月(例えば、8ヵ月と36ヵ月の間、例えば8ヵ月と24ヵ月の間(例えば、8ヵ月、9ヵ月、10ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、又は24ヵ月)の対象集団のPFS中央値をもたらす。いくつかの例では、処置は、約12.5ヶ月~約14.7ヶ月(例えば、12.5、12.7、12.9、13.1、13.3、13.5、13.7、13.9、14.1、14.3、14.5、又は14.7ヶ月、例えば、約12.5~13ヶ月、13~13.5ヶ月、13.5~14ヶ月、又は14~14.7ヶ月)の対象集団のPFS中央値をもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも10ヵ月のPFS中央値をもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも12ヵ月のPFS中央値をもたらす。 In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab). ) to a subject or population of subjects with lung cancer (eg, NSCLC) for more than 8.8 months (eg, at least 8.9 months, at least 9.0 months, at least 9.2 months, at least 9.0 months). 5 months, at least 10 months, at least 11 months, at least 12 months, at least 13 months, at least 14 months, at least 15 months, at least 16 months, at least 17 months, at least 18 months, at least 20 months, at least 24 months, at least 30 months , at least 36 months, at least 42 months, at least 48 months, at least 54 months, or such as about 8.9 months, about 9.0 months, about 9.2 months, about 9.5 months, about 10 months, about 11 months , about 12 months, about 13 months, about 14 months, about 15 months, about 16 months, about 17 months, about 18 months, about 20 months, about 24 months, about 30 months, about 36 months, about 42 months, about 48 months, about 54 months, or longer) yields a median PFS. In some examples, the treatment is for at least about 8 months (e.g., between 8 months and 36 months, such as between 8 months and 24 months (e.g., 8 months, 9 months, 10 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, or 24 months). Treatment is from about 12.5 months to about 14.7 months (eg, 12.5, 12.7, 12.9, 13.1, 13.3, 13.5, 13.7, 13.9, 14 months). .1, 14.3, 14.5, or 14.7 months, such as about 12.5-13 months, 13-13.5 months, 13.5-14 months, or 14-14.7 months) In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist as disclosed herein) by any of the methods described herein antibodies, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapeutic combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolites. (e.g., in combination with pembrolizumab) to a subject or subject population with lung cancer (e.g., NSCLC) results in a median PFS of at least 10 months, hi some embodiments, described herein. an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD such as atezolizumab), by any of the methods of -L1 antagonist antibody), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab)), subjects with lung cancer (e.g., NSCLC) or Administration to the subject population results in a median PFS of at least 12 months.
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及び化学療法の組み合わせの、肺がんを有する対象又は対象集団(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペメトレキセド)との組み合わせ)への投与は、ペンブロリズマブ及び化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド)及び白金系化学療法剤(例えば、カルボプラチン又はシスプラチン))の組み合わせによる処置と比較して、対象又は対象集団のOS(OS)中央値の増加をもたらす。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約4ヶ月(例えば、4ヶ月と12ヶ月の間(例えば、4ヶ月、5ヶ月、6ヶ月、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、又は12ヶ月))延長させる。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約5.5ヶ月~約8.0ヶ月(例えば、5.5、6.0、6.5、7.0、7.5、又は8.0ヶ月、例えば、5.5~6.5、6.5~7.5、又は7.5~8.0ヶ月)延長させる。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- administration of a combination of L1 antagonist antibody) and chemotherapy to a subject or subject population with lung cancer (e.g., a combination of a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) and an antimetabolite agent (e.g., pemetrexed)) , median OS (OS) in a subject or subject population compared to treatment with a combination of pembrolizumab and a chemotherapeutic agent (e.g., an antimetabolite (e.g., pemetrexed) and a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin)) Provides an increase in value. In some examples, the treatment reduces the OS of the subject or subject population by at least about 4 months (e.g., between 4 months and 12 months (e.g., 4 months, 5 months, 6 months, 7 months, 8 months, 9 months). , 10 months, 11 months, or 12 months)). In some examples, the treatment reduces the OS of the subject or subject population by at least about 5.5 months to about 8.0 months (eg, 5.5, 6.0, 6.5, 7.0, 7.5 , or 8.0 months, eg, 5.5-6.5, 6.5-7.5, or 7.5-8.0 months).
いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、22ヶ月を超える(例えば、少なくとも23、少なくとも24、少なくとも25、少なくとも26、少なくとも27、少なくとも28、少なくとも29、少なくとも30、少なくとも31、少なくとも32、少なくとも33、少なくとも34、少なくとも35、少なくとも36、少なくとも42、少なくとも48、少なくとも54、少なくとも60、少なくとも70、少なくとも80、少なくとも90、少なくとも100、少なくとも110、少なくとも120、少なくとも130、少なくとも140、少なくとも150、少なくとも160、少なくとも170、少なくとも180、少なくとも190、又は少なくとも200ヵ月、例えば約23、約24、約25、約26、約27、約28、約29、約30、約31、約32、約、33、約34、約35、約36、約40、約42、約48、約54、約60、約70、約80、約90、約100、約110、約120、約130、約140、約150、約160、約170、約180、約190、約200ヵ月)OS中央値をもたらす。いくつかの実施形態では、処置は、少なくとも約24ヶ月(例えば、24ヵ月と42ヵ月の間(例えば、24ヵ月と36ヵ月の間(例えば、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)))の対象集団のOS中央値をもたらす。いくつかの実施形態では、処置は、約27.5ヶ月~約32.0ヶ月(例えば、27.5、28.0、28.5、29.0、29.5、30.0、30.5、31.0、31.5、又は32.0 ヵ月(例えば、27.5~28.5、28.5~29.5、29.5~30.5、30.5~31.5、又は31.5~32ヵ月)の対象集団のOS中央値をもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び対象又は対象集団への化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも24ヵ月のOS中央値をもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも36ヵ月のOS中央値をもたらす。 In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab). ) to a subject or population of subjects with lung cancer (e.g., NSCLC) for more than 22 months (e.g., at least 23, at least 24, at least 25, at least 26, at least 27, at least 28, at least 29, at least 30 , at least 31, at least 32, at least 33, at least 34, at least 35, at least 36, at least 42, at least 48, at least 54, at least 60, at least 70, at least 80, at least 90, at least 100, at least 110, at least 120, at least 130, at least 140, at least 150, at least 160, at least 170, at least 180, at least 190, or at least 200 months, such as about 23, about 24, about 25, about 26, about 27, about 28, about 29, about 30, about 31, about 32, about, 33, about 34, about 35, about 36, about 40, about 42, about 48, about 54, about 60, about 70, about 80, about 90, about 100, about 110, about 120, about 130, about 140, about 150, about 160, about 170, about 180, about 190, about 200 months) results in a median OS. In some embodiments, the treatment is for at least about 24 months (eg, between 24 months and 42 months (eg, between 24 months and 36 months (eg, 24 months, 25 months, 26 months, 27 months, 28 months)). , 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months))) median OS for the subject population. In some embodiments, treatment is from about 27.5 months to about 32.0 months (eg, 27.5, 28.0, 28.5, 29.0, 29.5, 30.0, 30.0 months). 5, 31.0, 31.5, or 32.0 months (e.g., 27.5-28.5, 28.5-29.5, 29.5-30.5, 30.5-31.5, or 31.5-32 months) in the subject population.In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibodies, such as tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapeutic combinations to a subject or subject population (e.g., platinum Administration of a systemic chemotherapeutic agent (e.g., carboplatin or cisplatin) in combination with an antimetabolite (e.g., pembrolizumab) to a subject or subject population with lung cancer (e.g., NSCLC) results in a median OS of at least 24 months In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) by any of the methods described herein , PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab). ) to a subject or subject population with lung cancer (eg, NSCLC) results in a median OS of at least 36 months.
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書中に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブなどの抗PD-L 1アンタゴニスト抗体)および化学療法の組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチンまたはシスプラチン)と代謝拮抗剤(例えば、ペメトレキセド)との組み合わせ)の、それを必要とする対象または対象の集団への投与は、ペンブロリズマブおよび化学療法の組み合わせ(例えば、代謝拮抗物質(例えば、ペメトレキセド)および白金系化学療法剤(例えば、カルボプラチンまたはシスプラチン))による処置と比較して、対象または対象集団の全奏効率(ORR)の増加、例えば、ペンブロリズマブおよび化学療法の組み合わせ(例えば、代謝拮抗物質(例えば、ペメトレキセド)および白金系化学療法剤(例えば、カルボプラチンまたはシスプラチン))による処置と比較して、少なくとも10%のORRの増加(例えば、少なくとも15%、少なくとも20%、少なくとも25%、少なくとも30%、少なくとも35%、または少なくとも40%)をもたらす。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD such as atezolizumab) - L1 antagonist antibody) and a combination of chemotherapy (e.g., a combination of a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) and an antimetabolite (e.g., pemetrexed)) in a subject in need thereof or for a subject. Population administration may reduce the total number of subjects or subject population compared to treatment with a combination of pembrolizumab and chemotherapy (e.g., an antimetabolite (e.g., pemetrexed) and a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin)). Increased response rate (ORR), e.g., at least 10 compared to treatment with a combination of pembrolizumab and chemotherapy (e.g., an antimetabolite (e.g., pemetrexed) and a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin)) % ORR increase (eg, at least 15%, at least 20%, at least 25%, at least 30%, at least 35%, or at least 40%).
いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、47.5%超(例えば、少なくとも48%,少なくとも49%,少なくとも50%,少なくとも55%,少なくとも60%,少なくとも65%,少なくとも70%,少なくとも75%,少なくとも80%,少なくとも85%,少なくとも90%,少なくとも95%又は100%、例えば約48%、約49%、約50%、約55%、約60%、約65%、約70%、約75%、約80%、約85%、約90%、約95%、又は約100%)のORRをもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも50%のORRをもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも60%のORRをもたらす。いくつかの実施形態では、本明細書に記載の方法のいずれかによる、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、及び化学療法組み合わせ(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)と代謝拮抗剤(例えば、ペンブロリズマブ)との組み合わせ)の、肺がん(例えば、NSCLC)を有する対象又は対象集団への投与は、少なくとも70%のORRをもたらす。 In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab)). of subjects or populations of subjects with lung cancer (e.g., NSCLC) is more than 47.5% (e.g., at least 48%, at least 49%, at least 50%, at least 55%, at least 60%, at least 65% , at least 70%, at least 75%, at least 80%, at least 85%, at least 90%, at least 95% or 100%, such as about 48%, about 49%, about 50%, about 55%, about 60%, about 65%, about 70%, about 75%, about 80%, about 85%, about 90%, about 95%, or about 100%). In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab)). to a subject or subject population with lung cancer (eg, NSCLC) results in an ORR of at least 50%. In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab)). to a subject or subject population with lung cancer (eg, NSCLC) results in an ORR of at least 60%. In some embodiments, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab), and chemotherapy combinations (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and antimetabolite agents (e.g., pembrolizumab)). to a subject or subject population with lung cancer (eg, NSCLC) results in an ORR of at least 70%.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に4週間(例えば、各28日間投薬サイクルの1日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して、対象又は対象集団の無増悪生存の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、DORの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象又は対象集団のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject or subject population in need thereof for four weeks (e.g., each on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を、それを必要とする対象又は対象集団に2週間ごとに(例えば、各28日間投薬サイクルの1及び15日目に)投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団の無増悪生存期間の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). antibody) to a subject or population in need thereof every two weeks (eg, on
特定の例では、本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に2週間ごとに(例えば、各28日間投薬サイクルの1日目及び15日目に)投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して、対象又は対象集団の無増悪生存の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象又は対象集団のOSを延長する。
In certain examples, the invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject or subject population in need thereof. Methods and uses comprising administration on a weekly basis (eg, on
いくつかの例では、対象又は対象集団は、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を投与する1ヶ月以内に(例えば、PD-1軸結合アンタゴニストと抗TIGITアンタゴニスト抗体との投与の2ヶ月前以内、3ヶ月前以内、4ヶ月前以内、6ヶ月前以内、1年前、2年前、3年前、4年前、5年前、又は10年前)事前全身治療(例えば、治癒目的の事前全身治療、例えば化学療法)を受けたことがない。いくつかの例では、対象又は対象集団は化学療法未経験である。 In some examples, the subject or subject population is within one month of administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody (e.g., two months of administration of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody). prior to, within 3 months, within 4 months, within 6 months, 1, 2, 3, 4, 5, or 10 years ago) prior systemic treatment (e.g., healing No previous intended systemic therapy (e.g., chemotherapy). In some examples, the subject or subject population is chemotherapy naive.
いくつかの実施形態では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、化学療法と組み合わせて投与される。例えば、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の2週間に1回(Q2W)、3週間に1回(Q3W)又は4週間に1回(Q4W)の投薬レジメンを、1つ以上の化学療法剤と併せて投与することができる。1つ以上の化学療法剤は、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体の投与頻度と同じ頻度(Q2W、Q3W、又はQ4W)又は異なる頻度(例えば、3週間の投薬/1週間の休薬のスケジュール)で投与することができる。例えば、いくつかの実施形態では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を2週間ごとに投与し、1つ以上の化学療法剤を毎週、3週間の投薬/1週間の休薬、2週間ごと、3週間ごと、又は4週間ごとに投与する。あるいは、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を3週間ごとに投与し、1つ以上の化学療法剤を1週間ごと、2週間ごと、3週間ごと、又は4週間ごとに投与する。あるいは、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を4週間ごとに投与し、1つ以上の化学療法剤を毎週、3週間の投薬/1週間の休薬、2週間ごと、3週間ごと、又は4週間ごとに投与する。ある特定の例では、化学療法剤は、週に複数回(例えば、週に2、3、4、5、6又は7回(例えば、投薬サイクルの1日目、2日目及び3日目に))投与される。
In some embodiments, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody are administered in combination with chemotherapy. For example, a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody once every two weeks (Q2W), once every three weeks (Q3W) or once every four weeks (Q4W) dosing regimen may be administered with one or more chemical It can be administered in conjunction with a therapeutic agent. The one or more chemotherapeutic agents are administered at the same frequency (Q2W, Q3W, or Q4W) or at a different frequency (e.g., 3 weeks on/1 week off) than the dosing frequency of the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody. schedule). For example, in some embodiments, the PD-1 axis binding antagonist and the anti-TIGIT antagonist antibody are administered every 2 weeks and one or more chemotherapeutic agents are administered weekly for 3 weeks on/1 week off, 2 Administer weekly, every three weeks, or every four weeks. Alternatively, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody are administered every three weeks and one or more chemotherapeutic agents are administered every week, every two weeks, every three weeks, or every four weeks. Alternatively, a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody administered every 4 weeks and one or more chemotherapeutic agents weekly, on 3 weeks/1 week off, every 2 weeks, every 3 weeks, Or every 4 weeks. In certain instances, the chemotherapeutic agent is administered multiple times per week (e.g., 2, 3, 4, 5, 6, or 7 times per week (e.g., on
いくつかの実施形態では、化学療法剤の用量は、1回以上の初期用量(例えば、1回、2回、3回、4回、又はそれ以上の初期投与後)の後に減少する。例えば、化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチンまたはシスプラチン)および/または1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセドまたはゲムシタビン)のその後の用量は、初期用量の約95%、90%、85%、80%、75%、70%、65%、60%、55%、50%、45%、40%、35%、30%、25%、20%、15%、10%、または5%で投与することができる。例えば、約75mg/m2のシスプラチンの初期用量を、その後の用量では、例えば、70mg/m2、65mg/m2、60mg/m2、55mg/m2、50mg/m2、又は45mg/m2に減少させることができ、約500mg/m2のペメトレキセドの初期用量を、その後の用量では、例えば、450mg/m2、400mg/m2、350mg/m2、300mg/m2、250mg/m2、又は200mg/m2に減少させることができ、及び/又はAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチンの初期用量は、その後の用量、例えばAUC=4.5mg/ml/分、4.0mg/ml/分、3.5mg/ml/分、又は3.0mg/ml/分を達成するのに十分な用量まで減少させることができる。
In some embodiments, the dose of the chemotherapeutic agent is decreased after one or more initial doses (eg, after 1, 2, 3, 4, or more initial doses). Subsequent doses of, for example, a chemotherapeutic agent (e.g., a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., an antimetabolite (e.g., pemetrexed or gemcitabine)) is about 95%, 90%, 85%, 80%, 75%, 70%, 65%, 60%, 55%, 50%, 45%, 40%, 35%, 30%, 25% of the initial dose , 20%, 15%, 10%, or 5%, for example, an initial dose of cisplatin of about 75 mg/m 2 followed by doses of, for example, 70 mg/m 2 , 65 mg/m 2 . , 60 mg/m 2 , 55 mg/m 2 , 50 mg/m 2 , or 45 mg/m 2 , with an initial dose of pemetrexed of about 500 mg/m 2 followed by doses of, for example, 450 mg/
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、対象又は対象集団の無増悪生存期間の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)の投与は、対象又は対象集団のOSを延長させる。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- Administration of L1 antagonist antibodies), platinum-based chemotherapeutic agents (eg carboplatin or cisplatin) and antimetabolites (eg pemetrexed) result in CR or PR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and antimetabolite agents (eg, pemetrexed) result in increased progression-free survival in a subject or subject population. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD- L1 antagonist antibody), platinum-based chemotherapeutic agents (eg, carboplatin or cisplatin) and antimetabolite agents (eg, pemetrexed) prolong OS in a subject or subject population.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び代謝拮抗剤(例えば、ペメトレキセド)を投与されている対象又は対象集団は、肺がん、例えばNSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC)))の処置を受けている。 In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies such as atezolizumab). ), a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin), and an antimetabolite (e.g., pemetrexed), lung cancer, e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced undergoing treatment for sexually unresectable or metastatic non-squamous NSCLC (eg, stage IV non-squamous NSCLC).
薬剤の投薬
抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及び化学療法剤の投与は、セクションIII(K)に記載されている。
Drug Administration Administration of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists and chemotherapeutic agents is described in Section III(K).
がんの特性評価
本明細書に記載の方法、使用又は使用のための組成物のいずれにおいても、肺がんはNSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC)))であり得る。いくつかの例では、対象又は対象集団は、肺がんの事前全身治療を受けたことがない。
Characterization of Cancer In any of the methods, uses or compositions for use described herein, lung cancer is characterized by NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous) NSCLC (eg, stage IV non-squamous NSCLC)). In some examples, the subject or subject population has never received prior systemic treatment for lung cancer.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、上皮成長因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない。いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、EGFR遺伝子変異(例えば、感作EGFR遺伝子変異)又はALK遺伝子再編成を有しない。いくつかの例では、対象は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)を有する。 In some examples, in any of the methods, uses or compositions for use described herein, the subject has epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumors. No abnormalities. In some examples, in any of the methods, uses or compositions for use described herein, the subject has an EGFR gene mutation (e.g., a sensitizing EGFR gene mutation) or an ALK gene rearrangement. do not. In some examples, the subject has a US East Coast Clinical Trials Group (ECOG) Performance (PS) of 0 or 1.
突然変異状態EGFR及びALKを検出するための方法は当該技術分野で周知であり、それだけに限らないが、参照によりその全体が本明細書に組み込まれるFrampton et al.(Nature Biotechnology.31(11):1023-1033,2013)に記載されている標的遺伝子プルダウン及び配列決定法等の次世代配列決定法を使用して、臨床試料(例えば、腫瘍生検又は血液試料(例えば、血液中の循環腫瘍DNA))からのDNAを配列決定することが挙げられる。このような次世代配列決定方法は、小試料(例えば、小コア針生検、細針吸引、及び/又はセルブロック由来)又は固定試料(例えば、ホルマリン固定パラフィン包埋(FFPE)試料)の使用を可能にしながら、様々な突然変異(例えば、挿入、欠失、塩基置換、焦点遺伝子増幅、及び/又はホモ接合性遺伝子欠失)を検出する本明細書に開示される方法のいずれかと共に使用することができる。EGFR及びALKの突然変異状態を検出するための他の方法としては、蛍光インサイチュハイブリダイゼーション(FISH)法及び免疫組織化学(IHC)法が挙げられる。ALKの突然変異状態を検出するための例示的な方法は、参照によりその全体が本明細書に組み込まれる米国特許第9,651,555号に開示されている。いくつかの例では、VENTANA(登録商標)抗ALK(D5F3)IHCアッセイを使用して、ALK遺伝子の変異状態を決定する。 Methods for detecting mutational status EGFR and ALK are well known in the art and include, but are not limited to, Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013) using next-generation sequencing methods such as targeted gene pull-down and sequencing methods described in Clinical samples (e.g., tumor biopsies or blood samples). (eg, circulating tumor DNA in blood)). Such next-generation sequencing methods employ the use of small samples (e.g., from small core needle biopsies, fine needle aspirates, and/or cell blocks) or fixed samples (e.g., formalin-fixed paraffin-embedded (FFPE) samples). use with any of the methods disclosed herein to detect various mutations (e.g., insertions, deletions, base substitutions, focal gene amplifications, and/or homozygous gene deletions) while allowing be able to. Other methods for detecting EGFR and ALK mutational status include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods. An exemplary method for detecting the mutational status of ALK is disclosed in US Pat. No. 9,651,555, which is incorporated herein by reference in its entirety. In some examples, the VENTANA® Anti-ALK (D5F3) IHC assay is used to determine the mutational status of the ALK gene.
本明細書に記載される方法のいずれかのいくつかの例では、突然変異は感作EGFR突然変異である。感作EGFR突然変異は当該技術分野で周知であり、米国特許出願公開第2018/0235968号及びJuan et al.(Therapeutic Advances in Medical Oncology.9(3):201-216,2017)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、感作EGFR突然変異は、エクソン18~21(例えば、エクソン18、エクソン19、エクソン20及び/又はエクソン21における突然変異)のいずれか一つにおける突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン19の欠失(del19)である。他の例では、感作EGFR突然変異は、エクソン21中のL858R点突然変異である。いくつかの例では、感作EGFR変異は、エクソン18におけるG719X点変異であり、「X」は、最も一般的には、C、A又はSである。いくつかの例では、感作EGFR突然変異は、エクソン18におけるG719S点突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン18におけるG719A点突然変異である。いくつかの例では、感作EGFR突然変異は、エクソン18におけるS720F点突然変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861Q点変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861R点変異である。他の例では、感作EGFR突然変異はT790M点突然変異である。いくつかの例では、感作EGFR変異はE709X点変異であり、「X」は最も一般的にはK、A、又はHである。いくつかの例では、感作EGFR変異は、S768I点変異である。
In some examples of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are well known in the art and are described in US Patent Application Publication No. 2018/0235968 and Juan et al. (Therapeutic Advances in Medical Oncology. 9(3):201-216, 2017), which are incorporated herein by reference in their entirety. In some examples, the sensitizing EGFR mutation is a mutation in any one of exons 18-21 (eg, mutations in
本明細書に記載される方法のいずれかのいくつかの例では、突然変異はALK遺伝子再編成である。ALK遺伝子再編成は当該技術分野で周知であり、米国特許第9,651,555号及びDu et al.(Thoracic Cancer.9:423-430,2018)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、ALK遺伝子再構成は、下流のシグナル伝達経路を活性化して細胞増殖及び生存を増加させる発がん性ALKチロシンキナーゼの作製をもたらす。いくつかの例では、ALK遺伝子再編成は、融合がん遺伝子の形成をもたらす、EML4、KIF5B、KLC1、TFG、TPR、HIP1、STRN、DCTN1、SQSTM1、NPM1、BCL11A、BIRC6、RANBP2、ATIC、CLTC、TMP4、及びMSNからなる群から選択される遺伝子によるALK再編成である。いくつかの例では、ALK遺伝子再編成は、ALKとのEML4再編成であり、融合がん遺伝子EML4-ALKの形成をもたらす。 In some examples of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are well known in the art and are described in US Pat. No. 9,651,555 and Du et al. (Thoracic Cancer. 9:423-430, 2018), which are incorporated herein by reference in their entireties. In some instances, ALK gene rearrangement results in the creation of an oncogenic ALK tyrosine kinase that activates downstream signaling pathways to increase cell proliferation and survival. In some instances, the ALK gene rearrangement results in the formation of a fusion oncogene, EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC , TMP4, and MSN. In some instances, the ALK gene rearrangement is an EML4 rearrangement with ALK, resulting in the formation of the fusion oncogene EML4-ALK.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、NSCLCの肺リンパ上皮腫様癌腫サブタイプを有しない。NSCLCのサブタイプを検出するための方法は当該技術分野で周知であり、限定されないが、組織病理学的基準又は分子的特徴(例えば、バイオマーカー(例えば、特定の遺伝子又は該遺伝子によってコードされるタンパク質)の1つ又は組み合わせの発現を特徴とするサブタイプ)による決定方法を含む。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, in any of the methods, uses or compositions for use described herein, the subject does not have pulmonary lymphoepithelioma-like carcinoma subtype of NSCLC. Methods for detecting subtypes of NSCLC are well known in the art and include, but are not limited to, histopathological criteria or molecular characteristics (e.g., biomarkers (e.g., specific genes or (subtype) characterized by expression of one or a combination of proteins). In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample.
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、対象は、活動性エプスタイン・バー・ウイルス(EBV)感染を有していない、又は既知の慢性活動性EBV感染を有していない、若しくはその疑いがない。本明細書に記載の方法で使用するための活動性又は慢性活動性EBV感染の指標としては、限定されないが、EBV IgM、EBV IgG、Epstein-Barr核抗原(EBNA)、及び対象由来の試料(例えば、血液又は血清試料)中に検出されたEpstein-Barrウイルス粒子を挙げることができる。対象由来の試料中のEBV IgM、EBV IgG、Epstein-Barr核抗原(EBNA)、及びEpstein-Barrウイルス粒子を含む、活動性又は慢性活動性EBV感染の1つ以上の指標の存在を検出するための方法は、当該技術分野で周知であり、血清学的診断(例えば、EBV DNAの検出(例えば、EBVウイルス粒子を検出するための血液試料のPCR分析による)又はEBV抗原又は抗EBV抗体の検出(例えば、異種親和性抗体を用いたEBNA、EBV IgM又はEBV IgGの検出)を含む方法を含むが、これらに限定されない。いくつかの例では、試料は、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、対象はEBV IgMについて陰性であり、及び/又はEBV PCRによって陰性である。いくつかの例では、対象は、EBV IgMについて陰性であり、及び/又はEBV PCRについて陰性であり、かつEBV IgGについて陽性であり、及び/又はエプスタイン・バー核抗原(EBNA)について陽性である。他の例では、対象はEBV IgGについて陰性であり、及び/又はEBNAについて陰性である。いくつかの例では、対象はPD-L1選択腫瘍(例えば、SP 263若しくは22C3抗体を用いたIHCによって決定される最小PD-L1陽性腫瘍細胞分率又はTPS≧30%(例えば、50%以上)を有する腫瘍PD-L1発現、又はSP 142抗体を用いたIHCによって決定される腫瘍試料中のPD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合が1%以上である)を有する。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって30%以上(例えば、50%以上)のPD-L1陽性腫瘍細胞分率又はPD-L1 TPSを有すると判定された腫瘍である。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって、PD-L1発現免疫細胞(IC)が占める腫瘍面積の割合が1%以上であると判定された腫瘍である。いくつかの例では、IHCアッセイは、抗PD-L1抗体SP263、22C3、SP142又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、腫瘍試料は、50%以上のTPSを有すると判定されている。いくつかの例では、PD-L1陽性腫瘍細胞分率は、50%以上である(例えば、抗PD-L1抗体SP263による陽性染色によって決定される場合(例えば、Ventana assayを使用)、抗PD-L1抗体22C3による陽性染色によって決定される場合(例えば、pharmDxアッセイの使用)、又は抗PD-L1抗体28-8による陽性染色によって決定される場合)。いくつかの実施形態では、PD-L1陽性腫瘍細胞分率は、抗PD-L1抗体SP142を用いる陽性染色によって決定される場合、30%以上である。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)5%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)10%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上50%未満であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上30%未満であると判定されている。 In some examples, in any of the methods, uses, or compositions for use described herein, the subject does not have an active Epstein-Barr virus (EBV) infection; or no known or suspected chronic active EBV infection. Indicators of active or chronically active EBV infection for use in the methods described herein include, but are not limited to, EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and subject-derived samples ( Examples include Epstein-Barr virus particles detected in blood or serum samples). To detect the presence of one or more indicators of active or chronically active EBV infection, including EBV IgM, EBV IgG, Epstein-Barr nuclear antigen (EBNA), and Epstein-Barr virus particles in a sample from a subject are well known in the art and include serological diagnostics (e.g. detection of EBV DNA (e.g. by PCR analysis of blood samples to detect EBV virions) or detection of EBV antigens or anti-EBV antibodies (e.g., detection of EBNA, EBV IgM or EBV IgG using heterophilic antibodies) In some examples, the sample is a whole blood sample, a serum sample and a plasma sample. is selected from the group consisting of: In some examples, the subject is EBV IgM negative and/or is negative by EBV PCR, In some examples, the subject is EBV IgM negative and /or negative for EBV PCR and positive for EBV IgG and/or positive for Epstein-Barr nuclear antigen (EBNA) In other examples, the subject is negative for EBV IgG and/or Negative for EBNA In some instances, the subject has a PD-L1-selected tumor (e.g., minimal PD-L1-positive tumor cell fraction as determined by IHC using SP 263 or 22C3 antibody or TPS > 30% ( 50% or more), or 1% of the tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (IC) in the tumor sample as determined by IHC using the SP 142 antibody In some examples, the PD-L1-selected tumor has a PD-L1-positive tumor cell fraction of 30% or greater (eg, 50% or greater) or PD-L1-positive tumor cell fraction by immunohistochemistry (IHC) assay. Tumors determined to have L1 TPS In some instances, PD-L1-selected tumors have a percentage of tumor area occupied by PD-L1-expressing immune cells (IC) by immunohistochemistry (IHC) assay. A tumor determined to be greater than or equal to 1%.In some examples, the IHC assay uses the anti-PD-L1 antibody SP263, 22C3, SP142, or 28-8.In some examples, the IHC assay is The anti-PD-L1 antibody SP263 is used, hi some examples, the IHC assay uses the anti-PD-L1 antibody SP142. use. In some examples, the IHC assay uses the anti-PD-L1 antibody 22C3. In some instances, tumor samples have been determined to have a TPS of 50% or greater. In some examples, the PD-L1 positive tumor cell fraction is 50% or greater (e.g., as determined by positive staining with the anti-PD-L1 antibody SP263 (e.g., using the Ventana assay), anti-PD- as determined by positive staining with the L1 antibody 22C3 (eg using the pharmDx assay) or by positive staining with the anti-PD-L1 antibody 28-8). In some embodiments, the PD-L1 positive tumor cell fraction is 30% or greater as determined by positive staining with the anti-PD-L1 antibody SP142. In some instances, the IC has been determined to be 1% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, the IC has been determined to be 5% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some instances, the IC has been determined to be 10% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, the IC has been determined to be greater than or equal to 1% and less than 50% (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, the IC has been determined to be greater than or equal to 1% and less than 30% (eg, as determined using the Ventana (SP142) PD-L1 IHC assay).
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1タンパク質発現レベルを有する。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、IHCアッセイによって決定されたものである。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上5%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の5%以上50%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の50%以上において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上5%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の5%以上10%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の10%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 protein expression level. In some examples, the detectable PD-L1 protein expression level was determined by an IHC assay. In some examples, the IHC assay uses the anti-PD-L1 antibody SP142. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more and less than 5% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 5% or more and less than 50% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in 50% or more of the tumor cells in the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more and less than 5% of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 5% or more and less than 10% of the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 10% or more of the tumor sample.
いくつかの例では、対象は、PD-L1発現から評価されていない肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する。例えば、いくつかの例では、肺がんを有する対象は、50%(例えば、対象は、45%、40%、35%又は30%以上のPD-L1陽性腫瘍細胞画分を有すると判定されていない)以上のPD-L1陽性腫瘍細胞分率を有すると判定されていない。例えば、いくつかの例では、対象は、例えば、本明細書に記載される又は当該技術分野で公知のIHC方法のいずれかを使用して評定した場合に、50%以上のPD-L1陽性(例えば、対象は、45% PD-L1陽性、40% PD-L1陽性、35% PD-L1陽性又は30% PD-L1陽性以上のTPSを有すると判定されていない)のTPSを有すると判定されていない。 In some examples, the subject has lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non- with squamous NSCLC)))). For example, in some instances, a subject with lung cancer has not been determined to have a PD-L1 positive tumor cell fraction of 50% (e.g., 45%, 40%, 35%, or 30% or greater) ) has not been determined to have a PD-L1 positive tumor cell fraction of ≥ For example, in some instances, the subject is 50% or more PD-L1 positive (e.g., as assessed using any of the IHC methods described herein or known in the art) For example, a subject has not been determined to have TPS greater than or equal to 45% PD-L1 positive, 40% PD-L1 positive, 35% PD-L1 positive, or 30% PD-L1 positive or higher. not
いくつかの例では、肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する対象は、50%未満(例えば、1%~50%、1%~49%、5%~45%、10%~40%、15%~35%又は20%~30%、例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%又は45%~49%、例えば、49%未満、45%未満、40%未満、35%未満、30%未満、25%未満、20%未満、15%未満、10%未満、9%未満、8%未満、7%未満、6%未満、5%未満、4%未満、3%未満、2%未満、未満、1%未満又は約0%)のPD-L1陽性腫瘍細胞分率を有すると判定された。例えば、特定の例では、肺がんを有する対象は、1~49%(例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%、又は45%~49%)のPD-L1陽性腫瘍細胞分率を有すると判定されている。他の例では、肺がんを有する対象は、1%未満(例えば、約0%、又は検出不能なPD-L1発現)のPD-L1陽性腫瘍細胞分率を有すると判定されている。 In some examples, a subject with lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)))) , less than 50% (such as 1% to 50%, 1% to 49%, 5% to 45%, 10% to 40%, 15% to 35% or 20% to 30%, such as 1% to 5% , 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45% or 45 % to 49%, such as less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15%, less than 10%, less than 9%, less than 8% , less than 7%, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than, less than 1%, or about 0%) . For example, in certain instances, 1-49% of subjects with lung cancer (eg, 1%-5%, 5%-10%, 10%-15%, 15%-20%, 20%-25%, 25%-30%, 30%-35%, 35%-40%, 40%-45%, or 45%-49%). In other examples, a subject with lung cancer has been determined to have a PD-L1 positive tumor cell fraction of less than 1% (eg, about 0%, or undetectable PD-L1 expression).
例えば、いくつかの例では、肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する対象は、50%未満のPD-L1陽性(例えば、1%~50%、1%~49%、5%~45%、10%~40%、15%~35%、又は20%~30%PD-L1陽性、例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%、又は45%~49%PD-L1陽性、例えば、49%未満、45%未満、40%未満、35%未満、30%未満、25%未満、20%未満、15%未満、10%未満、9%未満、8%未満、7%未満、6%未満、5%未満、4%未満、3%未満、2%未満、1%、又は約0%PD-L1陽性)のTPSを有すると判定されている。例えば、特定の例では、肺がんを有する対象は、1~49%PD-L1陽性(例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%又は45%~49%のPD-L1陽性)のTPSを有すると判定されている。他の例では、肺がんを有する対象は、1%未満のPD-L1陽性(例えば、約0%、又は検出不能なPD-L1発現)のTPSを有すると判定されている。 For example, in some cases, having lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC))) Subjects are less than 50% PD-L1 positive (e.g., 1%-50%, 1%-49%, 5%-45%, 10%-40%, 15%-35%, or 20%-30% PD-L1 positive, e.g., 1%-5%, 5%-10%, 10%-15%, 15%-20%, 20%-25%, 25%-30%, 30%-35%, 35 %-40%, 40%-45%, or 45%-49% PD-L1 positive, e.g., <49%, <45%, <40%, <35%, <30%, <25%, 20% Less than, less than 15%, less than 10%, less than 9%, less than 8%, less than 7%, less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, 1%, or about 0% PD -L1 positive) has been determined to have TPS. For example, in certain instances, subjects with lung cancer are 1-49% PD-L1 positive (eg, 1%-5%, 5%-10%, 10%-15%, 15%-20%, 20% ~25%, 25%-30%, 30%-35%, 35%-40%, 40%-45%, or 45%-49% PD-L1 positive) of TPS. In another example, a subject with lung cancer has been determined to have TPS with less than 1% PD-L1 positive (eg, about 0% or undetectable PD-L1 expression).
特定の実施形態では、対象は、PD-L1発現から評価されていないNSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC)))を有する。例えば、いくつかの例では、NSCLCを有する対象は、50%(例えば、対象は、45%、40%、35%又は30%以上のPD-L1陽性腫瘍細胞画分を有すると判定されていない)以上のPD-L1陽性腫瘍細胞分率を有すると判定されていない。例えば、いくつかの例では、対象は、例えば、本明細書に記載される又は当該技術分野で公知のIHC方法のいずれかを使用して評定した場合に、50%以上のPD-L1陽性(例えば、対象は、45% PD-L1陽性、40% PD-L1陽性、35% PD-L1陽性又は30% PD-L1陽性以上のTPSを有すると判定されていない)のTPSを有すると判定されていない。 In certain embodiments, the subject has NSCLC that has not been evaluated for PD-L1 expression (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC) ))). For example, in some instances, a subject with NSCLC has not been determined to have a PD-L1 positive tumor cell fraction of 50% (e.g., the subject is 45%, 40%, 35%, or 30% or greater) ) has not been determined to have a PD-L1 positive tumor cell fraction of ≥ For example, in some instances, the subject is 50% or more PD-L1 positive (e.g., as assessed using any of the IHC methods described herein or known in the art) For example, a subject has not been determined to have TPS greater than or equal to 45% PD-L1 positive, 40% PD-L1 positive, 35% PD-L1 positive, or 30% PD-L1 positive or higher. not
いくつかの例では、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC)))を有する対象は、50%未満(例えば、1%~50%、1%~49%、5%~45%、10%~40%、15%~35%又は20%~30%、例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%又は45%~49%、例えば、49%未満、45%未満、40%未満、35%未満、30%未満、25%未満、20%未満、15%未満、10%未満、9%未満、8%未満、7%未満、6%未満、5%未満、4%未満、3%未満、2%未満、未満、1%未満又は約0%)のPD-L1陽性腫瘍細胞分率を有すると判定された。例えば、特定の例では、NSCLCを有する対象は、1~49%(例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%、又は45%~49%)のPD-L1陽性腫瘍細胞分率を有すると判定されている。他の例では、NSCLCを有する対象は、1%未満(例えば、約0%、又は検出不能なPD-L1発現)のPD-L1陽性腫瘍細胞分率を有すると判定されている。 In some instances, subjects with NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC))) are less than 50% ( For example, 1% to 50%, 1% to 49%, 5% to 45%, 10% to 40%, 15% to 35% or 20% to 30%, such as 1% to 5%, 5% to 10% %, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40% to 45% or 45% to 49%, For example, less than 49%, less than 45%, less than 40%, less than 35%, less than 30%, less than 25%, less than 20%, less than 15%, less than 10%, less than 9%, less than 8%, less than 7%, was determined to have a PD-L1 positive tumor cell fraction of less than 6%, less than 5%, less than 4%, less than 3%, less than 2%, less than 1%, or about 0%). For example, in certain instances, 1-49% of subjects with NSCLC (eg, 1%-5%, 5%-10%, 10%-15%, 15%-20%, 20%-25%, 25%-30%, 30%-35%, 35%-40%, 40%-45%, or 45%-49%). In other examples, a subject with NSCLC has been determined to have a PD-L1 positive tumor cell fraction of less than 1% (eg, about 0%, or undetectable PD-L1 expression).
例えば、いくつかの例では、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC)))を有する対象は、50%未満のPD-L1陽性(例えば、1%~50%、1%~49%、5%~45%、10%~40%、15%~35%、又は20%~30%PD-L1陽性、例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%、又は45%~49%PD-L1陽性、例えば、49%未満、45%未満、40%未満、35%未満、30%未満、25%未満、20%未満、15%未満、10%未満、9%未満、8%未満、7%未満、6%未満、5%未満、4%未満、3%未満、2%未満、1%、又は約0%PD-L1陽性)のTPSを有すると判定されている。例えば、特定の例では、NSCLCを有する対象は、1~49%PD-L1陽性(例えば、1%~5%、5%~10%、10%~15%、15%~20%、20%~25%、25%~30%、30%~35%、35%~40%、40%~45%又は45%~49%のPD-L1陽性)のTPSを有すると判定されている。他の例では、NSCLCを有する対象は、1%未満のPD-L1陽性(例えば、約0%、又は検出不能なPD-L1発現)のTPSを有すると判定されている。 For example, in some instances, subjects with NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC))) are 50% less than PD-L1 positive (e.g., 1%-50%, 1%-49%, 5%-45%, 10%-40%, 15%-35%, or 20%-30% PD-L1 positive, For example, 1% to 5%, 5% to 10%, 10% to 15%, 15% to 20%, 20% to 25%, 25% to 30%, 30% to 35%, 35% to 40%, 40%-45%, or 45%-49% PD-L1 positive, e.g., <49%, <45%, <40%, <35%, <30%, <25%, <20%, <15% , <10%, <9%, <8%, <7%, <6%, <5%, <4%, <3%, <2%, 1%, or about 0% PD-L1 positive) Have been determined to have TPS. For example, in certain instances, subjects with NSCLC are 1-49% PD-L1 positive (eg, 1%-5%, 5%-10%, 10%-15%, 15%-20%, 20% ~25%, 25%-30%, 30%-35%, 35%-40%, 40%-45%, or 45%-49% PD-L1 positive) of TPS. In another example, a subject with NSCLC has been determined to have TPS with less than 1% PD-L1 positive (eg, about 0% or undetectable PD-L1 expression).
いくつかの例では、個体から得られる腫瘍試料は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, the tumor sample obtained from the individual has a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
いくつかの例では、肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する対象から得られた腫瘍試料は、PD-L1の核酸発現レベルが低いか又は検出不能である。いくつかの例では、PD-L1の核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, from a subject with lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)))) The resulting tumor samples have low or undetectable levels of PD-L1 nucleic acid expression. In some examples, the nucleic acid expression level of PD-L1 is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. ing. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
本明細書に記載される方法のいずれかのいくつかの例では、肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する対象は、肺がん(例えば、治癒目的での事前の全身処置なし)の事前の全身処置を受けたことがない。特定の実施形態では、対象は局所進行性肺がんを有し、局所進行性肺がんの事前の全身処置を受けたことがない。いくつかの例では、対象はNSCLC(例えば、非扁平上皮NSCLC、例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC)を有し、NSCLCに対する以前の全身処置を受けたことがない(例えば、非扁平上皮NSCLC、例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC)。以前の全身処置には、以前のネオアジュバント、アジュバント化学療法、放射線療法、及び非転移性疾患に対する治癒目的の化学放射線療法が含まれる。 In some examples of any of the methods described herein, lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV Subjects with non-squamous NSCLC)))) have no prior systemic treatment for lung cancer (eg, no prior systemic treatment with curative intent). In certain embodiments, the subject has locally advanced lung cancer and has had no prior systemic treatment for locally advanced lung cancer. In some examples, the subject has NSCLC (e.g., non-squamous NSCLC, e.g., locally advanced unresectable or metastatic non-squamous NSCLC) and has no prior systemic treatment for NSCLC (e.g., , non-squamous NSCLC, eg locally advanced unresectable or metastatic non-squamous NSCLC). Prior systemic treatments include prior neoadjuvants, adjuvant chemotherapy, radiation therapy, and curative chemoradiation therapy for non-metastatic disease.
他の例では、肺がん(例えば、NSCLC(例えば、非扁平上皮NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))))を有する対象は、肺がんの事前の全身処置を受けたことがあり、本発明の方法のいずれかによる処置前に少なくとも12ヶ月の無治療期間を経験したことがある。 In other examples, a subject with lung cancer (e.g., NSCLC (e.g., non-squamous NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC))) is Has undergone prior systemic treatment for lung cancer and has undergone a treatment-free period of at least 12 months prior to treatment with any of the methods of the invention.
iv.切除可能な肺がんを処置するための方法及び使用
有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)の1回以上の投薬サイクルを対象に投与することを含む、対象の肺がん(例えば、早期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))を処置するための方法及び使用が本明細書で提供される。いくつかの例では、少なくとも1つの投薬サイクルがネオアジュバント処置として投与される。いくつかの例では、処置はネオアジュバント処置である。いくつかの例では、少なくとも1つの投薬サイクルがアジュバント処置として投与される。いくつかの例では、処置はアジュバント処置である。いくつかの例では、処置は、ネオアジュバント処置及びアジュバント処置を含む。いくつかの例では、肺がんは切除可能な肺がんである。いくつかの例では、肺がんは初期肺がん(例えば、II期、IIIA期又はIIIB期の肺がん)である。いくつかの例では、肺がんはNSCLC(例えば、扁平上皮又は非扁平上皮NSCLC)である。いくつかの例では、肺がんはPD-L1陽性である(例えば、PD-L1高)。いくつかの例では、肺がんは、上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない。いくつかの実施形態では、対象は、以前に肺がん(例えば、以前の手術、以前の免疫療法、以前の化学療法、又は以前の放射線療法)の処置を受けたことがない。いくつかの例では、対象は、白金系化学療法レジメンを受けるのに適格である。いくつかの例では、対象は、治癒目的でR0切除に適格である。対象は、好ましくはヒトである。
iv. Methods and Uses for Treating Resectable Lung Cancer lung cancer (e.g., early-stage lung cancer (e.g., resectable Provided herein are methods and uses for treating lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC)). In some examples, at least one dosing cycle is administered as a neoadjuvant treatment. In some examples, the treatment is a neoadjuvant treatment. In some examples, at least one dosing cycle is administered as an adjuvant treatment. In some examples, the treatment is adjuvant treatment. In some examples, treatment includes neoadjuvant treatment and adjuvant treatment. In some examples, the lung cancer is resectable lung cancer. In some examples, the lung cancer is early stage lung cancer (eg, stage II, IIIA, or IIIB lung cancer). In some examples, the lung cancer is NSCLC (eg, squamous or non-squamous NSCLC). In some examples, the lung cancer is PD-L1 positive (eg, PD-L1 high). In some instances, the lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations. In some embodiments, the subject has no prior treatment for lung cancer (eg, prior surgery, prior immunotherapy, prior chemotherapy, or prior radiation therapy). In some examples, the subject is eligible to receive a platinum-based chemotherapy regimen. In some examples, the subject is eligible for R0 resection for curative purposes. The subject is preferably human.
本発明は、切除可能な肺がん(例えば、切除可能なNSCLC(例えば、切除可能な扁平上皮又は非扁平上皮NSCLC))を有する対象を処置するための方法及び使用を含み、方法は、3週間ごとに(例えば、各21日間投薬サイクルの1日目に)約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに(例えば、各21日間投薬サイクルの1日目に)約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)の1回以上の投薬サイクルを対象に投与することを含む。いくつかの態様では、本方法は、3週間ごとに(例えば、各21日間投薬サイクルの1日目に)30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに(例えば、各21日間投薬サイクルの1日目に)80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)の1回以上の投薬サイクルを対象に投与することを含む。
The invention includes methods and uses for treating a subject with resectable lung cancer (e.g., resectable NSCLC (e.g., resectable squamous or non-squamous NSCLC)), wherein the method comprises: every 3 weeks (e.g., on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)を、それを必要とする対象に3週間(例えば、各21日間投薬サイクルの1日目に)毎に投与することを含む方法及び使用を含む。いくつかの例では、投薬サイクルの少なくとも1つは、ネオアジュバント処置として、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに600mgの用量)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、3週間ごとに約80mgと約1600mgの間の用量(例えば、3週間ごとに約1200mgの用量)の用量(例えば、固定用量)でPD-1軸結合アンタゴニストを対象に投与することを含む。いくつかの例では、投薬サイクルの少なくとも1つは、アジュバント処置として、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに600mgの用量)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、3週間ごとに約80mgと約1600mgの間の用量(例えば、3週間ごとに約1200mgの用量)の用量(例えば、固定用量)でPD-1軸結合アンタゴニストを対象に投与することを含む。いくつかの例では、投薬サイクルの少なくとも1つは、ネオアジュバント処置として、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mgの用量)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、3週間ごとに80mgと1600mgの間の用量(例えば、3週間ごとに1200mgの用量)の用量(例えば、固定用量)でPD-1軸結合アンタゴニストを対象に投与することを含む。いくつかの例では、投薬サイクルの少なくとも1つは、アジュバント処置として、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mgの用量)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、3週間ごとに80mgと1600mgの間の用量(例えば、3週間ごとに1200mgの用量)の用量(例えば、固定用量)でPD-1軸結合アンタゴニストを対象に投与することを含む。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). (e.g., an anti-PD-1 antagonist antibody, such as pembrolizumab) to a subject in need thereof every three weeks (e.g., on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を投与されている対象は、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))の処置を受けている。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab) ) is undergoing treatment for lung cancer (eg, early stage lung cancer (eg, resectable lung cancer (eg, NSCLC (eg, squamous or non-squamous NSCLC))).
PD-1軸結合アンタゴニスト抗TIGITアンタゴニスト抗体は、当該技術分野で公知の任意の適切な様式で投与され得る。例えば、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、連続的に(異なる日に)又は同時に(同日又は同じ処置サイクル中に)投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニストは、投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に投与される。いくつかの例では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、同日に投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体の前に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体の後に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同時に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、同日に投与される抗TIGITアンタゴニスト抗体の前に投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、同日に投与される抗TIGITアンタゴニスト抗体の後に投与され得る。更に他の例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同時に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体とは別の組成物中にある。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同じ組成物中にある。いくつかの例では、PD-1軸結合アンタゴニストは、同日に患者に投与される任意の他の治療剤とは別個の静脈内ラインを介して投与される。PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、同じ投与経路又は異なる投与経路によって投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、PD-1軸結合アンタゴニストは静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニストの投与後に第1の観察期間がある。いくつかの例では、PD-1軸結合アンタゴニストの投与後に第2の観察期間がある。いくつかの例では、抗TIGITアンタゴニスト抗体の投与後に第1の観察期間がある。いくつかの例では、抗TIGITアンタゴニスト抗体の投与後に第2の観察期間がある。いくつかの例では、観察期間は、約30分と約60分の間の長さである。いくつかの例では、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニストは、静脈内又は皮下に投与される。いくつかの例では、静脈内注入は、30±10分超及び/又は60±15分超である。一例では、アテゾリズマブは60分かけて静脈内投与され得、最初の注入が許容される場合、その後の注入は全て30分かけて送達され得る。いくつかの例では、PD-1軸結合アンタゴニストは、静脈内プッシュ又はボーラスとして投与されない。一例では、チラゴルマブは、60分間にわたって静脈内投与され得る。最初の注入が許容される場合、その後の注入は全て30分かけて送達され得る。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内プッシュ又はボーラスとして投与されない。
A PD-1 axis binding antagonist anti-TIGIT antagonist antibody may be administered in any suitable manner known in the art. For example, a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody can be administered sequentially (on different days) or simultaneously (on the same day or during the same treatment cycle). In some examples, the anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist is administered at about
先の例のいずれかにおいて、各投薬サイクルは、任意の適切な長さ、例えば、約7日間(約5、6、7、8、又は9日)、約14日間(例えば、約12、13、14、15、又は16日間)、約21日間(例えば、約18、19、20、21、22、23、又は24日間)、約28日間(約25、26、27、28、29、30、又は31日間)又はそれを超えてもよい。いくつかの例では、各投薬サイクルは約21日間である。 In any of the preceding examples, each dosing cycle is of any suitable length, such as about 7 days (about 5, 6, 7, 8, or 9 days), about 14 days (eg, about 12, 13 days). , 14, 15, or 16 days), about 21 days (e.g., about 18, 19, 20, 21, 22, 23, or 24 days), about 28 days (about 25, 26, 27, 28, 29, 30 , or 31 days) or longer. In some examples, each dosing cycle is about 21 days.
いくつかの例では、対象から得られる試料(例えば、腫瘍試料、血液試料(例えば、血漿試料)、又はリンパ試料)のPD-L1発現レベルが決定されている。いくつかの例では、試料は、検出可能なPD-L1発現レベル(例えば、PD-L1の検出可能なタンパク質及び/又は核酸発現レベル)を有すると判定されている。いくつかの例では、検出可能なPD-L1発現レベルは、検出可能なPD-L1タンパク質発現レベルである。いくつかの例では、検出可能なPD-L1発現レベルは、PD-L1陽性腫瘍細胞分率(例えば、50%以上のPD-L1陽性腫瘍細胞分率)である。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、染色に適した抗PD-L1抗体(例えば、抗PD-L1抗体SP 263)で染色することを含む免疫組織化学(IHC)アッセイによって決定されている。いくつかの例では、IHCアッセイは、Ventana SP263 IHCアッセイである。いくつかの例では、検出可能なPD-L1発現レベルは、検出可能なPD-L1核酸発現レベルである。いくつかの例では、上皮成長因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)の変異状態が決定される。いくつかの例では、方法は、対象から試料を得ることを更に含む。いくつかの例では、方法は、PD-L1の発現レベルを決定することを更に含む。 In some examples, the PD-L1 expression level of a sample (eg, tumor sample, blood sample (eg, plasma sample), or lymph sample) obtained from the subject is determined. In some examples, the sample has been determined to have a detectable PD-L1 expression level (eg, a detectable protein and/or nucleic acid expression level of PD-L1). In some examples, the detectable PD-L1 expression level is a detectable PD-L1 protein expression level. In some examples, the detectable PD-L1 expression level is a PD-L1 positive tumor cell fraction (eg, a PD-L1 positive tumor cell fraction of 50% or greater). In some examples, detectable PD-L1 protein expression levels are determined by an immunohistochemistry (IHC) assay comprising staining with an anti-PD-L1 antibody suitable for staining (e.g., anti-PD-L1 antibody SP 263). is determined by In some examples, the IHC assay is the Ventana SP263 IHC assay. In some examples, the detectable PD-L1 expression level is a detectable PD-L1 nucleic acid expression level. In some examples, the mutational status of epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) is determined. In some examples, the method further comprises obtaining a sample from the subject. In some examples, the method further comprises determining the expression level of PD-L1.
いくつかの例では、第1の投薬サイクルは、手術(例えば、区域切除術、肺葉切除術、二葉切除術、又は肺切除術)の前に開始される。いくつかの例では、1回以上の投薬サイクルが手術前に完了する。いくつかの例では、少なくとも1、2、3、又は4回の投薬サイクル(例えば、1、2、3、4、5、6、7、8、又はそれ以上の投薬サイクル)が手術前に完了する。いくつかの例では、手術の前に4回の投薬サイクルが完了する。いくつかの例では、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、又はそれ以上の投薬サイクル)が手術後に開始される。いくつかの例では、手術後に16回の投薬サイクルが完了する。いくつかの例では、処置は手術を含む。いくつかの例では、手術は、区域切除術、肺葉切除術、二葉切除術、又は肺切除術である。いくつかの例では、処置は放射線療法(例えば、術後放射線療法)を含む。 In some examples, the first dosing cycle is initiated prior to surgery (eg, segmentectomy, lobectomy, bilobectomy, or pneumonectomy). In some instances, one or more dosing cycles are completed prior to surgery. In some examples, at least 1, 2, 3, or 4 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, or more dosing cycles) are completed prior to surgery do. In some instances, four dosing cycles are completed prior to surgery. In some examples, one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18 , 19, 20, or more dosing cycles) are initiated after surgery. In some instances, 16 dosing cycles are completed after surgery. In some examples, treatment includes surgery. In some examples, the surgery is segmentectomy, lobectomy, bilobectomy, or pneumonectomy. In some examples, treatment includes radiation therapy (eg, postoperative radiation therapy).
いくつかの例では、処置は、基準病理学的著効(MPR)率と比較して、MPR率の増加をもたらす。いくつかの例では、処置は、病理学的完全奏効(pCR)及び/又は基準pCR率と比較したpCR率の増加をもたらす。いくつかの例では、処置は、基準無症候生存期間(EFS)時間と比較してEFSの増加をもたらす。いくつかの例では、処置は、基準OS時間と比較してOSの増加をもたらす。いくつかの例では、基準MPR率、基準pCR率、及び/又は基準EFS時間は、(a)抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト;及び/又は(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル及びベバシズマブを含む処置を受けたことがある対象集団のMPR率、pCR率、及び/又はEFS時間である。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、MPR率の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、pCRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、EFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、OSの増加をもたらす。 In some instances, the treatment results in an increased MPR rate compared to the baseline significant pathologic response (MPR) rate. In some examples, the treatment results in a pathological complete response (pCR) and/or an increase in the pCR rate compared to the baseline pCR rate. In some instances, treatment results in an increase in EFS compared to baseline symptom-free survival (EFS) time. In some examples, treatment results in an increase in OS compared to baseline OS time. In some examples, the baseline MPR rate, baseline pCR rate, and/or baseline EFS time are determined by (a) a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody; and/or (b) cisplatin and docetaxel or MPR rate, pCR rate, and/or EFS time in treatment-experienced subject populations including cisplatin, docetaxel, and bevacizumab. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in an increase in the MPR rate. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of L1 antagonist antibody) results in pCR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in an increase in EFS. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of L1 antagonist antibody) results in increased OS.
いくつかの例では、処置は、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル))を更に含む。いくつかの例では、ネオアジュバント及び/又はアジュバント処置は、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル))を更に含む。いくつかの例では、1つ以上の化学療法剤が、1つ以上の白金系化学療法剤及び/又は1つ以上の非白金系化学療法剤である。いくつかの例では、白金系化学療法剤はカルボプラチン又はシスプラチンである。いくつかの例では、非白金系化学療法剤は、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル)である。いくつかの例では、1つ以上の化学療法剤は、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル))である。いくつかの例では、少なくとも1つ以上の化学療法剤は、(a)カルボプラチン及びペメトレキセド;(b)カルボプラチン及びパクリタキセル;(c)シスプラチン及びペメトレキセド;(d)カルボプラチン及びゲムシタビン;又は(e)シスプラチン及びゲムシタビンである。いくつかの例では、非扁平上皮NSCLCの処置に使用される1つ以上の化学療法剤は、(a)カルボプラチン及びペメトレキセド、(b)カルボプラチン及びパクリタキセル、又は(c)シスプラチン及びペメトレキセドである。いくつかの例では、扁平上皮NSCLCの処置に使用される1つ以上の化学療法剤は、(a)カルボプラチン及びゲムシタビン、(b)カルボプラチン及びパクリタキセル、又は(c)シスプラチン及びゲムシタビンである。いくつかの例では、処置は、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル))を投与することを更に含む。いくつかの例では、1つ以上の化学療法剤を3週間ごとに投与する。いくつかの例では、1つ以上の化学療法剤は、1回以上の投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に投与される。いくつかの例では、1つ以上の化学療法剤が、1回以上の投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)及び約8日目(例えば、5日目、6日目、7日目、8日目、9日目、10日目、又は11日目)に投与される。いくつかの例では、投薬サイクルは、例えば、約7日間(約5、6、7、8、又は9日)、約14日間(例えば、約12、13、14、15、又は16日間)、約21日間(例えば、約18、19、20、21、22、23、又は24日間)、約28日間(約25、26、27、28、29、30、又は31日間)又はそれを超える。いくつかの例では、各投薬サイクルは約21日間である。いくつかの例では、1つ以上の化学療法剤は、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、1つ以上の化学療法剤は、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)及び/又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の後に投与される。いくつかの例では、非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル))は、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の前に投与される。
In some instances, treatment includes one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g. pemetrexed or gemcitabine) and/or taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) In some examples, the neoadjuvant and/or adjuvant treatment comprises one or more chemotherapeutic agents (e.g. platinum-based chemotherapeutic agents (e.g. carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g. antimetabolites (e.g. pemetrexed or gemcitabine) and/or taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) )) In some examples, the one or more chemotherapeutic agents is one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents. In some examples, the platinum-based chemotherapeutic agent is carboplatin or cisplatin, hi some examples, the non-platinum-based chemotherapeutic agent is an antimetabolite (eg, pemetrexed or gemcitabine) and/or a taxane (eg, paclitaxel, such as nab-paclitaxel). In some examples, the one or more chemotherapeutic agents are a platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) and a non-platinum-based chemotherapeutic agent (e.g., an antimetabolite agent (e.g., pemetrexed or gemcitabine). ) and/or taxanes (eg paclitaxel, eg nab-paclitaxel) In some examples, at least one or more chemotherapeutic agents are (a) carboplatin and pemetrexed; (d) carboplatin and gemcitabine, or (e) cisplatin and gemcitabine In some examples, the one or more chemotherapeutic agents used to treat non-squamous NSCLC are (a) (b) carboplatin and paclitaxel, or (c) cisplatin and pemetrexed In some examples, the one or more chemotherapeutic agents used to treat squamous NSCLC are (a) carboplatin and gemcitabine, (b) carboplatin and paclitaxel, or (c) cisplatin and gemcitabine In some examples, the treatment includes one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents). (e.g. carboplatin or cisplatin) and/or one or more non-platinum chemotherapeutic agents (e.g. antimetabolites (e.g. pemetrexed or gemcitabine) and/or taxanes (e.g. paclitaxel, e.g. nab-paclitaxel)) further includes In some examples, one or more chemotherapeutic agents are administered every three weeks. In some examples, one or more chemotherapeutic agents are administered at about day 1 (e.g., day -3, day -2, day -1,
本発明は、切除可能な肺がん(例えば、初期の切除可能な肺がん(例えば、切除可能なNSCLC(例えば、切除可能な扁平上皮又は非扁平上皮NSCLC)))を有する対象を処置するための方法及び使用を含み、方法は、3週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、3週間ごとに約80mgと約1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)、及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))の1回以上の投薬サイクルを対象に投与することを含む。いくつかの態様では、方法は、3週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))の1回以上の投薬サイクルを対象に投与することを含む。 The present invention provides methods and methods for treating subjects with resectable lung cancer (e.g., early resectable lung cancer (e.g., resectable NSCLC (e.g., resectable squamous or non-squamous NSCLC))). The method includes the use of a dose (e.g., fixed dose) of between about 30 mg and about 600 mg every three weeks of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or an anti-PD-1 antagonist such as, for example, pembrolizumab) at doses (e.g., fixed doses) of about 80 mg and about 1600 mg every 3 weeks antibodies), platinum-based chemotherapeutic agents (e.g., cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab-paclitaxel)). Including administering one or more dosing cycles to the subject. In some aspects, the method comprises administering a dose (e.g., a fixed dose) of between 30 mg and 600 mg every three weeks of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g. an anti-PD-L1 antagonist antibody such as atezolizumab or an anti-PD-1 antagonist such as e.g. antibodies), platinum-based chemotherapeutic agents (e.g., cisplatin or carboplatin) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab-paclitaxel)). administering to the subject the above dosing cycles.
本発明は、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))を有する対象を処置するための方法及び使用を含み、方法は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)、及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))の1回以上の投薬サイクルを対象に投与することを含み、投薬サイクルの少なくとも1つは、ネオアジュバント処置として、3週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)、及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))を対象に投与することを含む。いくつかの態様では、投薬サイクルの少なくとも1つは、ネオアジュバント処置として、3週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))を対象に投与することを含む。 The present invention includes methods and uses for treating a subject with lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer (e.g., NSCLC (e.g., squamous or non-squamous NSCLC))). is an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or e.g. pembrolizumab anti-PD-1 antagonist antibodies, etc.), platinum-based chemotherapeutic agents (e.g., cisplatin or carboplatin), and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab-paclitaxel)), wherein at least one of the dosing cycles is between about 30 mg and about 600 mg every three weeks as a neoadjuvant treatment (e.g., a fixed dose) of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of between about 80 mg and about 1600 mg every three weeks, a platinum-based chemotherapeutic agent (e.g., cisplatin or carboplatin), and Including administering to the subject a non-platinum chemotherapeutic agent (eg, an antimetabolite (eg, pemetrexed or gemcitabine) or a taxane (eg, paclitaxel or nab-paclitaxel)). In some aspects, at least one of the dosing cycles is anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) between 30 mg and 600 mg every 3 weeks, 80 mg and 1600 mg every 3 weeks as a neoadjuvant treatment. between doses (e.g., fixed dose) of a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent (e.g., cisplatin or carboplatin) and a non-platinum-based chemotherapeutic agent (e.g., an antimetabolite (e.g., pemetrexed or gemcitabine), or administering a taxane (eg, paclitaxel or nab-paclitaxel) to the subject.
本発明は、切除可能な肺がん(例えば、初期の切除可能な肺がん(例えば、切除可能なNSCLC(例えば、切除可能な扁平上皮又は非扁平上皮NSCLC)))を有する対象を処置するための方法及び使用を含み、方法は、3週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)と、(a)(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量の白金系化学療法剤(例えば、シスプラチン又はカルボプラチン);又は(ii)3週間ごとに約75mg/m2の用量の白金系化学療法剤(例えば、シスプラチン又はカルボプラチン);(b)(i)3週間ごとに約500mg/m2、又は各投薬サイクルの第1日及び第8日に約1000mg/m2若しくは約1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとに約100mg/m2、約175mg/m2、若しくは約200mg/m2の用量のタキサンの1回以上の投薬サイクルを対象に投与することを含む。いくつかの態様では、本方法は、3週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)と、(a)(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量での白金系化学療法剤(例えば、シスプラチン又はカルボプラチン);又は(ii)3週間ごとに75mg/m2の用量の白金系化学療法剤(例えば、シスプラチン又はカルボプラチン);(b)(i)3週間ごとに500mg/m2の用量、又は各投薬サイクルの第1日及び第8日に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとに100mg/m2、175mg/m2、又は200mg/m2の用量のタキサン、の1回以上の投薬サイクルを対象に投与することを含む。
The present invention provides methods and methods for treating subjects with resectable lung cancer (e.g., early resectable lung cancer (e.g., resectable NSCLC (e.g., resectable squamous or non-squamous NSCLC))). The method includes the use of a dose (e.g., fixed dose) of between about 30 mg and about 600 mg every three weeks of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or an anti-PD-L1 antagonist such as, 1 antagonist antibody) and (a)(i) a dose of a platinum-based chemotherapeutic agent (e.g., cisplatin) targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks or carboplatin); or (ii) a platinum-based chemotherapeutic agent (e.g., cisplatin or carboplatin) at a dose of about 75 mg/m 2 every 3 weeks; (b) (i) about 500 mg/m 2 every 3 weeks, or an antimetabolite at a dose of about 1000 mg / m2 or about 1250 mg/ m2 on
本発明は、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))を有する対象を処置するための方法及び使用を含み、方法は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)、白金系化学療法剤(例えば、シスプラチン又はカルボプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))の1回以上の投薬サイクルを対象に投与することを含み、投薬サイクルの少なくとも1つは、対象に、(a)3週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体;(b)3週間ごとの約80mgと約1600mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト;(c)白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量;又は(ii)約75mg/m2の用量で3週間ごとの白金系化学療法剤;及び(d)非白金系化学療法剤であって、(i)3週間ごとに500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとに100mg/m2、175mg/m2、又は200mg/m2の用量のタキサンである非白金系化学療法剤、を投与することを含み、処置はネオアジュバント処置である。いくつかの態様では、投薬サイクルの少なくとも1つは、対象に:(a)3週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体;(b)3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト;(c)白金系化学療法剤:(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量で;又は(ii)75mg/m2の用量で3週間ごとに;及び(d)非白金系化学療法剤であって、(i)3週間ごとに500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m 2の用量の代謝拮抗剤;又は(ii)3週間ごとに100mg/m2、175mg/m2、又は200mg/m2の用量のタキサンである非白金系化学療法剤、を投与することを含み、処置はネオアジュバント処置である。
The present invention includes methods and uses for treating a subject with lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer (e.g., NSCLC (e.g., squamous or non-squamous NSCLC))). is an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or e.g. pembrolizumab anti-PD-1 antagonist antibodies, etc.), platinum-based chemotherapeutic agents (e.g., cisplatin or carboplatin) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab - administering to the subject one or more dosing cycles of paclitaxel), wherein at least one of the dosing cycles comprises administering to the subject: (a) a dose of between about 30 mg and about 600 mg every 3 weeks (e.g., (b) a PD-1 axis binding antagonist at a dose (e.g., fixed dose) between about 80 mg and about 1600 mg every three weeks; (c) a platinum-based chemotherapeutic agent; (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/ min every 3 weeks; and (d) a non-platinum chemotherapeutic agent, which is (i) 500 mg/ m2 every 3 weeks, or 1000 mg/ m2 on days 1 and 8 of each dosing cycle, or or (ii) a dose of 100 mg/ m 2 , 175 mg/m 2 , or 200 mg/m 2 of a taxane non-platinum chemotherapeutic agent every 3 weeks. and the treatment is a neoadjuvant treatment. In some embodiments, at least one of the dosing cycles comprises: (a) anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) between 30 mg and 600 mg every 3 weeks; (b) every 3 weeks PD-1 axis binding antagonist at a dose (e.g., fixed dose) between 80 mg and 1600 mg; (c) platinum-based chemotherapeutic agent: (i) AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks or (ii) every 3 weeks at a dose of 75 mg/ m2 ; and (d) a non-platinum chemotherapeutic agent that (i) every 3
本発明は、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))を有する対象を処置するための方法及び使用を含み、方法は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含み、(a)投薬サイクルの少なくとも一方が、抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)で、ネオアジュバント処置として対象に投与することを含み;(b)投薬サイクルの少なくとも一方が、抗TIGITアンタゴニスト抗体を、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)で、アジュバント処置として対象に投与することを含む。いくつかの態様では、本方法は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含み、(a)投薬サイクルの少なくとも一方が、抗TIGITアンタゴニスト抗体を3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)で、ネオアジュバント処置として対象に投与することを含み;(b)投薬サイクルの少なくとも一方が、抗TIGITアンタゴニスト抗体を、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを、3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)で、アジュバント処置として対象に投与することを含む。 The present invention includes methods and uses for treating a subject with lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer (e.g., NSCLC (e.g., squamous or non-squamous NSCLC))). comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein (a) at least one of the dosing cycles comprises about 30 mg of the anti-TIGIT antagonist antibody every 3 weeks; and a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of between about 80 mg and about 1600 mg (e.g., fixed dose) every three weeks as a neoadjuvant treatment to the subject (b) at least one of the dosing cycles comprises an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose (e.g., fixed dose) between about 30 mg and about 1200 mg every three weeks; administering to the subject as an adjuvant treatment at a dose (eg, fixed dose) of between about 80 mg and about 1600 mg every 3 weeks. In some aspects, the method comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein (a) at least one of the dosing cycles comprises an anti-TIGIT antagonist; Neoadjuvant treatment with antibody at doses between 30 mg and 1200 mg every 3 weeks (e.g. fixed dose) and PD-1 axis binding antagonist at doses between 80 mg and 1600 mg every 3 weeks (e.g. fixed dose) (b) at least one of the dosing cycles is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every 3 weeks as a PD-1 axis binding antagonist as an adjuvant treatment to the subject at doses between 80 mg and 1600 mg (eg, fixed dose) every 3 weeks.
本発明は、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))を有する対象を処置するための方法及び使用を含み、方法は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含み、(I)投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、対象に、(a)3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体;(b)ネオアジュバント処置としての3週間ごとの約80mgと約1600mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト;(c)白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量;又は(ii)約75mg/m2の用量で3週間ごとの白金系化学療法剤;及び(d)非白金系化学療法剤であって、(i)3週間ごとに約500mg/m2、又は各投薬サイクルの第1日及び第8日に約1000mg/m 2若しくは約1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとに約100mg/m2、約175mg/m2、又は約200mg/m2の用量のタキサンである非白金系化学療法剤、を投与することを含み;(II)投薬サイクルの少なくとも一方が、抗TIGITアンタゴニスト抗体を、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)で、アジュバント処置として対象に投与することを含む。いくつかの態様では、本方法は、対象に、(a)3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体;(b)ネオアジュバント処置としての3週間ごとの80mgと1600mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト;(c)白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量;又は(ii)75mg/m2の用量で3週間ごとの白金系化学療法剤;及び(d)非白金系化学療法剤であって、(i)3週間ごとに500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとに100mg/m2、175mg/m2、又は200mg/m2の用量のタキサンである非白金系化学療法剤を投与することを含み;(II)投薬サイクルの少なくとも一方が、アジュバント処置として、抗TIGITアンタゴニスト抗体を3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)で、PD-1軸結合アンタゴニストを3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)で対象投与することを含む。
The present invention includes methods and uses for treating a subject with lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer (e.g., NSCLC (e.g., squamous or non-squamous NSCLC))). comprises administering to the subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein (I) at least one of the dosing cycles is a neoadjuvant treatment; a) a dose of between about 30 mg and about 1200 mg (e.g., fixed dose) of an anti-TIGIT antagonist antibody every three weeks; (c) a platinum-based chemotherapeutic agent that (i) achieves an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m every 3 weeks; and (d) a non-platinum-based chemotherapeutic agent, wherein (i) every 3 weeks an antimetabolite at a dose of about 500 mg/ m2 , or about 1000 mg/ m2 or about 1250 mg/ m2 on
いくつかの例では、処置は追加の治療を更に含み得る。当該技術分野で公知であるか又は本明細書に記載される任意の適切な追加の治療を使用することができる。追加の治療は、放射線療法(例えば、術後放射線療法)、外科手術、遺伝子療法、DNA療法、ウイルス療法、RNA療法、免疫療法、骨髄移植、ナノ療法、モノクローナル抗体療法、ガンマ線照射、又はこれらの組み合わせであり得る。 In some examples, treatment may further include additional therapies. Any suitable additional therapy known in the art or described herein can be used. Additional treatments may include radiation therapy (e.g., postoperative radiation therapy), surgery, gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, gamma irradiation, or any of these. It can be a combination.
いくつかの例では、追加の治療は、副作用制限剤(例えば、処置の副作用の発生及び/又は重症度を軽減することを意図した薬剤、例えば、抗悪心剤、コルチコステロイド(例えば、プレドニゾン又は同等物、例えば1~2mg/kg/日の用量)、ホルモン補充薬等)の投与である。 In some instances, the additional therapy is a side effect-limiting agent (e.g., an agent intended to reduce the occurrence and/or severity of side effects of treatment, e.g., anti-nausea drugs, corticosteroids (e.g., prednisone or equivalents, eg doses of 1-2 mg/kg/day), hormone replacement drugs, etc.).
有効量のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)及び/又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む処置レジメンを、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)及び/又はタキサン(例えばパクリタキセル、例えばnab-パクリタキセル)))及び/又はがん治療(例えば、手術及び/又は放射線療法)と組み合わせて対象に投与することを含む、対象における肺がんを処置するための方法も本明細書に提供される。例えば、PD-1軸結合アンタゴニストは、追加の化学療法若しくは化学療法剤(上記の定義を参照);標的化療法若しくは標的化治療剤;免疫療法若しくは免疫療法剤、例えばモノクローナル抗体;1つ以上の細胞傷害剤(上記の定義を参照);又はそれらの組み合わせと併せて投与され得る。 A treatment regimen comprising an effective amount of a PD-1 axis binding antagonist (e.g., atezolizumab) and/or an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., antimetabolite agents (e.g., pemetrexed or gemcitabine) and/or taxanes (e.g. paclitaxel, e.g. nab-paclitaxel)))) and/or cancer therapy (e.g. surgery and/or radiation therapy). provided in the book. For example, a PD-1 axis binding antagonist may include an additional chemotherapy or chemotherapeutic agent (see definition above); a targeted therapy or targeted therapeutic agent; an immunotherapy or immunotherapeutic agent, such as a monoclonal antibody; cytotoxic agents (see definition above); or combinations thereof.
薬剤の投薬
抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及び化学療法剤の投与は、セクションIII(K)に記載されている。
Drug Administration Administration of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists and chemotherapeutic agents is described in Section III(K).
がんの特性評価及び選択
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、肺がん(例えば、早期肺がん(例えば、切除可能な肺がん(例えば、NSCLC(例えば、扁平上皮又は非扁平上皮NSCLC))))は切除可能である(例えば、治癒目的でのR0切除に適格である)。いくつかの例では、肺がんはNSCLCである。いくつかの例では、NSCLCは、扁平上皮又は非扁平上皮NSCLCである。いくつかの例では、肺がんはPD-L1陽性である。いくつかの例では、肺がんはPD-L1高値である。いくつかの例では、肺がんは、上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK))のゲノム腫瘍異常を有しない。いくつかの例では、肺がんは、ステージII、IIIA又はIIIB肺がんである。
Characterization and Selection of Cancers In some examples, lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer (e.g., , NSCLC (eg, squamous or non-squamous NSCLC)))) is resectable (eg, eligible for R0 resection with curative intent). In some examples, the lung cancer is NSCLC. In some examples, the NSCLC is squamous or non-squamous NSCLC. In some examples, the lung cancer is PD-L1 positive. In some instances, lung cancer is PD-L1 elevated. In some instances, the lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations. In some examples, the lung cancer is stage II, IIIA or IIIB lung cancer.
いくつかの例では、本明細書に記載の使用のための方法、使用又は組成物のいずれかにおいて、対象は白金系化学療法に適格である。いくつかの例では、対象は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)を有する。いくつかの例では、対象は肺がんの事前治療(例えば、免疫療法、化学療法又は放射線療法)を受けたことがない。 In some examples, the subject is eligible for platinum-based chemotherapy in any of the methods, uses or compositions for use described herein. In some examples, the subject has a US East Coast Clinical Trials Group (ECOG) Performance (PS) of 0 or 1. In some examples, the subject has no prior lung cancer treatment (eg, immunotherapy, chemotherapy or radiation therapy).
いくつかの例では、本明細書に記載の使用のための方法、使用又は組成物のいずれかにおいて、循環腫瘍DNA(ctDNA)の存在又はレベルを評定することができる。いくつかの例では、ctDNAが、対象からの試料(例えば、血液試料(例えば、血漿試料))において評定される。いくつかの例では、ctDNAは、第1の投薬サイクル(例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの最初の投薬サイクル)の1日目の前に対象からの試料で評定される。いくつかの例では、ctDNAは、手術前の対象からの試料で評定される。いくつかの例では、ctDNAは、手術後の対象からの試料で評定される。
In some examples, the presence or level of circulating tumor DNA (ctDNA) can be assessed in any of the methods, uses or compositions for use described herein. In some examples, ctDNA is assessed in a sample (eg, blood sample (eg, plasma sample)) from the subject. In some examples, ctDNA is assessed in a sample from the subject prior to
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、免疫細胞(例えば、T細胞)の存在又はレベルが評定され得る。いくつかの例では、免疫細胞の存在又はレベルが、対象からの試料(例えば、血液試料、腫瘍組織試料又はリンパ節試料)において評定される。いくつかの例では、免疫細胞の存在又はレベルは、手術前の対象からの試料で評定される。いくつかの例では、免疫細胞の存在又はレベルは、手術後の対象からの試料で評定される。 In some examples, the presence or level of immune cells (eg, T cells) can be assessed in any of the methods, uses or compositions for use described herein. In some examples, the presence or level of immune cells is assessed in a sample (eg, blood sample, tumor tissue sample, or lymph node sample) from the subject. In some examples, the presence or level of immune cells is assessed in a sample from the subject prior to surgery. In some examples, the presence or level of immune cells is assessed in samples from post-operative subjects.
PD-L1発現の評定
PD-L1の発現は、セクションIII(L)に記載されるように評定され得る。
Assessment of PD-L1 Expression PD-L1 expression can be assessed as described in Section III(L).
EGFR及びALK異常の評定
変異状態EGFR及びALKを検出するための方法は、本明細書のセクションIII(N)に記載されている。
Assessment of EGFR and ALK Abnormalities Methods for detecting the mutational status EGFR and ALK are described in Section III(N) herein.
処置に対する応答
本明細書に記載される方法のいずれかのいくつかの実施形態では、治療に対する対象の応答は、1つ以上の尺度によって特徴付けることができる。いくつかの実施形態では、処置は、病理学的著効(MPR)率における増大をもたらす。いくつかの実施形態において、処置はpCRをもたらす。いくつかの実施形態において、処置は無症候生存期間(EFS)の増加をもたらす。いくつかの実施形態では、処置は患者報告の転帰の改善をもたらす。いくつかの実施形態では、処置は、EORTC-QLQ-C30によって測定されるように、患者報告の身体機能、役割機能、又はGHS/QoLの改善をもたらす。いくつかの実施形態では、処置は、EORTC-QLQ-LC13の使用によって測定されるように、咳、呼吸困難及び胸痛についての患者報告肺がん症状の改善をもたらす。
Response to Treatment In some embodiments of any of the methods described herein, a subject's response to treatment can be characterized by one or more measures. In some embodiments, treatment results in an increase in severe pathologic response (MPR) rate. In some embodiments, treatment results in pCR. In some embodiments, treatment results in increased symptom-free survival (EFS). In some embodiments, treatment results in improved patient-reported outcomes. In some embodiments, treatment results in improvement in patient-reported physical functioning, role functioning, or GHS/QoL as measured by the EORTC-QLQ-C30. In some embodiments, treatment results in improvement of patient-reported lung cancer symptoms of cough, dyspnea and chest pain as measured by use of the EORTC-QLQ-LC13.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のMPR率の増加をもたらす。いくつかの例では、処置は、例えば、化学療法(例えば、白金系のダブレット化学療法(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))))を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体による治療と比較して、対象のMPR率の増加をもたらす。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Comparatively, it results in an increase in the subject's MPR rate. In some instances, treatment includes, for example, chemotherapy (e.g., platinum-based doublet chemotherapy (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab-paclitaxel)))) compared to treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody to increase the rate of MPR in a subject Bring.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のpCRの増加をもたらす。いくつかの例では、処置は、例えば、化学療法(例えば、白金系のダブレット化学療法(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))))を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体による治療と比較して、対象のpCRの増加をもたらす。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. In comparison, it results in an increase in the subject's pCR. In some instances, treatment includes, for example, chemotherapy (e.g., platinum-based doublet chemotherapy (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (e.g., pemetrexed or gemcitabine) or taxanes (e.g., paclitaxel or nab-paclitaxel)))) results in an increase in pCR in a subject compared to treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody .
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSを延長する。いくつかの例では、処置は、例えば、化学療法(例えば、白金系のダブレット化学療法(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))))を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体による治療と比較して、対象のOSを延長する。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Compare and extend the target OS. In some instances, treatment includes, for example, chemotherapy (e.g., platinum-based doublet chemotherapy (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (eg, pemetrexed or gemcitabine) or taxanes (eg, paclitaxel or nab-paclitaxel)))) in subjects compared to treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象のEFSを延長する。いくつかの例では、処置は、例えば、化学療法(例えば、白金系のダブレット化学療法(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)又はタキサン(例えば、パクリタキセル又はnab-パクリタキセル))))を用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体による治療と比較して、対象のEFSを延長する。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. By comparison, prolong the subject's EFS. In some instances, treatment includes, for example, chemotherapy (e.g., platinum-based doublet chemotherapy (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin)) and non-platinum-based chemotherapeutic agents (e.g., antimetabolites (eg, pemetrexed or gemcitabine) or taxanes (eg, paclitaxel or nab-paclitaxel))))), prolongs the subject's EFS compared to treatment with a PD-uniaxial binding antagonist and an anti-TIGIT antagonist antibody.
いくつかの実施形態では、記載される処置は、MPR率を少なくとも1%(例えば、5%、10%、15%、20%、25%、30%、35%、40%、45%、50%、55%、60%、65%、70%、75%、80%、85%、90%、95%、又は100%)増加させる。 In some embodiments, the described treatments reduce the MPR rate by at least 1% (e.g., 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%). %, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100%).
いくつかの実施形態では、処置は、対象のpCRを少なくとも2ヵ月(例えば、2~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヶ月、5.0~48ヶ月、6.0~36ヶ月、8.0~24ヶ月、又は10~12ヶ月、例えば少なくとも約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、対象のpCRを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment reduces the subject's pCR for at least 2 months (eg, 2-120 months, 2.5-100 months, 3.0-80 months, 4.0-60 months, 5.0-60 months, 48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months , 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months , 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months , 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) . In some embodiments, treatment reduces the subject's pCR by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months months) to extend.
いくつかの実施形態では、処置は、対象のEFSを少なくとも2ヵ月(例えば、2~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヶ月、5.0~48ヶ月、6.0~36ヶ月、8.0~24ヶ月、又は10~12ヶ月、例えば少なくとも約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、対象のEFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment reduces the subject's EFS for at least 2 months (eg, 2-120 months, 2.5-100 months, 3.0-80 months, 4.0-60 months, 5.0-60 months, 48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months , 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months , 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months , 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months , 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months) . In some embodiments, treatment reduces the subject's EFS for at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months months) to extend.
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、対象のOSを少なくとも約2ヵ月(例えば2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約3.3ヶ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約5.3ヶ月(例えば5.3~120、6~60ヵ月、7~48ヵ月、8~36 ヵ月、又は10~24ヵ月、例えば、少なくとも約5.3ヵ月、5.5ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, the treatment reduces the subject's OS by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8 months). ~36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months, 2.7 months months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-3 months). 36 months, or 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 5.3 months (eg, 5.3-120, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months , 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
C.子宮頸がんに関する治療及び診断方法並びに使用
子宮頸がん
子宮頸がんは、4番目に高頻度に診断されるがんであり、がん関連死の4番目の主因である。世界中で毎年500,000人を超える女性が子宮頸がんと診断され、300,000人を超える死亡をもたらしている。子宮頸がんによる死亡のほぼ90%が発展途上国で発生している。米国では、毎年13,000例の浸潤性子宮頸がんの新規症例及び約4000例のがん関連死がある。
C. Treatment and diagnostic methods and uses for cervical cancer Cervical cancer Cervical cancer is the fourth most frequently diagnosed cancer and the fourth leading cause of cancer-related deaths. Worldwide, over 500,000 women are diagnosed with cervical cancer each year, resulting in over 300,000 deaths. Nearly 90% of deaths from cervical cancer occur in developing countries. There are 13,000 new cases of invasive cervical cancer and approximately 4000 cancer-related deaths each year in the United States.
早期及び局所進行性子宮頸がんの処置は、それぞれ手術及び根治的化学放射線療法からなり、寛解を誘発するのに非常に有効であり得る。しかしながら、がんが再発するか又は一次処置で消散しない場合、予後は非常に悪く、5年生存率は約15%であり、これはデノボ転移性疾患を有する患者の5年生存率に匹敵する。少数の例外を除いて、再発性、持続性又はデノボ転移性疾患の標準治療は、Gynecology Oncology Group 240治験に基づく化学療法+ベバシズマブであり、これは、化学療法に加えられたベバシズマブが化学療法単独と比較してOS中央値を改善したことを示した(それぞれ17ヶ月対13.3ヶ月)。 Treatment of early and locally advanced cervical cancer consists of surgery and definitive chemoradiation, respectively, and can be very effective in inducing remission. However, if the cancer recurs or is not resolved with primary treatment, the prognosis is very poor, with a 5-year survival rate of approximately 15%, which is comparable to that of patients with de novo metastatic disease. . With a few exceptions, the standard of care for recurrent, persistent, or de novo metastatic disease is Gynecology Oncology Group 240 trial-based chemotherapy plus bevacizumab, which means that bevacizumab added to chemotherapy is less than chemotherapy alone. showed improved median OS compared to 17 months versus 13.3 months, respectively.
現在、化学療法+ベバシズマブでの再発又は進行後に世界的に認められている標準治療は存在しない。したがって、これらの患者の処置選択肢は、主に、単剤又は組み合わせのいずれかとして投与される様々な細胞傷害性化学療法剤を含む。しかしながら、歴史的に約10%という低い奏効率-15%を考えると、細胞傷害性化学療法が、そのような薬剤が患者の生活の質に与えることができる影響及び負担を考慮して、最良の支持療法よりも許容可能な標準治療を表すかどうかにますます焦点が当てられている。 Currently, there is no globally accepted standard of care after relapse or progression on chemotherapy plus bevacizumab. Thus, treatment options for these patients primarily include various cytotoxic chemotherapeutic agents administered either as single agents or in combination. However, given the historically low response rate of about 10%-15%, cytotoxic chemotherapy is the best option given the impact and burden such agents can have on the patient's quality of life. There is an increasing focus on whether it represents an acceptable standard of care rather than supportive care for patients.
子宮頸部上皮細胞のHPV感染による免疫応答の関与と相まって、既存の治療の有効率が歴史的に低いため、子宮頸がんは新規免疫療法に基づくアプローチにとって特に魅力的な機会となる。 The historically low efficacy of existing treatments coupled with the involvement of an immune response by HPV infection of cervical epithelial cells makes cervical cancer a particularly attractive opportunity for novel immunotherapy-based approaches.
したがって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-1L陽性子宮頸がん)の処置のために有効な免疫療法及びそれを投与する方法の開発に対する当分野における満たされていない必要性がある。 Thus, for the treatment of cancer (e.g. cervical cancer, e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-1L positive cervical cancer) There is an unmet need in the art for the development of effective immunotherapies and methods of administering them.
子宮頸がんを処置するための方法及び使用
有効量の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを対象又は対象集団に投与することを含む、対象又は対象集団において検出可能なPD-L1発現レベル(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有するがんを処置するための方法及び使用が本明細書で提供される。
Methods and Uses for Treating Cervical Cancer MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) detectable in a subject or subject population, comprising administering to the subject or subject population one or more dosing cycles Cancers with PD-L1 expression levels (eg, cervical cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer) Methods and uses for treating are provided herein.
投薬レジメン及び投与
本明細書に記載される本発明の治療方法及び使用は、一態様では、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団に、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを投与し、それにより対象又は対象集団を処置することを含む。
Dosing Regimens and Administration The therapeutic methods and uses of the invention described herein are, in one aspect, cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic , recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1-positive cervical cancer), in an effective amount of an anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody, such as tiragolumab) and an effective amount of a PD-1 axis binding antagonist (such as an anti-PD-L1 antagonist antibody (such as atezolizumab) or an anti-PD-1 antagonist antibody (such as MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))), thereby treating the subject or population of subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約600mgの間(例えば、約50mgと600mgの間、例えば、約60mgと約600mgの間、例えば、約100mgと約600mgの間、例えば、約200mgと約600mgの間、例えば、約200mgと約550mgの間、例えば、約250mgと約500mgの間、例えば、約300mgと約450mgの間、例えば、約350mgと約400mgの間、例えば、約375mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ))の有効量は、3週間ごとに30mgと1200mgの間(例えば、30mgと1100mgの間、例えば、60mgと1000mgの間、例えば、100mgと900mgの間、例えば、200mgと800mgの間、例えば、300mgと800mgの間、例えば、400mgと800mgの間、例えば、400mgと750mgの間、例えば、450mgと750mgの間、例えば、500mgと700mgの間、例えば、550mgと650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、抗TIGITアンタゴニスト抗体(本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ))の有効量は、3週間ごとに30mgと600mgの間(例えば、50mgと600mgの間、例えば、60mgと600mgの間、例えば、100mgと600mgの間、例えば、200mgと600mgの間、例えば、200mgと550mgの間、例えば、250mgと500mgの間、例えば、300mgと450mgの間、例えば、350mgと400mgの間、例えば、375mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量(例えば、固定用量)である。いくつかの例では、併用療法(例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)、又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)若しくはMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))との併用処置)で投与される抗TIGITアンタゴニスト抗体(例えば、本明細書中に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg (e.g., about 30 mg) every three weeks. and about 1100 mg, for example between about 60 mg and about 1000 mg, for example between about 100 mg and about 900 mg, for example between about 200 mg and about 800 mg, for example between about 300 mg and about 800 mg, for example about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg) (eg, a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 600 mg (e.g., about 50 mg) every three weeks. and 600 mg, for example between about 60 mg and about 600 mg, for example between about 100 mg and about 600 mg, for example between about 200 mg and about 600 mg, for example between about 200 mg and about 550 mg, for example about 250 mg between about 500 mg, eg between about 300 mg and about 450 mg, eg between about 350 mg and about 400 mg, eg about 375 mg) (eg a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is a dose (e.g., fixed dose) of about 600 mg every 3 weeks . In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between 30 mg and 1200 mg (e.g., 30 mg) every three weeks. and 1100 mg, such as between 60 mg and 1000 mg, such as between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg between, such as between 450 mg and 750 mg, such as between 500 mg and 700 mg, such as between 550 mg and 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg , eg 600±1 mg, eg 600±0.5 mg, eg 600 mg) (eg a fixed dose). In some examples, the effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody (anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab)) is between 30 mg and 600 mg every 3 weeks. between 50 mg and 600 mg, such as between 60 mg and 600 mg, such as between 100 mg and 600 mg, such as between 200 mg and 600 mg, such as between 200 mg and 550 mg, such as between 250 mg and 500 mg, For example, between 300 mg and 450 mg, such as between 350 mg and 400 mg, such as 375 mg) (eg, fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg (eg, fixed dose) every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg (eg, fixed dose) every three weeks. In some examples, combination therapy (e.g., PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab), or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) administered with -3475 (pembrolizumab, formerly known as lambrolizumab)) The dose may be reduced compared to standard doses of anti-TIGIT antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約80mgと約2000mgの間(例えば、約80mgと約1950mgの間、例えば約80mgと約1900mgの間、例えば約80mgと約1800mgの間、例えば約100mgと約1700mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1400mgの間、例えば約400mgと約1300mgの間、例えば約500mgと約1200mgの間、例えば約600mgと約1100mgの間、例えば約700mgと約1000mgの間、例えば約740mgと約940mgの間、例えば約790mgと約890mgの間、例えば約815mgと約865mgの間、例えば約830mgと約850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約80mgと約2000mgの間(例えば、約100mgと約2000mgの間、例えば、約200mgと約1900mgの間、例えば、約300mgと約1700mgの間、例えば、約400mgと約1600mgの間、例えば、約500mgと約1600mgの間、例えば、約600mgと約1600mgの間、例えば、約700mgと約1600mgの間、例えば、約800mgと約1600mgの間、例えば、約900mgと約1500mgの間、例えば、約1000mgと約1400mgの間、例えば、約1050mgと約1350mgの間、例えば、約1100mgと約1300mgの間、例えば、約1150mgと約1250mgの間、例えば、約1175mgと約1225mgの間、例えば、約1190mgと約1210mgの間、例えば、1200mg±5mg、例えば、1200±2.5mg、例えば、1200±1.0mg、例えば、1200±0.5mg、例えば、1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約2000mgの間、例えば約300mgと約2000mgの間、例えば約400mgと約2000mgの間、例えば約500mgと約2000mgの間、例えば約600mgと約1900mgの間、例えば約700mgと約1800mgの間、例えば約800mgと約1800mgの間、例えば約900mgと約1800mgの間、例えば約1000mgと約1800mgの間、例えば約1100mgと約1800mgの間、例えば約1200mgと約1800mgの間、例えば約1300mgと約1800mgの間、例えば約1400mgと約1800mgの間、例えば約1500mgと約1800mgの間、例えば約1580mgと約1780mgの間、例えば約1630mgと約1730mgの間、例えば約1655mgと約1705mgの間、例えば約1670mgと約1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約1200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに80mgと2000mgの間(例えば、80mgと1950mgの間、例えば80mgと1900mgの間、例えば80mgと1800mgの間、例えば100mgと1700mgの間、例えば200mgと1600mgの間、例えば300mgと1400mgの間、例えば400mgと1300mgの間、例えば500mgと1200mgの間、例えば600mgと1100mgの間、例えば700mgと1000mgの間、例えば740mgと940mgの間、例えば790mgと890mgの間、例えば815mgと865mgの間、例えば830mgと850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと1900mgの間、例えば300mgと1700mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと2000mgの間、例えば300mgと2000mgの間、例えば400mgと2000mgの間、例えば500mgと2000mgの間、例えば600mgと1900mgの間、例えば700mgと1800mgの間、例えば800mgと1800mgの間、例えば900mgと1800mgの間、例えば1000mgと1800mgの間、例えば1100mgと1800mgの間、例えば1200mgと1800mgの間、例えば1300mgと1800mgの間、例えば1400mgと1800mgの間、例えば1500mgと1800mgの間、例えば1580mgと1780mgの間、例えば1630mgと1730mgの間、例えば1655mgと1705mgの間、例えば1670mgと1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに1200mgの固定用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに1200mgの固定用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 80 mg and about between about 80 mg and about 1900 mg, such as between about 80 mg and about 1800 mg, such as between about 100 mg and about 1700 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1400 mg, such as between about 400 mg and about 1300 mg, such as between about 500 mg and about 1200 mg, such as between about 600 mg and about 1100 mg, such as between about 700 mg and about 1000 mg, such as between about 740 mg and about 940 mg, such as between about 790 mg and about 890 mg between about 815 mg and about 865 mg, such as between about 830 mg and about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg) (eg, fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about between 2000 mg, such as between about 200 mg and about 1900 mg, such as between about 300 mg and about 1700 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg, such as between about 600 mg and about Between 1600 mg, such as between about 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about between 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as 1200 mg±5 mg; For example, a dose of 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about 2000 mg) every 4 weeks. between about 200 mg and about 2000 mg, such as between about 300 mg and about 2000 mg, such as between about 400 mg and about 2000 mg, such as between about 500 mg and about 2000 mg, such as between about 600 mg and about 1900 mg, such as about between 700 mg and about 1800 mg, such as between about 800 mg and about 1800 mg, such as between about 900 mg and about 1800 mg, such as between about 1000 mg and about 1800 mg, such as between about 1100 mg and about 1800 mg, such as between about 1200 mg and about 1800 mg between about 1300 mg and about 1800 mg, such as between about 1400 mg and about 1800 mg, such as between about 1500 mg and about 1800 mg, such as between about 1580 mg and about 1780 mg, such as between about 1630 mg and about 1730 mg, such as about 1655 mg and about 1705 mg, e.g. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between 80 mg and 2000 mg (eg, between 80 mg and 1950 mg, between 80 mg and 1900 mg, such as between 80 mg and 1800 mg, such as between 100 mg and 1700 mg, such as between 200 mg and 1600 mg, such as between 300 mg and 1400 mg, such as between 400 mg and 1300 mg, such as between 500 mg and 1200 mg, such as between 600 mg and 1100 mg, such as between 700 mg and 1000 mg, such as between 740 mg and 940 mg, such as between 790 mg and 890 mg, such as between 815 mg and 865 mg, such as between 830 mg and 850 mg, such as 840 mg±5 mg, such as 840±2 .5 mg, such as 840±1.0 mg, such as 840±0.5 mg, such as 840 mg) (eg, fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every three weeks, e.g. between 200 mg and 1900 mg, such as between 300 mg and 1700 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg, such as between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg, such as between 1190 mg and 1210 mg, such as 1200 mg ± 5 mg, such as 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every 4 weeks, e.g. between 200 mg and 2000 mg, such as between 300 mg and 2000 mg, such as between 400 mg and 2000 mg, such as between 500 mg and 2000 mg, such as between 600 mg and 1900 mg, such as between 700 mg and 1800 mg, such as between 800 mg and 1800 mg, such as 900 mg and 1800 mg, such as between 1000 mg and 1800 mg, such as between 1100 mg and 1800 mg, such as between 1200 mg and 1800 mg, such as between 1300 mg and 1800 mg, such as between 1400 mg and 1800 mg, such as between 1500 mg and 1800 mg, such as 1580 mg between 1780 mg, such as between 1630 mg and 1730 mg, such as between 1655 mg and 1705 mg, such as between 1670 mg and 1690 mg, such as 1680 mg±5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg , eg 1680 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a fixed dose of 1200 mg every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a fixed dose of 1200 mg every 3 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば、約0.1mg/kgと約40mg/kgの間、例えば、約1mg/kgと約35mg/kgの間、例えば、約2.5mg/kgと約30mg/kgの間、例えば、約5mg/kgと約25mg/kgの間、例えば、約10mg/kgと約20mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約15mg/kgの間、例えば、約10mg/kgと約15mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約14mg/kgと約15mg/kgの間、例えば、約15±1mg/kg、例えば、約15±0.5mg/kg、例えば、約15±0.2mg/kg、例えば、約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の有効量は、3週間ごとに投与される約15mg/kgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば、0.1mg/kgと40mg/kgの間、例えば、1mg/kgと35mg/kgの間、例えば、2.5mg/kgと30mg/kgの間、例えば、5mg/kgと25mg/kgの間、例えば、10mg/kgと20mg/kgの間、例えば、12.5mg/kgと15mg/kgの間、例えば、15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば、15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに対象の体重の0.01mg/kgと15mg/kgの間(例えば0.1mg/kgと15mg/kgの間、例えば0.5mg/kgと15mg/kgの間、例えば1mg/kgと15mg/kgの間、例えば2.5mg/kgと15mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば10mg/kgと15mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば14mg/kgと15mg/kgの間、例えば15±1mg/kg、例えば15±0.5mg/kg、例えば15±0.2mg/kg、例えば15±0.1mg/kg、例えば15mg/kg)の用量である。いくつかの例では、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の有効量は、3週間ごとに投与される15mg/kgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg, e.g., between about 1 mg/kg and about 35 mg/kg) such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as about 12 mg/kg. between 5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0 .1 mg/kg, eg about 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 15 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.1 mg/kg and about 15 mg/kg, e.g., between about 0.5 mg/kg and about 15 mg/kg, e.g., between about 1 mg/kg and about 15 mg/kg) between about 2.5 mg/kg and about 15 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 15 mg/kg, such as about between 10 mg/kg and about 15 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as between about 14 mg/kg and about 15 mg/kg, such as about 15±1 mg/kg; For example, about 15±0.5 mg/kg, such as about 15±0.2 mg/kg, such as about 15±0.1 mg/kg, such as about 15 mg/kg). In some examples, an effective amount of anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg administered every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 50 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.01 mg/kg and 45 mg/kg, e.g. between 0.1 mg/kg and 40 mg/kg, e.g. between 1 mg/kg and 35 mg/kg, e.g. 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg /kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0.1 mg/kg, such as 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 15 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.1 mg/kg and 15 mg/kg, such as between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 10 mg/kg and 15 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, between 14 mg/kg and 15 mg/kg, such as 15±1 mg/kg, such as 15±0.5 mg/kg, such as 15±0.2 mg/kg, such as 15±0.1 mg/kg, such as 15 mg/kg) is the dose of In some examples, an effective amount of anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of 15 mg/kg administered every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g., a PD-1 axis binding antagonist (e.g. , an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) administered as monotherapy, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist Antibodies (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) may be reduced compared to standard doses.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに約20mgと約1000mgの間(例えば約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約180mgと約250mgの間、例えば約180mgと約220mgの間、例えば約190mgと約210mgの間、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに20mgと1000mgの間(例えば40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば180mgと250mgの間、例えば180mgと220mgの間、例えば190mgと210mgの間、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに200mgの用量(例えば、固定用量)である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, penprolizumab)) is between about 20 mg and about 1000 mg (eg, about 40 mg and about 900 mg) every three weeks. between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as between about 120 mg and about 400 mg, such as about between 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 180 mg and about 250 mg, such as between about 180 mg and about 220 mg, such as between about 190 mg and about 210 mg between, eg 200±5 mg, eg 200±2.5 mg, eg 200±1.0 mg, eg 200±0.5 mg, eg 200 mg) (eg a fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., penprolizumab)) is between 20 mg and 1000 mg (e.g., between 40 mg and 900 mg) every three weeks, e.g. between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg, such as between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as 180 mg and 300 mg, such as between 180 mg and 250 mg, such as between 180 mg and 220 mg, such as between 190 mg and 210 mg, such as 200 mg±5 mg, such as 200±2.5 mg, such as 200±1.0 mg, such as 200±0. 5 mg, eg 200 mg) dose (eg fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, penprolizumab)) is a dose of 200 mg (eg, fixed dose) every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-1 antagonist antibody (eg, penprolizumab)) can be reduced compared to the standard dose of anti-PD-L1 antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに約20mgと約1000mgの間(例えば約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約200mgと約280mgの間、例えば約220mgと約260mgの間、例えば約230mgと約250mgの間、例えば240mg±5mg、例えば240±2.5mg、例えば240±1.0mg、例えば240±0.5mg、例えば240mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに約100mgと約1000mgの間(例えば約200mgと約900mgの間、例えば約300mgと約800mgの間、例えば約400mgと約700mgの間、例えば約400mgと約600mgの間、例えば約400mgと約550mgの間、例えば約420mgと約540mgの間、例えば約440mgと約520mgの間、例えば約460mgと約500mgの間、例えば約470mgと約490mgの間、例えば480mg±5mg、例えば480±2.5mg、例えば480±1.0mg、例えば480±0.5mg、例えば480mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに20mgと1000mgの間(例えば40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば200mgと280mgの間、例えば220mgと260mgの間、例えば230mgと250mgの間、例えば240mg±5mg、例えば240±2.5mg、例えば240±1.0mg、例えば240±0.5mg、例えば240mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに100mgと1000mgの間(例えば200mgと900mgの間、例えば300mgと800mgの間、例えば400mgと700mgの間、例えば400mgと600mgの間、例えば400mgと550mgの間、例えば420mgと540mgの間、例えば440mgと520mgの間、例えば460mgと500mgの間、例えば470mgと490mgの間、例えば480mg±5mg、例えば480±2.5mg、例えば480±1.0mg、例えば480±0.5mg、例えば480mg)の固定用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに480mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is between about 20 mg and about 1000 mg (eg, about 40 mg and about 900 mg) every two weeks. between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as between about 120 mg and about 400 mg, such as about between 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 200 mg and about 280 mg, such as between about 220 mg and about 260 mg, such as between about 230 mg and about 250 mg between, eg 240±5 mg, eg 240±2.5 mg, eg 240±1.0 mg, eg 240±0.5 mg, eg 240 mg) (eg a fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is between about 100 mg and about 1000 mg (eg, about 200 mg and about 900 mg) every 4 weeks. between about 300 mg and about 800 mg, such as between about 400 mg and about 700 mg, such as between about 400 mg and about 600 mg, such as between about 400 mg and about 550 mg, such as between about 420 mg and about 540 mg, such as about between 440 mg and about 520 mg, such as between about 460 mg and about 500 mg, such as between about 470 mg and about 490 mg, such as 480 mg±5 mg, such as 480±2.5 mg, such as 480±1.0 mg, such as 480±0.5 mg , eg 480 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., nivolumab)) is between 20 mg and 1000 mg (e.g., between 40 mg and 900 mg) every two weeks, e.g. between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg, such as between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as 180 mg and 300 mg, such as between 200 mg and 280 mg, such as between 220 mg and 260 mg, such as between 230 mg and 250 mg, such as 240 mg±5 mg, such as 240±2.5 mg, such as 240±1.0 mg, such as 240±0. 5 mg, eg 240 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., nivolumab)) is between 100 mg and 1000 mg (e.g., between 200 mg and 900 mg) every 4 weeks, e.g. between 300 mg and 800 mg, such as between 400 mg and 700 mg, such as between 400 mg and 600 mg, such as between 400 mg and 550 mg, such as between 420 mg and 540 mg, such as between 440 mg and 520 mg, such as between 460 mg and 500 mg, such as 470 mg and 490 mg, eg 480±5 mg, eg 480±2.5 mg, eg 480±1.0 mg, eg 480±0.5 mg, eg 480 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g., a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibodies (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-1 antagonist antibodies administered as monotherapy.
本発明の方法及び使用のいずれかにおいて、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投薬サイクルは、臨床上の利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約14~28日間(例えば、14日間、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間、24日間、25日間、26日間、27日間又は28日間)である。いくつかの例では、投薬サイクルの長さは、約21日間である。いくつかの例では、投薬サイクルの長さは、約14日間である。いくつかの例では、投薬サイクルの長さは、約28日間である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに600mgの用量で)静脈内投与される。同様に、いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))は、約200mgの用量で各21日間サイクルの1日目に(すなわち、約200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各14日間サイクルの1日目に約240mgの用量で(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各28日間サイクル(すなわち、4週間ごとに約480mgの用量で)の1日目に約480mgの用量で静脈内投与されることになる。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))は、約200mgの用量で各21日間サイクルの1日目に(すなわち、約200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各14日間サイクルの1日目に約240mgの用量で(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各28日間サイクル(すなわち、4週間ごとに約480mgの用量で)の1日目に約480mgの用量で静脈内投与されることになる。
In any of the methods and uses of the invention, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody) (e.g., atezolizumab)) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))) is administered for one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) dosing cycles may be associated with clinical benefit (e.g., confirmed disease progression, drug resistance, death, or unacceptable toxicity). In some examples, the length of each dosing cycle is about 14 to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days). days, 24 days, 25 days, 26 days, 27 days or 28 days). In some examples, the dosing cycle length is about 21 days. In some examples, the dosing cycle length is about 14 days. In some examples, the dosing cycle length is about 28 days. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered on about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約600mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、約600mgの固定用量で3週間ごとに)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ペンプロリズマブ))は、21日間サイクルの1日目に約200mgの用量で(すなわち、3週間ごとに約200mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、600mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、600mgの固定用量で3週間ごとに)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、1200mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、1200mgの用量で3週間ごとに)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)は、600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ペンプロリズマブ))は、200mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに200mgの用量で)静脈内投与される。
In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) on about
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、第1の投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約600mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、約600mgの固定用量で3週間ごとに)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、約240mgの用量(例えば、固定用量)で14日間の各サイクルの1日目に(すなわち、約240mgの用量で2週間ごとに)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、28日間サイクルの1日目に約480mgの用量で(すなわち、4週間ごとに約480mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、600mgの用量(例えば、固定用量)で21日間の各サイクルの1日目に(すなわち、600mgの固定用量で3週間ごとに)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、240mgの用量(例えば、固定用量)で14日間の各サイクルの1日目に(すなわち、240mgの用量で2週間ごとに)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)は、600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、480mgの用量で28日間の各サイクルの1日目に(すなわち、4週間ごとに480mgの用量で)静脈内投与される。
In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) on about
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約60±15分(例えば約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、又は約70分)わたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 60 ± 15 minutes (e.g., about 50 minutes, about 51 minutes, about 52 minutes, About 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) to the subject or population of subjects. In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly Pembrolizumab, formerly known as rambrolizumab))) is about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes) minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, by intravenous infusion over about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes). or administered to a target population.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)わたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes). , about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about administered to the subject or population of subjects by intravenous infusion over 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes). In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly lambrolizumab) Pembrolizumab))) was known as )) was about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes , about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or administered to a subject or population of subjects by intravenous infusion over approximately 40 minutes).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の前に対象又は対象集団に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、本方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第2の観察期間を更に含む。いくつかの例では、本方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間と、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分の長さである場合、本方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後それぞれ約30±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分の長さである場合、本方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後それぞれ約15±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) prior to administration to the subject or subject population. In some examples, for example, after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 ( Prior to administration of nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))), the method includes an intervening first observation period. In some examples, the method uses a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475). (pembrolizumab, formerly known as rambrolizumab)))). In some examples, the method includes a first observation period after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 Both include a second observation period following administration of an antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)). In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. If the first and second observation periods are each about 60 minutes long, the method includes the addition of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti-PD - about 30 ± 10 after administration of an L1 antagonistic antibody (e.g., atezolizumab) or an anti-PD-1 antagonistic antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)), respectively This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute. If the first and second observation periods are each about 30 minutes long, the method includes the addition of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti-PD - about 15 ± 10 after administration of an L1 antagonistic antibody (e.g., atezolizumab) or an anti-PD-1 antagonistic antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)), respectively This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute.
他の例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後及び抗TIGITアンタゴニスト抗体の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間を含む。いくつかの例では、本方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第1の観察期間と、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分の長さである場合、本方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後それぞれ約30±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分の長さである場合、本方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後それぞれ約15±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly known as lambrolizumab) Known pembrolizumab))) is administered to a subject or population of subjects prior to an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, for example, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly After administration of pembrolizumab, formerly known as rambrolizumab))) and before administration of the anti-TIGIT antagonist antibody, the method includes an intervening first observation period. In some examples, the method includes a second observation period after administration of the anti-TIGIT antagonist antibody. In some examples, the method uses a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475). (pembrolizumab, formerly known as rambrolizumab)))) and a second observation period following administration of an anti-TIGIT antagonist antibody. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. If the first and second observation periods are each about 60 minutes long, the method includes the addition of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody ( atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody, respectively. This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute. If the first and second observation periods are each about 30 minutes long, the method includes the addition of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody ( atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody, respectively. This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute.
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、対象又は対象集団に同時に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後、方法は観察期間を含む。いくつかの例では、観察期間は、約30分と約60分の間の長さである。観察期間が約60分の長さである場合、本方法は、観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後約30±10分で対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。観察期間が約30分の長さである場合、本方法は、観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後約15±10分で対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab ) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered to the subject or population of subjects concurrently. In some examples, for example, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or Following administration of MK-3475 (pembrolizumab, formerly known as rambrolizumab))), the method included an observation period. In some examples, the observation period is between about 30 minutes and about 60 minutes long. If the observation period is about 60 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., , MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) and an anti-TIGIT antagonist antibody at about 30±10 minutes after administration of the subject or subject population's vital signs (e.g., pulse rate , respiratory rate, blood pressure, and temperature). If the observation period is about 30 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., , MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) and an anti-TIGIT antagonist antibody at about 15±10 minutes after administration of the subject or subject population's vital signs (e.g., pulse rate , respiratory rate, blood pressure, and temperature).
別の態様では、本発明は、ステージIVB、転移性、再発性、又は持続性子宮頸がんを有する対象又は対象集団を処置する方法であって、以下に更に詳細に記載されるように、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することによる方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention provides a method of treating a subject or subject population having stage IVB, metastatic, recurrent, or persistent cervical cancer, comprising: 3 Administering to the subject or subject population one or more dosing cycles of a dose (e.g., fixed dose) of 600 mg of anti-TIGIT antagonist antibody every week and a dose (e.g., fixed dose) of 1200 mg of atezolizumab every three weeks. wherein the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、ステージIVB、転移性、再発性、又は持続性子宮頸がんを有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having stage IVB, metastatic, recurrent, or persistent cervical cancer, wherein the subject or subject population is administered 600 mg every three weeks of Provided are methods of administering a dose (eg, fixed dose) of tiragolumab and one or more dosing cycles of a dose (eg, fixed dose) of 1200 mg atezolizumab every 3 weeks.
別の態様では、本発明は、ステージIVB、転移性、再発性、又は持続性子宮頸がんを有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ及び3週間ごとに200mgの用量(例えば、固定用量)のペンプロリズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having stage IVB, metastatic, recurrent, or persistent cervical cancer, wherein the subject or subject population is administered 600 mg every three weeks of Methods are provided for administering one or more dosing cycles of a dose (eg, fixed dose) of tiragolumab and a dose (eg, fixed dose) of 200 mg of penprolizumab every 3 weeks.
別の態様では、本発明は、ステージIVB、転移性、再発性、又は持続性子宮頸がんを有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ及び2週間ごとに240mgの用量(例えば、固定用量)のニボルマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having stage IVB, metastatic, recurrent, or persistent cervical cancer, wherein the subject or subject population is administered 600 mg every three weeks of Methods of administering a dose (eg, fixed dose) of tiragolumab and one or more dosing cycles of a dose (eg, fixed dose) of nivolumab of 240 mg every two weeks are provided.
別の態様では、本発明は、ステージIVB、転移性、再発性、又は持続性子宮頸がんを有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ及び4週間ごとに480mgの用量(例えば、固定用量)のニボルマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having stage IVB, metastatic, recurrent, or persistent cervical cancer, wherein the subject or subject population is administered 600 mg every three weeks of Methods of administering a dose (eg, fixed dose) of tiragolumab and one or more dosing cycles of a dose (eg, fixed dose) of nivolumab of 480 mg every 4 weeks are provided.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を提供し、方法は、有効量の抗TIGITアンタゴニスト抗体及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonistic antibodies (e.g. atezolizumab) or anti-PD-1 antagonistic antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly known as rambrolizumab) pembrolizumab))), wherein the method comprises an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody ( For example, administering one or more dosing cycles of MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) to a subject or population of subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約600mgの間(例えば、約50mgと600mgの間、例えば、約60mgと約600mgの間、例えば、約100mgと約600mgの間、例えば、約200mgと約600mgの間、例えば、約200mgと約550mgの間、例えば、約250mgと約500mgの間、例えば、約300mgと約450mgの間、例えば、約350mgと約400mgの間、例えば、約375mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ))の有効量は、3週間ごとに30mgと1200mgの間(例えば、30mgと1100mgの間、例えば、60mgと1000mgの間、例えば、100mgと900mgの間、例えば、200mgと800mgの間、例えば、300mgと800mgの間、例えば、400mgと800mgの間、例えば、400mgと750mgの間、例えば、450mgと750mgの間、例えば、500mgと700mgの間、例えば、550mgと650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに30mgと600mgの間(例えば、50mgと600mgの間、例えば、60mgと600mgの間、例えば、100mgと600mgの間、例えば、200mgと600mgの間、例えば、200mgと550mgの間、例えば、250mgと500mgの間、例えば、300mgと450mgの間、例えば、350mgと400mgの間、例えば、375mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、併用療法で投与される(例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))との併用処置は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少され得る。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg (e.g., about 30 mg) every three weeks. and about 1100 mg, for example between about 60 mg and about 1000 mg, for example between about 100 mg and about 900 mg, for example between about 200 mg and about 800 mg, for example between about 300 mg and about 800 mg, for example about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg) (eg, a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 600 mg (e.g., about 50 mg) every three weeks. and 600 mg, for example between about 60 mg and about 600 mg, for example between about 100 mg and about 600 mg, for example between about 200 mg and about 600 mg, for example between about 200 mg and about 550 mg, for example about 250 mg between about 500 mg, such as between about 300 mg and about 450 mg, such as between about 350 mg and about 400 mg, such as about 375 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between 30 mg and 1200 mg (e.g., 30 mg) every three weeks. and 1100 mg, such as between 60 mg and 1000 mg, such as between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg between, such as between 450 mg and 750 mg, such as between 500 mg and 700 mg, such as between 550 mg and 650 mg, such as between 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg , eg 600±1 mg, eg 600±0.5 mg, eg 600 mg) (eg a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between 30 mg and 600 mg (e.g., 50 mg and 600 mg) every three weeks. between 60 mg and 600 mg, such as between 100 mg and 600 mg, such as between 200 mg and 600 mg, such as between 200 mg and 550 mg, such as between 250 mg and 500 mg, such as between 300 mg and 450 mg; For example, doses between 350 mg and 400 mg, eg 375 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 600 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg every 3 weeks. In some examples, a dose of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered in combination therapy (e.g., a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) Treatment may be reduced compared to standard doses of anti-TIGIT antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約80mgと約2000mgの間(例えば、約80mgと約1950mgの間、例えば約80mgと約1900mgの間、例えば約80mgと約1800mgの間、例えば約100mgと約1700mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1400mgの間、例えば約400mgと約1300mgの間、例えば約500mgと約1200mgの間、例えば約600mgと約1100mgの間、例えば約700mgと約1000mgの間、例えば約740mgと約940mgの間、例えば約790mgと約890mgの間、例えば約815mgと約865mgの間、例えば約830mgと約850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約80mgと約2000mgの間(例えば、約100mgと約2000mgの間、例えば、約200mgと約1900mgの間、例えば、約300mgと約1700mgの間、例えば、約400mgと約1600mgの間、例えば、約500mgと約1600mgの間、例えば、約600mgと約1600mgの間、例えば、約700mgと約1600mgの間、例えば、約800mgと約1600mgの間、例えば、約900mgと約1500mgの間、例えば、約1000mgと約1400mgの間、例えば、約1050mgと約1350mgの間、例えば、約1100mgと約1300mgの間、例えば、約1150mgと約1250mgの間、例えば、約1175mgと約1225mgの間、例えば、約1190mgと約1210mgの間、例えば、1200mg±5mg、例えば、1200±2.5mg、例えば、1200±1.0mg、例えば、1200±0.5mg、例えば、1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約2000mgの間、例えば約300mgと約2000mgの間、例えば約400mgと約2000mgの間、例えば約500mgと約2000mgの間、例えば約600mgと約1900mgの間、例えば約700mgと約1800mgの間、例えば約800mgと約1800mgの間、例えば約900mgと約1800mgの間、例えば約1000mgと約1800mgの間、例えば約1100mgと約1800mgの間、例えば約1200mgと約1800mgの間、例えば約1300mgと約1800mgの間、例えば約1400mgと約1800mgの間、例えば約1500mgと約1800mgの間、例えば約1580mgと約1780mgの間、例えば約1630mgと約1730mgの間、例えば約1655mgと約1705mgの間、例えば約1670mgと約1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに80mgと2000mgの間(例えば、80mgと1950mgの間、例えば80mgと1900mgの間、例えば80mgと1800mgの間、例えば100mgと1700mgの間、例えば200mgと1600mgの間、例えば300mgと1400mgの間、例えば400mgと1300mgの間、例えば500mgと1200mgの間、例えば600mgと1100mgの間、例えば700mgと1000mgの間、例えば740mgと940mgの間、例えば790mgと890mgの間、例えば815mgと865mgの間、例えば830mgと850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと1900mgの間、例えば300mgと1700mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと2000mgの間、例えば300mgと2000mgの間、例えば400mgと2000mgの間、例えば500mgと2000mgの間、例えば600mgと1900mgの間、例えば700mgと1800mgの間、例えば800mgと1800mgの間、例えば900mgと1800mgの間、例えば1000mgと1800mgの間、例えば1100mgと1800mgの間、例えば1200mgと1800mgの間、例えば1300mgと1800mgの間、例えば1400mgと1800mgの間、例えば1500mgと1800mgの間、例えば1580mgと1780mgの間、例えば1630mgと1730mgの間、例えば1655mgと1705mgの間、例えば1670mgと1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約1200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに1200mgの固定用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 80 mg and about between about 80 mg and about 1900 mg, such as between about 80 mg and about 1800 mg, such as between about 100 mg and about 1700 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1400 mg, such as between about 400 mg and about 1300 mg, such as between about 500 mg and about 1200 mg, such as between about 600 mg and about 1100 mg, such as between about 700 mg and about 1000 mg, such as between about 740 mg and about 940 mg, such as between about 790 mg and about 890 mg between about 815 mg and about 865 mg, such as between about 830 mg and about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg) (eg, fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about between 2000 mg, such as between about 200 mg and about 1900 mg, such as between about 300 mg and about 1700 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg, such as between about 600 mg and about Between 1600 mg, such as between about 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about between 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as 1200 mg±5 mg; For example, a dose of 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about 2000 mg) every 4 weeks. between about 200 mg and about 2000 mg, such as between about 300 mg and about 2000 mg, such as between about 400 mg and about 2000 mg, such as between about 500 mg and about 2000 mg, such as between about 600 mg and about 1900 mg, such as about between 700 mg and about 1800 mg, such as between about 800 mg and about 1800 mg, such as between about 900 mg and about 1800 mg, such as between about 1000 mg and about 1800 mg, such as between about 1100 mg and about 1800 mg, such as between about 1200 mg and about 1800 mg between about 1300 mg and about 1800 mg, such as between about 1400 mg and about 1800 mg, such as between about 1500 mg and about 1800 mg, such as between about 1580 mg and about 1780 mg, such as between about 1630 mg and about 1730 mg, such as about 1655 mg and about 1705 mg, e.g. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between 80 mg and 2000 mg (eg, between 80 mg and 1950 mg, between 80 mg and 1900 mg, such as between 80 mg and 1800 mg, such as between 100 mg and 1700 mg, such as between 200 mg and 1600 mg, such as between 300 mg and 1400 mg, such as between 400 mg and 1300 mg, such as between 500 mg and 1200 mg, such as between 600 mg and 1100 mg, such as between 700 mg and 1000 mg, such as between 740 mg and 940 mg, such as between 790 mg and 890 mg, such as between 815 mg and 865 mg, such as between 830 mg and 850 mg, such as 840 mg±5 mg, such as 840±2 .5 mg, such as 840±1.0 mg, such as 840±0.5 mg, such as 840 mg) (eg, fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every three weeks, e.g. between 200 mg and 1900 mg, such as between 300 mg and 1700 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg, such as between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg, such as between 1190 mg and 1210 mg, such as 1200 mg ± 5 mg, such as 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every 4 weeks, e.g. between 200 mg and 2000 mg, such as between 300 mg and 2000 mg, such as between 400 mg and 2000 mg, such as between 500 mg and 2000 mg, such as between 600 mg and 1900 mg, such as between 700 mg and 1800 mg, such as between 800 mg and 1800 mg, such as 900 mg and 1800 mg, such as between 1000 mg and 1800 mg, such as between 1100 mg and 1800 mg, such as between 1200 mg and 1800 mg, such as between 1300 mg and 1800 mg, such as between 1400 mg and 1800 mg, such as between 1500 mg and 1800 mg, such as 1580 mg between 1780 mg, such as between 1630 mg and 1730 mg, such as between 1655 mg and 1705 mg, such as between 1670 mg and 1690 mg, such as 1680 mg±5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg , eg 1680 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a fixed dose of 1200 mg every 3 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g., a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (eg, atezolizumab)) can be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに約20mgと約1000mgの間(例えば約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約180mgと約250mgの間、例えば約180mgと約220mgの間、例えば約190mgと約210mgの間、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに20mgと1000mgの間(例えば40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば180mgと250mgの間、例えば180mgと220mgの間、例えば190mgと210mgの間、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに約200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに200mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, penprolizumab)) is between about 20 mg and about 1000 mg (eg, about 40 mg and about 900 mg) every three weeks. between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as between about 120 mg and about 400 mg, such as about between 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 180 mg and about 250 mg, such as between about 180 mg and about 220 mg, such as between about 190 mg and about 210 mg between, eg 200±5 mg, eg 200±2.5 mg, eg 200±1.0 mg, eg 200±0.5 mg, eg 200 mg) (eg a fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., penprolizumab)) is between 20 mg and 1000 mg (e.g., between 40 mg and 900 mg) every three weeks, e.g. between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg, such as between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as 180 mg and 300 mg, such as between 180 mg and 250 mg, such as between 180 mg and 220 mg, such as between 190 mg and 210 mg, such as 200 mg±5 mg, such as 200±2.5 mg, such as 200±1.0 mg, such as 200±0. 5 mg, eg 200 mg) dose (eg fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, penprolizumab)) is a dose of about 200 mg every 3 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, penprolizumab)) is a dose of 200 mg every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-1 antagonist antibody (eg, penprolizumab)) can be reduced compared to the standard dose of anti-PD-L1 antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに約20mgと約1000mgの間(例えば約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約200mgと約280mgの間、例えば約220mgと約260mgの間、例えば約230mgと約250mgの間、例えば240mg±5mg、例えば240±2.5mg、例えば240±1.0mg、例えば240±0.5mg、例えば240mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに約240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約100mgと約1000mgの間(例えば約200mgと約900mgの間、例えば約300mgと約800mgの間、例えば約400mgと約700mgの間、例えば約400mgと約600mgの間、例えば約400mgと約550mgの間、例えば約420mgと約540mgの間、例えば約440mgと約520mgの間、例えば約460mgと約500mgの間、例えば約470mgと約490mgの間、例えば480mg±5mg、例えば480±2.5mg、例えば480±1.0mg、例えば480±0.5mg、例えば480mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに20mgと1000mgの間(例えば40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば200mgと280mgの間、例えば220mgと260mgの間、例えば230mgと250mgの間、例えば240mg±5mg、例えば240±2.5mg、例えば240±1.0mg、例えば240±0.5mg、例えば240mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに100mgと1000mgの間(例えば200mgと900mgの間、例えば300mgと800mgの間、例えば400mgと700mgの間、例えば400mgと600mgの間、例えば400mgと550mgの間、例えば420mgと540mgの間、例えば440mgと520mgの間、例えば460mgと500mgの間、例えば470mgと490mgの間、例えば480mg±5mg、例えば480±2.5mg、例えば480±1.0mg、例えば480±0.5mg、例えば480mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに約480mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに480mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is between about 20 mg and about 1000 mg (eg, about 40 mg and about 900 mg) every two weeks. between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as between about 120 mg and about 400 mg, such as about between 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 200 mg and about 280 mg, such as between about 220 mg and about 260 mg, such as between about 230 mg and about 250 mg between, eg 240±5 mg, eg 240±2.5 mg, eg 240±1.0 mg, eg 240±0.5 mg, eg 240 mg) (eg a fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 240 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, atezolizumab)) is between about 100 mg and about 1000 mg (eg, about 200 mg and about 900 mg) every 4 weeks. between about 300 mg and about 800 mg, such as between about 400 mg and about 700 mg, such as between about 400 mg and about 600 mg, such as between about 400 mg and about 550 mg, such as between about 420 mg and about 540 mg, such as about between 440 mg and about 520 mg, such as between about 460 mg and about 500 mg, such as between about 470 mg and about 490 mg, such as 480 mg±5 mg, such as 480±2.5 mg, such as 480±1.0 mg, such as 480±0.5 mg , eg 480 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., nivolumab)) is between 20 mg and 1000 mg (e.g., between 40 mg and 900 mg) every two weeks, e.g. between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg, such as between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as 180 mg and 300 mg, such as between 200 mg and 280 mg, such as between 220 mg and 260 mg, such as between 230 mg and 250 mg, such as 240 mg±5 mg, such as 240±2.5 mg, such as 240±1.0 mg, such as 240±0. 5 mg, eg 240 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-1 antagonist antibody (e.g., nivolumab)) is between 100 mg and 1000 mg (e.g., between 200 mg and 900 mg) every 4 weeks, e.g. between 300 mg and 800 mg, such as between 400 mg and 700 mg, such as between 400 mg and 600 mg, such as between 400 mg and 550 mg, such as between 420 mg and 540 mg, such as between 440 mg and 520 mg, such as between 460 mg and 500 mg, such as 470 mg and 490 mg, such as 480±5 mg, such as 480±2.5 mg, such as 480±1.0 mg, such as 480±0.5 mg, such as 480 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 480 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g., a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibodies (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-1 antagonist antibodies administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば、約0.1mg/kgと約40mg/kgの間、例えば、約1mg/kgと約35mg/kgの間、例えば、約2.5mg/kgと約30mg/kgの間、例えば、約5mg/kgと約25mg/kgの間、例えば、約10mg/kgと約20mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約15mg/kgの間、例えば、約10mg/kgと約15mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約14mg/kgと約15mg/kgの間、例えば、約15±1mg/kg、例えば、約15±0.5mg/kg、例えば、約15±0.2mg/kg、例えば、約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の有効量は、3週間ごとに投与される約15mg/kgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば、0.1mg/kgと40mg/kgの間、例えば、1mg/kgと35mg/kgの間、例えば、2.5mg/kgと30mg/kgの間、例えば、5mg/kgと25mg/kgの間、例えば、10mg/kgと20mg/kgの間、例えば、12.5mg/kgと15mg/kgの間、例えば、15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば、15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに対象の体重の0.01mg/kgと15mg/kgの間(例えば0.1mg/kgと15mg/kgの間、例えば0.5mg/kgと15mg/kgの間、例えば1mg/kgと15mg/kgの間、例えば2.5mg/kgと15mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば10mg/kgと15mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば14mg/kgと15mg/kgの間、例えば15±1mg/kg、例えば15±0.5mg/kg、例えば15±0.2mg/kg、例えば15±0.1mg/kg、例えば15mg/kg)の用量である。いくつかの例では、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の有効量は、3週間ごとに投与される15mg/kgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg, e.g., between about 1 mg/kg and about 35 mg/kg) such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as about 12 mg/kg. between 5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0 .1 mg/kg, eg about 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 15 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.1 mg/kg and about 15 mg/kg, e.g., between about 0.5 mg/kg and about 15 mg/kg, e.g., between about 1 mg/kg and about 15 mg/kg) between about 2.5 mg/kg and about 15 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 15 mg/kg, such as about between 10 mg/kg and about 15 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as between about 14 mg/kg and about 15 mg/kg, such as about 15±1 mg/kg; For example, about 15±0.5 mg/kg, such as about 15±0.2 mg/kg, such as about 15±0.1 mg/kg, such as about 15 mg/kg). In some examples, an effective amount of anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg administered every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 50 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.01 mg/kg and 45 mg/kg, e.g. between 0.1 mg/kg and 40 mg/kg, e.g. between 1 mg/kg and 35 mg/kg, e.g. 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg /kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0.1 mg/kg, such as 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 15 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.1 mg/kg and 15 mg/kg, such as between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 10 mg/kg and 15 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, between 14 mg/kg and 15 mg/kg, such as 15±1 mg/kg, such as 15±0.5 mg/kg, such as 15±0.2 mg/kg, such as 15±0.1 mg/kg, such as 15 mg/kg) is the dose of In some examples, an effective amount of anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of 15 mg/kg administered every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) doses PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly rambrolizumab) administered as drug therapy) may be reduced compared to the standard dose of pembrolizumab))), which was known as
抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投薬サイクルは、臨床上の利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約14~28日間(例えば、14日間、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間、24日間、25日間、26日間、27日間又は28日間)である。いくつかの例では、投薬サイクルの長さは、約21日間である。いくつかの例では、投薬サイクルの長さは、約14日間である。いくつかの例では、投薬サイクルの長さは、約28日間である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。同様に、いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量(例えば、固定用量)で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))は、各21日間サイクルの1日目に約200mgの用量で(すなわち、3週間ごとに約200mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各14日間サイクルの1日目に約240mgの用量で(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各28日間サイクル(すなわち、4週間ごとに約480mgの用量で)の1日目に約480mgの用量で静脈内投与されることになる。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、第1の投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、14日間サイクルの1日目に約240mgの用量で(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、28日間サイクルの1日目に約480mgの用量で(すなわち、4週間ごとに約480mgの用量で)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、21日間の各サイクル(すなわち、3週間ごとに1200mgの用量で)の1日目に1200mgの用量(例えば、固定用量)で静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))は、各21日間サイクル(すなわち、3週間ごとに200mgの用量で)の1日目に200mgの用量で静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各14日間サイクル(すなわち、2週間ごとに240mgの用量で)の1日目に240mgの用量で静脈内投与されることになる。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))は、各28日間サイクル(すなわち、4週間ごとに480mgの用量で)の1日目に480mgの用量で静脈内投与されることになる。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、各投薬サイクルの1日目(例えば、1日目±3日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))の両方を、第1の投薬サイクルの1日目(例えば、1日目±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)は、600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、240mgの用量で14日間の各サイクルの1日目に(すなわち、2週間ごとに240mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)は、600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))は、480mgの用量で28日間の各サイクルの1日目に(すなわち、4週間ごとに480mgの用量で)静脈内投与される。
an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) or anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) dosing cycles may be associated with clinical benefit (e.g., confirmed disease progression, drug resistance, death, or unacceptable toxicity). In some examples, the length of each dosing cycle is about 14 to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days). days, 24 days, 25 days, 26 days, 27 days or 28 days). In some examples, the dosing cycle length is about 21 days. In some examples, the dosing cycle length is about 14 days. In some examples, the dosing cycle length is about 28 days. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered on about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約60±15分(例えば約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、又は約70分)にわたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 60 ± 15 minutes (e.g., about 50 minutes, about 51 minutes, about 52 minutes, About 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) to the subject or population of subjects. In some examples, PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly Pembrolizumab (formerly known as lambrolizumab))) is about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes) minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes). or administered to a target population.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)わたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes). , about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about administered to a subject or population of subjects by intravenous infusion over 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes). In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly lambrolizumab) Pembrolizumab))) was known as )) was about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes , about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or administered to a subject or population of subjects by intravenous infusion over approximately 40 minutes).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の前に対象又は対象集団に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、本方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第2の観察期間を更に含む。いくつかの例では、本方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間と、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分の長さである場合、本方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後それぞれ約30±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分の長さである場合、本方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後それぞれ約15±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) prior to administration to the subject or subject population. In some examples, for example, after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 ( Prior to administration of nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))), the method includes an intervening first observation period. In some examples, the method uses a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475). (pembrolizumab, formerly known as rambrolizumab)))). In some examples, the method includes a first observation period after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or anti-PD-1 Both include a second observation period following administration of an antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)). In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. If the first and second observation periods are each about 60 minutes long, the method includes the addition of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti-PD - about 30 ± 10 after administration of an L1 antagonistic antibody (e.g., atezolizumab) or an anti-PD-1 antagonistic antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)), respectively This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute. When the first and second observation periods are each about 30 minutes long, the method includes the addition of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti-PD - about 15 ± 10 after administration of an L1 antagonistic antibody (e.g., atezolizumab) or an anti-PD-1 antagonistic antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)), respectively This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute.
他の例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後及び抗TIGITアンタゴニスト抗体の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間を含む。いくつかの例では、本方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後の第1の観察期間と、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分の長さである場合、本方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後それぞれ約30±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分の長さである場合、本方法は、第1及び第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後それぞれ約15±10分に対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly known as lambrolizumab) Known pembrolizumab))) is administered to a subject or population of subjects prior to an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, for example, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (MDX-1106 (nivolumab) or MK-3475 (formerly lambrolizumab After administration of pembrolizumab))) and prior to administration of the anti-TIGIT antagonist antibody, the method includes an intervening first observation period. In some examples, the method includes a second observation period after administration of the anti-TIGIT antagonist antibody. In some examples, the method uses a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475). (pembrolizumab, formerly known as rambrolizumab)))) and a second observation period following administration of an anti-TIGIT antagonist antibody. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. If the first and second observation periods are each about 60 minutes long, the method includes the addition of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody ( atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody, respectively. This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute. If the first and second observation periods are each about 30 minutes long, the method includes the addition of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody ( atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an anti-TIGIT antagonist antibody, respectively. This can include recording the subject's or subject population's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) every minute.
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、対象又は対象集団に同時に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与後、方法は観察期間を含む。いくつかの例では、観察期間は、約30分と約60分の間の長さである。観察期間が約60分の長さである場合、本方法は、観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後約30±10分で対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。観察期間が約30分の長さである場合、本方法は、観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体の投与後約15±10分で対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab ) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) is administered to the subject or population of subjects concurrently. In some examples, for example, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or Following administration of MK-3475 (pembrolizumab, formerly known as rambrolizumab))), the method included an observation period. In some examples, the observation period is between about 30 minutes and about 60 minutes long. If the observation period is about 60 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., , MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) and an anti-TIGIT antagonist antibody at approximately 30±10 minutes after administration of the subject's vital signs (e.g., pulse rate, respiratory rate, , blood pressure, and temperature). If the observation period is about 30 minutes long, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., , MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) and an anti-TIGIT antagonist antibody at approximately 15±10 minutes after administration of the subject's vital signs (e.g., pulse rate, respiratory rate, , blood pressure, and temperature).
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を提供し、以下に更に詳細に記載されるように、方法は、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメインを含み、VLドメインは配列番号19のアミノ酸配列を含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), and as described in more detail below, the method comprises administering to the subject or subject population every 3 weeks administering a dose (e.g., fixed dose) of 600 mg of an anti-TIGIT antagonist antibody and one or more dosing cycles of a dose (e.g., fixed dose) of atezolizumab of 1200 mg every three weeks, wherein the anti-TIGIT antagonist antibody is The VH domain comprises the amino acid sequence of SEQ ID NO:17 or 18 and the VL domain comprises the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))を提供し、以下に更に詳細に記載されるように、方法は、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに200mgの用量(例えば、固定用量)のペンブロリズマブの1回以上の投薬サイクルを投与することを含み、抗TIGITアンタゴニスト抗体が、配列番号17又は18のアミノ酸配列を含むVHドメインを含み、VLドメインは配列番号19のアミノ酸配列を含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) for use in methods of treating a subject or subject population and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., pembrolizumab)), and as described in more detail below, the method comprises administering to the subject or subject population every 3 weeks administering one or more dosing cycles of a dose (e.g., fixed dose) of 600 mg of an anti-TIGIT antagonist antibody and a dose (e.g., fixed dose) of 200 mg (e.g., fixed dose) of pembrolizumab every three weeks, wherein the anti-TIGIT antagonist antibody is The VH domain comprises the amino acid sequence of SEQ ID NO:17 or 18 and the VL domain comprises the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))を提供し、以下に更に詳細に記載されるように、方法は、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び2週間ごとに240mgの用量(例えば、固定用量)のニボルマブの1回以上の投薬サイクルを投与することを含み、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメインを含み、VLドメインは配列番号19のアミノ酸配列を含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., nivolumab)), and as described in more detail below, the method comprises administering to the subject or subject population every 3 weeks administering one or more dosing cycles of a dose (e.g., fixed dose) of 600 mg of an anti-TIGIT antagonist antibody and a dose (e.g., fixed dose) of 240 mg every two weeks of nivolumab, wherein the anti-TIGIT antagonist antibody comprises: The VH domain comprises the amino acid sequence of SEQ ID NO:17 or 18 and the VL domain comprises the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))を提供し、以下に更に詳細に記載されるように、方法は、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び4週間ごとに480mgの用量(例えば、固定用量)のニボルマブの1回以上の投薬サイクルを投与することを含み、抗TIGITアンタゴニスト抗体が、配列番号17又は18のアミノ酸配列を含むVHドメインを含み、VLドメインは配列番号19のアミノ酸配列を含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) for use in methods of treating a subject or subject population and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., nivolumab)), and as described in more detail below, the method comprises administering to the subject or subject population every 3 weeks administering one or more dosing cycles of a dose (e.g., fixed dose) of 600 mg of an anti-TIGIT antagonist antibody and a dose (e.g., fixed dose) of nivolumab of 480 mg every 4 weeks, wherein the anti-TIGIT antagonist antibody is The VH domain comprises the amino acid sequence of SEQ ID NO:17 or 18 and the VL domain comprises the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)を提供し、方法は、対象又は対象集団に、1回以上の投薬サイクルの3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ、及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブを投与することを含む。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (eg, atezolizumab), the method comprising administering to the subject or subject population a dose (eg, fixed dose) of 600 mg every 3 weeks for one or more dosing cycles (eg, a fixed dose), and 3 Administering a dose (eg, fixed dose) of 1200 mg weekly of atezolizumab.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、MK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))を提供し、方法は、対象又は対象集団に、1回以上の投薬サイクルの3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ、及び3週間ごとに200mgの用量(例えば、固定用量)のペンプロリズマブを投与することを含む。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., MK-3475 (pembrolizumab, formerly known as lambrolizumab)), the method comprising administering to the subject or subject population one or more times administering a 600 mg dose (eg, fixed dose) of tiragolumab every 3 weeks and a 200 mg dose (eg, fixed dose) of penprolizumab every 3 weeks for a dosing cycle of .
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ))を提供し、方法は、対象又は対象集団に、1回以上の投薬サイクルの3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ、及び2週間ごとに240mgの用量(例えば、固定用量)のニボルマブを投与することを含む。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab)), the method comprising administering to the subject or subject population every 3 weeks for one or more dosing cycles administering a 600 mg dose (eg, fixed dose) of tiragolumab and a 240 mg dose (eg, fixed dose) of nivolumab every two weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ))を提供し、方法は、対象又は対象集団に、1回以上の投薬サイクルの3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ、及び4週間ごとに480mgの用量(例えば、固定用量)のニボルマブを投与することを含む。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab)), the method comprising administering to the subject or subject population every 3 weeks for one or more dosing cycles administering a 600 mg dose (eg, fixed dose) of tiragolumab and a 480 mg dose (eg, fixed dose) of nivolumab every 4 weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、有効量の抗TIGITアンタゴニスト抗体及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture or preparation of a medicament for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist disclosed herein) tiragolumab) and PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonistic antibodies (e.g. atezolizumab) or anti-PD-1 antagonistic antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly pembrolizumab))), formerly known as rambrolizumab, the method comprising administering to a subject or subject population one or more dosing cycles of a medicament, the medicament comprising an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly known as lambrolizumab) pembrolizumab))).
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体の使用を提供し、方法は、対象又は対象集団に医薬及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを投与することを含み、医薬は、有効量の抗TIGITアンタゴニスト抗体及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer). and PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonistic antibodies (e.g. atezolizumab) or anti-PD-1 antagonistic antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly known as rambrolizumab) pembrolizumab)))), wherein the medicament comprises an effective amount of an anti-TIGIT antagonist antibody and an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))).
別の態様では、本発明は、検出可能なPD-L1発現レベル(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造におけるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するため、及び有効量の抗TIGITアンタゴニスト抗体を投与するように製剤化される。 In another aspect, the present invention provides detectable PD-L1 expression levels (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD). - a PD-1 axis binding antagonist (e.g. an anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD in the manufacture of a medicament for use in a method of treating a subject or subject population having L1-positive cervical cancer) -1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)), wherein the method comprises one or more comprising administering a dosing cycle to a subject or population of subjects, wherein the medicament is an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., It is formulated to administer MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)), and to administer an effective amount of an anti-TIGIT antagonist antibody.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約600mgの間(例えば約50mgと600mgの間、例えば約60mgと約600mgの間、例えば約100mgと約600mgの間、例えば約200mgと約600mgの間、例えば約200mgと約550mgの間、例えば約250mgと約500mgの間、例えば約300mgと約450mgの間、例えば約350mgと約400mgの間、例えば約375mg)(例えば30mgと1200mg(例えば30mgと1100mgの間、例えば60mgと1000mgの間、例えば100mgと900mgの間、例えば200mgと800mgの間、例えば300mgと800mgの間、例えば400mgと800mgの間、例えば400mgと750mgの間、例えば450mgと750mgの間、例えば500mgと700mgの間、例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体の間、例えば、チラゴルマブ)の有効量は、3週間ごとに30mgと600mgの間(例えば、50mgと600mgの間、例えば、60mgと600mgの間、例えば、100mgと600mgの間、例えば、200mgと600mgの間、例えば、200mgと550mgの間、例えば、250mgと500mgの間、例えば、300mgと450mgの間、例えば、350mgと400mgの間、例えば、375mg))の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、併用療法(例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))との併用処置)で投与され、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg (e.g., about 30 mg) every three weeks. and about 1100 mg, for example between about 60 mg and about 1000 mg, for example between about 100 mg and about 900 mg, for example between about 200 mg and about 800 mg, for example between about 300 mg and about 800 mg, for example about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg) (eg, a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between about 30 mg and about 600 mg (e.g., about between 50 mg and 600 mg, such as between about 60 mg and about 600 mg, such as between about 100 mg and about 600 mg, such as between about 200 mg and about 600 mg, such as between about 200 mg and about 550 mg, such as between about 250 mg and about 500 mg such as between about 300 mg and about 450 mg, such as between about 350 mg and about 400 mg, such as about 375 mg) (such as between 30 mg and 1200 mg (such as between 30 mg and 1100 mg, such as between 60 mg and 1000 mg, such as between 100 mg and 900 mg, between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg, such as between 450 mg and 750 mg, such as between 500 mg and 700 mg, such as between 550 mg and 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg).In some examples, an anti-TIGIT antagonist antibody ( For example, between the anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab, the effective amount is between 30 mg and 600 mg (e.g., between 50 mg and 600 mg, e.g., between 60 mg and 600 mg) every three weeks. between 100 mg and 600 mg, such as between 200 mg and 600 mg, such as between 200 mg and 550 mg, such as between 250 mg and 500 mg, such as between 300 mg and 450 mg, such as between 350 mg and 400 mg, such as , 375 mg)). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 600 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg every 3 weeks. In some examples, the dose of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is used in combination therapy (e.g., a PD-1 axis binding antagonist (e.g., anti-PD- L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., combination treatment with MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))); It may be reduced compared to standard doses of anti-TIGIT antagonist antibodies administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約80mgと約2000mgの間(例えば約80mgと約1950mgの間、例えば約80mgと約1900mgの間、例えば約80mgと約1800mgの間、例えば約100mgと約1700mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1400mgの間、例えば約400mgと約1300mgの間、例えば約500mgと約1200mgの間、例えば約600mgと約1100mgの間、例えば約700mgと約1000mgの間、例えば約740mgと約940mgの間、例えば約790mgと約890mgの間、例えば約815mgと約865mgの間、例えば約830mgと約850mgの間、例えば840mg±5mgの間、例えば840±2.5mgの間、例えば840±1.0mgの間、例えば840±0.5mgの間、例えば840mg)(例えば80mgと2000mg(例えば80mgと1950mgの間、例えば80mgと1900mgの間、例えば80mgと1800mgの間、例えば100mgと1700mgの間、例えば200mgと1600mgの間、例えば300mgと1400mgの間、例えば400mgと1300mgの間、例えば500mgと1200mgの間、例えば600mgと1100mgの間、例えば700mgと1000mgの間、例えば740mgと940mgの間、例えば790mgと890mgの間、例えば815mgと865mgの間、例えば830mgと850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg))の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約1900mgの間、例えば約300mgと約1700mgの間、例えば約400mgと約1600mgの間、例えば約500mgと約1600mgの間、例えば約600mgと約1600mgの間、例えば約700mgと約1600mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mg(例えば100mgと2000mgの間、例えば200mgと1900mgの間、例えば300mgと1700mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間)、例えば約1190mgと約1210mgの間(例えば1190mgと1210mgの間)、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約2000mgの間、例えば約300mgと約2000mgの間、例えば約400mgと約2000mgの間、例えば約500mgと約2000mgの間、例えば約600mgと約1900mgの間、例えば約700mgと約1800mgの間、例えば約800mgと約1800mgの間、例えば約900mgと約1800mgの間、例えば約1000mgと約1800mgの間、例えば約1100mgと約1800mgの間、例えば約1200mgと約1800mgの間、例えば約1300mgと約1800mgの間、例えば約1400mgと約1800mgの間、例えば約1500mgと約1800mgの間、例えば約1580mgと約1780mgの間、例えば約1630mgと約1730mgの間、例えば約1655mgと約1705mgの間、例えば約1670mgと約1690mg(例えば100mgと2000mgの間、例えば200mgと2000mgの間、例えば300mgと2000mgの間、例えば400mgと2000mgの間、例えば500mgと2000mgの間、例えば600mgと1900mgの間、例えば700mgと1800mgの間、例えば800mgと1800mgの間、例えば900mgと1800mgの間、例えば1000mgと1800mgの間、例えば1100mgと1800mgの間、例えば1200mgと1800mgの間、例えば1300mgと1800mgの間、例えば1400mgと1800mgの間、例えば1500mgと1800mgの間、例えば1580mgと1780mgの間、例えば1630mgと1730mgの間、例えば1655mgと1705mgの間、例えば1670mgと1690mgの間)、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約1200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに1200mgの固定用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 80 mg and about 1950 mg) every two weeks. between about 80 mg and about 1900 mg, such as between about 80 mg and about 1800 mg, such as between about 100 mg and about 1700 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1400 mg, such as about between 400 mg and about 1300 mg, such as between about 500 mg and about 1200 mg, such as between about 600 mg and about 1100 mg, such as between about 700 mg and about 1000 mg, such as between about 740 mg and about 940 mg, such as between about 790 mg and about 890 mg between about 815 mg and about 865 mg, such as between about 830 mg and about 850 mg, such as between 840 mg±5 mg, such as between 840±2.5 mg, such as between 840±1.0 mg, such as 840±0. between 80 mg and 2000 mg (eg between 80 mg and 1950 mg, such as between 80 mg and 1900 mg, such as between 80 mg and 1800 mg, such as between 100 mg and 1700 mg, such as between 200 mg and 1600 mg, such as between 200 mg and 1600 mg, such as 300 mg and 1400 mg, such as between 400 mg and 1300 mg, such as between 500 mg and 1200 mg, such as between 600 mg and 1100 mg, such as between 700 mg and 1000 mg, such as between 740 mg and 940 mg, such as between 790 mg and 890 mg, such as 815 mg at a dose (e.g. fixed dose) of between 865 mg, such as between 830 mg and 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg) be. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about 2000 mg) every three weeks. between about 200 mg and about 1900 mg, such as between about 300 mg and about 1700 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg, such as between about 600 mg and about 1600 mg, such as about between 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between 100 mg and 2000 mg, such as between 200 mg and 1900 mg, such as between 300 mg and 1700 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as between 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg), such as between about 1190 mg and about 1210 mg (eg between 1190 mg and 1210 mg), such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1 .0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about 2000 mg) every 4 weeks. between about 200 mg and about 2000 mg, such as between about 300 mg and about 2000 mg, such as between about 400 mg and about 2000 mg, such as between about 500 mg and about 2000 mg, such as between about 600 mg and about 1900 mg, such as about between 700 mg and about 1800 mg, such as between about 800 mg and about 1800 mg, such as between about 900 mg and about 1800 mg, such as between about 1000 mg and about 1800 mg, such as between about 1100 mg and about 1800 mg, such as between about 1200 mg and about 1800 mg between about 1300 mg and about 1800 mg, such as between about 1400 mg and about 1800 mg, such as between about 1500 mg and about 1800 mg, such as between about 1580 mg and about 1780 mg, such as between about 1630 mg and about 1730 mg, such as about 1655 mg and about 1705 mg, such as between about 1670 mg and about 1690 mg, such as between 100 mg and 2000 mg, such as between 200 mg and 2000 mg, such as between 300 mg and 2000 mg, such as between 400 mg and 2000 mg, such as between 500 mg and 2000 mg, such as 600 mg and 1900 mg, such as between 700 mg and 1800 mg, such as between 800 mg and 1800 mg, such as between 900 mg and 1800 mg, such as between 1000 mg and 1800 mg, such as between 1100 mg and 1800 mg, such as between 1200 mg and 1800 mg, such as 1300 mg between 1800 mg, such as between 1400 mg and 1800 mg, such as between 1500 mg and 1800 mg, such as between 1580 mg and 1780 mg, such as between 1630 mg and 1730 mg, such as between 1655 mg and 1705 mg, such as between 1670 mg and 1690 mg), such as 1680 mg ± 5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg, such as 1680 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a fixed dose of 1200 mg every 3 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) doses It may be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as drug therapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごとに約20mgと約1000mgの間(例えば約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約180mgと約250mgの間、例えば約180mgと約220mgの間、例えば約190mgと約210mg(例えば40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば180mgと250mgの間、例えば180mgと220mgの間、例えば190mgと210mgの間)、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに約200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の有効量は、3週間ごとに200mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, pembrolizumab)) is between about 20 mg and about 1000 mg (eg, about 40 mg and about 900 mg) every three weeks. between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as between about 120 mg and about 400 mg, such as about Between 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 180 mg and about 250 mg, such as between about 180 mg and about 220 mg, such as between about 190 mg and about 210 mg ( between 40 mg and 900 mg, such as between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg, such as between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as between 180 mg and 300 mg, such as between 180 mg and 250 mg, such as between 180 mg and 220 mg, such as between 190 mg and 210 mg), such as 200 mg ± 5 mg, such as 200 ± 2.5 mg, such as 200 ± 1.0 mg, such as 200±0.5 mg, such as 200 mg) (eg, fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, penprolizumab)) is a dose of about 200 mg every 3 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, penprolizumab)) is a dose of 200 mg every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-1 antagonist antibody (eg, penprolizumab)) can be reduced compared to the standard dose of anti-PD-L1 antagonist antibody administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに約20mgと約1000mgの間(例えば、20mg~1000mg)(例えば、約40mgと約900mgの間、例えば約60mgと約800mgの間、例えば約80mgと約700mgの間、例えば約80mgと約600mgの間、例えば約100mgと約500mgの間、例えば約120mgと約400mgの間、例えば約140mgと約300mgの間、例えば約160mgと約350mgの間、例えば約180mgと約300mgの間、例えば約200mgと約280mgの間、例えば約220mgと約260mgの間、例えば約230mgと約250mgの間(例えば、40mgと900mgの間、例えば60mgと800mgの間、例えば80mgと700mgの間、例えば80mgと600mgの間、例えば100mgと500mgの間、例えば120mgと400mgの間、例えば140mgと300mgの間、例えば160mgと350mgの間、例えば180mgと300mgの間、例えば200mgと280mgの間、例えば220mgと260mgの間、例えば230mgと250mgの間)、例えば240mg±5mg、例えば240±2.5mg、例えば240±1.0mg、例えば240±0.5mg、例えば240mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに約240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、2週間ごとに240mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに約100mgと約1000mgの間(例えば100mgと1000mgの間)(例えば約200mgと約900mgの間、例えば約300mgと約800mgの間、例えば約400mgと約700mgの間、例えば約400mgと約600mgの間、例えば約400mgと約550mgの間、例えば約420mgと約540mgの間、例えば約440mgと約520mgの間、例えば約460mgと約500mgの間、例えば約470mgと約490mgの間(例えば200mgと900mgの間、例えば300mgと800mgの間、例えば400mgと700mgの間、例えば400mgと600mgの間、例えば400mgと550mgの間、例えば420mgと540mgの間、例えば440mgと520mgの間、例えば460mgと500mgの間、例えば470mgと490mgの間)、例えば480mg±5mg、例えば480±2.5mg、例えば480±1.0mg、例えば480±0.5mg、例えば480mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに約480mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))の有効量は、4週間ごとに480mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is between about 20 mg and about 1000 mg (eg, 20 mg to 1000 mg) every two weeks (e.g., between about 40 mg and about 900 mg, such as between about 60 mg and about 800 mg, such as between about 80 mg and about 700 mg, such as between about 80 mg and about 600 mg, such as between about 100 mg and about 500 mg, such as about 120 mg and about 400 mg, such as between about 140 mg and about 300 mg, such as between about 160 mg and about 350 mg, such as between about 180 mg and about 300 mg, such as between about 200 mg and about 280 mg, such as between about 220 mg and about 260 mg between about 230 mg and about 250 mg, such as between 40 mg and 900 mg, such as between 60 mg and 800 mg, such as between 80 mg and 700 mg, such as between 80 mg and 600 mg, such as between 100 mg and 500 mg, such as between 120 mg and 400 mg between 140 mg and 300 mg, such as between 160 mg and 350 mg, such as between 180 mg and 300 mg, such as between 200 mg and 280 mg, such as between 220 mg and 260 mg, such as between 230 mg and 250 mg), such as 240 mg ± 5 mg , eg 240±2.5 mg, eg 240±1.0 mg, eg 240±0.5 mg, eg 240 mg) (eg a fixed dose). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 240 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 240 mg every two weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-1 antagonist antibody (eg, nivolumab)) is between about 100 mg and about 1000 mg (eg, between 100 mg and 1000 mg) every 4 weeks. ) (e.g. between about 200 mg and about 900 mg, such as between about 300 mg and about 800 mg, such as between about 400 mg and about 700 mg, such as between about 400 mg and about 600 mg, such as between about 400 mg and about 550 mg, such as about 420 mg and about 540 mg, such as between about 440 mg and about 520 mg, such as between about 460 mg and about 500 mg, such as between about 470 mg and about 490 mg (e.g. between 200 mg and 900 mg, such as between 300 mg and 800 mg, such as 400 mg and between 700 mg, such as between 400 mg and 600 mg, such as between 400 mg and 550 mg, such as between 420 mg and 540 mg, such as between 440 mg and 520 mg, such as between 460 mg and 500 mg, such as between 470 mg and 490 mg), such as 480 mg ± 5 mg, such as 480±2.5 mg, such as 480±1.0 mg, such as 480±0.5 mg, such as 480 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of about 480 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-1 antagonist antibody (eg, nivolumab)) is a dose of 480 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibodies (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-1 antagonist antibodies administered as monotherapy.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば、約0.1mg/kgと約40mg/kgの間、例えば、約1mg/kgと約35mg/kgの間、例えば、約2.5mg/kgと約30mg/kgの間、例えば、約5mg/kgと約25mg/kgの間、例えば、約10mg/kgと約20mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約15mg/kgの間、例えば、約10mg/kgと約15mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約14mg/kgと約15mg/kgの間、例えば、約15±1mg/kg、例えば、約15±0.5mg/kg、例えば、約15±0.2mg/kg、例えば、約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の有効量は、3週間ごとに投与される約15mg/kgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg, e.g., between about 1 mg/kg and about 35 mg/kg) such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as about 12 mg/kg. between 5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0 .1 mg/kg, eg about 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 0.01 mg/kg and about 15 mg/kg of body weight of the subject every three weeks. /kg (e.g., between about 0.1 mg/kg and about 15 mg/kg, e.g., between about 0.5 mg/kg and about 15 mg/kg, e.g., between about 1 mg/kg and about 15 mg/kg) between about 2.5 mg/kg and about 15 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 15 mg/kg, such as about between 10 mg/kg and about 15 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as between about 14 mg/kg and about 15 mg/kg, such as about 15±1 mg/kg; For example, about 15±0.5 mg/kg, such as about 15±0.2 mg/kg, such as about 15±0.1 mg/kg, such as about 15 mg/kg). In some examples, an effective amount of anti-PD-L1 antagonist antibody (eg, atezolizumab) is a dose of about 15 mg/kg administered every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) doses It may be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as drug therapy.
本発明の任意の使用において、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬の投薬サイクルは、臨床上の利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約14~28日間(例えば、14日間、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間、24日間、25日間、26日間、27日間又は28日間)である。いくつかの例では、投薬サイクルの長さは、約21日間である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、各21日間サイクル(すなわち、3週間ごとに約600mgの用量で)の1日目に約600mgの用量(例えば、固定用量)で静脈内投与される。同様に、いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を含む医薬は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、3週間ごとに約1200mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))を含む医薬は、各21日間サイクルの1日目に約200mgの用量で(すなわち、3週間ごとに約200mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))を含む医薬は、各14日間サイクルの1日目に約240mgの用量で(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ニボルマブ))を含む医薬は、各28日間サイクルの1日目に約480mgの用量で(すなわち、4週間ごとに約480mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の両方を含む医薬は、各投薬サイクルの1日目(例えば、1日目±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、約600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を含む医薬は、約1200mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約1200mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)を含む医薬は、約600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))を含む医薬は、約200mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約200mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)を含む医薬は、約600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))を含む医薬は、約240mgの用量で14日間の各サイクルの1日目に(すなわち、2週間ごとに約240mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、アテゾリズマブ)を含む医薬は、約600mgの用量で21日間の各サイクルの1日目に(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))を含む医薬は、約480mgの用量で28日間の各サイクルの1日目に(すなわち、4週間ごとに約480mgの用量で)静脈内投与される。
In any use of the invention, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) may be administered in one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) may provide clinical benefit (e.g., confirmation until no evidence of disease progression, drug resistance, death, or unacceptable toxicity). In some examples, the length of each dosing cycle is about 14 to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days). days, 24 days, 25 days, 26 days, 27 days or 28 days). In some examples, the dosing cycle length is about 21 days. In some examples, a medicament comprising an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、約60±15分(例えば、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、又は約70分)にわたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, a medicament comprising an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 60 ± 15 minutes (e.g., about 50 minutes, about 51 minutes, About 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) to the subject or population of subjects. In some examples, PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly Pembrolizumab, formerly known as rambrolizumab))), containing about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes , about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes, about 74 minutes or about 75 minutes) intravenously It is administered to a subject or population of subjects by injection.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象又は対象集団に投与される。 In some examples, a medicament comprising an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, About 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes) to the subject or population of subjects. In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly lambrolizumab) Pembrolizumab))) was known as pembrolizumab))) was administered for about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, About 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes minutes, or about 40 minutes) to the subject or population of subjects.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬の前に対象又は対象集団に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体を含む医薬の投与後及び抗PD-L1アンタゴニスト抗体を含む医薬の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、抗PD-L1アンタゴニスト抗体の投与後の第2の観察期間を更に含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を含む医薬の投与後の第1の観察期間及び抗PD-L1アンタゴニスト抗体を含む医薬の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分である例では、方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体を含む医薬及び抗PD-L1アンタゴニスト抗体を含む医薬の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分である例では、方法は、第1及び第2の観察期間中の抗TIGITアンタゴニスト抗体を含む医薬及び抗PD-L1アンタゴニスト抗体を含む医薬の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。 In some examples, a medicament comprising an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist Subject or subject population prior to medication containing antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) administered. In some examples, the method includes an intervening first observation period, eg, after administration of the medicament comprising the anti-TIGIT antagonist antibody and before administration of the medicament comprising the anti-PD-L1 antagonist antibody. In some examples, the method further comprises a second observation period after administration of the anti-PD-L1 antagonist antibody. In some examples, the method includes both a first observation period after administration of a medicament comprising an anti-TIGIT antagonist antibody and a second observation period after administration of a medicament comprising an anti-PD-L1 antagonist antibody. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. In examples where the first and second observation periods are each about 60 minutes, the method comprises administering a medicament comprising an anti-TIGIT antagonist antibody and a medicament comprising an anti-PD-L1 antagonist antibody during the first and second observation periods This may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) at about 30±10 minutes later. In examples where the first and second observation periods are each about 30 minutes, the method comprises administering a medicament comprising an anti-TIGIT antagonist antibody and a medicament comprising an anti-PD-L1 antagonist antibody during the first and second observation periods It may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) at about 15±10 minutes later.
他の例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、抗PD-L1アンタゴニスト抗体を含む医薬の投与後及び抗TIGITアンタゴニスト抗体を含む医薬の投与前に、本方法は、介在する第1の観察期間を含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を含む医薬の投与後の第2の観察期間を含む。いくつかの例では、方法は、抗PD-L1アンタゴニスト抗体を含む医薬の投与後の第1の観察期間及び抗TIGITアンタゴニスト抗体を含む医薬の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分である例では、方法は、第1及び第2の観察期間中の抗PD-L1アンタゴニスト抗体を含む医薬及び抗TIGITアンタゴニスト抗体を含む医薬の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分である例では、方法は、第1及び第2の観察期間中の抗PD-L1アンタゴニスト抗体を含む医薬及び抗TIGITアンタゴニスト抗体を含む医薬の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)をそれぞれ記録することを含み得る。 In other examples, PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly known as lambrolizumab) A medicament comprising known pembrolizumab))) is administered to a subject or population of subjects prior to an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab). In some examples, the method includes an intervening first observation period, eg, after administration of the medicament comprising the anti-PD-L1 antagonist antibody and before administration of the medicament comprising the anti-TIGIT antagonist antibody. In some examples, the method includes a second observation period after administration of the medicament comprising the anti-TIGIT antagonist antibody. In some examples, the method includes both a first observation period after administration of a medicament comprising an anti-PD-L1 antagonist antibody and a second observation period after administration of a medicament comprising an anti-TIGIT antagonist antibody. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. In examples where the first and second observation periods are each about 60 minutes, the method comprises administering a medicament comprising an anti-PD-L1 antagonist antibody and a medicament comprising an anti-TIGIT antagonist antibody during the first and second observation periods. This may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) at about 30±10 minutes later. In examples where the first and second observation periods are each about 30 minutes, the method comprises administering a medicament comprising an anti-PD-L1 antagonist antibody and a medicament comprising an anti-TIGIT antagonist antibody during the first and second observation periods. It may include recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) at about 15±10 minutes later.
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む医薬及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む医薬は、対象又は対象集団に同時に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体を含む医薬及び抗PD-L1アンタゴニスト抗体を含む医薬の投与後に、方法は観察期間を含む。いくつかの例では、観察期間は、約30分と約60分の間の長さである。観察期間が約60分の長さである場合、方法は、観察期間中、抗PD-L1アンタゴニスト抗体を含む医薬及び抗TIGITアンタゴニスト抗体を含む医薬の投与後約30±10分に、対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。観察期間が約30分の長さである場合、方法は、観察期間中、抗PD-L1アンタゴニスト抗体を含む医薬及び抗TIGITアンタゴニスト抗体を含む医薬の投与後約15±10分に、対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In other examples, a medicament comprising an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) is administered concurrently to the subject or subject population. be. In some examples, the method includes an observation period, eg, after administration of the medicament comprising the anti-TIGIT antagonist antibody and the medicament comprising the anti-PD-L1 antagonist antibody. In some examples, the observation period is between about 30 minutes and about 60 minutes long. If the observation period is about 60 minutes in length, the method includes measuring the subject's vital signs at about 30±10 minutes after administration of the medicament comprising the anti-PD-L1 antagonist antibody and the medicament comprising the anti-TIGIT antagonist antibody during the observation period It may include recording signs (eg, pulse rate, respiration rate, blood pressure, and temperature). If the observation period is about 30 minutes long, the method includes measuring the subject's vital signs at about 15±10 minutes after administration of the medicament comprising the anti-PD-L1 antagonist antibody and the medicament comprising the anti-TIGIT antagonist antibody during the observation period. It may include recording signs (eg, pulse rate, respiration rate, blood pressure, and temperature).
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、及び3週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)若しくはMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するために製剤化される In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture or preparation of a medicament for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist disclosed herein) Antibodies (e.g., tiragolumab) and anti-PD-L1 antagonist antibodies (e.g., atezolizumab) are provided, the methods comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every 3 weeks and between about 80 mg and about 2000 mg (e.g., PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab ) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))))
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、及び2週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)若しくはMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するために製剤化される In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture or preparation of a medicament for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist disclosed herein) Antibodies (e.g., tiragolumab) and anti-PD-L1 antagonist antibodies (e.g., atezolizumab) are provided, the methods comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every 3 weeks and between about 80 mg and about 2000 mg (e.g., PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab ) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))))
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、及び4週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)若しくはMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するために製剤化される In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture or preparation of a medicament for use in a method of treating a subject or subject population (e.g., an anti-TIGIT antagonist disclosed herein) Antibodies (e.g., tiragolumab) and anti-PD-L1 antagonist antibodies (e.g., atezolizumab) are provided, the methods comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at doses between about 30 mg and about 1200 mg (e.g., fixed dose) every 3 weeks and doses between about 80 mg and about 2000 mg (e.g., between 80 mg and 2000 mg) every 4 weeks ( PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (formerly lambrolizumab) at fixed doses). is formulated to administer pembrolizumab))), formerly known as
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer) in the manufacture of a medicament for use in a method of treating a subject or subject population with a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), the method comprising the use of the medicament and the anti-TIGIT antagonist antibody. administering one or more dosing cycles to a subject or subject population, wherein the medicament is administered at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg (e.g., between 80 mg and 2000 mg) every three weeks PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonist antibodies (e.g. atezolizumab) or anti-PD-1 antagonist antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) ))) and to administer the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every three weeks. be.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、4週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture of a medicament for use in a method of treating a subject or subject population (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), the method comprising the use of the medicament and the anti-TIGIT antagonist antibody. administering one or more dosing cycles to a subject or subject population, wherein the medicament is administered at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg (e.g., between 80 mg and 2000 mg) every 4 weeks PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonist antibodies (e.g. atezolizumab) or anti-PD-1 antagonist antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) ))) and to administer the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every three weeks. be.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、2週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer) in the manufacture of a medicament for use in a method of treating a subject or subject population with a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab ) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), the method comprising the use of the medicament and the anti-TIGIT antagonist antibody. comprising administering one or more dosing cycles to a subject or population of subjects, wherein the medicament is administered at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg (e.g., between 80 mg and 2000 mg) every two weeks PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonist antibodies (e.g. atezolizumab) or anti-PD-1 antagonist antibodies (e.g. MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab) ))) and to administer the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every three weeks. be.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体の使用を提供し、方法は、医薬及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)若しくはMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)で抗TIGITアンタゴニスト抗体を、及び3週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)で抗PD-L1アンタゴニスト抗体を投与するために製剤化される In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer) in the manufacture of a medicament for use in a method of treating a subject or subject population, the method comprising the medicament and the PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))) administering one or more dosing cycles to a subject or subject population, wherein the medicament is administered at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg (e.g., between 30 mg and 1200 mg) every three weeks formulated to administer the anti-TIGIT antagonist antibody and the anti-PD-L1 antagonist antibody at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg (e.g., between 80 mg and 2000 mg) every three weeks. Ru
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で、及びアテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, described in further detail below. As such, the method comprises administering to the subject or subject population one or more dosing cycles of the medicament, wherein the medicament is an anti-TIGIT antagonist antibody at a dose of 600 mg (e.g., a fixed dose) every three weeks, and atezolizumab at a dose of 1200 mg (e.g., fixed dose) every 3 weeks, wherein the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19 contains a VL domain containing In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びペンブロリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で、及びペンプロリズマブを3週間ごとに200mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), use of an anti-TIGIT antagonist antibody and pembrolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, described in further detail below. As such, the method comprises administering to the subject or subject population one or more dosing cycles of the medicament, wherein the medicament is an anti-TIGIT antagonist antibody at a dose of 600 mg (e.g., a fixed dose) every three weeks, and penprolizumab at a dose of 200 mg (e.g., fixed dose) every 3 weeks, wherein the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19 contains a VL domain containing In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で、及びニボルマブを2週間ごとに240mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), use of an anti-TIGIT antagonist antibody and nivolumab in the manufacture of a medicament for use in a method of treating a subject or subject population, described in further detail below. As such, the method comprises administering to the subject or subject population one or more dosing cycles of the medicament, wherein the medicament is an anti-TIGIT antagonist antibody at a dose of 600 mg (e.g., a fixed dose) every three weeks, and nivolumab at a dose of 240 mg (e.g., fixed dose) every two weeks, wherein the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19 contains a VL domain containing In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で、及びニボルマブを4週間ごとに480mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), use of an anti-TIGIT antagonist antibody and nivolumab in the manufacture of a medicament for use in a method of treating a subject or subject population, described in further detail below. As such, the method comprises administering to the subject or subject population one or more dosing cycles of the medicament, wherein the medicament is an anti-TIGIT antagonist antibody at a dose of 600 mg (e.g., a fixed dose) every three weeks, and nivolumab at a dose of 480 mg (e.g., fixed dose) every 4 weeks, wherein the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19 contains a VL domain containing In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and atezolizumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every three weeks. and atezolizumab administered at a dose of 1200 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びペンプロリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びペンプロリズマブを3週間ごとに200mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and penprolizumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every three weeks. and penprolizumab administered at a dose of 200 mg every three weeks (e.g., a fixed dose), wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬品の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬品及びニボルマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びニボルマブを2週間ごとに240mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬品の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬品及びニボルマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びニボルマブを4週間ごとに480mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and nivolumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every 3 weeks. and nivolumab administered at a dose of 240 mg (e.g., a fixed dose) every two weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and nivolumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every 3 weeks. and nivolumab administered at a dose of 480 mg (e.g., fixed dose) every 4 weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and atezolizumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every three weeks. and atezolizumab administered at a dose of 840 mg (e.g., fixed dose) every two weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬品の製造における抗TIGITアンタゴニスト抗体の使用を提供し、以下に更に詳細に記載されるように、方法は、医薬品及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを4週間ごとに1680mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. In addition, the method comprises administering to the subject or subject population one or more dosing cycles of a pharmaceutical agent and atezolizumab, wherein the pharmaceutical agent is administered an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every three weeks. and atezolizumab administered at a dose (e.g., fixed dose) of 1680 mg every 4 weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有する(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)がんを有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention has detectable levels of PD-L1 expression (eg, cervical cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent use of atezolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population having (PD-L1-positive cervical cancer) cancer, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers atezolizumab at a dose of 1200 mg (e.g., a fixed dose) every 3 weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), the use of atezolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers atezolizumab at a dose of 840 mg (e.g., a fixed dose) every two weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるペンブロリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、ペンブロリズマブを3週間ごとに200mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), the use of pembrolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers pembrolizumab at a dose of 200 mg (e.g., a fixed dose) every 3 weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有する(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)がんを有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、ニボルマブを2週間ごとに240mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention has detectable levels of PD-L1 expression (eg, cervical cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent and the use of nivolumab in the manufacture of a medicament for use in a method of treating a subject or subject population having (PD-L1-positive cervical cancer) cancer, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers nivolumab at a dose of 240 mg (e.g., a fixed dose) every two weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、ニボルマブを4週間ごとに480mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), the use of nivolumab in the manufacture of a medicament for use in a method of treating a subject or subject population, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers nivolumab at a dose of 480 mg (e.g., a fixed dose) every 4 weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., a fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを4週間ごとに1680mgの用量(例えば、固定用量)で投与するため、及び抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), the use of atezolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and an anti-TIGIT antagonist antibody, wherein the pharmaceutical agent administers atezolizumab at a dose (e.g., fixed dose) of 1680 mg every 4 weeks, and an anti-TIGIT antagonist antibody formulated to be administered at a dose of 600 mg (e.g., fixed dose) every three weeks, wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and SEQ ID NO: 19 A VL domain comprising the amino acid sequence of In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びアテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to the subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., a fixed dose) every 3 weeks and atezolizumab every 3 weeks is formulated for administration at a dose of 1200 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to the subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., a fixed dose) every 3 weeks and atezolizumab every 2 weeks is formulated for administration at a dose of 840 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to the subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., a fixed dose) every 3 weeks and atezolizumab every 2 weeks is formulated for administration at a dose of 840 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びペンブロリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びペンブロリズマブを3週間ごとに200mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to the subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., a fixed dose) every 3 weeks and pembrolizumab every 3 weeks is formulated for administration at a dose of 200 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びニボルマブを2週間ごとに240mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to a subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., a fixed dose) every 3 weeks and nivolumab every 2 weeks is formulated for administration at a dose of 240 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブ及びニボルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で、及びニボルマブを4週間ごとに480mgの用量(例えば、固定用量)で投与するために製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1 positive cervical cancer), as described in further detail below. , the method comprises administering to the subject or subject population one or more dosing cycles of a medicament, wherein the medicament is tiragolumab at a dose of 600 mg (e.g., fixed dose) every 3 weeks and nivolumab every 4 weeks is formulated for administration at a dose of 480 mg (eg, a fixed dose) to
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and atezolizumab, wherein the pharmaceutical agent is to administer tiragolumab at a dose of 600 mg every three weeks (e.g., a fixed dose) and atezolizumab It is formulated to be administered at a dose of 1200 mg (eg, fixed dose) every 3 weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and atezolizumab, wherein the pharmaceutical agent is to administer tiragolumab at a dose of 600 mg every three weeks (e.g., a fixed dose) and atezolizumab It is formulated to be administered at a dose of 840 mg (eg, fixed dose) every two weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical and atezolizumab, wherein the pharmaceutical is to administer tiragolumab at a dose of 600 mg every three weeks (e.g., a fixed dose) and atezolizumab It is formulated to be administered at a dose of 840 mg (eg, fixed dose) every two weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びペンブロリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びペンブロリズマブを3週間ごとに200mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical and pembrolizumab, wherein the pharmaceutical is to administer tiragolumab at a dose of 600 mg every three weeks (e.g., a fixed dose) and pembrolizumab It is formulated to be administered at a dose of 200 mg (eg, fixed dose) every 3 weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びペンブロリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びニボルマブを2週間ごとに240mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a drug and pembrolizumab, wherein the drug is tiragolumab to be administered at a dose of 600 mg every three weeks (e.g., a fixed dose) and nivolumab It is formulated to be administered at a dose of 240 mg (eg, fixed dose) every two weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びペンブロリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、チラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するため、及びニボルマブを4週間ごとに480mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a drug and pembrolizumab, wherein the drug is tiragolumab to be administered at a dose of 600 mg every three weeks (e.g., a fixed dose) and nivolumab It is formulated to be administered at a dose of 480 mg (eg, fixed dose) every 4 weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びチラゴルマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するため、及びチラゴルマブを3週間ごとに600mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), the use of atezolizumab in the manufacture of a medicament for use in a method of treating a subject or subject population, as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and tiragolumab, wherein the pharmaceutical agent is to administer atezolizumab at a dose of 1200 mg (e.g., a fixed dose) every 3 weeks; It is formulated to be administered at a dose of 600 mg (eg, fixed dose) every 3 weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びチラゴルマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するため、及びチラゴルマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and tiragolumab, wherein the pharmaceutical agent is to administer atezolizumab at a dose of 1200 mg (e.g., a fixed dose) every 3 weeks; It is formulated to be administered at a dose of 840 mg (eg, fixed dose) every two weeks.
別の態様では、本発明は、検出可能なPD-L1発現レベルを有するがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を処置する方法に使用するための医薬の製造におけるチラゴルマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬及びチラゴルマブの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、アテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するため、及びチラゴルマブを4週間ごとに1680mgの用量(例えば、固定用量)で投与するように製剤化される。 In another aspect, the present invention provides cancers with detectable levels of PD-L1 expression (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or or recurrent PD-L1-positive cervical cancer), as described in more detail below. comprises administering to a subject or subject population one or more dosing cycles of a pharmaceutical agent and tiragolumab, wherein the pharmaceutical agent is to administer atezolizumab at a dose of 1200 mg (e.g., a fixed dose) every 3 weeks; It is formulated to be administered at a dose of 1680 mg (eg, fixed dose) every 4 weeks.
本明細書に記載される使用のためのいずれか方法、使用又は組成物において、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))又はその医薬は、1つ以上の更なる抗がん治療剤(複数可)(例えば、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法/放射線治療、及び/又は抗ホルモン剤(例えば、本明細書中上記で列挙されるもの))と併せて(別々に又は一緒に)投与される。 In any method, use or composition for use described herein, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and PD-1 axis-binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))) or the medicament is one or more additional anti-cancer therapeutic agent(s) (e.g., chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapy, and/or antihormonal agents (e.g., those listed herein above))) in combination (either separately or together).
本明細書に記載される使用のためのいずれかの方法、使用又は組成物において、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))又はその医薬は、子宮頸がんを有する対象又は対象集団を処置するためのものである。いくつかの例では、子宮頸がんは、ステージIVB、転移性、再発性、又は持続性の子宮頸がんである。いくつかの例では、子宮頸がんは、転移性及び/又は再発性PD-L1陽性子宮頸がんである。がんは、初期又は後期段階であり得る。 In any method, use or composition for use described herein, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and PD- Uniaxial binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) ) or medicament thereof for treating a subject or subject population having cervical cancer. In some examples, the cervical cancer is stage IVB, metastatic, recurrent, or persistent cervical cancer. In some examples, the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer. Cancer can be in early or late stage.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、検出可能なPD-L1発現レベルは、検出可能なPD-L1タンパク質発現レベルである。いくつかの例では、検出可能なPD-L1タンパク質発現レベルを免疫組織化学(IHC)アッセイによって決定されている。いくつかの例では、PD-L1のタンパク質発現レベルは、染色に適した抗PD-L1抗体を使用して検出される。いくつかの例では、腫瘍試料は、ホルマリン固定パラフィン包埋(FFPE)腫瘍試料である。 In some examples, in any of the methods, uses or compositions for use described herein, the detectable PD-L1 expression level is a detectable PD-L1 protein expression level. In some instances, detectable PD-L1 protein expression levels have been determined by immunohistochemistry (IHC) assays. In some examples, PD-L1 protein expression levels are detected using an anti-PD-L1 antibody suitable for staining. In some examples, the tumor sample is a formalin-fixed paraffin-embedded (FFPE) tumor sample.
いくつかの例では、本明細書に記載される使用のための方法、使用又は組成物のいずれかにおいて、検出可能なPD-L1発現レベルは、検出可能なPD-L1核酸発現レベルである。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。 In some examples, in any of the methods, uses or compositions for use described herein, the detectable PD-L1 expression level is a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided.
いくつかの例では、本明細書に記載の使用のための方法、使用又は組成物のいずれかにおいて、子宮頸がんが扁平上皮癌腫、腺扁平上皮癌腫又は腺癌腫である。いくつかの例では、子宮頸がんは、ステージIVB、転移性、再発性、又は持続性である。いくつかの例では、子宮頸がんは、転移性及び/又は再発性PD-L1陽性子宮頸がんである。いくつかの例では、対象又は対象集団は、事前治療を受けたことがない。いくつかの例では、対象又は対象集団は、少なくとも1種類の事前治療を受けている。いくつかの例では、対象又は対象集団は、2種類の事前治療を受けている。いくつかの例では、対象又は対象集団は、少なくとも1つであるが2つ以下の事前全身治療を受けている、及び/又はこれらの対象に対する許容可能な標準治療が存在しない。いくつかの例では、対象又は対象集団は、3種類以上の事前治療を受けたことがない。いくつかの例では、事前治療は、化学療法、外科手術、及び/又は放射線療法である。いくつかの例では、事前治療は免疫療法である。 In some examples, in any of the methods, uses or compositions for use described herein, the cervical cancer is squamous cell carcinoma, adenosquamous carcinoma, or adenocarcinoma. In some examples, the cervical cancer is stage IVB, metastatic, recurrent, or persistent. In some examples, the cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer. In some examples, the subject or subject population has received no prior treatment. In some examples, the subject or subject population has received at least one prior treatment. In some examples, the subject or subject population has received two prior treatments. In some examples, the subject or subject population has received at least one but no more than two prior systemic treatments and/or there is no acceptable standard of care for these subjects. In some examples, the subject or subject population has never received 3 or more prior treatments. In some examples, prior treatment is chemotherapy, surgery, and/or radiation therapy. In some examples, the prior treatment is immunotherapy.
いくつかの例では、本明細書に記載される使用のためのいずれかの方法、使用又は組成物において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与は、臨床応答をもたらす。いくつかの例では、臨床応答は、基準ORRと比較した、対象又は対象集団の客観的奏効率(ORR)の増加である。いくつかの例では、基準ORRは、少なくとも約14.6%~約26%である。いくつかの例では、基準ORRは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のORR中央値である。いくつかの例では、臨床応答は、基準PFS時間と比較した場合の対象又は対象集団のPFSの増加である。いくつかの例では、基準PFSは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のPFS時間中央値である。いくつかの例では、臨床応答は、基準DOR時間と比較した対象又は対象集団の奏効期間(DOR)の増加である。いくつかの例では、基準DORは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のDOR時間中央値である。いくつかの例では、臨床応答はOSの増加である。 In some examples, in any method, use or composition for use described herein, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) results in clinical responses. In some examples, a clinical response is an increase in objective response rate (ORR) in a subject or subject population compared to a baseline ORR. In some examples, the reference ORR is at least about 14.6% to about 26%. In some examples, the reference ORR is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median ORR of the subject population. In some examples, a clinical response is an increase in PFS for a subject or subject population when compared to a baseline PFS time. In some examples, the reference PFS is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median PFS time in a subject population. In some examples, a clinical response is an increase in duration of response (DOR) for a subject or subject population compared to baseline DOR time. In some examples, the reference DOR is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median DOR time in a subject population. In some instances the clinical response is an increase in OS.
子宮頸がんに関する診断方法及び使用
本発明は、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団に対する治療を選択するための方法を提供し、治療は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。
Diagnostic methods and uses for cervical cancer A method is provided for selecting a treatment for a subject or subject population having positive cervical cancer), wherein the treatment is one or more in a sample (e.g., tumor sample or blood sample) obtained from the subject or subject population diagnostic methods comprising determining the presence and/or expression levels/amounts of biomarkers (eg, PD-L1, TIGIT, activated T cells or cytokines) of
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置から利益を得ることができるがん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法が本明細書で更に提供され、同定は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。 Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly as lambrolizumab) known pembrolizumab)))) (e.g. cervical cancer, e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or Further provided herein are methods for identifying a subject or subject population having recurrent PD-L1 positive cervical cancer), wherein the identification is a sample obtained from the subject or subject population (e.g., a tumor sample or A diagnostic method comprising determining the presence and/or expression level/amount of one or more biomarkers (eg, PD-L1, TIGIT, activated T cells or cytokines) in a blood sample).
更に、本明細書では、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団に対する治療に対する応答性を評定するための方法を提供し、更なる治療は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。 Further herein, cancer (eg, cervical cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer) in a sample (e.g., tumor sample or blood sample) obtained from the subject or subject population, wherein the additional treatment is one or more Guided by diagnostic methods including determining the presence and/or expression level/amount of biomarkers (eg PD-L1, TIGIT, activated T cells or cytokines).
更に、本明細書では、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団に対する治療を最適化するための方法を提供し、更なる治療は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。 Further herein, cancer (eg, cervical cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer) wherein the further treatment is one or more biomarkers in a sample (e.g., tumor sample or blood sample) obtained from the subject or subject population (eg PD-L1, TIGIT, activated T-cells or cytokines) is guided by diagnostic methods including determining the presence and/or expression level/amount.
本明細書に記載の方法で使用するためのバイオマーカーとしては、限定されないが、組織(例えば、腫瘍組織)又は血液(例えば、全血)でのPD-L1及び/又はTIGIT発現、WGS及び/又はNGSによって同定された、組織(例えば、腫瘍組織)からの及び/又は血液中の循環腫瘍DNA(限定されないが、突然変異負荷、MSI及びMMR欠陥を含む)からの生殖系列及び体細胞の変異、腫瘍免疫生物学(例えば、TEFF)に関連する遺伝子(例えば、CD 274)又は遺伝子シグネチャの分析、HPV変化、リンパ球亜集団、T細胞受容体レパートリー、T細胞活性化に関連するサイトカイン、並びに血漿由来サイトカインが含まれ得るが、これらに限定されない。いくつかの例では、バイオマーカーはPD-L1である。いくつかの例では、試料は腫瘍試料(例えば、ホルマリン固定パラフィン包埋(FFPE)腫瘍試料)である。 Biomarkers for use in the methods described herein include, but are not limited to, PD-L1 and/or TIGIT expression in tissue (eg, tumor tissue) or blood (eg, whole blood), WGS and/or or germline and somatic mutations from tissue (e.g., tumor tissue) and/or from circulating tumor DNA in the blood (including but not limited to mutation burden, MSI and MMR defects) identified by NGS , analysis of genes (e.g., CD274) or gene signatures associated with tumor immunobiology (e.g., TEFF), HPV alterations, lymphocyte subpopulations, T-cell receptor repertoires, cytokines associated with T-cell activation, and Plasma-derived cytokines can be included, but are not limited to. In some examples, the biomarker is PD-L1. In some examples, the sample is a tumor sample (eg, a formalin-fixed paraffin-embedded (FFPE) tumor sample).
いくつかの例では、本方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)での抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルと、3週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルとを対象又は対象集団に投与することとを含む。いくつかの例では、本方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600(例えば600mg)の用量(例えば、固定用量)での抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルと、2週間ごとに840mgの用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルとを対象又は対象集団に投与することとを含む。いくつかの例では、本方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600(例えば600mg)の用量(例えば、固定用量)での抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルと、3週間ごとに1200mgの用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルとを対象又は対象集団に投与することとを含む。いくつかの例では、本方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600(例えば600mg)の用量(例えば、固定用量)での抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルと、4週間ごとに1680mgの用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルとを対象又は対象集団に投与することとを含む。 In some examples, the methods detect the presence and/or presence of a biomarker (eg, PD-L1, TIGIT, activated T cells or cytokines) in a sample (eg, a tumor sample or blood sample) from a subject or subject population. or determining expression levels/amounts and anti-TIGIT antagonist antibodies (e.g., as described herein 1 or more dosing cycles (e.g., between 80 mg and 2000 mg) of an anti-TIGIT antagonist antibody disclosed in the literature (e.g., tiragolumab) and a dose (e.g., fixed dose ) and administering to the subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some examples, the methods detect the presence and/or presence of a biomarker (eg, PD-L1, TIGIT, activated T cells or cytokines) in a sample (eg, a tumor sample or blood sample) from a subject or subject population. or determining expression levels/amounts and anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, one or more dosing cycles of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of 840 mg every two weeks. administering one or more dosing cycles to a subject or population of subjects. In some examples, the methods detect the presence and/or presence of a biomarker (eg, PD-L1, TIGIT, activated T cells or cytokines) in a sample (eg, a tumor sample or blood sample) from a subject or subject population. or determining expression levels/amounts and anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, one or more dosing cycles of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of 1200 mg every 3 weeks. administering one or more dosing cycles to a subject or population of subjects. In some examples, the methods detect the presence and/or presence of a biomarker (eg, PD-L1, TIGIT, activated T cells or cytokines) in a sample (eg, a tumor sample or blood sample) from a subject or subject population. or determining expression levels/amounts and anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, one or more dosing cycles of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of 1680 mg every 4 weeks. administering one or more dosing cycles to a subject or population of subjects.
バイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量は、タンパク質、タンパク質フラグメント、DNA、mRNA、cDNA及び/又は遺伝子コピー数を含むがこれらに限定されない、当該技術分野で公知の任意の適切な基準に基づいて定性的及び/又は定量的に決定することができる。 The presence and/or expression level/amount of biomarkers (eg, PD-L1, TIGIT, activated T cells or cytokines) include, but are not limited to, proteins, protein fragments, DNA, mRNA, cDNA and/or gene copy number. It can be determined qualitatively and/or quantitatively based on any suitable criteria known in the art, without limitation.
いくつかの例では、バイオマーカーの発現レベル又は量は、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1タンパク質発現レベルである。いくつかの例では、PD-L1タンパク質発現レベルを免疫組織化学(IHC)アッセイによって決定した。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 protein expression level in a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects. In some instances, PD-L1 protein expression levels were determined by immunohistochemistry (IHC) assays. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)は、検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)は、腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects has been determined to have a detectable PD-L1 expression level. In some examples, a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects has been determined to have detectable levels of PD-L1 expression in tumor-infiltrating immune cells. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、バイオマーカーの発現レベル又は量は、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1核酸発現レベルである。いくつかの例では、PD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR、又はRT-qPCR、マイクロアレイ分析、遺伝子発現の連続分析(SAGE)、MassARRAY(登録商標)技術、in situハイブリダイゼーション(ISH)、又はそれらの組み合わせによって決定されている。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 nucleic acid expression level in a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects. In some examples, PD-L1 nucleic acid expression levels are measured by RNA-seq, RT-qPCR, qPCR, multiplex qPCR, or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY® technique, in situ hybridization (ISH), or a combination thereof. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量は、例えば、検出可能なPD-L1発現レベルが個体を選択するためのバイオマーカーである場合、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))による治療に適格である対象又は対象集団を選択する。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は腫瘍試料(例えば、FFPE腫瘍試料)である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, the presence and/or expression level/ The amount is, for example, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) when detectable PD-L1 expression levels are biomarkers for selecting individuals. ) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))). In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample (eg, FFPE tumor sample). In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof. In some examples, the tumor sample is an FFPE tumor sample.
一態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与されるチラゴルマブ及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In one aspect, the present invention involves obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, protein expression of PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining, anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detected levels and PD-L1 expression in the tumor sample detected. cancer (e.g., cervical cancer) by identifying a subject or subject population as likely to benefit from treatment comprising one or more dosing cycles of atezolizumab administered in a dose (e.g., fixed dose). (e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer) wherein the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Based on detecting expression levels and PD-L1 expression in tumor samples detected, tiragolumab administered at a dose of 600 mg every 3 weeks (e.g., fixed dose) and a dose of 1200 mg every 3 weeks ( cancer (e.g., cervical cancer, cervical cancer, A method for selecting a therapy for a subject or subject population, e.g., with stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer I will provide a. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与されるチラゴルマブ及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the tumor sample detected cancer (e.g., cervical Selecting a treatment for a subject or subject population with cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Based on detecting expression levels and PD-L1 expression in tumor samples detected, tiragolumab administered at a dose of 600 mg every 3 weeks (e.g., fixed dose) and a dose of 1200 mg every 3 weeks ( cancer (e.g., cervical cancer, cervical cancer, A method for selecting a therapy for a subject or subject population, e.g., with stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer I will provide a. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the tumor sample detected cancer (e.g., cervical Selecting a treatment for a subject or subject population with cancer, such as stage IVB, metastatic, recurrent or persistent cervical cancer, such as metastatic and/or recurrent PD-L1 positive cervical cancer The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the detected tumor samples. cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent) by identifying a subject or subject population as likely to benefit from treatment involving one or more dosing cycles. Methods are provided for selecting a treatment for a subject or subject population with cervical cancer, eg, metastatic and/or recurrent PD-L1 positive cervical cancer. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))))). identify a subject or subject population with (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer) The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) (e.g., cervical cancer, e.g., stage IVB, metastatic, Methods are provided for identifying a subject or subject population with recurrent or persistent cervical cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., atezolizumab) by identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, Methods are provided for identifying a subject or subject population with metastatic, recurrent or persistent cervical cancer (e.g., metastatic and/or recurrent PD-L1 positive cervical cancer), wherein the anti-TIGIT antagonist antibody is , a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18, and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) (e.g., cervical cancer, e.g., stage IVB, metastatic, Methods are provided for identifying a subject or subject population with recurrent or persistent cervical cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得ることができる、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., atezolizumab) by identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, Methods are provided for identifying a subject or subject population with metastatic, recurrent or persistent cervical cancer (e.g., metastatic and/or recurrent PD-L1 positive cervical cancer), wherein the anti-TIGIT antagonist antibody is , a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18, and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) (e.g., cervical cancer, e.g., stage IVB, metastatic, Methods are provided for identifying a subject or subject population with recurrent or persistent cervical cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., atezolizumab) by identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or A method is provided for assessing the responsiveness of a subject or subject population with persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer, wherein the anti-TIGIT antagonist antibody comprises SEQ ID NO: A VH domain comprising a 17 or 18 amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) Methods are provided for assessing responsiveness of a subject or population of subjects with cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., atezolizumab) by identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or A method is provided for assessing the responsiveness of a subject or subject population with persistent cervical cancer, e.g., metastatic and/or recurrent PD-L1 positive cervical cancer, wherein the anti-TIGIT antagonist antibody comprises SEQ ID NO: A VH domain comprising a 17 or 18 amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) Methods are provided for assessing responsiveness of a subject or population of subjects with cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定する方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団の応答性を評定する方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., atezolizumab) by identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or A method of assessing the responsiveness of a subject or subject population with persistent cervical cancer (e.g., metastatic and/or recurrent PD-L1 positive cervical cancer) is provided, wherein the anti-TIGIT antagonist antibody comprises SEQ ID NO: 17 or It includes a VH domain comprising an 18 amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))))) Methods of assessing responsiveness of a subject or population of subjects with cancer (eg, metastatic and/or recurrent PD-L1 positive cervical cancer) are provided. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. By identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody in subjects or subject populations with PD-L1-positive cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), wherein the anti-TIGIT antagonist antibody is SEQ ID NO: 17 or It includes a VH domain comprising an 18 amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD- L1-positive cervical cancer) in a subject or subject population with an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., Methods are provided for optimizing therapy involving MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. By identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody in subjects or subject populations with PD-L1-positive cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), wherein the anti-TIGIT antagonist antibody is SEQ ID NO: 17 or It includes a VH domain comprising an 18 amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD- L1-positive cervical cancer) in a subject or subject population with an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., Methods are provided for optimizing therapy involving MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化する方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、がん(例えば、子宮頸がん、例えばステージIVB、転移性、再発性又は持続性子宮頸がん、例えば転移性及び/又は再発性PD-L1陽性子宮頸がん)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and benefiting from a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. By identifying a subject or subject population as likely to obtain cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody in subjects or subject populations with PD-L1-positive cervical cancer) (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))), wherein the anti-TIGIT antagonist antibody is SEQ ID NO: 17 or 18 A VH domain comprising the amino acid sequence and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. cancer (e.g., cervical cancer, e.g., stage IVB, metastatic, recurrent or persistent cervical cancer, e.g., metastatic and/or recurrent PD- L1-positive cervical cancer) in a subject or subject population with an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., Methods are provided for optimizing therapy involving MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab))). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本明細書に記載される診断方法又は使用のいずれかにおいて、子宮頸がんは、ステージIVBの転移性、再発性又は持続性の子宮頸がんである。がんは、初期又は後期段階であり得る。 In some examples, in any of the diagnostic methods or uses described herein, the cervical cancer is stage IVB metastatic, recurrent or persistent cervical cancer. Cancer can be in early or late stage.
D.乳がんに関する治療方法及び使用
乳がん
乳がんは、女性において診断される最も頻度の高いがんであり、2018年に報告された推定世界的発生率は新規症例が208万である。乳がんは、全がん死の約15%(約626,700症例)を占め、女性におけるがん関連死亡の最も一般的な原因であり、転移診断後の5年生存率は約15%である。患者の大部分は限局性乳がんと診断される。しかしながら、約6%の患者がデノボ転移性疾患を示し、10%と40%の間の限局性乳がん患者が全身に再発する。乳がんの初期段階(I~III;早期乳がん)では、ほとんど無症候性の疾患は通常、手術可能であり、治癒目的で処置することができる。
D. Treatment Methods and Uses Related to Breast Cancer Breast Cancer Breast cancer is the most frequently diagnosed cancer in women, with an estimated global incidence of 2.08 million new cases reported in 2018. Breast cancer accounts for approximately 15% of all cancer deaths (approximately 626,700 cases) and is the most common cause of cancer-related death in women, with a 5-year survival rate of approximately 15% after diagnosis of metastasis. . The majority of patients are diagnosed with localized breast cancer. However, approximately 6% of patients exhibit de novo metastatic disease and between 10% and 40% of patients with localized breast cancer have systemic recurrence. In the early stages of breast cancer (I-III; early breast cancer), mostly asymptomatic disease is usually operable and can be treated with curative intent.
乳がんは、約15の異なるタイプの癌腫を包含する不均一な疾患であり、治療上の理由から、それらのエストロゲン受容体(ER)、プロゲステロン受容体(PR)及びヒト上皮成長因子受容体2(HER 2)の状態に従って更に分類される。これらのサブグループは、治療、処置転帰、再発率、及び死亡リスクの選択に重要な意味を有する。トリプルネガティブ乳がん(TNBC)は、ER、PR及びHER 2の発現の欠如を特徴とする。全体として、全乳がんの約15%~20%がTNBCとして分類される。大規模な包括的ゲノム解析は、TNBCの不均一性ならびにそれらの多様な遺伝子発現パターン及び基礎となるゲノム変化を特徴付けてきたが、これらの洞察は、現在実験室及び臨床研究中の臨床的に有効な標的療法の同定のための明確な指針をまだ提供していない。 Breast cancer is a heterogeneous disease encompassing about 15 different types of carcinoma, and for therapeutic reasons, their estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 ( It is further classified according to the status of HER 2). These subgroups have important implications for selection of therapy, treatment outcome, recurrence rate, and mortality risk. Triple-negative breast cancer (TNBC) is characterized by lack of expression of ER, PR and HER2. Overall, approximately 15% to 20% of all breast cancers are classified as TNBC. Although large-scale comprehensive genomic analyzes have characterized the heterogeneity of TNBC and their diverse gene expression patterns and underlying genomic alterations, these insights are currently being used in clinical studies in laboratory and clinical studies. does not yet provide clear guidance for the identification of effective targeted therapies for
TNBCは、高い増殖率等の攻撃的特徴を有する可能性がより高い。転移性TNBCを有する患者は、特に不良な臨床転帰を示し、一般に急速な進行及びOS率の中央値は約16ヶ月である。最近の処置の改善にもかかわらず、TNBC患者の予後は依然として最適ではなく、実際には転移診断後の5年生存率は約15%である。 TNBC are more likely to have aggressive characteristics such as high proliferation rates. Patients with metastatic TNBC have a particularly poor clinical outcome, generally with rapid progression and a median OS rate of about 16 months. Despite recent treatment improvements, the prognosis for TNBC patients remains suboptimal, with a 5-year survival rate of approximately 15% indeed after diagnosis of metastasis.
したがって、早期TNBC(eTNBC)を含む、TNBCの改善された医学的介入に対する満たされていないニーズが高い。 Therefore, there is a high unmet need for improved medical interventions for TNBC, including early TNBC (eTNBC).
肺がんを処置するための方法及び使用
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及び化学療法(例えば、タキサン(例えば、nab-パクリタキセル又はパクリタキセル))を受けている対象又は対象集団は、乳がん(例えば、HER2+乳がん及びTNBC)について処置されている。いくつかの例では、抗TIGITアンタゴニスト抗体はチラゴルマブである。いくつかの例では、PD-1軸結合アンタゴニストは抗PD-L1アンタゴニスト抗体である。いくつかの例では、抗PD-L1アンタゴニスト抗体はアテゾリズマブである。いくつかの例では、化学療法はタキサンである。いくつかの例では、タキサンは、nab-パクリタキセル又はパクリタキセルである。いくつかの例では、タキサンはnab-パクリタキセルである。いくつかの例では、乳がんはTNBCである。いくつかの例では、TNBCはPD-L1陽性TNBCである。いくつかの例では、TNBCは切除不能な局所進行性又は転移性である。いくつかの例では、PD-L1陽性TNBCは、切除不能な局所進行性又は転移性である。いくつかの例では、対象又は対象集団は、乳がんの事前全身治療を受けたことがない。いくつかの例では、対象又は対象集団は、転移性乳がんの事前全身治療を受けたことがない。
Methods and Uses for Treating Lung Cancer Subjects or populations of subjects receiving chemotherapy (e.g., taxanes (e.g., nab-paclitaxel or paclitaxel)) and anti-PD-L1 antagonist antibodies such as atezolizumab are being treated for breast cancer (e.g., HER2+ breast cancer and TNBC). there is In some examples, the anti-TIGIT antagonist antibody is tiragolumab. In some examples, the PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody. In some examples, the anti-PD-L1 antagonist antibody is atezolizumab. In some examples, the chemotherapy is a taxane. In some examples, the taxane is nab-paclitaxel or paclitaxel. In some examples, the taxane is nab-paclitaxel. In some examples, the breast cancer is TNBC. In some examples, the TNBC is PD-L1 positive TNBC. In some instances, TNBC is unresectable, locally advanced or metastatic. In some instances, the PD-L1 positive TNBC is unresectable, locally advanced or metastatic. In some examples, the subject or subject population has never received prior systemic treatment for breast cancer. In some examples, the subject or subject population has no prior systemic treatment for metastatic breast cancer.
eTNBCを処置するための方法及び使用
対象又は対象集団における早期TNBC(eTNBC)を処置するための方法及び使用であって、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与し、それにより、対象又は対象集団を処置することを含む方法及び使用が本明細書で提供される。
Methods and Uses for Treating eTNBC United States Patent Application 20070010003 Kind Code: A1 Methods and uses for treating early stage TNBC (eTNBC) in a subject or subject population, comprising an effective amount of an anti-TIGIT antagonist antibody (e.g., as disclosed herein) an anti-TIGIT antagonist antibody (e.g., tiragolumab) and an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab) or administering to a subject or population of subjects, thereby treating the subject or population of subjects, a dosing regimen comprising one or more dosing cycles of MK-3475 (pembrolizumab, formerly known as rambrolizumab))) and uses are provided herein.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を、それを必要とする対象又は対象集団に投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))を用いて、又は用いずに、それを必要とする対象又は対象集団に投与する。いくつかの例では、方法は、1回以上の手術(例えば、乳房切除術及び/又は腋窩リンパ節手術)を更に含む。いくつかの例では、手術は、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、1つ以上の化学療法剤、及び/又はG-CSFもしくはGM-CSFを含む投薬レジメンを投与した後に行われる。いくつかの例では、手術は、乳房切除術及び/又は腋窩リンパ節手術である。いくつかの例では、手術は、投薬レジメンの最後の投与後2週間と6週間の間(例えば、2週間、3週間、4週間、5週間及び6週間)に行われる。 The present invention provides an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, anti-PD-L1, such as atezolizumab). antagonist antibody) to a subject or population in need thereof. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab) ) with one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclophosphamide), taxanes (eg, paclitaxel, eg nab-paclitaxel) and/or topoisomerase II inhibitors (eg, doxorubicin))) with or without a subject or population in need thereof. In some examples, the method further comprises one or more surgeries (eg, mastectomy and/or axillary lymph node surgery). In some examples, surgery is performed after administering a dosing regimen comprising an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, one or more chemotherapeutic agents, and/or G-CSF or GM-CSF. In some examples, the surgery is mastectomy and/or axillary lymph node surgery. In some examples, surgery is performed between 2 weeks and 6 weeks (eg, 2 weeks, 3 weeks, 4 weeks, 5 weeks and 6 weeks) after the last administration of the dosing regimen.
いくつかの例では、対象又は対象集団においてeTNBCを処置するための方法及び使用のいずれかが、pCRをもたらし得る。いくつかの例では、対象又は対象集団においてeTNBCを処置するための方法及び使用のいずれも、OS又は無症候生存期間(EFS)の増加をもたらし得る。 In some instances, any of the methods and uses for treating eTNBC in a subject or subject population can result in pCR. In some examples, any of the methods and uses for treating eTNBC in a subject or subject population can result in increased OS or disease-free survival (EFS).
投薬レジメン及び投与
本明細書に記載される本発明の治療方法及び使用は、一態様では、eTNBCを有する対象又は対象集団に、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを投与することを含む。いくつかの例では、本明細書に記載される本発明の治療方法及び使用は、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))及び/又はG-CSFもしくはGM-CSFを用いて、又は用いずに、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを、eTNBCを有する対象又は対象集団に投与することを含む。いくつかの態様では、トポイソメラーゼII阻害剤はドキソルビシンである。いくつかの態様では、ドキソルビシンは約60mg/m2の用量で投与される。
Dosing Regimens and Administration The therapeutic methods and uses of the invention described herein, in one aspect, involve administering to a subject or subject population with eTNBC an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist). antibodies (eg, atezolizumab) or anti-PD-1 antagonist antibodies (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and anti-TIGIT antagonist antibodies (eg, tiragolumab) administering a treatment regimen comprising In some examples, the treatment methods and uses of the invention described herein include one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin))) and/or G-CSF or GM - an effective amount of a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX-1106 (nivolumab)), with or without CSF or administering a treatment regimen comprising MK-3475 (pembrolizumab, formerly known as rambrolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab) to a subject or population of subjects with eTNBC. In some aspects, the topoisomerase II inhibitor is doxorubicin. In some aspects, doxorubicin is administered at a dose of about 60 mg/m 2 .
本明細書に記載の医薬組成物は、セクションIII(K)に記載の投与のために製剤化することができる。 The pharmaceutical compositions described herein can be formulated for administration as described in Section III(K).
化学療法剤の投薬
様々な化学療法剤の治療有効量は当該技術分野で公知であり、本発明で企図される。特定の場合において、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))が、本明細書中のセクションIII(K)に列挙される用量に従って投与される。
Dosing of Chemotherapeutic Agents Therapeutically effective amounts of various chemotherapeutic agents are known in the art and contemplated by the present invention. In certain cases, one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclo phosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin))) are administered according to the doses listed in Section III(K) herein. .
がんの特性評価及び選択
本明細書に記載の使用のための方法、使用又は組成物のいずれにおいても、がんは乳がんであり得る。いくつかの例では、乳がんはTNBCである。いくつかの例では、TNBCはeTNBCである。いくつかの例では、eTNBCは、提示時にT2-4d TNBCである。いくつかの例では、eTNBCは、提示時にcT2-cT4、cN0-cN3、及びcM0 TNBCである。いくつかの例では、eTNBCはPD-L1陽性である。いくつかの例では、eTNBCはPD-L1陰性である。いくつかの例では、対象又は対象集団は、eTNBCについて以前に処置されたことがない。いくつかの例では、対象又は対象集団は、以前に乳がんの全身処置を受けたことがない(例えば、TNBC、例えば、eTNBC)。
Characterization and Selection of Cancer In any of the methods, uses or compositions for use described herein, the cancer can be breast cancer. In some examples, the breast cancer is TNBC. In some examples, the TNBC is eTNBC. In some examples, the eTNBC is a T2-4d TNBC at presentation. In some examples, the eTNBC are cT2-cT4, cN0-cN3, and cM0 TNBC at presentation. In some instances, eTNBC are PD-L1 positive. In some instances, eTNBC are PD-L1 negative. In some examples, the subject or subject population has not been previously treated for eTNBC. In some examples, the subject or subject population has no prior systemic treatment for breast cancer (eg, TNBC, eg, eTNBC).
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象又は対象集団はPD-L1選択腫瘍(例えば、PD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合は、SP 142抗体を用いたIHCによって決定される場合、腫瘍試料において1%以上である)を有する。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって、PD-L1発現(IC)が占める腫瘍面積の割合が1%以上であると判定された腫瘍である。いくつかの例では、IHCアッセイは、抗PD-L1抗体SP142、SP263、22C3又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上であると判定されている。いくつかの例では、PD-L1発現レベルは、抗PD-L1抗体22C3を使用して検出される。いくつかの例では、検出可能なPD-L1発現レベルは、対象からの試料で1以上の複合陽性スコア(CPS)である。 In some examples, in any of the methods, uses or compositions for use described herein, the subject or subject population is PD-L1-selected tumors (e.g., PD-L1-expressing tumor-infiltrating immune cells ( IC) is greater than or equal to 1% in tumor samples as determined by IHC using the SP 142 antibody). In some examples, a PD-L1-selected tumor is one that has 1% or more of the tumor area occupied by PD-L1 expression (IC) as determined by immunohistochemistry (IHC) assay. In some examples, the IHC assay uses anti-PD-L1 antibodies SP142, SP263, 22C3 or 28-8. In some examples, the IHC assay uses the anti-PD-L1 antibody SP142. In some instances, the IC has been determined to be 1% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, PD-L1 expression levels are detected using anti-PD-L1 antibody 22C3. In some examples, the detectable PD-L1 expression level is a composite positive score (CPS) of 1 or more in a sample from the subject.
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
いくつかの例では、対象又は対象集団からの腫瘍試料は、PD-L1陽性であると判定されている。いくつかの例では、対象又は対象集団からの腫瘍試料は、PD-L1陰性であると判定されている。いくつかの例では、対象又は対象集団からのほとんどの腫瘍試料は、PD-L1陰性であると判定されている。いくつかの例では、対象又は対象集団からの全ての腫瘍試料がPD-L1陰性であると判定されている。 In some examples, the tumor sample from the subject or population of subjects has been determined to be PD-L1 positive. In some examples, the tumor sample from the subject or population of subjects has been determined to be PD-L1 negative. In some instances, most tumor samples from a subject or subject population have been determined to be PD-L1 negative. In some examples, all tumor samples from a subject or subject population have been determined to be PD-L1 negative.
処置に対する応答
本明細書に記載される方法のいずれかのいくつかの実施形態では、治療に対する対象又は対象集団の応答は、1つ以上の尺度によって特徴付けることができる。いくつかの実施形態では、処置はCR又はPRをもたらす。
Response to Treatment In some embodiments of any of the methods described herein, the response of a subject or subject population to treatment can be characterized by one or more measures. In some embodiments, treatment results in CR or PR.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団の無症候生存期間の増加をもたらす。例えば、化学療法剤が投与されない(例えば、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)と組み合わせた抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)のみを投与する)実施形態では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団の無症候生存期間の増加をもたらし得る。抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)が1つ又はそれを超える化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))及び/又はG-CSFもしくはGM-CSFと組み合わせて投与される実施形態では、処置は、例えば、(i)抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストならびに1つ以上の化学療法剤及び/又はG-CSFもしくはGM-CSFによる処置と比較して;(ii)PD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体及び1つもしくはそれを超える化学療法剤及び/又はG-CSFもしくはGM-CSFによる処置と比較して;並びに/又は(iii)1つ以上の化学療法剤及び/又はG-CSFもしくはGM-CSFを用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体での処置と比較して、対象又は対象集団の無症候生存期間の増加をもたらし得る。 In some examples, the treatment is compared to treatment with a PD-1 axis binding antagonist, e.g., without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. resulting in increased symptom-free survival in a subject or population of subjects. For example, in embodiments in which no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tiragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), treatment may include, for example, anti-TIGIT Disease-free survival of a subject or population of subjects compared to treatment with a PD-1 axis binding antagonist without an antagonist antibody or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist can result in an increase in An anti-TIGIT antagonist antibody (e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., atezolizumab) with one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one one or more non-platinum chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin))) and/ or in embodiments administered in combination with G-CSF or GM-CSF, the treatment may comprise, for example, (i) a PD-1 axis binding antagonist and one or more chemotherapeutic agents without an anti-TIGIT antagonist antibody and/or or compared to treatment with G-CSF or GM-CSF; (ii) an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents and/or G-CSF or GM without a PD-1 axis binding antagonist. - compared to treatment with CSF; and/or (iii) treatment with PD-1 axis binding antagonists and anti-TIGIT antagonist antibodies without one or more chemotherapeutic agents and/or G-CSF or GM-CSF. may result in increased symptom-free survival of a subject or population of subjects compared to
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOSを延長する。例えば、化学療法剤が投与されない(例えば、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)と組み合わせた抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)のみを投与する)実施形態では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOSの増加をもたらし得る。抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)が1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))及び/又はG-CSFもしくはGM-CSFと組み合わせて投与される実施形態では、処置は、例えば、(i)抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト及び1つ以上の化学療法剤及び/又はG-CSFもしくはGM-CSFによる治療と比較して;(ii)PD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体及び1つ以上の化学療法剤及び/又はG-CSFもしくはGM-CSFによる処置と比較して;並びに/又は(iii)1つ以上の化学療法剤及び/又はG-CSFもしくはGM-CSFを用いない、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体での処置と比較して、対象又は対象集団のOSの増加をもたらし得る。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Comparatively prolongs the OS of a subject or subject population. For example, in embodiments in which no chemotherapeutic agent is administered (eg, only an anti-TIGIT antagonist antibody (eg, tiragolumab) in combination with a PD-1 axis binding antagonist (eg, atezolizumab) is administered), treatment may include, for example, anti-TIGIT an increase in OS of a subject or population of subjects compared to treatment with a PD-1 axis binding antagonist without an antagonist antibody or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist can bring an anti-TIGIT antagonist antibody (e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., atezolizumab) with one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin))) and/or G - In embodiments administered in combination with CSF or GM-CSF, the treatment is, for example, (i) a PD-1 axis binding antagonist and one or more chemotherapeutic agents without an anti-TIGIT antagonist antibody and/or G - compared to treatment with CSF or GM-CSF; (ii) treatment with an anti-TIGIT antagonist antibody and one or more chemotherapeutic agents and/or G-CSF or GM-CSF without a PD-1 axis binding antagonist. and/or (iii) treatment with a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody without one or more chemotherapeutic agents and/or G-CSF or GM-CSF , may result in an increase in OS in a subject or population of subjects.
Eisenhauer et al.,Eur.J.Cancer.2009,45:228-47に記載されているように、RECIST v 1.1基準に従って対象又は対象集団の無症候生存期間を測定することができる。いくつかの実施形態では、EFSは、処置の開始から、RECIST第1.1版の基準によって決定される疾患進行の初回発生までの期間として測定される。いくつかの実施形態では、EFSは、処置の開始から死亡時までの期間として測定される。 Eisenhauer et al. , Eur. J. Cancer. 2009, 45:228-47, disease-free survival of a subject or subject population can be measured according to RECIST v 1.1 criteria. In some embodiments, EFS is measured as the time from initiation of treatment to the first occurrence of disease progression as determined by the criteria of RECIST version 1.1. In some embodiments, EFS is measured as the time from initiation of treatment to death.
いくつかの実施形態では、処置は、対象又は対象集団のEFSを少なくとも2.4ヵ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヶ月、5.0~48ヶ月、6.0~36ヶ月、8.0~24ヶ月、又は10~12ヶ月、例えば少なくとも約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のEFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のEFSを少なくとも約2ヵ月(例えば2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, treatment reduces the subject's or subject population's EFS by at least 2.4 months (eg, 2.4-120 months, 2.5-100 months, 3.0-80 months, 4.0- 60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the subject's or subject population's EFS by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9 months). ~36 months, or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months; 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the subject's or subject population's EFS by at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-48 months, 36 months, or 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months,2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months).
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約2ヵ月(例えば2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約3.3ヶ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約5.3ヶ月(例えば5.3~120、6~60ヵ月、7~48ヵ月、8~36 ヵ月、又は10~24ヵ月、例えば、少なくとも約5.3ヵ月、5.5ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、少なくとも約20ヶ月(例えば、約20ヶ月と約36ヶ月の間(例えば、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月))の対象集団のOS中央値をもたらす。いくつかの実施形態では、処置は、約25.0ヶ月の対象集団のOS中央値をもたらす。 In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, treatment reduces the OS of a subject or subject population by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months). months, 8-36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the OS of the subject or subject population by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months). , 8 to 36 months, or 10 to 24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the OS of the subject or subject population by at least about 5.3 months (eg, 5.3-120, 6-60 months, 7-48 months, 8-36 months, or 10-24 months). , e.g., at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months , 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment is for at least about 20 months (e.g., between about 20 months and about 36 months (e.g., 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months)) median OS for the subject population. In some embodiments, treatment results in a median OS for the subject population of about 25.0 months.
いくつかの実施形態では、処置は、少なくとも約53%(例えば、約53%~約100%(例えば、約53%、54%、55%、56%、57%、58%、59%、60%、61%、62%、63%、64%、65%、66%、67%、68%、69%、70%、75%、80%、85%、90%、95%、又は100%))の対象集団のORRをもたらす。いくつかの実施形態では、処置は、少なくとも約53%(例えば、約65%~約100%(例えば、65%、65.5%、66%、66.5%、67%、67.5%、68%、68.5%、69%、69.5%、70%、71%、72%、73%、74%、75%、76%、77%、78%、79%、80%、85%、90%、95%、又は100%))の対象集団のORRをもたらす。いくつかの実施形態では、処置は、少なくとも約53%~少なくとも約67.5%(例えば、少なくとも約54%、55%、56%、57%、58%、59%、60%、61%、62%、63%、64%、65%、66%、67%、又は67.5%)の対象集団のORRをもたらす。 In some embodiments, treatment is at least about 53% (eg, about 53% to about 100% (eg, about 53%, 54%, 55%, 56%, 57%, 58%, 59%, 60%). %, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 75%, 80%, 85%, 90%, 95%, or 100% )) of the target population. In some embodiments, treatment is at least about 53% (eg, about 65% to about 100% (eg, 65%, 65.5%, 66%, 66.5%, 67%, 67.5%) , 68%, 68.5%, 69%, 69.5%, 70%, 71%, 72%, 73%, 74%, 75%, 76%, 77%, 78%, 79%, 80%, 85%, 90%, 95%, or 100%)) of the target population ORR. In some embodiments, treatment is at least about 53% to at least about 67.5% (eg, at least about 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, or 67.5%) of the subject population ORR.
E.頭頸部がんに関する治療方法及び診断方法ならびに使用
頭頸部がん
頭頸部がんは、有意な罹患率及び死亡率の原因であり、2018年には世界中で890,000例の新規症例及び450,000例の死亡を占めている。頭頸部がんは、上部気道消化管の粘膜表面で始まり、口腔、中咽頭、喉頭、下咽頭、及び鼻咽頭に影響を及ぼすがんを含む不均一な群である。優性組織型は扁平上皮癌腫(SCC)であり、身体の頭頸部領域における全ての悪性疾患の90%超を占める。
E. Therapeutic and Diagnostic Methods and Uses for Head and Neck Cancer Head and Neck Cancer Head and neck cancer is a cause of significant morbidity and mortality, with 890,000 new cases and 450 new cases worldwide in 2018. ,000 deaths. Head and neck cancers are a heterogeneous group that includes cancers that begin on the mucosal surfaces of the upper aerodigestive tract and affect the oral cavity, oropharynx, larynx, hypopharynx, and nasopharynx. The predominant histology is squamous cell carcinoma (SCC), which accounts for over 90% of all malignancies in the head and neck regions of the body.
早期又は局所進行性の頭頸部扁平上皮癌腫(SCCHN)の診断及び処置の進歩にもかかわらず、これらの患者の65%超が再発性又は転移性疾患を発症するであろう。更に、SCCHN患者の約10%は、初期診断時に転移性SCCHNを呈する。局所再発性疾患を有する患者の場合、サルベージ手術は、切除可能な局所領域再発を有する選択された患者に対してのみ治癒的であり、再照射は、以前の放射線治療歴ならびに関連する毒性及び罹患率によって制限されることが多い。結果として、再発性又は転移性SCCHNを有する患者にとって、全身療法は標準治療(SOC)療法であり、緩和の中心である。これらの患者については、予後は不良であり、患者及び疾患関連因子に応じて、ほとんどの臨床試験で生存期間中央値は6~15ヶ月である。 Despite advances in the diagnosis and treatment of early-stage or locally advanced squamous cell carcinoma of the head and neck (SCCHN), more than 65% of these patients will develop recurrent or metastatic disease. Furthermore, approximately 10% of SCCHN patients present with metastatic SCCHN at initial diagnosis. For patients with locally recurrent disease, salvage surgery is curative only for selected patients with resectable locoregional recurrence, and reirradiation is limited to prior radiotherapy history and associated toxicities and morbidity. often limited by rates. As a result, systemic therapy is the standard of care (SOC) therapy and the mainstay of palliative care for patients with recurrent or metastatic SCCHN. For these patients, the prognosis is poor, with median survival of 6-15 months in most clinical trials, depending on patient and disease-related factors.
したがって、頭頸部がん、特にSCCHNの改善された医学的介入に対する満たされていないニーズが高い。 Therefore, there is a high unmet need for improved medical interventions for head and neck cancer, particularly SCCHN.
頭頸部がんを処置するための方法及び使用
有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX 1106(ニボルマブ)、MK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)、MEDI-0680(AMP-514)、PDR 001(スパルタリズマブ)、REGN 2810(セミプリマブ)、BGB-108、プロロリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、又はトリパリマブ))及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルを含む投薬レジメンを対象又は対象集団に投与し、それにより対象又は対象集団を処置することを含む、対象又は対象集団においてSCCHN(例えば、再発性及び/又は転移性SCCHN(例えば、PD-L1陽性及び/又はHPV陽性の再発性及び/又は転移性SCCHN))を処置するための方法及び使用が本明細書で提供される。検出可能なPD-L1発現レベルを有するSCCHNを有する対象を処置するための方法であって、約30mg~約1200mgの用量で3週間ごとに抗TIGITアンタゴニスト抗体及び約80mg~約1600mgの用量で3週間ごとにPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象に投与することを含む方法も本明細書で提供される。また、検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを対象に投与することを含む方法が本明細書で提供される。
Methods and Uses for Treating Head and Neck Cancer An effective amount of a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX 1106 (nivolumab)) , MK-3475 (pembrolizumab, formerly known as rambrolizumab), MEDI-0680 (AMP-514), PDR 001 (spartalizumab), REGN 2810 (semiplimab), BGB-108, prololimab, canrelizumab, cintilimab, tislelizumab or tripalimab)) and an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered to the subject or population of subjects. SCCHN (e.g., recurrent and/or metastatic SCCHN (e.g., PD-L1 positive and/or HPV positive recurrent and/or metastatic Provided herein are methods and uses for treating sexual SCCHN)). A method for treating a subject having SCCHN with detectable PD-L1 expression levels comprising an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a dose of about 80 mg to about 1600 mg every 3 weeks. Also provided herein are methods comprising administering to the subject one or more dosing cycles of a PD-1 axis binding antagonist on a weekly basis. Also, a method for treating a subject having SCCHN with detectable PD-L1 expression levels comprising tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. Provided herein are methods that include administering one or more dosing cycles to a subject.
本発明は、有効量のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に投与することを含む方法及び使用を含む。いくつかの例では、本発明は、有効量のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に投与することを含む方法及び使用を含む。 The present invention provides effective amounts of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab) and an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject or population in need thereof. In some examples, the present invention provides effective amounts of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody such as atezolizumab) and an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antibody as disclosed herein). Methods and uses comprising administering a TIGIT antagonist antibody (eg, tiragolumab) to a subject or subject population in need thereof.
いくつかの例では、対象又は対象集団におけるSCCHNを処置するための方法及び使用のいずれかが、CR又はPRをもたらすことができる。いくつかの例では、対象又は対象集団においてSCCHNを処置するための方法及び使用のいずれもが、対象又は対象集団の客観的奏効率(ORR)の増加をもたらし得る。いくつかの例では、対象又は対象集団においてSCCHNを処置するための方法及び使用のいずれも、対象又は対象集団のPFS、奏効期間(DOR)及び/又はOSの増加をもたらし得る。 In some instances, any of the methods and uses for treating SCCHN in a subject or subject population can result in CR or PR. In some examples, any of the methods and uses for treating SCCHN in a subject or subject population can result in an increased objective response rate (ORR) of the subject or subject population. In some examples, any of the methods and uses for treating SCCHN in a subject or subject population can result in increased PFS, duration of response (DOR) and/or OS of the subject or subject population.
いくつかの例では、SCCHNは、検出可能なPD-L1発現レベルを有するSCCHNである。いくつかの例では、対象又は対象集団から得られた腫瘍試料は、検出可能なPD-L1発現レベル(例えば、PD-L1の検出可能なタンパク質及び/又は核酸発現レベル(例えば、5%以上の腫瘍関連免疫細胞(TIC)))を有すると判定されている。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、腫瘍試料中の5%以上(例えば、PD-L1陽性)、5%以上20%未満(例えば、PD-L1低)、又は20%以上(例えば、PD-L1高)のTICである。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、腫瘍試料中の10%以上、10%以上及び50%未満、又は50%以上のTICである。 In some examples, the SCCHN is SCCHN with detectable PD-L1 expression levels. In some examples, a tumor sample obtained from a subject or population of subjects has a detectable PD-L1 expression level (e.g., a detectable protein and/or nucleic acid expression level of PD-L1 (e.g., 5% or more have been determined to have tumor-associated immune cells (TIC)). In some examples, the detectable PD-L1 protein expression level is 5% or more (eg, PD-L1 positive), 5% or more and less than 20% (eg, PD-L1 low), or 20% or more in tumor samples. % TIC (eg, PD-L1 high). In some examples, the detectable PD-L1 protein expression level is 10% or more, 10% or more and 50% or less, or 50% or more TIC in the tumor sample.
いくつかの例では、処置は第一選択治療である。いくつかの例では、対象又は対象集団は、事前治療を受けたことがない。いくつかの例では、対象又は対象集団は、再発性及び/又は転移性疾患のための事前全身治療を受けたことがない。 In some instances, the treatment is first line therapy. In some examples, the subject or subject population has received no prior treatment. In some examples, the subject or subject population has not received prior systemic therapy for recurrent and/or metastatic disease.
投薬レジメン及び投与
本明細書に記載される本発明の治療方法及び使用は、一態様では、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の1回以上の投薬サイクル及び有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルを含む投薬レジメンを、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団に投与することを含む。
Dosing Regimens and Administration The therapeutic methods and uses of the invention described herein, in one aspect, comprise an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD -1 antagonist antibody (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)) and an effective amount of an anti-TIGIT antagonist antibody (e.g., herein administering to a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody, e.g., tiragolumab, as disclosed in including doing
本明細書に記載の医薬組成物は、セクションIII(K)に記載の投与のために製剤化することができる。 The pharmaceutical compositions described herein can be formulated for administration as described in Section III(K).
頭頸部がんの診断方法及び使用
本発明は、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の治療(例えば、第一選択療法)を選択するための方法を提供し、治療は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。
Head and Neck Cancer Diagnostic Methods and Uses The present invention provides methods for selecting treatment (e.g., first-line therapy) for subjects or subject populations with SCCHN (e.g., recurrent and/or metastatic SCCHN). and the treatment is determined by one or more biomarkers (e.g., PD-L1 (e.g., PD-L1 protein and/or nucleic acid expression) in a sample (e.g., tumor sample or blood sample) obtained from the subject or subject population. determined) or HPV status (eg, determined by p16 IHC, ISH or PCR)).
更に、本明細書では、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX 1106(ニボルマブ)、MK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)、MEDI-0680(AMP-514)、PDR 001(スパルタリズマブ)、REGN2810(セミプリマブ)、BGB-108、プロロリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、又はトリパリマブ))を含む処置から利益を得ることができるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法が提供され、同定は、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる。
Further herein, anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX 1106 (nivolumab), MK- 3475 (pembrolizumab, formerly known as lambrolizumab), MEDI-0680 (AMP-514), PDR 001 (spartalizumab), REGN2810 (semiplimab), BGB-108, prololimab, canrelizumab, cintilimab, tislelizumab, or tripalizumab) ) is provided for identifying a subject or subject population having SCCHN (e.g., recurrent and/or metastatic SCCHN) that can benefit from treatment, wherein the identification is obtained from the subject or subject population one or more biomarkers (eg, PD-L1 (eg, as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (eg,
SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団について治療に対する応答性を評定するための方法であって、更なる治療が、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる方法が本明細書で更に提供される。
A method for assessing responsiveness to treatment for a subject or subject population having SCCHN (e.g., recurrent and/or metastatic SCCHN), wherein additional treatment is administered to a sample obtained from the subject or subject population (e.g., , tumor sample or blood sample) or one or more biomarkers (e.g., PD-L1 (e.g., as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (e.g.,
SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団について治療を最適化するための方法であって、更なる治療が、対象又は対象集団から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することを含む診断方法によって導かれる方法が本明細書で更に提供される。
A method for optimizing treatment for a subject or subject population having SCCHN (e.g., recurrent and/or metastatic SCCHN), wherein the further treatment comprises a sample obtained from the subject or subject population (e.g., a tumor one or more biomarkers (e.g., PD-L1 (e.g., as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (e.g.,
本明細書に記載の方法で使用するためのバイオマーカーとしては、限定されないが、組織(例えば、腫瘍組織)又は血液(例えば、全血)でのPD-L1発現、WGS及び/又はNGSによって同定された、組織(例えば、腫瘍組織)からの及び/又は血液中の循環腫瘍DNA(限定されないが、突然変異負荷、MSI及びMMR欠陥を含む)からの生殖系列及び体細胞の変異、腫瘍免疫生物学に関連する遺伝子又は遺伝子シグネチャの分析、HPV変化、リンパ球亜集団、T細胞受容体レパートリー、T細胞活性化に関連するサイトカイン、並びに血漿由来サイトカインが含まれ得るが、これらに限定されない。いくつかの例では、バイオマーカーはPD-L1である。いくつかの例では、対象又は対象集団から得られた腫瘍試料は、検出可能なPD-L1発現レベル(例えば、PD-L1の検出可能なタンパク質及び/又は核酸発現レベル(例えば、5%以上の腫瘍関連免疫細胞(TIC)))を有すると判定されている。いくつかの例では、検出可能なPD-L1タンパク質発現レベル、腫瘍試料中の5%以上(例えば、PD-L1陽性)、5%以上20%未満(例えば、PD-L1低)、又は20%以上(例えば、PD-L1高)の腫瘍関連免疫細胞(TIC)である。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、腫瘍試料中の10%以上、10%以上及び50%未満、又は50%以上のTICである。いくつかの例では、試料は腫瘍試料(例えば、ホルマリン固定パラフィン包埋(FFPE)腫瘍試料)である。いくつかの例では、腫瘍試料は腫瘍組織試料である。 Biomarkers for use in the methods described herein include, but are not limited to, PD-L1 expression in tissue (eg, tumor tissue) or blood (eg, whole blood), identified by WGS and/or NGS germline and somatic mutations from tissues (e.g., tumor tissue) and/or from circulating tumor DNA in the blood (including but not limited to mutation burden, MSI and MMR defects), tumor immune organisms analysis of genes or gene signatures associated with physiology, HPV alterations, lymphocyte subpopulations, T-cell receptor repertoires, cytokines associated with T-cell activation, and plasma-derived cytokines. In some examples, the biomarker is PD-L1. In some examples, a tumor sample obtained from a subject or population of subjects has a detectable PD-L1 expression level (e.g., a detectable protein and/or nucleic acid expression level of PD-L1 (e.g., 5% or more have been determined to have tumor-associated immune cells (TIC)). In some examples, a detectable PD-L1 protein expression level of 5% or more (eg, PD-L1 positive), 5% or more and less than 20% (eg, PD-L1 low), or 20% in tumor samples. Tumor-associated immune cells (TIC) above (eg, PD-L1 high). In some examples, the detectable PD-L1 protein expression level is 10% or more, 10% or more and 50% or less, or 50% or more TIC in the tumor sample. In some examples, the sample is a tumor sample (eg, a formalin-fixed paraffin-embedded (FFPE) tumor sample). In some examples, the tumor sample is a tumor tissue sample.
いくつかの例では、方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中の(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mgと約1200mgの間(例えば、30mgと1200mgの間)の用量(例えば、固定用量)での抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクルと、3週間ごとに約80mgと約2000mgの間(例えば、80mgと2000mgの間)の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルとを対象又は対象集団に投与することとを含む。いくつかの例では、方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中の(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600mg(例えば、600mg)の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクル、及び2週間ごとに840mgの用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルを対象又は対象集団に投与することとを含む。いくつかの例では、方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中の(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600mg(例えば、600mg)の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクル、及び3週間ごとに1200mgの用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルを対象又は対象集団に投与することとを含む。いくつかの例では、方法は、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中の(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量を決定することと、3週間ごとに約600mg(例えば、600mg)の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の1回以上の投薬サイクル、及び4週間ごとに1680mgの用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルを対象又は対象集団に投与することとを含む。
In some examples, the method provides a sample (e.g., a tumor sample or a blood sample) from a subject or subject population (e.g., PD-L1 (e.g., as determined by PD-L1 protein and/or nucleic acid expression ) or HPV status (e.g., as determined by p16 IHC, ISH or PCR)) and determining the presence and/or expression level/amount (e.g., between about 30 mg and about 1200 mg (e.g., 30 mg and 1200 mg) with one or more dosing cycles of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) at a dose (e.g., a fixed dose) and every 3
(例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量は、タンパク質、タンパク質フラグメント、DNA、mRNA、cDNA及び/又は遺伝子コピー数を含むがこれらに限定されない、当該技術分野で公知の任意の適切な基準に基づいて定性的及び/又は定量的に決定することができる。
presence and/or expression of (e.g., PD-L1 (e.g., as determined by PD-L1 protein and/or nucleic acid expression) or HPV status (e.g., as determined by
いくつかの例では、バイオマーカーの発現レベル又は量は、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1タンパク質発現レベルである。いくつかの例では、PD-L1タンパク質発現レベルをIHCアッセイによって決定した。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 protein expression level in a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects. In some instances, PD-L1 protein expression levels were determined by IHC assay. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)は、検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)は、腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects has been determined to have a detectable PD-L1 expression level. In some examples, a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects has been determined to have detectable levels of PD-L1 expression in tumor-infiltrating immune cells. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、バイオマーカーの発現レベル又は量は、対象又は対象集団からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1核酸発現レベルである。いくつかの例では、PD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR、又はRT-qPCR、マイクロアレイ分析、遺伝子発現の連続分析(SAGE)、MassARRAY(登録商標)技術、in situハイブリダイゼーション(ISH)、又はそれらの組み合わせによって決定されている。いくつかの例では、腫瘍試料はFFPE腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 nucleic acid expression level in a tumor sample (eg, an FFPE tumor sample) from a subject or population of subjects. In some examples, PD-L1 nucleic acid expression levels are measured by RNA-seq, RT-qPCR, qPCR, multiplex qPCR, or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY® technique, in situ hybridization (ISH), or a combination thereof. In some examples, the tumor sample is an FFPE tumor sample.
いくつかの例では、対象又は対象集団からの試料(例えば、腫瘍試料又は血液試料)中の例えば、PD-L1(例えば、PD-L1タンパク質及び/又は核酸発現によって決定される場合)又はHPV状態(例えば、p 16 IHC、ISH又はPCRによって決定される場合))の存在及び/又は発現レベル/量は、例えば、検出可能なPD-L1発現レベルが個体を選択するためのバイオマーカーである場合、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))による治療に適格である対象又は対象集団を選択する。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は腫瘍試料(例えば、FFPE腫瘍試料)である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。いくつかの例では、組織試料は、腫瘍試料である。
In some examples, e.g., PD-L1 (e.g., as determined by PD-L1 protein and/or nucleic acid expression) or HPV status in a sample (e.g., tumor sample or blood sample) from a subject or subject population The presence and/or expression level/amount of (e.g., as determined by
一態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In one aspect, the present invention involves obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, protein expression of PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining, anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detected levels and PD-L1 expression in the tumor sample detected. SCCHN (e.g., relapsed and/or or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the detected tumor samples. for a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from treatment that includes one or more dosing cycles A method for selecting a treatment is provided. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the tumor sample detected SCCHN (e.g., relapsed and and/or methods for selecting a treatment for a subject or subject population with metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the detected tumor samples. for a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from treatment that includes one or more dosing cycles A method for selecting a treatment is provided. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。別の態様では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び検出された腫瘍試料中のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団のための治療法を選択するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable Anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the tumor sample detected SCCHN (e.g., relapsed and and/or methods for selecting a treatment for a subject or subject population with metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In another aspect, the present invention relates to obtaining a tumor sample (e.g., biopsy) from a subject or population of subjects, staining PD-L1 protein in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable 1 of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on detecting expression levels and PD-L1 expression in the detected tumor samples. for a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from treatment that includes one or more dosing cycles A method for selecting a treatment is provided. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))))) that may benefit from therapy ( For example, methods are provided for identifying a subject or subject population with recurrent and/or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX - Subjects with SCCHN (e.g., recurrent and/or metastatic SCCHN) who may benefit from treatment with -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)); or A method is provided for identifying a subject population. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与されるチラゴルマブ及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))))) that may benefit from therapy ( For example, methods are provided for identifying a subject or subject population with recurrent and/or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and one or more doses of tiragolumab administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g. anti-PD-L1 antagonist antibodies (e.g. atezolizumab ) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) that may benefit from treatment (e.g., relapsed SCCHN) Methods are provided for identifying a subject or subject population that has cerebrospinal and/or metastatic SCCHN). In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療から利益を得る可能性があるSCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団を同定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab))))) that may benefit from therapy ( For example, methods are provided for identifying a subject or subject population with recurrent and/or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX - Subjects with SCCHN (e.g., recurrent and/or metastatic SCCHN) who may benefit from treatment with -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)); or A method is provided for identifying a subject population. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., relapsed and/or or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) Provide a method for grading. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., relapsed and/or or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) Provide a method for grading. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定する方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療に対する、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団の応答性を評定する方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies ( SCCHN (e.g., relapsed and/or or metastatic SCCHN). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., MDX -1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)))) Provide a way to grade. In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; In a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from therapy comprising one or more dosing cycles, Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly as lambrolizumab) It provides a method for optimizing therapy involving known pembrolizumab))). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti Optimizing treatment with PD-L1 antagonistic antibodies (eg, atezolizumab) or anti-PD-1 antagonistic antibodies (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) provide a method for In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; In a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from therapy comprising one or more dosing cycles, Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly as lambrolizumab) Methods are provided for optimizing treatments involving known pembrolizumab))). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti Optimizing treatment with PD-L1 antagonistic antibodies (eg, atezolizumab) or anti-PD-1 antagonistic antibodies (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) provide a method for In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量(例えば、固定用量)で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量(例えば、固定用量)で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び1680mgの用量で4週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、治療は、600mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び840mgの用量で2週間ごとに投与されるアテゾリズマブの1回以上の投薬サイクルを含む。いくつかの例では、本発明は、対象又は対象集団から腫瘍試料(例えば、生検)を得ること、染色に適した抗PD-L1抗体を使用するIHCアッセイによって腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む療法から利益を得る可能性が高いものとして対象又は対象集団を同定することによって、SCCHN(例えば、再発性及び/又は転移性SCCHN)を有する対象又は対象集団において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む治療を最適化するための方法を提供する。いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. detecting protein expression levels and anti-TIGIT antagonist antibody administered at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab administered at a dose (e.g., fixed dose) of 1200 mg every three weeks; In a subject or subject population with SCCHN (e.g., recurrent and/or metastatic SCCHN) by identifying the subject or subject population as likely to benefit from therapy comprising one or more dosing cycles, Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist (e.g. anti-PD-L1 antagonist antibody (e.g. atezolizumab) or anti-PD-1 antagonist antibody (e.g. MDX-1106 (nivolumab) or MK-3475 (formerly as lambrolizumab) It provides a method for optimizing therapy involving known pembrolizumab))). In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 1680 mg every 4 weeks. In some examples, the treatment comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at a dose of 600 mg every 3 weeks and atezolizumab at a dose of 840 mg every 2 weeks. In some examples, the present invention involves obtaining a tumor sample (e.g., a biopsy) from a subject or population of subjects, determining PD-L1 in the tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining. Detecting protein expression levels and potentially benefiting from a therapy comprising one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., anti Optimizing treatment with PD-L1 antagonistic antibodies (eg, atezolizumab) or anti-PD-1 antagonistic antibodies (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) provide a method for In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28) or an OX-40 agonist, such as an OX-40 agonist antibody , CD27, CD137, HVEM and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may further comprise or be administered in conjunction therewith (either separately or together).
いくつかの例では、方法は、同定された対象又は対象集団に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の抗がん治療剤(複数可)(例えば、免疫調節剤(例えば、CTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY(登録商標)))等の1つ以上の免疫共阻害受容体(例えば、TIGIT、PD-L1、PD-1、CTLA-4、LAG3、TIM3、BTLA、及び/又はVISTAから選択される1つ以上の免疫共阻害受容体)を減少又は阻害する薬剤、又は、OX-40アゴニスト、例えばOX-40アゴニスト抗体等の1つ以上の免疫共刺激受容体(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM、及び/又はGITRから選択される1つ以上の免疫共刺激受容体)を増加又は活性化する薬剤)、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法(radiotherapy)/放射線療法(radiation therapy)、及び/又は抗ホルモン剤、例えば本明細書で上に列挙したもの)を更に含み得るか又はそれと併せて(別々に又は一緒に)投与され得る。 In some examples, the method further comprises administering a treatment to the identified subject or subject population. In some examples, the treatment includes one or more additional anti-cancer therapeutic agent(s) (e.g., immunomodulatory agents (e.g., CTLA-4 antagonists, e.g., anti-CTLA-4 antagonist antibodies (e.g., ipilimumab)). one or more immune co-inhibitory receptors such as YERVOY®) (e.g., one selected from TIGIT, PD-L1, PD-1, CTLA-4, LAG3, TIM3, BTLA, and/or VISTA) an agent that reduces or inhibits one or more co-immune co-inhibitory receptors (e.g., CD226, OX-40, CD28), or an OX-40 agonist, such as an OX-40 agonistic antibody; , CD27, CD137, HVEM, and/or GITR), chemotherapeutic agents, cytotoxic agents, growth inhibitors, radiotherapy )/radiation therapy, and/or anti-hormonal agents, such as those listed herein above), may be further included or administered in conjunction therewith (either separately or together).
いくつかの例では、本明細書に記載される診断方法又は使用のいずれかにおいて、SCCHNは、再発性及び/又は転移性SCCHNである。がんは、初期又は後期段階であり得る。いくつかの例では、治療は第一選択療法である。いくつかの例では、対象又は対象集団は、事前治療を受けたことがない。いくつかの例では、事前治療は、再発性及び/又は転移性疾患の事前全身治療である。 In some examples, in any of the diagnostic methods or uses described herein the SCCHN is recurrent and/or metastatic SCCHN. Cancer may be in early or late stage. In some instances, the treatment is first line therapy. In some examples, the subject or subject population has received no prior treatment. In some examples, prior treatment is prior systemic treatment of recurrent and/or metastatic disease.
がんの特性評価及び選択
本明細書に記載される使用のための方法、使用又は組成物のいずれにおいても、がんはSCCHN(例えば、再発性及び/又は転移性SCCHN)であり得る。いくつかの例では、SCCHNは、再発性及び/又は転移性SCCHNである。いくつかの例では、SCCHNはPD-L1陽性である。いくつかの例では、SCCHNはHPV陽性である。いくつかの例では、SCCHNはHPV陰性である。いくつかの例では、SCCHNはPD-L1陽性及びHPV陽性である。いくつかの例では、SCCHNはPD-L1陽性及びHPV陰性である。いくつかの例では、対象又は対象集団は、事前治療を受けたことがない。いくつかの例では、事前治療は、再発性及び/又は転移性疾患の事前全身治療である。
Characterization and Selection of Cancer In any of the methods, uses or compositions for use described herein, the cancer can be SCCHN (eg, recurrent and/or metastatic SCCHN). In some examples, the SCCHN is recurrent and/or metastatic SCCHN. In some instances SCCHN is PD-L1 positive. In some instances SCCHN is HPV positive. In some instances SCCHN is HPV negative. In some instances SCCHN is PD-L1 positive and HPV positive. In some instances SCCHN is PD-L1 positive and HPV negative. In some examples, the subject or subject population has received no prior treatment. In some examples, prior treatment is prior systemic treatment of recurrent and/or metastatic disease.
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象又は対象集団はPD-L1選択腫瘍(例えば、検検出可能なPD-L1発現レベルを有する腫瘍(例えば、検出可能なPD-L1タンパク質発現レベル(例えば、5%以上の腫瘍関連免疫細胞(TIC)))を有する。いくつかの例では、対象又は対象集団から得られる試料(例えば、腫瘍試料(例えば、腫瘍組織試料))は、検出可能なPD-L1タンパク質発現レベル(例えば、5%以上のTIC)を有する。いくつかの例では、PD-L1選択腫瘍は、検出可能なPD-L1発現レベル(例えば、検出可能なPD-L1タンパク質発現レベル(例えば、5%以上のTIC))を有する。いくつかの例では、検出可能なPD-L1発現レベルは、検出可能なPD-L1タンパク質発現レベル(例えば、5%以上のTIC)である。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、約5%以上(例えば、5%、6%、7%、8%、9%、10%、11%、12%、13%、14%、15%、16%、17%、18%、19%、20%、25%、30%、35%、40%、45%、50%、60%、70%、75%、80%、90%以上)のTICである。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、5%以上20%未満(例えば、5%、6%、7%、8%、9%、10%、11%、12%、13%、14%、15%、16%、17%、18%、19%、又は20%)のTICである。いくつかの例では、5%以上20%未満のTICは、PD-L1低と定義される。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、20%以上(例えば、20%、21%、22%、23%、24%、25%、26%、27%、28%、29%、30%、31%、32%、33%、34%、35%、40%、45%、50%、55%、60%、65%、70%、75%、80%、85%、90%、95%、99%、又は100%)のTICである。いくつかの例では、20%以上のTICは、PD-L1高として定義される。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、約10%以上(例えば、10%、11%、12%、13%、14%、15%、16%、17%、18%、19%、20%、25%、30%、35%、40%、45%、50%、60%、70%、75%、80%、90%以上)のTICである。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、10%以上50%未満(例えば、10%、11%、12%、13%、14%、15%、16%、17%、18%、19%、20%、21%、22%、23%、24%、25%、30%、35%、40%、45%、46%、47%、48%、49%、49.5%、49.9%又は49.99%)のTICである。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、50%以上(例えば、50%、51%、52%、53%、54%、55%、56%、57%、58%、59%、60%、61%、62%、63%、64%、65%、66%、67%、68%、69%、70%、71%、72%、73%、74%、75%、76%、77%、78%、79%、80%、81%、82%、83%、84%、85%、86%、87%、88%、89%、90%、95%、99%、又は99.99%)のTICである。 In some examples, in any of the methods, uses or compositions for use described herein, the subject or subject population is a PD-L1-selected tumor (e.g., a detectable PD-L1 expression level (e.g., a detectable PD-L1 protein expression level (e.g., 5% or more tumor-associated immune cells (TIC)).In some examples, a sample obtained from a subject or population of subjects (e.g., , a tumor sample (e.g., a tumor tissue sample) has a detectable PD-L1 protein expression level (e.g., a TIC of 5% or greater), hi some examples, a PD-L1-selected tumor has a detectable has a PD-L1 expression level (e.g., a detectable PD-L1 protein expression level (e.g., a TIC of 5% or greater), hi some examples, a detectable PD-L1 expression level is detectable PD-L1 expression level - L1 protein expression level (e.g., TIC of 5% or more) In some examples, the detectable PD-L1 protein expression level is about 5% or more (e.g., 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40% , 45%, 50%, 60%, 70%, 75%, 80%, 90% or more) TIC In some examples, the detectable PD-L1 protein expression level is 5% or more and 20% or more less than (e.g., 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, or 20%) TIC, hi some examples, a TIC of 5% or more and less than 20% is defined as PD-L1 low, hi some examples, a detectable PD-L1 protein expression level is 20% or more (e.g., 20%, 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34% , 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, 99%, or 100%) of TIC In some examples, a TIC of 20% or more is defined as PD-L1 high, hi some examples, detectable PD-L1 protein expression levels are about 10% or more (e.g., 10% , 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 6 0%, 70%, 75%, 80%, 90% or more) TIC. In some examples, the detectable PD-L1 protein expression level is greater than or equal to 10% and less than 50% (e.g., 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 46%, 47%, 48%, 49%, 49. 5%, 49.9% or 49.99%) TIC. In some examples, the detectable PD-L1 protein expression level is 50% or more (e.g., 50%, 51%, 52%, 53%, 54%, 55%, 56%, 57%, 58%, 59%, 60%, 61%, 62%, 63%, 64%, 65%, 66%, 67%, 68%, 69%, 70%, 71%, 72%, 73%, 74%, 75% , 76%, 77%, 78%, 79%, 80%, 81%, 82%, 83%, 84%, 85%, 86%, 87%, 88%, 89%, 90%, 95%, 99 %, or 99.99%).
いくつかの例では、IHCアッセイは、抗PD-L1抗体SP263、SP142、22C3又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)5%以上であると判定されている。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)5%以上及び20%未満であると判定されている。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)20%以上であると判定されている。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)10%以上であると判定されている。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)10%以上50%未満であると判定されている。いくつかの例では、TICは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを使用して)50%以上であると判定されている。 In some examples, the IHC assay uses anti-PD-L1 antibodies SP263, SP142, 22C3 or 28-8. In some examples, the IHC assay uses the anti-PD-L1 antibody SP263. In some instances, the TIC has been determined to be 5% or greater (eg, using the Ventana (SP263) PD-L1 IHC assay). In some instances, the TIC has been determined to be greater than or equal to 5% and less than 20% (eg, using the Ventana (SP263) PD-L1 IHC assay). In some instances, the TIC has been determined to be 20% or greater (eg, using the Ventana (SP263) PD-L1 IHC assay). In some instances, the TIC has been determined to be 10% or greater (eg, using the Ventana (SP263) PD-L1 IHC assay). In some instances, the TIC has been determined to be greater than or equal to 10% and less than 50% (eg, using the Ventana (SP263) PD-L1 IHC assay). In some instances, the TIC has been determined to be 50% or greater (eg, using the Ventana (SP263) PD-L1 IHC assay).
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象又は対象集団から得られる試料(例えば、腫瘍試料)は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, in any of the methods, uses or compositions for use described herein, a sample obtained from a subject or subject population (e.g., a tumor sample) contains detectable PD-L1 Has a nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象又は対象集団は、検出可能なHPVを有する腫瘍を有する。いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象又は対象集団は、検出可能なHPVを伴わない腫瘍を有する。いくつかの例では、HPVは直接的又は間接的に検出される。いくつかの例では、HPVはタンパク質発現レベル(例えば、p 16又はHPVウイルスタンパク質)によって検出される。いくつかの例では、HPVは核酸発現レベルによって検出される。いくつかの例では、HPVの状態は、p16 IHC、in situハイブリダイゼーション、又はPCRによって決定される。いくつかの例では、HPVはHPV16である。いくつかの例では、HPVはHPV18である。 In some examples, in any of the methods, uses or compositions for use described herein, the subject or subject population has a tumor with detectable HPV. In some examples, in any of the methods, uses or compositions for use described herein, the subject or subject population has a tumor without detectable HPV. In some examples, HPV is directly or indirectly detected. In some instances, HPV is detected by protein expression levels (eg, p16 or HPV viral proteins). In some examples, HPV is detected by nucleic acid expression levels. In some instances, HPV status is determined by p16 IHC, in situ hybridization, or PCR. In some examples, the HPV is HPV16. In some examples, the HPV is HPV18.
処置に対する応答
本明細書に記載される方法のいずれかのいくつかの実施形態では、治療に対する対象又は対象集団の応答は、1つ以上の尺度によって特徴付けることができる。いくつかの実施形態では、処置はCR又はPRをもたらす。いくつかの例では、対象又は対象集団においてSCCHNを処置するための方法及び使用のいずれもが、対象又は対象集団の客観的奏効率(ORR)の増加をもたらし得る。いくつかの例では、対象又は対象集団においてSCCHNを処置するための方法及び使用のいずれも、対象又は対象集団のPFS、奏効期間(DOR)及び/又はOSの増加をもたらし得る。
Response to Treatment In some embodiments of any of the methods described herein, the response of a subject or subject population to treatment can be characterized by one or more measures. In some embodiments, treatment results in CR or PR. In some examples, any of the methods and uses for treating SCCHN in a subject or subject population can result in an increased objective response rate (ORR) of the subject or subject population. In some examples, any of the methods and uses for treating SCCHN in a subject or subject population can result in increased PFS, duration of response (DOR) and/or OS of the subject or subject population.
いくつかの例では、本明細書中記載される使用のためのいずれかの方法、使用又は組成物において、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))の投与は、臨床応答をもたらす。いくつかの例では、臨床応答は、基準ORR時間と比較した場合の対象又は対象集団のORRの増加である。いくつかの例では、基準ORRは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のORR中央値である。いくつかの例では、基準ORRは、少なくとも約19%(例えば、約19%と約80%の間、例えば、約19%と約60%の間(例えば、20%、21%、22%、23%、24%、25%、30%、35%、40%、45%、50%、55%、又は60%))である。いくつかの例では、基準ORRは、少なくとも約36%(例えば、約36%と約80%の間、例えば、約36%と約60%の間(例えば、36%、37%、38%、39%、40%、45%、50%、55%又は60%))である。いくつかの例では、基準ORRは、少なくとも約19%~約36%である。いくつかの例では、臨床応答は、基準PFS時間と比較した場合の対象又は対象集団のPFSの増加である。いくつかの例では、参照PFSは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のPFS時間中央値である。いくつかの例では、臨床応答は、基準DOR時間と比較した対象又は対象集団のDORの増加である。いくつかの例では、参照DORは、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))を含む処置を受けたことがある対象集団のDOR時間中央値である。いくつかの例では、基準DOR時間は少なくとも約4ヶ月(例えば、約4ヶ月と約42ヶ月の間(例えば、約6ヶ月と約30ヶ月の間(例えば、6ヶ月、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、又は30ヶ月)))である。いくつかの例では、基準DOR時間は、少なくとも約6.7ヶ月(例えば、少なくとも約6.7ヶ月、6.8ヶ月、6.9ヶ月、7.0ヶ月、8.0ヶ月、9.0ヶ月、10.0ヶ月、11.0ヶ月、又は12.0ヶ月)である。いくつかの例では、基準DOR時間は、少なくとも約6.7ヶ月~約23.4ヶ月である。いくつかの例では、基準DOR時間は、少なくとも約23.4ヶ月(例えば、少なくとも約23.4ヶ月、23.5ヶ月、23.6ヶ月、23.7ヶ月、23.8ヶ月、23.9ヶ月、24ヶ月、25ヶ月、26ヶ月、28ヶ月、30ヶ月、又は32ヶ月)である。いくつかの例では、臨床応答はOSの増加である。 In some examples, in any method, use or composition for use described herein, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab) or an anti-PD-1 antagonist antibody (eg, MDX-1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as rambrolizumab)) results in clinical responses. In some examples, a clinical response is an increase in ORR for a subject or subject population when compared to a baseline ORR time. In some examples, the reference ORR is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median ORR of the subject population. In some examples, the reference ORR is at least about 19% (e.g., between about 19% and about 80%, e.g., between about 19% and about 60% (e.g., 20%, 21%, 22%, 23%, 24%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, or 60%)). In some examples, the reference ORR is at least about 36% (e.g., between about 36% and about 80%, e.g., between about 36% and about 60% (e.g., 36%, 37%, 38%, 39%, 40%, 45%, 50%, 55% or 60%)). In some examples, the reference ORR is at least about 19% to about 36%. In some examples, a clinical response is an increase in PFS for a subject or subject population when compared to a baseline PFS time. In some examples, the reference PFS is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median PFS time in a subject population. In some examples, a clinical response is an increase in DOR for a subject or subject population compared to a baseline DOR time. In some examples, the reference DOR is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., MDX- 1106 (nivolumab) or MK-3475 (pembrolizumab, formerly known as lambrolizumab)))) median DOR time in a subject population. In some examples, the baseline DOR time is at least about 4 months (e.g., between about 4 months and about 42 months (e.g., between about 6 months and about 30 months (e.g., 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months , 26 months, 27 months, 28 months, 29 months, or 30 months))). In some examples, the baseline DOR time is at least about 6.7 months (e.g., at least about 6.7 months, 6.8 months, 6.9 months, 7.0 months, 8.0 months, 9.0 months). months, 10.0 months, 11.0 months, or 12.0 months). In some examples, the baseline DOR time is at least about 6.7 months to about 23.4 months. In some examples, the baseline DOR time is at least about 23.4 months (e.g., at least about 23.4 months, 23.5 months, 23.6 months, 23.7 months, 23.8 months, 23.9 months). months, 24 months, 25 months, 26 months, 28 months, 30 months, or 32 months). In some instances the clinical response is an increase in OS.
いくつかの例では、処置は15%を超える(例えば、15%、16%、17%、18%、19%、20%、21%、22%、23%、24%、25%、26%、27%、28%、29%、30%、31%、32%、33%、34%、35%、36%、37%、38%、39%、40%、41%、42%、43%、44%、45%、50%、55%、60%、65%、70%、75%、80%、90%以上)ORRをもたらす。いくつかの例では、処置は、基準ORRよりも大きいORRをもたらす。いくつかの例では、基準ORRは19%である。いくつかの例では、基準ORRは24.4%である。いくつかの例では、基準ORRは28.8%である。いくつかの例では、基準ORRは35%である。 In some instances, treatment is greater than 15% (e.g., 15%, 16%, 17%, 18%, 19%, 20%, 21%, 22%, 23%, 24%, 25%, 26% , 27%, 28%, 29%, 30%, 31%, 32%, 33%, 34%, 35%, 36%, 37%, 38%, 39%, 40%, 41%, 42%, 43% %, 44%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 90% or more) result in ORR. In some instances, treatment results in an ORR that is greater than the baseline ORR. In some examples, the reference ORR is 19%. In some examples, the reference ORR is 24.4%. In some examples, the reference ORR is 28.8%. In some examples, the reference ORR is 35%.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のPFS、DOR、又はOSの増加をもたらす。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Comparatively, it results in an increase in PFS, DOR, or OS for a subject or subject population.
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約2ヵ月(例えば2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約3.3ヶ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、対象又は対象集団のOSを少なくとも約5.3ヶ月(例えば5.3~120、6~60ヵ月、7~48ヵ月、8~36 ヵ月、又は10~24ヵ月、例えば、少なくとも約5.3ヵ月、5.5ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、基準OS時間と比較してOSの増加をもたらす。いくつかの例では、基準OS時間は少なくとも約8ヶ月(例えば、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、又は18ヶ月)である。いくつかの例では、基準OS時間は少なくとも約14.9ヶ月(例えば、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、又は20ヶ月)である。いくつかの例では、基準OS時間は、少なくとも約11.6ヶ月~約14.9ヶ月である。 In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, treatment reduces the OS of a subject or subject population by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months). months, 8-36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months, 2.7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the OS of the subject or subject population by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months). , 8 to 36 months, or 10 to 24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the OS of the subject or subject population by at least about 5.3 months (eg, 5.3-120, 6-60 months, 7-48 months, 8-36 months, or 10-24 months). , e.g., at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months , 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, treatment results in an increase in OS compared to baseline OS time. In some examples, the baseline OS time is at least about 8 months (e.g., 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, or 18 months). ). In some examples, the baseline OS time is at least about 14.9 months (eg, 15 months, 16 months, 17 months, 18 months, 19 months, or 20 months). In some examples, the baseline OS time is at least about 11.6 months to about 14.9 months.
いくつかの実施形態では、処置は、対象又は対象集団のPFSを少なくとも2.4ヵ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヶ月、5.0~48ヶ月、6.0~36ヶ月、8.0~24ヶ月、又は10~12ヶ月、例えば少なくとも約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のPFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のPFSを少なくとも約2ヵ月(例えば2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, treatment reduces the subject's or subject population's PFS to at least 2.4 months (eg, 2.4-120 months, 2.5-100 months, 3.0-80 months, 4.0- 60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the subject's or subject population's PFS by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9 months). ~36 months, or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months; 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the subject's or subject population's PFS by at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-48 months, 36 months, or 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months,2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months).
いくつかの実施形態では、処置は、対象又は対象集団のDORを少なくとも2.4ヵ月(例えば、2.4~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヶ月、5.0~48ヶ月、6.0~36ヶ月、8.0~24ヶ月、又は10~12ヶ月、例えば少なくとも約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のDORを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.5ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象又は対象集団のDORを少なくとも約2ヵ月(例えば2~120ヵ月、3~100ヵ月、4~80ヵ月、6~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば少なくとも約2.0ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、約2.4ヶ月、2.5ヶ月、2.6ヶ月、2.7ヶ月、2.8ヶ月、2.9ヶ月、3.0ヶ月、3.1ヶ月、3.2ヶ月、3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.5ヶ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, treatment reduces the subject's or subject population's DOR by at least 2.4 months (eg, 2.4-120 months, 2.5-100 months, 3.0-80 months, 4.0- 60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months, or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the subject's or subject population's DOR by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9 months). ~36 months, or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months; 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months). In some embodiments, treatment reduces the DOR of a subject or subject population by at least about 2 months (eg, 2-120 months, 3-100 months, 4-80 months, 6-60 months, 8-48 months, 9-48 months, 36 months, or 10-24 months, such as at least about 2.0 months, 2.1 months, 2.2 months, 2.3 months, about 2.4 months, 2.5 months, 2.6 months,2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months. 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.6 months. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8. 5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months , or 36 months).
いくつかの例では、処置は、患者報告転帰測定情報システム(登録商標)(PROMIS(登録商標))アイテムバンクv 2.0-身体機能-ショートフォーム10 bによって測定されるように、患者報告の身体機能の低下が確認されるまでの時間(TTCD)の改善をもたらす。いくつかの例では、処置は、PROMIS(登録商標)tem Bank v2.0-Physical Functioning-Short Form 10b、PROMIS(登録商標)Item Bank v1.0-Fatigue-Short Form 4a、PROMIS(登録商標)Item Bank v1.0-Pain Interference Short Form 4a、及びPROMIS(登録商標)Numeric Rating Scale v1.0-Pain Intensity 1aによって評定される、物理的機能、疲労、及び/又は疼痛のベースラインからの改善をもたらす。 In some examples, the treatment is a patient-reported outcome measurement as measured by the Patient-Reported Outcomes Measurement Information System® (PROMIS®) Item Bank v 2.0-Physical Function-Short Form 10 b. Resulting in improved time to documented decline in physical function (TTCD). In some examples, the treatment is according to PROMIS® Item Bank v2.0—Physical Functionaling—Short Form 10b, PROMIS® Item Bank v1.0—Fatigue—Short Form 4a, PROMIS® Item Bank v1.0—Produces improvement from baseline in physical function, fatigue, and/or pain as assessed by the Pain Interference Short Form 4a and PROMIS® Numeric Rating Scale v1.0—Pain Intensity 1a .
A.肝臓がんに関する治療方法及び使用
肝臓がん
肝臓がんは、世界で5番目に多いがんであり、がん関連死の2番目に多い原因であり、年間854,000件の新規症例及び810,000件の死亡がある。診断時に、原発性肝臓がんを有するほとんどの患者は進行性疾患を有しており、治癒的療法による処置が推奨されない段階である。世界保健機関は、2030年に100万人を超える人々が肝臓がんで死亡すると推定しており、重大な世界的な公衆衛生問題を強調している。
A. Treatment methods and uses for liver cancer Liver cancer Liver cancer is the fifth most common cancer and the second leading cause of cancer-related deaths worldwide, with 854,000 new cases and 810,000 new cases annually. 000 deaths. At diagnosis, most patients with primary liver cancer have progressive disease, at a stage where treatment with curative therapies is not recommended. The World Health Organization estimates that more than 1 million people will die from liver cancer in 2030, highlighting a significant global public health problem.
肝細胞癌腫(HCC)は、原発性肝臓がんの最も一般的な形態であり、全ての原発性肝悪性腫瘍の約90%を占める。HCCは、任意の固形腫瘍の0.98という最も高い死亡率対発生率比を有する非常に致死的な疾患である。HCCを最初に示す患者の最大80%は、症状の出現が遅いため、切除不能又は転移性の疾患が進行している。米国では、HCC患者の5年OS率は17%であり、遠隔転移が存在する場合、実質的にわずか3%に低下する。 Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer, accounting for about 90% of all primary liver malignancies. HCC is a highly fatal disease with the highest mortality-to-incidence ratio of 0.98 of any solid tumor. Up to 80% of patients who first present with HCC have advanced unresectable or metastatic disease due to late onset of symptoms. In the United States, the 5-year OS rate for HCC patients is 17%, dropping substantially to only 3% when distant metastases are present.
したがって、肝臓がん、例えばHCC、例えば局所進行性HCC、転移性HCC、又は切除不能なHCCの処置のための有効な免疫療法の開発に対する現場でのニーズは満たされていない。 Thus, there is an unmet need on the ground for the development of effective immunotherapies for the treatment of liver cancer, such as HCC, such as locally advanced HCC, metastatic HCC, or unresectable HCC.
肝臓がんを処置するための方法及び使用
有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む治療レジメンを対象又は対象集団に投与することを含む、対象又は対象集団における、肝臓がん、例えば肝細胞癌腫(HCC)、局所進行性もしくは転移性及び/又は切除不能なHCCを処置する又は進行を遅延させるための方法及び使用であって、対象又は対象集団は肝臓がん(例えば、HCC)の全身治療を以前に受けたことがない方法及び使用が本明細書で提供される。有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを対象又は対象集団に投与することを含む、対象又は対象集団における、局所進行性もしくは転移性及び/又は切除不能なHCCを含む肝臓がん、例えばHCCを治療する又は進行を遅延させるための方法及び使用も本明細書で提供される。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。他の実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。
Methods and uses for treating liver cancer Treating or delaying progression of liver cancer, such as hepatocellular carcinoma (HCC), locally advanced or metastatic and/or unresectable HCC, in a subject or population of subjects, comprising administering to the subject or population of subjects Provided herein are methods and uses for, wherein the subject or subject population has not previously undergone systemic treatment for liver cancer (eg, HCC). effective amounts of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab) treating or delaying progression of liver cancer, including locally advanced or metastatic and/or unresectable HCC, e.g., HCC, in a subject or subject population comprising administering to the subject or subject population a treatment regimen comprising Methods and uses for are also provided herein. In some embodiments, the treatment regimen comprises an effective amount of one or more of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab) Including dosing cycles. In other embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and Including one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tiragolumab).
有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを対象又は対象集団に投与することを含む、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)を有する対象又は対象集団における免疫機能を増強する方法も本明細書で提供される。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 administering to the subject or population of subjects a treatment regimen comprising an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab); Also provided herein are methods of enhancing immune function in a subject or population of subjects with liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC). In some embodiments, the treatment regimen comprises an effective amount of one or more of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab) Including dosing cycles.
例えば、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを対象又は対象集団に投与することを含む、対象又は対象集団における、局所進行性もしくは転移性及び/又は切除不能なHCCを含む肝臓がん、例えばHCCを治療する又は進行を遅延させるための方法及び使用も本明細書で提供される。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 For example, administering to a subject or population of subjects a treatment regimen comprising an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab) Also provided herein are methods and uses for treating or delaying progression of liver cancer, including locally advanced or metastatic and/or unresectable HCC, e.g., HCC, in a subject or population of subjects, including be. In some embodiments, the treatment regimen comprises an effective amount of one or more of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab) Including dosing cycles.
対象又は対象集団の肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)の治療に使用するためのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を含む医薬組成物も本明細書で提供され、処置は、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)と組み合わせたPD-1軸結合アンタゴニストの投与を含む処置レジメンを含む。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 A PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody) for use in treating liver cancer (e.g., HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects (eg, atezolizumab)) are also provided herein, and treatment includes treatment regimens comprising administration of a PD-1 axis binding antagonist in combination with an anti-TIGIT antagonist antibody (eg, tiragolumab). In some embodiments, the treatment regimen includes an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab). Including dosing cycles.
対象又は対象集団の肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)の治療に使用するためのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を含む医薬組成物が本明細書で提供され、処置は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)と組み合わせたPD-1軸結合アンタゴニストの投与を含む処置レジメンを含む。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 A PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody) for use in treating liver cancer (e.g., HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects (e.g., atezolizumab)), wherein the treatment is PD in combination with a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and an anti-TIGIT antagonist antibody (e.g., tiragolumab) - Includes treatment regimens that include administration of a monoaxial binding antagonist. In some embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tiragolumab).
別の例では、対象又は対象集団の肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)の治療に使用するためのVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を含む医薬組成物が本明細書で提供され、処置は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)と組み合わせたVEGFアンタゴニストの投与を含む処置レジメンを含む。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 In another example, a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., , bevacizumab)), wherein the treatment is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, tiragolumab ) in combination with treatment regimens that include administration of a VEGF antagonist. In some embodiments, the treatment regimen includes an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tiragolumab).
別の例では、対象又は対象集団の肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)の治療に使用するための抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む医薬組成物が本明細書で提供され、処置は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))と組み合わせた抗TIGITアンタゴニスト抗体の投与を含む処置レジメンを含む。いくつかの実施形態では、処置レジメンは、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)の1回以上の投薬サイクルを含む。 In another example, an anti-TIGIT antagonist antibody (e.g., tiragolumab) for use in treating liver cancer (e.g., HCC, including locally advanced or metastatic and/or unresectable HCC) in a subject or population of subjects. Provided herein are pharmaceutical compositions comprising a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) ) in combination with an anti-TIGIT antagonist antibody. In some embodiments, the treatment regimen comprises an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and one or more dosing cycles of an anti-TIGIT antagonist antibody (eg, tiragolumab).
本明細書に記載の使用のための方法、使用又は医薬組成物のいずれかのいくつかの実施形態では、肝臓がんは初期又は後期段階であり得る。いくつかの実施形態では、肝臓がんは、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)である。いくつかの例では、肝臓がんは、局所進行性又は転移性及び/又は切除不能なHCCである。いくつかの実施形態では、肝臓がんは高リスク肝臓がん(例えば、高リスクの局所進行性又は転移性及び/又は切除不能なHCC)である。いくつかの実施形態では、高リスク肝臓がんは、次の1つ以上の特徴:VP4 PVTT、胆管浸潤及び/又は肝臓の≧50%の腫瘍占有を含む。 In some embodiments of any of the methods, uses or pharmaceutical compositions for use described herein, the liver cancer may be in early or late stage. In some embodiments, the liver cancer is HCC (eg, locally advanced or metastatic and/or unresectable HCC). In some examples, the liver cancer is locally advanced or metastatic and/or unresectable HCC. In some embodiments, the liver cancer is high-risk liver cancer (eg, high-risk locally advanced or metastatic and/or unresectable HCC). In some embodiments, high-risk liver cancer comprises one or more of the following characteristics: VP4 PVTT, bile duct invasion and/or >50% tumor occupancy of the liver.
本明細書中記載される使用のための方法、使用又は医薬組成物のいずれかのいくつかの実施形態では、処置は、処置後の対象又は対象集団において応答をもたらす。例えば、いくつかの実施形態では、処置は、例えば、基準治療と比較して、対象又は対象集団が客観的奏効を有する可能性を高め、対象又は対象集団のPFSを延ばし、対象又は対象集団のOSを延ばし、対象又は対象集団の放射線学的進行(radiographic progression)までの時間(TTRP)を延ばし、対象又は対象集団の奏効期間(DOR)を延ばし、及び/又は死亡のリスクを低下させる。いくつかの実施形態では、処置は、少なくとも約5.6ヶ月(例えば、5.6ヶ月と14ヶ月の間(例えば、5.6ヶ月、5.7ヶ月、5.8ヶ月、5.9ヶ月、6ヶ月、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、又は14ヶ月))の対象集団のPFS中央値をもたらす。いくつかの実施形態では、処置は、少なくとも約6.83ヶ月(例えば、6.9ヶ月、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、又は14ヶ月)の対象集団のPFS中央値をもたらす。いくつかの実施形態では、処置は、少なくとも約5.6ヶ月~少なくとも約6.83ヶ月(例えば、少なくとも約5.7、5.8、5.9、6.0、6.1、6.2、6.3、6.4、6.5、6.6、6.7、6.8、又は6.83ヶ月)の対象集団のPFS中央値をもたらす。いくつかの実施形態では、基準処置は現在の標準治療を含む。いくつかの実施形態では、参照処置は、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)及びVEGFアンタゴニスト(例えば、ベバシズマブ)を含む。いくつかの実施形態では、参照処置は、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストを含む。いくつかの実施形態では、基準処置は、PD-1軸結合アンタゴニストと、VEGFアンタゴニストを含まない抗TIGITアンタゴニスト抗体とを含む。いくつかの実施形態では、基準処置は、PD-1軸結合アンタゴニストを含まないVEGFアンタゴニスト及び抗TIGITアンタゴニスト抗体を含む。いくつかの実施形態では、基準処置は、VEGFアンタゴニストを含まないPD-1軸結合アンタゴニストと、抗TIGITアンタゴニスト抗体とを含む。いくつかの実施形態では、基準処置は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを含まないVEGFアンタゴニストを含む。いくつかの実施形態では、基準処置は、VEGFアンタゴニスト及びPD-1軸結合アンタゴニストを含まない抗TIGITアンタゴニスト抗体を含む。 In some embodiments of any of the methods, uses or pharmaceutical compositions for use described herein, the treatment produces a response in the subject or subject population following treatment. For example, in some embodiments, treatment increases the likelihood of a subject or subject population having an objective response, prolongs the subject or subject population's PFS, increases the subject's or subject population's It prolongs OS, prolongs the time to radiographic progression (TTRP) of a subject or subject population, prolongs the duration of response (DOR) of a subject or subject population, and/or reduces the risk of death. In some embodiments, the treatment is for at least about 5.6 months (e.g., between 5.6 months and 14 months (e.g., 5.6 months, 5.7 months, 5.8 months, 5.9 months). , 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months)). In some embodiments, the treatment is for at least about 6.83 months (e.g., 6.9 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months). Median PFS for the subject population is provided. In some embodiments, the treatment is for at least about 5.6 months to at least about 6.83 months (eg, for at least about 5.7, 5.8, 5.9, 6.0, 6.1, 6.6 months). 2, 6.3, 6.4, 6.5, 6.6, 6.7, 6.8, or 6.83 months). In some embodiments, the reference treatment comprises the current standard of care. In some embodiments, the reference treatment comprises a PD-1 axis binding antagonist (eg, atezolizumab) and a VEGF antagonist (eg, bevacizumab) without an anti-TIGIT antagonist antibody. In some embodiments, reference treatments include PD-1 axis binding antagonists and VEGF antagonists. In some embodiments, the reference treatment comprises a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody without a VEGF antagonist. In some embodiments, the reference treatment comprises a VEGF antagonist without a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody. In some embodiments, the reference treatment comprises a PD-1 axis binding antagonist without a VEGF antagonist and an anti-TIGIT antagonist antibody. In some embodiments, the reference treatment comprises a VEGF antagonist without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist. In some embodiments, the reference treatment comprises an anti-TIGIT antagonist antibody that is free of VEGF antagonists and PD-1 axis binding antagonists.
本明細書に記載の使用のための方法、使用又は医薬組成物のいずれかのいくつかの実施形態では、処置応答(複数可)は、任意の適切な標準治療がん療法と比較して改善され得る。いくつかの実施形態では、標準治療がん療法は、標準治療肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)療法である。いくつかの実施形態では、標準治療肝臓がん(例えば、HCC)療法がチロシンキナーゼ阻害剤を含む。いくつかの実施形態では、チロシンキナーゼ阻害剤はマルチキナーゼ阻害剤である。いくつかの実施形態では、マルチキナーゼ阻害剤はソラフェニブ又はレンバチニブである。いくつかの実施形態では、マルチキナーゼ阻害剤はソラフェニブである。 In some embodiments of any of the methods, uses or pharmaceutical compositions for use described herein, the treatment response(s) is improved compared to any suitable standard of care cancer therapy can be In some embodiments, the standard of care cancer therapy is standard of care liver cancer (eg, HCC, including locally advanced or metastatic and/or unresectable HCC) therapy. In some embodiments, standard of care liver cancer (eg, HCC) therapy comprises a tyrosine kinase inhibitor. In some embodiments, the tyrosine kinase inhibitor is a multikinase inhibitor. In some embodiments, the multikinase inhibitor is sorafenib or lenvatinib. In some embodiments, the multikinase inhibitor is sorafenib.
本明細書に記載される使用のための方法、使用、又は医薬組成物のいずれかのいくつかの実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))、又はそれらの医薬は、投与されてもよく、医薬の製造で使用されてもよく、又は1つ以上の追加の抗がん治療剤(例えば、化学療法剤、細胞傷害剤、成長阻害剤、放射線療法/放射線療法、及び/又は抗ホルモン剤(例えば、本明細書中上記で列挙されるもの))と組み合わせて(別々に又は一緒に)投与するために製剤化されてもよい。 In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein , e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)), VEGF antagonists (e.g., anti-VEGF antibodies (e.g., bevacizumab)), or pharmaceuticals thereof may be used in the manufacture of a medicament, or one or more additional anti-cancer therapeutic agents (e.g., chemotherapeutic agents, cytotoxic agents, growth inhibitory agents, radiotherapy/radiotherapy, and/or or antihormonal agents (eg, those listed hereinabove)) for administration in combination (either separately or together).
本明細書に記載の使用のための方法、使用、又は医薬組成物のいずれかのいくつかの実施形態では、対象又は対象集団は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)について以前に治療されていない。いくつかの例では、対象又は対象集団は、事前治療を受けたことがない。いくつかの例では、対象又は対象集団は、少なくとも1種類の事前治療を受けている。いくつかの例では、対象又は対象集団は、2種類の事前治療を受けている。いくつかの例では、対象又は対象集団は、少なくとも1つであるが2つ以下の事前全身治療を受けている、及び/又はこれらの対象に対する許容可能な標準治療が存在しない。いくつかの例では、対象又は対象集団は、3種類以上の事前治療を受けたことがない。いくつかの例では、事前治療は、化学療法、外科手術、及び/又は放射線療法である。いくつかの例では、事前治療は免疫療法である。いくつかの実施形態では、対象又は対象集団は、肝臓がん(例えば、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC))について以前に処置されていない。いくつかの実施形態では、対象又は対象集団は、HCCについて以前に処置されていない。いくつかの実施形態では、対象又は対象集団は、局所進行性もしくは転移性及び/又は切除不能なHCCについて以前に処置されていない。 In some embodiments of any of the methods, uses, or pharmaceutical compositions for uses described herein, the subject or subject population is liver cancer (e.g., locally advanced or metastatic and/or previously untreated for HCC, including unresectable HCC). In some examples, the subject or subject population has received no prior treatment. In some examples, the subject or subject population has received at least one prior treatment. In some examples, the subject or subject population has received two prior treatments. In some examples, the subject or subject population has received at least one but no more than two prior systemic treatments and/or there is no acceptable standard of care for these subjects. In some examples, the subject or subject population has never received 3 or more prior treatments. In some examples, prior treatment is chemotherapy, surgery, and/or radiation therapy. In some examples, the prior treatment is immunotherapy. In some embodiments, the subject or subject population has not been previously treated for liver cancer (eg, HCC (eg, locally advanced or metastatic and/or unresectable HCC)). In some embodiments, the subject or subject population has not been previously treated for HCC. In some embodiments, the subject or subject population has not been previously treated for locally advanced or metastatic and/or unresectable HCC.
本明細書に記載の使用のための方法、使用、又は医薬組成物のいずれかのいくつかの実施形態では、対象又は対象集団は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能なHCCを含むHCC)に対する事前全身治療を受けたことがない。いくつかの実施形態では、対象又は対象集団は、肝臓がん(例えば、HCC)に対する事前全身治療を受けたことがない。 In some embodiments of any of the methods, uses, or pharmaceutical compositions for uses described herein, the subject or subject population is liver cancer (e.g., locally advanced or metastatic and/or No prior systemic therapy for HCC (including unresectable HCC). In some embodiments, the subject or subject population has no prior systemic therapy for liver cancer (eg, HCC).
本明細書に記載される使用のための方法、使用、又は医薬組成物のいずれかのいくつかの実施形態では、対象又は対象集団は、PD-1軸結合アンタゴニスト、VEGFアンタゴニスト、又は抗TIGITアンタゴニスト抗体による事前の処置を受けたことがない。 In some embodiments of any of the methods, uses, or pharmaceutical compositions for use described herein, the subject or subject population is a PD-1 axis binding antagonist, a VEGF antagonist, or an anti-TIGIT antagonist Has never received prior treatment with antibodies.
本明細書中記載される使用のための方法、使用又は医薬組成物のいずれかのいくつかの実施形態では、対象又は対象集団は、任意の好適なChild-Pug肝機能を有し得る。例えば、いくつかの実施形態では、対照又は対象集団は、Child-PugクラスAの肝機能を有する。 In some embodiments of any of the methods, uses or pharmaceutical compositions for use described herein, the subject or subject population may have any suitable Child-Pug liver function. For example, in some embodiments, the control or subject population has Child-Pug class A liver function.
任意の適切なPD-1軸結合アンタゴニスト、VEGFアンタゴニスト又は抗TIGITアンタゴニスト抗体を、本明細書中記載される使用のための方法、使用又は医薬組成物において使用することができる。例えば、当該技術分野で公知であるか又は本明細書に記載されるPD-1軸結合アンタゴニスト、VEGFアンタゴニスト又は抗TIGITアンタゴニスト抗体のいずれかは、本明細書に記載される使用のための方法、使用又は医薬組成物において使用され得る。いくつかの実施形態では、PD-1軸結合アンタゴニストは、抗PD-L1抗体又は抗PD-1抗体である。いくつかの実施形態では、抗PD-L1抗体は、アテゾリズマブである。いくつかの実施形態では、VEGFアンタゴニストは、抗VEGF抗体である。いくつかの実施形態では、抗VEGF抗体は、ベバシズマブである。いくつかの実施形態では、抗TIGITアンタゴニスト抗体はチラゴルマブである。 Any suitable PD-1 axis binding antagonist, VEGF antagonist or anti-TIGIT antagonist antibody can be used in the methods, uses or pharmaceutical compositions for use described herein. For example, any of the PD-1 axis binding antagonists, VEGF antagonists or anti-TIGIT antagonist antibodies known in the art or described herein can be used in the methods for use described herein, use or in a pharmaceutical composition. In some embodiments, the PD-1 axis binding antagonist is an anti-PD-L1 antibody or an anti-PD-1 antibody. In some embodiments, the anti-PD-L1 antibody is atezolizumab. In some embodiments, the VEGF antagonist is an anti-VEGF antibody. In some embodiments, the anti-VEGF antibody is bevacizumab. In some embodiments, the anti-TIGIT antagonist antibody is tiragolumab.
例示的な方法
一態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、以下に更に詳細に記載されるように、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを対象又は対象集団に投与することによる方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、対象又は対象集団はHCC、例えば局所進行性もしくは転移性及び/又は切除不能なHCCについて以前に処置されていない。
Exemplary Methods In one aspect, the invention provides a method of treating a subject or subject population with HCC (e.g., locally advanced or metastatic and/or unresectable HCC), described in more detail below. subject to one or more dosing cycles of a dose (e.g., fixed dose) of 600 mg of an anti-TIGIT antagonist antibody every 3 weeks and a dose (e.g., fixed dose) of 1200 mg of atezolizumab every 3 weeks, or A method is provided by administering to a subject population, wherein the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19. In some examples, the subject or subject population has not been previously treated for HCC, eg, locally advanced or metastatic and/or unresectable HCC.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、以下に更に詳細に記載されるように、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブ、及び3週間ごとの15mg/kgの用量のベバシズマブの1回以上の投薬サイクルを対象又は対象集団に投与することによる方法を提供し、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC (e.g., locally advanced or metastatic and/or unresectable HCC), as described in more detail below. In addition, anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every 3 weeks, atezolizumab at a dose (e.g., fixed dose) of 1200 mg every 3 weeks, and bevacizumab at a dose of 15 mg/kg every 3 weeks. A method is provided by administering one or more dosing cycles to a subject or population of subjects, wherein the anti-TIGIT antagonist antibody comprises a VH domain having the amino acid sequence of SEQ ID NO: 17 or 18 and a VL domain having the amino acid sequence of SEQ ID NO: 19 have In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or subject population is given administering one or more dosing cycles of a 600 mg dose (eg, fixed dose) of tiragolumab and a 1200 mg dose (eg, fixed dose) of atezolizumab every 3 weeks.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブ、3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブ、及び3週間ごとに15mg/kgの用量のベバシズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or subject population is given 600 mg dose (e.g., fixed dose) of tiragolumab, 1200 mg dose (e.g., fixed dose) of atezolizumab every 3 weeks, and 15 mg/kg dose of bevacizumab every 3 weeks. provide a way to
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、2週間ごとに420mgの用量(例えば、固定用量)のチラゴルマブ及び2週間ごとに840mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or subject population is given administering one or more dosing cycles of a 420 mg dose (eg, fixed dose) of tiragolumab and a 840 mg dose (eg, fixed dose) of atezolizumab every two weeks.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、2週間ごとに420mgの用量(例えば、固定用量)のチラゴルマブ、2週間ごとに840mgの用量(例えば、固定用量)のアテゾリズマブ、及び2週間ごとに5mg/kg、7.5mg/kg又は10mg/kgの用量のベバシズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or subject population having HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or subject population is given tiragolumab at a dose (e.g., fixed dose) of 420 mg every 2 weeks, atezolizumab at a dose (e.g., fixed dose) of 840 mg every 2 weeks, and doses of 5 mg/kg, 7.5 mg/kg or 10 mg/kg every 2 weeks. Methods of administering one or more dosing cycles of bevacizumab are provided.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、4週間ごとに840mgの用量(例えば、固定用量)のチラゴルマブ及び4週間ごとに1680mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or population of subjects with HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or population of subjects is given administering a dose (eg, fixed dose) of 840 mg of tiragolumab and one or more dosing cycles of a dose (eg, fixed dose) of 1680 mg (eg, fixed dose) of atezolizumab every 4 weeks.
別の態様では、本発明は、HCC(例えば、局所進行性もしくは転移性及び/又は切除不能なHCC)を有する対象又は対象集団を処置する方法であって、対象又は対象集団に、4週間ごとに840mgの用量(例えば、固定用量)のチラゴルマブ、4週間ごとに1680mgの用量(例えば、固定用量)のアテゾリズマブ、及び2週間ごとに5mg/kg、7.5mg/kg又は10mg/kgの用量のベバシズマブの1回以上の投薬サイクルを投与する方法を提供する。 In another aspect, the invention provides a method of treating a subject or population of subjects with HCC (e.g., locally advanced or metastatic and/or unresectable HCC), wherein the subject or population of subjects is given tiragolumab at a dose (e.g., fixed dose) of 840 mg every 4 weeks; Methods of administering one or more dosing cycles of bevacizumab are provided.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を提供し、方法は、有効量の抗TIGITアンタゴニスト抗体及び有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) for , a method comprising administering to a subject or population of subjects an effective amount of an anti-TIGIT antagonist antibody and an effective amount of one or more dosing cycles of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) including doing
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を提供し、方法は、有効量の抗TIGITアンタゴニスト抗体、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及び有効量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) and VEGF antagonists for (e.g., an anti-VEGF antibody (e.g., bevacizumab)), the method comprising an effective amount of an anti-TIGIT antagonist antibody, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) and an effective amount of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) one or more dosing cycles to the subject or population of subjects.
例示的な医薬品及びその使用
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに約80mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される使用を提供する。いくつかの態様では、医薬は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに80mgと2000mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される。
Exemplary Medicaments and Uses Thereof In another aspect, the invention provides a subject or subject population having liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC). anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD - use of an L1 antagonistic antibody (e.g., atezolizumab), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament, wherein the medicament is about 30 mg every 3 weeks and about An anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 1200 mg and a PD-1 axis binding antagonist (e.g., an anti-PD- Uses formulated for administration of L1 antagonist antibodies (eg, atezolizumab) are provided. In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks and a dose (e.g., fixed dose) of between 80 mg and 2000 mg every three weeks PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)) are formulated for administration at .
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び3週間ごとに約0.1mg/kgと50mg/kgの間の用量(例えば、抗VEGF抗体(例えば、ベバシズマブ))のVEGFアンタゴニストを投与するために製剤化される。いくつかの態様では、医薬は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mgと2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び3週間ごとに約0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するために製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), wherein the method comprises administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg every three weeks, PD-1 axial binding at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg every three weeks Antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and VEGF at a dose between about 0.1 mg/kg and 50 mg/kg (eg, an anti-VEGF antibody (eg, bevacizumab)) every 3 weeks Formulated for administration of the antagonist. In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks, a dose (e.g., fixed dose) of between 80 mg and 2000 mg every three weeks A PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody) at a dose between about 0.1 mg/kg and 50 mg/kg every 3 weeks (eg, bevacizumab)).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、2週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに約80mgと約1200mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される使用を提供する。いくつかの態様では、医薬は、2週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに80mgと1200mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament, wherein the medicament is administered at a dose of between about 30 mg and about 600 mg every two weeks (e.g. , fixed dose) of an anti-TIGIT antagonist antibody (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab ))). In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 600 mg every two weeks and a dose (e.g., fixed dose) of between 80 mg and 1200 mg every two weeks are formulated for administration of PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)) in patients.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、2週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、2週間ごとに約80mgと約1200mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び2週間ごとに約0.1mg/kgと50mg/kgの間の用量(例えば、抗VEGF抗体(例えば、ベバシズマブ))のVEGFアンタゴニストを投与するために製剤化される。いくつかの態様では、医薬は、2週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、2週間ごとに80mgと1200mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び2週間ごとに0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するために製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), wherein the method comprises administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 600 mg every two weeks, PD-1 axial binding at a dose (e.g., fixed dose) of between about 80 mg and about 1200 mg every two weeks Antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and VEGF at a dose between about 0.1 mg/kg and 50 mg/kg (eg, an anti-VEGF antibody (eg, bevacizumab)) every two weeks Formulated for administration of the antagonist. In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 600 mg every two weeks; A PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., an anti-VEGF antibody (e.g., For example, it is formulated for administration of bevacizumab)).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、4週間ごとに約600mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び4週間ごとに約1200mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される使用を提供する。いくつかの態様では、医薬は、4週間ごとに600mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び4週間ごとに1200mgと2000mgの間の用量(例えば、固定用量)でのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するために製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies) in the manufacture or preparation of a medicament for atezolizumab)), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament, wherein the medicament is dosed between about 600 mg and about 1200 mg every 4 weeks (e.g. , fixed dose) of an anti-TIGIT antagonist antibody (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab ))). In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 600 mg and 1200 mg every 4 weeks and a dose (e.g., fixed dose) of between 1200 mg and 2000 mg every 4 weeks PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)) are formulated for administration at .
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造又は調製における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、4週間ごとに約600mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、4週間ごとに約1200mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び2週間ごとに約0.1mg/kgと50mg/kgの間の用量(例えば、抗VEGF抗体(例えば、ベバシズマブ))のVEGFアンタゴニストを投与するために製剤化される。いくつかの態様では、医薬は、4週間ごとに600mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、4週間ごとに1200mgと2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び2週間ごとに0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するために製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), wherein the method comprises administering to a subject or subject population one or more dosing cycles of the medicament, the medicament comprising: anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 600 mg and about 1200 mg every 4 weeks, PD-1 axis binding at a dose (e.g., fixed dose) of between about 1200 mg and about 2000 mg every 4 weeks Antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and VEGF at a dose between about 0.1 mg/kg and 50 mg/kg (eg, an anti-VEGF antibody (eg, bevacizumab)) every two weeks Formulated for administration of the antagonist. In some aspects, the medicament is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 600 mg and 1200 mg every four weeks; A PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., an anti-VEGF antibody (e.g., For example, it is formulated for administration of bevacizumab)).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、対象又は対象集団に医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを投与することを含み、医薬は、3週間ごとに約80mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。いくつかの態様では、医薬は、3週間ごとに80mgと2000mgの間の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) in the manufacture of medicaments for ), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament and an anti-TIGIT antagonist antibody, wherein the medicament is between about 80 mg and about 2000 mg every three weeks. to administer a dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a dose between about 30 mg and about 1200 mg (e.g., , fixed dose) of the anti-TIGIT antagonist antibody. In some aspects, the medicament administers a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) at a dose (eg, fixed dose) of between 80 mg and 2000 mg every 3 weeks. and to administer a dose of between 30 mg and 1200 mg (eg, a fixed dose) of the anti-TIGIT antagonist antibody every 3 weeks.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに約80mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに約0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。いくつかの態様では、医薬は、3週間ごとに80mgと2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab), in the manufacture of medicaments for ) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), the method comprising administering to a subject or population of subjects one or more dosing cycles of the medicament and an anti-TIGIT antagonist antibody, The medicament is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of between about 80 mg and about 2000 mg every three weeks, about An anti-TIGIT antagonist antibody at a dose of between 30 mg and about 1200 mg (e.g., a fixed dose) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., , bevacizumab)). In some aspects, the medicament is administered a dose (e.g., fixed dose) of between 80 mg and 2000 mg of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) every three weeks. anti-TIGIT antagonist antibody at doses between 30 mg and 1200 mg every 3 weeks (e.g., fixed dose) and VEGF antagonists at doses between 0.1 mg/kg and 50 mg/kg every 3 weeks (e.g., formulated to administer an anti-VEGF antibody (eg, bevacizumab).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、対象又は対象集団に医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを投与することを含み、医薬は、2週間ごとに約80mgと約1200mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び2週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。いくつかの態様では、医薬は、2週間ごとに80mgと1200mgの間の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び2週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) in the manufacture of medicaments for ), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament and an anti-TIGIT antagonist antibody, wherein the medicament is between about 80 mg and about 1200 mg every two weeks. to administer a dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a dose of between about 30 mg and about 600 mg (e.g., , fixed dose) of the anti-TIGIT antagonist antibody. In some aspects, the medicament administers a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) at a dose (eg, fixed dose) of between 80 mg and 1200 mg every two weeks. and to administer a dose of between 30 mg and 600 mg (eg, a fixed dose) of the anti-TIGIT antagonist antibody every two weeks.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、2週間ごとに約80mgと約1200mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、2週間ごとに約30mgと約600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに約0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。いくつかの態様では、医薬は、2週間ごとに80mgと1200mgの間の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、2週間ごとに30mgと600mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab), in the manufacture of medicaments for ) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), the method comprising administering to a subject or population of subjects one or more dosing cycles of the medicament and an anti-TIGIT antagonist antibody, The medicament is a dose (e.g., fixed dose) of between about 80 mg and about 1200 mg of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) every two weeks, about An anti-TIGIT antagonist antibody at a dose of between 30 mg and about 600 mg (e.g., a fixed dose) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., an anti-VEGF antibody, e.g., , bevacizumab))). In some aspects, the medicament administers a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) at a dose (eg, fixed dose) of between 80 mg and 1200 mg every two weeks. anti-TIGIT antagonist antibody at doses between 30 mg and 600 mg (e.g., fixed dose) every 2 weeks and VEGF antagonists at doses between 0.1 mg/kg and 50 mg/kg every 2 weeks (e.g., formulated to administer an anti-VEGF antibody (eg, bevacizumab).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の使用を提供し、方法は、対象又は対象集団に医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを投与することを含み、医薬は、4週間ごとに約1200mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び4週間ごとに約600mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。いくつかの態様では、医薬は、4週間ごとに1200mgと2000mgの間の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、及び4週間ごとに600mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) in the manufacture of medicaments for ), wherein the method comprises administering to a subject or subject population one or more dosing cycles of a medicament and an anti-TIGIT antagonist antibody, wherein the medicament is between about 1200 mg and about 2000 mg every 4 weeks. to administer a dose (e.g., a fixed dose) of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a dose between about 600 mg and about 1200 mg (e.g., , fixed dose) of the anti-TIGIT antagonist antibody. In some aspects, the medicament administers a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of between 1200 mg and 2000 mg every 4 weeks. and to administer a dose (eg, fixed dose) of between 600 mg and 1200 mg of anti-TIGIT antagonist antibody every 4 weeks.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の使用を提供し、方法は、医薬及び抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、4週間ごとに約1200mgと約2000mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、4週間ごとに約600mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに約0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。いくつかの態様では、医薬は、4週間ごとに1200mgと2000mgの間の用量(例えば、固定用量)でPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与するため、4週間ごとに600mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び2週間ごとに0.1mg/kgと50mg/kgの間の用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を投与するように製剤化される。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab), in the manufacture of medicaments for ) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), the method comprising administering to a subject or population of subjects one or more dosing cycles of the medicament and an anti-TIGIT antagonist antibody, The medicament is a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) at a dose (eg, fixed dose) of between about 1200 mg and about 2000 mg every 4 weeks, about An anti-TIGIT antagonist antibody at a dose between 600 mg and about 1200 mg (e.g., a fixed dose) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., an anti-VEGF antibody (e.g., , bevacizumab))). In some aspects, the medicament administers a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose (e.g., fixed dose) of between 1200 mg and 2000 mg every 4 weeks. anti-TIGIT antagonist antibody at doses between 600 mg and 1200 mg (e.g., fixed dose) every 4 weeks and VEGF antagonists at doses between 0.1 mg/kg and 50 mg/kg every 2 weeks (e.g., formulated to administer an anti-VEGF antibody (eg, bevacizumab).
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を3週間ごとに600mgの用量(例えば、固定用量)で、及びアテゾリズマブを3週間ごとに1200mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for , the method comprising administering one or more dosing cycles of the medicament to a subject or population of subjects, as described in more detail below. wherein the medicament is formulated for administration of the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 600 mg every three weeks and atezolizumab at a dose (e.g., fixed dose) of 1200 mg every three weeks; The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体、アテゾリズマブ、及びベバシズマブの使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、3週間ごとに600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブ、3週間ごとに15mg/kgの用量のベバシズマブを投与するために製剤化され、抗TIGITアンタゴニスト抗体は、以下に更に詳細に記載するように、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。
In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody, atezolizumab, and bevacizumab in the manufacture of a medicament for, the method comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament administered every 3
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を2週間ごとに420mgの用量(例えば、固定用量)で、及びアテゾリズマブを2週間ごとに840mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for , the method comprising administering one or more dosing cycles of the medicament to a subject or population of subjects, as described in more detail below. wherein the medicament is formulated for administration of the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 420 mg every two weeks and atezolizumab at a dose (e.g., fixed dose) of 840 mg every two weeks; The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体、アテゾリズマブ、及びベバシズマブの使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、2週間ごとに420mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、2週間ごとに840mgの用量(例えば、固定用量)のアテゾリズマブ、及び2週間ごとに5mg/kg、7.5mg/kg又は10mg/kgの用量のベバシズマブを投与するために製剤化され、抗TIGITアンタゴニスト抗体は、以下に更に詳細に記載するように、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody, atezolizumab, and bevacizumab in the manufacture of a medicament for, the method comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament administered every two weeks anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 420 mg every 2 weeks, atezolizumab at a dose (e.g., fixed dose) of 840 mg every 2 weeks, and 5 mg/kg, 7.5 mg/kg or 10 mg/kg every 2 weeks and the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19, as described in more detail below. VL domain containing In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用を提供し、以下に更に詳細に記載されるように、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、抗TIGITアンタゴニスト抗体を4週間ごとに840mgの用量(例えば、固定用量)で、及びアテゾリズマブを4週間ごとに1680mgの用量(例えば、固定用量)で投与するために製剤化され、抗TIGITアンタゴニスト抗体は、配列番号17又は18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for , the method comprising administering one or more dosing cycles of the medicament to a subject or population of subjects, as described in more detail below. wherein the medicament is formulated for administration of the anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 840 mg every 4 weeks and atezolizumab at a dose (e.g., fixed dose) of 1680 mg every 4 weeks; The anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
別の態様では、本発明は、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団を処置する方法で使用するための医薬の製造における抗TIGITアンタゴニスト抗体、アテゾリズマブ、及びベバシズマブの使用を提供し、方法は、医薬の1回以上の投薬サイクルを対象又は対象集団に投与することを含み、医薬は、4週間ごとに840mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、4週間ごとに1680mgの用量(例えば、固定用量)のアテゾリズマブ、2週間ごとに5mg/kg、7.5mg/kg又は10mg/kgの用量のベバシズマブを投与するために製剤化され、抗TIGITアンタゴニスト抗体は、以下に更に詳細に記載するように、配列番号17又は18のアミノ酸配列を含むVHドメイン、及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを含む。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を有するVHドメイン及び配列番号19のアミノ酸配列を有するVLドメインを有する。 In another aspect, the invention is used in a method of treating a subject or population of subjects with liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC) use of an anti-TIGIT antagonist antibody, atezolizumab, and bevacizumab in the manufacture of a medicament for, the method comprising administering to a subject or subject population one or more dosing cycles of the medicament, the medicament administered every 4 weeks anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 840 mg every 4 weeks; atezolizumab at a dose (e.g., fixed dose) of 1680 mg every 4 weeks; Formulated to administer a dose of bevacizumab, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18 and the amino acid sequence of SEQ ID NO: 19, as described in more detail below Contains the VL domain. In some examples, the anti-TIGIT antagonist antibody comprises a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has a VH domain having the amino acid sequence of SEQ ID NO:18 and a VL domain having the amino acid sequence of SEQ ID NO:19.
投薬レジメン及び投与
本明細書に記載される本発明の治療方法及び使用は、一態様では、肝臓がん(例えば、局所進行性もしくは転移性及び/又は切除不能のHCCを含む肝細胞癌腫(HCC))を有する対象又は対象集団に、有効量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)を含む処置レジメンを投与することを含む。
Dosing Regimens and Administration The therapeutic methods and uses of the invention described herein are, in one aspect, directed to liver cancer (e.g., hepatocellular carcinoma (HCC), including locally advanced or metastatic and/or unresectable HCC). )), an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and administering a treatment regimen comprising an anti-TIGIT antagonist antibody (eg, tiragolumab).
本明細書に記載の医薬組成物は、以下及びセクションIII(K)に記載の投与のために製剤化することができる。 The pharmaceutical compositions described herein can be formulated for administration as described below and in Section III(K).
有効投与量
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、併用療法(例えば、セクションIII(K)に記載されている用量のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))とのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))による併用処置)で投与され、用量は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストの投与は、セクションIII(K)に記載されている。
Effective Dosage In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is used in combination therapy (e.g., as described in Section III(K)). co-treatment with a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) at a dose of , may be decreased compared to standard doses of anti-TIGIT antagonist antibodies administered as monotherapy. Administration of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists and VEGF antagonists are described in Section III(K).
投薬サイクル投薬サイクル
本発明の方法及び使用のいずれにおいても、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、及び/又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投薬サイクルは、臨床上の利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約14~28日間(例えば、14日間、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間、24日間、25日間、26日間、27日間又は28日間)である。いくつかの例では、投薬サイクルの長さは、約21日間である。いくつかの例では、投薬サイクルの長さは、約14日間である。いくつかの例では、投薬サイクルの長さは、約28日間である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、各投薬サイクルの約1日目(例えば、1±3日目)に投与する。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、各投薬サイクルの約1日目(例えば、1±3日目)に投与する。例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、約15mg/kgの用量で(すなわち、3週間ごとに約15mg/kgの用量で)各21日間サイクルの1日目に静脈内投与する。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに600mgの用量で)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、各投薬サイクルの1日目(例えば、1±3日目)に投与する。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、1200mgの用量で各21日間サイクルの1日目に(すなわち、1200mgの用量で3週間ごとに)静脈内投与される。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、各投薬サイクルの1日目(例えば、1±3日目)に投与する。例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、15mg/kgの用量で(すなわち、3週間ごとに15mg/kgの用量で)各21日間サイクルの1日目に静脈内投与する。
Dosing Cycle Dosing Cycle In any of the methods and uses of the invention, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, anti-PD - L1 antagonist antibody (e.g., atezolizumab)) or VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) for one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7) , 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32 , 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) ), and/or a dosing cycle of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) lacks clinical benefit (e.g., documented disease progression, drug resistance, death, or unacceptable toxicity) continue until In some examples, the length of each dosing cycle is about 14 to 28 days (eg, 14 days, 15 days, 16 days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days). days, 24 days, 25 days, 26 days, 27 days or 28 days). In some examples, the dosing cycle length is about 21 days. In some examples, the dosing cycle length is about 14 days. In some examples, the dosing cycle length is about 28 days. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered on about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与する。
In some examples, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) are administered on about day 1 (eg,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間の各サイクルの第1日に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、21日間の各サイクルの第1日に約1200mgの用量で(すなわち、3週間ごとに約1200mgの用量で)静脈内投与され、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、21日間の各サイクルの第1日に約15mg/kgの用量で(すなわち、3週間ごとに約15mg/kgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間の各サイクルの第1日に600mgの用量で(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、21日間の各サイクルの第1日に1200mgの用量で(すなわち、3週間ごとに1200mgの用量で)静脈内投与され、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、21日間の各サイクルの第1日に15mg/kgの用量で(すなわち、3週間ごとに15mg/kgの用量で)静脈内投与される。
In some examples, the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered at a dose of about 600 mg on
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を14日間の各サイクルの1日目に約420mgの用量で(すなわち、2週間ごとに約420mgの用量で)静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を14日間の各サイクルの1日目に約840mgの用量で(すなわち、2週間ごとに約840mgの用量で)静脈内投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を14日間の各サイクルの1日目に約5mg/kg、7.5mg/kg、又は10mg/kgの用量で(すなわち、2週間ごとに約5mg/kg、7.5mg/kg、又は10mg/kgの用量で)静脈内投与する。他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を14日間の各サイクルの1日目に420mgの用量で(すなわち、2週間ごとに420mgの用量で)静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を14日間の各サイクルの1日目に840mgの用量で(すなわち、2週間ごとに840mgの用量で)静脈内投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を14日間の各サイクルの1日目に5mg/kg、7.5mg/kg、又は10mg/kgの用量で(すなわち、2週間ごとに5mg/kg、7.5mg/kg、又は10mg/kgの用量で)静脈内投与する。
In another example, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) at a dose of about 420 mg on
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を28日間の各サイクルの1日目に約840mgの用量で(すなわち、4週間ごとに約840mgの用量で)静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を28日間の各サイクルの1日目に約1680mgの用量で(すなわち、4週間ごとに約1680mgの用量で)静脈内投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を28日間の各サイクルの1日目及び15日目に約5mg/kg、7.5mg/kg、又は10mg/kgの用量で(すなわち、2週間ごとに約5mg/kg、7.5mg/kg、又は10mg/kgの用量で)静脈内投与する。他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を28日間の各サイクルの1日目に840mgの用量で(すなわち、4週間ごとに840mgの用量で)静脈内投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を28日間の各サイクルの1日目に1680mgの用量で(すなわち、4週間ごとに1680mgの用量で)静脈内投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を28日間の各サイクルの1日目及び15日目に5mg/kg、7.5mg/kg、又は10mg/kgの用量で(すなわち、2週間ごとに5mg/kg、7.5mg/kg、又は10mg/kgの用量で)静脈内投与する。
In another example, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered at a dose of about 840 mg on
投与順序及び観察期間
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び/又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。他の例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の前に対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を最初に対象又は対象集団に投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))をPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後に対象又は対象集団に投与し、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)をVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))アンタゴニストの投与後に対象又は対象集団に投与する。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を最初に対象又は対象集団に投与し、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)をPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後に対象又は対象集団に投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後に対象又は対象集団に投与する。
Dosing Sequence and Observation Period In some examples, the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is combined with a VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) and/or or administered to the subject or population of subjects prior to an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, for example, after administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) or anti-TIGIT Prior to administration of an antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), the method includes an intervening first observation period. In some examples, for example, following administration of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), the VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) A TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered to the subject or population of subjects prior to administration. In other examples, administration of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) followed by an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein) (eg, tiragolumab)) is administered to a subject or population of subjects prior to a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)). In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is first administered to a subject or population of subjects, and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab) )) to a subject or population of subjects following administration of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and an anti-TIGIT antagonist antibody (e.g., as disclosed herein an anti-TIGIT antagonist antibody (eg, tiragolumab) is administered to a subject or population of subjects after administration of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) antagonist. In some examples, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is first administered to a subject or population of subjects, followed by an anti-TIGIT antagonist antibody (e.g., disclosed herein). An anti-TIGIT antagonist antibody (e.g., tiragolumab) such as is administered to a subject or population of subjects after administration of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), and a VEGF antagonist (e.g., , an anti-VEGF antibody (eg, bevacizumab)) is administered to a subject or population of subjects after administration of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab).
いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第2の観察期間を更に含む。いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第3の観察期間を更に含む。 In some examples, the method involves the use of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) or an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab). A second post-administration observation period is further included. In some examples, the method uses a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and an anti-TIGIT antagonist antibody. Further includes a third observation period following administration of (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab).
いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第1の観察期間及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第2の観察期間の両方を含む。いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第1の観察期間、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第2の観察期間、ならびにTIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストの投与後の第3の観察期間を含む。いくつかの例では、第1、第2、及び/又は第3の観察期間は、それぞれ約30分と約120分の間の長さ(例えば、約30分と60分の間の長さ、60と90分の間の長さ、及び/又は90と120分の間の長さ)である。第1、第2及び第3の観察期間がそれぞれ約60分の長さである場合、方法は、第1、第2又は第3の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、又はVEGF抗体(例えば、抗VEGF抗体(ベバシズマブ))の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1、第2及び第3の観察期間がそれぞれ約30分の長さである場合、方法は、第1、第2又は第3の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、又はVEGF抗体(例えば、抗VEGF抗体(ベバシズマブ))の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, the methods include a first observation period following administration of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., , bevacizumab)) or a second observation period following administration of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) for a first observation period, a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., , bevacizumab)) or an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), and a second observation period following administration of the TIGIT antagonist antibody, PD-1 axis binding. A third observation period following administration of antagonist and VEGF antagonist is included. In some examples, the first, second, and/or third observation periods are each between about 30 minutes and about 120 minutes long (e.g., between about 30 minutes and 60 minutes long, between 60 and 90 minutes and/or between 90 and 120 minutes). If the first, second and third observation periods are each about 60 minutes long, the method includes treating the PD-1 axis binding antagonist (e.g., anti-PD - L1 antagonist antibody (e.g., atezolizumab)), anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), or VEGF antibody (e.g., anti-VEGF antibody (bevacizumab)) recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature) at about 30±10 minutes after administration of If the first, second and third observation periods are each about 30 minutes long, the method includes treating the PD-1 axis binding antagonist (e.g., anti-PD - L1 antagonist antibody (e.g., atezolizumab)), anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), or VEGF antibody (e.g., anti-VEGF antibody (bevacizumab)) recording the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and body temperature) at about 15±10 minutes after administration of the drug.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の前に対象又は対象集団に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab)) or a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) prior to administration to the subject or population of subjects.
いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の前に対象又は対象集団に投与される。他の例では、例えば、抗TIGITアンタゴニスト抗体の投与後、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の前に対象又は対象集団に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を最初に対象又は対象集団に投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後に対象又は対象集団に投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))をPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後に対象又は対象集団に投与する。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を最初に対象又は対象集団に投与し、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後に対象又は対象集団に投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))をVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後に対象又は対象集団に投与する。 In some examples, for example, after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab )), the method includes an intervening first observation period. In some instances, e.g., after administration of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) acts as a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) to the subject or subject population. In other examples, for example, following administration of an anti-TIGIT antagonist antibody, a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is administered to a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). )) to a subject or population of subjects. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is first administered to a subject or population of subjects, and a PD-1 axis binding antagonist (e.g., , an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) to a subject or population of subjects after administration of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab); A VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is administered to a subject or population of subjects after administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is first administered to a subject or population of subjects, and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) to a subject or population of subjects after administration of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), and a PD-1 axis binding antagonist ( For example, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to a subject or population of subjects after administration of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)).
いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第2の観察期間を更に含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第3の観察期間を更に含む。 In some examples, the method includes administering a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)). It further includes 2 observation periods. In some examples, the method uses an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody). (eg, atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), followed by a third observation period.
いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間、及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第2の観察期間の両方を含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第2の観察期間、ならびにTIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストの投与後の第3の観察期間を含む。いくつかの例では、第1、第2、及び第3の観察期間は、それぞれ約30分と約60分の間の長さである。第1、第2、及び第3の観察期間がそれぞれ約60分の長さである例では、方法は、第1、第2、又は第3の観察期間中の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後約30±10分で対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)の集団を記録することを含み得る。第1、第2、及び第3の観察期間がそれぞれ約30分の長さである例では、方法は、第1、第2、又は第3の観察期間中の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、又はVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後約15±10分で対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)の集団を記録することを含み得る。 In some examples, the method includes a first observation period after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) or a VEGF antagonist (eg, , a second observation period following administration of an anti-VEGF antibody (eg, bevacizumab). In some examples, the method includes a first observation period after administration of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) or a VEGF antagonist (eg, A second observation period following administration of an anti-VEGF antibody (eg, bevacizumab)) and a third observation period following administration of a TIGIT antagonist antibody, a PD-1 axis binding antagonist and a VEGF antagonist. In some examples, the first, second, and third observation periods are each between about 30 minutes and about 60 minutes long. In examples in which the first, second, and third observation periods are each about 60 minutes long, the method includes: Vital signs of the subject or subject population at about 30 ± 10 minutes after administration of the axially bound antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) (eg, pulse rate, respiration rate, blood pressure, and temperature). In examples in which the first, second, and third observation periods are each about 30 minutes long, the method includes: Vital signs of the subject or subject population about 15 ± 10 minutes after administration of the axially bound antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) (eg, pulse rate, respiration rate, blood pressure, and temperature).
いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の前に対象又は対象集団に投与される。いくつかの例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の前に対象又は対象集団に投与される。他の例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を対象又は対象集団に最初に投与し、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)をVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後に対象又は対象集団に投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後に対象又は対象集団に投与する。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を対象又は対象集団に最初に投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))をVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後に対象又は対象集団に投与し、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)をPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))アンタゴニストの投与後に対象又は対象集団に投与する。 In some examples, the VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) or PD- A monoaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered prior to the subject or population of subjects. In some examples, for example, after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab ) or a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)), the method includes an intervening first observation period. In some examples, for example, administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) followed by an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab ) is administered to a subject or population of subjects prior to a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In other examples, for example, following administration of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to anti-TIGIT An antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered to the subject or population of subjects prior to administration. In some examples, a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is first administered to the subject or subject population, and an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist as disclosed herein) is administered. An antibody (e.g., tiragolumab) is administered to a subject or population of subjects after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is administered to a subject or population of subjects after administration of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is first administered to the subject or subject population, and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) is administered to the subject or population of subjects first. )) to a subject or population of subjects after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., , tiragolumab) is administered to a subject or population of subjects following administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) antagonist.
いくつかの例では、方法は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第2の観察期間を更に含む。いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第3の観察期間を更に含む。 In some examples, the method uses an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) or a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody). (eg, atezolizumab)). In some examples, the method uses a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)), an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and Further includes a third observation period following administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第1の観察期間、及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第2の観察期間の両方を含む。いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第1の観察期間、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第2の観察期間、ならびにTIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストの投与後の第3の観察期間を含む。いくつかの例では、第1、第2、及び第3の観察期間は、それぞれ約30分と約60分の間の長さである。第1、第2、及び第3の観察期間がそれぞれ約60分の長さである場合、方法は、第1、第2、又は第3の観察期間中のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1、第2、及び第3の観察期間がそれぞれ約30分の長さである場合、方法は、第1、第2、又は第3の観察期間中のVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, the method includes a first observation period after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and an anti-TIGIT antagonist antibody (e.g., as disclosed herein). A second observation period following administration of both an anti-TIGIT antagonist antibody (eg, tiragolumab) or a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is included. In some examples, the method includes administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) for a first observation period, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antibody as disclosed herein). A second observation period following administration of a TIGIT antagonist antibody, e.g. tiragolumab) or a PD-1 axis binding antagonist (e.g. an anti-PD-L1 antagonist antibody (e.g. atezolizumab)) and a TIGIT antagonist antibody, PD-1 axis binding A third observation period following administration of antagonist and VEGF antagonist is included. In some examples, the first, second, and third observation periods are each between about 30 minutes and about 60 minutes long. If the first, second, and third observation periods are each about 60 minutes long, the method includes administering a VEGF antagonist (e.g., an anti-VEGF antibody ( bevacizumab)), an anti-TIGIT antagonist antibody (e.g. an anti-TIGIT antagonist antibody as disclosed herein, e.g. tiragolumab), or a PD-1 axis binding antagonist (e.g. an anti-PD-L1 antagonist antibody (e.g. , atezolizumab)) at about 30±10 minutes after administration of the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature). If the first, second, and third observation periods are each about 30 minutes long, the method includes administering a VEGF antagonist (e.g., an anti-VEGF antibody ( bevacizumab)), an anti-TIGIT antagonist antibody (e.g. an anti-TIGIT antagonist antibody as disclosed herein, e.g. tiragolumab), or a PD-1 axis binding antagonist (e.g. an anti-PD-L1 antagonist antibody (e.g. , atezolizumab)) at about 15±10 minutes after administration of the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature).
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を対象又は対象集団に同時に投与する。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後、方法は観察期間を含む。 In other examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is a subject or subject population. administered at the same time. In some examples, the method includes an observation period, eg, after administration of the anti-TIGIT antagonist antibody and the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)).
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、対象又は対象集団に同時に投与される。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後に、方法は観察期間を含む。 In other examples, anti-TIGIT antagonist antibodies (eg, anti-TIGIT antagonist antibodies disclosed herein, eg, tiragolumab) and PD-1 axis binding antagonists (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)). are administered simultaneously to a subject or population of subjects. In some examples, the method includes an observation period, eg, after administration of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
他の例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を対象又は対象集団に同時に投与する。いくつかの例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後、方法は観察期間を含む。 In other examples, a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) and a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) are administered simultaneously to a subject or population of subjects. . In some examples, for example, after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), the method is Including observation period.
いくつかの例では、観察期間は、約30分と約60分の間の長さである。観察期間が約60分の長さである場合、方法は、投与後約30±10分で対象又は対象集団のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。観察期間が約30分の長さである場合、方法は、投与後約15±10分で対象のバイタルサインの集団(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, the observation period is between about 30 minutes and about 60 minutes long. If the observation period is about 60 minutes long, the method includes recording the subject's or subject population's vital signs (e.g., pulse rate, respiratory rate, blood pressure, and temperature) at about 30±10 minutes after administration. can contain. If the observation period is about 30 minutes long, the method includes recording the subject's vital signs cluster (e.g., pulse rate, respiratory rate, blood pressure, and temperature) at about 15±10 minutes after administration. obtain.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の同時投与後に投与される。 In some examples, the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein; tiragolumab) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)), followed by co-administration.
いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の同時投与後に投与される。 In some examples, the VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is combined with an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, such as tiragolumab) and PD- It is administered after co-administration of a uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))及びVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の同時投与後に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab)) and a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)).
いくつかの例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後、方法は第2の観察期間を含む。いくつかの例では、例えば、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後、方法は第2の観察期間を含む。いくつかの例では、第2の観察期間は、約30分と約60分の間の長さである。第2の観察期間が約60分の長さである場合、方法は、投与後約30±10分で対象のバイタルサインの集団(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第2の観察期間が約30分の長さである場合、方法は、投与後約15±10分で対象のバイタルサインの集団(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, e.g., VEGF antagonists (e.g., anti-VEGF antibodies (e.g., bevacizumab)), anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies as disclosed herein, e.g., tiragolumab), and After administration of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)), the method includes a second observation period. In some examples, for example, after administration of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), the method is Includes a second observation period. In some examples, the second observation period is between about 30 minutes and about 60 minutes long. If the second observation period is about 60 minutes long, the method records the subject's vital signs cluster (e.g., pulse rate, respiratory rate, blood pressure, and temperature) at about 30±10 minutes after administration. can include If the second observation period is about 30 minutes long, the method records the subject's vital signs cluster (e.g., pulse rate, respiratory rate, blood pressure, and temperature) at about 15±10 minutes after administration. can include
B.尿路上皮がんに関する治療方法及び使用
尿路上皮癌腫
尿路上皮癌腫(UC)は、世界中で最も一般的な泌尿器系のがんである。症例の大部分は膀胱に由来する。UCは、非筋肉浸潤性、筋肉浸潤性、又は転移性疾患と診断することができ、3人に1人が新たに筋肉浸潤性疾患と診断される(腫瘍、リンパ節及び転移(TNM)分類によるcT2-T4a Nx M0)。筋肉浸潤性UC(MIUC)は、まとめて、筋肉浸潤性膀胱がん(MIBC)及び筋肉浸潤性尿路上皮がん(UTUC)を指す。2018年には、世界中で推定549,393例の膀胱がんの新規症例及び199,922例の死亡例があった。欧州では、197,110例の膀胱がんの新規症例及び64,970例の死亡があったと推定され、このうち164,450例の新規症例及び52,930例の死亡は欧州連合の28の会員国においてであった。米国では、2020年に膀胱がんの新規症例が81,400例あり、17,980例が死亡すると推定されている。米国でUCと診断された患者の年齢中央値は73であり、これは全ての腫瘍タイプの診断時の最高年齢である。
B. Methods of Treatment and Uses for Urothelial Cancer Urothelial Carcinoma Urothelial carcinoma (UC) is the most common cancer of the urinary system worldwide. The majority of cases originate in the bladder. UC can be diagnosed as non-muscle invasive, muscle invasive, or metastatic disease, with 1 in 3 newly diagnosed muscle invasive disease (tumor, node and metastasis (TNM) classification). cT2-T4a Nx M0). Muscle invasive UC (MIUC) collectively refers to muscle invasive bladder cancer (MIBC) and muscle invasive urothelial carcinoma (UTUC). In 2018, there were an estimated 549,393 new cases of bladder cancer and 199,922 deaths worldwide. In Europe, there were an estimated 197,110 new cases of bladder cancer and 64,970 deaths, of which 164,450 new cases and 52,930 deaths were attributed to 28 members of the European Union. in the country. In the United States, it is estimated that there will be 81,400 new cases of bladder cancer in 2020 and 17,980 deaths. The median age of patients diagnosed with UC in the United States is 73, the oldest age at diagnosis for any tumor type.
MIBCの処置のための治療アプローチに対する特に差し迫った必要性がある。MIBCは、新たな尿路上皮がん症例の約30%に相当する。MIBCは、25~50%の5年生存率を有し(欧州泌尿器科学会EAUガイドライン2013)、この疾患領域における有効な新しい処置 がないため、過去30年間ほとんど改善が見られなかった(Surveillance,Epidemiology,and End Results(SEER)Program.Cancer stat facts:bladder cancer,2020)。したがって、改善された医療介入に対する満たされていないニーズが高い。 There is a particularly urgent need for therapeutic approaches for the treatment of MIBC. MIBC represents approximately 30% of new urothelial cancer cases. MIBC has a 5-year survival rate of 25-50% (European Urological Association EAU Guidelines 2013) and has seen little improvement over the past 30 years due to the lack of effective new treatments in this disease area (Surveillance, Epidemiology, and End Results (SEER) Program. Cancer stats: bladder cancer, 2020). Therefore, there is a high unmet need for improved medical interventions.
尿路上皮癌腫を処置するための方法及び使用
有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)の1回以上の投薬サイクルを対象又は対象集団に投与することを含む、対象又は対象集団においてUC(例えば、膀胱がん(例えば、MIBC))を処置するための方法及び使用が本明細書で提供される。対象は、好ましくはヒトである。いくつかの実施形態では、対象又は対象集団は、以前にがん免疫療法で処置されたことがない。
Methods and Uses for Treating Urothelial Carcinoma UC (e.g., bladder Provided herein are methods and uses for treating cancer (eg, MIBC). The subject is preferably human. In some embodiments, the subject or subject population has not been previously treated with cancer immunotherapy.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)を、それを必要とする対象又は対象集団に3週間(例えば、各21日間の投薬サイクルの1日目に)毎に投与することを含む方法及び使用を含む。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). (e.g., an anti-PD-1 antagonist antibody, such as pembrolizumab) to a subject or population in need thereof every three weeks (e.g., on
本発明は、MIBCを有する対象又は対象集団を処置するための方法及び使用を含み、方法は、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストを1回以上の投薬サイクルで対象又は対象集団に投与することを含み、対象又は対象集団は、白金系化学療法剤(例えば、シスプラチン)による治療に適格ではない。いくつかの態様では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、対象又は対象集団は、白金系化学療法剤(例えば、シスプラチン)による処置に不適格である。 The present invention includes methods and uses for treating a subject or subject population with MIBC, wherein the method comprises an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg every three weeks; and administering to the subject or population of subjects in one or more dosing cycles a dose (e.g., fixed dose) of between about 80 mg and about 1600 mg every three weeks of a PD-1 axis binding antagonist; are not eligible for treatment with platinum-based chemotherapeutic agents (eg, cisplatin). In some aspects, the method comprises administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks and a dose (e.g., fixed dose) of between 80 mg and 1600 mg every three weeks. comprising administering one or more dosing cycles of a PD-1 axis binding antagonist to a subject or population of subjects, wherein the subject or population of subjects is ineligible for treatment with a platinum-based chemotherapeutic agent (eg, cisplatin).
本発明は、MIBCを有する対象又は対象集団を処置するための方法及び使用を含み、方法は、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、対象又は対象集団は、クレアチニンクリアランス<60mL/分、グレード2以上の難聴、及び/又はグレード2以上の神経障害を有する。いくつかの態様では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、対象又は対象集団は、クレアチニンクリアランス<60mL/分、グレード2以上の難聴、及び/又はグレード2以上の神経障害を有する。
The present invention includes methods and uses for treating a subject or subject population with MIBC, wherein the method comprises administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg every three weeks and administering to the subject or subject population one or more dosing cycles of a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of between about 80 mg and about 1600 mg every three weeks, wherein the subject or subject population is , creatinine clearance <60 mL/min,
本発明は、MIBCを有する対象又は対象集団を処置するための方法及び使用を含み、方法は、対象又は対象集団に、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、処置は周術期処置である。いくつかの態様では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含み、処置は周術期治療である。 The present invention includes methods and uses for treating a subject or subject population with MIBC, wherein the method administers to the subject or subject population a dose of between about 30 mg and about 1200 mg (e.g., fixed dose) every three weeks. and one or more dosing cycles of a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of between about 80 mg and about 1600 mg every 3 weeks; It is a temporary measure. In some aspects, the method comprises administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks and a dose (e.g., fixed dose) of between 80 mg and 1600 mg every three weeks. The treatment is perioperative therapy, comprising administering to the subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist.
本発明は、手術可能なMIBCを有する対象又は対象集団を処置するための方法及び使用を含み、方法は、対象又は対象集団に、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含む。いくつかの態様では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを対象又は対象集団に投与することを含む。 The present invention includes methods and uses for treating a subject or subject population with operable MIBC, wherein the method administers to the subject or subject population a dose of between about 30 mg and about 1200 mg every three weeks (e.g., administration of a fixed dose) of an anti-TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose (eg, fixed dose) of between about 80 mg and about 1600 mg every three weeks. In some aspects, the method comprises administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks and a dose (e.g., fixed dose) of between 80 mg and 1600 mg every three weeks. administering to the subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist.
PD-1軸結合アンタゴニスト抗TIGITアンタゴニスト抗体は、当該技術分野で公知の任意の適切な様式で投与され得る。例えば、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、連続的に(異なる日に)又は同時に(同日又は同じ処置サイクル中に)投与され得る。いくつかの例では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、同日に投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体の前に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体の後に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同時に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、同日に投与される抗TIGITアンタゴニスト抗体の前に投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、同日に投与される抗TIGITアンタゴニスト抗体の後に投与され得る。更に他の例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同時に投与される。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体とは別の組成物中にある。いくつかの例では、PD-1軸結合アンタゴニストは、抗TIGITアンタゴニスト抗体と同じ組成物中にある。いくつかの例では、PD-1軸結合アンタゴニストは、同日に患者に投与される任意の他の治療剤とは別個の静脈内ラインを介して投与される。PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、同じ投与経路又は異なる投与経路によって投与され得る。いくつかの例では、PD-1軸結合アンタゴニストは、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内に、筋肉内に、皮下に、局所的に、経口的に、経皮的に、腹腔内に、眼窩内に、移植により、吸入により、髄腔内に、脳室内に、又は鼻腔内に投与される。いくつかの例では、PD-1軸結合アンタゴニストの投与後に第1の観察期間がある。いくつかの例では、PD-1軸結合アンタゴニストの投与後に第2の観察期間がある。いくつかの例では、抗TIGITアンタゴニスト抗体の投与後に第1の観察期間がある。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第2の観察期間を含む。いくつかの例では、観察期間は、約30分と約60分の間の長さである。いくつかの例では、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニストは、静脈内又は皮下に投与される。いくつかの例では、静脈内注入は、30±10分超及び/又は60±15分超である。一例では、アテゾリズマブは60分かけて静脈内投与され得、最初の注入が許容される場合、その後の注入は全て30分かけて送達され得る。いくつかの例では、PD-1軸結合アンタゴニストは、静脈内プッシュ又はボーラスとして投与されない。一例では、チラゴルマブは、60分間にわたって静脈内投与され得る。最初の注入が許容される場合、その後の注入は全て30分かけて送達され得る。いくつかの例では、抗TIGITアンタゴニスト抗体は、静脈内プッシュ又はボーラスとして投与されない。 A PD-1 axis binding antagonist anti-TIGIT antagonist antibody may be administered in any suitable manner known in the art. For example, a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody can be administered sequentially (on different days) or simultaneously (on the same day or during the same treatment cycle). In some instances, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody can be administered on the same day. In some examples, the PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody. In some examples, the PD-1 axis binding antagonist is administered after the anti-TIGIT antagonist antibody. In some examples, the PD-1 axis binding antagonist is co-administered with the anti-TIGIT antagonist antibody. In some instances, the PD-1 axis binding antagonist can be administered prior to the anti-TIGIT antagonist antibody administered on the same day. In some instances, the PD-1 axis binding antagonist can be administered after the anti-TIGIT antagonist antibody administered on the same day. In still other examples, the PD-1 axis binding antagonist is co-administered with the anti-TIGIT antagonist antibody. In some examples, the PD-1 axis binding antagonist is in a separate composition from the anti-TIGIT antagonist antibody. In some examples, the PD-1 axis binding antagonist is in the same composition as the anti-TIGIT antagonist antibody. In some instances, the PD-1 axis binding antagonist is administered via a separate intravenous line from any other therapeutic agents administered to the patient on the same day. The PD-1 axis binding antagonist and anti-TIGIT antagonist antibody can be administered by the same route of administration or by different routes of administration. In some examples, the PD-1 axis binding antagonist is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, by implantation, by inhalation. administered intrathecally, intracerebroventricularly, or intranasally. In some examples, the anti-TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, by implantation, by inhalation, It is administered intrathecally, intracerebroventricularly, or intranasally. In some examples, the anti-TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, by implantation, by inhalation, It is administered intrathecally, intracerebroventricularly, or intranasally. In some examples, the anti-TIGIT antagonist antibody is administered intravenously, intramuscularly, subcutaneously, topically, orally, transdermally, intraperitoneally, intraorbitally, by implantation, by inhalation, It is administered intrathecally, intracerebroventricularly, or intranasally. In some examples, there is a first observation period following administration of the PD-1 axis binding antagonist. In some examples, there is a second observation period following administration of the PD-1 axis binding antagonist. In some examples, there is a first observation period after administration of the anti-TIGIT antagonist antibody. In some examples, the method includes a second observation period after administration of the anti-TIGIT antagonist antibody. In some examples, the observation period is between about 30 minutes and about 60 minutes long. In some examples, the anti-TIGIT antagonist antibody and/or PD-1 axis binding antagonist is administered intravenously or subcutaneously. In some examples, the intravenous infusion is over 30±10 minutes and/or over 60±15 minutes. In one example, atezolizumab may be administered intravenously over 60 minutes, and if the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some instances, the PD-1 axis binding antagonist is not administered as an intravenous push or bolus. In one example, tiragolumab can be administered intravenously over 60 minutes. If the first infusion is allowed, all subsequent infusions may be delivered over 30 minutes. In some instances, the anti-TIGIT antagonist antibody is not administered as an intravenous push or bolus.
いくつかの例では、第1の投薬サイクルは、手術の前に開始される。いくつかの例では、1回以上の投薬サイクルが手術前に完了する。いくつかの例では、少なくとも1、2、又は3回の投薬サイクル(例えば、1、2、3、4、5、6、7、8、又はそれ以上の投薬サイクル)が手術前に完了する。いくつかの例では、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、又はそれ以上の投薬サイクル)が手術後に開始される。いくつかの例では、1~17回の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、又は17回の投薬サイクル)が手術後に完了する。いくつかの例では、少なくとも1つの投薬サイクルは、手術後約4週間と6週間の間(例えば、約4週間、約5週間、又は約6週間)に開始される。いくつかの例では、処置は手術を含む。いくつかの例では、手術は膀胱切除術及び/又はリンパ節郭清術である。 In some examples, the first dosing cycle is initiated prior to surgery. In some instances, one or more dosing cycles are completed prior to surgery. In some examples, at least 1, 2, or 3 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, or more dosing cycles) are completed prior to surgery. In some examples, one or more dosing cycles (e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18 , 19, 20, or more dosing cycles) are initiated after surgery. In some examples, 1 to 17 dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, or 17 one dosing cycle) is completed after surgery. In some examples, at least one dosing cycle is initiated between about 4 and 6 weeks (eg, about 4 weeks, about 5 weeks, or about 6 weeks) after surgery. In some examples, treatment includes surgery. In some examples, the surgery is a cystectomy and/or a lymphadenectomy.
いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、pCRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、無再発生存期間(RFS)、例えばランドマークRFS(例えば、12、18、又は24ヶ月でのランドマークRFS)の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、無症候生存期間(EFS)、例えばランドマークEFS(例えば、12、18、又は24ヶ月でのランドマークEFS)の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、OS、例えばランドマークOS(例えば、12、18、又は24ヶ月でのランドマークOS)の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、病理的進展度の低下率の増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のpCRの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のEFS(例えば、ランドマークEFS)を延長する。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のRFS(例えば、ランドマークRFS)を延長する。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOS(例えば、ランドマークOS)を延長する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of L1 antagonist antibody) results in pCR. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in increased recurrence-free survival (RFS), eg, landmark RFS (eg, landmark RFS at 12, 18, or 24 months). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in increased symptom-free survival (EFS), eg, landmark EFS (eg, landmark EFS at 12, 18, or 24 months). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of an L1 antagonist antibody) results in an increase in OS, eg, landmark OS (eg, landmark OS at 12, 18, or 24 months). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). Administration of L1 antagonist antibody) results in an increased rate of reduction of pathological progression. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. resulting in an increase in pCR in a subject or population of subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. , to extend the EFS (eg, landmark EFS) of a subject or population of subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. , extend the RFS (eg, landmark RFS) of a subject or population of subjects. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) and a PD-1 axis binding antagonist (eg, an anti-PD-1, such as atezolizumab). L1 antagonist antibody), e.g., compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or compared to treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. , extends the OS (eg, landmark OS) of the subject or subject population.
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に4週間(例えば、各28日間の投薬サイクルの1日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を4週間(例えば、各28日間の投薬サイクルの1日目に)ごとに投与し、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ、又は抗PD-1アンタゴニスト抗体、例えば、ペンブロリズマブ)を2週間(例えば、各28日間投薬サイクルの1及び15日目に)ごと、3週間(例えば、各21日間の投薬サイクルの1日目に)ごと、又は4週間(例えば、各28日間の投薬サイクルの1日目に)ごとに投与する。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、CR又はPRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して、対象又は対象集団のpCRの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、EFS及び/又はRFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象又は対象集団のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject or subject population in need thereof for four weeks (e.g., each on
本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)を、それを必要とする対象又は対象集団に2週間(例えば、各28日間の投薬サイクルの1日目及び15日目に)ごとに投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、pCRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のEFS及び/又はRFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)の投与は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象又は対象集団のOSを延長する。
The present invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist such as atezolizumab). (e.g., an anti-PD-1 antagonist antibody such as pembrolizumab) to a subject or population in need thereof every two weeks (e.g., on
特定の例では、本発明は、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、それを必要とする対象又は対象集団に2週間ごとに(例えば、各28日間の投薬サイクルの1日目及び15日目に)投与することを含む方法及び使用を含む。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、pCRをもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、参照と比較して、対象又は対象集団のEFS及び/又はRFSの増加をもたらす。いくつかの例では、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与は、対象又は対象集団のOSを延長する。
In certain examples, the invention provides an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) to a subject or subject population in need thereof. Methods and uses comprising administration on a weekly basis (eg, on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)を投与されている対象又は対象集団は、MIBCについて処置されている。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab) ) is being treated for MIBC.
いくつかの例では、処置は追加の治療を更に含み得る。当該技術分野で公知であるか又は本明細書に記載される任意の適切な追加の治療を使用することができる。追加の治療は、放射線療法、外科手術(例えば、膀胱切除術)、遺伝子療法、DNA療法、ウイルス療法、RNA療法、免疫療法、骨髄移植、ナノ療法、モノクローナル抗体療法、ガンマ線照射、又はこれらの組み合わせであり得る。 In some examples, treatment may further include additional therapies. Any suitable additional therapy known in the art or described herein can be used. Additional treatments include radiotherapy, surgery (e.g., cystectomy), gene therapy, DNA therapy, viral therapy, RNA therapy, immunotherapy, bone marrow transplantation, nanotherapy, monoclonal antibody therapy, gamma radiation, or combinations thereof. can be
いくつかの例では、追加の治療は、副作用制限剤(例えば、処置の副作用の発生及び/又は重症度を軽減することを意図した薬剤、例えば、抗悪心剤、コルチコステロイド(例えば、プレドニゾン又は同等物、例えば1~2mg/kg/日の用量)、ホルモン補充薬等)の投与である。 In some instances, the additional therapy is a side effect-limiting agent (e.g., an agent intended to reduce the occurrence and/or severity of side effects of treatment, e.g., anti-nausea drugs, corticosteroids (e.g., prednisone or equivalents, eg, doses of 1-2 mg/kg/day), hormone replacement drugs, etc.).
先の例のいずれかにおいて、各投薬サイクルは、任意の適切な長さ、例えば、約7日間、約14日間、約21日間、約28日間又はそれを超えてもよい。いくつかの例では、各投薬サイクルは約21日間である。 In any of the preceding examples, each dosing cycle may be of any suitable length, such as about 7 days, about 14 days, about 21 days, about 28 days or more. In some examples, each dosing cycle is about 21 days.
有効量のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)及び/又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を含む治療レジメンを別の抗がん剤又はがん治療と組み合わせて対象又は対象集団に投与することを含む、対象又は対象集団においてMIBCを処置するための方法も本明細書で提供される。例えば、PD-1軸結合アンタゴニストは、追加の化学療法若しくは化学療法剤(上記の定義を参照);標的化療法若しくは標的化治療剤;免疫療法若しくは免疫療法剤、例えばモノクローナル抗体;1つ以上の細胞傷害剤(上記の定義を参照);又はそれらの組み合わせと併せて投与され得る。 A therapeutic regimen comprising an effective amount of a PD-1 axis binding antagonist (eg, atezolizumab) and/or an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) Also provided herein are methods for treating MIBC in a subject or population of subjects, comprising administering to the subject or population of subjects in combination with a cancer agent or cancer therapy. For example, a PD-1 axis binding antagonist may include an additional chemotherapy or chemotherapeutic agent (see definition above); a targeted therapy or targeted therapeutic agent; an immunotherapy or immunotherapeutic agent, such as a monoclonal antibody; cytotoxic agents (see definition above); or combinations thereof.
患者が転移性尿路上皮癌腫(mUC)を有し、mUCが白金含有療法の間又は後に進行したいくつかの例では、本明細書において提供される方法は、対象又は対象集団が疾患進行又は許容できない毒性を経験した後に、対象又は対象集団に第2の投薬レジメンを投与することを更に含む。いくつかの例では、第2の投薬レジメンは、PD-1軸結合アンタゴニスト、及び抗体-薬物コンジュゲート(ADC)の1回以上の投薬サイクルを含む。いくつかの例では、(a)ADCはエンフォルツマブベドチン又は(b)サシツズマブゴビテカンである。 In some examples in which the patient has metastatic urothelial carcinoma (mUC) and the mUC has progressed during or after platinum-containing therapy, the methods provided herein provide that the subject or subject population has disease progression or Further comprising administering a second dosing regimen to the subject or subject population after experiencing unacceptable toxicity. In some examples, the second dosing regimen includes one or more dosing cycles of the PD-1 axis binding antagonist and an antibody-drug conjugate (ADC). In some examples, (a) the ADC is enfortumab vedotin or (b) sacituzumab govitecan.
mUCを有する対象又は対象集団を処置するための方法も本明細書で提供され、方法は、対象又は対象集団に、第1の投薬レジメンとそれに続く第2の投薬レジメンとを投与することを含み、(a)第1の投薬レジメンは、3週間ごとに約600mgの用量(例えば、固定用量)のチラゴルマブを、及び3週間ごとに約1200mgの用量(例えば、固定用量)のアテゾリズマブを含み、(b)第2の投薬レジメンは、3週間ごとに約1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンは、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与され、又は(ii)サクツズマブゴビテカンは、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、第2の投薬レジメンは、第1の投薬レジメン中に対象又は対象集団が疾患進行又は許容できない毒性を経験した後に対象又は対象集団に投与される。いくつかの態様では、mUCを有する対象又は対象集団を処置するための方法が本明細書で提供され、方法は、対象又は対象集団に、第1の投薬レジメンとそれに続く第2の投薬レジメンとを投与することを含み、(a)第1の投薬レジメンは、3週間ごとに600mgの用量(例えば、固定用量)のチラゴルマブを、及び3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブを含み、(b)第2の投薬レジメンは、3週間ごとに1200mgの用量(例えば、固定用量)のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンは、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与され、又は(ii)サクツズマブゴビテカンは、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、第2の投薬レジメンは、第1の投薬レジメン中に対象又は対象集団が疾患進行又は許容できない毒性を経験した後に対象又は対象集団に投与される。 Also provided herein are methods for treating a subject or population of subjects with mUC, the methods comprising administering to the subject or population of subjects a first dosing regimen followed by a second dosing regimen. (a) the first dosing regimen comprises a dose (e.g., fixed dose) of about 600 mg every three weeks of tiragolumab and a dose (e.g., fixed dose) of about 1200 mg of atezolizumab every three weeks; b) the second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose (e.g., fixed dose) of about 1200 mg every 3 weeks; administered at a dose of 1.25 mg/kg weekly for 1 week off, or (ii) suctuzumab govitecan at 10 mg/kg weekly for 2 weeks on/1 week off A second dosing regimen is administered to a subject or subject population after the subject or subject population experiences disease progression or unacceptable toxicity during the first dosing regimen. In some aspects, provided herein are methods for treating a subject or population of subjects with mUC, the methods comprising administering to the subject or population of subjects a first dosing regimen followed by a second dosing regimen and (a) the first dosing regimen is tiragolumab at a dose (e.g., fixed dose) of 600 mg every 3 weeks and atezolizumab at a dose (e.g., fixed dose) of 1200 mg every 3 weeks (b) the second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose (e.g., fixed dose) of 1200 mg every 3 weeks; (i) enfortumab vedotin for 2 weeks or (ii) suctuzumab govitecan at 10 mg weekly for 2 weeks on/1 week off /kg, and the second dosing regimen is administered to a subject or subject population after the subject or subject population experiences disease progression or unacceptable toxicity during the first dosing regimen.
いくつかの例では、処置は、少なくとも約13.4%~少なくとも約15%(例えば、少なくとも約13.5%、14%、14.5%、又は15%)の対象集団のORRをもたらす。 In some examples, treatment results in an ORR of the subject population of at least about 13.4% to at least about 15% (eg, at least about 13.5%, 14%, 14.5%, or 15%).
いくつかの例では、処置は、少なくとも約7.9ヶ月(例えば、8.0ヶ月、8.1ヶ月、8.2ヶ月、8.3ヶ月、8.4ヶ月、8.5ヶ月、8.6ヶ月、8.7ヶ月、8.8ヶ月、8.9ヶ月、9ヶ月、9.5ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、又は14ヶ月)の対象集団のOS中央値をもたらす。いくつかの例では、処置は、少なくとも約8.6ヶ月(例えば、8.6ヶ月、8.7ヶ月、8.8ヶ月、8.9ヶ月、9ヶ月、9.5ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、又は16ヶ月)の対象集団のOS中央値をもたらす。いくつかの例では、処置は、約7.9ヶ月~約8.6ヶ月(例えば、約8.0ヶ月、8.1ヶ月、8.2ヶ月、8.3ヶ月、8.4ヶ月、8.5ヶ月、又は8.6ヶ月)の対象集団のOS中央値をもたらす。 In some examples, the treatment is for at least about 7.9 months (eg, 8.0 months, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8.5 months, 8.5 months, 6 months, 8.7 months, 8.8 months, 8.9 months, 9 months, 9.5 months, 10 months, 11 months, 12 months, 13 months, or 14 months). Bring. In some examples, the treatment is for at least about 8.6 months (e.g., 8.6 months, 8.7 months, 8.8 months, 8.9 months, 9 months, 9.5 months, 10 months, 11 months). (months, 12 months, 13 months, 14 months, 15 months, or 16 months). In some examples, the treatment is from about 7.9 months to about 8.6 months (eg, about 8.0 months, 8.1 months, 8.2 months, 8.3 months, 8.4 months, 8 months .5 months, or 8.6 months).
いくつかの例では、処置は、少なくとも約13.4%~少なくとも約31%(例えば、少なくとも約13.5%、14%、15%、18%、17%、18%、19%、20%、21%、22%、23%、24%、25%、26%、27%、28%、29%、30%又は31%)の対象集団のORRをもたらす。いくつかの例では、処置は、少なくとも約31% 31% 100%(例えば、35%、40%、45%、50%、55%、又は60%)の対象集団の31% ORR 60%をもたらす。
In some examples, the treatment is at least about 13.4% to at least about 31% (eg, at least about 13.5%, 14%, 15%, 18%, 17%, 18%, 19%, 20% , 21%, 22%, 23%, 24%, 25%, 26%, 27%, 28%, 29%, 30% or 31%) of the subject population. In some examples, the treatment results in a 31
いくつかの例では、処置は、少なくとも約7.9(例えば、約7.9ヶ月と約36ヶ月の間(例えば、約7.9ヶ月と約24ヶ月の間(例えば、8ヶ月、10ヶ月、12ヶ月、14ヶ月、16ヶ月、18ヶ月、20ヶ月、22ヶ月、又は24ヶ月)))の対象集団のOS中央値をもたらす。いくつかの例では、処置は、少なくとも約16.3(例えば、約16.3ヶ月と約36ヶ月の間(例えば、約16.3ヶ月と約24ヶ月の間(例えば、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、又は24ヶ月))の対象集団のOS中央値をもたらす。いくつかの例では、処置は、約7.9ヶ月~約16.3ヶ月(例えば、8ヶ月、8.5ヶ月、9ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、12.5ヶ月、13ヶ月、13.5ヶ月、14ヶ月、14.5ヶ月、15ヶ月、15.5ヶ月、16ヶ月、又は16.3ヶ月、例えば、7.9ヶ月~9ヶ月、9ヶ月~10ヶ月、10ヶ月~11ヶ月、11ヶ月~12ヶ月、12ヶ月~13ヶ月、13ヶ月~14ヶ月、14ヶ月~15ヶ月、15ヶ月~16ヶ月、又は16ヶ月超)の対象集団のOS中央値をもたらす。 In some examples, the treatment is at least about 7.9 (e.g., between about 7.9 months and about 36 months (e.g., between about 7.9 months and about 24 months (e.g., 8 months, 10 months) , 12 months, 14 months, 16 months, 18 months, 20 months, 22 months, or 24 months))). In some examples, the treatment is for at least about 16.3 (e.g., between about 16.3 months and about 36 months (e.g., between about 16.3 months and about 24 months (e.g., 16 months, 17 months) , 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, or 24 months. 16.3 months (e.g., 8 months, 8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 12.5 months, 13 months, 13.5 months, 14 months, 14.5 months, 15 months, 15.5 months, 16 months, or 16.3 months, such as 7.9 months to 9 months, 9 months to 10 months, 10 months to 11 months months, 11 months to 12 months, 12 months to 13 months, 13 months to 14 months, 14 months to 15 months, 15 months to 16 months, or over 16 months).
抗TIGITアンタゴニスト抗体の投薬
抗TIGITアンタゴニスト抗体の投与は、セクションIII(K)に記載されている。
Dosing of Anti-TIGIT Antagonist Antibodies Administration of anti-TIGIT antagonist antibodies is described in Section III(K).
PD-1軸結合アンタゴニストの投薬
PD-1軸結合アンタゴニストの投与は、セクションIII(K)に記載されている。
Dosing of PD-1 Axis Binding Antagonists Administration of PD-1 axis binding antagonists is described in Section III(K).
がんの特性評価及び選択
いくつかの例では、本明細書に記載の使用のための方法、使用、又は組成物のいずれかにおいて、UC(例えば、膀胱がん(例えば、MIBC))は外科的に操作可能である(例えば、膀胱切除術に適したUC(例えば、膀胱がん(例えば、MIBC)))。いくつかの例では、本明細書に記載の使用のための方法、使用、又は組成物のいずれかにおいて、MIBCは外科的に操作可能である(例えば、膀胱切除術に適したMIBC)。
Cancer Characterization and Selection In some examples, in any of the methods, uses, or compositions for use described herein, UC (e.g., bladder cancer (e.g., MIBC)) is surgical. (eg, UC suitable for cystectomy (eg, bladder cancer (eg, MIBC))). In some examples, the MIBC is surgically manipulable (eg, a MIBC suitable for cystectomy) in any of the methods, uses, or compositions for use described herein.
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、白金系化学療法に不適格(例えば、シスプラチン不適格)である。いくつかの例では、対象はシスプラチン不適格である。いくつかの例では、対象は60mL/分未満のクレアチニンクリアランスを有する。いくつかの例では、対象は30mL/分以上のクレアチニンクリアランスを有する。いくつかの例では、対象はグレード2以上の難聴を有する。いくつかの例では、対象はグレード2以上の神経障害を有する。いくつかの例では、クレアチニンクリアランス<60mL/分、グレード2以上の難聴、及び/又はグレード2以上の神経障害を有する対象は、シスプラチン不適格である。いくつかの例では、60mL/分未満のクレアチニンクリアランスを有する対象はシスプラチン不適格である。いくつかの例では、グレード2以上の難聴を有する対象はシスプラチン不適格である。いくつかの例では、グレード2以上の神経障害を有する対象はシスプラチン不適格である。いくつかの例では、シスプラチンに基づく化学療法を拒絶する対象は、シスプラチン不適格である。いくつかの例では、対象は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)を有する。
In some examples, the subject is ineligible for platinum-based chemotherapy (eg, cisplatin ineligible) in any of the methods, uses or compositions for use described herein. In some examples, the subject is cisplatin ineligible. In some examples, the subject has creatinine clearance of less than 60 mL/min. In some examples, the subject has creatinine clearance greater than or equal to 30 mL/min. In some examples, the subject has
いくつかの例では、本明細書に記載の使用のための方法、使用又は組成物のいずれかにおいて、循環腫瘍DNA(ctDNA)の存在又はレベルを評定することができる。いくつかの例では、ctDNAが、対象からの試料(例えば、血液試料)において評定される。いくつかの例では、ctDNAは、第1の投薬サイクル(例えば、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの最初の投薬サイクル)の1日目の前に対象からの試料で評定される。いくつかの例では、ctDNAは、手術(例えば、膀胱切除術)前の対象からの試料で評定される。いくつかの例では、ctDNAは、手術(例えば、膀胱切除術)後の対象からの試料で評定される。いくつかの例では、ctDNAは、手術(例えば、膀胱切除術)の4~6週間後(例えば、4週間、5週間、又は6週間)に対象からの試料で評定される。いくつかの例では、ctDNAは、手術の6ヶ月後(例えば、膀胱切除術)に対象からの試料で評定される。
In some examples, the presence or level of circulating tumor DNA (ctDNA) can be assessed in any of the methods, uses or compositions for use described herein. In some examples, ctDNA is assessed in a sample (eg, blood sample) from the subject. In some examples, ctDNA is assessed in a sample from the subject prior to
PD-L1発現の評定
PD-L1の発現は、セクションIII(L)に記載されるように評定され得る。
Assessment of PD-L1 Expression PD-L1 expression can be assessed as described in Section III(L).
処置に対する応答
本明細書に記載される方法のいずれかのいくつかの実施形態では、治療に対する対象の応答は、1つ以上の尺度によって特徴付けることができる。いくつかの実施形態では、処置はpCRをもたらす。いくつかの実施形態では、処置は、無再発生存期間(RFS)、無症候生存期間(EFS)、又はOSの増加をもたらす。いくつかの実施形態では、処置は、ランドマークRFS、ランドマークEFS、又はランドマークOSの増加をもたらす。いくつかの実施形態では、処置は、病理的進展度の低下率の増加をもたらす。
Response to Treatment In some embodiments of any of the methods described herein, a subject's response to treatment can be characterized by one or more measures. In some embodiments, treatment results in pCR. In some embodiments, treatment results in increased recurrence-free survival (RFS), disease-free survival (EFS), or OS. In some embodiments, treatment results in an increase in landmark RFS, landmark EFS, or landmark OS. In some embodiments, the treatment results in an increased rate of reduction of pathologic extent.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象のpCRの増加をもたらす。 In some examples, treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. In comparison, it results in an increase in the subject's pCR.
いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象のOSを延長する。いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象のEFSを延長する。いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象のRFSを延長する。いくつかの例では、処置は、例えば、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストによる処置と比較して、又はPD-1軸結合アンタゴニストを用いない、抗TIGITアンタゴニスト抗体による処置と比較して、対象の病理的進展度の低下率を増加させる。 In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Compare and extend the target OS. In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. By comparison, prolong the subject's EFS. In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Compare and prolong the subject's RFS. In some examples, the treatment is, for example, compared to treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or treatment with an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist. Comparatively, it increases the subject's rate of reduction in pathological progression.
いくつかの実施形態では、本明細書に記載される処置は、対象のpCRを少なくとも約2ヵ月(例えば、2~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月又は10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のpCRを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment described herein reduces the subject's pCR by at least about 2 months (eg, 2-120 months, 2.5-100 months, 3.0-80 months, 4.0 ~60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2 .7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3 months .7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4 months .7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5 months .7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9 months .5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment reduces the subject's pCR by at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、本明細書に記載される処置は、対象のEFSを少なくとも約2ヵ月(例えば、2~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月又は10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のEFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment described herein reduces the subject's EFS by at least about 2 months (eg, 2-120 months, 2.5-100 months, 3.0-80 months, 4.0 months). ~60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2 .7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3 months .7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4 months .7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5 months .7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9 months .5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, treatment reduces the subject's EFS for at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、本明細書に記載される処置は、対象のRFSを少なくとも約2ヵ月(例えば、2~120ヵ月、2.5~100ヵ月、3.0~80ヵ月、4.0~60ヵ月、5.0~48ヵ月、6.0~36ヵ月、8.0~24ヵ月又は10~12ヵ月、例えば、少なくとも約2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの実施形態では、処置は、対象のRFSを少なくとも約4ヶ月(例えば、4~120ヵ月、5~100ヵ月、6~80ヵ月、7~60ヵ月、8~48ヵ月、9~36ヵ月、又は10~24ヵ月、例えば、少なくとも約4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。 In some embodiments, treatment described herein reduces the subject's RFS by at least about 2 months (eg, 2-120 months, 2.5-100 months, 3.0-80 months, 4.0 months). ~60 months, 5.0-48 months, 6.0-36 months, 8.0-24 months or 10-12 months, such as at least about 2.4 months, 2.5 months, 2.6 months, 2 .7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3 months .7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4 months .7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5 months .7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9 months .5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some embodiments, the treatment reduces the subject's RFS for at least about 4 months (eg, 4-120 months, 5-100 months, 6-80 months, 7-60 months, 8-48 months, 9-36 months). , or 10-24 months, such as at least about 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months , 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months , 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months , 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
いくつかの実施形態では、OSは、処置の開始から死亡までの期間として測定される。いくつかの例では、処置は、対象のOSを少なくとも約2ヵ月(例えば、2~120ヵ月、3~110ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば、少なくとも約2ヵ月、2.1ヵ月、2.2ヵ月、2.3ヵ月、2.4ヵ月、2.5ヵ月、2.6ヵ月、2.7ヵ月、2.8ヵ月、2.9ヵ月、3.0ヵ月、3.1ヵ月、3.2ヵ月、3.3ヵ月、3.4ヵ月、3.5ヵ月、3.6ヵ月、3.7ヵ月、3.8ヵ月、3.9ヵ月、4.0ヵ月、4.1ヵ月、4.2ヵ月、4.3ヵ月、4.4ヵ月、4.5ヵ月、4.6ヵ月、4.7ヵ月、4.8ヵ月、4.9ヵ月、5.0ヵ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヵ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヵ月、6.5ヵ月、7.0ヵ月、7.5ヵ月、8.0ヵ月、8.5ヵ月、9.0ヵ月、9.5ヵ月、10ヵ月、10.5ヵ月、11ヵ月、11.5ヵ月、12ヵ月、13ヵ月、14ヵ月、15ヵ月、16ヵ月、17ヵ月、18ヵ月、19ヵ月、20ヵ月、21ヵ月、22ヵ月、23ヵ月、24ヵ月、25ヵ月、26ヵ月、27ヵ月、28ヵ月、29ヵ月、30ヵ月、31ヵ月、32ヵ月、33ヵ月、34ヵ月、35ヵ月、又は36ヵ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約3.3ヵ月(例えば3.3~120ヵ月、4~100ヵ月、5~80ヵ月、6~60ヵ月、7~48ヵ月、8~36ヵ月、又は10~24ヵ月、例えば少なくとも約3.3ヶ月、3.4ヶ月、3.5ヶ月、3.6ヶ月、3.7ヶ月、3.8ヶ月、3.9ヶ月、4.0ヶ月、4.1ヶ月、4.2ヶ月、4.3ヶ月、4.4ヶ月、4.5ヶ月、4.6ヶ月、4.7ヶ月、4.8ヶ月、4.9ヶ月、5.0ヶ月、5.1ヵ月、5.2ヵ月、5.3ヵ月、5.4ヵ月、5.5ヶ月、5.6ヵ月、5.7ヵ月、5.8ヵ月、5.9ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。いくつかの例では、処置は、対象のOSを少なくとも約5.3ヶ月(例えば5.3~120、6~60ヵ月、7~48ヵ月、8~36 ヵ月、又は10~24ヵ月、例えば、少なくとも約5.3ヵ月、5.5ヵ月、6.0ヶ月、6.5ヶ月、7.0ヶ月、7.5ヶ月、8.0ヶ月、8.5ヶ月、9.0ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、11.5ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、16ヶ月、17ヶ月、18ヶ月、19ヶ月、20ヶ月、21ヶ月、22ヶ月、23ヶ月、24ヶ月、25ヶ月、26ヶ月、27ヶ月、28ヶ月、29ヶ月、30ヶ月、31ヶ月、32ヶ月、33ヶ月、34ヶ月、35ヶ月、又は36ヶ月)延長する。 In some embodiments, OS is measured as the time from initiation of treatment to death. In some examples, the treatment reduces the subject's OS by at least about 2 months (eg, 2-120 months, 3-110 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 2 months, 2.1 months, 2.2 months, 2.3 months, 2.4 months, 2.5 months, 2.6 months,2. 7 months, 2.8 months, 2.9 months, 3.0 months, 3.1 months, 3.2 months, 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.6 months; 7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4. 7 months, 4.8 months, 4.9 months, 5.0 months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5. 7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9. 5 months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months months, 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 3.3 months (eg, 3.3-120 months, 4-100 months, 5-80 months, 6-60 months, 7-48 months, 8-3 months). 36 months, or 10-24 months, such as at least about 3.3 months, 3.4 months, 3.5 months, 3.6 months, 3.7 months, 3.8 months, 3.9 months, 4.0 months, 4.1 months, 4.2 months, 4.3 months, 4.4 months, 4.5 months, 4.6 months, 4.7 months, 4.8 months, 4.9 months, 5.0 months months, 5.1 months, 5.2 months, 5.3 months, 5.4 months, 5.5 months, 5.6 months, 5.7 months, 5.8 months, 5.9 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months, 10 months, 10.5 months, 11 months, 11 months. 5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months, 23 months, 24 months, 25 months, 26 months, 27 months , 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months). In some examples, the treatment reduces the subject's OS by at least about 5.3 months (eg, 5.3-120, 6-60 months, 7-48 months, 8-36 months, or 10-24 months, such as at least about 5.3 months, 5.5 months, 6.0 months, 6.5 months, 7.0 months, 7.5 months, 8.0 months, 8.5 months, 9.0 months, 9.5 months months, 10 months, 10.5 months, 11 months, 11.5 months, 12 months, 13 months, 14 months, 15 months, 16 months, 17 months, 18 months, 19 months, 20 months, 21 months, 22 months , 23 months, 24 months, 25 months, 26 months, 27 months, 28 months, 29 months, 30 months, 31 months, 32 months, 33 months, 34 months, 35 months, or 36 months).
C.膵臓がんに関する治療方法及び使用
膵臓がん
膵がん患者のうち、80%が初期診断時に進行性疾患を有している。根治的手術を受けた患者でさえ、疾患再発を有し、それぞれ、膵頭十二指腸切除術におけるリンパ節陰性及びリンパ節陽性疾患を有する患者において25%-30%及び10%の5年生存率をもたらす。局所進行性の切除不能な疾患を有する患者は、しばしば放射線化学療法を受け、9~13ヶ月のOS中央値をもたらすが、長期生存をもたらすことは稀である。
C. Treatment Methods and Uses for Pancreatic Cancer Pancreatic Cancer Of patients with pancreatic cancer, 80% have progressive disease at initial diagnosis. Even patients undergoing radical surgery have disease recurrence, resulting in 5-year survival rates of 25%-30% and 10% in patients with node-negative and node-positive disease on pancreaticoduodenectomy, respectively. . Patients with locally advanced, unresectable disease often receive chemotherapy radiotherapy, resulting in median OS of 9-13 months, but rarely long-term survival.
したがって、改善された医療介入に対する満たされていないニーズが高い。 Therefore, there is a high unmet need for improved medical interventions.
膵臓がんを処置するための方法及び使用
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)、代謝拮抗剤(例えば、ゲムシタビン)及びタキサン(例えば、パクリタキセル)を投与されている対象又は対象集団は、膵臓がん(例えば、膵管腺癌(PDAC)、例えば、転移性PDAC(mPDAC)))について処置されている。
Methods and Uses for Treating Pancreatic Cancer Subjects or populations of subjects receiving anti-PD-L1 antagonist antibodies, e.g., atezolizumab), antimetabolites (e.g., gemcitabine) and taxanes (e.g., paclitaxel) have pancreatic cancer (e.g., pancreatic ductal adenocarcinoma (PDAC)). ), eg, metastatic PDAC (mPDAC))).
本発明は、膵臓がんを有する対象又は対象集団を処置する方法であって、対象又は対象集団に、各28日間投薬サイクルの1日目及び15日目に約420mgの用量のチラゴルマブ、各28日間投薬サイクルの第1及び15日目に約840mgの用量のアテゾリズマブ、各28日間投薬サイクルの第1、8及び15日目に約1000mg/m2の用量のゲムシタビン、並びに各28日間投薬サイクルの第1、8及び15日目に約125mg/m2 の用量のnab-パクリタキセルの1回以上の28日間投薬サイクルを含む投薬レジメンを投与することを含む、方法を含む。。いくつかの例では、方法は、対象又は対象集団に、28日間の各投薬サイクルの第1及び15日目に420mgの用量のチラゴルマブ、28日間の各投薬サイクルの第1及び15日目に840mgの用量のアテゾリズマブ、28日間の各投薬サイクルの第1、8及び15日目に1000mg/m2の用量のゲムシタビン、ならびに28日間の各投薬サイクルの第1、8及び15日目に28mg/m2の用量のnab-パクリタキセルを含む1回以上の125日間投薬サイクルを含む投薬レジメンを投与することを含む。いくつかの例では、膵臓がんはPDAC、例えばmPDACである。いくつかの態様では、一又は複数の対象は、転移性PDACの事前全身治療受けたことがない。
The present invention provides a method of treating a subject or subject population having pancreatic cancer, wherein the subject or subject population is administered a dose of about 420 mg tiragolumab on
いくつかの例では、処置は、少なくとも約41.7%~約46.7%(例えば、42%、42.5%、43%、43.5%、44%、44.5%、45%、45.5%、46%、46.5%、又は46.7%(例えば、41.7%~43%、43%~45%、又は45%~46.7%)の対象集団のORRをもたらす。いくつかの例では、処置は、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを用いない、ゲムシタビン及びnab-パクリタキセルを含む処置と比較して、少なくとも約20%のORRの増加をもたらす。いくつかの例では、処置は、少なくとも約5.5ヶ月(例えば、5.5ヶ月と14ヶ月の間(例えば、6ヶ月、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、又は14ヶ月))の対象集団のPFS中央値をもたらす。いくつかの例では、処置は、少なくとも約7ヶ月(例えば、7ヶ月と14ヶ月の間(例えば、7ヶ月、8ヶ月、9ヶ月、10ヶ月、11ヶ月、12ヶ月、13ヶ月、又は14ヶ月))の対象集団のPFS中央値をもたらす。いくつかの例では、処置は、少なくとも約5.5ヶ月~約7ヶ月(例えば、6ヶ月、6.2ヶ月、6.4ヶ月、6.6ヶ月、6.8ヶ月、7ヶ月、又は7ヶ月超)の対象集団のPFS中央値をもたらす。いくつかの例では、処置は、少なくとも約8.5ヶ月(例えば、約8.5ヶ月と約16ヶ月の間(8.5ヶ月、9ヶ月、9.5ヶ月、10ヶ月、10.5ヶ月、11ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、又は16ヶ月))の対象集団のOS中央値をもたらす。いくつかの例では、処置は、少なくとも約10.6ヶ月(例えば、約10.6ヶ月と約16ヶ月の間(10.6ヶ月、11ヶ月、12ヶ月、13ヶ月、14ヶ月、15ヶ月、又は16ヶ月))の対象集団のOS中央値をもたらす。いくつかの例では、処置は、少なくとも約8.5ヶ月~約10.6ヶ月(例えば、8.7ヶ月、9.0ヶ月、9.2ヶ月、9.4ヶ月、9.6ヶ月、9.8ヶ月、10ヶ月、10.2ヶ月、10.4ヶ月、10.6ヶ月、又は10.6ヶ月超)の対象集団のOS中央値をもたらす。 In some examples, treatment is at least about 41.7% to about 46.7% (eg, 42%, 42.5%, 43%, 43.5%, 44%, 44.5%, 45% , 45.5%, 46%, 46.5%, or 46.7% (e.g., 41.7%-43%, 43%-45%, or 45%-46.7%) ORR of the subject population In some examples, the treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nab-paclitaxel without the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist In some examples, the treatment is for at least about 5.5 months (e.g., between 5.5 months and 14 months (e.g., 6 months, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months). months, 13 months, or 14 months), hi some examples, the treatment results in a median PFS for the subject population of at least about 7 months (eg, between 7 months and 14 months (eg, 7 months, 8 months, 9 months, 10 months, 11 months, 12 months, 13 months, or 14 months. provide a median PFS for a subject population of months (e.g., 6 months, 6.2 months, 6.4 months, 6.6 months, 6.8 months, 7 months, or more than 7 months). , the treatment is for at least about 8.5 months (e.g., between about 8.5 months and about 16 months (8.5 months, 9 months, 9.5 months, 10 months, 10.5 months, 11 months, 12 months). months, 13 months, 14 months, 15 months, or 16 months)), hi some examples, treatment is at least about 10.6 months (e.g., about 10.6 months and results in a median OS in the subject population for about 16 months (10.6 months, 11 months, 12 months, 13 months, 14 months, 15 months, or 16 months) In some examples, the treatment includes: at least about 8.5 months to about 10.6 months (eg, 8.7 months, 9.0 months, 9.2 months, 9.4 months, 9.6 months, 9.8 months, 10 months, 10. 2 months, 10.4 months, 10.6 months, or over 10.6 months).
薬剤の投薬
抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、代謝拮抗剤及びタキサンの投与は、セクションIII(K)に記載されている。
Drug Administration Administration of anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, antimetabolites and taxanes is described in Section III(K).
D.食道がんに関する治療方法及び使用
本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を含み、方法は、各投薬サイクルの1日目に約30mgと約1200mgの間(例えば約550mgと約650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間(例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む。いくつかの例では、方法は、各投薬サイクルの1日目に約500mgと約700mgの間(例えば約550mgと約650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間(例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む。いくつかの態様では、方法は、各投薬サイクルの1日目に500mgと700mgの間(例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に900mgと1500mgの間(例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含む。
D. Therapeutic Methods and Uses for Esophageal Cancer The present invention includes methods for treating a subject or population of subjects with advanced or metastatic esophageal cancer, the methods comprising about 30 mg and about a dose between 1200 mg (e.g. between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, such as 600 mg) (e.g., a fixed dose) of an anti-TIGIT antagonist antibody and between about 80 mg and about 1600 mg (e.g., between about 1000 mg and about 1400 mg, e.g., between about 1050 mg and about 1350 mg, e.g., about 1100 mg) on
本発明は、食道がんを有する対象又は対象集団を処置するための方法を含み、方法は、各投薬サイクルの1日目に約500mgと約700mgの間(例えば約550mgと約650mg、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mgの間、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間(例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、対象又は対象集団は、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある。いくつかの態様では、方法は、各投薬サイクルの1日目に500mgと700mgの間(例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に900mgと1500mgの間(例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、対象又は対象集団は、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある。
The invention includes a method for treating a subject or subject population with esophageal cancer, wherein the method comprises between about 500 mg and about 700 mg (e.g., about 550 mg and about 650 mg, e.g., 600 mg) on
いくつかの例では、対象又は対象集団は、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある。いくつかの例では、対象又は対象集団は、以前の処置中に疾患進行又は許容できない毒性を経験したことがある。 In some examples, the subject or subject population has been previously treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. In some instances, the subject or subject population has experienced disease progression or unacceptable toxicity during prior treatment.
いくつかの例では、21日間投薬サイクルは、白金系化学療法剤及び非白金系化学療法剤を更に含む。いくつかの例では、白金系化学療法剤は、6回の投薬後に投薬レジメンから省かれる。 In some examples, the 21-day dosing cycle further includes a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. In some instances, the platinum-based chemotherapeutic agent is omitted from the dosing regimen after 6 doses.
いくつかの例では、白金系化学療法剤はシスプラチンである。いくつかの例では、シスプラチンは、各投薬サイクルの1日目に約80mg/m2の用量で投与される。いくつかの例では、シスプラチンは、各投薬サイクルの1日目に80mg/m2の用量で投与される。
In some examples, the platinum-based chemotherapeutic agent is cisplatin. In some examples, cisplatin is administered at a dose of about 80 mg/m 2 on
いくつかの例では、非白金系化学療法剤は代謝拮抗剤である。いくつかの例では、代謝拮抗剤は5-フルオロウラシルである。いくつかの例では、5-フルオロウラシルを800mg/m2/24時間の用量で、各21日間サイクルの1~5日目に投与する。 In some examples, the non-platinum chemotherapeutic agent is an antimetabolite. In some examples, the antimetabolite is 5-fluorouracil. In some examples, 5-fluorouracil is administered at a dose of 800 mg/m 2 /24 hours on days 1-5 of each 21-day cycle.
いくつかの例では、食道がんは進行性又は転移性食道がんである。 In some examples, the esophageal cancer is advanced or metastatic esophageal cancer.
いくつかの例では、一又は複数の対象は、転移性食道がんの事前処置を受桁ことがなかった。 In some instances, one or more subjects have never received prior treatment for metastatic esophageal cancer.
本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を含み、方法は、対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量(例えば、固定用量)のチラゴルマブ、各投薬サイクルの1日目に約1200mgの用量(例えば、固定用量)のアテゾリズマブ、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に投薬レジメンからシスプラチンが省略される。いくつかの態様では、方法は、1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に、それぞれの投薬サイクルの1日目に600mgの用量(例えば、固定用量)のチラゴルマブ、それぞれの投薬サイクルの1日目に1200mgの用量(例えば、固定用量)のアテゾリズマブ、それぞれの投薬サイクルの1日目に80mg/m 2の用量のシスプラチン、及びそれぞれの21日間サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルを投与することを含み、シスプラチンは、6回の投薬後では投薬レジメンから省かれる。
The invention includes a method for treating a subject or subject population with advanced or metastatic esophageal cancer, wherein the method comprises administering to the subject or subject population a dose of about 600 mg on
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごと(Q2W)に約10mgと約1000mgの間(例えば約20mgと約1000mgの間、例えば約50mgと約900mgの間、例えば約100mgと約850mgの間、例えば約200mgと約800mgの間、例えば約300mgと約600mgの間、例えば約400mgと約500mgの間、例えば約405mgと約450mgの間、例えば約410mgと約430mgの間、例えば約420mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごと(Q2W)に約10mgと1000mgの間(例えば、20mgと1000mgの間、例えば、50mgと900mgの間、例えば、00mgと850mgの間、例えば、200mgと800mgの間、例えば、300mgと600mgの間、例えば、400mgと500mgの間、例えば、405mgと450mgの間、例えば、410mgと430mgの間、例えば、420mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごとに約420mg(例えば、420mg±10mg、例えば、420±6mg、例えば、420±5mg、例えば、420±3mg、例えば、420±1mg、例えば、420±0.5mg、例えば、2週間ごとに420mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 10 mg and about 1000 mg every two weeks (Q2W) (e.g., between about 20 mg and about 1000 mg, such as between about 50 mg and about 900 mg, such as between about 100 mg and about 850 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 600 mg, such as between about 400 mg and about 500 mg between about 405 mg and about 450 mg, such as between about 410 mg and about 430 mg, such as about 420 mg) (eg, a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 10 mg and 1000 mg every two weeks (Q2W) (e.g., between 20 mg and 1000 mg, such as between 50 mg and 900 mg, such as between 00 mg and 850 mg, such as between 200 mg and 800 mg, such as between 300 mg and 600 mg, such as between 400 mg and 500 mg, such as 405 mg between 450 mg, eg between 410 mg and 430 mg, eg 420 mg) (eg a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is about 420 mg (e.g., 420 mg ± 10 mg, e.g., 420 mg ± 10 mg) every two weeks. ±6 mg, such as 420±5 mg, such as 420±3 mg, such as 420±1 mg, such as 420±0.5 mg, such as 420 mg every two weeks).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに(Q4W)約200mgと約2000mgの間(例えば、約200mgと約1600mgの間、例えば、約250mgと約1600mgの間、例えば、約300mgと約1600mgの間、例えば、約400mgと約1500mgの間、例えば、約500mgと約1400mgの間、例えば、約600mgと約1200mgの間、例えば、約700mgと約1100mgの間、例えば、約800mgと約1000mgの間、例えば、約800mgと約900mgの間、例えば、約800、約810、約820、約830、約840、約850、約860、約870、約880、約890又は約900mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごと(Q4W)に200mgと2000mgの間(例えば、200mgと1600mgの間、例えば、250mgと1600mgの間、例えば、300mgと1600mgの間、例えば、400mgと1500mgの間、例えば、500mgと1400mgの間、例えば、600mgと1200mgの間、例えば、700mgと1100mgの間、例えば、800mgと1000mgの間、例えば、800mgと900mgの間、例えば、800、810、820、830、840、850、860、870、880、890mg又は900mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 200 mg and about 2000 mg every four weeks (Q4W) (e.g., between about 200 mg and about 1600 mg, such as between about 250 mg and about 1600 mg, such as between about 300 mg and about 1600 mg, such as between about 400 mg and about 1500 mg, such as between about 500 mg and about 1400 mg, such as , between about 600 mg and about 1200 mg, such as between about 700 mg and about 1100 mg, such as between about 800 mg and about 1000 mg, such as between about 800 mg and about 900 mg, such as about 800, about 810, about 820, about 830, about 840, about 850, about 860, about 870, about 880, about 890 or about 900 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between 200 mg and 2000 mg every four weeks (Q4W) (e.g., between 200 mg and 1600 mg, such as between 250 mg and 1600 mg, such as between 300 mg and 1600 mg, such as between 400 mg and 1500 mg, such as between 500 mg and 1400 mg, such as between 600 mg and 1200 mg, such as 700 mg and 1100 mg, e.g.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約80mgと約2000mgの間(例えば約80mgと約1950mgの間、例えば約80mgと約1900mgの間、例えば約80mgと約1800mgの間、例えば約100mgと約1700mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1400mgの間、例えば約400mgと約1300mgの間、例えば約500mgと約1200mgの間、例えば約600mgと約1100mgの間、例えば約700mgと約1000mgの間、例えば約740mgと約940mgの間、例えば約790mgと約890mgの間、例えば約815mgと約865mgの間、例えば約830mgと約850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約2000mgの間、例えば約300mgと約2000mgの間、例えば約400mgと約2000mgの間、例えば約500mgと約2000mgの間、例えば約600mgと約1900mgの間、例えば約700mgと約1800mgの間、例えば約800mgと約1800mgの間、例えば約900mgと約1800mgの間、例えば約1000mgと約1800mgの間、例えば約1100mgと約1800mgの間、例えば約1200mgと約1800mgの間、例えば約1300mgと約1800mgの間、例えば約1400mgと約1800mgの間、例えば約1500mgと約1800mgの間、例えば約1580mgと約1780mgの間、例えば約1630mgと約1730mgの間、例えば約1655mgと約1705mgの間、例えば約1670mgと約1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに80mgと2000mgの間(例えば80mgと1950mgの間、例えば80mgと1900mgの間、例えば80mgと1800mgの間、例えば100mgと1700mgの間、例えば200mgと1600mgの間、例えば300mgと1400mgの間、例えば400mgと1300mgの間、例えば500mgと1200mgの間、例えば600mgと1100mgの間、例えば700mgと1000mgの間、例えば740mgと940mgの間、例えば790mgと890mgの間、例えば815mgと865mgの間、例えば830mgと850mgの間、例えば840mg±5mg、例えば840±2.5mg、例えば840±1.0mg、例えば840±0.5mg、例えば840mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと2000mgの間、例えば300mgと2000mgの間、例えば400mgと2000mgの間、例えば500mgと2000mgの間、例えば600mgと1900mgの間、例えば700mgと1800mgの間、例えば800mgと1800mgの間、例えば900mgと1800mgの間、例えば1000mgと1800mgの間、例えば1100mgと1800mgの間、例えば1200mgと1800mgの間、例えば1300mgと1800mgの間、例えば1400mgと1800mgの間、例えば1500mgと1800mgの間、例えば1580mgと1780mgの間、例えば1630mgと1730mgの間、例えば1655mgと1705mgの間、例えば1670mgと1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量である。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 80 mg and about 1950 mg) every two weeks. between about 80 mg and about 1900 mg, such as between about 80 mg and about 1800 mg, such as between about 100 mg and about 1700 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1400 mg, such as about between 400 mg and about 1300 mg, such as between about 500 mg and about 1200 mg, such as between about 600 mg and about 1100 mg, such as between about 700 mg and about 1000 mg, such as between about 740 mg and about 940 mg, such as between about 790 mg and about 890 mg between about 815 mg and about 865 mg, such as between about 830 mg and about 850 mg, such as 840 mg±5 mg, such as 840±2.5 mg, such as 840±1.0 mg, such as 840±0.5 mg, such as 840 mg dose. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, about 100 mg and about 2000 mg) every 4 weeks. between about 200 mg and about 2000 mg, such as between about 300 mg and about 2000 mg, such as between about 400 mg and about 2000 mg, such as between about 500 mg and about 2000 mg, such as between about 600 mg and about 1900 mg, such as about between 700 mg and about 1800 mg, such as between about 800 mg and about 1800 mg, such as between about 900 mg and about 1800 mg, such as between about 1000 mg and about 1800 mg, such as between about 1100 mg and about 1800 mg, such as between about 1200 mg and about 1800 mg between about 1300 mg and about 1800 mg, such as between about 1400 mg and about 1800 mg, such as between about 1500 mg and about 1800 mg, such as between about 1580 mg and about 1780 mg, such as between about 1630 mg and about 1730 mg, such as about 1655 mg and about 1705 mg, e.g. In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 80 mg and 1950 mg) every two weeks, e.g. between 80 mg and 1900 mg, such as between 80 mg and 1800 mg, such as between 100 mg and 1700 mg, such as between 200 mg and 1600 mg, such as between 300 mg and 1400 mg, such as between 400 mg and 1300 mg, such as between 500 mg and 1200 mg, such as 600 mg and 1100 mg, such as between 700 mg and 1000 mg, such as between 740 mg and 940 mg, such as between 790 mg and 890 mg, such as between 815 mg and 865 mg, such as between 830 mg and 850 mg, such as 840 mg±5 mg, such as 840±2. 5 mg, such as 840±1.0 mg, such as 840±0.5 mg, such as 840 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every 4 weeks, e.g. between 200 mg and 2000 mg, such as between 300 mg and 2000 mg, such as between 400 mg and 2000 mg, such as between 500 mg and 2000 mg, such as between 600 mg and 1900 mg, such as between 700 mg and 1800 mg, such as between 800 mg and 1800 mg, such as 900 mg and 1800 mg, such as between 1000 mg and 1800 mg, such as between 1100 mg and 1800 mg, such as between 1200 mg and 1800 mg, such as between 1300 mg and 1800 mg, such as between 1400 mg and 1800 mg, such as between 1500 mg and 1800 mg, such as 1580 mg between 1780 mg, such as between 1630 mg and 1730 mg, such as between 1655 mg and 1705 mg, such as between 1670 mg and 1690 mg, such as 1680 mg±5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg , eg 1680 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks. In some examples, a PD-1 axis binding antagonist (e.g., a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as monotherapy.
本発明は、進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法を含み、方法は、対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、(a)第1の投薬レジメンが、各投薬サイクルの第1日目に約80mg/m 2の用量のシスプラチンと、各21日サイクルの第1~5日目に800mg/m2/24時間の用量の5-フルオロウラシルとの1回以上の21日間投薬サイクルを含み、シスプラチンが6回投与後に投薬レジメンから省略され(b)第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量での1回以上の21日間投薬サイクルのチラゴルマブと、各投薬サイクルの1日目に約1200mgの用量でのアテゾリズマブとを含む。
The present invention includes a method for treating a subject or subject population with advanced or metastatic esophageal cancer, comprising administering to the subject or subject population a first dosing regimen and a second dosing regimen. (a) the first dosing regimen comprises cisplatin at a dose of about 80 mg/m 2 on
上記の方法のいずれかのいくつかの態様では、処置は、対象集団の少なくとも約14%のORRをもたらす(例えば、少なくとも約14%、15%、16%、17%、18%、19%、20%、25%、30%、35%、40%、45%、50%、55%、60%、65%、70%、75%、80%、85%、90%、95%、又は100%のORR、例えば、14%~16%、16%~18%、18%~20%、20%~30%、30%~40%、40%~50%、50%~60%、60%~70%、70%~80%、80%~90%、又は90%~100%をもたらす)。 In some aspects of any of the above methods, the treatment results in an ORR of at least about 14% of the subject population (e.g., at least about 14%, 15%, 16%, 17%, 18%, 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100 % ORR, such as 14%-16%, 16%-18%, 18%-20%, 20%-30%, 30%-40%, 40%-50%, 50%-60%, 60% resulting in ~70%, 70%-80%, 80%-90%, or 90%-100%).
E.がんに関する診断方法及び使用 E. Diagnostic methods and uses for cancer
本発明は、がん(例えば、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLCもしくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性もしくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性もしくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC))を有する対象のための治療法を選択するための方法を提供し、治療法は、対象から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって誘導される。 The present invention provides cancer (e.g., lung cancer (e.g., early stage lung cancer (e.g., resectable lung cancer)), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC locally advanced unresectable). NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)), or stage IV NSCLC (e.g., subject is stage IV previously untreated for NSCLC))): cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (e.g. TNBC (e.g. eTNBC))) or HER2 positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer (e.g., HCC, e.g., locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g., MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g., PDAC). renal cancer or renal cancer (eg, RCC); melanoma; ovarian cancer; gastric cancer (eg, gastroesophageal junction cancer); or CRC (eg, MSS or MSI-Low CRC). )), wherein the treatment comprises one or more biomarkers (e.g., PD-L1, TIGIT, activated T cells or cytokines) by diagnostic methods including determining the presence and/or expression level/amount.
更に、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えばアテゾリズマブ、又は抗PD-1アンタゴニスト抗体、例えばペンプロリズマブ)を含む処置から利益を得る可能性がある、がん(例えば、肺がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLCもしくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性もしくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性もしくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC))を有する対象を同定するための方法が本明細書で提供され、同定は、対象から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって誘導される。 Additionally, anti-TIGIT antagonist antibodies (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab) and PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies, e.g., atezolizumab, or anti-PD-1 Cancers (e.g. lung cancer (e.g. early stage lung cancer (e.g. resectable lung cancer), SCLC (e.g. ES-SCLC), NSCLC (e.g. , squamous NSCLC or non-squamous NSCLC locally advanced unresectable NSCLC, stage IIIB NSCLC, recurrent or metastatic NSCLC (e.g. locally advanced unresectable or metastatic non-squamous NSCLC (e.g. stage IV non-squamous NSCLC) )), or stage IV NSCLC (e.g., subject has not been previously treated for stage IV NSCLC))): cervical cancer (e.g., stage IVB, metastatic, recurrent or persistent cervical cancer , e.g., metastatic and/or recurrent PD-L1-positive cervical cancer); breast cancer (e.g., TNBC (e.g., eTNBC))) or HER2-positive breast cancer); head and neck cancer (e.g., SCCHN, e.g., recurrent liver cancer (e.g. HCC, e.g. locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or pancreatic cancer (e.g. PDAC, e.g. metastatic PDAC); kidney cancer or renal cancer (e.g. RCC); melanoma; ovarian cancer; or CRC (e.g., MSS or MSI-Low CRC)), wherein the identification is a sample obtained from the subject (e.g., a tumor sample or a blood sample). ) by a diagnostic method comprising determining the presence and/or expression level/amount of one or more biomarkers (eg, PD-L1, TIGIT, activated T cells or cytokines).
更に、がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLCもしくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性もしくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性もしくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC))を有する対象のための治療法に対する応答性を評定するための方法が本明細書で提供され、更なる治療法は、対象から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって誘導される。 Furthermore, cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB NSCLC, Recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)), or stage IV NSCLC (e.g., subject previously treated for stage IV NSCLC) never been treated))): cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (e.g. TNBC (e.g. eTNBC)) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer (e.g. HCC, e.g. , locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g. PDAC, e.g. metastatic PDAC) renal cancer or renal cancer (e.g., RCC); melanoma; ovarian cancer; gastric cancer (e.g., gastroesophageal junction cancer); or CRC (e.g., MSS or MSI-Low CRC)) Provided herein are methods for assessing responsiveness to a therapy for , a further therapy comprising one or more biomarkers in a sample (e.g., tumor sample or blood sample) obtained from a subject (eg PD-L1, TIGIT, activated T-cells or cytokines) by diagnostic methods including determining the presence and/or expression level/amount.
更に、がん(例えば、初期肺がん(例えば、切除可能な肺がん)、SCLC(例えば、ES-SCLC)、NSCLC(例えば、扁平上皮NSCLCもしくは非扁平上皮NSCLC局所進行性切除不能NSCLC、ステージIIIB NSCLC、再発性もしくは転移性NSCLC(例えば、局所進行性切除不能又は転移性非扁平上皮NSCLC(例えば、ステージIV非扁平上皮NSCLC))、又はステージIV NSCLC(例えば、対象がステージIVのNSCLCについて以前に処置されたことがない))):子宮頸がん(例えば、ステージIVB、転移性、再発性又は持続性子宮頸がん、例えば、転移性及び/又は再発性PD-L1陽性子宮頸がん);乳がん(例えば、TNBC(例えば、eTNBC)))又はHER2陽性乳がん);頭頸部がん(例えば、SCCHN、例えば、再発性/転移性PD-L1陽性SCCHN);肝臓がん(例えば、HCC、例えば、局所進行性もしくは転移性HCC及び/又は切除不能HCC);膀胱がん(例えば、MIBC、局所進行性UC、又はmUC);食道がん;膵臓がん(例えば、PDAC、例えば転移性PDAC);腎臓がん若しくは腎がん(例えば、RCC);黒色腫;卵巣がん;胃がん(例えば、胃食道接合部がん);又はCRC(例えば、MSS又はMSI-Low CRC))を有する対象のための治療法を最適化するための方法が本明細書で提供され、更なる治療法は、対象から得られた試料(例えば、腫瘍試料又は血液試料)中の1つ以上のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することを含む診断方法によって誘導される。 Furthermore, cancer (e.g., early stage lung cancer (e.g., resectable lung cancer), SCLC (e.g., ES-SCLC), NSCLC (e.g., squamous NSCLC or non-squamous NSCLC, locally advanced unresectable NSCLC, stage IIIB NSCLC, Recurrent or metastatic NSCLC (e.g., locally advanced unresectable or metastatic non-squamous NSCLC (e.g., stage IV non-squamous NSCLC)), or stage IV NSCLC (e.g., subject previously treated for stage IV NSCLC) never been treated))): cervical cancer (e.g. stage IVB, metastatic, recurrent or persistent cervical cancer, e.g. metastatic and/or recurrent PD-L1 positive cervical cancer); breast cancer (e.g. TNBC (e.g. eTNBC)) or HER2-positive breast cancer); head and neck cancer (e.g. SCCHN, e.g. recurrent/metastatic PD-L1 positive SCCHN); liver cancer (e.g. HCC, e.g. , locally advanced or metastatic HCC and/or unresectable HCC); bladder cancer (e.g. MIBC, locally advanced UC, or mUC); esophageal cancer; pancreatic cancer (e.g. PDAC, e.g. metastatic PDAC) renal cancer or renal cancer (e.g., RCC); melanoma; ovarian cancer; gastric cancer (e.g., gastroesophageal junction cancer); or CRC (e.g., MSS or MSI-Low CRC)) Provided herein are methods for optimizing a therapeutic regimen for, further therapeutic regimens comprising one or more biomarkers (e.g., , PD-L1, TIGIT, activated T cells or cytokines).
本明細書に記載の方法で使用するためのバイオマーカーとしては、限定されないが、組織(例えば、腫瘍組織)又は血液(例えば、全血)でのPD-L1及び/又はTIGIT発現、WGS及び/又はNGSによって同定された、組織(例えば、腫瘍組織)からの及び/又は血液中の循環腫瘍DNA(限定されないが、突然変異負荷、MSI及びMMR欠陥を含む)からの生殖系列及び体細胞の変異、腫瘍免疫生物学(例えば、TEFF)に関連する遺伝子(例えば、CD274)又は遺伝子シグネチャの分析、リンパ球亜集団、T細胞受容体レパートリー、T細胞活性化に関連するサイトカイン、並びに血漿由来サイトカインが含まれ得るが、これらに限定されない。いくつかの例では、バイオマーカーはPD-L1である。いくつかの例では、試料は腫瘍試料(例えば、ホルマリン固定パラフィン包埋(FFPE)腫瘍試料)である。 Biomarkers for use in the methods described herein include, but are not limited to, PD-L1 and/or TIGIT expression in tissue (eg, tumor tissue) or blood (eg, whole blood), WGS and/or or germline and somatic mutations from tissue (e.g., tumor tissue) and/or from circulating tumor DNA in the blood (including but not limited to mutation burden, MSI and MMR defects) identified by NGS , analyzes of genes (e.g., CD274) or gene signatures associated with tumor immunobiology (e.g., TEFF), lymphocyte subpopulations, T-cell receptor repertoires, cytokines associated with T-cell activation, as well as plasma-derived cytokines may include, but are not limited to: In some examples, the biomarker is PD-L1. In some examples, the sample is a tumor sample (eg, a formalin-fixed paraffin-embedded (FFPE) tumor sample).
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定すること、ならびにセクションIII(A)に記載されている方法又は使用のいずれかに従って、有効量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又は例えばペンブロリズマブ等の抗PD-1アンタゴニスト抗体)の1回以上の投薬サイクルを対象に投与することを含む。 In some examples, the methods determine the presence and/or expression level/ An effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, such as , tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody, such as atezolizumab, or an anti-PD-1 antagonist antibody, such as, e.g., pembrolizumab) to the subject. .
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、4週間ごとに約700mg~約1000mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び4週間ごとに約1400mg~2000mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、投薬レジメンは、700mg~1000mgの用量(例えば、固定用量)で4週間ごとの抗TIGITアンタゴニスト抗体及び1400mg~2000mgの用量(例えば、固定用量)で4週間ごとのPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む。 In some examples, the methods determine the presence and/or expression level/ an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of about 700 mg to about 1000 mg every 4 weeks and PD-1 at a dose (e.g., fixed dose) of about 1400 mg to 2000 mg every 4 weeks; administering to the subject a dosing regimen comprising one or more dosing cycles of the axially bound antagonist. In some examples, the dosing regimen is anti-TIGIT antagonist antibody at a dose (eg, fixed dose) of 700 mg to 1000 mg every 4 weeks and PD-1 at a dose (eg, fixed dose) of 1400 mg to 2000 mg every 4 weeks. Including one or more dosing cycles of the axially bound antagonist.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、2週間ごとに約300mg~約600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び2週間ごとに約600mg~約1200mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、方法は、2週間ごとに300mg~600mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体及び2週間ごとに600mg~1200mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニストを含む1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In some examples, the methods determine the presence and/or expression level/ and anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of about 300 mg to about 600 mg every two weeks and PD- at a dose (e.g., fixed dose) of about 600 mg to about 1200 mg every two weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the monoaxial binding antagonist. In some examples, the method comprises administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 300 mg to 600 mg every two weeks and a PD-1 axis at a dose (e.g., fixed dose) of 600 mg to 1200 mg every two weeks. administering to the subject a dosing regimen comprising one or more dosing cycles comprising the binding antagonist.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mg~約1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80及び1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、方法は、3週間ごとに30mg~1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mg~1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In some examples, the methods determine the presence and/or expression level/ and anti-TIGIT antagonist antibody at doses (eg, fixed dose) of about 30 mg to about 1200 mg every 3 weeks, and PD-1 at doses (eg, fixed dose) of about 80 and 1600 mg every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of an axially-linked antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks. In some examples, the method comprises administering an anti-TIGIT antagonist antibody at a dose (eg, fixed dose) of 30 mg to 1200 mg every 3 weeks, PD-1 axis at a dose (eg, fixed dose) of 80 mg to 1600 mg every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of a binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体及び3週間ごとに約200mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含み、抗PD-1アンタゴニスト抗体はペンブロリズマブである。いくつかの例では、方法は、3週間ごとに30mg~1200mgの用量の抗TIGITアンタゴニスト抗体及び3週間ごとに200mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含み、抗PD-1アンタゴニスト抗体はペンブロリズマブである。 In some examples, the methods determine the presence and/or expression level/ and a dosing regimen comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every three weeks and an anti-PD-1 antagonist antibody at a dose of about 200 mg every three weeks. and administering to the subject, the anti-PD-1 antagonist antibody is pembrolizumab. In some examples, the method comprises one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of 30 mg to 1200 mg every three weeks and an anti-PD-1 antagonist antibody at a dose of 200 mg every three weeks. administering to the subject, wherein the anti-PD-1 antagonist antibody is pembrolizumab;
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、チラゴルマブ及びペンブロリズマブの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含み、ペンブロリズマブは、6週間ごとに約100mgと約1000mgの間の用量で投与される。いくつかの例では、ペンブロリズマブは、6週間ごとに約400mgの用量で投与される。 In some examples, the methods determine the presence and/or expression level/ and administering to the subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein pembrolizumab is administered at a dose of between about 100 mg and about 1000 mg every 6 weeks. be. In some examples, pembrolizumab is administered at a dose of about 400 mg every 6 weeks.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、及び3週間ごとに2週間/1週間間隔で1日2回の約10mg/m2と約10000mg/m2の間の用量(例えば、固定用量)の代謝拮抗剤の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mgと1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、及び3週間ごとに2週間の投薬/1週間の休薬で1日2回の10mg/m2と10000mg/m2の間の用量(例えば、固定用量)の代謝拮抗剤の1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。 In some examples, the methods determine the presence and/or expression level/ and anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg every three weeks; a dose of between about 80 mg and about 1600 mg (e.g., fixed dose) every three weeks; ) and an antimetabolite at a dose (e.g., fixed dose) between about 10 mg/m 2 and about 10,000 mg/m 2 twice daily at 2-week/1-week intervals every 3 weeks administering to the subject a dosing regimen comprising one or more dosing cycles of the agent. In some examples, the method includes administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks, PD- a monoaxial binding antagonist and an antimetabolite at a dose (e.g., fixed dose) between 10 mg/ m2 and 10000 mg/ m2 twice daily with 2 weeks on/1 week off every 3 weeks administering to the subject a dosing regimen comprising one or more dosing cycles.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとに約30mg~約1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80及び1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、ゲムシタビン、及びnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、方法は、3週間ごとに30mg~1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80及び1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、ゲムシタビン及びnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In some examples, the methods determine the presence and/or expression level/ and anti-TIGIT antagonist antibody at doses (eg, fixed dose) of about 30 mg to about 1200 mg every 3 weeks, and PD-1 at doses (eg, fixed dose) of about 80 and 1600 mg every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the axially bound antagonist, gemcitabine, and nab-paclitaxel. In some examples, the method includes anti-TIGIT antagonist antibody at doses (eg, fixed dose) of 30 mg to 1200 mg every 3 weeks, PD-1 axis at doses (eg, fixed dose) of 80 and 1600 mg every 3 weeks. administering to the subject a dosing regimen comprising one or more dosing cycles of the binding antagonist, gemcitabine and nab-paclitaxel.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、3週間ごとの約30mgと約1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、及び3週間ごとに約1mg/kgと約35mg/kgの間の用量のVEGFアンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することとを含む。いくつかの例では、方法は、3週間ごとに30mgと1200mgの間の用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mgと1600mgの間の用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、及び3週間ごとに1mg/kgと35mg/kgの間の用量のVEGFアンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む。 In some examples, the methods determine the presence and/or expression level/ and anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between about 30 mg and about 1200 mg every three weeks, a dose of between about 80 mg and about 1600 mg (e.g., fixed dose) every three weeks. ) and one or more dosing cycles of a VEGF antagonist at a dose between about 1 mg/kg and about 35 mg/kg every 3 weeks. . In some examples, the method includes administering an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of between 30 mg and 1200 mg every three weeks; administering to the subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist and a VEGF antagonist at a dose between 1 mg/kg and 35 mg/kg every 3 weeks.
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、導入期及び維持期を含む投薬レジメンを対象に投与することと、を含み、(a)導入期は、3週間ごとに約30mg~約1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約80mg~1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み;(b)維持期は、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、維持期は白金系化学療法剤の投与を含まない。いくつかの例では、(a)導入期は、3週間ごとに30mg~1200mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに80mg~1600mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み;(b)維持期は、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、維持期は白金系化学療法剤の投与を含まない。 In some examples, the methods determine the presence and/or expression level/ and administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein (a) the induction phase is a dose of about 30 mg to about 1200 mg every 3 weeks (e.g., fixed dose ), a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of about 80 mg to 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks. (b) a maintenance phase of anti-TIGIT antagonist antibody every 3 weeks, PD-1 axis binding antagonist every 3 weeks and non-platinum chemotherapeutic agent every 3 weeks; The maintenance phase does not include administration of platinum-based chemotherapeutic agents, including one or more additional dosing cycles. In some examples, (a) the induction phase is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 30 mg to 1200 mg every three weeks; comprising one or more dosing cycles of a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks; TIGIT antagonist antibody, PD-1 axis binding antagonist every 3 weeks and one or more additional dosing cycles of a non-platinum-based chemotherapeutic agent every 3 weeks, with a maintenance phase that does not include administration of a platinum-based chemotherapeutic agent .
いくつかの例では、方法は、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量を決定することと、導入期及び維持期を含む投薬レジメンを対象に投与することと、を含み、(a)導入期が、3週間ごとに約500mg~約700mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含み、(b)維持期が、4週間ごとに約700mg~約1000mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び4週間ごとに約1400mg~2000mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、維持期は、白金系化学療法剤又は非白金系化学療法剤の投与を含まない。いくつかの例では、(a)導入期が、3週間ごとに500mg~700mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、3週間ごとに900mg~1500mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニスト、3週間ごとに白金系化学療法剤、及び3週間ごとに非白金系化学療法剤の1回以上の投薬サイクルを含み、(b)維持期が、4週間ごとに700mg~1000mgの用量(例えば、固定用量)の抗TIGITアンタゴニスト抗体、及び4週間ごとに1400mg~2000mgの用量(例えば、固定用量)のPD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、維持期は、白金系化学療法剤又は非白金系化学療法剤の投与を含まない。 In some examples, the methods determine the presence and/or expression level/ and administering to the subject a dosing regimen comprising an induction phase and a maintenance phase, wherein (a) the induction phase is a dose of about 500 mg to about 700 mg every 3 weeks (e.g., fixed dose ), a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based (b) a maintenance phase of an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of about 700 mg to about 1000 mg every 4 weeks, and about 1400 mg every 4 weeks. One or more additional dosing cycles of a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of ~2000 mg, with a maintenance phase that does not include administration of a platinum-based or non-platinum-based chemotherapeutic agent . In some examples, (a) the induction phase is an anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of 500 mg to 700 mg every three weeks, a dose (e.g., fixed dose) of 900 mg to 1500 mg every three weeks; One or more dosing cycles of a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks, and (b) a maintenance phase of 700 mg every 4 weeks. An anti-TIGIT antagonist antibody at a dose (e.g., fixed dose) of ~1000 mg and one or more additional dosing cycles of a PD-1 axis binding antagonist at a dose (e.g., fixed dose) of 1400 mg to 2000 mg every 4 weeks. , the maintenance phase does not include administration of platinum-based chemotherapeutic agents or non-platinum-based chemotherapeutic agents.
バイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量は、タンパク質、タンパク質フラグメント、DNA、mRNA、cDNA及び/又は遺伝子コピー数を含むがこれらに限定されない、当該技術分野で公知の任意の適切な基準に基づいて定性的及び/又は定量的に決定することができる。いくつかの例では、バイオマーカーはPD-L1である。PD-L1発現は、セクションIII(L)に記載されているように評定され得る。いくつかの例では、バイオマーカーはTIGITである。TIGIT発現は、セクションIII(M)に記載されているように評定することができる。いくつかの例では、バイオマーカーは、EGFR及び/又はALK異常である。EGFR及び/又はALK異常は、セクションIII(N)に記載されているように評定することができる。 The presence and/or expression level/amount of biomarkers (eg, PD-L1, TIGIT, activated T cells or cytokines) include, but are not limited to, proteins, protein fragments, DNA, mRNA, cDNA and/or gene copy number. It can be determined qualitatively and/or quantitatively based on any suitable criteria known in the art, without limitation. In some examples, the biomarker is PD-L1. PD-L1 expression can be assessed as described in Section III(L). In some examples, the biomarker is TIGIT. TIGIT expression can be assessed as described in Section III(M). In some examples, the biomarkers are EGFR and/or ALK abnormalities. EGFR and/or ALK abnormalities can be assessed as described in Section III(N).
いくつかの例では、バイオマーカーの発現レベル又は量は、対象からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1タンパク質発現レベルである。いくつかの例では、PD-L1タンパク質発現レベルを免疫組織化学(IHC)アッセイによって決定した。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 protein expression level in a tumor sample (eg, an FFPE tumor sample) from the subject. In some instances, PD-L1 protein expression levels were determined by immunohistochemistry (IHC) assays. In some examples, the tissue sample is a tumor sample.
いくつかの例では、対象からの腫瘍試料(例えば、FFPE腫瘍試料)は、検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、対象からの腫瘍試料(例えば、FFPE腫瘍試料)は、腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, a tumor sample (eg, an FFPE tumor sample) from the subject has been determined to have a detectable PD-L1 expression level. In some examples, a tumor sample (eg, an FFPE tumor sample) from a subject has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells. In some examples, the tissue sample is a tumor sample.
いくつかの例では、バイオマーカーの発現レベル又は量は、対象からの腫瘍試料(例えば、FFPE腫瘍試料)中の検出可能なPD-L1核酸発現レベルである。いくつかの例では、PD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR、又はRT-qPCR、マイクロアレイ分析、遺伝子発現の連続分析(SAGE)、MassARRAY(登録商標)技術、in situハイブリダイゼーション(ISH)、又はそれらの組み合わせによって決定されている。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, the biomarker expression level or amount is a detectable PD-L1 nucleic acid expression level in a tumor sample (eg, an FFPE tumor sample) from the subject. In some examples, PD-L1 nucleic acid expression levels are measured by RNA-seq, RT-qPCR, qPCR, multiplex qPCR, or RT-qPCR, microarray analysis, serial analysis of gene expression (SAGE), MassARRAY® technique, in situ hybridization (ISH), or a combination thereof. In some examples, the tissue sample is a tumor sample.
いくつかの例では、対象からの試料(例えば、腫瘍試料又は血液試料)中のバイオマーカー(例えば、PD-L1、TIGIT、活性化T細胞又はサイトカイン)の存在及び/又は発現レベル/量は、例えば、検出可能なPD-L1発現レベルが個体を選択するためのバイオマーカーである場合、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体、又はペンブロリズマブ等の抗PD-1アンタゴニスト抗体)による治療に適格である対象を選択する。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は腫瘍試料(例えば、FFPE腫瘍試料)である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。いくつかの例では、組織試料は、腫瘍試料である。 In some examples, the presence and/or expression level/amount of a biomarker (e.g., PD-L1, TIGIT, activated T cells or cytokines) in a sample (e.g., tumor sample or blood sample) from the subject is For example, if the detectable PD-L1 expression level is a biomarker for selecting individuals, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab, or pembrolizumab, etc.) Subjects are selected who are eligible for treatment with an anti-PD-1 antagonist antibody). In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample (eg, FFPE tumor sample). In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof. In some examples, the tissue sample is a tumor sample.
いくつかの例では、方法は、同定された対象に治療を投与することを更に含む。いくつかの例では、治療は、1つ以上の追加の治療剤(例えば、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1抗体)、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム))を更に含むか又はそれと組み合わせて(別々に又は一緒に)投与することができる。 In some examples, the method further comprises administering a treatment to the identified subject. In some examples, treatment includes one or more additional therapeutic agents (e.g., anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists (e.g., anti-PD-L1 antibodies), VEGF antagonists, chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents or non-platinum-based chemotherapeutic agents), ADC (e.g., enfortumab vedotin or sacituzumab govitecan) or CSF (e.g., pegfilgrastim, filgrastim, or sargramostim)) It can be further included or administered in combination (separately or together).
いくつかの例では、本明細書に記載される診断方法又は使用のいずれかにおいて、がんは固形腫瘍及び/又は局所進行性もしくは転移性がんである。 In some examples, in any of the diagnostic methods or uses described herein the cancer is a solid tumor and/or locally advanced or metastatic cancer.
F.投薬
i.抗TIGITアンタゴニスト抗体の投薬
一般的な提案として、ヒトに投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の治療有効量は、1回以上の投与によるかどうかにかかわらず、患者の体重1 kg当たり約0.01~約50mgの範囲であろう。いくつかの実施形態では、ヒトに投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の治療有効量は、1回以上の投与によるかどうかにかかわらず、患者の体重1kg当たり0.01~50mgの範囲である。
F. Dosing i. Anti-TIGIT Antagonist Antibody Dosing As a general proposition, a therapeutically effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) administered to a human is The dosage may range from about 0.01 to about 50 mg/kg of patient body weight, whether or not with the above dosages. In some embodiments, a therapeutically effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) administered to a human is by one or more administrations. Regardless, it ranges from 0.01 to 50 mg/kg of patient body weight.
いくつかの例示的実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約0.01~約45mg/kg、約0.01~約40mg/kg、約0.01~約35mg/kg、約0.01~約30mg/kg、約0.01~約25mg/kg、約0.01~約20mg/kg、約0.01~約15mg/kg、約0.01~約10mg/kg、約0.01~約5mg/kg、又は約0.01~約1mg/kgの用量で投与され、例えば、毎日、毎週、2週間ごと、3週間ごと、又は4週間ごとに投与される。いくつかの例示的実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、0.01~45mg/kg、0.01~40mg/kg、0.01~35mg/kg、0.01~30mg/kg、0.01~25mg/kg、0.01~20mg/kg、0.01~15mg/kg、0.01~10mg/kg、0.01~5mg/kg、又は0.01~1mg/kgの用量で投与され、例えば、毎日、毎週、2週間ごと、3週間ごと、又は4週間ごとに投与される。 In some exemplary embodiments, the anti-TIGIT antagonist antibody (eg, anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is about 0.01 to about 45 mg/kg, about 0.01 to about 40 mg/kg, about 0.01 to about 35 mg/kg, about 0.01 to about 30 mg/kg, about 0.01 to about 25 mg/kg, about 0.01 to about 20 mg/kg, about 0.01 administered at a dose of to about 15 mg/kg, about 0.01 to about 10 mg/kg, about 0.01 to about 5 mg/kg, or about 0.01 to about 1 mg/kg, e.g., daily, weekly, for two weeks administered every, every three weeks, or every four weeks. In some exemplary embodiments, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 0.01-45 mg/kg, 0.01-40 mg/kg, kg, 0.01-35 mg/kg, 0.01-30 mg/kg, 0.01-25 mg/kg, 0.01-20 mg/kg, 0.01-15 mg/kg, 0.01-10 mg/kg, Dosages of 0.01-5 mg/kg, or 0.01-1 mg/kg are administered, for example, daily, weekly, every two weeks, every three weeks, or every four weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に投与する。
In some examples, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered at about day 1 (eg, day −3, −2) of the dosing cycle.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、段階的投薬レジメン(例えば、対象の体重(BW)又は体表面積(BSA)に基づく投薬)で(例えば、3週間ごとに)投与する。そのような投薬レジメンは、比較的低体重(例えば、40 kg以下(例えば、5 kg~40 kg、15 kg~40 kg、又は5 kg~15 kg))の対象の処置に利用することができ、成人データから推定された薬物動態パラメーターの外挿に基づくバイオシミュレーション研究を通じて開発されている。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered in a graded dosing regimen (e.g., subject body weight (BW) or body surface area ( BSA)-based dosing) (eg, every 3 weeks). Such dosing regimens can be utilized in the treatment of relatively low weight subjects (eg, 40 kg or less (eg, 5 kg to 40 kg, 15 kg to 40 kg, or 5 kg to 15 kg)). , being developed through biosimulation studies based on extrapolation of pharmacokinetic parameters estimated from adult data.
いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約250mgと約350mgの間の用量(例えば、3週間ごとに約300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約350mgと約450mgの間の用量(例えば、3週間ごとに約400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約550mgと約650mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgの用量で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgの用量で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約600mgの用量で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに250mgと350mgの間の用量(例えば、3週間ごとに300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに350mgと450mgの間の用量(例えば、3週間ごとに400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに550mgと650mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgの用量で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgの用量で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに600mgの用量で投与される。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is It is a tiered dose based on In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 300 mg every 3 weeks); (b) weighing more than 15 kg and 40 kg; or (c) greater than 40 kg and the anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every 3 weeks (e.g., about 400 mg every 3 weeks); , at doses between about 30 mg and about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between about 250 mg and about 350 mg every 3 weeks (e.g., about 300 mg every 3 weeks); (b) weighing more than 15 kg and 40 kg; or (c) greater than 40 kg and the anti-TIGIT antagonist antibody is administered at a dose of between about 350 mg and about 450 mg every 3 weeks (e.g., about 400 mg every 3 weeks); , at doses between about 550 mg and about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) weighing greater than 15 kg and ≤40 kg and the anti-TIGIT antagonist antibody is administered at about or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 300 mg every 3 weeks); (b) weighing more than 15 kg and 40 kg or less; , the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 400 mg every 3 weeks); and 1200 mg (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighs 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between 250 mg and 350 mg every 3 weeks (e.g., 300 mg every 3 weeks); (b) weighs more than 15 kg and ≤40 kg; or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of between 350 mg and 450 mg every 3 weeks (e.g., 400 mg every 3 weeks); and 650 mg (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体重が40kgを超える(例えば、40.5kg、41kg、42kg、43kg、44kg、45kg、46kg、47kg、48kg、49kg、50kg、51kg、52kg、53kg、54kg、55kg、56kg、57kg、58kg、59kg、60kg、61kg、62kg、63kg、64kg、65kg、66kg、67kg、68kg、69kg、70kg、75kg、80kg、85kg、90kg、95kg、100kg、110kg、120kg、130kg、140kg、150kg以上)対象について、3週間ごと(Q3W)に約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、40kgを超える体重を有する対象については、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体重が40kgを超える(例えば、40.5kg、41kg、42kg、43kg、44kg、45kg、46kg、47kg、48kg、49kg、50kg、51kg、52kg、53kg、54kg、55kg、56kg、57kg、58kg、59kg、60kg、61kg、62kg、63kg、64kg、65kg、66kg、67kg、68kg、69kg、70kg、75kg、80kg、85kg、90kg、95kg、100kg、110kg、120kg、130kg、140kg、150kg以上)対象について、3週間ごと(Q3W)に30mgと1200mgの間(例えば、30mgと1100mgの間、例えば、60mgと1000mgの間、例えば、100mgと900mgの間、例えば、200mgと800mgの間、例えば、300mgと800mgの間、例えば、400mgと800mgの間、例えば、400mgと750mgの間、例えば、450mgと750mgの間、例えば、500mgと700mgの間、例えば、550mgと650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、40kgを超える体重を有する対象については、3週間ごとに600mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is greater than 40 kg (e.g., 40.5 kg, 41 kg, 42 kg, 43kg, 44kg, 45kg, 46kg, 47kg, 48kg, 49kg, 50kg, 51kg, 52kg, 53kg, 54kg, 55kg, 56kg, 57kg, 58kg, 59kg, 60kg, 61kg, 62kg, 63kg, 64kg, 65kg, 66kg, 67kg, between about 30 mg and about 1200 mg (e.g., about between 30 mg and about 1100 mg, such as between about 60 mg and about 1000 mg, such as between about 100 mg and about 900 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 800 mg, such as about between about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ±10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is about 600 mg every 3 weeks for a subject weighing over 40 kg. is the dose of In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is greater than 40 kg (e.g., 40.5 kg, 41 kg, 42 kg, 43kg, 44kg, 45kg, 46kg, 47kg, 48kg, 49kg, 50kg, 51kg, 52kg, 53kg, 54kg, 55kg, 56kg, 57kg, 58kg, 59kg, 60kg, 61kg, 62kg, 63kg, 64kg, 65kg, 66kg, 67kg, 68 kg, 69 kg, 70 kg, 75 kg, 80 kg, 85 kg, 90 kg, 95 kg, 100 kg, 110 kg, 120 kg, 130 kg, 140 kg, 150 kg or more) between 30 mg and 1200 mg (e.g., 30 mg and 1100 mg) every 3 weeks (Q3W) between 60 mg and 1000 mg, such as between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg e.g. , 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is 600 mg every 3 weeks for a subject weighing over 40 kg. dose.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体重が15kg超40kg以下(例えば、15.1kg、15.2kg、15.3kg、15.4kg、15.5kg、16kg、17kg、18kg、19kg、20kg、21kg、22kg、23kg、24kg、25kg、26kg、27kg、28kg、29kg、30kg、31kg、32kg、33kg、34kg、35kg、36kg、37kg、38kg、39kg、又は39.5kg)の対象について、3週間ごと(Q3W)に約10mgと約1000mgの間(例えば約20mgと約1000mgの間、例えば約50mgと約900mgの間、例えば約100mgと約850mgの間、例えば約200mgと約700mgの間、例えば約250mgと約600mgの間、例えば約300mgと約500mgの間、例えば約350mgと約450mgの間、例えば約390mgと約410mgの間、例えば約400mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、15kg超40kg以下の体重を有する対象に対して3週間ごとに約400mg(例えば、400mg±10mg、例えば、400±6mg、例えば、400±5mg、例えば、400±3mg、例えば、400±1mg、例えば、400±0.5mg、例えば、3週間ごとに400mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えばチラゴルマブ)の有効量は、体重15kg超40kg以下(例えば15.1kg、15.2kg、15.3kg、15.4kg、15.5kg、16kg、17kg、18kg、19kg、20kg、21kg、22kg、23kg、24kg、25kg、26kg、27kg、28kg、29kg、30kg、31kg、32kg、33kg、34kg、35kg、36kg、37kg、38kg、39kg、又は39.5kg)の対象について、3週間(Q3W)ごとに10mgと1000mgの間(例えば20mgと1000mgの間、例えば50mgと900mgの間、例えば100mgと850mgの間、例えば200mgと700mgの間、例えば250mgと600mgの間、例えば300mgと500mgの間、例えば350mgと450mgの間、例えば390mgと410mgの間、例えば400mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、15kg超40kg以下の体重を有する対象に対して3週間ごとに400mg(例えば、400mg±10mg、例えば、400±6mg、例えば、400±5mg、例えば、400±3mg、例えば、400±1mg、例えば、400±0.5mg、例えば、3週間ごとに400mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is greater than 15 kg and 40 kg or less (e.g., 15.1 kg, 15 .2kg, 15.3kg, 15.4kg, 15.5kg, 16kg, 17kg, 18kg, 19kg, 20kg, 21kg, 22kg, 23kg, 24kg, 25kg, 26kg, 27kg, 28kg, 29kg, 30kg, 31kg, 32kg, 33kg , 34 kg, 35 kg, 36 kg, 37 kg, 38 kg, 39 kg, or 39.5 kg) every three weeks (Q3W) between about 10 mg and about 1000 mg (e.g., between about 20 mg and about 1000 mg, e.g., about 50 mg) between about 900 mg, such as between about 100 mg and about 850 mg, such as between about 200 mg and about 700 mg, such as between about 250 mg and about 600 mg, such as between about 300 mg and about 500 mg, such as between about 350 mg and about 450 mg; eg between about 390 mg and about 410 mg, eg about 400 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is 3 weeks for a subject having a weight of greater than 15 kg but 40 kg or less. about 400 mg every 3 weeks (e.g., 400 mg ± 10 mg, such as 400 ± 6 mg, such as 400 ± 5 mg, such as 400 ± 3 mg, such as 400 ± 1 mg, such as 400 ± 0.5 mg, such as 400 mg every 3 weeks ). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is greater than 15 kg and 40 kg or less (e.g., 15.1 kg, 15.2 kg, 15 .3kg, 15.4kg, 15.5kg, 16kg, 17kg, 18kg, 19kg, 20kg, 21kg, 22kg, 23kg, 24kg, 25kg, 26kg, 27kg, 28kg, 29kg, 30kg, 31kg, 32kg, 33kg, 34kg, 35kg , 36 kg, 37 kg, 38 kg, 39 kg, or 39.5 kg) between 10 mg and 1000 mg (e.g., between 20 mg and 1000 mg, such as between 50 mg and 900 mg, such as 100 mg and 850 mg) every three weeks (Q3W) between 200 mg and 700 mg, such as between 250 mg and 600 mg, such as between 300 mg and 500 mg, such as between 350 mg and 450 mg, such as between 390 mg and 410 mg, such as 400 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is 3 weeks for a subject having a weight of greater than 15 kg but 40 kg or less. 400 mg every 3 weeks (e.g., 400 mg ± 10 mg, such as 400 ± 6 mg, such as 400 ± 5 mg, such as 400 ± 3 mg, such as 400 ± 1 mg, such as 400 ± 0.5 mg, such as 400 mg every 3 weeks) is the dose of
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体重15kg以下(例えば、0.5kg、1kg、1.5kg、2.0kg、2.5kg、3.0kg、3.5kg、4.0kg、4.5kg、5.0kg、5.5kg、6.0kg、6.5kg、7.0kg、7.5kg、8.0kg、8.5kg、9.0kg、9.5kg、10.0kg、10.5kg、11.0kg、11.5kg、12.0kg、12.5kg、13.0kg、13.5kg、14.0kg、14.5kg、又は15.0kg)の対象について、3週間ごと(Q3W)に約10mgと約1000mgの間(例えば、約10mgと約900mgの間、例えば、約50mgと約900mgの間、例えば、約100mgと約750mgの間、例えば、約100mgと約600mgの間、例えば、約150mgと約500mgの間、例えば、約200mgと約400mgの間、例えば、約250mgと約350mgの間、例えば、約290mgと約310mgの間、例えば、約300mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、15kg以下の体重を有する対象に対して3週間ごとに約300mg(例えば、300mg±10mg、例えば、300±6mg、例えば、300±5mg、例えば、300±3mg、例えば、300±1mg、例えば、300±0.5mg、例えば、3週間ごとに300mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体重15kg以下(例えば、0.5kg、1kg、1.5kg、2.0kg、2.5kg、3.0kg、3.5kg、4.0kg、4.5kg、5.0kg、5.5kg、6.0kg、6.5kg、7.0kg、7.5kg、8.0kg、8.5kg、9.0kg、9.5kg、10.0kg、10.5kg、11.0kg、11.5kg、12.0kg、12.5kg、13.0kg、13.5kg、14.0kg、14.5kg、又は15.0kg)の対象について、3週間(Q3W)ごとに10mgと1000mgの間(例えば、10mgと900mgの間、例えば、50mgと900mgの間、例えば、100mgと750mgの間、例えば、100mgと600mgの間、例えば、150mgと500mgの間、例えば、200mgと400mgの間、例えば、250mgと350mgの間、例えば、290mgと310mgの間、例えば、300mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、15kg以下の体重を有する対象に対して3週間ごとに300mg(例えば、300mg±10mg、例えば、300±6mg、例えば、300±5mg、例えば、300±3mg、例えば、300±1mg、例えば、300±0.5mg、例えば、3週間ごとに300mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is less than or equal to 15 kg body weight (eg, 0.5 kg, 1 kg, 1. 5kg, 2.0kg, 2.5kg, 3.0kg, 3.5kg, 4.0kg, 4.5kg, 5.0kg, 5.5kg, 6.0kg, 6.5kg, 7.0kg, 7.5kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14. 0 kg, 14.5 kg, or 15.0 kg) every three weeks (Q3W) between about 10 mg and about 1000 mg (e.g., between about 10 mg and about 900 mg, e.g., between about 50 mg and about 900 mg; between about 100 mg and about 750 mg, such as between about 100 mg and about 600 mg, such as between about 150 mg and about 500 mg, such as between about 200 mg and about 400 mg, such as between about 250 mg and about 350 mg, For example, a dose of between about 290 mg and about 310 mg, eg, about 300 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered every 3 weeks to a subject having a weight of 15 kg or less. about 300 mg (e.g., 300±10 mg, such as 300±6 mg, such as 300±5 mg, such as 300±3 mg, such as 300±1 mg, such as 300±0.5 mg, such as 300 mg every 3 weeks) dose. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 15 kg or less of body weight (eg, 0.5 kg, 1 kg, 1. 5kg, 2.0kg, 2.5kg, 3.0kg, 3.5kg, 4.0kg, 4.5kg, 5.0kg, 5.5kg, 6.0kg, 6.5kg, 7.0kg, 7.5kg, 8.0 kg, 8.5 kg, 9.0 kg, 9.5 kg, 10.0 kg, 10.5 kg, 11.0 kg, 11.5 kg, 12.0 kg, 12.5 kg, 13.0 kg, 13.5 kg, 14. between 10 mg and 1000 mg (e.g., between 10 mg and 900 mg, e.g., between 50 mg and 900 mg, e.g., 100 mg and 750 mg) every three weeks (Q3W) for subjects weighing 0 kg, 14.5 kg, or 15.0 kg). between 100 mg and 600 mg, such as between 150 mg and 500 mg, such as between 200 mg and 400 mg, such as between 250 mg and 350 mg, such as between 290 mg and 310 mg, such as 300 mg). . In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered to a subject having a weight of 15 kg or less every 3 weeks. A dose of 300 mg (eg, 300±10 mg, such as 300±6 mg, such as 300±5 mg, such as 300±3 mg, such as 300±1 mg, such as 300±0.5 mg, such as 300 mg every 3 weeks) is.
いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間(例えば、3週間ごとに約300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約350mg)で投与され;(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約250mgと約350mgの間(例えば、3週間ごとに約300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgと約400mgの間の用量(例えば、3週間ごとに約350mg)で投与され;又は(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgと約500mgの間の用量(例えば、3週間ごとに約450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約550mgと約650mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgの用量で投与される;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgの用量で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに450mgの用量で投与し;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約600mgの用量で投与される。いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間(例えば、3週間ごとに300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに350mg)で投与され;(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに250mgと350mgの間(例えば、3週間ごとに300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgと400mgの間の用量(例えば、3週間ごとに350mg)で投与され;又は(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgと500mgの間の用量(例えば、3週間ごとに450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに550mgと650mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgの用量で投与される;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgの用量で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに450mgの用量で投与し;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに600mgの用量で投与される。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is the body surface area of the subject. It is a tiered dose based on In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 or less than 0.75 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 350 mg every 3 weeks); c) greater than 0.75 m 2 and less than or equal to 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 450 mg every 3 weeks); or ( d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 30 mg and about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between about 250 mg and about 350 mg every three weeks (eg, about 300 mg every three weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between about 300 mg and about 400 mg every 3 weeks (e.g., about 350 mg every 3 weeks); or (c) greater than 0.75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between about 400 mg and about 500 mg every 3 weeks (e.g., about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 550 mg and about 650 mg every three weeks (eg, about 600 mg every three weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) has a body surface area of 0.5 m2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; , the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks ; or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is the body surface area of the subject. It is a tiered dose based on In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between 10 mg and 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 350 mg every 3 weeks); (c) 0 greater than .75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 450 mg every 3 weeks); or (d) 1.25 m2 and the anti-TIGIT antagonist antibody is administered at a dose between 30 mg and 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between 250 mg and 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 300 mg and 400 mg every 3 weeks (e.g., 350 mg every 3 weeks); or (c) greater than 0.75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 400 mg and 500 mg every 3 weeks (e.g., 450 mg every 3 weeks); or (d) 1.25 m greater than 2 and the anti-TIGIT antagonist antibody is administered at a dose between 550 mg and 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) has a body surface area of 0.5 m2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; the anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体表面積が1.25m2超(例えば、1.25m2、1.35m2、1.45m2、1.50m2、1.55m2、1.60m2、1.65m2、1.70m2、1.75m2、1.80m2、1.85m2、1.90m2、1.95m2、2.0m2、2.1m2、2.2m2、2.3m2、2.4m2、2.5m2、2.6m2、2.7m2、2.8m2、2.9m2、3.0m2又はそれ以上)の対象について、3週間ごと(Q3W)に約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、1.25m2を超える体表面積を有する対象については、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、1.25m2超(例えば、1.25m2、1.35m2、1.45m2、1.50m2、1.55m2、1.60m2、1.65m2、1.70m2、1.75m2、1.80m2、1.85m2、1.90m2、1.95m2、2.0m2、2.1m2、2.2m2、2.3m2、2.4m2、2.5m2、2.6m2、2.7m2、2.8m2、2.9m2、3.0m2又はそれ以上)の体表面積を有する対象について、3週間ごと(Q3W)に30mgと1200mgの間(例えば、30mgと1100mgの間、例えば、60mgと1000mgの間、例えば、100mgと900mgの間、例えば、200mgと800mgの間、例えば、300mgと800mgの間、例えば、400mgと800mgの間、例えば、400mgと750mgの間、例えば、450mgと750mgの間、例えば、500mgと700mgの間、例えば、550mgと650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、1.25m2を超える体表面積を有する対象については、3週間ごとに600mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) has a body surface area greater than 1.25 m 2 (e.g., 1.25 m 2 , 1.35m2 , 1.45m2 , 1.50m2 , 1.55m2 , 1.60m2 , 1.65m2 , 1.70m2 , 1.75m2 , 1.80m2 , 1.85m2 , 1.90 m 2 , 1.95 m 2 , 2.0 m 2 , 2.1 m 2 , 2.2 m 2 , 2.3 m 2 , 2.4 m 2 , 2.5 m 2 , 2.6 m 2 , 2.7 m 2 , between about 30 mg and about 1200 mg (e.g. , between about 30 mg and about 1100 mg, e.g., about between 60 mg and about 1000 mg, such as between about 100 mg and about 900 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 800 mg, such as between about 400 mg and about 800 mg, such as about between 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as , 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is 3 weeks for a subject with a body surface area greater than 1.25 m2 . dose of about 600 mg per dose. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is greater than 1.25 m 2 (eg, 1.25 m 2 , 1.35 m 2 , 1.45m2 , 1.50m2 , 1.55m2 , 1.60m2 , 1.65m2, 1.70m2 , 1.75m2 , 1.80m2 , 1.85m2 , 1.90m 2 , 1.95 m 2 , 2.0 m 2 , 2.1 m 2 , 2.2 m 2 , 2.3 m 2 , 2.4 m 2 , 2.5 m 2 , 2.6 m 2 , 2.7 m 2 , 2.8 m 2 , 2.9 m 2 , 3.0 m 2 or greater), between 30 mg and 1200 mg (e.g., between 30 mg and 1100 mg, e.g., 60 mg and 1000 mg) every three weeks (Q3W) between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg, such as between 450 mg and 750 mg, between 500 mg and 700 mg, such as between 550 mg and 650 mg, such as 600 mg ± 10 mg, such as 600 ± 6 mg, such as 600 ± 5 mg, such as 600 ± 3 mg, such as 600 ± 1 mg, such as 600 ± 0.5 mg, eg 600 mg) dose. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is 3 weeks for a subject with a body surface area greater than 1.25 m2 . dose of 600 mg per dose.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、0.75m2を超え1.25m2以下(例えば、0.76m2、0.77m2、0.78m2、0.79m2、0.80m2、0.82m2、0.84m2、0.86m2、0.88m2、0.90m2、0.95m2、1.0m2、1.05m2、1.10m2、1.15m2、1.20m2、又は1.25m2)の体表面積を有する対象について、3週間ごと(Q3W)に約10mgと約1000mgの間(例えば、約20mgと約1000mgの間、例えば、約50mgと約900mgの間、例えば、約100mgと約850mgの間、例えば、約200mgと約700mgの間、例えば、約250mgと約600mgの間、例えば、約300mgと約500mgの間、例えば、約400mgと約500mgの間、例えば、約440mgと約460mgの間、例えば、約450mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体表面積が0.75m2を超え1.25m2以下の対象に対して3週間ごとに約450mg(例えば、450mg±10mg、例えば、450±6mg、例えば、450±5mg、例えば、450±3mg、例えば、450±1mg、例えば、450±0.5mg、例えば、3週間ごとに450mg)の用量である。 In some examples, the effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is greater than 0.75 m2 and no more than 1.25 m2 (e.g., 0.76m2 , 0.77m2 , 0.78m2 , 0.79m2 , 0.80m2, 0.82m2 , 0.84m2 , 0.86m2 , 0.88m2 , 0.90m2 , 0.95 m 2 , 1.0 m 2 , 1.05 m 2 , 1.10 m 2 , 1.15 m 2 , 1.20 m 2 , or 1.25 m 2 ) every 3 weeks (Q3W) between about 10 mg and about 1000 mg, such as between about 20 mg and about 1000 mg, such as between about 50 mg and about 900 mg, such as between about 100 mg and about 850 mg, such as between about 200 mg and about 700 mg, such as , between about 250 mg and about 600 mg, such as between about 300 mg and about 500 mg, such as between about 400 mg and about 500 mg, such as between about 440 mg and about 460 mg, such as about 450 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) has a body surface area greater than 0.75 m2 and less than or equal to 1.25 m2 . about 450 mg every 3 weeks for subjects with For example, a dose of 450 mg every 3 weeks).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、0.5m2を超え0.75m2以下(例えば、0.51m2、0.52m2、0.53m2、0.54m2、0.55m2、0.56m2、0.57m2、0.58m2、0.59m2、0.60m2、0.61m2、0.62m2、0.63m2、0.64m2、0.65m2、0.66m2、0.67m2、0.68m2、0.69m2、0.70m2、0.71m2、0.72m2、0.73m2、0.74m2、又は0.75m2)の体表面積を有する対象について、3週間ごと(Q3W)に約10mgと約1000mgの間(例えば約20mgと約1000mgの間、例えば約50mgと約900mgの間、例えば約100mgと約850mgの間、例えば約200mgと約700mgの間、例えば約250mgと約600mgの間、例えば約300mgと約500mgの間、例えば約300mgと約400mgの間、例えば約340mgと約360mgの間、例えば約350mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、体表面積が0.5 m2を超え0.75 m2以下の対象に対して3週間ごとに約350mg(例えば、350mg±10mg、例えば、350±6mg、例えば、350±5mg、例えば、350±3mg、例えば、350±1mg、例えば、350±0.5mg、例えば、3週間ごとに350mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is greater than 0.5 m2 and no more than 0.75 m2 (e.g., 0.51 m 2 , 0.52 m 2 , 0.53 m 2 , 0.54 m 2 , 0.55 m 2 , 0.56 m 2 , 0.57 m 2 , 0.58 m 2 , 0.59 m 2 , 0.60 m 2 , 0.61 m 2 , 0.62 m 2 , 0.63 m 2 , 0.64 m 2 , 0.65 m 2 , 0.66 m 2 , 0.67 m 2 , 0.68 m 2 , 0.69 m 2 , 0.70 m 2 , between about 10 mg and about 1000 mg every three weeks ( Q3W ) ( e.g. , between about 20 mg and about 1000 mg, such as between about 50 mg and about 900 mg, such as between about 100 mg and about 850 mg, such as between about 200 mg and about 700 mg, such as between about 250 mg and about 600 mg, such as between about 300 mg and about 500 mg between about 300 mg and about 400 mg, such as between about 340 mg and about 360 mg, such as about 350 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) has a body surface area of greater than 0.5 m2 to 0.75 m2. 350 mg every 3 weeks (eg, 350 mg±10 mg, such as 350±6 mg, such as 350±5 mg, such as 350±3 mg, such as 350±1 mg, such as 350±0. 5 mg, eg 350 mg every 3 weeks).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、0.5m2以下(例えば0.02m2、0.04m2、0.06m2、0.08m2、0.1m2、0.15m2、0.20m2、0.25m2、0.30m2、0.35m2、0.40m2、0.45m2、又は0.50m2)の体表面積を有する対象について、3週間ごと(Q3W)に約10mgと約1000mgの間(例えば約10mgと約900mgの間、例えば約50mgと約900mgの間、例えば約100mgと約750mgの間、例えば約100mgと約600mgの間、例えば約150mgと約500mgの間、例えば約200mgと約400mgの間、例えば約250mgと約350mgの間、例えば約290mgと約310mgの間、例えば約300mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、0.5m2の対表面積を有する対象に対して3週間ごとに約300mg(例えば、300mg±10mg、例えば、300±6mg、例えば、300±5mg、例えば、300±3mg、例えば、300±1mg、例えば、300±0.5mg、例えば、3週間ごとに300mg)の用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is 0.5 m 2 or less (eg, 0.02 m 2 , 0.5 m 2 or less). 04 m 2 , 0.06 m 2 , 0.08 m 2 , 0.1 m 2 , 0.15 m 2 , 0.20 m 2 , 0.25 m 2 , 0.30 m 2 , 0.35 m 2 , 0.40 m 2 , 0.4 m 2 between about 10 mg and about 1000 mg (e.g., between about 10 mg and about 900 mg, e.g., between about 50 mg and about 900 mg) every three weeks (Q3W) for a subject with a body surface area of 45 m 2 , or 0.50 m 2 ; for example between about 100 mg and about 750 mg, such as between about 100 mg and about 600 mg, such as between about 150 mg and about 500 mg, such as between about 200 mg and about 400 mg, such as between about 250 mg and about 350 mg, such as between about 290 mg and about between 310 mg, eg about 300 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is 3 to a subject having a surface area of 0.5 m 2 . about 300 mg per week (e.g., 300 mg ± 10 mg, such as 300 ± 6 mg, such as 300 ± 5 mg, such as 300 ± 3 mg, such as 300 ± 1 mg, such as 300 ± 0.5 mg, such as every 3 weeks 300 mg).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごと(Q2W)に約10mgと約1000mgの間(例えば約20mgと約1000mgの間、例えば約50mgと約900mgの間、例えば約100mgと約850mgの間、例えば約200mgと約800mgの間、例えば約300mgと約600mgの間、例えば約400mgと約500mgの間、例えば約405mgと約450mgの間、例えば約410mgと約430mgの間、例えば約420mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごとに約420mg(例えば、420mg±10mg、例えば、420±6mg、例えば、420±5mg、例えば、420±3mg、例えば、420±1mg、例えば、420±0.5mg、例えば、2週間ごとに420mg)の用量である。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を、2週間ごとに約300mg~約600mgの用量で対象又は対象集団に投与することを含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を、2週間ごとに300mg~600mgの用量で対象又は対象集団に投与することを含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を、2週間ごとに約420の用量で対象又は対象集団に投与することを含む。いくつかの例では、方法は、抗TIGITアンタゴニスト抗体を、2週間ごとに420の用量で対象又は対象集団に投与することを含む。いくつかの例では、抗TIGITアンタゴニスト抗体の用量は固定用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 10 mg and about 1000 mg every two weeks (Q2W) (e.g., between about 20 mg and about 1000 mg, such as between about 50 mg and about 900 mg, such as between about 100 mg and about 850 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 600 mg, such as between about 400 mg and about 500 mg between about 405 mg and about 450 mg, such as between about 410 mg and about 430 mg, such as about 420 mg) (eg, a fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is about 420 mg (e.g., 420 mg ± 10 mg, e.g., 420 mg ± 10 mg) every two weeks. ±6 mg, such as 420±5 mg, such as 420±3 mg, such as 420±1 mg, such as 420±0.5 mg, such as 420 mg every two weeks). In some examples, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at a dose of about 300 mg to about 600 mg every two weeks. In some examples, the method comprises administering the anti-TIGIT antagonist antibody to the subject or subject population at a dose of 300 mg to 600 mg every two weeks. In some examples, the method comprises administering the anti-TIGIT antagonist antibody to the subject or population of subjects at about 420 doses every two weeks. In some examples, the method comprises administering the anti-TIGIT antagonist antibody to the subject or subject population at 420 doses every two weeks. In some examples, the dose of anti-TIGIT antagonist antibody is a fixed dose.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごと(Q3W)に約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごと(Q3W)に約200mgと約2000mgの間(例えば約200mgと約2000mgの間、例えば約400mgと約1900mgの間、例えば約500mgと約1800mgの間、例えば約600mgと約1700mgの間、例えば約700mgと約1400mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば約1200mg、例えば1200mg±10mg、例えば1200±6mg、例えば1200±5mg、例えば1200±3mg、例えば1200±1mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約1200mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに1200mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg every three weeks (Q3W) (e.g., between about 30 mg and about 1100 mg, such as between about 60 mg and about 1000 mg, such as between about 100 mg and about 900 mg, such as between about 200 mg and about 800 mg, such as between about 300 mg and about 800 mg, such as between about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as , 600±10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 600 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between about 200 mg and about 2000 mg every three weeks (Q3W). (e.g. between about 200 mg and about 2000 mg, such as between about 400 mg and about 1900 mg, such as between about 500 mg and about 1800 mg, such as between about 600 mg and about 1700 mg, such as between about 700 mg and about 1400 mg, such as about 800 mg between about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg; for example between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as about 1200 mg, such as 1200 mg ± 10 mg, such as 1200 ± 6 mg, such as 1200 ± 5 mg, such as 1200 ± 3 mg, such as 1200 ± 1 mg, such as 1200 ± 0.5 mg, eg 1200 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 1200 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 1200 mg every 3 weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごと(Q4W)に約200mgと約2000mgの間(例えば約200と300mgの間、約300と400mgの間、約400と500mgの間、約500と600mgの間、約600と700mgの間、約700と800mgの間、約800と900mgの間、約900と1000mgの間、約1000と1100mgの間、約1100と1200mgの間、約1200と1300mgの間、約1300と1400mgの間、約1400と1500mgの間、約1500と1600mgの間、約1600と1700mgの間、約1700と1800mgの間、約1800と1900mgの間、又は約1900と2000mgの間、例えば約200mgと約1600mgの間、例えば約250mgと約1600mgの間、例えば約300mgと約1600mgの間、例えば約400mgと約1500mgの間、例えば約500mgと約1400mgの間、例えば約600mgと約1200mgの間、例えば約700mgと約1100mgの間、例えば約800mgと約1000mgの間、例えば約800mgと約900mgの間、例えば約200、約250、約300、約350、約400、約450、約500、約550、約600、約650、約700、約750、約800、約850、約900、約950、約1000、約1050、約1100、約1150、約1200、約1250、約1300、約1350、約1400、約1450、約1500、約1550、約1600mg、約1650mg、約1700mg、約1750mg、約1800mg、約1850mg、約1900mg、約1950mg、又は約2000mg、例えば約800、約810、約820、約830、約840、約850、約860、約870、約880、約890、又は約900mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約約700mg~約1000mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約700mg~1000mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約840mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに840mgの用量である。840mgのQ4Wの投薬レジメンは、PKモデリング及びシミュレーションならびに曝露-安全性分析の結果によって裏付けられる。簡潔には、840mgのQ4W投薬レジメン後の平均濃度は、以前の研究で評価された3週間ごとの600mg投薬レジメンの平均濃度と同様である。840mgのQ4W投薬レジメンのCmaxは、3週間ごとの600mgの投薬レジメンのCmaxと比較して、定常状態で28%高いとシミュレートされたが、診療所で観察された最高投与量(3週間ごとに1200mg)の曝露の範囲内である。以前の観察結果(単独療法として、又は3週間ごとに1200mgのアテゾリズマブと組み合わせて投与された3週間ごとの2-1200mgのチラゴルマブ用量)に基づくチラゴルマブの曝露-安全性関係の予備的分析は、チラゴルマブが平坦な曝露-安全性関係を示すことを示唆している。要約すると、予測される曝露が観察された有効な曝露の範囲内であり、チラゴルマブが平坦な曝露-安全性関係を示すことを考慮すると、840mgのQ4W投薬レジメンは、3週間ごとに600mgの投薬レジメンと同等の安全性及び有効性を提供し得る。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between about 200 mg and about 2000 mg every four weeks (Q4W). (e.g. between about 200 and 300 mg, between about 300 and 400 mg, between about 400 and 500 mg, between about 500 and 600 mg, between about 600 and 700 mg, between about 700 and 800 mg, between about 800 and 900 mg between about 900 and 1000 mg, between about 1000 and 1100 mg, between about 1100 and 1200 mg, between about 1200 and 1300 mg, between about 1300 and 1400 mg, between about 1400 and 1500 mg, between about 1500 and 1600 mg; between about 1600 and 1700 mg, between about 1700 and 1800 mg, between about 1800 and 1900 mg, or between about 1900 and 2000 mg, such as between about 200 mg and about 1600 mg, such as between about 250 mg and about 1600 mg, such as about 300 mg and about 1600 mg, such as between about 400 mg and about 1500 mg, such as between about 500 mg and about 1400 mg, such as between about 600 mg and about 1200 mg, such as between about 700 mg and about 1100 mg, such as between about 800 mg and about 1000 mg for example between about 800 mg and about 900 mg, for example about 200, about 250, about 300, about 350, about 400, about 450, about 500, about 550, about 600, about 650, about 700, about 750, about 800, about 850, about 900, about 950, about 1000, about 1050, about 1100, about 1150, about 1200, about 1250, about 1300, about 1350, about 1400, about 1450, about 1500, about 1550, about 1600 mg, about 1650 mg , about 1700 mg, about 1750 mg, about 1800 mg, about 1850 mg, about 1900 mg, about 1950 mg, or about 2000 mg, such as about 800, about 810, about 820, about 830, about 840, about 850, about 860, about 870, about 880 , about 890, or about 900 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 700 mg to about 1000 mg every 4 weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 700 mg to 1000 mg every 4 weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 840 mg every 4 weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 840 mg every 4 weeks. The 840 mg Q4W dosing regimen is supported by the results of PK modeling and simulation and exposure-safety analysis. Briefly, the mean concentrations following the 840 mg Q4W dosing regimen are similar to the mean concentrations for the 600 mg every 3 weeks dosing regimen evaluated in previous studies. The Cmax of the 840 mg Q4W dosing regimen was simulated to be 28% higher at steady state compared to the Cmax of the 600 mg every 3 weeks dosing regimen, although the highest dose observed in the clinic (every 3 weeks 1200 mg per day) exposure. A preliminary analysis of the exposure-safety relationship of indicate a flat exposure-safety relationship. In summary, given that the predicted exposures are within the observed efficacious exposures and that tiragolumab exhibits a flat exposure-safety relationship, the 840 mg Q4W dosing regimen was reduced to 600 mg every 3 weeks. It may provide safety and efficacy comparable to regimens.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約840mg(例えば、840mg±10mg、例えば、840±6mg、例えば、840±5mg、例えば、840±3mg、例えば、840±1mg、例えば、840±0.5mg、例えば、4週間ごとに840mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量はの間、4週間ごと(Q4W)に約200mgと約2000mgの間(例えば約200mgと約2000mgの間、例えば約400mgと約1900mgの間、例えば約500mgと約1800mgの間、例えば約600mgと約1700mgの間、例えば約700mgと約1400mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mg(例えば200mgと2000mgの間、例えば400mgと1900mgの間、例えば500mgと1800mgの間、例えば600mgと1700mgの間、例えば700mgと1400mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間)、例えば約1200mg、例えば1200mg±10mg、例えば1200±6mg、例えば1200±5mg、例えば1200±3mg、例えば1200±1mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約1200mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is about 840 mg (e.g., 840 mg ± 10 mg, e.g., 840 mg ± 10 mg) every 4 weeks. ±6 mg, such as 840±5 mg, such as 840±3 mg, such as 840±1 mg, such as 840±0.5 mg, such as 840 mg every 4 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is between about 200 mg and about 2000 mg every four weeks (Q4W) for between about 200 mg and about 2000 mg, such as between about 400 mg and about 1900 mg, such as between about 500 mg and about 1800 mg, such as between about 600 mg and about 1700 mg, such as between about 700 mg and about 1400 mg, such as about between 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as between 200 mg and 2000 mg, such as between 400 mg and 1900 mg, such as between 500 mg and 1800 mg, such as between 600 mg and 1700 mg, such as between 700 mg and 1400 mg between 800 mg and 1600 mg, such as between 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg between 1190 mg and 1210 mg), such as about 1200 mg, such as 1200 mg ± 10 mg, such as 1200 ± 6 mg, such as 1200 ± 5 mg, such as 1200 ± 3 mg, such as 1200 ± 1 mg, such as 1200 ± 0.5 mg, such as 1200 mg). dose. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 1200 mg every 4 weeks.
いくつかの例では、併用療法(例えば、抗PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)との併用処置)で投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。 In some examples, combination therapy (e.g., combination treatment with an anti-PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) The dose of anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) administered is compared to the standard dose of anti-TIGIT antagonist antibody administered as monotherapy. can decrease.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を静脈内投与する。あるいは、いくつかの実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を皮下投与する。いくつかの例では、チラゴルマブは、2週間ごとに約420mg、3週間ごとに約1200mg、又は4週間ごとに約1200mgの用量で患者に静脈内投与される。いくつかの例では、チラゴルマブ、2週間ごとに420mg、3週間ごとに1200mg、又は4週間ごとに1200mgの用量で患者に静脈内投与される。 In some examples, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered intravenously. Alternatively, in some embodiments, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered subcutaneously. In some examples, tiragolumab is administered intravenously to the patient at a dose of about 420 mg every 2 weeks, about 1200 mg every 3 weeks, or about 1200 mg every 4 weeks. In some examples, tiragolumab is administered intravenously to the patient at doses of 420 mg every 2 weeks, 1200 mg every 3 weeks, or 1200 mg every 4 weeks.
いくつかの例では、対象に、合計1~20の量、例えば1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19又は20用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を投与する。いくつかの例では、対象には、合計で1~50用量、例えば、1~50用量、1~45用量、1~40用量、1~35用量、1~30用量、1~25用量、1~20用量、1~15用量、1~10用量、1~5用量、2~50用量、2~45用量、2~40用量、2~35用量、2~30用量、2~25用量、2~20用量、2~15用量、2~10用量、2~5用量、3~50用量、3~45用量、3~40用量、3~35用量、3~30用量、3~25用量、3~20用量、3~15用量、3~10用量、3~5用量、4~50用量、4~45用量、4~40用量、4~35用量、4~30用量、4~25用量、4~20用量、4~15用量、4~10用量、4~5用量、5~50用量、5~45用量、5~40用量、5~35用量、5~30用量、5~25用量、5~20用量、5~15用量、5~10用量、10~50用量、10~45用量、10~40用量、10~35用量、10~30用量、10~25用量、10~20用量、10~15用量、15~50用量、15~45用量、15~40用量、15~35用量、15~30用量、15~25用量、15~20用量、20~50用量、20~45用量、20~40用量、20~35用量、20~30用量、20~25用量、25~50用量、25~45用量、25~40用量、25~35用量、25~30用量、30~50用量、30~45用量、30~40用量、30~35用量、35~50用量、35~45用量、35~40用量、40~50用量、40~45用量、又は45~50用量の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)が投与される。特定の例では、用量は静脈内投与され得る。 In some examples, the subject has a total amount of 1 to 20, such as 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17 , 18, 19 or 20 doses of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, the subject receives a total of 1-50 doses, such as 1-50 doses, 1-45 doses, 1-40 doses, 1-35 doses, 1-30 doses, 1-25 doses, 1 ~20 doses, 1-15 doses, 1-10 doses, 1-5 doses, 2-50 doses, 2-45 doses, 2-40 doses, 2-35 doses, 2-30 doses, 2-25 doses, 2 ~20 doses, 2-15 doses, 2-10 doses, 2-5 doses, 3-50 doses, 3-45 doses, 3-40 doses, 3-35 doses, 3-30 doses, 3-25 doses, 3 ~20 doses, 3-15 doses, 3-10 doses, 3-5 doses, 4-50 doses, 4-45 doses, 4-40 doses, 4-35 doses, 4-30 doses, 4-25 doses, 4 ~20 doses, 4-15 doses, 4-10 doses, 4-5 doses, 5-50 doses, 5-45 doses, 5-40 doses, 5-35 doses, 5-30 doses, 5-25 doses, 5 ~20 doses, 5-15 doses, 5-10 doses, 10-50 doses, 10-45 doses, 10-40 doses, 10-35 doses, 10-30 doses, 10-25 doses, 10-20 doses, 10 ~15 doses, 15-50 doses, 15-45 doses, 15-40 doses, 15-35 doses, 15-30 doses, 15-25 doses, 15-20 doses, 20-50 doses, 20-45 doses, 20 ~40 doses, 20-35 doses, 20-30 doses, 20-25 doses, 25-50 doses, 25-45 doses, 25-40 doses, 25-35 doses, 25-30 doses, 30-50 doses, 30 ~45 doses, 30-40 doses, 30-35 doses, 35-50 doses, 35-45 doses, 35-40 doses, 40-50 doses, 40-45 doses, or 45-50 doses of an anti-TIGIT antagonist antibody ( For example, an anti-TIGIT antagonist antibody disclosed herein (eg, tiragolumab) is administered. In certain instances, doses may be administered intravenously.
ii.PD-1軸結合アンタゴニストの投薬
一般的な提案として、ヒトに投与される治療有効量のPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、1回以上の投与によるかどうかにかかわらず、患者の体重の約0.01~約50mg/kgの範囲となる。
ii. PD-1 Axis Binding Antagonist Dosing As a general proposition, a therapeutically effective amount of a PD-1 axis binding antagonist (eg, atezolizumab) administered to a human, whether by one or more administrations, is It ranges from about 0.01 to about 50 mg/kg of body weight.
いくつかの例示的実施形態では、PD-1軸結合アンタゴニストは、約0.01~約45mg/kg、約0.01~約40mg/kg、約0.01~約35mg/kg、約0.01~約30mg/kg、約0.01~約25mg/kg、約0.01~約20mg/kg、約0.01~約15mg/kg、約0.01~約10mg/kg、約0.01~約5mg/kg、又は約0.01~約1mg/kgの用量で投与され、例えば、毎日、毎週、2週間ごと、3週間ごと、又は4週間ごとに投与される。いくつかの例示的実施形態では、PD-1軸結合アンタゴニストは、0.01~45mg/kg、0.01~40mg/kg、0.01~35mg/kg、0.01~30mg/kg、0.01~25mg/kg、0.01~20mg/kg、0.01~15mg/kg、0.01~10mg/kg、0.01~5mg/kg、又は0.01~1mg/kgの用量で投与され、例えば、毎日、毎週、2週間ごと、3週間ごと、又は4週間ごとに投与される。 In some exemplary embodiments, the PD-1 axis binding antagonist is about 0.01 to about 45 mg/kg, about 0.01 to about 40 mg/kg, about 0.01 to about 35 mg/kg, about 0.01 to about 45 mg/kg. 0.01 to about 30 mg/kg, about 0.01 to about 25 mg/kg, about 0.01 to about 20 mg/kg, about 0.01 to about 15 mg/kg, about 0.01 to about 10 mg/kg, about 0.01 to about 20 mg/kg. 01 to about 5 mg/kg, or about 0.01 to about 1 mg/kg, eg, every day, every week, every two weeks, every three weeks, or every four weeks. In some exemplary embodiments, the PD-1 axis binding antagonist is 0.01-45 mg/kg, 0.01-40 mg/kg, 0.01-35 mg/kg, 0.01-30 mg/kg, 0 at doses of 0.01-25 mg/kg, 0.01-20 mg/kg, 0.01-15 mg/kg, 0.01-10 mg/kg, 0.01-5 mg/kg, or 0.01-1 mg/kg administered, for example, daily, weekly, every two weeks, every three weeks, or every four weeks.
いくつかの例では、PD-1軸結合アンタゴニストは、投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に投与される。
In some examples, the PD-1 axis binding antagonist is administered at about day 1 (eg, day −3, day −2, day −1,
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、2週間ごとに(Q2W)、約20mgと約1600mgの間(例えば約40mgと約1500mgの間、例えば約200mgと約1400mgの間、例えば約300mgと約1400mgの間、例えば約400mgと約1400mgの間、例えば約500mgと約1300mgの間、例えば約600mgと約1200mgの間、例えば約700mgと約1100mgの間、例えば約800mgと約1000mgの間、例えば約800mgと約900mgの間、例えば約800、約810、約820、約830、約840、約850、約860、約870、約880、約890、又は約900mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、2週間ごと(Q2W)に、20mgと1600mgの間(例えば40mgと1500mgの間、例えば200mgと1400mgの間、例えば300mgと1400mgの間、例えば400mgと1400mgの間、例えば500mgと1300mgの間、例えば600mgと1200mgの間、例えば700mgと1100mgの間、例えば800mgと1000mgの間、例えば800mgと900mgの間、例えば800、810、820、830、840、850、860、870、880、890、又は900mg)の用量(例えば、固定用量)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、2週間ごとに、約840mg(例えば、840mg±10mg、例えば、840±6mg、例えば、840±5mg、例えば、840±3mg、例えば、840±1mg、例えば、840±0.5mg、例えば、2週間ごとに840mg)の用量である。いくつかの例では、アテゾリズマブの有効量は、2週間ごとに約840mgの用量である。
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間
In some examples, the effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is administered every two weeks (Q2W ), between about 20 mg and about 1600 mg, such as between about 40 mg and about 1500 mg, such as between about 200 mg and about 1400 mg, such as between about 300 mg and about 1400 mg, such as between about 400 mg and about 1400 mg, such as about 500 mg between about 1300 mg, such as between about 600 mg and about 1200 mg, such as between about 700 mg and about 1100 mg, such as between about 800 mg and about 1000 mg, such as between about 800 mg and about 900 mg, such as about 800, about 810, about 820 , about 830, about 840, about 850, about 860, about 870, about 880, about 890, or about 900 mg) (eg, a fixed dose). In some examples, the effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is administered every two weeks (Q2W) between 20 mg and 1600 mg, such as between 40 mg and 1500 mg, such as between 200 mg and 1400 mg, such as between 300 mg and 1400 mg, such as between 400 mg and 1400 mg, such as between 500 mg and 1300 mg, such as between 600 mg and 1200 mg; between 700 mg and 1100 mg, such as between 800 mg and 1000 mg, such as between 800 mg and 900 mg, such as 800, 810, 820, 830, 840, 850, 860, 870, 880, 890, or 900 mg) (e.g., fixed dose). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is about A dose of 840 mg (e.g., 840 mg ± 10 mg, such as 840 ± 6 mg, such as 840 ± 5 mg, such as 840 ± 3 mg, such as 840 ± 1 mg, such as 840 ± 0.5 mg, such as 840 mg every 2 weeks) is. In some examples, the effective amount of atezolizumab is a dose of about 840 mg every two weeks.
In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., pembrolizumab) or an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is administered to the subject every two weeks between about 0.01 mg/kg and about 50 mg/kg of body weight
(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約5mg/kgと約15mg/kgの間、例えば約7.5mg/kgと約12.5mg/kgの間、例えば約10±2mg/kg、約10±1mg/kg、約10±0.5mg/kg、約10±0.2mg/kg、又は約10±0.1mg/kg、例えば約10mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、対象の体重の約0.01mg/kgと約10mg/kgの間(例えば約0.1mg/kgと約10mg/kgの間、例えば約0.5mg/kgと約10mg/kgの間、例えば約1mg/kgと約10mg/kgの間、例えば約2.5mg/kgと約10mg/kgの間、例えば約5mg/kgと約10mg/kgの間、例えば約7.5mg/kgと約10mg/kgの間、例えば約8mg/kgと約10mg/kgの間、例えば約9mg/kgと約10mg/kgの間、例えば約9.5mg/kgと約10mg/kgの間、例えば約10±1mg/kg、例えば約10±0.5mg/kg、例えば約10±0.2mg/kg、例えば約10±0.1mg/kg、例えば約10mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと12.5mg/kgの間、例えば10±2mg/kg、10±1mg/kg、10±0.5mg/kg、10±0.2mg/kg、又は10±0.1mg/kg、例えば10mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、対象の体重の0.01mg/kgと10mg/kgの間(例えば0.1mg/kgと10mg/kgの間、例えば0.5mg/kgと10mg/kgの間、例えば1mg/kgと10mg/kgの間、例えば2.5mg/kgと10mg/kgの間、例えば5mg/kgと10mg/kgの間、例えば7.5mg/kgと10mg/kgの間、例えば8mg/kgと10mg/kgの間、例えば9mg/kgと10mg/kgの間、例えば9.5mg/kgと10mg/kgの間、例えば10±1mg/kg、例えば10±0.5mg/kg、例えば10±0.2mg/kg、例えば10±0.1mg/kg、例えば10mg/kg)の用量である。いくつかの例では、ペンブロリズマブの有効量は、2週間ごとに約10mg/kgの用量である。いくつかの例では、ペンブロリズマブの有効量は、2週間ごとに10mg/kgの用量である。 (e.g., between about 0.01 mg/kg and about 45 mg/kg, such as between about 0.1 mg/kg and about 40 mg/kg, such as between about 1 mg/kg and about 35 mg/kg, such as about 2.5 mg/kg). between about 5 mg/kg and about 25 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 12.5 mg/kg. between about 10±2 mg/kg, about 10±1 mg/kg, about 10±0.5 mg/kg, about 10±0.2 mg/kg, or about 10±0.1 mg/kg, such as about 10 mg/kg ). In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., pembrolizumab) or an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is administered to the subject every two weeks between about 0.01 mg/kg and about 10 mg/kg of body weight, such as between about 0.1 mg/kg and about 10 mg/kg, such as between about 0.5 mg/kg and about 10 mg/kg, such as about 1 mg /kg and about 10 mg/kg, such as between about 2.5 mg/kg and about 10 mg/kg, such as between about 5 mg/kg and about 10 mg/kg, such as between about 7.5 mg/kg and about 10 mg/kg between about 8 mg/kg and about 10 mg/kg, such as between about 9 mg/kg and about 10 mg/kg, such as between about 9.5 mg/kg and about 10 mg/kg, such as about 10±1 mg/kg kg, such as about 10±0.5 mg/kg, such as about 10±0.2 mg/kg, such as about 10±0.1 mg/kg, such as about 10 mg/kg). In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., pembrolizumab) or an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is administered to the subject every two weeks between 0.01 mg/kg and 50 mg/kg of body weight (such as between 0.01 mg/kg and 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 12.5 mg/kg between, eg, 10±2 mg/kg, 10±1 mg/kg, 10±0.5 mg/kg, 10±0.2 mg/kg, or 10±0.1 mg/kg, such as 10 mg/kg). In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-1 antagonist antibody (e.g., pembrolizumab) or an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is administered to the subject every two weeks between 0.01 and 10 mg/kg of body weight (e.g. between 0.1 and 10 mg/kg, such as between 0.5 and 10 mg/kg, such as between 1 and 10 mg/kg) between 2.5 mg/kg and 10 mg/kg, such as between 5 mg/kg and 10 mg/kg, such as between 7.5 mg/kg and 10 mg/kg, such as between 8 mg/kg and 10 mg/kg, between 9 mg/kg and 10 mg/kg, such as between 9.5 mg/kg and 10 mg/kg, such as 10±1 mg/kg, such as 10±0.5 mg/kg, such as 10±0.2 mg/kg, such as 10±0.1 mg/kg, eg 10 mg/kg). In some examples, the effective amount of pembrolizumab is a dose of about 10 mg/kg every two weeks. In some examples, the effective amount of pembrolizumab is a dose of 10 mg/kg every two weeks.
いくつかの例では、がんを有する対象を処置するためのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば、約0.1mg/kgと約40mg/kgの間、例えば、約1mg/kgと約35mg/kgの間、例えば、約2.5mg/kgと約30mg/kgの間、例えば、約5mg/kgと約25mg/kgの間、例えば、約10mg/kgと約20mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば約0.1mg/kgと約15mg/kgの間、例えば約0.5mg/kgと約15mg/kgの間、例えば約1mg/kgと約15mg/kgの間、例えば約2.5mg/kgと約15mg/kgの間、例えば約5mg/kgと約15mg/kgの間、例えば約7.5mg/kgと約15mg/kgの間、例えば約10mg/kgと約15mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約14mg/kgと約15mg/kgの間、例えば約15±1mg/kg、例えば約15±0.5mg/kg、例えば約15±0.2mg/kg、例えば約15±0.1mg/kg、例えば約15mg/kg)の用量である。いくつかの例では、がんを有する対象を処置するためのPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば、0.1mg/kgと40mg/kgの間、例えば、1mg/kgと35mg/kgの間、例えば、2.5mg/kgと30mg/kgの間、例えば、5mg/kgと25mg/kgの間、例えば、10mg/kgと20mg/kgの間、例えば、12.5mg/kgと15mg/kgの間、例えば、15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば、15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに対象の体重の0.01mg/kgと15mg/kgの間(例えば0.1mg/kgと15mg/kgの間、例えば0.5mg/kgと15mg/kgの間、例えば1mg/kgと15mg/kgの間、例えば2.5mg/kgと15mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば10mg/kgと15mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば14mg/kgと15mg/kgの間、例えば15±1mg/kg、例えば15±0.5mg/kg、例えば15±0.2mg/kg、例えば15±0.1mg/kg、例えば15mg/kg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに投与される約15mg/kgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに投与される約15mg/kgの用量であり、最大用量は3週間ごとに1200mgである。いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して減少し得る。いくつかの実施形態では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、3週間ごとに1200mgの最大用量で投与される。 In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) to treat a subject with cancer is weight loss of the subject every three weeks. between about 0.01 mg/kg and about 50 mg/kg (e.g., between about 0.01 mg/kg and about 45 mg/kg, such as between about 0.1 mg/kg and about 40 mg/kg, such as about Between 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg /kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0 .2 mg/kg, or about 15±0.1 mg/kg, eg about 15 mg/kg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is about 0.01 mg/kg and about 15 mg/kg of body weight of the subject every three weeks. between about 0.1 mg/kg and about 15 mg/kg, such as between about 0.5 mg/kg and about 15 mg/kg, such as between about 1 mg/kg and about 15 mg/kg, such as about 2. between 5 mg/kg and about 15 mg/kg, such as between about 5 mg/kg and about 15 mg/kg, such as between about 7.5 mg/kg and about 15 mg/kg, such as between about 10 mg/kg and about 15 mg/kg between about 12.5 mg/kg and about 15 mg/kg, such as between about 14 mg/kg and about 15 mg/kg, such as about 15±1 mg/kg, such as about 15±0.5 mg/kg, such as about 15±0.2 mg/kg, such as about 15±0.1 mg/kg, such as about 15 mg/kg). In some examples, an effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) to treat a subject with cancer is weight loss of the subject every three weeks. between 0.01 mg/kg and 50 mg/kg of between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg /kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0.1 mg/kg, such as 15 mg/kg) is the dose of In some examples, the effective amount of the PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is 0.01 mg/kg and 15 mg/kg of the subject's body weight every three weeks. between (e.g. between 0.1 mg/kg and 15 mg/kg, such as between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 10 mg/kg and 15 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, between 14 mg/kg and 15 mg/kg, such as 15±1 mg/kg, such as 15±0.5 mg/kg, such as 15±0.2 mg/kg, such as 15±0.1 mg/kg, such as 15 mg/kg) is the dose of In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 15 mg/kg administered every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 15 mg/kg administered every 3 weeks, with a maximum dose of is 1200 mg every 3 weeks. In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibodies (eg, atezolizumab)) may be reduced compared to standard doses of PD-1 axis binding antagonists administered as monotherapy. In some embodiments, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a maximum dose of 1200 mg every 3 weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))又は抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ)の有効量は、3週間ごと(Q3W)に、約80mgと約2000mgの間(例えば約100mgと約1600mgの間、例えば約200mgと約1600mgの間、例えば約300mgと約1600mgの間、例えば約400mgと約1600mgの間、例えば約500mgと約1600mgの間、例えば約600mgと約1600mgの間、例えば約700mgと約1600mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごとに、約1200mg(例えば、1200mg±10mg、例えば、1200±6mg、例えば、1200±5mg、例えば、1200±3mg、例えば、1200±1mg、例えば、1200±0.5mg、例えば、3週間ごとに1200mg)の用量である。いくつかの例では、アテゾリズマブの有効量は、3週間ごとに1200mgの用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) or anti-PD-1 antagonist antibody (e.g., penprolizumab) every three weeks (Q3W) is between about 80 mg and about 2000 mg, such as between about 100 mg and about 1600 mg, such as between about 200 mg and about 1600 mg, such as between about 300 mg and about 1600 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg between about 600 mg and about 1600 mg, such as between about 700 mg and about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as about between about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg, such as between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as between about 1200 mg±5 mg, such as 1200 ±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is about A dose of 1200 mg (e.g. 1200 mg ± 10 mg, such as 1200 ± 6 mg, such as 1200 ± 5 mg, such as 1200 ± 3 mg, such as 1200 ± 1 mg, such as 1200 ± 0.5 mg, such as 1200 mg every 3 weeks) is. In some examples, the effective amount of atezolizumab is a dose of 1200 mg every 3 weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごとに(Q3W)、約10mgと約800mgの間(例えば約10mgと約800mgの間、例えば約20mgと約700mgの間、例えば約50mgと約600mgの間、例えば約75mgと約500mgの間、例えば約100mgと約400mgの間、例えば約100mgと約300mgの間、例えば約125mgと約275mgの間、例えば約150mgと約250mgの間、例えば約175mgと約225mgの間、例えば約190mgと約210mgの間、例えば約200mg±10mg、例えば200mg±7.5mg、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごとに、約200mg(例えば、200mg±10mg、例えば、200±6mg、例えば、200±5mg、例えば、200±3mg、例えば、200±1mg、例えば、200±0.5mg、例えば、3週間ごとに200mg)の用量である。いくつかの例では、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)の有効量は、3週間ごとに、約200mg(例えば、200mg±10mg、例えば、200±6mg、例えば、200±5mg、例えば、200±3mg、例えば、200±1mg、例えば、200±0.5mg、例えば、3週間ごとに200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごと(Q3W)に、10mgと800mgの間(例えば10mgと800mgの間、例えば20mgと700mgの間、例えば50mgと600mgの間、例えば75mgと500mgの間、例えば100mgと400mgの間、例えば100mgと300mgの間、例えば125mgと275mgの間、例えば150mgと250mgの間、例えば175mgと225mgの間、例えば190mgと210mgの間、例えば200mg±10mg、例えば200mg±7.5mg、例えば200mg±5mg、例えば200±2.5mg、例えば200±1.0mg、例えば200±0.5mg、例えば200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、3週間ごとに、200mg(例えば、200mg±10mg、例えば、200±6mg、例えば、200±5mg、例えば、200±3mg、例えば、200±1mg、例えば、200±0.5mg、例えば、3週間ごとに200mg)の用量である。いくつかの例では、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)の有効量は、3週間ごとに、200mg(例えば、200mg±10mg、例えば、200±6mg、例えば、200±5mg、例えば、200±3mg、例えば、200±1mg、例えば、200±0.5mg、例えば、3週間ごとに200mg)の用量である。いくつかの例では、ペンブロリズマブの有効量は、3週間ごとに200mgの用量である。いくつかの例では、ペンブロリズマブの有効量は、3週間ごとに200mgの用量である。 In some examples, the effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is every 3 weeks (Q3W ), between about 10 mg and about 800 mg, such as between about 10 mg and about 800 mg, such as between about 20 mg and about 700 mg, such as between about 50 mg and about 600 mg, such as between about 75 mg and about 500 mg, such as between about 100 mg between about 400 mg, such as between about 100 mg and about 300 mg, such as between about 125 mg and about 275 mg, such as between about 150 mg and about 250 mg, such as between about 175 mg and about 225 mg, such as between about 190 mg and about 210 mg; for example about 200 mg±10 mg, such as 200 mg±7.5 mg, such as 200 mg±5 mg, such as 200±2.5 mg, such as 200±1.0 mg, such as 200±0.5 mg, such as 200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is about A dose of 200 mg (eg, 200±10 mg, such as 200±6 mg, such as 200±5 mg, such as 200±3 mg, such as 200±1 mg, such as 200±0.5 mg, such as 200 mg every 3 weeks) is. In some examples, the effective amount of the anti-PD-1 antagonist antibody (eg, pembrolizumab) is about 200 mg (eg, 200 mg±10 mg, such as 200±6 mg, such as 200±5 mg, such as 200±3 mg, eg 200±1 mg, eg 200±0.5 mg, eg 200 mg every 3 weeks). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is every 3 weeks (Q3W) between 10 mg and 800 mg, such as between 10 mg and 800 mg, such as between 20 mg and 700 mg, such as between 50 mg and 600 mg, such as between 75 mg and 500 mg, such as between 100 mg and 400 mg, such as between 100 mg and 300 mg; between 125 mg and 275 mg, such as between 150 mg and 250 mg, such as between 175 mg and 225 mg, such as between 190 mg and 210 mg, such as 200 mg±10 mg, such as 200 mg±7.5 mg, such as 200 mg±5 mg, such as 200±2. 5 mg, such as 200±1.0 mg, such as 200±0.5 mg, such as 200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is 200 mg every 3 weeks at a dose of (e.g., 200±10 mg, such as 200±6 mg, such as 200±5 mg, such as 200±3 mg, such as 200±1 mg, such as 200±0.5 mg, such as 200 mg every 3 weeks) be. In some examples, the effective amount of anti-PD-1 antagonist antibody (eg, pembrolizumab) is 200 mg (eg, 200 mg±10 mg, such as 200±6 mg, such as 200±5 mg, such as 200 mg every 3 weeks). ±3 mg, eg 200±1 mg, eg 200±0.5 mg, eg 200 mg every 3 weeks). In some examples, the effective amount of pembrolizumab is a dose of 200 mg every 3 weeks. In some examples, the effective amount of pembrolizumab is a dose of 200 mg every 3 weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、4週間ごと(Q4W)に、約80mgと約3000mgの間(例えば約80mgと200mgの間、約200mgと400mgの間、約400mgと600mgの間、約600mgと800mgの間、約800mgと1000mgの間、約1000mgと1200mgの間、約1200mgと1400mgの間、約1400mgと1600mgの間、約1600mgと1800mgの間、約1800mgと2000mgの間、約2200mgと2400mgの間、約2400mgと2600mgの間、約2600mgと2800mgの間、又は約2800mgと3000mgの間、例えば約100mgと約3000mgの間、例えば約200mgと約2900mgの間、例えば約500mgと約2800mgの間、例えば約600mgと約2700mgの間、例えば約650mgと約2600mgの間、例えば約700mgと約2500mgの間、例えば約1000mgと約2400mgの間、例えば約1100mgと約2300mgの間、例えば約1200mgと約2200mgの間、例えば約1300mgと約2100mgの間、例えば約1400mgと約2000mgの間、例えば約1500mgと約1900mgの間、例えば約1600mgと約1800mgの間、例えば約1620mgと約1700mgの間、例えば約1640mgと約1690mgの間、例えば約1660mgと約1680mgの間、約1680mg、例えば約80mg、約200mg、約400mg、約600mg、約800mg、約1000mg、約1200mg、約1400mg、約1600mg、約1800mg、約2000mg、約2200mg、約2400mg、約2600mg、約2800mg、又は約3000mg、例えば約1600mg、約1610mg、約1620mg、約1630mg、約1640mg、約1650mg、約1660mg、約1670mg、約1680mg、約1690mg、又は約1700mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、4週間ごと(Q4W)に、500mgと3000mgの間(例えば500mgと2800mgの間、例えば600mgと2700mgの間、例えば650mgと2600mgの間、例えば700mgと2500mgの間、例えば1000mgと2400mgの間、例えば1100mgと2300mgの間、例えば1200mgと2200mgの間、例えば1300mgと2100mgの間、例えば1400mgと2000mgの間、例えば1500mgと1900mgの間、例えば1600mgと1800mgの間、例えば1620mgと1700mgの間、例えば1640mgと1690mgの間、例えば1660mgと1680mgの間、1680mg、例えば1600mg、1610mg、1620mg、1630mg、1640mg、1650mg、1660mg、1670mg、1680mg、1690mg、又は1700mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の有効量は、4週間ごとに、1680mg(例えば、1680mg±10mg、例えば、1680±6mg、例えば、1680±5mg、例えば、1680±3mg、例えば、1680±1mg、例えば、1680±0.5mg、例えば、4週間ごとに1680mg)の用量である。いくつかの例では、アテゾリズマブの有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、アテゾリズマブの有効量は、4週間ごとに1680mgの用量である。 In some examples, the effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is every 4 weeks (Q4W) between about 80 mg and about 3000 mg (e.g. between about 80 mg and 200 mg, between about 200 mg and 400 mg, between about 400 mg and 600 mg, between about 600 mg and 800 mg, between about 800 mg and 1000 mg, between about 1000 mg and 1200 mg) between about 1200 mg and 1400 mg between about 1400 mg and 1600 mg between about 1600 mg and 1800 mg between about 1800 mg and 2000 mg between about 2200 mg and 2400 mg between about 2400 mg and 2600 mg between about 2600 mg and 2800 mg between about 2800 mg and 3000 mg, such as between about 100 mg and about 3000 mg, such as between about 200 mg and about 2900 mg, such as between about 500 mg and about 2800 mg, such as between about 600 mg and about 2700 mg, such as between about 650 mg between about 2600 mg, such as between about 700 mg and about 2500 mg, such as between about 1000 mg and about 2400 mg, such as between about 1100 mg and about 2300 mg, such as between about 1200 mg and about 2200 mg, such as between about 1300 mg and about 2100 mg; for example between about 1400 mg and about 2000 mg, for example between about 1500 mg and about 1900 mg, for example between about 1600 mg and about 1800 mg, for example between about 1620 mg and about 1700 mg, for example between about 1640 mg and about 1690 mg, for example between about 1660 mg and about between 1680 mg, about 1680 mg, such as about 80 mg, about 200 mg, about 400 mg, about 600 mg, about 800 mg, about 1000 mg, about 1200 mg, about 1400 mg, about 1600 mg, about 1800 mg, about 2000 mg, about 2200 mg, about 2400 mg, about 2600 mg; about 2800 mg, or about 3000 mg, such as about 1600 mg, about 1610 mg, about 1620 mg, about 1630 mg, about 1640 mg, about 1650 mg, about 1660 mg, about 1670 mg, about 1680 mg, about 1690 mg, or about 1700 mg). In some examples, the effective amount of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is every 4 weeks (Q4W) between 500 mg and 3000 mg, such as between 500 mg and 2800 mg, such as between 600 mg and 2700 mg, such as between 650 mg and 2600 mg, such as between 700 mg and 2500 mg, such as between 1000 mg and 2400 mg, such as between 1100 mg and 2300 mg; between 1200 mg and 2200 mg, such as between 1300 mg and 2100 mg, such as between 1400 mg and 2000 mg, such as between 1500 mg and 1900 mg, such as between 1600 mg and 1800 mg, such as between 1620 mg and 1700 mg, such as between 1640 mg and 1690 mg, such as between 1660 mg and 1680 mg, 1680 mg, such as 1600 mg, 1610 mg, 1620 mg, 1630 mg, 1640 mg, 1650 mg, 1660 mg, 1670 mg, 1680 mg, 1690 mg, or 1700 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is 1680 mg every 4 weeks at a dose of (e.g. 1680 mg ± 10 mg, such as 1680 ± 6 mg, such as 1680 ± 5 mg, such as 1680 ± 3 mg, such as 1680 ± 1 mg, such as 1680 ± 0.5 mg, such as 1680 mg every 4 weeks) be. In some examples, the effective amount of atezolizumab is a dose of about 1680 mg every 4 weeks. In some examples, the effective amount of atezolizumab is a dose of 1680 mg every 4 weeks.
いくつかの例では、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)の有効量は、6週間ごと(Q6W)に、約50mgと約2000mgの間(例えば約50mgと100mgの間、約100mgと250mgの間、約250mgと500mgの間、約500mgと750mgの間、約750mgと1000mgの間、約1000mgと1250mgの間、約1250mgと1500mgの間、約1500mgと1750mgの間、又は約1750mgと2000mgの間、例えば約100mgと約1000mgの間、約120mgと約900mgの間、約150mgと約800mgの間、約200mgと約700mgの間、約250mgと約600mgの間、約300mgと約500mgの間、又は約350mgと約450mgの間、例えば約50mgと約100mgの間、約100mgと約200mgの間、約200mgと約300mgの間、約300mgと約400mgの間、約400mgと約500mgの間、約500mgと約600mgの間、約600mgと約700mgの間、約700mgと約800mgの間、又は約800mgと約1000mgの間、例えば約50mg、約100mg、約250mg、約500mg、約750mg、約1000mg、約1250mg、約1500mg、約1750mg、又は約2000mg、例えば約300mg、約310mg、約320mg、約330mg、約340mg、約350mg、約360mg、約370mg、約380mg、約390mg、約400mg、約410mg、約420mg、約430mg、約440mg、約450mg、約460mg、約470mg、約480mg、約490mg、又は約500mg、例えば400mg)の用量である。いくつかの例では、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)の有効量は、6週間(Q6W)ごとに、50mgと2000mgの間(例えば100mgと1000mgの間、120mgと900mgの間、150mgと800mgの間、200mgと700mgの間、250mgと600mgの間、300mgと500mgの間、又は350mgと450mgの間、例えば50mgと100mgの間、100mgと200mgの間、200mgと300mgの間、300mgと400mgの間、400mgと500mgの間、500mgと600mgの間、600mgと700mgの間、700mgと800mgの間、又は800mgと1000mgの間、例えば300mg、310mg、320mg、330mg、340mg、350mg、360mg、370mg、380mg、390mg、400mg、410mg、420mg、430mg、440mg、450mg、460mg、470mg、480mg、490mg、又は500mg、例えば400mg)の用量である。いくつかの例では、抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)の有効量は、6週間ごとに、約400mg(例えば、400mg±10mg、例えば、400±6mg、例えば、400±5mg、例えば、400±3mg、例えば、400±1mg、例えば、400±0.5mg、例えば、6週間ごとに400mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニストの用量は固定用量である。いくつかの例では、ペンブロリズマブの有効量は、6週間ごとに約400mgの用量(例えば、固定用量)である。いくつかの例では、ペンブロリズマブの有効量は、6週間ごとの400mgの用量(例えば、固定用量)である。 In some examples, the effective amount of the anti-PD-1 antagonist antibody (eg, pembrolizumab) is between about 50 mg and about 2000 mg (eg, between about 50 mg and 100 mg, about 100 mg and 250 mg) every 6 weeks (Q6W). between about 250 mg and 500 mg, between about 500 mg and 750 mg, between about 750 mg and 1000 mg, between about 1000 mg and 1250 mg, between about 1250 mg and 1500 mg, between about 1500 mg and 1750 mg, or between about 1750 mg and 2000 mg between about 100 mg and about 1000 mg, between about 120 mg and about 900 mg, between about 150 mg and about 800 mg, between about 200 mg and about 700 mg, between about 250 mg and about 600 mg, between about 300 mg and about 500 mg between about 350 mg and about 450 mg, such as between about 50 mg and about 100 mg, between about 100 mg and about 200 mg, between about 200 mg and about 300 mg, between about 300 mg and about 400 mg, between about 400 mg and about 500 mg between about 500 mg and about 600 mg, between about 600 mg and about 700 mg, between about 700 mg and about 800 mg, or between about 800 mg and about 1000 mg, such as about 50 mg, about 100 mg, about 250 mg, about 500 mg, about 750 mg , about 1000 mg, about 1250 mg, about 1500 mg, about 1750 mg, or about 2000 mg, such as about 300 mg, about 310 mg, about 320 mg, about 330 mg, about 340 mg, about 350 mg, about 360 mg, about 370 mg, about 380 mg, about 390 mg, about 400 mg , about 410 mg, about 420 mg, about 430 mg, about 440 mg, about 450 mg, about 460 mg, about 470 mg, about 480 mg, about 490 mg, or about 500 mg, such as 400 mg). In some examples, the effective amount of the anti-PD-1 antagonist antibody (eg, pembrolizumab) is between 50 mg and 2000 mg (eg, between 100 mg and 1000 mg, between 120 mg and 900 mg, 150 mg) every 6 weeks (Q6W) and 800 mg, between 200 mg and 700 mg, between 250 mg and 600 mg, between 300 mg and 500 mg, or between 350 mg and 450 mg, such as between 50 mg and 100 mg, between 100 mg and 200 mg, between 200 mg and 300 mg, 300 mg and 400 mg, between 400 mg and 500 mg, between 500 mg and 600 mg, between 600 mg and 700 mg, between 700 mg and 800 mg, or between 800 mg and 1000 mg, such as 300 mg, 310 mg, 320 mg, 330 mg, 340 mg, 350 mg, 360 mg , 370 mg, 380 mg, 390 mg, 400 mg, 410 mg, 420 mg, 430 mg, 440 mg, 450 mg, 460 mg, 470 mg, 480 mg, 490 mg, or 500 mg, such as 400 mg). In some examples, the effective amount of anti-PD-1 antagonist antibody (eg, pembrolizumab) is about 400 mg (eg, 400 mg±10 mg, such as 400±6 mg, such as 400±5 mg, such as 400±3 mg, such as 400±1 mg, such as 400±0.5 mg, such as 400 mg every 6 weeks). In some examples, the dose of PD-1 axis binding antagonist is a fixed dose. In some examples, the effective amount of pembrolizumab is a dose (eg, fixed dose) of about 400 mg every 6 weeks. In some examples, the effective amount of pembrolizumab is a dose of 400 mg (eg, fixed dose) every 6 weeks.
いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して減少し得る。 In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (e.g., atezolizumab) or anti-PD-1 antagonist antibody (e.g., penprolizumab)) is reduced compared to standard doses of PD-1 axis binding antagonists administered as monotherapy. can.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンプロリズマブ))を静脈内投与する。あるいはまた、いくつかの実施形態では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))は、皮下投与される。いくつかの例では、アテゾリズマブは、2週間ごとに約840mg、3週間ごとに約1200mg、又は4週間ごとに約1680mgの用量で患者に静脈内投与される。いくつかの例では、アテゾリズマブは、2週間ごとに840mg、3週間ごとに1200mg、又は4週間ごとに1680mgの用量で患者に静脈内投与される。 In some examples, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, penprolizumab)) is administered intravenously. Alternatively, in some embodiments, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered subcutaneously. In some examples, atezolizumab is administered intravenously to the patient at a dose of about 840 mg every 2 weeks, about 1200 mg every 3 weeks, or about 1680 mg every 4 weeks. In some examples, atezolizumab is administered intravenously to the patient at a dose of 840 mg every 2 weeks, 1200 mg every 3 weeks, or 1680 mg every 4 weeks.
いくつかの例では、対象には、合計で1回~20回の用量のPD-1軸結合アンタゴニスト、例えば、1回、2回、3回、4回、5回、6回、7回、8回、9回、10回、11回、12回、13回、14回、15回、16回、17回、18回、19回又は20回の用量が投与される。いくつかの例では、対象には、合計で1~50用量、例えば、1~50用量、1~45用量、1~40用量、1~35用量、1~30用量、1~25用量、1~20用量、1~15用量、1~10用量、1~5用量、2~50用量、2~45用量、2~40用量、2~35用量、2~30用量、2~25用量、2~20用量、2~15用量、2~10用量、2~5用量、3~50用量、3~45用量、3~40用量、3~35用量、3~30用量、3~25用量、3~20用量、3~15用量、3~10用量、3~5用量、4~50用量、4~45用量、4~40用量、4~35用量、4~30用量、4~25用量、4~20用量、4~15用量、4~10用量、4~5用量、5~50用量、5~45用量、5~40用量、5~35用量、5~30用量、5~25用量、5~20用量、5~15用量、5~10用量、10~50用量、10~45用量、10~40用量、10~35用量、10~30用量、10~25用量、10~20用量、10~15用量、15~50用量、15~45用量、15~40用量、15~35用量、15~30用量、15~25用量、15~20用量、20~50用量、20~45用量、20~40用量、20~35用量、20~30用量、20~25用量、25~50用量、25~45用量、25~40用量、25~35用量、25~30用量、30~50用量、30~45用量、30~40用量、30~35用量、35~50用量、35~45用量、35~40用量、40~50用量、40~45用量、又は45~50用量のPD-1軸結合アンタゴニストが投与される。特定の例では、用量は静脈内投与され得る。 In some examples, the subject receives a total of 1 to 20 doses of the PD-1 axis binding antagonist, e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19 or 20 doses are administered. In some examples, the subject receives a total of 1-50 doses, such as 1-50 doses, 1-45 doses, 1-40 doses, 1-35 doses, 1-30 doses, 1-25 doses, 1 ~20 doses, 1-15 doses, 1-10 doses, 1-5 doses, 2-50 doses, 2-45 doses, 2-40 doses, 2-35 doses, 2-30 doses, 2-25 doses, 2 ~20 doses, 2-15 doses, 2-10 doses, 2-5 doses, 3-50 doses, 3-45 doses, 3-40 doses, 3-35 doses, 3-30 doses, 3-25 doses, 3 ~20 doses, 3-15 doses, 3-10 doses, 3-5 doses, 4-50 doses, 4-45 doses, 4-40 doses, 4-35 doses, 4-30 doses, 4-25 doses, 4 ~20 doses, 4-15 doses, 4-10 doses, 4-5 doses, 5-50 doses, 5-45 doses, 5-40 doses, 5-35 doses, 5-30 doses, 5-25 doses, 5 ~20 doses, 5-15 doses, 5-10 doses, 10-50 doses, 10-45 doses, 10-40 doses, 10-35 doses, 10-30 doses, 10-25 doses, 10-20 doses, 10 ~15 doses, 15-50 doses, 15-45 doses, 15-40 doses, 15-35 doses, 15-30 doses, 15-25 doses, 15-20 doses, 20-50 doses, 20-45 doses, 20 ~40 doses, 20-35 doses, 20-30 doses, 20-25 doses, 25-50 doses, 25-45 doses, 25-40 doses, 25-35 doses, 25-30 doses, 30-50 doses, 30 ~45 doses, 30-40 doses, 30-35 doses, 35-50 doses, 35-45 doses, 35-40 doses, 40-50 doses, 40-45 doses, or 45-50 doses of PD-1 axial binding An antagonist is administered. In certain instances, doses may be administered intravenously.
iii.抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの有効投与量
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごとに、約30mgと約600mgの間(例えば約50mgと600mgの間、例えば約60mgと約600mgの間、例えば約100mgと約600mgの間、例えば約200mgと約600mgの間、例えば約200mgと約550mgの間、例えば約250mgと約600mgの間、例えば約300mgと約500mgの間、例えば約350mgと約450mgの間、例えば約400mgと約440mgの間、例えば約410mgと約430mgの間、例えば、約420±10mg、例えば420±6mg、例えば420±5mg、例えば420±3mg、例えば420±1mg、例えば420±0.5mg、例えば420mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ))の有効量は、2週間ごとに、30mgと600mgの間(例えば50mgと600mgの間、例えば60mgと600mgの間、例えば100mgと600mgの間、例えば200mgと600mgの間、例えば200mgと550mgの間、例えば250mgと600mgの間、例えば300mgと500mgの間、例えば350mgと450mgの間、例えば400mgと440mgの間、例えば410mgと430mgの間、例えば420±10mg、例えば420±6mg、例えば420±5mg、例えば420±3mg、例えば420±1mg、例えば420±0.5mg、例えば420mg)の用量(例えば、固定用量)である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごとに約420mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、2週間ごとに420mgの用量である。
iii. Effective Dosages of Anti-TIGIT Antagonist Antibodies and PD-1 Axis Binding Antagonists In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is , every two weeks between about 30 mg and about 600 mg, such as between about 50 mg and 600 mg, such as between about 60 mg and about 600 mg, such as between about 100 mg and about 600 mg, such as between about 200 mg and about 600 mg, such as between about 200 mg and about 600 mg, such as between about 200 mg and about 550 mg, such as between about 250 mg and about 600 mg, such as between about 300 mg and about 500 mg, such as between about 350 mg and about 450 mg, such as between about 400 mg and about 440 mg, such as between about 410 mg and about 430 mg 420±10 mg, such as 420±6 mg, such as 420±5 mg, such as 420±3 mg, such as 420±1 mg, such as 420±0.5 mg, such as 420 mg) (e.g., fixed dose) between . In some examples, the effective amount of the anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody (e.g., tiragolumab)) is between 30 mg and 600 mg (e.g., between 50 mg and 600 mg, e.g., 60 mg and 600 mg) every two weeks. between 100 mg and 600 mg, such as between 200 mg and 600 mg, such as between 200 mg and 550 mg, such as between 250 mg and 600 mg, such as between 300 mg and 500 mg, such as between 350 mg and 450 mg, such as between 400 mg and 440 mg between, such as between 410 mg and 430 mg, such as 420±10 mg, such as 420±6 mg, such as 420±5 mg, such as 420±3 mg, such as 420±1 mg, such as 420±0.5 mg, such as 420 mg) (e.g. fixed dose). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 420 mg every two weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 420 mg every two weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約30mgと約1200mgの間(例えば、約30mgと約1100mgの間、例えば、約60mgと約1000mgの間、例えば、約100mgと約900mgの間、例えば、約200mgと約800mgの間、例えば、約300mgと約800mgの間、例えば、約400mgと約800mgの間、例えば、約400mgと約750mgの間、例えば、約450mgと約750mgの間、例えば、約500mgと約700mgの間、例えば、約550mgと約650mgの間、例えば、600mg±10mg、例えば、600±6mg、例えば、600±5mg、例えば、600±3mg、例えば、600±1mg、例えば、600±0.5mg、例えば、600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ))の有効量は、3週間ごとに30mgと1200mgの間(例えば30mgと1100mgの間、例えば60mgと1000mgの間、例えば100mgと900mgの間、例えば200mgと800mgの間、例えば300mgと800mgの間、例えば400mgと800mgの間、例えば400mgと750mgの間、例えば450mgと750mgの間、例えば500mgと700mgの間、例えば550mgと650mgの間、例えば600mg±10mg、例えば600±6mg、例えば600±5mg、例えば600±3mg、例えば600±1mg、例えば600±0.5mg、例えば600mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、3週間ごとに600mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 30 mg and about 1200 mg (e.g., about 30 mg) every three weeks. and about 1100 mg, for example between about 60 mg and about 1000 mg, for example between about 100 mg and about 900 mg, for example between about 200 mg and about 800 mg, for example between about 300 mg and about 800 mg, for example about 400 mg and about 800 mg, such as between about 400 mg and about 750 mg, such as between about 450 mg and about 750 mg, such as between about 500 mg and about 700 mg, such as between about 550 mg and about 650 mg, such as 600 mg ± 10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, the effective amount of the anti-TIGIT antagonist antibody (e.g., anti-TIGIT antagonist antibody (e.g., tiragolumab)) is between 30 mg and 1200 mg (e.g., between 30 mg and 1100 mg, e.g., between 60 mg and 1000 mg) every three weeks. between 100 mg and 900 mg, such as between 200 mg and 800 mg, such as between 300 mg and 800 mg, such as between 400 mg and 800 mg, such as between 400 mg and 750 mg, such as between 450 mg and 750 mg, such as between 500 mg and 700 mg, for example between 550 mg and 650 mg, such as 600±10 mg, such as 600±6 mg, such as 600±5 mg, such as 600±3 mg, such as 600±1 mg, such as 600±0.5 mg, such as 600 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 600 mg every three weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg every 3 weeks.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約600mgと約1200mgの間(例えば約600mgと約1100mgの間、例えば約600mgと約1000mgの間、例えば約700mgと約950mgの間、例えば約800mgと約900mgの間、例えば約820mgと約860mgの間、例えば約840±10mg、例えば840±6mg、例えば840±5mg、例えば840±3mg、例えば840±1mg、例えば840±0.5mg、例えば840mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに600mgと1200mgの間(例えば600mgと1100mgの間、例えば600mgと1000mgの間、例えば700mgと950mgの間、例えば800mgと900mgの間、例えば820mgと860mgの間、例えば840±10mg、例えば840±6mg、例えば840±5mg、例えば840±3mg、例えば840±1mg、例えば840±0.5mg、例えば840mg)の用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに約840mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、4週間ごとに840mgの用量である。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between about 600 mg and about 1200 mg (e.g., about 600 mg and about 1200 mg) every four weeks. between about 1100 mg, such as between about 600 mg and about 1000 mg, such as between about 700 mg and about 950 mg, such as between about 800 mg and about 900 mg, such as between about 820 mg and about 860 mg, such as about 840±10 mg, such as 840± 6 mg, such as 840±5 mg, such as 840±3 mg, such as 840±1 mg, such as 840±0.5 mg, such as 840 mg). In some examples, the effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is between 600 mg and 1200 mg (e.g., between 600 mg and 1100 mg) every four weeks. between 600 mg and 1000 mg, such as between 700 mg and 950 mg, such as between 800 mg and 900 mg, such as between 820 mg and 860 mg, such as 840±10 mg, such as 840±6 mg, such as 840±5 mg, such as 840±3 mg, such as 840±1 mg, such as 840±0.5 mg, such as 840 mg). In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 840 mg every 4 weeks. In some examples, an effective amount of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 840 mg every 4 weeks.
いくつかの例では、併用療法(例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ))による併用処置)で投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、単剤療法として投与される抗TIGITアンタゴニスト抗体の標準用量と比較して減少し得る。いくつかの例では、併用療法(例えば、1つ以上の白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えば、パクリタキセル又はnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン))を用いて又は用いずに、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))との併用処置)で投与される抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び/又はG-CSF若しくはGM-CSFの用量は、単独療法として投与される抗TIGITアンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の標準用量と比較して減少し得る。 In some examples, combination therapy (e.g., PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) or anti-PD-1 antagonist antibodies (e.g., MDX-1106 (nivolumab) or MK- 3475 (pembrolizumab, formerly known as lambrolizumab)) dose of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) administered at In some instances, combination therapy (e.g., one or more platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and /or with non-platinum chemotherapeutic agents (e.g. alkylating agents (e.g. cyclophosphamide), taxanes (e.g. paclitaxel or nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin)) or Anti-TIGIT antagonist antibody (e.g., as disclosed herein) administered without PD-1 axis binding antagonist (e.g., co-treatment with anti-PD-L1 antagonist antibody (e.g., atezolizumab)) Anti-TIGIT antagonist antibodies (eg, tiragolumab) and/or G-CSF or GM-CSF doses are standard for anti-TIGIT antagonist antibodies (eg, anti-PD-L1 antagonist antibodies (eg, atezolizumab)) administered as monotherapy. may be reduced relative to dose.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、約20mgと約1600mgの間(例えば約20と100mgの間、約100と200mgの間、約200と400mgの間、約400と600mgの間、約600と800mgの間、約800と1000mgの間、約1000と1200mgの間、約1200と1400mgの間、又は約1400と1600mgの間、例えば約80mgと約1200mgの間、例えば約100mgと約1200mgの間、例えば約200mgと約1200mgの間、例えば約300mgと約1200mgの間、例えば約400mgと約1200mgの間、例えば約500mgと約1200mgの間、例えば約600mgと約1100mgの間、例えば約700mgと約1000mgの間、例えば約740mgと約940mgの間、例えば約790mgと約890mgの間、例えば約815mgと約865mgの間、例えば約830mgと約850mgの間、例えば840mg±5mg,例えば840±2.5mg,例えば840±1.0mg,例えば840±0.5mg,例えば840mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに、80mgと1200mgの間(例えば、80mgと1200mgの間、例えば、100mgと1200mgの間、例えば、200mgと1200mgの間、例えば、300mgと1200mgの間、例えば、400mgと1200mgの間、例えば、500mgと1200mgの間、例えば、600mgと1100mgの間、例えば、700mgと1000mgの間、例えば、740mgと940mgの間、例えば、790mgと890mgの間、例えば、815mgと865mgの間、例えば、830mgと850mgの間、例えば、840mg±5mg、例えば、840±2.5mg、例えば、840±1.0mg、例えば、840±0.5mg、例えば、840mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約20mg、100mg、200mg、300mg、400mg、500mg、600mg、700mg、800mg、900mg、1000mg、1200mg、1400mg又は1600mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに約840mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、2週間ごとに840mgの用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 20 mg and about 1600 mg (eg, about 20 and 100 mg) every two weeks. between about 100 and 200 mg between about 200 and 400 mg between about 400 and 600 mg between about 600 and 800 mg between about 800 and 1000 mg between about 1000 and 1200 mg between about 1200 and 1400 mg between about 1400 and 1600 mg, such as between about 80 mg and about 1200 mg, such as between about 100 mg and about 1200 mg, such as between about 200 mg and about 1200 mg, such as between about 300 mg and about 1200 mg, such as between about 400 mg between about 1200 mg, such as between about 500 mg and about 1200 mg, such as between about 600 mg and about 1100 mg, such as between about 700 mg and about 1000 mg, such as between about 740 mg and about 940 mg, such as between about 790 mg and about 890 mg; at a dose of between about 815 mg and about 865 mg, such as between about 830 mg and about 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2.5 mg, such as 840 ± 1.0 mg, such as 840 ± 0.5 mg, such as 840 mg. be. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between 80 mg and 1200 mg (eg, between 80 mg and 1200 mg) every two weeks. between 100 mg and 1200 mg, such as between 200 mg and 1200 mg, such as between 300 mg and 1200 mg, such as between 400 mg and 1200 mg, such as between 500 mg and 1200 mg, such as between 600 mg and 1100 mg, such as , between 700 mg and 1000 mg, such as between 740 mg and 940 mg, such as between 790 mg and 890 mg, such as between 815 mg and 865 mg, such as between 830 mg and 850 mg, such as 840 mg ± 5 mg, such as 840 ± 2 .5 mg, eg 840±1.0 mg, eg 840±0.5 mg, eg 840 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is about 20 mg, 100 mg, 200 mg, 300 mg, 400 mg, 500 mg, 600 mg every two weeks , 700 mg, 800 mg, 900 mg, 1000 mg, 1200 mg, 1400 mg or 1600 mg. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 840 mg every two weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 840 mg every two weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ))の有効量は、3週間ごとに約80mgと約2000mgの間(例えば約100mgと約2000mgの間、例えば約200mgと約1900mgの間、例えば約300mgと約1700mgの間、例えば約400mgと約1600mgの間、例えば約500mgと約1600mgの間、例えば約600mgと約1600mgの間、例えば約700mgと約1600mgの間、例えば約800mgと約1600mgの間、例えば約900mgと約1500mgの間、例えば約1000mgと約1400mgの間、例えば約1050mgと約1350mgの間、例えば約1100mgと約1300mgの間、例えば約1150mgと約1250mgの間、例えば約1175mgと約1225mgの間、例えば約1190mgと約1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに80mgと2000mgの間(例えば100mgと2000mgの間、例えば200mgと1900mgの間、例えば300mgと1700mgの間、例えば400mgと1600mgの間、例えば500mgと1600mgの間、例えば600mgと1600mgの間、例えば700mgと1600mgの間、例えば800mgと1600mgの間、例えば900mgと1500mgの間、例えば1000mgと1400mgの間、例えば1050mgと1350mgの間、例えば1100mgと1300mgの間、例えば1150mgと1250mgの間、例えば1175mgと1225mgの間、例えば1190mgと1210mgの間、例えば1200mg±5mg、例えば1200±2.5mg、例えば1200±1.0mg、例えば1200±0.5mg、例えば1200mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに約1200mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、3週間ごとに1200mgの固定用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 80 mg and about 2000 mg (eg, between about 100 mg and about 2000 mg) every 3 weeks. such as between about 200 mg and about 1900 mg, such as between about 300 mg and about 1700 mg, such as between about 400 mg and about 1600 mg, such as between about 500 mg and about 1600 mg, such as between about 600 mg and about 1600 mg, such as about 700 mg between about 1600 mg, such as between about 800 mg and about 1600 mg, such as between about 900 mg and about 1500 mg, such as between about 1000 mg and about 1400 mg, such as between about 1050 mg and about 1350 mg, such as between about 1100 mg and about 1300 mg; for example between about 1150 mg and about 1250 mg, such as between about 1175 mg and about 1225 mg, such as between about 1190 mg and about 1210 mg, such as 1200 mg ± 5 mg, such as 1200 ± 2.5 mg, such as 1200 ± 1.0 mg, such as 1200 ± 0 .5 mg, eg 1200 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 80 mg and 2000 mg (e.g., between 100 mg and 2000 mg) every three weeks, e.g. between 200 mg and 1900 mg, such as between 300 mg and 1700 mg, such as between 400 mg and 1600 mg, such as between 500 mg and 1600 mg, such as between 600 mg and 1600 mg, such as between 700 mg and 1600 mg, such as between 800 mg and 1600 mg, such as 900 mg and 1500 mg, such as between 1000 mg and 1400 mg, such as between 1050 mg and 1350 mg, such as between 1100 mg and 1300 mg, such as between 1150 mg and 1250 mg, such as between 1175 mg and 1225 mg, such as between 1190 mg and 1210 mg, such as 1200 mg ± 5 mg, such as 1200±2.5 mg, such as 1200±1.0 mg, such as 1200±0.5 mg, such as 1200 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1200 mg every 3 weeks. In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a fixed dose of 1200 mg every 3 weeks.
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1200mgと約2000mgの間(例えば約1200mgと約1900mgの間、例えば約1200mgと約1800mgの間、例えば約1300mgと約1800mgの間、例えば約1400mgと約1800mgの間、例えば約1500mgと約1800mgの間、例えば約1580mgと約1780mgの間、例えば約1630mgと約1730mgの間、例えば約1655mgと約1705mgの間、例えば約1670mgと約1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1200mgと2000mgの間(例えば1200mgと1900mgの間、例えば1200mgと1800mgの間、例えば1300mgと1800mgの間、例えば1400mgと1800mgの間、例えば1500mgと1800mgの間、例えば1580mgと1780mgの間、例えば1630mgと1730mgの間、例えば1655mgと1705mgの間、例えば1670mgと1690mgの間、例えば1680mg±5mg、例えば1680±2.5mg、例えば1680±1.0mg、例えば1680±0.5mg、例えば1680mg)の用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに約1680mgの用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の有効量は、4週間ごとに1680mgの用量である。 In some examples, the effective amount of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is between about 1200 mg and about 2000 mg (eg, about 1200 mg and about 1900 mg) every 4 weeks. between about 1200 mg and about 1800 mg, such as between about 1300 mg and about 1800 mg, such as between about 1400 mg and about 1800 mg, such as between about 1500 mg and about 1800 mg, such as between about 1580 mg and about 1780 mg, such as about between 1630 mg and about 1730 mg, such as between about 1655 mg and about 1705 mg, such as between about 1670 mg and about 1690 mg, such as 1680 mg±5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg , eg 1680 mg). In some examples, the effective amount of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is between 1200 mg and 2000 mg (e.g., between 1200 mg and 1900 mg) every 4 weeks, e.g. between 1200 mg and 1800 mg, such as between 1300 mg and 1800 mg, such as between 1400 mg and 1800 mg, such as between 1500 mg and 1800 mg, such as between 1580 mg and 1780 mg, such as between 1630 mg and 1730 mg, such as between 1655 mg and 1705 mg, such as 1670 mg and 1690 mg, such as 1680±5 mg, such as 1680±2.5 mg, such as 1680±1.0 mg, such as 1680±0.5 mg, such as 1680 mg). In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of about 1680 mg every 4 weeks. In some examples, an effective amount of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a dose of 1680 mg every 4 weeks.
いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、ニボルマブ))の用量は、単剤療法として投与される抗PD-L1アンタゴニスト抗体の標準用量と比較して減少し得る。いくつかの例では、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))及び/又はG-CSFもしくはGM-CSFを伴う又は伴わない併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブとの併用処置)で投与されるPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して低減され得る。 In some examples, a PD-1 axis binding antagonist (e.g. , anti-PD-L1 antagonist antibody (eg, nivolumab)) can be reduced compared to standard doses of anti-PD-L1 antagonist antibody administered as monotherapy. In some examples, one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclophosphamide ), taxanes (e.g. paclitaxel, e.g. nab-paclitaxel) and/or topoisomerase II inhibitors (e.g. doxorubicin))) and/or combination therapy with or without G-CSF or GM-CSF (e.g. anti-TIGIT antagonist antibody , e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., combination treatment with tiragolumab)) can be reduced compared to standard doses of PD-1 axis binding antagonists administered as monotherapy.
iv.抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの投薬サイクル
本発明の方法及び使用のいずれにおいても、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び/又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、1回以上の投薬サイクル(例えば、1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17、18、19、20、21、22、23、24、25、26、27、28、29、30、31、32、33、34、35、36、37、38、39、40、41、42、43、44、45、46、47、48、49、又は50又はそれ以上の投薬サイクル)で投与され得る。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投薬サイクルは、臨床上の利益(例えば、確認された疾患進行、薬物耐性、死亡、又は許容できない毒性)が失われるまで継続する。いくつかの例では、各投薬サイクルの長さは、約7~42日間(例えば、7日間、8日間、9日間、10日間、11日間、12日間、13日間、14日間、15日間、16日間、17日間、18日間、19日間、20日間、21日間、22日間、23日間、24日間、25日間、26日間、27日間、28日間、29日間、30日間、31日間、32日間、33日間、34日間、35日間、36日間、37日間、38日間、39日間、41日間、42日間)である。いくつかの例では、投薬サイクルの長さは、約14日間である。いくつかの例では、投薬サイクルの長さは、約21日間である。いくつかの例では、投薬サイクルの長さは、約28日間である。いくつかの例では、投薬サイクルの長さは、約42日間である。いくつかの例では、投薬サイクルの長さは、約7日間である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約1日目(例えば、1±3日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約15日目(例えば、15±3日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約22日目(例えば、22±3日目)に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各投薬サイクルの約29日目(例えば、29±3日目)に投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各28日間サイクルの1日目及び15日目に約600mgの用量(例えば、固定用量)で(すなわち、2週間ごとに約420mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各42日間サイクルの1日目、15日目及び29日目に約600mgの用量(例えば、固定用量)で(すなわち、2週間ごとに約420mgの用量で)静脈内投与される。例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各42日間サイクルの1日目及び22日目に約600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに約600mgの用量で)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、各投薬サイクルの約15日目(例えば、15日目±3日目)に投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各21日間サイクルの1日目に(すなわち、約1200mgの用量で3週間ごとに)静脈内投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約1200mgの用量で各28日間サイクルの1日目及び15日目に(すなわち、約840mgの用量で2週間ごとに)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、各21日間サイクルの1日目に600mgの用量(例えば、固定用量)で(すなわち、3週間ごとに600mgの用量で)静脈内投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、MDX-1106(ニボルマブ)又はMK-3475(以前はラムブロリズマブとして知られていたペンブロリズマブ)))は、各投薬サイクルの1日目(例えば、1日目±3日目)に投与される。例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、1200mgの用量で各21日間サイクルの1日目に(すなわち、1200mgの用量で3週間ごとに)静脈内投与される。
iv. Anti-TIGIT Antagonist Antibody and PD-1 Axis Binding Antagonist Dosing Cycles In any of the methods and uses of the invention, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and/or or a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) for one or more dosing cycles (eg, 1, 2, 3, 4, 5, 6, 7, 8, 9 , 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34 , 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, or 50 or more dosing cycles). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) ) are continued until clinical benefit (eg, documented disease progression, drug resistance, death, or unacceptable toxicity) is lost. In some examples, the length of each dosing cycle is about 7 to 42 days (eg, 7 days, 8 days, 9 days, 10 days, 11 days, 12 days, 13 days, 14 days, 15 days, 16 days). days, 17 days, 18 days, 19 days, 20 days, 21 days, 22 days, 23 days, 24 days, 25 days, 26 days, 27 days, 28 days, 29 days, 30 days, 31 days, 32 days, 33 days, 34 days, 35 days, 36 days, 37 days, 38 days, 39 days, 41 days, 42 days). In some examples, the dosing cycle length is about 14 days. In some examples, the dosing cycle length is about 21 days. In some examples, the dosing cycle length is about 28 days. In some examples, the dosing cycle length is about 42 days. In some examples, the dosing cycle length is about 7 days. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered on about day 1 (e.g.,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の両方を、各投薬サイクルの約1日目(例えば、1日目±3日目)に投与する。
In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) are administered on about day 1 (eg,
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に約600mgの用量で(すなわち、3週間ごとに約600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、21日間サイクルの1日目に約1200mgの用量で(すなわち、3週間ごとに約1200mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、21日間サイクルの1日目に600mgの用量で(すなわち、3週間ごとに600mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、21日間サイクルの1日目に1200mgの用量で(すなわち、3週間ごとに1200mgの用量で)静脈内投与される。
In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered at a dose of about 600 mg on
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、14日間サイクルの1日目に約420mgの用量で(すなわち、2週間ごとに約420mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、14日間サイクルの1日目に約840mgの用量で(すなわち、2週間ごとに約840mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、14日間サイクルの1日目に420mgの用量で(すなわち、2週間ごとに約420mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、14日間サイクルの1日目に840mgの用量で(すなわち、2週間ごとに840mgの用量で)静脈内投与される。
In another example, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered at a dose of about 420 mg on
他の例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、28日間サイクルの1日目に約840mgの用量で(すなわち、4週間ごとに約840mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、28日間サイクルの1日目に約1680mgの用量で(すなわち、4週間ごとに約1680mgの用量で)静脈内投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、28日間サイクルの1日目に840mgの用量で(すなわち、4週間ごとに840mgの用量で)静脈内投与され、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、28日間サイクルの1日目に1680mgの用量で(すなわち、4週間ごとに1680mgの用量で)静脈内投与される。
In another example, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered at a dose of about 840 mg on
v.抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの静脈内注入及び皮下投与
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を静脈内投与する。あるいは、いくつかの実施形態では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を皮下投与する。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を静脈内投与する。あるいはまた、いくつかの実施形態では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を皮下投与する。
v. Intravenous Infusion and Subcutaneous Administration of Anti-TIGIT Antagonist Antibody and PD-1 Axis Binding Antagonist Administer intravenously. Alternatively, in some embodiments, an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab) is administered subcutaneously. In some examples, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered intravenously. Alternatively, in some embodiments, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered subcutaneously.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約60±10分(例えば約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、又は約70分)わたる静脈内注入によって対象又は対象集団に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)は、約60±15分(例えば、約45分、約46分、約47分、約48分、約49分、約50分、約51分、約52分、約53分、約54分、約55分、約56分、約57分、約58分、約59分、約60分、約61分、約62分、約63分、約64分、約65分、約66分、約67分、約68分、約69分、約70分、約71分、約72分、約73分、約74分又は約75分)にわたる静脈内注入によって対象に投与される。 In some examples, the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered for about 60 ± 15 minutes (e.g., about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes , about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about administered to a subject or population of subjects by intravenous infusion over a period of 72 minutes, about 73 minutes, about 74 minutes, or about 75 minutes). In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 60 ± 10 minutes (e.g., about 50 minutes, about 51 minutes, about 52 minutes, About 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, about 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, or about 70 minutes) to the subject or population of subjects. In some examples, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab) is administered for about 60±15 minutes (eg, about 45 minutes, about 46 minutes, about 47 minutes, about 48 minutes). minutes, about 49 minutes, about 50 minutes, about 51 minutes, about 52 minutes, about 53 minutes, about 54 minutes, about 55 minutes, about 56 minutes, about 57 minutes, about 58 minutes, about 59 minutes, about 60 minutes, About 61 minutes, about 62 minutes, about 63 minutes, about 64 minutes, about 65 minutes, about 66 minutes, about 67 minutes, about 68 minutes, about 69 minutes, about 70 minutes, about 71 minutes, about 72 minutes, about 73 minutes minutes, about 74 minutes, or about 75 minutes).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象に投与される。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、約30±10分(例えば、約20分、約21分、約22分、約23分、約24分、約25分、約26分、約27分、約28分、約29分、約30分、約31分、約32分、約33分、約34分、約35分、約36分、約37分、約38分、約39分、又は約40分)にわたる静脈内注入によって対象に投与される。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) is administered for about 30 ± 10 minutes (e.g., about 20 minutes, about 21 minutes, about 22 minutes). , about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes, about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes). In some examples, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered for about 30±10 minutes (eg, about 20 minutes, about 21 minutes, about 22 minutes, about 23 minutes, about 24 minutes, about 25 minutes, about 26 minutes, about 27 minutes, about 28 minutes, about 29 minutes, about 30 minutes, about 31 minutes, about 32 minutes, about 33 minutes, about 34 minutes, about 35 minutes , about 36 minutes, about 37 minutes, about 38 minutes, about 39 minutes, or about 40 minutes).
vi.投与順序及び観察期間
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの両方が対象又は対象集団に投与されるいくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の前に対象に投与される。
vi. Order of Administration and Observation Period In some examples where both an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist are administered to a subject or population of subjects, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antibody as disclosed herein) is administered to a subject or population of subjects. A TIGIT antagonist antibody (eg, tiragolumab) is administered to the subject prior to a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)). be.
いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後及びPD-1軸結合アンタゴニストの投与前に、方法は、介在する第1の観察期間を含む。いくつかの例では、例えば、抗TIGITアンタゴニスト抗体の投与後、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を対象に投与する。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を最初に対象に投与し、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後にPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を対象に投与する。 In some examples, the method includes an intervening first observation period, eg, after administration of the anti-TIGIT antagonist antibody and before administration of the PD-1 axis binding antagonist. In some examples, for example, a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to the subject after administration of the anti-TIGIT antagonist antibody. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is first administered to the subject, and an anti-TIGIT antagonist antibody (e.g., A PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered to the subject after administration of an anti-TIGIT antagonist antibody as disclosed (eg, tiragolumab).
いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第2の観察期間を更に含む。 In some examples, the method further comprises a second observation period following administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)).
いくつかの例では、方法は、抗TIGITアンタゴニスト抗体の投与後の第1の観察期間、及びPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分である場合、方法は、第1又は第2の観察期間中の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分である場合、方法は、第1又は第2の間の抗TIGITアンタゴニスト抗体又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, the method includes a first observation period after administration of an anti-TIGIT antagonist antibody and a second observation period after administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). Includes both observation periods. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. When the first and second observation periods are each about 60 minutes, the method includes anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody) during the first or second observation period. (eg, atezolizumab)) at about 30±10 minutes after administration of the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature). If the first and second observation periods are each about 30 minutes, the method includes anti-TIGIT antagonist antibody or PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody) between the first or second , atezolizumab)) at about 15±10 minutes after administration of the subject's vital signs (eg, pulse rate, respiratory rate, blood pressure, and temperature).
いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の前に対象又は対象集団に投与される。いくつかの例では、例えば、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与前に、方法は、介在する第1の観察期間を含む。 In some examples, the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) is an anti-TIGIT antagonist antibody (e.g., herein prior to administration of an anti-TIGIT antagonist antibody (eg, tiragolumab) as disclosed in the literature to the subject or population of subjects. In some examples, for example, after administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antibody as disclosed herein). Prior to administration of the TIGIT antagonist antibody (eg, tiragolumab), the method includes an intervening first observation period.
いくつかの例では、方法は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第2の観察期間を更に含む。 In some examples, the method further comprises a second observation period after administration of an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab).
いくつかの例では、方法は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の投与後の第1の観察期間、及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後の第2の観察期間の両方を含む。いくつかの例では、第1及び第2の観察期間はそれぞれ、約30分と約60分の間の長さである。第1及び第2の観察期間がそれぞれ約60分の長さである場合、方法は、第1又は第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))又は抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後約30±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。第1及び第2の観察期間がそれぞれ約30分の長さである場合、方法は、第1又は第2の観察期間中のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の投与後約15±10分での対象のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録することを含み得る。 In some examples, the methods include a first observation period following administration of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) and an anti-TIGIT antagonist antibody (eg, herein A second observation period after administration of an anti-TIGIT antagonist antibody (eg, tiragolumab) as disclosed in the literature. In some examples, the first and second observation periods are each between about 30 minutes and about 60 minutes long. If the first and second observation periods are each about 60 minutes long, the method includes the use of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab)) or the subject's vital signs (e.g., pulse rate, recording breathing rate, blood pressure, and temperature). If the first and second observation periods are each about 30 minutes long, the method includes the use of a PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., , atezolizumab)), the subject's vital signs (e.g., pulse rate, recording breathing rate, blood pressure, and temperature).
いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与を更に含む。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))及び抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の後に投与される。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))の投与後の第2の観察期間の後に投与される。 In some examples, the method further comprises administration of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)). In some examples, the VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody (e.g., pembrolizumab)) and an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody as disclosed herein, eg, tiragolumab). In some examples, the VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) or PD- A second observation period following administration of a uniaxial binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) is administered.
いくつかの例では、方法は、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の投与後の第3の観察期間を更に含む。いくつかの例では、第3の観察期間は、約30分と約120分の間の長さである。いくつかの例では、第1の観察期間、第2の観察期間、及び第3の観察期間がそれぞれ、約30分と約120分の間の長さである。 In some examples, the method further comprises a third observation period after administration of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)). In some examples, the third observation period is between about 30 minutes and about 120 minutes long. In some examples, the first observation period, the second observation period, and the third observation period are each between about 30 minutes and about 120 minutes long.
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの併用投与
いくつかの例では、例えばがんを有する対象の処置のための併用療法(例えば、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)とPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)との併用処置)では、有効量の用量の抗TIGITアンタゴニスト抗体(例えば、本明細書開中に示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)を、有効量の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))と共に投与する。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように2週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように2週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように2週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように3週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように2週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように4週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように2週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように6週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように3週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように2週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように3週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように3週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように3週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように4週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように3週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように6週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように4週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように2週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように4週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように3週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように4週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように4週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように4週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように6週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体は、本明細書のセクションIII(K)(i)に記載されるように2、3又は4週間ごとに投与され、PD-1軸結合アンタゴニストは、本明細書のセクションIII(K)(ii)に記載されるように2、3、4又は6週間ごとに投与される。
Combination Administration of Anti-TIGIT Antagonist Antibody and PD-1 Axis Binding Antagonist such as anti-TIGIT antagonist antibody (e.g., tiragolumab) and a PD-1 axis binding antagonist (e.g., combination treatment with an anti-PD-L1 antagonist antibody (e.g., atezolizumab)), an effective dose of the anti-TIGIT antagonist antibody (e.g., , an anti-TIGIT antagonist antibody (e.g., tiragolumab) as set forth herein, administered with an effective dose of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)). In some examples, the anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered herein In some examples, the anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(ii) of Section III(K)(ii) herein. and the PD-1 axis binding antagonist is administered every three weeks as described in Section III(K)(ii) herein. The anti-TIGIT antagonist antibody is administered every two weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(ii) herein. In some examples, the anti-TIGIT antagonist antibody is administered every 2 weeks as described in Section III(K)(i) herein. and the PD-1 axis binding antagonist is administered every 6 weeks as described in Section III(K)(ii) herein, hi some examples, the anti-TIGIT antagonist antibody is administered herein and the PD-1 axis binding antagonist is administered every 3 weeks as described in Section III(K)(i) of this specification, and the PD-1 axis binding antagonist is administered as described in Section III(K)(ii) herein. In some examples, the anti-TIGIT antagonist antibody is administered every three weeks as described in Section III(K)(i) herein, and P The D-1 axis binding antagonist is administered every three weeks as described in Section III(K)(ii) herein. In some examples, the anti-TIGIT antagonist antibody is administered every three weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 4 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every three weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 6 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 2 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 3 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 4 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every 4 weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered in Section III(K)(i) herein. Administered every 6 weeks as described in III(K)(ii). In some examples, the anti-TIGIT antagonist antibody is administered every 2, 3 or 4 weeks as described in Section III(K)(i) herein and the PD-1 axis binding antagonist is administered herein. Administered every 2, 3, 4 or 6 weeks as described in Section III(K)(ii) of the specification.
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、3週間ごとに約600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、3週間ごとに600mgの用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、段階的投薬レジメン(例えば、対象の体重(BW)又は体表面積(BSA)に基づく投薬)で(例えば、3週間ごとに)投与され、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、約0.01mg/kg~約50mg/kg(例えば、約15mg/kg)、最大1200mgの用量で、例えば3週間ごとに投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)は、段階的投薬レジメン(例えば、対象の体重(BW)又は体表面積(BSA)に基づく投薬)で(例えば、3週間ごとに)投与され、PD-1軸結合アンタゴニスト(例えば、アテゾリズマブ等の抗PD-L1アンタゴニスト抗体)は、0.01mg/kg~50mg/kg(例えば、15mg/kg)、最大1200mgの用量で、例えば3週間ごとに投与される。そのような投薬レジメンは、比較的低体重(例えば、40 kg以下(例えば、5 kg~40 kg、15 kg~40 kg、又は5 kg~15 kg))の対象の処置に利用することができ、成人データから推定された薬物動態パラメーターの外挿に基づくバイオシミュレーション研究を通じて開発されている。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量は、対象の体重(例えば、体重(BW)>40kg:600mg、BW>15kg及び≦40kg:400mg、BW≦15kg:300mg)に基づく段階的用量である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、対象の体重に基づく用量(例えば、15mg/kg)である。いくつかの例では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量は、対象の体表面積(例えば、体表面積(BSA)>1.25m2:600mg、BSA>0.75m2かつ≦1.25m2:450mg、BSA>0.5m2かつ≦0.75m2:350mg、及びBSA≦0.5m2:300mg)に基づく用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の用量(例えば、約600mg)を、対象の体重(例えば、15mg/kg)に基づいて3週間ごとにPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量と組み合わせて投与する。いくつかの例では、3週間ごとに、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の段階的用量(例えば、体重(BW)>40kg:600mg、BW>15kgかつ≦40kg:400mg、BW≦15kg:300mg)を、対象の体重に基づくPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量(例えば、15mg/kg)と組み合わせて投与する。いくつかの例では、3週間ごとに、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の段階的用量(例えば、体重(BW)>40kg:600mg、BW>15kgかつ≦40kg:400mg、BW≦15kg:300mg)を、対象の体表面積(例えば、BSA>1.25m2:600mg、BSA>0.75m2かつ≦1.25m2:450mg、BSA>0.5m2かつ≦0.75m2:350mg、及びBSA≦0.5m2:300mg)に基づくPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))の用量と組み合わせて投与する。いくつかの実施形態では、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))は、3週間ごとに1200mgの最大用量で投与される。いくつかの例では、併用療法は、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は非白金系化学療法剤(例えば、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン))とともに投与される。 In some examples, the dose of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of about 600 mg every 3 weeks. In some examples, the dose of the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) is a dose of 600 mg every 3 weeks. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered in a graded dosing regimen (e.g., subject body weight (BW) or body surface area ( (e.g., every 3 weeks) and the PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody such as atezolizumab) is administered from about 0.01 mg/kg to about 50 mg/kg (eg, about 15 mg/kg), administered at doses up to 1200 mg, eg, every 3 weeks. In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is administered in a graded dosing regimen (e.g., subject body weight (BW) or body surface area ( BSA)-based dosing) (e.g., every 3 weeks) and the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody such as atezolizumab) is administered at 0.01 mg/kg to 50 mg/kg (e.g., , 15 mg/kg), at doses up to 1200 mg, eg every 3 weeks. Such dosing regimens can be utilized in the treatment of relatively low weight subjects (eg, 40 kg or less (eg, 5 kg to 40 kg, 15 kg to 40 kg, or 5 kg to 15 kg)). , being developed through biosimulation studies based on extrapolation of pharmacokinetic parameters estimated from adult data. In some examples, the dose of the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is the body weight of the subject (e.g., body weight (BW) >40 kg: 600 mg; BW >15 kg and <40 kg: 400 mg; BW <15 kg: 300 mg). In some examples, the dose of the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is a subject weight-based dose (eg, 15 mg/kg). In some examples, the dose of the PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) is a subject's body surface area (e.g., body surface area (BSA) >1.25 m 2 : 600 mg , BSA>0.75 m 2 and ≦1.25 m 2 : 450 mg, BSA>0.5 m 2 and ≦0.75 m 2 : 350 mg, and BSA ≦0.5 m 2 : 300 mg). In some examples, a dose (e.g., about 600 mg) of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is added to a subject's body weight (e.g., 15 mg/kg ) every 3 weeks in combination with a dose of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some examples, graded doses (e.g., body weight (BW) >40 kg) of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) every 3 weeks: 600 mg, BW>15 kg and ≦40 kg: 400 mg, BW ≦15 kg: 300 mg) to a dose of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) based on the body weight of the subject (e.g., 15 mg/kg). In some examples, graded doses (e.g., body weight (BW) >40 kg) of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) every 3 weeks: 600 mg, BW>15 kg and ≦40 kg: 400 mg, BW ≦15 kg: 300 mg) to subject body surface area (e.g., BSA>1.25 m 2 : 600 mg, BSA>0.75 m 2 and ≦1.25 m 2 : 450 mg, PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody (e.g., atezolizumab)) based on BSA>0.5 m 2 and ≦0.75 m 2 : 350 mg, and BSA ≦0.5 m 2 : 300 mg) administered in combination with In some embodiments, the PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a maximum dose of 1200 mg every 3 weeks. In some instances, the combination therapy includes one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or non-platinum-based chemotherapeutic agents (e.g., antimetabolite agents (e.g., pemetrexed or gemcitabine))).
いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約250mgと約350mgの間の用量(例えば、3週間ごとに約300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約350mgと約450mgの間の用量(例えば、3週間ごとに約400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約550mgと約650mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgの用量で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgの用量で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約600mgの用量で投与される。いくつかの例では、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、対象の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の体重に基づく段階的用量と組み合わせて投与し、対象は、(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約400mg)で投与され;又は(c)体重が40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、体重が15kg以下の対象に、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約300mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、体重が15kg超40kg未満の対象に、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約400mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、体重が40kg超の対象に、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is The subject is (a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 300 mg every 3 weeks) (b) weighs more than 15 kg and less than or equal to 40 kg and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 400 mg every 3 weeks); or (c ) >40 kg, and the anti-TIGIT antagonist antibody is administered at a dose between about 30 mg and about 1200 mg every three weeks (eg, about 600 mg every three weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between about 250 mg and about 350 mg every 3 weeks (e.g., about 300 mg every 3 weeks); (b) weighing more than 15 kg and 40 kg; or (c) greater than 40 kg and the anti-TIGIT antagonist antibody is administered at a dose of between about 350 mg and about 450 mg every 3 weeks (e.g., about 400 mg every 3 weeks); , at doses between about 550 mg and about 650 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; (b) weighing greater than 15 kg and ≤40 kg and the anti-TIGIT antagonist antibody is administered at about or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every three weeks. In some examples, between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg). /kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as about 10 mg/kg. kg and about 20 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15 ± 0.2 mg/kg or about 15 ± 0.1 mg/kg, such as about 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) administered in combination with weight-based graded doses of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), wherein the subject (a) weighs 15 kg or less; , the anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every 3 weeks (e.g., about 300 mg every 3 weeks); is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 400 mg every 3 weeks); or (c) weighs over 40 kg and the anti-TIGIT antagonist antibody is administered at about Administered at doses between 30 mg and about 1200 mg (eg, about 600 mg every 3 weeks). In some examples, an anti-TIGIT antagonist antibody (e.g., as disclosed herein) is administered to a subject weighing 15 kg or less at a dose of between about 10 mg and about 1000 mg every three weeks (e.g., about 300 mg every three weeks). an anti-TIGIT antagonist antibody, e.g., tiragolumab, as administered and between about 0.01 mg/kg and about 50 mg/kg of the subject's body weight (e.g., about 0.01 mg/kg and about 45 mg/kg) every 3 weeks between about 0.1 mg/kg and about 40 mg/kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg. kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0.1 mg/kg, such as about 15 mg/kg) of a PD-1 axis binding antagonist (e.g., anti-PD - Administer an L1 antagonistic antibody (eg, atezolizumab). In some examples, a subject weighing more than 15 kg and less than 40 kg is administered an anti-TIGIT antagonist antibody (e.g., doses of between about 10 mg and about 1000 mg every 3 weeks (e.g., about 400 mg every 3 weeks), e.g., and between about 0.01 mg/kg and about 50 mg/kg of the subject's body weight (e.g., about 0.01 mg/kg and about 45 mg/kg) every 3 weeks. /kg, such as between about 0.1 mg/kg and about 40 mg/kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as about between 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15± 1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0.1 mg/kg, such as about 15 mg/kg) dose of a PD-1 axis binding antagonist (e.g., An anti-PD-L1 antagonist antibody (eg, atezolizumab) is administered. In some examples, an anti-TIGIT antagonist antibody (e.g., as disclosed herein) is administered to a subject weighing more than 40 kg at a dose of between about 30 mg and about 1200 mg every three weeks (e.g., about 600 mg every three weeks). an anti-TIGIT antagonist antibody, e.g., tiragolumab, as administered and between about 0.01 mg/kg and about 50 mg/kg of the subject's body weight (e.g., about 0.01 mg/kg and about 45 mg/kg) every 3 weeks between about 0.1 mg/kg and about 40 mg/kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg. kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0.1 mg/kg, such as about 15 mg/kg) of a PD-1 axis binding antagonist (e.g., anti-PD - Administer an L1 antagonistic antibody (eg, atezolizumab).
いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに250mgと350mgの間の用量(例えば、3週間ごとに300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに350mgと450mgの間の用量(例えば、3週間ごとに400mg)で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに550mgと650mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体重に基づく段階的用量であり、対象は(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgの用量で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgの用量で投与され;又は(c)40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに600mgの用量で投与される。いくつかの例では、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、対象の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の体重に基づく段階的用量と組み合わせて投与し、対象は、(a)体重が15kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの用量(例えば、3週間ごとに300mg)で投与され;(b)体重が15kg超40kg以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの用量(例えば、3週間ごとに400mg)で投与され;又は(c)体重が40kgを超え、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、体重が15kg以下の対象に、3週間ごとに10mgと1000mgの用量(例えば、3週間ごとに300mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、体重が15kg超40kg未満の対象に、3週間ごとに10mgと1000mgの用量(例えば、3週間ごとに400mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、体重が40kg超の対象に、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is ( b) weighing more than 15 kg and less than or equal to 40 kg, and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 400 mg every 3 weeks); The TIGIT antagonist antibody is administered at doses between 30 mg and 1200 mg every 3 weeks (eg 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighs 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose between 250 mg and 350 mg every 3 weeks (e.g., 300 mg every 3 weeks); (b) weighs more than 15 kg and ≤40 kg; or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of between 350 mg and 450 mg every 3 weeks (e.g., 400 mg every 3 weeks); and 650 mg (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on the weight of the subject, wherein the subject is ( a) weighing 15 kg or less and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; or (c) greater than 40 kg, the anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks. In some examples, between 0.01 mg/kg and 50 mg/kg of body weight of the subject (e.g., between 0.01 mg/kg and 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as 12.5 mg/kg kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg or 15±0.1 mg/kg, such as 15 mg/kg) of a dose of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) to a subject anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g. , tiragolumab) in combination with weight-based graded doses of the anti-TIGIT antagonist antibody (a) weighing 15 kg or less and anti-TIGIT antagonist antibody at doses of 10 mg and 1000 mg every 3 weeks (e.g. (b) weighing >15 kg and ≤40 kg and the anti-TIGIT antagonist antibody is administered at doses of 10 mg and 1000 mg every 3 weeks (e.g., 400 mg every 3 weeks); or (c ) weighs more than 40 kg and the anti-TIGIT antagonist antibody is administered at doses of 30 mg and 1200 mg every 3 weeks (eg 600 mg every 3 weeks). In some examples, subjects weighing 15 kg or less receive doses of 10 mg and 1000 mg every 3 weeks (e.g., 300 mg every 3 weeks) of an anti-TIGIT antagonist antibody (e.g., an anti TIGIT antagonist antibody, e.g., tiragolumab), and between 0.01 and 50 mg/kg of subject body weight (e.g., between 0.01 and 45 mg/kg, e.g., 0.1 mg/kg) every 3 weeks and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0. A dose of 1 mg/kg, eg, 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered. In some examples, a subject weighing more than 15 kg and less than 40 kg is administered an anti-TIGIT antagonist antibody (e.g., as disclosed herein) at doses of 10 mg and 1000 mg every 3 weeks (e.g., 400 mg every 3 weeks). anti-TIGIT antagonist antibody, e.g., tiragolumab), and between 0.01 mg/kg and 50 mg/kg of the subject's body weight (e.g., between 0.01 mg/kg and 45 mg/kg, e.g., 0.1 mg/kg) every 3 weeks /kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as 10 mg/kg and 20 mg /kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± A dose of 0.1 mg/kg, eg, 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered. In some examples, a subject weighing more than 40 kg is administered an anti-TIGIT antagonist antibody (e.g., as disclosed herein) at a dose between 30 mg and 1200 mg every 3 weeks (e.g., 600 mg every 3 weeks). anti-TIGIT antagonist antibody, e.g., tiragolumab), and between 0.01 mg/kg and 50 mg/kg of the subject's body weight (e.g., between 0.01 mg/kg and 45 mg/kg, e.g., 0.1 mg/kg) every 3 weeks /kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as 10 mg/kg and 20 mg /kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15 ± 2 mg/kg, 15 ± 1 mg/kg, 15 ± 0.5 mg/kg, 15 ± 0.2 mg/kg, or 15 ± A dose of 0.1 mg/kg, eg, 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered.
いくつかの例では、がんを有する対象を処置するための抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量である。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間(例えば、3週間ごとに約300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約350mg)で投与され;(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約250mgと約350mgの間(例えば、3週間ごとに約300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgと約400mgの間の用量(例えば、3週間ごとに約350mg)で投与され;又は(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgと約500mgの間の用量(例えば、3週間ごとに約450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約550mgと約650mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約300mgの用量で投与される;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約400mgの用量で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに450mgの用量で投与し;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約600mgの用量で投与される。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) for treating a subject with cancer is the body surface area of the subject. It is a tiered dose based on In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every 3 weeks (eg, about 300 mg every 3 weeks); (b) greater than 0.5 m 2 or less than 0.75 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 350 mg every 3 weeks); c) greater than 0.75 m 2 and less than or equal to 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 450 mg every 3 weeks); or ( d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 30 mg and about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between about 250 mg and about 350 mg every three weeks (eg, about 300 mg every three weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between about 300 mg and about 400 mg every 3 weeks (e.g., about 350 mg every 3 weeks); or (c) greater than 0.75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between about 400 mg and about 500 mg every 3 weeks (e.g., about 450 mg every 3 weeks); or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between about 550 mg and about 650 mg every three weeks (eg, about 600 mg every three weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) has a body surface area of 0.5 m2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks; , the anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks ; or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose of about 600 mg every 3 weeks.
いくつかの例では、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kg、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kg、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、対象の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の体表面積に基づく段階的用量と組み合わせて投与し、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの用量(例えば、3週間ごとに約300mg)で投与され;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約350mg)で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)で投与される。いくつかの例では、0.5m2以下の体表面積を有する対象に、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約300mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、0.5m2超0.75m2以下の体表面積を有する対象に、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約350mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、0.75m2超1.25m2以下の体表面積を有する対象に、3週間ごとに約10mgと約1000mgの間の用量(例えば、3週間ごとに約450mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間の間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、1.25m2超の体表面積を有する対象に、3週間ごとに約30mgと約1200mgの間の用量(例えば、3週間ごとに約600mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと45約mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。
In some examples, between about 0.01 mg/kg and about 50 mg/kg of body weight of the subject (e.g., between about 0.01 mg/kg and about 45 mg/kg, e.g., between about 0.1 mg/kg and about 40 mg/kg). /kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg, such as between about 5 mg/kg and about 25 mg/kg, such as about 10 mg/kg. between about 20 mg/kg, such as about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg, about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg /kg or about 15±0.1 mg/kg, such as about 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) to the subject's anti-TIGIT antagonist antibody. (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) in combination with graded doses based on body surface area, wherein the subject: (a) has a body surface area of 0.5 m 2 or less; and the anti-TIGIT antagonist antibody is administered at a dose of about 10 mg and about 1000 mg every three weeks (e.g., about 300 mg every three weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 ; the anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every three weeks (e.g., about 350 mg every three weeks); (c) greater than 0.75 m2 and less than or equal to 1.25 m2 ; The anti-TIGIT antagonist antibody is administered at a dose of between about 10 mg and about 1000 mg every 3 weeks (e.g., about 450 mg every 3 weeks); or (d) greater than 1.25 m2 and the anti-TIGIT antagonist antibody is , at doses between about 30 mg and about 1200 mg every 3 weeks (eg, about 600 mg every 3 weeks). In some examples, an anti- TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) and between about 0.01 mg/kg and about 50 mg/kg of body weight of a subject (e.g., about 0.01 mg/kg) every 3 weeks and about 45 mg/kg, such as between about 0.1 mg/kg and about 40 mg/kg, such as between about 1 mg/kg and about 35 mg/kg, such as between about 2.5 mg/kg and about 30 mg/kg such as between about 5 mg/kg and about 25 mg/kg, such as between about 10 mg/kg and about 20 mg/kg, such as between about 12.5 mg/kg and about 15 mg/kg, such as about 15±2 mg/kg; PD-1 axis binding antagonist at a dose of about 15±1 mg/kg, about 15±0.5 mg/kg, about 15±0.2 mg/kg, or about 15±0.1 mg/kg, such as about 15 mg/kg) (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some examples, anti-TIGIT at a dose between about 10 mg and about 1000 mg every 3 weeks (e.g., about 350 mg every 3 weeks) to a subject having a body surface area greater than 0.5 m 2 and less than or equal to 0.75
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間(例えば、3週間ごとに300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに350mg)で投与され;(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに250mgと350mgの間(例えば、3週間ごとに300mg)の用量で投与される。(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgと400mgの間の用量(例えば、3週間ごとに350mg)で投与され;又は(c)0.75m2超1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgと500mgの間の用量(例えば、3週間ごとに450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに550mgと650mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の有効量は、対象の体表面積に基づく段階的用量であり、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに300mgの用量で投与される;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに400mgの用量で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに450mgの用量で投与し;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに600mgの用量で投与される。 In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between 10 mg and 1000 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 350 mg every 3 weeks); (c) 0 greater than .75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 450 mg every 3 weeks); or (d) 1.25 m2 and the anti-TIGIT antagonist antibody is administered at a dose between 30 mg and 1200 mg every 3 weeks (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) have a body surface area of 0.5 m 2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of between 250 mg and 350 mg every 3 weeks (eg, 300 mg every 3 weeks); (b) greater than 0.5 m2 and less than or equal to 0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 300 mg and 400 mg every 3 weeks (e.g., 350 mg every 3 weeks); or (c) greater than 0.75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 400 mg and 500 mg every 3 weeks (e.g., 450 mg every 3 weeks); or (d) 1.25 m greater than 2 and the anti-TIGIT antagonist antibody is administered at a dose between 550 mg and 650 mg every 3 weeks (eg, 600 mg every 3 weeks). In some examples, an effective amount of an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab) is a graded dose based on a subject's body surface area, wherein the subject is (a) has a body surface area of 0.5 m2 or less, and the anti-TIGIT antagonist antibody is administered at a dose of 300 mg every 3 weeks; the anti-TIGIT antagonist antibody is administered at a dose of 400 mg every 3 weeks; or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose of 600 mg every 3 weeks.
いくつかの例では、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を、対象の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)の体表面積に基づく段階的用量と組み合わせて投与し、対象は、(a)0.5m2以下の体表面積を有し、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに300mg)で投与され;(b)0.5m2超0.75m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに350mg)で投与され;(c)0.75m2より大きく1.25m2以下であり、抗TIGITアンタゴニスト抗体は、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに450mg)で投与され;又は(d)1.25m2超であり、抗TIGITアンタゴニスト抗体は、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)で投与される。いくつかの例では、0.5m2以下の体表面積を有する対象に、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに300mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、0.5m2超0.75m2未満の体表面積を有する対象に、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに350mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、0.75m2超1.25m2以下の体表面積を有する対象に、3週間ごとに10mgと1000mgの間の用量(例えば、3週間ごとに450mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。いくつかの例では、1.25m2超の体表面積を有する対象に、3週間ごとに30mgと1200mgの間の用量(例えば、3週間ごとに600mg)の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示されるような抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)、及び3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば10mg/kgと20mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば15mg/kg)の用量のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を投与する。
In some examples, between 0.01 mg/kg and 50 mg/kg of body weight of the subject (e.g., between 0.01 mg/kg and 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as 12.5 mg/kg kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg or 15±0.1 mg/kg, such as 15 mg/kg) of a dose of a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab)) to a subject anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody as disclosed herein, e.g. , tiragolumab) in combination with graded doses based on body surface area, subjects (a) with a body surface area of ≤ 0.5 m2 and anti-TIGIT antagonist antibody doses between 10 mg and 1000 mg every 3 weeks (e.g., 300 mg every 3 weeks); (b) greater than 0.5 m2 and ≤0.75 m2 , and the anti-TIGIT antagonist antibody is administered at a dose of between 10 mg and 1000 mg every 3 weeks (e.g., (c) greater than 0.75 m2 and less than or equal to 1.25 m2 , and the anti-TIGIT antagonist antibody is administered at a dose between 10 mg and 1000 mg every 3 weeks (e.g., 350 mg every 3 weeks); or (d) greater than 1.25 m 2 and the anti-TIGIT antagonist antibody is administered at a dose between 30 mg and 1200 mg every 3 weeks (e.g., 600 mg every 3 weeks) . In some examples, a subject with a body surface area of 0.5 m 2 or less is administered an anti-TIGIT antagonist antibody (e.g., 300 mg every 3 weeks) at a dose of between 10 mg and 1000 mg every 3 weeks (e.g., 300 mg every 3 weeks). and an anti-TIGIT antagonist antibody, such as tiragolumab, as disclosed in US Pat. between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15±0.2 mg/kg kg, or 15±0.1 mg/kg, eg, 15 mg/kg) of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)). In some examples, an anti-TIGIT antagonist antibody (e.g., 350 mg every 3 weeks) at a dose of between 10 mg and 1000 mg every 3 weeks ( For example, an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), and between 0.01 mg/kg and 50 mg/kg (e.g., 0.01 mg/kg and between 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15 A dose of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a dose of ±0.2 mg/kg, or 15±0.1 mg/kg, eg, 15 mg/kg. In some examples, an anti-TIGIT antagonist antibody ( e.g. , 450 mg every 3 weeks) at a dose of between 10 mg and 1000 mg every 3 weeks ( For example, an anti-TIGIT antagonist antibody as disclosed herein, e.g., tiragolumab), and between 0.01 mg/kg and 50 mg/kg (e.g., 0.01 mg/kg and between 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as between 5 mg/kg and 25 mg/kg kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg, 15±0.5 mg/kg, 15 A dose of a PD-1 axis binding antagonist (eg, an anti-PD-L1 antagonist antibody (eg, atezolizumab)) is administered at a dose of ±0.2 mg/kg, or 15±0.1 mg/kg, eg, 15 mg/kg. In some examples, an anti-TIGIT antagonist antibody (e.g., 600 mg every 3 weeks) at a dose of between 30 mg and 1200 mg every 3 weeks (e.g., 600 mg every 3 weeks) to a subject with a body surface area greater than 1.25
化学療法剤の投薬
様々な化学療法剤の治療有効量は当該技術分野で公知であり、本発明で企図される。特定の場合において、1つ以上の化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び/又は1つ以上の非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン))が、本明細書に列挙される用量に従って投与される。
白金系化学療法剤
Dosing of Chemotherapeutic Agents Therapeutically effective amounts of various chemotherapeutic agents are known in the art and contemplated by the present invention. In certain cases, one or more chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and/or one or more non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclo phosphamide), taxanes (eg paclitaxel, eg nab-paclitaxel) and/or topoisomerase II inhibitors (eg doxorubicin)) are administered according to the doses recited herein.
platinum-based chemotherapeutic agent
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、1~50mg/ml/分(例えば、2~25mg/ml/分、3~15mg/ml/分、4~10mg/ml/分、又は5mg/ml/分、例えば、2mg/ml/分、3mg/ml/分、4mg/ml/分、5mg/ml/分、6mg/ml/分、7mg/ml/分、8mg/ml/分、9mg/ml/分、10mg/ml/分、11mg/ml/分、12mg/ml/分、13mg/ml/分、14mg/ml/分、15mg/ml/分、20mg/ml/分、25mg/ml/分、30mg/ml/分、35mg/ml/分、40mg/ml/分、45mg/ml/分、50mg/ml/分)のAUCを達成するのに十分な用量である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、AUC=5mg/ml/分を達成するのに十分な用量である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、AUC=6mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、AUC=5mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、AUC=6mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、21日間の投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、21日間の投薬サイクルの1日目にAUC=6mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、ペメトレキセド又はゲムシタビンの後に投与された場合にAUC=5mg/ml/分を達成するのに十分な用量である。いくつかの例では、カルボプラチンの有効量は、パクリタキセル後に投与した場合にAUC=6mg/ml/分を達成するのに十分な用量である。
AUCは、カルバート式(Calvert et al.,J.Clin.Oncol.1989,7:1748-56)を使用して計算することができる:
総投与量(mg)=(目標AUC)X(糸球体濾過率[GFR]+25)
In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 1-50 mg/ml/min (eg, 2-25 mg/ml/min, 3-15 mg/ml/min, 4 ~10 mg/ml/min, or 5 mg/ml/min, such as 2 mg/ml/min, 3 mg/ml/min, 4 mg/ml/min, 5 mg/ml/min, 6 mg/ml/min, 7 mg/ml/
AUC can be calculated using the Calvert formula (Calvert et al., J. Clin. Oncol. 1989, 7:1748-56):
Total Dose (mg) = (Target AUC) X (Glomerular Filtration Rate [GFR] + 25)
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、200mg~1500mg(例えば、300mg~1200mg、400mg~1100mg又は500mg~1000mg、例えば、300mg~400mg、400mg~500mg、500mg~600mg、600mg~700mg、700mg~750mg、750mg~800mg、800mg~900mg、900mg~1000mg、1000mg~1100mg又は1100mg~1200mg、例えば、約200mg、約300mg、約400mg、約500mg、約600mg、約700mg、約800mg、約900mg、約1000mg、約1100mg、約1200mg、約1300mg、1400mg又は約1500mg)である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、500mg~1000mg(例えば、約500mg、約600mg、約700mg、約800mg、約900mg、又は約1000mg)である。 In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 200 mg to 1500 mg (eg, 300 mg to 1200 mg, 400 mg to 1100 mg, or 500 mg to 1000 mg, such as 300 mg to 400 mg, 400 mg to 500 mg). , 500 mg to 600 mg, 600 mg to 700 mg, 700 mg to 750 mg, 750 mg to 800 mg, 800 mg to 900 mg, 900 mg to 1000 mg, 1000 mg to 1100 mg or 1100 mg to 1200 mg, such as about 200 mg, about 300 mg, about 400 mg, about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, about 1000 mg, about 1100 mg, about 1200 mg, about 1300 mg, 1400 mg or about 1500 mg). In some examples, the effective amount of the platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) is 500 mg to 1000 mg (e.g., about 500 mg, about 600 mg, about 700 mg, about 800 mg, about 900 mg, or about 1000 mg) .
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、約20mg/m2と約200mg/m2の間(例えば約20mg/m2と約150mg/m2の間、例えば約30mg/m2と約125mg/m2の間、例えば約40mg/m2と約110mg/m2の間、例えば約50mg/m2と約100mg/m2の間、例えば約60mg/m2と約90mg/m2の間、例えば約70mg/m2と約80mg/m2の間、例えば約75mg/m2、例えば75mg/m2)である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は約75mg/m2である。いくつかの例では、シスプラチンの有効量は約75mg/m2である。いくつかの例では、シスプラチンの有効量は、3週間ごとに約75mg/m2ある。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は、20mg/m2と200mg/m2の間(例えば20mg/m2と150mg/m2の間、例えば30mg/m2と125mg/m2の間、例えば40mg/m2と110mg/m2の間、例えば50mg/m2と100mg/m2の間、例えば60mg/m2と90mg/m2の間、例えば70mg/m2と80mg/m2の間、例えば75mg/m2、例えば75mg/m2)である。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)の有効量は75mg/m2である。いくつかの例では、シスプラチンの有効量は75mg/m2である。いくつかの例では、シスプラチンの有効量は、3週間ごとに75mg/m2ある。 In some examples, the effective amount of the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is between about 20 mg/m 2 and about 200 mg/m 2 (eg, between about 20 mg/m 2 and about 150 mg/m 2 ) . between about 30 mg/m 2 and about 125 mg/m 2 , such as between about 40 mg/m 2 and about 110 mg/m 2 , such as between about 50 mg/m 2 and about 100 mg/m 2 , such as about 60 mg /m 2 and about 90 mg/m 2 , such as between about 70 mg/m 2 and about 80 mg/m 2 , such as about 75 mg/m 2 , such as about 75 mg/m 2 ). In some examples, the effective amount of platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is about 75 mg/m 2 . In some examples, the effective amount of cisplatin is about 75 mg/ m2 . In some examples, the effective amount of cisplatin is about 75 mg/ m2 every 3 weeks. In some examples, the effective amount of the platinum-based chemotherapeutic agent (e.g., carboplatin or cisplatin) is between 20 mg/ m2 and 200 mg/ m2 (e.g., between 20 mg/ m2 and 150 mg/ m2 , e.g., 30 mg/m2). /m 2 and 125 mg/m 2 , such as between 40 mg/m 2 and 110 mg/m 2 , such as between 50 mg/m 2 and 100 mg/m 2 , such as between 60 mg/m 2 and 90 mg/m 2 , eg between 70 mg/m 2 and 80 mg/m 2 , eg 75 mg/m 2 , eg 75 mg/m 2 ). In some examples, the effective amount of platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is 75 mg/m 2 . In some examples, the effective amount of cisplatin is 75 mg/ m2 . In some examples, the effective amount of cisplatin is 75 mg/ m2 every 3 weeks.
いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)を対象又は対象集団に静脈内(例えば、30~120分かけて注入)投与する。いくつかの例では、カルボプラチンを30~60分間かけて静脈内投与する。いくつかの例では、シスプラチンは、60~120分の注入にわたって静脈内投与される。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)は、対象又は対象集団に3週間ごとに投与される。いくつかの例では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)は、21日間投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に対象又は対象集団に投与される。
In some examples, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered intravenously (eg, infused over 30-120 minutes) to the subject or population of subjects. In some examples, carboplatin is administered intravenously over 30-60 minutes. In some instances, cisplatin is administered intravenously over a 60-120 minute infusion. In some examples, a platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered to the subject or subject population every three weeks. In some examples, the platinum-based chemotherapeutic agent (eg, carboplatin or cisplatin) is administered at about day 1 (eg, day −3, day −2, day −1, day 1) of a 21-day dosing cycle. ,
タキサン
ヒトに投与されるタキサン(例えば、パクリタキセル又はnab-パクリタキセル(ABRAXANE(登録商標)))の治療有効量は、1回以上の投与によるかどうかにかかわらず、約25~約300mg/m2の範囲(例えば約25mg/m2、約50mg/m2、約75mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約125mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約175mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約225mg/m2、約250mg/m2、約275mg/m2、又は約300mg/m2(例えば25mg/m2、50mg/m2、75mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、125mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、175mg/m2、180mg/m2、190mg/m2、200mg/m2、225mg/m2、250mg/m2、275mg/m2、又は300mg/m2))となる 例えば、いくつかの実施形態では、約175mg/m2のパクリタキセルが投与される。いくつかの実施形態では、175mg/m2のパクリタキセルが投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに約175mg/m2から約200mg/m2の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに約175mg/m2の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに約200mg/m2の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに175mg/m2と200mg/m2の間の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに175mg/m2の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに200mg/m2の用量で投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに175mg/m2 IVで投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに175mg/m2 IVでアジア人種/民族の対象に投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに200mg/m2 IVで投与される。いくつかの実施形態では、パクリタキセルは、非アジア人種/民族の対象に、200mg/m2 IVで3週間ごとに投与される。いくつかの実施形態では、約100mg/m 2のnab-パクリタキセル(ABRAXANE(登録商標))が投与される。いくつかの実施形態では、100mg/m 2 のnab-パクリタキセル(ABRAXANE(登録商標))が投与される。いくつかの実施形態では、nab-パクリタキセル(ABRAXANE(登録商標))を、毎週100mg/m2 IVで投与する。いくつかの実施形態では、nab-パクリタキセル(ABRAXANE(登録商標))を、4週間ごとに3回(例えば、各28日間投薬サイクルの1、8及び15日目に)、100mg/m2 IVで投与する。いくつかの実施形態では、タキサン(例えば、パクリタキセル又はnab-パクリタキセル(ABRAXANE(登録商標))は、毎週、2週間ごと、3週間ごと、4週間ごと、各21日サイクルの1、8、及び15日目、又は各28日サイクルの1、8、及び15日目に投与され得る。
Taxanes A therapeutically effective amount of a taxane (e.g., paclitaxel or nab-paclitaxel (ABRAXANE®)) administered to humans, whether by one or more administrations, ranges from about 25 to about 300 mg/m 2 . ranges (e.g., about 25 mg/m 2 , about 50 mg/m 2 , about 75 mg/m 2 , about 80 mg/m 2 , about 90 mg/m 2 , about 100 mg/m 2 , about 110 mg/m 2 , about 120 mg/m 2 , about 125 mg/m 2 , about 130 mg/m 2 , about 140 mg/m 2 , about 150 mg/m 2 , about 160 mg/m 2 , about 170 mg/m 2 , about 175 mg/m 2 , about 180 mg/m 2 , about 190 mg/m 2 , about 200 mg/m 2 , about 225 mg/m 2 , about 250 mg/m 2 , about 275 mg/m 2 , or about 300 mg/m 2 (e.g. 25 mg/m 2 , 50 mg/m 2 , 75 mg/m 2 , 2 , 80 mg/ m2 , 90 mg/ m2 , 100 mg/ m2 , 110 mg/m2, 120 mg/ m2 , 125 mg/ m2 , 130 mg/ m2 , 140 mg/ m2 , 150 mg/ m2 , 160 mg/ m2 2 , 170 mg/ m2 , 175 mg/ m2 , 180 mg/ m2 , 190 mg/m2, 200 mg/ m2 , 225 mg/ m2 , 250 mg/ m2 , 275 mg/ m2 , or 300 mg/ m2 )) and For example, in some embodiments about 175 mg/m 2 of paclitaxel is administered. In some embodiments, 175 mg/m 2 paclitaxel is administered. In some embodiments, paclitaxel is administered at a dose of about 175 mg/m 2 to about 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of about 175 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of about 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose between 175 mg/m 2 and 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of 175 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at a dose of 200 mg/m 2 every 3 weeks. In some embodiments, paclitaxel is administered at 175 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered to subjects of Asian race/ethnicity at 175 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered at 200 mg/m 2 IV every 3 weeks. In some embodiments, paclitaxel is administered to subjects of non-Asian race/ethnicity at 200 mg/m 2 IV every 3 weeks. In some embodiments, about 100 mg/m 2 nab-paclitaxel (ABRAXANE®) is administered. In some embodiments, 100 mg/m 2 nab-paclitaxel (ABRAXANE®) is administered. In some embodiments, nab-paclitaxel (ABRAXANE®) is administered weekly at 100 mg/m 2 IV. In some embodiments, nab-paclitaxel (ABRAXANE®) at 100 mg/m 2 IV three times every 4 weeks (eg, on
いくつかの実施形態では、タキサン(例えば、パクリタキセル又はnab-パクリタキセル(ABRAXANE(登録商標)))は、対象又は対象集団に静脈内(例えば、3時間にわたる注入)投与される。いくつかの実施形態では、タキサンは、3週間ごとに対象又は対象集団に投与される。いくつかの実施形態では、タキサンは、21日間の投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に対象又は対象集団に投与される。いくつかの実施形態では、パクリタキセルは、3週間ごとに対象に投与される。いくつかの実施形態では、パクリタキセルは、21日間の投薬サイクルの約1日目に対象又は対象集団に投与される。いくつかの実施形態では、nab-パクリタキセル(ABRAXANE(登録商標))を、3週間ごとに対象又は対象集団に投与する。いくつかの実施形態では、nab-パクリタキセル(ABRAXANE(登録商標))は、21日間の投薬サイクルの約1日目に対象又は対象集団に投与される。
In some embodiments, the taxane (eg, paclitaxel or nab-paclitaxel (ABRAXANE®)) is administered intravenously (eg, infusion over 3 hours) to the subject or population of subjects. In some embodiments, the taxane is administered to the subject or subject population every three weeks. In some embodiments, the taxane is administered at about day 1 (e.g., day −3, day −2, day −1,
代謝拮抗剤
いくつかの例では、本明細書に記載の方法の一部として投与される代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は、10~10000mg/m2(例えば20~8000mg/m2、30~5000mg/m2、40~2500mg/m2、50~2000mg/m2、100~1500mg/m2、又は400~1200mg/m2、例えば約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、約1000mg/m2、約1100mg/m2、約1200mg/m2、約1250mg/m2、約1300mg/m2、約1400mg/m2、約1500mg/m2、約1750mg/m2、約2000mg/m2、約3000mg/m2、約4000mg/m2、約5000mg/m2、約6000mg/m2、約7000mg/m2、約8000mg/m2、約9000mg/m2、又は約10000mg/m2)である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は、約500mg/m2と約1250mg/m2の間(例えば20mg/m2、30mg/m2、40mg/m2、50mg/m2、60mg/m2、70mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、180mg/m2、190mg/m2、200mg/m2、250mg/m2、300mg/m2、400mg/m2、500mg/m2、600mg/m2、700mg/m2、800mg/m2、900mg/m2、1000mg/m2、1100mg/m2、1200mg/m2、1250mg/m2、1300mg/m2、1400mg/m2、1500mg/m2、1750mg/m2、2000mg/m2、3000mg/m2、4000mg/m2、5000mg/m2、6000mg/m2、7000mg/m2、8000mg/m2、9000mg/m2、又は10000mg/m2)である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は約500mg/m2である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は約1000mg/m2である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は約1250mg/m2である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は500mg/m2である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は1000mg/m2である。いくつかの例では、代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は1250mg/m2である。
Antimetabolites In some examples, an effective amount of an antimetabolite (eg, pemetrexed or gemcitabine) administered as part of the methods described herein is 10-10000 mg/m 2 (eg, 20-8000 mg/m2). m 2 , 30-5000 mg/m 2 , 40-2500 mg/m 2 , 50-2000 mg/m 2 , 100-1500 mg/m 2 , or 400-1200 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/ m2 , about 50 mg/ m2 , about 60 mg/ m2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/ m2 , about 100 mg/ m2 , about 110 mg/ m2 , about 120 mg/ m2 , about 130 mg/ m2 , about 140 mg/ m2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/ m2 , about 180 mg/ m2 , about 190 mg/ m2 , about 200 mg / m2 , about 250 mg/ m2 , about 300 mg/ m2 , about 400 mg/m2, about 500 mg/ m2 , about 600 mg/ m2 , about 700 mg/ m2 , about 800 mg/m2 , about 900 mg/m 2 , about 1000 mg/ m2 , about 1100 mg/ m2 , about 1200 mg/m2, about 1250 mg/ m2 , about 1300 mg/ m2 , about 1400 mg/ m2 , about 1500 mg/ m2 , about 1750 mg/ m2 , about 2000 mg/ m2 , about 3000 mg/ m2 , about 4000 mg/ m2 , about 5000 mg/ m2 , about 6000 mg/ m2 , about 7000 mg/ m2 , about 8000 mg/ m2 , about 9000 mg/ m2 , or about 10000 mg/m 2 ). In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is between about 500 mg/m 2 and about 1250 mg/m 2 (eg, 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 ) . , 50 mg/ m2 , 60 mg/ m2 , 70 mg/ m2 , 80 mg/m2, 90 mg/ m2 , 100 mg/ m2 , 110 mg/ m2 , 120 mg/ m2 , 130 mg/ m2 , 140 mg/ m2 , 150 mg/m 2 , 160 mg/m 2 , 170 mg/m 2 , 180 mg/m 2 , 190 mg/m 2 , 200 mg/m 2 , 250 mg/m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , 1000 mg/m 2 , 1100 mg/m 2 , 1200 mg/m 2 , 1250 mg/m 2 , 1300 mg/m 2 , 1400 mg/m 2 , 1500 mg/ m2 , 1750 mg/ m2 , 2000 mg/ m2 , 3000 mg/ m2 , 4000 mg/ m2 , 5000 mg/ m2 , 6000 mg/ m2 , 7000 mg/ m2 , 8000 mg/ m2 , 9000 mg/ m2 , or 10000 mg/m 2 ). In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 500 mg/m 2 . In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 1000 mg/m 2 . In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is about 1250 mg/m 2 . In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 500 mg/m 2 . In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 1000 mg/m 2 . In some examples, the effective amount of the antimetabolite (eg, pemetrexed or gemcitabine) is 1250 mg/m 2 .
いくつかの例では、本明細書に記載の方法の一部として投与されるパクリタキセルの有効量は、10~1000mg/m2(例えば、20~900mg/m2、30~800mg/m2、40~700mg/m2、50~650mg/m2、100~600mg/m2、又は200~550mg/m2、例えば、約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、又は約1000mg/m2)である。いくつかの例では、ペメトレキセドの有効量は約500mg/m2である。いくつかの例では、ペメトレキセドの有効量は3週間ごとに約500mg/m2である。いくつかの例では、ペメトレキセドの有効量は500mg/m2である。いくつかの例では、ペメトレキセドの有効量は3週間ごとに500mg/m2である。 In some examples, the effective amount of paclitaxel administered as part of the methods described herein is 10-1000 mg/m 2 (eg, 20-900 mg/m 2 , 30-800 mg/m 2 , 40 ~700 mg/ m2 , 50-650 mg / m2 , 100-600 mg/m2, or 200-550 mg/ m2 , such as about 20 mg/ m2 , about 30 mg/ m2 , about 40 mg/ m2 , about 50 mg / m2 , about 60 mg/ m2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/m2, about 100 mg /m2, about 110 mg/m2, about 120 mg/m2 , about 130 mg/m 2 , about 140 mg/ m2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/ m2 , about 180 mg/ m2 , about 190 mg/ m2 , about 200 mg/ m2 , about 250 mg/ m2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 ) be. In some examples, the effective amount of pemetrexed is about 500 mg/ m2 . In some examples, the effective amount of pemetrexed is about 500 mg/ m2 every 3 weeks. In some examples, the effective amount of pemetrexed is 500 mg/ m2 . In some examples, the effective amount of pemetrexed is 500 mg/ m2 every 3 weeks.
いくつかの実施形態では、ペメトレキセドは、対象又は対象集団に静脈内(例えば、10分間にわたる注入)投与される。いくつかの実施形態では、ペメトレキセドは、3週間ごとに対象又は対象集団に投与される。いくつかの実施形態では、ペメトレキセドは、21日間の投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に対象又は対象集団に投与される。
In some embodiments, pemetrexed is administered intravenously (eg, infusion over 10 minutes) to a subject or population of subjects. In some embodiments, pemetrexed is administered to the subject or subject population every three weeks. In some embodiments, pemetrexed is administered at about day 1 (eg, day −3, day −2, day −1,
いくつかの例では、本明細書に記載の方法の一部として投与される代謝拮抗剤(例えば、ペメトレキセド又はゲムシタビン)の有効量は、10~10000mg/m2(例えば20~8000mg/m2、30~5000mg/m2、40~2500mg/m2、50~2000mg/m2、100~1500mg/m2、又は400~1250mg/m2、例えば約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、約1000mg/m2、約1100mg/m2、約1200mg/m2、約1250mg/m2、約1300mg/m2、約1400mg/m2、約1500mg/m2、約1750mg/m2、約2000mg/m2、約3000mg/m2、約4000mg/m2、約5000mg/m2、約6000mg/m2、約7000mg/m2、約8000mg/m2、約9000mg/m2、又は約10000mg/m2(例えば20mg/m2、30mg/m2、40mg/m2、50mg/m2、60mg/m2、70mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、180mg/m2、190mg/m2、200mg/m2、250mg/m2、300mg/m2、400mg/m2、500mg/m2、600mg/m2、700mg/m2、800mg/m2、900mg/m2、1000mg/m2、1100mg/m2、1200mg/m2、1250mg/m2、1300mg/m2、1400mg/m2、1500mg/m2、1750mg/m2、2000mg/m2、3000mg/m2、4000mg/m2、5000mg/m2、6000mg/m2、7000mg/m2、8000mg/m2、9000mg/m2、又は10000mg/m2))である。いくつかの例では、ゲムシタビンの有効量は、約500mg/m2と約1250mg/m2の間である。いくつかの例では、ゲムシタビンの有効量は、約500mg/m2である。いくつかの例では、ゲムシタビンの有効量は、約1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、カルボプラチンの前に与えられる場合、約1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、約1250mg/m2である。いくつかの例では、ゲムシタビンの有効量は、シスプラチンの前に与えられる場合、約1250mg/m2である。いくつかの例では、ゲムシタビンの有効量は、21日間投薬サイクルの第1日目及び第8日目において約1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、21日間投薬サイクルの第1日目及び第8日目において約1250mg/m2である。いくつかの例では、ゲムシタビンの有効量は、1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、カルボプラチンの前に与えられる場合、1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、1250mg/m2である。いくつかの例では、シスプラチンの前に投与する場合、ゲムシタビンの有効量は1250mg/m2である。いくつかの例では、ゲムシタビンの有効量は、21日間投薬サイクルの第1日目及び第8日目において1000mg/m2である。いくつかの例では、ゲムシタビンの有効量は、21日間投薬サイクルの第1日目及び第8日目において1250mg/m2である。
In some examples, the effective amount of an antimetabolite (eg, pemetrexed or gemcitabine) administered as part of the methods described herein is 10-10000 mg/m 2 (eg, 20-8000 mg/m 2 , 30-5000 mg/m 2 , 40-2500 mg/m 2 , 50-2000 mg/m 2 , 100-1500 mg/m 2 , or 400-1250 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/ m2 , about 50 mg/ m2 , about 60 mg/ m2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/ m2 , about 100 mg/ m2 , about 110 mg/ m2 , about 120 mg/m2 m2 , about 130 mg/ m2 , about 140 mg/ m2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/ m2 , about 180 mg/ m2 , about 190 mg/ m2 , about 200 mg/ m2 , about 250 mg/m 2 , about 300 mg/m 2 , about 400 mg/m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , about 1000 mg/ m2 , about 1100 mg/ m2 , about 1200 mg/ m2 , about 1250 mg/m2, about 1300 mg/ m2 , about 1400 mg/ m2 , about 1500 mg/ m2 , about 1750 mg/ m2 , about 2000 mg/ m2 m2 , about 3000 mg/ m2 , about 4000 mg/ m2 , about 5000 mg/ m2 , about 6000 mg/ m2 , about 7000 mg/ m2 , about 8000 mg/ m2 , about 9000 mg/ m2 , or about 10000 mg/m2 2 (e.g. 20 mg/m 2 , 30 mg/m 2 , 40 mg/m 2 , 50 mg/m 2 , 60 mg/m 2 , 70 mg/m 2 , 80 mg/m 2 , 90 mg/m 2 , 100 mg/m 2 , 110 mg/m 2 ) m2 , 120 mg/ m2 , 130 mg/ m2 , 140 mg/m2, 150 mg/ m2 , 160 mg/ m2 , 170 mg/ m2 , 180 mg/ m2 , 190 mg/ m2 , 200 mg/ m2 , 250 mg/ m2 m 2 , 300 mg/m 2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 9 00 mg/m 2 , 1000 mg/m 2 , 1100 mg/m 2 , 1200 mg/m 2 , 1250 mg/m 2 , 1300 mg/m 2 , 1400 mg/m 2 , 1500 mg/m 2 , 1750 mg/m 2 , 2000 mg/m 2 , 3000 mg/ m2 , 4000 mg/ m2 , 5000 mg/ m2 , 6000 mg/ m2 , 7000 mg/ m2 , 8000 mg/ m2 , 9000 mg/ m2 , or 10000 mg/ m2 )). In some examples, the effective amount of gemcitabine is between about 500 mg/m 2 and about 1250 mg/m 2 . In some examples, the effective amount of gemcitabine is about 500 mg/ m2 . In some examples, the effective amount of gemcitabine is about 1000 mg/ m2 . In some examples, the effective amount of gemcitabine is about 1000 mg/m 2 when given before carboplatin. In some examples, the effective amount of gemcitabine is about 1250 mg/m 2 . In some examples, the effective amount of gemcitabine is about 1250 mg/m 2 when given before cisplatin. In some examples, the effective amount of gemcitabine is about 1000 mg/m 2 on
いくつかの実施形態では、ゲムシタビンは、対象又は対象集団に静脈内(例えば、30分間にわたる注入)投与される。いくつかの例では、ゲムシタビンは、21日間の投薬サイクルの約1日目(例えば、-3日目、-2日目、-1日目、1日目、2日目、又は3日目)に対象又は対象集団に投与される。いくつかの例では、ゲムシタビンは、21日間投薬サイクルの約1日目及び約8日目(例えば、5日目、6日目、7日目、8日目、9日目、10日目、又は11日目)に対象又は対象集団に投与される。
トポイソメラーゼII阻害剤
In some embodiments, gemcitabine is administered intravenously (eg, infused over 30 minutes) to a subject or population of subjects. In some examples, gemcitabine is administered at about day 1 (e.g., day -3, day -2, day -1,
Topoisomerase II inhibitor
いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、10~1000mg/m2(例えば20~800mg/m2、30~700mg/m2、40~500mg/m2、50~300mg/m2、75~200mg/m2、又は80~150mg/m2、例えば約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、又は約1000mg/m2(例えば20mg/m2、30mg/m2、40mg/m2、50mg/m2、60mg/m2、70mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、180mg/m2、190mg/m2、200mg/m2、250mg/m2、300mg/m2、400mg/m2、500mg/m2、600mg/m2、700mg/m2、800mg/m2、900mg/m2、又は1000mg/m2))である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、約100mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、3週間ごとに1~3日目に約100mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、エトポシド)の有効量は、3週間ごとに1~3日目に100mg/m2である。 In some examples, the effective amount of the topoisomerase II inhibitor (eg, etoposide) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 , 50 ~300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/ m2 , about 100 mg/ m2 , about 110 mg/ m2 , about 120 mg/ m2 , about 130 mg/ m2 , about 140 mg/ m2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/ m2 , about 180 mg/m2, about 190 mg/ m2 , about 200 mg/ m2 , about 250 mg/ m2 , about 300 mg/m2 , about 400 mg /m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 (e.g. 20 mg/m 2 , 30 mg/m 2 2 , 40 mg/ m2 , 50 mg/ m2 , 60 mg/ m2 , 70 mg/m2, 80 mg/ m2 , 90 mg/ m2 , 100 mg/ m2 , 110 mg/ m2 , 120 mg/ m2 , 130 mg/m2 2 , 140 mg/ m2 , 150 mg/ m2 , 160 mg/m2, 170 mg/ m2 , 180 mg/ m2 , 190 mg/ m2 , 200 mg/ m2 , 250 mg /m2 , 300 mg/ m2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , or 1000 mg/m 2 )). In some examples, an effective amount of topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 . In some examples, the effective amount of a topoisomerase II inhibitor (eg, etoposide) is about 100 mg/m 2 on days 1-3 every 3 weeks. In some examples, the effective amount of a topoisomerase II inhibitor (eg, etoposide) is 100 mg/m 2 on days 1-3 every 3 weeks.
いくつかの実施形態では、トポイソメラーゼII阻害剤(例えば、エトポシド)は、対象に静脈内(例えば、60分間にわたる注入)投与される。 In some embodiments, the topoisomerase II inhibitor (eg, etoposide) is administered to the subject intravenously (eg, infusion over 60 minutes).
いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の有効量は、10~1000mg/m2(例えば20~800mg/m2、30~700mg/m2、40~500mg/m2、50~300mg/m2、75~200mg/m2、又は80~150mg/m2、例えば約20mg/m2、約30mg/m2、約40mg/m2、約50mg/m2、約60mg/m2、約70mg/m2、約80mg/m2、約90mg/m2、約100mg/m2、約110mg/m2、約120mg/m2、約130mg/m2、約140mg/m2、約150mg/m2、約160mg/m2、約170mg/m2、約180mg/m2、約190mg/m2、約200mg/m2、約250mg/m2、約300mg/m2、約400mg/m2、約500mg/m2、約600mg/m2、約700mg/m2、約800mg/m2、約900mg/m2、又は約1000mg/m2(例えば20mg/m2、30mg/m2、40mg/m2、50mg/m2、60mg/m2、70mg/m2、80mg/m2、90mg/m2、100mg/m2、110mg/m2、120mg/m2、130mg/m2、140mg/m2、150mg/m2、160mg/m2、170mg/m2、180mg/m2、190mg/m2、200mg/m2、250mg/m2、300mg/m2、400mg/m2、500mg/m2、600mg/m2、700mg/m2、800mg/m2、900mg/m2、又は1000mg/m2))である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の有効量は、約60mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の有効量は、60mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の有効量は、約100mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の有効量は、100mg/m2である。いくつかの例では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)の用量は、毒性を回避するために減少又は遅延される。 In some examples, an effective amount of a topoisomerase II inhibitor (eg, doxorubicin) is 10-1000 mg/m 2 (eg, 20-800 mg/m 2 , 30-700 mg/m 2 , 40-500 mg/m 2 , 50 ~300 mg/m 2 , 75-200 mg/m 2 , or 80-150 mg/m 2 , such as about 20 mg/m 2 , about 30 mg/m 2 , about 40 mg/m 2 , about 50 mg/m 2 , about 60 mg/m 2 , about 70 mg/ m2 , about 80 mg/ m2 , about 90 mg/ m2 , about 100 mg/ m2 , about 110 mg/ m2 , about 120 mg/ m2 , about 130 mg/ m2 , about 140 mg/ m2 , about 150 mg/ m2 , about 160 mg/ m2 , about 170 mg/ m2 , about 180 mg/m2, about 190 mg/ m2 , about 200 mg/ m2 , about 250 mg/ m2 , about 300 mg/m2 , about 400 mg /m 2 , about 500 mg/m 2 , about 600 mg/m 2 , about 700 mg/m 2 , about 800 mg/m 2 , about 900 mg/m 2 , or about 1000 mg/m 2 (e.g. 20 mg/m 2 , 30 mg/m 2 2 , 40 mg/ m2 , 50 mg/ m2 , 60 mg/ m2 , 70 mg/m2, 80 mg/ m2 , 90 mg/ m2 , 100 mg/ m2 , 110 mg/ m2 , 120 mg/ m2 , 130 mg/m2 2 , 140 mg/ m2 , 150 mg/ m2 , 160 mg/m2, 170 mg/ m2 , 180 mg/ m2 , 190 mg/ m2 , 200 mg/ m2 , 250 mg /m2 , 300 mg/ m2 , 400 mg/m 2 , 500 mg/m 2 , 600 mg/m 2 , 700 mg/m 2 , 800 mg/m 2 , 900 mg/m 2 , or 1000 mg/m 2 )). In some examples, the effective amount of topoisomerase II inhibitor (eg, doxorubicin) is about 60 mg/m 2 . In some examples, the effective amount of topoisomerase II inhibitor (eg, doxorubicin) is 60 mg/m 2 . In some examples, an effective amount of topoisomerase II inhibitor (eg, doxorubicin) is about 100 mg/m 2 . In some examples, the effective amount of topoisomerase II inhibitor (eg, doxorubicin) is 100 mg/m 2 . In some instances, the dose of the topoisomerase II inhibitor (eg, doxorubicin) is reduced or delayed to avoid toxicity.
いくつかの実施形態では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)は、毎週、2週間ごと、3週間ごと、4週間ごと、各21日間のサイクルの第1、8及び15日目、又は各28日間のサイクルの第1、8及び15日目に投与され得る。いくつかの実施形態では、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)は、2週間ごとに投与され得る。
In some embodiments, the topoisomerase II inhibitor (e.g., doxorubicin) is administered weekly, every two weeks, every three weeks, every four weeks, on
いくつかの実施形態では、アルキル化剤(例えば、シクロホスファミド)は、3~5分にわたってIVボーラスとして対象に投与される。いくつかの実施形態では、アルキル化剤(例えば、シクロホスファミド)は、15~30分間にわたってIV注入として投与される。いくつかの実施形態では、トポイソメラーゼII阻害剤(例えば、ドキソルビシン)は、対象に静脈内(例えば、60分間にわたる注入)投与される。 In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject as an IV bolus over 3-5 minutes. In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered as an IV infusion over 15-30 minutes. In some embodiments, the topoisomerase II inhibitor (eg, doxorubicin) is administered to the subject intravenously (eg, infusion over 60 minutes).
アルキル化剤
ヒトに投与されるアルキル化剤(例えば、シクロホスファミド)の治療有効量は、1回以上の投与によるかどうかにかかわらず、約400~約800mg/m2(例えば約400mg/m2、約425mg/m2、約450mg/m2、約475mg/m2、約500mg/m2、約525mg/m2、約550mg/m2、約575mg/m2、約600mg/m2、約625mg/m2、約650mg/m2、約675mg/m2、約700mg/m2、約725mg/m2、約750mg/m2、約775mg/m2、又は約800mg/m2(例えば、400mg/m2、425mg/m2、450mg/m2、475mg/m2、500mg/m2、525mg/m2、550mg/m2、575mg/m2、600mg/m2、625mg/m2、650mg/m2、675mg/m2、700mg/m2、725mg/m2、750mg/m2、775mg/m2、又は800mg/m2))の範囲となる。例えば、いくつかの実施形態では、約600mg/m2のアルキル化剤(例えば、シクロホスファミド)が投与される。いくつかの実施形態では、約600mg/m2のアルキル化剤(例えば、シクロホスファミド)が、2週間ごとに投与される。いくつかの実施形態では、約600mg/m2のシクロホスファミドが投与される。いくつかの実施形態では、約600mg/m2のシクロホスファミドが2週間ごとに投与される。いくつかの実施形態では、600mg/m2のアルキル化剤(例えば、シクロホスファミド)が、2週間ごとに投与される。いくつかの実施形態では、アルキル化剤(例えば、シクロホスファミド)を、毎週、2週間ごと、3週間ごと、4週間ごと、各21日間サイクルの第1、8及び15日目、各28日間サイクルの第1及び22日目、又は各28日間サイクルの第1、8及び15日目に投与することができる。
Alkylating Agents A therapeutically effective amount of an alkylating agent (eg, cyclophosphamide) administered to a human is from about 400 to about 800 mg/m 2 (eg, about 400 mg/m2), whether or not by one or more administrations. m2 , about 425 mg/ m2 , about 450 mg/ m2 , about 475 mg/ m2 , about 500 mg/ m2 , about 525 mg/ m2 , about 550 mg/ m2 , about 575 mg/ m2 , about 600 mg/ m2 , about 625 mg/m 2 , about 650 mg/m 2 , about 675 mg/m 2 , about 700 mg/m 2 , about 725 mg/m 2 , about 750 mg/m 2 , about 775 mg/m 2 , or about 800 mg/m 2 ( For example, 400 mg/m 2 , 425 mg/m 2 , 450 mg/m 2 , 475 mg/m 2 , 500 mg/m 2 , 525 mg/m 2 , 550 mg/m 2 , 575 mg/m 2 , 600 mg/m 2 , 625 mg/m 2) , 650 mg/m 2 , 675 mg/m 2 , 700 mg/m 2 , 725 mg/m 2 , 750 mg/m 2 , 775 mg/m 2 , or 800 mg/m 2 ) . For example, in some embodiments about 600 mg/m 2 of alkylating agent (eg, cyclophosphamide) is administered. In some embodiments, about 600 mg/m 2 of alkylating agent (eg, cyclophosphamide) is administered every two weeks. In some embodiments, about 600 mg/m 2 of cyclophosphamide is administered. In some embodiments, about 600 mg/m 2 of cyclophosphamide is administered every two weeks. In some embodiments, 600 mg/m 2 of alkylating agent (eg, cyclophosphamide) is administered every two weeks. In some embodiments, the alkylating agent (e.g., cyclophosphamide) is administered weekly, every 2 weeks, every 3 weeks, every 4 weeks on
いくつかの実施形態では、アルキル化剤(例えば、シクロホスファミド)は、3~5分にわたってIVボーラスとして対象に投与される。いくつかの実施形態では、アルキル化剤(例えば、シクロホスファミド)は、IV注入として投与される。 In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered to the subject as an IV bolus over 3-5 minutes. In some embodiments, the alkylating agent (eg, cyclophosphamide) is administered as an IV infusion.
コロニー刺激因子の投薬
ヒトに投与されるコロニー刺激因子(CSF)(例えば、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム))の治療有効量は、約1~約100mg の範囲(例えば、約1mg、約2mg、約3mg、約4mg、約5mg、約6mg、約7mg、約8mg、約9mg、約10mg、約15mg、約20mg、約25mg、約30mg、約45mg、約50mg、約60mg、約70mg、約80mg、約90mg、又は約100mg)となる。例えば、いくつかの実施形態では、約6mgが投与される。いくつかの態様では、ヒトに投与されるコロニー刺激因子(CSF)(例えば、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム))の治療有効量は、1~100mgの範囲(例えば、1mg、2mg、3mg、4mg、5mg、6mg、7mg、8mg、9mg、10mg、15mg、20mg、25mg、30mg、45mg、50mg、60mg、70mg、80mg、90mg、又は100mg)となる。いくつかの実施形態では、ペグフィルグラスチム6mgが投与される。いくつかの実施形態では、コロニー刺激因子はペグフィルグラスチムである。いくつかの実施形態では、コロニー刺激因子はフィルグラスチムである。いくつかの実施形態では、約6mgのペグフィルグラスチムが投与される。
Colony Stimulating Factor Dosing A therapeutically effective amount of a colony stimulating factor (CSF) (e.g., G-CSF (e.g., pegfilgrastim or filgrastim) and GM-CSF (e.g., sargramostim)) administered to a human is about 1 to about 100 mg (eg, about 1 mg, about 2 mg, about 3 mg, about 4 mg, about 5 mg, about 6 mg, about 7 mg, about 8 mg, about 9 mg, about 10 mg, about 15 mg, about 20 mg, about 25 mg, about 30 mg, about 45 mg, about 50 mg, about 60 mg, about 70 mg, about 80 mg, about 90 mg, or about 100 mg). For example, in some embodiments about 6 mg is administered. In some aspects, a therapeutically effective amount of colony stimulating factor (CSF) (e.g., G-CSF (e.g., pegfilgrastim or filgrastim) and GM-CSF (e.g., sargramostim)) administered to a human is , in the range of 1-100 mg (e.g., 1 mg, 2 mg, 3 mg, 4 mg, 5 mg, 6 mg, 7 mg, 8 mg, 9 mg, 10 mg, 15 mg, 20 mg, 25 mg, 30 mg, 45 mg, 50 mg, 60 mg, 70 mg, 80 mg, 90 mg, or 100 mg). In some embodiments, 6 mg of pegfilgrastim is administered. In some embodiments, the colony stimulating factor is pegfilgrastim. In some embodiments, the colony stimulating factor is filgrastim. In some embodiments, about 6 mg pegfilgrastim is administered.
ヒトに投与されるコロニー刺激因子(例えば、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム))の治療有効量は、約1~約400mcg/kg/日の範囲(例えば、約1mcg/kg/日、約2mcg/kg/日、約3mcg/kg/日、約4mcg/kg/日、約5mcg/kg/日、約6mcg/kg/日、約7mcg/kg/日、約8mcg/kg/日、約9mcg/kg/日、約10mcg/kg/日、約15mcg/kg/日、約20mcg/kg/日、約25mcg/kg/日、約50mcg/kg/日、約75mcg/kg/日、約100mcg/kg/日、約125mcg/kg/日、約150mcg/kg/日、約175mcg/kg/日、約200mcg/kg/日、約225mcg/kg/日、約250mcg/kg/日、約275mcg/kg/日、約300mcg/kg/日、約325mcg/kg/日、約350mcg/kg/日、約375mcg/kg/日、又は約400mcg/kg/日)となる。例えば、いくつかの実施形態では、約250 mcg/m2/日が投与される。いくつかの実施形態では、ヒトに投与されるコロニー刺激因子(例えば、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム))の治療有効量は、1~400mcg/kg/日の範囲(例えば、1mcg/kg/日、2mcg/kg/日、3mcg/kg/日、4mcg/kg/日、5mcg/kg/日、6mcg/kg/日、7mcg/kg/日、8mcg/kg/日、9mcg/kg/日、10mcg/kg/日、15mcg/kg/日、20mcg/kg/日、25mcg/kg/日、50mcg/kg/日、75mcg/kg/日、100mcg/kg/日、125mcg/kg/日、150mcg/kg/日、175mcg/kg/日、200mcg/kg/日、225mcg/kg/日、250mcg/kg/日、275mcg/kg/日、300mcg/kg/日、325mcg/kg/日、350mcg/kg/日、375mcg/kg/日、又は400mcg/kg/日)となる。例えば、いくつかの実施形態では、250 mcg/m2/日が投与される。いくつかの実施形態では、コロニー刺激因子(例えば、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム))は、皮下注射として投与される。いくつかの実施形態では、コロニー刺激因子はサルグラモスチムである。いくつかの実施形態では、サルグラモスチムは、約250 mcg/m 2/日の用量でヒトに投与される。いくつかの実施形態では、サルグラモスチムは、250 mcg/m 2/日の用量でヒトに投与される。
A therapeutically effective amount of a colony-stimulating factor (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sargramostim)) administered to humans ranges from about 1 to about 400 mcg/kg/kg. daily range (e.g., about 1 mcg/kg/day, about 2 mcg/kg/day, about 3 mcg/kg/day, about 4 mcg/kg/day, about 5 mcg/kg/day, about 6 mcg/kg/day, about 7 mcg /kg/day, about 8 mcg/kg/day, about 9 mcg/kg/day, about 10 mcg/kg/day, about 15 mcg/kg/day, about 20 mcg/kg/day, about 25 mcg/kg/day, about 50 mcg/day kg/day, about 75 mcg/kg/day, about 100 mcg/kg/day, about 125 mcg/kg/day, about 150 mcg/kg/day, about 175 mcg/kg/day, about 200 mcg/kg/day, about 225 mcg/kg /day, about 250 mcg/kg/day, about 275 mcg/kg/day, about 300 mcg/kg/day, about 325 mcg/kg/day, about 350 mcg/kg/day, about 375 mcg/kg/day, or about 400 mcg/kg / day). For example, in some embodiments about 250 mcg/m 2 /day is administered. In some embodiments, the therapeutically effective amount of colony-stimulating factors (e.g., G-CSF (e.g., pegfilgrastim or filgrastim) and GM-CSF (e.g., sargramostim)) administered to humans is 1 ~400 mcg/kg/day range (e.g., 1 mcg/kg/day, 2 mcg/kg/day, 3 mcg/kg/day, 4 mcg/kg/day, 5 mcg/kg/day, 6 mcg/kg/day, 7 mcg/kg /day, 8mcg/kg/day, 9mcg/kg/day, 10mcg/kg/day, 15mcg/kg/day, 20mcg/kg/day, 25mcg/kg/day, 50mcg/kg/day, 75mcg/kg/day , 100 mcg/kg/day, 125 mcg/kg/day, 150 mcg/kg/day, 175 mcg/kg/day, 200 mcg/kg/day, 225 mcg/kg/day, 250 mcg/kg/day, 275 mcg/kg/day, 300 mcg /kg/day, 325 mcg/kg/day, 350 mcg/kg/day, 375 mcg/kg/day, or 400 mcg/kg/day). For example, in some embodiments 250 mcg/m 2 /day is administered. In some embodiments, the colony-stimulating factor (eg, G-CSF (eg, pegfilgrastim or filgrastim) and GM-CSF (eg, sargramostim)) is administered as a subcutaneous injection. In some embodiments, the colony stimulating factor is sargramostim. In some embodiments, sargramostim is administered to humans at a dose of about 250 mcg/
VEGFアンタゴニストの投与
いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごと(例えば、各21日間投薬サイクルの1日目(例えば、1日目±3日目))に、対象の体重の約0.01mg/kgと約50mg/kgの間(例えば、約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約10mg/kgと約20mg/kgの間、例えば約12.5mg/kgと約15mg/kgの間、例えば約15±2mg/kg、約15±1mg/kg、約15±0.5mg/kg、約15±0.2mg/kg、又は約15±0.1mg/kg、例えば約15mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約15mg/kgの間、例えば、約10mg/kgと約15mg/kgの間、例えば、約12.5mg/kgと約15mg/kgの間、例えば、約14mg/kgと約15mg/kgの間、例えば、約15±1mg/kg、例えば、約15±0.5mg/kg、例えば、約15±0.2mg/kg、例えば、約15±0.1mg/kg、例えば、約15mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごとに投与される約15mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごと(例えば、各14日間の投薬サイクルの1日目(例えば、1日目±3日目)、又は各15日間の投薬サイクルの1日目(例えば、1日目±3日目)及び28日目(例えば、15日目±3日目))に対象の体重の約0.01mg/kgと約50mg/kgの間(例えば約0.01mg/kgと約45mg/kgの間、例えば約0.1mg/kgと約40mg/kgの間、例えば約1mg/kgと約35mg/kgの間、例えば約2.5mg/kgと約30mg/kgの間、例えば約5mg/kgと約25mg/kgの間、例えば約7.5mg/kgと約20mg/kgの間、例えば約7.5mg/kgと約15mg/kgの間、例えば約7.5mg/kgと約12.5mg/kgの間、例えば約10±2mg/kg,約10±1mg/kg,約10±0.5mg/kg,約10±0.2mg/kg、又は約10±0.1mg/kg、例えば約10mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに、対象の体重の約0.01mg/kgと約15mg/kgの間(例えば、約0.1mg/kgと約15mg/kgの間、例えば、約0.5mg/kgと約15mg/kgの間、例えば、約1mg/kgと約15mg/kgの間、例えば、約2.5mg/kgと約15mg/kgの間、例えば、約5mg/kgと約15mg/kgの間、例えば、約7.5mg/kgと約12.5mg/kgの間、例えば、約8mg/kgと約12mg/kgの間、例えば、約9mg/kgと約11mg/kgの間、例えば、約9.5mg/kgと約10.5mg/kgの間、例えば、約10±1mg/kg、例えば、約10±0.5mg/kg、例えば、約10±0.2mg/kg、例えば、約10±0.1mg/kg、例えば、約10mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される約10mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される約5mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される約7.5mg/kgの用量である。
Administration of VEGF Antagonist In some examples, an effective amount of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) is administered every three weeks (e.g., on
いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば、0.01mg/kgと45mg/kgの間、例えば、0.1mg/kgと40mg/kgの間、例えば、1mg/kgと35mg/kgの間、例えば、2.5mg/kgと30mg/kgの間、例えば、5mg/kgと25mg/kgの間、例えば、10mg/kgと20mg/kgの間、例えば、12.5mg/kgと15mg/kgの間、例えば、15±2mg/kg、15±1mg/kg、15±0.5mg/kg、15±0.2mg/kg、又は15±0.1mg/kg、例えば、15mg/kg)の用量である。いくつかの例では、EGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごとに対象の体重の0.01mg/kgと15mg/kgの間(例えば0.1mg/kgと15mg/kgの間、例えば0.5mg/kgと15mg/kgの間、例えば1mg/kgと15mg/kgの間、例えば2.5mg/kgと15mg/kgの間、例えば5mg/kgと15mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば10mg/kgと15mg/kgの間、例えば12.5mg/kgと15mg/kgの間、例えば14mg/kgと15mg/kgの間、例えば15±1mg/kg、例えば15±0.5mg/kg、例えば15±0.2mg/kg、例えば15±0.1mg/kg、例えば15mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、3週間ごとに投与される15mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに、対象の体重の0.01mg/kgと50mg/kgの間(例えば0.01mg/kgと45mg/kgの間、例えば0.1mg/kgと40mg/kgの間、例えば1mg/kgと35mg/kgの間、例えば2.5mg/kgと30mg/kgの間、例えば5mg/kgと25mg/kgの間、例えば7.5mg/kgと20mg/kgの間、例えば7.5mg/kgと15mg/kgの間、例えば7.5mg/kgと12.5mg/kgの間、例えば10±2mg/kg、10±1mg/kg、10±0.5mg/kg、10±0.2mg/kg、又は10±0.1mg/kg、例えば10mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに、対象の体重の0.01mg/kgと15mg/kgの間(例えば、0.1mg/kgと15mg/kgの間、例えば、0.5mg/kgと15mg/kgの間、例えば、1mg/kgと15mg/kgの間、例えば、2.5mg/kgと15mg/kgの間、例えば、5mg/kgと15mg/kgの間、例えば、7.5mg/kgと12.5mg/kgの間、例えば、8mg/kgと12mg/kgの間、例えば、9mg/kgと11mg/kgの間、例えば、9.5mg/kgと10.5mg/kgの間、例えば、10±1mg/kg、例えば、10±0.5mg/kg、例えば、10±0.2mg/kg、例えば、10±0.1mg/kg、例えば、10mg/kg)の用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される10mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される5mg/kgの用量である。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の有効量は、2週間ごとに投与される7.5mg/kgの用量である。 In some examples, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is between 0.01 mg/kg and 50 mg/kg of body weight (eg, 0.5 mg/kg) of the subject's body weight every three weeks. between 0.1 mg/kg and 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg; between 5 mg/kg and 25 mg/kg, such as between 10 mg/kg and 20 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as 15±2 mg/kg, 15±1 mg/kg kg, 15±0.5 mg/kg, 15±0.2 mg/kg, or 15±0.1 mg/kg, such as 15 mg/kg). In some examples, the effective amount of the EGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) is between 0.01 mg/kg and 15 mg/kg of body weight of the subject (e.g., 0.1 mg/kg) every three weeks. between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg, such as between 5 mg/kg between 15 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 10 mg/kg and 15 mg/kg, such as between 12.5 mg/kg and 15 mg/kg, such as between 14 mg/kg and 15 mg/kg kg, such as 15±1 mg/kg, such as 15±0.5 mg/kg, such as 15±0.2 mg/kg, such as 15±0.1 mg/kg, such as 15 mg/kg). In some examples, an effective amount of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is a dose of 15 mg/kg administered every 3 weeks. In some examples, the effective amount of the VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) is between 0.01 mg/kg and 50 mg/kg of body weight of the subject (e.g., 0.01 mg/kg) every two weeks. /kg and 45 mg/kg, such as between 0.1 mg/kg and 40 mg/kg, such as between 1 mg/kg and 35 mg/kg, such as between 2.5 mg/kg and 30 mg/kg, such as 5 mg/kg and 25 mg/kg, such as between 7.5 mg/kg and 20 mg/kg, such as between 7.5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 12.5 mg/kg, such as 10 ±2 mg/kg, 10±1 mg/kg, 10±0.5 mg/kg, 10±0.2 mg/kg, or 10±0.1 mg/kg, such as 10 mg/kg). In some examples, the effective amount of the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is between 0.01 mg/kg and 15 mg/kg of body weight of the subject (eg, 0.01 mg/kg) every two weeks. between 1 mg/kg and 15 mg/kg, such as between 0.5 mg/kg and 15 mg/kg, such as between 1 mg/kg and 15 mg/kg, such as between 2.5 mg/kg and 15 mg/kg; between 5 mg/kg and 15 mg/kg, such as between 7.5 mg/kg and 12.5 mg/kg, such as between 8 mg/kg and 12 mg/kg, such as between 9 mg/kg and 11 mg/kg between, such as between 9.5 mg/kg and 10.5 mg/kg, such as 10±1 mg/kg, such as 10±0.5 mg/kg, such as 10±0.2 mg/kg, such as 10± 0.1 mg/kg, eg 10 mg/kg). In some examples, an effective amount of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is a dose of 10 mg/kg administered every two weeks. In some examples, an effective amount of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is a dose of 5 mg/kg administered every two weeks. In some examples, an effective amount of a VEGF antagonist (eg, an anti-VEGF antibody (eg, bevacizumab)) is a dose of 7.5 mg/kg administered every two weeks.
いくつかの例では、併用療法(例えば、抗TIGITアンタゴニスト抗体、例えば本明細書に開示される抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及び/又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ)による併用処置)で投与されるVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))の用量は、単剤療法として投与されるPD-1軸結合アンタゴニストの標準用量と比較して減少し得る。 In some examples, combination therapy (e.g., an anti-TIGIT antagonist antibody, such as an anti-TIGIT antagonist antibody disclosed herein (e.g., tiragolumab) and/or a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist A dose of a VEGF antagonist (e.g., an anti-VEGF antibody (e.g., bevacizumab)) administered with an antibody (e.g., atezolizumab) or co-treatment with an anti-PD-1 antagonist antibody (e.g., pembrolizumab) is administered as monotherapy. may be reduced compared to standard doses of PD-1 axis binding antagonists.
いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を静脈内投与する。いくつかの例では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、90±15分(例えば、約75分、約76分、約77分、約78分、約79分、約80分、約81分、約82分、約83分、約84分、約85分、約86分、約87分、約88分、約89分、約90分、約91分、約92分、約93分、約94分、約95分、約96分、約97分、約98分、約99分、約100分、約101分、約102分、約103分、約104分又は約105分)にわたって静脈内投与される。あるいは、いくつかの実施形態では、VEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))を皮下投与する。 In some examples, the VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered intravenously. In some examples, the VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) is administered for 90±15 minutes (e.g., about 75 minutes, about 76 minutes, about 77 minutes, about 78 minutes, about 79 minutes, about 80 minutes, about 81 minutes, about 82 minutes, about 83 minutes, about 84 minutes, about 85 minutes, about 86 minutes, about 87 minutes, about 88 minutes, about 89 minutes, about 90 minutes, about 91 minutes, about 92 minutes , about 93 minutes, about 94 minutes, about 95 minutes, about 96 minutes, about 97 minutes, about 98 minutes, about 99 minutes, about 100 minutes, about 101 minutes, about 102 minutes, about 103 minutes, about 104 minutes or about 105 min). Alternatively, in some embodiments, a VEGF antagonist (eg, anti-VEGF antibody (eg, bevacizumab)) is administered subcutaneously.
G.PD-L1発現の評定 G. Assessment of PD-L1 expression
PD-L1の発現は、本明細書中記載される使用のための方法、使用及び組成物のいずれかに従って処置される対象において評定され得る。使用のための方法、使用及び組成物は、対象から得られた生物学的試料(例えば、腫瘍試料)中のPD-L1の発現レベルを決定することを含み得る。いくつかの例では、患者は膀胱がんを有し、試料は膀胱腫瘍の経尿道切除(TURBT)試料である。いくつかの例では、試料は膀胱切除術又は腎尿管切除試料である。いくつかの例では、試料は、区域切除、肺葉切除、二葉切除又は肺切除試料である。いくつかの例では、試料はリンパ節郭清術試料である。他の例では、対象から得られた生物学的試料(例えば、腫瘍試料)中のPD-L1の発現レベルは、処置開始前又は処置開始後に決定されている。PD-L1発現は、任意の適切なアプローチを使用して決定され得る。例えば、PD-L1発現は、米国特許出願公開第20180030138号A1及び米国特許出願公開第20180037655号A1に記載されているように決定され得る。任意の適切な腫瘍試料、例えばホルマリン固定パラフィン包埋(FFPE)腫瘍試料、保管腫瘍試料、新鮮腫瘍試料又は凍結腫瘍試料を使用することができる。 PD-L1 expression can be assessed in a subject treated according to any of the methods, uses and compositions for use described herein. Methods, uses and compositions for use can include determining the expression level of PD-L1 in a biological sample (eg, tumor sample) obtained from a subject. In some examples, the patient has bladder cancer and the sample is a transurethral resection of bladder tumor (TURBT) sample. In some examples, the sample is a cystectomy or nephroureterectomy sample. In some examples, the sample is a segmentectomy, lobectomy, bilobectomy, or pneumonectomy sample. In some examples, the sample is a lymphadenectomy sample. In other examples, the level of expression of PD-L1 in a biological sample (eg, tumor sample) obtained from the subject has been determined before treatment or after treatment is initiated. PD-L1 expression can be determined using any suitable approach. For example, PD-L1 expression can be determined as described in US Patent Application Publication No. 20180030138A1 and US Patent Application Publication No. 20180037655A1. Any suitable tumor sample can be used, such as formalin-fixed paraffin-embedded (FFPE) tumor samples, archived tumor samples, fresh or frozen tumor samples.
例えば、PD-L1の発現は、検出可能なPD-L1発現レベルを発現する腫瘍浸潤免疫細胞に含まれる腫瘍試料の割合に関して、検出可能なPD-L1発現レベルを発現する腫瘍試料中の腫瘍浸潤免疫細胞の割合として、及び/又は検出可能なPD-L1発現レベルを発現する腫瘍試料中の腫瘍細胞の割合として決定され得る。前述の例のいずれにおいても、腫瘍浸潤免疫細胞によって構成される腫瘍試料のパーセンテージは、対象から得られた腫瘍試料の切片において、腫瘍浸潤免疫細胞によって覆われる腫瘍領域のパーセンテージ(例えば、抗PD-L1抗体(例えば、SP142抗体)を使用してIHCによって評定されるように)に関してであり得ることが理解されるべきである。例えば、SP142(Ventana)、SP263(Ventana)、22C3(Dako)、28-8(Dako)、E1L3N(Cell Signaling Technology)、4059(ProSci,Inc.)、h5H1(Advanced Cell Diagnostics)及び9A11を含む任意の適切な抗PD-L1抗体を使用することができる。いくつかの例では、抗PD-L1抗体はSP142である。他の例では、抗PD-L1抗体はSP263である。いくつかの例では、抗PD-L1抗体は22C3である。いくつかの例では、抗PD-L1抗体は28-8である。 For example, the expression of PD-L1 is relative to the percentage of tumor samples that are comprised of tumor-infiltrating immune cells that express detectable levels of PD-L1 expression, relative to tumor infiltration in tumor samples that express detectable levels of PD-L1 expression. It can be determined as a percentage of immune cells and/or as a percentage of tumor cells in a tumor sample that express a detectable level of PD-L1 expression. In any of the foregoing examples, the percentage of the tumor sample composed of tumor-infiltrating immune cells is the percentage of the tumor area covered by tumor-infiltrating immune cells (e.g., anti-PD- immune cells) in a section of the tumor sample obtained from the subject. as assessed by IHC using the L1 antibody (eg, the SP142 antibody). Any including, for example, SP142 (Ventana), SP263 (Ventana), 22C3 (Dako), 28-8 (Dako), E1L3N (Cell Signaling Technology), 4059 (ProSci, Inc.), h5H1 (Advanced Cell Diagnostics) and 9A11 of suitable anti-PD-L1 antibodies can be used. In some examples, the anti-PD-L1 antibody is SP142. In another example, the anti-PD-L1 antibody is SP263. In some examples, the anti-PD-L1 antibody is 22C3. In some examples, the anti-PD-L1 antibody is 28-8.
いくつかの例では、対象から得られる腫瘍試料は、腫瘍試料中の1%未満の腫瘍細胞、腫瘍試料中の1%以上の腫瘍細胞、腫瘍試料中の1%~5%未満の腫瘍細胞、腫瘍試料中の5%以上の腫瘍細胞、腫瘍試料中の5%~50%未満の腫瘍細胞又は腫瘍試料中の50%以上の腫瘍細胞において、検出可能なPD-L1発現レベルを有する。 In some examples, the tumor sample obtained from the subject has less than 1% tumor cells in the tumor sample, 1% or more tumor cells in the tumor sample, 1% to less than 5% tumor cells in the tumor sample, 5% or more of the tumor cells in the tumor sample, 5% to less than 50% of the tumor cells in the tumor sample, or 50% or more of the tumor cells in the tumor sample have detectable levels of PD-L1 expression.
いくつかの例では、対象から得られた腫瘍試料は、腫瘍試料の1%未満、腫瘍試料の1%超、腫瘍試料の1%~5%未満、腫瘍試料の5%超、腫瘍試料の5%~10%未満、又は腫瘍試料の10%超を構成する腫瘍浸潤免疫細胞中の検出可能なPD-L1発現レベルを有する。 In some examples, the tumor samples obtained from the subject are less than 1% of the tumor samples, more than 1% of the tumor samples, 1% to less than 5% of the tumor samples, more than 5% of the tumor samples, 5 of the tumor samples % to less than 10%, or greater than 10% of tumor samples with detectable PD-L1 expression levels in tumor-infiltrating immune cells.
いくつかの態様では、対象から得られる腫瘍試料は、腫瘍試料の5%~19%(例えば、TIC5%~19%)を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有し、例えば、PD-L1低であるPD-L1発現レベルを有する。いくつかの態様では、対象から得られる腫瘍試料は、腫瘍試料の≧20%(例えば、TIC≧20%)を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有し、例えば、PD-L1高であるPD-L1発現レベルを有する。いくつかの実施形態では、5%以上のTICを有すると判定された腫瘍試料は、1以上のCPSに匹敵する。
In some aspects, the tumor sample obtained from the subject has a detectable PD-L1 expression level in tumor-infiltrating immune cells that constitute 5%-19% (e.g.,
いくつかの例では、腫瘍試料は、表1及び/又は表2にそれぞれ示される診断評定のための基準に従って、腫瘍浸潤免疫細胞及び/又は腫瘍細胞におけるPD-L1陽性についてスコア化され得る。


いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象はPD-L1選択腫瘍(例えば、PD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合は、SP 142抗体を用いたIHCによって決定される場合、腫瘍試料において5%以上である)を有する。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって、PD-L1発現免疫細胞(IC)が占める腫瘍面積の割合が5%以上であると判定された腫瘍である。いくつかの例では、IHCアッセイは、抗PD-L1抗体SP142、SP263、22C3又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、IHCアッセイは、抗PD-L1抗体28-8を使用する。 In some examples, in any of the methods, uses or compositions for use described herein, the subject has a PD-L1-selected tumor (e.g., PD-L1-expressing tumor-infiltrating immune cells (ICs) The percentage of tumor area occupied is greater than or equal to 5% in tumor samples as determined by IHC using the SP 142 antibody. In some examples, a PD-L1-selected tumor is a tumor that has 5% or more of the tumor area occupied by PD-L1-expressing immune cells (ICs) as determined by an immunohistochemistry (IHC) assay. . In some examples, the IHC assay uses anti-PD-L1 antibodies SP142, SP263, 22C3 or 28-8. In some examples, the IHC assay uses the anti-PD-L1 antibody SP142. In some examples, the IHC assay uses the anti-PD-L1 antibody SP263. In some examples, the IHC assay uses the anti-PD-L1 antibody 22C3. In some examples, the IHC assay uses the anti-PD-L1 antibody 22C3. In some examples, the IHC assay uses the anti-PD-L1 antibody 28-8.
いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)5%以上であると判定されている。いくつかの例では、ICスコアは(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)2又は3であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)10%以上であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上50%未満であると判定されている。いくつかの例では、ICは、(例えば、Ventana(SP142)PD-L1 IHCアッセイを用いて決定した場合)1%以上30%未満であると判定されている。 In some examples, the IC has been determined to be 5% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some instances, the IC score has been determined to be 2 or 3 (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some instances, the IC has been determined to be 1% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some instances, the IC has been determined to be 10% or greater (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, the IC has been determined to be greater than or equal to 1% and less than 50% (eg, as determined using the Ventana (SP142) PD-L1 IHC assay). In some examples, the IC has been determined to be greater than or equal to 1% and less than 30% (eg, as determined using the Ventana (SP142) PD-L1 IHC assay).
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1タンパク質発現レベルを有する。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、IHCアッセイによって決定されたものである。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、腫瘍試料は、腫瘍試料の5%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上5%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の5%以上10%未満を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の10%以上を構成する腫瘍浸潤免疫細胞において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の1%以上5%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の5%以上50%未満において検出可能なPD-L1発現レベルを有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料中の腫瘍細胞の50%以上において検出可能なPD-L1発現レベルを有すると判定されている。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 protein expression level. In some examples, the detectable PD-L1 protein expression level was determined by an IHC assay. In some examples, the IHC assay uses the anti-PD-L1 antibody SP142. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 5% or more of the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 1% or more and less than 5% of the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 5% or more and less than 10% of the tumor sample. In some instances, the tumor sample has been determined to have detectable PD-L1 expression levels in tumor-infiltrating immune cells that constitute 10% or more of the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 1% or more and less than 5% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have a detectable PD-L1 expression level in 5% or more and less than 50% of the tumor cells in the tumor sample. In some examples, the tumor sample has been determined to have detectable PD-L1 expression levels in 50% or more of the tumor cells in the tumor sample.
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、PD-L1選択腫瘍(例えば、PD-L1高(例えば、SP 263抗体を用いたIHCによって決定される腫瘍試料中の50%以上のPD-L1腫瘍割合スコア(TPS))を有する。いくつかの例では、PD-L1選択腫瘍はPD-L1高選択腫瘍である。いくつかの例では、PD-L1選択腫瘍は、免疫組織化学(IHC)アッセイによって50%以上のTPSを有すると判定された腫瘍である。いくつかの例では、IHCアッセイは、抗PD-L1抗体SP263、SP142、22C3又は28-8を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体SP142を使用する。いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、TPSは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを用いて決定した場合)50%以上であると判定されている。いくつかの例では、TPSは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを用いて決定した場合)50%未満であると判定されている。いくつかの例では、TPSは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを用いて決定した場合)1%以上であると判定されている。いくつかの例では、TPSは、(例えば、Ventana(SP263)PD-L1 IHCアッセイを用いて決定した場合)1%以上50%未満であると判定されている。
In some examples, in any of the methods, uses or compositions for use described herein, the subject has a PD-L1-selected tumor (e.g., PD-L1 high (e.g.,
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1タンパク質発現レベルを有する。いくつかの例では、検出可能なPD-L1タンパク質発現レベルは、IHCアッセイによって決定されたものである。いくつかの例では、IHCアッセイは抗PD-L1抗体SP263を使用する。いくつかの例では、腫瘍試料は、腫瘍試料の50%以上のPD-L1陽性腫瘍細胞分率を有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の50%未満のPD-L1陽性腫瘍細胞分率を有すると判定されている。いくつかの例では、腫瘍試料は、腫瘍試料の1%以上50%未満のPD-L1陽性腫瘍細胞分率を有すると判定されている。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 protein expression level. In some examples, the detectable PD-L1 protein expression level was determined by an IHC assay. In some examples, the IHC assay uses the anti-PD-L1 antibody SP263. In some examples, the tumor sample has been determined to have a PD-L1 positive tumor cell fraction of 50% or greater of the tumor sample. In some examples, the tumor sample has been determined to have a PD-L1 positive tumor cell fraction of less than 50% of the tumor sample. In some examples, the tumor sample has been determined to have a PD-L1 positive tumor cell fraction of greater than or equal to 1% and less than 50% of the tumor sample.
いくつかの例では、IHCアッセイは抗PD-L1抗体22C3を使用する。いくつかの例では、IHCアッセイはpharmDx 22C3 IHCアッセイである。いくつかの例では、PD-L1陽性腫瘍細胞分率は、抗PD-L1抗体22C3による陽性染色によって決定される場合、50%以上である。いくつかの実施形態では、腫瘍試料は、例えばpharmDx 22C3 IHCアッセイの一部として抗PD-L1抗2体2C3を使用して決定される場合、腫瘍試料において10以上の複合陽性スコア(CPS)又は1%以上の腫瘍割合スコア(TPS)を有すると判定されている。いくつかの実施形態では、腫瘍試料は、例えばpharmDx 22C3 IHCアッセイの一部として抗PD-L1抗体22 C 3を使用して決定されるように、腫瘍試料中に10以上のCPS又は1%以上50%未満のTPSを有すると判定されている。いくつかの実施形態では、腫瘍試料は、例えばpharmDx 22C3 IHCアッセイの一部として抗PD-L1抗体22C3を使用して決定されるように、腫瘍試料において20以上のCPS又は50%以上のTPSを有すると判定されている。いくつかの実施形態では、1以上のCPSを有すると判定された腫瘍試料は、5%以上のTICに匹敵する。 In some examples, the IHC assay uses the anti-PD-L1 antibody 22C3. In some examples, the IHC assay is the pharmDx 22C3 IHC assay. In some examples, the PD-L1 positive tumor cell fraction is greater than or equal to 50% as determined by positive staining with the anti-PD-L1 antibody 22C3. In some embodiments, the tumor sample has a composite positive score (CPS) of 10 or greater in the tumor sample, eg, as determined using the anti-PD-L1 anti-2 body 2C3 as part of the pharmDx 22C3 IHC assay, or Determined to have a Tumor Proportion Score (TPS) of 1% or greater. In some embodiments, the tumor sample has 10 or more CPS or 1% or more in the tumor sample, eg, as determined using the anti-PD-L1 antibody 22C3 as part of the pharmDx 22C3 IHC assay. It has been determined to have a TPS of less than 50%. In some embodiments, the tumor sample exhibits 20 or more CPS or 50% or more TPS in the tumor sample, eg, as determined using the anti-PD-L1 antibody 22C3 as part of the pharmDx 22C3 IHC assay. determined to have In some embodiments, a tumor sample determined to have 1 or more CPS corresponds to a TIC of 5% or more.
いくつかの例では、IHCアッセイは、抗PD-L1抗体28-8を使用する。いくつかの例では、IHCアッセイはpharmDx 28-8 IHCアッセイである。いくつかの例では、PD-L1陽性腫瘍細胞分率は、抗PD-L1抗体28-8による陽性染色によって判定される場合、50%以上である。 In some examples, the IHC assay uses the anti-PD-L1 antibody 28-8. In some examples, the IHC assay is the pharmDx 28-8 IHC assay. In some examples, the PD-L1 positive tumor cell fraction is greater than or equal to 50% as determined by positive staining with anti-PD-L1 antibody 28-8.
いくつかの例では、本明細書に記載される方法、使用、又は、使用のための組成物のいずれかにおいて、個体から得られる腫瘍試料は、検出可能なPD-L1核酸発現レベルを有する。いくつかの例では、検出可能なPD-L1核酸発現レベルは、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている。いくつかの例では、試料は、組織試料、全血試料、血清試料及び血漿試料からなる群から選択される。いくつかの例では、組織試料は、腫瘍試料である。いくつかの例では、腫瘍試料は、腫瘍浸潤免疫細胞、腫瘍細胞、間質細胞、及びこれらの任意の組合せを含む。 In some examples, in any of the methods, uses, or compositions for use described herein, the tumor sample obtained from the individual has a detectable PD-L1 nucleic acid expression level. In some examples, the detectable PD-L1 nucleic acid expression level is determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or combinations thereof. has been decided. In some examples, the sample is selected from the group consisting of tissue samples, whole blood samples, serum samples and plasma samples. In some examples, the tissue sample is a tumor sample. In some examples, the tumor sample comprises tumor-infiltrating immune cells, tumor cells, stromal cells, and any combination thereof.
H.TIGIT発現の評定
TIGITの発現は、本明細書中記載される使用のための方法、使用及び組成物のいずれかに従って処置される対象において評定され得る。使用のための方法、使用及び組成物は、対象から得られた生物学的試料(例えば、腫瘍試料)中のTIGITの発現レベルを決定することを含み得る。他の例では、対象から得られた生物学的試料(例えば、腫瘍試料)中のTIGITの発現レベルは、処置開始前又は処置開始後に決定されている。TIGIT発現は、任意の適切なアプローチを使用して決定され得る。任意の適切な腫瘍試料、例えばホルマリン固定パラフィン包埋(FFPE)腫瘍試料、保管腫瘍試料、新鮮腫瘍試料又は凍結腫瘍試料を使用することができる。
H. Assessing TIGIT Expression Expression of TIGIT can be assessed in subjects treated according to any of the methods, uses and compositions for use described herein. Methods, uses and compositions for use can include determining the expression level of TIGIT in a biological sample (eg, tumor sample) obtained from a subject. In other examples, the level of expression of TIGIT in a biological sample (eg, tumor sample) obtained from the subject has been determined prior to or after treatment initiation. TIGIT expression can be determined using any suitable approach. Any suitable tumor sample can be used, such as formalin-fixed paraffin-embedded (FFPE) tumor samples, archived tumor samples, fresh or frozen tumor samples.
例えば、TIGITの発現は、TIGITの検出可能な発現レベルを発現する腫瘍浸潤免疫細胞に含まれる腫瘍試料の割合に関して、TIGITの検出可能な発現レベルを発現する腫瘍試料中の腫瘍浸潤免疫細胞の割合として、及び/又はTIGITの検出可能な発現レベルを発現する腫瘍試料中の腫瘍細胞の割合として決定され得る。前述の例のいずれかにおいて、腫瘍浸潤免疫細胞によって構成される腫瘍試料の割合は、例えば、抗TIGITアンタゴニスト抗体を使用してIHCによって評定される場合、対象から得られた腫瘍試料の切片中の腫瘍浸潤免疫細胞によって覆われた腫瘍面積の割合に関してであり得ることが理解されるべきである。任意の適切な抗TIGITアンタゴニスト抗体を使用することができる。いくつかの例では、抗TIGITアンタゴニスト抗体は10A7(国際公開第2009/126688号A3;米国特許第9,499,596号)である。 For example, the expression of TIGIT can be measured with respect to the percentage of tumor-infiltrating immune cells in a tumor sample that express a detectable expression level of TIGIT, relative to the percentage of tumor-infiltrating immune cells in a tumor sample that express a detectable expression level of TIGIT. and/or as the percentage of tumor cells in a tumor sample that express a detectable expression level of TIGIT. In any of the foregoing examples, the proportion of a tumor sample composed of tumor-infiltrating immune cells, e.g., as assessed by IHC using an anti-TIGIT antagonist antibody, is It should be understood that it may be in terms of the percentage of tumor area covered by tumor-infiltrating immune cells. Any suitable anti-TIGIT antagonist antibody can be used. In some examples, the anti-TIGIT antagonist antibody is 10A7 (WO 2009/126688 A3; US Patent No. 9,499,596).
I.EGFR及びALK異常の評定
いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、上皮成長因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない。いくつかの例では、本明細書中記載される使用のための方法、使用又は組成物のいずれかにおいて、対象は、EGFR遺伝子変異(例えば、感作又は活性化EGFR遺伝子変異)又はALK遺伝子再編成(例えば、ALK融合がん遺伝子)を有しない。いくつかの例では、対象は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンス(PS)を有する。
I. Assessment of EGFR and ALK Abnormalities In some examples, in any of the methods, uses, or compositions for use described herein, the subject has epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations. In some examples, in any of the methods, uses or compositions for use described herein, the subject has an EGFR gene mutation (e.g., a sensitizing or activating EGFR gene mutation) or an ALK gene rearrangement. No organization (eg, ALK fusion oncogene). In some examples, the subject has a US East Coast Clinical Trials Group (ECOG) Performance (PS) of 0 or 1.
突然変異状態EGFR及びALKを検出するための方法は当該技術分野で周知であり、それだけに限らないが、参照によりその全体が本明細書に組み込まれるFrampton et al.(Nature Biotechnology.31(11):1023-1033,2013)に記載されている標的遺伝子プルダウン及び配列決定法等の次世代配列決定法を使用して、臨床試料(例えば、腫瘍生検又は血液試料(例えば、血液中の循環腫瘍DNA))からのDNAを配列決定することが挙げられる。このような次世代配列決定方法は、小試料(例えば、小コア針生検、細針吸引、及び/又はセルブロック由来)又は固定試料(例えば、ホルマリン固定パラフィン包埋(FFPE)試料)の使用を可能にしながら、様々な突然変異(例えば、挿入、欠失、塩基置換、焦点遺伝子増幅、及び/又はホモ接合性遺伝子欠失)を検出する本明細書に開示される方法のいずれかと共に使用することができる。EGFR及びALKの突然変異状態を検出するための他の方法としては、蛍光in situハイブリダイゼーション(FISH)法及び免疫組織化学(IHC)法が挙げられる。ALKの突然変異状態を検出するための例示的な方法は、参照によりその全体が本明細書に組み込まれる米国特許第9,651,555号に開示されている。いくつかの例では、VENTANA(登録商標)抗ALK(D5F3)IHCアッセイを使用して、ALK遺伝子の変異状態を判定する。 Methods for detecting mutational status EGFR and ALK are well known in the art and include, but are not limited to, Frampton et al. (Nature Biotechnology. 31(11): 1023-1033, 2013) using next-generation sequencing methods such as targeted gene pull-down and sequencing methods described in Clinical samples (e.g., tumor biopsies or blood samples). (eg, circulating tumor DNA in blood)). Such next-generation sequencing methods employ the use of small samples (e.g., from small core needle biopsies, fine needle aspirates, and/or cell blocks) or fixed samples (e.g., formalin-fixed paraffin-embedded (FFPE) samples). use with any of the methods disclosed herein to detect various mutations (e.g., insertions, deletions, base substitutions, focal gene amplifications, and/or homozygous gene deletions) while allowing be able to. Other methods for detecting EGFR and ALK mutation status include fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) methods. An exemplary method for detecting the mutational status of ALK is disclosed in US Pat. No. 9,651,555, which is incorporated herein by reference in its entirety. In some examples, the VENTANA® anti-ALK (D5F3) IHC assay is used to determine the mutational status of the ALK gene.
本明細書中記載される方法のいずれかのいくつかの例では、突然変異は感作性EGFR突然変異である。感作性EGFR突然変異は当該技術分野で周知であり、米国特許出願公開第2018/0235968号及びJuan et al.(Therapeutic Advances in Medical Oncology.9(3):201-216,2017)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、感作性EGFR突然変異は、エクソン18~21(例えば、エクソン18、エクソン19、エクソン20及び/又はエクソン21における突然変異)のいずれか一つにおける突然変異である。いくつかの例では、感作性EGFR突然変異は、エクソン19の欠失(del19)である。他の例では、感作性EGFR突然変異は、エクソン21中のL858R点突然変異である。いくつかの例では、感作性EGFR突然変異はエクソン18中のG719X点突然変異であり、「X」は最も一般的にはC、A、又はSである。いくつかの例では、感作性EGFR突然変異は、エクソン18におけるG719S点突然変異である。いくつかの例では、感作性EGFR突然変異は、エクソン18におけるG719A点突然変異である。いくつかの例では、感作性EGFR突然変異は、エクソン18におけるS720F点突然変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861Q点変異である。いくつかの例では、感作EGFR変異は、エクソン21におけるL861R点変異である。他の例では、感作性EGFR突然変異はT790M点突然変異である。いくつかの例では、感作EGFR変異はE709X点変異であり、「X」は最も一般的にはK、A、又はHである。いくつか例では、感作EGFR変異は、S768I点変異である。
In some examples of any of the methods described herein, the mutation is a sensitizing EGFR mutation. Sensitizing EGFR mutations are well known in the art and are described in US Patent Application Publication No. 2018/0235968 and Juan et al. (Therapeutic Advances in Medical Oncology. 9(3):201-216, 2017), which are incorporated herein by reference in their entirety. In some examples, the sensitizing EGFR mutation is a mutation in any one of exons 18-21 (eg, mutations in
本明細書中記載される方法のいずれかのいくつかの例では、突然変異はALK遺伝子再編成である。ALK遺伝子再編成は当該技術分野で周知であり、米国特許第9,651,555号及びDu et al.(Thoracic Cancer.9:423-430,2018)に記載されているものが含まれ、それらの全体が参照により本明細書に組み込まれる。いくつかの例では、ALK遺伝子再構成は、下流のシグナル伝達経路を活性化して細胞増殖及び生存を増加させる発がん性ALKチロシンキナーゼの作製をもたらす。いくつかの例では、ALK遺伝子再編成は、融合がん遺伝子の形成をもたらす、EML4、KIF5B、KLC1、TFG、TPR、HIP1、STRN、DCTN1、SQSTM1、NPM1、BCL11A、BIRC6、RANBP2、ATIC、CLTC、TMP4、及びMSNからなる群から選択される遺伝子によるALK再編成である。いくつかの例では、ALK遺伝子再編成は、ALKとのEML4再編成であり、融合がん遺伝子EML4-ALKの形成をもたらす。 In some examples of any of the methods described herein, the mutation is an ALK gene rearrangement. ALK gene rearrangements are well known in the art and are described in US Pat. No. 9,651,555 and Du et al. (Thoracic Cancer. 9:423-430, 2018), which are incorporated herein by reference in their entireties. In some instances, ALK gene rearrangement results in the creation of an oncogenic ALK tyrosine kinase that activates downstream signaling pathways to increase cell proliferation and survival. In some instances, the ALK gene rearrangement results in the formation of a fusion oncogene, EML4, KIF5B, KLC1, TFG, TPR, HIP1, STRN, DCTN1, SQSTM1, NPM1, BCL11A, BIRC6, RANBP2, ATIC, CLTC , TMP4, and MSN. In some instances, the ALK gene rearrangement is an EML4 rearrangement with ALK, resulting in the formation of the fusion oncogene EML4-ALK.
IV.例示的な抗TIGIT抗アゴニスト抗体、PD-1軸結合アンタゴニスト、及び他の薬剤
本発明の使用のための方法、使用及び組成物に従ってがんを有する対象(例えば、ヒト)を処置するのに有用な例示的な抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、化学療法剤、コロニー刺激因子及びVEGFアンタゴニストが本明細書に記載される。
IV. Exemplary Anti-TIGIT Anti-Agonist Antibodies, PD-1 Axis Binding Antagonists, and Other Agents Useful for Treating Subjects (eg, Humans) Having Cancer According to the Methods, Uses and Compositions for Use of the Invention Exemplary anti-TIGIT antagonist antibodies, PD-1 axis binding antagonists, chemotherapeutic agents, colony stimulating factors and VEGF antagonists are described herein.
A.例示的な抗TIGITアンタゴニスト抗体
本発明は、対象(例えば、ヒト)のがんを処置するのに有用な抗TIGITアンタゴニスト抗体を提供する。
A. Exemplary Anti-TIGIT Antagonist Antibodies The present invention provides anti-TIGIT antagonist antibodies useful for treating cancer in a subject (eg, human).
いくつかの例では、抗TIGITアンタゴニスト抗体はチラゴルマブ(CAS登録番号:1918185-84-8)である。チラゴルマブ(Genentech)は、MTIG7192Aとしても既知である。 In some examples, the anti-TIGIT antagonist antibody is tiragolumab (CAS Registry Number: 1918185-84-8). Tiragolumab (Genentech) is also known as MTIG7192A.
特定の例では、抗TIGITアンタゴニスト抗体は、以下から選択される少なくとも1、2、3、4、5、又は6つのHVRを含む:(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1;(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2;(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3;(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1、(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2;及び/又は(f)QQYYSTPFTのアミノ酸配列(配列番号6)を含むHVR-L3、又は上記HVRの1つ以上の組合せ、並びに配列番号1~6のいずれか1つと少なくとも約90%の配列同一性(例えば、90%、91%、92%、93%、94%、95%、96%、97%、98%又は99%の同一性)を有する1つ以上のそのバリアント。 In certain examples, the anti-TIGIT antagonist antibody comprises at least 1, 2, 3, 4, 5, or 6 HVRs selected from: (a) a HVR comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1)- (b) HVR-H2 comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO:2); (c) HVR-H3 comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3); (d) the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO:4) (e) HVR-L2 comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and/or (f) HVR-L3 comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6), or one of the above HVRs Combinations of one or more, and at least about 90% sequence identity to any one of SEQ ID NOs: 1-6 (e.g., 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%) , 98% or 99% identity).
いくつかの例では、上記抗TIGITアンタゴニスト抗体のいずれかとしては、(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1;(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2;(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3;(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1、(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2;及び(f)QQYYSTPFTのアミノ酸配列(配列番号6)を含むHVR-L3を挙げることができる。いくつかの例では、抗TIGITアンタゴニスト抗体は、EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(配列番号17)と少なくとも90%(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%又は99%の配列同一性)を有するアミノ酸配列若しくはその配列、又はQVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(配列番号18)と少なくとも90%(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%又は99%の配列同一性)を有するアミノ酸配列若しくはその配列を有するVHドメイン、及び/又はDIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIK配列番号19)と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%又は99%の配列同一性)若しくはその配列を有するアミノ酸配列を含むVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17若しくはその配列と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVHドメイン、及び/又は配列番号19若しくはその配列と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号17のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18若しくはその配列と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVHドメイン、及び/又は配列番号19若しくはその配列と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVLドメインを有する。いくつかの例では、抗TIGITアンタゴニスト抗体は、配列番号18のアミノ酸配列を含むVHドメイン及び配列番号19のアミノ酸配列を含むVLドメインを有する。 In some examples, any of the anti-TIGIT antagonist antibodies include (a) HVR-H1 comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1); (b) HVR comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2) -H2; (c) HVR-H3 containing the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3); (d) HVR-L1 containing the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO:4), (e) the amino acids of WASTRES (SEQ ID NO:5) and (f) HVR-L3, which contains the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).いくつかの例では、抗TIGITアンタゴニスト抗体は、EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(配列番号17)と少なくとも90%(例えば、少なくとも91%、92%、93%、94%、95%、96%、97%、98%又は99%の配列同一性)を有するアミノ酸配列若しくはその配列、又はQVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSS(配列番号18)と少なくとも90%(例えば、少なくとも91%、92%、93%、94%、95%、96%、97% 、98%又は99%の配列同一性)を有するアミノ酸配列若しくはその配列を有するVHドメイン、及び/又はDIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIK配列番号19)と少なくとも90%の配列同一性(例えば、少なくとも91%、92%、93 %, 94%, 95%, 96%, 97%, 98% or 99% sequence identity) or an amino acid sequence having that sequence. In some examples, the anti-TIGIT antagonist antibody has at least 90% sequence identity to SEQ ID NO: 17 or a sequence thereof (e.g., at least 91%, 92%, 93%, 94%, 95%, 96%, 97% , 98%, or 99% sequence identity) and/or at least 90% sequence identity (e.g., at least 91%, 92%, 93%) with SEQ ID NO: 19 or a sequence thereof , 94%, 95%, 96%, 97%, 98%, or 99% sequence identity). In some examples, the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO:17 and a VL domain comprising the amino acid sequence of SEQ ID NO:19. In some examples, the anti-TIGIT antagonist antibody has at least 90% sequence identity with SEQ ID NO: 18 or a sequence thereof (e.g., at least 91%, 92%, 93%, 94%, 95%, 96%, 97% , 98%, or 99% sequence identity) and/or at least 90% sequence identity (e.g., at least 91%, 92%, 93%) with SEQ ID NO: 19 or a sequence thereof , 94%, 95%, 96%, 97%, 98%, or 99% sequence identity). In some examples, the anti-TIGIT antagonist antibody has a VH domain comprising the amino acid sequence of SEQ ID NO:18 and a VL domain comprising the amino acid sequence of SEQ ID NO:19.
いくつかの例では、抗TIGITアンタゴニスト抗体は、重鎖及び軽鎖配列を含み、(a)重鎖は、アミノ酸配列:EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK(配列番号33)を含み;(b)軽鎖は、アミノ酸配列:DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(配列番号34)を含む。 いくつかの例では、抗TIGITアンタゴニスト抗体は、重鎖及び軽鎖配列を含み、(a)重鎖は、アミノ酸配列:EVQLQQSGPGLVKPSQTLSLTCAISGDSVSSNSAAWNWIRQSPSRGLEWLGKTYYRFKWYSDYAVSVKGRITINPDTSKNQFSLQLNSVTPEDTAVFYCTRESTTYDLLAGPFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK(配列番号33)を含み;(b)軽鎖は、アミノ酸配列:DIVMTQSPDSLAVSLGERATINCKSSQTVLYSSNNKKYLAWYQQKPGQPPNLLIYWASTRESGVPDRFSGSGSGTDFTLTISSLQAEDVAVYYCQQYYSTPFTFGPGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(配列番号34)を含む。
いくつかの例では、抗TIGITアンタゴニスト抗体は、少なくとも1つ、2つ、3つ又は4つの以下の軽鎖可変領域フレームワーク領域(FR)を更に含む:DIVMTQSPDSLAVSLG ERATINCのアミノ酸配列を含むFR-L1(配列番号7);WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び/又はFGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、又は上記FRの1つ以上の組合せ、並びに配列番号7~10のいずれか1つと少なくとも約90%の配列同一性(例えば、90%、91%、92%、93%、94%、95%、96%、97%、98%又は99%の同一性)を有する1つ以上のそのバリアント。いくつかの例では、例えば、抗体は、DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1、WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2、GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3、及びFGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4を更に含む。 In some examples, the anti-TIGIT antagonist antibody further comprises at least one, two, three or four of the following light chain variable region framework regions (FR): FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLG ERATINC FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO:8); FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO:9); and/or comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO:10) FR-L4, or a combination of one or more of the above FRs, and at least about 90% sequence identity to any one of SEQ ID NOs: 7-10 (e.g., 90%, 91%, 92%, 93%, 94% , 95%, 96%, 97%, 98% or 99% identity) thereof. In some examples, for example, the antibody comprises FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO:7), FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO:8), GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO:9) and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
いくつかの例では、抗TIGITアンタゴニスト抗体は、以下の1つ、2つ、3つ、又は4つ重鎖可変領域FRを更に含む:X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)(X1はE又はQである)のアミノ酸配列を含むFR-H1:WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び/又はWGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、又は上記FRの1つ以上と、配列番号11~14のいずれか1つと少なくとも約90%の配列同一性(例えば、90%、91%、92%、93%、94%、95%、96%、97%、98%又は99%の同一性)を有するその1つ以上のバリアントとの組み合わせ。抗TIGITアンタゴニスト抗体は、例えば、以下の1つ、2つ、3つ、又は4つ重鎖可変領域FRを更に含み得る:EVQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号15)のアミノ酸配列を含むFR-H1:WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び/又はWGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、又は上記FRの1つ以上と、配列番号12~15のいずれか1つと少なくとも約90%の配列同一性(例えば、90%、91%、92%、93%、94%、95%、96%、97%、98%又は99%の同一性)を有するその1つ以上のバリアントとの組み合わせ。いくつかの例では、抗TIGITアンタゴニスト抗体は、EVQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号15)のアミノ酸配列を含むFR-H1、WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及びWGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4を含む。別の例では、例えば、抗TIGITアンタゴニスト抗体は、以下の1つ、2つ、3つ、又は4つ重鎖可変領域FRを更に含み得る:QVQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号16)のアミノ酸配列を含むFR-H1:WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び/又はWGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、又は上記FRの1つ以上と、配列番号12~14及び16のいずれか1つと少なくとも約90%の配列同一性(例えば、90%、91%、92%、93%、94%、95%、96%、97%、98%又は99%の同一性)を有するその1つ以上のバリアントとの組み合わせ。いくつかの例では、抗TIGITアンタゴニスト抗体は、QVQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号16)のアミノ酸配列を含むFR-H1、WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及びWGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4を含む。 In some examples, the anti-TIGIT antagonist antibody further comprises 1, 2, 3, or 4 heavy chain variable region FRs: X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11) (where X 1 is E or Q FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or WGQGTLVTVSS (SEQ ID NO: 14) ), or one or more of the above FRs, with at least about 90% sequence identity to any one of SEQ ID NOS: 11-14 (e.g., 90%, 91%, 92%, 93% %, 94%, 95%, 96%, 97%, 98% or 99% identity). The anti-TIGIT antagonist antibody can further comprise, for example, one, two, three, or four heavy chain variable region FRs: FR-H1 comprising the amino acid sequence of EVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 15): WIRQSPSRGLEWLG (sequence FR-H2 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14), or one of the above FRs. and at least about 90% sequence identity to any one of SEQ ID NOS: 12-15 (e.g., 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%) % or 99% identity) with one or more variants thereof. In some examples, the anti-TIGIT antagonist antibody is FR-H1 comprising the amino acid sequence of EVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO:15), FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO:12); RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO:13) FR-H3 containing the sequence; and FR-H4 containing the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14). In another example, for example, the anti-TIGIT antagonist antibody can further comprise 1, 2, 3, or 4 heavy chain variable region FRs: FR- H1: FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12); FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and/or FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14); or at least about 90% sequence identity with any one of SEQ ID NOs: 12-14 and 16 with one or more of the above FRs (e.g., 90%, 91%, 92%, 93%, 94%, 95%, A combination with one or more variants thereof having 96%, 97%, 98% or 99% identity). In some examples, the anti-TIGIT antagonist antibody comprises FR-H1 comprising the amino acid sequence of QVQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO:16), FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO:12); RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO:13) FR-H3 containing the sequence; and FR-H4 containing the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
別の態様では、抗TIGITアンタゴニスト抗体が提供され、抗体は、上記いずれかの例のようなVH及び上記いずれかの例のようなVLを含み、可変ドメイン配列の一方又は両方が翻訳後修飾を含む。 In another aspect, anti-TIGIT antagonist antibodies are provided, wherein the antibody comprises a VH as in any example above and a VL as in any example above, wherein one or both of the variable domain sequences are post-translationally modified. include.
いくつかの例では、上記の抗TIGITアンタゴニスト抗体のいずれか1つは、ヒトTIGITに加えてウサギTIGITに結合することができる。いくつかの例では、上記の抗TIGITアンタゴニスト抗体のいずれか1つは、ヒトTIGIT及びカニクイザル(cyno)TIGITの両方に結合することができる。いくつかの例では、上記の抗TIGITアンタゴニスト抗体のいずれか1つは、ヒトTIGIT、カニクイザルTIGIT及びウサギTIGITに結合することができる。いくつかの例では、上記の抗TIGITアンタゴニスト抗体のいずれか1つは、ヒトTIGIT、カニクイザルTIGIT及びウサギTIGITに結合することができるが、マウスTIGITには結合できない。 In some examples, any one of the anti-TIGIT antagonist antibodies described above can bind to rabbit TIGIT in addition to human TIGIT. In some examples, any one of the anti-TIGIT antagonist antibodies described above can bind to both human TIGIT and cynomolgus monkey (cyno) TIGIT. In some examples, any one of the anti-TIGIT antagonist antibodies described above can bind to human TIGIT, cynomolgus monkey TIGIT and rabbit TIGIT. In some examples, any one of the anti-TIGIT antagonist antibodies described above can bind to human TIGIT, cynomolgus TIGIT, and rabbit TIGIT, but not mouse TIGIT.
いくつかの例では、抗TIGITアンタゴニスト抗体は、約10nM以下のKDでヒトTIGITに結合し、約10nM以下のKDでカニクイザルTIGITに結合する(例えば、約0.1nM~約1nMのKDでヒトTIGITに結合し、約0.5nM~約1nMのKDでカニクイザルTIGITに結合し、例えば、約0.1nM以下のKDでヒトTIGITに結合し、約0.5nM以下のKDでカニクイザルTIGITに結合する)。 In some examples, the anti-TIGIT antagonist antibody binds human TIGIT with a K D of about 10 nM or less and binds cynomolgus monkey TIGIT with a K D of about 10 nM or less (eg, a K D of about 0.1 nM to about 1 nM). and binds to cynomolgus monkey TIGIT with a K D of about 0.5 nM to about 1 nM, for example, binds human TIGIT with a K D of about 0.1 nM or less and binds to human TIGIT with a K D of about 0.5 nM or less. binds to cynomolgus monkey TIGIT).
いくつかの例では、抗TIGITアンタゴニスト抗体は、TIGITに特異的に結合し、ポリオウイルス受容体(PVR)とのTIGIT相互作用を阻害又は遮断する(例えば、アンタゴニスト抗体は、PVRへのTIGIT結合によって媒介される細胞内シグナル伝達を阻害する)。いくつかの例では、アンタゴニスト抗体は、10nM以下のIC50値でヒトPVRへのヒトTIGITの結合を阻害又は遮断する(例えば、1nM~約10nM)。いくつかの例では、抗TIGITアンタゴニスト抗体は、TIGITに特異的に結合し、PVR-CD 226相互作用に影響を与えることなく、PVRとのTIGIT相互作用を阻害又は遮断する。いくつかの例では、アンタゴニスト抗体は、カニクイザルPVRへのカニクイザルTIGITの結合を50nM以下のIC50値で阻害又は遮断する(例えば、1nM~約50nM、例えば、1nM~約5nM)。いくつかの例では、抗TIGITアンタゴニスト抗体は、CD226とTIGITとの相互作用を阻害及び/又は遮断する。いくつかの例では、抗TIGITアンタゴニスト抗体は、TIGITがCD226ホモ二量体化を破壊する能力を阻害および/または遮断する。 In some examples, the anti-TIGIT antagonist antibody specifically binds to TIGIT and inhibits or blocks TIGIT interaction with the poliovirus receptor (PVR) (e.g., the antagonist antibody binds TIGIT to the PVR). mediated intracellular signaling). In some examples, the antagonist antibody inhibits or blocks binding of human TIGIT to human PVR with an IC50 value of 10 nM or less (eg, 1 nM to about 10 nM). In some examples, an anti-TIGIT antagonist antibody specifically binds to TIGIT and inhibits or blocks TIGIT interaction with PVR without affecting PVR-CD226 interaction. In some examples, the antagonist antibody inhibits or blocks binding of cynomolgus monkey TIGIT to cynomolgus monkey PVR with an IC50 value of 50 nM or less (eg, 1 nM to about 50 nM, eg, 1 nM to about 5 nM). In some examples, the anti-TIGIT antagonist antibody inhibits and/or blocks the interaction between CD226 and TIGIT. In some examples, an anti-TIGIT antagonist antibody inhibits and/or blocks the ability of TIGIT to disrupt CD226 homodimerization.
いくつかの例では、本明細書に記載の方法又は使用は、TIGITへの結合について上記の抗TIGITアンタゴニスト抗体のいずれかと競合する単離された抗TIGITアンタゴニスト抗体を使用又は投与することを含み得る。例えば、方法は、以下の6つのHVRを有する抗TIGITアンタゴニスト抗体とTIGITへの結合について競合する単離された抗TIGITアンタゴニスト抗体を投与することを含み得る:(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1;(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2;(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3;(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1、(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2;及び(f)QQYYSTPFTのアミノ酸配列(配列番号6)を含むHVR-L3が挙げられる。本明細書に記載の方法はまた、上記の抗TIGITアンタゴニスト抗体と同じエピトープに結合する単離された抗TIGITアンタゴニスト抗体を投与することを含み得る。 In some examples, the methods or uses described herein can comprise using or administering an isolated anti-TIGIT antagonist antibody that competes with any of the anti-TIGIT antagonist antibodies described above for binding to TIGIT. . For example, the method can include administering an isolated anti-TIGIT antagonist antibody that competes for binding to TIGIT with an anti-TIGIT antagonist antibody having the following six HVRs: (a) SNSAAWN (SEQ ID NO: 1); (b) HVR-H2 comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2); (c) HVR-H3 comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3); (d) KSSQTVLYSSSNNKKYLA (sequence (e) HVR-L2 containing the amino acid sequence of WASTRES (SEQ ID NO: 5); and (f) HVR-L3 containing the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6). be done. The methods described herein can also include administering an isolated anti-TIGIT antagonist antibody that binds to the same epitope as the anti-TIGIT antagonist antibody described above.
いくつかの態様では、抗TIGITアンタゴニスト抗体は、インタクトなFc媒介エフェクター機能(例えば、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS084448又はTJ-T6)又は増強されたエフェクター機能(例えば、SGN-TGT)を有する抗体である。 In some aspects, the anti-TIGIT antagonist antibody is an antibody with intact Fc-mediated effector functions (e.g., tiragolumab, vivostolimab, etiglimab, EOS084448 or TJ-T6) or enhanced effector functions (e.g., SGN-TGT). be.
他の態様では、抗TIGITアンタゴニスト抗体は、Fc媒介エフェクター機能を欠く抗体(例えば、ドムバナリマブ、BMS-986207、ASP8374、又はCOM902)である。 In other aspects, the anti-TIGIT antagonist antibody is an antibody that lacks Fc-mediated effector functions (eg, domvanalimab, BMS-986207, ASP8374, or COM902).
いくつかの態様では、抗TIGITアンタゴニスト抗体はIgG1クラスの抗体、例えば、チラゴルマブ、ビボストリマブ、ドムバナリマブ、BMS-986207、エチギリマブ、BGB-A1217、SGN-TGT、EOS084448(EOS-448)、TJ-T6、又はAB308である。 In some aspects, the anti-TIGIT antagonist antibody is an IgG1 class antibody, such as tiragolumab, vivostolimab, domvanalimab, BMS-986207, etigilimab, BGB-A1217, SGN-TGT, EOS084448 (EOS-448), TJ-T6, or AB308.
他の態様では、抗TIGITアンタゴニスト抗体は、IgG4クラス抗体、例えばASP8374又はCOM902である。 In other aspects, the anti-TIGIT antagonist antibody is an IgG4 class antibody, such as ASP8374 or COM902.
このような抗体を含有する組成物を含む、本発明において有用な抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)は、PD-1軸結合アンタゴニスト(例えば、PD-L1結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体、例えば、アテゾリズマブ)、PD-1結合アンタゴニスト(例えば、抗PD-1アンタゴニスト抗体、例えば、ペンブロリズマブ)及びPD-L2結合アンタゴニスト(例えば、抗PD-L2アンタゴニスト抗体))と組み合わせて使用され得る。 Anti-TIGIT antagonist antibodies (eg, tiragolumab) useful in the invention, including compositions containing such antibodies, are PD-1 axis binding antagonists (eg, PD-L1 binding antagonists (eg, anti-PD-L1 antagonists) antibodies (eg, atezolizumab), PD-1 binding antagonists (eg, anti-PD-1 antagonist antibodies, such as pembrolizumab) and PD-L2 binding antagonists (eg, anti-PD-L2 antagonist antibodies)).
いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、TIGITシグナル伝達を阻害するように機能する。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、その結合パートナーへのTIGITの結合を阻害する。例示的なTIGIT結合パートナーには、CD155(PVR)、CD112(PVRL2又はネクチン-2)及びCD113(PVRL3又はネクチン-3)が含まれる。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、TIGITとCD155との間の結合を阻害することができる。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、TIGITとCD112との間の結合を阻害し得る。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、TIGITとCD113との間の結合を阻害する。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、免疫細胞のTIGIT媒介性細胞シグナル伝達を阻害する。いくつかの実施形態では、抗TIGITアンタゴニスト抗体は、制御性T細胞(例えば、FcγR)を枯渇させることによってTIGITを阻害する。 In some embodiments, an anti-TIGIT antagonist antibody functions to inhibit TIGIT signaling. In some embodiments, an anti-TIGIT antagonist antibody inhibits binding of TIGIT to its binding partner. Exemplary TIGIT binding partners include CD155 (PVR), CD112 (PVRL2 or Nectin-2) and CD113 (PVRL3 or Nectin-3). In some embodiments, an anti-TIGIT antagonist antibody can inhibit binding between TIGIT and CD155. In some embodiments, an anti-TIGIT antagonist antibody can inhibit binding between TIGIT and CD112. In some embodiments, an anti-TIGIT antagonist antibody inhibits binding between TIGIT and CD113. In some embodiments, an anti-TIGIT antagonist antibody inhibits TIGIT-mediated cell signaling of immune cells. In some embodiments, an anti-TIGIT antagonist antibody inhibits TIGIT by depleting regulatory T cells (eg, FcγRs).
いくつかの実施形態では、抗TIGIT抗体はモノクローナル抗体である。いくつかの実施形態では、抗TIGIT抗体は、Fab、Fab’-SH、Fv、scFv及び(Fab’)2フラグメントからなる群より選択される抗体フラグメントである。いくつかの実施形態では、抗TIGIT抗体はヒト化抗体である。いくつかの実施形態では、抗TIGIT抗体はヒト抗体である。いくつかの実施形態では、本明細書に記載の抗TIGIT抗体は、ヒトTIGITに結合する。いくつかの実施形態では、抗TIGIT抗体はFc融合タンパク質である。 In some embodiments, the anti-TIGIT antibody is a monoclonal antibody. In some embodiments, the anti-TIGIT antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv and (Fab') 2 fragments. In some embodiments, the anti-TIGIT antibody is a humanized antibody. In some embodiments, the anti-TIGIT antibody is a human antibody. In some embodiments, an anti-TIGIT antibody described herein binds to human TIGIT. In some embodiments, the anti-TIGIT antibody is an Fc fusion protein.
いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ(MTIG7192A、RG6058又はRO7092284)、ビボストリマブ(MK-7684)、ASP8374(PTZ-201)、EOS884448(EOS-448)、SEA-TGT(SGN-TGT)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、IBI939、ドムバナリマブ(AB154)、M6223、AB308、AB154、TJ-T6、MG1131、NB6253、HLX301、HLX53、SL-9258(TIGIT-Fc-LIGHT)、STW264、及びYBL-012からなる群から選択される。いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ(MTIG7192A、RG6058又はRO7092284)、ビボストリマブ(MK-7684)、ASP8374(PTZ-201)、EOS-448、及びSEA-TGT(SGN-TGT)からなる群から選択される。抗TIGIT抗体は、チラゴルマブ(MTIG7192A、RG6058又はRO7092284)であり得る。 In some embodiments, the anti-TIGIT antibody is tiragolumab (MTIG7192A, RG6058 or RO7092284), vibostolimab (MK-7684), ASP8374 (PTZ-201), EOS884448 (EOS-448), SEA-TGT (SGN-TGT) , BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), IBI939, Dombanalimab (AB154), M6223, AB308, AB154, TJ-T6, MG1131, NB6253, HLX301, HLX53, SL-9258 TIGIT-Fc-LIGHT), STW264, and YBL-012. In some embodiments, the anti-TIGIT antibody consists of tiragolumab (MTIG7192A, RG6058 or RO7092284), vibostolimab (MK-7684), ASP8374 (PTZ-201), EOS-448, and SEA-TGT (SGN-TGT) Selected from the group. The anti-TIGIT antibody can be tiragolumab (MTIG7192A, RG6058 or RO7092284).
本明細書に開示される方法に有用な抗TIGIT抗体の非限定的な例及びその作製方法は、PCT公開公報の国際公開第2018183889号A1、国際公開第2019129261号A1、国際公開第2016106302号A9、国際公開第2018033798号A1、国際公開第2020020281号A1、国際公開第2019023504号A1、国際公開第2017152088号A1、国際公開第2016028656号A1、国際公開第2017030823号A2、国際公開第2018204405号A1、国際公開第2019152574号A1及び国際公開第2020041541号A2;米国特許第10,189,902号、米国特許第10,213,505号、米国特許第10,124,061号、米国特許第10,537,633号及び米国特許第10,618,958号;並びに米国特許出願公開第 2020/0095324号、第2019/0112375号、第2018/0371083号及び2020/0062859号に記載され、それらの各々が参照により本明細書に組み込まれる。本明細書に開示される方法に有用な抗TIGIT抗体の更なる非限定的な例及びその作製方法は、PCT公開公報の国際公開第2018204363号A1号、国際公開第2018047139号A1号、国際公開第2019175799号A2号、国際公開第2018022946号A1号、国際公開第2015143343号A2号、国際公開第2018218056号A1号、国際公開第2019232484号A1、国際公開第2019079777号A1号、国際公開第2018128939号A1号、国際公開第2017196867号A1号、国際公開第2019154415号A1号、国際公開第2019062832号A1号、国際公開第2018234793号A3号、国際公開第2018102536号A1号、国際公開第2019137548号A1号、国際公開第2019129221号A1号、国際公開第2018102746号A1号、国際公開第2018160704号A9号、国際公開第2020041541号A2号、国際公開第2019094637号A9号、国際公開第2017037707号A1号、国際公開第2019168382号A1号、国際公開第2006124667号A3号、国際公開第2017021526号A1号、国際公開第2017184619号A2号、国際公開第2017048824号A1号、国際公開第2019032619号A9号、国際公開第2018157162号A1号、国際公開第2020176718号A1号、国際公開第2020047329号A1号、国際公開第2020047329号A1号、国際公開第2018220446号A9;米国特許第9,617,338号、米国特許第9,567,399号、米国特許第10,604,576号及びUS9,994,637号;並びに米国特許出願公開第2018/0355040号、米国特許出願公開第2019/0175654号、米国特許出願公開第2019/0040154号、米国特許出願公開第2019/0382477号、米国特許出願公開第2019/0010246号、米国特許出願公開第2020/0164071号、米国特許出願公開第2020/0131267号、米国特許出願公開第2019/0338032号、米国特許出願公開第2019/0330351号、米国特許出願公開第2019/0202917号、米国特許出願公開第2019/0284269号、米国特許出願公開第2018/0155422号、米国特許出願公開第2020/0040082号、米国特許出願公開第2019/0263909号、米国特許出願公開第2018/0185480号、米国特許出願公開第2019/0375843号、米国特許出願公開第2017/0037133号、米国特許出願公開第2019/0077869号、米国特許出願公開第2019/0367579号、米国特許出願公開第2020/0222503号、米国特許出願公開第2020/0283496号、中国特許出願公開第109734806号A及び中国特許出願公開第110818795号Aに記載され、それらの各々が参照により本明細書に組み込まれる。 Non-limiting examples of anti-TIGIT antibodies useful in the methods disclosed herein and methods of making them can be found in PCT Publication Nos. WO2018183889A1, WO2019129261A1, WO2016106302A9 , WO2018033798A1, WO2020020281A1, WO2019023504A1, WO2017152088A1, WO2016028656A1, WO2017030823A2, WO2018204405A1, WO2019152574A1 and WO2020041541A2; US 10,189,902, US 10,213,505, US 10,124,061, US 10,537 , 633 and U.S. Patent No. 10,618,958; incorporated herein by. Further non-limiting examples of anti-TIGIT antibodies useful in the methods disclosed herein and methods of making the same can be found in PCT Publication Nos. WO2018204363A1, WO2018047139A1, No. 2019175799 A2, International Publication No. 2018022946 A1, International Publication No. 2015143343 A2, International Publication No. 2018218056 A1, International Publication No. 2019232484 A1, International Publication No. 2019079777 A1, International Publication No. 2018128939 A1, International Publication No. 2017196867 A1, International Publication No. 2019154415 A1, International Publication No. 2019062832 A1, International Publication No. 2018234793 A3, International Publication No. 2018102536 A1, International Publication No. 2019137548 A1 , International Publication No. 2019129221 A1, International Publication No. 2018102746 A1, International Publication No. 2018160704 A9, International Publication No. 2020041541 A2, International Publication No. 2019094637 A9, International Publication No. 2017037707 A1, International Publication No. 2019168382 A1, International Publication No. 2006124667 A3, International Publication No. 2017021526 A1, International Publication No. 2017184619 A2, International Publication No. 2017048824 A1, International Publication No. 2019032619 A9, International Publication No. 2018157162A1, WO2020176718A1, WO2020047329A1, WO2020047329A1, WO2018220446A9; U.S. Patent No. 9,617,338, U.S. Patent No. 9 , 567,399, U.S. Patent Nos. 10,604,576 and 9,994,637; US2019/0382477, US2019/0010246, US2020/0164071, US2020/0131267, US2019 /0338032, U.S. Patent Application Publication No. 2019/0330351, U.S. Patent Application Publication No. 2019/0202917, U.S. Patent Application Publication No. 2019/ 0284269, US2018/0155422, US2020/0040082, US2019/0263909, US2018/0185480, US2019/0185480 0375843, US2017/0037133, US2019/0077869, US2019/0367579, US2020/0222503, US2020/ 0283496, CN109734806A and CN110818795A, each of which is incorporated herein by reference.
本明細書に開示される方法において有用な抗TIGIT抗体には、ASP8374(PTZ-201)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、M6223、IBI939、EOS-448、ドムバナリマブ(AB154)、ビボストリマブ(MK-7684)及びSEA-TGT(SGN-TGT)が含まれる。本明細書に開示される方法において有用な更なる抗TIGIT抗体としては、AGEN1307;AGEN1777;抗体クローンpab2197及びpab2196(Agenus Inc.);抗体クローンTBB8、TDC8、3TB3、5TB10、及びD1Y1A(Anhui Anke Biotechnology Group Co.Ltd.)、抗体クローンMAB1、MAB2、MAB3、MAB4、MAB5、MAB6、MAB 7、MAB8、MAB9、MAB 10、MAB 11、MAB 12、MAB13、MAB 14、MAB 15、MAB 16、MAB 17、MAB 18、MAB19、MAB20、MAB21(Astellas Pharma/Potenza Therapeutics)、抗体クローンhu1217-1-1及びhu1217-2-2(BeiGene)、抗体クローン4D4及び19G(Brigham&Women’s Hospital)、抗体クローン11G11、10D7、15A6、22G2、TIGIT G2a、及びTIGIT G1 D265A、(改変重鎖定常領域を有するそのような抗体(Bristol-Myers Squibb)を含む);抗体クローン10A7、CPA.9.086、CPA.9.083.H4(S241P)、CPA.9.086.H4(S241P)、CHA.9.547.7.H4(S241P)及びCHA.9.547.13.H4(S241P)(Compugen);抗PVRIG/抗TIGIT 二重特異性抗体(Compugen)、抗体クローン315293、328189、350426、326504、及び331672(Fred Hutchinson Cancer Research Center);抗体クローンT-01、T-02、T-03、T-04、T-05、T-06、T-07、T-08、T-09、及びT-10(Gensun BioPharma Inc.);抗体クローン1H6、2B11、3A10、4A5、4A9、4H5、6A2、6B7、7F4、8E1、8G3、9F4、9G6、10C1、10F10、11G4、12B7、12C8、15E9、16C11、16D6、及び16E10(Hefei Ruida Immunological Drugs Research Institute Co.Ltd.);抗体クローンh3C5H1、h3C5H2、h3C5H3、h3C5H4、h3C5H3-1、h3C5H3-2、h3C5H3-3、h3C5L1、及びh3C5L2(IGM Biosciences Inc.);抗体クローン90D9、101E1、116H8、118A12、131A12、143B6、167F7、221F11、222H4、327C9、342A9、344F2、349H6、及び350D10(I-Mab Biopharma);抗体クローンADI-27238、ADI-30263、ADI-30267、ADI-30268、ADI-27243、ADI-30302、ADI-30336、ADI-27278、ADI-30193、ADI-30296、ADI-27291、ADI-30283、ADI-30286、ADI-30288、ADI27297、ADI-30272、ADI-30278、ADI-27301、ADI-30306、及びADI-30311(Innovent Biologics、Inc.);抗体クローン26518、29478、26452、29487、29489、31282、26486、29494、29499、26521、29513、26493、29520、29523、29527、31288、32919、32931、26432、及び32959(iTeos Therapeutics);抗体クローンm1707、m1708、m1709、m1710、m1711、h1707、h1708、h1709、h1710、及びh1711(Jiangsu Hengrui Medicine Co.Ltd.);抗体クローンTIG1、TIG2、及びTIG3(JN Biosciences LLC);抗体クローン(例えば、KY01、KY02、KY03、KY04、KY05、KY06、KY07、KY08、KY09、KY10、K11、K12、K13、K14、K15、K16、K17、K18、K19、K20、K21、K22、K23 Kymab TIGIT(抗体2)、及びTool TIGIT(抗体4)(Kymab Limited);二重特異性抗体1D05/1D05を有するin-house抗TIGIT(抗PD-L1)ネイティブ可変ドメイン及びKymab TIGIT抗原結合部位(ABS)ドメイン(二重特異性1)、Kymab TIGITネイティブ可変ドメイン及び1D05 ABSドメインを有するIn-house抗TIGIT/1D05(二重特異性2)、Toon抗TIGITネイティブ可変ドメイン及びTool抗PD-L1 ABSドメインを有するTool抗TIGIT/Tool抗PD-L1(二重特異性3)、Tool抗PD-L1ネイティブ可変ドメイン及びTool抗TIGIT ABSドメインを有するTool抗PD-L1/Tool抗TIGIT(二重特異性4)(Kymab Limited);抗体クローン及びクローン抗体14D7、26B10、Hu14D7、Hu26B10、14A6、Hu14A6、28H5、31C6、Hu31C6、25G10、MBS43、37D10、18G10、11A11、c18G10、及びLB155.14A6.G2.A8(Merck);エチジリマブ(OMP-313M32)(Mereo BioPharma);抗体クローン64G1E9B4、100C4E7D11、83G5H11C12、92E9D4B4、104G12E12G2、121C2F10B5、128E3F10F3F2、70A11A8E6、11D8E124A、16F10H12C11、8F2D8E7、48B5G4E12、139E2C2D2、128E3G7F5、AS19584、AS19852、AS19858、AS19886、AS19887、AS19888、AS20160、AS19584VH26、AS19584VH29、AS19584VH30、AS19584VH31、AS19886VH5、AS19886VH8、AS19886VH9、AS19886VH10、AS19886VH19、AS19886VH20、AS19584VH28-Fc、AS19886VH5-Fc、AS19886VH8-Fc、AS19584-Fc、及びAS19886-Fc(Nanjing Legend Biotechnology Co.Ltd.);抗体クローンAREクローン:Ab58、Ab69、Ab75、Ab133、Ab177、Ab122、Ab86、Ab180、Ab83、Ab26、Ab20、Ab147、Ab12、Ab66、Ab176、Ab96、Ab123、Ab109、Ab149、Ab34、Ab61、Ab64、Ab105、Ab108、Ab178、Ab166、Ab29、Ab135、Ab171、Ab194、Ab184、Ab164、Ab183、Ab158、Ab55、Ab136、Ab39、Ab159、Ab151、Ab139、Ab107、Ab36、Ab193、Ab115、Ab106、Ab13f8、Ab127、Ab165、Ab155、Ab19、Ab6、Ab187、Ab179、Ab65、Ab114、Ab102、Ab94、Ab163、Ab110、Ab80、Ab92、Ab117、Ab162、Ab121、Ab195、Ab84、Ab161、Ab198、Ab24、Ab98、Ab116、Ab174、Ab196、Ab51、Ab91、Ab185、Ab23、Ab7、Ab95、Ab100、Ab140、Ab145、Ab150、Ab168、Ab54、Ab77、Ab43、Ab160、Ab82、Ab189、Ab17、Ab103、Ab18、Ab130、Ab132、Ab134、Ab144;ARGクローン:Ab2、Ab47、Ab49、Ab31、Ab53、Ab40、Ab5、Ab9、Ab48、Ab4、Ab10、Ab37、Ab33、Ab42、Ab45;ARVクローン:Ab44、Ab97、Ab81、Ab188、Ab186、Ab62、Ab57、Ab192、Ab73、Ab60、Ab28、Ab32、Ab78、Ab14、Ab152、Ab72、Ab137、Ab128、Ab169、Ab87、Ab74、Ab172、Ab153、Ab120、Ab13、Ab113、Ab16、Ab56、Ab129、Ab50、Ab90、Ab99、Ab3、Ab148、Ab124、Ab22、Ab41、Ab119、Ab157、Ab27、Ab15、Ab191、Ab190、Ab79、Ab181、Ab146、Ab167、Ab88、Ab199、Ab71、Ab85、Ab59、Ab141、Ab68、Ab143、Ab46、Ab197、Ab175、Ab156、Ab63、Ab11、Ab182、Ab89、Ab8、Ab101、Ab25、Ab154、Ab21、Ab111、Ab118、Ab173、Ab38、Ab76、Ab131、Ab1、Ab67、Ab70、Ab170、Ab30、Ab93、Ab142、Ab104、Ab112、Ab35、Ab126、及びAb125(Rigel Pharmaceuticals、Inc.);CASC-674(Seattle Genetics);抗体クローン2、2C、3、5、13、13A、13B、13C、13D、14、16、16C、16D、16E、18、21、22、25、25A、25B、25C、25D、25E、27、54、13 IgG2a脱フコシル化、13 hIgG1野生型、及び13 LALA-PG(Seattle Genetics);JS006(Shanghai Junshi Biosciences Ltd.);抗TIGIT Fc抗体及び二重特異性抗体 PD1×TIGIT(Xencor)、抗体クローンVSIG9#1(Vsig9.01)及び258-CS1#4(#4)(Yissum Research Development Company of The Hebrew University Of Jerusalem Ltd.);YH29143(Yuhan Co、Ltd.);抗体クローンS02、S03、S04、S05、S06、S11、S12、S14、S19、S32、S39、S43、S62、S64、F01、F02、F03、F04、32D7、101H3、10A7、及び1F4(Yuhan Co、Ltd.);抗zB7R1クローン318.4.1.1(E9310)、318.28.2.1(E9296)、318.39.1.1(E9311)、318.59.3.1(E9400)、及び318.77.1.10(ZymoGenetics、Inc).が挙げられる。
Anti-TIGIT antibodies useful in the methods disclosed herein include ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS- 448, domvanalimab (AB154), vibostolimab (MK-7684) and SEA-TGT (SGN-TGT). Additional anti-TIGIT antibodies useful in the methods disclosed herein include AGEN 1307; AGEN 1777; antibody clones pab2197 and pab2196 (Agenus Inc.); antibody clones TBB8, TDC8, 3TB3, 5TB10, and D1Y1A (Anhui Anke Biotechnology Group Co. Ltd.), antibody clones MAB1, MAB2, MAB3, MAB4, MAB5, MAB6, MAB 7, MAB8, MAB9,
いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ、ASP8374(PTZ-201)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、M6223、IBI939、EOS884448(EOS-448)、ドムバナリマブ(AB154)、ビボストリマブ(MK-7684)、及びSEA-TGT(SGN-TGT)からなる群から選択される。ASP874(PTZ-201)は、PCT公開公報の国際公開第2018183889号A1及び米国特許出願公開第2020/0095324号に記載されている抗TIGITモノクローナル抗体である。BGB-A 1217は、PCT公開公報の国際公開第2019129261号A1に記載されている抗TIGIT抗体である。BMS-986207(ONO-4686)は、PCT公開公報の国際公開第2016106302号A9、米国特許第10,189,902号、及び米国特許出願公開第2019/0112375号に記載されている抗TIGIT抗体である。。COM902(CGEN-15137)は、PCT公開公報の国際公開第2018033798号A1、並びに米国特許第10,213,505号及び第10,124,061号に記載されている抗TIGIT抗体である。IBI939は、PCT公開公報の国際公開第2020020281号A1に記載されている抗TIGIT抗体である。EOS884448(EOS-448)は、PCT公開公報の国際公開第2019023504号A1に記載されている抗TIGIT抗体である。ドムバナリマブ(AB 154)は、PCT公開公報の国際公開第2017152088号A1及び米国特許第10,537,633号に記載されている抗TIGITモノクローナル抗体である。ビボストリマブ(MK-7684)は、PCT公開公報の国際公開第2016028656号A1、国際公開第2017030823号A2、国際公開第2018204405号A1、及び/又は国際公開第2019152574号A1、米国特許第10,618,958号及び米国特許第2018/0371083号に記載されている抗TIGIT抗体である。SEA-TGT(SGN-TGT)は、PCT公開公報の国際公開第2020041541号A2及び米国特許出願公開第2020/0062859号に記載されているような抗TIGIT抗体である。 In some embodiments, the anti-TIGIT antibody is tiragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS-448 ), domvanalimab (AB154), vibostolimab (MK-7684), and SEA-TGT (SGN-TGT). ASP874 (PTZ-201) is an anti-TIGIT monoclonal antibody described in PCT Publication No. WO2018183889A1 and US Patent Application Publication No. 2020/0095324. BGB-A 1217 is an anti-TIGIT antibody described in PCT Publication No. WO2019129261 A1. BMS-986207 (ONO-4686) is an anti-TIGIT antibody described in PCT Publication No. WO2016106302A9, US Patent No. 10,189,902, and US Patent Application Publication No. 2019/0112375 be. . COM902 (CGEN-15137) is an anti-TIGIT antibody described in PCT Publication No. WO2018033798A1 and US Pat. Nos. 10,213,505 and 10,124,061. IBI939 is an anti-TIGIT antibody described in PCT Publication No. WO2020020281A1. EOS884448 (EOS-448) is an anti-TIGIT antibody described in PCT Publication No. WO2019023504A1. Domvanalimab (AB 154) is an anti-TIGIT monoclonal antibody described in PCT Publication No. WO2017152088A1 and US Pat. No. 10,537,633. Vivostolimab (MK-7684) can be found in PCT Publication Nos. WO2016028656A1, WO2017030823A2, WO2018204405A1, and/or WO2019152574A1, U.S. Patent No. 10,618, 958 and the anti-TIGIT antibody described in US2018/0371083. SEA-TGT (SGN-TGT) is an anti-TIGIT antibody as described in PCT Publication No. WO2020041541A2 and US Patent Application Publication No. 2020/0062859.
いくつかの実施形態では、抗TIGITアンタゴニスト抗体はチラゴルマブ(CAS登録番号:1918185-84-8)である。チラゴルマブ(Genentech)は、MTIG7192A、RG6058又はRO7092284としても知られている。チラゴルマブは、国際公開第2003072305号A8、国際公開第2004024068号A3、国際公開第2004024072号A3、国際公開第2009126688号A2、国際公開第2015009856号A2、国際公開第2016011264号A1、国際公開第2016109546号A2、国際公開第2017053748号A2及び国際公開第2019165434号A1、並びに米国特許出願公開第2017/0044256号、第2017/0037127号、第2017/0145093号、第2017/260594号、第2017/0088613号、第2018/0186875号、第2019/0119376号、及び米国特許第9873740号B2、米国特許第10626174号B2、米国特許第10611836号B2、米国特許第9499596号B2、米国特許第8431350号B2、米国特許第10047158号B2及び米国特許第10017572号B2に記載されるアンタゴニスト性モノクローナル抗体である。 In some embodiments, the anti-TIGIT antagonist antibody is tiragolumab (CAS Registry Number: 1918185-84-8). Tiragolumab (Genentech) is also known as MTIG7192A, RG6058 or RO7092284. WO2003072305A8, WO2004024068A3, WO2004024072A3, WO2009126688A2, WO2015009856A2, WO2016011264A1, WO2016109546 A2, WO2017053748A2 and WO2019165434A1, and U.S. Patent Application Publication Nos. 2017/0044256, 2017/0037127, 2017/0145093, 2017/260594, 2017/0088613 , 2018/0186875, 2019/0119376, and US Pat. It is an antagonistic monoclonal antibody described in Patent No. 10047158 B2 and US Patent No. 10017572 B2.
いくつかの実施形態では、抗TIGIT抗体は、本明細書に開示される抗TIGIT抗体のいずれかの少なくとも1、2、3、4、5、又は6つの相補性決定領域(CDR)を含む。いくつかの実施形態では、抗TIGIT抗体は、本明細書に開示される抗TIGIT抗体のいずれかの6つのCDRを含む。いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ、ASP8374(PTZ-201)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、M6223、IBI939、EOS884448(EOS-448)、ドムバナリマブ(AB154)、ビボストリマブ(MK-7684)、及びSEA-TGT(SGN-TGT)からなる群から選択される抗体のいずれか1つの6つのCDRを含む。 In some embodiments, an anti-TIGIT antibody comprises at least 1, 2, 3, 4, 5, or 6 complementarity determining regions (CDRs) of any of the anti-TIGIT antibodies disclosed herein. In some embodiments, an anti-TIGIT antibody comprises the 6 CDRs of any of the anti-TIGIT antibodies disclosed herein. In some embodiments, the anti-TIGIT antibody is tiragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS-448 ), domvanarimab (AB154), vibostolimab (MK-7684), and SEA-TGT (SGN-TGT).
いくつかの実施形態では、抗TIGIT抗体は、重鎖及び軽鎖を含み、重鎖は、本明細書に開示される抗TIGIT抗体のいずれか1つの重鎖可変領域(VH)配列を含み、軽鎖は、同じ抗体の軽鎖可変領域(VL)を含む。いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ、ASP8374(PTZ-201)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、M6223、IBI939、EOS884448(EOS-448)、ドムバナリマブ(AB154)、ビボストリマブ(MK-7684)、及びSEA-TGT(SGN-TGT)からなる群から選択される抗TIGIT抗体のVH及びVLを含む。 In some embodiments, the anti-TIGIT antibody comprises a heavy chain and a light chain, the heavy chain comprising a heavy chain variable region (VH) sequence of any one of the anti-TIGIT antibodies disclosed herein; A light chain comprises the light chain variable region (VL) of the same antibody. In some embodiments, the anti-TIGIT antibody is tiragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS-448 ), domvanarimab (AB154), vivostolimab (MK-7684), and SEA-TGT (SGN-TGT).
いくつかの実施形態では、抗TIGIT抗体は、本明細書に開示される抗TIGIT抗体のいずれかの重鎖及び軽鎖を含む。いくつかの実施形態では、抗TIGIT抗体は、チラゴルマブ、ASP8374(PTZ-201)、BGB-A1217、BMS-986207(ONO-4686)、COM902(CGEN-15137)、M6223、IBI939、EOS884448(EOS-448)、ドムバナリマブ(AB154)、ビボストリマブ(MK-7684)、及びSEA-TGT(SGN-TGT)からなる群から選択される抗TIGIT抗体の重鎖及び軽鎖を含む。 In some embodiments, an anti-TIGIT antibody comprises the heavy and light chains of any of the anti-TIGIT antibodies disclosed herein. In some embodiments, the anti-TIGIT antibody is tiragolumab, ASP8374 (PTZ-201), BGB-A1217, BMS-986207 (ONO-4686), COM902 (CGEN-15137), M6223, IBI939, EOS884448 (EOS-448 ), domvanarimab (AB154), vivostolimab (MK-7684), and SEA-TGT (SGN-TGT).
いくつかの実施形態では、抗TIGITアンタゴニスト抗体(本明細書に記載される実施形態のいずれかによる)は、以下のセクションCに記載されるように、単独で又は組み合わせて特徴のいずれかを組み込むことができる。 In some embodiments, an anti-TIGIT antagonist antibody (according to any of the embodiments described herein) incorporates any of the features, alone or in combination, as described in Section C below be able to.
B.PD-1軸結合アンタゴニスト
有効量のPD-1軸結合アンタゴニストを対象に投与することを含む、対象(例えば、ヒト)のがんを処置するための方法が本明細書で提供される。PD-1軸結合アンタゴニストには、PD-L1結合アンタゴニスト、PD-1結合アンタゴニスト及びPD-L2結合アンタゴニストが含まれ得る。任意の適切なPD-1軸結合アンタゴニストが使用され得る。
B. PD-1 Axis Binding Antagonists Provided herein are methods for treating cancer in a subject (eg, human) comprising administering to the subject an effective amount of a PD-1 axis binding antagonist. PD-1 axis binding antagonists can include PD-L1 binding antagonists, PD-1 binding antagonists and PD-L2 binding antagonists. Any suitable PD-1 axis binding antagonist can be used.
1.PD-L1結合アンタゴニスト
いくつかの例では、PD-L1結合アンタゴニストは、PD-L1のそのリガンド結合パートナーのうちの1つ以上への結合を阻害する。他の例では、PD-L1結合アンタゴニストは、PD-L1のPD-1への結合を阻害する。更に他の例では、PD-L1結合アンタゴニストは、PD-L1のB7-1への結合を阻害する。いくつかの例では、PD-L1結合アンタゴニストは、PD-L1のPD-1及びB7-1両方への結合を阻害する。PD-L1結合アンタゴニストは、限定されないが、抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド又は小分子であり得る。いくつかの例では、PD-L1結合アンタゴニストは、PD-L1を阻害する小分子(例えば、GS-4224、INCB 086550、MAX-10181、INCB 090244、CA-170又はABSK 041)である。いくつかの例では、PD-L1結合アンタゴニストは、PD-L1及びVISTAを阻害する小分子である。いくつかの例では、PD-L1結合アンタゴニストはCA-170(AUPM-170としても知られる)である。いくつかの例では、PD-L1結合アンタゴニストは、PD-L1及びTIM3を阻害する小分子である。いくつかの例では、小分子は、国際公開第2015/033301号及び/又は国際公開第2015/033299号に記載されている化合物である。
1. PD-L1 Binding Antagonists In some examples, a PD-L1 binding antagonist inhibits binding of PD-L1 to one or more of its ligand binding partners. In another example, a PD-L1 binding antagonist inhibits binding of PD-L1 to PD-1. In yet another example, the PD-L1 binding antagonist inhibits binding of PD-L1 to B7-1. In some examples, the PD-L1 binding antagonist inhibits the binding of PD-L1 to both PD-1 and B7-1. PD-L1 binding antagonists can be, but are not limited to, antibodies, antigen-binding fragments thereof, immunoadhesins, fusion proteins, oligopeptides or small molecules. In some examples, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 (eg, GS-4224, INCB 086550, MAX-10181, INCB 090244, CA-170 or ABSK 041). In some examples, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 and VISTA. In some examples, the PD-L1 binding antagonist is CA-170 (also known as AUPM-170). In some examples, the PD-L1 binding antagonist is a small molecule that inhibits PD-L1 and TIM3. In some examples, the small molecule is a compound described in WO2015/033301 and/or WO2015/033299.
いくつかの例では、PD-L1結合アンタゴニストは抗PD-L1抗体である。様々な抗PD-L1抗体が本明細書において企図され、記載される。本明細書の例のいずれにおいても、単離された抗PD-L1抗体は、ヒトPD-L1、例えば、UniProtKB/Swiss-Prot受託番号Q9NZQ7-1に示されるようなヒトPD-L1、又はそのバリアントに結合することができる。いくつかの例では、抗PD-L1抗体は、PD-L1とPD-1との間及び/又はPD-L1とB7-1との間の結合を阻害することができる。いくつかの例では、抗PD-L1抗体は、モノクローナル抗体である。いくつかの例では、抗PD-L1抗体は、Fab、Fab’-SH、Fv、scFv、及び(Fab’)2フラグメントからなる群から選択される抗体フラグメントである。いくつかの例では、抗PD-L1抗体は、ヒト化抗体である。いくつかの例では、抗PD-L1抗体は、ヒト抗体である。例示的な抗PD-L1抗体としては、アテゾリズマブ、MDX-1105、MEDI4736(デュルバルマブ)、MSB0010718C(アベルマブ)、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007及びHS-636が挙げられる。本発明の方法及びそれらを作製する方法において有用な抗PD-L1抗体の例は、国際特許出願公開第2010/077634号及び米国特許第8,217,149号に記載されており、これらの各々は、参照によりその全体が本明細書に組み込まれる。 In some examples, the PD-L1 binding antagonist is an anti-PD-L1 antibody. Various anti-PD-L1 antibodies are contemplated and described herein. In any of the examples herein, the isolated anti-PD-L1 antibody is human PD-L1, eg, human PD-L1 as set forth in UniProtKB/Swiss-Prot Accession No. Q9NZQ7-1, or its Can be combined into variants. In some examples, anti-PD-L1 antibodies can inhibit binding between PD-L1 and PD-1 and/or between PD-L1 and B7-1. In some examples, the anti-PD-L1 antibody is a monoclonal antibody. In some examples, the anti-PD-L1 antibody is an antibody fragment selected from the group consisting of Fab, Fab'-SH, Fv, scFv, and (Fab') 2 fragments. In some examples, the anti-PD-L1 antibody is a humanized antibody. In some examples, the anti-PD-L1 antibody is a human antibody. Exemplary anti-PD-L1 antibodies include atezolizumab, MDX-1105, MEDI4736 (durvalumab), MSB0010718C (avelumab), SHR-1316, CS1001, embafolimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001 , KL-A167, APL-502, cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL -007 and HS-636. Examples of anti-PD-L1 antibodies useful in the methods of the invention and methods of making them are described in International Patent Application Publication No. 2010/077634 and US Pat. No. 8,217,149, each of which is incorporated herein by reference in its entirety.
いくつかの例では、抗PD-L1抗体(例えば、アテゾリズマブ)は、以下から選択される少なくとも1つ、2つ、3つ、4つ、5つ又は6つのHVRを含む:(a)HVR-H1配列はGFTFSDSWIH(配列番号20)であり;(b)HVR-H2配列はAWISPYGGSTYYADSVKG(配列番号21)であり;(c)HVR-H3配列はRHWPGGFDY(配列番号22)であり、(d)HVR-L1配列はRASQDVSTAVA(配列番号23)であり;(e)HVR-L2配列はSASFLYS(配列番号24)であり;(f)HVR-L3配列はQQYLYHPAT(配列番号25)である。 In some examples, the anti-PD-L1 antibody (eg, atezolizumab) comprises at least 1, 2, 3, 4, 5, or 6 HVRs selected from: (a) HVR- (b) HVR-H2 sequence is AWISPYGGSTYYADSVKG (SEQ ID NO:21); (c) HVR-H3 sequence is RHWPGGFDY (SEQ ID NO:22); (d) HVR -L1 sequence is RASQDVSTAVA (SEQ ID NO:23); (e) HVR-L2 sequence is SASFLYS (SEQ ID NO:24); (f) HVR-L3 sequence is QQYLYHPAT (SEQ ID NO:25).
いくつかの例では、抗PD-L1抗体は、
(a)それぞれ配列番号20、配列番号21及び配列番号22のHVR-H1、HVR-H2及びHVR-H3配列、ならびに
(b)それぞれ配列番号23、配列番号24及び配列番号25のHVR-L1、HVR-L2及びHVR-L3配列、を含む。
In some examples, the anti-PD-L1 antibody is
(a) HVR-H1, HVR-H2 and HVR-H3 sequences of SEQ ID NO:20, SEQ ID NO:21 and SEQ ID NO:22 respectively; and (b) HVR-L1 of SEQ ID NO:23, SEQ ID NO:24 and SEQ ID NO:25 respectively; HVR-L2 and HVR-L3 sequences.
いくつかの例では、抗PD-L1抗体(例えば、アテゾリズマブ)は、重鎖及び軽鎖配列を含み:(a)重鎖可変(VH)領域配列は、アミノ酸配列:EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSS(配列番号26);を含み、(b)軽鎖可変(VL)領域配列は、アミノ酸配列:DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKR(配列番号27)を含む。 いくつかの例では、抗PD-L1抗体(例えば、アテゾリズマブ)は、重鎖及び軽鎖配列を含み:(a)重鎖可変(VH)領域配列は、アミノ酸配列:EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSS(配列番号26); (b) the light chain variable (VL) region sequence comprises the amino acid sequence: DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKR (SEQ ID NO: 27).
いくつかの例では、抗PD-L1抗体(例えば、アテゾリズマブ)は、重鎖及び軽鎖配列を含み:(a)重鎖は、アミノ酸配列:EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYASTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPG(配列番号28)を含み;(b)軽鎖は、アミノ酸配列:DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(配列番号29)を含む。 いくつかの例では、抗PD-L1抗体(例えば、アテゾリズマブ)は、重鎖及び軽鎖配列を含み:(a)重鎖は、アミノ酸配列:EVQLVESGGGLVQPGGSLRLSCAASGFTFSDSWIHWVRQAPGKGLEWVAWISPYGGSTYYADSVKGRFTISADTSKNTAYLQMNSLRAEDTAVYYCARRHWPGGFDYWGQGTLVTVSSASTKGPSVFPLAPSSKSTSGGTAALGCLVKDYFPEPVTVSWNSGALTSGVHTFPAVLQSSGLYSLSSVVTVPSSSLGTQTYICNVNHKPSNTKVDKKVEPKSCDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYASTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSREEMTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPG(配列番号28)を含み;(b )軽鎖は、アミノ酸配列:DIQMTQSPSSLSASVGDRVTITCRASQDVSTAVAWYQQKPGKAPKLLIYSASFLYSGVPSRFSGSGSGTDFTLTISSLQPEDFATYYCQQYLYHPATFGQGTKVEIKRTVAAPSVFIFPPSDEQLKSGTASVVCLLNNFYPREAKVQWKVDNALQSGNSQESVTEQDSKDSTYSLSSTLTLSKADYEKHKVYACEVTHQGLSSPVTKSFNRGEC(配列番号29)を含む。
いくつかの例では、抗PD-L1抗体は、(a)配列番号26又は配列番号26の配列と少なくとも95%の配列同一性(例えば、少なくとも95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVHドメイン、(b)配列番号27又は配列番号27の配列と少なくとも95%の配列同一性(例えば、少なくとも95%、96%、97%、98%、又は99%の配列同一性)を有するアミノ酸配列を含むVLドメイン、又は(c)(a)に記載のVHドメイン及び(b)に記載のVLドメインを含む。一実施形態では、抗PD-L1抗体は、以下を含むアテゾリズマブを含む:(a)配列番号28の重鎖アミノ酸配列、及び(b)配列番号29の軽鎖アミノ酸配列。 In some examples, the anti-PD-L1 antibody has (a) at least 95% sequence identity to SEQ ID NO:26 or the sequence of SEQ ID NO:26 (e.g., at least 95%, 96%, 97%, 98%, or (b) SEQ ID NO: 27 or at least 95% sequence identity with the sequence of SEQ ID NO: 27 (e.g., at least 95%, 96%, 97%, 98% sequence identity); % or 99% sequence identity), or (c) a VH domain according to (a) and a VL domain according to (b). In one embodiment, the anti-PD-L1 antibody comprises atezolizumab comprising: (a) the heavy chain amino acid sequence of SEQ ID NO:28, and (b) the light chain amino acid sequence of SEQ ID NO:29.
いくつかの例では、抗PD-L1抗体はアベルマブ(CAS登録番号:1537032-82-8)である。MSB0010718Cとしても知られるアベルマブは、ヒトモノクローナルIgG1抗PD-L1抗体(Merck KGaA、Pfizer)である。 In some examples, the anti-PD-L1 antibody is avelumab (CAS Registry Number: 1537032-82-8). Avelumab, also known as MSB0010718C, is a human monoclonal IgG1 anti-PD-L1 antibody (Merck KGaA, Pfizer).
いくつかの例では、抗PD-L1抗体はデュルバルマブ(CAS登録番号:1428935-60-7)である。MEDI4736としても知られるデュルバルマブは、国際公開第2011/066389号及び米国特許出願公開第2013/034559号に記載されている、Fc最適化ヒトモノクローナルIgG1カッパ抗PD-L1抗体(MedImmune、AstraZeneca)である。 In some examples, the anti-PD-L1 antibody is durvalumab (CAS Registry Number: 1428935-60-7). Durvalumab, also known as MEDI4736, is an Fc-optimized human monoclonal IgG1 kappa anti-PD-L1 antibody (MedImmune, AstraZeneca) described in WO2011/066389 and US2013/034559. .
いくつかの例では、抗PD-L1抗体はMDX-1105(Bristol Myers Squibb)である。BMS-936559としても知られているMDX-1105は、国際公開第2007/005874号に記載されている抗PD-L1抗体である。 In some examples, the anti-PD-L1 antibody is MDX-1105 (Bristol Myers Squibb). MDX-1105, also known as BMS-936559, is an anti-PD-L1 antibody described in WO2007/005874.
いくつかの例では、抗PD-L1抗体はLY3300054(Eli Lilly)である。 In some examples, the anti-PD-L1 antibody is LY3300054 (Eli Lilly).
いくつかの例では、抗PD-L1抗体はSTI-A1014(Sorrento)である。STI-A1014はヒト抗PDL-1抗体である。 In some examples, the anti-PD-L1 antibody is STI-A1014 (Sorrento). STI-A1014 is a human anti-PDL-1 antibody.
いくつかの例では、抗PD-L1抗体はKN035(Suzhou Alphamab)である。KN035は、ラクダファージディスプレイライブラリーから生成されたシングルドメイン抗体(dAB)である。 In some examples, the anti-PD-L1 antibody is KN035 (Suzhou Alphamab). KN035 is a single domain antibody (dAB) generated from a camel phage display library.
いくつかの例では、抗PDL1抗体は、(例えば、腫瘍微小環境中のプロテアーゼによって)切断されると、抗体抗原結合ドメインを活性化して、例えば、非結合性立体部位を除去することによって、その抗原を結合させることができるようにする、切断可能な部位又はリンカーから構成される。いくつかの例では、抗PDL-1抗体はCX-072(CytomX Therapeutics)である。 In some examples, the anti-PDL1 antibody, when cleaved (e.g., by a protease in the tumor microenvironment), activates the antibody antigen-binding domain, e.g., by removing a non-binding steric moiety, thereby It consists of a cleavable site or linker that allows antigen to be attached. In some examples, the anti-PDL-1 antibody is CX-072 (CytomX Therapeutics).
いくつかの例では、抗PD-L1抗体は、6つのHVR配列(例えば、3つの重鎖HVR及び3つの軽鎖HVR)、及び/又は米国特許出願公開第20160108123号、国際公開第2016/000619号、国際公開第2012/145493号、米国特許第。国際公開第9,205,148号、国際公開第2013/181634号、又は国際公開第2016/061142号に記載される抗PD-L1抗体からの重鎖可変ドメイン及び軽鎖可変ドメインを含む。 In some examples, the anti-PD-L1 antibody comprises 6 HVR sequences (eg, 3 heavy chain HVRs and 3 light chain HVRs) and/or US Patent Application Publication No. 20160108123, WO2016/000619 No., WO2012/145493, U.S. Patent No. comprising heavy and light chain variable domains from an anti-PD-L1 antibody described in WO 9,205,148, WO 2013/181634, or WO 2016/061142.
なお更なる特定の態様では、抗PD-L1抗体は、低下した又は最小のエフェクター機能を有する。更に特定の態様では、「エフェクターレスFc変異(effector-less Fc mutation)」又は非グリコシル化(aglycosylation)変異に起因する。なお更なる例では、エフェクターなしのFc突然変異は、定常領域内のN297A又はD265A/N297A置換である。なお更なる例では、エフェクターなしのFc突然変異は、定常領域内のN297A置換である。いくつかの例では、単離された抗PD-L1抗体は、アグリコシル化される。抗体のグリコシル化は、典型的には、N結合型又はO結合型のいずれかである。N結合型とは、炭水化物部分のアスパラギン残基の側鎖への結合を指す。トリペプチド配列であるアスパラギン-X-セリン及びアスパラギン-X-トレオニン(式中、Xは、プロリン以外の任意のアミノ酸である)は、炭水化物部分のアスパラギン側鎖への酵素結合の認識配列である。したがって、ポリペプチド内でのこれらのトリペプチド配列のいずれかの存在により、潜在的なグリコシル化部位が作製される。O結合型グリコシル化とは、糖類、N-アセチルガラクトサミン、ガラクトース、又はキシロースのうちの1つのヒドロキシアミノ酸、最も一般的にはセリン又はトレオニンへの結合を指すが、5-ヒドロキシプロリン又は5-ヒドロキシリジンも使用され得る。抗体からのグリコシル化部位の除去は、(N結合型グリコシル化部位について)上述のトリペプチド配列のうちの1種が除去されるようにアミノ酸配列を改変することによって好都合に達成される。この改変は、グリコシル化部位内のアスパラギン、セリン、又はトレオニン残基の別のアミノ酸残基(例えば、グリシン、アラニン又は保存的置換)との置換によって行われ得る。
2.PD-1結合アンタゴニスト
In a still further particular aspect, the anti-PD-L1 antibody has reduced or minimal effector function. In a more particular aspect, it results from "effector-less Fc mutation" or aglycosylation mutation. In yet a further example, the effectorless Fc mutation is an N297A or D265A/N297A substitution within the constant region. In a still further example, the effectorless Fc mutation is an N297A substitution within the constant region. In some instances, the isolated anti-PD-L1 antibody is aglycosylated. Glycosylation of antibodies is typically either N-linked or O-linked. N-linked refers to attachment of the carbohydrate moiety to the side chain of the asparagine residue. The tripeptide sequences asparagine-X-serine and asparagine-X-threonine, where X is any amino acid except proline, are recognition sequences for enzymatic attachment of the carbohydrate moiety to the asparagine side chain. Thus, the presence of either of these tripeptide sequences within a polypeptide creates a potential glycosylation site. O-linked glycosylation refers to the attachment of one of the sugars, N-acetylgalactosamine, galactose, or xylose, to a hydroxyamino acid, most commonly serine or threonine, although 5-hydroxyproline or 5-hydroxy Lysine can also be used. Removal of glycosylation sites from the antibody is conveniently accomplished by altering the amino acid sequence such that one of the tripeptide sequences described above (for N-linked glycosylation sites) is removed. This modification may be accomplished by replacement of an asparagine, serine, or threonine residue within a glycosylation site with another amino acid residue (eg, glycine, alanine, or conservative substitution).
2. PD-1 binding antagonist
いくつかの例では、PD-1軸結合アンタゴニストは、PD-1結合アンタゴニストである。例えば、いくつかの例では、PD-1結合アンタゴニストは、PD-1のそのリガンド結合パートナーのうちの1つ以上への結合を阻害する。いくつかの例では、PD-1結合アンタゴニストは、PD-1のPD-L1への結合を阻害する。他の例では、PD-1結合アンタゴニストは、PD-1のPD-L2への結合を阻害する。更に他の例では、PD-1結合アンタゴニストは、PD-1のPD-L1及びPD-L2両方への結合を阻害する。PD-1結合アンタゴニストは、限定されないが、抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド又は小分子であり得る。いくつかの例では、PD-1結合アンタゴニストは、イムノアドヘシン(例えば、定常領域(例えば、免疫グロブリン配列のFc領域)に融合したPD-L1若しくはPD-L2の細胞外又はPD-1結合部分を含むイムノアドヘシン)である。例えば、いくつかの例では、PD-1結合アンタゴニストは、Fc融合タンパク質である。いくつかの例では、PD-1結合アンタゴニストはAMP-224である。AMP-224、別名B7-DCIgは、WO2010/027827及びWO2011/066342に記載されているPD-L2-Fc融合可溶性受容体である。いくつかの例では、PD-1結合アンタゴニストは、ペプチド又は低分子化合物である。いくつかの例では、PD-1結合アンタゴニストは、AUNP-12(PierreFabre/Aurigene)である。例えば、国際公開第2012/168944号、国際公開第2015/036927号、国際公開第2015/044900号、国際公開第2015/033303号、国際公開第2013/144704号、国際公開第2013/132317号及び国際公開第2011/161699号を参照されたい。いくつかの例では、PD-1結合アンタゴニストは、PD-1を阻害する小分子である。 In some examples, the PD-1 axis binding antagonist is a PD-1 binding antagonist. For example, in some instances, a PD-1 binding antagonist inhibits binding of PD-1 to one or more of its ligand binding partners. In some examples, the PD-1 binding antagonist inhibits binding of PD-1 to PD-L1. In another example, the PD-1 binding antagonist inhibits binding of PD-1 to PD-L2. In yet another example, a PD-1 binding antagonist inhibits the binding of PD-1 to both PD-L1 and PD-L2. PD-1 binding antagonists can be, but are not limited to, antibodies, antigen binding fragments thereof, immunoadhesins, fusion proteins, oligopeptides or small molecules. In some examples, the PD-1 binding antagonist is an immunoadhesin, such as an extracellular or PD-1 binding portion of PD-L1 or PD-L2 fused to a constant region (eg, the Fc region of an immunoglobulin sequence) immunoadhesins, including For example, in some instances the PD-1 binding antagonist is an Fc fusion protein. In some examples, the PD-1 binding antagonist is AMP-224. AMP-224, also known as B7-DCIg, is a PD-L2-Fc fusion soluble receptor described in WO2010/027827 and WO2011/066342. In some examples, the PD-1 binding antagonist is a peptide or small molecule compound. In some examples, the PD-1 binding antagonist is AUNP-12 (PierreFabre/Aurigene). For example, WO 2012/168944, WO 2015/036927, WO 2015/044900, WO 2015/033303, WO 2013/144704, WO 2013/132317 and See WO2011/161699. In some examples, the PD-1 binding antagonist is a small molecule that inhibits PD-1.
いくつかの例では、PD-1結合拮抗薬は、抗PD-1抗体である。様々な抗PD-1抗体が、本明細書に開示される方法及び使用において利用され得る。本明細書の例のいずれかでは、PD-1抗体はヒトPD-1又はそのバリアントに結合することができる。いくつかの例では、抗PD-1抗体はモノクローナル抗体である。いくつかの例では、抗PD-1抗体は、Fab、Fab’、Fab’-SH、Fv、scFv、及び(Fab’)2フラグメントからなる群から選択される抗体フラグメントである。いくつかの例では、抗PD-1抗体は、ヒト化抗体である。他の例では、抗PD-1抗体はヒト抗体である。例示的な抗PD-1アンタゴニスト抗体としては、ニボルマブ、ペンブロリズマブ、MEDI-0680、PDR001(スパルタリズマブ)、REGN2810(セミプリマブ)、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103及びhAb21が挙げられる。 In some examples, the PD-1 binding antagonist is an anti-PD-1 antibody. Various anti-PD-1 antibodies can be utilized in the methods and uses disclosed herein. In any of the examples herein, the PD-1 antibody can bind human PD-1 or a variant thereof. In some examples, the anti-PD-1 antibody is a monoclonal antibody. In some examples, the anti-PD-1 antibody is an antibody fragment selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab') 2 fragments. In some examples, the anti-PD-1 antibody is a humanized antibody. In other examples, the anti-PD-1 antibody is a human antibody. Exemplary anti-PD-1 antagonist antibodies include nivolumab, pembrolizumab, MEDI-0680, PDR001 (spartalizumab), REGN2810 (semiplimab), BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifanlimab, sasanlimab, penplimab, CS1003, HLX10, SCT-I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budikarimab, AMG404, CX-188, JTX-4014, 609A, LZM0219, LZM0219, SG001, AM0001, ENUM 244C8, ENUM 388D4, STI-1110, AK-103 and hAb21.
いくつかの例では、抗PD-1抗体はニボルマブ(CAS登録番号:946414-94-4)である。ニボルマブ(Bristol-Myers Squibb/Ono)、別名、MDX-1106-04、MDX-1106、ONO-4538、BMS-936558、及びOPDIVO(登録商標)は、国際公開第2006/121168号に記載の抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is nivolumab (CAS Registry Number: 946414-94-4). Nivolumab (Bristol-Myers Squibb/Ono), also known as MDX-1106-04, MDX-1106, ONO-4538, BMS-936558, and OPDIVO® are anti-PD -1 antibody.
いくつかの例では、抗PD-1抗体はペンブロリズマブ(CAS登録番号:1374853-91-4)である。ペンブロリズマブ(Merck)は、MK-3475、Merck 3475、ラムブロリズマブ、KEYTRUDA(登録商標)、及びSCH-900475としても知られており、国際公開第2009/114335号に記載の抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is pembrolizumab (CAS Registry Number: 1374853-91-4). Pembrolizumab (Merck), also known as MK-3475, Merck 3475, lambrolizumab, KEYTRUDA®, and SCH-900475, is an anti-PD-1 antibody described in WO2009/114335.
いくつかの例では、抗PD-1抗体は、MEDI-0680(AMP-514;AstraZeneca)である。MEDI-0680はヒト化IgG4抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is MEDI-0680 (AMP-514; AstraZeneca). MEDI-0680 is a humanized IgG4 anti-PD-1 antibody.
いくつかの例では、抗PD-1抗体は、PDR 001(CAS登録番号1859072-53-9;Novartis)である。PDR 001は、PD-1に対するPD-L1及びPD-L2の結合を遮断するヒト化IgG 4抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is PDR 001 (CAS Registry Number 1859072-53-9; Novartis). PDR 001 is a humanized IgG4 anti-PD-1 antibody that blocks the binding of PD-L1 and PD-L2 to PD-1.
いくつかの例では、抗PD-1抗体は、REGN 2810(Regeneron)である。REGN 2810は、ヒト抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is REGN 2810 (Regeneron). REGN 2810 is a human anti-PD-1 antibody.
いくつかの例では、抗PD-1抗体はBGB-108(BeiGene)である。 In some examples, the anti-PD-1 antibody is BGB-108 (BeiGene).
いくつかの例では、抗PD-1抗体はBGB-A 317(BeiGene)である。 In some examples, the anti-PD-1 antibody is BGB-A 317 (BeiGene).
いくつかの例では、抗PD-1抗体は、JS-001(Shanghai Junshi)である。JS-001はヒト化抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is JS-001 (Shanghai Junshi). JS-001 is a humanized anti-PD-1 antibody.
いくつかの例では、抗PD-1抗体はSTI-A 1110(Sorrento)である。STI-A 1110は、ヒト抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is STI-A 1110 (Sorrento). STI-A 1110 is a human anti-PD-1 antibody.
いくつかの例では、抗PD-1抗体は、INCSHR-1210(Incyte)である。INCSHR-1210は、ヒトIgG4抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is INCSHR-1210 (Incyte). INCSHR-1210 is a human IgG4 anti-PD-1 antibody.
いくつかの例では、抗PD-1抗体は、PF-06801591(Pfizer)である。 In some examples, the anti-PD-1 antibody is PF-06801591 (Pfizer).
いくつかの例では、抗PD-1抗体は、TSR-042(ANB 011としても知られている;Tesaro/AnaptysBio)である。 In some examples, the anti-PD-1 antibody is TSR-042 (also known as ANB 011; Tesaro/AnaptysBio).
いくつかの例では、抗PD-1抗体はAM 0001(ARMO Biosciences)である。 In some examples, the anti-PD-1 antibody is AM 0001 (ARMO Biosciences).
いくつかの例では、抗PD-1抗体は、ENUM 244C8(Enumeral Biomedical Holdings)である。ENUM 244 C 8は、PD-1へのPD-L1の結合を遮断することなくPD-1機能を阻害する抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is ENUM 244C8 (Enumeral Biomedical Holdings). ENUM 244 C8 is an anti-PD-1 antibody that inhibits PD-1 function without blocking PD-L1 binding to PD-1.
いくつかの例では、抗PD-1抗体は、ENUM 388D4(Enumeral Biomedical Holdings)である。ENUM 388 D4は、PD-1に対するPD-L1の結合を競合的に阻害する抗PD-1抗体である。 In some examples, the anti-PD-1 antibody is ENUM 388D4 (Enumeral Biomedical Holdings). ENUM 388 D4 is an anti-PD-1 antibody that competitively inhibits the binding of PD-L1 to PD-1.
いくつかの例では、抗PD-1抗体は、国際公開第2015/112800号、国際公開第2015/112805号、国際公開第2015/112900号、米国特許出願公開第20150210769号、国際公開第2016/089873号、国際公開第2015/035606号、国際公開第2015/085847号、国際公開第2014/206107号、国際公開第2012/145493号、米国特許第9,205,148号、国際公開第2015/119930号、国際公開第2015/119923号、国際公開第2016/032927号、国際公開第2014/179664号、国際公開第2016/106160号、及び国際公開第2014/194302に記載される抗PD-1抗体由来の6つのHVR配列(例えば、3つの重鎖HVR及び3つの軽鎖HVR)及び/又は重鎖可変ドメイン及び軽鎖可変ドメインを含む。 In some examples, the anti-PD-1 antibody is WO2015/112800, WO2015/112805, WO2015/112900, US20150210769, WO2016/ 089873, WO2015/035606, WO2015/085847, WO2014/206107, WO2012/145493, U.S. Patent No. 9,205,148, WO2015/ 119930, WO2015/119923, WO2016/032927, WO2014/179664, WO2016/106160, and WO2014/194302 It includes 6 HVR sequences (eg, 3 heavy chain HVRs and 3 light chain HVRs) and/or a heavy chain variable domain and a light chain variable domain from an antibody.
なお更なる特定の態様では、抗PD-1抗体は、Fc媒介エフェクター機能が低下しているか又は最小である。なお更なる特定の態様では、最小のFc媒介エフェクター機能は、「エフェクターレスFc変異」又はアグリコシル化変異に起因する。なお更なる例では、エフェクターなしのFc突然変異は、定常領域内のN297A又はD265A/N297A置換である。いくつかの例では、単離された抗PD-1抗体は、アグリコシル化されている。 In a still further specific aspect, the anti-PD-1 antibody has reduced or minimal Fc-mediated effector functions. In a still further specific aspect, minimal Fc-mediated effector function is due to "effectorless Fc mutations" or aglycosylation mutations. In a still further example, the effectorless Fc mutation is an N297A or D265A/N297A substitution within the constant region. In some instances, the isolated anti-PD-1 antibody is aglycosylated.
3.PD-L2結合アンタゴニスト
いくつかの例では、PD-1軸結合アンタゴニストはPD-L2結合アンタゴニストである。いくつかの例では、PD-L2結合アンタゴニストは、PD-L2のそのリガンド結合パートナーへの結合を阻害する分子である。特定の態様では、PD-L2結合リガンドパートナーはPD-1である。PD-L2結合アンタゴニストは、限定されないが、抗体、その抗原結合フラグメント、イムノアドヘシン、融合タンパク質、オリゴペプチド又は小分子であり得る。
3. PD-L2 Binding Antagonists In some examples, the PD-1 axis binding antagonist is a PD-L2 binding antagonist. In some examples, a PD-L2 binding antagonist is a molecule that inhibits the binding of PD-L2 to its ligand binding partner. In certain aspects, the PD-L2 binding ligand partner is PD-1. PD-L2 binding antagonists can be, but are not limited to, antibodies, antigen-binding fragments thereof, immunoadhesins, fusion proteins, oligopeptides or small molecules.
いくつかの例では、PD-L2結合アンタゴニストは抗PD-L2抗体である。本明細書の例のいずれかでは、抗PD-L2抗体は、ヒトPD-L2又はそのバリアントに結合することができる。いくつかの例では、抗PD-L2抗体はモノクローナル抗体である。いくつかの例では、抗PD-L2抗体は、Fab、Fab’、Fab’-SH、Fv、scFv、及び(Fab’)2フラグメントからなる群から選択される抗体フラグメントである。いくつかの例では、抗PD-L2抗体はヒト化抗体である。他の例では、抗PD-L2抗体はヒト抗体である。なお更なる特定の態様では、抗PD-L2抗体は、低下した又は最小のエフェクター機能を有する。更に特定の態様では、「エフェクターレスFc変異(effector-less Fc mutation)」又は非グリコシル化(aglycosylation)変異に起因する。なお更なる例では、エフェクターなしのFc突然変異は、定常領域内のN297A又はD265A/N297A置換である。いくつかの例では、単離された抗PD-L2抗体は、非グリコシル化されている。 In some examples, the PD-L2 binding antagonist is an anti-PD-L2 antibody. In any of the examples herein, an anti-PD-L2 antibody can bind to human PD-L2 or a variant thereof. In some examples, the anti-PD-L2 antibody is a monoclonal antibody. In some examples, the anti-PD-L2 antibody is an antibody fragment selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab') 2 fragments. In some examples, the anti-PD-L2 antibody is a humanized antibody. In other examples, the anti-PD-L2 antibody is a human antibody. In a still further specific aspect, the anti-PD-L2 antibody has reduced or minimal effector function. In a more particular aspect, it results from "effector-less Fc mutation" or aglycosylation mutation. In a still further example, the effectorless Fc mutation is an N297A or D265A/N297A substitution within the constant region. In some examples, the isolated anti-PD-L2 antibody is non-glycosylated.
そのような分子を含有する組成物を含む、本発明において有用なPD-1軸結合アンタゴニスト(例えば、アテゾリズマブ)は、抗TIGITアンタゴニスト抗体と組み合わせて使用され得る。 PD-1 axis binding antagonists (eg, atezolizumab) useful in the invention, including compositions containing such molecules, can be used in combination with anti-TIGIT antagonist antibodies.
更なる態様では、PD-1軸結合アンタゴニストは、上記の例のいずれかによるPD-1軸結合アンタゴニスト抗体であり、以下のセクションCに記載されるように、単独で又は組み合わせて任意の特徴を組み込むことができる。 In a further aspect, the PD-1 axis binding antagonist is a PD-1 axis binding antagonist antibody according to any of the above examples and any of the characteristics, alone or in combination, as described in Section C below. can be incorporated.
C.抗体の形態及び特性
1.抗体親和性
特定の例では、本明細書中提供される抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体、又は抗PD-1アンタゴニスト抗体)、抗VEGF抗体、及び/又は抗IL-6R抗体)は、1μM以下、100nM以下、10nM以下、1nM以下、0.1nM以下、0.01nM以下、又は0.001nM以下(例えば、10-8M以下、例えば10-8M~10-13M、例えば、10-9M~10-13M)の解離定数(KD)を有する。
C. Forms and Properties of
一例では、KDは、放射標識抗原結合アッセイ(RIA)によって測定される。一例では、RIAは、目的の抗体及びその抗原のFabバージョンを用いて実施される。例えば、抗原に対するFabの溶液結合親和性は、非標識抗原の滴定系の存在下で、最小濃度の(125I)標識抗原によりFabを平衡化し、次いで、結合した抗原を抗Fab抗体でコーティングしたプレートで捕捉することにより測定する(例えばChenら、J.Mol.Biol.293:865~881(1999)を参照されたい)。アッセイの条件を確立するために、MICROTITER(登録商標)マルチウェルプレート(Thermo Scientific)を、50mMの炭酸ナトリウム(pH9.6)中の5μg/mLの捕捉用抗Fab抗体(Cappel Labs)で一晩コーティングし、その後、PBS中の2%(w/v)ウシ血清アルブミンで2~5時間、室温(およそ23℃)でブロッキングする。非吸着性プレート(Nunc#269620)中で、100pM又は26pMの[125I]-抗原を、関心のあるFabの連続希釈物と混合する(例えば、Presta et al.,Cancer Res.57:4593-4599(1997)における抗VEGF抗体Fab-12の評定と一致する)。次いで、関心のあるFabを一晩インキュベートする;しかしながら、平衡に達することを達するために、インキュベーションをより長い期間(例えば、約65時間)継続してもよい。その後、室温でのインキュベーション(例えば、1時間)のために混合物を捕捉プレートに移す。次いで、溶液を除去し、プレートを、PBS中の0.1%のポリソルベート20(TWEEN-20(登録商標))で8回洗浄する。プレートが乾燥したら、150μL/ウェルのシンチラント(MICROSCINT-20(商標)、Packard)を添加し、プレートを10分間、TOPCOUNT(商標)ガンマカウンター(Packard)上で計数する。最大結合の20%以下をもたらす各Fabの濃度を、競合結合アッセイにおける使用のために選択する。 In one example, KD is measured by a radiolabeled antigen binding assay (RIA). In one example, RIA is performed using the antibody of interest and the Fab version of its antigen. For example, the solution binding affinity of Fabs for antigen was evaluated by equilibrating the Fabs with a minimal concentration of ( 125 I)-labeled antigen in the presence of a titration system of unlabeled antigen and then coating the bound antigen with anti-Fab antibody. Measured by plate capture (see, eg, Chen et al., J. Mol. Biol. 293:865-881 (1999)). To establish assay conditions, MICROTITER® multiwell plates (Thermo Scientific) were treated overnight with 5 μg/mL capture anti-Fab antibody (Cappel Labs) in 50 mM sodium carbonate, pH 9.6. Coat and then block with 2% (w/v) bovine serum albumin in PBS for 2-5 hours at room temperature (approximately 23°C). 100 pM or 26 pM of [ 125 I]-antigen is mixed with serial dilutions of the Fab of interest in non-adsorbing plates (Nunc#269620) (see, eg, Presta et al., Cancer Res. 57:4593- 4599 (1997) for the anti-VEGF antibody Fab-12). The Fab of interest is then incubated overnight; however, incubation may be continued for longer periods (eg, about 65 hours) to reach equilibrium. The mixture is then transferred to a capture plate for incubation (eg, 1 hour) at room temperature. The solution is then removed and the plate washed 8 times with 0.1% polysorbate 20 (TWEEN-20®) in PBS. Once the plates are dry, 150 μL/well of scintillant (MICROSCINT-20™, Packard) is added and the plates are counted for 10 minutes on a TOPCOUNT™ gamma counter (Packard). Concentrations of each Fab that yield 20% or less of maximal binding are selected for use in competitive binding assays.
別の一例によると、KDは、BIACORE(登録商標)表面プラズモン共鳴アッセイを使用して測定される。例えば、BIACORE(登録商標)-2000又はBIACORE(登録商標)-3000(BIAcore,Inc.,Piscataway,NJ)を使用するアッセイを、約10の反応単位(RU)で、固定化された抗原CM5チップによって25℃で実行する。一例では、カルボキシメチル化デキストランバイオセンサーチップ(CM5、BIACORE,Inc.)は、供給業者の指示に従って、N-エチル-N’-(3-ジメチルアミノプロピル)-カルボジイミドヒドロクロリド(EDC)及びN-ヒドロキシスクシンイミド(NHS)を用いて活性化される。抗原を、pH4.8の10mMの酢酸ナトリウムによって、5μg/ml(約0.2μM)に希釈した後、5μl/分の流速でインジェクトし、カップリングされたタンパク質のおよそ10応答ユニット(RU)を達成する。抗原のインジェクション後、1Mのエタノールアミンをインジェクトして、未反応基をブロックする。キネティクス測定のために、Fab(0.78nM~500nM)の2倍段階希釈物(0.05%のポリソルベート20(TWEEN-20(商標))界面活性剤(PBST)を有するPBS中)を、25℃で、およそ25μL/分の流速でインジェクトする。会合速度(kon)及び解離速度(koff)を、会合センサグラム及び解離センサグラムを同時に適合することによって、単純1対1Langmuir結合モデル(BIACORE(登録商標)Evaluation Software第3.2版)を使用して計算する。平衡解離定数(KD)は、koff/kon比として計算される。例えば、Chen et al.,J.Mol.Biol.293:865-881(1999)を参照されたい。オン速度が上記の表面プラズモン共鳴アッセイによって106M-1s-1を超える場合、このオン速度は、撹拌されたキュベットを備えるストップフロー装着分光光度計(Aviv Instruments)又は8000シリーズSLM-AMINCO(商標)分光光度計(ThermoSpectronic)等の分光計において測定される、漸増濃度の抗原の存在下で、25℃でのPBS(pH7.2)中の20nM抗-抗原抗体(Fab型)の蛍光発光強度(励起=295nm、発光=340nm、16nm帯域通過)の増加又は減少を測定する、蛍光クエンチ技法を使用することによって、判定することができる。
2.抗体フラグメント
According to another example, K D is measured using the BIACORE® surface plasmon resonance assay. For example, assays using BIACORE®-2000 or BIACORE®-3000 (BIAcore, Inc., Piscataway, NJ) can be performed at about 10 response units (RU) on immobilized antigen on a CM5 chip. at 25° C. by In one example, a carboxymethylated dextran biosensor chip (CM5, BIACORE, Inc.) was prepared with N-ethyl-N'-(3-dimethylaminopropyl)-carbodiimide hydrochloride (EDC) and N- Activated with hydroxysuccinimide (NHS). Antigen was diluted with 10 mM sodium acetate, pH 4.8, to 5 μg/ml (approximately 0.2 μM) before injection at a flow rate of 5 μl/min, resulting in approximately 10 response units (RU) of coupled protein. to achieve After injection of antigen, 1M ethanolamine is injected to block unreacted groups. For kinetic measurements, two-fold serial dilutions of Fabs (0.78 nM to 500 nM) in PBS with 0.05% polysorbate 20 (TWEEN-20™) detergent (PBST) were added to 25 °C and inject at a flow rate of approximately 25 μL/min. A simple one-to-one Langmuir binding model (BIACORE® Evaluation Software Version 3.2) was developed by simultaneously fitting the association rate (k on ) and dissociation rate (k off ) to the association and dissociation sensorgrams. Calculate using The equilibrium dissociation constant (K D ) is calculated as the ratio k off /k on . For example, Chen et al. , J. Mol. Biol. 293:865-881 (1999). If the on-rate exceeds 10 6 M- 1 s- 1 by the surface plasmon resonance assay described above, the on-rate can be measured using a stop-flow-equipped spectrophotometer (Aviv Instruments) with a stirred cuvette or an 8000 series SLM-AMINCO ( Fluorescence emission of 20 nM anti-antigen antibody (Fab type) in PBS (pH 7.2) at 25° C. in the presence of increasing concentrations of antigen as measured in a spectrometer such as the ThermoSpectronic™. It can be determined by using a fluorescence quenching technique that measures the increase or decrease in intensity (Excitation=295 nm, Emission=340 nm, 16 nm bandpass).
2. antibody fragment
特定の例では、本明細書中提供される抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)は、抗体フラグメントである。抗体フラグメントとしては、Fab、Fab’、Fab’-SH、F(ab’)2、Fv、及びscFvフラグメント、及び以下に記載する他のフラグメントが挙げられるがこれらに限定されない。特定の抗体フラグメントの総説としては、Hudson et al.Nat.Med.9:129-134(2003)を参照されたい。scFvフラグメントの参照には、例えばPluckthuen,in The Pharmacology of Monoclonal Antibodies,vol.113,Rosenburg and Moore eds.,(Springer-Verlag,New York),pp.269-315(1994)を参照されたい;また、国際公開第93/16185号を参照されたい;及び米国特許第5,571,894号及び同第5,587,458号も参照されたい。サルベージ受容体結合エピトープ残基を構成し、かつin vivo半減期を増加させたFab及びF(ab’)2フラグメントの議論については、米国特許第5,869,046号を参照されたい。 In certain examples, the anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) provided herein are antibody fragments. Antibody fragments include, but are not limited to, Fab, Fab', Fab'-SH, F(ab') 2 , Fv, and scFv fragments, and other fragments described below. Reviews of particular antibody fragments include Hudson et al. Nat. Med. 9:129-134 (2003). References to scFv fragments include, for example, Pluckthuen, in The Pharmacology of Monoclonal Antibodies, vol. 113, Rosenburg and Moore eds. , (Springer-Verlag, New York), pp. 269-315 (1994); see also WO 93/16185; and see also US Pat. Nos. 5,571,894 and 5,587,458. See US Pat. No. 5,869,046 for a discussion of Fab and F(ab') 2 fragments that constitute salvage receptor binding epitope residues and have increased in vivo half-lives.
ダイアボディは、二価又は二重特異性であり得る2つの抗原結合部位を有する抗体フラグメントである。例えば、欧州特許第404,097号、国際公開第1993/01161号、Hudson et al.Nat.Med.9:129-134(2003);and Hollinger et al.Proc.Natl.Acad.Sci.USA 90:6444-6448(1993)を参照されたい。トリアボディ及びテトラボディはまた、Hudson et al.Nat.Med.9:129-134(2003)においても説明されている。 Diabodies are antibody fragments with two antigen-binding sites that can be bivalent or bispecific. See, for example, EP 404,097, WO 1993/01161, Hudson et al. Nat. Med. 9:129-134 (2003); and Hollinger et al. Proc. Natl. Acad. Sci. See USA 90:6444-6448 (1993). Triabodies and tetrabodies are also described in Hudson et al. Nat. Med. 9:129-134 (2003).
単一ドメイン抗体は、抗体の重鎖可変ドメインの全て又は一部又は軽鎖可変ドメインの全て又は一部を含む抗体フラグメントである。特定の例では、単一ドメイン抗体は、ヒト単一ドメイン抗体である(Domantis,Inc.、マサチューセッツ州ウォルサム、例えば米国特許第6,248,516号B1を参照)。 Single domain antibodies are antibody fragments that contain all or part of the heavy chain variable domain or all or part of the light chain variable domain of an antibody. In a particular example, the single domain antibody is a human single domain antibody (Domantis, Inc., Waltham, Mass., see, eg, US Pat. No. 6,248,516 B1).
抗体フラグメントは、本明細書に記載されるように、組み換え宿主細胞(例えばE.coli又はファージ)による、インタクトな抗体のタンパク分解、及び産生を含むがこれらに限定されない各種技術により製造可能である。
3.キメラ抗体及びヒト化抗体
Antibody fragments can be produced by a variety of techniques including, but not limited to, proteolysis and production of intact antibodies by recombinant host cells (e.g., E. coli or phage) as described herein. .
3. Chimeric and humanized antibodies
特定の例では、本明細書中提供される抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)は、キメラ抗体である。特定のキメラ抗体は、例えば、米国特許第4,816,567号;及びMorrison et al.Proc.Natl.Acad.Sci.USA,81:6851-6855(1984))に記載されている。一例では、キメラ抗体は、非ヒト可変領域(例えば、マウス、ラット、ハムスター、ウサギ、又はサル等の非ヒト霊長類に由来する可変領域)とヒト定常領域を含む。更なる例では、キメラ抗体は、クラス又はサブクラスが親抗体のそれらから変更されている「クラススイッチ」抗体である。キメラ抗体は、その抗原結合フラグメントを含む。 In certain examples, the anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) provided herein are chimeric antibodies. Certain chimeric antibodies are described, for example, in US Pat. No. 4,816,567; and Morrison et al. Proc. Natl. Acad. Sci. USA, 81:6851-6855 (1984)). In one example, a chimeric antibody comprises a non-human variable region (eg, a variable region derived from a non-human primate such as mouse, rat, hamster, rabbit, or monkey) and a human constant region. In a further example, chimeric antibodies are "class-switched" antibodies in which the class or subclass has been altered from that of the parent antibody. A chimeric antibody includes an antigen-binding fragment thereof.
特定の例では、キメラ抗体は、ヒト化抗体である。典型的には、非ヒト抗体は、ヒトに対する免疫原性を低減する一方で、親非ヒト抗体の特異性及び親和性は保持するようにヒト化される。一般に、ヒト化抗体は、HVR、例えば、CDR(又はその一部)が非ヒト抗体由来であり、かつFR(又はその一部)がヒト抗体配列由来である1つ以上の可変ドメインを含む。ヒト化抗体はまた、任意に、ヒト定常領域の少なくとも一部を含む。いくつかの例では、ヒト化抗体中のいくつかのFR残基は、例えば、抗体特異性又は親和性を復元又は改善するために、非ヒト抗体(例えば、HVR残基が由来する抗体)由来の対応する残基で置換される。 In certain examples, a chimeric antibody is a humanized antibody. Typically, non-human antibodies are humanized to reduce their immunogenicity to humans while retaining the specificity and affinity of the parent non-human antibody. Generally, humanized antibodies comprise one or more HVRs, eg, variable domains in which the CDRs (or portions thereof) are derived from a non-human antibody and the FRs (or portions thereof) are derived from human antibody sequences. A humanized antibody optionally also will comprise at least a portion of a human constant region. In some instances, some FR residues in the humanized antibody are derived from a non-human antibody (e.g., the antibody from which the HVR residues are derived), e.g., to restore or improve antibody specificity or affinity. is substituted with the corresponding residue of
ヒト化抗体及びそれらの製造方法は、例えばAlmagro and Fransson,Front.Biosci.13:1619-1633(2008)にて総説されており、更にRiechmann et al.,Nature 332:323-329(1988);Queen et al.,Proc.Nat’l Acad.Sci.USA 86:10029-10033(1989);米国特許第5,821,337号、第7,527,791号、第6,982,321号及び第7,087,409号;Kashmiri et al.,Methods 36:25-34(2005)(特異性決定領域(SDR)の移植を記載);Padlan,Mol.Immunol.28:489-498(1991)(「リサーフェシング」を記載);Dall’Acqua et al.,Methods 36:43-60(2005)(「FRシャッフリング」を記載)、並びにOsbourn et al.,Methods 36:61-68(2005)及び Klimka et al.,Br.J.Cancer,83:252-260(2000)(FRシャッフリングに対する「誘導選択」手法を記載)に詳述されている。 Humanized antibodies and methods for their production are described, for example, in Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008) and further in Riechmann et al. , Nature 332:323-329 (1988); Queen et al. , Proc. Nat'l Acad. Sci. USA 86:10029-10033 (1989); US Patent Nos. 5,821,337, 7,527,791, 6,982,321 and 7,087,409; Kashmiri et al. , Methods 36:25-34 (2005) (describing the transplantation of the specificity determining region (SDR)); Padlan, Mol. Immunol. 28:489-498 (1991) (describing "resurfacing"); Dall'Acqua et al. , Methods 36:43-60 (2005) (describing "FR shuffling"), and Osbourn et al. , Methods 36:61-68 (2005) and Klimka et al. , Br. J. Cancer, 83:252-260 (2000) (describing a "guided selection" approach to FR shuffling).
ヒト化に用い得るヒトフレームワーク領域としては、以下が挙げられるが、これらに限定されない:「ベストフィット」法を用いて選択したフレームワーク領域(例えば、Sims et al.J.Immunol.151:2296(1993)を参照されたい);重鎖又は軽鎖可変領域の特定の亜型のヒト抗体コンセンサス配列に由来するフレームワーク領域(例えば、Carter et al.Proc.Natl.Acad.Sci.USA,89:4285(1992);及びPresta et al.J.Immunol.,151:2623(1993)を参照されたい);ヒト成熟(体細胞突然変異)フレームワーク領域又はヒト生殖系列フレームワーク領域(例えば、Almagro and Fransson,Front.Biosci.13:1619-1633(2008)を参照されたい);並びにFRライブラリのスクリーニングに由来するフレームワーク領域(例えば、Baca et al.,J.Biol.Chem.272:10678-10684(1997)及びRosok et al.,J.Biol.Chem.271:22611-22618(1996)を参照されたい)。 Human framework regions that can be used for humanization include, but are not limited to: framework regions selected using the "best fit" method (e.g., Sims et al. J. Immunol. 151:2296 (1993)); framework regions derived from human antibody consensus sequences of a particular subtype of the heavy or light chain variable region (e.g., Carter et al. Proc. Natl. Acad. Sci. USA, 89). :4285 (1992); and Presta et al., J. Immunol., 151:2623 (1993)); human mature (somatic mutation) framework regions or human germline framework regions (e.g., Almagro and Fransson, Front. Biosci. 13:1619-1633 (2008)); 10684 (1997) and Rosok et al., J. Biol. Chem. 271:22611-22618 (1996)).
4.ヒト抗体
特定の例では、本明細書中提供される抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)は、ヒト抗体である。ヒト抗体は、当該技術分野で公知の様々な技法を使用して作製され得る。ヒト抗体は一般的に、van Dijk and van de Winkel,Curr.Opin.Pharmacol.5:368-74(2001)及びLonberg,Curr.Opin.Immunol.20:450-459(2008)に記載されている。
4. Human Antibodies In certain examples, the anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) provided herein are human antibodies. be. Human antibodies can be made using various techniques known in the art. Human antibodies are generally described in van Dijk and van de Winkel, Curr. Opin. Pharmacol. 5:368-74 (2001) and Lonberg, Curr. Opin. Immunol. 20:450-459 (2008).
ヒト抗体は、抗原チャレンジに応答して、インタクトなヒト抗体又はヒト可変領域を有するインタクトな抗体を産生するように改変されたトランスジェニック動物に免疫原を投与することによって調製することができる。そのような動物は、典型的には、内因性免疫グロブリン遺伝子座に取って代わるか、又は染色体外に存在するか、又は動物の染色体にランダムに組み込まれるヒト免疫グロブリン遺伝子座の全部又は一部を含有する。そのようなトランスジェニックマウスでは、内因性免疫グロブリン遺伝子座は、一般的に不活性化されている。トランスジェニック動物からヒト抗体を得るための方法の総説については、Lonberg,Nat.Biotech.23:1117-1125(2005)を参照。また、例えば、XENOMOUSE(商標)技術を記載する米国特許第6,075,181号及び同第6,150,584号;HuMab(登録商標)技術を記載する米国特許第5,770,429号;K-M MOUSE(登録商標)技術を記載する米国特許第7,041,870号;及び、VelociMouse(登録商標)技術を記載する米国特許出願公開第2007/0061900号も参照されたい。そのような動物によって生成されるインタクトな抗体からのヒト可変領域は、例えば、異なるヒト定常領域と組み合わせることによって更に改変されてもよい。 Human antibodies can be prepared by administering an immunogen to transgenic animals that have been engineered to produce intact human antibodies or intact antibodies with human variable regions in response to antigenic challenge. Such animals typically have all or part of the human immunoglobulin loci replacing the endogenous immunoglobulin loci, or existing extrachromosomally, or randomly integrated into the animal's chromosomes. contains In such transgenic mice, the endogenous immunoglobulin loci are generally inactivated. For a review of methods for obtaining human antibodies from transgenic animals, see Lonberg, Nat. Biotech. 23:1117-1125 (2005). Also, for example, U.S. Pat. Nos. 6,075,181 and 6,150,584 describing XENOMOUSE™ technology; U.S. Pat. No. 5,770,429 describing HuMab® technology; See also US Pat. No. 7,041,870, which describes KM MOUSE® technology; and US Patent Application Publication No. 2007/0061900, which describes VelociMouse® technology. Human variable regions from intact antibodies produced by such animals may be further modified, for example, by combining with a different human constant region.
ヒト抗体は、ハイブリドーマに基づく方法によっても作製することができる。ヒトモノクローナル抗体を産生するためのヒト骨髄腫及びマウス-ヒト異種骨髄腫細胞株が記載されている。(例えば、Kozbor J.Immunol.,133:3001(1984);Brodeur et al.,Monoclonal Antibody Production Techniques and Applications,pp.51-63(Marcel Dekker,Inc.,New York,1987);及びBoerner et al.,J.Immunol.,147:86(1991)を参照。)ヒトB細胞ハイブリドーマ技術を介して生成されたヒト抗体もまた、Li et al.,Proc.Natl.Acad.Sci.USA,103:3557-3562(2006)に記載されている。更なる方法は、例えば、米国特許第7,189,826号(ハイブリドーマ細胞株由来のモノクローナルヒトIgM抗体の産生を記載する)、及びNi,Xiandai Mianyixue,26(4):265-268(2006)(ヒト-ヒトハイブリドーマを記載する)を含む。ヒトハイブリドーマ技術(トリオーマ技術)はまた、Histology and Histopathology,20(3):927-937(2005)及びVollmers and Brandlein,Methods and Findings in Experimental and Clinical Pharmacology,27(3):185-91(2005)にも記載されている。 Human antibodies can also be made by hybridoma-based methods. Human myeloma and mouse-human xenomyeloma cell lines have been described for the production of human monoclonal antibodies. (eg, Kozbor J. Immunol., 133:3001 (1984); Brodeur et al., Monoclonal Antibody Production Techniques and Applications, pp. 51-63 (Marcel Dekker, Inc., New York 7 et al.) and B198; , J. Immunol., 147:86 (1991).) Human antibodies generated via human B-cell hybridoma technology have also been described by Li et al. , Proc. Natl. Acad. Sci. USA, 103:3557-3562 (2006). Additional methods are described, for example, in US Pat. No. 7,189,826 (describing the production of monoclonal human IgM antibodies from hybridoma cell lines), and Ni, Xiandai Mianyixue, 26(4):265-268 (2006). (describing human-human hybridomas). Human hybridoma technology (trioma technology) is also described in Histology and Histopathology, 20(3):927-937 (2005) and Vollmers and Brandlein, Methods and Findings in Experimental and Clinical Pharmacology, 1805-1 (525-9). is also described.
ヒト抗体は、ヒト由来のファージディスプレイライブラリから選択されるFvクローン可変ドメイン配列を単離することによっても作製され得る。その後、そのような可変ドメイン配列は、所望のヒト定常ドメインと組み合わせられ得る。抗体ライブラリからヒト抗体を選択するための技術を以下に記載する。
5.ライブラリ由来の抗体
Human antibodies may also be generated by isolating Fv clone variable domain sequences selected from human-derived phage display libraries. Such variable domain sequences can then be combined with the desired human constant domain. Techniques for selecting human antibodies from antibody libraries are described below.
5. Antibodies from libraries
本発明の抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)は、所望の一又は複数の活性を有する抗体についてコンビナトリアルライブラリをスクリーニングすることによって単離され得る。例えば、ファージディスプレイライブラリを生成し、所望の結合特性を有する抗体についてそのようなライブラリをスクリーニングするための様々な方法が当該技術分野で知られている。そのような方法については、例えば、Hoogenboom et al.in Methods in Molecular Biology 178:1-37(O’Brien et al.,ed.,Human Press,Totowa,NJ,2001)で概説し、McCafferty et al.,Nature 348:552-554;Clackson et al.,Nature 352:624-628(1991);Marks et al.,J.Mol.Biol.222:581-597(1992);Marks and Bradbury,in Methods in Molecular Biology 248:161-175(Lo,ed.,Human Press,Totowa,NJ,2003);Sidhu et al.,J.Mol.Biol.338(2):299-310(2004);Lee et al.,J.Mol.Biol.340(5):1073-1093(2004);Fellouse,Proc.Natl.Acad.Sci.USA 101(34):12467-12472(2004);及びLee et al.,J.Immunol.Methods 284(1-2):119-132(2004)に更に記載されている。 Anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) of the invention screen combinatorial libraries for antibodies having the desired activity or activities. can be isolated by For example, various methods are known in the art for generating phage display libraries and screening such libraries for antibodies with desired binding properties. Such methods are described, for example, in Hoogenboom et al. in Methods in Molecular Biology 178:1-37 (O'Brien et al., ed., Human Press, Totowa, NJ, 2001); , Nature 348:552-554; Clackson et al. , Nature 352:624-628 (1991); Marks et al. , J. Mol. Biol. 222:581-597 (1992); Marks and Bradbury, in Methods in Molecular Biology 248:161-175 (Lo, ed., Human Press, Totowa, NJ, 2003); Sidhu et al. , J. Mol. Biol. 338(2):299-310 (2004); Lee et al. , J. Mol. Biol. 340(5):1073-1093 (2004); Fellowe, Proc. Natl. Acad. Sci. USA 101(34):12467-12472 (2004); and Lee et al. , J. Immunol. Methods 284(1-2):119-132 (2004).
特定のファージディスプレイ法では、VH及びVL遺伝子のレパートリーは、ポリメラーゼ連鎖反応(PCR)によって別個にクローニングされ、ファージライブラリ中でランダムに再結合され、次いで、Winter et al.,Ann.Rev.Immunol.,12:433-455(1994)に記載されているように抗原結合ファージのスクリーニングを行うことができる。ファージは、典型的には、抗体フラグメントを一本鎖Fv(scFv)フラグメント又はFabフラグメントのいずれかとしてディスプレイする。免疫源からのライブラリは、ハイブリドーマを構築する必要なしに、免疫原に対する高親和性抗体を提供する。代替的に、ナイーブレパートリは、Griffiths et al.,EMBO J,12:725-734(1993)によって記載されているように、免疫化を行わずに、広範囲の非自己抗原及びまた自己抗原に対する抗体の単一の供給源を提供するために、(例えば、ヒトから)クローン化することができる。最後に、ナイーブライブラリは、幹細胞から再配列されていないV遺伝子セグメントをクローニングし、ランダムな配列を含むPCRプライマーを使用して、非常に可変的なCDR3領域をコードし、Hoogenboom and Winter,J.Mol.Biol.,227:381-388(1992)に記載されているように、in vitroで再配列を達成することによって、合成的に作製することもできる。ヒト抗体ファージライブラリについて記載する特許公報としては、例えば:米国特許第5,750,373号、並びに米国特許出願公開第2005/0079574号、同第2005/0119455号、同第2005/0266000号、同第2007/0117126号、同第2007/0160598号、同第2007/0237764号、同第2007/0292936号、及び同第2009/0002360号が挙げられる。 In a particular phage display method, repertoires of VH and VL genes are separately cloned by polymerase chain reaction (PCR), randomly recombined in a phage library, and then used as described by Winter et al. , Ann. Rev. Immunol. , 12:433-455 (1994). Phage typically display antibody fragments, either as single-chain Fv (scFv) or Fab fragments. Libraries from immunogens provide high affinity antibodies to immunogens without the need to construct hybridomas. Alternatively, a naive repertoire can be found in Griffiths et al. , EMBO J, 12:725-734 (1993), to provide a single source of antibodies against a wide range of non-self and also self antigens without immunization. It can be cloned (eg, from humans). Finally, a naive library was created by cloning unrearranged V-gene segments from stem cells and using PCR primers containing random sequences to encode the highly variable CDR3 region, Hoogenboom and Winter, J. Am. Mol. Biol. , 227:381-388 (1992), by effecting rearrangements in vitro. Patent publications describing human antibody phage libraries include, for example: US Pat. 2007/0117126, 2007/0160598, 2007/0237764, 2007/0292936, and 2009/0002360.
抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体)又はヒト抗体ライブラリから単離された抗体フラグメントは、本明細書ではヒト抗体又はヒト抗体フラグメントとみなされる。 Anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies) or antibody fragments isolated from human antibody libraries are considered human antibodies or human antibody fragments herein. .
6.抗体バリアント
特定の例では、本発明の抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)のアミノ酸配列バリアントが意図される。本明細書で詳細に記載されるように、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体)は、所望の構造的及び機能的特性に基づいて最適化され得る。例えば、抗体の結合親和性及び/又は他の生物学的特性を改善することが望ましい場合がある。抗体のアミノ酸配列バリアントは、抗体をコードするヌクレオチド配列中に適正な修飾を導入することによって、又はペプチド合成によって調製されてもよい。このような改変としては、例えば、抗体のアミノ酸配列内の残基からの欠失、及び/又は抗体のアミノ酸配列内の残基への挿入、及び/又は抗体のアミノ酸配列内の残基の置換が挙げられる。欠失、挿入、及び置換の任意の組合せにより、最終構築物に到達することができるが、但し、最終構築物が所望される特徴、例えば、抗原結合を保有することを条件とする。
6. Antibody Variants In certain examples, amino acid sequence variants of anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (eg, anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) of the invention are contemplated. As described in detail herein, anti-TIGIT antagonist antibodies and PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies) are optimized based on desired structural and functional properties. obtain. For example, it may be desirable to improve the binding affinity and/or other biological properties of an antibody. Amino acid sequence variants of the antibody may be prepared by introducing appropriate modifications into the nucleotide sequence encoding the antibody, or by peptide synthesis. Such modifications include, for example, deletions from, and/or insertions into, and/or substitutions of residues within the amino acid sequences of the antibody. are mentioned. Any combination of deletion, insertion, and substitution can be made to arrive at the final construct, provided that the final construct possesses the desired characteristics, eg, antigen binding.
I.置換、挿入、及び欠失バリアント
特定の例では、1つ以上のアミノ酸置換を有する抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)バリアントが提供される。置換による突然変異誘発に関して目的の部位には、HVR及びFRが含まれる。保存的置換は、表3において、「好ましい置換」の見出しの下に示される。より実質的な変化は、表3において、「例示的な置換」の見出しの下に提供され、またアミノ酸側鎖クラスを参照して以下に更に記載される通りである。アミノ酸置換は、目的の抗体中に導入され得、その産物は、所望の活性、例えば、保持/改善された抗原結合、減少した免疫原性、又は改善されたADCC若しくはCDCについてスクリーニングされ得る。

アミノ酸は共通の側鎖特性に従ってグループ化することができる。
(1)疎水性:ノルロイシン、Met、Ala、Val、Leu、Ile;
(2)中性親水性:Cys、Ser、Thr、Asn、Gln;
(3)酸性:Asp、Glu;
(4)塩基性:His、Lys、Arg;
(5)鎖配向に影響を及ぼす残基:Gly、Pro;
(6)芳香族:Trp、Tyr、Phe。
Amino acids can be grouped according to common side chain properties.
(1) Hydrophobic: Norleucine, Met, Ala, Val, Leu, Ile;
(2) neutral hydrophilicity: Cys, Ser, Thr, Asn, Gln;
(3) acidic: Asp, Glu;
(4) basic: His, Lys, Arg;
(5) residues affecting chain orientation: Gly, Pro;
(6) Aromatics: Trp, Tyr, Phe.
非保存的置換は、これらのクラスの1つのメンバーを別のクラスと交換することを伴うであろう。 Non-conservative substitutions will entail exchanging a member of one of these classes for another class.
1つの種類の置換型バリアントは、親抗体(例えば、ヒト化抗体又はヒト抗体)の1つ以上の超可変領域残基を置換することを伴う。一般に、更なる試験ために選択される結果として生じるバリアント(複数可)は、親抗体と比較して特定の生物学的特性(例えば、親和性の増加、免疫原性の低減)の修正(例えば、改善)を有し、かつ/又は実質的に保持された親抗体の特定の生物学的特性を有する。例示的な置換型バリアントは、親和性成熟した抗体であり、例えば、本明細書に記載されるようなファージディスプレイに基づく親和性成熟技法を使用して、簡便に生成され得る。要するに、1つ以上のHVR残基が変異され、バリアント抗体がファージにディスプレイされ、特定の生物活性(例えば、結合親和性)についてスクリーニングされる。 One type of substitutional variant involves substituting one or more hypervariable region residues of a parent antibody (eg, a humanized or human antibody). Generally, the resulting variant(s) selected for further testing are modified (e.g. , improvement) and/or have substantially retained certain biological properties of the parent antibody. Exemplary substitutional variants are affinity matured antibodies, which can be conveniently generated using, for example, phage display-based affinity maturation techniques as described herein. Briefly, one or more HVR residues are mutated and the variant antibodies are displayed on phage and screened for a particular biological activity (eg, binding affinity).
変更(例えば、置換)は、抗体親和性を改善するために、例えば、HVRにおいて行われてもよい。そのような改変は、HVR「ホットスポット」、すなわち、体細胞成熟プロセス中に高頻度で突然変異を受けるコドンによってコードされる残基(例えば、Chowdhury,Methods Mol.Biol.207:179-196(2008)を参照されたい)、及び/又は抗原と接触する残基内で行われ得、結果として得られるバリアントVH又はVLが結合親和性について試験される。二次ライブラリを構築し、それから再選択することによる親和性成熟が、例えば、Hoogenboom et al.in Methods in Molecular Biology 178:1-37(O’Brien et al.,ed.,Human Press,Totowa,NJ,(2001))に記載されている。親和性成熟のいくつかの例では、多様な方法(例えば、エラープローンPCR、鎖シャッフリング、又はオリゴヌクレオチド指向性突然変異誘発)のいずれかによって、成熟のために選択される可変遺伝子に多様性が導入される。次いで、二次ライブラリが作製される。その後、このライブラリがスクリーニングされて、所望の親和性を有する任意の抗体バリアントを特定する。多様性を導入するための別の方法は、いくつかのHVR残基(例えば、一度に4~6個の残基)をランダム化する、HVR指向性アプローチを含む。抗原結合に関与するHVR残基は、例えば、アラニンスキャニング変異誘発又はモデリングを使用して、特異的に特定され得る。特にCDR-H3及びCDR-L3が標的とされることが多い。 Alterations (eg, substitutions) may be made, eg, in HVRs, to improve antibody affinity. Such alterations are made by HVR "hotspots", i.e., residues encoded by codons that are frequently mutated during the somatic maturation process (e.g., Chowdhury, Methods Mol. Biol. 207:179-196). 2008)), and/or within residues that contact the antigen, and the resulting variant VH or VL is tested for binding affinity. Affinity maturation by constructing secondary libraries and reselecting from them is described, for example, in Hoogenboom et al. in Methods in Molecular Biology 178:1-37 (O'Brien et al., ed., Human Press, Totowa, NJ, (2001)). In some examples of affinity maturation, diversity is introduced into the variable genes selected for maturation by any of a variety of methods (e.g., error-prone PCR, strand shuffling, or oligonucleotide-directed mutagenesis). be introduced. A secondary library is then created. This library is then screened to identify any antibody variants with the desired affinity. Another method for introducing diversity involves an HVR-directed approach that randomizes several HVR residues (eg, 4-6 residues at a time). HVR residues involved in antigen binding can be specifically identified using, for example, alanine scanning mutagenesis or modeling. In particular, CDR-H3 and CDR-L3 are often targeted.
特定の例では、置換、挿入、又は欠失は、そのような改変が抗体の抗原に結合する能力を実質的に低減させない限り、1つ以上のHVR内で生じ得る。例えば、結合親和性を実質的に低下させない保存的改変(例えば、本明細書に提供される保存的置換)が、HVR中で行われてよい。そのような変化は、例えば、HVR内の抗原接触残基の外側であり得る。上述のバリアントVH及びVL配列の特定の例では、各HVRは、改変されていないか又は1つ、2つ、若しくは3つ以下のアミノ酸置換を有するかのいずれかである。 In certain instances, substitutions, insertions, or deletions may occur within one or more HVRs, so long as such modifications do not substantially reduce the ability of the antibody to bind antigen. For example, conservative modifications (eg, conservative substitutions provided herein) that do not substantially reduce binding affinity may be made in HVRs. Such changes can be, for example, outside the antigen contacting residues within the HVR. In the specific examples of variant VH and VL sequences described above, each HVR is either unmodified or has no more than 1, 2, or 3 amino acid substitutions.
変異導入の標的となり得る抗体の残基又は領域を同定するための有用な方法は、Cunningham and Wells(1989)Science,244:1081-1085に記載されているように「アラニンスキャニング変異導入」と呼ばれる。この方法では、抗体と抗原との相互作用が影響を受けるかどうかを判定するために、残基又は標的残基群(例えば、荷電残基、例えば、Arg、Asp、His、Lys及びGlu)が同定され、中性又は負に荷電したアミノ酸(例えば、アラニン又はポリアラニン)によって置き換えられる。更なる置換が、初期置換に対する機能的感受性を示すアミノ酸位置に導入されてもよい。あるいは、又は加えて、抗体と抗原との間の接点を特定するための抗原-抗体複合体の結晶構造。そのような接触残基及び隣接残基は、置換の候補として標的とされるか又は除去されてもよい。バリアントを、所望の特性を有するか否かを判定するためにスクリーニングしてもよい。 A useful method for identifying residues or regions of an antibody that can be targeted for mutagenesis is called "alanine scanning mutagenesis" as described in Cunningham and Wells (1989) Science, 244:1081-1085. . In this method, a residue or group of target residues (e.g., charged residues such as Arg, Asp, His, Lys, and Glu) are used to determine whether antibody-antigen interaction is affected. Identified and replaced by a neutral or negatively charged amino acid (eg, alanine or polyalanine). Further substitutions may be introduced at amino acid positions demonstrating functional sensitivity to the initial substitutions. Alternatively, or additionally, a crystal structure of the antigen-antibody complex to identify contact points between the antibody and the antigen. Such contact residues and flanking residues may be targeted as candidates for substitution or removed. Variants may be screened to determine whether they possess the desired property.
アミノ酸配列挿入には、1個の残基から100個以上の残基を含むポリペプチドまでの長さの範囲のアミノ末端及び/又はカルボキシル末端融合、並びに1個又は複数のアミノ酸残基の配列内挿入が含まれる。末端挿入の例には、N末端メチオニル残基を有する抗体が含まれる。抗体分子の他の挿入バリアントとしては、抗体の血清半減期を増加させる酵素(例えば、ADEPTのための)又はポリペプチドへの抗体のN末端又はC末端の融合が挙げられる。 Amino acid sequence insertions include amino- and/or carboxyl-terminal fusions ranging in length from one residue to polypeptides containing a hundred or more residues, as well as intrasequence of one or more amino acid residues. Includes inserts. Examples of terminal insertions include antibodies with N-terminal methionyl residues. Other insertional variants of the antibody molecule include N- or C-terminal fusions of the antibody to enzymes (eg, for ADEPT) or polypeptides that increase the serum half-life of the antibody.
II.グリコシル化バリアント
特定の例では、本発明の抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)は、抗体がグリコシル化される程度を増加又は減少させるように変更することができる。本発明の抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体)へのグリコシル化部位の付加又は欠失は、1つ以上のグリコシル化部位を作り出すか又は除去するように、アミノ酸配列を変化させることによって、簡便に達成されることができる。
II. Glycosylation Variants In certain examples, the anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies) of the invention are glycosylated. Modifications can be made to increase or decrease the degree. Addition or deletion of glycosylation sites to the anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies) of the invention creates one or more glycosylation sites or It can be conveniently accomplished by altering the amino acid sequence so as to remove it.
抗体がFc領域を含む場合、それに付着した炭水化物が改変され得る。哺乳動物細胞によって産生された天然抗体は、典型的には、N結合によってFc領域のCH2ドメインのAsn297に一般に付着される分岐状の二分岐オリゴ糖を含む。例えば、Wright et al.TIBTECH15:26-32(1997)を参照されたい。オリゴ糖には、様々な炭水化物、例えば、マンノース、N-アセチルグルコサミン(GlcNAc)、ガラクトース、及びシアル酸、並びに二分岐オリゴ糖構造の「幹」のGlcNAcに付着したフコースが含まれ得る。いくつかの例では、特定の特性が改善された抗体バリアントを作製するために、本発明の抗体中におけるオリゴ糖の修飾が行われる。 Where the antibody contains an Fc region, the carbohydrate attached to it may be modified. Natural antibodies produced by mammalian cells typically contain branched, biantennary oligosaccharides commonly attached to Asn297 of the CH2 domain of the Fc region by an N-linkage. For example, Wright et al. See TIBTECH 15:26-32 (1997). Oligosaccharides can include a variety of carbohydrates, such as mannose, N-acetylglucosamine (GlcNAc), galactose, and sialic acid, as well as fucose attached to the "stem" GlcNAc of the biantennary oligosaccharide structure. In some instances, oligosaccharide modifications in the antibodies of the invention are made to generate antibody variants with improved specific properties.
一例では、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)のバリアントは、Fc領域に(直接的又は間接的に)付着したフコースを欠く炭水化物構造を有するものが提供される。例えば、そのような抗体内のフコースの量は、1%~80%、1%~65%、5%~65%又は20%~40%であり得る。フコースの量は、例えば、国際公開第2008/077546号に記載されているように、MALDI-TOF質量分析法によって測定されたように、Asn297(例えば、複合体構造、ハイブリッド構造、及び高マンノース構造)に付着した全ての糖鎖構造の合計に対するAsn297における糖鎖内のフコースの平均量を計算することによって判定される。Asn297は、Fc領域の約297位に位置するアスパラギン残基を指す(Fc領域残基のEUナンバリング);ただし、Asn297はまた、抗体のマイナーな配列変化のために、位置297の上流又は下流、すなわち位置294と300の間の約±3個のアミノ酸に位置していてもよい。このようなフコシル化バリアントは、ADCCの機能を改善している可能性がある。例えば、米国特許出願公開第2003/0157108号(Presta,L.);同第2004/0093621号(Kyowa Hakko Kogyo Co.,Ltd)を参照されたい。「脱フコシル化」又は「フコース欠乏」抗体バリアントに関する刊行物の例としては:米国特許出願公開第2003/0157108号;国際公開第2000/61739号;同第2001/29246号;米国特許出願公開第2003/0115614号;同第2002/0164328号;同第2004/0093621号;同第2004/0132140号;同第2004/0110704号;同第2004/0110282号;同第2004/0109865号;国際公開第2003/085119号;同第2003/084570号;同第2005/035586号;同第2005/035778号;同第2005/053742号;同第2002/031140号;Okazaki et al.J.Mol.Biol.336:1239-1249(2004);Yamane-Ohnuki et al.Biotech.Bioeng.87:614(2004)が挙げられる。デフコシル化抗体を産生することができる細胞株の例としては、タンパク質フコシル化を欠損するLec13 CHO細胞(Ripka et al.Arch.Biochem.Biophys.249:533-545(1986);米国特許出願公開第2003/0157108号A1,Presta,L;及び国際公開第2004/056312号A1,Adams et al.,特に実施例11)、及びノックアウト細胞株、例えばα-1,6-フコシルトランスフェラーゼ遺伝子、FUT8、ノックアウトCHO細胞(例えば、Yamane-Ohnuki et al.Biotech.Bioeng.87:614(2004);Kanda,Y.et al.,Biotechnol.Bioeng.,94(4):680-688(2006);及び国際公開第2003/085107号を参照されたい)。
In one example, a variant of an anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (e.g., an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody) is attached (directly or indirectly) to the Fc region Carbohydrate structures lacking fucose are provided. For example, the amount of fucose in such antibodies can be 1%-80%, 1%-65%, 5%-65% or 20%-40%. The amount of fucose is determined by MALDI-TOF mass spectrometry, for example as described in WO 2008/077546, Asn297 (e.g. complex, hybrid and high mannose structures). ) by calculating the average amount of fucose within the sugar chain at Asn297 for the sum of all sugar chain structures attached to . Asn297 refers to the asparagine residue located at about position 297 of the Fc region (EU numbering of Fc region residues); That is, it may be located at about ±3 amino acids between
上記を考慮して、いくつかの例では、本発明の方法は、非グリコシル化部位突然変異を含む抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えばアテゾリズマブ)又は抗PD-1アンタゴニスト抗体)バリアントを、分割された用量漸増投薬レジメンの状況で対象に投与することを含む。いくつかの例では、アグリコシル化部位突然変異は、抗体のエフェクター機能を低下させる。いくつかの例では、アグリコシル化部位の突然変異は、置換突然変異である。いくつかの例では、抗体は、エフェクター機能を低下させるFc領域における置換突然変異を含む。いくつかの例では、置換突然変異は、アミノ酸残基N297、L234、L235、及び/又はD265(EUナンバリング)におけるものである。いくつかの例では、置換突然変異は、N297G、N297A、L234A、L235A、D265A、及びP329Gからなる群から選択される。いくつかの例では、置換突然変異は、アミノ酸残基N297におけるものである。好ましい例では、置換突然変異は、N297Aである。 In view of the above, in some examples, the methods of the invention include anti-TIGIT antagonist antibodies comprising non-glycosylation site mutations (e.g., anti-TIGIT antagonist antibodies disclosed herein (e.g., tiragolumab) and /or administering a PD-1 axis binding antagonist antibody (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody) variant to the subject in the context of a divided dose escalating dosing regimen. In some examples, the aglycosylation site mutations reduce the effector function of the antibody.In some examples, the aglycosylation site mutations are substitution mutations.In some examples, the aglycosylation site mutations are substitution mutations. The antibodies comprise substitution mutations in the Fc region that reduce effector function, hi some examples, the substitution mutations are at amino acid residues N297, L234, L235, and/or D265 (EU numbering). In some examples, the substitution mutation is selected from the group consisting of N297G, N297A, L234A, L235A, D265A, and P329G In some examples, the substitution mutation is at amino acid residue N297 In a preferred example, the substitution mutation is N297A.
二分されたオリゴ糖類を有する、例えば、抗体のFc領域に結合した二分岐オリゴ糖がGlcNAcによって二分されている、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体抗PD-1アンタゴニスト抗体)バリアントが更に提供される。そのような抗体バリアントは、低減されたフコシル化及び/又は改善されたADCC機能を有し得る。そのような抗体バリアントの例は、例えば、国際公開第2003/011878(Jean-Mairet et al.);米国特許第6,602,684号(Umana et al.);及び米国特許出願公開第2005/0123546号(Umana et al)に記載されている。Fc領域に付着したオリゴ糖の少なくとも1つのガラクトース残基を有する抗体バリアントも提供される。そのような抗体バリアントは、改善されたCDC機能を有し得る。このような抗体バリアントは、例えば、国際公開第1997/30087号(Patel et al.);国際公開第1998/58964号(Raju,S.);及び国際公開第1999/22764号(Raju,S.)に記載されている。 Anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 Further provided are antagonist antibody (anti-PD-1 antagonist antibody) variants. Such antibody variants may have reduced fucosylation and/or improved ADCC function. Examples of such antibody variants are, for example, WO 2003/011878 (Jean-Mairet et al.); US Patent No. 6,602,684 (Umana et al.); 0123546 (Umana et al). Antibody variants having at least one galactose residue of the oligosaccharide attached to the Fc region are also provided. Such antibody variants may have improved CDC function. Such antibody variants are described, for example, in WO 1997/30087 (Patel et al.); WO 1998/58964 (Raju, S.); and WO 1999/22764 (Raju, S.; )It is described in.
III.Fc領域バリアント
特定の例では、1つ以上のアミノ酸修飾が、本発明の抗TIGITアンタゴニスト(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体)のFc領域に導入され、それにより、Fc領域バリアントが作製される(例えば、米国特許出願公開第2012/0251531号明細書を参照)。Fc領域バリアントは、1つ以上のアミノ酸位置にアミノ酸修飾(例えば、置換)を含むヒトFc領域配列(例えば、ヒトIgG1、IgG2、IgG3、又はIgG4 Fc領域)を含み得る。
III. Fc Region Variants In certain examples, one or more amino acid modifications are associated with an anti-TIGIT antagonist (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab) antibody of the invention and/or PD-1 axis binding. introduced into the Fc region of an antagonist antibody (e.g., an anti-PD-L1 antagonist antibody (e.g., atezolizumab) or an anti-PD-1 antagonist antibody), thereby creating an Fc region variant (e.g., US Patent Application Publication No. 2012 /0251531). An Fc region variant can include a human Fc region sequence (eg, a human IgG1, IgG2, IgG3, or IgG4 Fc region) with amino acid modifications (eg, substitutions) at one or more amino acid positions.
特定の例では、本発明は、全てではないが、いくつかのエフェクター機能を有することにより、in vivoでの抗体の半減期が重要ではあるが、特定のエフェクター機能(補体及びADCC等)が不要又は有害である用途に望ましい候補となる、抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体バリアントを企図する。CDC及び/又はADCC活性の低下/消失を確認するために、in vitro及び/又はin vivoの細胞毒性アッセイを実施することができる。例えば、Fc受容体(FcR)結合アッセイを実行して、抗体がFcγR結合を欠いている(そのため、ADCC活性を欠いている可能性が高い)が、FcRn結合能力を保持することを確認することができる。ADCCを媒介するための主要な細胞であるNK細胞は、Fc(RIIIのみを発現するが、一方で単球は、Fc(RI、Fc(RII、及びFc(RIIIを発現する。造血細胞でのFcR発現は、Ravetch及びKinet、Annu.Rev.Immunol.、9:457~492(1991)の464頁、表3にまとめられている。目的の分子のADCC活性を評定するためのin vitroアッセイの非限定的な例は、米国特許第5,500,362号(例えば、Hellstrom,I.et al.Proc.Nat’l Acad.Sci.USA 83:7059-7063(1986)を参照)及びHellstrom,I et al.,Proc.Nat’l Acad.Sci.USA 82:1499-1502(1985);5,821,337(Bruggemann,M.et al.,J.Exp.Med.166:1351-1361(1987)を参照)に記載されている。或いは、非放射性アッセイ方法を使用してもよい(例えば、フローサイトメトリー(CellTechnology、Inc.、カナダ、マウンテンビュー)のためのACTI(商標)非放射性細胞傷害アッセイ、及びCYTOTOX 96(登録商標)非放射性細胞傷害アッセイ(Promega、ワイオミング州マディソン))。そのようなアッセイに有用なエフェクター細胞としては、末梢血単核細胞(PBMC)及びナチュラルキラー(NK)細胞が挙げられる。代替的又は追加的に、関心のある分子のADCC活性は、in vivo、例えば、Clynes et al.Proc.Nat’l Acad.Sci.USA 95:652-656(1998)に開示されているような動物モデルで評定することができる。また、抗体がC1qに結合することができず、CDC活性を欠いていることを確認するために、C1q結合アッセイを実施してもよい。例えば、国際公開第2006/029879号及び国際公開第2005/100402号における、C1q及びC3c結合ELISAを参照されたい。補体活性化を評定するため、CDCアッセイを実施してもよい(例えば、Gazzano-Santoro et al.J.Immunol.Methods 202:163(1996);Cragg,M.S.et al.Blood.101:1045-1052(2003);及びCragg,M.S.and M.J.Glennie Blood.103:2738-2743(2004)を参照)。FcRn結合及びin vivoクリアランス/半減期の決定はまた、当該技術分野で知られている方法を用いて行うことができる(例えば、Petkova,S.B.et al.Int’l.Immunol.18(12):1759-1769(2006)参照)。 In certain instances, the present invention provides that by having some, but not all, effector functions, the half-life of antibodies in vivo is important, but certain effector functions (such as complement and ADCC) are important. Anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibody variants) are contemplated as desirable candidates for unwanted or harmful uses. Reduced/absence of CDC and/or ADCC activity. In vitro and/or in vivo cytotoxicity assays can be performed to confirm, for example, performing Fc receptor (FcR) binding assays to determine if the antibody lacks FcγR binding (thus NK cells, which are the primary cells for mediating ADCC, express Fc (RIII only), but retain FcRn binding capacity. , whereas monocytes express Fc(RI, Fc(RII, and Fc(RIII). FcR expression in hematopoietic cells has been reported by Ravetch and Kinet, Annu. 464, Table 3. Non-limiting examples of in vitro assays for assessing ADCC activity of a molecule of interest are described in US Pat. et al., Proc. Nat'l Acad. Sci. USA 83:7059-7063 (1986)) and Hellstrom, I et al., Proc. 5, 821, 337 (see Bruggemann, M. et al., J. Exp. Med. 166:1351-1361 (1987). Alternatively, non-radioactive assay methods may be used. (e.g., ACTI™ Non-Radioactive Cytotoxicity Assay for Flow Cytometry (CellTechnology, Inc., Mountain View, Canada) and CYTOTOX 96® Non-Radioactive Cytotoxicity Assay (Promega, Madison, WY)) Useful effector cells for such assays include peripheral blood mononuclear cells (PBMC) and natural killer (NK) cells. The ADCC activity of the molecule is determined in vivo, eg, by Clynes et al. Proc. Nat'l Acad. Sci. USA 95:652-656 (1998) can be evaluated in animal models. A C1q binding assay may also be performed to confirm that the antibody is incapable of binding C1q and lacks CDC activity. See, for example, C1q and C3c binding ELISAs in WO2006/029879 and WO2005/100402. CDC assays may be performed to assess complement activation (eg, Gazzano-Santoro et al. J. Immunol. Methods 202:163 (1996); Cragg, M. S. et al. Blood. 101 : 1045-1052 (2003); and Cragg, M. S. and M. J. Glennie Blood. 103:2738-2743 (2004)). Determination of FcRn binding and in vivo clearance/half-life can also be performed using methods known in the art (e.g., Petkova, SB et al. Int'l. Immunol. 18 ( 12): 1759-1769 (2006)).
エフェクター機能が低下した抗体には、Fc領域残基238、265、269、270、297、327及び329の1つ以上が置換されたものが含まれる(米国特許第6,737,056号及び同第8,219,149号)。このようなFc突然バリアントとしては、アラニンへの残基265及び297の置換を有するいわゆる「DANA」Fc突然バリアントを含む、アミノ酸265位、269位、270位、297位、及び327位のうちの2つ以上において置換を有するFc突然バリアントが挙げられる(米国特許第7,332,581号及び同第8,219,149号)。 Antibodies with reduced effector function include those in which one or more of Fc region residues 238, 265, 269, 270, 297, 327 and 329 have been substituted (U.S. Pat. Nos. 6,737,056 and ibid.). 8,219,149). Such Fc mutations include the so-called "DANA" Fc mutations with substitutions of residues 265 and 297 to alanine at amino acid positions 265, 269, 270, 297 and 327. Fc mutations with substitutions in more than one are included (US Pat. Nos. 7,332,581 and 8,219,149).
特定の例では、抗体中の野生型ヒトFc領域の位置329のプロリンは、Fcのプロリン329とFcgRIII(Sondermann et al.:Nature 406,267-273(20 Jul.2000))のトリプトファン残基Trp87及びTrp110との間に形成されるFc/Fc.γ.受容体界面内のプロリンサンドイッチを破壊するのに十分な大きさのアミノ酸残基、又はグリシン若しくはアルギニンで置換される。特定の例では、抗体は、少なくとも1つのアミノ酸置換を更に含む。一例では、更なるアミノ酸置換は、S228P、E233P、L234A、L235A、L235E、N297A、N297D、又はP331Sであり、更に別の例では、少なくとも1つの更なるアミノ酸置換は、ヒトIgG1 Fc領域のL234A及びL235A、又はヒトIgG4 Fc領域のS228P及びL235E(例えば、米国特許出願公開第2012/0251531号を参照されたい)であり、また更に別の例では、少なくとも1つの更なるアミノ酸置換は、ヒトIgG1 Fc領域のL234A及びL235A及びP329Gである。 In a particular example, the proline at position 329 of the wild-type human Fc region in the antibody is combined with proline 329 of Fc and the tryptophan residue Trp87 of FcgRIII (Sondermann et al.: Nature 406, 267-273 (20 Jul. 2000)). and Fc/Fc. γ. Amino acid residues large enough to disrupt the proline sandwich within the receptor interface, or substituted with glycine or arginine. In certain examples, the antibody further comprises at least one amino acid substitution. In one example, the additional amino acid substitution is S228P, E233P, L234A, L235A, L235E, N297A, N297D, or P331S, and in yet another example, the at least one additional amino acid substitution is L234A of the human IgG1 Fc region and L235A, or S228P and L235E of the human IgG4 Fc region (see, e.g., US Patent Application Publication No. 2012/0251531), and in yet another example, the at least one additional amino acid substitution is human IgG1 Fc Regions L234A and L235A and P329G.
FcRに対する結合が改善又は減少した特定の抗体バリアントが記載される。(例えば、米国特許第6,737,056号;国際公開第2004/056312号,及びShields et al.,J.Biol.Chem.9(2):6591-6604(2001)を参照されたい。) Specific antibody variants with improved or decreased binding to FcRs are described. (See, eg, U.S. Pat. No. 6,737,056; WO 2004/056312, and Shields et al., J. Biol. Chem. 9(2):6591-6604 (2001).)
特定の例では、抗体バリアントは、ADCCを改善する1つ以上のアミノ酸置換、例えば、Fc領域の298、333、及び/又は334位(残基のEUナンバリング)での置換を有するFc領域を含む。 In certain examples, antibody variants comprise an Fc region having one or more amino acid substitutions that improve ADCC, e.g., substitutions at positions 298, 333, and/or 334 (EU numbering of residues) of the Fc region. .
いくつかの例では、例えば米国特許第6,194,551号、国際公開第99/51642号、及びIdusogie et al.J.Immunol.164:4178-4184(2000)に記載されているように、C1q結合及び/又は補体依存性細胞傷害(CDC)の変化(即ち向上又は低下のいずれか)をもたらすFc領域内で変化が起こる。 Some examples include, for example, US Pat. No. 6,194,551, WO 99/51642, and Idusogie et al. J. Immunol. 164:4178-4184 (2000), changes occur within the Fc region that result in altered (i.e., either increased or decreased) C1q binding and/or complement dependent cytotoxicity (CDC). .
半減期が増大し、母体IgGを胎児に移入する役割を果たす新生児型Fc受容体(FcRn)(Guyer et al.,J.Immunol.117:587(1976)及びKim et al.,J.Immunol.24:249(1994))への結合が向上した抗体が、米国特許出願公開第2005/0014934号A1(Hinton et al.)に記載されている。それらの抗体は、Fc領域とFcRnとの結合を改善する1つ以上の置換をその中に有するFc領域を含む。このようなFcバリアントとしては、Fc領域残基:238、256、265、272、286、303、305、307、311、312、317、340、356、360、362、376、378、380、382、413、424又は434のうち1つ以上における置換、例えば、Fc領域残基434の置換を伴うもの(米国特許第7,371,826号)が挙げられる。 The neonatal Fc receptor (FcRn), which has an increased half-life and plays a role in transferring maternal IgG to the fetus (Guyer et al., J. Immunol. 117:587 (1976) and Kim et al., J. Immunol. 24:249 (1994)) are described in US Patent Application Publication No. 2005/0014934 Al (Hinton et al.). Those antibodies comprise an Fc region having one or more substitutions therein that improve binding between the Fc region and FcRn. Such Fc variants include Fc region residues: , 413, 424 or 434, eg, with substitution of Fc region residue 434 (US Pat. No. 7,371,826).
Fc領域のバリアントの他の例に関して、Duncan&Winter,Nature 322:738-40(1988);米国特許第5,648,260号;米国特許第5,624,821号;及び国際公開第94/29351号も参照されたい。 For other examples of Fc region variants, Duncan & Winter, Nature 322:738-40 (1988); US Patent No. 5,648,260; US Patent No. 5,624,821; See also
いくつかの態様では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び/又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)は、N297G変異を含むFc領域を含む(EUナンバリング)。 In some aspects, the anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and/or the anti-PD-L1 antagonist antibody (e.g., atezolizumab) has an Fc Includes regions (EU numbering).
いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ)及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体)は、1つ以上の重鎖定常ドメインを含み、1つ以上の重鎖定常ドメインは、第1のCH1(CH11)ドメイン、第1のCH2(CH21)ドメイン、第1のCH3(CH31)ドメイン、第2のCH1(CH12)ドメイン、第2のCH2(CH22)ドメイン、及び第2のCH3(CH32)ドメインから選択される。いくつかの例では、1つ以上の重鎖定常ドメインの少なくとも1つは、別の重鎖定常ドメインと対になっている。いくつかの例では、CH31及びCH32ドメインは、突起又は空洞を各含み、CH31ドメイン内の突起又は空洞は、それぞれ、CH32ドメイン内の空洞又は突起中に配置可能である。いくつかの例では、CH31及びCH32ドメインは、当該突起と空洞との間の界面で会合する。いくつかの例では、CH21及びCH22ドメインはそれぞれ、突起又は空洞を構成し、ここで、CH21ドメインにおける突起又は空洞が、CH22ドメインにおける空洞又は突起にそれぞれ位置決め可能である。他の例では、CH21及びCH22ドメインは、当該突起と空隙との間の境界面において接触する。いくつかの例では、抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ及び/又は抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)は、IgG1抗体である。 In some examples, an anti-TIGIT antagonist antibody (e.g., an anti-TIGIT antagonist antibody disclosed herein, e.g., tiragolumab) and/or a PD-1 axis binding antagonist antibody (e.g., an anti-PD-L1 antagonist antibody (e.g., , atezolizumab) or anti-PD-1 antagonist antibody) comprises one or more heavy chain constant domains, wherein the one or more heavy chain constant domains are a first CH1 (CH1 1 ) domain, a first CH2 (CH2 1 ) domain, a first CH3 (CH3 1 ) domain, a second CH1 (CH1 2 ) domain, a second CH2 (CH2 2 ) domain, and a second CH3 (CH3 2 ) domain. In some examples, at least one of the one or more heavy chain constant domains is paired with another heavy chain constant domain. In some examples, the CH3 1 and CH3 2 domains each include a protrusion or cavity, and the protrusion or cavity within the CH3 1 domain can be positioned within the cavity or protrusion within the CH3 2 domain, respectively. In some examples, the CH3 1 and CH3 2 domains associate at the interface between the protrusion and the cavity. In some examples, the CH2 1 and CH2 2 domains each constitute a protrusion or cavity, wherein the protrusion or cavity in the CH2 1 domain can be positioned with the cavity or protrusion in the CH2 2 domain, respectively. In other examples, the CH2 1 and CH2 2 domains meet at the interface between the protrusion and the cavity. In some examples, the anti-TIGIT antagonist antibody (eg, an anti-TIGIT antagonist antibody disclosed herein, eg, tiragolumab and/or an anti-PD-L1 antagonist antibody (eg, atezolizumab) is an IgG1 antibody.
IV.システイン操作抗体バリアント
特定の例では、システイン操作された抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)、例えば、抗体の1つ以上の残基がシステイン残基で置換された「チオMAb」を作製することが望ましい。特定の例では、置換された残基は、抗体の利用しやすい部位で生じる。これらの残基をシステインで置換することによって、反応性チオール基が抗体の接近可能部位に配置され、それは、本明細書で更に説明するように、例えば薬物部分又はリンカー-薬物部分等の他の部分に抗体をコンジュゲートさせて免疫コンジュゲートを作製するために使用されうる。特定の例では、以下の残基のうちの任意の1つ以上を、システインで置換される:軽鎖のV205(Kabatナンバリング)、重鎖のA118(EUナンバリング)、及び重鎖Fc領域のS400(EUナンバリング)。システイン人工抗体は、例えば、米国特許第7,521,541号に記載されているように生成することができる。
IV. Cysteine Engineered Antibody Variants In certain examples, a cysteine engineered anti-TIGIT antagonist antibody and/or a PD-1 axis binding antagonist antibody (e.g., an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody), e.g. It may be desirable to generate "thio MAbs" in which one or more residues are replaced with cysteine residues. In certain instances, substituted residues occur at accessible sites in the antibody. By replacing these residues with cysteines, reactive thiol groups are placed at accessible sites on the antibody, which can be used to bind other residues, such as drug moieties or linker-drug moieties, as further described herein. The moieties can be used to conjugate antibodies to make immunoconjugates. In particular examples, any one or more of the following residues are replaced with cysteines: V205 of the light chain (Kabat numbering), A118 of the heavy chain (EU numbering), and S400 of the heavy chain Fc region. (EU numbering). Cysteine engineered antibodies can be generated, for example, as described in US Pat. No. 7,521,541.
V.抗体誘導体
あつ特定の例では、本発明の抗TIGITアンタゴニスト抗体(例えば、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)又はそのバリアント)及び/又は本発明のPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ又はそのバリアント))は、当該技術分野で公知であり容易に入手可能な追加の非タンパク質性部分を含むように更に修飾される。抗体の誘導体化に適した部位としては、水溶性ポリマーが挙げられるが、これらに限定されるものではない。水溶性ポリマーの非限定的な例としては、限定されないが、ポリエチレングリコール(PEG)、エチレングリコール/プロピレングリコールのコポリマー、カルボキシメチルセルロース、デキストラン、ポリビニルアルコール、ポリビニルピロリドン、ポリ-1,3-ジオキソラン、ポリ-1,3,6-トリオキサン、エチレン/無水マレイン酸コポリマー、ポリアミノ酸(ホモポリマー又はランダムコポリマーのいずれか)、及びデキストラン又はポリ(n-ビニルピロリドン)ポリエチレングリコール、ポリプロピレングリコールホモポリマー、ポリプロピレンオキシド/エチレンオキシドコポリマー、ポリオキシエチル化ポリオール(例えば、グリセロール)、ポリビニルアルコール、及びこれらの混合物が挙げられる。ポリエチレングリコールプロピオンアルデヒドは、水中でのその安定性のため、製造時に有利であり得る。ポリマーは、任意の分子量であってもよく、分岐していても、分岐していなくてもよい。抗体に付着しているポリマーの数は様々であり、複数のポリマーが付着している場合には、それらは同じ分子であっても、異なった分子であってもよい。一般に、誘導体化のために使用されるポリマーの数及び/又は種類は、限定するものではないが、改良される抗体の特定の特性又は機能、抗体誘導体が定義される条件下で治療に使用されるかどうか等を含む考慮事項に基づいて判定することができる。
V. Antibody Derivatives In a particular example, an anti-TIGIT antagonist antibody of the invention (e.g., an anti-TIGIT antagonist antibody (e.g., tiragolumab) or a variant thereof) and/or a PD-1 axis binding antagonist antibody of the invention (e.g., anti-PD- L1 antagonist antibodies (eg, atezolizumab or variants thereof) are further modified to contain additional non-proteinaceous moieties that are known and readily available in the art. Suitable sites for antibody derivatization include, but are not limited to, water-soluble polymers. Non-limiting examples of water-soluble polymers include, but are not limited to, polyethylene glycol (PEG), copolymers of ethylene glycol/propylene glycol, carboxymethylcellulose, dextran, polyvinyl alcohol, polyvinylpyrrolidone, poly-1,3-dioxolane, poly - 1,3,6-trioxane, ethylene/maleic anhydride copolymer, polyamino acid (either homopolymer or random copolymer), and dextran or poly(n-vinylpyrrolidone) polyethylene glycol, polypropylene glycol homopolymer, polypropylene oxide/ Ethylene oxide copolymers, polyoxyethylated polyols (eg, glycerol), polyvinyl alcohol, and mixtures thereof. Polyethylene glycol propionaldehyde may have manufacturing advantages due to its stability in water. The polymer can be of any molecular weight and can be branched or unbranched. The number of polymers attached to the antibody may vary, and when multiple polymers are attached, they may be the same molecule or different molecules. In general, the number and/or type of polymers used for derivatization is not limiting, and the particular property or function of the antibody that is to be improved is defined under the conditions under which the antibody derivative is used therapeutically. can be determined based on considerations including whether
別の例では、放射線への曝露によって選択的に加熱され得る抗体及び非タンパク質性部分の複合体が提供される。一例では、非タンパク質性部分はカーボンナノチューブである(Kam et al.,Proc.Natl.Acad.Sci.USA 102:11600-11605(2005))。放射線は、任意の波長であってもよく、通常の細胞に害を与えないが、抗体非保護性部位に近位の細胞が死滅する温度まで非保護性部位を加熱する波長を含むが、これらに限定されない。 In another example, conjugates of antibodies and non-proteinaceous moieties are provided that can be selectively heated by exposure to radiation. In one example, the non-proteinaceous portion is a carbon nanotube (Kam et al., Proc. Natl. Acad. Sci. USA 102:11600-11605 (2005)). The radiation can be of any wavelength, including wavelengths that do not harm normal cells but that heat the non-protected site to a temperature at which cells proximal to the antibody-unprotected site are killed. is not limited to
組換え生産方法
本発明の抗TIGITアンタゴニスト抗体(例えば、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、チラゴルマブ及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体)は、例えば、参照によりその全体が本明細書に組み込まれる米国特許第4,816,567号に記載されるように、組換え方法及び組成物を使用して産生され得る。
Recombinant Production Methods Anti-TIGIT antagonist antibodies of the invention (e.g., anti-TIGIT antagonist antibodies disclosed herein, e.g., tiragolumab and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies, e.g. , atezolizumab) or anti-PD-1 antagonist antibodies) using recombinant methods and compositions, for example, as described in US Pat. No. 4,816,567, which is incorporated herein by reference in its entirety. can be produced as
抗TIGITアンタゴニスト抗体及び/又はPD-1軸結合アンタゴニスト抗体(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)の組換え産生のため、抗体をコードする核酸を単離し、宿主細胞における更なるクローニング及び/又は発現のために1つ以上のベクターに挿入する。このような核酸は、従来の手順を用い(例えば、抗体の重鎖及び軽鎖をコードする遺伝子に特異的に結合することが可能なオリゴヌクレオチドプローブを用いることによって)、容易に単離され、配列決定されてもよい。 For recombinant production of anti-TIGIT antagonist antibodies and/or PD-1 axis binding antagonist antibodies (e.g., anti-PD-L1 antagonist antibodies or anti-PD-1 antagonist antibodies), nucleic acids encoding the antibodies are isolated and grown in host cells. Insert into one or more vectors for further cloning and/or expression. Such nucleic acids are readily isolated using conventional procedures (e.g., by using oligonucleotide probes capable of specifically binding to the genes encoding the heavy and light chains of the antibody), may be sequenced.
抗体コード化ベクターのクローニング又は発現のための好適な宿主細胞には、本明細書に記載の原核細胞又は真核細胞が含まれる。例えば、抗体は、特に糖鎖修飾やFcエフェクター機能を必要としない場合には、細菌中で産生されてもよい。細菌における抗体フラグメント及びポリペプチドの発現については、例えば、米国特許第5,648,237号、同第5,789,199号、及び同第5,840,523号を参照。(E.coliにおける抗体フラグメントの発現を記載するCharlton,Methods in Molecular Biology,Vol.248(B.K.C.Lo,ed.,Humana Press,Totowa,NJ,2003),pp.245-254も参照されたい)発現後、本発明の抗体は、細菌細胞ペーストから可溶性画分で単離されてもよく、更に精製されてもよい。 Suitable host cells for cloning or expression of antibody-encoding vectors include prokaryotic or eukaryotic cells described herein. For example, antibodies may be produced in bacteria, particularly if they do not require glycosylation or Fc effector functions. See, eg, US Pat. Nos. 5,648,237, 5,789,199, and 5,840,523 for expression of antibody fragments and polypeptides in bacteria. (See also Charlton, Methods in Molecular Biology, Vol. 248 (B.K.C. Lo, ed., Humana Press, Totowa, NJ, 2003), pp. 245-254 describing the expression of antibody fragments in E. coli. See) After expression, the antibodies of the invention may be isolated in the soluble fraction from the bacterial cell paste and further purified.
原核生物に加えて、糸状菌や酵母等の真核生物は、抗体をコードするベクターのクローニング又は発現宿主として適しており、その中には、グリコシル化経路が「ヒト化」された菌株や酵母株が含まれ、その結果、部分的又は完全にヒトのグリコシル化パターンを有する抗体が産生される。Gerngross,Nat.Biotech.22:1409-1414(2004),and Li et al.,Nat.Biotech.24:210-215(2006)を参照されたい。 In addition to prokaryotes, eukaryotes such as filamentous fungi and yeast are suitable cloning or expression hosts for antibody-encoding vectors, including strains and yeasts in which the glycosylation pathway has been "humanized." Strains are included that produce antibodies with a partially or fully human glycosylation pattern. Gerngross, Nat. Biotech. 22:1409-1414 (2004), and Li et al. , Nat. Biotech. 24:210-215 (2006).
また、グリコシル化抗体を発現させるのに適した宿主細胞は、多細胞生物(無脊椎動物及び脊椎動物)に由来する。無脊椎動物細胞の例としては、植物細胞及び昆虫細胞が挙げられる。多数のバキュロウイルス株が同定されており、昆虫細胞と組み合わせて使用することができ、特にスポドプテラ・フルギペルダ(Spodoptera frugiperda)細胞のトランスフェクションに使用することができる。 Suitable host cells for the expression of glycosylated antibodies are also derived from multicellular organisms (invertebrates and vertebrates). Examples of invertebrate cells include plant cells and insect cells. A number of baculovirus strains have been identified and can be used in conjunction with insect cells, particularly for transfection of Spodoptera frugiperda cells.
植物細胞培養物も、宿主として利用することができる。例えば、米国特許第5,959,177号、同第6,040,498号、同第6,420,548号、同第7,125,978号、及び同第6,417,429号(トランスジェニック植物で抗体を産生するためのPLANTIBODIES(商標)技術を記載)を参照されたい。 Plant cell cultures can also be used as hosts. For example, US Pat. Nos. 5,959,177, 6,040,498, 6,420,548, 7,125,978, and 6,417,429 (trans. See PLANTIBODIES™ Technology for Producing Antibodies in Genetic Plants).
脊椎動物細胞も、宿主として使用されてもよい。例えば、懸濁液中で増殖するように適合されている哺乳動物細胞株は有用であり得る。有用な哺乳動物宿主細胞株の他の例は、SV40(COS-7)により形質転換されたサル腎臓CV1株;ヒト胚性腎臓株(例えば、Graham et al.,J.Gen Virol.36:59(1977))に記載される293又は293細胞);ベビーハムスター腎細胞(BHK);マウスセルトリ細胞(例えば、Mather,Biol.Reprod.23:243-251(1980)に記載されるTM4細胞);サル腎臓細胞(CV1);アフリカ緑猿腎臓細胞(VERO-76);ヒト子宮頸がん細胞(HELA);イヌ腎臓細胞(MDCK);水牛ラット肝臓細胞(BRL 3A);ヒト肺細胞(W138);ヒト肝細胞(Hep G2);マウス乳腺腫瘍(MMT 060562);例えば、Mather et al.,Annals N.Y.Acad.Sci.383:44-68(1982)に記載されるTRI細胞;MRC 5細胞;及びFS4細胞である。他の有用な哺乳動物宿主細胞株としては、DHFR-CHO細胞(Urlaub et al.,Proc.Natl.Acad.Sci.USA 77:4216(1980))を含むチャイニーズハムスター卵巣(CHO)細胞、並びにY0、NS0、及びSp2/0等の骨髄腫細胞株が挙げられる。抗体産生に好適な特定の哺乳動物宿主細胞株の概説については、例えば、Yazaki and Wu,Methods in Molecular Biology,Vol.248(B.K.C.Lo,ed.,Humana Press,Totowa,NJ),pp.255-268(2003)、
Vertebrate cells may also be used as hosts. For example, mammalian cell lines adapted to grow in suspension may be useful. Other examples of useful mammalian host cell lines are the monkey kidney CV1 strain transformed with SV40 (COS-7); (1977))); baby hamster kidney cells (BHK); mouse Sertoli cells (e.g., TM4 cells as described in Mather, Biol. Reprod. 23:243-251 (1980)); African Green Monkey Kidney Cells (VERO-76); Human Cervical Cancer Cells (HELA); Canine Kidney Cells (MDCK); Buffalo Rat Liver Cells (BRL 3A); Human Lung Cells (W138) human hepatocytes (Hep G2); mouse mammary tumors (MMT 060562); see, eg, Mather et al. , Annals N.; Y. Acad. Sci. 383:44-68 (1982);
免疫コンジュゲート
本明細書に記載の方法又は使用に使用するための、本明細書に開示される抗TIGITアンタゴニスト抗体、例えば、化学療法剤又は薬物、増殖阻害剤、毒素(例えば、タンパク質毒素、細菌、真菌、植物もしくは動物起源の酵素的に活性な毒素、又はそのフラグメント)、又は放射性同位体等の1つ以上の細胞傷害剤にコンジュゲートされたチラゴルマブ及び/又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ)又は抗PD-1アンタゴニスト抗体(例えば、ペンブロリズマブ))を含む免疫コンジュゲートも提供される。
Immunoconjugates Anti-TIGIT antagonist antibodies disclosed herein, such as chemotherapeutic agents or drugs, growth inhibitors, toxins (e.g., protein toxins, bacterial , enzymatically active toxins of fungal, plant or animal origin, or fragments thereof), or tiragolumab and/or PD-1 axis binding antagonists conjugated to one or more cytotoxic agents such as radioisotopes (e.g. , an anti-PD-L1 antagonist antibody (eg, atezolizumab) or an anti-PD-1 antagonist antibody (eg, pembrolizumab)) are also provided.
いくつかの例では、免疫コンジュゲートは抗体薬剤抱合体(ADC)であり、抗体が、これらに限定されるわけではないが、マイタンシノイド(米国特許第5,208,020号、同第5,416,064号、及び欧州特許第0425235B1号を参照されたい);モノメチルオーリスタチン薬剤部分DE及びDF(MMAE及びMMAF)等のオーリスタチン(米国特許第5,635,483号、同第5,780,588号、及び同第7,498,298号を参照されたい);ドラスタチン;カリケアマイシン又はその誘導体(米国特許第5,712,374号、同第5,714,586号、同第5,739,116号、同第5,767,285号、同第5,770,701号、同第5,770,710号、同第5,773,001号、及び同第5,877,296号;Hinman et al.,Cancer Res.53:3336-3342(1993);並びにLode et al.,Cancer Res.58:2925-2928(1998)を参照されたい);ダウノマイシン及びドキソルビシン等のアントラサイクリン(例えばKratz et al.,Current Med.Chem.13:477-523(2006);Jeffrey et al.,Bioorganic&Med.Chem.Letters 16:358-362(2006);Torgov et al.,Bioconj.Chem.16:717-721(2005);Nagy et al.,Proc.Natl.Acad.Sci.USA 97:829-834(2000);Dubowchik et al.,Bioorg.&Med.Chem.Letters 12:1529-1532(2002);King et al.,J.Med.Chem.45:4336-4343(2002);及び米国特許第6,630,579号を参照されたい);メトトレキサート;ビンデシン;ドセタキセル、パクリタキセル、ラロタキセル、テセタキセル、及びオルタタキセル等のタキサン;トリコテセン;並びにCC1065を含む1つ以上の薬剤に結合している。 In some examples, the immunoconjugate is an antibody drug conjugate (ADC) and the antibody is a maytansinoid (U.S. Pat. Nos. 5,208,020, 5), including but not limited to , 416,064, and EP 0425235B1); auristatins such as monomethyl auristatin drug moieties DE and DF (MMAE and MMAF) (U.S. Pat. Nos. 5,635,483, 5, 780,588, and 7,498,298); dolastatin; calicheamicin or its derivatives (U.S. Pat. Nos. 5,712,374, 5,714,586, 5,739,116, 5,767,285, 5,770,701, 5,770,710, 5,773,001, and 5,877, 296; Hinman et al., Cancer Res.53:3336-3342 (1993); and Lode et al., Cancer Res.58:2925-2928 (1998)); (eg Kratz et al., Current Med. Chem. 13:477-523 (2006); Jeffrey et al., Bioorganic & Med. Chem. Letters 16:358-362 (2006); Torgov et al., Bioconj. Chem. 16 USA 97:829-834 (2000); Dubowchik et al., Bioorg. & Med. Chem. Letters 12:1529-1532 (2002). 45:4336-4343 (2002); and US Patent No. 6,630,579); methotrexate; vindesine; and taxanes such as ortataxel; trichothecenes; and CC1065.
別の例では、免疫コンジュゲートは、ジフテリアA鎖、ジフテリア毒素の非結合活性フラグメント、外毒素A鎖(Pseudomonas aeruginosa由来)、リシンA鎖、アブリンA鎖、モデシンA鎖、アルファ-サルシン、Aleurites fordiiタンパク質、ジアンシンタンパク質、Phytolaca americanaタンパク質(PAPI、PAPII、及びPAP-S)、momordica charantia阻害剤、クルシン、クロチン、sapaonaria officinalis阻害剤、ゲロニン、ミトゲリン、レストリクトシン、フェノマイシン、エノマイシン、及びトリコテセンを含むがこれらに限定されない酵素活性毒素又はそのフラグメントにコンジュゲートされた、本明細書に記載の抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)又はPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))を含む。 In another example, the immunoconjugate is diphtheria A chain, non-binding active fragment of diphtheria toxin, exotoxin A chain (from Pseudomonas aeruginosa), ricin A chain, abrin A chain, modeccin A chain, alpha-sarcin, Aleurites fordii protein, diancin protein, Phytolaca americana protein (PAPI, PAPII, and PAP-S), momordica charantia inhibitor, curcin, crotin, sapaonaria officinalis inhibitor, gelonin, mitgerin, restrictocin, phenomycin, enomycin, and trichothecene An anti-TIGIT antagonist antibody (e.g., tiragolumab) or a PD-1 axis binding antagonist (e.g., an anti-PD-L1 antagonist antibody) described herein conjugated to an enzymatically active toxin or fragment thereof, including but not limited to For example, atezolizumab)).
別の例では、免疫コンジュゲートは、放射性原子にコンジュゲートして放射性コンジュゲートを形成する本明細書に記載の抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)及び/又は本明細書に記載のPD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体)(例えば、アテゾリズマブ)を含む。放射性コンジュゲートの生成には、様々な放射性同位体が利用可能である。例としては、At211、I131、I125、Y90、Re186、Re188、Sm153、Bi212、P32、Pb212、及びLuの放射性同位元素が挙げられる。放射性物質が検出のために使用される場合、それは、シンチグラフィ研究のための放射性原子、例えばtc99m又はI123、又は核磁気共鳴(nuclear magnetic resonance:NMR)イメージング(別名、磁気共鳴イメージング、MRI)のためのスピンラベル、例えば再びヨウ素123、ヨウ素131、インジウム111、フッ素19、炭素13、窒素15、酸素17、ガドリニウム、マンガン又は鉄を含んでいてもよい。 In another example, the immunoconjugate is an anti-TIGIT antagonist antibody described herein (eg, tiragolumab) and/or PD-1 described herein conjugated to a radioactive atom to form a radioactive conjugate. Axis binding antagonists (eg, anti-PD-L1 antagonist antibodies) (eg, atezolizumab). A variety of radioactive isotopes are available for the production of radioconjugates. Examples include radioactive isotopes of At 211 , I 131 , I 125 , Y 90 , Re 186 , Re 188 , Sm 153 , Bi 212 , P 32 , Pb 212 , and Lu. When a radioactive substance is used for detection, it may be a radioactive atom such as tc99m or I123 for scintigraphic studies, or nuclear magnetic resonance (NMR) imaging (aka magnetic resonance imaging, MRI). spin labels for, eg, again iodine-123, iodine-131, indium-111, fluorine-19, carbon-13, nitrogen-15, oxygen-17, gadolinium, manganese or iron.
抗体と細胞毒性剤とのコンジュゲートは、例えば、各種の二官能性タンパク質カップリング剤を用いて作製することができる:N-スクシンイミジル-3-(2-ピリジルジチオ)プロピオネート(SPDP)、スクシンイミジル-4-(N-マレイミドメチル)シクロヘキサン-1-カルボキシレート(SMCC)、イミノチオラン(IT)、イミドエステルの二官能性誘導体(ジメチルアジピミデートHCl等)、活性エステル(スベリン酸ジスクシンイミジル等)、アルデヒド(グルタルアルデヒド等)、ビスアジド化合物(ビス(p-アジドベンゾイル)ヘキサンジアミン等)、ビス-ジアゾニウム誘導体(ビス-(p-ジアゾニウムベンゾイル)-エチレンジアミン等)、ジイソシアネート(トルエン2,6-ジイソシアネート等)、及び二活性フッ素化合物(1,5-ジフルオロ-2,4-ジニトロベンゼン等)。例えば、Vitetta et al.,Science 238:1098(1987)に記載されているように、リシン免疫トキシンを調製することができる。炭素14標識1-イソチオシアナトベンジル-3-メチルジエチレントリアミンペンタ酢酸(MX-DTPA)は、抗体にラジヌクレオチドを共役させるための例示的なキレート剤である。国際公開第94/11026号を参照されたい。リンカーは、細胞内での細胞傷害性薬物の放出を促進する「開裂性リンカー」であってもよい。例えば、酸-解離性リンカー、ペプチダーゼ感受性リンカー、光解離性リンカー、ジメチルリンカー又はジスルフィド含有リンカー(Chari et al.,Cancer Res.52:127-131(1992);米国特許第5,208,020号)を使用することができる。
Conjugates of antibodies and cytotoxic agents can be made using, for example, various bifunctional protein coupling agents: N-succinimidyl-3-(2-pyridyldithio)propionate (SPDP), succinimidyl- 4-(N-maleimidomethyl)cyclohexane-1-carboxylate (SMCC), iminothiolane (IT), bifunctional derivatives of imide esters (dimethyladipimidate HCl, etc.), active esters (disuccinimidyl suberate, etc.) ), aldehydes (glutaraldehyde, etc.), bisazide compounds (bis(p-azidobenzoyl)hexanediamine, etc.), bis-diazonium derivatives (bis-(p-diazoniumbenzoyl)-ethylenediamine, etc.), diisocyanates (
本明細書のイムノコンジュゲート又はADCは、市販されている(例えば、Pierce Biotechnology,Inc.、Rockford、IL.、U.S.Aから)、BMPS、EMCS、GMBS、HBVS、LC-SMCC、MBS、MPBH、SBAP、SIA、SIAB、SMCC、SMPB、SMPH、スルホ-EMCS、スルホ-GMBS、スルホ-KMUS、スルホ-MBS、スルホ-SIAB、スルホ-SMCC、及びスルホ-SMPB、並びにSVSB(スクシンイミジル-(4-ビニルスルホン)ベンゾエート)を含むが、これらに限定されない架橋剤試薬で調製される、このような複合体を明示的に企図するが、これらに限定されない。 Immunoconjugates or ADCs herein are commercially available (eg from Pierce Biotechnology, Inc., Rockford, Ill., USA), BMPS, EMCS, GMBS, HBVS, LC-SMCC, MBS , MPBH, SBAP, SIA, SIAB, SMCC, SMPB, SMPH, sulfo-EMCS, sulfo-GMBS, sulfo-KMUS, sulfo-MBS, sulfo-SIAB, sulfo-SMCC, and sulfo-SMPB, and SVSB (succinimidyl-( It is expressly contemplated, but not limited to, such conjugates prepared with crosslinker reagents including, but not limited to, 4-vinylsulfone)benzoate).
抗TIGITアンタゴニスト抗体又はPD-1軸結合アンタゴニストを含まないADCもまた、本明細書中記載される方法において使用され得る。いくつかの例では、ADCはエンフォルツマブベドチン又はサシツズマブゴビテカンである。 ADCs that do not contain anti-TIGIT antagonist antibodies or PD-1 axis binding antagonists can also be used in the methods described herein. In some examples, the ADC is enfortumab vedotin or sacituzumab govitecan.
D.化学療法剤
1.白金系化学療法剤
白金系化学療法剤には、分子の不可欠な部分として白金を含有する有機化合物が含まれる。典型的には、白金系化学療法剤は、白金の配位錯体である。薬剤としては、カルボプラチン、シスプラチン及びオキサリプラチンが挙げられるが、これらに限定されない。
白金系化学療法剤(シスプラチン、カルボプラチン、オキサリプラチン、スターラプラチン等)は、モノアダクト、鎖間クロスリンク、鎖内クロスリンク、又はDNAタンパク質クロスリンクとしてDNAの架橋を引き起こす、広く使用されている抗腫瘍剤である。白金系化学療法剤は、典型的にはグアニンの隣接するN-7位に作用し、1,2鎖内架橋を形成する(Poklar et al.(1996).Proc.Natl.Acad.Sci.U.S.A.93(15):7606-11;Rudd et al.(1995).Cancer Chemother.Pharmacol.35(4):323-6)。結果として生じる架橋は、がん細胞におけるDNA修復及び/又はDNA合成を阻害する。 Platinum-based chemotherapeutic agents (such as cisplatin, carboplatin, oxaliplatin, starlaplatin) are widely used anti-tumor agents that cause cross-linking of DNA as monoadducts, interstrand cross-links, intrastrand cross-links, or DNA protein cross-links. is an agent. Platinum-based chemotherapeutic agents typically act on the adjacent N-7 positions of guanine, forming 1,2 intrastrand cross-links (Poklar et al. (1996). Proc. Natl. Acad. Sci. U SA 93(15):7606-11; Rudd et al.(1995).Cancer Chemother.Pharmacol.35(4):323-6). The resulting crosslinks inhibit DNA repair and/or DNA synthesis in cancer cells.
カルボプラチンは、本明細書に記載の方法で使用される例示的な白金配位化合物である。カルボプラチンの化学名は、白金,ジアミン[l,l-cyclobutanedicarboxylato(2-)-0,0’]-、(SP-4-2)であり、カルボプラチンは次の構造式:

カルボプラチンは、C6H12N2O4Ptの分子式及び371.25の分子量を有する結晶性粉末である。これは約14mg/mLの速度で水に可溶性であり、1%溶液のpHは5~7である。エタノール、アセトン、及びジメチルアセトアミドにはほとんど溶けない。カルボプラチンは主に鎖間DNA架橋を生成し、この効果は細胞周期に非特異的である。カルボプラチンは、PARAPLATIN(登録商標)、BIOCARN、BLASTOCARB、BLASTOPLATIN、CARBOKEM、CARBOMAX、CARBOPA、CARBOPLAN、CARBOTEEN、CARBOTINAL、CYTOCARB、DUCARB、KARPLAT、KEMOCARB、NAPROPLAT、NEOPLATIN、NISCARBO、ONCOCARBIN、TEVACARB、及びWOMASTIN等として市販されている。 Carboplatin is a crystalline powder with a molecular formula of C6H12N2O4Pt and a molecular weight of 371.25. It is soluble in water at a rate of about 14 mg/mL and has a pH of 5-7 for a 1% solution. It is practically insoluble in ethanol, acetone, and dimethylacetamide. Carboplatin primarily produces interstrand DNA crosslinks and this effect is non-specific to the cell cycle.カルボプラチンは、PARAPLATIN(登録商標)、BIOCARN、BLASTOCARB、BLASTOPLATIN、CARBOKEM、CARBOMAX、CARBOPA、CARBOPLAN、CARBOTEEN、CARBOTINAL、CYTOCARB、DUCARB、KARPLAT、KEMOCARB、NAPROPLAT、NEOPLATIN、NISCARBO、ONCOCARBIN、TEVACARB、及びWOMASTIN等として市販It is
本発明の方法において有用な別の例示的な白金系化学療法剤はシスプラチンであり、これは以下の構造:

2.非白金系化学療法剤
非白金系化学療法剤は、本明細書に記載の方法、使用及び組成物の一部として有用な別のクラスの化学療法剤である。例示的な非白金系化学療法剤としては、代謝拮抗剤(例えば、ペメトレキセド及びゲムシタビン)、トポイソメラーゼII阻害剤(例えば、ドキソルビシン、エトポシド、テニポシド、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸又はHU-331)、アルキル化剤(例えば、シクロホスファミド)及びタキサン(例えば、パクリタキセル(例えば、ナノ粒子-アルブミン結合(nab)-パクリタキセル)、ドセタキセル、ラロタキセル、カバジタキセル、ミラタキセル、テセタキセル、及び/又はオラタキセル)が挙げられる。
2. Non-Platinum Chemotherapeutic Agents Non-platinum chemotherapeutic agents are another class of chemotherapeutic agents useful as part of the methods, uses and compositions described herein. Exemplary non-platinum chemotherapeutic agents include antimetabolites (e.g., pemetrexed and gemcitabine), topoisomerase II inhibitors (e.g., doxorubicin, etoposide, teniposide, daunorubicin, mitoxantrone, amsacrine, ellipticine, orintricarboxylic acid or HU-331), alkylating agents (e.g., cyclophosphamide) and taxanes (e.g., paclitaxel (e.g., nanoparticles-albumin-bound (nab)-paclitaxel), docetaxel, larotaxel, cabazitaxel, mirataxel, tesetaxel, and/or Orataxel).
3.代謝拮抗剤
代謝拮抗剤は、細胞(例えば、がん細胞)内の内因性(正常)代謝プロセスを干渉し、(全体的又は部分的に)阻害する。代謝拮抗剤としては、ゲムシタビン、ペメトレキセド、カペシタビン、ヒドロキシ尿素、メトトレキサート、フルオロウラシル、クラドリビン、メルカプトプリン及びプララトレキセートが挙げられる。
3. Antimetabolites Antimetabolites interfere with and inhibit (totally or partially) endogenous (normal) metabolic processes within cells (eg, cancer cells). Antimetabolites include gemcitabine, pemetrexed, capecitabine, hydroxyurea, methotrexate, fluorouracil, cladribine, mercaptopurine and pralatrexate.
ゲムシタビンは、本明細書に記載の方法で使用される例示的な代謝拮抗剤であり、以下の構造:

いくつかの例では、ペメトレキセドを本発明の方法の一部として投与することができる。ペメトレキセドは以下の構造:

4.トポイソメラーゼII阻害剤
トポイソメラーゼIIの阻害剤(例えば、エトポシド(VP-16)、テニポシド、ドキソルビシン、ダウノルビシン、マイトキサントロン、アムサクリン、エリプチン、オーリントリカルボン酸、及びHU-331)もまた、酵素媒介DNA切断の形成後に、トポイソメラーゼIEDNA 共有結合複合体(すなわち、「開裂複合体」)を安定化させる、広く使用されている抗腫瘍剤である。そのような切断複合体の蓄積は、細胞死経路を誘導する。
4. Topoisomerase II Inhibitors Inhibitors of topoisomerase II (e.g., etoposide (VP-16), teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, elliptin, orintricarboxylic acid, and HU-331) are also effective inhibitors of enzyme-mediated DNA cleavage. It is a widely used antitumor agent that stabilizes the topoisomerase IE DNA covalent complex (ie, the “cleavage complex”) after formation. Accumulation of such cleavage complexes induces cell death pathways.
アントラサイクリンは、ストレプトマイセス菌から抽出されるトポイソメラーゼII阻害剤の一種である。例としては、ドキソルビシン(アドリアマイシン)、ダウノルビシン(ダウノマイシン)、エピルビシン、イダルビシン、ロドマイシン、ピラルビシン、バルルビシン、N-トリフルオロ-アセチルドキソルビシン-14-バレレート、アクラシノマイシン、モルホリノドキソルビシン(モルホリノ-DOX)、シアノモルホリノ-ドキソルビシン(シアノモルホリノ-DOX)、2-ピロリノドキソルビシン(2-PDOX)、5-イミノダウノマイシン、ミトキサントロン及びアクラシノマイシンA(アクラルビシン)が挙げられる。いくつかの実施形態では、アントラサイクリンはアルキル化剤、例えばシクロホスファミドと組み合わせたドキソルビシン(ACによる処置)と組み合わせて投与される。 Anthracycline is a type of topoisomerase II inhibitor extracted from Streptomyces. Examples include doxorubicin (adriamycin), daunorubicin (daunomycin), epirubicin, idarubicin, rhodomycin, pirarubicin, valrubicin, N-trifluoro-acetyldoxorubicin-14-valerate, aclacinomycin, morpholinodoxorubicin (morpholino-DOX), cyanomorpholino -doxorubicin (cyanomorpholino-DOX), 2-pyrrolinodoxorubicin (2-PDOX), 5-iminodaunomycin, mitoxantrone and aclacinomycin A (acrubicin). In some embodiments, an anthracycline is administered in combination with an alkylating agent such as doxorubicin in combination with cyclophosphamide (treatment with AC).
ドキソルビシン(アドリアマイシン(登録商標))は、本明細書に記載の方法で使用される例示的なトポイソメラーゼII阻害剤である。これは、化学名10-[(3-アミノ-2,3,6トリデオキシ-α-L-リキソ-ヘキソピラノシル)オキシ]-7,8,9,10テトラヒドロ-6,8,11トリヒドロキシ-8-(2-ヒドロキシアセチル)-1-メトキシ-(8S,10S)-5,12-ナフタセンジオンを有する。ドキソルビシンは以下の構造:

エトポシドは、本明細書に記載の方法で使用される例示的なトポイソメラーゼII阻害剤である。エトポシドは、通常、プロドラッグであるエトポシドリン酸塩として投与されるが、その化学名は以下の通りである:4’-デメチレピポフィロトキシン9-[4,6-0-(R)-エチリデン-Dグルコピラノシド],4’(リン酸二水素)。 Etoposide is an exemplary topoisomerase II inhibitor for use in the methods described herein. Etoposide is usually administered as the prodrug etoposide phosphate, whose chemical name is 4′-demethylepipophyllotoxin 9-[4,6-0-(R)- ethylidene-D-glucopyranoside], 4' (dihydrogen phosphate).
エトポシドリン酸塩は、以下の構造:

エトポシドのリン酸エステルであるエトポシドリン酸塩は、ポドフィロトキシンの半合成誘導体であり、脱リン酸化によりエトポシドに変換される。エトポシドは、DNAトポイソメラーゼIIとの相互作用やフリーラジカルの形成によりDNA鎖切断を誘導し、細胞周期停止(主に細胞周期のG2段階)や細胞死を引き起こす。エトポシドは以下として市販されている:ETOPOPHOS(登録商標)、TOPOSAR(商標)、VP-16、VEPESID(登録商標)、ACTITOP、ASIDE、BIOPOSIDE、CTOP、CYTOP、EPOSED、ESIDE、ETHOPUL、ETOLON、ETONIS、ETOPLAST、ETOSID、ETOVEL、FYTOP、FYTOSID、LASTET、NZYTOP、ONCOSIDE、PLACID、POSID、RETOPSON、TEVASIDE、TOPOK、TOPOSIDE等。 Etoposide phosphate, the phosphate ester of etoposide, is a semi-synthetic derivative of podophyllotoxin that is converted to etoposide by dephosphorylation. Etoposide induces DNA strand breaks through interaction with DNA topoisomerase II and formation of free radicals, leading to cell cycle arrest (mainly the G2 phase of the cell cycle) and cell death. Etoposide is marketed as: ETOPOPHOS®, TOPOSAR®, VP-16, VEPESID®, ACTITOP, ASIDE, BIOPOSIDE, CTOP, CYTOP, EPOSED, ESIDE, ETHOPUL, ETOLON, ETONIS, ETOPLAST, ETOSID, ETOVEL, FYTOP, FYTOSID, LASTET, NZYTOP, ONCOSIDE, PLACID, POSID, RETOPSON, TEVASIDE, TOPOK, TOPOSIDE and the like.
5.タキサン
タキサンは、チューブリンに結合し、微小管集合及び安定化を促進し、及び/又は微小管解重合を防止し得る化学療法剤である。本明細書に含まれるタキサンは、タキソイド10-デアセチルバッカチンIII及び/又はその誘導体を含む。例示的なタキサンとしては、パクリタキセル(すなわち、TAXOL(登録商標)、CAS#33069-62-4)、ドセタキセル(すなわち、TAXOTERE(登録商標)、CAS#114977-28-5)、ラロタキセル、カバジタキセル、ミラタキセル、テセタキセル、及び/又はオルタタキセル(orataxel)が挙げられるが、これらに限定されない。いくつかの実施形態では、タキサンは、アルブミンコーティングされたナノ粒子(例えば、ナノ-アルブミン結合(nab)-パクリタキセル、すなわち、ABRAXANE(登録商標)及び/又はnab-ドセタキセル、ABI-008)である。いくつかの実施形態では、タキサンは、nab-パクリタキセル(ABRAXANE(登録商標))である。いくつかの実施形態では、タキサンは、CREMAPHOR(登録商標)(例えば、TAXOL(登録商標))及び/又はTween、例えば、ポリソルベート80(例えば、TAXOTERE(登録商標))に製剤化される。いくつかの実施形態では、タキサンは、リポソームに封入されたタキサンである。いくつかの実施形態では、タキサンは、プロドラッグの形態及び/又はタキサンのコンジュゲート形態(例えば、パクリタキセル、パクリタキセルポリグルメクス、及び/又は炭酸リノレイル-パクリタキセルに共有結合的にコンジュゲートしたDHA)である。いくつかの実施形態では、パクリタキセルは、実質的に界面活性剤なしで(例えば、CREMAPHOR及び/又はTweenの不在下で-TOCOSOL(登録商標)パクリタキセル等)製剤化される。
いくつかの例では、パクリタキセルは、本発明の方法の一部として投与される。パクリタキセルは、以下の構造:

In some examples, paclitaxel is administered as part of the methods of the invention. Paclitaxel has the following structure:
いくつかの例では、方法又は使用は、ナノアルブミン結合(nab)-パクリタキセルの投与を含む。 In some examples, the method or use comprises administration of nanoalbumin binding (nab)-paclitaxel.
6.アルキル化剤
アルキル化剤は、DNA損傷を引き起こす化学療法剤である。アルキル化剤には、ナイトロジェンマスタード、ニトロソウレア及びアルキルスルホネートが含まれた。例示的なアルキル化剤としては、シクロホスファミド、1,3-ビス(2-クロロエチル)-1-ニトロソウレア、1,4-ブタンジオールジメタンスルホネート、(2S)-2-アミノ-3-{4-[ビス(2-クロロエチル)アミノ]フェニル}プロパン酸、3-(2-クロロエチル)-2-[(2-クロロエチル)アミノ]テトラヒドロ-2H-1,3,2-オキサザホスホリン2-オキシド及び1-(2-クロロエチル)-3-シクロヘキシル-1-ニトロソウレアが挙げられるが、これらに限定されない。いくつかの実施形態では、アルキル化剤はシクロホスファミドである。シクロホスファミドは、以下の構造:

当業者は、上述の化学療法剤のいずれも、本発明の一部として企図される塩形態等の様々な形態で投与することができることを理解するであろう。 Those skilled in the art will appreciate that any of the chemotherapeutic agents described above can be administered in a variety of forms, including salt forms, which are contemplated as part of this invention.
E.例示的なコロニー刺激因子
コロニー刺激因子は、細胞の増殖を刺激するタンパク質である。コロニー刺激因子には、G-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)及びGM-CSF(例えば、サルグラモスチム)が含まれる。いくつかの実施形態では、コロニー刺激因子はG-CSF(例えば、ペグフィルグラスチム又はフィルグラスチム)である。いくつかの実施形態では、G-CSFはペグフィルグラスチムである。いくつかの実施形態では、G-CSFはフィルグラスチムである。いくつかの実施形態では、コロニー刺激因子はGM-CSF(例えば、サルグラモスチム)である。いくつかの実施形態では、GM-CSFはサルグラモスチムである。
E. Exemplary Colony Stimulating Factors Colony stimulating factors are proteins that stimulate cell proliferation. Colony stimulating factors include G-CSF (eg pegfilgrastim or filgrastim) and GM-CSF (eg sargramostim). In some embodiments, the colony stimulating factor is G-CSF (eg, pegfilgrastim or filgrastim). In some embodiments, the G-CSF is pegfilgrastim. In some embodiments, the G-CSF is filgrastim. In some embodiments, the colony stimulating factor is GM-CSF (eg, sargramostim). In some embodiments, GM-CSF is sargramostim.
F.例示的なVEGFアンタゴニスト
本発明は、対象(例えば、ヒト)のがんを処置するのに有用なVEGFアンタゴニストを提供する。本発明のVEGFアンタゴニストには、VEGFと結合する、VEGF発現レベルを低減する、又はVEGFの生物活性を中和する、遮断する、阻害する、無効化する、低減する、もしくはそれに干渉することができる任意の分子が含まれる。例示的なヒトVEGFは、UniProtKB/Swiss-Prot受託番号P15692、Gene ID(NCBI):7422として示される。
F. Exemplary VEGF Antagonists The present invention provides VEGF antagonists useful for treating cancer in a subject (eg, human). VEGF antagonists of the invention are capable of binding VEGF, reducing VEGF expression levels, or neutralizing, blocking, inhibiting, abolishing, reducing, or interfering with VEGF biological activity. Any molecule is included. An exemplary human VEGF is shown as UniProtKB/Swiss-Prot Accession No. P15692, Gene ID (NCBI):7422.
いくつかの例では、VEGFアンタゴニストは抗VEGF抗体である。いくつかの実施形態では、抗VEGF抗体は、「rhuMab VEGF」又は「AVASTIN(登録商標)」としても公知のベバシズマブである。ベバシズマブは、Presta et al.(Cancer Res.57:4593-4599,1997)に従って生成される組換えヒト化抗VEGFモノクローナル抗体である。これは、変異型ヒトIgG1フレームワーク領域と、ヒトVEGFの、その受容体への結合を遮断するマウス抗hVEGFモノクローナル抗体A.4.6.1由来の抗原結合相補性決定領域とを含む。フレームワーク領域の大部分を含む、ベバシズマブのアミノ酸配列の約93%は、ヒトIgG1に由来し、配列の約7%は、マウス抗体A4.6.1に由来する。ベバシズマブは、分子量が約149,000ダルトンであり、グリコシル化されている。ベバシズマブ及び他のヒト化抗VEGF抗体は、2005年2月26日に発行された米国特許第6,884,879号に更に記載されており、その開示全体は、参照により本明細書に明示的に組み込まれる。いくつかの例では、抗VEGF抗体は、ベバシズマブの重鎖可変(VH)領域配列及び軽鎖可変(VL)領域配列を含む。 In some examples, the VEGF antagonist is an anti-VEGF antibody. In some embodiments, the anti-VEGF antibody is bevacizumab, also known as "rhuMab VEGF" or "AVASTIN®." Bevacizumab has been described by Presta et al. (Cancer Res. 57:4593-4599, 1997). This consists of a mutated human IgG1 framework region and a murine anti-hVEGF monoclonal antibody, A., which blocks the binding of human VEGF to its receptor. and the antigen binding complementarity determining region from 4.6.1. Approximately 93% of the amino acid sequence of bevacizumab, including most of the framework regions, is derived from human IgG1 and approximately 7% of the sequence is derived from the murine antibody A4.6.1. Bevacizumab has a molecular weight of approximately 149,000 Daltons and is glycosylated. Bevacizumab and other humanized anti-VEGF antibodies are further described in U.S. Pat. No. 6,884,879, issued Feb. 26, 2005, the entire disclosure of which is expressly incorporated herein by reference. incorporated into. In some examples, the anti-VEGF antibody comprises a heavy chain variable (VH) region sequence and a light chain variable (VL) region sequence of bevacizumab.
追加の好ましい抗体としては、PCT出願公開第WO2005/012359号に記載されているG6又はB20シリーズ抗体(例えば、G6-31、B20-4.1)が挙げられる。追加の好ましい抗体については、米国特許第7,060,269号、同第6,582,959号、同第6,703,020号、同第6,054,297号、WO98/45332、WO96/30046、WO94/10202、EP0666868B1、米国特許出願公開第2006009360号、同第20050186208号、同第20030206899号、同第20030190317号、同第20030203409号、及び同第20050112126号、ならびにPopkovら(Journal of Immunological Methods288:149~164,2004)を参照されたい。他の好ましい抗体としては、残基F17、M18、D19、Y21、Y25、Q89、191、K101、E103、及びC104を含むか、又はあるいは残基F17、Y21、Q22、Y25、D63、183、及びQ89を含む、ヒトVEGF上の機能的エピトープに結合する抗体が挙げられる。 Additional preferred antibodies include the G6 or B20 series antibodies (eg, G6-31, B20-4.1) described in PCT Application Publication No. WO2005/012359. For additional preferred antibodies see U.S. Pat. 30046、WO94/10202、EP0666868B1、米国特許出願公開第2006009360号、同第20050186208号、同第20030206899号、同第20030190317号、同第20030203409号、及び同第20050112126号、ならびにPopkovら(Journal of Immunological Methods288 : 149-164, 2004). Other preferred antibodies include residues F17, M18, D19, Y21, Y25, Q89, 191, K101, E103, and C104, or alternatively residues F17, Y21, Q22, Y25, D63, 183, and Antibodies that bind to functional epitopes on human VEGF including Q89 are included.
他の例では、VEGFアンタゴニストは、抗VEGFR2抗体又は関連する分子(例えば、ラムシルマブ、タニビルマブ、アフリベルセプト);抗VEGFR1抗体又は関連する分子(例えば、イクルクマブ、アフリベルセプト(VEGF Trap-Eye;EYLEA(登録商標))、又はジブ-アフリベルセプト(ziv-aflibercept)(VEGF Trap;ZALTRAP(登録商標)));二重特異性VEGF抗体(例えば、MP-0250、バヌシズマブ(VEGF-ANG2)、又はUS2001/0236388に開示されている二重特異性抗体);抗VEGFアーム、抗VEGFR1アーム、及び抗VEGFR2のうちの2つの組み合わせを含む二重特異性抗体;抗VEGFA抗体(例えば、ベバシズマブ、セバシズマブ);抗VEGFB抗体;抗VEGFC抗体(例えば、VGX-100)、抗VEGFD抗体;又は非ペプチド小分子VEGFアンタゴニスト(例えば、パゾパニブ、アキシチニブ、バンデタニブ、スチバーガ、カボザンチニブ、レンバチニブ、ニンテダニブ、オランチニブ、テラチニブ、ドビチニグ(dovitinig)、セジラニブ、モテサニブ、スルファチニブ、アパチニブ、フォレチニブ、ファミチニブ、及びチボザニブ)である。 In other examples, the VEGF antagonist is an anti-VEGFR2 antibody or related molecule (e.g. ramucirumab, tanivirumab, aflibercept); an anti-VEGFR1 antibody or related molecule (e.g. ®), or ziv-aflibercept (VEGF Trap; ZALTRAP®)); bispecific VEGF antibodies (e.g., MP-0250, vanucizumab (VEGF-ANG2), or US2001/0236388); bispecific antibodies comprising a combination of two of an anti-VEGF arm, an anti-VEGFR1 arm and an anti-VEGFR2; anti-VEGFA antibodies (e.g. bevacizumab, sevacizumab) anti-VEGFB antibodies; anti-VEGFC antibodies (e.g., VGX-100), anti-VEGFD antibodies; or non-peptide small molecule VEGF antagonists (e.g., pazopanib, axitinib, vandetanib, stivarga, cabozantinib, lenvatinib, nintedanib, orantinib, teratinib, dovitinig ( dovitinig), cediranib, motesanib, sulfatinib, apatinib, foretinib, famitinib, and tivozanib).
更なる態様では、上記のいずれかの例によるVEGFアンタゴニスト(例えば、抗VEGF抗体(例えば、ベバシズマブ))は、上記のセクションCに記載されているように、任意の特徴を単独で又は組み合わせて組み込むことができる。 In a further aspect, the VEGF antagonist (e.g., anti-VEGF antibody (e.g., bevacizumab)) according to any of the examples above incorporates any of the features, singly or in combination, as described in Section C above. be able to.
G.追加の治療剤
本発明において使用され得る追加の治療剤(例えば、抗TIGITアンタゴニスト抗体と組み合わせて使用される)としては、アレムツズマブ(Campath)、ベバシズマブ(AVASTIN(登録商標)、Genentech)、セツキシマブ(ERBITUX(登録商標)、Imclone)、パニツムマブ(VECTIBIX(登録商標)、Amgen)、リツキシマブ(RITUXAN(登録商標)、Genentech/Biogen Idec)、ペルツズマブ(OMNITARG(登録商標)、2C4、Genentech)、トラスツズマブ(HERCEPTIN(登録商標)、Genentech)、トシツモマブ(Bexxar、Corixia)、及び抗体-薬物コンジュゲート、ゲムツズマブオゾガマイシン(MYLOTARG(登録商標)、Wyeth)が挙げられる。記載される化合物と組み合わせた薬剤としての治療可能性を有する追加のヒト化モノクローナル抗体としては、アポリズマブ、アセリズマブ、アトリズマブ、バピヌズマブ、ビバツズマブメルタンシン、カンツズマブメルタンシン、セデリズマブ、セロリズマブペゴール、シドフシツズマブ、シドツズマブ、ダクリズマブ、エクリズマブ、エファリズマブ、エプラツズマブ、エルリズマブ、フェルビズマブ、フォントリズマブ、ゲムツズマブオゾガマイシン、イノツズマブオゾガマイシン、イピリムマブ、ラベツズマブ、リンツズマブ、マッツズマブ、メポリズマブ、モタビズマブ、モトビズマブ、ナタリズマブ、ニモツズマブ、ノロビズマブ、ヌマビズマブ、オクレリズマブ、オマリズマブ、パリビズマブ、パスコリズマブ、ペクフシツズマブ、ペクセリズマブ、ペクセリズマブ、ラリビズマブ、ラニビズマブ、レスリビズマブ、レスリズマブ、レスリビズマブ、ロベリズマブ、ルピズマブ、シブロツズマブ、シプリズマブ、ソンツズマブ、タカタツズマブテトラキセタン、タドキシズマブ、タリズマブ、テフィバズマブ、トシリズマブ、トラリズマブ、ツコツズマブセルモレウキン、ツクシツズマブ、ウマビズマブ、ウルトキサズマブ、ウステキヌマブ、ビジリズマブ、及びインターロイキン-12 p40タンパク質を認識するように遺伝子組換えされた、ヒト配列のみの完全長IgG1λ抗体である抗インターロイキン-12(ABT-874/J695、Wyeth Research及びAbbott Laboratories)が挙げられる。
G. Additional Therapeutic Agents Additional therapeutic agents that may be used in the present invention (e.g., used in combination with an anti-TIGIT antagonist antibody) include alemtuzumab (Campath), bevacizumab (AVASTIN®, Genentech), cetuximab (ERBITUX). ®, Imclone), panitumumab (VECTIBIX®, Amgen), rituximab (RITUXAN®, Genentech/Biogen Idec), pertuzumab (OMNITARG®, 2C4, Genentech), trastuzumab (HERCEPTIN ( ®, Genentech), tositumomab (Bexxar, Corixia), and the antibody-drug conjugate, gemtuzumab ozogamicin (MYLOTARG®, Wyeth). Additional humanized monoclonal antibodies with therapeutic potential as drugs in combination with the described compounds include apolizumab, acerizumab, atolizumab, bapinuzumab, vivatuzumab mertansine, cantuzumab mertansine, cedelizumab, celolizumab Pegor, cidovucizumab, sidtuzumab, daclizumab, eculizumab, efalizumab, epratuzumab, erulizumab, feluvizumab, vontolizumab, gemtuzumab ozogamicin, inotuzumab ozogamicin, ipilimumab, labetuzumab, lintuzumab, mattuzumab, mepolizumab, motavizumab 、モトビズマブ、ナタリズマブ、ニモツズマブ、ノロビズマブ、ヌマビズマブ、オクレリズマブ、オマリズマブ、パリビズマブ、パスコリズマブ、ペクフシツズマブ、ペクセリズマブ、ペクセリズマブ、ラリビズマブ、ラニビズマブ、レスリビズマブ、レスリズマブ、レスリビズマブ、ロベリズマブ、ルピズマブ、シブロツズマブ、シプリズマブ、ソンツズマブ、タカタツズマブテトラxetan, tadoxizumab, talizumab, tefibazumab, tocilizumab, tralizumab, tuktuzumab sermoreukin, tuktuzumab, umabizumab, ultoxazumab, ustekinumab, vigilizumab, and human sequences genetically engineered to recognize the interleukin-12 p40 protein and anti-interleukin-12 (ABT-874/J695, Wyeth Research and Abbott Laboratories), a full-length IgG1λ antibody only.
治療用抗体には、EGFRに結合する抗体も含まれる。EGFRに結合する抗体の例としては、以下のものが挙げられる:MAb 579(ATCC CRL HB 8506)、MAb 455(ATCC CRL HB8507)、Mab 225(ATCC CRL 8508)、MAb 528(ATCC CRL 8509)(米国特許第4,943,533号、Mendelsohn et al.を参照)及びそのバリアント、例えばキメラ化225(C225又はセツキシマブ;ERBUTIX(登録商標))及びリシェイプヒト225(H225)(国際公開第96/40210号、Imclone Systems Inc.を参照);完全ヒトEGFR標的化抗体IMC-11F8(Imclone);II型突然バリアントEGFRを結合する抗体(米国特許第5,212,290号);米国特許第5,891,996号に記載されているようなEGFRを結合するヒト化抗体及びキメラ抗体;及びABX-EGF又はPanitumumabのようなEGFRと結合するヒト抗体(国際公開第98/50433号、Abgenix/Amgenを参照);EMD 55900(Stragliottoら、EurCancer 32A:636-640(1996));EGFR結合のためにEGF及びTGF-αの両方と競合するEGFRに対するヒト化EGFR抗体であるEMD7200(マツズマブ)(EMD/Merck);ヒトEGFR抗体、HuMax-EGFR(GenMab);E1.1、E2.4、E2.5、E6.2、E6.4、E2.11、E6.3及びE7.6.3として知られており米国特許第6,235,883号に記載される完全ヒト抗体;MDX-447(Medarex Inc);及びmAb 806又はヒト化mAb 806(Johns et al.,J.Biol.Chem.279(29):30375-30384(2004))。抗EGFR抗体は、細胞毒性剤にコンジュゲートされ、それによりイムノコンジュゲートを生成し得る(例えば、EP659,439A2、Merck Patent GmbHを参照されたい)。 Therapeutic antibodies also include antibodies that bind EGFR. Examples of antibodies that bind EGFR include: MAb 579 (ATCC CRL HB 8506), MAb 455 (ATCC CRL HB8507), Mab 225 (ATCC CRL 8508), MAb 528 (ATCC CRL 8509) ( See U.S. Pat. No. 4,943,533, Mendelsohn et al.) and variants thereof such as chimerized 225 (C225 or cetuximab; ERBUTIX®) and reshaped human 225 (H225) (WO 96/40210). Imclone Systems Inc.); the fully human EGFR-targeting antibody IMC-11F8 (Imclone); an antibody that binds the type II mutant EGFR (U.S. Pat. No. 5,212,290); U.S. Pat. , 996; and human antibodies that bind EGFR, such as ABX-EGF or Panitumumab (see WO 98/50433, Abgenix/Amgen). ); EMD 55900 (Stragliotto et al., EurCancer 32A:636-640 (1996)); EMD7200 (matuzumab), a humanized EGFR antibody against EGFR that competes with both EGF and TGF-α for EGFR binding (EMD/Merck ); human EGFR antibody, HuMax-EGFR (GenMab); known as E1.1, E2.4, E2.5, E6.2, E6.4, E2.11, E6.3 and E7.6.3 MDX-447 (Medarex Inc); and mAb 806 or humanized mAb 806 (Johns et al., J. Biol. Chem. 279 (29)). : 30375-30384 (2004)). Anti-EGFR antibodies may be conjugated to cytotoxic agents thereby generating immunoconjugates (see, eg, EP 659,439 A2, Merck Patent GmbH).
本明細書で提供される方法、組成物及び使用で使用され得る更なる治療剤としては、共阻害標的(例えば、CTLA-4、LAG3、TIM3、BTLA及び/又はVISTA)を標的とする薬剤、例えばCTLA-4アンタゴニスト、例えば抗CTLA-4アンタゴニスト抗体(例えば、イピリムマブ(YERVOY));共刺激標的を標的とする薬剤(例えば、CD226、OX-40、CD28、CD27、CD137、HVEM及び/又はGITR);放射線治療;抗血管形成剤;アポトーシス剤;及び抗チューブリン剤が挙げられる。 Additional therapeutic agents that can be used in the methods, compositions and uses provided herein include agents that target co-inhibitory targets such as CTLA-4, LAG3, TIM3, BTLA and/or VISTA; For example, CTLA-4 antagonists, such as anti-CTLA-4 antagonist antibodies (eg, ipilimumab (YERVOY)); agents that target co-stimulatory targets (eg, CD226, OX-40, CD28, CD27, CD137, HVEM and/or GITR); ); radiotherapy; antiangiogenic agents; apoptotic agents; and antitubulin agents.
V.医薬組成物、製剤及びキット
本明細書に記載の任意の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体)、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤(例えば、カルボプラチン又はシスプラチン)及び非白金系化学療法剤(例えば、アルキル化剤(例えば、シクロホスファミド)、タキサン(例えばパクリタキセル、例えばnab-パクリタキセル)及び/又はトポイソメラーゼII阻害剤(例えば、ドキソルビシン)))、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)、及び/又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム)を医薬組成物及び製剤に使用することができる。抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体)、VEGFアンタゴニスト、1つ以上の化学療法剤、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)及び/又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム)の医薬組成物及び製剤は、凍結乾燥製剤又は水溶液の形態で、所望の純度を有する1つ、2つ、3つ、4つ、又は4つを超える薬剤を1つ以上の任意の薬学的に許容される担体(Remington’s Pharmaceutical Sciences 16th edition,Osol,A.Ed.(1980))と混合することによって調製することができる。薬学的に許容される担体は、一般に、用いられる投薬量及び濃度ではレシピエントに非毒性であり、それらとしては、リン酸、クエン酸、及び他の有機酸等の緩衝剤;アスコルビン酸及びメチオニンを含む抗酸化物質;防腐剤(例えば、塩化オクタデシルジメチルベンジルアンモニウム、塩化ヘキサメトニウム、塩化ベンザルコニウム、塩化ベンゼトニウム;フェノール、ブチル、若しくはベンジルアルコール;メチル若しくはプロピルパラベン等のアルキルパラベン;カテコール;レゾルシノール;シクロヘキサノール;3-ペンタノール;及びm-クレゾール);低分子量(約10残基未満)ポリペプチド;血清アルブミン、ゼラチン、又は免疫グロブリン等のタンパク質;ポリビニルピロリドン等の親水性ポリマー;グリシン、グルタミン、アスパラギン、ヒスチジン、アルギニン、若しくはリジン等のアミノ酸;単糖類、二糖類、及びグルコース、マンノース、若しくはデキストリンを含む他の炭水化物;EDTA等のキレート剤;スクロース、マンニトール、トレハロース、若しくはソルビトール等の糖類;ナトリウム等の塩形成対イオン;金属錯体(例えば、Zn-タンパク質錯体);ならびに/又はポリエチレングリコール(PEG)等の非イオン性界面活性剤が挙げられるが、これらに限定されない。本明細書における例示的な薬学的に許容され得る担体には、可溶性の中性活性ヒアルロニダーゼ糖タンパク質(sHASEGP)、例えば、rHuPH20(HYLENEX(登録商標)、Baxter International,Inc.)等のヒト可溶性PH-20ヒアルロニダーゼ糖タンパク質等の介在性薬物分散剤が更に含まれる。rHuPH20を含む、特定の例示的なsHASEGP及び使用方法は、米国特許出願公開第2005/0260186号及び同第2006/0104968号に記載される。一態様では、sHASEGPを、1つ以上の追加のグリコサミノグリカナーゼ(例えば、コンドロイチナーゼ)と組み合わせる。
V. Pharmaceutical Compositions, Formulations and Kits Any anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (e.g., anti-PD-L1 antagonist antibody or anti-PD-1 antagonist antibody), VEGF antagonist, chemotherapeutic agent described herein (e.g., platinum-based chemotherapeutic agents (e.g., carboplatin or cisplatin) and non-platinum-based chemotherapeutic agents (e.g., alkylating agents (e.g., cyclophosphamide), taxanes (e.g., paclitaxel, e.g., nab-paclitaxel) and/or a topoisomerase II inhibitor (e.g., doxorubicin))), an ADC (e.g., enfortumab vedotin or sacituzumab govitecan), and/or CSF (e.g., pegfilgrastim, filgrastim, or sargramostim) It can be used in pharmaceutical compositions and formulations. anti-TIGIT antagonist antibody, PD-1 axis binding antagonist (eg, anti-PD-L1 antagonist antibody), VEGF antagonist, one or more chemotherapeutic agents, ADC (eg, enfortumab vedotin or sacituzumab govitecan) and/or pharmaceutical compositions and formulations of CSF (e.g., pegfilgrastim, filgrastim, or sargramostim) in the form of lyophilized formulations or aqueous solutions having the desired
例示的な凍結乾燥抗体製剤は、米国特許第6,267,958号に記載されている。水性抗体製剤としては、米国特許第6,171,586号及び国際公開第2006/044908号に記載されるものが挙げられ、後者の製剤は、酢酸ヒスチジン緩衝液を含む。 An exemplary lyophilized antibody formulation is described in US Pat. No. 6,267,958. Aqueous antibody formulations include those described in US Pat. No. 6,171,586 and WO 2006/044908, the latter formulation comprising a histidine acetate buffer.
例示的なアテゾリズマブ製剤は、5.8のpHを有する氷酢酸、L-ヒスチジン、ポリソルベート20及びスクロースを含む。例えば、アテゾリズマブは、氷酢酸(16.5mg)、L-ヒスチジン(62mg)、ポリソルベート20(8mg)及びスクロース(821.6mg)中に製剤化された1200mgのアテゾリズマブを含有する20mLバイアルで提供され得、pHは5.8である。別の例では、アテゾリズマブは、氷酢酸(11.5mg)、L-ヒスチジン(43.4mg)、ポリソルベート20(5.6mg)及び(575.1mg)中に製剤化された840mgのアテゾリズマブを含有する14mLバイアルで提供されることができ、pHは5.8である。
An exemplary atezolizumab formulation comprises glacial acetic acid, L-histidine,
例示的なチラゴルマブ製剤は、ポリソルベート20、スクロース、L-メチオニン及びWFIを含有するヒスチジン溶液を含む。チラゴルマブは、60mg/mLのチラゴルマブ抗体のおおよその濃度で10mLのチラゴルマブ製剤を含有する15mLバイアルで提供され得る。
An exemplary tiragolumab formulation comprises a histidine
本明細書における製剤はまた、処置される特定の適応症に必要な2つ以上の活性成分、好ましくは互いに悪影響を及ぼさない相補的活性を有するものを含有してもよい。例えば、追加の治療剤を更に提供することが望ましい場合がある。そのような有効成分は、意図される目的に有効な量で組み合わせて好適に存在する。 The formulations herein may also contain two or more active ingredients as required for the particular indication being treated, preferably those with complementary activities that do not adversely affect each other. For example, it may be desirable to further provide an additional therapeutic agent. Such active ingredients are suitably present in combination in amounts that are effective for the purpose intended.
活性成分はまた、例えば、コアセルベーション技術によって、又は界面重合によって調製されたマイクロカプセル、例えば、それぞれ、ヒドロキシメチルセルロース若しくはゼラチンマイクロカプセル及びポリ-(メチルメタクリレート)マイクロカプセルにより、コロイド薬物送達系(例えば、リポソーム、アルブミンマイクロスフェア、マイクロ乳濁液、ナノ粒子、及びナノカプセル)内、又はマクロ乳濁液中にも取り込まれ得る。そのような技術が、Remington’s Pharmaceutical Sciences 16th edition,Osol,A.Ed.(1980)に開示されている。 Active ingredients are also available in colloidal drug delivery systems (e.g., microcapsules prepared by coacervation techniques or by interfacial polymerization, such as hydroxymethylcellulose or gelatin microcapsules and poly-(methyl methacrylate) microcapsules, respectively). , liposomes, albumin microspheres, microemulsions, nanoparticles, and nanocapsules) or in macroemulsions. Such techniques are described in Remington's Pharmaceutical Sciences 16th edition, Osol, A.; Ed. (1980).
徐放性調製物を調製してもよい。持続放出調製物の好適な例としては、本抗体を含有する固体疎水性ポリマーの半透性マトリックスが挙げられ、これらのマトリックスは、成形物品、例えば、フィルム、又はマイクロカプセルの形態である。in vivo投与に使用される製剤は一般に、滅菌される。滅菌状態は、例えば滅菌濾過膜を通す濾過により容易に達成することができる。 Sustained-release preparations may be prepared. Suitable examples of sustained-release preparations include semipermeable matrices of solid hydrophobic polymers containing the antibody, which matrices are in the form of shaped articles, eg films, or microcapsules. Formulations to be used for in vivo administration are generally sterile. Sterility can be readily accomplished, for example, by filtration through sterile filtration membranes.
本発明は、例えば、本明細書中記載される方法のいずれかに従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含むキットを提供する。 The invention provides kits comprising anti-TIGIT antagonist antibodies for use in combination with PD-1 axis binding antagonists, eg, to treat a subject with cancer according to any of the methods described herein. do.
本発明の別の実施形態では、本明細書に記載の方法のいずれかに従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含むキットが提供される。いくつかの例では、キットは、PD-1軸結合アンタゴニストを更に含む。いくつかの例では、製品又はキットは、更に、抗TIGITアンタゴニスト抗体をPD-1軸結合アンタゴニストと組み合わせて使用して、がん(例えば、患者におけるがん)を処置するため又はがんの進行を遅延させるための説明書を含む添付文書を含む。 In another embodiment of the invention, a kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject with cancer according to any of the methods described herein is provided. In some examples, the kit further comprises a PD-1 axis binding antagonist. In some examples, the article of manufacture or kit further uses an anti-TIGIT antagonist antibody in combination with a PD-1 axis binding antagonist to treat cancer (eg, cancer in a patient) or prevent cancer progression. including a package insert containing instructions for delaying
本発明の別の実施形態では、本明細書に記載の方法のいずれかに従ってがんを有する対象を処置するための抗TIGITアンタゴニスト抗体と組み合わせて使用するためのPD-1軸結合アンタゴニストを含むキットが提供される。いくつかの例では、キットは抗TIGITアンタゴニスト抗体を更に含む。いくつかの例では、製品又はキットは、患者のがんを処置又は進行を遅延させるために、抗TIGITアンタゴニスト抗体(例えば、チラゴルマブ)と組み合わせてPD-1軸結合アンタゴニストを使用するための説明書を含む添付文書を更に含む。 In another embodiment of the invention, a kit comprising a PD-1 axis binding antagonist for use in combination with an anti-TIGIT antagonist antibody to treat a subject with cancer according to any of the methods described herein is provided. In some examples, the kit further comprises an anti-TIGIT antagonist antibody. In some examples, the article of manufacture or kit includes instructions for using the PD-1 axis binding antagonist in combination with an anti-TIGIT antagonist antibody (eg, tiragolumab) to treat or delay cancer progression in a patient. further including a package insert containing
別の実施形態では、キットは、本明細書に記載の方法のいずれかに従ってがんを有する対象を処置するためにアテゾリズマブと組み合わせて使用するためのチラゴルマブを含む。いくつかの実施形態では、キットはアテゾリズマブを更に含む。いくつかの例では、製造品又はキットは、患者のがんを処置又はその進行を遅延させるために、アテゾリズマブと組み合わせてチラゴルマブを使用するための説明書を含む添付文書を更に含む。 In another embodiment, the kit comprises tiragolumab for use in combination with atezolizumab to treat a subject with cancer according to any of the methods described herein. In some embodiments, the kit further comprises atezolizumab. In some examples, the article of manufacture or kit further comprises a package insert containing instructions for using tiragolumab in combination with atezolizumab to treat or delay progression of cancer in a patient.
別の実施形態では、キットは、本明細書に記載の方法のいずれかに従ってがんを有する対象を処置するための、チラゴルマブと組み合わせて使用するためのアテゾリズマブを含む。いくつかの実施形態では、キットは、チラゴルマブを更に含む。いくつかの例では、製造品又はキットは、患者のがんを処置又はその進行を遅延させるために、チラゴルマブと組み合わせてアテゾリズマブを使用するための説明書を含む添付文書を更に含む。 In another embodiment, the kit comprises atezolizumab for use in combination with tiragolumab to treat a subject with cancer according to any of the methods described herein. In some embodiments, the kit further comprises tiragolumab. In some examples, the article of manufacture or kit further comprises a package insert containing instructions for using atezolizumab in combination with tiragolumab to treat or delay progression of cancer in a patient.
いくつかの例では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体は、同じ容器又は別々の容器に入っている。好適な容器としては、例えば、ボトル、バイアル、袋、及びシリンジが挙げられる。容器は、ガラス、プラスチック(ポリ塩化ビニル若しくはポリオレフィン等)、又は金属合金(ステンレス鋼若しくはハステロイ等)等の様々な材料から形成され得る。いくつかの例では、容器は、製剤を保持し、容器上のラベル又は容器に関連するラベルは、使用上の指示を示し得る。製品又はキットは、他の緩衝液、希釈剤、フィルタ、針、シリンジ、及び使用上の指示を有する添付文書等の商業的視点及び使用者の視点から望ましい他の材料を更に含み得る。いくつかの例では、製造品は、1つ以上の別の薬剤(例えば、更なる化学療法剤又は抗新生物剤)を更に含む。1つ以上の薬剤に好適な容器としては、例えば、ボトル、バイアル、袋、及びシリンジが挙げられる。 In some examples, the PD-1 axis binding antagonist and anti-TIGIT antagonist antibody are in the same container or in separate containers. Suitable containers include, for example, bottles, vials, bags, and syringes. The container can be formed from a variety of materials such as glass, plastic (such as polyvinyl chloride or polyolefin), or metal alloys (such as stainless steel or Hastelloy). In some instances, the container holds the formulation and a label on or associated with the container may indicate directions for use. The product or kit may further include other materials desirable from a commercial and user standpoint, such as other buffers, diluents, filters, needles, syringes, and package inserts with directions for use. In some examples, the article of manufacture further comprises one or more additional agents (eg, additional chemotherapeutic or anti-neoplastic agents). Suitable containers for one or more medicaments include, for example, bottles, vials, bags, and syringes.
いくつかの実施形態では、PD-1軸結合アンタゴニスト及び抗TIGITアンタゴニスト抗体を含むキットは、VEGFアンタゴニスト、化学療法剤(例えば、白金系化学療法剤又は非白金系化学療法剤)、ADC(例えば、エンフォルツマブベドチン又はサシツズマブゴビテカン)及び/又はCSF(例えば、ペグフィルグラスチム、フィルグラスチム、又はサルグラモスチム)を更に含む。 In some embodiments, a kit comprising a PD-1 axis binding antagonist and an anti-TIGIT antagonist antibody is a VEGF antagonist, a chemotherapeutic agent (e.g., a platinum-based chemotherapeutic agent or a non-platinum-based chemotherapeutic agent), an ADC (e.g., enfortumab vedotin or sacituzumab govitecan) and/or CSF (eg, pegfilgrastim, filgrastim, or sargramostim).
本明細書に記載されるPD-1軸結合アンタゴニスト及び/又は抗TIGITアンタゴニスト抗体のいずれも、製造品又はキットに含まれ得る。任意の製造品又はキットは、本明細書中記載される方法のいずれかに従って対象にPD-1軸結合アンタゴニスト及び/又は抗TIGITアンタゴニスト抗体を投与するための説明書を含み得る。 Any of the PD-1 axis binding antagonists and/or anti-TIGIT antagonist antibodies described herein can be included in an article of manufacture or kit. Any article of manufacture or kit can include instructions for administering a PD-1 axis binding antagonist and/or an anti-TIGIT antagonist antibody to a subject according to any of the methods described herein.
VI.実施例

以下は、本発明の方法の実施例である。上記の一般的な説明を前提として、他の様々な実施形態を実施できることが理解される。 The following are examples of the method of the present invention. It is understood that various other embodiments may be practiced, given the general description above.
実施例1.局所進行性又は転移性腫瘍を有する患者において化学療法を用いて及び用いずに投与される、単剤としての及びアテゾリズマブと組み合わせたチラゴルマブの安全性及び薬物動態の第Ia/Ib相非盲検用量漸増試験
この試験は、局所進行性又は転移性腫瘍を有する患者において、単剤として投与した場合(第Ia相)又は化学療法を用いて又は用いずにアテゾリズマブと組み合わせて投与した場合(第Ib相)の、チラゴルマブ(MTIG7192A)の安全性、PK、薬力学及び予備的抗腫瘍活性を評価する。本試験の具体的な目的及び対応評価項目を表5に概説する。


A.試験計画
これは、標準治療が存在しない、無効若しくは忍容性がないことが証明されている、又は不適切と考えられている、又は治験薬の臨床試験が認識された標準治療である局所進行性、再発性、又は転移性の治癒不能の腫瘍を有する単剤入院患者としてのチラゴルマブの安全性、忍容性、及びPKを評価するように設計された、ヒト初回投与第I相非盲検、多施設、グローバル、用量漸増試験である。この試験はまた、標準治療が存在しない、無効若しくは忍容性がないことが証明されている、若しくは不適切と考えられている、又は治験薬の臨床試験が認識されている標準治療である、又は抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と考えられている局所進行性、再発性、又は転移性の治癒不能腫瘍を有する患者において、化学療法を用いて、又は用いずにアテゾリズマブと共に投与した場合のチラゴルマブの安全性、忍容性、及びPKの評価を可能にするように設計されている。
A. Study design This is a local progression for which no standard treatment exists, has been proven to be ineffective or intolerable, or is considered inadequate, or for which clinical trials of investigational agents are a recognized standard of care. A first-in-human, phase I, open-label study designed to evaluate the safety, tolerability, and PK of tiragolumab as a single-agent hospitalized patient with incurable, recurrent, or metastatic tumors. , a multicenter, global, dose escalation study. The trial also indicates that no standard of care exists, has been proven to be ineffective or intolerable, or is considered inappropriate, or is a recognized standard of care for clinical trials of an investigational drug; or with chemotherapy in patients with locally advanced, recurrent, or metastatic incurable tumors for whom clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are considered an acceptable treatment option; It is designed to allow evaluation of the safety, tolerability, and PK of tiragolumab when administered with atezolizumab without or with atezolizumab.
図1は、第Ib相化学療法拡大及び第Ib相Q4W投与拡大を示すフローチャートである。用量漸増段階の間、およそ3~6名の患者のコホートをそれぞれ漸増用量レベルで評価して、単剤としての又はアテゾリズマブと組み合わせたチラゴルマブのMTD又は最大投与用量(MAD)を決定する。 FIG. 1 is a flow chart showing Phase Ib chemotherapy expansion and Phase Ib Q4W dosing expansion. During the dose escalation phase, cohorts of approximately 3-6 patients are evaluated at each escalating dose level to determine the MTD or maximum administered dose (MAD) of tiragolumab as a single agent or in combination with atezolizumab.
用量拡大段階では、患者が登録され、単剤としてのチラゴルマブのMTD若しくはMAD未満で(第Ia相)、又は化学療法を用いて若しくは用いずにアテゾリズマブと組み合わせて(第Ib相)処置される。単剤としてのチラゴルマブ(第Ia相)又はチラゴルマブとアテゾリズマブとの組み合わせ(化学療法なしの第Ib相コホート)は、各21日間サイクルの1日目又は各28日間サイクルの1日目にIV注入によって投与され(第Ib相Q4W投与拡大)、化学療法なしの第Ib相コホートでは、チラゴルマブはアテゾリズマブの前に投与される。許容できない毒性又は疾患進行の臨床的に説得力のある証拠がない場合、治験責任医師による有益性及びリスクの好ましい評定に基づいて、チアゴルマブ(第Ia相)又はアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)のいずれかによる処置をサイクル1を超えて継続する。
In the dose expansion phase, patients are enrolled and treated below the MTD or MAD of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib). Tiragolumab as a single agent (Phase Ia) or combination of tiragolumab and atezolizumab (Phase Ib cohort without chemotherapy) by IV infusion on
第Ib相化学療法拡大コホート及び第Ib相Q4W投薬拡大コホート(図1)では、3人の患者の安全性ランインが完了している。安全性ランインからの全ての関連する安全性データは、登録が継続される前にIMC及び治験責任医師によって十分に再検討される。 The phase Ib chemotherapy expansion cohort and the phase Ib Q4W dosing expansion cohort (Figure 1) have completed the safety run-in of three patients. All relevant safety data from the safety run-in will be fully reviewed by the IMC and investigator before enrollment continues.
化学療法拡大コホートでは、チラゴルマブ及びアテゾリズマブは、3つのコホート:コホートAではカルボプラチン又はシスプラチン及びペメトレキセド、コホートBではカルボプラチン及びパクリタキセル、並びにコホートCではカルボプラチン又はシスプラチン及びエトポシドのそれぞれにおける特定の化学療法レジメンと組み合わされる(図1参照)。各コホートにおいて、処置は導入期及び維持期を含む。導入期では、チラゴルマブ及びアテゾリズマブと化学療法との組み合わせを、コホートA及びBでは4~6サイクル、コホートCでは4サイクル、21日間のサイクルでIV注入によって投与する。コホートA及びBの導入処置のサイクル数は治験責任医師の裁量による。 In the chemotherapy expansion cohorts, tiragolumab and atezolizumab were combined with specific chemotherapy regimens in each of three cohorts: carboplatin or cisplatin and pemetrexed in cohort A, carboplatin and paclitaxel in cohort B, and carboplatin or cisplatin and etoposide in cohort C. (See Figure 1). In each cohort, treatment includes an induction phase and a maintenance phase. In the run-in phase, tiragolumab and atezolizumab in combination with chemotherapy will be administered by IV infusion for 4-6 cycles in Cohorts A and B and 4 cycles in Cohort C in 21-day cycles. The number of cycles of induction treatment for Cohorts A and B is at the investigator's discretion.
導入期の後、疾患の進行又は許容できない毒性を経験したことがない患者は、維持療法による処置を継続する。維持期の間、コホートB及びCの患者は、チラゴルマブ及びアテゾリズマブのみを継続し、一方、コホートAの患者は、ペメトレキセドと共にチラゴルマブ及びアテゾリズマブを継続する。全ての化学療法拡大コホートにおいて、アテゾリズマブは、チラゴルマブの前に投与される。化学療法を施す場合、アテゾリズマブ及びチラゴルマブの後に投与される。 After the induction phase, patients who have not experienced disease progression or unacceptable toxicity continue treatment with maintenance therapy. During the maintenance phase, patients in Cohorts B and C continue on tiragolumab and atezolizumab alone, while patients in Cohort A continue on tiragolumab and atezolizumab along with pemetrexed. Atezolizumab is administered prior to tiragolumab in all chemotherapy expansion cohorts. If chemotherapy is administered, it is administered after atezolizumab and tiragolumab.
全ての患者は、試験を通して、及び試験処置の最後の用量の後又は別の全身性抗がん治療の開始までの少なくとも90日間(いずれか早く発生する方)、有害事象について綿密に監視される。有害事象は、NCI CTCAE、バージョン4.0に従って等級付けされる。 All patients will be closely monitored for adverse events throughout the study and for at least 90 days after the last dose of study treatment or until initiation of another systemic anticancer therapy (whichever occurs first). . Adverse events are graded according to the NCI CTCAE, version 4.0.
単剤(第Ia相)としての、又は化学療法を伴う又は伴わないアテゾリズマブとの組み合わせ(第Ib相)としてのチラゴルマブのPK特性、免疫原性応答、及び薬力学的効果を特性評価するために、投与前後の様々な時点で血液試料を採取する。中間PK分析の結果に応じて、PKサンプリングの頻度は試験の後半に減少し得る。 To characterize the PK properties, immunogenic responses, and pharmacodynamic effects of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) , blood samples are taken at various time points before and after dosing. Depending on the results of the interim PK analysis, the frequency of PK sampling may decrease later in the study.
患者は、スクリーニング時及び試験中に腫瘍評定を受け、これは、固形腫瘍の標準的奏効評定基準(RECIST)v 1.1基準によって測定される。疾患の進行のための標準的なRECIST v 1.1基準が試験の第Ia相部分又は第Ib相部分において満たされている場合であっても、継続した処置のための基準を満たすならば、患者は試験処置を継続することを許される場合がある。試験の第Ia相部分を中止する患者は、クロスオーバーの基準を満たし、アクセス可能な病変の生検に同意することを条件として、試験の第Ib相部分に移り、アテゾリズマブと組み合わせたチラゴルマブによる処置を受けることができる。 Patients underwent tumor assessments at screening and during the study, as measured by the Standard Response Rating Criteria for Solid Tumors (RECIST) v 1.1 criteria. Even if standard RECIST v 1.1 criteria for disease progression are met in the Phase Ia or Phase Ib portion of the trial, if criteria for continued treatment are met, Patients may be allowed to continue study treatment. Patients who discontinue the Phase Ia portion of the trial, provided they meet crossover criteria and consent to biopsy of accessible lesions, will proceed to the Phase Ib portion of the trial and be treated with tiragolumab in combination with atezolizumab. can receive
利用可能な標準治療後に進行した局所進行性、再発性又は転移性の治癒不能の悪性腫瘍を有する約60~320人の患者;又は標準治療が無効若しくは忍容できないことが証明されているか、又は不適切であると考えられている患者;又は治験薬の臨床試験が認識された標準治療である場合には、試験の拡大コホートに登録される。試験の第Ib相部分では、化学療法を用いて又は用いずに抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容される処置選択肢とみなされる患者が、拡大コホートに登録され得る。 Approximately 60-320 patients with locally advanced, recurrent, or metastatic incurable malignancies that have progressed after available standard therapy; or standard therapy has proven ineffective or intolerable, or Patients considered unsuitable; or enrolled in a trial expansion cohort if a clinical trial of an investigational drug is a recognized standard of care. In the Phase Ib portion of the study, patients for whom clinical trials of an investigational drug in combination with anti-PD-L1 antibodies with or without chemotherapy are considered an acceptable treatment option may be enrolled in an expansion cohort.
この拡大段階には、特定のがんの状況における単剤(第Ia相)としての、又は化学療法を伴う又は伴わないアテゾリズマブ(第Ib相)と組み合わせた、チラゴルマブの安全性、忍容性、PK変動性、薬力学的活性、及び予備抗腫瘍活性をより良好に特性評価するための患者の定義されたコホートが含まれる。安全性、忍容性、PK、薬力学及び抗腫瘍活動性データの蓄積の評定に基づいて、試験の治験責任医師によって決定されたように、単剤としてのチラゴルマブ(第Ia相)又は化学療法を用いる又は用いずにアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)のMAD又はMTD以下の選択された用量レベルで、拡大コホートの登録を開始する。 This expansion phase will focus on the safety, tolerability, A defined cohort of patients is included to better characterize PK variability, pharmacodynamic activity, and preliminary anti-tumor activity. Tiragolumab as a single agent (Phase Ia) or chemotherapy, as determined by the study investigator based on assessment of safety, tolerability, PK, pharmacodynamic and pooling antitumor activity data Enrollment of the expansion cohort will begin at selected dose levels below the MAD or MTD of tiragolumab (Phase Ib) in combination with atezolizumab with or without .
試験の第Ia相部分では、最大約40人の患者が、NSCLC、RCC、TNBC、黒色腫、HNSCC、OC、GEJがんを含むGC、UBC、及びMSS又はMSI-LowであるCRCを含むCRCを含む、PD-L1選択及び/又はTIGIT選択の複数の腫瘍適応症の計画された拡大コホートに登録される。 In the Phase Ia portion of the study, up to about 40 patients will have NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC including GEJ cancer, UBC, and CRC including CRC that is MSS or MSI-Low. A planned expansion cohort of PD-L1-selected and/or TIGIT-selected multiple tumor indications, including
試験の第Ib相部分(化学療法なし)では、約20~40人の患者が以下の計画された適応症特異的拡大コホートのそれぞれに登録される。NSCLC:がん免疫療法(CIT)ナイーブ(例えば、抗PD-L1/PD-1による事前の処置なし);NSCLC:CIT処理(例えば、抗PD-L1/PD-1による事前の処置を含む);RCC;TNBC;黒色腫;HNSCC;OC;GEJがんを含むGC;UBC;MSS又はMSI-LowであるCRCを含むCRC;黒色腫、OC、RCC及びUBCを含む特定の腫瘍適応症の生検コホート。 In the Phase Ib portion of the trial (without chemotherapy), approximately 20-40 patients will be enrolled in each of the following planned indication-specific expansion cohorts. NSCLC: cancer immunotherapy (CIT) naïve (eg, no prior treatment with anti-PD-L1/PD-1); NSCLC: CIT-treated (eg, with prior treatment with anti-PD-L1/PD-1) GC including GEJ cancer; UBC; CRC including CRC that is MSS or MSI-Low; survival of specific tumor indications including melanoma, OC, RCC and UBC probate cohort.
試験の第Ib相化学療法拡大部分では、約20~40人の患者が以下の計画された化学療法拡大コホート(図1参照)のそれぞれに登録される。
コホートA:
-導入期-アテゾリズマブ及びチラゴルマブとの併用
シスプラチン又はカルボプラチン及びペメトレキセド
-維持期-アテゾリズマブとチラゴルマブとの併用
ペメトレキセド
コホートB:
-導入期-アテゾリズマブ及びチラゴルマブとの併用
カルボプラチン及びパクリタキセル
-維持期-アテゾリズマブ及びチラゴルマブ
コホートC:
-導入期-アテゾリズマブ及びチラゴルマブとの併用
シスプラチン又はカルボプラチン及びエトポシド
-維持期-アテゾリズマブ及びチラゴルマブ
In the Phase Ib chemotherapy expansion portion of the trial, approximately 20-40 patients will be enrolled in each of the following planned chemotherapy expansion cohorts (see Figure 1).
Cohort A:
- Run-in - combination with atezolizumab and tiragolumab Cisplatin or carboplatin and pemetrexed - Maintenance - combination of atezolizumab and tiragolumab Pemetrexed Cohort B:
- Induction - in combination with atezolizumab and tiragolumab Carboplatin and paclitaxel - Maintenance - atezolizumab and tiragolumab Cohort C:
- Induction phase - combination with atezolizumab and tiragolumab Cisplatin or carboplatin and etoposide - Maintenance phase - atezolizumab and tiragolumab
各コホートにおける処置の組み合わせを表6に示す。

B.第Ib相化学療法拡大コホート:投薬及び投与
導入期では、特定の化学療法拡大コホートの患者は以下を受ける:
コホートAは、21日ごとのサイクルの第1日に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いてシスプラチン75mg/m2IV又は6mg/mL・分IVのカルボプラチンAUC及びペメトレキセド500mg/m2IVの組み合わせを受ける。4~6サイクルの導入期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
コホートBは、21日ごとのサイクルの1日目に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いて6mg/mL・分IVのカルボプラチンAUCとパクリタキセル200mg/m2のIVを受ける。4~6サイクルの導入期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
コホートCは、21日間ごとのサイクルの1日目に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いてシスプラチン75mg/m2 IV、又はカルボプラチンAUC 5mg/mL・分 IV、次いで21日間ごとのサイクルの1日目~3日目にエトポシド100mg/m2 IVを受ける。4サイクルの導入期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
B. Phase Ib Chemo Expansion Cohorts: Dosing and Administration In the run-in phase, patients in certain chemotherapy expansion cohorts will receive:
Cohort A received atezolizumab 1200 mg IV, followed by
Cohort B receives atezolizumab 1200 mg IV, followed by
Cohort C received atezolizumab 1200 mg IV, followed by
導入期の後、患者との潜在的なリスク及び利益の慎重な評定及び徹底的な議論の後に治験責任医師の裁量で、許容できない毒性、臨床的に説得力のある疾患の進行、及び/又は臨床的利益の不在下で、処置が維持期に継続される。維持期では、特定の化学療法拡大コホートの患者は以下を受ける:
コホートAは、21日ごとのサイクルの1日目に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いて、ペメトレキセド500mg/m2 IVを受け;コホートBは、21日ごとのサイクルの1日目に、アテゾリズマブ1200mg IV、次いで、チラゴルマブ600mg IVを受け;コホートCは、21日ごとのサイクルの1日目に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IVを受ける。
After the run-in period, unacceptable toxicity, clinically plausible disease progression, and/or at the investigator's discretion after careful assessment and thorough discussion of potential risks and benefits with the patient Treatment is continued in the maintenance phase in the absence of clinical benefit. In the maintenance phase, patients in certain chemotherapy expansion cohorts receive:
Cohort A received atezolizumab 1200 mg IV, followed by
毒性及び疾患進行がない場合、個々の化学療法剤又は免疫療法剤は独立して中止される。 In the absence of toxicity and disease progression, individual chemotherapeutic or immunotherapeutic agents are discontinued independently.
C.第Ib相Q4W投与拡大コホート C. Phase Ib Q4W Dosing Expansion Cohort
第IbQ4W相用量拡大コホートの目的は、安全性、忍容性、PK及び予備的有効性データをより良好に特性評価すること、並びに4週間(28日)ごとの投与スケジュールでアテゾリズマブ1680mg IVと組み合わせたチラゴルマブ840mg IVで処置された患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。 The objectives of the Phase IbQ4W dose expansion cohort were to better characterize the safety, tolerability, PK and preliminary efficacy data, and in combination with atezolizumab 1680 mg IV on a dosing schedule of every 4 weeks (28 days). To explore potential tumor biomarkers of pharmacodynamic activity in patients treated with tiragolumab 840 mg IV.
第Ib相Q4Wコホートには、スクリーニング又は再スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1選択及び/又はTIGIT選択され得る腫瘍を有する約20~40人の患者が含まれる。治験責任医師との議論に基づいてメディカルモニターがそうであると判断した場合、保管組織が不十分又は入手不可能な患者は、このコホートへの登録に適格であり得る。抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる腫瘍型の患者は、これらの拡大コホートに登録され得る。 The Phase Ib Q4W cohort includes approximately 20-40 patients with tumors who can be selected for PD-L1 and/or TIGIT selection based on prospective testing of tumor tissue during screening or rescreening. Patients with insufficient or unavailable archive tissue may be eligible for enrollment in this cohort if the medical monitor determines so based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are considered an acceptable treatment option may be enrolled in these expansion cohorts.
D.第Ib相の各指標特異的拡大コホートにおける患者の追加の選択基準 D. Additional Inclusion Criteria for Patients in Each Index-Specific Expansion Cohort of Phase Ib
NSCLCコホート(CIT-ナイーブ)には、抗PD-L1/PD-1及び/又は抗CTLA-4を含む、CIT(治験薬又は承認済み)で以前に処置されていない組織学的に確認された治癒不能の進行性NSCLCを有する患者であって、CIT(抗PD-L1/PD-1剤を含む)がNSCLCの処置として現地の規制当局によって承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢とみなされる患者が含まれる。腫瘍が既知の感作性上皮成長因子受容体(EGFR)変異を有する患者は、疾患進行(治療中若しくは処置後)、又はEGFRチロシンキナーゼ阻害剤(複数可)での処置に対する不耐性も経験していなければならない;腫瘍が既知の未分化リンパ腫キナーゼ(ALK)再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はALKチロシンキナーゼ阻害剤(複数可)での処置に対する不耐性も経験していなければならない;腫瘍が既知のROS1再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はROS1チロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;腫瘍が既知のBRAFV600E変異を有する患者は、疾患進行(処置中若しくは処置後)、又はトラメチニブと組み合わせたダブラフェニブによる処置に対する不耐性も経験していなければならない; NSCLC cohort (CIT-naive) had histologically confirmed no prior treatment with CIT (investigational or approved), including anti-PD-L1/PD-1 and/or anti-CTLA-4 In patients with incurable advanced NSCLC, in combination with anti-PD-L1 antibody if CIT (including anti-PD-L1/PD-1 agents) is approved by local regulatory authorities for treatment of NSCLC Includes patients for whom a clinical trial of an investigational drug is considered an acceptable treatment option. Patients whose tumors have known sensitizing epidermal growth factor receptor (EGFR) mutations also experience disease progression (on or after treatment) or intolerance to treatment with EGFR tyrosine kinase inhibitor(s). Patients whose tumors have known anaplastic lymphoma kinase (ALK) rearrangements also have disease progression (during or after treatment) or intolerance to treatment with ALK tyrosine kinase inhibitor(s). Patients whose tumors have known ROS1 rearrangements must also not experience disease progression (during or after treatment) or intolerance to treatment with ROS1 tyrosine kinase inhibitor(s). patients whose tumors have a known BRAFV600E mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with dabrafenib in combination with trametinib;
NSCLCコホート(CIT処置)には、抗PD-L1/PD-1を含むCIT(治験中又は承認済み)で以前に処置された組織学的に確認された治癒不能な進行性NSCLCを有する患者が含まれる。腫瘍が既知の感作EGFR変異を有する患者は、疾患進行(処置中若しくは処置後)、又はEGFRチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;腫瘍が既知のALK再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はALKチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;腫瘍が既知のROS1再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はROS1チロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;腫瘍が既知のBRAFV600E変異を有する患者は、疾患進行(処置中若しくは処置後)、又はトラメチニブと組み合わせたダブラフェニブによる処置に対する不耐性も経験していなければならない;患者は、以前の抗PD-L1/PD-1を含んでいなければならない、CIT単独療法及び/又は併用療法(治験中又は承認済み)で文書化された疾患進行を経験していなければならない。 The NSCLC cohort (CIT treatment) included patients with histologically confirmed incurable advanced NSCLC previously treated with CIT (investigational or approved) containing anti-PD-L1/PD-1. included. Patients with known sensitizing EGFR mutations whose tumors must also experience disease progression (during or after treatment) or intolerance to treatment with EGFR tyrosine kinase inhibitor(s); Patients with ALK rearrangements must also experience disease progression (during or after treatment) or intolerance to treatment with ALK tyrosine kinase inhibitor(s); tumor has known ROS1 rearrangement Patients must also experience disease progression (during or after treatment) or intolerance to treatment with ROS1 tyrosine kinase inhibitor(s); during or after treatment), or intolerance to treatment with dabrafenib in combination with trametinib; patients must have prior anti-PD-L1/PD-1, CIT monotherapy and/or have documented disease progression on concomitant therapy (investigational or approved).
以前の抗PD-L1/PD-1を単剤療法又は併用療法として受けている間に、いつでもRECIST v1.1による治験責任医師による評定で確認されたPR又はCRの文書化された最良効果を経験した少なくとも約10人の患者が登録され得る。以前の抗PD-L1/PD-1を単剤療法及び/又は併用療法として受けている間に、RECIST v1.1による治験責任医師が評定したSDの文書化された最良効果をいつでも経験した少なくとも約10人の患者が登録され得る。以前の抗PD-L1/PD-1を単剤療法及び/又は併用療法として受けている間に、RECIST v1.1による治験責任医師が評定した進行性疾患(PD)の文書化された最良効果をいつでも経験した少なくとも約10人の患者が登録され得る。単剤療法及び/又は併用療法としての以前の抗PD-L1/PD-1は、この拡大コホートへの登録前に投与された最新の全身性抗がん治療とならなければならない。主に毒性又は不耐性のために以前の抗PD-L1/PD-1単剤療法及び/又は併用療法を中止した患者は、この拡大コホートへの登録に適格ではない。 Best documented response of PR or CR confirmed by investigator assessment by RECIST v1.1 at any time while receiving prior anti-PD-L1/PD-1 as monotherapy or combination therapy At least about 10 experienced patients may be enrolled. At least the best documented effect of Investigator-rated SD by RECIST v1.1 experienced at any time while receiving prior anti-PD-L1/PD-1 as monotherapy and/or combination therapy About 10 patients can be enrolled. Investigator-assessed best documented response to progressive disease (PD) by RECIST v1.1 while receiving prior anti-PD-L1/PD-1 as monotherapy and/or combination therapy At any time, at least about 10 patients who have experienced Previous anti-PD-L1/PD-1 as monotherapy and/or combination therapy must be the most recent systemic anti-cancer therapy administered prior to enrollment in this expansion cohort. Patients who discontinued prior anti-PD-L1/PD-1 monotherapy and/or combination therapy primarily due to toxicity or intolerance are not eligible for enrollment in this expansion cohort.
TNBCコホートには、乳房の組織学的に確認された治癒不能な進行性エストロゲン受容体(ER)陰性、プロゲステロン受容体(PgR)陰性、及びヒトEGFR2(HER2)陰性腺癌(トリプルネガティブ)を有する患者が含まれる。トリプルネガティブ状態は、米国臨床腫瘍学会米国病理学者協会(ASCO-CAP)ガイドラインによって定義されるように文書化されなければならない:1%未満の腫瘍細胞核がERについて免疫反応性であり、1%未満の腫瘍細胞核がプロゲステロン受容体について免疫反応性であり、HER2検査はIHC1+、IHC0、又はin situハイブリダイゼーション(ISH)陰性を実証するCRCコホートには、組織学的に確認された治癒不能で進行性の結腸又は直腸の腺癌を有する患者が含まれる。虫垂起源の腫瘍を有する患者は適格ではない。 The TNBC cohort has histologically confirmed incurable advanced estrogen receptor (ER)-negative, progesterone receptor (PgR)-negative, and human EGFR2 (HER2)-negative adenocarcinoma (triple-negative) of the breast Patients included. Triple-negative status must be documented as defined by the American Society of Clinical Oncology-American Society of Pathologists (ASCO-CAP) guidelines: less than 1% of tumor cell nuclei are immunoreactive for ER and less than 1% of tumor cell nuclei immunoreactive for the progesterone receptor and HER2 testing demonstrating IHC1+, IHC0, or negative in situ hybridization (ISH). patients with adenocarcinoma of the colon or rectum are included. Patients with tumors of appendiceal origin are not eligible.
GCコホートには、組織学的に確認された手術不能な、局所進行性若しくは転移性又は再発性の胃腺癌又はGEJ腺癌を有し、治癒的療法に適していない患者が含まれる。腫瘍中心が解剖学的食道胃接合部上1~5cm以内に位置する遠位食道の腺癌としてRuediger Siewert et al.(2000)によって定義された1型GEJ腫瘍を有する患者が試験に適格である。食道がん(扁平上皮癌腫又は腺癌)を有する患者は、メディカルモニターとの議論の後に適格となり得る。腫瘍が既知のHER2陽性を有する患者は、疾患進行(処置中若しくは処置後)、又はHER2標的化抗体/HER2阻害剤(複数可)による処置に対する不耐性も経験していなければならない;HER 2陽性は、原発腫瘍又は転移性病変に対する現地の検査室の検査によって評定されるIHC3+又はIHC2+/ISH+(ISH陽性は、2以上のHER2:CEP17比として定義される)のいずれかとして定義される。組織が不十分又は利用できない(例えば、保管及び/又は生検)ためにHER2検査を受けておらず、したがって腫瘍のHER2状態が不明である患者は依然として適格であり得る。
The GC cohort includes patients with histologically confirmed inoperable, locally advanced or metastatic or recurrent gastric or GEJ adenocarcinoma who are not amenable to curative therapy. Ruediger Siewert et al., as adenocarcinoma of the distal esophagus with the tumor center located within 1-5 cm above the anatomical esophagogastric junction. (2000) are eligible for the study with
HNSCCコホートには、組織学的に確認された、治癒的療法を受け入れることができない手術不能な、局所進行性又は転移性の、再発性又は持続性の頭頸部扁平上皮癌腫(口腔、中咽頭、下咽頭、又は喉頭)を有する患者が含まれる。頭頸部における任意の他の原発解剖学的位置のHNSCC患者、原発不明のHNSCC患者、又は非扁平上皮組織の腫瘍を有する患者は、適格ではない。鼻咽頭のHNSCC患者は適格であり得る。HNSCCのHPV状態を知らなければならない。 The HNSCC cohort included histologically confirmed inoperable, locally advanced or metastatic, recurrent or persistent squamous cell carcinoma of the head and neck (oral, oropharyngeal, Included are patients with hypopharynx, or larynx. HNSCC patients of any other primary anatomical location in the head and neck, HNSCC patients of unknown primary, or patients with tumors of non-squamous tissue are not eligible. Nasopharyngeal HNSCC patients may be eligible. The HPV status of HNSCC must be known.
UBCコホートには、尿路上皮(腎盂、尿管、膀胱、及び尿道を含む)の組織学的に確認された治癒不能な進行性移行細胞癌腫を有する患者が含まれる。混合組織型の患者は、優勢な移行細胞パターンを有する必要がある。 The UBC cohort includes patients with histologically confirmed, incurable, advanced transitional cell carcinoma of the urothelium (including the renal pelvis, ureter, bladder, and urethra). Patients with mixed histology should have a predominant transitional cell pattern.
黒色腫のコホートには、組織学的に確認された治癒不能な進行性転移性黒色腫を有する患者が含まれる。CIT(抗PD-L1/PD-1剤及び/又は抗CTLA-4剤を含む)が黒色腫の処置として地域の規制当局によって承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる黒色腫を有する患者。腫瘍が既知のBRAFV 600変異を有する患者はまた、疾患の進行(処置中又は治療後)又はBRAF阻害剤及び/又はMEK阻害剤による不耐性を経験していなければならない。このコホートの患者の約20%以下が眼(ブドウ膜)黒色腫の患者であるように、登録が管理される。
The melanoma cohort includes patients with histologically confirmed incurable advanced metastatic melanoma. Investigational drug in combination with anti-PD-L1 antibody if CIT (including anti-PD-L1/PD-1 and/or anti-CTLA-4 agents) is approved by the local regulatory agency for the treatment of melanoma Patients with melanoma for whom clinical trials are considered an acceptable treatment option. Patients whose tumors have known
OCコホートには、組織学的に確認された治癒不能な進行性上皮性卵巣がん、ファロピウス管がん、又は原発性腹膜がんを有する患者が含まれる。境界線上の卵巣上皮新生物(例えば、低悪性度の腫瘍、非定型増殖性腫瘍)は除外される。 The OC cohort includes patients with histologically confirmed incurable advanced epithelial ovarian cancer, fallopian tube carcinoma, or primary peritoneal cancer. Borderline ovarian epithelial neoplasms (eg, low-grade tumors, atypical proliferative tumors) are excluded.
RCCコホートには、明細胞組織学の構成要素及び/又は肉腫様組織学の構成要素を有する、組織学的に確認された治癒不能進行性RCCを有する患者が含まれる。CIT(抗PD-L1/PD-1剤を含む)が地域の規制当局によってRCCの処置として承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされるRCCを有する患者。 The RCC cohort includes patients with histologically confirmed incurable advanced RCC with a clear cell histology component and/or a sarcomatoid histology component. If CITs (including anti-PD-L1/PD-1 agents) are approved by local regulatory authorities for the treatment of RCC, clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are an acceptable treatment option. Patients with considered RCC.
E.投薬及び投与 E. Dosing and Administration
この試験の第Ib相部分において、チラゴルマブと組み合わせて投与されるアテゾリズマブの用量は、アテゾリズマブ1680mgのIVQ4Wが投与される第Ib相Q4W投与コホートを除いて、3週間ごとに1200mgのIVである。この用量は固定されており、体重に依存しない。化学療法を用いない全ての第Ib相コホートにおいて、アテゾリズマブは、チラゴルマブ注入及びその後の観察期間の後に投与される。第Ib相化学療法拡大コホートでは、アテゾリズマブは、チラゴルマブの前に投与される。 In the Phase Ib portion of the study, the dose of atezolizumab administered in combination with tiragolumab is 1200 mg IV every 3 weeks, except for the Phase Ib Q4W dose cohort, which receives atezolizumab 1680 mg IVQ4W. This dose is fixed and independent of body weight. In all Phase Ib cohorts without chemotherapy, atezolizumab will be administered after tiragolumab infusion and a subsequent observation period. Atezolizumab is administered prior to tiragolumab in the Phase Ib chemotherapy expansion cohort.
アテゾリズマブの初回用量は、60(±10)分かけて送達される。注入に関連する有害事象なしに1回目の注入が許容される場合、2回目の注入は30(±10)分かけて送達され得る。30分間の注入が十分に許容される場合、その後の注入は全て30(±10)分かけて送達され得る。サイクル1では、アテゾリズマブの投与後、90分間の観察期間が続く。その後の全てのアテゾリズマブ注入の後に、30分間の観察期間を設けてもよい。別の臨床試験で以前にアテゾリズマブを受けたことがある患者は、以前に忍容された最も速い速度で初期用量を受けることができる。
The initial dose of atezolizumab is delivered over 60 (±10) minutes. If the first infusion is tolerated without infusion-related adverse events, the second infusion may be delivered over 30 (±10) minutes. If a 30 minute infusion is well tolerated, all subsequent infusions may be delivered over 30 (±10) minutes. In
第Ib相拡大コホートにおける化学療法
化学療法は、アテゾリズマブ及びチラゴルマブ注入及びその後の観察期間の後に投与される。導入期の間、化学療法サイクルは、少なくとも1つの化学療法成分が21日間のサイクルの間に少なくとも1回投与されている限り、予め指定された数の導入化学療法サイクルに向かってカウントする。化学療法成分が投与されないサイクルは、導入化学療法サイクルの総数にカウントされない。
Chemotherapy in the Phase Ib Expansion Cohort Chemotherapy will be administered after atezolizumab and tiragolumab infusions followed by an observation period. During the induction phase, chemotherapy cycles count toward the prespecified number of induction chemotherapy cycles as long as at least one chemotherapy component has been administered at least once during the 21-day cycle. Cycles in which no chemotherapy component is administered are not counted in the total number of induction chemotherapy cycles.
患者は、現地の標準治療及び製造業者の指示に従って、化学療法剤の制吐剤及びIV水分補給を受ける。しかしながら、ステロイドの免疫調節効果のために、ステロイドによる前投薬は、臨床的に実施可能な程度に最小限にしなければならない。 Patients receive chemotherapeutic antiemetics and IV hydration according to local standard of care and manufacturer's instructions. However, due to the immunomodulatory effects of steroids, premedication with steroids should be minimized as clinically practicable.
コホートA-アテゾリズマブ+チラゴルマブ+カルボプラチン/シスプラチン+ペメトレキセド
各21日間のサイクルの1日目に、全ての適格患者は、以下の順序で薬物注入を受ける。
Cohort A—Atezolizumab + Tiragolumab + Carboplatin/Cisplatin +
導入:アテゾリズマブ>チラゴルマブ>ペメトレキセド>カルボプラチン又はシスプラチン
導入期の4~6サイクル後、患者は以下の投与順序で維持療法を開始する。
Induction: atezolizumab > tiragolumab > pemetrexed > carboplatin or cisplatin After 4-6 cycles of the induction phase, patients begin maintenance therapy with the following dosing sequence.
維持:アテゾリズマブ>チラゴルマブ>ペメトレキセド

表8は、導入期中のペメトレキセド及びカルボプラチン又はシスプラチンの処置投与のための、及び維持期中のペメトレキセドのための推奨される注入時間を列挙する。

コホートB-アテゾリズマブ+チラゴルマブ+カルボプラチン+パクリタキセル
各21日間のサイクルの1日目に、全ての適格患者は、以下の順序で薬物注入を受ける:
Cohort B—Atezolizumab + Tiragolumab + Carboplatin +
導入;アテゾリズマブ>チラゴルマブ>パクリタキセル>カルボプラチン In-licensing; atezolizumab > tiragolumab > paclitaxel > carboplatin
表8は、コホートBの患者の導入処置のための推奨される前投薬を列挙している。表9は、導入期中のパクリタキセル及びカルボプラチンの処置投与のための推奨注入時間を列挙している。

コホートC-アテゾリズマブ+チラゴルマブ+カルボプラチン又はシスプラチン+エトポシド
各21サイクルの1日目に、全ての適格患者に以下の順序で試験薬注入を行う。
Cohort C—Atezolizumab + Tiragolumab + Carboplatin or Cisplatin +
導入:アテゾリズマブ>チラゴルマブ>シスプラチン又はカルボプラチン>エトポシド
導入期の後、患者は以下の投与順序で維持療法を開始する。
Induction: atezolizumab > tiragolumab > cisplatin or carboplatin > etoposide After the induction phase, patients will begin maintenance therapy with the following dosing sequence.
維持:アテゾリズマブ>チラゴルマブ Maintenance: atezolizumab > tiragolumab
表10は、導入期中のカルボプラチン又はシスプラチン及びエトポシドの処置投与のための推奨注入時間を列挙している。

シスプラチン
異なるコホートにおけるシスプラチンの投与のためのガイドラインを表11に示す。

カルボプラチン
異なるコホートにおけるシスプラチンの投与のためのガイドラインを表12に示す。

この試験の目的のために、GFRは、計算されたクレアチニンクリアランス(CrCl)と同等であると考えられる。CrClは、施設のガイドラインによって、又は以下の式を使用してCockcroft及びGault(1976)の方法によって計算される。

年齢=年単位の患者の年齢
体重=kg単位の患者の体重
Scr=血清クレアチニン(mg/dL)
For the purposes of this study, GFR is considered equivalent to calculated creatinine clearance (CrCl). CrCl is calculated by institutional guidelines or by the method of Cockcroft and Gault (1976) using the following formula.
異常に低い血清クレアチニンレベルを有する患者については、0.8mg/dLの最小クレアチニンレベルを使用してGFRを推定するか、又は125mL/分で推定GFRを制限する。 For patients with abnormally low serum creatinine levels, a minimum creatinine level of 0.8 mg/dL is used to estimate GFR or limit estimated GFR at 125 mL/min.
患者のGFRが同位体希釈質量分析法による血清クレアチニン測定に基づいて推定される場合、米国FDAは、医師が過剰投与による潜在的な毒性を回避するために所望の曝露(AUC)のためにカルボプラチンの用量をキャッピングすることを検討することを推奨する。カルボプラチン標識に記載されているCalvert式に基づいて、最大用量を以下のように計算することができる。 When a patient's GFR is estimated based on serum creatinine measurements by isotope dilution mass spectrometry, the U.S. FDA recommends that physicians use carboplatin for desired exposure (AUC) to avoid potential toxicity from overdose. It is recommended that consideration be given to capping the dose of Based on the Calvert formula described in the carboplatin label, the maximum dose can be calculated as follows.
最大カルボプラチン用量(mg)=標的AUC(mg・分/mL)×(GFR+25mL/分)。 Maximum Carboplatin Dose (mg) = Target AUC (mg-min/mL) x (GFR + 25 mL/min).
最大用量は、正常な腎機能を有する患者について150mL/分で上限を定めたGFR推定値に基づく。より高い推定GFR値を使用すべきではない。 Maximum dose is based on GFR estimates capped at 150 mL/min for patients with normal renal function. Higher estimated GFR values should not be used.
標的AUC=6の場合、最大用量は6×150=900mgである。 For target AUC=6, the maximum dose is 6×150=900 mg.
標的AUC=5の場合、最大用量は5×150=750mgである。 For target AUC=5, the maximum dose is 5×150=750 mg.
標的AUC=4の場合、最大用量は4×150=600mgである。 For target AUC=4, the maximum dose is 4×150=600 mg.
ペメトレキセド
コホートAにおけるペメトレキセドの投与のためのガイドラインを表13に示す。

投与される投薬前用量は処方情報に従う。ペメトレキセド療法に適格な全ての患者は、ペメトレキセド投与の少なくとも5日前、当日および投与後少なくとも2日の間、半減期が長い非ステロイド性抗炎症薬の服用を避けるべきである。 The pre-dosing dose administered is according to the prescribing information. All patients eligible for pemetrexed therapy should avoid taking non-steroidal anti-inflammatory drugs with long half-lives for at least 5 days before, on the day of, and for at least 2 days after administration of pemetrexed.
パクリタキセル
コホートBのパクリタキセル投与のガイドラインを表14に示す。

アジア人種/民族の患者は、3時間にわたる175mg/m2 IVでのより低い開始用量のパクリタキセルを有する。パクリタキセルのより低い開始用量は、肺がん臨床試験の内部安全性の再検討中に観察されるように、非アジア諸国の患者と比較して、アジア諸国の患者における血液毒性のより高い全発生率に基づく。本試験で使用される場合、アジアの人種/民族とは、東アジア、東南アジア、又は南アジアに居住するか、又は祖先の起源を有する多様な集団を含む汎民族/人種グループを指す。特定の患者におけるそのような用語の適用可能性は、処置を行う治験責任医師の裁量であり、患者の臨床的特徴及び起源国に基づくべきである。 Patients of Asian race/ethnicity have a lower starting dose of paclitaxel at 175 mg/m2 IV over 3 hours. A lower starting dose of paclitaxel is associated with a higher overall incidence of hematologic toxicity in patients from Asian countries compared with patients from non-Asian countries, as observed during the internal safety review of lung cancer clinical trials. based on As used in this study, Asian race/ethnicity refers to a pan-ethnic/racial group that includes diverse populations residing in or having ancestral origins in East Asia, Southeast Asia, or South Asia. The applicability of such terms in a particular patient is at the discretion of the treating investigator and should be based on the patient's clinical characteristics and country of origin.
エトポシド
コホートCにおけるエトポシドの投与のためのガイドラインを表15に示す。

実施例2.アテゾリズマブ及びチラゴルマブと組み合わせた化学療法の第Ib/II相非盲検無作為化試験
本試験は、転移性膵管腺癌(PDAC)の事前全身治療を受けたことがない患者における、チラゴルマブと組み合わせたアテゾリズマブ及び化学療法(ナノ粒子アルブミン結合パクリタキセル(nab-パクリタキセル)及びゲムシタビン)の有効性、安全性及び薬物動態を評価する。この試験は、転移性PDACを有する患者における免疫療法に基づく処置の組み合わせの有効性、安全性、及び薬物動態を評価する。
Example 2. Phase Ib/II, open-label, randomized study of chemotherapy in combination with atezolizumab and tiragolumab Efficacy, safety and pharmacokinetics of atezolizumab and chemotherapy (nanoparticle albumin-bound paclitaxel (nab-paclitaxel) and gemcitabine) are evaluated. This study evaluates the efficacy, safety, and pharmacokinetics of immunotherapy-based treatment combinations in patients with metastatic PDAC.
A.試験計画
コホート1の患者を、対照群(化学療法)又はアテゾリズマブ及びチラゴルマブと組み合わせた化学療法からなる実験群に無作為に割り当てる。実験群内への登録は、予備期とそれに続く拡大期の2期で行われる。予備期中に約20人の患者が登録される。無作為化を中断して、最低6人の患者における安全性評価を可能にする。安全性評定は、少なくとも1用量の処置(すなわち、所与の組み合わせに対して各薬剤の1回の用量)を受け、少なくとも1つの完全な処置サイクル中に安全性フォローアップ評定を完了した最低6人の患者からの安全性データに基づく。組み合わせが十分に安全であると判定された場合、その群で登録が再開される。予備段階中に実験群で臨床活性が観察される場合、拡大相中に約25人の追加の患者がその群に登録され得る。さらなるサブグループ分析を可能にするために、潜在的な予測バイオマーカーを含む人口統計学的及びベースライン特性に関して処置群間のバランスを確保するために、さらなる患者を登録することができる。
A. Study Design Patients in
患者は処置群に無作為に割り当てられ、無作為化率は、登録のために開いている実験群の数(例えば、予備期からの結果の分析を待って、群が追加されるか、又は群への登録が中断される場合)に依存し、対照群に割り当てられる可能性は35%以下であるという規定がある。 Patients were randomly assigned to treatment groups, and the randomization rate was determined by the number of experimental groups open for enrollment (e.g., whether groups were added pending analysis of results from the preliminary phase, or There is a stipulation that the chance of being assigned to the control group is 35% or less, depending on when enrollment in the group is discontinued).
この試験の最後は、最後の患者が最後の来院(LPLV)を完了した日(電話又はクリニックで行われる生存フォローアップ来院を含む)として定義される。最初の患者のスクリーニングから試験終了までの試験の全長は、約3~5年である。 The end of the study is defined as the date the last patient completed the last visit (LPLV), including a survival follow-up visit conducted by phone or in the clinic. The total length of the trial, from initial patient screening to study termination, is approximately 3-5 years.
活動スケジュールを表16に示す。


処置日には、特に明記しない限り、全ての評定を投与前に行わなければならない。 On treatment days, all assessments must be performed prior to dosing unless otherwise specified.
a休日、休暇又は他の状況のために来院が除外される場合、メディカルモニターの同意が得られている場合には、指定されたウィンドウ外で訪問が行われる可能性がある。 a If a visit is excluded due to a holiday, vacation, or other circumstances, the visit may occur outside of the designated window if the medical monitor agrees.
bランダム化後7日以内に処置を開始することが推奨される。 bIt is recommended to start treatment within 7 days after randomization.
c患者は、試験処置の最後の投与後30日以内に処置中止来院のために診療所に戻る。疾患の進行が確認された訪問は、処置中止来院として使用され得る。次いで、患者はフォローアップ評定を受ける。 cPatients return to the clinic for a treatment discontinuation visit within 30 days after the last dose of study treatment. A visit with confirmed disease progression may be used as a treatment discontinuation visit. The patient then undergoes follow-up evaluations.
dバイタルサインには、呼吸数、脈拍数、並びに患者が座位にある間の収縮期及び拡張期血圧、パルスオキシメトリ、及び体温が含まれる。有害事象eCRFに新たな又は悪化した臨床的に有意な異常を記録する。アテゾリズマブの最初の注入のために、バイタルサインは、注入前の60分以内に、臨床上適応がある場合、注入中15(±5)分及び注入後30(±10)分ごとに測定しなければならない。その後の注入のために、注入前の60分以内にバイタルサインを測定し、臨床的に適応がある場合、又は以前の注入中に症状が発生した場合、注入中及び注入後30(±10)分以内にバイタルサインを測定しなければならない。チラゴルマブの初回注入では、注入前の60分以内、注入中15(±5)及び注入後30(±10)分毎にバイタルサインを測定しなければならない。チラゴルマブのその後の注入のために、注入前の60分以内にバイタルサインを測定し、臨床的に適応がある場合、又は以前の注入中に症状が発生した場合、注入中及び注入後15(±10)分以内にバイタルサインを測定しなければならない。 dVital signs include respiratory rate, pulse rate, and systolic and diastolic blood pressure, pulse oximetry, and temperature while the patient is seated. Record new or worsening clinically significant abnormalities on the Adverse Events eCRF. For the first infusion of atezolizumab, vital signs should be measured within 60 minutes prior to infusion and, if clinically indicated, every 15 (±5) minutes during infusion and every 30 (±10) minutes after infusion. must. For subsequent infusions, vital signs will be measured within 60 minutes prior to infusion and 30 (±10) during and after infusion if clinically indicated or if symptoms occurred during the previous infusion Vital signs must be measured within minutes. For the first infusion of tiragolumab, vital signs must be measured within 60 minutes prior to infusion, 15 (±5) during infusion, and every 30 (±10) minutes after infusion. For subsequent infusions of tiragolumab, vital signs were measured within 60 minutes prior to infusion and, if clinically indicated or symptoms occurred during the previous infusion, during and 15 (± 15) post-infusion 10) Vital signs must be measured within minutes.
e完全な身体検査には、頭部、眼、耳、鼻、及び咽喉、並びに心臓血管系、皮膚系、筋骨格系、呼吸器系、胃腸系、泌尿生殖器系、及び神経系の評価が含まれる。有害事象eCRFに新たな又は悪化した臨床的に有意な異常を記録する。 e A complete physical examination includes evaluation of the head, eyes, ears, nose, and throat, as well as the cardiovascular, skin, musculoskeletal, respiratory, gastrointestinal, genitourinary, and nervous systems. be Record new or worsening clinically significant abnormalities on the Adverse Events eCRF.
f指定された時点で、及び他の時点で臨床上適応があるように、限定的な症状指向検査を実施する。有害事象eCRFに新たな又は悪化した臨床的に有意な異常を記録する。 f Perform limited symptom-directed testing at designated time points and at other time points as clinically indicated. Record new or worsening clinically significant abnormalities on the Adverse Events eCRF.
g患者は、ECG記録の前に少なくとも10分間、仰臥位で安静にすることが推奨される。 gPatients are recommended to rest in supine position for at least 10 minutes prior to ECG recording.
h血液学には、WBC数、RBC数、ヘモグロビン、ヘマトクリット、血小板数、及び分類数(好中球、好酸球、好塩基球、単球、リンパ球、他の細胞)が含まれる。 hHematology includes WBC counts, RBC counts, hemoglobin, hematocrit, platelet counts, and differential counts (neutrophils, eosinophils, basophils, monocytes, lymphocytes, other cells).
i検査室での検査は、サイクル1の1日目の前の96時間以内、及び処置期間中の指定されたその後の来院の前の24時間以内に行われなければならない。
i Laboratory tests must occur within 96 hours prior to
jーニング検査室評定がサイクル1の1日目の前の96時間以内に行われた場合、それらを繰り返す必要はない。
If the training laboratory assessments were performed within 96 hours prior to
k化学パネル(血清又は血漿)には、重炭酸塩又は総二酸化炭素(その領域に対する標準治療と考えられる場合)、ナトリウム、カリウム、マグネシウム、塩化物、グルコース、BUN又は尿素、クレアチニン、総タンパク質、アルブミン、リン、カルシウム、総ビリルビン、ALP、ALT、及びASTが含まれる。 k Chemistry panel (serum or plasma) includes bicarbonate or total carbon dioxide (if considered standard of care for the area), sodium, potassium, magnesium, chloride, glucose, BUN or urea, creatinine, total protein, Included are albumin, phosphorus, calcium, total bilirubin, ALP, ALT, and AST.
lTSH、遊離T3(又は遊離T3が実施されていない部位については総T3)及び遊離T4を、スクリーニング時並びにサイクル1の1日目及びその後は3サイクルごとに評定する(すなわち、サイクル4、7、10等)。
l TSH, free T3 (or total T3 for sites where free T3 has not been performed) and free T4 are assessed at screening and on
mスクリーニング時に定量的HBV DNAが陽性である患者(適格基準当たり500IU/mL未満でなければならない)は、処置中止時(±7日)、並びに処置中止後3、6、9、及び12ヶ月目(各時点で±14日)に、3回目のサイクルごと(すなわち、サイクル3、6、9等)の1日目に追加のHBV DNA検査を受ける。HBV DNAが処理されている間に試験処置及び手順を進めることができるが、結果は入手可能になったらすぐに治験責任医師によって再検討しなければならない。HBV DNAが500IU/mL未満に増加した場合、試験処置の継続前にメディカルモニターに相談する必要があり、B型肝炎を専門とする肝臓専門医又は胃腸科医に相談することが推奨される。
mPatients with positive quantitative HBV DNA at screening (must be <500 IU/mL per eligibility criteria) at treatment discontinuation (±7 days) and at 3, 6, 9, and 12 months after treatment discontinuation (±14 days at each time point), receive an additional HBV DNA test on
n妊娠可能な全ての女性は、治療中の指定された来院時並びに試験処置の最後の用量の3ヶ月後及び6ヶ月後に実施された尿又は血清の妊娠検査を行う。尿妊娠検査が陽性である場合、それは血清妊娠検査によって確認されなければならない。 n All women of childbearing potential will have a urine or serum pregnancy test performed at designated visits during treatment and 3 and 6 months after the last dose of study treatment. If the urine pregnancy test is positive, it must be confirmed by a serum pregnancy test.
opH、比重、グルコース、タンパク質、ケトン、及び血液を含む;ディップスティックが許可されている。 o Includes pH, specific gravity, glucose, protein, ketones, and blood; dipsticks are allowed.
p自己抗体分析には、抗核抗体、抗二本鎖DNA、循環抗好中球細胞質抗体、及び核周囲抗好中球細胞質抗体が含まれる。 P- autoantibody assays include antinuclear antibodies, anti-double-stranded DNA, circulating antineutrophil cytoplasmic antibodies, and perinuclear antineutrophil cytoplasmic antibodies.
q自己免疫疾患を示唆する徴候又は症状を発症する患者については、自己抗体分析を繰り返さなければならない(例えば、紅斑性狼瘡)。 qAutoantibody assays should be repeated for patients who develop signs or symptoms suggestive of an autoimmune disease (eg, lupus erythematosus).
rRBRサンプリングの承認を受けていない施設には適用できない。参加するための書面によるインフォームドコンセントを提供した参加施設の患者に対してのみ実施した。 r Not applicable to establishments not licensed for RBR sampling. Performed only on patients from participating centers who provided written informed consent to participate.
s患者は、治験責任医師が臨床的に実施可能であると判断した場合、治験責任医師が決定した許容できない毒性又は臨床的利益の喪失時に腫瘍生検試料収集を受ける。生検は、許容できない毒性又は臨床的利益の喪失の判定後、又は次の抗がん治療の前のいずれか早い方の40日以内に行和なければならない。更に、拡大期に登録された患者は、同じCITの組み合わせで処置された最低15人の患者から処置中の組織試料が既に採取され、評価可能であると判定されていない限り、治療開始後4週間(±7日)で腫瘍生検試料の収集を受ける(臨床上実施可能と考えられる場合)。 sPatients will undergo tumor biopsy sample collection at the time of Investigator-determined unacceptable toxicity or loss of clinical benefit, if deemed clinically feasible by the Investigator. A biopsy must be performed within 40 days after determination of unacceptable toxicity or loss of clinical benefit or before the next anticancer therapy, whichever comes first. In addition, patients enrolled in the expansion phase will be treated 4 days after initiation of treatment unless an in-treatment tissue sample has already been obtained from a minimum of 15 patients treated with the same CIT combination and determined to be evaluable. Tumor biopsy samples will be collected weekly (±7 days) (if considered clinically feasible).
t任意の生検に同意した患者は、治療開始後4週間(±7日)で腫瘍生検試料の収集を受け、臨床的に実施可能と判断された場合(既に処置中の生検を受けている拡大期に登録された患者には適用されない)、治験責任医師の裁量で他の時点で追加の処置中の生検を受けることができる。 tPatients who consented to a voluntary biopsy had a tumor biopsy sample collected 4 weeks (± 7 days) after initiation of treatment and if clinically feasible (biopsy already under treatment). (not applicable to patients enrolled in an expansion phase who are currently enrolled) and may undergo additional in-treatment biopsies at other time points at the discretion of the Investigator.
u患者は、放射線学的疾患進行後に処置を継続する患者の場合を除いて、RECIST v 1.1による放射線学的疾患進行まで、ベースライン時、処置開始後最初の48週間は6週間ごと(±1週間)、その後は用量遅延にかかわらず12週間毎(±2週間)に腫瘍評定を受け、そのような患者は、治験責任医師によって決定される臨床的利益の喪失まで、6週間ごと(±1週間)に腫瘍評定を受ける。したがって、腫瘍評定は、疾患の進行以外の理由で処置を中断する患者において、たとえ彼らが新たな治験実施計画書に規定されていない抗がん治療を開始したとしても、スケジュールに従って継続しなければならない。 uPatients will be followed until radiographic disease progression by RECIST v 1.1 at baseline and every 6 weeks for the first 48 weeks after starting treatment, except for patients continuing treatment after radiographic disease progression ( ± 1 week), then every 12 weeks (± 2 weeks) regardless of dose delay, and such patients will undergo tumor assessments every 6 weeks ( ± 1 week) to undergo tumor assessment. Therefore, tumor assessment should continue on schedule in patients who discontinue treatment for reasons other than disease progression, even if they start new non-protocol-specified anticancer therapy. not.
vベースラインで特定された全ての測定可能及び/又は評価可能な病変は、上記の腫瘍評定スケジュールに従って、その後の各腫瘍評定で再評定価しなければならない(付記「t」を参照)。スクリーニングで疾患部位を評定するために使用されるのと同じX線撮影手順を、その後の腫瘍評定(例えば、CTスキャンのための同じコントラスト治験実施計画書)に使用しなければならない。 vAll measurable and/or evaluable lesions identified at baseline must be reassessed at each subsequent tumor assessment according to the tumor assessment schedule described above (see appendix "t"). The same radiographic procedure used to assess disease sites at screening should be used for subsequent tumor assessment (eg, same contrast protocol for CT scan).
w試験処置の開始の10日前から処置中止の来院までの治験実施計画書が定めた試験処置に加えて、患者が使用した任意の薬物(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)が含まれる。 wAny drugs (e.g., prescription drugs, over-the-counter drugs, vaccines, herbal remedies, or therapy, dietary supplements).
x試験処置の開始後、試験処置の最後の用量の30日後又は新しい全身性抗がん治療の開始までのいずれか早い方まで全ての有害事象が報告され、試験処置の最後の用量の135日後又は新しい全身性抗がん治療の開始までのいずれか早く発生する方まで特に興味深い重篤な有害事象及び有害事象が継続して報告される。この期間の後、原因にかかわらず、全ての死亡を報告しなければならない。治験責任医師は、各有害事象を、事象がベースライングレード以上に解消するまで、事象が治験責任医師によって安定であると評定されるまで、患者が追跡調査に失敗するまで、又は患者が同意を撤回するまでフォローアップしなければならない。最終結果が報告され得るまで、試験処置又は試験関連手順に関連すると考えられる全ての重篤な有害事象を追跡するためにあらゆる努力を払わなければならない。 x All adverse events reported after initiation of study treatment, 30 days after last dose of study treatment or until initiation of new systemic anti-cancer therapy, whichever comes first, 135 days after last dose of study treatment Serious adverse events and adverse events of particular interest continue to be reported until the start of a new systemic anticancer therapy, whichever occurs first. After this period, all deaths, regardless of cause, must be reported. The investigator will track each adverse event until the event resolves to ≥ baseline grade, until the event is rated stable by the investigator, until the patient fails follow-up, or until the patient gives consent. You must follow up until you withdraw. Every effort should be made to follow up all serious adverse events considered related to study treatment or study-related procedures until final results can be reported.
y各28日間サイクルの第1及び15日目に、アテゾリズマブを840mgの固定用量でIV注入によって投与する。アテゾリズマブの初回用量は、60(±15)分かけて送達される。その後の注入は、以前の注入が注入関連有害事象なしで許容された場合は30(±10)分にわたって、又は患者が以前の注入で注入関連有害事象を経験した場合は60(±15)分にわたって送達される。
y Atezolizumab is administered by IV infusion at a fixed dose of 840 mg on
z処置は、治験責任医師によって決定された許容できない毒性又は臨床的利益の喪失まで継続する。 zTreatment is continued until unacceptable toxicity or loss of clinical benefit as determined by the Investigator.
aa各28日サイクルの第1及び15日目に、420mgの固定用量でIV注入によって投与する。チラゴルマブの初回用量は、60(±10)分かけて送達される。その後の注入は、以前の注入が注入関連有害事象なしで許容された場合は30(±10)分にわたって、又は患者が以前の注入で注入関連有害事象を経験した場合は60(±10)分にわたって送達される。第1サイクルの1日目に、アテゾリズマブ注入の完了の60分後にチラゴルマブを投与する。その後の注入間の間隔は、以前のアテゾリズマブ注入がIRRを伴わずに忍容された場合は30分、又は患者が以前のアテゾリズマブ注入でIRRを経験した場合は60分である。
aa A fixed dose of 420 mg is administered by IV infusion on
bb1、8及び15日目に、患者は、30(±5)分かけてIV注入によって投与されるnab-パクリタキセル125mg/m2を受け、続いて30(±5)分かけてIV注入によって投与されるゲムシタビン1000mg/m2を受ける。第1サイクルの1日目に、チラゴルマブ注入終了60分後にnab-パクリタキセルを投与して、チラゴルマブ投与後の観察を可能にする。その後の注入間の間隔は、以前のチラゴルマブ注入がIRRを伴わずに忍容された場合は30分、又は患者が以前のチラゴルマブ注入でIRRを経験した場合は60分である。
bb On
cc処置中止後、生存フォローアップ及び新しい抗がん治療(標的療法及び免疫療法を含む)に関する情報は、死亡するまで(患者が同意を取り下げるか、又は試験が終了しない限り)およそ3ヶ月ごとに、電話、患者の医療記録、及び/又はクリニックの来院を介して収集される。患者がフォローアップからの離脱を要求する場合、この要求はソース文書に文書化され、治験責任医師が署名しなければならない。患者が試験から離脱する場合、試験スタッフは、公開情報源(例えば、郡記録)を使用して生存状態に関する情報のみを取得することができる。 After cessation of cc treatment, survival follow-up and information on new anticancer therapies (including targeted therapies and immunotherapies) will be provided approximately every 3 months until death (unless patient withdraws consent or study ends) , phone calls, patient medical records, and/or clinic visits. If a patient requests withdrawal from follow-up, this request must be documented in the source document and signed by the investigator. If a patient is withdrawn from the study, study staff can only obtain information on survival status using public sources (eg, county records).
評定及びモニタリング
全ての患者は、試験を通して有害事象について綿密に監視され、有害事象は、国立がん試験所有害事象共通用語規準(National Cancer Institute Common Terminology Criteria for Adverse Events,Version 4.0(NCI CTCAE v4.0))に従って等級付けされる。患者は、最初の48週間の間は6週間ごとに(サイクル1の1日目から)、その後は6週間ごと又は12週間ごとに腫瘍評定を受ける。応答は、RECIST v1.1を使用して治験責任医師によって評定される。免疫ベースの治療剤(iRECIST)に対する修正RECIST v 1.1あたりの応答は、治験責任医師が評定した個々の病変データに基づいてプログラムで決定される。臨床活性が実験群で実証される場合、その群の腫瘍評定スキャンは、独立した再検討施設による評定のために提出され得る。
Assessment and Monitoring All patients were closely monitored for adverse events throughout the study, and adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE). v4.0)). Patients undergo tumor assessments every 6 weeks (starting on
ベースライン腫瘍組織試料は、例えば、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、メディカルモニターの承認が得られた後に腫瘍組織の保管を提出してもよく、ただし、組織が登録前3ヶ月以内に得られ、患者が生検の時点からいかなる抗がん治療も受けたことがないことを条件とする。治験責任医師が臨床的に実施可能であると判断した場合、許容できない毒性、RECIST v 1.1による疾患進行、又は治験責任医師が決定した臨床的利益の喪失のためにステージ1を中止する患者の腫瘍組織を収集する。拡大期の間に実験群に登録された患者については、処置中の組織試料が既に収集されており、同じCITの組み合わせで処置された最低15人の患者から評価可能であると判定されない限り、処置中の腫瘍組織試料がステージ1の処置の開始後4週間で収集される(臨床的に実施可能な場合)。これらの試料は、バイオマーカー試験のために利用される(バイオマーカー評定の理論的解釈を参照)。
A baseline tumor tissue sample is collected from all patients, eg, by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, tumor tissue storage may be submitted after obtaining Medical Monitor approval, provided that the tissue was obtained within 3 months prior to enrollment, Provided that the patient had not received any anticancer therapy from the time of biopsy. Patients who discontinue
アテゾリズマブ及び他の治療剤の薬物動態(PK)特性及び/又は免疫原性を特性評価するために、試験処置投与の前及び間の様々な時点で血液試料を採取する(表17)。リアルタイムの安全性データ及び利用可能なPKデータの再検討に基づいて、処置レジメンを修正することができる。

実験室、バイオマーカー、及び他の生物学的試料
探索的バイオマーカー試験には、腫瘍免疫生物学に関連する遺伝子又は遺伝子シグネチャ、PD-L1、T細胞活性化に関連するサイトカイン、T細胞受容体レパートリー、がん胎児性抗原、又は免疫細胞及びそのサブセットの密度、局在及び活性化状態の分析が含まれるが、これらに限定されず、DNA又はRNA抽出、体細胞変異の分析、及びNGS(WESを含む)の使用が含まれ得る。
Laboratory, Biomarkers, and Other Biological Samples Exploratory biomarker studies include genes or gene signatures associated with tumor immunobiology, PD-L1, cytokines associated with T cell activation, T cell receptors including, but not limited to, analysis of repertoire, carcinoembryonic antigen, or density, localization and activation state of immune cells and their subsets, DNA or RNA extraction, analysis of somatic mutations, and NGS ( WES) may be included.
以下の臨床検査のための試料を、分析のために試験施設のローカル検査室に送る:
・血液学:WBC数、RBC数、ヘモグロビン、ヘマトクリット、血小板数、及び分画数(好中球、好酸球、好塩基球、単球、リンパ球、他の細胞)
・化学パネル(血清又は血漿):CPK、重炭酸塩又は二酸化炭素(その領域に対する標準治療と考えられる場合)、ナトリウム、カリウム、マグネシウム、塩化物、グルコース、BUN又は尿素、クレアチニン、総タンパク質、アルブミン、リン、カルシウム、総ビリルビン、ALP、ALT、及びAST。
・凝固:INR及びaPTT。
・甲状腺機能検査:甲状腺刺激ホルモン、遊離トリヨードチロニン(T3)(又は遊離T3が実施されない部位については総T3)、及び遊離チロキシン(T4としても知られる)
・フェリチン及びγ-グルタミルトランスフェラーゼ
・地域の規制に従って許可されない限り、HIV血清学
・HAV血清学:HAV IgM
・HBV血清学:HBsAg、総HBcAb、及び(HBsAg検査が陰性であり、総HBcAb検査が陽性である場合)HBV DNA。
患者がスクリーニング時にHBsAg検査陰性及び総HBcAb検査陽性を有する場合、患者がHBV感染症を有するかどうかを判定するためにHBV DNA検査も実施しなければならない。
・HCV血清学:HCV抗体及び(HCV抗体検査が陽性である場合)HCV RNA。
患者がスクリーニング時にHCV抗体検査が陽性であれば、活動性HCV RNA試験も行ってHCV感染の有無を判定しなければならない。
・HEV血清学:HEV IgM
・C反応性タンパク質
・LDH
・CA19-9
・EBV血清学:
-EBV VCA IgM
-EBV VCA IgG又はEBNA IgG
-EBV PCR(臨床的に必要な場合のみ)
・妊娠検査
妊娠可能な全ての女性は、ステージ1スクリーニングで血清妊娠検査を受けている。その後の指定の来院時に血清妊娠検査を実施した。尿妊娠検査が陽性である場合、それは血清妊娠検査によって確認されなければならない。
女性は、初経後であり、閉経後状態に到達しておらず(閉経以外の原因が同定されていない、連続12ヶ月以上の無月経)、かつ、外科的不妊(卵巣及び/又は子宮の切除)を受けたことがない場合に、懐胎の可能性があるとみなされる。
・尿検査(pH、比重、グルコース、タンパク質、ケトン類、血液)
ディップスティック尿検査は可能である。しかしながら、スクリーニング時のディップスティック尿検査で2+以上のタンパク質を有する患者は、登録のためにベバシズマブ含有群が開いている場合、タンパク質について24時間の尿収集を受けなければならない。
Samples for the following clinical tests will be sent to the testing facility's local laboratory for analysis:
Hematology: WBC counts, RBC counts, hemoglobin, hematocrit, platelet counts, and differential counts (neutrophils, eosinophils, basophils, monocytes, lymphocytes, other cells)
Chemistry panel (serum or plasma): CPK, bicarbonate or carbon dioxide (if considered standard of care for that area), sodium, potassium, magnesium, chloride, glucose, BUN or urea, creatinine, total protein, albumin , phosphorus, calcium, total bilirubin, ALP, ALT, and AST.
• Coagulation: INR and aPTT.
Thyroid function tests: thyroid stimulating hormone, free triiodothyronine (T3) (or total T3 for sites where free T3 is not performed), and free thyroxine (also known as T4)
Ferritin and γ-glutamyltransferase HIV serology unless permitted according to local regulations HAV serology: HAV IgM
• HBV serology: HBsAg, total HBcAb, and (if HBsAg test negative and total HBcAb test positive) HBV DNA.
If a patient has a negative HBsAg test and a positive total HBcAb test at screening, an HBV DNA test must also be performed to determine if the patient has HBV infection.
• HCV serology: HCV antibody and (if HCV antibody test positive) HCV RNA.
If a patient tests positive for HCV antibodies at screening, an active HCV RNA test should also be performed to determine the presence or absence of HCV infection.
・HEV serology: HEV IgM
・C-reactive protein ・LDH
・CA19-9
EBV serology:
- EBV VCA IgM
- EBV VCA IgG or EBNA IgG
- EBV PCR (only if clinically indicated)
• Pregnancy Testing All women of childbearing potential undergo a serum pregnancy test for
Females must be postmenopausal, have not reached a postmenopausal state (>12 consecutive months of amenorrhea with no identified cause other than menopause), and be surgically infertile (removal of the ovaries and/or uterus). ) is considered to be of possible gestation.
・Urinalysis (pH, specific gravity, glucose, protein, ketones, blood)
A dipstick urine test is possible. However, patients with a dipstick urine test at screening of 2+ or higher protein must undergo a 24-hour urine collection for protein if the bevacizumab-containing arm is open for enrollment.
以下の検査室試験のための試料は、分析のために中央検査室又は検査現場の現地検査室に送られる。
・可溶性CD25
Samples for the following laboratory tests are sent to a central laboratory or local laboratory at the test site for analysis.
・Soluble CD25
以下の試料は、分析のために1つ若しくはいくつかの中央検査室又は試験依頼者に送られる。
・自己抗体の分析のための血清試料:抗核抗体、抗二本鎖DNA、循環抗好中球細胞質抗体、及び核周囲抗好中球細胞質抗体
・検証されたアッセイの使用によるPK分析のための血漿又は血清試料
・検証されたアッセイの使用による免疫原性分析のための血漿又は血清試料
・バイオマーカーの探索的試験のための血漿、血清及び末梢血単核細胞(PBMC)試料
・PD-L1発現の決定及びバイオマーカーに関する調査試験のためにベースラインで採取した腫瘍組織試料
原発病変又は転移病変からのベースライン腫瘍組織試料は、好ましくは試験登録時に行われる生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、メディカルモニターの承認が得られた後に腫瘍組織の保管を提出してもよく、ただし、組織が登録前3ヶ月以内に行われた生検から得られ、患者が生検の時点からいかなる抗がん治療も受けたことがないことを条件とする。
パラフィンブロック(好ましい)における代表的なFFPE腫瘍標本、又は染色されていない新たに切断された連続切片を含む少なくとも16枚のスライドを、関連する病理報告とともに提出しなければならない。10~15枚のスライドしか入手できない場合、メディカルモニターの承認が得られた後、患者は依然として試験に適格であり得る。
腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならない。試料は、針ゲージ又は回収方法にかかわらず、細胞状況及び組織構造を保存する最低50個の生存腫瘍細胞を含まなければならない。摘出、コア針生検(単一のパラフィンブロックに埋め込まれた少なくとも3つのコア、18ゲージ針以上 [16ゲージ針が好ましい])、又は切除生検、切開生検、パンチ生検、若しくは鉗子生検によって採取された試料が許容される。細針吸引(組織構造を保存せず、細胞懸濁液及び/又は塗抹を生じない試料として定義される)、ブラッシング、胸水からの細胞ペレット、及び洗浄液試料は許容されない。脱灰された骨転移からの腫瘍組織は許容されない。
残りの腫瘍組織の保管ブロックは、要求に応じて、又は試験データベースの最終閉鎖から18ヶ月後のいずれか早く発生する方で現場に戻される。
・拡大期に実験群に登録した患者:バイオマーカーの探索試験のために処置開始後4週間(±7日)(治験責任医師が臨床上に実施可能と考える場合)に採取した腫瘍組織試料
同じCITの組み合わせで治療された最低15人の患者から処置中の組織試料が既に収集され、評価可能であると判定された場合、試料は収集されない。
摘出、コア針生検(少なくとも3つのコアが好ましい)、又は切除、切開、パンチ若しくは鉗子生検によって収集された試料が好ましい。
・バイオマーカーに関する調査試験のために、許容できない毒性、RECIST v1.1による疾患進行、又は治験責任医師によって臨床的に実施可能であるとみなされた場合、治験責任医師によって決定された臨床的利益の喪失の時点で収集された腫瘍組織試料
生検は、許容できない毒性、疾患進行、又は臨床的利益の喪失の判定後、又は次の抗がん治療の前のいずれか早い方の40日以内に行わなければならない。摘出、コア針生検(少なくとも3つのコアが好ましい)、又は切除、切開、パンチ若しくは鉗子生検によって収集された試料が好ましい。
The following samples are sent to one or several central laboratories or sponsors for analysis.
Serum samples for analysis of autoantibodies: antinuclear antibodies, anti-double-stranded DNA, circulating antineutrophil cytoplasmic antibodies, and perinuclear antineutrophil cytoplasmic antibodies For PK analysis using validated assays Plasma or serum samples for immunogenicity analysis using validated assays Plasma, serum and peripheral blood mononuclear cell (PBMC) samples for biomarker exploratory testing PD- Tumor Tissue Samples Collected at Baseline for Determination of L1 Expression and Research Studies for Biomarkers Baseline tumor tissue samples from primary or metastatic lesions are obtained from all patients, preferably by biopsy performed at study enrollment. Collected. If a biopsy is not considered feasible by the Investigator, tumor tissue storage may be submitted after obtaining medical monitor approval, provided that the tissue was performed within 3 months prior to enrollment. Obtained from a biopsy, provided that the patient has not received any anticancer therapy since the time of biopsy.
A representative FFPE tumor specimen in paraffin block (preferred) or at least 16 slides containing unstained freshly cut serial sections must be submitted along with the relevant pathology report. If only 10-15 slides are available, the patient may still be eligible for the study after obtaining medical monitor approval.
Tumor tissue must be of good quality based on total tumor content and viable tumor content. Samples must contain a minimum of 50 viable tumor cells preserving cellular context and histology, regardless of stylus gauge or collection method. Excision, core needle biopsy (at least 3 cores embedded in a single paraffin block, 18-gauge needle or larger [16-gauge needle preferred]), or excisional, incisional, punch, or forceps biopsy Samples taken by Fine-needle aspirations (defined as samples that do not preserve tissue architecture and yield cell suspensions and/or smears), brushings, cell pellets from pleural effusions, and lavage fluid samples are not permitted. Tumor tissue from demineralized bone metastases is not permitted.
The remaining tumor tissue archive blocks will be returned to the site on demand or 18 months after the final closure of the study database, whichever occurs first.
Patients enrolled in the exploratory arm during the expansion phase: Tumor tissue samples collected 4 weeks (± 7 days) after the start of treatment (if deemed clinically feasible by the investigator) for exploratory biomarker studies Same If an in-treatment tissue sample has already been collected from a minimum of 15 patients treated with the CIT combination and determined to be evaluable, the sample will not be collected.
Samples collected by excision, core needle biopsy (at least three cores are preferred), or excision, incision, punch or forceps biopsy are preferred.
- Unacceptable toxicity, disease progression according to RECIST v1.1, or clinical benefit as determined by the investigator if deemed clinically feasible by the investigator for research studies on biomarkers Tumor tissue sample collected at time of loss of biopsy within 40 days after determination of unacceptable toxicity, disease progression, or loss of clinical benefit, or prior to next anticancer therapy, whichever comes first must go to Samples collected by excision, core needle biopsy (at least three cores are preferred), or excision, incision, punch or forceps biopsy are preferred.
アテゾリズマブの用量及びスケジュール
アテゾリズマブは、2週間ごとに840mg(Q2W)の固定用量で投与される(各28日サイクルの第1及び15日目に840mg)。
Atezolizumab Dose and Schedule Atezolizumab is administered at a fixed dose of 840 mg (Q2W) every 2 weeks (840 mg on
チラゴルマブの用量及びスケジュール
チラゴルマブは、420mg Q2Wの固定用量で投与される(各28日間サイクルの1日目及び15日目に420mg)。420mg Q2W用量後の平均濃度は、3週間毎の600mgの平均濃度(Q3W)と同等であると予想される。患者が単剤のチラゴルマブ又はチラゴルマブ+アテゾリズマブを受けたGO30103試験からの利用可能な薬物動態(PK)、有効性、及び安全性データに基づいて、600mgのIV Q3Wの固定されたチラゴルマブ用量を選択した。MTDに到達せず、2~1200mg Q3Wの用量のチラゴルマブ単独療法又はアテゾリズマブ1200mg Q3Wと組み合わせたチラゴルマブではDLTは観察されなかった。加えて、チラゴルマブに対する抗薬物抗体(ADA)の発生が、チラゴルマブ(2~600mgQ3Wの用量)をアテゾリズマブとの併用で受けている145名の評価可能な患者のうちの3名において認められた。CD4+、CD8+、及びNK細胞上の末梢TIGIT受容体の完全な占有が、30mg Q3W用量のチラゴルマブで開始して観察され、全てのより高い用量で持続したままであった。アテゾリズマブ1200mg Q3Wと組み合わせて投与した場合、30~600mg Q3Wのチラゴルマブ用量で抗腫瘍活性(放射線学的部分奏効)が観察された。
投与量及び投与
Tiragolumab Dose and Schedule Tiragolumab will be administered at a fixed dose of 420 mg Q2W (420 mg on
Dosage and Administration
患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、概説される処置を受ける。 Patients will be screened by the investigator after integrated assessment of radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as pain secondary to disease). Receive treatment as outlined until determined unacceptable toxicity or loss of clinical benefit.
参加者は、表18に概説される指示に従って、各28日間サイクルの第1及び15日目にアテゾリズマブ840mgのIV注入を受ける。
Participants will receive an IV infusion of atezolizumab 840 mg on
参加者は、表19に概説されている指示に従って、各28日間サイクルの第1及び15日目にチラゴルマブ420mgのIV注入を受ける。第1サイクルの1日目に、アテゾリズマブ注入の完了の60分後にチラゴルマブを投与する。その後の注入間の間隔は、以前のアテゾリズマブ注入が前投薬なしで与えられ、注入関連反応(IRR)なしで許容された場合は30分、又は患者が以前のアテゾリズマブ注入でIRRを経験した場合は60分である。
Participants will receive an IV infusion of tiragolumab 420 mg on
参加者は、各28日間サイクルの1、8、及び15日目にnab-パクリタキセル125mg/m2のIV注入を受け、30(±5)分かけてIV注入によって投与され、続いてゲムシタビン1000mg/m2を受け、30(±10)分かけてIV注入によって投与される。第1サイクルの1日目に、チラゴルマブ注入終了60分後にnab-パクリタキセルを投与する。その後の注入間の間隔は、以前のチラゴルマブ注入がIRRを伴わずに忍容された場合は30分、又は患者が以前のチラゴルマブ注入でIRRを経験した場合は60分である。


用量の変更
この試験では、アテゾリズマブ又はチラゴルマブの用量変更はない。薬物関連毒性を管理するために、表20に概説されるように、nab-パクリタキセルの用量を最大で25mg/m2(1用量レベル)、ゲムシタビンの用量を最大で200mg/m 2(1用量レベル)減少させることができる。
Dose Modifications There were no dose modifications of atezolizumab or tiragolumab in this study. To manage drug-related toxicity, doses of nab-paclitaxel up to 25 mg/m 2 (1 dose level) and gemcitabine up to 200 mg/m 2 (1 dose level) were increased as outlined in Table 20. ) can be reduced.
2回の用量減少後にnab-パクリタキセル及び/又はゲムシタビンについてさらなる用量減少が示される場合、その薬物(又は該当する場合は両方の薬物)は中断されるが、患者は治験責任医師の裁量で他の試験処置を継続することができる。用量減少後、治験責任医師の裁量で、その後の投与中に用量を漸増してもよい。

併用療法
併用療法には、試験処置の開始の10日前から処置中止の来院までの治験実施計画書が定めた試験処置に加えて、患者が使用した任意の薬物(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)が含まれた。
Concomitant Therapy Concomitant therapy includes any drug used by the patient (e.g., prescription drug, over-the-counter drug, vaccines, herbal or homeopathic remedies, dietary supplements).
患者は、試験中に以下の治療法を使用することが許される:
●現地の診療/試験所のガイドライン又は米国臨床腫瘍学会の造血CSFに関する(Smith et al.2006)及び米国血液学会/米国臨床腫瘍学会ESAに関するガイドライン(Rizzo et al.2010)による、コロニー刺激因子(CSF)、例えば顆粒球コロニー刺激因子(G-CSF)、及び赤血球生成刺激剤(ESA)。
毎週の化学療法(すなわち、nab-パクリタキセル)を受けている患者における長時間作用性(PEG化)形態のG-CSFの使用を支持する証拠は限られている。したがって、治験責任医師は、G-CSFの従来の製剤を優先することを考慮しなければならない。
●経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●試験処置の開始後に食欲刺激剤として投与された酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与される吸入コルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●前立腺がんに対するゴナドトロピン放出ホルモンアゴニスト又はアンタゴニストを用いたホルモン療法
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。nab-パクリタキセル及びゲムシタビンによる処置は、緩和的放射線療法中は控えなければならない。アテゾリズマブ及びチラゴルマブによる処置は、緩和放射線療法中に継続され得る。
●以下に概説する脳への放射線療法:
頭蓋外腫瘍量が安定しているか又は試験処置に応答しており、その後3つ以下の脳転移を有することが判明した患者は、以下の基準の全てが満たされるならば、脳への放射線療法(定位的放射線手術又は全脳放射線療法のいずれか)を受けることができる。
-患者は、CNS向け治療の完了後に進行又は出血の証拠がない。
-患者は、CNS疾患の治療としてのコルチコステロイドに対する継続的な要求がない。
放射線療法の完了後7日を超えてコルチコステロイド療法を必要とする患者は、試験処置を中止しなければならない。
-抗痙攣療法は、必要に応じて、安定な用量で投与される。
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ及びチラゴルマブ注入のためにのみ投与され得る。
Patients are allowed to use the following therapies during the study:
colony-stimulating factors ( CSF), such as granulocyte colony stimulating factor (G-CSF), and erythropoiesis stimulating agents (ESA).
There is limited evidence to support the use of the long-acting (PEGylated) form of G-CSF in patients receiving weekly chemotherapy (ie nab-paclitaxel). Therefore, investigators should consider prioritizing conventional formulations of G-CSF.
● Oral contraceptives ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable dose warfarin or low molecular weight heparin)
Inactivated influenza vaccination Megestrol acetate administered as an appetite stimulant after initiation of study treatment Mineralcorticoids (eg fludrocortisone)
Inhaled corticosteroids given for chronic obstructive pulmonary disease or asthma Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency Gonadotropin-releasing hormone agonists or antagonists for prostate cancer hormonal therapy using palliative radiation therapy (e.g. treatment of known bone metastases or symptomatic relief of pain) as outlined below:
Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with nab-paclitaxel and gemcitabine should be withheld during palliative radiotherapy. Treatment with atezolizumab and tiragolumab may be continued during palliative radiotherapy.
● Radiation therapy to the brain as outlined below:
Patients with stable extracranial tumor burden or responding to study treatment who are subsequently found to have ≤3 brain metastases will receive radiation therapy to the brain if all of the following criteria are met: (either stereotactic radiosurgery or whole-brain radiotherapy).
- Patient has no evidence of progression or bleeding after completion of CNS-directed therapy.
- Patient has no ongoing need for corticosteroids as treatment for CNS disease.
Patients requiring corticosteroid therapy more than 7 days after completion of radiation therapy must discontinue study treatment.
- Anticonvulsant therapy is administered at stable doses as needed.
Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent atezolizumab and tiragolumab infusions at the investigator's discretion.
一般に、治験責任医師らは、現地の標準診療に従って、臨床上適応のある支持療法を用いて患者のケアを管理しなければならない。注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理されなければならない。 In general, investigators should manage patient care using clinically indicated supportive care according to local standard practice. Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine) or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2- adrenergic must be administered by a sexual agonist).
選択基準
患者は以下の基準を満たす:
●署名時の年齢が18歳以上
●ECOGパフォーマンスステータス0又は1
●組織学的又は細胞学的に確認された転移性PDAC
転移性PDACの確定診断は、臨床データ及び放射線学的データの文脈内で組織病理学的データを評価することによって行われる。
内分泌又は腺房膵癌腫を有する患者は、試験に適格ではない。
●PDACの事前の全身処置なし
●治験責任医師が決定した平均余命≧3ヶ月
●中央検査によるPD-L1及び/又はさらなるバイオマーカーの状態の決定に適した代表的な腫瘍標本の入手可能性
ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、メディカルモニターの承認が得られた後に腫瘍組織の保管を提出してもよく、ただし、組織が登録前3ヶ月以内に行われた生検から得られ、患者が生検の時点からいかなる抗がん治療も受けたことがないことを条件とする。
パラフィンブロック(好ましい)又は未染色の新たに切断した連続切片を含む少なくとも16枚のスライド中のホルマリン固定パラフィン包埋腫瘍標本は、試験登録前に関連する病理報告と共に提出しなければならない。10~15枚のスライドしか入手できない場合、メディカルモニターの承認が得られた後、患者は依然として試験に適格であり得る。
●署名済みインフォームドコンセントフォーム
●治験責任医師の判断による、試験治験実施計画書を遵守する能力
●RECIST v 1.1による測定可能な疾患(少なくとも1つの標的病変)
以前に放射線照射された病変は、放射線照射後にその部位で進行性疾患が明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。
●試験処置の開始の前、14日以内に得られた、以下の検査試験結果によって定義される適切な血液学的機能及び終末器官機能:
-スクリーニング検査試験前の14日以内に顆粒球コロニー刺激因子の支援なしでANC≧1.5×109/L(1500/μL)
-WBC数≧2.5×109/L(2500/μL)
-リンパ球数≧0.5×109/L(500/μL)
-スクリーニング検査室試験前の7日以内に輸血なしで血小板数≧100×109/L(100,000/μL)
-ヘモグロビン≧90g/L(9.0g/dL)
患者は、メディカルモニターとの検討の後に、この基準を満たすように輸血され得る。
-以下を除いて、AST、ALT及びALPが正常値の上限(ULN)の2.5倍以下である:
文書化された肝臓転移を有する患者:AST及びALT≦5×ULN
文書化された肝臓転移又は骨転移を有する患者:ALP≦5×ULN
-以下の例外を除いて、血清ビリルビン≦1.5×ULN:
既知のギルバート病患者:血清ビリルビン値≦3×ULN
-クレアチニンクリアランス≧50mL/分(Cockcroft-Gault式を使用して計算)
-血清アルブミン≧25g/L(2.5g/dL)
-抗凝固療法を受けていない患者について:INR又はaPTT≦1.5×ULN
●治療的抗凝固薬を投与されている患者:安定な抗凝固薬レジメン
●生検にアクセス可能な腫瘍
●妊娠の可能性のある女性の場合:禁欲(異性間の性交を控える)又は避妊手段を使用することの合意、及び卵の提供を控えることの合意
●男性の場合:禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることに同意すること。
Inclusion Criteria Patients meet the following criteria:
●
- Histologically or cytologically confirmed metastatic PDAC
A definitive diagnosis of metastatic PDAC is made by evaluating histopathological data within the context of clinical and radiological data.
Patients with endocrine or acinar pancreatic carcinoma are not eligible for the study.
No prior systemic treatment for PDAC Investigator-determined life expectancy ≥3 months Availability of representative tumor specimens suitable for determination of PD-L1 and/or further biomarker status by central laboratory Base Line tumor tissue samples are preferably collected from all patients by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, tumor tissue storage may be submitted after obtaining medical monitor approval, provided that the tissue was performed within 3 months prior to enrollment. Obtained from a biopsy, provided that the patient has not received any anticancer therapy since the time of biopsy.
Formalin-fixed, paraffin-embedded tumor specimens in paraffin blocks (preferred) or at least 16 slides containing unstained freshly cut serial sections must be submitted with relevant pathology reports prior to study enrollment. If only 10-15 slides are available, the patient may still be eligible for the study after obtaining medical monitor approval.
- Signed informed consent form - Ability to comply with study protocol, as determined by investigator - Measurable disease (at least 1 target lesion) per RECIST v 1.1
Previously irradiated lesions can be considered measurable disease only if progressive disease is clearly documented at the site after irradiation.
- Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to initiation of study treatment:
- ANC ≥ 1.5 x 10 9 /L (1500/μL) without granulocyte colony stimulating factor support within 14 days prior to screening test test
- WBC count ≧2.5×10 9 /L (2500/μL)
- Lymphocyte count ≧0.5×10 9 /L (500/μL)
- Platelet count ≥ 100 x 10 9 /L (100,000/μL) without transfusion within 7 days prior to screening laboratory test
- hemoglobin ≥ 90 g/L (9.0 g/dL)
Patients may be transfused to meet this criteria after review with a medical monitor.
- AST, ALT and ALP ≤2.5 times the upper limit of normal (ULN) except for:
Patients with documented liver metastases: AST and ALT ≤ 5 x ULN
Patients with documented liver or bone metastases: ALP ≤ 5 x ULN
- Serum bilirubin ≤ 1.5 x ULN, with the following exceptions:
Patients with known Gilbert's disease: Serum bilirubin level < 3 x ULN
- Creatinine clearance ≥ 50 mL/min (calculated using the Cockcroft-Gault formula)
- Serum albumin ≥25 g/L (2.5 g/dL)
- For patients not receiving anticoagulant therapy: INR or aPTT ≤ 1.5 x ULN
• Patients receiving therapeutic anticoagulants: stable anticoagulant regimen • Tumors accessible for biopsy • For women of childbearing potential: abstinence (abstinence from heterosexual intercourse) or contraceptive measures and agree to refrain from donating eggs For men: maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and refrain from donating sperm you agree to
安全性
この試験に参加する患者の安全性を確保するために、厳格な選択基準及び除外基準の使用、並びに試験中の患者の綿密な監視を含む対策がとられる。試験処置の投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び薬剤に直ちにアクセスできる監視された状況で行われる。有害事象は記載されているように報告される。
Safety Measures are taken to ensure the safety of patients participating in this study, including the use of strict inclusion and exclusion criteria and close monitoring of patients during the study. Administration of the study treatment will occur in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions. Adverse events will be reported as described.
言語有害事象用語は、Medical Dictionary for Regulatory Activities thesaurus termsにマッピングされ、有害事象重症度はNCI CTCAE v 4.0に従って等級付けされる。 Verbal adverse event terms are mapped to the Medical Dictionary for Regulatory Activities thesaurus terms and adverse event severity is graded according to NCI CTCAE v 4.0.
安全性は、有害事象の要約、検査室での検査結果の変化、バイタルサイン及びECGの変化、及び試験薬への曝露を通して評定される。併用処置への曝露及び安全性フォローアップの長さは、各段階内の処置群によって要約される。 Safety will be assessed through a summary of adverse events, changes in laboratory results, changes in vital signs and ECG, and exposure to study drug. Exposure to combination treatment and length of safety follow-up are summarized by treatment group within each phase.
処置開始後に起こる処置時発生有害事象を要約する。各患者について、各有害事象の最大報告重症度を重症度グレードごとに要約に使用する。全てのn処置下で発現する有害事象、重篤な有害事象、試験処置の中止につながる有害事象、グレード3の有害事象、死亡、及び死因を列挙し、マッピングされた用語、適切な類義語レベル、及びNCI CTCAE重症度グレードによって要約する。関連する検査室、バイタルサイン(脈拍数、呼吸数、血圧、パルスオキシメトリ、及び体温)、及びECGデータは、必要に応じて識別されたグレードと共に時間によって表示される。更に、選択された検査室での検査のシフトテーブルを使用して、ベースライン及びベースライン後の最大重症度グレードを要約する。バイタルサイン及びECGの変化を要約する。
Treatment-emergent adverse events occurring after treatment initiation will be summarized. For each patient, the maximum reported severity of each adverse event will be used in the summary by severity grade. List all n treatment emergent adverse events, serious adverse events, adverse events leading to study treatment discontinuation,
アテゾリズマブは、以下のようなリスクと関連している:IRR及び免疫介在性肝炎、肺臓炎、大腸炎、膵炎、真性糖尿病、甲状腺機能低下症、甲状腺機能亢進症、副腎機能不全、下垂体炎、ギラン・バレー症候群、筋無力症症候群又は重症筋無力症、髄膜脳炎、心筋炎、腎炎及び筋炎。免疫介在性反応は、任意の器官系を伴い得、血球貪食性リンパ組織球増加症及びマクロファージ活性化症候群(アテゾリズマブの潜在的リスクであると考えられる)をもたらし得る。 Atezolizumab is associated with the following risks: IRR and immune-mediated hepatitis, pneumonitis, colitis, pancreatitis, diabetes mellitus, hypothyroidism, hyperthyroidism, adrenal insufficiency, hypophysitis, Guillain-Barre syndrome, myasthenia syndrome or myasthenia gravis, meningoencephalitis, myocarditis, nephritis and myositis. Immune-mediated reactions can involve any organ system and can lead to hemophagocytic lymphohistiocytosis and macrophage activation syndrome (considered potential risks of atezolizumab).
以下は、PDAC患者においてnab-パクリタキセルで観察される最も一般的な有害事象である:好中球減少症、疲労、末梢神経障害、悪心、脱毛症、末梢浮腫、下痢、発熱、嘔吐、食欲不振、発疹、及び脱水。以下の有害事象も観察されている:骨髄抑制(主に好中球減少症、貧血、血小板減少症)、脳神経麻痺、過敏反応、肺臓炎、筋肉痛、関節痛、心毒性(心筋障害、心不全、狭心症、頻脈、心室性不整脈)、類嚢胞黄斑浮腫、スティーブンス・ジョンソン症候群/中毒性表皮壊死症、敗血症、注入部位反応/血管外漏出、肝毒性(薬物誘発性肝損傷)、急性腎不全、溶血性尿毒症症候群、及び薬物誘発性エリテマトーデス。 The following are the most common adverse events observed with nab-paclitaxel in PDAC patients: neutropenia, fatigue, peripheral neuropathy, nausea, alopecia, peripheral edema, diarrhea, fever, vomiting, anorexia. , rash, and dehydration. The following adverse events have also been observed: myelosuppression (mainly neutropenia, anemia, thrombocytopenia), cranial nerve palsy, hypersensitivity reactions, pneumonitis, myalgia, arthralgia, cardiotoxicity (myocardial injury, heart failure). , angina pectoris, tachycardia, ventricular arrhythmias), cystoid macular edema, Stevens-Johnson syndrome/toxic epidermal necrolysis, sepsis, injection site reactions/extravasation, hepatotoxicity (drug-induced liver injury), Acute renal failure, hemolytic uremic syndrome, and drug-induced lupus erythematosus.
ゲムシタビンで観察される最も一般的な有害事象は、悪心/嘔吐、貧血、肝トランスアミネート、好中球減少症、ALP増加、タンパク尿、発熱、血液尿、発疹、血小板減少症、呼吸困難及び末梢浮腫である。 The most common adverse events observed with gemcitabine were nausea/vomiting, anemia, hepatic transaminates, neutropenia, increased ALP, proteinuria, pyrexia, hematuria, rash, thrombocytopenia, dyspnea and Peripheral edema.
IRRは、チラゴルマブについて同定されたリスクである。チラゴルマブの臨床評価は限定的であり、全てのリスクが知られているわけではないが、TIGITのアンタゴニストとして、チラゴルマブはT細胞及びNK細胞の増殖、生存、及び機能を増強すると予想される。したがって、チラゴルマブは、自己免疫性炎症(免疫媒介性有害事象としても記載される)のリスクを高める可能性がある。更に、チラゴルマブのインタクトなFcエフェクター機能のために、抗体依存性細胞傷害(ADCC)を介したリンパ球減少症は理論上のリスクである。 IRR is a risk identified for tiragolumab. Although clinical evaluation of tiragolumab is limited and not all risks are known, as an antagonist of TIGIT, tiragolumab is expected to enhance T cell and NK cell proliferation, survival, and function. Therefore, tiragolumab may increase the risk of autoimmune inflammation (also described as immune-mediated adverse events). Furthermore, due to the intact Fc effector function of tiragolumab, antibody-dependent cellular cytotoxicity (ADCC)-mediated lymphopenia is a theoretical risk.
チラゴルマブは治療用モノクローナル抗体であり、免疫細胞を標的とするので、過敏反応、標的媒介性サイトカイン放出、及び/又は緊急性のADAに関連するIRRが起こり得る。そのような反応の臨床的徴候及び症状には、体温低下、悪寒、喘鳴、掻痒、潮紅、発疹、低血圧、低酸素血症及び発熱が含まれ得る。IRRは、チラゴルマブ単独又はアテゾリズマブとの組み合わせで処置された患者において報告されている。大部分の事象は軽度から中程度で管理可能であった。 Because tiragolumab is a therapeutic monoclonal antibody and targets immune cells, hypersensitivity reactions, target-mediated cytokine release, and/or acute ADA-associated IRR can occur. Clinical signs and symptoms of such reactions may include hypothermia, chills, wheezing, pruritus, flushing, rash, hypotension, hypoxemia and fever. IRR has been reported in patients treated with tiragolumab alone or in combination with atezolizumab. Most events were mild to moderate and manageable.
IRRのリスク及び続発症を最小限に抑えるために、チラゴルマブの初回用量を60分間にわたって投与し、続いて60分間の観察期間を設ける。後続の注入及び観察時間は、先行する注入が十分に許容された場合に短縮され得る。全てのチラゴルマブの注入は、適切な医療環境で投与される。 To minimize the risk of IRR and sequelae, the initial dose of tiragolumab is administered over 60 minutes followed by a 60 minute observation period. Subsequent injections and observation times can be shortened if the preceding injections are well tolerated. All tiragolumab infusions are administered in an appropriate medical setting.
非臨床モデルは、自己免疫におけるTIGITシグナル伝達の中断の役割を示唆している。ノックアウトモデル(TIGIT-/-)では、TIGITシグナル伝達の喪失は、過剰増殖性T細胞応答及び実験的自己免疫性脳炎(EAE)の増悪をもたらした。TIGIT-/-及び野生型B6マウスを最適以下の用量のミエリンオリゴデンドロサイト糖タンパク質ペプチドで免疫して、EAEを誘導した。野生型B 6マウスとは対照的に、TIGIT-/-マウスの大部分は重度のEAEを発症した(Joller et al.2011)。 Non-clinical models suggest a role for disruption of TIGIT signaling in autoimmunity. In a knockout model (TIGIT-/-), loss of TIGIT signaling resulted in exacerbation of hyperproliferative T-cell responses and experimental autoimmune encephalitis (EAE). TIGIT-/- and wild-type B6 mice were immunized with suboptimal doses of myelin oligodendrocyte glycoprotein peptides to induce EAE. In contrast to wild-type B6 mice, the majority of TIGIT-/- mice developed severe EAE (Joller et al. 2011).
抗腫瘍T細胞応答を増強することを意図した治療薬による臨床経験は、自己免疫性炎症状態の発症が一般的なリスクであり、したがって、チラゴルマブの潜在的なリスクと考えられ得ることを実証した。そのような免疫介在性有害事象は、事実上全ての器官系について記載されており、限定されないが、大腸炎、肝炎、肺臓炎、内分泌不全症、眼毒性、膵臓毒性、神経毒性、心筋炎、腎炎、筋炎及び発疹が挙げられる。 Clinical experience with therapeutics intended to enhance anti-tumor T cell responses has demonstrated that the development of autoimmune inflammatory conditions is a common risk and thus could be considered a potential risk for tiragolumab. . Such immune-mediated adverse events have been described for virtually all organ systems, including but not limited to colitis, hepatitis, pneumonitis, endocrine insufficiency, ocular toxicity, pancreatic toxicity, neurotoxicity, myocarditis, Nephritis, myositis and rash are included.
自己免疫疾患の病歴を有する患者は、この試験から除外される。更に、以前の免疫療法に関連する重度の免疫介在性有害事象又は以前の免疫療法の中止後にベースラインまで回復しなかった有害事象の病歴を有する患者は、この試験から除外される。 Patients with a history of autoimmune disease are excluded from this study. In addition, patients with a history of severe immune-mediated adverse events related to prior immunotherapy or adverse events that did not resolve to baseline after discontinuation of prior immunotherapy are excluded from the study.
この試験では、特定の免疫媒介性有害事象は、特別な関心のある有害事象と見なされ、それに応じて捕捉される。 In this study, certain immune-mediated adverse events are considered adverse events of special interest and captured accordingly.
インタクトFcエフェクター機能を有するチラゴルマブのIgG1骨格を考えると、リンパ球数のADCC媒介性減少は潜在的なリスクである。しかしながら、カニクイザルにおける反復投与毒性試験では、全体的なリンパ球数におけるチラゴルマブ関連の減少はなかった。 Given the IgG1 backbone of tiragolumab with intact Fc effector function, ADCC-mediated reduction in lymphocyte counts is a potential risk. However, in repeated-dose toxicity studies in cynomolgus monkeys, there was no tiragolumab-related decrease in global lymphocyte counts.
固形腫瘍における第I相試験(GO 30103試験)において、単独で又はアテゾリズマブと組み合わせて、チラゴルマブで処置れた患者において、臨床的続発症を伴わない一過性リンパ球数の減少が観察されている。チラゴルマブがリンパ球減少症を誘発するこの潜在的なリスクのために、リンパ球数<0.5×109/L(500/μL)の患者は試験から除外される。全血球数を試験全体を通して監視する。 A transient decrease in lymphocyte counts without clinical sequelae has been observed in patients treated with tiragolumab, alone or in combination with atezolizumab, in a phase I trial in solid tumors (GO 30103 study) . Because of this potential risk of tiragolumab inducing lymphopenia, patients with lymphocyte counts <0.5×10 9 /L (500/μL) are excluded from the study. Complete blood counts are monitored throughout the study.
以下の有害事象は、アテゾリズマブ、nab-パクリタキセル、ゲムシタビン、及びチラゴルマブの併用に関連する潜在的な重複毒性である:血球貪食性リンパ組織球増加症、マクロファージ活性化症候群等を含む免疫媒介毒性、胃腸毒性、血液毒性、及び皮膚毒性。 The following adverse events are potential overlapping toxicities associated with the combination of atezolizumab, nab-paclitaxel, gemcitabine, and tiragolumab: hemophagocytic lymphohistiocytosis, immune-mediated toxicities including macrophage activation syndrome, gastrointestinal Toxicity, hematotoxicity, and skin toxicity.
各サイクルの1日目に、患者は、nab-パクリタキセル及びゲムシタビンによる処置を受けるために、1.5×109/L(1500/μL)以上のANC及び100×109/L(100,000/μL)以上の血小板数を有する必要がある。
毒性のための処置中断
On
Treatment interruption for toxicity
アテゾリズマブ及び/又はチラゴルマブは、試験処置に関連すると考えられる毒性を経験している患者において一時的に中断され得る。毒性の処置のためにコルチコステロイドを開始する場合、コルチコステロイドは、薬物を再開することができる前に、1ヶ月以上にわたって10mg/日以下の経口プレドニゾン又は等価物まで漸減しなければならない。アテゾリズマブ又はチラゴルマブが12週間超にわたって保留される場合、患者はその薬物を中止される。しかしながら、患者が処置を再開する前にコルチコステロイドを漸減させることを可能にするために、薬物を12週間超にわたって保留してもよい。患者が臨床的利益を得る可能性が高いとメディカルモニターが認める場合、アテゾリズマブ又はチラゴルマブを12週間超にわたって保留した後に再開することができる。 Atezolizumab and/or tiragolumab may be temporarily discontinued in patients experiencing toxicity considered related to study treatment. When corticosteroids are initiated for the treatment of toxicity, corticosteroids must be tapered to no more than 10 mg/day oral prednisone or equivalent over 1 month before drug can be restarted. If atezolizumab or tiragolumab is held for more than 12 weeks, patients will be discontinued from the drug. However, drug may be withheld for more than 12 weeks to allow patients to taper corticosteroids before resuming treatment. Atezolizumab or tiragolumab may be held for more than 12 weeks and then resumed if the medical monitor believes the patient is likely to experience clinical benefit.
作用機序の利用可能な特性評価に基づいて、チラゴルマブは、アテゾリズマブと類似しているが独立した有害事象を引き起こす可能性がある。チラゴルマブはまた、アテゾリズマブ関連有害事象の頻度又は重症度を悪化させ得るか、又はアテゾリズマブと重複しない毒性を有し得る。これらのシナリオは臨床現場では互いに区別できない可能性があるため、免疫介在性有害事象は一般に両方の薬剤に起因するはずであり、免疫介在性有害事象に応答した投薬中断又は処置中止は、チラゴルマブとアテゾリズマブの両方に適用しなければならない。 Based on the available characterization of mechanism of action, tiragolumab may cause similar but independent adverse events to atezolizumab. Tiragolumab may also exacerbate the frequency or severity of atezolizumab-related adverse events or have toxicities that do not overlap with atezolizumab. Because these scenarios may be indistinguishable from each other in clinical practice, immune-mediated adverse events should generally be attributed to both agents, and drug interruption or treatment discontinuation in response to immune-mediated adverse Must apply to both atezolizumab.
試験処置に関連すると考えられる毒性を経験している患者では、Nab-パクリタキセル及び/又はゲムシタビン処置を一時的に中断することができる。nab-パクリタキセル又はゲムシタビンが毒性のために56日間超にわたって保留された場合、患者は両方の化学療法剤を中止しなければならない。しかしながら、患者が臨床的利益を得る可能性が高いとメディカルモニターが認める場合、nab-パクリタキセル又はゲムシタビンを56日間超にわたって保留した後に再開することができる。 Nab-paclitaxel and/or gemcitabine treatment may be temporarily discontinued in patients experiencing toxicity considered related to study treatment. If nab-paclitaxel or gemcitabine are withheld for more than 56 days due to toxicity, patients must discontinue both chemotherapy agents. However, nab-paclitaxel or gemcitabine can be held for more than 56 days and then resumed if the medical monitor believes that the patient is likely to experience clinical benefit.
アテゾリズマブが中止される場合、チラゴルマブも中止されなければならないが、治験責任医師によって決定されるように、患者が臨床的利益を得る可能性がある場合、nab-パクリタキセル及びゲムシタビンは継続され得る。nab-パクリタキセル、ゲムシタビン又はチラゴルマブを中止する場合、治験責任医師によって決定されるように、患者が臨床的利益を得る可能性がある場合、他の薬物を継続することができる。
統計
If atezolizumab is discontinued, tiragolumab should also be discontinued, but nab-paclitaxel and gemcitabine may be continued if the patient is likely to benefit clinically, as determined by the investigator. When discontinuing nab-paclitaxel, gemcitabine, or tiragolumab, other drugs may be continued if the patient is likely to benefit clinically, as determined by the investigator.
statistics
最終試験分析は、試験の中止を通して収集された患者データに基づく。特に明記しない限り、有効性分析は、割り当てられた治療レジメンに対して各薬物の少なくとも1回の用量を受けた全ての患者として定義される有効性評価可能な集団に基づき、安全性分析は、任意の量の試験処置を受けた全ての患者として定義される安全性評価可能な集団に基づく。 Final study analysis is based on patient data collected through study discontinuation. Unless otherwise stated, efficacy analyzes were based on the efficacy evaluable population defined as all patients who received at least one dose of each drug on their assigned treatment regimen; Based on a safety evaluable population defined as all patients who received any amount of study treatment.
データは、試料サイズによって保証されるように記載され、要約される。連続変数は、平均、標準偏差、中央値、及び範囲を使用して要約される。カテゴリ変数は、カウント及びパーセンテージの使用によって要約される。試料サイズが小さい場合、表の代わりにリストを使用する。 Data are described and summarized as warranted by sample size. Continuous variables are summarized using mean, standard deviation, median and range. Categorical variables are summarized by the use of counts and percentages. If the sample size is small, use lists instead of tables.
この試験は、仮説検定のための明示的なパワー及びタイプI誤差を考慮するように設計されていない。代わりに、この試験は、転移性PDACを有する患者に投与した場合の免疫療法に基づく処置の組み合わせに関する予備的な有効性、安全性、及びPKデータを得るように設計されている。 This test was not designed to account for explicit power and Type I errors for hypothesis testing. Instead, this study is designed to obtain preliminary efficacy, safety, and PK data for immunotherapy-based treatment combinations when administered to patients with metastatic PDAC.
表21は、実験群と対照群との間のORRの推定差を、漸近正規性を仮定して、予備期のそれぞれ15人の患者の試料サイズでの90%信頼区間と共に示す。

表22は、実験群と対照群との間のORRの推定差を90%信頼区間と共に示し、漸近正規性を仮定して、予備期と拡大期のそれぞれの40人の患者の試料サイズを組み合わせている。

目的及び評価項目
この試験の目的及び対応する評価項目の概要を表23に示す。


1つの時点での全奏効が、RECIST v 1.1を使用して治験責任医師によって評定される。iRECISTによる全奏効はeCRFでは捕捉されないが、eCRFに記録された治験責任医師が評定した個々の病変データに基づいてプログラムで計算される。 Overall response at one time point will be assessed by the investigator using RECIST v 1.1. Overall response by iRECIST is not captured in the eCRF, but is calculated programmatically based on individual investigator-assessed lesion data recorded in the eCRF.
有効性分析
主要有効性評価項目は客観的奏効である。完全奏効又は部分奏効を有する患者の割合であるORRを、90%信頼区間(Clopper-Pearson法)と共に各群について計算する。実験群と対照群との間のORRの差を、90%信頼区間と共に計算する。信頼区間は、試料サイズに応じて、漸近滴正規性法によって推定される。
Efficacy analysis The primary efficacy endpoint is objective response. ORR, the proportion of patients with a complete or partial response, is calculated for each group with 90% confidence intervals (Clopper-Pearson method). Differences in ORR between experimental and control groups are calculated with 90% confidence intervals. Confidence intervals are estimated by the asymptotic droplet normality method, depending on the sample size.
副次的有効性評価項目は、PFS、OS、特定の時点でのOS(例えば、6ヶ月)、奏効期間(DOR)であり、疾患対照PFS、DOR及び疾患対照は、RECIST v 1.1に従って治験責任医師によって決定される。DORを、完全奏効又は部分奏効を有する有効性評価可能な患者について導出する。試験段階で疾患の進行又は死亡が文書化されていない患者については、PFS及びDORを最後の腫瘍評定の日に打ち切る。OS分析時にまだ生存している患者は、生存していることが知られていた最後の日に打ち切る。 Secondary efficacy endpoints are PFS, OS, OS at a specified time point (e.g., 6 months), duration of response (DOR); Determined by the Investigator. DOR is derived for efficacy evaluable patients with complete or partial response. For patients with no documented disease progression or death during the study phase, PFS and DOR will be censored on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day known to be alive.
Kaplan-Meier法を使用してPFS、OS、及びDORの中央値を推定し、90%信頼区間をBrookmeyer及びCrowley法の使用によって構築する。特定の時点でのOS率は、Kaplan-Meier法を用いて推定され、90%信頼区間は、分散についてのGreenwoodの推定値に基づいて計算される。疾患対照率、12週間以上にわたって安定した疾患、部分奏効、又は完全奏効を有する患者の割合が各処置群について計算され、90%信頼区間は、Clopper-Pearsonの正確な方法の使用によって推定される。 The Kaplan-Meier method is used to estimate median PFS, OS, and DOR, and 90% confidence intervals are constructed by using the Brookmeyer and Crowley method. The OS rates at specific time points are estimated using the Kaplan-Meier method and 90% confidence intervals are calculated based on Greenwood's estimate of the variance. Disease-control rate, proportion of patients with stable disease, partial response, or complete response over 12 weeks is calculated for each treatment group, and 90% confidence intervals are estimated by use of the Clopper-Pearson exact method. .
探索的有効性評価項目は、iRECISTに従って治験責任医師が決定した客観的奏効、PFS、DOR及び疾患対照であり、両段階中のその後の時点でのCA19-9のベースラインからの変化である。DORを、完全奏効又は部分奏効を有する有効性評価可能な患者について導出する。経時的なベースラインからのCA19-9の変化を要約する。更に、CA19-9のベースラインから50%以上の最大減少又は他の閾値を有する患者の割合を各処置群について計算することができ、90%信頼区間は、Clopper-Pearsonの正確な方法の使用によって推定される。 Exploratory efficacy endpoints were investigator-determined objective response, PFS, DOR, and disease control according to iRECIST, the change from baseline in CA19-9 at subsequent time points during both phases. DOR is derived for efficacy evaluable patients with complete or partial response. The change in CA19-9 from baseline over time is summarized. In addition, the proportion of patients with a maximal reduction of ≥50% from baseline in CA19-9 or other thresholds can be calculated for each treatment group, with 90% confidence intervals using the Clopper-Pearson exact method. estimated by
薬物動態分析
アテゾリズマブ(少なくとも1用量のアテゾリズマブを受けた患者)及びアテゾリズマブと組み合わせて投与された指定の薬物(少なくとも1用量の薬物を受けた患者)の潜在的なPK分析のために、まばらな試料を収集することができる。様々な試験薬物の血清又は血漿濃度は、個々の値として報告され、処置群によって、並びに適切な場合及びデータが許す場合はサイクル及び日によって要約(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)され得る。様々な試験薬物の個々の及び中央の血清又は血漿濃度は、処置群及びサイクル及び日によってプロットされ得る。配合剤のPKデータを、内部試験及び公表された以前の試験からの利用可能な履歴データと比較することができる。アテゾリズマブ濃度データは、クリアランス、分布容積及び曲線下面積等のPKパラメーターを導出するために、確立された集団PKモデルを使用して他の試験からのデータと共にプールされ得る。
Pharmacokinetic Analysis Sparse samples for potential PK analysis of atezolizumab (patients who received atezolizumab at least 1 dose) and the indicated drug administered in combination with atezolizumab (patients who received at least 1 dose of drug) can be collected. Serum or plasma concentrations of various study drugs were reported as individual values and summarized (mean, standard deviation, coefficient of variation, median, range) by treatment group and, where appropriate and data permitted, by cycle and day. , geometric mean, and geometric mean coefficient of variation). Individual and median serum or plasma concentrations of various study drugs can be plotted by treatment group and cycle and day. PK data for formulations can be compared to available historical data from internal and previous published studies. Atezolizumab concentration data can be pooled with data from other studies using established population PK models to derive PK parameters such as clearance, volume of distribution and area under the curve.
免疫原性分析
免疫原性は、必要に応じてアテゾリズマブ及び他の試験処置について評定され得る(詳細については群の特定の添付物を参照)。免疫原性分析には、少なくとも1つの抗薬物抗体(ADA)評定を受けた全ての患者が含まれる。患者は、受けた処置に従って、又は試験中止前に処置を受けていない場合は割り当てられた処置に従ってグループ分けされる。
Immunogenicity Analysis Immunogenicity may be assessed for atezolizumab and other test treatments as appropriate (see group specific appendix for details). Immunogenicity analysis included all patients who had at least one anti-drug antibody (ADA) assessment. Patients are grouped according to the treatment received or assigned treatment if they had not received treatment prior to study discontinuation.
アテゾリズマブについては、ベースライン(ベースライン有病率)及びベースライン後(ベースライン発生後)のADA陽性患者及びADA陰性患者の数及び割合を処置グループ別に要約する。ベースライン後の発生率を決定するとき、患者は、ADA陰性であるか、又はベースラインでデータが欠落しているが、試験薬物曝露後にADA応答を発症する場合(処置誘発性ADA応答)、又は患者がベースラインでADA陽性であり、1つ以上のベースライン後の試料の力価がベースライン試料の力価よりも少なくとも0.60力価単位大きい場合(処置増強ADA応答)、ADA陽性であるとみなされる。患者がADA陰性であるか若しくはベースラインでデータが欠落しており、全てのベースライン後の試料が陰性である場合、又は患者がベースラインでADA陽性であるが、ベースライン試料の力価よりも少なくとも0.60力価単位大きい力価を有するベースライン後の試料を有さない(処置は影響を受けない)場合、患者はADA陰性であるとみなされる。 For atezolizumab, baseline (baseline prevalence) and post-baseline (post-baseline incidence) number and proportion of ADA-positive and ADA-negative patients will be summarized by treatment group. When determining post-baseline incidence, if a patient is ADA-negative or has missing data at baseline but develops an ADA response after study drug exposure (treatment-induced ADA response), or ADA positive if the patient is ADA positive at baseline and the titer of one or more post-baseline samples is at least 0.60 titer units greater than the titer of the baseline sample (treatment-enhanced ADA response) is considered to be If the patient is ADA-negative or has missing data at baseline and all post-baseline samples are negative, or if the patient is ADA-positive at baseline but the titer of the baseline sample is higher than Patients are considered ADA-negative if they have no post-baseline sample with a titer at least 0.60 titer units greater (treatment is unaffected).
ADAが検査される他の試験処置については、ADA陽性は、これらの薬物の以前の試験のために確立された標準的な方法に従って決定される。ADAの状態と安全性、有効性、PK、及びバイオマーカー評価項目との間の関係は、記述統計学によって分析及び報告され得る。 For other test treatments that test for ADA, ADA positivity is determined according to standard methods established for previous testing of these drugs. Relationships between ADA status and safety, efficacy, PK, and biomarker endpoints can be analyzed and reported by descriptive statistics.
実施例3.トリプルネガティブ乳がんを有する患者におけるアテゾリズマブ及び化学療法と組み合わせたチラゴルマブの安全性、有効性、及び薬物動態の第Ib相非盲検多施設試験
本実施例は、転移性トリプルネガティブ乳がん(TNBC)患者におけるアテゾリズマブ及び化学療法と組み合わせたチラゴルマブの安全性、有効性及び薬物動態を評価するように設計された第Ib相非盲検多施設試験を記載する。この試験は、以下のコホートからなる:
・コホートAは、転移性乳がんの事前全身治療を受けたことがない切除不能、局所進行性、又は転移性のプログラム死リガンド1(PD-L1)陽性TNBC(一次転移性TNBC)患者を登録する。患者は、アテゾリズマブ及びnab-パクリタキセルと組み合わせてチラゴルマブを受ける。
Example 3. A phase Ib, open-label, multicenter study of the safety, efficacy, and pharmacokinetics of atezolizumab and tiragolumab in combination with chemotherapy in patients with triple-negative breast cancer. A phase Ib, open-label, multicenter study designed to evaluate the safety, efficacy and pharmacokinetics of tiragolumab in combination with atezolizumab and chemotherapy is described. This trial will consist of the following cohorts:
Cohort A will enroll patients with unresectable, locally advanced, or metastatic programmed death ligand 1 (PD-L1)-positive TNBC (primary metastatic TNBC) who have not received prior systemic therapy for metastatic breast cancer . Patients receive tiragolumab in combination with atezolizumab and nab-paclitaxel.
A.試験計画
この第Ib相多施設非盲検多施設世界的試験は、転移性乳がんの事前全身治療を受けたことがない切除不能な局所進行性又は転移性PD-L1陽性TNBC患者(コホートA、転移性TNBCと呼ばれる)におけるアテゾリズマブ及びnab-パクリタキセルと組み合わせたチラゴルマブの安全性及び忍容性、予備的有効性、並びに薬物動態を調査するように設計されている。PD-L1陽性を、SP142 PD-L1 IHCアッセイを使用して評定する。図2は、コホートAの試験計画を示す。
A. STUDY DESIGN This Phase Ib, multicenter, open-label, multicenter global study will evaluate patients with unresectable, locally advanced or metastatic PD-L1-positive TNBC who have received no prior systemic treatment for metastatic breast cancer (Cohort A, It is designed to investigate the safety and tolerability, preliminary efficacy, and pharmacokinetics of tiragolumab in combination with atezolizumab and nab-paclitaxel in metastatic TNBC). PD-L1 positivity is assessed using the SP142 PD-L1 IHC assay. FIG. 2 shows the study design for Cohort A.
適格患者(すなわち、PD-L1陽性患者)を、チラゴルマブ(840mg)及びアテゾリズマブ(1680mg)を28日間サイクルごとの1日目にIV注入によって受けることに加えて、nab-パクリタキセル(100mg/m2)を28日間サイクルごとの1日目、8日目、及び15日目にIV注入によって患者に投与されることを登録する。
Eligible patients (ie, PD-L1 positive patients) received tiragolumab (840 mg) and atezolizumab (1680 mg) by IV infusion on
疾患の進行又は許容できない毒性がない場合、nab-パクリタキセルは、最大ではなく、少なくとも6サイクルの標的に対して投与される。 In the absence of disease progression or unacceptable toxicity, nab-paclitaxel is administered to target for at least 6 cycles, but not maximally.
腫瘍微小環境における薬物の組合せの作用機序及び可能性のある耐性機序を評定するために、腫瘍組織は、任意に、サイクル2の1日目に投与前に収集され得る。
Tumor tissue may optionally be collected on
腫瘍微小環境における薬物併用に対する耐性の機序を検査するために、全ての患者は、RECIST v1.1に従って治験責任医師によって評定されるように(新しい抗がん処置の開始前に)、疾患進行の最初の証拠で必須の腫瘍生検収集(臨床上に実施可能な場合)を受ける。 To examine mechanisms of resistance to drug combinations in the tumor microenvironment, all patients will undergo disease progression as assessed by the investigator according to RECIST v1.1 (prior to initiation of new anticancer treatment). undergo mandatory tumor biopsy collection (if clinically feasible) at first evidence of
患者は、処置の遅れにかかわらず、第1サイクルの1日目の後、最初の48週間にわたって、ベースライン時及び8週間(±7日)ごとに腫瘍評定を受ける。48週目の腫瘍評定の完了後、腫瘍評定は、RECIST v1.1に従って治験責任医師が決定した疾患進行までの処置の遅れ、同意の撤回、死亡、又は試験終了(いずれか早く発生する方)にかかわらず、12週間ごと(±7日)に必要とされる。
Patients undergo tumor assessments at baseline and every 8 weeks (±7 days) after
試験処置は、RECIST v 1.1に従って治験責任医師によって決定されるように、疾患進行時に中止される。進行の明確な所見(例えば、非常に小さい又は不確実な新しい病変又はリンパ節;既存の病変における嚢胞性変化又は壊死)については、治験責任医師が評定したRECIST v1.1に従って、次の予定された評定まで処置を継続してもよい。次の予定された評定で進行が確認された場合、進行の日付は、進行が疑われたより早い日付であるべきである。 Study treatment will be discontinued upon disease progression as determined by the investigator according to RECIST v 1.1. For definite evidence of progression (e.g., very small or equivocal new lesions or lymph nodes; cystic changes or necrosis in pre-existing lesions), follow the investigator-assessed RECIST v1.1 for the next scheduled Treatment may be continued until evaluation is completed. If progression is confirmed at the next scheduled assessment, the date of progression should be the earlier date when progression was suspected.
B.投薬及び投与
処置レジメンを図2に要約する。
B. Dosing and Administration The treatment regimen is summarized in FIG.
アテゾリズマブ、チラゴルマブ及び化学療法の予定された注入の日に、化学療法は、アテゾリズマブ及びチラゴルマブの注入後に投与される。 On the day of the scheduled infusion of atezolizumab, tiragolumab and chemotherapy, chemotherapy is administered after infusion of atezolizumab and tiragolumab.
アテゾリズマブ注入(1680mg)後、患者は840mgのチラゴルマブを受ける。 After atezolizumab infusion (1680 mg), the patient receives 840 mg of tiragolumab.
アテゾリズマブ、チラゴルマブ、及び化学療法の投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び医薬に直ちにアクセスできる監視された設定で行われる。 Administration of atezolizumab, tiragolumab, and chemotherapy will occur in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
製剤、保存及び投与に関する詳細な説明については、治験薬管理手順書を参照されたい。
チラゴルマブ及びアテゾリズマブ
Refer to the Investigational Product Control Procedures for detailed instructions regarding formulation, storage, and administration.
Tiragolumab and atezolizumab
コホートAの患者は、各28日間サイクルの1日目にIV注入Q4Wによって投与される1680mgの固定用量のアテゾリズマブを受け、続いて各28日間サイクルの1日目にIV注入Q4Wによって投与される840mgの固定用量のチラゴルマブを受ける。チラゴルマブ及びアテゾリズマブの用量は固定されており、体重に依存しない。チラゴルマブ及びアテゾリズマブの注入(観察期間を含む)は、表24に概説される指示に従って投与される。


Nab-パクリタキセル
Nab-パクリタキセルは、現地の処方情報に従って投与される。この試験におけるnab-パクリタキセルの開始用量レベルは、100mg/m2であり、各28日間サイクルの1、8、及び15日目に30分間かけて患者に静脈内投与される(3週間on/1週間offのスケジュール)。nab-パクリタキセルを、アテゾリズマブ及びチラゴルマブの後に投与しなければならない。Nab-パクリタキセルは、各サイクルの8日目及び15日目に単独で投与される。nab-パクリタキセルの用量は、7日ごとよりも頻繁に投与すべきではない。
Nab-paclitaxel Nab-paclitaxel will be administered according to local prescribing information. The starting dose level of nab-paclitaxel in this study was 100 mg/m 2 administered intravenously over 30 minutes to patients on
現場は、肥満である患者のnab-パクリタキセル用量を決定するため、及び患者の体重変化の場合の用量調整のための施設の標準治療に従わなければならない。注入部位を、薬物投与中に起こり得る浸潤について厳密に監視しなければならない。 Sites must follow the institution's standard of care for determining nab-paclitaxel doses for patients who are obese and for dose adjustments in the event of patient weight change. The injection site must be closely monitored for possible infiltration during drug administration.
疾患の進行又は許容できない毒性がない場合、nab-パクリタキセルは、最大ではなく、少なくとも6サイクルの標的に対して投与される。 In the absence of disease progression or unacceptable toxicity, nab-paclitaxel is administered to target for at least 6 cycles, but not maximally.
nab-パクリタキセルの調製及び投与に関するさらなる詳細については、局所処方情報を参照されたい。 See topical prescribing information for additional details regarding the preparation and administration of nab-paclitaxel.
用量の変更 Dose change
この試験では、アテゾリズマブ又はチラゴルマブの用量変更はない。nab-パクリタキセル(すなわち、用量変更及び処置中断規則)の管理については、表25を参照されたい。

C.併用療法
併用療法は、試験薬の開始の7日前から処置中止の来院までの治験実施計画書に定められた処置に加えて、患者によって使用される任意の医薬(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)からなる。
C. Concomitant Therapy Concomitant therapy is any medication used by the patient (e.g., prescription, over-the-counter, vaccines, herbal or homeopathic remedies, dietary supplements).
許可された治療
患者は、試験中に以下の治療法を使用することが許される:
●失敗率が年間1%未満の経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与されるコルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●骨格事象の予防のためのビスホスホネート
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。チラゴルマブ及びアテゾリズマブによる処置は、緩和放射線療法中に継続され得る。nab-パクリタキセルによる処置を、施設の標準治療に従って中断しなければならない。
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ及びチラゴルマブ注入のためにのみ投与され得る。
Allowed Treatments Patients will be allowed to use the following treatments during the study:
● Oral contraceptives with an annual failure rate of less than 1% ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable-dose warfarin or low molecular weight heparin)
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
o Corticosteroids given for chronic obstructive pulmonary disease or asthma o Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency o Bisphosphonates for the prevention of skeletal events o For the following: Palliative radiotherapy outlined (e.g. treatment of known bone metastases or symptomatic relief of pain):
Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with tiragolumab and atezolizumab may be continued during palliative radiotherapy. Treatment with nab-paclitaxel must be discontinued according to institutional standard of care.
Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent atezolizumab and tiragolumab infusions at the investigator's discretion.
注意を要する治療
全身性コルチコステロイド及びTNF-α阻害剤は、アテゾリズマブによる処置の潜在的に有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物を検討しなければならない・ 代替が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。
Treatments requiring caution Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines must be considered If alternatives are not feasible, corticosteroids and TNF-α inhibitors Systemic administration of agents can be at the discretion of the investigator.
アテゾリズマブ治療に関連する場合、特定の有害事象の処置のために、治験責任医師の裁量で、全身コルチコステロイドが推奨される。 Systemic corticosteroids are recommended at the investigator's discretion for treatment of specific adverse events when associated with atezolizumab therapy.
禁止される治療法
以下の併用療法の使用は、以下に記載されるように禁止される:
●がん(限定されないが、化学療法、ホルモン療法、免疫療法、放射線療法、及びハーブ療法を含む)の処置を目的とした併用療法であって、保健当局承認済みであるか実験的であるかにかかわらず、試験処置を開始する前の様々な期間、薬剤に応じて、及び試験処置中、疾患の進行が文書化され、患者が緩和的放射線療法を除く試験処置を中止するまでの併用療法
●治験治療の開始前28日以内及び試験処置中の試験処置
●試験処置開始前4週間以内、アテゾリズマブ処置中及び試験処置の最終用量後5ヶ月間の生弱毒化ワクチン(例えば、FLUMIST(登録商標))
●アテゾリズマブ及びチラゴルマブと組み合わせて投与した場合、自己免疫症状のリスクを潜在的に増加させる可能性があるため、試験処置の開始前及び試験処置中の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫賦活剤(限定されないが、インターフェロン及びIL-2を含む)
試験処置中の全身免疫抑制薬(限定されないが、アザチオプリン、メトトレキサート、及びサリドマイドを含む)(これらの薬剤がアテゾリズマブ及びチラゴルマブの有効性及び安全性を潜在的に変化させる可能性があるため)
●化学療法誘発性好中球減少症の減少のために試験されている新しい分子であるプリナブリンは、G-CSF/GMCSFの代替として許容されていない。
Prohibited Therapies The use of the following concomitant therapies is prohibited as described below:
Any health authority-approved or experimental combination therapy for the treatment of cancer (including, but not limited to, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy). Concomitant therapy for various periods prior to initiation of study treatment, depending on drug, and during study treatment until disease progression is documented and patient discontinues study treatment, excluding palliative radiation therapy, regardless of • Study treatment within 28 days prior to initiation of study treatment and during study treatment • Live attenuated vaccine (e.g., FLUMIST®) within 4 weeks prior to initiation of study treatment, during atezolizumab treatment and 5 months after the last dose of study treatment ))
Due to the potential increased risk of autoimmune symptoms when administered in combination with atezolizumab and tiragolumab, no drug elimination half-lives (either within 4 weeks or 5 during study treatment) or longer), systemic immunostimulants (including but not limited to interferon and IL-2)
Systemic immunosuppressants (including but not limited to azathioprine, methotrexate, and thalidomide) during study treatment (as these agents may potentially alter the efficacy and safety of atezolizumab and tiragolumab)
• Plinabulin, a new molecule being tested for the reduction of chemotherapy-induced neutropenia, has not been accepted as an alternative to G-CSF/GMCSF.
D.選択基準
患者は、試験参加のための以下の一般的な基準を満たさなければならない:
●署名済みインフォームドコンセントフォーム
●インフォームドコンセント用紙に署名した時点で≧18歳の女性及び男性
●試験治験実施計画書を遵守する能力
●ECOGパフォーマンスステータス0又は1
●試験処置(サイクル1の1日目)開始前14日以内に得られた以下の検査室結果として定義される、十分な血液学的機能及び終末器官機能
-サイクル1の1日目の前2週間以内にG-CSF支援なしでANC≧1.5X109/L(1500/μL)
-リンパ球数≧0.5X109/L(≧500/μL)
-サイクル1の1日目の前2週間以内に輸血なしで血小板数≧100X109/L(≧100,000/μL)
-ヘモグロビン≧90g/L(≧9g/dL)。
患者は、この基準を満たすために輸血又は赤血球造血処置を受けることができる
-AST、ALT、ALP≦2.5X正常値上限(ULN)
-血清ビリルビン≦1.5XULN、但し以下の例外がある:
血清ビリルビン値≦3XULNを有する既知のギルバート病患者を登録することができる。
-INR及びaPTT ≦1.5XULN
これは、治療的抗凝固療法を受けていない患者にのみ適用され、治療的抗凝固療法を受けている患者は、安定した用量であるべきである。
-クレアチニンクリアランス≧30mL/分(Cockcroft-Gault式を用いて計算)
-血清アルブミン≧25g/L(≧2.5g/dL)
●スクリーニング時の陰性HIV検査
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時のB型肝炎表面抗体(HBsAb)検査陽性、又は以下のいずれかを伴うスクリーニング時にHBsAb陰性:
-総B型肝炎コア抗体(HBcAb)陰性
-陽性の全HBcAb検査とそれに続く定量的B型肝炎ウイルス(HBV)DNA
<500 IU/mL
HBV DNA検査は、HBsAg検査陰性、HBsAb検査陰性、及び総HBcAb検査陽性の患者に対してのみ実施される。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。
HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:以下に定義するように、禁欲(異性間の性交を控える)又は避妊方法を使用することの同意、及び卵の提供を控えることの同意:
女性は、処置期間中及びアテゾリズマブの最終投与後少なくとも5ヶ月間、チラゴルマブの最終投与後90日間、nab-パクリタキセルの最終投与後1ヶ月間、カルボプラチン若しくはドキソルビシンの最終投与後6ヶ月間、又はシクロホスファミドの最終投与後12ヶ月間のいずれか遅い方で、禁欲を維持するか、又は年間<1%の失敗率をもたらす避妊方法を使用しなければならない。女性は、この同じ期間中に卵を提供することを控えなければならない。
女性は、初経後であり、閉経後状態に到達しておらず(閉経以外の原因が同定されていない、連続≧12ヶ月の無月経)、かつ、外科的不妊(卵巣及び/又は子宮の切除)を受けたことがない場合に、懐胎の可能性があるとみなされる。
年間失敗率<1%の避妊方法の例としては、一貫して正しく使用される場合、排卵の阻害に関連する併用(エストロゲン及びプロゲストゲン含有)ホルモン避妊、排卵の阻害に関連するプロゲストゲンのみのホルモン避妊、両側卵管閉塞、男性不妊;子宮内避妊器具;子宮内ホルモン放出システム;及び性的禁欲が挙げられる。
性的禁欲の信頼性は、臨床試験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。
試験処置の中止後に妊娠することを望む女性は、化学療法による処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に卵母細胞の保存についての助言を求めるべきである。
●男性の場合:以下に定義するように、禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることに同意すること:
妊娠可能な女性パートナー又は妊娠中の女性パートナーの場合、処置期間中及びチラゴルマブの最終投与後90日間、又はnab-パクリタキセル、カルボプラチン、ドキソルビシン、又はシクロホスファミドの最終投与後6ヶ月間のいずれか遅い方で、男性は禁欲を維持するか、又はコンドームと併せて、年間<1%の失敗率をもたらす追加の避妊方法を使用しなければならない。男性は、同期間中は精子提供をやめなければならない。
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。
試験処置の開始後に子供を持ちたい男性は、化学療法による処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に精子保存についての助言を求めるべきである。
●閉経後(≧12ヶ月の非治療誘発性無月経)でないか、又は避妊手術を受けたことがある女性では、試験処置の開始前14日以内に陰性血清妊娠検査結果が必要である。
●予定された来院、処置計画、検査室の検査、及び他の試験手順を遵守する意思及び能力
D. Inclusion Criteria Patients must meet the following general criteria for study entry:
● Signed informed consent form ● Females and males ≥18 years of age at the time of signing the informed consent form ● Ability to comply with the study protocol ●
Adequate hematologic and end-organ function, defined as the following laboratory results obtained within 14 days prior to the start of study treatment (
- Lymphocyte count ≥0.5 X 109/L (≥500/μL)
- Platelet count ≥100 X 109/L (≥100,000/μL) without transfusion within 2 weeks prior to
- Hemoglobin ≧90 g/L (≧9 g/dL).
Patients can receive blood transfusions or erythropoietic procedures to meet this criterion - AST, ALT, ALP ≤ 2.5X upper limit of normal (ULN)
- serum bilirubin ≤ 1.5 XULN, with the following exceptions:
Known Gilbert's disease patients with serum bilirubin levels < 3XULN can be enrolled.
- INR and aPTT ≤ 1.5XULN
This applies only to patients not receiving therapeutic anticoagulant therapy, and patients receiving therapeutic anticoagulant therapy should be on stable doses.
- Creatinine clearance ≥ 30 mL/min (calculated using the Cockcroft-Gault formula)
- serum albumin ≥25 g/L (≥2.5 g/dL)
A negative HIV test at screening A negative hepatitis B surface antigen (HBsAg) test at screening A positive hepatitis B surface antibody (HBsAb) test at screening or negative HBsAb at screening with any of the following:
- total hepatitis B core antibody (HBcAb) negative - positive total HBcAb test followed by quantitative hepatitis B virus (HBV) DNA
<500 IU/mL
HBV DNA testing is performed only for patients with negative HBsAg, negative HBsAb, and positive total HBcAb tests.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening.
HCV RNA testing is performed only for patients who test positive for HCV antibodies.
For women of childbearing potential: Consent to abstinence (abstinence from heterosexual intercourse) or use of contraceptive methods, and consent to abstain from donating eggs, as defined below:
Women should be treated during treatment and for at least 5 months after the last dose of atezolizumab, 90 days after the last dose of tiragolumab, 1 month after the last dose of nab-paclitaxel, 6 months after the last dose of carboplatin or doxorubicin, or For 12 months after the last dose of Famide, whichever is later, must maintain abstinence or use a contraceptive method that results in a failure rate of <1% per year. Females should refrain from donating eggs during this same period.
Females are post-menopausal, have not reached a post-menopausal state (>12 consecutive months of amenorrhea, no other cause identified), and are surgically infertile (removal of ovaries and/or uterus). ) is considered to be of possible gestation.
Examples of methods of contraception with an annual failure rate of <1% include combined (estrogen- and progestogen-containing) hormonal contraception associated with inhibition of ovulation, progestogens associated with inhibition of ovulation when used consistently and correctly. hormonal contraception alone, bilateral fallopian tube obstruction, male infertility; intrauterine devices; intrauterine hormone releasing systems; and sexual abstinence.
The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle.
Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
Women who wish to become pregnant after discontinuing study treatment should seek advice on oocyte storage prior to initiation of study treatment due to possible irreversible infertility resulting from chemotherapy treatment. .
For men: agreeing to maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and to abstain from donating sperm, as defined below:
For female partners of childbearing potential or pregnant, either during the treatment period and for 90 days after the last dose of tiragolumab or 6 months after the last dose of nab-paclitaxel, carboplatin, doxorubicin, or cyclophosphamide Later, men must maintain abstinence or use additional methods of contraception in conjunction with condoms that result in failure rates of <1% per year. Men must stop donating sperm during the same period.
The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle.
Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
Men who wish to have children after initiation of study treatment should seek advice on sperm storage prior to initiation of study treatment due to the potential for irreversible infertility resulting from treatment with chemotherapy.
• Females who are not postmenopausal (≥12 months of non-treatment-induced amenorrhea) or who have undergone surgical sterilization must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
Willingness and ability to comply with scheduled visits, treatment plans, laboratory tests, and other testing procedures
コホートAの患者は、試験参加のための以下のがん特異的基準を満たさなければならない:
●平均余命≧12週間
●転移性又は局所進行性の切除不能な組織学的に文書化されたTNBC(局所検査によって決定されるHER2、ER及びプロゲステロン受容体(PgR)発現の非存在)
HER2陰性は、現地の検査室の評定によって以下の(Wolff et al.2018)のいずれかとして定義される:
in situハイブリダイゼーション(ISH)非増幅(HER2対CEP 17の比<2.0又は単一プローブ平均HER2遺伝子コピー数<4シグナル/細胞)、又はIHC 0若しくはIHC 1+。
ER及びPgR陰性は、IHC分析によって決定されるように、ホルモン受容体を発現する細胞の<1%として定義される。
●中央で検査され、PD-L1陽性であることが見出された転移性TNBC腫瘍を有する患者のみが登録される
Patients in Cohort A must meet the following cancer-specific criteria for study entry:
- Life expectancy ≥12 weeks - Metastatic or locally advanced unresectable histologically documented TNBC (absence of HER2, ER and progesterone receptor (PgR) expression as determined by local examination)
HER2-negative is defined as either of the following (Wolff et al. 2018) by local laboratory assessment:
In situ hybridization (ISH) unamplified (HER2 to CEP 17 ratio <2.0 or single probe average HER2 gene copy number <4 signals/cell), or
ER and PgR negative is defined as <1% of cells expressing hormone receptors as determined by IHC analysis.
- Only patients with metastatic TNBC tumors that are centrally tested and found to be PD-L1 positive will be enrolled
臨床的に実施可能であれば、(適用可能であれば)再発性転移性又は局所進行性疾患から得られた腫瘍標本を提出しなければならない。 Tumor specimens from recurrent metastatic or locally advanced disease (if applicable) should be submitted, if clinically feasible.
パラフィンブロック(好ましい)又は少なくとも20枚の染色されていないスライド中の代表的なFFPE腫瘍標本(保管標本又は再発性疾患からの新鮮な前処理組織のいずれか) Representative FFPE tumor specimens in paraffin blocks (preferred) or at least 20 unstained slides (either archival specimens or fresh pretreated tissue from recurrent disease)
腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならず、登録前にVentana(SP142)PD-L1 IHCアッセイを使用して決定した場合にPD-L1発現について評価しなければならず、陽性は、中央検査室によって決定された任意の強度のPD-L1発現腫瘍浸潤免疫細胞が占める腫瘍面積の1%以上として定義される。腫瘍組織がPD-L1発現について評価可能でない患者は、適格ではない。 Tumor tissue must be of good quality based on total tumor content and viable tumor content and assessed for PD-L1 expression as determined using the Ventana (SP142) PD-L1 IHC assay prior to enrollment. Positivity is defined as ≥1% of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells of any intensity as determined by a central laboratory. Patients whose tumor tissue was not evaluable for PD-L1 expression were not eligible.
複数の腫瘍標本が提出される場合、少なくとも1つの標本が評価可能であり、PD-L1発現について陽性である場合(組織が保管標本由来であるか再発性疾患由来であるかにかかわらず)、患者は適格であり得る。 If multiple tumor specimens are submitted, if at least one specimen is evaluable and positive for PD-L1 expression (whether the tissue is from archival specimens or from recurrent disease); Patients may be eligible.
許容され得る試料には、深部腫瘍組織のためのコア針生検(最低3つのコア)、又は皮膚、皮下、若しくは粘膜病変のための切除、切開、パンチ、若しくは鉗子生検が含まれる。 Acceptable samples include core needle biopsies (minimum of 3 cores) for deep tumor tissue, or excision, incision, punch, or forceps biopsies for cutaneous, subcutaneous, or mucosal lesions.
パラフィンブロック中のFFPE腫瘍標本が好ましい。 FFPE tumor specimens in paraffin blocks are preferred.
細針吸引、ブラッシング、胸水からの細胞ペレット、骨転移、及び洗浄液試料は許容されない。骨転移由来の腫瘍組織は、PD-L1発現について評価することができず、したがって許容されない。
●手術不能、局所進行性、又は転移性TNBCのための事前の化学療法又は標的全身療法なし
Fine needle aspirations, brushings, cell pellets from pleural effusions, bone metastases, and lavage fluid samples are not permitted. Tumor tissue from bone metastases cannot be assessed for PD-L1 expression and is therefore unacceptable.
- No prior chemotherapy or targeted systemic therapy for inoperable, locally advanced, or metastatic TNBC
転移性疾患に対する事前の放射線療法は許容される。放射線療法に必要な最小ウォッシュアウト期間はない。患者は、放射線の影響から回復されなければならない。 Prior radiation therapy for metastatic disease is permissible. There is no minimum washout period required for radiation therapy. Patients must recover from the effects of radiation.
試験処置の開始の≧12ヶ月前に治療が完了した場合、ネオアジュバント又はアジュバント療法における事前化学療法(タキサンを含む)及び/又はCIT(抗PD-L1剤又は抗PD-1剤のみ)が許容される。
●RECIST v1.1に従って治験責任医師が評定した測定可能な疾患
Prior chemotherapy (including taxanes) and/or CIT (anti-PD-L1 agents or anti-PD-1 agents only) in neoadjuvant or adjuvant therapy acceptable if therapy was completed ≥12 months prior to initiation of study treatment be done.
- Investigator-assessed measurable disease according to RECIST v1.1
以前に放射線照射された病変は、放射線照射後にその部位で疾患の進行が明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。 Previously irradiated lesions can be considered measurable disease only if there is clearly documented disease progression at the site after irradiation.
E.除外基準
以下の基準のいずれかを満たす患者は試験から除外される:
●試験処置中、チラゴルマブ処置後90日以内、アテゾリズマブ処置後5ヶ月以内、nab-パクリタキセル、カルボプラチン若しくはドキソルビシン処置後6ヶ月以内、又はシクロホスファミド処置後12ヶ月以内(いずれか長い方)に妊娠若しくは授乳、又は妊娠する意図
E. Exclusion Criteria Patients meeting any of the following criteria will be excluded from the study:
Pregnancy during study treatment, within 90 days after tiragolumab treatment, within 5 months after atezolizumab treatment, within 6 months after nab-paclitaxel, carboplatin or doxorubicin treatment, or within 12 months after cyclophosphamide treatment (whichever is longer) or breastfeeding, or intending to become pregnant
妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
●治験実施計画書の遵守又は重大な肝疾患(例えば、肝硬変、制御不能な大発作性障害、又は上大静脈症候群)を含む結果の解釈に影響を及ぼし得る有意な制御されない同時発症疾患の証拠
●試験処置開始前3ヶ月以内の重大な心血管疾患、例えば、ニューヨーク心臓病(クラスII以上)、心筋梗塞、不安定性不整脈又は不安定狭心症
LVEF<53%が既知の患者は除外する。
上記の基準を満たさない既知の冠動脈疾患又はうっ血性心不全を有する患者。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)
●試験処置開始前2週間以内の経口又はIV抗生物質による処置
定期的な抗生物質予防(例えば、慢性閉塞性肺疾患の増悪を予防するため、又は抜歯のために)を受けている患者は適格である。
●試験処置の開始前28日以内の大きな外科的処置、又は診断以外の試験中の大きな外科的処置の必要性の予想
中心静脈アクセスカテーテル(複数可)(例えば、ポート等)の配置は、大きな外科的処置とは考えられておらず、したがって許容される。
●キメラ抗体若しくはヒト化抗体、又は融合タンパク質に対する重度のアレルギー性、アナフィラキシー性、又は他の超過敏反応の病歴。
●CHO細胞で産生される生物製剤又はチラゴルマブ若しくはアテゾリズマブ製剤の任意の成分に対する既知の過敏症又はアレルギー
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質症候群に関連する血管血栓症、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、多発性硬化症、血管炎、又は糸球体腎炎を含むがこれらに限定されない活動性の自己免疫疾患又はその病歴
安定用量の甲状腺補充ホルモンで自己免疫介在性甲状腺機能低下症の病歴を有する患者は、この試験に適格である。
安定したインスリン投薬レジメンで制御された1型糖尿病患者はこの試験に適格である。
湿疹、乾癬、慢性単純性苔癬又は皮膚症状のみを有する白斑(例えば、乾癬性関節炎なし)を有する患者は、以下の条件を満たすならば許可される:
-発疹が覆っている体表面積は<10%でなければならない
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない
-別の免疫賦活性抗がん剤を投与されている間に重度又は生命を脅かす皮膚有害反応を以前に経験した患者に対してアテゾリズマブを検討する場合は注意を払うべきである
●事前の同種異系幹細胞又は固形臓器移植
●スクリーニング時の胸部コンピューター断層撮影(CT)スキャンでの特発性肺線維症(肺臓炎を含む)、薬物誘発性肺臓炎、器質化肺炎(すなわち、閉塞性細気管支炎、潜在性器質化肺炎)の病歴、又は活動性肺臓炎の証拠
放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●スクリーニング時の陽性EBVウイルスカプシド抗原(VCA)IgM検査
活動性感染又は慢性活動性感染の疑いをスクリーニングするために、EBVポリメラーゼ連鎖反応(PCR)検査を臨床的に適応されるように実施しなければならない。
EBV PCR検査が陽性の患者は除外する。
●活動性結核(TB)
●試験処置の開始前4週間以内に生弱毒化ワクチンを受けること、又はそのような生弱毒化ワクチンが試験中に必要であると予想すること
患者は、試験処置の開始前28日以内、処置中、又は試験処置の最終用量後5ヶ月以内に生弱毒化ワクチン(例えば、FLUMIST(登録商標))を受けないことに同意しなければならない。
●抗PD-1又は抗PD-L1治療抗体を除く、抗CTLA-4を含むCD137アゴニスト又は免疫チェックポイント遮断療法による事前処置
●試験処置の開始前の4週間以内又は薬物の5つの薬物除去半減期(いずれか長い方)以内の全身免疫刺激剤(インターフェロン又はIL-2を含むが、これらに限定されない)による処置
●試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、
プレドニゾン、デキサメタゾン、アザチオプリン、メトトレキサート、サリドマイド及び抗腫瘍壊死因子[抗TNF]剤)による処置、又は試験中の全身免疫抑制薬が必要と予想される
急性低用量全身免疫抑制薬(例えば、悪心のためのデキサメタゾンの1回投与)を受けた患者は試験に登録され得る。
ステロイド前処置を必要とするIV造影剤に対するアレルギー反応の病歴を有する患者は、磁気共鳴画像法(MRI)を用いて行われるベースライン及びその後の腫瘍評定を受けなくてはならない。
慢性閉塞性肺疾患のための吸入コルチコステロイド、起立性低血圧患者のためのミネラルコルチコイド(例えば、フルドロコルチゾン)、及び副腎皮質機能不全のための低用量補充コルチコステロイドの使用が許容される。
以下のがん特異的排除基準のいずれかを満たすコホートAの患者は、試験の参加から除外される:
●SP142 PD-L1 IHCアッセイで測定されるPD-L1陰性のFFPE腫瘍組織、陽性は任意の強度のPD-L1発現腫瘍浸潤免疫細胞が占有する腫瘍面積の≧1%以上として定義されるFFPE腫瘍組織
●手術及び/又は放射線で確定的に処置されていない脊髄圧迫、又は以前に診断及び処置された脊髄圧迫であって、試験処置の開始前の>2週間、疾患が臨床的に安定しているという証拠がない脊髄圧迫
●処置された無症候性CNS転移を除いて、以下の基準の全てが満たされるならば、既知の中枢神経系(CNS)疾患:
-テント上(supratentorial)及び小脳転移のみが許容された(すなわち、中脳、橋、延髄又は脊髄への転移なし)
-CNS疾患の治療としてのコルチコステロイドの継続的な必要性はない
-試験処置開始前7日間以内に定位放射線照射なし、又は14日間以内に全脳照射
-CNSに向けられた治療の完了とスクリーニングX線試験との間の暫定的な進行の証拠はない
注:スクリーニング検査で新たに無症候性CNS転移が検出された患者は、CNS転移に対する放射線療法及び/又は手術を受けていなければならない。処置後、これらの患者は、他の基準の全てが満たされる場合、登録前に追加の脳スキャンを必要とせずに適格となり得る。
●軟髄膜疾患
●制御されない胸水、心膜滲出、又は腹水
留置カテーテル(例えば、PLEURX(登録商標))を有する患者は許容される。
●制御されない腫瘍関連疼痛
麻薬性鎮痛剤を必要とする患者は、試験登録時に安定したレジメンでなければならない。
緩和的放射線療法に適した症候性病変(例えば、神経インピンジメントを引き起こす骨転移又は転移)は、登録前に処置しなければならない。患者は、放射線の影響から回復されなければならない。必要とされる最低限の回復期間はない。
そのさらなる成長が機能不全又は難治性疼痛を引き起こす可能性がある無症候性転移病変(脊髄圧迫に現在は関連付けられていない硬膜外転移)は、適切である場合、登録前に局所領域的療法について検討されなければならない;
●制御されない高カルシウム血症(>1.5mmol/Lのイオン化カルシウム若しくはカルシウム>12mg/dL又はULNより大きい補正血清カルシウム)又はビスホスホネート療法の継続的な使用を必要とする症候性高カルシウム血症
特に骨格事象を予防するためにビスホスホネート療法を受けており、臨床的に有意な高カルシウム血症の病歴がない患者が適格である。
●試験処置の開始前5年以内のTNBC以外の悪性腫瘍、ただし、転移又は死亡のリスクが無視できるもの(例えば、>90%の5年OS)、及び予測される治癒的転帰を伴って処置されたもの(例えば、適切に処置された子宮頸部上皮内癌腫又は基底の限局性前立腺がん又は扁平上皮皮膚がん)を除く
●nab-パクリタキセル又はその賦形剤のいずれかに対する既知の過敏症
Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
- Evidence of significant uncontrolled comorbidities that could affect interpretation of results, including protocol compliance or significant liver disease (e.g., cirrhosis, uncontrolled grand paroxysmal disorder, or superior vena cava syndrome) • Significant cardiovascular disease within 3 months prior to initiation of study treatment, eg New York heart disease (class II or greater), myocardial infarction, unstable arrhythmia or unstable angina Pectoris with known LVEF <53% are excluded.
Patients with known coronary artery disease or congestive heart failure who do not meet the above criteria.
- Severe infection within 4 weeks prior to initiation of study treatment (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia)
Oral or IV antibiotic treatment within 2 weeks prior to study treatment initiation Patients receiving routine antibiotic prophylaxis (e.g., to prevent exacerbation of chronic obstructive pulmonary disease or for tooth extraction) are eligible is.
Anticipation of need for major surgical procedure within 28 days prior to initiation of study procedure, or non-diagnostic procedure during study Placement of central venous access catheter(s) (e.g., ports, etc.) It is not considered a surgical procedure and is therefore acceptable.
• History of severe allergic, anaphylactic, or other hypersensitivity reactions to chimeric or humanized antibodies, or fusion proteins.
Known hypersensitivity or allergy to CHO cell-produced biologics or any component of tiragolumab or atezolizumab formulations Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, Active autoimmune disease including, but not limited to, vascular thrombosis associated with antiphospholipid syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barre syndrome, multiple sclerosis, vasculitis, or glomerulonephritis; or Their History Patients with a history of autoimmune-mediated hypothyroidism on stable doses of thyroid replacement hormone are eligible for this trial.
Patients with
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin symptoms only (e.g., no psoriatic arthritis) are allowed if they meet the following conditions:
- Rash must cover <10% body surface area - Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UV within the last 12 months No occurrence of acute exacerbation of underlying symptoms requiring A-irradiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors, or high-potency or oral corticosteroids - Administration of another immunostimulatory anticancer agent Caution should be exercised when considering atezolizumab in patients who have previously experienced severe or life-threatening cutaneous adverse reactions while being treated Prior allogeneic stem cell or solid organ transplantation Thoracic at screening History or activity of idiopathic pulmonary fibrosis (including pneumonitis), drug-induced pneumonitis, organizing pneumonia (ie, bronchiolitis obliterans, subclinical organizing pneumonia) on computed tomography (CT) scan Evidence of pneumonitis A history of radiation pneumonitis (fibrosis) in the radiation field is acceptable.
Positive EBV viral capsid antigen (VCA) IgM test at screening EBV polymerase chain reaction (PCR) testing should be performed as clinically indicated to screen for suspected active or chronic active infection. must.
Patients with a positive EBV PCR test are excluded.
● Active tuberculosis (TB)
- Receiving a live-attenuated vaccine within 4 weeks prior to initiation of study treatment, or anticipating need for such a live-attenuated vaccine during the study Patients will receive treatment within 28 days prior to initiation of study treatment Must agree not to receive a live attenuated vaccine (eg, FLUMIST®) during or within 5 months after the last dose of study treatment.
- Pretreatment with CD137 agonists or immune checkpoint blockade therapy, including anti-CTLA-4, excluding anti-PD-1 or anti-PD-L1 therapeutic antibodies - Within 4 weeks prior to initiation of study treatment or 5 drug elimination halves of drug Treatment with systemic immunostimulating agents (including but not limited to interferon or IL-2) within the period (whichever is longer) Systemic immunosuppressive agents (including but not limited to,
Prednisone, dexamethasone, azathioprine, methotrexate, thalidomide, and anti-tumor necrosis factor [anti-TNF] agents) or investigational systemic immunosuppressants expected to require acute low-dose systemic immunosuppressants (e.g., for nausea) of dexamethasone) may be enrolled in the study.
Patients with a history of allergic reactions to IV contrast agents requiring steroid pretreatment should undergo baseline and subsequent tumor assessments performed using magnetic resonance imaging (MRI).
The use of inhaled corticosteroids for chronic obstructive pulmonary disease, mineralocorticoids (eg, fludrocortisone) for patients with orthostatic hypotension, and low-dose supplemental corticosteroids for adrenocortical insufficiency is permissible. be.
Patients in Cohort A who meet any of the following cancer-specific exclusion criteria are excluded from study participation:
- FFPE tumor tissues that are PD-L1 negative as measured by the SP142 PD-L1 IHC assay, with FFPE tumors defined as ≥1% of tumor area occupied by PD-L1 expressing tumor-infiltrating immune cells of any intensity Tissues - Spinal cord compression not definitively treated with surgery and/or radiation or previously diagnosed and treated spinal cord compression with clinically stable disease >2 weeks prior to initiation of study treatment. Spinal cord compression with no evidence of having known central nervous system (CNS) disease, provided all of the following criteria are met, except for treated asymptomatic CNS metastases:
- Only supratentorial and cerebellar metastases were allowed (ie no midbrain, pons, medulla oblongata or spinal cord metastases)
- No ongoing need for corticosteroids as treatment for CNS disease - No stereotactic radiation within 7 days or whole brain radiation within 14 days prior to initiation of study treatment - Completion of CNS-directed therapy and No evidence of interim progression between screening radiographs Note: Patients with new asymptomatic CNS metastases detected on screening must have undergone radiotherapy and/or surgery for CNS metastases . After treatment, these patients may be eligible without the need for additional brain scans prior to enrollment if all other criteria are met.
• Leptomeningeal disease • Uncontrolled pleural effusion, pericardial effusion, or ascites Patients with indwelling catheters (eg, PLEURX®) are permitted.
• Uncontrolled tumor-related pain Patients requiring narcotic analgesics must be on a stable regimen at study entry.
Symptomatic lesions amenable to palliative radiotherapy (eg bone metastases or metastases causing nerve impingement) must be treated prior to enrollment. Patients must recover from the effects of radiation. There is no minimum recovery period required.
Asymptomatic metastatic lesions (epidural metastases not currently associated with spinal cord compression) whose further growth may cause dysfunction or intractable pain should be treated with locoregional therapy prior to enrollment, if appropriate. must be considered;
Uncontrolled hypercalcemia (>1.5 mmol/L ionized calcium or calcium >12 mg/dL or corrected serum calcium > ULN) or symptomatic hypercalcemia requiring continued use of bisphosphonate therapy, especially Patients receiving bisphosphonate therapy to prevent skeletal events and with no history of clinically significant hypercalcemia are eligible.
- Malignancies other than TNBC within 5 years prior to initiation of study treatment, but with negligible risk of metastasis or death (e.g., >90% 5-year OS) and treatment with expected curative outcome known hypersensitivity to nab-paclitaxel or any of its excipients disease
F.分析
安全性分析を全ての患者で行う。
F. Analysis A safety analysis will be performed in all patients.
有効性分析は、コホートA及びBのためのITTアプローチを使用し、患者が割り当てられた試験薬物を受けているかどうかにかかわらず、任意の登録患者が分析に含まれる。ITT集団のサブセットに基づく分析も行われ得る。 Efficacy analyzes will use the ITT approach for Cohorts A and B, and any enrolled patient will be included in the analysis regardless of whether the patient is receiving their assigned study drug. Analysis based on subsets of the ITT population can also be performed.
仮説検定は、特に指示しない限り、両側性である。 Hypothesis tests are two-sided unless otherwise indicated.
試料サイズ
コホートAの目的は、客観的奏効として定義される主要有効性評価項目に対する、アテゾリズマブ及びnab-パクリタキセルと組み合わせたチラゴルマブの効果を推定することである。過去のデータと比較して、応答の割合は、さらなる開発のために有望であるか又は有望でないと考えられる。正式な仮説検定はない。統計を両側90% CIで示す。開発の継続又は停止を推奨する場合、PFS、OS、及びサブグループの分析結果を含むがこれらに限定されない副次的有効性評価項目の結果を含むデータ全体が考慮される。
Sample Size The purpose of Cohort A is to estimate the effect of tiragolumab in combination with atezolizumab and nab-paclitaxel on the primary efficacy endpoint defined as objective response. Compared to historical data, the proportion of responses is considered either promising or unpromising for further development. There are no formal hypothesis tests. Statistics are presented as two-sided 90% CI. When recommending continuation or cessation of development, the overall data, including the results of secondary efficacy endpoints, including but not limited to PFS, OS, and subgroup analyses, will be considered.
主要な有効性分析は、CR又はPRを得ると予想される患者の真の割合の推定である(すなわち、ORR)。類似の疾患状況における完了した試験及び進行中の試験からのデータを、比較のための歴史的対照として使用することができる。現在利用可能なデータは、局所進行性の切除不能又は転移性PD-L1陽性TNBCにおいて、過去に確認された奏効率が約53%(TECENTRIQ(登録商標)米国添付文書)であることを示している。 The primary efficacy analysis is an estimate of the true proportion of patients expected to have a CR or PR (ie, ORR). Data from completed and ongoing trials in similar disease settings can be used as historical controls for comparison. Currently available data show a historically confirmed response rate of approximately 53% (TECENTRIQ® US Package Insert) in locally advanced, unresectable or metastatic PD-L1-positive TNBC there is
40人の患者の試料サイズは、観察された奏効率を67.5%と仮定して、53%未満の臨床的に関心のない奏効確率を除外するための点推定及び両側90% CIの下限の適切な精度を提供するのに十分であると考えられる。具体的には、40人の患者のうち少なくとも27人が応答を達成した場合、応答率は53%より高いと結論付けることができる。奏効を達成すると予想される患者の割合の更新された推定値は、有効性分析の時点までに進行中の試験から入手可能であると予想され、基準データとして使用される。 A sample size of 40 patients was used, assuming an observed response rate of 67.5%, point estimates and lower bounds for a two-sided 90% CI to exclude clinically irrelevant response probabilities of less than 53%. is considered sufficient to provide adequate accuracy of Specifically, if at least 27 out of 40 patients achieve a response, it can be concluded that the response rate is greater than 53%. Updated estimates of the proportion of patients expected to achieve a response are expected to be available from ongoing trials by the time of efficacy analysis and will be used as baseline data.
表26は、40人の患者の試料に基づくある範囲の観察された割合について応答を達成する真の確率についての両側90%Clopper-Pearsonの正確なCIを列挙している。様々な閾値下でのORRの観察された点推定値並びに基礎となる真のORRに基づいて正及び負のシグナルを検出する確率を表27及び表28に示す。



安全性解析
安全性評定には、有害事象の発生率、性質及び重症度、治験実施計画書に定められたバイタルサイン、検査異常、及び、試験の安全性評価にとって重要であると考えられる他の治験実施計画書に規定された試験が含まれる。有害事象はNCI CTCAE v5.0に従って等級付けされる。
Safety analysis Safety assessments should include the incidence, nature and severity of adverse events, protocol-specified vital signs, laboratory abnormalities, and other factors considered important to the safety evaluation of the study. Includes protocol-specified studies. Adverse events are graded according to NCI CTCAE v5.0.
安全性は、ADAによって測定され、処置群によって提示される有害事象、検査室での検査結果の変化、バイタルサインの変化、試験処置曝露及び免疫原性の要約によって評定される。 Safety is measured by the ADA and assessed by treatment group presented adverse events, changes in laboratory test results, changes in vital signs, study treatment exposure and immunogenicity summaries.
有害事象の言語記述をMedDRA用語にマッピングする。 Verbal descriptions of adverse events are mapped to MedDRA terminology.
処置下で発現する事象(試験処置の最初の用量で又はその後に起こる事象として定義される)は、治験責任医師によって評定される試験薬との関係に関係なく、MedDRA用語、適切なMedDRAレベル、及びNCI CTCAE v5.0グレードによって要約される。各患者について、同じ有害事象の複数の発生が起こる場合、報告された最大重症度を要約に使用する。 A treatment-emergent event (defined as an event occurring at or after the first dose of study treatment), regardless of relationship to study drug as assessed by the Investigator, is a MedDRA term, an appropriate MedDRA level, and summarized by the NCI CTCAE v5.0 grade. For each patient, if multiple occurrences of the same adverse event occur, the maximum severity reported will be used for summaries.
以下の処置下で発現する有害事象を別々に要約する:試験薬の中止につながる有害事象、用量の減少又は中断につながる有害事象、グレード≧3の有害事象、グレード5の有害事象、重篤な有害事象、及び特別な関心のある有害事象。
The following treatment-emergent adverse events will be summarized separately: adverse events leading to discontinuation of study drug, adverse events leading to dose reduction or interruption, grade ≥3 adverse events,
全ての死亡及び死亡原因を要約する。 Summarize all deaths and causes of death.
関連する検査値を時点によって要約し、NCI CTCAEグレード3及びグレード4の値を適宜同定する。NCI CTCAEグレードの変化を処置群によって集計する。
曝露、有害事象、検査及びバイタルサインデータの分析
Relevant laboratory values are summarized by time point and
Analysis of exposure, adverse events, laboratory and vital signs data
安全性は、試験処置への曝露、有害事象、検査室での検査結果の変化、並びにバイタルサイン及びECGの変化の要約を通して評定される。 Safety is assessed through a summary of exposure to study treatment, adverse events, changes in laboratory results, and changes in vital signs and ECG.
試験処置曝露(例えば、処置期間、受けた総用量、並びにサイクル数及び用量変更)を記述統計学によって要約する。 Study treatment exposure (eg, duration of treatment, total dose received, and number of cycles and dose modifications) will be summarized by descriptive statistics.
全ての逐語的有害事象用語をMedDRAシソーラス用語にマッピングし、有害事象重症度をNCI CTCAE v5.0に従って等級付けする。試験処置の初回用量(すなわち、処置下で発現した有害事象)のとき又はその後に起こる全ての有害事象、重篤な有害事象、死亡につながる有害事象、特別な関心のある有害事象、及び試験処置の中止につながる有害事象を、マッピングされた用語、適切な類義語レベル、及び重症度によって要約する。様々な重症度の事象について、最高グレードが要約に使用される。死亡及び死亡原因を要約する。 All verbatim adverse event terms are mapped to MedDRA thesaurus terms and adverse event severity is graded according to the NCI CTCAE v5.0. All adverse events occurring at or after the first dose of study treatment (i.e., treatment-emergent adverse events), serious adverse events, adverse events leading to death, adverse events of special interest, and study treatment Adverse events leading to discontinuation of study will be summarized by mapped terms, appropriate synonym levels, and severity. For events of varying severity, the highest grade is used for summaries. Summarize deaths and causes of death.
関連する検査室、バイタルサイン(脈拍数、呼吸数、血圧、パルスオキシメトリ、及び体温)、及びECGデータは、必要に応じて識別されたグレードと共に時間によって表示される。更に、選択された検査室での検査のシフトテーブルを使用して、ベースライン及びベースライン後の最大重症度グレードを要約する。バイタルサイン及びECGの変化を要約する。 Relevant laboratory, vital signs (pulse rate, respiratory rate, blood pressure, pulse oximetry, and temperature), and ECG data are displayed by time with grades identified as appropriate. In addition, baseline and post-baseline maximum severity grades will be summarized using shift tables for selected laboratory tests. Summarize changes in vital signs and ECG.
有効性分析
主要有効性目的
コホートAの主要な有効性目的は、以下の評価項目に基づいて、アテゾリズマブ及びnab-パクリタキセルと組み合わせたチラゴルマブの有効性を評定することである。
●ORR、RECIST v1.1を用いて治験責任医師が決定したCR又はPRを有する患者の割合として定義される
Efficacy Analysis Primary Efficacy Objectives The primary efficacy objective for Cohort A is to assess the efficacy of tiragolumab in combination with atezolizumab and nab-paclitaxel based on the following endpoints.
ORR, defined as the proportion of patients with an investigator-determined CR or PR using RECIST v1.1
PR又はCRの確認が必要である。ベースライン後の腫瘍評定を受けていない患者を含む、この基準を満たさない患者は、非応答者とみなされる。ORRは、客観的奏効を有する患者の割合として定義される。 Confirmation of PR or CR is required. Patients who do not meet this criteria, including those who do not have a post-baseline tumor assessment, are considered non-responders. ORR is defined as the proportion of patients with an objective response.
有効性データの最も早い観察は、全ての患者が少なくとも2つの腫瘍評定を受けた後に行われる。 The earliest observation of efficacy data will be made after all patients have had at least two tumor assessments.
副次的有効性目的
コホートAの副次的有効性目的は、以下の評価項目に基づいて、アテゾリズマブ及びnab-パクリタキセルと組み合わせたチラゴルマブの有効性に関する予備データを得ることである。
●PFS、登録から疾患進行の最初の発生までの時間又はRECIST v 1.1に従って治験責任医師によって決定された任意の原因による死亡(いずれか早く発生する方)と定義される
Secondary Efficacy Objectives The secondary efficacy objectives for Cohort A are to obtain preliminary data on the efficacy of tiragolumab in combination with atezolizumab and nab-paclitaxel based on the following endpoints.
- PFS, defined as the time from enrollment to the first occurrence of disease progression or death from any cause as determined by the investigator according to RECIST v 1.1 (whichever occurs first)
疾患の進行を経験したことがないか又は死亡した患者のデータは、それぞれの分析の臨床的カットオフ日の前又はその時点で生存しており無増悪であることが最後に分かった日に打ち切られる。ベースライン後の情報がない患者は、登録日に打ち切られる。
●DOR:RECIST v1.1に従って治験責任医師が決定した、疾患進行又は何らかの原因による死亡に対する文書化された客観的奏効の最初の発生からの時間(いずれか早く発生する方)として定義される
Data for patients who have never experienced disease progression or who have died are censored on the date of the last known survival and progression-free prior to or at the clinical cut-off date for each analysis. be done. Patients with no post-baseline information will be censored on the day of enrollment.
DOR: defined as the time from the first occurrence of documented objective response to disease progression or death from any cause (whichever occurs first) as determined by the investigator according to RECIST v1.1
疾患の進行を経験したことがないか又は死亡した患者のデータは、最後の腫瘍評定日に打ち切られる。CR又はPRの最初の発生日以降に腫瘍評定が行われない場合、DORはCR又はPRの最初の発生日に打ち切られる。
●OS、任意の原因からの登録から死亡までの時間として定義される
Data for patients who have never experienced disease progression or died are censored at the date of the last tumor assessment. If no tumor assessment is performed after the date of first occurrence of CR or PR, DOR will be censored at the date of first occurrence of CR or PR.
- OS, defined as the time from enrollment to death from any cause
分析時に死亡したと報告されていない患者は、最後に生存していることが分かった日に打ち切られる。ベースライン後に情報を有さない患者は、登録日に打ち切られる。 Patients not reported dead at the time of analysis are censored on the date they were last known alive. Patients with no information after baseline will be censored on the day of enrollment.
薬物動態学的分析
PK分析のために試料を収集し、この試験における曝露を以前の試験で得られた曝露と比較する。チラゴルマブ及びアテゾリズマブの血清濃度並びにnab-パクリタキセル、カルボプラチン、ドキソルビシン及びシクロホスファミドの血漿濃度は、適切な場合及びデータが許す場合、処置群及びサイクルによって個々の値として報告され、要約される(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)。
Pharmacokinetic Analysis Samples are collected for PK analysis and exposures in this study are compared to those obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab and plasma concentrations of nab-paclitaxel, carboplatin, doxorubicin and cyclophosphamide, where appropriate and data permitting, are reported as individual values by treatment arm and cycle and summarized (mean , standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean coefficient of variation).
個々の及び血清中のチラゴルマブ及びアテゾリズマブ濃度の中央値を、処置群及び日ごとにプロットする。チラゴルマブ及びアテゾリズマブの濃度データを、確立された集団PKモデルを使用して他の試験からのデータと共にプールして、データによって保証されるクリアランス、分布容積及びAUC等のPKパラメーターを導出することができる。関連するPKパラメーターと用量、安全性、有効性又はバイオマーカーの結果との潜在的な相関関係を調べることができる。 Median individual and serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be pooled with data from other studies using established population PK models to derive data-assured PK parameters such as clearance, volume of distribution and AUC. . Potential correlations between relevant PK parameters and dose, safety, efficacy or biomarker outcomes can be examined.
免疫原性分析
免疫原性分析には、任意のADA評定を受けた患者が含まれ、受けた処置に従って患者がグループ分けされる。処置中及びフォローアップ期間中の処置下で発現したADA陽性患者及びADA陰性患者の数及び割合を処置群によって要約する。
Immunogenicity Analysis The immunogenicity analysis includes patients with any ADA assessment and groups the patients according to the treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients during treatment and follow-up are summarized by treatment group.
ADAの状態と安全性、有効性及びPK評価項目との間の関係は、記述統計学を用いて分析及び報告され得る。 Relationships between ADA status and safety, efficacy and PK endpoints can be analyzed and reported using descriptive statistics.
バイオマーカー分析
探索的バイオマーカーの正式な統計分析は行われていないが、データは、この試験の文脈で、及び他の試験からのデータとまとめて分析することができる。
Biomarker Analysis Although no formal statistical analysis of the exploratory biomarkers has been performed, the data can be analyzed in the context of this study and together with data from other studies.
実施例4.局所進行性又は転移性腫瘍を有する患者における、単剤としての、アテゾリズマブ及び/又は他の抗がん治療と組み合わせた、チラゴルマブの安全性及び薬物動態の第Ia/Ib相非盲検用量漸増試験
本実施例は、以下を評価するように設計されたヒト初回投与第I相非盲検、多施設、グローバル、用量漸増試験を記載する:
(第Ia相)標準処置が存在しない、無効若しくは忍容性がないことが証明されている、又は不適切と考えられている、又は治験薬の臨床試験が認識された標準治療である局所進行性、再発性、又は転移性の治癒不能の腫瘍を有する単剤入院患者としてのチラゴルマブの安全性、忍容性、及びPK;並びに
(第Ib相)標準治療が存在しない、無効若しくは忍容性がないことが証明されている、若しくは不適切と考えられている、又は治験薬の臨床試験が認識されている標準治療である、又は抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と考えられている局所進行性、再発性、又は転移性の治癒不能腫瘍を有する患者において、標準処置療法と組み合わせて投与した場合のチラゴルマブの安全性、忍容性、及びPK。
Example 4. A Phase Ia/Ib, Open-label, Dose Escalation Study of the Safety and Pharmacokinetics of Tiragolumab in Combination with Atezolizumab and/or Other Anticancer Therapy as a Single Agent in Patients With Locally Advanced or Metastatic Tumors This example describes a first-in-human, Phase I, open-label, multicenter, global, dose escalation study designed to evaluate:
(Phase Ia) Local progression for which no standard treatment exists, has been proven to be ineffective or intolerable, or is considered inappropriate, or clinical trials of investigational agents are the recognized standard of care Safety, tolerability, and PK of tiragolumab as single-agent hospitalized patients with incurable, recurrent, or metastatic tumors; proven to be absent or considered inappropriate, clinical trials of investigational drugs are recognized standard of care, or clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are acceptable Safety, tolerability, and PK of tiragolumab when administered in combination with standard of care therapy in patients with locally advanced, recurrent, or metastatic incurable tumors that are considered viable treatment options.
A.試験計画 A. test plan
このヒト初回投与第I相非盲検、多施設、グローバル、用量漸増試験は、標準治療が存在しない、無効若しくは忍容性がないことが証明されている、又は不適切と考えられている、又は治験薬の臨床試験が認識された標準治療である局所進行性、再発性、又は転移性の治癒不能の腫瘍を有する単剤入院患者としてのチラゴルマブの安全性、忍容性、及びPKを評価するように設計されている。これは、試験の第Ia相部分で評定される。 This first-in-human, Phase I, open-label, multicenter, global, dose escalation study demonstrated that no standard of care exists, has proven to be ineffective or intolerable, or is considered inappropriate. or Investigational Clinical Trials to assess the safety, tolerability, and PK of tiragolumab as single-agent hospitalized patients with locally advanced, recurrent, or metastatic incurable tumors, a recognized standard of care is designed to This will be assessed in the Phase Ia portion of the trial.
この試験はまた、標準治療が存在しない、無効若しくは忍容性がないことが証明されている、若しくは不適切と考えられている、又は治験薬の臨床試験が認識されている標準治療である、又は抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と考えられている局所進行性、再発性、又は転移性の治癒不能腫瘍を有する患者において、標準処置療法と組み合わせて投与した場合のチラゴルマブの安全性、忍容性、及びPKの評価を可能にするように設計されている。これは、試験の第Ib相部分の複数のコホートで試験されている。
●第Ib相:チラゴルマブ及びアテゾリズマブ用量漸増コホート(図4)
●第Ib相:チラゴルマブ及びアテゾリズマブ適応症特異的拡大コホート(図4)
●第Ib相:チラゴルマブ及びアテゾリズマブの連続生検コホート(図4)
●第Ib相:チラゴルマブ及びアテゾリズマブ4週間毎(Q4W)投薬拡大コホート(図4)
●第Ib相:化学療法拡大コホートと組み合わせたチラゴルマブ及びアテゾリズマブ(コホートA~D;図5)
●第Ib相:非化学療法拡大コホートと組み合わせたチラゴルマブ(コホートNC 1及びNC 2;図6)
The trial also indicates that no standard of care exists, has been proven to be ineffective or intolerable, or is considered inappropriate, or is a recognized standard of care for clinical trials of an investigational drug; or in combination with standard treatment therapy in patients with locally advanced, recurrent, or metastatic incurable tumors for whom a clinical trial of an investigational drug in combination with an anti-PD-L1 antibody is considered an acceptable treatment option It is designed to allow assessment of the safety, tolerability, and PK of tiragolumab when administered. It is being tested in multiple cohorts in the Phase Ib portion of the trial.
Phase Ib: Tiragolumab and Atezolizumab Dose Escalation Cohort (Figure 4)
Phase Ib: Tiragolumab and Atezolizumab Indication-Specific Expansion Cohort (Figure 4)
- Phase Ib: Serial biopsy cohort of tiragolumab and atezolizumab (Figure 4)
Phase 1b: Tiragolumab and Atezolizumab every 4 weeks (Q4W) dosing expansion cohort (Figure 4)
Phase Ib: Tiragolumab and Atezolizumab in Combination with Chemotherapy Expansion Cohort (Cohorts AD; Figure 5)
Phase Ib: Tiragolumab in combination with non-chemotherapy expansion cohorts (
この試験の第Ib相部分は、少なくとも2つの用量レベルの単剤のチラゴルマブのDLT評価が完了した後に活性化され、全ての関連する単剤の安全性データが治験責任医師及びIMCによって十分に再検討されている。適切であると考えられる場合、第Ib相部分は、第Ia相部分の場合と同じ用量漸増スキーム及び包括的な安全性監視計画を使用して、初期チラゴルマブ用量レベル以下の用量レベルで開始する。更に、単剤のチラゴルマブを用いて試験の第Ia相部分で進行する患者には、試験の第Ib相部分に交差する選択肢が与えられ得る。 The Phase Ib portion of the study was activated after the DLT evaluation of single-agent tiragolumab at at least two dose levels was completed and all relevant single-agent safety data had been fully reviewed by the investigator and the IMC. being considered. If deemed appropriate, the Phase Ib portion will begin at dose levels equal to or lower than the initial tiragolumab dose level using the same dose escalation scheme and comprehensive safety monitoring plan as for the Phase Ia portion. Additionally, patients progressing in the Phase Ia portion of the trial using single agent tiragolumab may be given the option of crossing over to the Phase Ib portion of the trial.
試験の第Ia相部分と第Ib相部分の両方は、スクリーニング期間、処置期間、及び処置後フォローアップ期間からなる。患者は、用量漸増段階及び用量拡大段階の2つの段階で登録され、第Ia相及び第Ib相については、それぞれ図3及び図4を参照されたい。図4は、連続生検及びQ4Wコホートを更に示し、図5は、第Ib相化学療法拡大コホートを示し、図6は、第Ib相非化学療法拡大コホートを示す。用量漸増段階の間、およそ3~6名の患者のコホートをそれぞれ漸増用量レベルで評価して、単剤としての又はアテゾリズマブと組み合わせたチラゴルマブのMTD又は最大投与用量(MAD)を決定する。さらなる安全性及び薬力学データを取得して、拡大コホートの用量選択をより完全に知らせるために、さらなる患者を登録して、以下に記載される用量漸増基準に基づいて、関連するMTDを超えないことが示されている用量レベルでコホートを埋め戻してもよい。用量漸増決定の目的のために、これらの患者はDLT評価可能集団の一部として含まれない。 Both the Phase Ia and Phase Ib portions of the study consist of a screening period, a treatment period, and a post-treatment follow-up period. Patients are enrolled in two phases, a dose escalation phase and a dose expansion phase, see Figures 3 and 4 for Phases Ia and Ib, respectively. Figure 4 further shows the serial biopsy and Q4W cohorts, Figure 5 shows the Phase Ib chemotherapy expansion cohort, and Figure 6 shows the Phase Ib no-chemo expansion cohort. During the dose escalation phase, cohorts of approximately 3-6 patients are evaluated at each escalating dose level to determine the MTD or maximum administered dose (MAD) of tiragolumab as a single agent or in combination with atezolizumab. To obtain additional safety and pharmacodynamic data to more fully inform dose selection for the expansion cohort, additional patients will be enrolled to not exceed the relevant MTD based on the dose escalation criteria described below. Cohorts may be backfilled at dose levels as indicated. For purposes of dose escalation decisions, these patients will not be included as part of the DLT evaluable population.
用量拡大段階では、患者が登録され、単剤としての(第Ia相)又はアテゾリズマブ及び/又は他の抗がん治療と組み合わせた(第Ib相)、チラゴルマブのMTD又はMAD以下で処置される。 In the dose expansion phase, patients are enrolled and treated at or below the MTD or MAD of tiragolumab, either as a single agent (Phase Ia) or in combination with atezolizumab and/or other anticancer therapies (Phase Ib).
単剤としてのチラゴルマブ(第Ia相)、又はチラゴルマブとアテゾリズマブとの組み合わせ、チラゴルマブとアテゾリズマブとベバシズマブとの組み合わせ、又はチラゴルマブとペンブロリズマブとの組み合わせ(化学療法なしの第Ib相コホート)は、各21日間サイクルの1日目又は各28日間サイクルの1日目にIV注入によって投与される(第Ib相Q4W投薬拡大)。化学療法なしの第Ib相コホートでは、アテゾリズマブ、ベバシズマブ、又はペンブロリズマブの前に、チラゴルマブを投与する。許容できない毒性又は疾患進行の臨床上説得力のある証拠がない場合、治験責任医師による有益性及びリスクの好ましい評定に基づいて、第1サイクルを超えて、アテゾリズマブ及び/又は他の抗がん治療と組み合わせたチラゴルマブ(第Ia相)又はチラゴルマブ(第Ib相拡大コホート)のいずれかによる処置を継続することができる。
Tiragolumab as a single agent (Phase Ia), or a combination of tiragolumab and atezolizumab, a combination of tiragolumab and atezolizumab and bevacizumab, or a combination of tiragolumab and pembrolizumab (Phase Ib cohort without chemotherapy) each for 21 days Administered by IV infusion on
第Ib相化学療法及び非化学療法拡大コホート並びに第Ib相Q4W投薬拡大コホートでは、3名の患者の安全性ラン-インが完了する。安全性ラン-インからの全ての関連する安全性データは、登録が継続される前にIMC及び治験責任医師によって十分に再検討される。 The Phase Ib chemotherapy and no-chemo expansion cohorts and the Phase Ib Q4W dosing expansion cohort complete a safety run-in of 3 patients. All relevant safety data from the safety run-in will be reviewed thoroughly by the IMC and investigator before enrollment continues.
チラゴルマブ及びアテゾリズマブは、4つの化学療法拡大コホート:コホートAではカルボプラチン又はシスプラチン及びペメトレキセド、コホートBではカルボプラチン及びパクリタキセル、コホートCではカルボプラチン又はシスプラチン及びエトポシド、並びにコホートDではカペシタビンのそれぞれにおける特定の化学療法レジメンと組み合わされる。コホートA、B及びCでは、処置は導入期及び維持期からなる。導入期では、チラゴルマブ及びアテゾリズマブと化学療法との組み合わせを、コホートA及びBでは4~6サイクル、コホートCでは4サイクル、21日間のサイクルでIV注入によって投与する。コホートA及びBの導入処置のサイクル数は治験責任医師の裁量による。 Tiragolumab and atezolizumab were included in specific chemotherapy regimens in each of four chemotherapy expansion cohorts: carboplatin or cisplatin and pemetrexed in cohort A, carboplatin and paclitaxel in cohort B, carboplatin or cisplatin and etoposide in cohort C, and capecitabine in cohort D. is combined with In cohorts A, B and C, treatment consisted of an induction phase and a maintenance phase. In the run-in phase, tiragolumab and atezolizumab in combination with chemotherapy will be administered by IV infusion for 4-6 cycles in Cohorts A and B and 4 cycles in Cohort C in 21-day cycles. The number of cycles of induction treatment for Cohorts A and B is at the investigator's discretion.
導入期の後、疾患の進行又は許容できない毒性を経験したことがない患者は、維持療法による処置を継続する。維持期の間、コホートB及びCの患者は、チラゴルマブ及びアテゾリズマブのみを継続し、一方、コホートAの患者は、ペメトレキセドと共にチラゴルマブ及びアテゾリズマブを継続する。 After the induction phase, patients who have not experienced disease progression or unacceptable toxicity continue treatment with maintenance therapy. During the maintenance phase, patients in Cohorts B and C continue on tiragolumab and atezolizumab alone, while patients in Cohort A continue on tiragolumab and atezolizumab along with pemetrexed.
維持期では、コホートAは、アテゾリズマブ、チラゴルマブ及びペメトレキセドと共に21日間のサイクルで継続する。コホートBでは、治験実施計画書GO30103バージョン4の下で登録した患者は、アテゾリズマブ及びチラゴルマブを用いて21日間のサイクルを継続する。コホートBでは、治験実施計画書GO30103バージョン5以降に登録した患者は、アテゾリズマブ及びチラゴルマブを用いて28日間のサイクルを開始する。コホートCは、アテゾリズマブ及びチラゴルマブを用いて28日間のサイクルを開始する。
In the maintenance phase, Cohort A continues with atezolizumab, tiragolumab and pemetrexed in 21-day cycles. In Cohort B, patients enrolled under
コホートDでは、患者は、治験責任医師によって決定された許容できない毒性又は臨床的利益の喪失まで、チラゴルマブ、アテゾリズマブ、及びカペシタビンによる処置を受ける。患者は、1250mg/m2の用量のカペシタビンを1日2回(BID)、各21日間サイクルの1日目~14日目に経口で受ける。サイクル1の1日目に、最初の用量のカペシタビンを、アテゾリズマブ及びチラゴルマブ注入の前に診療所で投与する。チラゴルマブとアテゾリズマブとの組み合わせは、21日間のサイクルでIV注入によって投与される。
In Cohort D, patients receive treatment with tiragolumab, atezolizumab, and capecitabine until unacceptable toxicity or loss of clinical benefit as determined by the investigator. Patients receive capecitabine at a dose of 1250 mg/m 2 orally twice daily (BID) on days 1-14 of each 21-day cycle. On
全ての化学療法拡大コホートにおいて、アテゾリズマブは、チラゴルマブの前に投与される。 Atezolizumab is administered prior to tiragolumab in all chemotherapy expansion cohorts.
全ての患者は、試験を通して有害事象について綿密に監視される。有害事象は、NCI CTCAE、バージョン4.0に従って等級付けされる。 All patients will be closely monitored for adverse events throughout the study. Adverse events are graded according to the NCI CTCAE, version 4.0.
単剤(第Ia相)としての、又は化学療法を伴う又は伴わないアテゾリズマブとの組み合わせ(第Ib相)としてのチラゴルマブのPK特性、免疫原性応答、及び薬力学的効果を特性評価するために、投与前後の様々な時点で血液試料を採取する。中間PK分析の結果に応じて、PKサンプリングの頻度は試験の後半に減少し得る。 To characterize the PK properties, immunogenic responses, and pharmacodynamic effects of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab with or without chemotherapy (Phase Ib) , blood samples are taken at various time points before and after dosing. Depending on the results of the interim PK analysis, the frequency of PK sampling may decrease later in the study.
患者は、スクリーニング時及び試験中に腫瘍評定を受け、これは、固形腫瘍の標準的奏効評価基準(RECIST)v 1.1基準によって測定される。 Patients will undergo tumor assessments at screening and during the study, as measured by the Standard Response Evaluation Criteria for Solid Tumors (RECIST) v 1.1 criteria.
疾患の進行のための標準的なRECIST v 1.1基準が試験の第Ia相部分又は第Ib相部分において満たされている場合であっても、継続した処置のための基準を満たすならば、患者は試験処置を継続することを許される場合がある(図7)。試験の第Ia相部分を中止する患者は、クロスオーバーの基準を満たし、アクセス可能な病変の生検に同意することを条件として、試験の第Ib相部分に移り、アテゾリズマブと組み合わせたチラゴルマブによる処置を受けることができる(図8)。 Even if standard RECIST v 1.1 criteria for disease progression are met in the Phase Ia or Phase Ib portion of the trial, if criteria for continued treatment are met, Patients may be allowed to continue study treatment (Figure 7). Patients who discontinue the Phase Ia portion of the trial, provided they meet crossover criteria and consent to biopsy of accessible lesions, will proceed to the Phase Ib portion of the trial and be treated with tiragolumab in combination with atezolizumab. (Fig. 8).
チラゴルマブ(第Ia相)又はチラゴルマブ及びアテゾリズマブ、化学療法を伴うチラゴルマブ及びアテゾリズマブ、ベバシズマブを伴うチラゴルマブ及びアテゾリズマブ、又はチラゴルマブ及びペンブロリズマブ(第Ib相)を恒久的に中止した患者は、試験処置の最後の投与後30日以内に処置中止来院のためにクリニックに戻ることになる。特別な関心のある有害事象のさらなる監視及び記録は、別の全身抗がん治療の開始にかかわらず、試験処置の最後の投与後90日間まで行われる。他の全ての有害事象の監視及び記録は、試験処置の最後の投与後又は別の全身抗がん治療の開始のいずれか早く発生する方までの90日間まで行われる。この試験の全ての患者は、患者が追跡調査から撤回することを要求しない限り、死亡、フォローアップの喪失、又は試験終了まで約3カ月毎に生存期間及びその後の抗がん治療情報についてフォローアップされる。 Patients who permanently discontinue tiragolumab (Phase Ia) or tiragolumab and atezolizumab, tiragolumab and atezolizumab with chemotherapy, tiragolumab and atezolizumab with bevacizumab, or tiragolumab and pembrolizumab (Phase Ib) will receive the last dose of study treatment They will return to the clinic for a treatment discontinuation visit within the next 30 days. Further monitoring and recording of adverse events of special interest will occur for up to 90 days after the last dose of study treatment, regardless of initiation of another systemic anticancer therapy. Monitoring and recording of all other adverse events will occur for up to 90 days following the last dose of study treatment or initiation of another systemic anti-cancer therapy, whichever occurs first. All patients in this study were followed up for survival and subsequent anticancer treatment information approximately every 3 months until death, loss of follow-up, or termination of the study, unless the patient requested withdrawal from follow-up. be done.
IMCは、この試験で処置された全ての患者からの累積安全性データを定期的に評価する。安全性要約データは、試験の第Ia相(単剤チラゴルマブ)部分の最初の2つの用量コホートについてDLT評定が完了した後にIMCによって評価される。IMCは安全性データを再検討して、第Ia相の治験実施計画書を変更せずに登録を継続するかどうか、安全性ランインコホートからの安全性データを再検討し、第Ib相化学療法拡大コホート、非化学療法拡大コホート及びQ4W投与拡大コホートへの登録を継続するかどうか、安全性監視及び/又は適格性を修正するかどうか、新たに発生している安全性の問題に対処するための追加の安全性再検討を追加するかどうか、又は試験を終了するかどうかを推奨するために、アテゾリズマブと組み合わせたチラゴルマブとの試験の第Ib相部分への登録を開始するかどうかを推奨する。それを妨げる安全上の懸念がない場合、安全性分析が進行している間、試験の第Ia相の部分では増加が続く。 The IMC will periodically evaluate cumulative safety data from all patients treated in this study. Safety summary data will be evaluated by the IMC after completion of DLT assessments for the first two dose cohorts of the Phase Ia (single-agent tiragolumab) portion of the study. The IMC will review the safety data to determine whether to continue enrollment without changing the Phase Ia protocol, to review the safety data from the safety run-in cohort and to review the Phase Ib Chemistry Whether to continue enrollment in therapy expansion cohorts, non-chemotherapy expansion cohorts and Q4W treatment expansion cohorts, whether to modify safety monitoring and/or eligibility, address emerging safety issues recommend whether to initiate enrollment in the phase 1b portion of the study with tiragolumab in combination with atezolizumab to recommend whether to add an additional safety review for do. If there are no safety concerns preventing it, the Phase Ia portion of the trial will continue to ramp up while the safety analysis is ongoing.
潜在的な予想外の有害事象のリスクを更に軽減するために、IMCはまた、試験の第Ia相部分及び第Ib相部分の拡大コホートに参加した患者からの安全性データを定期的に再検討し、具体的には、試験処置を受けている間に患者の安全性を確実にするために、新たな試験安全性データに基づいて試験実施に関する推奨を行う。第Ia相及び第Ib相の拡大コホートでは、IMCによる無駄に関する中間分析も行われる。更に、メディカルモニターは、追加の安全性レポートを要求することができ、リスクと利益のバランスのために進行中の安全性データを再検討するために、試験中のいつでもIMCの臨時会議を呼び出すことができる。 To further reduce the risk of potential unanticipated adverse events, the IMC will also periodically review safety data from patients enrolled in the expansion cohorts of the Phase Ia and Phase Ib portions of the study. Specifically, to ensure patient safety while undergoing study treatment, make study conduct recommendations based on emerging study safety data. An interim analysis of IMC waste will also be performed in the Phase Ia and Phase Ib expansion cohorts. In addition, medical monitors can request additional safety reports and call ad hoc meetings of the IMC at any time during the study to review ongoing safety data for a balance of risks and benefits. can be done.
用量漸増段階の間、少なくとも3人の患者が、以下に記載される用量漸増規則に従って各チラゴルマブ用量レベルで治療されて、単剤又はアテゾリズマブと組み合わせたチラゴルマブのMTD又はMADを決定する。第Ia相又は第Ib相における新たな用量レベルのチラゴルマブを試験する各新たな用量漸増コホートにおける最初の3名の患者の登録は、それらのそれぞれのサイクル1、1日目の処置が≧7日間隔で投与されるようにずらして行われる。全ての患者は、21日間(サイクル1の1-21日目)として定義されるDLT評定期間中に有害事象について綿密に監視される。
During the dose escalation phase, at least 3 patients will be treated at each tiragolumab dose level according to the dose escalation rules described below to determine the MTD or MAD of tiragolumab alone or in combination with atezolizumab. Enrollment of the first 3 patients in each new dose escalation cohort testing a new dose level of tiragolumab in Phase Ia or Phase Ib will be subject to ≥7 days of treatment on
DLT以外の理由でDLT評定ウィンドウを完了しない用量漸増患者は、用量漸増決定及びMTD評定のために評価不可能であると考えられ、その同じ用量レベルで追加の患者によって置き換えられる場合がある。DLTの評定を混乱させる(後述の支持療法を含まない)DLT評定ウィンドウの間に支持療法を受け、DLTを経験していない患者は、メディカルモニターの裁量で置き換えられる場合がある。次の計画された用量の投与が7日を超えて遅延されるようなDLT以外の理由でDLT評定ウィンドウ中に保持された試験処置の任意の成分を有する患者は、用量漸増決定及びMTD又はMAD評定のために評価不可能であると考えられ、その同じ用量レベルで追加の患者によって置き換えられる場合がある。 Dose escalation patients who do not complete the DLT assessment window for reasons other than DLT are considered non-evaluable for dose escalation decisions and MTD assessment and may be replaced by additional patients at that same dose level. DLT-naive patients receiving supportive care during the DLT assessment window (not including supportive care as described below) that disrupt the assessment of DLT may be replaced at the discretion of the medical monitor. Patients with any component of study treatment held during the DLT assessment window for reasons other than DLT such that administration of the next planned dose is delayed for more than 7 days will be subject to dose escalation decisions and MTD or MAD Considered non-evaluable for assessment and may be replaced by additional patients at that same dose level.
試験の第Ia相部分で処置され、チラゴルマブ単独で疾患進行を発症する患者は、クロスオーバーのための特定の適格基準が満たされるならば、試験の第Ib相部分(図8)で処置を受けるのに適格であり得る。 Patients treated in the Phase Ia portion of the trial who develop disease progression on tiragolumab alone will receive treatment in the Phase Ib portion of the trial (Figure 8), provided certain eligibility criteria for crossover are met may be eligible for
用量制限毒性の定義
試験の第Ia相部分及び第Ib相部分の両方において、以下の事象のいずれか1つがDLT評定ウィンドウの間に発生し、治験責任医師によって試験処置に関連すると評定される場合、DLTとみなされる。
●グレード≧3の非血液学的、非肝臓有害事象、ただし以下の例外がある。
-3日間の標準処置療法でグレード≦2に回復するグレード≦3の悪心、嘔吐又は下痢
-≦3日間でグレード≦2に回復するグレード3の疲労
-グレード3の発熱(>40℃で≦24時間と定義)
-≦7日以内にグレード≦2になるグレード3の腫瘍フレア(局所疼痛、かぶれ、又は既知又は疑われる腫瘍の部位に局在する発疹として定義される)の有害事象;
-無症候性であり、治験責任医師によって臨床的に有意でないと考えられるグレード3の臨床検査異常
-プレドニゾン10mg/日以下と同等の治療で≦7日以内にグレード≦2になるグレード3の発疹;
-支持療法で適切に管理することができる、又は7日以内にグレード≦2に回復するグレード3の関節痛
-グレード3自己免疫性甲状腺炎又は全身性コルチコステロイドの開始を必要としない内分泌療法によって管理することができる他の内分泌異常(副腎機能不全のための補充ステロイドを除く)
●>7日間続くグレード≧4の好中球減少症(絶対好中球数(ANC)<500/μL)
●グレード≧3発熱性好中球減少症
●グレード≧4の貧血
●グレード≧4の血小板減少、又は臨床的に有意な出血に関連付けられるグレード3の血小板減少;
●>7日間続く血清肝臓トランスアミナーゼ(ALT又はAST)のグレード≧3上昇
肝転移の結果としてベースラインでグレード1のALT又はAST上昇を有する患者では、≧3倍Xベースラインが>7日持続するグレード≧3の上昇のみがDLTとみなされた。
●グレード≧3血清総ビリルビン上昇
ALT又はAST>3X正常値上限(ULN)及び総ビリルビン>2XULN
Definition of Dose-Limiting Toxicities In both the Phase Ia and Phase Ib portions of the study, if any one of the following events occurs during the DLT assessment window and is assessed by the Investigator to be related to study treatment: , DLT.
• Grade ≥3 non-hematologic, non-hepatic adverse events, with the following exceptions.
-
- Adverse event of
-
-
o Grade ≥4 neutropenia (absolute neutrophil count (ANC) <500/μL) lasting >7 days
- Grade ≥3 febrile neutropenia - Grade ≥4 anemia - Grade ≥4 thrombocytopenia or
• Grade ≥3 elevations in serum liver transaminase (ALT or AST) lasting >7 days Patients with
Grade ≥3 serum total bilirubin elevation ALT or AST >3X upper limit of normal (ULN) and total bilirubin >2XULN
用量漸増規則
登録は、試験の第Ia相部分で最初に開始する。チラゴルマブの開始用量は2mgであり、21日ごとにIV投与される。チラゴルマブの用量は、連続する用量レベル間で≦4倍増加し、チラゴルマブの評価のための提案されたおおよその用量レベルは、2mg、8mg、30mg、100mg、400mg、及び1200mgである。連続する用量レベル間の最大用量増加を減少させることができる。新興の非臨床有効性、臨床安全性、及び/又は臨床PKデータに基づいて、追加の中間用量レベルのチラゴルマブを評価することができる。
Dose Escalation Rule Enrollment will first begin in the Phase Ia portion of the study. The starting dose of tiragolumab is 2 mg administered IV every 21 days. The dose of tiragolumab increases ≤4-fold between successive dose levels, and the approximate dose levels proposed for the evaluation of tiragolumab are 2 mg, 8 mg, 30 mg, 100 mg, 400 mg, and 1200 mg. Maximum dose increments between successive dose levels can be decreased. Additional intermediate dose levels of tiragolumab can be evaluated based on emerging preclinical efficacy, clinical safety, and/or clinical PK data.
任意のDLTに加えて、他の利用可能な関連する人口統計学、有害事象、検査室、用量投与、PK(利用可能な場合)及び薬力学(利用可能な場合)データは、用量漸増決定の前に再検討され、用量漸増決定は、治験責任医師並びに安全科学者、統計学者、PK科学者及び/又は臨床試験マネージャから構成されるがこれらに限定されない委員会と協議してメディカルモニターによって行われる。 In addition to any DLT, other available relevant demographic, adverse event, laboratory, dosing, PK (if available) and pharmacodynamic (if available) data should be included in dose escalation decisions. Dose escalation decisions will be made by the medical monitor in consultation with the investigator and a committee consisting of, but not limited to, safety scientists, statisticians, PK scientists and/or clinical trial managers. will be
用量漸増は、以下に列挙する規則に従って行われる。
●最低3人の患者が各用量レベル(コホート)で登録される。
●最初の3人のDLT評価可能な患者のいずれもがDLT評定ウィンドウの間にDLTを経験しない場合、上記のように決定された増加した用量レベルでの次のコホートの登録を進めることができる。
●所与のコホートにおける最初の3人のDLT評価可能な患者のうちの1人がDLTを経験する場合、少なくとも3人のさらなる患者が同じ用量レベル(例えば、コホートを6人の患者に拡大する)で登録される。評価可能な患者の1/3未満がDLTを経験する場合(例えば、6人中<2人の患者)、用量漸増が継続し、増加した用量レベルでの次のコホートの登録が進行し得る。
●コホートにおける用量レベルあたりのDLT評価可能な患者の少なくとも1/3でDLTが観察された場合(例えば、6人中≧2人の患者)、MTDを超え、用量漸増を停止する。先のコホートは、6人の患者が既にそのレベルで評価されていない限り、最低6人の患者に拡大される。しかしながら、MTDを超える用量レベルが先行する用量レベルよりも≧2倍高い場合、6人の患者が中間用量レベルで評価され得る。
●任意の用量レベルでMTDを超える場合、DLT評価可能な患者の3分の1未満(すなわち、6人の患者のうち<2人)がDLTを経験する最高用量がMTDと宣言される。
●いかなる用量レベルでもMTDを超えなかった場合、この試験において投与された最高用量がMADと見なされる。
●MTDを超えないことが示されている任意の用量レベルは、サイクル1の後に起こる事象及び拡大コホートで観察された事象を含む非DLT有害事象の治験責任医師の評価に基づいて正当化される場合、拡大され得る。
Dose escalation is performed according to the rules listed below.
• A minimum of 3 patients will be enrolled at each dose level (cohort).
- If none of the first 3 DLT-evaluable patients experience a DLT during the DLT assessment window, then enrollment of the next cohort at the escalating dose level determined as above can proceed .
- If 1 of the first 3 DLT-evaluable patients in a given cohort experiences a DLT, at least 3 additional patients at the same dose level (e.g., expand the cohort to 6 patients) ). If less than ⅓ of evaluable patients experience DLT (eg, <2 patients out of 6), dose escalation will continue and enrollment of the next cohort at the increased dose level may proceed.
• DLT per dose level in a cohort If DLT is observed in at least ⅓ of evaluable patients (eg, ≧2 patients out of 6), MTD is exceeded and dose escalation is stopped. Prior cohorts will be expanded to a minimum of 6 patients unless 6 patients have already been evaluated at that level. However, 6 patients may be evaluated at the intermediate dose level if the dose level above the MTD is ≧2-fold higher than the preceding dose level.
• If the MTD is exceeded at any dose level, the highest dose at which less than one-third of DLT-evaluable patients (ie, <2 out of 6 patients) experience DLT is declared the MTD.
• If the MTD is not exceeded at any dose level, the highest dose administered in this study will be considered the MAD.
Any dose level shown not to exceed the MTD is justified based on the investigator's assessment of non-DLT adverse events, including events occurring after
利用可能な予備的リアルタイム安全性データ及び利用可能な予備的PKデータ(第Ia相及び/又は第Ib相試験のいずれかから収集される)の再検討に基づいて、第Ia相及び/又は第Ib相における用量漸増は、必要に応じて中止又は制限され得る。 Based on review of available preliminary real-time safety data and available preliminary PK data (collected from either Phase Ia and/or Phase Ib studies), Phase Ia and/or Dose escalation in Phase Ib may be stopped or limited as needed.
試験の第Ia相部分における最初の2つの投与コホートについてDLT評定が完了した後、安全性データが治験責任医師及びIMCによって再検討され、試験の第Ib相部分を活性化するかどうかが推奨される。第Ib相を活性化することが適切であると考えられる場合、次いで、試験の両方の部分で同時に登録を進めることができる。アテゾリズマブと組み合わせたチラゴルマブの開始用量は2mgであり、アテゾリズマブは1200mg IVの固定用量で投与され、両薬物は21日ごとに投与される。試験の第Ib相部分のチラゴルマブの用量は、試験の第Ia相部分のMTDを超えないことが示されている最高用量を決して超えない。試験の第Ib相部分のコホート1で組み合わせMTDを超える場合、アテゾリズマブと組み合わせて、より低用量のチラゴルマブを考慮してもよい。
After completing the DLT assessment for the first two dose cohorts in the Phase Ia portion of the study, safety data were reviewed by the investigator and the IMC to recommend whether to activate the Phase Ib portion of the study. be. If it is deemed appropriate to activate Phase Ib, then enrollment can proceed simultaneously in both parts of the trial. The starting dose of tiragolumab in combination with atezolizumab is 2 mg, with atezolizumab administered at a fixed dose of 1200 mg IV, both drugs administered every 21 days. The dose of tiragolumab in the Phase Ib portion of the study will never exceed the highest dose shown not to exceed the MTD in the Phase Ia portion of the study. Lower doses of tiragolumab may be considered in combination with atezolizumab if the combination MTD is exceeded in
さらなる安全性及び薬力学データを取得して、拡大コホートの用量選択をより完全に知らせるために、追加の患者を、上記の用量漸増基準に基づいてMTD又はMADを超えないことが示された試験の第Ia相部分及び/又は第Ib相部分の用量レベルで登録することができる。用量漸増決定の目的のために、これらの患者はDLT評価可能集団の一部とはみなされない。これらの患者は、安全にアクセス可能な腫瘍を有していなければならず、生検に同意しなければならない。薬力学の評定を知らせるために、スクリーニング又は事前スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1及び/又はTIGITを発現する腫瘍を有する患者が登録される。更に、用量拡大段階を開始する前に追加の安全性データを提供するために、最大約12人の追加の患者が、MTD又はMAD以下での第Ia相又は第Ib相試験において選択された用量レベルで登録され得る。 To obtain additional safety and pharmacodynamic data to more fully inform dose selection for the expansion cohort, additional patients were included in studies that were shown not to exceed the MTD or MAD based on the above dose escalation criteria. can be enrolled at dose levels for the Phase Ia portion and/or Phase Ib portion of For purposes of dose escalation decisions, these patients will not be considered part of the DLT evaluable population. These patients must have safely accessible tumors and consent to biopsy. Patients with tumors expressing PD-L1 and/or TIGIT based on prospective studies of tumor tissue during screening or pre-screening will be enrolled to inform the pharmacodynamic assessment. In addition, up to about 12 additional patients at the selected dose in the Phase Ia or Phase Ib study at or below the MTD or MAD to provide additional safety data before initiating the dose expansion phase level can be registered.
試験の第Ia相部分のみでは、放射線学的進行を発症した患者及び/又は単剤チラゴルマブから臨床的利益をもはや得ていない患者は、安全に入手可能な腫瘍を有し、生検に同意し、交差のための指定基準を満たすならば、試験の第Ib相部分で処置を受けるのに適格となり得る。 For the Phase Ia portion of the trial only, patients who developed radiographic progression and/or no longer receiving clinical benefit from single-agent tiragolumab had tumors that were safely available and consented to biopsy. , may be eligible to receive treatment in the Phase Ib portion of the trial if they meet the designated criteria for crossover.
第Ia相及び第Ib相のための拡大段階
利用可能な標準治療後に進行した局所進行性、再発性又は転移性の治癒不能な悪性腫瘍を有する患者;又は標準治療が無効若しくは忍容できないことが証明されているか、又は不適切であると考えられている患者;又は治験薬の臨床試験が認識された標準治療である場合には、試験の拡大コホートに登録される。試験の第Ib相部分のみについて、化学療法又は抗VEGF抗体を伴う又は伴わない抗PD-L1/PD-1抗体と組み合わせた治験薬の臨床試験が許容される処置選択肢と見なされる患者が、拡大コホートに登録され得る。
Expansion Phase for Phase Ia and Phase Ib Patients with locally advanced, recurrent, or metastatic incurable malignancies that have progressed after available standard therapy; Patients who are proven or considered unsuitable; or enrolled in a study expansion cohort if the clinical trial of the investigational drug is a recognized standard of care. For the Phase Ib portion of the study only, patients for whom clinical trials of an investigational drug in combination with anti-PD-L1/PD-1 antibodies with or without chemotherapy or anti-VEGF antibodies are considered an acceptable treatment option were expanded. be enrolled in a cohort.
この拡大段階は、特定のがん状況において、単剤として(第Ia相)、又はアテゾリズマブ、アテゾリズマブと化学療法、アテゾリズマブとベバシズマブ若しくはペンプロリズマブとの組み合わせで(第Ib相)チラゴルマブの安全性、忍容性、PK変動性、薬力学的活性、及び予備抗腫瘍活性をより良好に特性評価するための患者の定義されたコホートからなる。拡大コホートへの登録は、安全性、忍容性、PK、薬力学、及び抗腫瘍活性データの蓄積の評定に基づいて、単剤としてのチラゴルマブ(第Ia相)又はアテゾリズマブ、アテゾリズマブと化学療法、アテゾリズマブとベバシズマブ、若しくはペンブロリズマブ(第Ib相)と組み合わせたチラゴルマブのMAD又はMTD以下の選択された用量レベルで開始される。 This expansion phase will explore the safety, tolerability and efficacy of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab, atezolizumab plus chemotherapy, atezolizumab plus bevacizumab or penprolizumab (Phase Ib) in certain cancer settings. A defined cohort of patients to better characterize sex, PK variability, pharmacodynamic activity, and preliminary anti-tumor activity. Enrollment in the expansion cohort is based on assessment of safety, tolerability, PK, pharmacodynamics, and pooling anti-tumor activity data, with tiragolumab (Phase Ia) or atezolizumab as single agents, atezolizumab plus chemotherapy, Atezolizumab plus bevacizumab or tiragolumab in combination with pembrolizumab (Phase Ib) will be initiated at a selected dose level below the MAD or MTD.
試験の第Ia相部分では、最大約40人の患者が、NSCLC、RCC、TNBC、黒色腫、HNSCC、OC、GEJがんを含むGC、UBC、及びMSS又はMSI-LowであるCRCを含むCRCを含む、PD-L1選択及び/又はTIGIT選択の複数の腫瘍適応症の計画された拡大コホートに登録される。 In the Phase Ia portion of the study, up to about 40 patients will have NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC including GEJ cancer, UBC, and CRC including CRC that is MSS or MSI-Low. A planned expansion cohort of PD-L1-selected and/or TIGIT-selected multiple tumor indications, including
試験の第Ib相部分(化学療法なし)では、以下の計画された適応症特異的拡大コホートのそれぞれを含む、約20-40人の患者が複数の腫瘍適応症に登録され得る:
●NSCLC:がん免疫療法(CIT)未経験(例えば、抗PD-L1/PD-1による事前の処置なし)
●NSCLC:CIT処置(例えば、抗PD-L1/PD-1による事前の処置を含む)
●RCC
●TNBC
●黒色腫
●HNSCC
●OC
●GEJがんを含むGC
●UBC
●MSS又はMSI-LowであるCRCを含むCRC
●黒色腫、OC、RCC及びUBCを含む特定の腫瘍適応症の生検コホート
In the Phase Ib portion of the trial (no chemotherapy), approximately 20-40 patients may be enrolled in multiple tumor indications, including each of the following planned indication-specific expansion cohorts:
NSCLC: cancer immunotherapy (CIT) naïve (eg, no prior treatment with anti-PD-L1/PD-1)
- NSCLC: CIT treatment (eg, including prior treatment with anti-PD-L1/PD-1)
●RCC
● TNBC
●Melanoma ●HNSCC
●OC
● GC including GEJ cancer
●UBC
● CRC including CRC that is MSS or MSI-Low
- Biopsy cohorts for specific tumor indications including melanoma, OC, RCC and UBC
試験の第Ib相化学療法拡大部分では、約20-40人の患者が以下の計画された化学療法拡大コホート(図5参照)のそれぞれに登録され得る:
●コホートA:
-導入期-シスプラチン又はカルボプラチン及びペメトレキセドと組み合わせたアテゾリズマブ及びチラゴルマブ
-維持期-ペメトレキセドと組み合わせたアテゾリズマブ及びチラゴルマブ
●コホートB
-導入期-カルボプラチン及びパクリタキセルと組み合わせたアテゾリズマブ及びチラゴルマブ
-維持期-アテゾリズマブ及びチラゴルマブ
●コホートC:
-導入期-シスプラチン又はカルボプラチン及びエトポシドと組み合わせたアテゾリズマブ及びチラゴルマブ
-維持期-アテゾリズマブ及びチラゴルマブ
●コホートD:
-カペシタビンと組み合わせたアテゾリズマブ及びチラゴルマブ
In the Phase Ib chemotherapy expansion portion of the trial, approximately 20-40 patients may be enrolled in each of the following planned chemotherapy expansion cohorts (see Figure 5):
● Cohort A:
- Run-in - Atezolizumab and tiragolumab in combination with cisplatin or carboplatin and pemetrexed - Maintenance - Atezolizumab and tiragolumab in combination with pemetrexed Cohort B
- Induction phase - Atezolizumab and tiragolumab in combination with carboplatin and paclitaxel - Maintenance phase - Atezolizumab and tiragolumab Cohort C:
- Induction phase - Atezolizumab and tiragolumab in combination with cisplatin or carboplatin and etoposide - Maintenance phase - Atezolizumab and tiragolumab Cohort D:
- Atezolizumab and tiragolumab in combination with capecitabine
本試験の第Ib Q4W相用量拡大部分では、約20-40人の患者が計画されたコホート(図4を参照)に登録され得る。 Approximately 20-40 patients may be enrolled in the planned cohort (see Figure 4) in the Phase Ib Q4W dose expansion portion of the study.
試験の第Ib相非化学療法拡大部分では、約20-40人の患者が以下の計画された非化学療法拡大コホート(図6を参照)のそれぞれに登録され得る。
●コホートNC 1:
-ピラゴルマブ及びベバシズマブを伴うアテゾリズマブ
●コホートNC 2:
-チラゴルマブ及びペンブロリズマブ
In the Phase Ib non-chemo expansion portion of the trial, approximately 20-40 patients may be enrolled in each of the following planned non-chemo expansion cohorts (see Figure 6).
- Cohort NC 1:
- Atezolizumab with pyragolumab and bevacizumab Cohort NC 2:
- tiragolumab and pembrolizumab
抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされるCIT未経験患者のみが、試験の第Ib相部分の関連する拡大コホートへの登録に適格であると見なされる。そうでなければ、患者は、治験責任医師の裁量に基づいて、試験の第Ia相又は第Ib相部分の利用可能な拡大スロットに割り当てられる。 Only CIT-naive patients for whom clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are considered an acceptable treatment option will be considered eligible for enrollment in the relevant expansion cohort for the Phase Ib portion of the trial. Otherwise, patients will be assigned to an available expansion slot in the Phase Ia or Phase Ib portion of the study at the discretion of the Investigator.
用量漸増段階における患者の評価後に、単剤としてのチラゴルマブ(第Ia相)又はアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)の安全性プロファイルが完全には特性評価されない可能性があることを考えると、潜在的な有害事象又はそれらの発生の可能性の全てが、拡大コホートへの登録時に知られ得るわけではない。全ての利用可能な安全性データを継続的に評価して、試験した用量レベルの忍容性を評定する。潜在的な予想外の有害事象のリスクを更に軽減するために、IMCは、試験の第Ia相部分及び第Ib相部分の拡大コホートに登録された全ての患者からの安全性データを定期的に再検討し、患者の安全性に関連する試験実施に関する推奨を行う。グレード3若しくはグレード4の毒性又は拡大段階コホートで観察された他の許容できない毒性の頻度が、第Ia相又は第Ib相においてその用量レベルでMTDを超えたことを示唆する場合、その用量レベルでの集積は停止される。次いで、より低い用量レベルでの拡大段階への登録の再開が検討される。加えて、安全性、忍容性、PK又は薬力学データの蓄積により、拡大コホートにおける用量レベルが、単剤としてのチラゴルマブ(第Ia相)又はアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)の予備的抗腫瘍活性の評価に最適以下であることが示唆される場合、そのコホートに新しい患者を異なる用量レベルに登録することが考慮される。第Ia相又は第Ib相の拡大段階で試験された用量レベルは、第Ia相又は第Ib相のそれぞれの用量漸増段階でMTDを超えないことが示されている最高用量レベルを決して超えない。
Given that the safety profile of tiragolumab as a single agent (Phase Ia) or in combination with atezolizumab (Phase Ib) may not be fully characterized after evaluation of patients in the dose escalation phase, Not all potential adverse events or their likelihood of occurrence may be known at the time of enrollment in the expansion cohort. All available safety data are continually evaluated to assess tolerability of the dose levels tested. To further reduce the risk of potential unanticipated adverse events, the IMC will periodically review safety data from all patients enrolled in the expansion cohorts of the Phase Ia and Phase Ib portions of the study. Review and make recommendations for conducting studies relevant to patient safety. If the frequency of
第Ib相化学療法拡大コホート、第Ib相Q4W投与拡大コホート及び第Ib相非化学療法拡大コホートでは、各コホートの最初の3人の患者が安全性ランイン中に試験処置の1サイクルを全て完了した後、IMCは初期安全性も監視する(図7参照)。IMCは、そのコホートの最初の3人の患者の全ての安全性データを再検討して、試験処置が忍容性であるかどうかを決定し、患者が投薬を継続することを可能にするためのIMC及び治験責任医師によるリスクの許容可能な評定がある。試験処置が各コホートにおける安全性ランインにおいて忍容性であると考えられる場合、安全性についての中間解析まで、各コホートにおける同じ用量のチラゴルマブで登録を継続することができる。これは、安全性ランインの患者を含む約20人の患者が登録された後に起こる。 In the Phase Ib Chemo Expansion Cohort, Phase Ib Q4W Dose Expansion Cohort, and Phase Ib Non-Chemo Expansion Cohort, the first 3 patients in each cohort completed a full cycle of study treatment during the safety run-in. Later, the IMC also monitors initial safety (see Figure 7). The IMC will review all safety data for the first 3 patients in that cohort to determine if the study treatment was tolerable and to allow patients to continue dosing. There is an acceptable assessment of risk by the IMC and Investigator of the If study treatment is considered tolerable in the safety run-in in each cohort, enrollment can continue at the same dose of tiragolumab in each cohort until interim analysis for safety. This occurs after approximately 20 patients have been enrolled, including those in the safety run-in.
IMCはまた、各コホートの約20人の患者が最初の腫瘍評定を完了した後に中間解析を行うことによって、試験の第Ia相部分及び第Ib相部分の拡大コホートにおける有効性を監視する。治験責任医師ごとの抗腫瘍活動性及び/又は臨床的利益がその拡大コホートで検出されない場合、試験の治験責任医師と相談してIMCが決定して、登録を停止することができる。治験責任医師ごとの抗腫瘍活性及び/又は臨床的利益がその拡大コホートの患者で検出された場合、IMCは、約40人の患者に登録を継続することを可能にし得る。40人を超える評価可能な患者への拡大コホートの試料サイズの増加はない。連続生検に同意したが評価可能な試料を有していない患者は、各拡大コホートに登録される最大40人の評価可能な患者の一部として置き換えられる場合がある。
相Ia拡大コホート
The IMC will also monitor efficacy in the expansion cohorts of the Phase Ia and Phase Ib portions of the trial by conducting an interim analysis after approximately 20 patients in each cohort have completed initial tumor assessments. If anti-tumor activity and/or clinical benefit per investigator is not detected in its expansion cohort, enrollment may be terminated as determined by the IMC in consultation with the study investigator. If anti-tumor activity and/or clinical benefit per investigator is detected in patients in its expansion cohort, the IMC may allow approximately 40 patients to remain enrolled. There is no increase in sample size for expansion cohorts beyond 40 evaluable patients. Patients who consent to serial biopsies but do not have evaluable samples may be replaced as part of the maximum of 40 evaluable patients enrolled in each expansion cohort.
Phase Ia expansion cohort
第Ia相拡大コホートの目的は、安全性、忍容性、PK、及び予備的有効性データをより良好に特性評価すること、並びにその単一薬剤MTD又はMAD以下の用量レベルのチラゴルマブで処置された患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。このコホートは、PD-L1選択及び/又はTIGIT選択された腫瘍を有する約20-40人の患者からなる。登録は、最初は以下の腫瘍型の患者に限定される:NSCLC、RCC、TNBC、黒色腫、HNSCC、OC、GEJがんを含むGC、UBC、並びにMSS及びMSI-Lowを含むCRC。治験責任医師による抗腫瘍活性及び/又は臨床的利益が、この試験において他の腫瘍型を有する患者において観察される場合、登録は、他の適応症を含むように拡大及び/又は修正され得る。 The objective of the Phase Ia expansion cohort is to better characterize the safety, tolerability, PK, and preliminary efficacy data and to To explore potential tumor biomarkers of pharmacodynamic activity in patients with This cohort consists of approximately 20-40 patients with PD-L1-selected and/or TIGIT-selected tumors. Enrollment is initially limited to patients with the following tumor types: NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC including GEJ cancer, UBC, and CRC including MSS and MSI-Low. Enrollment may be expanded and/or modified to include other indications if anti-tumor activity and/or clinical benefit by the investigator is observed in patients with other tumor types in this study.
第Ia相のこのコホートに登録された患者の最大約半分は、安全にアクセス可能な腫瘍病変を有し、処置前及び処置中の生検(コアニードル、パンチ、鉗子、又は切除/切開)に同意しなければならない。このコホートの患者の約半分が十分な生存可能な腫瘍内容物を有する評価可能な連続生検を有することを確実にするために、追加の患者を登録することができる。 Up to about half of the patients enrolled in this cohort in Phase Ia had safely accessible tumor lesions and had pre- and intra-procedural biopsies (core needle, punch, forceps, or excision/incision). I have to agree. Additional patients can be enrolled to ensure that approximately half of the patients in this cohort have evaluable serial biopsies with adequate viable tumor content.
放射線学的進行を発症した患者及び/又はこの第Ia相拡大コホートにおいて単剤チラゴルマブから臨床的利益をもはや得ていない患者は、患者が安全にアクセス可能な腫瘍を有し、生検に同意し、クロスオーバーのための指定基準を満たすならば、クロスオーバーに適格であり得、試験の第Ib相部分(図8)で処置を受け得る。
相Ib適応症特異的拡大コホート
Patients who developed radiological progression and/or no longer receiving clinical benefit from single-agent tiragolumab in this Phase Ia expansion cohort must have a safely accessible tumor and consent to biopsy. , may be eligible for crossover and receive treatment in the Phase Ib portion of the study (FIG. 8) if they meet the specified criteria for crossover.
Phase Ib indication-specific expansion cohort
第Ib相適応症特異的拡大コホートの目的は、安全性、忍容性、PK及び予備的有効性データをより良好に特性評価すること、並びにアテゾリズマブと組み合わせたそのMTD又はMADに等しい又はそれ未満の用量レベルでのチラゴルマブで処置された特定のがんのタイプを有する患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。各適応症特異的拡大コホートは、最初に、スクリーニング又は予備スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1選択及び/又はTIGIT選択され、以下の腫瘍型を含む複数の腫瘍適応症を含む腫瘍を有する約20人までの患者を登録する。
●NSCLC:CIT未経験
●これらの患者は、抗PD-L1/PD-1及び/又は抗CTLA-4を含む事前のCIT(治験中又は承認済み)を受けたことがなく、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と考えられる場合にのみ登録され得る。
●NSCLC:CIT処置あり
これらの患者は、抗PD-L1/PD-1を含む事前のCIT(治験中又は承認済み)を受けている。
●TNBC
●RCC
●CRC
●胃がん(GC)、胃食道接合部(GEJ)がんを含む
●HNSCC
●UBC
●黒色腫
●OC
The aim of the Phase Ib indication-specific expansion cohort is to better characterize the safety, tolerability, PK and preliminary efficacy data and its MTD or MAD in combination with atezolizumab equal to or less than To explore potential tumor biomarkers of pharmacodynamic activity in patients with specific cancer types treated with tiragolumab at dose levels of . Each indication-specific expansion cohort is initially PD-L1-selected and/or TIGIT-selected based on prospective testing of tumor tissue during screening or prescreening and includes multiple tumor indications, including the following tumor types: Up to approximately 20 patients with tumors will be enrolled.
NSCLC: CIT-naive These patients had no prior CIT (investigational or approved) including anti-PD-L1/PD-1 and/or anti-CTLA-4 and had no anti-PD-L1 antibodies may be enrolled only if a clinical trial of an investigational drug in combination with is considered an acceptable treatment option.
• NSCLC: With CIT treatment These patients have received prior CIT (investigational or approved) including anti-PD-L1/PD-1.
● TNBC
● RCC
●CRC
● Including gastric cancer (GC) and gastroesophageal junction (GEJ) cancer ● HNSCC
●UBC
●Melanoma ●OC
20人の患者の登録後、IMCは、およそ40人の患者への登録を継続するために、治験責任医師によって評定された抗腫瘍活性及び/又は臨床的利益の証拠があるかどうかを決定するための中間解析を行うために会議を行う。 After enrollment of 20 patients, the IMC will determine whether there is evidence of anti-tumor activity and/or clinical benefit assessed by the investigator to continue enrollment in approximately 40 patients A meeting will be held to conduct an interim analysis for
第Ib相のこれらの適応症特異的拡大コホートのそれぞれに登録された患者の最大約半分は、安全にアクセス可能な腫瘍病変を有し、処置前及び処置中の生検(例えば、コアニードル、パンチ、鉗子、又は切除/切開生検)に同意しなければならない。このコホートの患者の約半分が十分な生存可能な腫瘍内容物を有する評価可能な連続生検を有することを確実にするために、追加の患者を登録することができる。 Up to about half of the patients enrolled in each of these indication-specific expansion cohorts in Phase Ib had safely accessible tumor lesions and were punch, forceps, or excisional/incisional biopsy). Additional patients can be enrolled to ensure that approximately half of the patients in this cohort have evaluable serial biopsies with adequate viable tumor content.
第Ib相連続生検拡大コホート
第Ib相連続生検拡大コホートの目的は、薬力学的活性の潜在的な腫瘍バイオマーカーを調査し、アテゾリズマブと組み合わせたMTD又はMAD以下の用量レベルのチラゴルマブで処置された特定のがんのタイプを有する患者における安全性、忍容性、PK、及び予備的有効性データをより良好に特性評価することである。コホートは、スクリーニング又は事前スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1選択及び/又はTIGIT選択され、以下の腫瘍型を含み得る腫瘍を有する約20-40人の患者からなる。
●黒色腫
●RCC
●OC
●UBC
Phase Ib Serial Biopsy Expansion Cohort The purpose of the Phase Ib serial biopsy expansion cohort is to investigate potential tumor biomarkers of pharmacodynamic activity and treatment with tiragolumab at dose levels below the MTD or MAD in combination with atezolizumab. To better characterize safety, tolerability, PK, and preliminary efficacy data in patients with specific cancer types that have been identified. The cohort consists of approximately 20-40 patients with tumors who are PD-L1-selected and/or TIGIT-selected based on prospective testing of tumor tissue during screening or pre-screening and may include the following tumor types.
●Melanoma ●RCC
●OC
●UBC
この連続生検拡大コホートに登録された患者は、2回の腫瘍生検を受ける必要があるため、安全にアクセス可能な腫瘍病変を有していなければならない:1)前処置生検:全ての適格基準(利用可能な保管組織の要件を除く)が満たされた後、試験薬の投与前のベースライン時、及び2)処置中生検:アテゾリズマブと組み合わせたチラゴルマブの初回投与後約2週間(サイクル1の15-21日目又はその間)。RECIST標的病変は生検の対象としない。
Patients enrolled in this serial biopsy expansion cohort must have safely accessible tumor lesions, as they will be required to undergo two tumor biopsies: 1) Pretreatment biopsies: all; After eligibility criteria (excluding the requirement of available archived tissue) are met, at baseline prior to administration of study drug, and 2) an in-treatment biopsy: approximately 2 weeks after the first dose of tiragolumab in combination with atezolizumab ( Days 15-21 of
組織生検方法は、コアニードル、パンチ、鉗子、又は切除/切開生検を含み得る。必要とされる新鮮な生検を提供する患者は、利用可能であれば保管腫瘍標本も提出しなければならない。 Tissue biopsy methods may include core needle, punch, forceps, or excisional/incisional biopsy. Patients who provide the required fresh biopsy must also submit an archival tumor specimen, if available.
この連続生検コホートでは、以下の状況下で、新鮮なベースライン生検の代わりに最近の保管検体を使用することができる。
●試料は試料基準を満たす(例えば、コアの数又はパンチのサイズ)。
●試験片は、提案されたサイクル1、1日目の3ヶ月以内、又はメディカルモニターによって承認された間隔内に収集した。
●検体は、最新の全身療法及び/又は関連する解剖学的領域に投与された任意の放射線療法の後に収集された。
●検体は、処置中の生検の提案された部位と同じ病変又は器官に由来する。
In this serial biopsy cohort, a recent archival specimen can be used in lieu of a fresh baseline biopsy under the following circumstances:
• The sample meets the sample criteria (eg number of cores or punch size).
• Specimens were collected within 3 months of proposed
• Specimens were collected after most recent systemic therapy and/or any radiotherapy administered to relevant anatomic regions.
• The specimen is from the same lesion or organ as the proposed site for biopsy during the procedure.
ベースライン生検が評価不可能であることが分かった患者(すなわち、試料中の不十分な材料又は腫瘍細胞の欠如に起因して)は、依然として試験処置を受けており、処置中の生検が検討される。そのような患者、並びに、処置中の生検が評価不可能であることが判明している患者、又は十分な生存腫瘍内容物を有しない生検を有する任意の患者は、連続生検評定の目的のために置き換えられる場合がある。追加の任意の生検は、治験責任医師の裁量で、患者の同意を得て、好ましくはX線写真の応答又は進行時に収集することができる。 Patients whose baseline biopsy was found to be non-evaluable (i.e., due to insufficient material or lack of tumor cells in the sample) were still receiving study treatment and had an in-treatment biopsy. is considered. Such patients, as well as those for whom an intraprocedural biopsy is found to be non-evaluable, or for any patient with a biopsy that does not have adequate viable tumor content, should be considered for serial biopsy evaluation. May be replaced for purposes. Additional optional biopsies may be collected at the investigator's discretion and with patient consent, preferably upon radiographic response or progression.
拡大コホートにおける任意の生検
拡大コホートに登録されている患者は、単剤又はアテゾリズマブと組み合わせたチラゴルマブの活性に関連する薬力学的変化を調べるために、任意の生検(例えば、コアニードル、パンチ、鉗子、又は切除/切開生検)を検討するように求められる。各拡大コホートの登録は、発生患者の約半分までが安全にアクセス可能な腫瘍病変を有し、これらの任意の生検を受けることに同意した患者であるように管理される。このシナリオの下で推奨される生検時点は上記と同じである:全ての適格基準(利用可能な保管組織の要件を除く)が満たされた後のベースライン、及びチラゴルマブの最初の投与から約2週間後(サイクル1の15-21日目又はその間)。
Optional Biopsies in the Expansion Cohort Patients enrolled in the expansion cohort may undergo an optional biopsy (e.g., core needle, punch) to investigate pharmacodynamic changes related to the activity of tiragolumab alone or in combination with atezolizumab. , forceps, or excisional/incisional biopsy) to be considered. Enrollment in each expansion cohort will be managed so that up to about half of the incident patients have safely accessible tumor lesions and consent to undergo any of these biopsies. Recommended biopsy time points under this scenario are the same as above: baseline after all eligibility criteria (except the requirement for available archived tissue) are met, and approximately from the first dose of tiragolumab. After 2 weeks (Days 15-21 of
ベースライン試料が評価不可能であり、比較のために最近の保管検体が利用できない場合、処置中の生検は必要ない。評価不可能なベースライン又は処置中の生検(すなわち、生検は生存腫瘍含有量が不十分である)を有する患者は、連続生検評定の目的で置き換えられる場合がある。 If the baseline sample is not evaluable and no recent archival specimen is available for comparison, no intraprocedural biopsy is required. Patients with non-evaluable baseline or on-treatment biopsies (ie, biopsies with insufficient viable tumor content) may be replaced for serial biopsy evaluation purposes.
任意のベースライン生検を提供する患者は、利用可能であれば、保管腫瘍標本も提出する。 Patients who provide any baseline biopsy will also submit an archival tumor specimen, if available.
第Ib相化学療法拡大コホート
第Ib相化学療法拡大コホートの目的は、安全性、忍容性、薬物動態及び予備的有効性データをより良好に特性評価し、アテゾリズマブ及び化学療法と組み合わせたチラゴルマブで処置された患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。
Phase Ib Chemotherapy Expansion Cohort The purpose of the Phase Ib Chemotherapy Expansion Cohort is to better characterize the safety, tolerability, pharmacokinetics and preliminary efficacy data for tiragolumab in combination with atezolizumab and chemotherapy. To explore potential tumor biomarkers of pharmacodynamic activity in treated patients.
各コホートは、スクリーニング又は事前スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1-選択及び/又はTIGIT選択され得る腫瘍を有する約20-40人の患者からなる。治験責任医師との議論に基づいてメディカルモニターがそうであると判断した場合、保管組織が不十分又は入手不可能な患者は、このコホートへの登録に適格であり得る。化学療法を伴う抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容される処置選択肢と見なされる腫瘍型の患者は、これらの拡大コホートに登録され得る。特定の腫瘍タイプ(例えば、NSCLC、SCLC、TNBC)を有する患者又は特定の処置歴(例えば、CITナイーブ)を有する患者の数は、各試験コホートにおいて限定され得る。 Each cohort consists of approximately 20-40 patients with tumors who may be PD-L1-selected and/or TIGIT-selected based on prospective testing of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archived tissue may be eligible for enrollment in this cohort if the medical monitor determines so based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational drugs in combination with anti-PD-L1 antibodies with chemotherapy are considered an acceptable treatment option may be enrolled in these expansion cohorts. The number of patients with a particular tumor type (eg, NSCLC, SCLC, TNBC) or with a particular treatment history (eg, CIT naive) may be limited in each study cohort.
各コホートにおける処置の組み合わせを表29に示す。

各コホートは、3人の患者(図5を参照)の初期安全性ランインを有する。コホート内の最初の3人の患者が21日間の試験処置(すなわち、サイクル1の1-21日目)を完了した後、IMCはそのコホートの全ての安全性データを再検討して試験処置が忍容性であるかどうかを判定し、患者がアテゾリズマブ及びチラゴルマブ及び化学療法の投与を継続することを可能にするためのIMC及び治験責任医師によるリスクの許容可能な評定がある。処置関連毒性以外の理由で最初の21日間の処置を完了しない患者は、同じ用量レベルで追加の患者に置き換えられる場合がある。最低3人の患者が登録し、21日間の試験処置を完了した後、IMCによるコホートの安全性ランインにおいて試験処置が許容されると考えられる場合、合計約20人の患者が登録されるまでそのコホートに登録を継続することができる。IMCは、安全性及び有効性を評価するために、各コホートの最初の約20人の患者の有効性データを再検討する。IMCが好ましい有益リスクがあると判定した場合、そのコホートへの登録は、合計約40人の患者まで継続することができる。 Each cohort has an initial safety run-in of 3 patients (see Figure 5). After the first 3 patients in a cohort have completed 21 days of study treatment (i.e., Days 1-21 of Cycle 1), the IMC will review all safety data for that cohort to ensure that study treatment is There is an acceptable assessment of risk by the IMC and investigator to determine if tolerability and allow patients to continue on atezolizumab and tiragolumab and chemotherapy. Patients who do not complete the first 21 days of treatment for reasons other than treatment-related toxicity may be replaced by additional patients at the same dose level. After a minimum of 3 patients have been enrolled and have completed 21 days of study treatment, if study treatment is considered acceptable in the cohort safety run-in by the IMC, it will continue until a total of approximately 20 patients have been enrolled. You can continue to enroll in the cohort. The IMC will review the efficacy data of approximately the first 20 patients in each cohort to assess safety and efficacy. Enrollment in the cohort may continue up to a total of approximately 40 patients if the IMC determines that there is a favorable benefit risk.
任意のコホートにおける安全性ランイン中に600mg用量のチラゴルマブが忍容されない場合、そのコホートに登録された3人以上の患者に対して、より低用量のチラゴルマブでの安全性ランインを開始することができる。この低用量グループの安全性データは、そのコホートの最初の3人の患者が21日間の試験処置(サイクル1の1-21日目)を完了した後に評価される。次いで、このより低い用量でのチラゴルマブの安全性及び忍容性を更に評定するために、安全性ランインにおける約3人のさらなる患者が登録される。チラゴルマブの用量のみを減少させることができる;アテゾリズマブの用量は変化しない。化学療法の用量調整は、必要に応じて、以下のガイドラインに従う:この低用量での試験処置が忍容される場合、低用量安全性ランイン中の患者を含む合計約20人の患者が各コホートに登録されるまで、登録は低用量で継続する。IMCは、安全性及び有効性を評価するために各コホートの20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクがあると判定した場合、そのコホートへの登録は、より低用量で合計約40人の患者まで継続することができる。 If the 600 mg dose of tiragolumab is not tolerated during the safety run-in in any cohort, a safety run-in with a lower dose of tiragolumab can be initiated for 3 or more patients enrolled in that cohort. . Safety data for this low dose group will be evaluated after the first 3 patients in the cohort have completed 21 days of study treatment (Days 1-21 of Cycle 1). Approximately 3 additional patients in the safety run-in will then be enrolled to further assess the safety and tolerability of tiragolumab at this lower dose. Only the tiragolumab dose can be decreased; the atezolizumab dose remains unchanged. Chemotherapy dose adjustments, if necessary, follow the guidelines: If study treatment at this low dose is tolerated, a total of approximately 20 patients, including those in the low-dose safety run-in, will be included in each cohort. Enrollment will continue at lower doses until enrolled in . The IMC will review data from 20 patients in each cohort to assess safety and efficacy. If the IMC determines there is a favorable benefit-risk, enrollment in that cohort may continue at lower doses, up to a total of approximately 40 patients.
安全性ランイン中にチラゴルマブの600mg用量が十分に忍容され、新たな臨床PKデータ(例えば、PKデータは化学療法と異なる)及び/又は薬力学データ(例えば、受容体占有)が、より高用量のチラゴルマブが使用されることを示唆する場合、各コホートに登録された次の3人の患者に対して、より高用量のチラゴルマブでの安全性ランインを開始する。このより高い用量は、この試験の第Ia相部分及び第Ib相部分の両方におけるMTG7192Aの最大評定用量である3週間ごとに1200mgを超えず、3週間ごとに1200mgの用量レベルで観察されたものよりも大きい最大濃度(Cmax)は観察されなかった。この高用量のチラゴルマブでの試験処置が許容される場合、最低6人の患者が登録し、21日間の試験処置を完了するまで、高用量での安全性ランインへの登録を継続する。この高用量での試験処置がIMCによる安全性ランインにおいて忍容可能であると考えられる場合、合計約20人の患者が各コホートに登録されるまで、この高用量のチラゴルマブで登録を継続することができる。IMCは、安全性及び有効性を評価するために各コホートの最初の20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクプロファイルがあると判断した場合、そのコホートへの登録は、より高用量で合計約40人の患者まで継続することができる。 The 600 mg dose of tiragolumab was well tolerated during the safety run-in, and new clinical PK data (e.g. PK data differing from chemotherapy) and/or pharmacodynamic data (e.g. receptor occupancy) supported higher doses. of tiragolumab will be used, initiate a safety run-in with the higher dose of tiragolumab for the next 3 patients enrolled in each cohort. This higher dose did not exceed the maximum rated dose of 1200 mg every 3 weeks for MTG7192A in both the Phase Ia and Ib portions of the study, which was observed at the dose level of 1200 mg every 3 weeks. No maximum concentration (C max ) greater than was observed. If study treatment at this high dose of tiragolumab is allowed, a minimum of 6 patients will be enrolled and will continue to be enrolled in the high dose safety run-in until they have completed 21 days of study treatment. If study treatment at this higher dose is deemed tolerable in the safety run-in by the IMC, continue enrollment at this higher dose of tiragolumab until a total of approximately 20 patients are enrolled in each cohort. can be done. The IMC will review data from the first 20 patients in each cohort to assess safety and efficacy. If the IMC determines there is a favorable benefit-risk profile, enrollment in that cohort may continue at higher doses up to a total of approximately 40 patients.
第Ib相化学療法拡大コホート:投薬及び投与
コホートA、B及びCの患者は、2つの相:導入期及び維持期で処置を受ける場合がある。導入期では、特定の化学療法拡大コホートの患者は以下を受ける:
●コホートAは、21日間サイクルの1日に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いてペメトレキセド500mg/m2 IV、続いてシスプラチン75mg/m2 IV、又は6mg/mL分 IVのカルボプラチンAUCを受ける。4~6サイクルの導入-期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
●コホートBは、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いてパクリタキセル200mg/m2 IV、続いて21日間サイクルの1日目に6mg/mL分 IV のカルボプラチンAUCを受ける。4~6サイクルの導入期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
●コホートCは、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いて、シスプラチン75mg/m2 IV、又は5mg/mL分 IVのカルボプラチンAUCを21日間サイクルの1日目に受け、次いで、エトポシド100mg/m2 IVを21日間サイクルの1-3日間目に受ける。4サイクルの導入期処置を、疾患進行又は許容できない毒性の非存在下で投与する。
Phase Ib Chemotherapy Expansion Cohort: Dosing and Administration Patients in Cohorts A, B and C may receive treatment in two phases: induction and maintenance. In the induction phase, patients in certain chemotherapy expansion cohorts receive:
Cohort A received atezolizumab 1200 mg IV, followed by
• Cohort B will receive atezolizumab 1200 mg IV, followed by
Cohort C received atezolizumab 1200 mg IV followed by
コホートA及びCの場合、シスプラチン又はカルボプラチンの選択が治験責任医師の決定であるが、特定の白金系化学療法剤を受ける患者の数は限定され得る。コホートA及びBの場合、導入期に投与されるサイクル数(4~6)が治験責任医師の決定である。 For Cohorts A and C, the choice of cisplatin or carboplatin is an investigator's decision, although the number of patients receiving a particular platinum-based chemotherapy agent may be limited. For Cohorts A and B, the number of cycles (4-6) administered in the run-in phase is at the investigator's discretion.
導入期の後、患者との潜在的なリスク及び利益の慎重な評定及び徹底的な議論の後に治験責任医師の裁量で、許容できない毒性、臨床的に説得力のある疾患の進行、及び/又は臨床的利益の不在下で、処置が維持期に継続され得る。 After the run-in period, unacceptable toxicity, clinically plausible disease progression, and/or at the investigator's discretion after careful assessment and thorough discussion of potential risks and benefits with the patient Treatment may be continued in the maintenance phase in the absence of clinical benefit.
維持期では、試験処置は、コホートA、治験実施計画書バージョン4に登録されたコホートB及びコホートDについてはQ 3 Wごとに継続するか、又は治験実施計画書バージョン5以降に登録されたコホートB及びコホートCについてはQ4Wごとに継続する。
In the maintenance phase, study treatment will continue every Q3W for Cohort A, Cohort B and Cohort D enrolled in
維持期では、特定の化学療法拡大コホートの患者は以下を受ける:
●コホートAは、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IV、続いてペメトレキセド500mg/m2 IVを-21日間サイクルごとの1日目に受ける。
●コホートBは、-28日間サイクルごとの1日目に、アテゾリズマブ1680mg IV、次いでチラゴルマブ840mg IVを受ける。患者がGO 30103バージョン4に登録された場合、コホートBの患者は、-21日間サイクルの1日目に、アテゾリズマブ1200mg IV、次いでチラゴルマブ600mg IVを受け続ける。
●コホートCは、-28日間サイクルごとの1日目に、アテゾリズマブ1680mg IV、次いでチラゴルマブ840mg IVを受ける。
In the maintenance phase, patients in certain chemotherapy expansion cohorts receive:
• Cohort A will receive atezolizumab 1200 mg IV followed by
• Cohort B will receive atezolizumab 1680 mg IV followed by tiragolumab 840 mg IV on
• Cohort C will receive atezolizumab 1680 mg IV followed by tiragolumab 840 mg IV on
コホートDの患者は、治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、カペシタビン、アテゾリズマブ、及びチラゴルマブによる処置を受ける。患者は、1250mg/m2 BIDの用量のカペシタビンを、各21日間サイクルの1日目~14日目に経口で受ける。サイクル1の1日目に、最初の用量のカペシタビンを、アテゾリズマブ及びチラゴルマブ注入の前に診療所で投与する。アテゾリズマブとチラゴルマブとの組み合わせは、21日間サイクルでIV注入によって投与される。
Patients in Cohort D receive treatment with capecitabine, atezolizumab, and tiragolumab until unacceptable toxicity or loss of clinical benefit as determined by the investigator. Patients receive a dose of 1250 mg/m 2 BID of capecitabine orally on days 1-14 of each 21-day cycle. On
毒性及び疾患の進行又は臨床的利益の喪失がない場合、個々の化学療法剤又は免疫療法剤を独立して中止することができる。しかしながら、アテゾリズマブ単独又はチラゴルマブ単独(化学療法を用いる又は用いない)による処置は、禁忌がなく、メディカルモニターとの議論の後にのみ考慮することができる。 Individual chemotherapeutic or immunotherapeutic agents can be discontinued independently in the absence of toxicity and disease progression or loss of clinical benefit. However, treatment with atezolizumab alone or tiragolumab alone (with or without chemotherapy) has no contraindications and can only be considered after discussion with a medical monitor.
第Ib相Q4W投与拡大コホート
第IbQ4W相用量拡大コホートの目的は、安全性、忍容性、PK及び予備的有効性データをより良好に特性評価すること、並びに4週間(28日;Q4W)ごとの投与スケジュールでアテゾリズマブ1680mg IVと組み合わせたチラゴルマブ840mg IVで処置された患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。
Phase Ib Q4W Dose Expansion Cohort The objectives of the Phase Ib Q4W dose expansion cohort are to better characterize safety, tolerability, PK and preliminary efficacy data, and every 4 weeks (28 days; Q4W). To explore potential tumor biomarkers of pharmacodynamic activity in patients treated with tiragolumab 840 mg IV in combination with atezolizumab 1680 mg IV on a dosing schedule of .
第Ib相Q4Wコホートは、スクリーニング又は事前スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1-選択及び/又はTIGIT選択され得る腫瘍を有する約20-40人の患者からなる。治験責任医師との議論に基づいてメディカルモニターがそうであると判断した場合、保管組織が不十分又は入手不可能な患者は、このコホートへの登録に適格であり得る。抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる腫瘍型の患者は、これらの拡大コホートに登録され得る。特定の腫瘍タイプ(例えば、NSCLC、SCLC)を有する患者又は特定の処置歴(例えば、CIT-ナイーブ)を有する患者の数は、各試験コホートにおいて限定され得る。 The Phase Ib Q4W cohort will consist of approximately 20-40 patients with tumors who may be PD-L1-selected and/or TIGIT-selected based on prospective testing of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archived tissue may be eligible for enrollment in this cohort if the medical monitor determines so based on discussion with the investigator. Patients with tumor types for which clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are considered an acceptable treatment option may be enrolled in these expansion cohorts. The number of patients with a particular tumor type (eg, NSCLC, SCLC) or with a particular treatment history (eg, CIT-naive) may be limited in each study cohort.
このコホートは、3人の患者(図4参照)の初期安全性ランインを有する。コホート内の最初の3人の患者が28日間の試験処置(すなわち、サイクル1の1-28日目)を完了した後、IMCはそのコホートの全ての安全性データを再検討して試験処置が忍容性であるかどうかを判定し、IMC及び治験責任医師によるリスクの許容可能な評定が存在して、患者がアテゾリズマブによるチラゴルマブの投与を継続することを可能にする。処置関連毒性以外の理由で最初の28日間の処置を完了しない患者は、同じ用量レベルで追加の患者に置き換えられる場合がある。最低3人の患者が登録し、28日間の試験処置を完了した後、IMCによるコホートの安全性ランインにおいて試験処置が許容されると考えられる場合、合計約20人の患者が登録されるまでそのコホートに登録を継続することができる。IMCは、安全性及び有効性を評価するために、各コホートの最初の約20人の患者の有効性データを再検討する。IMCが好ましい有益リスクがあると判定した場合、そのコホートへの登録は、合計約40人の患者まで継続することができる。 This cohort has an initial safety run-in of 3 patients (see Figure 4). After the first three patients in a cohort have completed 28 days of study treatment (i.e., Days 1-28 of Cycle 1), the IMC will review all safety data for that cohort to ensure that study treatment is Determined if tolerable, there is an acceptable assessment of risk by the IMC and investigator to allow the patient to continue on tiragolumab with atezolizumab. Patients who do not complete the first 28 days of treatment for reasons other than treatment-related toxicity may be replaced by additional patients at the same dose level. After a minimum of 3 patients have been enrolled and have completed 28 days of study treatment, if study treatment is considered acceptable in the cohort safety run-in by the IMC, it will continue until a total of approximately 20 patients have been enrolled. You can continue to enroll in the cohort. The IMC will review the efficacy data of approximately the first 20 patients in each cohort to assess safety and efficacy. Enrollment in the cohort may continue up to a total of approximately 40 patients if the IMC determines that there is a favorable benefit risk.
任意のコホートにおける安全性ランイン中に840mg用量のチラゴルマブが忍容されない場合、そのコホートに登録された3人以上の患者に対して、より低用量のチラゴルマブでの安全性ランインを開始することができる。この低用量グループの安全性データは、そのコホートの最初の3人の患者が28日間の試験処置(サイクル1の1-28日目)を完了した後に評価される。この低用量でのチラゴルマブの安全性及び忍容性を更に評定するために、およそ3人の追加の患者が安全性ランインに登録されることになる。チラゴルマブの用量のみを減少させることができる;アテゾリズマブの用量は変化しない。この低用量での試験処置が忍容される場合、低用量安全性ランイン中の患者を含む合計約20人の患者が各コホートに登録されるまで、登録は低用量で継続する。IMCは、安全性及び有効性を評価するために各コホートの20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクがあると判定した場合、そのコホートへの登録は、より低用量で合計約40人の患者まで継続することができる。 If the 840 mg dose of tiragolumab is not tolerated during the safety run-in in any cohort, a safety run-in with a lower dose of tiragolumab can be initiated for 3 or more patients enrolled in that cohort. . Safety data for this low dose group will be evaluated after the first 3 patients in the cohort have completed 28 days of study treatment (Days 1-28 of Cycle 1). Approximately three additional patients will be enrolled in the safety run-in to further evaluate the safety and tolerability of tiragolumab at this lower dose. Only the tiragolumab dose can be decreased; the atezolizumab dose remains unchanged. If study treatment at this lower dose is tolerated, enrollment will continue at the lower dose until a total of approximately 20 patients are enrolled in each cohort, including patients in the low-dose safety run-in. The IMC will review data from 20 patients in each cohort to assess safety and efficacy. If the IMC determines there is a favorable benefit-risk, enrollment in that cohort may continue at lower doses, up to a total of approximately 40 patients.
安全性ランイン中にチラゴルマブの840mg用量が十分に忍容され、新たな臨床PKデータ及び/又は薬力学データ(例えば、受容体占有)が、より高用量のチラゴルマブが使用されることを示唆する場合、各コホートに登録された次の3人の患者に対して、より高用量のチラゴルマブでの安全性ランインを開始する。このより高い用量は、この試験の第Ia相部分及び第Ib相部分の両方におけるMTG7192Aの最大評定用量である1200mgを超えず、3週間ごとに1200mgの用量レベルで観察されたものよりも大きい最大濃度(Cmaxは観察されなかった。この高用量のチラゴルマブでの試験処置が許容される場合、最低6人の患者が登録し、28日間の試験処置を完了するまで、高用量での安全性ランインへの登録を継続する。この高用量での試験処置がIMCによる安全性ランインにおいて忍容可能であると考えられる場合、合計約20人の患者が各コホートに登録されるまで、この高用量のチラゴルマブで登録を継続することができる。IMCは、安全性及び有効性を評価するために各コホートの最初の20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクがあると判定した場合、そのコホートへの登録は、より高用量で合計約40人の患者まで継続する。
第Ib相非化学療法拡大コホート
If the 840 mg dose of tiragolumab is well tolerated during the safety run-in and new clinical PK and/or pharmacodynamic data (e.g., receptor occupancy) suggest higher doses of tiragolumab are used , to initiate a safety run-in at the higher dose of tiragolumab for the next 3 patients enrolled in each cohort. This higher dose did not exceed the maximum rated dose of 1200 mg for MTG7192A in both the Phase Ia and Ib portions of the study, and did not exceed the maximum dose level observed at the 1200 mg every 3 weeks dose level. Concentration (C max was not observed. If study treatment at this high dose of tiragolumab is allowed, safety at the high dose will continue until a minimum of 6 patients are enrolled and complete 28 days of study treatment. Continue enrollment in run-in: If study treatment at this high dose is deemed tolerable in the safety run-in by the IMC, continue at this high dose until a total of approximately 20 patients are enrolled in each cohort. of tiragolumab can continue.The IMC will review data from the first 20 patients in each cohort to assess safety and efficacy.The IMC will determine favorable benefit-risk If so, enrollment in that cohort will continue at the higher doses to a total of approximately 40 patients.
Phase Ib non-chemotherapy expansion cohort
第Ib相非化学療法拡大コホートの目的は、安全性、忍容性、及び予備有効性データをより良好に特性評価し、ベバシズマブを伴うチラゴルマブ及びアテゾリズマブ、並びにペンブロリズマブと組み合わせたチラゴルマブで処置された患者における薬力学的活性の潜在的な腫瘍バイオマーカーを探索することである。 The objective of the Phase Ib non-chemotherapy expansion cohort was to better characterize the safety, tolerability, and preliminary efficacy data, patients treated with tiragolumab and atezolizumab with bevacizumab, and tiragolumab in combination with pembrolizumab To explore potential tumor biomarkers of pharmacodynamic activity in .
各コホートは、スクリーニング又は事前スクリーニング中の腫瘍組織の前向き試験に基づいてPD-L1-選択及び/又はTIGIT選択され得る腫瘍を有する約20-40人の患者からなる。治験責任医師との議論に基づいてメディカルモニターがそうであると判断した場合、保管組織が不十分又は入手不可能な患者は、このコホートへの登録に適格であり得る。治験責任医師の判断により、ベバシズマブを伴う又は伴わない抗PD-L1/PD-1と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる腫瘍型を有する患者は、これらの拡大コホートに登録され得る。特定の腫瘍型(例えば、HCC、メラノーマ)を有する患者又は特定の処置歴(例えば、CITナイーブ)を有する患者の数は、各試験コホートにおいて限定され得る。 Each cohort consists of approximately 20-40 patients with tumors who may be PD-L1-selected and/or TIGIT-selected based on prospective testing of tumor tissue during screening or prescreening. Patients with insufficient or unavailable archived tissue may be eligible for enrollment in this cohort if the medical monitor determines so based on discussion with the investigator. Patients with tumor types for which, at the investigator's discretion, a clinical trial of an investigational drug in combination with anti-PD-L1/PD-1 with or without bevacizumab would be considered an acceptable treatment option are included in these expansion cohorts. can be registered. The number of patients with a particular tumor type (eg HCC, melanoma) or with a particular treatment history (eg CIT naive) may be limited in each study cohort.
各コホートにおける処置の組み合わせを表30に示す。

各コホートは、約3人の患者(図6)の初期安全性ランインを有する。コホート内の最初の3人の患者が3週間(21日間)の試験処置(すなわち、サイクル1の1-21日目)を完了した後、IMCはそのコホートの全ての安全性データを再検討して、試験処置が忍容性であるかどうかを判定し、IMC及び治験責任医師によるリスクの許容可能な評定があり、患者がベバシズマブ(コホートNC 1)又はチラゴルマブ及びペンブロリズマブ(コホートNC 2)とのチラゴルマブ及びアテゾリズマブの投与を継続することを可能にする。処置関連毒性以外の理由で最初の3週間間の処置を完了しない患者は、同じ用量レベルで追加の患者に置き換えられる場合がある。最低3人の患者が登録し、3週間の試験処置を完了した後、IMCによるコホートの安全性ランインにおいて試験処置が許容されると考えられる場合、合計約20人の患者が登録されるまでそのコホートに登録を継続することができる。IMCは、安全性及び有効性を評価するために、各コホートの最初の約20人の患者の有効性データを再検討する。IMCが好ましい有益リスクがあると判定した場合、そのコホートへの登録は、合計約40人の患者まで継続することができる。 Each cohort has an initial safety run-in of approximately 3 patients (Figure 6). After the first 3 patients in a cohort have completed 3 weeks (21 days) of study treatment (i.e., Days 1-21 of Cycle 1), the IMC will review all safety data for that cohort. to determine if the study treatment was tolerable, with an acceptable assessment of risk by the IMC and investigator, and if patients were treated with bevacizumab (cohort NC 1) or tiragolumab and Tiragolumab and atezolizumab can be continued. Patients who do not complete the first 3 weeks of treatment for reasons other than treatment-related toxicity may be replaced by additional patients at the same dose level. After a minimum of 3 patients have been enrolled and have completed 3 weeks of study treatment, if study treatment is deemed acceptable in the cohort safety run-in by the IMC, it will continue until a total of approximately 20 patients have been enrolled. You can continue to enroll in the cohort. The IMC will review the efficacy data of approximately the first 20 patients in each cohort to assess safety and efficacy. Enrollment in the cohort may continue up to a total of approximately 40 patients if the IMC determines that there is a favorable benefit risk.
任意のコホートにおける安全性ランイン中に600mg用量のチラゴルマブが忍容されない場合、そのコホートに登録されたおよそ3人の患者に対して、より低用量のチラゴルマブでの安全性ランインを開始することができる。この低用量グループの安全性データは、そのコホートの最初の3人の患者が3週間の試験処置を完了した後(サイクル1の1-21日目)に評価される。次いで、このより低い用量でのチラゴルマブの安全性及び忍容性を更に評定するために、安全性ランインにおける約3人のさらなる患者が登録される。チラゴルマブの用量のみを減少させることができる;ベバシズマブとのペンブロリズマブ又はアテゾリズマブの用量は変化しない。この低用量での試験処置が忍容される場合、低用量安全性ランイン中の患者を含む合計約20人の患者が各コホートに登録されるまで、登録は低用量で継続する。IMCは、安全性及び有効性を評価するために各コホートの20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクがあると判定した場合、そのコホートへの登録は、より低用量で合計約40人の患者まで継続することができる。 If the 600 mg dose of tiragolumab is not tolerated during the safety run-in in any cohort, a safety run-in with a lower dose of tiragolumab can be initiated for approximately 3 patients enrolled in that cohort. . Safety data for this low dose group will be evaluated after the first 3 patients in the cohort have completed 3 weeks of study treatment (Days 1-21 of Cycle 1). Approximately 3 additional patients in the safety run-in will then be enrolled to further assess the safety and tolerability of tiragolumab at this lower dose. Only the dose of tiragolumab can be reduced; the dose of pembrolizumab or atezolizumab with bevacizumab remains unchanged. If study treatment at this lower dose is tolerated, enrollment will continue at the lower dose until a total of approximately 20 patients are enrolled in each cohort, including patients in the low-dose safety run-in. The IMC will review data from 20 patients in each cohort to assess safety and efficacy. If the IMC determines there is a favorable benefit-risk, enrollment in that cohort may continue at lower doses, up to a total of approximately 40 patients.
安全性ラン-イン中に600mg用量のチラゴルマブが十分に忍容される場合、各コホートに登録された次の約3人の患者に対して、より高用量のチラゴルマブでの安全性ランインを開始することができる。このより高い用量は、3週間毎に1200mgを超えず、これは、この試験の第Ia相部分及び第Ib相部分の両方におけるチラゴルマブの最大評定用量であり、観察された最大濃度(Cmax)は、3週間毎の用量レベルで1200mgで観察されたものより大きくはならない。この高用量のチラゴルマブでの試験処置が許容される場合、最低6人の患者が登録し、3週間の試験処置を完了するまで、高用量での安全性ランインへの登録を継続する。この高用量での試験処置がIMCによる安全性ランインにおいて忍容可能であると考えられる場合、合計約20人の患者が各コホートに登録されるまで、この高用量のチラゴルマブで登録を継続することができる。IMCは、安全性及び有効性を評価するために各コホートの最初の20人の患者のデータを再検討する。IMCが好ましいベネフィット-リスクプロファイルがあると判断した場合、そのコホートへの登録は、より高用量で合計約40人の患者まで継続することができる。 If the 600 mg dose of tiragolumab is well tolerated during the safety run-in, initiate a safety run-in with the higher dose of tiragolumab for approximately the next 3 patients enrolled in each cohort be able to. This higher dose did not exceed 1200 mg every 3 weeks, which was the maximum rated dose of tiragolumab in both the Phase Ia and Ib portions of the study, and the maximum concentration observed ( Cmax ). is no greater than that observed at the 1200 mg every 3 weeks dose level. If study treatment at this high dose of tiragolumab is allowed, a minimum of 6 patients will be enrolled and will continue to be enrolled in the high dose safety run-in until they have completed 3 weeks of study treatment. If study treatment at this higher dose is deemed tolerable in the safety run-in by the IMC, continue enrollment at this higher dose of tiragolumab until a total of approximately 20 patients are enrolled in each cohort. can be done. The IMC will review data from the first 20 patients in each cohort to assess safety and efficacy. If the IMC determines there is a favorable benefit-risk profile, enrollment in that cohort may continue at higher doses up to a total of approximately 40 patients.
チラゴルマブ及びアテゾリズマブ並びに他の非化学療法剤の用量減少
一般に、この試験では、チラゴルマブの用量減少はない。しかしながら、入手可能な累積安全性データが、単剤として最初に選択された(第Ia相)又はアテゾリズマブと組み合わせた(第Ib相)チラゴルマブの用量レベルがMTD又はMADを超えることを示唆している場合、その用量レベルでの集積は停止され得、適用可能であれば、さらなる用量漸増は停止される。
Dose Reductions of Tiragolumab and Atezolizumab and Other Non-Chemotherapeutic Agents In general, there were no dose reductions of tiragolumab in this study. However, available cumulative safety data suggest that dose levels of tiragolumab initially selected as single agent (Phase Ia) or in combination with atezolizumab (Phase Ib) exceed the MTD or MAD. If so, accumulation at that dose level can be stopped and, if applicable, further dose escalation is stopped.
この状況では、以下の基準を満たす場合、個々の患者は、新たな用量レベルのチラゴルマブへの用量減少の選択肢を有する。
●患者の最初に割り当てられた用量は、さらなる登録のために閉じられている用量レベルに等しい(又はそれより大きい)。
●全体的な利益/リスクバランスは、治験責任医師の意見では、第Ia相又は第Ib相での継続処置に有利である。
In this situation, individual patients have the option of dose reduction to a new dose level of tiragolumab if the following criteria are met:
• The patient's initially assigned dose is equal to (or greater than) the dose level that is closed for further enrollment.
• The overall benefit/risk balance favors continued treatment in Phase Ia or Phase Ib, in the investigator's opinion.
アテゾリズマブの場合、患者内用量の減少はない;アテゾリズマブは、21日ごとに1200mg又は28日ごとに1680mgの固定用量で投与されなければならない(Q4W投薬拡大コホート)。 For atezolizumab, there is no intra-patient dose reduction; atezolizumab must be administered at a fixed dose of 1200 mg every 21 days or 1680 mg every 28 days (Q4W dosing expansion cohort).
ベバシズマブについては、患者内用量の減少はない;ベバシズマブは15mg/kgの固定用量で3週間ごとに投与されることになる。 There will be no intra-patient dose reductions for bevacizumab; bevacizumab will be administered at a fixed dose of 15 mg/kg every 3 weeks.
ペンブロリズマブの場合、患者内用量の減少はない;ペンブロリズマブは、3週間ごとに200mgの固定用量で投与されることになる。 For pembrolizumab, there will be no intra-patient dose reduction; pembrolizumab will be administered at a fixed dose of 200 mg every 3 weeks.
疾患進行後の処置
進行性疾患に対する標準的なRECIST v 1.1基準が、メディカルモニターとの議論の後、治験責任医師の裁量で満たされた後、患者は試験の第Ia相又は第Ib相部分で試験処置を継続することができ、ただし、患者が以下の基準を満たす(図7を参照):
●疾患の明確な進行を示す症状及び徴候(検査値の悪化、例えば、新たな又は悪化する高カルシウム血症を含む)がないこと
●米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータスの低下がないこと
●反復投与の前に、治験実施計画書で許可された医学的介入によって容易に管理及び安定化することができない重要な解剖学的部位における腫瘍進行がないこと 重要な解剖学的部位には、CNS、中央気道、大血管、並びに腫瘍進行に次ぐ機能障害が重度及び/若しくは不可逆的な障害若しくは死亡を急性的にもたらすことが予想される他の器官又は組織が含まれる。
Treatment after disease progression After standard RECIST v 1.1 criteria for progressive disease have been met at the discretion of the Investigator after discussion with the medical monitor, patients will enter Phase Ia or Phase Ib of the study. Partial study treatment can be continued provided the patient meets the following criteria (see Figure 7):
Absence of symptoms and signs of definite disease progression (including worsening laboratory values, e.g., new or worsening hypercalcemia) Decreased US East Coast Cancer Clinical Trials Group (ECOG) performance status No tumor progression in critical anatomic sites that cannot be readily controlled and stabilized by protocol-approved medical intervention prior to repeat dosing It includes the CNS, central airways, great blood vessels, and other organs or tissues where dysfunction secondary to tumor progression is expected to acutely lead to severe and/or irreversible disability or death.
患者は、放射線学的進行を超えて試験処置を継続することのベネフィット-リスクバランスについて治療治験責任医師との議論を承認するために同意を与えなければならない。 Patients must give consent to authorize discussion with the treating investigator of the benefit-risk balance of continuing study treatment beyond radiological progression.
第Ia相又は第Ib相でのその後の腫瘍評定で放射線学的疾患の進行が確認された場合、以下の少なくとも1つによって証明されるように、患者が上記の基準を満たし続け、臨床的利益を継続している場合、治験責任医師の裁量で、メディカルモニターとの議論後に、継続した試験処置を検討することができる。
●1つ以上の評価可能な病変の腫瘍縮小(ベースラインからの直径の少なくとも30%の減少)
●治験責任医師が評定した、根底にあるがん(例えば、疼痛に対する麻薬の要求の減少、胸水に関連する呼吸困難の減少、体重増加)に起因する1つ以上の症状又は徴候の改善
If subsequent tumor assessment in Phase Ia or Phase Ib confirms radiological disease progression, the patient continues to meet the above criteria and clinical benefit as evidenced by at least one of the following: continued study treatment may be considered at the Investigator's discretion after discussion with the Medical Monitor.
- Tumor reduction (at least 30% reduction in diameter from baseline) of one or more evaluable lesions
Investigator-assessed improvement in one or more symptoms or signs attributed to the underlying cancer (e.g., decreased need for narcotics for pain, decreased dyspnea associated with pleural effusion, weight gain)
試験の第Ia相部分のみでは、進行性疾患を発症する及び/又は臨床的利益をもはや導出していない単剤チラゴルマブで処置された患者は、上に概説したように、患者が安全にアクセス可能な腫瘍を有し、生検に同意し、交差のための指定基準を満たすならば、アテゾリズマブと組み合わせたチラゴルマブによる試験の第Ib相部分での処置を受ける資格があり得る。 In the Phase Ia portion of the trial alone, patients treated with single-agent tiragolumab who developed progressive disease and/or no longer elicited clinical benefit were treated with safe access to the patient, as outlined above. Patients with tiragolumab in combination with atezolizumab may be eligible for treatment in the phase Ib portion of the trial if they have tumors of moderate size, consent to biopsy, and meet designated criteria for crossover.
化学療法拡大コホートA、B、C及びDでは、疾患進行後の処置は、化学療法を伴う又は伴わない免疫療法(アテゾリズマブ及び/又はチラゴルマブ)を含まなければならず、化学療法単独ではあり得ない。 In chemotherapy expansion cohorts A, B, C and D, treatment after disease progression must include immunotherapy (atezolizumab and/or tiragolumab) with or without chemotherapy and cannot be chemotherapy alone. .
進行時の単剤チラゴルマブ処置からチラゴルマブとアテゾリズマブとの組み合わせへのクロスオーバー
進行性疾患を発症する、及び/又は臨床的利益をもはや得ていない、試験の第Ia相部分の単剤としてのチラゴルマブで処置された患者は、以下の条件が満たされるならば、試験の第Ib相部分(図8参照)でアテゾリズマブと組み合わせたチラゴルマブによる処置を受けるのに適格であり得る。
●患者は、試験の第Ia相部分において、胸部、腹部及び骨盤のCTスキャンを含めて、X線写真で文書化された疾患進行を有していなければならない。
●患者は、チラゴルマブ処置の中止を必要とする毒性を経験していてはならず、第Ib相試験におけるチラゴルマブとアテゾリズマブとの組み合わせによる処置を妨げる試験処置の最後の投薬中に毒性を経験していてはならない。
●患者は、全ての選択基準及び除外基準を満たさなければならない。
●いかなるチラゴルマブ関連有害事象も、試験の第Ib相部分における処置の1日目又はそれ以前にグレード1≦又はベースライングレードに解消していなければならない。治験責任医師(複数可)による患者とのベネフィット-リスクバランスの慎重な評定及び議論の後、メディカルモニターの承認を得て、例外が許可されてもよい。
●単一薬剤のチラゴルマブでの進行後のチラゴルマブ及びアテゾリズマブによる処置は、治験責任医師(複数可)による患者との利益-リスクバランスの慎重な評定及び議論の後決定されるように、またメディカルモニターからの承認を得て許容可能とみなされなければならない。
Crossover from single agent tiragolumab treatment at progression to combination of tiragolumab and atezolizumab Developing progressive disease and/or no longer gaining clinical benefit with tiragolumab as single agent in the Phase Ia portion of the study Treated patients may be eligible to receive treatment with tiragolumab in combination with atezolizumab in the Phase Ib portion of the study (see Figure 8) if the following conditions are met.
• Patients must have radiographically documented disease progression, including CT scans of the chest, abdomen, and pelvis in the Phase Ia portion of the study.
- Patients must not have experienced toxicity requiring discontinuation of tiragolumab treatment and have experienced toxicity during the last dose of study treatment that would prevent treatment with the combination of tiragolumab and atezolizumab in a Phase Ib trial. must not.
• Patients must meet all inclusion and exclusion criteria.
• Any tiragolumab-related adverse event must resolve to
Treatment with tiragolumab and atezolizumab after progression on single-agent tiragolumab should be determined after careful assessment and discussion of the benefit-risk balance with the patient by the investigator(s) and by the medical monitor. shall be deemed acceptable with approval from
安全にアクセス可能な疾患部位(複数可)を有する患者には腫瘍生検が必要である。この生検は、第Ib相試験におけるチラゴルマブ及びアテゾリズマブの投与前の任意の時点で行われ得る。任意の処置中の生検はまた、チラゴルマブ及びアテゾリズマブの投与後のサイクル1の15-21日目又はその間に収集され得る。RECIST標的病変は生検対象としない。
Patients with safely accessible disease site(s) require a tumor biopsy. This biopsy can be performed at any time prior to administration of tiragolumab and atezolizumab in the Phase Ib trial. An optional in-treatment biopsy may also be collected on or during
第Ib相試験におけるアテゾリズマブと組み合わせたチラゴルマブによるクロスオーバー処置の用量及びスケジュールは、メディカルモニターの承認を必要とする。一般に、試験の第Ib相部分に参加した患者は、アテゾリズマブと組み合わせてそのMTDを超えないことが既に示されている最高用量でチラゴルマブを受ける(図7)。したがって、第Ib相試験で評価されるチラゴルマブの用量レベルは、第Ia相試験で同じ患者で評価される用量レベルとは異なる場合がある。第Ia相試験で単剤としてのチラゴルマブの用量及び/又はスケジュールに変更を受けた患者は、その用量のチラゴルマブがアテゾリズマブを伴うチラゴルマブのMTDを超えないことが以前に示されている限り、第Ib相で同じ用量及び/又はスケジュールでのチラゴルマブの投与を継続する。 The dose and schedule of crossover treatment with tiragolumab in combination with atezolizumab in the Phase Ib trial requires medical monitor approval. Generally, patients enrolled in the Phase Ib portion of the trial receive tiragolumab at the highest dose previously shown not to exceed its MTD in combination with atezolizumab (Figure 7). Therefore, the dose level of tiragolumab evaluated in the Phase Ib trial may differ from the dose level evaluated in the same patient in the Phase Ia trial. Patients undergoing a change in dose and/or schedule of tiragolumab as a single agent in a Phase Ia trial should be treated with a Phase Ib study as long as the dose of tiragolumab has not previously been shown to exceed the MTD of tiragolumab with atezolizumab. Continue administration of tiragolumab at the same dose and/or schedule in phases.
試験の第Ia相部分から試験の第Ib相部分にクロスオーバーする患者を以下のように処置する。
●第Ia相の試験処置中止来院時に得られた評定は、試験の第Ib相部分の併用処置のスクリーニング評定として使用することができる。ベースライン前処置の臨床的及び疾患状態を再確立するために、併用レジメンでの治療開始1日目の2週間以内に以下の再スクリーニング評定を繰り返さなければならない(標的化身体検査、ECOG状態、血液学及び血清化学検査室試験、凝固パネル、アミラーゼ、リパーゼ、甲状腺機能試験、及び尿分析)。
●B型肝炎、C型肝炎、HIV、サイトメガロウイルス(CMV)及びEBVのスクリーニング検査は、第Ia相試験のスクリーニング中に最後に実施されたため、これらの検査結果の陽性について臨床的疑いがない限り、繰り返す必要はない。
●胸部、腹部及び骨盤のCTスキャンを含む放射線腫瘍評定も、疾患進行を文書化するために既に行われていない限り、この評定が第Ib相試験に参加する患者の新しいベースラインスキャンになるため、第Ib相試験で併用処置を開始する1日前の6週間以内に行われなければならない。
●患者は、初回試験処置で進行性疾患、臨床的悪化、併用処置に対する不耐性、及び/又は併用処置からの臨床上の利益の喪失を文書化した腫瘍評定と比較して第2の疾患進行事象まで、第Ib相試験でチラゴルマブとアテゾリズマブの組み合わせで処置される。前述のように、進行性疾患に対する標準的なRECIST v1.1基準が、治験責任医師の裁量による第Ib相試験においてメディカルモニターとの議論後に満たされた後、患者は試験処置を継続することができ、規定された全ての基準を満たすことが提供される。
●クロスオーバー患者を安全性及び有効性について評価する。
Patients crossing over from the Phase Ia portion of the study to the Phase Ib portion of the study will be treated as follows.
• Ratings obtained at the Study Treatment Discontinuation Visit in Phase Ia can be used as screening endpoints for concomitant treatments in the Phase Ib portion of the study. To re-establish baseline pretreatment clinical and disease status, the following rescreening assessments must be repeated within 2 weeks of
There is no clinical suspicion of positive test results for hepatitis B, hepatitis C, HIV, cytomegalovirus (CMV), and EBV because they were last performed during screening of the Phase Ia trial As long as it doesn't need to be repeated.
- Radiation oncology assessment, including CT scans of the chest, abdomen, and pelvis, as this assessment will be the new baseline scan for patients entering the Phase Ib trial, unless it has also been previously performed to document disease progression. , within 6 weeks prior to commencing combination treatment in a Phase Ib study.
Patients had secondary disease progression compared to tumor assessment documenting progressive disease, clinical deterioration, intolerance to concomitant treatment, and/or loss of clinical benefit from concomitant treatment at initial study treatment Until event, treated with a combination of tiragolumab and atezolizumab in a Phase Ib trial. As previously described, patients may continue study treatment after standard RECIST v1.1 criteria for progressive disease have been met after discussion with the medical monitor in a Phase Ib study at the discretion of the investigator. provided that it can and meets all the specified criteria.
• Evaluate crossover patients for safety and efficacy.
第Ia相から第Ib相へのクロスオーバー処置の前に得られた腫瘍生検から得られた臨床データ及び探索的データを継続的に監視する。 Clinical and exploratory data from tumor biopsies obtained prior to crossover treatment from Phase Ia to Phase Ib will be monitored continuously.
第Ia相部分からの第Ib相試験への交差登録は、いつでも制限又は中断することができる。この理由には、安全性、不十分な患者登録、及び/又は不完全なデータ記録が含まれ得る。 Cross-enrollment from the Phase Ia portion to Phase Ib trials may be restricted or suspended at any time. Reasons for this may include safety, inadequate patient enrollment, and/or incomplete data recording.
A.試験処置
投薬及び投与
単剤としてのチラゴルマブ(第Ia相)又はアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)の投与は、救急医療施設を備え、救命救急ユニット及び医療緊急事態を監視し、それに対応するように訓練されたスタッフにアクセスできる環境で行われる。
A. Study Treatment Dosing and Administration Administration of tiragolumab (Phase Ia) as a single agent or in combination with atezolizumab (Phase Ib) should be provided with critical care facilities, critical care units and medical emergencies to monitor and respond to. conducted in an environment accessible to staff trained to
試験の第Ib相部分(化学療法なしのコホート)での治療のために、試験処置注入予定日に、観察期間を挟んで、チラゴルマブをアテゾリズマブの前に投与する。 For treatments in the Phase Ib portion of the study (the chemotherapy-free cohort), tiragolumab is administered prior to atezolizumab, with an observation period in between, on the scheduled study treatment infusion days.
第Ib相化学療法拡大コホートでの処置のために、試験処置注入の予定日に、アテゾリズマブを、観察期間を挟んで、チラゴルマブの前に投与する。化学療法は、アテゾリズマブ及びチラゴルマブの後に投与され、チラゴルマブの観察期間が介在する。 For treatment in the Phase Ib chemotherapy expansion cohort, atezolizumab will be administered prior to tiragolumab with an observation period on the scheduled day of study treatment infusion. Chemotherapy is administered after atezolizumab and tiragolumab, with an intervening observation period for tiragolumab.
第Ib相非化学療法拡大コホートにおける処置のために、予定された試験処置注入の日に、チラゴルマブは、ベバシズマブを伴うアテゾリズマブ(コホートNC 1)又はペンブロリズマブ(コホートNC 2)の前に投与され、観察期間が介在する。ベバシズマブは、ベバシズマブの観察期間を挟んで、チラゴルマブ及びアテゾリズマブの後に投与される。 For treatment in the Phase Ib non-chemotherapy expansion cohort, on the day of scheduled study treatment infusion, tiragolumab was administered prior to atezolizumab (cohort NC 1) or pembrolizumab (cohort NC 2) with bevacizumab and observed. A period intervenes. Bevacizumab is administered after tiragolumab and atezolizumab with an observation period for bevacizumab.
チラゴルマブ、アテゾリズマブ、又はベバシズマブの用量調製及び投与指示の詳細については、それぞれの治験責任医師のパンフレット及びGO 30103治験薬管理手順書を参照されたい。 Please refer to the respective Investigator's brochure and GO 30103 Investigational Product Management Protocol for details on dosage preparation and dosing instructions for tiragolumab, atezolizumab, or bevacizumab.
シスプラチン、カルボプラチン、ペメトレキセド、パクリタキセル、カペシタビン、エトポシド及びペンブロリズマブについての用量調製及び投与説明書の詳細については、添付文書又はSmPCを参照されたい。 See package inserts or SmPC for detailed dosage preparation and dosing instructions for cisplatin, carboplatin, pemetrexed, paclitaxel, capecitabine, etoposide, and pembrolizumab.
第Ia相及び第Ib相のチラゴルマブ
この試験の第Ia相部分及び第Ib相部分で評価されるチラゴルマブのおおよその用量レベルは、IV注入によって3週間ごとに投与される2mg、8mg、30mg、100mg、400mg、及び1200mgである。第Ia相若しくは第Ib相のMTDを超えない他の用量レベル、又は第Ia相及び/若しくは第Ib相のチラゴルマブの新しい投与スケジュールは、参加治験責任医師と相談した後、新しい非臨床有効性、臨床安全性、及び臨床PKデータに基づいて評価され得る。チラゴルマブ1200mgを超える用量レベルの評価には、裏付けとなる理論的根拠を伴う治験実施計画書の修正が必要である。第Ib相化学療法及び非化学療法拡大コホートの場合、チラゴルマブ600mgは、IV注入によって3週間ごとに投与される初期用量である。Q4W維持を伴う第Ib相化学療法コホートB及びコホートCの場合、チラゴルマブ用量は維持時に840mgに変更される。第Ib相Q4W投与コホートの場合、840mgのチラゴルマブが、IV注入によってQ4Wで投与される初期用量である。用量は体重に依存しない。
Tiragolumab in Phase Ia and Phase Ib Approximate dose levels of tiragolumab evaluated in the Phase Ia and Ib portions of this study are 2 mg, 8 mg, 30 mg, 100 mg administered every 3 weeks by IV infusion , 400 mg, and 1200 mg. Other dose levels that do not exceed the Phase Ia or Phase Ib MTD, or new dosing schedules for Phase Ia and/or Phase Ib tiragolumab, are subject to new nonclinical efficacy, It can be evaluated based on clinical safety and clinical PK data. Evaluation of dose levels above 1200 mg of tiragolumab will require a protocol amendment with a supporting rationale. For Phase Ib chemotherapy and non-chemotherapy expansion cohorts, tiragolumab 600 mg is the initial dose given every 3 weeks by IV infusion. For Phase Ib chemotherapy Cohort B and Cohort C with Q4W maintenance, the tiragolumab dose is changed to 840 mg at maintenance. For the Phase Ib Q4W dose cohort, 840 mg of tiragolumab is the initial dose administered Q4W by IV infusion. Dosage is independent of body weight.
840mgのQ4Wの投薬レジメンは、PKモデリング及びシミュレーション並びに曝露-安全性分析の結果によって裏付けられる。840mg Q4W投薬レジメン後の平均濃度は、GO30103試験及びGO40290試験で評価された3週間ごとの600mg投薬レジメンの平均濃度に匹敵する。840mg Q4W投薬レジメンのCmaxは、3週間ごとの600mgの投薬レジメンのCmaxと比較して定常状態で28%高いが、診療所で観察される最高投与量の曝露の範囲内である(GO30103試験では3週間ごとに1200mg)。試験GO 30103からのデータ(単剤療法として、又は3週間ごとに1200mgのアテゾリズマブと組み合わせて投与された、3週間ごとに2-1200mgのチラゴルマブ用量)に基づくチラゴルマブの曝露-安全性関係の予備的分析は、チラゴルマブが平坦な曝露-安全性関係を示すことを示唆している。要約すると、曝露が観察された有効な曝露の範囲内であり、チラゴルマブが曝露-安全関係が平坦であると思われることを考慮すると、840mg 4W投薬レジメンは、600mgの3週間ごとの投薬レジメンと同等の安全性及び有効性を有する。
The 840 mg Q4W dosing regimen is supported by the results of PK modeling and simulation and exposure-safety analysis. Mean concentrations following the 840 mg Q4W dosing regimen are comparable to those of the 600 mg every 3 weeks dosing regimen evaluated in studies GO30103 and GO40290. The Cmax for the 840 mg Q4W dosing regimen was 28% higher at steady state compared to the Cmax for the 600 mg every 3 weeks dosing regimen, but within the highest dose exposure observed in the clinic (in
試験の第Ia相のチラゴルマブの初回用量を90(±10)分かけて送達し(ただし、注入に関連する症状を経験する患者では注入を減速又は中断してもよい)、続いて240分間観察する。試験の第Ib相におけるチラゴルマブの初回用量を60(±10)分にわたって送達し、続いて60分間の観察期間を設ける。注入関連有害事象なしに初回注入が忍容される場合、第Ia相の2回目の注入を60(±10)分にわたって送達し、続いて60分間の観察期間を設けてもよく、第Ib相の2回目の注入を30(±10)分にわたって送達し、続いて30分間の観察期間を設けてもよい。第Ia相の60分間の注入が十分に忍容される場合、第Ia相の3回目の注入は、30(±10)分間にわたって送達され得、その後、30分間の観察期間が続く。第Ia相での3回目の注入又は第Ib相での2回目の注入が十分に許容される場合、第Ia相又は第Ib相でのその後の注入は全て、30(±10)分にわたって送達され、その後、30分間の観察期間が続く。以前に第Ia相で単剤のチラゴルマブを受けており、現在は第Ib相でアテゾリズマブと組み合わせてチラゴルマブを投与されている患者は、以前に忍容された最も速い速度で第Ib相で初回用量を受けることができる。 The initial dose of tiragolumab in Phase Ia of the study will be delivered over 90 (±10) minutes (although infusion may be slowed or interrupted in patients experiencing infusion-related symptoms) followed by 240 minutes of observation. do. The initial dose of tiragolumab in Phase Ib of the study is delivered over 60 (±10) minutes, followed by a 60 minute observation period. If the first infusion is tolerated without infusion-related adverse events, a second infusion of Phase Ia may be delivered over 60 (±10) minutes followed by a 60 minute observation period; A second infusion of is delivered over 30 (±10) minutes, followed by a 30 minute observation period. If the 60-minute infusion of Phase Ia is well tolerated, the third infusion of Phase Ia can be delivered over 30 (±10) minutes, followed by a 30-minute observation period. If the third infusion in Phase Ia or the second infusion in Phase Ib is well tolerated, all subsequent infusions in Phase Ia or Phase Ib will be delivered over 30 (±10) minutes followed by a 30 minute observation period. Patients previously receiving single-agent tiragolumab in Phase Ia and currently receiving tiragolumab in combination with atezolizumab in Phase Ib will receive the first dose in Phase Ib at the fastest rate previously tolerated. can receive
明記されている場合を除き、この試験(第Ia相又は第Ib相)では、チラゴルマブの用量減少はない。チラゴルマブの投与量の変更及び処置の中断又は中止のためのガイドラインが提供される。特定の有害事象の管理との関連での試験薬物投与に関するガイダンスが提供される。 There will be no dose reductions of tiragolumab in this study (Phase Ia or Phase Ib) unless specified. Guidelines for modifying the dose of tiragolumab and interrupting or discontinuing treatment are provided. Guidance is provided regarding study drug administration in the context of managing specific adverse events.
試験薬の過剰投与又は誤った投与に関連する有害事象を記録する。 Adverse events related to overdose or misadministration of study drug will be recorded.
第Ib相のアテゾリズマブ
この試験の第Ib相部分でチラゴルマブと組み合わせて投与されるアテゾリズマブの用量は、3週間ごとに1200mg IVである。Q4Wの維持を伴う第Ib相化学療法コホートB及びコホートCの場合、アテゾリズマブ用量は維持時に1680mgに変更される。第Ib相Q4W投薬コホートでは、アテゾリズマブ1680mg IV Q4Wが投与される。この用量は固定されており、体重に依存しない。
Atezolizumab in Phase Ib The dose of atezolizumab administered in combination with tiragolumab in the Phase Ib portion of this study is 1200 mg IV every 3 weeks. For Phase Ib chemotherapy Cohort B and Cohort C with Q4W maintenance, the atezolizumab dose is changed to 1680 mg at maintenance. The Phase Ib Q4W dosing cohort will receive atezolizumab 1680 mg IV Q4W. This dose is fixed and independent of body weight.
化学療法を用いない全ての第Ib相コホートにおいて、アテゾリズマブは、チラゴルマブ注入及びその後の観察期間の後に投与される。第Ib相化学療法拡大コホートでは、アテゾリズマブは、チラゴルマブの前に投与される。 In all Phase Ib cohorts without chemotherapy, atezolizumab will be administered after tiragolumab infusion and a subsequent observation period. Atezolizumab is administered prior to tiragolumab in the Phase Ib chemotherapy expansion cohort.
アテゾリズマブの初回用量は60(±10)分かけて送達される。注入に関連する有害事象なしに1回目の注入が許容される場合、2回目の注入は30(±10)分かけて送達され得る。30分間の注入が十分に許容される場合、その後の注入は全て30(±10)分かけて送達され得る。サイクル1では、アテゾリズマブの投与後、60分間の観察期間が続く。その後の全てのアテゾリズマブ注入の後に、30分間の観察期間を設けてもよい。別の臨床試験で以前にアテゾリズマブを受けたことがある患者は、以前に忍容された最も速い速度で初期用量を受けることができる。
The initial dose of atezolizumab is delivered over 60 (±10) minutes. If the first infusion is tolerated without infusion-related adverse events, the second infusion may be delivered over 30 (±10) minutes. If a 30 minute infusion is well tolerated, all subsequent infusions may be delivered over 30 (±10) minutes. In
この試験では、アテゾリズマブの用量減少はない。投与量の変更及び処置の中断又は中止のためのガイドラインが提供される。特定の有害事象の管理との関連での試験薬物投与に関するガイダンスが提供される。 There were no dose reductions of atezolizumab in this trial. Guidelines are provided for modifying dosage and interrupting or discontinuing treatment. Guidance is provided regarding study drug administration in the context of managing specific adverse events.
試験薬の過剰投与又は誤った投与に関連する有害事象を記録する。 Adverse events related to overdose or misadministration of study drug will be recorded.
第Ib相拡大における非化学療法コホート
コホートNC1:ベバシズマブを伴うチラゴルマブ及びアテゾリズマブ
チラゴルマブ及びアテゾリズマブ及びベバシズマブコホートの患者は、統合評定後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、表31に概説される処置を受ける。登録後7日以内に治療を開始することが推奨される;しかし、試験処置の最初の用量は、コア生検又は他の外科的処置後7日以内に行われるべきではない。

コホートNC2:チラゴルマブ及びペンブロリズマブ
チラゴルマブ及びペンブロリズマブコホートの患者は、統合評定後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、表32に概説される処置を受ける。登録後7日以内に治療を開始することが推奨される;しかし、試験処置の最初の用量は、コア生検又は他の外科的処置後7日以内に行われるべきではない。

第Ib相非化学療法拡大コホート:投薬及び投与
コホートNC1の患者は、3週間ごとのサイクルの1日目に、チラゴルマブ600mg IV、次いでアテゾリズマブ1200mg IV、次いでベバシズマブ15mg/kg IV受ける。治験責任医師が決定した許容できない毒性又は臨床的利益の喪失まで処置を行う。
Phase Ib Non-Chemotherapy Expansion Cohort: Dosing and Administration Patients in cohort NC1 receive
コホートNC 2の患者は、3週間ごとのサイクルの1日目に、チラゴルマブ600mg IV、次いでペンブロリズマブ200mg IVを受ける 治験責任医師が決定した許容できない毒性又は臨床的利益の喪失まで処置を行う。
Patients in Cohort NC 2 will receive
毒性及び臨床的利益の喪失の場合、個々の免疫療法剤を独立して中止することができる。しかしながら、ペムブロリズマブ若しくはベバシズマブ若しくはアテゾリズマブ若しくはチラゴルマブ単独による処置は、禁忌がなく、メディカルモニターとの議論後にのみ考慮することができる。 In the event of toxicity and loss of clinical benefit, individual immunotherapeutic agents can be discontinued independently. However, treatment with pembrolizumab or bevacizumab or atezolizumab or tiragolumab alone has no contraindications and can only be considered after discussion with a medical monitor.
第Ib相拡大コホートにおけるベバシズマブ
ベバシズマブは、各21日間サイクルの1日目に15mg/kgの固定用量でIV注入によって投与される。ベバシズマブの投与は、訓練された人員並びに潜在的に重篤な反応を管理するための適切な機器及び薬剤に直ちにアクセスできる監視された設定で行われる。毒性のための投薬量の変更及び処置の中断又は中止のためのガイドラインが提供される。
Bevacizumab in Phase Ib Expansion Cohort Bevacizumab will be administered by IV infusion at a fixed dose of 15 mg/kg on
最初のベバシズマブ注入の前に前投薬は許可されない。患者が以前の薬物注入でIRRを経験した場合、抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬を治験責任医師の裁量で投与することができる。バイタルサイン(脈拍数、呼吸数、血圧、体温)を注入前の60分以内に測定する。ベバシズマブの初期用量は90(±10)分かけて送達される。注入に関連する有害事象なしに1回目の注入が許容される場合、2回目の注入は60(±10)分かけて送達され得る。60分間の注入が十分に許容される場合、その後の注入は全て30(±10)分かけて送達され得る。サイクル1では、ベバシズマブの投与の後に60分間の観察期間が続く。ベバシズマブの全てのその後の注入の後に30分間の観察期間が続く場合がある。以前にベバシズマブを受けたことがある患者は、以前に忍容された最も速い速度で初期用量を受けることができる。患者は、注入後の症状の遅延の可能性について知らされ、そのような症状を発症した場合、試験医師に連絡するように指示される。生体情報測定に関する指示が提供される。
No premedication is allowed before the first bevacizumab infusion. If a patient has experienced IRR with previous drug infusions, premedication with antihistamines, antipyretics, and/or analgesics can be administered at the investigator's discretion. Vital signs (pulse rate, respiratory rate, blood pressure, temperature) are measured within 60 minutes prior to infusion. The initial dose of bevacizumab is delivered over 90 (±10) minutes. If the first infusion is tolerated without infusion-related adverse events, the second infusion may be delivered over 60 (±10) minutes. If a 60 minute infusion is well tolerated, all subsequent infusions may be delivered over 30 (±10) minutes. In
第Ib相拡大コホートにおけるペンブロリズマブ
本試験の第Ib相非化学療法拡大コホートにおいて、チラゴルマブと組み合わせて投与されるペンブロリズマブの用量は、3週間ごとに200mg IVである。この用量は固定されており、体重に依存しない。
Pembrolizumab in the Phase Ib Expansion Cohort In the Phase Ib non-chemotherapy expansion cohort of this study, the dose of pembrolizumab administered in combination with tiragolumab is 200 mg IV every 3 weeks. This dose is fixed and independent of body weight.
ペンブロリズマブの用量調製、保存、投与、及び処置の中断又は中止の指示のガイダンスについては、ペンブロリズマブ処方情報を参照されたい。 Refer to the pembrolizumab prescribing information for guidance on dosing, storage, administration, and instructions for interrupting or discontinuing treatment of pembrolizumab.
第Ib相拡大コホートにおける化学療法
化学療法(カペシタビンを除く)は、アテゾリズマブ及びチラゴルマブ注入及びその後の観察期間の後に投与される。
Chemotherapy in Phase Ib Expansion Cohort Chemotherapy (excluding capecitabine) will be administered after atezolizumab and tiragolumab infusion followed by an observation period.
導入期の間、化学療法サイクルは、少なくとも1つの化学療法成分が21日間のサイクルの間に少なくとも1回投与されている限り、予め指定された数の導入化学療法サイクルに向かってカウントする。化学療法成分が投与されないサイクルは、導入化学療法サイクルの総数にカウントされない。 During the induction phase, chemotherapy cycles count toward the prespecified number of induction chemotherapy cycles as long as at least one chemotherapy component has been administered at least once during the 21-day cycle. Cycles in which no chemotherapy component is administered are not counted in the total number of induction chemotherapy cycles.
治療(導入又は維持)中、臨床的利益の証拠を示す患者は、PDのRECIST v 1.1基準が満たされた後、処置を継続することが許可される。 Patients who demonstrate evidence of clinical benefit during treatment (induction or maintenance) will be allowed to continue treatment after RECIST v 1.1 criteria for PD are met.
患者は、現地の標準治療及び製造業者の指示に従って、化学療法剤の制吐剤及びIV水分補給を受ける。しかしながら、ステロイドの免疫調節効果のために、ステロイドによる前投薬は、臨床的に実施可能な程度に最小限に抑えられる。 Patients receive chemotherapeutic antiemetics and IV hydration according to local standard of care and manufacturer's instructions. However, due to the immunomodulatory effects of steroids, premedication with steroids is minimized to the extent clinically feasible.
化学療法のための用量変更及び処置の中断又は中止のためのガイドラインが提供される。 Guidelines for dose modification and treatment interruption or discontinuation for chemotherapy are provided.
コホートA:アテゾリズマブ+チラゴルマブ+カルボプラチン/シスプラチン+ペメトレキセド
各21日間のサイクルの1日目に、全ての適格患者は、以下の順序で薬物注入を受ける:
導入:アテゾリズマブ→チラゴルマブ→ペメトレキセド→カルボプラチン又はシスプラチン
導入期の4~6サイクル後、患者は以下の投与順序で維持療法を開始する。
維持:アテゾリズマブ→チラゴルマブ→ペメトレキセド
Cohort A: Atezolizumab + Tiragolumab + Carboplatin/Cisplatin + Pemetrexed On
Induction: atezolizumab→tiragolumab→pemetrexed→carboplatin or cisplatin After 4-6 cycles of the induction phase, patients will begin maintenance therapy with the following dosing sequence.
Maintenance: atezolizumab → tiragolumab → pemetrexed
表33は、ペメトレキセドに対する提案された前投薬を列挙する。表7は、導入期中のペメトレキセド及びカルボプラチン又はシスプラチンの処置投与のための、及び維持期中のペメトレキセドのための推奨される注入時間を列挙する。

コホートB:アテゾリズマブ+チラゴルマブ+カルボプラチン+パクリタキセル
各21日間のサイクルの1日目に、全ての適格患者は、以下の順序で薬物注入を受ける:
導入:アテゾリズマブ→チラゴルマブ→パクリタキセル→カルボプラチン
導入期の4~6サイクル後、患者は、治験実施計画書バージョン4に登録した場合は各21日間サイクルの1日目に、又は治験実施計画書バージョン5以降に登録した場合は各28日間サイクルの1日目に維持療法を開始する。全ての適格患者は、以下の投与順序で薬物注入を受ける:
維持:アテゾリズマブ→チラゴルマブ
Cohort B: Atezolizumab + Tiragolumab + Carboplatin + Paclitaxel On
Run-in: atezolizumab → tiragolumab → paclitaxel → carboplatin After 4-6 cycles of the run-in phase, patients will be enrolled on
Maintenance: atezolizumab → tiragolumab
表8は、コホートBの患者の導入処置のための推奨される前投薬を列挙している。表9は、導入期中のパクリタキセル及びカルボプラチンの処置投与のための推奨注入時間を列挙している。 Table 8 lists the recommended premedications for the induction treatment of Cohort B patients. Table 9 lists recommended infusion times for treatment administration of paclitaxel and carboplatin during the induction phase.
コホートC:アテゾリズマブ+チラゴルマブ+カルボプラチン又はシスプラチン
各21サイクルの1日目に、全ての適格患者に以下の順序で試験薬注入を行う。
導入:アテゾリズマブ→チラゴルマブ→シスプラチン又はカルボプラチン→エトポシド
導入期の後、患者は、以下の投与順序で各28日間サイクルの1日目に維持療法を開始する。
維持:アテゾリズマブ→チラゴルマブ
Cohort C: Atezolizumab + Tiragolumab + Carboplatin or Cisplatin On
Run-in: atezolizumab→tiragolumab→cisplatin or carboplatin→etoposide After the run-in phase, patients begin maintenance therapy on
Maintenance: atezolizumab → tiragolumab
表10は、導入期中のカルボプラチン又はシスプラチン及びエトポシドの処置投与のための推奨注入時間を列挙している。
コホートD:カペシタビン+アテゾリズマブ+チラゴルマブ
各21日間サイクルの1日目に、全ての適格患者に以下の順序で試験薬を投与する:
カペシタビン→アテゾリズマブ→チラゴルマブ
Table 10 lists recommended infusion times for treatment administration of carboplatin or cisplatin and etoposide during the induction phase.
Cohort D: Capecitabine + Atezolizumab +
Capecitabine → atezolizumab → tiragolumab
表34は、カペシタビンの処置投与のための推奨される長さ、用量経路及びレジメンを列挙している。

シスプラチン
異なるコホートにおけるシスプラチンの投与のためのガイドラインを表11に示す。
Cisplatin Guidelines for administration of cisplatin in different cohorts are shown in Table 11.
カルボプラチン
異なるコホートにおけるカルボプラチンの投与のためのガイドラインを表12に示す。
Carboplatin Guidelines for administration of carboplatin in different cohorts are shown in Table 12.
ペメトレキセド
コホートAにおけるペメトレキセドの投与のためのガイドラインを表13に示す。
Guidelines for administration of pemetrexed in Pemetrexed Cohort A are shown in Table 13.
パクリタキセル
コホートBにおけるパクリタキセル投与のガイドラインを表14に示す。
Guidelines for paclitaxel dosing in Paclitaxel Cohort B are shown in Table 14.
エトポシド
コホートCにおけるエトポシドの投与のためのガイドラインを表15に示す。
Etoposide Guidelines for administration of etoposide in Cohort C are shown in Table 15.
カペシタビン
カペシタビンは、150mg及び500mgの錠剤として供給される。患者は、治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、表35に概説される処置を受ける。

カペシタビンを水と共に、食事後30分以内に摂取する。患者は、使用済み及び未使用の薬物を試験施設に戻すように指示される。 Take capecitabine with water within 30 minutes after meals. Patients will be instructed to return used and unused medication to the study site.
B.併用療法 B. Combination therapy
併用療法には、スクリーニングの7日前から処置中止来院までに患者が使用した任意の薬物(例えば、処方薬、市販薬、ハーブ又はホメオパシー薬、及び/又は栄養補助食品)が含まれる。 Concomitant therapy includes any drug (eg, prescription drug, over-the-counter drug, herbal or homeopathic drug, and/or dietary supplement) used by the patient from 7 days prior to screening until the discontinuation visit.
許可された治療
この試験で注入関連症状を経験する患者(第Ia相又は第Ib相)は、標準診療(米国以外の地域については、同等の医薬を現地の診療により置き換えてもよい)に従って、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン及び/又はラニチジン又は別のH2受容体アンタゴニストで症候的に処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理する。抗ヒスタミン剤による前投薬は、処置する医師の裁量により、第Ia相又は第Ib相のサイクル≧2に対して投与され得る。
Allowed Treatments Patients experiencing infusion-related symptoms in this study (Phase Ia or Phase Ib) should be treated according to standard practice (for regions outside the United States, equivalent medication may be substituted by local practice) It can be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine and/or ranitidine or another H2 receptor antagonist. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2-adrenergic agonist). Premedication with an antihistamine may be administered for cycles ≧2 of Phase Ia or Phase Ib, at the discretion of the treating physician.
全身性コルチコステロイド、免疫抑制薬及びTNFαアンタゴニストは、単剤としてのチラゴルマブ又は抗PD-L1/PD-1と組み合わせたチラゴルマブによる治療の潜在的に有益な免疫学的効果を減弱させる可能性があるが、緊急時又はメディカルモニターとの相談後に、処置する医師の裁量で投与され得る。実施可能であれば、コルチコステロイド、免疫抑制薬又はTNFαアンタゴニストの代替物が考慮される。チラゴルマブ、アテゾリズマブ、ベバシズマブ、及びペンブロリズマブの前投薬は、メディカルモニターに相談した後、処置する医師の裁量でサイクル≧2に対して投与され得る。.吸入コルチコステロイド及びミネラルコルチコイド(例えば、起立性低血圧又は副腎皮質機能不全を有する患者のためのフルドロコルチゾン)の使用は認められる。副腎不全のためのコルチコステロイドの生理学的用量は認められる。食欲増進剤として投与されるメゲストロールも認められる。他の薬剤の計画された使用は、メディカルモニターと議論される。 Systemic corticosteroids, immunosuppressants and TNFα antagonists may attenuate the potentially beneficial immunological effects of treatment with tiragolumab as a single agent or in combination with anti-PD-L1/PD-1. However, it may be administered at the discretion of the treating physician in an emergency or after consultation with a medical monitor. Alternatives to corticosteroids, immunosuppressants or TNFα antagonists are considered where feasible. Tiragolumab, atezolizumab, bevacizumab, and pembrolizumab premedication may be administered for cycles ≧2 at the discretion of the treating physician after consulting the medical monitor. . The use of inhaled corticosteroids and mineralocorticoids (eg fludrocortisone for patients with orthostatic hypotension or adrenocortical insufficiency) is permitted. Physiological doses of corticosteroids for adrenal insufficiency are allowed. Megestrol, administered as an appetite stimulant, is also recognized. Planned use of other medications will be discussed with the medical monitor.
第Ib相化学療法拡大コホートの患者については、制吐剤及び全身ステロイドを以下の状況で与えることもできる。
●適切な制吐薬予防が投与される。5-HT3受容体及びNK1Rアンタゴニストからなる非ステロイド性制吐薬レジメンの使用は、実施可能であれば奨励される(Hesketh et al.J Clin Oncol 2017;35:3240-3261)。
●デキサメタゾン(又は等価物)による前処置は、皮膚反応の発生率及び重症度を低下させるために、ペメトレキセドを受けているコホートAの全患者に与えられ得る。臨床試験では、ペメトレキセド投与の前日、当日及び翌日にデキサメタゾン4mgを経口BIDで投与した。
●デキサメタゾン(又は等価物)による前処置は、パクリタキセルを受けているコホートBの全ての患者に与えられ得る。臨床試験では、パクリタキセル投与の12時間前及び6時間前にデキサメタゾン20mgを経口投与した。
For patients in the Phase Ib chemotherapy expansion cohort, antiemetics and systemic steroids may also be given in the following circumstances.
• Appropriate antiemetic prophylaxis is administered. The use of nonsteroidal antiemetic regimens consisting of 5-HT3 receptor and NK1R antagonists is encouraged when feasible (Hesketh et al. J Clin Oncol 2017;35:3240-3261).
• Pretreatment with dexamethasone (or equivalent) may be given to all patients in Cohort A receiving pemetrexed to reduce the incidence and severity of skin reactions. In the clinical trial, 4 mg of dexamethasone was administered orally BID on the day before, the day of, and the day after pemetrexed administration.
• Pretreatment with dexamethasone (or equivalent) may be given to all patients in Cohort B receiving paclitaxel. In clinical trials, 20 mg of dexamethasone was given orally 12 hours and 6 hours before paclitaxel administration.
予防的抗生物質(例えば、外科的介入後)の計画された使用は、メディカルモニターと議論される。試験薬物処置は、抗生物質経過が終了するまで保持される。 Planned use of prophylactic antibiotics (eg, after surgical intervention) will be discussed with the medical monitor. Study drug treatment is maintained until the antibiotic course is completed.
経口避妊薬、ホルモン補充療法、予防的若しくは治療的抗凝固療法(例えば、安定用量レベルでの低分子量ヘパリン若しくはワルファリン)、又は非悪性の適応症のための他の維持療法を使用する患者は、その使用を継続しなければならない。生殖能力のある男性及び女性は、非常に有効な避妊手段を使用しなければならない。 Patients using oral contraceptives, hormone replacement therapy, prophylactic or therapeutic anticoagulant therapy (e.g., low molecular weight heparin or warfarin at stable dose levels), or other maintenance therapy for non-malignant indications, must continue to use it. Men and women of reproductive potential must use highly effective means of contraception.
化学療法拡大コホートの患者については、以下の薬剤を使用して注意を払う:
●ペメトレキセド(コホートA)を受けている軽度から中等度の腎機能不全(クレアチニンクリアランス[CrCl]が45~79mL/分)の患者に非ステロイド系抗炎症薬(NSAID)を投与する場合には注意を払う。排泄半減期が短いNSAID(例えば、ジクロフェナク、インドメタシン)は、ペメトレキセドの投与の2日前、当日及び投与の2日後の期間にわたって回避される。ペメトレキセドと半減期がより長いNSAID(例えば、メロキシカム、ナブメトン)との間の潜在的な相互作用に関するデータがない場合、これらのNSAIDを服用している患者は、ペメトレキセドの前の少なくとも5日間、その日及びその2日後に投薬を中断することになる。NSAIDの同時投与が必要な場合、毒性、特に骨髄抑制、腎臓及び胃腸毒性について患者を綿密に監視する。
●アミノグリコシド及びループ利尿薬等の耳毒性薬は、シスプラチン又はカルボプラチンを投与されている患者において耳毒性を増強し得る。シスプラチンによる抗ヒスタミン剤の使用は、これらがめまい及び耳鳴り等の耳毒性症状をマスクするかのうせいがあるので、綿密に再検討される。リチウム及び抗痙攣薬(フェニトインを含む)のレベルは、シスプラチン又はカルボプラチンを投与されている患者において綿密に監視される。INRは、経口抗凝固剤及びシスプラチンを服用している患者において厳密に監視される。
●ベースラインINRを超える増加によって証明されるような凝固時間の上昇が、ワーファリンをエトポシドと同時に服用している患者において報告されている(コホートC)。エトポシドを用いてワーファリンを投与されている患者は、頻繁なINRで綿密に監視される。
●カペシタビン(コホートD)及び経口クマリン誘導体抗凝固剤療法を併用している患者を、抗凝固剤用量を適宜調整するために、抗凝固剤応答(INR又はプロトロンビン時間)を頻繁に監視しなければならない。カペシタビンをクマリン誘導体抗凝固剤(例えば、ワルファリン及びフェンプロクモン等)と同時に服用している患者において、変化した凝固パラメーター並びに/又は出血及び死亡が報告されている。CYP2C9基質であるロイコボリン及びフェニトインを服用しているカペシタビン(コホートD)を服用している患者には、さらなる予防措置が必要である。
For patients in the chemotherapy expansion cohort, use the following agents with caution:
Caution when administering non-steroidal anti-inflammatory drugs (NSAIDs) to patients with mild to moderate renal insufficiency (creatinine clearance [CrCl] 45-79 mL/min) receiving pemetrexed (Cohort A). pay the NSAIDs with short elimination half-lives (eg, diclofenac, indomethacin) are avoided for a period of 2 days before, on, and 2 days after administration of pemetrexed. In the absence of data on potential interactions between pemetrexed and NSAIDs with longer half-lives (e.g., meloxicam, nabumetone), patients taking these NSAIDs should be treated for at least 5 days prior to pemetrexed on that day. and 2 days later dosing will be discontinued. Patients are closely monitored for toxicity, particularly myelosuppression, renal and gastrointestinal toxicity, if co-administration of NSAIDs is required.
• Ototoxic agents such as aminoglycosides and loop diuretics can increase ototoxicity in patients receiving cisplatin or carboplatin. The use of antihistamines with cisplatin is closely reviewed as they may mask ototoxic symptoms such as vertigo and tinnitus. Levels of lithium and anticonvulsants (including phenytoin) are closely monitored in patients receiving cisplatin or carboplatin. INR is closely monitored in patients taking oral anticoagulants and cisplatin.
• Elevated clotting times, as evidenced by increases over baseline INR, have been reported in patients taking warfarin concurrently with etoposide (Cohort C). Patients receiving warfarin with etoposide are closely monitored for frequent INR.
• Patients on concomitant capecitabine (Cohort D) and oral coumarin derivative anticoagulant therapy should be monitored frequently for anticoagulant response (INR or prothrombin time) to appropriately adjust the anticoagulant dose. not. Altered coagulation parameters and/or bleeding and death have been reported in patients taking capecitabine concomitantly with coumarin derivative anticoagulants such as warfarin and phenprocoumon. Patients on capecitabine (Cohort D) taking the CYP2C9 substrates leucovorin and phenytoin require additional precautions.
非化学療法拡大コホートの患者については、以下の薬剤を使用して注意を払う:
●顎の骨壊死が、主にビスホスホネートと組み合わせてベバシズマブを投与された患者において報告されている。したがって、併用ビスホスホネートを受けている患者においてベバシズマブを使用する際には注意を払わなければならない。
For patients in non-chemotherapy expansion cohorts, use the following agents with caution:
• Osteonecrosis of the jaw has been reported primarily in patients receiving bevacizumab in combination with bisphosphonates. Therefore, caution must be exercised when using bevacizumab in patients receiving concomitant bisphosphonates.
禁止される治療法
以下の治療法の使用は試験中禁止する:
●(限定されないが)化学療法、ホルモン療法、免疫療法、放射線療法、治験薬、又はハーブ療法を含む、保険当局が承認したか実験的かにかかわらず、がんの処置を目的とした任意の併用療法
Prohibited Therapies The following treatments are prohibited during the study:
Any drug, whether approved by health authorities or experimental, for the treatment of cancer, including (but not limited to) chemotherapy, hormone therapy, immunotherapy, radiation therapy, investigational drugs, or herbal therapies. combination therapy
患者が他の様式で利益を得る場合、痛みの緩和のため(例えば、既知の骨転移の処置)に放射線療法が検討され得る。第Ia相又は第Ib相の用量漸増コホートの患者については、DLT評定ウィンドウの完了まで緩和的放射線療法を延期する。試験処置投与は、メディカルモニターの同意を得て、放射線療法中に中断してもよい。 Radiation therapy may be considered for pain relief (eg, treatment of known bone metastases) if the patient would benefit otherwise. For patients in the Phase Ia or Phase Ib dose escalation cohorts, defer palliative radiotherapy until completion of the DLT assessment window. Study treatment administration may be discontinued during radiotherapy with the consent of the medical monitor.
混合した応答を経験する患者は、メディカルモニターによる承認を得て、3つ以下の病変の制御のための局所療法(例えば、手術、定位放射線手術、放射線療法、ラジオ波焼灼術)を受けてもよい; Patients experiencing a mixed response may receive local therapy (e.g., surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) for control of no more than three lesions with approval by the medical monitor. good;
標的病変に対する放射線療法又は標的病変の摘出を受けた患者は、その後、その標的病変がRECIST v1.1による応答決定のために評価不能になる。
●生弱毒化ワクチン(例えば、FluMist(登録商標)インフルエンザワクチン)は、試験中のいつでも、及び試験処置の最後の投与後5ヶ月間禁止する。
●患者は、試験全体の間、IFN-α、IFN-γ又はIL-2を含むがこれらに限定されない免疫賦活剤を受けることができない。これらの薬剤は、アテゾリズマブと組み合わせて、自己免疫症状のリスクを潜在的に増加させる可能性がある。
●伝統的なハーブ薬(典型的には、これらの特徴が不完全であり、毒性の評定を引き起こすか又は混乱させる可能性がある予期しない薬物-薬物相互作用をもたらす可能性があるため)。
Patients who have undergone radiation therapy to the target lesion or resection of the target lesion subsequently have the target lesion non-evaluable for response determination by RECIST v1.1.
• Live attenuated vaccines (eg, FluMist® influenza vaccine) are prohibited at any time during the study and for 5 months after the last dose of study treatment.
• Patients cannot receive immunostimulants, including but not limited to IFN-α, IFN-γ or IL-2, during the entire study. These agents in combination with atezolizumab may potentially increase the risk of autoimmune conditions.
• Traditional herbal medicines (typically because these characteristics are imperfect and can lead to unanticipated drug-drug interactions that can cause or confound assessments of toxicity).
コホートNC1について検討されているHCC患者に特異的な禁止治療:
●全用量の抗凝固剤、治療用量での血栓溶解療法、及び抗血小板療法の現在の使用は禁止されている。
Prohibited therapies specific for HCC patients being studied for cohort NC1:
• Current use of full-dose anticoagulants, therapeutic-dose thrombolytic therapy, and antiplatelet therapy is prohibited.
抗凝固剤又は血栓溶解療法の予防的使用のための局所ラベル推奨用量が許容される。 Local label recommended doses for prophylactic use of anticoagulant or thrombolytic therapy are acceptable.
低用量アスピリン(<325mg/日)が許容される。プロトンポンプ阻害剤の同時投与は、潜在的な胃腸損傷を軽減するために強く推奨される。 Low-dose aspirin (<325 mg/day) is permitted. Co-administration of proton pump inhibitors is strongly recommended to reduce potential gastrointestinal damage.
患者が依然として試験薬物処置を受けている間に静脈血栓塞栓症事象を経験した場合、患者は抗凝固処置にもかかわらず試験薬を継続することが依然として可能であり得る。
●ワルファリン又はクマジン様製品(予防的使用を含む)の現在の使用は禁止されている。
If a patient experiences a venous thromboembolic event while still receiving study drug treatment, the patient may still be allowed to continue study drug despite anticoagulation.
• Current use of warfarin or coumadin-like products (including prophylactic use) is prohibited.
低用量抗凝固療法、未分画ヘパリン又はLMWHの予防的使用が許容される。抗凝固処置のための好ましい選択は、ASCOガイドライン(Lyman GH et al.J Clin Oncol 2015;33:654-6)によるLMWHである。 Prophylactic use of low-dose anticoagulant therapy, unfractionated heparin, or LMWH is permitted. A preferred choice for anticoagulant treatment is LMWH according to ASCO guidelines (Lyman GH et al. J Clin Oncol 2015;33:654-6).
試験薬を受けている間のNSAIDの併用慢性使用は、慢性低用量アスピリン(<325mg/日)を除いて禁止される。ただし、医学的症状(例えば、頭痛、発熱)の症候的軽減のために、潜在的な胃腸損傷を軽減するためにプロトンポンプ阻害剤と同時投与される場合、経口NSAIDの断続的又は短期間の摂取が許容される。
D.選択基準
患者は次の試験登録基準を満たさなければならない:
一般的な基準
●署名済みインフォームドコンセントフォーム(ICF)
●年齢≧18歳
●試験の治験実施計画書を遵守できると治験責任医師が判断すること
●0又は1の、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス
●平均余命≧12週間
●最初の試験処置(サイクル1、1日目)の14日前以内に得られた以下の臨床検査結果によって定義される、適切な血液学的及び終末器官機能:
●絶対好中球数(ANC)≧1,500細胞/μL
●白血球(WBC)数≧2,500/μL
●リンパ球数≧500/μL
●血小板数≧100,000/μL(サイクル1、1日目の前の14日間以内に輸血なし)
●ヘモグロビン≧9g/dL
●患者は輸血されてもよく、又は局所標準治療に従って赤血球造血処置を受けてもよい。
●総ビリルビン≦1.5X正常値の上限(ULN)
●パクリタキセルを投与されている患者(コホートB)は、総ビリルビンが≦1.25XULNでなければならない。
●AST及びALT≦3XULN
●アルカリホスファターゼ≦2.5XULN、ただし、以下の例外がある:
●文書化された肝臓又は骨転移を有する患者は、アルカリホスファターゼ≦5XULNを有し得る。
●血清アルブミン≧2.5g/dL
●PT及び活性化部分トロンボプラスチン時間(aPTT)≦1.5XULN
これは、治療的抗凝固療法を受けていない患者にのみ適用される。
治療的抗凝固療法を受けている患者は安定した用量である。
●Cockcroft-Gault糸球体濾過量推定に基づいて測定又は計算されたクレアチニンクリアランス≧50mL/分:

●血清妊娠検査(卵管結紮術を受けた女性を含む、妊娠の可能性がある女性のため)が行い、第1サイクルの1日目の前の14日以内に陰性として文書化されなければならない;
●妊娠の可能性のある女性の場合:以下に定義するように、禁欲(異性間の性交を控える)又は避妊を使用することの同意、及び卵の提供を控えることの同意:
●女性は、処置期間中及びチラゴルマブの最終投薬後90日間、アテゾリズマブの最終投薬後5ヶ月間、ペンブロリズマブの最終投薬後4ヶ月間、並びにベバシズマブ及び化学療法(ペメトレキセド、シスプラチン、カルボプラチン、パクリタキセル、エトポシド及びカペシタビン)の最終投与後6ヶ月間、禁欲を維持するか、又は年間<1%の失敗率の避妊方法を使用しなければならない。女性は、この同じ期間中に卵を提供することを控えなければならない。
●女性は、月経後であり、閉経後の状態に達しておらず(閉経以外の特定された原因のない≧12ヶ月間の無月経)、外科的滅菌(卵巣、卵管、及び/又は子宮の除去)又は治験責任医師によって決定される別の原因(例えば、ミュラー誘発)を受けたことがない場合、妊娠可能性があると考えられる。出産可能性の定義は、地域のガイドライン又は規制との整合に適合させることができる。
●年間失敗率<1%の避妊方法の例としては、両側卵管結紮術、男性の不妊手術、排卵を阻害するホルモン避妊具、ホルモン放出子宮内避妊具、及び銅付加子宮内避妊具が挙げられる。
●ホルモン避妊法は、バリア法によって補完されなければならない。
●性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価される。周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。
●男性の場合:以下に定義するように、禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることに同意すること:
●妊娠していない妊娠可能性のある女性パートナーの場合、外科的に避妊していない男性は、処置期間中及びチラゴルマブの最後の投薬後90日間、カペシタビンの最後の投薬後3ヶ月間、及び任意の他の化学療法薬の最後の投薬後6ヶ月間、禁欲を維持するか、又は合わせて年間<1%の失敗率をもたらすコンドーム及び追加の避妊方法を使用しなければならない。男性は、同期間中は精子提供をやめなければならない。
●妊娠中の女性パートナーの場合、男性は、処置期間中及びチラゴルマブの最終投薬後90日間、カペシタビンの最終投薬後3ヶ月間、及び化学療法の最終投薬後6ヶ月間は、胚曝露を回避するため、禁欲を維持するか、又はコンドームを使用しなければならない。
●性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価される。周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。
Concomitant chronic use of NSAIDs while receiving study drug is prohibited, except for chronic low-dose aspirin (<325 mg/day). However, for symptomatic relief of medical symptoms (e.g., headache, fever), intermittent or short-term use of oral NSAIDs when co-administered with proton pump inhibitors to reduce potential gastrointestinal damage. Ingestion is permissible.
D. Inclusion Criteria Patients must meet the following study entry criteria:
General Criteria Signed Informed Consent Form (ICF)
Age ≥ 18 years As determined by the investigator to be able to comply with the study's protocol U.S. East Coast Oncology Group (ECOG) performance status of 0 or 1 Life expectancy ≥ 12 weeks Initial Adequate hematology and end-organ function as defined by the following laboratory test results obtained within 14 days prior to study treatment (
● Absolute neutrophil count (ANC) ≥ 1,500 cells/μL
● White blood cell (WBC) count ≥ 2,500/μL
●Lymphocyte count≧500/μL
- Platelet count ≥ 100,000/μL (
● Hemoglobin ≥ 9g/dL
• Patients may be transfused or undergo erythropoietic procedures according to local standard of care.
● Total bilirubin ≤ 1.5 x upper limit of normal (ULN)
• Patients receiving paclitaxel (Cohort B) must have total bilirubin < 1.25 XULN.
● AST and ALT ≤ 3XULN
- alkaline phosphatase ≤ 2.5 XULN, with the following exceptions:
• Patients with documented liver or bone metastases may have alkaline phosphatase < 5XULN.
● Serum albumin ≥ 2.5 g/dL
PT and activated partial thromboplastin time (aPTT) < 1.5 XULN
This applies only to patients not receiving therapeutic anticoagulant therapy.
Patients receiving therapeutic anticoagulant therapy are dose stable.
- Creatinine clearance ≥50 mL/min measured or calculated based on the Cockcroft-Gault glomerular filtration rate estimate:
A serum pregnancy test (for women of childbearing potential, including those who have undergone tubal ligation) must be performed and documented as negative within 14 days prior to
For women of childbearing potential: Consent to abstinence (abstinence from heterosexual intercourse) or use of contraception, and consent to abstain from donating eggs, as defined below:
- Women were allowed to receive treatment during the treatment period and for 90 days after the last dose of tiragolumab, 5 months after the last dose of atezolizumab, 4 months after the last dose of Must maintain abstinence or use a method of contraception with an annual failure rate of <1% for 6 months after the last dose of capecitabine. Females should refrain from donating eggs during this same period.
Females are postmenopausal, have not achieved postmenopausal status (≥12 months of amenorrhea with no identified cause other than menopause), have undergone surgical sterilization (ovaries, fallopian tubes, and/or uterus) Pregnancy potential is considered if the patient has not had any prior causes (e.g., Müller induction)) or another cause as determined by the Investigator. Fertility definitions can be adapted to match local guidelines or regulations.
● Examples of contraceptive methods with an annual failure rate of <1% include bilateral tubal ligation, male sterilization, hormonal contraceptives that inhibit ovulation, hormone-releasing intrauterine devices, and copper-enriched intrauterine devices. be done.
• Hormonal contraception must be complemented by barrier methods.
- Reliability of sexual abstinence will be assessed in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle. Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
For men: agreeing to maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and to abstain from donating sperm, as defined below:
In the case of nonpregnant female partners of childbearing potential, males who are not surgically contraceptive should receive a must maintain abstinence for 6 months after the last dose of any other chemotherapeutic agent or use condoms and additional methods of contraception that together result in a failure rate of <1% per year. Men must stop donating sperm during the same period.
For pregnant female partners, men avoid embryo exposure during treatment and for 90 days after last dose of tiragolumab, 3 months after last dose of capecitabine, and 6 months after last dose of chemotherapy Therefore, they must remain abstinent or use condoms.
- Reliability of sexual abstinence will be assessed in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle. Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
E.がん特異的選択基準
●少なくとも1つの利用可能な標準治療後に進行した局所進行性、再発性又は転移性の治癒不能な悪性腫瘍の組織学的な文書化を有する患者;又は標準治療が無効若しくは忍容できないことが証明されているか、又は不適切であると考えられている患者;又は治験薬の治験が認められている標準治療である者。
●少なくとも1つの利用可能な標準治療後に進行した患者が、利用可能な追加の承認された標準処置の選択肢を有する場合、試験医師は、この試験に参加するためのインフォームドコンセントが得られる前に、これらの処置のリスク及び利益を議論しなければならない。この議論は、患者の文書化に文書化されなければならない。
●第Ib相試験のみの拡大コホートについては、化学療法用いて又は用いずに抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容される処置選択肢と見なされる局所進行性、再発性又は転移性の治癒不能な悪性腫瘍の組織学的な文書化を有する患者も適格であり得る。
●ホルマリン固定パラフィン包埋(FFPE)ブロック(好ましい)又は≧15枚の未染色スライドにおいて代表的な腫瘍標本の入手可能性が確認された患者及び関連する病理報告。
●許容可能な試料はまた、深部腫瘍組織に対するコアニードル生検(最低3個のコア)又は、皮膚、皮下、又は粘膜病変に対する切除生検、切開生検、パンチ生検、又は鉗子生検を含み得る。
●微細針吸引(FNA)試料、ブラッシング(brushing)、滲出液又は腹水からの細胞ペレット、及び洗浄液試料は許容されない。
●骨転移からの腫瘍組織は、PD-L1及び/又はTIGIT(Ig及びITIMドメインを有するT細胞免疫受容体)発現について評価することができず、したがって許容されない。
●異なる時点(例えば、初期診断時及び疾患再発時)及び/又は複数の転移腫瘍からの適切な組織が利用可能である場合、最近に採取された(理想的には、最近の全身性療法に続いて)組織が優先しなければならない。利用可能性に基づき、所与の患者から複数の試料が採取され得るが、ブロック又は≧15以上の染色されていないスライドの要件は、単一の生検又は摘出検体によって満たされなければならない。
●主試験インフォームドコンセント用紙(ICF)に署名する前に、患者は事前スクリーニングICFに署名して、保管又は新鮮な腫瘍標本の収集及び検査を特に可能にすることができる。
●保管用組織が不十分又は利用不可能な患者は、メディカルモニターとの議論の上、患者が以下のいずれかを満たす場合に適格となり得る:
●少なくとも10枚の染色されていない連続スライドを提供することができる
●前処置コア、パンチ、又は腫瘍の切除/切開生検試料の収集に同意し、それを受ける意思がある(許容可能な試料については上記参照)
●用量漸増コホートに登録される
●化学療法拡大コホートに登録される(第Ib相)
●Q4W投薬拡大コホート(第Ib相)に登録される
●バックフィルコホート又は拡大コホートの患者については、提出された保管腫瘍組織を、登録前にPD-L1及び/又はTIGIT発現について評価しなければならない。
●RECIST v 1.1による測定可能な疾患を有する患者
●以前に照射された病変は、標的病変としてカウントされる。
●生検を意図する病変は、標的病変としてカウントされない。
E. Cancer-specific inclusion criteria Patients with histologically documented locally advanced, recurrent, or metastatic incurable malignancies that have progressed after at least one available standard therapy; Patients who have proven intolerable or are considered unsuitable; or who are the approved standard of care for clinical trials of investigational agents.
If a patient who has progressed after at least one available standard treatment has additional approved standard treatment options available, the study physician should be advised before informed consent to participate in this study is obtained. , the risks and benefits of these procedures must be discussed. This discussion must be documented in patient documentation.
For Phase Ib-only expansion cohorts, locally advanced, recurrent, or metastatic disease for which clinical trials of investigational agents in combination with anti-PD-L1 antibodies, with or without chemotherapy, are considered acceptable treatment options Patients with histologic documentation of incurable malignancies may also be eligible.
• Patients and associated pathology reports with confirmed availability of representative tumor specimens in formalin-fixed paraffin-embedded (FFPE) blocks (preferred) or ≧15 unstained slides.
Acceptable specimens also include core needle biopsy (minimum of 3 cores) for deep tumor tissue or excisional, incisional, punch, or forceps biopsy for cutaneous, subcutaneous, or mucosal lesions. can contain.
• Fine needle aspiration (FNA) samples, brushings, cell pellets from exudates or ascites, and lavage fluid samples are not allowed.
• Tumor tissue from bone metastases cannot be assessed for PD-L1 and/or TIGIT (T cell immunoreceptor with Ig and ITIM domains) expression and is therefore unacceptable.
If appropriate tissue from different time points (e.g., at initial diagnosis and at disease recurrence) and/or from multiple metastatic tumors is available, recently harvested (ideally following recent systemic therapy). subsequently) must be prioritized by the organization. Multiple samples may be taken from a given patient based on availability, but the requirement for a block or >15 or more unstained slides must be met by a single biopsy or excision.
• Prior to signing the Main Study Informed Consent Form (ICF), patients may sign a pre-screening ICF to specifically allow collection and examination of archival or fresh tumor specimens.
Patients with insufficient or unavailable archival tissue may be eligible if, upon discussion with the medical monitor, the patient either:
- Able to provide at least 10 unstained serial slides - Consent and willing to have excisional/incisional biopsy specimens of pretreatment core, punch, or tumor collected (acceptable specimens) See above for
• Enrolled in a dose escalation cohort • Enrolled in a chemotherapy expansion cohort (Phase Ib)
Enrolled in the Q4W dosing expansion cohort (Phase Ib) For backfill or expansion cohort patients, submitted archived tumor tissue must be assessed for PD-L1 and/or TIGIT expression prior to enrollment not.
• Patients with measurable disease by RECIST v 1.1 • Previously irradiated lesions are counted as target lesions.
• Lesions intended for biopsy are not counted as target lesions.
F.第Ia相及び第Ib相の明確なコホートを埋め戻した患者の追加の選択基準
●バックフィルコホート登録は、腫瘍がPD-L1及び/又はTIGIT発現を有する患者に限定される。したがって、腫瘍組織の保管品を提出し、登録前にPD-L1及び/又はTIGIT発現について評価しなければならない。したがって、腫瘍組織の保管品を提出し、登録前にPD-L1及び/又はTIGIT発現について評価しなければならない。PD-L1及び/又はTIGITの発現は、免疫浸潤細胞又は腫瘍細胞のいずれかにおいて評価され得る。複数の腫瘍標本が提出される場合(例えば、再発性疾患からの保管標本及び組織)、少なくとも1つの標本がPD-L1及び/又はTIGITについて評価可能である場合、患者は適格であり得る。患者のPD-L1及び/又はTIGITスコアは、それぞれ試料間の最大PD-L1及び/又はTIGITスコアである。
●患者は、以下の腫瘍タイプのうちの1つのPD-L1選択腫瘍及び/又はTIGIT選択腫瘍を有していなければならない:非小細胞肺がん(NSCLC)、腎細胞がん(RCC)、トリプル-ネガティブ乳がん(TNBC)、黒色腫、頭頸部扁平上皮癌腫(HNSCC)、卵巣がん(OC)、胃食道接合部(GEJ)がんを含む胃がん(GC)、尿路上皮膀胱がん(UBC)、及びマイクロサテライト安定性(MSS)及びマイクロサテライト不安定性低(MSI-Low)を含む結腸直腸がん(CRC)。
●患者は、重大な処置上の合併症の許容できないリスクなしに、合計1~2回の生検(前処置及び処置中)又は1回の生検(処置前の生検の代わりに保管組織を提出することができる場合、処置中)を可能にするアクセス可能な病変を有していなければならない。
●許容される試料には、深部腫瘍組織若しくはリンパ節のためのコア針生検、又は皮膚、皮下、若しくは粘膜病変のための切除、切開、パンチ、若しくは鉗子生検が含まれる。FNA、浸出液又は腹水からの細胞ペレット、洗浄液試料、及び骨生検は許可されない。コア針生検のために考慮される標的病変は、所与の時点(最小直径18-ゲージ)で最低3つ、理想的には5つのコアの回収に適していると考えられる。
●複数の病変が利用可能である場合、同じ腫瘍病変は、実施可能であれば、腫瘍又は転移部位に関連する不均一性の導入を回避するために、全ての時点で生検されなければならない。
F. Additional Inclusion Criteria for Patients Who Have Backfilled Defined Phase Ia and Phase Ib Cohorts • Backfill cohort enrollment is limited to patients whose tumors have PD-L1 and/or TIGIT expression. Therefore, an archive of tumor tissue must be submitted and assessed for PD-L1 and/or TIGIT expression prior to enrollment. Therefore, an archive of tumor tissue must be submitted and assessed for PD-L1 and/or TIGIT expression prior to enrollment. PD-L1 and/or TIGIT expression can be assessed in either immune-infiltrating cells or tumor cells. If multiple tumor specimens are submitted (eg, archival specimens and tissues from recurrent disease), patients may be eligible if at least one specimen is evaluable for PD-L1 and/or TIGIT. A patient's PD-L1 and/or TIGIT score is the maximum PD-L1 and/or TIGIT score between samples, respectively.
- Patients must have a PD-L1-selected tumor and/or a TIGIT-selected tumor of one of the following tumor types: non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), triple- Negative breast cancer (TNBC), melanoma, head and neck squamous cell carcinoma (HNSCC), ovarian cancer (OC), gastric cancer (GC) including gastroesophageal junction (GEJ) cancer, urothelial bladder cancer (UBC) , and colorectal cancer (CRC), including microsatellite stable (MSS) and microsatellite instability low (MSI-Low).
Patients may receive a total of 1-2 biopsies (pretreatment and during treatment) or 1 biopsy (archive tissue instead of pretreatment biopsy) without unacceptable risk of significant procedural complications. must have accessible lesions to allow for treatment (if available).
• Acceptable samples include core needle biopsy for deep tumor tissue or lymph nodes, or excision, incision, punch, or forceps biopsy for skin, subcutaneous, or mucosal lesions. FNA, cell pellets from exudates or ascites, lavage fluid samples, and bone biopsies are not permitted. Target lesions considered for core needle biopsy are considered suitable for retrieval of a minimum of 3 and ideally 5 cores at a given time point (18-gauge minimum diameter).
- If multiple lesions are available, the same tumor lesion must be biopsied at all time points, if feasible, to avoid introducing heterogeneity related to tumor or metastatic sites .
G.拡大コホートの患者の追加の選択基準
●拡大コホートへの登録は、腫瘍がPD-L1及び/又はTIGITが選択された患者に限定される。したがって、腫瘍組織の保管品を提出し、登録前にPD-L1及び/又はTIGIT発現について評価しなければならない。腫瘍組織がPD-L1及び/又はTIGIT発現について評価可能でない患者は、適格ではない。PD-L1及び/又はTIGITの発現は、免疫浸潤細胞又は腫瘍細胞のいずれかにおいて評価され得る。複数の腫瘍標本が提出される場合(例えば、再発性疾患からの保管標本及び組織)、少なくとも1つの標本がPD-L1及び/又はTIGIT発現について評価可能である場合、患者は適格であり得る。患者のPD-L1及び/又はTIGITスコアは、それぞれ試料間の最大PD-L1及び/又はTIGITスコアである。
●登録は、各拡大コホートにおける約半数までの発生患者が任意の生検を受けることに同意した患者であるように管理される。
●第Ib相の連続生検拡大コホートに登録された患者については、生検が必要である。
G. Additional Inclusion Criteria for Patients in the Expansion Cohort • Enrollment in the expansion cohort is limited to patients whose tumors were selected for PD-L1 and/or TIGIT. Therefore, an archive of tumor tissue must be submitted and assessed for PD-L1 and/or TIGIT expression prior to enrollment. Patients whose tumor tissue is not evaluable for PD-L1 and/or TIGIT expression are not eligible. PD-L1 and/or TIGIT expression can be assessed in either immune-infiltrating cells or tumor cells. If multiple tumor specimens are submitted (eg, archival specimens and tissues from recurrent disease), patients may be eligible if at least one specimen is evaluable for PD-L1 and/or TIGIT expression. A patient's PD-L1 and/or TIGIT score is the maximum PD-L1 and/or TIGIT score between samples, respectively.
• Enrollment will be managed so that up to approximately half of the incident patients in each expansion cohort are those who consent to undergo a voluntary biopsy.
• A biopsy is required for patients enrolled in the Phase Ib serial biopsy expansion cohort.
H.第Ia相の拡大コホートにおける患者の追加の選択基準
●患者は、以下の腫瘍型を含むPD-L1選択腫瘍及び/又はTIGIT選択腫瘍を有さなければならない:NSCLC、RCC、TNBC、黒色腫、HNSCC、OC、GEJがんを含むGC、UBC及びCRC
H. Additional Inclusion Criteria for Patients in the Phase Ia Expansion Cohort Patients must have PD-L1-selected tumors and/or TIGIT-selected tumors, including the following tumor types: NSCLC, RCC, TNBC, melanoma, HNSCC, OC, GC including GEJ cancer, UBC and CRC
I.第Ib相の各指標特異的拡大コホートにおける患者の追加の選択基準
●NSCLCコホート(CIT未経験):抗PD-L1/PD-1及び/又は抗CTLA-4(細胞傷害性Tリンパ球関連タンパク質4)を含む、CIT(治験薬又は承認済み)で以前に処置されていない組織学的に確認された治癒不能の進行性NSCLCを有する患者であって、CIT(抗PD-L1/PD-1剤を含む)がNSCLCの処置として現地の規制当局によって承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢とみなされる患者が含まれる。
●腫瘍が既知の感作EGFR変異を有する患者は、疾患進行(処置中若しくは処置後)、又はEGFRチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知の未分化リンパ腫キナーゼ(ALK)再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はALKチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知のROS1再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はROS1チロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知のBRAFV600E変異を有する患者は、疾患進行(処置中若しくは処置後)、又はトラメチニブと組み合わせたダブラフェニブによる処置に対する不耐性も経験していなければならない;
●NSCLCコホート(CIT処置):抗PD-L1/PD-1を含むCIT(治験中又は承認済み)で以前に処置された組織学的に確認された治癒不能の進行性NSCLC患者
●腫瘍が既知の感作EGFR変異を有する患者は、疾患進行(処置中若しくは処置後)、又はEGFRチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知のALK再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はALKチロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知のROS1再編成を有する患者は、疾患進行(処置中若しくは処置後)、又はROS1チロシンキナーゼ阻害剤(複数可)による処置に対する不耐性も経験していなければならない;
●腫瘍が既知のBRAFV600E変異を有する患者は、疾患進行(処置中若しくは処置後)、又はトラメチニブと組み合わせたダブラフェニブによる処置に対する不耐性も経験していなければならない;
●患者は、以前の抗PD-L1/PD-1を含んでいなければならない、CIT単独療法及び/又は併用療法(治験中又は承認済み)で文書化された疾患進行を経験していなければならない。
●単剤療法及び/又は併用療法としての以前の抗PD-L1/PD-1は、この拡大コホートへの登録前に投与された最新の全身性抗がん治療とならなければならない。
●以前の抗PD-L1/PD-1を単剤療法又は併用療法として受けている間に、いつでもRECIST v1.1による治験責任医師の評定による確認された部分奏効(PR)又は完全奏効(CR)の文書化された最良効果を経験した少なくとも約10人の患者が登録され得る。
●以前の抗PD-L1/PD-1を単剤療法として及び/又は併用療法として受けている間に、RECIST v 1.1ごとに治験責任医師が評定した安定疾患(SD)の文書化された最良効果をいつでも経験した少なくとも約10人の患者が登録され得る。
●以前の抗PD--L1/PD-1を単剤療法及び/又は併用療法として受けている間に、RECIST v1.1による治験責任医師が評定した進行性疾患(PD)の文書化された最良効果をいつでも経験した少なくとも約10人の患者が登録され得る。
●単剤療法及び/又は併用療法としての以前の抗PD-L1/PD-1は、この拡大コホートへの登録前に投与された最新の全身性抗がん治療とならなければならない。
●主に毒性又は不耐性のために以前の抗PD-L1/PD-1単剤療法及び/又は併用療法を中止した患者は、この拡大コホートへの登録に適格ではない。
●TNBCコホート:乳房の組織学的に確認された治癒不能の進行性エストロゲン受容体(ER)-陰性、プロゲステロン受容体陰性、及びヒト上皮成長因子受容体2(HER2)陰性腺癌(トリプルネガティブ)を有する患者
●三重陰性状態は、米国臨床腫瘍学会(American Society of Clinical Oncology-College of American Pathologists)(ASCO-CAP)ガイドラインによって定義されるように文書化されなければならない:
●<1%の腫瘍細胞核がERについて免疫反応性であり、<1%の腫瘍細胞核がプロゲステロン受容体について免疫反応性であり、
かつ
●HER2検査は、免疫組織化学(IHC)1+、IHC0、又はin situハイブリダイゼーション(ISH)陰性を実証する。
●CRCコホート:結腸又は直腸の組織学的に確認された治癒不能の進行性腺癌を有する患者
●虫垂起源の腫瘍を有する患者は適格ではない。
●GCコホート:組織学的に確認された手術不能な、局所進行性若しくは転移性又は再発性の胃腺癌又はGEJ腺癌を有し、治癒的療法に適していない患者
●腫瘍中心が解剖学的食道胃接合部上1~5cm以内に位置する遠位食道の腺癌として定義された1型GEJ腫瘍を有する患者が試験に適格である。
●食道がん(扁平上皮癌腫又は腺癌)を有する患者は、メディカルモニターとの議論の後に適格となり得る。
●腫瘍が既知のHER2陽性を有する患者は、疾患進行(処置中若しくは処置後)、又はHER2-標的化抗体/HER2阻害剤(複数可)による処置に対する不耐性も経験していなければならない。
●HER 2陽性は、原発腫瘍又は転移性病変に対する現地の検査室での検査によって評定されるIHC3+又はIHC 2+/ISH+(ISH陽性は、≧2のHER2:CEP17比として定義される)のいずれかとして定義される。
●組織が不十分であるか又は利用できない(例えば、保管及び/又は生検)ためにHER2検査を受けておらず、したがって腫瘍のHER2状態が不明である患者は、メディカルモニターとの議論後に依然として適格であり得る。
●HNSCCコホート:組織学的に確認された、治癒的療法を受け入れることができない手術不能な、局所進行性又は転移性の、再発性又は持続性の頭頸部扁平上皮癌腫(口腔、中咽頭、下咽頭、又は喉頭)を有する患者
●頭頸部における任意の他の原発解剖学的位置のHNSCC患者、原発不明のHNSCC患者、又は非扁平上皮組織の腫瘍を有する患者は、適格ではない。
●鼻咽頭のHNSCC患者は、メディカルモニターとの議論の後に適格となり得る。
●HNSCCのHPV状態を知らなければならない。
●UBCコホート:尿路上皮(腎盂、尿管、膀胱、及び尿道を含む)の組織学的に確認された治癒不能な進行性移行細胞癌腫を有する患者
●混合組織型の患者は、優勢な移行細胞パターンを有する必要がある。
●黒色腫コホート:組織学的に確認された治癒不能な進行性転移性黒色腫を有する患者
●CIT(抗PD-L1/PD-1剤及び/又は抗CTLA-4剤を含む)が黒色腫の処置として地域の規制当局によって承認されている場合、抗PD-L1/PD-1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる黒色腫を有する患者。
●腫瘍が既知のBRAFV 600変異を有する患者はまた、疾患の進行(処置中又は治療後)又はBRAF阻害剤及び/又はマイトジェン活性化プロテインキナーゼ(MEK)阻害剤による不耐性を経験していなければならない。
●このコホートの患者の約20%以下が眼(ブドウ膜)黒色腫の患者であるように、登録が管理される。
●OCコホート:組織学的に確認された治癒不能進行性上皮性卵巣がん、ファロピウス管がん、又は原発性腹膜がんを有する患者
●境界線上の卵巣上皮新生物(例えば、低悪性度の腫瘍、非定型増殖性腫瘍)は除外される。
●RCCコホート:明細胞病理学の成分及び/又は肉腫様組織学の成分を有する、組織学的に確認された治癒不能進行性RCCを有する患者;
●CIT(抗PD-L1/PD-1剤を含む)が地域の規制当局によってRCCの処置として承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされるRCCを有する患者。
I. Additional inclusion criteria for patients in each index-specific expansion cohort of phase Ib NSCLC cohort (CIT-naive): anti-PD-L1/PD-1 and/or anti-CTLA-4 (cytotoxic T lymphocyte-associated protein 4) Patients with histologically confirmed incurable advanced NSCLC not previously treated with CIT (investigational or approved), including CIT (anti-PD-L1/PD-1 agent ) is approved by local regulatory authorities for the treatment of NSCLC, patients for whom a clinical trial of an investigational drug in combination with an anti-PD-L1 antibody is considered an acceptable treatment option are included.
• Patients whose tumors have a known sensitizing EGFR mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with an EGFR tyrosine kinase inhibitor(s);
- Patients whose tumors have known anaplastic lymphoma kinase (ALK) rearrangements must also not experience disease progression (during or after treatment) or intolerance to treatment with an ALK tyrosine kinase inhibitor(s). not;
• Patients whose tumors have known ROS1 rearrangements must also experience disease progression (during or after treatment) or intolerance to treatment with ROS1 tyrosine kinase inhibitor(s);
- Patients whose tumors have a known BRAF V600E mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with dabrafenib in combination with trametinib;
NSCLC cohort (CIT treatment): Histologically confirmed incurable advanced NSCLC patients previously treated with CIT (investigational or approved) containing anti-PD-L1/PD-1 Known tumor patients with sensitizing EGFR mutations must also have experienced disease progression (during or after treatment) or intolerance to treatment with an EGFR tyrosine kinase inhibitor(s);
• Patients whose tumors have known ALK rearrangements must also experience disease progression (during or after treatment) or intolerance to treatment with an ALK tyrosine kinase inhibitor(s);
• Patients whose tumors have known ROS1 rearrangements must also experience disease progression (during or after treatment) or intolerance to treatment with ROS1 tyrosine kinase inhibitor(s);
- Patients whose tumors have a known BRAF V600E mutation must also have experienced disease progression (during or after treatment) or intolerance to treatment with dabrafenib in combination with trametinib;
Patients must have had prior anti-PD-L1/PD-1 containing, CIT monotherapy and/or combination therapy (investigational or approved) with documented disease progression not.
• Previous anti-PD-L1/PD-1 as monotherapy and/or combination therapy must be the most recent systemic anticancer therapy administered prior to enrollment in this expansion cohort.
Investigator-assessed confirmed partial response (PR) or complete response (CR) at any time while receiving prior anti-PD-L1/PD-1 as monotherapy or combination therapy ) can be enrolled at least about 10 patients who experienced the best documented response to
Documented Investigator-rated stable disease (SD) per RECIST v 1.1 while receiving prior anti-PD-L1/PD-1 as monotherapy and/or as combination therapy At least about 10 patients who experienced the best response at any given time can be enrolled.
Documented Investigator-rated progressive disease (PD) by RECIST v1.1 while receiving prior anti-PD--L1/PD-1 as monotherapy and/or combination therapy At least about 10 patients who experienced the best response at any given time can be enrolled.
• Previous anti-PD-L1/PD-1 as monotherapy and/or combination therapy must be the most recent systemic anticancer therapy administered prior to enrollment in this expansion cohort.
• Patients who discontinued prior anti-PD-L1/PD-1 monotherapy and/or combination therapy primarily due to toxicity or intolerance are not eligible for enrollment in this expansion cohort.
TNBC cohort: histologically confirmed incurable advanced estrogen receptor (ER)-negative, progesterone receptor-negative, and human epidermal growth factor receptor 2 (HER2)-negative adenocarcinoma of the breast (triple-negative) Triple-negative status must be documented as defined by the American Society of Clinical Oncology-College of American Pathologists (ASCO-CAP) guidelines:
- <1% of tumor cell nuclei are immunoreactive for ER and <1% of tumor cell nuclei are immunoreactive for progesterone receptor;
and • HER2 testing demonstrates immunohistochemistry (IHC) 1+, IHC0, or in situ hybridization (ISH) negative.
• CRC cohort: patients with histologically confirmed incurable advanced adenocarcinoma of the colon or rectum • Patients with tumors of appendiceal origin are not eligible.
GC cohort: Patients with histologically confirmed inoperable, locally advanced or metastatic or recurrent gastric or GEJ adenocarcinoma who are not amenable to curative therapy Tumor center anatomic Patients with
• Patients with esophageal cancer (squamous cell carcinoma or adenocarcinoma) may be eligible after discussion with the medical monitor.
• Patients with known HER2-positive tumors must also have experienced disease progression (during or after treatment) or intolerance to treatment with HER2-targeting antibody/HER2 inhibitor(s).
HER2 positivity is either IHC3+ or IHC2+/ISH+ (ISH positivity is defined as a HER2:CEP17 ratio ≥2) as assessed by local laboratory testing for primary tumor or metastatic disease defined as
• Patients who have not undergone HER2 testing due to insufficient or unavailable tissue (e.g. storage and/or biopsy) and therefore whose tumor HER2 status is unknown may still may be eligible.
HNSCC cohort: Histologically confirmed inoperable, locally advanced or metastatic, recurrent or persistent squamous cell carcinoma of the head and neck (oral, oropharyngeal, inferior) not amenable to curative therapy HNSCC of any other primary anatomical location in the head and neck, HNSCC of unknown primary, or patients with tumors of non-squamous tissue are not eligible.
• Patients with nasopharyngeal HNSCC may be eligible after discussion with the medical monitor.
• The HPV status of HNSCC must be known.
UBC Cohort: Patients with histologically confirmed incurable advanced transitional cell carcinoma of the urothelium (including renal pelvis, ureters, bladder, and urethra) Patients with mixed histology were predominantly transitional Must have a cell pattern.
- Melanoma cohort: Patients with histologically confirmed incurable advanced metastatic melanoma - CIT (including anti-PD-L1/PD-1 and/or anti-CTLA-4 agents) melanoma Patients with melanoma for whom clinical trials of investigational drugs in combination with anti-PD-L1/PD-1 antibodies are considered an acceptable treatment option if approved by local regulatory authorities for the treatment of.
- Patients whose tumors have a known
• Enrollment will be managed so that approximately 20% or less of the patients in this cohort are patients with ocular (uveal) melanoma.
OC cohort: Patients with histologically confirmed incurable advanced epithelial ovarian cancer, fallopian tube carcinoma, or primary peritoneal cancer Borderline ovarian epithelial neoplasms (e.g., low-grade tumors, atypical proliferative tumors) are excluded.
- RCC cohort: patients with histologically confirmed incurable progressive RCC with components of clear cell pathology and/or sarcomatoid histology;
If CIT (including anti-PD-L1/PD-1 agents) is approved by local regulatory authorities for the treatment of RCC, clinical trials of investigational drugs in combination with anti-PD-L1 antibodies are an acceptable treatment option Patients with RCC considered as
J.第Ib相の連続生検拡大コホートにおける患者の追加の選択基準
●患者は、以下の腫瘍タイプを含み得るPD-L1選択腫瘍及び/又はTIGIT選択腫瘍を有しなければならない:黒色腫、OC、RCC及びUBC
●CIT(抗PD-L1/PD-1剤を含む)が地域の規制当局によってこれらの適応症(複数可)の処置として承認されている場合、抗PD-L1抗体と組み合わせた治験薬の臨床試験が許容可能な処置選択肢と見なされる黒色腫又はRCCの患者。
●患者は、重大な処置上の合併症の許容できないリスクなしに、合計1~2回の生検(前処置及び処置中)又は1回の生検(処置前の生検の代わりに保管組織を提出することができる場合、処置中)を可能にするアクセス可能な病変を有していなければならない。
●許容される試料には、深部腫瘍組織若しくはリンパ節のためのコア針生検、又は皮膚、皮下、若しくは粘膜病変のための切除、切開、パンチ、若しくは鉗子生検が含まれる。FNA、浸出液又は腹水からの細胞ペレット、洗浄液試料、及び骨生検は許可されない。コア針生検のために考慮される標的病変は、所与の時点(最小直径18-ゲージ)で最低3つ、理想的には5つのコアの回収に適していると考えられる。
J. Additional Inclusion Criteria for Patients in the Phase Ib Serial Biopsy Expansion Cohort Patients must have PD-L1-selected tumors and/or TIGIT-selected tumors, which may include the following tumor types: melanoma, OC, RCC and UBC
If CITs (including anti-PD-L1/PD-1 agents) are approved by local regulatory authorities for the treatment of these indication(s), clinical trials of investigational drugs in combination with anti-PD-L1 antibodies Patients with melanoma or RCC for whom testing is considered an acceptable treatment option.
Patients may receive a total of 1-2 biopsies (pretreatment and during treatment) or 1 biopsy (archive tissue instead of pretreatment biopsy) without unacceptable risk of significant procedural complications must have accessible lesions to allow for treatment (if available).
• Acceptable samples include core needle biopsy for deep tumor tissue or lymph nodes, or excision, incision, punch, or forceps biopsy for skin, subcutaneous, or mucosal lesions. FNA, cell pellets from exudates or ascites, lavage fluid samples, and bone biopsies are not permitted. Target lesions considered for core needle biopsy are considered suitable for retrieval of a minimum of 3 and ideally 5 cores at a given time point (18-gauge minimum diameter).
複数の病変が利用可能である場合、同じ腫瘍病変は、実施可能であれば、腫瘍又は転移部位に関連する不均一性の導入を回避するために、全ての時点で生検されなければならない。 If multiple lesions are available, the same tumor lesion should be biopsied at all time points, if feasible, to avoid the introduction of tumor- or metastatic site-related heterogeneity.
K.除外基準
以下の基準のいずれかを満たす患者は除外される:
一般的な除外基準
●試験及びフォローアップの手続きを遵守することができないこと
●妊娠、授乳又は母乳栄養
●重大な心血管疾患、例えば、New York Heart Associationの心臓病(クラスII以上)、過去3カ月以内の心筋梗塞、不安定不整脈、及び/又は不安定狭心症。
●活動性のウイルス性、アルコール性又は他の肝炎、肝硬変、及び遺伝性肝疾患又は現在のアルコール乱用を含む、既知の臨床的に重要な肝疾患
●スクリーニングヘモグロビンA1C≧8%又は空腹時血漿グルコース≧160mg/dL(又は8.8mmol/L)として定義されるコントロール不良の2型糖尿病
●サイクル1の1日目の前の28日以内の主要な外科的処置、又は試験の経過中での主要な外科的処置の必要になるという予想
●治験の薬の使用に禁忌を示す疾患又は症状の合理的な疑いを与えるか、結果の解釈に影響を及ぼし得るか、及び/又は患者を処置合併症に対して高リスクにする可能性がある任意の他の疾患、代謝機能障害、健康診断所見、又は臨床試験所見
K. Exclusion Criteria Patients meeting any of the following criteria are excluded:
General Exclusion Criteria ● Inability to comply with study and follow-up procedures ● Pregnancy, lactation or breastfeeding ● Significant cardiovascular disease, e.g., New York Heart Association heart disease (class II or higher), past 3 Myocardial infarction, unstable arrhythmia, and/or unstable angina pectoris within months.
- Known clinically significant liver disease, including active viral, alcoholic or other hepatitis, cirrhosis, and inherited liver disease or current alcohol abuse - Screen hemoglobin A1 C ≥8% or fasting plasma
L.がん特異的除外基準
●試験処置の開始前3週間以内の、化学療法、ホルモン療法、及び/又は放射線療法を含む任意の抗がん治療(治験中であるか承認されているかを問わない)、ただし、以下の例外がある:
●前立腺がんのためのゴナドトロピン放出ホルモン(GnRH)アゴニスト又はアンタゴニストでのホルモン療法;
●ホルモン補充療法又は経口避妊薬;
●サイクル1、1日目の>7日前に中止されたがんの処置のために地元の規制当局によって承認されたチロシンキナーゼ阻害剤(TKI);以前のTKIの中止後にベースラインスキャンを取得しなければならず、以前のがん治療に起因する有害事象に関する基準を満たさなければならない
●サイクル1、1日目の>1週間前のハーブ療法
●サイクル1、1日目の2週間前>の、感受性が高い可能性のある場所(例えば、硬膜外腔)における有痛性の転移又は転移に対する姑息的放射線治療
●この試験の第Ia相部分から、チラゴルマブ及びアテゾリズマブを用いた第Ib相試験にクロスオーバーする患者は、第Ib相試験に入る前に、単剤としてのチラゴルマブで処置されていてもよい。
●CITによる以前の処置に基づく適格性は、以下に記載されるように、薬物の機構的クラス及び患者が考慮されているコホートに依存する。更に、以前のがん治療に起因する有害事象に関する全ての基準を満たさなければならない。
L. Cancer-Specific Exclusion Criteria Any anti-cancer therapy (whether investigational or approved) including chemotherapy, hormone therapy, and/or radiation therapy within 3 weeks prior to initiation of study treatment , with the following exceptions:
- hormone therapy with gonadotropin releasing hormone (GnRH) agonists or antagonists for prostate cancer;
● hormone replacement therapy or oral contraceptives;
• Eligibility based on prior treatment with CIT depends on the mechanistic class of the drug and the cohort in which the patient is being considered, as described below. Additionally, all criteria for adverse events attributable to prior cancer therapy must be met.
第Ia相及び第Ib相の全てのコホート(用量漸増、バックフィル及び拡大):
●以前の抗TIGIT剤は、以下の例外を除いて許可されない:
●第Ia相試験でチラゴルマブで処置された患者は、指定された基準が満たされていれば、第Ib相試験に登録することができる。
●少なくとも6週間又は5半減期のいずれか短い方の薬物が、最終用量と提案されたサイクル1、1日目との間で経過していれば、がんワクチン及び/又はサイトカインによる事前の処置は可能である。
●最小のウォッシュアウトは、任意の以前の全身のがん治療に対して3週間である。
●この治験実施計画書に明示的に記載されていない以前のがん免疫療法について、潜在的適格性を判定するためにメディカルモニターと議論すべきである;
All Phase Ia and Phase Ib cohorts (dose escalation, backfill and expansion):
- No previous anti-TIGIT agents are allowed with the following exceptions:
• Patients treated with tiragolumab in a Phase Ia trial may be enrolled in a Phase Ib trial if specified criteria are met.
- Prior treatment with cancer vaccines and/or cytokines if at least 6 weeks or 5 half-lives of the drug, whichever is shorter, have elapsed between the final dose and proposed
• The minimum washout is 3 weeks for any previous systemic cancer therapy.
- Prior cancer immunotherapy not explicitly listed in this protocol should be discussed with the medical monitor to determine potential eligibility;
第Ia相及び第Ib相における用量漸増及びバックフィルコホート(用量漸増中の登録):
●免疫チェックポイント阻害剤(例えば、抗PD-L1/PD-1)、免疫調節性MAb及び/又はMAb由来療法による事前の処置は、薬物の少なくとも5つの消失半減期が最終用量と提案されたサイクル1、1日目との間で経過していることを条件として許容される。
●toll様受容体(TLR)アゴニスト、インドールアミン2,3-ジオキシゲナーゼ若しくはトリプトファン-2,3-ジオキシゲナーゼ(IDO/TDO)の阻害剤、又はOX40のアゴニストを含む免疫調節剤による事前の処置は、最後の投与と、提案されたサイクル1、1日目との間に少なくとも6週間が経過していることを条件として許容される。
Dose escalation and backfill cohorts in Phase Ia and Phase Ib (enrollment during dose escalation):
- Prior treatment with immune checkpoint inhibitors (e.g., anti-PD-L1/PD-1), immunomodulatory MAbs and/or MAb-derived therapies with at least 5 elimination half-lives of the drug suggested as the
Prior treatment with immunomodulatory agents, including toll-like receptor (TLR) agonists, inhibitors of
第Ia相及び第Ib相における用量拡大及びバックフィルコホート(用量拡大中の登録):
●免疫チェックポイント阻害剤、免疫調節性MAb及び/又はMAb由来療法による事前の処置は、最終用量と提案されたサイクル1、1日目との間に少なくとも6週間が経過していることを条件として許容され、ただし、下記の例外がある:
事前の抗PD-L1/PD-1を少なくとも3週間のウォッシュアウト期間に供する
事前の抗CTLA-4を6週間のウォッシュアウト期間に供する
●第Ib相のNSCLC CIT処置拡大コホートでは、最新の全身処置は、単剤療法又は組み合わせとしての抗PD-L1/PD-1であった
●第Ib相のNSCLC CITナイーブ拡大コホートでは、免疫チェックポイント阻害剤(抗PD-L1/PD-1等)、免疫調節性MAb、及び/又はMAb由来療法による事前の処置は許可されていない。
Dose Expansion and Backfill Cohorts in Phase Ia and Phase Ib (enrollment during dose expansion):
- Prior treatment with an immune checkpoint inhibitor, immunomodulatory MAb and/or MAb-derived therapy, provided that at least 6 weeks have elapsed between the final dose and proposed
Prior anti-PD-L1/PD-1 with at least a 3-week washout period Prior anti-CTLA-4 with a 6-week washout period In the Phase Ib NSCLC CIT treatment expansion cohort, current systemic Treatment was anti-PD-L1/PD-1 as monotherapy or combination In the Phase Ib NSCLC CIT naive expansion cohort, immune checkpoint inhibitors (such as anti-PD-L1/PD-1), Prior treatment with immunomodulatory MAbs and/or MAb-derived therapies is not permitted.
TLRアゴニスト、IDO/TDOの阻害剤又はOX 40のアゴニストを含む免疫調節剤による事前の処置は、事前の処置の最後の用量と提案されたサイクル1、1日目との間に、以下の例外を除いて、薬物の少なくとも5半減期又は最低3週間が経過していることを条件として許容される。
Prior treatment with an immunomodulatory agent, including a TLR agonist, an inhibitor of IDO/TDO or an agonist of OX40, between the last dose of prior treatment and the proposed
第Ib相のNSCLC CITナイーブ拡大コホートでは、他の免疫調節薬による事前の処置は許容されない。
●以前のがん免疫療法に起因する免疫介在性グレード4有害事象の病歴(補充療法で管理される内分泌不全症又は血清アミラーゼ若しくはリパーゼの無症候性上昇以外)
●以前の免疫療法剤の永続的な中止をもたらした及び/又はサイクル1、1日目の≦6ヶ月前に発生した、以前のがん免疫療法に起因する免疫介在性グレード3有害事象(置換療法で管理された内分泌不全症、又は血清アミラーゼ若しくはリパーゼの無症候性上昇以外)の病歴。
●補充療法で管理された脱毛症、白斑又は内分泌障害を除いてグレード≦1に回復していない以前の抗がん治療からの有害事象
●以前のがん免疫療法に関連する全ての免疫介在性有害事象(置換療法又は安定白斑で管理される内分泌不全症以外)は、ベースラインまで完全に消散していなければならない。
●免疫介在性有害事象のためにコルチコステロイドで処置された患者は、コルチコステロイドの中止後≧4週間、関連する症候又は徴候がないことを示さなければならない。
●NSCLCの肺リンパ上皮腫様癌腫亜型を有する患者
●原発性CNS悪性腫瘍、未処置CNS転移、又は活動性CNS転移(進行しているか、又は症候性制御のためにコルチコステロイドを必要とする)
CNS転移の処置歴を有する患者は適格であるが、但し、以下の基準の全てを満たすことを条件とする:
●CNS外の測定可能な疾患
●CNS転移の治療としてのコルチコステロイドの継続的な必要性はなく、コルチコステロイドは登録前に≧2週間中止され、CNS転移に起因する進行中の症状はない
●安定な用量の抗痙攣剤が許容される。
●CNS指向性治療の完了時の改善のX線による実証及びCNS指向性治療の完了とスクリーニングX線試験との間の暫定的な進行の証拠なし
●スクリーニングCNS X線試験は放射線療法の完了後≧4週間である
●軟髄膜疾患
●制御されない腫瘍関連疼痛
●姑息的放射線療法を受けることができる症候性病変(例えば、骨転移又は神経インピンジメントを引き起こす転移)は、登録前に処置されなければならない。
●そのさらなる成長が機能不全又は難治性疼痛を引き起こす可能性がある無症候性転移病変(脊髄圧迫に現在は関連付けられていない硬膜外転移)は、適切である場合、登録前に局所領域的療法について検討されるべきである;
●制御されない胸水、心膜滲出液、又は再発性排液処置を必要とする腹水(毎月1回又はより頻繁に)
●留置カテーテル(例えば、PleurXカテーテル)を有する患者は許容される。
●転移又は死亡の無視できるリスクを有するもの(例えば、適切に処置された非浸潤性子宮頸癌腫、基底細胞若しくは扁平上皮皮膚がん、限局性前立腺がん、又は非浸潤性乳管癌腫)を除く、サイクル1の1日目の前5年以内の試験下にある疾患以外の悪性腫瘍
●制御されない高カルシウム血症(>1.5mmol/Lのイオン化カルシウム若しくはCa>12mg/dL若しくは補正血清カルシウム≧ULN)又はビスホスホネート療法若しくはデノスマブの継続的な使用を必要とする症候性高カルシウム血症。
No prior treatment with other immunomodulatory agents is permitted in the Phase Ib NSCLC CIT naive expansion cohort.
- History of immune-mediated
- Immune-mediated
- Adverse events from previous anticancer therapy that have not resolved to Grade ≤ 1, except for alopecia, vitiligo or endocrine disorders managed with replacement therapy - Any immune-mediated event associated with previous cancer immunotherapy Adverse events (other than replacement therapy or endocrine insufficiency managed with stable vitiligo) must have resolved completely to baseline.
• Patients treated with corticosteroids for immune-mediated adverse events must demonstrate no associated symptoms or signs for >4 weeks after discontinuation of corticosteroids.
- Patients with pulmonary lymphoepithelioma-like carcinoma subtype of NSCLC - Primary CNS malignancies, untreated CNS metastases, or active CNS metastases (advanced or requiring corticosteroids for symptomatic control) do)
Patients with prior treatment for CNS metastases are eligible provided they meet all of the following criteria:
No ongoing need for corticosteroids as treatment for CNS metastases, corticosteroids were discontinued ≥2 weeks prior to enrollment, no ongoing symptoms attributed to CNS metastases No • Stable doses of anticonvulsants are acceptable.
X-ray demonstration of improvement at completion of CNS-directed therapy and no interim evidence of progression between completion of CNS-directed therapy and screening X-ray study Screening CNS X-ray study after completion of radiotherapy Leptomeningeal disease Uncontrolled tumor-related pain Symptomatic lesions amenable to palliative radiotherapy (e.g., bone metastases or metastases causing nerve impingement) must be treated prior to enrollment. must.
Asymptomatic metastatic lesions (epidural metastases not currently associated with spinal cord compression) whose further growth may cause dysfunction or intractable pain should be treated locoregionally prior to enrollment, if appropriate. therapy should be considered;
- Uncontrolled pleural effusion, pericardial effusion, or ascites requiring recurrent drainage (monthly or more frequently)
• Patients with indwelling catheters (eg, PleurX catheter) are allowed.
Exclude those with negligible risk of metastasis or death (e.g., appropriately treated cervical carcinoma in situ, basal or squamous skin cancer, localized prostate cancer, or ductal carcinoma in situ) , malignancy other than disease under study within 5 years prior to
特に骨格事象を予防するためにビスホスホネート療法又はデノスマブを受けており、臨床的に有意な高カルシウム血症の病歴がない患者が適格である。ただし、デノスマブの患者は、試験中にデノスマブの代わりにビスホスホネートを受ける意思及び資格がなければならない。
●患者は、疾患がスクリーニング前の≧2週間にわたって臨床的に安定しているという証拠なしに、手術及び/又は放射線で確定的に処置されていない、又は以前に診断及び処置された脊髄圧迫を有する。
Specifically, patients receiving bisphosphonate therapy or denosumab to prevent skeletal events and no history of clinically significant hypercalcemia are eligible. However, denosumab patients must be willing and eligible to receive a bisphosphonate instead of denosumab during the study.
Patients who have not been definitively treated with surgery and/or radiation or have previously diagnosed and treated spinal cord compression without evidence that their disease has been clinically stable for ≥2 weeks prior to Screening. have.
M.処置特異的除外基準
●全身性エリテマトーデス、リウマチ性関節炎、炎症性腸疾患、抗リン脂質抗体症候群に関連付けられる血管血栓症、ウェゲナー肉芽腫症、シェーグレン症候群、ベル麻痺(自己免疫病因のみ)、ギラン・バレー症候群、多発性硬化症、血管炎、又は糸球体腎炎を含むがこれらに限定されない自己免疫疾患の病歴、以下の注意点を伴う:
M. Treatment-specific exclusion criteria Systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, vascular thrombosis associated with antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Bell's palsy (autoimmune etiology only), Guillain- History of autoimmune disease, including but not limited to Barré syndrome, multiple sclerosis, vasculitis, or glomerulonephritis, with the following caveats:
安定した用量の甲状腺補充ホルモンを受ける、自己免疫甲状腺機能低下症の病歴を有する患者は、適格であり得る。 Patients with a history of autoimmune hypothyroidism who receive stable doses of thyroid replacement hormone may be eligible.
湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを有する白斑(例えば、乾癬性関節炎なし)を有する患者は、以下の条件を満たすならば適格であり得る。
●発疹が覆っている体表面積は10%未満でなければならない。
●疾患はベースラインで十分に制御されており、低効力の局所ステロイドのみを必要とする
●過去12ヶ月以内に基礎症状の急性増悪はない(例えば、ソラレン+紫外線A照射(PUVA)、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、高効力又は経口のステロイドを必要としない)
●サイクル1、1日目の前の2週間以内の全身免疫抑制薬(限定されないが、プレドニゾン>10mg/日、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び腫瘍壊死因子-α[TNF-α]アンタゴニストを含む)による処置
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin symptoms only (eg, no psoriatic arthritis) may be eligible if they meet the following conditions:
• Less than 10% of the body surface area must be covered by the rash.
- Disease is well controlled at baseline, requiring only low-potency topical steroids - No acute exacerbation of underlying symptoms within the past 12 months (e.g., psoralen plus ultraviolet A radiation (PUVA), methotrexate, does not require retinoids, biologics, oral calcineurin inhibitors, high-potency or oral steroids)
- Systemic immunosuppressants (including but not limited to prednisone >10 mg/day, cyclophosphamide, azathioprine, methotrexate, thalidomide and tumor necrosis factor-α [TNF-α] within 2 weeks prior to
急性の低用量の全身性免疫抑制薬(例えば、悪心のためのデキサメタゾンの1回用量)を受けた患者は、メディカルモニターと協議及び承認後に試験に登録することができる: Patients receiving acute low-dose systemic immunosuppressants (e.g., single dose of dexamethasone for nausea) may be enrolled in the study after consultation and approval with the medical monitor:
吸入コルチコステロイド(例えば、慢性閉塞性肺疾患のためのフルチカゾン)の使用は許容される Use of inhaled corticosteroids (e.g. fluticasone for chronic obstructive pulmonary disease) is permissible
経口ミネラルコルチコイド(例えば、起立性低血圧患者のためのフルドロコルチゾン)の使用は許容される Use of oral mineralocorticoids (e.g. fludrocortisone for patients with orthostatic hypotension) is permissible
副腎不全のためのコルチコステロイドの生理学的用量は認められる。
●特発性肺線維症、肺臓炎(薬物誘発性を含む)、器質化肺炎(すなわち、閉塞性細気管支炎、潜在性器質化肺炎等)の病歴、又は胸部CTスキャンのスクリーニングでの活動性肺臓炎の病歴。
Physiological doses of corticosteroids for adrenal insufficiency are allowed.
History of idiopathic pulmonary fibrosis, pneumonitis (including drug-induced), organizing pneumonia (ie, bronchiolitis obliterans, subclinical organizing pneumonia, etc.), or active lung on screening chest CT scan A history of inflammation.
放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●HIV感染症の陽性検査
●活動性B型肝炎(スクリーニング時に陽性B型肝炎表面抗原[HBsAg]検査を有すると定義される)。
A history of radiation pneumonitis (fibrosis) in the radiology area is acceptable.
• Positive test for HIV infection • Active hepatitis B (defined as having a positive hepatitis B surface antigen [HBsAg] test at screening).
過去に又は解決されたB型肝炎感染を有した患者(陰性HBsAg検査及びB型肝炎コア抗原に対する陽性IgG抗体[抗HBc]を有すると定義される)は適格である。B型肝炎ウイルス(HBV)DNAは、これらの患者においてサイクル1、1日目の前に取得されなければならず、活動性感染を示さなければならない。
●活動性C型肝炎
C型肝炎ウイルス(HCV)抗体について陽性の患者は、ポリメラーゼ連鎖反応(PCR)がHCV RNAについて陰性である場合にのみ適格である。
●スクリーニング時の活動性EBV感染及び既知又は疑われる慢性活動性EBV感染
Patients with previous or resolved hepatitis B infection (defined as having a negative HBsAg test and positive IgG antibodies to hepatitis B core antigen [anti-HBc]) are eligible. Hepatitis B virus (HBV) DNA must be obtained in these patients prior to
• Active Hepatitis C Patients who are positive for hepatitis C virus (HCV) antibodies are eligible only if the polymerase chain reaction (PCR) is negative for HCV RNA.
Active EBV infection at screening and known or suspected chronic active EBV infection
EBV IgG及び/又はEBNAについて陽性の患者は、EBV IgM及び/又はEBV PCRが陰性である場合にのみ適格である。
●活動性結核
●感染症、菌血症、又は重度の肺炎の合併症を含むがこれらに限定されない、サイクル1の1日目の前4週間以内の重度の感染症
●以下を含む、重度の感染症の上記基準を満たさない最近の感染症:
●サイクル1、1日目の前の2週間以内の感染の徴候又は症候
●サイクル1、1日目の前の2週間以内に経口又はIV抗生物質を受けた
●予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の予防のため)を受ける患者は適格である;
●事前の同種骨髄移植又は事前の固形臓器移植
●サイクル1、1日目の4週間前以内の生弱毒化ワクチンの投与、又はそのような生弱毒化ワクチンが試験中に必要とされることの予想。
●インフルエンザワクチン接種は、インフルエンザシーズンにのみ行わなければならない。患者は、サイクル1、1日目の前の4週間以内、又は試験中のいつでも、及び最後の試験処置後5ヶ月間、生弱毒化インフルエンザワクチン(例えば、FluMist(登録商標))を受けてはならない。
●キメラ抗体若しくはヒト化抗体、又は融合タンパク質に対する重度のアレルギー性、アナフィラキシー性、又は他の超過敏反応の病歴。
●CHO細胞産物に対する既知の過敏性
●アテゾリズマブ製剤の成分に対するアレルギー又は過敏症
Patients positive for EBV IgG and/or EBNA are eligible only if EBV IgM and/or EBV PCR are negative.
- Active tuberculosis - Severe infection within the 4 weeks prior to
o Signs or symptoms of infection within the 2 weeks prior to
- Prior allogeneic bone marrow transplantation or prior solid organ transplantation - Administration of a live attenuated vaccine within 4 weeks prior to
• Influenza vaccination should be given only during the influenza season. Patients may not receive a live attenuated influenza vaccine (e.g., FluMist®) within 4 weeks prior to
• History of severe allergic, anaphylactic, or other hypersensitivity reactions to chimeric or humanized antibodies, or fusion proteins.
- Known hypersensitivity to CHO cell products - Allergy or hypersensitivity to components of atezolizumab preparations
N.化学療法拡大コホートに特異的な除外基準
●白金又は白金含有化合物に対する既知の重度のアレルギー又は過敏症
●シスプラチンに特異的な除外基準
●聴覚障害が知られている患者(シスプラチン処置のみ)
●NCI CTCAE v 4.0基準によって定義したグレード≧2末梢神経障害(シスプラチン処置のみ)
●Cockcroft-Gault GFR推定に基づいて測定又は計算されたクレアチニンクリアランス≦60mL/分(シスプラチン処置のみ):

- Grade ≥ 2 peripheral neuropathy as defined by NCI CTCAE v 4.0 criteria (cisplatin treatment only)
- Creatinine clearance < 60 mL/min measured or calculated based on Cockcroft-Gault GFR estimates (cisplatin treatment only):
O.コホートAに特異的な除外基準
●ペメトレキセドに対する既知の重度のアレルギー又は過敏症
O. Exclusion criteria specific to Cohort A Known severe allergy or hypersensitivity to pemetrexed
P.コホートBに特異的な除外基準
●パクリタキセルに対する既知の重度のアレルギー又は過敏症
●Cremophor(登録商標)ELを含有する製品に対する重度の過敏反応の既知の病歴(例えば、注射濃縮物用のシクロスポリン及び注射濃縮物用のテニポシド)
P. Exclusion Criteria Specific to Cohort B Known severe allergy or hypersensitivity to paclitaxel Known history of severe hypersensitivity reaction to products containing Cremophor® EL (e.g., cyclosporine for injection concentrate and injection teniposide for concentrates)
Q.コホートCに特異的な除外基準
●エトポシドに対する既知の重度のアレルギー又は過敏症
Q. Exclusion criteria specific to Cohort C Known severe allergy or hypersensitivity to etoposide
R.コホートDに特異的な除外基準
●カペシタビン製剤の任意の成分に対する過敏性
●丸薬を嚥下することができない
●吸収不良症候群、胃腸機能に有意に影響する疾患、胃若しくは小腸の摘出、又は潰瘍性大腸炎
●既知のジヒドロピリミジンデヒドロゲナーゼ欠損症又はフルオロピリミジン療法に対する重度及び予想外の反応の病歴
●抗ウイルス薬ソリブジン(抗ウイルス薬)又は化学的に関連する類似体、例えばブリブジンの同時使用の要件(これらの薬物の使用は、カペシタビンを含む試験処置の開始から4週間以内には許容されない)
R. Exclusion criteria specific to Cohort D Hypersensitivity to any component of the capecitabine formulation Inability to swallow pills Malabsorption syndrome, disease significantly affecting gastrointestinal function, resection of the stomach or small bowel, or ulcerative colon inflammation history of known dihydropyrimidine dehydrogenase deficiency or severe and unexpected response to fluoropyrimidine therapy requirement for concomitant use of the antiviral agent sorivudine (an antiviral agent) or chemically related analogues such as brivudine drug use is not permitted within 4 weeks of initiation of study treatment, including capecitabine)
S.コホートNC1に特異的な除外基準
●≧2つのセッションでの≧3つの血圧測定値の平均に基づく、不十分に制御された高血圧(収縮期血圧>150mmHg及び/又は拡張期血圧>100mmHgとして定義される);これらのパラメーターを達成するための降圧療法が許容される
●高血圧性クリーゼ又は高血圧性脳症の病歴
●試験処置開始前6ヶ月以内の有意な血管疾患(例えば、外科的修復を必要とする大動脈瘤又は最近の末梢動脈血栓症)
●試験処置開始前1ヶ月以内の喀血の病歴(1エピソード当たり≧2.5mLの鮮赤血)
●出血性素因又は有意な凝固障害の証拠(治療的抗凝固療法の非存在下)
●アスピリン(>325mg/日)又はクロピドグレル(>75mg/日)の現在又は最近(試験処置開始の≦10日前)の使用
●注:治療目的のための全用量経口又は非経口抗凝固薬の使用は、INR及び/又はaPTTが試験処置の開始前7日以内に(施設の基準に従って)治療限界内にあり、患者が試験処置の開始前≧2週間安定用量の抗凝固薬を投与されている限り許可され、抗凝固剤の予防的使用が許容される
●試験処置の開始前3日以内の、血管アクセスデバイスの配置を除くコア生検又は他の軽微な外科的処置
●試験処置の開始前6ヶ月以内の腹部又は気管食道瘻、胃腸穿孔、又は腹腔内膿瘍の病歴
●試験処置の開始前6ヶ月以内、又は試験処置の開始前6ヶ月以内の日常的な非経口水和、非経口栄養若しくは経管栄養の必要性の病歴及び/又は基礎疾患に関連する亜閉塞性若しくは閉塞性症候群を含む胃腸閉塞の臨床徴候若しくは症状
●初期診断時に閉塞下又は閉塞症候群の徴候又は症状を有するか、又は腸閉塞を有する患者は、症状解消のために最終的な(外科的)処置を受けた場合に登録され得る。
●穿刺又は最近の外科的処置によって説明されない腹部遊離空気の証拠
●重篤な非治癒性又は裂開性の創傷、活動性潰瘍、又は未処置の骨折
●ディップスティック尿検査での≧2+タンパク質及び24時間の尿収集での≧1.0gのタンパク質によって実証されるグレード≧2のタンパク尿
●スクリーニング時のディップスティック尿検査で≧2+タンパク質を有する全ての患者は、タンパク質について24時間の尿収集を受けなければならない。
●ディップスティック尿検査で<2+タンパク質を有する患者が試験に適格である。
●大気道若しくは大血管、又は大容積の中央に位置する縦隔腫瘤(気管分岐部から<30 mm)を伴う転移性疾患
●限定されないが、消化性潰瘍疾患、憩室炎又は大腸炎を含む、試験処置の開始前6ヶ月以内の腹腔内炎症過程の病歴
●試験処置開始前の28日以内の放射線療法又は60日以内の腹部/骨盤放射線療法
●試験処置の開始前28日以内の主要な外科的処置、切開生検、又は重大な外傷性損傷;又は試験処置の開始前60日以内の腹部手術、腹部介入又は重大な腹部外傷性損傷;又は、試験の過程における主要な外科的処置の必要性の予測、又はそのような処置の副作用からの回復の欠如
S. Exclusion Criteria Specific to Cohort NC1 Poorly controlled hypertension (defined as systolic BP >150 mmHg and/or diastolic BP >100 mmHg based on the mean of ≥3 blood pressure measurements in ≥2 sessions antihypertensive therapy to achieve these parameters is acceptable History of hypertensive crisis or hypertensive encephalopathy Significant vascular disease (e.g., requiring surgical repair) within 6 months prior to initiation of study treatment aortic aneurysm or recent peripheral arterial thrombosis)
- History of hemoptysis (≥2.5 mL bright red blood per episode) within 1 month prior to initiation of study treatment
Bleeding diathesis or evidence of significant coagulopathy (in the absence of therapeutic anticoagulation)
- Current or recent (≤10 days prior to initiation of study treatment) use of aspirin (>325 mg/day) or clopidogrel (>75 mg/day) - Note: Use of full-dose oral or parenteral anticoagulants for therapeutic purposes INR and/or aPTT are within therapeutic limits (according to institutional criteria) within 7 days prior to initiation of study treatment and patient is on a stable dose of anticoagulant for ≥2 weeks prior to initiation of study treatment A core biopsy or other minor surgical procedure, excluding placement of a vascular access device, within 3 days prior to the start of the study procedure. Before the start of the study procedure. History of abdominal or tracheoesophageal fistula, gastrointestinal perforation, or intra-abdominal abscess within 6 months Routine parenteral hydration, parenteral nutrition within 6 months prior to initiation of study treatment or within 6 months prior to initiation of study treatment or clinical signs or symptoms of gastrointestinal obstruction, including sub-obstructive or obstructive syndromes related to history of need for tube feeding and/or underlying disease Have signs or symptoms of obstructive or obstructive syndrome at initial diagnosis or Alternatively, patients with intestinal obstruction may be enrolled if they undergo definitive (surgical) treatment for symptom relief.
- Evidence of abdominal free air not accounted for by puncture or recent surgical procedure - Serious non-healing or dehiscent wound, active ulcer, or untreated fracture - ≥2+ protein and protein on dipstick urinalysis Grade ≥2 proteinuria as demonstrated by ≥1.0 g protein on 24 hour urine collection All patients with ≥2+ protein on dipstick urine test at screening will have a 24 hour urine collection for protein have to receive.
• Patients with <2+ protein on dipstick urinalysis are eligible for the study.
- Metastatic disease with airways or great vessels, or a large volume of centrally located mediastinal mass (<30 mm from carina) - Including, but not limited to, peptic ulcer disease, diverticulitis or colitis History of an intra-abdominal inflammatory process within 6 months prior to initiation of study treatment Radiation therapy within 28 days or abdominal/pelvic radiation therapy within 60 days prior to initiation of study treatment Major surgery within 28 days prior to initiation of study treatment surgical procedure, incisional biopsy, or significant traumatic injury; or abdominal surgery, abdominal intervention, or significant abdominal traumatic injury within 60 days prior to the start of study procedures; or the need for major surgical procedures during the course of the study. lack of anticipation of sex or recovery from side effects of such treatment
T.評定
患者は、安全性及び忍容性について綿密にモニターされ、単剤としてのチラゴルマブ(第Ia相)又は以下と組み合わせたチラゴルマブの各投薬の前に毒性について評定される:アテゾリズマブ、アテゾリズマブと化学療法、アテゾリズマブとベバシズマブ、又はペンブロリズマブ(第Ib相)。投与は、臨床評定及び局所検査結果が許容される場合にのみ行われる。
T. Assessment Patients will be closely monitored for safety and tolerability and evaluated for toxicity prior to each dose of tiragolumab as a single agent (Phase Ia) or in combination with: atezolizumab, atezolizumab plus chemotherapy. , atezolizumab and bevacizumab, or pembrolizumab (Phase Ib). Dosing will occur only if clinical evaluation and local laboratory results are acceptable.
時間ウィンドウが指定されていない限り、全ての評定は来院予定日に行われる。試験処置の日に予定された評定は、特に明記しない限り、試験薬物の注入前に実施される。 All assessments will occur on the scheduled visit unless a time window is specified. Assessments scheduled on the day of study treatment will be performed prior to study drug infusion unless otherwise specified.
病歴、ベースライン症状、併用薬及び人口統計データ
病歴には、がんの病歴(以前のがん治療及び/又は以前のCIT及び処置並びに腫瘍の特徴、例えばホルモン受容体の状態又は変異状態が含まれるが、これらに限定されない)、他の臨床的に重要な疾患、外科手術、喫煙歴、アルコール及び/又は乱用薬物の使用、生殖状態及びスクリーニング来院前7日以内に患者によって使用された全ての薬物(例えば、処方薬、市販薬、ハーブ又はホメオパシー薬、及び栄養補助食品)が含まれる。
Medical history, baseline symptoms, concomitant medications and demographic data Medical history includes cancer history (previous cancer therapy and/or previous CIT and procedures and tumor characteristics such as hormone receptor status or mutational status). (including but not limited to), other clinically significant disease, surgery, smoking history, alcohol and/or drug use of abuse, reproductive status, and any other clinically significant disease used by the patient within 7 days prior to the Screening Visit. Drugs (eg, prescription drugs, over-the-counter drugs, herbal or homeopathic drugs, and dietary supplements) are included.
試験の第Ia相から第Ib相部分にクロスオーバーする患者について、疾患進行時の治療再開始時の再スクリーニング病歴には、治験実施計画書で指定されたフォローアップ中に取得されなかった、最初の治療中止後に発生したがん関連処置又は試験処置に関連する有害事象が含まれる。 For patients crossing over from the Phase Ia to Phase Ib portion of the trial, the rescreening history at reinitiation of treatment at disease progression should include: including cancer-related or study treatment-related adverse events that occurred after discontinuation of treatment for
人口統計データには、年齢、性別、及び自己報告の人種/民族性が含まれる。観察されたPK、薬力学、毒性、及び/又は処置に対する応答の差に対するこの変数の潜在的寄与のために、人種/民族性が記録される。 Demographic data includes age, gender, and self-reported race/ethnicity. Race/ethnicity is recorded because of the potential contribution of this variable to observed differences in PK, pharmacodynamics, toxicity, and/or response to treatment.
バイタルサイン
バイタルサインは、患者が座位にある間の体温、呼吸数、脈拍数、並びに収縮期及び拡張期血圧の測定を含む。
Vital Signs Vital signs include measurement of temperature, respiratory rate, pulse rate, and systolic and diastolic blood pressure while the patient is in a sitting position.
試験処置日に、その日の最初の試験薬物注入前の60分以内にバイタルサインを測定する。 On study treatment days, vital signs are measured within 60 minutes prior to the first study drug infusion of the day.
第Ia相のチラゴルマブの初回注入では、注入中15(±5)分ごと、注入終了時(±5分)、並びに注入終了後30(±10)分、120(±15)分、及び240(±15)分毎にバイタルサインを測定する。 The first infusion of Phase Ia tiragolumab was administered every 15 (±5) minutes during the infusion, at the end of the infusion (±5 min), and at 30 (±10), 120 (±15), and 240 (±15) minutes after the end of the infusion. ±15) Measure vital signs every minute.
第Ib相のチラゴルマブの初回注入では、注入中15(±5)分ごと、注入終了時(±5分)、及び注入終了後30分(±10分)毎にバイタルサインを測定する。化学療法を用いない全ての第Ib相コホートについて、アテゾリズマブ又はペンブロリズマブの初回注入は、チラゴルマブ注入の完了の60分後に投与される。ベバシズマブの最初の注入はアテゾリズマブ注入の完了の60分後に投与される。 For the first infusion of tiragolumab in Phase Ib, vital signs will be measured every 15 (±5) minutes during the infusion, at the end of the infusion (±5 min), and every 30 min (±10 min) after the end of the infusion. For all Phase Ib cohorts without chemotherapy, the first infusion of atezolizumab or pembrolizumab will be administered 60 minutes after completion of the tiragolumab infusion. The first infusion of bevacizumab is administered 60 minutes after completion of the atezolizumab infusion.
化学療法を用いる第Ib相コホートの場合、チラゴルマブの初回注入は、アテゾリズマブ注入の完了後60分で投与される。 For Phase Ib cohorts with chemotherapy, the first infusion of tiragolumab is administered 60 minutes after completion of the atezolizumab infusion.
アテゾリズマブ及びペンブロリズマブの最初の注入及びその後のチラゴルマブの注入のために、バイタルサインは、臨床上適応がある場合、又は以前の注入で症状が生じた場合、注入中及び注入後30(±10)分に測定される。 For the first infusion of atezolizumab and pembrolizumab and subsequent infusion of tiragolumab, vital signs will be taken during and 30 (±10) minutes after the infusion if clinically indicated or if symptoms occurred on the previous infusion. is measured to
ベバシズマブの最初の注入のために、バイタルサインは、臨床上適応がある場合、又は以前の注入で症状が生じた場合、注入中、注入終了時(±5分)、及び注入後30分(±10分)に測定される。 For the first infusion of bevacizumab, vital signs were taken during the infusion, at the end of the infusion (± 5 min), and 30 min after the infusion (± 10 minutes).
その後のチラゴルマブとアテゾリズマブ若しくはペンブロリズマブとの間、又はアテゾリズマブとベバシズマブとの間(化学療法を用いない全ての第Ib相コホートの場合)、又はアテゾリズマブとチラゴルマブとの間(化学療法を用いる第Ib相コホートの場合)の注入間隔は、以前のチラゴルマブ又はアテゾリズマブ注入がIRRなしで許容された場合は30分、又は患者が以前のチラゴルマブ又はアテゾリズマブ注入でIRRを経験した場合は60分である。 Between subsequent tiragolumab and atezolizumab or pembrolizumab, or between atezolizumab and bevacizumab (for all Phase Ib cohorts without chemotherapy), or between atezolizumab and tiragolumab (Phase Ib cohorts with chemotherapy) ) is 30 minutes if the previous tiragolumab or atezolizumab infusion was tolerated without IRR, or 60 minutes if the patient experienced an IRR on the previous tiragolumab or atezolizumab infusion.
化学療法拡大A、B及びCコホートでは、追加のバイタルサインを測定し、最後の化学療法注入の完了後30(±10)分以内にサイクル1で記録する(例えば、コホートA:カルボプラチン又はシスプラチンの後、コホートB:カルボプラチンの後、コホートC:エトポシドの後)。その後のサイクルで、臨床上適応がある場合、化学療法注入後にさらなるバイタルサインが測定され、記録される。
In chemotherapy expansion A, B, and C cohorts, additional vital signs are measured and recorded in
スクリーニング来院時に収集したバイタルサインを記録する。その後の各来院について、その日の最初の試験薬物注入の前に得られたか、又は有害事象(例えば、発熱時の温度)若しくは有害事象の主要症状(例えば、注入関連反応に関連する血圧又は不整脈に関連する心拍数)を構成するバイタルサインのみを記録する。治験実施計画書ごとに収集された全てのバイタルサインは、患者の医療文書化に文書化される。 Vital signs collected at the screening visit will be recorded. For each subsequent visit, any adverse event (e.g. fever temperature) or cardinal symptom of an adverse event (e.g. blood pressure or arrhythmia related to infusion-related reaction) obtained prior to the first study drug infusion of the day Record only the vital signs that make up the associated heart rate). All vital signs collected per protocol will be documented in the patient's medical documentation.
血中酸素飽和度は、パルスオキシメトリによってベースラインで測定される。 Blood oxygen saturation is measured at baseline by pulse oximetry.
身体検査
スクリーニング時に行われる完全な身体検査には、頭部、目、鼻、及び喉、並びに心臓血管系、皮膚科学系、筋骨格系、呼吸器系、消化器系、泌尿生殖器系、及び神経系が含まれる。
Physical Exam A complete physical exam performed at Screening includes head, eyes, nose, and throat, as well as cardiovascular, dermatological, musculoskeletal, respiratory, digestive, genitourinary, and neurological systems. system is included.
ECOGパフォーマンスステータスを評定する。 Assess ECOG performance status.
その後の来院で(又は臨床的に示されるように)、限定的な症状指向性の身体検査を行う。ベースライン異常からの変化を、患者の医療記録に記録する。新規又は悪化した臨床的に有意な異常を、有害事象として記録する。 At subsequent visits (or as clinically indicated), a limited symptom-directed physical examination is performed. Changes from baseline abnormalities are recorded in the patient's medical record. New or worsening clinically significant abnormalities are recorded as adverse events.
腫瘍評定の一部として、身体検査には、リンパ節症、脾腫、肝腫、及び皮膚新生物又は転移の評定も含まれる。全ての患者をCNS転移の症状についてモニターし、そのような報告された症状の後に完全な神経学的検査を行う。脳磁気共鳴画像法(MRI)スキャン又は造影増強頭部CTスキャンを臨床的に示されるように行って、新たな又は悪化する脳関与を確認又は否定する。 As part of the tumor evaluation, the physical examination also includes assessment of lymphadenopathy, splenomegaly, hepatomegaly, and cutaneous neoplasms or metastases. All patients are monitored for symptoms of CNS metastases and undergo a complete neurological examination after such reported symptoms. A magnetic resonance imaging (MRI) scan or contrast-enhanced head CT scan is performed as clinically indicated to confirm or rule out new or worsening brain involvement.
腫瘍及び反応の評価
スクリーニング
疾患の全ての既知の部位を、スクリーニング時に文書化し、その後の各腫瘍評価時に再評定しなければならない。
Tumor and Response Assessment Screening All known sites of disease must be documented at screening and reevaluated at each subsequent tumor assessment.
スクリーニング及びその後の腫瘍評定には、CTスキャン(禁忌でない限りIV造影剤、及び施設標準に従い適切な場合経口造影剤を用いる)又は胸部、腹部、及び骨盤のMRIスキャンを含まなければならない。腫瘍評定のためのCTスキャンが陽電子放射断層撮影(PET)/CTスキャナーで行われる場合、CT取得は、完全造影CTスキャンの標準と一致しなければならない。 Screening and subsequent tumor assessment should include a CT scan (with IV contrast unless contraindicated, and oral contrast when appropriate according to institutional standards) or MRI scans of the chest, abdomen, and pelvis. If CT scans for tumor assessment are performed on a Positron Emission Tomography (PET)/CT scanner, the CT acquisition should conform to the standard for full contrast-enhanced CT scans.
処置された脳転移を有する患者、及び新規又は悪化したCNS転移を示す症状若しくは兆候に基づいて臨床上適応がある場合、脳撮像(MRI又は造影CTのいずれか)がスクリーニング時に必要とされる。曖昧な頭部CTの場合、疑わしい脳転移の存在又は程度を明らかにするために脳MRIが必要とされる。 Brain imaging (either MRI or CT with contrast) is required at screening for patients with treated brain metastases and if clinically indicated based on symptoms or signs indicative of new or worsening CNS metastases. In the case of equivocal head CT, a brain MRI is required to clarify the presence or extent of suspected brain metastases.
頸部の骨スキャン及びCTスキャン等のさらなる調査もまた、基礎疾患(例えば、頭頸部CTスキャンが、HNSCCの患者について示される)によって示されるように、及び上に列挙した評定の最小スケジュールによって実証され得ない任意の部位で疾患の臨床的疑いがある場合に実施される。治験責任医師の裁量で、RECIST v1.1に従う測定可能な疾患の評定の他の方法を使用してもよい。 Further investigations, such as neck bone scans and CT scans, are also demonstrated by the underlying disease (e.g., head and neck CT scans are indicated for patients with HNSCC) and by the minimum schedule of assessments listed above. It is performed when there is clinical suspicion of disease at any site that cannot be At the investigator's discretion, other methods of measurable disease assessment according to RECIST v1.1 may be used.
スクリーニング時に疾患部位を評定するために使用されたものと同じ放射線学的手順が、試験を通して使用されなければならない(例えば、CTスキャンの同じ造影治験実施計画書)。安定な脳転移は、ベースライン試験と同じX線検査手順を用いて各腫瘍評定で評価しなければならない。脳転移のない患者は、臨床上正当化されない限り、腫瘍評定のための脳スキャンを必要としない。応答は、RECIST v1.1を使用して、身体検査及び上に詳述したイメージングモダリティに基づいて治験責任医師によって評定される。全ての時点における全腫瘍奏功の治験責任医師の評定は、RECIST v1.1のみに基づく。評定は、来院間の内部一貫性を保証するために、可能であれば同じ評定者によって行われる。 The same radiological procedure used to assess disease sites at screening must be used throughout the study (eg, same imaging protocol for CT scan). Stable brain metastases must be evaluated at each tumor assessment using the same radiographic procedure as the baseline study. Patients without brain metastases do not require brain scans for tumor evaluation unless clinically justified. Responses will be assessed by the investigator using RECIST v1.1 based on physical examination and imaging modalities detailed above. Investigator assessment of overall tumor response at all time points is based solely on RECIST v1.1. Ratings will be performed by the same raters where possible to ensure internal consistency between visits.
以下の評定を行う:治験責任医師の裁量で、PDが疑われる場合はいつでもスキャンを実施することができる。 The following assessments will be made: At the discretion of the Investigator, scans can be performed whenever PD is suspected.
最初の試験処置中止後(中止が疾患進行以外の理由によるものであった場合)、死亡、疾患進行、別の全身性抗がん治療の開始、追跡不能、同意の撤回、又は試験終了のいずれか早く発生する方までフォローアップ腫瘍評定を行う。 After discontinuation of first study treatment (if discontinuation was for reasons other than disease progression), either death, disease progression, initiation of another systemic anticancer therapy, lost to follow-up, consent withdrawal, or study termination A follow-up tumor assessment is performed until the tumor occurs sooner.
RECIST v1.1による放射線学的疾患進行の後に処置を継続する患者は、6(±2)週間後(すなわち、スキャン頻度が2サイクル毎である場合、次の予定された腫瘍評定時、又はスキャン頻度が4サイクル毎である場合、予定外の腫瘍評定として)、又は臨床上適応がある場合にはそれより早くフォローアップスキャンで監視する。腫瘍評定は、その後2サイクル毎に、2つの連続したスキャンが、安定又は放射線学的疾患進行を示した最初のスキャンと比べた改善を示すまで継続されるべきであり、その時点でスキャン頻度は適用可能であれば4サイクル毎に戻すか移行される。全ての時点における全腫瘍奏功の治験責任医師の評定は、RECIST 1.1のみに基づく。 Patients continuing treatment after radiological disease progression by RECIST v1.1 will be scheduled after 6 (±2) weeks (i.e., at the next scheduled tumor assessment if the scan frequency is every 2 cycles, or at the scan If the frequency is every 4 cycles, as an unscheduled tumor assessment) or sooner as clinically indicated with follow-up scans. Tumor assessment should continue every 2 cycles thereafter until 2 consecutive scans show improvement over the first scan showing stable or radiological disease progression, at which point the scan frequency should be Return or transition every 4 cycles if applicable. Investigator assessment of overall tumor response at all time points is based solely on RECIST 1.1.
実験室、バイオマーカー、及び他の生物学的試料
第Ia相及び第Ib相の現地の検査室での試験
以下の検査室での試験は、検査施設の現地実験室で行われる。
Laboratory, Biomarkers, and Other Biological Specimens Phase Ia and Phase Ib Local Laboratory Testing The following laboratory testing is performed in the laboratory's local laboratory.
●血液学(WBC数、RBC数、ヘモグロビン、ヘマトクリット、血小板数、及び分類数(好中球、好酸球、好塩基球、単球、リンパ球、他の細胞)を含むCBC)。
●血清/血漿化学(ナトリウム、カリウム、塩化物、重炭酸塩、BUN又は尿素、クレアチニン、グルコース、カルシウム、マグネシウム、リン、総ビリルビン、ALT、AST、アルカリホスファターゼ、LDH、総タンパク質及びアルブミン)
●血清フェリチン及びC反応性タンパク質(CRP)
●凝固(PT、aPTT、及びINR)
●アミラーゼ及びリパーゼ
●妊娠検査。妊娠の可能性がある全ての女性(卵管結紮術を受けたことがある女性を含む)は、スクリーニング時に血清妊娠検査を受ける。尿妊娠検査は、試験処置の期間中、一定の間隔で行われる。尿妊娠検査結果が陽性である場合、患者の状態が血清妊娠検査によって判定されるまで投与を遅らせる。
●尿検査(比重、pH、グルコース、タンパク質、ケトン類、血液)
●甲状腺機能検査(甲状腺刺激ホルモン[TSH]、遊離T3及び遊離T4)
●EBV血清学(EBV IgM、EBV IgG及び/又はEBNA])及び/又はEBV PCR
• Hematology (CBC including WBC count, RBC count, hemoglobin, hematocrit, platelet count, and differential counts (neutrophils, eosinophils, basophils, monocytes, lymphocytes, other cells)).
Serum/plasma chemistry (sodium, potassium, chloride, bicarbonate, BUN or urea, creatinine, glucose, calcium, magnesium, phosphorus, total bilirubin, ALT, AST, alkaline phosphatase, LDH, total protein and albumin)
● Serum ferritin and C-reactive protein (CRP)
Coagulation (PT, aPTT, and INR)
● amylase and lipase ● pregnancy test. All women of childbearing potential (including those who have had tubal ligation) have a serum pregnancy test at screening. Urine pregnancy tests are performed at regular intervals throughout the study treatment. If the urine pregnancy test result is positive, dosing is delayed until the patient's status is determined by serum pregnancy test.
Urinalysis (specific gravity, pH, glucose, protein, ketones, blood)
Thyroid function tests (thyroid stimulating hormone [TSH], free T3 and free T4)
EBV serology (EBV IgM, EBV IgG and/or EBNA]) and/or EBV PCR
EBV IgM検査及び/又はEBV PCR検査は、患者がEBV IgG及び/又はEBNAについて陽性血清学を有する場合の適格性を考慮するために、サイクル1の1日目の前に必要である。
●CMV血清学(CMV IgG)
●HBV血清学(HBsAg、HBsAgに対する抗体、B型肝炎コア抗原)
An EBV IgM test and/or an EBV PCR test is required prior to
●CMV serology (CMV IgG)
HBV serology (HBsAg, antibodies against HBsAg, hepatitis B core antigen)
HBV DNA検査は、患者が抗HBcについて陽性血清学を有する場合、サイクル1、1日目の前に取得しなければならない。
●HCV血清学(抗HCV)
HBV DNA test must be obtained before
● HCV serology (anti-HCV)
患者が抗HCVについて陽性血清学を有する場合、適格性を考慮するために、サイクル1、1日目の前にHCV RNA検査が必要である。
●全ての患者は、試験への組み入れ前にHIVについて検査され、HIV陽性患者は試験から除外される。
●限定されないが、CA-125、CA19-9、がん胎児性抗原(CEA)、前立腺特異抗原(PSA)、ベータ-hCG、AFP、CA15-3及びCA27.29を含む腫瘍マーカー(適用可能かつ有益である場合)
If a patient has positive serology for anti-HCV, an HCV RNA test is required prior to
• All patients will be tested for HIV prior to inclusion in the study and HIV-positive patients will be excluded from the study.
- Tumor markers (as applicable and beneficial)
第Ia相及び第Ib相の中央検査
以下に列挙する試験は、中央検査室で行われる。PK又はADA分析のために収集された試料は、さらなる免疫原性特性評価、PK、バイオマーカー、及び/又は免疫原性アッセイの開発及び検証のために必要とされ得、したがって、それらの試料は、最終的な臨床試験報告書が完成してから5年以内に、又は地域の規制に応じてより早く破壊される。
Central Laboratory for Phase Ia and Phase Ib The studies listed below are conducted in the central laboratory. Samples collected for PK or ADA analysis may be required for further immunogenicity characterization, PK, biomarker, and/or immunogenicity assay development and validation; , within five years of completion of the final clinical study report, or sooner depending on local regulations.
血液試料に対して行われる評定
●ADAアッセイ
Ratings performed on blood samples ADA assay
検証されたアッセイ(第Ia相及び第Ib相)を使用して、チラゴルマブに対するADAの測定のために血清試料を得る。 Serum samples are obtained for measurement of ADA to tiragolumab using validated assays (Phase Ia and Phase Ib).
検証されたアッセイ(第Ib相のみ)を使用して、アテゾリズマブに対するADAの測定のために血清試料を得る。
●PKアッセイ
Serum samples will be obtained for measurement of ADA to atezolizumab using validated assays (Phase Ib only).
● PK assay
検証されたアッセイ(第Ia相及び第Ib相)を使用して、チラゴルマブ濃度の測定のために血清試料を得る。 Serum samples are obtained for determination of tiragolumab concentrations using validated assays (Phase Ia and Phase Ib).
検証されたアッセイ(第Ib相のみ)を使用してアテゾリズマブ濃度の測定のために血清試料を得る。 Serum samples will be obtained for determination of atezolizumab concentrations using validated assays (Phase Ib only).
検証されたアッセイを使用して、シスプラチン、カルボプラチン、ペメトレキセド、パクリタキセル、カペシタビン及びエトポシド濃度の測定のために血漿試料を得る(第Ib相化学療法拡大コホートのみ)。
●自己抗体検査
Plasma samples are obtained for determination of cisplatin, carboplatin, pemetrexed, paclitaxel, capecitabine and etoposide concentrations using validated assays (Phase Ib chemotherapy expansion cohort only).
● Autoantibody test
血清試料は、必ずしも限定されないが、抗核抗体、抗二本鎖DNA、抗好中球細胞質抗体、及び甲状腺ペルオキシダーゼ抗体を含む 自己抗体検査のために得られ、個々の患者又は試験集団のいずれかにおいて、試験中の臨床事象に基づいて実施される。
●血液中のバイオマーカーアッセイ
Serum samples are obtained for autoantibody testing including, but not necessarily limited to, antinuclear antibodies, anti-double-stranded DNA, antineutrophil cytoplasmic antibodies, and thyroid peroxidase antibodies, either for individual patients or study populations. , based on clinical events during the study.
●Biomarker assay in blood
スクリーニング来院時及び処置中に、全ての適格患者からバイオマーカー評価のために血液試料を得る。
●全ゲノム配列決定(WGS)
Blood samples for biomarker evaluation will be obtained from all eligible patients at screening visits and during treatment.
● Whole Genome Sequencing (WGS)
WGSのために単一の血液試料を採取し、分析のために1つ以上の検査室に送ることができる。WGSデータ及び関連する臨床データは、試験に参加していない試験者と共有されてもよく、又はヒトの健康及び疾患に関する試験を行うために他の試験者と広く共有するために政府又は他の健康試験データベースに提出されてもよい。試験参加者は、名前又は他の個人識別情報によって識別されない。 A single blood sample can be taken for WGS and sent to one or more laboratories for analysis. WGS data and related clinical data may be shared with testers not participating in the trial, or may be approved by governments or other parties for broad sharing with other testers to conduct human health and disease studies. May be submitted to a health test database. Study participants are not identified by name or other personally identifiable information.
WGSは、各サイトのIRB/EC及び該当する場合は適切な規制機関による再検討及び承認を条件とする。当該施設がWGSの承認を受けていない場合、この評定は当該施設では適用されない。 WGS is subject to review and approval by each site's IRB/EC and, where applicable, appropriate regulatory bodies. If the facility is not WGS approved, this rating is not applicable at the facility.
WGSデータは、この試験の文脈で分析され、疾患病理生物学をよりよく理解し、新しい治療アプローチの開発を導くために、他の試験とまとめて調査される。これらの分析の複雑さ及び探索的性質を考慮すると、WGSデータ及び分析は試験目的のみのためであり、治験責任医師又は試験参加者と共有されない。 The WGS data will be analyzed in the context of this study and will be explored together with other studies to better understand disease pathobiology and guide the development of new therapeutic approaches. Given the complexity and exploratory nature of these analyses, WGS data and analyzes are for study purposes only and will not be shared with investigators or study participants.
これらの試料は、枯渇するまで、又は患者が試料の破壊を要求するまで、無期限に保存される。 These samples are stored indefinitely until exhausted or until the patient requests destruction of the sample.
腫瘍試料に対して行われる評定
免疫関連及び腫瘍関連バイオマーカー(限定されないが、特定の細胞型上でのPD-L1、TIGIT、PVR及び/又はCD 226の発現を含む;及び浸潤性T細胞の有病率及び/又は活性化)の状態は、保管及び新鮮腫瘍試料の両方で、IHC、IF、及びqRT-PCRを含むがこれらに限定されない方法を使用して評価することができる。腫瘍RNA及び/又はDNAを精製し、RNA配列決定及びWGSによる特性評価に供することができる。臨床データ及び非臨床データによって導かれる場合、追加の探索的バイオマーカーも評定することができる。
●保管腫瘍組織:試験に登録した全ての患者について
Assessments performed on tumor samples Immune-related and tumor-related biomarkers, including but not limited to PD-L1, TIGIT, PVR and/or CD 226 expression on specific cell types; prevalence and/or activation) status can be assessed in both archived and fresh tumor samples using methods including, but not limited to, IHC, IF, and qRT-PCR. Tumor RNA and/or DNA can be purified and subjected to RNA sequencing and characterization by WGS. Additional exploratory biomarkers can also be assessed when guided by clinical and non-clinical data.
Archived tumor tissue: for all patients enrolled in the study
利用可能であれば、他の目的のために本試験の外部で得られた保管腫瘍組織試料を全ての患者から収集する(パラフィンブロックが好ましい;少なくとも15枚の染色されていないスライドが許容される)。第Ia相又は第Ib相の全ての患者について、試験に入る前に保管腫瘍組織の利用可能性を確認しなければならない。細針吸引物、浸出液又は腹水からの細胞ペレット、洗浄液試料、及び骨生検は、保管組織の要件を満たさない。 If available, archive tumor tissue samples obtained outside of the study for other purposes will be collected from all patients (paraffin blocks preferred; at least 15 unstained slides acceptable ). For all Phase Ia or Phase Ib patients, the availability of archived tumor tissue must be confirmed prior to entry into the study. Fine needle aspirates, cell pellets from exudates or ascites, lavage samples, and bone biopsies do not meet archival tissue requirements.
異なる時点(例えば、初期診断時及び疾患再発時)及び/又は複数の転移腫瘍からの適切な組織が利用可能である場合、最近に採取された(理想的には、最近の全身性療法に続いて)組織が優先しなければならない。 If appropriate tissue from different time points (e.g., at initial diagnosis and at disease recurrence) and/or from multiple metastatic tumors is available, recently harvested (ideally following recent systemic therapy). organization).
保管組織が不十分又は利用できない患者は依然として適格であり得る。 Patients with insufficient or unavailable archive tissue may still be eligible.
回収腫瘍組織は、タンパク質、RNA及びDNAの分析のための特性評価されたアッセイを使用して、潜在的な予測バイオマーカーを評価するために使用される。
●必要な腫瘍生検:第Ib相の連続生検拡大コホートに登録された患者の場合
Harvested tumor tissue is used to evaluate potential predictive biomarkers using characterized assays for protein, RNA and DNA analysis.
Required tumor biopsy: For patients enrolled in the Phase Ib serial biopsy expansion cohort
時点:連続生検を2つの時点で得る:1)全ての適格基準が満たされた後、ベースライン時に処置前-生検を得る、2)チラゴルマブ及びアテゾリズマブの両方の最初の投与後約2週間で処置中生検を得る(すなわち、サイクル1の15-21日目又はその間)。
Time points: Serial biopsies will be obtained at 2 time points: 1) pretreatment-biopsies will be obtained at baseline after all eligibility criteria are met, 2) approximately 2 weeks after the first dose of both tiragolumab and atezolizumab. Obtain in-treatment biopsies at (ie, on or during
追加の任意の生検は、治験責任医師の裁量により、好ましくはX線写真進行時(特に偽進行が疑われる場合)又は応答時に収集され得る。 Additional optional biopsies may be collected at the discretion of the investigator, preferably at radiographic progression (particularly if pseudoprogression is suspected) or at response.
連続腫瘍生検は、タンパク質、RNA及びDNAの分析のための特性評価されたアッセイを使用して、腫瘍薬力学バイオマーカー及び潜在的な予測バイオマーカーを評価するために使用される。
●第Ia相から第Ib相へのクロスオーバーのための進行時の腫瘍組織生検:治験責任医師が評定した放射線学的疾患進行後の試験の第Ia相から第Ib相へのクロスオーバーを検討している患者にのについて
Serial tumor biopsies are used to evaluate tumor pharmacodynamic and potential predictive biomarkers using characterized assays for protein, RNA and DNA analysis.
In-progress tumor tissue biopsy for crossover from Phase Ia to Phase Ib: Investigator-assessed crossover from Phase Ia to Phase Ib of the study after radiological disease progression about the patient under consideration
進行時の生検は、試料収集が治験責任医師によって臨床的に実施可能であると考えられる場合、及び患者が書面によるインフォームドコンセントを提供した場合に必要とされる。深部腫瘍組織若しくはリンパ節のコアニードル生検、又は皮膚、皮下若しくは粘膜病変の切除生検、切開生検、パンチ生検若しくは鉗子生検からなる腫瘍組織試料を得る。 A progression biopsy is required if sample collection is deemed clinically feasible by the investigator and if the patient provides written informed consent. Tumor tissue samples are obtained consisting of core needle biopsies of deep tumor tissue or lymph nodes, or excisional, incisional, punch or forceps biopsies of skin, subcutaneous or mucosal lesions.
進行時の生検は、タンパク質、RNA及びDNAの分析のための特性評価されたアッセイを使用して、腫瘍薬力学バイオマーカー及び潜在的な予測バイオマーカーの評価に使用される。
●任意の腫瘍生検:特に第Ia相又は第Ib相の拡大コホートに登録された患者の最大半数において、任意の生検を受けるための特定のインフォームドコンセントを提供する患者について
Biopsies at progression are used for evaluation of tumor pharmacodynamic and potential predictive biomarkers using characterized assays for protein, RNA and DNA analysis.
Optional tumor biopsy: For patients who provide specific informed consent to undergo an optional biopsy, especially in up to half of patients enrolled in Phase Ia or Phase Ib expansion cohorts
任意の生検に同意した患者は、全ての適格基準が満たされた後、及び単剤としてのチラゴルマブの初回投与後約2週間(第Ia相)又はチラゴルマブ及びアテゾリズマブの初回投与後約2週間(第Ib相)(すなわち、サイクル1の15-21日目又はその間)にベースラインで腫瘍生検を提供する。 Patients who consented to a voluntary biopsy were selected after all eligibility criteria were met and approximately 2 weeks after the first dose of tiragolumab as a single agent (Phase Ia) or approximately 2 weeks after the first dose of tiragolumab and atezolizumab (Phase Ia). Provide a tumor biopsy at baseline during or during Phase Ib) (ie, Days 15-21 of Cycle 1).
アクセス可能な残留塊を有する確認された長期CR及び/又はPR(例えば、約1年の期間)を有する患者については、その残留塊の生検が生存腫瘍細胞(対線維性組織又は壊死組織)について評定するために推奨される。 For patients with documented long-term CR and/or PR (e.g., duration of about 1 year) with accessible residual mass, a biopsy of the residual mass should be evaluated for viable tumor cells (vs. fibrotic or necrotic tissue). recommended for grading.
腫瘍組織試料は、コアニードル、パンチ、切除生検(上記のように)、又は鉗子生検を用いて収集することができる。選択された生検技術に関連するさらなる指針については、必須の腫瘍生検について上記の試料の仕様を参照されたい。 Tumor tissue samples can be collected using core needle, punch, excisional biopsy (as described above), or forceps biopsy. See the sample specifications above for required tumor biopsies for additional guidance related to the selected biopsy technique.
任意の腫瘍生検は、タンパク質、RNA及びDNAの分析のための特性評価されたアッセイを使用して、腫瘍薬力学バイオマーカー及び潜在的な予測バイオマーカーを評価するために使用される。
●試料の仕様:第Ia相及び第Ib相の全ての患者について、必要な及び任意の生検は、以下の試料要件を満たすものとする。
Any tumor biopsy is used to evaluate tumor pharmacodynamics biomarkers and potential predictive biomarkers using characterized assays for protein, RNA and DNA analysis.
• Specimen Specifications: For all Phase Ia and Ib patients, required and optional biopsies must meet the following specimen requirements.
深部腫瘍組織若しくはリンパ節のコアニードル生検、又は皮膚、皮下若しくは粘膜病変の切除生検、切開生検、パンチ生検若しくは鉗子生検からなる腫瘍組織試料を得る。細針吸引物、滲出液又は腹水からの細胞ペレット、洗浄液試料、及び骨生検は許可されない。コア針生検のために考慮される標的病変は、所与の時点(18-ゲージの最小直径)での少なくとも3つのコアの回収に適していると考えられる。可能であれば、同じ病変を通る連続パスは≧1cm離れていることになる。 Tumor tissue samples are obtained consisting of core needle biopsies of deep tumor tissue or lymph nodes, or excisional, incisional, punch or forceps biopsies of skin, subcutaneous or mucosal lesions. Fine needle aspirates, cell pellets from exudates or ascites, lavage samples, and bone biopsies are not permitted. Target lesions considered for core needle biopsy are considered suitable for retrieval of at least 3 cores at a given time point (minimum diameter of 18-gauge). If possible, consecutive paths through the same lesion will be ≧1 cm apart.
複数の病変が利用可能である場合、実施可能であれば、転移部位に関連する不均一性の導入を回避するために、前処置生検と同じ病変(又は器官)から処置中生検を得ることが好ましい。 If multiple lesions are available, obtain a periprocedural biopsy from the same lesion (or organ) as the pretreatment biopsy, if practicable, to avoid introducing heterogeneity related to metastatic sites is preferred.
RECIST標的病変は生検対象としない。 RECIST target lesions are not biopsied.
組織試料及びそれらの誘導体(DNA及びRNA等)は、無期限に又は使い切るまで、又は患者がそれらの試料の破壊を要求するまで保存される。
●第Ia相及び第Ib相の全患者に対する残りの試料の使用
Tissue samples and their derivatives (such as DNA and RNA) are stored indefinitely or until exhausted or until the patient requests destruction of the samples.
Use of Remaining Samples for All Phase Ia and Phase Ib Patients
患者が試験の経過中のいつでも医学的に指定される手順(すなわち、気管支鏡検査、食道胃十二指腸鏡検査、大腸鏡検査等)を受けて、単剤としてのチラゴルマブ(第Ia相)、又は化学療法を用いて若しくは用いずにアテゾリズマブと組み合わせたチラゴルマブ(第Ib相)の活性(抗腫瘍又は自己免疫のいずれか)を知らせ得る腫瘍組織又は他の組織が得られる場合、医学的診断に必要ではない残りの試料又は試料の一部(体液試料又は残存腫瘍組織)を探索分析のために得ることができる。患者は、これらの試料を収集して評価するために、特定のインフォームドコンセントを提供しなければならない。 Tiragolumab as a single agent (Phase Ia), or chemo Not required for medical diagnosis if tumor tissue or other tissue is available that may signal the activity (either antitumor or autoimmune) of tiragolumab (Phase Ib) in combination with atezolizumab with or without therapy. The remaining sample or portion of the sample (bodily fluid sample or residual tumor tissue) can be obtained for exploratory analysis. Patients must provide specific informed consent for these samples to be collected and evaluated.
残りの腫瘍試料は、タンパク質、RNA及びDNAの分析のための特性評価されたアッセイを使用して、腫瘍薬力学バイオマーカー及び潜在的な予測バイオマーカーの評価に使用される。 Remaining tumor samples are used for evaluation of tumor pharmacodynamic biomarkers and potential predictive biomarkers using characterized assays for protein, RNA and DNA analysis.
心電図
3連のECG記録を、チラゴルマブ単独(第Ia相)の用量漸増コホート及びバックフィルコホートについての指定された時点で得て、他の全ての患者については1回のECG記録を得る。異なる日に取得されたECGは、実施可能な限り厳密に時間が一致する。3つの解釈可能なECG記録(例えば、アーチファクトなし)を各時点(±5分)で取得しなければならない。3つの読み取り値の平均を使用して、ECG間隔を決定する(例えば、PR、QRS、QT)。臨床的に示されるように、予定外の時点で追加のECGを得ることができる。
Electrocardiogram Triplicate ECG recordings will be obtained at the indicated time points for the dose escalation and backfill cohorts of tiragolumab alone (Phase Ia) and one ECG recording will be obtained for all other patients. ECGs acquired on different days are time-matched as closely as practicable. Three interpretable ECG recordings (eg, no artifact) must be acquired at each time point (±5 minutes). An average of the three readings is used to determine the ECG interval (eg PR, QRS, QT). Additional ECGs can be obtained at unscheduled time points as clinically indicated.
全てのECG記録は、コンピュータベースの間隔測定値を備えた標準的な高品質の高忠実度デジタル心電計を使用して行われなければならない。リードの配置は可能な限り一貫している。ECG記録は、患者が少なくとも10分間仰臥位で安静にした後に行われなければならない。全てのECGは、同時にスケジュールされた他の手順(例えば、生体情報測定、採血)の前に取得されるべきであり、食事後3時間以内に取得されるべきではない。このガイダンスに従うことが患者にとって困難であり得る場合、食事摂取とECG記録との間の時間は、全ての時点で同じ最小時間が維持される限り、2.5時間又は施設の基準に短縮され得る。環境的注意散漫(例えば、テレビ、ラジオ、会話)を含む、心拍数の変化を誘発し得る状況は、プレECG休止期間中及びECG記録中に回避されなければならない。 All ECG recordings must be made using a standard, high quality, high fidelity digital electrocardiograph with computer-based interval measurements. Lead placement is as consistent as possible. ECG recordings must be taken after the patient has rested in the supine position for at least 10 minutes. All ECGs should be obtained prior to other concurrently scheduled procedures (eg, biometric measurements, blood draws) and should not be obtained within 3 hours after meals. If it may be difficult for the patient to follow this guidance, the time between meal intake and ECG recording may be shortened to 2.5 hours or institutional standards as long as the same minimum time is maintained at all time points. . Situations that can induce heart rate changes, including environmental distractions (eg, television, radio, talking) must be avoided during the pre-ECG rest period and during ECG recording.
安全性を監視する目的で、治験責任医師は全てのECG記録を再検討し、署名し、日付を付けなければならない。臨床的意義の有無にかかわらず、ECGの正常又は異常としての全体的な評定を記録する。ECG記録の紙又は電子コピーは、現場で患者の恒久的な試験ファイルの一部として保持される。 For safety monitoring purposes, the investigator must review, sign, and date all ECG records. An overall rating of the ECG as normal or abnormal, whether clinically relevant or not, is recorded. A paper or electronic copy of the ECG record is maintained on site as part of the patient's permanent test file.
特定の投与後時点において、フリデリシアの式(QTcF)を使用して補正された平均QT間隔がベースライン値よりも>500 ms及び/又は>60 ms長い場合、理想的には次の5分以内に別のECGを記録しなければならず、ECGモニタリングは、QTcFが2つの連続するECGで安定するまで継続する。治験責任医師の裁量により、標準治療処置を開始してもよい。PK試料がその時点で予定されていない場合、予定されていないPK試料が得られる。治験責任医師は、潜在的な同時危険因子(例えば、電解質異常、QT間隔を延長することが知られている共投薬、重度の徐脈)について患者を評価する。 If the mean QT interval corrected using the Fridericia formula (QTcF) is >500 ms and/or >60 ms longer than the baseline value at a given post-dose time point, ideally within the next 5 minutes Another ECG must be recorded at 10:00 a.m. and ECG monitoring continues until QTcF is stable in two consecutive ECGs. At the discretion of the Investigator, standard of care treatment may be initiated. If a PK sample is not scheduled at that time, an unscheduled PK sample is obtained. The investigator will evaluate the patient for potential co-risk factors (eg, electrolyte imbalances, co-medications known to prolong the QT interval, severe bradycardia).
がんに関連する処置
がん関連の医学的、外科的及び放射線処置の収集は、1日目に開始し、試験の第Ia相部分及び第Ib相部分の両方において、処置期間を通して及び生存フォローアップ期間中に実施する。
Cancer-Related Treatments Cancer-related medical, surgical and radiological treatment collections began on
抗薬物抗体検査
チラゴルマブ及び/又はアテゾリズマブは、それ自体に対する免疫応答を誘発し得る。検証されたスクリーニング、確認及び力価アッセイを使用して、第Ia相の単剤としてのチラゴルマブによる処置前、処置中及び処置後、又は第Ib相の化学療法の有無にかかわらず、チラゴルマブとアテゾリズマブとの組み合わせによる処置後の複数の時点でADAを検出する。ADA応答は、その臨床的意義を理解するために関連する臨床評価項目と相関する。ADA応答を更に特性評価するために、追加のADAアッセイ(例えば、中和抗体アッセイ)を使用することができる。
Anti-Drug Antibody Testing Tiragolumab and/or atezolizumab can induce an immune response against themselves. Tiragolumab and atezolizumab before, during and after treatment with tiragolumab as single agents in Phase Ia or with or without chemotherapy in Phase Ib using validated screening, confirmation and potency assays ADA is detected at multiple time points after treatment in combination with ADA responses are correlated with relevant clinical endpoints to understand their clinical significance. Additional ADA assays (eg, neutralizing antibody assays) can be used to further characterize the ADA response.
U.患者及び試験処置の中止
患者の中止
試験からの患者の中止は、試験処置の中止とは区別され、患者が死亡したとき、フォローアップに失敗したとき、又はフ追跡の同意を取り下げるときに起こる。
U.S.A. Withdrawal of Patients and Study Treatment Patient withdrawal Patient withdrawal from a study is distinct from discontinuation of study treatment and occurs when a patient dies, fails follow-up, or withdraws consent for follow-up.
患者は、何らかの理由でいつでも試験から自発的に離脱する権利を有する。更に、治験責任医師は、患者を試験からいつでも離脱させる権利を有する。試験からの離脱の理由には、限定されないが、以下が含まれ得る:
●同意の任意の時点での患者の離脱
●治験責任医師が試験を継続する場合、治験責任医師が患者の安全性を危険にさらす可能性があると判断した医学的症状
●治験責任医師が患者にとって最も有益であるとの判断
Patients have the right to voluntarily withdraw from the study at any time for any reason. Additionally, the investigator has the right to withdraw a patient from the study at any time. Reasons for withdrawal from the study may include, but are not limited to:
- patient withdrawal at any time of consent - any medical condition that the investigator determines may jeopardize the patient's safety if the investigator continues the study - the investigator does not determined to be most beneficial to
試験から離脱する患者に関する情報を得るためにあらゆる努力がなされる。試験又はフォローアップからの離脱の主な理由が文書化されている。しかしながら、同意が取り消された後、患者はいかなる理由でも追跡されない。試験から離脱する患者は置き換えられない。 Every effort will be made to obtain information regarding patients withdrawing from the study. The primary reason for withdrawal from the study or follow-up is documented. However, patients are not followed for any reason after consent is revoked. Patients who withdraw from the study are not replaced.
試験処置の中止
患者は、以下のいずれかを経験した場合、試験処置を中止しなければならない:
●全てのX線写真データ、生検結果及び臨床状態の統合評定後に治験責任医師によって決定された疾患進行に起因する症候性悪化(すなわち、疾患又は管理不能な腹水等に続発する制御不能な疼痛)。
●個々の患者の治療に対する潜在的応答及び事象の重症度を考慮すると、許容できないと治験責任医師が判断した免疫介在性有害事象の発生を含む、試験処置に関連する許容できない毒性
●治験責任医師が試験処置を継続する場合、治験責任医師が患者の安全性を危険にさらす可能性があると判断した医学的症状
●非治験実施計画書全身性抗がん治療の使用
●妊娠
患者は、何らかの理由でいつでも試験処置を自発的に中止する権利を有する。更に、治験責任医師は、患者を試験処置からいつでも引き抜く権利を有する。試験処置からの離脱の理由には、限定されないが、以下が含まれ得る:
●治験責任医師が患者にとって最も有益であるとの判断
●患者のノンコンプライアンス
Discontinuation of Study Treatment Patients must discontinue study treatment if they experience any of the following:
- Symptomatic exacerbation due to disease progression as determined by the investigator after integrated assessment of all radiographic data, biopsy results and clinical status (i.e., uncontrolled pain secondary to disease or uncontrolled ascites, etc.) ).
- Unacceptable treatment-related toxicities, including the occurrence of immune-mediated adverse events that the investigator deems unacceptable given the individual patient's potential response to treatment and the severity of the event - Investigator Any medical condition that the investigator determines may jeopardize the patient's safety if the patient continues study treatment Use of a non-protocol systemic anticancer therapy Pregnancy You have the right to voluntarily discontinue study treatment at any time for any reason. Additionally, the investigator has the right to withdraw a patient from study treatment at any time. Reasons for withdrawal from study treatment may include, but are not limited to:
● Investigator's decision to be in the best interest of the patient ● Patient non-compliance
主に疾患進行以外の理由で試験処置を中止する患者は腫瘍評定を継続し、試験処置を中止する全ての患者は、同意が取り消されない限り、3ヶ月ごとに生存のために追跡され続ける。 Patients who discontinue study treatment primarily for reasons other than disease progression will continue to have tumor assessments, and all patients who discontinue study treatment will continue to be followed for survival every 3 months unless consent is revoked.
試験処置を中止した患者は、試験処置の最後の投与の≦30日後に処置中止の来院のために診療所に戻るように求められる。 Patients who discontinue study treatment will be asked to return to the clinic for a treatment discontinuation visit ≤30 days after the last dose of study treatment.
応答評定がPDを示す来院(これは、チラゴルマブ(第Ia相)の中止又はチラゴルマブとアテゾリズマブとの組み合わせ、チラゴルマブとアテゾリズマブとベバシズマブとの組み合わせ、又はチラゴルマブとペンブロリズマブとの組み合わせ(第Ib相)の中止をもたらす)が、必要に応じて処置中止来院として使用され得、その場合、処置中止来院に関連する全ての評定がその時点で行われる。 A visit with a response rating of PD (which is discontinuation of tiragolumab (Phase Ia) or tiragolumab in combination with atezolizumab, tiragolumab in combination with atezolizumab in combination with bevacizumab, or tiragolumab in combination with pembrolizumab (Phase Ib)) ) can optionally be used as a discontinuation visit, where all assessments associated with the discontinuation visit are made at that time.
試験処置の中止後、全患者を生存及びその後の抗がん治療について追跡する。生存及びその後の抗がん治療療法のフォローアップ情報は、患者がフォローアップからの中止を要求しない限り、死亡、フォローアップの喪失、又は試験終了まで、およそ3ヶ月毎に電話、患者の医療記録、及び/又はクリニック来院を介して収集される。その後の抗がん治療に関する情報には、全身療法(例えば、化学療法、標的療法、ホルモン療法、又はCIT)、手術(例えば、転移性疾患の摘出)、及び放射線処置(例えば、腫瘍病変に対する放射線療法)が含まれる。 After discontinuation of study treatment, all patients are followed for survival and subsequent anticancer therapy. Survival and subsequent anticancer therapy follow-up information will be obtained by phone call, patient's medical records approximately every 3 months until death, loss of follow-up, or study termination, unless the patient requests discontinuation from follow-up. , and/or collected via clinic visits. Information regarding subsequent anticancer therapy includes systemic therapy (eg, chemotherapy, targeted therapy, hormone therapy, or CIT), surgery (eg, removal of metastatic disease), and radiation treatment (eg, radiation to tumor lesions). therapy).
患者が試験から離脱する場合、現場のスタッフは、公開情報源(例えば、郡記録)を使用して生存状態に関する情報のみを取得することができる。 If a patient is withdrawn from the study, site staff can only obtain information on survival status using public sources (eg, county records).
V.分析
目的及び評価項目
この試験は、局所進行性又は転移性腫瘍を有する患者において、単剤として(第Ia相)又はアテゾリズマブ若しくは他の抗がん治療と組み合わせて(第Ib相)投与した場合のチラゴルマブの安全性、PK、薬力学及び予備抗腫瘍活性を評価する。本試験の具体的な目的及び対応評価項目を表36に概説する。


活性分析
以下に記載される分析は、RECIST v 1.1による客観的奏効の定義に基づく。
Activity Analysis The analysis described below is based on the definition of objective response according to RECIST v 1.1.
応答評定データ、客観的奏効期間、PFS及びOSは、適切な場合には、全ての処置患者について用量レベル又は腫瘍タイプによって列挙される。 Response rating data, duration of objective response, PFS and OS are listed by dose level or tumor type for all treated patients, as appropriate.
客観的奏効率
ORRの分析には、任意の量の試験処置を受け、ベースラインで測定可能な疾患を有する第Ia相又は第Ib相試験の患者が含まれる。客観的奏効は、治験責任医師の評定によって決定され、最初の文書化の≧4週間後の反復評定によって確認されるCR又はPRとして定義される。ベースラインが欠けているか又は応答評定がない患者は、非応答者として分類される。客観的奏効率は、腫瘍タイプ及び適用可能であれば用量によって推定及び要約される。
Objective Response Rate The ORR analysis includes Phase Ia or Phase Ib patients who have received any amount of study treatment and who have measurable disease at baseline. An objective response is defined as a CR or PR as determined by the investigator's assessment and confirmed by a repeat assessment >4 weeks after initial documentation. Patients with missing baselines or no response ratings are classified as non-responders. Objective response rates are estimated and summarized by tumor type and dose, if applicable.
奏効期間
客観的奏効を有する患者の中で、客観的奏効の期間は、最初の完全奏効又は部分奏効から疾患進行又は死亡(いずれか早く発生する方)までの時間として定義される。試験の終了前に死亡していないか、又は疾患進行を経験していないか、又はフォローアップ不能になっている患者については、客観的奏効期間が最後の腫瘍評定の日に打ち消されるものとする。
Duration of Response Among patients with an objective response, the duration of objective response is defined as the time from the first complete or partial response to disease progression or death (whichever occurs first). For patients who do not die, experience disease progression, or are lost to follow-up before the end of the study, the duration of objective response shall be canceled on the date of the last tumor assessment. .
無増悪生存期間
PFSの分析には、任意の量の試験処置を受けた患者が含まれる。PFSは、試験処置の最初の日から、文書化された疾患進行又は死亡まで(いずれか早く発生する方)の時間として定義される。試験の終了前にPD又は死亡が文書化されていない患者、又はフォローアップに失敗した患者については、PFSは最後の腫瘍評定の日に打ち切られる。ベースライン後の腫瘍評定がない患者については、試験処置の1日目にPFSを打ち切られる。
Progression-Free Survival The analysis of PFS included patients who received any dose of study treatment. PFS is defined as the time from the first day of study treatment to documented disease progression or death (whichever occurs first). For patients with no documented PD or death before the end of the study, or who fail to follow up, PFS will be censored on the day of the last tumor assessment. Patients with no post-baseline tumor assessment will have PFS censored on
全生存期間
OSの分析には、任意の量の試験処置を受けた患者が含まれる。OSは、任意の試験処置の最初の投与から試験中の任意の原因による死亡までの時間として定義される。試験の終了前に死亡しなかった患者又はフォローアップを失った患者については、生存していることが最後に分かった日にOSを打ち切る。
Overall Survival The analysis of OS includes patients who received any amount of study treatment. OS is defined as the time from the first dose of any study treatment to death from any cause during the study. For patients who do not die before the end of the study or are lost to follow-up, OS is censored on the last known alive date.
安全性解析
安全性は、DLT、有害事象、臨床検査結果の変化、バイタルサイン及びECGの変化、及び任意の試験処置(チラゴルマブ、アテゾリズマブ、ベバシズマブ、ペンブロリズマブ、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル、カペシタビン、エトポシド)への曝露の要約を通して評定される。任意量の試験処置を受ける患者は全員、安全性分析に含められる。
Safety Analysis Safety was measured by DLTs, adverse events, laboratory changes, vital signs and ECG changes, and any study treatments (tiragolumab, atezolizumab, bevacizumab, pembrolizumab, carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine, etoposide). ) through a summary of exposure to All patients who receive any dose of study treatment will be included in the safety analysis.
有害事象の言語記述を類義語にマッピングする。有害事象データは、試験部位、必要に応じて用量コホート又は腫瘍タイプ、患者番号及び試験日によって列挙される。1日目の処置時又は処置後に発生した事象を、マッピングされた用語、適切な類義語レベル、及びNCI CTCAE v 4.0グレードによって要約する。更に、死亡を含む重篤な有害事象を別々に列挙し、要約する。
Map verbal descriptions of adverse events to synonyms. Adverse event data are listed by study site, dose cohort or tumor type as appropriate, patient number and study date. Events occurring during or after treatment on
処置中止につながる有害事象を列挙する。DLT以外の理由でDLT評定ウィンドウを完了する前に試験から離脱した患者は、DLT及びMTD評定について評価不可能であると考えられる。 Adverse events leading to treatment discontinuation will be listed. Patients who withdraw from the study for reasons other than DLT before completing the DLT assessment window will be considered non-evaluable for DLT and MTD assessment.
関連する検査室、バイタルサイン、及びECGデータを、必要に応じてNCI CTCAEグレード3及びグレード4の値を特定して時間順に表示する。ADA応答(血清抗チラゴルマブ又は抗アテゾリズマブの存在)の発生率、並びにPK、薬力学、及び安全性パラメーターとの潜在的な相関を評定することができる。
Relevant laboratory, vital signs, and ECG data are displayed in chronological order specifying
薬物動態分析
第Ia相試験では、個別及び平均血清チラゴルマブ濃度対時間データを集計し、用量レベルによってプロットする。チラゴルマブの薬物動態は、総AUC、Cmax、Cmin、総CL、Vss、及び終末期半減期(収集されたデータに適切な場合)を推定することによって要約される。これらのパラメーターの推定値を集計し、要約する(平均、標準偏差、及び変動係数)。患者間の変動性及び薬物蓄積を評価する。
Pharmacokinetic Analysis For the Phase Ia study, individual and mean serum tiragolumab concentration versus time data will be aggregated and plotted by dose level. The pharmacokinetics of tiragolumab are summarized by estimating total AUC, C max , C min , total CL, V ss , and terminal half-life (if appropriate for collected data). Estimates of these parameters are tabulated and summarized (mean, standard deviation, and coefficient of variation). Patient-to-patient variability and drug accumulation are assessed.
第Ib相試験では、血清チラゴルマブ及びアテゾリズマブ濃度データ(Cmax及びCmin)を集計し、収集した各サイクルの用量レベルによって要約する。記述統計学には、必要に応じて、平均、中央値、標準偏差、及び範囲が含まれる。他のPKパラメーターを決定し、データ正当性として要約することができる。これらの結果は、チラゴルマブ又はアテゾリズマブPKが他の薬剤の同時投与によって変化するかどうかに関する予備的情報を提供するので、データを歴史的データと比較することができる。 In Phase Ib studies, serum tiragolumab and atezolizumab concentration data (C max and C min ) will be aggregated and summarized by dose level for each cycle collected. Descriptive statistics include mean, median, standard deviation, and range as appropriate. Other PK parameters can be determined and summarized as data validity. These results provide preliminary information as to whether tiragolumab or atezolizumab PK is altered by co-administration of other agents, so the data can be compared with historical data.
第Ib相化学療法拡大コホートでは、チラゴルマブ及びアテゾリズマブの血清濃度並びにカルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル、カペシタビン及びエトポシドの血漿濃度を収集する。チラゴルマブ、アテゾリズマブ、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル、カペシタビン及びエトポシドの濃度は、上記のように記述統計を使用して要約される。これらの結果は、チラゴルマブ、アテゾリズマブ、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル、カペシタビン及びエトポシドPKが他の薬剤の同時投与によって変化するかどうかに関する予備的情報を提供するので、データを履歴データと比較する。 In the Phase Ib chemotherapy expansion cohort, serum concentrations of tiragolumab and atezolizumab and plasma concentrations of carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide will be collected. Concentrations of tiragolumab, atezolizumab, carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide are summarized using descriptive statistics as described above. These results provide preliminary information as to whether tiragolumab, atezolizumab, carboplatin, cisplatin, pemetrexed, paclitaxel, capecitabine and etoposide PK are altered by co-administration of other agents, and the data are compared with historical data.
薬力学的分析は、入手可能な場合、腫瘍組織及び血液の両方における薬力学的バイオマーカーの評定を含む。追加のPK及び薬力学的分析を適宜行う。バイオマーカーサンプリング時間の潜在的な調整は、以前の患者において観察されたバイオマーカー応答に基づいて、必要に応じて適用され得る。 Pharmacodynamic analysis includes evaluation of pharmacodynamic biomarkers in both tumor tissue and blood, when available. Additional PK and pharmacodynamic analyzes are performed as appropriate. Potential adjustments to biomarker sampling times may be applied as needed based on biomarker responses observed in previous patients.
免疫原性分析
患者は、ベースラインでADA陰性であり、その後、試験薬物投与後にADA応答を発症する場合、処置誘発性ADA応答を有すると考えられる。患者がベースラインでADA陽性であり、1つ以上のベースライン後の試料の力価がベースライン試料の力価よりも少なくとも4倍大きい(すなわち、≧0.60タイターユニット)場合、患者は処置によって増強されたADA応答を有すると考えられる。患者は、全ての時点でADA陰性である場合、ADAについて陰性であるとみなされる。患者は、ベースラインでADA陽性であるが、ベースライン試料の力価より少なくとも4倍大きい力価を有するベースライン後の試料を有していない場合、処置に影響されないと考えられる。
Immunogenicity Analysis Patients are considered to have a treatment-induced ADA response if they are ADA negative at baseline and subsequently develop an ADA response after administration of study drug. If the patient is ADA-positive at baseline and the titer of one or more post-baseline samples is at least 4-fold greater than the titer of the baseline sample (i.e., ≧0.60 titer units), the patient is eligible for treatment. is thought to have an enhanced ADA response by Patients are considered negative for ADA if they are ADA negative at all time points. Patients are considered unaffected by treatment if they are ADA positive at baseline but do not have a post-baseline sample with a titer that is at least 4-fold greater than the baseline sample titer.
チラゴルマブ及びアテゾリズマブについてのADAの結果を要約し、試験の第Ia相部分及び第Ib相部分についての患者及びサイクルによって列挙する。 The ADA results for tiragolumab and atezolizumab are summarized and listed by patient and cycle for the Phase Ia and Ib portions of the study.
相Ia及び相Ibの拡大コホートにおける中間解析
活性の証拠がない場合、登録の早期停止の可能性を導くために、段階Ia及び段階Ibの各拡大コホートについてIMCによって中間分析を行う。拡大コホートに登録された約20人の患者が1-2の腫瘍評定を完了した後、IMCが会議を開いて中間解析を行う。中間解析が、化学療法を伴う又は伴わない、チラゴルマブ(第Ia相)又はアテゾリズマブと組み合わせたチラゴルマブ、又はアテゾリズマブ及びベバシズマブと組み合わせたチラゴルマブ、又はペンブロリズマブと組み合わせたチラゴルマブ(第Ib相)による客観的腫瘍応答によって示される活性が、その患者グループのための関心の閾値未満であることを示唆する場合(例えば、最初の20人の患者において応答が観察されない場合、)、IMCは、拡大コホートへの登録を中止することを推奨し得る。
Interim Analysis in the Phase Ia and Phase Ib Expansion Cohorts An interim analysis will be conducted by the IMC on each of the Phase Ia and Phase Ib expansion cohorts to guide possible early termination of enrollment in the absence of evidence of activity. After approximately 20 patients enrolled in the expansion cohort have completed 1-2 tumor assessments, the IMC will convene for an interim analysis. Interim analysis of objective tumor response with tiragolumab (Phase Ia) or tiragolumab in combination with atezolizumab, or tiragolumab in combination with atezolizumab and bevacizumab, or tiragolumab in combination with pembrolizumab (Phase Ib), with or without chemotherapy suggests that the activity indicated by is below the threshold of interest for that patient group (e.g., no response is observed in the first 20 patients), the IMC will consider enrollment in the expansion cohort. Discontinuation may be recommended.
例えば、真のORRが5%である場合、最初の20人の患者において応答が観察されない約35%の確率があり、真のORRが10%である場合、最初の20人の患者において応答が観察されない約12%の確率がある。 For example, if the true ORR is 5%, there is approximately a 35% chance that no response will be observed in the first 20 patients, and if the true ORR is 10%, there will be no response in the first 20 patients. There is about a 12% chance of not being observed.
IMCはまた、活性の証拠がある場合、又は十分な評価を可能にするのに十分な特定の患者が登録していない場合(例えば、特定の腫瘍タイプ、特定の腫瘍PD-L1及び/若しくはTIGIT発現状態、並びに/又は特定のCIT病歴を有する患者)、その拡大コホートで登録を継続することを推奨し得る。 IMC may also be used if there is evidence of activity or if not enough specific patients are enrolled to allow adequate evaluation (e.g., specific tumor types, specific tumor PD-L1 and/or TIGIT expression status, and/or a specific history of CIT), it may be recommended to continue enrollment in the expansion cohort.
全ての場合において、無駄に基づいて拡大コホートへの登録を停止する決定は、試験の治験責任医師と相談して、メディカルモニターによるIMC推奨に従って行われる。メディカルモニターはまた、第Ia相又は第Ib相の各拡大コホートにおける進行中のデータを再検討するために、IMCの追加の臨時会議を要求することができる。 In all cases, the decision to discontinue enrollment in the expansion cohort on the basis of futility will be made in consultation with the study investigator and according to IMC recommendations by the medical monitor. The medical monitor may also request an additional ad hoc meeting of the IMC to review ongoing data in each of the Phase Ia or Phase Ib expansion cohorts.
W.チラゴルマブの臨床試験の概要
局所進行性腫瘍又は転移性腫瘍を有する患者におけるチラゴルマブを評価するこの進行中の試験(GO30103)から、予備的な臨床データが利用可能である。2019年12月2日の臨床的カットオフ日の時点で、GO 30103試験には190人の登録患者がおり、42人の患者が第Ia相部分に登録され、171人の患者が第Ib相部分に登録され、23人の患者が疾患進行後に第Ia相からクロスオーバーした。
W. Overview of Tiragolumab Clinical Trials Preliminary clinical data are available from this ongoing trial (GO30103) evaluating tiragolumab in patients with locally advanced or metastatic tumors. As of the clinical cut-off date of December 2, 2019, the GO 30103 study had 190 patients enrolled, with 42 patients enrolled in the Phase Ia portion and 171 patients in the Phase Ib portion. Partially enrolled, 23 patients crossed over from Phase Ia after disease progression.
進行中の第II相試験(CITYSCAPEとも呼ばれるGO40290)は、感作性上皮増殖因子受容体(EGFR)変異又はALK転座を有する患者を除いて、局所進行性の切除不能又は転移性PD-L1-選択NSCLCを有する化学療法未経験患者における、プラセボ+アテゾリズマブと比較した、チラゴルマブ及びアテゾリズマブの有効性及び安全性を評価している。 An ongoing phase II trial (GO40290, also called CITYSCAPE) is investigating locally advanced unresectable or metastatic PD-L1, except in patients with sensitizing epidermal growth factor receptor (EGFR) mutations or ALK translocations. - Evaluating the efficacy and safety of tiragolumab and atezolizumab compared to placebo plus atezolizumab in chemotherapy-naive patients with elective NSCLC.
臨床薬物動態及び免疫原性
2019年12月2日のデータカットオフ日の時点で、入手可能なデータ(試験GO 30103の第Ia相部分では3週間ごとに投与される2-1200mgのチラゴルマブ及び第Ib相部分では3週間ごとに投与される1200mgのアテゾリズマブと組み合わせて3週間ごとに投与される2-1200mgのチラゴルマブ)に基づいて、標準的な非コンパートメントPK法を用いて予備PK解析を実施した。アテゾリズマブと組み合わせたチラゴルマブの薬物動態は、単剤として投与されたチラゴルマブの薬物動態と一致するようであった。予備的な集団-PK分析は、単独療法として、又は3週間ごとに1200mgのアテゾリズマブと組み合わせて、3週間ごとに100mg~1200mgの範囲の用量でのIV投与後に、チラゴルマブ曝露がほぼ用量比例的に増加したことを示している。予備的集団PK分析は、約15日の線形薬物除去半減期で0.28 L/日のチラゴルマブクリアランスを推定した。試験GO 30103の第Ib相部分では、チラゴルマブに対する抗薬物抗体(ADA)の発生が154人の評価可能な患者中3人(1.9%)で観察された。予備的データは、チラゴルマブADAがPKに及ぼす明らかな影響がなかったことを示唆している。しかしながら、少数の陽性ADA患者は、チラゴルマブの薬物動態に対するADAの影響を評定するのに十分ではなかった。
Clinical Pharmacokinetics and Immunogenicity As of the data cut-off date of December 2, 2019, available data (tiragolumab 2-1200 mg every 3 weeks for Phase Ia portion of study GO 30103 and Preliminary PK analysis was performed using standard non-compartmental PK methodology (based on 2-1200 mg tiragolumab given every 3 weeks in combination with 1200 mg atezolizumab given every 3 weeks for the Phase Ib portion). . The pharmacokinetics of tiragolumab in combination with atezolizumab appeared to be consistent with that of tiragolumab administered as a single agent. Preliminary population-PK analysis showed that tiragolumab exposure was nearly dose-proportional following IV administration at doses ranging from 100 mg to 1200 mg every 3 weeks as monotherapy or in combination with 1200 mg atezolizumab every 3 weeks. increased. A preliminary population PK analysis estimated a tiragolumab clearance of 0.28 L/day with a linear drug elimination half-life of approximately 15 days. In the Phase Ib portion of study GO 30103, development of anti-drug antibodies (ADA) to tiragolumab was observed in 3 of 154 evaluable patients (1.9%). Preliminary data suggest that tiragolumab ADA had no apparent effect on PK. However, the small number of positive ADA patients was not sufficient to assess the impact of ADA on the pharmacokinetics of tiragolumab.
臨床上の安全性
2019年12月2日のデータカットオフ日の時点で、安全性データは、試験GO 30103の第Ia相部分の42名の患者について利用可能であった。第Ia相で一般的に報告されている有害事象(全患者の≧10%で報告されている)には、チラゴルマブとの関係にかかわらず、疲労、便秘、嘔吐、食欲不振、貧血、咳、呼吸困難、頭痛、注入関連反応(IRR)、悪性新生物進行、悪心及び掻痒症が含まれた。チラゴルマブに関連する一般的に報告された有害事象(患者の≧10%で報告)には、疲労及びIRRが含まれた。
Clinical Safety As of the data cut-off date of December 2, 2019, safety data were available for 42 patients in the Phase Ia portion of study GO 30103. Commonly reported adverse events in Phase Ia (reported in ≥10% of all patients) included fatigue, constipation, vomiting, anorexia, anemia, cough, Included were dyspnea, headache, infusion-related reactions (IRR), malignant neoplasm progression, nausea and pruritus. Commonly reported adverse events associated with tiragolumab (reported in >10% of patients) included fatigue and IRR.
試験薬物の帰属にかかわらず、グレード≧3の有害事象(国立がん試験所有害事象共通用語規準バージョン4.0[NCI CTCAE v4.0]に基づく)がGO30103試験の第Ia相部分の16名の患者(38.1%)で報告され、3名の患者(7.1%)が処置関連グレード≧3の有害事象を経験した。治験責任医師によってチラゴルマブに関連すると考えられたグレード≧3の有害事象には、アミラーゼ増加、血中クレアチニン増加、肝不全(後述)、IRR及び発疹が含まれた。 Grade ≥3 adverse events (based on the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0 [NCI CTCAE v4.0]), regardless of study drug attribution, in 16 patients in the phase Ia portion of study GO30103 patients (38.1%), and 3 patients (7.1%) experienced treatment-related Grade ≥3 adverse events. Grade ≧3 adverse events considered by the investigator to be related to tiragolumab included increased amylase, increased blood creatinine, liver failure (described below), IRR and rash.
2019年12月2日のデータカットオフ日の時点で、疾患進行後に第Ia相から交差した23名の患者を含む171名の患者が試験GO30103の第Ib相部分に登録された。第Ib相で処置された171名の患者のうち、163名の患者(95.9%)が少なくとも1つの有害事象を経験し、これには少なくとも1つの処置関連有害事象を経験した110名の患者(64.7%)が含まれる。チラゴルマブとの関係にかかわらず、第Ib相で一般的に報告された有害事象(全患者の≧10%で報告)には、掻痒症、発熱、貧血、発疹、悪性新生物進行、便秘、食欲不振、下痢、咳、無力症、嘔吐及び疲労が含まれた。チラゴルマブ及び/又はアテゾリズマブに関連する一般的に報告されている有害事象(患者の≧10%で報告されている)には、掻痒症及び発疹が含まれた。 As of the data cut-off date of December 2, 2019, 171 patients were enrolled in the Phase Ib portion of study GO30103, including 23 patients who crossed out from Phase Ia after disease progression. Of the 171 patients treated in Phase Ib, 163 patients (95.9%) experienced at least one adverse event, including 110 patients who experienced at least one treatment-related adverse event. Patients (64.7%) are included. Regardless of relationship to tiragolumab, commonly reported adverse events in phase Ib (reported in ≥10% of all patients) included pruritus, fever, anemia, rash, malignant neoplastic progression, constipation, appetite Included were malaise, diarrhea, cough, asthenia, vomiting and fatigue. Commonly reported adverse events associated with tiragolumab and/or atezolizumab (reported in >10% of patients) included pruritus and rash.
試験薬物の帰属にかかわらず、グレード≧3の有害事象(NCI CTCAE v4.0に準拠)がGO30103試験の第Ib相部分の91名の患者(53.5%)で報告され、21名の患者(12.4%)が処置関連グレード≧3の有害事象を経験した。治験責任医師によってチラゴルマブ及び/又はアテゾリズマブに関連すると考えられたグレード≧3の有害事象には、リンパ球数の減少、リパーゼの増加、リンパ球減少症、アミラーゼの増加、副腎機能不全、無力症、心タンポナーデ、頭痛、高血糖症、高脂血症、高トランスアミナーゼ血症、肺臓炎、掻痒性発疹、横紋筋融解症、糖尿病、糖尿病性ケトアシドーシス、及びリパーゼが含まれた。 Grade ≥3 adverse events (according to NCI CTCAE v4.0) were reported in 91 patients (53.5%) and 21 patients in the phase Ib portion of the GO30103 study, regardless of study drug attribution (12.4%) experienced treatment-related grade ≧3 adverse events. Grade ≥3 adverse events considered by the investigator to be related to tiragolumab and/or atezolizumab included decreased lymphocyte count, increased lipase, lymphopenia, increased amylase, adrenal insufficiency, asthenia, Included were cardiac tamponade, headache, hyperglycemia, hyperlipidemia, hypertransaminasemia, pneumonitis, pruritic rash, rhabdomyolysis, diabetes, diabetic ketoacidosis, and lipase.
GO30103試験の第Ia相単独療法拡大コホートに登録された患者において、致命的な肝不全に至る肝毒性の致死的な症例が発生した。スクリーニング時、患者のトランスアミナーゼは正常範囲内であった。投与前のC1D1において、AST及びALTはグレード1に上昇していた。C1D1へのチラゴルマブ投与中、患者は、用量の中断及び標準的な処置に応答する注入反応を発症し、患者は、およそ733mgの意図された1200mg用量のチラゴルマブを受けた。試験8日目に、ALT/ASTはグレード3に上昇し、これはグレード3の発疹に関連しており、患者を毎日60mgのプレドニゾンで処置した。試験12日目までに、発疹は改善していたが、AST及びALTはグレード4(正常ビリルビン及びPT-国際正常化比(INR))であり、第2の免疫抑制剤(アザチオプリン)を追加した。患者は、2つの免疫抑制剤の使用にもかかわらず次第に悪化し、ビリルビン上昇を伴う明白な肝不全及び進行性肝性脳症を発症し、最終的に試験30日目に死亡した。ウイルス(HBV、HCV)、併用薬、又は解剖学的異常を含む肝炎の複数の代替病因を除外した。試験16日目に実施した肝生検は、コンフルエントな亜大量壊死を示し、わずかな炎症性浸潤物が毒性肝炎と解釈された。
Fatal cases of hepatotoxicity leading to fatal liver failure occurred in patients enrolled in the Phase Ia monotherapy expansion cohort of the GO30103 trial. At screening, the patient's transaminases were within normal limits. AST and ALT were elevated to
この事象の後、安全性データの分析は、有害事象所見に対する有意な変化を示さず、GO30103試験の第Ia相部分及び第Ib相部分で投与された対象について新たな有意な有害事象は認められなかった。 After this event, analysis of safety data showed no significant changes to adverse event findings, and no new significant adverse events were noted for subjects dosed in the Phase Ia and Ib portions of study GO30103. I didn't.
2019年6月30日のデータカットオフ日の時点で、第II相盲検試験GO 40290では、安全性評価可能な135人の患者に、アテゾリズマブと組み合わせたチラゴルマブ(3週間ごとに600mg)又はアテゾリズマブと組み合わせたプラセボのいずれかを投与した。チラゴルマブ及びアテゾリズマブの安全性プロファイルは、全グレード有害事象(98.5%対95.6%)、グレード≧3 AE(41.8%対44.1%)、重篤AE(34.3%対35.3%)、及び処置中止に至るAE(7.5%対10.3%)について、プラセボ及びアテゾリズマブの安全性プロファイルと類似していた。特に興味深い有害事象は、チラゴルマブ群及びアテゾリズマブ群では47.8%の患者で報告され、プラセボ+アテゾリズマブ群では32.4%の患者で報告された。2019年12月の更新データは、同様の安全性プロファイルを示した。 As of the data cut-off date of June 30, 2019, the phase II blinded study GO 40290 enrolled 135 safety-evaluable patients with tiragolumab (600 mg every 3 weeks) in combination with atezolizumab or atezolizumab either placebo in combination with The safety profiles of tiragolumab and atezolizumab included all grade adverse events (98.5% vs. 95.6%), grade ≥3 AEs (41.8% vs. 44.1%), serious AEs (34.3% vs. 35.3%) and AEs leading to treatment discontinuation (7.5% vs. 10.3%) were similar to the safety profiles of placebo and atezolizumab. Adverse events of particular interest were reported in 47.8% of patients in the tiragolumab and atezolizumab groups and 32.4% of patients in the placebo plus atezolizumab group. The December 2019 update data showed a similar safety profile.
EBV再活性化及び続発性血球貪食性リンパ組織球増加症(HLH)の可能性のある致死的な症例が、NSCLCの転移性リンパ上皮腫様癌腫亜型(PD-L1陽性)を有する台湾の69歳の男性において報告され、これはアジア人患者におけるEBV感染に関連し得る。スクリーニング時に、患者は血清Epstein-Barr核抗原(EBNA)抗体検査が陽性であったが、処置の治験責任医師によって確認されたように活動性EBV感染の臨床兆候はなかった。サイクル1の1日目に、患者は、試験薬物、アテゾリズマブ及びチラゴルマブの両方を受け、処置に十分に忍容性であった。10日目に、患者は上気道感染に起因すると考えられる発熱を発症し、これを抗生物質で処置した。サイクル2の1日目に、患者はアテゾリズマブを受け、注入の20分後にグレード2の発熱を発症した。発熱はアテゾリズマブIRRであると推定されたので、チラゴルマブはサイクル2で投与しなかった。患者は発熱のために入院したが、感染原因の精密検査は陰性であった。発熱が解消すると、患者はサイクル2の8日目に退院した。サイクル2の15日目に、患者は断続的な熱のために再び入院し、低血圧を伴うショック、代謝性アシドーシス、急性腎障害、汎血球減少症、凝固障害、出血、精神状態の変化、トランスアミナーゼ炎、高ビリルビン血症及び呼吸不全を発症したので集中治療室に搬送された。患者は血液中の高いEBV力価を有し、骨髄生検はHLHと一致していた。他の感染性病因についての培養は陰性であった。ステロイド及び複数の免疫抑制薬(トシリズマブ、ヒドロキシクロロキン及びエタネルセプト)による処置にもかかわらず、患者は悪化し、サイクル2の31日目に死亡した。合計で、患者は、1用量のチラゴルマブ(サイクル1)及び2用量のアテゾリズマブ(サイクル1及び2)を受けていた。この修正の時点では事象の正確な原因は不明であり、調査は進行中であるが、入手可能な情報は、この患者が稀な組織学的サブタイプのNSCLCを有し、慢性活動性EBV感染が疑われ、これがチラゴルマブ及びアテゾリズマブの投与で再活性化したことを示唆している。試験薬曝露と患者の臨床経過との間の時間的関係を考慮すると、患者は二次性HLHを発症したと思われる。肺リンパ上皮腫様癌腫患者におけるEBV再活性化のこの指標症例のため、安全性データは慎重に再検討されており、第II相試験(GO40290)又は現在の第I相試験(GO30103)ではウイルス再活性化の他の症例は観察されていない。
A potentially fatal case of EBV reactivation and secondary hemophagocytic lymphohistiocytosis (HLH) occurred in a Taiwanese patient with metastatic lymphoepithelioma-like carcinoma subtype (PD-L1 positive) of NSCLC. It was reported in a 69-year-old man, which may be related to EBV infection in Asian patients. At screening, the patient had a positive serum Epstein-Barr nuclear antigen (EBNA) antibody test, but had no clinical signs of active EBV infection as confirmed by the treatment investigator. On
2019年12月2日のデータカットオフ日の時点で、42人の患者がチラゴルマブ単剤で処置されている。単剤のチラゴルマブを投与された患者は、IRRを経験したことがある。第Ia相では、5名の患者(12%)がIRRを経験した。IRRに関連する徴候及び症状は一般に軽度であり、発熱、悪寒、潮紅、高血圧、リンパ節症、悪心、筋痛症及び皮膚病変が含まれた。IRRの全ての症例が、支持的処置によって首尾よく処置された。患者の12%において単一薬剤のチラゴルマブの注入中及び注入後に発生するIRRのために、IRRは潜在的なリスクから特定されたリスクに移行した。チラゴルマブにはさらなる特定されたリスクはないが、TIGIT共阻害経路の関与は、チラゴルマブが単剤として投与された場合、自己免疫性炎症のリスクを増加させ得る。したがって、単一薬剤としてのチラゴルマブは、アテゾリズマブと同様の有害事象を引き起こす可能性がある。そのような免疫媒介性有害事象は、抗CTLA-4及び抗PD-L1/PD-1等の他の免疫チェックポイント阻害剤について十分に特性評価されている。 As of the data cutoff date of December 2, 2019, 42 patients are being treated with tiragolumab alone. Patients receiving single-agent tiragolumab have experienced IRR. In Phase Ia, 5 patients (12%) experienced IRR. Signs and symptoms associated with IRR were generally mild and included fever, chills, flushing, hypertension, lymphadenopathy, nausea, myalgia and skin lesions. All cases of IRR were successfully treated with supportive treatment. IRR moved from potential to identified risk due to IRR occurring during and after infusion of single-agent tiragolumab in 12% of patients. Although tiragolumab has no further identified risks, involvement of the TIGIT co-inhibition pathway may increase the risk of autoimmune inflammation when tiragolumab is administered as a single agent. Therefore, tiragolumab as a single agent may cause adverse events similar to atezolizumab. Such immune-mediated adverse events have been well characterized for other immune checkpoint inhibitors such as anti-CTLA-4 and anti-PD-L1/PD-1.
これは、抗-PD-L1/PD-1剤と組み合わせたチラゴルマブの最初の臨床評価である。アテゾリズマブと組み合わせたチラゴルマブの臨床評価は限定的であり、全てのリスクが知られているわけではないが、2019年12月2日現在、200人を超える患者がアテゾリズマブと組み合わせたチラゴルマブで処置されている。現在のところ、アテゾリズマブと併用して投与されるチラゴルマブに固有の特定されたリスクはないが、TIGIT共阻害経路の関与は、チラゴルマブがアテゾリズマブと併用して投与される場合、HLH及びMASを含むいくつかの免疫反応のリスクを増加させ得る。したがって、アテゾリズマブと共に投与された場合、チラゴルマブは、アテゾリズマブ関連有害事象を悪化させ得るか、又はアテゾリズマブと重複しない毒性を有し得る。 This is the first clinical evaluation of tiragolumab in combination with an anti-PD-L1/PD-1 agent. Although clinical evaluation of tiragolumab in combination with atezolizumab is limited and not all risks are known, as of December 2, 2019, over 200 patients have been treated with tiragolumab in combination with atezolizumab. there is Although there are currently no identified risks specific to tiragolumab administered in combination with atezolizumab, involvement of the TIGIT co-inhibition pathway has been implicated in several risks, including HLH and MAS, when tiragolumab is administered in combination with atezolizumab. may increase the risk of some immune reactions. Thus, when administered with atezolizumab, tiragolumab may exacerbate atezolizumab-related adverse events or have toxicities that do not overlap with atezolizumab.
適応免疫の相補的調節因子の組み合わせに関するこれまでの最大の臨床経験は、ニボルマブと組み合わせたイピリムマブの試験から得られる。別の抗TIGIT抗体MK-7684(ビボストリマブ)は、ペンブロリズマブと組み合わせた場合、進行性腫瘍を有する患者において許容可能な安全性プロファイル及び有望な抗腫瘍活性を示した。これらのデータに基づいて、免疫媒介性有害事象の頻度及び重症度は、いずれかの単一薬剤阻害剤と比較した場合、組み合わせで増加し得るが、組み合わせ免疫介在性有害事象は、臨床現場でのモニタリング及び管理が容易になると予想される。 The greatest clinical experience to date with combinations of complementary regulators of adaptive immunity comes from trials of ipilimumab in combination with nivolumab. Another anti-TIGIT antibody MK-7684 (vivostolimab) showed an acceptable safety profile and promising anti-tumor activity in patients with advanced tumors when combined with pembrolizumab. Based on these data, the frequency and severity of immune-mediated adverse events may be increased with combination when compared to either single agent inhibitor, although combined immune-mediated adverse events are is expected to be easier to monitor and manage.
臨床的有効性
2019年12月2日のデータカットオフ日の時点で、GO30103試験の第Ia相部分に登録された患者について客観的奏効は報告されておらず、最良の効果は、試験中の腫瘍評定で42人中8人の患者において安定疾患(SD)であった。試験の第Ib相部分では、NSCLC、HNSCC及びトリプルネガティブ乳がんを含む複数の腫瘍型によるがん免疫療法(CIT)に対して未経験の患者において、171人中4人の患者における完全奏効(CR)及び171人中23人の患者における部分奏効(PR)を含む客観的奏効が観察された。
Clinical Efficacy As of the data cut-off date of December 2, 2019, no objective responses have been reported for patients enrolled in the Phase Ia portion of the GO30103 study, with the best response being There was stable disease (SD) in 8 of 42 patients at tumor assessment. Complete response (CR) in 4 of 171 patients in cancer immunotherapy (CIT)-naïve patients with multiple tumor types including NSCLC, HNSCC and triple-negative breast cancer in the Phase Ib portion of the study and objective responses including partial responses (PR) in 23 of 171 patients were observed.
2019年6月30日のデータカットオフ日の時点で、盲検無作為化第II相試験GO 40290からのデータは、ITT集団において、チラゴルマブとアテゾリズマブとの組み合わせがプラセボとアテゾリズマブと比較してORR及びPFSを改善したことを示した。チラゴルマブ及びアテゾリズマブのORRは、プラセボ及びアテゾリズマブの16.2%(95% CI:19.5~43.2)と比較して、31.3%(95% CI:6.7~25.7)であった。治験責任医師が評定したチラゴルマブ及びアテゾリズマブのPFSは5.4ヶ月(95% CI:4.2、未到達)であったのに対して、プラセボ及びアテゾリズマブのPFSは3.6ヶ月(95% CI:2.7~4.4)であり、HRは0.57(95% CI:0.37~0.90)であった。 As of the data cut-off date of June 30, 2019, data from the blinded, randomized phase II study GO 40290 showed that the combination of tiragolumab and atezolizumab compared to placebo and atezolizumab in the ITT population had an ORR and improved PFS. ORR for tiragolumab and atezolizumab was 31.3% (95% CI: 6.7-25.7) compared to 16.2% for placebo and atezolizumab (95% CI: 19.5-43.2) Met. Investigator-assessed PFS for tiragolumab and atezolizumab was 5.4 months (95% CI: 4.2, not reached) compared to 3.6 months (95% CI : 2.7-4.4) and the HR was 0.57 (95% CI: 0.37-0.90).
チラゴルマブ及び化学療法を伴うアテゾリズマブによる第Ib相
進行性固形腫瘍の複数の大規模ランダム化第III相試験では、標準化学療法への抗PD-L1/PD-1の追加は、化学療法単独と比較して患者のOS及びPFSを改善した。これらの試験では、非扁平上皮NSCLC(Gandhi et al.N Engl J Med 2018;378:2078-92)におけるペメトレキセド及び白金ベースの化学療法への、並びに扁平上皮NSCLC(Paz-Ares et al.N Engl J Med 2018;379:2040-51)におけるカルボプラチン及びパクリタキセル又はnab-パクリタキセルへの抗PD-1の追加を試験した。これらの試験はまた、進展型SCLCにおけるカルボプラチン及びエトポシド(Horn et al.N Engl J Med 2018;379:2220-9)and to nab-paclitaxel in TNBC(Schmid et al.N Engl J Med 2018;379:2108-21)への抗PD-L1の添加を調査した。これらの試験の結果として、化学療法と組み合わせた抗PD-L1/PD-1は、進行性がん患者に対してFDA及びEMAによって承認されている。非臨床データは、同時の抗TIGIT及び抗PD-L1/PD-1が単剤の抗PD-L1/PD-1単独よりも抗腫瘍免疫応答を増強することを示唆しているので、化学療法と組み合わせた抗PD-L1/PD-1への抗TIGITの添加は、化学療法への抗PD-L1/PD-1の添加よりも有効であり得ると仮定される。
Phase Ib with Tiragolumab and Atezolizumab with Chemotherapy In multiple large randomized phase III trials in advanced solid tumors, the addition of anti-PD-L1/PD-1 to standard chemotherapy compared with chemotherapy alone improved the patient's OS and PFS. In these studies, pemetrexed and platinum-based chemotherapy in non-squamous NSCLC (Gandhi et al. N
抗PD-L1/PD-1と化学療法を組み合わせることから生じる安全性プロファイルは、一般に、進行性固形腫瘍の複数の臨床試験で観察された各薬剤の既知の毒性効果と一致している(Gandhi et al.N Engl J Med 2018;378:2078-92;Horn et al.N Engl J Med 2018;379:2220-9;Paz-Ares et al.N Engl J Med 2018;379:2040-51;Schmid et al.N Engl J Med 2018;379:2108-21)。チラゴルマブとアテゾリズマブとの間の作用機序の類似性を考えると、アテゾリズマブ及び化学療法と組み合わせて投与されたチラゴルマブの安全性プロファイルは、抗TIGIT及び抗PD-L1を組み合わせた免疫関連毒性及び個々の化学療法剤の毒性と一致し得ることが予想される。したがって、第Ib相化学療法拡大コホートのための設計及び安全性管理計画は、化学療法による広範な臨床経験、並びに抗TIGITを抗PD-L1と組み合わせて参加患者に対する潜在的リスクを低減するために記載された考慮事項を組み込む。
The safety profile resulting from combining anti-PD-L1/PD-1 with chemotherapy is generally consistent with the known toxic effects of each agent observed in multiple clinical trials in advanced solid tumors (Gandhi et al. Horn et al.N
チラゴルマブ、及びベバシズマブを伴うアテゾリズマブによる第Ib相
強力な科学的根拠及び新たな臨床データは、PD-L1、VEGF及びTIGITの併用阻害がいくつかの腫瘍型において臨床的に有益であり得ることを示唆している。
Phase Ib with Tiragolumab and Atezolizumab with Bevacizumab Strong Evidence and Emerging Clinical Data Suggest that Combined Inhibition of PD-L1, VEGF and TIGIT May Be Clinically Beneficial in Several Tumor Types are doing.
ステージIV NSCLCを有する化学療法未経験患者において、GO29436試験(IMpower150)の結果は、アテゾリズマブ+ベバシズマブ及び化学療法が、ベバシズマブ及び化学療法単独と比較して有意に長いOSをもたらすことを示している(Socinski et al.N Engl J Med 2018;378:2288-301)。手術不能、局所進行性、又は転移性RCCを有する患者について、試験の国際公開第29637号(IMmotion 151)からの結果は、処置未経験患者集団においてスニチニブと比較して、アテゾリズマブとベバシズマブとの組み合わせによる処置後に改善されたPFSを実証した(Motzer et al.J Clin Oncol 2018;36(6_suppl):578,Rini et al.Lancet 2019;393:2404-15)。フロントラインHCCにおける第Ib相GO30140試験は、病因、地理、ベースラインアルファフェトプロテインのレベル、及び肝外拡散にわたって、23人の評価可能な患者において65%のORRを見出した(Stein et al.J Clin Oncol 2018;36(Suppl 15):4074,Lee et al.Lancet Oncol.2020 Jun;21(6):808-820)。これらの結果に基づいて、この処置は画期的治療薬の指定(breakthrough designation)を付与され、結果は無作為化第III相試験、YO40245(IMbrave150)試験で確認された。事前の全身処置を受けていない進行性又は転移性HCC患者におけるアテゾリズマブ及びベバシズマブ対ソラフェニブの有効性及び安全性を評価するために、YO40245試験(IMbrave 150)を設計した。この試験には、2:1の比で無作為化された501人の患者が登録された。最近の試験結果は、PFS及びOSの統計的に有意で臨床的に有意な改善を実証した。死亡リスクは、ソラフェニブ群と比較してアテゾリズマブ+ベバシズマブ群では42%低下した(層別HR=0.58(95% CI:0.42~0.79);OS中央値、NE対13.24ヶ月)。固形腫瘍における応答評価基準(RECIST)v 1.1による独立した再検討容易性評定PFSは、併用処置を支持する改善を実証した(層別HR=0.59(95% CI:0.47から0.76);PFSの中央値、6.83ヶ月対4.27ヶ月)(Cheng et al.Ann Oncol 2019;30:ix186-ix187、Finn et al.N Engl J Med 2020;382:1894-1905)。
In chemotherapy-naive patients with stage IV NSCLC, results from the GO29436 trial (IMpower150) show that atezolizumab plus bevacizumab and chemotherapy lead to significantly longer OS compared to bevacizumab and chemotherapy alone (Socinski et al.N
これらは、異なる腫瘍タイプにおけるアテゾリズマブとベバシズマブとの間の潜在的な相乗効果の例であり、これは、チラゴルマブとの組み合わせのさらなる探求を支持する。 These are examples of potential synergistic effects between atezolizumab and bevacizumab in different tumor types, which support further exploration of the combination with tiragolumab.
実施例5.進行性固形腫瘍を有する患者における単剤としての、アテゾリズマブと組み合わせた抗TIGIT抗体チラゴルマブの第Ia/Ib相用量漸増試験における薬物動態、薬力学、安全性及び有効性
A.患者の特徴
試験の第Ia相部分及び第Ib相部分の患者のベースライン特性を表37に示す。第Ia相及び第Ib相の両方の患者は、重度に前処置された集団を含み、第Ia相の患者の42%及び第Ib相の患者の37%が4つ以上の以前のがん治療を有する。第Ia相及び第Ib相の患者は、同様のベースライン特性を共有する。

試験の第Ia相部分及び第Ib相部分のほとんどの患者は、疾患の進行のための処置を中止した(第Ia相の42%及び第Ib相の76%)。第Ib相交差患者のいずれも応答を示さなかった。患者の状態を表38に示す。

B.チラゴルマブの薬物動態及び薬力学
単剤(第Ia相)としての、及びアテゾリズマブと組み合わせた(第Ib相)、チラゴルマブの薬物動態を測定した。チラゴルマブの曝露は、単剤として用量とともに、アテゾリズマブと組み合わせて増加した(図9)。チラゴルマブの薬物動態は、アテゾリズマブと組み合わせて変化しない
B. Pharmacokinetics and Pharmacodynamics of Tiragolumab The pharmacokinetics of tiragolumab as a single agent (Phase Ia) and in combination with atezolizumab (Phase Ib) were determined. Tiragolumab exposure increased with dose as a single agent and in combination with atezolizumab (Figure 9). Tiragolumab pharmacokinetics are unchanged in combination with atezolizumab
単剤としてのチラゴルマブ(第Ia相)の薬力学を測定した(図10)。CD8+T細胞上及びNK細胞上の末梢TIGIT受容体の占有を、3週間ごとに2mg、8mg、30mg、100mg、400mg、600mg、及び1200mgの用量で測定した。2日目(C1D2)後の末梢TIGIT受容体の完全かつ持続的な占有が、30mg以上のチラゴルマブ用量で観察された。 The pharmacodynamics of tiragolumab (Phase Ia) as a single agent were determined (Figure 10). Peripheral TIGIT receptor occupancy on CD8 + T cells and on NK cells was measured at doses of 2 mg, 8 mg, 30 mg, 100 mg, 400 mg, 600 mg and 1200 mg every 3 weeks. Complete and sustained occupancy of peripheral TIGIT receptors after day 2 (C1D2) was observed at tiragolumab doses of 30 mg and above.
C.安全性 C. safety
有害事象の要約を表39に示す。グレード3~5の有害事象の全体的な割合は、第Ia相部分及び第Ib相部分について低く、いずれもグレード5の有害事象を有していなかった。単剤又はアテゾリズマブと組み合わせたチラゴルマブについては、用量制限毒性は観察されなかった。第Ia相及び第Ib相の患者の10%以上に存在する全ての有害事象をそれぞれ図11及び図12に示す。全ての免疫媒介性有害事象を表40に示す。チラゴルマブは、単剤として、アテゾリズマブと組み合わせて良好に忍容された。


D.有効性
第Ia相及び第Ib相用量漸増試験に対して予備的有効性分析を行った。第Ia相部分では、神経内分泌がん、卵巣がん及び直腸がんで腫瘍サイズの減少が観察された(図13)。試験の第Ia相部分では客観的奏効はなかったが、ほとんどの患者は、がん免疫療法(CIT)に典型的に応答しない腫瘍型を有していたか、PD-L1発現の低い腫瘍を有していたか、又は重度に前処置されていた。客観的奏効が、NSCLC、TNBC、HNSCC及び食道がんタイプにおける試験の第Ib相部分において認められた(図14)。
D. Efficacy A preliminary efficacy analysis was performed for the Phase Ia and Phase Ib dose escalation studies. In the Phase Ia portion, a decrease in tumor size was observed in neuroendocrine, ovarian and rectal cancers (Figure 13). Although there were no objective responses in the Phase Ia portion of the trial, most patients either had tumor types that typically do not respond to cancer immunotherapy (CIT) or had tumors with low PD-L1 expression. or had been heavily pretreated. Objective responses were seen in the phase Ib portion of the trial in NSCLC, TNBC, HNSCC and esophageal cancer types (Figure 14).
CIT未経験腫瘍を含むPD-L1陽性NSCLC腫瘍のサイズは、アテゾリズマブと組み合わせたチラゴルマブで処置された患者において大きく減少した(図14)。アテゾリズマブと組み合わせたチラゴルマブで処置されたCIT未経験PD-L1陽性NSCLCは、46%の全奏効率を有し、これには2つの完全奏効及び永続性を示すいくつかの応答が含まれた(図15及び図16)。 The size of PD-L1-positive NSCLC tumors, including CIT-naive tumors, was greatly reduced in patients treated with tiragolumab in combination with atezolizumab (FIG. 14). CIT-naïve PD-L1-positive NSCLC treated with tiragolumab in combination with atezolizumab had an overall response rate of 46%, including two complete responses and some responses that were durable (Fig. 15 and Figure 16).
実施例6:進行性肝臓がんのためのチアゴルマブ及びベバシズマブと組み合わせたアテゾリズマブ
肝臓がんは、世界で5番目に多いがんであり、がん関連死の2番目に多い原因であり、年間854,000件の新規症例及び810,000件の死亡がある。肝細胞癌腫(HCC)は、原発性肝臓がんの最も一般的な形態であり、全ての原発性肝悪性腫瘍の約90%を占める。あまり一般的でない原発性肝臓がんには、肝内胆管がん(iCCA)、血管肉腫及び肝芽腫が含まれる。
Example 6: Atezolizumab in combination with tiagorumab and bevacizumab for advanced liver cancer Liver cancer is the fifth most common cancer and the second most common cause of cancer-related deaths worldwide, with 854,500 per year. 000 new cases and 810,000 deaths. Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer, accounting for about 90% of all primary liver malignancies. Less common primary liver cancers include intrahepatic cholangiocarcinoma (iCCA), angiosarcoma and hepatoblastoma.
YO40245試験(IMbrave150)は、進行性又は転移性HCCを有する患者における第一選択処置として、アテゾリズマブ+ベバシズマブ対ソラフェニブを評価する進行中の無作為化第III相試験である。この試験は、ソラフェニブとの直接比較における新規な処置の組み合わせについて、OS及び無増悪生存期間(PFS)における統計学的に有意で臨床的に有意な改善を実証した最初の試験である。一次解析の時点で、死亡リスクはソラフェニブ群と比較してアテゾリズマブ+ベバシズマブ群で42%低下した(層別ハザード比[HR]=0.58[95%CI:0.42~0.79];p=0.0006;OS中央値、推定不能[NE]対13.24ヶ月)。RECIST v 1.1による独立した-再検討の試験施設で評定されたPFSもまた、併用処置を支持する統計学的に有意で臨床的に有意な改善を実証した(層別HR=0.59[95%CI:0.47~0.76];p<0.0001;PFS中央値、6.83ヶ月対4.27ヶ月)。全体として、HCCにおけるアテゾリズマブ+ベバシズマブの組み合わせは、管理可能な毒性で一般に良好に忍容され、安全性プロファイルは、個々の試験処置の既知のリスク及び基礎疾患と一致した(Cheng et al.IMbrave150:Efficacy and Safety Results From a Ph 3 Study Evaluating Atezolizumab(atezo)+Bevacizumab(bev)vs Sorafenib(Sor)as First Treatment(tx)for Patients(pts)With Unresectable Hepatocellular Carcinoma(HCC).Proceedings of ESMO Asia 2019:22-24 November 2019[cited:27 November 2019];Singapore.
The YO40245 trial (IMbrave150) is an ongoing randomized Phase III trial evaluating atezolizumab plus bevacizumab versus sorafenib as first-line treatment in patients with advanced or metastatic HCC. This trial is the first to demonstrate a statistically significant and clinically significant improvement in OS and progression-free survival (PFS) for a novel treatment combination in head-to-head comparisons with sorafenib. At the time of the primary analysis, the risk of death was reduced by 42% in the atezolizumab + bevacizumab group compared to the sorafenib group (stratified hazard ratio [HR] = 0.58 [95% CI: 0.42-0.79]; p=0.0006; median OS, not estimable [NE] vs. 13.24 months). Independent-review trial site-assessed PFS by RECIST v 1.1 also demonstrated a statistically significant and clinically significant improvement in favor of combination treatment (stratified HR = 0.59 [95% CI: 0.47-0.76]; p<0.0001; median PFS, 6.83 vs. 4.27 months). Overall, the combination of atezolizumab plus bevacizumab in HCC was generally well tolerated with manageable toxicity, and the safety profile was consistent with the known risks and underlying disease of the individual study treatments (Cheng et al. IMbrave150: Efficacy and Safety Results From a
これは、疾患のための事前全身治療を受けたことがない局所進行性又は転移性肝細胞がん(HCC)患者における第Ib/II相非盲検多施設無作為化包括的試験である。 This is a Phase Ib/II, open-label, multicenter, randomized, comprehensive study in patients with locally advanced or metastatic hepatocellular carcinoma (HCC) who have not received prior systemic therapy for their disease.
患者を無作為に対照群(アテゾリズマブ+ベバシズマブ[Atezo+Bev])又はチラゴルマブと組み合わせたアテゾリズマブ及びベバシズマブからなる処置群(Atezo+Bev+Tira)に割り当てる。 Patients are randomized to a control group (atezolizumab + bevacizumab [Atezo + Bev]) or a treatment group consisting of atezolizumab and bevacizumab in combination with tiragolumab (Atezo + Bev + Tira).
対照群(Atezo+Bev) Control group (Atezo + Bev)
アテゾリズマブ+ベバシズマブ(Atezo+Bev)群の患者は、以下の表に概説される処置を受ける。

アテゾリズマブ+ベバシズマブ+チラゴルマブ(Atezo +Bev +Tira)群の患者は、以下の表に概説される処置を受ける。

B.選択基準
患者は以下の基準の全てを満たさなければならない:
●年齢≧18歳。
●処置前7日以内の0又は1のECOGパフォーマンスステータス。
●肝硬変患者における組織学/細胞学によって、又は臨床的にAASLD基準によって確認された診断を伴う局所進行性若しくは転移性及び/又は切除不能HCC
診断の組織学的確認がない肝硬変患者については、AASLD基準に従って臨床的確認が必要である。
●無作為化前7日以内のChild-PughクラスA
●治癒的外科療法及び/又は局所領域療法に適していない疾患
外科的及び/又は局所領域療法後に進行性疾患を有する患者が適格である。
●HCCに対する以前の全身処置(全身治験薬を含む)なし
ラベルに記載されている抗がん活性を有する伝統的な漢方薬を含むハーブ療法による事前の処置は、これらの薬剤がランダム化前に中止されることを条件として許容される。
●平均余命≧3ヶ月。
B. Inclusion Criteria Patients must meet all of the following criteria:
● Age ≥ 18 years old.
• ECOG performance status of 0 or 1 within 7 days prior to procedure.
- Locally advanced or metastatic and/or unresectable HCC with diagnosis confirmed by histology/cytology or clinically by AASLD criteria in patients with cirrhosis
Patients with cirrhosis without histologic confirmation of diagnosis require clinical confirmation according to AASLD criteria.
- Child-Pug Class A within 7 days prior to randomization
• Disease not amenable to curative surgery and/or locoregional therapy Patients with progressive disease after surgical and/or locoregional therapy are eligible.
No prior systemic treatment (including systemic investigational drugs) for HCC Prior treatment with herbal remedies containing traditional herbal medicines with labeled anticancer activity, discontinuing these agents prior to randomization permissible provided that
● Life expectancy ≧3 months.
有効性及び安全性の目的及び評価項目を以下の表に記載する。本明細書におけるAtezo+Bev+Tiraの三重の組み合わせで処置された患者は、プラセボAtezo+Bev(すなわち、Tiraなし)と比較して、許容される毒性を有しながら、1つ以上の有効性評価項目(ORR、PFS、OS、DOR及び/又は疾患対照)を達成すると予想される。


実施例7.未処置の進展型小細胞肺がん患者における、チラゴルマブを用いる又は用いないアテゾリズマブ+カルボプラチン及びエトポシドの第III相無作為化二重盲検プラセボ対照試験
本実施例では、OS、PFS、ORR及びDORによって測定される、アテゾリズマブ+化学療法の抗腫瘍効果が、ES-SCLCを有する患者におけるアテゾリズマブ及び化学療法への抗TIGIT抗体チラゴルマブの添加によって改善され得るかどうかを評価するために設計された無作為化第III相グローバル多施設二重盲検プラセボ対照試験を記載する。ES-SCLCを有し、その進展型疾患について化学療法未経験である患者において、アテゾリズマブ及びCEと組み合わせたチラゴルマブの安全性及び有効性を、アテゾリズマブ及びCEと組み合わせたプラセボによる処置と比較する。
Example 7. Phase III, randomized, double-blind, placebo-controlled study of atezolizumab plus carboplatin and etoposide with or without tiragolumab in patients with previously untreated extensive-stage small cell lung cancer, as measured by OS, PFS, ORR and DOR in this example A randomized trial designed to assess whether the antitumor effects of atezolizumab plus chemotherapy could be improved by the addition of the anti-TIGIT antibody tiragolumab to atezolizumab and chemotherapy in patients with ES-SCLC. A Phase III global, multicenter, double-blind, placebo-controlled study is described. To compare the safety and efficacy of tiragolumab in combination with atezolizumab and CE to treatment with placebo in combination with atezolizumab and CE in patients with ES-SCLC who are chemotherapy-naïve for their extensive-stage disease.
A.試験計画
ES-SCLCを有し、その進展型疾患について化学療法未経験である患者において、アテゾリズマブ及びCEと組み合わせたプラセボによる処置と比較した、アテゾリズマブ及びCEと組み合わせたチラゴルマブの安全性及び有効性を評価するための無作為化第III相多施設二重盲検プラセボ対照試験の詳細を以下に記載する。図17は、試験計画を示す。
A. Study Design To evaluate the safety and efficacy of tiragolumab in combination with atezolizumab and CE compared to treatment with placebo in combination with atezolizumab and CE in patients with ES-SCLC who are chemotherapy naive for their extensive-stage disease. Details of a randomized Phase III, multicenter, double-blind, placebo-controlled study to Figure 17 shows the study plan.
適格患者を、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス(0対1)、LDH(≦正常値の上限(ULN)対>ULN)、及び脳転移の有無又は病歴(あり対なし)によって層別化し、1:1の比で無作為化して、表46に示されるような以下の処置レジメンの1つを受ける。ECOG性能状態に関するさらなる詳細は、Oken et al.,Am.J.Clin Oncol.1982,5:649-655に提供される。 Eligible patients were evaluated according to US East Coast Clinical Trials Group (ECOG) performance status (0 vs. 1), LDH (≦upper limit of normal (ULN) vs. >ULN), and presence or history of brain metastases (yes vs. no). and randomized in a 1:1 ratio to receive one of the following treatment regimens as shown in Table 46. Further details regarding ECOG performance states can be found in Oken et al. , Am. J. Clin Oncol. 1982, 5:649-655.
合計で約470人の患者が本試験において無作為化される。一次集団(PP)は、ベースラインでの脳転移の存在又は病歴の有病率が15%であると仮定して、約400人の患者を含む。処置意図(ITT)集団は、全ての患者を含む。

導入処置を21日間サイクルで4サイクル投与した。導入期の後、患者は、アテゾリズマブ+チラゴルマブ(A群)又はアテゾリズマブ+プラセボ(B群)のいずれかによる維持療法を継続する。維持期の間、予防的頭蓋照射(PCI)は現地の標準治療ごとに許可され、予防的頭蓋照射電子症例報告書(eCRF)に報告されている。対症療法のための緩和的放射線が許容される。表46の処置レジメンの投薬及び投与スケジュールを以下の表47に提供する。

各サイクルの1日目に、全ての適格患者に以下の順序で試験薬注入を投与する:
群A:アテゾリズマブ、チラゴルマブ、カルボプラチン及びエトポシド
群B:アテゾリズマブ、プラセボ、カルボプラチン及びエトポシド
On
Group A: atezolizumab, tiragolumab, carboplatin and etoposide Group B: atezolizumab, placebo, carboplatin and etoposide
患者は、局所標準治療及び製造業者の指示に従って、カルボプラチン及びエトポシドの制吐剤及びIV水分補給を受けることができる。コルチコステロイドによる前投薬は、臨床上実施可能な程度に最小限に抑えられる。全ての医薬品は、適切な併用医薬eCRFに記録される。 Patients can receive carboplatin and etoposide antiemetics and IV hydration according to the local standard of care and manufacturer's instructions. Premedication with corticosteroids is minimized to the extent clinically feasible. All medications will be recorded on the appropriate Concomitant Medications eCRF.
導入期の間、試験処置を以下の方法で1日目に投与しなければならない:
1.アテゾリズマブ1200mgを60(±15)分かけて静脈内投与し(初回注入の場合、その後の注入では30[±10]分に短縮)(表48を参照)、続いて、
2.チラゴルマブ/プラセボ600mgを60(±15)分かけて静脈内投与し(初回注入の場合、及びその後の注入の場合は30[±10]分に短縮)(表48を参照)、続いて、
3.カルボプラチンを30-60分かけて静脈内投与し、5mg/mL/分の濃度時間曲線(AUC)で初期目標面積を達成し(Calvert式投与)、
4.60分かけて静脈内投与されるエトポシド(100mg/m2)が続く。導入期の間、2日目及び3日目にエトポシド(100mg/m2)も60分かけて静脈内投与される。
During the run-in phase, study treatment must be administered on
1.
2. Tiragolumab/
3. Carboplatin was administered intravenously over 30-60 minutes to achieve an initial target area with a concentration-time curve (AUC) of 5 mg/mL/minute (Calvert dosing);
4. Followed by etoposide (100 mg/m 2 ) administered intravenously over 60 minutes. Etoposide (100 mg/m 2 ) is also administered intravenously over 60 minutes on
化学療法が行われないサイクルは、導入導化学療法サイクルの総数にカウントされない。導入期の後、患者はアテゾリズマブ+チラゴルマブ/プラセボによる維持療法を開始する。カルボプラチン及びエトポシドについて提案された注入時間は、現地の標準治療に従って適合される。アテゾリズマブ及びチラゴルマブ/プラセボの投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び薬剤に直ちにアクセスできる監視された状況で行われる。 Cycles without chemotherapy are not counted in the total number of induction chemotherapy cycles. After the run-in phase, patients will begin maintenance therapy with atezolizumab plus tiragolumab/placebo. Suggested infusion times for carboplatin and etoposide are adapted according to local standard of care. Administration of atezolizumab and tiragolumab/placebo will be conducted in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
RECIST v1.1による放射線学的疾患進行まで、又は患者が治験責任医師によって評定されるように臨床的利益を経験している限り、放射線学的データ、生検結果(利用可能な場合)、及び臨床状態の統合評定後の疾患進行に起因する許容できない毒性又は症候性悪化がない限り、処置を継続する。RECIST v1.1による疾患進行の基準を満たす患者は、全ての選択基準を満たす場合、試験処置(チラゴルマブ+アテゾリズマブ又はプラセボ+アテゾリズマブ)を継続することが許可される。 Radiological data, biopsy results (if available), and Treatment is continued unless there is unacceptable toxicity or symptomatic exacerbation due to disease progression after integrated assessment of clinical status. Patients meeting criteria for disease progression by RECIST v1.1 will be allowed to continue study treatment (tiragolumab + atezolizumab or placebo + atezolizumab) if all inclusion criteria are met.
アテゾリズマブ
患者は、各21日間サイクルの1日目にIV注入によって投与される1200mgのアテゾリズマブを受ける。アテゾリズマブ用量は固定され、体重に依存しない。アテゾリズマブ注入は、表48に概説される指示に従って投与される。アテゾリズマブ用量は変更されない。アテゾリズマブの用量調製、保存及び投与指示のさらなる詳細は、治験薬管理手順書及び/又はアテゾリズマブ治験責任医師のパンフレットに見出すことができる。
Atezolizumab Patients receive 1200 mg atezolizumab administered by IV infusion on
チラゴルマブ/プラセボ
アテゾリズマブの投与及び観察期間(表48参照)の後、患者は、各21日間サイクルの第1日にIV注入によって投与される600mgのチラゴルマブ/プラセボを受ける。チラゴルマブ/プラセボの用量は固定されており、体重に依存しない。チラゴルマブ/プラセボ注入は、表48に概説される指示に従って投与される。チラゴルマブ/プラセボの用量は変更されない。チラゴルマブ/プラセボの用量調製、保存、及び投与指示のさらなる詳細は、治験薬管理手順書及び/又は治験責任医師のパンフレットに見出すことができる。


カルボプラチン
導入期の間、カルボプラチンは、現地の診療ガイドラインによる標準的な制吐剤を用いて5mg/mL/分(Calvert式投薬)の初期標的AUCを達成するために、30-60分間にわたるIV注入によるチラゴルマブ/プラセボの完了後に投与される。コルチコステロイドによる前投薬は、臨床上実施可能な程度に最小限に抑えられ得る。カルボプラチン注入時間は、局所標準治療に従って適合される。
Carboplatin During the run-in phase, carboplatin is administered by IV infusion over 30-60 minutes to achieve an initial target AUC of 5 mg/mL/min (Calvert regimen) with standard antiemetics according to local clinical practice guidelines. Administered after completion of tiragolumab/placebo. Premedication with corticosteroids can be minimized to the extent clinically feasible. Carboplatin infusion times are adapted according to local standard of care.
AUC 5のカルボプラチン用量は、Calvert式(Calvert et al.,J.Clin.Oncol.1989,7:1748-56)を使用して計算される:
Calvert式:
総投与量(mg)=(目標AUC)X(糸球体濾過率[GFR]+25)
注:AUCベースの投与量を計算するためにCalvert式で使用されるGFRは、125mL/分を超えてはならない。
The
Calvert formula:
Total Dose (mg) = (Target AUC) X (Glomerular Filtration Rate [GFR] + 25)
Note: The GFR used in the Calvert formula to calculate AUC-based dose should not exceed 125 mL/min.
本明細書で使用される場合、GFRはクレアチニンクリアランス(CRCL)と同等であると考えられる。CRCLは、以下の式を使用して、施設のガイドラインによって、又はCockcroft and Gault,Nephron 1976,16:31-41の方法によって計算される:
CRCL=(140-年齢)X(体重)
(女性の場合、X0.85)
72XScr
式中:CRCL=mL/分単位のクレアチニンクリアランス
年齢=年単位の患者の年齢
体重=kg単位の患者の体重
Scr=mg/dL単位の血清クレアチニン
注:異常に低い血清クレアチニンレベルを有する患者については、0.8mg/dLの最小クレアチニンレベルを使用してGFRを推定するか、又は推定GFRを125mL/分でキャップする。
As used herein, GFR is considered equivalent to creatinine clearance (CRCL). CRCL is calculated by institutional guidelines or by the method of Cockcroft and Gault, Nephron 1976, 16:31-41, using the following formula:
CRCL = (140-age) X (weight)
(For women, X0.85)
72X Scr
Where: CRCL = creatinine clearance in mL/min Age = patient age in years Weight = patient weight in kg Scr = serum creatinine in mg/dL Note: For patients with abnormally low serum creatinine levels , use a minimum creatinine level of 0.8 mg/dL to estimate GFR, or cap the estimated GFR at 125 mL/min.
患者のGFRが同位体希釈質量分析法による血清クレアチニン測定に基づいて推定される場合、医師は、過剰投与による潜在的な毒性を回避するために所望の曝露(AUC)のためにカルボプラチンの用量をキャッピングすることを検討する。カルボプラチンのラベルに記載されているCalvert式に基づいて、最大用量を以下のように計算することができる:
最大カルボプラチン用量(mg)=標的AUC(mgX分/mL)X(GFR+25mL/分)
If a patient's GFR is estimated based on serum creatinine measurements by isotope dilution mass spectrometry, the physician should titrate the dose of carboplatin for the desired exposure (AUC) to avoid potential toxicity from overdose. Consider capping. Based on the Calvert formula on the carboplatin label, the maximum dose can be calculated as follows:
Maximum Carboplatin Dose (mg) = Target AUC (mgX min/mL) X (GFR + 25 mL/min)
最大用量は、正常な腎機能を有する患者について125mL/分で上限を定めたGFR推定値に基づく。より高い推定GFR値を使用すべきではない。 Maximum dose is based on GFR estimates capped at 125 mL/min for patients with normal renal function. Higher estimated GFR values should not be used.
標的AUC=5の場合、最大用量は5×(125+25)=5X150=750mgである。 For target AUC=5, the maximum dose is 5×(125+25)=5×150=750 mg.
標的AUC=4の場合、最大用量は4×(125+25)=4X150=600mgである。 For target AUC=4, the maximum dose is 4×(125+25)=4×150=600 mg.
エトポシド
導入期の間、各サイクルの1日目に、カルボプラチン投与後60分間にわたってエトポシド(100mg/m2)をIV注入によって投与する。各サイクルの2日目及び3日目に、エトポシド(100mg/m2)を60分かけてIV注入によって投与する。前投薬は、現地の標準治療に従って投与される。コルチコステロイドによる前投薬は、臨床上実施可能な程度に最小限に抑えられ得る。エトポシド注入時間は、現地の標準治療に従って適合させることができる。
Etoposide During the induction phase, on
ベースライン時に脳転移のない患者を評価する根拠(統計分析のための一次集団)
脳は、ES-SCLC患者の転移の一般的な部位であり、いくつかの試験は、診断時に脳転移を有する患者の18%もの高さを示し、診断後の最初の2年間に最大80%が脳疾患の関与を有すると予想される(Seute et al.,Cancer,100:801-806,2004;Pacheco and Bunn,Clin Lung Cancer,20:148-160,2019)。一般に、免疫療法と化学療法の併用からの利益は、ES-SCLC患者において示されている。しかし、IMpower 133試験で見られるように、この患者サブグループのハザード比(HR)は1.07であり、脳転移のない患者のHRは0.68であったのに対して、ベースラインで脳転移を有する患者ではこの利益が弱まる可能性がある(Horn et al.,New Engl J Med,379:2220-2229,2018)。
Rationale for Evaluating Patients Without Brain Metastases at Baseline (Primary Population for Statistical Analysis)
The brain is a common site of metastasis in ES-SCLC patients, with some studies showing as high as 18% of patients with brain metastases at diagnosis and up to 80% during the first 2 years after diagnosis. are expected to have brain disease involvement (Seute et al., Cancer, 100:801-806, 2004; Pacheco and Bunn, Clin Lung Cancer, 20:148-160, 2019). In general, benefit from a combination of immunotherapy and chemotherapy has been shown in ES-SCLC patients. However, as seen in the IMpower 133 trial, the hazard ratio (HR) for this patient subgroup was 1.07, compared to a HR of 0.68 for patients without brain metastases at baseline. This benefit may be attenuated in patients with brain metastases (Horn et al., New Engl J Med, 379:2220-2229, 2018).
KEYNOTE-604は別の第3相試験であり、診断時に脳転移を有するES-SCLC患者は、第一選択の免疫療法+化学療法に対して、それを有しない患者と比較して、全生存利益を達成し得ないか、又は達成し得ないことを示唆している。実際、脳転移を有する患者のOS HRは1.32であったのに対して、脳転移を有しない患者のOS HRは0.75であった(Rudin et al.,J Clin Oncology,38:2369-2379,2020)。CASPIAN試験は、脳転移を有する患者において0.69のOS HRを最初に報告したが、更新された分析ではHRは0.79になった。最初の報告及び更新された報告における脳転移のない患者のOS HRは、それぞれ 0.74及び0.76であったPaz-Ares et al.,N Engl J Med,379:2040-2051,2018;Paz-Ares et al.,Am Soc Clin Oncol 2020,abstract 9002,2020)。
KEYNOTE-604 is another
両方の患者サブグループにおける試験レジメンの利益を理解することが重要であり、したがって、試験統計的検定階層を、最初にPPを検定し、次にITTを検定するために実施した。 It was important to understand the benefit of the trial regimen in both patient subgroups, therefore a trial statistical test hierarchy was performed to test PP first and then ITT.
B.評定
患者は、第1サイクル、第1日後の48週間にわたって、ベースライン及び6週間毎(±7日)に腫瘍評定を受ける。ランダム化の前又は後4週間以内に、前処置腫瘍組織(保管又は新たに得た)試料を提出する。この標本は、関連する病理報告を伴う。任意の入手可能な腫瘍組織試料を提出することができるが、パラフィンブロック 中の代表的な腫瘍標本(好ましくは)又は10(又はそれ以上)の連続的な新たに切断された未染色スライドをバイオマーカー分析用(例えば、PD-L1の状態、免疫又はSCLCの生物学に関連するマーカー、例えば、T細胞マーカー、又は抽出されたDNA、RNA若しくは他の生物学的分子上のNGSによって同定される非遺伝性バイオマーカー)に提出することが推奨される。例示的な試料の種類としては、摘出、コアニードル、切除、切開、パンチ、鉗子生検、細針吸引及び細胞ペレット標本(例えば、胸水及び洗浄液試料から)から調製されたホルマリン固定パラフィン包埋(FFPE)試料が挙げられる。腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならない。脱灰の対象となる骨転移からの腫瘍組織は推奨できない。
B. Assessments Patients undergo tumor assessments at baseline and every 6 weeks (±7 days) for 48 weeks after
48週目の腫瘍評定の完了後、その後9週間毎(±7日)に腫瘍評定を行う。RECIST v1.1による疾患進行を超えて処置された患者は、処置が中止されるまで腫瘍評定を受ける。RECIST v1.1(例えば、毒性、症候性悪化)による放射線学的疾患進行以外の理由で処置を中止する患者は、患者が新たな抗がん治療を開始するかどうかにかかわらず、第1サイクル、1日目の後48週間、次いで9週間ごと(±7日)、その後6週間ごと(±7日)に予定された腫瘍評定を継続する。
After completion of the Week 48 tumor assessment, tumor assessments will be performed every 9 weeks (±7 days) thereafter. Patients treated beyond disease progression by RECIST v1.1 will undergo tumor assessments until treatment is discontinued. Patients who discontinue treatment for reasons other than radiographic disease progression according to RECIST v1.1 (e.g., toxicity, symptomatic worsening) are eligible for
血清試料を採取して、チラゴルマブ及びアテゾリズマブの薬物動態を監視する。選択された患者において、血漿試料を化学療法薬物動態学のために収集する。安全性評定には、有害事象の発生率、性質及び重症度、治験実施計画書に定められたバイタルサイン、及び検査異常が含まれる。 Serum samples are collected to monitor the pharmacokinetics of tiragolumab and atezolizumab. Plasma samples are collected for chemotherapy pharmacokinetics in selected patients. Safety assessments will include the incidence, nature and severity of adverse events, protocol defined vital signs, and laboratory abnormalities.
腫瘍生検は、放射線学的進行時に行われる。例示的な試料の種類として、摘出、コアニードル、切除、切開、パンチ、鉗子生検、細針吸引、及び細胞ペレット標本(例えば、胸水及び洗浄液試料から)から調製されたFFPE試料が挙げられる。組織からのDNA及び/又はRNA抽出を行うことができる。 A tumor biopsy is performed at radiological progression. Exemplary sample types include FFPE samples prepared from excision, core needle, dissection, incision, punch, forceps biopsy, fine needle aspiration, and cell pellet specimens (eg, from pleural fluid and lavage fluid samples). DNA and/or RNA extraction from tissue can be performed.
C.患者の報告された転帰
患者の報告された転帰(Patent Reported Outcome(PRO))データを、処置効果を文書化し、チラゴルマブ+アテゾリズマブの臨床プロファイルをより完全に特性評価するために収集する。PROデータは、以下の機器を使用して収集される:EORTC QLQ-C30、単一項目EORTC IL46、PRO-CTCAEからの選択項目、及びEQ-5D-5L。
C. Patient Reported Outcomes Patent Reported Outcomes (PRO) data will be collected to document treatment efficacy and to more fully characterize the clinical profile of tiragolumab plus atezolizumab. PRO data are collected using the following instruments: EORTC QLQ-C30, single-item EORTC IL46, selected items from PRO-CTCAE, and EQ-5D-5L.
EORTC QLQ-C30は、患者の機能の5つの側面(身体的、感情的、役割、認知的、及び社会的)、3つの症状尺度(疲労、悪心及び嘔吐、疼痛)、全身の健康状態/生活の質、及び6つの単一項目(呼吸困難、不眠症、食欲不振、便秘、下痢、及び金銭的困難)を評定する30の質問からなる、検証され信頼性の高い自己報告尺度である(Aaronson et al.,J.Natl.Cancer Inst.1993,85:365-76;Fitzsimmons et al.,Eur.J.Cancer 1999,35:939-41)。複数項目スケールについてスケールスコアを得ることができる。 The EORTC QLQ-C30 measures five aspects of patient functioning (physical, emotional, role, cognitive, and social), three symptom scales (fatigue, nausea and vomiting, pain), general health/life and six single items (dyspnea, insomnia, anorexia, constipation, diarrhea, and financial difficulties). et al., J. Natl. Cancer Inst. 1993, 85:365-76; Fitzsimmons et al., Eur. J. Cancer 1999, 35:939-41). Scale scores can be obtained for multiple-item scales.
EORTC QLQ-C30モジュールは、完了するのに約15分かかる。更に、単一項目EORTC IL46を回収する。この検証された単一項目の質問は、全体的な副作用の影響を評定する。
The EORTC QLQ-C30 module takes approximately 15 minutes to complete. In addition, the single
PRO-CTCAEは、78の患者報告可能な対症処置毒性(Basch et al.,J.Natl Cancer Inst.2014,106:1-11;Dueck et al.,JAMA Oncol.2015,1:1051-52)の存在、頻度、重症度、及び日常機能への干渉を特性評価するために使用される有効なアイテムバンクである。PROCTCAEは、5段階リッカート尺度(周波数、重大度及び干渉)又は2分法(有無)のいずれかで評価される124の質問を含む。含まれる処置毒性用語は、観察可能な成分(例えば、それぞれ嘔吐及び悪心)の有無にかかわらず主観的であり得るか、又は主観的な成分(例えば、発疹)で主に観察可能であり得る。標準PRO-CTCAEリコール期間は「過去7日間」である。現在の処置に最も適用可能であると考えられる3つの症状のサブセットをこの試験のために選択した。 PRO-CTCAE had 78 patient-reportable symptomatic treatment toxicities (Basch et al., J. Natl Cancer Inst. 2014, 106:1-11; Dueck et al., JAMA Oncol. 2015, 1:1051-52). is a validated item bank used to characterize the presence, frequency, severity, and interference with daily functioning of The PROCTCAE contains 124 questions rated on either a 5-point Likert scale (frequency, severity and interference) or dichotomous (presence or absence). Treatment toxicity terms included can be subjective with or without observable components (eg, vomiting and nausea, respectively) or can be primarily observable with subjective components (eg, rash). The standard PRO-CTCAE recall period is "last 7 days". Three subsets of symptoms were selected for this study that were considered most applicable to current treatment.
EQ-5D-5Lは、複合型の患者の健康状態の構築するために使用される、可動性、セルフケア、通常の活動、痛み/不快感、及び不安/抑うつに関する質問を含む一般的な選好に基づく健康効用尺度である。EQ-5D-5Lは、完了するのに約2分かかる。EQ-5D-5Lは、経済モデル化のためにこの試験で利用される。 The EQ-5D-5L are used to construct a composite patient well-being survey of general preferences including questions on mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. It is a health utility measure based on EQ-5D-5L takes about 2 minutes to complete. EQ-5D-5L will be utilized in this study for economic modeling.
PRO機器の紙バージョンは処置来院中に自己回答され、面接者は現場の担当者によってフォローアップ来院中の患者に電話で回答するため、患者の臨床現場への移動を要求することなくデータを収集することができる。PROデータは、現場担当者によって試験データベースに入力される。 The paper version of the PRO device is self-answered during the procedure visit, and the interviewer answers the patient by phone during the follow-up visit by on-site personnel, thus collecting data without requiring the patient to travel to the clinical site can do. PRO data are entered into the trial database by field personnel.
器具の有効性及びデータ規格が保健当局の要件を満たすことを確実にするために、診療所来院中に回答するようにスケジュールされた質問票は、特に明記しない限り、疾患状態に関する情報を受け取る前、患者の答えにバイアスをかける可能性がある非PRO評定の実施前、及び試験処置の投与前に、患者によってその全体が完成される。 To ensure device efficacy and data specifications meet health authority requirements, questionnaires scheduled to be completed during clinic visits should be completed prior to receiving information on disease status, unless otherwise specified. , completed in its entirety by the patient, prior to administration of non-PRO assessments that may bias the patient's responses, and prior to administration of study treatment.
試験薬の投与前のサイクル1、1日目(ベースライン)の導入期中に質問票(EORTC QLQ-C30、EORTC IL46、PRO-CTCAE(選択項目)、及びEQ-5 D-5L)を完成させ、次いで、各試験処置サイクルで、試験薬物の投与前(すなわち、サイクル2、1日目;サイクル3、1日目;サイクル4、1日目)に完成させる。維持期の間、試験薬の投与前の1回おきの試験処置サイクル(すなわち、サイクル5、1日目;サイクル7、1日目;サイクル9、1日目等)及び試験処置中止来院時に質問票を完成させる。生存フォローアップ中、3ヶ月での最初の生存追跡(±30日)及び6ヶ月での2回目の生存追跡(±30日)でPROを収集する。RECIST v1.1(例えば、毒性、症候性悪化)による放射線学的疾患進行以外の何らかの理由で試験処置を中断した患者は、RECIST v1.1による放射線学的疾患進行、死亡、フォローアップの喪失、同意の撤回、又は試験依頼者による試験終了(いずれか早く発生する方)まで、各腫瘍評定来院時にEORTC QLQ-C30、PRO-CTCAE(選択項目)及びEQ-5 D-5Lを完成する。質問票でネイティブ言語が利用できない患者は、全てのPRO評定を完了することを免除される。
Completed questionnaires (EORTC QLQ-C30, EORTC IL46, PRO-CTCAE (optional), and EQ-5 D-5L) during the run-in phase on
有害事象報告はPROデータから導き出されていない。 No adverse event reports were derived from PRO data.
D.評価項目
治験責任医師が評定したPFS(RECIST v 1.1に従って発明者が評定した)及びPP中のOSは、この試験の共主要評価項目である。PP及びITT集団における客観的奏効率、PP及びITT集団における奏効期間、並びにITT集団におけるPFS及びOSは副次評価項目である。
D. Endpoints Investigator-assessed PFS (assessed by the inventors according to RECIST v 1.1) and OS in PP are co-primary endpoints of this study. Objective response rate in the PP and ITT population, duration of response in the PP and ITT population, and PFS and OS in the ITT population are secondary endpoints.
無増悪生存期間
PFSは、ランダム化の日付と最初に文書化された疾患進行(RECIST v1.1に従って治験責任医師によって評定された場合)又は死亡の日付との間(いずれか早く発生する方)の時間である。疾患の進行を経験したことがない、又はデータカットオフ日までに死亡しなかった患者は、最後の腫瘍評定時に打ち切られる。ベースライン後の腫瘍評定がない患者は、ランダム化の日付で打ち切られる。
Progression-Free Survival PFS is measured between the date of randomization and the date of first documented disease progression (as assessed by the investigator according to RECIST v1.1) or the date of death, whichever occurs first. It's time for Patients who have never experienced disease progression or who do not die by the data cutoff date will be censored at the last tumor assessment. Patients with no post-baseline tumor assessment will be censored at the date of randomization.
評価項目としてのPFSは腫瘍成長を反映することができ、生存利益の決定の前に評定することができ、更に、その決定は、一般に、その後の治療によって混同されない。PFSの改善が直接的な臨床的利益を表すか、又は臨床的利益の代用物を表すかは、利用可能な治療法と比較した新しい処置の効果及びベネフィット-リスクの大きさに依存する(U.S.Food and Drug Administration(2007)Guidance for Industry:Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics)。 PFS as an endpoint can reflect tumor growth, can be assessed prior to determination of survival benefit, and that determination is generally not confounded by subsequent treatment. Whether improvement in PFS represents a direct clinical benefit or a surrogate for clinical benefit depends on the efficacy and benefit-risk magnitude of the new treatment compared to available therapies (U S. Food and Drug Administration (2007) Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologies).
治験責任医師が評定したPFSを主要評価項目としての有効性を確実にするために、多くの測定が実施されている:利益の実質的な目標規模及びベネフィット-リスクの堅牢な評価を可能にする試験評定(両方の処置群で同一である一定の評定間隔で放射線学的疾患進行を定義するための従来のRECIST v1.1基準、及びPFSの堅牢な定義、並びに感度分析を含むPFSを評定、定量化、及び分析するための予測的に定義された方法)。 To ensure efficacy of investigator-assessed PFS as the primary endpoint, a number of measures have been performed: enabling a robust target size of benefit and benefit-risk assessment. Study assessment (conventional RECIST v1.1 criteria for defining radiographic disease progression at regular assessment intervals that are identical in both treatment arms, and robust definition of PFS, as well as PFS assessment including sensitivity analysis; predictively defined methods for quantification and analysis).
PFSの共主要評価項目の主要分析は、PPで約300のPFS事象(400人の患者の75%)が観察されたときに行われる。これは、以下に基づいて、0.001の両側有意レベルでPFSの目標HR 0.56を検出するための96%検定力を提供する。PFS曲線は指数分布に従う;PFS中央値は、プラセボ+アテゾリズマブ+EC群では5.2ヶ月であり、チラゴルマブ+アテゾリズマブ+EC群では9.2ヶ月である(0.56の目標HRに相当);脱落率がPFSについて12ヶ月にわたって5%である;及びPFSの暫定分析なし。 The primary analysis of the co-primary endpoint of PFS will be performed when approximately 300 PFS events (75% of 400 patients) were observed in PP. It provides 96% power to detect the target HR of 0.56 for PFS at a two-sided significance level of 0.001 based on: PFS curves follow an exponential distribution; median PFS is 5.2 months in the placebo + atezolizumab + EC group and 9.2 months in the tiragolumab + atezolizumab + EC group (equivalent to a target HR of 0.56); dropout rate is 5% for PFS over 12 months; and no interim analysis for PFS.
PFSについて観察された0.68以上のHRは、処置群間の統計学的に有意な差に対応する。すなわち、0.68のHRは、分析のための最小検出可能差である。これは、PFS中央値の2.4ヶ月の改善に相当し、プラセボ+アテゾリズマブ+CE群の5.2ヶ月から、チラゴルマブ+アテゾリズマブ+CE群の7.6ヶ月までである。 An observed HR of 0.68 or greater for PFS corresponds to a statistically significant difference between treatment groups. Thus, an HR of 0.68 is the minimum detectable difference for analysis. This corresponds to a median PFS improvement of 2.4 months, from 5.2 months in the placebo + atezolizumab + CE group to 7.6 months in the tiragolumab + atezolizumab + CE group.
カプラン・マイヤー法を用いて各処置群のPFS中央値を推定し、カプラン・マイヤー曲線を構築して処置群間の差を視覚的に説明する。Brookmeyer-Crowley方法論を使用して、各処置群の中央値PFSの95% CIを構築する(Brookmeyer and Crowley,Biometrics 1982,38:29-41)。 The Kaplan-Meier method is used to estimate the median PFS for each treatment group and construct Kaplan-Meier curves to visually illustrate differences between treatment groups. A 95% CI for the median PFS for each treatment group is constructed using the Brookmeyer-Crowley methodology (Brookmeyer and Crowley, Biometrics 1982, 38:29-41).
無作為化の6ヶ月後及び1年後のPFS率は、Greenwoodの式から導出された標準誤差を使用して計算された95% CIと共に、各処置群のKaplan-Meier法を使用して推定される。2つの処置群間のPFS率の差の95% CIは、通常の近似法を使用して推定される。 PFS rates at 6 months and 1 year after randomization were estimated using the Kaplan-Meier method for each treatment group, with 95% CIs calculated using standard errors derived from the Greenwood equation. be done. The 95% CI for the difference in PFS rates between the two treatment groups is estimated using routine approximation.
全生存期間
OSは、この試験における共主要評価項目である。OSは、ランダム化の日付と任意の原因による死亡との間の時間である。OSの改善は、一般に、進行性/切除不能又は転移性肺がんを有する患者の臨床的利益の最良の尺度として受け入れられている。
Overall survival OS is the co-primary endpoint in this trial. OS is the time between the date of randomization and death from any cause. Improvement in OS is generally accepted as the best measure of clinical benefit for patients with advanced/unresectable or metastatic lung cancer.
PFS及びOSを、層別化ログランク検定を使用して処置群間で比較する。PFS及びOSのHRは、層別化Cox比例ハザードモデルを使用して推定される。HRの95% CIが提供される。層別化係数は、IxRS(すなわち、ECOGパフォーマンスステータス及び乳酸デヒドロゲナーゼ(LDH))からの無作為化に用いたものである。過層別化のリスクがある場合、層別化因子(複数可)を層別化分析から除去してもよい。IxRS記録とeCRF記録との間にかなりの不一致が観察された場合、電子症例報告書(eCRF)に記録された層別化因子に基づく分析も提供される。非層別化分析の結果も提供される。 PFS and OS are compared between treatment groups using a stratified log-rank test. HR for PFS and OS are estimated using a stratified Cox proportional hazards model. A 95% CI for HR is provided. Stratification factors were used for randomization from IxRS (ie, ECOG performance status and lactate dehydrogenase (LDH)). If there is a risk of over-stratification, the stratification factor(s) may be removed from the stratification analysis. Analysis based on stratification factors recorded on electronic case report forms (eCRFs) is also provided if substantial discrepancies between IxRS and eCRF records are observed. Results of non-stratified analyzes are also provided.
OSの共主要評価項目の最終分析は、およそ288人の死亡(400人の72%)がPPにおいて観察されたときに行われる。これは、以下に基づいて、両側有意性レベル0.049でOSの目標HR 0.70を検出するための85%検定力を提供する。OS曲線は指数分布に従う;プラセボ+アテゾリズマブ+EC群では12.3ヶ月、チラゴルマブ+アテゾリズマブ+EC群では17.6ヶ月のOS中央値(0.70の目標HRに相当);脱落率がOSについて24ヶ月にわたって5%である;及びO’Brien-Fleming関数のLan-DeMets近似に基づいて決定された統計学的有意性の暫定境界を用いて、情報フラクションの約70%でのOSの1つの計画された暫定分析。
A final analysis of the co-primary endpoint of OS will be performed when approximately 288 deaths (72% of 400) were observed in PP. This provides 85% power to detect a target HR of 0.70 for OS at a two-sided significance level of 0.049 based on: OS curves follow an exponential distribution; median OS of 12.3 months for the placebo + atezolizumab + EC group and 17.6 months for the tiragolumab + atezolizumab + EC group (equivalent to a target HR of 0.70); dropout rate of 24 months for
PPにおけるOSについて観察された0.789以上のHRは、処置群間の統計学的に有意な差に対応する。すなわち、0.789のHRは、分析のための最小検出可能差であり、これは、OS中央値の3.3ヶ月の改善に相当し、プラセボ+アテゾリズマブ+CE群の12.3ヶ月から、チラゴルマブ+アテゾリズマブ+CE群の15.6ヶ月までである。 An observed HR of 0.789 or greater for OS in PP corresponds to a statistically significant difference between treatment groups. That is, an HR of 0.789 was the minimal detectable difference for analysis, corresponding to a median OS improvement of 3.3 months, from 12.3 months in the placebo + atezolizumab + CE group to tiragolumab + up to 15.6 months in the atezolizumab + CE arm.
OSの中間解析及び最終解析のタイミングを以下の表49に要約し、発生の追加の仮定を示す。

OS暫定分析は、最終PFS分析時に行う。Kaplan-Meier法を用いて各処置群のOS中央値を推定し、Kaplan-Meier曲線を構築して処置群間の差を視覚的に説明する。Brookmeyer-Crowley方法論を使用して、各処置群の中央値OSの95% CIを構築する(Brookmeyer and Crowley,Biometrics 1982,38:29-41)。 A preliminary OS analysis is performed during the final PFS analysis. The Kaplan-Meier method is used to estimate median OS for each treatment group, and Kaplan-Meier curves are constructed to visually illustrate differences between treatment groups. A 95% CI for median OS for each treatment group is constructed using the Brookmeyer-Crowley methodology (Brookmeyer and Crowley, Biometrics 1982, 38:29-41).
無作為化の1ヶ月後及び2年後のOS率は、Greenwoodの式から導出された標準誤差を使用して計算された95% CIと共に、各処置群のKaplan-Meier法を使用して推定される。2つの処置群間のOS率の差の95% CIは、通常の近似法を使用して推定される。 OS rates at 1 month and 2 years after randomization were estimated using the Kaplan-Meier method for each treatment group, with 95% CIs calculated using standard errors derived from the Greenwood equation. be done. The 95% CI for the difference in OS rates between the two treatment groups is estimated using routine approximation.
副次的有効性評価項目
処置意図集団における無増悪生存期間及び全生存期間
PP中のOSの差が統計的に有意である場合、PFS及びOSを、上記の共主要有効性評価項目の分析のための同じα割り当て比(1:49)及びαリサイクル戦略に従って、ITT集団で検定する。ITT集団中のPFS及びOSを、3つ全ての層別化を除いて上記と同じ方法を用いてPPと同時に分析する。
Secondary Efficacy Endpoints Progression-free survival and overall survival in the intent-to-treat population. following the same α assignment ratio (1:49) and α recycling strategy for ITT population. PFS and OS in the ITT population are analyzed simultaneously with PP using the same method as above except for all three stratifications.
IxRSからのランダム化に使用される因子(すなわち、ECOGパフォーマンスステータス、LDH、及び脳転移の存在又は履歴)は、ITT集団の層別解析に含まれる。過層別化のリスクがある場合、層別化因子(複数可)を層別化分析から除去してもよい。 Factors used for randomization from IxRS (ie, ECOG performance status, LDH, and presence or history of brain metastases) are included in the stratified analysis of the ITT population. If there is a risk of over-stratification, the stratification factor(s) may be removed from the stratification analysis.
確認された客観的奏効率
確認された客観的奏効は、RECIST v 1.1を使用して治験責任医師によって決定されるように、4週間以上離れた2回の連続した機会における確認されたCR又はPRのいずれかであり得る。ベースライン後の腫瘍評定を受けていない患者を含む、これらの基準を満たさない患者は、非応答者とみなされる。
Confirmed Objective Response Rate A confirmed objective response is a confirmed CR on two consecutive occasions ≥4 weeks apart, as determined by the investigator using RECIST v 1.1. or PR. Patients who do not meet these criteria, including those who do not have a post-baseline tumor assessment, are considered non-responders.
確認されたORRは、確認された客観的奏効を有した患者の割合として定義される。確認されたORRについての分析集団は、ベースラインで測定可能な疾患を有するPP及びITT集団である。確認されたORR及びその95% CIの推定値を、各処置群についてClopper-Pearson法を使用して計算する。2つの処置群間の確認されたORRの差のCIは、二項分布の正規近似を使用して決定される。 Confirmed ORR is defined as the proportion of patients with a confirmed objective response. Analysis populations for confirmed ORR are PP and ITT populations with measurable disease at baseline. Estimates of the confirmed ORR and its 95% CI are calculated using the Clopper-Pearson method for each treatment group. The CI of the confirmed ORR difference between the two treatment groups is determined using the normal approximation of the binomial distribution.
奏効期間
確認された応答のDORが、PP集団及びITT集団においてRECIST v 1.1を使用して治験責任医師によって決定されるような確認された客観的奏効を有した患者において評定される。確認された応答のDORは、確認された客観的奏効の最初の発生の日付から、RECIST v1.1に従って治験責任医師によって決定された進行性疾患又は死亡が文書化される最初の日付(いずれか早く発生する方)までの時間間隔である。分析時に進行しておらず死亡していない患者は、最後の腫瘍評定日の時点で打ち切られる。DORは、患者の非ランダム化サブセット(具体的には、客観的奏効を達成した患者)に基づく;したがって、この評価項目に対して正式な仮説検定は行われない。処置群間の比較は、説明のために行われる。PFS分析について詳述された方法論は、DOR分析に使用される。
Duration of Response The DOR of confirmed response will be assessed in patients with a confirmed objective response as determined by the investigator using RECIST v 1.1 in the PP and ITT populations. The DOR for a confirmed response is calculated from the date of first occurrence of a confirmed objective response to the first date of documented progressive disease or death as determined by the investigator according to RECIST v1.1 (either whichever occurs earlier). Patients who have not progressed and died at the time of analysis will be censored at the date of the last tumor assessment. DOR is based on a non-randomized subset of patients (specifically those who achieve an objective response); therefore, no formal hypothesis testing is performed for this endpoint. Comparisons between treatment groups are made for illustration. The methodology detailed for PFS analysis is used for DOR analysis.
層別化因子
層別化因子は、IxRSからのランダム化に使用されるものである(すなわち、ECOGパフォーマンスステータス、LDH、及び脳転移の存在又は履歴)。少なくとも1つの階層(すなわち、ECOGパフォーマンスステータス[0対1]、LDH[≦ULN対>ULN]、及びIxRSあたりの脳転移の存在又は履歴[ある対なし]にわたる層別化因子レベルの組み合わせ)が10未満の事象(PFS又はOS事象)を有する場合、層別化因子(3つの層別化因子のうちの1つ:患者数が最も少ないレベルを含むECOGパフォーマンスステータス、LDH及びIxRSあたりの脳転移の存在又は履歴)を層別化分析から除外する。層別化因子の除去は、10事象未満の階層(PFS又はOS事象)がなくなるまで継続する。層別解析に用いる最終層別因子セットは、層別解析を計画する全ての評価項目に適用する。IxRS記録とeCRF記録との間にかなりの不一致が観察された場合、電子症例報告書(eCRF)に記録された層別化因子に基づく分析も提供される。
Stratification Factors Stratification factors are those used for randomization from IxRS (ie, ECOG performance status, LDH, and presence or history of brain metastases). At least one stratum (i.e., a combination of stratification factor levels across ECOG performance status [0 vs. 1], LDH [≤ULN vs. >ULN], and presence or history of brain metastases per IxRS [with vs. no]) If having <10 events (PFS or OS events), stratification factor (1 of 3 stratification factors: ECOG performance status including lowest number of patients, brain metastases per LDH and IxRS) (presence or history of ) are excluded from the stratification analysis. Removal of stratification factors continues until there are no strata (PFS or OS events) with less than 10 events. The final stratification factor set used for stratification analysis will be applied to all endpoints for which stratification analysis is planned. Analysis based on stratification factors recorded on electronic case report forms (eCRFs) is also provided if substantial discrepancies between IxRS and eCRF records are observed.
E.適格性
患者は、ES-SCLCに対して化学療法を受けておらず、以下のような適格基準を満たしている場合に適格となる:18歳以上;治験責任医師の判断で試験治験実施計画書に従う能力;ECOGパフォーマンスステータスが0又は1;組織学的又は細胞学的に確認されたES-SCLC(修正Veterans Administration Lung Study Group(VALG)の病期分類システム(Micke et al.,Lung Cancer 2002,37:271-6)による;ES-SCLCに対する事前の全身処置なし;限局型SCLCに対して以前に化学放射線療法を受けたことがある患者は、治癒を目的とした処置を受けたことがあり、化学療法、胸部放射線療法、又は化学放射線療法の最終投薬/サイクルとES-SCLCの診断との間で少なくとも6ヵ月間の無治療期間がなければならない;RECIST v1.1で定義されている測定可能な疾患(以前に照射された病変は、(1)放射線療法以降、その部位で疾患の進行が明確に文書化されており、(2)以前に照射された病変が測定可能な疾患の唯一の部位ではない場合にのみ、測定可能な疾患と見なすことができる);処置前の腫瘍組織試料の提出;治療的抗凝固療法を受けている患者の場合:安定した抗凝固レジメン;スクリーニング時のHIV検査陰性、スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性;試験処置開始前(サイクル1の1日目)の14日以内に得られた、以下の臨床検査結果によって定義される、適切な血液学的及び臓器末端機能:顆粒球コロニー刺激因子支援なしの絶対好中球数(ANC)≧1.5×109/L(1500/μL);リンパ球数≧0.5×109/L(500/μL);血小板数≧100×109/L(100,000/μL)、輸血なし;ヘモグロビン≧90g/L(9g/dL)(この基準を満たすために、患者は輸血されるか、又は地域の標準治療に従って赤血球形成療法を受けることができる);INR又はaPTT≦1.5×ULN(治療的抗凝固薬、INR、又はaPTT≦1.5×ULNを受けていない患者の場合);AST、ALT、及びALP≦2.5×ULN。ただし、次の例外を含む:(文書化された肝転移の患者:AST及び/又はALT≦5×ULN;文書化された肝臓又は骨転移を有する患者:ALP≦5×ULN);ビリルビン≦1.5×ULN(ただし、以下の例外:既知のギルバート病患者:ビリルビン≦3×ULN);クレアチニン≦1.5×ULN;アルブミン≧25g/L(2.5g/dL)。
E. Eligibility Patients are eligible if they are naive to chemotherapy for ES-SCLC and meet the following eligibility criteria: 18 years of age or older; ECOG performance status 0 or 1; histologically or cytologically confirmed ES-SCLC (modified Veterans Administration Lung Study Group (VALG) staging system (Micke et al., Lung Cancer 2002, 37:271-6); no prior systemic treatment for ES-SCLC; , there must be a treatment-free interval of at least 6 months between the last dose/cycle of chemotherapy, thoracic radiotherapy, or chemoradiation and the diagnosis of ES-SCLC; measures as defined in RECIST v1.1 Possible disease (previously irradiated lesions are the only disease in which (1) disease progression is clearly documented at the site since radiotherapy and (2) previously irradiated lesions are measurable) can be considered measurable disease only if it is not at the site of the tumor); submission of pretreatment tumor tissue samples; for patients on therapeutic anticoagulation: stable anticoagulant regimen; Negative HIV test, negative hepatitis B surface antigen (HBsAg) test at Screening; Adequate, as defined by the following laboratory results obtained within 14 days prior to initiation of study treatment (Day 1 of Cycle 1) hematological and organ end function: absolute neutrophil count (ANC) ≥1.5 x 10 9 /L (1500/μL) without granulocyte colony stimulating factor support; lymphocyte count ≥ 0.5 x 10 9 platelet count ≧100×10 9 /L (100,000/μL), no transfusion; hemoglobin ≧90 g/L (9 g/dL) (to meet this criterion, patients were INR or aPTT ≤ 1.5 x ULN (Patients not on therapeutic anticoagulants, INR, or aPTT ≤ 1.5 x ULN) AST, ALT, and ALP ≤ 2.5 x ULN, with the following exceptions: (Patients with documented liver metastases: AST and/or ALT ≤ 5 x ULN; documented liver or patients with bone metastases: ALP ≤ 5 bilirubin ≤ 1.5 x ULN (with the following exceptions: patients with known Gilbert's disease: bilirubin ≤ 3 x ULN); creatinine ≤ 1.5 x ULN; albumin ≥ 25 g/L (2.5 g/dL) ).
除外基準は以下を含む:症候性又は活発に進行中のCNS転移(注:処置済み(すなわち、局所CNS指向療法)又は未処置のCNS病変を有する無症候性の患者は、以下の基準を全て満たす場合に適格である:RECIST v1.1よれば、測定可能な病変はCNSの外に存在する;患者にはCNS病変による頭蓋内出血又は脊髄出血の既往がない;転移は小脳又はテント上領域に限られる(すなわち、中脳、血管、髄質、又は脊髄への転移はない);患者には中枢神経系疾患による症状はない(すなわち、頭痛、吐き気、嘔吐、けいれん、麻痺等);患者は中枢神経系疾患に対する抗けいれん薬を継続して必要としていない;患者は、中枢神経系疾患に対するデキサメタゾン/コルチコステロイドを継続して必要としていない(以前に処置を受けていない患者も、CNS疾患に対してデキサメタゾン/コルチコステロイドの必要又は投与歴があってはならない);以前に治療されたCNS転移を有する患者の場合、CNS指向療法の完了とランダム化の間に中枢神経系の中間的な進行の証拠はない;以前に処置されていない患者の場合、CNS病変に関連する脳浮腫(例えば、血管原性浮腫)の証拠がない;以前に処置されていない患者では、スクリーニング時に造影剤を用いた脳磁気共鳴画像法(MRI)スキャンが必要であり、その後の全ての予定されたフォローアップ腫瘍評定では好ましい様式である(注:以下の基準が満たされる場合、造影剤を用いたコンピューター断層撮影(CT)スキャンは、その後の全ての予定されたフォローアップで許容可能となり得る:未処置の中枢神経系疾患を評定するために、スクリーニング時に脳MRI及び造影剤を用いたCTスキャンの両方を実施しなければならない;造影剤を用いたCTスキャンは、造影剤を用いたスクリーニングMRIで同定された病変を確実に評価するために使用できる;造影剤を用いたCTスキャンを使用して、スクリーニングMRIで同定された病変を造影剤を用いて確実に評価できない場合には、その後の全ての予定されたフォローアップ腫瘍評定に対して造影剤を用いたMRIスキャンを用いる必要がある;及び全ての腫瘍評定で同じ様式を使用する;手術及び/又は放射線による確定的処置を受けていない脊髄圧迫、又はランダム化前の1週間以上臨床的に安定していたという証拠のない脊髄圧迫の診断及び処置を受けた脊髄圧迫;軟髄膜疾患;制御不能な胸水、心膜液貯留、又は再発性排液処置を必要とする腹水(月に1回又はそれ以上の頻度);留置カテーテル(例えば、PLEURX(登録商標))を装着した患者は、排液頻度に関係なく許可される;制御されない又は症候性の高カルシウム血症(イオン化カルシウム>1.5mmol/L、総血清カルシウム>12mg/dL、又は補正カルシウム >ULN);ウイルス性、アルコール性、その他の肝炎、肝硬変、遺伝性肝疾患、又は現在のアルコール乱用等、臨床的に重要な既知の肝疾患;ランダム化前の5年以内にSCLC以外の悪性腫瘍、ただし、転移又は死亡のリスクがごくわずかで(例えば、5年OSが90%を超えると予想される)、治癒的転帰が期待されるものを除く(適切に治療された子宮頸部上皮内癌腫、基底又は扁平上皮細胞皮膚がん、治癒目的で外科的に処置された限局性前立腺がん、治癒目的で外科的に処置された非浸潤性乳管癌腫等);自己免疫疾患又は免疫不全の活動性又は病歴、ただし、以下の例外がある:(甲状腺補充ホルモン療法を受けている自己免疫関連甲状腺機能低下症の病歴のある患者はこの試験に適格である;インスリンレジメンを受けている制御された1型糖尿病の患者は、試験に適格である;湿疹、乾癬、単純苔癬、又は皮膚科症状のみを伴う白斑の患者(例えば、乾癬性関節炎の患者は除外される)は、次の条件を満たす場合、試験に適格である:発疹は体表面積の10%未満を覆っていなければならない;疾患はベースラインで十分に制御されなければならず、低効力の局所コルチコステロイドのみを必要とする;過去12ヶ月以内に、ソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的製剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎疾患の急性悪化が起こっていない;特発性肺線維症、組織化性肺炎(例、閉塞性細気管支炎)、薬物誘発性肺炎、若しくは特発性肺炎の病歴、又は胸部CTスキャンのスクリーニングにおける活動性肺炎の証拠;放射線野における放射線性肺炎の病歴(線維症)は許可される;スクリーニング時の活動性EBV感染又は既知又は疑われる慢性活動性EBV感染;EBV IgG及び/又はEBV核抗原(EBNA)陽性の患者は、EBV IgM及び/又はEBVポリメラーゼ連鎖反応(PCR)が陰性の場合にのみ適格である;活動性結核;感染症、菌血症、又は重度の肺炎の合併症のための入院を含むがこれらに限定されない、ランダム化時の重度の感染症;ニューヨーク心臓協会の心臓病(クラスII以上)、心筋梗塞、又はランダム化前の3か月以内の脳血管障害、不安定な不整脈、又は不安定狭心症等の重大な心血管疾患;既知の冠動脈疾患、上記の基準を満たさないうっ血性心不全、又は左心室駆出率が50%未満の患者は、必要に応じて心臓専門医と相談して、処置を行う医師の意見に基づいて最適化された安定した医療レジメンを受けなければならない;ランダム化前の28日以内の診断以外の大きな外科的処置、又は試験の過程における大きな外科的処置の必要性が予想される場合;以前の同種骨髄移植又は固形臓器移植;治験薬の使用を禁じる、又は結果の解釈に影響を与える、又は患者を処置の合併症の高いリスクにさらす可能性のある疾患又は症状の合理的な疑いを与えるその他の疾患、代謝機能障害、身体検査所見、又は臨床検査所見;治験手順を理解し、従うこと、及び/又は遵守する能力を妨げる疾病又は症状を有する患者;試験処置開始前28日以内の他の治験薬による処置;HBV又はHCVに対する抗ウイルス療法による現在の処置;無作為化前の4週間以内の弱毒化生ワクチンの投与、又はそのような弱毒化生ワクチンが試験中に必要になるという予想;患者は無作為化前の4週間以内、治療中、及び試験処置の最終投薬から5ヵ月間、弱毒化生インフルエンザワクチン(例えば、FLUMIST(登録商標))を受けてはならない;CD137アゴニスト又は免疫チェックポイント遮断療法、抗CTLA-4、抗TIGIT、抗PD-1、及び抗PD-L1治療抗体による事前処置;ランダム化前の4週間又は5回の薬物排泄半減期(いずれか長い方)以内の全身免疫賦活剤(インターフェロン及びインターロイキン2(IL-2)を含むがこれらに限定されない)による処置;ランダム化前又は治験治療中の全身免疫抑制薬の必要性が予想される1週間以内の全身性免疫抑制薬(コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド、及び抗腫瘍壊死因子(抗TNF)剤を含むがこれらに限定されない)による処置、ただし以下を除く:急性、低用量の全身免疫抑制薬、又は全身免疫抑制薬(例えば、造影剤アレルギーの場合は48時間のコルチコステロイド)のパルス投与を受けた患者は、メディカルモニターの確認が得られた後に試験に適格である;ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患(COPD)又は喘息に対するコルチコステロイド、又は起立性低血圧のための低用量ミネラルコルチコイド、又は副腎不全のための低用量ミネラルコルチコイド及びコルチコステロイドを投与された患者は、この試験に適格である;キメラ抗体若しくはヒト化抗体、又は融合タンパク質に対する重度のアレルギー性アナフィラキシー反応の病歴;チャイニーズハムスター卵巣細胞生成物、又はチラゴルマブ若しくはアテゾリズマブ製剤の任意の成分に対する既知の過敏症;カルボプラチン又はエトポシドに対するアレルギー反応の病歴;妊娠又は授乳中、又は試験処置中、又はチラゴルマブ若しくはプラセボの最終投与後90日以内、アテゾリズマブの最終投与後5か月以内、又はカルボプラチン若しくはエトポシドの最終投与後6か月間に妊娠する意図;妊娠可能性のある女性は、試験処置開始前の14日以内に血清妊娠検査結果が陰性でなければならない。 Exclusion criteria include: Asymptomatic patients with symptomatic or actively developing CNS metastases Eligible if: Measurable disease exists outside the CNS according to RECIST v1.1; patient has no history of intracranial or spinal cord hemorrhage due to CNS lesions; metastasis to cerebellum or supratentorial region Limited (ie, no midbrain, vascular, medulla, or spinal cord metastases); patient has no symptoms of CNS disease (ie, headache, nausea, vomiting, seizures, paralysis, etc.); No ongoing need for anticonvulsants for neurological disease; patient has no ongoing need for dexamethasone/corticosteroids for central nervous system disease intermediate progression of the central nervous system between completion of CNS-directed therapy and randomization for patients with previously treated CNS metastases; no evidence of cerebral edema (e.g., vasogenic edema) associated with CNS lesions in previously untreated patients; contrast agents used at screening in previously untreated patients; A brain magnetic resonance imaging (MRI) scan is required and is the preferred modality for all subsequent scheduled follow-up tumor assessments (CT) scans may be acceptable at all subsequent scheduled follow-ups: both brain MRI and CT scan with contrast at Screening to assess untreated central nervous system disease contrast-enhanced CT scan can be used to reliably evaluate lesions identified by contrast-enhanced screening MRI; contrast-enhanced MRI scans should be used for all subsequent scheduled follow-up tumor assessments, unless lesions identified in 2010-2011 can be reliably assessed with contrast; Use the same modalities for assessment; spinal cord compression without definitive treatment with surgery and/or radiation or without evidence of clinical stability >1 week prior to randomization. received spinal cord compression; leptomeningeal disease; uncontrolled pleural effusion, pericardial effusion, or ascites requiring recurrent drainage (monthly or more frequently); Wearing patients are allowed regardless of drainage frequency; uncontrolled or symptomatic hypercalcemia (ionized calcium >1.5 mmol/L, total serum calcium >12 mg/dL, or corrected calcium >ULN); Known clinically significant liver disease, such as viral, alcoholic, other hepatitis, cirrhosis, hereditary liver disease, or current alcohol abuse; malignancy other than SCLC within 5 years prior to randomization, provided that Except those with negligible risk of metastasis or death (e.g., 5-year OS expected >90%) and expected curative outcome (adequately treated cervical carcinoma in situ, baseline or squamous cell skin cancer, localized prostate cancer surgically treated with curative intent, ductal carcinoma in situ surgically treated with curative intent, etc.); autoimmune disease or active immunodeficiency or medical history, with the following exceptions: (Patients with a history of autoimmune-related hypothyroidism receiving thyroid replacement hormone therapy are eligible for this study; Patients with type diabetes are eligible for the study; patients with eczema, psoriasis, lichen simplex, or vitiligo with dermatologic symptoms only (e.g., patients with psoriatic arthritis are excluded) meet the following conditions: is eligible for the study if: rash must cover less than 10% of body surface area; disease must be well controlled at baseline and require only low-potency topical corticosteroids; No acute exacerbation of underlying disease requiring psoralen plus UV A radiation, methotrexate, retinoids, biologics, oral calcineurin inhibitors, or high-potency or oral corticosteroids within the past 12 months; idiopathic History of pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis obliterans), drug-induced pneumonia, or idiopathic pneumonia, or evidence of active pneumonia on screening chest CT scan; history (fibrosis) allowed; active EBV infection at screening or known or suspected chronic active EBV infection; Eligible only if polymerase chain reaction (PCR) is negative active tuberculosis; severe infection at randomization, including but not limited to hospitalization for complications of infection, bacteremia, or severe pneumonia; New York Heart Association cardiology (Class II or above), myocardial infarction, or significant cardiovascular disease such as cerebrovascular disease, unstable arrhythmia, or unstable angina within 3 months prior to randomization; known coronary artery disease, not meeting the above criteria Patients with congestive heart failure or left ventricular ejection fraction less than 50% should receive a stable medical regimen optimized in the opinion of the treating physician, in consultation with a cardiologist if necessary. non-diagnostic major surgical procedure within 28 days prior to randomization, or anticipation of need for major surgical procedure during the course of the study; prior allogeneic bone marrow or solid organ transplantation; use of study drug other diseases, metabolic dysfunctions, physical examination findings, which impair the interpretation of results or give reasonable suspicion of a disease or condition that may put the patient at increased risk for procedural complications; or laboratory findings; patients with a disease or condition that interferes with their ability to understand, follow, and/or adhere to study procedures; treatment with other investigational agents within 28 days prior to initiation of study treatment; antiviral against HBV or HCV Current treatment with therapy; Administration of live attenuated vaccine within 4 weeks prior to randomization, or anticipation that such live attenuated vaccine will be required during the study; Patients will be administered within 4 weeks prior to randomization , during treatment, and for 5 months after the last dose of study treatment, should not receive a live attenuated influenza vaccine (e.g., FLUMIST®); Pretreatment with TIGIT, anti-PD-1, and anti-PD-L1 therapeutic antibodies; systemic immunostimulants (interferon and interleukin-2) within 4 weeks or 5 drug elimination half-lives (whichever is longer) prior to randomization (including but not limited to IL-2)); systemic immunosuppressants (corticosteroids, cyclo treatment with fosphamide, azathioprine, methotrexate, thalidomide, and anti-tumor necrosis factor (anti-TNF) agents), except: acute, low-dose systemic immunosuppressants, or systemic immunosuppression Medications (eg, corticosteroids for 48 hours for contrast allergy) ) are eligible for the study after obtaining medical monitor confirmation; mineralocorticoids (e.g., fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose mineralocorticoids for orthostatic hypotension, or low-dose mineralocorticoids and corticosteroids for adrenal insufficiency are eligible for this study; chimeric or humanized antibodies, or fusions History of severe allergic anaphylactic reaction to protein; Known hypersensitivity to Chinese Hamster Ovary Cell Products or any component of tiragolumab or atezolizumab formulations; History of allergic reaction to carboplatin or etoposide; Pregnancy or lactation, or study treatment Intention to become pregnant during or within 90 days after the last dose of tiragolumab or placebo, within 5 months after the last dose of atezolizumab, or within 6 months after the last dose of carboplatin or etoposide; A negative serum pregnancy test result must be obtained within 14 days prior to initiation.
F.サイトカイン放出症候群
チラゴルマブ/プラセボ又はアテゾリズマブのサイクル1の投与のための前投薬は示されていない。しかしながら、チラゴルマブ/プラセボ又はアテゾリズマブによるサイトカイン放出症候群(CRS)を経験する患者は、その後の注入のために抗ヒスタミン剤、解熱剤及び/又は鎮痛剤(例えば、アセトアミノフェン)による前投薬を受け得る。CRSは、内因性又は注入されたT細胞及び/又は他の免疫エフェクター細胞の活性化又は関与をもたらす任意の免疫療法の投与後の超生理学的応答として定義される。症状は進行性であり得、常に発症時の発熱を含み、低血圧、毛細血管漏出(低酸素症)、及び終末器官機能不全を含み得る(Lee et al.,Biol Blood Marrow Transplant,25(4):625-638,2019)。CRSは、キメラ抗原受容体T細胞療法及び二重特異性T細胞エンゲージャー抗体療法で十分に文書化されているが、アテゾリズマブを含むPD-1又はPD-L1を標的とする免疫療法でも報告されている(Rotz et al.,Pediatr Blood Cancer,64:e26642,2017;Adashek and Feldman,J Oncol Practice,15:502-504,2019)。
F. Cytokine Release Syndrome No premedication for
実施例8.以前に処置されていない進行性非扁平上皮非小細胞肺がんの患者における、アテゾリズマブ+ペメトレキセド及びカルボプラチン/シスプラチン対ペンブロリズマブ+ペメトレキセド及びカルボプラチン/シスプラチンと組み合わせたチラゴルマブの第II相無作為化二重盲検プラセボ対照試験
本実施例は、以前に治療されていない局所進行性切除不能又は転移性非扁平上皮非小細胞肺がん(NSCLC)を有する患者において、アテゾリズマブ+ペメトレキセド及びカルボプラチン/シスプラチンと組み合わせたチラゴルマブの有効性及び安全性を、ペンブロリズマブ+ペメトレキセド及びカルボプラチン/シスプラチンと組み合わせたプラセボと比較して評価するように設計された無作為化第II相グローバル多施設二重盲検試験を記載する。
Example 8. Phase II, Randomized, Double-Blind, Placebo of Tiragolumab in Combination with Atezolizumab + Pemetrexed and Carboplatin/Cisplatin Versus Pembrolizumab + Pemetrexed and Carboplatin/Cisplatin in Patients With Previously Untreated Advanced Non-Squamous Non-Small Cell Lung Cancer Controlled Study This example demonstrates the efficacy of tiragolumab in combination with atezolizumab plus pemetrexed and carboplatin/cisplatin in patients with previously untreated locally advanced unresectable or metastatic non-squamous non-small cell lung cancer (NSCLC). A randomized, phase II, global, multicenter, double-blind study designed to evaluate pembrolizumab plus pemetrexed and safety compared to placebo in combination with carboplatin/cisplatin is described.
A.試験計画 A. test plan
この試験の適格患者には、EGFR又はALKのゲノム異常を有さず、局所進行性切除不能又は転移性の非扁平上皮NSCLCを有する、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス(0対1)を有する≧18歳の以前に処置されていない男性及び女性の患者が含まれる。 Eligible patients for this study had locally advanced unresectable or metastatic non-squamous NSCLC with no EGFR or ALK genomic aberrations, US East Coast Cancer Clinical Trials Group (ECOG) Performance Status (0 Previously untreated male and female patients ≧18 years of age with pair 1) are included.
腫瘍が既知のEGFR又はALK再編成を有する患者は、この試験から除外される。 Patients whose tumors have known EGFR or ALK rearrangements are excluded from this study.
EGFR又はALKの突然変異状態が不明である腫瘍を有する患者は、登録前に検査する必要がある。適格患者を、PD-L1発現(局所アッセイ又は中央アッセイによる腫瘍割合スコア(TPS)/腫瘍細胞(TC)<1%対1%-49%対≧50%)、地理的地域(アジア対非アジア)及びECOGパフォーマンスステータス(0対1)によって層別化し、以下の処置レジメンを受けるために1:1に無作為化する。
群A:アテゾリズマブ+ペメトレキセド及びシスプラチン/カルボプラチンと組み合わせたチラゴルマブ;
群B:ペンブロリズマブ+ペメトレキセド及びシスプラチン/カルボプラチンと組み合わせたプラセボ。
Patients with tumors with unknown EGFR or ALK mutational status should be tested prior to enrollment. Eligible patients were evaluated for PD-L1 expression (tumor percentage score (TPS)/tumor cell (TC) <1% vs. 1%-49% vs. ≧50% by local or central assay), geographic region (Asia vs. non-Asia ) and ECOG performance status (0 vs. 1) and randomized 1:1 to receive the following treatment regimens.
Group A: Tiragolumab in combination with atezolizumab + pemetrexed and cisplatin/carboplatin;
Group B: Pembrolizumab + pemetrexed and placebo in combination with cisplatin/carboplatin.
カルボプラチン又はシスプラチンの選択は、治験責任医師の選択による。カルボプラチン又はシスプラチンの選択はランダム化の前に行われ、サイクル1の1日目後に変更することはできない。
The choice of carboplatin or cisplatin is at the investigator's choice. The choice of carboplatin or cisplatin was made prior to randomization and cannot be changed after
ランダム化スキームは、全てのPD-L1発現サブグループ(TPS/TC <1%、1%-49%、及び≧50%)の適切な提示を有するほぼ等しい数の患者が登録されることを確実にするように設計される。一次NSCLC患者で観察されるPD-L1発現の自然な分布を反映するために、各PD-L1サブグループに登録された患者の割合は、治験VENTANA PD-L1(SP263)Companion Diagnostics(CDx)アッセイを用いた中央検査当たり約80人の患者(計画された総登録の約40%)に制限される。局所結果と中央結果との差を説明するために、中央結果によって定義されるサブグループへの登録が上限を超える軌道上にある場合、局所PD-L1状態に基づく選択的登録が実施される。 The randomization scheme ensures that approximately equal numbers of patients with adequate presentation of all PD-L1 expressing subgroups (TPS/TC <1%, 1%-49%, and ≧50%) are enrolled designed to be To reflect the natural distribution of PD-L1 expression observed in primary NSCLC patients, the proportion of patients enrolled in each PD-L1 subgroup was calculated using the investigational VENTANA PD-L1 (SP263) Companion Diagnostics (CDx) assay. Limited to approximately 80 patients (approximately 40% of planned total enrollment) per central study using To account for differences between local and central results, selective enrollment based on local PD-L1 status will be performed if enrollment into the subgroup defined by the central outcome is on track to exceed the upper bound.
群A及び群Bの導入処置を21日間のサイクルで4サイクル投与する。導入期の後、患者は、以下に概説されるように維持療法を継続する。
●群A:アテゾリズマブ+ペメトレキセドと組み合わせたチラゴルマブ
●群B:ペンブロリズマブ+ペメトレキセドと組み合わせたプラセボ
Induction treatments in Groups A and B are administered in 21-day cycles for 4 cycles. After the induction phase, patients continue maintenance therapy as outlined below.
Arm A: tiragolumab in combination with atezolizumab + pemetrexed Arm B: pembrolizumab + placebo in combination with pemetrexed
患者は、処置投薬の遅延にかかわらず、第1サイクル、第1日後の48週間にわたって、ベースライン及び6週間毎(±7日間)に腫瘍評定を受ける。48週目の腫瘍評定の完了後、RECIST v 1.1による放射線学的疾患進行、同意の撤回、試験終了又は死亡(いずれか早く発生する方)まで、その後は用量遅延にかかわらず、9週間(±7日)毎に腫瘍評定が必要とされる。RECIST v1.1による疾患進行を超えて処置された患者は、試験処置が中止されるまで、上記の頻度で腫瘍評定を受ける。RECIST v 1.1(例えば、毒性、症候性悪化)による放射線学的疾患進行以外の理由で処置を中止する患者は、患者が新しい抗がん治療を開始するかどうかにかかわらず、患者が試験処置を継続していた場合(すなわち、サイクル1、1日目の後の48週間にわたって6週間ごとに[±7日間]、その後は9週間ごとに[±7日間]、RECIST v 1.1による放射線学的疾患進行、同意の撤回、試験終了又は死亡のいずれか早く発生する方まで)と同じ頻度で予定された腫瘍評定を継続する。
Patients undergo tumor assessments at baseline and every 6 weeks (±7 days) for 48 weeks after
患者は、処置中、試験処置の中止時、及び試験処置の中止来院時に、患者が報告した転帰に関する質問票(EORTC QLQ-C30、EORTC QLQ-LC13及びEORTC IL46)を記入するように求められる。 Patients will be asked to complete patient-reported outcome questionnaires (EORTC QLQ-C30, EORTC QLQ-LC13 and EORTC IL46) during treatment, at study treatment discontinuation, and at the study treatment discontinuation visit.
試験来院時の安全性評定には、有害事象の発生率、性質及び重症度、治験実施計画書に定められたバイタルサイン、検査異常、及び、試験の安全性評定にとって重要であると考えられる他の治験実施計画書に規定された試験が含まれる。 Safety assessments at study visits should include the incidence, nature and severity of adverse events, protocol-specified vital signs, laboratory abnormalities, and other factors considered important to the safety assessment of the study. included protocol-specified studies.
試験中、血清試料を収集して、チラゴルマブ及びアテゾリズマブの薬物動態を監視し、チラゴルマブ及びアテゾリズマブに対する抗体の存在を検出する。 During the study, serum samples will be collected to monitor the pharmacokinetics of tiragolumab and atezolizumab and to detect the presence of antibodies to tiragolumab and atezolizumab.
保管及び新鮮な腫瘍組織、血清、血漿、及び血液試料を含む患者試料が、探索的バイオマーカー評定のために収集される。 Patient samples, including archival and fresh tumor tissue, serum, plasma, and blood samples, are collected for exploratory biomarker assessment.
試験中、RECIST v 1.1による疾患進行の基準を満たし、臨床的利益の証拠を示す患者は、患者が以下の基準の全てを満たすならば、治験責任医師の裁量で、チラゴルマブ/プラセボ及びアテゾリズマブ/ペンブロリズマブによる処置を継続することができる。
●治験責任医師によって評定される臨床的利益の証拠
●疾患の明確な進行を示す症状及び徴候(検査値の悪化(例えば、新たな又は悪化する高カルシウム血症)を含む)がないこと
●疾患進行に起因し得るECOGパフォーマンスステータスの低下なし
●治験実施計画書で許可された医学的介入によって管理することができない重要な解剖学的部位(例えば、軟髄膜疾患)における腫瘍進行の欠如
●患者は、RECIST v 1.1による最初の放射線学的進行時に試験処置を継続するために、他の処置選択肢を延期することを承認するための書面によるインフォームドコンセントを提供しなければならない。
During the study, patients who met criteria for disease progression by RECIST v 1.1 and demonstrated evidence of clinical benefit were allowed to receive tiragolumab/placebo and atezolizumab at the investigator's discretion, provided the patient met all of the following criteria: / Treatment with pembrolizumab can be continued.
- Evidence of clinical benefit as assessed by the investigator - Absence of symptoms and signs of definite disease progression (including deterioration of laboratory values (e.g., new or worsening hypercalcemia) - Disease No decline in ECOG performance status that could be attributed to progression Lack of tumor progression in critical anatomical sites (e.g., leptomeningeal disease) that cannot be managed by protocol-allowed medical intervention Patients must provide written informed consent to approve deferment of other treatment options in order to continue study treatment at first radiographic progression per RECIST v 1.1.
全ての時点での全腫瘍応答の治験責任医師による評定は、RECIST v 1.1のみに基づく。iRECISTによる客観的奏効を、各特定の時点での個々の病変の治験責任医師の評定に基づいてプログラムで計算する。 Investigator assessment of overall tumor response at all time points is based solely on RECIST v 1.1. The objective response by iRECIST is calculated by the program based on the investigator's assessment of individual lesions at each specified time point.
B.投薬及び投与
処置レジメンを図18に要約する。
アテゾリズマブ及びペンブロリズマブ
B. Dosing and Administration The treatment regimen is summarized in FIG.
atezolizumab and pembrolizumab
患者は、各21日間のサイクルの1日目に、群Aでは20mL(1200mg)の固定用量のアテゾリズマブ、又は群Bでは8mL(200mg)のペンブロリズマブを受ける。アテゾリズマブ/ペンブロリズマブ注入は、表50に概説される指示に従って投与される。


チラゴルマブ及びプラセボ
患者は、21日間の各サイクルの1日目に、群Aに10mL(600mg)の固定用量のチラゴルマブ又は群Bに10mLのプラセボを受ける。チラゴルマブ/プラセボ注入は、表50に概説される指示に従って投与される。
Tiragolumab and Placebo Patients will receive 10 mL (600 mg) fixed dose tiragolumab in Group A or 10 mL placebo in Group B on
ペメトレキセド、シスプラチン及びカルボプラチン
表51は、ペメトレキセド、カルボプラチン又はシスプラチンの処置投与のための用量及び推奨される注入時間を列挙する。

患者は、局所標準治療及び製造業者の指示に従って、白金-ペメトレキセド処置のための制吐剤及びIV水分補給を受ける。ただし、これらの免疫調節効果のために、ステロイドによる前投薬は臨床上実施可能な場合に限られた。更に、ペメトレキセド関連皮膚発疹の場合、臨床的に実施可能であるときはいつでも、局所ステロイド使用がフロントライ処置として推奨される。 Patients receive antiemetics and IV hydration for platinum-pemetrexed treatment according to local standard of care and manufacturer's instructions. However, because of these immunomodulatory effects, steroid premedication was limited to cases where it was clinically feasible. Additionally, for pemetrexed-related skin rashes, topical steroid use is recommended as a front-line treatment whenever clinically feasible.
表52は、ペメトレキセドに対する提案された前投薬を列挙する。

導入期の間、化学療法サイクルは、少なくとも1つの白金系化学療法成分が21日間のサイクルの間に少なくとも1回投与されている限り、4サイクルの導入化学療法に向かってカウントする。化学療法が行われないサイクルは、導入導化学療法サイクルの総数にカウントされない。 During the induction phase, chemotherapy cycles count toward 4 cycles of induction chemotherapy as long as at least one platinum-based chemotherapy component is administered at least once during the 21-day cycle. Cycles without chemotherapy are not counted in the total number of induction chemotherapy cycles.
用量の変更
ペメトレキセド及びシスプラチン/カルボプラチンの用量変更は、処方情報及び局所標準治療に従って毒性に対して許容される。
Dose Modifications Dose modifications of pemetrexed and cisplatin/carboplatin are acceptable for toxicity according to prescribing information and local standard of care.
用量変更ガイドラインを以下に提供する。一旦減少すると、用量を100%に戻すことはできない。 Dose modification guidelines are provided below. Once reduced, the dose cannot be returned to 100%.
ペメトレキセド又はシスプラチン/カルボプラチンによる治療は、患者が何らかの血液学的又は非血液学的グレード3又はグレード4の毒性を経験した場合、2回の用量減少又は処置が毒性のために63日間を超えて遅延した後に中止される。
Treatment with pemetrexed or cisplatin/carboplatin was 2 dose reductions or treatment delayed >63 days due to toxicity if the patient experienced any hematologic or
血液毒性
各サイクルの開始時に、ANCは≧1500/μLであり、血小板数は≧100,000/μLである。回復のための十分な時間を可能にするために、処置を最大63日間遅らせることができた。成長因子は、米国臨床腫瘍学会(ASCO)及びNCCNガイドライン(Smith et al.2015;NCCN 2019)に従って使用することができる。回復したら、前のサイクルからの最低の血小板及び好中球の値に基づいて、次のサイクルの開始時の用量調整を行う(表53)。ANC及び血小板の両方について用量調整が必要な場合、患者はより低い用量を受ける。

治験責任医師らは、これらの合併症が迅速かつ適切に管理され得るように、骨髄抑制、感染症又は発熱性好中球減少症の早期かつ明白な徴候に注意し、警告する。患者はこれらの徴候を認識し、できるだけ早い機会に医療処置を求めるように促される。 Investigators should be alert and alert to early and overt signs of myelosuppression, infection or febrile neutropenia so that these complications can be managed promptly and appropriately. Patients are encouraged to recognize these symptoms and seek medical attention at the earliest opportunity.
血液学的毒性のために化学療法を控える場合、全血球計算(WBC分画を含む)を、概説したように、計数が処置の下限に達するまで毎週取得する。その後、処置を再開する。 If chemotherapy is withheld due to hematologic toxicity, complete blood counts (including WBC differentials) are obtained weekly as outlined until counts reach the lower limit of treatment. Then resume treatment.
貧血のための用量減少は推奨されない。患者は、治験責任医師の施設のガイドラインに従って支援される。 Dose reduction for anemia is not recommended. Patients will be assisted according to the investigator's institutional guidelines.
非血液毒性
非血液学的毒性(表54)の場合、処置は、患者のベースライン値(又は患者がベースラインでその毒性を有していなかった場合はグレード≦1)以下に回復するまで最大63日間遅延される。次のサイクルの開始時の用量減少は、前のサイクルで投与された用量からの非血液学的毒性に基づいて行われる。表54は、非血液学的毒性に対する推奨される用量変更を提供する。

下痢は、適切な止瀉薬で制御される。悪心及び/又は嘔吐は、適切な制吐剤で制御することができる。グレード3又は4については、神経毒性化学療法を、(治験責任医師の臨床判断に基づいて)改善後に以前の用量の50%で再開するか、又は直ちに中止する。
Diarrhea is controlled with appropriate antidiarrheals. Nausea and/or vomiting can be controlled with appropriate antiemetics. For
C.併用療法 C. Combination therapy
併用療法は、試験薬の開始の7日前から試験中止来院までの治験実施計画書に定められた処置に加えて、患者によって使用される任意の医薬(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)からなる。そのような薬剤は全て、治験責任医師に報告され、記録される。 Concomitant therapy includes any medication used by the patient (e.g., prescription or over-the-counter medication, vaccine, herbal therapeutic or homeopathic remedies, dietary supplements). All such medications will be reported to the investigator and recorded.
許可された治療
患者は、試験中に以下の治療法を使用することが許される。
●年間失敗率<1%の経口避妊薬
●ホルモン補充療法
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
Allowed Treatments Patients will be allowed to use the following treatments during the study.
● Oral contraceptives with <1% annual failure rate ● Hormone replacement therapy ● Palliative radiation therapy (eg, treatment of known bone metastases or symptomatic relief of pain) as outlined below:
放射線学的疾患進行の文書化がない患者では、対症療法のための支持療法を最大化し、腫瘍標的病変の評定を妨げる放射線療法を回避することが強く奨励される。チラゴルマブ/プラセボ及びアテゾリズマブ/ペンブロリズマブによる処置は、緩和放射線療法中に継続され得る。
●骨密度を増加させるための核因子κBリガンド標的療法の受容体活性化因子
●骨量減少の進行を遅らせるためのビスホスホネート
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えばフルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与される吸入又は低用量コルチコステロイド
●起立性低血圧のために投与される低用量ミネラルコルチコイド、又は副腎皮質機能不全のための低用量ミネラルコルチコイド及びコルチコステロイド
In patients without documented radiographic disease progression, maximizing supportive care for symptomatic treatment and avoiding radiation therapy that interferes with assessment of tumor target lesions is strongly encouraged. Treatment with tiragolumab/placebo and atezolizumab/pembrolizumab may be continued during palliative radiotherapy.
- Receptor activator of nuclear factor κB ligand-targeted therapy to increase bone density - Bisphosphonates to slow progression of bone loss - Prophylactic or therapeutic anticoagulant therapy (such as stable dose warfarin or low molecular weight heparin) )
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
Inhaled or low-dose corticosteroids given for chronic obstructive pulmonary disease or asthma Low-dose mineralocorticoids given for orthostatic hypotension or low-dose mineralocorticoids for adrenal cortical insufficiency and corticosteroid
ペメトレキセド及びシスプラチン又はカルボプラチンのための前投薬が許容される。抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ/ペンブロリズマブ及びチラゴルマブ/プラセボ注入のためにのみ投与され得る。 Premedication for pemetrexed and cisplatin or carboplatin is permitted. Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent atezolizumab/pembrolizumab and tiragolumab/placebo infusions at the investigator's discretion.
一般に、治験責任医師は、現地の標準診療に従って、臨床上適応がある注意療法又は禁止療法として定義されているもの以外の支持療法を用いて患者のケアを管理する。注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理する。 In general, the investigator will manage patient care according to local standard practice, using supportive care other than those defined as clinically indicated attentional or prohibitive care. Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine) or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2-adrenergic agonist).
注意を要する治療
全身性コルチコステロイド及びTNF-α阻害剤は、チラゴルマブ及び/又はアテゾリズマブによる処置の潜在的に有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物が検討される。代替法が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。
Treatments requiring caution Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with tiragolumab and/or atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines are considered. If alternatives are not feasible, systemic corticosteroids and TNF-α inhibitors can be administered at the investigator's discretion.
チラゴルマブ及び/又はアテゾリズマブ治療に関連する場合、特定の有害事象の処置のために、治験責任医師の裁量で、全身コルチコステロイドが推奨される。 Systemic corticosteroids are recommended at the Investigator's discretion for the treatment of specific adverse events when associated with tiragolumab and/or atezolizumab therapy.
禁止される治療法
以下の併用療法の使用は、以下に記載されるように禁止される:
●試験治療(治験実施計画書で定められた試験処置以外)は、試験処置の開始前28日以内及び試験処置中に禁止される。
●がんの処置(限定されるものではないが、化学療法、ホルモン療法、免疫療法、放射線療法、及び薬草療法を含む)を目的とした併用療法は、薬剤に応じて、試験処置を開始する前の様々な期間、及び試験処置中、疾患の進行が文書化され、特定の状況下での緩和的放射線療法を除いて患者が試験処置を中止するまで禁止される。
●生弱毒化ワクチンは、試験処置の開始前4週間以内、試験処置中及び試験処置の最終用量後5ヶ月間禁止する。
●試験処置と組み合わせて投与した場合、自己免疫症状のリスクを潜在的に増加させる可能性があるため、試験処置の開始前及び試験処置中の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫調節剤(限定されないが、インターフェロン及びIL-2を含む)
●試験処置中の全身免疫抑制剤(限定されないが、シクロホスファミド、アザチオプリン、メトトレキサート及びサリドマイドを含む)(薬剤が試験処置の有効性及び安全性を潜在的に変化させる可能性があるため)
Prohibited Therapies The use of the following concomitant therapies is prohibited as described below:
• Study treatment (other than protocol-defined study treatment) is prohibited within 28 days prior to and during study treatment.
- Combination therapy for the treatment of cancer (including but not limited to chemotherapy, hormonal therapy, immunotherapy, radiotherapy, and herbal therapy), depending on the drug, to initiate study treatment At various times prior to and during study treatment, disease progression is documented and is prohibited until the patient discontinues study treatment, with the exception of palliative radiotherapy under certain circumstances.
• Live-attenuated vaccines are prohibited within 4 weeks prior to initiation of study treatment, during study treatment, and 5 months after the final dose of study treatment.
o Within 4 weeks or 5 drug elimination half-lives (either within 4 weeks prior to initiation of study treatment and during study treatment due to potential increased risk of autoimmune symptoms when administered in combination with study treatment) systemic immunomodulators (including but not limited to interferon and IL-2) within the longer term)
- Systemic immunosuppressants (including but not limited to cyclophosphamide, azathioprine, methotrexate, and thalidomide) during study treatment (because drugs can potentially alter the efficacy and safety of study treatment)
D.選択基準
患者は次の試験登録基準を満たさなければならない:
●署名済みインフォームドコンセントフォーム
●インフォームドコンセント書類の署名時の年齢が≧18歳
●試験治験実施計画書を遵守する能力
●ECOGパフォーマンスステータス0又は1
●組織学的又は細胞学的に文書化された局所進行性切除不能又は転移性非扁平上皮NSCLC
D. Inclusion Criteria Patients must meet the following study entry criteria:
● A signed informed consent form ● Age ≥18 years at the time of signing the informed consent document ● Ability to comply with the study protocol ●
- Histologically or cytologically documented locally advanced unresectable or metastatic nonsquamous NSCLC
混合型NSCLC組織学の腫瘍を有する患者は、主要な組織学的成分に基づいて非扁平上皮として分類されなければならない。混合型NSCLC及び小細胞肺がんを有する患者は試験に適格ではない。
●転移性非扁平上皮NSCLCに対する事前の全身処置なし
Patients with tumors of mixed NSCLC histology must be classified as non-squamous based on major histologic components. Patients with mixed NSCLC and small cell lung cancer are not eligible for the study.
No prior systemic treatment for metastatic non-squamous NSCLC
非転移性疾患に対する治癒目的でネオアジュバント、アジュバント化学療法、放射線療法又は化学放射線療法を以前に受けたことがある患者は、最後の化学療法の投薬及び/又は最後の放射線療法以来、ランダム化から少なくとも12ヶ月無治療期間を経験していなければならない。
●承認された局所試験が利用可能でない場合、現地の保健当局承認済みアッセイ(SP263[好ましい]、又はSP263が利用できない場合にのみ22C3)の使用、又は中央検査室アッセイ(治験用VENTANA[SP263]CDxアッセイ)による既知の腫瘍PD-L1の状態
Patients who have previously received neoadjuvant, adjuvant chemotherapy, radiotherapy or chemoradiotherapy with curative intent for non-metastatic disease will be excluded from randomization since the last chemotherapy dose and/or last radiotherapy. Must have experienced a treatment-free period of at least 12 months.
Use of a local health authority approved assay (SP263 [preferred], or 22C3 only if SP263 is not available) or a central laboratory assay (Investigational VENTANA [SP263]) if an approved local test is not available Known tumor PD-L1 status by CDx assay)
ホルマリン固定、パラフィン包埋(FFPE)ブロック(好ましい)又は少なくとも15-20枚の染色されていない連続スライドにおいて、関連する病理報告とともに代表的な腫瘍標本の利用可能性を確認した。EGFR突然変異及び/又はALK転座についての中央検査が必要な場合、更に5枚の未染色スライドを提供しなければならない。 The availability of representative tumor specimens along with relevant pathology reports was confirmed in formalin-fixed, paraffin-embedded (FFPE) blocks (preferred) or at least 15-20 unstained serial slides. If central testing for EGFR mutations and/or ALK translocations is required, an additional 5 unstained slides must be provided.
腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質である(すなわち、細胞状況及び組織構造が保存された最小数の100個の生存腫瘍細胞)。許容可能な試料には、摘出に由来する試料、深部腫瘍組織(新たに収集した生検のための最低3つのコアを有する)のに関するコアニードル生検、又は皮膚、皮下若しくは粘膜病変に関する切除生検、切開生検、パンチ生検若しくは鉗子生検、又は気管支腔内超音波(EBUS)コアニードル生検が含まれる。 Tumor tissue is of good quality based on total tumor content and viable tumor content (ie, a minimum number of 100 viable tumor cells with preserved cellular context and histology). Acceptable specimens include specimens from excisions, core needle biopsies of deep tumor tissue (with a minimum of 3 cores for freshly collected biopsies), or excisional biopsies of cutaneous, subcutaneous, or mucosal lesions. Includes biopsy, incisional biopsy, punch or forceps biopsy, or endobronchial ultrasound (EBUS) core needle biopsy.
気管支腔内超音波:経気管支針吸引(EBUS-TBNA)は、細針吸引と呼ばれることもあるが、(特に、より大きなゲージ針が用いられる場合は)組織が上記のように良質であれば許容され得る(すなわち、細胞内容物及び組織構造が保存された最小数が100個の生存腫瘍細胞)。針の吸引の場合、18ゲージ以上の針が推奨される。 Endobronchial Ultrasound: Transbronchial Needle Aspiration (EBUS-TBNA), sometimes referred to as fine needle aspiration (especially when larger gauge needles are used), should the tissue be of good quality as described above. acceptable (ie, a minimum number of 100 viable tumor cells with preservation of cellular contents and tissue architecture). For needle aspiration, an 18 gauge or larger needle is recommended.
組織構造を保存せず、細胞懸濁液及び/又は細胞スメア、ブラシ、胸水からの細胞ペレット、及び洗浄液試料を保存しない細針吸引は許容されない。 Fine-needle aspiration, which does not preserve tissue architecture and does not preserve cell suspensions and/or cell smears, brushes, cell pellets from pleural effusions, and lavage fluid samples, is not acceptable.
骨転移からの腫瘍組織は、IHCによる腫瘍PD-L1発現について評価することができず、したがって許容されない。 Tumor tissue from bone metastases cannot be assessed for tumor PD-L1 expression by IHC and is therefore not accepted.
保管組織が不十分又は利用できない場合、生検部位に安全にアクセスできる場合、患者はスクリーニング時に生検を受けることができる。生検を提供することができない場合、≧10枚の染色されていない連続スライドを提供することができれば、患者は、メディカルモニターとの議論の際に依然として適格であり得る。
●RECIST v 1.1によって定義される測定可能な疾患
If archival tissue is insufficient or unavailable, patients may undergo a biopsy at screening if the biopsy site is safely accessible. If a biopsy cannot be provided, the patient may still be eligible during discussion with the medical monitor if ≧10 consecutive unstained slides can be provided.
- Measurable disease as defined by RECIST v 1.1
以前に放射線照射された病変は、放射線及び以前に放射線照射された病変が測定可能な疾患の唯一の部位ではないため、疾患の進行がその部位で明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。
●平均余命≧12週間
●試験処置の開始(サイクル1の1日目)の前、14日以内に得られた、以下の検査試験結果によって定義される適切な血液学的機能及び終末器官機能:
-顆粒球コロニー刺激因子支持なしでANC≧1.5X109/L(≧1500/μL)
-リンパ球数≧0.5X109/L(≧500/μL)
-輸血なしで血小板数≧100X109/L(≧100,000/μL)
-ヘモグロビン≧90g/L(≧9g/dL)。
Previously irradiated lesions should only be measured if disease progression is clearly documented at that site, as radiation and previously irradiated lesions are not the only sites of disease measurable. can be considered a possible disease.
- Life expectancy ≥ 12 weeks - Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to initiation of study treatment (
- ANC ≧1.5×109/L (≧1500/μL) without granulocyte colony stimulating factor support
- Lymphocyte count ≥0.5 X 109/L (≥500/μL)
- Platelet count ≥100 X 109/L (≥100,000/μL) without transfusion
- Hemoglobin ≧90 g/L (≧9 g/dL).
患者は、この基準を満たすために、地域の標準治療に従って輸血又は赤血球造血処置を受けることができる。
-以下を除く、AST、ALT及びALP≦2.5X正常値の上限(ULN):
文書化された肝臓転移を有する患者:AST及びALT≦5XULN
文書化された肝臓転移又は骨転移を有する患者:ALP≦5XULN
-総ビリルビン≦1.5XULN、但し以下の例外がある:
既知のギルバート病患者:ビリルビン値≦3XULN
-Cockcroft-Gault式(Cockcroft and Gault 1976)を用いて、又はCrClを決定するための24時間の尿収集によって計算した、クレアチニンクリアランス(CrCl)≧40mL/分(シスプラチンに必要な≧60mL/分)
-アルブミン≧25g/L(≧2.5g/dL)
●治療的抗凝固療法を受けていない患者の場合:INR及びaPTT≦1.5XULN
●治療的抗凝固薬を投与されている患者:安定な抗凝固薬レジメン
●スクリーニング時の陰性HIV検査
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時のB型肝炎表面抗体(HBsAb)陽性検査、又は以下のいずれかを伴うスクリーニング時のHBsAb陰性:
-総B型肝炎コア抗体(HBcAb)陰性
-総HBcAb検査陽性、引き続いてB型肝炎ウイルス(HBV)DNA検査陰性(地域の検査定義による)。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:以下に定義するように、禁欲(異性間の性交を控える)又は避妊を使用することの同意、及び卵の提供を控えることの同意:
Patients can receive blood transfusions or erythropoietic procedures according to local standard of care to meet this criterion.
- AST, ALT and ALP ≤ 2.5X upper limit of normal (ULN), excluding:
Patients with documented liver metastases: AST and ALT ≤ 5XULN
Patients with documented liver or bone metastases: ALP ≤ 5XULN
- Total bilirubin ≤ 1.5 XULN, with the following exceptions:
Patients with known Gilbert's disease: bilirubin level ≤ 3XULN
- Creatinine clearance (CrCl) ≥ 40 mL/min (≥ 60 mL/min required for cisplatin), calculated using the Cockcroft-Gault formula (Cockcroft and Gault 1976) or by 24-hour urine collection to determine CrCl
- Albumin ≥25 g/L (≥2.5 g/dL)
- For patients not receiving therapeutic anticoagulation: INR and aPTT ≤ 1.5XULN
● Patients receiving therapeutic anticoagulants: stable anticoagulant regimen ● Negative HIV test at screening ● Negative hepatitis B surface antigen (HBsAg) test at screening ● Hepatitis B surface antibody (HBsAg) test at screening HBsAb) positive test or HBsAb negative at screening with any of the following:
- total hepatitis B core antibody (HBcAb) negative - total HBcAb test positive followed by hepatitis B virus (HBV) DNA test negative (according to local laboratory definitions).
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening. HCV RNA testing is performed only for patients who test positive for HCV antibodies.
For women of childbearing potential: Consent to abstinence (abstinence from heterosexual intercourse) or use of contraception, and consent to abstain from donating eggs, as defined below:
女性は、処置期間中、並びにチラゴルマブ又はプラセボの最終投与後90日間、アテゾリズマブ又はペンブロリズマブの最終投与後5ヶ月間、ペメトレキセド及びカルボプラチン又はシスプラチンの最終投与後6ヶ月間、年間<1%の失敗率で禁酒したままであるか、又は避妊方法を使用しなければならない。女性は、この同じ期間中に卵を提供することを控えなければならない。 Women had a <1% failure rate per year during the treatment period and for 90 days after the last dose of tiragolumab or placebo, 5 months after the last dose of atezolizumab or pembrolizumab, and 6 months after the last dose of pemetrexed and carboplatin or cisplatin. Must remain abstinent from alcohol or use contraceptive methods. Females should refrain from donating eggs during this same period.
女性は、月経後であり、閉経後の状態(連続≧12ヶ月の閉経以外の特定された原因のない無月経)に達しておらず、手術(すなわち、卵巣、卵管、及び/又は子宮の除去)又は治験責任医師によって決定される別の原因(例えば、ミュラー管無発生)のために永久に不妊ではない場合、妊娠可能性があるとみなされる。出産可能性の定義は、地域のガイドライン又は規制との整合に適合させることができる。 Females are postmenopausal, have not achieved postmenopausal status (amenorrhea with no identified cause other than menopause for ≧12 consecutive months), and have had surgery (i.e., ovarian, fallopian tube, and/or uterine Ablation) or another cause determined by the Investigator (eg, Müllerian agenesis) is considered fertile if not permanently infertile. Fertility definitions can be adapted to match local guidelines or regulations.
年間失敗率<1%の避妊方法の例としては、両側卵管結紮術、男性の不妊手術、排卵を阻害するホルモン避妊具、ホルモン放出子宮内避妊具、及び銅付加子宮内避妊具が挙げられる。 Examples of contraceptive methods with an annual failure rate of <1% include bilateral tubal ligation, male sterilization, hormonal devices that inhibit ovulation, hormone-releasing intrauterine devices, and copper-added intrauterine devices. .
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価される。 Reliability of sexual abstinence will be assessed in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle.
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、適切な避妊方法ではない。 Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not suitable methods of contraception.
試験処置の中止後に妊娠することを望む女性は、カルボプラチンによる処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に卵母細胞の保存についての助言を求めなければならない。
●男性の場合:以下に定義するように、禁欲を維持する(異性間の性交を控える)こと、又は避妊方法を使用すること、及び精子の提供を控えることに同意すること:
Women who wish to become pregnant after discontinuation of study treatment should seek advice regarding oocyte storage prior to initiation of study treatment due to the potential for irreversible infertility resulting from treatment with carboplatin.
For men: agreeing to maintain abstinence (abstain from heterosexual intercourse) or use contraceptive methods and to abstain from donating sperm, as defined below:
妊娠していない妊娠の可能性がある女性パートナーの場合、外科的に避妊していない男性は、胚曝露及び/又は遺伝毒性を回避するために、処置期間中、並びにチラゴルマブ又はプラセボの最終投与後90日間、アテゾリズマブ又はペンブロリズマブの最終投与後4ヶ月間、ペメトレキセド及びカルボプラチン又はシスプラチンの最終投与後6ヶ月間、禁欲を維持するか、又はコンドームと合わせて年間<1%の失敗率をもたらす追加の避妊方法を使用しなければならない。男性は、同期間中は精子提供をやめなければならない。 For non-pregnant female partners of childbearing potential, non-surgically contraceptive males should receive 100 mg/kg during the treatment period and after the last dose of tiragolumab or placebo to avoid embryo exposure and/or genotoxicity. Maintain abstinence for 90 days, 4 months after the last dose of atezolizumab or pembrolizumab, 6 months after the last dose of pemetrexed and carboplatin or cisplatin, or add-on contraception combined with a condom that results in <1% failure rate per year method must be used. Men must stop donating sperm during the same period.
妊婦のパートナーの場合、男性は、処置間中、及び胚が曝露されるのを回避するために、チラゴルマブ又はプラセボの最終投与後90日間、アテゾリズマブ又はペンブロリズマブの最終投与後4ヶ月間、カルボプラチン及びパクリタキセル又はnab-パクリタキセルの最終投与後6ヶ月間、禁欲を維持するか、又はコンドームを使用しなければならない。 For pregnant partners, men receive carboplatin and paclitaxel throughout the procedure and for 90 days after the last dose of tiragolumab or placebo and 4 months after the last dose of atezolizumab or pembrolizumab to avoid embryo exposure. OR must maintain abstinence or use a condom for 6 months after the last dose of nab-paclitaxel.
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価される。 Reliability of sexual abstinence will be assessed in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle.
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、適切な避妊方法ではない。 Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not suitable methods of contraception.
試験処置の開始後に子供を持ちたい男性は、ペメトレキセド、シスプラチン又はカルボプラチンによる処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に精子保存についての助言を求めるべきである。 Men who wish to have children after initiation of study treatment should seek advice on sperm storage prior to initiation of study treatment due to the potential for irreversible infertility resulting from treatment with pemetrexed, cisplatin, or carboplatin.
E.除外基準
EGFR遺伝子又はALK融合がん遺伝子に変異を有することが知られているNSCLCを有する患者は、試験参加から除外される。EGFR又はALKの状態が不明である非扁平上皮NSCLC患者を、事前スクリーニング又はスクリーニングで検査する。EGFR及び/又はALKの状態を現地の又は中央の検査室で評定する。局所的に評定されるEGFRの状態が、エクソン18-21における変異を検出する、検証された保健当局承認済みの検査を使用して、組織又は細胞学に対して行われる。試料を中央EGFR及び/又はALK検査に供する場合、追加のスライドを提供する。
E. Exclusion Criteria Patients with NSCLC known to have mutations in the EGFR gene or the ALK fusion oncogene are excluded from study participation. Patients with non-squamous NSCLC with unknown EGFR or ALK status are examined at pre-screening or screening. EGFR and/or ALK status will be assessed by a local or central laboratory. A local assessment of EGFR status is performed on tissue or cytology using a validated, health authority-approved test that detects mutations in exons 18-21. Additional slides are provided if the sample is subjected to central EGFR and/or ALK testing.
F.評定
患者は、試験を通して安全性及び忍容性について綿密に監視される。患者は、各投与の前に毒性について評定される;投薬は、臨床評定及び地域の臨床検査値が許容できる場合にのみ実施する。
F. Assessments Patients will be closely monitored for safety and tolerability throughout the study. Patients will be assessed for toxicity prior to each dose; dosing will be administered only if clinical evaluation and local laboratory values are acceptable.
病歴、ベースライン症状、併用薬及び人口統計データ
臨床的に重要な疾患、外科手術、がん病歴(以前のがん治療及び処置を含む)及び肺がん突然変異状態(例えば、EGFR及びALK)、生殖状態、喫煙歴、並びにアルコール及び乱用薬物の使用を含む病歴をベースライン時に記録する。更に、試験処置の開始前7日以内に患者によって使用された全ての薬物(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)を記録する。各フォローアップ健康診断時に、インターバルの病歴を取得し、投薬及びアレルギーの変化を記録する。
Medical history, baseline symptoms, concomitant medications and demographic data Clinically significant disease, surgery, cancer history (including previous cancer therapies and procedures) and lung cancer mutational status (e.g., EGFR and ALK), reproductive Medical history, including condition, smoking history, and alcohol and drug use of abuse are recorded at baseline. In addition, all drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, dietary supplements) used by the patient within 7 days prior to initiation of study treatment are recorded. At each follow-up check-up, an interval medical history is obtained and changes in medications and allergies are recorded.
人口統計データには、年齢、性別、及び自己報告の人種/民族性が含まれる。 Demographic data includes age, gender, and self-reported race/ethnicity.
身体検査
スクリーニング時に完全な身体検査を行い、これには頭部、目、鼻、及び喉、並びに心臓血管系、皮膚科学系、筋骨格系、呼吸器系、消化器系、泌尿生殖器系、及び神経系が含まれる。ベースラインで特定された異常を記録する。
Physical Exam A complete physical exam is performed at Screening, including the head, eyes, nose, and throat, as well as the cardiovascular, dermatological, musculoskeletal, respiratory, digestive, genitourinary, and genitourinary systems. Includes nervous system. Record any abnormalities identified at baseline.
限定的には、症状に応じた理学的検査が、指定されたベースライン後の来院で、臨床上示されるように実施される。ベースライン異常からの変化は、患者ノートに記録される。新たな又は悪化した臨床的に有意な異常が記録される。 Limited, symptomatic physical examinations will be performed as clinically indicated at designated post-baseline visits. Changes from baseline abnormalities are recorded in patient notes. New or worsening clinically significant abnormalities are recorded.
バイタルサイン
バイタルサインは、呼吸数、脈拍数、並びに患者が座位にある間の収縮期及び拡張期血圧、並びに体温の測定を含む。
Vital Signs Vital signs include measurements of respiratory rate, pulse rate, and systolic and diastolic blood pressure and body temperature while the patient is in a sitting position.
一般的病歴及びベースライン症状のeCRFでベースライン時に観察された異常を記録する。その後の来院時に、新たな又は悪化した臨床上に有意な異常を記録する。 Any abnormalities observed at baseline on the General Medical History and Baseline Symptom eCRF will be recorded. New or worsening clinically significant abnormalities are recorded at subsequent visits.
ECOGパフォーマンスステータス
パフォーマンスステータスを、ベースラインでECOGパフォーマンスステータスを使用して測定され、試験全体を通して一定の間隔で評定する。
ECOG Performance Status Performance status will be measured using the ECOG Performance Status at baseline and assessed at regular intervals throughout the study.
腫瘍及び反応の評価
スクリーニング及びその後の腫瘍評定には、腹部及び胸部のCTスキャンが含まれなければならない(禁忌でない限りIV造影剤及び施設基準に従って適切な経口造影剤を用いる)。骨盤の造影剤を用いたCTスキャンは、スクリーニング時に、及び臨床上適応があるように、又はその後の応答評価での局所標準治療に従って必要とされる。造影剤を用いたCTスキャンが禁忌である(すなわち、ヨウ素系造影剤アレルギー又は腎クリアランス障害を有する患者)患者は、胸部の非造影CTスキャンによる胸部、腹部、及び骨盤の造影剤を用いたMRIスキャンが使用され得る。
Tumor and Response Assessment Screening and subsequent tumor assessment must include a CT scan of the abdomen and chest (using IV contrast unless contraindicated and appropriate oral contrast according to institutional standards). A CT scan with contrast of the pelvis is indicated at screening and as clinically indicated or according to local standard of care with subsequent response assessment. Patients for whom contrast-enhanced CT scans are contraindicated (i.e., patients with iodine-based contrast allergy or impaired renal clearance) should receive contrast-enhanced MRI of the chest, abdomen, and pelvis with a non-contrast CT scan of the chest. Scanning can be used.
全ての患者のCNS転移を評価するために、スクリーニング時に頭部のCT(造影剤を用いる)又は造影剤を用いるMRIスキャン(CT造影剤が禁忌である場合)を行わなければならない。造影剤を用いたCTが行われ、脳転移の存在が明確でないと考えられる場合、ベースラインでのCNS転移の診断を確認又は否定するために頭部のMRIが必要である。 A CT of the head (with contrast) or MRI with contrast (if CT is contraindicated) must be performed at screening to assess CNS metastases in all patients. If a CT with contrast agent is performed and the presence of brain metastases is considered ambiguous, an MRI of the head is required to confirm or rule out the diagnosis of CNS metastases at baseline.
腫瘍評定のためのCTスキャンが陽電子放射断層撮影(PET)/CTスキャナーで行われる場合、CT取得は、完全造影診断CTスキャンの標準と一致しなければならない。 If CT scans for tumor assessment are performed on a Positron Emission Tomography (PET)/CT scanner, the CT acquisition must conform to the standard for full contrast-enhanced diagnostic CT scans.
臨床上適応がある場合、頸部の骨スキャン及びCTスキャン等のさらなる調査が行われる。治験責任医師の裁量で、RECIST v1.1に従う測定可能な疾患の評定の他の方法を使用してもよい。 Further investigations such as bone and CT scans of the neck are performed if clinically indicated. At the investigator's discretion, other methods of measurable disease assessment according to RECIST v1.1 may be used.
検査を繰り返すのではなく、インフォームドコンセントを得る前及びサイクル1の1日目の28日以内に標準治療として行われる腫瘍評定を使用することができる。測定可能及び/又は測定不可能な疾患を含む全ての疾患の既知の部位は、スクリーニング時に文書化され、その後の各腫瘍評価時に再評定されなければならない。
Tumor assessments performed prior to obtaining informed consent and within 28 days of
患者は、処置の遅れにかかわらず、第1サイクルの1日目の後、48週間にわたって、ベースライン時及び6週間(±7日)ごとに腫瘍評定を受ける。48週目の腫瘍評定の完了後、RECIST v 1.1(又はRECIST v 1.1による疾患進行後に試験処置を継続する患者の臨床的利益の喪失)による放射線学的疾患進行、同意の撤回、死亡又は試験終了(いずれか早く発生する方)まで、処置の遅れに関係なく、9週間毎(±7日間)に腫瘍評定が必要とされる。治験責任医師の裁量により、進行性疾患又は臨床的利益の喪失が疑われる場合はいつでもスキャンを実施され得る。
Patients undergo tumor assessments at baseline and every 6 weeks (±7 days) for 48 weeks after
奏効は、RECIST v1.1を用いて、上で詳述した画像診断に対して治験責任医師によって評定される。全ての時点における全腫瘍奏功の治験責任医師の評定は、RECIST v1.1のみに基づく。評定は、来院間の内部一貫性を保証するために、可能であれば同じ評価者によって行われる。結果は次のサイクルでの投与の前に治験責任医師によって再検討されなければならない。 Response will be assessed by the investigator for imaging as detailed above using RECIST v1.1. Investigator assessment of overall tumor response at all time points is based solely on RECIST v1.1. Ratings will be performed by the same rater when possible to ensure internal consistency between visits. Results should be reviewed by the investigator prior to dosing in the next cycle.
X線写真データ、生検結果(利用可能な場合)、及び臨床状態の統合評定後、疾患進行に起因する許容できない毒性又は症候性悪化がない状態で治験責任医師によって評評定された臨床的利益を患者が経験している限り、チラゴルマブ/プラセボ及びアテゾリズマブ/ペンブロリズマブによる試験処置を継続することができる。RECIST v 1.1による疾患進行の基準を満たす患者は、指定された基準の全てを満たし、書面による同意を提供する場合、試験処置を継続することが許可される。 Clinical benefit assessed by the investigator in the absence of unacceptable toxicity or exacerbation due to disease progression after integrated assessment of radiographic data, biopsy results (if available), and clinical status Study treatment with tiragolumab/placebo and atezolizumab/pembrolizumab can continue as long as the patient experiences Patients who meet the criteria for disease progression according to RECIST v 1.1 will be allowed to continue study treatment if they meet all of the specified criteria and provide written consent.
RECIST v1.1による放射線学的疾患の進行以外の理由(例えば、毒性、症候性悪化)で処置を中止する患者は、RECIST v1.1による放射線学的疾患の進行、同意の撤回、死亡又は試験終了(いずれか早く発生する方)まで、予定された腫瘍評定を上記の頻度で継続する。RECIST v1.1による放射線学的疾患の進行の非存在下で新たな抗がん治療を開始する患者は、RECIST v1.1による放射線学的疾患の進行、同意の撤回、死亡、又は試験終了(いずれか早く発生する方)まで、上記頻度で腫瘍評定を継続する。 Patients who discontinue treatment for reasons other than radiological disease progression according to RECIST v1.1 (e.g., toxicity, worsening of symptoms) will be assessed for radiological disease progression, withdrawal of consent, death, or study Scheduled tumor assessments will continue at the above frequency until termination (whichever occurs first). Patients starting new anticancer therapy in the absence of radiographic disease progression by RECIST v1.1 will be assessed for radiographic disease progression by RECIST v1.1, withdrawal of consent, death, or study end ( Tumor evaluations will continue at the above frequency until (whichever occurs first).
全ての時点における全腫瘍奏功の治験責任医師の評定は、RECIST v1.1のみに基づく。全体的な腫瘍評定は、iRECISTによるものであり、全ての標的病変、非標的病変、及び新しい病変のエントリーに基づく。iRECISTによる応答の評価を容易にするために、腫瘍評定を、進行を超えて試験処置を受けた患者について、RECIST v1.1による疾患進行後に継続しなければならない。これには、標的病変の継続的な測定、非標的病変の評価(明確な進行を示した任意の非標的病変のさらなる悪化の監視を含む)、及びその後の全ての評定での任意の新たに同定された病変(病変が測定可能である場合、測定値を含む)の評価が含まれる。 Investigator assessment of overall tumor response at all time points is based solely on RECIST v1.1. Global tumor ratings are from iRECIST and are based on entries of all target lesions, non-target lesions, and new lesions. To facilitate assessment of response by iRECIST, tumor assessment should be continued after disease progression by RECIST v1.1 for patients who received study treatment beyond progression. This includes continuous measurement of target lesions, assessment of non-target lesions (including monitoring for further deterioration of any non-target lesion that has demonstrated definite progression), and any new Evaluation of identified lesions (including measurements if lesions are measurable) is included.
心電図
スクリーニング時及び臨床的に適応がある場合、ECGが必要である。各患者のECGは、可能な限り同じ機械から取得される。リードの配置は可能な限り一貫している。ECG記録は、患者が少なくとも10分間仰臥位で安静にした後に行われなければならない。
Electrocardiogram An ECG is required at screening and when clinically indicated. Each patient's ECG is obtained from the same machine whenever possible. Lead placement is as consistent as possible. ECG recordings must be taken after the patient has rested in the supine position for at least 10 minutes.
安全性監視の目的で、治験責任医師は全てのECG記録を再検討しなければならない。ECG記録のコピーは、現場で患者の恒久的な試験ファイルの一部として保持される。任意の形態学的波形変化又は他のECG異常を文書化しなければならない。 For safety monitoring purposes, the investigator must review all ECG recordings. A copy of the ECG recording is kept on site as part of the patient's permanent test file. Any morphological waveform changes or other ECG abnormalities must be documented.
臨床転帰評定
処置の利益を文書化し、パクリタキセル/nab-パクリタキセルを用いたチラゴルマブ及びアテゾリズマブ+カルボプラチンの臨床プロファイルをより完全に特性評価するために、PRO機器が完成される。PROデータは、以下の機器を使用して収集される:EORTC QLQ-C30、EORTC QLQ-LC13、及びEORTC IL46からの単一項目。
Clinical Outcome Assessment A PRO instrument will be completed to document treatment benefit and more fully characterize the clinical profile of tiragolumab and atezolizumab plus carboplatin with paclitaxel/nab-paclitaxel. PRO data are collected using the following instruments: single items from EORTC QLQ-C30, EORTC QLQ-LC13, and EORTC IL46.
質問票(EORTC QLQ-C30、EORTC QLQ-LC13及びEORTC IL46)は、試験薬の投与前のサイクル1(ベースライン)の1日目に完了し、その後、サイクル4まで各処置サイクルの1日目(すなわち、サイクル2、1日目;サイクル3、1日目;サイクル4、1日目)に試験薬を投与する。
Questionnaires (EORTC QLQ-C30, EORTC QLQ-LC13 and EORTC IL46) will be completed on
サイクル5では、試験薬の投与(すなわち、サイクル5、1日目に;サイクル7、1日目;サイクル9、1日目;以下同様)の1日前から試験処置中止来院まで、及び試験処置中止来院時に、1回おきの試験処置サイクルで質問票を完了する。
In
全ゲノムシーケンシング又は全エクソームシーケンシングのための血液試料
参加施設では、血液試料をDNA抽出のために収集して、WGS又はWESが試験薬に対する応答を予測する、より重篤な疾患状態への進行に関連する、試験薬に対する獲得耐性に関連する、有害事象の発生に対する感受性に関連する、有害事象の監視又は調査の改善をもたらすことができる、又は疾患生物学及び薬物安全性の知識及び理解を高めることができるバリアントを同定することを可能にする。血液から抽出されたDNAを組織から抽出されたDNAと比較して、生殖系列変異体を体細胞バリアントと区別することによって体細胞バリアントを同定することができる。試料を、分析のために1つ以上の検査室に送ることができる。
Blood Samples for Whole Genome Sequencing or Whole Exome Sequencing At participating centers, blood samples will be collected for DNA extraction to more severe disease states where WGS or WES predicts response to study drug. associated with the progression of disease, associated with acquired resistance to the study drug, associated with susceptibility to the occurrence of adverse events, can lead to improved monitoring or investigation of adverse events, or knowledge and understanding of disease biology and drug safety It allows us to identify variants that can enhance our understanding. Somatic variants can be identified by comparing DNA extracted from blood to DNA extracted from tissue to distinguish germline variants from somatic variants. Samples can be sent to one or more laboratories for analysis.
WGS又はWESのための血液試料の収集及び提出は、各施設のIRB/EC及び該当する場合は適切な規制機関による調査試験の再検討及び承認を条件とする。 Collection and submission of blood samples for WGS or WES is subject to review and approval of the investigative study by each institution's IRB/EC and, where applicable, appropriate regulatory bodies.
ゲノミクスは、疾患病理生物学の試験者の理解をますます促している。WGS及びWESは、それぞれゲノム及びエクソームの包括的な特性評価を提供し、この試験で収集された臨床データと共に、有効性及び安全性を監視するため、又はどの患者が薬物に応答するか若しくは有害事象を発症する可能性がより高いかを予測するための新しい治療アプローチ又は新しい方法を開発する機会を増やす可能性がある。データは、この試験に関連して分析されるが、他の試験からのデータとまとめて調査することもできる。より大きなデータセットの利用可能性は、将来の薬物開発を支援するための重要なバイオマーカー及び経路の同定及び特性評価に役立つであろう。 Genomics is increasingly facilitating investigator's understanding of disease pathobiology. WGS and WES provide comprehensive genomic and exome characterization, respectively, along with the clinical data collected in this trial, to monitor efficacy and safety, or to determine which patients will respond to drug or adverse events. It may increase opportunities to develop new therapeutic approaches or new methods to predict whether an event is more likely to develop. Data will be analyzed in relation to this study, but can also be examined together with data from other studies. The availability of larger data sets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
WGS又はWESのために収集された血液試料は、もはや必要とされなくなるまで、又は使い果たされるまで保存しなければならない。 Blood samples collected for WGS or WES must be stored until no longer needed or until exhausted.
Research Biosample Repositoryのための試料
Research Biosample Repository(RBR)は、体液、固形組織及びそれらの誘導体(例えば、DNA、RNA、タンパク質、ペプチド)を含むヒト生体試料の長期保存に使用される集中管理型の施設グループである。RBR試料の収集、保存、及び分析は、新しい医薬品の合理的な設計及び診断検査の開発を容易にし、将来の患者のための個別化された薬物療法を可能にし得る。
Samples for the Research Biosample Repository The Research Biosample Repository (RBR) is a centralized repository used for long-term storage of human biological samples, including body fluids, solid tissues and their derivatives (e.g. DNA, RNA, proteins, peptides). Facility group. The collection, storage, and analysis of RBR samples may facilitate the rational design of new pharmaceuticals and development of diagnostic tests, enabling personalized drug therapy for future patients.
RBRの試料は、この任意の試験に参加することに具体的に同意した患者から収集される。RBR試料は、以下の目的のうちの1つ以上を達成するために分析される:
●バイオマーカーと有効性又は疾患進行との関連性を試験すること
●有害事象の発生に対する感受性に関連するか、又は有害事象のモニタリング若しくは調査の改善をもたらし得る安全性バイオマーカーを同定すること
●疾患生物学及び薬物安全性の知識及び理解を高めること
●薬物効果並びに薬物の吸収及び配置のプロセスを含む薬物応答を試験すること
●バイオマーカー又は診断アッセイを開発し、これらのアッセイの性能特性を確立すること
RBR samples are collected from patients who specifically consent to participate in this optional study. RBR samples are analyzed to achieve one or more of the following objectives:
• To test the association of biomarkers with efficacy or disease progression • To identify safety biomarkers that are associated with susceptibility to adverse event development or that may lead to improved monitoring or surveillance of adverse events • To enhance knowledge and understanding of disease biology and drug safety To test drug effects and drug responses, including processes of drug absorption and disposition To develop biomarker or diagnostic assays and characterize the performance of these assays to establish
試料収集
以下の試料は、RBRに保存され、限定されないが、チラゴルマブ、アテゾリズマブ、非扁平上皮NSCLC、又は薬物安全性に関連するバイオマーカーに関する試験を含む試験目的に使用される。
●試験過程中に治験責任医師の裁量で行われた医学的に指定される手順(例えば、気管支鏡検査、食道胃十二指腸鏡検査、大腸鏡検査)からの残留組織試料を含む、残留血液、血清、血漿及び腫瘍組織試料(現場に戻される残りの保管組織ブロックを除く)並びにその任意の導出物(例えば、DNA、RNA、タンパク質、ペプチド)
●サイクル1、1日目及びサイクル2、15日目の投与前及びサイクル3、1日目の投与前に収集した、任意の便試料。これらの試料を、家庭で収集してもよい。
Sample Collection The following samples will be stored in the RBR and used for testing purposes, including but not limited to testing for tiragolumab, atezolizumab, non-squamous NSCLC, or biomarkers related to drug safety.
- Residual blood, serum, including residual tissue samples from medically designated procedures (e.g., bronchoscopy, esophagogastroduodenoscopy, colonoscopy) performed at the discretion of the Investigator during the course of the study , plasma and tumor tissue samples (excluding remaining archival tissue blocks returned to the field) and any derivatives thereof (e.g. DNA, RNA, proteins, peptides)
• Any stool sample collected pre-dose on
上記の試料は、WGS、WES、又は他のゲノム分析方法による生殖系列又は体細胞変異体の分析のために1つ以上の検査室に送られ得る。ゲノミクスは、疾患病理生物学の試験者の理解をますます促している。WGS及びWESは、それぞれゲノム及びエクソームの包括的な特性評価を提供し、この試験で収集された臨床データと共に、有効性及び安全性を監視するため、又はどの患者が薬物に応答するか若しくは有害事象を発症する可能性がより高いかを予測するための新しい治療アプローチ又は新しい方法を開発する機会を増やす可能性がある。 The samples can be sent to one or more laboratories for analysis of germline or somatic variants by WGS, WES, or other genomic analysis methods. Genomics is increasingly facilitating investigator's understanding of disease pathobiology. WGS and WES provide comprehensive genomic and exome characterization, respectively, along with the clinical data collected in this trial, to monitor efficacy and safety, or to determine which patients will respond to drug or adverse events. It may increase opportunities to develop new therapeutic approaches or new methods to predict whether an event is more likely to develop.
RBR試料から生成されたデータは、この試験に関連して分析されるが、他の試験からのデータとまとめて調査することもできる。より大きなデータセットの利用可能性は、将来の薬物開発を支援するための重要なバイオマーカー及び経路の同定及び特性評価に役立つであろう。 Data generated from the RBR samples are analyzed in conjunction with this study, but can also be examined together with data from other studies. The availability of larger data sets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
G.処置及び患者の中止
処置の中止
患者は、以下のいずれかを経験した場合、試験処置を恒久的に中止しなければならない:
●個々の患者の治療に対する潜在的応答及び事象の重症度を考慮すると、許容できないと治験責任医師が判断した免疫介在性有害事象の発生を含む、試験処置に関連する許容できない毒性
●患者が試験処置を受け続ける場合、彼又は彼女の安全性を危険にさらす可能性があると治験責任医師が判断する任意の医学的症状
●処置の中止が患者にとって最も有益であるという治験責任医師の判断
●妊娠
●非治験実施計画書指定抗がん治療の使用
●RECIST v1.1による放射線学的疾患進行(試験処置が放射線学的進行を超えて継続されない限り)
●放射線学的疾患進行を超えて処置された患者については、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、症候性悪化)の統合評定の後に治験責任医師によって決定される臨床的利益の喪失(チラゴルマブ/プラセボ及びアテゾリズマブ/ペンブロリズマブによる処置が放射線学的疾患進行を超えて継続される場合)
G. Treatment and Patient Discontinuation Treatment Discontinuation Patients must permanently discontinue study treatment if they experience any of the following:
- unacceptable treatment-related toxicity, including the occurrence of immune-mediated adverse events that the investigator judged to be unacceptable given the individual patient's potential response to treatment and the severity of the event; Any medical condition that the investigator determines may endanger his or her safety if he or she continues to receive treatment. Pregnancy Use of non-protocol anticancer therapy Radiographic disease progression per RECIST v1.1 (unless study treatment continues beyond radiographic progression)
For patients treated beyond radiographic disease progression, a combined assessment of radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., symptomatic worsening). Loss of clinical benefit later determined by the investigator (if treatment with tiragolumab/placebo and atezolizumab/pembrolizumab is continued beyond radiographic disease progression)
試験処置の中止の主な理由は、適切なeCRFに文書化される。試験処置を早期に中止する患者は置き換えられない。 The primary reason for discontinuing study treatment will be documented in the appropriate eCRF. Patients who discontinue study treatment early are not replaced.
患者は、試験薬の最終投与の≦30日後に処置中止来院のために診療所に戻る。応答評定が進行性疾患を示す来院は、処置中止来院として使用され得る。進行性疾患又は臨床的利益の喪失以外の何らかの理由で試験処置を中止する患者(放射線学的疾患進行を超えて処置を継続する患者)は、腫瘍応答評定及びPRO評定を受け続ける。 Patients return to the clinic for a treatment discontinuation visit ≤30 days after the last dose of study drug. Visits where response ratings indicate progressive disease may be used as treatment discontinuation visits. Patients who discontinue study treatment for any reason other than progressive disease or loss of clinical benefit (patients continuing treatment beyond radiological disease progression) will continue to receive tumor response assessments and PRO assessments.
RECIST v1.1による試験処置の中止及び疾患の進行後、生存フォローアップ及び新しい抗がん治療に関する情報は、死亡までおよそ3ヶ月ごとに電話、患者の医療記録及び/又はクリニック来院を介して収集される(患者が同意を取り下げる場合を除く)。 After discontinuation of study treatment and disease progression per RECIST v1.1, information regarding survival follow-up and new anti-cancer therapy will be collected via telephone, patient medical records and/or clinic visits approximately every 3 months until death. (unless the patient withdraws consent).
H.分析
有効性分析
有効性分析は、ランダム化処置に従ってグループ化された患者を有するITT集団で行われる。2つの処置群とPFS HRとの間のORRの差の推定値が、それらの95%CIと共に計算される。
H. Analysis Efficacy analysis Efficacy analysis will be performed in the ITT population with patients grouped according to randomized treatment. Estimates of the ORR difference between the two treatment groups and PFS HR are calculated with their 95% CIs.
共主要有効性評価項目のn仮説検定もITT集団で行う。 n-hypothesis tests for co-primary efficacy endpoints are also performed in the ITT population.
疾患進行及び客観的奏効の全ての一次解析は、RECIST v1.1を使用した腫瘍評定の治験責任医師の再検討に基づく。 All primary analyzes of disease progression and objective response are based on the investigator's review of tumor assessments using RECIST v1.1.
主要有効性評価項目
共主要有効性評価項目は、ORR及びPFSで確認される。
Primary Efficacy Endpoints Co-primary efficacy endpoints will be identified with ORR and PFS.
確認されたORRは、CR又はPRを特徴とする客観的奏効を≧4週間の間隔で2回連続して達成した患者の割合として定義される。 Confirmed ORR is defined as the proportion of patients who achieved two consecutive objective responses characterized by CR or PR, ≧4 weeks apart.
客観的奏効が処置群によって評価され、ベースライン後の全奏効評定を行わない患者が非奏効者としてカウントされる。 Objective response will be assessed by treatment arm, and patients who do not have a post-baseline overall response assessment will be counted as non-responders.
2つの群におけるORR間の差の推定値が、その95%CIと共に計算される。Mantel-Haenszel検定を使用して、治験実施計画書で定義された層別化因子によって層別化された5%の両側有意水準で2つの処置群間のORRを比較する。 An estimate of the difference between the ORRs in the two groups is calculated with its 95% CI. The Mantel-Haenszel test will be used to compare the ORR between the two treatment groups at a two-sided significance level of 5% stratified by protocol-defined stratification factors.
PFSは、ランダム化の日付と最初に文書化された疾患進行又は死亡の日付との間のいずれか早く発生する方の時間として定義される。疾患の進行を経験したことがない患者又は分析時に死亡していない患者は、最後の腫瘍評定時に打ち切られる。ベースライン後の腫瘍評定がない患者は、ランダム化の日付で打ち切られる。 PFS is defined as the time between the date of randomization and the date of first documented disease progression or death, whichever occurs first. Patients who have never experienced disease progression or who have not died at the time of analysis will be censored at the last tumor assessment. Patients with no post-baseline tumor assessment will be censored at the date of randomization.
PFSを、層別化ログランク検定を使用して処置群間で比較する。 PFS will be compared between treatment groups using a stratified log-rank test.
PFSのHR及びその95%CIは、層別化Cox比例ハザードモデルを使用して推定される。 The HR of PFS and its 95% CI are estimated using a stratified Cox proportional hazards model.
カプラン・マイヤー法を使用して、各処置群のPFS中央値を推定し、カプラン・マイヤー曲線を構築して、処置群間の差の視覚的説明を提供する。 The Kaplan-Meier method is used to estimate median PFS for each treatment group and construct Kaplan-Meier curves to provide a visual description of differences between treatment groups.
副次的有効性評価項目
全生存期間
OSは、ランダム化から死に至るまでの時間として定義される。データカットオフの時点で生存している患者のデータは、生存していることが分かっていた最後の日に打ち切られる。ベースライン後の情報のない患者からのデータは、ランダム化の日付で打ち切られる。層別化Cox比例ハザードモデルを使用して、OS HR及びその95%CIを推定する。カプラン-マイヤー法を使用して、各処置群のOS曲線及びOS中央値を推定する。
Secondary Efficacy Endpoints Overall Survival OS is defined as the time from randomization to death. Data for patients alive at the time of data cutoff are censored on the last day known to be alive. Data from patients with no post-baseline information are censored at the date of randomization. A stratified Cox proportional hazards model is used to estimate the OS HR and its 95% CI. The Kaplan-Meier method is used to estimate the OS curve and median OS for each treatment group.
確認応答の持続時間
DORは、疾患進行に対する文書化された客観的奏功の最初の発生からの時間又はいずれかの原因による脂肪(いずれか早く発生する方)として定義される。DORの分析には、試験処置に対する客観的奏効を達成した患者のみが含まれる。DORは、カプラン-マイヤー法を用いて推定される。DORの決定は患者の非ランダム化サブセットに基づくため、正式な仮説検定は行われない。
Duration of Acknowledgment DOR is defined as the time from the first occurrence of a documented objective response to disease progression or fat due to any cause (whichever occurs first). Only patients who achieved an objective response to study treatment were included in the DOR analysis. DOR is estimated using the Kaplan-Meier method. No formal hypothesis testing is performed as the determination of DOR is based on a non-randomized subset of patients.
患者の報告された転帰
EORTC QLQ-LC13、GHS/QoL、及びEORTC QLQ-C30を使用した身体機能を使用した咳、呼吸困難、及び胸痛症状のTTCDは、ランダム化の日付から最初に確認された臨床的に意味のある悪化までの時間として定義される。症状の確認された臨床的に意味のある悪化は、少なくとも2回の連続評定のために保持されなければならない症状スコアのベースラインから≧10ポイントのスコア増加、又はベースラインから≧10ポイントの初期増加とそれに続く死亡と定義される。GHS/QoL及び身体機能について確認された臨床的に有意な低下は、GHS/QoLのベースラインから≧10ポイントのスコア低下、又は少なくとも2回の連続評定のために保持されなければならない身体機能スケールスコア、又はベースラインからの最初の≧10ポイントの低下とそれに続く死亡として定義される。
Patient Reported Outcomes TTCD with cough, dyspnea, and chest pain symptoms using physical functions using the EORTC QLQ-LC13, GHS/QoL, and EORTC QLQ-C30 were first confirmed from the date of randomization. Defined as time to clinically meaningful deterioration. Confirmed clinically meaningful worsening of symptoms must be retained for at least 2 consecutive assessments of symptom score ≥ 10 point score increase from baseline or initial score ≥ 10 points from baseline Defined as an increase followed by death. Confirmed clinically significant decline in GHS/QoL and physical functioning must be maintained for ≥10 point score reduction from baseline in GHS/QoL or at least 2 consecutive assessments of the physical functioning scale Defined as the score, or the first >10 point drop from baseline followed by death.
TTCDの場合、患者のデータは、臨床カットオフ日に臨床的に意味のある確認された劣化事象を経験したことがない場合、患者が評定を完了した最後の時点で打ち切られる。ベースライン又はベースライン後の評定が行われない場合、患者はランダム化日に打ち切られる。 For TTCD, patient data will be censored at the last time the patient completes the assessment if they have not experienced a confirmed clinically meaningful deteriorating event on the clinical cut-off date. If no baseline or post-baseline assessments are made, patients will be censored on the randomization day.
EORTCスケールを使用するTTCDは、PFSと同じ方法を使用して分析される。 TTCD using the EORTC scale is analyzed using the same method as PFS.
EORTCスコアリングのマニュアルガイドラインに従って、EORTC QLQ-C30、EORTC QLQ-LC13、及びEORTC IL46(副作用に悩まされるという項目)の質問票の項目及びサブスケールの全てについて、要約統計及び線形変換スコアのベースラインからの平均変化を報告する。 Baseline summary statistics and linear transformation scores for all questionnaire items and subscales of the EORTC QLQ-C30, EORTC QLQ-LC13, and EORTC IL46 (Suffering from Side Effects Item) according to manual guidelines for EORTC scoring. Report the mean change from .
安全性解析
安全性分析には、任意の量の試験処置を受けた無作為化患者として定義される全ての治療患者が含まれる。
Safety Analysis The safety analysis included all treated patients, defined as randomized patients who received any amount of study treatment.
安全性分析は、処置群によって実施され、受けた実際の処置に基づく。具体的には、ランダム化時の初期処置割り当てにかかわらず、患者が任意の量のチラゴルマブ又はアテゾリズマブを受けた場合、患者は安全性分析において群Aに含まれる。 Safety analyzes are performed by treatment group and are based on the actual treatment received. Specifically, patients are included in Group A in the safety analysis if they receive any dose of tiragolumab or atezolizumab, regardless of initial treatment assignment at randomization.
薬物曝露を、持続時間、投薬量及び用量強度を含めて要約する。有害事象の言語記述は、MedDRAシソーラス用語にマッピングされる。 Drug exposure is summarized including duration, dosage and dose intensity. Verbal descriptions of adverse events are mapped to MedDRA thesaurus terms.
全ての有害事象の重症度は、NCI CTCAE v5.0に従って治験責任医師によって等級付けされ、CRSの重症度も、ASTCTコンセンサス等級スケールに従って治験責任医師によって等級付けされる。全ての有害事象を処置群及びNCI CTCAEグレードによって要約する。また、CRSを、処置群及びASTCTコンセンサスグレードによって要約する。更に、試験処置の中断又は中止につながる重篤な有害事象及び有害事象を適宜要約する。同じ事象の複数の発生は、最大重症度で1回カウントする。正常範囲外の値を有する実験データが特定される。更に、ADA結果を含む選択された実験データを処置群によって要約する。死亡及び死亡原因を要約する。 The severity of all adverse events will be graded by the investigator according to the NCI CTCAE v5.0, and the severity of CRS will also be graded by the investigator according to the ASTCT consensus grading scale. All adverse events will be summarized by treatment group and NCI CTCAE grade. CRS is also summarized by treatment group and ASTCT consensus grade. In addition, serious adverse events and adverse events leading to interruption or discontinuation of study treatment will be summarized as appropriate. Multiple occurrences of the same event are counted once at maximum severity. Experimental data with values outside the normal range are identified. In addition, selected experimental data, including ADA results, are summarized by treatment group. Summarize deaths and causes of death.
薬物動態分析
PK分析のためにPK試料を収集し、この試験における曝露を以前の試験で得られた曝露と比較する。チラゴルマブ及びアテゾリズマブの血清濃度は、個々の値として報告され、適切な場合及びデータが許す場合、処置群及びサイクルによって要約される(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)。
Pharmacokinetic Analysis PK samples are collected for PK analysis and exposures in this study are compared to those obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab are reported as individual values and summarized by treatment group and cycle (mean, standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean coefficient of variation).
個々の及び血清中のチラゴルマブ及びアテゾリズマブ濃度の中央値を、処置群及び日ごとにプロットする。チラゴルマブ及びアテゾリズマブの濃度データを、確立された集団PKモデルを使用して他の試験からのデータと共にプールして、データによって保証されるクリアランス、分布容積及びAUC等のPKパラメーターを導出することができる。関連するPKパラメーターと安全性、有効性又はバイオマーカーの結果との潜在的な相関関係を調べることができる。 Median individual and serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be pooled with data from other studies using established population PK models to derive data-assured PK parameters such as clearance, volume of distribution and AUC. . Potential correlations between relevant PK parameters and safety, efficacy or biomarker outcomes can be examined.
免疫原性分析
免疫原性分析には、任意のADA評定を受けた患者が含まれ、受けた処置に従って患者がグループ分けされる。チラゴルマブ及びアテゾリズマブの両方についての処置下で発現したADA陽性患者及びADA陰性患者の数及び割合を処置群によって要約する。ADAの状態と安全性、有効性及びPK評価項目との間の関係は、記述統計学によって分析及び報告され得る。
Immunogenicity Analysis The immunogenicity analysis includes patients with any ADA assessment and groups the patients according to the treatment received. The numbers and percentages of treatment-emergent ADA-positive and ADA-negative patients for both tiragolumab and atezolizumab are summarized by treatment group. Relationships between ADA status and safety, efficacy and PK endpoints can be analyzed and reported by descriptive statistics.
バイオマーカー分析
バイオマーカー分析は、関連マーカー(例えば、TIGIT)と試験処置の有効性との関連を理解するために行われ得る。有効性転帰は、IHC及び/又はRNA分析によって決定されるように、腫瘍が高いバイオマーカー発現を有する患者の集団において調査され得る。WGSデータの探索的分析は、この試験の文脈で実施され、疾患病理生物学の試験者の理解を高め、新しい治療アプローチの開発を導くために、他の試験からのデータとまとめて調査され得る。WGSは、WGSサンプリングの規制上の承認を受けたことがない施設には適用されない。
Biomarker Analysis Biomarker analysis can be performed to understand the association between relevant markers (eg, TIGIT) and efficacy of the study treatment. Efficacy outcomes can be investigated in a population of patients whose tumors have high biomarker expression as determined by IHC and/or RNA analysis. Exploratory analysis of WGS data will be conducted in the context of this study and can be explored together with data from other studies to enhance the investigator's understanding of disease pathobiology and guide the development of new therapeutic approaches. . WGS does not apply to establishments that have never received regulatory approval for WGS sampling.
探索的分析
人口統計学的特性(例えば、年齢、性別、及び人種/民族性)及びベースライン予後特性(例えば、中央検査室検査によるPD-L1発現、地理的地域、及びECOG)によって定義されたサブグループにおける試験結果の一貫性を評定するために、これらのサブグループにおけるORR及びPFSを確認した共主要有効性評価項目を調べる。確認されたORR及びPFSの要約を、2つの処置群間の比較のためにカテゴリ変数のレベルごとに別々に作成する。
Exploratory Analysis Defined by demographic characteristics (e.g., age, sex, and race/ethnicity) and baseline prognostic characteristics (e.g., central laboratory PD-L1 expression, geographic region, and ECOG). Co-primary efficacy endpoints that confirmed ORR and PFS in these subgroups will be examined to assess the consistency of study results in these subgroups. Confirmed ORR and PFS summaries are generated separately for each level of the categorical variable for comparison between the two treatment groups.
中間分析
累積安全性データの定期的な分析をこの試験について計画する。PFSの有効性中間解析は、およそ86のPFS事象がITT集団において観察されたときに行われる。これは、最初の患者が無作為化されてから約19ヶ月後に起こると予測される。約120人の患者が少なくとも2つの腫瘍評定を受けた場合にも、ORRの早期分析を行う。これは、最初の患者が無作為化されてから約14ヶ月後に起こると予測される。
Interim Analysis Periodic analyzes of cumulative safety data are planned for this study. The PFS efficacy interim analysis will be performed when approximately 86 PFS events were observed in the ITT population. This is expected to occur approximately 19 months after the first patient is randomized. Early analysis of ORR will also be performed when approximately 120 patients have had at least two tumor assessments. This is expected to occur approximately 14 months after the first patient is randomized.
実施例9.以前に処置されていない局所進行性の切除可能なステージII、IIIA又は選択されたIIIB非小細胞肺がんを有する患者における、白金系化学療法を用いる又は用いない、ネオアジュバント及びアジュバントであるチラゴルマブ+アテゾリズマブの安全性及び有効性を評価する第II相非盲検多施設試験
A.試験計画の概要
GO42501は、以前に処置されていない、組織学的若しくは細胞学的に確認された切除可能なステージII、IIIA又は選択されたIIIB(T3N2のみ)NSCLC患者における、白金ベースの化学療法(Chemo)を用いて又は用いずに、ネオアジュバント及びアジュバントであるアテゾリズマブ(Atezo)+チラゴルマブ(Tira)の安全性及び有効性を評価する世界的な第II相非盲検多施設試験である。この試験は、Atezo+Tira又はAtezo+Tira+Chemoによるネオアジュバント処置が安全であり、忍容性があり、早期切除可能NSCLC患者の外科的転帰に対して臨床上有意な負の効果を有しないという概念実証臨床データを確立するように設計されている。この試験はまた、病理学的著効(MPR)によって測定されるような、ネオアジュバントであるAtezo+Tira又はAtezo+Tira+Chemoの潜在的な抗腫瘍効果を評価するために設計される。試験は、新しい処置の組み合わせが利用可能になるにつれて新しいコホートを開く柔軟性を伴って設計される。
Example 9. Neoadjuvant and adjuvant tiragolumab plus atezolizumab with or without platinum-based chemotherapy in patients with previously untreated locally advanced resectable stage II, IIIA or selected IIIB non-small cell lung cancer A Phase II, Open-label, Multicenter Study Evaluating the Safety and Efficacy of A. Study Design Overview GO42501 is a platinum-based chemotherapy in previously untreated, histologically or cytologically confirmed resectable stage II, IIIA, or selected IIIB (T3N2 only) NSCLC patients. A global phase II, open-label, multicenter study evaluating the safety and efficacy of the neoadjuvants and adjuvants atezolizumab (Atezo) plus tiragolumab (Tira) with or without (Chemo). This study provides proof-of-concept clinical data that neoadjuvant treatment with Atezo + Tira or Atezo + Tira + Chemo is safe, tolerable, and has no clinically significant negative effects on surgical outcomes in patients with early resectable NSCLC. Designed to establish This study is also designed to assess the potential anti-tumor effects of the neoadjuvants Atezo+Tira or Atezo+Tira+Chemo as measured by significant pathological response (MPR). The trial is designed with the flexibility to open new cohorts as new treatment combinations become available.
投与された試験処置を表55に示す。この治験実施計画書では、「試験処置」は、この試験の一部として患者に割り当てられた治療の組み合わせを指す(すなわち、Atezo+Tira、Atezo+Tira+Chemo、又は化学療法)。

図19は、試験計画の概要を示す。患者をPD-L1状態に基づいてコホートに割り当て、以下のように処置を受ける。 Figure 19 shows an overview of the study plan. Patients are assigned to cohorts based on PD-L1 status and receive treatment as follows.
コホートA(PD-L1高):4サイクルのネオアジュバントAtezo+Tira後、外科的摘出、及び16サイクルのアジュバントAtezo+Tira又は4サイクルのアジュバント化学療法のいずれかが続く。 Cohort A (PD-L1 High): 4 cycles of neoadjuvant Atezo + Tira followed by surgical excision and either 16 cycles of adjuvant Atezo + Tira or 4 cycles of adjuvant chemotherapy.
コホートB(PD-L1 all comer):4サイクルのネオアジュバントAtezo+Tira+Chemo後、16サイクルの外科的摘出、及びアジュバントAtezo+Tiraが続く。 Cohort B (PD-L1 all comers): 4 cycles of neoadjuvant Atezo+Tira+Chemo followed by 16 cycles of surgical excision and adjuvant Atezo+Tira.
白金系化学療法レジメンの選択は、組織学的サブタイプ及び開始時に文書化されたものに基づいて、治験責任医師の裁量による。この試験では、以下の白金系化学療法の選択肢が許容される。
●非扁平上皮NSCLCの場合:
-シスプラチン+ペメトレキセド
-カルボプラチン+ペメトレキセド
-カルボプラチン+パクリタキセル
●扁平上皮NSCLCの場合:
-シスプラチン+ゲムシタビン
-カルボプラチン+ゲムシタビン
-カルボプラチン+パクリタキセル
The choice of platinum-based chemotherapy regimen is at the investigator's discretion, based on histologic subtype and documented at initiation. The following platinum-based chemotherapy options are allowed in this trial:
●For non-squamous NSCLC:
- cisplatin + pemetrexed - carboplatin + pemetrexed - carboplatin + paclitaxel For squamous NSCLC:
- cisplatin + gemcitabine - carboplatin + gemcitabine - carboplatin + paclitaxel
外科標本は、独立した中央病理検査室並びに治験責任医師の施設の病理検査室によって、病理学的応答(MPR及び病理学的完全奏効(pCR))について評定される。更に、探索的バイオマーカー分析を、残った外科標本(原発腫瘍組織及び切除リンパ節)に対して行うことができる。 Surgical specimens will be evaluated for pathologic response (MPR and pathologic complete response (pCR)) by an independent central pathology laboratory as well as by the investigator's institutional pathology laboratory. In addition, exploratory biomarker analyzes can be performed on surviving surgical specimens (primary tumor tissue and resected lymph nodes).
術後放射線療法(PORT)は、外科的摘出(ypN2及び/又はR1/R2)時に存在する確認された病理学的N2+疾患又は陽性腫瘍マージンを有する患者に許容され、アジュバントAtezo+Tira処置の前又はアジュバント白金系化学療法剤の後に投与されなければならない。 Postoperative radiation therapy (PORT) is acceptable for patients with confirmed pathological N2+ disease or positive tumor margins present at surgical resection (ypN2 and/or R1/R2) prior to adjuvant Atezo+Tira treatment or adjuvant Must be administered after platinum-based chemotherapeutic agents.
すべての患者が、スクリーニング時のコンピューター断層撮影(CT)及び陽電子放射断層撮影(PET)の両方によって、並びにネオアジュバント処置のサイクル2及び4の後にのみCTによって、胸部及び腹部の予定された腫瘍評定を完了する。腫瘍評定は、手術後に再発するまで継続する。疾患フォローアップ評定が疾患再発の証拠を示す場合、それは病理学的に及び/又はスキャンからの明確な放射線学的証拠によって確認されなければならない。スキャンが明確な所見を示す場合(例えば、縦隔節は、短軸で<1.5cmの大きさであり、肺実質病変又は内臓病変は、最長直径で<1cmの大きさである)、生検を行うべきである。生検は、次の抗がん治療を開始する前に行わなければならない。疾患再発確認のための生検を実施する場合、残った生検組織は、探索的バイオマーカー研究に提出することが強く推奨される。生検が実施可能又は安全でない場合、4~8週間以内に確認スキャンを再度行わなければならない。
All patients had scheduled tumor assessments of the chest and abdomen by both computed tomography (CT) and positron emission tomography (PET) at screening and by CT only after
生検が疾患再発の証拠を示さない場合(例えば、非悪性浸潤物)、患者は予定された試験処置、評定及び/又はフォローアップを継続してもよい。疾患再発がない場合、疾患フォローアップ評定は、疾患再発、同意の撤回、死亡、フォローアップ不能又は試験依頼者による試験終了のいずれか早く発生する方まで継続すべきである。 If the biopsy shows no evidence of disease recurrence (eg, non-malignant infiltrates), the patient may continue with scheduled study treatment, evaluation and/or follow-up. In the absence of disease recurrence, disease follow-up assessment should continue until disease recurrence, withdrawal of consent, death, loss of follow-up, or sponsor termination of the study, whichever occurs first.
すべての患者が、ネオアジュバント処置段階(両方のコホート)及びアジュバント処置期において各サイクルの1日目に安全性、忍容性及び探索的評定を受ける。処置中止後、生存状態及び任意の追加の抗がん処置のために患者のフォローアップを定期的に行う。安全性評定には、有害事象の発生率、性質及び重症度、治験実施計画書に定められたバイタルサイン、検査異常、及び、試験の安全性評価にとって重要であると考えられる他の治験実施計画書に規定された試験が含まれる。有害事象は、米国国立がん研究所(NCI)の有害事象共通用語規準(CTCAE)、バ^ジョン5.0(v5.0)に従って治験責任医師により等級付けされる。
All patients undergo safety, tolerability and exploratory assessments on
保管及び新鮮な腫瘍及び/又はリンパ節組織、並びに
血清、血漿及び血液を含む患者試料を、将来の探索的バイオマーカー評定のために収集する。更に、患者は、探索的微生物叢研究のための任意の便の収集に同意する機会を提供される。
Archived and fresh tumor and/or lymph node tissue and patient samples including serum, plasma and blood will be collected for future exploratory biomarker assessments. In addition, patients are provided the opportunity to consent to the collection of any stool for exploratory microbiota studies.
本試験の具体的な目的及び対応評価項目を表56に概説する。


B.処置割り当て及び安全リードイン
患者は、スクリーニング時に治癒目的のR0摘出に適格でなければならず、本明細書で指定されるすべての適格基準を満たさなければならない。この試験への参加基準を満たさない患者(スクリーニング失敗)は、治験責任医師の裁量で2回の再スクリーニング機会(参加者あたり合計3回のスクリーニング)の資格を得る場合がある。
B. Treatment Allocation and Safety Lead-in Patients must be eligible for curative R0 extraction at screening and must meet all eligibility criteria specified herein. Patients who do not meet the entry criteria for this study (screen failure) may be eligible for two rescreening opportunities (a total of 3 screens per participant) at the investigator's discretion.
腫瘍PD-L1状態に基づく処置割り当て及び安全性リードイン
インフォームドコンセントを提供した後、患者は、SP263免疫組織化学(IHC)(腫瘍細胞(TC)ベースのアッセイによるPD-L1状態の中心的評定を含むスクリーニング手順を受ける。
After providing treatment assignment and safety lead-in informed consent based on tumor PD-L1 status, patients underwent SP263 immunohistochemistry (IHC), a central assessment of PD-L1 status by tumor cell (TC)-based assay. undergo screening procedures, including
登録は、以下のように段階的に完了し(図20を参照)、各コホートに約41人の患者が登録された: Enrollment was completed in stages as follows (see Figure 20), with approximately 41 patients enrolled in each cohort:
1.最初に安全性リードインがある。
-スクリーニング時にPD-L1腫瘍割合スコア(TPS)≧50%を有する腫瘍を有する6人の患者をコホートA(PD-L1高コホート)に登録する。
-コホートB(PD-L1 all-comerコホート)は、PD-L1 TPS<50%を有する腫瘍を有する6人の患者の登録から開始する。
1. First there is the safety lead-in.
- Six patients with tumors with a PD-L1 Tumor Proportion Score (TPS) > 50% at screening will be enrolled in Cohort A (PD-L1 High Cohort).
- Cohort B (PD-L1 all-comer cohort) will start with enrollment of 6 patients with tumors with PD-L1 TPS<50%.
2.各コホートの安全性を評価し、安全であると考えられる場合:
-PD-L1 TPS≧50%を有する腫瘍を有する患者を含む患者は、PD-L1 TPS≧50%を有する腫瘍を有する8人の患者がコホートに登録されるまで、コホートB(PD-L1 all comer)にのみ登録される。
-次いで、コホートB患者の残りは、PD-L1 TPS<50%を有する腫瘍を有する患者を含む。
2. Evaluate the safety of each cohort and if considered safe:
- Patients including patients with tumors with PD-L1 TPS ≥50% will be enrolled in Cohort B (PD-L1 all comer) only.
- The remainder of Cohort B patients then includes patients with tumors with PD-L1 TPS<50%.
3.PD-L1 TPS≧50%を有する腫瘍を有する合計8人の患者がコホートB(PD-L1 all comer)に登録された後、コホートA(PD-L1高)への登録を再開し、PD-L1 TPS≧50%を有する腫瘍を有するすべてのその後の患者をそのコホートに登録する。 3. After a total of 8 patients with tumors with PD-L1 TPS ≥ 50% were enrolled in Cohort B (PD-L1 all comers), enrollment resumed in Cohort A (PD-L1 high) and PD- All subsequent patients with tumors with L1 TPS≧50% will be enrolled in the cohort.
安全性リードイン
試験処置に関連する潜在的な外科的遅延、がん化又は合併症を説明するために、各コホート内の登録を一時停止して、約6人の患者がネオアジュバント処置を完了し、手術を完了した後又は手術計画を変更した後の安全性評価を可能にする。コホートは同じ速度で登録することはできず、各コホートは別々に独立して評価される。
Safety lead-in Approximately 6 patients completed neoadjuvant treatment, suspending enrollment within each cohort to account for potential surgical delays, malignant transformation or complications associated with the study procedure and allow safety assessment after surgery is completed or after a change in surgical plan. Cohorts will not be enrolled at the same rate and each cohort will be evaluated separately and independently.
安全性評価は、安全性及び手術データに基づく。データの再検討に基づいて、そのコホートへの登録を継続するか、又はコホートを終了することが推奨される。安全リードイン期間中、患者は、特別な関心又は疾患進行の有害事象以外の理由で手術に進まない場合、交換され得る。 Safety evaluations are based on safety and surgical data. Based on review of the data, it is recommended to continue enrolling in the cohort or terminate the cohort. During the safety lead-in period, patients may be replaced if they do not proceed to surgery for reasons other than special concerns or adverse events of disease progression.
手術及びアジュバント処置
患者は、4サイクルのネオアジュバント治療の完了時に腫瘍の外科的摘出を受ける。手術の前に、主治医及び腫瘍内科医は患者を再評定する。
Surgery and Adjuvant Treatment Patients will undergo surgical excision of the tumor upon completion of 4 cycles of neoadjuvant therapy. Prior to surgery, the attending physician and medical oncologist will reassess the patient.
術前来院は、ネオアジュバント処置の最後の投与後30日以内に行われるべきである;肺機能検査(PFT)(臨床上適応がある場合)を繰り返し、並びに関連する評定を、現地の施設内慣行に従って行うべきである。外科的処置は、主治医及び腫瘍内科医の両方によって臨床上実施可能であると判断された場合、手術前来院から30日以内に実施されるべきである。 A preoperative visit should occur within 30 days after the last dose of neoadjuvant treatment; Practice should be followed. Surgery should be performed within 30 days of the preoperative visit if judged clinically feasible by both the attending physician and the medical oncologist.
予定された腫瘍評定(サイクル2及びサイクル4の後)又はネオアジュバント処置中の任意の時点で疾患進行が認められ、依然として切除可能及び非転移性であると考えられる患者は、すべての試験処置及び評価に適しており、資格があるままである場合、手術に進む。
Patients with disease progression at scheduled tumor assessments (after
治験責任医師が、4サイクルすべてのネオアジュバント処置を完了する前に、疾患の進行がない状態で患者を手術に進めることを計画している場合、メディカルモニターに相談しなければならない。 If the investigator plans to proceed to surgery in the absence of disease progression before completing all four cycles of neoadjuvant treatment, the medical monitor should be consulted.
疾患の進行のためにネオアジュバント処置を早期に中止し、手術に進まない患者は、追加の臨床試験手順から中止され、治験責任医師によって決定された他の処置を受けることに進む。このような患者は、生存フォローアップのために試験に残る。ネオアジュバント治療に応答しているが、予期せぬ医学的問題(例えば、肺塞栓症又は心筋梗塞)により手術に進めない患者の場合、患者は、化学療法(コホートA[PD-L1高])、又はAtezo+Tira(コホートA又はB)及び放射線療法等の治験実施計画書に定められた処置を継続することができる。 Patients who discontinue neoadjuvant treatment early due to disease progression and do not proceed to surgery will be discontinued from additional clinical trial procedures and proceed to receive other treatments as determined by the investigator. Such patients remain in the study for survival follow-up. For patients responding to neoadjuvant therapy but not proceeding to surgery due to unforeseen medical problems (e.g., pulmonary embolism or myocardial infarction), patients will receive chemotherapy (Cohort A [PD-L1 high]) or continue protocol-specified treatments such as Atezo + Tira (Cohort A or B) and radiotherapy.
外科的摘出後、患者は、以下のうち1つが生じるまで、アジュバントAtezo+Tira又はアジュバント化学療法(コホートA[PD-L1高]のみ)を受け続ける:現地の標準治療(SOC)当たり最大4サイクルのアジュバント化学療法の投与、16サイクルのアジュバントのAtezo+Tira、許容できない毒性、疾患再発、死亡、又は試験処置を中止する患者及び/又は医師の決定。 After surgical excision, patients continue to receive adjuvant Atezo + Tira or adjuvant chemotherapy (Cohort A [PD-L1 high] only) until one of the following occurs: up to 4 cycles of adjuvant per local standard of care (SOC). Administration of chemotherapy, 16 cycles of adjuvant Atezo+Tira, unacceptable toxicity, disease recurrence, death, or patient and/or physician decision to discontinue study treatment.
試験終了及び試験期間
この試験の終わりは、最後の患者が最後に来院した日付として定義され、これは、最後の患者が手術後に試験薬の最終用量を受けた約3年後に起こる。
Study End and Study Duration The end of the study was defined as the date of the last patient's last visit, which occurs approximately three years after the last patient received the last dose of study drug after surgery.
最初の患者のスクリーニングから試験終了までの試験の全長は、約5-6年である。 The total length of the trial from initial patient screening to study termination is approximately 5-6 years.
C.試験計画の理論的根拠
この試験は、以前に治療されていない局所進行性NSCLC患者のためのネオアジュバント処置としてのAtezo+Tira又はAtezo+Tira+Chemoの外科的安全性及び実行可能性を評価する。この試験はまた、ネオアジュバントであるAtezo+Tira又はAtezo+Tira+Chemo、続いてアジュバントであるAtezo+Tira又はアジュバント化学療法の有効性、薬物動態、免疫原性及び安全性を評価する。
C. Rationale for Study Design This study evaluates the surgical safety and feasibility of Atezo+Tira or Atezo+Tira+Chemo as a neoadjuvant treatment for previously untreated patients with locally advanced NSCLC. This study also evaluates the efficacy, pharmacokinetics, immunogenicity and safety of neoadjuvant Atezo+Tira or Atezo+Tira+Chemo followed by adjuvant Atezo+Tira or adjuvant chemotherapy.
アテゾリズマブ+チラゴルマブの用量及びスケジュールの理論的根拠
アテゾリズマブは、処方情報に概説されているように、アテゾリズマブの承認された投与量である1200mg Q3W(各21日間サイクルの1日目に1200mg)の固定用量で投与される。抗腫瘍活性は、1mg/kg~20mg/kg Q 3 Wの範囲の用量にわたって観察されている。GO27381試験(PCD 4989 g)では、アテゾリズマブの最大耐量に達しておらず、用量制限毒性(DLT)はいずれの用量でも観察されなかった。非臨床試験(Deng et al.,MAbs,8:593-603,2016)並びに利用可能な臨床薬物動態、有効性及び安全性データの両方に基づいて、1200mg Q3Wの固定用量(平均体重-に基づく用量15mg/kg Q3Wと同等)を選択した。
Atezolizumab + Tiragolumab Dose and Schedule Rationale Atezolizumab is a fixed dose of 1200 mg Q3W (1200 mg on
チラゴルマブは、21日間の各サイクルの1日目に、600mg Q3Wの固定用量で静脈内投与される。患者が単剤チラゴルマブ又はチラゴルマブ+アテゾリズマブを受けたGO30103試験からの利用可能な臨床薬物動態、有効性、及び安全性データに基づいて、チラゴルマブ600mg IV Q3Wの固定用量を選択した。試験GO30103では、最大耐量に到達せず、チラゴルマブ単独療法又はアテゾリズマブ1200mg Q3W(2~1200mg Q3Wのチラゴルマブ用量範囲)と組み合わせたDLTは観察されなかった。CD4+、CD8+及びNK細胞上の末梢TIGIT受容体の完全な占有は、30mgQ3Wのチラゴルマブ用量レベルで開始して観察され、すべてのより高い用量で持続したままであった。アテゾリズマブ1200mg Q3Wと組み合わせて投与した場合、チラゴルマブについて、30-600mg Q3Wの用量範囲で抗腫瘍活性(放射線部分奏効(PR)によって評定)が観察された。
Tiragolumab is administered intravenously at a fixed dose of 600 mg Q3W on
第II相GO40290試験では、アテゾリズマブ+チラゴルマブ群に登録した全ての患者は、600mgのチラゴルマブを受けた。この用量では、チラゴルマブは忍容され、アテゾリズマブ+チラゴルマブの組み合わせは、アテゾリズマブと組み合わせたプラセボと比較して、PFSの臨床上有意な改善及びより高いORRをもたらした。600mgで観察された好ましいベネフィット-リスク比を考慮して、この同じ用量のチラゴルマブをこの試験に使用する。 In the Phase II GO40290 trial, all patients enrolled in the atezolizumab plus tiragolumab arm received 600 mg tiragolumab. At this dose, tiragolumab was well tolerated and the combination of atezolizumab plus tiragolumab resulted in clinically significant improvement in PFS and higher ORR compared to placebo in combination with atezolizumab. Given the favorable benefit-risk ratio observed at 600 mg, this same dose of tiragolumab will be used in this study.
患者集団の理論的根拠
この試験は、切除可能なステージII、IIIAの患者を登録し、スクリーニングで決定されたIIIB(T3N2のみ)NSCLCを選択する。高いPD-L1発現(中央実験室でSP 263による免疫組織化学[IHC]によって決定した場合、TPS≧50%)を有する腫瘍を有する患者は、コホートA(PD-L1高)に登録されるが、全ての参加者(PD-L1発現レベルにかかわらず)は、コホートB(PD-L1 all comer)に登録される。
Patient Population Rationale This trial will enroll patients with resectable stage II, IIIA and select screen-determined IIIB (T3N2 only) NSCLC. Patients with tumors with high PD-L1 expression (TPS≧50% as determined by immunohistochemistry [IHC] with
ネオアジュバント化学療法及びアジュバント化学療法は、早期切除可能NSCLC患者に対して有意であるが中程度の利益を示しているが、この処置状況での転帰の改善に対する実質的な満たされていない必要性が依然として存在する。 Neoadjuvant and adjuvant chemotherapy have shown significant but moderate benefit for patients with early resectable NSCLC, but there is a substantial unmet need for improved outcomes in this treatment setting. still exists.
細胞傷害性化学療法による腫瘍細胞の死滅は、免疫系を高レベルの腫瘍抗原に曝露し得る。PD-L1及びTIGIT経路を遮断することによるこの状況での腫瘍特異的T細胞免疫のブーストは、標準的な化学療法単独で観察されるものよりも深く、より永続的な応答をもたらし得(Merritt et al.,J Thorac Cardiovasc Surg,126:1609-1617,2003;Apetoh et al.,Nat Med,13:1050-1059,2007)、これはPD-L1発現にかかわらず腫瘍で合理的に起こり得る。 Killing tumor cells by cytotoxic chemotherapy can expose the immune system to high levels of tumor antigens. Boosting tumor-specific T cell immunity in this setting by blocking the PD-L1 and TIGIT pathways could result in deeper and more durable responses than those observed with standard chemotherapy alone (Merritt et al. et al., J Thorac Cardiovasc Surg, 126:1609-1617, 2003; Apetoh et al., Nat Med, 13:1050-1059, 2007), which could reasonably occur in tumors regardless of PD-L1 expression. .
PD-L1 TPS≧50%集団における利益の大きさを示すCITISCAPEからの強力なデータ、及び切除可能な早期NSCLC患者の生存率を改善し、再発率を低下させる必要性を考慮して、この試験は、化学療法非併用選択肢としての Atezo+Tiraの組み合わせの有効性を調べる。切除可能なNSCLCを有する患者のための化学療法を用いない選択肢は、患者のためのランドマーク的な改善であり得、白金系化学療法に関連する早期及び後期の毒性を患者に与えないであろう。 Given the strong data from CITISCAPE showing the magnitude of benefit in the PD-L1 TPS≧50% population and the need to improve survival and reduce recurrence rates in resectable early-stage NSCLC patients, this trial will examine the efficacy of the combination of Atezo + Tira as a non-chemotherapy option. A chemotherapy-free option for patients with resectable NSCLC could be a landmark improvement for the patient, without the early and late toxicities associated with platinum-based chemotherapy. deaf.
主要評価項目としての病理学的著効の理論的根拠
本試験の主要な有効性目的は、中央病理検査室で評定した病理学的著効(MPR)によって測定したとき、切除可能なステージII、IIIA又は選択IIIB(T3N2のみ)NSCLCを有する患者におけるAtezo+Tira又はAtezo+Tira+Chemoによるネオアジュバント処置の有効性を評価することである。
Rationale for Pathological Response as Primary Endpoint The primary efficacy objective of the study was resectable Stage II, To evaluate the efficacy of neoadjuvant treatment with Atezo+Tira or Atezo+Tira+Chemo in patients with IIIA or selected IIIB (T3N2 only) NSCLC.
全生存期間(OS)が、アジュバントNSCLC試験及びネオアジュバントNSCLC試験における臨床的有用性を評価する際の標準である一方で、OSの読み出しは、特に初期段階の疾患において、しばしば長い年月を要する。したがって、意味のある代用評価項目を採用することは、新しい処置の評価を迅速化し、新しい処置をNSCLC患者に早くもたらすことができる。NSCLCの外科的摘出後の病理学的応答は、OSの代用評価項目として提案されている(Hellmann et al.,Lancet Oncol,15:e42-50,2014)。Hellmann et al.(2014)は、評価項目が「臨床的利益を予測する可能性がかなり高い」はずである代替評価項目の米国食品医薬品局(FDA)の定義を引用した。彼らは、ネオアジュバント状況において病理学的応答を使用することが、3つの所見に基づいてこの定義を満たすことを主張する:1)病理学的応答はOSと強く相関する;2)病理学的応答はネオアジュバント化学療法を反映している;3)病理学的応答の程度はOS利益の程度と相関する。 While overall survival (OS) is the standard for evaluating clinical utility in adjuvant and neoadjuvant NSCLC trials, OS readouts often take many years, especially in early-stage disease. . Employing meaningful surrogate endpoints can therefore expedite the evaluation of new treatments and bring new treatments to NSCLC patients sooner. Pathological response after surgical resection of NSCLC has been proposed as a surrogate endpoint for OS (Hellmann et al., Lancet Oncol, 15:e42-50, 2014). Hellmann et al. (2014) cited the US Food and Drug Administration's (FDA) definition of an alternative endpoint in which the endpoint should be "very likely to predict clinical benefit." They argue that using pathological response in the neoadjuvant setting meets this definition based on three observations: 1) pathological response is strongly correlated with OS; Response reflects neoadjuvant chemotherapy; 3) degree of pathological response correlates with degree of OS benefit.
代理評価項目としての病理学的応答の使用は、先例がないわけではない。乳がんの治験では、ネオアジュバント処置の有効性を評価するために病理学的完全奏効(pCR)が使用されている。しかしながら、pCR率は、ネオアジュバントNSCLC研究において変動している。更に、NSCLCで報告される比較的低いpCR率は、臨床上有意なOS利益につながらない可能性があり、したがって、NSCLC治験における代理生存評価項目としてのpCRの有用性を制限する。実際、pCR率が低いため(割合の中央値4%)、NSCLCにおけるpCRの結果としての生存データを報告した試験はほとんどない(Hellmann et al.,Lancet Oncol,15:e42-50,2014)。
The use of pathological response as a surrogate endpoint is not without precedent. Pathologic complete response (pCR) is used to assess efficacy of neoadjuvant treatment in breast cancer trials. However, pCR rates are variable in neoadjuvant NSCLC studies. Furthermore, the relatively low pCR rates reported in NSCLC may not translate into clinically significant OS benefits, thus limiting the usefulness of pCR as a surrogate survival endpoint in NSCLC trials. Indeed, few studies have reported survival data as a result of pCR in NSCLC due to the low rate of pCR (
pCRの代わりに、Hellman et al.は、ネオアジュバント化学療法処置を受けている切除可能なNSCLC患者の生存代用として、≦10%生存腫瘍組織として定義されるMPRの使用を提案した(Hellmann et al.,Lancet Oncol,15:e42-50,2014)。これは、治験責任医師らが、NSCLCにおけるpCRの希少性の認識において、代理生存評価項目としての残存生存腫瘍を含む病理学的応答の他の定義を検討した研究に基づいている。Junker et al.(J Cancer Res Clin Oncol,123:469-477,1997)は、一連のネオアジュバント化学療法処置、化学放射線療法、及び外科的摘出を受けたステージIIIA及びIIIB疾患を有する患者由来の40個の腫瘍の病理学的分析を行った。この群の≦10%の残存腫瘍を有する患者は36ヶ月の生存期間中央値を有し、>10%の残存生存腫瘍組織を有する患者は14ヶ月の生存期間中央値を有した。 Instead of pCR, Hellman et al. proposed the use of MPR, defined as ≤10% viable tumor tissue, as a survival surrogate for resectable NSCLC patients undergoing neoadjuvant chemotherapy treatment (Hellmann et al., Lancet Oncol, 15:e42- 50, 2014). This is based on a study in which investigators examined other definitions of pathologic response, including residual viable tumor as a surrogate survival endpoint, in recognition of the rarity of pCR in NSCLC. Junker et al. (J Cancer Res Clin Oncol, 123:469-477, 1997) reviewed 40 tumors from patients with stage IIIA and IIIB disease who underwent a series of neoadjuvant chemotherapy treatments, chemoradiation, and surgical excision. pathological analysis was performed. Patients in this group with <10% residual tumor had a median survival of 36 months, and those with >10% residual viable tumor tissue had a median survival of 14 months.
2つの前向き試験は、NSCLCにおけるネオアジュバント化学療法で約22%のMPR率を報告した。最初の試験では、ネオアジュバント化学療法(シスプラチン+ドセタキセル)を受けたステージIIIA疾患を有する90人の患者のうち、病理学的応答の中央値(腫瘍壊死及び線維症の量)は≦60%であり、OSの中央値は61ヶ月であったのに対して、病理学的応答が60%の患者では22ヶ月であった(Betticher et al.,Br J Cancer,94(8):1099-1106,2006)。別の試験は、ベバシズマブと組み合わせてネオアジュバント化学療法(シスプラチン+ドセタキセル)を受けた50人の患者のうち、MPRを有する患者は、MPRを達成しなかった患者(それぞれ61ヶ月対22ヶ月)と比較して有意に長い3年生存率を有することを示した(Chaft et al.,J Thorac Oncol,8:1084-1090,2013)。William及び同僚によるMD Anderson Cancer Centerからの遡及的試験(William et al.,J Thorac Oncol,8:222-228,2013)は、ネオアジュバント白金ベースの化学療法を受けた160人の患者において、MPRが固形腫瘍における臨床応答評価基準(RECIST)応答よりもOSの強力な予測因子であることを示した。 Two prospective studies reported an MPR rate of approximately 22% with neoadjuvant chemotherapy in NSCLC. In the first study, among 90 patients with stage IIIA disease who received neoadjuvant chemotherapy (cisplatin + docetaxel), the median pathological response (amount of tumor necrosis and fibrosis) was < 60%. with a median OS of 61 months compared to 22 months in patients with 60% pathological response (Betticher et al., Br J Cancer, 94(8):1099-1106). , 2006). Another study showed that among 50 patients who received neoadjuvant chemotherapy (cisplatin + docetaxel) in combination with bevacizumab, patients with MPR were compared with those who did not achieve MPR (61 vs. 22 months, respectively). have been shown to have significantly longer 3-year survival rates in comparison (Chaft et al., J Thorac Oncol, 8:1084-1090, 2013). A retrospective study from the MD Anderson Cancer Center by William and colleagues (William et al., J Thorac Oncol, 8:222-228, 2013) found that MPR was a stronger predictor of OS than the Clinical Response Evaluation Criteria (RECIST) response in solid tumors.
治験依頼者は、OSの改善の大きさとの相関に基づいて、代理評価項目としてのMPRの使用には大きな理論的根拠があると考えている。現在、MPRを一次又は二次目的として評定する化学療法+PD-L1/PD-1阻害剤対化学療法単独の世界的な第III相ネオアジュバント登録試験が進行中である。代替評価項目としてのMPRの使用は、臨床試験の有効性を高め、NSCLC患者のための新しい治療を加速する可能性を有する。 Sponsors believe there is a strong rationale for using MPR as a surrogate endpoint, based on its correlation with the magnitude of improvement in OS. A global Phase III neoadjuvant registry trial of chemotherapy plus a PD-L1/PD-1 inhibitor versus chemotherapy alone evaluating MPR as a primary or secondary objective is currently underway. The use of MPR as a surrogate endpoint has the potential to enhance the effectiveness of clinical trials and accelerate new treatments for NSCLC patients.
実施例10.GO42501試験のための材料及び方法
ステージII、IIIA又は選択されたIIIB(T3N2のみ)を有する約82人の患者がGO42501試験に登録される。
Example 10. Materials and Methods for the GO42501 Trial Approximately 82 patients with stage II, IIIA or selected IIIB (T3N2 only) will be enrolled in the GO42501 trial.
A.選択基準
患者は、試験参加に適格であるために、以下に列挙する選択基準を満たさなければならない:
●インフォームドコンセント書類の署名時の年齢が≧18歳
●試験治験実施計画書を遵守する能力
●組織学的若しくは細胞学的に確認されたステージII、IIIA、又は扁平上皮若しくは非扁平上皮組織のIIIB(T3N2のみ)非小細胞肺がん(NSCLC)を選択する。病期分類は、第8版のAmerican Joint Committee on Cancer/Union Internationale Contre le Cancer NSCLC病期分類システムに基づくべきである。
-T4原発性NSCLCの患者は、サイズ(腫瘍>7cm)のみに基づいて適格である。横隔膜、縦隔、心臓、大血管、気管、再発性喉頭神経、食道、椎体、気管分岐部、及び異なる同側葉の別個の腫瘍結節の浸潤を有する患者は適格ではない。
-混合組織(扁平上皮及び非扁平上皮)のNSCLC患者が適格であり、主要な組織学的成分(非扁平上皮又は扁平上皮)に基づいて分類されなければならない。
A. Inclusion Criteria Patients must meet the inclusion criteria listed below to be eligible for study participation:
- Age ≥ 18 years at the time of signing the informed consent document - Ability to comply with the study protocol - Histologically or cytologically confirmed stage II, IIIA, or squamous or non-squamous tissue Select IIIB (T3N2 only) non-small cell lung cancer (NSCLC). Staging should be based on the 8th edition of the American Joint Committee on Cancer/Union International Contre le Cancer NSCLC staging system.
- Patients with T4 primary NSCLC are eligible based on size (tumor >7 cm) only. Patients with separate tumor nodule involvement of the diaphragm, mediastinum, heart, great vessels, trachea, recurrent laryngeal nerves, esophagus, vertebral bodies, tracheal carina, and different ipsilateral lobes are not eligible.
- NSCLC patients with mixed histology (squamous and non-squamous) must be eligible and classified based on the major histologic component (non-squamous or squamous).
患者は臨床病期に基づいてスクリーニングされ得るが、PET陽性N 2リンパ節については、侵襲的縦隔病期分類(例えば、CT誘導生検、気管支腔内超音波、縦隔鏡検査)によるN2リンパ節浸潤の必須の術前の文書化が必要である。レベル5及びレベル6の節の術前病期分類は任意である。
●純粋なすりガラス影(GGO)の出現を伴わないCTスキャン上のNSCLCの充実型又は亜充実型の出現。亜充実型病変については、GGO成分を除いて、固形成分のみに基づいて腫瘍サイズ(すなわち、臨床T段階)を測定すべきである。
●スクリーニング時に治癒目的のR0摘出に適格であり、試験登録前に主治医及び関与する腫瘍内科医によって確認される。
●肺機能検査(PFT)によって評定される、治癒目的の外科的摘出に適格であるのに十分な肺機能(肺容積、肺活量測定及び拡散能を含む)が、計画された切除の6ヶ月以内に行われ、臨床上適応がある場合、スクリーニング時に繰り返され、これは以下の基準の少なくとも1つを満たす:
-術後予測(ppo)1秒間努力呼気容量(FEV1)、及び一酸化炭素に対する肺のppo拡散能力(DLCO)≧40%。
-最大酸素消費量(VO2max)≧15mL/kg/分。
Patients can be screened based on clinical stage, but for PET-positive N2 lymph nodes, N2 by invasive mediastinal staging (e.g., CT-guided biopsy, endobronchial ultrasound, mediastinoscopy) Mandatory preoperative documentation of nodal involvement is required. Preoperative staging of
• Appearance of solid or subsolid form of NSCLC on CT scan without appearance of pure ground-glass opacity (GGO). For subsolid lesions, tumor size (ie, clinical T stage) should be measured based on the solid component only, excluding the GGO component.
• Eligible for curative R0 extraction at screening and confirmed by the attending physician and participating medical oncologist prior to study enrollment.
Sufficient pulmonary function (including lung volume, spirometry and diffusing capacity) to be eligible for curative surgical resection as assessed by pulmonary function test (PFT) within 6 months of planned resection and repeated at Screening if clinically indicated, which meets at least 1 of the following criteria:
- Post-operative prediction (ppo) forced expiratory volume in 1 second (FEV1) and lung ppo diffusing capacity for carbon monoxide (DL CO ) >40%.
- Maximum oxygen consumption (VO 2 max) ≧15 mL/kg/min.
o ppoFEV1又はppoDLCOのいずれかが<40%であるか、又は肺切除術が計画されている場合、心肺運動検査を実施しなければならず、VO2max≧15mL/kg/分でなければならない。 If either o ppoFEV 1 or ppoDL CO <40% or if pneumonectomy is planned, cardiopulmonary exercise testing must be performed and VO 2 max ≧15 mL/kg/min. must.
o PFTが6ヶ月の計画された摘出の前に実施されたか、又は以前に実施されていない場合、それらはスクリーニング期間中に実施されなければならない。
●白金系化学療法レジメンを受ける適格性。各患者の意図するレジメンにおける各個々の化学療法処置(すなわち、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル又はゲムシタビン)の処方情報の警告及び注意のセクションは、適格性を判定するために使用される。
●RECIST v 1.1に従って治験責任医師によって評定された測定可能な疾患。
●PD-L1状態及び中央検査による他の探索的バイオマーカーの決定に適した代表的な腫瘍標本の入手可能性。
●0又は1の、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス
●肺がん死亡リスクを除く、通常の平均余命。
●試験処置の開始の前、14日以内に得られた、以下の臨床検査結果によって定義される適切な血液学的機能及び終末器官機能:
-顆粒球コロニー刺激因子の支持なしで、絶対好中球数(ANC)≧1.5X109/L(1500/μL)。
-リンパ球数≧0.5X109/L(500/μL)。
-輸血なしで血小板数≧100X109/L(100,000/μL)。
-ヘモグロビン≧90g/L(9g/dL)。この基準を満たすために患者を輸血することができる。
-アスパラギン酸トランスアミナーゼ(AST)、アラニントランスアミナーゼ(ALT)及びアルカリホスファターゼ(ALP)≦2.5X正常値上限(ULN)。
-総ビリルビン≦1.5XULN、ただし、以下を除く:既知のギルバート病患者:総ビリルビン≦3XULN.
-クレアチニンクリアランス≧45mL/分(Cockcroft-Gault式を用いて計算)。シスプラチンを受けることを意図した患者:クレアチニンクリアランス≧60mL/分。
-血清アルブミン≧25g/L(2.5g/dL)
-治療的抗凝固療法を受けていない患者の場合:INR又はaPTT≦1.5XULN
●治療的抗凝固薬を投与されている患者:安定な抗凝固薬レジメン
●スクリーニング時の陰性HIV検査。
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時のB型肝炎表面抗体(HBsAb)陽性検査、又は以下のいずれかを伴うスクリーニング時のHBsAb陰性:
-総B型肝炎コア抗体(HBcAb)陰性
-陽性の全HBcAb検査とそれに続く定量的B型肝炎ウイルス(HBV)DNA<500 IU/mL HBV DNA検査は、HBsAg検査陰性、HBsAb検査陰性、及び総HBcAb検査陽性の患者に対してのみ実施される。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:禁欲(異性間の性交を控える)又は避妊を使用することの合意、及び卵の提供を控えることの同意。
●男性の場合:禁欲(異性との性交を控える)又はコンドームの使用の同意、及び精子の提供を控える旨の同意。
o If PFTs were performed 6 months before the planned extirpation or were not previously performed, they must be performed during the screening period.
• Eligibility to receive a platinum-based chemotherapy regimen. The WARNINGS and PRECAUTIONS sections of the prescribing information for each individual chemotherapeutic treatment (ie, carboplatin, cisplatin, pemetrexed, paclitaxel, or gemcitabine) in each patient's intended regimen are used to determine eligibility.
• Measurable disease as assessed by the investigator according to RECIST v 1.1.
• Availability of representative tumor specimens suitable for determination of PD-L1 status and other exploratory biomarkers by central laboratory.
• US East Coast Cancer Clinical Trials Group (ECOG) performance status of 0 or 1 • Normal life expectancy, excluding lung cancer mortality risk.
- Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to initiation of study treatment:
- Absolute neutrophil count (ANC) ≥ 1.5 x 109 /L (1500/μL) without the support of granulocyte colony stimulating factor.
- Lymphocyte count ≧0.5×10 9 /L (500/μL).
- Platelet count ≧100×10 9 /L (100,000/μL) without transfusion.
- Hemoglobin > 90 g/L (9 g/dL). Patients can be transfused to meet this criterion.
- Aspartate transaminase (AST), alanine transaminase (ALT) and alkaline phosphatase (ALP) < 2.5X upper limit of normal (ULN).
- total bilirubin ≤ 1.5 X ULN, except: patients with known Gilbert's disease: total bilirubin ≤ 3 X ULN.
- Creatinine clearance ≧45 mL/min (calculated using the Cockcroft-Gault formula). Patients intending to receive cisplatin: creatinine clearance ≧60 mL/min.
- Serum albumin ≥25 g/L (2.5 g/dL)
- For patients not receiving therapeutic anticoagulation: INR or aPTT ≤ 1.5XULN
• Patients on therapeutic anticoagulants: stable anticoagulant regimen • Negative HIV test at screening.
- Hepatitis B surface antigen (HBsAg) test negative at screening - Hepatitis B surface antibody (HBsAb) positive test at screening or HBsAb negative at screening with any of the following:
- total hepatitis B core antibody (HBcAb) negative - positive total HBcAb test followed by quantitative hepatitis B virus (HBV) DNA <500 IU/mL Only performed for patients with a positive HBcAb test.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening. HCV RNA testing is performed only for patients who test positive for HCV antibodies.
• For women of childbearing potential: consent to abstinence (abstinence from heterosexual intercourse) or use of contraception, and consent to refrain from donating eggs.
●For men: Consent to abstinence (refrain from sexual intercourse with the opposite sex) or consent to use condoms, and consent to refrain from donating sperm.
B.除外基準
以下に列挙する基準のいずれかを満たす患者は、試験参加から除外される:
●大細胞神経内分泌癌腫、肉腫様癌腫、又は他に特定されないNSCLCの組織学を有するNSCLC。
●小細胞肺がん(SCLC)の組織学又はSCLCの任意の構成要素を有するNSCLC。
●患者が試験手順を理解、遵守、及び/又は遵守する能力を妨げ得る疾患又は症状。
●免疫療法、化学療法、又は放射線療法を含む、肺がんのための任意の事前治療。
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質抗体症候群、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、又は多発性硬化症を含むがこれらに限定されない自己免疫疾患又は免疫不全活動が活動性であるもの、又はその病歴、ただし、以下を除く:甲状腺補充ホルモンを服用している自己免疫関連甲状腺機能低下症の病歴を有する患者は試験に適格である。インスリンレジメンを受けている制御された1型糖尿病患者は試験に適格である。
B. Exclusion Criteria Patients meeting any of the criteria listed below will be excluded from study participation:
- NSCLC with large cell neuroendocrine carcinoma, sarcomatoid carcinoma, or NSCLC histology not otherwise specified.
- Histology of small cell lung cancer (SCLC) or NSCLC with any component of SCLC.
• A disease or condition that may interfere with the patient's ability to understand, comply with, and/or comply with study procedures.
- Any prior treatment for lung cancer, including immunotherapy, chemotherapy, or radiation therapy.
Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barré syndrome, or multiple sclerosis Active or history of autoimmune disease or immunodeficiency activity, including but not limited to, excluding: patients with a history of autoimmune-related hypothyroidism taking thyroid replacement hormones are eligible for testing. Patients with controlled
湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを伴う白斑(例えば、乾癬性関節炎を有する患者は除外される)を有する患者は、以下の条件の全てが満たされるならば、試験に適格である。
-発疹が覆っている体表面積は<10%でなければならない。
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない
●特発性肺線維症、器質化肺炎(例えば、閉塞性細気管支炎)、薬物誘発性間質性肺炎、若しくは特発性間質性肺炎の病歴、又はスクリーニング胸部CTスキャンでの活動性間質性肺炎の証拠。
●活動性結核。
●試験処置の開始前3ヶ月以内の有意な心血管疾患(New York Heart Association Class II以上の心疾患、心筋梗塞、脳血管障害等)、不安定な不整脈又は不安定狭心症。
●試験処置の開始前4週間以内の大きな外科的処置、又は試験中の大きな外科的処置の必要性の予想
●活性化EGFR 変異又はALK 融合がん遺伝子を有するNSCLC。非扁平上皮NSCLCの組織型を有する患者の場合:EGFR 及び/又はALK の状態が不明であるため、スクリーニング時の検査が必要である。ALK 及び/又はEGFR の状態は、現地で評定され得るか、又は中央臨床検査に提出され得る。
●既知のc-rosがん遺伝子1(ROS1)再編成。スクリーニング時のROS1 検査は試験参加に必要ではない;ただし、既知のROS1再編成を有する患者は除外される。
●適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚癌腫、限局性前立腺がん、上皮内乳管癌腫、又はステージI子宮がん等、転移又は死亡のリスクが無視できる(例えば、5年OS率>90%)悪性腫瘍を除いて、スクリーニング前5年以内のNSCLC以外の悪性腫瘍の病歴。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)、又は治験責任医師の見解では患者の安全性に影響を及ぼし得る任意の活動性感染症。
●試験処置開始前2週間以内の治療用経口又はIV抗生物質による処置 予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の増悪を予防するため)を受ける患者は試験に適格である;
●事前の同種異系幹細胞又は固形臓器移植
●治験薬の使用を禁忌にする任意の他の疾患、代謝機能不全、身体検査所見、又は臨床検査所見は、結果の解釈に影響を及ぼす可能性があり、又は患者を処置の合併症のリスクが高くなる可能性がある。
●試験処置の開始前4週間以内の生弱毒化ワクチンによる処置、若しくは試験処置中のそのようなワクチンの必要性の予想、チラゴルマブの最終投与後90日以内、又はアテゾリズマブの最終投与後5ヶ月以内の生弱毒化ワクチンによる処置。化学療法(すなわち、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル又はゲムシタビン)で処置されている患者は生ワクチンを受けるべきではない。
●HBVのための抗ウイルス療法による現在の処置。
●スクリーニング時のエプスタイン・バーウイルスウイルス(EBV)ウイルスカプシド抗原免疫グロブリンM(IgM)検査陽性。EBV PCR検査を、急性感染又は疑われる慢性活動性感染をスクリーニングするために臨床上適応がある場合、実施すべきである。EBV PCR検査が陽性の患者は除外する。
●試験処置の開始前42日以内の治験治療による処置。
●抗-CTLA-4、抗-PD-1、抗-TIGIT及び抗-PD-L1治療用抗体を含むCD137アゴニスト又は免疫チェックポイント遮断療法による事前処置。
●試験処置の開始前の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫刺激剤(限定されないが、インターフェロン及びIL-2を含む)による処置。
●以下の例外を除いて、試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び抗-腫瘍壊死因子-α[TNF-α]剤を含む)による処置、又は試験処置中の全身免疫抑制薬の必要性の予測:
-急性低用量の全身免疫抑制薬、又は1回のパルス用量の全身免疫抑制薬(例えば、造影剤アレルギーのための48時間のコルチコステロイド)を受けた患者は試験に適格である。
-ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患(COPD)若しくは喘息のためのコルチコステロイド、又は起立性低血圧若しくは副腎機能不全のための低用量コルチコステロイドを受けた患者は試験に適格である。
●キメラ若しくはヒト化抗体又は融合タンパク質に対する重度のアレルギーアナフィラキシー反応の病歴。
●チャイニーズハムスター卵巣細胞生成物又はアテゾリズマブ又はチラゴルマブ製剤の任意の成分に対する既知の過敏症。
●試験中に患者が受ける可能性のある化学療法レジメンの任意の成分に対する既知のアレルギー又は過敏症。
●妊娠若しくは授乳、又は試験処置中、チラゴルマブの最終投与後90日以内、アテゾリズマブの最終投与後5ヶ月以内、又はペメトレキセド、ゲムシタビン、パクリタキセル、カルボプラチン若しくはシスプラチンの最終投与後6ヶ月以内に妊娠する意図。妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin manifestations only (e.g., patients with psoriatic arthritis are excluded) are eligible for the study if all of the following conditions are met: is.
- The rash must cover <10% of body surface area.
- Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UVA radiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors within the past 12 months , or no acute exacerbation of underlying symptoms requiring high-potency or oral corticosteroids Idiopathic pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis obliterans), drug-induced interstitial pneumonia, or history of idiopathic interstitial pneumonia or evidence of active interstitial pneumonia on screening chest CT scan.
● Active tuberculosis.
- Significant cardiovascular disease (New York Heart Association Class II or greater heart disease, myocardial infarction, cerebrovascular accident, etc.), unstable arrhythmia or unstable angina pectoris within 3 months prior to initiation of study treatment.
• Major surgery within 4 weeks prior to initiation of study treatment, or anticipation of need for major surgery during study • NSCLC with activating EGFR mutation or ALK fusion oncogene. For patients with non-squamous NSCLC histology: EGFR and/or ALK status is unknown, requiring investigation at screening. ALK and/or EGFR status can be assessed locally or submitted to a central laboratory.
• A known c-ros oncogene 1 (ROS1) rearrangement. ROS1 testing at screening is not required for study entry; however, patients with known ROS1 rearrangements are excluded.
Appropriately treated cervical carcinoma in situ, nonmelanoma cutaneous carcinoma, localized prostate cancer, ductal carcinoma in situ, or stage I uterine cancer with negligible risk of metastasis or death (e.g., 5-year OS rate >90%) History of malignancy other than NSCLC within 5 years prior to screening, excluding malignancies.
- Severe infection (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia) within 4 weeks prior to initiation of study treatment, or opinion of investigator Any active infection that may affect patient safety.
Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of study treatment be;
- Prior allogeneic stem cell or solid organ transplantation - Any other disease, metabolic dysfunction, physical examination findings, or laboratory findings that contraindicate study drug use may affect interpretation of results or may put the patient at increased risk of procedural complications.
- Treatment with a live-attenuated vaccine within 4 weeks prior to initiation of study treatment, or anticipation of need for such vaccine during study treatment, within 90 days after last dose of tiragolumab, or within 5 months after last dose of atezolizumab treatment with live attenuated vaccines. Patients being treated with chemotherapy (ie carboplatin, cisplatin, pemetrexed, paclitaxel or gemcitabine) should not receive live vaccines.
• Current treatment with antiviral therapy for HBV.
• Positive Epstein-Barr virus (EBV) virus capsid antigen immunoglobulin M (IgM) test at screening. EBV PCR testing should be performed when clinically indicated to screen for acute infection or suspected chronic active infection. Patients with a positive EBV PCR test are excluded.
- Treatment with study therapy within 42 days prior to initiation of study treatment.
- Pretreatment with CD137 agonist or immune checkpoint blockade therapy including anti-CTLA-4, anti-PD-1, anti-TIGIT and anti-PD-L1 therapeutic antibodies.
• Treatment with systemic immune stimulants (including but not limited to interferon and IL-2) within 4 weeks or 5 drug elimination half-lives (whichever is longer) prior to initiation of study treatment.
- Systemic immunosuppressants (including but not limited to corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide and anti-tumor necrosis factor-α [TNF] within 2 weeks prior to initiation of study treatment, with the following exceptions - Prediction of the need for systemic immunosuppressive drugs during treatment with (including α] agents) or study treatment:
- Patients who received acute low-dose systemic immunosuppressants or single pulse doses of systemic immunosuppressants (eg, 48-hour corticosteroids for contrast allergy) are eligible for the study.
- patients who have received mineralocorticoids (e.g. fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency Eligible for testing.
• History of severe allergic anaphylactic reactions to chimeric or humanized antibodies or fusion proteins.
• Known hypersensitivity to Chinese Hamster Ovary Cell Products or any component of the atezolizumab or tiragolumab formulations.
• Known allergy or hypersensitivity to any component of the chemotherapy regimen that the patient may experience during the study.
Pregnancy or lactation, or intention to become pregnant during the study treatment, within 90 days after the last dose of tiragolumab, within 5 months after the last dose of atezolizumab, or within 6 months after the last dose of pemetrexed, gemcitabine, paclitaxel, carboplatin, or cisplatin. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
C.処置の割り当て
この試験は非盲検試験である。
高いPD-L1発現(中央実験室でSP 263 IHCによって決定した場合、TPS≧50%)を有する患者はコホートA(PD-L1高)に登録され、全参加者(all comer)(PD-L1発現レベルにかかわらず)はコホートB(PD-L1 all comer)に登録される。登録は、以下のように段階的に完了し(図20を参照)、各コホートに約41人の患者が登録された:
C. Treatment Allocation This study is an open-label study.
Patients with high PD-L1 expression (TPS≧50% as determined by
1.最初に安全性リードインがある:
-スクリーニング時にPD-L1 TPS≧50%を有する腫瘍を有する6人の患者をコホートA(PD-L1高コホート)に登録する。
-コホートB(PD-L1 all-comerコホート)は、PD-L1 TPS<50%を有する腫瘍を有する6人の患者の登録から開始する。
1. First there is the safety lead-in:
- Six patients with tumors with PD-L1 TPS > 50% at screening will be enrolled in cohort A (PD-L1 high cohort).
- Cohort B (PD-L1 all-comer cohort) will start with enrollment of 6 patients with tumors with PD-L1 TPS<50%.
2.各コホートの安全性を評価し、安全であると考えられる場合:
-PD-L1 TPS≧50%を有する腫瘍を有する患者を含む患者は、PD-L1 TPS≧50%を有する腫瘍を有する8人の患者がコホートに登録されるまで、コホートB(PD-L1 all comer)にのみ登録される。
-次いで、コホートB患者の残りは、PD-L1 TPS<50%を有する腫瘍を有する患者を含む。
2. Evaluate the safety of each cohort and if considered safe:
- Patients including patients with tumors with PD-L1 TPS ≥50% will be enrolled in Cohort B (PD-L1 all comer) only.
- The remainder of Cohort B patients then includes patients with tumors with PD-L1 TPS<50%.
3.PD-L1 TPS≧50%を有する腫瘍を有する合計8人の患者がコホートB(PD-L1 all comer)に登録された後、コホートA(PD-L1高)への登録を再開し、PD-L1 TPS≧50%を有する腫瘍を有するすべてのその後の患者をそのコホートに登録する。 3. After a total of 8 patients with tumors with PD-L1 TPS ≥ 50% were enrolled in Cohort B (PD-L1 all comers), enrollment resumed in Cohort A (PD-L1 high) and PD- All subsequent patients with tumors with L1 TPS≧50% will be enrolled in the cohort.
D.試験処置の投与量、投与及びコンプライアンス D. Study Treatment Dosage, Administration and Compliance
各試験処置成分は、表57に指定される用量及び頻度で投与される。

ネオアジュバント処置期は、4サイクルのAtezo+Tira又はAtezo+Tira+Chemoからなる。各サイクルの期間は21日間である。各サイクルの第1日目に、全ての適格患者に以下の順序で試験薬注入が行われる。
●コホートA(PD-L1高):(1)アテゾリズマブ、(2)チラゴルマブ。
●コホートB(PD-L1 all comer):治験責任医師は、組織学的サブタイプ及び現地SOCに基づいて列挙されたレジメンの1つを投与する。
-(1)アテゾリズマブ、(2)チラゴルマブ、(3)パクリタキセル、(4)カルボプラチン
-(1)アテゾリズマブ、(2)チラゴルマブ、(3)ペメトレキセド、(4)(カルボプラチン又はシスプラチン)
-(1)アテゾリズマブ、(2)チラゴルマブ、(3)ゲムシタビン、(4)(カルボプラチン又はシスプラチン)
The neoadjuvant treatment phase consisted of 4 cycles of Atezo+Tira or Atezo+Tira+Chemo. The duration of each cycle is 21 days. On
• Cohort A (PD-L1 high): (1) atezolizumab, (2) tiragolumab.
• Cohort B (PD-L1 all comers): Investigator will receive one of the listed regimens based on histologic subtype and local SOC.
- (1) atezolizumab, (2) tiragolumab, (3) paclitaxel, (4) carboplatin - (1) atezolizumab, (2) tiragolumab, (3) pemetrexed, (4) (carboplatin or cisplatin)
- (1) atezolizumab, (2) tiragolumab, (3) gemcitabine, (4) (carboplatin or cisplatin)
アテゾリズマブ(1200mg)及びチラゴルマブ(600mg)は、固定用量で投与される。患者は、可能であれば登録日に初回用量の試験処置を受ける。登録日の処置が不可能である場合、初回用量は登録後5日以内に行われる。 Atezolizumab (1200 mg) and tiragolumab (600 mg) will be administered at fixed doses. Patients will receive the first dose of study treatment on the day of enrollment if possible. If treatment on the day of enrollment is not possible, the first dose will be administered within 5 days after enrollment.
サイクル1では、アテゾリズマブ及びチラゴルマブの一次予防(抗ヒスタミン剤、解熱剤及び/又は鎮痛剤)のための前投薬は許可されない。患者は、現地SOC及び製造業者の指示に従って、選択された化学療法のバックボーンレジメンのための制吐剤及びIV水分補給を受けなくてはならない。しかしながら、コルチコステロイドの免疫調節効果のために、コルチコステロイドによる前投薬は、臨床上実施可能な程度に最小限にしなければならない。
No premedication for primary prophylaxis (antihistamines, antipyretics and/or analgesics) for atezolizumab and tiragolumab is allowed in
Atezo+Tiraによるアジュバント処置は、手術後14~60日以内又は最後のPORT治療後7-42日以内に開始する。アジュバント化学療法を投与する場合、処置は、手術後28-72日以内に開始し、続いてPORT(選択された場合)をアジュバント化学療法後21-60日以内に開始する。術後アジュバント処置の間、注入は以下の順序で投与される(患者ごとに1レジメン)。コホートA(PD-L1高)レジメンの選択は、各患者について治験責任医師の裁量による。 Adjuvant treatment with Atezo+Tira is initiated within 14-60 days after surgery or within 7-42 days after the last PORT treatment. If adjuvant chemotherapy is administered, treatment is initiated within 28-72 days after surgery, followed by PORT (if selected) within 21-60 days after adjuvant chemotherapy. During postoperative adjuvant treatment, infusions will be administered in the following order (one regimen per patient). Selection of the Cohort A (PD-L1 High) regimen is at the investigator's discretion for each patient.
●コホートA(PD-L1高):治験責任医師は、以下に列挙するレジメンの1つを投与する。
-(1)アテゾリズマブ、(2)チラゴルマブ
-(1)パクリタキセル、(2)カルボプラチン
-(1)ペメトレキセド、(2)(カルボプラチン又はシスプラチン)
-(1)ゲムシタビン、(2)(カルボプラチン又はシスプラチン)
●コホートB(PD-L1 all comer):(1)アテゾリズマブ、(2)チラゴルマブ
• Cohort A (PD-L1 High): Investigator will administer one of the regimens listed below.
- (1) atezolizumab, (2) tiragolumab - (1) paclitaxel, (2) carboplatin - (1) pemetrexed, (2) (carboplatin or cisplatin)
- (1) gemcitabine, (2) (carboplatin or cisplatin)
- Cohort B (PD-L1 all comers): (1) atezolizumab, (2) tiragolumab
アテゾリズマブ及びチラゴルマブ
アテゾリズマブは、各21日間サイクルの1日目に1200mgの固定用量でIV注入によって投与される。アテゾリズマブの用量は固定されており、体重に依存しない。用量の減少は許容されない。
Atezolizumab and Tiragolumab Atezolizumab is administered by IV infusion at a fixed dose of 1200 mg on
アテゾリズマブの投与及び観察期間の後、患者は、各21日間サイクルの第1日にIV注入によって投与される600mgのチラゴルマブを受ける。チラゴルマブ用量は固定され、体重に依存しない。用量の減少は許容されない。
After administration of atezolizumab and an observation period, patients receive 600 mg of tiragolumab administered by IV infusion on
試験処置の投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び薬剤に直ちにアクセスできる監視された状況で行われる。アテゾリズマブ及びチラゴルマブの注入は、 Administration of study treatment will occur in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions. Infusion of atezolizumab and tiragolumab
表58に概説される指示に従って投与される。


アテゾリズマブ及びチラゴルマブの投薬遅延
アテゾリズマブもチラゴルマブも永続的に中止されていない限り、以下の規則が適用される:
●処置サイクルは通常、各21日間サイクルの1日目にアテゾリズマブ及びチラゴルマブを投与することから始まる。いずれかの試験薬物が関連する毒性のために遅延される場合、アテゾリズマブ及びチラゴルマブの安全性プロファイルが類似しているので、他の試験薬物も遅延されることが推奨される。
●薬物関連毒性のための1つの試験薬の投与が遅延し、他方の試験薬が計画通り投与される場合、遅延されている試験薬を次の予定された注入(すなわち、次の予定された21日サイクル)で投与することが推奨される。
Atezolizumab and Tiragolumab Dose Delays Unless atezolizumab or tiragolumab are permanently discontinued, the following rules apply:
• Treatment cycles generally begin with administration of atezolizumab and tiragolumab on
- If the administration of one study drug is delayed for drug-related toxicity and the other study drug is administered as planned, the delayed 21-day cycles) are recommended.
化学療法
施設は、以下の情報及び現地の処方情報に従うべきである。一般に、施設はまた、患者の体重変化の場合に用量調整を決定するために施設内及び局所SOCに従うべきである。化学療法レジメンのいずれかの成分に起因する毒性のために処置サイクルが遅延又は中断された場合、両方の化学療法成分は保留されるべきであり、再開された場合、両方は同期したままにするために再開されるべきである。
Chemotherapy centers should follow the information below and local prescribing information. In general, institutions should also follow institutional and local SOCs to determine dose adjustments in the event of patient weight change. If a treatment cycle is delayed or interrupted due to toxicity due to either component of the chemotherapy regimen, both chemotherapy components should be held and when restarted both remain synchronized should be reopened for
パクリタキセル
アジア人種/民族の患者は、3時間にわたる175mg/m2IVでのより低い開始用量のパクリタキセルを受ける。アジア人種/民族の患者に対するパクリタキセルのより低い開始用量は、非アジア諸国の患者と比較して、アジア諸国の患者における血液毒性のより高い全発生率に基づいており、これは独立したデータモニタリング委員会によるIMpower 150及びIMpower 131試験結果の安全性の再検討中に観察された。「アジア人種/民族」という用語は、東アジア、東南アジア、又は南アジアに住むか、又はこれらに祖先の起源を有する多様な集団を含む汎民族/人種を指す。特定の患者におけるこの用語の適用可能性は、処置を行う治験責任医師の裁量であり、患者の臨床的特徴及び起源国に基づくべきである。
Paclitaxel Asian race/ethnicity patients receive a lower starting dose of paclitaxel at 175 mg/m 2 IV over 3 hours. The lower starting dose of paclitaxel for patients of Asian race/ethnicity was based on the higher overall incidence of hematologic toxicity in patients from Asian countries compared with patients from non-Asian countries, which was supported by independent data monitoring. Observed during the safety review of the IMpower 150 and IMpower 131 trial results by the panel. The term "Asian race/ethnicity" refers to a pan-ethnic/ethnic group that includes diverse populations living in or having ancestral origins in East Asia, Southeast Asia, or South Asia. The applicability of this term in a particular patient is at the discretion of the treating investigator and should be based on the patient's clinical characteristics and country of origin.
パクリタキセル注射は、注入前に希釈しなければならない。パクリタキセルは0.9%塩化ナトリウムUSP;5%デキストロース注射液、USP;5%デキストロース及び0.9%塩化ナトリウム注射液、USPで希釈するか、又は5%デキストロースを最終濃度0.3~1.2mg/mLになるようにリンガー注射液に添加すべきである。注入部位を、薬物投与中に起こり得る浸潤について厳密に監視しなければならない。 Paclitaxel injections must be diluted prior to injection. Paclitaxel is diluted with 0.9% sodium chloride USP; 5% dextrose injection, USP; 5% dextrose and 0.9% sodium chloride injection, USP, or 5% dextrose at a final concentration of 0.3-1. 2 mg/mL should be added to Ringer's Injection. The injection site must be closely monitored for possible infiltration during drug administration.
希釈されていない濃縮物と、注入用溶液を調製するために使用される可塑化ポリ塩化ビニル(PVC)機器又は装置との接触は推奨されない。パクリタキセルは、0.22μm以下の微孔膜を有するインラインフィルタを通して投与しなければならない。短い入口及び出口PVC-被覆管を組み込んだIVEX-2(登録商標)フィルタ等のフィルタ装置の使用は、フタル酸ビス(2-エチルヘキシル)の著しい漏出をもたらさなかった。 Contact of undiluted concentrate with plasticized polyvinyl chloride (PVC) equipment or equipment used to prepare infusion solutions is not recommended. Paclitaxel must be administered through an in-line filter with a microporous membrane of 0.22 μm or less. The use of filter devices such as the IVEX-2® filter incorporating short inlet and outlet PVC-clad tubes did not result in significant leakage of bis(2-ethylhexyl) phthalate.
現場は、患者の体重変化の場合のパクリタキセル用量調整を決定するために施設のSOCガイドラインに従うべきである。パクリタキセル注入の場合、3時間の注入時間の例外は、パクリタキセルをより迅速に(90分かけて)又はよりゆっくり(最初の注入については最大4時間)注入する施設の方針を有する現場について許容される。 Sites should follow institutional SOC guidelines to determine paclitaxel dose adjustments in the event of patient weight change. For paclitaxel infusions, an exception to the 3-hour infusion time is allowed for sites with institutional policies to infuse paclitaxel more quickly (over 90 minutes) or more slowly (up to 4 hours for the first infusion). .
ペメトレキセド
施設は、ペメトレキセドの標準的な投与手順に従うべきである。ペメトレキセドの投与は、少なくとも10分間にわたってIV注入によって投与されるべきである。投与される投薬前用量は、処方情報に従うべきである。ペメトレキセド療法に適格なすべての患者は、ペメトレキセド投与の前、当日、及び少なくとも2日後の少なくとも5日間、薬物除去半減期が長い非ステロイド性抗炎症薬の服用を避けるべきである。
Pemetrexed Institutions should follow standard administration procedures for pemetrexed. Administration of pemetrexed should be administered by IV infusion over at least 10 minutes. The pre-medication dose administered should comply with the prescribing information. All patients eligible for pemetrexed therapy should avoid taking non-steroidal anti-inflammatory drugs with a long drug elimination half-life for at least 5 days before, on the day of, and at least 2 days after pemetrexed administration.
ゲムシタビン
ゲムシタビンは、カルボプラチン又はシスプラチンの前に30分間にわたってIV注入によって投与されなくてはならない。ゲムシタビンの用量は、カルボプラチンの前に投与した場合とシスプラチンの前に投与した場合とで異なることに留意されたい(表57)。ゲムシタビンは、注入前に希釈しなければならない。
Gemcitabine Gemcitabine must be administered by IV infusion over 30 minutes prior to carboplatin or cisplatin. Note that the dose of gemcitabine was different when administered before carboplatin and before cisplatin (Table 57). Gemcitabine must be diluted prior to infusion.
ゲムシタビンの再構成のための推奨される希釈剤は、保存剤を含まない0.9%塩化ナトリウム注射液、USPである。ゲムシタビンの投与は、現地の診療及び処方情報に従って行われるべきである。 The recommended diluent for reconstitution of gemcitabine is 0.9% preservative-free sodium chloride injection, USP. Gemcitabine should be administered according to local clinical practice and prescribing information.
カルボプラチン
カルボプラチンを、6mg/mL/分(Calvert式投薬)の濃度時間曲線下面積(AUC)を達成するために、パクリタキセル又はペメトレキセド投与の完了直後に15~30分間にわたってIV注入によって、及び現地の診療ガイドラインによる標準的な制吐剤とともに投与すべきである。
Carboplatin Carboplatin was administered by IV infusion over 15-30 minutes immediately after completion of paclitaxel or pemetrexed administration and by local clinical practice to achieve a concentration-time curve (AUC) of 6 mg/mL/min (Calvert dosing). It should be administered with standard antiemetics according to guidelines.
AUC 6mg/mL/分のカルボプラチン用量は、Calvert式
(Calvert et al.,J Clin Oncol,7:1748-1756,1989)を使用して計算される:
総投与量(mg)=(目標AUC)X(糸球体濾過率[GFR]+25)
A Carboplatin dose of
Total Dose (mg) = (Target AUC) X (Glomerular Filtration Rate [GFR] + 25)
AUCベースの投与量を計算するためにCalvert式で使用されるGFRは、125mL/分を超えてはならない。この試験の目的のために、GFRは、クレアチニンクリアランス(CrCl)と同等であると考えられる。CrClは、施設のガイドライン又は以下の方法によって計算される。
以下の式を使用するCockcroft and Gault(Nephron,16:31-41,(1976)):
女性の場合、CrCl=((140-年齢)(重量)/(72XScr))X0.85
式中:CrCl=mL/分単位のクレアチニンクリアランス;年齢=患者の年齢;wt=kg単位の患者の体重;
Scr=g/dL単位の血清クレアチニン
The GFR used in the Calvert formula to calculate AUC-based dose should not exceed 125 mL/min. For the purposes of this study, GFR is considered equivalent to creatinine clearance (CrCl). CrCl is calculated according to institutional guidelines or the following method.
Cockcroft and Gault (Nephron, 16:31-41, (1976)) using the following formula:
For females, CrCl = ((140-age)(weight)/(72XScr)) X 0.85
where: CrCl = creatinine clearance in mL/min; age = patient age; wt = patient weight in kg;
Scr = serum creatinine in g/dL
異常に低い血清クレアチニンレベルを有する患者については、0.8mg/dLの最小クレアチニンレベルを使用してGFRを推定するか、又は125mL/分で推定GFRを制限すべきである。患者のGFRが同位体希釈質量分析法による血清クレアチニン測定に基づいて推定される場合、FDAは、医師が過剰投与による潜在的な毒性を回避するために所望の曝露(AUC)のためにカルボプラチンの用量をキャッピングすることを検討することを推奨する。カルボプラチン標識に記載されているCalvert式に基づいて、最大用量を以下のように計算することができる。
最大カルボプラチン用量(mg)=標的AUC(mg・分/mL)(GFRX25mL/分)
For patients with abnormally low serum creatinine levels, a minimum creatinine level of 0.8 mg/dL should be used to estimate GFR or limit estimated GFR at 125 mL/min. When a patient's GFR is estimated based on serum creatinine measurements by isotope dilution mass spectrometry, the FDA recommends that physicians use carboplatin for the desired exposure (AUC) to avoid potential toxicity from overdose. We recommend that you consider dose capping. Based on the Calvert formula described in the carboplatin label, the maximum dose can be calculated as follows.
Maximum Carboplatin Dose (mg) = Target AUC (mg min/mL) (
最大用量は、正常な腎機能を有する患者について125mL/分で上限を定めたGFR推定値に基づく。より高い推定GFR値を使用すべきではない。標的AUC=6の場合、最大用量は6X(125+25)=900mgである。標的AUC=5の場合、最大用量は5X(125+25)=750mgである。標的AUC=4の場合、最大用量は4X(125+25)=600mgである。 Maximum dose is based on GFR estimates capped at 125 mL/min for patients with normal renal function. Higher estimated GFR values should not be used. For target AUC=6, the maximum dose is 6×(125+25)=900 mg. For target AUC=5, the maximum dose is 5×(125+25)=750 mg. For target AUC=4, the maximum dose is 4×(125+25)=600 mg.
シスプラチン
シスプラチンは、ペメトレキセド又はゲムシタビン注入の完了のおよそ30分後に、75mg/m2の用量で1~2時間にわたって、又は施設でのSOCごとに、IV注入によって投与される。患者は、シスプラチンを投与する前及び投与した後に、適切な制吐処置及び適切な水分補給を受けなければならない。
Cisplatin Cisplatin is administered by IV infusion at a dose of 75 mg/m 2 over 1-2 hours or as per SOC at the center approximately 30 minutes after completion of the pemetrexed or gemcitabine infusion. Patients must receive adequate antiemetic treatment and adequate hydration prior to and after administration of cisplatin.
E.外科的処置計画 E. surgical planning
早期切除可能NSCLCの経験を有する主治医は、スクリーニング時に患者を評価して、外科的適応度及び外科的摘出の適格性を決定する。患者は、スクリーニング時に治癒目的のR0摘出に適格でなければならない。患者を手術可能にするために段階を下げる意図は許可されない。 An attending physician with experience with early resectable NSCLC will evaluate the patient at screening to determine surgical suitability and eligibility for surgical excision. Patients must be eligible for curative R0 extraction at screening. No intent to downgrade to make the patient operable is permitted.
スクリーニングでは、患者は、選択基準に概説されているように、肺機能検査(PFT)に基づいて手術適応性について確認されなければならない。ppoFEV1及びppoDLCOは、以下の方法論を用いて計算される(Brunelli et al.,Chest,143(5Suppl):e166S-e190S,2013):
●灌流法(肺換気/灌流スキャン(VQスキャン):
ppoFEV1又はppoDLCO=術前FEV1又はDLCOX(1-x)
式中、x=切除された肺の全灌流の割合
●解剖学的方法:
ppoFEV1又はppoDLCO=術前FEV1又はDLCOX(1-(y/z))
式中、y=除去されるべき機能的又は非閉塞性肺セグメントの数;z=19、機能的肺セグメントの総数。なお、機能的肺セグメント(19)の総数は、右肺に10セグメント(上葉に3つ、中葉に2つ、及び下葉に5つ)及び左肺に9セグメント(上葉に5つ、及び下葉に4つ)で表される。
At screening, patients must be confirmed for surgical suitability based on pulmonary function testing (PFT) as outlined in the inclusion criteria. ppoFEV 1 and ppoDL CO are calculated using the following methodology (Brunelli et al., Chest, 143(5Suppl): e166S-e190S, 2013):
Perfusion method (lung ventilation/perfusion scan (VQ scan):
ppoFEV 1 or ppoDL CO = preoperative FEV 1 or DL CO X(1−x)
where x = percentage of total perfusion of the resected lung Anatomical method:
ppoFEV 1 or ppoDL CO = preoperative FEV 1 or DLCOX (1 - (y/z))
where y = number of functional or non-obstructive lung segments to be removed; z = 19, total number of functional lung segments. It should be noted that the total number of functional lung segments (19) is 10 segments in the right lung (3 upper, 2 middle and 5 lower lobes) and 9 segments in the left lung (5 upper and 5 lower lobes). and four in the lower lobe).
患者は、ネオアジュバント処置の完了後及び外科医及び腫瘍内科医による手術の前に再評定される。限定されないが、血液検査、凝固、心臓検査又はPFT(指定される場合)、麻酔評定、及び他の評価手順を含む術前評価は、局所SOCごとに行われるべきである。 Patients will be reassessed after completion of neoadjuvant treatment and prior to surgery by the surgeon and medical oncologist. Preoperative evaluations, including but not limited to blood tests, coagulation, cardiac tests or PFT (if specified), anesthesia evaluations, and other evaluation procedures should be performed for each local SOC.
外科的処置は、可能な限り術前来院から30日以内に行われるべきである。この時間枠内に手術を行うことができない場合(例えば、長期の有害事象のために)、メディカルモニターに相談すべきである。手術前来院から30日を超えて手術が計画されている場合、計画された手術の前に反復CTスキャンを得るべきである。 Surgical procedures should be performed within 30 days of the preoperative visit whenever possible. If surgery cannot be performed within this time frame (eg, due to long-term adverse events), a medical monitor should be consulted. If surgery is planned more than 30 days from the preoperative visit, a repeat CT scan should be obtained prior to the planned surgery.
摘出は、開放処置又は低侵襲処置(例えば、開胸、胸骨切開、クラムシェル若しくはヘミクラムシェル切開、又はビデオ支援胸部手術[VATS]又はロボット支援VATS)によって達成されるべきである。 Extraction should be accomplished by an open or minimally invasive procedure (eg, thoracotomy, sternotomy, clamshell or hemiclamshell incision, or video-assisted thoracic surgery [VATS] or robot-assisted VATS).
原発腫瘍及び関与するリンパ節(R 0)の病理学的完全摘出を行うべきである。区域切除、肺葉切除、二葉切除又は肺切除による解剖学的摘出が必要である。すべての摘出について、すべての解剖学的構造の区分(例えば、動脈、気管支、静脈)が含まれなくてはならない。楔状切除術は許容されない。前述の解剖学的詳細を提供しない区域(例えば、尖端域又は上部の区域の楔形切除)を含む深部楔状切除術(deep wedge resections)は、区域切除としてカウントされない。 Complete pathologic resection of the primary tumor and involved lymph nodes (R0) should be performed. Anatomical excision by segmentectomy, lobectomy, bilobectomy, or pneumonectomy is required. For all excisions, all anatomical segments (eg, arteries, bronchi, veins) must be included. Wedge resection is not permitted. Deep wedge resections, including areas that do not provide the aforementioned anatomical details (eg, wedge resections of the apical or superior areas), do not count as segmentectomy.
門部及び縦隔のリンパ節郭清術又はサンプリングは必須である。右側摘出の場合、これは少なくともレベル4R、7、10R及び11Rのリンパ節を含む。 Hilar and mediastinal lymphadenectomy or sampling is mandatory. For right-sided resections, this includes at least the lymph nodes at levels 4R, 7, 10R and 11R.
レベル2Rのリンパ節を含めることが推奨される。左側摘出の場合、これは少なくともレベル5/6、7、10L及び11Lのリンパ節を含む。下葉摘出の場合、レベル8又は9を含むことが推奨される。
Inclusion of level 2R lymph nodes is recommended. For left-sided resections, this includes at least the lymph nodes at
F.術後放射線療法
術後放射線療法(PORT)は、外科的摘出時に存在する確認された病理学的N 2+疾患(ypN2)又は陽性腫瘍周縁部(R1又はR2)を有する患者に許容され、アジュバントであるAtezo+Tira処置の前又はアジュバントである白金系化学療法剤の後に投与されなければならない。
F. Postoperative Radiation Therapy Postoperative radiation therapy (PORT) is tolerated in patients with confirmed pathological N2+ disease (ypN2) or positive tumor margins (R1 or R2) present at the time of surgical excision, with adjuvant It must be administered before certain Atezo+Tira treatments or after adjuvant platinum-based chemotherapeutic agents.
1.8-2Gyのフラクション中の50-66グレイ(Gy)の推奨線量に対するコンフォーマル3次元又は強度変調放射線療法は、施設及び/又は国際ガイドラインに従って投与されるべきである。強く推奨される制約には、肺葉切除後に31%を超えない肺への平均線量≦20 Gy及びV20(20Gy以上の放射線量を受ける肺体積の割合)、又は肺切除後に8 Gy及びV20≦5%の平均肺線量が含まれる。 Conformal 3D or intensity-modulated radiation therapy to recommended doses of 50-66 Grays (Gy) in fractions of 1.8-2 Gy should be administered according to institutional and/or international guidelines. Strongly recommended constraints include mean dose to lung < 20 Gy and V20 (percentage of lung volume receiving 20 Gy or more radiation dose) not exceeding 31% after lobectomy, or 8 Gy and V20 < 5 after pneumonectomy. % mean lung dose is included.
G.併用療法 G. Combination therapy
併用療法は、試験薬の開始の7日前から処置中止の来院までの治験実施計画書に定められた処置に加えて、患者によって使用される任意の医薬(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)からなる。 Concomitant therapy includes any drug used by the patient (e.g., prescription drug, over-the-counter drug, vaccine, herbal or homeopathic remedies, dietary supplements).
許可された治療
患者は、試験中に以下の治療法を使用することが許される。
●年間失敗率<1%の経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●COPD又は喘息のために投与されるコルチコステロイド。
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
Allowed Treatments Patients will be allowed to use the following treatments during the study.
● Oral contraceptives with <1% annual failure rate ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable-dose warfarin or low-molecular-weight heparin)
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
• Corticosteroids administered for COPD or asthma.
Low-dose corticosteroids given for orthostatic hypotension or adrenocortical insufficiency
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent atezolizumab infusions, at the discretion of the Investigator.
一般に、治験責任医師は、臨床上適応がある場合、現地の標準診療に従って、注意療法又は禁止療法として定義されるもの以外の支持療法で患者のケア(既存の症状を含む)を管理すべきである。 In general, investigators should manage patient care (including pre-existing symptoms) with supportive care other than those defined as attention or prohibitive care, as clinically indicated, and in accordance with local standard practice. be.
注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧、喘鳴、気管支攣縮、頻脈、酸素飽和度の低下、または呼吸困難によって現れる重篤な注入関連事象は、臨床的に示されるような支持療法(例えば、補充酸素およびβ2-アドレナリン作動薬)で管理されるべきである。 Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine) or equivalent drugs according to local standard practice. can be done. Serious infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, desaturation, or dyspnea should be treated with supportive care as clinically indicated (e.g., supplemental oxygen and β2- should be managed with adrenergic agonists).
アテゾリズマブ及びチラゴルマブで処置された患者のための注意療法
コルチコステロイド及びTNFα阻害剤
全身性コルチコステロイド及びTNF-α阻害剤は、アテゾリズマブによる処置の潜在的に有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物を検討しなければならない。代替法が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。
Cautionary Therapy for Patients Treated with Atezolizumab and Tiragolumab Corticosteroids and TNFα Inhibitors Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab . Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines must be considered. If alternatives are not feasible, systemic corticosteroids and TNF-α inhibitors can be administered at the investigator's discretion.
アテゾリズマブ及び/又はチラゴルマブ治療に関連する場合、特定の有害事象の処置のために、治験責任医師の裁量で、全身コルチコステロイドが推奨される。 Systemic corticosteroids are recommended at the investigator's discretion for treatment of specific adverse events when associated with atezolizumab and/or tiragolumab therapy.
禁止される治療法
以下の併用療法の使用は、以下に記載されるように禁止される:
●がん(限定されるものではないが、化学療法、ホルモン療法、免疫療法、放射線療法、及び薬草療法を含む)の処置を目的とした併用療法は、保健当局が-承認したものであろうと実験的なものであろうと、薬剤に応じて、試験処置を開始する前の様々な期間、及び試験処置中、疾患の進行が文書化され、患者が試験処置を中止するまで禁止される。
●試験処置の開始前42日以内及び試験処置中の治験治療。
●生弱毒化ワクチン(例えば、FLUMIST(登録商標))は、試験処置の開始前4週間以内、試験処置中、チラゴルマブの最終投与後90日間、及びアテゾリズマブの最終投与後5ヶ月間禁止する。化学療法(すなわち、カルボプラチン、シスプラチン、ペメトレキセド、パクリタキセル又はゲムシタビン)により処置されている患者は、生ワクチンを受けてはならない。
●アテゾリズマブ及びチラゴルマブと組み合わせて投与した場合、自己免疫症状のリスクを潜在的に増加させる可能性があるため、試験処置の開始前及び試験処置中の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫賦活剤(限定されないが、インターフェロン及びIL-2を含む)は禁止される。
●試験処置中の全身免疫抑制剤(限定されないが、シクロホスファミド、アザチオプリン、メトトレキサート及びサリドマイドを含む)(薬剤が試験処置の有効性及び安全性を潜在的に変化させる可能性があるため)
Prohibited Therapies The use of the following concomitant therapies is prohibited as described below:
• Combination therapies for the treatment of cancer (including, but not limited to, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy), if approved by health authorities. Depending on the drug, whether experimental, it is prohibited for various periods of time before starting study treatment and during study treatment until disease progression is documented and the patient discontinues study treatment.
• Study treatment within 42 days prior to initiation of study treatment and during study treatment.
• Live attenuated vaccines (eg, FLUMIST®) are prohibited within 4 weeks prior to initiation of study treatment, during study treatment, 90 days after the last dose of tiragolumab, and 5 months after the last dose of atezolizumab. Patients being treated with chemotherapy (ie carboplatin, cisplatin, pemetrexed, paclitaxel or gemcitabine) should not receive live vaccines.
Due to the potential increased risk of autoimmune symptoms when administered in combination with atezolizumab and tiragolumab, no more than 4 weeks or 5 drug elimination half-lives (either within 4 weeks prior to initiation of study treatment and during study treatment) or longer) are prohibited (including but not limited to interferon and IL-2).
- Systemic immunosuppressants (including but not limited to cyclophosphamide, azathioprine, methotrexate, and thalidomide) during study treatment (because drugs can potentially alter the efficacy and safety of study treatment)
H.試験評定
患者は、試験を通して安全性及び忍容性について綿密に監視される。患者は、各投与の前に毒性について評定され、投薬は、臨床評定及び地域の臨床検査値が許容できる場合にのみ実施されなければならない。
H. Study Assessment Patients will be closely monitored for safety and tolerability throughout the study. Patients should be assessed for toxicity prior to each dose and doses administered only if clinical evaluation and local laboratory values are acceptable.
全ての処置来院は、特に明記しない限り、予定日から±3日に行わなければならない。時間枠が指定されていない限り、全ての評定は指定された来院日に実施されなければならない。患者は、各投与の前に毒性について評定され、投薬は、臨床評定及び現地の臨床検査値が許容できる場合にのみ実施されなければならない。試験処置投与の日に予定される評定は、特に明記しない限り、投与前に行わなければならない。 All treatment visits must occur ±3 days from the scheduled date unless otherwise specified. All assessments must be performed on the designated visits unless a time frame is designated. Patients should be assessed for toxicity prior to each dose and doses administered only if clinical evaluation and local laboratory values are acceptable. Assessments scheduled on the day of study treatment administration must be performed prior to dosing unless otherwise specified.
以下の評定を、各サイクルの1日目の≦4日前に行うことができる:
●限定的な身体検査
●現地の臨床検査
The following assessments can be performed ≤4 days prior to
● limited physical examination ● local clinical examination
腫瘍定を除いて、サイクル1の1日目の≦4日前に実施されたスクリーニング評定をサイクル1の1日目に繰り返す必要はない。
Screening assessments performed ≤4 days prior to
休日、週末、又は他の事象が予定された投与を妨げる場合、投与を最も早い次の日に延期し、その後の投与を21日間のスケジュールで継続してもよい。処置が3日未満にわたって延期される場合、患者は元のスケジュールを再開することができる。 If holidays, weekends, or other events interfere with scheduled dosing, dosing may be postponed to the next earliest day and subsequent dosing may continue on the 21-day schedule. If treatment is delayed for less than 3 days, the patient can resume their original schedule.
I.腫瘍応答及び疾患状態のフォローアップ評価
手術後及びアジュバント処置期の間、疾患状態のフォローアップ評定は、最初の1年間はIV造影剤を用いた胸部CT(肝臓及び副腎を含む)によって手術日から4ヶ月ごとに、次いで2年目は6ヶ月ごとに、すべての患者(両方のコホート)で実施される。造影剤を用いたCTスキャンが禁忌である場合(例えば、腎クリアランスが損なわれた患者において)、胸部の非造影CTスキャンを実施することができる。疾患の再発を経験していない患者は、手後3-5年の間にIV造影剤を用いた胸部CTスキャン(肝臓及び副腎を含む)によって6ヶ月ごとに疾患状態のフォローアップ評定を受ける。
I. Follow-up Assessment of Tumor Response and Disease Status During the postoperative and adjuvant treatment phases, follow-up assessment of disease status will be performed from the day of surgery by chest CT (including liver and adrenal glands) with IV contrast for the first year. Every 4 months, then every 6 months for the second year, in all patients (both cohorts). If a CT scan with contrast is contraindicated (eg, in patients with impaired renal clearance), a non-contrast CT scan of the chest can be performed. Patients who have not experienced recurrence of disease have a follow-up assessment of disease status every 6 months by chest CT scan (including liver and adrenal glands) with IV contrast for 3-5 years afterward.
疾患状態のフォローアップ評定は、予定されたフォローアップ評価の許容時間枠内で行われなくてはならない。疾患状態フォローアップ評定のために許容される時間枠は、1年目では±7日間、2-3年目では±14日間、及びその後±4週間である。
Follow-up assessments of disease status must occur within the acceptable timeframe for scheduled follow-up assessments. The timeframes allowed for disease status follow-up assessment are ±7 days at
手術後の疾患再発は、病理学的に及び/又は明確な放射線学的証拠によって確認されなくてはならない。スキャンが明確な所見を示す場合(例えば、縦隔節は、短軸で<1.5cmの大きさであり、肺実質病変又は内臓病変は、最長直径で<1cmの大きさである)、生検を行うべきである。生検が実施可能又は安全でない場合、4~8週間以内に確認スキャンを再度行わなければならない。確認スキャンで疾患の再発が確認された場合、その事象を、曖昧な事象を示した以前の確認検査日に文書化しなければならない。 Disease recurrence after surgery must be confirmed pathologically and/or by clear radiological evidence. If the scan shows clear findings (e.g., mediastinal nodes measure <1.5 cm on the short axis and pulmonary parenchymal or visceral lesions measure <1 cm on the longest diameter), the patient is considered alive. should be examined. If biopsy is not feasible or safe, confirmatory scans should be repeated in 4-8 weeks. If a confirmatory scan confirms disease recurrence, the event must be documented on the date of the previous confirmatory examination that showed an equivocal event.
生検は、次の抗がん療法を開始する前に行わなければならない。生検が疾患再発の証拠を示さない場合(例えば、非悪性浸潤物)、患者は予定された試験処置、評定及び/又はフォローアップを継続してもよい。 A biopsy must be performed before starting the next anticancer therapy. If the biopsy shows no evidence of disease recurrence (eg, non-malignant infiltrates), the patient may continue with scheduled study treatment, evaluation and/or follow-up.
腫瘍又は疾患状態のフォローアップ評定は、疾患の進行又は再発以外の理由で(例えば、毒性のために)早期に処置を中止する患者において継続すべきである。疾患の進行又は再発がない場合、腫瘍又は疾患の状態のフォローアップ評定は、すべての患者において、新しい抗がん治療を開始するかどうかにかかわらず、疾患の進行又は再発、同意の撤回、死亡、フォローアップの喪失、又は試験依頼者による試験の終了のいずれか早く発生する方まで継続すべきである。 Follow-up assessment of tumor or disease status should continue in patients who discontinue treatment prematurely for reasons other than disease progression or recurrence (eg, due to toxicity). In the absence of disease progression or recurrence, follow-up assessment of tumor or disease status should include disease progression or recurrence, withdrawal of consent, and death in all patients, whether or not new anticancer therapy is initiated. , loss of follow-up, or termination of the study by the sponsor, whichever occurs first.
J.試験処置の中止
患者は、以下のいずれかを経験した場合、試験処置を恒久的に中止しなければならない:
●個々の患者の治療に対する潜在的応答及び事象の重症度を考慮すると、許容できないと治験責任医師が判断した免疫介在性有害事象の発生を含む、アテゾリズマブ又はチラゴルマブに関連する許容できない毒性 ネオアジュバント処置期の間にアテゾリズマブ及びチラゴルマブを中止した場合、化学療法を継続してもよい。
●試験処置の他の成分に関連する許容できない毒性。ネオアジュバント処置期の間に化学療法関連毒性のために、いずれか又はすべての化学療法剤が中止された場合、Atezo+Tiraを依然として投与すべきである。
●患者が試験処置を継続する場合、患者の安全性を危うくする可能性がある任意の医学的症状。
●処置の中止が患者にとって最も有益であるという治験責任医師又は試験依頼者の判断
●別の非治験実施計画書規定抗がん治療の使用。
●妊娠。
●ネオアジュバント処置期の間のRECIST v1.1による不均一な放射線学的疾患進行。
●アジュバント処置期の間の疾患再発の病理学的に確認された又は明確な放射線学的証拠。
J. Discontinuation of Study Treatment Patients must permanently discontinue study treatment if they experience any of the following:
- Unacceptable toxicities associated with atezolizumab or tiragolumab, including the occurrence of immune-mediated adverse events that the investigator judged to be unacceptable given the individual patient's potential response to treatment and severity of events Neoadjuvant treatment Chemotherapy may be continued if atezolizumab and tiragolumab are discontinued during the phase.
• Unacceptable toxicity associated with other components of the study treatment. If any or all chemotherapy agents are discontinued due to chemotherapy-related toxicity during the neoadjuvant treatment phase, Atezo+Tira should still be administered.
• Any medical condition that may jeopardize patient safety if the patient continues study treatment.
• Investigator's or sponsor's judgment that discontinuation of treatment would be most beneficial to the patient • Use of another non-protocol prescribed anti-cancer therapy.
● Pregnancy.
• Heterogeneous radiographic disease progression by RECIST v1.1 during the neoadjuvant treatment phase.
• Pathologically confirmed or clear radiological evidence of disease recurrence during the adjuvant treatment phase.
少なくとも2サイクルのネオアジュバント処置を受け、試験処置を早期に中止する患者は交換されない。早期の処置中止の理由が、特に注目すべき有害事象又は疾患進行ではない場合、2サイクル未満のネオアジュバント処置を受ける患者を交換することができる。 Patients who receive at least 2 cycles of neoadjuvant treatment and discontinue study treatment prematurely are not replaced. Patients receiving less than 2 cycles of neoadjuvant treatment can be replaced if the reason for early treatment discontinuation is not a particularly notable adverse event or disease progression.
4サイクルを受ける前にネオアジュバント試験処置を中止する患者(例えば、処置不耐性又は応答の欠如のため)は、外科的摘出又は非外科的標準治療の治療措置(手術に適していない場合)のために処置を行う腫瘍内科医及び主治医によって評定される。計画された治験実施計画書に規定された手術を進める患者は、すべての術後試験処置及び手続きに適格なままである。 Patients who discontinue neoadjuvant study treatment before receiving 4 cycles (e.g., due to treatment intolerance or lack of response) may undergo surgical excision or non-surgical standard-of-care treatment regimens (if not suitable for surgery). It will be assessed by the treating oncologist and attending physician. Patients who proceed with surgery as specified in the planned protocol remain eligible for all post-operative study treatments and procedures.
患者は、試験処置の最終投薬の≦30日後に処置中止来院のために診療所に戻る。疾患評定が進行性疾患を示すか又は疾患再発を確認する来院は、処置中止来院として使用され得る。進行性疾患又は再発以外の何らかの理由で試験処置を中止する患者は、腫瘍又は疾患状態の評定を受け続ける。 Patients return to the clinic for a treatment discontinuation visit ≤30 days after the last dose of study treatment. Visits where disease assessment indicates progressive disease or confirms disease recurrence may be used as discontinuation visits. Patients who discontinue study treatment for any reason other than progressive disease or recurrence continue to undergo tumor or disease status assessments.
実施例11.GO42501試験の安全性の評定
A.安全性計画
Example 11. SAFETY ASSESSMENT OF THE GO42501 STUDY A. safety plan
この試験における患者の安全性計画は、予想される作用機序、非臨床試験の結果、同様の分子に関する公開データ、第I相及び第II相試験におけるチラゴルマブ単独及びアテゾリズマブとの併用での臨床経験、並びにアテゾリズマブの臨床安全性プロファイルに基づく。 The patient safety plan for this study includes the expected mechanism of action, results of nonclinical studies, published data on similar molecules, and clinical experience with tiragolumab alone and in combination with atezolizumab in phase I and II trials. , as well as the clinical safety profile of atezolizumab.
この試験に参加する患者の安全性を確保するために、厳格な選択基準及び除外基準の使用、並びに試験中の患者の綿密な監視を含む対策がとられる。アテゾリズマブ及びチラゴルマブの投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び薬剤に直ちにアクセスできる監視された状況で行われる。 Measures are taken to ensure the safety of patients entering this study, including the use of strict inclusion and exclusion criteria, and close monitoring of patients during the study. Atezolizumab and tiragolumab are administered in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
B.有害事象の管理
用量変更
試験において、アテゾリズマブ又はチラゴルマブについて、用量減少を含む用量変更はない。
B. Management of Adverse Events Dose Modifications There were no dose modifications, including dose reductions, for atezolizumab or tiragolumab in the study.
処置中断
試験処置は、毒性の管理のために必要に応じて一時的に保留されてもよい。作用機序の利用可能な特性評価に基づいて、チラゴルマブは、アテゾリズマブと類似しているが無関係の有害事象を引き起こす可能性があり、アテゾリズマブ関連有害事象の頻度又は重症度を悪化させる可能性があり、又はアテゾリズマブと重複しない毒性を有する可能性がある。これらのシナリオは臨床現場では互いに区別されない可能性があるため、免疫介在性有害事象は一般に両方の試験薬に起因すると考えられ得、免疫介在性有害事象に応じた用量中断又は処置中止はアテゾリズマブ及びチラゴルマブの両方に適用されるべきである。
Treatment Interruption Study treatment may be temporarily withheld as necessary to manage toxicity. Based on available characterization of mechanism of action, tiragolumab may cause similar but unrelated adverse events to atezolizumab and may exacerbate the frequency or severity of atezolizumab-related adverse events. , or may have toxicities that do not overlap with atezolizumab. Because these scenarios may be indistinguishable from one another in clinical practice, immune-mediated adverse events can generally be attributed to both study drugs, and dose interruptions or treatment discontinuations in response to immune-mediated adverse events are atezolizumab and Should apply to both tiragolumab.
アジュバント設定では、アテゾリズマブ及びチラゴルマブは、最大12週間保持され得る。何らかの理由でチラゴルマブが>12週間中断された場合、患者はチラゴルマブ処置を恒久的に中止しなければならないが、禁忌がなく、毒性がチラゴルマブ及び/又は組み合わせに関連すると考えられるかどうかを判定するための議論の後に、アテゾリズマブを継続することができる。治験責任医師の判断において、患者が>12週間の保留後にチラゴルマブを再開することによって臨床的利益を得る可能性が高い場合、例外を設けることができる。この場合、チラゴルマブを再開してもよい。アテゾリズマブが>12週間中断された場合、患者はアテゾリズマブを恒久的に中止しなければならない。 In the adjuvant setting, atezolizumab and tiragolumab may be maintained for up to 12 weeks. If tiragolumab is discontinued for >12 weeks for any reason, patients must permanently discontinue tiragolumab treatment, but without contraindications, to determine if toxicity is considered related to tiragolumab and/or the combination. After discussion, atezolizumab can be continued. Exceptions can be made if, at the investigator's discretion, the patient is likely to gain clinical benefit from resuming tiragolumab after >12 weeks of hold. In this case, tiragolumab may be restarted. If atezolizumab is discontinued for >12 weeks, patients must permanently discontinue atezolizumab.
しかしながら、治験責任医師の判断において、患者が>12週間の保留後にアテゾリズマブから臨床的利益を得る可能性が高い場合、アテゾリズマブは再開され得る。単剤のアテゾリズマブを患者に継続的に投与するには、他のすべての試験適格基準を満たし続ける必要がある。 However, atezolizumab may be restarted if, at the investigator's discretion, the patient is likely to gain clinical benefit from atezolizumab after >12 weeks of hold. All other study eligibility criteria must continue to be met for patients to continue receiving single-agent atezolizumab.
アテゾリズマブの永続的な中止後の単剤チラゴルマブの継続投与は許可されない。 Continuation of single-agent tiragolumab after permanent discontinuation of atezolizumab is not permitted.
患者が、有害事象を処置するために使用されるステロイドから漸減しなければならない場合、アテゾリズマブ及び/又はチラゴルマブは、最後の投薬から≧12週間を超えて更に長く保留されてもよく、チラゴルマブは、ステロイドが中断されるまで、又はステロイドがプレドニゾン用量(又は用量等価物)≦10mg/日に減らされるまで、最後の投薬から≧12週間を超えて更に長く保留されてもよい。毒性以外の理由(複数可)による用量中断が許容され得る。両方の試験処置を中止した後、患者を安全性及び有効性について監視する。 Atezolizumab and/or tiragolumab may be held longer than >12 weeks from the last dose if the patient must be tapered off steroids used to treat the adverse event, and tiragolumab is It may be held longer than ≧12 weeks from the last dose until the steroid is discontinued or the steroid is reduced to a prednisone dose (or dose equivalent) ≦10 mg/day. Dose interruptions for reason(s) other than toxicity may be tolerated. After discontinuing both study treatments, patients are monitored for safety and efficacy.
C.安全性パラメーター及び定義 C. Safety parameters and definitions
安全性評定は、有害事象(重篤な有害事象及び特に関心のある有害事象を含む)のモニタリング及び記録、治験実施計画書指定の安全性臨床検査評定の実施、治験実施計画書指定のバイタルサインの測定、及び試験の安全性評価にとって重要であると考えられる他の治験実施計画書指定の試験の実施からなる。 Safety assessment includes monitoring and recording of adverse events (including serious adverse events and adverse events of particular interest), conducting protocol-specified safety laboratory evaluations, and protocol-specified vital signs. and other protocol-specified studies considered important to the safety evaluation of the study.
有害事象
臨床試験の実施(Good Clinical Practice)のためのICHガイドラインによれば、有害事象は、原因の属性にかかわらず、医薬品を投与された臨床試験対象における何らかの不都合な医学的事象である。したがって、有害事象は、以下のいずれかであり得る:
●医薬に関連すると考えられるか否かにかかわらず、医薬品の使用に一時的に関連するあらゆる好ましくない意図しない徴候(異常な検査所見を含む)、症候又は疾患
●新規疾患又は既存疾患の増悪(既知の症状の特徴、頻度、又は重症度の悪化)
●ベースラインに存在しない間欠的な医学的症状(例えば、頭痛)の再発
●症候に関連した、又は試験処置若しくは併用治療の変更、又は試験処置からの中止をもたらす、実験値又は他の臨床検査(例えば、ECG、X線)の低下
●治験実施計画書に規定された介入に関連する有害事象、例えば試験処置の割り当て前に発生するもの(例えば、生検等の侵襲的手順のスクリーニング)
Adverse Event According to the ICH Guidelines for Good Clinical Practice, an adverse event is any untoward medical occurrence in a clinical trial subject administered a drug, regardless of the causal attribute. Adverse events can therefore be any of the following:
any unfavorable and unintended signs (including abnormal laboratory findings), symptoms or diseases temporally related to the use of the drug, whether or not considered drug-related, new disease or exacerbation of an existing disease ( exacerbation of known symptom characteristics, frequency, or severity)
• Intermittent recurrence of medical symptoms (e.g., headache) not present at baseline • Laboratory values or other laboratory tests related to symptoms or leading to change in study treatment or concomitant therapy, or discontinuation from study treatment (e.g., ECG, X-ray) Protocol-specified intervention-related adverse events, e.g., occurring prior to study treatment assignment (e.g., screening for invasive procedures such as biopsies)
重篤な有害事象
重篤な有害事象は、以下の基準のいずれかを満たす任意の有害事象である:
●致命的である(すなわち、有害事象が実際に死を引き起こすか、又は死に至る)。
●生命を脅かす(すなわち、有害事象は、治験責任医師の観点から、患者を死亡の即時リスクにさらす)。これには、より重度の形態で発生したか、又は継続された場合、死を引き起こした可能性がある有害事象は含まれない。
●入院患者の入院を必要とするか、又は延長する。
●持続的又は有意な障害/無能力をもたらす(すなわち、有害事象は、正常な生活機能を行う患者の能力の実質的な破壊をもたらす)。
●試験処置に曝露された母親から生まれた新生児/乳児における先天異常/出生時欠損である。
●治験責任医師の判断において重大な医学的事象である(例えば、患者を危険にさらす可能性があり、又は上に列挙した結果のうちの1つを防ぐために医学的/外科的介入を必要とする可能性がある)。
Serious Adverse Event A serious adverse event is any adverse event that meets any of the following criteria:
• Fatal (ie, the adverse event actually causes or leads to death).
• Life-threatening (ie, the adverse event puts the patient at immediate risk of death from the investigator's perspective). This does not include adverse events that may have caused death if they occurred or continued in more severe forms.
• Require or prolong hospitalization of inpatients.
• Result in persistent or significant disability/incapacity (ie, the adverse event results in substantial disruption of the patient's ability to perform normal life functions).
• Congenital anomalies/birth defects in neonates/infants born to mothers exposed to the study treatment.
Is a significant medical event in the investigator's judgment (e.g., may endanger the patient or require medical/surgical intervention to prevent one of the consequences listed above) there's a possibility that).
「重度」及び「重篤」という用語は、同義語ではない。重症度は、有害事象の強度(例えば、軽度、中等度、若しくは重度と評価されるか、又はNCI CTCAEに従って)を指し、事象自体は、比較的医学的に重要でない可能性がある(さらなる所見のない重度の頭痛等)。 The terms "severe" and "serious" are not synonymous. Severity refers to the intensity of the adverse event (e.g., rated as mild, moderate, or severe, or according to the NCI CTCAE) and the event itself may be relatively medically insignificant (further findings severe headache without pain, etc.).
特に注目すべき有害事象
この試験にとって特に注目すべき有害事象は以下の通りである:
●Hyの法則によって定義される、ビリルビン上昇又は臨床的黄疸のいずれかと組み合わせたALT又はAST上昇を含む潜在的な薬物誘発性肝損傷の症例。
●以下に定義される試験処置による感染病原体の伝播の疑い:
Adverse Events of Special Note Adverse events of particular note for this study were:
• Cases of potential drug-induced liver injury, including elevated ALT or AST in combination with either elevated bilirubin or clinical jaundice, as defined by Hy's law.
Suspected transmission of infectious agents by study procedures defined below:
病原性又は非病原性の任意の生物、ウイルス又は感染性粒子(例えば、伝染性海綿状脳症を伝達するプリオンタンパク質)は、感染病原体と考えられる。感染病原体の伝播は、医薬品に曝露された患者における感染を示す臨床症状又は検査所見から疑われ得る。この用語は、試験処置の汚染が疑われる場合にのみ適用される。
●間質性肺炎
●大腸炎
●内分泌不全症:真性糖尿病、膵炎、副腎機能不全、甲状腺機能亢進症、及び下垂体炎。
●AST又はALT>10XULNを含む肝炎。
●全身性エリテマトーデス。
●神経障害:ギラン・バレー症候群、筋無力症症候群又は重症筋無力症、及び髄膜脳炎。
●過敏症、注入関連反応、サイトカイン放出症候群、血球貪食性リンパ組織球増加症、及びマクロファージ活性化症候群を示唆する事象。
●腎炎。
●眼毒性(例えば、ブドウ膜炎、網膜炎、視神経炎)。
●筋炎。
●横紋筋融解症を含むミオパシー。
●グレード≧2の心臓障害(例えば、心房細動、心筋炎、心膜炎)。
●血管炎。
●自己免疫性溶血性貧血。
●重度の皮膚反応(例えば、スティーブンス・ジョンソン症候群、水疱性皮膚炎、中毒性表皮壊死症)。
Any pathogenic or non-pathogenic organism, virus or infectious particle (eg, the prion protein that transmits infectious spongiform encephalopathy) is considered an infectious agent. Transmission of infectious agents can be suspected from clinical symptoms or laboratory findings indicative of infection in patients exposed to the drug. This term applies only when contamination of the study procedure is suspected.
● interstitial pneumonia ● colitis ● endocrine insufficiency: diabetes mellitus, pancreatitis, adrenal insufficiency, hyperthyroidism, and hypophysitis.
- Hepatitis with AST or ALT>10XULN.
● Systemic lupus erythematosus.
• Neuropathy: Guillain-Barré syndrome, myasthenia syndrome or myasthenia gravis, and meningoencephalitis.
• Events suggestive of hypersensitivity, infusion-related reactions, cytokine release syndrome, hemophagocytic lymphohistiocytosis, and macrophage activation syndrome.
- Nephritis.
o ocular toxicity (eg uveitis, retinitis, optic neuritis);
●Myositis.
• Myopathy, including rhabdomyolysis.
• Cardiac disorders of grade ≧2 (eg, atrial fibrillation, myocarditis, pericarditis).
• Vasculitis.
● Autoimmune hemolytic anemia.
• Severe skin reactions (eg Stevens-Johnson syndrome, bullous dermatitis, toxic epidermal necrolysis).
有害事象の重症度の評定
NCI CTCAE(v5.0)の有害事象重症度等級スケールは、有害事象重症度を評定するために使用される。CRSの重症度を報告するときには、NCI CTCAE v5.0に加えて、米国移植細胞療法学会(ASTCT)CRSコンセンサス等級スケールを使用すべきである。
Adverse Event Severity Rating The NCI CTCAE (v5.0) Adverse Event Severity Rating Scale is used to rate adverse event severity. The American Society for Transplantation and Cell Therapy (ASTCT) CRS consensus grading scale should be used in addition to the NCI CTCAE v5.0 when reporting the severity of CRS.
実施例12.GO42501試験の統計的考察及び分析計画
有効性及び安全性分析を、各コホートについて、試験薬物の少なくとも1つの投薬を受けたGO42501試験に登録されたすべての患者で行う。
Example 12. Statistical Considerations and Analytical Plan for the GO42501 Study Efficacy and safety analyzes will be performed in all patients enrolled in the GO42501 study who received at least one dose of study drug for each cohort.
試料サイズの決定
この試験の主要な有効性目的は、病理学的著効答(MPR)率を評価することである。およそ41人の患者が試験の各コホートに登録される。観測されたMPR率を61%と仮定すると、この試料サイズは、両側95%CIの下限が46%を超える各コホートにおけるMPR率の点推定のための十分な精度を提供し、この比率は、この設定における併用療法のさらなる調査を正当化し得る。
Determination of sample size The primary efficacy objective of this study is to assess the significant pathological response (MPR) rate. Approximately 41 patients will be enrolled in each cohort of the trial. Assuming an observed MPR rate of 61%, this sample size provides sufficient precision for point estimates of the MPR rate in each cohort with a lower bound of 46% for the two-sided 95% CI, and this ratio is Further investigation of combination therapy in this setting may be warranted.
試験実施の概要
試験に参加する、試験を中止する、又は試験を完了する患者の数を要約する。早期試験中止の理由を列挙し、要約する。各処置コホートについて、登録及び主要な治験実施計画書の逸脱を列挙する。
Summary of study conduct Summarize the number of patients entering, withdrawing from, or completing the study. List and summarize reasons for early study termination. Enrollment and major protocol deviations are listed for each treatment cohort.
A.人口統計学的特性及びベースライン特性を要約する。
年齢及び人種等の人口統計情報を集計を集計する。連続パラメーターの平均、標準偏差、及び範囲、並びにカテゴリパラメータのパーセンテージ及び頻度を含む記述統計が提示される。全体集団及び各処置コホートについて要約を提示する。ベースライン測定値は、特に明記しない限り、患者が試験薬の任意の成分の最初の用量を受ける前に得られた最後の利用可能なデータである。
A. Summarize demographic and baseline characteristics.
Aggregate demographic information such as age and race. Descriptive statistics including mean, standard deviation, and range for continuous parameters and percentages and frequencies for categorical parameters are presented. Summaries are presented for the overall population and each treatment cohort. Baseline measurements are the last available data obtained before the patient received their first dose of any component of study drug, unless otherwise stated.
B.安全性分析 B. Safety analysis
各コホートについて、安全性分析は、少なくとも1用量の試験処置を受けるすべての登録患者を含む。 For each cohort, safety analyzes include all enrolled patients who receive at least one dose of study treatment.
治療期間、投薬量及び用量強度を含む試験処置曝露を要約する。 Summarize study treatment exposure, including duration of treatment, dosage and dose intensity.
試験処置治に関連する外科的遅延の発生率及び長さ、手術及び術後合併症の発生率、及び/又は外科的キャンセルの数を、各コホートについて評価する。 The incidence and length of surgical delays associated with study treatment, the incidence of surgical and postoperative complications, and/or the number of surgical cancellations will be assessed for each cohort.
有害事象の言語記述は、MedDRAシソーラス用語にマッピングされる。全ての有害事象の重症度は、NCI CTCAE v5.0に従って治験責任医師によって等級付けされ、CRSの重症度も、ASTCTコンセンサス等級スケールに従って治験責任医師によって等級付けされる。これらの要約は、処置群によって提示される。全ての有害事象を処置群及びNCI CTCAEグレードによって要約する。また、CRSを、処置群及びASTCTコンセンサスグレードによって要約する。更に、試験処置の離脱につながる、用量の減少又は中断につながる、試験処置に関連する処置下で発現した有害事象、重度の(すなわち、グレード≧3の有害事象)、致死的有害事象(すなわち、グレード5)、及び重篤な有害事象、並びに特に興味深い有害事象も要約する。同じ事象の複数の発生は、最大重症度で1回カウントする。正常範囲外の値を有する実験データが特定される。更に、ADA結果を含む選択された実験データ、及びバイタルサインの変化を処置アームによって要約する。死亡及び死亡原因を要約する。 Verbal descriptions of adverse events are mapped to MedDRA thesaurus terms. The severity of all adverse events will be graded by the investigator according to the NCI CTCAE v5.0, and the severity of CRS will also be graded by the investigator according to the ASTCT consensus grading scale. These summaries are presented by treatment group. All adverse events will be summarized by treatment group and NCI CTCAE grade. CRS is also summarized by treatment group and ASTCT consensus grade. In addition, treatment-emergent adverse events related to study treatment, severe (i.e., grade ≥ 3 adverse events), fatal adverse events (i.e., Grade 5), and serious adverse events and adverse events of particular interest are also summarized. Multiple occurrences of the same event are counted once at maximum severity. Experimental data with values outside the normal range are identified. In addition, selected experimental data, including ADA results, and changes in vital signs are summarized by treatment arm. Summarize deaths and causes of death.
C.有効性分析 C. Effectiveness analysis
有効性分析集団は、少なくとも1用量の試験処置を受けたすべての登録患者を含む。 The efficacy analysis population includes all enrolled patients who received at least one dose of study treatment.
主要有効性評価項目
MPR率は、MPRを達成した患者の割合として定義され、有効性分析集団の各処置コホートについて推定される。MPRは、中央病理検査室によって評定されるように、原発腫瘍における外科的摘出時の≦10%残存生存腫瘍として定義される。手術に進まない患者は、MPRに対するノンレスポンダーとみなされる。Clopper-Pearson法を用いて算出したMPR率の両側95% CIを報告する。
Primary Efficacy Endpoints MPR rate, defined as the proportion of patients achieving MPR, is estimated for each treatment cohort in the efficacy analysis population. MPR is defined as ≤10% residual viable tumor at surgical excision in the primary tumor, as assessed by the Central Pathology Laboratory. Patients who do not proceed to surgery are considered non-responders to MPR. Two-sided 95% CIs for MPR rates calculated using the Clopper-Pearson method are reported.
副次的有効性評価項目
病理学的完全奏効(pCR)率は、pCRを達成した患者の割合として定義される。pCRは、中央病理検査室によって評定されるように、外科的摘出時に生存可能な原発腫瘍が存在しないこととして定義される。pCR率は、有効性分析集団についての各処置コホートについてのMPR率と同じ統計学的方法を用いて分析される。
Secondary Efficacy Endpoints Pathologic complete response (pCR) rate is defined as the proportion of patients achieving pCR. pCR is defined as the absence of a viable primary tumor at the time of surgical excision, as assessed by a central pathology laboratory. pCR rates are analyzed using the same statistical methods as MPR rates for each treatment cohort for the efficacy analysis population.
無症候生存期間(EFS)は、試験薬の初回投与から、次のいずれかの事象が最初に起こる(いずれか早く発生する方)までの時間と定義される:RECIST v 1.1に従って治験責任医師によって評定された手術を妨げる疾患進行;局所再発又は遠隔疾患再発(新たな原発性NSCLCの発生を含む);又は何らかの原因による死亡。手術、局所若しくは遠隔疾患再発を妨げる疾患進行を経験していないか、又は分析時に死亡した患者は、最後の腫瘍又は疾患のフォローアップ評定の再に打ち切られる。ベースライン後の腫瘍評定がない患者は、試験薬物の最初の用量の日付で打ち切られる。EFSは、有効性分析集団の各処置コホートについてKaplan-Meier法を用いて評価する。 Symptom-free survival (EFS) is defined as the time from the first dose of study drug to the first occurrence (whichever occurs first) of any of the following: Investigator according to RECIST v 1.1 Physician-assessed disease progression precluding surgery; local or distant disease recurrence (including new primary NSCLC development); or death from any cause. Patients who have not experienced disease progression precluding surgery, local or distant disease recurrence, or who die at the time of analysis will be censored at the last tumor or disease follow-up assessment. Patients with no post-baseline tumor assessment will be censored on the date of the first dose of study drug. EFS will be assessed using the Kaplan-Meier method for each treatment cohort in the efficacy analysis population.
D.薬物動態分析 D. Pharmacokinetic analysis
PK分析のために試料を収集し、この試験における曝露を以前の試験で得られた曝露と比較する。チアテゾリズマブ及びチラゴルマブの血清濃度は、個々の値として報告され、適切な場合及びデータが許す場合、コホート及びサイクルによって要約される(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)。 Samples are collected for PK analysis and exposures in this study are compared to exposures obtained in previous studies. Serum concentrations of tiatezolizumab and tiragolumab are reported as individual values and summarized by cohort and cycle where appropriate and data permit (mean, standard deviation, coefficient of variation, median, range, geometric mean and geometric mean). mean coefficient of variation).
アテゾリズマブ及びチラゴルマブの個々の血清濃度及び血清中濃度の中央値をコホート及び日ごとにプロットする。アテゾリズマブ及びチラゴルマブの濃度データを、確立された集団PKモデルを使用して他の試験からのデータと共にプールして、データによって保証されるクリアランス、分布容積及びAUC等のPKパラメーターを導出することができる。関連するPKパラメーターと安全性、有効性又はバイオマーカーの結果との潜在的な相関関係を調べることができる。 Individual serum and median serum concentrations of atezolizumab and tiragolumab are plotted by cohort and day. Atezolizumab and tiragolumab concentration data can be pooled with data from other studies using established population PK models to derive data-assured PK parameters such as clearance, volume of distribution and AUC. . Potential correlations between relevant PK parameters and safety, efficacy or biomarker outcomes can be examined.
E.免疫原性分析 E. Immunogenicity analysis
免疫原性分析には、任意の抗薬物抗体(ADA)評定を受けた患者が含まれ、受けた処置に従って患者がグループ分けされる。アテゾリズマブ及びチラゴルマブの両方についての処置下で発現したADA陽性患者及びADA陰性患者の数及び割合をコホートによって要約する。ADAの状態と安全性、有効性及びPK評価項目との間の関係は、記述統計学によって分析及び報告され得る。 Immunogenicity analyzes include patients who have received any anti-drug antibody (ADA) assessment and group patients according to the treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients for both atezolizumab and tiragolumab are summarized by cohort. Relationships between ADA status and safety, efficacy and PK endpoints can be analyzed and reported by descriptive statistics.
F.バイオマーカー分析 F. Biomarker analysis
探索的バイオマーカー分析は、これらの患者におけるがんの複数の病理学的、免疫学的、及びゲノム特性と臨床成績との間の関係を調べるために行われる。これらの分析には、腫瘍微小環境及び/又は末梢における免疫細胞及びctDNAの特性評価が含まれるが、これらに限定されない。MPR、pCR、及びEFSを含む臨床的有効性転帰は、実施可能であれば処置利益を評価するためにバイオマーカーサブグループ(例えば、PD-L1及びTIGITの状態に基づく)で分析される。 Exploratory biomarker analyzes are conducted to investigate the relationship between multiple pathological, immunological, and genomic characteristics of cancer and clinical outcome in these patients. These analyzes include, but are not limited to, characterization of immune cells and ctDNA in the tumor microenvironment and/or periphery. Clinical efficacy outcomes, including MPR, pCR, and EFS, will be analyzed in biomarker subgroups (eg, based on PD-L1 and TIGIT status) to assess treatment benefit, if feasible.
実施例13.子宮頸がん患者におけるPD-1軸結合アンタゴニストと組み合わせた抗TIGITアンタゴニスト抗体の有効性
少なくとも1つの白金系であるが2回以下の事前全身治療からの進行又は再発後の転移性及び/又は再発性PD-L1-陽性(腫瘍細胞及び腫瘍関連免疫細胞[TIC]≧5%)子宮頸がんを有する患者における、PD-1軸結合アンタゴニスト(例えば、抗PD-L1アンタゴニスト抗体(例えば、アテゾリズマブ))と組み合わせた抗TIGITアンタゴニスト抗体(例えば、本明細書中に開示される抗TIGIT抗体、例えば、チラゴルマブ)による処置、及びアテゾリズマブ単剤療法の有効性及び安全性を評価する。適格であるためには、患者は、0又は1の米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス及び転移性及び/又は再発性PD-L1陽性子宮頸がんを有していなければならない。
Example 13. Efficacy of Anti-TIGIT Antagonist Antibodies in Combination with PD-1 Axis Binding Antagonists in Patients With Cervical Cancer Metastatic and/or relapse after progression or relapse from at least one platinum-based but no more than two prior systemic treatments PD-1 axis binding antagonists (e.g., anti-PD-L1 antagonist antibodies (e.g., atezolizumab) in patients with cervical cancer that are PD-L1-positive (tumor cells and tumor-associated immune cells [TIC] >5%) to assess the efficacy and safety of treatment with an anti-TIGIT antagonist antibody (eg, an anti-TIGIT antibody disclosed herein, eg, tiragolumab) in combination with ) and atezolizumab monotherapy. To be eligible, patients must have an East Coast Cancer Trials Group (ECOG) performance status of 0 or 1 and metastatic and/or recurrent PD-L1 positive cervical cancer .
臨床試験は、以下に詳細に記載され、図21に示されるように、単相からなる。 The clinical trial consisted of a single phase, as described in detail below and shown in FIG.
ランダム化
この試験では、約160人の患者が登録され、アテゾリズマブ又はアテゾリズマブ単剤療法と組み合わせたチラゴルマブの2つの処置群のうちの一方に割り当てられる。ランダム化は、各処置群へのバランスのとれた割り当てを確実にするために、順列ブロックランダム化法を使用することによって3:1の比で行われる。ランダム化は、ECOGパフォーマンスステータス(0対1)、化学放射線療法又は放射線療法の以前の使用(あり対なし)、及び処置歴(持続性対再発性疾患)に従って層別化される。
Randomization In this trial, approximately 160 patients will be enrolled and assigned to one of two treatment arms of atezolizumab or tiragolumab in combination with atezolizumab monotherapy. Randomization is performed in a 3:1 ratio by using a permuted block randomization method to ensure balanced allocation to each treatment group. Randomization is stratified according to ECOG performance status (0 vs. 1), previous use of chemoradiation or radiotherapy (yes vs. no), and treatment history (persistent vs. recurrent disease).
適格性
この試験には、以下の参加基準に従って最低年齢18歳の女性患者が登録されている:
-全身化学療法、手術及び/又は放射線療法による治癒的処置に適していない1~2種類の事前全身化学療法後の子宮頸部(神経内分泌組織、明細胞組織及び肉腫組織は許容されない)の組織学的に確認された再発性又は持続性扁平上皮癌腫、腺扁平上皮癌腫、又は腺癌。
-先行する少なくとも1種類の白金系全身化学療法-放射線療法と共に投与されるシスプラチンの放射線増感は、全身化学療法のラインとは見なされない。
-放射線測定可能な疾患
-0又は1の、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス
-試験分析用の子宮頸がん組織(保管又は新鮮生検検体)
-少なくとも12週間の平均余命
-適切な血液学的及び臓器機能
-妊娠可能な女性は、適切な避妊を遵守する意思がなければならない
Eligibility This study enrolls female patients with a minimum age of 18 years according to the following entry criteria:
- Tissues of the cervix (neuroendocrine, clear cell and sarcoma tissues are not allowed) after 1-2 prior systemic chemotherapy not amenable to curative treatment with systemic chemotherapy, surgery and/or radiotherapy Clinically confirmed recurrent or persistent squamous cell carcinoma, adenosquamous carcinoma, or adenocarcinoma.
- At least one prior platinum-based systemic chemotherapy - Cisplatin radiosensitization administered with radiotherapy is not considered a line of systemic chemotherapy.
- radiomeasurable disease - East Coast Cancer Trials Group (ECOG) performance status of 0 or 1 - cervical cancer tissue for study analysis (archived or fresh biopsy specimen)
- Life expectancy of at least 12 weeks - Adequate hematologic and organ function - Women of childbearing potential must be willing to adhere to adequate contraception
患者は、以下の基準に基づいて登録から除外される:
-ランダム化前28日以内及び試験処置中の治療目的の治験療法による処置
-任意の中枢神経系(CNS)又は脳の転移
-自己免疫疾患又は免疫不全の活動性又は病歴
-活動性結核
-既知の臨床上重要な肝疾患
-ランダム化時の治験責任医師判断による重症感染
-CD 137アゴニスト又は免疫チェックポイント遮断療法、抗CTLA-4、抗TIGIT、抗PD-1及び抗PD-L1治療抗体による事前の処置
-ランダム化前の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫賦活剤による処置
-ランダム化前の1週間以内の全身免疫抑制薬による処置、又は試験中の全身免疫抑制薬の必要性の予測
-妊娠中又は授乳中の女性。
-チラゴルマブ又はアテゾリズマブ製剤の任意の成分に対する既知の過敏症
Patients are excluded from enrollment based on the following criteria:
- Treatment with a therapeutic investigational therapy within 28 days prior to randomization and during study treatment - Any central nervous system (CNS) or brain metastasis - Active or history of autoimmune disease or immunodeficiency - Active tuberculosis - Known of clinically significant liver disease - Investigator-determined severe infection at randomization - CD 137 agonist or immune checkpoint blockade therapy, anti-CTLA-4, anti-TIGIT, anti-PD-1 and anti-PD-L1 therapeutic antibodies Prior treatment - Treatment with systemic immunostimulants within 4 weeks or 5 drug elimination half-lives (whichever is longer) prior to randomization - Treatment with systemic immunosuppressants within 1 week prior to randomization, or study Prediction of need for systemic immunosuppressants during pregnancy - women who are pregnant or breastfeeding.
- Known hypersensitivity to any component of the tiragolumab or atezolizumab formulations
A.試験処置投薬量及び投与
処置中、患者は、固定用量の1200mgのアテゾリズマブ若しくは固定用量の1200mgのアテゾリズマブ及び固定用量の600mgのチラゴルマブを受ける。アテゾリズマブは、1200mg Q3Wの固定用量(各21日間サイクルの1日目に1200mg)で投与される。アテゾリズマブと組み合わせたチラゴルマブは、600mg IV Q3Wの固定用量で各21日間サイクルの1日目に実験群の全患者に投与される。
A. Study Treatment Dosage and Administration During treatment, patients receive a fixed dose of 1200 mg atezolizumab or a fixed dose of 1200 mg atezolizumab and a fixed dose of 600 mg tiragolumab. Atezolizumab will be administered at a fixed dose of 1200 mg Q3W (1200 mg on
別の試験では、投与日に、アテゾリズマブは、表59に概説されている指示に従って単剤療法として投与される。最初の注入の前に、注入を開始する60分以内に患者のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録する。アテゾリズマブの最初の注入は60(±15)分かけて投与され、その間、患者のバイタルサインは注入中15(±5)分毎に、そして注入後30(±10)分に記録される。最初の注入中に注入関連有害事象が経験されない場合、その後の注入は30(±10)分かけて投与することができる。バイタルサインの注入前記録は、アテゾリズマブの注入開始前60分以内に記録し続けるものとする。

別の試験では、投与日に、アテゾリズマブは、表60に概説されている指示に従ってチラゴルマブの前に投与される。最初の注入の前に、注入を開始する60分以内に患者のバイタルサイン(例えば、脈拍数、呼吸数、血圧、及び体温)を記録する。アテゾリズマブの最初の注入は60(±15)分かけて投与され、その間、患者のバイタルサインは注入中15(±5)分毎に、そして注入後30(±10)分に記録される。抗TIGIT抗体(例えば、本明細書中に開示される抗TIGIT抗体、例えば、チラゴルマブ)の初回注入は、60(±10)分かけて投与され、その間、患者のバイタルサインは、注入中15(±5)分ごと及び注入後30(±10)分に記録される。最初の注入中に注入関連有害事象が経験されない場合、その後の注入は30(±10)分かけて投与することができる。バイタルサインの注入前記録は、アテゾリズマブの注入開始前60分以内に記録し続けるものとする。 In another study, on dosing days, atezolizumab is administered prior to tiragolumab according to the instructions outlined in Table 60. Prior to the first infusion, the patient's vital signs (eg, pulse rate, respiration rate, blood pressure, and temperature) are recorded within 60 minutes of starting the infusion. The first infusion of atezolizumab is administered over 60 (±15) minutes, during which patient vital signs are recorded every 15 (±5) minutes during the infusion and 30 (±10) minutes after the infusion. The first infusion of an anti-TIGIT antibody (e.g., an anti-TIGIT antibody disclosed herein, e.g., tiragolumab) is administered over 60 (±10) minutes, during which the patient's vital signs are 15 ( Recorded every ±5) minutes and 30 (±10) minutes after injection. Subsequent infusions can be administered over 30 (±10) minutes if no infusion-related adverse events are experienced during the first infusion. Pre-infusion recording of vital signs shall be maintained within 60 minutes prior to initiation of atezolizumab infusion.
処置は、X線写真データ、生検結果、及び臨床状態の統合評定後に疾患進行に起因する許容できない毒性又は症候性悪化がない場合、臨床的利益を患者が経験している限り継続され得る。独立審査委員会(IRC)により決定されたRECIST v1.1による明確でない疾患進行の基準を満たす患者は、指定された基準のすべてを満たす場合、処置(アテゾリズマブ若しくはアテゾリズマブ単独と組み合わせたチラゴルマブ)を継続することが許可される。


B.併用療法
特定の併用療法が許容される。併用療法には、試験処置の開始の7日前から処置中止の来院までの治験実施計画書が定めた試験処置に加えて、患者が使用した任意の薬物(例えば、経口避妊薬、ホルモン補充療法、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)が含まれる。患者は、試験中に以下の併用療法を使用することが許される。
B. Concomitant Therapies Certain combination therapies are permissible. Concomitant therapy includes protocol-defined study treatment from 7 days prior to the start of study treatment until the discontinuation visit, plus any medications the patient has used (e.g., oral contraceptives, hormone replacement therapy, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, dietary supplements). Patients are allowed to use the following concomitant therapies during the study.
全身性コルチコステロイド及びTNF-α阻害剤は、アテゾリズマブによる処置の潜在的に有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物を検討しなければならない。代替法が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。 Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines must be considered. If alternatives are not feasible, systemic corticosteroids and TNF-α inhibitors can be administered at the investigator's discretion.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降の試験処置注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent study treatment infusions, at the discretion of the Investigator.
C.有効性の評価項目
アテゾリズマブ単独療法と比較したアテゾリズマブと組み合わせたチラゴルマブの有効性を評価するため、4週間以上離れた2回の連続した機会(RECIST v 1.1に従って治験責任医師が決定)に完全奏効(CR)又は部分奏効(PR)を経験した患者の割合として定義されるORRを伴う客観的奏効率(ORR)を主要評価項目として測定する。主要な有効性分析は、すべての患者が登録され、ORR評定のフォローアップを継続している患者の中で約6ヶ月の最小限のフォローアップが達成された後に行われる。一次分析では、ORR評定が欠落していた患者は、応答を達成していないとカウントされる。比率についての1サンプルz検定を使用して、アテゾリズマブ群と組み合わせたチラゴルマブのORRを歴史的参照と比較する。ORR及びその95%CI(Clopper-Pearson;Clopper and Pearson 1934)の推定値を各処置群について計算する。併用群おけるORRの95%CIの下端(表61)及び単剤療法群における観察されたORR(表62)は、基準点を除外すべきであると予想される。


この試験の副次的有効性目的は、奏効期間(DOR)、病勢制御率(DCR)、最良臨床応答(BCR)、無増悪生存期間(PFS)及び全生存期間(OS)に基づいて、アテゾリズマブと組み合わせたチラゴルマブ及びアテゾリズマブ単剤療法の有効性を評価することである。DORは、RECIST v1.1に従ってIRCによって判定される場合、客観的奏効を有していた患者については、文書化された客観的奏効(CR又はPR)の最初の発生から疾患進行の日又は何らかの原因による死亡の日(いずれか早く発生する方)までの時間として定義される。DCRは、RECIST v1.1に従ってIRCによって決定されるCR、PR又はSDを有する患者の割合として定義される。BCRは、治験責任医師が決定したCR、PR又はSDを有する患者の割合として定義される。PFSは、RECIST v1.1に従ってIRCによって決定される場合、ランダム化から疾患進行又は何らかの原因による死の最初の発生(いずれか早く発生する方)までの時間として定義される。OSは、ランダム化から何らかの原因による死亡までの時間として定義される。 The secondary efficacy objectives of this study were based on duration of response (DOR), disease control rate (DCR), best clinical response (BCR), progression-free survival (PFS), and overall survival (OS). To evaluate the efficacy of tiragolumab and atezolizumab monotherapy in combination with DOR is the date of disease progression from the first occurrence of a documented objective response (CR or PR) or any Defined as the time to date of death from cause (whichever occurs first). DCR is defined as the proportion of patients with CR, PR or SD as determined by IRC according to RECIST v1.1. BCR is defined as the proportion of patients with an investigator-determined CR, PR or SD. PFS is defined as the time from randomization to first occurrence of disease progression or death from any cause (whichever occurs first) as determined by IRC according to RECIST v1.1. OS is defined as the time from randomization to death from any cause.
さらなる探索的有効性評価項目には、RECIST v1.1に従って治験責任医師が決定した病勢制御(≧6週間にわたるSD又はCR又はPRとして定義される)が更に含まれ得る。 Additional exploratory efficacy endpoints may further include investigator-determined disease control (defined as SD or CR or PR over ≧6 weeks) according to RECIST v1.1.
アテゾリズマブ単独療法と比較したアテゾリズマブと組み合わせたチラゴルマブの安全性及び忍容性を評価するために、有害事象(AE)(例えば、国立がん研究所有害事象共通用語規準(National Cancer Institute Common Terminology Criteria for Adverse Events)バージョン5.0(NCI CTCAE v 5.0)に従って等級付けされるAE)の発生率、性質及び重症度を測定する(NCI CTCAEに具体的に列挙されていない有害事象を表63に従って測定する)。サイトカイン放出症候群(CRS)の重症度もまた、米国移植細胞療法学会CRSコンセンサス等級スケールに従って決定される。更に、アテゾリズマブ単独療法と比較して、アテゾリズマブと組み合わせたチラゴルマブの投与中及び投与後のベースラインからのバイタルサイン、身体所見、及び臨床検査結果の臨床上有意な変化も測定される。

主要評価項目の尺度である客観的奏効率(ORR)の時間枠は、文書化された客観的奏効から疾患の進行又は何らかの原因による死亡(いずれか早く発生する方)の日付まで(最大36ヶ月)となる。副次的結果の測定の時間枠を表64に示す。

D.バイオマーカー
保管腫瘍組織を含む患者試料、並びに血清、血漿、全血及び便を、ランダム化試験における全ての患者の探索的バイオマーカー評定のために収集する。PD-L1状態の評定に加えて、チラゴルマブ及び/又はアテゾリズマブの耐性、疾患進行、及び臨床的利益に関連するバイオマーカーを分析する。例えば、チラゴルマブ及び/又はアテゾリズマブの臨床的利益及び安全性に関連する潜在的な予測及び予後バイオマーカーが分析される。
D. Biomarkers Patient samples, including archived tumor tissue, as well as serum, plasma, whole blood and stool, will be collected for exploratory biomarker assessment of all patients in the randomized trial. In addition to assessment of PD-L1 status, biomarkers associated with tiragolumab and/or atezolizumab resistance, disease progression, and clinical benefit will be analyzed. For example, potential predictive and prognostic biomarkers associated with clinical benefit and safety of tiragolumab and/or atezolizumab are analyzed.
ベースラインで収集された腫瘍組織及び血液試料(治験責任医師が臨床上実施可能と判断した場合は、疾患進行時に採取した腫瘍組織)は、全エクソームシーケンシング(WES)及び/又は次世代シーケンシング(NGS)を可能にして、試験処置に対する応答を予測する、より重篤な疾患状態への進行に関連する、試験処置に対する獲得耐性に関連する、有害事象の発生に対する感受性に関連する、又は疾患生物学の知識及び理解を高めることができる体細胞変異を同定する。 Tumor tissue and blood samples collected at baseline (or tumor tissue collected at disease progression, if deemed clinically feasible by the investigator) will be subjected to whole exome sequencing (WES) and/or next-generation sequencing. predicts response to a study treatment, is associated with progression to a more severe disease state, is associated with acquired resistance to a study treatment, is associated with susceptibility to the occurrence of adverse events, or Identify somatic mutations that can enhance our knowledge and understanding of disease biology.
バイオマーカーには、限定されないが、腫瘍組織上のPD-L1及び/又はTIGIT発現、WGS及び/又はNGSによって同定された、腫瘍組織及び/又は血液中の循環腫瘍DNA(限定されないが、突然変異負荷、MSI及びMMR欠陥を含む)からの生殖系列及び体細胞変異、腫瘍免疫生物学に関連する遺伝子(例えば、CD274)又は遺伝子シグネチャの分析、例えば、Tエフェクター遺伝子、PD-L1、TIGIT、HPV変化、リンパ球亜集団、T細胞受容体レパートリー、T細胞及びNK細胞活性化に関連するサイトカイン、並びに血漿由来サイトカインが含まれる。 Biomarkers include, but are not limited to, PD-L1 and/or TIGIT expression on tumor tissue, circulating tumor DNA in tumor tissue and/or blood identified by WGS and/or NGS (including but not limited to mutations). Germline and somatic mutations (including burden, MSI and MMR defects), analyzes of genes (e.g. CD274) or gene signatures associated with tumor immunobiology, e.g. T effector genes, PD-L1, TIGIT, HPV Included are alterations, lymphocyte subpopulations, T cell receptor repertoire, cytokines associated with T cell and NK cell activation, and plasma-derived cytokines.
一次患者集団におけるORR、PFS、DOR、及び/又はOSに対するPD-L1/PD-1経路の効果を評定するために、有効性、安全性、PK、免疫原性、及び患者報告の転帰(PRO)に対する、タンパク質、RNA、DNA、腫瘍変異負荷量、及び腫瘍組織及び/又は血液中の他の探索的バイオマーカーの間の関係を評価することができる。更に、一次集団におけるORR、PFS、DOR及び/又はOSに対するTIGIT経路の効果を評定するために、ORR、DOR、PFS及びOSを、腫瘍がタンパク質及び/又はRNA発現によって定義されるTIGIT発現を有する患者集団において評価することができる。 To assess the effects of the PD-L1/PD-1 pathway on ORR, PFS, DOR, and/or OS in primary patient populations, efficacy, safety, PK, immunogenicity, and patient-reported outcomes (PRO ) can be assessed between protein, RNA, DNA, tumor mutational burden, and other exploratory biomarkers in tumor tissue and/or blood. In addition, to assess the effect of the TIGIT pathway on ORR, PFS, DOR and/or OS in primary populations, ORR, DOR, PFS and OS were measured using tumors with TIGIT expression defined by protein and/or RNA expression. It can be evaluated in a patient population.
探索的バイオマーカー分析は、これらのマーカー(例えば、TIGIT IHC状態)と試験処置の有効性との関連を理解しようとして行われ得る。有効性転帰は、IHC及び/又はRNA分析によって決定される、腫瘍が高いTIGIT発現を有する患者の集団において調査され得る。WGSデータの探索的分析は、この試験の文脈で実施され、疾患病理生物学の研究者の理解を高め、新しい治療アプローチの開発を導くために、他の試験からのデータとまとめて調査され得る。 Exploratory biomarker analyzes can be performed in an attempt to understand the association between these markers (eg, TIGIT IHC status) and efficacy of study treatments. Efficacy outcomes can be investigated in a population of patients whose tumors have high TIGIT expression as determined by IHC and/or RNA analysis. Exploratory analysis of WGS data will be conducted in the context of this trial and can be explored together with data from other trials to enhance researchers' understanding of disease pathobiology and guide the development of new therapeutic approaches. .
E.免疫原性分析
チラゴルマブ及びアテゾリズマブに対する免疫応答を評定するために、処置下で発現した抗薬物抗体(ADA)の発生率、並びに安全性、有効性及び薬物動態(PK)に対するそれらの潜在的影響を評価する。
E. Immunogenicity Analysis To assess immune responses to tiragolumab and atezolizumab, the incidence of treatment-developed anti-drug antibodies (ADAs) and their potential impact on safety, efficacy and pharmacokinetics (PK) was evaluated. evaluate.
GO30103試験の第Ia相部分の2019年12月時点では、チラゴルマブに対する処置下で発現した抗薬物抗体(ADA)は検出されなかった。GO30103試験の第Ib相部分では、評価可能な154人中3人(1.9%)の患者が、チラゴルマブに対する処置下で発現したADAについて陽性であった。GO40290試験の2019年10月時点で、評価した66人中1人(1.5%)の患者が、チラゴルマブに対する処置下で緊急のADAについて陽性であった。GO40290試験の2019年10月時点で、評価した66人中1人(1.5%)の患者が、チラゴルマブに対する処置下で発現したADAについて陽性であり、患者は一時点でのみ陽性であった。 As of December 2019 in the Phase Ia portion of the GO30103 study, no treatment-developed anti-drug antibodies (ADA) to tiragolumab were detected. In the Phase Ib portion of the GO30103 trial, 3 of 154 (1.9%) evaluable patients were positive for treatment-emergent ADAs for tiragolumab. As of October 2019 in the GO40290 study, 1 of 66 (1.5%) patients evaluated were positive for emergent ADA on treatment for tiragolumab. As of October 2019 in the GO40290 study, 1 of 66 (1.5%) patients evaluated were positive for treatment-emergent ADAs for tiragolumab, and patients were positive at only one time point .
F.薬物動態学的分析
アテゾリズマブと組み合わせて投与した場合のチラゴルマブの薬物動態を特性評価するために、異なる時点で対象からチラゴルマブの血清濃度を決定する。更に、アテゾリズマブがチラゴルマブと組み合わせて又は単剤療法として投与された場合のアテゾリズマブの薬物動態を特性評価するために、アテゾリズマブの血漿濃度を試験中の異なる時点で対象から得る。
F. Pharmacokinetic Analysis To characterize the pharmacokinetics of tiragolumab when administered in combination with atezolizumab, serum concentrations of tiragolumab are determined from subjects at different time points. Additionally, plasma concentrations of atezolizumab are obtained from subjects at different time points during the study to characterize the pharmacokinetics of atezolizumab when atezolizumab is administered in combination with tiragolumab or as monotherapy.
実施例14.トリプルネガティブ乳がんを有する患者におけるアテゾリズマブ及び化学療法と組み合わせたチラゴルマブの安全性、有効性、及び薬物動態の第Ib相非盲検多施設試験
本実施例は、初期トリプルネガティブ乳がん(eTNBC)患者におけるアテゾリズマブ及び化学療法と組み合わせたチラゴルマブの安全性、有効性及び薬物動態を評価するように設計された第Ib相非盲検多施設試験を記載する。この試験は、以下のコホートからなる:
●コホートBは、手術に適格な臨床上評定エされたT2-4d TNBCの患者(PD-L1 all-commr集団)を登録する。患者を以下の2つの処置群の1つに1:1の比でランダム化する。
-A群:アテゾリズマブ、nab-パクリタキセル、及びカルボプラチンと組み合わせたチラゴルマブ、続いてアテゾリズマブ、ドキソルビシン、及びシクロホスファミドと組み合わせたチラゴルマブ(チラゴルマブ及びアテゾリズマブ+nab-pac-carbo-ACと呼ばれる)
-B群:アテゾリズマブ、nab-パクリタキセルと組み合わせたチラゴルマブ、続いてアテゾリズマブ、ドキソルビシン、及びシクロホスファミドと組み合わせたチラゴルマブ(チラゴルマブ及びアテゾリズマブ+nab-pac-ACと呼ばれる)
Example 14. Phase 1b, open-label, multicenter study of the safety, efficacy, and pharmacokinetics of atezolizumab and tiragolumab in combination with chemotherapy in patients with triple-negative breast cancer. A Phase Ib, open-label, multi-center study designed to evaluate the safety, efficacy and pharmacokinetics of tiragolumab in combination with chemotherapy is described. This trial will consist of the following cohorts:
• Cohort B enrolls patients with clinically assessed T2-4d TNBC who are eligible for surgery (PD-L1 all-commr population). Patients are randomized in a 1:1 ratio to one of the following two treatment groups.
- Group A: tiragolumab in combination with atezolizumab, nab-paclitaxel, and carboplatin, followed by tiragolumab in combination with atezolizumab, doxorubicin, and cyclophosphamide (termed tiragolumab and atezolizumab + nab-pac-carbo-AC)
- Arm B: atezolizumab, tiragolumab in combination with nab-paclitaxel, followed by atezolizumab, doxorubicin, and tiragolumab in combination with cyclophosphamide (termed tiragolumab and atezolizumab + nab-pac-AC)
更に、AC及びG-CSF(例えば、フィルグラスチム又はペグフィルグラスチム)又はGM-CSFを、nab-パクリタキセル後のバックグラウンド処置としてコホートBの患者に投与する。 In addition, AC and G-CSF (eg, filgrastim or pegfilgrastim) or GM-CSF are administered to patients in Cohort B as background treatment after nab-paclitaxel.
この試験は、最初に臨床上評定されたT2-4d TNBCを用いて手術に適格な患者における、アテゾリズマブ、nab-パクリタキセル及びカルボプラチンと組み合わせたネオアジュバントであるチラゴルマブ、続いてアテゾリズマブ、nab-パクリタキセルと組み合わせたAC又はネオアジュバントであるチラゴルマブ、続いてACの安全性及び忍容性、予備的有効性、並びに薬物動態の評定を可能にするように設計されている。 This study initially evaluated the neoadjuvant tiragolumab in combination with atezolizumab, nab-paclitaxel, and carboplatin, followed by atezolizumab, in combination with nab-paclitaxel, in patients eligible for surgery with clinically assessed T2-4d TNBC. It is designed to allow assessment of the safety and tolerability, preliminary efficacy, and pharmacokinetics of AC or the neoadjuvant tiragolumab followed by AC.
A.試験計画
この第Ib相多施設非盲検多施設世界的試験は、最初に臨床上評定されたT2-4d TNBC(PD-L1 all comer集団)で手術に適格な患者における、アテゾリズマブ、nab-パクリタキセル、及びカルボプラチンと組み合わせたネオアジュバントであるチラゴルマブ、引き続いてドキソルビシン及びシクロホスファミド(AC)、又はアテゾリズマブ、nab-パクリタキセルと組み合わせたネオアジュバントであるチラゴルマブ、続いてACによる安全性及び忍容性、予備的有効性、及び薬物動態を調査するように設計されている。図22は、コホートBの試験計画を示す。
A. Study Design This Phase Ib, multicenter, open-label, multicenter global study will investigate atezolizumab, nab-paclitaxel in patients eligible for surgery with first clinically assessed T2-4d TNBC (PD-L1 all comer population). , and the neoadjuvant tiragolumab in combination with carboplatin, followed by doxorubicin and cyclophosphamide (AC), or atezolizumab, safety and tolerability with the neoadjuvant tiragolumab in combination with nab-paclitaxel, followed by AC, It is designed to investigate preliminary efficacy and pharmacokinetics. FIG. 22 shows the Cohort B study plan.
同意し適格である患者を以下の2つの処置群の1つに1:1の比でランダム化する:
-A群(最大約20人の患者):チラゴルマブ(420mg)及びアテゾリズマブ(840mg)は、IV注入によりQWで投与されるnab-パクリタキセル(125mg/m2)及び静脈内注入でQ3Wで投与されるカルボプラチン(濃度時間曲線下面積[AUC]:5mg/mL/分])と組み合わせてIV注入によりQ2Wで4サイクルにわたって投与され、続いて、顆粒球コロニー刺激因子(G-CSF;例えば、フィルグラスチム又はペグフィルグラスチム)又は顆粒球マクロファージコロニー刺激因子(GM-CSF)の支持を伴う静脈内注入によってドキソルビシン(60mg/m2)及びシクロホスファミド(600mg/m2)と組み合わせて、チラゴルマブ(420mg)及びアテゾリズマブ(840mg)が、Q2Wで4用量にわたって投与される。
-B群(最大約20人の患者):チラゴルマブ(420mg)及びアテゾリズマブ(840mg)は、12週間にわたるIV注入QWによって投与されるnab-パクリタキセル(125mg/m2)と組み合わせたIV注入Q2Wによって投与され、続いて、G-CSF(例えば、フィルグラスチム又はペグフィルグラスチム)又はGM-CSF支持を伴うIV注入によってQ2Wで投与されるドキソルビシン(60mg/m2)及びシクロホスファミド(600mg/m2)と組み合わせたチラゴルマブ(420mg)及びアテゾリズマブ(840mg)が、4用量にわたって投与される。
Consent and eligible patients will be randomized in a 1:1 ratio to one of the following two treatment groups:
- Group A (up to approximately 20 patients): tiragolumab (420 mg) and atezolizumab (840 mg) administered QW by IV infusion and nab-paclitaxel (125 mg/m 2 ) administered Q3W by intravenous infusion administered Q2W for 4 cycles by IV infusion in combination with carboplatin (area under the concentration-time curve [AUC]: 5 mg/mL/min]), followed by granulocyte colony-stimulating factor (G-CSF; e.g., filgrastim) or pegfilgrastim) or granulocyte-macrophage colony-stimulating factor (GM-CSF) in combination with doxorubicin (60 mg/m 2 ) and cyclophosphamide (600 mg/m 2 ) by intravenous infusion with tiragolumab ( 420 mg) and atezolizumab (840 mg) are administered Q2W over 4 doses.
Arm B (up to approximately 20 patients): tiragolumab (420 mg) and atezolizumab (840 mg) administered by IV infusion Q2W in combination with nab-paclitaxel (125 mg/m 2 ) administered by IV infusion QW for 12 weeks followed by doxorubicin (60 mg/m 2 ) and cyclophosphamide (600 mg/m2) administered Q2W by IV infusion with G-CSF (eg, filgrastim or pegfilgrastim) or GM-CSF support. Tiragolumab (420 mg) and atezolizumab (840 mg) in combination with m 2 ) are administered over 4 doses.
探索的評価項目(病理学的完全奏効(pCR);乳房及びリンパ節の両方からの浸潤性腫瘍の根絶(ypT0/はypN0である))は、ネオアジュバント治療及び手術の完了後の現地の再検討によって確立される。手術は、ネオアジュバント治療の最終投薬の14日後以降、6週間後までに行われるべきである。血小板数は、手術前に確認すべきであり、75,000細胞/μL以上でなくてはならない。 Exploratory endpoints (pathologic complete response (pCR); eradication of invasive tumor from both breast and lymph nodes (ypT0/is ypN0)) were evaluated in local recurrence after completion of neoadjuvant treatment and surgery. Established by review. Surgery should be performed no later than 14 days and no later than 6 weeks after the last dose of neoadjuvant therapy. Platelet counts should be confirmed prior to surgery and should be greater than or equal to 75,000 cells/μL.
術後患者管理には、臨床上適応がある場合、放射線療法が含まれ得、pCRを達成しない患者の管理は、現在の標準治療ガイドラインに従うべきである。 Postoperative patient management may include radiotherapy if clinically indicated, and management of patients who do not achieve pCR should follow current standard of care guidelines.
身体検査又はベースラインでの任意の放射線画像撮影によって評定された臨床上陽性の腋窩リンパ節を有する患者は、ランダム化の前に細針吸引又はコア針生検を受けること、及びリンパ節郭清術(ALND)又は少なくともセンチネルリンパ節生検(SLNB)が根治手術時に行われることが推奨される。ベースライン細針吸引又はコア針生検の結果を使用して、リンパ節病期分類(Union for International Cancer Control/American Joint Committee on Cancer[UICC/AJCC]第8版のAnatomic Stage Groupsに従う)を決定し、生検結果が陽性の患者はリンパ節陽性(N1~N3c)として病期分類されるべきであり、生検結果が陰性又は明確でない患者は、他の臨床測定に関係なくリンパ節陰性(N0)として病期分類されるべきである。 Patients with clinically positive axillary lymph nodes as assessed by physical examination or any radiographic imaging at baseline will undergo fine-needle aspiration or core needle biopsy and lymphadenectomy prior to randomization. (ALND) or at least sentinel lymph node biopsy (SLNB) is recommended at the time of definitive surgery. Baseline fine needle aspiration or core needle biopsy results were used to determine lymph node staging (according to the Anatomic Stage Groups of the Union for International Cancer Control/American Joint Committee on Cancer [UICC/AJCC] 8th edition). , patients with positive biopsies should be staged as node-positive (N1-N3c), and patients with negative or equivocal biopsies should be node-negative (N0 ).
臨床的又は細針生検又はコア針生検で証明された陰性腋窩リンパ節をベースラインに有する患者の場合、ネオアジュバント治療の完了後の腋窩外科管理には、SLNB又はALNDが含まれ得る。SLNBを実施する場合、2つ以上のリンパ節(最低2~3個)を摘除し、陽性リンパ節の数にかかわらず、センチネルリンパ節に陽性の巨大転移を有するすべての患者がALNDを受けるべきであることが強く推奨される。 For patients with clinical or fine- or core-needle biopsy-proven negative axillary lymph nodes at baseline, axillary surgical management after completion of neoadjuvant therapy may include SLNB or ALND. If SLNB is performed, all patients with 2 or more lymph nodes (minimum 2-3) removed and sentinel node-positive bulky metastases should receive ALND regardless of the number of positive nodes is strongly recommended.
患者は、試験中に予定された間隔で臨床的及び放射線学的腫瘍評定の両方を受ける。 Patients undergo both clinical and radiological tumor assessments at scheduled intervals during the study.
腫瘍微小環境における薬物の組合せの作用機序及び可能性のある耐性機序を評価するために、腫瘍組織は、サイクル2の1日目に投与前に収集され得る。
To assess the mechanism of action and possible resistance mechanisms of the drug combination in the tumor microenvironment, tumor tissue may be collected on
腫瘍組織は、臨床的に実施不可能でない限り、治験責任医師によって評定及び文書化された通り、及び疾患進行の最初の証拠時(新しい抗がん処置の開始前)に、生検によって収集される。試料は、アテゾリズマブと組み合わせたチラゴルマブの耐性又は疾患進行及び臨床的利益に関連する腫瘍組織バイオマーカーの分析を可能にするために使用される。 Tumor tissue will be collected by biopsy as assessed and documented by the investigator and at the first evidence of disease progression (prior to initiation of new anticancer treatment) unless clinically infeasible. be. Samples are used to allow analysis of tumor tissue biomarkers associated with resistance or disease progression and clinical benefit of tiragolumab in combination with atezolizumab.
B.投薬及び投与 B. Dosing and Administration
処置レジメンを図22に要約する。 The treatment regimen is summarized in FIG.
アテゾリズマブ、チラゴルマブ及び化学療法の予定された注入の日に、化学療法は、アテゾリズマブ及びチラゴルマブの注入後に投与される。 On the day of the scheduled infusion of atezolizumab, tiragolumab and chemotherapy, chemotherapy is administered after infusion of atezolizumab and tiragolumab.
アテゾリズマブ注入(840mg)後、患者は420mgのチラゴルマブを受ける。 After atezolizumab infusion (840 mg), patients receive 420 mg of tiragolumab.
アテゾリズマブ、チラゴルマブ、及び化学療法の投与は、潜在的に重篤な反応を管理するための訓練された人員並びに適切な機器及び医薬に直ちにアクセスできる監視された設定で行われる。 Administration of atezolizumab, tiragolumab, and chemotherapy will occur in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
製剤、保存及び投与に関する詳細な説明については、治験薬管理手順書を参照されたい。
チラゴルマブ及びアテゾリズマブ
Refer to the Investigational Product Control Procedures for detailed instructions regarding formulation, storage, and administration.
Tiragolumab and atezolizumab
コホートBの患者は、各28日間サイクルの1日目及び15日目にIV注入Q2Wによって投与される840mgの固定用量のアテゾリズマブを受け、続いて各28日間サイクルの1日目及び15日目にもIV注入Q2Wによって投与される420mgの固定用量のチラゴルマブを受ける(図22を参照)。チラゴルマブ及びアテゾリズマブの用量は固定されており、体重に依存しない。チラゴルマブ及びアテゾリズマブの注入(観察期間を含む)は、表65に概説される指示に従って投与される。


Nab-パクリタキセル
Nab-パクリタキセルは、30分かけて投与されるIV注入として患者に投与される。
Nab-paclitaxel Nab-paclitaxel is administered to patients as an IV infusion administered over 30 minutes.
nab-パクリタキセルを、アテゾリズマブ及びチラゴルマブの後に投与しなければならない。nab-パクリタキセルの用量は125mg/m2であり、12週間にわたるIV注入QWによって患者に投与される。nab-パクリタキセルの用量は、7日ごとよりも頻繁に投与すべきではない。 Nab-paclitaxel should be administered after atezolizumab and tiragolumab. The dose of nab-paclitaxel is 125 mg/m 2 and is administered to patients by IV infusion QW for 12 weeks. Doses of nab-paclitaxel should not be administered more frequently than every 7 days.
現場は、患者の体重が変化した場合にnab-パクリタキセルの用量調整を決定するための施設標準治療に従わなければならない。注入部位を、試験薬物投与中に起こり得る浸潤について厳密に監視しなければならない。 Sites must follow institutional standard of care for determining dose adjustments of nab-paclitaxel if patient weight changes. The injection site must be closely monitored for possible infiltration during study drug administration.
nab-パクリタキセルの調製及び投与に関するさらなる詳細については、現地の処方情報を参照されたい。 Refer to your local prescribing information for additional details regarding the preparation and administration of nab-paclitaxel.
カルボプラチン
カルボプラチンは、4用量について3週間ごとに5mg/mL/分のAUCを目標とするために、15~60分間にわたる短期IV注入によってnab-パクリタキセル投与の完了後に投与される。
Carboplatin Carboplatin will be administered after completion of nab-paclitaxel administration by brief IV infusion over 15-60 minutes to target an AUC of 5 mg/mL/min every 3 weeks for 4 doses.
カルボプラチン過剰投与に対する既知の解毒剤はない。必要に応じて、患者は、骨髄抑制並びに腎機能、肝機能及び聴覚機能の障害に関する支持処置を必要とする場合がある。最大1600mg/m2の用量は、下痢及び脱毛症を発症して極度に体調が悪い患者に関連している。推奨されるよりも高用量のカルボプラチンの使用もまた、視力喪失に関連している。さらなる詳細については、カルボプラチンの現地の処方情報を参照されたい。 There is no known antidote for carboplatin overdose. If necessary, patients may require supportive treatment for myelosuppression and impaired renal, hepatic and hearing function. Doses up to 1600 mg/m2 have been associated with extremely ill patients with diarrhea and alopecia. Use of carboplatin at doses higher than recommended has also been associated with vision loss. Refer to your local prescribing information for carboplatin for additional details.
シクロホスファミド
シクロホスファミドは、3~5分間にわたるIVボーラスとして、又は現地の標準治療に従ってIV注入として与えられるべきである。ACは、アテゾリズマブ及びチラゴルマブの後に投与しなければならない。シクロホスファミドの用量は、静脈内投与される600mg/m2である。毒性のための用量遅延及び用量減少が許容される。シクロホスファミドを、G-CSF又はGM-CSF の指示とともに4回用量(用量高密度AC)Q2Wで投与する。注:経口シクロホスファミドは許容されない。
Cyclophosphamide Cyclophosphamide should be given as an IV bolus over 3-5 minutes or as an IV infusion according to local standard of care. AC must be administered after atezolizumab and tiragolumab. The dose of cyclophosphamide is 600 mg/ m2 administered intravenously. Dose delays and dose reductions for toxicity are acceptable. Cyclophosphamide is administered in 4 doses (Dose Density AC) Q2W with either G-CSF or GM-CSF as indicated. Note: Oral cyclophosphamide is not allowed.
化学療法によって誘発される悪心及び嘔吐の予防及び処置は、臨床上適応がある場合、投与されるべきである。全身性コルチコステロイドは、アテゾリズマブ及びチラゴルマブによる処置の潜在的な有益な免疫学的効果を減弱させる可能性があるため、臨床上実施可能な場合は代替薬剤を考慮すべきである。 Prevention and treatment of chemotherapy-induced nausea and vomiting should be administered when clinically indicated. Because systemic corticosteroids may attenuate the potentially beneficial immunological effects of treatment with atezolizumab and tiragolumab, alternative agents should be considered when clinically feasible.
シクロホスファミドの調製及び投与に関する詳細については、現地の処方情報を参照されたい。 Refer to your local prescribing information for details regarding the preparation and administration of cyclophosphamide.
ドキソルビシン
ドキソルビシンは、現地の標準治療に従って、3~5分間にわたるIVボーラスとして、又は15~30分間にわたるIV注入として投与されるべきである。ACは、アテゾリズマブ及びチラゴルマブの後に投与しなければならない。ドキソルビシンの用量は、IV注入によって患者に投与される60mg/m2である。用量遅延及び毒性の低減が許容される。ドキソルビシンを、G-CSF又はGM-CSF 支持を伴う4用量(用量高密度AC)についてQ2Wで投与する。
Doxorubicin Doxorubicin should be administered as an IV bolus over 3-5 minutes or as an IV infusion over 15-30 minutes according to local standard of care. AC must be administered after atezolizumab and tiragolumab. The dose of doxorubicin is 60 mg/ m2 administered to the patient by IV infusion. Dose delays and reduced toxicity are acceptable. Doxorubicin is administered Q2W for 4 doses (dose density AC) with G-CSF or GM-CSF support.
ドキソルビシンの調製及び投与に関する詳細については、現地の処方情報を参照されたい。 Refer to your local prescribing information for details regarding the preparation and administration of doxorubicin.
前投薬及び支持療法
一般に、化学療法支持療法は、米国臨床腫瘍学会(ASCO)、欧州がん研究治療機構(EORTC)、又はESMOガイドライン、又は現地の標準治療に従って投与されるべきである。
Premedication and Supportive Care In general, chemotherapy supportive care should be administered according to American Society of Clinical Oncology (ASCO), European Organization for Research and Treatment of Cancer (EORTC), or ESMO guidelines, or local standards of care.
化学療法によって誘発される悪心及び嘔吐の予防及び処置は、臨床上適応がある場合、投与されるべきである。全身性コルチコステロイドは、アテゾリズマブ及びチラゴルマブによる処置の潜在的な有益な免疫学的効果を減弱させる可能性があるので、治験実施計画書で提供される指針を除いて、臨床上実施可能な場合は代替薬剤を考慮すべきである。 Prevention and treatment of chemotherapy-induced nausea and vomiting should be administered when clinically indicated. Systemic corticosteroids may attenuate the potentially beneficial immunological effects of treatment with atezolizumab and tiragolumab, so unless clinically feasible, except for guidance provided in the protocol should consider alternative agents.
予防的G-CSF又はGM-CSFは、局所的な方針に従って血液毒性のリスクを軽減するために使用され得、化学療法のAC部分の間に必要とされる。G-CSF又はGM-CSFによる好中球減少症の処置は、現地の方針に従って許可される。 Prophylactic G-CSF or GM-CSF may be used to reduce the risk of hematologic toxicity according to local policy and is required during the AC portion of chemotherapy. Treatment of neutropenia with G-CSF or GM-CSF is permitted according to local policy.
用量の変更
この試験では、アテゾリズマブ又はチラゴルマブの用量変更はない。nab-パクリタキセル(すなわち、用量変更及び処置中断規則)の管理については、表25を参照されたい。カルボプラチン、ドキソルビシン又はシクロホスファミド関連毒性の管理(すなわち、用量変更及び処置中断規則)に関するガイドラインについては、各薬剤のそれぞれの現地の処方情報を参照されたい。
Dose Modifications There were no dose modifications of atezolizumab or tiragolumab in this study. See Table 25 for administration of nab-paclitaxel (ie dose modification and treatment interruption rules). Refer to each agent's respective local prescribing information for guidelines regarding the management of carboplatin-, doxorubicin-, or cyclophosphamide-related toxicities (ie, dose modification and treatment interruption rules).
C.併用療法 C. Combination therapy
併用療法は、試験薬の開始の7日前から処置中止の来院までの治験実施計画書に定められた処置に加えて、患者によって使用される任意の医薬(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)からなる。 Concomitant therapy includes any drug used by the patient (e.g., prescription drug, over-the-counter drug, vaccine, herbal or homeopathic remedies, dietary supplements).
許可された治療
患者は、試験中に以下の治療法を使用することが許される:
●失敗率が年間1%未満の経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与されるコルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●骨格事象の予防のためのビスホスホネート
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。チラゴルマブ及びアテゾリズマブによる処置は、緩和放射線療法中に継続され得る。nab-パクリタキセルによる処置を、施設の標準治療に従って中断しなければならない。
●化学療法(nab-パクリタキセル)を受けている患者に許可され、化学療法のAC部分の間に必要とされるG-CSF(例えば、フィルグラスチム又はペグフィルグラスチム)又はGM-CSF処置
Allowed Treatments Patients are allowed to use the following treatments during the study:
● Oral contraceptives with an annual failure rate of less than 1% ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable-dose warfarin or low molecular weight heparin)
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
o Corticosteroids given for chronic obstructive pulmonary disease or asthma o Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency o Bisphosphonates for the prevention of skeletal events o For the following: Palliative radiotherapy outlined (e.g. treatment of known bone metastases or symptomatic relief of pain):
Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with tiragolumab and atezolizumab may be continued during palliative radiotherapy. Treatment with nab-paclitaxel must be discontinued according to institutional standard of care.
- G-CSF (eg, filgrastim or pegfilgrastim) or GM-CSF treatment permitted for patients receiving chemotherapy (nab-paclitaxel) and required during the AC portion of chemotherapy
一次予防は、ASCO、EORTC、若しくはESMOのガイドラインに従って、又は現地の標準診療に従って患者に投与されるべきである(すなわち、≧60歳及び/又は併存症を有する患者において)(Smith et al.2006;Crawford et al.2010;Aapro et al.2011)。 Primary prophylaxis should be administered to patients according to ASCO, EORTC, or ESMO guidelines or according to local standard practice (i.e., in patients ≥60 years and/or with comorbidities) (Smith et al. 2006 Crawford et al. 2010; Aapro et al. 2011).
毎週nab-パクリタキセルを投与されている患者におけるG-CSFの長時間作用型(ペグ化)形態の使用を支持する証拠は限られており、治験責任医師はG-CSFの従来の製剤を優先することを検討すべきである。 Evidence supporting the use of long-acting (pegylated) forms of G-CSF in patients receiving weekly nab-paclitaxel is limited and investigators prefer conventional formulations of G-CSF should be considered.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ及びチラゴルマブ注入のためにのみ投与され得る。
注意を要する治療
Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent atezolizumab and tiragolumab infusions at the investigator's discretion.
Sensitive treatment
全身性コルチコステロイド及びTNF-α阻害剤は、アテゾリズマブによる処置の潜在的に有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物が検討される。代替が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。 Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines are considered. If alternatives are not feasible, systemic corticosteroids and TNF-α inhibitors can be administered at the investigator's discretion.
アテゾリズマブ治療に関連する場合、特定の有害事象の処置のために、治験責任医師の裁量で、全身コルチコステロイドが推奨される。 Systemic corticosteroids are recommended at the investigator's discretion for treatment of specific adverse events when associated with atezolizumab therapy.
禁止される治療
以下の併用療法の使用は、以下に記載されるように禁止される:
●がん(限定されないが、化学療法、ホルモン療法、免疫療法、放射線療法、及びハーブ療法を含む)の処置を目的とした併用療法であって、保健当局承認済みであるか実験的であるかにかかわらず、試験処置を開始する前の様々な期間、薬剤に応じて、及び試験処置中、疾患の進行が文書化され、患者が緩和的放射線療法を除く試験処置を中止するまでの併用療法
●試験処置の開始前28日以内及び試験処置中の治験治療
●試験処置開始前4週間以内、アテゾリズマブ処置中及び試験処置の最終用量後5ヶ月間の生弱毒化ワクチン(例えば、FLUMIST(登録商標))
●アテゾリズマブ及びチラゴルマブと組み合わせて投与した場合、自己免疫症状のリスクを潜在的に増加させる可能性があるため、試験処置の開始前及び試験処置中の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫賦活剤(限定されないが、インターフェロン及びIL-2を含む)
●試験処置中の全身免疫抑制薬(限定されないが、アザチオプリン、メトトレキサート、及びサリドマイドを含む)(これらの薬剤がアテゾリズマブ及びチラゴルマブの有効性及び安全性を潜在的に変化させる可能性があるため)
Prohibited Therapies The use of the following concomitant therapies is prohibited as described below:
Any health authority-approved or experimental combination therapy for the treatment of cancer (including, but not limited to, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy). Concomitant therapy for various periods prior to initiation of study treatment, depending on drug, and during study treatment until disease progression is documented and patient discontinues study treatment, excluding palliative radiation therapy, regardless of - Study treatment within 28 days prior to initiation of study treatment and during study treatment - Live attenuated vaccine (e.g., FLUMIST®) within 4 weeks prior to initiation of study treatment, during atezolizumab treatment and 5 months after the last dose of study treatment ))
Due to the potential increased risk of autoimmune symptoms when administered in combination with atezolizumab and tiragolumab, no drug elimination half-lives (either within 4 weeks or 5 during study treatment) or longer), systemic immunostimulants (including but not limited to interferon and IL-2)
- Systemic immunosuppressants (including but not limited to azathioprine, methotrexate, and thalidomide) during study treatment (because these agents can potentially alter the efficacy and safety of atezolizumab and tiragolumab)
カルボプラチン化学療法に関連する追加の制限
●黄熱病ワクチンの併用は禁止され、他の弱毒生ワクチンとのワクチン接種は避けるべきである。
●死滅又は不活化ワクチンが投与され得るが、そのようなワクチンに対する応答は減少し得る。
●フェニトイン又はホスフェニトインの併用は、痙攣の悪化のリスク、毒性増強のリスク、又は細胞傷害性薬物の有効性の喪失のために推奨されない。
●以下の薬剤の併用には注意を払うべきである:シクロスポリン、腎毒性又は耳毒性薬(例えば、アミノグリコシド、バンコマイシン、カプレオマイシン及び利尿薬、例えばループ利尿薬[増大した毒性、悪化した毒性、又は累積的な毒性のリスク])。
●同時(一緒に又は≦7日間隔で与えられる)放射線療法は避けるべきである。
Additional Restrictions Related to Carboplatin Chemotherapy • Concomitant use of yellow fever vaccine is prohibited and vaccination with other live attenuated vaccines should be avoided.
• Killed or inactivated vaccines may be administered, but responses to such vaccines may be diminished.
• Concomitant use of phenytoin or fosphenytoin is not recommended due to the risk of exacerbation of convulsions, risk of increased toxicity, or loss of efficacy of cytotoxic drugs.
Caution should be exercised in concomitant use of the following drugs: cyclosporine, nephrotoxic or ototoxic agents (e.g. aminoglycosides, vancomycin, capreomycin and diuretics, e.g. loop diuretics [increased toxicity, exacerbated toxicity, or risk of cumulative toxicity]).
• Concurrent radiotherapy (given together or <7 days apart) should be avoided.
D.選択基準
患者は、試験参加のための以下の一般的な基準を満たさなければならない:
●署名したインフォームドコンセントフォーム
●インフォームドコンセント用紙に署名した時点で≧18歳の女性及び男性
●試験治験実施計画書を遵守する能力
●ECOGパフォーマンスステータスが0又は1(添付物5を参照)
●試験処置(サイクル1の1日目)開始前14日以内に得られた以下の検査室結果として定義される、十分な血液学的機能及び終末器官機能
-サイクル1の1日目の前2週間以内にG-CSF支持なしでANC≧1.5X109/L(1500/μL)
-リンパ球数≧0.5X109/L(≧500/μL)
-サイクル1の1日目の前2週間以内に輸血なしで血小板数≧100X109/L(≧100,000/μL)
-ヘモグロビン≧90g/L(≧9g/dL)。
D. Inclusion Criteria Patients must meet the following general criteria for study entry:
A signed informed consent form Females and males ≥18 years of age at the time of signing the informed consent form Ability to comply with the study protocol ECOG performance status of 0 or 1 (see Appendix 5)
Adequate hematologic and end-organ function, defined as the following laboratory results obtained within 14 days prior to the start of study treatment (
- Lymphocyte count ≥0.5 X 109/L (≥500/μL)
- Platelet count ≥100 X 109/L (≥100,000/μL) without transfusion within 2 weeks prior to
- Hemoglobin ≧90 g/L (≧9 g/dL).
患者は、この基準を満たすために輸血又は赤血球造血処置を受けることができる
-AST、ALT、ALP≦2.5X正常値上限(ULN)
-血清ビリルビン≦1.5XULN、ただし以下を除く:
血清ビリルビン値≦3XULNを有する既知のギルバート病患者を登録することができる。
-INR及びaPTT≦1.5XULN
これは、治療的抗凝固療法を受けたことがない患者にのみ適用され、治療的抗凝固療法を受けている患者は、安定した用量であるべきである。
-クレアチニンクリアランス≧30mL/分(Cockcroft-Gault式を用いて計算)
-血清アルブミン≧25g/L(≧2.5g/dL)
●スクリーニング時の陰性HIV検査。
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時のB型肝炎表面抗体(HBsAb)検査陽性、又は以下のいずれかを伴うスクリーニング時にHBsAb陰性:
-総B型肝炎コア抗体(HBcAb)陰性
-陽性の全HBcAb検査とそれに続く定量的B型肝炎ウイルス(HBV)DNA<500 IU/mL
Patients can receive blood transfusions or erythropoietic procedures to meet this criterion - AST, ALT, ALP ≤ 2.5X upper limit of normal (ULN)
- Serum bilirubin ≤ 1.5 XULN, except:
Known Gilbert's disease patients with serum bilirubin levels < 3XULN can be enrolled.
-INR and aPTT≤1.5XULN
This applies only to patients who have not received therapeutic anticoagulation therapy; patients receiving therapeutic anticoagulation therapy should be on a stable dose.
- Creatinine clearance ≥ 30 mL/min (calculated using the Cockcroft-Gault formula)
- serum albumin ≥25 g/L (≥2.5 g/dL)
• Negative HIV test at screening.
- Negative hepatitis B surface antigen (HBsAg) test at screening - Positive hepatitis B surface antibody (HBsAb) test at screening or negative HBsAb at screening with any of the following:
- total hepatitis B core antibody (HBcAb) negative - positive total HBcAb test followed by quantitative hepatitis B virus (HBV) DNA <500 IU/mL
HBV DNA検査は、HBsAg検査陰性、HBsAb検査陰性、及び総HBcAb検査陽性の患者に対してのみ実施される。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。
HBV DNA testing is performed only for patients with negative HBsAg, negative HBsAb, and positive total HBcAb tests.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening.
HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:以下に定義するように、禁欲(異性間の性交を控える)又は避妊方法を使用することの同意、及び卵の提供を控えることの同意:
HCV RNA testing is performed only for patients who test positive for HCV antibodies.
For women of childbearing potential: Consent to abstinence (abstinence from heterosexual intercourse) or use of contraceptive methods, and consent to abstain from donating eggs, as defined below:
女性は、処置期間中及びアテゾリズマブの最終投与後少なくとも5ヶ月間、チラゴルマブの最終投与後90日間、nab-パクリタキセルの最終投与後1ヶ月間、カルボプラチン若しくはドキソルビシンの最終投与後6ヶ月間、又はシクロホスファミドの最終投与後12ヶ月間のいずれか遅い方で、禁欲を維持するか、又は年間<1%の失敗率をもたらす避妊方法を使用しなければならない。女性は、この同じ期間中に卵を提供することを控えなければならない。 Women should be treated during treatment and for at least 5 months after the last dose of atezolizumab, 90 days after the last dose of tiragolumab, 1 month after the last dose of nab-paclitaxel, 6 months after the last dose of carboplatin or doxorubicin, or For 12 months after the last dose of Famide, whichever is later, must maintain abstinence or use a contraceptive method that results in a failure rate of <1% per year. Females should refrain from donating eggs during this same period.
女性は、初経後であり、閉経後状態に到達しておらず(閉経以外の原因が同定されていない、連続≧12ヶ月の無月経)、かつ、外科的不妊(卵巣及び/又は子宮の切除)を受けたことがない場合に、懐胎の可能性があるとみなされる。 Females are post-menopausal, have not reached a post-menopausal state (>12 consecutive months of amenorrhea, no other cause identified), and are surgically infertile (removal of ovaries and/or uterus). ) is considered to be of possible gestation.
年間失敗率<1%の避妊方法の例としては、一貫して正しく使用される場合、排卵の阻害に関連する併用(エストロゲン及びプロゲストゲン含有)ホルモン避妊、排卵の阻害に関連するプロゲストゲンのみのホルモン避妊、両側卵管閉塞、男性不妊;子宮内避妊器具;子宮内ホルモン放出システム;及び性的禁欲が挙げられる。 Examples of methods of contraception with an annual failure rate of <1% include combined (estrogen- and progestogen-containing) hormonal contraception associated with inhibition of ovulation, progestogens associated with inhibition of ovulation when used consistently and correctly. hormonal contraception alone, bilateral fallopian tube obstruction, male infertility; intrauterine devices; intrauterine hormone releasing systems; and sexual abstinence.
性的禁欲の信頼性は、臨床試験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。 The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and normal lifestyle.
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。 Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
試験処置の中止後に妊娠することを望む女性は、化学療法による処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に卵母細胞の保存についての助言を求めるべきである。
●男性の場合:以下に定義するように、禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることに同意すること:
Women who wish to become pregnant after discontinuation of study treatment should seek advice regarding oocyte storage prior to initiation of study treatment due to the potential for irreversible infertility resulting from treatment with chemotherapy. .
For men: agreeing to maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and to abstain from donating sperm, as defined below:
妊娠可能な女性パートナー又は妊娠中の女性パートナーの場合、処置期間中及びチラゴルマブの最終投与後90日間、又はnab-パクリタキセル、カルボプラチン、ドキソルビシン、又はシクロホスファミドの最終投与後6ヶ月間のいずれか遅い方で、男性は禁欲を維持するか、又はコンドームと併せて、年間<1%の失敗率をもたらす追加の避妊方法を使用しなければならない。男性は、同期間中は精子提供をやめなければならない。 For female partners of childbearing potential or pregnant, either during the treatment period and for 90 days after the last dose of tiragolumab or 6 months after the last dose of nab-paclitaxel, carboplatin, doxorubicin, or cyclophosphamide Later, men must maintain abstinence or use additional methods of contraception in conjunction with condoms that result in failure rates of <1% per year. Men must stop donating sperm during the same period.
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。 The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle.
周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、許容される避妊方法ではない。 Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not acceptable methods of contraception.
試験処置の開始後に子供を持ちたい男性は、化学療法による処置に起因する不可逆的不妊症の可能性があるため、試験処置の開始前に精子保存についての助言を求めるべきである。
●閉経後(≧12ヶ月の非治療誘発性無月経)でないか、又は避妊手術を受けたことがある女性では、試験処置の開始前14日以内に陰性血清妊娠検査結果が必要である。
●予定された来院、処置計画、臨床検査、及び他の試験手順を遵守する意思及び能力
Men who wish to have children after initiation of study treatment should seek advice on sperm storage prior to initiation of study treatment due to the potential for irreversible infertility resulting from treatment with chemotherapy.
• Females who are not postmenopausal (≥12 months of non-treatment-induced amenorrhea) or who have undergone surgical sterilization must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
Willingness and ability to comply with scheduled visits, treatment plans, laboratory tests, and other study procedures
患者は、以下の登録のためのがん特異的適格基準を満たさなければならない:
●組織学的に文書化されたTNBC(現地の検査によって評定した場合のHER2、ER及びPRの陰性状態)
HER2陰性は、現地の検査室の評定によって以下の(Wolff et al.2018)のいずれかとして定義される:
ISH非増幅(HER2 対CEP 17比<2.0、又は単一プローブ平均HER2 遺伝子コピー数<4シグナル/細胞、又はIHC 0若しくはIHC 1+ER、及びPgR陰性はIHC分析でホルモン受容体を発現する細胞の<1%と定義される。
Patients must meet the following cancer-specific eligibility criteria for enrollment:
- Histologically documented TNBC (negative status for HER2, ER and PR as assessed by local laboratory)
HER2-negative is defined as either of the following (Wolff et al. 2018) by local laboratory assessment:
ISH unamplified (HER2 to CEP 17 ratio <2.0, or single-probe average HER2 gene copy number <4 signals/cell, or
少なくとも1つの焦点がTNBCとしてサンプリングされ、現地で確認され、文書化されるならば、多巣性腫瘍(原発腫瘍と同じ象限に限定された2つ以上の別個の腫瘍)を有する患者が適格である。 Patients with multifocal tumors (two or more separate tumors confined to the same quadrant as the primary tumor) are eligible if at least one focus is sampled as TNBC, confirmed locally, and documented. be.
すべての個別の病変がサンプリングされ、現地で確認され、TNBCとして文書化されるならば、多中心性腫瘍(2つ以上の個別の四分円を含む複数の腫瘍)を有する患者が適格である。
●パラフィンブロック(好ましい)又は少なくとも20枚の非染色スライドにおける代表的なFFPE腫瘍組織標本の中央検査を通して文書化された確認済みの腫瘍PD-L1評価
Patients with multicentric tumors (multiple tumors involving two or more separate quadrants) are eligible if all individual lesions are sampled, confirmed locally, and documented as TNBC .
- Confirmed tumor PD-L1 assessment documented through central examination of representative FFPE tumor tissue specimens on paraffin blocks (preferred) or at least 20 unstained slides
腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならず、登録前にVentana(SP142)PD-L1 IHCアッセイを使用して決定した場合にPD-L1発現について評価しなければならず、陽性は、中央検査室によって決定された任意の強度のPD-L1発現腫瘍浸潤免疫細胞が占める腫瘍面積の≧1%以上として定義される。腫瘍組織がPD-L1発現について評価可能でない患者は、適格ではない。 Tumor tissue must be of good quality based on total tumor content and viable tumor content and assessed for PD-L1 expression as determined using the Ventana (SP142) PD-L1 IHC assay prior to enrollment. Positivity is defined as ≧1% of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells of any intensity as determined by a central laboratory. Patients whose tumor tissue was not evaluable for PD-L1 expression were not eligible.
複数の腫瘍標本が提出される場合、少なくとも1つの標本がPD-L1について評価可能である場合、患者は適格であり得る。許容され得る試料には、深部腫瘍組織のためのコア針生検(最低3つのコア)、又は皮膚、皮下、若しくは粘膜病変のための切除、切開、パンチ、若しくは鉗子生検が含まれる。 If multiple tumor specimens are submitted, patients may be eligible if at least one specimen is evaluable for PD-L1. Acceptable samples include core needle biopsies (minimum of 3 cores) for deep tumor tissue, or excision, incision, punch, or forceps biopsies for cutaneous, subcutaneous, or mucosal lesions.
パラフィンブロック中のFFPE腫瘍標本が好ましい。 FFPE tumor specimens in paraffin blocks are preferred.
細針吸引、ブラッシング、胸水からの細胞ペレット、骨転移、及び洗浄液試料は許容されない。
●少なくとも1つのX線又は臨床測定で>2cmの原発性乳房腫瘍サイズ
●提示時のステージ:cT2-cT4、cN0-cN3、及びcM0
●ネオアジュバント処置の完了後に適切な外科的管理(例えば、腋窩リンパ節手術及び部分的又は全乳房切除術を含む)を受けることに対する患者の同意
●心エコー図(ECHO)又はマルチゲート収集(MUGA)スキャンで測定した場合のベースライン左室駆出率(LVEF)≧53%
Fine needle aspirations, brushings, cell pellets from pleural effusions, bone metastases, and lavage fluid samples are not permitted.
- Primary breast tumor size >2 cm by at least one radiographic or clinical measurement - Stage at presentation: cT2-cT4, cN0-cN3, and cM0
Patient consent to undergo appropriate surgical management (e.g., including axillary lymph node surgery and partial or total mastectomy) after completion of neoadjuvant treatment Echocardiogram (ECHO) or multigated acquisition (MUGA) ) baseline left ventricular ejection fraction (LVEF) ≥53% as measured by scan
E.除外基準
以下の基準のいずれかを満たす患者は試験から除外される:
●試験処置中、チラゴルマブ処置後90日以内、アテゾリズマブ処置後5ヶ月以内、nab-パクリタキセル、カルボプラチン若しくはドキソルビシン処置後6ヶ月以内、又はシクロホスファミド処置後12ヶ月以内(いずれか長い方)に妊娠若しくは授乳、又は妊娠する意図
E. Exclusion Criteria Patients meeting any of the following criteria will be excluded from the study:
Pregnancy during study treatment, within 90 days after tiragolumab treatment, within 5 months after atezolizumab treatment, within 6 months after nab-paclitaxel, carboplatin or doxorubicin treatment, or within 12 months after cyclophosphamide treatment (whichever is longer) or breastfeeding, or intending to become pregnant
妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
●治験実施計画書の遵守又は重大な肝疾患(例えば、肝硬変、制御不能な大発作性障害、又は上大静脈症候群)を含む結果の解釈に影響を及ぼし得る有意な制御されない同時発症疾患の証拠
●試験処置開始前3ヶ月以内の重大な心血管疾患、例えば、ニューヨーク心臓病(クラスII以上)、心筋梗塞、不安定性不整脈又は不安定狭心症
Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
- Evidence of significant uncontrolled comorbidities that could affect interpretation of results, including protocol compliance or significant liver disease (e.g., cirrhosis, uncontrolled grand paroxysmal disorder, or superior vena cava syndrome) - Significant cardiovascular disease within 3 months prior to initiation of study treatment, e.g. New York heart disease (class II or greater), myocardial infarction, unstable arrhythmia or unstable angina pectoris
LVEF<53%が既知の患者は除外する。 Patients with known LVEF <53% are excluded.
上記の基準を満たさない既知の冠動脈疾患又はうっ血性心不全を有する患者。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)
●試験処置開始前2週間以内の経口又はIV抗生物質による処置
Patients with known coronary artery disease or congestive heart failure who do not meet the above criteria.
- Severe infection within 4 weeks prior to initiation of study treatment (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia)
- Treatment with oral or IV antibiotics within 2 weeks prior to initiation of study treatment
定期的な抗生物質予防(例えば、慢性閉塞性肺疾患の増悪を予防するため、又は抜歯のために)を受けている患者は適格である。
●試験処置の開始前28日以内の大きな外科的処置、又は診断以外の試験中の大きな外科的処置の必要性の予想
Patients receiving routine antibiotic prophylaxis (eg, to prevent exacerbation of chronic obstructive pulmonary disease or for tooth extraction) are eligible.
- Anticipation of need for major surgery within 28 days prior to initiation of study procedure or non-diagnostic major surgery during study
中心静脈アクセスカテーテル(複数可)(例えば、ポート等)の配置は、大きな外科的処置とは考えられておらず、したがって許容される。
●キメラ抗体若しくはヒト化抗体、又は融合タンパク質に対する重度のアレルギー性、アナフィラキシー性、又は他の超過敏反応の病歴。
●CHO細胞で産生される生物製剤又はチラゴルマブ若しくはアテゾリズマブ製剤の任意の成分に対する既知の過敏症又はアレルギー
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質症候群に関連する血管血栓症、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、多発性硬化症、血管炎、又は糸球体腎炎を含むがこれらに限定されない活動性の自己免疫疾患又はその病歴
Placement of a central venous access catheter(s) (eg, ports, etc.) is not considered a major surgical procedure and is therefore acceptable.
• History of severe allergic, anaphylactic, or other hypersensitivity reactions to chimeric or humanized antibodies, or fusion proteins.
Known hypersensitivity or allergy to any component of CHO cell-produced biologics or tiragolumab or atezolizumab preparations Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, Active autoimmune disease including, but not limited to, vascular thrombosis associated with antiphospholipid syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barre syndrome, multiple sclerosis, vasculitis, or glomerulonephritis; or its medical history
安定用量の甲状腺補充ホルモンで自己免疫介在性甲状腺機能低下症の病歴を有する患者は、この試験に適格である。 Patients with a history of autoimmune-mediated hypothyroidism on stable doses of thyroid replacement hormone are eligible for this trial.
安定したインスリン投薬レジメンで制御された1型糖尿病患者はこの試験に適格である。
Patients with
湿疹、乾癬、慢性単純性苔癬又は皮膚症状のみを有する白斑(例えば、乾癬性関節炎なし)を有する患者は、以下の条件を満たすならば許可される:
-発疹が覆っている体表面積は<10%でなければならない
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない
●事前の同種異系幹細胞又は固形臓器移植
●スクリーニング時の胸部コンピューター断層撮影(CT)スキャンでの特発性肺線維症(肺臓炎を含む)、薬物誘発性肺臓炎、器質化肺炎(すなわち、閉塞性細気管支炎、潜在性器質化肺炎)の病歴、又は活動性肺臓炎の証拠
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin symptoms only (e.g., no psoriatic arthritis) are allowed if they meet the following conditions:
- Rash must cover <10% body surface area - Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UV within the last 12 months No occurrence of acute exacerbation of underlying symptoms requiring A-irradiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors, or high-potency or oral corticosteroids Prior allogeneic stem cell or solid organ transplantation Idiopathic pulmonary fibrosis (including pneumonitis), drug-induced pneumonitis, organizing pneumonia (ie, bronchiolitis obliterans, subclinical organizing pneumonia) on screening chest computed tomography (CT) scan History or evidence of active pneumonitis
放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●スクリーニング時の陽性EBVウイルスカプシド抗原(VCA)IgM検査
A history of radiation pneumonitis (fibrosis) in the radiology area is acceptable.
●Positive EBV viral capsid antigen (VCA) IgM test at screening
活動性感染又は慢性活動性感染の疑いをスクリーニングするために、EBVポリメラーゼ連鎖反応(PCR)検査を臨床上適応される場合、実施しなければならない。 To screen for active or suspected chronic active infection, an EBV polymerase chain reaction (PCR) test should be performed when clinically indicated.
EBV PCR検査が陽性の患者は除外する。
●活動性結核
●試験処置の開始前4週間以内に生弱毒化ワクチンを受けること、又はそのような生弱毒化ワクチンが試験中に必要であると予想すること
Patients with a positive EBV PCR test are excluded.
- Active tuberculosis - Receiving a live-attenuated vaccine within 4 weeks prior to initiation of study treatment, or anticipating that such a live-attenuated vaccine will be needed during the study
患者は、試験処置の開始前28日以内、処置中、又は試験処置の最終用量後5ヶ月以内に生弱毒化ワクチン(例えば、FluMist(登録商標))を受けないことに同意しなければならない。
●抗PD-1又は抗PD-L1治療抗体を除く、抗CTLA-4を含むCD 137アゴニスト又は免疫チェックポイント遮断療法による事前処置
●試験処置の開始前の4週間以内又は薬物の5つの薬物除去半減期(いずれか長い方)以内の全身免疫刺激剤(インターフェロン又はIL-2を含むが、これらに限定されない)による処置
●試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、プレドニゾン、デキサメタゾン、アザチオプリン、メトトレキサート、サリドマイド及び抗-腫瘍壊死因子[抗TNF]剤)による処置、又は試験中の全身免疫抑制薬が必要と予想される
Patients must agree not to receive a live attenuated vaccine (eg, FluMist®) within 28 days prior to initiation of study treatment, during treatment, or within 5 months after the final dose of study treatment.
- Pretreatment with a CD 137 agonist or immune checkpoint blockade therapy, including anti-CTLA-4, excluding anti-PD-1 or anti-PD-L1 therapeutic antibodies - Within 4 weeks prior to initiation of study treatment or 5 drug withdrawals of drug Treatment with systemic immunostimulants (including but not limited to interferon or IL-2) within half-life (whichever is longer) Systemic immunosuppressants (including but not limited to, Treatment with prednisone, dexamethasone, azathioprine, methotrexate, thalidomide and anti-tumor necrosis factor [anti-TNF] agents) or investigational systemic immunosuppressants expected to be required
急性低用量全身免疫抑制薬(例えば、悪心のためのデキサメタゾンの1回投与)を受けた患者は試験に登録され得る。 Patients receiving acute low-dose systemic immunosuppressants (eg, a single dose of dexamethasone for nausea) may be enrolled in the study.
慢性閉塞性肺疾患のための吸入コルチコステロイド、起立性低血圧患者のためのミネラルコルチコイド(例えば、フルドロコルチゾン)、及び副腎皮質機能不全のための低用量補充コルチコステロイドの使用が許容される。
●浸潤性乳がんの病歴
●ステージIV(転移性)乳がん
●乳がんの処置及び予防のための事前全身治療
●任意の悪性腫瘍に対するアントラサイクリン、白金又はタキサンによる以前の治療
注:非多形性LCIS(未処置又は手術で処置)を有する患者は適格である。
●同期両側性浸潤性乳がん
●原発腫瘍及び/又は腋窩リンパ節の以前の切開生検及び/又は切除生検
●ネオアジュバント療法の開始前の腋窩リンパ節郭清術
●適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚がん、限局性前立腺がん、又はステージI子宮がん等、転移又は死亡のリスクが無視できるほどでないもの(例えば、>90%の5年OS)を除いて、スクリーニング前5年以内の他の悪性腫瘍の病歴
●試験処置開始前12ヶ月以内の脳血管障害の病歴
●試験処置の開始前の以下のいずれかとして定義される心肺機能不全:
-NCI CTCAE v 5.0 グレード≧3症候性うっ血性心不全又はニューヨーク心臓病学会クラスII以上の心疾患の病歴
-抗狭心症薬を必要とする狭心症、適切な投薬によって制御されない重篤な心不整脈、重篤な伝導異常、又は臨床上重要な弁膜疾患
-高リスクの制御されない不整脈(すなわち、安静時の心拍数が>100拍/分の心房性頻拍、有意な心室性不整脈[心室性頻拍]、高悪性度の房室[AV]ブロック[第2度AVブロックタイプ2[Mobitz 2]、又は第3度AVブロック])
-左室機能不全、不整脈又は心虚血に関する有意な症状(グレード≧2)
-試験処置開始前12ヶ月以内の心筋梗塞
-制御されない高血圧(収縮期血圧>180 mmHg及び/又は拡張期血圧>100 mmHg)
-ECGでの経壁梗塞の証拠
-酸素療法の要求
●nab-パクリタキセル、シクロホスファミド、ドキソルビシン又はカルボプラチン製剤の成分に対する既知のアレルギー又は過敏症
●G-CSF又はGM-CSF製剤に対する既知のアレルギー又は過敏症
The use of inhaled corticosteroids for chronic obstructive pulmonary disease, mineralocorticoids (eg, fludrocortisone) for patients with orthostatic hypotension, and low-dose supplemental corticosteroids for adrenocortical insufficiency is permissible. be.
● History of invasive breast cancer ● Stage IV (metastatic) breast cancer ● Prior systemic therapy for the treatment and prevention of breast cancer ● Previous treatment with anthracyclines, platinum or taxanes for any malignancy Note: non-pleomorphic LCIS ( Patients with no treatment or surgically treated) are eligible.
Synchronous bilateral invasive breast cancer Prior incisional and/or excisional biopsy of primary tumor and/or axillary lymph nodes Axillary lymph node dissection prior to initiation of neoadjuvant therapy Appropriately prepared cervix Carcinoma in situ, non-melanoma skin cancer, localized prostate cancer, or stage I uterine cancer, unless the risk of metastasis or death is not negligible (e.g., >90% 5-year OS) history of other malignancies within 5 years prior to Screening history of cerebrovascular disease within 12 months prior to initiation of study treatment cardiopulmonary insufficiency defined as any of the following prior to initiation of study treatment:
- History of NCI CTCAE v 5.0 grade ≥ 3 symptomatic congestive heart failure or New York Heart Association class II or greater heart disease - Angina pectoris requiring antianginal medication, severe not controlled by appropriate medication cardiac arrhythmias, severe conduction abnormalities, or clinically significant valvular disease ventricular tachycardia], high-grade atrioventricular [AV] block [second-degree AV block type 2 [Mobitz 2], or third-degree AV block])
- Significant symptoms (grade ≥2) related to left ventricular dysfunction, arrhythmias or cardiac ischemia
- Myocardial infarction within 12 months prior to initiation of study treatment - Uncontrolled hypertension (systolic blood pressure >180 mmHg and/or diastolic blood pressure >100 mmHg)
- evidence of transmural infarction on ECG - requirement for oxygen therapy known allergy or hypersensitivity to components of nab-paclitaxel, cyclophosphamide, doxorubicin or carboplatin preparations known allergy to G-CSF or GM-CSF preparations or hypersensitivity
F.分析
安全性分析
患者をコホートBの2つの群のうちの1つに1:1の比でランダム化して、チラゴルマブ及びアテゾリズマブ+nab-pac+ACに対するアテゾリズマブ+nab-pac-carboーACの安全性プロファイルを評定する。主要安全性評価項目について正式な統計的比較は行われず、安全性分析は記述的である。したがって、形式電力計算は実行されなかった。試料サイズは、チラゴルマブ及びアテゾリズマブ+nab-pac-ACに対するアテゾリズマブ+nab-pac-carbo-ACの忍容性を評定するための記述的安全性分析を提供するのに十分であると考えられる。計画された試料サイズは、各処置群及び組み合わせた両群にわたる許容可能な確率で、≧10%の真の発生率を有する有害事象の観察を可能にする(表66を参照)。

安全性評定には、有害事象の発生率、性質及び重症度、治験実施計画書に定められたバイタルサイン、検査異常、及び、試験の安全性評価にとって重要であると考えられる他の治験実施計画書に規定された試験が含まれる。有害事象はNCI CTCAE v5.0に従って等級付けされる。 Safety assessment should include the incidence, nature and severity of adverse events, protocol-specified vital signs, laboratory abnormalities, and other protocol considerations considered important to the safety assessment of the study. including tests specified in the Adverse events are graded according to NCI CTCAE v5.0.
安全性は、ADAによって測定され、処置群によって提示される有害事象、臨床検査結果の変化、バイタルサインの変化、試験処置曝露及び免疫原性の要約によって評定される。 Safety is measured by the ADA and assessed by summaries of adverse events, laboratory test changes, vital sign changes, study treatment exposure and immunogenicity presented by treatment group.
有害事象の言語記述をMedDRA用語にマッピングする。 Verbal descriptions of adverse events are mapped to MedDRA terminology.
処置下で発現する事象(試験処置の最初の用量で又はその後に起こる事象として定義される)は、治験責任医師によって評定される試験薬との関係に関係なく、MedDRA用語、適切なMedDRAレベル、及びNCI CTCAE v5.0グレードによって要約される。各患者について、同じ有害事象の複数の発生が起こる場合、報告された最大重症度を要約に使用する。 A treatment-emergent event (defined as an event occurring at or after the first dose of study treatment), regardless of relationship to study drug as assessed by the Investigator, is a MedDRA term, an appropriate MedDRA level, and summarized by the NCI CTCAE v5.0 grade. For each patient, if multiple occurrences of the same adverse event occur, the maximum severity reported will be used for summaries.
以下の処置下で発現する有害事象を別々に要約する:試験薬の中止につながる有害事象、用量の減少又は中断につながる有害事象、グレード≧3の有害事象、グレード5の有害事象、重篤な有害事象、及び特別な関心のある有害事象。
The following treatment-emergent adverse events will be summarized separately: adverse events leading to discontinuation of study drug, adverse events leading to dose reduction or interruption, grade ≥3 adverse events,
全ての死亡及び死亡原因を要約する。 Summarize all deaths and causes of death.
関連する検査値を時点によって要約し、NCI CTCAEグレード3及びグレード4の値を適宜同定する。NCI CTCAEグレードの変化を処置群によって集計する。
曝露、有害事象、検査及びバイタルサインデータの分析
Relevant laboratory values are summarized by time point and
Analysis of exposure, adverse events, laboratory and vital signs data
安全性は、試験処置への曝露、有害事象、臨床検査結果の変化、並びにバイタルサイン及びECGの変化の要約を通して評定される。 Safety will be assessed through summaries of exposure to study treatment, adverse events, laboratory changes, and changes in vital signs and ECG.
試験処置曝露(例えば、処置期間、受けた総用量、並びにサイクル数及び用量変更)を記述統計学によって要約する。 Study treatment exposure (eg, duration of treatment, total dose received, and number of cycles and dose modifications) will be summarized by descriptive statistics.
全ての逐語的有害事象用語をMedDRAシソーラス用語にマッピングし、有害事象重症度をNCI CTCAE v5.0に従って等級付けする。試験処置の初回用量(すなわち、処置下で発現した有害事象)のとき又はその後に起こる全ての有害事象、重篤な有害事象、死亡につながる有害事象、特別な関心のある有害事象、及び試験処置の中止につながる有害事象を、マッピングされた用語、適切な類義語レベル、及び重症度によって要約する。様々な重症度の事象について、最高グレードが要約に使用される。死亡及び死亡原因を要約する。 All verbatim adverse event terms are mapped to MedDRA thesaurus terms and adverse event severity is graded according to the NCI CTCAE v5.0. All adverse events occurring at or after the first dose of study treatment (i.e., treatment-emergent adverse events), serious adverse events, adverse events leading to death, adverse events of special interest, and study treatment Adverse events leading to discontinuation of study will be summarized by mapped terms, appropriate synonym levels, and severity. For events of varying severity, the highest grade is used for summaries. Summarize deaths and causes of death.
関連する検査室、バイタルサイン(脈拍数、呼吸数、血圧、パルスオキシメトリ、及び体温)、及びECGデータは、必要に応じて識別されたグレードと共に時間によって表示される。更に、選択された臨床検査のシフトテーブルを使用して、ベースライン及びベースライン後の最大重症度グレードを要約する。バイタルサイン及びECGの変化を要約する。 Relevant laboratory, vital signs (pulse rate, respiratory rate, blood pressure, pulse oximetry, and temperature), and ECG data are displayed by time with grades identified as appropriate. In addition, baseline and post-baseline maximum severity grades will be summarized using a shift table of selected laboratory tests. Summarize changes in vital signs and ECG.
有効性分析
有効性分析はITTアプローチを使用し、患者が割り当てられた試験薬を受けているかどうかにかかわらず、登録された患者は分析に含まれ、コホートBの患者はランダム化時に割り当てられた処置に従って1:1の比でグループ化される。ITT集団のサブセットに基づく分析も行われ得る。仮説検定は、特に指示しない限り、両側性である。
Efficacy Analysis The efficacy analysis used an ITT approach, enrolled patients were included in the analysis whether or not they received their assigned study drug, patients in Cohort B were assigned at randomization Grouped in a 1:1 ratio according to treatment. Analysis based on subsets of the ITT population can also be performed. Hypothesis tests are two-sided unless otherwise indicated.
コホートBの調査有効性目的は、以下の評価項目に基づいて、チラゴルマブ及びアテゾリズマブ+nab-pac-carbo-ACに対するチラゴルマブ及びアテゾリズマブ+nab-pac-ACの有効性を調査することである。
●pCR、乳房及びリンパ節の両方からの腫瘍の根絶として定義される(ypT0/はypN0である)。
The study efficacy objective for Cohort B is to investigate the efficacy of tiragolumab and atezolizumab + nab-pac-AC versus tiragolumab and atezolizumab + nab-pac-carbo-AC based on the following endpoints.
• pCR, defined as tumor eradication from both breast and lymph nodes (ypT0/ is ypN0).
この有効性評価項目は、ネオアジュバント治療及び手術の完了後に確立される。pCR評定が欠落している患者は、pCRを達成していないとカウントされる。
●EFS、ランダム化から、文書化された疾患再発、進行、又は何らかの原因による死亡までの時間として定義される。
This efficacy endpoint is established after completion of neoadjuvant treatment and surgery. Patients with missing pCR scores are counted as not achieving pCR.
• EFS, defined as the time from randomization to documented disease recurrence, progression, or death from any cause.
分析時に無症候の患者は、最後に生存していて無症候と分かった日に打ち切られる。 Patients who are asymptomatic at the time of analysis are censored on the last known alive and asymptomatic day.
ベースライン後の情報がない患者は、ランダム化の日に打ち切られる。
●OS、ランダム化から任意の原因による死亡日までの時間として定義される。
Patients with no post-baseline information will be censored on the day of randomization.
• OS, defined as the time from randomization to the date of death from any cause.
分析時に死亡したと報告されていない患者は、最後に生存していることが分かった日に打ち切られる。ベースライン後に情報を有さない患者は、ランダム化の日付で打ち切られる。 Patients not reported dead at the time of analysis are censored on the date they were last known alive. Patients with no information after baseline will be censored at the date of randomization.
薬物動態学的分析
PK分析のために試料を収集し、この試験における曝露を以前の試験で得られた曝露と比較する。チラゴルマブ及びアテゾリズマブの血清濃度並びにnab-パクリタキセル、カルボプラチン、ドキソルビシン及びシクロホスファミドの血漿濃度は、適切な場合及びデータが許す場合、処置群及びサイクルによって個々の値として報告され、要約される(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)。
Pharmacokinetic Analysis Samples are collected for PK analysis and exposures in this study are compared to those obtained in previous studies. Serum concentrations of tiragolumab and atezolizumab and plasma concentrations of nab-paclitaxel, carboplatin, doxorubicin and cyclophosphamide, where appropriate and data permitting, are reported as individual values by treatment arm and cycle and summarized (mean , standard deviation, coefficient of variation, median, range, geometric mean, and geometric mean coefficient of variation).
個々の及び血清中のチラゴルマブ及びアテゾリズマブ濃度の中央値を、処置群及び日ごとにプロットする。チラゴルマブ及びアテゾリズマブの濃度データを、確立された集団PKモデルを使用して他の試験からのデータと共にプールして、データによって保証されるクリアランス、分布容積及びAUC等のPKパラメーターを導出することができる。関連するPKパラメーターと用量、安全性、有効性又はバイオマーカーの結果との潜在的な相関関係を調べることができる。 Median individual and serum tiragolumab and atezolizumab concentrations are plotted by treatment group and day. Tiragolumab and atezolizumab concentration data can be pooled with data from other studies using established population PK models to derive data-assured PK parameters such as clearance, volume of distribution and AUC. . Potential correlations between relevant PK parameters and dose, safety, efficacy or biomarker outcomes can be examined.
免疫原性分析
免疫原性分析には、任意のADA評定を受けた患者が含まれ、受けた処置に従って患者がグループ分けされる。処置中及びフォローアップ期間中の処置下で発現したADA陽性患者及びADA陰性患者の数及び割合を処置群によって要約する。
Immunogenicity Analysis The immunogenicity analysis includes patients with any ADA assessment and groups the patients according to the treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients during treatment and the follow-up period are summarized by treatment group.
ADAの状態と安全性、有効性及びPK評価項目との間の関係は、記述統計学を用いて分析及び報告され得る。 Relationships between ADA status and safety, efficacy and PK endpoints can be analyzed and reported using descriptive statistics.
バイオマーカー分析
探索的バイオマーカーの正式な統計分析は行われていないが、データは、この試験の文脈で、及び他の試験からのデータとまとめて分析することができる。
Biomarker Analysis Although no formal statistical analysis of the exploratory biomarkers has been performed, the data can be analyzed in the context of this study and together with data from other studies.
実施例15.頭頸部の再発性/転移性PD-L1陽性扁平上皮癌腫を有する患者における第1選択処置としてのアテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボの第II相ランダム化二重盲検試験
本実施例は、頭頸部の再発性/転移性PD-L1陽性扁平上皮癌腫(SCCHN)における一次(1L)処置としてのアテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボの有効性及び安全性を評価するために設計された第II相ランダム化二重盲検グローバル試験を記載する。この試験は、以下の群からなる:
群A:患者は、3週間ごと(Q3W)のIV注入によって投与される1200mgの固定用量のアテゾリズマブを各21日間サイクルの1日目に受け、続いて、Q3WのIVの注入によって患者に投与される600mgの固定用量のチラゴルマブを各21日間サイクルの1日目に受ける。
群B:患者は、Q3WのIV注入によって投与される1200mgの固定用量のアテゾリズマブを各21日間サイクルの1日目に受け、続いて、Q3WのIV注入によって投与されるプラセボを各21日間サイクルの1日目に受ける。
Example 15. A phase II randomized, double-blind study of atezolizumab plus tiragolumab and atezolizumab plus placebo as first-line treatment in patients with recurrent/metastatic PD-L1-positive squamous cell carcinoma of the head and neck. A phase II randomization designed to evaluate the efficacy and safety of atezolizumab + tiragolumab and atezolizumab + placebo as first-line (1L) treatment in recurrent/metastatic PD-L1-positive squamous cell carcinoma (SCCHN) A double-blind global study is described. This study consists of the following groups:
Group A: Patients received a fixed dose of 1200 mg of atezolizumab administered by IV infusion every 3 weeks (Q3W) on
Group B: Patients received 1200 mg fixed dose atezolizumab administered by IV infusion Q3W on
A.試験計画
この第II相ランダム化二重盲検グローバル試験は、再発性/転移性PD-L1陽性SCCHNにおける1L処置としてのアテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボの有効性及び安全性を評価するように設計されている。適格患者には、根治目的の局所療法に適していない再発性疾患及び/又は転移性PD-L1陽性SCCHN(腫瘍関連免疫細胞(TIC)≧5%)を有し、再発性/転移性疾患の事前全身治療を受けたことがない、米国東海岸がん臨床試験グループ(ECOG)のパフォーマンスステータスが0又は1の18歳以上の男性及び女性の患者が含まれる。
A. Study Design This Phase II, randomized, double-blind, global study is designed to evaluate the efficacy and safety of atezolizumab + tiragolumab and atezolizumab + placebo as 1L treatment in recurrent/metastatic PD-L1-positive SCCHN It is Eligible patients must have recurrent disease and/or metastatic PD-L1-positive SCCHN (tumor-associated immune cells (TIC) ≥5%) not amenable to local therapy with curative intent, and no recurrent/metastatic disease. Male and female patients aged 18 years and older with US East Coast Cancer Clinical Trials Group (ECOG) performance status of 0 or 1 who have not received prior systemic therapy are included.
スクリーニング中に、各潜在的に適格な患者由来の腫瘍標本を、治験VENTANA PD-L1(SP 263)Companion Diagnostics(CDx)アッセイを使用して、中央検査室によって評定されるように、PD-L1発現について前向きに試験する。中央で評定された5%以上のTICを有するPD-L1陽性の患者のみが適格である。PD-L1発現は、5%~19%のTICを有するPD-L1低及び20%以上のTICを有するPD-L1高として定義される。 During screening, tumor specimens from each potentially eligible patient were tested for PD-L1 as assessed by a central laboratory using the investigational VENTANA PD-L1 (SP 263) Companion Diagnostics (CDx) assay. Test prospectively for expression. Only PD-L1 positive patients with a centrally assessed TIC of ≥5% are eligible. PD-L1 expression is defined as PD-L1 low with TICs between 5% and 19% and PD-L1 high with TICs greater than or equal to 20%.
適格患者を、中咽頭がんについてのヒトパピローマウイルス(HPV)状態(HPV陽性中咽頭がん:有対無)及びPD-L1状態(PD-L1:低対高)によって層別化する。各PD-L1サブグループ(PD-L1低[TIC5%-19%]及びPD-L1高[TIC≧20%])への登録は、計画された全登録の約55%で制限される(すなわち、約66人の患者)。
Eligible patients will be stratified by human papillomavirus (HPV) status for oropharyngeal cancer (HPV-positive oropharyngeal cancer: present vs. absent) and PD-L1 status (PD-L1: low vs. high). Enrollment in each PD-L1 subgroup (PD-L1 low [
適格患者を2:1の比でランダム化して、アテゾリズマブ+チラゴルマブ(群A)又はアテゾリズマブ+プラセボ(群B)のいずれかを受ける。 Eligible patients are randomized in a 2:1 ratio to receive either atezolizumab plus tiragolumab (Arm A) or atezolizumab plus placebo (Arm B).
群A:患者は、3週間ごと(Q3W)のIV注入によって投与される1200mgの固定用量のアテゾリズマブを各21日間サイクルの1日目に受け、続いて、Q3WのIVの注入によって患者に投与される600mgの固定用量のチラゴルマブを各21日間サイクルの1日目に受ける。
Group A: Patients received a fixed dose of 1200 mg of atezolizumab administered by IV infusion every 3 weeks (Q3W) on
群B:患者は、Q3WのIV注入によって投与される1200mgの固定用量のアテゾリズマブを各21日間サイクルの1日目に受け、続いて、Q3WのIV注入によって投与されるプラセボを各21日間サイクルの1日目に受ける。
Group B: Patients received 1200 mg fixed dose atezolizumab administered by IV infusion Q3W on
患者は、ベースライン、サイクル1の1日目の後の最初の30週間の6週間ごと(±7日)、及び30週目の腫瘍評定の完了後9週間ごと(±7日)に腫瘍評定を受ける。腫瘍評定は、RECIST v1.1による放射線学的疾患進行又はRECIST v1.1による放射線学的疾患進行後の試験処置を継続する患者についての臨床的利益の喪失、同意の撤回、死亡又は試験依頼者による試験の終了のいずれか早く発生する方まで、処置の遅延にかかわらず、スケジュールごとに継続する。治験責任医師の裁量により、進行性疾患又は臨床的利益の喪失が疑われる場合はいつでもスキャンを実施しなければならない。
Patients will have tumor assessments at baseline, every 6 weeks (±7 days) for the first 30 weeks after
RECIST v 1.1による放射線学的疾患進行がない場合に試験処置(限定されないが、臨床的低下又は毒性を含む何らかの理由で、)を中止する患者は、RECIST v1.1による放射線学的疾患進行、同意の撤回、死亡、又は試験依頼者による試験終了のいずれか早く発生する方まで、予定された腫瘍評定を上記の頻度で継続する。RECIST v1.1による、放射線学的疾患の進行がない場合、患者が新しい抗がん治療を開始するかどうかにかかわらず、腫瘍評定を継続すべきである。単一の時点での客観的奏効は、RECIST v1.1に従って治験責任医師によって決定される。 Patients who discontinue study treatment (for any reason, including but not limited to clinical decline or toxicity) in the absence of radiographic disease progression by RECIST v1.1 will have radiographic disease progression by RECIST v1.1. , scheduled tumor assessments will continue at the above frequency until withdrawal of consent, death, or sponsor termination of the study, whichever occurs first. In the absence of radiographic disease progression by RECIST v1.1, tumor assessment should continue regardless of whether the patient begins new anticancer therapy. Objective response at a single time point will be determined by the investigator according to RECIST v1.1.
血清試料を採取して、アテゾリズマブ及びチラゴルマブPKをモニタリングし、アテゾリズマブ及びチラゴルマブに対する抗体の存在を検出する。保管及び新鮮な腫瘍組織、血漿、及び血液試料を含む患者試料が、探索的バイオマーカー評定のために収集される。 Serum samples are collected to monitor atezolizumab and tiragolumab PK and to detect the presence of antibodies to atezolizumab and tiragolumab. Patient samples, including archival and fresh tumor tissue, plasma, and blood samples, are collected for exploratory biomarker assessment.
安全性評定には、有害事象の発生率、性質及び重症度、並びに試験の安全性評価にとって重要であると考えられる検査異常等の他の治験実施計画書指定の試験が含まれる。 Safety assessments include other protocol-specified studies such as the incidence, nature and severity of adverse events, and laboratory abnormalities considered important to the study's safety assessment.
試験処置の中止後、生存フォローアップ情報は、死亡、フォローアップ不能、又は試験依頼者による試験終了のいずれか早く発生する方まで、およそ3ヶ月毎に電話、患者の医療記録、及び/又はクリニック来院によって収集される。すべての患者は、患者が生存フォローアップから撤退することを要求(この要求は、ソース文書に文書化され、治験責任医師によって署名されなければならない)しない限り、生存及び新しい抗がん治療情報について定期的に連絡を受けることになる。患者が生存フォローアップから離脱する場合、試験スタッフは、公開されている情報源(例えば、郡記録)を使用して生存状態に関する情報を得ることができる。 After discontinuation of study treatment, survival follow-up information will be obtained by telephone, patient medical records, and/or clinic visit approximately every 3 months until death, loss of follow-up, or termination of the study by the sponsor, whichever occurs first. Collected by hospital visit. All patients will be discontinued for survival and new anticancer therapy information unless the patient requests withdrawal from survival follow-up (this request must be documented in the source document and signed by the investigator). You will be contacted regularly. If a patient is withdrawn from survival follow-up, study staff can obtain information on survival status using publicly available sources (eg, county records).
処置は、X線写真データ、生検結果(利用可能な場合)、及び臨床状態の統合評定後に疾患進行に起因する許容できない毒性又は症候性悪化がない場合、治験責任医師によって評定される臨床的利益を患者が経験している限り継続され得る。RECIST v 1.1による疾患進行の基準を満たすが臨床的利益を有し続ける患者は、概説された基準のすべてを満たし、書面による同意を提供する場合、処置(アテゾリズマブ+チラゴルマブ又はアテゾリズマブ+プラセボ)を継続することが許可される。 Treatment will be clinically assessed by the investigator if there is no unacceptable toxicity or exacerbation due to disease progression after integrated assessment of radiographic data, biopsy results (if available), and clinical status. It can be continued as long as the patient experiences the benefits. Patients who meet criteria for disease progression by RECIST v 1.1 but continue to have clinical benefit will be treated (atezolizumab + tiragolumab or atezolizumab + placebo) if they meet all outlined criteria and provide written informed consent. is allowed to continue.
B.投薬及び投与
処置レジメンを図23に要約する。
B. Dosing and Administration The treatment regimen is summarized in FIG.
アテゾリズマブ
全ての患者は、各21日間サイクルの1日目にIV注入によって投与される1200mgのアテゾリズマブを受ける。アテゾリズマブ用量は固定され、体重に依存しない。アテゾリズマブ注入は、表67に概説される指示に従って投与される。

チラゴルマブ及びプラセボ
アテゾリズマブの投与及び観察期間(表67参照)の後、患者は、各21日間サイクルの第1日にIV注入によって投与される600mgのチラゴルマブ/プラセボを受ける。チラゴルマブ/プラセボの用量は固定されており、体重に依存しない。チラゴルマブ/プラセボ注入は、表68に概説される指示に従って投与される。

アテゾリズマブ及びチラゴルマブ/プラセボ
アテゾリズマブもチラゴルマブ/プラセボも永続的に中止されていない限り、以下の規則が適用される:
●処置サイクルは通常、各21日間サイクルの1日目にアテゾリズマブ及びチラゴルマブ/プラセボを投与することから始まる。いずれかの試験薬物が薬物関連毒性のために遅延される場合、アテゾリズマブ及びチラゴルマブの安全性プロファイルは類似しているので、他方の試験薬物も遅延されることが推奨される。しかし、サイクルは、治験責任医師の裁量で適切と考えられる場合、他の試験薬の投与から開始してもよい。
●薬物関連毒性のための1つの試験薬の投与が遅延し、他方の試験薬が計画通り投与される場合、遅延されている試験薬を次の予定された注入(すなわち、次の予定された21日サイクル)で投与することが推奨される。
Atezolizumab and Tiragolumab/Placebo Unless atezolizumab or tiragolumab/placebo are permanently discontinued, the following rules apply:
• Treatment cycles generally begin with administration of atezolizumab and tiragolumab/placebo on
- If the administration of one study drug is delayed for drug-related toxicity and the other study drug is 21-day cycles) are recommended.
用量の変更
この試験では、アテゾリズマブ又はチラゴルマブ/プラセボについて用量減少を含む用量変更はない。
Dose Modifications There are no dose modifications, including dose reductions, for atezolizumab or tiragolumab/placebo in this study.
C.併用療法
併用療法は、試験処置の開始の7日前から処置中止の来院までの治験実施計画書に定められた処置に加えて、患者によって使用される任意の医薬(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)からなる。
C. Concomitant Therapy Concomitant therapy is any medication used by the patient (e.g., prescription, over-the-counter, vaccines, herbal or homeopathic remedies, dietary supplements).
許可された治療
患者は、試験中に以下の治療法を使用することが許される。
●年間失敗率<1%の経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●COPD又は喘息のために投与される吸入又は低用量コルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
Allowed Treatments Patients will be allowed to use the following treatments during the study.
● Oral contraceptives with <1% annual failure rate ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable-dose warfarin or low-molecular-weight heparin)
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
Inhaled or low-dose corticosteroids given for COPD or asthma Low-dose corticosteroids given for orthostatic hypotension or adrenocortical insufficiency Palliative radiotherapy as outlined below (e.g., Treatment of known bone metastases or symptomatic relief of pain):
RECIST v1.1による放射線学的疾患進行の文書化がない患者では、対症療法のための支持療法を最大化し、腫瘍標的病変の評定を妨げる放射線療法を回避することが強く奨励される。 In patients without documented radiographic disease progression by RECIST v1.1, maximizing supportive care for symptomatic treatment and avoiding radiation therapy that interferes with assessment of tumor target lesions is strongly encouraged.
アテゾリズマブ及びチラゴルマブ/プラセボによる処置は、緩和放射線療法中に継続され得る。 Treatment with atezolizumab and tiragolumab/placebo may be continued during palliative radiotherapy.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ及びチラゴルマブ/プラセボ注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may only be administered for the second and subsequent atezolizumab and tiragolumab/placebo infusions at the investigator's discretion.
一般に、治験責任医師は、臨床上適応がある場合、現地の標準診療に従って、注意療法又は禁止療法として定義されるもの以外の支持療法で患者のケア(既存の症状を含む)を管理すべきである。注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びββ2アドレナリン作用性アゴニスト)によって管理されなければならない。 In general, investigators should manage patient care (including pre-existing symptoms) with supportive care other than those defined as attention or prohibitive care, as clinically indicated, and in accordance with local standard practice. be. Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine) or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and ββ2-adrenergic agonist).
注意を要する治療
全身性コルチコステロイド及びTNF-α阻害剤は、アテゾリズマブ及び/又はチラゴルマブによる処置の潜在的な有益な免疫学的効果を減弱させ得る。したがって、全身性コルチコステロイド又はTNF-α阻害剤が日常的に投与される状況では、抗ヒスタミン剤を含む代替物を検討する。代替が実施可能でない場合、コルチコステロイド及びTNF-α阻害剤の全身投与を治験責任医師の裁量で行うことができる。
Treatments requiring caution Systemic corticosteroids and TNF-α inhibitors may attenuate the potentially beneficial immunological effects of treatment with atezolizumab and/or tiragolumab. Therefore, in situations where systemic corticosteroids or TNF-α inhibitors are routinely administered, alternatives including antihistamines are considered. If alternatives are not feasible, systemic corticosteroids and TNF-α inhibitors can be administered at the investigator's discretion.
アテゾリズマブ及び/又はチラゴルマブ治療に関連する場合、特定の有害事象の処置のために、治験責任医師の裁量で、全身コルチコステロイドが推奨される。 Systemic corticosteroids are recommended at the investigator's discretion for treatment of specific adverse events when associated with atezolizumab and/or tiragolumab therapy.
禁止される治療
以下の併用療法の使用は、以下に記載されるように禁止される:
●がん(限定されるものではないが、手術、化学療法、ホルモン療法、免疫療法、放射線療法、及び薬草療法を含む)の処置を目的とした併用療法は、保健当局が-承認したものであろうと実験的なものであろうと、薬剤に応じて、試験処置を開始する前の様々な期間、及び試験処置中、疾患の進行が文書化され、患者が試験処置を中止するまで、特定の状況下での緩和的放射線療法及び局所療法を除いて禁止される。
●治験治療は、試験処置の開始前28日以内及び試験処置中に禁止される。
●生弱毒化ワクチン(例えば、FLUMIST(登録商標))は、試験処置の開始前4週間以内、試験処置中、及びアテゾリズマブの最終投与後5ヶ月間及びチラゴルマブ/プラセボの最終投与後90日間は禁止する。
●試験処置と組み合わせて投与した場合、自己免疫症状のリスクを潜在的に増加させる可能性があるため、試験処置の開始前及び試験処置中の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫賦活剤(限定されないが、インターフェロン及びIL-2を含む)は禁止される。
●全身免疫抑制薬(限定されないが、シクロホスファミド、アザチオプリン、メトトレキサート及びサリドマイドを含む)は、これらの薬剤が試験処置の有効性及び安全性を潜在的に変化させる可能性があるため、試験処置中は禁止される。
Prohibited Therapies The use of the following concomitant therapies is prohibited as described below:
Any combination therapy for the treatment of cancer (including, but not limited to, surgery, chemotherapy, hormone therapy, immunotherapy, radiation therapy, and herbal therapy) is approved by health authorities. Depending on the drug, whether experimental or experimental, for various periods prior to initiation of study treatment, and during study treatment, until disease progression is documented and the patient discontinues study treatment, a specific Prohibited except for palliative radiotherapy and local therapy under certain circumstances.
• Study treatment is prohibited within 28 days prior to initiation of study treatment and during study treatment.
- Live attenuated vaccines (e.g., FLUMIST®) are prohibited within 4 weeks prior to initiation of study treatment, during study treatment, and for 5 months after final dose of atezolizumab and 90 days after final dose of tiragolumab/placebo do.
o Within 4 weeks or 5 drug elimination half-lives (either within 4 weeks prior to initiation of study treatment and during study treatment due to potential increased risk of autoimmune symptoms when administered in combination with study treatment) Systemic immunostimulants (including but not limited to interferon and IL-2) within the longer term) are prohibited.
- Systemic immunosuppressants (including but not limited to cyclophosphamide, azathioprine, methotrexate, and thalidomide) should not be used in studies because these agents can potentially alter the efficacy and safety of study treatments. Prohibited during treatment.
D.選択基準
患者は次の試験登録基準を満たさなければならない:
●署名済みインフォームドコンセントフォーム
●インフォームドコンセント書類の署名時の年齢が≧18歳
●試験治験実施計画書を遵守する能力
●組織学的又は細胞学的に確認された、中咽頭、口腔、喉頭又は下咽頭を含む再発性/転移性SCCHNであって、局所療法によって治癒不能であると考えられるもの
D. Inclusion Criteria Patients must meet the following study entry criteria:
- Signed informed consent form - Age ≥18 years at the time of signing the informed consent document - Ability to comply with the study protocol - Histologically or cytologically confirmed oropharynx, oral cavity, larynx or recurrent/metastatic SCCHN involving the hypopharynx, considered incurable by local therapy
任意の組織学の鼻咽頭又は耳下腺に腫瘍の原発部位を有する患者は適格ではない。
●p16免疫組織化学(IHC)、インサイチュハイブリダイゼーション又はポリメラーゼ連鎖に基づくアッセイによって局所的に決定される中咽頭癌腫のHPV状態の検査からの既知の結果
注:口腔がん、喉頭がん及び下咽頭がんのHPV検査は必要ではない。
●転移性及び/又は再発性SCCHNに対する事前全身治療なし
Patients with a primary site of tumor in the nasopharynx or parotid gland of any histology are not eligible.
• Known results from testing for HPV status in oropharyngeal carcinoma locally determined by p16 immunohistochemistry (IHC), in situ hybridization or polymerase chain-based assays Note: oral cavity cancer, laryngeal cancer and hypopharyngeal cancer HPV testing for cancer is not required.
- No prior systemic therapy for metastatic and/or recurrent SCCHN
局所進行性疾患に対するマルチモーダル処置(例えば、同時化学放射線)の一部として与えられる全身療法を受け、全身治療の最後の用量がランダム化の≧6ヶ月前であった患者が許可される。
●RECIST v 1.1による測定可能な疾患
Patients who received systemic therapy given as part of multimodal treatment (eg, concurrent chemoradiation) for locally advanced disease and whose last dose of systemic therapy was ≧6 months prior to randomization are permitted.
●Measurable disease according to RECIST v1.1
以前に放射線照射された病変は、放射線照射後にその部位で進行性疾患が明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。
●先に得られた保管腫瘍組織又は予備スクリーニング/スクリーニングでの生検から得られた組織のいずれかにおいて、治験VENTANA PD-L1(SP263)CDxアッセイによって決定され、代表的な腫瘍組織標本の中央検査により文書化された、TIC≧5%である腫瘍PD-L1発現。約66人の患者(全予定登録の55%)がPD-L1サブグループ(PD-L1低(TIC 5%-19%)及びPD-L1高(TIC≧20%))のいずれかに登録された後、PD-L1サブグループにおいて追加の患者は登録されない。
Previously irradiated lesions can be considered measurable disease only if progressive disease is clearly documented at the site after irradiation.
- median of representative tumor tissue specimens, as determined by the investigational VENTANA PD-L1 (SP263) CDx assay, either in previously obtained archival tumor tissue or in tissue obtained from prescreening/screening biopsies; Tumor PD-L1 expression with TIC > 5% documented by laboratory. Approximately 66 patients (55% of all planned enrollments) were enrolled in one of the PD-L1 subgroups (PD-L1 low (
ホルマリン固定パラフィン包埋(FFPE)ブロック(好ましい)又は関連する病理報告と共に染色されていない新たに切断した連続切片を含む少なくとも20枚のスライドにおける代表的な腫瘍標本の確認された利用可能性 15-19枚のスライドしか利用できない場合、メディカルモニターの確認が得られた後、患者は依然として試験に適格であり得る。 Confirmed availability of representative tumor specimens in formalin-fixed paraffin-embedded (FFPE) blocks (preferred) or at least 20 slides containing unstained freshly cut serial sections with relevant pathology reports. If only 19 slides are available, the patient may still be eligible for the study after obtaining medical monitor confirmation.
保管腫瘍組織が利用できないか、又は必要な検査に適さないと判定された場合、腫瘍組織は、事前スクリーニング/スクリーニングで行われた生検から得なければならない。患者の保管組織検査結果が適格基準を満たさない場合、事前スクリーニング/スクリーニングで生検を実施することもできる。
●ECOGパフォーマンスステータス0又は1
●平均余命≧12週間
●ランダム化前14日以内に得られた以下の臨床検査結果によって定義される、適切な血液学的機能及び終末器官機能:
-顆粒球コロニー刺激因子支持なしでANC≧1.5X109/L(1500/μL)
-リンパ球数≧0.5X109/L(500/μL)
-輸血なしで血小板数≧100X109/L(100,000/μL)
-ヘモグロビン≧90g/L(9g/dL)。
If archival tumor tissue is unavailable or determined to be unsuitable for the required testing, tumor tissue must be obtained from a biopsy performed at prescreening/screening. A biopsy may also be performed at pre-screening/screening if the patient's archival tissue test results do not meet eligibility criteria.
●
- Life expectancy ≥ 12 weeks - Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to randomization:
- ANC ≧1.5×109/L (1500/μL) without granulocyte colony stimulating factor support
- Lymphocyte count ≧0.5×109/L (500/μL)
- Platelet count ≥100 X 109/L (100,000/μL) without transfusion
- Hemoglobin > 90 g/L (9 g/dL).
患者は、この基準を満たすために、現地のSOCに従って輸血又は赤血球造血処置を受けることができる。
-AST、ALT及びアルカリホスファターゼ(ALP)≦2.5X正常値の上限(ULN)、ただし、以下の例外を除く:
文書化された肝臓転移を有する患者:AST及びALT≦5XULN
文書化された肝臓転移又は骨転移を有する患者:ALP≦5XULN
-総ビリルビン≦1.5XULN、ただし、以下を除く:
既知のギルバート病患者:総ビリルビン≦3XULN
-クレアチニン≦1.5XULN
-アルブミン≧25g/L(2.5g/dL)
-治療的抗凝固療法を受けていない患者の場合:INR及びaPTT≦1.5XULN
●治療的抗凝固薬を投与されている患者:安定な抗凝固薬
●スクリーニング時の陰性HIV検査
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時のB型肝炎表面抗体(HBsAb)陽性検査、又は以下のいずれかを伴うスクリーニング時のHBsAb陰性:
-総B型肝炎コア抗体(HBcAb)陰性
-陽性の全HBcAb検査とそれに続く定量的B型肝炎ウイルス(HBV)DNA<500 IU/mL
Patients may receive blood transfusions or erythropoietic procedures according to local SOC to meet this criterion.
- AST, ALT and alkaline phosphatase (ALP) < 2.5X upper limit of normal (ULN), with the following exceptions:
Patients with documented liver metastases: AST and ALT ≤ 5XULN
Patients with documented liver or bone metastases: ALP ≤ 5XULN
- total bilirubin ≤ 1.5 XULN, except:
Patients with known Gilbert's disease: total bilirubin < 3XULN
- creatinine ≤ 1.5 XULN
- albumin ≥ 25 g/L (2.5 g/dL)
- For patients not receiving therapeutic anticoagulation: INR and aPTT ≤ 1.5XULN
Patients receiving therapeutic anticoagulants: stable anticoagulants Negative HIV test at screening Negative hepatitis B surface antigen (HBsAg) test at screening Hepatitis B surface antibody (HBsAb) at screening ) positive test or negative for HBsAb at screening with any of the following:
- total hepatitis B core antibody (HBcAb) negative - positive total HBcAb test followed by quantitative hepatitis B virus (HBV) DNA <500 IU/mL
HBV DNA検査を、HBsAg検査陰性、HBsAb検査陰性、及び総HBcAb検査陽性の患者に対して実施しなければならない。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。
-HCV RNA検査を、HCV抗体検査が陽性の患者に対して行われなければならない。
●妊娠可能な女性の場合:以下に定義されるように、禁欲したままである(異性間の性交を控える)か、又は避妊を使用することの同意:
HBV DNA tests must be performed on patients with negative HBsAg tests, negative HBsAb tests, and positive total HBcAb tests.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening.
- HCV RNA testing should be performed for patients with a positive HCV antibody test.
For women of childbearing potential: consent to remain abstinent (abstain from heterosexual intercourse) or to use contraception, as defined below:
女性は、処置期間中、並びにアテゾリズマブの最終投与後5ヶ月間及びチラゴルマブ/プラセボの最終投与後90日間、禁欲を維持するか、又は年間<1%の失敗率の避妊方法を使用しなければならない。 Women must remain abstinent or use a contraceptive method with an annual failure rate of <1% during the treatment period and for 5 months after the last dose of atezolizumab and 90 days after the last dose of tiragolumab/placebo. .
女性は、月経後であり、閉経後の状態(連続≧12ヶ月の閉経以外の特定された原因のない無月経)に達しておらず、手術(すなわち、卵巣、卵管、及び/又は子宮の除去)又は治験責任医師によって決定される別の原因(例えば、ミュラー管無発生)のために永久に不妊ではない場合、妊娠可能性があるとみなされる。出産可能性の定義は、地域のガイドライン又は規制との整合に適合させることができる。 Females are postmenopausal, have not achieved postmenopausal status (amenorrhea with no identified cause other than menopause for ≧12 consecutive months), and have had surgery (i.e., ovarian, fallopian tube, and/or uterine Ablation) or another cause determined by the Investigator (eg, Müllerian agenesis) is considered fertile if not permanently infertile. Fertility definitions can be adapted to match local guidelines or regulations.
年間失敗率<1%の避妊方法の例としては、両側卵管結紮術、男性の不妊手術、排卵を阻害するホルモン避妊具、ホルモン放出子宮内避妊具、及び銅付加子宮内避妊具が挙げられる。 Examples of contraceptive methods with an annual failure rate of <1% include bilateral tubal ligation, male sterilization, hormonal devices that inhibit ovulation, hormone-releasing intrauterine devices, and copper-added intrauterine devices. .
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。周期性禁欲(例えば暦、排卵、症候体温法、又は排卵後法)及び禁断は、適切な避妊方法ではない。地域のガイドライン又は規制に従って要求される場合、地域で認められている適切な避妊方法及び禁欲の信頼性に関する情報は、地域のインフォームドコンセント用紙に記載される。
●男性の場合:以下に定義されるように、禁欲(異性との性交を控える)又はコンドームの使用の同意、及び精子の提供を控える旨の同意
The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle. Cyclic abstinence (eg, calendar, ovulatory, symptomothermic, or postovulatory) and abstinence are not suitable methods of contraception. When required according to local guidelines or regulations, information regarding the reliability of locally accepted methods of appropriate contraception and abstinence is provided on the local informed consent form.
For men: Consent to abstinence (abstinence from heterosexual intercourse) or condom use, and consent to refrain from donating sperm, as defined below.
妊娠可能な女性パートナー又は妊娠中の女性パートナーの場合、男性は、胚に曝露させないように、チラゴルマブ/プラセボによる処置中、及びチラゴルマブ/プラセボの最終投与後90日間、禁欲を維持するか、又はコンドームを使用しなければならない。男性は、同期間中は精子提供をやめなければならない。 For female partners of childbearing potential or pregnant, males should remain abstinent or use a condom during treatment with tiragolumab/placebo and for 90 days after the last dose of tiragolumab/placebo to avoid exposing the embryos. must be used. Men must stop donating sperm during the same period.
性的禁欲の信頼性は、臨床治験の期間、並びに、患者の好ましい、及び通常のライフスタイルに関連して評価されなければならない。周期的な禁欲(例えば、カレンダー法、排卵法、症候体温法、又は排卵後法)及び中絶性交は、薬物曝露を防止する適切な方法ではない。地域のガイドライン又は規制に従って要求される場合、禁欲の信頼性に関する情報は、地域のインフォームドコンセント用紙に記載される。 The reliability of sexual abstinence must be evaluated in relation to the duration of the clinical trial and the patient's preferred and usual lifestyle. Cyclic abstinence (eg, calendar, ovulatory, symptomatic, or postovulatory) and abortive intercourse are not adequate methods to prevent drug exposure. If required according to local guidelines or regulations, information regarding the reliability of abstinence will be provided on the local informed consent form.
E.除外基準
以下の基準のいずれかを満たす患者は試験から除外される:
●根治目的の局所療法に適した疾患
●局所進行性SCCHNのための治癒目的の全身処置の最後の用量から6ヶ月以内の進行性又は再発性疾患
●手術又は他の事前治療に関連するグレード≧2の未解消の毒性≦グレード2の脱毛症又は神経障害を有する患者は許容される。
E. Exclusion Criteria Patients meeting any of the following criteria will be excluded from the study:
- Disease amenable to local therapy with curative intent - Progressive or recurrent disease within 6 months of last dose of systemic treatment with curative intent for locally advanced SCCHN - Grade ≥ related to surgery or other prior therapy Patients with 2 unresolved toxicities <
大きな手術を受けた患者は、介入に関連するあらゆる合併症からの回復を含め、十分に回復していなければならない。 Patients undergoing major surgery should be well recovered, including recovery from any complications associated with the intervention.
管理されており、試験薬物処置によって悪化すると予想されない不可逆的毒性を有する患者は、メディカルモニターに相談した後に含めることができる。
●症候性、未処置、又は活発に進行する中枢神経系(CNS)転移。
処置されたCNS病変を有する無症候性患者は、以下の基準の全てが満たされるならば適格である:
-RECIST v1.1による測定可能な疾患はCNS外に存在しなければならない
-患者は頭蓋内出血又は脊髄出血の病歴がない。
-患者は、ランダム化前の7日以内に定位放射線療法を受けておらず、ランダム化前の14日間以内に全脳放射線療法を受けておらず、又はランダム化前の28日間以内に神経外科的摘出を受けたことがない。
-患者は、CNS疾患の治療としてのコルチコステロイドに対する継続的な要求がない。安定な用量での抗痙攣療法が許容される。
●軟髄膜疾患の病歴
●制御されない腫瘍関連疼痛
Patients with irreversible toxicities that are controlled and not expected to be exacerbated by study drug treatment can be included after consulting a medical monitor.
• Symptomatic, untreated, or actively progressing central nervous system (CNS) metastases.
Asymptomatic patients with treated CNS lesions are eligible if all of the following criteria are met:
- Measurable disease by RECIST v1.1 must be present outside the CNS - Patient has no history of intracranial or spinal cord hemorrhage.
- Patient has not received stereotactic radiotherapy within 7 days prior to randomization, has not received whole-brain radiotherapy within 14 days prior to randomization, or received neurosurgical therapy within 28 days prior to randomization I have never had a surgical resection.
- Patient has no ongoing need for corticosteroids as treatment for CNS disease. Anticonvulsant therapy at stable doses is acceptable.
history of leptomeningeal disease uncontrolled tumor-related pain
鎮痛薬を必要とする患者は、試験登録時に安定したレジメンでなければならない。 Patients requiring analgesics must be on a stable regimen at study entry.
緩和的放射線療法に適した症候性病変(例えば、神経インピンジメントを引き起こす骨転移又は転移)は、登録前に処置しなければならない。 Symptomatic lesions amenable to palliative radiotherapy (eg bone metastases or metastases causing nerve impingement) must be treated prior to enrollment.
患者は、放射線の影響から回復されなければならない。必要とされる最低限の回復期間はない。 Patients must recover from the effects of radiation. There is no minimum recovery period required.
更なる成長(例えば、脊髄圧迫に現在関連していない硬膜外転移)を伴う機能障害又は難治性疼痛を引き起こす可能性が高い無症候性転移性病変は、登録前に適切な場合、局所領域治療について検討されるべきである。
●制御不能又は症候性の高カルシウム血症
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質抗体症候群、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、又は多発性硬化症を含むがこれらに限定されない自己免疫疾患又は免疫不全活動が活動性であるもの、又はその病歴、ただし、以下を除く:
Asymptomatic metastatic lesions likely to cause functional impairment or intractable pain with further growth (e.g., epidural metastases not currently associated with spinal cord compression) should be treated with locoregional, if appropriate, prior to enrollment. Treatment should be considered.
● Uncontrolled or symptomatic hypercalcemia ● Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Active or history of autoimmune disease or immunodeficiency activity, including but not limited to Guillain-Barré syndrome, or multiple sclerosis, with the exception of:
甲状腺補充ホルモンを服用している自己免疫関連甲状腺機能低下症の病歴を有する患者が試験に適格である。 Patients with a history of autoimmune-related hypothyroidism taking thyroid replacement hormone are eligible for the study.
インスリンレジメンを受けている制御された1型糖尿病患者は試験に適格である。
Patients with controlled
湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを伴う白斑(例えば、乾癬性関節炎を有する患者は除外される)を有する患者は、以下の条件の全てが満たされるならば、試験に適格である。
-発疹が覆っている体表面積は<10%でなければならない
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない
●特発性肺線維症、器質化肺炎(例えば、閉塞性細気管支炎)、薬物誘発性間質性肺炎、若しくは特発性間質性肺炎の病歴、又はスクリーニング胸部コンピューター断層撮影(CT)スキャンでの活動性間質性肺炎の証拠。
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin manifestations only (e.g., patients with psoriatic arthritis are excluded) are eligible for the study if all of the following conditions are met: is.
- Rash must cover <10% body surface area - Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UV within the last 12 months No acute exacerbation of underlying symptoms requiring A-irradiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors, or high-potency or oral corticosteroids Idiopathic pulmonary fibrosis, organizing pneumonia (e.g. , bronchiolitis obliterans), drug-induced interstitial pneumonia, or idiopathic interstitial pneumonia, or evidence of active interstitial pneumonia on screening chest computed tomography (CT) scan.
放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●活動性結核
●試験処置の開始前3ヶ月以内の有意な心血管疾患(New York Heart Association Class II以上の心疾患、心筋梗塞、脳血管障害等)、不安定な不整脈又は不安定狭心症。
●診断以外の、試験処置の開始前4週間以内の大きな外科的処置、試験中の大きな外科的処置の計画された又は予想される必要性
●ランダム化前5年以内のSCCHN以外のさらなる悪性腫瘍の病歴、ただし、転移又は死亡のリスクが無視できる程度(例えば、5年OS率>90%)の悪性腫瘍、例えば、適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚がん、限局性前立腺がん、上皮内乳管癌腫、又はステージI子宮がんは除く。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)
●試験処置開始前2週間以内の治療用経口又はIV抗生物質による処置
A history of radiation pneumonitis (fibrosis) in the radiology area is acceptable.
● Active tuberculosis ● Significant cardiovascular disease (New York Heart Association Class II or higher heart disease, myocardial infarction, cerebrovascular accident, etc.), unstable arrhythmia or unstable angina pectoris within 3 months before the start of study treatment .
Major surgical procedure other than diagnosis within 4 weeks prior to initiation of study procedure, planned or anticipated need for major surgical procedure during study Additional malignancy other than SCCHN within 5 years prior to randomization malignancies with negligible risk of metastasis or death (e.g., 5-year OS >90%), e.g., appropriately treated cervical carcinoma in situ, non-melanoma skin cancer, Excludes localized prostate cancer, ductal carcinoma in situ, or stage I uterine cancer.
- Severe infection within 4 weeks prior to initiation of study treatment (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia)
- Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of study treatment
予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の増悪を予防するため)を受ける患者は試験に適格である;
●事前の同種異系幹細胞又は固形臓器移植
●治験薬の使用を禁忌にする任意の他の疾患、代謝機能不全、身体検査所見、又は臨床検査所見は、結果の解釈に影響を及ぼす可能性があり、又は患者を治療合併症のリスクが高くなる可能性がある。
●試験処置の開始前4週間以内の生弱毒化ワクチンによる処置、又は試験処置中のそのようなワクチンの必要性の予想、アテゾリズマブの最終投与後5ヶ月以内、又はチラゴルマブ/プラセボの最終投与後90日以内の生弱毒化ワクチンによる処置。
●HBV又はHCVに対する抗ウイルス療法による現在の処置
●スクリーニング時の陽性エプスタイン・バーウイルスウイルス(EBV)ウイルスカプシド抗原(VCA)IgM検査
Patients receiving prophylactic antibiotics (e.g., to prevent exacerbations of urinary tract infections or chronic obstructive pulmonary disease) are eligible for the study;
- Prior allogeneic stem cell or solid organ transplantation - Any other disease, metabolic dysfunction, physical examination findings, or laboratory findings that contraindicate study drug use may affect interpretation of results or may put the patient at increased risk of treatment complications.
- Treatment with a live-attenuated vaccine within 4 weeks prior to initiation of study treatment, or anticipated need for such vaccine during study treatment, within 5 months after last dose of atezolizumab, or 90 after last dose of tiragolumab/placebo Treatment with live attenuated vaccine within days.
Current treatment with antiviral therapy for HBV or HCV Positive Epstein-Barr virus (EBV) viral capsid antigen (VCA) IgM test at screening
急性感染又は慢性活動性感染の疑いをスクリーニングするために、EBVポリメラーゼ連鎖反応(PCR)検査を、臨床上適応さがある場合、実施しなければならない。EBV PCR検査が陽性の患者は除外する。
●試験処置の開始前28日以内の治験療法による処置。
●抗-CTLA-4、抗TIGIT、抗-PD-L1及び抗-PD-1治療用抗体を含むCD137アゴニスト又は免疫チェックポイント遮断療法による事前処置
●試験処置の開始前の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫刺激剤(限定されないが、インターフェロン及びインターロイキン2[IL-2]を含む)による処置。
●以下を除いて、試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び抗-TNF-α剤を含む)による処置、又は試験処置中の全身免疫抑制薬の必要性の予測:
-急性低用量の全身免疫抑制薬又は1回パルス用量の全身免疫抑制薬(例えば、造影剤アレルギーのための48時間のコルチコステロイド)を受けた患者は、メディカルモニターの確認が得られた後、試験に適格である。
-ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患若しくは喘息のための吸入若しくは低用量コルチコステロイド、又は起立性低血圧若しくは副腎機能不全のための低用量コルチコステロイドを受けた患者は試験に適格である。
●キメラ若しくはヒト化抗体又は融合タンパク質に対する重度のアレルギーアナフィラキシー反応の病歴。
●チャイニーズハムスター卵巣細胞生成物又はアテゾリズマブ又はチラゴルマブ製剤の任意の成分に対する既知の過敏症。
●妊娠若しくは授乳、又は試験処置中、アテゾリズマブの最終投与後5ヶ月以内、又はチラゴルマブ/プラセボの最終投薬後90日以内に妊娠する意図。
To screen for suspected acute or chronic active infection, an EBV polymerase chain reaction (PCR) test should be performed when clinically indicated. Patients with a positive EBV PCR test are excluded.
- Treatment with study therapy within 28 days prior to initiation of study treatment.
- Pretreatment with a CD137 agonist or immune checkpoint blockade therapy, including anti-CTLA-4, anti-TIGIT, anti-PD-L1 and anti-PD-1 therapeutic antibodies - Within 4 weeks or 5 prior to initiation of study treatment Treatment with systemic immune stimulants (including but not limited to interferon and interleukin-2 [IL-2]) within the drug elimination half-life (whichever is longer).
- Treatment with systemic immunosuppressants (including but not limited to corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide and anti-TNF-α agents) within 2 weeks prior to initiation of study treatment, except for: , or prediction of need for systemic immunosuppressants during study treatment:
- Patients who received acute low-dose systemic immunosuppressants or single pulse-dose systemic immunosuppressants (e.g., 48-hour corticosteroids for contrast allergy) after obtaining medical monitor confirmation , are eligible for the test.
- Patients who received mineralocorticoids (eg fludrocortisone), inhaled or low-dose corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency are eligible for testing.
• History of severe allergic anaphylactic reactions to chimeric or humanized antibodies or fusion proteins.
• Known hypersensitivity to Chinese Hamster Ovary Cell Products or any component of the atezolizumab or tiragolumab formulations.
- Pregnancy or lactation, or intention to become pregnant during study treatment, within 5 months after last dose of atezolizumab, or within 90 days after last dose of tiragolumab/placebo.
妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。 Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
F.評定 F. Grade
患者は、試験を通して安全性及び忍容性について綿密に監視される。患者は、各投与の前に毒性について評定される;投薬は、臨床評定及び地域の臨床検査値が許容できる場合にのみ実施する。 Patients will be closely monitored for safety and tolerability throughout the study. Patients will be assessed for toxicity prior to each dose; dosing will be administered only if clinical evaluation and local laboratory values are acceptable.
病歴、ベースライン症状、併用薬及び人口統計データ
臨床的に重要な疾患、外科手術、がんの病歴(以前のがん治療及び処理を含む)、生殖状態、喫煙歴、並びにアルコール及び乱用薬物の使用を含む病歴をベースラインで記録する。更に、試験処置の開始前7日以内に患者によって使用された全ての薬物(例えば、処方薬、市販薬、ワクチン、ハーブ療法又はホメオパシー療法、栄養補助食品)を記録する。各フォローアップ健康診断時に、インターバルの病歴を取得し、投薬及びアレルギーの変化を記録する。
Medical history, baseline symptoms, concomitant medications and demographic data Clinically significant illness, surgery, history of cancer (including previous cancer treatments and treatments), reproductive status, smoking history, and use of alcohol and drugs of abuse Medical history including use will be recorded at baseline. In addition, all drugs (eg, prescription drugs, over-the-counter drugs, vaccines, herbal or homeopathic remedies, dietary supplements) used by the patient within 7 days prior to initiation of study treatment are recorded. At each follow-up check-up, an interval medical history is obtained and changes in medications and allergies are recorded.
人口統計データには、年齢、性別、及び自己報告の人種/民族性が含まれる。 Demographic data includes age, gender, and self-reported race/ethnicity.
ECOGパフォーマンスステータス
パフォーマンスステータスは、ECOGパフォーマンスステータススケールを使用して測定される。
ECOG Performance Status Performance Status is measured using the ECOG Performance Status Scale.
身体検査
完全な身体検査をスクリーニング時に行和なければならず、これは頭部、眼、耳、鼻、及び咽喉、並びに心臓血管系、皮膚系、筋骨格系、呼吸器系、胃腸系、泌尿生殖器系、及び神経系の評価を含むべきである。ベースラインで特定されたあらゆる異常は記録されるべきである。
Physical Examination A complete physical examination must be performed at Screening, which includes the head, eyes, ears, nose, and throat, as well as the cardiovascular, skin, musculoskeletal, respiratory, gastrointestinal, and urinary systems. Reproductive and nervous system evaluations should be included. Any abnormalities identified at baseline should be recorded.
限定的には、指定のベースライン後の来院時及び臨床的に示されているように、症候に応じた理学的検査を行うべきである。ベースライン異常からの変化を、患者ノートに記録すべきである。新規又は悪化した臨床的に有意な異常は、有害事象として記録されるべきである。 Limited, physical examination should be performed at designated post-baseline visits and as clinically indicated, according to symptoms. Changes from baseline abnormalities should be recorded in patient notes. New or worsening clinically significant abnormalities should be recorded as adverse events.
身体検査
バイタルサインは、呼吸数、脈拍数、並びに患者が座位にある間の収縮期及び拡張期血圧、並びに体温の測定を含む。ベースライン時及びその後の来院時に観察された異常、新たな又は悪化した臨床的に有意な異常が記録される。
Physical Examination Vital signs include measurement of respiratory rate, pulse rate, and systolic and diastolic blood pressure while the patient is seated, and body temperature. Abnormalities observed at baseline and at subsequent visits, new or worsening clinically significant abnormalities are recorded.
腫瘍及び反応の評価
スクリーニング評定及びその後の腫瘍評定には、胸部及び腹部のCTスキャン(経口又はIV造影剤を用いる)、又は頭頸部(頭蓋底から鎖骨)のCTスキャン(経口又はIV造影剤を用いる)若しくは磁気共鳴画像法(MRI)(造影剤を用いる)が含まれなければならない。骨盤の造影剤を用いたCTスキャンは、臨床上適応がある場合、又はスクリーニング及びその後の応答評価での局所SOCに従って実施されるべきである。造影剤を用いたCTスキャンが禁忌である場合(例えば、腎クリアランスが損なわれた患者において)、胸部の非造影CTスキャンを実施することができ、頭頸部、腹部、及び骨盤の造影剤を用いたMRIスキャン(該当する場合)を実施しなければならない。ベースライン及びその後の応答評価で臨床的に示される場合、骨スキャン等のさらなる調査も行うべきである。
Tumor and Response Assessment The screening evaluation and subsequent tumor evaluation included a CT scan of the chest and abdomen (with oral or IV contrast) or a CT scan of the head and neck (base of skull to clavicle) (with oral or IV contrast). (using contrast agents) or magnetic resonance imaging (MRI) (using contrast agents). Pelvic CT scan with contrast should be performed as clinically indicated or according to local SOC at screening and subsequent response assessment. If CT scans with contrast are contraindicated (e.g., in patients with impaired renal clearance), non-contrast CT scans of the chest can be performed, and contrast-enhanced CT scans of the head and neck, abdomen, and pelvis can be performed. A complete MRI scan (if applicable) must be performed. Further investigations such as bone scans should also be performed if clinically indicated at baseline and subsequent response assessments.
スクリーニング時及びその後の応答評価時にCNS転移を評価するために、脳の造影剤を用いたCTスキャン又は造影剤を用いたMRIスキャン(造影剤を用いたCTが禁忌である場合)を臨床上適応がある場合に行うべきである。造影剤を用いたCTスキャンが行われ、脳転移の存在が明確でないと考えられる場合、ベースラインでのCNS転移の診断を確認又は否定するために頭部のMRIスキャンが必要である。活性又は未処置のCNS転移を有する患者は、この試験に適格ではない。スクリーニング時に放射線照射された脳転移の病歴を有する患者は、臨床上適応がない限り、その後の応答評価時に脳スキャンを受ける必要はない。 Clinically indicated for brain contrast CT scan or contrast MRI scan (if contrast CT is contraindicated) to assess CNS metastases at screening and subsequent response assessment should be done if there is If a contrast-enhanced CT scan is performed and the presence of brain metastases is considered ambiguous, an MRI scan of the head is required to confirm or rule out the diagnosis of CNS metastases at baseline. Patients with active or untreated CNS metastases are not eligible for this study. Patients with a history of brain metastases who were irradiated at screening do not need to undergo brain scans at subsequent response assessment unless clinically indicated.
腫瘍評定のためのCTスキャンが陽電子放射断層撮影(PET)/CTスキャナーで行われる場合、CT取得は、完全造影診断CTスキャンの標準と一致しなければならない。 If CT scans for tumor assessment are performed on a Positron Emission Tomography (PET)/CT scanner, the CT acquisition must conform to the standard for full contrast-enhanced diagnostic CT scans.
インフォームドコンセントを得る前にSOCとして行われる腫瘍評定は、スキャンが診断品質であり、ランダム化の28日以内に行われるならば、検査を繰り返さずに使用され得る。 Tumor assessments performed as SOC prior to obtaining informed consent may be used without repeat testing if the scans are of diagnostic quality and are performed within 28 days of randomization.
スクリーニングで使用されるのと同じ放射線モダリティ(例えば、造影剤を用いたCTスキャン)及び手順(例えば、CTスキャンのための同じコントラストプロトコル)を、その後のすべての腫瘍評定に使用しなければならない。測定可能及び/又は測定不可能な疾患を含む全ての疾患の既知の部位は、スクリーニング時に文書化され、その後の各腫瘍評価時に再評定されなければならない。 The same radiation modality (eg, CT scan with contrast agent) and procedure (eg, same contrast protocol for CT scan) used in screening must be used for all subsequent tumor assessments. All known sites of disease, including measurable and/or non-measurable disease, must be documented at screening and reevaluated at each subsequent tumor evaluation.
患者は、ベースライン、サイクル1の1日目の後の最初の30週間の6週間ごと(±7日)、及び30週目の腫瘍評定の完了後9週間ごと(±7日)に腫瘍評定を受ける。腫瘍評定は、RECIST v1.1による放射線学的疾患進行又はRECIST v1.1による放射線学的疾患進行後の試験処置を継続する患者についての臨床的利益の喪失、同意の撤回、死亡又は試験依頼者による試験の終了のいずれか早く発生する方まで、処置の遅延にかかわらず、スケジュールごとに継続する。また、治験責任医師の裁量により、進行性疾患又は臨床的利益の喪失が疑われる場合はいつでもスキャンを実施しなければならない。
Patients will have tumor assessments at baseline, every 6 weeks (±7 days) for the first 30 weeks after
RECIST v.1.1による放射線学的疾患進行の非存在下で試験処置(それだけに限らないが、臨床的低下又は毒性を含む、何らかの理由で)を中断する患者は、新しい抗がん治療が開始されるかどうかにかかわらず、上記のスケジュールに従って腫瘍応答評定を受け続ける。腫瘍評定は、RECIST v1.1による放射線学的疾患進行、同意の撤回、死亡、又は試験依頼者による試験終了のいずれか早く発生する方まで継続すし、最初の応答は、RECIST v1.1を使用して、上に詳述したイメージングモダリティについて治験責任医師によって評定される。全ての時点における全腫瘍奏効の治験責任医師の評定は、RECIST v1.1にのみ基づくべきである。評定は、来院間の内部一貫性を保証するために、可能であれば同じ評価者によって行われるべきである。 RECIST v. 1. Patients who discontinue study treatment (for any reason, including but not limited to clinical Regardless, continue to undergo tumor response assessment according to the schedule above. Tumor assessment will continue until radiological disease progression, withdrawal of consent, death, or sponsor termination of the study by RECIST v1.1, whichever occurs first, and initial response will use RECIST v1.1. and assessed by the Investigator for the imaging modalities detailed above. Investigator assessment of overall tumor response at all time points should be based solely on RECIST v1.1. Ratings should be performed by the same rater if possible to ensure internal consistency between visits.
全ての時点における全腫瘍奏効の治験責任医師の評定は、RECIST 1.1のみに基づく。腫瘍評定を、進行を超えて試験処置を受けた患者について、RECIST v1.1による疾患進行後に継続しなければならない。これには、標的病変の継続的な測定、非標的病変の評価、及びその後のすべての評定で新たに同定された病変の評価が含まれる。 Investigator assessment of overall tumor response at all time points is based solely on RECIST 1.1. Tumor assessment must continue after disease progression by RECIST v1.1 for patients who received study treatment beyond progression. This includes continuous measurement of target lesions, evaluation of non-target lesions, and evaluation of newly identified lesions at all subsequent assessments.
実験室、バイオマーカー、及び他の生物学的試料
以下の臨床検査のための試料を、分析のために試験施設の現地の検査室に送る:
●血液学:WBC数、RBC数、ヘモグロビン、ヘマトクリット、血小板数及び分化数(好中球、好酸球、好塩基球、単球、リンパ球)。
●化学パネル(血清又は血漿):重炭酸塩又は総二酸化炭素(その領域についてSOCと考えられる場合)、ナトリウム、カリウム、塩化物、グルコース、BUN又は尿素、クレアチニン、総タンパク質、アルブミン、リン酸塩、カルシウム、総ビリルビン、ALP、ALT、AST及びLDH
●凝固:INR及びaPTT
●甲状腺機能検査:甲状腺刺激ホルモン、遊離トリヨードチロニン(T3)(又は遊離T 3が実施されない部位については総T3)、及び遊離チロキシン(T4としても知られる)
●以下を含むEBV血清学
o EBV VCA IgM
o EBV VCA IgG又はエプスタイン・バー・ウイルス核抗原(EBNA)IgG
o 臨床上適応がある場合:EBV PCR
●HIV血清学
●以下からなるHBV血清学:
o 全患者のHBsAg、HBsAb及び総HBcAb
o HBsAg及びHBsAb検査が陰性であり、総HBcAb検査が陽性である患者のHBV DNA
Laboratory, Biomarkers, and Other Biological Samples Samples for the following clinical tests will be sent to the test facility's local laboratory for analysis:
• Hematology: WBC counts, RBC counts, hemoglobin, hematocrit, platelet counts and differential counts (neutrophils, eosinophils, basophils, monocytes, lymphocytes).
Chemistry panel (serum or plasma): bicarbonate or total carbon dioxide (if considered SOC for that area), sodium, potassium, chloride, glucose, BUN or urea, creatinine, total protein, albumin, phosphate , calcium, total bilirubin, ALP, ALT, AST and LDH
Coagulation: INR and aPTT
Thyroid function tests: thyroid stimulating hormone, free triiodothyronine (T3) (or total T3 for sites where free T3 is not performed), and free thyroxine (also known as T4)
o EBV serology including o EBV VCA IgM
o EBV VCA IgG or Epstein-Barr Virus Nuclear Antigen (EBNA) IgG
o If clinically indicated: EBV PCR
● HIV serology ● HBV serology consisting of:
o HBsAg, HBsAb and total HBcAb for all patients
o HBV DNA from patients with negative HBsAg and HBsAb tests and positive total HBcAb tests
スクリーニング時に定量的HBV DNAが陽性である患者(適格基準当たり<500 IU/mLでなければならない)は、活動スケジュールに概説されているように追加のHBV DNA検査を受ける。
●HCV血清学:HCV抗体及び(HCV抗体検査が陽性である場合)HCV RNA。
●中咽頭に関与するSCCHNを有する患者の場合:p16 IHC、in situハイブリダイゼーション、又はPCRに基づくアッセイによって決定された腫瘍組織のHPV状態
●妊娠検査
Patients with positive quantitative HBV DNA at screening (must be <500 IU/mL per eligibility criteria) will undergo an additional HBV DNA test as outlined in the Activity Schedule.
• HCV serology: HCV antibody and (if HCV antibody test positive) HCV RNA.
For patients with SCCHN involving the oropharynx: HPV status of tumor tissue as determined by p16 IHC, in situ hybridization, or PCR-based assay Pregnancy test
妊娠可能な全ての女性は、スクリーニング時に血清妊娠検査を受ける。試験処置中、尿妊娠検査を、各サイクルの1日目に行う。尿妊娠検査を処置中止来院時にも行う。尿妊娠検査が陽性である場合、それは血清妊娠検査によって確認されなければならない。
All women of childbearing potential will have a serum pregnancy test at screening. During study treatment, a urine pregnancy test is performed on
女性は、月経後であり、閉経後の状態(連続≧12ヶ月の閉経以外の特定された原因のない無月経)に達しておらず、手術(すなわち、卵巣、卵管、及び/又は子宮の除去)又は治験責任医師によって決定される別の原因(例えば、ミュラー管無発生)のために永久に不妊ではない場合、妊娠可能性があるとみなされる。
●尿検査(pH、比重、グルコース、タンパク質、ケトン類、血液);ディップスティックは許可されている
Females are postmenopausal, have not achieved postmenopausal status (amenorrhea with no identified cause other than menopause for ≧12 consecutive months), and have had surgery (i.e., ovarian, fallopian tube, and/or uterine Ablation) or another cause determined by the Investigator (eg, Müllerian agenesis) is considered fertile if not permanently infertile.
Urinalysis (pH, specific gravity, glucose, protein, ketones, blood); dipsticks allowed
以下の試料は、分析のために1つ以上の中央検査室、又は試験依頼者若しくは指名された人に送られる。
●自己抗体の分析のための血清試料:抗核抗体、抗-二本鎖DNA、循環抗好中球細胞質抗体、及び核周囲抗好中球細胞質抗体
●C反応性タンパク質の血清試料
●検証されたアッセイの使用によるアテゾリズマブ及びチラゴルマブPK分析のための血清試料
●検証されたアッセイの使用によるアテゾリズマブ及びチラゴルマブに対するADAの評定のための血清試料
●バイオマーカーの探索研究のための血液及び血漿試料
The following samples are sent to one or more central laboratories or to the sponsor or designee for analysis.
• Serum samples for analysis of autoantibodies: antinuclear antibodies, anti-double-stranded DNA, circulating antineutrophil cytoplasmic antibodies, and perinuclear antineutrophil cytoplasmic antibodies • Serum samples for C-reactive protein • Validated Serum samples for atezolizumab and tiragolumab PK analysis using a validated assay Serum samples for assessment of ADAs for atezolizumab and tiragolumab using validated assays Blood and plasma samples for biomarker discovery studies
血液試料を処理して、末梢血単核細胞(PBMC)及び他の誘導体(例えば、RNA、DNA等)を得ることができる。
●PD-L1発現の決定及びバイオマーカーに関する調査研究のためにベースラインで得られた保管又は新たに収集された腫瘍組織試料
Blood samples can be processed to obtain peripheral blood mononuclear cells (PBMC) and other derivatives (eg, RNA, DNA, etc.).
Archived or freshly collected tumor tissue samples obtained at baseline for determination of PD-L1 expression and biomarker research studies
パラフィンブロック(好ましい)又は未染色の新たに切断した連続切片を含む少なくとも20枚のスライド中の代表的なFFPE腫瘍標本は、試験登録前に関連する病理報告と共に提出しなければならない。15-19枚のスライドしか入手できない場合、メディカルモニターの承認が得られた後、患者は依然として試験に適格であり得る。 Representative FFPE tumor specimens in at least 20 slides containing paraffin blocks (preferred) or unstained freshly cut serial sections must be submitted with relevant pathology reports prior to study enrollment. If only 15-19 slides are available, patients may still be eligible for the study after obtaining medical monitor approval.
腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならない。 Tumor tissue must be of good quality based on total tumor content and viable tumor content.
試料は、針ゲージ又は回収方法にかかわらず、細胞状況及び組織構造を保存する最低50個の生存TCを含まなければならない。 Samples must contain a minimum of 50 viable TCs preserving cellular context and tissue architecture, regardless of needle gauge or collection method.
摘出、コア針生検(単一のパラフィンブロックに埋め込まれた少なくとも3つのコア)、又は切除生検、切開生検、パンチ生検、若しくは鉗子生検によって採取された試料が許容される。細針吸引(組織構造を保存せず、細胞懸濁液及び/又は塗抹を生じない試料として定義される)、ブラッシング、胸水からの細胞ペレット、及び洗浄液試料は許容されない。脱灰された骨転移からの腫瘍組織は許容されない。 Specimens obtained by excision, core needle biopsy (at least 3 cores embedded in a single paraffin block), or excisional, incisional, punch, or forceps biopsy are acceptable. Fine-needle aspirations (defined as samples that do not preserve tissue architecture and yield cell suspensions and/or smears), brushings, cell pellets from pleural effusions, and lavage fluid samples are not permitted. Tumor tissue from demineralized bone metastases is not permitted.
保管腫瘍組織が利用できないか、又は必要な検査に適さないと判定された場合、前処置腫瘍生検が必要である。患者の保管組織検査の結果が適格基準を満たさない場合、前処置腫瘍生検も実施され得る。
●バイオマーカーの探索的研究のために、進行時に得られた腫瘍組織試料(臨床的に実施可能と考えられる場合)
A pretreatment tumor biopsy is required if archival tumor tissue is unavailable or determined to be unsuitable for the required testing. A pretreatment tumor biopsy may also be performed if the patient's archival tissue examination results do not meet eligibility criteria.
- Tumor tissue samples obtained at progression for biomarker exploratory studies (if considered clinically feasible)
進行時の生検は、進行後40日以内又は次の抗がん治療の前のいずれか早い方で行うべきである。 A biopsy at progression should be performed within 40 days of progression or before the next anticancer therapy, whichever comes first.
摘出、コア針生検(少なくとも3つのコアが好ましい)、又は切除、切開、パンチ若しくは鉗子生検によって収集された試料が好ましい。 Samples collected by excision, core needle biopsy (at least three cores are preferred), or excision, incision, punch or forceps biopsy are preferred.
NGSは、Foundation Medicineによって実施され得る。Foundation Medicineによって実施される場合、治験責任医師、Foundation Medicineのウェブポータルを介してNGS報告を取得することができる。現地の法律によって許可されている場合、治験責任医師は、患者がそうでないことを選択しない限り、結果を患者と共有し、議論することができる。NGS報告は、研究目的のために作成され、将来の処置決定を導く目的では提供されない。検査基準を満たさない試料については結果を入手することができない。 NGS can be performed by Foundation Medicine. If performed by Foundation Medicine, the NGS report can be obtained via the Investigator, Foundation Medicine's web portal. Where permitted by local law, the investigator may share and discuss results with the patient unless the patient chooses otherwise. NGS reports are produced for research purposes and are not provided for the purpose of guiding future treatment decisions. No results are available for samples that do not meet the test criteria.
探索的バイオマーカー研究には、腫瘍遺伝子変化、腫瘍免疫生物学に関連するHPV状態又は遺伝子シグネチャ、PD-L1、TIGIT、リンパ球亜集団、及びT細胞受容体レパートリーの分析が含まれ得るが、これらに限定されない。研究は、DNA、無細胞DNA又はRNAの抽出;変異及び他の腫瘍特異的ゲノム変異体の分析;並びに包括的な遺伝子パネルのNGSの使用によるゲノムプロファイリングを含み得る。血液から抽出されたDNAを組織から抽出されたDNAと比較して、生殖系列変異体を体細胞バリアントと区別することによって体細胞バリアントを同定することができる。NGS法は、組織及び血液試料のWGS又はWESを含み得るが、血液試料のWGS又はWESは、関与部位でのみ行われる。 Exploratory biomarker studies may include analysis of tumor genetic alterations, HPV status or gene signatures associated with tumor immunobiology, PD-L1, TIGIT, lymphocyte subpopulations, and T cell receptor repertoires, It is not limited to these. Studies may include extraction of DNA, cell-free DNA or RNA; analysis of mutations and other tumor-specific genomic variants; and genomic profiling through the use of NGS of comprehensive gene panels. Somatic variants can be identified by comparing DNA extracted from blood to DNA extracted from tissue to distinguish germline variants from somatic variants. NGS methods may include WGS or WES of tissue and blood samples, but WGS or WES of blood samples are performed only at the site of interest.
サンプリング手順、保管条件及び輸送指示については、実験室マニュアルを参照されたい。 Please refer to the laboratory manual for sampling procedures, storage conditions and transport instructions.
患者が自らの使い残した試料を任意の探索的研究のために保存することについて具体的な同意を与えない限り、生物学的試料は、以下の例外を除いて、最終臨床試験報告書の完了時までに破棄される。
●PK又は免疫原性分析のために収集された血清試料は、さらなる免疫原性特性評価のために、並びにPK又は免疫原性アッセイの開発及び検証のために必要とされ得るため、これらの試料は、最終臨床試験報告書が完成してから5年以内に破棄される。
●バイオマーカー研究のために収集された血液、血漿及びPBMC試料は、WGS又はWESを受けた組織試料を除いて、最終臨床試験報告が完了してから5年以内に破棄され、それらはもはや必要とされなくなるまで、又はそれらが使い尽くされるまで保存される。ただし、保管期間は、IRB/EC承認インフォームドコンセント用紙及び適用法令(例えば、保健当局の要求)に従う。
●登録された患者の場合、残りの保管組織ブロックは、要求に応じて、又は最終臨床試験報告から18ヶ月以内のいずれか早く発生する方で現場に戻される。登録されていない患者については、残りの保管組織ブロックを適格性判定後6週間以内に現場に戻す。
Unless the patient has given specific consent to have their leftover samples retained for any exploratory research, biological samples are not included in the final clinical study report completion, with the following exceptions: destroyed by time.
• Serum samples collected for PK or immunogenicity analysis may be required for further immunogenicity characterization and for the development and validation of PK or immunogenicity assays; shall be destroyed within 5 years after the completion of the final clinical study report.
- Blood, plasma and PBMC samples collected for biomarker studies, with the exception of tissue samples that underwent WGS or WES, will be destroyed within 5 years after the final clinical study report is completed and they are no longer needed. are stored until they are no longer needed or until they are exhausted. However, the retention period is subject to the IRB/EC approved informed consent form and applicable legislation (eg, requirements of health authorities).
• For enrolled patients, the remaining archival tissue blocks will be returned to the site upon request or within 18 months of the final clinical study report, whichever occurs first. For unenrolled patients, the remaining archival tissue blocks will be returned to the site within 6 weeks after eligibility determination.
患者が試験から離脱する場合、患者が試料を破壊することを特に要求しない限り、又は現地の法律が試料の破棄を要求しない限り、離脱日より前に収集された試料を依然として分析することができる。しかしながら、試料が回収前に検査されている場合、それらの検査結果は、全体的な研究データの一部として残る。 If a patient withdraws from the study, samples collected prior to the withdrawal date may still be analyzed unless the patient specifically requests that the sample be destroyed or local law requires sample destruction. . However, if samples were tested prior to collection, those test results remain part of the overall study data.
探索的バイオマーカー分析の複雑さ及び探索的性質を考慮すると、これらの分析に由来するデータは、一般に、法律によって要求されない限り、試験の治験責任医師又は患者に提供されない(疾患進行時に得られた生検にのみ適用可能なFoundation Medicineからの報告を除く)。実施された研究の全体的な結果は、試験データ出版に関する有効な主催者の方針に従って入手可能である。 Given the complexity and exploratory nature of exploratory biomarker analyzes, data derived from these analyzes are generally not provided to trial investigators or patients unless required by law (not obtained at disease progression). (except reports from Foundation Medicine, which are applicable only to biopsies). The overall results of the studies conducted are available in accordance with the sponsor's policy on publication of trial data in effect.
心電図
スクリーニング時及び試験中の他の時点で臨床的に示されるように、ECGが必要である。各患者のECGは、可能な限り同じ機械から取得されるべきである。リードの配置は、可能な限り一貫しているべきである。ECG記録は、患者が少なくとも10分間仰臥位で安静にした後に行われなければならない。
Electrocardiogram An ECG is required as clinically indicated at screening and at other times during the study. Each patient's ECG should be obtained from the same machine whenever possible. Lead placement should be as consistent as possible. ECG recordings must be taken after the patient has rested in the supine position for at least 10 minutes.
安全性を監視する目的で、治験責任医師は全てのECG記録を再検討し、署名し、日付を付けなければならない。ECG記録のコピーは、現場で患者の恒久的な試験ファイルの一部として保持される。形態学的波形の変化又は他のECG異常は、eCRFに文書化されなければならない。 For safety monitoring purposes, the investigator must review, sign, and date all ECG records. A copy of the ECG recording is kept on site as part of the patient's permanent test file. Morphological waveform changes or other ECG abnormalities must be documented on the eCRF.
臨床転帰評定
アテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボの臨床プロファイルをより完全に特性評価するために、PRO尺度が完成される。更に、PRO尺度は、アテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボによる各患者の直接的な経験の捕捉を可能にする。
Clinical Outcome Assessment PRO scales will be completed to more fully characterize the clinical profiles of atezolizumab + tiragolumab and atezolizumab + placebo. In addition, the PRO scale allows capture of each patient's direct experience with atezolizumab + tiragolumab and atezolizumab + placebo.
PROデータは、以下の尺度を使用して収集される:
●PROMIS(登録商標)Item Bank v2.0-身体機能-ショートフォーム10b
●PROMIS(登録商標)Item Bank v1.0-疲労-ショートフォーム4a
●PROMIS(登録商標)Item Bank v1.1-疼痛による支障-ショートフォーム4a
●PROMIS(登録商標)数値評価スケールv1.0-疼痛強度1a
●重症度に関する患者全般印象度(PGI-S)
●変化及びその重要性の患者全般印象度(PGI-CI)
●最も重要な症状(MIS)
●PRO-CTCAE
PRO data will be collected using the following scales:
●PROMIS® Item Bank v2.0-Physical Functions-Short Form 10b
● PROMIS (registered trademark) Item Bank v1.0-fatigue-short form 4a
● PROMIS® Item Bank v1.1-Disturbed by Pain-Short Form 4a
● PROMIS® Numerical Rating Scale v1.0—Pain Intensity 1a
●Patient Global Impressions of Severity (PGI-S)
-Patient Global Impression of Change and its Importance (PGI-CI)
● Most important symptoms (MIS)
●PRO-CTCAE
PRO質問票(すなわち、PROMIS(登録商標)、PGI-S/PGI-CI、MIS、及びPRO-CTCAE)は、処置中及び処置中止来院時に完了する。 PRO questionnaires (ie, PROMIS®, PGI-S/PGI-CI, MIS, and PRO-CTCAE) are completed during the treatment and at the treatment discontinuation visit.
臨床転帰評定ためのデータ収集方法
アテゾリズマブ+チラゴルマブ及びアテゾリズマブ+プラセボの臨床プロファイルを特性評価するために使用されるPRO尺度は、試験中の特定の時点で診療所で自己で適用するか、又は面接者が(必要に応じて)適用する。PROMIS(登録商標)、PGI-S/PGI-CI、MIS、及びPRO-CTCAE質問票の使用によって得られたPROデータ。
Data Collection Methods for Clinical Outcome Assessment PRO scales used to characterize the clinical profile of atezolizumab + tiragolumab and atezolizumab + placebo were either self-administered at the clinic or interviewed at specific time points during the study. apply (if necessary). PRO data obtained through the use of PROMIS®, PGI-S/PGI-CI, MIS, and PRO-CTCAE questionnaires.
診療所では、尺度は、特に明記しない限り、患者が疾患状態に関する情報を受ける前、非PRO評定の実施前、及び試験処置の投与前に適用される。 In the clinic, scales will be applied before patients receive information about disease status, before non-PRO assessments are performed, and before administration of study treatment, unless otherwise specified.
必要に応じて現地語に翻訳され、診療所来院中の投与が予定されている書面のPRO質問票は、他の試験評定の前及び試験処置の投与の前に、可能な限り評定バイアスを回避するために、診療所訪問の開始時に試験施設で患者によって完成されなければならない。患者は、現場スタッフによって提供される紙バージョンの質問票を完成させる。面接者の評定は許可されているが、自分で測定を完了することができない患者のために診療所スタッフのみが行うことができる。 Written PRO questionnaires, translated into the local language as necessary and scheduled to be administered during the clinic visit, prior to other study assessments and prior to administration of study treatment, to avoid assessment bias as much as possible. must be completed by the patient at the study site at the beginning of the clinic visit. Patients complete a paper version of the questionnaire provided by the site staff. Interviewer ratings are permitted, but can only be done by clinic staff for patients who are unable to complete the measurements themselves.
試験担当者は、患者が治験施設を出る前に、完全性のためにすべての質問票を再検討すべきである。 Investigators should review all questionnaires for completeness before the patient leaves the study site.
診療所来院中、PRO尺度は、以下に概説されるよう適用しなければならない:
●患者の健康状態は、尺度の適用前に議論されるべきではない。
●現場は、試験依頼者が提供する各尺度の公式版を管理しなければならない。尺度は治験実施計画書からコピーしてはならない。
●部位は、患者が尺度を完成させるのに十分な時間を許容すべきであり、サイクル1及び2の1日目では15分であり、その後の各サイクルでは10分未満であると推定される。
●現場は、気をそらすもの及び混乱させるものを最小限にし、静かなエリアで尺度を適用すべきである。
●患者は、自身の能力を最大限に発揮するように質問に答えるように指導されるべきであり、正解も不正解もない。
●現場スタッフは、質問を解釈又は説明すべきではなく、要求に応じて質問を逐語的に読んでもよい。
●患者は、尺度を完成させる際に、他者(例えば、家族又は友人)からの助言又は支援を得てはならない。
●現場スタッフは、すべての完成した尺度を確認、適切な場所に明確にマークされていない応答を修正するように患者に依頼する必要がある。応答が欠落している場合、現場スタッフは、患者に項目を完成させるか、項目が意図的に空白のままであったことを確認するように求めるべきである。
During clinic visits, the PRO scale must be applied as outlined below:
• The patient's health status should not be discussed prior to application of the scale.
• Sites must maintain official versions of each sponsor-supplied scale. Scales should not be copied from the protocol.
• The site should allow sufficient time for the patient to complete the scale, estimated to be 15 minutes on
• The site should minimize distractions and distractions and apply the scale in a quiet area.
• Patients should be instructed to answer questions to the best of their ability; there are no right or wrong answers.
• Field staff should not interpret or explain questions and may read questions verbatim upon request.
• Patients should not seek advice or assistance from others (eg, family members or friends) in completing the scale.
• Site staff should review all completed scales and ask patients to correct responses that are not clearly marked in the appropriate location. If responses are missing, site staff should ask the patient to complete the item or confirm that the item was intentionally left blank.
臨床転帰評定尺度の説明
PROMIS(登録商標)Item Bank v2.0-身体機能-ショートフォーム10b
PROMIS(登録商標)Item Bank v2.0-身体機能-ショートフォーム10bは、上肢(器用さ)、下肢(歩行又は可動性)、及び中央領域(首、背中)の機能、並びに手段的日常生活動作を含む身体活動の自己報告能力を測定するように設計された10の質問からなる。全ての質問は1-5段階でスコア化され、5のスコアは患者の最高の機能能力に等しく、1のスコアは患者の最低の機能能力に等しい。リコール期間は7日間 である。
Clinical Outcome Rating Scale Description PROMIS® Item Bank v2.0-Physical Function-Short Form 10b
PROMIS® Item Bank v2.0-Physical Functions-Short Form 10b measures upper extremity (dexterity), lower extremity (gait or mobility), and central area (neck, back) functions, as well as instrumental activities of daily living. It consists of 10 questions designed to measure the self-reported ability of physical activity, including All questions are scored on a scale of 1-5, with a score of 5 equaling the patient's best functional ability and a score of 1 equaling the patient's worst functional ability. The recall period is 7 days.
PROMIS(登録商標)Item Bank v1.0-疲労ショートフォーム4a
PROMIS(登録商標)Item Bank v1.0-疲労-ショートフォーム4aは、自己申告による一連の疲労症状及び患者の日常生活を実行する能力を評定するように設計された4つの項目からなる。アンケートの項目は、過去7日間に経験した患者の疲労度を質問する。項目は1-5段階でスコア化され、5のスコアは患者が経験した最高レベルの疲労に等しく、1のスコアは患者が経験した最低レベルの疲労に等しい。リコール期間は7日間である。
PROMIS® Item Bank v1.0 - Fatigue Short Form 4a
The PROMIS® Item Bank v1.0-Fatigue-Short Form 4a consists of four items designed to assess a self-reported spectrum of fatigue symptoms and the patient's ability to carry out daily activities. A questionnaire item asks the patient's degree of fatigue experienced in the past 7 days. Items are scored on a scale of 1-5, with a score of 5 equaling the highest level of fatigue experienced by the patient and a score of 1 equaling the lowest level of fatigue experienced by the patient. The recall period is 7 days.
PROMIS(登録商標)Item Bank v1.1-疼痛による支障-ショートフォーム4a
PROMIS(登録商標)Item Bank v1.1-疼痛による支障-ショートフォーム4aは、患者の生活の関連する態様に対する疼痛の影響/支障を評定するように設計された自己報告式の尺度に関する4つの質問からなる。全ての質問は1-5段階でスコア化され、5のスコアは疼痛からの支障の最高レベルに等しく、1のスコアは患者が経験する疼痛からの支障の最低レベルに等しい。リコール期間は7日間である。
PROMIS® Item Bank v1.1 - Disturbed by Pain - Short Form 4a
PROMIS® Item Bank v1.1-Pain Disturbance-Short Form 4a is a 4-question self-report scale designed to assess the impact/disturbance of pain on relevant aspects of a patient's life. consists of All questions are scored on a scale of 1-5, with a score of 5 equaling the highest level of pain disturbance and a score of 1 equaling the lowest level of pain disturbance experienced by the patient. The recall period is 7 days.
PROMIS(登録商標)数値評価尺度v 1.0-疼痛強度1a
PROMIS(登録商標)Numeric評価尺度v1.0-疼痛強度1aは、患者の平均疼痛レベルを評定するように設計された自己申告式尺度での1つの質問からなる。
PROMIS® Numerical Rating Scale v 1.0—Pain Intensity 1a
The PROMIS® Numeric Rating Scale v1.0—Pain Intensity 1a consists of one question on a self-report scale designed to rate a patient's average pain level.
質問は1-10段階でスコア付けされ、10のスコアは「考えられる最も悪い痛み」に相当し、1のスコアは「痛みなし」に相当する。リコール期間は7日間である。 The questions are scored on a scale of 1-10, with a score of 10 corresponding to "worst possible pain" and a score of 1 corresponding to "no pain". The recall period is 7 days.
重症度に関する患者全般印象度(PGI-S)
重症度に関する患者全般印象度(PGI-S)は、前の7日間の患者の全体的な症状の重症度に関する患者の印象を評定するために使用される1項目の自己申告式の尺度である。PGI-Sは、5点応答尺度を利用し、5のスコアは「非常に重度」に等しく、1のスコアは「なし」に等しい(Guy et al.1976から適合)。
Patient Global Impression of Severity (PGI-S)
The Patient Global Impression of Severity (PGI-S) is a one-item self-report scale used to rate the patient's impression of the severity of his or her overall symptoms over the previous 7 days. . The PGI-S utilizes a 5-point response scale, with a score of 5 equating to "very severe" and a score of 1 equating to "none" (adapted from Guy et al. 1976).
変化及びその重要性の患者全般印象度(PGI-CI)
変化に関する患者の全般的印象は、患者が試験を開始したときと比較して、患者の症状の変化に関する患者の印象を評定するために使用される一項目の自己申告測定である。これは、7点の応答尺度を利用し、7のスコアは「非常に悪い」と等しく、1のスコアは「非常に改善された」と等しい(Guy et al.1976から適合)。変化に関する患者の全般的印象に対する次の質問では、経験した変化が患者にとって重要であったかどうかを示すように患者に求められ、患者が変化を経験しなかった場合、応答選択肢は「はい」、「いいえ」、又は「該当せず」である。
Patient Global Impression of Change and its Significance (PGI-CI)
The Patient's Global Impression of Change is a one-item self-reported measure used to rate a patient's impression of a change in their symptoms compared to when they entered the study. It utilizes a 7-point response scale, with a score of 7 equating to 'very bad' and a score of 1 equating to 'much improved' (adapted from Guy et al. 1976). In the following question on the patient's global impression of change, the patient was asked to indicate whether the change experienced was significant to the patient, and if the patient did not experience the change, the response options were yes, No” or “Not Applicable”.
最も重要な症状(MIS)
最も重要な症状アンケートの目的は、どの症状が過去7日間に患者にとって最も面倒であったかを特定することである。MISは、University of Washington Quality of Life Questionnaire Scale 2.0以降の重要度評価尺度に基づいており、疾患及び/又は処置に関連するいくつかの症状(Rogers et al.2002)を追加している。患者は、過去1週間で最も面倒であった4つの症状をピックアップするように求められる。
Most Important Symptoms (MIS)
The purpose of the Most Important Symptom Questionnaire is to identify which symptoms have been most troublesome to the patient in the past 7 days. The MIS is based on the University of Washington Quality of Life Questionnaire Scale 2.0 and later severity rating scales and adds several disease and/or treatment related symptoms (Rogers et al. 2002). Patients are asked to pick the 4 most troublesome symptoms in the past week.
PRO-CTCAE
PRO-CTCAEは、78の患者報告可能な対症処置毒性の存在、発生頻度、重症度、及び/又は日常機能への干渉の程度を特性評価するために使用される検証された項目バンクである(Basch et al.2014;Dueck et al.2015)。PRO-CTCAEは、二分法(存在対非存在の決定のため)又は5段階のスケール(発生頻度、重大度、及び日常機能への干渉を判定するため)のいずれかで評価される124の質問を含む。処置毒性は、観察可能な徴候(例えば、嘔吐)又は観察不可能な症状(例えば、悪心)で起こり得る。
PRO-CTCAE
PRO-CTCAE is a validated item bank used to characterize the presence, frequency, severity, and/or degree of interference with daily functioning of 78 patient-reportable symptomatic toxicities ( Basch et al. 2014; Dueck et al. 2015). The PRO-CTCAE consists of 124 questions rated either dichotomously (to determine presence versus absence) or on a 5-point scale (to determine frequency of occurrence, severity, and interference with daily functioning). including. Treatment toxicity can occur with observable signs (eg vomiting) or unobservable symptoms (eg nausea).
標準PRO-CTCAEリコール期間は、その前の7日間である。 The standard PRO-CTCAE recall period is the preceding 7 days.
現在の処置に最も適用可能であると考えられる11の症状のサブセットをこの試験のために選択した。症状は、アテゾリズマブ+チラゴルマブ(Rodriguez-Abreu et al.2020)を用いた以前の試験、患者及び臨床医によって報告された免疫療法に関連する対症処置毒性(Hansen et al.2020、並びに頭頸部がんで測定すべき症状に関する推奨(Cella et al.2011;Chera et la.2014)に基づいて選択されている。 A subset of 11 symptoms considered most applicable to current treatment was selected for this study. Symptoms were consistent with previous studies with atezolizumab plus tiragolumab (Rodriguez-Abreu et al. 2020), symptomatic treatment toxicities associated with immunotherapy reported by patients and clinicians (Hansen et al. 2020, and in head and neck cancer). Selected based on recommendations for symptoms to be measured (Cella et al. 2011; Chera et al. 2014).
全ゲノムシーケンシング又は全エクソームシーケンシングのための血液試料
参加部位では、DNA抽出のために血液試料を採取して、WGS又はWESが、試験薬に対する応答を予測し、より重篤な疾患状態への進行に関連する腫瘍に特異的に発生する変異体を同定することを可能にする。血液から抽出されたDNAを組織から抽出されたDNAと比較して、生殖系列変異体を体細胞バリアントと区別することによって体細胞バリアントを同定することができる。試料を、分析のために1つ以上の検査室に送ることができる。
Blood Samples for Whole Genome Sequencing or Whole Exome Sequencing At participating sites, blood samples will be taken for DNA extraction to allow WGS or WES to predict response to study drug and more severe disease states. It allows us to identify tumor-specifically occurring variants associated with progression to . Somatic variants can be identified by comparing DNA extracted from blood to DNA extracted from tissue to distinguish germline variants from somatic variants. Samples can be sent to one or more laboratories for analysis.
WGS又はWESのための血液試料の収集及び提出は、各施設のIRB/EC及び該当する場合は適切な規制機関による調査試験の再検討及び承認を条件とする。施設がWGS又はWESの承認を受けていない場合、治験実施計画書のこのセクションはその施設には適用されない。 Collection and submission of blood samples for WGS or WES is subject to review and approval of the investigative study by each institution's IRB/EC and, where applicable, appropriate regulatory bodies. If a site is not WGS or WES approved, this section of the protocol will not apply to that site.
ゲノミクスは、疾患病理生物学の試験者の理解をますます促している。WGS及びWESは、それぞれゲノム及びエクソームの包括的な特性評価を提供し、この試験で収集された臨床データと共に、有効性及び安全性を監視するため、又はどの患者が薬物に応答するか若しくは有害事象を発症する可能性がより高いかを予測するための新しい治療アプローチ又は新しい方法を開発する機会を増やす可能性がある。データは、この試験に関連して分析されるが、他の試験からのデータとまとめて調査することもできる。より大きなデータセットの利用可能性は、将来の薬物開発を支援するための重要なバイオマーカー及び経路の同定及び特性評価に役立つ。 Genomics is increasingly facilitating investigator's understanding of disease pathobiology. WGS and WES provide comprehensive genomic and exome characterization, respectively, along with the clinical data collected in this trial, to monitor efficacy and safety, or to determine which patients will respond to drug or adverse events. It may increase opportunities to develop new therapeutic approaches or new methods to predict whether an event is more likely to develop. Data will be analyzed in relation to this study, but can also be examined together with data from other studies. The availability of larger datasets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
サンプリング手順、保管条件及び輸送指示については、実験室マニュアルを参照されたい。 Please refer to the laboratory manual for sampling procedures, storage conditions and transport instructions.
WGS又はWESのために収集された血液試料は、もはや必要とされなくなるまで、又は使い果たされるまで保存しなければならない。ただし、保管期間は、IRB/EC承認インフォームドコンセント用紙及び適用法令(例えば、保健当局の要求)に従う。 Blood samples collected for WGS or WES must be stored until no longer needed or until exhausted. However, the retention period is subject to the IRB/EC approved informed consent form and applicable legislation (eg, requirements of health authorities).
研究用バイオサンプルリポジトリのための試料
Research Biosample Repository(RBR)は、体液、固形組織及びそれらの誘導体(例えば、DNA、RNA、タンパク質、ペプチド)を含むヒト生体試料の長期保存に使用される集中管理型の施設グループである。RBR試料の収集、保存、及び分析は、新しい医薬品の合理的な設計及び診断検査の開発を容易にし、将来の患者のための個別化された薬物治療を可能にし得る。
Specimens for Research Biosample Repository The Research Biosample Repository (RBR) is a centralized management system used for long-term storage of human biological samples, including body fluids, solid tissues and their derivatives (e.g. DNA, RNA, proteins, peptides). It is a facility group of type. The collection, storage, and analysis of RBR samples may facilitate the rational design of new pharmaceuticals and development of diagnostic tests, enabling personalized drug therapy for future patients.
RBRの試料は、この任意の試験に参加することに具体的に同意した患者から収集される。RBR試料は、以下の目的のうちの1つ以上を達成するために分析される:
●バイオマーカーと有効性又は疾患進行との関連性を試験すること
●有害事象の発生に対する感受性に関連するか、又は有害事象のモニタリング若しくは調査の改善をもたらし得る安全性バイオマーカーを同定すること
●疾患生物学及び薬物安全性の知識及び理解を高めること
●薬物効果並びに薬物の吸収及び配置のプロセスを含む薬物応答を試験すること
●バイオマーカー又は診断アッセイを開発し、これらのアッセイの性能特性を確立すること
RBR samples are collected from patients who specifically consent to participate in this optional study. RBR samples are analyzed to achieve one or more of the following objectives:
• To test the association of biomarkers with efficacy or disease progression • To identify safety biomarkers that are associated with susceptibility to adverse event development or that may lead to improved monitoring or surveillance of adverse events • To enhance knowledge and understanding of disease biology and drug safety To test drug effects and drug responses, including processes of drug absorption and disposition To develop biomarker or diagnostic assays and characterize the performance of these assays to establish
試料収集
以下の試料は、RBRに保存され、限定されないが、アテゾリズマブ、チラゴルマブ、頭頸部がん、又は薬物安全性に関連するバイオマーカーに関する研究を含む研究目的に使用される。
●試験過程中に治験責任医師の裁量で行われた医学的に指定される手順(例えば、気管支鏡検査、食道胃十二指腸鏡検査、大腸鏡検査)からの残留組織試料を含む、残留血液、血漿、PBMC、及び腫瘍組織試料(現場に戻される残りの保管組織ブロックを除く)並びにその任意の導出物(例えば、DNA、RNA、タンパク質、ペプチド)
●試験中の任意の時点で収集されたDNA抽出のための任意の血液試料
●サイクル1、1日目及びサイクル2、15日目の投与前及びサイクル3、1日目の投与前に収集した、任意の便試料。これらの試料を、家庭で収集してもよい。
Sample Collection The following samples will be stored in RBR and used for research purposes, including but not limited to studies on atezolizumab, tiragolumab, head and neck cancer, or biomarkers related to drug safety.
- Residual blood, plasma, including residual tissue samples from medically designated procedures (e.g., bronchoscopy, esophagogastroduodenoscopy, colonoscopy) performed at the discretion of the Investigator during the course of the study , PBMCs, and tumor tissue samples (excluding remaining archival tissue blocks returned to the scene) and any derivatives thereof (e.g., DNA, RNA, proteins, peptides)
- Optional blood samples for DNA extraction collected at any time during the study - Collected pre-dose on
上記の試料は、WGS、WES、又は他のゲノム分析方法を介して、全メタゲノムシーケンシング、微生物培養、生殖系列又は体細胞変異体による微生物集団の分析のために1つ以上の検査室に送られ得る。ゲノミクスは、疾患病理生物学の試験者の理解をますます促している。WGS及びWESは、それぞれゲノム及びエクソームの包括的な特性評価を提供し、この試験で収集された臨床データと共に、有効性及び安全性を監視するため、又はどの患者が薬物に応答するか若しくは有害事象を発症する可能性がより高いかを予測するための新しい治療アプローチ又は新しい方法を開発する機会を増やす可能性がある。 The above samples are sent to one or more laboratories for analysis of the microbial population by whole metagenomic sequencing, microbial culture, germline or somatic mutation via WGS, WES, or other genomic analysis method. can be Genomics is increasingly facilitating investigator's understanding of disease pathobiology. WGS and WES provide comprehensive genomic and exome characterization, respectively, along with the clinical data collected in this trial, to monitor efficacy and safety, or to determine which patients will respond to drug or adverse events. It may increase opportunities to develop new therapeutic approaches or new methods to predict whether an event is more likely to develop.
RBR試料から生成されたデータは、この試験に関連して分析されるが、他の試験からのデータとまとめて調査することもできる。より大きなデータセットの利用可能性は、将来の薬物開発を支援するための重要なバイオマーカー及び経路の同定及び特性評価に役立つ。 Data generated from the RBR samples are analyzed in conjunction with this study, but can also be examined together with data from other studies. The availability of larger datasets will aid in the identification and characterization of important biomarkers and pathways to support future drug development.
RBR試料は、もはや必要とされなくなるまで、又は使い果たされるまで保存されるべきである。ただし、RBR保管期間は、IRB/EC承認のインフォームドコンセント用紙及び適用法令(例えば、保健当局の要求)に従う。 RBR samples should be stored until no longer needed or exhausted. However, the RBR retention period is subject to IRB/EC approved informed consent forms and applicable legislation (eg, requirements of health authorities).
G.処置及び患者の中止
処置の中止
患者は、以下のいずれかを経験した場合、試験処置を恒久的に中止しなければならない:
●個々の患者の治療に対する潜在的応答及び事象の重症度を考慮すると、許容できないと治験責任医師が判断した免疫介在性有害事象の発生を含む、試験処置に関連する許容できない毒性
●患者が試験処置を継続する場合、患者の安全性を危うくする可能性がある任意の医学的症状。
●処置の中止が患者にとって最も有益であるという治験責任医師又は試験依頼者の判断
●別の非治験実施計画書抗がん治療の使用
●妊娠
●RECIST v 1.1による放射線疾患進行
G. Treatment and Patient Discontinuation Treatment Discontinuation Patients must permanently discontinue study treatment if they experience any of the following:
- unacceptable treatment-related toxicity, including the occurrence of immune-mediated adverse events that the investigator judged to be unacceptable given the individual patient's potential response to treatment and the severity of the event; Any medical condition that may compromise patient safety if treatment is continued.
- Investigator's or sponsor's judgment that discontinuation of treatment would be most beneficial to the patient - Use of another non-protocol anticancer therapy - Pregnancy - Radiation disease progression by RECIST v 1.1
例外:患者は、進行性疾患についてのRECIST v1.1基準が満たされた後、放射線学的進行を超える処置について概説された基準のすべてを満たすならば、試験処置を継続することを許される。
●RECIST v1.1による放射線学的進行を超えて処置された患者の場合:放射線学的データ、生検結果(利用可能な場合)及び臨床状態の統合評定後に治験責任医師によって決定された臨床的利益の喪失
Exception: Patients are allowed to continue study treatment after RECIST v1.1 criteria for progressive disease are met, provided they meet all of the criteria outlined for treatment beyond radiographic progression.
For patients treated beyond radiological progression by RECIST v1.1: clinical as determined by the investigator after integrated assessment of radiological data, biopsy results (if available) and clinical status loss of profit
試験処置の中止の主な理由は、適切なeCRFに文書化されるべきである。試験処置を早期に中止する患者は置き換えられない。 The primary reason for discontinuing study treatment should be documented in the appropriate eCRF. Patients who discontinue study treatment early are not replaced.
患者は、試験処置の最終投薬の≦30日後に処置中止来院のために診療所に戻る。応答評定が進行性疾患を示す来院を処置中止来院として使用することができ、その場合、処置中止来院に関連するすべての評定をその時点で行うべきである。 Patients return to the clinic for a treatment discontinuation visit ≤30 days after the last dose of study treatment. A visit where a response rating indicates progressive disease can be used as a discontinuation visit, in which case all ratings associated with the discontinuation visit should be made at that time.
患者が試験処置に関連すると考えられる有害事象(特別な関心のある有害事象を含む)のために試験処置を中止し、その事象が試験処置の最後の投与の30日後に進行中である場合、その事象は、事象が安定又は不可逆的になったという治験責任医師による解消又は判定まで追跡されなければならない。 If the patient discontinued study treatment for an adverse event considered related to study treatment (including adverse events of special interest) and the event is ongoing 30 days after the last dose of study treatment, The event must be followed until resolution or determination by the investigator that the event has become stable or irreversible.
フォローアップ評定
腫瘍評定
RECIST v.1.1による放射線学的疾患進行の非存在下で試験処置(限定されないが、臨床的低下又は毒性を含む、何らかの理由で)を中止する患者は、患者が新たな抗がん治療を開始するかどうかにかかわらず、RECIST v1.1による放射線学的疾患進行、同意の撤回、死亡又は試験依頼者による終了のいずれか早く発生する方まで、活動スケジュールに概説されている腫瘍応答評定を受け続けなければならない。治験責任医師の裁量により、進行性疾患が疑われる場合はいつでもスキャンを実施しなければならない。
Follow-up assessment Tumor assessment RECIST v. Patients who discontinue study treatment (for any reason, including but not limited to clinical decline or toxicity) in the absence of radiographic disease progression according to 1.1 will allow the patient to start a new anti-cancer therapy. Continue to receive tumor response assessment as outlined in the activity schedule until radiological disease progression, withdrawal of consent, death or sponsor termination, whichever occurs first, regardless of whether There must be. At the investigator's discretion, scans should be performed whenever progressive disease is suspected.
生存及びその後の治療
処置中止後、生存フォローアップ及び新たな抗がん治療に関する情報は、死亡するまで(患者が生存フォローアップの同意を取り下げるか、又は試験依頼人が試験を終了しない限り)およそ3ヶ月毎に電話、患者の医療記録及び/又はクリニック来院によって収集される。
Survival and Subsequent Treatment After treatment discontinuation, information regarding survival follow-up and new anticancer therapy will be available approximately until death (unless the patient withdraws consent for survival follow-up or the sponsor terminates the study). Collected by phone, patient medical records and/or clinic visits every 3 months.
その後の抗がん治療に関する情報には、全身療法(例えば、化学療法、標的療法、免疫療法)、手術(例えば、局所及び/又は転移性疾患の摘出)、及び放射線処置(例えば、腫瘍病変に対する放射線療法)が含まれる。 Information regarding subsequent anticancer therapy includes systemic therapy (e.g., chemotherapy, targeted therapy, immunotherapy), surgery (e.g., removal of local and/or metastatic disease), and radiation treatment (e.g., for tumor lesions). radiation therapy).
患者の中止
患者は、何らかの理由でいつでも試験から自発的に離脱する権利を有する。更に、治験責任医師は、患者を試験からいつでも離脱させる権利を有する。
Patient Withdrawal Patients have the right to voluntarily withdraw from the study at any time for any reason. Additionally, the investigator has the right to withdraw a patient from the study at any time.
試験からの患者の中止の理由には、以下が含まれ得るが、これらに限定されない:
●患者の同意の撤回
●試験終了又は施設閉鎖
●フォローアップの喪失
●患者の不遵守、治験責任医師又は試験依頼者によって決定された治験実施計画書要件を遵守していないと定義される
Reasons for patient withdrawal from the study may include, but are not limited to:
● patient withdrawal of consent ● study termination or site closure ● loss of follow-up ● patient non-compliance, defined as non-compliance with protocol requirements as determined by the investigator or sponsor
試験から患者の中止の理由を得るためにあらゆる努力を払うべきである。試験を中止する主な理由は、適切なeCRFで文書化されるべきである。患者が試験からの中止を要求する場合(すなわち、すべての生存フォローアップからの離脱要求)、この要求はソース文書に文書化され、治験責任医師が署名しなければならない。試験から離脱する患者(すなわち、生存フォローアップ)は交換されない。 Every effort should be made to obtain the patient's reason for discontinuation from the trial. The primary reason for study discontinuation should be documented in the appropriate eCRF. If a patient requests withdrawal from the study (ie, a request to withdraw from all living follow-up), this request must be documented in the source document and signed by the investigator. Patients who leave the study (ie, survival follow-up) will not be replaced.
患者が試験から離脱する場合(すなわち、生存フォローアップ)、試験スタッフは、公開されている情報源(例えば、郡記録)を使用して生存状態に関する情報を得ることができる。 If a patient discontinues from the study (ie, survival follow-up), study staff can obtain information on survival status using publicly available sources (eg, county records).
H.分析
有効性分析
主要有効性評価項目
主要な有効性評価項目は、確認されたORRである。確認された客観的奏効は、RECIST v 1.1を使用して治験責任医師によって決定された場合、≧4週間離れた2回の連続した機会のCR又はPRのいずれかとして定義される。ベースライン後の腫瘍評定を受けていない患者を含む、これらの基準を満たさない患者は、非レスポンダーとみなされる。確認されたORRは、確認された客観的奏効を有した患者の割合として定義される。
H. Analysis Efficacy Analysis Primary Efficacy Endpoint The primary efficacy endpoint is confirmed ORR. A confirmed objective response is defined as either CR or PR on two consecutive occasions >4 weeks apart, as determined by the investigator using RECIST v1.1. Patients who do not meet these criteria, including those who do not have a post-baseline tumor assessment, are considered non-responders. Confirmed ORR is defined as the proportion of patients with a confirmed objective response.
主要な有効性分析は、すべての患者が登録され、ORR評定のフォローアップを継続している患者の中で約5ヶ月の最小限のフォローアップが達成された後に行われる。 The primary efficacy analysis will be performed after all patients have been enrolled and a minimum follow-up of approximately 5 months has been achieved among patients with ongoing follow-up for ORR assessment.
一次有効性分析集団は、割り当てられた処置に従ってグループ分けされた全てのランダム化患者からなる。ORR及びその95% CIの推定値を、各処置群についてClopper-Pearson法を使用して計算する。 The primary efficacy analysis population consisted of all randomized patients grouped according to assigned treatment. Estimates of the ORR and its 95% CI are calculated using the Clopper-Pearson method for each treatment group.
副次的有効性評価項目
奏効期間
DORは、RECIST v1.1に従って治験責任医師によって決定されるように、確認された客観的奏効を達成した患者において評定される。DORは、確認された客観的奏効の最初の発生の日から、RECIST v1.1に従って治験責任医師によって決定される進行性疾患の最初の日又は何らかの原因による死亡のいずれか早く発生する方までの時間間隔として定義される。進行しておらず、分析時に死亡していない患者は、最後の腫瘍評定日の時点で打ち切られる。Kaplan-Meier法を用いて各処置アームの中央値DORを推定し、Kaplan-Meier曲線を作成する Brookmeyer-Crowley方法論を使用して、各処置アームのDOR中央値に対して95%Clを構築する。
Secondary Efficacy Endpoints Duration of Response DOR will be assessed in patients who achieve a confirmed objective response as determined by the Investigator according to RECIST v1.1. DOR is measured from the date of first confirmed objective response to the first date of progressive disease or death from any cause, whichever occurs first, as determined by the investigator according to RECIST v1.1. Defined as a time interval. Patients who have not progressed and who have not died at the time of analysis will be censored at the date of the last tumor assessment. Estimate the median DOR for each treatment arm using the Kaplan-Meier method and generate a Kaplan-Meier curve Use the Brookmeyer-Crowley methodology to construct the 95% Cl for the median DOR for each treatment arm .
6ヶ月での無増悪生存率を含む無増悪生存期間
PFSは、ランダム化の日付と、RECIST v1.1に従って治験責任医師によって評定される、最初に文書化された疾患進行又は死亡の日付との間(いずれか早く発生する方)の時間と定義される。疾患の進行を経験したことがない、又はデータカットオフ日までに死亡しなかった患者は、最後の腫瘍評定時に打ち切られる。ベースライン後の腫瘍評定がない患者は、ランダム化の日付で打ち切られる。
Progression-free survival, including progression-free survival at 6 months PFS is defined as the date of randomization and the date of first documented disease progression or death as assessed by the investigator according to RECIST v1.1. defined as the time between (whichever occurs first). Patients who have never experienced disease progression or who do not die by the data cutoff date will be censored at the last tumor assessment. Patients with no post-baseline tumor assessment will be censored at the date of randomization.
Kaplan-Meier法を用いて各処置アームの中央値PFSを推定し、Kaplan-Meier曲線を作成する Brookmeyer-Crowley方法論を使用して、各処置アームのPFS中央値に対して95%Clを構築する。ランダム化の6ヶ月後のPFS率は、Greenwoodの式から導出された標準誤差を使用して計算された95% CIと共に、各処置群のKaplan-Meier法を使用して推定される。
6ヶ月及び12ヶ月での全生存率を含む全生存率
Estimate the median PFS for each treatment arm using the Kaplan-Meier method and generate a Kaplan-Meier curve Use the Brookmeyer-Crowley methodology to construct the 95% Cl for the median PFS for each treatment arm .
Overall survival including overall survival at 6 months and 12 months
OSは、ランダム化の日付と何らかの原因による死亡との間の時間として定義される。データカットオフ日までに死亡したと報告されていない患者のデータは、最後に生存していることが分かった日に打ち切られる。ベースライン後の情報を有していない患者のデータは、ランダム化の日付で打ち切られる。6ヶ月及び12ヶ月でのOS及びOS率を、PFSについて記載したのと同じ方法を用いて分析する。 OS is defined as the time between the date of randomization and death from any cause. Data for patients not reported to have died by the data cutoff date will be censored on the date they were last known to be alive. Data for patients with no post-baseline information will be censored at the date of randomization. OS and OS rates at 6 months and 12 months are analyzed using the same methods as described for PFS.
患者の報告された転帰
PROMIS(登録商標)Item Bank v 2.0-身体機能-ショートフォーム10bを使用した物理的機能のためのTTCDは、ランダム化の日付から最初に確認された臨床的に意味のある劣化までの時間として定義される。確認された臨床的に意味のある身体機能の低下は、少なくとも2回の連続評定のために保持されなければならないベースラインからの臨床的に意味のある減少、又はベースラインを超える最初の臨床的に意味のある増加とそれに続く死亡と定義される。4点を超えるTスコア変化は、身体機能サブスケールスコアにとって臨床的に有意であると考えられる。
Patient Reported Outcomes PROMIS® Item Bank v 2.0 - Physical Function - TTCD for Physical Function Using Short Form 10b was first confirmed clinically relevant from date of randomization defined as the time to a certain degradation of A confirmed clinically meaningful decline in physical function must be maintained for at least two consecutive assessments or the first clinically meaningful decrease from baseline over baseline. defined as a meaningful increase in A T-score change of greater than 4 points is considered clinically significant for the physical function subscale scores.
TTCDをITT集団で評定する。臨床的カットオフ日に確認された臨床的に意味のある悪化を経験していない患者は、評定を完了した最後の時点で打ち切られる。ベースライン又はベースライン後の評定が行われない場合、患者はランダム化日に打ち切られる。PROMIS(登録商標)スケールを使用するTTCDは、PFSと同じ方法を使用して分析される。 TTCD is assessed in the ITT population. Patients who have not experienced clinically meaningful deterioration confirmed at the clinical cut-off date will be censored at the end of completing the assessment. If no baseline or post-baseline assessments are made, patients will be censored on the randomization day. TTCD using the PROMIS® scale is analyzed using the same method as PFS.
PROMIS(登録商標)スケール(疼痛、疲労及び身体機能)の探索的分析には、PROMIS(登録商標)疼痛、PROMIS(登録商標)疲労及びPROMIS(登録商標)身体機能質問票の使用によって報告され、PROMIS(登録商標)スコアリングマニュアルに従って計算されたITT集団の要約統計及びベースラインからの平均変化が含まれる。 An exploratory analysis of the PROMIS® Scale (Pain, Fatigue and Physical Function) reported by use of the PROMIS® Pain, PROMIS® Fatigue and PROMIS® Physical Function Questionnaire, ITT population summary statistics and mean change from baseline calculated according to the PROMIS® Scoring Manual are included.
カウント及び割合を含む要約統計が、PGI-CI、PGI-S及び最も重要な症状について提示され、それらは探索的である。 Summary statistics including counts and rates are presented for PGI-CI, PGI-S and most important symptoms and they are exploratory.
PRO-CTCAEの分析は、試験中の疾患及び対症処置の毒性のパターンを特性評価することに焦点を当てて、本質的に探索的であり、主に記述的である。これらの探索的分析の結果は、他の安全性分析とは別に提示される。PRO-CTCAEデータは、データ処理のための現在のNCI勧告に沿って項目レベルで分析される。各処置群について、「頻度」、「重症度」、「干渉」、及び「存在」カテゴリによって症状を報告している患者の数(パーセンテージ)が各評定で報告される。 Analyzes of PRO-CTCAEs are exploratory in nature and primarily descriptive, with a focus on characterizing the toxicity patterns of the disease and symptomatic treatments under study. The results of these exploratory analyzes are presented separately from other safety analyses. PRO-CTCAE data will be analyzed at the item level in line with current NCI recommendations for data processing. For each treatment group, the number (percentage) of patients reporting symptoms by "frequency," "severity," "interference," and "presence" categories are reported at each rating.
更に、症状の頻度を症状の重症度と交差集計して、症状が発生したときの症状の影響を調べる。処置群による試験中に症状の重症度を「重症」又は「非常に重症」として報告した患者の割合の要約表も提供される。 In addition, symptom frequency is cross-tabulated with symptom severity to examine the impact of symptoms when they occur. A summary table of the proportion of patients reporting symptom severity as "severe" or "very severe" during the study by treatment group is also provided.
安全性分析
安全性分析集団は、少なくとも1回の用量のアテゾリズマブ又はチラゴルマブ/プラセボを受けた全てのランダム化患者からなる。
Safety Analysis The safety analysis population consists of all randomized patients who received atezolizumab or tiragolumab/placebo at least one dose.
安全性分析は、処置群によって実施され、受けた実際の処置に基づく。具体的には、ランダム化の際の最初の処置割り当てに関係なく、患者が任意の量のチラゴルマブを受けた場合、患者は安全性分析においてアテゾリズマブ+チラゴルマブ群に含まれる。 Safety analyzes are performed by treatment group and are based on the actual treatment received. Specifically, patients are included in the atezolizumab plus tiragolumab group in the safety analysis if they received any dose of tiragolumab, regardless of their initial treatment assignment at randomization.
薬物曝露を、持続時間、投薬量及び用量強度を含めて要約する。 Drug exposure is summarized including duration, dosage and dose intensity.
有害事象の言語記述は、MedDRA類義語にマッピングされ、NCI CTCAE v5.0に従って等級付けされ、CRSの重症度もASTCTコンセンサス等級付けスケールに従って治験責任医師によって等級付けされる。全ての有害事象を処置群及びNCI CTCAEグレードによって要約する。また、CRSを、処置群及びASTCTコンセンサスグレードによって要約する。更に、重篤な有害事象、免疫介在性有害事象、及び試験処置の中止又は中断につながる有害事象を適宜要約する。同じ事象の複数の発生は、最大重症度で1回カウントする。 Verbal descriptions of adverse events will be mapped to MedDRA synonyms and graded according to the NCI CTCAE v5.0, and the severity of CRS will also be graded by investigators according to the ASTCT consensus grading scale. All adverse events will be summarized by treatment group and NCI CTCAE grade. CRS is also summarized by treatment group and ASTCT consensus grade. In addition, serious adverse events, immune-mediated adverse events, and adverse events leading to discontinuation or discontinuation of study treatment will be summarized as appropriate. Multiple occurrences of the same event are counted once at maximum severity.
全ての死亡及び死亡の原因を処置群によって要約する。 All deaths and causes of death are summarized by treatment group.
正常範囲外の値を有する実験データが特定される。更に、ADA結果を含む選択された実験データを要約する。 Experimental data with values outside the normal range are identified. In addition, selected experimental data including ADA results are summarized.
薬物動態学的分析
本試験では、チラゴルマブ及びアテゾリズマブのPK試料を収集する。チラゴルマブ及びアテゾリズマブの血清濃度データ(最小血清濃度及び最大血清濃度)を集計し、要約する。
Pharmacokinetic Analysis In this study, PK samples of tiragolumab and atezolizumab are collected. Tiragolumab and atezolizumab serum concentration data (minimum and maximum serum concentrations) will be collected and summarized.
記述統計学には、必要に応じて、平均値、中央値、範囲及び標準偏差が含まれる。 Descriptive statistics include mean, median, range and standard deviation as appropriate.
データの入手可能性に基づいて、必要に応じて、さらなるPK分析を行う。 Further PK analysis will be performed as needed based on data availability.
免疫原性分析
免疫原性分析には、任意のADA評定を受けた患者が含まれ、受けた処置に従って患者がグループ分けされる。処置下で発現したADA陽性患者及びADA陰性患者の数及び割合を処置群によって要約する。
Immunogenicity Analysis The immunogenicity analysis includes patients with any ADA assessment and groups the patients according to the treatment received. The number and proportion of treatment-emergent ADA-positive and ADA-negative patients are summarized by treatment group.
ADAの状態と安全性、有効性及びPK評価項目との間の関係は、記述統計学を用いて分析及び報告され得る。 Relationships between ADA status and safety, efficacy and PK endpoints can be analyzed and reported using descriptive statistics.
バイオマーカー分析
バイオマーカー分析は探索的である。記述統計学は、バイオマーカーサブグループ及びそれらの有効性評価項目との関係を要約するために使用される。データは、この試験の状況において、及び他の試験からのデータと併せて分析することができる。
Biomarker Analysis Biomarker analysis is exploratory. Descriptive statistics are used to summarize biomarker subgroups and their relationship to efficacy endpoints. Data can be analyzed in the context of this study and in conjunction with data from other studies.
暫定分析
有効性の暫定分析を計画し、約60人の患者を登録し、約少なくとも5ヶ月間フォローアップされる機会を得たときにIMCによって再検討する。
Interim Analysis An interim analysis of efficacy is planned to enroll approximately 60 patients and be reviewed by the IMC when given the opportunity to be followed up for approximately at least 5 months.
実施例16.筋層浸潤性膀胱がん(MIBC)患者における複数の免疫療法に基づく処置及び組み合わせの有効性及び安全性を評価する第Ib/II相非盲検多施設ランダム化包括的試験
筋層浸潤性膀胱がん(MIBC)の診断から膀胱切除術までの時間は、典型的には4~8週間であり、再発率及びOSを改善するためのネオアジュバント療法を患者に提供する機会のウィンドウを提供する。ネオアジュバント化学療法の利益は中程度であり、膀胱切除術単独と比較して、ネオアジュバント化学療法で処置された患者の全生存(OS)は5%増加する(Vale et al.,Eur Urol,48:202-205,2005)。病理学的完全奏効(pCR)を達成した患者は、ネオアジュバントであるシスプラチンベースの化学療法を受けたことから最も利益を受け、5年追跡調査時に80~90%が生存しているが、患者の50%までが、手術時に残存する高リスク疾患(pT 2以上)を有する場合があり、5年生存率は50%未満である(Rosenblatt et al.,Eur Urol,61:1229-1238,2011;Bhindi et al.,Eur Urol,72:660-664,2017)。したがって、pCRは、MIBCのためのネオアジュバント療法における有効性及び生存率増加の代用マーカーとなり得る。
Example 16. A Phase Ib/II, Open-label, Multicenter, Randomized, Comprehensive Study Evaluating the Efficacy and Safety of Multiple Immunotherapy-Based Treatments and Combinations in Patients with Muscle-Invasive Bladder Cancer (MIBC) Muscle-invasive Bladder The time from cancer (MIBC) diagnosis to cystectomy is typically 4-8 weeks, providing a window of opportunity to provide patients with neoadjuvant therapy to improve recurrence rates and OS. . Benefits of neoadjuvant chemotherapy are moderate, with a 5% increase in overall survival (OS) in patients treated with neoadjuvant chemotherapy compared to cystectomy alone (Vale et al., Eur Urol, 48:202-205, 2005). Patients who achieved a pathological complete response (pCR) benefited most from receiving neoadjuvant cisplatin-based chemotherapy, with 80-90% surviving at 5-year follow-up, although patients up to 50% of patients may have residual high-risk disease (
WO39613は、シスプラチン不適格MIBCを有する患者における複数の免疫療法ベースの処置及び組み合わせの有効性及び安全性を評価する第Ib/II相非盲検多施設ランダム化包括的試験である。この試験は、新しい処置が利用可能になるにつれて新しい処置群を開き、最小限の臨床活性又は許容できない毒性を示す既存の処置群を閉じ、又は患者集団を変更する(例えば、以前の抗がん処置又はバイオマーカーの状態に関して)ための柔軟性を備えて設計される。患者をランダムに対照群(アテゾリズマブ(Atezo))又はチラゴルマブと組み合わせたアテゾリズマブ(Atezo+Tira)からなる実験群(図24及び表69)に割り当てる。

アテゾリズマブ及びチラゴルマブについての目標及び提案された作用機序分類を表70に要約する。

本試験の具体的な目的及び対応評価項目を表71に概説する。


1つの時点での全奏効が、RECIST v 1.1を使用して治験責任医師によって評定される。iRECISTによる全奏効は、治験責任医師が評定した個々の病変データに基づいて、試験依頼者がプログラムによって計算する。 Overall response at one time point will be assessed by the investigator using RECIST v 1.1. Overall response by iRECIST will be calculated programmatically by the sponsor based on investigator-assessed individual lesion data.
約150~350人の患者が登録され、MIBCコホート1(PD-L1+)とMIBCコホート2(PD-L1-)に分けられる。実験群内への登録は、予備期とそれに続く拡大期の2期で行われる。すべての処置アームは、予備期の間、MIBCコホート1(PD-L1+)及びMIBCコホート2(PD-L1-)について同じである。VENTANA PD-L1(SP142)アッセイを使用した膀胱腫瘍(TURBT)試料の経尿道切除の中央PD-L1検査後に、患者をMIBCコホート1(PD-L1+)又はMIBCコホート2(PD-L1-)のいずれかに割り当てる。腫瘍細胞、関連する腫瘍内及び隣接する腫瘍周囲間質によって占められる腫瘍面積の5%以上を覆う腫瘍浸潤免疫細胞における任意の強度の識別可能なPD-L1染色の存在に対応する、2又は3(IC2/3)のPD-L1免疫細胞(IC)スコアを有する患者を、MIBCコホート1(PD-L1+)に割り当てる。腫瘍細胞、関連する腫瘍内、及び隣接する腫瘍周囲間質によって占められる腫瘍領域の5%以下を覆う腫瘍浸潤免疫細胞における任意の強度の識別可能なPD-L1染色の存在に対応する、0又は1のICスコアを有する患者(IC0/1)をMIBCコホート2(PD-L1-)に割り当てる。 Approximately 150-350 patients are enrolled and divided into MIBC Cohort 1 (PD-L1+) and MIBC Cohort 2 (PD-L1-). Enrollment within the experimental group is conducted in two phases, a preliminary phase followed by an expansion phase. All treatment arms are the same for MIBC cohort 1 (PD-L1+) and MIBC cohort 2 (PD-L1-) during the preliminary phase. After central PD-L1 examination of transurethral resection of bladder tumor (TURBT) specimens using the VENTANA PD-L1 (SP142) assay, patients were assigned to MIBC Cohort 1 (PD-L1+) or MIBC Cohort 2 (PD-L1-). Assign to either. 2 or 3, corresponding to the presence of any intensity of discernible PD-L1 staining in tumor cells, tumor-infiltrating immune cells covering 5% or more of the tumor area occupied by associated intratumoral and adjacent peritumoral stroma. Patients with a PD-L1 immune cell (IC) score of (IC2/3) are assigned to MIBC cohort 1 (PD-L1+). 0 or 0, corresponding to the presence of any intensity of discernible PD-L1 staining in tumor-infiltrating immune cells covering up to 5% of the tumor area occupied by tumor cells, associated intratumoral, and adjacent peritumoral stroma Patients with an IC score of 1 (IC0/1) are assigned to MIBC cohort 2 (PD-L1-).
予備期中、MIBC PD-L1コホートのそれぞれについて、最大30人の患者がAtezo+Tiraアームに登録され、約15人の患者が他のすべてのアームに登録される。予備期中に実験群で臨床活性が観察される場合、拡大期中に約25人の追加の患者がその群に登録される。 During the preliminary phase, up to 30 patients will be enrolled in the Atezo+Tira arm and approximately 15 patients in all other arms for each of the MIBC PD-L1 cohorts. If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients will be enrolled in that group during the expansion phase.
試験依頼者は、所与の治処置群内への登録を遅延又は一時停止することを決定し得る。不十分な臨床活性又は許容できない毒性を有する実験群は拡大されない。さらなるサブグループ分析を可能にするために、潜在的な予測バイオマーカーを含む人口統計学的及びベースライン特性に関して処置群間のバランスを確保するために、さらなる患者を登録することができる。 Sponsors may decide to delay or suspend enrollment within a given treatment arm. Experimental groups with inadequate clinical activity or unacceptable toxicity will not be expanded. Additional patients can be enrolled to ensure balance between treatment groups with respect to demographic and baseline characteristics, including potential predictive biomarkers, to allow for further subgroup analysis.
ランダム化は、利用可能な実験群の数(例えば、予備期からの結果の分析を待って、群が追加されるか、又は群への登録が一時停止される場合)に依存し、対照群に割り当てられる可能性は35%以下であるという規定がある。ランダム化は、群特異的排除基準を考慮に入れる。患者は、その群について概説された除外基準のいずれかを満たす場合(下記を参照)、特定の群について不適格である。 Randomization will depend on the number of experimental groups available (e.g., if groups are added or group enrollment is suspended pending analysis of results from the preliminary phase) and the control group There is a provision that the probability of being assigned to is 35% or less. Randomization takes into account group-specific exclusion criteria. Patients are ineligible for a particular group if they meet any of the exclusion criteria outlined for that group (see below).
アテゾリズマブ対照群及び実験群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで処置される。患者は、術後最大1年間の処置を受けた後、2年間の3ヶ月のフォローアップ評定を受ける。 Patients in the atezolizumab control and experimental groups will be integrated with radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening symptoms such as pain secondary to disease). Treatment is until unacceptable toxicity or loss of clinical benefit as determined by the Investigator after evaluation. Patients will undergo treatment for up to 1 year postoperatively, followed by 3-month follow-up assessments for 2 years.
A.評定及びモニタリング A. Rating and monitoring
全ての患者は、試験を通して有害事象について綿密に監視され、有害事象は、国立がん試験所有害事象共通用語規準(National Cancer Institute Common Terminology Criteria for Adverse Events,Version 4.0(NCI CTCAE v4.0))に従って等級付けされる。患者は、最初の54週間は9週間毎に(サイクル1の1日目から開始して)、その後は12週間毎に腫瘍評定を受ける。応答は、
RECIST v 1.1を使用して治験責任医師によって評定されるEisenhauer et al.,Eur J Cancer,45:228-247,2009))。臨床活性が実験群において実証される場合、提供者は、そのための腫瘍評定スキャンを要求し得る。
All patients were closely monitored for adverse events throughout the study, and adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). )). Patients undergo tumor assessments every 9 weeks for the first 54 weeks (starting on
Eisenhauer et al., assessed by investigators using RECIST v 1.1. , Eur J Cancer, 45:228-247, 2009)). If clinical activity is demonstrated in the experimental group, the donor may request a tumor assessment scan for it.
その群の腫瘍評定スキャンが独立した読み取り施設による評価に提出されることを要求し得る。 It may be required that the group's tumor assessment scans be submitted for evaluation by an independent reading center.
ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、腫瘍組織の保管を提出することができる。腫瘍組織はまた、治験責任医師によって決定されるように(治験責任医師によって臨床的に実施可能であると考えられる場合)、許容できない毒性又は臨床的利益の喪失のためにステージ1を中止する患者から収集される。これらの試料、並びに試験中に採取された血液試料は、バイオマーカー研究に利用される。
Baseline tumor tissue samples are collected from all patients, preferably by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, archiving of tumor tissue may be submitted.
アテゾリズマブ及び他の治療剤の薬物動態(PK)特性及び/又は免疫原性を特性評価するために、試験処置投与の前及び間の様々な時点で血液試料を取得する。 To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points before and during study treatment administration.
B.試験終了及び試験期間 B. End of test and test period
試験の終了は、両方のステージでの最後の患者が最後の来院を完了した日(電話又は現場での来院によって行われる生存フォローアップ来院を含む)として定義される。 End of study is defined as the date the last patient in both stages completed the last visit (including survival follow-up visits conducted by telephone or on-site visit).
最初の患者のスクリーニングから試験終了までの試験の全長は、約3~5年である。 The total length of the trial, from initial patient screening to study termination, is approximately 3-5 years.
C.試験計画の理論的根拠
試験の理論的根拠及び利益-リスク評定
C. RATIONALE OF THE STUDY DESIGN RATIONALE AND BENEFITS OF THE STUDY - RISK ASSESSMENT
この試験は、シスプラチン不適格MIBC患者における初期シグナルを同定し、概念実証臨床データを確立することによって、がん免疫療法(CIT)の組み合わせの開発を加速するように設計されている。 This study is designed to accelerate the development of cancer immunotherapy (CIT) combinations by identifying early signals and establishing proof-of-concept clinical data in cisplatin-ineligible MIBC patients.
白金ベースのネオアジュバント化学療法はOSの改善に関連するが、少数の患者にのみ適している。シスプラチン不適格MIBCを有する患者の処置選択肢が比較的限られており、更に局所進行性又は転移性UCの処置に関連する予後不良及び潜在的毒性を考慮すると、これらの集団は処置選択肢を必要としており、したがって新規治療候補の試験に適していると考えられる。現在普及しているCITアプローチは、プログラム死リガンド1(PD-L1)/プログラム死1(PD-1)等のT細胞阻害因子を標的とすることによって、免疫回避機構を回避し、抗腫瘍応答を再活性化することである。 Platinum-based neoadjuvant chemotherapy is associated with improved OS, but is suitable for only a minority of patients. Given the relatively limited treatment options for patients with cisplatin-ineligible MIBC, and the poor prognosis and potential toxicity associated with treatment of locally advanced or metastatic UC, these populations are in need of treatment options. and therefore considered suitable for testing new therapeutic candidates. Current prevalent CIT approaches target T cell inhibitors such as programmed death ligand 1 (PD-L1)/programmed death 1 (PD-1) to circumvent immune evasion mechanisms and enhance anti-tumor responses. is to reactivate
CITは明確な臨床的有効性を実証しており、複数の進行性悪性腫瘍にわたって有意な生存利益が観察されており、PD-1/PD-L1チェックポイント遮断がUC患者においてpCR及び永続的応答を生成し得るという証拠がある(Powles et al.,Nat Med,25:1706-1714,2019;Necchi et al.,Int J Clin Oncol,36:3353-3360,2018)。これらの標的は様々ながん適応症について顕著な臨床的成功をもたらしたが、進行中の研究は、一連の段階的事象が有効な抗腫瘍免疫応答の生成に必要であることを示している(Chen and Mellman,Immunity,39:1-10,2013)。各事象は有効な応答にとって重要であり、それぞれがいくつかの腫瘍免疫回避機構の影響を受けやすい。したがって、有効な抗がん免疫応答の欠如又は回避を説明する様々な因子を同定及び回避する必要性は、がん免疫を伝播し、CITの分野を進歩させるために重要である。アテゾリズマブと、異なる免疫回避機構又は新規な第2世代CPIを標的とする薬剤との組み合わせは、この集団における奏効率を増加させ、疾患再発率を更に低下させ得る。 CIT has demonstrated clear clinical efficacy, with significant survival benefits observed across multiple advanced malignancies, and PD-1/PD-L1 checkpoint blockade demonstrated pCR and durable responses in UC patients. (Powles et al., Nat Med, 25:1706-1714, 2019; Necchi et al., Int J Clin Oncol, 36:3353-3360, 2018). Although these targets have provided remarkable clinical success for a variety of cancer indications, ongoing research indicates that a series of stepwise events are required to generate an effective anti-tumor immune response. (Chen and Mellman, Immunity, 39:1-10, 2013). Each event is critical for an effective response and each is susceptible to several tumor immune evasion mechanisms. Therefore, the need to identify and evade various factors that account for the lack or evasion of effective anti-cancer immune responses is critical to propagating cancer immunity and advancing the field of CIT. Combining atezolizumab with agents that target different immune evasion mechanisms or novel second-generation CPIs may increase response rates and further reduce disease relapse rates in this population.
MIBC患者の潜在的なリスクは、試験処置に関連する有害事象に関連する。ほとんどの国において、患者は、尿路上皮がんの診断を確立するのと手術との間に平均4~8週間待つ。術前処置を含むこの治験への参加は、参加者にとって手術の関連する遅延をもたらすとは予想されない。更に、アテゾリズマブは、手術適応に影響を及ぼさず、ABACUS試験における手術に関連するリスクを増加させなかった(Powles et al.,Nat Med,25:1706-1714,2019)。 A potential risk for MIBC patients is associated with adverse events related to study treatment. In most countries, patients wait an average of 4-8 weeks between establishing a diagnosis of urothelial carcinoma and surgery. Participation in this trial, including preoperative treatment, is not expected to result in associated delays in surgery for participants. Furthermore, atezolizumab did not affect surgical indications or increase surgery-related risks in the ABACUS trial (Powles et al., Nat Med, 25:1706-1714, 2019).
筋層浸潤性膀胱がんにおける周術期処置の理論的根拠
ネオアジュバント療法及び手術後の維持療法の治療的寄与は不明である。WO39613の試験は、処置有効性を評定し、連続する患者組織に対して広範なバイオマーカー分析を行うように設計されている。
Rationale for Perioperative Treatment in Muscle-Invasive Bladder Cancer The therapeutic contribution of neoadjuvant therapy and postoperative maintenance therapy is unclear. The WO39613 trial is designed to assess treatment efficacy and perform extensive biomarker analysis on serial patient tissues.
IMVigor010は、外科的摘出及びリンパ節郭清術後にアジュバント療法としてアテゾリズマブ対観察を受けるようにMIBCを有する患者をランダムに割り当てた第III相ランダム化試験である。この試験は、処置企図集団においてアテゾリズマブアジュバント治療による無病生存利益を示すというその主要評価項目を満たしていなかったが、T3及びT4患者のサブグループ分析、並びに非臨床データ(Liu et al.,Cancer Discov,6:1382-1399,2016;Pai et al.,Immunity,50:477-492,2019;Hussain et al.,J Clin Oncol,38(15 Suppl.):5000,2020)は、免疫療法が、患者がチェックポイント免疫療法について残存疾患又は活動性疾患を有することが有効となることを必要とし得ることを示唆する。 IMVigor010 is a phase III randomized trial that randomly assigned patients with MIBC to receive atezolizumab versus observation as adjuvant therapy after surgical excision and lymphadenectomy. Although this trial did not meet its primary endpoint of demonstrating a disease-free survival benefit with atezolizumab adjuvant therapy in the intention-to-treat population, subgroup analyzes of T3 and T4 patients and nonclinical data (Liu et al. Pai et al., Immunity, 50:477-492, 2019; Hussain et al., J Clin Oncol, 38 (15 Suppl.): 5000, 2020). It is suggested that therapy may require that patients with residual or active disease be effective for checkpoint immunotherapy.
D.シスプラチンに基づく化学療法に適格でない筋浸潤性膀胱がんを有する患者における免疫療法の証拠 D. Evidence for immunotherapy in patients with muscle-invasive bladder cancer who are not eligible for cisplatin-based chemotherapy
MIBCを有する患者の約50%は、シスプラチンに基づくネオアジュバント化学療法を受けるのに不適格であり、これらの患者に推奨される周術期全身処置は現在存在せず、両側骨盤リンパ節郭清術を伴う膀胱切除術が標準治療である。更に、ネオアジュバント化学療法に適格であるMIBCを有する患者の半数未満が、個人の好み又は他の併存症のためにそれを受けるであろう。したがって、MIBC患者の転帰を改善するための新しい治療法が必要である。 Approximately 50% of patients with MIBC are ineligible to receive cisplatin-based neoadjuvant chemotherapy, and there is currently no perioperative systemic treatment recommended for these patients, bilateral pelvic lymphadenectomy Cystectomy with surgery is the standard treatment. Moreover, less than half of patients with MIBC who are eligible for neoadjuvant chemotherapy will receive it due to personal preference or other comorbidities. Therefore, new therapeutic modalities are needed to improve the outcome of MIBC patients.
PD-1/PD-L1チェックポイント免疫療法は、mUCに対する化学療法で進行した全ての患者、及び1LのmUCを有する患者であって、腫瘍がPD-L1+である場合、白金ベースの化学療法に不適格であるか又はシスプラチンベースの化学療法に不適格である患者に対して承認されている。MIBC患者におけるPD-1/PD-L1チェックポイントネオアジュバント免疫療法の安全性及び有効性を調査する最大の研究は、ABACUS及びPURE-01研究であった(Powles et al.,Nat Med,25:1706-1714,2019;Necchi et al.,Int J Clin Oncol,36:3353-3360,2018)。 PD-1/PD-L1 checkpoint immunotherapy for all patients who progressed on chemotherapy to mUC and patients with 1 L mUC to platinum-based chemotherapy if the tumor is PD-L1+ Approved for patients who are ineligible or ineligible for cisplatin-based chemotherapy. The largest studies investigating the safety and efficacy of PD-1/PD-L1 checkpoint neoadjuvant immunotherapy in MIBC patients were the ABACUS and PURE-01 studies (Powles et al., Nat Med, 25: 1706-1714, 2019; Necchi et al., Int J Clin Oncol, 36:3353-3360, 2018).
E.主要評価項目としての病理学的完全寛解の理論的根拠 E. Rationale for complete pathologic response as the primary endpoint
病理学的完全寛解(pCR)並びに病理的進展度の低下(探索的評価項目)は、永続的な無寛解生存との関連のために、この状況における活動性の代用マーカーとして検証されている(Rosenblatt et al.,Eur Urol,61:1229-1238,2011;Bhindi et al.,Eur Urol,72:660-664,2017)。 Complete pathologic response (pCR) as well as reduction in pathologic extent (exploratory endpoints) have been validated as surrogate markers of activity in this setting due to their association with durable remission-free survival ( Rosenblatt et al., Eur Urol, 61:1229-1238, 2011; Bhindi et al., Eur Urol, 72:660-664, 2017).
ベースラインCD8 T細胞浸潤及びPD-L1+疾患の増加は、ネオアジュバント環境における免疫療法によるpCRの確率を増加させることが示されている(Powles et al.,Nat Med,25:1706-1714,2019)。 An increase in baseline CD8 T-cell infiltration and PD-L1+ disease has been shown to increase the probability of pCR with immunotherapy in a neoadjuvant setting (Powles et al., Nat Med, 25:1706-1714, 2019). ).
F.比較対象としてアテゾリズマブを使用する理論的根拠 F. Rationale for using atezolizumab as a comparator
シスプラチンベースのネオアジュバント化学療法を拒否するか又は不適格なMIBC患者に外科的摘出の前又は後に全身療法を提供するための標準治療は存在しない。 There is no standard treatment for providing systemic therapy before or after surgical excision in MIBC patients who refuse or are ineligible for cisplatin-based neoadjuvant chemotherapy.
アテゾリズマブは、ABACUS及びPURE-01研究が、PD-1/PD-L1チェックポイント免疫療法がMIBC患者において有効かつ安全であり、シスプラチンに基づく化学療法で歴史的に観察された奏効率に匹敵する奏効率であることを示したことから、比較処置として選択した。ABACUS及びPURE-01データに基づいて、mUCと比較して、MIBCは典型的にはより多くの炎症を起こしており、したがってPD-L1発現がIMVigor211及びKN-045試験でそれぞれmUCについて処置された患者の25%及び28.5%のみで観察されたことから、PD-1/PD-L1チェックポイント免疫療法から利益を得る可能性が高い。 Atezolizumab demonstrated that ABACUS and PURE-01 studies demonstrated that PD-1/PD-L1 checkpoint immunotherapy was efficacious and safe in MIBC patients, with response rates comparable to those historically observed with cisplatin-based chemotherapy. It was selected as a comparison treatment because it showed efficacy. Based on ABACUS and PURE-01 data, compared to mUC, MIBC are typically more inflamed and thus PD-L1 expression was treated for mUC in IMVigor211 and KN-045 studies, respectively. Observed in only 25% and 28.5% of patients, it is likely to benefit from PD-1/PD-L1 checkpoint immunotherapy.
免疫療法の組み合わせを評価するランダム化試験は、シスプラチンに基づく化学療法に不適格なMIBCを有する患者のための安全で効果的な治療法の特定を可能にする一方で、がん生物学の理解を著しく高め、MIBCを有するすべての患者のための新しい試験及び処置を設計する際に反復する能力を改善する。この試験はまた、十分な臨床的安全性が実証されている免疫療法の組み合わせを使用する可能性のある将来の群及びコホートを含み得る。 Randomized trials evaluating combinations of immunotherapies may allow the identification of safe and effective treatments for patients with MIBC who are ineligible for cisplatin-based chemotherapy, while improving our understanding of cancer biology. and improve the ability to iterate in designing new tests and treatments for all patients with MIBC. This study may also include potential future groups and cohorts using immunotherapeutic combinations that have demonstrated sufficient clinical safety.
G.別々の PD-L1+及びPD-L1-コホートの理論的根拠 G. Rationale for separate PD-L1+ and PD-L1− cohorts
PD-1/PD-L1遮断は、2L mUCについて、及びシスプラチンに基づく化学療法を受けることに不適格なPD-L1+mUCの患者についてはFDAによって承認されているが、MIBCの患者については承認されていない。ABACUS試験におけるpCRの利益は、PD-L1-(24.5%;n=12/49)疾患よりもPD-L1+(37.1%;n=13/35)でアテゾリズマブ処置された患者において大きかったが、PD-L1-疾患を有する一部の患者は、アテゾリズマブ又は免疫療法の組み合わせから依然として利益を得る可能性がある。試験の設計により、試験依頼者は、これらの患者サブセットにおけるアテゾリズマブ及び他の免疫療法の組み合わせの有効性を別々に評価し、他のコホートにおける調査に影響を及ぼすことなく、利益の証拠がない各コホートにおける群への登録を終了することが可能になる。 PD-1/PD-L1 blockade has been approved by the FDA for 2L mUC and for patients with PD-L1+mUC who are ineligible to receive cisplatin-based chemotherapy, but not for patients with MIBC. do not have. The benefit of pCR in the ABACUS trial was greater in atezolizumab-treated patients with PD-L1+ (37.1%; n=13/35) than PD-L1- (24.5%; n=12/49) disease. However, some patients with PD-L1- disease may still benefit from a combination of atezolizumab or immunotherapy. The study design allowed the sponsor to separately assess the efficacy of atezolizumab and other immunotherapy combinations in these patient subsets, and to evaluate each patient for which there was no evidence of benefit without affecting investigations in other cohorts. Enrollment in groups in the cohort can be terminated.
H.筋肉浸潤性膀胱がんコホートに対するctDNAに対する周術期治療の影響の調査の理論的根拠 H. Rationale for Investigating the Impact of Perioperative Treatment on ctDNA for a Muscle-Invasive Bladder Cancer Cohort
経時的な循環腫瘍DNA(ctDNA)濃度の変化は、疾患再発を検出するために使用され得る(Moding et al.,Nat Cancer,1:176-183,2020)。がん細胞から末梢血中に放出されたctDNAを非侵襲的に収集し、腫瘍特異的変異の存在について検査することができる。UCのいくつかの特徴は、ctDNA検査を利用した疾患再発の予後診断のための強力な候補となる。 Changes in circulating tumor DNA (ctDNA) levels over time can be used to detect disease recurrence (Moding et al., Nat Cancer, 1:176-183, 2020). CtDNA released into peripheral blood from cancer cells can be collected non-invasively and tested for the presence of tumor-specific mutations. Several features of UC make it a strong candidate for prognosis of disease recurrence using ctDNA testing.
●UCは高い体細胞変異率を有する;したがって、非常に少数の遺伝子又は標的化領域は、疾患特性を予測するために非常に有益であり得る(Todenhoefer et al.,Bladder Cancer,4:1929,2018)。
●UCにおける転移性再発はクローン起源を有することが観察されており、変異分析において元の腫瘍と有意に異ならない(Thomsen et al.,Sci Rep,7:11702,2017)。
●UCにおける対の腫瘍の分析では、サブクローンがほとんど同定されず、根治療法後の長期ctDNA検査の予後の可能性が裏付けられた(Lamy et al.,Cancer Res,76:5894,2016;Nodentoft et al.,Cell Rep,7:1649-1663,2014)。
●ネオアジュバント化学療法を受け、膀胱切除術を受けたMIBC患者68人から長手方向に採取した試料に対して、Natera Signatera ctDNAアッセイを使用して分析を行った。この分析により、膀胱切除術後の任意の時点で試料がctDNA陽性であった患者は、膀胱切除術後にctDNA陰性を維持した患者(フォローアップ期間の中央値21ヶ月)に対して76%対0%の全再発率を有することが分かった(Christiensen et al.J Clin Oncol.37(18):1547-1557,2019)。
• UC has a high somatic mutation rate; therefore, a very small number of genes or targeted regions can be highly informative for predicting disease traits (Todenhoefer et al., Bladder Cancer, 4:1929, 2018).
• Metastatic recurrences in UC have been observed to have a clonal origin and are not significantly different from the original tumor in mutational analysis (Thomsen et al., Sci Rep, 7:11702, 2017).
Analysis of paired tumors in UC identified few subclones, supporting the prognostic potential of long-term ctDNA testing after definitive therapy (Lamy et al., Cancer Res, 76:5894, 2016; Nodentoft et al., Cell Rep, 7:1649-1663, 2014).
• Longitudinal samples from 68 MIBC patients who received neoadjuvant chemotherapy and underwent cystectomy were analyzed using the Natera Signatera ctDNA assay. This analysis showed that patients whose specimens were ctDNA positive at any time after cystectomy versus those who remained ctDNA negative after cystectomy (median follow-up of 21 months) were 76% It was found to have an overall recurrence rate of 0% (Christiensen et al. J Clin Oncol. 37(18):1547-1557, 2019).
これらのデータは、緊急の処置選択肢に対する満たされていないニーズが高いMIBC患者のバイオマーカー選択亜集団を提示する。しかしながら、現在のところ、1)尿路上皮がん患者における膀胱切除術前後のctDNAに対するネオアジュバント免疫療法の影響;2)維持免疫療法が、ネオアジュバント免疫療法で処置された患者における膀胱切除後の尿路上皮がんの再発を予防するのに役立つかどうか;3)維持免疫療法が These data present a biomarker-selected subpopulation of MIBC patients with a high unmet need for acute treatment options. However, currently there are 1) effects of neoadjuvant immunotherapy on ctDNA before and after cystectomy in patients with urothelial cancer; 2) maintenance immunotherapy after cystectomy in patients treated with neoadjuvant immunotherapy; whether maintenance immunotherapy helps prevent recurrence of urothelial carcinoma;
ネオアジュバント免疫療法で処置された患者が膀胱切除術後に測定可能なctDNAを有していた場合、疾患の再発リスクを減少するかどうか、に関するデータはない。 There are no data regarding whether patients treated with neoadjuvant immunotherapy have a reduced risk of disease recurrence if they have measurable ctDNA after cystectomy.
この試験の一部として、以下の4つの時点でアテゾリズマブ及びアテゾリズマブ+チラコルマブで処置されたPD-L1+MIBCを有する全ての患者においてctDNAを遡及的に測定する:1)サイクル1の1日目前;2)膀胱切除術前;3)膀胱切除後4~6週間;4)膀胱切除術の6ヶ月後。これらの時点でのctDNA結果と無症候生存期間(EFS)及びOSとの間の関連を調べる。これらの結果は、ネオアジュバントの影響、並びに
As part of this study, ctDNA will be measured retrospectively in all patients with PD-L1 + MIBC treated with atezolizumab and atezolizumab plus tiracolumab at four time points: 1)
チェックポイント免疫療法を受けている患者における維持療法価値に関する将来の試験の設計の情報を伝える。これらの調査の結果及び他の群で観察された臨床活性を保留して、試験の他の群でこれらの時点でctDNAを調査した。 To inform the design of future trials of maintenance therapy value in patients receiving checkpoint immunotherapy. Pending the results of these studies and the clinical activity observed in other groups, ctDNA was investigated at these time points in other groups of the study.
この設計及びctDNAの使用は、1)ctDNAに対するネオアジュバント療法の影響及び病理学的応答;2)ネオアジュバント免疫療法後の残存ctDNAに対する手術の影響;並びに3)維持免疫療法が、手術後のMIBC患者におけるctDNA及び疾患再発のリスクを低下させるかどうかの評価を可能にする。 This design and use of ctDNA has been shown to: 1) impact of neoadjuvant therapy on ctDNA and pathological responses; 2) impact of surgery on residual ctDNA after neoadjuvant immunotherapy; Allows assessment of ctDNA in patients and whether it reduces the risk of disease recurrence.
実施例17.WO39613の試験のための材料及び方法
A.選択基準
患者は以下の基準の全てを満たさなければならない:
●年齢≧18歳。
●治験責任医師の判断による、治験実施計画書を遵守する能力
●0又は1の、米国東海岸がん臨床試験グループ(ECOG)パフォーマンスステータス
●ネオアジュバントであるシスプラチンベースの化学療法を拒絶する患者、又はネオアジュバントであるシスプラチンベースの療法が適切でない患者。この試験に不適格なシスプラチンは、クレアチニンクリアランス<60mL/分及び/又はグレード≧2の難聴及び/又はグレード≧2の神経障害によって定義される。
●適合し、膀胱切除術が予定されている。
●TCC又は膀胱の尿路上皮細胞癌腫とも呼ばれる、組織学的に文書化されたMIBC(pT2-4、N0、M0)。
〇TURBT後の残存疾患(外科的所見、膀胱鏡検査/内視鏡検査又は放射線学的存在)。
〇混合組織型の患者は、優勢な移行細胞パターンを有する必要がある。
●中央検査によるPD-L1及びさらなるバイオマーカーの状態の決定に適したTURBT検体の入手可能性。
〇TURBT検体は、関連する病理報告とともに提出されなければならない。腫瘍組織は、2つの異なる方法(すなわち、パラフィン固定組織と新鮮組織は別々のバイオマーカー分析に必要である)によって処理される。膀胱又は上部尿路の腫瘍組織は、全体及び生存可能な腫瘍内容物に基づいて良好な品質を有するべきであり、現地の病理再検討によって検証された腫瘍の筋浸潤成分(すなわち、T2以上)を含有しなければならない。
〇MIBCの経過中に異なる時間に行われた処置からの追加の組織試料(例えば、以前のTURBTからの試料)を有する患者は、これらの試料を中央検査にも提出するように要求される(ただし、必要ではない)。
●CT又はMRIによるN0又はM0疾患(登録から4週間以内)。
●試験処置の開始の前、14日以内に得られた、以下の臨床検査結果によって定義される適切な血液学的機能及び終末器官機能:
-G-CSF支持なしで、絶対好中球数(ANC)≧1.5×109/L(1500/μL)
-白血球(WBC)数≧2.5×109/L(2500/μL)
-リンパ球数≧0.5×109/L(500/μL).
-輸血なしで血小板数≧100X109/L(100,000/μL)
-ヘモグロビン≧90g/L(9.0g/dL)
Example 17. Materials and methods for testing of WO39613A. Inclusion Criteria Patients must meet all of the following criteria:
● Age ≥ 18 years old.
- Ability to comply with the protocol, as determined by the investigator - East Coast Cancer Trials Group (ECOG) performance status of 0 or 1 - Patients who refuse neoadjuvant cisplatin-based chemotherapy, or patients who are not suitable for neoadjuvant cisplatin-based therapy. Cisplatin ineligible for this study is defined by creatinine clearance <60 mL/min and/or grade ≧2 hearing loss and/or grade ≧2 neuropathy.
• Conforms and is scheduled for cystectomy.
• Histologically documented MIBC (pT2-4, N0, M0), also called TCC or urothelial cell carcinoma of the bladder.
o Residual disease after TURBT (surgical findings, cystoscopy/endoscopy or radiological presence).
o Patients with mixed histology should have a predominant transitional cell pattern.
• Availability of TURBT specimens suitable for determination of PD-L1 and further biomarker status by central laboratories.
o TURBT specimens must be submitted with relevant pathology reports. Tumor tissue is processed by two different methods (ie, paraffin-fixed and fresh tissue are required for separate biomarker analyses). Bladder or upper urinary tract tumor tissue should be of good quality based on total and viable tumor content, muscle-invasive component of tumor verified by local pathology review (i.e., T2 or greater) must contain
o Patients with additional tissue samples from procedures performed at different times during the course of MIBC (e.g., samples from previous TURBT) are required to submit these samples to central review as well ( but not required).
• NO or M0 disease by CT or MRI (within 4 weeks of enrollment).
- Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to initiation of study treatment:
- Absolute neutrophil count (ANC) ≥ 1.5 x 10 9 /L (1500/μL) without G-CSF support
- white blood cell (WBC) count ≥ 2.5 x 10 9 /L (2500/μL)
- Lymphocyte count ≧0.5×10 9 /L (500/μL).
- Platelet count ≧100×10 9 /L (100,000/μL) without transfusion
- hemoglobin ≥ 90 g/L (9.0 g/dL)
患者は輸血されてもよいが、適格性について臨床検査をスクリーニングしてから2週間以内は、輸血は許容されない。 Patients may be transfused, but transfusions are not permitted within 2 weeks of clinical screening for eligibility.
単腎疾患又はエリスロポエチン産生が低い慢性腎臓疾患を有する患者は、エリスロポエチン刺激剤を使用してもよい。
-AST、ALT及びアルカリホスファターゼ(ALP)≦2.5×正常値の上限(ULN)
-ビリルビン≦1.5×ULN、ただし以下を除く:
既知のギルバート病患者:ビリルビンレベル≦3×ULN。
-アルブミン≧25g/L(2.5g/dL)。
-クレアチニンクリアランス≧30mL/分(Cockcroft-Gault式を使用して計算)
-治療的抗凝固療法を受けていない患者の場合:
部分トロンボプラスチン時間(PTT)又はaPTT≦1.5×ULN
プロトロンビン時間(PT)又は国際標準化比(INR)≦1.5×ULN
●スクリーニング時の陰性HIV検査。
〇事前の陽性HIV検査結果がない患者は、地域の規制によって許可されない限り、スクリーニング時にHIV検査を受ける。
●スクリーニング時の全B型肝炎コア抗体(HBcAb)検査陰性、又はスクリーニング時の全HBcAb検査陽性、続いてスクリーニング時の定量的B型肝炎ウイルス(HBV)DNA<500IU/mL。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。
●妊娠の可能性のある女性の場合:禁欲(異性間の性交を控える)又は避妊手段を使用することの合意、及び卵の提供を控えることの同意。
●男性の場合:禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることの同意。
Patients with single kidney disease or chronic kidney disease with low erythropoietin production may use erythropoietin stimulants.
- AST, ALT and alkaline phosphatase (ALP) < 2.5 x upper limit of normal (ULN)
- Bilirubin ≤ 1.5 x ULN, except:
Patients with known Gilbert's disease: bilirubin level < 3 x ULN.
- Albumin > 25 g/L (2.5 g/dL).
- Creatinine clearance ≧30 mL/min (calculated using the Cockcroft-Gault formula)
- In patients not receiving therapeutic anticoagulation:
Partial thromboplastin time (PTT) or aPTT ≤ 1.5 x ULN
Prothrombin Time (PT) or International Normalized Ratio (INR) < 1.5 x ULN
• Negative HIV test at screening.
o Patients without prior positive HIV test results will be tested for HIV at screening unless permitted by local regulations.
• Negative total hepatitis B core antibody (HBcAb) test at screening or positive total HBcAb test at screening followed by quantitative hepatitis B virus (HBV) DNA <500 IU/mL at screening.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening.
• For women of childbearing potential: consent to abstinence (abstinence from heterosexual intercourse) or use of contraceptive means, and consent to refrain from donating eggs.
• For men: Consent to maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and to refrain from donating sperm.
B.除外基準
以下の基準のいずれかを満たす患者は除外される:除外基準における事象グレードはNCI CTCAE v 4.0に基づく。
●試験処置の開始前の全身免疫刺激剤(限定されないが、CTLA-4、インターフェロン及びインターロイキン2を標的とする薬剤を含む)による事前治療
●対照群のみの適格性
●事前の同種異系幹細胞又は固形臓器移植
●以下の例外を除いて、試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び抗腫瘍壊死因子-α剤を含む)による処置、又は試験処置中の全身免疫抑制薬の必要性の予測:
B. Exclusion Criteria Patients meeting any of the following criteria will be excluded: Event grading in exclusion criteria is based on NCI CTCAE v4.0.
- Prior treatment with systemic immunostimulants (including but not limited to agents targeting CTLA-4, interferon and interleukin-2) prior to initiation of study treatment - Eligibility for control arm only - Prior allogeneic stem cells or solid organ transplantation Systemic immunosuppressants (including but not limited to corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide and anti-tumor necrosis factor) within 2 weeks prior to initiation of study treatment, with the following exceptions- treatment with alpha agents) or prediction of need for systemic immunosuppressants during study treatment:
急性低用量の全身免疫抑制薬、又は1回のパルス用量の全身免疫抑制薬(例えば、造影剤アレルギーのための48時間のコルチコステロイド)を受けた患者は試験に適格である。 Patients who received an acute low-dose systemic immunosuppressant or a single pulse dose of systemic immunosuppressant (eg, 48-hour corticosteroids for contrast allergy) are eligible for the study.
ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患若しくは喘息のためのコルチコステロイド、又は起立性低血圧若しくは副腎機能不全のための低用量コルチコステロイドを受けた患者は試験に適格である。
●試験処置の開始前4週間以内、又はアテゾリズマブ処置中若しくはアテゾリズマブの最終投薬後5ヶ月以内の生弱毒化ワクチンによる処置
●制御されない腫瘍関連疼痛。鎮痛薬を必要とする患者は、試験登録時に安定したレジメンでなければならない。
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質抗体症候群、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、又は多発性硬化症を含むがこれらに限定されない自己免疫疾患又は免疫不全活動が活動性であるもの、又はその病歴、ただし、以下を除く:
Patients receiving mineralocorticoids (e.g., fludrocortisone), corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency are eligible for the study. be.
• Treatment with a live attenuated vaccine within 4 weeks prior to initiation of study treatment or during atezolizumab treatment or within 5 months after the last dose of atezolizumab • Uncontrolled tumor-related pain. Patients requiring analgesics must be on a stable regimen at study entry.
Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barré syndrome, or multiple sclerosis Active or history of autoimmune disease or immunodeficiency activity, including but not limited to, excluding:
甲状腺補充ホルモンを服用している自己免疫関連甲状腺機能低下症の病歴を有する患者が試験に適格である。 Patients with a history of autoimmune-related hypothyroidism taking thyroid replacement hormone are eligible for the study.
安定なインスリンレジメンを受けている制御された1型糖尿病患者は試験に適格である。
Patients with controlled
湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを伴う白斑(例えば、乾癬性関節炎を有する患者は除外される)を有する患者は、以下の条件の全てが満たされるならば、試験に適格である。
-発疹が覆っている体表面積は<10%でなければならない。
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない。
●特発性肺線維症、器質化肺炎(例えば、閉塞性細気管支炎)、薬物誘発性間質性肺炎、若しくは特発性間質性肺炎の病歴、又はスクリーニング胸部コンピューター断層撮影(CT)スキャンでの活動性間質性肺炎の証拠。
●適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚癌腫、限局性前立腺がん、上皮内乳管癌腫、又はステージI子宮がん等、転移又は死亡のリスクが無視できる(例えば、5年OS率>90%)悪性腫瘍を除いて、スクリーニング前2年以内のUC以外の悪性腫瘍の病歴。治癒目的で処置され、PSA再発のない限局性前立腺がん(ステージ≦pT2c、Gleasonスコア≦7及び前立腺がん診断時の前立腺特異抗原(PSA)≦20 ng/mLとして定義される)患者が適格である。処置未経験であり、積極的監視療法を受けている既存の低リスク前立腺がん(ステージcT 1/T 2a、Gleasonスコア≦6、及びPSA≦10 ng/mLと定義)を有する患者が適格である。
●活動性結核(TB)(すなわち、TBの徴候及び症状を有する)。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)、又は治験責任医師の見解では患者の安全性に影響を及ぼし得る任意の活動性感染症。
●試験処置開始前2週間以内の治療用経口又はIV抗生物質による処置 予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の増悪を予防するため)を受ける患者は試験に適格である;
●ランダム化前3ヶ月以内のNew York Heart Association心疾患(クラスIII以上)、心筋梗塞又は脳血管障害、不安定不整脈又は不安定狭心症等の有意な心血管疾患。
●制御されない高血圧(収縮期血圧>140 mmHg及び/又は拡張期血圧>95 mmHgとして定義される)。これらのパラメーターを達成するための降圧療法が許容される。
●試験処置の開始前28日以内のグレード3以上の出血又は出血事象。
●試験処置の開始前4週間以内の診断以外の大きな外科的処置、又は試験中の膀胱切除術若しくは腎尿管摘出術以外の大きな外科的処置の必要性の予想。中心静脈アクセスカテーテル(例えば、ポート等)の配置は、大きな外科的処置とは考えられておらず、したがって許容される。
●治験薬の使用を禁忌にする任意の他の疾患、代謝機能不全、身体検査所見、又は臨床検査所見は、結果の解釈に影響を及ぼし得るか、患者が試験に参加する能力を損ない得るか、又は患者を処置合併症のリスクを高くし得る。
●キメラ若しくはヒト化抗体又は融合タンパク質に対する重度のアレルギー反応の病歴。
●チャイニーズハムスター卵巣細胞生成物又は組換えヒト抗体に対する既知の過敏症。
●賦形剤の試験薬物のいずれかに対する既知の不耐性又は過敏症(ヒスチジン、トレハロース二水和物、及びポリソルベート20を含む)。
●前投薬に必要な任意の薬物に対する既知の不耐性(アセトアミノフェン、ラニチジン、ジフェンヒドラミン、メチルプレドニゾロン)。
●妊娠若しくは授乳、又は試験中に妊娠する意図。妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin manifestations only (e.g., patients with psoriatic arthritis are excluded) are eligible for the study if all of the following conditions are met: is.
- The rash must cover <10% of body surface area.
- Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UVA radiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors within the past 12 months , or no acute exacerbation of underlying symptoms requiring high-potency or oral corticosteroids.
A history of idiopathic pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis obliterans), drug-induced interstitial pneumonia, or idiopathic interstitial pneumonia, or a screening chest computed tomography (CT) scan Evidence of active interstitial pneumonia.
Appropriately treated cervical carcinoma in situ, nonmelanoma cutaneous carcinoma, localized prostate cancer, ductal carcinoma in situ, or stage I uterine cancer with negligible risk of metastasis or death (e.g., 5-year OS rate >90%) History of non-UC malignancy within 2 years prior to screening, excluding malignancies. Patients with localized prostate cancer (defined as stage ≤ pT2c, Gleason score ≤ 7 and prostate specific antigen (PSA) ≤ 20 ng/mL at diagnosis of prostate cancer) treated with curative intent and without PSA recurrence are eligible is. Patients with pre-existing low-risk prostate cancer (
- Active tuberculosis (TB) (ie, having signs and symptoms of TB).
- Severe infection (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia) within 4 weeks prior to initiation of study treatment, or opinion of investigator Any active infection that may affect patient safety.
Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of study treatment be;
• Significant cardiovascular disease such as New York Heart Association heart disease (class III or higher), myocardial infarction or cerebrovascular disease, unstable arrhythmia or unstable angina pectoris within 3 months prior to randomization.
- Uncontrolled hypertension (defined as systolic blood pressure >140 mmHg and/or diastolic blood pressure >95 mmHg). Antihypertensive therapy to achieve these parameters is acceptable.
-
• Expected need for major non-diagnostic surgery within 4 weeks prior to initiation of study procedure or major surgical procedure other than cystectomy or nephroureterectomy during study. Placement of a central venous access catheter (eg, port, etc.) is not considered a major surgical procedure and is therefore acceptable.
Any other disease, metabolic dysfunction, physical examination findings, or laboratory findings that contraindicate the use of the study drug may affect the interpretation of results or impair the patient's ability to participate in the study. , or may put the patient at increased risk for procedural complications.
• History of severe allergic reaction to chimeric or humanized antibodies or fusion proteins.
• Known hypersensitivity to Chinese hamster ovary cell products or recombinant human antibodies.
• Known intolerance or hypersensitivity to any of the excipient study drugs (including histidine, trehalose dihydrate, and polysorbate 20).
• Known intolerance to any drug required for premedication (acetaminophen, ranitidine, diphenhydramine, methylprednisolone).
• Pregnancy or lactation, or intention to become pregnant during the study. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
アテゾリズマブ+チラゴルマブ群の追加の除外基準
以下の基準のいずれかを満たす患者は、アテゾリズマブ+チラゴルマブ群から除外される:
●スクリーニング時の活動性エプスタイン・バー・ウイルス(EBV)感染及び既知又は疑われる慢性活動性EBV感染
Additional Exclusion Criteria for Atezolizumab + Tiragolumab Arm Patients meeting any of the following criteria will be excluded from the atezolizumab + tiragolumab arm:
Active Epstein-Barr virus (EBV) infection at screening and known or suspected chronic active EBV infection
スクリーニング時にEBVウイルスカプシド抗原(VCA)IgM検査が陽性であった患者は、この群から除外される。活動性感染又は慢性活動性感染の疑いをスクリーニングするために、EBVポリメラーゼ連鎖反応(PCR)検査を臨床的に適応されるように実施しなければならない。陽性EBV PCR検査を有する患者は、この群から除外される。 Patients with a positive EBV viral capsid antigen (VCA) IgM test at screening are excluded from this group. To screen for suspected active or chronically active infection, an EBV polymerase chain reaction (PCR) test must be performed as clinically indicated. Patients with a positive EBV PCR test are excluded from this group.
C.許可された治療
患者は、試験中に以下の治療法を使用することが許される。
●経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(ワーファリン又は低分子量ヘパリン等)
●施設の基準に従って投与される予防的抗生物質又は抗ウイルス処置
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与されるコルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●前立腺がんに対するゴナドトロピン放出ホルモンアゴニスト又はアンタゴニストを用いたホルモン療法
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
2サイクルの処置後。緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。アテゾリズマブによる処置は、緩和放射線療法中に継続され得る。
●以下に概説されるような局所療法(例えば、外科手術、定位的放射線手術、放射線療法、高周波アブレーション):
3つ以下の病変の制御のために局所療法を必要とする混合応答を経験している患者は、メディカルモニターの承認が得られた後も試験処置を継続するのに依然として適格であり得る。標的病変に向けた局所療法を受けている患者は、もはや放射線学的応答については評価可能ではないが、進行については評価可能なままである。
C. Allowed Treatments Patients will be allowed to use the following treatments during the study.
● Oral contraceptives ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (warfarin or low molecular weight heparin, etc.)
● Prophylactic antibiotics or antiviral treatment administered according to institutional standards ● Inactivated influenza vaccination ● Megestrol acetate given as an appetite stimulant ● Mineralcorticoids (eg, fludrocortisone)
o Corticosteroids given for chronic obstructive pulmonary disease or asthma o Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency o Gonadotropin-releasing hormone agonists or antagonists for prostate cancer Hormonal therapy used Palliative radiation therapy (e.g. treatment of known bone metastases or symptomatic relief of pain) outlined below:
After 2 cycles of treatment. Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with atezolizumab may be continued during palliative radiotherapy.
- Local therapy (e.g., surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) as outlined below:
Patients experiencing a mixed response requiring local therapy for control of 3 or fewer lesions may still be eligible to continue study treatment after obtaining medical monitor approval. Patients receiving local therapy directed at target lesions are no longer evaluable for radiological response, but remain evaluable for progression.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent atezolizumab infusions, at the discretion of the Investigator.
注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理されなければならない。 Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine) or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2- adrenergic should be administered by a sexual agonist).
D.アテゾリズマブ群の材料及び方法
アテゾリズマブは、承認された投与量(TECENTRIQ(登録商標)米国添付文書;TECENTRIQ(登録商標)SmPC)である3週間ごとに1200mg(Q3W)(各21日間サイクルの1日目に1200mg)の固定用量で投与される(表72)。抗腫瘍活性は、1~20mg/kg Q3Wの範囲の用量にわたって観察された。PCD4989g試験では、アテゾリズマブの最大耐量に到達せず、用量制限毒性はいずれの用量でも観察されなかった。非臨床試験(Deng et al.,MAbs,8:593-603,2016)並びに利用可能な臨床薬物動態、有効性及び安全性データの両方に基づいて、1200mg Q3Wの固定用量(平均体重に基づく用量15mg/kg Q3Wと同等)を選択した。
D. Atezolizumab Group Materials and Methods Atezolizumab was administered at the approved dose (TECENTRIQ® US Prescribing; 1200 mg per day) (Table 72). Anti-tumor activity was observed over doses ranging from 1-20 mg/kg Q3W. In the PCD4989g study, the maximum tolerated dose of atezolizumab was not reached and no dose-limiting toxicity was observed at any dose. Based on both nonclinical studies (Deng et al., MAbs, 8:593-603, 2016) and available clinical pharmacokinetic, efficacy and safety data, a fixed dose of 1200 mg Q3W (mean weight-based dose 15 mg/kg Q3W) was selected.
アテゾリズマブ対照群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、処置を受ける。処置は、処置割り当て後7日以内に開始しなければならない。患者はサイクル3の後に手術を受け、第4サイクルの処置を、手術の4~6週間後に再開すべきである。

アテゾリズマブの投与は、訓練された人員並びに潜在的に重篤な反応を管理するための適切な機器及び薬剤に直ちにアクセスできる監視された設定で行われる。 Administration of atezolizumab occurs in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
アテゾリズマブ注入は、表73に概説される指示に従って投与される。

D.アテゾリズマブ+チラゴルマブ群の材料及び方法
アテゾリズマブは上記のように投与される(表73を参照)。
D. Materials and Methods for Atezolizumab + Tiragolumab Group Atezolizumab will be administered as described above (see Table 73).
チラゴルマブは、600mg IV Q3Wの固定用量(21日間の各サイクルの1日目に600mg)で投与される。600mg IV Q3Wの固定用量は、アテゾリズマブと組み合わせた単剤のチラゴルマブ又はチラゴルマブと組み合わせた第Ia相/第Ib相のGO30103試験からの利用可能な臨床PK、有効性、及び安全性データに基づいて選択した。単剤としてのチラゴルマブを用いた試験の第Ia相部分では、MTDに到達せず、用量漸増でDLTは観察されなかった。臨床上のカットオフ日
Tiragolumab is administered at a fixed dose of 600 mg IV Q3W (600 mg on
について、チラゴルマブに対する抗薬物抗体(ADA)は、全ての用量レベルにわたって、第Ia相部分又は第Ib相部分で稀であった。400mgで開始したチラゴルマブ用量で、試験の第Ia相部分の患者において長期安定疾患が観察された。チラゴルマブ+アテゾリズマブを用いた試験の第Ib相部分では、MTDに達しなかった。放射線部分奏効によって測定される抗腫瘍活性は、1200mgのアテゾリズマブと組み合わせて30mgから開始して600mgまでの範囲のチラゴルマブについて用量を超えて観察された。 , anti-drug antibodies (ADA) to tiragolumab were rare in Phase Ia or Phase Ib portions across all dose levels. Long-term stable disease was observed in patients in the Phase Ia portion of the study at tiragolumab doses starting at 400 mg. The MTD was not reached in the phase Ib portion of the trial with tiragolumab plus atezolizumab. Anti-tumor activity, as measured by radiation partial response, was observed across doses for tiragolumab ranging from 30 mg to 600 mg in combination with 1200 mg atezolizumab.
アテゾリズマブ+チラゴルマブ群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、表74に概説される処置を受ける。患者はサイクル3の後に手術を受け、第4サイクルの処置を、手術の4~6週間後に再開する。

チラゴルマブは、表75に記載のように、各21日間サイクルの1日目に600mgの固定用量でIV注入によって投与され、注入後観察期間を有する。チラゴルマブの投与は、訓練された人員並びに潜在的に重篤な反応を管理するための適切な機器及び薬剤に直ちにアクセスできる監視された設定で行われる。

実施例18.WO39613の試験の安全性の評定
A.安全性パラメーター及び定義
Example 18. SAFETY ASSESSMENT OF THE WO39613 TRIAL A.1. Safety parameters and definitions
安全性評定は、有害事象(重篤な有害事象及び特に関心のある有害事象を含む)のモニタリング及び記録、治験実施計画書指定の安全性臨床検査評定の実施、治験実施計画書指定のバイタルサインの測定、及び試験の安全性評価にとって重要であると考えられる他の治験実施計画書指定の試験の実施からなる。 Safety assessment includes monitoring and recording of adverse events (including serious adverse events and adverse events of particular interest), conducting protocol-specified safety laboratory evaluations, and protocol-specified vital signs. and other protocol-specified studies considered important to the safety evaluation of the study.
B.有害事象
臨床試験の実施(Good Clinical Practice)のための医薬品規制調和国際会議(ICH)ガイドラインによれば、有害事象は、原因の属性にかかわらず、医薬品を投与された臨床試験対象における何らかの不都合な医学的事象である。有害事象は、
B. Adverse Events According to the International Council for Harmonization (ICH) Guidelines for Good Clinical Practice, an adverse event is any adverse event in a clinical trial subject receiving a drug, regardless of the causal attribute. Medical event. Adverse events are
したがって、有害事象は、以下のいずれかであり得る: Adverse events can therefore be any of the following:
●医薬に関連すると考えられるか否かにかかわらず、医薬品の使用に一時的に関連するあらゆる好ましくない意図しない徴候(異常な検査所見を含む)、症候又は疾患。
●新規疾患又は既存疾患の増悪(既知の症状の特徴、頻度、又は重症度の悪化)。
●ベースラインに存在しない間欠的な医学的症状(例えば、頭痛)の再発。
●症候に関連した、又は試験処置若しくは併用治療の変更、又は試験処置からの中止をもたらす、実験値又は他の臨床検査(例えば、ECG、X線)の低下。
●治験実施計画書に規定された介入に関連する有害事象、例えば試験処置の割り当て前に発生するもの(例えば、生検等の侵襲的手順のスクリーニング)。
• Any unfavorable and unintended signs (including abnormal laboratory findings), symptoms or diseases temporally associated with the use of the medicinal product, whether or not considered medicinal-related.
• New disease or exacerbation of existing disease (worsening of known symptom features, frequency, or severity).
- Recurrence of intermittent medical symptoms (eg, headache) not present at baseline.
• Decrease in laboratory values or other laboratory tests (eg, ECG, X-ray) related to symptoms or leading to change in study treatment or concomitant therapy, or discontinuation from study treatment.
• Protocol-specified intervention-related adverse events, eg, those that occur prior to study treatment assignment (eg, screening for invasive procedures such as biopsies).
重篤な有害事象
重篤な有害事象は、以下の基準のいずれかを満たす任意の有害事象である:
●致命的である(すなわち、有害事象が実際に死を引き起こすか、又は死に至る)。
●生命を脅かす(すなわち、有害事象は、治験責任医師の観点から、患者を死亡の即時リスクにさらす)。これには、より重度の形態で発生したか、又は継続された場合、死を引き起こした可能性がある有害事象は含まれない。
●入院患者の入院を必要とするか、又は延長する。
●持続的又は有意な障害/無能力をもたらす(すなわち、有害事象は、正常な生活機能を行う患者の能力の実質的な破壊をもたらす)。
●試験処置に曝露された母親から生まれた新生児/乳児における先天異常/出生時欠損である。
●治験責任医師の判断において重大な医学的事象である(例えば、患者を危険にさらす可能性があり、又は上に列挙した結果のうちの1つを防ぐために医学的/外科的介入を必要とする可能性がある)。
Serious Adverse Event A serious adverse event is any adverse event that meets any of the following criteria:
• Fatal (ie, the adverse event actually caused or resulted in death).
• Life-threatening (ie, the adverse event puts the patient at immediate risk of death from the investigator's perspective). This does not include adverse events that may have caused death if they occurred or continued in more severe forms.
• Require or prolong hospitalization of inpatients.
• Result in persistent or significant disability/incapacity (ie, the adverse event results in substantial disruption of the patient's ability to perform normal life functions).
• Congenital anomalies/birth defects in neonates/infants born to mothers exposed to the study treatment.
Is a significant medical event in the investigator's judgment (e.g., may endanger the patient or require medical/surgical intervention to prevent one of the consequences listed above) there's a possibility that).
「重度」及び「重篤」という用語は、同義語ではない。重症度は、有害事象の強度(例えば、軽度、中等度、若しくは重度と評価されるか、又はNCI CTCAEに従って)を指し、事象自体は、比較的医学的に重要でない可能性がある(さらなる所見のない重度の頭痛等)。 The terms "severe" and "serious" are not synonymous. Severity refers to the intensity of the adverse event (e.g., rated as mild, moderate, or severe, or according to the NCI CTCAE) and the event itself may be relatively medically insignificant (further findings severe headache without pain, etc.).
特に注目すべき有害事象
アテゾリズマブ+チラゴルマブ群にとって特に注目すべき有害事象は以下の通りである:
●Hyの法則によって定義される、ビリルビン上昇又は臨床的黄疸のいずれかと組み合わせたALT又はAST上昇を含む潜在的な薬物誘発性肝損傷の症例。
●以下に定義される試験処置による感染病原体の伝播の疑い:
病原性又は非病原性の任意の生物、ウイルス又は感染性粒子(例えば、伝染性海綿状脳症を伝達するプリオンタンパク質)は、感染病原体と考えられる。感染病原体の伝播は、医薬品に曝露された患者における感染を示す臨床症状又は検査所見から疑われ得る。この用語は、試験処置の汚染が疑われる場合にのみ適用される。
●間質性肺炎。
●大腸炎。
●内分泌不全症:真性糖尿病、膵炎、副腎機能不全、及び下垂体炎。
●肝炎(AST又はALTを含む)>10×正常値の上限。
●全身性エリテマトーデス。
●神経障害:ギラン・バレー症候群、筋無力症症候群又は重症筋無力症、及び髄膜脳炎。
●過敏症、IRR、サイトカイン放出症候群、インフルエンザ様疾患、HLH及びMASを示唆する事象。
●腎炎。
●眼毒性(例えば、ブドウ膜炎、網膜炎、視神経炎)。
●筋炎。
●横紋筋融解症を含むミオパシー。
●グレード≧2の心臓障害(例えば、心房細動、心筋炎、心膜炎)。
●血管炎。
●自己免疫性溶血性貧血。
●重度の皮膚反応(例えば、スティーブンス・ジョンソン症候群、水疱性皮膚炎、中毒性表皮壊死症)。
Adverse Events of Special Note Adverse events of particular note for the atezolizumab plus tiragolumab arm were:
• Cases of potential drug-induced liver injury, including elevated ALT or AST combined with either elevated bilirubin or clinical jaundice, as defined by Hy's law.
Suspected transmission of infectious agents by study procedures defined below:
Any pathogenic or non-pathogenic organism, virus or infectious particle (eg, the prion protein that transmits infectious spongiform encephalopathy) is considered an infectious agent. Transmission of infectious agents can be suspected from clinical symptoms or laboratory findings indicative of infection in patients exposed to the drug. This term applies only when contamination of the study procedure is suspected.
● Interstitial pneumonia.
●Colitis.
• Endocrine insufficiency: diabetes mellitus, pancreatitis, adrenal insufficiency, and hypophysitis.
• Hepatitis (including AST or ALT) >10 x upper limit of normal.
● Systemic lupus erythematosus.
• Neuropathy: Guillain-Barré syndrome, myasthenia syndrome or myasthenia gravis, and meningoencephalitis.
• Events suggestive of hypersensitivity, IRR, cytokine release syndrome, influenza-like illness, HLH and MAS.
- Nephritis.
o ocular toxicity (eg uveitis, retinitis, optic neuritis);
●Myositis.
• Myopathy, including rhabdomyolysis.
• Cardiac disorders of grade ≧2 (eg, atrial fibrillation, myocarditis, pericarditis).
• Vasculitis.
●Autoimmune hemolytic anemia.
• Severe skin reactions (eg Stevens-Johnson syndrome, bullous dermatitis, toxic epidermal necrolysis).
実施例19.WO39613の試験の統計的考察及び分析計画
WO39613の試験分析は、試験の中止によって収集された患者データに基づいている。特に明記しない限り、有効性分析は、割り当てられた治療レジメンに対して各薬物の少なくとも1回の用量を受けた全ての患者として定義される有効性評価可能な集団に基づき、安全性分析は、任意の量の試験処置を受けた全ての患者として定義される安全性評価可能な集団に基づく。
Example 19. Statistical Considerations and Analysis Plan for the WO39613 Study The WO39613 study analysis is based on patient data collected by study discontinuation. Unless otherwise stated, efficacy analyzes were based on the efficacy evaluable population defined as all patients who received at least one dose of each drug on their assigned treatment regimen; Based on a safety evaluable population defined as all patients who received any amount of study treatment.
分析結果は、患者が実際に受けた処置によって要約される。データは、試料サイズによって保証されるように記載され、要約される。連続変数は、平均、標準偏差、中央値、並びに最小値及び最大値の使用によって要約される。カテゴリ変数は、カウント及びパーセンテージの使用によって要約される。試料サイズが小さい場合、表の代わりにリストを使用する。 Analysis results are summarized by the treatment actually received by the patient. Data are described and summarized as warranted by sample size. Continuous variables are summarized by using mean, standard deviation, median, and minimum and maximum values. Categorical variables are summarized by the use of counts and percentages. If the sample size is small, use lists instead of tables.
A.試料サイズの決定
WO39613の試験は、仮説検定のための明示的なパワー及びタイプI誤差を考慮するように設計されていない。
A. Determination of Sample Size The WO39613 test was not designed to take into account explicit power and Type I errors for hypothesis testing.
代わりに、この試験は、シスプラチン不適格MIBCを有する患者に投与した場合の免疫療法ベースの処置の組み合わせに関する予備的な有効性、安全性、及びPKデータを得るように設計されている。試験中、約150~350人の患者をランダムに対照群及び実験群に割り付ける。 Instead, this study is designed to obtain preliminary efficacy, safety, and PK data for immunotherapy-based treatment combinations when administered to patients with cisplatin-ineligible MIBC. Approximately 150-350 patients are randomly assigned to control and experimental groups during the study.
B.有効性分析
主要有効性評価項目
有効性の主要評価項目は、病理学的完全奏効(pCR)であり、これは完全に切除された標本の残存浸潤がんを有しない患者の割合として定義される。pCR率は、90%信頼区間と共に各群について計算される。実験群と対照群との間のpCRの差も、90%信頼区間と共に計算される。信頼区間は、試料サイズに応じて、正確な方法又はWald法によって推定される。応答評定が欠落しているか又は応答評価がない患者は、非応答者として分類される。
B. Efficacy Analysis Primary Efficacy Endpoint The primary efficacy endpoint was pathologic complete response (pCR), defined as the proportion of patients without residual invasive cancer in completely resected specimens . pCR rates are calculated for each group with 90% confidence intervals. Differences in pCR between experimental and control groups are also calculated with 90% confidence intervals. Confidence intervals are estimated by the exact method or the Wald method, depending on the sample size. Patients with missing or no response ratings are classified as non-responders.
副次的有効性評価項目
副次的有効性評価項目は、それぞれ特定の時点におけるランドマーク無再発生存期間(RFS)、ランドマーク無症候生存期間(EFS)及びランドマーク全生存期間(OS)である(例えば、12、18、24ヶ月)。これらの評価項目について以下に説明する。ランドマークRFS率、ランドマークEFS率、及びランドマークOS率は、Kaplan-Meier法を使用して各試験群について推定され、90% CIはGreenwoodの式を使用して計算される。
Secondary Efficacy Endpoints Secondary efficacy endpoints are landmark recurrence-free survival (RFS), landmark disease-free survival (EFS), and landmark overall survival (OS) at specific time points, respectively. Yes (eg, 12, 18, 24 months). These evaluation items are described below. Landmark RFS, landmark EFS, and landmark OS rates are estimated for each study group using the Kaplan-Meier method and 90% CIs are calculated using the Greenwood formula.
探索有効性評価項目
探索的有効性評価項目は、RFS、EFS、OS、及び病理的進展度の低下率である。
Exploratory Efficacy Endpoints Exploratory efficacy endpoints are RFS, EFS, OS, and percent reduction in pathologic progression.
無再発生存期間(RFS)は、手術後の最初のサイクルにおける1日目から、疾患の最初に文書化された再発までの時間又は任意の原因による死亡までの時間として定義される。疾患の再発又は死亡が文書化されていない患者については、RFSは手術後の最後の腫瘍評定の日に打ち切られる。
Recurrence-free survival (RFS) is defined as the time from
無症候生存期間(EFS)は、ランダム化から、治験責任医師によって評定される手術を妨げる疾患進行;局所又は遠隔疾患再発;又は何らかの原因による死亡の事象のいずれか(いずれか早く発生する方)までの時間として定義される。そのような事象を経験していない患者は、最後の腫瘍後腫瘍評定時に打ち切られる。 Disease-free survival (EFS) is defined as disease progression precluding surgery as assessed by the investigator from randomization; local or distant disease recurrence; or death from any cause, whichever event occurs first. defined as the time to Patients who have not experienced such an event will be censored at the last post-tumor tumor assessment.
全生存(OS)は、ランダム化から何らかの原因による死亡までの時間として定義される。死亡していない患者に関するデータは、生存していることが知られている最終日に打ち切られる。 Overall survival (OS) is defined as the time from randomization to death from any cause. Data for non-deceased patients are censored at the last date known to be alive.
病理的進展度の低下率は、膀胱切除術の時に≦pT1 pN0に達する患者の割合として定義される。 Rate of reduction in pathologic extent is defined as the proportion of patients reaching ≤ pT1 pN0 at the time of cystectomy.
Kaplan-Meier法を使用して、各試験群のRFS、EFS及びOSの中央値を推定する。Brookmeyer及びCrowley法を使用して、各試験アームのRFS、EFS及びOSの中央値の90%CIを構築する。 The Kaplan-Meier method is used to estimate the median RFS, EFS and OS for each study group. The Brookmeyer and Crowley method is used to construct the 90% CI for the median RFS, EFS and OS for each study arm.
C.安全性分析
言語有害事象用語は、Medical Dictionary for Regulatory Activities thesaurus termsにマッピングされ、有害事象重症度はNCI CTCAE v 4.0に従って等級付けされる。
C. Safety Analysis Verbal adverse event terms are mapped to the Medical Dictionary for Regulatory Activities thesaurus terms and adverse event severity is graded according to the NCI CTCAE v 4.0.
安全性は、有害事象の要約、臨床検査結果の変化、バイタルサイン及びECGの変化、及び試験薬への曝露を通して評定される。併用処置への曝露及び安全性フォローアップの長さを、各段階内の処置群によって要約する。 Safety will be assessed through a summary of adverse events, changes in laboratory test results, changes in vital signs and ECG, and exposure to study drug. Exposure to combination treatment and length of safety follow-up are summarized by treatment group within each phase.
処置開始後に起こる処置時発生有害事象を要約する。各患者について、各有害事象の最大報告重症度を重症度グレードごとに要約に使用する。全てのn処置下で発現する有害事象、重篤な有害事象、試験処置の中止につながる有害事象、グレード≧3の有害事象、死亡、及び死因を列挙し、マッピングされた用語、適切な類義語レベル、及びNCI CTCAE重症度グレードによって要約する。 Treatment-emergent adverse events occurring after treatment initiation will be summarized. For each patient, the maximum reported severity of each adverse event will be used in the summary by severity grade. List all n treatment emergent adverse events, serious adverse events, adverse events leading to discontinuation of study treatment, grade ≥3 adverse events, deaths, and causes of death, mapped terms, appropriate synonym level , and by NCI CTCAE severity grade.
関連する検査室、バイタルサイン(脈拍数、呼吸数、血圧、パルスオキシメトリ、及び体温)、及びECGデータは、必要に応じて識別されたグレードと共に時間によって表示される。更に、選択された臨床検査結果のシフトテーブルを使用して、ベースライン及びベースライン後の最大重症度グレードを要約する。バイタルサインの変化を要約する。 Relevant laboratory, vital signs (pulse rate, respiratory rate, blood pressure, pulse oximetry, and temperature), and ECG data are displayed by time with grades identified as appropriate. In addition, a shift table of selected laboratory test results will be used to summarize baseline and post-baseline maximum severity grades. Summarize changes in vital signs.
D.薬物動態分析 D. Pharmacokinetic analysis
アテゾリズマブ(少なくとも1用量のアテゾリズマブを受けた患者)及びアテゾリズマブと組み合わせて投与された薬物(少なくとも1用量の薬物を受けた患者)のPK分析のために、まばらな試料を収集する。様々な試験薬物の血清又は血漿濃度は、個々の値として報告され、処置群によって、並びに適切な場合及びデータが許す場合はサイクル及び日によって要約(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)される。様々な試験薬物の個々の及び中央の血清又は血漿濃度は、処置群、及びサイクル、及び日によってプロットされる。配合剤のPKデータを、内部試験及び公表された以前の試験からの利用可能な履歴データと比較することができる。濃度データは、クリアランス、分布容積及び曲線下面積等のPKパラメーターを導出するために、確立された集団PKモデルを使用して他の試験からのデータと共にプールされ得る。 Sparse samples are collected for PK analysis of atezolizumab (patients who received at least 1 dose of atezolizumab) and drugs administered in combination with atezolizumab (patients who received at least 1 dose of drug). Serum or plasma concentrations of various study drugs were reported as individual values and summarized (mean, standard deviation, coefficient of variation, median, range) by treatment group and, where appropriate and data permitted, by cycle and day. , the geometric mean, and the geometric mean coefficient of variation). Individual and median serum or plasma concentrations of the various study drugs are plotted by treatment group and cycle and day. PK data for formulations can be compared to available historical data from internal and previous published studies. Concentration data can be pooled with data from other studies using established population PK models to derive PK parameters such as clearance, volume of distribution and area under the curve.
PKパラメーターと安全性、有効性、PK、及びバイオマーカー評価項目との間の関係は、記述統計学によって分析及び報告され得る。 Relationships between PK parameters and safety, efficacy, PK, and biomarker endpoints can be analyzed and reported by descriptive statistics.
E.免疫原性分析 E. Immunogenicity analysis
免疫原性を、アテゾリズマブ及び必要に応じて他の試験処置について評定する。免疫原性分析には、少なくとも1つの抗薬物抗体(ADA)評定を受けた全ての患者が含まれる。患者は、受けた処置に従って、又は試験中止前に処置を受けていない場合は割り当てられた処置に従ってグループ分けされる。 Immunogenicity is assessed for atezolizumab and other study treatments as appropriate. Immunogenicity analysis included all patients who had at least one anti-drug antibody (ADA) assessment. Patients are grouped according to the treatment received or assigned treatment if they had not received treatment prior to study discontinuation.
アテゾリズマブについては、ベースライン(ベースライン有病率)及び薬物投与後(ベースライン発生後)のADA陽性患者及びADA陰性患者の数及び割合を処置グループ別に要約する。ベースライン後の発生率を決定するとき、患者は、ADA陰性であるか、又はベースラインでデータが欠落しているが、試験薬物曝露後にADA応答を発症する場合(処置誘発性ADA応答)、又は患者がベースラインでADA陽性であり、1つ以上のベースライン後の試料の力価がベースライン試料の力価よりも少なくとも0.60力価単位大きい場合(処置増強ADA応答)、ADA陽性であるとみなされる。患者がADA陰性であるか若しくはベースラインでデータが欠落しており、全てのベースライン後の試料が陰性である場合、又は患者がベースラインでADA陽性であるが、ベースライン試料の力価よりも少なくとも0.60力価単位大きい力価を有するベースライン後の試料を有さない(処置は影響を受けない)場合、患者はADA陰性であるとみなされる。 For atezolizumab, the numbers and percentages of ADA-positive and ADA-negative patients at baseline (baseline prevalence) and after drug administration (post-baseline incidence) are summarized by treatment group. When determining post-baseline incidence, if a patient is ADA-negative or has missing data at baseline but develops an ADA response after study drug exposure (treatment-induced ADA response), or ADA positive if the patient is ADA positive at baseline and the titer of one or more post-baseline samples is at least 0.60 titer units greater than the titer of the baseline sample (treatment-enhanced ADA response) is considered to be If the patient is ADA-negative or has missing data at baseline and all post-baseline samples are negative, or if the patient is ADA-positive at baseline but the titer of the baseline sample is higher than Patients are considered ADA-negative if they have no post-baseline sample with a titer at least 0.60 titer units greater (treatment is unaffected).
ADAを検査する他の試験処置については、陽性は、その薬物の以前の試験で確立された標準的な方法に従って決定される。 For other test procedures that test for ADA, positivity is determined according to standard methods established in previous testing of that drug.
ADAの状態と安全性、有効性、PK、及びバイオマーカー評価項目との関係は、記述統計学を介して分析及び報告することができる。 Relationships between ADA status and safety, efficacy, PK, and biomarker endpoints can be analyzed and reported via descriptive statistics.
F.バイオマーカー分析 F. Biomarker analysis
探索的バイオマーカー分析は、有効性、安全性、PK、免疫原性、及び他のバイオマーカーの評価項目を考慮して、これらのバイオマーカーと試験薬に対する応答との関連性を理解しようとして行われる。 Exploratory biomarker analyzes should be conducted to understand the association between these biomarkers and response to study drug, considering efficacy, safety, PK, immunogenicity, and other biomarker endpoints. will be
G.暫定分析
暫定分析は試験中に行われ、少なくとも1つの実験群が予備期での登録を完了し、患者が術後pCR評定を完了したときに、最も早い暫定分析が行われる。さらなる暫定分析は、試験依頼者が適切と判断した場合に実施してもよい。事後確率を使用して、対照群と比較した実験群における臨床活性の暫定分析に基づいてさらなる登録を導くことができる。暫定分析が、実験群の活性が対照群の活性よりも高いことを示唆する場合、各MIBCコホートについて、実験群に更に25人の患者を登録することができる(拡大期)。第1b相試験を拡大及び終了する最終決定は、事象までの時間評価項目及び安全性データを含む全体的な利益-リスクバランス及び全体的なデータ、並びに新たな外部情報を考慮して行われる。
G. Interim Analyzes Interim analyzes will be performed during the study, with the earliest interim analysis performed when at least one study arm has completed pre-enrollment and patients have completed postoperative pCR assessments. Further interim analyzes may be performed as deemed appropriate by the sponsor. Posterior probabilities can be used to guide further enrollment based on interim analyzes of clinical activity in the experimental group compared to the control group. For each MIBC cohort, an additional 25 patients can be enrolled in the experimental group (expansion phase) if the interim analysis suggests that the activity in the experimental group is higher than that in the control group. The final decision to expand and terminate the Phase 1b trial will take into consideration the overall benefit-risk balance and overall data, including time-to-event endpoints and safety data, as well as new external information.
実施例20.転移性尿路上皮癌腫(mUC)を有する患者におけるアテゾリズマブと組み合わせたチラゴルマブの有効性及び安全性を評価する第Ib/II相非盲検多施設ランダム化包括的試験
WO39613は、白金含有レジメン中又は後に進行した局所進行性又は転移性UCを有する患者におけるアテゾリズマブと組み合わせたチラゴルマブの有効性及び安全性を評価する第Ib/II相非盲検多施設ランダム化包括的試験である。この試験は、新しい処置が利用可能になるにつれて新しい処置群を開き、最小限の臨床活性又は許容できない毒性を示す既存の処置群を閉じ、又は患者集団を変更する(例えば、以前の抗がん治療又はバイオマーカーの状態に関して)ための柔軟性を備えて設計される。適格患者を最初にいくつかの処置群(図25参照)のうちの1つに割り当てる。ステージ1の間に臨床的利益の喪失又は許容できない毒性を経験する患者は、ステージ2のための異なる処置レジメン(図25参照)による処置を継続するのに適格であり得る。
Example 20. WO39613 is a phase Ib/II, open-label, multicenter, randomized, comprehensive study evaluating the efficacy and safety of tiragolumab in combination with atezolizumab in patients with metastatic urothelial carcinoma (mUC) in platinum-containing regimens or A Phase Ib/II, open-label, multicenter, randomized, global study evaluating the efficacy and safety of tiragolumab in combination with atezolizumab in patients with later-advanced locally advanced or metastatic UC. This trial will open new treatment arms as new treatments become available, close existing treatment arms showing minimal clinical activity or unacceptable toxicity, or alter the patient population (e.g., prior anticancer designed with flexibility for therapeutic or biomarker status). Eligible patients are initially assigned to one of several treatment groups (see Figure 25). Patients who experience loss of clinical benefit or unacceptable toxicity during
A.ステージ1
ステージ1の間、患者をランダムに対照群(アテゾリズマブ[Atezo])又はチラゴルマブと組み合わせたアテゾリズマブからなる実験群(Atezo+Tira)(図25及び表76を参照)に割り当てる。
During


実験群内への登録は、予備期とそれに続く拡大期の2期で行われる。予備期中に約15人の患者が登録される。予備期中に実験群で臨床活性が観察される場合、拡大期中に約25人の追加の患者がその群に登録され得る。 Enrollment within the experimental group is conducted in two phases, a preliminary phase followed by an expansion phase. Approximately 15 patients will be enrolled during the preliminary phase. If clinical activity is observed in the experimental group during the preliminary phase, approximately 25 additional patients may be enrolled in that group during the expansion phase.
試験依頼者は、所与の治処置群内への登録を遅延又は一時停止することを決定し得る。不十分な臨床活性又は許容できない毒性を有する実験群は拡大されない。さらなるサブグループ分析を可能にするために、潜在的な予測バイオマーカーを含む人口統計学的及びベースライン特性に関して処置群間のバランスを確保するために、さらなる患者を登録することができる。治験実施計画書を修正することによって、試験中に新しい実験群を追加することができる。 Sponsors may decide to delay or suspend enrollment within a given treatment arm. Experimental groups with inadequate clinical activity or unacceptable toxicity will not be expanded. Additional patients can be enrolled to ensure balance between treatment groups with respect to demographic and baseline characteristics, including potential predictive biomarkers, to allow for further subgroup analysis. New experimental groups can be added during a trial by amending the protocol.
ステージ2の処置群を除いて、患者を処置群にランダムに割り当てる。ランダム化はまた、利用可能な実験群の数(例えば、予備期からの結果の分析を待って、群が追加されるか、又は群への登録が一時停止される場合)に依存し、対照群に割り当てられる可能性は35%以下であるという規定がある。ランダム化は、群特異的排除基準を考慮に入れる。患者は、その群について概説された除外基準のいずれかを満たす場合(下記を参照)、特定の群について不適格である。
Patients are randomly assigned to treatment groups, with the exception of the
アテゾリズマブ対照群及び実験群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで処置される。がん免疫療法(CIT)(アテゾリズマブ等)によるT細胞応答(偽進行と呼ばれる)の状況では、免疫細胞浸潤によって引き起こされる腫瘍負荷の初期増加の可能性のために、Response Evaluation Criteria in Solid Tumors、バージョン1.1(RECIST v1.1)による放射線学的進行は、真の疾患進行を示さない可能性がある。許容できない毒性がない場合、CIT薬物による処置を受けている間にRECIST v1.1による疾患進行の基準を満たす患者は、以下の基準の全てを満たす場合、試験処置を継続することが許可される:
●すべての利用可能なデータの再検討後に治験責任医師によって決定される臨床的利益の証拠。
●疾患の明確な進行を示す症状及び徴候(検査値、例えば、新たな又は悪化する高カルシウム血症を含む)がないこと。
●疾患進行に起因し得るECOG PSの低下がないこと
●治験実施計画書で許可された医学的介入によって管理することができない重要な解剖学的部位(例えば、軟髄膜疾患)における腫瘍進行の欠如
Patients in the atezolizumab control and experimental groups will be integrated with radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening symptoms such as pain secondary to disease). Treatment is until unacceptable toxicity or loss of clinical benefit as determined by the Investigator after evaluation. In the context of cancer immunotherapy (CIT)-induced T-cell responses (called pseudoprogression), due to the possibility of an initial increase in tumor burden caused by immune cell infiltration, Response Evaluation Criteria in Solid Tumors, Radiographic progression by version 1.1 (RECIST v1.1) may not indicate true disease progression. In the absence of unacceptable toxicity, patients who meet the criteria for disease progression by RECIST v1.1 while receiving treatment with a CIT drug are allowed to continue study treatment if they meet all of the following criteria: :
• Evidence of clinical benefit as determined by the investigator after review of all available data.
• Absence of symptoms and signs (including laboratory values, eg, new or worsening hypercalcemia) of definite disease progression.
No decline in ECOG PS that could be attributed to disease progression No tumor progression in critical anatomic sites (e.g., leptomeningeal disease) that cannot be controlled by protocol-allowed medical interventions lack
B.ステージ2
ステージ1の間、治験責任医師によって決定された臨床的利益の損失又は許容できない毒性を経験したことがある患者は、適格基準を満たすならば、ステージ2の間に異なる処置の組み合わせを受ける資格があり得る(図25を参照)。2つ以上の処置群に対して適格であるステージ2の患者は、治験責任医師によって処置群治験責任医師に割り当てられる。
Patients who have experienced loss of clinical benefit or unacceptable toxicity as determined by the investigator during
ステージ2の処置は、患者が臨床的利益の喪失又は許容できない毒性を経験した後3ヶ月以内に開始しなければならず、治験責任医師によって決定された臨床的利益の喪失又は許容できない毒性まで継続する。患者は可能な限り早くステージ2の処置を開始することが推奨される。
試験依頼者は、必要に応じて、安全性データ、予備的有効性データ及び支援情報(例えば、バイオマーカー研究データ)の再検討に基づいて、ステージ2の処置群への登録を保留又は中止することを決定し得る。
Sponsor withholds or discontinues enrollment in
C.試験計画の理論的根拠
患者集団及びアテゾリズマブ対照群の理論的根拠
C. Rationale for Study Design Patient population and atezolizumab control arm rationale
この試験は、白金含有レジメン中又はそれに続いて進行した局所進行性又は転移性UCを有する患者を登録する。 This trial will enroll patients with locally advanced or metastatic UC who have progressed during or following a platinum-containing regimen.
アテゾリズマブ(Tecentriq(登録商標))は、白金含有レジメン、非小細胞肺がん、小細胞肺がん、トリプルネガティブ乳がん、肝細胞癌腫及び黒色腫中又はその後に進行した患者のUCの処置に承認されている。以前の白金含有レジメンに従って進行したUC患者の第二選択処置の承認は、進行中の第II相試験GO 29293(IMvigor 210)のコホート2からのデータに基づき、その後、IMvigor210と第III相GO29294試験(IMvigor211)の両方の結果に基づいて、欧州で同じ適応症で完全承認が続いた。IMvigor 210コホート2では、2017年7月12日現在で、310人の患者が登録されており、16%(95% CI:13、21)のORR及び7%の完全奏効(CR)率、並びに24.8ヶ月の奏効期間中央値(DOR)が観察された(95% CI:13.8、30.4)。安全性評価により、患者の8%が処置中止につながる有害事象を有し、患者の16%が最も一般的な事象である疲労、下痢及び掻痒症である、処置関連のグレード3又は4の有害事象を有した。免疫介在事象は全体で患者の12%で発生し、患者の7%はグレード3又は4の免疫介在事象を有していた(グレード3又は4の発疹[1%]、ALT増加[2%]、血中ビリルビン増加[2%]、及び横紋筋融解症[1%])。IMvigor211では、2017年3月13日現在で、処置意図(ITT)集団において8.6ヶ月のOS中央値、13.4%のORR(10.5,16.9)及び21.7ヶ月のDOR中央値が観察された。
Atezolizumab (Tecentriq®) is approved for the treatment of UC in patients who have progressed during or after platinum-containing regimens, non-small cell lung cancer, small cell lung cancer, triple-negative breast cancer, hepatocellular carcinoma and melanoma. Approval for second-line treatment of UC patients who progressed on previous platinum-containing regimens was based on data from
単剤チェックポイント阻害の見込みにもかかわらず、比較的少数の患者のみが利益を経験し、免疫療法の併用の必要性を強調している。この試験における複数の組み合わせパートナーは、アテゾリズマブの利益を手術不能な局所進行性及び転移性UCのより大きな集団に拡大する目的で、様々な機構を介して免疫系を賦活すると予想される。 Despite the promise of single-agent checkpoint inhibition, only a relatively small number of patients experience benefit, underscoring the need for concomitant immunotherapy. Multiple combination partners in this trial are expected to stimulate the immune system through various mechanisms with the aim of extending the benefit of atezolizumab to the larger population of inoperable locally advanced and metastatic UC.
ステージ2の理論的根拠
免疫療法の出現により、30年で初めてmUCにおいて実際の進歩が明らかになった。この進歩にもかかわらず、より大きな割合の患者に利益を拡大するためには、実質的により多くの作業を行う必要がある。免疫療法を進める能力の鍵は、基礎となる腫瘍免疫環境及び処置のシーケンシングが応答にどのように影響するかのより良い理解を得ることであろう。
Rationale for
この試験のステージ2の部分により、一部の患者は、CITレジメンに応答しないか又はCITレジメンを進めることができない患者における免疫回避機構の科学的理解を進めるために、疾患進行後にその後のCITの併用を進めることが可能になる。ステージ2に登録する患者の能力にとって重要なのは、ステージ1の処置中に起こり得る免疫環境及び任意の変化の評価を可能にするために生検を受ける患者の能力である。ステージ2への参加により、患者及び提供者は、従来の化学療法では利用できない永続的応答及び改善された毒性プロファイルの可能性を有する処置の選択肢にアクセスすることができる。ステージ2の処置は、他の潜在的により標準的な選択肢による処置を不可能にするため、患者は、ステージ2の同意プロセス中に、ステージ2に登録することによって、生存利益を有し得る前述する治療であることを知らされる。
The
ステージ2におけるAtezo+EV及びAtezo+SG群の理論的根拠
患者は、臨床的利益を失った後に、Atezo+EV又はAtezo+SGによるステージ2の処置を受ける機会を与えられ得る。
Rationale for Atezo+EV and Atezo+SG Groups in
Atezo+EVの組み合わせは、以前にCPI処置を受けたことがある単剤エンフォルツマブベドチンを受けた患者で文書化された強い処置応答のために、ステージ2に対して選択された。具体的には、エンフォルツマブベドチンの第I相試験では、推奨される第II相エンフォルツマブベドチン用量で処置された転移性膀胱を有する17人中8人(47%;95% CI:23、72.2)の患者がPRを得た(Petrylak et al.,J Clin Oncol,35(15 Suppl):106,2017)。これらの知見は、エンフォルツマブベドチンがCPI後空間において利益をもたらし得ることを示唆している。エンフォルツマブベドチンへのアテゾリズマブの添加は、応答耐久性を改善する可能性を有する。更に、微小管破壊療法は、免疫原性細胞死を誘導し、抗腫瘍免疫応答を開始する可能性を有する。
The Atezo+EV combination was selected for
Atezo+SGの組み合わせは、白金ベースの治療及びチェックポイント阻害剤治療で進行した、単剤サシツズマブゴビテカンを投与されたmUC患者で観察された強い処置応答のため、ステージ2に対して選択された。具体的には、第II相TROPHY-U-01試験で、サシツズマブゴビテカンは、35人の患者で29%のORRを示し、これには肝転移を有する患者で25.0%のORRが含まれる(Tagawa et al.,J Clin Oncol,37(7 Suppl):3199-3212,2019)。これらの所見は、サクツズマブゴビテカンがCPI後空間において利益をもたらし得ることを示唆している。化学療法及び免疫療法後に進行した患者におけるアテゾリズマブとサシツズマブゴビテカンとの組み合わせは、アテゾリズマブがサクツズマブゴビテカンの抗腫瘍活性によって媒介される炎症に由来する抗腫瘍免疫応答を増強することを可能にすることによって、相乗効果を提供し得る。
The Atezo+SG combination was selected for
初期の放射線学的進行を超える免疫療法に基づく処置の理論的根拠
免疫療法剤の研究では、CR、部分奏効(PR)、及び安定疾患はそれぞれ、腫瘍量の明らかな増加の放射線学的証拠の後に起こることが示されている。T細胞応答の状況における免疫細胞浸潤によって引き起こされる腫瘍負荷のこの初期の増加は、偽進行と呼ばれている(Hales et al.,Ann Oncol,21:1944-1951,2010)。
Rationale for Immunotherapy-Based Treatment Beyond Early Radiological Progression In immunotherapeutic studies, CR, partial response (PR), and stable disease have each been associated with radiological evidence of a clear increase in tumor burden. shown to occur later. This initial increase in tumor burden caused by immune cell infiltration in the context of a T cell response is called pseudoprogression (Hales et al., Ann Oncol, 21:1944-1951, 2010).
PCD4989g試験では、いくつかの腫瘍型において腫瘍成長とそれに続く応答の証拠が観察された。更に、進行の放射線学的証拠を有するいくつかの応答患者において、新たな病変又は既存の病変における新たな成長領域の生検により、免疫細胞が明らかにされ、生存可能ながん細胞は明らかにされなかった。偽進行後の応答の可能性のために、この試験は、免疫療法に基づく処置群にランダムに割り当てられた患者が、RECIST v 1.1による明らかな放射線学的進行後に併用処置を継続することを可能にするが、ただし、ベネフィット-リスク比が、治験責任医師が好都合であると判断した場合に限る。放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態の統合評定の後に治験責任医師によって決定された許容できない毒性又は臨床的利益の喪失の場合は、患者を中止すべきである。 In the PCD4989g study, evidence of tumor growth and subsequent response was observed in several tumor types. Moreover, in some responding patients with radiological evidence of progression, biopsies of new lesions or areas of new growth in existing lesions reveal immune cells and viable cancer cells. it wasn't. Because of the potential for responses after pseudoprogression, this study evaluated whether patients randomly assigned to immunotherapy-based treatment groups continued on combination treatment after overt radiological progression by RECIST v 1.1. possible, but only if the benefit-risk ratio is deemed favorable by the investigator. In the event of unacceptable toxicity or loss of clinical benefit as determined by the investigator after integrated assessment of radiological and biochemical data, local biopsy results (if available), and clinical status, patients will be should be discontinued.
試験の具体的な目的及び対応する評価項目を表78及び79に概説する。



D.評定及びモニタリング D. Rating and monitoring
全ての患者は、試験を通して有害事象について綿密に監視され、有害事象は、国立がん試験所有害事象共通用語規準(National Cancer Institute Common Terminology Criteria for Adverse Events,Version 4.0(NCI CTCAE v4.0))に従って等級付けされる。患者は、最初の54週間は9週間毎に(サイクル1の1日目から開始して)、その後は12週間毎に腫瘍評定を受ける。応答は、RECIST v 1.1を使用して治験責任医師によって評定される(Eisenhauer et al.,Eur J Cancer,45:228-247,2009))。臨床活性が実験群で実証された場合、試験依頼者は、その群の腫瘍評定スキャンが独立した読み取り施設による評価に提出されることを要求し得る。
All patients were closely monitored for adverse events throughout the study, and adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE v4.0). )). Patients undergo tumor assessments every 9 weeks for the first 54 weeks (starting on
ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、腫瘍組織の保管を提出することができる。腫瘍組織はまた、治験責任医師によって決定されるように(治験責任医師によって臨床的に実施可能であると考えられる場合)、許容できない毒性又は臨床的利益の喪失のためにステージ1を中止する患者から収集される。これらの試料、並びに試験中に採取された血液試料は、バイオマーカー研究に利用される。
Baseline tumor tissue samples are collected from all patients, preferably by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, archiving of tumor tissue may be submitted.
アテゾリズマブ及び他の治療剤の薬物動態(PK)特性及び/又は免疫原性を特性評価するために、試験処置投与の前及び間の様々な時点で血液試料を取得する。 To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points before and during study treatment administration.
E.試験終了及び試験期間
試験の終了は、両方のステージでの最後の患者が最後の来院を完了した日(電話又は現場での来院によって行われる生存フォローアップ来院を含む)として定義される。
E. End of Study and Study Duration End of study is defined as the date the last patient in both stages completed the last visit (including survival follow-up visits conducted by telephone or on-site visit).
最初の患者のスクリーニングから試験終了までの試験の全長は、約3~5年である。 The total length of the trial, from initial patient screening to study termination, is approximately 3-5 years.
実施例21.WO39613のmUC試験のための材料及び方法
A.ステージ1の選択基準
患者は、ステージ1に適格であるためには、以下に概説される基準の全てを満たさなければならない:
●署名時の年齢が≧18歳。
●治験責任医師が決定した平均余命≧3ヶ月。
●組織学的に文書化された、局所進行性(T4b、任意のN;又は任意のT、N2-N3)又は転移性UC(M1、ステージIV)(TCC又は尿路の尿路上皮細胞癌腫とも呼ばれる;腎盂、尿管、膀胱、及び尿道を含む)。混合組織型の患者は、優勢な移行細胞パターンを有する必要がある。局所進行性膀胱がんは、骨盤側壁又は隣接する内臓の浸潤に基づいて手術不能でなければならない(臨床病期T4b)か、又は巨大リンパ節転移(N2-N3)でなければならない
●中央検査によるPD-L1及び/又はさらなるバイオマーカーの状態の決定に適した代表的な腫瘍標本の入手可能性。ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。
Example 21. Materials and methods for mUC testing of WO39613A. Inclusion Criteria for
● Age at the time of signature is ≧18 years old.
• Investigator-determined life expectancy ≧3 months.
- Histologically documented locally advanced (T4b, any N; or any T, N2-N3) or metastatic UC (M1, stage IV) (TCC or urothelial cell carcinoma of the urinary tract) also called; includes renal pelvis, ureter, bladder, and urethra). Patients with mixed histology should have a predominant transitional cell pattern. Locally advanced bladder cancer must be inoperable based on pelvic sidewall or adjacent visceral involvement (clinical stage T4b) or must be large lymph node metastasis (N2-N3) Central examination Availability of representative tumor specimens suitable for determination of PD-L1 and/or additional biomarker status by. A baseline tumor tissue sample is preferably collected from all patients by biopsy performed at study enrollment.
パラフィンブロック(好ましい)中のホルマリン固定パラフィン包埋(FFPE)腫瘍標本又は未染色の新たに切断した連続切片を含む少なくとも16枚のスライドは、関連する病理報告と共に提出しなければならない。10-15枚のスライドしか利用できない場合、患者は依然として試験に適格であり得る。腫瘍組織は、総腫瘍含有量及び生存腫瘍含有量に基づいて良質でなければならない。 At least 16 slides containing formalin-fixed paraffin-embedded (FFPE) tumor specimens in paraffin blocks (preferred) or unstained freshly cut serial sections must be submitted along with the relevant pathology report. Patients may still be eligible for the study if only 10-15 slides are available. Tumor tissue must be of good quality based on total tumor content and viable tumor content.
細針吸引、ブラッシング、胸水からの細胞ペレット、骨転移、及び洗浄液試料は許容されない。コア針生検検体の場合、少なくとも3つのコアを評価に供するべきである。利用可能なコアが3つ未満の患者は依然として適格であり得る。TURBT検体は、局所病理の再検討によって検証された膀胱腫瘍の筋浸潤成分(すなわち、T2以上)を含まなければならない。TURBT標本が筋浸潤成分を含まない場合、膀胱切除術/腎尿管切除術又は転移拡散時に得られた標本(すなわち、転移性病変からの試料)がランダム化の前に必要とされる。
●手術不能な、局所進行性又は転移性のUC又は疾患再発のための1つ以下の白金含有レジメン(例えば、GC、MVAC、CarboGem)による処置中又は処置後の疾患進行。レジメンは、患者が少なくとも2サイクルの白金含有レジメンを受けることにより定義される。事前のアジュバント/ネオアジュバント化学療法を受け、白金含有アジュバント/ネオアジュバント療法による処置の12ヶ月以内に進行した患者は、第二選択患者とみなされる。患者は、進行性又は転移性UCに対して、2つ以下の事前の処置レジメン(必要な白金系のレジメンを含む)を受けたことがあってもよい。患者は、以前のすべてのレジメン(複数可)の間又は後に疾患の進行を実証していなければならない。化学放射線療法後に疾患が進行した患者は、以前の放射線療法ポート外での進行を実証しなければならない。
Fine needle aspirations, brushings, cell pellets from pleural effusions, bone metastases, and lavage fluid samples are not permitted. For core needle biopsy specimens, at least three cores should be submitted for evaluation. Patients with less than 3 cores available may still be eligible. TURBT specimens must contain a muscle-invasive component of bladder tumor (ie, T2 or greater) verified by review of local pathology. If the TURBT specimen does not contain a muscle-infiltrating component, specimens obtained at the time of cystectomy/nephroureterectomy or metastatic spread (ie, specimens from metastatic lesions) are required prior to randomization.
• Disease progression during or after treatment with no more than one platinum-containing regimen (eg, GC, MVAC, CarboGem) for inoperable, locally advanced or metastatic UC or disease recurrence. A regimen is defined by the patient receiving at least two cycles of a platinum-containing regimen. Patients who received prior adjuvant/neoadjuvant chemotherapy and progressed within 12 months of treatment with platinum-containing adjuvant/neoadjuvant therapy are considered second-line patients. Patients may have received no more than two prior treatment regimens (including required platinum-based regimens) for advanced or metastatic UC. Patients must have documented disease progression during or after all previous regimen(s). Patients with disease progression after chemoradiation must demonstrate progression outside the previous radiotherapy port.
B.ステージ1及びステージ2の選択基準
患者は、ステージ1又は2に適格であるためには、以下に概説される基準の全てを満たさなければならない:
●治験責任医師の判断による、試験治験実施計画書を遵守する能力
●ECOG PSが0又は1。
●RECIST v 1.1による測定可能な疾患(少なくとも1つの標的病変)以前に放射線照射された病変は、放射線照射後にその部位で進行性疾患が明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。
●試験処置の開始前14日以内に得られた以下の臨床検査結果によって定義される、適切な血液学的機能及び終末器官機能:
-顆粒球コロニー刺激因子支持なしでANC≧1.5X109/L(1500/μL)。
-WBC数≧2.5X109/L(2500/μL)。
-リンパ球数≧0.5X109/L(500/μL)。
-輸血なしで血小板数≧100X109/L(100,000/μL)。
-ヘモグロビン≧90g/L(9.0g/dL)。
B. Inclusion Criteria for
• Ability to comply with the study protocol, as determined by the investigator •
- Measurable disease (at least one target lesion) according to RECIST v 1.1 Previously irradiated lesions are only measurable if progressive disease is clearly documented at the site after irradiation can be considered a disease.
- Adequate hematologic and end-organ function as defined by the following laboratory results obtained within 14 days prior to initiation of study treatment:
- ANC ≧1.5×10 9 /L (1500/μL) without granulocyte colony stimulating factor support.
- WBC count ≧2.5×10 9 /L (2500/μL).
- Lymphocyte count ≧0.5×10 9 /L (500/μL).
- Platelet count ≧100×10 9 /L (100,000/μL) without transfusion.
- Hemoglobin > 90 g/L (9.0 g/dL).
患者は輸血されてもよいが、適格性について臨床検査をスクリーニングしてから2週間以内は、輸血は許容されない。 Patients may be transfused, but transfusions are not permitted within 2 weeks of clinical screening for eligibility.
単腎疾患又はエリスロポエチン産生が低い慢性腎臓疾患を有する患者は、エリスロポエチン刺激剤を使用してもよい。
-AST、ALT及びアルカリホスファターゼ(ALP)≦2.5X正常値の上限(ULN)、ただし、以下の例外を除く:
文書化された肝臓転移を有する患者:AST及び/又はALT≦5XULN
文書化された肝臓転移又は骨転移を有する患者:ALP≦5XULN
-以下を除く、ビリルビン≦1.5XULN:
既知のギルバート病患者:ビリルビン値≦3XULN。
-アルブミン≧25g/L(2.5g/dL)。
-クレアチニンクリアランス≧30mL/分(Cockcroft-Gault式を用いて計算)。
-治療的抗凝固療法を受けていない患者の場合:
PTT又はPTT≦1.5XULN
PT又はINR≦1.5XULN。
●治療的抗凝固療法を受けている患者の場合:試験処置の開始前の14日間の安定した抗凝固療法レジメン。
●スクリーニング時の陰性HIV検査。事前の陽性HIV検査結果がない患者は、地域の規制によって許可されない限り、スクリーニング時にHIV検査を受ける。
●スクリーニング時の全B型肝炎コア抗体(HBcAb)検査陰性、又はスクリーニング時の全HBcAb検査陽性、続いてスクリーニング時の定量的B型肝炎ウイルス(HBV)DNA<500IU/mL。HBV DNA検査は、全HBcAb検査が陽性である患者に対してのみ実施される。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:禁欲(異性間の性交を控える)又は避妊手段を使用することの合意、及び卵の提供を控えることの同意。
●男性の場合:禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることの同意。
Patients with single kidney disease or chronic kidney disease with low erythropoietin production may use erythropoietin stimulants.
- AST, ALT and alkaline phosphatase (ALP) < 2.5X upper limit of normal (ULN), with the following exceptions:
Patients with documented liver metastases: AST and/or ALT ≤ 5XULN
Patients with documented liver or bone metastases: ALP ≤ 5XULN
- Bilirubin ≤ 1.5 XULN, except:
Patients with known Gilbert's disease: bilirubin level < 3XULN.
- Albumin > 25 g/L (2.5 g/dL).
- Creatinine clearance ≧30 mL/min (calculated using the Cockcroft-Gault formula).
- In patients not receiving therapeutic anticoagulation:
PTT or PTT≤1.5XULN
PT or INR≤1.5XULN.
• For patients on therapeutic anticoagulation: a stable anticoagulation regimen for 14 days prior to initiation of study treatment.
• Negative HIV test at screening. Patients without prior positive HIV test results will undergo HIV testing at screening unless permitted by local regulations.
• Negative total hepatitis B core antibody (HBcAb) test at screening or positive total HBcAb test at screening followed by quantitative hepatitis B virus (HBV) DNA <500 IU/mL at screening. HBV DNA testing is performed only on patients with a positive overall HBcAb test.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening. HCV RNA testing is performed only for patients who test positive for HCV antibodies.
• For women of childbearing potential: consent to abstinence (abstinence from heterosexual intercourse) or use of contraceptive means, and consent to refrain from donating eggs.
• For men: Consent to maintain abstinence (abstain from heterosexual intercourse) or use contraceptives and to refrain from donating sperm.
C.ステージ2の選択基準
患者は、ステージ2に適格であるためには、以下の基準の全てを満たさなければならない:
●アテゾリズマブ対照群の患者:対照処置を受けている間に治験責任医師によって決定された臨床的利益の損失後3ヶ月以内にステージ2処置を開始する能力。
●ステージ1の間の実験群の患者:ステージ1の処置を受けている間に治験責任医師によって決定された、アテゾリズマブに関連しない許容できない毒性又は臨床的利益の喪失を経験した後、3ヶ月以内にステージ2の処置を開始する能力。
●ステージ1の中止時に行われた生検からの腫瘍標本の入手可能性。
C. Inclusion Criteria for
• Patients in the atezolizumab control arm: Ability to initiate
Patients in the experimental arm during Stage 1: Within 3 months after experiencing unacceptable toxicity or loss of clinical benefit unrelated to atezolizumab as determined by the Investigator while receiving
• Availability of tumor specimens from biopsies performed at
D.除外基準 D. Exclusion criteria
以下の基準のいずれかを満たす患者は、ステージ1及びステージ2の間の登録から除外される:除外基準における事象グレードはNCI CTCAE v 4.0に基づく。
Patients meeting any of the following criteria are excluded from enrollment during
ステージ1の除外基準
以下の基準のいずれかを満たす患者は、ステージ1から除外される:
●T細胞共刺激療法又は抗-CTLA-4、抗-PD-1及び抗-PD-L1治療用抗体を含むCPIによる事前処置。
●ポリ(アデノシン二リン酸[ADP]-リボース)ポリメラーゼ(PARP)阻害剤、ネクチン-4標的化剤、シグナル調節タンパク質α-標的化剤、TIGIT標的化剤、Trop-2標的化剤、FAP標的化療法、4-1 BB(CD 137)標的化療法、又はトポイソメラーゼ1阻害剤による処置を含む、治験実施計画書に指定された試験処置のいずれかによる事前処置。
●試験処置の開始前28日以内の治験療法による処置。
●試験処置の開始前3週間以内の化学療法又はホルモン療法を含む任意の承認された抗がん治療;以下の例外が許容される:
-骨転移又は軟部組織病変に対する緩和的放射線療法は、ベースラインイメージングの>14日前に完了すべきである。
-ホルモン補充療法又は経口避妊薬
●対照群のみの適格性
- Prior treatment with T cell costimulatory therapy or CPIs including anti-CTLA-4, anti-PD-1 and anti-PD-L1 therapeutic antibodies.
Poly(adenosine diphosphate [ADP]-ribose) polymerase (PARP) inhibitors, Nectin-4 targeting agents, Signal regulatory protein α-targeting agents, TIGIT targeting agents, Trop-2 targeting agents, FAP targets Prior treatment with any protocol-specified study treatment, including chemotherapy, 4-1 BB (CD 137) targeted therapy, or treatment with a
- Treatment with study therapy within 28 days prior to initiation of study treatment.
- Any approved anticancer therapy, including chemotherapy or hormone therapy, within 3 weeks prior to initiation of study treatment; the following exceptions are allowed:
- Palliative radiotherapy for bone metastases or soft tissue lesions should be completed >14 days before baseline imaging.
- Hormone replacement therapy or oral contraceptives Eligibility for control group only
ステージ1及びステージ2の除外基準
以下の基準のいずれかを満たす患者は、ステージ1及びステージ2から除外される:
●事前の同種異系幹細胞又は固形臓器移植
●試験処置の開始前の薬物の4週間以内又は5半減期(いずれか長い方)以内の全身免疫刺激剤(限定されないが、インターフェロン及びインターロイキン2を含む)による処置。
●以下の例外を除いて、試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び抗腫瘍壊死因子-α剤を含む)による処置、又は試験処置中の全身免疫抑制薬の必要性の予測:
Exclusion Criteria for
- Prior allogeneic stem cell or solid organ transplantation - Systemic immune stimulants (including but not limited to interferon and interleukin-2) within 4 weeks or 5 half-lives (whichever is longer) of drug prior to initiation of study treatment ) treatment.
- Systemic immunosuppressants (including but not limited to corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide and anti-tumor necrosis factor-alpha agents) within 2 weeks prior to initiation of study treatment, with the following exceptions ) or prediction of need for systemic immunosuppressants during study treatment:
急性低用量の全身免疫抑制薬、又は1回のパルス用量の全身免疫抑制薬(例えば、造影剤アレルギーのための48時間のコルチコステロイド)を受けた患者は試験に適格である。 Patients who received an acute low-dose systemic immunosuppressant or a single pulse dose of systemic immunosuppressant (eg, 48-hour corticosteroids for contrast allergy) are eligible for the study.
ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患若しくは喘息のためのコルチコステロイド、又は起立性低血圧若しくは副腎機能不全のための低用量コルチコステロイドを受けた患者は試験に適格である。
●試験処置の開始前4週間以内、又はアテゾリズマブ処置中若しくはアテゾリズマブの最終投薬後5ヶ月以内の生弱毒化ワクチンによる処置
●制御されない胸水、心膜滲出液、又は再発性排液処置を必要とする腹水(毎月1回又はより頻繁に)留置カテーテル(例えば、PLEURX(登録商標))の使用が許容される。
●制御されない腫瘍関連疼痛。鎮痛薬を必要とする患者は、試験登録時に安定したレジメンでなければならない。緩和的放射線療法に適した症候性病変(例えば、神経インピンジメントを引き起こす骨転移又は転移)は、登録前に処置しなければならない。患者は、放射線の影響から回復されなければならない。必要とされる最低限の回復期間はない。さらなる成長(例えば、脊髄圧迫に現在関連していない硬膜外転移)を伴う機能障害又は難治性疼痛を引き起こす可能性がある無症候性転移性病変は、登録前に適切な場合、局所領域療法について検討されるべきである。
●制御不能又は症候性の高カルシウム血症(イオン化カルシウム>1.5mmol/L、カルシウム>12mg/dL又は補正血清カルシウム>ULN)。
●症候性、未処置又は活発に進行するCNS転移。処置されたCNS病変を有する無症候性患者は、以下の基準の全てが満たされるならば適格である:
-RECIST v1.1による測定可能な疾患はCNS外に存在しなければならない
-患者は頭蓋内出血又は脊髄出血の病歴がない。
-患者は、試験処置の開始前7日間以内の定位放射線療法、試験処置の開始前14日間以内の全脳放射線療法、又は試験処置の開始前28日間以内の神経外科的摘出を受けたことがない。
-患者は、CNS疾患の治療としてのコルチコステロイドに対する継続的な要求がない。安定な用量での抗痙攣療法が許容される。
●軟髄膜疾患の病歴。
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質抗体症候群、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、又は多発性硬化症を含むがこれらに限定されない自己免疫疾患又は免疫不全活動が活動性であるもの、又はその病歴、ただし、以下を除く:
Patients receiving mineralocorticoids (e.g., fludrocortisone), corticosteroids for chronic obstructive pulmonary disease or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency are eligible for the study. be.
- Treatment with a live attenuated vaccine within 4 weeks prior to initiation of study treatment or during atezolizumab treatment or within 5 months after the last dose of atezolizumab - Requires uncontrolled pleural effusion, pericardial effusion, or recurrent drainage treatment Ascites (monthly or more frequently) use of an indwelling catheter (eg, PLEURX®) is permitted.
• Uncontrolled tumor-related pain. Patients requiring analgesics must be on a stable regimen at study entry. Symptomatic lesions amenable to palliative radiotherapy (eg bone metastases or metastases causing nerve impingement) must be treated prior to enrollment. Patients must recover from the effects of radiation. There is no minimum recovery period required. Asymptomatic metastatic lesions that may cause functional impairment with further growth (e.g., epidural metastases not currently associated with spinal cord compression) or intractable pain should be treated with locoregional therapy, if appropriate, prior to enrollment. should be considered.
• Uncontrolled or symptomatic hypercalcemia (ionized calcium >1.5 mmol/L, calcium >12 mg/dL or corrected serum calcium > ULN).
• Symptomatic, untreated or actively progressing CNS metastases. Asymptomatic patients with treated CNS lesions are eligible if all of the following criteria are met:
- Measurable disease by RECIST v1.1 must be present outside the CNS - Patient has no history of intracranial or spinal cord hemorrhage.
- Patient has had stereotactic radiotherapy within 7 days prior to the start of study treatment, whole brain radiotherapy within 14 days prior to the start of study treatment, or neurosurgical resection within 28 days prior to the start of study treatment do not have.
- Patient has no ongoing need for corticosteroids as treatment for CNS disease. Anticonvulsant therapy at stable doses is acceptable.
A history of leptomeningeal disease.
Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barré syndrome, or multiple sclerosis Active or history of autoimmune disease or immunodeficiency activity, including but not limited to, excluding:
甲状腺補充ホルモンを服用している自己免疫関連甲状腺機能低下症の病歴を有する患者が試験に適格である。安定なインスリンレジメンを受けている制御された1型糖尿病患者は試験に適格である。湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを伴う白斑(例えば、乾癬性関節炎を有する患者は除外される)を有する患者は、以下の条件の全てが満たされるならば、試験に適格である。
-発疹が覆っている体表面積は<10%でなければならない。
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない。
●特発性肺線維症、器質化肺炎(例えば、閉塞性細気管支炎)、薬物誘発性間質性肺炎、若しくは特発性間質性肺炎の病歴、又はスクリーニング胸部コンピューター断層撮影(CT)スキャンでの活動性間質性肺炎の証拠。放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚癌腫、限局性前立腺がん、上皮内乳管癌癌腫、又はステージI子宮がん等、転移又は死亡のリスクが無視できる(例えば、5年全生存[OS]率>90%)悪性腫瘍を除いて、スクリーニング前2年以内のUC以外の悪性腫瘍の病歴。治癒目的で処置され、PSA再発のない限局性前立腺がん(ステージ≦pT2c、Gleasonスコア≦7及び前立腺がん診断時の前立腺特異抗原(PSA)≦20 ng/mLとして定義される)患者が適格である。処置未経験であり、積極的監視療法を受けている既存の低リスク前立腺がん(ステージcT 1/T2a、Gleasonスコア≦6、及びPSA≦10 ng/mLと定義)を有する患者が適格である。
●活動性結核(TB)(すなわち、TBの徴候及び症状を有する)。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)、又は治験責任医師の見解では患者の安全性に影響を及ぼし得る任意の活動性感染症。
●試験処置開始前2週間以内の治療用経口又はIV抗生物質による処置
Patients with a history of autoimmune-related hypothyroidism taking thyroid replacement hormone are eligible for the study. Patients with controlled
- The rash must cover <10% of body surface area.
- Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UVA radiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors within the past 12 months , or no acute exacerbation of underlying symptoms requiring high-potency or oral corticosteroids.
A history of idiopathic pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis obliterans), drug-induced interstitial pneumonia, or idiopathic interstitial pneumonia, or a screening chest computed tomography (CT) scan Evidence of active interstitial pneumonia. A history of radiation pneumonitis (fibrosis) in the radiology area is acceptable.
Appropriately treated cervical carcinoma in situ, nonmelanoma cutaneous carcinoma, localized prostate cancer, ductal carcinoma in situ, or stage I uterine cancer with negligible risk of metastasis or death (e.g., , 5-year overall survival [OS] >90%) History of malignancy other than UC within 2 years prior to screening, excluding malignancy. Patients with localized prostate cancer (defined as stage ≤ pT2c, Gleason score ≤ 7 and prostate specific antigen (PSA) ≤ 20 ng/mL at diagnosis of prostate cancer) treated with curative intent and without PSA recurrence are eligible is. Patients with preexisting low-risk prostate cancer (
- Active tuberculosis (TB) (ie, having signs and symptoms of TB).
- Severe infection (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia) within 4 weeks prior to initiation of study treatment, or opinion of investigator Any active infection that may affect patient safety.
- Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of study treatment
予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の増悪を予防するため)を受ける患者は試験に適格である;
●ランダム化前3ヶ月以内のNew York Heart Association心疾患(クラスIII以上)、心筋梗塞又は脳血管障害、不安定不整脈又は不安定狭心症等の有意な心血管疾患。
●制御されない高血圧(収縮期血圧>140 mmHg及び/又は拡張期血圧>95 mmHgとして定義される)。これらのパラメーターを達成するための降圧療法が許容される。
●試験処置の開始前28日以内のグレード≧3の出血又は出血事象。
●試験処置の開始前4週間以内の大きな外科的処置(診断以外)、又は試験中の大きな外科的処置の必要性の予想 中心静脈アクセスカテーテル(例えば、ポート等)の配置は、大きな外科的処置とは考えられておらず、したがって許容される。
●任意のグレードの脱毛症及びグレード≦2の末梢神経障害を除いて、グレード≦1以上に改善していない以前の抗がん治療からの有害事象。
●治験薬の使用を禁忌にする任意の他の疾患、代謝機能不全、身体検査所見、又は臨床検査所見は、結果の解釈に影響を及ぼし得るか、患者が試験に参加する能力を損ない得るか、又は患者を処置合併症のリスクを高くし得る。
●キメラ若しくはヒト化抗体又は融合タンパク質に対する重度のアレルギー反応の病歴。
●チャイニーズハムスター卵巣細胞生成物又は組換えヒト抗体に対する既知の過敏症。
●賦形剤の試験薬物のいずれかに対する既知の不耐性又は過敏症(ヒスチジン、トレハロース二水和物、及びポリソルベート20を含む)。
●前投薬に必要な任意の薬物に対する既知の不耐性(アセトアミノフェン、ラニチジン、ジフェンヒドラミン、メチルプレドニゾロン)。
●ステージ2に入る患者:ステージ1の間、アテゾリズマブに忍容性がない。
●妊娠若しくは授乳、又は試験中に妊娠する意図。妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
●ステージ2に入る患者:以下の例外を除いて、同意時にグレード1以上又はベースラインまで回復していない免疫療法関連有害事象:補充療法で適切に管理されている進行中の内分泌事象を有する患者が適格である。
Patients receiving prophylactic antibiotics (e.g., to prevent exacerbations of urinary tract infections or chronic obstructive pulmonary disease) are eligible for the study;
• Significant cardiovascular disease such as New York Heart Association heart disease (class III or higher), myocardial infarction or cerebrovascular disease, unstable arrhythmia or unstable angina pectoris within 3 months prior to randomization.
- Uncontrolled hypertension (defined as systolic blood pressure >140 mmHg and/or diastolic blood pressure >95 mmHg). Antihypertensive therapy to achieve these parameters is acceptable.
• Grade ≥3 bleeding or bleeding event within 28 days prior to initiation of study treatment.
- Major surgical procedure (non-diagnostic) within 4 weeks prior to initiation of study procedure, or anticipation of need for major surgical procedure during study Placement of central venous access catheter (e.g., port, etc.) is not considered and is therefore permissible.
• Adverse events from previous anti-cancer therapy that have not improved to grade ≤ 1, except for any grade of alopecia and grade ≤ 2 peripheral neuropathy.
Any other disease, metabolic dysfunction, physical examination findings, or laboratory findings that contraindicate the use of the study drug may affect the interpretation of results or impair the patient's ability to participate in the study. , or may put the patient at increased risk for procedural complications.
• History of severe allergic reaction to chimeric or humanized antibodies or fusion proteins.
• Known hypersensitivity to Chinese hamster ovary cell products or recombinant human antibodies.
• Known intolerance or hypersensitivity to any of the excipient study drugs (including histidine, trehalose dihydrate, and polysorbate 20).
• Known intolerance to any drug required for premedication (acetaminophen, ranitidine, diphenhydramine, methylprednisolone).
• Patients entering Stage 2: During
• Pregnancy or lactation, or intention to become pregnant during the study. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
Patients entering Stage 2: Immunotherapy-related adverse events ≥
ステージ1中のAtezo+Tira群の追加の除外基準
以下の基準のいずれかを満たす患者は、ステージ1の間、Atezo+Tira群から除外される。
●スクリーニング時の活動性EBV感染及び既知又は疑われる慢性活動性EBV感染 スクリーニング時にEBVウイルスカプシド抗原IgM検査が陽性であった患者は、この群から除外される。活動性感染又は慢性活動性感染の疑いをスクリーニングするために、EBVポリメラーゼ連鎖反応(PCR)検査を臨床的に適応されるように実施される。陽性EBV PCR検査を有する患者は、この群から除外される。
Additional Exclusion Criteria for the Atezo+Tira Group During
• Active EBV infection at screening and known or suspected chronic active EBV infection Patients with a positive EBV viral capsid antigen IgM test at screening are excluded from this group. An EBV polymerase chain reaction (PCR) test is performed as clinically indicated to screen for suspected active or chronically active infection. Patients with a positive EBV PCR test are excluded from this group.
E.許可された治療 E. Allowed treatment
患者は、試験中に以下の治療法を使用することが許される。
●経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(ワーファリン又は低分子量ヘパリン等)
●施設の基準に従って投与される予防的抗生物質又は抗ウイルス処置
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与されるコルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●前立腺がんに対するゴナドトロピン放出ホルモンアゴニスト又はアンタゴニストを用いたホルモン療法
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
2サイクルの処置後。緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。アテゾリズマブによる処置は、緩和放射線療法中に継続され得る。
●以下に概説されるような局所療法(例えば、外科手術、定位的放射線手術、放射線療法、高周波アブレーション):
3つ以下の病変の制御のために局所療法を必要とする混合応答を経験している患者は、メディカルモニターの承認が得られた後も試験処置を継続するのに依然として適格であり得る。標的病変に向けた局所療法を受けている患者は、もはや放射線学的応答については評価可能ではないが、進行については評価可能なままである。
Patients will be allowed to use the following therapies during the study.
● Oral contraceptives ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (warfarin or low molecular weight heparin, etc.)
● Prophylactic antibiotics or antiviral treatment administered according to institutional standards ● Inactivated influenza vaccination ● Megestrol acetate given as an appetite stimulant ● Mineralcorticoids (eg, fludrocortisone)
o Corticosteroids given for chronic obstructive pulmonary disease or asthma o Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency o Gonadotropin-releasing hormone agonists or antagonists for prostate cancer Hormonal therapy used Palliative radiation therapy (e.g. treatment of known bone metastases or symptomatic relief of pain) outlined below:
After 2 cycles of treatment. Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with atezolizumab may be continued during palliative radiotherapy.
- Local therapy (e.g., surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) as outlined below:
Patients experiencing a mixed response requiring local therapy for control of 3 or fewer lesions may still be eligible to continue study treatment after obtaining medical monitor approval. Patients receiving local therapy directed at target lesions are no longer evaluable for radiological response, but remain evaluable for progression.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent atezolizumab infusions, at the discretion of the Investigator.
注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理されなければならない。 Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2- adrenergic must be administered by a sexual agonist).
D.アテゾリズマブ群の材料及び方法
アテゾリズマブは、承認された投与量(TECENTRIQ(登録商標)米国添付文書;TECENTRIQ(登録商標)SmPC)である3週間ごとに1200mg(Q3W)(各21日間サイクルの1日目に1200mg)の固定用量で投与される(表80)。抗腫瘍活性は、1~20mg/kg Q3Wの範囲の用量にわたって観察された。PCD4989g試験では、アテゾリズマブの最大耐量に到達せず、用量制限毒性はいずれの用量でも観察されなかった。非臨床試験(Deng et al.,MAbs,8:593-603,2016)並びに利用可能な臨床薬物動態、有効性及び安全性データの両方に基づいて、1200mg Q3Wの固定用量(平均体重に基づく用量15mg/kg Q3Wと同等)を選択した。
D. Atezolizumab Group Materials and Methods Atezolizumab was administered at the approved dose (TECENTRIQ® US Prescribing; 1200 mg per day) (Table 80). Anti-tumor activity was observed over doses ranging from 1-20 mg/kg Q3W. In the PCD4989g study, the maximum tolerated dose of atezolizumab was not reached and no dose-limiting toxicity was observed at any dose. Based on both nonclinical studies (Deng et al., MAbs, 8:593-603, 2016) and available clinical pharmacokinetic, efficacy and safety data, a fixed dose of 1200 mg Q3W (mean weight-based dose 15 mg/kg Q3W) was selected.
アテゾリズマブ対照群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、処置を受ける。処置は、処置割り当て後7日以内に開始しなければならない。患者はサイクル3の後に手術を受け、第4サイクルの処置を、手術の4~6週間後に再開すべきである。

アテゾリズマブの投与は、訓練された人員並びに潜在的に重篤な反応を管理するための適切な機器及び薬剤に直ちにアクセスできる監視された設定で行われる。 Administration of atezolizumab occurs in a monitored setting with ready access to trained personnel and appropriate equipment and medications to manage potentially serious reactions.
アテゾリズマブ注入は、表81に概説される指示に従って投与される。

F.アテゾリズマブ+チラゴルマブ群の材料及び方法
アテゾリズマブは上記のように投与される(表81を参照)。
F. Materials and Methods for Atezolizumab + Tiragolumab Group Atezolizumab will be administered as described above (see Table 81).
チラゴルマブは、600mg IV Q3Wの固定用量(21日間の各サイクルの1日目に600mg)で投与される。600mg IV Q3Wの固定用量は、アテゾリズマブと組み合わせた単剤のチラゴルマブ又はチラゴルマブと組み合わせた第Ia相/第Ib相のGO30103試験からの利用可能な臨床PK、有効性、及び安全性データに基づいて選択した。単剤としてのチラゴルマブを用いた試験の第Ia相部分では、MTDに到達せず、用量漸増でDLTは観察されなかった。臨床上のカットオフ日について、チラゴルマブに対する抗薬物抗体(ADA)は、全ての用量レベルにわたって、第Ia相部分又は第Ib相部分で稀であった。長期安定疾患は、試験の第Ia相部分の患者において、
Tiragolumab is administered at a fixed dose of 600 mg IV Q3W (600 mg on
400mgで開始するチラゴルマブ用量で観察された。チラゴルマブ+アテゾリズマブを用いた試験の第Ib相部分では、MTDに達しなかった。放射線部分奏効によって測定される抗腫瘍活性は、1200mgのアテゾリズマブと組み合わせて30mgから開始して600mgまでの範囲のチラゴルマブについて用量を超えて観察された。 Observed at tiragolumab doses starting at 400 mg. The MTD was not reached in the phase Ib portion of the trial with tiragolumab plus atezolizumab. Anti-tumor activity, as measured by radiation partial response, was observed across doses for tiragolumab ranging from 30 mg to 600 mg in combination with 1200 mg atezolizumab.
アテゾリズマブ+チラゴルマブ群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、表82に概説される処置を受ける。患者はサイクル3の後に手術を受け、第4サイクルの処置を、手術の4~6週間後に再開する。

チラゴルマブは、表83に記載のように、各21日間サイクルの1日目に600mgの固定用量でIV注入によって投与され、注入後観察期間を有する。チラゴルマブの投与は、訓練された人員並びに潜在的に重篤な反応を管理するための適切な機器及び薬剤に直ちにアクセスできる監視された設定で行われる。

WO39613のmUC試験の安全性評定を、実施例18に記載されているように行う。 Safety assessment of the WO39613 mUC test is performed as described in Example 18.
実施例22.WO39613のmUC試験の統計的考察及び分析計画
WO39613の試験分析は、試験の中止によって収集された患者データに基づいている。特に明記しない限り、有効性分析は、割り当てられた治療レジメンに対して各薬物の少なくとも1回の用量を受けた全ての患者として定義される有効性評価可能な集団に基づき、安全性分析は、任意の量の試験処置を受けた全ての患者として定義される安全性評価可能な集団に基づく。
Example 22. Statistical Considerations and Analysis Plan for the WO39613 mUC Study The WO39613 study analysis is based on patient data collected by study discontinuation. Unless otherwise stated, efficacy analyzes were based on the efficacy evaluable population defined as all patients who received at least one dose of each drug on their assigned treatment regimen; Based on a safety evaluable population defined as all patients who received any amount of study treatment.
分析結果は、患者が実際に受けている処置及び適用可能であればステージ(ステージ1又はステージ2)によって要約される。データは、試料サイズによって保証されるように記載され、要約される。連続変数は、平均、標準偏差、中央値、並びに最小値及び最大値の使用によって要約される。カテゴリ変数は、カウント及びパーセンテージの使用によって要約される。試料サイズが小さい場合、表の代わりにリストを使用する。
Analysis results are summarized by the treatment the patient is actually undergoing and by stage (
A.試料サイズの決定
WO39613号の試験は、仮説検定のための明示的なパワー及びタイプI誤差を考慮するように設計されていない。
A. Determination of Sample Size The WO39613 test was not designed to take into account explicit power and Type I errors for hypothesis testing.
代わりに、試験を、白金含有レジメン中又は後に進行した局所進行性又は転移性UCを有する患者に投与した場合の免疫療法に基づく処置の組み合わせに関する予備的な有効性、安全性及びPKデータを得るように設計する。試験中、約160~385人の患者をランダムに対照群及び実験群に割り付ける。 Instead, the study will provide preliminary efficacy, safety and PK data for immunotherapy-based treatment combinations when administered to patients with locally advanced or metastatic UC who have progressed on or after platinum-containing regimens. designed to Approximately 160-385 patients are randomly assigned to control and experimental groups during the study.
B.有効性分析 B. Effectiveness analysis
有効性の主要評価項目は、RECIST v 1.1に従って治験責任医師が決定し、上で定義したステージ1での客観的奏効率(ORR)である(表78を参照)。応答評定が欠落しているか又は応答評価がない患者は、非応答者として分類される。
The primary efficacy endpoint is the objective response rate (ORR) at
ORRは、CR又はPRを有する患者の割合として定義され、90%CIと共に各群について計算される(Clopper-Pearson正確法)。実験群と対照群との間のORRの差も、90%CIと共に計算される。CIは、試料サイズに応じて、正確法又はWald法によって推定される。 ORR is defined as the proportion of patients with CR or PR and is calculated for each group with a 90% CI (Clopper-Pearson exact method). The difference in ORR between experimental and control groups is also calculated with a 90% CI. CI is estimated by the exact method or the Wald method, depending on the sample size.
副次的有効性評価項目
副次的有効性評価項目は、無増悪生存期間(PFS)、OS、特定の時点でのOS(例えば、12ヶ月)、DOR、及び上に定義されるステージ1の間の病勢制御である(表78を参照)。PFS、DOR及び病勢制御は、RECIST v1.1に従って治験責任医師によって決定される。
Secondary Efficacy Endpoints Secondary efficacy endpoints are progression-free survival (PFS), OS, OS at a specified time point (e.g., 12 months), DOR, and
DORは、CR又はPRを有する有効性評価可能な患者について導出される。 DOR is derived for efficacy evaluable patients with CR or PR.
試験段階で疾患の進行又は死亡が文書化されていない患者については、PFS及びDORを最後の腫瘍評定の日に打ち切る。OS分析時にまだ生存している患者は、生存していることが知られていた最後の日に打ち切る。 For patients with no documented disease progression or death during the study phase, PFS and DOR will be censored on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day known to be alive.
Kaplan-Meier法を使用してPFS、OS、及びDORの中央値を推定し、90%CIをBrookmeyer及びCrowley法の使用によって構築する。特定の時点でのOS率もKaplan-Meier法を用いて推定され、90% CIは分散のGreenwood推定値に基づいて計算される。 Median PFS, OS, and DOR are estimated using the Kaplan-Meier method, and 90% CIs are constructed using the Brookmeyer and Crowley method. The OS rate at specific time points is also estimated using the Kaplan-Meier method and the 90% CI is calculated based on the Greenwood estimate of variance.
病勢制御率は、≧18週間にわたって安定した疾患、PR又はCRを有する患者の割合として定義され、各処置アームについて計算され、90% CIは、Clopper-Pearson正確法の使用によって推定される。 Disease control rate is defined as the proportion of patients with stable disease, PR or CR for ≧18 weeks and is calculated for each treatment arm, with 90% CIs estimated by use of the Clopper-Pearson exact method.
探索有効性評価項目
探索的有効性評価項目は、iRECISTに従って治験責任医師が決定したステージ1でのORR、PFS、DOR及び病勢制御、並びにRECIST v 1.1及びiRECISTに従って治験責任医師が決定したステージ2での客観的奏効、PFS、DOR及び病勢制御である。ORR、PFS、DOR及び病勢制御を
Exploratory Efficacy Endpoints The exploratory efficacy endpoints are ORR, PFS, DOR and disease control at Investigator-
上述したものと同じ方法の使用によって分析する DORは、CR又はPRを有する有効性評価可能な患者について導出される。 DOR analyzed by use of the same method as described above is derived for evaluable patients with CR or PR.
C.暫定分析
暫定分析は試験中に行われ、少なくとも1つの実験群がステージ1予備期への登録を完了し、患者を最低9週間追跡したときに、最も早い暫定分析を行う。必要に応じて、さらなる暫定分析を行ってもよい。事後確率を使用して、対照群と比較した実験群における臨床活性の暫定分析に基づいてさらなる登録を導くことができる。暫定分析が、実験群の活性が対照群の活性よりも高いことを示唆する場合、実験群に更に25人の患者を登録することができる(拡大期)。最終決定
C. Interim Analyzes Interim analyzes will be conducted during the study, with the earliest interim analysis occurring when at least one study arm has completed enrollment in
この第1b相試験を拡大及び終了するために、事象までの時間評価項目及び安全性データ、並びに新たな外部情報を含む全体的な利益-リスクバランス及び全データを考慮して行われる。 The expansion and completion of this Phase 1b study will take into account the overall benefit-risk balance and overall data including time-to-event endpoints and safety data, as well as new external information.
約15人の患者をステージ2の処置群に登録し、最低9週間追跡した後、暫定分析も行う。ステージ2の処置群で臨床活性が観察されない場合、その群へのさらなる登録を停止する。
Approximately 15 patients will be enrolled in the
D.他の分析
安全性分析、薬物動態分析、免疫原性分析、及びバイオマーカー分析は、実施例19に記載されているように行う。
D. Other Analyzes Safety, pharmacokinetic, immunogenicity, and biomarker analyzes are performed as described in Example 19.
実施例23.局所進行性又は転移性食道がんを有する患者における免疫療法に基づく処置併用の有効性及び安全性を評価する第Ib/II相非盲検多施設ランダム化包括的試験
A.試験計画の概要
YO39609は、食道がん患者における免疫療法に基づく処置の組み合わせの有効性、安全性、及び薬物動態を評価する第Ib/II相非盲検多施設ランダム化包括的試験である。この試験は、食道がん患者に投与した場合の免疫療法に基づく処置の組み合わせに関する予備的な有効性、安全性、及びPKデータを得るように設計されている。この試験はまた、新しい処置が利用可能になるにつれて新しい処置群を開き、最小限の臨床活性又は許容できない毒性を示す既存の処置群を閉じ、又は患者集団を変更する(例えば、以前の抗がん治療又はバイオマーカーの状態に関して)ための柔軟性を備えて設計される。
Example 23. A Phase Ib/II, Open-label, Multicenter, Randomized, Comprehensive Study Evaluating the Efficacy and Safety of Combination Immunotherapy-Based Treatments in Patients With Locally Advanced or Metastatic Esophageal Cancer. Study Design Overview YO39609 is a Phase Ib/II, open-label, multicenter, randomized, comprehensive study evaluating the efficacy, safety, and pharmacokinetics of immunotherapy-based treatment combinations in patients with esophageal cancer. This study is designed to obtain preliminary efficacy, safety, and PK data for immunotherapy-based treatment combinations when administered to patients with esophageal cancer. The trial may also open new treatment arms as new treatments become available, close existing treatment arms showing minimal clinical activity or unacceptable toxicity, or alter the patient population (e.g. designed with flexibility for cancer therapy or biomarker status).
疾患の事前の全身処置を受けたことがない食道がん患者をこの試験に登録する。適格患者を3つの処置群のうちの1つにランダム化する。ステージ1の間に疾患進行又は許容できない毒性を経験する対照群の患者は、ステージ2の異なる処置レジメンによる処置を継続するのに適格であり得る。
Esophageal cancer patients who have had no prior systemic treatment for their disease are enrolled in this study. Eligible patients are randomized to one of three treatment groups. Patients in the control group who experience disease progression or unacceptable toxicity during
ステージ1処置
ステージ1の間、食道がんを有する患者を、化学療法対照群(シスプラチン+5-FU)又は2つの実験群:チラゴルマブ及び化学療法と組み合わせたアテゾリズマブ(Atezo+チラゴルマブ+シスプラチン+5-FU)又は化学療法と組み合わせたアテゾリズマブ(Atezo+シスプラチン+5-FU)のうちの1つにランダムに割り当てる。ステージ1の処置レジメンの詳細を表84に示す。

本試験のステージ1の具体的な目的及び対応評価項目を表85に概説する。


2つの実験群の登録は2つの期で行われる:予備期、その後続く拡大期。 Enrollment of the two experimental groups occurs in two phases: a preliminary phase followed by an expansion phase.
ステージ1の間に約100~165人の患者が登録される。この亜集団内の利益及びリスクの評価を容易にするのに十分な数のTIGIT及びPD-L1発現の高い患者を確保するために、予備期中に最大約40人の患者が2つの実験群に登録される。予備期中に実験群で臨床活性が観察される場合、拡大期中に約25人の追加の患者がその群に登録され得る。試験依頼者は、所与の治処置群内への登録を遅延又は一時停止することを決定し得る。
Approximately 100-165 patients are enrolled during
最小限の臨床活性又は許容できない毒性を有する実験群は、拡大を受けない。治験実施計画書を修正することによって、試験中に新しい実験群を追加することができる。 Experimental groups with minimal clinical activity or unacceptable toxicity will not receive expansion. New experimental groups can be added during a trial by amending the protocol.
ステージ1の患者は処置群にランダムに割り当てられ、ランダム化率は、利用可能な実験群の数(例えば、予備期からの結果の分析を待って、群が追加されるか、又は群への登録が一時停止される場合)に依存し、対照群に割り当てられる可能性は35%以下であるという規定がある。有望な臨床活性を実証した実験群への登録を増加させるために、ランダム化の比率を変更することができる。ランダム化は、群特異的排除基準を考慮に入れる。患者は、その群について概説された除外基準のいずれかを満たす場合、特定の群に対して不適格である。
Patients in
対照群の患者は、RECIST v1.1に従って許容できない毒性又は疾患進行まで処置される。実験群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで処置される。がん免疫療法(CIT)(アテゾリズマブ等)によるT細胞応答(偽進行と呼ばれる)の状況では、免疫細胞浸潤によって引き起こされる腫瘍負荷の初期増加の可能性のために、RECIST v1.1による放射線学的進行は、真の疾患進行を示さない可能性がある。許容できない毒性がない場合、CIT薬物による処置を受けている間にRECIST v1.1による疾患進行の基準を満たす患者は、以下の基準の全てを満たす場合、試験処置を継続することが許可される:
-すべての利用可能なデータの再検討後に治験責任医師によって決定される臨床的利益の証拠。
-疾患の明確な進行を示す症状及び徴候(検査値、例えば、新たな又は悪化する高カルシウム血症を含む)がないこと
-疾患進行に起因し得るECOGパフォーマンスステータスの低下がないこと
-治験実施計画書で許可された医学的介入によって管理することができない重要な解剖学的部位(例えば、軟髄膜疾患)における腫瘍進行の欠如
-最初の疾患進行時に試験処置を継続するために他の処置選択肢を延期することを承認する患者の書面による同意。
Patients in the control group are treated until unacceptable toxicity or disease progression according to RECIST v1.1. Patients in the experimental group will be enrolled in the study after integrated assessment of radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as pain secondary to disease). Treat until unacceptable toxicity or loss of clinical benefit as determined by the attending physician. In the context of cancer immunotherapy (CIT)-induced T-cell responses (called pseudoprogression), radiology according to RECIST v1.1 is recommended due to the possibility of an initial increase in tumor burden caused by immune cell infiltration. progressive progression may not represent true disease progression. In the absence of unacceptable toxicity, patients who meet the criteria for disease progression by RECIST v1.1 while receiving treatment with a CIT drug are allowed to continue study treatment if they meet all of the following criteria: :
- Evidence of clinical benefit as determined by the investigator after review of all available data.
- Absence of symptoms and signs (including laboratory values, e.g., new or worsening hypercalcemia) indicative of definite disease progression - Absence of decline in ECOG performance status attributable to disease progression - Conducting the study Absence of tumor progression in critical anatomic sites (e.g., leptomeningeal disease) that cannot be managed by protocol-allowed medical intervention - other treatments to continue study treatment at initial disease progression Written consent of the patient authorizing deferment of choice.
ステージ2の処置
RECIST v1.1による疾患進行を経験した対照群の患者は、適格基準を満たし、ステージ2群が登録のためにオープンであるならば、ステージ2の間に異なる処置の組み合わせを受ける選択肢が与えられる。ステージ2の処置レジメンは、アテゾリズマブ+チラゴルマブである。
許容できない毒性を経験した対照群の患者は、メディカルモニターの承認が得られた後、ステージ2の処置に適格となり得る。ステージ2の処置は、患者がステージ1のRECIST v1.1又は許容できない毒性による疾患進行を経験した後3ヶ月以内に開始しなければならず、治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで継続する。
Patients in the control group who experience unacceptable toxicity may be eligible for
本試験のステージ2の具体的な目的及び対応評価項目を表86に概説する。


ステージ2の処置は、患者がステージ1のRECIST v1.1又は許容できない毒性による疾患進行を経験した後3ヶ月以内に開始しなければならず、治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで継続する。しかしながら、患者は可能な限り早くステージ2の処置を開始することが推奨される。
試験依頼者はまた、必要に応じて、安全性データ、予備的有効性データ及び支援情報(例えば、バイオマーカー研究データ)の再検討に基づいて、ステージ2の処置群への登録を中止することを決定し得る。
Sponsors may also discontinue enrollment in
A.試験終了及び試験期間
試験の終了は、最後の患者が最後の来院を完了した日(電話又は現場での来院によって行われる生存フォローアップ来院を含む)として定義される。
A. End of Study and Study Duration End of study is defined as the date the last patient completed the last visit (including survival follow-up visits conducted by telephone or on-site visit).
最初の患者のスクリーニングから試験終了までの試験の全長は、約3~6年である。 The total length of the trial, from initial patient screening to study termination, is approximately 3-6 years.
B.試験計画の根拠及び患者集団
この試験は、食道がん患者における初期シグナルを同定し、概念実証臨床データを確立することによって、がん免疫療法(CIT)の組み合わせの開発を加速するように設計されている。
B. Study Design Rationale and Patient Population This study is designed to accelerate the development of cancer immunotherapy (CIT) combinations by identifying early signals and establishing proof-of-concept clinical data in patients with esophageal cancer. ing.
CITは、並外れた成功を実証しており、複数の進行性悪性腫瘍にわたって有意な生存利益が観察されている。現在、普及しているCITアプローチは、CTLA-4及びPD-L1/PD-1等のT細胞共阻害性表面受容体を同定及び標的化することによって、免疫回避機構を回避し、抗腫瘍応答を再活性化することである。これらの標的は様々ながん適応症について顕著な臨床的成功をもたらしたが、進行中の研究は、連続的な抗腫瘍免疫応答の生成に必要な一連の段階的事象を示している(Chen and Mellman,Immunity,39:1-10,2013)。各事象は有効な応答にとって重要であり、それぞれがいくつかの腫瘍免疫回避機構の影響を受けやすい。したがって、腫瘍免疫回避に関与する様々な因子を同定し回避する必要性は、抗腫瘍免疫応答を伝播し、おそらく併用レジメンによってCITの分野を進歩させるために重要である。 CIT has demonstrated extraordinary success, with significant survival benefits observed across multiple advanced malignancies. Currently popular CIT approaches circumvent immune evasion mechanisms by identifying and targeting T-cell co-inhibitory surface receptors, such as CTLA-4 and PD-L1/PD-1, to circumvent immune evasion mechanisms and enhance anti-tumor responses. is to reactivate Although these targets have provided remarkable clinical success for a variety of cancer indications, ongoing research indicates a series of stepwise events required to generate a continuous anti-tumor immune response (Chen and Mellman, Immunity, 39:1-10, 2013). Each event is critical for an effective response and each is susceptible to several tumor immune evasion mechanisms. Therefore, the need to identify and evade various factors involved in tumor immune evasion is important for propagating anti-tumor immune responses and possibly advancing the field of CIT through combination regimens.
食道がんは、5年生存率が転移性疾患の状況では5%、局所進行性疾患の状況では24%である、満たされていない医学的ニーズの高い疾患である。進行性又は転移性食道がんを有する患者の処置選択肢は限られており、予後不良であり、全生存利益は最小限である。したがって、この患者集団に対して、より効果的でより忍容性の高い処置が引き続き必要とされている。 Esophageal cancer is a disease of high unmet medical need, with a 5-year survival rate of 5% in the setting of metastatic disease and 24% in the setting of locally advanced disease. Patients with advanced or metastatic esophageal cancer have limited treatment options, poor prognosis, and minimal overall survival benefit. Therefore, there is a continuing need for more effective and better tolerated treatments for this patient population.
実施例24.YO試験39609試験のための材料及び方法
この設定で事前全身治療を受けたことがない食道がん患者約100~165人を、YO 39609試験中に対照群及び実験群にランダム化する。
Example 24. Materials and Methods for the YO Study 39609 Study Approximately 100-165 patients with esophageal cancer who have not received prior systemic therapy in this setting are randomized into control and experimental groups during the YO 39609 study.
A.ステージ1の選択基準
患者は、ステージ1に適格であるためには、以下に概説される以下の基準の全てを満たさなければならない:
●署名時の年齢が18歳以上
●ECOGパフォーマンスステータスが0又は1
●局所進行性又は転移性疾患における扁平上皮癌腫又は食道の腺癌の組織学的又は細胞学的に確認された診断。
-転移性食道がんの確定診断は、臨床データ及び放射線データに関連して組織病理学的データを評価することによって行われる。
●以下を除いて、食道がんの事前の全身処置なし:
-局所進行性の状況で化学療法で処置された患者:化学療法の最後の投薬から6ヶ月後の転移の発生。
●腺癌を有する患者について:疾患の最初の診断時に以前に収集され評定された腫瘍組織においてISH陰性であると文書化されたHER2発現のがないこと。
-HER2陰性状態を、ISH非増幅(HER2対CEP17の比<2.0又は単一プローブ平均HER2遺伝子コピー数<4シグナル/細胞)IHC 0又はIHC 1+(複数の検査結果が利用可能であり、すべての結果が包含基準の定義を満たしていない場合、患者の適格性を確立するために、すべての結果をメディカルモニターと議論すべきである)に基づいて決定する。
●治験責任医師が決定した平均余命≧3ヶ月
●クレアチニンクリアランス(CrCl)≧50mL/分(Cockcroft-Gault式を使用して計算)
●遡及的中央検査によるIHC及び/又はさらなるバイオマーカー状態によるPD-L1及びTIGITレベルの決定に適した代表的な腫瘍標本の入手可能性。
-ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、メディカルモニターの承認後に腫瘍組織の保管を提出してもよく、ただし、組織が登録前6ヶ月以内に行われた生検から得られ、患者が生検の時点からいかなる抗がん治療も受けたことがないことを条件とする。
-パラフィンブロック(好ましい)におけるFFPE腫瘍標本、又は染色されていない新たに切断された連続切片を含む少なくとも16枚のスライドを、関連する病理報告とともに提出しなければならない。10~15枚のスライドしか入手できない場合、メディカルモニターの承認後、患者は依然として試験に適格であり得る。
A. Inclusion Criteria for
● Age at the time of signature is 18 years or older ● ECOG performance status is 0 or 1
- Histologically or cytologically confirmed diagnosis of squamous cell carcinoma or adenocarcinoma of the esophagus in locally advanced or metastatic disease.
- A definitive diagnosis of metastatic esophageal cancer is made by evaluating histopathological data in conjunction with clinical and radiological data.
- No prior systemic treatment for esophageal cancer, except for:
- Patients treated with chemotherapy in a locally advanced setting: occurrence of
• For patients with adenocarcinoma: no documented ISH-negative HER2 expression in tumor tissue previously collected and assessed at initial diagnosis of disease.
- HER2-negative status defined as ISH unamplified (HER2 to CEP17 ratio <2.0 or single-probe average HER2 gene copy number <4 signals/cell)
Investigator-determined life expectancy ≥3 months Creatinine clearance (CrCl) ≥50 mL/min (calculated using the Cockcroft-Gault formula)
• Availability of representative tumor specimens suitable for determination of PD-L1 and TIGIT levels by IHC and/or further biomarker status by retrospective central examination.
- A baseline tumor tissue sample is collected from all patients, preferably by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, archival tumor tissue may be submitted after medical monitor approval, provided that the tissue was obtained from a biopsy performed within 6 months prior to enrollment. provided that the patient had not received any anticancer therapy from the time of biopsy.
- FFPE tumor specimens in paraffin blocks (preferred) or at least 16 slides containing unstained freshly cut serial sections must be submitted along with the relevant pathology report. Patients may still be eligible for the study after medical monitor approval if only 10-15 slides are available.
B.ステージ1及びステージ2の選択基準
患者は、ステージ1及び2に適格であるためには、以下に概説される以下の基準の全てを満たさなければならない:
●署名済みインフォームドコンセントフォーム
●治験責任医師の判断による、試験治験実施計画書を遵守する能力
●RECIST v1.1による測定可能な疾患 以前に放射線照射された病変は、放射線照射後にその部位で進行性疾患が明確に文書化されている場合にのみ、測定可能な疾患とみなすことができる。
●試験処置の開始の前、14日以内に得られた、以下の臨床検査結果によって定義される適切な血液学的機能及び終末器官機能:
-顆粒球コロニー刺激因子支持なしでANC≧1.5×109/L(1500/μL)
-リンパ球数≧0.5×109/L(500/μL).
-輸血なしで血小板数≧100×109/L(100,000/μL)
-ヘモグロビン≧90g/L(9g/dL)この基準を満たすために患者を輸血することができる。
-AST、ALT及びアルカリホスファターゼ(ALP)≦2.5×正常値の上限(ULN)、ただし、以下の例外を除く:
文書化された肝臓転移を有する患者:AST及びALT≦5×ULN
文書化された肝臓転移又は骨転移を有する患者:ALP≦5×ULN。
-ビリルビン≦1.5×ULN、ただし以下を除く:
既知のギルバート病患者:ビリルビンレベル≦3×ULN。
-アルブミン≧25g/L(2.5g/dL)。
-治療的抗凝固療法を受けていない患者の場合:INR又はaPTT≦1.5×ULN。
-治療的抗凝固薬を投与されている患者:安定な抗凝固薬レジメン
●以下の例外を除いて、スクリーニング時のHIV検査陰性:スクリーニング時のHIV検査陽性の患者は、抗レトロウイルス療法で安定しており、CD4数が200/μL以上であり、検出不能なウイルス量を有するという条件で適格である。
●スクリーニング時のB型肝炎表面抗原(HBsAg)検査陰性
●スクリーニング時の全B型肝炎コア抗体(HBcAb)検査陰性、又はスクリーニング時の全HBcAb検査陽性、続いてスクリーニング時の定量的B型肝炎ウイルス(HBV)DNA<500IU/mL。HBV DNA検査は、全HBcAb検査が陽性である患者に対してのみ実施される。
●スクリーニング時にC型肝炎ウイルス(HCV)抗体検査陰性、又はスクリーニング時にHCV抗体検査陽性後、HCV RNA検査陰性。HCV RNA検査は、HCV抗体検査陽性の患者に対してのみ行う。
●妊娠の可能性のある女性の場合:禁欲(異性間の性交を控える)又は避妊手段を使用することの合意、及び卵の提供を控えることの同意
●男性の場合:禁欲を維持する(異性間の性交を控える)こと、又は避妊手段を使用すること、及び精子の提供を控えることの同意
B. Inclusion Criteria for
- Signed informed consent form - Ability to comply with the study protocol, as determined by the investigator - Measurable disease by RECIST v1.1 - Previously irradiated lesions progressing at the site after irradiation A sexually transmitted disease can only be considered a measurable disease if it is clearly documented.
- Adequate hematologic and end-organ function as defined by the following laboratory test results obtained within 14 days prior to initiation of study treatment:
- ANC ≧1.5×10 9 /L (1500/μL) without granulocyte colony stimulating factor support
- Lymphocyte count ≧0.5×10 9 /L (500/μL).
- Platelet count ≧100×10 9 /L (100,000/μL) without transfusion
- Hemoglobin ≥ 90 g/L (9 g/dL) Patients can be transfused to meet this criterion.
- AST, ALT and alkaline phosphatase (ALP) < 2.5 x upper limit of normal (ULN), with the following exceptions:
Patients with documented liver metastases: AST and ALT ≤ 5 x ULN
Patients with documented liver or bone metastases: ALP ≤ 5 x ULN.
- Bilirubin ≤ 1.5 x ULN, except:
Patients with known Gilbert's disease: bilirubin level < 3 x ULN.
- Albumin > 25 g/L (2.5 g/dL).
- For patients not receiving therapeutic anticoagulation: INR or aPTT ≤ 1.5 x ULN.
- Patients on therapeutic anticoagulants: Stable anticoagulant regimen Negative HIV test at screening, with the following exceptions: Patients with a positive HIV test at screening are stable on antiretroviral therapy Eligible if they have a CD4 count of ≥200/μL and have an undetectable viral load.
Negative hepatitis B surface antigen (HBsAg) test at screening Negative total hepatitis B core antibody (HBcAb) test at screening or positive total HBcAb test at screening followed by quantitative hepatitis B virus at screening (HBV) DNA <500 IU/mL. HBV DNA testing is performed only on patients with a positive overall HBcAb test.
●Negative hepatitis C virus (HCV) antibody test at screening, or negative HCV RNA test after positive HCV antibody test at screening. HCV RNA testing is performed only for patients who test positive for HCV antibodies.
For women of childbearing potential: consent to abstinence (abstinence from heterosexual intercourse) or use contraceptives, and consent to refrain from donating eggs consent to refrain from sexual intercourse) or to use contraceptives and to refrain from donating sperm
C.ステージ2の選択基準
患者は、ステージ2に適格であるためには、以下に概説される以下の基準の全てを満たさなければならない:
●ECOGパフォーマンスステータスが0、1、又は2。
●ステージ1の間に対照群にランダムに割り当てられた患者:ステージ2に入ることについてのメディカルモニターの承認が得られているならば、許容できない毒性、又は対照処置を受けている間のRECIST v 1.1による疾患進行を経験した後3ヶ月以内にステージ2の処置を開始する能力。
●クレアチニン≦1.5×ULN又はCrCl≧30mL/分(Cockcroft-Gault式を使用して計算)。
●RECIST v1.1による許容できない毒性又は疾患進行のためにステージ1の中止時に実施された生検からの腫瘍標本の入手可能性(臨床的に実施可能とみなされる場合)。
C. Inclusion Criteria for
• ECOG performance status of 0, 1, or 2;
• Patients randomly assigned to the control arm during Stage 1: Unacceptable toxicity, if medical monitor approval for entry into
• Creatinine ≤ 1.5 x ULN or CrCl ≥ 30 mL/min (calculated using the Cockcroft-Gault formula).
• Availability of tumor specimens from biopsies performed at
D.除外基準
以下の基準のいずれかを満たす患者は、ステージ1及びステージ2の間の登録から除外される:
D. Exclusion Criteria Patients meeting any of the following criteria are excluded from enrollment between
ステージ1の除外基準
以下の基準のいずれかを満たす患者は、ステージ1から除外される:
●治験実施計画書に規定された試験処置のいずれかによる事前処置。
●既知の聴覚障害を有する患者。
●NCI CTCAE v4.0基準によって定義されるグレード≧2の末梢神経障害。
●患者が5-FU毒性になりやすい既知のジヒドロピリミジンデヒドロゲナーゼ欠損症又はチミジル酸シンターゼ遺伝子多型。
• Prior treatment with any protocol-specified study treatment.
●Patients with known hearing impairment.
• Grade ≥2 peripheral neuropathy as defined by the NCI CTCAE v4.0 criteria.
• Known dihydropyrimidine dehydrogenase deficiency or thymidylate synthase gene polymorphism that predisposes the patient to 5-FU toxicity.
ステージ1及びステージ2の除外基準
以下の基準のいずれかを満たす患者は、ステージ1及びステージ2から除外される:
●過去の病歴又は食道瘻孔の随伴症状、又は内視鏡超音波によるT4分類等の臨床評定又は画像化によって食道瘻孔を発症する高いリスク。
●症候性、未処置、又は活発に進行する中枢神経系(CNS)転移。処置されたCNS病変を有する無症候性患者は、以下の基準の全てが満たされるならば適格である:
-RECIST v1.1による測定可能な疾患はCNS外に存在しなければならない
-患者は頭蓋内出血又は脊髄出血の病歴がない。
-患者は、試験処置の開始前7日間以内の定位放射線療法、試験処置の開始前14日間以内の全脳放射線療法、又は試験処置の開始前28日間以内の神経外科的摘出を受けたことがない。
-患者は、CNS疾患の治療としてのコルチコステロイドに対する継続的な要求がない。安定な用量での抗痙攣療法が許容される。
-転移は小脳又はテント上領域(すなわち、中脳、橋、延髄、又は脊髄への転移がない)に限定される。
-CNSに向けられた治療の完了と試験処置の開始との間の暫定進行の証拠はない。
-スクリーニング時に新たに検出されたCNS転移を有する無症候性患者は、放射線療法又は手術を受けた後に試験に適格であり、スクリーニング脳スキャンを繰り返す必要はない。
●スクリーニング時の活動性EBV感染及び既知又は疑われる慢性活動性EBV感染 EBV IgG及び/又はエプスタイン・バー・ウイルス核抗原(EBNA)について陽性である患者は、EBV IgM及び/又はEBV PCRが陰性である場合にのみ適格である。
●軟髄膜疾患の病歴。
●制御されない腫瘍関連疼痛。鎮痛薬を必要とする患者は、試験登録時に安定したレジメンでなければならない。緩和的放射線療法に適した症候性病変(例えば、神経インピンジメントを引き起こす骨転移又は転移)は、登録前に処置しなければならない。患者は、放射線の影響から回復されなければならない。必要とされる最低限の回復期間はない。更なる成長(例えば、脊髄圧迫に現在関連していない硬膜外転移)を伴う機能障害又は難治性疼痛を引き起こす可能性が高い無症候性転移性病変は、登録前に適切な場合、局所領域治療について検討されるべきである。
●制御されない胸水、心膜滲出液、又は再発性排液処置を必要とする腹水(毎月1回又はより頻繁に)留置カテーテル(例えば、PLEURX(登録商標))を有する患者は許容される。
●制御不能又は症候性の高カルシウム血症(イオン化カルシウム>1.5mmol/L、カルシウム>12mg/dL、又は補正カルシウム>ULN)。
●重症筋無力症、筋炎、自己免疫性肝炎、全身性エリテマトーデス、関節リウマチ、炎症性腸疾患、抗リン脂質抗体症候群、ウェゲナー肉芽腫症、シェーグレン症候群、ギラン・バレー症候群、又は多発性硬化症を含むがこれらに限定されない自己免疫疾患又は免疫不全活動が活動性であるもの、又はその病歴、ただし、以下を除く:
Exclusion Criteria for
• High risk of developing an esophageal fistula by prior medical history or concomitant symptoms of an esophageal fistula, or by clinical assessment or imaging such as T4 classification by endoscopic ultrasound.
• Symptomatic, untreated, or actively progressing central nervous system (CNS) metastases. Asymptomatic patients with treated CNS lesions are eligible if all of the following criteria are met:
- Measurable disease by RECIST v1.1 must be present outside the CNS - Patient has no history of intracranial or spinal cord hemorrhage.
- Patient has had stereotactic radiotherapy within 7 days prior to the start of study treatment, whole brain radiotherapy within 14 days prior to the start of study treatment, or neurosurgical resection within 28 days prior to the start of study treatment do not have.
- Patient has no ongoing need for corticosteroids as treatment for CNS disease. Anticonvulsant therapy at stable doses is acceptable.
- Metastases are restricted to the cerebellar or supratentorial regions (ie, no metastases to the midbrain, pons, medulla oblongata, or spinal cord).
- No evidence of interim progression between completion of CNS-directed therapy and initiation of study treatment.
- Asymptomatic patients with newly detected CNS metastases at screening are eligible for the study after undergoing radiotherapy or surgery and do not require repeat screening brain scans.
Active EBV infection at screening and known or suspected chronic active EBV infection Patients who are positive for EBV IgG and/or Epstein-Barr virus nuclear antigen Eligible only in some cases.
A history of leptomeningeal disease.
• Uncontrolled tumor-related pain. Patients requiring analgesics must be on a stable regimen at study entry. Symptomatic lesions amenable to palliative radiotherapy (eg bone metastases or metastases causing nerve impingement) must be treated prior to enrollment. Patients must recover from the effects of radiation. There is no minimum recovery period required. Asymptomatic metastatic lesions likely to cause functional impairment or intractable pain with further growth (e.g., epidural metastases not currently associated with spinal cord compression) should be treated with locoregional, if appropriate, prior to enrollment. Treatment should be considered.
• Patients with uncontrolled pleural effusions, pericardial effusions, or ascites requiring recurrent drainage procedures (monthly or more frequently) with indwelling catheters (eg, PLEURX®) are permitted.
• Uncontrolled or symptomatic hypercalcemia (ionized calcium >1.5 mmol/L, calcium >12 mg/dL, or corrected calcium > ULN).
Myasthenia gravis, myositis, autoimmune hepatitis, systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease, antiphospholipid antibody syndrome, Wegener's granulomatosis, Sjögren's syndrome, Guillain-Barré syndrome, or multiple sclerosis Active or history of autoimmune disease or immunodeficiency activity, including but not limited to, excluding:
甲状腺補充ホルモンを服用している自己免疫関連甲状腺機能低下症の病歴を有する患者が試験に適格である。 Patients with a history of autoimmune-related hypothyroidism taking thyroid replacement hormone are eligible for the study.
インスリンレジメンを受けている制御された1型糖尿病患者は試験に適格である。
Patients with controlled
湿疹、乾癬、慢性単純性苔癬、又は皮膚症状のみを伴う白斑(例えば、乾癬性関節炎を有する患者は除外される)を有する患者は、以下の条件の全てが満たされるならば、試験に適格である。
-発疹が覆っている体表面積は10%未満でなければならない。
-疾患はベースラインで十分に制御されており、低効力の局所コルチコステロイドのみを必要とする
-過去12ヶ月以内にソラレン+紫外線A照射、メトトレキサート、レチノイド、生物学的薬剤、経口カルシニューリン阻害剤、又は高効力若しくは経口コルチコステロイドを必要とする基礎症状の急性増悪の発生がない
●特発性肺線維症、器質化肺炎(例えば、閉塞性細気管支炎)、薬物誘発性間質性肺炎、若しくは特発性間質性肺炎の病歴、又はスクリーニング胸部コンピューター断層撮影(CT)スキャンでの活動性間質性肺炎の証拠。放射線領域における放射線肺臓炎(線維症)の病歴は許容される。
●活動性結核。
●試験処置の開始前3ヶ月以内の有意な心血管疾患(New York Heart Association Class II以上の心疾患、心筋梗塞、脳血管障害等)、不安定な不整脈又は不安定狭心症。
●試験処置の開始前4週間以内の大きな外科的処置(診断以外)、又は試験中の大きな外科的処置の必要性の予想
●適切に処置された子宮頸部上皮内癌腫、非黒色腫皮膚がん、限局性前立腺がん、上皮内乳管癌腫、又はステージI子宮がん等、転移又は死亡のリスクが無視できる(例えば、5年OS率>90%)悪性腫瘍を除いて、スクリーニング前2年以内の食道がん以外の悪性腫瘍の病歴。
●試験処置の開始前4週間以内の重度の感染症(感染症、菌血症、又は重度の肺炎の合併症のための入院が含まれるが、これらに限定されない)
●試験処置開始前2週間以内の治療用経口又はIV抗生物質による処置
●予防用抗生物質(例えば、尿路感染症又は慢性閉塞性肺疾患の増悪を予防するため)を受ける患者は試験に適格である;
●事前の同種異系幹細胞又は固形臓器移植
●治験薬の使用を禁忌にする任意の他の疾患、代謝機能不全、身体検査所見、又は臨床検査所見は、結果の解釈に影響を及ぼす可能性があり、又は患者を処置合併症のリスクが高くなる可能性がある。
●試験処置の開始前4週間以内、又はアテゾリズマブ処置中若しくはアテゾリズマブの最終投薬後5ヶ月以内の生弱毒化ワクチンによる処置
●HBVのための抗ウイルス療法による現在の処置。
●試験薬又はその賦形剤のいずれかに対する既知のアレルギー又は過敏症。
●試験処置の開始前28日以内の治験療法による処置。
●抗CTLA-4、抗PD-1、抗PD-L1及び抗TIGIT治療抗体を含むCD137アゴニスト又は免疫チェックポイント遮断療法による事前処置。
●試験処置の開始前の4週間以内又は5つの薬物除去半減期(いずれか長い方)以内の全身免疫刺激剤(限定されないが、インターフェロン及びインターロイキン2[IL-2]を含む)による処置。
●以下を除いて、試験処置の開始前2週間以内の全身免疫抑制薬(限定されないが、コルチコステロイド、シクロホスファミド、アザチオプリン、メトトレキサート、サリドマイド及び抗TNF-α剤を含む)による処置、又は試験処置中の全身免疫抑制薬の必要性の予測:
-急性低用量の全身免疫抑制薬又は1回パルス用量の全身免疫抑制薬(例えば、造影剤アレルギーのための48時間のコルチコステロイド)を受けた患者は、メディカルモニターの承認が得られた後、試験に適格である。
-ミネラルコルチコイド(例えば、フルドロコルチゾン)、慢性閉塞性肺疾患(COPD)若しくは喘息のためのコルチコステロイド、又は起立性低血圧若しくは副腎機能不全のための低用量コルチコステロイドを受けた患者は試験に適格である。
●キメラ若しくはヒト化抗体又は融合タンパク質に対する重度のアレルギーアナフィラキシー反応の病歴。
●チャイニーズハムスター卵巣細胞生成物又はアテゾリズマブ及びチラゴルマブ製剤の任意の成分に対する既知の過敏症。
●妊娠若しくは授乳、又は試験処置中又はアテゾリズマブの最終投与後5ヶ月以内及びチラゴルマブの最終投与後5ヶ月以内に妊娠する意図。妊娠可能な女性は、試験処置の開始前14日以内に血清妊娠検査結果が陰性でなければならない。
Patients with eczema, psoriasis, lichen simplex chronicus, or vitiligo with skin manifestations only (e.g., patients with psoriatic arthritis are excluded) are eligible for the study if all of the following conditions are met: is.
- The rash must cover less than 10% of body surface area.
- Disease is well controlled at baseline, requiring only low-potency topical corticosteroids - Psoralen + UVA radiation, methotrexate, retinoids, biologic agents, oral calcineurin inhibitors within the past 12 months , or no acute exacerbation of underlying symptoms requiring high-potency or oral corticosteroids Idiopathic pulmonary fibrosis, organizing pneumonia (e.g., bronchiolitis obliterans), drug-induced interstitial pneumonia, or history of idiopathic interstitial pneumonia or evidence of active interstitial pneumonia on screening chest computed tomography (CT) scan. A history of radiation pneumonitis (fibrosis) in the radiology area is acceptable.
● Active tuberculosis.
- Significant cardiovascular disease (New York Heart Association Class II or greater heart disease, myocardial infarction, cerebrovascular accident, etc.), unstable arrhythmia or unstable angina pectoris within 3 months prior to initiation of study treatment.
o Major surgical intervention (other than diagnosis) within 4 weeks prior to initiation of study procedure or anticipation of need for major surgical procedure during study o Appropriately treated cervical carcinoma in situ, non-melanoma skin pre-screening2, except for malignancies with negligible risk of metastasis or death (e.g., 5-year OS >90%) such as cancer, localized prostate cancer, ductal carcinoma in situ, or stage I uterine cancer History of malignancy other than esophageal cancer within 1 year.
- Severe infection within 4 weeks prior to initiation of study treatment (including, but not limited to, hospitalization for complications of infection, bacteremia, or severe pneumonia)
- Treatment with therapeutic oral or IV antibiotics within 2 weeks prior to initiation of study treatment - Patients receiving prophylactic antibiotics (e.g., to prevent exacerbation of urinary tract infection or chronic obstructive pulmonary disease) are eligible for the study is;
- Prior allogeneic stem cell or solid organ transplantation - Any other disease, metabolic dysfunction, physical examination findings, or laboratory findings that contraindicate study drug use may affect interpretation of results or may put the patient at increased risk of procedural complications.
• Treatment with a live attenuated vaccine within 4 weeks prior to initiation of study treatment or during atezolizumab treatment or within 5 months after the last dose of atezolizumab • Current treatment with antiviral therapy for HBV.
• Known allergy or hypersensitivity to the study drug or any of its excipients.
- Treatment with study therapy within 28 days prior to initiation of study treatment.
- Pretreatment with CD137 agonist or immune checkpoint blockade therapy including anti-CTLA-4, anti-PD-1, anti-PD-L1 and anti-TIGIT therapeutic antibodies.
• Treatment with systemic immune stimulants (including but not limited to interferon and interleukin-2 [IL-2]) within 4 weeks or 5 drug elimination half-lives (whichever is longer) prior to initiation of study treatment.
- Treatment with systemic immunosuppressants (including but not limited to corticosteroids, cyclophosphamide, azathioprine, methotrexate, thalidomide, and anti-TNF-α agents) within 2 weeks prior to initiation of study treatment, except: or prediction of need for systemic immunosuppressants during study treatment:
- Patients who received acute low-dose systemic immunosuppressants or single pulse-dose systemic immunosuppressants (e.g., 48-hour corticosteroids for contrast allergy) after obtaining medical monitor approval , are eligible for the test.
- patients who have received mineralocorticoids (e.g. fludrocortisone), corticosteroids for chronic obstructive pulmonary disease (COPD) or asthma, or low-dose corticosteroids for orthostatic hypotension or adrenal insufficiency Eligible for testing.
• History of severe allergic anaphylactic reactions to chimeric or humanized antibodies or fusion proteins.
• Known hypersensitivity to Chinese Hamster Ovary Cell Products or any component of Atezolizumab and Tiragolumab formulations.
- Pregnancy or lactation, or intention to become pregnant during study treatment or within 5 months after the last dose of atezolizumab and within 5 months after the last dose of tiragolumab. Women of childbearing potential must have a negative serum pregnancy test result within 14 days prior to initiation of study treatment.
E.許可された治療
患者は、試験中に以下の治療法を使用することが許される。
●経口避妊薬
●ホルモン補充療法
●予防的又は治療的抗凝固療法(安定用量のワーファリン又は低分子量ヘパリン等)
●不活化インフルエンザワクチン接種
●食欲刺激剤として投与される酢酸メゲストロール
●ミネラルコルチコイド(例えば、フルドロコルチゾン)
●慢性閉塞性肺疾患又は喘息のために投与されるコルチコステロイド
●起立性低血圧又は副腎皮質機能不全のために投与される低用量コルチコステロイド
●以下に概説する緩和的放射線療法(例えば、既知の骨転移の処置又は疼痛の症候性軽減):
E. Allowed Treatments Patients will be allowed to use the following treatments during the study.
● Oral contraceptives ● Hormone replacement therapy ● Prophylactic or therapeutic anticoagulant therapy (such as stable-dose warfarin or low-molecular-weight heparin)
Inactivated influenza vaccination Megestrol acetate given as an appetite stimulant Mineralcorticoids (eg fludrocortisone)
o Corticosteroids given for chronic obstructive pulmonary disease or asthma o Low-dose corticosteroids given for orthostatic hypotension or adrenal insufficiency o Palliative radiation therapy as outlined below (e.g., Treatment of known bone metastases or symptomatic relief of pain):
緩和的放射線療法は、腫瘍標的病変(例えば、照射される病変は、測定可能な疾患の唯一の部位であってはならない)の評定を妨げない限り許容される。アテゾリズマブによる処置は、緩和放射線療法中に継続され得る。
●以下に概説されるような局所療法(例えば、外科手術、定位的放射線手術、放射線療法、高周波アブレーション):
3つ以下の病変の制御のために局所療法を必要とする混合応答を経験している患者は、メディカルモニターの承認が得られた後も試験処置を継続するのに依然として適格であり得る。標的病変に向けた局所療法を受けている患者は、もはや放射線学的応答については評価可能ではないが、進行については評価可能なままである。
Palliative radiotherapy is permissible as long as it does not interfere with the assessment of tumor target lesions (eg, the irradiated lesion should not be the only site of measurable disease). Treatment with atezolizumab may be continued during palliative radiotherapy.
- Local therapy (e.g., surgery, stereotactic radiosurgery, radiotherapy, radiofrequency ablation) as outlined below:
Patients experiencing a mixed response requiring local therapy for control of 3 or fewer lesions may still be eligible to continue study treatment after obtaining medical monitor approval. Patients receiving local therapy directed at target lesions are no longer evaluable for radiological response but remain evaluable for progression.
抗ヒスタミン剤、解熱剤、及び/又は鎮痛剤による前投薬は、治験責任医師の裁量で、2回目以降のアテゾリズマブ注入のためにのみ投与され得る。 Premedication with antihistamines, antipyretics, and/or analgesics may be administered only for the second and subsequent atezolizumab infusions, at the discretion of the Investigator.
注入に関連する症状を経験する患者は、アセトアミノフェン、イブプロフェン、ジフェンヒドラミン、及び/又はH2受容体アンタゴニスト(例えば、ファモチジン、シメチジン)、又は現地の標準診療による同等の薬物で対症療法で処置することができる。呼吸困難、低血圧症、喘鳴、気管支痙攣、頻脈、酸素飽和度低下、又は呼吸促拍によって現れる重度の注入関連事象は、臨床上適応がある支持療法(例えば、酸素補充及びβ2アドレナリン作用性アゴニスト)によって管理されなければならない。 Patients experiencing infusion-related symptoms should be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or H2 receptor antagonists (e.g., famotidine, cimetidine), or equivalent drugs according to local standard practice. can be done. Severe infusion-related events manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, oxygen desaturation, or rapid breathing should be treated with clinically indicated supportive care (e.g., supplemental oxygen and β2- adrenergic must be administered by a sexual agonist).
F.投薬及び投与
以下の処置群の患者は、放射線学的及び生化学的データ、局所生検結果(利用可能な場合)、及び臨床状態(例えば、疾患に続発する疼痛等の症候性の悪化)の統合評定の後に治験責任医師によって決定される許容できない毒性又は臨床的利益の喪失まで、概説される処置を受ける。
F. Dosing and Administration Patients in the following treatment groups will be provided with radiological and biochemical data, local biopsy results (if available), and clinical status (e.g., worsening of symptoms such as pain secondary to disease). Receive the treatment outlined until unacceptable toxicity or loss of clinical benefit as determined by the Investigator after the pooled assessment.
アテゾリズマブ+チラゴルマブ+シスプラチン+5-フルオロウラシル群
アテゾリズマブ+チラゴルマブ+シスプラチン+5-FU群の患者は、表87に概説される処置を受ける。

アテゾリズマブ+シスプラチン+5-フルオロウラシル群
アテゾリズマブ+シスプラチン+5-FU群の患者は、表88に概説される処置を受ける。

対照群(シスプラチン+5-FU)
シスプラチンは、最初の6つの21日間サイクルの1日目に80mg/m2の用量で120分間にわたってIV注入によって投与される。5-FUを、各21日間サイクルの1日目から開始して800mg/m2/24時間の用量で1~5日目(120時間)にわたって連続IV注入によって投与する。シスプラチン治療は、許容できない毒性が生じない限り、又は患者が何らかの理由で試験処置から離脱しない限り、合計6サイクル継続する。シスプラチン+5-FU対照群の患者は、RECIST v1.1による許容できない毒性又は疾患進行まで処置を受ける。
Control group (cisplatin + 5-FU)
Cisplatin is administered by IV infusion over 120 minutes at a dose of 80 mg/m 2 on
対照群(アテゾリズマブ+チラゴルマブ)のステージ2の処置
アテゾリズマブ+チラゴルマブ群の患者は、表89に概説される処置を受ける。

RECIST v1.1による疾患進行を経験した患者は、適格基準を満たし、試験のステージ2群が登録のためにオープンであるならば、ステージ2の間に異なる処置の組み合わせを受ける選択肢が与えられる。
Patients who experience disease progression according to RECIST v1.1 will be given the option to receive different treatment combinations during
許容できない毒性を経験した患者は、適格基準を満たし、メディカルモニターの承認が得られた後であれば、ステージ2の間に処置を受けるのに適格となり得る。ステージ2の処置は、患者が疾患の進行又は許容できない毒性を経験した後3ヶ月以内に開始しなければならない。ステージ1の間の疾患進行又は許容できない毒性の前又はその時点で行われる腫瘍評定は、主要評定がステージ2の処置開始(すなわち、サイクル1の1日目)前28日以内に行われるならば、ステージ2のベースライン評定として機能し得る。ステージ2の処置は、治験責任医師によって決定された許容できない毒性又は臨床的利益の喪失まで継続する。
Patients who experience unacceptable toxicity may be eligible to receive treatment during
アテゾリズマブ注入は、表90に概説される指示に従って投与される。

チラゴルマブ注入は、表91に概説される指示に従って投与される。

G.安全性評価相
アテゾリズマブ+チラゴルマブ+シスプラチン+5-FUアームにおける潜在的な重複毒性を説明するために、安全性評価を可能にするために約6人の患者が登録された後、登録を中断する。安全性評定は、少なくとも1用量の処置(すなわち、所与の組み合わせに対して各薬剤の1回の用量)を受け、少なくとも1つの完全な処置サイクル中に安全性フォローアップを完了した最低6人の患者からの安全性データに基づく。組み合わせが十分に安全であると判定された場合、その群で登録が再開される。
G. Safety Evaluation Phase To account for potential overlapping toxicities in the atezolizumab + tiragolumab + cisplatin + 5-FU arm, enrollment will be discontinued after approximately 6 patients have been enrolled to allow for safety assessment. Safety assessment will consist of a minimum of 6 subjects who received at least 1 dose of treatment (i.e., 1 dose of each drug for a given combination) and who completed safety follow-up during at least 1 full treatment cycle. based on safety data from patients with If the combination is determined to be sufficiently safe, enrollment will resume in that group.
H.評定及びモニタリング
全ての患者は、試験を通して有害事象について綿密に監視され、有害事象は、国立がん試験所有害事象共通用語規準(National Cancer Institute Common Terminology Criteria for Adverse Events,Version 4.0(NCI CTCAE v4.0))に従って等級付けされる。患者は、最初の12ヶ月間は6週間毎(サイクル1の1日目から)、その後は6週間毎又は12週間毎に腫瘍評定を受ける。応答は、RECIST v1.1(Eisenhauer et al.,Eur J Cancer,45:228-247,2009)を使用して治験責任医師によって評定される。免疫ベースの治療薬(iRECIST)に対する修正RECIST v1.1あたりの応答は、治験責任医師が評定した個々の病変データに基づいてプログラムで決定される(Seymour et al.,Lancet Oncol,18:e143-152,2017)。臨床活性が実験群で実証された場合、試験依頼者は、その群の腫瘍評定スキャンが独立した読み取り施設による評価に提出されることを要求し得る。
H. Assessment and Monitoring All patients were closely monitored for adverse events throughout the study, and adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events, Version 4.0 (NCI CTCAE). v4.0)). Patients undergo tumor assessments every 6 weeks (starting on
ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。生検が治験責任医師によって実施可能であると考えられない場合、腫瘍組織の保管を提出することができる。治験責任医師が臨床的に実施可能であると判断した場合、許容できない毒性、RECIST v 1.1(対照群)による疾患進行、又は治験責任医師が決定した臨床的利益の喪失(実験群)のためにステージ1を中止する患者から腫瘍組織を収集する。拡大期の間に実験群に登録された患者については、処置中の組織試料が既に収集されており、同じCITの組み合わせで処置された最低15人の患者から評価可能であると判定されない限り、処置中の腫瘍組織試料がステージ1の処置の開始後4週間で収集される(臨床的に実施可能な場合)。これらの試料、並びに試験中に採取された血液試料は、バイオマーカー研究に利用される。
Baseline tumor tissue samples are collected from all patients, preferably by biopsy performed at study enrollment. If a biopsy is not considered feasible by the Investigator, archiving of tumor tissue may be submitted. Unacceptable toxicity, disease progression by RECIST v 1.1 (control arm), or loss of clinical benefit (experimental arm) as determined by the investigator, if deemed clinically feasible Tumor tissue is collected from patients who discontinue
アテゾリズマブ及び他の治療剤の薬物動態(PK)特性及び/又は免疫原性を特性評価するために、試験処置投与の前及び間の様々な時点で血液試料を取得する。
腫瘍及び応答評価
To characterize the pharmacokinetic (PK) properties and/or immunogenicity of atezolizumab and other therapeutic agents, blood samples are obtained at various time points before and during study treatment administration.
Tumor and response assessment
患者は、放射線学的疾患進行後に処置を継続する患者の場合を除いて、RECIST v 1.1による放射線学的疾患進行まで、ベースライン時、処置開始後最初の12ヵ月は6週間ごと(±1週間)、その後は用量遅延にかかわらず12週間毎(±2週間)に腫瘍評定を受け、そのような患者は、治験責任医師によって決定される臨床的利益の喪失まで、8週間ごと(±1週間)に腫瘍評定を受ける。 Patients were evaluated until radiographic disease progression by RECIST v 1.1 at baseline and every 6 weeks for the first 12 months after starting treatment (± 1 week), then every 12 weeks (± 2 weeks) regardless of dose delay, and such patients will undergo tumor assessments every 8 weeks (± 1 week) to undergo tumor assessment.
したがって、腫瘍評定は、疾患の進行又は臨床的利益の喪失以外の理由で処置を中止する患者については、たとえ患者が新たな非治験実施計画書指定の抗がん治療を開始したとしても、スケジュールに従って継続されるべきである。治験責任医師の裁量により、進行性疾患が疑われる場合はいつでも腫瘍評定を繰り返すことができる。 Therefore, for patients who discontinue treatment for reasons other than disease progression or loss of clinical benefit, tumor assessment should be performed on schedule, even if the patient starts a new non-protocol-specified anticancer therapy. should be continued in accordance with At the investigator's discretion, tumor assessments can be repeated whenever progressive disease is suspected.
ステージ2のベースライン腫瘍評定は、ステージ2の処置開始前28日以内(すなわち、サイクル1の1日目)に行われなければならない。ステージ2に適格な患者については、ステージ1中のRECIST v1.1(対照群)又は臨床的利益の喪失(実験群)による許容できない毒性若しくは疾患進行の前又はその時点で行われる腫瘍評定が、ステージ2の処置開始前28日以内に行われるならば、ステージ2のベースライン評定として機能し得る。
A
すべての測定可能及び評価可能な病変は、スクリーニング(ステージ1及びステージ2の両方)で評定及び文書化されるべきである。放射線療法又は手術で処置された脳転移は、測定可能又は評価可能であるとは考えられないが、転移性疾患の部位として文書化される。インフォームドコンセントを得る前及び試験処置の開始前28日以内に標準治療として行われる腫瘍評定は、スクリーニング時に繰り返す必要はない。
All measurable and evaluable lesions should be assessed and documented at screening (both
スクリーニング評定には、胸部、腹部及び骨盤のCTスキャン(経口及び/又はIV造影剤を用いる)又は磁気共鳴画像法(MRI)スキャンが含まれなければならない。胸部のスパイラルCTスキャンを得ることができるが、これは要件ではない。造影剤を用いたCTスキャンが禁忌である場合(すなわち、造影剤アレルギー又は腎クリアランス障害を有する患者において)、胸部の非造影CTスキャンを実施してもよく、腹部及び骨盤のMRIスキャン(実施可能であれば、IV造影剤を用いて)を実施すべきである。臨床的に必要な場合、骨スキャン及び首のCTスキャンもまた行われるべきである。治験責任医師の裁量により、RECIST v1.1による測定可能な疾患の評定の他の方法が使用され得る。 Screening evaluations must include CT scans (with oral and/or IV contrast) or magnetic resonance imaging (MRI) scans of the chest, abdomen, and pelvis. A spiral CT scan of the chest can be obtained, but this is not a requirement. If contrast-enhanced CT scans are contraindicated (i.e., in patients with contrast allergy or impaired renal clearance), a non-contrast CT scan of the chest may be performed and an MRI scan of the abdomen and pelvis (if available). with IV contrast) should be performed. A bone scan and a CT scan of the neck should also be performed if clinically indicated. Other methods of measurable disease assessment according to RECIST v1.1 may be used at the investigator's discretion.
腫瘍評定のためのCTスキャンが陽電子放射断層撮影/CTスキャナーで行われる場合、CT取得は、完全造影診断CTスキャンの標準と一致しなければならない。 If CT scans for tumor assessment are performed on a positron emission tomography/CT scanner, the CT acquisition must conform to the standard for full contrast-enhanced diagnostic CT scans.
ベースラインで特定されたすべての測定可能及び/又は評価可能な病変は、その後の腫瘍評定で再評価されるべきである。放射線療法又は手術で処置されたことがあるベースラインで同定された脳転移は、脳内に疾患の進行が疑われない限り(すなわち、患者は症候性になる)、測定可能又は評価可能とはみなされない。したがって、臨床的に示されない限り、その後の頭部CTスキャンは必要ない。スクリーニングで疾患部位を評定するために使用されるのと同じX放射線手順を、その後の腫瘍評定(例えば、CTスキャンのための同じコントラストプロトコル)に使用すべきである。iRECISTによる応答の評価を容易にするために、腫瘍評定を、進行を超えて処置を受けた患者について、RECIST v1.1による疾患進行後に継続しなければならない。これには、標的病変の継続的な測定、非標的病変の評価(明確な進行を示した任意の非標的病変のさらなる悪化の監視を含む)、及びその後の全ての評定での任意の新たに同定された病変(病変が測定可能である場合、測定値を含む)の評価が含まれる。1つの時点での全奏効が、RECIST v1.1を使用して治験責任医師によって評定される。 All measurable and/or evaluable lesions identified at baseline should be re-evaluated at subsequent tumor assessments. Baseline-identified brain metastases that have been treated with radiotherapy or surgery are not measurable or assessable unless disease progression in the brain is suspected (i.e., the patient becomes symptomatic). not considered. Therefore, no subsequent head CT scan is necessary unless clinically indicated. The same X-radiation procedure used to assess disease sites at screening should be used for subsequent tumor assessment (eg, same contrast protocol for CT scan). To facilitate assessment of response by iRECIST, tumor assessment should be continued after disease progression by RECIST v1.1 for patients treated beyond progression. This includes continuous measurement of target lesions, assessment of non-target lesions (including monitoring for further deterioration of any non-target lesion that has demonstrated definite progression), and any new Evaluation of identified lesions (including measurements if lesions are measurable) is included. Overall response at one time point will be assessed by the investigator using RECIST v1.1.
バイオマーカー評定
探索的バイオマーカー研究には、限定されないが、腫瘍分子サブタイプ及び腫瘍免疫生物学、PD-L1、リンパ球亜集団、T細胞受容体レパートリー、IC及びそれらのサブセットのT細胞活性化又は密度、局在化及び活性化状態に関連するサイトカインに関連する遺伝子又は遺伝子シグネチャの分析が含まれ得、DNA又はRNA抽出、体細胞変異の分析、及び次世代シーケンシング(NGS)(全エクソームシーケンシング(WES)を含む)の使用が含まれ得る。
Biomarker assessment Exploratory biomarker studies include, but are not limited to, tumor molecular subtypes and tumor immunobiology, PD-L1, lymphocyte subpopulations, T cell receptor repertoire, T cell activation of IC and subsets thereof or analysis of genes or gene signatures associated with cytokines related to density, localization and activation state, including DNA or RNA extraction, analysis of somatic mutations, and next generation sequencing (NGS) (whole experiment). The use of some-body sequencing (WES)) may be included.
バイオマーカー評定のための血液試料をベースライン時及び試験中に収集する。血液中のバイオマーカーの変化は、特定の処置の組み合わせの生物学的活性の証拠を提供し得る。血液中の代用バイオマーカー(腫瘍負荷マーカー、サイトカイン、ケモカイン、IC亜集団、遺伝子発現、及び循環腫瘍DNA等)と薬物用量、有効性、及び安全性評価項目との間の相関は、どの患者が特定の治療の組み合わせから恩恵を受ける可能性がより高いかを予測し得る将来の処置を定義するのに役立つ血液ベースのバイオマーカーの開発を可能にし得る。 Blood samples for biomarker assessment are collected at baseline and during the study. Changes in biomarkers in blood can provide evidence of biological activity of a particular treatment combination. Correlations between surrogate biomarkers in blood (such as tumor burden markers, cytokines, chemokines, IC subpopulations, gene expression, and circulating tumor DNA) and drug dose, efficacy, and safety endpoints are It may allow the development of blood-based biomarkers that help define future treatments that may predict whether they are more likely to benefit from a particular combination of treatments.
ベースライン腫瘍組織試料は、好ましくは、試験登録時に行われた生検によって、全ての患者から収集される。PD-L1及びTIGIT発現の決定及びバイオマーカーに関する調査試験のために、ベースラインで収集した腫瘍組織試料を使用する。治験責任医師によって臨床的に実施可能であると考えられる場合、腫瘍組織は、許容できない毒性、RECIST v1.1による疾患進行、又は治験責任医師によって決定された臨床的利益の喪失のためにステージ1の間に中断した患者から収集され、試験処置の耐性、疾患進行、及び臨床的利益に関連する腫瘍組織バイオマーカーの分析を可能にする。
Baseline tumor tissue samples are collected from all patients, preferably by biopsy performed at study enrollment. Tumor tissue samples collected at baseline are used for determination of PD-L1 and TIGIT expression and for exploratory studies for biomarkers. If deemed clinically viable by the Investigator, the tumor tissue is
治験責任医師によって臨床的に実施可能であると考えられる場合、拡大期中に実験群に登録された患者は、同じCITの組み合わせで治療された最低15人の患者から処置中の組織試料が既に収集され、評価可能であると判定されていない限り、ステージ1治療の開始後4週間(±7日)で処置中の生検を受ける。処置中の組織試料は、CITの組合せ(免疫回避を含む)による処置中に生じる潜在的な生物学的変化をよりよく理解しようとして、薬力学的効果の証拠を提供しようとして、又は仮定される作用機序を確認しようとして収集される。
If deemed clinically feasible by the Investigator, patients enrolled in the experimental arm during the expansion phase must have already collected on-treatment tissue samples from a minimum of 15 patients treated with the same CIT combination. Undergo an in-
腫瘍試料を、腫瘍浸潤IC、PD-L1、TIGIT及びCD8等のバイオマーカーについて評価する。腫瘍浸潤ICの数及び機能状態の変化を含む、各群内の処置に応答した腫瘍微小環境の評価は、仮定された作用機序の検証、並びに特定の処置の組み合わせのための適切な用量及び曝露が達成されたことの確認を提供し得る。 Tumor samples are evaluated for biomarkers such as tumor infiltration IC, PD-L1, TIGIT and CD8. Evaluation of the tumor microenvironment in response to treatment within each group, including changes in the number of tumor-infiltrating ICs and functional status, will allow validation of postulated mechanisms of action, as well as appropriate doses and doses for specific treatment combinations. It can provide confirmation that exposure has been achieved.
腫瘍組織及び血液試料を、WESを含むNGSの使用によって分析して、試験薬に対する応答を予測する、より重度の疾患状態への進行に関連する、試験薬に対する獲得耐性に関連する、有害事象の発生に対する感受性に関連する、又は疾患生物学の知識及び理解を高めることができる体細胞変異を同定することができる。 Tumor tissue and blood samples are analyzed by use of NGS, including WES, to predict response to study drug, associated with progression to more severe disease states, associated with acquired resistance to study drug, of adverse events. Somatic mutations can be identified that are associated with developmental susceptibility or that can enhance knowledge and understanding of disease biology.
実施例25.YO39609試験の統計的考察及び分析計画
最終試験分析は、試験の中止を通して収集された患者データに基づく。特に明記しない限り、有効性分析は、割り当てられた治療レジメンに対して各薬物の少なくとも1回の用量を受けた全ての患者として定義される有効性評価可能な集団に基づき、安全性分析は、任意の量の試験処置を受けた全ての患者として定義される安全性評価可能な集団に基づく。
Example 25. Statistical Considerations and Analysis Plan for the YO39609 Study Final study analysis is based on patient data collected through study discontinuation. Unless otherwise stated, efficacy analyzes were based on the efficacy evaluable population defined as all patients who received at least one dose of each drug on their assigned treatment regimen; Based on a safety evaluable population defined as all patients who received any amount of study treatment.
分析結果は、患者が実際に受けた処置によって要約される。ステージ2の処置が利用可能な場合はいつでも、結果をステージ(ステージ1又は2)によって要約する。データは、試料サイズによって保証されるように記載され、要約される。連続変数を、平均、標準偏差、中央値、範囲、及び四分位範囲を使用して要約する。カテゴリ変数は、カウント及びパーセンテージの使用によって要約される。試料サイズが小さい場合、表の代わりにリストを使用する。
Analysis results are summarized by the treatment actually received by the patient. Results are summarized by stage (
ステージ2の有効性及び安全性分析のために新しいベースライン値が確立される。腫瘍応答の評価のために、新しいベースライン腫瘍評定が確立される。他の評価項目(例えば、バイタルサイン又は臨床検査結果のベースラインからの変化)については、ステージ2中の患者の最初の投与前の最後の欠落していない値が新しいベースラインとして機能する。
New baseline values will be established for
試料サイズの決定
この試験は、仮説検定のための明示的な検定力及びタイプIエラーを考慮するように設計されていない。代わりに、この試験は、食道がん患者に投与した場合の免疫療法に基づく処置の組み合わせに関する予備的な有効性、安全性、及びPKデータを得るように設計されている。
Determination of Sample Size This test was not designed to take explicit power and Type I errors into account for hypothesis testing. Instead, this study is designed to obtain preliminary efficacy, safety, and PK data for immunotherapy-based treatment combinations when administered to patients with esophageal cancer.
この試験には、この状況で事前全身治療を受けたことがない食道がん患者が登録されている。約100~165人の患者を、試験中に対照群及び実験群にランダムに割り当てる。 The trial enrolls patients with esophageal cancer who have never received prior systemic therapy in this setting. Approximately 100-165 patients are randomly assigned to control and experimental groups during the study.
A.有効性分析
有効性評価可能な集団は、割り当てられた処置レジメンのために各薬物の少なくとも1つの用量を受けた全ての患者として定義される。有効性評価項目を実際の処置群によって要約する。
A. Efficacy Analysis The efficacy evaluable population is defined as all patients who received at least one dose of each drug for their assigned treatment regimen. Efficacy endpoints will be summarized by actual treatment group.
主要有効性評価項目
有効性の主要評価項目は、客観的奏効が得られた患者の割合として定義される、RECIST v1.1に基づくステージ1の間の客観的奏効率(ORR)である。客観的奏効は、治験責任医師がRECIST v 1.1を使用して決定した場合に、4週間以上離れた2回の連続した機会の完全奏効又は部分奏効として定義される。ベースライン後の腫瘍評定を受けていない患者を含む、この基準を満たさない患者は、非応答者であるとみなされる。ORR並びにその95%CI(Clopper-Pearson法)を要約する。ORRの分析集団は、有効性評価可能な集団である。
Primary Efficacy Endpoint The primary efficacy endpoint is the Objective Response Rate (ORR) during
副次的有効性評価項目
表77に定義されるように、副次的有効性評価項目は、PFS、OS、特定の時点でのOS(例えば、6ヶ月及び12ヶ月)、奏効期間(DOR)、ステージ1の間の病勢制御、TIGIT陽性腫瘍を有する患者における客観的奏効、及びPD-L1陽性腫瘍を有する患者における客観的奏効である。PFS、DOR及び病勢制御は、RECIST v1.1に従って治験責任医師によって決定される。
Secondary Efficacy Endpoints As defined in Table 77, the secondary efficacy endpoints were PFS, OS, OS at specified time points (e.g., 6 months and 12 months), duration of response (DOR) , disease control during
DORを、確認された完全奏効又は部分奏効を有する有効性評価可能な患者について導出する。試験段階で疾患の進行又は死亡が文書化されていない患者については、PFS及びDORを最後の腫瘍評定の日に打ち切る。OS分析時にまだ生存している患者は、生存していることが知られていた最後の日に打ち切る。 DOR is derived for efficacy evaluable patients with confirmed complete or partial response. For patients with no documented disease progression or death during the study phase, PFS and DOR will be censored on the day of the last tumor assessment. Patients still alive at the time of OS analysis are censored on the last day known to be alive.
Kaplan-Meier法を使用してPFS、OS、及びDORの中央値を推定し、90%信頼区間(CI)をBrookmeyer及びCrowley法の使用によって構築する。特定の時点でのOS率もまた、Kaplan-Meier法を用いて推定され、90%CIは、分散についてのGreenwoodの推定値に基づいて計算される。 The Kaplan-Meier method is used to estimate median PFS, OS, and DOR, and 90% confidence intervals (CI) are constructed by using the Brookmeyer and Crowley method. The OS rate at a particular time point was also estimated using the Kaplan-Meier method and the 90% CI is calculated based on Greenwood's estimate of variance.
病勢制御率、16週間以上にわたって安定した疾患、部分奏効、又は完全奏効を有する患者の割合として定義され、各処置群について計算され、90%CIはClopper-Pearsonの正確な方法の使用によって推定される。 Disease control rate, defined as the proportion of patients with stable disease, partial response, or complete response over 16 weeks, was calculated for each treatment group, and 90% CIs were estimated by using the Clopper-Pearson exact method. be.
探索有効性評価項目
探索的有効性評価項目は、iRECISTに従って治験責任医師が決定したステージ1での客観的奏効、PFS、DOR及び病勢制御、並びにRECIST v 1.1及びiRECISTに従って治験責任医師が決定したステージ2での客観的奏効、PFS、DOR及び病勢制御である。
Exploratory Efficacy Endpoints Exploratory efficacy endpoints were objective response, PFS, DOR and disease control at
B.安全性分析
安全性分析には、試験処置の任意の成分の少なくとも1つの用量を受けた全ての患者が含まれる。試験処置への曝露は、全体的に、及び各段階内の実際の処置群によって要約される。
B. Safety Analysis The safety analysis includes all patients who received at least one dose of any component of the study treatment. Exposure to study treatments is summarized overall and by actual treatment group within each phase.
言語有害事象用語は、Medical Dictionary for Regulatory Activities thesaurus termsにマッピングされ、有害事象重症度はNCI CTCAE v 4.0に従って等級付けされる。 Verbal adverse event terms are mapped to the Medical Dictionary for Regulatory Activities thesaurus terms and adverse event severity is graded according to NCI CTCAE v 4.0.
安全性は、有害事象の要約、臨床検査結果の変化、バイタルサイン及びECGの変化、及び試験薬への曝露を通して評定される。併用処置への曝露及び安全性フォローアップの長さは、各段階内の処置群によって要約される。 Safety will be assessed through a summary of adverse events, changes in laboratory test results, changes in vital signs and ECG, and exposure to study drug. Exposure to combination treatment and length of safety follow-up are summarized by treatment group within each phase.
処置開始後に起こる処置時発生有害事象を要約する。各患者について、各有害事象の最大報告重症度を重症度グレードごとに要約に使用する。全てのn処置下で発現する有害事象、重篤な有害事象、試験処置の中止につながる有害事象、グレード≧3の有害事象、死亡、及び死因を列挙し、マッピングされた用語、適切な類義語レベル、及びNCI CTCAE重症度グレードによって要約する。 Treatment-emergent adverse events occurring after treatment initiation will be summarized. For each patient, the maximum reported severity of each adverse event will be used in the summary by severity grade. List all n treatment emergent adverse events, serious adverse events, adverse events leading to discontinuation of study treatment, grade ≥3 adverse events, deaths, and causes of death, mapped terms, appropriate synonym level , and by NCI CTCAE severity grade.
関連する検査室、バイタルサイン(脈拍数、呼吸数、パルスオキシメトリ、血圧、及び体温)、及びECGデータは、必要に応じて識別されたグレードと共に時間によって表示される。更に、選択された臨床検査のシフトテーブルを使用して、ベースライン及びベースライン後の最大重症度グレードを要約する。バイタルサイン及びECGの変化を要約する。 Relevant laboratory, vital signs (pulse rate, respiratory rate, pulse oximetry, blood pressure, and temperature), and ECG data are displayed by time with grades identified as appropriate. In addition, baseline and post-baseline maximum severity grades will be summarized using a shift table of selected laboratory tests. Summarize changes in vital signs and ECG.
C.薬物動態分析
アテゾリズマブ(少なくとも1用量のアテゾリズマブを受けた患者)及びアテゾリズマブと組み合わせて投与された指定の薬物(少なくとも1用量の薬物を受けた患者)のPK分析のために、まばらな試料を収集する。様々な試験薬物の血清又は血漿濃度は、個々の値として報告され、処置群によって、並びに適切な場合及びデータが許す場合はサイクル及び日によって要約(平均、標準偏差、変動係数、中央値、範囲、幾何平均、及び幾何平均変動係数)される。様々な試験薬物の個々の及び中央の血清又は血漿濃度は、処置群、サイクル及び日によってプロットされる。配合剤のPKデータを、内部試験及び公表された以前の試験からの利用可能な履歴データと比較することができる。アテゾリズマブ濃度データは、クリアランス、分布容積及び濃度時間曲線下面積等のPKパラメーターを導出するために、確立された集団PKモデルを使用して他の試験からのデータと共にプールされ得る。
C. Pharmacokinetic Analysis Collect sparse samples for PK analysis of atezolizumab (patients who received atezolizumab at least 1 dose) and the indicated drugs administered in combination with atezolizumab (patients who received at least 1 dose of drug) . Serum or plasma concentrations of various study drugs were reported as individual values and summarized (mean, standard deviation, coefficient of variation, median, range) by treatment group and, where appropriate and data permitted, by cycle and day. , the geometric mean, and the geometric mean coefficient of variation). Individual and median serum or plasma concentrations of various study drugs are plotted by treatment group, cycle and day. PK data for formulations can be compared to available historical data from internal and previous published studies. Atezolizumab concentration data can be pooled with data from other studies using established population PK models to derive PK parameters such as clearance, volume of distribution and area under the concentration-time curve.
D.免疫原性分析
免疫原性を、アテゾリズマブ及び必要に応じて他の試験処置について評定する。アテゾリズマブの免疫原性分析には、少なくとも1つの抗薬物抗体(ADA)評定を受けた全ての患者が含まれる。患者は、受けた処置に従って、又は試験中止前に処置を受けていない場合は割り当てられた処置に従ってグループ分けされる。アテゾリズマブについては、ベースライン(ベースライン有病率)及びベースライン後(ベースライン発生後)のADA陽性患者及びADA陰性患者の数及び割合を処置グ群別に要約する。ADAが検査される他の試験処置については、ADA陽性は、これらの薬物の以前の試験のために確立された標準的な方法に従って決定される。ADAの状態と安全性、有効性、PK、及びバイオマーカー評価項目との間の関係は、記述統計学を用いて分析及び報告され得る。
D. Immunogenicity Analysis Immunogenicity is assessed for atezolizumab and other study treatments as appropriate. The atezolizumab immunogenicity analysis includes all patients with at least one anti-drug antibody (ADA) assessment. Patients are grouped according to the treatment received or assigned treatment if they had not received treatment prior to study discontinuation. For atezolizumab, baseline (baseline prevalence) and post-baseline (post-baseline incidence) numbers and percentages of ADA-positive and ADA-negative patients are summarized by treatment group. For other test treatments that test for ADA, ADA positivity is determined according to standard methods established for previous testing of these drugs. Relationships between ADA status and safety, efficacy, PK, and biomarker endpoints can be analyzed and reported using descriptive statistics.
E.バイオマーカー分析
探索的バイオマーカー分析は、有効性及び安全性評価項目を考慮して、これらのバイオマーカーと試験薬に対する応答との関連性を理解使用として行われる。
E. Biomarker Analyzes Exploratory biomarker analyzes are performed to understand the association between these biomarkers and response to study drug in view of efficacy and safety endpoints.
F.暫定分析
暫定分析は試験の過程にわたって行われ、少なくとも1つの実験アームが予備期での登録を完了し、患者を最低6週間追跡したときに、最も早い(段階1)暫定分析が行われる。事後確率を使用して、対照群と比較した実験群における臨床活性の暫定分析に基づいて、処置群へのさらなる登録を導くことができる。暫定分析が、実験群の活性が対照群の活性よりも高いことを示唆する場合、実験群に更に25人の患者が登録され得る。約15人の患者がステージ2の処置群に登録され、最低6週間追跡された後、暫定分析も行われる。ステージ2の処置群で臨床活性が観察されない場合、その群へのさらなる登録を停止する。
F. Interim Analyzes Interim analyzes will occur over the course of the study, with the earliest (Phase 1) interim analyzes occurring when at least one study arm has completed pre-phase enrollment and patients have been followed for a minimum of 6 weeks. Posterior probabilities can be used to guide further enrollment into treatment groups based on interim analysis of clinical activity in experimental groups compared to controls. If the interim analysis suggests that the activity of the experimental group is higher than that of the control group, an additional 25 patients can be enrolled in the experimental group. Approximately 15 patients will be enrolled in the
実施例26.チラゴルマブ+アテゾリズマブ処置の予測バイオマーカーとしてのPD-L1
第Ib相試験(GO30103;NCT02794571号)では、複数の固形腫瘍タイプにおいて、単独療法として、及びアテゾリズマブと組み合わせて、チラゴルマブは忍容性が高かった。1L NSCLCにおけるランダム化第II相CITYSCAPE試験(NCT03563716)では、処置意図(ITT)集団において、プラセボ+アテゾリズマブに対するチラゴルマブ+アテゾリズマブを用いたORR及びPFSにおいて臨床上意味のある改善が見られた。PD-L1腫瘍割合スコア(TPS)≧50%のサブグループでより大きな改善が見られた(PharmDx 22C3 IHCアッセイを用いて評定した場合;データ遮断2019年12月;フォローアップ中央値10.9ヶ月)。
Example 26. PD-L1 as a predictive biomarker for tiragolumab plus atezolizumab treatment
In a phase Ib trial (GO30103; NCT02794571), tiragolumab was well tolerated as monotherapy and in combination with atezolizumab in multiple solid tumor types. The randomized phase II CITYSCAPE trial (NCT03563716) in 1L NSCLC showed clinically meaningful improvements in ORR and PFS with tiragolumab + atezolizumab versus placebo + atezolizumab in the intention-to-treat (ITT) population. Greater improvement was seen in the subgroup with PD-L1 Tumor Proportion Score (TPS) ≥50% (as assessed using the PharmDx 22C3 IHC assay; data cut-off December 2019; median follow-up 10.9 months). ).
チラゴルマブ+アテゾリズマブ処置の予測バイオマーカーとしてのPD-L1の値は、異なるPD-L1アッセイにわたって一貫していることが分かった。pharmDx 22C3アッセイ(ITT集団)及びConformite Europeenne(欧州適合性)in vitro診断(CE-IVD 0 VENTANA SP 263 IHCアッセイ(バイオマーカー評価可能集団)を使用して、全ての利用可能な患者試料についてPD-L1タンパク質発現を評価するためにIHCを実施し、PD-L1発現のレベルを、各アッセイについて確立されたアルゴリズムを使用してスコア化した。BEP集団及びITT集団のベースライン特性は類似していた(表92)。

PD-L1サブグループの有病率は、2つのIHCアッセイ間で同程度であった(図26)。PD-L1 22C3アッセイの場合、高TPをTPS≧50%として分類し、低TPSをTPS 1~49%として分類した。SP263 IHCアッセイの場合、高TCをTC≧50%に分類し、低TCをTC1~49%として分類した。SP263によって定義されたPD-L1陽性(TC≧1%)サブグループ(PFS HR 0.56、95%CI:0.34-0.92)と22C3によって定義されたPD-L1陽性(TPS≧1%)サブグループ(図27A、27B、28A、28B)との間で、チラゴルマブ+アテゾリズマブ対アテゾリズマブ単独療法による同等のORR及びPFSの改善が見られた。SP263によって定義されたPD-L1高(TC≧50%)サブグループ(PFS HR 0.23、95%CI:0.10-0.53)と22C3によって定義されたPD-L1高(TPS≧50%)サブグループ(図29A、29B、30A、30B)との間でも、チラゴルマブ+アテゾリズマブ対アテゾリズマブ単独療法による同等のORR及びPFSの改善が見られた。 The prevalence of the PD-L1 subgroup was similar between the two IHC assays (Figure 26). For the PD-L1 22C3 assay, high TP was classified as TPS≧50% and low TPS as TPS 1-49%. For the SP263 IHC assay, high TC was classified as TC≧50% and low TC as TC1-49%. PD-L1-positive (TC ≥ 1%) subgroup defined by SP263 (PFS HR 0.56, 95% CI: 0.34-0.92) and PD-L1-positive (TPS ≥ 1%) defined by 22C3 %) subgroups (Figures 27A, 27B, 28A, 28B) with comparable ORR and PFS improvements with tiragolumab plus atezolizumab versus atezolizumab monotherapy. PD-L1 high (TC ≥ 50%) subgroup defined by SP263 (PFS HR 0.23, 95% CI: 0.10-0.53) and PD-L1 high (TPS ≥ 50%) defined by 22C3 %) subgroups (Figures 29A, 29B, 30A, 30B) also showed comparable ORR and PFS improvements with tiragolumab plus atezolizumab versus atezolizumab monotherapy.
22C3又はSP263 IHCのいずれかによって評定される高いPD-L1発現は、チラゴルマブ+アテゾリズマブ併用療法の重要な予測バイオマーカーであり得る。 High PD-L1 expression as assessed by either 22C3 or SP263 IHC may be an important predictive biomarker for tiragolumab plus atezolizumab combination therapy.
VII.他の実施形態 VII. Other embodiment
本明細書に記載の技術のいくつかの実施形態は、実施形態セットA、B、及びCの以下の番号付けされた実施形態のいずれかに従って定義することができる。 Some embodiments of the technology described herein can be defined according to any of the following numbered embodiments of embodiment sets A, B, and C.
実施形態のセットA:
1.がんを有する対象を処置する方法であって、前記方法が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤を含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。
Embodiment set A:
1. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every three weeks, PD-1 axis at a dose of about 900 mg to about 1500 mg every three weeks. administering to said subject a dosing regimen comprising one or more dosing cycles comprising a binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
2.がんを有する対象を処置する方法であって、前記方法が、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 2. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis at a dose of about 1400 mg to 2000 mg every 4 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
3.がんを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約600mg~1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 3. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and a PD-1 axis at a dose of about 600 mg to about 1200 mg every two weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
4.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態2又は3に記載の方法。
4. 4. The method of
5.前記抗TIGITアンタゴニスト抗体がIgGクラス抗体、特にIgG1サブクラス抗体である、実施形態1~4のいずれかに記載の方法。 5. The method of any of embodiments 1-4, wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
(f)QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、
を含む、実施形態1~5のいずれか一項に記載の方法。
6. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3);
(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO:5); and (f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO:6).
6. The method of any one of embodiments 1-5, comprising
7.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
(a)DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
(b)WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
(c)GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
(d)FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、並びに
以下の重鎖可変領域FR:
(a)X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
(b)WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
(c)RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
(d)WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4
を更に含む、実施形態1~6のいずれか一項に記載の方法。
7. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and (d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and the following heavy chain variable region FRs:
(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), where X1 is E or Q;
(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and (d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
7. The method of any one of embodiments 1-6, further comprising
8.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)配列番号17若しくは18のアミノ酸配列を含むVHドメインと、配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態1~7のいずれか一項に記載の方法。
8. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or (c) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18. , SEQ ID NO:19.
9.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態1~8のいずれか一項に記載の方法。 9. The method of any one of embodiments 1-8, wherein said anti-TIGIT antagonist antibody is tiragolumab.
10.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト又はPD-1結合アンタゴニストである、実施形態1~9のいずれか一項に記載の方法。 10. The method of any one of embodiments 1-9, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
11.前記PD-1軸結合アンタゴニストが、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体である、実施形態1~10のいずれか一項に記載の方法。 11. The method of any one of embodiments 1-10, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
12.前記PD-1軸結合アンタゴニストが、抗PD-L1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の方法。 12. The method of any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
13.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態12に記載の方法。
13. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 13. The method of
14.前記PD-1軸結合アンタゴニストが、モノクローナル抗体である、実施形態1~13のいずれか一項に記載の方法。 14. The method of any one of embodiments 1-13, wherein said PD-1 axis binding antagonist is a monoclonal antibody.
15.前記PD-1軸結合アンタゴニストが抗PD-1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の方法。 15. The method of any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
16.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態15に記載の方法。 16. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21.
17.前記方法が、有効量の白金系化学療法剤及び非白金系化学療法剤を前記対象に投与することを含む、実施形態2~16のいずれか一項に記載の方法。 17. The method of any one of embodiments 2-16, wherein said method comprises administering to said subject an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
18.前記非白金系化学療法剤がトポイソメラーゼII阻害剤である、実施形態1又は17に記載の方法。
18. 18. The method of
19.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331、特にエトポシドである、実施形態18に記載の方法。
19. 19. The method of
20.前記トポイソメラーゼII阻害剤が100mg/m2の用量で投与される、実施形態18又は19に記載の方法。
20. 20. The method of
21.前記白金系化学療法剤がカルボプラチン又はシスプラチン、特にカルボプラチンである、実施形態17~20のいずれか一項に記載の方法。 21. 21. The method of any one of embodiments 17-20, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin, particularly carboplatin.
22.前記白金系化学療法剤が、投与日にAUC=5mg/ml/分を達成するのに十分な用量で投与される、実施形態17~21のいずれか一項に記載の方法。 22. The method of any one of embodiments 17-21, wherein said platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
23.前記方法が、導入期及び維持期を含む投薬レジメンを含む、実施形態1~22のいずれか一項に記載の方法。 23. The method of any one of embodiments 1-22, wherein said method comprises a dosing regimen comprising an induction phase and a maintenance phase.
24.前記導入期が4回の初期投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤が4回の初期投薬サイクルの各々で投与される、実施形態23に記載の方法。
24. wherein the induction phase comprises four initial dosing cycles, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles; 24. The method of
25.前記維持期が、前記白金系化学療法剤及び/又は非白金系化学療法剤の投与を含まない、実施形態23又は24に記載の方法。
25. 25. The method of
26.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、実施形態1~25のいずれか一項に記載の方法。 26. 26. The method of any one of embodiments 1-25, wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody.
27.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の全生存期間を延長する、実施形態1~26のいずれか一項に記載の方法。 27. The method of any one of embodiments 1-26, wherein said treatment prolongs overall survival of said subject compared to treatment without said anti-TIGIT antagonist antibody.
28.前記がんが肺がんである、実施形態1~27のいずれか一項に記載の方法。 28. 28. The method of any one of embodiments 1-27, wherein said cancer is lung cancer.
29.前記肺がんが小細胞肺がん(SCLC)、特に進展型SCLC(ES-SCLC)である、実施形態28に記載の方法。 29. 29. The method of embodiment 28, wherein said lung cancer is small cell lung cancer (SCLC), particularly extensive-stage SCLC (ES-SCLC).
30.前記肺がんが、非小細胞肺がん(NSCLC)、特に局所進行性切除不能NSCLC(ステージIIIB NSCLC)である、実施形態28に記載の方法。 30. 29. The method of embodiment 28, wherein said lung cancer is non-small cell lung cancer (NSCLC), particularly locally advanced unresectable NSCLC (stage IIIB NSCLC).
31.前記肺がんが局所進行性切除不能又は転移性の非扁平上皮NSCLCである、実施形態28に記載の方法。 31. 29. The method of embodiment 28, wherein said lung cancer is locally advanced, unresectable or metastatic non-squamous NSCLC.
32.前記肺がんが切除可能な肺がんである、実施形態28に記載の方法。 32. 29. The method of embodiment 28, wherein said lung cancer is resectable lung cancer.
33.前記がんが子宮頸がんである、実施形態1~27のいずれか一項に記載の方法。 33. 28. The method of any one of embodiments 1-27, wherein said cancer is cervical cancer.
34.前記がんが早期トリプルネガティブ乳がん(eTNBC)である、実施形態1~27のいずれか一項に記載の方法。 34. 28. The method of any one of embodiments 1-27, wherein said cancer is early triple negative breast cancer (eTNBC).
35.前記がんが頭頸部がんである、実施形態1~27のいずれか一項に記載の方法。 35. 28. The method of any one of embodiments 1-27, wherein the cancer is head and neck cancer.
36.前記がんが肝臓がん、特に肝細胞癌腫(HCC)である、実施形態1~27のいずれか一項に記載の方法。 36. 28. The method of any one of embodiments 1-27, wherein said cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
37.前記がんが膀胱がんである、実施形態1~27のいずれか一項に記載の方法。 37. 28. The method of any one of embodiments 1-27, wherein said cancer is bladder cancer.
38.前記がんが尿路上皮癌腫(UC)、特に転移性尿路上皮癌腫(mUC)である、実施形態37に記載の方法。
38. 38. The method of
39.前記がんが膵臓がん、特に膵管腺癌(PDAC)である、実施形態1~27のいずれか一項に記載の方法。 39. 28. The method of any one of embodiments 1-27, wherein said cancer is pancreatic cancer, in particular pancreatic ductal adenocarcinoma (PDAC).
40.前記がんが食道がん、特に進行性又は転移性食道がんである、実施形態1~27のいずれか一項に記載の方法。 40. 28. The method of any one of embodiments 1-27, wherein said cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
41.実施形態1~40のいずれか一項に記載の方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含む、キット。 41. A kit comprising an anti-TIGIT antagonist antibody for use in combination with a PD-1 axis binding antagonist to treat a subject with cancer according to the method of any one of embodiments 1-40.
42.前記キットが、1つ以上の化学療法剤を更に含む、実施形態41に記載のキット。
42. 42. The kit of
43.がんを有する対象を処置する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が実施形態1~40のいずれか一項に記載されるものである、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 43. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein the method is as described in any one of embodiments 1-40. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
44.PD-1軸結合アンタゴニストと組み合わせてがんを有する対象を処置するための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、前記処置が実施形態1~40のいずれか一項に記載の方法によるものである、使用。 44. 41. Use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject with cancer in combination with a PD-1 axis binding antagonist, said treatment being a method according to any one of embodiments 1-40. is due to use.
45.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態44に記載の使用。
45. 45. Use according to
46.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態44に記載の使用。
46. 45. Use according to
47.がんを有する対象を処置する方法であって、前記方法が、4週間ごとの約200mg~約2000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 47. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis at a dose of about 80 mg to 2000 mg every 4 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
48.がんを有する対象を処置する方法であって、前記方法が、4週間ごとの約200mg~約2000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約20mg~1600mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 48. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and a PD-1 axis at a dose of about 20 mg to 1600 mg every 4 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
49.がんを有する対象を処置する方法であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約20mg~1600mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 49. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks and a PD-1 axis at a dose of about 20 mg to about 1600 mg every two weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
50.がんを有する対象を処置する方法であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 50. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every 2 weeks and a PD-1 axis at a dose of about 80 mg to 2000 mg every 4 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
51.がんを有する対象を処置する方法であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、及び6週間ごとの約100mg~1000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 51. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks and a PD-1 axis at a dose of about 100 mg to 1000 mg every 6 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist.
52.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態47~51のいずれか一項に記載の方法。 52. The method of any one of embodiments 47-51, wherein said method further comprises administering to said subject one or more chemotherapeutic agents.
53.前記方法が、白金系化学療法剤及び非白金系化学療法剤を前記対象に投与することを含む、実施形態52に記載の方法。 53. 53. The method of embodiment 52, wherein said method comprises administering to said subject a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
54.がんを有する対象を処置する方法であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤を含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 54. A method of treating a subject with cancer, said method comprising an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis at a dose of about 80 mg to about 1600 mg every 3 weeks. administering to said subject a dosing regimen comprising one or more dosing cycles comprising a binding antagonist, a platinum-based chemotherapeutic agent every three weeks, and a non-platinum-based chemotherapeutic agent every three weeks.
55.前記方法が、導入期及び維持期を含む、実施形態53又は54に記載の方法。 55. 55. The method of embodiment 53 or 54, wherein said method comprises an induction phase and a maintenance phase.
56.前記導入期及び維持期がそれぞれ、1回以上の投薬サイクルを含む、実施形態55に記載の方法。 56. 56. The method of embodiment 55, wherein said induction phase and maintenance phase each comprise one or more dosing cycles.
57.前記維持期が、前記白金系化学療法剤の投与を含まない、実施形態55又は56に記載の方法。
57. 57. The method of
58.前記維持期が、前記非白金系化学療法剤の投与を含まない、実施形態55~57のいずれか一項に記載の方法。 58. 58. The method of any one of embodiments 55-57, wherein said maintenance phase does not comprise administration of said non-platinum chemotherapeutic agent.
59.前記維持期が、4週間ごとの約200mg~約2000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~約2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む、実施形態58に記載の方法。 59. The maintenance phase comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at doses of about 200 mg to about 2000 mg every 4 weeks and the PD-1 axis binding antagonist at doses of about 80 mg to about 2000 mg every 4 weeks. , embodiment 58.
60.がんを有する対象を処置する方法であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mg~約1600mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含み、前記抗PD-1アンタゴニスト抗体がペンブロリズマブである、方法。 60. A method of treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every three weeks and an anti-PD- administering to said subject a dosing regimen comprising one or more dosing cycles of an antagonist antibody, wherein said anti-PD-1 antagonist antibody is pembrolizumab.
61.がんを有する対象を処置する方法であって、前記方法が、チラゴルマブ及びペンブロリズマブの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含み、前記ペンブロリズマブが、6週間ごとに約100mgと約1000mgの間の用量で投与される、方法。 61. A method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, wherein said pembrolizumab is administered about every 6 weeks A method wherein a dose of between 100 mg and about 1000 mg is administered.
62.がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び2週間の投薬/1週間の休薬の間、3週間ごとの1日2回の経口の約10mg/m2と約10000mg/m2の間の用量の代謝拮抗剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 62. A method for treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks, between about 80 mg and about 1600 mg every three weeks A PD-1 axis binding antagonist at a dose and an antimetabolite at a dose between about 10 mg/m2 and about 10000 mg/m2 orally twice daily every 3 weeks for 2 weeks on/1 week off. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of an agent.
63.がんを有する対象を処置する方法であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、ゲムシタビン及びnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 63. A method of treating a subject with cancer, said method comprising an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis at a dose of about 80 mg to about 1600 mg every 3 weeks. A method comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a binding antagonist, gemcitabine and nab-paclitaxel.
64.前記1つ以上の化学療法剤がゲムシタビン及びnab-パクリタキセルである、実施形態52に記載の方法。 64. 53. The method of embodiment 52, wherein said one or more chemotherapeutic agents are gemcitabine and nab-paclitaxel.
65.がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約1mg/kgと約35mg/kgの間の用量のVEGFアンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 65. A method for treating a subject with cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks, between about 80 mg and about 1600 mg every three weeks administering to said subject a dosing regimen comprising a dose of a PD-1 axis binding antagonist and one or more dosing cycles of a VEGF antagonist at a dose between about 1 mg/kg and about 35 mg/kg every three weeks. ,Method.
66.がんを有する対象を処置する方法であって、前記方法が、導入期及び維持期を含む投薬レジメンを前記対象に投与することを含み、
(a)前記導入期が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤の投与を含まない、方法。
66. 1. A method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase,
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding antagonist every 3 weeks and a non-platinum chemotherapeutic agent every 3 weeks; The method, wherein said maintenance phase does not include administration of said platinum-based chemotherapeutic agent.
67.がんを有する対象を処置する方法であって、前記方法が、導入期及び維持期を含む投薬レジメンを前記対象に投与することを含み、
(a)前記導入期が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、4週間ごとの約200mg~約2000mgの用量の前記抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~約2000mgの用量の前記PD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤又は前記非白金系化学療法剤の投与を含まない、方法。
67. 1. A method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase,
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more times of said anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and said PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks; wherein said maintenance phase does not comprise administration of said platinum-based chemotherapeutic agent or said non-platinum-based chemotherapeutic agent.
68.前記導入期が、4~6回の投薬サイクルを含む、実施形態56~59、66及び67のいずれか一項に記載の方法。 68. The method of any one of embodiments 56-59, 66 and 67, wherein said induction phase comprises 4-6 dosing cycles.
69.実施形態53~59及び66~68のいずれか一項に記載の方法であって、
(a)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、又は
(c)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がエトポシドである、
実施形態53~59及び66~68のいずれか一項に記載の方法。
69. The method of any one of embodiments 53-59 and 66-68, wherein
(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel, or (c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is etoposide,
The method of any one of embodiments 53-59 and 66-68.
70.前記がんが固形腫瘍である、実施形態47~69のいずれか一項に記載の方法。 70. 70. The method of any one of embodiments 47-69, wherein said cancer is a solid tumor.
71.前記がんが局所進行性又は転移性である、実施形態47~70のいずれか一項に記載の方法。 71. 71. The method of any one of embodiments 47-70, wherein said cancer is locally advanced or metastatic.
72.前記がんが、肺がん、膵臓がん、子宮頸がん、乳がん、頭頸部がん、肝臓がん、膀胱がん、食道がん、胃がん、結腸直腸がん、腎臓がん、腎がん、黒色腫、又は卵巣がんである、実施形態47~71のいずれか一項に記載の方法。 72. the cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, renal cancer, 72. The method of any one of embodiments 47-71, which is melanoma, or ovarian cancer.
73.前記がんが、肺がんである、実施形態72に記載の方法。
73. 73. The method of
74.前記肺がんがNSCLC、特に局所進行性切除不能NSCLCである、実施形態73に記載の方法。
74. 74. The method of
75.前記NSCLCが、ステージIIIBのNSCLCである、実施形態74に記載の方法。 75. 75. The method of embodiment 74, wherein the NSCLC is stage IIIB NSCLC.
76.前記肺がんが再発性又は転移性NSCLCである、実施形態73~75のいずれか一項に記載の方法。 76. 76. The method of any one of embodiments 73-75, wherein said lung cancer is recurrent or metastatic NSCLC.
77.前記NSCLCが、ステージIVのNSCLCである、実施形態76に記載の方法。
77. 77. The method of
78.前記対象が、ステージIVのNSCLCについて以前に処置されたことがない、実施形態77に記載の方法。 78. 78. The method of embodiment 77, wherein said subject has not been previously treated for Stage IV NSCLC.
79.前記肺がんが小細胞肺がん(SCLC)である、実施形態73に記載の方法。
79. 74. The method of
80.肺がんを有する対象又は対象集団を処置する方法であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、方法。 80. A method of treating a subject or population of subjects having lung cancer, said method comprising administering an effective amount of one or more of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. administering to said subject or population of subjects a dosing regimen comprising cycles, wherein said treatment comprises said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor, without said anti-TIGIT antagonist antibody. A method of prolonging progression-free survival (PFS) of said subject compared to treatment with an agent.
81.肺がんを有する対象集団を処置する方法であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象集団に投与することを含み、前記処置が、約8.2ヶ月~約9.2ヶ月の前記対象集団のPFS中央値をもたらす、方法。 81. A method of treating a subject population with lung cancer, said method comprising one or more dosing cycles of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. administering to said subject population a dosing regimen comprising said subject population, wherein said treatment results in a median PFS of said subject population of from about 8.2 months to about 9.2 months.
82.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の全生存期間(OS)を延長する、実施形態80又は81に記載の方法。
82. said treatment compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody, overall survival of said subject or subject population ( 82. The method of
83.前記処置が、抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のPFSを少なくとも約2.4ヶ月延長する、実施形態80~82のいずれか一項に記載の方法。 83. said treatment reduces the PFS of said subject or subject population by at least about 2 compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without an anti-TIGIT antagonist antibody; 83. The method of any one of embodiments 80-82, wherein the method is extended for 4 months.
84.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の前記PFSを少なくとも約3ヶ月~約4ヶ月延長する、実施形態83に記載の方法。 84. said treatment reduces said PFS of said subject or subject population at least as compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without said anti-TIGIT antagonist antibody 84. The method of embodiment 83, extended from about 3 months to about 4 months.
85.肺がんを有する対象又は対象集団を処置する方法であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象のOSを延長する、方法。 85. A method of treating a subject or population of subjects having lung cancer, said method comprising administering an effective amount of one or more of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. administering to said subject or population of subjects a dosing regimen comprising cycles, wherein said treatment comprises said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor, without said anti-TIGIT antagonist antibody. A method of prolonging OS in said subject compared to treatment with an agent.
86.肺がんを有する対象集団を処置する方法であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象集団に投与することを含み、前記処置が、約15.3ヶ月~約17.6ヶ月の前記対象集団の中央値OSをもたらす、方法。 86. A method of treating a subject population having lung cancer, said method comprising one or more dosing cycles of an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor. administering to said subject population a dosing regimen comprising said subject population, wherein said treatment results in a median OS of said subject population of from about 15.3 months to about 17.6 months.
87.前記処置が、抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3.3ヶ月延長する、実施形態82~86のいずれか一項に記載の方法。 87. said treatment reduces the OS of said subject or subject population by at least about 3, compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without an anti-TIGIT antagonist antibody; 87. The method of any one of embodiments 82-86, wherein the method is extended for 3 months.
88.前記処置が、抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3ヶ月~約5.3ヵ月延長する、実施形態82~86のいずれか一項に記載の方法。 88. said treatment reduced the OS of said subject or subject population by at least about 3, compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without an anti-TIGIT antagonist antibody; 87. The method of any one of embodiments 82-86, extending from months to about 5.3 months.
89.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が、4回の初期投薬サイクルの各々で投与される、実施形態80~88のいずれか一項に記載の方法。 89. 89. According to any one of embodiments 80-88, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered in each of four initial dosing cycles. the method of.
90.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが、前記第4の初期投薬サイクルに続いて1回以上の追加のサイクルで更に投与される、実施形態80~89のいずれか一項に記載の方法。 90. 89. Any one of embodiments 80-89, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are further administered in one or more additional cycles following said fourth initial dosing cycle. the method of.
91.前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤が、前記1回以上の追加の投薬サイクルの各々から省略される、実施形態90に記載の方法。
91. 91. The method of
92.前記白金系化学療法剤がカルボプラチンであり、前記トポイソメラーゼII阻害剤がエトポシドである、実施形態80~91のいずれか一項に記載の方法。 92. The method of any one of embodiments 80-91, wherein said platinum-based chemotherapeutic agent is carboplatin and said topoisomerase II inhibitor is etoposide.
93.前記肺がんが小細胞肺がん(SCLC)である、実施形態80~92のいずれか一項に記載の方法。 93. The method of any one of embodiments 80-92, wherein said lung cancer is small cell lung cancer (SCLC).
94.前記SCLCが進展型SCLC(ES-SCLC)である、実施形態93に記載の方法。 94. 94. The method of embodiment 93, wherein said SCLC is extensive SCLC (ES-SCLC).
95.前記一又は複数の対象が、ES-SCLCに対して処置未経験である、実施形態94に記載の方法。 95. 95. The method of embodiment 94, wherein said one or more subjects are treatment-naive for ES-SCLC.
96.前記一又は複数の対象が脳転移の存在又は病歴を有していない、実施形態80~95のいずれか一項に記載の方法。 96. 96. The method of any one of embodiments 80-95, wherein said one or more subjects do not have the presence or history of brain metastases.
97.前記肺がんがPD-L1発現について選択されていない、実施形態80~96のいずれか一項に記載の方法。 97. 97. The method of any one of embodiments 80-96, wherein said lung cancer is not selected for PD-L1 expression.
98.前記肺がんがPD-L1発現について選択される、実施形態80~96のいずれか一項に記載の方法。 98. The method of any one of embodiments 80-96, wherein said lung cancer is selected for PD-L1 expression.
99.前記肺がんが、検出可能なPD-L1発現レベルによってPD-L1発現について選択される、実施形態98に記載の方法。 99. 99. The method of embodiment 98, wherein said lung cancer is selected for PD-L1 expression by a detectable level of PD-L1 expression.
100.前記肺がんが転移性である、実施形態80~99のいずれか一項に記載の方法。 100. 99. The method of any one of embodiments 80-99, wherein said lung cancer is metastatic.
101.前記肺がんが脳、肝臓、リンパ節及び/又は副腎に転移したことがある、実施形態100に記載の方法。
101. 101. The method of
102.前記肺がんが脳に転移したことがない、実施形態100又は101に記載の方法。
102. 102. The method of
103.前記処置が完全奏効(CR)又は部分奏効(PR)をもたらす、実施形態100~102のいずれか一項に記載の方法。 103. 103. The method of any one of embodiments 100-102, wherein said treatment results in a complete response (CR) or partial response (PR).
104.前記抗TIGITアンタゴニスト抗体が、2週間、3週間又は4週間ごとに約30mg~約1200mgの用量で投与される、実施形態80~103のいずれか一項に記載の方法。 104. 104. The method of any one of embodiments 80-103, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 2, 3 or 4 weeks.
105.前記PD-1軸結合アンタゴニストが、2週間、3週間又は4週間ごとに約80mg~約2000mgの用量で投与される、実施形態80~104のいずれか一項に記載の方法。 105. 105. The method of any one of embodiments 80-104, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 2, 3 or 4 weeks.
106.前記PD-1軸結合アンタゴニスト、抗TIGITアンタゴニスト抗体、白金系化学療法剤及びトポイソメラーゼII阻害剤を連続的に投与する、実施形態80~105のいずれか一項に記載の方法。 106. 106. The method of any one of embodiments 80-105, wherein said PD-1 axis binding antagonist, anti-TIGIT antagonist antibody, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered sequentially.
107.前記PD-1軸結合アンタゴニストが前記抗TIGITアンタゴニスト抗体の前に投与され、前記抗TIGITアンタゴニスト抗体が前記白金系化学療法剤の前に投与され、前記白金剤がトポイソメラーゼII阻害剤の前に投与される、実施形態106に記載の方法。 107. The PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered prior to the platinum-based chemotherapeutic agent, and the platinum agent is administered prior to the topoisomerase II inhibitor. 107. The method of embodiment 106, wherein
108.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が静脈内投与される、実施形態80~107のいずれか一項に記載の方法。 108. 108. The method of any one of embodiments 80-107, wherein said anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered intravenously.
109.前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤のうち1つ以上が皮下投与される、実施形態80~108のいずれか一項に記載の方法。 109. 109. Any one of embodiments 80-108, wherein one or more of said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are administered subcutaneously. Method.
110.SCLCを有する対象を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約80mg~約1600mgの用量のアテゾリズマブ、各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドの1回以上の21日間投薬サイクルを前記対象に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いないアテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、方法。
110. A method for treating a subject with SCLC, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
111.SCLCを有する対象を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約300mg~約800mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約900mg~約1500mgの用量のアテゾリズマブ、各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドの1回以上の21日間投薬サイクルを前記対象に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いないアテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、方法。
111. A method for treating a subject with SCLC, said method comprising administering an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 800 mg on
112.各追加の投薬サイクルの1日目に約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体と、各追加の投薬サイクルの1日目に約80mg~約1600mgの用量のアテゾリズマブとの1回以上の追加の21日間の投薬サイクルを前記対象に投与することを更に含み、カルボプラチン及びエトポシドが1回以上の追加の投薬サイクルのそれぞれから省略される、実施形態110又は111に記載の方法。
112. One or more additions of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
113.ES-SCLCを有する対象又は対象集団を処置するための方法であって、前記方法が、4回の初期投薬サイクルと、それに続く1回以上の追加の投薬サイクルとを前記対象又は対象集団に投与することを含み、
(a)前記4回の初期投薬サイクルが、各初期投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各初期投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各初期投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各初期投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量のエトポシドを投与することを含み、
(b)前記1回以上の追加の投薬サイクルが、各追加の投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各追加の投薬サイクルの1日目に約1200mgの用量のアテゾリズマブを投与することを含み、
前記4回の初期投薬サイクル及び前記1回以上の追加の投薬サイクルが、それぞれ21日間投薬サイクルであり、前記処置が、前記チラゴルマブを用いないアテゾリズマブ、カルボプラチン及びエトポシドを含む処置と比較して、前記対象又は対象集団のPFS及び/又はOSを延長する、方法。
113. A method for treating a subject or subject population with ES-SCLC, said method administering to said subject or subject population four initial dosing cycles followed by one or more additional dosing cycles. including
(a) the four initial dosing cycles are tiragolumab at a dose of about 600 mg on
(b) said one or more additional dosing cycles administering a dose of about 600 mg tiragolumab on
each of the four initial dosing cycles and the one or more additional dosing cycles is a 21-day dosing cycle, and the treatment is compared to a treatment comprising atezolizumab, carboplatin and etoposide without the tiragolumab; A method of prolonging PFS and/or OS of a subject or subject population.
114.肺がんを有する対象又は対象集団を処置する方法であって、前記方法が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤である第1の化学療法剤、及び非白金系化学療法剤である第2の化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、方法。 114. 1. A method of treating a subject or population of subjects having lung cancer, said method comprising: an anti-TIGIT antagonist antibody; a PD-1 axis binding antagonist; a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent; administering to said subject or population of subjects a dosing regimen comprising one or more dosing cycles of a second chemotherapeutic agent that is a therapeutic agent.
115.前記肺がんがPD-L1発現について評価されていない、実施形態114に記載の方法。 115. 115. The method of embodiment 114, wherein said lung cancer has not been evaluated for PD-L1 expression.
116.前記一又は複数の対象が、50%以上のPD-L1陽性腫瘍細胞分率を有すると決定されていない、実施形態114又は115に記載の方法。 116. 116. The method of embodiment 114 or 115, wherein said one or more subjects have not been determined to have a PD-L1 positive tumor cell fraction of 50% or greater.
117.前記一又は複数の対象が50%未満のPD-L1陽性腫瘍細胞分率を有すると決定されている、実施形態116に記載の方法。 117. 117. The method of embodiment 116, wherein said one or more subjects have been determined to have a PD-L1 positive tumor cell fraction of less than 50%.
118.前記PD-L1陽性腫瘍細胞分率が、抗PD-L1抗体を用いる陽性染色によって決定され、前記抗PD-L1抗体がSP263又は22C3である、実施形態116又は117に記載の方法。 118. 118. The method of embodiment 116 or 117, wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, said anti-PD-L1 antibody is SP263 or 22C3.
119.前記一又は複数の対象が、上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態114~118のいずれか一項に記載の方法。 119. 119. The method of any one of embodiments 114-118, wherein the one or more subjects do not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations.
120.前記一又は複数の対象が、前記肺がんに対する事前全身治療を受けたことがない、実施形態114~119のいずれか一項に記載の方法。 120. 120. The method of any one of embodiments 114-119, wherein said one or more subjects have not received prior systemic therapy for said lung cancer.
121.前記肺がんが局所進行性肺がんである、実施形態114~120のいずれか一項に記載の方法。 121. 121. The method of any one of embodiments 114-120, wherein said lung cancer is locally advanced lung cancer.
122.前記肺がんがNSCLC、特に局所進行性切除不能又は転移性非扁平上皮NSCLCである、実施形態114~121のいずれか一項に記載の方法。 122. 122. The method of any one of embodiments 114-121, wherein said lung cancer is NSCLC, particularly locally advanced unresectable or metastatic non-squamous NSCLC.
123.前記非扁平上皮NSCLCがステージIV非扁平上皮NSCLCである、実施形態122に記載の方法。 123. 123. The method of embodiment 122, wherein said non-squamous NSCLC is stage IV non-squamous NSCLC.
124.前記投薬レジメンが、4回の投薬サイクルを含む導入期を含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記非白金系化学療法剤が、前記導入期の各投薬サイクルの1日目に投与される、実施形態114~123のいずれか一項に記載の方法。
124. The dosing regimen comprises an induction phase comprising four dosing cycles, wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent and the non-platinum-based chemotherapeutic agent are in the induction phase 124. The method of any one of embodiments 114-123, administered on
125.前記投薬レジメンが、前記導入期に続いて維持期を含み、前記維持期が1回以上の投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト及び前記非白金系化学療法剤が、前記維持期の各投薬サイクルの1日目に投与される、実施形態124に記載の方法。
125. wherein said dosing regimen comprises a maintenance phase following said induction phase, said maintenance phase comprising one or more dosing cycles, said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist and said non-platinum chemotherapeutic agent is administered on
126.前記維持期の前記1回以上の投薬サイクルが、前記白金系化学療法剤の投与を含まない、実施形態125に記載の方法。 126. 126. The method of embodiment 125, wherein said one or more dosing cycles of said maintenance phase do not include administration of said platinum-based chemotherapeutic agent.
127.前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、実施形態114~126のいずれか一項に記載の方法。 127. 127. The method of any one of embodiments 114-126, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin and said non-platinum-based chemotherapeutic agent is pemetrexed.
128.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法であって、前記方法が、前記対象又は対象集団に、チラゴルマブ、アテゾリズマブ、カルボプラチン又はシスプラチン及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンを投与することを含み、前記4回の21日間投薬サイクルの各々の1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与され、前記カルボプラチンが3週間ごとにAUC=5mg/ml/分を達成するのに十分な用量で投与されるか又は前記シスプラチンが3週間ごとに75mg/m2の用量で投与され、前記ペメトレキセドが3週間ごとに約500mg/m2の用量で投与される、方法。
128. A method of treating a subject or subject population with advanced non-squamous NSCLC, said method comprising administering to said subject or subject population four 21-day dosing cycles of tiragolumab, atezolizumab, carboplatin or cisplatin and pemetrexed. administering a dosing regimen wherein, on
129.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法であって、前記方法が、前記対象又は対象集団に、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル
で投与することを含み、
前記対象又は対象集団が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、方法。
129. 1. A method of treating a subject or subject population having advanced non-squamous NSCLC, said method comprising:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin. including
The method, wherein said subject or subject population has not received prior systemic therapy for said advanced non-squamous NSCLC.
130.進行性非扁平上皮NSCLCを有する対象を処置する方法であって、前記方法が、前記対象に、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル、
で投与することを含み、
前記対象が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、方法。
130. A method of treating a subject with advanced non-squamous NSCLC, said method comprising:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin;
administering with
The method, wherein said subject has no prior systemic therapy for said advanced non-squamous NSCLC.
131.進行性非扁平上皮NSCLCを有する対象を処置する方法であって、前記方法が、前記対象に、チラゴルマブ、アテゾリズマブ、カルボプラチン又はシスプラチン及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンを投与することを含み、前記4回の21日間投薬サイクルの各々の1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与され、前記シスプラチンが75mg/m2の用量で投与され、前記ペメトレキセドが約500mg/m2の用量で投与される、方法。
131. A method of treating a subject with advanced non-squamous NSCLC, said method administering to said subject a dosing regimen comprising four 21-day dosing cycles of tiragolumab, atezolizumab, carboplatin or cisplatin and pemetrexed. wherein on
132.前記処置が、前記対象又は対象集団のPFSを少なくとも約3.5ヶ月又は約4.7ヶ月延長する、実施形態114~131のいずれか一項に記載の方法。 132. 132. The method of any one of embodiments 114-131, wherein said treatment prolongs PFS of said subject or population of subjects by at least about 3.5 months or about 4.7 months.
133.前記処置が、約12.5ヶ月~約14.7ヶ月の前記対象集団のPFS中央値をもたらす、実施形態114~132のいずれか一項に記載の方法。 133. The method of any one of embodiments 114-132, wherein said treatment results in a median PFS for said subject population of about 12.5 months to about 14.7 months.
134.前記処置が、前記対象又は対象集団のOSを少なくとも約5.5ヶ月又は約8.0ヶ月延長する、実施形態114~133のいずれか一項に記載の方法。 134. 134. The method of any one of embodiments 114-133, wherein said treatment prolongs OS of said subject or population of subjects by at least about 5.5 months or about 8.0 months.
135.前記処置が、約27.5ヶ月~約32.0ヶ月の前記対象集団のOS中央値をもたらす、実施形態114~134のいずれか一項に記載の方法。 135. 135. The method of any one of embodiments 114-134, wherein said treatment results in a median OS for said subject population of from about 27.5 months to about 32.0 months.
136.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 136. A method for treating a subject with resectable lung cancer, said method comprising anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every 3 weeks and about 80 mg and about 1600 mg every 3 weeks. administering to said subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose between .
137.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 137. A method for treating a subject with resectable lung cancer, said method comprising anti-TIGIT antagonist antibody at a dose between about 300 mg and about 800 mg every 3 weeks and about 900 mg and about 1500 mg every 3 weeks. administering to said subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose between .
138.肺がんを有する対象を処置するための方法であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600mgの間の用量で前記対象に投与することを含む、方法。 138. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, at least one of said anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every 3 weeks and said PD-1 axis binding antagonist between about 80 mg and about 1600 mg every 3 weeks as a neoadjuvant treatment. administering to said subject at a dose of
139.肺がんを有する対象を処置するための方法であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約300mgと約800mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約900mgと約1500mgの間の用量で前記対象に投与することを含む、方法。 139. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, at least one of said anti-TIGIT antagonist antibody at a dose between about 300 mg and about 800 mg every 3 weeks and said PD-1 axis binding antagonist between about 900 mg and about 1500 mg every 3 weeks as a neoadjuvant treatment. administering to said subject at a dose of
140.前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600の間の用量で前記対象に投与することを含む、実施形態138又は139に記載の方法。 140. At least one of said dosing cycles comprises, as an adjuvant treatment, said anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks and said PD-1 axis binding antagonist at a dose between about 80 mg and about every three weeks. 140. The method of embodiment 138 or 139, comprising administering to said subject at a dose of between 1600.
141.前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約500mgと約700mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約900mgと約1500の間の用量で前記対象に投与することを含む、実施形態140に記載の方法。 141. At least one of said dosing cycles comprises, as an adjuvant treatment, said anti-TIGIT antagonist antibody at a dose between about 500 mg and about 700 mg every 3 weeks and said PD-1 axis binding antagonist at a dose between about 900 mg and about 900 mg every 3 weeks. 141. The method of embodiment 140, comprising administering to said subject at a dose of between 1500.
142.前記肺がんが切除可能な肺がんである、実施形態138~141のいずれか一項に記載の方法。 142. 142. The method of any one of embodiments 138-141, wherein said lung cancer is resectable lung cancer.
143.前記肺がんが初期肺がんである、実施形態136~142のいずれか一項に記載の方法。 143. 143. The method of any one of embodiments 136-142, wherein said lung cancer is early stage lung cancer.
144.前記肺がんが、ステージII、IIIA又はIIIBの肺がんである、実施形態136~143のいずれか一項に記載の方法。 144. 144. The method of any one of embodiments 136-143, wherein said lung cancer is stage II, IIIA or IIIB lung cancer.
145.前記肺がんが上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態136~144のいずれか一項に記載の方法。 145. 145. The method of any one of embodiments 136-144, wherein said lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations.
146.前記対象が治癒目的でのR0摘出術に適格である、実施形態136~145のいずれか一項に記載の方法。 146. 146. The method of any one of embodiments 136-145, wherein said subject is eligible for R0 enucleation with curative intent.
147.前記対象が肺がんの事前治療を受けたことがない、実施形態136~146のいずれか一項に記載の方法。 147. 147. The method of any one of embodiments 136-146, wherein said subject has no prior treatment for lung cancer.
148.前記事前治療が免疫療法、化学療法、又は放射線療法である、実施形態147に記載の方法。 148. 148. The method of embodiment 147, wherein said prior treatment is immunotherapy, chemotherapy, or radiation therapy.
149.前記対象が白金系化学療法レジメンを受けるのに適格である、実施形態136~148のいずれか一項に記載の方法。 149. The method of any one of embodiments 136-148, wherein said subject is eligible to undergo a platinum-based chemotherapy regimen.
150.前記第1の投薬サイクルが手術の前に開始される、実施形態136~149のいずれか一項に記載の方法。 150. 149. The method of any one of embodiments 136-149, wherein said first dosing cycle is initiated prior to surgery.
151.少なくとも1、2、3又は4回の投薬サイクルが前記手術の前に完了する、実施形態150に記載の方法。 151. 151. The method of embodiment 150, wherein at least 1, 2, 3 or 4 dosing cycles are completed prior to said surgery.
152.4回の投薬サイクルが前記手術の前に完了する、実施形態150又は151に記載の方法。 152. The method of embodiment 150 or 151, wherein 4 dosing cycles are completed prior to said surgery.
153.少なくとも1回の投薬サイクルが手術後に開始される、実施形態136~152のいずれか一項に記載の方法。 153. 153. The method of any one of embodiments 136-152, wherein at least one dosing cycle is initiated after surgery.
154.16回の投薬サイクルが前記手術後に完了する、実施形態153に記載の方法。 154. The method of embodiment 153, wherein 16 dosing cycles are completed after said surgery.
155.前記手術が、区域切除術、肺葉切除術、二葉切除術、又は肺切除術である、実施形態150~154のいずれか一項に記載の方法。 155. 155. The method of any one of embodiments 150-154, wherein said surgery is segmentectomy, lobectomy, bilobectomy, or pneumonectomy.
156.前記方法が放射線療法を更に含む、実施形態136~155のいずれか一項に記載の方法。 156. 156. The method of any one of embodiments 136-155, wherein said method further comprises radiation therapy.
157.前記放射線療法が術後放射線療法である、実施形態156に記載の方法。 157. 157. The method of embodiment 156, wherein said radiation therapy is postoperative radiation therapy.
158.前記方法が、1つ以上の化学療法剤を投与することを更に含む、実施形態136~157のいずれか一項に記載の方法。 158. 158. The method of any one of embodiments 136-157, wherein said method further comprises administering one or more chemotherapeutic agents.
159.前記1つ以上の化学療法剤が手術後に投与される、実施形態158に記載の方法。 159. 159. The method of embodiment 158, wherein said one or more chemotherapeutic agents are administered post-operatively.
160.前記1つ以上の化学療法剤が、前記手術後に4回の投薬サイクルで投与される、実施形態159に記載の方法。 160. 160. The method of embodiment 159, wherein said one or more chemotherapeutic agents are administered in four dosing cycles after said surgery.
161.前記1つ以上の化学療法剤が、白金系化学療法剤及び非白金系化学療法剤である、実施形態158~160のいずれか一項に記載の方法。 161. 161. The method of any one of embodiments 158-160, wherein said one or more chemotherapeutic agents are platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents.
162.(a)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
(c)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、
(d)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、又は
(e)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
実施形態161に記載の方法。
162. (a) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine. is
162. The method of embodiment 161.
163.前記処置が、基準病理学的著効(MPR)率と比較してMPR率の増加をもたらす、実施形態136~162のいずれか一項に記載の方法。 163. 163. The method of any one of embodiments 136-162, wherein said treatment results in an increase in MPR rate compared to the baseline significant pathological response (MPR) rate.
164.前記基準MPR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のMPR率である、実施形態163に記載の方法。
164. The reference MPR rate is
MPR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 164. The method of embodiment 163, wherein
165.前記処置が、病理学的完全奏効(pCR)及び/又は基準pCR率と比較したpCR率の増加をもたらす、実施形態136~164のいずれか一項に記載の方法。 165. 165. The method of any one of embodiments 136-164, wherein said treatment results in pathological complete response (pCR) and/or increased pCR rate compared to baseline pCR rate.
166.前記基準pCR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のpCR率である、実施形態165に記載の方法。
166. The reference pCR rate is
pCR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 166. The method of embodiment 165, wherein
167.前記処置が、基準無症候生存期間(EFS)と比較して、EFS時間の増加をもたらす、実施形態136~166のいずれか一項に記載の方法。 167. 167. The method of any one of embodiments 136-166, wherein said treatment results in increased EFS time compared to baseline symptom-free survival (EFS).
168.前記基準EFS時間が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のEFS時間である、実施形態167に記載の方法。
168. the reference EFS time,
EFS time in a subject population that has received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 168. The method of embodiment 167, wherein
169.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約600mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 169. A method for treating a subject with resectable lung cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 600 mg every three weeks and between about 80 mg and about 1600 mg every three weeks. administering to said subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose between .
170.肺がんを有する対象を処置するための方法であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約600mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600mgの間の用量で前記対象に投与することを含む、方法。 170. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, at least one of said anti-TIGIT antagonist antibody at a dose between about 30 mg and about 600 mg every 3 weeks and said PD-1 axis binding antagonist between about 80 mg and about 1600 mg every 3 weeks as a neoadjuvant treatment. administering to said subject at a dose of
171.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含む、方法。 171. A method for treating a subject with resectable lung cancer, said method comprising: an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every 3 weeks; administering to said subject one or more dosing cycles of between doses of a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent.
172.肺がんを有する対象を処置するための方法であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとの約30mgと約1200mgの間の用量の前記抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤を前記対象に投与することを含む、方法。 172. A method for treating a subject with lung cancer, said method comprising one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent. wherein at least one of said dosing cycles comprises administering to said subject a dose of said anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg every 3 weeks, about 80 mg every 3 weeks and about 80 mg every 3 weeks as a neoadjuvant treatment. administering to said subject a dose of between about 1600 mg of said PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent.
173.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストと、(a)(i)3週間ごとの5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量の白金系化学療法剤;又は(ii)3週間ごとの約75mg/m2の用量の白金系化学療法剤と、(b)(i)3週間ごとの約500mg/m2、各投薬サイクルの第1日及び第8日に約1000mg/m2若しくは約1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとの約100mg/m2、約175mg/m2、若しくは約200mg/m2の用量のタキサンと、の1回以上の投薬サイクルを対象に投与することを含む、方法。
173. A method for treating a subject with resectable lung cancer, said method comprising: an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every 3 weeks; and (a)(i) a dose of a platinum-based chemical aimed at achieving an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks. or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m2 every three weeks and (b)(i) about 500 mg/m2 every three weeks on
174.肺がんを有する対象を処置するための方法であって、前記方法が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、少なくとも1つの前記投薬サイクルが、前記対象に、(a)3週間ごとの約30mgと約600mgの間の用量の前記抗TIGITアンタゴニスト抗体と、(b)3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニストと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量、又は(ii)3週間ごとの約75mg/m2の用量の前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のタキサンである非白金系化学療法剤と、を投与することを含み、前記処置がネオアジュバント処置である、方法。
174. A method for treating a subject with lung cancer, said method comprising administering one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. administering to said subject, wherein at least one said dosing cycle comprises: (a) said anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 600 mg every 3 weeks; and (b) for 3 weeks. (c) said platinum-based chemotherapeutic agent, wherein (i) an AUC of 5 mg/mL/min or 6 mg every 3 weeks; (ii) a dose of about 75 mg/m every 3 weeks of the platinum-based chemotherapeutic agent; and (d) the non-platinum-based chemotherapeutic agent. (i) an antimetabolite at a dose of 500 mg/m2 every 3 weeks, or 1000 mg/m2 or 1250 mg/m2 on
175.切除可能な肺がんを有する対象を処置するための方法であって、前記方法が、前記対象に、3週間ごとの約600mgの用量のチラゴルマブと、3週間ごとの約1200mgの用量のアテゾリズマブと、
(a)
(i)3週間ごとの5mg/mL/分のAUC若しくは6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は
(ii)3週間ごとの約75mg/m2の用量のシスプラチンと、
(b)
(i)3週間ごとの約500mg/m2の用量のペメトレキセド、又は各投薬サイクルの1日目及び8日目に約1000mg/m2若しくは約1250mg/m2の用量のゲムシタビン、又は
(ii)3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセルと、の1回以上の投薬サイクルを投与することを含む、方法。
175. A method for treating a subject with resectable lung cancer, said method comprising administering to said subject tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks;
(a)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and,
(b)
(i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks, or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on
176.肺がんを有する対象を処置するための方法であって、前記方法が、チラゴルマブ、アテゾリズマブ、白金系化学療法剤及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、少なくとも1つの前記投薬サイクルが、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブと、(b)3週間ごとの約1200mgの用量のアテゾリズマブと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は(ii)3週間ごとの約75mg/m2の用量のシスプラチンである、前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量のペメトレキセド、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のパクリタキセルである非白金系化学療法剤と、を投与することを含み、前記処置がネオアジュバント処置である、方法。
176. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. wherein at least one of said dosing cycles administered to said subject (a) tiragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks; A therapeutic agent which is (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) about 75 mg every 3 weeks (d) the non-platinum-based chemotherapeutic agent, which is (i) 500 mg/m2 every 3 weeks or on
177.非扁平上皮NSCLC有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(a)前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとの約600mgの用量のチラゴルマブ及び3週間ごとの1200mgの用量のアテゾリズマブを前記対象に投与することを含み、(b)前投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量の前記アテゾリズマブを投与することを含む、方法。 177. A method for treating a subject with non-squamous NSCLC, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab, (a) at least one of said dosing cycles (b) at least one of the premedication cycles comprises administering to said subject a dose of about 600 mg of tiragolumab every 3 weeks and atezolizumab at a dose of 1200 mg every 3 weeks as neoadjuvant treatment; administering to said subject a dose of about 600 mg of tiragolumab every 3 weeks and a dose of about 1200 mg of said atezolizumab every 3 weeks.
178.非扁平上皮NSCLCを有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ;(b)ネオアジュバント処置として3週間ごとの約1200mgの用量のアテゾリズマブ;(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセド;(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2又は約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドを投与することを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストを投与すること、含む、方法。 178. A method for treating a subject with non-squamous NSCLC, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab, wherein (I) at least One is a neoadjuvant treatment, wherein the subject is given (a) tiragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment; i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; (ii) 6 mg/mL/min every 3 weeks; carboplatin at a dose targeted to achieve a minute AUC and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and administering pemetrexed at a dose of about 500 mg/m2 every 3 weeks; and administering a dose of an anti-TIGIT antagonist antibody between about 80 mg and about 1600 mg every three weeks of a PD-1 axis binding antagonist.
179.肺がんを有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブを投与することを含む、方法。 179. 1. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab, wherein (I) at least one of the dosing cycles comprises: (a) tiragolumab at a dose of about 600 mg every 3 weeks, (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment, (c) (i) 3 carboplatin at a dose targeted to achieve a weekly AUC of 5 mg/mL/min and gemcitabine at a dose of approximately 1000 mg/m2 on days 1 and 8 of each dosing cycle, (ii) every 3 weeks Carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min of and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii) about 75 mg/m2 every 3 weeks m and a dose of gemcitabine of about 1250 mg/m on days 1 and 8 of each dosing cycle, and (II) at least one of said dosing cycles comprises, as an adjuvant treatment, administering to said subject a dose of tiragolumab between about 30 mg and about 1200 mg every three weeks and atezolizumab at a dose of between about 80 mg and about 1600 mg every three weeks.
180.肺がんを有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、
(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、
(a)3週間ごとの約1200mgの用量のチラゴルマブと、
(b)ネオアジュバント処置として3週間ごとの約1200mgの用量のアテゾリズマブと、
(c)
(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの第1日及び第8日に約1000mg/m2の用量のゲムシタビン、
(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は
(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの1日目及び8日目に約1250mg/m2の用量のゲムシタビン、を投与することを含み、
(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に、3週間ごとの約300mgと約800mgの間の用量のチラゴルマブ、及び3週間ごとの約900mgと約1500mgの間の用量のアテゾリズマブを投与することを含む、方法。
180. 1. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab,
(I) at least one of said dosing cycles is a neoadjuvant treatment, wherein said subject comprises:
(a) tiragolumab at a dose of about 1200 mg every 3 weeks;
(b) atezolizumab at a dose of about 1200 mg every 3 weeks as a neoadjuvant treatment;
(c)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
(ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii)3 administering a weekly dose of cisplatin of about 75 mg/m2 and a dose of gemcitabine of about 1250 mg/m2 on
(II) at least one of said dosing cycles comprises, as an adjuvant treatment, giving said subject tiragolumab at a dose of between about 300 mg and about 800 mg every three weeks and a dose of between about 900 mg and about 1500 mg every three weeks; A method comprising administering atezolizumab.
181.肺がんを有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの訳600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブを投与することを含む、方法。
181. 1. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab, wherein (I) at least one of the dosing cycles comprises: (a) tiragolumab at a dose of about 600 mg every 3 weeks, (b) atezolizumab at a dose of about 1200 mg every 3 weeks as neoadjuvant treatment, (c) (i) 3 carboplatin at a dose targeted to achieve a weekly AUC of 5 mg/mL/min and gemcitabine at a dose of approximately 1000 mg/m2 on
182.切除可能な扁平上皮NSCLCを有する対象を処置するための方法であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの訳600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブを投与することを含む、方法。
182. 1. A method for treating a subject with resectable squamous NSCLC, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab; at least one is a neoadjuvant treatment, wherein the subject is administered (a) tiragolumab at a dose of about 600 mg every 3 weeks; (b) atezolizumab at a dose of about 1200 mg every 3 weeks as a neoadjuvant treatment; ) (i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
183.抗PD-L1抗体SP263による染色を含むIHCアッセイによって検出可能なPD-L1タンパク質発現レベルが決定される、実施形態136~182のいずれか一項に記載の方法。 183. The method of any one of embodiments 136-182, wherein detectable PD-L1 protein expression levels are determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP263.
184.前記検出可能なPD-L1タンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態183に記載の方法。 184. 184. The method of embodiment 183, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 50% or greater.
185.前記肺がんがNSCLCである、実施形態73、114~121、及び136~184のいずれか一項に記載の方法。
185. The method of any one of
186.NSCLCが、扁平上皮NSCLCである、実施形態185に記載の方法。 186. 186. The method of embodiment 185, wherein the NSCLC is squamous NSCLC.
187.NSCLCが、非扁平上皮NSCLCである、実施形態185に記載の方法。 187. 186. The method of embodiment 185, wherein the NSCLC is non-squamous NSCLC.
188.前記がんが、子宮頸がんである、実施形態72に記載の方法。
188. 73. The method of
189.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、方法。 189. A method for treating a subject or subject population having cervical cancer with detectable levels of PD-L1 expression, said method comprising anti-TIGIT at a dose between about 30 mg and about 1200 mg every 3 weeks. administering to said subject or population of subjects one or more dosing cycles of an antagonist antibody and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks.
190.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法であって、前記方法が、3週間ごとに約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとに約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、方法。 190. A method for treating a subject or subject population having cervical cancer with detectable levels of PD-L1 expression, said method comprising anti-TIGIT at a dose of between about 300 mg and about 800 mg every three weeks. administering to said subject or population of subjects one or more dosing cycles of an antagonist antibody and a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every three weeks.
191.子宮頸がんを有する対象に対して治療を選択する方法であって、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、約30mgと約1200mgの間の用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び約80mgと約1600mgの間の用量で3週間ごとに投与されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
191. A method of selecting treatment for a subject with cervical cancer, comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - for said subject with an L1 expression level, an anti-TIGIT antagonist antibody administered every three weeks at a dose of between about 30 mg and about 1200 mg based on detected PD-L1 expression on tumor cells and about 80 mg and selecting a treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist administered every three weeks at a dose of between about 1600 mg.
192.前記子宮頸がんが扁平上皮癌腫、腺扁平上皮癌腫、又は腺癌である、実施形態189~191のいずれか一項に記載の方法。 192. 192. The method of any one of embodiments 189-191, wherein said cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
193.前記子宮頸がんがステージIVB、転移性、再発性又は持続性である、実施形態189~191のいずれか一項に記載の方法。 193. 192. The method of any one of embodiments 189-191, wherein said cervical cancer is stage IVB, metastatic, recurrent or persistent.
194.前記子宮頸がんが転移性及び/又は再発性PD-L1陽性子宮頸癌腫である、実施形態189~193のいずれか一項に記載の方法。 194. 194. The method of any one of embodiments 189-193, wherein said cervical cancer is metastatic and/or recurrent PD-L1 positive cervical carcinoma.
195.前記一又は複数の対象が、少なくとも1種類の事前治療を受けたことがある、実施形態189~194のいずれか一項に記載の方法。 195. 195. The method of any one of embodiments 189-194, wherein said one or more subjects have received at least one prior treatment.
196.前記一又は複数の対象が、2種類の事前治療を受けたことがある、実施形態189~195のいずれか一項に記載の方法。 196. 196. The method of any one of embodiments 189-195, wherein said one or more subjects have received two prior treatments.
197.前記一又は複数の対象が、3種類以上の事前治療を受けたことがない、実施形態189~196のいずれか一項に記載の方法。 197. 197. The method of any one of embodiments 189-196, wherein said one or more subjects have not received 3 or more prior treatments.
198.前記一又は複数の対象が事前治療を受けたことがない、実施形態189~194のいずれか一項に記載の方法。 198. 195. The method of any one of embodiments 189-194, wherein said one or more subjects have no prior treatment.
199.前記事前治療が、化学療法、外科手術及び/又は放射線療法である、実施形態195~198のいずれか一項に記載の方法。 199. 199. The method of any one of embodiments 195-198, wherein said prior treatment is chemotherapy, surgery and/or radiotherapy.
200.前記処置が臨床応答をもたらす、実施形態189及び192~199のいずれか一項に記載の方法。 200. The method of any one of embodiments 189 and 192-199, wherein said treatment results in a clinical response.
201.前記臨床応答が、基準客観的奏効率(ORR)と比較した前記対象集団のORRの増加である、実施形態200に記載の方法。
201. 201. The method of
202.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態201に記載の方法。 202. 202. The method of embodiment 201, wherein said baseline ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
203.前記基準ORRが、少なくとも約14.6%~約26%である、実施形態200に記載の方法。
203. 201. The method of
204.前記臨床応答がCR又はPRである、実施形態200に記載の方法。
204. 201. The method of
205.前記臨床応答が、基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象のOS時間の増加である、実施形態200~204のいずれか一項に記載の方法。 205. wherein said clinical response is increased in said subject's PFS time compared to baseline progression-free survival (PFS), increased in said subject's DOR time compared to baseline duration of response (DOR), or baseline overall survival (OS) 205. The method of any one of embodiments 200-204, wherein the increase in OS time of the compared subjects.
206.実施形態205に記載の方法であって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
方法。
206. 206. The method of embodiment 205, wherein:
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
Method.
207.[実施形態177]検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法であって、前記方法が、前記対象に、3週間ごとの600mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、方法。 207. [Embodiment 177] A method for treating a subject having cervical cancer with detectable levels of PD-L1 expression, said method comprising administering to said subject anti-TIGIT at a dose of 600 mg every three weeks. A method comprising administering an antagonist antibody and one or more dosing cycles of atezolizumab at a dose of 1200 mg every 3 weeks.
208.抗TIGITアンタゴニスト抗体及びアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い子宮頸がんを有する対象を同定する方法であって、前記方法が、
(a)前記対象からの腫瘍試料提供すること、
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、を含む、方法。
208. A method of identifying a subject with cervical cancer who is likely to benefit from treatment comprising an anti-TIGIT antagonist antibody and one or more dosing cycles of atezolizumab, said method comprising:
(a) providing a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (c) PD-L1 expression on the detected tumor cells. based on the likely benefit from treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. A method comprising identifying a subject.
209.子宮頸がんを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、方法。
209. A method of selecting treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on tumor cells detected for said subject with L1 expression level selecting a treatment comprising one or more dosing cycles of atezolizumab administered.
210.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法であって、前記方法が、前記対象に、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、方法。 210. A method for treating a subject having cervical cancer with detectable levels of PD-L1 expression, said method comprising administering to said subject tiragolumab at a dose of about 600 mg every 3 weeks and administering one or more dosing cycles of atezolizumab at a dose of about 1200 mg.
211.子宮頸がんを有する対象を処置する方法であって、前記方法が、
(a)前記対象からの腫瘍試料提供すること、
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、方法。
211. A method of treating a subject with cervical cancer, said method comprising:
(a) providing a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) based on detected PD-L1 expression on tumor cells, one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. and (d) administering said treatment to said identified subject.
212.子宮頸がんを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、方法。
212. A method of selecting treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks for said subjects with L1 expression levels based on detected PD-L1 expression on tumor cells selecting a treatment comprising one or more dosing cycles of
213.転移性及び/又は再発性子宮頸がんを有する対象を処置する方法であって、前記方法が、
(a)前記対象からの腫瘍試料提供すること、
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、方法。
213. A method of treating a subject with metastatic and/or recurrent cervical cancer, said method comprising:
(a) providing a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) based on detected PD-L1 expression on tumor cells, one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. and (d) administering said treatment to said identified subject.
214.転移性及び/又は再発性子宮頸がんを有する対象のための治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、方法。
214. A method of selecting a treatment for a subject with metastatic and/or recurrent cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks for said subjects with L1 expression levels based on detected PD-L1 expression on tumor cells selecting a treatment comprising one or more dosing cycles of
215.前記対象が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態189~214のいずれか一項に記載の方法。 215. The method of any one of embodiments 189-214, wherein said subject is identified as likely to benefit from said treatment based on detected PD-L1 expression on tumor cells.
216.PD-L1発現レベルが抗PD-L1抗体SP263を使用して検出される、実施形態189~215のいずれか一項に記載の方法。 216. The method of any one of embodiments 189-215, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
217.前記検出可能なPD-L1発現レベルが、前記対象からの試料において5%以上の腫瘍関連免疫細胞(TIC)である、実施形態189~216のいずれか一項に記載の方法。 217. 217. The method of any one of embodiments 189-216, wherein said detectable PD-L1 expression level is 5% or more tumor-associated immune cells (TIC) in a sample from said subject.
218.PD-L1発現レベルが抗PD-L1抗体22C3を使用して検出される、実施形態189~215のいずれか一項に記載の方法。 218. The method of any one of embodiments 189-215, wherein PD-L1 expression level is detected using anti-PD-L1 antibody 22C3.
219.前記検出可能なPD-L1発現レベルが、前記対象からの試料において1以上の複合陽性スコア(CPS)である、実施形態189~216のいずれか一項に記載の方法。 219. 217. The method of any one of embodiments 189-216, wherein said detectable PD-L1 expression level is a composite positive score (CPS) of 1 or more in a sample from said subject.
220.前記がんが乳がんである、実施形態72に記載の方法。
220. 73. The method of
221.乳がんを有する対象又は対象集団を処置する方法であって、4週間ごとの約840mgの用量のチラゴルマブ、4週間ごとの約1680mgの用量のアテゾリズマブ、及び3週間の投薬/1週間の休薬で約100mg/m2の用量のnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、方法。 221. A method of treating a subject or subject population having breast cancer, comprising tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and about 3 weeks on/1 week off. administering to said subject or subject population a dosing regimen comprising one or more dosing cycles of nab-paclitaxel at a dose of 100 mg/m2.
222.前記乳がんがトリプルネガティブ乳がん(TNBC)である、実施形態220又は221に記載の方法。 222. 222. The method of embodiment 220 or 221, wherein said breast cancer is triple negative breast cancer (TNBC).
223.前記TNBCが、切除不能な局所進行性又は転移性TNBCである、実施形態222に記載の方法。 223. 223. The method of embodiment 222, wherein said TNBC is unresectable locally advanced or metastatic TNBC.
224.前記対象が転移性乳がんのための事前全身治療を受けたことがない、実施形態220~223のいずれか一項に記載の方法。 224. 224. The method of any one of embodiments 220-223, wherein said subject has had no prior systemic therapy for metastatic breast cancer.
225.前記処置が、少なくとも約53%~約67.5%の対象集団のORRをもたらす、実施形態220~224のいずれか一項に記載の方法。 225. The method of any one of embodiments 220-224, wherein said treatment results in an ORR of the subject population of at least about 53% to about 67.5%.
226.前記処置が、約25.0ヵ月の前記対象集団のOS中央値をもたらす、実施形態222~225のいずれか一項に記載の方法。 226. The method of any one of embodiments 222-225, wherein said treatment results in a median OS for said subject population of about 25.0 months.
227.初期トリプルネガティブ乳がん(eTNBC)を有する対象を処置する方法であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約20mg~1600mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、方法。 227. A method of treating a subject with early triple negative breast cancer (eTNBC), said method comprising an anti-TIGIT antagonist antibody at a dose of about 10 mg to about 1000 mg every two weeks and a dose of about 20 mg to 1600 mg every two weeks. administering to said subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist of.
228.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態227に記載の方法。 228. 228. The method of embodiment 227, wherein said method further comprises administering one or more chemotherapeutic agents to said subject.
229.前記1つ以上の化学療法剤が、白金系化学療法剤、タキサン、トポイソメラーゼII阻害剤又はアルキル化剤である、実施形態228に記載の方法。 229. 229. The method of embodiment 228, wherein said one or more chemotherapeutic agents is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
230.前記方法が、(a)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、タキサンと、又はタキサン及び白金系化学療法剤との1回以上の投薬サイクル、並びに(b)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、トポイソメラーゼII阻害剤と、アルキル化剤と、顆粒球コロニー刺激因子(G-CSF)又は顆粒球マクロファージコロニー刺激因子(GM-CSF)との1回以上の投薬サイクル、を投与することを更に含む、実施形態227に記載の方法。 230. The method comprises (a) one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, a taxane, or a taxane and a platinum-based chemotherapeutic agent, and (b) the anti-TIGIT One dose of an antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony-stimulating factor (G-CSF) or granulocyte-macrophage colony-stimulating factor (GM-CSF) 228. The method of embodiment 227, further comprising administering the above dosing cycle.
231.前記アルキル化剤がシクロホスファミドである、実施形態229又は230に記載の方法。 231. 231. The method of embodiment 229 or 230, wherein said alkylating agent is cyclophosphamide.
232.前記シクロホスファミドが約600mg/m2の用量で投与される、実施形態231に記載の方法。 232. 232. The method of embodiment 231, wherein said cyclophosphamide is administered at a dose of about 600 mg/m2.
233.前記方法が、G-CSF又はGM-CSFを前記対象に更に投与することを含む、実施形態227~229、231、及び232のいずれか一項に記載の方法。 233. The method of any one of embodiments 227-229, 231, and 232, wherein said method further comprises administering G-CSF or GM-CSF to said subject.
234.前記G-CSFがペグフィルグラスチム又はフィルグラスチムである、実施形態230又は233に記載の方法。 234. 234. The method of embodiment 230 or 233, wherein said G-CSF is pegfilgrastim or filgrastim.
235.前記G-CSFがペグフィルグラスチムである、実施形態234に記載の方法。 235. 235. The method of embodiment 234, wherein said G-CSF is pegfilgrastim.
236.前記ペグフィルグラスチムが約6mgの用量で投与される、実施形態235に記載の方法。 236. 236. The method of embodiment 235, wherein said pegfilgrastim is administered at a dose of about 6 mg.
237.前記方法が、前記1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFの1つ以上の後続用量を前記対象に更に投与することを含む、実施形態228、229、及び231~236のいずれか一項に記載の方法。 237. Embodiments 228, 229, and 231-236, wherein said method further comprises administering said one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF to said subject The method according to any one of .
238.前記1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFがそれぞれ、週に1回、2週間に1回、又は3週間に1回投与される、実施形態228、229、及び231~237のいずれか一項に記載の方法。 238. Embodiments 228, 229, and 231, wherein said one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once weekly, once every two weeks, or once every three weeks, respectively 237. The method of any one of clauses 1-237.
239.前記白金系化学療法剤が3週間ごとに投与され、前記タキサンが毎週投与され、前記トポイソメラーゼII阻害剤が2週間ごとに投与され、前記アルキル化剤が2週間ごとに投与され、前記G-CSF又はGM-CSFが2週間ごとに投与される、実施形態229~238のいずれか一項に記載の方法。 239. The platinum-based chemotherapeutic agent is administered every three weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every two weeks, the alkylating agent is administered every two weeks, and the G-CSF Or the method of any one of embodiments 229-238, wherein GM-CSF is administered every two weeks.
240.前記タキサン、又は前記タキサン及び前記白金系化学療法剤が、前記投薬レジメンの最初の12週間投与される、実施形態229~239のいずれか一項に記載の方法。 240. 239. The method of any one of embodiments 229-239, wherein said taxane, or said taxane and said platinum-based chemotherapeutic agent are administered for the first 12 weeks of said dosing regimen.
241.前記トポイソメラーゼII阻害剤、前記アルキル化剤、及び前記G-CSF又はGM-CSFが、前記投薬レジメンの第13週~第19週の間投与される、実施形態229~240いずれか一項に記載の方法。
241. 240. Any one of embodiments 229-240, wherein the topoisomerase II inhibitor, the alkylating agent, and the G-CSF or GM-CSF are administered during
242.前記投薬レジメンの全長が19週間である、実施形態227~241のいずれか一項に記載の方法。 242. The method of any one of embodiments 227-241, wherein the total length of said dosing regimen is 19 weeks.
243.前記方法がネオアジュバント処置である、実施形態227~242のいずれか一項に記載の方法。 243. The method of any one of embodiments 227-242, wherein said method is a neoadjuvant treatment.
244.前記投薬レジメンに続いて手術が行われる、実施形態227~243のいずれか一項に記載の方法。 244. 244. The method of any one of embodiments 227-243, wherein said dosing regimen is followed by surgery.
245.前記手術が、前記投薬レジメンの最後の投与後2週間と6週間の間に行われる、実施形態244に記載の方法。 245. 245. The method of embodiment 244, wherein said surgery is performed between 2 and 6 weeks after the last administration of said dosing regimen.
246.前記手術が乳房切除術を含む、実施形態244又は245に記載の方法。 246. 246. The method of embodiment 244 or 245, wherein said surgery comprises a mastectomy.
247.前記手術が腋窩リンパ節手術を含む、実施形態244~246のいずれか一項に記載の方法。 247. 247. The method of any one of embodiments 244-246, wherein said surgery comprises axillary lymph node surgery.
248.前記トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の方法。 248. The method of any one of embodiments 229-247, wherein said topoisomerase II inhibitor is doxorubicin.
249.前記タキサンがnab-パクリタキセルであり、前記白金系化学療法剤がカルボプラチンであり、前記トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の方法。 249. 248. The method of any one of embodiments 229-247, wherein the taxane is nab-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin.
250.ドキソルビシンが約60mg/m2の用量で投与される、実施形態248又は249に記載の方法。 250. The method of embodiment 248 or 249, wherein doxorubicin is administered at a dose of about 60 mg/m2.
251.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~1200mgの用量のPD-1軸結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
251. A method of treating a subject with eTNBC, said method comprising anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and PD-1 axis binding at a dose of about 600 mg to about 1200 mg every two weeks. an antagonist, and
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
252.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~1200mgの用量のPD-L1結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
252. A method of treating a subject with eTNBC, said method comprising an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and a PD-L1 binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks. and,
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
253.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~1200mgの用量の抗PD-1アンタゴニスト抗体と、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
253. A method of treating a subject with eTNBC, said method comprising an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and an anti-PD-1 antagonist at a dose of about 600 mg to about 1200 mg every two weeks. an antibody;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
254.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量のチラゴルマブと、2週間ごとの約600mg~1200mgの用量の抗PD-1アンタゴニスト抗体と、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
254. A method of treating a subject with eTNBC, said method comprising tiragolumab at a dose of about 300 mg to about 600 mg every two weeks and an anti-PD-1 antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
255.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
255. A method of treating a subject with eTNBC, said method comprising an anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks and atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
256.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとの約300mg~約600mgの用量のチラゴルマブと、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
256. A method of treating a subject with eTNBC, said method comprising tiragolumab at a dose of about 300 mg to about 600 mg every two weeks and atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
257.eTNBCを有する対象を処置する方法であって、前記方法が、2週間ごとに約420mgの用量のチラゴルマブと、2週間ごとに約840mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、方法。
257. A method of treating a subject with eTNBC, said method comprising tiragolumab at a dose of about 420 mg every two weeks and atezolizumab at a dose of about 840 mg every two weeks;
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and administering to said subject a dosing regimen comprising: and said method further comprising surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen.
258.前記対象からの腫瘍試料中の検出可能なPD-L1タンパク質発現レベルが、抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される、実施形態220~257のいずれか一項に記載の方法。 258. 258. The method of any one of embodiments 220-257, wherein the detectable PD-Ll protein expression level in a tumor sample from said subject is determined by an IHC assay comprising staining with the anti-PD-Ll antibody SP142. .
259.前記腫瘍試料中のPD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合が1%以上である、実施形態258に記載の方法。 259. 259. The method of embodiment 258, wherein the percentage of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (ICs) in said tumor sample is 1% or more.
260.前記eTNBCが、提示時にT2-4d TNBCである、実施形態227~259のいずれか一項に記載の方法。 260. 260. The method of any one of embodiments 227-259, wherein said eTNBC is T2-4d TNBC when presented.
261.前記eTNBCが、提示時にcT2-cT4、cN0-cN3、及びcM0 TNBCである、実施形態227~260のいずれか一項に記載の方法。 261. 261. The method of any one of embodiments 227-260, wherein said eTNBCs are cT2-cT4, cN0-cN3, and cM0 TNBCs when presented.
262.前記対象が以前にeTNBCの処置を受けたことがない、実施形態227~261のいずれか一項に記載の方法。 262. 262. The method of any one of embodiments 227-261, wherein said subject has no previous treatment for eTNBC.
263.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態227~262のいずれか一項に記載の方法。 263. 263. The method of any one of embodiments 227-262, wherein said treatment results in a pathological complete response (pCR).
264.前記処置が、全生存期間(OS)又は無症候生存期間(EFS)の増加をもたらす、実施形態227~263のいずれか一項に記載の方法。 264. 264. The method of any one of embodiments 227-263, wherein said treatment results in increased overall survival (OS) or symptom-free survival (EFS).
265.前記がんが頭頸部がんである、実施形態72に記載の方法。
265. 73. The method of
266.前記頭頸部がんが頭頸部の扁平上皮癌腫(SCCHN)である、実施形態265に記載の方法。 266. 266. The method of embodiment 265, wherein said head and neck cancer is squamous cell carcinoma of the head and neck (SCCHN).
267.検出可能なPD-L1発現レベルを伴うnSCCHNを有する対象又は対象集団を処置するための方法であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、方法。 267. A method for treating a subject or subject population having nSCCHN with detectable PD-L1 expression levels, said method comprising administering an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks; and administering to said subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks.
268.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置するための方法であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、方法。 268. 1. A method for treating a subject or subject population having SCCHN with detectable PD-L1 expression levels, said method comprising administering an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every three weeks; and administering to said subject or population of subjects one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every three weeks.
269.SCCHNを有する対象又は対象集団に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象又は対象集団について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
269. A method of selecting a treatment for a subject or subject population with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg every 3 weeks, based on detected PD-L1 expression, for said subject or subject population having a level of selecting a treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 1200 mg.
270.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、方法。 270. A method for treating a subject or population of subjects having SCCHN with detectable levels of PD-L1 expression, said method comprising administering to said subject or population of subjects tiragolumab at a dose of about 600 mg every three weeks, and administering one or more dosing cycles of atezolizumab at a dose of about 1200 mg every three weeks.
271.前記一又は複数の対象から得られた腫瘍試料が、検出可能なPD-L1発現レベルを有すると判定されている、実施形態267~270のいずれか一項に記載の方法。 271. 271. The method of any one of embodiments 267-270, wherein the tumor sample obtained from said one or more subjects has been determined to have a detectable level of PD-Ll expression.
272.前記SSCHNがヒトパピローマウイルス(HPV)陽性である、実施形266~271いずれか一項に記載の方法。 272. 272. The method of any one of embodiments 266-271, wherein said SSCHN is human papillomavirus (HPV) positive.
273.前記SSCHNがHPV陰性である、実施形態266~272のいずれか一項に記載の方法。 273. 273. The method of any one of embodiments 266-272, wherein said SSCHN is HPV negative.
274.HPVの状態が、p16 IHC、in situハイブリダイゼーション又はPCRによって判定される、実施形態272又は273に記載の方法。 274. 274. The method of embodiment 272 or 273, wherein HPV status is determined by p16 IHC, in situ hybridization or PCR.
275.前記SCCHNが、再発性及び/又は転移性SCCHNである、実施形態266~274ずれか一項に記載の方法。 275. 275. The method of any one of embodiments 266-274, wherein said SCCHN is recurrent and/or metastatic SCCHN.
276.前記一又は複数の対象が事前治療を受けたことがない、実施形態265~275のいずれか一項に記載の方法。 276. 276. The method of any one of embodiments 265-275, wherein said one or more subjects have no prior treatment.
277.前記事前治療が、再発性及び/又は転移性疾患のための事前全身治療である、実施形態276に記載の方法。 277. 277. The method of embodiment 276, wherein said prior treatment is prior systemic therapy for recurrent and/or metastatic disease.
278.前記処置がCR又はPRをもたらす、実施形態265~268及び270~277のいずれか一項に記載の方法。 278. The method of any one of embodiments 265-268 and 270-277, wherein said treatment results in CR or PR.
279.前記処置が、基準客観的奏効率(ORR)と比較して前記対象集団のORRの増加をもたらす、実施形態265~268及び270~277のいずれか一項に記載の方法。 279. The method of any one of embodiments 265-268 and 270-277, wherein said treatment results in an increase in ORR in said subject population compared to a baseline objective response rate (ORR).
280.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態279に記載の方法。 280. 280. The method of embodiment 279, wherein said baseline ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
281.前記基準ORRが約19%~約36%である、実施形態279又は280に記載の方法。 281. 281. The method of embodiment 279 or 280, wherein said baseline ORR is from about 19% to about 36%.
282.前記処置が、基準無増悪生存期間(PFS)と比較した前記対象又は対象集団のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象又は対象集団のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象又は対象集団のOS時間の増加をもたらす、実施形態265~268及び270~281のいずれか一項に記載の方法。 282. wherein said treatment increases PFS time of said subject or subject population compared to baseline progression-free survival (PFS), increases DOR time of said subject or subject population compared to baseline duration of response (DOR), or baseline overall survival The method of any one of embodiments 265-268 and 270-281, which results in an increase in OS time for said subject or subject population compared to duration (OS).
283.実施形態282に記載の方法であって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
方法。
283. 283. The method of embodiment 282, wherein:
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
Method.
284.前記基準DOR時間が、少なくとも約6.7ヶ月~約23.4ヶ月である、実施形態282に記載の方法。 284. 283. The method of embodiment 282, wherein the baseline DOR time is from at least about 6.7 months to about 23.4 months.
285.前記基準OS時間が少なくとも約11.6ヶ月~約14.9ヶ月である、実施形態282に記載の方法。 285. 283. The method of embodiment 282, wherein the baseline OS time is at least about 11.6 months to about 14.9 months.
286.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、前記方法が、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、方法。 286. A method for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising administering a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks; and administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks.
287.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、前記方法が、3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、方法。 287. A method for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising administering a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and about administering to said subject one or more dosing cycles of a 600 mg dose of an anti-TIGIT antagonist antibody.
288.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、前記方法が、3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、方法。 288. A method for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising administering a PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks; administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg weekly.
289.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、前記方法が、3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 289. A method for treating a subject having SCCHN with detectable levels of PD-L1 expression, said method comprising administering atezolizumab at a dose between about 80 mg and about 1600 mg every 3 weeks and about administering to said subject one or more dosing cycles of tiragolumab at a dose of between 30 mg and about 1200 mg.
290.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法であって、前記方法が、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 290. A method for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. administering to said subject one or more dosing cycles of
291.SCCHNを有する対象を処置する方法であって、前記方法が、
(a)前記対象からの腫瘍試料提供すること、
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、方法。
291. A method of treating a subject with SCCHN, said method comprising:
(a) providing a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable PD-L1 expression level.
292.SCCHNを有する対象を処置する方法であって、前記方法が、
(a)前記対象からの腫瘍試料提供すること、
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、方法。
292. A method of treating a subject with SCCHN, said method comprising:
(a) providing a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) may benefit from treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable PD-L1 expression level.
293.SCCHNを有する対象を処置する方法であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、方法。
293. A method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) potential to benefit from treatment comprising one or more dosing cycles of atezolizumab at doses between about 80 mg and about 1600 mg every 3 weeks and tiragolumab at doses between about 30 mg and about 1200 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable level of PD-L1 expression.
294.SCCHNを有する対象を処置する方法であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、方法。
294. A method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) identifying subjects likely to benefit from treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks; (d) administering said treatment to said identified subject having a detectable PD-L1 expression level.
295.SCCHNを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
295. A method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg and about 1200 mg every 3 weeks, based on detected PD-L1 expression, for said subjects with levels of selecting a treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at between doses.
296.SCCHNを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
296. A method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. 1 of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks, based on detected PD-L1 expression, for said subjects with levels of selecting a treatment comprising one or more dosing cycles.
297.SCCHNを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
297. A method of selecting treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. atezolizumab at a dose between about 80 mg and about 1600 mg every 3 weeks, and tiragolumab at a dose between about 30 mg and about 1200 mg every 3 weeks for said subjects with levels of selecting a treatment comprising one or more dosing cycles of
298.SCCHNを有する対象に対して治療を選択する方法であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含む方法。
298. A method of selecting treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on detected PD-L1 expression for said subject with a level selecting a.
299.前記検出可能なPD-L1発現レベルが、抗PD-L1抗体SP263で染色することを含む免疫組織化学(IHC)アッセイによって決定される検出可能なPD-L1タンパク質発現レベルである、実施形態267~298のずれか一項に記載の方法。 299. Embodiment 267- wherein said detectable PD-L1 expression level is a detectable PD-L1 protein expression level determined by an immunohistochemistry (IHC) assay comprising staining with anti-PD-L1 antibody SP263 298;
300.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中、
(a)5%以上、
(b)5%以上20%未満、又は
(c)20%以上
の腫瘍関連免疫細胞(TIC)である、実施形態299に記載の方法。
300. the detectable PD-L1 protein expression level in the tumor sample is
(a) 5% or more,
299. The method of embodiment 299, wherein (b) 5% or more and less than 20%, or (c) 20% or more tumor-associated immune cells (TIC).
301.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、方法。 301. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. A method of identifying a subject as likely to benefit from a treatment comprising a dosing cycle, said method comprising detecting PD in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining. - a method comprising determining the L1 protein expression level, wherein a TIC PD-L1 protein expression level of 5% or more identifies said subject as likely to benefit from said treatment.
302.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上かつ20%未満のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、方法。 302. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. A method of identifying a subject as likely to benefit from a treatment comprising a dosing cycle, said method comprising detecting PD in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining. - a method comprising determining the L1 protein expression level, wherein a TIC PD-L1 protein expression level of 5% or more and less than 20% identifies said subject as likely to benefit from said treatment. .
303.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、20%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、方法。 303. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. A method of identifying a subject as likely to benefit from a treatment comprising a dosing cycle, said method comprising detecting PD in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining. - a method comprising determining the L1 protein expression level, wherein a TIC PD-L1 protein expression level of 20% or more identifies said subject as likely to benefit from said treatment.
304.前記対象が治療から利益を得る可能性が高いと同定され、前記方法が、前記対象に治療を投与することを更に含む、実施形態301~303のいずれか一項に記載の方法。 304. The method of any one of embodiments 301-303, wherein said subject is identified as likely to benefit from treatment, said method further comprising administering treatment to said subject.
305.前記TICが、Ventana SP263 IHCアッセイを使用して決定される、実施形態301~304のいずれか一項に記載の方法。 305. 305. The method of any one of embodiments 301-304, wherein said TIC is determined using the Ventana SP263 IHC assay.
306.前記対象又は対象集団が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態267~305のいずれか一項に記載の方法。 306. 306. The method of any one of embodiments 267-305, wherein said subject or subject population is identified as likely to benefit from said treatment based on detected PD-Ll expression on tumor cells. .
307.前記がんが肝臓がんである、実施形態72に記載の方法。
307. 73. The method of
308.前記肝臓がんが肝細胞癌腫(HCC)である、実施形態307に記載の方法。 308. 308. The method of embodiment 307, wherein said liver cancer is hepatocellular carcinoma (HCC).
309.肝細胞癌腫(HCC)を有する対象又は対象集団を処置する方法であって、前記対象又は対象集団に抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象又は対象集団がHCCの事前全身治療を受けたことがない、方法。 309. A method of treating a subject or population of subjects with hepatocellular carcinoma (HCC) comprising administering to said subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist. , the subject or subject population has not received prior systemic therapy for HCC.
310.前記対象又は対象集団にVEGFアンタゴニストを投与する工程を更に含む、実施形態309に記載の方法。 310. 310. The method of embodiment 309, further comprising administering a VEGF antagonist to said subject or population of subjects.
311.HCCを有する対象又は対象集団を処置する方法であって、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、及びVEGFアンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、方法。 311. A method of treating a subject or population of subjects with HCC, comprising administering to said subject or population of subjects one or more dosing cycles of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist, Method.
312.前記VEGFアンタゴニストが、3週間ごとの約5mg/kg~約25mg/kgの用量で投与される、実施形態310及び311に記載の方法。 312. The method of embodiments 310 and 311, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every three weeks.
313.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約1200mgの用量で投与される、実施形態309~312のいずれか一項に記載の方法。 313. The method of any one of embodiments 309-312, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every three weeks.
314.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約800mgの用量で投与される、実施形態313に記載の方法。 314. 314. The method of embodiment 313, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 800 mg every three weeks.
315.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約600mgの固定用量で投与される、実施形態309~314のいずれか一項に記載の方法。 315. The method of any one of embodiments 309-314, wherein said anti-TIGIT antagonist antibody is administered at a fixed dose of about 30 mg to about 600 mg every three weeks.
316.前記PD-1軸結合アンタゴニストが、3週間ごとの約80mg~約1600mgの用量で投与される、実施形態309~315のいずれか一項に記載の方法。 316. The method of any one of embodiments 309-315, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 1600 mg every three weeks.
317.前記PD-1軸結合アンタゴニストが、3週間ごとの約900mg~約1500mgの用量で投与される、実施形態309~316のいずれか一項に記載の方法。 317. The method of any one of embodiments 309-316, wherein said PD-1 axis binding antagonist is administered at a dose of about 900 mg to about 1500 mg every three weeks.
318.前記VEGFアンタゴニストが、2週間ごとの約1mg/kg~約20mg/kgの用量で投与される、実施形態310又は311に記載の方法。 318. The method of embodiment 310 or 311, wherein said VEGF antagonist is administered at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
319.前記VEGFアンタゴニストが、2週間ごとの約5mg/kg~約10mg/kgの用量で投与される、実施形態318に記載の方法。 319. 319. The method of embodiment 318, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
320.前記VEGFアンタゴニストが、2週間ごとの約5mg/kg、約7.5mg/kg又は約10.0mg/kgの用量で投与される、実施形態319に記載の方法。 320. 320. The method of embodiment 319, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10.0 mg/kg every two weeks.
321.前記抗TIGITアンタゴニスト抗体が、2週間ごとの約10mg~約1000mgの用量で投与される、実施形態309~311及び318~320のいずれか一項に記載の方法。 321. The method of any one of embodiments 309-311 and 318-320, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks.
322.前記PD-1軸結合アンタゴニストが、2週間ごとの約20mg~約1600mgの用量で投与される、実施形態309~311及び318~321のいずれか一項に記載の方法。 322. The method of any one of embodiments 309-311 and 318-321, wherein said PD-1 axis binding antagonist is administered at a dose of about 20 mg to about 1600 mg every two weeks.
323.前記抗TIGITアンタゴニスト抗体が、4週間ごとの約200mg~約2000mgの用量で投与される、実施形態309~311に記載の方法。 323. The method of embodiments 309-311, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks.
324.前記PD-1軸結合アンタゴニストが、4週間ごとの約80mg~約2000mgの用量で投与される、実施形態309~311及び323のいずれか一項に記載の方法。 324. The method of any one of embodiments 309-311 and 323, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 4 weeks.
325.前記PD-1軸結合アンタゴニストが、4週間ごとの約1400mg~約2000mgの用量で投与される、実施形態309~311、323及び324のいずれか一項に記載の方法。 325. The method of any one of embodiments 309-311, 323 and 324, wherein said PD-1 axis binding antagonist is administered at a dose of about 1400 mg to about 2000 mg every 4 weeks.
326.前記HCCが局所進行性又は転移性HCCである、実施形態309~325のいずれか一項に記載の方法。 326. 326. The method of any one of embodiments 309-325, wherein said HCC is locally advanced or metastatic HCC.
327.前記HCCが切除不能なHCCである、実施形態309~326のいずれか一項に記載の方法。 327. The method of any one of embodiments 309-326, wherein said HCC is unresectable HCC.
328.前記一又は複数の対象が、適切な肝機能を有すると判定されている、実施形態309~327のいずれか一項に記載の方法。 328. 328. The method of any one of embodiments 309-327, wherein said one or more subjects have been determined to have adequate liver function.
329.前記適切な肝機能がChild-PughクラスAとして特徴付けられる、実施形態328に記載の方法。 329. 329. The method of embodiment 328, wherein said adequate liver function is characterized as Child-Pugh class A.
330.前記一又は複数の対象から得られたHCC腫瘍試料が、検出可能なPD-L1発現レベルを有すると判定されている、実施形態309~329のいずれか一項に記載の方法。 330. The method of any one of embodiments 309-329, wherein the HCC tumor sample obtained from said one or more subjects has been determined to have a detectable PD-L1 expression level.
331.前記方法が、前記対象又は対象集団に少なくとも4回の投薬サイクルを投与することを含む、実施形態309~330のいずれか一項に記載の方法。 331. 331. The method of any one of embodiments 309-330, wherein said method comprises administering to said subject or subject population at least four dosing cycles.
332.前記対象又は対象集団に少なくとも16回の投薬サイクルを投与することを含む、実施形態331に記載の方法。 332. 332. The method of embodiment 331, comprising administering at least 16 dosing cycles to said subject or subject population.
333.HCCを有する対象又は対象集団を処置する方法であって、前記方法が、3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約15mg/kgの用量のベバシズマブの1回以上の投薬サイクルを前記対象に投与することを含む、方法。 333. A method of treating a subject or subject population with HCC, said method comprising tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and about 15 mg/kg every 3 weeks. administering to said subject one or more dosing cycles of bevacizumab at a dose of
334.前記一又は複数の対象が、HCCに対する以前の全身処置を受けたことがない、実施形態311~333のいずれか一項に記載の方法。 334. 334. The method of any one of embodiments 311-333, wherein said one or more subjects have no prior systemic treatment for HCC.
335.前記処置が、少なくとも約5.6ヶ月~少なくとも約6.83ヶ月の前記対象集団のPFS中央値をもたらす、実施形態309~334のいずれか一項に記載の方法。 335. The method of any one of embodiments 309-334, wherein said treatment results in a median PFS of said subject population of at least about 5.6 months to at least about 6.83 months.
336.前記がんが膀胱がんである、実施形態72に記載の方法。
336. 73. The method of
337.前記膀胱がんが筋層浸潤性膀胱がん(MIBC)である、実施形態336に記載の方法。 337. 337. The method of embodiment 336, wherein said bladder cancer is muscle invasive bladder cancer (MIBC).
338.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象が白金系化学療法剤による処置に不適格である、方法。 338. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent, comprising administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per dose.
339.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象が白金系化学療法剤による処置に不適格である、方法。 339. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every three weeks and for three weeks. wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent, comprising administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg per dose.
340.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 340. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per day, wherein said treatment is perioperative treatment.
341.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 341. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every three weeks and for three weeks. administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg per day, wherein said treatment is perioperative treatment.
342.前記一又は複数の対象が60mL/分未満のクレアチニンクリアランスを有する、実施形態338~341に記載の方法。 342. The method of embodiments 338-341, wherein said one or more subjects have a creatinine clearance of less than 60 mL/min.
343.前記一又は複数の対象が、グレード2以上の難聴を有する、実施形態338~342のいずれか一項に記載の方法。
343. 343. The method of any one of embodiments 338-342, wherein the one or more subjects have
344.前記一又は複数の対象がグレード2以上の神経障害を有する、実施形態338~343のいずれか一項に記載の方法。
344. 344. The method of any one of embodiments 338-343, wherein said one or more subjects have
345.前記一又は複数の対象が白金系化学療法剤による処置を拒否した、実施形態338~344のいずれか一項に記載の方法。 345. 345. The method of any one of embodiments 338-344, wherein said one or more subjects have refused treatment with a platinum-based chemotherapeutic agent.
346.前記白金系化学療法剤がシスプラチンである、実施形態338又は342~345のいずれか一項に記載の方法。 346. The method of any one of embodiments 338 or 342-345, wherein said platinum-based chemotherapeutic agent is cisplatin.
347.前記MIBCが外科的に操作可能である、実施形態338~346のいずれか一項に記載の方法。 347. 347. The method of any one of embodiments 338-346, wherein said MIBC is surgically manipulable.
348.前記方法が手術を更に含む、実施形態347に記載の方法。 348. 348. The method of embodiment 347, wherein said method further comprises surgery.
349.少なくとも1つの投薬サイクルが前記手術の前に開始される、実施形態348に記載の方法。 349. 349. The method of embodiment 348, wherein at least one dosing cycle is initiated prior to said surgery.
350.少なくとも1、2、又は3回の投薬サイクルが前記手術の前に完了する、実施形態348又は349に記載の方法。 350. The method of embodiment 348 or 349, wherein at least 1, 2, or 3 dosing cycles are completed prior to said surgery.
351.少なくとも1回の投薬サイクルが、前記手術後4週間と6週間の間に開始される、実施形態348~350のいずれか一項に記載の方法。 351. 351. The method of any one of embodiments 348-350, wherein at least one dosing cycle is initiated between 4 and 6 weeks after said surgery.
352.1~17回の投薬サイクルが前記手術後に完了する、実施形態351に記載の方法。 352. The method of embodiment 351, wherein 1-17 dosing cycles are completed after said surgery.
353.前記手術が膀胱切除術及び/又はリンパ節郭清術である、実施形態348~352いずれか一項に記載の方法。 353. 353. The method of any one of embodiments 348-352, wherein said surgery is cystectomy and/or lymphadenectomy.
354.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態338~353のいずれか一項に記載の方法。 354. 354. The method of any one of embodiments 338-353, wherein said treatment results in a pathological complete response (pCR).
355.前記処置が、基準無再発生存期間(RFS)と比較した前記一又は複数の対象のRFS時間の増加、基準無症候生存期間(EFS)と比較した前記一又は複数の対象のEFS時間の増加、又はOSと比較した前記一又は複数の対象のOS時間の増加をもたらす、実施形態338~354のいずれか一項に記載の方法。 355. said treatment increases RFS time of said one or more subjects compared to baseline recurrence-free survival (RFS); increases EFS time of said one or more subjects compared to baseline disease-free survival (EFS); 355. The method of any one of embodiments 338-354, resulting in an increase in OS time of said one or more subjects compared to OS.
356.実施形態355に記載の方法であって、
(a)前記基準RFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のRFS時間の中央値である、
(b)前記基準EFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のEFS時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、方法。
356. 356. The method of embodiment 355, wherein:
(a) said baseline RFS time is the median RFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline EFS time is the median EFS time of a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
357.前記処置が病理的進展度の低下をもたらす、実施形態338~356のいずれか一項に記載の方法。 357. 357. The method of any one of embodiments 338-356, wherein said treatment results in a reduction in pathological extent.
358.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、方法。 358. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per dose, wherein said subject is cisplatin ineligible.
359.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 359. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and administering one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per day, wherein said treatment is perioperative treatment.
360.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、方法。 360. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and administering one or more dosing cycles of a PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg per dose, wherein said subject is cisplatin ineligible.
361.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 361. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and administering one or more dosing cycles of a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg per day, wherein said treatment is perioperative treatment.
362.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、方法。 362. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population a dose of tiragolumab between about 30 mg and about 1200 mg every three weeks and about administering one or more dosing cycles of atezolizumab at doses of 80 mg and about 1600 mg, wherein said subject is cisplatin ineligible.
363.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 363. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population a dose of tiragolumab between about 30 mg and about 1200 mg every three weeks and about administering one or more dosing cycles of atezolizumab at doses of 80 mg and about 1600 mg, wherein said treatment is perioperative treatment.
364.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記一又は複数の対象がシスプラチン不適格である、方法。 364. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. wherein said one or more subjects are cisplatin ineligible.
365.MIBCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 365. A method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. wherein said treatment is perioperative treatment.
366.前記処置が、少なくとも約13.4%~約15%の対象集団のORRをもたらす、実施形態338~365のいずれか一項に記載の方法。 366. The method of any one of embodiments 338-365, wherein said treatment results in an ORR of the subject population of at least about 13.4% to about 15%.
367.前記処置が、少なくとも約7.9ヶ月~約8.6ヶ月の対象集団のOS中央値をもたらす、実施形態338~366のいずれか一項に記載の方法。 367. 367. The method of any one of embodiments 338-366, wherein said treatment results in a median OS for the subject population of at least about 7.9 months to about 8.6 months.
368.抗PD-L1抗体SP142による染色を含むIHCアッセイによって検出可能なPD-L1タンパク質発現レベルが決定される、実施形態338~367のいずれか一項に記載の方法。 368. The method of any one of embodiments 338-367, wherein detectable PD-L1 protein expression levels are determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142.
369.前記検出可能なPD-L1タンパク質発現レベルが、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合が5%以上であるPD-L1陽性腫瘍細胞分率である、実施形態368に記載の方法。 369. Embodiment 368, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction in which 5% or more of the tumor area is occupied by PD-L1-expressing tumor-infiltrating immune cells (ICs) The method described in .
370.膀胱がんが尿路上皮癌腫(UC)である、実施形態336に記載の方法。 370. 337. The method of embodiment 336, wherein the bladder cancer is urothelial carcinoma (UC).
371.前記UCが転移性尿路上皮癌腫(mUC)である、実施形態370に記載の方法。 371. 371. The method of embodiment 370, wherein said UC is metastatic urothelial carcinoma (mUC).
372.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法。 372. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and for three weeks. administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per dose.
373.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法。 373. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every three weeks and for three weeks. administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg per dose.
374.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含み、前記対象が事前のがん免疫療法を受けたことがない、方法。 374. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and for three weeks. administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg per day, wherein said subject has received prior cancer immunotherapy no way.
375.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含み、前記処置が第二選択処置である、方法。 375. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and for three weeks. administering a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg per dose, wherein said treatment is a second line treatment.
376.前記一又は複数の対象が事前のがん免疫療法を受けたことがない、実施形態372、372及び375に記載の方法。 376. 376. The method of embodiments 372, 372 and 375, wherein said one or more subjects have not received prior cancer immunotherapy.
377.前記処置が第二選択処置である、実施形態372~374のいずれか一項に記載の方法。 377. 375. The method of any one of embodiments 372-374, wherein said treatment is a second line treatment.
378.前記mUCが、白金含有療法の間又は後に進行した、実施形態372~377のいずれか一項に記載の方法。 378. 378. The method of any one of embodiments 372-377, wherein said mUC progressed during or after platinum-containing therapy.
379.前記一又は複数の対象が疾患進行性又は許容できない毒性を経験した後、第2の投薬レジメンを前記対象又は対象集団に投与することを更に含む、実施形態372~378のいずれか一項に記載の方法。 379. 379. According to any one of embodiments 372-378, further comprising administering a second dosing regimen to said subject or population of subjects after said one or more subjects experience disease progression or unacceptable toxicity. the method of.
380.前記第2の投薬レジメンが、PD-1軸結合アンタゴニスト、及び抗体-薬物コンジュゲート(ADC)の1回以上の投薬サイクルを含む、実施形態379に記載の方法。 380. 379. The method of embodiment 379, wherein said second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist and an antibody-drug conjugate (ADC).
381.前記ADCが、(a)エンフォルツマブベドチン又は(b)サクツズマブゴビテカンである、実施形態380に記載の方法。 381. 381. The method of embodiment 380, wherein said ADC is (a) enfortumab vedotin or (b) suctuzumab govitecan.
382.(a)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(b)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与される、実施形態381に記載の方法。 382. (a) enfortumab vedotin administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (b) sactuzumab govitecan administered at 2 382. The method of embodiment 381, administered at a dose of 10 mg/kg weekly for weekly on/weekly off.
383.(a)エンフォルツマブベドチンが1.25mg/kgの用量で各21日間サイクルの1日目及び8日目に投与されるか、又は(b)サクツズマブゴビテカンが10mg/kgの用量で各21日間サイクルの1日目及び8日目に投与される、実施形態381又は382に記載の方法。
383. (a) enfortumab vedotin at a dose of 1.25 mg/kg on
384.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法。 384. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and for three weeks. administering a dosing regimen comprising one or more dosing cycles of a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg per dose.
385.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの用量のアテゾリズマブの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、方法。 385. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population a dose of tiragolumab between about 30 mg and about 1200 mg every three weeks and about administering a dosing regimen comprising one or more dosing cycles of atezolizumab at doses of 80 mg and about 1600 mg.
386.mUCを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、方法。 386. A method for treating a subject or subject population having mUC, said method comprising administering to said subject or subject population tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks. A method comprising administering one or more dosing cycles of
387.mUCを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象又は対象集団が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象又は対象集団に投与される、方法。
387. 1. A method for treating a subject or population of subjects with mUC comprising administering to said subject or population of subjects a first dosing regimen followed by a second dosing regimen,
(a) said first dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks and PD-1 axis binding at a dose of between about 80 mg and about 1600 mg every 3 weeks; comprising one or more dosing cycles of the antagonist;
(b) said second dosing regimen comprises one or more dosing cycles of said PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks; (i) enfortumab vedotin; is administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (ii) suctuzumab govitecan is administered for 2 weeks on/1 week off administered at a dose of 10 mg/kg weekly during drug administration, wherein said second dosing regimen is administered to said subject or subject after said subject or subject population experiences disease progression or unacceptable toxicity during said first dosing regimen; A method administered to a subject population.
388.mUCを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約80mgと約1600mgの間の用量の前記PD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、方法。
388. 1. A method for treating a subject or population of subjects with mUC comprising administering to said subject or population of subjects a first dosing regimen followed by a second dosing regimen,
(a) the first dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks; comprising one or more dosing cycles of
(b) said second dosing regimen comprises one or more dosing cycles of said PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks, and (i) enfortumab vedotin is , 2 weeks on/1 week off, or (ii) suctuzumab govitecan administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off and the second dosing regimen is administered to the subject after the subject experiences disease progression or unacceptable toxicity during the first dosing regimen. Method.
389.mUCを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約600mgの用量のチラゴルマブ及び約3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約1200用量のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、方法。
389. 1. A method for treating a subject or population of subjects with mUC comprising administering to said subject or population of subjects a first dosing regimen followed by a second dosing regimen,
(a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of 1200 mg about every 3 weeks;
(b) said second dosing regimen comprises one or more dosing cycles of about 1200 doses of atezolizumab every 3 weeks, and (i) enfortumab vedotin 2 weeks on/1 week off or (ii) suctuzumab govitecan administered at a dose of 10 mg/kg weekly for 2 weeks on/1 week off and wherein said second dosing regimen is administered to said subject after said subject experiences disease progression or unacceptable toxicity during said first dosing regimen.
390.前記処置が、少なくとも約13.4%~少なくとも約31%の対象集団のORRをもたらす、実施形態372~389のいずれか一項に記載の方法。 390. The method of any one of embodiments 372-389, wherein said treatment results in an ORR of the subject population of at least about 13.4% to at least about 31%.
391.前記処置が、約7.9ヶ月~約16.3ヶ月の対象集団のOS中央値をもたらす、実施形態372~390のいずれか一項に記載の方法。 391. 391. The method of any one of embodiments 372-390, wherein said treatment results in a median OS for the subject population of from about 7.9 months to about 16.3 months.
392.前記がんが膵臓がんである、実施形態72に記載の方法。
392. 73. The method of
393.膵臓がんを有する対象又は対象集団を処置する方法であって、前記方法が、前記対象又は対象集団に、各28日間投薬サイクルの1日目及び15日目に約420mgの用量のチラゴルマブ、各28日間投薬サイクルの1及び15日目に約840mgの用量のアテゾリズマブ、各28日間投薬サイクルの1、8及び15日目に約1000mg/m2の用量のゲムシタビン、並びに各28日間投薬サイクルの1、8及び15日目に約125mg/m2の用量のnab-パクリタキセルの1回以上の28日間投薬サイクルを含む投薬レジメンを投与することを含む、方法。
393. A method of treating a subject or population of subjects with pancreatic cancer, said method comprising administering to said subject or population of subjects a dose of about 420 mg tiragolumab on
394.前記膵臓がんが膵管腺癌(PDAC)である、実施形態392又は393に記載の方法。 394. 394. The method of embodiment 392 or 393, wherein said pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395.前記PDACが転移性PDACである、実施形態394に記載の方法。 395. 395. The method of embodiment 394, wherein said PDAC is metastatic PDAC.
396.前記一又は複数の対象が転移性PDACに対する事前全身治療を受けたことがない、実施形態392~395のいずれか一項に記載の方法。 396. 396. The method of any one of embodiments 392-395, wherein said one or more subjects have had no prior systemic therapy for metastatic PDAC.
397.前記処置が、少なくとも約41.7%~約46.7%の対象集団のORRをもたらす、実施形態392~396のいずれか一項に記載の方法。 397. The method of any one of embodiments 392-396, wherein said treatment results in an ORR of the subject population of at least about 41.7% to about 46.7%.
398.前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを用いないゲムシタビン及びnab-パクリタキセルを含む処置と比較して、少なくとも約20%のORRの増加をもたらす、実施形態392~397のいずれか一項に記載の方法。
398. Any of embodiments 392-397, wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nab-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist The method according to
399.前記処置が、少なくとも約5.5ヶ月~約7ヶ月の対象集団のPFS中央値をもたらす、実施形態392~398のいずれか一項に記載の方法。 399. The method of any one of embodiments 392-398, wherein said treatment results in a median PFS for the subject population of at least about 5.5 months to about 7 months.
400.前記処置が、少なくとも約8.5ヶ月~約10.6ヶ月の対象集団のOS中央値をもたらす、実施形態392~399のいずれか一項に記載の方法。 400. The method of any one of embodiments 392-399, wherein said treatment results in a median OS for the subject population of at least about 8.5 months to about 10.6 months.
401.前記がんが食道がんである、実施形態72に記載の方法。
401. 73. The method of
402.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、方法。
402. A method for treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
403.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、方法。
403. A method for treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
404.[実施形態321]食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記対象が白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、方法。
404. [Embodiment 321] A method for treating a subject or subject population with esophageal cancer, said method comprising anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
405.食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、各投薬サイクルの1日目に約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記対象が白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、方法。
405. A method for treating a subject or subject population with esophageal cancer, said method comprising administering an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg on
406.前記一又は複数の対象が、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、実施形態402又は403に記載の方法。 406. 404. The method of embodiment 402 or 403, wherein the one or more subjects have been previously treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
407.前記一又は複数の対象が、以前の処置中に疾患進行性又は許容できない毒性を経験したことがある、実施形態404~406のいずれか一項に記載の方法。 407. 407. The method of any one of embodiments 404-406, wherein said one or more subjects have experienced disease progression or unacceptable toxicity during prior treatment.
408.前記21日間の投薬サイクルが、白金系化学療法剤及び非白金系化学療法剤を更に含む、実施形態402又は403に記載の方法。 408. 404. The method of embodiment 402 or 403, wherein the 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409.前記白金系化学療法剤が、6回の投薬後に前記投薬レジメンから省略される、実施形態408に記載の方法。 409. 409. The method of embodiment 408, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
410.前記白金系化学療法剤がシスプラチンである、実施形態404~409のいずれか一項に記載の方法。 410. The method of any one of embodiments 404-409, wherein said platinum-based chemotherapeutic agent is cisplatin.
411.シスプラチンが、各投薬サイクルの1日目に約80mg/m2の用量で投与される、実施形態410に記載の方法。
411. 411. The method of embodiment 410, wherein cisplatin is administered at a dose of about 80 mg/m2 on
412.前記非白金系化学療法剤が代謝拮抗剤である、実施形態404~411のいずれか一項に記載の方法。 412. The method of any one of embodiments 404-411, wherein said non-platinum chemotherapeutic agent is an antimetabolite.
413.前記代謝拮抗剤が5-フルオロウラシルである、実施形態412に記載の方法。 413. 413. The method of embodiment 412, wherein said antimetabolite is 5-fluorouracil.
414.5-フルオロウラシルを800mg/m2/24時間の用量で、各21日間サイクルの1~5日目に投与する、実施形態413に記載の方法。 414. The method of embodiment 413, wherein 5-fluorouracil is administered at a dose of 800 mg/m2/24 hours on days 1-5 of each 21-day cycle.
415.前記食道がんが進行性又は転移性食道がんである、実施形態404~414のいずれか一項に記載の方法。 415. 415. The method of any one of embodiments 404-414, wherein said esophageal cancer is advanced or metastatic esophageal cancer.
416.前記一又は複数の対象が転移性食道がんの事前処置を受けたことがない、実施形態402、403、408及び409に記載の方法。 416. The method of embodiments 402, 403, 408, and 409, wherein said one or more subjects have no prior treatment for metastatic esophageal cancer.
417.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、各投薬サイクルの1日目に約80mg/m2の用量の白金系化学療法剤、及び各21日間サイクルの1~5日目に800mg/m2/24時間の用量の非白金系化学療法剤の1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、前記白金系化学療法剤が6回の投薬後に前記投薬レジメンから省略される、方法。
417. A method for treating a subject or subject population with advanced or metastatic esophageal cancer comprising: an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
418.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約1200mgの用量のPD-1軸結合アンタゴニスト、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に前記投薬レジメンからシスプラチンが省略される、方法。
418. A method for treating a subject or subject population having advanced or metastatic esophageal cancer, said method comprising administering to said subject or subject population a dose of about 600 mg of anti-TIGIT on
419.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記方法が、前記対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に前記投薬レジメンからシスプラチンが省略される、方法。
419. 1. A method for treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising administering to said subject or subject population a dose of tiragolumab of about 600 mg on
420.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、白金系化学療法剤及び非白金系化学療法剤の1回以上の21日間投薬サイクルを含み、前記白金系化学療法剤が6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、方法。
420. 1. A method for treating a subject or population of subjects with advanced or metastatic esophageal cancer comprising administering to said subject or population of subjects a first dosing regimen and a second dosing regimen,
(a) the first dosing regimen comprises one or more 21-day dosing cycles of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent is omitted from
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
421.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンは、各投薬サイクルの1日目に約80mg/m2の用量の白金系化学療法剤と、及び各21日間サイクルの1~5日目に800mg/m2/24時間の用量の非白金系化学療法剤の1回以上の21日間投薬サイクル含み、前記白金系化学療法剤が、6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、方法。
421. 1. A method for treating a subject or population of subjects with advanced or metastatic esophageal cancer comprising administering to said subject or population of subjects a first dosing regimen and a second dosing regimen,
(a) the first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
422.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日間サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含み、6回の投薬後にシスプラチンが投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブの1回以上の21日間投薬サイクルを含む、方法。
422. 1. A method for treating a subject or population of subjects with advanced or metastatic esophageal cancer comprising administering to said subject or population of subjects a first dosing regimen and a second dosing regimen,
(a) said first dosing regimen comprises cisplatin at a dose of about 80 mg/m2 on
(b) said second dosing regimen is one or more 21-day dosing cycles of tiragolumab at a dose of about 600 mg on
423.前記処置が、少なくとも約14%の対象集団のORRをもたらす、実施形態402~422のいずれか一項に記載の方法。 423. The method of any one of embodiments 402-422, wherein said treatment results in an ORR of the subject population of at least about 14%.
424.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、を含む、実施形態47~423のいずれか一項に記載の方法。
424. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO:5); and HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO:6). .
425.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、を更に含む、実施形態424に記載の方法。
425. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
425. The method of embodiment 424, further comprising FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO:9); and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO:10).
426.前記抗TIGITアンタゴニスト抗体が、以下の重鎖可変領域FR:
X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、を更に含む、実施形態424に記載の方法。
426. The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11) (wherein X1 is E or Q);
FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
425. The method of embodiment 424, further comprising FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
427.X1がEである、実施形態426に記載の方法。 427. 427. The method of embodiment 426, wherein X1 is E.
428.X1がQである、実施形態426に記載の方法。 428. 427. The method of embodiment 426, wherein X1 is Q.
429.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態424~428のいずれか一項に記載の方法。
429. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 19; or (c) a VH domain according to (a) and (b) 429. The method of any one of embodiments 424-428, comprising the described VL domain.
430.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~429に記載の方法。
430. wherein said anti-TIGIT antagonist antibody:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
431.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~427、429及び430のいずれか一項に記載の方法。
431. wherein said anti-TIGIT antagonist antibody:
The method of any one of embodiments 424-427, 429 and 430, comprising (a) a VH domain comprising the amino acid sequence of SEQ ID NO:17; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
432.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号33のアミノ酸配列を含む重鎖;及び
(b)配列番号34のアミノ酸配列を含む軽鎖、
を含む、実施形態424~427及び429~431のいずれか一項に記載の方法。
432. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:33; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:34,
The method of any one of embodiments 424-427 and 429-431, comprising
433.抗TIGITアンタゴニスト抗体がモノクローナル抗体である、実施形態424~432のいずれか一項に記載の方法。 433. The method of any one of embodiments 424-432, wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
434.前記抗TIGITアンタゴニスト抗体がヒト抗体である、実施形態424~433のいずれか一項に記載の方法。 434. The method of any one of embodiments 424-433, wherein said anti-TIGIT antagonist antibody is a human antibody.
435.抗TIGITアンタゴニスト抗体が完全長抗体である、実施形態424~434のいずれか一項に記載の方法。 435. The method of any one of embodiments 424-434, wherein the anti-TIGIT antagonist antibody is a full length antibody.
436.抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態424~427及び429~436のいずれか一項に記載の方法。 436. The method of any one of embodiments 424-427 and 429-436, wherein the anti-TIGIT antagonist antibody is tiragolumab.
437.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチジリマブ、EOS084448、SGN-TGT、又はTJ-T6である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291,292,295,296、301~332、336~361、370~384、387,388、401~418、420,421、及び424~436のいずれか一項に記載の方法。 437. embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, wherein said anti-TIGIT antagonist antibody is tiragolumab, vivostolimab, etidilimab, EOS084448, SGN-TGT, or TJ-T6; 265 to 269, 286 to 288, 291, 292, 295, 296, 301 to 332, 336 to 361, 370 to 384, 387, 388, 401 to 418, 420, 421, and 424 to 436 described method.
438.前記抗TIGITアンタゴニスト抗体がインタクトなFc媒介エフェクター機能を有する、実施形態437に記載の方法。 438. 438. The method of embodiment 437, wherein said anti-TIGIT antagonist antibody has intact Fc-mediated effector functions.
439.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を増強している、実施形態437又は438に記載の方法。 439. The method of embodiment 437 or 438, wherein said anti-TIGIT antagonist antibody enhances Fc-mediated effector function.
440.前記抗TIGITアンタゴニスト抗体がSGN-TGTである、実施形態437~439のいずれか一項に記載の方法。 440. The method of any one of embodiments 437-439, wherein said anti-TIGIT antagonist antibody is SGN-TGT.
441.前記抗TIGITアンタゴニスト抗体が、ドムバナリマブ、BMS-986207、ASP8374又はCOM902である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291,292,295,296、301~332、336~361、370~384、387,388、401~418、420及び421のいずれか一項に記載の方法。 441. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-288 wherein said anti-TIGIT antagonist antibody is domvanalimab, BMS-986207, ASP8374 or COM902 , 291, 292, 295, 296, 301-332, 336-361, 370-384, 387, 388, 401-418, 420 and 421.
442.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を有しない、実施形態424~431及び441のいずれか一項に記載の方法。 442. The method of any one of embodiments 424-431 and 441, wherein said anti-TIGIT antagonist antibody has no Fc-mediated effector functions.
443.抗TIGITアンタゴニスト抗体がIgGクラス抗体である、実施形態47~442のいずれか一つに記載の方法。 443. The method of any one of embodiments 47-442, wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444.IgGクラス抗体がIgG1サブクラス抗体である、実施形態443に記載の方法。 444. 444. The method of embodiment 443, wherein the IgG class antibody is an IgG1 subclass antibody.
445.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS084448、SGN-TGT、TJ-T6、BGB-A1217、AB308、ドムバナリマブ又はBMS-986207である、実施形態444に記載の方法。 445. 445. The method of embodiment 444, wherein said anti-TIGIT antagonist antibody is tiragolumab, vibostolimab, etiglimab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, domvanalimab or BMS-986207.
446.前記IgGクラス抗体がIgG4サブクラス抗体である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291、292、295、296、301~332、336~361、370~384、387,388、401~418、420及び421のいずれか一項に記載の方法。 446. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-288, 291, 292, 295, 296, wherein said IgG class antibody is an IgG4 subclass antibody , 301-332, 336-361, 370-384, 387, 388, 401-418, 420 and 421.
447.前記抗TIGITアンタゴニスト抗体がASP8374又はCOM902である、実施形態446に記載の方法。 447. 447. The method of embodiment 446, wherein said anti-TIGIT antagonist antibody is ASP8374 or COM902.
448.前記抗TIGITアンタゴニスト抗体が、Fab、ビス-Fab、Fab’、Fab’-SH、Fv、単鎖可変断片(scFv)及び(Fab’)2フラグメントからなる群から選択されるTIGITに結合する抗体フラグメントである、実施形態424~434のいずれか一項に記載の方法。 448. an antibody fragment wherein said anti-TIGIT antagonist antibody binds to TIGIT selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv) and (Fab')2 fragment 435. The method of any one of embodiments 424-434, wherein the method is
449.前記抗TIGITアンタゴニスト抗体が単一特異性抗体である、実施形態424~448のいずれか一項に記載の方法。 449. The method of any one of embodiments 424-448, wherein said anti-TIGIT antagonist antibody is a monospecific antibody.
450.前記抗TIGITアンタゴニスト抗体が多重特異性抗体である、実施形態424~448のいずれか一項に記載の方法。 450. The method of any one of embodiments 424-448, wherein said anti-TIGIT antagonist antibody is a multispecific antibody.
451.前記多重特異性抗体が二重特異性抗体である、実施形態450に記載の方法。 451. The method of embodiment 450, wherein said multispecific antibody is a bispecific antibody.
452.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト、PD-1結合アンタゴニスト、及びPD-L2結合アンタゴニストからなる群から選択される、実施形態424~451のいずれか一項に記載の方法。 452. The method of any one of embodiments 424-451, wherein said PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
453.前記PD-1軸結合アンタゴニストがPD-L1結合アンタゴニストである、実施形態452に記載の方法。 453. The method of embodiment 452, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist.
454.前記PD-L1結合アンタゴニストが、PD-L1のそのリガンド結合パートナーのうちの1つ以上への結合を阻害する、実施形態453に記載の方法。 454. 454. The method of embodiment 453, wherein said PD-Ll binding antagonist inhibits binding of PD-Ll to one or more of its ligand binding partners.
455.前記PD-L1結合アンタゴニストが、PD-L1の、PD-1、B7-1、又はPD-1及びB7-1の両方への結合を阻害する、実施形態454に記載の方法。 455. The method of embodiment 454, wherein said PD-L1 binding antagonist inhibits binding of PD-L1 to PD-1, B7-1, or both PD-1 and B7-1.
456.前記PD-L1結合アンタゴニストが抗PD-L1アンタゴニスト抗体である、実施形態453~455のいずれか一項に記載の方法。 456. The method of any one of embodiments 453-455, wherein said PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態456に記載の方法。 457. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 , embodiment 456.
458.抗PD-L1アンタゴニスト抗体がアテゾリズマブである、実施形態457に記載の方法。 458. The method of embodiment 457, wherein the anti-PD-L1 antagonist antibody is atezolizumab.
459.前記抗PD-L1アンタゴニスト抗体が、以下のHVR:
GFTFSDSWIH(配列番号20)のアミノ酸配列を含むHVR-H1配列;
AWISPYGGSTYYADSVKG(配列番号21)のアミノ酸配列を含むHVR-H2配列;
RHWPGGFDY(配列番号22)のアミノ酸配列を含むHVR-H3配列;
RASQDVSTAVA(配列番号23)のアミノ酸配列を含むHVR-L1配列;
SASFLYS(配列番号24)のアミノ酸配列を含むHVR-L2配列;及び
QQYLYHPAT(配列番号25)のアミノ酸配列を含むHVR-L3配列
459. The anti-PD-L1 antagonist antibody is a HVR that:
an HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
an HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
an HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
an HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
HVR-L2 sequence comprising the amino acid sequence of SASFLYS (SEQ ID NO:24); and HVR-L3 sequence comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
を含む、実施形態456に記載の方法。 457. The method of embodiment 456, comprising
460.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)配列番号26のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号27のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態459に記載の方法。
460. wherein said anti-PD-L1 antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or (c) a VH domain according to (a) and (b) 460. The method of embodiment 459, comprising the described VL domains.
461.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)配列番号26のアミノ酸配列を含むVHドメイン;及び
(b)配列番号27のアミノ酸配列を含むVLドメインを含む、
実施形態460に記載の方法。
461. wherein said anti-PD-L1 antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:27,
460. The method of embodiment 460.
462.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)(a)配列番号28のアミノ酸配列を含む重鎖;及び
(b)(b)配列番号29のアミノ酸配列を含む軽鎖、
を含む、実施形態461に記載の方法。
462. wherein said anti-PD-L1 antagonist antibody is:
(a) (a) a heavy chain comprising the amino acid sequence of SEQ ID NO:28; and (b) (b) a light chain comprising the amino acid sequence of SEQ ID NO:29,
462. The method of embodiment 461, comprising
463.前記抗PD-L1アンタゴニスト抗体がモノクローナル抗体である、実施形態459~462のいずれか一項に記載の方法。 463. The method of any one of embodiments 459-462, wherein said anti-PD-L1 antagonist antibody is a monoclonal antibody.
464.前記抗PD-L1アンタゴニスト抗体がヒト化抗体である、実施形態459~463のいずれか一項に記載の方法。 464. The method of any one of embodiments 459-463, wherein said anti-PD-L1 antagonist antibody is a humanized antibody.
465.前記抗PD-L1アンタゴニスト抗体が完全長抗体である、実施形態463又は464に記載の方法。 465. The method of embodiment 463 or 464, wherein said anti-PD-L1 antagonist antibody is a full length antibody.
466.前記抗PD-L1アンタゴニスト抗体が、Fab、Fab’、Fab’-SH、Fv、scFv及び(Fab’)2フラグメントからなる群から選択されるPD-L1に結合する抗体フラグメントである、実施形態459~464のいずれか一項に記載の方法。 466. Embodiment 459, wherein said anti-PD-Ll antagonist antibody is an antibody fragment that binds PD-Ll selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv and (Fab')2 fragments. 464. The method of any one of paragraphs 1-464.
467.前記抗PD-L1アンタゴニスト抗体がIgGクラス抗体である、実施形態459~465のいずれか一項に記載の方法。 467. The method of any one of embodiments 459-465, wherein said anti-PD-L1 antagonist antibody is an IgG class antibody.
468.IgGクラス抗体がIgG1サブクラス抗体である、実施形態467に記載の方法。 468. 468. The method of embodiment 467, wherein the IgG class antibody is an IgG1 subclass antibody.
469.前記PD-1軸結合アンタゴニストが、PD-1結合アンタゴニストである、実施形態452に記載の方法。 469. The method of embodiment 452, wherein said PD-1 axis binding antagonist is a PD-1 binding antagonist.
470.前記PD-1結合アンタゴニストが、PD-Lのそのリガンド結合パートナーのうちの1つ以上への結合を阻害する、実施形態469に記載の方法。 470. The method of embodiment 469, wherein said PD-1 binding antagonist inhibits binding of PD-L to one or more of its ligand binding partners.
471.前記PD-1結合アンタゴニストが、PD-1のPD-L1、PD-L2、又はPD-L1とPD-L2の両方への結合を阻害する、実施形態470に記載の方法。 471. The method of embodiment 470, wherein said PD-1 binding antagonist inhibits binding of PD-1 to PD-L1, PD-L2, or both PD-L1 and PD-L2.
472.前記PD-1結合アンタゴニストが抗PD-1アンタゴニスト抗体である、実施形態469~471のいずれか一項に記載の方法。 472. The method of any one of embodiments 469-471, wherein said PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態472に記載の方法。 473. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21.
474.前記PD-1結合アンタゴニストがFc融合タンパク質である、実施形態469~471のいずれか一項に記載の方法。 474. The method of any one of embodiments 469-471, wherein said PD-1 binding antagonist is an Fc fusion protein.
475.Fc融合タンパク質がAMP-224である、実施形態474に記載の方法。 475. 475. The method of embodiment 474, wherein the Fc fusion protein is AMP-224.
476.前記方法が、前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体を3週間ごとの約30mgと約1200mgの間の用量で投与することを含む、実施形態80~112、114~127及び309~312のいずれか一項に記載の方法。 476. of embodiments 80-112, 114-127 and 309-312, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or subject population at a dose of between about 30 mg and about 1200 mg every three weeks. A method according to any one of paragraphs.
477.前記方法が、3週間ごとの約600mgの用量で前記抗TIGITアンタゴニスト抗体を前記対象に投与することを含む、実施形態51、54、60、62、63、65~67、80~112、114~127、136~140、169~174、189、191、267、269、286、288、291、295、301、302、303、313、315、338、340、358~361、372、384、387、388、402~404、417、420、421及び476のいずれか一項に記載の方法。
477.
478.前記方法が、以下の前記対象の体重に基づく段階的用量で前記抗TIGITアンタゴニスト抗体を対象又は対象集団に投与することを含む、実施形態51、54、60、62、63、65-67、80-112、114-127、136-140、169-174、189、191、267、269、286、288、291、295、301、302、303、309、313、315、338、340、358-361、372、384、387、388、402-404、417、420、421、及び476のいずれか一項に記載の方法:
(a)15kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとの約300mgの用量で投与される;
(b)15kg超40kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとの約400mgの用量で投与される;又は
(c)40kgを超え、前記抗TIGITアンタゴニスト抗体は、3週間ごとの約600mgの用量で投与される。
478.
(a) is 15 kg or less and said anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks;
(b) greater than 15 kg and less than or equal to 40 kg and said anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 40 kg and said anti-TIGIT antagonist antibody is administered at about It is administered at a dose of 600 mg.
479.前記方法が、前記抗TIGITアンタゴニスト抗体を、4週間ごとに約700mg~約1000mgの用量で前記対象又は対象集団に投与することを含む、実施形態47,48、77、78、82、及び83のいずれか一項に記載の方法。 479. of embodiments 47, 48, 77, 78, 82, and 83, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects at a dose of about 700 mg to about 1000 mg every four weeks. A method according to any one of paragraphs.
480.前記方法が、前記抗TIGITアンタゴニスト抗体を4週間ごとの約840mgの用量で前記対象に投与することを含む、実施形態47、48、59、67,323、及び479のいずれか一項に記載の方法。
480. 479. The method of any one of
481.前記抗TIGITアンタゴニスト抗体を、前記対象又は対象集団に、2週間ごとの約300mg~約600mgの用量で投与することを含む、実施形態49、50、及び104のいずれか一項に記載の方法。
481. The method of any one of
482.前記方法が、前記対象に、2週間ごとの約420mgの用量で前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態49、50、227、251~253、255、及び481のいずれか一項に記載の方法。
482. Any one of
483.前記抗TIGITアンタゴニスト抗体の用量が固定用量である、実施形態47~482のいずれか一項に記載の方法。 483. The method of any one of embodiments 47-482, wherein the dose of said anti-TIGIT antagonist antibody is a fixed dose.
484.前記方法が、前記対象又は対象集団に、3週間ごとの約900mgと約1500mgの間の用量の前記PD-1軸結合アンタゴニストを投与することを含む、実施形態54、62、63、65~67、80~109、及び27~2698のいずれか一項に記載の方法。
484.
485.前記方法が、前記対象に、3週間ごとの約1200mgの用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態54、60、62、63、65~67、80~112、114~127、136~140、169~172、189、191、267、269、286、288、291、295、301~303、309、311、313、315、338、340、358~361、372~375、384、387、388、402~405、417、420、421及び484のいずれか一項に記載の方法。
485.
486.前記方法が、前記対象又は対象集団に、4週間ごとの前記PD-1軸結合アンタゴニストを約1400mg~2000mgの用量で投与することを含む、実施形態47、50、80~109、及び324のいずれか一項に記載の方法。
486. Any of
487.前記方法が、前記対象に、4週間ごとの約1680mgの用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態47、50、59、67、324、及び479のいずれか一項に記載の方法。
487. Any one of
488.前記方法が、前記対象又は対象集団に、2週間ごとの約600mgと約1200mgの間の用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態48、49、80~109、及び481のいずれか一項に記載の方法。 488. Embodiments 48, 49, 80-109, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects at a dose of between about 600 mg and about 1200 mg every two weeks, and 481. The method according to any one of paragraphs 481 to 481.
489.前記PD-1軸結合アンタゴニストを、2週間ごとに約840mgの用量で前記対象に投与することを含む、実施形態48、49、80~109、227、251~253、及び481のいずれか一項に記載の方法。 489. Any one of embodiments 48, 49, 80-109, 227, 251-253, and 481, comprising administering said PD-1 axis binding antagonist to said subject at a dose of about 840 mg every two weeks. The method described in .
490.前記PD-1軸結合アンタゴニストの用量が固定用量である、実施形態47~489のいずれか一項に記載の方法。 490. The method of any one of embodiments 47-489, wherein the dose of PD-1 axis binding antagonist is a fixed dose.
491.前記方法が、前記対象に、3週間ごとの約200mg又は6週間ごとの400mgの固定用量でペンブロリズマブを投与することを含む、実施形態60又は61に記載の方法。
491. 62. The method of
492.前記1回以上の投薬サイクルのそれぞれの長さが21日間である、実施形態54、60、62、63、65、80~109、及び191のいずれか一項に記載の方法。
492. 192. The method of any one of
493.前記1回以上の投薬サイクルの各々の長さが28日間である、実施形態47、59、67、80~109、及び309~311のいずれか一項に記載の方法。
493. The method of any one of
494.前記1回以上の投薬サイクルの各々の長さが14日間である、実施形態49、80~109、及び309~311のいずれか一項に記載の方法。 494. The method of any one of embodiments 49, 80-109, and 309-311, wherein each of said one or more dosing cycles is 14 days in length.
495.前記方法が、前記1回以上の投薬サイクルのそれぞれの約1日目に、前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態47~494のいずれか一項に記載の方法。
495. 495. Any one of embodiments 47-494, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects on about
496.前記1回以上の投薬サイクルのそれぞれの約1日目に、前記PD-1軸結合アンタゴニストを前記対象又は対象集団に投与することを含む、、実施形態47~495いずれか一項に記載の方法。
496. 496. The method of any one of embodiments 47-495, comprising administering said PD-1 axis binding antagonist to said subject or population of subjects on about
497.前記方法が、前記1回以上の投薬サイクルのそれぞれの約15日目に、前記抗TIGITアンタゴニスト抗体を前記対象に投与することを含む、実施形態321又は493に記載の方法。 497. The method of embodiment 321 or 493, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject on about day 15 of each of said one or more dosing cycles.
498.前記1回以上の投薬サイクルのそれぞれの約15日目に、前記PD-1軸結合アンタゴニストを前記対象に投与することを含む、実施形態322又は493に記載の方法。 498. The method of embodiment 322 or 493, comprising administering said PD-1 axis binding antagonist to said subject on about day 15 of each of said one or more dosing cycles.
499.前記方法が、対象又は対象集団に、前記抗TIGITアンタゴニスト抗体の前にPD-1軸結合アンタゴニストを投与すること、又は前記PD-1軸結合アンタゴニストの前に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態47~498のいずれか一項に記載の方法。 499. The method comprises administering to the subject or population of subjects a PD-1 axis binding antagonist prior to the anti-TIGIT antagonist antibody, or administering the anti-TIGIT antagonist antibody prior to the PD-1 axis binding antagonist. 499. The method of any one of embodiments 47-498, comprising:
500.前記方法が、前記PD-1軸結合アンタゴニスト又は前記抗TIGITアンタゴニスト抗体の投与後の第1の観察期間を含む、実施形態499に記載の方法。 500. 499. The method of embodiment 499, wherein said method comprises a first observation period after administration of said PD-1 axis binding antagonist or said anti-TIGIT antagonist antibody.
501.前記第1の観察期間が、約30分と約60分の間の長さである、実施形態500に記載の方法。
501. 500. The method of
502.前記方法が、前記抗TIGITアンタゴニスト抗体又は前記PD-1軸結合アンタゴニストの投与後の第2観察期間を含む、実施形態500又は501に記載の方法。
502. 502. The method of
503.前記第2の観察期間が、約30分と約60分の間の長さである、実施形態502に記載の方法。 503. 503. The method of embodiment 502, wherein the second observation period is between about 30 minutes and about 60 minutes long.
504.前記方法が、前記対象又は対象集団に前記PD-1軸結合アンタゴニストを前記抗TIGITアンタゴニスト抗体と同時に投与することを含む実施形態47~503のいずれか一項に記載の方法。 504. 504. The method of any one of embodiments 47-503, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects concurrently with said anti-TIGIT antagonist antibody.
505.前記抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを前記対象又は対象集団に静脈内投与することを含む、実施形態47~504のいずれか一項に記載の方法。 505. 505. The method of any one of embodiments 47-504, comprising administering said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist to said subject or population of subjects intravenously.
506.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記PD-1軸結合アンタゴニストを投与することを含む、実施形態505に記載の方法。 506. 506. The method of embodiment 505, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or subject population by intravenous infusion over 30±10 minutes and/or 60±10 minutes. .
507.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態505又は506に記載の方法。 507. The method of embodiment 505 or 506, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or subject population by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes. .
508.前記一又は複数の対象から得られた腫瘍試料のPD-L1発現レベルが決定されている、実施形態47~114及び116~507のいずれか一項に記載の方法。 508. The method of any one of embodiments 47-114 and 116-507, wherein the tumor sample obtained from said one or more subjects has its PD-L1 expression level determined.
509.前記一又は複数の対象から得られた前記腫瘍試料が検出可能なPD-L1発現レベルを有すると決定されている、実施形態508に記載の方法。 509. 509. The method of embodiment 508, wherein said tumor sample obtained from said one or more subjects has been determined to have a detectable PD-Ll expression level.
510.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1タンパク質発現レベルである、実施形態509に記載の方法。 510. 510. The method of embodiment 509, wherein said detectable PD-Ll expression level is a detectable PD-Ll protein expression level.
511.前記検出可能なPD-L1タンパク質発現レベルが、染色に適した抗PD-L1抗体による染色を含む免疫組織化学(IHC)アッセイによって決定されている、実施形態510に記載の方法。 511. 511. The method of embodiment 510, wherein said detectable PD-L1 protein expression level is determined by an immunohistochemistry (IHC) assay comprising staining with an anti-PD-L1 antibody suitable for staining.
512.染色に適した前記抗PD-L1抗体が抗PD-L1抗体SP263、SP142、22C3又は28-8である、実施形態511に記載の方法。 512. 512. The method of embodiment 511, wherein said anti-PD-Ll antibody suitable for staining is anti-PD-Ll antibody SP263, SP142, 22C3 or 28-8.
513.前記検出可能なPD-L1タンパク質発現レベルが、Ventana SP263 IHCアッセイ、pharmDx 22C3 IHCアッセイ、Ventana SP142 IHCアッセイ、又はpharmDx 28-8 IHCアッセイを使用して決定される、実施形態511又は512に記載の方法。 513. 513. According to embodiment 511 or 512, wherein the detectable PD-L1 protein expression level is determined using the Ventana SP263 IHC assay, pharmDx 22C3 IHC assay, Ventana SP142 IHC assay, or pharmDx 28-8 IHC assay. Method.
514.抗PD-L1抗体SP263による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~109、188、220~265、及び307~423のいずれか一項に記載の方法。
514. Any of embodiments 47-109, 188, 220-265, and 307-423, wherein detectable PD-L1 protein expression levels as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP263 have been determined The method according to
515.抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~220、265~338、及び370~423のいずれか一項に記載の方法。 515. Any one of embodiments 47-220, 265-338, and 370-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142 has been determined The method described in .
516.抗PD-L1抗体SP22C3による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~113、136~187、及び220~423のいずれか一項に記載の方法。 516. Any one of embodiments 47-113, 136-187, and 220-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP22C3 has been determined The method described in .
517.抗PD-L1抗体28-8による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~114、及び116~423のいずれか一項に記載の方法。 517. According to any one of embodiments 47-114 and 116-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody 28-8 has been determined. the method of.
518.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上の腫瘍関連免疫細胞(TIC)である、実施形態514に記載の方法。 518. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more tumor-associated immune cells (TIC) in said tumor sample.
519.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上20%未満のTICである、実施形態514に記載の方法。 519. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more and less than 20% TIC in said tumor sample.
520.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上のTICである、実施形態514に記載の方法。 520. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more TIC in said tumor sample.
521.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の20%以上のTICである、実施形態514に記載の方法。 521. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 20% or more TIC in said tumor sample.
522.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上50%未満のTICである、実施形態514に記載の方法。 522. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more and less than 50% TIC in said tumor sample.
523.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の50%以上のTICである、実施形態514に記載の方法。 523. 515. The method of embodiment 514, wherein said detectable PD-L1 protein expression level is 50% or more TIC in said tumor sample.
524.前記検出可能なPD-L1タンパク質発現レベルが、1%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の方法。 524. The method of any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or greater.
525.前記検出可能なPD-L1タンパク質発現レベルが、30%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の方法。 525. The method of any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 30% or greater.
526.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の1%以上50%未満のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517いずれか一項に記載の方法。 526. The method of any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or more and less than 50% in said tumor sample. .
527.前記検出可能なPD-L1タンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の方法。 527. The method of any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 50% or greater.
528.前記PD-L1陽性腫瘍細胞分率が、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合である、実施形態515に記載の方法。 528. 516. The method of embodiment 515, wherein said PD-L1 positive tumor cell fraction is the percentage of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (IC).
529.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が1%以上である、実施形態515に記載の方法。 529. 516. The method of embodiment 515, wherein the percentage of tumor area occupied by said PD-L1-expressing tumor-infiltrating IC is 1% or more.
530.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が5%以上である、実施形態515に記載の方法。 530. 516. The method of embodiment 515, wherein the percentage of tumor area occupied by said PD-L1-expressing tumor-infiltrating IC is 5% or more.
531.前記検出可能なPD-L1タンパク質発現レベルが、1以上の複合陽性スコア(CPS)である、実施形態516に記載の方法。 531. 517. The method of embodiment 516, wherein said detectable PD-L1 protein expression level is a composite positive score (CPS) of 1 or more.
532.前記検出可能なPD-L1タンパク質発現レベルが、10以上のCPSである、実施形態516に記載の方法。 532. 517. The method of embodiment 516, wherein said detectable PD-L1 protein expression level is 10 or more CPS.
533.前記検出可能なPD-L1タンパク質発現レベルが、20以上のCPSである、実施形態516に記載の方法。 533. 517. The method of embodiment 516, wherein said detectable PD-L1 protein expression level is 20 or more CPS.
534.前記IHCアッセイが、Ventana SP142 IHCアッセイである、実施形態528~530のいずれか一項に記載の方法。 534. The method of any one of embodiments 528-530, wherein said IHC assay is the Ventana SP142 IHC assay.
535.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1核酸発現レベルである、実施形態509に記載の方法。 535. 510. The method of embodiment 509, wherein said detectable PD-Ll expression level is a detectable PD-Ll nucleic acid expression level.
536.前記検出可能なPD-L1核酸発現レベルが、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている、実施形態535に記載の方法。 536. said detectable PD-L1 nucleic acid expression level has been determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof; 535. The method of embodiment 535.
537.前記処置が、基準全生存期間(OS)と比較した前記対象のOS時間及び/又は基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加をもたらす、実施形態47~423のいずれか一項に記載の方法。
537. 424. Any of embodiments 47-423, wherein said treatment results in an increase in said subject's OS time compared to baseline overall survival (OS) and/or said subject's PFS time compared to baseline progression-free survival (PFS) or the method described in
538.実施形態537に記載の方法であって、
(a)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のOS時間の中央値である、及び/又は
(b)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のPFS時間の中央値である、方法。
538. 538. The method of embodiment 537, wherein:
(a) a subject whose baseline OS time has undergone a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or a treatment comprising an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist; and/or (b) the baseline PFS time is a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or an anti-PD-1 axis binding antagonist without a PD-1 axis binding antagonist. Method, median PFS time in a subject population that has received treatment comprising a TIGIT antagonist antibody.
539.前記1つ以上の化学療法剤が、1つ以上の白金系化学療法剤及び/又は1つ以上の非白金系化学療法剤である、実施形態52、158及び228のいずれか一項に記載の方法。 539. 229. According to any one of embodiments 52, 158 and 228, wherein said one or more chemotherapeutic agents is one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents. Method.
540.前記白金系化学療法剤がカルボプラチン又はシスプラチンである、実施形態539に記載の方法。 540. 539. The method of embodiment 539, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541.前記カルボプラチンが、AUC=5mg/ml/分又はAUC=6mg/ml/分を達成するのに十分な用量で投与される、実施形態69、92、127、131、249、及び540に記載の方法。 541. The method of embodiments 69, 92, 127, 131, 249, and 540, wherein said carboplatin is administered at a dose sufficient to achieve AUC = 5 mg/ml/min or AUC = 6 mg/ml/min .
542.前記シスプラチンが約75mg/m2又は80mg/m2の用量で投与される、実施形態69、127、162、164、166、168及び540に記載の方法。 542. The method of embodiments 69, 127, 162, 164, 166, 168, and 540, wherein said cisplatin is administered at a dose of about 75 mg/m2 or 80 mg/m2.
543.前記1つ以上の非白金系化学療法剤が、代謝拮抗剤、タキサン又はトポイソメラーゼII阻害剤である、実施形態539~542のいずれか一項に記載の方法。 543. 543. The method of any one of embodiments 539-542, wherein said one or more non-platinum-based chemotherapeutic agents are antimetabolites, taxanes or topoisomerase II inhibitors.
544.前記代謝拮抗剤が、ペメトレキセド、ゲムシタビン、カペシタビン又は5-フルオロウラシルである、実施形態62、173、174、及び543のいずれか一項に記載の方法。 544. The method of any one of embodiments 62, 173, 174, and 543, wherein said antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
545.前記ペメトレキセドが約500mg/m2の用量で投与される、実施形態69、127、162及び544のいずれか一項に記載の方法。 545. The method of any one of embodiments 69, 127, 162 and 544, wherein said pemetrexed is administered at a dose of about 500 mg/m2.
546.前記ゲムシタビンが約1000mg/m2又は約1250mg/m2の用量で投与される、実施形態63、64、162、398、及び544のいずれか一項に記載の実施形態の方法。
546. The method of any one of
547.前記代謝拮抗剤がカペシタビンである、実施形態544に記載の方法。 547. 545. The method of embodiment 544, wherein said antimetabolite is capecitabine.
548.前記カペシタビンが約1250mg/m2の用量で投与される、実施形態544又は547に記載の方法。 548. The method of embodiment 544 or 547, wherein said capecitabine is administered at a dose of about 1250 mg/m2.
549.前記タキサンがパクリタキセル又はnab-パクリタキセルである、実施形態173、174、229、230、239、240及び543~548のいずれか一項に記載の方法。 549. The method of any one of embodiments 173, 174, 229, 230, 239, 240 and 543-548, wherein said taxane is paclitaxel or nab-paclitaxel.
550.前記パクリタキセルが約175mg/m2又は約200mg/m2の用量で投与される、実施形態69、162、及び549のいずれか一項に記載の方法。 550. The method of any one of embodiments 69, 162, and 549, wherein said paclitaxel is administered at a dose of about 175 mg/m2 or about 200 mg/m2.
551.前記nab-パクリタキセルが約100mg/m2の用量で投与される、実施形態63、64、249、398、及び549のいずれか一項に記載の方法。
551. The method of any one of
552.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331である、実施形態80~91、229、230、239、241、251~255、及び543~551のいずれか一項に記載の方法。 552. Embodiments 80-91, 229, 230, 239, 241, 251- wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticine, orintricarboxylic acid, or HU-331 255, and the method of any one of 543-551.
553.前記エトポシドが約100mg/m2の用量で投与される、実施形態69、92、及び552のいずれか一項に記載の方法。 553. The method of any one of embodiments 69, 92, and 552, wherein said etoposide is administered at a dose of about 100 mg/m2.
554.前記1つ以上の化学療法剤がそれぞれ、1週間ごとに1回、2週間ごとに1回、3週間ごとに1回、3週間ごとに2回、4週間ごとに1回、4週間ごとに2回、又は4週間ごとに3回投与される、実施形態543~553のいずれか一項に記載の方法。 554. each of said one or more chemotherapeutic agents once every week, once every two weeks, once every three weeks, twice every three weeks, once every four weeks, every four weeks 554. The method of any one of embodiments 543-553, administered twice, or three times every four weeks.
555.前記1つ以上の化学療法剤が、1回以上の投薬サイクルの1日目に投与される、実施形態543~554のいずれか一項に記載の方法。
555. 555. The method of any one of embodiments 543-554, wherein said one or more chemotherapeutic agents are administered on
556.前記ゲムシタビンが4週間ごとに3回投与される、実施形態544~555のいずれか一項に記載の方法。 556. 556. The method of any one of embodiments 544-555, wherein said gemcitabine is administered three times every four weeks.
557.前記ゲムシタビンが、1回以上の投薬サイクルの1、8及び/又は15日目に投与される、実施形態544~556のいずれか一項に記載の方法。
557. 556. The method of any one of embodiments 544-556, wherein said gemcitabine is administered on
558.前記カペシタビンが2週間ごと日投与される、実施形態544~557のいずれか一項に記載の方法。 558. The method of any one of embodiments 544-557, wherein said capecitabine is administered daily every two weeks.
559.前記カペシタビンが、1回以上の投薬サイクルの1~14日目に投与される、実施形態544~558のいずれか一項に記載の方法。 559. The method of any one of embodiments 544-558, wherein said capecitabine is administered on days 1-14 of one or more dosing cycles.
560.前記nab-パクリタキセルが4週間ごとに3回投与される、実施形態549~559のいずれか一項に記載の方法。 560. 559. The method of any one of embodiments 549-559, wherein said nab-paclitaxel is administered three times every four weeks.
561.前記nab-パクリタキセルが、1回以上の投薬サイクルの1、8及び/又は15日目に投与される、実施形態549~560のいずれか一項に記載の方法。
561. 561. The method of any one of embodiments 549-560, wherein said nab-paclitaxel is administered on
562.前記エトポシドが3週間ごとに1~3日目に投与される、実施形態552~561のいずれか一項に記載の方法。 562. The method of any one of embodiments 552-561, wherein said etoposide is administered on days 1-3 every 3 weeks.
563.前記エトポシドが、1回以上の投薬サイクルの1~3日目に投与される、実施形態552~562のいずれか一項に記載の方法。 563. 563. The method of any one of embodiments 552-562, wherein said etoposide is administered on days 1-3 of one or more dosing cycles.
564.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の前に投与される、実施形態543~563のいずれか一項に記載の方法。 564. 564. The method of any one of embodiments 543-563, wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
565.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の後に投与される、実施形態543~564のいずれか一項に記載の方法。 565. 564. The method of any one of embodiments 543-564, wherein said one or more chemotherapeutic agents are administered subsequent to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
566.前記1つ以上の化学療法剤が静脈内又は経口投与される、実施形態543~565のいずれか一項に記載の方法。 566. 566. The method of any one of embodiments 543-565, wherein said one or more chemotherapeutic agents are administered intravenously or orally.
567.前記VEGFアンタゴニストが、3週間ごとに約5mg/kg~約25mg/kgの用量で投与される、実施形態65、310、及び311のいずれか一項に記載の方法。
567. The method of any one of
568.前記VEGFアンタゴニストが、3週間ごとに約10mg/kg~約20mg/kgの用量で投与される、実施形態312又は567に記載の方法。 568. The method of embodiment 312 or 567, wherein said VEGF antagonist is administered at a dose of about 10 mg/kg to about 20 mg/kg every three weeks.
569.前記VEGFアンタゴニストが、3週間ごとに約15mg/kgの用量で投与される、実施形態318又は568に記載の方法。 569. The method of embodiment 318 or 568, wherein said VEGF antagonist is administered at a dose of about 15 mg/kg every three weeks.
570.前記VEGFアンタゴニストが抗VEGF抗体である、実施形態65、310~312、318~320、及び567~569のいずれか一項に記載の方法。
570. The method of any one of
571.前記抗VEGF抗体がベバシズマブのVHドメイン及びVLドメインを含む、実施形態570に記載の方法。 571. The method of embodiment 570, wherein said anti-VEGF antibody comprises the VH and VL domains of bevacizumab.
572.前記抗VEGF抗体が、ベバシズマブである、実施形態570又は571に記載の方法。 572. The method of embodiment 570 or 571, wherein said anti-VEGF antibody is bevacizumab.
573.前記抗TIGITアンタゴニスト抗体がチラゴルマブであり、前記PD-1軸結合アンタゴニストがアテゾリズマブであり、前記VEGFアンタゴニストがベバシズマブである、実施形態65、310~312、及び318~320のいずれか一項に記載の方法。
573. according to any one of
574.前記方法が、1回以上の投薬サイクルの1日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態65、310~312、318~320、及び567~573のいずれか一項に記載の方法。
574. any one of
575.前記方法が、1回以上の投薬サイクルの15日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態318~320のいずれか一項に記載の方法。 575. The method of any one of embodiments 318-320, wherein said method comprises administering said VEGF antagonist to said subject on day 15 of one or more dosing cycles.
576.前記VEGFアンタゴニストが静脈内投与される、実施形態65、310~312、及び318~320、及び567~575いずれか一項に記載の方法。
576. The method of any one of
577.前記VEGFアンタゴニストが、90±15分間かけて静脈内注入によって前記対象に投与される、実施形態576に記載の方法。 577. 577. The method of embodiment 576, wherein said VEGF antagonist is administered to said subject by intravenous infusion over 90±15 minutes.
578.前記方法が、前記対象に、前記VEGFアンタゴニストの前に前記PD-1軸結合アンタゴニストを投与し、前記抗TIGITアンタゴニスト抗体の前に前記VEGFアンタゴニストを投与することを含む、実施形態65、310~312、318~320、及び567~577のいずれか一項に記載の方法。
578.
579.前記方法が、前記PD-1軸結合アンタゴニストの投与後の第1の観察期間、前記VEGFアンタゴニストの投与後の第2の観察期間、及び前記抗TIGITアンタゴニスト抗体の投与後の第3の観察期間を含む、実施形態578に記載の方法。 579. The method comprises a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody. 578. The method of embodiment 578, comprising:
580.前記第1の観察期間、前記第2の観察期間、及び前記第3の観察期間がそれぞれ、約30分と約120分の間の長さである、実施形態579に記載の方法。 580. 579. The method of embodiment 579, wherein the first observation period, the second observation period, and the third observation period are each between about 30 minutes and about 120 minutes in length.
581.前記チラゴルマブ及びアテゾリズマブが、投与前にIVバッグにおいて組み合わされる、実施形態113、128、129~131、175~182、210~214、221、256、257、270、289、290、293、294、297、298、333、362~365、385、386、389、393、419、及び422のいずれか一項に記載の方法。 581. Embodiments 113, 128, 129-131, 175-182, 210-214, 221, 256, 257, 270, 289, 290, 293, 294, 297, wherein said tiragolumab and atezolizumab are combined in an IV bag prior to administration , 298, 333, 362-365, 385, 386, 389, 393, 419, and 422.
582.該対象が、ヒトである、実施形態47~581のいずれか一項に記載の方法。 582. The method of any one of embodiments 47-581, wherein said subject is a human.
583.実施形態47~190、192~208、210~211、213、215~268、270~294、及び299~582のいずれか一項に記載の方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニスト及び/又は抗TIGITアンタゴニスト抗体を含む、キット。 583. PD for treating a subject with cancer according to the method of any one of embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-582- A kit comprising a uniaxial binding antagonist and/or an anti-TIGIT antagonist antibody.
584.実施形態47~190、192~208、210~211、213、215~268、270~294、及び299~582のいずれか一項に記載の方法に従ってがんを有する対象を処置するための抗TIGITアンタゴニスト抗体と組み合わせて使用するためのPD-1軸結合アンタゴニストを含む、キット。 584. Anti-TIGIT for treating a subject with cancer according to the method of any one of embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-582 A kit comprising a PD-1 axis binding antagonist for use in combination with an antagonist antibody.
585.抗TIGITアンタゴニスト抗体を更に含む、実施形態584に記載のキット。 585. The kit of embodiment 584, further comprising an anti-TIGIT antagonist antibody.
586.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態583~585のいずれか一項に記載のキット。 586. The kit of any one of embodiments 583-585, wherein said anti-TIGIT antagonist antibody is tiragolumab.
587.前記PD-1軸結合アンタゴニストが、モノクローナル抗体である、実施形態583~586のいずれか一項に記載のキット。 587. The kit of any one of embodiments 583-586, wherein said PD-1 axis binding antagonist is a monoclonal antibody.
588.実施形態47~190、192~208、210~211、213、215~268、270~294、及び299~582のいずれか一項に記載の方法に従ってがんを有する対象を処置するためのPD-1軸結合アンタゴニストと組み合わせて使用するための抗TIGITアンタゴニスト抗体を含む、キット。 588. PD for treating a subject with cancer according to the method of any one of embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-582- A kit comprising an anti-TIGIT antagonist antibody for use in combination with a uniaxial binding antagonist.
589.前記キットが、PD-1軸結合アンタゴニストを更に含む、実施形態588に記載のキット。 589. The kit of embodiment 588, wherein said kit further comprises a PD-1 axis binding antagonist.
590.前記PD-1軸結合アンタゴニストがアテゾリズマブである、実施形態588又は589に記載のキット。 590. The kit of embodiment 588 or 589, wherein said PD-1 axis binding antagonist is atezolizumab.
591.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態588~590のいずれか一項に記載のキット。 591. The kit of any one of embodiments 588-590, wherein said anti-TIGIT antagonist antibody is tiragolumab.
592.前記キットが、1つ以上の化学療法剤を更に含む、実施形態583~591のいずれか一項に記載のキット。 592. The kit of any one of embodiments 583-591, wherein said kit further comprises one or more chemotherapeutic agents.
593.前記1つ以上の化学療法剤が、1つ以上の白金系化学療法剤及び/又は1つ以上の非白金系化学療法剤である、実施形態592に記載のキット。 593. 593. The kit of embodiment 592, wherein said one or more chemotherapeutic agents are one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents.
594.前記1つ以上の白金系化学療法剤がカルボプラチン又はシスプラチンである、実施形態593に記載のキット。 594. The kit of embodiment 593, wherein said one or more platinum-based chemotherapeutic agents is carboplatin or cisplatin.
595.前記1つ以上の非白金系化学療法剤が、代謝拮抗剤、タキサン又はトポイソメラーゼII阻害剤である、実施形態593又は594に記載のキット。 595. The kit of embodiment 593 or 594, wherein said one or more non-platinum chemotherapeutic agents are antimetabolites, taxanes or topoisomerase II inhibitors.
596.前記代謝拮抗剤が、ペメトレキセド、ゲムシタビン、カペシタビン又は5-フルオロウラシルである、実施形態595に記載のキット。 596. 596. The kit of embodiment 595, wherein said antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
597.前記タキサンがパクリタキセル又はnab-パクリタキセルである、実施形態595又は596に記載のキット。 597. The kit of embodiment 595 or 596, wherein said taxane is paclitaxel or nab-paclitaxel.
598.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331である、実施形態595~597のいずれか一項に記載のキット。 598. 598. The kit of any one of embodiments 595-597, wherein the topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticine, orintricarboxylic acid, or HU-331.
599.前記VEGFアンタゴニストを更に含む、実施形態583~598のいずれか一項に記載のキット。 599. The kit of any one of embodiments 583-598, further comprising said VEGF antagonist.
600.前記VEGFアンタゴニストが、抗VEGF抗体である、実施形態599に記載のキット。 600. The kit of embodiment 599, wherein said VEGF antagonist is an anti-VEGF antibody.
601.前記抗VEGF抗体が、ベバシズマブである、実施形態600に記載のキット。
601. The kit of
602.前記方法が、実施形態47~190、192~208、210~211、213、215~268、270~294、及び299~582のいずれか一項に記載のものである、がんを有する対象又は対象集団を処置する方法における使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 602. A subject with cancer, wherein the method is according to any one of embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-582; or Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in methods of treating a subject population.
603.前記処置が実施形態47~190、192~208、210~211、213、215~268、270~294、及び299~582のいずれか一項に記載の方法によるものである、PD-1軸結合アンタゴニストと組み合わせてがんを有する対象又は対象集団を処置するための医薬の製造における抗TIGITアンタゴニスト抗体の使用。 603. PD-1 axial binding, wherein said treating is by the method of any one of embodiments 47-190, 192-208, 210-211, 213, 215-268, 270-294, and 299-582 Use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for treating a subject or subject population with cancer in combination with an antagonist.
604.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態603に記載の使用。 604. Use according to embodiment 603, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in separate formulations.
605.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態603に記載の使用。 605. The use of embodiment 603, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in a single formulation.
実施形態のセットB:
1.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約500mg~約700mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約900mg~約1500mgの用量で投与するために製剤化され、前記処置が、3週間ごとの白金系化学療法剤及び3週間ごとの非白金系化学療法剤の使用を更に含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
Embodiment set B:
1. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment comprises administering said anti-TIGIT antagonist antibody and said PD-1 in one or more dosing cycles. comprising the use of a uniaxial binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 500 mg to about 700 mg every 3 weeks; an anti-TIGIT antagonist antibody formulated for administration at a dose of 900 mg to about 1500 mg, wherein said treatment further comprises use of a platinum-based chemotherapeutic agent every 3 weeks and a non-platinum-based chemotherapeutic agent every 3 weeks; and PD-1 axis binding antagonist.
2.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、4週間ごとに約700mg~約1000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、4週間ごとに約1400mg~2000mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 2. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment comprises administering said anti-TIGIT antagonist antibody and said PD- in one or more dosing cycles. comprising the use of a uniaxial binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 700 mg to about 1000 mg every 4 weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of 1400 mg to 2000 mg.
3.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、2週間ごとに約600mg~約1200mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 3. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment comprises administering said anti-TIGIT antagonist antibody and said PD- in one or more dosing cycles. comprising the use of a uniaxial binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 600 mg every 2 weeks; said PD-1 Axis binding antagonist is administered at about An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of 600 mg to about 1200 mg.
4.前記処置が1つ以上の化学療法剤の使用を更に含む、実施形態2又は3に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
4. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
5.前記抗TIGITアンタゴニスト抗体がIgGクラス抗体、特にIgG1サブクラス抗体である、実施形態1~4のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 5. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-4, wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
(f)QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、
を含む、実施形態1~5のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
6. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3);
(d) a HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO:5); and (f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO:6).
An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-5, comprising:
7.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
(a)DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
(b)WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
(c)GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
(d)FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、並びに
以下の重鎖可変領域FR:
(a)X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
(b)WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
(c)RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
(d)WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4
を含む、実施形態1~6のいずれか一項に記載の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
7. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and (d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and the following heavy chain variable region FRs:
(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), where X1 is E or Q;
(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and (d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
The anti-TIGIT antagonist antibody and PD-1 axis binding antagonist of any one of embodiments 1-6, comprising:
8.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)配列番号17若しくは18のアミノ酸配列を含むVHドメインと、配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態1~7のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
8. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or (c) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18. , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-7, comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
9.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである実施形態1~8のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 9. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-8, wherein said anti-TIGIT antagonist antibody is tiragolumab.
10.PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト又はPD-1結合アンタゴニストである、実施形態1~9のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 10. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-9, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist .
11.前記PD-1軸結合アンタゴニストが抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体である、実施形態1~10のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 11. Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 1-10, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody Binding antagonist.
12.前記PD-1軸結合アンタゴニストが抗PD-L1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 12. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
13.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態12に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
13. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
14.前記PD-1軸結合アンタゴニストがアテゾリズマブである、実施形態1~13のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 14. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-13, wherein said PD-1 axis binding antagonist is atezolizumab.
15.前記PD-1軸結合アンタゴニストが抗PD-1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 15. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
16.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態15に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 16. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21.
17.前記処置が、有効量の白金系化学療法剤及び非白金系化学療法剤の使用を更に含む、実施形態2~16のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 17. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 2-16, wherein said treatment further comprises the use of an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent. Axis binding antagonist.
18.前記非白金系化学療法剤がトポイソメラーゼII阻害剤である、実施形態1又は17に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
18. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
19.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331、特にエトポシドである、実施形態18に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
19. Anti-TIGIT antagonist for use according to
20.前記トポイソメラーゼII阻害剤が100mg/m2の用量での投与のために製剤化される、実施形態18又は19に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
20. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
21.前記白金系化学療法剤がカルボプラチン又はシスプラチン、特にカルボプラチンである、実施形態17~20のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 21. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 17-20, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin.
22.前記白金系化学療法剤が、投与日にAUC=5mg/ml/分を達成するのに十分な用量で投与される、実施形態17~21のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 22. Anti-TIGIT for use according to any one of embodiments 17-21, wherein said platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
23.前記方法が、導入期及び維持期を含む投薬レジメンを含む、実施形態1~22のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 23. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 1-22, wherein said method comprises a dosing regimen comprising an induction phase and a maintenance phase.
24.前記導入期が4回の初期投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤が4回の初期投薬サイクルの各々で投与される、実施形態23に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
24. wherein the induction phase comprises four initial dosing cycles, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles; an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
25.前記維持期が、前記白金系化学療法剤及び/又は非白金系化学療法剤の投与を含まない、実施形態23又は24に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
25. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
26.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、実施形態1~25のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 26. Antibody for use according to any one of embodiments 1-25, wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody. TIGIT antagonist antibody and PD-1 axis binding antagonist.
27.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の全生存期間を延長する、実施形態1~26のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 27. 27. An anti-TIGIT antagonist antibody for use according to any one of embodiments 1-26, wherein said treatment prolongs overall survival of said subject compared to treatment without said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
28.前記がんが肺がんである、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 28. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is lung cancer.
29.前記肺がんが、小細胞肺がん(SCLC)、特に進展型SCLC(ES-SCLC)である、実施形態28に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 29. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 28, wherein said lung cancer is small cell lung cancer (SCLC), in particular extensive-stage SCLC (ES-SCLC).
30.前記肺がんが、非小細胞肺がん(NSCLC)、特に局所進行性切除不能NSCLC(ステージIIIB NSCLC)である、実施形態28に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 30. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 28, wherein said lung cancer is non-small cell lung cancer (NSCLC), in particular locally advanced unresectable NSCLC (Stage IIIB NSCLC).
31.前記肺がんが局所進行性の切除不能又は転移性の非扁平上皮NSCLCである、実施形態28に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 31. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 28, wherein said lung cancer is locally advanced, unresectable or metastatic non-squamous NSCLC.
32.前記肺がんが切除可能な肺がんである、実施形態28に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 32. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 28, wherein said lung cancer is resectable lung cancer.
33.前記がんが子宮頸がんである、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 33. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is cervical cancer.
34.前記がんが初期トリプルネガティブ乳がん(eTNBC)である、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 34. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is early triple negative breast cancer (eTNBC).
35.前記がんが頭頸部がんである、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 35. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is head and neck cancer.
36.前記がんが肝臓がん、特に肝細胞癌腫(HCC)である、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 36. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is liver cancer, in particular hepatocellular carcinoma (HCC).
37.前記がんが膀胱がんである、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 37. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is bladder cancer.
38.前記がんが尿路上皮癌腫(UC)、特に転移性尿路上皮癌腫(mUC)である、実施形態37に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
38. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
39.前記がんが、膵臓がん、特に膵管腺癌(PDAC)である、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 39. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is pancreatic cancer, in particular pancreatic ductal adenocarcinoma (PDAC).
40.前記がんが食道がん、特に進行性又は転移性食道がんである、実施形態1~27のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 40. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 1-27, wherein said cancer is esophageal cancer, in particular advanced or metastatic esophageal cancer.
41.がんを有する対象を処置する方法で使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、3週間ごとに約500mg~約700mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量で投与するための製剤化されたPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤を含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 41. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said method is formulated for administration at a dose of about 500 mg to about 700 mg every three weeks. a formulated anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist formulated for administration at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, comprising administering to said subject a dosing regimen comprising one or more dosing cycles comprising a non-platinum chemotherapeutic agent.
42.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、4週間ごとに約700mg~約1000mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び4週間ごとに約1400mg~2000mgの用量で投与するために製剤化されたPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 42. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said method is formulated for administration at a dose of about 700 mg to about 1000 mg every four weeks. administering to said subject a dosing regimen comprising a formulated anti-TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist formulated to be administered at a dose of about 1400 mg to 2000 mg every 4 weeks. an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, comprising:
43.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び2週間ごとに約600mg~約1200mgの用量で投与するために製剤化されたPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 43. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said method is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks. and one or more dosing cycles of a PD-1 axis binding antagonist formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks. an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, comprising administering.
44.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、(a)前記方法が、3週間ごとに約500mg~約700mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、3週間ごとに約900mg~約1500mgの用量で投与するために製剤化されたPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、(b)前記方法が、4週間ごとに約700mg~約1000mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び4週間ごと約1400mg~2000mgの用量でに投与するために製剤化されたPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、又は(c)前記方法が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び2週間ごとに約600mg~約1200mgの用量で投与するために製剤化されたPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 44. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, said method administering (a) at a dose of about 500 mg to about 700 mg every three weeks a PD-1 axis binding antagonist formulated to be administered at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and 3 (b) said method comprises administering to said subject a dosing regimen comprising one or more weekly dosing cycles of a non-platinum chemotherapeutic agent, wherein (b) said method is administered at a dose of about 700 mg to about 1000 mg every 4 weeks; and one or more dosing cycles of a PD-uniaxial binding antagonist formulated to be administered at a dose of about 1400 mg to 2000 mg every 4 weeks. or (c) the method comprises administering to said subject an anti-TIGIT antagonist antibody formulated for administration at a dose of about 300 mg to about 600 mg every two weeks, and about 600 mg to about 600 mg every two weeks. anti-TIGIT antagonist antibody and PD-1 axis binding, comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a PD-1 axis binding antagonist formulated for administration at a dose of about 1200 mg. antagonist.
45.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態44に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
45. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
46.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態44に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
46. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
47.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、4週間ごとに約200mg~約2000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、4週間ごとに約80mg~約2000mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 47. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks, said PD-1 axis binding antagonist is administered 4 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 80 mg to about 2000 mg weekly.
48.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、4週間ごとに約200mg~約2000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、2週間ごとに約20mg~約1600mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 48. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks, said PD-1 axis binding antagonist is administered 2 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 20 mg to about 1600 mg weekly.
49.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、2週間ごとに約10mg~約1000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、2週間ごとに約20mg~約1600mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 49. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 10 mg to about 1000 mg every two weeks, said PD-1 axis binding antagonist is An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 20 mg to about 1600 mg weekly.
50.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、2週間ごとに約10mg~約1000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、4週間ごとに約80mg~約2000mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 50. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 10 mg to about 1000 mg every two weeks, said PD-1 axis binding antagonist is An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 80 mg to about 2000 mg weekly.
51.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、6週間ごとに約100mg~約1000mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 51. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, said PD-1 axis binding antagonist is An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 100 mg to about 1000 mg weekly.
52.前記処置が1つ以上の化学療法剤の使用を更に含む、実施形態47~51のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 52. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 47-51, wherein said treatment further comprises the use of one or more chemotherapeutic agents.
53.前記処置が、白金系化学療法剤及び非白金系化学療法剤の使用を更に含む、実施形態52に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 53. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 52, wherein said treatment further comprises the use of platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents.
54.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約80mg~約1600mgの用量で投与するために製剤化され、3週間ごとの白金系化学療法剤及び3週間ごとの非白金系化学療法剤を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 54. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, said PD-1 axis binding antagonist is administered for 3 An anti-TIGIT antagonist antibody and PD-1 formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks, comprising a platinum-based chemotherapeutic agent every 3 weeks and a non-platinum-based chemotherapeutic agent every 3 weeks. Axis binding antagonist.
55.前記方法が導入期及び維持期を含む、実施形態53又は54に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 55. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 53 or 54, wherein said method comprises an induction phase and a maintenance phase.
56.前記導入期及び維持期がそれぞれ1回以上の投薬サイクルを含む、実施形態55に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 56. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 55, wherein said induction phase and maintenance phase each comprise one or more dosing cycles.
57.前記維持期が白金系化学療法剤の投与を含まない、実施形態55又は56に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
57. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
58.前記維持期が非白金系化学療法剤の投与を含まない、実施形態55~57のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 58. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 55-57, wherein said maintenance phase does not comprise administration of a non-platinum chemotherapeutic agent.
59.前記維持期が、4週間ごとに約200mg~約2000mgの用量での投与するために製剤化される抗TIGITアンタゴニスト抗体、及び4週間ごとに約80mg~約2000mgの用量で投与するために製剤化されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む、実施形態58に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 59. said maintenance phase anti-TIGIT antagonist antibody formulated to be administered at a dose of about 200 mg to about 2000 mg every 4 weeks and formulated to be administered at a dose of about 80 mg to about 2000 mg every 4 weeks anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 58, comprising one or more dosing cycles of the PD-1 axis binding antagonist.
60.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及び抗PD-1アンタゴニスト抗体であって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化され、抗PD-1アンタゴニスト抗体が、3週間ごとに約80mg~約1600mgの用量で投与するために製剤化され、前記抗PD-1アンタゴニスト抗体がペンブロリズマブである、抗TIGITアンタゴニスト抗体及び抗PD-1アンタゴニスト抗体。 60. An anti-TIGIT antagonist antibody and an anti-PD-1 antagonist antibody for use in a method of treating a subject with cancer, wherein said treatment comprises one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, and said anti-PD-1 antagonist antibody is administered for 3 weeks An anti-TIGIT antagonist antibody and an anti-PD-1 antagonist antibody formulated for administration at a dose of about 80 mg to about 1600 mg per dose, wherein said anti-PD-1 antagonist antibody is pembrolizumab.
61.がんを有する対象を処置する方法に使用するためのチラゴルマブ及びペンブロリズマブであって、前記処置が、チラゴルマブ及びペンブロリズマブの1回以上の投薬サイクルを含む投薬レジメンにおけるチラゴルマブ及びペンブロリズマブの使用を含み、前記ペンブロリズマブが、6週間ごとに約100mgと約1000mgの間の用量で投与するために製剤化される、チラゴルマブ及びペンブロリズマブ。 61. Tiragolumab and pembrolizumab for use in a method of treating a subject with cancer, said treatment comprising the use of tiragolumab and pembrolizumab in a dosing regimen comprising one or more dosing cycles of tiragolumab and pembrolizumab, said pembrolizumab tiragolumab and pembrolizumab formulated for administration at doses between about 100 mg and about 1000 mg every 6 weeks.
62.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で3週間ごとに製剤化され、及び代謝拮抗剤が、2週間の投薬/1週間の休薬の間、3週間ごとの1日2回の経口の約10mg/m2と約10000mg/m2の間の用量で投与するために製剤される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 62. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist antibody is formulated at a dose of between about 80 mg and about 1600 mg every 3 weeks every 3 weeks, and the antimetabolite is administered twice a day every 3 weeks for 2 weeks on/1 week off. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 10 mg/m2 and about 10000 mg/m2 per oral dose.
63.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとの約80mg~約1600mgの用量であり、ゲムシタビン及びnab-パクリタキセルである、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 63. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 3 weeks, said PD-1 axis binding antagonist is administered for 3 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist that is gemcitabine and nab-paclitaxel at a dose of about 80 mg to about 1600 mg weekly.
64.前記1つ以上の化学療法剤がゲムシタビン及びnab-パクリタキセルである、実施形態52に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 64. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 52, wherein said one or more chemotherapeutic agents are gemcitabine and nab-paclitaxel.
65.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で3週間ごとに投与するために製剤化され、及びVEGFアンタゴニストが3週間ごとに約1mg/kgと約35mg/kgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 65. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment is in a dosing regimen comprising one or more dosing cycles. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist antibody is formulated for administration every 3 weeks at a dose of between about 80 mg and about 1600 mg every 3 weeks, and the VEGF antagonist is administered every 3 weeks at a dose of between about 1 mg/kg and about 35 mg/kg An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration.
66.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、導入期及び維持期を含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記導入期が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量の前記PD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤の投与を含まない、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
66. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment comprises said anti-TIGIT antagonist antibody and a dosing regimen comprising an induction phase and a maintenance phase. comprising the use of said PD-1 axis binding antagonist;
(a) said anti-TIGIT antagonist antibody formulated for administration in said induction phase at a dose of about 30 mg to about 1200 mg every 3 weeks; said PD-1 at a dose of about 80 mg to about 1600 mg every 3 weeks; one or more dosing cycles of an axially bound antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks;
(b) said maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding antagonist every 3 weeks and a non-platinum chemotherapeutic agent every 3 weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said maintenance phase does not include administration of said platinum-based chemotherapeutic agent.
67.がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、導入期及び維持期を含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記導入期が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量の前記PD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、4週間ごとに約200mg~約2000mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体、及び4週間ごとに約80mg~約2000mgの用量で投与するために製剤化された前記PD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤又は前記非白金系化学療法剤の投与を含まない、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
67. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with cancer, wherein said treatment comprises said anti-TIGIT antagonist antibody and a dosing regimen comprising an induction phase and a maintenance phase. comprising the use of said PD-1 axis binding antagonist;
(a) said anti-TIGIT antagonist antibody formulated for administration in said induction phase at a dose of about 30 mg to about 1200 mg every 3 weeks; said PD-1 at a dose of about 80 mg to about 1600 mg every 3 weeks; one or more dosing cycles of an axially bound antagonist, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks;
(b) said anti-TIGIT antagonist antibody formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks during said maintenance phase, and for administration at a dose of about 80 mg to about 2000 mg every 4 weeks; wherein said maintenance phase does not comprise administration of said platinum-based chemotherapeutic agent or said non-platinum-based chemotherapeutic agent. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
68.前記導入期が4~6回の投薬サイクルを含む、実施形態56~59、66、及び67のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 68. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 56-59, 66 and 67, wherein said induction phase comprises 4-6 dosing cycles.
69.実施形態53~59及び66~68のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、又は
(c)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がエトポシドである、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
69. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 53-59 and 66-68, wherein
(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel, or (c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is etoposide,
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
70.前記がんが固形腫瘍である、実施形態47~69のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 70. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-69, wherein said cancer is a solid tumor.
71.前記がんが局所進行性又は転移性である、実施形態47~70のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 71. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-70, wherein said cancer is locally advanced or metastatic.
72.前記がんが、肺がん、膵臓がん、子宮頸がん、乳がん、頭頸部がん、肝臓がん、膀胱がん、食道がん、胃がん、結腸直腸がん、腎臓がん、腎がん、黒色腫、又は卵巣がんである、実施形態47~71のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 72. the cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, renal cancer, Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-71, which is melanoma, or ovarian cancer.
73.前記がんが肺がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
73. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
74.肺がんがNSCLC、特に局所進行性切除不能NSCLCである、実施形態73に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
74. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
75.前記NSCLCがステージIIIB NSCLCである、実施形態74に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 75. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 74, wherein said NSCLC is stage IIIB NSCLC.
76.前記肺がんが再発性又は転移性NSCLCである、実施形態73~75のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 76. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 73-75, wherein said lung cancer is recurrent or metastatic NSCLC.
77.前記NSCLCがステージIV NSCLCである、実施形態76に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
77. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
78.前記対象がステージIVのNSCLCについて以前に処置されたことがない、実施形態77に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 78. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 77, wherein said subject has not been previously treated for stage IV NSCLC.
79.前記肺がんが小細胞肺がん(SCLC)である、実施形態73に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
79. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
80.肺がんを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤を含む処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 80. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer, said treatment comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising one or more dosing cycles of a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment comprises said anti-TIGIT antagonist antibody. an anti-TIGIT antagonist antibody that prolongs progression-free survival (PFS) of said subject compared to treatment comprising said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without and PD-1 axis binding antagonists.
81.肺がんを有する対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記処置が、約8.2ヶ月~約9.2ヶ月の前記対象集団のPFS中央値をもたらす、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 81. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject population having lung cancer, said treatment comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising one or more dosing cycles of a chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment lasts from about 8.2 months to about 9. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist that produced a median PFS in the subject population of 2 months.
82.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の全生存期間(OS)を延長する、実施形態80又は81に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
82. The treatment compared the overall survival (OS 82. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
83.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のPFSを少なくとも約2.4ヶ月延長する、実施形態80~82のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 83. said treatment prolongs PFS of said subject or subject population by at least about 2.4 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-82.
84.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の前記PFSを少なくとも約3ヶ月~約4ヶ月延長する、実施形態83に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 84. said treatment reduces said PFS of said subject or subject population by at least about Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 83, extending from 3 months to about 4 months.
85.肺がんを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤を含む処置と比較して、前記対象のOSを延長する、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 85. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer, said treatment comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising one or more dosing cycles of a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment comprises said anti-TIGIT antagonist antibody. an anti-TIGIT antagonist antibody and PD-1 axis binding that prolongs OS in said subject compared to treatment comprising said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor without antagonist.
86.肺がんを有する対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記処置が、約15.3ヶ月~約17.6ヶ月の前記対象集団のOS中央値をもたらす、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 86. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject population having lung cancer, said treatment comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of a chemotherapeutic agent and a topoisomerase II inhibitor, said treatment for about 15.3 months to about 17.6 months. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist that yielded a median OS in the subject population of .
87.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3.3ヶ月延長する、実施形態82~86のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 87. said treatment prolongs OS of said subject or subject population by at least about 3.3 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 82-86.
88.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3ヶ月~約5.3ヵ月延長する、実施形態82~86のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 88. said treatment reduces the OS of said subject or subject population by at least about 3 months to about 5 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 82-86, extended for 3 months.
89.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が、4回の初期投薬サイクルの各々で投与される、実施形態80~88のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 89. 89. According to any one of embodiments 80-88, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered in each of four initial dosing cycles. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in.
90.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが、前記第4の初期投薬サイクルに続いて1回以上の追加のサイクルで更に投与される、実施形態80~89のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 90. 89. Any one of embodiments 80-89, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are further administered in one or more additional cycles following said fourth initial dosing cycle. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in.
91.前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤が、前記1回以上の追加の投薬サイクルの各々から省略される、実施形態90に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
91. An anti-TIGIT antagonist antibody and PD-1 axis binding for use according to
92.前記白金系化学療法剤がカルボプラチンであり、前記トポイソメラーゼII阻害剤がエトポシドである、実施形態80~91のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 92. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-91, wherein said platinum-based chemotherapeutic agent is carboplatin and said topoisomerase II inhibitor is etoposide.
93.前記肺がんが小細胞肺がん(SCLC)である、実施形態80~92のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 93. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-92, wherein said lung cancer is small cell lung cancer (SCLC).
94.前記SCLCが、進展型SCLC(ES-SCLC)である、実施形態93に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 94. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 93, wherein said SCLC is extended-stage SCLC (ES-SCLC).
95.前記一又は複数の対象がES-SCLCに対して処置未経験である、実施形態94に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 95. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 94, wherein said one or more subjects are treatment naive for ES-SCLC.
96.前記一又は複数の対象が脳転移の存在又は病歴を有しない、実施形態80~95のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 96. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-95, wherein said one or more subjects do not have the presence or history of brain metastases.
97.前記肺がんがPD-L1発現について選択されていない、実施形態80~96のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 97. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-96, wherein said lung cancer is not selected for PD-L1 expression.
98.前記肺がんがPD-L1発現について選択される、実施形態80~96のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 98. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 80-96, wherein said lung cancer is selected for PD-L1 expression.
99.前記肺がんが、検出可能なPD-L1発現レベルによってPD-L1発現について選択される、実施形態98に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 99. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 98, wherein said lung cancer is selected for PD-L1 expression by a detectable level of PD-L1 expression.
100.前記肺がんが転移性である、実施形態80~99のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 100. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 80-99, wherein said lung cancer is metastatic.
101.前記肺がんが脳、肝臓、リンパ節、及び/又は副腎に転移している、実施形態100に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
101. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
102.前記肺がんが脳に転移したことがない、実施形態100又は101に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
102. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
103.前記処置が完全奏効(CR)又は部分奏効(PR)をもたらす、実施形態100~102のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 103. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 100-102, wherein said treatment results in a complete response (CR) or a partial response (PR).
104.前記抗TIGITアンタゴニスト抗体が、2週間、3週間又は4週間ごとに約30mg~約1200mgの用量で投与するために製剤化される、実施形態80~103のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 104. For use according to any one of embodiments 80-103, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every 2, 3 or 4 weeks. anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
105.前記PD-1軸結合アンタゴニストが、2週間、3週間又は4週間ごとに約80mg~約2000mgの用量で投与するために製剤化される、実施形態80~104のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 105. 105. Use according to any one of embodiments 80-104, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 2000 mg every 2, 3 or 4 weeks. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
106.前記PD-1軸結合アンタゴニスト、抗TIGITアンタゴニスト抗体、白金系化学療法剤及びトポイソメラーゼII阻害剤を連続的に投与する、実施形態80~105のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 106. Anti-TIGIT antagonist for use according to any one of embodiments 80-105, wherein said PD-1 axis binding antagonist, anti-TIGIT antagonist antibody, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered sequentially. Antibodies and PD-1 axis binding antagonists.
107.前記PD-1軸結合アンタゴニストが前記抗TIGITアンタゴニスト抗体の前に投与され、前記抗TIGITアンタゴニスト抗体が前記白金系化学療法剤の前に投与され、前記白金剤がトポイソメラーゼII阻害剤の前に投与される、実施形態106に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 107. The PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered prior to the platinum-based chemotherapeutic agent, and the platinum agent is administered prior to the topoisomerase II inhibitor. an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 106.
108.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が静脈内投与される、実施形態80~107のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 108. 108. Anti-TIGIT antagonist for use according to any one of embodiments 80-107, wherein said anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered intravenously. Antibodies and PD-1 axis binding antagonists.
109.前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤のうち1つ以上が皮下投与される、実施形態80~108のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 109. 109. Any one of embodiments 80-108, wherein one or more of said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are administered subcutaneously. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
110.SCLCを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記処置が、前記抗TIGITアンタゴニスト抗体の1回以上の21日間投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が各投薬サイクルの1日目に約30mg~約1200mgの用量で投与するために製剤化され、アテゾリズマブが各投薬サイクルの1日目に約80mg~約1600mgの用量で投与するために製剤化され、カルボプラチンが各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量で製剤化され、エトポシドが各投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量で投与するために製剤化され、前記処置が、前記抗TIGITアンタゴニストを用いないアテゾリズマブ、カルボシド及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、抗TIGITアンタゴニスト抗体及びアテゾリズマブ。
110. An anti-TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with SCLC, wherein said treatment comprises one or more 21-day dosing cycles of said anti-TIGIT antagonist antibody and said comprising the use of a PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg on
111.SCLCを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記処置が、前記抗TIGITアンタゴニスト抗体の1回以上の21日間投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が各投薬サイクルの1日目に約300mg~約800mgの用量で投与するために製剤化され、アテゾリズマブが各投薬サイクルの1日目に約900mg~約1500mgの用量で投与するために製剤化され、カルボプラチンが各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量で製剤化され、エトポシドが各投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量で投与するために製剤化され、前記処置が、前記抗TIGITアンタゴニストを用いないアテゾリズマブ、カルボシド及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、抗TIGITアンタゴニスト抗体及びアテゾリズマブ。
111. An anti-TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with SCLC, wherein said treatment comprises one or more 21-day dosing cycles of said anti-TIGIT antagonist antibody and said comprising the use of a PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg to about 800 mg on
112.前記処置が、各追加の投薬サイクルの1日目に約30mg~約1200mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び各追加の投薬サイクルの1日目に約80mg~約1600mgの用量で投与するために製剤化されたアテゾリズマブの1回以上の追加の21日間投薬サイクルを更に含み、カルボプラチン及びエトポシドが1回以上の追加の投薬サイクルのそれぞれから省略される、実施形態110又は111に記載の使用のための抗TIGITアンタゴニスト抗体及びアテゾリズマブ。
112. The treatment comprises an anti-TIGIT antagonist antibody formulated for administration at a dose of about 30 mg to about 1200 mg on
113.ES-SCLCを有する対象又は対象集団を処置するための方法において使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの4回の初期投薬サイクルと、それに続く1回以上の追加の投薬サイクルでの使用を含み、
(a)前記4回の初期投薬サイクルが、各初期投薬サイクルの1日目に約600mgの用量で投与するために製剤化されたチラゴルマブ、各初期投薬サイクルの1日目に約1200mgの用量で投与するために製剤化されたアテゾリズマブ、各初期投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各初期投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量のエトポシドを含み、
(b)前記1回以上の追加の投薬サイクルが、各追加の投薬サイクルの1日目に約600mgの用量で投与するために製剤化されたチラゴルマブ、及び各追加の投薬サイクルの1日目に約1200mgの用量で投与するために製剤化されたアテゾリズマブを含み、
前記4回の初期投薬サイクル及び前記1回以上の追加の投薬サイクルが、それぞれ21日間投薬サイクルであり、前記処置が、前記チラゴルマブを用いないアテゾリズマブ、カルボプラチン及びエトポシドを含む処置と比較して、前記対象又は対象集団のPFS及び/又はOSを延長する、チラゴルマブ及びアテゾリズマブ。
113. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with ES-SCLC, said treatment comprising four initial dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist , including use in one or more additional dosing cycles followed by
(a) tiragolumab formulated for the four initial dosing cycles to be administered at a dose of about 600 mg on
(b) said one or more additional dosing cycles are formulated to be administered at a dose of about 600 mg on
each of the four initial dosing cycles and the one or more additional dosing cycles is a 21-day dosing cycle, and the treatment is compared to a treatment comprising atezolizumab, carboplatin and etoposide without the tiragolumab; Tiragolumab and atezolizumab that prolong PFS and/or OS in a subject or subject population.
114.肺がんを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤である第1の化学療法剤、及び非白金系化学療法剤である第2の化学療法剤の1回以上の投薬サイクルを含む投薬レジメンにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 114. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having lung cancer, said treatment comprising an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, a platinum-based chemical said anti-TIGIT antagonist antibody and said PD-1 axis binding in a dosing regimen comprising one or more dosing cycles of a first chemotherapeutic agent that is a therapeutic agent and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists, including the use of antagonists.
115.前記肺がんがPD-L1発現について評価されていない、実施形態114に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 115. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 114, wherein said lung cancer has not been evaluated for PD-L1 expression.
116.前記一又は複数の対象が、50%以上のPD-L1陽性腫瘍細胞分率を有すると決定されていない、実施形態114又は115に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 116. 116. An anti-TIGIT antagonist antibody and PD-1 axis binding for use according to embodiment 114 or 115, wherein said one or more subjects have not been determined to have a PD-L1 positive tumor cell fraction of 50% or greater antagonist.
117.前記一又は複数の対象が50%未満のPD-L1陽性腫瘍細胞分率を有すると決定されている、実施形態116に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 117. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 116, wherein said one or more subjects have been determined to have a PD-L1 positive tumor cell fraction of less than 50%.
118.前記PD-L1陽性腫瘍細胞分率が、抗PD-L1抗体での陽性染色によって決定され、前記抗PD-L1抗体がSP263又は22C3である、実施形態116又は117に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 118. 118. An anti-tumor for use according to embodiment 116 or 117, wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, and said anti-PD-L1 antibody is SP263 or 22C3. TIGIT antagonist antibody and PD-1 axis binding antagonist.
119.前記一又は複数の対象が、上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態114~118のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 119. Antibiotic for use according to any one of embodiments 114-118, wherein said one or more subjects do not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations. TIGIT antagonist antibody and PD-1 axis binding antagonist.
120.前記一又は複数の対象が肺がんの事前全身治療を受けたことがない、実施形態114~119のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 120. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 114-119, wherein said one or more subjects have no prior systemic treatment for lung cancer.
121.前記肺がんが局所進行性肺がんである、実施形態114~120のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 121. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 114-120, wherein said lung cancer is locally advanced lung cancer.
122.前記肺がんがNSCLC、特に局所進行性の切除不能又は転移性の非扁平上皮NSCLCである、実施形態114~121のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 122. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 114 to 121, wherein said lung cancer is NSCLC, in particular locally advanced unresectable or metastatic non-squamous NSCLC antagonist.
123.前記非扁平上皮NSCLCが、ステージIV非扁平上皮NSCLCである、実施形態122に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 123. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 122, wherein said non-squamous NSCLC is stage IV non-squamous NSCLC.
124.前記投薬レジメンが、4回の投薬サイクルを含む導入期を含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記非白金系化学療法剤が、前記導入期の各投薬サイクルの1日目に投与される、実施形態114~123のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
124. The dosing regimen comprises an induction phase comprising four dosing cycles, wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent and the non-platinum-based chemotherapeutic agent are in the induction phase 124. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 114-123, administered on
125.前記投薬レジメンが、前記導入期に続いて維持期を含み、前記維持期が1回以上の投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト及び前記非白金系化学療法剤が、前記維持期の各投薬サイクルの1日目に投与される、実施形態124に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
125. wherein said dosing regimen comprises a maintenance phase following said induction phase, said maintenance phase comprising one or more dosing cycles, said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist and said non-platinum chemotherapeutic agent is administered on
126.前記維持期の前記1回以上の投薬サイクルが、前記白金系化学療法剤の投与を含まない、実施形態125に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 126. 126. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 125, wherein said one or more dosing cycles of said maintenance phase does not comprise administration of said platinum-based chemotherapeutic agent.
127.前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、非白金系化学療法剤がペメトレキセドである、実施形態114~126のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 127. Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 114-126, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed Binding antagonist.
128.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの、チラゴルマブ、アテゾリズマブ、カルボプラチン若しくはシスプラチン、及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンでの使用を含み、ペメトレキセドが4回の21日間投薬サイクルのそれぞれの1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与するために製剤化され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与するために製剤化され、カルボプラチンが3週間ごとにAUC=5mg/ml/分を達成するのに十分な用量で投与され、又はシスプラチンが3週間ごとに75mg/m2の用量で投与するために製剤化され、ペメトレキセドが3週間ごとに約500mg/m2の用量で投与するために製剤化される、チラゴルマブ及びアテゾリズマブ。
128. Tiragolumab and atezolizumab for use in a method of treating a subject or subject population with advanced non-squamous NSCLC, said treatment comprising an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist tiragolumab, atezolizumab, carboplatin or cisplatin, and pemetrexed in a dosing regimen comprising four 21-day dosing cycles, wherein pemetrexed on
129.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル、
での抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、
前記対象又は対象集団が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、チラゴルマブ及びアテゾリズマブ。
129. Tiragolumab and atezolizumab for use in a method of treating a subject or subject population with advanced non-squamous NSCLC, said treatment comprising
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin;
including the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in
Tiragolumab and atezolizumab, wherein said subject or subject population has not received prior systemic therapy for said advanced non-squamous NSCLC.
130.進行性非扁平上皮NSCLCを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル、
での抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、
前記対象が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、チラゴルマブ及びアテゾリズマブ。
130. Tiragolumab and atezolizumab for use in a method of treating a subject with advanced non-squamous NSCLC, said treatment comprising
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin;
including the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in
tiragolumab and atezolizumab, wherein said subject was naive to prior systemic therapy for said advanced non-squamous NSCLC.
131.進行性非扁平上皮NSCLCを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの、チラゴルマブ、アテゾリズマブ、カルボプラチン若しくはシスプラチン、及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンでの使用を含み、ペメトレキセドが4回の21日間投薬サイクルのそれぞれの1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与するために製剤化され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与するために製剤化され、シスプラチンが3週間ごとに75mg/m2の用量で投与するために製剤化され、ペメトレキセドが約500mg/m2の用量で投与するために製剤化される、チラゴルマブ及びアテゾリズマブ。
131. Tiragolumab and atezolizumab for use in a method of treating a subject with advanced non-squamous NSCLC, said treatment comprising an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist tiragolumab, atezolizumab, carboplatin or cisplatin; and pemetrexed on
132.前記処置が、前記対象又は対象集団のPFSを少なくとも約3.5ヶ月又は約4.7ヶ月延長させる、実施形態114~131のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 132. Anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 114-131, wherein said treatment prolongs PFS of said subject or population of subjects by at least about 3.5 months or about 4.7 months - uniaxial binding antagonists.
133.前記処置が、約12.5ヶ月~約14.7ヶ月の前記対象集団のPFS中央値をもたらす、実施形態114~132のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 133. The anti-TIGIT antagonist antibody and PD-antibody for use according to any one of embodiments 114-132, wherein said treatment results in a median PFS of said subject population of about 12.5 months to about 14.7 months. Uniaxial binding antagonist.
134.前記処置が、前記対象又は対象集団のOSを少なくとも約5.5ヶ月又は約8.0ヶ月延長させる、実施形態114~133のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 134. An anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 114-133, wherein said treatment prolongs OS of said subject or population of subjects by at least about 5.5 months or about 8.0 months - uniaxial binding antagonists.
135.前記処置が約27.5ヵ月~約32.0ヵ月の前記対象集団のOS中央値をもたらす、実施形態114~134のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 135. 135. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 114-134, wherein said treatment results in a median OS for said subject population of about 27.5 months to about 32.0 months Axis binding antagonist.
136.切除可能な肺がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 136. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects having resectable lung cancer, said treatment comprising said anti-TIGIT antibody in one or more dosing cycles. comprising the use of a TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the binding antagonist antibody is formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks.
137.切除可能な肺がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 137. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects having resectable lung cancer, said treatment comprising said anti-TIGIT antibody in one or more dosing cycles. comprising the use of a TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 300 mg and about 800 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the binding antagonist antibody is formulated for administration at a dose of between about 900 mg and about 1500 mg every three weeks.
138.肺がんを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体、及び3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される前記PD-1軸結合アンタゴニストを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 138. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with lung cancer, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist. wherein at least one of said dosing cycles is administered at a dose between about 30 mg and about 1200 mg every 3 weeks as a neoadjuvant treatment and PD-uniaxial binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks. - uniaxial binding antagonists.
139.肺がんを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を含み、前記PD-1軸結合アンタゴニストが3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 139. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject with lung cancer, said treatment comprising one or more of the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist. comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in dosing cycles, wherein at least one of said dosing cycles is administered at a dose of between about 300 mg and about 800 mg every 3 weeks as a neoadjuvant treatment. wherein said PD-1 axis binding antagonist is formulated for administration at a dose of between about 900 mg and about 1500 mg every three weeks. and PD-1 axis binding antagonists.
140.前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を含み、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、実施形態138又は139に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 140. at least one of said dosing cycles comprises said anti-TIGIT antagonist antibody formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks as an adjuvant treatment, wherein said PD-1 axis binding antagonist is 140. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 138 or 139, formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks.
141.前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとに約500mgと約700mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を含み、前記PD-1軸結合アンタゴニストが3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化される、実施形態140に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 141. at least one of said dosing cycles comprises said anti-TIGIT antagonist antibody formulated for administration at a dose of between about 500 mg and about 700 mg every three weeks as an adjuvant treatment, wherein said PD-1 axis binding antagonist is Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 140, formulated for administration at a dose of between about 900 mg and about 1500 mg every 3 weeks.
142.前記肺がんが切除可能な肺がんである、実施形態138~141のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 142. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 138-141, wherein said lung cancer is resectable lung cancer.
143.前記肺がんが初期がんである、実施形態136~142のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 143. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 136-142, wherein said lung cancer is early stage cancer.
144.前記肺がんが、ステージII、IIIA又はIIIB肺がんである、実施形態136~143のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 144. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 136-143, wherein said lung cancer is stage II, IIIA or IIIB lung cancer.
145.前記肺がんが上皮成長因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態136~144のいずれか一項に記載のしようのための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 145. 145. Anti-TIGIT antagonist antibody and PD for any one of embodiments 136-144, wherein said lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations - uniaxial binding antagonists.
146.前記対象が治癒目的でのR0摘出に適格である、実施形態136~145のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 146. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 136-145, wherein said subject is eligible for R0 ablation for curative purposes.
147.前記対象が肺がんの事前治療を受けたことがない、実施形態136~146のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 147. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 136-146, wherein said subject has no prior treatment for lung cancer.
148.前記事前治療が免疫療法、化学療法、又は放射線療法である、実施形態147に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 148. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 147, wherein said prior treatment is immunotherapy, chemotherapy or radiotherapy.
149.前記対象が白金系化学療法レジメンを受けるのに適格である、実施形態136~148のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 149. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 136-148, wherein said subject is eligible to undergo a platinum-based chemotherapy regimen.
150.前記第1の投薬サイクルが手術前に開始される、実施形態136~149のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 150. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 136-149, wherein said first dosing cycle is initiated prior to surgery.
151.少なくとも1、2、3、又は4回の投薬サイクルが手術前に完了する、実施形態150に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 151. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 150, wherein at least 1, 2, 3, or 4 dosing cycles are completed prior to surgery.
152.4回の投薬サイクルが手術前に完了する、実施形態150又は151に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 152. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiments 150 or 151, wherein 4 dosing cycles are completed prior to surgery.
153.少なくとも1回の投薬サイクルが手術後に開始される、実施形態136~152のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 153. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 136-152, wherein at least one dosing cycle is initiated after surgery.
154.16回の投薬サイクルが手術後に完了する、実施形態153に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 154. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 153, wherein 16 dosing cycles are completed after surgery.
155.前記手術が、区域切除術、肺葉切除術、二葉切除術、又は肺切除術である、実施形態150~154のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 155. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 150-154, wherein said surgery is segmentectomy, lobectomy, bilobectomy, or pneumonectomy antagonist.
156.前記方法が放射線療法を更に含む、実施形態136~155のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 156. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 136-155, wherein said method further comprises radiotherapy.
157.前記放射線療法が術後放射線療法である、実施形態156に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 157. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 156, wherein said radiotherapy is post-operative radiotherapy.
158.前記処置が1つ以上の化学療法剤の使用を更に含む、実施形態136~157のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 158. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 136-157, wherein said treatment further comprises the use of one or more chemotherapeutic agents.
159.前記1つ以上の化学療法剤が手術後に投与される、実施形態158に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 159. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 158, wherein said one or more chemotherapeutic agents are administered post-operatively.
160.前記1つ以上の化学療法剤が、手術後に4回の投薬サイクルで投与される、実施形態159に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 160. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 159, wherein said one or more chemotherapeutic agents are administered in four dosing cycles after surgery.
161.前記1つ以上化学療法剤が、白金系化学療法剤及び非白金系化学療法剤である、実施形態158~160のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
162.実施形態161に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
(c)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、
(d)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、又は
(e)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
161. Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 158-160, wherein said one or more chemotherapeutic agents are platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents Binding antagonist.
162. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 161, wherein
(a) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine. is
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
163.前記処置が、基準病理学的著効(MPR)率と比較してMPR率の増加をもたらす、実施形態136~162のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 163. 163. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 136-162, wherein said treatment results in an increase in MPR rate compared to the baseline significant pathologic response (MPR) rate Axis binding antagonist.
164.前記基準MPR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のMPR率である、実施形態163に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
164. The reference MPR rate is
MPR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 164. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 163 which is .
165.前記処置が、病理学的完全奏効(pCR)及び/又は基準pCR率と比較したpCR率の増加をもたらす、実施形態136~164のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 165. 165. An anti-TIGIT antagonist antibody for use according to any one of embodiments 136-164, wherein said treatment results in a pathological complete response (pCR) and/or an increase in the pCR rate compared to the baseline pCR rate and PD-1 axis binding antagonist.
166.前記基準pCR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のpCR率である、実施形態165に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
166. The reference pCR rate is
pCR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 165. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 165 which is .
167.前記処置、基準EFS時間と比較して、無症候生存期間(EFS)の増加をもたらす、実施形態136~166のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 167. 167. An anti-TIGIT antagonist antibody for use according to any one of embodiments 136-166, wherein said treatment results in an increase in symptom-free survival (EFS) compared to baseline EFS time and PD-1 axis binding antagonist.
168.前記基準EFS率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のEFS時間である、実施形態167に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
168. The reference EFS rate is
EFS time in a subject population that has received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 167. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 167 which is .
169.切除可能な肺がんを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約600mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 169. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having resectable lung cancer, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist. antibody and said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 600 mg every 3 weeks, said PD-1 axis binding antagonist An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the antibody is formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks.
170.肺がんを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体及び-1軸結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとに約30mgと約600mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を含み、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 170. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject with lung cancer, said treatment comprising one or more doses of the anti-TIGIT antagonist antibody and the -1 axis binding antagonist comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in cycles, wherein at least one of said dosing cycles administers as a neoadjuvant treatment at a dose of between about 30 mg and about 600 mg every three weeks. wherein the PD-1 axis binding antagonist is formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks; and PD-1 axis binding antagonist.
171.切除可能な肺がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約1600mgの間の用量で3週間ごとに投与するために製剤化される前記PD-1軸結合アンタゴニスト抗体、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 171. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects having resectable lung cancer, said treatment comprising about 30 mg and about 1200 mg every 3 weeks. said anti-TIGIT antagonist antibody formulated for administration at a dose between about 80 mg and about 1600 mg every 3 weeks for administration every 3 weeks at a dose of between about 80 mg and about 1600 mg every 3 weeks anti-TIGIT antagonist antibody and PD-, including the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of an antagonist antibody, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent. Uniaxial binding antagonist.
172.肺がんを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される前記PD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 172. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject with lung cancer, said treatment comprising an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, platinum-based chemotherapy and the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of a non-platinum chemotherapeutic agent, at least one of said dosing cycles as a neoadjuvant treatment, 3 said anti-TIGIT antagonist antibody formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; said anti-TIGIT antagonist antibody formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks; Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists, including PD-1 axis binding antagonists, platinum-based chemotherapeutic agents, and non-platinum-based chemotherapeutic agents.
173.切除可能な肺がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される前記PD-1軸結合アンタゴニスト抗体と、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化されるPD-1軸結合アンタゴニストと、(a)(i)3週間ごとの5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量の白金系化学療法剤;又は(ii)3週間ごとの約75mg/m2の用量の白金系化学療法剤と、(b)(i)3週間ごとの約500mg/m2、各投薬サイクルの第1日及び第8日に約1000mg/m2若しくは約1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとの約100mg/m2、約175mg/m2、若しくは約200mg/m2の用量のタキサンと、の1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
173. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects having resectable lung cancer, said treatment comprising about 30 mg and about 1200 mg every 3 weeks. said PD-1 axis binding antagonist antibody formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks. and (a) (i) a platinum-based chemotherapeutic agent at a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; or (ii) every 3 weeks and (b)(i) about 500 mg/m2 every three weeks, about 1000 mg/m2 or about 1250 mg/m2 on
174.肺がんを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、チラゴルマブ、アテゾリズマブ、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルにおける抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、(a)3週間ごとの約30mgと約600mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体と、(b)3週間ごとの約80mgと約1600mgの間の用量で投与するために製剤化された前記PD-1軸結合アンタゴニストと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量、又は(ii)3週間ごとの約75mg/m2の用量の前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のタキサンである非白金系化学療法剤とを含み、前記処置がネオアジュバント処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 174. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject with lung cancer, said treatment comprising tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapy comprising use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in one or more dosing cycles of the agent, at least one of said dosing cycles comprising: (a) at a dose of between about 30 mg and about 600 mg every 3 weeks; (b) said PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks; c) the platinum-based chemotherapeutic agent (i) at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) for 3 weeks (d) said non-platinum-based chemotherapeutic agent (i) 500 mg/m every 3 weeks, or on day 1 of each dosing cycle and a non-platinum chemotherapeutic agent that is an antimetabolite at a dose of 1000 mg/m2 or 1250 mg/m2 on day 8, or (ii) a taxane at a dose of 100 mg/m2, 175 mg/m2 or 200 mg/m2 every 3 weeks. and wherein said treatment is a neoadjuvant treatment, an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
175.切除可能な肺がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとの約600mgの用量のチラゴルマブと、3週間ごとの約1200mgの用量のアテゾリズマブと、
(a)
(i)3週間ごとの5mg/mL/分のAUC若しくは6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は
(ii)3週間ごとの約75mg/m2の用量のシスプラチンと、
(b)
(i)3週間ごとの約500mg/m2の用量のペメトレキセド、又は各投薬サイクルの1日目及び8日目に約1000mg/m2若しくは約1250mg/m2の用量のゲムシタビン、又は
(ii)3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセルと、
の1回以上の投薬サイクルでの抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。
175. Tiragolumab and atezolizumab for use in a method for treating a subject with resectable lung cancer, said treatment comprising tiragolumab at a dose of about 600 mg every 3 weeks and tiragolumab at a dose of about 1200 mg every 3 weeks. atezolizumab and
(a)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and,
(b)
(i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks, or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on
tiragolumab and atezolizumab, including the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in one or more dosing cycles of
176.肺がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ、アテゾリズマブ、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルにおける抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、前記投薬サイクルの少なくとも1つが、(a)3週間ごとの約600mgの用量で投与するために製剤化されるチラゴルマブと、(b)3週間ごとの約1200mgの用量で投与するために製剤化されるアテゾリズマブと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は(ii)3週間ごとの約75mg/m2の用量のシスプラチンである、前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量のペメトレキセド、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のパクリタキセルである非白金系化学療法剤と、を投与することを含み、前記処置がネオアジュバント処置である、チラゴルマブ及びアテゾリズマブ。
176. Tiragolumab and atezolizumab for use in a method for treating a subject with lung cancer, said treatment comprising one or more dosing cycles of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent wherein at least one of said dosing cycles comprises (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks; ) atezolizumab formulated for administration at a dose of about 1200 mg every 3 weeks; (ii) cisplatin at a dose of about 75 mg/m2 every three weeks; A platinum-based chemotherapeutic agent that is (i) pemetrexed at a dose of 500 mg/m2 every 3 weeks, or 1000 mg/m2 or 1250 mg/m2 on
177.非扁平上皮NSCLCを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、(a)前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとに約600mgの用量で投与するために製剤化されたチラゴルマブと、3週間ごとに1200mgの用量で投与するために製剤化されたアテゾリズマブとを含み、(b)前記投薬サイクルの少なくとも1つが、アジュバント処置として、約600mgの用量で3週間ごとに投与するために製剤化されたチラゴルマブと、約1200mgの用量で3週間ごとに投与するために製剤化されたアテゾリズマブとを含む、チラゴルマブ及びアテゾリズマブ。 177. Tiragolumab and atezolizumab for use in a method for treating a subject with non-squamous NSCLC, said treatment comprising said anti-TIGIT antagonist antibody and said PD-1 in one or more dosing cycles of tiragolumab and atezolizumab (a) at least one of said dosing cycles, as a neoadjuvant treatment, tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks and 1200 mg every 3 weeks; atezolizumab formulated for administration in doses, wherein at least one of said dosing cycles is tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks as an adjuvant treatment; tiragolumab and atezolizumab, including atezolizumab formulated for administration at a dose of about 1200 mg every three weeks.
178.非扁平上皮NSCLCを有する対象を処置するための方法に使用するためのチラゴルマブ抗体及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、(I)前記投薬サイクルの少なくとも1つがネオアジュバント処置であって、(a)3週間ごとの約600mgの用量で投与するために製剤化されたチラゴルマブ;(b)ネオアジュバント処置として3週間ごとの約1200mgの用量で投与するために製剤化されたのアテゾリズマブ;(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセド;(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2又は約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとの約30mgと約1200mgの間の用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量で投与するために製剤化されたアテゾリズマブを含む、チラゴルマブ抗体及びアテゾリズマブ。 178. Tiragolumab antibody and atezolizumab for use in a method for treating a subject with non-squamous NSCLC, said treatment comprising said anti-TIGIT antagonist antibody and said PD- tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks comprising the use of a uniaxial binding antagonist, wherein (I) at least one of said dosing cycles is a neoadjuvant treatment; (b) ) atezolizumab formulated to be administered at a dose of approximately 1200 mg every 3 weeks as a neoadjuvant treatment; (c) (i) with the goal of achieving an AUC of 5 mg/mL/min every 3 weeks (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks, and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; paclitaxel at a dose of 175 mg/m2 or about 200 mg/m2, or (iii) cisplatin at a dose of about 75 mg/m2 every three weeks and pemetrexed at a dose of about 500 mg/m2 every three weeks; At least one of the dosing cycles is tiragolumab formulated to be administered at a dose of between about 30 mg and about 1200 mg every 3 weeks as an adjuvant treatment, and at a dose of between about 80 mg and about 1600 mg every 3 weeks. Tiragolumab antibodies and atezolizumab, including atezolizumab formulated for administration.
179.肺がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、(I)前記投薬サイクルの少なくとも1つが、ネオアジュバント処置であり、(a)3週間ごとの約600mgの用量で投与するために製剤化されたチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量で投与するために製剤化されたアテゾリズマブ、及び(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとの約30mgと約1200mgの間の用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量で投与するために製剤化されたアテゾリズマブを含む、チラゴルマブ及びアテゾリズマブ。
179. Tiragolumab and atezolizumab for use in a method for treating a subject with lung cancer, said treatment comprising said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is neoadjuvant treatment, (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks, (b) neoadjuvant treatment atezolizumab formulated to be administered at a dose of approximately 1200 mg every 3 weeks as and (c)(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
180.肺がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(I)前記投薬サイクルの少なくとも1つがネオアジュバント処置であって、
(a)3週間ごとに約1200mgの用量で投与するために製剤化されたチラゴルマブと、
(b)ネオアジュバント処置として3週間ごとに約1200mgの用量で投与するために製剤化されたアテゾリズマブと、
(c)
(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの第1日及び第8日に約1000mg/m2の用量のゲムシタビン、
(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は
(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの1日目及び8日目に約1250mg/m2の用量のゲムシタビンと、を含み、
(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとの約300mgと約800mgの間の用量で投与するために製剤化されたチラゴルマブと、3週間ごとの約900mgと約1500mgの間の用量で投与するために製剤化されたアテゾリズマブとを含む、チラゴルマブ及びアテゾリズマブ。
180. Tiragolumab and atezolizumab for use in a method for treating a subject with lung cancer, said treatment comprising said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab including the use of
(I) at least one of said dosing cycles is a neoadjuvant treatment;
(a) tiragolumab formulated for administration at a dose of about 1200 mg every 3 weeks;
(b) atezolizumab formulated for administration at a dose of about 1200 mg every three weeks as a neoadjuvant treatment;
(c)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
(ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii)3 cisplatin at a dose of about 75 mg/m2 weekly and gemcitabine at a dose of about 1250 mg/m2 on
(II) at least one of said dosing cycles comprises, as an adjuvant treatment, tiragolumab formulated for administration at a dose of between about 300 mg and about 800 mg every 3 weeks and about 900 mg and about 1500 mg every 3 weeks; Tiragolumab and atezolizumab, including atezolizumab formulated for administration at doses between.
181.肺がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、(I)前記投薬サイクルの少なくとも1つがネオアジュバント処置であって、(a)3週間ごとの約600mgの用量で投与するために製剤化されたチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量で投与するために製剤化されたアテゾリズマブ、及び(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとの約600mgの用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとの約1200mgの用量で投与するために製剤化されたアテゾリズマブを含む、チラゴルマブ及びアテゾリズマブ。
181. Tiragolumab and atezolizumab for use in a method for treating a subject with lung cancer, said treatment comprising said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is neoadjuvant treatment, (a) tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks, (b) neoadjuvant treatment atezolizumab formulated to be administered at a dose of approximately 1200 mg every 3 weeks as and (c)(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
182.切除可能な扁平上皮NSCLCを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、(I)前記投薬サイクルの少なくとも1つがネオアジュバント処置であって、(a)3週間ごとの約600mgの用量で投与するために製剤化されたチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量で投与するために製剤化されたアテゾリズマブ、及び(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとの約600mgの間の用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとの約1200mgの間の用量で投与するために製剤化されたアテゾリズマブを含む、チラゴルマブ及びアテゾリズマブ。
182. Tiragolumab and atezolizumab for use in a method for treating a subject with resectable squamous NSCLC, said treatment comprising said anti-TIGIT antagonist antibody and said PD in one or more dosing cycles of tiragolumab and atezolizumab - tiragolumab formulated for administration at a dose of about 600 mg every 3 weeks, comprising the use of a monoaxial binding antagonist, wherein (I) at least one of said dosing cycles is a neoadjuvant treatment, (a) b) Atezolizumab formulated to be administered at a dose of approximately 1200 mg every 3 weeks as a neoadjuvant treatment, and (c) (i) with the goal of achieving an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of approximately 1000 mg/m2 on
183.抗PD-L1抗体SP263による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態136~182のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 183. Anti-TIGIT for use according to any one of embodiments 136-182, wherein detectable PD-L1 protein expression levels as determined by an IHC assay including staining with the anti-PD-L1 antibody SP263 have been determined. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
184.検出可能なPD-L1タンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態183に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 184. 184. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 183, wherein the detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 50% or greater.
185.前記肺がんがNSCLCである、実施形態73、114~121、及び136~184のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
185. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of
186.NSCLCが扁平上皮NSCLCである、実施形態185に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 186. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 185, wherein the NSCLC is squamous NSCLC.
187.前記NSCLCが非扁平上皮NSCLCである、実施形態185に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 187. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 185, wherein said NSCLC is non-squamous NSCLC.
188.前記がんが子宮頸がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
188. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
189.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で3週間ごとに投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 189. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population having cervical cancer with detectable levels of PD-L1 expression, said treatment comprising comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of between about 30 mg and about 1200 mg every three weeks. wherein said PD-1 axis binding antagonist antibody is formulated for administration every 3 weeks at a dose of between about 80 mg and about 1600 mg every 3 weeks Axis binding antagonist.
190.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約900mgと約1500mgの間の用量で3週間ごとに投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 190. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population having cervical cancer with detectable levels of PD-L1 expression, said treatment comprising comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of between about 300 mg and about 800 mg every three weeks. wherein said PD-1 axis binding antagonist antibody is formulated for administration every 3 weeks at a dose of between about 900 mg and about 1500 mg every 3 weeks Axis binding antagonist.
191.子宮頸がんを有する対象のための治療を選択する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化されたPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む治療を選択すること、を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
191. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - an anti-TIGIT antagonist formulated for administration at a dose of between about 30 mg and about 1200 mg every 3 weeks for said subject with L1 expression levels, based on detected PD-L1 expression on tumor cells. selecting a treatment comprising an antibody and one or more dosing cycles of a PD-1 axis binding antagonist formulated to be administered at a dose of between about 80 mg and about 1600 mg every 3 weeks; TIGIT antagonist antibody and PD-1 axis binding antagonist.
192.前記子宮頸がんが扁平上皮癌腫、腺扁平上皮癌腫又は腺癌腫である、実施形態189~191のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 192. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 189-191, wherein said cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma or adenocarcinoma.
193.前記子宮頸がんがステージIVB、転移性、再発性、又は持続性である、実施形態189~191のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 193. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 189-191, wherein said cervical cancer is stage IVB, metastatic, recurrent or persistent.
194.前記子宮頸がんが転移性及び/又は再発性のPD-L1陽性子宮頸がんである、実施形態189~193のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 194. Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 189-193, wherein said cervical cancer is metastatic and/or recurrent PD-L1 positive cervical cancer Binding antagonist.
195.前記一又は複数の対象が、少なくとも1種類の事前治療を受けたことがある、実施形態189~194のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 195. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 189-194, wherein said one or more subjects have received at least one prior treatment.
196.前記一又は複数の対象が、2種類の事前治療を受けたことがある、実施形態189~195のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 196. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 189-195, wherein said one or more subjects have received two prior treatments.
197.前記一又は複数の対象が3つ以上の事前治療を受けたことがない、実施形態189~196のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 197. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 189-196, wherein said one or more subjects have not received 3 or more prior treatments.
198.前記一又は複数の対象が事前治療を受けたことがない、実施形態189~194のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 198. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 189-194, wherein said one or more subjects have no prior treatment.
199.前記事前治療が化学療法、外科手術及び/又は放射線療法である、実施形態195~198のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 199. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 195-198, wherein said prior treatment is chemotherapy, surgery and/or radiotherapy.
200.前記処置が臨床応答をもたらす、実施形態189及び192~199のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 200. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 189 and 192-199, wherein said treatment results in a clinical response.
201.前記臨床応答が、基準客観的奏効率(ORR)と比較した前記対象集団のORRの増加である、実施形態200に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
201. 201. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
202.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態201に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 202. An anti-TIGIT antagonist for use according to embodiment 201, wherein said reference ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody Antibodies and PD-1 axis binding antagonists.
203.前記基準ORRが少なくとも約14.6%~約26%である、実施形態200に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
203. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
204.前記臨床応答がCR又はPRである、実施形態200に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
204. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to
205.前記臨床応答が、基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象のOS時間の増加である、実施形態200~204のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 205. wherein said clinical response is increased in said subject's PFS time compared to baseline progression-free survival (PFS), increased in said subject's DOR time compared to baseline duration of response (DOR), or baseline overall survival (OS) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 200-204, which is an increase in OS time of said subjects compared.
206.実施形態205に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
206. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 205, wherein
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
207.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記処置が、3週間ごとに600mgの用量で投与するために製剤化される前記PD-1軸結合アンタゴニスト、及び3週間ごとに1200mgの用量で製剤化されるアテゾリズマブの1回以上の投薬サイクルでの抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含む、抗TIGITアンタゴニスト抗体及びアテゾリズマブ。 207. An anti-TIGIT antagonist antibody and atezolizumab for use in a method for treating a subject having cervical cancer with detectable levels of PD-L1 expression, said treatment being at a dose of 600 mg every 3 weeks. The PD-1 axis binding antagonist formulated for administration and the anti-TIGIT antagonist antibody and PD-1 axis binding antagonist at one or more dosing cycles of atezolizumab formulated at a dose of 1200 mg every 3 weeks. anti-TIGIT antagonist antibodies and atezolizumab, including the use of
208.抗TIGITアンタゴニスト抗体及びアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い子宮頸がんを有する対象を同定する方法における使用のための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び3週間ごとに1200mgの用量で投与で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、を含む、抗TIGITアンタゴニスト抗体及びアテゾリズマブ。
208. An anti-TIGIT antagonist antibody and atezolizumab for use in a method of identifying subjects with cervical cancer who are likely to benefit from treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab, comprising: the method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (c) PD-L1 expression on the detected tumor cells. Based on identifying subjects likely to benefit from treatment, including dosing cycles, anti-TIGIT antagonist antibodies and atezolizumab.
209.子宮頸がんを有する対象のための治療を選択する方法において使用するための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体、及び3週間ごとに1200mgの用量で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、抗TIGITアンタゴニスト抗体及びアテゾリズマブ。
209. An anti-TIGIT antagonist antibody and atezolizumab for use in a method of selecting a treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - an anti-TIGIT antagonist antibody formulated for administration at a dose of 600 mg every 3 weeks, based on detected PD-L1 expression on tumor cells, for said subject with L1 expression levels, and every 3 weeks selecting a treatment comprising one or more dosing cycles of atezolizumab formulated to be administered at a dose of 1200 mg to .
210.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。 210. Tiragolumab and atezolizumab for use in a method for treating a subject having cervical cancer with detectable levels of PD-L1 expression, said treatment comprising tiragolumab at a dose of about 600 mg every 3 weeks; and tiragolumab and atezolizumab, including the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks.
211.子宮頸がんを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとに1200mgの用量で投与で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、チラゴルマブ及びアテゾリズマブ。
211. Tiragolumab and atezolizumab for use in a method of treating a subject with cervical cancer, said method comprising
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) Tiragolumab formulated to be administered at a dose of 600 mg every 3 weeks and to be administered at a dose of 1200 mg every 3 weeks based on detected PD-L1 expression on tumor cells and (d) administering said treatment to said identified subject. and atezolizumab.
212.子宮頸がんを有する対象のための治療を選択する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとに1200mgの用量で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、チラゴルマブ及びアテゾリズマブ。
212. Tiragolumab and atezolizumab for use in a method of selecting treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - for said subjects with L1 expression levels, tiragolumab formulated to be administered at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detected PD-L1 expression on tumor cells; selecting a treatment comprising one or more dosing cycles of atezolizumab formulated to be administered in doses.
213.転移性及び/又は再発性子宮頸がんを有する対象を処置する方法における使用のためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとに1200mgの用量で投与で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、チラゴルマブ及びアテゾリズマブ。
213. Tiragolumab and atezolizumab for use in a method of treating a subject with metastatic and/or recurrent cervical cancer, said method comprising
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) Tiragolumab formulated to be administered at a dose of 600 mg every 3 weeks and to be administered at a dose of 1200 mg every 3 weeks based on detected PD-L1 expression on tumor cells and (d) administering said treatment to said identified subject. and atezolizumab.
214.転移性及び/又は再発性子宮頸がんを有する対象のための治療を選択する方法における使用のためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与するために製剤化されたチラゴルマブ、及び3週間ごとに1200mgの用量で投与するために製剤化されたアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、チラゴルマブ及びアテゾリズマブ。
214. Tiragolumab and atezolizumab for use in a method of selecting treatment for a subject with metastatic and/or recurrent cervical cancer, said method comprising
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - for said subjects with L1 expression levels, tiragolumab formulated to be administered at a dose of 600 mg every 3 weeks and 1200 mg every 3 weeks based on detected PD-L1 expression on tumor cells; selecting a treatment comprising one or more dosing cycles of atezolizumab formulated to be administered in doses.
215.前記対象が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態189~214のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 215. 215. For use according to any one of embodiments 189-214, wherein said subject is identified as likely to benefit from said treatment based on detected PD-L1 expression on tumor cells Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
216.PD-L1発現レベルが抗PD-L1抗体SP263を使用して検出される、実施形態189~215のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 216. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 189-215, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
217.前記検出可能なPD-L1発現レベルが、前記対象からの試料において5%以上の腫瘍関連免疫細胞(TIC)である、実施形態189~216のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 217. Anti-TIGIT for use according to any one of embodiments 189-216, wherein said detectable PD-L1 expression level is 5% or more tumor-associated immune cells (TIC) in a sample from said subject Antagonist Antibodies and PD-1 Axis Binding Antagonists.
218.PD-L1発現レベルが抗PD-L1抗体22C3を使用して検出される、実施形態189~215のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 218. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 189-215, wherein PD-L1 expression level is detected using anti-PD-L1 antibody 22C3.
219.前記検出可能なPD-L1発現レベルが、前記対象からの試料で1以上の複合陽性スコア(CPS)である、実施形態189~216のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 219. Anti-TIGIT antagonist antibody for use according to any one of embodiments 189-216, wherein said detectable PD-L1 expression level is a composite positive score (CPS) of 1 or more in a sample from said subject and PD-1 axis binding antagonists.
220.前記がんが乳がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
220. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
221.乳がんを有する対象又は対象集団を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間の投薬/1週間の休薬の間、4週間ごとの約840mgの用量のチラゴルマブ、4週間ごとの約1680mgの用量のアテゾリズマブ、及び約100mg/m2の用量のnab-パクリタキセルを含む1回以上の投薬サイクルを含む投薬レジメンにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。 221. Tiragolumab and atezolizumab for use in a method of treating a subject or subject population having breast cancer, wherein said treatment comprises tiragolumab at a dose of about 840 mg every 4 weeks for 3 weeks on/1 week off. , atezolizumab at a dose of about 1680 mg every 4 weeks, and nab-paclitaxel at a dose of about 100 mg/m2, in a dosing regimen comprising one or more dosing cycles. Tiragolumab and atezolizumab, including use.
222.前記乳がんがトリプルネガティブ乳がん(TNBC)である、実施形態220又は221に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 222. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 220 or 221, wherein said breast cancer is triple negative breast cancer (TNBC).
223.前記TNBCが切除不能な局所進行性又は転移性TNBCである、実施形態222に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 223. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 222, wherein said TNBC is unresectable locally advanced or metastatic TNBC.
224.前記対象が転移性乳がんに対する事前全身治療を受けたことがない、実施形態220~223のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 224. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 220-223, wherein said subject has had no prior systemic therapy for metastatic breast cancer.
225.前記処置が、少なくとも約53%~約67.5%の対象集団のORRをもたらす、実施形態220~224のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 225. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 220-224, wherein said treatment results in an ORR of the subject population of at least about 53% to about 67.5% .
226.前記処置が約25.0ヶ月の対象集団のOS中央値をもたらす、実施形態222~225のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 226. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 222-225, wherein said treatment results in a median OS for the subject population of about 25.0 months.
227.初期トリプルネガティブ乳がん(eTNBC)を有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、2週間ごとに約10mg~約1000mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが2週間ごとに約20mg~約1600mgの用量で投与するための製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 227. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with early stage triple negative breast cancer (eTNBC), wherein said treatment is in a dosing regimen comprising one or more dosing cycles comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 10 mg to about 1000 mg every two weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of about 20 mg to about 1600 mg of the binding antagonist every two weeks.
228.前記処置が1つ以上の化学療法剤の使用を更に含む、実施形態227に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 228. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 227, wherein said treatment further comprises use of one or more chemotherapeutic agents.
229.前記1つ以上の化学療法剤が、白金系化学療法剤、タキサン、トポイソメラーゼII阻害剤又はアルキル化剤である、実施形態228に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 229. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 228, wherein said one or more chemotherapeutic agents is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor or an alkylating agent .
230.前記方法が、(a)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、タキサンと、又はタキサン及び白金系化学療法剤との1回以上の投薬サイクル、並びに(b)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、トポイソメラーゼII阻害剤と、アルキル化剤と、顆粒球コロニー刺激因子(G-CSF)又は顆粒球マクロファージコロニー刺激因子(GM-CSF)との1回以上の投薬サイクルを更に含む、実施形態227に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 230. The method comprises (a) one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, a taxane, or a taxane and a platinum-based chemotherapeutic agent, and (b) the anti-TIGIT One dose of an antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony-stimulating factor (G-CSF) or granulocyte-macrophage colony-stimulating factor (GM-CSF) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 227, further comprising the above dosing cycles.
231.前記アルキル化剤がシクロホスファミドである、実施形態229又は230に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 231. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 229 or 230, wherein said alkylating agent is cyclophosphamide.
232.前記シクロホスファミドが、約600mg/m2の用量での投与のために製剤化される、実施形態231に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 232. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 231, wherein said cyclophosphamide is formulated for administration at a dose of about 600 mg/m2.
233.前記処置がG-CSF又はGM-CSFの使用を更に含む、実施形態227~229、231、及び232のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 233. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 227-229, 231 and 232, wherein said treatment further comprises use of G-CSF or GM-CSF.
234.前記G-CSFがペグフィルグラスチム又はフィルグラスチムである、実施形態230又は233に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 234. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiments 230 or 233, wherein said G-CSF is pegfilgrastim or filgrastim.
235.前記G-CSFがペグフィルグラスチムである、実施形態234に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 235. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 234, wherein said G-CSF is pegfilgrastim.
236.前記ペグフィルグラスチムが約6mgの用量での投与のために製剤化される、実施形態235に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 236. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 235, wherein said pegfilgrastim is formulated for administration at a dose of about 6 mg.
237.前記処置が、1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFの1つ以上のその後の用量の使用を更に含む、実施形態228、229及び231~236のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 237. 237. Any one of embodiments 228, 229 and 231-236, wherein said treatment further comprises the use of one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for the uses described.
238.前記1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFがそれぞれ、週に1回、2週間に1回、又は3週間に1回投与される、実施形態228、229、及び231~237のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 238. Embodiments 228, 229, and 231, wherein said one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once weekly, once every two weeks, or once every three weeks, respectively Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of paragraphs 1-237.
239.前記白金系化学療法剤が3週間ごとに投与され、前記タキサンが毎週投与され、前記トポイソメラーゼII阻害剤が2週間ごとに投与され、前記アルキル化剤が2週間ごとに投与され、前記G-CSF又はGM-CSFが2週間ごとに投与される、実施形態229~238のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 239. The platinum-based chemotherapeutic agent is administered every three weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every two weeks, the alkylating agent is administered every two weeks, and the G-CSF or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 229-238, wherein GM-CSF is administered every two weeks.
240.前記タキサン、又は前記タキサン及び前記白金系化学療法剤が、前記投薬レジメンの最初の12週間投与される、実施形態229~239のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 240. Anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 229-239, wherein said taxane, or said taxane and said platinum-based chemotherapeutic agent are administered for the first 12 weeks of said dosing regimen - uniaxial binding antagonists.
241.前記トポイソメラーゼII阻害剤、アルキル化剤、及びG-CSF又はGM-CSFが、投薬レジメンの第13週~第19週の間に投与される、実施形態229~240のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 241. 241. According to any one of embodiments 229-240, wherein the topoisomerase II inhibitor, alkylating agent, and G-CSF or GM-CSF are administered between weeks 13-19 of the dosing regimen. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
242.前記投薬レジメンの全長が19週間である、実施形態227~241のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 242. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 227-241, wherein the total length of said dosing regimen is 19 weeks.
243.前記方法がネオアジュバント処置である、実施形態227~242のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 243. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 227-242, wherein said method is neoadjuvant treatment.
244.前記投薬レジメンの後に手術が続く、実施形態227~243のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 244. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 227-243, wherein said dosing regimen is followed by surgery.
245.前記手術が、前記投薬レジメンの最後の投与後2週間と6週間の間に行われる、実施形態244に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 245. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 244, wherein said surgery is performed between 2 and 6 weeks after the last administration of said dosing regimen.
246.前記手術が乳房切除術を含む、実施形態244又は245の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 246. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 244 or 245, wherein said surgery comprises a mastectomy.
247.前記手術が腋窩リンパ節手術を含む、実施形態244~246のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 247. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 244-246, wherein said surgery comprises axillary lymph node surgery.
248.前記トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 248. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 229-247, wherein said topoisomerase II inhibitor is doxorubicin.
249.前記タキサンがnab-パクリタキセルであり、白金系化学療法剤がカルボプラチンであり、トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 249. an anti-TIGIT antagonist antibody for use according to any one of embodiments 229-247, wherein the taxane is nab-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin; and PD-1 axis binding antagonist.
250.前記ドキソルビシンが約60mg/m2の用量での投与のために製剤化される、実施形態248又は249に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 250. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 248 or 249, wherein said doxorubicin is formulated for administration at a dose of about 60 mg/m2.
251.eTNBCを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量の前記PD-1軸結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む、投薬レジメンでの抗TIGITアンタゴニスト抗体及び抗PD-L1アンタゴニスト抗体使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
251. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with eTNBC, wherein said treatment is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks and said PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
using an anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody in a dosing regimen comprising: Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
252.eTNBCを有する対象を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量の前記PD-L1結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む、投薬レジメンでの抗TIGITアンタゴニスト抗体及び抗PD-L1アンタゴニスト抗体使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
252. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with eTNBC, wherein said treatment is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks and the PD-L1 binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
using an anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody in a dosing regimen comprising: Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
253.eTNBCを有する対象を処置する方法において使用するための抗TIGITアンタゴニスト抗体及び抗PD-L1アンタゴニスト抗体であって、前記処置が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体と、2週間ごとに約600mg~約1200mgの用量で投与するために製剤化される抗PD-L1アンタゴニスト抗体と、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む、投薬レジメンでの抗TIGITアンタゴニスト抗体及び抗PD-L1アンタゴニスト抗体使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
253. An anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody for use in a method of treating a subject with eTNBC, wherein said treatment is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks and an anti-PD-L1 antagonist antibody formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
using an anti-TIGIT antagonist antibody and an anti-PD-L1 antagonist antibody in a dosing regimen comprising: use.
254.eTNBCを有する対象を処置する方法において使用するためのチラゴルマブ及び抗PD-L1アンタゴニスト抗体であって、前記処置が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化される前記チラゴルマブと、2週間ごとに約600mg~約1200mgの用量で投与するために製剤化される抗PD-L1アンタゴニスト抗体と、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンでの抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
255.eTNBCを有する対象を処置する方法において使用するための抗TIGITアンタゴニスト抗体及びアテゾリズマブであって、前記処置が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化される前記抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンでの抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
256.eTNBCを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、2週間ごとの約300mg~約600mgの用量のチラゴルマブと、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
を含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
254. Tiragolumab and an anti-PD-L1 antagonist antibody for use in a method of treating a subject with eTNBC, wherein said treatment is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks. tiragolumab and an anti-PD-L1 antagonist antibody formulated for administration at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen, use.
255. An anti-TIGIT antagonist antibody and atezolizumab for use in a method of treating a subject with eTNBC, wherein said anti-TIGIT treatment is formulated for administration at a dose of about 300 mg to about 600 mg every two weeks. an antagonist antibody and atezolizumab at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen, use.
256. Tiragolumab and atezolizumab for use in a method of treating a subject with eTNBC, wherein said treatment comprises tiragolumab at a dose of about 300 mg to about 600 mg every two weeks and a dose of about 600 mg to about 1200 mg every two weeks. of atezolizumab and
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week over the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
wherein said method further comprises surgery between 2 weeks and 6 weeks after the last dose of said dosing regimen ,use.
257.eTNBCを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、2週間ごとの約420mgの用量のチラゴルマブと、2週間ごとの約840mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
とを含む投薬レジメンにおける抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
257. Tiragolumab and atezolizumab for use in a method of treating a subject with eTNBC, wherein said treatment comprises tiragolumab at a dose of about 420 mg every two weeks and atezolizumab at a dose of about 840 mg every two weeks;
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and the method further comprising surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen. .
258.前記対象からの腫瘍試料中の検出可能なPD-L1タンパク質発現レベルが、抗PD-L1抗体SP 142による染色を含むIHCアッセイによって決定されている、実施形態220~257のいずれか1つに記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 258. 258. According to any one of embodiments 220-257, wherein the detectable PD-L1 protein expression level in a tumor sample from said subject is determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP 142. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in.
259.前記腫瘍試料中のPD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合が1%以上である、実施形態258に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 259. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 258, wherein the percentage of tumor area occupied by PD-L1 expressing tumor-infiltrating immune cells (IC) in said tumor sample is 1% or more .
260.前記eTNBCが、提示時にT2-4d TNBCである、実施形態227~259のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 260. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 227-259, wherein said eTNBC are T2-4d TNBC when presented.
261.前記eTNBCが、提示時にcT2~cT4、cN0-cN3及びcM0 TNBCである、実施形態227~260のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 261. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 227-260, wherein said eTNBCs are cT2-cT4, cN0-cN3 and cM0 TNBCs when presented.
262.前記対象がeTNBCについて以前に処置さたことがない、実施形態227~261のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 262. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 227-261, wherein said subject has not been previously treated for eTNBC.
263.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態227~262のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 263. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 227-262, wherein said treatment results in a complete pathological response (pCR).
264.前記処置が全生存期間(OS)又は無症候生存期間(EFS)の増加をもたらす、実施形態227~263のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 264. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 227-263, wherein said treatment results in increased overall survival (OS) or symptom-free survival (EFS) .
265.前記がんが頭頸部がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
265. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
266.前記頭頸部がんが頭頸部の扁平上皮癌腫(SCCHN)である、実施形態265に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 266. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 265, wherein said head and neck cancer is squamous cell carcinoma of the head and neck (SCCHN).
267.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約80mgと約1600mgの間の用量で3週間ごとに投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 267. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects having SCCHN with detectable PD-L1 expression levels, said treatment comprising one or more doses comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said PD-1 axis binding antagonist antibody is formulated for administration every three weeks at a dose of between about 80 mg and about 1600 mg every three weeks.
268.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニスト抗体が、3週間ごとに約900mgと約1500mgの間の用量で3週間ごとに投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 268. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects having SCCHN with detectable levels of PD-L1 expression, wherein said treatment comprises one or more wherein the anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 300 mg and about 800 mg every three weeks. and wherein said PD-1 axis binding antagonist antibody is formulated for administration every three weeks at a dose of between about 900 mg and about 1500 mg every three weeks. .
269.SCCHNを有する対象又は対象集団のための治療を選択する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象又は対象集団について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
269. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a treatment for a subject or subject population with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg every 3 weeks, based on detected PD-L1 expression, for said subject or subject population having a level of selecting a treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody formulated to be administered at a dose of between about 1200 mg.
270.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、前記チラゴルマブが、3週間ごとに約600mgの用量で投与するための製剤化され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与するために製剤化される、チラゴルマブ及びアテゾリズマブ。 270. Tiragolumab and atezolizumab for use in a method for treating a subject or population of subjects having SCCHN with detectable levels of PD-L1 expression, said treatment comprising tiragolumab and atezolizumab in one or more dosing cycles wherein said tiragolumab is formulated for administration at a dose of about 600 mg every 3 weeks and said atezolizumab is formulated for administration at a dose of about 1200 mg every 3 weeks .
271.前記一又は複数の対象から得られた腫瘍試料が、検出可能なPD-L1発現レベルを有すると決定されている、実施形態267~270のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 271. Anti-TIGIT antagonist for use according to any one of embodiments 267-270, wherein the tumor sample obtained from said one or more subjects has been determined to have a detectable level of PD-L1 expression Antibodies and PD-1 axis binding antagonists.
272.前記SSCHNがヒトパピローマウイルス(HPV)陽性である、実施形態266~271のいずれか一項に記載の使用のための記載の抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 272. The anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 266-271, wherein said SSCHN is human papillomavirus (HPV) positive.
273.前記SSCHNがHPV陰性である、実施形態266~272のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 273. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 266-272, wherein said SSCHN is HPV negative.
274.HPVの状態が、p16 IHC、in situハイブリダイゼーション又はPCRによって判定される、実施形態272又は273に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 274. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 272 or 273, wherein HPV status is determined by p16 IHC, in situ hybridization or PCR.
275.前記SCCHNが再発性及び/又は転移性SCCHNである、実施形態266~274のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 275. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 266-274, wherein said SCCHN is recurrent and/or metastatic SCCHN.
276.前記一又は複数の対象が事前治療を受けたことがない、実施形態265~275のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 276. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 265-275, wherein said one or more subjects have no prior treatment.
277.前記事前治療が再発性及び/又は転移性疾患のための事前全身治療である、実施形態276に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 277. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 276, wherein said prior treatment is prior systemic therapy for recurrent and/or metastatic disease.
278.前記処置がCR又はPRをもたらす、実施形態265~268及び270~277のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 278. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 265-268 and 270-277, wherein said treatment results in CR or PR.
279.前記処置が、基準客観的奏効率(ORR)と比較して前記対象集団のORRの増加をもたらす、実施形態265~268及び270~277のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 279. Anti-TIGIT antagonist for use according to any one of embodiments 265-268 and 270-277, wherein said treatment results in an increase in said subject population's ORR compared to a baseline objective response rate (ORR) Antibodies and PD-1 axis binding antagonists.
280.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態279に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 280. Anti-TIGIT antagonist for use according to embodiment 279, wherein said reference ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody Antibodies and PD-1 axis binding antagonists.
281.前記基準ORRが約19%~約36%である、実施形態279又は280に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 281. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 279 or 280, wherein said baseline ORR is from about 19% to about 36%.
282.前記処置が、基準無増悪生存期間(PFS)と比較した前記対象又は対象集団のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象又は対象集団のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象又は対象集団のOS時間の増加をもたらす、実施形態265~268及び270~281のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 282. wherein said treatment increases PFS time of said subject or subject population compared to baseline progression-free survival (PFS), increases DOR time of said subject or subject population compared to baseline duration of response (DOR), or baseline overall survival Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 265-268 and 270-281, which results in an increase in OS time of said subject or subject population compared to duration (OS) Binding antagonist.
283.実施形態282に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
283. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 282, wherein
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment containing a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
284.前記基準DOR時間が少なくとも約6.7ヶ月~約23.4ヶ月である、実施形態282に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 284. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 282, wherein said baseline DOR time is from at least about 6.7 months to about 23.4 months.
285.前記基準OS時間が少なくとも約11.6ヶ月~約14.9ヶ月である、実施形態282に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 285. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 282, wherein said baseline OS time is at least about 11.6 months to about 14.9 months.
286.検出可能なPD-L1発現レベル伴うSCCHNを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、3週間ごとに約80mgと約1600mgの間の用量でPD-1軸結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 286. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject having SCCHN with detectable levels of PD-L1 expression, said treatment comprising about 80 mg every 3 weeks. said anti-TIGIT antagonist antibody and use of said PD-1 axis binding antagonist in one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 1600 mg, said anti-TIGIT antagonist antibody being administered every 3 weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, formulated for administration at a dose of between about 30 mg and about 1200 mg per day.
287.検出可能なPD-L1発現レベル伴うSCCHNを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、3週間ごとに約1200mgの用量でPD-1軸結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約600mgの用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 287. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject having SCCHN with detectable levels of PD-L1 expression, said treatment comprising about 1200 mg of said anti-TIGIT antagonist antibody and the use of said PD-1 axis binding antagonist in one or more dosing cycles of a PD-1 axis binding antagonist at a dose, said anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, formulated for administration at .
288.検出可能なPD-L1発現レベル伴うSCCHNを有する対象を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、3週間ごとに約80mgと約1600mgの間の用量でPD-L1結合アンタゴニストの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 288. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject having SCCHN with detectable levels of PD-L1 expression, said treatment comprising about 80 mg every 3 weeks. comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of a PD-L1 binding antagonist at a dose of between about 1600 mg, said anti-TIGIT antagonist antibody being administered every 3 weeks An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 30 mg and about 1200 mg.
289.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとに約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとに約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。 289. Tiragolumab and atezolizumab for use in a method for treating a subject having SCCHN with detectable levels of PD-L1 expression, said treatment comprising a dose of between about 80 mg and about 1600 mg every 3 weeks. Tiragolumab and atezolizumab, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist at one or more dosing cycles of atezolizumab and tiragolumab at a dose of between about 30 mg and about 1200 mg every 3 weeks.
290.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとに約600mgの用量のチラゴルマブ、及び3週間ごとに約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。
291.SCCHNを有する対象を処置する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量ので投与するために製剤化された前記抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
290. Tiragolumab and atezolizumab for use in a method for treating a subject having SCCHN with detectable PD-L1 expression levels, said treatment comprising tiragolumab at a dose of about 600 mg every 3 weeks and 3 weeks Tiragolumab and atezolizumab, comprising the use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in one or more dosing cycles of atezolizumab at a dose of about 1200 mg per dose.
291. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) said PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and said anti-drug formulated for administration at a dose of between about 30 mg and about 1200 mg every 3 weeks; identifying a subject likely to benefit from a treatment comprising one or more dosing cycles of a TIGIT antagonist antibody; and (d) administering said treatment to said identified subject having a detectable PD-L1 expression level. an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, comprising administering.
292.SCCHNを有する対象を処置する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量の前記PD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量ので投与するために製剤化された前記抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
292. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) one or more dosing cycles of said PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and said anti-TIGIT antagonist antibody formulated to be administered at a dose of about 600 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable PD-L1 expression level. and PD-1 axis binding antagonists.
293.SCCHNを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、チラゴルマブ及びアテゾリズマブ。
293. Tiragolumab and atezolizumab for use in a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) potential to benefit from treatment comprising one or more dosing cycles of atezolizumab at doses between about 80 mg and about 1600 mg every 3 weeks and tiragolumab at doses between about 30 mg and about 1200 mg every 3 weeks; and (d) administering said treatment to said identified subject with a detectable level of PD-L1 expression.
294.SCCHNを有する対象を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、チラゴルマブ及びアテゾリズマブ。
294. Tiragolumab and atezolizumab for use in a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) identifying subjects likely to benefit from treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks; (d) tiragolumab and atezolizumab, comprising administering said treatment to said identified subject with a detectable PD-L1 expression level.
295.SCCHNを有する対象のための治療を選択する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
295. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg and about 1200 mg every 3 weeks, based on detected PD-L1 expression, for said subjects with levels of selecting a treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody formulated to be administered at doses between the anti-TIGIT antagonist antibody and the PD-1 axis binding antagonist.
296.SCCHNを有する対象のための治療を選択する方法において使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとに約600mgの用量で投与するために製剤化される抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
296. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of selecting a treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and a dose of about 600 mg every 3 weeks based on detected PD-L1 expression for said subject with a level of selecting a treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist.
297.SCCHNを有する対象のための治療を選択する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、チラゴルマブ及びアテゾリズマブ。
297. Tiragolumab and atezolizumab for use in a method of selecting a treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. atezolizumab at a dose between about 80 mg and about 1600 mg every 3 weeks, and tiragolumab at a dose between about 30 mg and about 1200 mg every 3 weeks for said subjects with levels of selecting a treatment comprising one or more dosing cycles of tiragolumab and atezolizumab.
298.SCCHNを有する対象のための治療を選択する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含むチラゴルマブ及びアテゾリズマブ。
298. Tiragolumab and atezolizumab for use in a method of selecting a treatment for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on detected PD-L1 expression for said subject with a level tiragolumab and atezolizumab.
299.前記検出可能なPD-L1発現レベルが、抗PD-L1抗体SP263による染色を含む免疫組織化学(IHC)アッセイによって決定される検出可能なPD-L1タンパク質発現レベルである、実施形態267~298のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 299. of embodiments 267-298, wherein said detectable PD-L1 expression level is a detectable PD-L1 protein expression level determined by an immunohistochemistry (IHC) assay including staining with the anti-PD-L1 antibody SP263 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of claims.
300.前記検出可能なPD-L1タンパク質発現レベルが、
(a)5%以上、
(b)5%以上20%未満、又は
(c)20%以上
の腫瘍関連免疫細胞(TIC)である、実施形態299に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
300. wherein the detectable PD-L1 protein expression level is
(a) 5% or more;
(b) 5% or more and less than 20%, or (c) 20% or more tumor-associated immune cells (TIC).
301.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量で投与するために製剤化された抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 301. A PD-1 axis binding antagonist formulated to administer subjects with SCCHN at doses between about 80 mg and about 1600 mg every three weeks, doses between about 30 mg and about 1200 mg every three weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a method of identifying subjects likely to benefit from treatment comprising one or more dosing cycles of a TIGIT antagonist antibody, said method being suitable for staining determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody, wherein a TIC of 5% or more PD-L1 protein expression level is determined in said subject as likely to benefit from said treatment.
302.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量で投与するために製剤化された抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上かつ20%未満のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 302. A PD-1 axis binding antagonist formulated to administer subjects with SCCHN at doses between about 80 mg and about 1600 mg every three weeks, doses between about 30 mg and about 1200 mg every three weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a method of identifying subjects likely to benefit from treatment comprising one or more dosing cycles of a TIGIT antagonist antibody, said method being suitable for staining determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody, wherein the protein expression level of PD-L1 of TIC is greater than or equal to 5% and less than 20%. identifies said subject as likely to benefit from said treatment.
303.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量で投与するために製剤化された抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、20%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 303. A PD-1 axis binding antagonist formulated to administer subjects with SCCHN at doses between about 80 mg and about 1600 mg every three weeks, doses between about 30 mg and about 1200 mg every three weeks. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in a method of identifying subjects likely to benefit from treatment comprising one or more dosing cycles of a TIGIT antagonist antibody, said method being suitable for staining determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody, wherein a PD-L1 protein expression level of 20% or more of the TICs of said subject as likely to benefit from said treatment.
304.前記対象が治療から利益を得る可能性が高いと同定され、前記方法が、前記対象に治療を投与することを更に含む、実施形態301~303のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 304. 304. Antibiotics for use according to any one of embodiments 301-303, wherein said subject is identified as likely to benefit from treatment and said method further comprises administering treatment to said subject. TIGIT antagonist antibody and PD-1 axis binding antagonist.
305.前記TICが、Ventana SP263 IHCアッセイを使用して決定される、実施形態301~304のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 305. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 301-304, wherein said TIC is determined using the Ventana SP263 IHC assay.
306.前記対象又は対象集団が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態267~305のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 306. Use according to any one of embodiments 267-305, wherein said subject or subject population is identified as likely to benefit from said treatment based on detected PD-L1 expression on tumor cells. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
307.前記がんが肝臓がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
307. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
308.前記肝臓がんが肝細胞癌腫(HCC)である、実施形態307に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 308. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 307, wherein said liver cancer is hepatocellular carcinoma (HCC).
309肝細胞癌腫(HCC)を有する対象又は対象集団を処置する方法における使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの1回以上の投薬サイクルでの使用を含み、前記抗TIGITアンタゴニスト抗体が投与のために製剤化され、及びPD-1軸結合アンタゴニスト、前記対象又は対象集団がHCCの事前の全身治療を受けたことがない、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or population of subjects with 309 hepatocellular carcinoma (HCC), said treatment comprising said anti-TIGIT antagonist antibody and said PD- wherein the anti-TIGIT antagonist antibody is formulated for administration and the PD-uniaxial binding antagonist, wherein the subject or subject population has a prior systemic history of HCC; Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist, naive to treatment.
310.前記処置がVEGFアンタゴニストの使用を更に含む、実施形態309に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 310. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 309, wherein said treatment further comprises use of a VEGF antagonist.
311.HCCを有する対象又は対象集団を処置する方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト及びVEGFアンタゴニストの1回以上の投薬サイクルにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 311. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method of treating a subject or subject population with HCC, wherein said treatment comprises an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist and a VEGF antagonist. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists, including using said anti-TIGIT antagonist antibodies and said PD-1 axis binding antagonists in one or more dosing cycles.
312.前記VEGFアンタゴニストが、3週間ごとに約5mg/kg~約25mg/kgの用量での投与するために製剤化される、実施形態310及び311に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 312. Anti-TIGIT antagonist antibody and PD- for use according to embodiments 310 and 311, wherein said VEGF antagonist is formulated for administration at a dose of about 5 mg/kg to about 25 mg/kg every 3 weeks. Uniaxial binding antagonist.
313.前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約1200mgの用量で投与するために製剤化される、実施形態309~312のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 313. An anti-TIGIT antagonist antibody for use according to any one of embodiments 309-312, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 1200 mg every three weeks and PD-1 axis binding antagonist.
314.前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mg~約800mgの用量で投与するために製剤化される、実施形態313に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 314. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 313, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 30 mg to about 800 mg every three weeks.
315.前記抗TIGITアンタゴニスト抗体が、3週間ごとに約600mgの用量で投与するために製剤化される、実施形態309~314のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 315. Anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 309-314, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 600 mg every three weeks Axis binding antagonist.
316.前記PD-1軸結合アンタゴニストが、3週間ごとに約80mg~約1600mgの用量で投与するために製剤化される、実施形態309~315のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 316. Anti-TIGIT antagonist for use according to any one of embodiments 309-315, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 1600 mg every 3 weeks Antibodies and PD-1 axis binding antagonists.
317.前記PD-1軸結合アンタゴニストが、3週間ごとに約900mg~約1500mgの用量で投与するために製剤化される、実施形態309~316のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 317. Anti-TIGIT antagonist for use according to any one of embodiments 309-316, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 900 mg to about 1500 mg every three weeks Antibodies and PD-1 axis binding antagonists.
318.前記VEGFアンタゴニストが、2週間ごとに約1mg/kg~約20mg/kgの用量での投与するために製剤化される、実施形態310又は311に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 318. Anti-TIGIT antagonist antibody and PD- for use according to embodiment 310 or 311, wherein said VEGF antagonist is formulated for administration at a dose of about 1 mg/kg to about 20 mg/kg every two weeks Uniaxial binding antagonist.
319.前記VEGFアンタゴニストが、2週間ごとに約5mg/kg~約10mg/kgの用量での投与するために製剤化される、実施形態318に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 319. Anti-TIGIT antagonist antibody and PD-1 axis for use according to embodiment 318, wherein said VEGF antagonist is formulated for administration at a dose of about 5 mg/kg to about 10 mg/kg every two weeks Binding antagonist.
320.前記VEGFアンタゴニストが、2週間ごとに約5mg/kg、約7.5mg/kg、又は約10mg/kgの用量での投与するために製剤化される、実施形態319に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 320. Antibiotics for use according to embodiment 319, wherein said VEGF antagonist is formulated for administration at a dose of about 5 mg/kg, about 7.5 mg/kg, or about 10 mg/kg every two weeks. TIGIT antagonist antibody and PD-1 axis binding antagonist.
321.前記抗TIGITアンタゴニスト抗体が、2週間ごとに約10mg~約1000mgの用量で投与するために製剤化される、実施形態309~311及び318~320のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 321. Antibody for use according to any one of embodiments 309-311 and 318-320, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 10 mg to about 1000 mg every two weeks. TIGIT antagonist antibody and PD-1 axis binding antagonist.
322.前記PD-1軸結合アンタゴニストが、2週間ごとに約20mg~約1600mgの用量で投与するために製剤化される、実施形態309~311及び318~321のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 322. For use according to any one of embodiments 309-311 and 318-321, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 20 mg to about 1600 mg every two weeks anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
323.前記抗TIGITアンタゴニスト抗体が、4週間ごとに約200mg~約2000mgの用量で投与するために製剤化される、実施形態309~311に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 323. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to embodiments 309-311, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 200 mg to about 2000 mg every 4 weeks antagonist.
324.前記PD-1軸結合アンタゴニストが、4週間ごとに約80mg~約2000mgの用量で投与するために製剤化される、実施形態309~311及び323のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 324. Antibiotic for use according to any one of embodiments 309-311 and 323, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 80 mg to about 2000 mg every 4 weeks. TIGIT antagonist antibody and PD-1 axis binding antagonist.
325.前記PD-1軸結合アンタゴニストが、4週間ごとに約1400mg~約2000mgの用量で投与するために製剤化される、実施形態309~311、323及び324のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 325. For use according to any one of embodiments 309-311, 323 and 324, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of about 1400 mg to about 2000 mg every 4 weeks anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
326.前記HCCが局所進行性又は転移性HCCである、実施形態309~325のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 326. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 309-325, wherein said HCC is locally advanced or metastatic HCC.
327.前記HCCが切除不能なHCCである、実施形態309~326のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 327. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 309-326, wherein said HCC is unresectable HCC.
328.前記一又は複数の対象が、適切な肝機能を有すると判定されている、実施形態309~327のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 328. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 309-327, wherein said one or more subjects have been determined to have adequate liver function.
329.適切な肝機能がChild-PughクラスAとして特徴付けられる、実施形態328に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 329. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 328, wherein adequate liver function is characterized as Child-Pugh class A.
330.前記一又は複数の対象から得られたHCC腫瘍試料が、検出可能なPD-L1発現レベルを有すると判定されている、実施形態309~329のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 330. Anti-TIGIT for use according to any one of embodiments 309-329, wherein the HCC tumor sample obtained from said one or more subjects has been determined to have a detectable level of PD-L1 expression. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
331.前記方法が、対象又は対象集団に少なくとも4回の投薬サイクルを投与することを含む、実施形態309~330のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 331. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 309-330, wherein said method comprises administering at least four dosing cycles to a subject or population of subjects .
332.前記方法が、対象又は対象集団に少なくとも16回の投薬サイクルを投与することを含む、実施形態331に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 332. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 331, wherein said method comprises administering to the subject or population of subjects at least 16 dosing cycles.
333.HCCを有する対象又は対象集団を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約15mg/kgの用量のベバシズマブの1回以上の投薬サイクルでの抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。 333. Tiragolumab and atezolizumab for use in a method of treating a subject or subject population with HCC, wherein said treatment comprises tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and Tiragolumab and atezolizumab, including the use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist with one or more dosing cycles of bevacizumab at a dose of about 15 mg/kg every 3 weeks.
334.前記一又は複数の対象がHCCに対する以前の全身処置を受けたことがない、実施形態311~333のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 334. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 311-333, wherein said one or more subjects have no prior systemic treatment for HCC.
335.前記処置が、少なくとも約5.6ヶ月~少なくとも約6.83ヶ月の対象集団のPFS中央値をもたらす、実施形態309~334のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 335. Anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 309-334, wherein said treatment results in a median PFS of the subject population of at least about 5.6 months to at least about 6.83 months - Uniaxial binding antagonists.
336.前記がんが膀胱がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
336. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
337.前記膀胱がんが筋層浸潤性膀胱がん(MIBC)である、実施形態336に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 337. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 336, wherein said bladder cancer is muscle invasive bladder cancer (MIBC).
338.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象が、白金系化学療法剤による治療に不適格である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 338. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist , an anti-TIGIT antagonist antibody and PD-1 axis binding, formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks, wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent. antagonist.
339.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化され、前記対象が、白金系化学療法剤による治療に不適格である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 339. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 300 mg and about 800 mg every three weeks, said PD-1 axis binding antagonist is , an anti-TIGIT antagonist antibody and PD-1 axis binding, formulated for administration at a dose of between about 900 mg and about 1500 mg every 3 weeks, wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent. antagonist.
340.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記処置が周術期処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 340. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment.
341.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化され、前記処置が周術期処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 341. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 300 mg and about 800 mg every three weeks, said PD-1 axis binding antagonist is , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 900 mg and about 1500 mg every 3 weeks, wherein said treatment is perioperative treatment.
342.前記一又は複数の対象が、60mL/分未満のクレアチニンクリアランスを有する、実施形態338~341のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 342. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 338-341, wherein said one or more subjects have a creatinine clearance of less than 60 mL/min.
343.前記一又は複数の対象が、グレード2以上の難聴を有する、実施形態338~342のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
343. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 338-342, wherein said one or more subjects have
344.前記一又は複数の対象がグレード2以上の神経障害を有する、実施形態338~343のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
344. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 338-343, wherein said one or more subjects have a neuropathy of
345.前記一又は複数の対象が白金系化学療法剤による処置を拒否したことがある、実施形態338~344のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 345. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 338-344, wherein said one or more subjects have refused treatment with a platinum-based chemotherapeutic agent.
346.前記白金系化学療法剤がシスプラチンである、実施形態338又は342~345のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 346. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 338 or 342-345, wherein said platinum-based chemotherapeutic agent is cisplatin.
347.MIBCが外科的に手術可能である、実施形態338~346のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 347. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 338-346, wherein the MIBC is surgically operable.
348.前記方法が手術を更に含む、実施形態347に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 348. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 347, wherein said method further comprises surgery.
349.前記少なくとも1回の投薬サイクルが手術前に開始される、実施形態348に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 349. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 348, wherein said at least one dosing cycle is initiated prior to surgery.
350.前記少なくとも1、2、又は3回の投薬サイクルが手術前に完了する、実施形態348又は349に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 350. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 348 or 349, wherein said at least 1, 2 or 3 dosing cycles are completed prior to surgery.
351.少なくとも1回の投薬サイクルが手術後4週間と6週間の間に開始される、実施形態348~350のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 351. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 348-350, wherein at least one dosing cycle is initiated between 4 and 6 weeks after surgery.
352.1~17回の投薬サイクルが手術後に完了する、実施形態351に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 352. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 351, wherein 1-17 dosing cycles are completed after surgery.
353.前記手術が膀胱切除術及び/又はリンパ節郭清術である、実施形態348~352のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 353. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 348-352, wherein said surgery is cystectomy and/or lymphadenectomy.
354.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態338~353のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 354. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 338-353, wherein said treatment results in a complete pathological response (pCR).
355.前記処置が、基準無再発生存期間(RFS)と比較した前記一又は複数の対象のRFS時間の増加、基準無症候生存期間(EFS)と比較した前記一又は複数の対象のEFS時間の増加、又はOSと比較した前記一又は複数の対象のOS時間の増加をもたらす、実施形態338~354のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 355. said treatment increases RFS time of said one or more subjects compared to baseline recurrence-free survival (RFS); increases EFS time of said one or more subjects compared to baseline disease-free survival (EFS); or an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 338-354, which results in an increase in OS time in said one or more subjects compared to OS.
356.実施形態355に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記基準RFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のRFS時間の中央値である、
(b)前記基準EFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のEFS時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
356. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 355, wherein
(a) said baseline RFS time is the median RFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline EFS time is the median EFS time of a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
357.前記処置が病理的進展度の低下をもたらす、実施形態338~356のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 357. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 338-356, wherein said treatment results in a reduction in pathological extent.
358.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象がシスプラチン不適格である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 358. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks and wherein said subject is cisplatin ineligible.
359.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記処置が周術期処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 359. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-1 axis binding antagonist , an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment.
360.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-L1結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象がシスプラチン不適格である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 360. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-L1 binding antagonist comprising: An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks, wherein said subject is cisplatin ineligible.
361.MIBCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の投薬サイクルでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-L1結合アンタゴニストが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記処置が周術期処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 361. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with MIBC, wherein said treatment comprises one or more dosing cycles of said anti-TIGIT antagonist antibody. and the use of said PD-1 axis binding antagonist, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks, said PD-L1 binding antagonist comprising: An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks, wherein said treatment is perioperative treatment.
362.MIBCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、チラゴルマブが、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、アテゾリズマブが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象がシスプラチン不適格である、チラゴルマブ及びアテゾリズマブ。 362. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with MIBC, said treatment comprising the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is administered for 3 weeks atezolizumab is formulated to be administered at a dose of between about 80 mg and about 1600 mg every three weeks, and the subject is cisplatin insoluble; Eligible, tiragolumab and atezolizumab.
363.MIBCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、チラゴルマブが、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、アテゾリズマブが、3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記処置が周術期処置である、チラゴルマブ及びアテゾリズマブ。 363. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with MIBC, said treatment comprising the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is administered for 3 weeks atezolizumab is formulated to be administered at a dose of between about 80 mg and about 1600 mg every three weeks, and said treatment is administered perioperatively; tiragolumab and atezolizumab, as early treatment.
364.MIBCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、チラゴルマブが、3週間ごとに約600mgの用量で投与するために製剤化され、アテゾリズマブが、3週間ごとに約1200mgの用量で投与するために製剤化され、前記一又は複数の対象がシスプラチン不適格である、チラゴルマブ及びアテゾリズマブ。 364. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with MIBC, said treatment comprising the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is administered for 3 weeks tiragolumab, wherein atezolizumab is formulated to be administered at a dose of about 1200 mg every 3 weeks, and wherein the one or more subjects are cisplatin ineligible; Atezolizumab.
365.MIBCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、チラゴルマブが、3週間ごとに約600mgの用量で投与するために製剤化され、アテゾリズマブが、3週間ごとに約1200mgの用量で投与するために製剤化され、前記処置が周術期処置である、チラゴルマブ及びアテゾリズマブ。 365. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with MIBC, said treatment comprising the use of tiragolumab and atezolizumab in one or more dosing cycles, wherein tiragolumab is administered for 3 weeks tiragolumab and atezolizumab formulated to be administered at a dose of about 600 mg every 3 weeks, wherein atezolizumab is formulated to be administered at a dose of about 1200 mg every 3 weeks and said treatment is perioperative treatment.
366.前記処置が、少なくとも約13.4%~約15%の対象集団のORRをもたらす、実施形態338~365のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 366. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 338-365, wherein said treatment results in an ORR of the subject population of at least about 13.4% to about 15% .
367.前記処置が、少なくとも約7.9ヶ月~約8.6ヶ月の対象集団のOS中央値をもたらす、実施形態338~366のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 367. 367. Anti-TIGIT antagonist antibody and PD-antibody for use according to any one of embodiments 338-366, wherein said treatment results in a median OS for the subject population of at least about 7.9 months to about 8.6 months Uniaxial binding antagonist.
368.抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態338~367のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 368. Anti-TIGIT for use according to any one of embodiments 338-367, wherein detectable PD-L1 protein expression levels as determined by an IHC assay including staining with the anti-PD-L1 antibody SP142 have been determined. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
369.前記検出可能なPD-L1タンパク質発現レベルが、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合が5%以上であるPD-L1陽性腫瘍細胞分率である、実施形態368に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 369. Embodiment 368, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction in which 5% or more of the tumor area is occupied by PD-L1-expressing tumor-infiltrating immune cells (ICs) Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use as described in .
370.前記膀胱がんが尿路上皮癌腫(UC)である、実施形態336に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 370. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 336, wherein said bladder cancer is urothelial carcinoma (UC).
371.前記UCが転移性尿路上皮癌腫(mUC)である、実施形態370に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 371. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 370, wherein said UC is metastatic urothelial carcinoma (mUC).
372.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 372. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with mUC, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks.
373.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が3週間ごとに約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 373. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with mUC, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 300 mg and about 800 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of between about 900 mg and about 1500 mg every three weeks.
374.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象が事前のがん免疫療法を受けたことがない、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 374. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with mUC, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; an anti-TIGIT antagonist antibody wherein said PD-1 axis binding antagonist is formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks and said subject has not received prior cancer immunotherapy. and PD-1 axis binding antagonists.
375.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化され、前記処置が二次処置である、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 375. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with mUC, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein said PD-1 axis binding antagonist is formulated for administration at a dose of between about 80 mg and about 1600 mg every 3 weeks and said treatment is a secondary treatment .
376.前記一又は複数の対象が以前にがん免疫療法を受けたことがない、実施形態372,372及び375のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 376. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 372, 372 and 375, wherein said one or more subjects have not previously received cancer immunotherapy .
377.前記処置が第二選択処置である、実施形態372~374のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 377. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 372-374, wherein said treatment is a second line treatment.
378.前記mUCが白金含有療法の期間中又はその後に進行している、実施形態372~377のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 378. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 372-377, wherein said mUC is progressing during or after platinum-containing therapy.
379.前記一又は複数の対象が疾患進行性又は許容できない毒性を経験した後、第2の投薬レジメンを前記対象又は対象集団に投与することを更に含む、実施形態372~378のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 379. 379. According to any one of embodiments 372-378, further comprising administering a second dosing regimen to said subject or population of subjects after said one or more subjects experience disease progression or unacceptable toxicity. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in.
380.前記第2の投薬レジメンが、PD-1軸結合アンタゴニスト及び抗体-薬物コンジュゲート(ADC)の1回以上の投薬サイクルを含む、実施形態379に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 380. Anti-TIGIT antagonist antibody and PD-1 for use according to embodiment 379, wherein said second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist and an antibody-drug conjugate (ADC). Uniaxial binding antagonist.
381.前記ADCが、(a)エンフォルツマブベドチン又は(b)サクツズマブゴビテカンである、実施形態380に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 381. 380. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 380, wherein said ADC is (a) enfortumab vedotin or (b) suctuzumab govitecan.
382.(a)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与するために製剤化されるか、又は(b)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与するために製剤化される、実施形態381に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 382. (a) enfortumab vedotin is formulated for administration at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (b) suctuzumab Anti-TIGIT antagonist antibody for use according to embodiment 381 and PD- Uniaxial binding antagonist.
383.(a)エンフォルツマブベドチンが、各21日間サイクルの1日目及び8日目に1.25mg/kgの用量で投与するために製剤化されるか、又は(b)サクツズマブゴビテカンが、各21日間サイクルの1日目及び8日目に10mg/kgの用量で投与するために製剤化される、実施形態381又は382に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
383. (a) enfortumab vedotin is formulated for administration at a dose of 1.25 mg/kg on
384.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、PD-L1結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 384. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or subject population with mUC, said treatment comprising one or more dosing cycles of the anti-TIGIT antagonist antibody comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist, wherein the PD-L1 binding antagonist is formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks.
385.mUCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブの1回以上の投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。 385. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with mUC, wherein said treatment comprises tiragolumab at a dose of between about 30 mg and about 1200 mg every 3 weeks and Tiragolumab and atezolizumab, comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising one or more dosing cycles of atezolizumab at a dose between about 80 mg and about 1600 mg.
386.mUCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、1回以上の投薬サイクルでのチラゴルマブ及びアテゾリズマブの使用を含み、前記チラゴルマブが、3週間ごとに約600mgの用量で投与するための製剤化され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与するために製剤化される、チラゴルマブ及びアテゾリズマブ。 386. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with mUC, said treatment comprising the use of tiragolumab and atezolizumab in one or more dosing cycles, said tiragolumab Tiragolumab and atezolizumab, formulated for administration at a dose of about 600 mg every 3 weeks, said atezolizumab being formulated for administration at a dose of about 1200 mg every 3 weeks.
387.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、第1の投薬レジメンに続いて第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンは、前記抗TIGITアンタゴニスト抗体が3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが3週間ごとに約80mgと約1600mgの間の用量で投与するために製剤化される、1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとに約80mgと約1600mgの間の用量での投与のために製剤化されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量での投与のために製剤化されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量での投与のために製剤化され、前記第2の投薬レジメンが、前記第1の投薬レジメン中に前記対象又は対象集団が疾患進行性又は許容できない毒性を経験した後に前記対象又は対象集団に投与される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
387. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with mUC, wherein said treatment comprises a first dosing regimen followed by a second dosing regimen using said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in
(a) said first dosing regimen is formulated for administration of said anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks and said PD-1 axis binding antagonist every 3 weeks; one or more dosing cycles formulated for administration at a dose of between about 80 mg and about 1600 mg to
(b) said second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist formulated for administration at a dose of between about 80 mg and about 1600 mg every three weeks; (i) enfortumab vedotin is formulated for administration at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (ii) Mabgovitecan is formulated for administration at a dose of 10 mg/kg weekly for 2 weeks on/1 week off, wherein said second dosing regimen is during said first dosing regimen An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist administered to said subject or subject population after said subject or subject population experiences disease progression or unacceptable toxicity.
388.mUCを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、第1の投薬レジメンに続いて第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンが、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化される抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約80mgと約1600mgの間の用量の前記PD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与するために製剤化されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与するために製剤化され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
388. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with mUC, wherein said treatment comprises a first dosing regimen followed by a second dosing regimen using said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in
(a) an anti-TIGIT antagonist antibody wherein said first dosing regimen is formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks and between about 80 mg and about 1600 mg every three weeks; one or more dosing cycles of a PD-L1 binding antagonist at a dose of
(b) said second dosing regimen comprises one or more dosing cycles of said PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks; , 2 weeks on/1 week off, or (ii) suctuzumab govitecan is formulated to be administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off; formulated to be administered at a dose of 10 mg/kg weekly with a one-week rest period, wherein said second dosing regimen is effective if said subject has disease progression or unacceptable toxicity during said first dosing regimen. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist administered to said subject after experiencing.
389.mUCを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、第1の投薬レジメンに続いて第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンが、3週間ごとの約600mgの用量のチラゴルマブ及び約3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与するために製剤化されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与するために製剤化され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
389. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with mUC, wherein said treatment comprises a first dosing regimen followed by said anti-TIGIT antagonist antibody in a second dosing regimen and comprising the use of said PD-1 axis binding antagonist;
(a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of 1200 mg about every 3 weeks;
(b) said second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks; (ii) suctuzumab govitecan was formulated to be administered at a dose of 1.25 mg/kg weekly during drug administration, or (ii) suctuzumab govitecan was administered at 10 mg weekly for 2 weeks on/1 week off /kg, wherein the second dosing regimen is administered to the subject after the subject experiences disease progression or unacceptable toxicity during the first dosing regimen; Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
390.前記処置が、少なくとも約13.4%~約31%の対象集団のORRをもたらす、実施形態372~389のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 390. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 372-389, wherein said treatment results in an ORR of the subject population of at least about 13.4% to about 31% .
391.前記処置が約7.9ヵ月~約16.3ヵ月の前記対象集団のOS中央値をもたらす、実施形態372~390のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 391. 391. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 372-390, wherein said treatment results in a median OS for said subject population of about 7.9 months to about 16.3 months Axis binding antagonist.
392.前記がんが膵臓がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
392. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
393.膵臓がんを有する対象又は対象集団を処置する方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、各28日間投薬サイクルの1及び15日目に約420mgの用量でのチラゴルマブ、各28日間投薬サイクルの1及び15日目に約840mgの用量でのアテゾリズマブ、各28日間投薬サイクルの1、8及び15日目に約1000mg/m2の用量でのゲムシタビン、並びに各28日間投薬サイクルの1、8及び15日目に約125mg/m2の用量でのnab-パクリタキセルを含む1回以上の28日間投薬サイクルを含む投薬レジメンにおける抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用を含む、チラゴルマブ及びアテゾリズマブ。
393. Tiragolumab and atezolizumab for use in a method of treating a subject or subject population having pancreatic cancer, said treatment comprising tiragolumab at a dose of about 420 mg on
394.前記膵臓がんが膵管腺癌腫(PDAC)である、実施形態392又は393に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 394. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 392 or 393, wherein said pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395.前記PDACが転移性PDACである、実施形態394に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 395. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 394, wherein said PDAC is a metastatic PDAC.
396.前記一又は複数の対象が転移性PDACのための事前全身治療を受けたことがない、実施形態392~395のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 396. An anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 392-395, wherein said one or more subjects have not received prior systemic therapy for metastatic PDAC antagonist.
397.前記処置が少なくとも約41.7~約46.7%の対象集団のORRをもたらす、実施形態392~396のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 397. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 392-396, wherein said treatment results in an ORR of the subject population of at least about 41.7 to about 46.7% .
398.前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを用いないゲムシタビン及びnab-パクリタキセルを含む処置と比較して、少なくとも約20%のORRの増加をもたらす、実施形態392~397のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
398. Any of embodiments 392-397, wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nab-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
399.前記処置が、少なくとも約5.5ヶ月~約7ヶ月の対象集団のOS中央値をもたらす、実施形態392~398のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 399. Anti-TIGIT antagonist antibody and PD-1 axis for use according to any one of embodiments 392-398, wherein said treatment results in a median OS for the subject population of at least about 5.5 months to about 7 months Binding antagonist.
400.前記処置が、少なくとも約8.5ヶ月~約10.6ヶ月の対象集団のOS中央値をもたらす、実施形態392~399のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 400. The anti-TIGIT antagonist antibody and PD-antibody for use according to any one of embodiments 392-399, wherein said treatment results in a median OS of the subject population of at least about 8.5 months to about 10.6 months. Uniaxial binding antagonist.
401.前記がんが食道がんである、実施形態72に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
401. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
402.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンでの使用を含み、前記抗TIGITアンタゴニスト抗体が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、各投薬サイクルの1日目に約80mgと約1600mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
402. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein said treatment comprises said anti-TIGIT antagonist antibody and use of said PD-1 axis binding antagonist in a dosing regimen comprising one or more 21-day dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of between about 30 mg and about 1200 mg on
403.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンでの使用を含み、前記抗TIGITアンタゴニスト抗体が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、各投薬サイクルの1日目に約900mgと約1500mgの間の用量で投与するために製剤化される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
403. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein said treatment comprises said anti-TIGIT antagonist antibody and use of said PD-1 axis binding antagonist in a dosing regimen comprising one or more 21-day dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of between about 30 mg and about 1200 mg on
404.食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の21日間投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が各投薬サイクルの1日目に約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが各投薬サイクルの1日目に約80mgと約1600mgの間の用量で投与するために製剤化され、前記対象が、白金系化学療法剤及び非白金系化学療法剤で以前に治療されたことがある、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
404. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with esophageal cancer, wherein said treatment comprises one or more treatments of the anti-TIGIT antagonist antibody for 21 days. use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising dosing cycles, wherein said anti-TIGIT antagonist antibody is administered on
405.食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、抗TIGITアンタゴニスト抗体の1回以上の21日間投薬サイクルを含む投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が各投薬サイクルの1日目に約300mgと約800mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが各投薬サイクルの1日目に約900mgと約1500mgの間の用量で投与するために製剤化され、前記対象が、白金系化学療法剤及び非白金系化学療法剤で以前に治療されたことがある、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
405. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with esophageal cancer, wherein said treatment comprises one or more treatments of the anti-TIGIT antagonist antibody for 21 days. use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising dosing cycles, wherein said anti-TIGIT antagonist antibody is administered on
406.前記一又は複数の対象が、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、実施形態402又は403に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 406. An anti-TIGIT antagonist antibody and PD-1 for use according to embodiment 402 or 403, wherein said one or more subjects have been previously treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent Axis binding antagonist.
407.前記一又は複数の対象が、以前の処置中に疾患進行性又は許容できない毒性を経験したことがある、実施形態404~406のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 407. Anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 404-406, wherein said one or more subjects have experienced disease progression or unacceptable toxicity during prior treatment - uniaxial binding antagonists.
408.前記21日間投薬サイクルが、白金系化学療法剤及び非白金系化学療法剤を更に含む、実施形態402又は403に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 408. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 402 or 403, wherein said 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409.前記白金系化学療法剤が6回投与後の投薬レジメンから省略される、実施形態408に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 409. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 408, wherein said platinum-based chemotherapeutic agent is omitted from the dosing regimen after 6 doses.
410.前記白金系化学療法剤がシスプラチンである、実施形態404~409のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 410. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 404-409, wherein said platinum-based chemotherapeutic agent is cisplatin.
411.シスプラチンが、各投薬サイクルの1日目に約80mg/m2の用量で投与するために製剤化される、実施形態410に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
411. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 410, wherein cisplatin is formulated for administration at a dose of about 80 mg/m2 on
412.前記非白金系化学療法剤が代謝拮抗剤である、実施形態404~411のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 412. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 404-411, wherein said non-platinum chemotherapeutic agent is an antimetabolite.
413.前記代謝拮抗剤が5-フルオロウラシルである、実施形態412に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 413. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 412, wherein said antimetabolite is 5-fluorouracil.
414.5-フルオロウラシルが、各21日間サイクルの1~5日目に800mg/m2/24時間の用量で投与するために製剤化される、実施形態413に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 414.5-Fluorouracil is formulated for administration at a dose of 800 mg/m2/24 hours on days 1-5 of each 21-day cycle, anti-TIGIT antagonist antibody for use according to embodiment 413 and PD-1 axis binding antagonists.
415.前記食道がんが進行性又は転移性食道がんである、実施形態404~414のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 415. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 404-414, wherein said esophageal cancer is advanced or metastatic esophageal cancer.
416.前記一又は複数の対象が転移性食道がんのための以前の処置を行ったことがない、実施形態402、403、408及び409のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 416. An anti-TIGIT antagonist antibody for use according to any one of embodiments 402, 403, 408 and 409, wherein said one or more subjects have no prior treatment for metastatic esophageal cancer and PD-1 axis binding antagonists.
417.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンにおける使用を含み、前記抗TIGITアンタゴニスト抗体が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、各投薬サイクルの1日目に約80mgと約1600mgの間の用量で製剤化され、白金系化学療法剤が各投薬サイクルの1日目に約80mg/m2の用量で投与するために製剤化され、非白金系化学療法剤が各21日間サイクルの1日目~5日目に800mg/m2/24時間の用量で投与するために製剤化され、6回の投薬後に前記白金系化学療法剤が前記投薬レジメンから省略される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
417. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein said treatment comprises said anti-TIGIT antagonist antibody and use of said PD-1 axis binding antagonist in a dosing regimen comprising one or more 21-day dosing cycles, wherein said anti-TIGIT antagonist antibody is administered at a dose of between about 30 mg and about 1200 mg on
418.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、1回以上の21日間投薬サイクルを含む投薬レジメンにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、前記抗TIGITアンタゴニスト抗体が、各投薬サイクルの1日目に約600mgの用量で投与するために製剤化され、前記PD-1軸結合アンタゴニストが、各投薬サイクルの1日目に約1200mgの用量で投与するために製剤化され、シスプラチンが、各投薬サイクルの1日目に約80mg/m2の用量で投与するために製剤化され、5-フルオロウラシルが、各21日間サイクルの1~5日目に800mg/m2/24時間の用量で投与するために製剤化され、6回投与後の前記投薬レジメンからシスプラチンが省略される、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
418. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein said treatment is performed one or more times for 21 days. use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a dosing regimen comprising dosing cycles, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 600 mg on
419.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、各21日間サイクルの1~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間投薬サイクルを含む投薬レジメンにおける前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、6回投与後の前記投薬レジメンからシスプラチンが省略される、チラゴルマブ及びアテゾリズマブ。
419. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with advanced or metastatic esophageal cancer, wherein said treatment comprises tiragolumab at a dose of about 600 mg on
420.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、第1の投薬レジメン及び第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンが、白金系化学療法剤及び非白金系化学療法剤の1回以上の21日間投薬サイクルを含み、前記白金系化学療法剤が6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
420. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, said treatment comprising a first dosing regimen and comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a second dosing regimen;
(a) the first dosing regimen comprises one or more 21-day dosing cycles of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent is omitted from
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
421.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、前記処置が、第1の投薬レジメン及び第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンは、各投薬サイクルの1日目に約80mg/m2の用量の白金系化学療法剤と、及び各21日間サイクルの1~5日目に800mg/m2/24時間の用量の非白金系化学療法剤の1回以上の21日間投薬サイクル含み、前記白金系化学療法剤が、6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
421. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use in a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, said treatment comprising a first dosing regimen and comprising use of said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist in a second dosing regimen;
(a) the first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
422.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法に使用するためのチラゴルマブ及びアテゾリズマブであって、前記処置が、第1の投薬レジメン及び第2の投薬レジメンでの前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストの使用を含み、
(a)前記第1の投薬レジメンが、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日間サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含み、6回の投薬後にシスプラチンが投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブの1回以上の21日間投薬サイクルを含む、チラゴルマブ及びアテゾリズマブ。
422. Tiragolumab and atezolizumab for use in a method for treating a subject or subject population with advanced or metastatic esophageal cancer, said treatment comprising said comprising the use of an anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist;
(a) said first dosing regimen comprises cisplatin at a dose of about 80 mg/m2 on
(b) said second dosing regimen is one or more 21-day dosing cycles of tiragolumab at a dose of about 600 mg on
423.前記処置が少なくとも約14%の対象集団のORRをもたらす、実施形態402~422のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 423. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 402-422, wherein said treatment results in an ORR of the subject population of at least about 14%.
424.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、を含む、実施形態47~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
424. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6). anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
425.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、を更に含む、実施形態424に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
425. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
an anti-TIGIT antagonist antibody for use according to embodiment 424, further comprising FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10); PD-1 axis binding antagonist.
426.前記抗TIGITアンタゴニスト抗体が、以下の重鎖可変領域FR:
X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、を更に含む、実施形態424に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
426. The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11) (wherein X1 is E or Q);
FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14); and PD-1 axis binding antagonist.
427.X1がEである、実施形態426に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 427. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 426, wherein X1 is E.
428.X1がQである、実施形態426に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 428. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 426, wherein X1 is Q.
429.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態424~428のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
429. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 19; or (c) a VH domain according to (a) and (b) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-428, comprising a VL domain as described.
430.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~429のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
430. wherein said anti-TIGIT antagonist antibody:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO: 17 or 18; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO: 19. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
431.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~427、429及び430のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
431. wherein said anti-TIGIT antagonist antibody:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
432.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号33のアミノ酸配列を含む重鎖;及び
(b)配列番号34のアミノ酸配列を含む軽鎖、
を含む、実施形態424~427及び429~431のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
432. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:33; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:34,
An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-427 and 429-431, comprising:
433.抗TIGITアンタゴニスト抗体がモノクローナル抗体である、実施形態424~432のいずれか一つに記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 433. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-432, wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
434.抗TIGITアンタゴニスト抗体がヒト化抗体である、実施形態424~433のいずれか一つに記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 434. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-433, wherein the anti-TIGIT antagonist antibody is a humanized antibody.
435.抗TIGITアンタゴニスト抗体が完全長抗体である、実施形態424~434のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 435. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-434, wherein the anti-TIGIT antagonist antibody is a full length antibody.
436.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである実施形態424~427及び429~436のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 436. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-427 and 429-436, wherein said anti-TIGIT antagonist antibody is tiragolumab.
437.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS 084448、SGN-TGT又はTJ-T 6である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291,292,295,296、301~332、336~361、370~384、387,388、401~418、420、421及び424~436のいずれか1つに記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
437. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, wherein said anti-TIGIT antagonist antibody is tiragolumab, vivostrimab, etiglimab, EOS 084448, SGN-TGT or TJ-
438.抗TIGITアンタゴニスト抗体がインタクトなFc媒介エフェクター機能を有する、実施形態437に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 438. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 437, wherein the anti-TIGIT antagonist antibody has intact Fc-mediated effector functions.
439.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を増強している、実施形態437又は438に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 439. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 437 or 438, wherein said anti-TIGIT antagonist antibody enhances Fc-mediated effector function.
440.前記抗TIGITアンタゴニスト抗体がSGN-TGTである、実施形態437~439のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 440. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 437-439, wherein said anti-TIGIT antagonist antibody is SGN-TGT.
441.前記抗TIGITアンタゴニスト抗体が、ドムバナリマブ、BMS-986207、ASP8374、又はCOM902である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291、292、295、296、301~332、336~361、370~384、387、388、401~418、420、及び421のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 441. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-, wherein said anti-TIGIT antagonist antibody is domvanalimab, BMS-986207, ASP8374, or COM902 288, 291, 292, 295, 296, 301-332, 336-361, 370-384, 387, 388, 401-418, 420, and 421, anti-TIGIT antagonist antibody for use according to any one of and PD-1 axis binding antagonists.
442.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を有しない、実施形態424~431及び441のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 442. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 424-431 and 441, wherein said anti-TIGIT antagonist antibody has no Fc-mediated effector functions.
443.抗TIGITアンタゴニスト抗体がIgGクラス抗体である、実施形態47~442のいずれか一つに記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 443. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-442, wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444.IgGクラス抗体がIgG1サブクラス抗体である、実施形態443に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 444. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 443, wherein the IgG class antibody is an IgG1 subclass antibody.
445.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS084448、SGN-TGT、TJ-T6、BGB-A1217、AB308、ドムバナリマブ又はBMS-986207である、実施形態444に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 445. Anti-TIGIT antagonist for use according to embodiment 444, wherein said anti-TIGIT antagonist antibody is tiragolumab, vivostolimab, etiglimab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, domvanalimab or BMS-986207 Antibodies and PD-1 axis binding antagonists.
446.前記IgGクラス抗体がIgG4サブクラス抗体である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291、292、295、296、301~332、336~361、370~384、387,388、401~418、420及び421のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 446. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-288, 291, 292, 295, 296, wherein said IgG class antibody is an IgG4 subclass antibody , 301-332, 336-361, 370-384, 387, 388, 401-418, 420 and 421.
447.抗TIGITアンタゴニスト抗体がASP8374又はCOM902である、実施形態446に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 447. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 446, wherein the anti-TIGIT antagonist antibody is ASP8374 or COM902.
448.抗TIGITアンタゴニスト抗体が、Fab、ビス-Fab、Fab’、Fab’-SH、Fv、一本鎖可変断片(scFv)、及び(Fab’)2フラグメントからなる群から選択されるTIGITに結合する抗体フラグメントである、実施形態424~434のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 448. an antibody that binds to TIGIT, wherein the anti-TIGIT antagonist antibody is selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single-chain variable fragment (scFv), and (Fab')2 fragment An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 424-434, which is a fragment.
449.抗TIGITアンタゴニスト抗体が単一特異性抗体である、実施形態424~448のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 449. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-448, wherein the anti-TIGIT antagonist antibody is a monospecific antibody.
450.抗TIGITアンタゴニスト抗体が多重特異性抗体である、実施形態424~448のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 450. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 424-448, wherein the anti-TIGIT antagonist antibody is a multispecific antibody.
451.多重特異性抗体が二重特異性抗体である、実施形態450に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 451. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 450, wherein the multispecific antibody is a bispecific antibody.
452.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト、PD-1結合アンタゴニスト、及びPD-L2結合アンタゴニストからなる群から選択される、実施形態424~451のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 452. 452. Use according to any one of embodiments 424-451, wherein said PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist. anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
453.PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニストである、実施形態452に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 453. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 452, wherein the PD-1 axis binding antagonist is a PD-L1 binding antagonist.
454.前記PD-L1結合アンタゴニストが、PD-L1のそのリガンド結合パートナーのうちの1つ以上の結合を阻害する、実施形態453に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 454. 454. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 453, wherein said PD-L1 binding antagonist inhibits binding of PD-L1 to one or more of its ligand binding partners.
455.PD-L1結合アンタゴニストが、PD-L1の、PD-1、B7-1、又はPD-1とB7-1の両方への結合を阻害する、実施形態454に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 455. Anti-TIGIT antagonist for use according to embodiment 454, wherein the PD-L1 binding antagonist inhibits binding of PD-L1 to PD-1, B7-1, or both PD-1 and B7-1 Antibodies and PD-1 axis binding antagonists.
456.前記PD-L1結合アンタゴニストが抗PD-L1アンタゴニスト抗体である、実施形態453~455のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 456. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 453-455, wherein said PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態456に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 457. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 , embodiment 456. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 456.
458.抗PD-L1アンタゴニスト抗体がアテゾリズマブである、実施形態457に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 458. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 457, wherein the anti-PD-L1 antagonist antibody is atezolizumab.
459.前記抗PD-L1アンタゴニスト抗体が、以下のHVR:
GFTFSDSWIH(配列番号20)のアミノ酸配列を含むHVR-H1配列;
AWISPYGGSTYYADSVKG(配列番号21)のアミノ酸配列を含むHVR-H2配列;
RHWPGGFDY(配列番号22)のアミノ酸配列を含むHVR-H3配列;
RASQDVSTAVA(配列番号23)のアミノ酸配列を含むHVR-L1配列;
SASFLYS(配列番号24)のアミノ酸配列を含むHVR-L2配列;及び
QQYLYHPAT(配列番号25)のアミノ酸配列を含むHVR-L3配列
を含む、実施形態456に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
459. The anti-PD-L1 antagonist antibody is a HVR that:
an HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
an HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
an HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
an HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
an anti-TIGIT antagonist antibody for use according to embodiment 456 comprising a HVR-L2 sequence comprising the amino acid sequence of SASFLYS (SEQ ID NO:24); and a HVR-L3 sequence comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25); PD-1 axis binding antagonist.
460.前記抗PD-L1アンタゴニスト抗体が、
(a)配列番号26のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号27のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態459に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
460. The anti-PD-L1 antagonist antibody is
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or (c) a VH domain according to (a) and (b) An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 459 comprising the VL domain as described.
461.前記抗PD-L1アンタゴニスト抗体が、
(a)配列番号26のアミノ酸配列を含むVHドメイン;及び
(b)配列番号27のアミノ酸配列を含むVLドメインを含む、
実施形態460に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
461. The anti-PD-L1 antagonist antibody is
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:27,
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 460.
462.前記抗PD-L1アンタゴニスト抗体が、
(a)配列番号28のアミノ酸配列を含む重鎖;及び
(b)配列番号29のアミノ酸配列を含む軽鎖、
を含む、実施形態461に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
462. The anti-PD-L1 antagonist antibody is
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:28; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:29,
An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 461, comprising:
463.抗PD-L1アンタゴニスト抗体がモノクローナル抗体である、実施形態459~462のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 463. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 459-462, wherein the anti-PD-L1 antagonist antibody is a monoclonal antibody.
464.抗PD-L1アンタゴニスト抗体がヒト化抗体である、実施形態459~463のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 464. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 459-463, wherein the anti-PD-L1 antagonist antibody is a humanized antibody.
465.前記抗PD-L1アンタゴニスト抗体が完全長抗体である、実施形態463又は464に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 465. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 463 or 464, wherein said anti-PD-L1 antagonist antibody is a full length antibody.
466.前記抗PD-L1アンタゴニスト抗体が、Fab、Fab’、Fab’-SH、Fv、scFv、及び(Fab’)2フラグメントからなる群から選択されるPD-L1に結合する抗体フラグメントである、実施形態459~464のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 466. An embodiment wherein said anti-PD-L1 antagonist antibody is an antibody fragment that binds PD-L1 selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv, and (Fab')2 fragments. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of 459-464.
467.抗PD-L1アンタゴニスト抗体がIgGクラス抗体である、実施形態459~465のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 467. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 459-465, wherein the anti-PD-L1 antagonist antibody is an IgG class antibody.
468.IgGクラス抗体がIgG1サブクラス抗体である、実施形態467に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 468. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 467, wherein the IgG class antibody is an IgG1 subclass antibody.
469.前記PD-1軸結合アンタゴニストがPD-1結合アンタゴニストである、実施形態452に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 469. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 452, wherein said PD-1 axis binding antagonist is a PD-1 binding antagonist.
470.前記PD-1結合アンタゴニストが、PD-1のそのリガンド結合パートナーのうちの1つ以上の結合を阻害する、実施形態469に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 470. 469. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 469, wherein said PD-1 binding antagonist inhibits binding of PD-1 to one or more of its ligand binding partners.
471.前記PD-1結合アンタゴニストが、PD-L1、PD-L2、又はPD-L1とPD-L2の両方に対するPD-1の結合を阻害する、実施形態470に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 471. Anti-TIGIT antagonist antibody for use according to embodiment 470, wherein said PD-1 binding antagonist inhibits binding of PD-1 to PD-L1, PD-L2, or both PD-L1 and PD-L2 and PD-1 axis binding antagonists.
472.前記PD-1結合アンタゴニストが抗PD-1アンタゴニスト抗体である、実施形態469~471のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 472. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 469-471, wherein said PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態472に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 473. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21, and an anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 472.
474.前記PD-1結合アンタゴニストがFc融合タンパク質である、実施形態469~471のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 474. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 469-471, wherein said PD-1 binding antagonist is an Fc fusion protein.
475.前記Fc融合タンパク質がAMP-224である、実施形態474に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 475. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 474, wherein said Fc fusion protein is AMP-224.
476.前記方法が、3週間ごとに約30mgと約1200mgの間の用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態80~112、114~127及び309~312のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 476. Embodiments 80-112, wherein the method comprises administering to the subject or subject population the anti-TIGIT antagonist antibody formulated for administration at a dose of between about 30 mg and about 1200 mg every three weeks; Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of 114-127 and 309-312.
477.前記方法が、3週間ごとに約600mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体を対象に投与することを含む、実施形態51、54、60、62、63、65~67、80-112、114-127、136-140、169~174、189、191、267、269、286、288、291、295、301、302、303、313、315、338、340、358~361、372、384、387、388、402~404、417、420、421及び476のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
477.
478.前記方法が、以下の前記対象の体重に基づく段階的用量で前記抗TIGITアンタゴニスト抗体を対象又は対象集団に投与することを含む、実施形態51、54、60、62、63、65-67、80-112、114-127、136-140、169-174、189、191、267、269、286、288、291、295、301、302、303、309、313、315、338、340、358-361、372、384、387、388、402-404、417、420、421、及び476のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト:
(a)15kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約300mgの用量で投与するために製剤化される;
(b)15kg超40kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとに約400mgの用量で投与するために製剤化される;又は
(c)40kgを超え、前記抗TIGITアンタゴニスト抗体は、3週間ごとに約600mgの用量で投与するために製剤化される。
478.
(a) weighing 15 kg or less and wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 300 mg every three weeks;
(b) greater than 15 kg and less than or equal to 40 kg, wherein said anti-TIGIT antagonist antibody is formulated for administration at a dose of about 400 mg every 3 weeks; or (c) greater than 40 kg, wherein said anti-TIGIT antagonist antibody is: It is formulated for administration at a dose of approximately 600 mg every 3 weeks.
479.前記方法が、4週間ごとに約700mg~約1000mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態47、48、77、78、82、及び83のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 479. Embodiments 47, 48, 77, wherein the method comprises administering to the subject or subject population the anti-TIGIT antagonist antibody formulated for administration at a dose of about 700 mg to about 1000 mg every four weeks; Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of 78, 82 and 83.
480.前記方法が、4週間ごとに約840mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を前記対象に投与することを含む、実施形態47、48、59、67、323、及び479のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
480.
481.前記方法が、2週間ごとに約300mg~約600mgの用量で投与するために製剤化された前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態49、50、及び104のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
481.
482.前記方法が、2週間ごとに約420mgの用量で投与するために製剤化された抗TIGITアンタゴニスト抗体を対象に投与することを含む、実施形態49、50、227、251~253、255、及び481のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
482.
483.前記抗TIGITアンタゴニスト抗体の用量が固定用量である、実施形態47~482のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 483. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 47-482, wherein the dose of said anti-TIGIT antagonist antibody is a fixed dose.
484.前記方法が、対象又は対象集団に、3週間ごとに約900mgと約1500mgの間の用量で投与するために製剤化されたPD-1軸結合アンタゴニストを投与することを含む、実施形態54、62、63、65~67、80~109、及び27~2698のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 484. Embodiments 54, 62, wherein the method comprises administering to the subject or subject population a PD-1 axis binding antagonist formulated for administration at a dose of between about 900 mg and about 1500 mg every three weeks. , 63, 65-67, 80-109, and 27-2698.
485.前記方法が、3週間ごとに約1200mgの用量で投与するために製剤化される前記PD-1軸結合アンタゴニストを前記対象に投与することを含む、実施形態54、60、62、63、65~67、80~112、114~127、136~140、169~172、189、191、267、269、286、288、291、295、301~303、309、311、313、315、338、340、358~361、372~375、384、387、388、402~405、417、420、421、及び484のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
485.
486.前記方法が、4週間ごとに約1400mg~2000mgの用量で投与するために製剤化される前記PD-1軸結合アンタゴニストを前記対象又は対象集団に投与することを含む、実施形態47、50、80~109、及び324のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
486.
487.前記方法が、4週間ごとに約1680mgの用量で投与するために製剤化される前記PD-1軸結合アンタゴニストを前記対象に投与することを含む、実施形態47、50、59、67、324、及び479のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
487.
488.前記方法が、2週間ごとに約600mgと約1200mgの間の用量で投与するために製剤化された前記PD-1軸結合アンタゴニストを前記対象又は対象集団に投与することを含む、実施形態48、49、80~109、及び481に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 488. Embodiment 48, wherein the method comprises administering to the subject or population of subjects the PD-1 axis binding antagonist formulated for administration at a dose of between about 600 mg and about 1200 mg every two weeks; 49, 80-109, and 481 anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists.
489.前記方法が、2週間ごとに約840mgの用量で投与するために製剤化される前記PD-1軸結合アンタゴニストを前記対象に投与することを含む、実施形態48、49、80~109、227、251~253、及び481のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 489. embodiments 48, 49, 80-109, 227, wherein said method comprises administering to said subject said PD-1 axis binding antagonist formulated for administration at a dose of about 840 mg every two weeks; 251-253, and anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of paragraphs 481-481.
490.前記PD-1軸結合アンタゴニストの用量が固定用量である、実施形態47~489のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 490. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 47-489, wherein the dose of said PD-1 axis binding antagonist is a fixed dose.
491.前記方法が、3週間ごとに約200mg又は6週間ごとに400mgの固定用量でペンブロリズマブを前記対象に投与することを含む、実施形態60又は61に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト又はペンブロリズマブ。
491. 62. An anti-TIGIT antagonist antibody and PD- for use according to
492.前記1回以上の投薬サイクルの各々の長さが21日間である、実施形態54、60、62、63、65、80~109、及び191のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
492. 192. Anti-TIGIT for use according to any one of
493.前記1回以上の投薬サイクルの各々の長さが28日間である、実施形態47、59、67、80~109、及び309~311のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
493. An anti-TIGIT antagonist antibody for use according to any one of
494.前記1回以上の投薬サイクルの各々の長さが14日間である、実施形態49、80~109、及び309~311のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 494. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 49, 80-109, and 309-311, wherein each of said one or more dosing cycles is 14 days in length Axis binding antagonist.
495.前記方法が、1回以上の投薬サイクルのそれぞれの約1日目に前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態47~494のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
495. 495. Use according to any one of embodiments 47-494, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects on about
496.前記方法が、前記1回以上の投薬サイクルのそれぞれの約1日目に前記対象又は対象集団に前記PD-1軸結合アンタゴニストを投与することを含む、実施形態47~495のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
496. 496. according to any one of embodiments 47-495, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects on about
497.前記方法が、前記抗TIGITアンタゴニスト抗体を前記1回以上の投薬サイクルのそれぞれの約15日目に前記対象に投与することを含む、実施形態321又は493に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 497. Anti-TIGIT antagonist antibody for use according to embodiment 321 or 493, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject on about day 15 of each of said one or more dosing cycles and PD-1 axis binding antagonists.
498.前記方法が、前記PD-1軸結合アンタゴニストを前記1回以上の投薬サイクルのそれぞれの約15日目に前記対象に投与することを含む、実施形態321又は493に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 498. Anti-TIGIT for use according to embodiment 321 or 493, wherein said method comprises administering said PD-1 axis binding antagonist to said subject on about day 15 of each of said one or more dosing cycles Antagonist Antibodies and PD-1 Axis Binding Antagonists.
499.前記方法が、対象又は対象集団に、前記抗TIGITアンタゴニスト抗体の前にPD-1軸結合アンタゴニストを投与すること、又は前記PD-1軸結合アンタゴニストの前に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態47~498のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 499. The method comprises administering to the subject or population of subjects a PD-1 axis binding antagonist prior to the anti-TIGIT antagonist antibody, or administering the anti-TIGIT antagonist antibody prior to the PD-1 axis binding antagonist. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 47-498.
500.前記方法が、前記PD-1軸結合アンタゴニスト又は前記抗TIGITアンタゴニスト抗体の投与後の第1の観察期間を含む、実施形態499に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 500. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 499, wherein said method comprises a first observation period after administration of said PD-1 axis binding antagonist or said anti-TIGIT antagonist antibody .
501.第1の観察期間が約30分と約60分の間の長さである、実施形態500に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
501. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
502.前記方法が、前記抗TIGITアンタゴニスト抗体又は前記PD-1軸結合アンタゴニストの投与後の第2観察期間を含む、実施形態500又は501に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
502. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to
503.第2の観察期間が約30分と約60分の間の長さである、実施形態502に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 503. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 502, wherein the second observation period is between about 30 minutes and about 60 minutes long.
504.前記方法が、前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体と同時に前記PD-1軸結合アンタゴニストを投与することを含む、実施形態47~503のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 504. Anti-TIGIT for use according to any one of embodiments 47-503, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects concurrently with said anti-TIGIT antagonist antibody. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
505.前記方法が、前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを静脈内投与することを含む、実施形態47~504のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 505. Anti-TIGIT for use according to any one of embodiments 47-504, wherein said method comprises administering said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist intravenously to said subject or population of subjects Antagonist Antibodies and PD-1 Axis Binding Antagonists.
506.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記PD-1軸結合アンタゴニストを投与することを含む、実施形態505に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 506. Use according to embodiment 505, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or subject population by intravenous infusion over 30±10 minutes and/or 60±10 minutes. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
507.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態505又は506に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 507. Use according to embodiment 505 or 506, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or subject population by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
508.前記一又は複数の対象から得られた腫瘍試料のPD-L1発現レベルが決定されている、実施形態47~114及び116~507のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 508. an anti-TIGIT antagonist antibody for use according to any one of embodiments 47-114 and 116-507, wherein the PD-L1 expression level of a tumor sample obtained from said one or more subjects has been determined; and PD-1 axis binding antagonist.
509.前記一又は複数の対象から得られた前記腫瘍試料が検出可能なPD-L1発現レベルを有すると決定されている、実施形態508に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 509. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to embodiment 508, wherein said tumor sample obtained from said one or more subjects has been determined to have a detectable PD-L1 expression level antagonist.
510.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1タンパク質発現レベルである、実施形態509に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 510. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 509, wherein said detectable PD-L1 expression level is a detectable PD-L1 protein expression level.
511.前記検出可能なPD-L1タンパク質発現レベルが、染色に適した抗PD-L1抗体による染色を含む免疫組織化学(IHC)アッセイによって決定されている、実施形態510に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 511. Anti-TIGIT for use according to embodiment 510, wherein said detectable PD-L1 protein expression level has been determined by an immunohistochemistry (IHC) assay comprising staining with an anti-PD-L1 antibody suitable for staining. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
512.染色に適した前記抗PD-L1抗体が抗PD-L1抗体SP263、SP142、22C3又は28-8である、実施形態511に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 512. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 511, wherein said anti-PD-L1 antibody suitable for staining is anti-PD-L1 antibody SP263, SP142, 22C3 or 28-8.
513.前記検出可能なPD-L1タンパク質発現レベルが、Ventana SP263 IHCアッセイ、pharmDx 22C3 IHCアッセイ、Ventana SP142 IHCアッセイ、又はpharmDx 28-8 IHCアッセイを使用して決定される、実施形態511又は512に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 513. 513. According to embodiment 511 or 512, wherein the detectable PD-L1 protein expression level is determined using the Ventana SP263 IHC assay, pharmDx 22C3 IHC assay, Ventana SP142 IHC assay, or pharmDx 28-8 IHC assay. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
514.抗PD-L1抗体SP263による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~109、188、220~265、及び307~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
514. Any of embodiments 47-109, 188, 220-265, and 307-423, wherein detectable PD-L1 protein expression levels as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP263 have been determined An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
515.抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~220、265~338、及び370~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 515. Any one of embodiments 47-220, 265-338, and 370-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142 has been determined Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use as described in .
516.抗PD-L1抗体SP22C3による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~113、136~187、及び220~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 516. Any one of embodiments 47-113, 136-187, and 220-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP22C3 has been determined Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use as described in .
517.抗PD-L1抗体28-8による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~114、及び116~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 517. According to any one of embodiments 47-114 and 116-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody 28-8 has been determined. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use in.
518.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上の腫瘍関連免疫細胞(TIC)である、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 518. Anti-TIGIT antagonist antibody and PD-1 axis for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more tumor-associated immune cells (TIC) in said tumor sample Binding antagonist.
519.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上20%未満のTICである、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 519. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more and less than 20% TIC in said tumor sample.
520.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上のTICである、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 520. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more TIC in said tumor sample.
521.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の20%以上のTICである、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 521. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 20% or more TIC in said tumor sample.
522.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上50%未満のTICである、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 522. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more and less than 50% TIC in said tumor sample.
523.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の50%以上のTICである、実施形態514に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 523. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 50% or more TIC in said tumor sample.
524.前記検出可能なPD-L1タンパク質発現レベルが、1%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 524. Anti-TIGIT antagonist antibody for use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or more and PD-1 axis binding antagonists.
525.前記検出可能なPD-L1タンパク質発現レベルが、30%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 525. Anti-TIGIT antagonist antibody for use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 30% or more and PD-1 axis binding antagonists.
526.前記検出可能なPD-L1タンパク質発現レベルが、腫瘍試料中の1%以上50%未満のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 526. Use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or more and less than 50% in the tumor sample. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
527.前記PD-L1の検出可能なタンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 527. Anti-TIGIT antagonist for use according to any one of embodiments 514, 516 and 517, wherein said detectable protein expression level of PD-L1 is a PD-L1 positive tumor cell fraction of 50% or more Antibodies and PD-1 axis binding antagonists.
528.前記PD-L1陽性腫瘍細胞分率が、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合である、実施形態515に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 528. Anti-TIGIT antagonist antibody and PD-1 for use according to embodiment 515, wherein said PD-L1 positive tumor cell fraction is the percentage of tumor area occupied by PD-L1 expressing tumor-infiltrating immune cells (IC) Axis binding antagonist.
529.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が1%以上である、実施形態515に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 529. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 515, wherein the percentage of tumor area occupied by said PD-L1 expressing tumor infiltrating IC is 1% or more.
530.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が5%以上である、実施形態515に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 530. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 515, wherein the percentage of tumor area occupied by said PD-L1 expressing tumor infiltrating IC is 5% or more.
531.前記検出可能なPD-L1タンパク質発現レベルが、1以上の複合陽性スコア(CPS)である、実施形態516に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 531. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 516, wherein said detectable PD-L1 protein expression level is a composite positive score (CPS) of 1 or greater.
532.前記検出可能なPD-L1タンパク質発現レベルが、10以上のCPSである、実施形態516に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 532. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 516, wherein said detectable PD-L1 protein expression level is 10 or more CPS.
533.前記検出可能なPD-L1タンパク質発現レベルが、20以上のCPSである、実施形態516に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 533. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 516, wherein said detectable PD-L1 protein expression level is 20 or more CPS.
534.前記IHCアッセイがVentana SP 142 IHCアッセイである、実施形態528~530のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 534. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 528-530, wherein said IHC assay is the Ventana SP 142 IHC assay.
535.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1核酸発現レベルである、実施形態509に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 535. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 509, wherein said detectable PD-L1 expression level is a detectable PD-L1 nucleic acid expression level.
536.前記検出可能なPD-L1核酸発現レベルが、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている、実施形態535に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 536. said detectable PD-L1 nucleic acid expression level has been determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof; Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 535.
537.前記処置が、基準全生存期間(OS)と比較した前記対象のOS時間及び/又は基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加をもたらす、実施形態47~423のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
537. 424. Any of embodiments 47-423, wherein said treatment results in an increase in said subject's OS time compared to baseline overall survival (OS) and/or said subject's PFS time compared to baseline progression-free survival (PFS) An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to
538.実施形態537に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストであって、
(a)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のOS時間の中央値である、及び/又は
(b)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のPFS時間の中央値である、
抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
538. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 537, wherein
(a) a subject whose baseline OS time has undergone treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment comprising an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist; and/or (b) the baseline PFS time is a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or an anti-PD-1 axis binding antagonist without a PD-1 axis binding antagonist. median PFS time in a subject population that has received treatment containing a TIGIT antagonist antibody;
Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist.
539.前記1つ以上の化学療法剤が、1つ以上の白金系化学療法剤及び/又は1つ以上の非白金系化学療法剤である、実施形態52、158及び228のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 539. 229. According to any one of embodiments 52, 158 and 228, wherein said one or more chemotherapeutic agents is one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents. Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for use.
540.前記白金系化学療法剤がカルボプラチン又はシスプラチンである、実施形態539に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 540. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 539, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541.前記カルボプラチンが、AUC=5mg/ml/分又はAUC=6mg/ml/分を達成するのに十分な用量で投与される、実施形態69、92、127、131、249、及び540に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 541. Use according to embodiments 69, 92, 127, 131, 249, and 540, wherein said carboplatin is administered at a dose sufficient to achieve AUC = 5 mg/ml/min or AUC = 6 mg/ml/min Anti-TIGIT antagonist antibodies and PD-1 axis binding antagonists for.
542.前記シスプラチンが、約75mg/m2又は80mg/m2の用量での投与のために製剤化される、実施形態69、127、162、164、166、168及び540に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 542. Anti-TIGIT antagonist for use according to embodiments 69, 127, 162, 164, 166, 168 and 540, wherein said cisplatin is formulated for administration at a dose of about 75 mg/m2 or 80 mg/m2 Antibodies and PD-1 axis binding antagonists.
543.前記1つ以上の非白金系化学療法剤が、代謝拮抗剤、タキサン、又はトポイソメラーゼII阻害剤である、実施形態539~542のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 543. Anti-TIGIT antagonist antibody and PD for use according to any one of embodiments 539-542, wherein said one or more non-platinum chemotherapeutic agents are antimetabolites, taxanes, or topoisomerase II inhibitors - uniaxial binding antagonists.
544.前記代謝拮抗剤が、ペメトレキセド、ゲムシタビン、カペシタビン又は5-フルオロウラシルである、実施形態62、173、174、及び543のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 544. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 62, 173, 174 and 543, wherein said antimetabolite is pemetrexed, gemcitabine, capecitabine or 5-fluorouracil antagonist.
545.前記ペメトレキセドが、約500mg/m2の用量での投与のために製剤化される、実施形態69、127、162及び544のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 545. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 69, 127, 162 and 544, wherein said pemetrexed is formulated for administration at a dose of about 500 mg/m2 Axis binding antagonist.
546.前記ゲムシタビンが、約1000mg/m2又は約1250mg/m2の用量での投与のために製剤化される、実施形態63、64、162、398、及び544のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
546. For use according to any one of
547.前記代謝拮抗剤がカペシタビンである、実施形態544に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 547. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 544, wherein said antimetabolite is capecitabine.
548.前記カペシタビンが約1250mg/m2の用量での投与のために製剤化される、実施形態544又は547に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 548. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 544 or 547, wherein said capecitabine is formulated for administration at a dose of about 1250 mg/m2.
549.前記タキサンがパクリタキセル又はnab-パクリタキセルである、実施形態173、174、229、230、239、240及び543~548のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 549. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 173, 174, 229, 230, 239, 240 and 543-548, wherein said taxane is paclitaxel or nab-paclitaxel antagonist.
550.前記パクリタキセルが、約175mg/m2又は約200mg/m2の用量での投与のために製剤化される、実施形態69、162及び549のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 550. an anti-TIGIT antagonist antibody for use according to any one of embodiments 69, 162 and 549, wherein said paclitaxel is formulated for administration at a dose of about 175 mg/m2 or about 200 mg/m2; and PD-1 axis binding antagonist.
551.前記nab-パクリタキセルが、約100mg/m2の用量での投与のために製剤化される、実施形態63、64、249、398、及び549のいずれか一項の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
551. and the anti-TIGIT antagonist antibody for use according to any one of
552.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリンカルボン酸又はHU-331である、実施形態80-91、229、230、239、241、251-255及び543~551のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 552. Embodiments 80-91, 229, 230, 239, 241, 251-255 wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticine, aurincarboxylic acid or HU-331 and anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of 543-551.
553.前記エトポシドが約100mg/m2の用量での投与のために製剤化される、実施形態69、92、及び552のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 553. Anti-TIGIT antagonist antibody and PD-1 axis binding for use according to any one of embodiments 69, 92, and 552, wherein said etoposide is formulated for administration at a dose of about 100 mg/m2 antagonist.
554.前記1つ以上の化学療法剤がそれぞれ、1週間ごとに1回、2週間ごとに1回、3週間ごとに1回、3週間ごとに2回、4週間ごとに1回、4週間ごとに2回、又は4週間ごとに3回投与される、実施形態543~553のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 554. each of said one or more chemotherapeutic agents once every week, once every two weeks, once every three weeks, twice every three weeks, once every four weeks, every four weeks Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 543-553, administered twice, or three times every four weeks.
555.前記1つ以上の化学療法剤が、1回以上の投薬サイクルの1日目に投与される、実施形態543~554のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
555. An anti-TIGIT antagonist antibody and PD-1 for use according to any one of embodiments 543-554, wherein said one or more chemotherapeutic agents are administered on
556.前記ゲムシタビンが4週間ごとに3回投与される、実施形態544~555のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 556. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 544-555, wherein said gemcitabine is administered three times every four weeks.
557.前記ゲムシタビンが、1回以上の投薬サイクルの1、8、及び/又は15日目に投与される、実施形態544~556のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
557. Anti-TIGIT antagonist antibody and PD-antibody for use according to any one of embodiments 544-556, wherein said gemcitabine is administered on
558.前記カペシタビンが2週間にわたって毎日投与される、実施形態544~557のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 558. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 544-557, wherein said capecitabine is administered daily for two weeks.
559.前記カペシタビンを1回以上の投薬サイクルの1~14日目に投与する、実施形態544~558のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 559. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 544-558, wherein said capecitabine is administered on days 1-14 of one or more dosing cycles.
560.前記nab-パクリタキセルが4週間ごとに3回投与される、実施形態549~559のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 560. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 549-559, wherein said nab-paclitaxel is administered three times every four weeks.
561.前記nab-パクリタキセルが、1回以上の投薬サイクルの1、8、及び15日目に投与される、実施形態549~560のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
561. Anti-TIGIT antagonist antibody and PD-antibody for use according to any one of embodiments 549-560, wherein said nab-paclitaxel is administered on
562.前記エトポシドが3週間ごとに1~3日目に投与される、実施形態552~561のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 562. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 552-561, wherein said etoposide is administered on days 1-3 every 3 weeks.
563.前記エトポシドが1回以上の投薬サイクルの1~3日目に投与される、実施形態552~562のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 563. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 552-562, wherein said etoposide is administered on days 1-3 of one or more dosing cycles.
564.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の前に投与される、実施形態543~563のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 564. Antibodies for use according to any one of embodiments 543-563, wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody. TIGIT antagonist antibody and PD-1 axis binding antagonist.
565.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の後に投与される、実施形態543~564のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 565. Anti-TIGIT for use according to any one of embodiments 543-564, wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody. Antagonist Antibodies and PD-1 Axis Binding Antagonists.
566.前記1つ以上の化学療法剤が静脈内又は経口投与される、実施形態543~565のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 566. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to any one of embodiments 543-565, wherein said one or more chemotherapeutic agents are administered intravenously or orally.
567.前記VEGFアンタゴニストが、3週間ごとに約5mg/kg~約25mg/kgの用量で投与するために製剤化される、実施形態65、310及び311のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
567. Antibodies for use according to any one of
568.前記VEGFアンタゴニストが、3週間ごとに約10mg/kg~約20mg/kgの用量での投与するために製剤化される、実施形態312又は567に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 568. Anti-TIGIT antagonist antibody for use according to embodiment 312 or 567, wherein said VEGF antagonist is formulated for administration at a dose of about 10 mg/kg to about 20 mg/kg every 3 weeks Uniaxial binding antagonist.
569.前記VEGFアンタゴニストが、3週間ごとに約15mg/kgの用量での投与するために製剤化される、実施形態318又は568に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 569. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 318 or 568, wherein said VEGF antagonist is formulated for administration at a dose of about 15 mg/kg every three weeks.
570.前記VEGFアンタゴニストが抗VEGF抗体である、実施形態65、310~312、318~320及び567~569のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
570. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of
571.前記抗VEGF抗体がベバシズマブのVHドメイン及びVLドメインを含む、実施形態570に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 571. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 570, wherein said anti-VEGF antibody comprises the VH and VL domains of bevacizumab.
572.前記抗VEGF抗体がベバシズマブである、実施形態570又は571に記載の使使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 572. An anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to embodiment 570 or 571, wherein said anti-VEGF antibody is bevacizumab.
573.前記抗TIGITアンタゴニスト抗体がチラゴルマブであり、前記PD-1軸結合アンタゴニストがアテゾリズマブであり、前記VEGFアンタゴニストがベバシズマブである、実施形態65、310~312、及び318~320のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
573. according to any one of
574.前記方法が、1回以上の投薬サイクルの1日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態65、310~312、318~320、及び567~573のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
574. any one of
575.前記方法が、1回以上の投薬サイクルの15日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態318~320のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 575. an anti-TIGIT antagonist antibody for use according to any one of embodiments 318-320, wherein said method comprises administering said VEGF antagonist to said subject on day 15 of one or more dosing cycles; and PD-1 axis binding antagonist.
576.前記VEGFアンタゴニストが静脈内投与される、実施形態65、310~312、及び318~320、及び567~575のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
576. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of
577.前記VEGFアンタゴニストが90±15分間にわたる静脈内注入によって前記対象に投与される、実施形態576に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 577. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 576, wherein said VEGF antagonist is administered to said subject by intravenous infusion over 90±15 minutes.
578.前記方法が、前記VEGFアンタゴニストの前に前記PD-1軸結合アンタゴニストを投与し、前記抗TIGITアンタゴニスト抗体の前に前記VEGFアンタゴニストを投与することを含む、実施形態65、310~312、318~320、及び567~577のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。
578.
579.前記方法が、前記PD-1軸結合アンタゴニストの投与後の第1の観察期間、前記VEGFアンタゴニストの投与後の第2の観察期間、及び前記抗TIGITアンタゴニスト抗体の投与後の第3の観察期間を含む、実施形態578に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 579. The method comprises a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody. An anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist for use according to embodiment 578, comprising:
580.前記第1の観察期間、前記第2の観察期間、及び前記第3の観察期間がそれぞれ、約30分と約120分の間の長さである、実施形態579に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 580. 579. The resistance for use according to embodiment 579, wherein the first observation period, the second observation period, and the third observation period are each between about 30 minutes and about 120 minutes in length. TIGIT antagonist antibody and PD-1 axis binding antagonist.
581.前記チラゴルマブ及びアテゾリズマブが、投与前にIVバッグにおいて組み合わされる、実施形態113、128、129~131、175~182、210~214、221、256、257、270、289、290、293、294、297、298、333、362~365、385、386、389、393、419、及び422のいずれか一項に記載の使用のためのチラゴルマブ及びアテゾリズマブ。 581. Embodiments 113, 128, 129-131, 175-182, 210-214, 221, 256, 257, 270, 289, 290, 293, 294, 297, wherein said tiragolumab and atezolizumab are combined in an IV bag prior to administration , 298, 333, 362-365, 385, 386, 389, 393, 419, and 422.
582.前記対象がヒトである、実施形態47~581のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 582. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-581, wherein said subject is a human.
583.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態47~582のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 583. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-582, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in separate formulations .
584.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態47~582のいずれか一項に記載の使用のための抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト。 584. Anti-TIGIT antagonist antibody and PD-1 axis binding antagonist for use according to any one of embodiments 47-582, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in a single formulation. .
実施形態のセットC:
1.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。
Set C of embodiments:
1. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 500 mg to about 700 mg of the anti-TIGIT every 3 weeks. One or more doses of a TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks. A use comprising administering to said subject a dosing regimen comprising cycles.
2.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 2. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 700 mg to about 1000 mg of the anti-TIGIT every four weeks. A use comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a TIGIT antagonist antibody and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks.
3.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約600mg~約1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 3. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 300 mg to about 600 mg of the anti-TIGIT antagonist every two weeks. A use comprising administering to said subject a dosing regimen comprising a TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks.
4.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態2又は3に記載の使用。
4. 4. Use according to
5.前記抗TIGITアンタゴニスト抗体がIgGクラス抗体、特にIgG1サブクラス抗体である、実施形態1~4のいずれかに記載の使用。
6.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
(f)QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、
を含む、実施形態1~5のいずれか一項に記載の使用。
5. Use according to any of embodiments 1-4, wherein said anti-TIGIT antagonist antibody is an IgG class antibody, in particular an IgG1 subclass antibody.
6. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3);
(d) an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and (f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
The use according to any one of embodiments 1-5, comprising
7.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
(a)DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
(b)WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
(c)GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
(d)FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、並びに
以下の重鎖可変領域FR:
(a)X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
(b)WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
(c)RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
(d)WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4
を含む、実施形態1~6のいずれか一項に記載の使用。
8.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)配列番号17若しくは18のアミノ酸配列を含むVHドメインと、配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態1~7のいずれか一項に記載の使用。
7. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and (d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and the following heavy chain variable region FRs:
(a) FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), where X1 is E or Q;
(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and (d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
The use according to any one of embodiments 1-6, comprising
8. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or (c) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18. , SEQ ID NO:19.
9.前記抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態1~8のいずれか一項に記載の使用。 9. Use according to any one of embodiments 1-8, wherein said anti-TIGIT antagonist antibody is tiragolumab.
10.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト又はPD-1結合アンタゴニストである、実施形態1~9のいずれか一項に記載の使用。 10. Use according to any one of embodiments 1-9, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist or a PD-1 binding antagonist.
11.前記PD-1軸結合アンタゴニストが、抗PD-L1アンタゴニスト抗体又は抗PD-1アンタゴニスト抗体である、実施形態1~10のいずれか一項に記載の使用。 11. Use according to any one of embodiments 1-10, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody or an anti-PD-1 antagonist antibody.
12.前記PD-1軸結合アンタゴニストが、抗PD-L1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の使用。 12. Use according to any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-L1 antagonist antibody.
13.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態12に記載の使用。
13. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 ,
14.前記PD-1軸結合アンタゴニストが、モノクローナル抗体である、実施形態1~13のいずれか一項に記載の使用。 14. Use according to any one of embodiments 1-13, wherein said PD-1 axis binding antagonist is a monoclonal antibody.
15.前記PD-1軸結合アンタゴニストが、抗PD-1アンタゴニスト抗体である、実施形態1~11のいずれか一項に記載の使用。 15. Use according to any one of embodiments 1-11, wherein said PD-1 axis binding antagonist is an anti-PD-1 antagonist antibody.
16.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態15に記載の使用。 16. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21.
17.前記方法が、有効量の白金系化学療法剤及び非白金系化学療法剤を前記対象に投与することを含む、実施形態2~16のいずれか一項に記載の使用。 17. 17. Use according to any one of embodiments 2-16, wherein said method comprises administering to said subject an effective amount of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
18.前記非白金系化学療法剤がトポイソメラーゼII阻害剤である、実施形態1又は17に記載の使用。
18. 18. Use according to
19.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331、特にエトポシドである、実施形態18に記載の使用。
19. 19. Use according to
20.前記トポイソメラーゼII阻害剤が100mg/m2の用量で投与される、実施形態18又は19に記載の使用。
20. 20. Use according to
21.前記白金系化学療法剤がカルボプラチン又はシスプラチン、特にカルボプラチンである、実施形態17~20のいずれか一項に記載の使用。 21. 21. Use according to any one of embodiments 17-20, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin, in particular carboplatin.
22.前記白金系化学療法剤が、投与日にAUC=5mg/ml/分を達成するのに十分な用量で投与される、実施形態17~21のいずれか一項に記載の使用。 22. Use according to any one of embodiments 17-21, wherein said platinum-based chemotherapeutic agent is administered at a dose sufficient to achieve AUC=5 mg/ml/min on the day of administration.
23.前記方法が、導入期及び維持期を含む投薬レジメンを含む、実施形態1~22のいずれか一項に記載の使用。 23. Use according to any one of embodiments 1-22, wherein said method comprises a dosing regimen comprising an induction phase and a maintenance phase.
24.前記導入期が4回の初期投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤が4回の初期投薬サイクルの各々で投与される、実施形態23に記載の使用。
24. wherein the induction phase comprises four initial dosing cycles, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and non-platinum-based chemotherapeutic agent are administered in each of the four initial dosing cycles; 24. The use according to
25.前記維持期が、前記白金系化学療法剤及び/又は非白金系化学療法剤の投与を含まない、実施形態23又は24に記載の使用。
25. 25. Use according to
26.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、実施形態1~25のいずれか一項に記載の使用。 26. 26. The use of any one of embodiments 1-25, wherein said treatment prolongs progression-free survival (PFS) of said subject compared to treatment without said anti-TIGIT antagonist antibody.
27.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない処置と比較して、前記対象の全生存期間を延長する、実施形態1~26のいずれか一項に記載の使用。 27. 27. The use of any one of embodiments 1-26, wherein said treatment prolongs overall survival of said subject compared to treatment without said anti-TIGIT antagonist antibody.
28.前記がんが肺がんである、実施形態1~27のいずれか一項に記載の使用。 28. 28. Use according to any one of embodiments 1-27, wherein said cancer is lung cancer.
29.前記肺がんが小細胞肺がん(SCLC)、特に進展型SCLC(ES-SCLC)である、実施形態28に記載の使用。 29. 29. Use according to embodiment 28, wherein said lung cancer is small cell lung cancer (SCLC), in particular extensive-stage SCLC (ES-SCLC).
30.前記肺がんが、非小細胞肺がん(NSCLC)、特に局所進行性切除不能NSCLC(ステージIIIB NSCLC)である、実施形態28に記載の使用。 30. 29. Use according to embodiment 28, wherein said lung cancer is non-small cell lung cancer (NSCLC), in particular locally advanced unresectable NSCLC (stage IIIB NSCLC).
31.前記肺がんが局所進行性切除不能又は転移性の非扁平上皮NSCLCである、実施形態28に記載の使用。 31. 29. Use according to embodiment 28, wherein said lung cancer is locally advanced unresectable or metastatic non-squamous NSCLC.
32.前記肺がんが切除可能な肺がんである、実施形態28に記載の使用。 32. 29. Use according to embodiment 28, wherein said lung cancer is resectable lung cancer.
33.前記がんが子宮頸がんである、実施形態1~27のいずれか一項に記載の使用。 33. 28. Use according to any one of embodiments 1-27, wherein said cancer is cervical cancer.
34.前記がんが早期トリプルネガティブ乳がん(eTNBC)である、実施形態1~27のいずれか一項に記載の使用。 34. 28. Use according to any one of embodiments 1-27, wherein said cancer is early triple negative breast cancer (eTNBC).
35.前記がんが頭頸部がんである、実施形態1~27のいずれか一項に記載の使用。 35. 28. Use according to any one of embodiments 1-27, wherein said cancer is head and neck cancer.
36.前記がんが肝臓がん、特に肝細胞癌腫(HCC)である、実施形態1~27のいずれか一項に記載の使用。
36. Use according to any one of
37.前記がんが膀胱がんである、実施形態1~27のいずれか一項に記載の使用。 37. 28. Use according to any one of embodiments 1-27, wherein said cancer is bladder cancer.
38.前記がんが尿路上皮癌腫(UC)、特に転移性尿路上皮癌腫(mUC)である、実施形態37に記載の使用。
38. 38. Use according to
39.前記がんが膵臓がん、特に膵管腺癌(PDAC)である、実施形態1~27のいずれか一項に記載の使用。
39. Use according to any one of
40.前記がんが食道がん、特に進行性又は転移性食道がんである、実施形態1~27のいずれか一項に記載の使用。
40. Use according to any one of
41.PD-1軸結合アンタゴニストと組み合わせてがんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、前記方法が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤を、及び3週間ごとの非白金系化学療法剤を含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 41. Use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for a method of treating a subject with cancer in combination with a PD-1 axis binding antagonist, said method comprising a dose of about 500 mg to about 700 mg every 3 weeks a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum-based chemotherapeutic agent every 3 weeks1 A use comprising administering to said subject a dosing regimen comprising one or more dosing cycles.
42.PD-1軸結合アンタゴニストと組み合わせてがんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、前記方法が、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストを含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 42. Use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for a method of treating a subject with cancer in combination with a PD-1 axis binding antagonist, said method comprising a dose of about 700 mg to about 1000 mg every 4 weeks and one or more dosing cycles comprising a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks.
43.PD-1軸結合アンタゴニストと組み合わせてがんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体の使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約600mg~約1200mgの用量のPD-1軸結合アンタゴニストを含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 43. Use of an anti-TIGIT antagonist antibody in the manufacture of a medicament for a method of treating a subject with cancer in combination with a PD-1 axis binding antagonist, said method comprising a dose of about 300 mg to about 600 mg every two weeks and one or more dosing cycles comprising a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks.
44.抗TIGITアンタゴニスト抗体と組み合わせてがんを有する対象を処置する方法のための医薬の製造におけるPD-1軸結合アンタゴニストの使用であって、(a)前記方法が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤及び3週間ごとのn非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、(b)前記方法が、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストを含む1回以上の投薬サイクルを含む投薬レジメンを対象に投与することを含む、又は(c)前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約600mg~約1200mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、使用。 44. Use of a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer in combination with an anti-TIGIT antagonist antibody, said method comprising: (a) said method comprising from about 500 mg to about anti-TIGIT antagonist antibody at a dose of 700 mg, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks and a non-platinum-based chemotherapeutic agent every 3 weeks. (b) the method comprises administering to said subject a dosing regimen comprising one or more dosing cycles, wherein said method comprises administering a dose of about 700 mg to about 1000 mg of anti-TIGIT antagonist antibody every 4 weeks and about administering to the subject a dosing regimen comprising one or more dosing cycles comprising a dose of 1400 mg to 2000 mg of a PD-1 axis binding antagonist, or (c) the method comprises about 300 mg to about 600 mg every two weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks.
45.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態44に記載の使用。
45. 45. Use according to
46.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態44に記載の使用。
46. 45. Use according to
47.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、4週間ごとの約200mg~約1200mgの用量の抗TIGITアンタゴニスト抗体及び4週間ごとの約80mg~約2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 47. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 200 mg to about 1200 mg of the anti-TIGIT every four weeks. A use comprising administering to said subject a dosing regimen comprising one or more dosing cycles of a TIGIT antagonist antibody and a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every four weeks.
48.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、4週間ごとの約200mg~約2000mgの用量の抗TIGITアンタゴニスト抗体及び2週間ごとの約20mg~約1600mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 48. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 200 mg to about 2000 mg of the anti-TIGIT every four weeks. administering to said subject a dosing regimen comprising one or more dosing cycles of a TIGIT antagonist antibody and a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every two weeks.
49.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約20mg~約1600mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 49. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 10 mg to about 1000 mg of the anti-TIGIT antagonist every two weeks. A use comprising administering to said subject a dosing regimen comprising a TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 20 mg to about 1600 mg every two weeks.
50.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~約2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 50. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 10 mg to about 1000 mg of the anti-TIGIT antagonist every two weeks. A use comprising administering to said subject a dosing regimen comprising a TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every four weeks.
51.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、及び6週間ごとの約100mg~約1000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 51. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 30 mg to about 1200 mg of the anti-TIGIT every 3 weeks. A use comprising administering to said subject a dosing regimen comprising a TIGIT antagonist antibody and one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 100 mg to about 1000 mg every 6 weeks.
52.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態47~51のいずれか一項に記載の使用。 52. 52. Use according to any one of embodiments 47-51, wherein said method further comprises administering to said subject one or more chemotherapeutic agents.
53.前記方法が、白金系化学療法剤及び非白金系化学療法剤を前記対象に投与することを含む、実施形態52に記載の使用。 53. 53. Use according to embodiment 52, wherein said method comprises administering to said subject a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
54.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 54. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 30 mg to about 1200 mg of the anti-TIGIT every 3 weeks. One or more doses of a TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent every 3 weeks, and a non-platinum chemotherapeutic agent every 3 weeks. A use comprising administering to said subject a dosing regimen comprising cycles.
55.前記方法が、導入期及び維持期を含む、実施形態53又は54に記載の使用。 55. 55. Use according to embodiment 53 or 54, wherein said method comprises an induction phase and a maintenance phase.
56.前記導入期及び維持期がそれぞれ、1回以上の投薬サイクルを含む、実施形態55に記載の使用。 56. 56. Use according to embodiment 55, wherein said induction phase and maintenance phase each comprise one or more dosing cycles.
57.前記維持期が、前記白金系化学療法剤の投与を含まない、実施形態55又は56に記載の使用。
57. 57. Use according to
58.前記維持期が、前記非白金系化学療法剤の投与を含まない、実施形態55~57のいずれか一項に記載の使用。 58. 58. Use according to any one of embodiments 55-57, wherein said maintenance phase does not comprise administration of said non-platinum chemotherapeutic agent.
59.前記維持期が、4週間ごとの約200mg~約2000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~約2000mgの用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む、実施形態58に記載の使用。 59. The maintenance phase comprises one or more dosing cycles of the anti-TIGIT antagonist antibody at doses of about 200 mg to about 2000 mg every 4 weeks and the PD-1 axis binding antagonist at doses of about 80 mg to about 2000 mg every 4 weeks. , embodiment 58.
60.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mg~約1600mgの用量の抗PD-1アンタゴニスト抗体の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含み、前記抗PD-1アンタゴニスト抗体がペンブロリズマブである、使用。 60. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 30 mg to about 1200 mg of the anti-TIGIT every 3 weeks. administering to said subject a dosing regimen comprising one or more dosing cycles of a TIGIT antagonist antibody and an anti-PD-1 antagonist antibody at a dose of about 80 mg to about 1600 mg every three weeks; Use wherein the antibody is pembrolizumab.
61.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、チラゴルマブ及びペンブロリズマブの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含み、前記ペンブロリズマブが、6週間ごとに約100mgと約1000mgの間の用量で投与される、使用。 61. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising one or more dosing cycles of tiragolumab and pembrolizumab. administering a regimen to said subject, wherein said pembrolizumab is administered at a dose of between about 100 mg and about 1000 mg every 6 weeks.
62.がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び2週間の投薬/1週間の休薬の間、3週間ごとの1日2回の経口の約10mg/m2と約10000mg/m2の間の用量の代謝拮抗剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 62. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with cancer, said method comprising between about 30 mg and about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks, and 2 daily for 2 weeks on/1 week off. administering to said subject a dosing regimen comprising one or more dosing cycles of an antimetabolite at a dose of between about 10 mg/m2 and about 10000 mg/m2 orally.
63.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、ゲムシタビン及びnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 63. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering a dose of about 30 mg to about 1200 mg of the anti-TIGIT every 3 weeks. administering to said subject a dosing regimen comprising one or more dosing cycles of a TIGIT antagonist antibody, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every three weeks, gemcitabine and nab-paclitaxel. .
64.前記1つ以上の化学療法剤がゲムシタビン及びnab-パクリタキセルである、実施形態52に記載の使用。 64. 53. Use according to embodiment 52, wherein said one or more chemotherapeutic agents are gemcitabine and nab-paclitaxel.
65.がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約1mg/kgと約35mg/kgの間の用量のVEGFアンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 65. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with cancer, said method comprising between about 30 mg and about 1200 mg every 3 weeks a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and a VEGF antagonist at a dose of between about 1 mg/kg and about 35 mg/kg every 3 weeks. administering to said subject a dosing regimen comprising one or more dosing cycles of
66.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象に、導入期及び維持期を含む投薬レジメンを投与することを含み、
(a)前記導入期が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤の投与を含まない、使用。
66. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase administering
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding antagonist every 3 weeks and a non-platinum chemotherapeutic agent every 3 weeks; Use, wherein said maintenance phase does not include administration of said platinum-based chemotherapeutic agent.
67.がんを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象に、導入期及び維持期を含む投薬レジメンを投与することを含み、
(a)前記導入期が、3週間ごとの約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mg~約1600mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、4週間ごとの約200mg~約2000mgの用量の前記抗TIGITアンタゴニスト抗体、及び4週間ごとの約80mg~約2000mgの用量の前記PD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤又は前記非白金系化学療法剤の投与を含まない、使用。
67. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase administering
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 80 mg to about 1600 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more times of said anti-TIGIT antagonist antibody at a dose of about 200 mg to about 2000 mg every 4 weeks and said PD-1 axis binding antagonist at a dose of about 80 mg to about 2000 mg every 4 weeks; and wherein said maintenance phase does not comprise administration of said platinum-based chemotherapeutic agent or said non-platinum-based chemotherapeutic agent.
68.前記導入期が、4~6回の投薬サイクルを含む、実施形態56~59、66、及び67のいずれか一項に記載の使用。 68. The use according to any one of embodiments 56-59, 66, and 67, wherein said induction phase comprises 4-6 dosing cycles.
69.実施形態53~59及び66~68のいずれか一項に記載の使用であって、
(a)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、又は
(c)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がエトポシドである、
使用。
69. The use according to any one of embodiments 53-59 and 66-68, wherein
(a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin and the non-platinum-based chemotherapeutic agent is paclitaxel, or (c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is etoposide,
use.
70.前記がんが固形腫瘍である、実施形態47~69のいずれか一項に記載の使用。 70. Use according to any one of embodiments 47-69, wherein said cancer is a solid tumor.
71.前記がんが局所進行性又は転移性である、実施形態47~70のいずれか一項に記載の使用。 71. 71. Use according to any one of embodiments 47-70, wherein said cancer is locally advanced or metastatic.
72.前記がんが、肺がん、膵臓がん、子宮頸がん、乳がん、頭頸部がん、肝臓がん、膀胱がん、食道がん、胃がん、結腸直腸がん、腎臓がん、腎がん、黒色腫、又は卵巣がんである、実施形態47~71のいずれか一項に記載の使用。 72. the cancer is lung cancer, pancreatic cancer, cervical cancer, breast cancer, head and neck cancer, liver cancer, bladder cancer, esophageal cancer, stomach cancer, colorectal cancer, kidney cancer, renal cancer, 72. Use according to any one of embodiments 47-71, which is melanoma, or ovarian cancer.
73.前記がんが、肺がんである、実施形態72に記載の使用。
73. 73. Use according to
74.前記肺がんがNSCLC、特に局所進行性切除不能NSCLCである、実施形態73に記載の使用。
74. 74. Use according to
75.前記NSCLCが、ステージIIIBのNSCLCである、実施形態74に記載の使用。 75. 75. The use according to embodiment 74, wherein said NSCLC is stage IIIB NSCLC.
76.前記肺がんが再発性又は転移性NSCLCである、実施形態73~75のいずれか一項に記載の使用。 76. 76. Use according to any one of embodiments 73-75, wherein said lung cancer is recurrent or metastatic NSCLC.
77.前記NSCLCが、ステージIVのNSCLCである、実施形態76に記載の使用。
77. 77. The use according to
78.前記対象が、ステージIVのNSCLCについて以前に処置されたことがない、実施形態77に記載の使用。 78. 78. Use according to embodiment 77, wherein said subject has not been previously treated for stage IV NSCLC.
79.前記肺がんが小細胞肺がん(SCLC)である、実施形態73に記載の使用。
79. 74. Use according to
80.肺がんを有する対象又は対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象の無増悪生存期間(PFS)を延長する、使用。 80. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having lung cancer, said method comprising an effective amount of an anti-TIGIT antagonist antibody, PD-1 administering to said subject or population of subjects a dosing regimen comprising one or more dosing cycles of an axial binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment does not use said anti-TIGIT antagonist antibody. , which prolongs progression-free survival (PFS) of said subject compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor.
81.肺がんを有する対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象集団に投与することを含み、前記処置が、約8.2ヶ月~約9.2ヶ月の前記対象集団のPFS中央値をもたらす、使用。 81. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject population having lung cancer, said method comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding administering to said subject population a dosing regimen comprising one or more dosing cycles of an antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment lasts from about 8.2 months to about 9.2 months. A use that provides a median PFS for said subject population.
82.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の全生存期間(OS)を延長する、実施形態80又は81に記載の使用。 82. The treatment compared the overall survival (OS ) is extended.
83.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のPFSを少なくとも約2.4ヶ月延長する、実施形態80~82のいずれか一項に記載の使用。 83. said treatment prolongs PFS of said subject or subject population by at least about 2.4 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody The use according to any one of embodiments 80-82.
84.前記処置が、前記抗TIGITアンタゴニスト抗体を用いない前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団の前記PFSを少なくとも約3ヶ月~約4ヶ月延長する、実施形態83に記載の使用。 84. said treatment reduces said PFS of said subject or subject population by at least about 84. Use according to embodiment 83, extending from 3 months to about 4 months.
85.肺がんを有する対象又は対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いない、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤による処置と比較して、前記対象のOSを延長する、使用。 85. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having lung cancer, said method comprising an effective amount of an anti-TIGIT antagonist antibody, PD-1 administering to said subject or population of subjects a dosing regimen comprising one or more dosing cycles of an axial binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment does not use said anti-TIGIT antagonist antibody. , which prolongs OS in said subject compared to treatment with said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor.
86.肺がんを有する対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、有効量の抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象集団に投与することを含み、前記処置が、約15.3ヶ月~約17.6ヶ月の前記対象集団のOS中央値をもたらす、使用。 86. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject population having lung cancer, said method comprising an effective amount of an anti-TIGIT antagonist antibody, a PD-1 axis binding administering to said subject population a dosing regimen comprising one or more dosing cycles of an antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor, wherein said treatment lasts from about 15.3 months to about 17.6 months. A use that results in median OS for said subject population.
87.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3.3ヶ月延長する、実施形態82~86のいずれか一項に記載の使用。 87. said treatment prolongs OS of said subject or subject population by at least about 3.3 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody 87. Use according to any one of embodiments 82-86.
88.前記処置が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤による処置と比較して、前記対象又は対象集団のOSを少なくとも約3ヶ月~約5.3ヵ月延長する、実施形態82~86のいずれか一項に記載の使用。 88. said treatment reduces the OS of said subject or subject population by at least about 3 months to about 5 months compared to treatment with a PD-1 axis binding antagonist, a platinum-based chemotherapeutic agent and a topoisomerase II inhibitor without an anti-TIGIT antagonist antibody; .The use according to any one of embodiments 82-86, extended for 3 months.
89.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が、4回の初期投薬サイクルの各々で投与される、実施形態80~88のいずれか一項に記載の使用。 89. 89. According to any one of embodiments 80-88, wherein the anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered in each of four initial dosing cycles. Use of.
90.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが、前記第4の初期投薬サイクルに続いて1回以上の追加のサイクルで更に投与される、実施形態80~89のいずれか一項に記載の使用。 90. 89. Any one of embodiments 80-89, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are further administered in one or more additional cycles following said fourth initial dosing cycle. Use of.
91.前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤が、前記1回以上の追加の投薬サイクルの各々から省略される、実施形態90に記載の使用。
91. 91. Use according to
92.前記白金系化学療法剤がカルボプラチンであり、前記トポイソメラーゼII阻害剤がエトポシドである、実施形態80~91のいずれか一項に記載の使用。 92. 92. Use according to any one of embodiments 80-91, wherein said platinum-based chemotherapeutic agent is carboplatin and said topoisomerase II inhibitor is etoposide.
93.前記肺がんが小細胞肺がん(SCLC)である、実施形態80~92のいずれか一項に記載の使用。 93. Use according to any one of embodiments 80-92, wherein said lung cancer is small cell lung cancer (SCLC).
94.前記SCLCが進展型SCLC(ES-SCLC)である、実施形態93に記載の使用。 94. 94. Use according to embodiment 93, wherein said SCLC is extensive SCLC (ES-SCLC).
95.前記一又は複数の対象が、ES-SCLCに対して処置未経験である、実施形態94に記載の使用。 95. 95. Use according to embodiment 94, wherein said one or more subjects are treatment-naive for ES-SCLC.
96.前記一又は複数の対象が脳転移の存在又は病歴を有していない、実施形態80~95のいずれか一項に記載の使用。 96. 96. Use according to any one of embodiments 80-95, wherein said one or more subjects do not have the presence or history of brain metastases.
97.前記肺がんがPD-L1発現について選択されていない、実施形態80~96のいずれか一項に記載の使用。 97. 97. Use according to any one of embodiments 80-96, wherein said lung cancer is not selected for PD-L1 expression.
98.前記肺がんがPD-L1発現について選択される、実施形態80~96のいずれか一項に記載の使用。 98. 97. Use according to any one of embodiments 80-96, wherein said lung cancer is selected for PD-L1 expression.
99.前記肺がんが、検出可能なPD-L1発現レベルによってPD-L1発現について選択される、実施形態98に記載の使用。 99. 99. Use according to embodiment 98, wherein said lung cancer is selected for PD-L1 expression by a detectable level of PD-L1 expression.
100.前記肺がんが転移性である、実施形態80~99のいずれか一項に記載の使用。 100. 99. Use according to any one of embodiments 80-99, wherein said lung cancer is metastatic.
101.前記肺がんが脳、肝臓、リンパ節及び/又は副腎に転移したことがある、実施形態100に記載の使用。
101. 101. Use according to
102.前記肺がんが脳に転移したことがない、実施形態100又は101に記載の使用。
102. 102. Use according to
103.前記処置が完全奏効(CR)又は部分奏効(PR)をもたらす、実施形態100~102のいずれか一項に記載の使用。 103. Use according to any one of embodiments 100-102, wherein said treatment results in a complete response (CR) or partial response (PR).
104.前記抗TIGITアンタゴニスト抗体が、2週間、3週間又は4週間ごとに約30mg~約1200mgの用量で投与される、実施形態80~103のいずれか一項に記載の使用。 104. 104. Use according to any one of embodiments 80-103, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every 2, 3 or 4 weeks.
105.前記PD-1軸結合アンタゴニストが、2週間、3週間又は4週間ごとに約80mg~約2000mgの用量で投与される、実施形態80~104のいずれか一項に記載の使用。 105. 105. Use according to any one of embodiments 80-104, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 2, 3 or 4 weeks.
106.前記PD-1軸結合アンタゴニスト、抗TIGITアンタゴニスト抗体、白金系化学療法剤及びトポイソメラーゼII阻害剤を連続的に投与する、実施形態80~105のいずれか一項に記載の使用。 106. 106. Use according to any one of embodiments 80-105, wherein said PD-1 axis binding antagonist, anti-TIGIT antagonist antibody, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered sequentially.
107.前記PD-1軸結合アンタゴニストが前記抗TIGITアンタゴニスト抗体の前に投与され、前記抗TIGITアンタゴニスト抗体が前記白金系化学療法剤の前に投与され、前記白金剤がトポイソメラーゼII阻害剤の前に投与される、実施形態106に記載の使用。 107. The PD-1 axis binding antagonist is administered prior to the anti-TIGIT antagonist antibody, the anti-TIGIT antagonist antibody is administered prior to the platinum-based chemotherapeutic agent, and the platinum agent is administered prior to the topoisomerase II inhibitor. 107. The use according to embodiment 106, wherein.
108.前記抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及びトポイソメラーゼII阻害剤が静脈内投与される、実施形態80~107のいずれか一項に記載の使用。 108. 108. Use according to any one of embodiments 80-107, wherein said anti-TIGIT antagonist antibody, PD-1 axis binding antagonist, platinum-based chemotherapeutic agent and topoisomerase II inhibitor are administered intravenously.
109.前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記トポイソメラーゼII阻害剤のうち1つ以上が皮下投与される、実施形態80~108のいずれか一項に記載の使用。 109. 109. Any one of embodiments 80-108, wherein one or more of said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist, said platinum-based chemotherapeutic agent and said topoisomerase II inhibitor are administered subcutaneously. use.
110.SCLCを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約80mg~約1600mgの用量のアテゾリズマブ、各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドの1回以上の21日間投薬サイクルを前記対象に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いないアテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、使用。
110. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with SCLC, said method comprising from about 30 mg to about Anti-TIGIT antagonist antibody at a dose of 1200 mg, atezolizumab at a dose of about 80 mg to about 1600 mg on
111.SCLCを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約300mg~約800mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約900mg~約1500mgの用量のアテゾリズマブ、各投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各投薬サイクルの1日目、2日目、及び3日目のそれぞれに100mg/m2の用量のエトポシドの1回以上の21日間投薬サイクルを前記対象に投与することを含み、前記処置が、前記抗TIGITアンタゴニスト抗体を用いないアテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、前記対象のPFS及び/又はOSを延長する、使用。
111. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with SCLC, said method comprising from about 300 mg to about Anti-TIGIT antagonist antibody at a dose of 800 mg, atezolizumab at a dose of about 900 mg to about 1500 mg on
112.各追加の投薬サイクルの1日目に約30mg~約1200mgの用量の抗TIGITアンタゴニスト抗体と、各追加の投薬サイクルの1日目に約80mg~約1600mgの用量のアテゾリズマブとの1回以上の追加の21日間の投薬サイクルを前記対象に投与することを更に含み、カルボプラチン及びエトポシドが1回以上の追加の投薬サイクルのそれぞれから省略される、実施形態110又は111に記載の使用。
112. One or more additions of an anti-TIGIT antagonist antibody at a dose of about 30 mg to about 1200 mg on
113.ES-SCLCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、4回の初期投薬サイクルと、それに続く1回以上の追加の投薬サイクルとを前記対象又は対象集団に投与することを含み、
(a)前記4回の初期投薬サイクルが、各初期投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各初期投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各初期投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各初期投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量のエトポシドを投与することを含み、
(b)前記1回以上の追加の投薬サイクルが、各追加の投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各追加の投薬サイクルの1日目に約1200mgの用量のアテゾリズマブを投与することを含み、
前記4回の初期投薬サイクル及び前記1回以上の追加の投薬サイクルが、それぞれ21日間投薬サイクルであり、前記処置が、前記チラゴルマブを用いないアテゾリズマブ、カルボプラチン及びエトポシドを含む処置と比較して、前記対象又は対象集団のPFS及び/又はOSを延長する、使用。
113. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population with ES-SCLC, said method comprising four initial dosing cycles followed by one or more additional and administering to said subject or subject population a dosing cycle of
(a) the four initial dosing cycles are tiragolumab at a dose of about 600 mg on
(b) said one or more additional dosing cycles administering a dose of about 600 mg tiragolumab on
each of the four initial dosing cycles and the one or more additional dosing cycles is a 21-day dosing cycle, and the treatment is compared to a treatment comprising atezolizumab, carboplatin and etoposide without the tiragolumab; A use that prolongs PFS and/or OS in a subject or subject population.
114.肺がんを有する対象又は対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤である第1の化学療法剤、及び非白金系化学療法剤である第2の化学療法剤の1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。 114. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having lung cancer, said method comprising an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist administering to said subject or population of subjects a dosing regimen comprising one or more dosing cycles of a first chemotherapeutic agent that is a platinum-based chemotherapeutic agent and a second chemotherapeutic agent that is a non-platinum-based chemotherapeutic agent use, including
115.前記肺がんがPD-L1発現について評価されていない、実施形態114に記載の使用。 115. 115. Use according to embodiment 114, wherein said lung cancer has not been evaluated for PD-L1 expression.
116.前記一又は複数の対象が、50%以上のPD-L1陽性腫瘍細胞分率を有すると決定されていない、実施形態114又は115に記載の使用。 116. 116. Use according to embodiment 114 or 115, wherein said one or more subjects have not been determined to have a PD-L1 positive tumor cell fraction of 50% or greater.
117.前記一又は複数の対象が50%未満のPD-L1陽性腫瘍細胞分率を有すると決定されている、実施形態116に記載の使用。 117. 117. Use according to embodiment 116, wherein said one or more subjects have been determined to have a PD-L1 positive tumor cell fraction of less than 50%.
118.前記PD-L1陽性腫瘍細胞分率が、抗PD-L1抗体を用いる陽性染色によって決定され、前記抗PD-L1抗体がSP263又は22C3である、実施形態116又は117に記載の使用。 118. 118. Use according to embodiment 116 or 117, wherein said PD-L1 positive tumor cell fraction is determined by positive staining with an anti-PD-L1 antibody, said anti-PD-L1 antibody being SP263 or 22C3.
119.前記一又は複数の対象が、上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態114~118のいずれか一項に記載の使用。 119. 119. Use according to any one of embodiments 114-118, wherein said one or more subjects do not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations.
120.前記一又は複数の対象が、前記肺がんに対する事前全身治療を受けたことがない、実施形態114~119のいずれか一項に記載の使用。 120. 120. Use according to any one of embodiments 114-119, wherein said one or more subjects have not received prior systemic therapy for said lung cancer.
121.前記肺がんが局所進行性肺がんである、実施形態114~120のいずれか一項に記載の使用。 121. Use according to any one of embodiments 114-120, wherein said lung cancer is locally advanced lung cancer.
122.前記肺がんがNSCLC、特に局所進行性切除不能又は転移性非扁平上皮NSCLCである、実施形態114~121のいずれか一項に記載の使用。 122. Use according to any one of embodiments 114 to 121, wherein said lung cancer is NSCLC, in particular locally advanced unresectable or metastatic non-squamous NSCLC.
123.前記非扁平上皮NSCLCがステージIV非扁平上皮NSCLCである、実施形態122に記載の使用。 123. 123. Use according to embodiment 122, wherein said non-squamous NSCLC is stage IV non-squamous NSCLC.
124.前記投薬レジメンが、4回の投薬サイクルを含む導入期を含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト、前記白金系化学療法剤及び前記非白金系化学療法剤が、前記導入期の各投薬サイクルの1日目に投与される、実施形態114~123のいずれか一項に記載の使用。
124. The dosing regimen comprises an induction phase comprising four dosing cycles, wherein the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, the platinum-based chemotherapeutic agent and the non-platinum-based chemotherapeutic agent are in the induction phase 124. Use according to any one of embodiments 114-123, administered on
125.前記投薬レジメンが、前記導入期に続いて維持期を含み、前記維持期が1回以上の投薬サイクルを含み、前記抗TIGITアンタゴニスト抗体、前記PD-1軸結合アンタゴニスト及び前記非白金系化学療法剤が、前記維持期の各投薬サイクルの1日目に投与される、実施形態124に記載の使用。
125. wherein said dosing regimen comprises a maintenance phase following said induction phase, said maintenance phase comprising one or more dosing cycles, said anti-TIGIT antagonist antibody, said PD-1 axis binding antagonist and said non-platinum chemotherapeutic agent is administered on
126.前記維持期の前記1回以上の投薬サイクルが、前記白金系化学療法剤の投与を含まない、実施形態125に記載の使用。 126. 126. Use according to embodiment 125, wherein said one or more dosing cycles of said maintenance phase do not comprise administration of said platinum-based chemotherapeutic agent.
127.前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、実施形態114~126のいずれか一項に記載の使用。 127. 127. Use according to any one of embodiments 114-126, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin and said non-platinum-based chemotherapeutic agent is pemetrexed.
128.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、チラゴルマブ、アテゾリズマブ、カルボプラチン又はシスプラチン及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンを投与することを含み、前記4回の21日間投薬サイクルの各々の1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与され、前記カルボプラチンが3週間ごとにAUC=5mg/ml/分を達成するのに十分な用量で投与されるか又は前記シスプラチンが3週間ごとに75mg/m2の用量で投与され、前記ペメトレキセドが3週間ごとに約500mg/m2の用量で投与される、使用・
129.進行性非扁平上皮NSCLCを有する対象又は対象集団を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル、
で投与することを含み、
前記対象又は対象集団が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、使用。
128. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population with advanced non-squamous NSCLC, said method comprising administering to said subject or subject population tiragolumab, atezolizumab, carboplatin or cisplatin and pemetrexed for four 21-day dosing cycles, wherein on
129. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population with advanced non-squamous NSCLC, said method comprising:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin;
administering with
Use, wherein said subject or subject population has never received prior systemic therapy for said advanced non-squamous NSCLC.
130.進行性非扁平上皮NSCLCを有する対象を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル、
で投与することを含み、
前記対象が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、使用。
130. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with advanced non-squamous NSCLC, said method comprising:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) atezolizumab at a dose of about 1200 mg every 3 weeks, and (ii) one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/m2, wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin;
administering with
Use wherein said subject has had no prior systemic therapy for said advanced non-squamous NSCLC.
131.進行性非扁平上皮NSCLCを有する対象を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ、アテゾリズマブ、カルボプラチン又はシスプラチン及びペメトレキセドの4回の21日間投薬サイクルを含む投薬レジメンを投与することを含み、前記4回の21日間投薬サイクルの各々の1日目に、前記チラゴルマブが3週間ごとに約600mgの用量で投与され、前記アテゾリズマブが3週間ごとに約1200mgの用量で投与され、前記シスプラチンが75mg/m2の用量で投与され、前記ペメトレキセドが約500mg/m2の用量で投与される、使用。
131. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with advanced non-squamous NSCLC, said method comprising administering to said subject four doses of tiragolumab, atezolizumab, carboplatin or cisplatin and pemetrexed administering a dosing regimen comprising a 21-day dosing cycle, wherein on
132.前記処置が、前記対象又は対象集団のPFSを少なくとも約3.5ヶ月又は約4.7ヶ月延長する、実施形態114~131のいずれか一項に記載の使用。 132. 132. Use according to any one of embodiments 114-131, wherein said treatment prolongs the PFS of said subject or population of subjects by at least about 3.5 months or about 4.7 months.
133.前記処置が、約12.5ヶ月~約14.7ヶ月の前記対象集団のPFS中央値をもたらす、実施形態114~132のいずれか一項に記載の使用。 133. 133. Use according to any one of embodiments 114-132, wherein said treatment results in a median PFS for said subject population of about 12.5 months to about 14.7 months.
134.前記処置が、前記対象又は対象集団のOSを少なくとも約5.5ヶ月又は約8.0ヶ月延長する、実施形態114~133のいずれか一項に記載の使用。 134. 134. Use according to any one of embodiments 114-133, wherein said treatment prolongs OS of said subject or population of subjects by at least about 5.5 months or about 8.0 months.
135.前記処置が、約27.5ヶ月~約32.0ヶ月の前記対象集団のOS中央値をもたらす、実施形態114~134のいずれか一項に記載の使用。 135. 135. Use according to any one of embodiments 114-134, wherein said treatment results in a median OS for said subject population of from about 27.5 months to about 32.0 months.
136.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、使用。 136. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising about 30 mg and about 1200 mg every 3 weeks and administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose between about 80 mg and about 1600 mg every three weeks.
137.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、使用。 137. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising about 300 mg and about 800 mg every 3 weeks and administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose between about 900 mg and about 1500 mg every three weeks.
138.肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600mgの間の用量で前記対象に投与することを含む、使用。 138. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising: administering to said subject one or more dosing cycles, wherein at least one of said dosing cycles includes said anti-TIGIT antagonist antibody as a neoadjuvant treatment at a dose of between about 30 mg and about 1200 mg every three weeks; and administering said PD-1 axis binding antagonist to said subject at a dose of between about 80 mg and about 1600 mg every three weeks.
139.肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約300mgと約800mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約900mgと約1500mgの間の用量で前記対象に投与することを含む、使用。 139. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising: administering to said subject one or more dosing cycles, wherein at least one of said dosing cycles includes said anti-TIGIT antagonist antibody as a neoadjuvant treatment at a dose of between about 300 mg and about 800 mg every three weeks; and administering said PD-1 axis binding antagonist to said subject at a dose of between about 900 mg and about 1500 mg every three weeks.
140.前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約1200mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600の間の用量で前記対象に投与することを含む、実施形態138又は139に記載の使用。 140. At least one of said dosing cycles comprises, as an adjuvant treatment, said anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks and said PD-1 axis binding antagonist at a dose between about 80 mg and about every three weeks. 140. Use according to embodiment 138 or 139, comprising administering to said subject at a dose of between 1600.
141.前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約500mgと約700mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約900mgと約1500の間の用量で前記対象に投与することを含む、実施形態140に記載の使用。 141. At least one of said dosing cycles comprises, as an adjuvant treatment, said anti-TIGIT antagonist antibody at a dose between about 500 mg and about 700 mg every 3 weeks and said PD-1 axis binding antagonist at a dose between about 900 mg and about 900 mg every 3 weeks. 141. Use according to embodiment 140, comprising administering to said subject at a dose of between 1500.
142.前記肺がんが切除可能な肺がんである、実施形態138~141のいずれか一項に記載の使用。 142. 142. Use according to any one of embodiments 138-141, wherein said lung cancer is resectable lung cancer.
143.前記肺がんが初期肺がんである、実施形態136~142のいずれか一項に記載の使用。 143. 143. Use according to any one of embodiments 136-142, wherein said lung cancer is early stage lung cancer.
144.前記肺がんが、ステージII、IIIA又はIIIBの肺がんである、実施形態136~143のいずれか一項に記載の使用。 144. 144. Use according to any one of embodiments 136-143, wherein said lung cancer is stage II, IIIA or IIIB lung cancer.
145.前記肺がんが上皮増殖因子受容体(EGFR)又は未分化リンパ腫キナーゼ(ALK)のゲノム腫瘍異常を有しない、実施形態136~144のいずれか一項に記載の使用。 145. 145. Use according to any one of embodiments 136-144, wherein said lung cancer does not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations.
146.前記対象が治癒目的でのR0摘出術に適格である、実施形態136~145のいずれか一項に記載の使用。 146. 146. Use according to any one of embodiments 136-145, wherein said subject is eligible for R0 enucleation with curative intent.
147.前記対象が肺がんの事前治療を受けたことがない、実施形態136~146のいずれか一項に記載の使用。 147. 147. Use according to any one of embodiments 136-146, wherein said subject has no prior treatment for lung cancer.
148.前記事前治療が免疫療法、化学療法、又は放射線療法である、実施形態147に記載の使用。 148. 148. Use according to embodiment 147, wherein said prior treatment is immunotherapy, chemotherapy or radiotherapy.
149.前記対象が白金系化学療法レジメンを受けるのに適格である、実施形態136~148のいずれか一項に記載の使用。 149. 149. Use according to any one of embodiments 136-148, wherein said subject is eligible to receive a platinum-based chemotherapy regimen.
150.前記第1の投薬サイクルが手術の前に開始される、実施形態136~149のいずれか一項に記載の使用。 150. 149. Use according to any one of embodiments 136-149, wherein said first dosing cycle is initiated prior to surgery.
151.少なくとも1、2、3又は4回の投薬サイクルが前記手術の前に完了する、実施形態150に記載の使用。 151. 151. Use according to embodiment 150, wherein at least 1, 2, 3 or 4 dosing cycles are completed prior to said surgery.
152.4回の投薬サイクルが前記手術の前に完了する、実施形態150又は151に記載の使用。 152. Use according to embodiment 150 or 151, wherein 4 dosing cycles are completed prior to said surgery.
153.少なくとも1回の投薬サイクルが手術後に開始される、実施形態136~152のいずれか一項に記載の使用。 153. 153. Use according to any one of embodiments 136-152, wherein at least one dosing cycle is initiated after surgery.
154.16回の投薬サイクルが前記手術後に完了する、実施形態153に記載の使用。 154. Use according to embodiment 153, wherein 16 dosing cycles are completed after said surgery.
155.前記手術が、区域切除術、肺葉切除術、二葉切除術、又は肺切除術である、実施形態150~154のいずれか一項に記載の使用。 155. 155. Use according to any one of embodiments 150-154, wherein said surgery is segmentectomy, lobectomy, bilobectomy, or pneumonectomy.
156.前記方法が放射線療法を更に含む、実施形態136~155のいずれか一項に記載の使用。 156. 156. Use according to any one of embodiments 136-155, wherein said method further comprises radiotherapy.
157.前記放射線療法が術後放射線療法である、実施形態156に記載の使用。 157. 157. Use according to embodiment 156, wherein said radiotherapy is post-operative radiotherapy.
158.前記方法が、1つ以上の化学療法剤を投与することを更に含む、実施形態136~157のいずれか一項に記載の使用。 158. 158. Use according to any one of embodiments 136-157, wherein said method further comprises administering one or more chemotherapeutic agents.
159.前記1つ以上の化学療法剤が手術後に投与される、実施形態158に記載の使用。 159. 159. Use according to embodiment 158, wherein said one or more chemotherapeutic agents are administered after surgery.
160.前記1つ以上の化学療法剤が、前記手術後に4回の投薬サイクルで投与される、実施形態159に記載の使用。 160. 159. Use according to embodiment 159, wherein said one or more chemotherapeutic agents are administered in four dosing cycles after said surgery.
161.前記1つ以上の化学療法剤が、白金系化学療法剤及び非白金系化学療法剤である、実施形態158~160のいずれか一項に記載の使用。
162.実施形態161の使用であって、
(a)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がペメトレキセドである、
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
(c)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、
(d)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、又は
(e)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
使用。
161. 161. Use according to any one of embodiments 158-160, wherein said one or more chemotherapeutic agents are platinum-based chemotherapeutic agents and non-platinum-based chemotherapeutic agents.
162. 161. The use of embodiment 161, comprising:
(a) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine. is
use.
163.前記処置が、基準病理学的著効(MPR)率と比較してMPR率の増加をもたらす、実施形態136~162のいずれか一項に記載の使用。 163. 163. Use according to any one of embodiments 136-162, wherein said treatment results in an increased MPR rate compared to the baseline significant pathological response (MPR) rate.
164.前記基準MPR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のMPR率である、実施形態163に記載の使用。
164. The reference MPR rate is
MPR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 164. The use according to embodiment 163, which is.
165.前記処置が、病理学的完全奏効(pCR)及び/又は基準pCR率と比較したpCR率の増加をもたらす、実施形態136~164のいずれか一項に記載の使用。 165. 165. Use according to any one of embodiments 136-164, wherein said treatment results in a pathological complete response (pCR) and/or an increase in the pCR rate compared to the baseline pCR rate.
166.前記基準pCR率が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のpCR率である、実施形態165に記載の使用。
166. The reference pCR rate is
pCR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 165. The use according to embodiment 165, which is.
167.前記処置が、基準無症候生存期間(EFS)と比較して、EFS時間の増加をもたらす、実施形態136~166のいずれか一項に記載の使用。 167. 167. Use according to any one of embodiments 136-166, wherein said treatment results in increased EFS time compared to baseline symptom-free survival (EFS).
168.前記基準EFS時間が、
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブ
を含む処置を受けたことがある対象集団のEFS時間である、実施形態167に記載の使用。
168. the reference EFS time,
EFS time in a subject population that has received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 168. The use according to embodiment 167, which is.
169.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約600mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含む、使用。 169. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising about 30 mg and about 600 mg every 3 weeks and administering to said subject one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose between about 80 mg and about 1600 mg every three weeks.
170.肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、前記抗TIGITアンタゴニスト抗体を3週間ごとに約30mgと約600mgの間の用量で、及び前記PD-1軸結合アンタゴニストを3週間ごとに約80mgと約1600mgの間の用量で前記対象に投与することを含む、使用。 170. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising: administering to said subject one or more dosing cycles, wherein at least one of said dosing cycles includes said anti-TIGIT antagonist antibody as a neoadjuvant treatment at a dose of between about 30 mg and about 600 mg every three weeks; and administering said PD-1 axis binding antagonist to said subject at a dose of between about 80 mg and about 1600 mg every three weeks.
171.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含む、使用。 171. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising about 30 mg and about 1200 mg every 3 weeks one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between, a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent to said subject.
172.肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとの約30mgと約1200mgの間の用量の前記抗TIGITアンタゴニスト抗体、3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニスト、白金系化学療法剤、及び非白金系化学療法剤を前記対象に投与することを含む、使用。 172. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising: an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist; administering to said subject one or more dosing cycles of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein at least one of said dosing cycles is about 30 mg every 3 weeks as a neoadjuvant treatment; said anti-TIGIT antagonist antibody at a dose of between about 1200 mg, said PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks, a platinum-based chemotherapeutic agent, and a non-platinum-based chemotherapeutic agent. Use, including administering to a subject.
173.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体と、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストと、(a)(i)3週間ごとの5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量の白金系化学療法剤;又は(ii)3週間ごとの約75mg/m2の用量の白金系化学療法剤と、(b)(i)3週間ごとの約500mg/m2、各投薬サイクルの第1日及び第8日に約1000mg/m2若しくは約1250mg/m2の用量の代謝拮抗剤;又は(ii)3週間ごとの約100mg/m2、約175mg/m2、若しくは約200mg/m2の用量のタキサンと、の1回以上の投薬サイクルを対象に投与することを含む、使用。
173. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising about 30 mg and about 1200 mg every 3 weeks an anti-TIGIT antagonist antibody at a dose of between and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks; and (a)(i) an AUC of 5 mg/mL/min every 3 weeks. or a platinum-based chemotherapeutic agent at a dose targeted to achieve an AUC of 6 mg/mL/min; or (ii) a platinum-based chemotherapeutic agent at a dose of about 75 mg/m every three weeks; i) an antimetabolite at a dose of about 500 mg/m2 every 3 weeks, about 1000 mg/m2 or about 1250 mg/m2 on
174.肺がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、白金系化学療法剤及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、少なくとも1つの前記投薬サイクルが、前記対象に、(a)3週間ごとの約30mgと約600mgの間の用量の前記抗TIGITアンタゴニスト抗体と、(b)3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニストと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量、又は(ii)3週間ごとの約75mg/m2の用量の前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量の代謝拮抗剤、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のタキサンである非白金系化学療法剤と、を投与することを含み、前記処置がネオアジュバント処置である、使用。
174. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising: an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, administering to said subject one or more dosing cycles of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein at least one said dosing cycle provides said subject with: (a) about 30 mg every 3 weeks; (b) the PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks; (c) the platinum-based chemotherapeutic agent (i) a dose targeted to achieve an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks, or (ii) a dose of about 75 mg/m2 every 3 weeks and (d) the non-platinum-based chemotherapeutic agent, which is (i) 500 mg/m2 every three weeks, or 1000 mg/m2 on
175.切除可能な肺がんを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、3週間ごとに約600mgの用量のチラゴルマブと、3週間ごとに約1200mgの用量のアテゾリズマブと、
(a)
(i)3週間ごとの5mg/mL/分のAUC若しくは6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は
(ii)3週間ごとの約75mg/m2の用量のシスプラチンと、
(b)
(i)3週間ごとの約500mg/m2の用量のペメトレキセド、又は各投薬サイクルの1日目及び8日目に約1000mg/m2若しくは約1250mg/m2の用量のゲムシタビン、又は
(ii)3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセルと、の1回以上の投薬サイクルを投与することを含む、使用。
175. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with resectable lung cancer, said method comprising administering to said subject a dose of tiragolumab of about 600 mg every 3 weeks; atezolizumab at a dose of about 1200 mg weekly;
(a)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) cisplatin at a dose of about 75 mg/m2 every 3 weeks and,
(b)
(i) pemetrexed at a dose of about 500 mg/m2 every 3 weeks, or gemcitabine at a dose of about 1000 mg/m2 or about 1250 mg/m2 on
176.肺がんを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、チラゴルマブ、アテゾリズマブ、白金系化学療法剤及び非白金系化学療法剤の1回以上の投薬サイクルを前記対象に投与することを含み、少なくとも1つの前記投薬サイクルが、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブと、(b)3週間ごとの約1200mgの用量のアテゾリズマブと、(c)前記白金系化学療法剤であって、(i)3週間ごとに5mg/mL/分のAUC又は6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は(ii)3週間ごとの約75mg/m2の用量のシスプラチンである、前記白金系化学療法剤と、(d)前記非白金系化学療法剤であって、(i)3週間ごとの500mg/m2、又は各投薬サイクルの1日目及び8日目に1000mg/m2若しくは1250mg/m2の用量のペメトレキセド、又は(ii)3週間ごとの100mg/m2、175mg/m2若しくは200mg/m2の用量のパクリタキセルである非白金系化学療法剤と、を投与することを含み、前記処置がネオアジュバント処置である、使用。
176. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising one or more of tiragolumab, atezolizumab, a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent wherein at least one of said dosing cycles administers to said subject (a) a dose of tiragolumab of about 600 mg every 3 weeks; and (b) a dose of about 1200 mg every 3 weeks of (c) said platinum-based chemotherapeutic agent, (i) at a dose aimed at achieving an AUC of 5 mg/mL/min or an AUC of 6 mg/mL/min every 3 weeks; (ii) cisplatin at a dose of about 75 mg/m every 3 weeks; and (d) the non-platinum-based chemotherapeutic agent, wherein (i) every 3 weeks Pemetrexed at doses of 500 mg/m2, or 1000 mg/m2 or 1250 mg/m2 on
177.非扁平上皮NSCLCを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(a)前記投薬サイクルの少なくとも1つが、ネオアジュバント処置として、3週間ごとの約600mgの用量のチラゴルマブ及び3週間ごとの1200mgの用量のアテゾリズマブを前記対象に投与することを含み、(b)前投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量の前記アテゾリズマブを投与することを含む、使用。 177. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with non-squamous NSCLC, said method administering to said subject one or more dosing cycles of tiragolumab and atezolizumab (a) at least one of said dosing cycles administering to said subject a dose of about 600 mg of tiragolumab every 3 weeks and a dose of 1200 mg of atezolizumab every 3 weeks as neoadjuvant treatment; (b) use wherein at least one of the premedication cycles comprises administering to said subject a dose of about 600 mg of tiragolumab every three weeks and a dose of about 1200 mg of said atezolizumab every three weeks as an adjuvant treatment.
178.非扁平上皮NSCLCを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ;(b)ネオアジュバント処置として3週間ごとの約1200mgの用量のアテゾリズマブ;(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセド;(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2又は約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドを投与することを含み、(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストを投与すること、含む、使用。 178. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with non-squamous NSCLC, said method administering to said subject one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is neoadjuvant treatment, and said subject is administered (a) tiragolumab at a dose of about 600 mg every 3 weeks; (b) every 3 weeks as neoadjuvant treatment (c)(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks, and pemetrexed at a dose of about 500 mg/m every 3 weeks (ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii) administering cisplatin at a dose of about 75 mg/m2 every 3 weeks and pemetrexed at a dose of about 500 mg/m2 every 3 weeks; and (II) at least one of said dosing cycles as adjuvant treatment; administering an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks to use .
179.肺がんを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブを投与することを含む、使用。
179. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is neoadjuvant treatment, and said subject receives (a) tiragolumab at a dose of about 600 mg every 3 weeks; atezolizumab at a dose of 1200 mg, (c)(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks, and approximately 1000 mg on
180.肺がんを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、
(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、
(a)3週間ごとの約1200mgの用量のチラゴルマブと、
(b)ネオアジュバント処置として3週間ごとの約1200mgの用量のアテゾリズマブと、
(c)
(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの第1日及び第8日に約1000mg/m2の用量のゲムシタビン、
(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は
(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの1日目及び8日目に約1250mg/m2の用量のゲムシタビンとを投与することを含み、
(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、前記対象に、3週間ごとの約300mgと約800mgの間の用量のチラゴルマブ、及び3週間ごとの約900mgと約1500mgの間の用量のアテゾリズマブを投与することを含む、使用。
180. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab ,
(I) at least one of said dosing cycles is a neoadjuvant treatment, wherein said subject comprises:
(a) tiragolumab at a dose of about 1200 mg every 3 weeks;
(b) atezolizumab at a dose of about 1200 mg every 3 weeks as a neoadjuvant treatment;
(c)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/m2 on
(ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/m2 or about 200 mg/m2 every 3 weeks, or (iii)3 administering a weekly dose of cisplatin of about 75 mg/m2 and a dose of gemcitabine of about 1250 mg/m2 on
(II) at least one of said dosing cycles comprises, as an adjuvant treatment, giving said subject tiragolumab at a dose of between about 300 mg and about 800 mg every three weeks and a dose of between about 900 mg and about 1500 mg every three weeks; Uses, including administering atezolizumab.
181.肺がんを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの訳600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブを投与することを含む、使用。
181. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is neoadjuvant treatment, and said subject receives (a) tiragolumab at a dose of about 600 mg every 3 weeks; atezolizumab at a dose of 1200 mg, (c)(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks, and approximately 1000 mg on
182.切除可能な扁平上皮NSCLCを有する対象を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象に、チラゴルマブ及びアテゾリズマブの1回以上の投薬サイクルを投与することを含み、(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、(a)3週間ごとの約600mgの用量のチラゴルマブ、(b)ネオアジュバント処置として、3週間ごとの約1200mgの用量のアテゾリズマブ、(c)(i)3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに各投薬サイクルの1日目及び8日目に約1000mg/m2の用量のゲムシタビン、(ii)3週間ごとの6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとの約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は(iii)3週間ごとの約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの第1日及び第8日に約1250mg/m2の用量のゲムシタビンを投与することを含み、(II)前記投薬サイクルの少なくとも1つは、アジュバント処置として、前記対象に、3週間ごとの訳600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブを投与することを含む、使用。
182. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject with resectable squamous NSCLC, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab (I) at least one of said dosing cycles is a neoadjuvant treatment, wherein said subject is administered (a) tiragolumab at a dose of about 600 mg every three weeks, (b) as neoadjuvant treatment, Atezolizumab at a dose of approximately 1200 mg every 3 weeks, (c)(i) Carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks, and
183.抗PD-L1抗体SP263による染色を含むIHCアッセイによって検出可能なPD-L1タンパク質発現レベルが決定される、実施形態136~182のいずれか一項に記載の使用。 183. 183. Use according to any one of embodiments 136-182, wherein the detectable PD-L1 protein expression level is determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP263.
184.前記検出可能なPD-L1タンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態183に記載の使用。 184. 184. Use according to embodiment 183, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 50% or more.
185.前記肺がんがNSCLCである、実施形態73、114~121、及び136~184のいずれか一項に記載の使用。
185. Use according to any one of
186.NSCLCが、扁平上皮NSCLCである、実施形態185に記載の使用。 186. 186. Use according to embodiment 185, wherein the NSCLC is squamous NSCLC.
187.NSCLCが、非扁平上皮NSCLCである、実施形態185に記載の使用。 187. 186. Use according to embodiment 185, wherein the NSCLC is non-squamous NSCLC.
188.前記がんが、子宮頸がんである、実施形態72に記載の使用。
188. 73. Use according to
189.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、使用。 189. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having cervical cancer with detectable PD-L1 expression levels, comprising: The method comprises one or more doses of an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks and a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks. A use comprising administering a cycle to said subject or population of subjects.
190.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、使用。 190. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having cervical cancer with detectable PD-L1 expression levels, comprising: The method comprises one or more dosings of an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every three weeks and a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every three weeks. A use comprising administering a cycle to said subject or population of subjects.
191.子宮頸がんを有する対象のための治療を選択する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、約30mgと約1200mgの間の用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び約80mgと約1600mgの間の用量で3週間ごとに投与されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む治療を選択すること、を含む、使用。
191. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting therapy for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - for said subject with an L1 expression level, an anti-TIGIT antagonist antibody administered every three weeks at a dose of between about 30 mg and about 1200 mg based on detected PD-L1 expression on tumor cells and about 80 mg and selecting a treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist administered every three weeks at a dose of between about 1600 mg.
192.前記子宮頸がんが扁平上皮癌腫、腺扁平上皮癌腫、又は腺癌である、実施形態189~191のいずれか一項に記載の使用。 192. 192. Use according to any one of embodiments 189-191, wherein said cervical cancer is squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma.
193.前記子宮頸がんがステージIVB、転移性、再発性又は持続性である、実施形態189~191のいずれか一項に記載の使用。 193. 192. Use according to any one of embodiments 189-191, wherein said cervical cancer is stage IVB, metastatic, recurrent or persistent.
194.前記子宮頸がんが転移性及び/又は再発性PD-L1陽性子宮頸癌腫である、実施形態189~193のいずれか一項に記載の使用。 194. 194. Use according to any one of embodiments 189-193, wherein said cervical cancer is metastatic and/or recurrent PD-L1 positive cervical carcinoma.
195.前記一又は複数の対象が、少なくとも1種類の事前治療を受けたことがある、実施形態189~194のいずれか一項に記載の使用。 195. 195. Use according to any one of embodiments 189-194, wherein said one or more subjects have received at least one prior treatment.
196.前記一又は複数の対象が、2種類の事前治療を受けたことがある、実施形態189~195のいずれか一項に記載の使用。 196. 196. Use according to any one of embodiments 189-195, wherein said one or more subjects have received two prior treatments.
197.前記一又は複数の対象が、3種類以上の事前治療を受けたことがない、実施形態189~196のいずれか一項に記載の使用。 197. 197. Use according to any one of embodiments 189-196, wherein said one or more subjects have not received 3 or more prior treatments.
198.前記一又は複数の対象が事前治療を受けたことがない、実施形態189~194のいずれか一項に記載の使用。 198. 195. Use according to any one of embodiments 189-194, wherein said one or more subjects have no prior treatment.
199.前記事前治療が、化学療法、外科手術及び/又は放射線療法である、実施形態195~198のいずれか一項に記載の使用。 199. 199. Use according to any one of embodiments 195-198, wherein said prior treatment is chemotherapy, surgery and/or radiotherapy.
200.前記処置が臨床応答をもたらす、実施形態189及び192~199のいずれか一項に記載の使用。 200. Use according to any one of embodiments 189 and 192-199, wherein said treatment results in a clinical response.
201.前記臨床応答が、基準客観的奏効率(ORR)と比較した前記対象集団のORRの増加である、実施形態200に記載の使用。
201. 201. Use according to
202.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態201に記載の使用。 202. 202. Use according to embodiment 201, wherein said reference ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
203.前記基準ORRが、少なくとも約14.6%~約26%である、実施形態200に記載の使用。
203. 201. Use according to
204.前記臨床応答がCR又はPRである、実施形態200に記載の使用。
204. 201. Use according to
205.前記臨床応答が、基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象のOS時間の増加である、実施形態200~204のいずれか一項に記載の使用。 205. wherein said clinical response is increased in said subject's PFS time compared to baseline progression-free survival (PFS), increased in said subject's DOR time compared to baseline duration of response (DOR), or baseline overall survival (OS) 205. Use according to any one of embodiments 200-204, which is an increase in OS time for the subjects compared.
206.実施形態205の使用であって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
使用。
206. The use of embodiment 205, comprising:
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
use.
207.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用であって、前記方法が、3週間ごとの600mgの用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを前記対象に投与することを含む、使用。 207. Use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method for treating a subject with cervical cancer with detectable PD-L1 expression levels, said method comprising: every 3 weeks A use comprising administering to said subject one or more dosing cycles of a dose of 600 mg of an anti-TIGIT antagonist antibody and one or more dosing cycles of a dose of atezolizumab of 1200 mg every three weeks.
208.抗TIGITアンタゴニスト抗体及びアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い子宮頸がんを有する対象を同定する方法のための医薬品の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、及び
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、を含む、使用。
209.子宮頸がんを有する対象のための治療を選択する方法のための医薬品の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与される抗TIGITアンタゴニスト抗体及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、使用。
208. Use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of identifying subjects with cervical cancer who are likely to benefit from treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody and atezolizumab wherein the method comprises
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (c) PD-L1 expression on detected tumor cells. based on the likely benefit from treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. Uses, including identifying a subject.
209. Use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of selecting therapy for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Anti-TIGIT antagonist antibody administered at a dose of 600 mg every 3 weeks and a dose of 1200 mg every 3 weeks based on PD-L1 expression on detected tumor cells for said subject with L1 expression level selecting a treatment comprising one or more dosing cycles of atezolizumab administered.
210.検出可能なPD-L1発現レベルを伴う子宮頸がんを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、使用。 210. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject with cervical cancer with detectable PD-L1 expression levels, said method comprising administering to said subject one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
211.子宮頸がんを有する対象を処置する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、使用。
211. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with cervical cancer, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) based on detected PD-L1 expression on tumor cells, one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks. and (d) administering said treatment to said identified subject.
212.子宮頸がんを有する対象のための治療を選択する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、使用。
212. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting treatment for a subject with cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks for said subjects with L1 expression levels based on detected PD-L1 expression on tumor cells selecting a treatment comprising one or more dosing cycles of
213.転移性及び/又は再発性子宮頸がんを有する対象を処置する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)前記同定された対象に前記治療を投与することを含む、使用。
213. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with metastatic and/or recurrent cervical cancer, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) one or more dosing cycles of tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks based on detected PD-L1 expression on tumor cells; and (d) administering said treatment to said identified subject.
214.転移性及び/又は再発性子宮頸がんを有する対象のための治療を選択する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、3週間ごとに600mgの用量で投与されるチラゴルマブ及び3週間ごとに1200mgの用量で投与されるアテゾリズマブの1回以上の投薬サイクルを含む治療を選択すること、を含む、使用。
214. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting treatment for a subject with metastatic and/or recurrent cervical cancer, said method comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - Tiragolumab administered at a dose of 600 mg every 3 weeks and atezolizumab administered at a dose of 1200 mg every 3 weeks for said subjects with L1 expression levels based on detected PD-L1 expression on tumor cells selecting a treatment comprising one or more dosing cycles of
215.前記対象が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態189~214のいずれか一項に記載の使用。 215. 215. Use according to any one of embodiments 189-214, wherein said subject is identified as likely to benefit from said treatment based on detected PD-Ll expression on tumor cells.
216.PD-L1発現レベルが抗PD-L1抗体SP263を使用して検出される、実施形態189~215のいずれか一項に記載の使用。 216. Use according to any one of embodiments 189-215, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody SP263.
217.前記検出可能なPD-L1発現レベルが、前記対象からの試料において5%以上の腫瘍関連免疫細胞(TIC)である、実施形態189~216のいずれか一項に記載の使用。 217. 217. Use according to any one of embodiments 189-216, wherein said detectable PD-L1 expression level is 5% or more tumor-associated immune cells (TIC) in a sample from said subject.
218.PD-L1発現レベルが抗PD-L1抗体22C3を使用して検出される、実施形態189~215のいずれか一項に記載の使用。 218. Use according to any one of embodiments 189-215, wherein the PD-L1 expression level is detected using the anti-PD-L1 antibody 22C3.
219.前記検出可能なPD-L1発現レベルが、前記対象からの試料において1以上の複合陽性スコア(CPS)である、実施形態189~216のいずれか一項に記載の使用。 219. 217. Use according to any one of embodiments 189-216, wherein said detectable PD-L1 expression level is a composite positive score (CPS) of 1 or more in a sample from said subject.
220.前記がんが乳がんである、実施形態72に記載の使用。
220. 73. Use according to
221.乳がんを有する対象又は対象集団を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、4週間ごとの約840mgの用量のチラゴルマブ、4週間ごとの約1680mgの用量のアテゾリズマブ、及び3週間の投薬/1週間の休薬で約100mg/m2の用量のnab-パクリタキセルの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。 221. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population having breast cancer, comprising tiragolumab at a dose of about 840 mg every 4 weeks, atezolizumab at a dose of about 1680 mg every 4 weeks, and administering to said subject or population of subjects a dosing regimen comprising one or more dosing cycles of nab-paclitaxel at a dose of about 100 mg/m2 with 3 weeks on/1 week off.
222.前記乳がんがトリプルネガティブ乳がん(TNBC)である、実施形態220又は221に記載の使用。 222. 222. Use according to embodiment 220 or 221, wherein said breast cancer is triple negative breast cancer (TNBC).
223.前記TNBCが、切除不能な局所進行性又は転移性TNBCである、実施形態222に記載の使用。 223. 223. Use according to embodiment 222, wherein said TNBC is unresectable locally advanced or metastatic TNBC.
224.前記対象が転移性乳がんのための事前全身治療を受けたことがない、実施形態220~223のいずれか一項に記載の使用。 224. 224. Use according to any one of embodiments 220-223, wherein said subject has no prior systemic therapy for metastatic breast cancer.
225.前記処置が、少なくとも約53%~約67.5%の対象集団のORRをもたらす、実施形態220~224のいずれか一項に記載の使用。 225. 225. Use according to any one of embodiments 220-224, wherein said treatment results in an ORR of the subject population of at least about 53% to about 67.5%.
226.前記処置が、約25.0ヵ月の前記対象集団のOS中央値をもたらす、実施形態222~225のいずれか一項に記載の使用。 226. 226. Use according to any one of embodiments 222-225, wherein said treatment results in a median OS for said subject population of about 25.0 months.
227.初期トリプルネガティブ乳がん(eTNBC)を有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約10mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び2週間ごとの約20mg~約1600mgの用量のPD-1軸結合アンタゴニストを含む1回以上の投薬サイクルを含む投薬レジメンを前記対象に投与することを含む、使用。 227. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with early triple negative breast cancer (eTNBC), said method comprising from about 10 mg to about administering to said subject a dosing regimen comprising a dose of 1000 mg of an anti-TIGIT antagonist antibody and one or more dosing cycles comprising a dose of about 20 mg to about 1600 mg of a PD-1 axis binding antagonist every two weeks; use.
228.前記方法が、1つ以上の化学療法剤を前記対象に更に投与することを含む、実施形態227に記載の使用。 228. 228. Use according to embodiment 227, wherein said method further comprises administering to said subject one or more chemotherapeutic agents.
229.前記1つ以上の化学療法剤が、白金系化学療法剤、タキサン、トポイソメラーゼII阻害剤又はアルキル化剤である、実施形態228に記載の使用。 229. 229. Use according to embodiment 228, wherein said one or more chemotherapeutic agents is a platinum-based chemotherapeutic agent, a taxane, a topoisomerase II inhibitor, or an alkylating agent.
230.前記方法が、(a)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、タキサンと、又はタキサン及び白金系化学療法剤との1回以上の投薬サイクル、並びに(b)前記抗TIGITアンタゴニスト抗体と、前記PD-1軸結合アンタゴニストと、トポイソメラーゼII阻害剤と、アルキル化剤と、顆粒球コロニー刺激因子(G-CSF)又は顆粒球マクロファージコロニー刺激因子(GM-CSF)との1回以上の投薬サイクル、を投与することを更に含む、実施形態227に記載の使用。 230. The method comprises (a) one or more dosing cycles of the anti-TIGIT antagonist antibody, the PD-1 axis binding antagonist, a taxane, or a taxane and a platinum-based chemotherapeutic agent, and (b) the anti-TIGIT One dose of an antagonist antibody, said PD-1 axis binding antagonist, a topoisomerase II inhibitor, an alkylating agent, and granulocyte colony-stimulating factor (G-CSF) or granulocyte-macrophage colony-stimulating factor (GM-CSF) 228. Use according to embodiment 227, further comprising administering the above dosing cycle.
231.前記アルキル化剤がシクロホスファミドである、実施形態229又は230に記載の使用。 231. 231. Use according to embodiment 229 or 230, wherein said alkylating agent is cyclophosphamide.
232.前記シクロホスファミドが約600mg/m2の用量で投与される、実施形態231に記載の使用。 232. 232. Use according to embodiment 231, wherein said cyclophosphamide is administered at a dose of about 600 mg/m2.
233.前記使用が、G-CSF又はGM-CSFを前記対象に更に投与することを含む、実施形態227~229、231、及び232のいずれか一項に記載の使用。 233. The use of any one of embodiments 227-229, 231, and 232, wherein said use further comprises administering G-CSF or GM-CSF to said subject.
234.前記G-CSFがペグフィルグラスチム又はフィルグラスチムである、実施形態230又は233に記載の使用。 234. 234. Use according to embodiment 230 or 233, wherein said G-CSF is pegfilgrastim or filgrastim.
235.前記G-CSFがペグフィルグラスチムである、実施形態234に記載の使用。 235. 235. Use according to embodiment 234, wherein said G-CSF is pegfilgrastim.
236.前記ペグフィルグラスチムが約6mgの用量で投与される、実施形態235に記載の使用。 236. 236. Use according to embodiment 235, wherein said pegfilgrastim is administered at a dose of about 6 mg.
237.前記方法が、前記1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFの1つ以上の後続用量を前記対象に更に投与することを含む、実施形態228、229、及び231~236のいずれか一項に記載の使用。 237. Embodiments 228, 229, and 231-236, wherein said method further comprises administering said one or more chemotherapeutic agents and/or one or more subsequent doses of G-CSF or GM-CSF to said subject Use according to any one of
238.前記1つ以上の化学療法剤及び/又はG-CSF若しくはGM-CSFがそれぞれ、週に1回、2週間に1回、又は3週間に1回投与される、実施形態228、229、及び231~237のいずれか一項に記載の使用。 238. Embodiments 228, 229, and 231, wherein said one or more chemotherapeutic agents and/or G-CSF or GM-CSF are administered once weekly, once every two weeks, or once every three weeks, respectively 237. Use according to any one of clauses 1-237.
239.前記白金系化学療法剤が3週間ごとに投与され、前記タキサンが毎週投与され、前記トポイソメラーゼII阻害剤が2週間ごとに投与され、前記アルキル化剤が2週間ごとに投与され、前記G-CSF又はGM-CSFが2週間ごとに投与される、実施形態229~238のいずれか一項に記載の使用。 239. The platinum-based chemotherapeutic agent is administered every three weeks, the taxane is administered weekly, the topoisomerase II inhibitor is administered every two weeks, the alkylating agent is administered every two weeks, and the G-CSF Or the use according to any one of embodiments 229-238, wherein GM-CSF is administered every two weeks.
240.前記タキサン、又は前記タキサン及び前記白金系化学療法剤が、前記投薬レジメンの最初の12週間投与される、実施形態229~239のいずれか一項に記載の使用。 240. 239. Use according to any one of embodiments 229-239, wherein said taxane, or said taxane and said platinum-based chemotherapeutic agent are administered for the first 12 weeks of said dosing regimen.
241.前記トポイソメラーゼII阻害剤、前記アルキル化剤、及び前記G-CSF又はGM-CSFが、前記投薬レジメンの第13週~第19週の間投与される、実施形態229~240いずれか一項に記載の使用。
241. 240. Any one of embodiments 229-240, wherein the topoisomerase II inhibitor, the alkylating agent, and the G-CSF or GM-CSF are administered during
242.前記投薬レジメンの全長が19週間である、実施形態227~241のいずれか一項に記載の使用。 242. 242. Use according to any one of embodiments 227-241, wherein the total length of said dosing regimen is 19 weeks.
243.前記方法がネオアジュバント処置である、実施形態227~242のいずれか一項に記載の使用。 243. Use according to any one of embodiments 227-242, wherein said method is neoadjuvant treatment.
244.前記投薬レジメンに続いて手術が行われる、実施形態227~243のいずれか一項に記載の使用。 244. 244. Use according to any one of embodiments 227-243, wherein said dosing regimen is followed by surgery.
245.前記手術が、前記投薬レジメンの最後の投与後2週間と6週間の間に行われる、実施形態244に記載の使用。 245. 245. Use according to embodiment 244, wherein said surgery is performed between 2 and 6 weeks after the last administration of said dosing regimen.
246.前記手術が乳房切除術を含む、実施形態244又は245に記載の使用。 246. 246. Use according to embodiment 244 or 245, wherein said surgery comprises a mastectomy.
247.前記手術が腋窩リンパ節手術を含む、実施形態244~246のいずれか一項に記載の使用。 247. 247. Use according to any one of embodiments 244-246, wherein said surgery comprises axillary lymph node surgery.
248.前記トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の使用。 248. 248. Use according to any one of embodiments 229-247, wherein said topoisomerase II inhibitor is doxorubicin.
249.前記タキサンがnab-パクリタキセルであり、前記白金系化学療法剤がカルボプラチンであり、前記トポイソメラーゼII阻害剤がドキソルビシンである、実施形態229~247のいずれか一項に記載の使用。 249. 248. Use according to any one of embodiments 229-247, wherein the taxane is nab-paclitaxel, the platinum-based chemotherapeutic agent is carboplatin, and the topoisomerase II inhibitor is doxorubicin.
250.ドキソルビシンが約60mg/m2の用量で投与される、実施形態248又は249に記載の使用。 250. Use according to embodiment 248 or 249, wherein doxorubicin is administered at a dose of about 60 mg/m2.
251.eTNBCを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のPD-1軸結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
251. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering anti-TIGIT at a dose of about 300 mg to about 600 mg every two weeks. an antagonist antibody and a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
252.eTNBCを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のPD-L1結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
252. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering anti-TIGIT at a dose of about 300 mg to about 600 mg every two weeks. an antagonist antibody and a PD-L1 binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
253.eTNBCを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量の抗PD-L1アンタゴニスト抗体と、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
253. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering anti-TIGIT at a dose of about 300 mg to about 600 mg every two weeks. an antagonist antibody and an anti-PD-L1 antagonist antibody at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
254.eTNBCを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のPD-1軸結合アンタゴニストと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
254. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering anti-TIGIT at a dose of about 300 mg to about 600 mg every two weeks. an antagonist antibody and a PD-1 axis binding antagonist at a dose of about 600 mg to about 1200 mg every two weeks;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
255.eTNBCを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びアテゾリズマブの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量の抗TIGITアンタゴニスト抗体と、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量の白金剤、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)前記投薬レジメンの最初の12週間にわたって、毎週の約125mg/m2の用量のタキサン、並びに
(ii)前記投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のトポイソメラーゼII阻害剤、2週間ごとの約600mg/m2の用量のアルキル化剤、及び2週間ごとのG-CSF又はGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
255. 1. Use of an anti-TIGIT antagonist antibody and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising: anti-TIGIT antagonist antibody at a dose of about 300 mg to about 600 mg every two weeks; atezolizumab at a weekly dose of about 600 mg to about 1200 mg;
(a)
(i) a taxane at a dose of about 125 mg/m2 weekly over the first 12 weeks of said dosing regimen and a platinum agent at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; (ii) a topoisomerase II inhibitor at a dose of about 60 mg/m2 every 2 weeks, an alkylating agent at a dose of about 600 mg/m2 every 2 weeks, and for 2 weeks over
(i) a taxane at a dose of about 125 mg/m2 weekly for the first 12 weeks of said dosing regimen; a topoisomerase II inhibitor at a dose, an alkylating agent at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
256.eTNBCを有する対象を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、2週間ごとの約300mg~約600mgの用量のチラゴルマブと、2週間ごとの約600mg~約1200mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
256. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering tiragolumab at a dose of about 300 mg to about 600 mg every 2 weeks and about 600 mg to about 600 mg every 2 weeks. atezolizumab at a dose of about 1200 mg;
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
257.eTNBCを有する対象を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、2週間ごとの約420mgの用量のチラゴルマブと、2週間ごとの約840mgの用量のアテゾリズマブと、
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、
とを含む投薬レジメンを前記対象に投与することを含み、前記方法が、前記投薬レジメンの最後の投薬の2週間後と6週間後の間の手術を更に含む、使用。
257. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with eTNBC, said method comprising administering tiragolumab at a dose of about 420 mg every two weeks and atezolizumab at a dose of about 840 mg every two weeks. and,
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m every week for the first 12 weeks of said dosing regimen and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks; ii) doxorubicin at a dose of about 60 mg/m every 2 weeks, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G- every 2 weeks for
(i) nab-paclitaxel at a dose of about 125 mg/m2 weekly for the first 12 weeks of the dosing regimen, and (ii) a dose of about 60 mg/m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin, cyclophosphamide at a dose of about 600 mg/m every 2 weeks, and G-CSF or GM-CSF every 2 weeks;
and wherein the method further comprises surgery between 2 weeks and 6 weeks after the last dose of the dosing regimen.
258.前記対象からの腫瘍試料中の検出可能なPD-L1タンパク質発現レベルが、抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される、実施形態220~257のいずれか一項に記載の使用。 258. Use according to any one of embodiments 220-257, wherein the detectable PD-L1 protein expression level in a tumor sample from said subject is determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142. .
259.前記腫瘍試料中のPD-L1発現腫瘍浸潤免疫細胞(IC)が占める腫瘍面積の割合が1%以上である、実施形態258に記載の使用。 259. 259. Use according to embodiment 258, wherein the percentage of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (IC) in said tumor sample is 1% or more.
260.前記eTNBCが、提示時にT2-4d TNBCである、実施形態227~259のいずれか一項に記載の使用。 260. 259. Use according to any one of embodiments 227-259, wherein said eTNBC is T2-4d TNBC when presented.
261.前記eTNBCが、提示時にcT2-cT4、cN0-cN3、及びcM0 TNBCである、実施形態227~260のいずれか一項に記載の使用。 261. 261. The use according to any one of embodiments 227-260, wherein said eTNBC are cT2-cT4, cN0-cN3, and cM0 TNBC when presented.
262.前記対象が以前にeTNBCの処置を受けたことがない、実施形態227~261のいずれか一項に記載の使用。 262. 262. Use according to any one of embodiments 227-261, wherein said subject has not previously been treated for eTNBC.
263.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態227~262のいずれか一項に記載の使用。 263. 263. Use according to any one of embodiments 227-262, wherein said treatment results in a pathological complete response (pCR).
264.前記処置が、全生存期間(OS)又は無症候生存期間(EFS)の増加をもたらす、実施形態227~263のいずれか一項に記載の使用。 264. 264. Use according to any one of embodiments 227-263, wherein said treatment results in increased overall survival (OS) or symptom-free survival (EFS).
265.前記がんが頭頸部がんである、実施形態72に記載の使用。
265. 73. Use according to
266.前記頭頸部がんが頭頸部の扁平上皮癌腫(SCCHN)である、実施形態265に記載の使用。 266. 266. Use according to embodiment 265, wherein said head and neck cancer is squamous cell carcinoma of the head and neck (SCCHN).
267.検出可能なPD-L1発現レベルを伴うnSCCHNを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、使用。 267. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or subject population having nSCCHN with detectable PD-L1 expression levels, said method comprising , an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks, and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks. Use, including administering to a subject or population of subjects.
268.検出可能なPD-L1発現レベルを伴うnSCCHNを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、使用。 268. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject or subject population having nSCCHN with detectable PD-L1 expression levels, said method comprising , an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every 3 weeks, and a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every 3 weeks. Use, including administering to a subject or population of subjects.
269.SCCHNを有する対象又は対象集団に対する治療を選択する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象又は対象集団について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む使用。
269. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting therapy for a subject or subject population with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg every 3 weeks, based on detected PD-L1 expression, for said subject or subject population having levels of selecting a treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 1200 mg.
270.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、使用。 270. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having SCCHN with detectable PD-L1 expression levels, said method comprising administering to said subject or population of subjects one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
271.前記一又は複数の対象から得られた腫瘍試料が、検出可能なPD-L1発現レベルを有すると判定されている、実施形態267~270のいずれか一項に記載の使用。 271. 271. Use according to any one of embodiments 267-270, wherein the tumor sample obtained from said one or more subjects has been determined to have a detectable level of PD-Ll expression.
272.前記SSCHNがヒトパピローマウイルス(HPV)陽性である、実施形態266~271いずれか一項に記載の使用。 272. 272. Use according to any one of embodiments 266-271, wherein said SSCHN is human papillomavirus (HPV) positive.
273.前記SSCHNがHPV陰性である、実施形態266~272のいずれか一項に記載の使用。 273. 273. Use according to any one of embodiments 266-272, wherein said SSCHN is HPV negative.
274.HPVの状態が、p16 IHC、in situハイブリダイゼーション又はPCRによって判定される、実施形態272又は273に記載の使用。 274. 274. Use according to embodiment 272 or 273, wherein HPV status is determined by p16 IHC, in situ hybridization or PCR.
275.前記SCCHNが、再発性及び/又は転移性SCCHNである、実施形態266~274ずれか一項に記載の使用。 275. 275. Use according to any one of embodiments 266-274, wherein said SCCHN is recurrent and/or metastatic SCCHN.
276.前記一又は複数の対象が事前治療を受けたことがない、実施形態265~275のいずれか一項に記載の使用。 276. 276. Use according to any one of embodiments 265-275, wherein said one or more subjects have no prior treatment.
277.前記事前治療が、再発性及び/又は転移性疾患のための事前全身治療である、実施形態276に記載の使用。 277. 277. Use according to embodiment 276, wherein said prior treatment is prior systemic treatment for recurrent and/or metastatic disease.
278.前記処置がCR又はPRをもたらす、実施形態265~268及び270~277のいずれか一項に記載の使用。 278. Use according to any one of embodiments 265-268 and 270-277, wherein said treatment results in CR or PR.
279.前記処置が、基準客観的奏効率(ORR)と比較して前記対象集団のORRの増加をもたらす、実施形態265~268及び270~277のいずれか一項に記載の使用。 279. Use according to any one of embodiments 265-268 and 270-277, wherein said treatment results in an increase in ORR in said subject population compared to a baseline objective response rate (ORR).
280.前記基準ORRが、抗TIGITアンタゴニスト抗体を用いない、PD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のORR中央値である、実施形態279に記載の使用。 280. 280. Use according to embodiment 279, wherein said reference ORR is the median ORR of a subject population that has undergone treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
281.前記基準ORRが約19%~約36%である、実施形態279又は280に記載の使用。 281. 281. Use according to embodiment 279 or 280, wherein said baseline ORR is from about 19% to about 36%.
282.前記処置が、基準無増悪生存期間(PFS)と比較した前記対象又は対象集団のPFS時間の増加、基準奏効期間(DOR)と比較した前記対象又は対象集団のDOR時間の増加、又は基準全生存期間(OS)と比較した前記対象又は対象集団のOS時間の増加をもたらす、実施形態265~268及び270~281のいずれか一項に記載の使用。 282. wherein said treatment increases PFS time of said subject or subject population compared to baseline progression-free survival (PFS), increases DOR time of said subject or subject population compared to baseline duration of response (DOR), or baseline overall survival Use according to any one of embodiments 265-268 and 270-281, which results in an increase in OS time of said subject or subject population compared to duration (OS).
283.実施形態282に記載の使用であって、
(a)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のPFS時間の中央値である、
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
使用。
283. 283. The use according to embodiment 282, wherein:
(a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment containing a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
use.
284.前記基準DOR時間が、少なくとも約6.7ヶ月~約23.4ヶ月である、実施形態282に記載の使用。 284. 283. Use according to embodiment 282, wherein the baseline DOR time is from at least about 6.7 months to about 23.4 months.
285.前記基準OS時間が、少なくとも約11.6ヶ月~約14.9ヶ月である、実施形態282に記載の使用。 285. 283. Use according to embodiment 282, wherein the baseline OS time is from at least about 11.6 months to about 14.9 months.
286.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、使用。 286. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising: administering to said subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks and an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks. use, including
287.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、使用。 287. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising: administering to said subject one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every three weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every three weeks.
288.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-L1結合アンタゴニストの使用であって、前記方法が、3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを前記対象に投与することを含む、使用。 288. Use of an anti-TIGIT antagonist antibody and a PD-L1 binding antagonist in the manufacture of a medicament for a method for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising: every 3 weeks administering to said subject one or more dosing cycles of a PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg of and an anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg every three weeks including, use.
289.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象に、3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを投与することを含む、使用。 289. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising: administering one or more dosing cycles of atezolizumab at a dose between about 80 mg and about 1600 mg every 3 weeks and tiragolumab at a dose between about 30 mg and about 1200 mg every 3 weeks.
290.検出可能なPD-L1発現レベルを伴うSCCHNを有する対象を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、使用。 290. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for treating a subject having SCCHN with detectable PD-L1 expression levels, said method comprising: administering one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks.
291.SCCHNを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、使用。
291. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) one or more dosing cycles of a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable PD-L1 expression level.
292.SCCHNを有する対象を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、使用。
292. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) may benefit from treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable level of PD-L1 expression.
293.SCCHNを有する対象を処置する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、使用。
293. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) potential to benefit from treatment comprising one or more dosing cycles of atezolizumab at doses between about 80 mg and about 1600 mg every 3 weeks and tiragolumab at doses between about 30 mg and about 1200 mg every 3 weeks; and (d) administering said treatment to said identified subject having a detectable level of PD-L1 expression.
294.SCCHNを有する対象を処置する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)前記対象から腫瘍試料を取得すること;
(b)染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、
(c)3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象を同定すること、並びに
(d)検出可能なPD-L1発現レベルを有する前記同定された対象に前記治療を投与することを含む、使用。
294. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject with SCCHN, said method comprising:
(a) obtaining a tumor sample from said subject;
(b) detecting the protein expression level of PD-L1 in said tumor sample by an IHC assay using an anti-PD-L1 antibody suitable for staining;
(c) identifying subjects likely to benefit from treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks; (d) a use comprising administering said treatment to said identified subject having a detectable PD-L1 expression level.
295.SCCHNを有する対象のための治療を選択する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む使用。
295. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks, and about 30 mg and about 1200 mg every 3 weeks, based on detected PD-L1 expression, for said subjects with levels of selecting a treatment comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at an intermediate dose.
296.SCCHNを有する対象のための治療を選択する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約600mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療を選択すること、を含む使用。
296. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. 1 of a PD-1 axis binding antagonist at a dose of about 1200 mg every 3 weeks and an anti-TIGIT antagonist antibody at a dose of about 600 mg every 3 weeks, based on detected PD-L1 expression, for said subjects with levels of Selecting a treatment that includes one or more dosing cycles.
297.SCCHNを有する対象のための治療を選択する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブ、及び3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含む使用。
297. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. atezolizumab at doses between about 80 mg and about 1600 mg every 3 weeks, and tiragolumab at doses between about 30 mg and about 1200 mg every 3 weeks, for said subjects with levels of selecting a treatment comprising one or more dosing cycles of
298.SCCHNを有する対象のための治療を選択する方法のための医薬品の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出されたPD-L1発現に基づいて、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約600mgの用量のチラゴルマブの1回以上の投薬サイクルを含む治療を選択すること、を含む使用。
298. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of selecting therapy for a subject with SCCHN, said method comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD-L1 expression. treatment comprising one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks and tiragolumab at a dose of about 600 mg every 3 weeks based on detected PD-L1 expression for said subject with a level use, including selecting
299.前記検出可能なPD-L1発現レベルが、抗PD-L1抗体SP263で染色することを含む免疫組織化学(IHC)アッセイによって決定される検出可能なPD-L1タンパク質発現レベルである、実施形態267~298のずれか一項に記載の使用。 299. Embodiment 267- wherein said detectable PD-L1 expression level is a detectable PD-L1 protein expression level determined by an immunohistochemistry (IHC) assay comprising staining with anti-PD-L1 antibody SP263 298. Use according to any one of clauses 298-298.
300.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中、
(a)5%以上、
(b)5%以上20%未満、又は
(c)20%以上
の腫瘍関連免疫細胞(TIC)である、実施形態299に記載の使用。
300. the detectable PD-L1 protein expression level in the tumor sample is
(a) 5% or more;
299. Use according to embodiment 299, wherein (b) 5% or more and less than 20%, or (c) 20% or more tumor-associated immune cells (TIC).
301.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法のための医薬製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 301. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying subjects likely to benefit from a treatment comprising a dosing cycle, said method comprising an anti-TIGIT antibody suitable for staining. determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using a PD-L1 antibody, wherein a PD-L1 protein expression level of 5% or more TIC indicates said subject. A use that identifies a likely person to benefit from said treatment.
302.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法のための医薬製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、5%以上かつ20%未満のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 302. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying subjects likely to benefit from a treatment comprising a dosing cycle, said method comprising an anti-TIGIT antibody suitable for staining. determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using a PD-L1 antibody, wherein the protein expression level of PD-L1 of 5% or more and less than 20% of the TIC is , identifying said subject as likely to benefit from said treatment.
303.SCCHNを有する対象を、3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療から利益を得る可能性が高い対象として同定する方法のための医薬製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、染色に適した抗PD-L1抗体を使用するIHCアッセイによって前記対象からの腫瘍試料中のPD-L1のタンパク質発現レベルを決定することを含み、20%以上のTICのPD-L1のタンパク質発現レベルが、前記対象を前記治療から利益を得る可能性が高いと同定する、使用。 303. Subjects with SCCHN were given one or more doses of a PD-1 axis binding antagonist at doses between about 80 mg and about 1600 mg every 3 weeks, anti-TIGIT antagonist antibodies at doses between about 30 mg and about 1200 mg every 3 weeks. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of identifying subjects likely to benefit from a treatment comprising a dosing cycle, said method comprising an anti-TIGIT antibody suitable for staining. determining the protein expression level of PD-L1 in a tumor sample from said subject by an IHC assay using a PD-L1 antibody, wherein 20% or more of said PD-L1 protein expression level of TIC indicates said subject. A use that identifies a likely person to benefit from said treatment.
304.前記対象が治療から利益を得る可能性が高いと同定され、前記方法が、前記対象に治療を投与することを更に含む、実施形態301~303のいずれか一項に記載の使用。 304. 304. Use according to any one of embodiments 301-303, wherein said subject is identified as likely to benefit from treatment and said method further comprises administering treatment to said subject.
305.前記TICが、Ventana SP263 IHCアッセイを使用して決定される、実施形態301~304のいずれか一項に記載の使用。 305. 305. Use according to any one of embodiments 301-304, wherein said TIC is determined using the Ventana SP263 IHC assay.
306.前記対象又は対象集団が、検出された腫瘍細胞上のPD-L1発現に基づく前記処置から利益を得る可能性が高いものとして同定される、実施形態267~305のいずれか一項に記載の使用。 306. Use according to any one of embodiments 267-305, wherein said subject or subject population is identified as likely to benefit from said treatment based on detected PD-L1 expression on tumor cells. .
307.前記がんが肝臓がんである、実施形態72に記載の使用。
307. 73. Use according to
308.前記肝臓がんが肝細胞癌腫(HCC)である、実施形態307に記載の使用。 308. 308. Use according to embodiment 307, wherein said liver cancer is hepatocellular carcinoma (HCC).
309.肝細胞癌腫(HCC)を有する対象又は対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記対象又は対象集団に抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象又は対象集団がHCCの事前全身治療を受けたことがない、使用。 309. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population having hepatocellular carcinoma (HCC), wherein said subject or subject population is treated with the anti-TIGIT antagonist antibody and administering one or more dosing cycles of a PD-1 axis binding antagonist, wherein said subject or population of subjects has no prior systemic treatment for HCC.
310.前記対象又は対象集団にVEGFアンタゴニストを投与する工程を更に含む、実施形態309に記載の使用。 310. 309. Use according to embodiment 309, further comprising administering to said subject or population of subjects a VEGF antagonist.
311.HCCを有する対象又は対象集団を処置する方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用抗TIGITアンタゴニスト抗体、PD-1軸結合アンタゴニスト、及びVEGFアンタゴニストの1回以上の投薬サイクルを前記対象又は対象集団に投与することを含む、使用。 311. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population with HCC One or more of an anti-TIGIT antagonist antibody, a PD-1 axis binding antagonist, and a VEGF antagonist to said subject or population of subjects.
312.前記VEGFアンタゴニストが、3週間ごとの約5mg/kg~約25mg/kgの用量で投与される、実施形態310及び311に記載の使用。 312. Use according to embodiments 310 and 311, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg to about 25 mg/kg every three weeks.
313.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約1200mgの用量で投与される、実施形態309~312のいずれか一項に記載の使用。 313. 313. Use according to any one of embodiments 309-312, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 1200 mg every three weeks.
314.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約800mgの用量で投与される、実施形態313に記載の使用。 314. 314. Use according to embodiment 313, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 30 mg to about 800 mg every three weeks.
315.前記抗TIGITアンタゴニスト抗体が、3週間ごとの約30mg~約600mgの固定用量で投与される、実施形態309~314のいずれか一項に記載の使用。 315. 315. Use according to any one of embodiments 309-314, wherein said anti-TIGIT antagonist antibody is administered at a fixed dose of about 30 mg to about 600 mg every three weeks.
316.前記PD-1軸結合アンタゴニストが、3週間ごとの約80mg~約1600mgの用量で投与される、実施形態309~315のいずれか一項に記載の使用。 316. 316. Use according to any one of embodiments 309-315, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 1600 mg every three weeks.
317.前記PD-1軸結合アンタゴニストが、3週間ごとの約900mg~約1500mgの用量で投与される、実施形態309~316のいずれか一項に記載の使用。 317. 317. Use according to any one of embodiments 309-316, wherein said PD-1 axis binding antagonist is administered at a dose of about 900 mg to about 1500 mg every three weeks.
318.前記VEGFアンタゴニストが、2週間ごとの約1mg/kg~約20mg/kgの用量で投与される、実施形態310又は311に記載の使用。 318. Use according to embodiment 310 or 311, wherein said VEGF antagonist is administered at a dose of about 1 mg/kg to about 20 mg/kg every two weeks.
319.前記VEGFアンタゴニストが、2週間ごとの約5mg/kg~約10mg/kgの用量で投与される、実施形態318に記載の使用。 319. 319. Use according to embodiment 318, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg to about 10 mg/kg every two weeks.
320.前記VEGFアンタゴニストが、2週間ごとの約5mg/kg、約7.5mg/kg又は約10.0mg/kgの用量で投与される、実施形態319に記載の使用。 320. 320. Use according to embodiment 319, wherein said VEGF antagonist is administered at a dose of about 5 mg/kg, about 7.5 mg/kg or about 10.0 mg/kg every two weeks.
321.前記抗TIGITアンタゴニスト抗体が、2週間ごとの約10mg~約1000mgの用量で投与される、実施形態309~311及び318~320のいずれか一項に記載の使用。 321. The use of any one of embodiments 309-311 and 318-320, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 10 mg to about 1000 mg every two weeks.
322.前記PD-1軸結合アンタゴニストが、2週間ごとの約20mg~約1600mgの用量で投与される、実施形態309~311及び318~321のいずれか一項に記載の使用。 322. Use according to any one of embodiments 309-311 and 318-321, wherein said PD-1 axis binding antagonist is administered at a dose of about 20 mg to about 1600 mg every two weeks.
323.前記抗TIGITアンタゴニスト抗体が、4週間ごとの約200mg~約2000mgの用量で投与される、実施形態309~311に記載の使用。 323. Use according to embodiments 309-311, wherein said anti-TIGIT antagonist antibody is administered at a dose of about 200 mg to about 2000 mg every 4 weeks.
324.前記PD-1軸結合アンタゴニストが、4週間ごとの約80mg~約2000mgの用量で投与される、実施形態309~311及び323のいずれか一項に記載の使用。 324. Use according to any one of embodiments 309-311 and 323, wherein said PD-1 axis binding antagonist is administered at a dose of about 80 mg to about 2000 mg every 4 weeks.
325.前記PD-1軸結合アンタゴニストが、4週間ごとの約1400mg~約2000mgの用量で投与される、実施形態309~311、323、及び324のいずれか一項に記載の使用。 325. The use of any one of embodiments 309-311, 323, and 324, wherein said PD-1 axis binding antagonist is administered at a dose of about 1400 mg to about 2000 mg every 4 weeks.
326.前記HCCが局所進行性又は転移性HCCである、実施形態309~325のいずれか一項に記載の使用。 326. 326. Use according to any one of embodiments 309-325, wherein said HCC is locally advanced or metastatic HCC.
327.前記HCCが切除不能なHCCである、実施形態309~326のいずれか一項に記載の使用。 327. 327. Use according to any one of embodiments 309-326, wherein said HCC is unresectable HCC.
328.前記一又は複数の対象が、適切な肝機能を有すると判定されている、実施形態309~327のいずれか一項に記載の使用。 328. 328. Use according to any one of embodiments 309-327, wherein said one or more subjects have been determined to have adequate liver function.
329.前記適切な肝機能がChild-PughクラスAとして特徴付けられる、実施形態328に記載の使用。 329. 329. Use according to embodiment 328, wherein said adequate liver function is characterized as Child-Pugh class A.
330.前記一又は複数の対象から得られたHCC腫瘍試料が、検出可能なPD-L1発現レベルを有すると判定されている、実施形態309~329のいずれか一項に記載の使用。 330. 329. Use according to any one of embodiments 309-329, wherein the HCC tumor sample obtained from said one or more subjects has been determined to have a detectable PD-L1 expression level.
331.前記方法が、前記対象又は対象集団に少なくとも4回の投薬サイクルを投与することを含む、実施形態309~330のいずれか一項に記載の使用。 331. 331. Use according to any one of embodiments 309-330, wherein said method comprises administering to said subject or subject population at least four dosing cycles.
332.前記対象又は対象集団に少なくとも16回の投薬サイクルを投与することを含む、実施形態331に記載の使用。 332. 332. Use according to embodiment 331, comprising administering at least 16 dosing cycles to said subject or population of subjects.
333.HCCを有する対象又は対象集団を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約15mg/kgの用量のベバシズマブの1回以上の投薬サイクルを前記対象に投与することを含む、使用。 333. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population with HCC, said method comprising administering tiragolumab at a dose of about 600 mg every 3 weeks, a dose of about 1200 mg every 3 weeks and one or more dosing cycles of bevacizumab at a dose of about 15 mg/kg every 3 weeks to said subject.
334.前記一又は複数の対象が、HCCに対する以前の全身処置を受けたことがない、実施形態311~333のいずれか一項に記載の使用。 334. 334. Use according to any one of embodiments 311-333, wherein said one or more subjects have no prior systemic treatment for HCC.
335.前記処置が、少なくとも約5.6ヶ月~少なくとも約6.83ヶ月の前記対象集団のPFS中央値をもたらす、実施形態309~334のいずれか一項に記載の使用。 335. 335. Use according to any one of embodiments 309-334, wherein said treatment results in a median PFS of said subject population of at least about 5.6 months to at least about 6.83 months.
336.前記がんが膀胱がんである、実施形態72に記載の使用。
336. 73. Use according to
337.前記膀胱がんが筋層浸潤性膀胱がん(MIBC)である、実施形態336に記載の使用。 337. 337. Use according to embodiment 336, wherein said bladder cancer is muscle invasive bladder cancer (MIBC).
338.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象が白金系化学療法剤による処置に不適格である、使用。 338. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks. wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
339.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象が白金系化学療法剤による処置に不適格である、使用。 339. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every 3 weeks. wherein said subject is ineligible for treatment with a platinum-based chemotherapeutic agent.
340.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、使用。 340. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks. A use, including, wherein said treatment is a perioperative treatment.
341.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、方法。 341. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg every 3 weeks and a PD-1 axis binding antagonist at a dose of between about 900 mg and about 1500 mg every 3 weeks. wherein said treatment is a perioperative treatment.
342.前記一又は複数の対象が60mL/分未満のクレアチニンクリアランスを有する、実施形態338~341に記載の使用。 342. Use according to embodiments 338-341, wherein said one or more subjects have a creatinine clearance of less than 60 mL/min.
343.前記一又は複数の対象が、グレード2以上の難聴を有する、実施形態338~342のいずれか一項に記載の使用
343. 343. Use according to any one of embodiments 338-342, wherein said one or more subjects have a hearing loss of
344.前記一又は複数の対象がグレード2以上の神経障害を有する、実施形態338~343のいずれか一項に記載の使用。
344. 344. Use according to any one of embodiments 338-343, wherein said one or more subjects have
345.前記一又は複数の対象が白金系化学療法剤による処置を拒否した、実施形態338~344のいずれか一項に記載の使用。 345. 345. Use according to any one of embodiments 338-344, wherein said one or more subjects have refused treatment with a platinum-based chemotherapeutic agent.
346.前記白金系化学療法剤がシスプラチンである、実施形態338又は342~345のいずれか一項に記載の使用。 346. Use according to any one of embodiments 338 or 342-345, wherein said platinum-based chemotherapeutic agent is cisplatin.
347.前記MIBCが外科的に操作可能である、実施形態338~346のいずれか一項に記載の使用。 347. 347. Use according to any one of embodiments 338-346, wherein said MIBC is surgically manipulable.
348.前記方法が手術を更に含む、実施形態347に記載の使用。 348. 348. Use according to embodiment 347, wherein said method further comprises surgery.
349.少なくとも1つの投薬サイクルが前記手術の前に開始される、実施形態348に記載の使用。 349. 349. Use according to embodiment 348, wherein at least one dosing cycle is initiated prior to said surgery.
350.少なくとも1、2、又は3回の投薬サイクルが前記手術の前に完了する、実施形態348又は349に記載の使用。 350. 349. Use according to embodiment 348 or 349, wherein at least 1, 2, or 3 dosing cycles are completed prior to said surgery.
351.少なくとも1回の投薬サイクルが、前記手術後4週間と6週間の間に開始される、実施形態348~350のいずれか一項に記載の使用。 351. 351. Use according to any one of embodiments 348-350, wherein at least one dosing cycle is initiated between 4 and 6 weeks after said surgery.
352.1~17回の投薬サイクルが前記手術後に完了する、実施形態351に記載の使用。 352. Use according to embodiment 351, wherein 1-17 dosing cycles are completed after said surgery.
353.前記手術が膀胱切除術及び/又はリンパ節郭清術である、実施形態348~352いずれか一項に記載の使用。 353. 353. Use according to any one of embodiments 348-352, wherein said surgery is cystectomy and/or lymphadenectomy.
354.前記処置が病理学的完全奏効(pCR)をもたらす、実施形態338~353のいずれか一項に記載の使用。 354. 354. Use according to any one of embodiments 338-353, wherein said treatment results in a pathological complete response (pCR).
355.前記処置が、基準無再発生存期間(RFS)と比較した前記一又は複数の対象のRFS時間の増加、基準無症候生存期間(EFS)と比較した前記一又は複数の対象のEFS時間の増加、又はOSと比較した前記一又は複数の対象のOS時間の増加をもたらす、実施形態338~354のいずれか一項に記載の使用。
356.実施形態355に記載の使用であって、
(a)前記基準RFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のRFS時間の中央値である、
(b)前記基準EFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のEFS時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
使用。
355. said treatment increases RFS time of said one or more subjects compared to baseline recurrence-free survival (RFS); increases EFS time of said one or more subjects compared to baseline disease-free survival (EFS); 355. Use according to any one of embodiments 338-354, resulting in an increase in OS time of said one or more subjects compared to OS.
356. 356. The use according to embodiment 355, comprising:
(a) said baseline RFS time is the median RFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline EFS time is the median EFS time of a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment containing a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
use.
357.前記処置が病理的進展度の低下をもたらす、実施形態338~356のいずれか一項に記載の使用。 357. 357. Use according to any one of embodiments 338-356, wherein said treatment results in a reduction in pathological extent.
358.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、使用。 358. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks. and wherein said subject is cisplatin ineligible.
359.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、使用。 359. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-1 axis binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks. A use, including, wherein said treatment is a perioperative treatment.
360.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、使用。 360. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks , use wherein said subject is cisplatin ineligible.
361.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、使用。 361. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population for 3 weeks administering one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every three weeks and a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg every three weeks , the use wherein said treatment is a perioperative treatment.
362.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記対象がシスプラチン不適格である、使用。 362. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population about 30 mg and about 1200 mg every three weeks tiragolumab at a dose of between and one or more dosing cycles of atezolizumab at a dose of about 80 mg and about 1600 mg every 3 weeks, wherein said subject is cisplatin ineligible.
363.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、使用。 363. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population about 30 mg and about 1200 mg every three weeks and one or more dosing cycles of between about 80 mg and about 1600 mg of atezolizumab every three weeks, wherein said treatment is perioperative treatment.
364.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であってであって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記一又は複数の対象がシスプラチン不適格である、使用。 364. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population about 600 mg every 3 weeks A dose of tiragolumab and one or more dosing cycles of atezolizumab at a dose of about 1200 mg every three weeks, wherein said one or more subjects are cisplatin ineligible.
365.MIBCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であってであって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含み、前記処置が周術期処置である、使用。 365. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or subject population with MIBC, said method comprising administering to said subject or subject population about 600 mg every 3 weeks A dose of tiragolumab and one or more dosing cycles of a dose of atezolizumab of about 1200 mg every three weeks, wherein said treatment is perioperative treatment.
366.前記処置が、少なくとも約13.4%~約15%の対象集団のORRをもたらす、実施形態338~365のいずれか一項に記載の使用。 366. 366. Use according to any one of embodiments 338-365, wherein said treatment results in an ORR of the subject population of at least about 13.4% to about 15%.
367.前記処置が、少なくとも約7.9ヶ月~約8.6ヶ月の対象集団のOS中央値をもたらす、実施形態338~366のいずれか一項に記載の使用。 367. 367. Use according to any one of embodiments 338-366, wherein said treatment results in a median OS for the subject population of at least about 7.9 months to about 8.6 months.
368.抗PD-L1抗体SP142による染色を含むIHCアッセイによって検出可能なPD-L1タンパク質発現レベルが決定される、実施形態338~367のいずれか一項に記載の使用。 368. Use according to any one of embodiments 338-367, wherein detectable PD-L1 protein expression levels are determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142.
369.前記検出可能なPD-L1タンパク質発現レベルが、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合が5%以上であるPD-L1陽性腫瘍細胞分率である、実施形態368に記載の使用。 369. Embodiment 368, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction in which 5% or more of the tumor area is occupied by PD-L1-expressing tumor-infiltrating immune cells (ICs) Use as described.
370.膀胱がんが尿路上皮癌腫(UC)である、実施形態336に記載の使用。 370. 337. Use according to embodiment 336, wherein the bladder cancer is urothelial carcinoma (UC).
371.前記UCが転移性尿路上皮癌腫(mUC)である、実施形態370に記載の使用。 371. 371. Use according to embodiment 370, wherein said UC is metastatic urothelial carcinoma (mUC).
372.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。 372. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising about 30 mg and about 1200 mg every 3 weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks to said subject or population of subjects. use, including
373.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。 373. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising about 300 mg and about 800 mg every 3 weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 900 mg and about 1500 mg every three weeks to said subject or population of subjects. use, including
374.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記対象が事前のがん免疫療法を受けたことがない、使用。 374. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising about 30 mg and about 1200 mg every 3 weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks to said subject or population of subjects. and wherein said subject has no prior cancer immunotherapy.
375.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記処置が第二選択処置である使用。 375. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising about 30 mg and about 1200 mg every 3 weeks and one or more dosing cycles of a PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks to said subject or population of subjects. and wherein said treatment is a second line treatment.
376.前記一又は複数の対象が事前のがん免疫療法を受けたことがない、実施形態372、372及び375に記載の使用。 376. Use according to embodiments 372, 372 and 375, wherein said one or more subjects have not received prior cancer immunotherapy.
377.前記処置が第二選択処置である、実施形態372~374のいずれか一項に記載の使用。 377. 375. Use according to any one of embodiments 372-374, wherein said treatment is a second line treatment.
378.前記mUCが、白金含有療法の間又は後に進行した、実施形態372~377のいずれか一項に記載の使用。 378. 378. Use according to any one of embodiments 372-377, wherein said mUC progressed during or after platinum-containing therapy.
379.前記一又は複数の対象が疾患進行性又は許容できない毒性を経験した後、第2の投薬レジメンを前記対象又は対象集団に投与することを更に含む、実施形態372~378のいずれか一項に記載の使用。 379. 379. According to any one of embodiments 372-378, further comprising administering a second dosing regimen to said subject or population of subjects after said one or more subjects experience disease progression or unacceptable toxicity. Use of.
380.前記第2の投薬レジメンが、PD-1軸結合アンタゴニスト、及び抗体-薬物コンジュゲート(ADC)の1回以上の投薬サイクルを含む、実施形態379に記載の使用。 380. 379. Use according to embodiment 379, wherein said second dosing regimen comprises one or more dosing cycles of a PD-1 axis binding antagonist and an antibody-drug conjugate (ADC).
381.前記ADCが、(a)エンフォルツマブベドチン又は(b)サクツズマブゴビテカンである、実施形態380に記載の使用。 381. 381. Use according to embodiment 380, wherein said ADC is (a) enfortumab vedotin or (b) suctuzumab govitecan.
382.(a)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(b)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与される、実施形態381に記載の使用。 382. (a) enfortumab vedotin administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (b) sactuzumab govitecan administered at 2 382. Use according to embodiment 381, administered at a dose of 10 mg/kg weekly for weekly on/weekly off.
383.(a)エンフォルツマブベドチンが1.25mg/kgの用量で各21日間サイクルの1日目及び8日目に投与されるか、又は(b)サクツズマブゴビテカンが10mg/kgの用量で各21日間サイクルの1日目及び8日目に投与される、実施形態381又は382に記載の使用。
383. (a) enfortumab vedotin at a dose of 1.25 mg/kg on
384.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。 384. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising about 30 mg and about 1200 mg every 3 weeks and one or more dosing cycles of a PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg every 3 weeks to said subject or population of subjects. use, including
385.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であってであって、前記方法が、前記対象又は対象集団に、3週間ごとの約30mgと約1200mgの間の用量のチラゴルマブ、及び3週間ごとの約80mgと約1600mgの間の用量のアテゾリズマブの1回以上の投薬サイクルを含む投薬レジメンを投与することを含む、使用。 385. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising administering to said subject or subject population about 30 mg every 3 weeks A use comprising administering a dosing regimen comprising one or more dosing cycles of tiragolumab at a dose of between about 1200 mg and atezolizumab at a dose of between about 80 mg and about 1600 mg every three weeks.
386.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、3週間ごとの約600mgの用量のチラゴルマブ、及び3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを投与することを含む、使用。 386. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with mUC, said method comprising administering to said subject or subject population for 3 weeks administration of one or more dosing cycles of tiragolumab at a dose of about 600 mg every three weeks and atezolizumab at a dose of about 1200 mg every three weeks.
387.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約80mgと約1600mgの間の用量の前記PD-1軸結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象又は対象集団が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象又は対象集団に投与される、使用。
387. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having mUC, comprising administering to said subject or subject population a first dosing regimen and administering a subsequent second dosing regimen;
(a) said first dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks and PD-1 axis binding at a dose of between about 80 mg and about 1600 mg every 3 weeks; comprising one or more dosing cycles of the antagonist;
(b) said second dosing regimen comprises one or more dosing cycles of said PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks; (i) enfortumab vedotin; is administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off, or (ii) suctuzumab govitecan is administered for 2 weeks on/1 week off administered at a dose of 10 mg/kg weekly during drug administration, wherein said second dosing regimen is administered to said subject or subject after said subject or subject population experiences disease progression or unacceptable toxicity during said first dosing regimen; A use administered to a target population.
388.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び3週間ごとの約80mgと約1600mgの間の用量のPD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約80mgと約1600mgの間の用量の前記PD-L1結合アンタゴニストの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、使用。
388. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having mUC, comprising administering to said subject or subject population a first dosing regimen and administering a subsequent second dosing regimen;
(a) said first dosing regimen comprises an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg every 3 weeks and a PD-L1 binding antagonist at a dose of between about 80 mg and about 1600 mg every 3 weeks; comprising one or more dosing cycles of
(b) said second dosing regimen comprises one or more dosing cycles of said PD-L1 binding antagonist at a dose between about 80 mg and about 1600 mg every three weeks; , 2 weeks on/1 week off, or (ii) suctuzumab govitecan administered at a dose of 1.25 mg/kg weekly for 2 weeks on/1 week off and the second dosing regimen is administered to the subject after the subject experiences disease progression or unacceptable toxicity during the first dosing regimen. use.
389.mUCを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記対象又は対象集団に第1の投薬レジメンとそれに続く第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、3週間ごとの約600mgの用量のチラゴルマブ及び約3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約1200用量のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間の投薬/1週間の休薬の間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サクツズマブゴビテカンが、2週間の投薬/1週間の休薬の間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象が前記第1の投薬レジメン中に疾患進行性又は許容できない毒性を経験した後に前記対象に投与される、使用。
389. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or population of subjects with mUC, wherein said subject or population of subjects is administered a first dosing regimen followed by a second dosing regimen including doing
(a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of 1200 mg about every 3 weeks;
(b) said second dosing regimen comprises one or more dosing cycles of about 1200 doses of atezolizumab every 3 weeks, and (i) enfortumab vedotin 2 weeks on/1 week off or (ii) suctuzumab govitecan administered at a dose of 10 mg/kg weekly for 2 weeks on/1 week off and wherein said second dosing regimen is administered to said subject after said subject experiences disease progression or unacceptable toxicity during said first dosing regimen.
390.前記処置が、少なくとも約13.4%~少なくとも約31%の対象集団のORRをもたらす、実施形態372~389のいずれか一項に記載の使用。 390. 389. Use according to any one of embodiments 372-389, wherein said treatment results in an ORR of the subject population of at least about 13.4% to at least about 31%.
391.前記処置が、約7.9ヶ月~約16.3ヶ月の対象集団のOS中央値をもたらす、実施形態372~390のいずれか一項に記載の使用。 391. 391. Use according to any one of embodiments 372-390, wherein said treatment results in a median OS for the subject population of about 7.9 months to about 16.3 months.
392.前記がんが膵臓がんである、実施形態72に記載の使用。
392. 73. Use according to
393.膵臓がんを有する対象又は対象集団を処置する方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、各28日間投薬サイクルの1日目及び15日目に約420mgの用量のチラゴルマブ、各28日間投薬サイクルの1及び15日目に約840mgの用量のアテゾリズマブ、各28日間投薬サイクルの1、8及び15日目に約1000mg/m2の用量のゲムシタビン、並びに各28日間投薬サイクルの1、8及び15日目に約125mg/m2の用量のnab-パクリタキセルの1回以上の28日間投薬サイクルを含む投薬レジメンを投与することを含む、使用。
393. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population having pancreatic cancer, said method comprising administering to said subject or subject population on
394.前記膵臓がんが膵管腺癌(PDAC)である、実施形態392又は393に記載の使用。 394. 394. Use according to embodiment 392 or 393, wherein said pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC).
395.前記PDACが転移性PDACである、実施形態394に記載の使用。 395. 395. Use according to embodiment 394, wherein said PDAC is a metastatic PDAC.
396.前記一又は複数の対象が転移性PDACに対する事前全身治療を受けたことがない、実施形態392~395のいずれか一項に記載の使用。 396. 396. Use according to any one of embodiments 392-395, wherein said one or more subjects have not received prior systemic therapy for metastatic PDAC.
397.前記処置が、少なくとも約41.7%~約46.7%の対象集団のORRをもたらす、実施形態392~396のいずれか一項に記載の使用。 397. 397. Use according to any one of embodiments 392-396, wherein said treatment results in an ORR of the subject population of at least about 41.7% to about 46.7%.
398.前記処置が、抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを用いないゲムシタビン及びnab-パクリタキセルを含む処置と比較して、少なくとも約20%のORRの増加をもたらす、実施形態392~397のいずれか一項に記載の使用。
398. Any of embodiments 392-397, wherein said treatment results in an increase in ORR of at least about 20% compared to treatment comprising gemcitabine and nab-paclitaxel without an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist Use as set forth in
399.前記処置が、少なくとも約5.5ヶ月~約7ヶ月の対象集団のPFS中央値をもたらす、実施形態392~398のいずれか一項に記載の使用。 399. Use according to any one of embodiments 392-398, wherein said treatment results in a median PFS for the subject population of at least about 5.5 months to about 7 months.
400.前記処置が、少なくとも約8.5ヶ月~約10.6ヶ月の対象集団のOS中央値をもたらす、実施形態392~399のいずれか一項に記載の使用。 400. 399. Use according to any one of embodiments 392-399, wherein said treatment results in a median OS for the subject population of at least about 8.5 months to about 10.6 months.
401.前記がんが食道がんである、実施形態72に記載の使用。
401. 73. Use according to
402.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。
402. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising: An anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
403.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含む、使用。
403. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method of treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising: anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
404.食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記対象が白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、使用。
404. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having esophageal cancer, said method comprising: one or more 21-day dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 30 mg and about 1200 mg on
405.食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、各投薬サイクルの1日目に約300mgと約800mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約900mgと約1500mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む投薬レジメンを前記対象又は対象集団に投与することを含み、前記対象が白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、使用。
405. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having esophageal cancer, said method comprising: one or more 21-day dosing cycles of an anti-TIGIT antagonist antibody at a dose of between about 300 mg and about 800 mg on
406.前記一又は複数の対象が、白金系化学療法剤及び非白金系化学療法剤で以前に処置されたことがある、実施形態402又は403に記載の使用。 406. 404. Use according to embodiment 402 or 403, wherein said one or more subjects have been previously treated with a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
407.前記一又は複数の対象が、以前の処置中に疾患進行性又は許容できない毒性を経験したことがある、実施形態404~406のいずれか一項に記載の使用。 407. 407. Use according to any one of embodiments 404-406, wherein said one or more subjects have experienced disease progression or unacceptable toxicity during prior treatment.
408.前記21日間の投薬サイクルが、白金系化学療法剤及び非白金系化学療法剤を更に含む、実施形態402又は403に記載の使用。 408. 404. Use according to embodiment 402 or 403, wherein said 21-day dosing cycle further comprises a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent.
409.前記白金系化学療法剤が、6回の投薬後に前記投薬レジメンから省略される、実施形態408に記載の使用。 409. 409. Use according to embodiment 408, wherein said platinum-based chemotherapeutic agent is omitted from said dosing regimen after 6 doses.
410.前記白金系化学療法剤がシスプラチンである、実施形態404~409のいずれか一項に記載の使用。 410. 409. Use according to any one of embodiments 404-409, wherein said platinum-based chemotherapeutic agent is cisplatin.
411.シスプラチンが、各投薬サイクルの1日目に約80mg/m2の用量で投与される、実施形態410に記載の使用。
411. 411. Use according to embodiment 410, wherein cisplatin is administered at a dose of about 80 mg/m2 on
412.前記非白金系化学療法剤が代謝拮抗剤である、実施形態404~411のいずれか一項に記載の使用。 412. Use according to any one of embodiments 404-411, wherein said non-platinum chemotherapeutic agent is an antimetabolite.
413.前記代謝拮抗剤が5-フルオロウラシルである、実施形態412に記載の使用。 413. 413. Use according to embodiment 412, wherein said antimetabolite is 5-fluorouracil.
414.5-フルオロウラシルを800mg/m2/24時間の用量で、各21日間サイクルの1~5日目に投与する、実施形態413に記載の使用。 414. Use according to embodiment 413, wherein 5-fluorouracil is administered at a dose of 800 mg/m2/24 hours on days 1-5 of each 21-day cycle.
415.前記食道がんが進行性又は転移性食道がんである、実施形態404~414のいずれか一項に記載の使用。 415. Use according to any one of embodiments 404-414, wherein said esophageal cancer is advanced or metastatic esophageal cancer.
416.前記一又は複数の対象が転移性食道がんの事前処置を受けたことがない、実施形態402、403、408及び409に記載の使用。 416. Use according to embodiments 402, 403, 408 and 409, wherein said one or more subjects have no prior treatment for metastatic esophageal cancer.
417.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニスト、各投薬サイクルの1日目に約80mg/m2の用量の白金系化学療法剤、及び各21日間サイクルの1~5日目に800mg/m2/24時間の用量の非白金系化学療法剤の1回以上の21日間投薬サイクルを含む投薬レジメンを対象又は対象集団に投与することを含み、前記白金系化学療法剤が6回の投薬後に前記投薬レジメンから省略される、使用。
417. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with advanced or metastatic esophageal cancer, comprising 1 day of each dosing cycle anti-TIGIT antagonist antibody at a dose between about 30 mg and about 1200 mg in the eye, PD-1 axis binding antagonist at a dose between about 80 mg and about 1600 mg on
418.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記方法が、前記対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量の抗TIGITアンタゴニスト抗体、各投薬サイクルの1日目に約1200mgの用量のPD-1軸結合アンタゴニスト、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に前記投薬レジメンからシスプラチンが省略される、方法。
418. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising: or to the subject population, anti-TIGIT antagonist antibody at a dose of about 600 mg on
419.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記方法が、前記対象又は対象集団に、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含む投薬レジメンを投与することを含み、6回の投薬後に前記投薬レジメンからシスプラチンが省略される、方法。
419. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method of treating a subject or subject population with advanced or metastatic esophageal cancer, said method comprising administering to said subject or subject population each dosing cycle tiragolumab at a dose of about 600 mg on
420.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、白金系化学療法剤及び非白金系化学療法剤の1回以上の21日間投薬サイクルを含み、前記白金系化学療法剤が6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、使用。
420. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having advanced or metastatic esophageal cancer, said subject or subject population comprising: administering a first dosing regimen and a second dosing regimen;
(a) the first dosing regimen comprises one or more 21-day dosing cycles of a platinum-based chemotherapeutic agent and a non-platinum-based chemotherapeutic agent, wherein the platinum-based chemotherapeutic agent is omitted from
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
421.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造における抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストの使用であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンは、各投薬サイクルの1日目に約80mg/m2の用量の白金系化学療法剤と、及び各21日間サイクルの1~5日目に800mg/m2/24時間の用量の非白金系化学療法剤の1回以上の21日間投薬サイクル含み、前記白金系化学療法剤が、6回の投薬後に前記投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約30mgと約1200mgの間の用量の抗TIGITアンタゴニスト抗体、及び各投薬サイクルの1日目に約80mgと約1600mgの間の用量のPD-1軸結合アンタゴニストの1回以上の21日間投薬サイクルを含む、使用。
422.進行性又は転移性食道がんを有する対象又は対象集団を処置するための方法のための医薬の製造におけるチラゴルマブ及びアテゾリズマブの使用であって、前記対象又は対象集団に第1の投薬レジメン及び第2の投薬レジメンを投与することを含み、
(a)前記第1の投薬レジメンが、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日間サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含み、6回の投薬後にシスプラチンが投薬レジメンから省略され、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブの1回以上の21日間投薬サイクルを含む、使用。
421. Use of an anti-TIGIT antagonist antibody and a PD-1 axis binding antagonist in the manufacture of a medicament for a method for treating a subject or subject population having advanced or metastatic esophageal cancer, said subject or subject population comprising: administering a first dosing regimen and a second dosing regimen;
(a) the first dosing regimen comprises a platinum-based chemotherapeutic agent at a dose of about 80 mg/m2 on
(b) said second dosing regimen comprises a dose of the anti-TIGIT antagonist antibody between about 30 mg and about 1200 mg on
422. Use of tiragolumab and atezolizumab in the manufacture of a medicament for a method for treating a subject or population of subjects with advanced or metastatic esophageal cancer, wherein said subject or population of subjects comprises a first dosing regimen and a second administering a dosing regimen of
(a) said first dosing regimen comprises cisplatin at a dose of about 80 mg/m2 on
(b) said second dosing regimen is one or more 21-day dosing cycles of tiragolumab at a dose of about 600 mg on
423.前記処置が、少なくとも約14%の対象集団のORRをもたらす、実施形態402~422のいずれか一項に記載の使用。 423. Use according to any one of embodiments 402-422, wherein said treatment results in an ORR of the subject population of at least about 14%.
424.前記抗TIGITアンタゴニスト抗体が、以下の超可変領域(HVR):
SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、を含む、実施形態47~423のいずれか一項に記載の使用。
424. The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6). .
425.前記抗TIGITアンタゴニスト抗体が、以下の軽鎖可変領域フレームワーク領域(FR):
DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、を更に含む、実施形態424に記載の使用。
425. The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
425. Use according to embodiment 424, further comprising FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10).
426.抗TIGITアンタゴニスト抗体が、以下の重鎖可変領域FR:
X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4、を更に含む、実施形態424に記載の方法。
426. The anti-TIGIT antagonist antibody has the following heavy chain variable region FRs:
FR-H1 comprising the amino acid sequence of X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11) (wherein X1 is E or Q);
FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
425. The method of embodiment 424, further comprising FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
427.X1がEである、実施形態426に記載の使用。 427. 427. The use according to embodiment 426, wherein X1 is E.
428.X1がQである、実施形態426に記載の使用。 428. 427. The use according to embodiment 426, wherein X1 is Q.
429.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態424~428のいずれか一項に記載の使用。
429. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 19; or (c) a VH domain according to (a) and (b) Use according to any one of embodiments 424-428, comprising a VL domain as described.
430.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17又は18のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~429のいずれか一項に記載の使用。
430. wherein said anti-TIGIT antagonist antibody:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
431.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号17のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、実施形態424~427、429及び430のいずれか一項に記載の使用。
431. wherein said anti-TIGIT antagonist antibody:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
432.前記抗TIGITアンタゴニスト抗体が:
(a)配列番号33のアミノ酸配列を含む重鎖;及び
(b)配列番号34のアミノ酸配列を含む軽鎖、
を含む、実施形態424~427及び429~431のいずれか一項に記載の使用。
432. wherein said anti-TIGIT antagonist antibody:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:33; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:34,
The use according to any one of embodiments 424-427 and 429-431, comprising
433.抗TIGITアンタゴニスト抗体がモノクローナル抗体である、実施形態424~432のいずれか一項に記載の使用。 433. Use according to any one of embodiments 424-432, wherein the anti-TIGIT antagonist antibody is a monoclonal antibody.
434.前記抗TIGITアンタゴニスト抗体がヒト抗体である、実施形態424~433のいずれか一項に記載の使用。 434. Use according to any one of embodiments 424-433, wherein said anti-TIGIT antagonist antibody is a human antibody.
435.抗TIGITアンタゴニスト抗体が完全長抗体である、実施形態424~434のいずれか一項に記載の使用。 435. Use according to any one of embodiments 424-434, wherein the anti-TIGIT antagonist antibody is a full length antibody.
436.抗TIGITアンタゴニスト抗体が、チラゴルマブである、実施形態424~427及び429~436のいずれか一項に記載の使用。 436. Use according to any one of embodiments 424-427 and 429-436, wherein the anti-TIGIT antagonist antibody is tiragolumab.
437.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチジリマブ、EOS084448、SGN-TGT、又はTJ-T6である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291,292,295,296、301~332、336~361、370~384、387,388、401~418、420,421、及び424~436のいずれか一項に記載の使用。 437. embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, wherein said anti-TIGIT antagonist antibody is tiragolumab, vivostolimab, etidilimab, EOS084448, SGN-TGT, or TJ-T6; 265 to 269, 286 to 288, 291, 292, 295, 296, 301 to 332, 336 to 361, 370 to 384, 387, 388, 401 to 418, 420, 421, and 424 to 436 Use as indicated.
438.前記抗TIGITアンタゴニスト抗体がインタクトなFc媒介エフェクター機能を有する、実施形態437に記載の使用。 438. 438. Use according to embodiment 437, wherein said anti-TIGIT antagonist antibody has intact Fc-mediated effector functions.
439.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を増強している、実施形態437又は438に記載の使用。 439. Use according to embodiment 437 or 438, wherein said anti-TIGIT antagonist antibody enhances Fc-mediated effector function.
440.前記抗TIGITアンタゴニスト抗体がSGN-TGTである、実施形態437~439のいずれか一項に記載の使用。 440. The use according to any one of embodiments 437-439, wherein said anti-TIGIT antagonist antibody is SGN-TGT.
441.前記抗TIGITアンタゴニスト抗体が、ドムバナリマブ、BMS-986207、ASP8374又はCOM902である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291,292,295,296、301~332、336~361、370~384、387,388、401~418、420及び421のいずれか一項に記載の使用。 441. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-288 wherein said anti-TIGIT antagonist antibody is domvanalimab, BMS-986207, ASP8374 or COM902 , 291, 292, 295, 296, 301-332, 336-361, 370-384, 387, 388, 401-418, 420 and 421.
442.前記抗TIGITアンタゴニスト抗体がFc媒介エフェクター機能を有しない、実施形態424~431及び441のいずれか一項に記載の使用。 442. Use according to any one of embodiments 424-431 and 441, wherein said anti-TIGIT antagonist antibody has no Fc-mediated effector functions.
443.抗TIGITアンタゴニスト抗体がIgGクラス抗体である、実施形態47~442のいずれか一つに記載の使用。 443. Use according to any one of embodiments 47-442, wherein the anti-TIGIT antagonist antibody is an IgG class antibody.
444.IgGクラス抗体がIgG1サブクラス抗体である、実施形態443に記載の使用。 444. Use according to embodiment 443, wherein the IgG class antibody is an IgG1 subclass antibody.
445.前記抗TIGITアンタゴニスト抗体が、チラゴルマブ、ビボストリマブ、エチグリマブ、EOS084448、SGN-TGT、TJ-T6、BGB-A1217、AB308、ドムバナリマブ又はBMS-986207である、実施形態444に記載の使用。 445. 445. Use according to embodiment 444, wherein said anti-TIGIT antagonist antibody is tiragolumab, vibostolimab, etiglimab, EOS084448, SGN-TGT, TJ-T6, BGB-A1217, AB308, domvanalimab or BMS-986207.
446.前記IgGクラス抗体がIgG4サブクラス抗体である、実施形態47~112、114~127、136~174、188~209、227~253、255、265~269、286~288、291、292、295、296、301~332、336~361、370~384、387,388、401~418、420及び421のいずれか一項に記載の使用。 446. Embodiments 47-112, 114-127, 136-174, 188-209, 227-253, 255, 265-269, 286-288, 291, 292, 295, 296, wherein said IgG class antibody is an IgG4 subclass antibody , 301-332, 336-361, 370-384, 387, 388, 401-418, 420 and 421.
447.前記抗TIGITアンタゴニスト抗体がASP8374又はCOM902である、実施形態446に記載の使用。 447. 447. Use according to embodiment 446, wherein said anti-TIGIT antagonist antibody is ASP8374 or COM902.
448.前記抗TIGITアンタゴニスト抗体が、Fab、ビス-Fab、Fab’、Fab’-SH、Fv、単鎖可変断片(scFv)及び(Fab’)2フラグメントからなる群から選択されるTIGITに結合する抗体フラグメントである、実施形態424~434のいずれか一項に記載の使用。 448. an antibody fragment wherein said anti-TIGIT antagonist antibody binds to TIGIT selected from the group consisting of Fab, bis-Fab, Fab', Fab'-SH, Fv, single chain variable fragment (scFv) and (Fab')2 fragment 435. Use according to any one of embodiments 424-434, wherein the
449.前記抗TIGITアンタゴニスト抗体が単一特異性抗体である、実施形態424~448のいずれか一項に記載の使用。 449. Use according to any one of embodiments 424-448, wherein said anti-TIGIT antagonist antibody is a monospecific antibody.
450.前記抗TIGITアンタゴニスト抗体が多重特異性抗体である、実施形態424~448のいずれか一項に記載の使用。 450. Use according to any one of embodiments 424-448, wherein said anti-TIGIT antagonist antibody is a multispecific antibody.
451.前記多重特異性抗体が二重特異性抗体である、実施形態450に記載の使用。 451. 451. Use according to embodiment 450, wherein said multispecific antibody is a bispecific antibody.
452.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニスト、PD-1結合アンタゴニスト、及びPD-L2結合アンタゴニストからなる群から選択される、実施形態424~451のいずれか一項に記載の使用。 452. 452. Use according to any one of embodiments 424-451, wherein said PD-1 axis binding antagonist is selected from the group consisting of a PD-L1 binding antagonist, a PD-1 binding antagonist, and a PD-L2 binding antagonist.
453.前記PD-1軸結合アンタゴニストが、PD-L1結合アンタゴニストである、実施形態452に記載の使用。 453. 453. Use according to embodiment 452, wherein said PD-1 axis binding antagonist is a PD-L1 binding antagonist.
454.前記PD-L1結合アンタゴニストが、PD-L1のそのリガンド結合パートナーのうちの1つ以上への結合を阻害する、実施形態453に記載の使用。 454. 454. Use according to embodiment 453, wherein said PD-Ll binding antagonist inhibits binding of PD-Ll to one or more of its ligand binding partners.
455.前記PD-L1結合アンタゴニストが、PD-L1の、PD-1、B7-1、又はPD-1及びB7-1の両方への結合を阻害する、実施形態454に記載の使用。 455. 455. Use according to embodiment 454, wherein said PD-L1 binding antagonist inhibits binding of PD-L1 to PD-1, B7-1, or both PD-1 and B7-1.
456.前記PD-L1結合アンタゴニストが抗PD-L1アンタゴニスト抗体である、実施形態453~455のいずれか一項に記載の使用。 456. Use according to any one of embodiments 453-455, wherein said PD-L1 binding antagonist is an anti-PD-L1 antagonist antibody.
457.前記抗PD-L1アンタゴニスト抗体が、アテゾリズマブ、MDX-1105、デュルバルマブ、アベルマブ、SHR-1316、CS1001、エンバホリマブ、TQB2450、ZKAB001、LP-002、CX-072、IMC-001、KL-A167、APL-502、コシベリマブ、ロダポリマブ、FAZ053、TG-1501、BGB-A333、BCD-135、AK-106、LDP、GR1405、HLX20、MSB2311、RC98、PDL-GEX、KD036、KY1003、YBL-007又はHS-636である、実施形態456に記載の使用。 457. The anti-PD-L1 antagonist antibody is atezolizumab, MDX-1105, durvalumab, avelumab, SHR-1316, CS1001, emvaforimab, TQB2450, ZKAB001, LP-002, CX-072, IMC-001, KL-A167, APL-502 , cosibelimab, rhodapolimab, FAZ053, TG-1501, BGB-A333, BCD-135, AK-106, LDP, GR1405, HLX20, MSB2311, RC98, PDL-GEX, KD036, KY1003, YBL-007 or HS-636 , embodiment 456.
458.抗PD-L1アンタゴニスト抗体がアテゾリズマブである、実施形態457に記載の使用。 458. Use according to embodiment 457, wherein the anti-PD-L1 antagonist antibody is atezolizumab.
459.前記抗PD-L1アンタゴニスト抗体が、以下のHVR:
GFTFSDSWIH(配列番号20)のアミノ酸配列を含むHVR-H1配列;
AWISPYGGSTYYADSVKG(配列番号21)のアミノ酸配列を含むHVR-H2配列;
RHWPGGFDY(配列番号22)のアミノ酸配列を含むHVR-H3配列;
RASQDVSTAVA(配列番号23)のアミノ酸配列を含むHVR-L1配列;
SASFLYS(配列番号24)のアミノ酸配列を含むHVR-L2配列;及び
QQYLYHPAT(配列番号25)のアミノ酸配列を含むHVR-L3配列
を含む、実施形態456に記載の方法。
459. The anti-PD-L1 antagonist antibody is a HVR that:
an HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
an HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
an HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
an HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
457. The method of embodiment 456, comprising an HVR-L2 sequence comprising the amino acid sequence of SASFLYS (SEQ ID NO:24); and a HVR-L3 sequence comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
460.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)配列番号26のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号27のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、実施形態459に記載の方法。
460. wherein said anti-PD-L1 antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or (c) a VH domain according to (a) and (b) 460. The method of embodiment 459, comprising the described VL domains.
461.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)配列番号26のアミノ酸配列を含むVHドメイン;及び
(b)配列番号27のアミノ酸配列を含むVLドメインを含む、
実施形態460に記載の方法。
461. wherein said anti-PD-L1 antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:27,
460. The method of embodiment 460.
462.前記抗PD-L1アンタゴニスト抗体が、以下:
(a)配列番号28のアミノ酸配列を含む重鎖;及び
(b)配列番号29のアミノ酸配列を含む軽鎖、
を含む、実施形態461に記載の方法。
462. wherein said anti-PD-L1 antagonist antibody is:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:28; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:29,
462. The method of embodiment 461, comprising
463.前記抗PD-L1アンタゴニスト抗体がモノクローナル抗体である、実施形態459~462のいずれか一項に記載の使用。 463. Use according to any one of embodiments 459-462, wherein said anti-PD-L1 antagonist antibody is a monoclonal antibody.
464.前記抗PD-L1アンタゴニスト抗体がヒト化抗体である、実施形態459~463のいずれか一項に記載の使用。 464. Use according to any one of embodiments 459-463, wherein said anti-PD-L1 antagonist antibody is a humanized antibody.
465.前記抗PD-L1アンタゴニスト抗体が完全長抗体である、実施形態463又は464に記載の使用。 465. Use according to embodiment 463 or 464, wherein said anti-PD-L1 antagonist antibody is a full length antibody.
466.前記抗PD-L1アンタゴニスト抗体が、Fab、Fab’、Fab’-SH、Fv、scFv及び(Fab’)2フラグメントからなる群から選択されるPD-L1に結合する抗体フラグメントである、実施形態459~464のいずれか一項に記載の使用。 466. Embodiment 459, wherein said anti-PD-Ll antagonist antibody is an antibody fragment that binds PD-Ll selected from the group consisting of Fab, Fab', Fab'-SH, Fv, scFv and (Fab')2 fragments. 464. Use according to any one of clauses 1-464.
467.前記抗PD-L1アンタゴニスト抗体がIgGクラス抗体である、実施形態459~465のいずれか一項に記載の使用。 467. Use according to any one of embodiments 459-465, wherein said anti-PD-L1 antagonist antibody is an IgG class antibody.
468.IgGクラス抗体がIgG1サブクラス抗体である、実施形態467に記載の使用。 468. 468. Use according to embodiment 467, wherein the IgG class antibody is an IgG1 subclass antibody.
469.前記PD-1軸結合アンタゴニストが、PD-1結合アンタゴニストである、実施形態452に記載の使用。 469. 453. Use according to embodiment 452, wherein said PD-1 axis binding antagonist is a PD-1 binding antagonist.
470.前記PD-1結合アンタゴニストが、PD-Lのそのリガンド結合パートナーのうちの1つ以上への結合を阻害する、実施形態469に記載の使用。 470. 469. Use according to embodiment 469, wherein said PD-1 binding antagonist inhibits binding of PD-L to one or more of its ligand binding partners.
471.前記PD-1結合アンタゴニストが、PD-1のPD-L1、PD-L2、又はPD-L1とPD-L2の両方への結合を阻害する、実施形態470に記載の使用。 471. 471. Use according to embodiment 470, wherein said PD-1 binding antagonist inhibits binding of PD-1 to PD-L1, PD-L2, or both PD-L1 and PD-L2.
472.前記PD-1結合アンタゴニストが抗PD-1アンタゴニスト抗体である、実施形態469~471のいずれか一項に記載の使用。 472. Use according to any one of embodiments 469-471, wherein said PD-1 binding antagonist is an anti-PD-1 antagonist antibody.
473.前記抗PD-1アンタゴニスト抗体が、ニボルマブ、ペンブロリズマブ、MEDI-0680、スパルタリズマブ、セミプリマブ、BGB-108、プロルゴリマブ、カンレリズマブ、シンチリマブ、チスレリズマブ、トリパリマブ、ドスタリマブ、レチファンリマブ、ササンリマブ、ペンプリマブ、CS1003、HLX10、SCT-I10A、ジンベレリマブ、バルスチリマブ、ゲノリムズマブ、BI754091、セトレリマブ、YBL-006、BAT1306、HX008、ブジカリマブ、AMG404、CX-188、JTX-4014、609A、Sym021、LZM009、F520、SG001、AM0001、ENUM 244C8、ENUM 388D4、STI-1110、AK-103又はhAb21である、実施形態472に記載の使用。 473. The anti-PD-1 antagonist antibody is nivolumab, pembrolizumab, MEDI-0680, spartalizumab, semiplimab, BGB-108, prorgolimab, canrelizumab, cintilimab, tislelizumab, tripalimab, dostarimab, retifantlimab, sasanlimab, penplimab, CS1003, HLX10, SCT - I10A, gimberelimab, valsutilimab, genolimuzumab, BI754091, cetrelimab, YBL-006, BAT1306, HX008, budicarimab, AMG404, CX-188, JTX-4014, 609A, Sym021, LZM009, F520, SG001, AM48ENUM38ENUM48ENUM40001 , STI-1110, AK-103 or hAb21.
474.前記PD-1結合アンタゴニストがFc融合タンパク質である、実施形態469~471のいずれか一項に記載の使用。 474. Use according to any one of embodiments 469-471, wherein said PD-1 binding antagonist is an Fc fusion protein.
475.Fc融合タンパク質がAMP-224である、実施形態474に記載の使用。 475. 475. Use according to embodiment 474, wherein the Fc fusion protein is AMP-224.
476.前記方法が、前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体を3週間ごとの約30mgと約1200mgの間の用量で投与することを含む、実施形態80~112、114~127及び309~312のいずれか一項に記載の使用。 476. of embodiments 80-112, 114-127 and 309-312, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or subject population at a dose of between about 30 mg and about 1200 mg every three weeks. Use according to any one of the paragraphs.
477.前記方法が、3週間ごとの約600mgの用量で前記抗TIGITアンタゴニスト抗体を前記対象に投与することを含む、実施形態51、54、60、62、63、65~67、80~112、114~127、136~140、169~174、189、191、267、269、286、288、291、295、301、302、303、313、315、338、340、358~361、372、384、387、388、402~404、417、420、421及び476のいずれか一項に記載の使用。
477.
478.前記方法が、以下の前記対象の体重に基づく段階的用量で前記抗TIGITアンタゴニスト抗体を対象又は対象集団に投与することを含む、実施形態51、54、60、62、63、65-67、80-112、114-127、136-140、169-174、189、191、267、269、286、288、291、295、301、302、303、309、313、315、338、340、358-361、372、384、387、388、402-404、417、420、421、及び476のいずれか一項に記載の使用:
(a)15kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとの約300mgの用量で投与される;
(b)15kg超40kg以下であり、前記抗TIGITアンタゴニスト抗体が、3週間ごとの約400mgの用量で投与される;又は
(c)40kgを超え、前記抗TIGITアンタゴニスト抗体は、3週間ごとの約600mgの用量で投与される。
478.
(a) is 15 kg or less and said anti-TIGIT antagonist antibody is administered at a dose of about 300 mg every 3 weeks;
(b) greater than 15 kg and less than or equal to 40 kg and said anti-TIGIT antagonist antibody is administered at a dose of about 400 mg every 3 weeks; or (c) greater than 40 kg and said anti-TIGIT antagonist antibody is administered at about It is administered at a dose of 600 mg.
479.前記方法が、前記抗TIGITアンタゴニスト抗体を、4週間ごとに約700mg~約1000mgの用量で前記対象又は対象集団に投与することを含む、実施形態47,48、77、78、82、及び83のいずれか一項に記載の使用。 479. of embodiments 47, 48, 77, 78, 82, and 83, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects at a dose of about 700 mg to about 1000 mg every four weeks. Use according to any one of the paragraphs.
480.前記方法が、前記抗TIGITアンタゴニスト抗体を4週間ごとの約840mgの用量で前記対象に投与することを含む、実施形態47、48、59、67,323、及び479のいずれか一項に記載の使用。
480. 479. The method of any one of
481.前記抗TIGITアンタゴニスト抗体を、前記対象又は対象集団に、2週間ごとの約300mg~約600mgの用量で投与することを含む、実施形態49、50、及び104のいずれか一項に記載の使用。
481. The use of any one of
482.前記方法が、前記対象に、2週間ごとの約420mgの用量で前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態49、50、227、251~253、255、及び481のいずれか一項に記載の使用。
482. Any one of
483.前記抗TIGITアンタゴニスト抗体の用量が固定用量である、実施形態47~482のいずれか一項に記載の使用。 483. Use according to any one of embodiments 47-482, wherein the dose of said anti-TIGIT antagonist antibody is a fixed dose.
484.前記方法が、前記対象又は対象集団に、3週間ごとの約900mgと約1500mgの間の用量の前記PD-1軸結合アンタゴニストを投与することを含む、実施形態54、62、63、65~67、80~109、及び27~2698のいずれか一項に記載の使用。
484.
485.前記方法が、前記対象に、3週間ごとの約1200mgの用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態54、60、62、63、65~67、80~112、114~127、136~140、169~172、189、191、267、269、286、288、291、295、301~303、309、311、313、315、338、340、358~361、372~375、384、387、388、402~405、417、420、421及び484のいずれか一項に記載の使用。
485.
486.前記方法が、前記対象又は対象集団に、4週間ごとの前記PD-1軸結合アンタゴニストを約1400mg~2000mgの用量で投与することを含む、実施形態47、50、80~109、及び324のいずれか一項に記載の使用。
486. Any of
487.前記方法が、前記対象に、4週間ごとの約1680mgの用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態47、50、59、67、324、及び479のいずれか一項に記載の使用。
487. Any one of
488.前記方法が、前記対象又は対象集団に、2週間ごとの約600mgと約1200mgの間の用量で前記PD-1軸結合アンタゴニストを投与することを含む、実施形態48、49、80~109、及び481のいずれか一項に記載の使用。 488. Embodiments 48, 49, 80-109, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects at a dose of between about 600 mg and about 1200 mg every two weeks, and 481. Use according to any one of clauses 481 to 481.
489.前記PD-1軸結合アンタゴニストを、前記対象に、2週間ごとの約840mgの用量で投与することを含む、実施形態48、49、80~109、227、251~253、及び481のいずれか一項に記載の使用。 489. Any one of embodiments 48, 49, 80-109, 227, 251-253, and 481, comprising administering said PD-1 axis binding antagonist to said subject at a dose of about 840 mg every two weeks. Use as described in section.
490.前記PD-1軸結合アンタゴニストの用量が固定用量である、実施形態47~489のいずれか一項に記載の使用。 490. 489. Use according to any one of embodiments 47-489, wherein the dose of said PD-1 axis binding antagonist is a fixed dose.
491.前記方法が、前記対象に、3週間ごとの約200mg又は6週間ごとの400mgの固定用量でペンブロリズマブを投与することを含む、実施形態60又は61に記載の使用。
491. 62. Use according to
492.前記1回以上の投薬サイクルのそれぞれの長さが21日間である、実施形態54、60、62、63、65、80~109、及び191のいずれか一項に記載の使用。
492. 192. Use according to any one of
493.前記1回以上の投薬サイクルの各々の長さが28日間である、実施形態47、59、67、80~109、及び309~311のいずれか一項に記載の使用。
493. The use according to any one of
494.前記1回以上の投薬サイクルの各々の長さが14日間である、実施形態49、80~109、及び309~311のいずれか一項に記載の使用。 494. The use according to any one of embodiments 49, 80-109, and 309-311, wherein each of said one or more dosing cycles is 14 days in length.
495.前記方法が、前記1回以上の投薬サイクルのそれぞれの約1日目に、前記抗TIGITアンタゴニスト抗体を前記対象又は対象集団に投与することを含む、実施形態47~494のいずれか一項に記載の使用。
495. 495. Any one of embodiments 47-494, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or population of subjects on about
496.前記1回以上の投薬サイクルのそれぞれの約1日目に、前記PD-1軸結合アンタゴニストを前記対象又は対象集団に投与することを含む、、実施形態47~495いずれか一項に記載の使用。
496. 496. Use according to any one of embodiments 47-495, comprising administering said PD-1 axis binding antagonist to said subject or population of subjects on about
497.前記方法が、前記1回以上の投薬サイクルのそれぞれの約15日目に、前記抗TIGITアンタゴニスト抗体を前記対象に投与することを含む、実施形態321又は493に記載の使用。 497. Use according to embodiment 321 or 493, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject on about day 15 of each of said one or more dosing cycles.
498.前記1回以上の投薬サイクルのそれぞれの約15日目に、前記PD-1軸結合アンタゴニストを前記対象に投与することを含む、実施形態321又は493に記載の使用。 498. Use according to embodiment 321 or 493, comprising administering said PD-1 axis binding antagonist to said subject on about day 15 of each of said one or more dosing cycles.
499.前記方法が、対象又は対象集団に、前記抗TIGITアンタゴニスト抗体の前にPD-1軸結合アンタゴニストを投与すること、又は前記PD-1軸結合アンタゴニストの前に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態47~498のいずれか一項に記載の使用。 499. The method comprises administering to the subject or population of subjects a PD-1 axis binding antagonist prior to the anti-TIGIT antagonist antibody, or administering the anti-TIGIT antagonist antibody prior to the PD-1 axis binding antagonist. 498. Use according to any one of embodiments 47-498, comprising
500.前記方法が、前記PD-1軸結合アンタゴニスト又は前記抗TIGITアンタゴニスト抗体の投与後の第1の観察期間を含む、実施形態499に記載の使用。 500. 499. Use according to embodiment 499, wherein said method comprises a first observation period after administration of said PD-1 axis binding antagonist or said anti-TIGIT antagonist antibody.
501.前記第1の観察期間が、約30分と約60分の間の長さである、実施形態500に記載の使用。
501. 500. The use according to
502.前記方法が、前記抗TIGITアンタゴニスト抗体又は前記PD-1軸結合アンタゴニストの投与後の第2観察期間を含む、実施形態500又は501に記載の使用。
502. Use according to
503.前記第2の観察期間が、約30分と約60分の間の長さである、実施形態502に記載の使用。 503. 503. The use according to embodiment 502, wherein the second observation period is between about 30 minutes and about 60 minutes long.
504.前記方法が、前記対象又は対象集団に前記PD-1軸結合アンタゴニストを前記抗TIGITアンタゴニスト抗体と同時に投与することを含む実施形態47~503のいずれか一項に記載の使用。 504. 504. Use according to any one of embodiments 47-503, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or population of subjects simultaneously with said anti-TIGIT antagonist antibody.
505.前記抗TIGITアンタゴニスト抗体及びPD-1軸結合アンタゴニストを前記対象又は対象集団に静脈内投与することを含む、実施形態47~504のいずれか一項に記載の使用。 505. 505. Use according to any one of embodiments 47-504, comprising administering said anti-TIGIT antagonist antibody and PD-1 axis binding antagonist to said subject or population of subjects intravenously.
506.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記PD-1軸結合アンタゴニストを投与することを含む、実施形態505に記載の使用。 506. Use according to embodiment 505, wherein said method comprises administering said PD-1 axis binding antagonist to said subject or subject population by intravenous infusion over 30±10 minutes and/or 60±10 minutes. .
507.前記方法が、30±10分かけて及び/又は60±10分かけて静脈内注入によって前記対象又は対象集団に前記抗TIGITアンタゴニスト抗体を投与することを含む、実施形態505又は506に記載の使用。 507. Use according to embodiment 505 or 506, wherein said method comprises administering said anti-TIGIT antagonist antibody to said subject or subject population by intravenous infusion over 30 ± 10 minutes and/or 60 ± 10 minutes. .
508.前記一又は複数の対象から得られた腫瘍試料のPD-L1発現レベルが決定されている、実施形態47~114及び116~507のいずれか一項に記載の使用。 508. Use according to any one of embodiments 47-114 and 116-507, wherein the PD-L1 expression level of a tumor sample obtained from said one or more subjects has been determined.
509.前記一又は複数の対象から得られた前記腫瘍試料が検出可能なPD-L1発現レベルを有すると決定されている、実施形態508に記載の使用。 509. 509. Use according to embodiment 508, wherein said tumor sample obtained from said one or more subjects has been determined to have a detectable PD-L1 expression level.
510.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1タンパク質発現レベルである、実施形態509に記載の使用。 510. 509. Use according to embodiment 509, wherein said detectable PD-L1 expression level is a detectable PD-L1 protein expression level.
511.前記検出可能なPD-L1タンパク質発現レベルが、染色に適した抗PD-L1抗体による染色を含む免疫組織化学(IHC)アッセイによって決定されている、実施形態510に記載の使用。 511. 511. Use according to embodiment 510, wherein said detectable PD-L1 protein expression level is determined by an immunohistochemistry (IHC) assay comprising staining with an anti-PD-L1 antibody suitable for staining.
512.染色に適した前記抗PD-L1抗体が抗PD-L1抗体SP263、SP142、22C3又は28-8である、実施形態511に記載の使用。 512. 512. Use according to embodiment 511, wherein said anti-PD-Ll antibody suitable for staining is anti-PD-Ll antibody SP263, SP142, 22C3 or 28-8.
513.前記検出可能なPD-L1タンパク質発現レベルが、Ventana SP263 IHCアッセイ、pharmDx 22C3 IHCアッセイ、Ventana SP142 IHCアッセイ、又はpharmDx 28-8 IHCアッセイを使用して決定される、実施形態511又は512に記載の使用。 513. 513. According to embodiment 511 or 512, wherein the detectable PD-L1 protein expression level is determined using the Ventana SP263 IHC assay, pharmDx 22C3 IHC assay, Ventana SP142 IHC assay, or pharmDx 28-8 IHC assay. use.
514.抗PD-L1抗体SP263による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~109、188、220~265、及び307~423のいずれか一項に記載の使用。
514. Any of embodiments 47-109, 188, 220-265, and 307-423, wherein detectable PD-L1 protein expression levels as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP263 have been determined Use as set forth in
515.抗PD-L1抗体SP142による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~220、265~338、及び370~423のいずれか一項に記載の使用。 515. Any one of embodiments 47-220, 265-338, and 370-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with the anti-PD-L1 antibody SP142 has been determined Use as described.
516.抗PD-L1抗体SP22C3による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~113、136~187、及び220~423のいずれか一項に記載の使用。 516. Any one of embodiments 47-113, 136-187, and 220-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody SP22C3 has been determined Use as described.
517.抗PD-L1抗体28-8による染色を含むIHCアッセイによって決定される検出可能なPD-L1タンパク質発現レベルが決定されている、実施形態47~114、及び116~423のいずれか一項に記載の使用。 517. According to any one of embodiments 47-114 and 116-423, wherein the detectable PD-L1 protein expression level as determined by an IHC assay comprising staining with anti-PD-L1 antibody 28-8 has been determined. Use of.
518.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上の腫瘍関連免疫細胞(TIC)である、実施形態514に記載の使用。 518. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more tumor-associated immune cells (TIC) in said tumor sample.
519.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の5%以上20%未満のTICである、実施形態514に記載の使用。 519. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 5% or more and less than 20% TIC in said tumor sample.
520.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上のTICである、実施形態514に記載の使用。 520. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more TIC in said tumor sample.
521.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の20%以上のTICである、実施形態514に記載の使用。 521. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 20% or more TIC in said tumor sample.
522.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の10%以上50%未満のTICである、実施形態514に記載の使用。 522. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 10% or more and less than 50% TIC in said tumor sample.
523.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の50%以上のTICである、実施形態514に記載の使用。 523. 515. Use according to embodiment 514, wherein said detectable PD-L1 protein expression level is 50% or more TIC in said tumor sample.
524.前記検出可能なPD-L1タンパク質発現レベルが、1%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用。 524. Use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or greater.
525.前記検出可能なPD-L1タンパク質発現レベルが、30%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用。 525. Use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 30% or more.
526.前記検出可能なPD-L1タンパク質発現レベルが、前記腫瘍試料中の1%以上50%未満のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517いずれか一項に記載の使用。 526. Use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 1% or more and less than 50% in said tumor sample. .
527.前記検出可能なPD-L1タンパク質発現レベルが、50%以上のPD-L1陽性腫瘍細胞分率である、実施形態514、516及び517のいずれか一項に記載の使用。 527. Use according to any one of embodiments 514, 516 and 517, wherein said detectable PD-L1 protein expression level is a PD-L1 positive tumor cell fraction of 50% or more.
528.前記PD-L1陽性腫瘍細胞分率が、PD-L1発現腫瘍浸潤免疫細胞(IC)によって占められる腫瘍面積の割合である、実施形態515に記載の使用。 528. 516. Use according to embodiment 515, wherein said PD-L1 positive tumor cell fraction is the percentage of tumor area occupied by PD-L1-expressing tumor-infiltrating immune cells (IC).
529.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が1%以上である、実施形態515に記載の使用。 529. 516. Use according to embodiment 515, wherein the percentage of tumor area occupied by said PD-L1-expressing tumor-infiltrating IC is 1% or more.
530.前記PD-L1発現腫瘍浸潤ICが占める腫瘍面積の割合が5%以上である、実施形態515に記載の使用。 530. 516. Use according to embodiment 515, wherein the percentage of tumor area occupied by said PD-L1-expressing tumor-infiltrating IC is 5% or more.
531.前記検出可能なPD-L1タンパク質発現レベルが、1以上の複合陽性スコア(CPS)である、実施形態516に記載の使用。 531. 517. Use according to embodiment 516, wherein said detectable PD-L1 protein expression level is a composite positive score (CPS) of 1 or more.
532.前記検出可能なPD-L1タンパク質発現レベルが、10以上のCPSである、実施形態516に記載の使用。 532. 517. Use according to embodiment 516, wherein said detectable PD-L1 protein expression level is 10 or more CPS.
533.前記検出可能なPD-L1タンパク質発現レベルが、20以上のCPSである、実施形態516に記載の使用。 533. 517. Use according to embodiment 516, wherein said detectable PD-L1 protein expression level is 20 or more CPS.
534.前記IHCアッセイが、Ventana SP142 IHCアッセイである、実施形態528~530のいずれか一項に記載の使用。 534. Use according to any one of embodiments 528-530, wherein said IHC assay is the Ventana SP142 IHC assay.
535.前記検出可能なPD-L1発現レベルが、検出可能なPD-L1核酸発現レベルである、実施形態509に記載の使用。 535. 509. Use according to embodiment 509, wherein said detectable PD-L1 expression level is a detectable PD-L1 nucleic acid expression level.
536.前記検出可能なPD-L1核酸発現レベルが、RNA-seq、RT-qPCR、qPCR、マルチプレックスqPCR若しくはRT-qPCR、マイクロアレイ解析、SAGE、MassARRAY技術、ISH、又はそれらの組合せによって決定されている、実施形態535に記載の使用。 536. said detectable PD-L1 nucleic acid expression level has been determined by RNA-seq, RT-qPCR, qPCR, multiplex qPCR or RT-qPCR, microarray analysis, SAGE, MassARRAY technology, ISH, or a combination thereof; A use according to embodiment 535.
537.前記処置が、基準全生存期間(OS)と比較した前記対象のOS時間及び/又は基準無増悪生存期間(PFS)と比較した前記対象のPFS時間の増加をもたらす、実施形態47~423のいずれか一項に記載の使用。
537. 424. Any of embodiments 47-423, wherein said treatment results in an increase in said subject's OS time compared to baseline overall survival (OS) and/or said subject's PFS time compared to baseline progression-free survival (PFS) or the use described in
538.実施形態537に記載の使用であって、
(a)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のOS時間の中央値である、及び/又は
(b)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のPFS時間の中央値である、
ペプチド。
538. 538. The use according to embodiment 537, comprising:
(a) a subject whose baseline OS time has undergone treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or treatment comprising an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist; and/or (b) the baseline PFS time is a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or an anti-PD-1 axis binding antagonist without a PD-1 axis binding antagonist. median PFS time in a subject population that has received treatment containing a TIGIT antagonist antibody;
peptide.
539.前記1つ以上の化学療法剤が、1つ以上の白金系化学療法剤及び/又は1つ以上の非白金系化学療法剤である、実施形態52、158及び228のいずれか一項に記載の使用。 539. 229. According to any one of embodiments 52, 158 and 228, wherein said one or more chemotherapeutic agents is one or more platinum-based chemotherapeutic agents and/or one or more non-platinum-based chemotherapeutic agents. use.
540.前記白金系化学療法剤がカルボプラチン又はシスプラチンである、実施形態539に記載の使用。 540. 539. Use according to embodiment 539, wherein said platinum-based chemotherapeutic agent is carboplatin or cisplatin.
541.前記カルボプラチンが、AUC=5mg/ml/分又はAUC=6mg/ml/分を達成するのに十分な用量で投与される、実施形態69、92、127、131、249、及び540に記載の使用。 541. Use according to embodiments 69, 92, 127, 131, 249, and 540, wherein said carboplatin is administered at a dose sufficient to achieve AUC = 5 mg/ml/min or AUC = 6 mg/ml/min .
542.前記シスプラチンが約75mg/m2又は80mg/m2の用量で投与される、実施形態69、127、162、164、166、168及び540に記載の使用。 542. Use according to embodiments 69, 127, 162, 164, 166, 168 and 540, wherein said cisplatin is administered at a dose of about 75 mg/m2 or 80 mg/m2.
543.前記1つ以上の非白金系化学療法剤が、代謝拮抗剤、タキサン又はトポイソメラーゼII阻害剤である、実施形態539~542のいずれか一項に記載の使用。 543. 543. Use according to any one of embodiments 539-542, wherein said one or more non-platinum chemotherapeutic agents are antimetabolites, taxanes or topoisomerase II inhibitors.
544.前記代謝拮抗剤が、ペメトレキセド、ゲムシタビン、カペシタビン又は5-フルオロウラシルである、実施形態62、173、174、及び543のいずれか一項に記載の使用。 544. Use according to any one of embodiments 62, 173, 174, and 543, wherein said antimetabolite is pemetrexed, gemcitabine, capecitabine, or 5-fluorouracil.
545.前記ペメトレキセドが約500mg/m2の用量で投与される、実施形態69、127、162及び544のいずれか一項に記載の使用。 545. Use according to any one of embodiments 69, 127, 162 and 544, wherein said pemetrexed is administered at a dose of about 500 mg/m2.
546.前記ゲムシタビンが約1000mg/m2又は約1250mg/m2の用量で投与される、実施形態63、64、162、398、及び544のいずれか一項に記載の実施形態の使用。
546. Use of any one of
547.前記代謝拮抗剤がカペシタビンである、実施形態544に記載の使用。 547. 545. Use according to embodiment 544, wherein said antimetabolite is capecitabine.
548.前記カペシタビンが約1250mg/m2の用量で投与される、実施形態544又は547に記載の使用。 548. Use according to embodiment 544 or 547, wherein said capecitabine is administered at a dose of about 1250 mg/m2.
549.前記タキサンがパクリタキセル又はnab-パクリタキセルである、実施形態173、174、229、230、239、240及び543~548のいずれか一項に記載の使用。 549. The use according to any one of embodiments 173, 174, 229, 230, 239, 240 and 543-548, wherein said taxane is paclitaxel or nab-paclitaxel.
550.前記パクリタキセルが約175mg/m2又は約200mg/m2の用量で投与される、実施形態69、162、及び549のいずれか一項に記載の使用。 550. 549. Use according to any one of embodiments 69, 162, and 549, wherein said paclitaxel is administered at a dose of about 175 mg/m2 or about 200 mg/m2.
551.前記nab-パクリタキセルが約100mg/m2の用量で投与される、実施形態63、64、249、398、及び549のいずれか一項に記載の使用。
551. Use according to any one of
552.前記トポイソメラーゼII阻害剤が、エトポシド、テニポシド、ドキソルビシン、ダウノルビシン、ミトキサントロン、アムサクリン、エリプチシン、オーリントリカルボン酸、又はHU-331である、実施形態80~91、229、230、239、241、251~255、及び543~551のいずれか一項に記載の使用。 552. Embodiments 80-91, 229, 230, 239, 241, 251- wherein said topoisomerase II inhibitor is etoposide, teniposide, doxorubicin, daunorubicin, mitoxantrone, amsacrine, ellipticine, orintricarboxylic acid, or HU-331 255, and use according to any one of 543-551.
553.前記エトポシドが約100mg/m2の用量で投与される、実施形態69、92、及び552のいずれか一項に記載の使用。 553. 553. Use according to any one of embodiments 69, 92, and 552, wherein said etoposide is administered at a dose of about 100 mg/m2.
554.前記1つ以上の化学療法剤がそれぞれ、1週間ごとに1回、2週間ごとに1回、3週間ごとに1回、3週間ごとに2回、4週間ごとに1回、4週間ごとに2回、又は4週間ごとに3回投与される、実施形態543~553のいずれか一項に記載の使用。 554. each of said one or more chemotherapeutic agents once every week, once every two weeks, once every three weeks, twice every three weeks, once every four weeks, every four weeks Use according to any one of embodiments 543-553, administered twice, or three times every four weeks.
555.前記1つ以上の化学療法剤が、1回以上の投薬サイクルの1日目に投与される、実施形態543~554のいずれか一項に記載の使用。
555. 555. Use according to any one of embodiments 543-554, wherein said one or more chemotherapeutic agents are administered on
556.前記ゲムシタビンが4週間ごとに3回投与される、実施形態544~555のいずれか一項に記載の使用。 556. 556. Use according to any one of embodiments 544-555, wherein said gemcitabine is administered three times every four weeks.
557.前記ゲムシタビンが、1回以上の投薬サイクルの1、8及び/又は15日目に投与される、実施形態544~556のいずれか一項に記載の使用。
557. 556. Use according to any one of embodiments 544-556, wherein said gemcitabine is administered on
558.前記カペシタビンが2週間ごと日投与される、実施形態544~557のいずれか一項に記載の使用。 558. The use according to any one of embodiments 544-557, wherein said capecitabine is administered daily every two weeks.
559.前記カペシタビンが、1回以上の投薬サイクルの1~14日目に投与される、実施形態544~558のいずれか一項に記載の使用。 559. Use according to any one of embodiments 544-558, wherein said capecitabine is administered on days 1-14 of one or more dosing cycles.
560.前記nab-パクリタキセルが4週間ごとに3回投与される、実施形態549~559のいずれか一項に記載の使用。 560. 559. Use according to any one of embodiments 549-559, wherein said nab-paclitaxel is administered three times every four weeks.
561.前記nab-パクリタキセルが、1回以上の投薬サイクルの1、8及び/又は15日目に投与される、実施形態549~560のいずれか一項に記載の使用。
561. 561. Use according to any one of embodiments 549-560, wherein said nab-paclitaxel is administered on
562.前記エトポシドが3週間ごとに1~3日目に投与される、実施形態552~561のいずれか一項に記載の使用。 562. 562. Use according to any one of embodiments 552-561, wherein said etoposide is administered on days 1-3 every 3 weeks.
563.前記エトポシドが、1回以上の投薬サイクルの1~3日目に投与される、実施形態552~562のいずれか一項に記載の使用。 563. 563. Use according to any one of embodiments 552-562, wherein said etoposide is administered on days 1-3 of one or more dosing cycles.
564.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の前に投与される、実施形態543~563のいずれか一項に記載の使用。 564. 564. Use according to any one of embodiments 543-563, wherein said one or more chemotherapeutic agents are administered prior to said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
565.前記1つ以上の化学療法剤が、前記PD-1軸結合アンタゴニスト及び/又は前記抗TIGITアンタゴニスト抗体の後に投与される、実施形態543~564のいずれか一項に記載の使用。 565. 564. Use according to any one of embodiments 543-564, wherein said one or more chemotherapeutic agents are administered after said PD-1 axis binding antagonist and/or said anti-TIGIT antagonist antibody.
566.前記1つ以上の化学療法剤が静脈内又は経口投与される、実施形態543~565のいずれか一項に記載の使用。 566. 566. Use according to any one of embodiments 543-565, wherein said one or more chemotherapeutic agents are administered intravenously or orally.
567.前記VEGFアンタゴニストが、3週間ごとに約5mg/kg~約25mg/kgの用量で投与される、実施形態65、310、及び311のいずれか一項に記載の使用。
567. Use according to any one of
568.前記VEGFアンタゴニストが、3週間ごとに約10mg/kg~約20mg/kgの用量で投与される、実施形態312又は567に記載の使用。 568. Use according to embodiment 312 or 567, wherein said VEGF antagonist is administered at a dose of about 10 mg/kg to about 20 mg/kg every three weeks.
569.前記VEGFアンタゴニストが、3週間ごとに約15mg/kgの用量で投与される、実施形態318又は568に記載の使用。 569. Use according to embodiment 318 or 568, wherein said VEGF antagonist is administered at a dose of about 15 mg/kg every three weeks.
570.前記VEGFアンタゴニストが抗VEGF抗体である、実施形態65、310~312、318~320、及び567~569のいずれか一項に記載の使用。
570. Use according to any one of
571.前記抗VEGF抗体がベバシズマブのVHドメイン及びVLドメインを含む、実施形態570に記載の使用。 571. 571. Use according to embodiment 570, wherein said anti-VEGF antibody comprises the VH and VL domains of bevacizumab.
572.前記抗VEGF抗体が、ベバシズマブである、実施形態570又は571に記載の使用。 572. Use according to embodiment 570 or 571, wherein said anti-VEGF antibody is bevacizumab.
573.前記抗TIGITアンタゴニスト抗体がチラゴルマブであり、前記PD-1軸結合アンタゴニストがアテゾリズマブであり、前記VEGFアンタゴニストがベバシズマブである、実施形態65、310~312、及び318~320のいずれか一項に記載の使用。
573. according to any one of
574.前記使用が、1回以上の投薬サイクルの1日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態65、310~312、318~320、及び567~573いずれか一項に記載の使用。
574. Any one of
575.前記方法が、1回以上の投薬サイクルの15日目に前記VEGFアンタゴニストを前記対象に投与することを含む、実施形態318~320のいずれか一項に記載の使用。 575. 321. Use according to any one of embodiments 318-320, wherein said method comprises administering said VEGF antagonist to said subject on day 15 of one or more dosing cycles.
576.前記VEGFアンタゴニストが静脈内投与される、実施形態65、310~312、及び318~320、及び567~575いずれか一項に記載の使用。
576. Use according to any one of
577.前記VEGFアンタゴニストが、90±15分間かけて静脈内注入によって前記対象に投与される、実施形態576に記載の使用。 577. 577. Use according to embodiment 576, wherein said VEGF antagonist is administered to said subject by intravenous infusion over 90±15 minutes.
578.前記使用が、前記対象に、前記VEGFアンタゴニストの前に前記PD-1軸結合アンタゴニストを投与し、前記抗TIGITアンタゴニスト抗体の前に前記VEGFアンタゴニストを投与することを含む、実施形態65、310~312、318~320、及び567~577のいずれか一項に記載の使用。
578.
579.前記方法が、前記PD-1軸結合アンタゴニストの投与後の第1の観察期間、前記VEGFアンタゴニストの投与後の第2の観察期間、及び前記抗TIGITアンタゴニスト抗体の投与後の第3の観察期間を含む、実施形態578に記載の使用。 579. The method comprises a first observation period after administration of the PD-1 axis binding antagonist, a second observation period after administration of the VEGF antagonist, and a third observation period after administration of the anti-TIGIT antagonist antibody. 578. The use according to embodiment 578, comprising:
580.前記第1の観察期間、前記第2の観察期間、及び前記第3の観察期間がそれぞれ、約30分と約120分の間の長さである、実施形態579に記載の使用。 580. 579. The use according to embodiment 579, wherein the first observation period, the second observation period, and the third observation period are each between about 30 minutes and about 120 minutes long.
581.前記チラゴルマブ及びアテゾリズマブが、投与前にIVバッグにおいて組み合わされる、実施形態113、128、129~131、175~182、210~214、221、256、257、270、289、290、293、294、297、298、333、362~365、385、386、389、393、419、及び422のいずれか一項に記載の使用。 581. Embodiments 113, 128, 129-131, 175-182, 210-214, 221, 256, 257, 270, 289, 290, 293, 294, 297, wherein said tiragolumab and atezolizumab are combined in an IV bag prior to administration , 298, 333, 362-365, 385, 386, 389, 393, 419, and 422.
582.該対象が、ヒトである、実施形態47~581のいずれか一項に記載の使用。 582. Use according to any one of embodiments 47-581, wherein said subject is a human.
583.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが別々の製剤で提供される、実施形態47~582のいずれか一項に記載の使用に記載の使用。 583. Use according to any one of embodiments 47-582, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in separate formulations.
584.前記抗TIGITアンタゴニスト抗体及び前記PD-1軸結合アンタゴニストが単一製剤で提供される、実施形態47~582のいずれか一項に記載の使用に記載の使用。 584. Use according to any one of embodiments 47-582, wherein said anti-TIGIT antagonist antibody and said PD-1 axis binding antagonist are provided in a single formulation.
上述の発明は、理解を明確にする目的のために説明及び実施例によってある程度詳細に記載されているが、これらの記載及び実施例は、本発明の範囲を限定するものとして解釈されるべきではない。本明細書に引用される全ての特許及び科学文献の開示は、その全体が参考として明示的に組み込まれる。 Although the foregoing invention has been described in some detail by way of illustration and example for purposes of clarity of understanding, these descriptions and examples should not be construed as limiting the scope of the invention. do not have. The disclosures of all patent and scientific literature cited herein are expressly incorporated by reference in their entirety.
Claims (503)
(a)SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
(b)KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
(c)ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
(d)KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
(e)WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
(f)QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列、
を含む、請求項1~5のいずれか一項に記載の方法。 The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
(a) an HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
(b) an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
(c) an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO:3);
(d) a HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
(e) an HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and (f) an HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
The method according to any one of claims 1 to 5, comprising
(a)DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
(b)WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
(c)GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
(d)FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4、並びに
以下の重鎖可変領域FR:
(a)X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
(b)WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
(c)RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
(d)WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4
を更に含む、請求項1~6のいずれか一項に記載の方法。 The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
(a) FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
(b) FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
(c) FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and (d) FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10), and the following heavy chain variable region FRs:
(a) FR-H1 comprising the amino acid sequence of X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), where X 1 is E or Q;
(b) FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
(c) FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and (d) FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14).
The method of any one of claims 1-6, further comprising
(a)配列番号17若しくは18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)配列番号17若しくは18のアミノ酸配列を含むVHドメインと、配列番号19のアミノ酸配列を含むVLドメイン
を含む、請求項1~7のいずれか一項に記載の方法。 The anti-TIGIT antagonist antibody is
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:19; or (c) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18. , comprising a VL domain comprising the amino acid sequence of SEQ ID NO:19.
(a)前記導入期が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、3週間ごとの抗TIGITアンタゴニスト抗体、3週間ごとのPD-1軸結合アンタゴニスト及び3週間ごとの非白金系化学療法剤の1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤の投与を含まない、
方法。 A method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase,
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more additional dosing cycles of an anti-TIGIT antagonist antibody every 3 weeks, a PD-1 axis binding antagonist every 3 weeks and a non-platinum chemotherapeutic agent every 3 weeks; The maintenance period does not include administration of the platinum-based chemotherapeutic agent,
Method.
(a)前記導入期が、3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、3週間ごとの白金系化学療法剤、及び3週間ごとの非白金系化学療法剤の1回以上の投薬サイクルを含み、
(b)前記維持期が、4週間ごとの約700mg~約1000mgの用量の抗TIGITアンタゴニスト抗体、及び4週間ごとの約1400mg~2000mgの用量のPD-1軸結合アンタゴニストの1回以上の追加の投薬サイクルを含み、前記維持期が前記白金系化学療法剤又は前記非白金系化学療法剤の投与を含まない、
方法。 A method of treating a subject with cancer, said method comprising administering to said subject a dosing regimen comprising an induction phase and a maintenance phase,
(a) the induction phase comprises an anti-TIGIT antagonist antibody at a dose of about 500 mg to about 700 mg every 3 weeks, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, platinum-based every 3 weeks; chemotherapeutic agents, and one or more dosing cycles of non-platinum chemotherapeutic agents every 3 weeks;
(b) said maintenance phase comprises one or more additions of an anti-TIGIT antagonist antibody at a dose of about 700 mg to about 1000 mg every 4 weeks and a PD-1 axis binding antagonist at a dose of about 1400 mg to 2000 mg every 4 weeks; comprising a dosing cycle, wherein the maintenance phase does not include administration of the platinum-based chemotherapeutic agent or the non-platinum-based chemotherapeutic agent;
Method.
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、又は
(c)前記白金系化学療法剤がカルボプラチン又はシスプラチンであり、前記非白金系化学療法剤がエトポシドである、
請求項50~56及び63~65のいずれか一項に記載の方法。 (a) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel, or (c) the platinum-based chemotherapeutic agent is carboplatin or cisplatin, and the non-platinum-based chemotherapeutic agent is etoposide,
The method of any one of claims 50-56 and 63-65.
(a)前記4回の初期投薬サイクルが、各初期投薬サイクルの1日目に約600mgの用量のチラゴルマブ、各初期投薬サイクルの1日目に約1200mgの用量のアテゾリズマブ、各初期投薬サイクルの1日目にAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、並びに各初期投薬サイクルの1日目、2日目及び3日目のそれぞれに100mg/m2の用量のエトポシドを投与することを含み、
(b)前記1回以上の追加の投薬サイクルが、各追加の投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各追加の投薬サイクルの1日目に約1200mgの用量のアテゾリズマブを投与することを含み、
前記4回の初期投薬サイクル及び前記1回以上の追加の投薬サイクルが、それぞれ21日間投薬サイクルであり、前記処置が、前記チラゴルマブを用いない、アテゾリズマブ、カルボプラチン及びエトポシドによる処置と比較して、前記対象又は対象集団のPFS及び/又はOSを延長する、方法。 A method for treating a subject or subject population with ES-SCLC, said method administering to said subject or subject population four initial dosing cycles followed by one or more additional dosing cycles. including
(a) the four initial dosing cycles are tiragolumab at a dose of about 600 mg on day 1 of each initial dosing cycle, atezolizumab at a dose of about 1200 mg on day 1 of each initial dosing cycle, and 1 of each initial dosing cycle; Carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min on Day 1 and etoposide at a dose of 100 mg/m2 on each of Days 1, 2 and 3 of each initial dosing cycle. administering
(b) said one or more additional dosing cycles administering a dose of about 600 mg tiragolumab on day 1 of each additional dosing cycle and atezolizumab at a dose of about 1200 mg on day 1 of each additional dosing cycle; including
each of the four initial dosing cycles and the one or more additional dosing cycles is a 21-day dosing cycle, and the treatment is compared to treatment with atezolizumab, carboplatin, and etoposide without the tiragolumab; A method of prolonging PFS and/or OS of a subject or subject population.
(i)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、3週間ごとのAUC=5mg/ml/分を達成するのに十分な用量のカルボプラチン、及び3週間ごとの約500mg/m2の用量のペメトレキセドの4回の導入期投薬サイクル、並びに
(ii)3週間ごとの約600mgの用量のチラゴルマブ、3週間ごとの約1200mgの用量のアテゾリズマブ、及び3週間ごとの約500mg/m2の用量のペメトレキセドの1回以上の維持期投薬サイクルであって、前記維持期の1回以上の21日間投薬サイクルがカルボプラチンの投与を含まない、維持期投薬サイクル
で投与することを含み、
前記対象又は対象集団が、前記進行性非扁平上皮NSCLCに対する事前全身治療を受けたことがない、方法。 1. A method of treating a subject or subject population having advanced non-squamous NSCLC, said method comprising:
(i) tiragolumab at a dose of about 600 mg every 3 weeks, atezolizumab at a dose of about 1200 mg every 3 weeks, carboplatin at a dose sufficient to achieve AUC = 5 mg/ml/min every 3 weeks, and 3 weeks and (ii) tiragolumab at a dose of about 600 mg every 3 weeks , atezolizumab at a dose of about 1200 mg every 3 weeks, and every 3 weeks. one or more maintenance dosing cycles of pemetrexed at a dose of about 500 mg/ m2 , wherein said one or more 21-day maintenance dosing cycles do not include administration of carboplatin including
The method, wherein said subject or subject population has not received prior systemic therapy for said advanced non-squamous NSCLC.
(b)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がゲムシタビンである、
(c)前記白金系化学療法剤がカルボプラチンであり、前記非白金系化学療法剤がパクリタキセルである、
(d)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がペメトレキセドである、又は
(e)前記白金系化学療法剤がシスプラチンであり、前記非白金系化学療法剤がゲムシタビンである、請求項144に記載の方法。 (a) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is pemetrexed;
(b) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is gemcitabine;
(c) the platinum-based chemotherapeutic agent is carboplatin, and the non-platinum-based chemotherapeutic agent is paclitaxel;
(d) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is pemetrexed; or (e) the platinum-based chemotherapeutic agent is cisplatin and the non-platinum-based chemotherapeutic agent is gemcitabine. 145. The method of claim 144, wherein
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブを含む処置
を受けたことがある対象集団のMPR率である、請求項146に記載の方法。 The reference MPR rate is
MPR rates in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel and bevacizumab 147. The method of claim 146, wherein
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブを含む処置
を受けたことがある対象集団のpCR率である、請求項148に記載の方法。 The reference pCR rate is
pCR rates in subject populations who have received (a) treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, and/or (b) treatment with cisplatin and docetaxel or cisplatin, docetaxel, and bevacizumab 149. The method of claim 148, wherein
(a)抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、及び/又は
(b)シスプラチン及びドセタキセル又はシスプラチン、ドセタキセル、及びベバシズマブを含む処置
を受けたことがある対象集団のEFS時間である、請求項150に記載の方法。 the reference EFS time,
EFS time in subject populations who have received (a) treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody and/or (b) treatment comprising cisplatin and docetaxel or cisplatin, docetaxel and bevacizumab 151. The method of claim 150, wherein
(a)
(i)3週間ごとに5mg/mL/分のAUC若しくは6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、又は
(ii)3週間ごとに約75mg/m2の用量のシスプラチンと、
(b)
(i)3週間ごとに約500mg/m2の用量のペメトレキセド、又は各投薬サイクルの1日目及び8日目に約1000mg/m2若しくは約1250mg/m2の用量のゲムシタビン、又は
(ii)3週間ごとに約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、
の1回以上の投薬サイクルを投与すること
を含む、方法。 A method for treating a subject with resectable lung cancer, said method comprising administering to said subject tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of about 1200 mg every 3 weeks;
(a)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min or 6 mg/mL/min every 3 weeks, or (ii) a dose of about 75 mg/ m2 every 3 weeks cisplatin, and
(b)
(i) pemetrexed at a dose of about 500 mg/ m2 every 3 weeks, or gemcitabine at a dose of about 1000 mg/ m2 or about 1250 mg/ m2 on days 1 and 8 of each dosing cycle, or (ii) paclitaxel at a dose of about 175 mg/ m2 or about 200 mg/ m2 every 3 weeks;
A method comprising administering one or more dosing cycles of
(I)前記投薬サイクルの少なくとも1つは、ネオアジュバント処置であり、前記対象に、
(a)3週間ごとに約1200mgの用量のチラコルマブと、
(b)ネオアジュバント処置として3週間ごとに約1200mgの用量のアテゾリズマブと、
(c)
(i)3週間ごとに5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン及び各投薬サイクルの第1日及び第8日に約1000mg/m2の用量のゲムシタビン、
(ii)3週間ごとに6mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、及び3週間ごとに約175mg/m2若しくは約200mg/m2の用量のパクリタキセル、又は
(iii)3週間ごとに約75mg/m2の用量のシスプラチン、並びに各投薬サイクルの1日目及び8日目に約1250mg/m2の用量のゲムシタビン
を投与することを含み、
(II)前記投薬サイクルの少なくとも1つが、アジュバント処置として、3週間ごとに約500mg~約700mgの用量のチラゴルマブ、及び3週間ごとに約900mg~約1500mgの用量のアテゾリズマブを前記対象に投与することを含む、
方法。 1. A method for treating a subject with lung cancer, said method comprising administering to said subject one or more dosing cycles of tiragolumab and atezolizumab,
(I) at least one of said dosing cycles is a neoadjuvant treatment, wherein said subject comprises:
(a) tilacolumab at a dose of about 1200 mg every 3 weeks;
(b) atezolizumab at a dose of about 1200 mg every 3 weeks as a neoadjuvant treatment;
(c)
(i) carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks and gemcitabine at a dose of about 1000 mg/ m2 on days 1 and 8 of each dosing cycle;
(ii) carboplatin at a dose targeted to achieve an AUC of 6 mg/mL/min every 3 weeks and paclitaxel at a dose of about 175 mg/ m2 or about 200 mg/ m2 every 3 weeks, or (iii) ) administering cisplatin at a dose of about 75 mg/ m2 every 3 weeks and gemcitabine at a dose of about 1250 mg/ m2 on days 1 and 8 of each dosing cycle;
(II) at least one of said dosing cycles administering tiragolumab at a dose of about 500 mg to about 700 mg every 3 weeks and atezolizumab at a dose of about 900 mg to about 1500 mg every 3 weeks as an adjuvant treatment; including,
Method.
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象の腫瘍試料からの腫瘍細胞上のPD-L1のタンパク質発現レベルを検出すること、及び
(b)検出可能なPD-L1発現レベルを有する前記対象について、検出された腫瘍細胞上のPD-L1発現に基づいて、約500mg~約700mgの用量で3週間ごとに投与される抗TIGITアンタゴニスト抗体及び約900mg~約1500mgの用量で3週間ごとに投与されるPD-1軸結合アンタゴニストの1回以上の投薬サイクルを含む治療を選択すること
を含む方法。 A method of selecting treatment for a subject with cervical cancer, comprising:
(a) detecting protein expression levels of PD-L1 on tumor cells from a tumor sample of said subject by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - anti-TIGIT antagonist antibody administered every three weeks at a dose of about 500 mg to about 700 mg and about 900 mg to about 1500 mg for said subject with L1 expression levels, based on detected PD-L1 expression on tumor cells A method comprising selecting a treatment comprising one or more dosing cycles of a PD-1 axis binding antagonist administered every three weeks at a dose of
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
請求項175に記載の方法。 (a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment containing a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
176. The method of claim 175.
(a)
(i)前記投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル及び3週間ごとの5mg/mL/分のAUCを達成することを目標とした用量のカルボプラチン、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF、又は
(b)
(i)投薬レジメンの最初の12週間にわたって、毎週約125mg/m2の用量のnab-パクリタキセル、並びに
(ii)投薬レジメンの第13週~第19週にわたって、2週間ごとの約60mg/m2の用量のドキソルビシン、2週間ごとの約600mg/m2の用量のシクロホスファミド、及び2週間ごとのG-CSF若しくはGM-CSF
とを含む投薬レジメンで前記対象に投与することを含み、
前記方法が、前記投薬レジメンの最後の投与の2週間後と6週間後の間の手術を更に含む、方法。 A method of treating a subject with eTNBC, said method comprising tiragolumab at a dose of about 420 mg every two weeks and atezolizumab at a dose of about 840 mg every two weeks;
(a)
(i) nab-paclitaxel at a dose of about 125 mg/m 2 weekly and carboplatin at a dose targeted to achieve an AUC of 5 mg/mL/min every 3 weeks over the first 12 weeks of said dosing regimen; and (ii) doxorubicin at a dose of about 60 mg/ m2 every 2 weeks, cyclophosphamide at a dose of about 600 mg/ m2 every 2 weeks, and every 2 weeks for weeks 13 through 19 of the dosing regimen; G-CSF or GM-CSF of, or (b)
(i) nab-paclitaxel at a dose of about 125 mg/ m2 weekly for the first 12 weeks of the dosing regimen, and (ii) about 60 mg/ m2 every two weeks for weeks 13-19 of the dosing regimen. doxorubicin at a dose of , cyclophosphamide at a dose of about 600 mg/m 2 every 2 weeks, and G-CSF or GM-CSF every 2 weeks
administering to said subject with a dosing regimen comprising
The method further comprising surgery between 2 weeks and 6 weeks after the last administration of the dosing regimen.
(a)染色に適した抗PD-L1抗体を使用するIHCアッセイによって、前記対象又は対象集団からの腫瘍試料中のPD-L1のタンパク質発現レベルを検出すること、並びに
(b)検出可能なPD-L1発現レベルを有する前記対象又は対象集団について、検出されたPD-L1発現に基づいて、3週間ごとの約900mg~約1500mgの用量のPD-1軸結合アンタゴニスト、及び3週間ごとの約500mg~約700mgの用量の抗TIGITアンタゴニスト抗体の1回以上の投薬サイクルを含む治療法を選択すること、
を含む方法。 A method of selecting a treatment for a subject or subject population with SCCHN, comprising:
(a) detecting the protein expression level of PD-L1 in a tumor sample from said subject or subject population by an IHC assay using an anti-PD-L1 antibody suitable for staining; and (b) detectable PD. - for said subject or population of subjects with L1 expression levels, a PD-1 axis binding antagonist at a dose of about 900 mg to about 1500 mg every 3 weeks, and about 500 mg every 3 weeks, based on detected PD-L1 expression; selecting a therapy comprising one or more dosing cycles of an anti-TIGIT antagonist antibody at a dose of ~700 mg;
method including.
(b)前記基準DOR時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のDOR時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、
請求項238に記載の方法。 (a) said baseline PFS time is the median PFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline DOR time is the median DOR time of a subject population that has been treated with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. is the median OS time in a subject population that has received treatment containing a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
239. The method of claim 238.
(a)5%以上、
(b)5%以上20%未満、又は
(c)20%以上の腫瘍関連免疫細胞(TIC)
である、請求項242に記載の方法。 wherein the detectable PD-L1 protein expression level is in a tumor sample,
(a) 5% or more,
(b) greater than or equal to 5% and less than 20%, or (c) greater than or equal to 20% tumor-associated immune cells (TIC)
243. The method of claim 242, wherein
(b)前記基準EFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のEFS時間の中央値である、又は
(c)前記基準OS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置を受けたことがある対象集団のOS時間の中央値である、請求項287に記載の方法。 (a) said baseline RFS time is the median RFS time of a subject population that has received treatment with a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody;
(b) said baseline EFS time is the median EFS time of a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody, or (c) said baseline OS time. 288. The method of claim 287, wherein is the median OS time in a subject population that has received treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody.
(a)前記第1の投薬レジメンが、3週間ごとの約600mgの用量のチラゴルマブ及び約3週間ごとの1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、
(b)前記第2の投薬レジメンが、3週間ごとの約1200mgの用量のアテゾリズマブの1回以上の投薬サイクルを含み、(i)エンフォルツマブベドチンが、2週間のon/1週間のoffの間、毎週1.25mg/kgの用量で投与されるか、又は(ii)サシツズマブゴビテカンが、2週間のon/1週間のoffの間、毎週10mg/kgの用量で投与され、前記第2の投薬レジメンが、前記対象又は対象集団が前記第1の投薬レジメン中に疾患進行又は許容できない毒性を経験した後に前記対象又は対象集団に投与される、方法。 1. A method for treating a subject or population of subjects with mUC comprising administering to said subject or population of subjects a first dosing regimen followed by a second dosing regimen,
(a) said first dosing regimen comprises one or more dosing cycles of tiragolumab at a dose of about 600 mg every 3 weeks and atezolizumab at a dose of 1200 mg about every 3 weeks;
(b) said second dosing regimen comprises one or more dosing cycles of atezolizumab at a dose of about 1200 mg every 3 weeks, and (i) enfortumab vedotin 2 weeks on/1 week off or (ii) sacituzumab govitecan administered at a dose of 10 mg/kg weekly for 2 weeks on/1 week off. , wherein said second dosing regimen is administered to said subject or subject population after said subject or subject population experiences disease progression or unacceptable toxicity during said first dosing regimen.
(a)前記第1の投薬レジメンが、各投薬サイクルの1日目に約80mg/m2の用量のシスプラチン、及び各21日間サイクルの1日目~5日目に800mg/m2/24時間の用量の5-フルオロウラシルの1回以上の21日間の投薬サイクルを含み、6回の投薬後にシスプラチンを投薬レジメンから省略する、
(b)前記第2の投薬レジメンが、各投薬サイクルの1日目に約600mgの用量のチラゴルマブ、及び各投薬サイクルの1日目に約1200mgの用量のアテゾリズマブの1回以上の21日間投薬サイクルを含む、
方法。 1. A method for treating a subject or population of subjects with advanced or metastatic esophageal cancer comprising administering to said subject or population of subjects a first dosing regimen and a second dosing regimen,
(a) said first dosing regimen comprises cisplatin at a dose of about 80 mg/m 2 on Day 1 of each dosing cycle and 800 mg/m 2 /24 hours on Days 1-5 of each 21-day cycle; and omitting cisplatin from the dosing regimen after 6 doses of 5-fluorouracil for one or more 21-day dosing cycles
(b) said second dosing regimen is one or more 21-day dosing cycles of tiragolumab at a dose of about 600 mg on day 1 of each dosing cycle and atezolizumab at a dose of about 1200 mg on day 1 of each dosing cycle; including,
Method.
SNSAAWN(配列番号1)のアミノ酸配列を含むHVR-H1配列;
KTYYRFKWYSDYAVSVKG(配列番号2)のアミノ酸配列を含むHVR-H2配列;
ESTTYDLLAGPFDY(配列番号3)のアミノ酸配列を含むHVR-H3配列;
KSSQTVLYSSNNKKYLA(配列番号4)のアミノ酸配列を含むHVR-L1配列;
WASTRES(配列番号5)のアミノ酸配列を含むHVR-L2配列;及び
QQYYSTPFT(配列番号6)のアミノ酸配列を含むHVR-L3配列
を含む、請求項47~335のいずれか一項に記載の方法。 The anti-TIGIT antagonist antibody comprises the following hypervariable regions (HVR):
HVR-H1 sequence comprising the amino acid sequence of SNSAAWN (SEQ ID NO: 1);
an HVR-H2 sequence comprising the amino acid sequence of KTYYRFKWYSDYAVSVKG (SEQ ID NO: 2);
an HVR-H3 sequence comprising the amino acid sequence of ESTTYDLLAGPFDY (SEQ ID NO: 3);
an HVR-L1 sequence comprising the amino acid sequence of KSSQTVLYSSNNKKYLA (SEQ ID NO: 4);
HVR-L2 sequence comprising the amino acid sequence of WASTRES (SEQ ID NO: 5); and HVR-L3 sequence comprising the amino acid sequence of QQYYSTPFT (SEQ ID NO: 6).
DIVMTQSPDSLAVSLGERATINC(配列番号7)のアミノ酸配列を含むFR-L1;
WYQQKPGQPPNLLIY(配列番号8)のアミノ酸配列を含むFR-L2;
GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC(配列番号9)のアミノ酸配列を含むFR-L3;及び
FGPGTKVEIK(配列番号10)のアミノ酸配列を含むFR-L4
を更に含む、請求項336に記載の方法。 The anti-TIGIT antagonist antibody comprises the following light chain variable region framework regions (FR):
FR-L1 comprising the amino acid sequence of DIVMTQSPDSLAVSLGERATINC (SEQ ID NO: 7);
FR-L2 comprising the amino acid sequence of WYQQKPGQPPNLLIY (SEQ ID NO: 8);
FR-L3 comprising the amino acid sequence of GVPDRFSGSGSGTDFTLTISSLQAEDVAVYYC (SEQ ID NO: 9); and FR-L4 comprising the amino acid sequence of FGPGTKVEIK (SEQ ID NO: 10)
337. The method of claim 336, further comprising:
X1VQLQQSGPGLVKPSQTLSLTCAISGDSVS(配列番号11)のアミノ酸配列を含むFR-H1(配列中、X1はE又はQである);
WIRQSPSRGLEWLG(配列番号12)のアミノ酸配列を含むFR-H2;
RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR(配列番号13)のアミノ酸配列を含むFR-H3;及び
WGQGTLVTVSS(配列番号14)のアミノ酸配列を含むFR-H4
を更に含む、請求項336に記載の方法。 The anti-TIGIT antagonist antibody comprises the following heavy chain variable region FRs:
FR-H1 comprising the amino acid sequence of X 1 VQLQQSGPGLVKPSQTLSLTCAISGDSVS (SEQ ID NO: 11), in which X 1 is E or Q;
FR-H2 comprising the amino acid sequence of WIRQSPSRGLEWLG (SEQ ID NO: 12);
FR-H3 comprising the amino acid sequence of RITINPDTSKNQFSLQLNSVTPEDTAVFYCTR (SEQ ID NO: 13); and FR-H4 comprising the amino acid sequence of WGQGTLVTVSS (SEQ ID NO: 14)
337. The method of claim 336, further comprising:
(a)配列番号17又は18のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号19のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、請求項336~340のいずれか一項に記載の方法。 wherein said anti-TIGIT antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 17 or 18;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO: 19; or (c) a VH domain according to (a) and (b) 341. The method of any one of claims 336-340, comprising the VL domain of claim 336-340.
(a)配列番号17又は18のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、請求項336~341に記載の方法。 wherein said anti-TIGIT antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17 or 18; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
(a)配列番号17のアミノ酸配列を含むVHドメイン;及び
(b)配列番号19のアミノ酸配列を含むVLドメイン
を含む、請求項336~339、341及び342に記載の方法。 wherein said anti-TIGIT antagonist antibody is:
(a) a VH domain comprising the amino acid sequence of SEQ ID NO:17; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:19.
(a)配列番号33のアミノ酸配列を含む重鎖;及び
(b)配列番号34のアミノ酸配列を含む軽鎖
を含む、請求項336~339及び341~343のいずれか一項に記載の方法。 wherein said anti-TIGIT antagonist antibody is:
(a) a heavy chain comprising the amino acid sequence of SEQ ID NO:33; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:34.
GFTFSDSWIH(配列番号20)のアミノ酸配列を含むHVR-H1配列;
AWISPYGGSTYYADSVKG(配列番号21)のアミノ酸配列を含むHVR-H2配列;
RHWPGGFDY(配列番号22)のアミノ酸配列を含むHVR-H3配列;
RASQDVSTAVA(配列番号23)のアミノ酸配列を含むHVR-L1配列;
SASFLYS(配列番号24)のアミノ酸配列を含むHVR-L2配列;及び
QQYLYHPAT(配列番号25)のアミノ酸配列を含むHVR-L3配列
を含む、請求項357に記載の方法。 The anti-PD-L1 antagonist antibody is a HVR that:
an HVR-H1 sequence comprising the amino acid sequence of GFTFSDSWIH (SEQ ID NO: 20);
an HVR-H2 sequence comprising the amino acid sequence of AWISPYGGSTYYADSVKG (SEQ ID NO: 21);
an HVR-H3 sequence comprising the amino acid sequence of RHWPGGFDY (SEQ ID NO: 22);
an HVR-L1 sequence comprising the amino acid sequence of RASQDVSTAVA (SEQ ID NO: 23);
HVR-L2 sequence comprising the amino acid sequence of SASFLYS (SEQ ID NO:24); and HVR-L3 sequence comprising the amino acid sequence of QQYLYHPAT (SEQ ID NO:25).
(a)配列番号26のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む重鎖可変(VH)ドメイン;
(b)配列番号27のアミノ酸配列に対して少なくとも95%の配列同一性を有するアミノ酸配列を含む軽鎖可変(VL)ドメイン;又は
(c)(a)に記載のVHドメインと(b)に記載のVLドメイン
を含む、請求項360に記載の方法。 wherein said anti-PD-L1 antagonist antibody is:
(a) a heavy chain variable (VH) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:26;
(b) a light chain variable (VL) domain comprising an amino acid sequence having at least 95% sequence identity to the amino acid sequence of SEQ ID NO:27; or (c) a VH domain according to (a) and (b) 361. The method of claim 360, comprising a VL domain as described.
(a)配列番号26のアミノ酸配列を含むVHドメイン;及び
(b)配列番号27のアミノ酸配列を含むVLドメイン
を含む、請求項361に記載の方法。 wherein said anti-PD-L1 antagonist antibody is:
362. The method of claim 361, comprising (a) a VH domain comprising the amino acid sequence of SEQ ID NO:26; and (b) a VL domain comprising the amino acid sequence of SEQ ID NO:27.
(a)配列番号28のアミノ酸配列を含む重鎖;及び
(b)配列番号29のアミノ酸配列を含む軽鎖
を含む、請求項362に記載の方法。 wherein said anti-PD-L1 antagonist antibody is:
363. The method of claim 362, comprising (a) a heavy chain comprising the amino acid sequence of SEQ ID NO:28; and (b) a light chain comprising the amino acid sequence of SEQ ID NO:29.
(b)前記基準PFS時間が、抗TIGITアンタゴニスト抗体を用いないPD-1軸結合アンタゴニストを含む処置、若しくはPD-1軸結合アンタゴニストを用いない抗TIGITアンタゴニスト抗体を含む処置を受けたことがある対象集団のPFS時間の中央値である、
請求項436に記載の方法。 (a) a subject whose baseline OS time has undergone a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or a treatment comprising an anti-TIGIT antagonist antibody without a PD-1 axis binding antagonist; and/or (b) the baseline PFS time is a treatment comprising a PD-1 axis binding antagonist without an anti-TIGIT antagonist antibody or an anti-PD-1 axis binding antagonist without a PD-1 axis binding antagonist. median PFS time in a subject population that has received treatment containing a TIGIT antagonist antibody;
437. The method of claim 436.
Applications Claiming Priority (29)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US202062966448P | 2020-01-27 | 2020-01-27 | |
| US62/966,448 | 2020-01-27 | ||
| US202062985822P | 2020-03-05 | 2020-03-05 | |
| US62/985,822 | 2020-03-05 | ||
| US202062994272P | 2020-03-24 | 2020-03-24 | |
| US62/994,272 | 2020-03-24 | ||
| PCT/US2020/024526 WO2021194481A1 (en) | 2020-03-24 | 2020-03-24 | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies |
| USPCT/US2020/024526 | 2020-03-24 | ||
| US202063059054P | 2020-07-30 | 2020-07-30 | |
| US63/059,054 | 2020-07-30 | ||
| US202063059960P | 2020-07-31 | 2020-07-31 | |
| US63/059,960 | 2020-07-31 | ||
| US202063074827P | 2020-09-04 | 2020-09-04 | |
| US202063074807P | 2020-09-04 | 2020-09-04 | |
| US63/074,807 | 2020-09-04 | ||
| US63/074,827 | 2020-09-04 | ||
| PCT/US2020/049415 WO2022050954A1 (en) | 2020-09-04 | 2020-09-04 | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies |
| USPCT/US2020/049415 | 2020-09-04 | ||
| US202063085890P | 2020-09-30 | 2020-09-30 | |
| US63/085,890 | 2020-09-30 | ||
| US202063105198P | 2020-10-23 | 2020-10-23 | |
| US63/105,198 | 2020-10-23 | ||
| US202063114517P | 2020-11-16 | 2020-11-16 | |
| US63/114,517 | 2020-11-16 | ||
| US202063124693P | 2020-12-11 | 2020-12-11 | |
| US63/124,693 | 2020-12-11 | ||
| US202063127109P | 2020-12-17 | 2020-12-17 | |
| US63/127,109 | 2020-12-17 | ||
| PCT/US2021/015143 WO2021154761A1 (en) | 2020-01-27 | 2021-01-26 | Methods for treatment of cancer with an anti-tigit antagonist antibody |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| JP2023511595A true JP2023511595A (en) | 2023-03-20 |
| JPWO2021154761A5 JPWO2021154761A5 (en) | 2024-02-05 |
Family
ID=74626264
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| JP2022545057A Pending JP2023511595A (en) | 2020-01-27 | 2021-01-26 | Methods for treating cancer using anti-TIGIT antagonist antibodies |
Country Status (10)
| Country | Link |
|---|---|
| EP (1) | EP4096646A1 (en) |
| JP (1) | JP2023511595A (en) |
| KR (1) | KR20220133243A (en) |
| CN (1) | CN115315256A (en) |
| AU (1) | AU2021212662A1 (en) |
| CA (1) | CA3165187A1 (en) |
| IL (1) | IL294800A (en) |
| MX (1) | MX2022009170A (en) |
| TW (1) | TW202142230A (en) |
| WO (1) | WO2021154761A1 (en) |
Families Citing this family (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2023531406A (en) * | 2020-06-16 | 2023-07-24 | ジェネンテック, インコーポレイテッド | Methods and compositions for treating triple-negative breast cancer |
| KR20240028452A (en) * | 2021-07-02 | 2024-03-05 | 제넨테크, 인크. | Methods and compositions for treating cancer |
| WO2023010094A2 (en) * | 2021-07-28 | 2023-02-02 | Genentech, Inc. | Methods and compositions for treating cancer |
| WO2023018675A1 (en) * | 2021-08-10 | 2023-02-16 | Merck Sharp & Dohme Llc | A therapeutic combination comprising a tigit antagonist, a pd-1 antagonist, and lenvatinib |
| KR20240047393A (en) * | 2021-08-10 | 2024-04-12 | 머크 샤프 앤드 돔 엘엘씨 | A therapeutic combination comprising a TIGIT antagonist, a PD-1 antagonist and a chemotherapy agent(s) |
| WO2023040804A1 (en) * | 2021-09-14 | 2023-03-23 | 信达生物制药(苏州)有限公司 | Pharmaceutical composition of anti-pd-1 antibody and chemotherapy agent and method for using same |
| CN117940453A (en) * | 2021-09-15 | 2024-04-26 | 江苏恒瑞医药股份有限公司 | Protein capable of specifically binding to PD-1 and medical application thereof |
| WO2023122665A1 (en) * | 2021-12-22 | 2023-06-29 | Genentech, Inc. | Clinical formulations of anti-tigit antibodies |
| CN114181310B (en) * | 2022-02-14 | 2022-07-05 | 中山康方生物医药有限公司 | anti-TIGIT antibody, and pharmaceutical composition and use thereof |
Family Cites Families (38)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816567A (en) | 1983-04-08 | 1989-03-28 | Genentech, Inc. | Recombinant immunoglobin preparations |
| US6548640B1 (en) | 1986-03-27 | 2003-04-15 | Btg International Limited | Altered antibodies |
| DE3920358A1 (en) | 1989-06-22 | 1991-01-17 | Behringwerke Ag | BISPECIFIC AND OLIGO-SPECIFIC, MONO- AND OLIGOVALENT ANTI-BODY CONSTRUCTS, THEIR PRODUCTION AND USE |
| US6150584A (en) | 1990-01-12 | 2000-11-21 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| US6075181A (en) | 1990-01-12 | 2000-06-13 | Abgenix, Inc. | Human antibodies derived from immunized xenomice |
| EP0617706B1 (en) | 1991-11-25 | 2001-10-17 | Enzon, Inc. | Multivalent antigen-binding proteins |
| AU661533B2 (en) | 1992-01-20 | 1995-07-27 | Astrazeneca Ab | Quinazoline derivatives |
| GB9314893D0 (en) | 1993-07-19 | 1993-09-01 | Zeneca Ltd | Quinazoline derivatives |
| IL112248A0 (en) | 1994-01-25 | 1995-03-30 | Warner Lambert Co | Tricyclic heteroaromatic compounds and pharmaceutical compositions containing them |
| US5679683A (en) | 1994-01-25 | 1997-10-21 | Warner-Lambert Company | Tricyclic compounds capable of inhibiting tyrosine kinases of the epidermal growth factor receptor family |
| IL112249A (en) | 1994-01-25 | 2001-11-25 | Warner Lambert Co | Pharmaceutical compositions containing di and tricyclic pyrimidine derivatives for inhibiting tyrosine kinases of the epidermal growth factor receptor family and some new such compounds |
| EP0772609B1 (en) | 1994-07-21 | 1999-02-24 | Akzo Nobel N.V. | Cyclic ketone peroxide formulations |
| US5804396A (en) | 1994-10-12 | 1998-09-08 | Sugen, Inc. | Assay for agents active in proliferative disorders |
| CA2216796C (en) | 1995-03-30 | 2003-09-02 | Pfizer Inc. | Quinazoline derivatives |
| US5641870A (en) | 1995-04-20 | 1997-06-24 | Genentech, Inc. | Low pH hydrophobic interaction chromatography for antibody purification |
| GB9508565D0 (en) | 1995-04-27 | 1995-06-14 | Zeneca Ltd | Quiazoline derivative |
| GB9508538D0 (en) | 1995-04-27 | 1995-06-14 | Zeneca Ltd | Quinazoline derivatives |
| US5747498A (en) | 1996-05-28 | 1998-05-05 | Pfizer Inc. | Alkynyl and azido-substituted 4-anilinoquinazolines |
| KR100437582B1 (en) | 1995-07-06 | 2004-12-17 | 노파르티스 아게 | Pyrrolopyrimidines and Processes for the Preparation Thereof |
| US5760041A (en) | 1996-02-05 | 1998-06-02 | American Cyanamid Company | 4-aminoquinazoline EGFR Inhibitors |
| GB9603095D0 (en) | 1996-02-14 | 1996-04-10 | Zeneca Ltd | Quinazoline derivatives |
| CA2249446C (en) | 1996-04-12 | 2008-06-17 | Warner-Lambert Company | Irreversible inhibitors of tyrosine kinases |
| WO1998002434A1 (en) | 1996-07-13 | 1998-01-22 | Glaxo Group Limited | Fused heterocyclic compounds as protein tyrosine kinase inhibitors |
| ID18494A (en) | 1996-10-02 | 1998-04-16 | Novartis Ag | PIRAZOLA DISTRIBUTION IN THE SEQUENCE AND THE PROCESS OF MAKING IT |
| US6002008A (en) | 1997-04-03 | 1999-12-14 | American Cyanamid Company | Substituted 3-cyano quinolines |
| UA73073C2 (en) | 1997-04-03 | 2005-06-15 | Уайт Холдінгз Корпорейшн | Substituted 3-cyan chinolines |
| WO1998050038A1 (en) | 1997-05-06 | 1998-11-12 | American Cyanamid Company | Use of quinazoline compounds for the treatment of polycystic kidney disease |
| ZA986732B (en) | 1997-07-29 | 1999-02-02 | Warner Lambert Co | Irreversible inhibitiors of tyrosine kinases |
| ZA986729B (en) | 1997-07-29 | 1999-02-02 | Warner Lambert Co | Irreversible inhibitors of tyrosine kinases |
| TW436485B (en) | 1997-08-01 | 2001-05-28 | American Cyanamid Co | Substituted quinazoline derivatives |
| WO1999024037A1 (en) | 1997-11-06 | 1999-05-20 | American Cyanamid Company | Use of quinazoline derivatives as tyrosine kinase inhibitors for treating colonic polyps |
| EP1034298B1 (en) | 1997-12-05 | 2011-11-02 | The Scripps Research Institute | Humanization of murine antibody |
| PT1131304E (en) | 1998-11-19 | 2003-04-30 | Warner Lambert Co | N-4- (3-CHLORO-4-FLUORO-PHENYLAMINO) -7- (3-MORFOLIN-4-IL-PROPOXY) -QUINAZOLIN-6-IL | -ACRYLAMIDE AN IRREVERSIVAL INJECTOR OF TYROSOS KINASES |
| EP1766068A4 (en) | 2004-06-04 | 2010-03-03 | Genentech Inc | Egfr mutations |
| EP2898329B1 (en) | 2012-09-24 | 2017-05-17 | Ventana Medical Systems, Inc. | Method of identifying treatment responsive non-small cell lung cancer using anaplastic lymphoma kinase (alk) as a marker |
| PT3294770T (en) | 2015-05-12 | 2020-12-04 | Hoffmann La Roche | Therapeutic and diagnostic methods for cancer |
| IL255372B (en) | 2015-05-29 | 2022-07-01 | Genentech Inc | Therapeutic and diagnostic methods for cancer |
| EP3759141A1 (en) * | 2018-02-26 | 2021-01-06 | F. Hoffmann-La Roche AG | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies |
-
2021
- 2021-01-26 MX MX2022009170A patent/MX2022009170A/en unknown
- 2021-01-26 CA CA3165187A patent/CA3165187A1/en active Pending
- 2021-01-26 WO PCT/US2021/015143 patent/WO2021154761A1/en unknown
- 2021-01-26 IL IL294800A patent/IL294800A/en unknown
- 2021-01-26 JP JP2022545057A patent/JP2023511595A/en active Pending
- 2021-01-26 TW TW110102913A patent/TW202142230A/en unknown
- 2021-01-26 EP EP21705841.1A patent/EP4096646A1/en active Pending
- 2021-01-26 KR KR1020227029306A patent/KR20220133243A/en unknown
- 2021-01-26 AU AU2021212662A patent/AU2021212662A1/en active Pending
- 2021-01-26 CN CN202180022830.2A patent/CN115315256A/en active Pending
Also Published As
| Publication number | Publication date |
|---|---|
| CN115315256A (en) | 2022-11-08 |
| WO2021154761A1 (en) | 2021-08-05 |
| EP4096646A1 (en) | 2022-12-07 |
| IL294800A (en) | 2022-09-01 |
| CA3165187A1 (en) | 2021-08-05 |
| TW202142230A (en) | 2021-11-16 |
| KR20220133243A (en) | 2022-10-04 |
| AU2021212662A1 (en) | 2022-08-11 |
| MX2022009170A (en) | 2022-08-17 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| TWI775781B (en) | Therapeutic and diagnostic methods for cancer | |
| JP2023511595A (en) | Methods for treating cancer using anti-TIGIT antagonist antibodies | |
| US20180346586A1 (en) | Methods of treating cancer using anti-ox40 antibodies | |
| JP2018518483A (en) | Methods of treating cancer using anti-OX40 antibodies and PD-1 axis binding antagonists | |
| KR20230082632A (en) | Dosing for Treatment with Anti-FCRH5/Anti-CD3 Bispecific Antibodies | |
| US20220016243A1 (en) | Methods for treatment of cancer with an anti-tigit antagonist antibody | |
| KR20210133237A (en) | Dosing for treatment with anti-TIGIT and anti-CD20 or anti-CD38 antibodies | |
| KR20210034622A (en) | Lung cancer treatment method using PD-1 axis binding antagonist, anti-metabolite, and platinum agent | |
| JP2023531200A (en) | Treatment with anti-TIGIT antibody and PD-1 axis binding antagonist | |
| JP2022548978A (en) | Dosing for Treatment with Drugs Anti-TIGIT and Anti-PD-L1 Antagonist Antibodies | |
| WO2021092171A1 (en) | Diagnostic and therapeutic methods for treatment of hematologic cancers | |
| WO2022050954A1 (en) | Dosing for treatment with anti-tigit and anti-pd-l1 antagonist antibodies | |
| TWI836278B (en) | Dosing for treatment with anti-fcrh5/anti-cd3 bispecific antibodies | |
| TW202320848A (en) | Methods and compositions for treating cancer | |
| JP2023523450A (en) | Methods and compositions for non-small cell lung cancer immunotherapy | |
| KR20240028452A (en) | Methods and compositions for treating cancer | |
| CN117940452A (en) | Methods and compositions for treating cancer | |
| TW202321308A (en) | Methods for treatment of hematologic cancers using anti-tigit antibodies, anti-cd38 antibodies, and pd-1 axis binding antagonists | |
| CN117715936A (en) | Methods and compositions for treating cancer | |
| WO2024049949A1 (en) | Therapeutic and diagnostic methods for bladder cancer |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| A521 | Request for written amendment filed |
Free format text: JAPANESE INTERMEDIATE CODE: A523 Effective date: 20240126 |
|
| A621 | Written request for application examination |
Free format text: JAPANESE INTERMEDIATE CODE: A621 Effective date: 20240126 |