ES2745352B2 - GDF15 in urine as a biomarker of chronic kidney disease - Google Patents
GDF15 in urine as a biomarker of chronic kidney disease Download PDFInfo
- Publication number
- ES2745352B2 ES2745352B2 ES201830849A ES201830849A ES2745352B2 ES 2745352 B2 ES2745352 B2 ES 2745352B2 ES 201830849 A ES201830849 A ES 201830849A ES 201830849 A ES201830849 A ES 201830849A ES 2745352 B2 ES2745352 B2 ES 2745352B2
- Authority
- ES
- Spain
- Prior art keywords
- gdf15
- urine
- patients
- ckd
- levels
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Active
Links
Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Immunology (AREA)
- Engineering & Computer Science (AREA)
- Molecular Biology (AREA)
- Biomedical Technology (AREA)
- Chemical & Material Sciences (AREA)
- Hematology (AREA)
- Urology & Nephrology (AREA)
- Biotechnology (AREA)
- Microbiology (AREA)
- Cell Biology (AREA)
- Food Science & Technology (AREA)
- Medicinal Chemistry (AREA)
- Physics & Mathematics (AREA)
- Analytical Chemistry (AREA)
- Biochemistry (AREA)
- General Health & Medical Sciences (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Investigating Or Analysing Biological Materials (AREA)
Description
GDF15 en orina como biomarcador de enfermedad renal crónicaGDF15 in urine as a biomarker of chronic kidney disease
Campo de la técnicaTechnical field
La presente invención se refiere a un método y a un kit para el diagnóstico y/o pronóstico de daño renal que comprende analizar una muestra de orina obtenida de un paciente y determinar los niveles urinarios del factor 15 de crecimientoy diferenciación (GDF15).The present invention relates to a method and a kit for the diagnosis and/or prognosis of kidney damage that comprises analyzing a urine sample obtained from a patient and determining the urinary levels of growth and differentiation factor 15 (GDF15).
Antecedentes de la invenciónBackground of the invention
La enfermedad renal crónica (ERC) o insuficiencia renal crónica (IRC) es una pérdida progresiva (por tres meses o más) e irreversible de las funciones renales, cuyo grado de afección se determina con un filtrado glomerular (FG) <60 ml/min/1.73 m2. Como consecuencia, los riñones pierden su capacidad para eliminar desechos, concentrar la orina y conservar los electrolitos en la sangre.Chronic kidney disease (CKD) or chronic kidney failure (CKD) is a progressive (for three months or more) and irreversible loss of kidney functions, the degree of which is determined by a glomerular filtration rate (GFR) <60 ml/min. /1.73 m2. As a result, the kidneys lose their ability to eliminate waste, concentrate urine, and preserve electrolytes in the blood.
Los síntomas de un deterioro de la función renal son inespecíficos y pueden incluir una sensación de malestar general y una reducción del apetito.Symptoms of impaired kidney function are nonspecific and may include a feeling of general malaise and a reduction in appetite.
A menudo, la ERC se diagnostica como resultado del estudio en personas en las que se sabe que están en riesgo de problemas renales, tales como aquellos con presión arterial alta o diabetes y aquellos con parientes con ERC. La insuficiencia renal crónica también puede ser identificada cuando conduce a una de sus reconocidas complicaciones, como las enfermedades cardiovasculares, anemia o pericarditis. CKD is often diagnosed as a result of screening in people who are known to be at risk for kidney problems, such as those with high blood pressure or diabetes and those with relatives with CKD. Chronic kidney failure can also be identified when it leads to one of its recognized complications, such as cardiovascular diseases, anemia or pericarditis.
Las causas más comunes de ERC son la nefropatía diabética, hipertensión arterial, y glomerulonefritis. Juntas, causan aproximadamente el 75% de todos los casos en adultos de ERC. En la práctica clínica, la mayoría de las nefropatías progresan lentamente hacia la pérdida definitiva de la función renal. Históricamente, las enfermedades del riñón han sido clasificadas según la parte de la anatomía renal que está implicada:The most common causes of CKD are diabetic nephropathy, high blood pressure, and glomerulonephritis. Together, they cause approximately 75% of all adult cases of CKD. In clinical practice, most nephropathies progress slowly toward permanent loss of renal function. Historically, kidney diseases have been classified according to the part of the kidney anatomy that is involved:
- Vascular, incluye enfermedades de los grandes vasos sanguíneos, como estenosis de la arteria renal bilateral, y enfermedades de los vasos sanguíneos pequeños, como nefropatía isquémica, síndrome urémico hemolítico y vasculitis.- Vascular, includes diseases of large blood vessels, such as bilateral renal artery stenosis, and diseases of small blood vessels, such as ischemic nephropathy, hemolytic uremic syndrome, and vasculitis.
- Glomerular, abarcando a un grupo diverso y subclasificado en: Enfermedad glomerular primaria, como glomeruloesclerosis focal y segmentaria y nefropatía por IgA.- Glomerular, covering a diverse group subclassified into: Primary glomerular disease, such as focal and segmental glomerulosclerosis and IgA nephropathy.
- Enfermedad glomerularsecundaria, como nefropatía diabética y nefritis lupus. - Secondary glomerular disease, such as diabetic nephropathy and lupus nephritis.
- Túbulo intersticial, incluyendo enfermedad poliquística renal, nefritis tubulointersticial crónica inducida por drogas o toxinas, y nefropatía de reflujo.- Interstitial tubule, including polycystic kidney disease, chronic tubulointerstitial nephritis induced by drugs or toxins, and reflux nephropathy.
- Obstructiva, por ejemplo, con piedras del riñón bilateralesy enfermedades de la próstata.- Obstructive, for example, with bilateral kidney stones and prostate diseases.
Los pacientes de ERC sufren de aterosclerosis acelerada y tienen incidencia más alta de enfermedades cardiovasculares, con un pronóstico más pobre. Inicialmente no presentan síntomas específicos y solamente puede ser detectada como un aumento en la creatinina del plasma sanguíneo. A medida que la función del riñón disminuye:CKD patients suffer from accelerated atherosclerosis and have a higher incidence of cardiovascular diseases, with a poorer prognosis. Initially they do not present specific symptoms and can only be detected as an increase in blood plasma creatinine. As kidney function declines:
- La presión arterial está incrementada debido a la sobrecarga de líquidos y a la producción de hormonas vasoactivas que conducen a la hipertensión y a una insuficiencia cardíaca congestiva. - La urea se acumula, conduciendo a la azoemia y en última instancia a la uremia (los síntomas van desde el letargo a la pericarditis y a la encefalopatía).- Blood pressure is increased due to fluid overload and the production of vasoactive hormones leading to hypertension and congestive heart failure. - Urea accumulates, leading to azotemia and ultimately uremia (symptoms range from lethargy to pericarditis to encephalopathy).
- El potasio se acumula en la sangre (lo que se conoce como hiperpotasemia), con síntomas que van desde malestar genera la arritmias cardiacas fatales.- Potassium accumulates in the blood (known as hyperkalemia), with symptoms ranging from discomfort to fatal cardiac arrhythmias.
- Se disminuye la síntesis de eritropoyetina (conduciendo a la anemia y causando fatiga)- Erythropoietin synthesis is decreased (leading to anemia and causing fatigue)
- Sobrecarga de volumen de líquido, los síntomas van desde edema suave al edema agudo de pulmón peligroso para la vida.- Fluid volume overload, symptoms range from mild edema to life-threatening acute lung edema.
- La hiperfosfatemia, debido a la retención de fosfato que conlleva a la hipocalcemia (asociado además con la deficiencia de vitamina D3 activa) y al hiperparatiroidismo secundario, que conduce a la osteoporosis renal, osteítis fibrosa y a la calcificación vascular.- Hyperphosphatemia, due to phosphate retention that leads to hypocalcemia (also associated with active vitamin D3 deficiency) and secondary hyperparathyroidism, which leads to renal osteoporosis, osteitis fibrosa and vascular calcification.
- La acidosis metabólica, debido a la generación disminuida de bicarbonato por el riñón, conduce a respiración incómoda y después al empeoramiento de la salud de los huesos.- Metabolic acidosis, due to decreased bicarbonate generation by the kidney, leads to uncomfortable breathing and then worsening bone health.
En las etapas iniciales de la ERC, cuando las manifestaciones clínicas y resultados de laboratorio son mínimos o inexistentes, el diagnóstico puede ser sugerido por la asociación de manifestaciones inespecíficas por parte del paciente, tales como fatiga, anorexia, pérdida de peso, picazón, náuseas, hipertensión, poliuria, nicturia, hematuria o edema. Otros síntomas son: oliguria, debilidad, , vómito, insomnios, calambres, palidez cutánea, xerosis, miopatía proximal, dismenorrea y/o amenorrea, atrofia testicular, impotencia, déficit cognitivos o de atención, confusión, somnolencia, obnubilación y coma. Sin embargo, aún existe la necesidad de identificar y validar nuevos biomarcadores de daño renal, más precisos, cuya determinación además sea rápida, sencilla y sin necesidad de biopsiar al paciente y que permitan determinar la causa del daño renal, más concretamente del daño renal crónico.In the initial stages of CKD, when clinical manifestations and laboratory results are minimal or non-existent, the diagnosis can be suggested by the association of non-specific manifestations by the patient, such as fatigue, anorexia, weight loss, itching, nausea , hypertension, polyuria, nocturia, hematuria or edema. Other symptoms are: oliguria, weakness, vomiting, insomnia, cramps, skin pallor, xerosis, proximal myopathy, dysmenorrhea and/or amenorrhea, testicular atrophy, impotence, cognitive or attention deficits, confusion, drowsiness, obtundation and coma. However, there is still a need to identify and validate new, more precise biomarkers of kidney damage, whose determination is also quick, simple and without the need to biopsy the patient and that allow determining the cause of kidney damage, more specifically chronic kidney damage. .
Además, se hace notar que durante la última década se han desarrollado modelos conceptuales separados para la ERC y el fracaso renal agudo (FRA; también denominado Lesión Renal Aguda o en inglés, Acute Kidney Injury; AKI) que facilitan enfoques organizados para la investigación y los ensayos clínicos. Sin embargo, estudios epidemiológicos y mecanicistas recientes indican que los dos síndromes no son entidades diferentes sino que están estrechamente interconectados—la ERC es un factor de riesgo de FRA, y el FRA es un factor de riesgo para el desarrollo de la ERC; a su vez, ambos síndromes son factores de riesgo de enfermedad cardiovascular. Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. N Engl J Med. 2014 Jul 3;371(l):58-66 Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease . Kidney International Supplements 2013;3: 1-150. En este sentido, la presente invención proporciona nuevos biomarcadores de daño renal, tanto de ERC como de fracaso renal agudo, dichas biomarcadores han demostrado ser útiles para diagnosticar y pronosticar ambos síndromes en virtud de la interconexión que parecen tener ambos.Furthermore, it is noted that during the last decade separate conceptual models have been developed for CKD and acute kidney injury (AKI; also called Acute Kidney Injury or in English, Acute Kidney Injury; AKI) that facilitate organized approaches to research and clinical trials. However, recent epidemiological and mechanistic studies indicate that the two syndromes are not different entities but are closely interconnected—CKD is a risk factor for AKI, and AKI is a risk factor for the development of CKD; In turn, both syndromes are risk factors for cardiovascular disease. Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. N Engl J Med. 2014 Jul 3;371(l):58-66 Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150. In this sense, the present invention provides new biomarkers of kidney damage, both CKD and acute kidney failure, these biomarkers have proven to be useful for diagnosing and prognosticating both syndromes by virtue of the interconnection that both seem to have.
Breve descripción de la invenciónBrief description of the invention
En base a los resultados experimentales aportados a lo largo de la descripción, la presente invención versa sobre los siguientes aspectos expuestos de forma resumida y general:Based on the experimental results provided throughout the description, the present invention deals with the following aspects presented in a summarized and general manner:
a. los niveles urinarios de GDF15 están alterados, en concreto se encuentran incrementados, en varios modelos de daño renal, tanto agudo y crónico y, por tanto, constituyen un biomarcador de daño renal;to. urinary levels of GDF15 are altered, specifically they are increased, in several models of kidney damage, both acute and chronic, and therefore constitute a biomarker of kidney damage;
b. los niveles urinarios de GDF15 contribuyen a diferenciar la causa del daño renal en pacientes diabéticos, diferenciando entre pacientes diabéticos con nefropatía diabética y sin nefropatía diabética; yb. urinary GDF15 levels contribute to differentiating the cause of kidney damage in diabetic patients, differentiating between diabetic patients with diabetic nephropathy and without diabetic nephropathy; and
c. los niveles urinarios de GDF15 identifican pacientes ya diagnosticados de ERC que tienen un altísimo riesgo de muerte, en concreto el 100% de los pacientes con GDF15 urinario >13,8ng/mg fallecieron durante un seguimiento medio de 30 meses.c. Urinary GDF15 levels identify patients already diagnosed with CKD who have a very high risk of death, specifically 100% of patients with urinary GDF15 >13.8ng/mg died during a mean follow-up of 30 months.
Breve descripción de las figurasBrief description of the figures
Figura 1. Correlaciones de GDF15 en orina con FG y Albuminuria (coc MAU/Cr = cociente microalbuminuria/creatinina). Figure 1. Correlations of GDF15 in urine with GFR and Albuminuria (coc MAU/Cr = microalbuminuria/creatinine ratio).
Figura 2. GDF15 en orina de pacientes diabéticos con riñón nativo, es decir aquel riñón que no ha sido trasplantado, con y sin nefropatía diabética. Figure 2. GDF15 in urine of diabetic patients with a native kidney, that is, a kidney that has not been transplanted, with and without diabetic nephropathy.
Figura 3. Árbol de clasificación de evolución de los pacientes: diálisis (D), vivo (V) o muerto (M). Figure 3. Patient evolution classification tree: dialysis (D), alive (V) or dead (M).
Figura 4. Curva ROC de GDF15 en orina, mortalidad, diálisis y muerte diálisis. Figure 4. ROC curve of GDF15 in urine, mortality, dialysis and dialysis death.
Figura 5. Comportamiento de GDF15 en suero como predictor de mortalidad. Figure 5. Behavior of GDF15 in serum as a predictor of mortality.
Figura 6. Curva ROC de GDF15 en orina como biomarcador de nefropatía diabética en pacientes diabéticos. (N=13) Figure 6. ROC curve of GDF15 in urine as a biomarker of diabetic nephropathy in diabetic patients. (N=13)
Descripción de la invenciónDescription of the invention
Los autores de la presente invención, en un estudio transcriptómico de un modelo preclínico de daño renal determinaron que el gen de la familia de GDF más sobre expresado fue el factor 15 de crecimiento y diferenciación (ver GDF 15 en la tabla 1 mostrada abajo). Es más, los autores de la presente invención confirmaron que dicho aumento de expresión de GDF15 se producía en varios modelos de daño renal agudo y crónico, de diversas etiologías (Tablas 2,3 y 4).The authors of the present invention, in a transcriptomic study of a preclinical model of kidney damage, determined that the most overexpressed GDF family gene was growth and differentiation factor 15 (see GDF 15 in Table 1 shown below). Furthermore, the authors of the present invention confirmed that said increase in GDF15 expression occurred in several models of acute and chronic kidney damage, of various etiologies (Tables 2, 3 and 4).
Tabla 1. Expresión renal de ARNm de genes de la familia GDF en el fracaso renal agudo experimental inducido p or ácido fótico, analizado por transcriptómico, técnica deArrays. Datos expresados como media ± error estándar de la media. Los niveles de mRNA fueron analizados a las 72h de la inducción del daño.Table 1. Renal mRNA expression of GDF family genes in experimental acute renal failure induced by photic acid, analyzed by transcriptomics, Arrays technique. Data expressed as mean ± standard error of the mean. The mRNA levels were analyzed 72 h after the induction of damage.


Tabla 2. Expresión renal de ARNm de genes de la familia CDF en el modelo de daño renal por proteinurla (Inducido por administración BSA o Albúmina desuero bovino). Analizado por Transcriptómica, técnica de RNA-seq. Los niveles de mRNA fueron analizados a los 7 días de la inducción del daño. Table 2. Renal mRNA expression of CDF family genes in the proteinurla kidney injury model ( Induced by administration of BSA or bovine serum albumin). Analyzed by Transcriptomics, RNA-seq technique. The mRNA levels were analyzed 7 days after the induction of damage.

Tabla 3. Expresión renal de ARNm de genes de la familia GDF en inflamación, analizado por transcriptómica, técnica RNA -seq. Datos expresados comomedia± error estándar de la media. Losniveles de mRNA fueron analizadosa los 7 días de la inducción del daño mediante la Inyección de la citoquina inflamatoria Tweak. Table 3. Renal mRNA expression of GDF family genes in inflammation, analyzed by transcriptomics, RNA-seq technique. Data expressed as mean ± standard error of the mean. The mRNA levels were analyzed 7 days after the induction of damage by injection of the inflammatory cytokine Tweak.


Tabla 4 Expresión GDF15 ARNm (UA) en el riñón completo de ratones MRL/lpr 6 semanas (control) vs ratones M RL/lprl4 -18 semanas (nefritis lúpica). Datos expresados como media ± error estándar de la media. NL: nefritis lúpica Table 4 GDF15 mRNA expression ( UA) in the whole kidney of MRL/lpr mice 6 weeks ( control) vs M RL/lprl4 mice -18 weeks ( lupus nephritis). Data expressed as mean ± standard error of the mean. LN: lupus nephritis


*Escalasemicuantitativadel+a 4+*Semiquantitative scale from+ to 4+
En base a estos resultados, se estableció que GDF15 era un biomarcador de enfermedad renal, aumentando la expresión de este marcador en el riñón en diversos modelos de daño renal agudoy crónico. Además, se confirmó que GDF15 aumenta en orina de pacientes con daño renal agudo. Esto se ve confirmado tal y como se ilustra a continuación:Based on these results, it was established that GDF15 was a biomarker of kidney disease, increasing the expression of this marker in the kidney in various models of acute and chronic kidney damage. Furthermore, GDF15 was confirmed to be increased in urine from patients with acute kidney injury. This is confirmed as illustrated below:
N iveles de GDF15 en orina de pacientes con fracaso renal agudo (AKI)GDF15 levels in urine of patients with acute kidney injury (AKI)

n= 20 AKIn= 20 AKI
n= 7 Controlesn= 7 Controls
Además, con el objeto de poder confirmar estos resultados también en daño renal crónico, se realizó un estudio prospectivo, en el que se analizó mediante ELISA los niveles de e GDF15 en muestras de orina de 73 pacientes y plasma de 82 pacientes, que se sometieron a biopsia renal entre septiembre 2012 y marzo 2017, en el Hospital Universitario Fundación Jiménez Díaz. Todos ellos tenían un diagnóstico de ERC basado en el filtrado glomerular y la albuminuria. Estos valores fueron correlacionados con datos clínicos básales y con seguimiento de los pacientes a los 29 ± 17 meses. Tal y como se puede comprobar en la tabla 5, los niveles urinarios de GDF15 en orina estaban aumentados de forma significativa en pacientes con ERC, en comparación con controles sanos.Furthermore, in order to confirm these results also in chronic kidney damage, a prospective study was carried out, in which the levels of GDF15 were analyzed by ELISA in urine samples from 73 patients and plasma from 82 patients, who underwent to kidney biopsy between September 2012 and March 2017, at the Fundación Jiménez Díaz University Hospital. All of them had a diagnosis of CKD based on glomerular filtration rate and albuminuria. These values were correlated with baseline clinical data and with patient follow-up at 29 ± 17 months. As can be seen in Table 5, urinary GDF15 levels in urine were significantly increased in patients with CKD, compared to healthy controls.
Tabla 5 Valores de GDF15 en orina, pacientes y controles. Datos expresados como media ± desviación estándar.Table 5 GDF15 values in urine, patients and controls. Data expressed as mean ± standard deviation.

(Pacientes=73 Sujetos con ERC a los que se iba a hacer una biopsia renal) (Controles= 7 Sujetos control)(Patients=73 Subjects with CKD who were going to have a kidney biopsy) (Controls= 7 Control subjects)
La ERC se diagnostica en base a niveles de Filtrado Glomerular (FG) y Albuminuria (A), lo que a su vez identifica a personas con alto riesgo de muerte prematura. Los niveles de GDF15 en orina no se modifican en función del Filtrado Glomerular (FG) ni Albuminuria (A) (tablas 6 y 7). En la Figura 1 se muestra la correlación con estasvariables.CKD is diagnosed based on levels of Glomerular Filtration (GFR) and Albuminuria (A), which in turn identifies people at high risk of premature death. GDF15 levels in urine are not They modify depending on the Glomerular Filtration (GFR) or Albuminuria (A) (tables 6 and 7). Figure 1 shows the correlation with these variables.
Tabla 6 GDF15 orina por categoría de ERC dependiente de FG: G l, G2, G3 y G4-G5. Datos expresados como media ± desviación estándar.Table 6 GDF15 urine by GFR-dependent CKD category: G l, G2, G3 and G4-G5. Data expressed as mean ± standard deviation.

Donde G l, G2, G3, G4-G5 son los distintos niveles de estratificación ERC en función de FG (filtrado glomerular). Las categorías G l-a G5 provienen de un consenso internacional (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150) y se definen de la siguiente manera: G l (>90); G2 (60-89), G3a (45-59), G3b (30-44), G4 (15-29), G5 (<15). Los números entre paréntesis se refieren a filtrado glomerular (FG) expresado en ml/min/1.73 m2. Además, nos gustaría señalar que en la página 52 de la referencia Rev Nefrol Dial Trasμl. 2017; 37 (1): 48-61), se describe la estratificación de la nefropatía diabética en función de niveles FG y/o albuminuria (página 52).Where G l, G2, G3, G4-G5 are the different levels of CKD stratification based on GFR (glomerular filtration rate). The categories G l-a G5 come from an international consensus (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150) and are defined as follows: G l (>90); G2 (60-89), G3a (45-59), G3b (30-44), G4 (15-29), G5 (<15). The numbers in parentheses refer to glomerular filtration rate (GFR) expressed in ml/min/1.73 m2. Additionally, we would like to point out that on page 52 of the reference Rev Nefrol Dial Trasμl. 2017; 37 (1): 48-61), the stratification of diabetic nephropathy based on GFR levels and/or albuminuria is described (page 52).
Tabla 7 GDF15 orina por categoría de ERC dependiente de Albuminuria: A l, A2 yA3. Datos expresados como media ± desviación estándar. Table 7 GDF15 urine by CKD category dependent on Albuminuria: A l, A2 and A3. Data expressed as mean ± standard deviation.

Donde A l, A2, A3 son los distintos niveles de estratificación ERC en función de A (albuminuria). Las categorías A l a A3 provienen de un consenso internacional (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150) y se definen de la siguiente manera: A l (<30); A2 (30-300), A3 (>300). Los números entre paréntesis se refieren a cociente albuminuria: creatinuria (creatinina en orina) expresado en mg/g. Placemos notar que los valores de diferentes analitos en orina se normalizan por mg o g de creatinina en orina, ya que la eliminación urinaria de creatinina es constante en 24 h, como ejemplifica las unidades de albuminuria (mg/g de creatinuria), como indican las guías internacionales (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150). A lo largo del texto, hemos normalizado de la misma manera la eliminación urinaria de GDF15, expresando los valores en ng de GDF15 urinario por mg de creatinina urinaria (ng/mg). En este sentido, se desaconseja expresar las proteínas (albúmina, GDF15) en orina por unidad de volumen (vg mg/ml), ya que el volumen depende fundamentalmente de la ingesta de agua y varía de minuto a minuto (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease . Kidney International Supplements 2013;3: 1-150; Ortiz A, Sanchez-Niño MD, Sanz AB. The meaning of urinary creatinine concentration. Kidney Int. 2011 Apr;79(7):791).Where A l, A2, A3 are the different levels of CKD stratification based on A (albuminuria). Categories A to A3 come from an international consensus (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150) and are defined as follows: A l (<30); A2 (30-300), A3 (>300). The numbers in parentheses refer to the albuminuria: creatinuria (creatinine in urine) ratio expressed in mg/g. We note that the values of different analytes in urine are normalized by mg or g of creatinine in urine, since the urinary elimination of creatinine is constant in 24 hours, as exemplified by the units of albuminuria (mg/g of creatinuria), as indicated by the international guidelines (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150). Throughout the text, we have The urinary elimination of GDF15 was normalized in the same way, expressing the values in ng of urinary GDF15 per mg of urinary creatinine (ng/mg). In this sense, it is not recommended to express proteins (albumin, GDF15) in urine per unit of volume (eg mg/ml), since the volume depends fundamentally on water intake and varies from minute to minute (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 2013;3: 1-150; Ortiz A, Sanchez-Niño MD, Sanz AB. The meaning of urinary creatinine concentration. Kidney Int. 2011 Apr;79(7):791).
Fruto de los resultados del estudio prospectivo se identificaron los siguientes aspectos:As a result of the results of the prospective study, the following aspects were identified:
1. Existe una asociación entre niveles de GDF15 urinario con el diagnóstico de nefropatía diabética en pacientes con diabetes.1. There is an association between urinary GDF15 levels and the diagnosis of diabetic nephropathy in patients with diabetes.
Se observó que la nefropatía diabética es la causa de ERC en la que existen mayores niveles de GDF15 en orina con respecto a otras causas (tabla 8)It was observed that diabetic nephropathy is the cause of CKD in which there are higher levels of GDF15 in urine compared to other causes (table 8).
Tabla 8. GDF1S en suero ng/ml y orina ng/mg según diagnósticos, organizado en orden de frecuencia del diagnóstico. Datos expresados como media ± desviación estándar (n). Los valores obtenidos de uno o dos pacientes se indican en paréntesis. Los datos obtenidos de un paciente no tienen desviación estándar por tratarse de un solo valor.Table 8. GDF1S in serum ng/ml and urine ng/mg according to diagnoses, organized in order of frequency of diagnosis. Data expressed as mean ± standard deviation (n). Values obtained from one or two patients are indicated in parentheses. The data obtained from a patient does not have a standard deviation because it is a single value.


Tabla 9. GDF15 en orina en pacientes diabéticas can riñones nativos (no trasplantados) con nefropatía diabética versus con otros diagnósticos diferentes de nefropatía diabética Table 9. GDF15 in urine in diabetic patients with native (non-transplanted) kidneys with diabetic nephropathy versus diagnoses other than diabetic nephropathy.
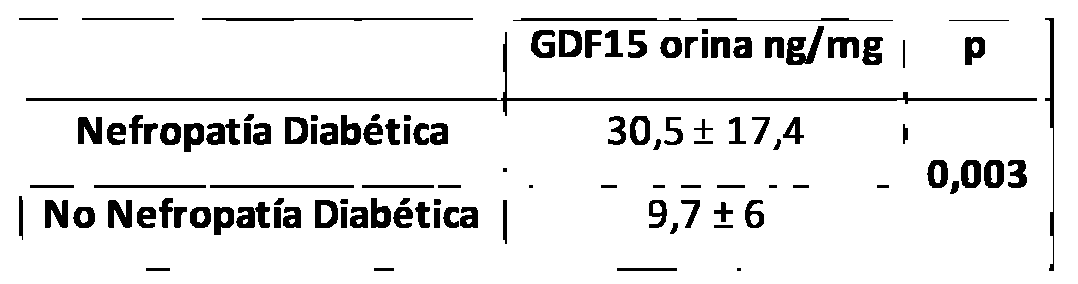
Asimismo, se observó que los pacientes con diagnóstico de diabetes y de ERC (Enfermedad renal crónica) basado en el filtrado glomerular y la albuminuria, que fueron diagnosticados de nefropatía diabética en la biopsia comparados con los pacientes biopsiados con diagnóstico de diabetes y de ERC (Enfermedad renal crónica) basado en el filtrado glomerular y la albuminuria sin nefropatía diabética en la biopsia, tenían niveles significativamente más altos de GDF15 en orina (figura 2 y tabla 9), por loque los valores de GDF15 urinario contribuyen a diferenciar la causa del daño renal en pacientes diabéticos con ERC (Enfermedad renal crónica) basado en el filtrado glomerular y la albuminuria.Likewise, it was observed that patients with a diagnosis of diabetes and CKD (Chronic Kidney Disease) based on glomerular filtration rate and albuminuria, who were diagnosed with diabetic nephropathy in the biopsy compared to patients biopsied with a diagnosis of diabetes and CKD ( Chronic kidney disease) based on glomerular filtration rate and albuminuria without diabetic nephropathy in the biopsy, had significantly higher levels of GDF15 in urine (figure 2 and table 9), so urinary GDF15 values contribute to differentiating the cause of the damage kidney in diabetic patients with CKD (Chronic Kidney Disease) based on glomerular filtration and albuminuria.
2. Existe una asociación entre niveles de GDF15 urinario con mortalidad 2. There is an association between urinary GDF15 levels and mortality
Se realizaron árboles de clasificación para valorar si los valores de GDF15 en suero y orina podían predecir la evolución de pacientes con supervivencia sin diálisis, supervivencia con diálisis o muerte. De acuerdo a esta clasificación, la única variable que predijo la evolución de los pacientes fue el valor de GDF15 en orina, que si era mayor de 19.9 ng/mg se asociaba a aumento de mortalidad: mortalidad 83% entre pacientes con valores de GDF15 urinario > 20 ng/mg de creatinina en orina (figura 3). Adicionalmente, para valorar el aporte de GDF15 sobre la evolución de los pacientes, se realizaron modelos de regresión logística (tabla 10).Classification trees were made to assess whether GDF15 values in serum and urine could predict the outcome of patients with survival without dialysis, survival with dialysis or death. According to this classification, the only variable that predicted the evolution of the patients was the value of GDF15 in urine, which if it was greater than 19.9 ng/mg was associated with increased mortality: mortality 83% among patients with urinary GDF15 values > 20 ng/mg creatinine in urine (figure 3). Additionally, to assess the contribution of GDF15 on patient outcomes, logistic regression models were performed (Table 10).
Tabla 10. Modelos de regresión logística para predecir evolución: muerte, diálisis o vivo, valoradas por separado las variables GDF1S en suero y orina. Table 10. Logistic regression models to predict outcome: death, dialysis or alive, with the GDF1S variables in serum and urine assessed separately.

Unidades en las que fueron medidas las variables: GFF15 suero ng/ml, GDF15 orina ng/ml. Edad (años). Sexo (mas/fem), MAU/Cr (albuminuria:creatinuria) mg/gr, FG ml/min/l,73m2.Units in which the variables were measured: GFF15 serum ng/ml, GDF15 urine ng/ml. Age (years). Sex (mas/fem), MAU/Cr (albuminuria:creatinuria) mg/gr, GFR ml/min/l,73m2.
En todos los modelos: multivariables, árboles de clasificación y regresión logística, se aprecia una relación de GDF15 en orina con mortalidad. En relación con el GDF15 en suero, solo apreciamos relación con mortalidad en el modelo de regresión logística, esto podría deberse a que en este último el GDF15 en suero no fue incluido en las variables independientes al mismo tiempo que el GDF15 en orina, como en los modelos de árboles de clasificación. Esto indica que la relación con mortalidad es más fuerte con los niveles de GDF15 en orina. Para demostrar esto realizamos dos modelos multivariables adicionales en los que incluimos a la vez como variables independientes: GDF15 en suero, GDF15 en orina y edad, que fueron las variables asociadas con mortalidad en la tabla 10. En estos modelos se aprecia como GDF15 en suero queda excluido al ser comparado con GDF15 en orina como predictor de mortalidad (ver tabla 11).In all models: multivariable, classification trees and logistic regression, a relationship between GDF15 in urine and mortality is seen. In relation to GDF15 in serum, we only saw a relationship with mortality in the logistic regression model; this could be due to the fact that in the latter, GDF15 in serum was not included in the independent variables at the same time as GDF15 in urine, as in classification tree models. This indicates that the relationship with mortality is stronger with urinary GDF15 levels. To demonstrate this, we performed two additional multivariable models in which we included as independent variables: GDF15 in serum, GDF15 in urine and age, which were the variables associated with mortality in table 10. These models show how GDF15 in serum is excluded when compared with GDF15 in urine as a predictor of mortality (see table 11).
Tabla 11. Modelos de regresión logística para predecir evolución: muerte, diálisis o vivo, valoradas a la vez las variables GDF1S en suero y orina. Table 11. Logistic regression models to predict outcome: death, dialysis or alive, simultaneously assessing the GDF1S variables in serum and urine.

Unidades en lasque fueron medidas las variables: GFF15 suero ng/ml, GDF15 orina ng/ml. Edad (años).Units in which the variables were measured: GFF15 serum ng/ml, GDF15 urine ng/ml. Age (years).
Dada esta importante relación entre GDF15 en orina y los eventos no deseados de mortalidad, se realizaron unas curvas ROC para representar gráficamente la sensibilidad y especificidad que tiene GDF15 en orina para predecir el estado final del paciente: muerte, diálisis o muerte diálisis (figura 4). Las curvas ROC obtenidas indican que GDF15 tiene un buen índice de calidad diagnóstica para predecir mortalidad, con un área bajo la curva (AUC) de 0,952 (IC 95% 0,9-1; p <0,001). Se utilizó el índice de Youden para decidir el valor de corte que maximice la diferencia entre sensibilidad y (1 - especificidad). Mediante este índice se determinó el punto de corte: GDF15 en orina 13,83 ng/mg. Lo que indica que el test es positivo si el valor es superior de 13,83 ng/mg con una sensibilidad de 100% y especificidad de 81%. Los valores de área bajo la curva son menores para predecir mortalidad diálisis: AUC 0,777 (IC 95% 0,6-0,9; p=0,001) y no fue significativo para predecir diálisis por separado: AUC 0,541 (IC 95% 0,3 0,7; p=0,695).Given this important relationship between GDF15 in urine and unwanted mortality events, ROC curves were made to graphically represent the sensitivity and specificity of GDF15 in urine to predict the final state of the patient: death, dialysis, or death on dialysis (Figure 4 ). The ROC curves obtained indicate that GDF15 has a good diagnostic quality index for predicting mortality, with an area under the curve (AUC) of 0.952 (95% CI 0.9-1; p <0.001). Youden's index was used to decide the cut-off value that maximizes the difference between sensitivity and (1 - specificity). Using this index, the cut-off point was determined: GDF15 in urine 13.83 ng/mg. Which indicates that the test is positive if the value is greater than 13.83 ng/mg with a sensitivity of 100% and specificity of 81%. The area under the curve values are lower to predict dialysis mortality: AUC 0.777 (95% CI 0.6-0.9; p=0.001) and were not significant to predict dialysis separately: AUC 0.541 (95% CI 0. 3 0.7; p=0.695).
Por lo tanto, y en base a los dos análisis estadísticos explicitados en este apartado podemos concluir que a mayor GDF15 en orina, mayor mortalidad. Explicar que la forma tradicional de identificar un punto de corte es la curva ROC que identifica el punto óptimo asociado a mayor sensibilidad y especificad. El punto de corte de 13,8 ng/mg identificado en el párrafo precedente, se trata del punto de corte ideal para identificar a todos los pacientes de alto riesgo. El punto de corte de 19.9 ng/mg mencionado en los párrafos iniciales de esta sección, solo identifica a alrededor del 80% de aquellos pacientes que van a morir.Therefore, and based on the two statistical analyzes explained in this section, we can conclude that the higher GDF15 in urine, the higher mortality. Explain that the traditional way of identifying a cut-off point is the ROC curve that identifies the optimal point associated with greater sensitivity and specificity. He cut-off point of 13.8 ng/mg identified in the preceding paragraph, this is the ideal cut-off point to identify all high-risk patients. The cut-off point of 19.9 ng/mg mentioned in the opening paragraphs of this section only identifies about 80% of those patients who will die.
En cualquier caso y dados estos hallazgos, podemos afirmar que los niveles urinarios de GDF15 identifican pacientes ya diagnosticados de ERC que tienen un altísimo riesgo de muerte. En concreto el 100% de los pacientes con GDF15 urinario >13,8ng/mg falleció durante un seguimiento medio de 30 meses.In any case and given these findings, we can affirm that urinary GDF15 levels identify patients already diagnosed with CKD who have a very high risk of death. Specifically, 100% of patients with urinary GDF15 >13.8ng/mg died during a mean follow-up of 30 months.
Por lo tanto, y en base a los resultados experimentales aportados hasta el momento, podemos concluir que:Therefore, and based on the experimental results provided so far, we can conclude that:
a. los niveles urinarios de GDF15 se incrementan en varios modelos de daño renal agudo y crónico y, por tanto, constituyen un biomarcador de daño renal;to. urinary GDF15 levels are increased in several models of acute and chronic kidney damage and, therefore, constitute a biomarker of kidney damage;
b. los niveles urinarios de GDF15 contribuyen a diferenciar la causa del daño renal en pacientes diabéticos, diferenciando entre pacientes diabéticos con nefropatía diabética y sin nefropatía diabética; yb. urinary GDF15 levels contribute to differentiating the cause of kidney damage in diabetic patients, differentiating between diabetic patients with diabetic nephropathy and without diabetic nephropathy; and
c. los niveles urinarios de GDF15 identifican pacientes ya diagnosticados de ERC que tienen un altísimo riesgo de muerte, en concreto el 100% de los pacientes con GDF15 urinario >13,8ng/mg falleció durante un seguimiento medio de 30 meses.c. urinary GDF15 levels identify patients already diagnosed with CKD who have a very high risk of death, specifically 100% of patients with urinary GDF15 >13.8ng/mg died during a mean follow-up of 30 months.
Por otro lado, la elección de determinar niveles urinarios de GDF15 en vez de niveles séricos de GDF15 no es causal, tal y como se muestra en los ejemplos. GDF15 es una proteína pequeña de 25KDa que atraviesa fácilmente la barrera de filtración glomerular. Sin embargo, en condiciones normales, las células tubulares proximales debieran reabsorber el GDF15 filtrado, y no debiera aparecer en orina. La existencia de GDF15en orina podría deberse a las siguientes razones:On the other hand, the choice to determine urinary GDF15 levels instead of serum GDF15 levels is not causal, as shown in the examples. GDF15 is a small 25KDa protein that easily crosses the glomerular filtration barrier. However, under normal conditions, filtered GDF15 should be reabsorbed by proximal tubular cells, and it should not appear in urine. The existence of GDF15 in urine could be due to the following reasons:
• Que exista una exagerada producción sistémica de GDF15 que exceda la capacidad de reabsorción de las células tubulares.• That there is an exaggerated systemic production of GDF15 that exceeds the reabsorption capacity of the tubular cells.
• Que el GDF15 urinario provenga de un aumento de síntesis a nivel local, secundario al daño renal, al igual que aumenta la síntesis de otras citoquinas y mediadores en el contexto del estado inflamatorio de la uremia.• That urinary GDF15 comes from an increase in synthesis at a local level, secondary to kidney damage, just as it increases the synthesis of other cytokines and mediators in the context of the inflammatory state of uremia.
Sin perjuicio de lo anterior, determinar niveles urinarios de GDF15 en vez de niveles séricos de GDF15, proporciona (ver ejemplo 1) valores notablemente más altos de sensibilidad y especificidad como biomarcador predictor de mortalidad a 30 meses en pacientes que padecen de ERC. Los pacientes con ERC tienen un alto riesgo de mortalidad prematura. Sin embargo, dentro de la ERC diferentes pacientes pueden tener un riesgo diferente de mortalidad prematura, la incapacidad para identificar estos pacientes de altísimo riesgo tiene un impacto negativo sobre la selección de pacientes para ensayos clínicos. En general, los ensayos clínicos en pacientes con ERC que tienen un punto final primario de eventos graves o mortalidad han fracasado. En al menos algunos de ellos, la razón del fracaso fue un escaso enriquecimiento en paciente de alto riesgo. La posibilidad que brindan los niveles de GDF15 en orina de identificar pacientes con altísimo riesgo de muerte puede ayudar a diseñar ensayos clínicos centrados en estos pacientes que permitan identificar nuevos tratamientos que disminuyan la mortalidad. En este sentido, hemos de recalcar que GDF15 en orina predijo la alta mortalidad en pacientes seguidos en unidades de nefrología, esto es en pacientes tratados, según el estado del arte actual. Ello implica que los tratamientos actuales son incapaces de evitar la mortalidad asociada a altos niveles de GDF15 en orina.Without prejudice to the above, determining urinary levels of GDF15 instead of serum levels of GDF15, provides (see example 1) notably higher values of sensitivity and specificity as biomarker predictor of 30-month mortality in patients suffering from CKD. Patients with CKD have a high risk of premature mortality. However, within CKD different patients may have a different risk of premature mortality, the inability to identify these very high risk patients has a negative impact on the selection of patients for clinical trials. In general, clinical trials in patients with CKD who have a primary end point of serious events or mortality have failed. In at least some of them, the reason for failure was poor enrichment in high-risk patients. The possibility that GDF15 levels in urine offer to identify patients with a very high risk of death can help design clinical trials focused on these patients that allow the identification of new treatments that reduce mortality. In this sense, we must emphasize that GDF15 in urine predicted high mortality in patients followed up in nephrology units, that is, in patients treated, according to the current state of the art. This implies that current treatments are unable to avoid the mortality associated with high levels of GDF15 in urine.
Por otro lado, determinar niveles urinarios de GDF15 en vez de niveles séricos de GDF15, permite diferenciar entre pacientes diabéticos que sufren de nefropatía diabética de aquellos que no cuando los niveles séricos de GDF15 no permiten esta diferenciación (ver ejemplo 2). Por lo tanto y en este sentido, la utilidad clínica de la determinación de GDF15 en orina, para apoyar o descartar la existencia de nefropatía diabética sería de gran interés, porque evitaría realizar la biopsia de tejido renal, un procedimiento altamente invasivo, en pacientes con alta sospecha clínica de nefropatía diabética y un GDF15 en orina alto. Por otro lado, una alta sospecha clínica de nefropatía diabética y un GDF15 en orina bajo, podría sugerir realizar biopsia renal para descartar otra causa de ERC que requiera un tratamiento diferente al del manejo general de la ERC, como por ejemplo un tratamiento inmunosupresor.On the other hand, determining urinary levels of GDF15 instead of serum levels of GDF15 allows us to differentiate between diabetic patients who suffer from diabetic nephropathy from those who do not, when serum levels of GDF15 do not allow this differentiation (see example 2). Therefore, and in this sense, the clinical usefulness of determining GDF15 in urine, to support or rule out the existence of diabetic nephropathy, would be of great interest, because it would avoid performing a kidney tissue biopsy, a highly invasive procedure, in patients with high clinical suspicion of diabetic nephropathy and a high urinary GDF15. On the other hand, a high clinical suspicion of diabetic nephropathy and a low GDF15 in urine could suggest performing a kidney biopsy to rule out another cause of CKD that requires a different treatment than the general management of CKD, such as immunosuppressive treatment.
Así pues, la presente invención proporciona un método no invasivo para el diagnóstico y/o pronóstico de daño renal, fácilmente utilizable en la práctica clínica diaria, mediante un test sencillo, rápido y económico que permite la determinación en serie de un alto volumen de muestras.Thus, the present invention provides a non-invasive method for the diagnosis and/or prognosis of kidney damage, easily usable in daily clinical practice, through a simple, rapid and economical test that allows the serial determination of a high volume of samples. .
Así pues, en un primer aspecto, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de la proteína GDF15, opcionalmente previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador de diagnóstico y/o pronóstico de daño renal. Por daño renal en la presente invención nos referimos, sin limitarnos, a cualquier anormalidad funcional o estructural de diversa etiología ya sea por una disminución en la perfusión renal o intrarrenal, por una agresión tóxica u obstrucción del túbulo renal, por inflamación tubulointersticial y edema o por una reducción en la capacidad de filtración del glomérulo. En una realización más preferida de la presente invención, el daño renal que se puede diagnosticar y/o pronosticar es un daño renal agudo o crónico, más preferiblemente el daño renal que se puede diagnosticar y/o pronosticar es un daño renal crónico (ERC).Thus, in a first aspect, the present invention refers to the use of at least the urinary levels or concentration of the GDF15 protein, optionally before, after or simultaneously with the determination of the glomerular filtration rate and/or albuminuria, preferably after the determination of glomerular filtration rate and/or albuminuria, as a diagnostic and/or prognostic marker of kidney damage. By kidney damage in the present invention we refer, without limitation, to any functional or structural abnormality of diverse etiology, whether due to a decrease in renal or intrarenal perfusion, due to toxic aggression or obstruction of the renal tubule, due to inflammation. tubulointerstitial and edema or by a reduction in the filtration capacity of the glomerulus. In a more preferred embodiment of the present invention, the kidney damage that can be diagnosed and/or predicted is acute or chronic kidney damage, more preferably the kidney damage that can be diagnosed and/or predicted is chronic kidney damage (CKD). .
Por daño renal agudo en la presente invención nos referimos a un daño renal cuya anormalidad funcional o estructural que lo produce está presente durante menos de tres meses consecutivos. Más de tres meses consecutivos de dicha anormalidad funcional o estructural produciría un daño renal crónico (Kidney Disease: ImprovingGlobalBy acute kidney injury in the present invention we refer to kidney damage whose functional or structural abnormality that produces it is present for less than three consecutive months. More than three consecutive months of said functional or structural abnormality would produce chronic kidney damage (Kidney Disease: ImprovingGlobal
Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and ManagementofChronic Kidney Disease. Kidney InternationalSupplements 2013;3:1-150).Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney InternationalSupplements 2013;3:1-150).
Se hace notar que, de acuerdo a cualquiera de los aspectos de la presente invención, los niveles de GDF15 se pueden medir o determinar por si mismos o se pueden normalizar con respecto a los niveles urinarios de creatinina.It is noted that, according to any of the aspects of the present invention, GDF15 levels can be measured or determined by themselves or can be normalized with respect to urinary creatinine levels.
En una realización preferida del primer aspecto de la invención, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador de diagnóstico de nefropatía diabética. Preferiblemente, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador de diagnóstico diferencial de la causa etiológica del daño renal en pacientes diabéticos. Más preferiblemente, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador de diagnóstico diferencial de la causa etiológica del daño renal en pacientes diabéticos, diferenciando entre pacientes diabéticos con nefropatía diabética y sin nefropatía diabética, donde dichos pacientes diabéticos preferiblemente habían sido previamente diagnosticados con ERCen base a la determinación del filtrado glomerulary/o la albuminuria.In a preferred embodiment of the first aspect of the invention, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate. and/or albuminuria, preferably the urinary levels or concentration of GDF15 are determined subsequent to the determination of glomerular filtration rate and/or albuminuria, as a diagnostic marker of diabetic nephropathy. Preferably, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate and/or albuminuria, preferably the levels or urinary GDF15 concentrations are determined after determining glomerular filtration rate and/or albuminuria, as a differential diagnostic marker of the etiological cause of kidney damage in diabetic patients. More preferably, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate and/or albuminuria, preferably the Urinary levels or concentration of GDF15 are determined after the determination of glomerular filtration rate and/or albuminuria, as a differential diagnostic marker of the etiological cause of kidney damage in diabetic patients, differentiating between diabetic patients with diabetic nephropathy and without diabetic nephropathy, where said patients Diabetics preferably had been previously diagnosed with CKD based on the determination of glomerular filtration rate and/or albuminuria.
En otra realización preferida del primer aspecto de la invención, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador pronóstico de mortalidad de aquellos enfermos o pacientes diagnosticados con daño renal, ya sea éste daño agudo o crónico. Preferiblemente, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico. Más preferiblemente, la presente invención se refiere al uso de al menos los niveles o concentración urinarios de GDF15, opcionalmente dichos niveles o concentración urinarios de GDF15 se determinan previa, posterior o simultáneamente a la determinación del filtrado glomerular y/o la albuminuria, preferiblemente los niveles o concentración urinarios de GDF15 se determinan posteriormente a la determinación del filtrado glomerular y/o la albuminuria, como marcador pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico; donde por pronóstico de mortalidad se entiende la muerte del paciente en un periodo menor a 5 años, preferiblemente menor a 3 años, más preferiblemente menor a 30 a meses, desde la determinación de la concentración incrementada de GDF15 en la orina del paciente. Preferiblemente, dichos enfermos habían sido previamente diagnosticados con ERC en base a la determinación del filtrado glomerular y/o la albuminuria.In another preferred embodiment of the first aspect of the invention, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate. and/or albuminuria, preferably the urinary levels or concentration of GDF15 are determined after the determination of the glomerular filtration rate and/or albuminuria, as a prognostic marker of mortality for those patients or patients diagnosed with kidney damage, whether this damage is acute or chronic. Preferably, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate and/or albuminuria, preferably the levels or urinary concentrations of GDF15 are determined after the determination of glomerular filtration rate and/or albuminuria, as a prognostic marker of mortality in those patients diagnosed with chronic kidney damage. More preferably, the present invention relates to the use of at least the urinary levels or concentration of GDF15, optionally said urinary levels or concentration of GDF15 are determined before, after or simultaneously with the determination of the glomerular filtration rate and/or albuminuria, preferably the Urinary levels or concentration of GDF15 are determined after the determination of glomerular filtration rate and/or albuminuria, as a prognostic marker of mortality in those patients diagnosed with chronic kidney damage; where mortality prognosis means the death of the patient in a period of less than 5 years, preferably less than 3 years, more preferably less than 30 months, from the determination of the increased concentration of GDF15 in the patient's urine. Preferably, said patients had previously been diagnosed with CKD based on the determination of glomerular filtration rate and/or albuminuria.
En un segundo aspecto, la presente invención se refiere a un método para la obtención de datos útiles en el diagnóstico y/o pronóstico de daño renal que comprende determinar en una muestra aislada de orina los niveles o concentración urinarios de GDF15. En una realización particular, dicho nivel o concentración se determina mediante análisis fluorométrico o mediante cualquier tipo de inmunoensayo (incluyendo ELISA) o mediante espectrometría de masas. En una realización preferida del segundo aspecto de la invención, el método es para la obtención de datos útiles en el diagnóstico de nefropatía diabética. Preferiblemente, el método es para la obtención de datos útiles en el diagnóstico diferencial de la causa etiológica del daño renal en pacientes diabéticos. Más preferiblemente, el método es para la obtención de datos útiles en el diagnóstico diferencial de la causa etiológica del daño renal en pacientes diabéticos, aportando datos que ayudan en la diferenciación entre pacientes diabéticos que padecen de ERC, preferiblemente dicho diagnóstico de ERC se hace en base al filtrado glomerulary/o la albuminuria, con nefropatía diabética y sin nefropatía diabética.In a second aspect, the present invention refers to a method for obtaining data useful in the diagnosis and/or prognosis of kidney damage that comprises determining the urinary levels or concentration of GDF15 in an isolated urine sample. In a particular embodiment, said level or concentration is determined by fluorometric analysis or by any type of immunoassay (including ELISA) or by mass spectrometry. In a preferred embodiment of the second aspect of the invention, the method is for obtaining data useful in the diagnosis of diabetic nephropathy. Preferably, the method is for obtaining data useful in the differential diagnosis of the etiological cause of kidney damage in diabetic patients. More preferably, the This method is for obtaining useful data in the differential diagnosis of the etiological cause of kidney damage in diabetic patients, providing data that helps in the differentiation between diabetic patients who suffer from CKD, preferably said diagnosis of CKD is made based on glomerular filtration. /or albuminuria, with diabetic nephropathy and without diabetic nephropathy.
En otra realización preferida del segundo aspecto de la invención, el método es para la obtención de datos útiles en el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal, ya sea este daño agudo o crónico. Preferiblemente, el método es para la obtención de datos útiles en el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico. Más preferiblemente, el método es para la obtención de datos útiles en el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico, preferiblemente dicho diagnóstico de ERC se hace en base al filtrado glomerular y/o la albuminuria , donde por pronóstico de mortalidad se entiende la muerte del paciente en un periodo menor a 5 años, preferiblemente menor a 3 años, más preferiblemente menor a 30 a meses, desde la determinación de la concentración incrementada de GDF15en la orina del paciente.In another preferred embodiment of the second aspect of the invention, the method is for obtaining data useful in the prognosis of mortality of those patients diagnosed with kidney damage, whether this damage is acute or chronic. Preferably, the method is for obtaining data useful in the mortality prognosis of those patients diagnosed with chronic kidney damage. More preferably, the method is for obtaining useful data in the mortality prognosis of those patients diagnosed with chronic kidney damage, preferably said diagnosis of CKD is made based on glomerular filtration and/or albuminuria, where for mortality prognosis, means the death of the patient in a period of less than 5 years, preferably less than 3 years, more preferably less than 30 months, from the determination of the increased concentration of GDF15 in the patient's urine.
En un tercer aspecto, la presente invención se refiere a un método para el diagnóstico y/o pronóstico de daño renal que comprende analizar una muestra de orina obtenida de un paciente, determinar al menos los niveles o concentración urinarios de GDF15, y comparar dicho nivel o concentración con un valor control, donde la alteración de dicho nivel o concentración, donde preferiblemente dicha alteración constituye un incremento con respecto al valor control, es indicativa de daño renal. En una realización preferida del tercer aspecto de la invención, el método es para el diagnóstico de nefropatía diabética, donde se determina al menos los niveles o concentración urinarios de GDF15, y se compara dicho nivel o concentración con un valor control, donde la alteración de dicho nivel o concentración, donde preferiblemente dicha alteración constituye un incremento con respecto al valor control, es indicativa de nefropatía diabética. Preferiblemente, el método es para el diagnóstico diferencial de nefropatía diabética en un paciente diabético diagnosticado con ERC, preferiblemente dicho diagnóstico de ERC se hace en base al filtrado glomerular y/o la albuminuria , donde se determina al menos los niveles o concentración urinarios de GDF15, y se compara dicho nivel o concentración con un valor control, donde la alteración de dicho nivel concentración, donde preferiblemente dicha alteración constituye un incremento con respecto al valor control, es indicativa de que la causa etiológica del daño renal en dicho pacientes diabético es la nefropatía diabética.In a third aspect, the present invention relates to a method for the diagnosis and/or prognosis of kidney damage that comprises analyzing a urine sample obtained from a patient, determining at least the urinary levels or concentration of GDF15, and comparing said level. or concentration with a control value, where the alteration of said level or concentration, where preferably said alteration constitutes an increase with respect to the control value, is indicative of kidney damage. In a preferred embodiment of the third aspect of the invention, the method is for the diagnosis of diabetic nephropathy, where at least the urinary levels or concentration of GDF15 are determined, and said level or concentration is compared with a control value, where the alteration of Said level or concentration, where preferably said alteration constitutes an increase with respect to the control value, is indicative of diabetic nephropathy. Preferably, the method is for the differential diagnosis of diabetic nephropathy in a diabetic patient diagnosed with CKD, preferably said diagnosis of CKD is made based on glomerular filtration and/or albuminuria, where at least the urinary levels or concentration of GDF15 are determined. , and said level or concentration is compared with a control value, where the alteration of said concentration level, where preferably said alteration constitutes an increase with respect to the control value, is indicative that the etiological cause of kidney damage in said diabetic patients is diabetic nephropathy.
En otra realización preferida del tercer aspecto de la invención, el método es para el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal, ya sea éste daño agudo o crónico, que comprende analizar una muestra de orina aislada obtenida del paciente, determinaral menos los niveles o concentración urinarios de GDF15, y comparar dicho nivel o concentración con un valor control, donde la alteración de dicho nivel o concentración, donde preferiblemente dicha alteración constituye un incremento con respecto al valor control, es indicativo de un pronóstico de muerte del paciente en un periodo menor a 5 años, preferiblemente menor a 3 años, más preferiblemente menor a 30 a meses, desde la determinación de la concentración incrementada de GDF15 en la orina del paciente. Preferiblemente, el método es para el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico, donde preferiblemente dicho diagnóstico de ERC se hace en base al filtrado glomerulary/o la albuminuria.In another preferred embodiment of the third aspect of the invention, the method is for the prognosis of mortality of those patients diagnosed with kidney damage, whether this damage is acute or chronic, which It comprises analyzing an isolated urine sample obtained from the patient, determining at least the urinary levels or concentration of GDF15, and comparing said level or concentration with a control value, where the alteration of said level or concentration, where preferably said alteration constitutes an increase with respect to at the control value, it is indicative of a prognosis of death of the patient in a period of less than 5 years, preferably less than 3 years, more preferably less than 30 months, from the determination of the increased concentration of GDF15 in the patient's urine. Preferably, the method is for the mortality prognosis of those patients diagnosed with chronic kidney damage, where preferably said diagnosis of CKD is made based on glomerular filtration and/or albuminuria.
Por otro lado, la caracterización del GDF15 urinario sirve no sólo para dilucidar el diagnóstico o pronóstico de la enfermedad renal, ayudar a identificar el mecanismo del daño renal, y/o indicar el sitio y la severidad del daño, sino que debe ayudar a monitorizar la respuesta al tratamiento, para cribar o seleccionar pacientes y para tratar aquellos pacientes conforme a la selección o cribado efectuado. On the other hand, the characterization of urinary GDF15 serves not only to elucidate the diagnosis or prognosis of kidney disease, help identify the mechanism of kidney damage, and/or indicate the site and severity of damage, but should also help to monitor the response to treatment, to screen or select patients and to treat those patients in accordance with the selection or screening carried out.
Por tanto, un cuarto aspecto de la invención se refiere a un método de monitorización de la respuesta al tratamiento de un paciente diagnosticado con daño renal y que esté actualmente sujeto a tratamiento, que comprende analizar una muestra de orina obtenida del paciente, determinaral menos los niveles o concentración urinarios de GDF15 en dicha muestra, y comparar dicho nivel o concentración con el nivel o concentración de GDF15 en una muestra de orina obtenida en un momento anterior en el tiempo del mismo paciente, donde la alteración de dicho nivel o concentración de forma que dicha alteración constituya una reducción con respecto al valor anterior, es indicativa de una progresión favorable del paciente; y donde la alteración de dicho nivel o concentración de forma que dicha alteración constituya un incremento con respecto al valor anterior, es indicativa de una progresión desfavorable del paciente. En una realización preferida del cuarto aspecto de la invención, el paciente ha sido diagnosticado con ERC. En otra realización preferida del cuarto aspecto de la invención el paciente es diabético diagnosticado con ERC y con nefropatía diabética.Therefore, a fourth aspect of the invention relates to a method of monitoring the response to treatment of a patient diagnosed with kidney damage and who is currently subject to treatment, which comprises analyzing a urine sample obtained from the patient, determining at least the urinary levels or concentration of GDF15 in said sample, and comparing said level or concentration with the level or concentration of GDF15 in a urine sample obtained at a previous moment in time from the same patient, where the alteration of said level or concentration of form That said alteration constitutes a reduction with respect to the previous value is indicative of a favorable progression of the patient; and where the alteration of said level or concentration so that said alteration constitutes an increase with respect to the previous value, is indicative of an unfavorable progression of the patient. In a preferred embodiment of the fourth aspect of the invention, the patient has been diagnosed with CKD. In another preferred embodiment of the fourth aspect of the invention, the patient is a diabetic diagnosed with CKD and diabetic nephropathy.
En un quinto aspecto, la invención se refiere a un método de cribado de pacientes diabéticos que padecen o han sido diagnosticados con ERC, preferiblemente dicho diagnóstico de ERC se hace en base al FG y/o a la A, que comprende analizar una muestra de orina obtenida del paciente, determinar al menos los niveles o concentración urinarios de GDF15, y comparar dicho nivel o concentración con un valor control, donde si existe una alteración de dicho nivel o concentración y dicha alteración constituye un incremento con respecto al valor control, el paciente se clasifica como un paciente diabético que padece de nefropatía diabética; y donde si no existe una alteración de dicho nivel o concentración o si dicha alteración constituye una reducción con respecto al valor control, el paciente se clasifica como un paciente diabético que padece de una ERC distinta a la nefropatía diabética. Aquellos pacientes que padezcan de una ERC distinta a la nefropatía diabética, normalmente serán objeto de una biopsia para determinar la causa de la ERC. Aquellos pacientes que padezcan de nefropatía diabética, no serán objeto de una biopsia al haberse determinado la causa de la ERC.In a fifth aspect, the invention relates to a method for screening diabetic patients who suffer from or have been diagnosed with CKD, preferably said diagnosis of CKD is made based on the GFR and/or A, which comprises analyzing a urine sample. obtained from the patient, determine at least the urinary levels or concentration of GDF15, and compare said level or concentration with a control value, where if there is an alteration of said level or concentration and said alteration constitutes an increase with respect to the control value, the patient is classified as a diabetic patient suffering from diabetic nephropathy; and where if there is no alteration of said level or concentration or if This alteration constitutes a reduction with respect to the control value, the patient is classified as a diabetic patient who suffers from CKD other than diabetic nephropathy. Patients with CKD other than diabetic nephropathy will usually undergo a biopsy to determine the cause of the CKD. Those patients who suffer from diabetic nephropathy will not undergo a biopsy once the cause of CKD has been determined.
En una realización preferida del quinto aspecto de la invención, al paciente que padece de diabetes ya sea ésta diabetes mellitus tipo I o II y se clasifica de acuerdo al quinto aspecto de la invención como un paciente que padece de nefropatía diabética, se le trata con al menos una composición farmacéutica seleccionada de las siguientes: estatinas, antiplaqueta ríos, inhibidores del cotransportador de sodioglucosa tipo 2 (SGLT2) tales como empagliflozina o canagliflozina, o con análogos del péptido similar al glucagón-1 (GLP-1) tales como el liraglutido. Preferiblemente si el paciente padece de diabetes mellitus tipo II y se clasifica de acuerdo al quinto aspecto de la invención como un paciente que padece de nefropatía diabética, se le trata con inhibidores del cotransportador de sodio-glucosa tipo 2 (SGLT2) tales como empagliflozina o canagliflozina.In a preferred embodiment of the fifth aspect of the invention, the patient who suffers from diabetes, whether diabetes mellitus type I or II and is classified according to the fifth aspect of the invention as a patient suffering from diabetic nephropathy, is treated with at least one pharmaceutical composition selected from the following: statins, antiplatelet drugs, sodium glucose cotransporter type 2 (SGLT2) inhibitors such as empagliflozin or canagliflozin, or glucagon-like peptide-1 (GLP-1) analogues such as liraglutide . Preferably if the patient suffers from type II diabetes mellitus and is classified according to the fifth aspect of the invention as a patient suffering from diabetic nephropathy, he is treated with sodium-glucose cotransporter 2 (SGLT2) inhibitors such as empagliflozin or canagliflozin.
Un sexto aspecto de la invención se refiere a un método de cribado de pacientes con alto riesgo de muerte y que padecen o han sido diagnosticados con enfermedad renal, preferiblemente de ERC y donde preferiblemente dicho diagnóstico de ERC se hace en base al filtrado glomerular y/o la albuminuria , que comprende analizar una muestra de orina aislada obtenida del paciente, determinar al menos los niveles o concentración urinarios de GDF15, y comparar dicho nivel o concentración con un valor control, donde si existe una alteración de dicho nivel o concentración y dicha alteración constituye un incremento con respecto al valor control, el paciente se selecciona como un paciente con pronóstico de muerte en un periodo menor a 5 años, preferiblemente menor a 3 años, más preferiblemente menor a 30 a meses, desde la determinación de la concentración incrementada de GDF15 en la orina del paciente. Preferiblemente, el método es para el pronóstico de mortalidad de aquellos enfermos diagnosticados con daño renal crónico, donde preferiblemente dicho diagnóstico de ERC se hace en base al FG y/o a la A. En una realización preferida del sexto aspecto de la invención el paciente, diabético o no, que padece de enfermedad renal, preferiblemente de ERC y donde preferiblemente dicho diagnóstico de ERC se hace en base al FG y/o a la A, y se clasifica de acuerdo al sexto aspecto de la invención como un paciente con pronóstico de muerte en un periodo menor a 5 años, se le trata con al menos una composición farmacéutica seleccionada de las siguientes: estatinas, antiplaqueta ríos, inhibidores del cotransportador de sodio-glucosa tipo 2 (SGLT2) tales como empagliflozina o canagliflozina, o con análogos del péptido similar al glucagón-1 (GLP-1) tales como el liraglutido.. A sixth aspect of the invention refers to a method of screening patients with a high risk of death and who suffer from or have been diagnosed with kidney disease, preferably CKD and where preferably said diagnosis of CKD is made based on glomerular filtration and/or or albuminuria, which includes analyzing an isolated urine sample obtained from the patient, determining at least the urinary levels or concentration of GDF15, and comparing said level or concentration with a control value, where if there is an alteration of said level or concentration and said alteration constitutes an increase with respect to the control value, the patient is selected as a patient with a prognosis of death in a period of less than 5 years, preferably less than 3 years, more preferably less than 30 months, from the determination of the increased concentration. of GDF15 in the patient's urine. Preferably, the method is for the mortality prognosis of those patients diagnosed with chronic kidney damage, where preferably said diagnosis of CKD is made based on the GFR and/or the A. In a preferred embodiment of the sixth aspect of the invention, the patient, diabetic or not, who suffers from kidney disease, preferably CKD and where preferably said diagnosis of CKD is made based on the GFR and/or the A, and is classified according to the sixth aspect of the invention as a patient with a prognosis of death. In a period of less than 5 years, it is treated with at least one pharmaceutical composition selected from the following: statins, antiplatelet drugs, sodium-glucose cotransporter 2 (SGLT2) inhibitors such as empagliflozin or canagliflozin, or with peptide analogues. similar to glucagon-1 (GLP-1) such as liraglutide.
En un séptimo aspecto, la presente invención se refiere a un kit o dispositivo, de ahora en adelante kit o dispositivo de la invención, para el diagnóstico y/o pronóstico de daño renal según cualquiera de los métodos descritos anteriormente, que comprende los reactivos necesarios para determinar el nivel o concentración de GDF15 en una muestra de orina tales como anticuerpos anti-GDF15, o fragmentos de los mismos o aptámeros anti-GDF15 o fluorocromos. En una realización preferida, el kit comprende los sustratos necesarios para determinar cuantitativamente la concentración o al nivel de GDF15 mediante un método fluorométrico o mediante cualquier tipo de inmunoensayo (tal y como un ELISA) utilizando anticuerpos anti-GDF15 o fragmentos de los mismos o aptámeros anti-GDF15. En un quinto aspecto, la presente invención se refiere al uso dicho kit para el diagnóstico y pronóstico del daño renal, preferiblemente para llevar a cabo cualquiera de los métodos descritos en los aspectos segundo a sexto de la presente invención.In a seventh aspect, the present invention refers to a kit or device, hereinafter kit or device of the invention, for the diagnosis and/or prognosis of kidney damage according to any of the methods described above, which comprises the necessary reagents to determine the level or concentration of GDF15 in a urine sample such as anti-GDF15 antibodies, or fragments thereof or anti-GDF15 aptamers or fluorochromes. In a preferred embodiment, the kit comprises the substrates necessary to quantitatively determine the concentration or level of GDF15 by a fluorometric method or by any type of immunoassay (such as an ELISA) using anti-GDF15 antibodies or fragments thereof or aptamers. anti-GDF15. In a fifth aspect, the present invention refers to the use of said kit for the diagnosis and prognosis of kidney damage, preferably to carry out any of the methods described in the second to sixth aspects of the present invention.
Los siguientes ejemplos meramente ilustran, pero en ningún caso limitan la presente invención.The following examples merely illustrate, but in no way limit the present invention.
EjemplosExamples
Ejemplo 1. Curvas ROC GDF15Example 1. GDF15 ROC curves
Las curvas ROC mostradas en las figuras 4 y 5 justifican que GDF15 en orina es un biomarcador predictor de mortalidad significativamente mejor que en suero.The ROC curves shown in Figures 4 and 5 justify that GDF15 in urine is a significantly better predictive biomarker of mortality than in serum.
Los datos de la figura 4 ilustran el comportamiento de GDF15 en orina como predictor de mortalidad: The data in Figure 4 illustrate the behavior of GDF15 in urine as a predictor of mortality:
AUC: 0,952 (p<0,001)AUC: 0.952 (p<0.001)
índice de Youden: 0,810Youden index: 0.810
Punto de corte: 13,83 ng/mgCutoff point: 13.83 ng/mg
Sensibilidad: 1Sensitivity: 1
1-Especificidad: 0,1901-Specificity: 0.190
Los datos de la figura 5 ilustran el comportamiento de GDF15en suero como predictor de mortalidad: AUC: 0,896 (p<0,001)The data in Figure 5 illustrate the behavior of GDF15 in serum as a predictor of mortality: AUC: 0.896 (p<0.001)
índice de Youden: 0,701Youden index: 0.701
Punto de corte: 2,98 ng/mlCutoff point: 2.98 ng/ml
Sensibilidad: 0,889Sensitivity: 0.889
I-Especificidad: 0,188I-Specificity: 0.188
Ejemplo 2. Comparación entre determinar niveles urinarios de GDF15 en vez de niveles séricos de GDF15, para el diagnósticode nefropatía diabéticaExample 2. Comparison between determining urinary levels of GDF15 instead of serum levels of GDF15, for the diagnosis of diabetic nephropathy
Se analizaron los valores de GDF15 séricos y en orina, observando que los pacientes con valores de GDF15 más altos correspondían a pacientes con diagnóstico de nefropatía diabética, en sangre eran 2 veces más altos y en orina 3 veces más altos en pacientes con nefropatía diabética comparados con otros diagnósticos.Serum and urine GDF15 values were analyzed, observing that patients with higher GDF15 values corresponded to patients with a diagnosis of diabetic nephropathy, in blood they were 2 times higher and in urine 3 times higher in patients with diabetic nephropathy compared with other diagnoses.
Sin embargo, comprobar si un paciente padece o no de nefropatía diabética resulta especialmente útil en pacientes diabéticos, para poder diferenciar la causa de la enfermedad renal crónica. Por eso se compararon los niveles de GDF15 urinario entre los pacientes diabéticos con nefropatía diabética y los pacientes diabéticos sin nefropatía diabética: los pacientes diabéticos con nefropatía diabética tuvieron niveles de GDF15 urinario 3 veces más altos y no se vio diferencia alguna con el GDF15 sérico (ver figura 2 ). However, checking whether or not a patient suffers from diabetic nephropathy is especially useful in diabetic patients, in order to differentiate the cause of chronic kidney disease. Therefore, urinary GDF15 levels were compared between diabetic patients with diabetic nephropathy and diabetic patients without diabetic nephropathy: diabetic patients with diabetic nephropathy had urinary GDF15 levels 3 times higher and no difference was seen with serum GDF15 ( see figure 2 ).
La utilidad clínica de la determinación de GDF15 en orina, para apoyar o descartar la existencia de nefropatía diabética sin realizar biopsia renal podría ser de gran interés, porque evitaría realizar la biopsia, un procedimiento invasivo, en pacientes con alta sospecha clínica de nefropatía diabética y un GDF15 en orina alto. Por otro lado, una alta sospecha clínica de nefropatía diabética y un GDF15 en orina bajo, podría sugerir realizar biopsia renal para descartar otra causa de ERC que requiera un tratamiento diferente al del manejo general de la ERC, como por ejemplo un tratamiento inmunosupresor.The clinical usefulness of determining GDF15 in urine, to support or rule out the existence of diabetic nephropathy without performing a renal biopsy, could be of great interest, because it would avoid performing the biopsy, an invasive procedure, in patients with a high clinical suspicion of diabetic nephropathy and a high GDF15 in urine. On the other hand, a high clinical suspicion of diabetic nephropathy and a low GDF15 in urine could suggest performing a kidney biopsy to rule out another cause of CKD that requires a different treatment than the general management of CKD, such as immunosuppressive treatment.
En la figura 6 se ilustra la curva ROC de GDF15 en orina como biomarcador de nefropatía diabética en pacientes diabéticos: (N=13)Figure 6 illustrates the ROC curve of GDF15 in urine as a biomarker of diabetic nephropathy in diabetic patients: (N=13)
AUC: 0,900 (p=0,0i9) AUC: 0.900 (p=0.0i9)
índice de Youden: 0,750Youden index: 0.750
Punto de corte: 10,486 ng/mgCutoff point: 10,486 ng/mg
Sensibilidad: 1,000Sensitivity: 1,000
I-Especificidad: 0,250 I-Specificity: 0.250
Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| ES201830849A ES2745352B2 (en) | 2018-08-28 | 2018-08-28 | GDF15 in urine as a biomarker of chronic kidney disease |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| ES201830849A ES2745352B2 (en) | 2018-08-28 | 2018-08-28 | GDF15 in urine as a biomarker of chronic kidney disease |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| ES2745352A1 ES2745352A1 (en) | 2020-02-28 |
| ES2745352B2 true ES2745352B2 (en) | 2023-08-10 |
Family
ID=69628206
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| ES201830849A Active ES2745352B2 (en) | 2018-08-28 | 2018-08-28 | GDF15 in urine as a biomarker of chronic kidney disease |
Country Status (1)
| Country | Link |
|---|---|
| ES (1) | ES2745352B2 (en) |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP6753861B2 (en) * | 2014-11-25 | 2020-09-09 | エフ.ホフマン−ラ ロシュ アーゲーF. Hoffmann−La Roche Aktiengesellschaft | Biomarker of rapid progression of chronic kidney disease |
-
2018
- 2018-08-28 ES ES201830849A patent/ES2745352B2/en active Active
Also Published As
| Publication number | Publication date |
|---|---|
| ES2745352A1 (en) | 2020-02-28 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| ES2380440T3 (en) | Marker for graft failure and mortality | |
| ES2933570T3 (en) | Methods and compositions for the diagnosis and prognosis of kidney injury and kidney failure | |
| ES2706403T3 (en) | Methods to diagnose and predict kidney disease | |
| Yang et al. | Urine neutrophil gelatinase-associated lipocalin: an independent predictor of adverse outcomes in acute kidney injury | |
| Giasson et al. | Neutrophil gelatinase-associated lipocalin (NGAL) as a new biomarker for non-acute kidney injury (AKI) diseases | |
| KR20140076571A (en) | Method for monitoring, diagnosis and/or prognosis of acute kidney injury in early stage | |
| US11041864B2 (en) | Method for prediction of prognosis of sepsis | |
| Singal et al. | Biomarkers of renal injury in cirrhosis: association with acute kidney injury and recovery after liver transplantation | |
| ES2622361T3 (en) | Biomarkers of kidney disease | |
| Devarajan et al. | Biomarkers in acute kidney injury: are we ready for prime time? | |
| Yepes-Calderón et al. | Urinary liver-type fatty acid-binding protein is independently associated with graft failure in outpatient kidney transplant recipients | |
| Fiorentino et al. | Plasma biomarkers in predicting renal recovery from acute kidney injury in critically ill patients | |
| JP2007163151A (en) | Method of determining physiological state of target organism | |
| ES2745352B2 (en) | GDF15 in urine as a biomarker of chronic kidney disease | |
| RU2520753C1 (en) | Method for prediction of developing complicated systemic inflammation response in patients with septic endocarditis | |
| WO2011105474A1 (en) | Method for examining acute renal disorder | |
| Thorlacius et al. | High‐sensitive troponinT, interleukin‐8, and interleukin‐6 link with post‐surgery risk in infant heart surgery | |
| Iseki et al. | C-reactive protein is a predictor for developing proteinuria in a screened cohort | |
| JP6062439B2 (en) | Evaluation markers for early kidney injury and methods for measuring them | |
| ES2529018T3 (en) | Methods and use for the evaluation of the severity of chronic obstructive pulmonary disease (COPD) | |
| Maravić-Stojković et al. | Levels of presepsin and midregion-proadrenomedullin in septic patients with end-stage renal disease after cardiovascular surgery: 1-year follow up study | |
| Al-Barshomy et al. | Value of serum copeptin estimation for the diagnosis of diabetic nephropathy in type 2 diabetes mellitus patients | |
| El-Kafrawy et al. | Study and Clinical Significance of Urinary Levels of Glypican 5 in Diabetic Patients | |
| RU2691937C1 (en) | Method for predicting the risk of developing ischemic heart disease in patients with type 2 diabetes mellitus combined with subclinical hypothyroidism | |
| JP7300642B2 (en) | Prognostic method for idiopathic pulmonary fibrosis |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| BA2A | Patent application published |
Ref document number: 2745352 Country of ref document: ES Kind code of ref document: A1 Effective date: 20200228 |
|
| FG2A | Definitive protection |
Ref document number: 2745352 Country of ref document: ES Kind code of ref document: B2 Effective date: 20230810 |