WO2020176797A1 - Immunotherapeutic combination for treating cancer - Google Patents
Immunotherapeutic combination for treating cancer Download PDFInfo
- Publication number
- WO2020176797A1 WO2020176797A1 PCT/US2020/020224 US2020020224W WO2020176797A1 WO 2020176797 A1 WO2020176797 A1 WO 2020176797A1 US 2020020224 W US2020020224 W US 2020020224W WO 2020176797 A1 WO2020176797 A1 WO 2020176797A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- cancer
- vaccine
- cells
- dna vaccine
- cell
- Prior art date
Links
- 206010028980 Neoplasm Diseases 0.000 title claims abstract description 295
- 201000011510 cancer Diseases 0.000 title claims abstract description 92
- 230000001024 immunotherapeutic effect Effects 0.000 title description 18
- 210000001744 T-lymphocyte Anatomy 0.000 claims abstract description 235
- 229960005486 vaccine Drugs 0.000 claims abstract description 160
- 238000000034 method Methods 0.000 claims abstract description 117
- 229940076838 Immune checkpoint inhibitor Drugs 0.000 claims abstract description 65
- 239000012274 immune-checkpoint protein inhibitor Substances 0.000 claims abstract description 65
- 150000001875 compounds Chemical class 0.000 claims abstract description 47
- 239000000203 mixture Substances 0.000 claims abstract description 28
- 230000010261 cell growth Effects 0.000 claims abstract description 10
- 238000002255 vaccination Methods 0.000 claims description 117
- 238000011282 treatment Methods 0.000 claims description 89
- 230000005867 T cell response Effects 0.000 claims description 84
- 230000000890 antigenic effect Effects 0.000 claims description 71
- 108010002350 Interleukin-2 Proteins 0.000 claims description 59
- 102000000588 Interleukin-2 Human genes 0.000 claims description 59
- 108010041986 DNA Vaccines Proteins 0.000 claims description 54
- 229940021995 DNA vaccine Drugs 0.000 claims description 54
- 229920001223 polyethylene glycol Polymers 0.000 claims description 51
- 230000001093 anti-cancer Effects 0.000 claims description 47
- 238000004519 manufacturing process Methods 0.000 claims description 44
- 108090000623 proteins and genes Proteins 0.000 claims description 38
- 102000004169 proteins and genes Human genes 0.000 claims description 36
- 230000008685 targeting Effects 0.000 claims description 35
- -1 9h-fluorene-9-yl Chemical group 0.000 claims description 33
- 238000006471 dimerization reaction Methods 0.000 claims description 32
- 230000006698 induction Effects 0.000 claims description 32
- 206010009944 Colon cancer Diseases 0.000 claims description 26
- 239000002773 nucleotide Substances 0.000 claims description 24
- 125000003729 nucleotide group Chemical group 0.000 claims description 24
- 239000002202 Polyethylene glycol Substances 0.000 claims description 22
- DHMQDGOQFOQNFH-UHFFFAOYSA-N Glycine Chemical compound NCC(O)=O DHMQDGOQFOQNFH-UHFFFAOYSA-N 0.000 claims description 19
- 125000002496 methyl group Chemical group [H]C([H])([H])* 0.000 claims description 19
- 230000001965 increasing effect Effects 0.000 claims description 18
- 239000013612 plasmid Substances 0.000 claims description 16
- 239000004471 Glycine Substances 0.000 claims description 15
- 108040006849 interleukin-2 receptor activity proteins Proteins 0.000 claims description 15
- 201000001441 melanoma Diseases 0.000 claims description 15
- 125000003827 glycol group Chemical group 0.000 claims description 14
- 239000000556 agonist Substances 0.000 claims description 13
- 150000003839 salts Chemical group 0.000 claims description 13
- 208000029742 colonic neoplasm Diseases 0.000 claims description 12
- MTCFGRXMJLQNBG-UHFFFAOYSA-N Serine Natural products OCC(N)C(O)=O MTCFGRXMJLQNBG-UHFFFAOYSA-N 0.000 claims description 10
- 108700025316 aldesleukin Proteins 0.000 claims description 9
- 229960005310 aldesleukin Drugs 0.000 claims description 9
- 208000002154 non-small cell lung carcinoma Diseases 0.000 claims description 9
- 208000029729 tumor suppressor gene on chromosome 11 Diseases 0.000 claims description 9
- 208000006265 Renal cell carcinoma Diseases 0.000 claims description 8
- SOWBFZRMHSNYGE-UHFFFAOYSA-N Monoamide-Oxalic acid Natural products NC(=O)C(O)=O SOWBFZRMHSNYGE-UHFFFAOYSA-N 0.000 claims description 7
- 210000000987 immune system Anatomy 0.000 claims description 7
- 229940002612 prodrug Drugs 0.000 claims description 6
- 239000000651 prodrug Substances 0.000 claims description 6
- 206010044412 transitional cell carcinoma Diseases 0.000 claims description 6
- 208000003174 Brain Neoplasms Diseases 0.000 claims description 5
- 206010006187 Breast cancer Diseases 0.000 claims description 5
- 208000026310 Breast neoplasm Diseases 0.000 claims description 5
- 206010061902 Pancreatic neoplasm Diseases 0.000 claims description 5
- 206010041067 Small cell lung cancer Diseases 0.000 claims description 5
- 208000015486 malignant pancreatic neoplasm Diseases 0.000 claims description 5
- 201000002528 pancreatic cancer Diseases 0.000 claims description 5
- 208000008443 pancreatic carcinoma Diseases 0.000 claims description 5
- 208000000587 small cell lung carcinoma Diseases 0.000 claims description 5
- 206010005003 Bladder cancer Diseases 0.000 claims description 4
- 206010008342 Cervix carcinoma Diseases 0.000 claims description 4
- 208000001333 Colorectal Neoplasms Diseases 0.000 claims description 4
- 208000017604 Hodgkin disease Diseases 0.000 claims description 4
- 208000010747 Hodgkins lymphoma Diseases 0.000 claims description 4
- 208000008839 Kidney Neoplasms Diseases 0.000 claims description 4
- 206010033128 Ovarian cancer Diseases 0.000 claims description 4
- 206010061535 Ovarian neoplasm Diseases 0.000 claims description 4
- 206010060862 Prostate cancer Diseases 0.000 claims description 4
- 208000000236 Prostatic Neoplasms Diseases 0.000 claims description 4
- 206010038389 Renal cancer Diseases 0.000 claims description 4
- 208000007097 Urinary Bladder Neoplasms Diseases 0.000 claims description 4
- 208000006105 Uterine Cervical Neoplasms Diseases 0.000 claims description 4
- 125000003277 amino group Chemical group 0.000 claims description 4
- 208000026900 bile duct neoplasm Diseases 0.000 claims description 4
- 201000010881 cervical cancer Diseases 0.000 claims description 4
- 201000010982 kidney cancer Diseases 0.000 claims description 4
- 201000005112 urinary bladder cancer Diseases 0.000 claims description 4
- 208000006468 Adrenal Cortex Neoplasms Diseases 0.000 claims description 3
- 206010005949 Bone cancer Diseases 0.000 claims description 3
- 208000018084 Bone neoplasm Diseases 0.000 claims description 3
- 208000000461 Esophageal Neoplasms Diseases 0.000 claims description 3
- 108010060632 Interleukin-2 Receptor beta Subunit Proteins 0.000 claims description 3
- 102000008193 Interleukin-2 Receptor beta Subunit Human genes 0.000 claims description 3
- 206010025323 Lymphomas Diseases 0.000 claims description 3
- 208000005450 Maxillary Sinus Neoplasms Diseases 0.000 claims description 3
- 206010030155 Oesophageal carcinoma Diseases 0.000 claims description 3
- 208000005718 Stomach Neoplasms Diseases 0.000 claims description 3
- 208000024770 Thyroid neoplasm Diseases 0.000 claims description 3
- 239000000654 additive Substances 0.000 claims description 3
- 230000000996 additive effect Effects 0.000 claims description 3
- 208000035250 cutaneous malignant susceptibility to 1 melanoma Diseases 0.000 claims description 3
- 201000004101 esophageal cancer Diseases 0.000 claims description 3
- 206010017758 gastric cancer Diseases 0.000 claims description 3
- 201000007270 liver cancer Diseases 0.000 claims description 3
- 208000014018 liver neoplasm Diseases 0.000 claims description 3
- 201000004488 maxillary sinus cancer Diseases 0.000 claims description 3
- 208000019303 maxillary sinus carcinoma Diseases 0.000 claims description 3
- 239000007787 solid Substances 0.000 claims description 3
- 206010041823 squamous cell carcinoma Diseases 0.000 claims description 3
- 201000011549 stomach cancer Diseases 0.000 claims description 3
- 210000003128 head Anatomy 0.000 claims description 2
- 201000010536 head and neck cancer Diseases 0.000 claims description 2
- 208000014829 head and neck neoplasm Diseases 0.000 claims description 2
- 208000023747 urothelial carcinoma Diseases 0.000 claims description 2
- 210000003739 neck Anatomy 0.000 claims 1
- 229940031732 DNA cancer vaccine Drugs 0.000 abstract description 58
- 241000699670 Mus sp. Species 0.000 description 86
- 125000005647 linker group Chemical group 0.000 description 69
- 108020004414 DNA Proteins 0.000 description 46
- 102000053602 DNA Human genes 0.000 description 46
- 235000001014 amino acid Nutrition 0.000 description 44
- 210000004027 cell Anatomy 0.000 description 40
- 150000001413 amino acids Chemical class 0.000 description 36
- 229940022399 cancer vaccine Drugs 0.000 description 35
- 235000018102 proteins Nutrition 0.000 description 34
- 230000004044 response Effects 0.000 description 34
- 108090000765 processed proteins & peptides Proteins 0.000 description 32
- 230000028993 immune response Effects 0.000 description 28
- 210000000952 spleen Anatomy 0.000 description 28
- 102000004196 processed proteins & peptides Human genes 0.000 description 25
- 241000699666 Mus <mouse, genus> Species 0.000 description 24
- 210000004988 splenocyte Anatomy 0.000 description 24
- 210000004881 tumor cell Anatomy 0.000 description 24
- 229920000642 polymer Polymers 0.000 description 21
- 230000001225 therapeutic effect Effects 0.000 description 21
- 229920001184 polypeptide Polymers 0.000 description 20
- 230000004614 tumor growth Effects 0.000 description 19
- 238000002347 injection Methods 0.000 description 18
- 239000007924 injection Substances 0.000 description 18
- 210000004369 blood Anatomy 0.000 description 17
- 239000008280 blood Substances 0.000 description 17
- 238000009566 cancer vaccine Methods 0.000 description 17
- 238000009169 immunotherapy Methods 0.000 description 17
- 239000000427 antigen Substances 0.000 description 15
- 108091007433 antigens Proteins 0.000 description 15
- 102000036639 antigens Human genes 0.000 description 15
- 238000001574 biopsy Methods 0.000 description 15
- 230000035772 mutation Effects 0.000 description 15
- 102000040430 polynucleotide Human genes 0.000 description 15
- 108091033319 polynucleotide Proteins 0.000 description 15
- 239000002157 polynucleotide Substances 0.000 description 15
- 230000000694 effects Effects 0.000 description 14
- 229960002449 glycine Drugs 0.000 description 14
- 238000002648 combination therapy Methods 0.000 description 13
- 239000003814 drug Substances 0.000 description 13
- 230000002163 immunogen Effects 0.000 description 13
- 210000003289 regulatory T cell Anatomy 0.000 description 13
- 239000000523 sample Substances 0.000 description 13
- 230000004083 survival effect Effects 0.000 description 13
- 210000000612 antigen-presenting cell Anatomy 0.000 description 12
- 238000010172 mouse model Methods 0.000 description 12
- 229940124597 therapeutic agent Drugs 0.000 description 12
- 238000004458 analytical method Methods 0.000 description 11
- 238000002474 experimental method Methods 0.000 description 11
- 125000003983 fluorenyl group Chemical group C1(=CC=CC=2C3=CC=CC=C3CC12)* 0.000 description 11
- 230000001681 protective effect Effects 0.000 description 11
- 238000002560 therapeutic procedure Methods 0.000 description 11
- 210000001266 CD8-positive T-lymphocyte Anatomy 0.000 description 10
- 102100040678 Programmed cell death protein 1 Human genes 0.000 description 10
- 101710089372 Programmed cell death protein 1 Proteins 0.000 description 10
- 125000003275 alpha amino acid group Chemical group 0.000 description 10
- 238000013459 approach Methods 0.000 description 10
- 201000010099 disease Diseases 0.000 description 10
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 description 10
- 238000012216 screening Methods 0.000 description 10
- 108010076504 Protein Sorting Signals Proteins 0.000 description 9
- 208000000102 Squamous Cell Carcinoma of Head and Neck Diseases 0.000 description 9
- 230000003111 delayed effect Effects 0.000 description 9
- 201000000459 head and neck squamous cell carcinoma Diseases 0.000 description 9
- 230000007246 mechanism Effects 0.000 description 9
- 238000003384 imaging method Methods 0.000 description 8
- 231100000636 lethal dose Toxicity 0.000 description 8
- 230000005923 long-lasting effect Effects 0.000 description 8
- 229960003301 nivolumab Drugs 0.000 description 8
- 230000037361 pathway Effects 0.000 description 8
- 230000002829 reductive effect Effects 0.000 description 8
- 230000002195 synergetic effect Effects 0.000 description 8
- 210000001519 tissue Anatomy 0.000 description 8
- 102000005962 receptors Human genes 0.000 description 7
- 108020003175 receptors Proteins 0.000 description 7
- 230000008093 supporting effect Effects 0.000 description 7
- 230000008901 benefit Effects 0.000 description 6
- 230000008859 change Effects 0.000 description 6
- 230000005847 immunogenicity Effects 0.000 description 6
- 238000001727 in vivo Methods 0.000 description 6
- 238000007619 statistical method Methods 0.000 description 6
- 229940045513 CTLA4 antagonist Drugs 0.000 description 5
- 241000282412 Homo Species 0.000 description 5
- 101001002657 Homo sapiens Interleukin-2 Proteins 0.000 description 5
- 101001055144 Homo sapiens Interleukin-2 receptor subunit alpha Proteins 0.000 description 5
- 102100026878 Interleukin-2 receptor subunit alpha Human genes 0.000 description 5
- 108700018351 Major Histocompatibility Complex Proteins 0.000 description 5
- 230000000875 corresponding effect Effects 0.000 description 5
- 239000012636 effector Substances 0.000 description 5
- 239000002955 immunomodulating agent Substances 0.000 description 5
- 230000002401 inhibitory effect Effects 0.000 description 5
- 238000007918 intramuscular administration Methods 0.000 description 5
- 235000005772 leucine Nutrition 0.000 description 5
- 239000013642 negative control Substances 0.000 description 5
- 210000003819 peripheral blood mononuclear cell Anatomy 0.000 description 5
- 230000006641 stabilisation Effects 0.000 description 5
- 238000011105 stabilization Methods 0.000 description 5
- 238000007920 subcutaneous administration Methods 0.000 description 5
- 230000020382 suppression by virus of host antigen processing and presentation of peptide antigen via MHC class I Effects 0.000 description 5
- 238000012360 testing method Methods 0.000 description 5
- 229940022511 therapeutic cancer vaccine Drugs 0.000 description 5
- 208000001382 Experimental Melanoma Diseases 0.000 description 4
- 102000002689 Toll-like receptor Human genes 0.000 description 4
- 108020000411 Toll-like receptor Proteins 0.000 description 4
- 230000004913 activation Effects 0.000 description 4
- 230000004071 biological effect Effects 0.000 description 4
- 238000007912 intraperitoneal administration Methods 0.000 description 4
- 238000002595 magnetic resonance imaging Methods 0.000 description 4
- 238000012423 maintenance Methods 0.000 description 4
- WCYWZMWISLQXQU-UHFFFAOYSA-N methyl Chemical class [CH3] WCYWZMWISLQXQU-UHFFFAOYSA-N 0.000 description 4
- 208000015347 renal cell adenocarcinoma Diseases 0.000 description 4
- 238000009097 single-agent therapy Methods 0.000 description 4
- 229940021747 therapeutic vaccine Drugs 0.000 description 4
- 238000011277 treatment modality Methods 0.000 description 4
- NHBKXEKEPDILRR-UHFFFAOYSA-N 2,3-bis(butanoylsulfanyl)propyl butanoate Chemical compound CCCC(=O)OCC(SC(=O)CCC)CSC(=O)CCC NHBKXEKEPDILRR-UHFFFAOYSA-N 0.000 description 3
- 108010074708 B7-H1 Antigen Proteins 0.000 description 3
- 102000008096 B7-H1 Antigen Human genes 0.000 description 3
- 102000008203 CTLA-4 Antigen Human genes 0.000 description 3
- 108010021064 CTLA-4 Antigen Proteins 0.000 description 3
- LFQSCWFLJHTTHZ-UHFFFAOYSA-N Ethanol Chemical compound CCO LFQSCWFLJHTTHZ-UHFFFAOYSA-N 0.000 description 3
- PEDCQBHIVMGVHV-UHFFFAOYSA-N Glycerine Chemical compound OCC(O)CO PEDCQBHIVMGVHV-UHFFFAOYSA-N 0.000 description 3
- 101000746783 Homo sapiens Cytochrome b-c1 complex subunit 6, mitochondrial Proteins 0.000 description 3
- 101001057504 Homo sapiens Interferon-stimulated gene 20 kDa protein Proteins 0.000 description 3
- 108091008874 T cell receptors Proteins 0.000 description 3
- 102000016266 T-Cell Antigen Receptors Human genes 0.000 description 3
- 238000007792 addition Methods 0.000 description 3
- 230000002411 adverse Effects 0.000 description 3
- 230000004075 alteration Effects 0.000 description 3
- 238000003556 assay Methods 0.000 description 3
- AFYNADDZULBEJA-UHFFFAOYSA-N bicinchoninic acid Chemical compound C1=CC=CC2=NC(C=3C=C(C4=CC=CC=C4N=3)C(=O)O)=CC(C(O)=O)=C21 AFYNADDZULBEJA-UHFFFAOYSA-N 0.000 description 3
- 239000000872 buffer Substances 0.000 description 3
- 238000002619 cancer immunotherapy Methods 0.000 description 3
- 239000003937 drug carrier Substances 0.000 description 3
- 238000004520 electroporation Methods 0.000 description 3
- 238000003379 elimination reaction Methods 0.000 description 3
- 238000011156 evaluation Methods 0.000 description 3
- 238000000684 flow cytometry Methods 0.000 description 3
- 239000001963 growth medium Substances 0.000 description 3
- 102000055277 human IL2 Human genes 0.000 description 3
- 102000048638 human UQCRH Human genes 0.000 description 3
- 230000002209 hydrophobic effect Effects 0.000 description 3
- 238000001802 infusion Methods 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- 230000000977 initiatory effect Effects 0.000 description 3
- 238000010255 intramuscular injection Methods 0.000 description 3
- 239000007927 intramuscular injection Substances 0.000 description 3
- 238000001990 intravenous administration Methods 0.000 description 3
- 238000002955 isolation Methods 0.000 description 3
- 230000003902 lesion Effects 0.000 description 3
- 150000002614 leucines Chemical class 0.000 description 3
- 230000003278 mimic effect Effects 0.000 description 3
- 150000007522 mineralic acids Chemical class 0.000 description 3
- 210000000822 natural killer cell Anatomy 0.000 description 3
- 150000007524 organic acids Chemical class 0.000 description 3
- 230000036961 partial effect Effects 0.000 description 3
- 230000002093 peripheral effect Effects 0.000 description 3
- 239000002953 phosphate buffered saline Substances 0.000 description 3
- 238000002360 preparation method Methods 0.000 description 3
- 230000008569 process Effects 0.000 description 3
- 238000012163 sequencing technique Methods 0.000 description 3
- 230000000392 somatic effect Effects 0.000 description 3
- 230000002459 sustained effect Effects 0.000 description 3
- 238000012384 transportation and delivery Methods 0.000 description 3
- 206010069754 Acquired gene mutation Diseases 0.000 description 2
- BPYKTIZUTYGOLE-IFADSCNNSA-N Bilirubin Chemical compound N1C(=O)C(C)=C(C=C)\C1=C\C1=C(C)C(CCC(O)=O)=C(CC2=C(C(C)=C(\C=C/3C(=C(C=C)C(=O)N\3)C)N2)CCC(O)=O)N1 BPYKTIZUTYGOLE-IFADSCNNSA-N 0.000 description 2
- 0 CCCC(*)NC(OCC1c2cc(C(NCCO**)=O)ccc2-c(cc2)c1cc2C(NCC*(C)N)=O)=O Chemical compound CCCC(*)NC(OCC1c2cc(C(NCCO**)=O)ccc2-c(cc2)c1cc2C(NCC*(C)N)=O)=O 0.000 description 2
- 102000000013 Chemokine CCL3 Human genes 0.000 description 2
- 102000009410 Chemokine receptor Human genes 0.000 description 2
- 108050000299 Chemokine receptor Proteins 0.000 description 2
- 102000019034 Chemokines Human genes 0.000 description 2
- 108010012236 Chemokines Proteins 0.000 description 2
- 108020004705 Codon Proteins 0.000 description 2
- 102000004127 Cytokines Human genes 0.000 description 2
- 108090000695 Cytokines Proteins 0.000 description 2
- 238000011510 Elispot assay Methods 0.000 description 2
- LYCAIKOWRPUZTN-UHFFFAOYSA-N Ethylene glycol Chemical group OCCO LYCAIKOWRPUZTN-UHFFFAOYSA-N 0.000 description 2
- 108010040721 Flagellin Proteins 0.000 description 2
- WQZGKKKJIJFFOK-GASJEMHNSA-N Glucose Natural products OC[C@H]1OC(O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-GASJEMHNSA-N 0.000 description 2
- 102100029966 HLA class II histocompatibility antigen, DP alpha 1 chain Human genes 0.000 description 2
- 101000864089 Homo sapiens HLA class II histocompatibility antigen, DP alpha 1 chain Proteins 0.000 description 2
- 101000930802 Homo sapiens HLA class II histocompatibility antigen, DQ alpha 1 chain Proteins 0.000 description 2
- 101000968032 Homo sapiens HLA class II histocompatibility antigen, DR beta 3 chain Proteins 0.000 description 2
- 101000669447 Homo sapiens Toll-like receptor 4 Proteins 0.000 description 2
- VEXZGXHMUGYJMC-UHFFFAOYSA-N Hydrochloric acid Chemical compound Cl VEXZGXHMUGYJMC-UHFFFAOYSA-N 0.000 description 2
- ROHFNLRQFUQHCH-YFKPBYRVSA-N L-leucine Chemical compound CC(C)C[C@H](N)C(O)=O ROHFNLRQFUQHCH-YFKPBYRVSA-N 0.000 description 2
- ROHFNLRQFUQHCH-UHFFFAOYSA-N Leucine Natural products CC(C)CC(N)C(O)=O ROHFNLRQFUQHCH-UHFFFAOYSA-N 0.000 description 2
- 206010058467 Lung neoplasm malignant Diseases 0.000 description 2
- 102000009571 Macrophage Inflammatory Proteins Human genes 0.000 description 2
- 108010009474 Macrophage Inflammatory Proteins Proteins 0.000 description 2
- 206010027476 Metastases Diseases 0.000 description 2
- 206010027480 Metastatic malignant melanoma Diseases 0.000 description 2
- 241001465754 Metazoa Species 0.000 description 2
- 108700001237 Nucleic Acid-Based Vaccines Proteins 0.000 description 2
- 229910019142 PO4 Inorganic materials 0.000 description 2
- 102000011923 Thyrotropin Human genes 0.000 description 2
- 108010061174 Thyrotropin Proteins 0.000 description 2
- 102100039360 Toll-like receptor 4 Human genes 0.000 description 2
- XSQUKJJJFZCRTK-UHFFFAOYSA-N Urea Chemical compound NC(N)=O XSQUKJJJFZCRTK-UHFFFAOYSA-N 0.000 description 2
- 239000002253 acid Substances 0.000 description 2
- 208000009956 adenocarcinoma Diseases 0.000 description 2
- 239000002671 adjuvant Substances 0.000 description 2
- 150000001408 amides Chemical class 0.000 description 2
- 229960003852 atezolizumab Drugs 0.000 description 2
- 230000005784 autoimmunity Effects 0.000 description 2
- WPYMKLBDIGXBTP-UHFFFAOYSA-N benzoic acid Chemical compound OC(=O)C1=CC=CC=C1 WPYMKLBDIGXBTP-UHFFFAOYSA-N 0.000 description 2
- 230000015572 biosynthetic process Effects 0.000 description 2
- 230000037396 body weight Effects 0.000 description 2
- 230000001413 cellular effect Effects 0.000 description 2
- 239000003795 chemical substances by application Substances 0.000 description 2
- 238000002512 chemotherapy Methods 0.000 description 2
- HVYWMOMLDIMFJA-DPAQBDIFSA-N cholesterol Chemical compound C1C=C2C[C@@H](O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@H]([C@H](C)CCCC(C)C)[C@@]1(C)CC2 HVYWMOMLDIMFJA-DPAQBDIFSA-N 0.000 description 2
- 238000002591 computed tomography Methods 0.000 description 2
- 238000012790 confirmation Methods 0.000 description 2
- 238000010276 construction Methods 0.000 description 2
- DDRJAANPRJIHGJ-UHFFFAOYSA-N creatinine Chemical compound CN1CC(=O)NC1=N DDRJAANPRJIHGJ-UHFFFAOYSA-N 0.000 description 2
- 210000001151 cytotoxic T lymphocyte Anatomy 0.000 description 2
- 238000012217 deletion Methods 0.000 description 2
- 230000037430 deletion Effects 0.000 description 2
- 210000004443 dendritic cell Anatomy 0.000 description 2
- 230000001419 dependent effect Effects 0.000 description 2
- 238000013461 design Methods 0.000 description 2
- 238000011161 development Methods 0.000 description 2
- 230000004069 differentiation Effects 0.000 description 2
- 239000003085 diluting agent Substances 0.000 description 2
- 210000003162 effector t lymphocyte Anatomy 0.000 description 2
- 230000008030 elimination Effects 0.000 description 2
- 239000003623 enhancer Substances 0.000 description 2
- 230000002708 enhancing effect Effects 0.000 description 2
- 238000003114 enzyme-linked immunosorbent spot assay Methods 0.000 description 2
- 210000003743 erythrocyte Anatomy 0.000 description 2
- 230000002068 genetic effect Effects 0.000 description 2
- 150000002333 glycines Chemical class 0.000 description 2
- 230000012010 growth Effects 0.000 description 2
- 230000036541 health Effects 0.000 description 2
- 239000000710 homodimer Substances 0.000 description 2
- 230000005746 immune checkpoint blockade Effects 0.000 description 2
- 230000001506 immunosuppresive effect Effects 0.000 description 2
- 230000001939 inductive effect Effects 0.000 description 2
- 230000010354 integration Effects 0.000 description 2
- 238000001361 intraarterial administration Methods 0.000 description 2
- 238000007913 intrathecal administration Methods 0.000 description 2
- 210000000265 leukocyte Anatomy 0.000 description 2
- 230000021633 leukocyte mediated immunity Effects 0.000 description 2
- 239000003446 ligand Substances 0.000 description 2
- 201000005202 lung cancer Diseases 0.000 description 2
- 208000020816 lung neoplasm Diseases 0.000 description 2
- 210000004698 lymphocyte Anatomy 0.000 description 2
- 239000008176 lyophilized powder Substances 0.000 description 2
- 239000000463 material Substances 0.000 description 2
- 239000002609 medium Substances 0.000 description 2
- 210000003071 memory t lymphocyte Anatomy 0.000 description 2
- 230000009401 metastasis Effects 0.000 description 2
- 230000001394 metastastic effect Effects 0.000 description 2
- 208000021039 metastatic melanoma Diseases 0.000 description 2
- 206010061289 metastatic neoplasm Diseases 0.000 description 2
- 208000037843 metastatic solid tumor Diseases 0.000 description 2
- 125000001570 methylene group Chemical group [H]C([H])([*:1])[*:2] 0.000 description 2
- 238000012544 monitoring process Methods 0.000 description 2
- NIHNNTQXNPWCJQ-UHFFFAOYSA-N o-biphenylenemethane Natural products C1=CC=C2CC3=CC=CC=C3C2=C1 NIHNNTQXNPWCJQ-UHFFFAOYSA-N 0.000 description 2
- 230000001717 pathogenic effect Effects 0.000 description 2
- 230000006320 pegylation Effects 0.000 description 2
- 229960002621 pembrolizumab Drugs 0.000 description 2
- 210000005259 peripheral blood Anatomy 0.000 description 2
- 239000011886 peripheral blood Substances 0.000 description 2
- 229940038309 personalized vaccine Drugs 0.000 description 2
- NBIIXXVUZAFLBC-UHFFFAOYSA-K phosphate Chemical compound [O-]P([O-])([O-])=O NBIIXXVUZAFLBC-UHFFFAOYSA-K 0.000 description 2
- 239000010452 phosphate Substances 0.000 description 2
- 230000004962 physiological condition Effects 0.000 description 2
- 230000035755 proliferation Effects 0.000 description 2
- 230000005855 radiation Effects 0.000 description 2
- 230000009467 reduction Effects 0.000 description 2
- 230000003362 replicative effect Effects 0.000 description 2
- 230000003248 secreting effect Effects 0.000 description 2
- 230000028327 secretion Effects 0.000 description 2
- 230000035945 sensitivity Effects 0.000 description 2
- DAEPDZWVDSPTHF-UHFFFAOYSA-M sodium pyruvate Chemical compound [Na+].CC(=O)C([O-])=O DAEPDZWVDSPTHF-UHFFFAOYSA-M 0.000 description 2
- 239000000243 solution Substances 0.000 description 2
- 230000037439 somatic mutation Effects 0.000 description 2
- 241000894007 species Species 0.000 description 2
- 210000004989 spleen cell Anatomy 0.000 description 2
- 238000005728 strengthening Methods 0.000 description 2
- UCSJYZPVAKXKNQ-HZYVHMACSA-N streptomycin Chemical compound CN[C@H]1[C@H](O)[C@@H](O)[C@H](CO)O[C@H]1O[C@@H]1[C@](C=O)(O)[C@H](C)O[C@H]1O[C@@H]1[C@@H](NC(N)=N)[C@H](O)[C@@H](NC(N)=N)[C@H](O)[C@H]1O UCSJYZPVAKXKNQ-HZYVHMACSA-N 0.000 description 2
- 239000000126 substance Substances 0.000 description 2
- 238000006467 substitution reaction Methods 0.000 description 2
- 208000024891 symptom Diseases 0.000 description 2
- 231100000419 toxicity Toxicity 0.000 description 2
- 230000001988 toxicity Effects 0.000 description 2
- VZCYOOQTPOCHFL-UHFFFAOYSA-N trans-butenedioic acid Natural products OC(=O)C=CC(O)=O VZCYOOQTPOCHFL-UHFFFAOYSA-N 0.000 description 2
- 230000005909 tumor killing Effects 0.000 description 2
- PGOHTUIFYSHAQG-LJSDBVFPSA-N (2S)-6-amino-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-4-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-5-amino-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S,3R)-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S,3R)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-5-amino-2-[[(2S)-1-[(2S,3R)-2-[[(2S)-2-[[(2S)-2-[[(2R)-2-[[(2S)-2-[[(2S)-2-[[2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-1-[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-amino-4-methylsulfanylbutanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-5-carbamimidamidopentanoyl]amino]propanoyl]pyrrolidine-2-carbonyl]amino]-3-methylbutanoyl]amino]-4-methylpentanoyl]amino]-4-methylpentanoyl]amino]acetyl]amino]-3-hydroxypropanoyl]amino]-4-methylpentanoyl]amino]-3-sulfanylpropanoyl]amino]-4-methylsulfanylbutanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-hydroxybutanoyl]pyrrolidine-2-carbonyl]amino]-5-oxopentanoyl]amino]-3-hydroxypropanoyl]amino]-3-hydroxypropanoyl]amino]-3-(1H-imidazol-5-yl)propanoyl]amino]-4-methylpentanoyl]amino]-3-hydroxybutanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-5-carbamimidamidopentanoyl]amino]-5-oxopentanoyl]amino]-3-hydroxybutanoyl]amino]-3-hydroxypropanoyl]amino]-3-carboxypropanoyl]amino]-3-hydroxypropanoyl]amino]-5-oxopentanoyl]amino]-5-oxopentanoyl]amino]-3-phenylpropanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-methylbutanoyl]amino]-4-methylpentanoyl]amino]-4-oxobutanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-4-carboxybutanoyl]amino]-5-oxopentanoyl]amino]hexanoic acid Chemical compound CSCC[C@H](N)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C)C(=O)N1CCC[C@H]1C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(=O)NCC(=O)N[C@@H](CO)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CS)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H]([C@@H](C)O)C(=O)N1CCC[C@H]1C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CO)C(=O)N[C@@H](Cc1cnc[nH]1)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](Cc1ccccc1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCCCN)C(O)=O PGOHTUIFYSHAQG-LJSDBVFPSA-N 0.000 description 1
- 108091032973 (ribonucleotides)n+m Proteins 0.000 description 1
- LDMOEFOXLIZJOW-UHFFFAOYSA-N 1-dodecanesulfonic acid Chemical class CCCCCCCCCCCCS(O)(=O)=O LDMOEFOXLIZJOW-UHFFFAOYSA-N 0.000 description 1
- JKMHFZQWWAIEOD-UHFFFAOYSA-N 2-[4-(2-hydroxyethyl)piperazin-1-yl]ethanesulfonic acid Chemical compound OCC[NH+]1CCN(CCS([O-])(=O)=O)CC1 JKMHFZQWWAIEOD-UHFFFAOYSA-N 0.000 description 1
- 125000005273 2-acetoxybenzoic acid group Chemical group 0.000 description 1
- QTBSBXVTEAMEQO-UHFFFAOYSA-M Acetate Chemical compound CC([O-])=O QTBSBXVTEAMEQO-UHFFFAOYSA-M 0.000 description 1
- 108010088751 Albumins Proteins 0.000 description 1
- 102000009027 Albumins Human genes 0.000 description 1
- 102000002260 Alkaline Phosphatase Human genes 0.000 description 1
- 108020004774 Alkaline Phosphatase Proteins 0.000 description 1
- 201000003076 Angiosarcoma Diseases 0.000 description 1
- 206010003571 Astrocytoma Diseases 0.000 description 1
- 238000011725 BALB/c mouse Methods 0.000 description 1
- 208000005440 Basal Cell Neoplasms Diseases 0.000 description 1
- 206010004146 Basal cell carcinoma Diseases 0.000 description 1
- 206010004593 Bile duct cancer Diseases 0.000 description 1
- 241000283690 Bos taurus Species 0.000 description 1
- COVZYZSDYWQREU-UHFFFAOYSA-N Busulfan Chemical compound CS(=O)(=O)OCCCCOS(C)(=O)=O COVZYZSDYWQREU-UHFFFAOYSA-N 0.000 description 1
- 102100031172 C-C chemokine receptor type 1 Human genes 0.000 description 1
- 101710149814 C-C chemokine receptor type 1 Proteins 0.000 description 1
- 102100024167 C-C chemokine receptor type 3 Human genes 0.000 description 1
- 101710149862 C-C chemokine receptor type 3 Proteins 0.000 description 1
- 102100035875 C-C chemokine receptor type 5 Human genes 0.000 description 1
- 101710149870 C-C chemokine receptor type 5 Proteins 0.000 description 1
- 102100032367 C-C motif chemokine 5 Human genes 0.000 description 1
- 108010074051 C-Reactive Protein Proteins 0.000 description 1
- 102100032752 C-reactive protein Human genes 0.000 description 1
- 238000011740 C57BL/6 mouse Methods 0.000 description 1
- 102000004500 CCR1 Receptors Human genes 0.000 description 1
- 108010017319 CCR1 Receptors Proteins 0.000 description 1
- 102000004499 CCR3 Receptors Human genes 0.000 description 1
- 108010017316 CCR3 Receptors Proteins 0.000 description 1
- 102000004274 CCR5 Receptors Human genes 0.000 description 1
- 108010017088 CCR5 Receptors Proteins 0.000 description 1
- 108010029697 CD40 Ligand Proteins 0.000 description 1
- 102100032937 CD40 ligand Human genes 0.000 description 1
- 210000001239 CD8-positive, alpha-beta cytotoxic T lymphocyte Anatomy 0.000 description 1
- OYPRJOBELJOOCE-UHFFFAOYSA-N Calcium Chemical compound [Ca] OYPRJOBELJOOCE-UHFFFAOYSA-N 0.000 description 1
- 241000282465 Canis Species 0.000 description 1
- KXDHJXZQYSOELW-UHFFFAOYSA-M Carbamate Chemical compound NC([O-])=O KXDHJXZQYSOELW-UHFFFAOYSA-M 0.000 description 1
- 208000005623 Carcinogenesis Diseases 0.000 description 1
- 201000009030 Carcinoma Diseases 0.000 description 1
- 108010055166 Chemokine CCL5 Proteins 0.000 description 1
- VEXZGXHMUGYJMC-UHFFFAOYSA-M Chloride anion Chemical compound [Cl-] VEXZGXHMUGYJMC-UHFFFAOYSA-M 0.000 description 1
- 102000003914 Cholinesterases Human genes 0.000 description 1
- 108090000322 Cholinesterases Proteins 0.000 description 1
- 208000005243 Chondrosarcoma Diseases 0.000 description 1
- 201000009047 Chordoma Diseases 0.000 description 1
- 208000006332 Choriocarcinoma Diseases 0.000 description 1
- KRKNYBCHXYNGOX-UHFFFAOYSA-K Citrate Chemical compound [O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O KRKNYBCHXYNGOX-UHFFFAOYSA-K 0.000 description 1
- 208000009798 Craniopharyngioma Diseases 0.000 description 1
- 102000004420 Creatine Kinase Human genes 0.000 description 1
- 108010042126 Creatine kinase Proteins 0.000 description 1
- 229920000089 Cyclic olefin copolymer Polymers 0.000 description 1
- XUIIKFGFIJCVMT-GFCCVEGCSA-N D-thyroxine Chemical compound IC1=CC(C[C@@H](N)C(O)=O)=CC(I)=C1OC1=CC(I)=C(O)C(I)=C1 XUIIKFGFIJCVMT-GFCCVEGCSA-N 0.000 description 1
- FEWJPZIEWOKRBE-JCYAYHJZSA-N Dextrotartaric acid Chemical compound OC(=O)[C@H](O)[C@@H](O)C(O)=O FEWJPZIEWOKRBE-JCYAYHJZSA-N 0.000 description 1
- MYMOFIZGZYHOMD-UHFFFAOYSA-N Dioxygen Chemical group O=O MYMOFIZGZYHOMD-UHFFFAOYSA-N 0.000 description 1
- 206010061818 Disease progression Diseases 0.000 description 1
- 238000002965 ELISA Methods 0.000 description 1
- 102000004190 Enzymes Human genes 0.000 description 1
- 108090000790 Enzymes Proteins 0.000 description 1
- 206010014967 Ependymoma Diseases 0.000 description 1
- 241000283073 Equus caballus Species 0.000 description 1
- OTMSDBZUPAUEDD-UHFFFAOYSA-N Ethane Chemical compound CC OTMSDBZUPAUEDD-UHFFFAOYSA-N 0.000 description 1
- IAYPIBMASNFSPL-UHFFFAOYSA-N Ethylene oxide Chemical compound C1CO1 IAYPIBMASNFSPL-UHFFFAOYSA-N 0.000 description 1
- 208000006168 Ewing Sarcoma Diseases 0.000 description 1
- 241000282324 Felis Species 0.000 description 1
- 201000008808 Fibrosarcoma Diseases 0.000 description 1
- VZCYOOQTPOCHFL-OWOJBTEDSA-N Fumaric acid Chemical compound OC(=O)\C=C\C(O)=O VZCYOOQTPOCHFL-OWOJBTEDSA-N 0.000 description 1
- 108020004206 Gamma-glutamyltransferase Proteins 0.000 description 1
- 208000032612 Glial tumor Diseases 0.000 description 1
- 206010018338 Glioma Diseases 0.000 description 1
- 239000007995 HEPES buffer Substances 0.000 description 1
- 208000001258 Hemangiosarcoma Diseases 0.000 description 1
- 108700019828 Hinge Exons Proteins 0.000 description 1
- 208000021519 Hodgkin lymphoma Diseases 0.000 description 1
- 101000946889 Homo sapiens Monocyte differentiation antigen CD14 Proteins 0.000 description 1
- CPELXLSAUQHCOX-UHFFFAOYSA-N Hydrogen bromide Chemical compound Br CPELXLSAUQHCOX-UHFFFAOYSA-N 0.000 description 1
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical compound C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 1
- 229940123776 Immuno-oncology therapy Drugs 0.000 description 1
- 208000026350 Inborn Genetic disease Diseases 0.000 description 1
- 102000037984 Inhibitory immune checkpoint proteins Human genes 0.000 description 1
- 108091008026 Inhibitory immune checkpoint proteins Proteins 0.000 description 1
- 102000018682 Interleukin Receptor Common gamma Subunit Human genes 0.000 description 1
- 108010066719 Interleukin Receptor Common gamma Subunit Proteins 0.000 description 1
- 102000003812 Interleukin-15 Human genes 0.000 description 1
- 108090000172 Interleukin-15 Proteins 0.000 description 1
- 102000003855 L-lactate dehydrogenase Human genes 0.000 description 1
- 108700023483 L-lactate dehydrogenases Proteins 0.000 description 1
- JVTAAEKCZFNVCJ-UHFFFAOYSA-M Lactate Chemical compound CC(O)C([O-])=O JVTAAEKCZFNVCJ-UHFFFAOYSA-M 0.000 description 1
- 208000018142 Leiomyosarcoma Diseases 0.000 description 1
- 102000004882 Lipase Human genes 0.000 description 1
- 108090001060 Lipase Proteins 0.000 description 1
- 239000004367 Lipase Substances 0.000 description 1
- 102000043129 MHC class I family Human genes 0.000 description 1
- 108091054437 MHC class I family Proteins 0.000 description 1
- 206010064912 Malignant transformation Diseases 0.000 description 1
- 241000124008 Mammalia Species 0.000 description 1
- 208000000172 Medulloblastoma Diseases 0.000 description 1
- 206010027406 Mesothelioma Diseases 0.000 description 1
- AFVFQIVMOAPDHO-UHFFFAOYSA-N Methanesulfonic acid Chemical compound CS(O)(=O)=O AFVFQIVMOAPDHO-UHFFFAOYSA-N 0.000 description 1
- 102100035877 Monocyte differentiation antigen CD14 Human genes 0.000 description 1
- 208000034578 Multiple myelomas Diseases 0.000 description 1
- 241001529936 Murinae Species 0.000 description 1
- 101100438957 Mus musculus Cd8a gene Proteins 0.000 description 1
- GDIHDSKOVXEJQQ-UHFFFAOYSA-N NC(O)=O.NC(O)=O.NC(O)=O.N Chemical group NC(O)=O.NC(O)=O.NC(O)=O.N GDIHDSKOVXEJQQ-UHFFFAOYSA-N 0.000 description 1
- 229910002651 NO3 Inorganic materials 0.000 description 1
- 208000034176 Neoplasms, Germ Cell and Embryonal Diseases 0.000 description 1
- 206010029260 Neuroblastoma Diseases 0.000 description 1
- NHNBFGGVMKEFGY-UHFFFAOYSA-N Nitrate Chemical compound [O-][N+]([O-])=O NHNBFGGVMKEFGY-UHFFFAOYSA-N 0.000 description 1
- 208000015914 Non-Hodgkin lymphomas Diseases 0.000 description 1
- 108091028043 Nucleic acid sequence Proteins 0.000 description 1
- 201000010133 Oligodendroglioma Diseases 0.000 description 1
- 108700026244 Open Reading Frames Proteins 0.000 description 1
- 239000012270 PD-1 inhibitor Substances 0.000 description 1
- 239000012668 PD-1-inhibitor Substances 0.000 description 1
- 239000012271 PD-L1 inhibitor Substances 0.000 description 1
- 229930182555 Penicillin Natural products 0.000 description 1
- JGSARLDLIJGVTE-MBNYWOFBSA-N Penicillin G Chemical compound N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)CC1=CC=CC=C1 JGSARLDLIJGVTE-MBNYWOFBSA-N 0.000 description 1
- 208000007641 Pinealoma Diseases 0.000 description 1
- 206010035226 Plasma cell myeloma Diseases 0.000 description 1
- 229920003171 Poly (ethylene oxide) Polymers 0.000 description 1
- ZLMJMSJWJFRBEC-UHFFFAOYSA-N Potassium Chemical compound [K] ZLMJMSJWJFRBEC-UHFFFAOYSA-N 0.000 description 1
- 108010026552 Proteome Proteins 0.000 description 1
- 238000003559 RNA-seq method Methods 0.000 description 1
- 239000012980 RPMI-1640 medium Substances 0.000 description 1
- 201000000582 Retinoblastoma Diseases 0.000 description 1
- 102000001712 STAT5 Transcription Factor Human genes 0.000 description 1
- 108010029477 STAT5 Transcription Factor Proteins 0.000 description 1
- 201000010208 Seminoma Diseases 0.000 description 1
- FAPWRFPIFSIZLT-UHFFFAOYSA-M Sodium chloride Chemical compound [Na+].[Cl-] FAPWRFPIFSIZLT-UHFFFAOYSA-M 0.000 description 1
- QAOWNCQODCNURD-UHFFFAOYSA-L Sulfate Chemical compound [O-]S([O-])(=O)=O QAOWNCQODCNURD-UHFFFAOYSA-L 0.000 description 1
- 230000006044 T cell activation Effects 0.000 description 1
- 230000024932 T cell mediated immunity Effects 0.000 description 1
- 208000024313 Testicular Neoplasms Diseases 0.000 description 1
- 206010057644 Testis cancer Diseases 0.000 description 1
- 108010000499 Thromboplastin Proteins 0.000 description 1
- AUYYCJSJGJYCDS-LBPRGKRZSA-N Thyrolar Chemical compound IC1=CC(C[C@H](N)C(O)=O)=CC(I)=C1OC1=CC=C(O)C(I)=C1 AUYYCJSJGJYCDS-LBPRGKRZSA-N 0.000 description 1
- 102100030859 Tissue factor Human genes 0.000 description 1
- 102000004142 Trypsin Human genes 0.000 description 1
- 108090000631 Trypsin Proteins 0.000 description 1
- LEHOTFFKMJEONL-UHFFFAOYSA-N Uric Acid Chemical compound N1C(=O)NC(=O)C2=C1NC(=O)N2 LEHOTFFKMJEONL-UHFFFAOYSA-N 0.000 description 1
- TVWHNULVHGKJHS-UHFFFAOYSA-N Uric acid Natural products N1C(=O)NC(=O)C2NC(=O)NC21 TVWHNULVHGKJHS-UHFFFAOYSA-N 0.000 description 1
- 208000014070 Vestibular schwannoma Diseases 0.000 description 1
- 208000008383 Wilms tumor Diseases 0.000 description 1
- 230000002159 abnormal effect Effects 0.000 description 1
- 238000009825 accumulation Methods 0.000 description 1
- 229940022663 acetate Drugs 0.000 description 1
- 208000004064 acoustic neuroma Diseases 0.000 description 1
- 230000003213 activating effect Effects 0.000 description 1
- 230000001464 adherent effect Effects 0.000 description 1
- 230000001270 agonistic effect Effects 0.000 description 1
- 238000010171 animal model Methods 0.000 description 1
- 230000006023 anti-tumor response Effects 0.000 description 1
- 238000011394 anticancer treatment Methods 0.000 description 1
- 230000014102 antigen processing and presentation of exogenous peptide antigen via MHC class I Effects 0.000 description 1
- 230000009118 appropriate response Effects 0.000 description 1
- 239000012062 aqueous buffer Substances 0.000 description 1
- 238000000149 argon plasma sintering Methods 0.000 description 1
- 229950002916 avelumab Drugs 0.000 description 1
- 230000001580 bacterial effect Effects 0.000 description 1
- 230000004888 barrier function Effects 0.000 description 1
- 229940121413 bempegaldesleukin Drugs 0.000 description 1
- 230000009286 beneficial effect Effects 0.000 description 1
- WQZGKKKJIJFFOK-VFUOTHLCSA-N beta-D-glucose Chemical compound OC[C@H]1O[C@@H](O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-VFUOTHLCSA-N 0.000 description 1
- 230000000975 bioactive effect Effects 0.000 description 1
- 238000004159 blood analysis Methods 0.000 description 1
- 238000004820 blood count Methods 0.000 description 1
- 210000001124 body fluid Anatomy 0.000 description 1
- 230000036760 body temperature Effects 0.000 description 1
- 239000007975 buffered saline Substances 0.000 description 1
- 239000011575 calcium Substances 0.000 description 1
- 229910052791 calcium Inorganic materials 0.000 description 1
- FATUQANACHZLRT-KMRXSBRUSA-L calcium glucoheptonate Chemical compound [Ca+2].OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C(O)C([O-])=O.OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C(O)C([O-])=O FATUQANACHZLRT-KMRXSBRUSA-L 0.000 description 1
- 230000036952 cancer formation Effects 0.000 description 1
- 239000004202 carbamide Substances 0.000 description 1
- 231100000504 carcinogenesis Toxicity 0.000 description 1
- 230000020411 cell activation Effects 0.000 description 1
- 230000032823 cell division Effects 0.000 description 1
- 230000004663 cell proliferation Effects 0.000 description 1
- 229940121420 cemiplimab Drugs 0.000 description 1
- 238000006243 chemical reaction Methods 0.000 description 1
- 239000003153 chemical reaction reagent Substances 0.000 description 1
- 208000006990 cholangiocarcinoma Diseases 0.000 description 1
- 235000012000 cholesterol Nutrition 0.000 description 1
- 229940048961 cholinesterase Drugs 0.000 description 1
- 230000008711 chromosomal rearrangement Effects 0.000 description 1
- 238000010367 cloning Methods 0.000 description 1
- 230000035071 co-translational protein modification Effects 0.000 description 1
- 238000011220 combination immunotherapy Methods 0.000 description 1
- 230000021615 conjugation Effects 0.000 description 1
- 230000002596 correlated effect Effects 0.000 description 1
- 229940109239 creatinine Drugs 0.000 description 1
- 238000005138 cryopreservation Methods 0.000 description 1
- 150000001925 cycloalkenes Chemical class 0.000 description 1
- 208000002445 cystadenocarcinoma Diseases 0.000 description 1
- 230000006378 damage Effects 0.000 description 1
- 230000002498 deadly effect Effects 0.000 description 1
- 230000006735 deficit Effects 0.000 description 1
- 230000001934 delay Effects 0.000 description 1
- 239000008121 dextrose Substances 0.000 description 1
- 238000002059 diagnostic imaging Methods 0.000 description 1
- 230000003205 diastolic effect Effects 0.000 description 1
- 238000010790 dilution Methods 0.000 description 1
- 239000012895 dilution Substances 0.000 description 1
- 239000013024 dilution buffer Substances 0.000 description 1
- LOKCTEFSRHRXRJ-UHFFFAOYSA-I dipotassium trisodium dihydrogen phosphate hydrogen phosphate dichloride Chemical compound P(=O)(O)(O)[O-].[K+].P(=O)(O)([O-])[O-].[Na+].[Na+].[Cl-].[K+].[Cl-].[Na+] LOKCTEFSRHRXRJ-UHFFFAOYSA-I 0.000 description 1
- 230000008034 disappearance Effects 0.000 description 1
- 230000005750 disease progression Effects 0.000 description 1
- POULHZVOKOAJMA-UHFFFAOYSA-M dodecanoate Chemical compound CCCCCCCCCCCC([O-])=O POULHZVOKOAJMA-UHFFFAOYSA-M 0.000 description 1
- 239000002552 dosage form Substances 0.000 description 1
- 229940079593 drug Drugs 0.000 description 1
- 230000009977 dual effect Effects 0.000 description 1
- 229950009791 durvalumab Drugs 0.000 description 1
- 201000002246 embryonal cancer Diseases 0.000 description 1
- 238000005516 engineering process Methods 0.000 description 1
- 229940088598 enzyme Drugs 0.000 description 1
- 230000008995 epigenetic change Effects 0.000 description 1
- 230000001973 epigenetic effect Effects 0.000 description 1
- 235000020776 essential amino acid Nutrition 0.000 description 1
- 239000003797 essential amino acid Substances 0.000 description 1
- 238000009472 formulation Methods 0.000 description 1
- 230000037433 frameshift Effects 0.000 description 1
- 230000006870 function Effects 0.000 description 1
- 238000010230 functional analysis Methods 0.000 description 1
- 125000000524 functional group Chemical group 0.000 description 1
- 108020001507 fusion proteins Proteins 0.000 description 1
- 102000037865 fusion proteins Human genes 0.000 description 1
- 102000006640 gamma-Glutamyltransferase Human genes 0.000 description 1
- 238000005227 gel permeation chromatography Methods 0.000 description 1
- 208000016361 genetic disease Diseases 0.000 description 1
- 239000008103 glucose Substances 0.000 description 1
- 238000003306 harvesting Methods 0.000 description 1
- 201000002222 hemangioblastoma Diseases 0.000 description 1
- 238000005534 hematocrit Methods 0.000 description 1
- 206010073071 hepatocellular carcinoma Diseases 0.000 description 1
- IPCSVZSSVZVIGE-UHFFFAOYSA-M hexadecanoate Chemical compound CCCCCCCCCCCCCCCC([O-])=O IPCSVZSSVZVIGE-UHFFFAOYSA-M 0.000 description 1
- QAOWNCQODCNURD-UHFFFAOYSA-M hydrogensulfate Chemical compound OS([O-])(=O)=O QAOWNCQODCNURD-UHFFFAOYSA-M 0.000 description 1
- UWYVPFMHMJIBHE-OWOJBTEDSA-N hydroxymaleic acid group Chemical group O/C(/C(=O)O)=C/C(=O)O UWYVPFMHMJIBHE-OWOJBTEDSA-N 0.000 description 1
- 230000002519 immonomodulatory effect Effects 0.000 description 1
- 210000002865 immune cell Anatomy 0.000 description 1
- 230000009851 immunogenic response Effects 0.000 description 1
- 238000000099 in vitro assay Methods 0.000 description 1
- 238000011065 in-situ storage Methods 0.000 description 1
- 208000015181 infectious disease Diseases 0.000 description 1
- 230000003993 interaction Effects 0.000 description 1
- 230000003834 intracellular effect Effects 0.000 description 1
- 230000002601 intratumoral effect Effects 0.000 description 1
- 238000011835 investigation Methods 0.000 description 1
- 229960005386 ipilimumab Drugs 0.000 description 1
- 229940099584 lactobionate Drugs 0.000 description 1
- JYTUSYBCFIZPBE-AMTLMPIISA-N lactobionic acid Chemical compound OC(=O)[C@H](O)[C@@H](O)[C@@H]([C@H](O)CO)O[C@@H]1O[C@H](CO)[C@H](O)[C@H](O)[C@H]1O JYTUSYBCFIZPBE-AMTLMPIISA-N 0.000 description 1
- 229940070765 laurate Drugs 0.000 description 1
- 208000032839 leukemia Diseases 0.000 description 1
- 230000000670 limiting effect Effects 0.000 description 1
- 235000019421 lipase Nutrition 0.000 description 1
- 206010024627 liposarcoma Diseases 0.000 description 1
- 238000004811 liquid chromatography Methods 0.000 description 1
- 239000012669 liquid formulation Substances 0.000 description 1
- 230000007774 longterm Effects 0.000 description 1
- 210000001165 lymph node Anatomy 0.000 description 1
- 208000037829 lymphangioendotheliosarcoma Diseases 0.000 description 1
- 208000012804 lymphangiosarcoma Diseases 0.000 description 1
- 210000004324 lymphatic system Anatomy 0.000 description 1
- 238000011418 maintenance treatment Methods 0.000 description 1
- VZCYOOQTPOCHFL-UPHRSURJSA-N maleic acid Chemical compound OC(=O)\C=C/C(O)=O VZCYOOQTPOCHFL-UPHRSURJSA-N 0.000 description 1
- 230000036212 malign transformation Effects 0.000 description 1
- 230000036210 malignancy Effects 0.000 description 1
- 238000005259 measurement Methods 0.000 description 1
- 230000001404 mediated effect Effects 0.000 description 1
- 206010027191 meningioma Diseases 0.000 description 1
- 208000037819 metastatic cancer Diseases 0.000 description 1
- 208000011575 metastatic malignant neoplasm Diseases 0.000 description 1
- 230000004048 modification Effects 0.000 description 1
- 238000012986 modification Methods 0.000 description 1
- 125000000896 monocarboxylic acid group Chemical group 0.000 description 1
- 239000000178 monomer Substances 0.000 description 1
- 238000011201 multiple comparisons test Methods 0.000 description 1
- 208000001611 myxosarcoma Diseases 0.000 description 1
- 231100000252 nontoxic Toxicity 0.000 description 1
- 230000003000 nontoxic effect Effects 0.000 description 1
- QIQXTHQIDYTFRH-UHFFFAOYSA-N octadecanoic acid Chemical compound CCCCCCCCCCCCCCCCCC(O)=O QIQXTHQIDYTFRH-UHFFFAOYSA-N 0.000 description 1
- 229940049964 oleate Drugs 0.000 description 1
- ZQPPMHVWECSIRJ-KTKRTIGZSA-N oleic acid Chemical compound CCCCCCCC\C=C/CCCCCCCC(O)=O ZQPPMHVWECSIRJ-KTKRTIGZSA-N 0.000 description 1
- 238000011275 oncology therapy Methods 0.000 description 1
- 235000005985 organic acids Nutrition 0.000 description 1
- 230000003204 osmotic effect Effects 0.000 description 1
- 201000008968 osteosarcoma Diseases 0.000 description 1
- 239000001301 oxygen Substances 0.000 description 1
- 229910052760 oxygen Inorganic materials 0.000 description 1
- 238000006213 oxygenation reaction Methods 0.000 description 1
- IPCSVZSSVZVIGE-UHFFFAOYSA-N palmitic acid group Chemical group C(CCCCCCCCCCCCCCC)(=O)O IPCSVZSSVZVIGE-UHFFFAOYSA-N 0.000 description 1
- 208000004019 papillary adenocarcinoma Diseases 0.000 description 1
- 238000007911 parenteral administration Methods 0.000 description 1
- 229940121655 pd-1 inhibitor Drugs 0.000 description 1
- 229940121656 pd-l1 inhibitor Drugs 0.000 description 1
- 229940049954 penicillin Drugs 0.000 description 1
- 230000007414 peripheral immune response Effects 0.000 description 1
- 239000000546 pharmaceutical excipient Substances 0.000 description 1
- WLJVXDMOQOGPHL-UHFFFAOYSA-N phenylacetic acid Chemical compound OC(=O)CC1=CC=CC=C1 WLJVXDMOQOGPHL-UHFFFAOYSA-N 0.000 description 1
- 230000026731 phosphorylation Effects 0.000 description 1
- 238000006366 phosphorylation reaction Methods 0.000 description 1
- 208000024724 pineal body neoplasm Diseases 0.000 description 1
- 201000004123 pineal gland cancer Diseases 0.000 description 1
- 238000002600 positron emission tomography Methods 0.000 description 1
- 230000004481 post-translational protein modification Effects 0.000 description 1
- 239000011591 potassium Substances 0.000 description 1
- 229910052700 potassium Inorganic materials 0.000 description 1
- 229960003975 potassium Drugs 0.000 description 1
- 230000003389 potentiating effect Effects 0.000 description 1
- 230000002265 prevention Effects 0.000 description 1
- 229940021993 prophylactic vaccine Drugs 0.000 description 1
- 229940023143 protein vaccine Drugs 0.000 description 1
- 230000002685 pulmonary effect Effects 0.000 description 1
- 238000001959 radiotherapy Methods 0.000 description 1
- 238000002271 resection Methods 0.000 description 1
- 238000011268 retreatment Methods 0.000 description 1
- 201000009410 rhabdomyosarcoma Diseases 0.000 description 1
- 238000005070 sampling Methods 0.000 description 1
- 208000018964 sebaceous gland cancer Diseases 0.000 description 1
- 238000000926 separation method Methods 0.000 description 1
- 210000002966 serum Anatomy 0.000 description 1
- 230000011664 signaling Effects 0.000 description 1
- 239000011734 sodium Substances 0.000 description 1
- 229910052708 sodium Inorganic materials 0.000 description 1
- 229940083542 sodium Drugs 0.000 description 1
- 239000011780 sodium chloride Substances 0.000 description 1
- 229940054269 sodium pyruvate Drugs 0.000 description 1
- 210000001082 somatic cell Anatomy 0.000 description 1
- 125000006850 spacer group Chemical group 0.000 description 1
- 208000017572 squamous cell neoplasm Diseases 0.000 description 1
- 238000010186 staining Methods 0.000 description 1
- 238000011301 standard therapy Methods 0.000 description 1
- 230000004936 stimulating effect Effects 0.000 description 1
- 229960005322 streptomycin Drugs 0.000 description 1
- KDYFGRWQOYBRFD-UHFFFAOYSA-L succinate(2-) Chemical compound [O-]C(=O)CCC([O-])=O KDYFGRWQOYBRFD-UHFFFAOYSA-L 0.000 description 1
- 230000001629 suppression Effects 0.000 description 1
- 238000001356 surgical procedure Methods 0.000 description 1
- 201000008759 sweat gland cancer Diseases 0.000 description 1
- 206010042863 synovial sarcoma Diseases 0.000 description 1
- 229940095064 tartrate Drugs 0.000 description 1
- 201000003120 testicular cancer Diseases 0.000 description 1
- 229940034208 thyroxine Drugs 0.000 description 1
- XUIIKFGFIJCVMT-UHFFFAOYSA-N thyroxine-binding globulin Natural products IC1=CC(CC([NH3+])C([O-])=O)=CC(I)=C1OC1=CC(I)=C(O)C(I)=C1 XUIIKFGFIJCVMT-UHFFFAOYSA-N 0.000 description 1
- JOXIMZWYDAKGHI-UHFFFAOYSA-N toluene-4-sulfonic acid Chemical compound CC1=CC=C(S(O)(=O)=O)C=C1 JOXIMZWYDAKGHI-UHFFFAOYSA-N 0.000 description 1
- 238000003325 tomography Methods 0.000 description 1
- 238000011200 topical administration Methods 0.000 description 1
- 230000000699 topical effect Effects 0.000 description 1
- 230000002110 toxicologic effect Effects 0.000 description 1
- 231100000759 toxicological effect Toxicity 0.000 description 1
- 238000001890 transfection Methods 0.000 description 1
- 230000009466 transformation Effects 0.000 description 1
- 230000001052 transient effect Effects 0.000 description 1
- 238000013519 translation Methods 0.000 description 1
- 229950007217 tremelimumab Drugs 0.000 description 1
- 150000003626 triacylglycerols Chemical class 0.000 description 1
- 229940035722 triiodothyronine Drugs 0.000 description 1
- 239000012588 trypsin Substances 0.000 description 1
- 239000000439 tumor marker Substances 0.000 description 1
- 238000007492 two-way ANOVA Methods 0.000 description 1
- 238000005199 ultracentrifugation Methods 0.000 description 1
- 230000004222 uncontrolled growth Effects 0.000 description 1
- 210000000689 upper leg Anatomy 0.000 description 1
- 229940116269 uric acid Drugs 0.000 description 1
- 238000002562 urinalysis Methods 0.000 description 1
- 229940070710 valerate Drugs 0.000 description 1
- NQPDZGIKBAWPEJ-UHFFFAOYSA-N valeric acid Chemical compound CCCCC(O)=O NQPDZGIKBAWPEJ-UHFFFAOYSA-N 0.000 description 1
- 239000003981 vehicle Substances 0.000 description 1
- 210000003462 vein Anatomy 0.000 description 1
- 238000000196 viscometry Methods 0.000 description 1
- 230000000007 visual effect Effects 0.000 description 1
- 238000005406 washing Methods 0.000 description 1
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Substances O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 description 1
- 229920003169 water-soluble polymer Polymers 0.000 description 1
- 238000007482 whole exome sequencing Methods 0.000 description 1
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/39—Medicinal preparations containing antigens or antibodies characterised by the immunostimulating additives, e.g. chemical adjuvants
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/0005—Vertebrate antigens
- A61K39/0011—Cancer antigens
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/0005—Vertebrate antigens
- A61K39/0011—Cancer antigens
- A61K39/00119—Melanoma antigens
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
- A61K39/39533—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals
- A61K39/3955—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals against proteinaceous materials, e.g. enzymes, hormones, lymphokines
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2803—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily
- C07K16/2818—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against the immunoglobulin superfamily against CD28 or CD152
-
- A—HUMAN NECESSITIES
- A01—AGRICULTURE; FORESTRY; ANIMAL HUSBANDRY; HUNTING; TRAPPING; FISHING
- A01K—ANIMAL HUSBANDRY; CARE OF BIRDS, FISHES, INSECTS; FISHING; REARING OR BREEDING ANIMALS, NOT OTHERWISE PROVIDED FOR; NEW BREEDS OF ANIMALS
- A01K2207/00—Modified animals
- A01K2207/12—Animals modified by administration of exogenous cells
-
- A—HUMAN NECESSITIES
- A01—AGRICULTURE; FORESTRY; ANIMAL HUSBANDRY; HUNTING; TRAPPING; FISHING
- A01K—ANIMAL HUSBANDRY; CARE OF BIRDS, FISHES, INSECTS; FISHING; REARING OR BREEDING ANIMALS, NOT OTHERWISE PROVIDED FOR; NEW BREEDS OF ANIMALS
- A01K2227/00—Animals characterised by species
- A01K2227/10—Mammal
- A01K2227/105—Murine
-
- A—HUMAN NECESSITIES
- A01—AGRICULTURE; FORESTRY; ANIMAL HUSBANDRY; HUNTING; TRAPPING; FISHING
- A01K—ANIMAL HUSBANDRY; CARE OF BIRDS, FISHES, INSECTS; FISHING; REARING OR BREEDING ANIMALS, NOT OTHERWISE PROVIDED FOR; NEW BREEDS OF ANIMALS
- A01K2267/00—Animals characterised by purpose
- A01K2267/03—Animal model, e.g. for test or diseases
- A01K2267/0331—Animal model for proliferative diseases
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/51—Medicinal preparations containing antigens or antibodies comprising whole cells, viruses or DNA/RNA
- A61K2039/53—DNA (RNA) vaccination
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/555—Medicinal preparations containing antigens or antibodies characterised by a specific combination antigen/adjuvant
- A61K2039/55511—Organic adjuvants
- A61K2039/55522—Cytokines; Lymphokines; Interferons
- A61K2039/55527—Interleukins
- A61K2039/55533—IL-2
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/555—Medicinal preparations containing antigens or antibodies characterised by a specific combination antigen/adjuvant
- A61K2039/55511—Organic adjuvants
- A61K2039/55561—CpG containing adjuvants; Oligonucleotide containing adjuvants
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/57—Medicinal preparations containing antigens or antibodies characterised by the type of response, e.g. Th1, Th2
- A61K2039/572—Medicinal preparations containing antigens or antibodies characterised by the type of response, e.g. Th1, Th2 cytotoxic response
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/70—Multivalent vaccine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/80—Vaccine for a specifically defined cancer
- A61K2039/82—Colon
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/80—Vaccine for a specifically defined cancer
- A61K2039/876—Skin, melanoma
Definitions
- cancer immunotherapy and in a particular aspect, cancer immunotherapy, and involves the treatment of an individual having cancer by administering to the individual an anticancer vaccine such as a DNA neoantigen vaccine, in combination with a T cell expander, optionally further combined with a checkpoint inhibitor.
- an anticancer vaccine such as a DNA neoantigen vaccine
- Cancer is a genetic disorder that results from genetic or epigenetic alternations in the somatic cells and represents one of the most deadly diseases in the developed world.
- Tumorigenesis in humans is a multistep process which involves various genetic or epigenetic changes that ultimately drive the malignant transformation of normal cells. While our understanding of mechanisms leading to malignancy continues to make enormous strides, the complexity of the processes that drive the development, growth and spread of cancer make the development of new and effective treatments particularly challenging.
- Therapeutic cancer vaccines represent a class of substances that work by stimulating or restoring a subject’s immune system’s ability to fight infections and disease.
- Therapeutic vaccines as opposed to preventative or prophylactic vaccines, are used to treat an existing cancer by boosting the body’s natural immune response against the cancer and represent a type of immunotherapy.
- Cancer treatment vaccines are designed to activate cytotoxic T cells and direct them to recognize and act against specific types of cancer or to induce production of antibodies that bind to molecules on the surface of cancer cells.
- tumor-associated antigens are antigens that are expressed at low levels in normal tissues, but are expressed at much higher levels in tumor tissue.
- producing effective therapeutic vaccines that bind to tumor-associated antigens has proven to be a challenging endeavor, at least in part, because the vaccine intervention must combat the body’s immune system that is restrained by mechanisms that work to sustain the cancer.
- therapeutic approaches based upon tumor- associated antigen-based vaccines may also lead to toxicities due to normal cell destruction.
- a therapeutic cancer vaccine must not only stimulate a specific immune response against an intended target, but must also be powerful enough to overcome the barriers that cancer cells utilize to protect themselves from attack by killer T cells.
- Therapeutic vaccines have been evaluated, for example, in patients with breast cancer, lung cancer, melanoma, pancreatic cancer, colorectal cancer, and renal cancer (Melero, I., et al, Nat Rev Clin Oncol, 2014, 11 (9), 509-524), although such therapeutic anticancer vaccines have met with limited success.
- neoantigen-based DNA cancer vaccine a compound effective to stimulate/expand production of T cells (i.e., effector T cells,“a T cell expander”).
- the disclosure provides a method for treating a subject having cancer, the method comprising administering to the subject, (i) an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, (ii) a compound effective to stimulate/expand production of T cells, and optionally, (iii) a checkpoint inhibitor.
- the neoepitopes comprised in the DNA vaccine are presented to the immune system as a dimeric protein called a vaccibody (to be described in greater detail herein), i.e., in such embodiments, the vaccine is referred to as a vaccibody DNA vaccine.
- a vaccibody DNA vaccine i.e., in such embodiments, the vaccine is referred to as a vaccibody DNA vaccine.
- WO 2004/076489 describes dimeric proteins called vaccibodies in detail.
- Targeting units are described in detail in WO 2011/161244.
- the neoantigen-based DNA cancer vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding (i) a targeting unit, (ii) a dimerization unit, (iii) a first linker and (iv) an antigenic unit, where the antigenic unit comprises n-1 antigenic subunits (where n is an integer of from about 3 to 50), each subunit comprising at least a part of a cancer neoepitope sequence and a second linker, and further comprising a final cancer neoepitope sequence.
- the neoantigen-based DNA cancer vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding an antigenic unit.
- the antigenic unit comprises n-1 antigenic subunits, where each subunit comprises at least a part of a cancer neoepitope sequence and a linker, and further comprises a final cancer neoepitope sequence, wherein n is an integer of from 3 to 50.
- the vaccine is a vaccibody DNA vaccine comprising from 10 to 50 neoepitopes, or from 15 to 40 neoepitopes, or from 10 to 30 neoepitopes, or from 10-20 neoepitopes.
- the vaccine comprises a DNA polynucleotide comprising a nucleotide sequence encoding an antigenic unit as described above, wherein the linker is an amino acid linker.
- linkers include, for example, glycine/serine-rich linkers. Further exemplary linkers include, for example, the linkers identified as SEQ ID NO:67-76.
- Exemplary mouse neoantigen-based DNA cancer vaccines comprising
- VB10.NEO pDNA constructs VB4011 and VB4061, are described in the supporting examples.
- the vaccine comprises a DNA
- the vaccine comprises a DNA pVBlO.NEO plasmid backbone sequence as provided in FIG. 12.
- the T cell expander when administered in combination with the neoantigen-based DNA cancer vaccine is effective to enhance specific clonal T cell expansion to vaccine epitopes over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander to a degree that is greater than additive.
- the T cell expander is a prodrug of an interleukin-2 (e.g., aldesleukin, des-alanyl-1, serine-125 human interleukin-2), wherein the interleukin-2 is modified by releasable covalent attachment of multiple polyethylene glycol moieties.
- the T cell expander is an interleukin-2 receptor beta (IL-2R_ ) selective agonist.
- the T cell expander is an IL-2R]3-selective agonist composition, multi(2,7-(bis-methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 (also referred to herein as“RSLAIL-2”), comprising compounds of Formula (I),
- IL-2 is interleukin-2 (such as, for example, aldesleukin)
- -NH-IL-2 represents an amino group of interleukin-2
- each integer (n) has a value from about 200-300; or pharmaceutically acceptable salt forms thereof.
- “n” in each of the polyethylene glycol chains is about 227 (i.e., where each polyethylene glycol chain extending from the central fluorenyl core has a weight average molecular weight of about 10,000 daltons, such that the weight average molecular weight of each overall branched PEG moiety is about 20,000 daltons).
- the T cell expander is (2,7-(bis- methoxyPEGiok d -carboxyamide)(9h-fluorene-9-yl)methyl N-carbamate)6 avg interleukin-2.
- numbers of neoantigen-based DNA cancer vaccine-induced T cells in the tumor are increased in number over such T cells determined upon following administration of one or more doses of the neoantigen-based DNA cancer vaccine alone, when evaluated in either a clinical or a preclinical setting.
- the cancer is a solid cancer.
- the cancer is selected from, for example, the group consisting of breast cancer, ovarian cancer, colon cancer, prostate cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer (SCLC), non-small cell lung cancer (NSCLC), pancreatic cancer, thyroid cancers, kidney cancer, e.g., renal cell carcinoma, cancer of the bile duct, cancer of the head and neck (e.g., squamous cell carcinomas of the head and neck), brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer (e.g., urothelial carcinoma), esophageal cancer, Hodgkin's disease and adrenocortical cancer, among others.
- SCLC small cell lung cancer
- NSCLC non-small cell lung cancer
- pancreatic cancer thyroid cancers
- kidney cancer e.g., renal cell carcinoma, cancer of the bile duct, cancer of the head and neck (e.g., s
- the cancer is selected from locally advanced or metastatic melanoma, non-small cell lung cancer, clear renal cell carcinoma, urothelial cancer, and squamous cell carcinoma of the head and neck.
- the cancer is melanoma or colon cancer.
- the neoantigen-based DNA cancer vaccine and the T cell expander, and optionally a checkpoint inhibitor may be administered concurrently or sequentially, and in any order, and via the same and/or different routes of administration. More particularly, the therapeutic components of the combination therapy may each be administered on the same day, on different days, or, a mixture of both (two immunotherapeutic components administered on the same day and one immunotherapeutic component administered on a different day).
- treatment may comprise a single cycle of therapy, or may comprise multiple cycles, including one or more doses of each of the neoantigen-based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor.
- treatment may comprise a mixture of single cycle and multiple cycles, such as, for example at least one of the neoantigen-based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor is administered for a single cycle and one or more of the neoantigen- based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor is administered for multiple cycles.
- the T cell expander is administered following administration of the neoantigen-based DNA cancer vaccine.
- the T cell expander is administered following the neoantigen-based DNA cancer vaccine induction phase, wherein such induction phase may span one or more administrations of the vaccine, e.g., 1, 2, 3, 4 or more vaccinations over a given time period.
- the time following the induction phase is a time, following one or more vaccinations, at which the neoepitope- specific T cell response has substantially levelled off, that is, is no longer significantly increasing.
- such time is within a time frame in which the neoepitope-specific T cell response has reached its maximum, or is within +25% of its maximum, or is within + 15% of its maximum, or is within about + 10% of its maximum.
- the T cell expander may be administered within about 3-20 days following the last vaccination of the induction period, or within about 3-15 days following the last vaccination of the induction period, or within about 7-20 days following the last vaccination of the induction period, such as within about 7-15 days or within 7-12 days. Additional ranges are also contemplated. In some embodiments, the T cell expander is administered at least 3 days following the last vaccine administration of the induction period.
- the T cell expander may, for example, first be administered within about 4-20 weeks following initiation of the vaccination(s) (i.e., following the first vaccination of the induction period), or within about 6-16 weeks following the first vaccination of the induction period, or within about 8-12 weeks following the first vaccination of the induction period, such as, e.g., 11 weeks following the first vaccination of the induction period.
- administration comprises administration of each of the neoepitope-specific DNA-based cancer vaccine and the T cell expander to align or substantially align the peak T cell responses of both the neoepitope-specific DNA-based cancer vaccine and the T cell expander to thereby achieve an optimized (and preferably synergistic) T cell response.
- the T cell expander is administered at a period of time following administration of one or more doses of the neoantigen-based DNA cancer vaccine, e.g., following 1-5 doses (i.e., vaccinations), or following 1-4 doses (vaccinations), or following 1-3 doses (vaccinations), or following 1-2 doses (vaccinations) e.g., to thereby result in an enhancement of the specific T cell response.
- the T cell expander is administered following 2 or 3 vaccinations or 4 vaccinations.
- the T cell expander is administered following 4 vaccinations.
- the T cell expander is administered from 1-20 days following the last vaccination of the induction period.
- the T cell is initially administered on day 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19 or 20 days following the last vaccination of the induction period.
- the vaccination period comprises 4 vaccinations
- the first dose of the T cell expander is administered from 5-10 days following the 4 th vaccination, e.g., e.g., 5, 6, 7, 8, 9, or 10 days following the 4 th vaccination, e.g., on day 7.
- the vaccine and the T cell expander are administered on either the same day or on different days.
- the vaccine and the T cell expander are administered on the same day.
- the vaccine induction period as described above comprises more than one vaccination, each subsequent vaccination separated by 1 week, 2 weeks, 3 weeks, or 4 weeks or more following the first administration.
- the vaccination induction period comprises 4 separate vaccinations, each separated by from 1-8 weeks, or from 2-8 weeks, or from 2-6 weeks, or from 3-8 weeks, or from 4-8 weeks, or from 4-6 weeks.
- the vaccine is administered every 3 weeks for the first one, two or three or four doses, following by a longer interval between vaccinations, e.g., every 4 weeks, or every 5 weeks or every 6 weeks, or longer.
- the checkpoint inhibitor when comprised in the combination therapy, is administered, for one or for multiple rounds (i) on the same day as the neoantigen-based DNA cancer vaccine is administered, (ii) on the same day as the T cell expander is administered (iii) following administering of the neoantigen- based DNA cancer vaccine, (iv) following administering of the T cell expander, (v) following administering of the neoantigen-based DNA cancer vaccine but before administering of the T cell expander.
- an exemplary order of administration is neoantigen-based DNA cancer vaccine, T cell expander, followed by checkpoint inhibitor.
- the checkpoint inhibitor such as an anti-PD-1 antibody or other suitable CPI
- the checkpoint inhibitor is administered more than once over the course of treatment.
- the checkpoint inhibitor is initially administered following an initial vaccination and following administration of the T cell expander.
- the checkpoint inhibitor is initially administered following an initial vaccination but prior to administration of the T cell expander.
- the check point inhibitor when comprised in the combination therapy, is administered prior to first vaccination (i.e., administration) of the neoantigen-based DNA cancer vaccine and prior to the first administration of the T cell expander.
- Exemplary checkpoint inhibitors include, e.g., an anti -PD- 1 antibody, an anti-
- CTLA-4 antibody or an anti-PD-Ll antibody.
- the cancer comprises a cancerous tumor and the method is effective to reduce the size of the cancerous tumor when compared to the size of the tumor prior to treatment.
- the cancer comprises a cancerous tumor, and the method is effective to reduce the size of the cancerous tumor by at least about 30% (partial response), or by at least about 40%, or by at least about 50%, or by at least about 60%, or by at least about 70%, or at least about 80%, or at least about 90%, or to result in complete tumor regression, when compared to the size of the tumor prior to the administering.
- the cancer comprises a cancerous tumor and the method is effective to result in complete tumor regression.
- FIG. 1 provides the amino acid sequence of the exemplary VB10.NEO pDNA mouse construct, VB4011 (SEQ ID NO: l), encoding 10 neoepitopes from B16, wherein each peptide is separated by a ten amino acid linker (GGGGS)2 (SEQ ID NO:33), as described in Table 2.
- FIGs. 2A-2D illustrate, as described in Example 1, that administration of a T cell expander such as RSLAIL-2 boosts the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO in a B16 mouse melanoma model.
- FIG. 2A is a graph of the total T cell responses (number of IFN-y+ spots/10 6 splenocytes) in a B16 tumor model after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- FIG. 1 is a graph of the total T cell responses (number of IFN-y+ spots/10 6 splenocytes) in a B16 tumor model after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine.
- FIG. 2B is a graph of the total T cell responses per spleen, that is the number of IFN-y+ spots/spleen, after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- FIG. 2C is a graph of the total CD8+ T cell responses (splenocytes depleted of CD4+ T cells using anti-CD4 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- 2D is a graph of the total CD4+ T cell responses (splenocytes depleted of CD8+ T cells using anti-CD8 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- the T cell expander synergizes vaccine induced neoepitope-specific IFN-g T cell responses in a mouse melanoma model.
- FIGs. 3A-3D illustrate, as described in Example 2, that administration of a T cell expander boosts the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO in a CT26 mouse colon carcinoma model.
- FIG. 3A is a graph of the total T cell responses (number of IFN-y+ spots/10 6 splenocytes) in a CT26 tumor model after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL- 2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- FIG. 3A is a graph of the total T cell responses (number of IFN-y+ spots/10 6 splenocytes) in a CT26 tumor model after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL- 2), or the combination of
- 3B is a graph of the total T cell responses per spleen, that is the number of IFN-y+ spots/spleen, after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), and the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- 3C is a graph of the total CD8+ T cell responses (splenocytes depleted of CD4+ T cells using anti-CD4 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- VB1026 the total CD8+ T cell responses
- VB4061 the vaccine alone
- RSLAIL-2 T cell expander alone
- 3D is a graph of the total CD4+ T cell responses (splenocytes depleted of CD8+ T cells using anti-CD8 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2).
- the T cell expander synergizes vaccine induced neoepitope-specific IFN-g T cell responses in a mouse colon carcinoma model.
- FIGs. 4A-4D illustrate, as described in Example 3, that administration of a T cell expander boosts the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine,
- FIG. 4A is a graph of the tumor growth shown as tumor volume (cm 3 ) for 5-25 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti -PD 1 Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2) in a CT26 mouse colon carcinoma model.
- FIG. 4A is a graph of the tumor growth shown as tumor volume (cm 3 ) for 5-25 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti -PD 1 Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2) in a CT26 mouse colon carcinoma model.
- 4B is a graph of the percentage of tumor-free mice (i.e., mice that never established a tumor) for 0-49 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti-PDl Ab), or the combination of the vaccine, an anti- PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2).
- Tuor take refers to mice that never established a tumor, which differs from mice that established a tumor which then later regressed or was cleared.
- 4C is a graph of the % survival of mice for 0-80 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti- PDl Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2).
- VB4061 the combination of the vaccine and an anti-PD-1 antibody
- a T cell expander VB4061 + anti-PDl Ab + RSLAIL-2).
- 4D is a graph of the percentage of tumor-free mice for 0-70 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti- PDl Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2) after re-challenge with 5xl0 4 CT26 tumor cells without retreatment.
- VB4061 + anti-PDl Ab + RSLAIL-2 T cell expander
- FIGs. 5A-5C provide the results of administration of a T cell expander that is postponed after one or more administrations of an anticancer vaccine as described further in Example 1.
- FIG. 5A is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a B 16 tumor model after treatment with a control (VB1026), the vaccine alone (VB4011) administered on day 1, or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2) administered on day 11 or day 14 after the anticancer vaccine.
- T cell response was analyzed at days 14, 18 or 21 after anticancer vaccine, and 7 days after dosing the T cell expander.
- FIG. 5B is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a CT26 tumor model after treatment with a control (VB1026), the vaccine alone (VB4061) on days 1 and 21 and the combination of the T cell expander and the vaccine (VB4061 + RSLAIL-2) administered on day 21 (same day as 2 nd vaccination) or day 24 (3 days post 2 nd vaccination).
- ELISpot was performed 7 days following administration of RSLAIL-2 (e.g., 21 + 7 or 24 +
- the day in the figure refers to when splenocytes were analyzed in ELISpot. (Vaccine is administered day 1).
- Vaccine is administered day 1.
- RSLAIL-2 d21 administration of both the vaccine and RSLAIL-2 (second doses) occurred on the same day.
- VB4061 + RSLAIL-2 d28 RSLAIL-2 was administered three days (day 24) following the second administration of the vaccine (on day 21).
- FIG. 1 The day in the figure refers to when splenocytes were analyzed in ELISpot.
- 5C is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a B16 tumor model after treatment with three administrations of a control (3x VB1026), three administrations of the vaccine alone (3xVAC), three administrations of the vaccine with administration of the T cell expander on the same day as the third vaccine (3xVAC + RSLAIL-2 d35), and three administrations of the vaccine with administration of the T cell expander three days following the third vaccine dose (3x VAC + RSLAIL-2).
- This figure indicates that when RSLAIL-2 is administered as late as the 3 rd vaccination, the difference between same day and 3-days postponed is no longer present. Postponed administration of the T cell expander appears to synergize the specific T cell response.
- FIGS. 6A-6C provide graphs of the tumor length (mm), where the T cell expander was administered days 0, 9, 18, 27 (dotted lines) starting when the tumor burden at first administration is 1-5 mm (FIG. 6A), 6-10 mm (FIG. 6B), or >10 mm (FIG. 6C) in a CT26 mouse colon carcinoma model.
- Mice were treated with the vaccine VB4061 + anti- PD-1 antibody in addition (red, green and blue legend), or VB4061 + anti.PD-1 only (black legend).
- Pink lines in FIGs. 6A and 6C corresponds to RSLAIL-2 at day 32. A complete response was observed in a greater number of mice where the tumor size was ⁇ 6 mm at the time of the first administration of the T cell expander.
- FIGs. 7A-7B illustrate that administration of a T cell expander provides rapid, complete and long lasting regression of relatively small tumors and long lasting stabilization of larger tumors when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB4061, and an anti-PD-1 antibody in a CT26 mouse colon carcinoma model.
- FIG. 7A is a graph of the tumor growth shown as tumor length (mm) for 0-42 days post injection of CT26 tumor cells as a control.
- FIG. 7B is a graph of the tumor growth shown as tumor length (mm) for 0-56 days post injection of CT26 tumor cells after administration of a combination of the vaccine (VB4061), an anti-PD-1 antibody, and a T cell expander in a CT26 mouse colon carcinoma model.
- FIG. 8 provides the amino acid sequence of the VB10.NEO pDNA mouse construct, VB4061 (SEQ ID NO:2), encoding 20 neoepitopes from CT26, wherein each peptide is separated by a ten amino acid glycine/serine rich linker (GGGGS)2, as described in Table 2.
- FIG. 9 provides the amino acid sequences of the individual neoepitopes from
- CT26 (SEQ ID NOs:3-22) included in the VB4061 mouse construct.
- FIG. 10 provides the amino acid sequences of the individual neoepitopes from
- FIGs. 11A-D provide an outline of dosing and assessments performed throughout the clinical study described in Example 4.
- FIG. 12 provides a complete pVBlO.NEO plasmid backbone sequence including coding sequences of the targeting module (hMIP-la, nucleotides 1143-1421) and the dimerization module (hi and h4 and CH3 domains of hIgG3, nucleotides 1422-1853) of the expression product (SEQ ID NO:77).
- the grey blocks are the internal Sfll cloning sites (nucleotides 1854-1866 and 1869-1881). Italic sequences are the flanking Notl/Bglll restriction sites (nucleotides 1884-1889).
- Underlined sequences are glycine/serine-rich linkers (nucleotides 1503-1532 and 1854-1868). The nucleotide numbering does not include the neoantigenic module nucleotides).
- FIG. 13 provides a pVBlO.NEO plasmid map.
- the instant disclosure relates to (among other things) the field of
- T cell expander a T cell expanding compound
- a personalized neoantigen DNA cancer vaccine in combination with a T cell expanding compound (“T cell expander”), i.e., a compound capable of driving specific clonal T cell expansion to vaccine epitopes, optionally further combined with a checkpoint inhibitor.
- T cell expander i.e., a compound capable of driving specific clonal T cell expansion to vaccine epitopes, optionally further combined with a checkpoint inhibitor.
- references to a range or sub-range is meant to expressly recite sub-ranges formed by any two members of a disclosed range.
- a range described as being from 20 to 50, or from 10 to 30, will thereby expressly include ranges from 10 to 20, 20 to 30, 10 to 50, 30 to 50, and so forth.
- substantially or “essentially” means nearly totally or completely, for instance, about 95% or greater of a given quantity.
- PEG polyethylene glycol
- a "PEG polymer” or a polyethylene glycol is one in which substantially all (preferably all) monomeric subunits are ethylene oxide subunits, though, the polymer may contain distinct end capping moieties or functional groups, e.g., for conjugation.
- PEG polymers for use in the moieties described herein will typically comprise one of the two following structures: "-(CEhCEhOV or "-(CH2CH 2 0)n-iCH 2 CH2-,” depending upon whether or not the terminal oxygen(s) has been displaced, e.g., during a synthetic transformation.
- variable (n) will typically fall within a range from about 3 to 4000, and the terminal groups and architecture of the overall PEG can vary.
- Preferred ranges /values for (n) for the T cell expander, RSLAIL-2 (described in greater detail below), e.g., in reference to Formulas (I), (II), (III) and (IV), include from about 200 to 300, and about 227.
- Additional exemplary ranges for (n) are those suitable to provide a branched polymer such as provided in Formulas (I), (II), (III) and (IV), having an overall weight average molecular weight in a range of from about 250 daltons to about 90,000 daltons.
- Additional exemplary ranges for (n) are those suitable to provide a branched polymer such as provided in Formulas (I), (II), (III) and (IV), having an overall weight average molecular weight in a range selected from about 1,000 daltons to about 60,000 daltons, in a range of from about 5,000 daltons to about 60,000 daltons, in a range of about 10,000 daltons to about 55,000 daltons, in a range of from about 15,000 daltons to about 50,000 daltons, and in a range of from about 20,000 daltons to about 50,000 daltons.
- Branched in reference to the geometry or overall structure of a polymer, optionally forming part of a polymer-conjugate, refers to a polymer having two or more polymer "arms” or“chains” extending from a branch point or central structural feature.
- a branched polymer comprises two polymer arms or chains emanating from a central structural feature.
- a covalent“releasable” linkage for example, in the context of a polyethylene glycol that is covalently attached to an active moiety such as an interleukin-2 (e.g., aldesleukin), is one that releases under physiological conditions by any suitable release mechanism to thereby release or detach the polyethylene glycol polymer from the active moiety.
- an interleukin-2 e.g., aldesleukin
- Molecular weight in the context of a water-soluble polymer can be expressed as either a number average molecular weight or a weight average molecular weight. Unless otherwise indicated, all references to molecular weight herein refer to the weight average molecular weight. Both molecular weight determinations, number average and weight average, can be measured using gel permeation chromatography or other liquid chromatography techniques.
- PEG polymers are typically polydisperse (i.e., number average molecular weight and weight average molecular weight of the polymers are not equal), possessing low polydispersity values of preferably less than about 1.2, more preferably less than about 1.15, still more preferably less than about 1.10, yet still more preferably less than about 1.05, and most preferably less than about 1.03.
- protein protein
- polypeptide peptide
- peptide refers to any peptide-linked chain of amino acids, regardless of length, co- translational or post-translational modification.
- “Pharmaceutically acceptable excipient” or “pharmaceutically acceptable carrier” refers to a component that may be included in the compositions described herein and causes no significant adverse toxicological effects to a subject.
- patient refers to a living organism suffering from or prone to a condition that can be prevented or treated by administration of a compound or composition or combination as provided herein, such as a cancer, and includes both humans and animals.
- Subjects include, but are not limited to, mammals (e.g., murines, simians, equines, bovines, porcines, canines, felines, and the like), and preferably are human.
- administering refers to the delivery of a therapeutic agent to a subject, using any of the various methods and delivery systems known to those skilled in the art.
- Exemplary routes of administration include intravenous, intramuscular, subcutaneous, intraperitoneal, spinal or other parenteral routes of administration, for example by injection or infusion.
- parenteral administration as used herein means modes of
- administration other than enteral and topical administration usually by injection, and includes, without limitation, intravenous, intramuscular, intraarterial, intrathecal,
- a therapeutic agent can be administered via a non-parenteral route, or orally.
- Other non-parenteral routes include a topical, epidermal or mucosal route of administration, for example, intranasally, vaginally, rectally, sublingually or topically.
- Administering of one or more therapeutic agents can also be performed for each of the therapeutic agents, for example, once, a plurality of times, and/or over one or more extended periods.
- a “cancer” refers a broad group of various diseases characterized by the uncontrolled growth of abnormal cells in the body.
- a “cancer” or “cancer tissue” includes a tumor, and as used herein, encompasses both a solid tumor as well as tumor cells found in a bodily fluid such as blood, and includes metastatic cancer. Unregulated cell division and growth results in the formation of malignant tumors that can invade neighboring tissues and can also metastasize to distant parts of the body through the lymphatic system or
- the distal tumors can be said to be "derived from” a pre metastasis tumor.
- immunotherapy refers to the treatment of a subject by a method comprising inducing, enhancing, suppressing, or otherwise modifying an immune response.
- tumor specific antigen comprising one or more mutations as compared to the host’s exome and is used
- tumor antigen any immunogenic mutation in a tumor antigen and is used synonymously herein with the term,“cancer neoepitope”.
- A“tumor neoepitope sequence” as used herein is the sequence comprising the neoepitope in an antigenic subunit, and is used synonymously with the term,“cancer neoepitope sequence”.
- a“plurality” refers to 3 or more of a given item.
- therapeutic anticancer vaccine and“therapeutic cancer vaccine” are used synonymously to describe a vaccine that is used for destroying or reducing the number of tumor cells already present in a patient.
- a "therapeutically effective amount” or “therapeutically effective dosage” of a therapeutic agent is any amount of an agent, when used alone or in combination with another therapeutic agent, that is effective to, for example, protect a subject against the onset of a disease such as cancer or promote disease regression evidenced by a decrease in severity of disease symptoms, an increase in frequency and duration of disease symptom-free periods, or a prevention of impairment or disability due to the disease affliction.
- the ability of a therapeutic agent to promote disease regression can be evaluated using a variety of methods known to the skilled practitioner, such as in human subjects during clinical trials, in animal model systems predictive of efficacy in humans, or by assaying the activity of the agent in in vitro assays. See, for instance, the supporting examples.
- substantially homologous or“substantially identical” means that a particular subject sequence, for example, a mutant sequence, varies from a reference sequence by one or more substitutions, deletions, or additions, the net effect of which does not result in an adverse functional dissimilarity between the reference and subject sequences.
- a sequence having greater than 95 percent homology (identity), equivalent biological activity (although not necessarily equivalent strength of biological activity), and equivalent expression characteristics to a given sequence is considered to be substantially homologous (identical).
- truncation of the mature sequence should be disregarded.
- the phrase "at least 80% sequence identity" may be used herein. This expression refers to a sequence identity of at least 80%, at least 81%, at least 82%, at least 83%, at least 84%, at least 85%, at least 86%, at least 87%, at least 88%, at least 89%, at least 90%, at least 91%, at least 92%, at least 93%, at least 94%, at least 95%, at least 96%, at least 97%, at least 98%, or at least 99% to the respective reference polypeptide or to the respective reference
- polypeptide in question and the reference polypeptide exhibit the indicated sequence identity over a continuous stretch of 20, 30, 40, 45, 50, 60, 70, 80, 90, 100 or more amino acids or over the entire length of the reference polypeptide.
- polynucleotide in question and the reference polynucleotide exhibit the indicated sequence identity over a continuous stretch of 60, 90, 120, 135, 150, 180, 210, 240, 270, 300 or more nucleotides or over the entire length of the reference polypeptide.
- a combination immunotherapy method based upon administration of a personalized neoantigen-based DNA cancer vaccine and a T cell expander, i.e., an entity that is effective to drive specific clonal T cell expansion to the vaccine epitopes.
- IL-2 stimulates immune cell proliferation and activation through a receptor signaling complex containing alpha (IL2Ra, CD25), beta (IL2R , CD122) and common gamma chain receptors (y C’ CD 132).
- IL-2 binds to heterodimeric IL2R.Py receptor leading to desired expansion of tumor killing CD8+ memory effector T (CD8 T) cells.
- CD8 T memory effector T
- IL-2 also binds to its heterotrimeric receptor IL2Ro y with greater affinity, which expands immunosuppressive CD4+, CD25+ regulatory T cells (Tregs), which may lead to an undesirable effect for cancer immunotherapy.
- a treatment modality that combines a neoantigen-based DNA cancer vaccine against tumor specific antigens with administration of a T cell expander.
- the T cell expander is an IL-2Raf -biased agonist.
- the treatment methods provided herein comprise administering (i) a vaccine, i.e., an anti cancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens (“neoantigen-based DNA cancer vaccine”), and (ii) a compound effective to stimulate/expand production of T cells (i.e., effector T cells,“a T cell expander”) for treating a patient having cancer, optionally in combination with a check point inhibitor.
- a vaccine i.e., an anti cancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens (“neoantigen-based DNA cancer vaccine”)
- a compound effective to stimulate/expand production of T cells i.e., effector T cells,“a T cell expander”
- compositions, combinations, and methods provided herein find use in, among other things, both clinical and pre-clinical applications.
- administration of a T cell expander, such as RSLAIL-2 in combination with a neoantigen- based DNA cancer vaccine, optionally further combined with a checkpoint inhibitor, is effective to significantly expand/enhance the T cell response to vaccine-encoded neoantigens in a subject, to thereby provide a strong-neoantigen focused immune response for fighting cancer.
- VB10.NEO alone. Mice treated with VB10.NEO in combination with the T cell expander, RSLAIL-2, showed both a stronger response to each neoepitope and to increased numbers of neoepitopes, demonstrating that both the breadth and depth of the immune response were elevated as a result of the combination therapy.
- the VB10.NEO and RSLAIL-2 combination produced an even greater effect on CD8+ T cell responses as the combination elicited a neoepitope-specific CD8+ T cell response to more neoepitopes compared to either immunotherapeutic agent when administrated alone, further strengthening the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses.
- mice treated with the exemplary triple immunotherapeutic combination of VB10.NEO, RSLAIL-2 and an anti-PD- 1 antibody (as representative of a combination therapy comprising administration of a personalized neoantigen-based DNA cancer vaccine, a T cell expander, and optionally, a checkpoint inhibitor), further demonstrating the advantages of combining such reagents to thereby activate non-overlapping mechanisms of immunotherapy and create an effective treatment of established tumors.
- therapeutic anticancer neoepitope vaccines suitable for use in the methods provided herein are described in U.S. Patent Publication No. 2019/0022202, along with methods describing their preparation and use, which is incorporated herein by reference.
- the therapeutic neoepitope vaccine is an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens.
- the neoepitopes comprised in the individualized DNA vaccine are presented to the immune system as a dimeric protein called a vaccibody.
- Dimeric proteins called vaccibodies are described in detail in WO 2004/076489, which is incorporated herein by reference.
- the neoantigen-based DNA cancer vaccine may comprise an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding at least (i) a targeting unit (also referred to as a targeting module), (ii) a dimerization unit (also referred to as a dimerization module), (iii) a first linker and (iv) an antigenic unit (also referred to as an antigenic module), wherein the antigenic unit comprises n-1 antigenic subunits; n is an integer of from 3 to 50.
- Each antigenic subunit comprises at least a part of a cancer neoepitope sequence and a second linker. Additionally, the antigenic unit further comprises a final cancer neoepitope sequence.
- the vaccines suitable for use in the instant methods are designed to evoke a cell-mediated immune response through activation of T cells against the neoantigens.
- T cells recognize neoepitopes when they have been processed and presented complexed to a MHC molecule.
- the neoantigen vaccine comprises a DNA polynucleotide encoding a polypeptide comprising three units, i.e. a targeting unit (or module), a dimerization unit (or module) and an antigenic unit (or module). Due to the dimerization unit, the polypeptide forms a dimeric protein called a vaccibody.
- the genes encoding the three units are genetically engineered to be expressed as one gene.
- the poly peptides/ dimeric proteins target antigen presenting cells (APCs), which results in enhanced vaccine potency compared to identical non-targeted antigens. See, for example, FIG. 13 which provides an exemplary plasmid map illustrating different functional elements.
- the antigenic unit comprises antigenic subunits, wherein each subunit comprises a cancer neoepitope sequence or at least a part of a cancer neoepitope sequence.
- the neoepitope sequence is obtained by sequencing tumor DNA (or RNA) and identifying tumor specific mutations representing neoantigens.
- a personalized neoantigen vaccine is obtained that specifically targets the identified tumor antigens.
- the therapeutic anticancer neoepitope vaccine comprises an immunologically effective amount of a polynucleotide comprising a nucleotide sequence encoding (i) a targeting unit, (ii) a dimerization unit, (iii) a first linker, (iv) an antigenic unit, wherein the antigenic unit comprises n-1 antigenic subunits, and each subunit comprises at least a part of a cancer neoepitope sequence and a second linker, where the antigenic unit further comprises a final cancer neoepitope sequence, wherein n is an integer of from 3 to 50.
- the vaccine comprises n neoepitopes or neoepitope sequences and n-1 second linkers, wherein n is an integer from 3 to 50 (with additional exemplary sub-ranges provided below).
- the antigenic unit comprises a plurality of tumor neoepitopes, wherein each neoepitope corresponds to a mutation identified in a tumor neoantigen in a specific patient. That is to say, all selected neoantigens are unique and specific for the individual patient.
- the mutation may be any mutation leading to a change in at least one amino acid.
- the mutation may be one of the following: a non-synonymous mutation leading to a change in the amino acid, a mutation leading to a frame shift and thereby a completely different open reading frame in the direction after the mutation, a read-through mutation in which a stop codon is modified or deleted leading to a longer protein with a tumor-specific neoepitope, splice mutations that lead to a unique tumor-specific protein sequence, chromosomal rearrangements that give rise to a chimeric protein with a tumor-specific neoepitope at the junction of the two proteins.
- each subunit consists of a tumor neoepitope sequence and a second linker, whereas the last subunit comprises a neoepitope only, i.e. no second linker.
- each neoepitope is presented in an optimal way to the immune system.
- the cancer neoepitope sequence preferably has a length suitable for presentation by the MHC molecules.
- the cancer neoepitope is from 7 to 30 amino acids long. More preferred are cancer neoepitope sequences having a length of from 7 to 10 amino acids or cancer neoepitope sequences having a length of from 13 to 30 amino acids, e.g., from 20 to 30 amino acids, e.g., comprised of 27 amino acids.
- a plurality of different neoepitopes are included in the antigenic unit.
- a preferred approach is to include as many neoepitopes as possible into the vaccine to thereby attack the tumor efficiently whilst not compromising the vaccine’s ability to activate T cells against the neoepitopes due to dilution of the desired T cell effect. Also, to secure that all neoepitopes are loaded efficiently to the same antigen presenting cell, the neoepitopes are arranged as one amino acid chain instead of as discrete peptides.
- the tumor exome is analyzed to identify neoantigens and select the most antigenic neoepitopes.
- at least 3 neoepitopes are incorporated into the vaccine, preferably at least 5 neoepitopes, more preferably at least 7 neoepitopes, such as at least 10 neoepitopes, etc., in order to efficiently be able to target substantially all tumor cells.
- the vaccine comprises at least 10 neoepitopes.
- the vaccine comprises at least 15 neoepitopes, such as at least 20 neoepitopes.
- the vaccine may comprise from 3 to 50 neoepitopes, or from 3 to 30 neoepitopes, or from 3 to 20 neoepitopes, or from 3 to 15 neoepitopes, such as from 3 to 10 neoepitopes, and consequently n is preferably an integer of from 3 to 50, such as from 3 to 30, such as from 5 to 25, such as from 3 to 20, such as from 3 to 15, such as from 3 to 10.
- the vaccine comprises from 10 to 20 neoepitopes.
- the antigenic unit may, for example, comprise one copy of each cancer neoepitope, so that when 10 neoepitopes are included in the vaccine, a cell-mediated immune response against 10 different neoepitopes can be elicited.
- the antigenic unit may comprise at least two copies of at least one neoepitope in order to strengthen the immune response to these neoepitopes.
- the length of the antigenic unit is primarily determined by the length of the neoepitopes and the number of neoepitopes arranged in the antigenic unit, and is from, for example, about 21 to 1500, preferably from about 30 amino acids to about a 1000 amino acids, more preferably from about 50 to about 500 amino acids, such as from about 100 to about 400 amino acids, from about 100 to about 300 amino acids.
- the neoepitopes may be ordered in the antigenic unit as described below, in order to enhance the immune response.
- the antigenic subunits may be arranged in the order of more antigenic to less antigenic in the direction from the first linker towards the final neoepitope.
- the hydrophilicity/hydrophobicity varies greatly among the neoepitopes, it is preferred that the most hydrophobic antigenic subunit(s) is/are substantially positioned in the middle of the antigenic unit and the most hydrophilic antigenic subunit(s) is/are positioned at the beginning and/or end of the antigenic unit.
- the neoepitopes may be arranged alternating between a hydrophilic and a hydrophobic neoepitope.
- the GC rich neoepitopes are spaced so that GC clusters are avoided, preferably GC rich neoepitopes are spaced by at least one subunit.
- the second linker is designed to be non-immunogenic and is preferably also a flexible linker, whereby the tumor neoepitopes, in spite of the high numbers of antigenic subunits present in the antigenic unit, are presented in an optimal manner to the T cells.
- the length of the second linker is from 4 to 20 amino acids to secure the flexibility.
- the length of the second linker is from 8 to 20 amino acids, such as from 8 to 15 amino acids, for example 8 to 12 amino acids or such as for example from 10 to 15 amino acids.
- the length of the second linker is 10 amino acids.
- the vaccine encodes a protein comprised of a neoepitope antigenic unit comprising 10 neoepitopes, wherein the second linkers have a length of from 8 to 20 amino acids, such as from 8 to 15 amino acids, for example 8 to 12 amino acids or such as, for example, from 10 to 15 amino acids.
- the vaccine encodes a protein comprised of a neoepitope antigenic unit comprising 10 neoepitopes, where the second linkers have a length of 10 amino acids.
- the DNA vaccine encodes a protein comprised of a neoepitope antigenic unit comprising from 10-20 neoepitopes, each of 27 amino acids, where the second linkers have a length of 10 amino acids.
- the second linker is preferably identical in all antigenic subunits. If, however, one or more of the neoepitopes comprise an amino acid motif similar to the linker, it may be an advantage to substitute the neighboring second linkers with a second linker of a different sequence. Also, if a neoepitope-second linker junction is predicted to constitute an epitope in itself, then a second linker of a different sequence might be used.
- the second linker is preferably a serine-glycine rich linker, such as a flexible GGGGS (SEQ ID NO:34) linker, such as, for example, GGGSS (SEQ ID NO:35), GGGSG (SEQ ID NO:36), GGGGS (SEQ ID NO:34) or multiple variants thereof such as GGGGSGGGGS (SEQ ID NO:33) or (GGGGS)m, (GGGSS)m, (GGGSG)m.
- m is an integer from 1 to 5 (e.g., 1, 2, 3, 4, or 5), from 1 to 4 or from 1 to 3. In some preferred embodiments, m is 2.
- the serine-glycine linker further comprises at least one leucine (L), such as at least 2 or at least 3 leucines.
- L leucine
- the serine-glycine linker may for example comprise 1, 2, 3 or 4 leucines. In some instances, the serine-glycine linker comprises 1 leucine or 2 leucines.
- second linkers include the following: for example, the second linker may comprise or consist of the sequence LGGGS (SEQ ID NO:37), GLGGS (SEQ ID NO:38), GGLGS (SEQ ID NO:39), GGGLS (SEQ ID NO:40) or GGGGL (SEQ ID NO:41); alternatively, the second linker may comprise or consist of a sequence LGGSG (SEQ ID NO:42), GLGSG (SEQ ID NO:43), GGLSG (SEQ ID NO:44), GGGLG (SEQ ID NO:45) or GGGSL (SEQ ID NO:46); or the second linker may comprise or consist of the sequence LGGSS (SEQ ID NO:47), GLGSS (SEQ ID NO:48), GGLSS (SEQ ID NO:49), GGGLS (SEQ ID NO:50) or GGGSL (SEQ ID NO:51).
- the second linker may comprises or consist of the sequence LGLGS (SEQ ID NO:52), GLGLS (SEQ ID NO:53), GLLGS (SEQ ID NO:54), LGGLS (SEQ ID NO:55) or GLGGL (SEQ ID NO:56), or may comprise or consist of the sequence LGLSG (SEQ ID NO:57), GLLSG (SEQ ID NO:58), GGLSL (SEQ ID NO:59), GGLLG (SEQ ID NO:60) or GLGSL (SEQ ID NO:61), or may comprise or consist of the sequence LGLSS (SEQ ID NO:62), GLGLS (SEQ ID NO:63), GGLLS (SEQ ID NO:64), or GLGSL (SEQ ID NO:65).
- Additional exemplary second linkers for use in the neoepitope antigenic unit separating the neoepitopes include serine-glycine rich linkers such as the following:
- the second linker is selected from linkers of SEQ ID NO:67 to SEQ ID NO:76.
- the second linker is selected from linkers of SEQ ID NO:67 to SEQ ID NO:76, in order of preference with a linker of SEQ ID NO:67 being more preferred than a linker of SEQ ID NO: 68, and so forth.
- the linkers may change from construct to construct for the various individualized vaccines, because in assembling the neoepitope antigenic unit for the construct, the junctional sequences are evaluated.
- a first preferred linker may be replaced with another candidate linker that excludes a junctional epitope that resembles a sequence found in the human proteome.
- Preferred serine/gly cine-rich linkers e.g., 10 amino acid linkers, contain from 6 to 9 glycines (e.g., 6, 7, 8 or 9), or from 6 to 8 glycines. In some preferred embodiments, the remaining non-glycine amino acids contained in the linker are serine(s).
- Examples of preferred vaccines include those comprising at least 10 neoepitopes that are separated by 10 amino acid linkers, or those comprising at least 15 neoepitopes that are separated by 10 amino acid linkers, such as at least 20 neoepitopes that are separated by 10 amino acid linkers.
- targeting unit refers to a unit that delivers the polypeptide/protein with its antigen to an antigen presenting cell for MHC class Il-restricted presentation to CD4+ T cells or for providing cross presentation to CD8+ T cells by MHC class I restriction.
- the targeting unit is connected through the dimerization unit to the antigenic unit, wherein the latter is in either the COOH-terminal or the ML-terminal end of the poly peptide/ dimeric protein. It is preferred that the antigenic unit is in the COOH- terminal end of the polypeptide/dimeric protein.
- the targeting unit is designed to target the polypeptide/dimeric protein to surface molecules expressed on the relevant antigen presenting cells, such as molecules expressed exclusively on subsets of dendritic cells (DC).
- DC dendritic cells
- HLA human leukocyte antigen
- CD 14 cluster of differentiation 14
- CD40 cluster of differentiation 40
- TLRs Toll-like receptors
- HLA is a major histocompatibility complex (MHC) in humans.
- the Toll-like receptors may for example include TLR-2, TLR-4 and/or TLR-5.
- the polypeptide/dimeric protein can be targeted to such surface molecules by means of targeting units comprising for example antibody binding regions with specificity for CD14, CD40, or Toll- like receptor; ligands, e.g. soluble CD40 ligand; natural ligands like chemokines, e.g. RANTES or MIP-la; or bacterial antigens like for example flagellin.
- An illustrative targeting unit has affinity for an MHC class II protein.
- the nucleotide sequence encoding the targeting unit encodes the antibody variable domains (VL and VH) with specificity for MHC class II proteins, selected from the group consisting of anti-HLA-DP, anti-HLA-DR and anti-HLA-II.
- the targeting unit has affinity for a surface molecule selected from the group consisting of CD40, TLR-2, TLR-4 and TLR-5.
- the nucleotide sequence encoding the targeting unit encodes the antibody variable domains (VL and VH) with specificity for anti- CD40, anti-TLR-2, anti-TLR-4 and anti-TLR-5.
- the nucleotide sequence encoding the targeting unit encodes flagellin, which has affinity for TLR-5.
- the targeting unit has affinity for a chemokine receptor selected from CCR1, CCR3 and CCR5.
- the nucleotide sequence encoding the targeting unit encodes the human chemokine macrophage inflammatory protein- 1 alpha, hMIP-la (LD78beta), which binds to its cognate receptors, CCR1, CCR3 and CCR5 expressed on the cell surface of antigen- presenting cells (APCs). See, e.g., FIG. 12, which includes the nucleotide sequence encoding the VBIO.NEO protein with the targeting unit identified therein (see, e.g., nucleotides 1143- 1421).
- the term“dimerization unit” as used herein, refers to a sequence of amino acids between the antigenic unit and the targeting unit.
- the dimerization unit serves to connect the antigenic unit and the targeting unit and facilitates dimerization of two monomeric polypeptides into a dimeric protein.
- the dimerization unit also provides the flexibility in the polypeptide/dimeric protein to allow optimal binding of the targeting unit to the surface molecules on the antigen presenting cells (APCs), even if they are located at variable distances.
- the dimerization unit may be any unit that fulfils these requirements.
- the term "hinge region” refers to a peptide sequence of the dimeric protein that facilitates the dimerization.
- the hinge region functions as a flexible spacer between the units allowing the two targeting units to bind simultaneously to two target molecules on APCs, even if they are expressed with variable distances.
- the hinge region may be Ig derived, such as derived from IgG3.
- the hinge region may contribute to the dimerization through the formation of covalent bond(s), e.g. disulfide bridge(s).
- the hinge region has the ability to form one or more covalent bonds.
- the covalent bond can for example be a disulfide bridge.
- the dimerization unit consists of hinge exons hi and h4 connected through a third linker to a CH3 domain of human IgG3. See, for example, FIG. 12, and the illustrative dimerization unit identified therein (hi and h4 and CH3 domains of hIgG3, nucleotides 1422-1853).
- the dimerization unit may have any orientation with respect to antigenic unit and targeting unit.
- the antigenic unit is in the COOH- terminal end of the dimerization unit with the targeting unit in the N-terminal end of the dimerization unit.
- the antigenic unit is in the N-terminal end of the dimerization unit with the targeting unit in the COOH-terminal end of the dimerization unit. It is preferred that the antigenic unit is in the COOH end of the dimerization unit.
- the antigenic unit and the dimerization unit are preferably connected through a first linker.
- the first linker may comprise a restriction site in order to facilitate the construction of the polynucleotide. It is, in some instances, preferred that the first linker is a GLGGL (SEQ ID NO:56) linker or a GLSGL (SEQ ID NO:66) linker.
- the polynucleotide may further comprise a nucleotide sequence encoding a signal peptide.
- the signal peptide is constructed to allow secretion of the polypeptide encoded by the polynucleotide in the cells transfected with said polynucleotide. Any suitable signal peptide may be used. Examples of suitable peptides are an Ig VH signal peptide, a human TPA signal peptide, and a signal peptide.
- the polynucleotide typically comprises a DNA nucleotide sequence, either double stranded or single stranded.
- the polynucleotide is optimized to the desired species to express a polypeptide, i.e. it is preferred that the polynucleotide sequence is human codon optimized.
- Exemplary mouse neoantigen-based DNA cancer vaccines comprising VB10.NEO pDNA constructs, VB4011 and VB4061, are described in the supporting examples. Additionally, an exemplary human neoantigen-based DNA cancer vaccine is described in Example 4. An illustrative pVBlO.NEO plasmid map is shown in FIG. 13.
- the vaccine may further comprise a pharmaceutically acceptable carrier, diluent, adjuvant or buffer.
- Pharmaceutically acceptable carriers, diluents, and buffers include, but are not limited to, saline, buffered saline, dextrose, water, glycerol, ethanol, sterile isotonic aqueous buffer, and combinations thereof.
- a carrier may include molecules that ease transfection of cells and adjuvants and may include plasmids comprising nucleotide sequences encoding chemokines or cytokines in order to enhance the immune response.
- the vaccine may be formulated into any suitable formulation, such as a liquid formulation for intradermal or intramuscular injection.
- the vaccine may be administered in any suitable way for either a polypeptide/protein vaccine or a polynucleotide vaccine, such as administered by injection intradermally, intramuscular, subcutaneously, or by mucosal or epithelial application, such as intranasally, orally, enteral or to the bladder.
- the vaccine is preferably administered intramuscular or intradermally when the vaccine is a polynucleotide vaccine.
- the vaccine is administered by intranodal injection.
- the term“intranodal injection” means that the vaccine is injected into the lymph nodes.
- a T cell expander is a compound or composition effective to stimulate/expand production of T cells.
- the T cell expander when administered in combination with the neoantigen-based DNA cancer vaccine, is effective to enhance specific clonal T cell expansion to vaccine epitopes.
- the T cell expander is effective to enhance specific clonal T cell expansion to vaccine epitopes over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander to a degree that is greater than additive, and the combination is not limited in this regard.
- the T cell expander is effective to enhance specific clonal T cell expansion to vaccine epitopes in a synergistic fashion over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander.
- Illustrative T cell expanders include interleukin-2 (e.g., aldesleukin), interleukin-15, and interferon-a, and an anti-CD3 antibody such as, e.g., OKT3.
- the T cell expander is a prodrug of an interleukin-2 (e.g., aldesleukin, chemical name, des-alanyl-1, serine- 125 human interleukin-2), wherein the interleukin-2 is modified by releasable covalent attachment of multiple polyethylene glycol moieties.
- the prodrug is essentially inactive upon administration, and following administration, the polyethylene glycol moieties are slowly released to provide bioactive species, thereby avoiding overstimulation of the immune system.
- Conjugates of an interleukin-2 moiety modified by covalent attachment of one or more polyethylene glycol moieties are described, for example, in U.S. Patent No. 9,861,705.
- the T cell expander is an interleukin-2 receptor beta (IL-2R ) selective agonist as described, for example, in U.S. Patent No. 10,101,587, and generally referred to therein as RSLAIL-2.
- IL-2R interleukin-2 receptor beta
- the releasable PEG comprised in RSLAIL-2 is based upon a 2,7,9-substituted fluorene as shown below, with poly (ethylene glycol) chains extending from the 2- and 7- positions on the fluorene ring via amide linkages (fluorene-C(O)-NH-), and having releasable covalent attachments to interleukin-2 via attachment to a carbamate nitrogen atom attached via a methylene group (-CH2-) to the 9-position of the fluorene ring.
- the T cell expander is a composition comprising compounds encompassed by the following formula:
- IL-2 is an interleukin-2; or pharmaceutically acceptable salts thereof, where each“n” is an integer from about 3 to about 4000, or more preferably is an integer from about 200- 300.
- RSLAIL-2 or multi(2,7-(bis- methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2.
- RSLAIL-2 is a composition comprising compounds encompassed by formula (I), that is, having four, five or six branched PEG moieties as shown above, i.e., 2,7-(bis-methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate moieties, releasably covalently attached to amino groups of IL-2.
- “n” in each of the polyethylene glycol chains has a value, on average, of about 227 (i.e., where each polyethylene glycol chain extending from the central fluorenyl core has a weight average molecular weight of about 10,000 daltons, such that the weight average molecular weight of the overall branched PEG moiety is about 20,000 daltons), i.e., referred to herein more particularly as multi(2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9- yl)methyl N-carbamate)interleukin-2 or as (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H- fluorene-9-yl)methyl N-carbamate)4-6interleukin-2.
- the value of“n” in each of the polyethylene glycol chains is substantially the same, that is to say that, for example, the two PEG chains extending from the central fluorenyl core
- multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 comprises compounds encompassed by the following formula:
- multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 comprises compounds encompassed by the following formula:
- Formula (III) wherein the average number of branched PEG moieties having a structure as shown and releasably covalently attached to the IL-2 moiety is six, i.e., (2,7-(bis-methoxyPEGiokd- carboxyamide)(9h-fluorene-9-yl)methyl N-carbamate)6 avg interleukin-2, also referred to in some instances as falling within the designation“RSLAIL-2” (releasable IL-2).
- T cell expander compounds and compositions encompassed by Formulae (I), (II), and (III) are generally designated“RSLAIL-2”.
- the releasable PEG moiety(moieties) comprised in RSLAIL-2 is based upon a 2,7,9-substituted fluorene with poly(ethylene glycol) chains extending from the 2- and 7- positions of the fluorene ring via amide linkages (fluorene-C(O)-NH-), to provide a branched PEG.
- the fluorenyl-based branched PEG moieties are releasably covalently attached to amino groups of the interleukin-2 moiety.
- the linkage between interleukin-2 amino groups and the fluorenyl-based branched PEG moiety is a carbamate linkage attached via a methylene group (-CH2-) to the 9-position of the fluorene ring.
- Releasable PEGs having this general structure typically undergo a b-elimination reaction under physiological conditions to slowly release the PEG moieties that are covalently attached to IL-2. It is believed that the PEG moieties release sequentially following administration.
- the IL-2R -biased agonist composition contains no more than 10% (based on a molar amount), and preferably no more than 5% (based on a molar amount), of compounds encompassed by the following formula:
- IL-2 is an interleukin-2 (e.g., aldesleukin), and“m” (referring to the number of branched polyethylene glycol moieties attached to IL-2) is an integer selected from the group consisting of 1, 2, 3, 7 and >7; or pharmaceutically acceptable salts thereof.
- interleukin-2 e.g., aldesleukin
- m referring to the number of branched polyethylene glycol moieties attached to IL-2
- m is an integer selected from the group consisting of 1, 2, 3, 7 and >7; or pharmaceutically acceptable salts thereof.
- the IL- 2R -biased agonist possesses on average about six branched polyethylene glycol moieties releasably attached to IL-2. See, for example, Formula (III).
- the IL-2R - selective agonist is generally considered to be an inactive prodrug, i.e., that is inactive upon administration, and by virtue of slow release of the polyethylene glycol moieties in vivo following administration, provides active conjugated forms of interleukin-2 having fewer PEG moieties attached than in the conjugate that is initially administered.
- references to“multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2” or“RSLAIL-2” is expressly intended to encompass compounds and compositions as set forth in Formula (I), Formula (II), and/or Formula (III), including compositions encompassed by Formula (IV) in reference to any one or more of Formulae (I), (II) and (III).
- RSLAIL-2 is considered to be an IL-2R -biased (i.e., selective) agonist.
- RSLAIL-2 referenced in the accompanying examples exhibits about a 60-fold decrease in affinity to IL-2Ra.p relative to IL-2, but only about a 5- fold decrease in affinity IL-2R relative to IL-2. See, for example, Example 20 in PCT Publication No. WO 2018/132496 describing the binding affinity of RSLAIL-2 to IL-2Ra and IL-2R .
- the protein is quantified by a method such as a bicinchoninic acid (BCA) assay or by UV analysis, to determine moles of protein in the sample.
- BCA bicinchoninic acid
- the PEG moieties are then released by exposing the sample to conditions in which the PEG moieties are released, and the released PEG is then quantified (e.g., by BCA or UV) and correlated with moles protein to determine average degree of PEGylation.
- RSLAIL-2 can be considered to be an inactive prodrug, i.e., it is inactive upon administration, and by virtue of slow release of the polyethylene glycol moieties in vivo, provides active conjugated forms of interleukin-2 that are effective to achieve sustained concentrations at a tumor site.
- Additional exemplary compositions of RSLAIL-2 comprise compounds in accordance with the above formulae wherein the overall polymer portion of the molecule has a weight average molecular weight in a range of from about 250 daltons to about 90,000 daltons. Additional suitable ranges include weight average molecular weights in a range selected from about 1,000 daltons to about 60,000 daltons, in a range of from about 5,000 daltons to about 60,000 daltons, in a range of about 10,000 daltons to about 55,000 daltons, in a range of from about 15,000 daltons to about 50,000 daltons, and in a range of from about 20,000 daltons to about 50,000 daltons.
- Additional illustrative weight-average molecular weights for the polyethylene glycol polymer portion include about 200 daltons, about 300 daltons, about 400 daltons, about 500 daltons, about 600 daltons, about 700 daltons, about 750 daltons, about 800 daltons, about 900 daltons, about 1,000 daltons, about 1,500 daltons, about 2,000 daltons, about 2,200 daltons, about 2,500 daltons, about 3,000 daltons, about 4,000 daltons, about 4,400 daltons, about 4,500 daltons, about 5,000 daltons, about 5,500 daltons, about 6,000 daltons, about 7,000 daltons, about 7,500 daltons, about 8,000 daltons, about 9,000 daltons, about 10,000 daltons, about 11,000 daltons, about 12,000 daltons, about 13,000 daltons, about 14,000 daltons, about 15,000 daltons, about 20,000 daltons, about 22,500 daltons, about 25,000 daltons,
- RSLAIL-2 may be in the form of a pharmaceutically- acceptable salt.
- such salts are formed by reaction with a pharmaceutically- acceptable acid or an acid equivalent.
- pharmaceutically-acceptable salt in this respect, will generally refer to the relatively non-toxic, inorganic and organic acid addition salts. These salts can be prepared in situ in the administration vehicle or the dosage form manufacturing process, or by separately reacting a long-acting interleukin-2 as described herein with a suitable organic or inorganic acid, and isolating the salt thus formed.
- Representative salts include the hydrobromide, hydrochloride, sulfate, bisulfate, phosphate, nitrate, acetate, valerate, oleate, palmitate, stearate, laurate, benzoate, lactate, phosphate, tosylate, citrate, maleate, fumarate, succinate, tartrate, napthylate, oxylate, mesylate, glucoheptonate, lactobionate, and laurylsulphonate salts and the like. (See, for example,
- salts as described may be derived from inorganic acids such as hydrochloride, hydrobromic, sulfuric, sulfamic, phosphoric, nitric, and the like; or prepared from organic acids such as acetic, propionic, succinic, glycolic, stearic, lactic, malic, tartaric, citric, ascorbic, palmitic, maleic, hydroxymaleic, phenylacetic, glutamic, benzoic, salicyclic, sulfanilic, 2-acetoxybenzoic, fumaric, toluenesulfonic, methanesulfonic, ethane disulfonic, oxalic, isothionic, and the like.
- inorganic acids such as hydrochloride, hydrobromic, sulfuric, sulfamic, phosphoric, nitric, and the like
- organic acids such as acetic, propionic, succinic, glycolic, stearic, lactic, malic,
- IL-2 refers to a moiety having human IL-2 activity.
- the term,‘residue’ in the context of residue of IL-2, means the portion of the IL-2 molecule that remains following covalent attachment to a polymer such as a polyethylene glycol, at one or more covalent attachment sites, as shown in the formula above. It will be understood that when the unmodified IL-2 is attached to a polymer such as polyethylene glycol, the IL-2 is slightly altered due to the presence of one or more covalent bonds associated with linkage to the polymer(s). This slightly altered form of the IL-2 attached to another molecule is sometimes referred to a "residue" of the IL-2.
- Proteins having an amino acid sequence corresponding to any one of SEQ ID NOs: 1 through 4 described in International Patent Publication No. WO 2012/065086 are exemplary IL-2 proteins.
- the term substantially homologous means that a particular subject sequence, for example, a mutant sequence, varies from a reference sequence by one or more substitutions, deletions, or additions, the net effect of which does not result in an adverse functional dissimilarity between the reference and subject sequences.
- sequences having greater than 95 percent homology, equivalent biological activity (although not necessarily equivalent strength of biological activity), and equivalent expression characteristics are considered substantially homologous.
- truncation of the mature sequence should be disregarded.
- the IL-2 may be naturally-occurring or may be recombinantly produced.
- the IL-2 can be derived from human sources, animal sources, and plant sources. Most preferably, the IL-2 is aldesleukin.
- RSLAIL-2 is generally referred to as long-acting.
- the long acting nature of an IL-2R biased agonist is typically determined using flow cytometry to measure STAT5 phosphorylation in lymphocytes at various time points after
- the signal is lost by around 24 hours with IL-2, but is sustained for a period greater than that for a long-acting IL- 2R -biased agonist.
- the signal is sustained over several days for (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2.
- RSLAIL-2 possesses immunomodulating properties - in the tumor environment, RSLAIL-2 preferentially activates CD8+ effector T and natural killer (NK) cells over suppressive regulatory T cells (Tregs), such as CD4+ Tregs, by targeting CD 122 receptors found on the surfaces of cancer-fighting cells.
- Tregs suppressive regulatory T cells
- RSLAIL-2 also induces CD4+ T cell activation and promotes proliferation of CD4+, CD8+, and NK cells in the peripheral blood.
- RSLAIL-2 is effective to preferentially activate and expand effector CD8+ T- and NK-cells over Tregs, it is suitable for use as a T cell expander as described herein.
- RLSAIL-2 is provided in an IL-2R -activating amount, to thereby result in T cell expansion activity.
- One of ordinary skill in the art can determine how much RSLAIL-2 is sufficient to provide clinically relevant agonistic activity at IL-2R .
- the IL-2R -activating amount of RSLAIL- 2 is an amount encompassed by one or more of the following ranges expressed in amount of protein: from about 0.01 to 100 mg/kg; from about 0.01 mg/kg to about 75 mg/kg; from about 0.02 mg/kg to about 60 mg/kg; from about 0.03 mg/kg to about 50 mg/kg; from about 0.05 mg/kg to about 40 mg/kg; from about 0.05 mg/kg to about 30 mg/kg; from about 0.05 mg/kg to about 25 mg/kg; from about 0.05 mg/kg to about 15 mg/kg; from about 0.05 mg/kg to about 10 mg/kg; from about 0.05 mg/kg to about 5 mg/kg; from about 0.05 mg/kg to about 1 mg/kg.
- Particular illustrative dosing ranges include for example, from about 0.1 mg/kg to about 10 mg/kg, or from about 0.2 mg/kg to about 7 mg/kg or from about 0.2 mg/kg to less than about
- the IL-2R -activating amount of RSLAIL-2 is from about 0.0005 to 0.3 mg/kg; from about 0.001 mg/kg to about 0.3 mg/kg; from about 0.001 mg/kg to about 0.25 mg/kg; from about 0.001 mg/kg to about 0.15 mg/kg; from about 0.001 mg/kg to about 0.05 mg/kg; from about 0.001 mg/kg to about 0.01 mg/kg; from about 0.001 mg/kg to about 0.008 mg/kg; from about 0.001 mg/kg to about 0.005 mg/kg; from about 0.002 mg/kg to about 0.005 mg/kg; from about 0.002 mg/kg to about 0.004 mg/kg, or from about 0.003 mg/kg to about 0.006 mg/kg.
- RSLAIL-2 is administered at a dose of about 0.006 mg/kg.
- the amount and extent of the activation can vary widely and still be effective when coupled with administration of a neoantigen-based DNA cancer vaccine, optionally with a checkpoint inhibitor, such as an anti-PD-1 antibody, to effectively drive expansion of neoepitope-specific T cells.
- the combination therapy may also comprise administration of an additional immunotherapeutic agent such as a checkpoint inhibitor.
- Checkpoint inhibitors suitable for use in the method provided herein include antibodies, such as for example, monoclonal antibodies, that target PD-1, PD-L1, or CTLA-4.
- the checkpoint inhibitor is an anti-PD-1 antibody or an anti-PD-Ll antibody.
- exemplary PD-1 inhibitors include but are not limited to pembrolizumab, nivolumab, and cemiplimab.
- Representative PD-L1 inhibitors include, for example, atezolizumab, avelumab, and durvalumab.
- ipilimumab or tremelimumab anti-CTLA-4 monoclonal antibodies
- Both are fully humanized anti-CTLA- 4 monoclonal antibodies of IgGl and IgG2, respectively.
- a PD-1 pathway-inhibiting amount of an anti-PD-1 antibody such as nivolumab may be administered.
- One of ordinary skill in the art can determine how much anti-PD-1 antibody, such as nivolumab, or anti-PD-Ll antibody, is sufficient to provide clinically relevant inhibition of the PD-1 pathway or the PD-L1 pathway, respectively.
- one of ordinary skill in the art can refer to the literature and/or administer a series of increasing amounts of nivolumab or another anti-PD-1 or anti-PD-Ll antibody to determine which amount or amounts provide clinically relevant inhibition of the PD-1 or PD-L1 pathway.
- a CTLA-4 pathway-inhibiting amount of an anti-CTLA-4 antibody may be administered.
- a PD-1 pathway-inhibiting amount of the anti-PD-1 antibody is encompassed by one or more of the following ranges: from about 1 mg/kg to about 1000 mg/kg; from about 2 mg/kg to about 900 mg/kg; from about 3 mg/kg to about 800 mg/kg; from about 4 mg/kg to about 700 mg/kg; from about 5 mg/kg to about 600 mg/kg; from about 6 mg/kg to about 550 mg/kg; from about 7 mg/kg to about 500 mg/kg; from about 8 mg/kg to about 450 mg/kg; from about 9 mg/kg to about 400 mg/kg; from about 5 mg/kg to about 200 mg/kg; from about 2 mg/kg to about 150 mg/kg; from about 5 mg/kg to about 100 mg/kg; from about 10 mg/kg to about 100 mg/kg; and from about 10 mg/kg to about 60 mg/kg. Further guidance
- an anti -PD-1 antibody such as nivolumab, or other suitable checkpoint inhibitor
- the amount and extent of the inhibition can vary widely and can still be effective, even when combined with administration of a T cell expander and the neoantigen-based DNA cancer vaccine.
- an amount of an anti-PD-1 antibody, i.e., nivolumab, that only minimally inhibits the PD-1 pathway can still be an inhibiting amount as used herein so long as the method results in a clinically meaningful response.
- the actual dose to be administered, for each of the immunotherapeutic components will vary depend upon the age, weight, and general condition of the subject as well as the severity of the cancer being treated, the judgment of the health care professional, and the particular identities and properties of each of the immunotherapeutic components.
- the subject has received one, two, three, four, five or more prior cancer treatments.
- the subject is treatment-naive.
- the subject has progressed on other cancer treatments.
- the prior cancer treatment comprised an immunotherapy.
- the prior cancer treatment comprised a chemotherapy.
- the tumor has reoccurred.
- the tumor is metastatic. In yet other embodiments, the tumor is not metastatic.
- the subject has received a prior therapy to treat the tumor and the tumor is relapsed or refractory. In some embodiments, the subject has received a prior immuno-oncology therapy to treat the tumor and the tumor is relapsed or refractory. In some embodiments, the subject has received more than one prior therapy to treat the tumor and the subject is relapsed or refractory.
- a neoantigen-based DNA cancer vaccine is first administered to generate a neoantigen-specific immune response in the subject, followed by one or more subsequent administrations of the neoantigen-based DNA cancer vaccine (induction period).
- the subsequent administrations of the neoantigen-based DNA cancer vaccine may be administered within 1 week, 2 weeks, 3 weeks or 4 weeks or more following the first administering.
- Non limiting parameters that indicate the treatment method is effective include any one or more of the following: tumor shrinkage (in terms of weight and/or volume); a decrease in the number of individual tumor colonies; tumor elimination; and progression-free survival. Change in tumor size may be determined by any suitable method such as imaging.
- Various diagnostic imaging modalities can be employed, such as computed tomography (CT scan), dual energy CDT, positron emission tomography and MRI.
- the frequency and schedule of administering the neoantigen- based DNA cancer vaccine and the T cell expander optionally combined with a checkpoint inhibitor
- a clinician can decide to administer the neoantigen-based DNA cancer vaccine, either as a single dose or in a series of doses, e.g., over the course of several days or weeks.
- the T cell expander is administered, either concurrently with the neoantigen-based DNA cancer vaccine, prior to vaccination, or following administration of the cancer vaccine.
- the T cell expander e.g., RSL AIL-2
- the T cell expander is administered following the vaccination induction period.
- RSL AIL-2 such composition may be administered relatively infrequently (e.g., once every four weeks, once every three weeks, once every two weeks, one every 8-10 days, once every week, etc.).
- dosing of the neoepitope-specific DNA-based cancer vaccine and the T cell expander are scheduled to align or substantially align the peak T cell responses of both therapeutic agents, to thereby achieve an optimized (and preferably synergistic) response.
- initial administration of a T cell expander is subsequent to one or more administrations of a neoepitope- specific DNA-based cancer vaccine, and is preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander.
- a treatment protocol includes a time period for screening and manufacture of a therapeutic neoantigen-based DNA cancer vaccine against tumor-specific neoantigens, a vaccination induction period where the anticancer vaccine is administered, and a vaccination maintenance period where a T cell expander is administered.
- the anticancer vaccine is preferably administered one or more times concurrently with or separate from the T cell expander.
- the anticancer vaccine may be prepared by any means as known in the art.
- the anticancer vaccine against tumor-specific neoantigens is prepared by sequencing the genome, or exome of a tumor; identifying tumor neoantigens comprising neoepitopes from the tumor; and selecting neoepitopes based on a predicted antigenicity.
- An exemplary method of preparing such an anticancer vaccine is described in U.S. Patent Publication No. 2019/0022202, the methods of preparation being incorporated by reference herein. After screening the tumor and manufacture of the anticancer vaccine, e.g.
- the neoantigen-based DNA cancer vaccine against tumor-specific neoantigens and/or T cell expander are administered according to a dosing schedule or protocol that provides a peak response for one or both of the anticancer vaccine and the T cell expander.
- the neoantigen-based DNA cancer vaccine may initially be administered for a period of time (e.g. 4-8 weeks or longer) as a vaccination induction.
- the patient may be vaccinated one or more times with the neoantigen- based DNA cancer vaccine during the induction period.
- the T cell expander is administered one or more times with or without administration of additional or maintenance anticancer vaccine.
- the T cell expander and/or the neoantigen-based DNA cancer vaccine may be administered for a period of time as needed for treatment (e.g. 1-12 months or longer).
- An exemplary administration schedule for treatment is provided below: [00153] Table 1. Exemplary Administration Schedule
- Exemplary lengths of time associated with the course of therapy include about one week; about two weeks; about three weeks; about four weeks; about five weeks; about six weeks; about seven weeks; about eight weeks; about nine weeks; about ten weeks; about eleven weeks; about twelve weeks; about thirteen weeks; about fourteen weeks; about fifteen weeks; about sixteen weeks; about seventeen weeks; about eighteen weeks; about nineteen weeks; about twenty weeks; about twenty-one weeks; about twenty-two weeks; about twenty- three weeks; about twenty four weeks; about seven months; about eight months; about nine months; about ten months; about eleven months; about twelve months; about thirteen months; about fourteen months; about fifteen months; about sixteen months; about seventeen months; about eighteen months; about nineteen months; about twenty months; about twenty one months; about twenty-two months; about twenty-three months; about twenty-four months; about thirty months; about three years; about four years and about five years.
- treatment methods described herein are typically continued for as long as the clinician overseeing the patient's care deems the treatment method to be effective, i.e., that the patient is responding to treatment, including no further progression of the disease, e.g., cancer.
- Non-limiting parameters that indicate the treatment method is effective may include one or more of the following: tumor shrinkage (in terms of weight and/or volume and/or visual appearance); a decrease in the number of individual tumor colonies; tumor elimination; progression-free survival; appropriate response by a suitable tumor marker (if applicable), increased number of NK (natural killer) cells, increased number of T cells, increased number of memory T cells, increased number of central memory T cells, reduced numbers of regulatory T cells such as CD4+ Tregs, CD25+ Tregs, and FoxP3+ Tregs.
- tumor shrinkage in terms of weight and/or volume and/or visual appearance
- a decrease in the number of individual tumor colonies may include one or more of the following: tumor shrinkage (in terms of weight and/or volume and/or visual appearance); a decrease in the number of individual tumor colonies; tumor elimination; progression-free survival; appropriate response by a suitable tumor marker (if applicable), increased number of NK (natural killer) cells, increased number of T cells, increased number of memory T cells, increased number of central memory T cells, reduced numbers
- patients may be responsive to the neoantigen-based DNA alone, as well as the combination with the T cell expander, optionally with a checkpoint inhibitor (CPI), but are more responsive to administration of the combination.
- CPI checkpoint inhibitor
- patients may be non-responsive or only marginally responsive to the neoantigen-based DNA cancer vaccine, or the T cell expander, or the checkpoint inhibitor, but are more responsive to the combination.
- patients may be non-responsive to the neoantigen-based DNA cancer vaccine or to the T cell expander or to the checkpoint inhibitor alone, but are responsive to the combination.
- Administration e.g., of the neoantigen-based DNA cancer vaccine and/or the T cell expander (e.g., RSLAIL-2) and/or the checkpoint inhibitor is typically via injection.
- Other modes of administration are also contemplated, such as pulmonary, nasal, buccal, rectal, sublingual and transdermal.
- parenteral includes subcutaneous, intravenous, intra-arterial, intratumoral, intralymphatic, intraperitoneal, intracardiac, intrathecal, and intramuscular injection, as well as infusion injections.
- cancers such as, for example, fibrosarcoma, myxosarcoma, liposarcoma, chondrosarcoma, osteogenic sarcoma, chordoma, angiosarcoma, endotheliosarcoma, lymphangiosarcoma,
- lymphangioendotheliosarcoma synovioma, mesothelioma, Ewing's tumor, leiomyosarcoma, rhabdomyosarcoma, colon carcinoma, pancreatic cancer, brain cancer, breast cancer, ovarian cancer, prostate cancer, squamous cell cancer, basal cell cancer, adenocarcinoma, sweat gland cancer, sebaceous gland cancer, papillary cancer, papillary adenocarcinomas,
- cystadenocarcinoma medullary cancer, bronchogenic cancer, renal cell cancer, hepatoma, bile duct cancer, choriocarcinoma, seminoma, embryonal cancer, Wilms' tumor, cervical cancer, Hodgkin lymphoma, non-Hodgkin lymphoma, testicular cancer, lung cancer, small cell lung cancer, brain cancer, bladder cancer, epithelial cancer, glioma, astrocytoma, medulloblastoma, craniopharyngioma, ependymoma, pinealoma, hemangioblastoma, acoustic neuroma, oligodendroglioma, meningioma, melanoma, multiple myeloma, neuroblastoma, retinoblastoma and leukemias.
- the cancer to be treated is a solid cancer, such as for example, breast cancer, ovarian cancer, colon cancer, prostate cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer, non-small cell lung cancer, pancreatic cancer, thyroid cancers, kidney cancer, cancer of the bile duct, brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer, esophageal cancer, Hodgkin's disease and adrenocortical cancer.
- a solid cancer such as for example, breast cancer, ovarian cancer, colon cancer, prostate cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer, non-small cell lung cancer, pancreatic cancer, thyroid cancers, kidney cancer, cancer of the bile duct, brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer, esophageal cancer, Hodgkin's disease and ad
- the present methods, combinations and compositions are useful for enhancing the therapeutic effectiveness of a neoantigen-based DNA cancer vaccine, for example, by improving the subject’s immune response to the neoantigen-based DNA cancer vaccine composition.
- An enhanced response may be evaluated at any suitable time point during treatment, after a single round of treatment, after 2-3 cycles of treatment, etc., and by any of a number of suitable methods, including shrinkage of a tumor (partial response), i.e., an evaluation of tumor size or volume, disappearance of a tumor, a reduction in disease progression (cancer has not progressed), and analysis of one or more tumor test markers if appropriate.
- the methods, kits, compositions and the like provided herein are also useful for reducing tumor growth or size (or volume) in a subject undergoing treatment.
- Treatment by administering a therapeutically combination as described herein is effective, in one or more embodiments, to reduce tumor growth or size in the subject.
- one or more cycles of treatment is effective to reduce tumor size by about 25%, or by about 30%, or by about 40%, or by about 50%, or even by about 60%, or by about 70% or more when compared to the size of the tumor prior to treatment.
- the methods, compositions and the like provided herein are effective to inhibit accumulation of regulatory T cells (Tregs) in a subject undergoing treatment for cancer.
- the methods, compositions and the like provided herein are effective to stimulate T cell and/or NK cell activity and/or proliferation in a subject.
- the method is effective, for example, when evaluated in a cancer mouse model of the corresponding cancer, for increasing the number of CD8+ T cells and/or CD4 T cells in the subject when compared to vaccination with a neoantigen-based DNA cancer vaccine alone.
- the subject’s CD8+ T cells may be increased by 2-fold or more, or 3-fold or more, or even 4-fold or more, when compared to treatment with the neoantigen-based DNA cancer vaccine alone.
- the treatment may, in some embodiments, be effective to increase the subject’s CD8+ T cells or CD4 T cells against the neoantigens by at least 2-fold or more, or 3 -fold or more, or even 4- fold or more, or 5-fold or more, or 6-fold or more when compared to an untreated subject.
- the supporting preclinical studies provide an indication of the synergistic effect arising from the administration of a neoantigen-based DNA cancer vaccine when accompanied by administration of the exemplary T cell expander, RSLAIL-2, and optionally, a checkpoint inhibitor.
- Example 1 As illustrated in Example 1, it was discovered that administration of the exemplary T cell expander, RSLAIL-2, in combination with an exemplary individualized anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, e.g., VB4011, is effective to not only increase the frequency, but to also increase the total numbers of neoepitope-specific T cells when evaluated in a preclinical melanoma model in mice.
- tumor neoantigens e.g., VB4011
- vaccination with the therapeutic neoepitope-specific DNA-based cancer vaccine is effective to induce a neoepitope-specific T cell response, which is then further expanded by administration of a T cell expander such as RSLAIL-2, effective to further expand the existing T cell population unspecifically.
- a T cell expander such as RSLAIL-2
- an optimized (and preferably synergistic) response could be achieved. See, for example, the results shown in FIGs.
- T cell expander such as RSLAIL-2 subsequent to one or more administrations of a neoepitope- specific DNA-based cancer vaccine, and preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander.
- RSLAIL-2 administration of the T cell expander
- the timing of administration of the T cell expander, RSLAIL-2, relative to the timing of administration of a second dose of the neoepitope- specific DNA-based cancer vaccine affected the T cell response. That is to say, as shown in FIG. 5B, administration of RSLAIL-2 at a period of time following administration of a second dose of the vaccine, in this case, 3 days later, resulted in a notable enhancement of the specific T cell response.
- FIG. 5C provides the results of administering RSLAIL-2 at various stages of the exemplary vaccination schedule, e.g., same day administration of the 3rd vaccine dose and RSLAIL-2, as well as administration of the 3 rd vaccine dose with delayed administration of RSLAIL-2. If two or more vaccinations, RSLAIL-2 administration was delayed by 3 days; in the case of a single vaccination, administration of RSLAIL-2 was delayed 7, 11 or 14 days.
- T cell expander such as RSLAIL-2 following the neoepitope-specific DNA-based cancer vaccine induction phase (e.g., following more than one vaccination, e.g., following 2 or 3 or 4 or more vaccinations) to thereby synergize or at least maximize the specific T cell response, preferably with reduced sensitivity to timing of administration of the T cell expander.
- T cell expander (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9- yl)methyl N-carbamate)6 avg interleukin-2 (“RLSAIL-2”), could boost the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary T cell expander, (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9- yl)methyl N-carbamate)6 avg interleukin-2 (“RLSAIL-2”), could boost the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary
- VB10.NEO and the T cell expander, RSLAIL-2, significantly synergizes to boost neoepitope-specific T cells responses, resulting in up to 5-fold increase in the number of neoepitope-specific T cell responses compared to VBIO.NEO monotherapy.
- Example 3 explores whether the T cell expander, RSLAIL-2, could increase tumor protective immune responses in VB4061 and anti-PD-1 antibody vaccinated mice (as illustrative of a subject undergoing cancer treatment with a checkpoint inhibitor further combined with administration of an individualized neoantigen-based DNA cancer vaccine) in a CT26 tumor model.
- Treatment with VB4061 alone and in combination with anti-PD-1 induces tumor protective responses (data not shown).
- vaccination could induce tumor protective immune responses (FIGs. 4A-4D).
- mice vaccinated with VB4061 and anti-PD-l were further and notably boosted when administered in combination with the T cell expander, RSLAIL-2.
- Reduced tumor growth was observed in the triple-therapy VB4061 + anti-PD-1 antibody + RSLAIL-2 treated group, where 50% of triple-treated mice remained tumor free and never did establish tumors.
- only 20% of mice receiving VB4061 + anti-PD-1 antibody without RSLAIL-2 (FIG. 4B) were protected.
- tumor regression of established tumors was observed, and overall survival was 70% and 80% in each of the VB4061 + anti-PD-1, and VB4061 + anti-PD-1 + RSLAIL-2 treated groups, respectively (FIG. 4C).
- both treatment groups were fully protective against the lethal dose of CT26 cells and both groups were statistically different from the control group both in tumor growth and in overall survival.
- RSLAIL-2 was diluted in dilution buffer to a concentration of 0.1 mg/ml and the volume determined to arrive at a final dose of 0.8 mg/kg, based upon the weight of the mouse, and injected into the tail vein of the mice.
- RSLAIL-2 is provided as a sterile white to yellow lyophilized powder for reconstitution as described in Example 4.
- VBIO.NEO pDNA constructs VB4011 and VB4061, were used as illustrative neoantigen- based DNA anticancer vaccines.
- the pDNA constructs, VB4011 and VB4061 encode 10 neoepitopes from B16 and 20 neoepitopes from CT26, respectively, as described in Table 2 below. Vaccination of mice was performed in combination with electroporation.
- FIG. 13 different functional elements of the pVBlO.NEO plasmids are shown in FIG. 13.
- Anti-PD-1 antibody precbnical experiments: InVivoMAb anti-mouse PD- 1, Clone RMP1-14. Cat no: BE0146 (Bio X Cell®).
- GGGGSE 10 amino acid linker
- amino acid sequence of VB4011 corresponds to SEQ ID NO: 1 (FIG. 1).
- the amino acid sequence of VB4061 corresponds to SEQ ID NO:2 (FIG. 8).
- a listing of the twenty neoepitopes included in the VB4061 mouse construct is shown in FIG. 9 and correspond to SEQ ID NOs:3-22.
- a listing of the ten individual neoepitopes included in the VB4011 construct is shown in FIG. 10 and correspond to SEQ ID NOs:23-32.
- IFN-Y ELISpot assay Briefly, splenocytes, CD4+ or CD8+ T cell depleted splenocytes were re-suspended to a cell concentration of 6xl0 5 cells. The cells were plated in triplicates (if limited number of cells duplicates were used) and re-stimulated for 24 hours with 2 pg/ml of individual peptides corresponding to the neoepitopes in the original VB10.NEO constructs (Table 2) used during vaccination. Immunogenicity was analyzed by IFN-g ELISpot Plus kit (Mabtech AB, Sweden) following the manufacturer’s instructions.
- SPU Spot-forming units
- CT26 tumor cells (# CRL-2638, ATCC) were cultured in bottles with culture medium (RPMI 1640, 10 mM HEPES, 1 mM sodium pyruvate, 1% non-essential amino acid solution, 1% penicillin/streptomycin, 10% FBS). Prior to injection, the cells were washed twice in lx PBS while still adherent to the flask and then trypsin treated, washed and resuspended in lx PBS to a final concentration of 5xl0 5 cell/ml. BALB/cJRj mice were injected s.c.
- VBIO.NEO non-replicative, non-integrating, genetically stable and non-pathogenic naked, covalently closed, circular and supercoiled double-stranded deoxyribonucleic acid (DNA) plasmid of 6297-7407 base pairs, dependent on the number of neoepitopes included in the personalized human vaccine.
- DNA deoxyribonucleic acid
- the DNA plasmid is based on the pUMVC4a vector backbone encoding a single recombinant homodimer protein that includes three modules: the targeting, the dimerization and the neoepitope antigenic module.
- the targeting module encodes the human chemokine macrophage inflammatory protein- 1 alpha (hMIP-la), which binds to its cognate receptors on the cell surface of antigen presenting cells (APCs), while the dimerization module encodes the upper and lower hinge regions and the constant heavy chain 3 (CH3) domain from human IgG3.
- the lower hinge region links two vaccibody monomers by disulfide bridges and the CH3 domain contributes to dimerization by hydrophobic interactions.
- the upper hinge region facilitates flexible bivalent binding of the targeting module to its cognate receptors to thereby enhance the immunogenicity of the vaccine.
- the neoepitope antigenic module consists of multiple (10-20) patient-specific neoepitopes including the somatic mutation/alteration spanning a total length of several (14 - 27) amino acids to form the neoepitope sequence and linked together by 10 amino acid flexible glycine/serine-rich linkers.
- the glycine/serine rich linkers typically change from construct to construct for the individualized vaccines based upon an evaluation of junctional sequences, such that a selected linker will typically excludes a junctional epitope that resembles a sequence found in the human schooleome.
- the neoepitope antigenic module is linked to the natural human chemokine macrophage inflammatory protein- la (targeting module) via a dimerization module derived from human IgG3 as described above.
- the transcript is translated to a 603-973 amino acid-containing protein of approximately 100 kDa, which forms an approximately 200 kDa dimeric protein.
- pVBlO. NEO Once delivered by i.m. administration to a patient, pVBlO. NEO is taken up by cells and leads to local and transient production, and secretion of the VBIO.NEO protein.
- the structure of the encoded protein is designed and selected to support the induction of strong cellular immune responses against patient-specific neoantigens.
- the pVBlO.NEO DNA backbone sequence (with a general indicator for the neoepitope antigenic module) is shown in FIG. 12 and provided as SEQ ID NO: 77.
- the different functional elements of the pVBlO.NEO plasmids are shown in FIG. 13.
- T cell expander (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2
- VB10.NEO an exemplary immunotherapeutic DNA-based neoantigen vaccine
- B16 model C56B1/6 mice were vaccinated 3x at day 0, 21 and 35 with either
- ELISpot Results in the B16 Melanoma Mouse Model Administration of RSLAIL-2 in combination with VB4011 was effective to boost neoepitope-specific IFN-g T cell responses as shown in FIG. 2A and Table 4).
- the neoepitopes M2, M3, M4, M7, M9 and M10 were immunogenic (Table 4 (immunogenic responses shown in grey boxes) and FIG. 2A).
- the neoepitopes M2, M4, M6, M7, M9 and M10 were immunogenic.
- a stronger immune response was observed in mice treated with the VB4011 + RSLAIL-2 combination therapy compared to VB4011 monotherapy.
- the criterium for an immunogenic epitope was defined as >25 IFN-g + spots/10 6 cells and > IFN-g + spots/10 6 cells than average negative control (pDNA VB1026) +2xSD. However, in this experiment since splenocytes were pooled (5 mice), 2xSD could not be used.
- the numbers represent average of triplicates in ELISpot and are presented as SPU/10 6 splenocytes. The average number of SPU in the medium control was subtracted from the average SPU elicited against each neoepitope. Wells with spot count ⁇ 0 are
- Criteria of an immunogenic epitope was defined as >25 SPU/10 6 cells.
- Epitopes determined to be immunogenic are boxed in grey.
- neoepitope-specific T cells increased in mice treated with RSLAIL-2 + VB4011 (doublet). In the doublet-treated mice, it was observed that spleens were enlarged typically 2-3-fold when compared to VB4011 vaccinated mice (Table 5). Thus, in mice treated with the VB4011 - RSLAIL-2 combination, the total number of neoepitope-specific T cells also increased. To accommodate this increase, the total number of IFN-g + secreting T cells (SPU) per spleen was calculated (Table 5), and as a result, a 3.7-fold increase of neoepitope-specific T cells was determined (see also FIG. 2B). This increase was evident for both CD8+ T cells and
- CD4+ T cells (FIGs. 2C and 2D, respectively). This finding demonstrates that administration of RSLAIL-2 in combination with VB4011 is effective to not only increase the frequency, but to also increase the total numbers of neoepitope-specific T cells in a preclinical melanoma model in mice.
- a neoepitope specific T vaccine-induced T cell response that is, following vaccination (i.e., of a first, second, or subsequent dose of the vaccine).
- vaccination with the therapeutic neoepitope-specific DNA-based cancer vaccine is effective to induce a neoepitope-specific T cell response, which is then further expanded by administration of a T cell expander such as RSLAIL-2, effective to further expand the existing T cell population unspecifically.
- a T cell expander such as RSLAIL-2
- FIGs. 5A and 5B which support, based upon this preclinical cancer model, administration of a T cell expander such as RSLAIL-2 subsequent to one or more administrations of a neoepitope-specific DNA-based cancer vaccine, and preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander.
- a T cell expander such as RSLAIL-2 subsequent to one or more administrations of a neoepitope-specific DNA-based cancer vaccine
- peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander.
- an optimal response was observed when administration of the T cell expander, RSLAIL-2, occurred 11 days following administration of the vaccine.
- FIG. 5C provides the results of administering RSLAIL-2 at various stages of the vaccination schedule, e.g., same day administration of the 3rd vaccine dose and RSLAIL-2, as well as administration of the 3 rd vaccine dose with delayed administration of RSLAIL-2. If two or more vaccinations, RSLAIL-2 administration was delayed by 3 days; in the case of a single vaccination, administration of RSLAIL-2 was delayed 7, 11 or 14 days. Based upon these results in the B16 model, it appears that administration of the T cell expander, RSLAIL-2, with a second dose of the vaccine modestly synergizes the specific T cell response, and that in this same model, administration of RSLAIL-2 with the 3 rd dose of vaccine does appear to
- T cell expander such as RSLAIL-2 following the neoepitope-specific DNA- based cancer vaccine induction phase (e.g., following more than one vaccination, e.g.,
- T cell expander (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6 avg interleukin-2
- VBIO.NEO immunotherapeutic DNA-based neoantigen vaccine
- CT26 model In the CT26 model, BALB/c mice were vaccinated lx with either 50 pg control pDNA VB1026 or 50 pg VB4061. RSLAIL-2 (0.8 mg/kg) was
- mice pDNA 50 mg ELISpot tumor cells 0.8 mg/kg
- Day 0 VB4061 day 7 Day 14 Day 21 may also consider tumor day as occurring on day (-)7, vaccination occurring on day 0 and administration of RSLAIL-2 on day 7. [00197] Other vaccination/administration schedules were also explored.
- ELISpot in CT26 colon cancer model In line with the strong synergism observed in the exemplary B16 melanoma model described in Example 1 above, the neoepitope-specific IFN-g T cell responses were also significantly elevated for the combination of VB4061 and RSLAIL-2 in the CT26 mouse tumor model (FIGs. 3A-3D and Table 7).
- mice vaccinated with VB4061 immune responses against the neoepitopes Ml, M30, Ml 03 and Ml 06 were elicited (FIG. 3A and Table 7, immunogenic epitopes are indicated in grey boxes).
- mice treated with VB4061 + RSLAIL-2 6 more neoepitopes induced immune responses (M2, M8, M65, Ml 12 and Ml 25).
- the splenocytes isolated from RSLAIL-2 monotherapy-treated mice elicited immune responses only against the neoepitope Ml 12.
- Splenocytes of individual mice were analyzed in the ELISpot assay and the criteria for an immunogenic epitope was defined to be >25 IFN-g + spots/10 6 cells and > average negative control (VB1026) +2xSD (Table 7, the numbers of average negative control (VB1026+2xSD) are shadowed in the second column.
- the numbers represent duplicates of individual mice in ELISpot and presented as SPU/10 6 splenocytes.
- the average number of SPU in the medium control was subtracted from the average of SPU elicited against each neoepitope for each sample. Samples with spot counts ⁇ 0 are reported as 0.
- An immunogenic epitope is defined as>25 SPU/10 6 splenocytes and > average negative control (VB1026) +2xSD. Epitopes deemed immunogenic are indicated by a grey box.
- mice treated with RSLAIL-2 were treated with RSLAIL-2.
- IFN-g + secreting T cells per spleen was calculated.
- a 4-fold increase in total number of neoepitope-specific T cells was observed in RSLAIL-2 + VB4061 treated mice (FIG. 3B).
- lymphocytes such as NK and effector CD8+ T cells above CD4+ T cells, due to their
- exemplary neoepitope cancer vaccine VB10.NEO, and RSLAIL-2 significantly synergizes to boost neoepitope-specific T cells responses, resulting in up to 5-fold increase in the number of neoepitope-specific T cell responses compared to VB10.NEO monotherapy. Mice treated with VB10.NEO in combination with RSLAIL-2 exhibited a stronger response to each
- neoepitope and also to more neoepitopes, demonstrating that the combination increased both the breadth and depth of the immune response.
- both frequency and total number of neoepitope-specific T cells were elevated.
- the synergistic effect was even more profound on the CD8+ T cell responses compared with CD4+ T cell responses supporting the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses.
- VB4061 encodes 20 neoepitopes from CT26 as shown above in Table 2 above and in FIGs. 7 and 8.
- mice All Balb/c mice were challenged with a lethal dose of 5xl0 4 CT26 tumor cells at day 0. 50 pg VB4061 was administered intramuscularly (i.m.) with electroporation at day 0, 3, 7, 10, 14, 27 and 64. 200 pg of an anti-PD-1 antibody was injected intraperitoneally
- VB4061 alone and in combination with anti-PD-1 induces tumor protective responses (data not shown).
- vaccination could induce tumor protective immune responses (FIGs. 4A-4D).
- the results of this experiment illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-1 was further boosted when administered in combination with RSLAIL-2. Tumor growth, tumor take and overall survival are shown in FIGs. 4A-4C.
- Re-challenge The Balb/c mice in both treatment arms that were tumor-free on day 56 were re-challenged with a second lethal dose of 5xl0 4 CT26 tumor cells without further treatment.
- FIG. 7A-7B Tumor length for untreated mice (control) and mice treated with VB4061 + anti-PD-1 + RSLAIL-2 groups was further monitored regularly by measuring the tumor length size (mm) using an electronic caliper. In this study, it was confirmed that vaccination could induce tumor regression and stabilization in a CT26 colon carcinoma mouse model (FIGs. 7A-7B).
- the results of this experiment illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-1 was further boosted when administered in combination with RSLAIL-2.
- Fig. 7B vaccination of mice with VB4061 and anti-PD-1 in combination with administration of RSLAIL-2 resulted in rapid, complete and long lasting tumor regression in mice with relatively small tumors (e.g. tumors less than about 5-6 mm) as well as long lasting stabilization of larger tumors (e.g. tumors larger than about 5-6 mm and even larger than about 10 mm).
- Objectives The primary objective of this Phase l/2a study is to assess the safety/tolerability of (i) multiple doses of 3 mg VB10.NEO immunotherapy and of (ii) multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2. Secondary objectives include (i) assessment of the immunogenicity of multiple doses of 3 mg VB10.NEO immunotherapy and of multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2, and (ii) additional preliminary assessments of the efficacy of multiple doses of 3 mg VB10.NEO immunotherapy and of multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2.
- Additional exploratory objects include, for example, an investigation of the immune signature alterations during therapy, and exploration of the correlation between immunological response and clinical efficacy after VB10.NEO immunotherapy alone or in combination with RSLAIL-2.
- Rationale Pre-clinical studies (above) have shown that the combination of VBIO.NEO and RSL AIL-2 synergizes to boost neoepitope-specific T cells responses, resulting in a 5-fold increase in the number of neoepitope-specific T cell responses compared to VBIO.NEO alone.
- mice treated with VBIO.NEO in combination with RSLAIL-2 showed both a stronger response to each neoepitope and to increased numbers of neoepitopes, showing that both the breadth and depth of the immune response were elevated.
- the combination showed an even more evident effect on CD8+ T cell responses as the combination elicited a neoepitope-specific CD8+ T cell response to more neoepitopes compared to either drug when administrated alone, further strengthening the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses.
- this open-label first-in-human phase l/2a study is designed to evaluate the safety and efficacy of multiple dosing with individualised VBIO.NEO or VBIO.NEO and RSLAIL- 2 immunotherapy in combination, in patients with locally advanced or metastatic solid tumors including melanoma, NSCLC (non-small cell lung cancer), clear-cell RCC (renal cell cancer), urothelial cancer or SCCHN (squamous cell carcinoma of the head and neck), who did not reach complete responses with current standard of care (i.e., checkpoint inhibitor therapy, CPI).
- CPI standard of care includes, e.g., nivolumab, pembrolizumab or atezolizumab. This study protocol may be amended during the course of the study.
- Part A of the study consists of 6 arms in 5 different tumor entities. All patients are administered VBIO.NEO on the background of CPI therapy. Patients receive CPI at least from the commencement of vaccine manufacturing (arms 1, 5 A and 5B) or for additional > 12 weeks (arms 2-4). Arm 5 (SCCHN) is divided into arm 5 A and arm 5B. Arm 5 A is administered VBIO.NEO whereas arm 5B receives the combination of VBIO.NEO and RSLAIL-2.
- Part B of the study will be opened after a certain number of patients have been enrolled and analysed in part A.
- the expansion part B will include up to 3 tumor-specific expansion cohorts.
- the study is divided into 3 periods: a screening and manufacturing period, a treatment period, and a long-term follow-up period.
- the neoantigenic vaccine is a non-replicative, non-integrating, genetically stable and non-pathogenic naked, covalently closed, circular and supercoiled double-stranded deoxyribonucleic acid (DNA) plasmid of 6297-7407 base pairs, dependent on the number of neoepitopes included in the personalized vaccine. It encodes a single recombinant homodimer protein consisting of 3 modules: the targeting, the dimerization and the neoepitope antigenic module.
- DNA deoxyribonucleic acid
- the latter consists of multiple (10-20) patient-specific neoepitopes including the somatic mutation/alteration spanning a total length of several (14 - 27) amino acids to form the neoepitope sequence and linked together by 10 amino acid flexible glycine/serine-rich linkers.
- the neoepitope antigenic module is linked to the natural human chemokine macrophage inflammatory protein- la (targeting module) via a dimerization module derived from human IgG3.
- the transcript is translated to a 603-973 amino acid-containing protein of approximately 100 kDa, which forms an approximately 200 kDa dimeric protein. See FIG. 12.
- the glycine/serine-rich linkers used between the neoepitopes typically change from construct to construct for the different patient vaccines based upon evaluation of junctional sequences such that a preferred linker is one that excludes a junctional epitope that resembles a sequence found in the human genome.
- Illustrative linkers that may be used between the neoepitopes include those provided in SEQ ID NOs:67-76.
- VBIO.NEO Screening, manufacturing, and delivery of VBIO.NEO vaccine: VBIO.NEO is supplied as a sterile, ready to use solution at a concentration of 3 mg/mL in phosphate buffered saline pH 7.4 in 2 mL sterile cyclo-olefin copolymer vials. The vials are stored at - 20°C ( ⁇ 5°C). The vaccine is administered using a needle-free injection system,
- neoepitopes are selected based on qualified algorithms identifying immunogenic neoepitopes with low risk of inducing autoimmunity.
- the individual VBIO.NEO vaccine is then synthesized; it is estimated that the process from tumor sampling to administration will take approximately 12 to 16 weeks, preferably from 6-10 weeks, and more preferably from 4-6 weeks.
- the vaccinations are given by intramuscular injection.
- Arm 1-4 Patients screened must have been receiving for at least 12 weeks a checkpoint inhibitor (anti-PD-1 or anti-PD-Ll) as the patient’s standard of care and according to currently approved indications.
- a checkpoint inhibitor anti-PD-1 or anti-PD-Ll
- Arms 5 A and 5B Patients can be screened as long as CPI treatments have been started as the patient’s standard of care for SCCHN.
- eligible patients provide a blood sample and at least 1 tumor specimen.
- the blood sample and the tumor specimen are mandatory. Once an adequate tumor specimen is available, the patient is enrolled, and the individualized neoantigen vaccine manufacturing period starts (approximately 12-16 weeks).
- the blood and tissue samples are included into the exome-sequencing program where the exome sequenced from the blood and the tumor sample/s are compared to identify the patients’ individual somatic tumor-specific mutations (neoepitopes).
- the blood and tissue samples are included into the exome-sequencing program where the exome sequenced from the blood and the screening tumor sample/s are compared to identify the patient’s individual somatic tumor-specific mutations (neoepitopes).
- Neoepitopes found in more than one sample fresh biopsies, available archival tumor specimens and cell free (cf)DNA from blood
- the tumor samples are subjected to RNA sequencing to select neoepitopes found in expressed proteins in the tumor.
- the blood sample is used for HLA typing to select neoepitopes that bind the individual patient’s HLA molecules.
- Vaccinations with individualized VBIO.NEO immunotherapy are commenced as soon as the patient- specific VBIO.NEO vaccine is available and if the patient-specific vaccine meets all pre specified product-release criteria after manufacturing.
- RSLAIL-2 provided as a lyophilized powder, is reconstituted by the clinician prior to administration, and each patient’s dose is determined by the patient’s weight in kilograms. RSLAIL-2 is administered IV over 30 ( ⁇ 5) minutes at a starting dose of
- RSLAIL-2 is administered on the same day as VBIO.NEO.
- the vaccination occurs first, and the RSLAIL- 2 administration occurs 2 hours later. If treatment with CPI occurs on the same day, then the dosing is in the following order with the time interval between: (1) VBIO.NEO (wait 2 hours); (2) RSLAIL-2 (wait 30 minutes) (3) CPI.
- RSLAIL-2 Dose delays and reductions are permitted for RSLAIL-2. Administration of RSLAIL-2 may be delayed or the dose reduced to 0.003 mg/kg based on observed drug-related toxicities. If the RSLAIL-2 dose is reduced to 0.003 mg/kg, the dose level should remain at this level throughout the remainder of the study.
- Vaccinations start at visit 1. Patients will have received CPI at least from the start of manufacturing (arms 5 A and 5B) or for additional > 12 weeks (arms 1-4).
- Patients receive a maximum of 14 vaccinations of each 3 mg VBIO.NEO at pre-specified time points for up to 1 year from first vaccination in addition to CPI.
- the VBIO.NEO vaccine is added to this continuing CPI treatment and will not replace, omit, postpone or terminate the standard therapy.
- patients receive 3 vaccinations of 3 mg VBIO.NEO Q3W in addition to their CPI. From week 10, patients will receive maintenance treatment with vaccinations Q4W for up to 1 year from the first vaccination in addition to their CPI.
- RSLAIL-2 (arm 5B): Dosing with RSLAIL-2 starts at week 11 (visit 8A), 1 week after the fourth VBIO.NEO vaccination and when VBIO.NEO is expected to have created a robust neoantigen-specific T cell response. Patients with SCCHN who are enrolled into arm 5A can, if willing to and fulfil all inclusion criteria for arm 5B, move into arm 5B (upon investigator’s and sponsor’s agreement) and start treatment with RSLAIL-2 at week 11 or 1 week after any later VBIO.NEO vaccination visit in the maintenance period up to week 34 (i.e. VBIO.NEO dose 10, week 18 + 1 week). Patients who have received at least 1 dose of VBIO.NEO vaccination are eligible for RSLAIL-2 administration.
- VBIO.NEO VBIO.NEO and CPI.
- the first 2 doses of RSLAIL-2 4 are administered in a Q3W interval and following doses in Q4W intervals. Treatment continues until end of treatment (EoT) at visit 18 (week 50). Depending on the time point of the RSLAIL-2 start, patients receive a maximum of 11 doses of RSLAIL-2. Except for the first RSLAIL-2 dose, all following doses are administrated on the same day as VBIO.NEO.
- Arms 1-4 To capture changes between screening and the first VBIO.NEO vaccination as well as in response to VBIO.NEO vaccination, up to 3 biopsies are taken at visit 1 (first VBIO.NEO vaccination) and 1 biopsy at visit 10 (week 18). This leads to a total maximum of 10 biopsies (3 at screening, 3 at visit 1, 1 at visit 10, and up to 3 additional biopsies at any timepoint after the first vaccination).
- Arms 5A and 5B To characterize changes before and after RSLAIL-2 administration, patients are asked to provide optional biopsies within 7 days prior and 15-21 days after the first administration of RSLAIL-2. In addition, biopsies can be taken at visit 1. At each of these time points, up to 3 biopsies are taken. This leads to a total maximum of 13 biopsies (3 at screening, 3 at visit 1, 3 at 1 week prior to the first RSLAIL-2 dose, 3 at 15-21 days after the first administration, and 1 additional biopsy at any timepoint after the first vaccination).
- tumor material is be secured for further analysis.
- PBMC peripheral blood monocytic cell
- PBMC peripheral neoepitope-specific T cell responses induced by the T cell expander, RSLAIL-2.
- VB10.NEO vaccination (visit 7A/week 7) and 7 days after first RSLAIL-2 administration (visit 8B/week 12) in order to fine characterize neoepitope-specific T cells.
- Functional analyses may include, for example, flow cytometry, ELISpot, enzyme-linked immunosorbent assay, and cytotox assays and will be compared with T cell clones isolated from tumor tissue/specimens.
- Efficacy to treatment is assessed as follows. Tumor response to VB10.NEO and RSLAIL-2 is assessed by means of iRECIST at regular intervals according to standard of practice. The imaging procedure is performed as part of the standard patient care and the patient is not exposed to any further radiation due to participation in this study.
- the imaging performed within 4 weeks of visit 1 is the baseline for tumor assessments according to iRECIST.
- an imaging assessment should preferably be carried out as close as possible prior to the first dose of RSLAIL-2.
- the same method of assessment (imaging modality, e.g., MRI or CT) is ideally be used to characterise each identified and reported lesion at baseline and during all follow-up examinations for an individual patient according to the individual site's practices of standard of care.
- imaging modality e.g., MRI or CT
- Efficacy analysis Early signs of efficacy of VB10.NEO immunotherapy alone or in combination with RSLAIL-2 will be based on Overall Response Rate (ORR), Duration of response (DOR), Progression-free survival (PFS), Overall survival (OS).
- ORR Overall Response Rate
- DOR Duration of response
- PFS Progression-free survival
- OS Overall survival
- Efficacy analyses will be done separately for each tumor entity-specific cohort in part A and part B.
- the efficacy endpoints will be analyzed descriptively including 95% confidence intervals for proportions wherever applicable.
- the DOR, PFS and OS will be analyzed using the Kaplan-Meier product-limit method.
- Additional assessments to be conducted include vital signs (body temperature, oxygenation, pulse rate, and systolic and diastolic BP, monitoring of BP, pulse and ECG, as well as blood assessments.
- Blood analysis includes the following: differential leukocyte analysis, haemoglobin, haematocrit, red blood cell count, platelet count, urea, calcium, chloride, phosphorus-inorganic, potassium, sodium, creatinine, uric acid, C-reactive protein, ALT, AST, gamma glutamyltransferase, bilirubin, lipase, alkaline phosphatase, lactate dehydrogenase, thyroid stimulating hormone (TSH), free triiodothyronine (fT3), free thyroxine (fT4), glucose, protein, albumin, partial thromboplastin time, international normalized ratio, cholesterol, triglycerides, cholinesterase, creatine kinase. Serum will also be
- the peripheral immune response of the individualized VBIO.NEO vaccine strategy will be measured by IFN-g enzyme-linked immunospot assay (ELISpot), a surrogate for T cell activity.
- IFN-g enzyme-linked immunospot assay a surrogate for T cell activity.
- the immune response to each neoepitope included in the vaccines will be assessed individually.
- further analysis may be performed by flow cytometry analysis of cellular surface markers, tetramer analysis and intracellular cytokine staining to characterize the T cell profile.
- TCR T cell receptor
Abstract
Provided herein are methods, combinations, and compositions for treating a subject having cancer by administering to the subject an individualized neoantigen DNA cancer vaccine in combination with a T cell expanding compound ("T cell expander"), i.e., a compound capable of driving specific clonal T cell expansion to vaccine epitopes, optionally further combined with a checkpoint inhibitor.
Description
IMMUNOTHERAPEUTIC COMBINATION FOR TREATING CANCER
CROSS REFERENCE TO RELATED APPLICATIONS
[0001] This application claims the benefit of priority under 35 U.S.C. §119(e) to U.S.
Provisional Patent Application No. 62/811,459, filed February 27, 2019; U.S. Provisional Patent Application No. 62/825,487, filed March 28, 2019; U.S. Provisional Patent
Application No. 62/838,180, filed April 24, 2019 and U.S. Provisional Patent Application No. 62/881,832, filed August 1, 2019, the disclosures of which are each incorporated herein by reference.
FIELD
[0002] The instant application relates to (among other things) the field of
immunotherapy, and in a particular aspect, cancer immunotherapy, and involves the treatment of an individual having cancer by administering to the individual an anticancer vaccine such as a DNA neoantigen vaccine, in combination with a T cell expander, optionally further combined with a checkpoint inhibitor.
BACKGROUND
[0003] Cancer is a genetic disorder that results from genetic or epigenetic alternations in the somatic cells and represents one of the most deadly diseases in the developed world. Tumorigenesis in humans is a multistep process which involves various genetic or epigenetic changes that ultimately drive the malignant transformation of normal cells. While our understanding of mechanisms leading to malignancy continues to make enormous strides, the complexity of the processes that drive the development, growth and spread of cancer make the development of new and effective treatments particularly challenging.
[0004] Conventional approaches to cancer treatment include surgery, radiotherapy and traditional chemotherapy, each of which has its own well-known advantages and drawbacks. More recently, therapeutic cancer vaccines have been explored as an alternative approach for treating cancer. Therapeutic cancer vaccines represent a class of substances that
work by stimulating or restoring a subject’s immune system’s ability to fight infections and disease. Therapeutic vaccines, as opposed to preventative or prophylactic vaccines, are used to treat an existing cancer by boosting the body’s natural immune response against the cancer and represent a type of immunotherapy. Cancer treatment vaccines are designed to activate cytotoxic T cells and direct them to recognize and act against specific types of cancer or to induce production of antibodies that bind to molecules on the surface of cancer cells. One type of such molecules, referred to as tumor-associated antigens, are antigens that are expressed at low levels in normal tissues, but are expressed at much higher levels in tumor tissue. However, producing effective therapeutic vaccines that bind to tumor-associated antigens has proven to be a challenging endeavor, at least in part, because the vaccine intervention must combat the body’s immune system that is restrained by mechanisms that work to sustain the cancer. Additionally, therapeutic approaches based upon tumor- associated antigen-based vaccines may also lead to toxicities due to normal cell destruction. To be effective, a therapeutic cancer vaccine must not only stimulate a specific immune response against an intended target, but must also be powerful enough to overcome the barriers that cancer cells utilize to protect themselves from attack by killer T cells. Over the last several years there have been substantial efforts in developing therapeutic cancer vaccines encompassing various platforms. Therapeutic vaccines have been evaluated, for example, in patients with breast cancer, lung cancer, melanoma, pancreatic cancer, colorectal cancer, and renal cancer (Melero, I., et al, Nat Rev Clin Oncol, 2014, 11 (9), 509-524), although such therapeutic anticancer vaccines have met with limited success.
[0005] Recently, immunotherapeutic approaches for treating cancer have expanded to vaccination against tumor-specific neoantigens derived from random somatic variations in tumors. Vaccination against tumor-specific neoantigens can minimize the potential induction of central and peripheral tolerance as well as the risk of autoimmunity.
[0006] While knowledge of the mechanisms involved in immune-mediated tumor control continues to grow at a rapid pace, successful translation of immunotherapies into the clinic remains a challenge. Although there have been substantial efforts in developing therapeutic vaccines encompassing various platforms to date, there remains a need to identify and provide new and more effective immunotherapeutic approaches such as vaccine-related treatment modalities that can effectively target tumor-specific antigens, and provide potent
and robust antitumor responses. Thus, the present disclosure seeks to address these and other needs.
SUMMARY
[0007] The present disclosure provides a new and surprisingly beneficial
immunotherapeutic approach for treating a subject having cancer. More particularly, provided herein is a method for treating a subject having cancer, the method comprising administering to the subject, (i) an anticancer DNA vaccine directed to a plurality of neoepitopes from a patient’s own tumor-specific antigens, referred to as“neoantigens” (“neoantigen-based DNA cancer vaccine”), and (ii) a compound effective to stimulate/expand production of T cells (i.e., effector T cells,“a T cell expander”).
[0008] In yet another aspect, the disclosure provides a method for treating a subject having cancer, the method comprising administering to the subject, (i) an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, (ii) a compound effective to stimulate/expand production of T cells, and optionally, (iii) a checkpoint inhibitor.
[0009] In one or more embodiments, the neoepitopes comprised in the DNA vaccine are presented to the immune system as a dimeric protein called a vaccibody (to be described in greater detail herein), i.e., in such embodiments, the vaccine is referred to as a vaccibody DNA vaccine. WO 2004/076489 describes dimeric proteins called vaccibodies in detail. Targeting units (comprised within the vaccine and described below) are described in detail in WO 2011/161244.
[0010] In yet one or more further embodiments, the neoantigen-based DNA cancer vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding (i) a targeting unit, (ii) a dimerization unit, (iii) a first linker and (iv) an antigenic unit, where the antigenic unit comprises n-1 antigenic subunits (where n is an integer of from about 3 to 50), each subunit comprising at least a part of a cancer neoepitope sequence and a second linker, and further comprising a final cancer neoepitope sequence. Representative neoantigen-based DNA cancer vaccines, as well as methods of making, i.e., constructing and expressing, and using such vaccines, are described in U.S. Patent Publication No. US 2019/0022202, incorporated herein by reference.
[0011] In some further embodiments, the neoantigen-based DNA cancer vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding an antigenic unit. The antigenic unit comprises n-1 antigenic subunits, where each subunit comprises at least a part of a cancer neoepitope sequence and a linker, and further comprises a final cancer neoepitope sequence, wherein n is an integer of from 3 to 50.
[0012] In some further embodiments, the vaccine is a vaccibody DNA vaccine comprising from 10 to 50 neoepitopes, or from 15 to 40 neoepitopes, or from 10 to 30 neoepitopes, or from 10-20 neoepitopes.
[0013] In yet some additional embodiments, the vaccine comprises a DNA polynucleotide comprising a nucleotide sequence encoding an antigenic unit as described above, wherein the linker is an amino acid linker. Exemplary linkers include, for example, glycine/serine-rich linkers. Further exemplary linkers include, for example, the linkers identified as SEQ ID NO:67-76.
[0014] Exemplary mouse neoantigen-based DNA cancer vaccines comprising
VB10.NEO pDNA constructs, VB4011 and VB4061, are described in the supporting examples.
[0015] In some additional embodiments, the vaccine comprises a DNA
polynucleotide sequence that is human. In yet some further embodiments, the vaccine comprises a DNA pVBlO.NEO plasmid backbone sequence as provided in FIG. 12.
[0016] In yet some further embodiments, the T cell expander, when administered in combination with the neoantigen-based DNA cancer vaccine is effective to enhance specific clonal T cell expansion to vaccine epitopes over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander to a degree that is greater than additive.
[0017] In one or more particular embodiments, the T cell expander is a prodrug of an interleukin-2 (e.g., aldesleukin, des-alanyl-1, serine-125 human interleukin-2), wherein the interleukin-2 is modified by releasable covalent attachment of multiple polyethylene glycol moieties. In yet one or more additional embodiments, the T cell expander is an interleukin-2 receptor beta (IL-2R_ ) selective agonist.
[0018] In yet some further embodiments, the T cell expander is an IL-2R]3-selective agonist composition, multi(2,7-(bis-methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 (also referred to herein as“RSLAIL-2”), comprising compounds of Formula (I),

Formula (I), wherein IL-2 is interleukin-2 (such as, for example, aldesleukin), “-NH-IL-2” represents an amino group of interleukin-2, each integer (n) has a value from about 200-300; or pharmaceutically acceptable salt forms thereof. In certain embodiments,“n” in each of the polyethylene glycol chains is about 227 (i.e., where each polyethylene glycol chain extending from the central fluorenyl core has a weight average molecular weight of about 10,000 daltons, such that the weight average molecular weight of each overall branched PEG moiety is about 20,000 daltons).
[0019] In yet some further embodiments, the T cell expander is (2,7-(bis- methoxyPEGiokd-carboxyamide)(9h-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2.
[0020] In one or more embodiments of the method wherein the cancer comprises a cancerous tumor, numbers of neoantigen-based DNA cancer vaccine-induced T cells in the tumor, such as CD4 and CD8 T cells reactive to each of the vaccine-encoded neoantigens, are increased in number over such T cells determined upon following administration of one or more doses of the neoantigen-based DNA cancer vaccine alone, when evaluated in either a clinical or a preclinical setting.
[0021] In some embodiments, the cancer is a solid cancer.
[0022] In yet some further embodiments of the method, the cancer is selected from, for example, the group consisting of breast cancer, ovarian cancer, colon cancer, prostate
cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer (SCLC), non-small cell lung cancer (NSCLC), pancreatic cancer, thyroid cancers, kidney cancer, e.g., renal cell carcinoma, cancer of the bile duct, cancer of the head and neck (e.g., squamous cell carcinomas of the head and neck), brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer (e.g., urothelial carcinoma), esophageal cancer, Hodgkin's disease and adrenocortical cancer, among others.
[0023] In some further embodiments, the cancer is selected from locally advanced or metastatic melanoma, non-small cell lung cancer, clear renal cell carcinoma, urothelial cancer, and squamous cell carcinoma of the head and neck.
[0024] In one or more further embodiments, the cancer is melanoma or colon cancer.
[0025] By way of clarity, with regard to the sequence of administering, the neoantigen-based DNA cancer vaccine and the T cell expander, and optionally a checkpoint inhibitor, may be administered concurrently or sequentially, and in any order, and via the same and/or different routes of administration. More particularly, the therapeutic components of the combination therapy may each be administered on the same day, on different days, or, a mixture of both (two immunotherapeutic components administered on the same day and one immunotherapeutic component administered on a different day).
Moreover, treatment may comprise a single cycle of therapy, or may comprise multiple cycles, including one or more doses of each of the neoantigen-based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor. It will be appreciated that treatment may comprise a mixture of single cycle and multiple cycles, such as, for example at least one of the neoantigen-based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor is administered for a single cycle and one or more of the neoantigen- based DNA cancer vaccine, the T cell expander, and the optional checkpoint inhibitor is administered for multiple cycles.
[0026] In some embodiments, the T cell expander is administered following administration of the neoantigen-based DNA cancer vaccine.
[0027] In some more particular embodiments, the T cell expander is administered following the neoantigen-based DNA cancer vaccine induction phase, wherein such induction phase may span one or more administrations of the vaccine, e.g., 1, 2, 3, 4 or more vaccinations over a given time period. In some embodiments, the time following the
induction phase is a time, following one or more vaccinations, at which the neoepitope- specific T cell response has substantially levelled off, that is, is no longer significantly increasing. For example, in one or more embodiments, such time is within a time frame in which the neoepitope-specific T cell response has reached its maximum, or is within +25% of its maximum, or is within + 15% of its maximum, or is within about + 10% of its maximum. For example, the T cell expander may be administered within about 3-20 days following the last vaccination of the induction period, or within about 3-15 days following the last vaccination of the induction period, or within about 7-20 days following the last vaccination of the induction period, such as within about 7-15 days or within 7-12 days. Additional ranges are also contemplated. In some embodiments, the T cell expander is administered at least 3 days following the last vaccine administration of the induction period. Measured in an alternative fashion, the T cell expander may, for example, first be administered within about 4-20 weeks following initiation of the vaccination(s) (i.e., following the first vaccination of the induction period), or within about 6-16 weeks following the first vaccination of the induction period, or within about 8-12 weeks following the first vaccination of the induction period, such as, e.g., 11 weeks following the first vaccination of the induction period.
[0028] In yet some further embodiments, administration comprises administration of each of the neoepitope-specific DNA-based cancer vaccine and the T cell expander to align or substantially align the peak T cell responses of both the neoepitope-specific DNA-based cancer vaccine and the T cell expander to thereby achieve an optimized (and preferably synergistic) T cell response.
[0029] In some further embodiments, the T cell expander is administered at a period of time following administration of one or more doses of the neoantigen-based DNA cancer vaccine, e.g., following 1-5 doses (i.e., vaccinations), or following 1-4 doses (vaccinations), or following 1-3 doses (vaccinations), or following 1-2 doses (vaccinations) e.g., to thereby result in an enhancement of the specific T cell response. In some particular embodiments, the T cell expander is administered following 2 or 3 vaccinations or 4 vaccinations. In yet some other embodiments, the T cell expander is administered following 4 vaccinations. In yet some more particular embodiments, the T cell expander is administered from 1-20 days following the last vaccination of the induction period. For example, the T cell is initially administered on day 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19 or 20 days following the last vaccination of the induction period. In some cases, the vaccination period
comprises 4 vaccinations, and the first dose of the T cell expander is administered from 5-10 days following the 4th vaccination, e.g., e.g., 5, 6, 7, 8, 9, or 10 days following the 4th vaccination, e.g., on day 7. In yet some further embodiments, following the initial dose of the T cell expander, the vaccine and the T cell expander are administered on either the same day or on different days. In some particular embodiments, following the initial dose of the T cell expander, the vaccine and the T cell expander are administered on the same day.
[0030] In yet some additional embodiments, the vaccine induction period as described above comprises more than one vaccination, each subsequent vaccination separated by 1 week, 2 weeks, 3 weeks, or 4 weeks or more following the first administration. In some further embodiments, the vaccination induction period comprises 4 separate vaccinations, each separated by from 1-8 weeks, or from 2-8 weeks, or from 2-6 weeks, or from 3-8 weeks, or from 4-8 weeks, or from 4-6 weeks. For example, in some particular embodiments, the vaccine is administered every 3 weeks for the first one, two or three or four doses, following by a longer interval between vaccinations, e.g., every 4 weeks, or every 5 weeks or every 6 weeks, or longer.
[0031] In some embodiments related to the foregoing, the checkpoint inhibitor, when comprised in the combination therapy, is administered, for one or for multiple rounds (i) on the same day as the neoantigen-based DNA cancer vaccine is administered, (ii) on the same day as the T cell expander is administered (iii) following administering of the neoantigen- based DNA cancer vaccine, (iv) following administering of the T cell expander, (v) following administering of the neoantigen-based DNA cancer vaccine but before administering of the T cell expander. In some embodiments in which the therapeutic components are all administered on the same day, an exemplary order of administration is neoantigen-based DNA cancer vaccine, T cell expander, followed by checkpoint inhibitor.
[0032] In yet some additional embodiments, the checkpoint inhibitor (CPI), such as an anti-PD-1 antibody or other suitable CPI, is administered more than once over the course of treatment. In yet some other further embodiments, the checkpoint inhibitor is initially administered following an initial vaccination and following administration of the T cell expander. In yet some other further embodiments, the checkpoint inhibitor is initially administered following an initial vaccination but prior to administration of the T cell expander.
[0033] In yet some further embodiments, the check point inhibitor, when comprised in the combination therapy, is administered prior to first vaccination (i.e., administration) of the neoantigen-based DNA cancer vaccine and prior to the first administration of the T cell expander.
[0034] Exemplary checkpoint inhibitors include, e.g., an anti -PD- 1 antibody, an anti-
CTLA-4 antibody, or an anti-PD-Ll antibody.
[0035] In yet additional embodiments, the cancer comprises a cancerous tumor and the method is effective to reduce the size of the cancerous tumor when compared to the size of the tumor prior to treatment. In some more particular embodiments, the cancer comprises a cancerous tumor, and the method is effective to reduce the size of the cancerous tumor by at least about 30% (partial response), or by at least about 40%, or by at least about 50%, or by at least about 60%, or by at least about 70%, or at least about 80%, or at least about 90%, or to result in complete tumor regression, when compared to the size of the tumor prior to the administering. In yet some further embodiments of the method, the cancer comprises a cancerous tumor and the method is effective to result in complete tumor regression.
[0036] Additional aspects and embodiments are set forth in the following description, including the examples, and the claims.
BRIEF DESCRIPTION OF THE DRAWINGS
[0037] FIG. 1 provides the amino acid sequence of the exemplary VB10.NEO pDNA mouse construct, VB4011 (SEQ ID NO: l), encoding 10 neoepitopes from B16, wherein each peptide is separated by a ten amino acid linker (GGGGS)2 (SEQ ID NO:33), as described in Table 2.
[0038] FIGs. 2A-2D illustrate, as described in Example 1, that administration of a T cell expander such as RSLAIL-2 boosts the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO in a B16 mouse melanoma model. FIG. 2A is a graph of the total T cell responses (number of IFN-y+ spots/106 splenocytes) in a B16 tumor model after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 2B is a graph of the total T cell responses per spleen, that is the number of IFN-y+ spots/spleen, after treatment with a control
(VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 2C is a graph of the total CD8+ T cell responses (splenocytes depleted of CD4+ T cells using anti-CD4 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 2D is a graph of the total CD4+ T cell responses (splenocytes depleted of CD8+ T cells using anti-CD8 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4011) or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). As shown, the T cell expander synergizes vaccine induced neoepitope-specific IFN-g T cell responses in a mouse melanoma model.
[0039] FIGs. 3A-3D illustrate, as described in Example 2, that administration of a T cell expander boosts the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO in a CT26 mouse colon carcinoma model. FIG. 3A is a graph of the total T cell responses (number of IFN-y+ spots/106 splenocytes) in a CT26 tumor model after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL- 2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 3B is a graph of the total T cell responses per spleen, that is the number of IFN-y+ spots/spleen, after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), and the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 3C is a graph of the total CD8+ T cell responses (splenocytes depleted of CD4+ T cells using anti-CD4 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). FIG. 3D is a graph of the total CD4+ T cell responses (splenocytes depleted of CD8+ T cells using anti-CD8 Ab coated Dynabeads) as the number of IFN-y+ spots/spleen after treatment with a control (VB1026), the vaccine alone (VB4061), the T cell expander alone (RSLAIL-2), or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2). As shown, the T cell expander synergizes vaccine induced neoepitope-specific IFN-g T cell responses in a mouse colon carcinoma model.
[0040] FIGs. 4A-4D illustrate, as described in Example 3, that administration of a T cell expander boosts the neoepitope-specific IFN-g T cell response when administered in
combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine,
VB4061, and an anti-PD-1 antibody in a CT26 mouse colon carcinoma model. FIG. 4A is a graph of the tumor growth shown as tumor volume (cm3) for 5-25 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti -PD 1 Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2) in a CT26 mouse colon carcinoma model. FIG. 4B is a graph of the percentage of tumor-free mice (i.e., mice that never established a tumor) for 0-49 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti-PDl Ab), or the combination of the vaccine, an anti- PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2). “Tumor take” refers to mice that never established a tumor, which differs from mice that established a tumor which then later regressed or was cleared. FIG. 4C is a graph of the % survival of mice for 0-80 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti- PDl Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2). FIG. 4D is a graph of the percentage of tumor-free mice for 0-70 days post injection of CT26 tumor cells after administration of the vaccine alone (VB4061), the combination of the vaccine and an anti-PD-1 antibody (VB4061 + anti- PDl Ab), or the combination of the vaccine, an anti-PD-1 antibody, and a T cell expander (VB4061 + anti-PDl Ab + RSLAIL-2) after re-challenge with 5xl04 CT26 tumor cells without retreatment. As shown, tumor protection in mice vaccinated with an individualized DNA anticancer vaccine and an anti-PDl antibody is further strengthened by administration of the T cell expander.
[0041] FIGs. 5A-5C provide the results of administration of a T cell expander that is postponed after one or more administrations of an anticancer vaccine as described further in Example 1. FIG. 5A is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a B 16 tumor model after treatment with a control (VB1026), the vaccine alone (VB4011) administered on day 1, or the combination of the T cell expander and the vaccine (VB4011 + RSLAIL-2) administered on day 11 or day 14 after the anticancer vaccine. T cell response was analyzed at days 14, 18 or 21 after anticancer vaccine, and 7 days after dosing the T cell expander. Optimal response was observed when the T cell expander was administered 11 days after the anticancer vaccine (the maximum T cell response as indicated by the arrow).
FIG. 5B is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a CT26 tumor model after treatment with a control (VB1026), the vaccine alone (VB4061) on days 1 and 21 and the combination of the T cell expander and the vaccine (VB4061 + RSLAIL-2) administered on day 21 (same day as 2nd vaccination) or day 24 (3 days post 2nd vaccination). ELISpot was performed 7 days following administration of RSLAIL-2 (e.g., 21 + 7 or 24 +
7). The day in the figure refers to when splenocytes were analyzed in ELISpot. (Vaccine is administered day 1). For VB4061 + RSLAIL-2 d21, administration of both the vaccine and RSLAIL-2 (second doses) occurred on the same day. For VB4061 + RSLAIL-2 d28, RSLAIL-2 was administered three days (day 24) following the second administration of the vaccine (on day 21). FIG. 5C is a graph of the total T cell responses (number of IFN-y+ spots/spleen) in a B16 tumor model after treatment with three administrations of a control (3x VB1026), three administrations of the vaccine alone (3xVAC), three administrations of the vaccine with administration of the T cell expander on the same day as the third vaccine (3xVAC + RSLAIL-2 d35), and three administrations of the vaccine with administration of the T cell expander three days following the third vaccine dose (3x VAC + RSLAIL-2). This figure indicates that when RSLAIL-2 is administered as late as the 3rd vaccination, the difference between same day and 3-days postponed is no longer present. Postponed administration of the T cell expander appears to synergize the specific T cell response.
[0042] FIGs. 6A-6C. As described in Example 3, the tumor burden at the time of the first administration of the T cell expander appears to be predictive of response (reduced tumor growth). FIGS. 6A-6C provide graphs of the tumor length (mm), where the T cell expander was administered days 0, 9, 18, 27 (dotted lines) starting when the tumor burden at first administration is 1-5 mm (FIG. 6A), 6-10 mm (FIG. 6B), or >10 mm (FIG. 6C) in a CT26 mouse colon carcinoma model. Mice were treated with the vaccine VB4061 + anti- PD-1 antibody in addition (red, green and blue legend), or VB4061 + anti.PD-1 only (black legend). Pink lines in FIGs. 6A and 6C corresponds to RSLAIL-2 at day 32. A complete response was observed in a greater number of mice where the tumor size was <6 mm at the time of the first administration of the T cell expander.
[0043] FIGs. 7A-7B. As described in Example 3, FIGs. 7A-7B illustrate that administration of a T cell expander provides rapid, complete and long lasting regression of relatively small tumors and long lasting stabilization of larger tumors when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine,
VB4061, and an anti-PD-1 antibody in a CT26 mouse colon carcinoma model. FIG. 7A is a graph of the tumor growth shown as tumor length (mm) for 0-42 days post injection of CT26 tumor cells as a control. FIG. 7B is a graph of the tumor growth shown as tumor length (mm) for 0-56 days post injection of CT26 tumor cells after administration of a combination of the vaccine (VB4061), an anti-PD-1 antibody, and a T cell expander in a CT26 mouse colon carcinoma model. The lines 1-10 in each graph represent tumor length of individual mice (n=10) over the time period.
[0044] FIG. 8 provides the amino acid sequence of the VB10.NEO pDNA mouse construct, VB4061 (SEQ ID NO:2), encoding 20 neoepitopes from CT26, wherein each peptide is separated by a ten amino acid glycine/serine rich linker (GGGGS)2, as described in Table 2.
[0045] FIG. 9 provides the amino acid sequences of the individual neoepitopes from
CT26 (SEQ ID NOs:3-22) included in the VB4061 mouse construct.
[0046] FIG. 10 provides the amino acid sequences of the individual neoepitopes from
B16 (SEQ ID NOs:23-32) included in the VB4011 mouse construct.
[0047] FIGs. 11A-D provide an outline of dosing and assessments performed throughout the clinical study described in Example 4.
[0048] FIG. 12 provides a complete pVBlO.NEO plasmid backbone sequence including coding sequences of the targeting module (hMIP-la, nucleotides 1143-1421) and the dimerization module (hi and h4 and CH3 domains of hIgG3, nucleotides 1422-1853) of the expression product (SEQ ID NO:77). The grey blocks are the internal Sfll cloning sites (nucleotides 1854-1866 and 1869-1881). Italic sequences are the flanking Notl/Bglll restriction sites (nucleotides 1884-1889). Underlined sequences are glycine/serine-rich linkers (nucleotides 1503-1532 and 1854-1868). The nucleotide numbering does not include the neoantigenic module nucleotides).
[0049] FIG. 13 provides a pVBlO.NEO plasmid map.
DETAILED DESCRIPTION
[0050] The instant disclosure relates to (among other things) the field of
immunotherapy, and in a particular aspect, cancer immunotherapy, and generally involves the
treatment of a patient having cancer by administering to the patient a personalized neoantigen DNA cancer vaccine in combination with a T cell expanding compound (“T cell expander”), i.e., a compound capable of driving specific clonal T cell expansion to vaccine epitopes, optionally further combined with a checkpoint inhibitor.
Definitions
[0051] In describing and claiming certain features of this disclosure, the following terminology will be used in accordance with the definitions described below unless indicated otherwise.
[0052] As used in this specification, the singular forms "a," "an," and "the" include plural referents unless the context clearly dictates otherwise.
[0053] Reference to a range or sub-range is meant to expressly recite sub-ranges formed by any two members of a disclosed range. For example, a range described as being from 20 to 50, or from 10 to 30, will thereby expressly include ranges from 10 to 20, 20 to 30, 10 to 50, 30 to 50, and so forth.
[0054] "Substantially" or "essentially" means nearly totally or completely, for instance, about 95% or greater of a given quantity.
[0055] Similarly,“about” or“approximately” as used herein means within plus or minus 5% of a given quantity.
[0056] It is understood that wherever aspects are described herein with the language
"comprising," otherwise analogous aspects described in terms of "consisting of' and/or "consisting essentially of' are also provided.
[0057] "PEG" or "polyethylene glycol," as used herein, is meant to encompass any water-soluble poly(ethylene oxide). Unless otherwise indicated, a "PEG polymer" or a polyethylene glycol is one in which substantially all (preferably all) monomeric subunits are ethylene oxide subunits, though, the polymer may contain distinct end capping moieties or functional groups, e.g., for conjugation. PEG polymers for use in the moieties described herein will typically comprise one of the two following structures: "-(CEhCEhOV or "-(CH2CH20)n-iCH2CH2-," depending upon whether or not the terminal oxygen(s) has been displaced, e.g., during a synthetic transformation. As stated above, for a PEG-based polymer
or a PEG-based polymer conjugate, the variable (n) will typically fall within a range from about 3 to 4000, and the terminal groups and architecture of the overall PEG can vary. Preferred ranges /values for (n) for the T cell expander, RSLAIL-2 (described in greater detail below), e.g., in reference to Formulas (I), (II), (III) and (IV), include from about 200 to 300, and about 227. Additional exemplary ranges for (n) are those suitable to provide a branched polymer such as provided in Formulas (I), (II), (III) and (IV), having an overall weight average molecular weight in a range of from about 250 daltons to about 90,000 daltons. Additional exemplary ranges for (n) are those suitable to provide a branched polymer such as provided in Formulas (I), (II), (III) and (IV), having an overall weight average molecular weight in a range selected from about 1,000 daltons to about 60,000 daltons, in a range of from about 5,000 daltons to about 60,000 daltons, in a range of about 10,000 daltons to about 55,000 daltons, in a range of from about 15,000 daltons to about 50,000 daltons, and in a range of from about 20,000 daltons to about 50,000 daltons.
[0058] "Branched" in reference to the geometry or overall structure of a polymer, optionally forming part of a polymer-conjugate, refers to a polymer having two or more polymer "arms" or“chains” extending from a branch point or central structural feature. In some embodiments, a branched polymer comprises two polymer arms or chains emanating from a central structural feature.
[0059] A covalent“releasable” linkage, for example, in the context of a polyethylene glycol that is covalently attached to an active moiety such as an interleukin-2 (e.g., aldesleukin), is one that releases under physiological conditions by any suitable release mechanism to thereby release or detach the polyethylene glycol polymer from the active moiety.
[0060] Molecular weight in the context of a water-soluble polymer, such as PEG, can be expressed as either a number average molecular weight or a weight average molecular weight. Unless otherwise indicated, all references to molecular weight herein refer to the weight average molecular weight. Both molecular weight determinations, number average and weight average, can be measured using gel permeation chromatography or other liquid chromatography techniques. Other methods for measuring molecular weight values can also be used, such as the use of end-group analysis or the measurement of colligative properties (e.g., freezing-point depression, boiling-point elevation, or osmotic pressure) to determine number average molecular weight or the use of light scattering techniques,
ultracentrifugation, or viscometry to determine weight average molecular weight. PEG polymers are typically polydisperse (i.e., number average molecular weight and weight average molecular weight of the polymers are not equal), possessing low polydispersity values of preferably less than about 1.2, more preferably less than about 1.15, still more preferably less than about 1.10, yet still more preferably less than about 1.05, and most preferably less than about 1.03.
[0061] The terms "protein", "polypeptide" and "peptide" are used interchangeably herein and refer to any peptide-linked chain of amino acids, regardless of length, co- translational or post-translational modification.
[0062] "Pharmaceutically acceptable excipient" or "pharmaceutically acceptable carrier" refers to a component that may be included in the compositions described herein and causes no significant adverse toxicological effects to a subject.
[0063] The term "patient," or“subject” as used herein refers to a living organism suffering from or prone to a condition that can be prevented or treated by administration of a compound or composition or combination as provided herein, such as a cancer, and includes both humans and animals. Subjects include, but are not limited to, mammals (e.g., murines, simians, equines, bovines, porcines, canines, felines, and the like), and preferably are human.
[0064] “Administering" refers to the delivery of a therapeutic agent to a subject, using any of the various methods and delivery systems known to those skilled in the art.
Exemplary routes of administration include intravenous, intramuscular, subcutaneous, intraperitoneal, spinal or other parenteral routes of administration, for example by injection or infusion. The phrase "parenteral administration" as used herein means modes of
administration other than enteral and topical administration, usually by injection, and includes, without limitation, intravenous, intramuscular, intraarterial, intrathecal,
intralymphatic, intralesional, intracapsular, intraorbital, intracardiac, intradermal,
intraperitoneal, transtracheal, subcutaneous, subcuticular, intraarticular, subcapsular, subarachnoid, intraspinal, epidural and intrastemal injection and infusion, as well as in vivo electroporation. A therapeutic agent can be administered via a non-parenteral route, or orally. Other non-parenteral routes include a topical, epidermal or mucosal route of administration, for example, intranasally, vaginally, rectally, sublingually or topically. Administering of one
or more therapeutic agents can also be performed for each of the therapeutic agents, for example, once, a plurality of times, and/or over one or more extended periods.
[0065] A "cancer" refers a broad group of various diseases characterized by the uncontrolled growth of abnormal cells in the body. A "cancer" or "cancer tissue" includes a tumor, and as used herein, encompasses both a solid tumor as well as tumor cells found in a bodily fluid such as blood, and includes metastatic cancer. Unregulated cell division and growth results in the formation of malignant tumors that can invade neighboring tissues and can also metastasize to distant parts of the body through the lymphatic system or
bloodstream. Following metastasis, the distal tumors can be said to be "derived from" a pre metastasis tumor.
[0066] The term "immunotherapy" refers to the treatment of a subject by a method comprising inducing, enhancing, suppressing, or otherwise modifying an immune response.
[0067] The term,“tumor neoantigen”, is used to describe any tumor specific antigen comprising one or more mutations as compared to the host’s exome and is used
synonymously herein with the term,“cancer neoantigen”.
[0068] The term,“tumor neoepitope”, is used for any immunogenic mutation in a tumor antigen and is used synonymously herein with the term,“cancer neoepitope”.
[0069] A“tumor neoepitope sequence” as used herein is the sequence comprising the neoepitope in an antigenic subunit, and is used synonymously with the term,“cancer neoepitope sequence”.
[0070] As used herein, a“plurality” refers to 3 or more of a given item.
[0071] The terms,“therapeutic anticancer vaccine” and“therapeutic cancer vaccine” are used synonymously to describe a vaccine that is used for destroying or reducing the number of tumor cells already present in a patient.
[0072] A "therapeutically effective amount" or "therapeutically effective dosage" of a therapeutic agent is any amount of an agent, when used alone or in combination with another therapeutic agent, that is effective to, for example, protect a subject against the onset of a disease such as cancer or promote disease regression evidenced by a decrease in severity of disease symptoms, an increase in frequency and duration of disease symptom-free periods, or
a prevention of impairment or disability due to the disease affliction. The ability of a therapeutic agent to promote disease regression can be evaluated using a variety of methods known to the skilled practitioner, such as in human subjects during clinical trials, in animal model systems predictive of efficacy in humans, or by assaying the activity of the agent in in vitro assays. See, for instance, the supporting examples.
[0073] The term "substantially homologous" or“substantially identical” means that a particular subject sequence, for example, a mutant sequence, varies from a reference sequence by one or more substitutions, deletions, or additions, the net effect of which does not result in an adverse functional dissimilarity between the reference and subject sequences. For purposes herein, a sequence having greater than 95 percent homology (identity), equivalent biological activity (although not necessarily equivalent strength of biological activity), and equivalent expression characteristics to a given sequence is considered to be substantially homologous (identical). For purposes of determining homology, truncation of the mature sequence should be disregarded.
[0074] With regard to polypeptide and polynucleotide sequence comparisons, the phrase "at least 80% sequence identity" may be used herein. This expression refers to a sequence identity of at least 80%, at least 81%, at least 82%, at least 83%, at least 84%, at least 85%, at least 86%, at least 87%, at least 88%, at least 89%, at least 90%, at least 91%, at least 92%, at least 93%, at least 94%, at least 95%, at least 96%, at least 97%, at least 98%, or at least 99% to the respective reference polypeptide or to the respective reference
polynucleotide. Preferably, the polypeptide in question and the reference polypeptide exhibit the indicated sequence identity over a continuous stretch of 20, 30, 40, 45, 50, 60, 70, 80, 90, 100 or more amino acids or over the entire length of the reference polypeptide. Preferably, the polynucleotide in question and the reference polynucleotide exhibit the indicated sequence identity over a continuous stretch of 60, 90, 120, 135, 150, 180, 210, 240, 270, 300 or more nucleotides or over the entire length of the reference polypeptide.
Overview
[0075] In an effort to address at least some of the shortcomings associated with current anti-cancer vaccine strategies, such as for example, weak immune responses due to suppression in T cell growing capacity by a cancerous tumor itself, provided herein is a combination immunotherapy method based upon administration of a personalized
neoantigen-based DNA cancer vaccine and a T cell expander, i.e., an entity that is effective to drive specific clonal T cell expansion to the vaccine epitopes.
[0076] IL-2 stimulates immune cell proliferation and activation through a receptor signaling complex containing alpha (IL2Ra, CD25), beta (IL2R , CD122) and common gamma chain receptors (yC’ CD 132). At high doses, IL-2 binds to heterodimeric IL2R.Py receptor leading to desired expansion of tumor killing CD8+ memory effector T (CD8 T) cells. However, IL-2 also binds to its heterotrimeric receptor IL2Ro y with greater affinity, which expands immunosuppressive CD4+, CD25+ regulatory T cells (Tregs), which may lead to an undesirable effect for cancer immunotherapy. Thus, in an effort to overcome one or more drawbacks associated with IL-2-based anti-cancer vaccination strategies, provided herein is a treatment modality that combines a neoantigen-based DNA cancer vaccine against tumor specific antigens with administration of a T cell expander. In one or more preferred embodiments, the T cell expander is an IL-2Raf -biased agonist. Without being bound by theory, it has been discovered that by utilizing a long-acting IL-2 compound in which a region that interacts with the IL2Ra subunit responsible for activating immunosuppressive Tregs is masked (i.e., its activity suppressed or dampened), e.g., RSLAIL-2, optionally further combined with a checkpoint inhibitor, vaccination-induced epitope specific T cell responses can be expanded to achieve superior therapeutic efficacy, as will become apparent from the instant disclosure and the supporting examples.
Vaccines
[0077] The treatment methods provided herein comprise administering (i) a vaccine, i.e., an anti cancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens (“neoantigen-based DNA cancer vaccine”), and (ii) a compound effective to stimulate/expand production of T cells (i.e., effector T cells,“a T cell expander”) for treating a patient having cancer, optionally in combination with a check point inhibitor.
[0078] The compositions, combinations, and methods provided herein find use in, among other things, both clinical and pre-clinical applications. As demonstrated in the supporting pre-clinical examples conducted in established in vivo models of cancer, administration of a T cell expander, such as RSLAIL-2, in combination with a neoantigen- based DNA cancer vaccine, optionally further combined with a checkpoint inhibitor, is effective to significantly expand/enhance the T cell response to vaccine-encoded neoantigens
in a subject, to thereby provide a strong-neoantigen focused immune response for fighting cancer.
[0079] More particularly, pre-clinical studies described in the accompanying examples illustrate that the combination of the exemplary neoantigen-based DNA cancer vaccine, VB10.NEO, administered in combination with the exemplary T cell expander, RSLAIL-2, appears to synergistically boost neoepitope-specific T cells responses, resulting in a 5-fold increase in the number of neoepitope-specific T cell responses compared to
VB10.NEO alone. Mice treated with VB10.NEO in combination with the T cell expander, RSLAIL-2, showed both a stronger response to each neoepitope and to increased numbers of neoepitopes, demonstrating that both the breadth and depth of the immune response were elevated as a result of the combination therapy. The VB10.NEO and RSLAIL-2 combination produced an even greater effect on CD8+ T cell responses as the combination elicited a neoepitope-specific CD8+ T cell response to more neoepitopes compared to either immunotherapeutic agent when administrated alone, further strengthening the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses. In a therapeutic tumor model, an increased number of complete responders was observed in mice treated with the exemplary triple immunotherapeutic combination of VB10.NEO, RSLAIL-2 and an anti-PD- 1 antibody (as representative of a combination therapy comprising administration of a personalized neoantigen-based DNA cancer vaccine, a T cell expander, and optionally, a checkpoint inhibitor), further demonstrating the advantages of combining such reagents to thereby activate non-overlapping mechanisms of immunotherapy and create an effective treatment of established tumors.
[0080] Therapeutic anticancer neoepitope vaccines suitable for use in the methods provided herein are described in U.S. Patent Publication No. 2019/0022202, along with methods describing their preparation and use, which is incorporated herein by reference. Briefly, the therapeutic neoepitope vaccine is an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens. The neoepitopes comprised in the individualized DNA vaccine are presented to the immune system as a dimeric protein called a vaccibody. Dimeric proteins called vaccibodies are described in detail in WO 2004/076489, which is incorporated herein by reference.
[0081] For example, the neoantigen-based DNA cancer vaccine may comprise an immunologically effective amount of a DNA polynucleotide comprising a nucleotide
sequence encoding at least (i) a targeting unit (also referred to as a targeting module), (ii) a dimerization unit (also referred to as a dimerization module), (iii) a first linker and (iv) an antigenic unit (also referred to as an antigenic module), wherein the antigenic unit comprises n-1 antigenic subunits; n is an integer of from 3 to 50. Each antigenic subunit comprises at least a part of a cancer neoepitope sequence and a second linker. Additionally, the antigenic unit further comprises a final cancer neoepitope sequence.
[0082] The vaccines suitable for use in the instant methods are designed to evoke a cell-mediated immune response through activation of T cells against the neoantigens. T cells recognize neoepitopes when they have been processed and presented complexed to a MHC molecule.
[0083] Preferably, the neoantigen vaccine comprises a DNA polynucleotide encoding a polypeptide comprising three units, i.e. a targeting unit (or module), a dimerization unit (or module) and an antigenic unit (or module). Due to the dimerization unit, the polypeptide forms a dimeric protein called a vaccibody. The genes encoding the three units are genetically engineered to be expressed as one gene. When expressed in vivo, the poly peptides/ dimeric proteins target antigen presenting cells (APCs), which results in enhanced vaccine potency compared to identical non-targeted antigens. See, for example, FIG. 13 which provides an exemplary plasmid map illustrating different functional elements.
[0084] In the vaccines described herein, the antigenic unit comprises antigenic subunits, wherein each subunit comprises a cancer neoepitope sequence or at least a part of a cancer neoepitope sequence. The neoepitope sequence is obtained by sequencing tumor DNA (or RNA) and identifying tumor specific mutations representing neoantigens. As a result, a personalized neoantigen vaccine is obtained that specifically targets the identified tumor antigens.
[0085] In some embodiments, the therapeutic anticancer neoepitope vaccine comprises an immunologically effective amount of a polynucleotide comprising a nucleotide sequence encoding (i) a targeting unit, (ii) a dimerization unit, (iii) a first linker, (iv) an antigenic unit, wherein the antigenic unit comprises n-1 antigenic subunits, and each subunit comprises at least a part of a cancer neoepitope sequence and a second linker, where the antigenic unit further comprises a final cancer neoepitope sequence, wherein n is an integer of from 3 to 50. Thus, in this embodiment, the vaccine comprises n neoepitopes or
neoepitope sequences and n-1 second linkers, wherein n is an integer from 3 to 50 (with additional exemplary sub-ranges provided below).
[0086] The antigenic unit comprises a plurality of tumor neoepitopes, wherein each neoepitope corresponds to a mutation identified in a tumor neoantigen in a specific patient. That is to say, all selected neoantigens are unique and specific for the individual patient. The mutation may be any mutation leading to a change in at least one amino acid. For example, the mutation may be one of the following: a non-synonymous mutation leading to a change in the amino acid, a mutation leading to a frame shift and thereby a completely different open reading frame in the direction after the mutation, a read-through mutation in which a stop codon is modified or deleted leading to a longer protein with a tumor-specific neoepitope, splice mutations that lead to a unique tumor-specific protein sequence, chromosomal rearrangements that give rise to a chimeric protein with a tumor-specific neoepitope at the junction of the two proteins.
[0087] In the antigenic unit, all but the last of the tumor neoepitopes are arranged in antigenic subunits, wherein each subunit consists of a tumor neoepitope sequence and a second linker, whereas the last subunit comprises a neoepitope only, i.e. no second linker.
Due to the separation of the tumor neoepitope sequences by the second linker, each neoepitope is presented in an optimal way to the immune system.
[0088] The cancer neoepitope sequence preferably has a length suitable for presentation by the MHC molecules. Thus, in a preferred embodiment, the cancer neoepitope is from 7 to 30 amino acids long. More preferred are cancer neoepitope sequences having a length of from 7 to 10 amino acids or cancer neoepitope sequences having a length of from 13 to 30 amino acids, e.g., from 20 to 30 amino acids, e.g., comprised of 27 amino acids. Preferably, a plurality of different neoepitopes are included in the antigenic unit.
Accordingly, a preferred approach is to include as many neoepitopes as possible into the vaccine to thereby attack the tumor efficiently whilst not compromising the vaccine’s ability to activate T cells against the neoepitopes due to dilution of the desired T cell effect. Also, to secure that all neoepitopes are loaded efficiently to the same antigen presenting cell, the neoepitopes are arranged as one amino acid chain instead of as discrete peptides.
[0089] To prepare the vaccine, the tumor exome is analyzed to identify neoantigens and select the most antigenic neoepitopes. Generally, at least 3 neoepitopes are incorporated
into the vaccine, preferably at least 5 neoepitopes, more preferably at least 7 neoepitopes, such as at least 10 neoepitopes, etc., in order to efficiently be able to target substantially all tumor cells.
[0090] More preferably, the vaccine comprises at least 10 neoepitopes. In another preferred embodiment, the vaccine comprises at least 15 neoepitopes, such as at least 20 neoepitopes. For example, the vaccine may comprise from 3 to 50 neoepitopes, or from 3 to 30 neoepitopes, or from 3 to 20 neoepitopes, or from 3 to 15 neoepitopes, such as from 3 to 10 neoepitopes, and consequently n is preferably an integer of from 3 to 50, such as from 3 to 30, such as from 5 to 25, such as from 3 to 20, such as from 3 to 15, such as from 3 to 10. In some preferred embodiments the vaccine comprises from 10 to 20 neoepitopes.
[0091] The antigenic unit may, for example, comprise one copy of each cancer neoepitope, so that when 10 neoepitopes are included in the vaccine, a cell-mediated immune response against 10 different neoepitopes can be elicited. Alternatively, if however only a few relevant antigenic mutations are identified, then the antigenic unit may comprise at least two copies of at least one neoepitope in order to strengthen the immune response to these neoepitopes.
[0092] The length of the antigenic unit is primarily determined by the length of the neoepitopes and the number of neoepitopes arranged in the antigenic unit, and is from, for example, about 21 to 1500, preferably from about 30 amino acids to about a 1000 amino acids, more preferably from about 50 to about 500 amino acids, such as from about 100 to about 400 amino acids, from about 100 to about 300 amino acids.
[0093] The neoepitopes may be ordered in the antigenic unit as described below, in order to enhance the immune response. For example, depending on the selected neoepitopes, the antigenic subunits may be arranged in the order of more antigenic to less antigenic in the direction from the first linker towards the final neoepitope. Alternatively, particularly if the hydrophilicity/hydrophobicity varies greatly among the neoepitopes, it is preferred that the most hydrophobic antigenic subunit(s) is/are substantially positioned in the middle of the antigenic unit and the most hydrophilic antigenic subunit(s) is/are positioned at the beginning and/or end of the antigenic unit. Alternatively, the neoepitopes may be arranged alternating between a hydrophilic and a hydrophobic neoepitope. Preferably, the GC rich neoepitopes
are spaced so that GC clusters are avoided, preferably GC rich neoepitopes are spaced by at least one subunit.
[0094] The second linker is designed to be non-immunogenic and is preferably also a flexible linker, whereby the tumor neoepitopes, in spite of the high numbers of antigenic subunits present in the antigenic unit, are presented in an optimal manner to the T cells. Preferably, the length of the second linker is from 4 to 20 amino acids to secure the flexibility. In another preferred embodiment, the length of the second linker is from 8 to 20 amino acids, such as from 8 to 15 amino acids, for example 8 to 12 amino acids or such as for example from 10 to 15 amino acids. In a particular embodiment, the length of the second linker is 10 amino acids.
[0095] For example, in a specific embodiment, the vaccine encodes a protein comprised of a neoepitope antigenic unit comprising 10 neoepitopes, wherein the second linkers have a length of from 8 to 20 amino acids, such as from 8 to 15 amino acids, for example 8 to 12 amino acids or such as, for example, from 10 to 15 amino acids. In a particular embodiment, the vaccine encodes a protein comprised of a neoepitope antigenic unit comprising 10 neoepitopes, where the second linkers have a length of 10 amino acids.
[0096] In yet another illustrative example, the DNA vaccine encodes a protein comprised of a neoepitope antigenic unit comprising from 10-20 neoepitopes, each of 27 amino acids, where the second linkers have a length of 10 amino acids.
[0097] The second linker is preferably identical in all antigenic subunits. If, however, one or more of the neoepitopes comprise an amino acid motif similar to the linker, it may be an advantage to substitute the neighboring second linkers with a second linker of a different sequence. Also, if a neoepitope-second linker junction is predicted to constitute an epitope in itself, then a second linker of a different sequence might be used. The second linker is preferably a serine-glycine rich linker, such as a flexible GGGGS (SEQ ID NO:34) linker, such as, for example, GGGSS (SEQ ID NO:35), GGGSG (SEQ ID NO:36), GGGGS (SEQ ID NO:34) or multiple variants thereof such as GGGGSGGGGS (SEQ ID NO:33) or (GGGGS)m, (GGGSS)m, (GGGSG)m. where m is an integer from 1 to 5 (e.g., 1, 2, 3, 4, or 5), from 1 to 4 or from 1 to 3. In some preferred embodiments, m is 2. In some other preferred embodiments, the serine-glycine linker further comprises at least one leucine (L), such as at
least 2 or at least 3 leucines. The serine-glycine linker may for example comprise 1, 2, 3 or 4 leucines. In some instances, the serine-glycine linker comprises 1 leucine or 2 leucines.
[0098] Examples of second linkers include the following: for example, the second linker may comprise or consist of the sequence LGGGS (SEQ ID NO:37), GLGGS (SEQ ID NO:38), GGLGS (SEQ ID NO:39), GGGLS (SEQ ID NO:40) or GGGGL (SEQ ID NO:41); alternatively, the second linker may comprise or consist of a sequence LGGSG (SEQ ID NO:42), GLGSG (SEQ ID NO:43), GGLSG (SEQ ID NO:44), GGGLG (SEQ ID NO:45) or GGGSL (SEQ ID NO:46); or the second linker may comprise or consist of the sequence LGGSS (SEQ ID NO:47), GLGSS (SEQ ID NO:48), GGLSS (SEQ ID NO:49), GGGLS (SEQ ID NO:50) or GGGSL (SEQ ID NO:51). As further examples, the second linker may comprises or consist of the sequence LGLGS (SEQ ID NO:52), GLGLS (SEQ ID NO:53), GLLGS (SEQ ID NO:54), LGGLS (SEQ ID NO:55) or GLGGL (SEQ ID NO:56), or may comprise or consist of the sequence LGLSG (SEQ ID NO:57), GLLSG (SEQ ID NO:58), GGLSL (SEQ ID NO:59), GGLLG (SEQ ID NO:60) or GLGSL (SEQ ID NO:61), or may comprise or consist of the sequence LGLSS (SEQ ID NO:62), GLGLS (SEQ ID NO:63), GGLLS (SEQ ID NO:64), or GLGSL (SEQ ID NO:65).
[0099] Additional exemplary second linkers for use in the neoepitope antigenic unit separating the neoepitopes include serine-glycine rich linkers such as the following:
SGGGGSGGGG (SEQ ID NO:67), GSGGGGSGGG (SEQ ID NO:68), GGSGGGGSGG (SEQ ID NO:69), GGGSGGGGSG (SEQ ID NO:70), GGGSSGGGSS (SEQ ID NO:71), SGGGSSGGGS (SEQ ID NO:72), SSGGGSSGGG (SEQ ID NO:73), GSSGGGSSGG (SEQ ID NO:74), GGSSGGGSSG (SEQ ID NO:75), and GGGSSGGGSG (SEQ ID NO:76). In some preferred embodiments, the second linker is selected from linkers of SEQ ID NO:67 to SEQ ID NO:76. In some other embodiments, the second linker is selected from linkers of SEQ ID NO:67 to SEQ ID NO:76, in order of preference with a linker of SEQ ID NO:67 being more preferred than a linker of SEQ ID NO: 68, and so forth. As described above, the linkers may change from construct to construct for the various individualized vaccines, because in assembling the neoepitope antigenic unit for the construct, the junctional sequences are evaluated. As a result, a first preferred linker may be replaced with another candidate linker that excludes a junctional epitope that resembles a sequence found in the human proteome. Preferred serine/gly cine-rich linkers, e.g., 10 amino acid linkers, contain
from 6 to 9 glycines (e.g., 6, 7, 8 or 9), or from 6 to 8 glycines. In some preferred embodiments, the remaining non-glycine amino acids contained in the linker are serine(s).
[00100] Further illustrative sequences for the second linker are described in U.S.
Patent Publication No. 2019/0022202.
[00101] Examples of preferred vaccines include those comprising at least 10 neoepitopes that are separated by 10 amino acid linkers, or those comprising at least 15 neoepitopes that are separated by 10 amino acid linkers, such as at least 20 neoepitopes that are separated by 10 amino acid linkers.
[00102] The term "targeting unit" as used herein refers to a unit that delivers the polypeptide/protein with its antigen to an antigen presenting cell for MHC class Il-restricted presentation to CD4+ T cells or for providing cross presentation to CD8+ T cells by MHC class I restriction. The targeting unit is connected through the dimerization unit to the antigenic unit, wherein the latter is in either the COOH-terminal or the ML-terminal end of the poly peptide/ dimeric protein. It is preferred that the antigenic unit is in the COOH- terminal end of the polypeptide/dimeric protein. The targeting unit is designed to target the polypeptide/dimeric protein to surface molecules expressed on the relevant antigen presenting cells, such as molecules expressed exclusively on subsets of dendritic cells (DC).
[00103] Examples of such target surface molecules on APC are human leukocyte antigen (HLA), cluster of differentiation 14 (CD 14), cluster of differentiation 40 (CD40), chemokine receptors and Toll-like receptors (TLRs). HLA is a major histocompatibility complex (MHC) in humans. The Toll-like receptors may for example include TLR-2, TLR-4 and/or TLR-5. The polypeptide/dimeric protein can be targeted to such surface molecules by means of targeting units comprising for example antibody binding regions with specificity for CD14, CD40, or Toll- like receptor; ligands, e.g. soluble CD40 ligand; natural ligands like chemokines, e.g. RANTES or MIP-la; or bacterial antigens like for example flagellin.
[00104] An illustrative targeting unit has affinity for an MHC class II protein. Thus, in one embodiment, the nucleotide sequence encoding the targeting unit encodes the antibody variable domains (VL and VH) with specificity for MHC class II proteins, selected from the group consisting of anti-HLA-DP, anti-HLA-DR and anti-HLA-II. Alternatively, the targeting unit has affinity for a surface molecule selected from the group consisting of CD40, TLR-2, TLR-4 and TLR-5. Thus, in one embodiment the nucleotide sequence encoding the
targeting unit encodes the antibody variable domains (VL and VH) with specificity for anti- CD40, anti-TLR-2, anti-TLR-4 and anti-TLR-5. In one embodiment the nucleotide sequence encoding the targeting unit encodes flagellin, which has affinity for TLR-5. Preferably, the targeting unit has affinity for a chemokine receptor selected from CCR1, CCR3 and CCR5. More preferably, the nucleotide sequence encoding the targeting unit encodes the human chemokine macrophage inflammatory protein- 1 alpha, hMIP-la (LD78beta), which binds to its cognate receptors, CCR1, CCR3 and CCR5 expressed on the cell surface of antigen- presenting cells (APCs). See, e.g., FIG. 12, which includes the nucleotide sequence encoding the VBIO.NEO protein with the targeting unit identified therein (see, e.g., nucleotides 1143- 1421).
[00105] The term“dimerization unit” as used herein, refers to a sequence of amino acids between the antigenic unit and the targeting unit. Thus, the dimerization unit serves to connect the antigenic unit and the targeting unit and facilitates dimerization of two monomeric polypeptides into a dimeric protein. Furthermore, the dimerization unit also provides the flexibility in the polypeptide/dimeric protein to allow optimal binding of the targeting unit to the surface molecules on the antigen presenting cells (APCs), even if they are located at variable distances. The dimerization unit may be any unit that fulfils these requirements.
[00106] The term "hinge region" refers to a peptide sequence of the dimeric protein that facilitates the dimerization. The hinge region functions as a flexible spacer between the units allowing the two targeting units to bind simultaneously to two target molecules on APCs, even if they are expressed with variable distances. The hinge region may be Ig derived, such as derived from IgG3. The hinge region may contribute to the dimerization through the formation of covalent bond(s), e.g. disulfide bridge(s). Thus, in one embodiment the hinge region has the ability to form one or more covalent bonds. The covalent bond can for example be a disulfide bridge.
[00107] In a preferred embodiment, the dimerization unit consists of hinge exons hi and h4 connected through a third linker to a CH3 domain of human IgG3. See, for example, FIG. 12, and the illustrative dimerization unit identified therein (hi and h4 and CH3 domains of hIgG3, nucleotides 1422-1853).
[00108] The dimerization unit may have any orientation with respect to antigenic unit and targeting unit. In one embodiment, the antigenic unit is in the COOH- terminal end of the dimerization unit with the targeting unit in the N-terminal end of the dimerization unit. In another embodiment, the antigenic unit is in the N-terminal end of the dimerization unit with the targeting unit in the COOH-terminal end of the dimerization unit. It is preferred that the antigenic unit is in the COOH end of the dimerization unit.
[00109] The antigenic unit and the dimerization unit are preferably connected through a first linker. The first linker may comprise a restriction site in order to facilitate the construction of the polynucleotide. It is, in some instances, preferred that the first linker is a GLGGL (SEQ ID NO:56) linker or a GLSGL (SEQ ID NO:66) linker.
[00110] The polynucleotide may further comprise a nucleotide sequence encoding a signal peptide. The signal peptide is constructed to allow secretion of the polypeptide encoded by the polynucleotide in the cells transfected with said polynucleotide. Any suitable signal peptide may be used. Examples of suitable peptides are an Ig VH signal peptide, a human TPA signal peptide, and a signal peptide.
[00111] In reference to polynucleotide sequences, the polynucleotide typically comprises a DNA nucleotide sequence, either double stranded or single stranded. Preferably, the polynucleotide is optimized to the desired species to express a polypeptide, i.e. it is preferred that the polynucleotide sequence is human codon optimized.
[00112] Exemplary mouse neoantigen-based DNA cancer vaccines comprising VB10.NEO pDNA constructs, VB4011 and VB4061, are described in the supporting examples. Additionally, an exemplary human neoantigen-based DNA cancer vaccine is described in Example 4. An illustrative pVBlO.NEO plasmid map is shown in FIG. 13.
[00113] The vaccine may further comprise a pharmaceutically acceptable carrier, diluent, adjuvant or buffer. Pharmaceutically acceptable carriers, diluents, and buffers include, but are not limited to, saline, buffered saline, dextrose, water, glycerol, ethanol, sterile isotonic aqueous buffer, and combinations thereof.
[00114] In particular, for vaccines comprising polynucleotides, a carrier may include molecules that ease transfection of cells and adjuvants and may include plasmids comprising
nucleotide sequences encoding chemokines or cytokines in order to enhance the immune response.
[00115] The vaccine may be formulated into any suitable formulation, such as a liquid formulation for intradermal or intramuscular injection. The vaccine may be administered in any suitable way for either a polypeptide/protein vaccine or a polynucleotide vaccine, such as administered by injection intradermally, intramuscular, subcutaneously, or by mucosal or epithelial application, such as intranasally, orally, enteral or to the bladder. The vaccine is preferably administered intramuscular or intradermally when the vaccine is a polynucleotide vaccine. In some embodiments, the vaccine is administered by intranodal injection. As used herein, the term“intranodal injection” means that the vaccine is injected into the lymph nodes.
T cell Expander
[00116] The therapeutic combinations, methods and the like described herein comprise as a T cell expander. As described above, a T cell expander is a compound or composition effective to stimulate/expand production of T cells. Preferably, the T cell expander, when administered in combination with the neoantigen-based DNA cancer vaccine, is effective to enhance specific clonal T cell expansion to vaccine epitopes. Preferably, the T cell expander is effective to enhance specific clonal T cell expansion to vaccine epitopes over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander to a degree that is greater than additive, and the combination is not limited in this regard. Even more preferably, the T cell expander is effective to enhance specific clonal T cell expansion to vaccine epitopes in a synergistic fashion over that achieved upon administration of the neoantigen-based DNA cancer vaccine in the absence of the T cell expander.
[00117] Illustrative T cell expanders include interleukin-2 (e.g., aldesleukin), interleukin-15, and interferon-a, and an anti-CD3 antibody such as, e.g., OKT3. In one or more particular embodiments, the T cell expander is a prodrug of an interleukin-2 (e.g., aldesleukin, chemical name, des-alanyl-1, serine- 125 human interleukin-2), wherein the interleukin-2 is modified by releasable covalent attachment of multiple polyethylene glycol moieties. In some particular embodiments, the prodrug is essentially inactive upon administration, and following administration, the polyethylene glycol moieties are slowly
released to provide bioactive species, thereby avoiding overstimulation of the immune system. Conjugates of an interleukin-2 moiety modified by covalent attachment of one or more polyethylene glycol moieties are described, for example, in U.S. Patent No. 9,861,705.
[00118] In yet one or more particular embodiments, the T cell expander is an interleukin-2 receptor beta (IL-2R ) selective agonist as described, for example, in U.S. Patent No. 10,101,587, and generally referred to therein as RSLAIL-2.
[00119] The releasable PEG comprised in RSLAIL-2, is based upon a 2,7,9-substituted fluorene as shown below, with poly (ethylene glycol) chains extending from the 2- and 7- positions on the fluorene ring via amide linkages (fluorene-C(O)-NH-), and having releasable covalent attachments to interleukin-2 via attachment to a carbamate nitrogen atom attached via a methylene group (-CH2-) to the 9-position of the fluorene ring. In this regard, in some embodiments, the T cell expander is a composition comprising compounds encompassed by the following formula:

Formula (I) wherein IL-2 is an interleukin-2; or pharmaceutically acceptable salts thereof, where each“n” is an integer from about 3 to about 4000, or more preferably is an integer from about 200- 300. The foregoing composition is referred to generally as RSLAIL-2 or multi(2,7-(bis- methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2. In reference to the foregoing formula, RSLAIL-2 is a composition comprising compounds encompassed by formula (I), that is, having four, five or six branched PEG moieties as shown above, i.e., 2,7-(bis-methoxyPEG-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate moieties, releasably covalently attached to amino groups of IL-2. In certain preferred embodiments,“n” in each of the polyethylene glycol chains has a value, on average, of about 227 (i.e., where each polyethylene glycol chain extending from the central fluorenyl core has a weight average molecular weight of about 10,000 daltons, such that the weight average
molecular weight of the overall branched PEG moiety is about 20,000 daltons), i.e., referred to herein more particularly as multi(2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9- yl)methyl N-carbamate)interleukin-2 or as (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H- fluorene-9-yl)methyl N-carbamate)4-6interleukin-2. In one or more embodiments, the value of“n” in each of the polyethylene glycol chains is substantially the same, that is to say that, for example, the two PEG chains extending from the central fluorenyl core have substantially the same weight average molecular weight.
[00120] In reference to the embodiment described above, multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 comprises compounds encompassed by the following formula:

Formula (II), where the average molecular weight of each polyethylene chain comprised in the branched PEG moiety is about 10,000 daltons, such that the overall molecular weight of each branched PEG moiety is about 20,000 daltons.
[00121] In other related embodiments, multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2 comprises compounds encompassed by the following formula:

Formula (III), wherein the average number of branched PEG moieties having a structure as shown and releasably covalently attached to the IL-2 moiety is six, i.e., (2,7-(bis-methoxyPEGiokd-
carboxyamide)(9h-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2, also referred to in some instances as falling within the designation“RSLAIL-2” (releasable IL-2). T cell expander compounds and compositions encompassed by Formulae (I), (II), and (III) are generally designated“RSLAIL-2”.
[00122] The releasable PEG moiety(moieties) comprised in RSLAIL-2 is based upon a 2,7,9-substituted fluorene with poly(ethylene glycol) chains extending from the 2- and 7- positions of the fluorene ring via amide linkages (fluorene-C(O)-NH-), to provide a branched PEG. The fluorenyl-based branched PEG moieties are releasably covalently attached to amino groups of the interleukin-2 moiety. The linkage between interleukin-2 amino groups and the fluorenyl-based branched PEG moiety is a carbamate linkage attached via a methylene group (-CH2-) to the 9-position of the fluorene ring. Releasable PEGs having this general structure typically undergo a b-elimination reaction under physiological conditions to slowly release the PEG moieties that are covalently attached to IL-2. It is believed that the PEG moieties release sequentially following administration.
[00123] In one or more embodiments, the IL-2R -biased agonist composition, RSLAIL-2, contains no more than 10% (based on a molar amount), and preferably no more than 5% (based on a molar amount), of compounds encompassed by the following formula:

Formula (IV) wherein IL-2 is an interleukin-2 (e.g., aldesleukin), and“m” (referring to the number of branched polyethylene glycol moieties attached to IL-2) is an integer selected from the group consisting of 1, 2, 3, 7 and >7; or pharmaceutically acceptable salts thereof.
[00124] In some embodiments, e.g., in reference to Formula (I) or Formula (II), the IL- 2R -biased agonist possesses on average about six branched polyethylene glycol moieties releasably attached to IL-2. See, for example, Formula (III). In some further particular embodiments, e.g., in reference to Formula (I), Formula (II), Formula (III), the IL-2R -
selective agonist is generally considered to be an inactive prodrug, i.e., that is inactive upon administration, and by virtue of slow release of the polyethylene glycol moieties in vivo following administration, provides active conjugated forms of interleukin-2 having fewer PEG moieties attached than in the conjugate that is initially administered.
[00125] As provided herein, reference to“multi(2,7-(bis-methoxyPEG- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)interleukin-2” or“RSLAIL-2” is expressly intended to encompass compounds and compositions as set forth in Formula (I), Formula (II), and/or Formula (III), including compositions encompassed by Formula (IV) in reference to any one or more of Formulae (I), (II) and (III).
[00126] As described herein, RSLAIL-2 is considered to be an IL-2R -biased (i.e., selective) agonist. For example, RSLAIL-2 referenced in the accompanying examples, exhibits about a 60-fold decrease in affinity to IL-2Ra.p relative to IL-2, but only about a 5- fold decrease in affinity IL-2R relative to IL-2. See, for example, Example 20 in PCT Publication No. WO 2018/132496 describing the binding affinity of RSLAIL-2 to IL-2Ra and IL-2R .
[00127] To determine average degree of PEGylation for a composition such as described in the formula above, typically the protein is quantified by a method such as a bicinchoninic acid (BCA) assay or by UV analysis, to determine moles of protein in the sample. The PEG moieties are then released by exposing the sample to conditions in which the PEG moieties are released, and the released PEG is then quantified (e.g., by BCA or UV) and correlated with moles protein to determine average degree of PEGylation.
[00128] RSLAIL-2 can be considered to be an inactive prodrug, i.e., it is inactive upon administration, and by virtue of slow release of the polyethylene glycol moieties in vivo, provides active conjugated forms of interleukin-2 that are effective to achieve sustained concentrations at a tumor site.
[00129] Additional exemplary compositions of RSLAIL-2 comprise compounds in accordance with the above formulae wherein the overall polymer portion of the molecule has a weight average molecular weight in a range of from about 250 daltons to about 90,000 daltons. Additional suitable ranges include weight average molecular weights in a range selected from about 1,000 daltons to about 60,000 daltons, in a range of from about 5,000 daltons to about 60,000 daltons, in a range of about 10,000 daltons to about 55,000 daltons, in
a range of from about 15,000 daltons to about 50,000 daltons, and in a range of from about 20,000 daltons to about 50,000 daltons.
[00130] Additional illustrative weight-average molecular weights for the polyethylene glycol polymer portion include about 200 daltons, about 300 daltons, about 400 daltons, about 500 daltons, about 600 daltons, about 700 daltons, about 750 daltons, about 800 daltons, about 900 daltons, about 1,000 daltons, about 1,500 daltons, about 2,000 daltons, about 2,200 daltons, about 2,500 daltons, about 3,000 daltons, about 4,000 daltons, about 4,400 daltons, about 4,500 daltons, about 5,000 daltons, about 5,500 daltons, about 6,000 daltons, about 7,000 daltons, about 7,500 daltons, about 8,000 daltons, about 9,000 daltons, about 10,000 daltons, about 11,000 daltons, about 12,000 daltons, about 13,000 daltons, about 14,000 daltons, about 15,000 daltons, about 20,000 daltons, about 22,500 daltons, about 25,000 daltons, about 30,000 daltons, about 35,000 daltons, about 40,000 daltons, about 45,000 daltons, about 50,000 daltons, about 55,000 daltons, about 60,000 daltons, about 65,000 daltons, about 70,000 daltons, and about 75,000 daltons. In some embodiments, the weight-average molecular weight of the branched polyethylene glycol polymer is about 20,000 daltons.
[00131] As described above, RSLAIL-2 may be in the form of a pharmaceutically- acceptable salt. Typically, such salts are formed by reaction with a pharmaceutically- acceptable acid or an acid equivalent. The term "pharmaceutically-acceptable salt" in this respect, will generally refer to the relatively non-toxic, inorganic and organic acid addition salts. These salts can be prepared in situ in the administration vehicle or the dosage form manufacturing process, or by separately reacting a long-acting interleukin-2 as described herein with a suitable organic or inorganic acid, and isolating the salt thus formed.
Representative salts include the hydrobromide, hydrochloride, sulfate, bisulfate, phosphate, nitrate, acetate, valerate, oleate, palmitate, stearate, laurate, benzoate, lactate, phosphate, tosylate, citrate, maleate, fumarate, succinate, tartrate, napthylate, oxylate, mesylate, glucoheptonate, lactobionate, and laurylsulphonate salts and the like. (See, for example,
Berge et al. (1977) "Pharmaceutical Salts", J. Pharm. Sci. 66: 1-19). Thus, salts as described may be derived from inorganic acids such as hydrochloride, hydrobromic, sulfuric, sulfamic, phosphoric, nitric, and the like; or prepared from organic acids such as acetic, propionic, succinic, glycolic, stearic, lactic, malic, tartaric, citric, ascorbic, palmitic, maleic,
hydroxymaleic, phenylacetic, glutamic, benzoic, salicyclic, sulfanilic, 2-acetoxybenzoic, fumaric, toluenesulfonic, methanesulfonic, ethane disulfonic, oxalic, isothionic, and the like.
[00132] In reference to RSLAIL-2, the term "IL-2" as used herein, refers to a moiety having human IL-2 activity. The term,‘residue’, in the context of residue of IL-2, means the portion of the IL-2 molecule that remains following covalent attachment to a polymer such as a polyethylene glycol, at one or more covalent attachment sites, as shown in the formula above. It will be understood that when the unmodified IL-2 is attached to a polymer such as polyethylene glycol, the IL-2 is slightly altered due to the presence of one or more covalent bonds associated with linkage to the polymer(s). This slightly altered form of the IL-2 attached to another molecule is sometimes referred to a "residue" of the IL-2.
[00133] Proteins having an amino acid sequence corresponding to any one of SEQ ID NOs: 1 through 4 described in International Patent Publication No. WO 2012/065086 are exemplary IL-2 proteins. The term substantially homologous means that a particular subject sequence, for example, a mutant sequence, varies from a reference sequence by one or more substitutions, deletions, or additions, the net effect of which does not result in an adverse functional dissimilarity between the reference and subject sequences. For the purposes herein, sequences having greater than 95 percent homology, equivalent biological activity (although not necessarily equivalent strength of biological activity), and equivalent expression characteristics are considered substantially homologous. For purposes of determining homology, truncation of the mature sequence should be disregarded. The IL-2 may be naturally-occurring or may be recombinantly produced. In addition, the IL-2 can be derived from human sources, animal sources, and plant sources. Most preferably, the IL-2 is aldesleukin.
[00134] RSLAIL-2 is generally referred to as long-acting. For the purposes herein, the long acting nature of an IL-2R biased agonist is typically determined using flow cytometry to measure STAT5 phosphorylation in lymphocytes at various time points after
administration of the agonist to be evaluated in mice. As a reference, the signal is lost by around 24 hours with IL-2, but is sustained for a period greater than that for a long-acting IL- 2R -biased agonist. As an illustration, the signal is sustained over several days for (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2.
[00135] RSLAIL-2 possesses immunomodulating properties - in the tumor environment, RSLAIL-2 preferentially activates CD8+ effector T and natural killer (NK) cells over suppressive regulatory T cells (Tregs), such as CD4+ Tregs, by targeting CD 122 receptors found on the surfaces of cancer-fighting cells. See, for example, Example 20 in PCT Publication No. WO 2018/132496, also describing certain immunotherapeutic properties of RSLAIL-2. Among other things, RSLAIL-2 also induces CD4+ T cell activation and promotes proliferation of CD4+, CD8+, and NK cells in the peripheral blood. Thus, since RSLAIL-2 is effective to preferentially activate and expand effector CD8+ T- and NK-cells over Tregs, it is suitable for use as a T cell expander as described herein.
[00136] In accordance with the methods, compositions, and combinations described herein, RLSAIL-2 is provided in an IL-2R -activating amount, to thereby result in T cell expansion activity. One of ordinary skill in the art can determine how much RSLAIL-2 is sufficient to provide clinically relevant agonistic activity at IL-2R .
[00137] In one or more instances, however, the IL-2R -activating amount of RSLAIL- 2 is an amount encompassed by one or more of the following ranges expressed in amount of protein: from about 0.01 to 100 mg/kg; from about 0.01 mg/kg to about 75 mg/kg; from about 0.02 mg/kg to about 60 mg/kg; from about 0.03 mg/kg to about 50 mg/kg; from about 0.05 mg/kg to about 40 mg/kg; from about 0.05 mg/kg to about 30 mg/kg; from about 0.05 mg/kg to about 25 mg/kg; from about 0.05 mg/kg to about 15 mg/kg; from about 0.05 mg/kg to about 10 mg/kg; from about 0.05 mg/kg to about 5 mg/kg; from about 0.05 mg/kg to about 1 mg/kg. Particular illustrative dosing ranges include for example, from about 0.1 mg/kg to about 10 mg/kg, or from about 0.2 mg/kg to about 7 mg/kg or from about 0.2 mg/kg to less than about 0.7 mg/kg.
[00138] In some preferred embodiments, the IL-2R -activating amount of RSLAIL-2 is from about 0.0005 to 0.3 mg/kg; from about 0.001 mg/kg to about 0.3 mg/kg; from about 0.001 mg/kg to about 0.25 mg/kg; from about 0.001 mg/kg to about 0.15 mg/kg; from about 0.001 mg/kg to about 0.05 mg/kg; from about 0.001 mg/kg to about 0.01 mg/kg; from about 0.001 mg/kg to about 0.008 mg/kg; from about 0.001 mg/kg to about 0.005 mg/kg; from about 0.002 mg/kg to about 0.005 mg/kg; from about 0.002 mg/kg to about 0.004 mg/kg, or from about 0.003 mg/kg to about 0.006 mg/kg. In some particular embodiments, RSLAIL-2 is administered at a dose of about 0.006 mg/kg.
[00139] For confirmation, with respect to RSL AIL-2, the amount and extent of the activation can vary widely and still be effective when coupled with administration of a neoantigen-based DNA cancer vaccine, optionally with a checkpoint inhibitor, such as an anti-PD-1 antibody, to effectively drive expansion of neoepitope-specific T cells.
Checkpoint Inhibitors
[00140] The combination therapy may also comprise administration of an additional immunotherapeutic agent such as a checkpoint inhibitor. Checkpoint inhibitors suitable for use in the method provided herein include antibodies, such as for example, monoclonal antibodies, that target PD-1, PD-L1, or CTLA-4. In certain therapeutic combinations as provided herein, the checkpoint inhibitor is an anti-PD-1 antibody or an anti-PD-Ll antibody. For example, exemplary PD-1 inhibitors include but are not limited to pembrolizumab, nivolumab, and cemiplimab. Representative PD-L1 inhibitors include, for example, atezolizumab, avelumab, and durvalumab.
[00141] Alternatively, ipilimumab or tremelimumab, anti-CTLA-4 monoclonal antibodies, may also be used in the treatment method. Both are fully humanized anti-CTLA- 4 monoclonal antibodies of IgGl and IgG2, respectively.
[00142] As an example, a PD-1 pathway-inhibiting amount of an anti-PD-1 antibody such as nivolumab may be administered. One of ordinary skill in the art can determine how much anti-PD-1 antibody, such as nivolumab, or anti-PD-Ll antibody, is sufficient to provide clinically relevant inhibition of the PD-1 pathway or the PD-L1 pathway, respectively. For example, one of ordinary skill in the art can refer to the literature and/or administer a series of increasing amounts of nivolumab or another anti-PD-1 or anti-PD-Ll antibody to determine which amount or amounts provide clinically relevant inhibition of the PD-1 or PD-L1 pathway. Similarly, a CTLA-4 pathway-inhibiting amount of an anti-CTLA-4 antibody may be administered.
[00143] In one or more instances, however, a PD-1 pathway-inhibiting amount of the anti-PD-1 antibody, e.g., nivolumab, or anti-PD-Ll antibody is encompassed by one or more of the following ranges: from about 1 mg/kg to about 1000 mg/kg; from about 2 mg/kg to about 900 mg/kg; from about 3 mg/kg to about 800 mg/kg; from about 4 mg/kg to about 700 mg/kg; from about 5 mg/kg to about 600 mg/kg; from about 6 mg/kg to about 550 mg/kg; from about 7 mg/kg to about 500 mg/kg; from about 8 mg/kg to about 450 mg/kg; from about
9 mg/kg to about 400 mg/kg; from about 5 mg/kg to about 200 mg/kg; from about 2 mg/kg to about 150 mg/kg; from about 5 mg/kg to about 100 mg/kg; from about 10 mg/kg to about 100 mg/kg; and from about 10 mg/kg to about 60 mg/kg. Further guidance may be provided based upon the current standard of care for administration of immune check point inhibitors in cancer therapy.
Treatment
[00144] For confirmation, as used herein with regard to a PD-1 pathway-inhibiting amount of an anti -PD-1 antibody such as nivolumab, or other suitable checkpoint inhibitor, the amount and extent of the inhibition can vary widely and can still be effective, even when combined with administration of a T cell expander and the neoantigen-based DNA cancer vaccine. For example, an amount of an anti-PD-1 antibody, i.e., nivolumab, that only minimally inhibits the PD-1 pathway can still be an inhibiting amount as used herein so long as the method results in a clinically meaningful response. The actual dose to be administered, for each of the immunotherapeutic components, will vary depend upon the age, weight, and general condition of the subject as well as the severity of the cancer being treated, the judgment of the health care professional, and the particular identities and properties of each of the immunotherapeutic components.
[00145] In certain embodiments of the combination therapy, the subject has received one, two, three, four, five or more prior cancer treatments. In other embodiments, the subject is treatment-naive. In some embodiments, the subject has progressed on other cancer treatments. In certain embodiments, the prior cancer treatment comprised an immunotherapy. In other embodiments, the prior cancer treatment comprised a chemotherapy. In some embodiments, the tumor has reoccurred. In some embodiments, the tumor is metastatic. In yet other embodiments, the tumor is not metastatic.
[00146] In some embodiments, the subject has received a prior therapy to treat the tumor and the tumor is relapsed or refractory. In some embodiments, the subject has received a prior immuno-oncology therapy to treat the tumor and the tumor is relapsed or refractory. In some embodiments, the subject has received more than one prior therapy to treat the tumor and the subject is relapsed or refractory.
[00147] In some treatment modalities, a neoantigen-based DNA cancer vaccine is first administered to generate a neoantigen-specific immune response in the subject, followed by
one or more subsequent administrations of the neoantigen-based DNA cancer vaccine (induction period). The subsequent administrations of the neoantigen-based DNA cancer vaccine may be administered within 1 week, 2 weeks, 3 weeks or 4 weeks or more following the first administering.
[00148] The treatment methods described herein can continue for as long as the clinician overseeing the patient's care deems the treatment method to be effective. Non limiting parameters that indicate the treatment method is effective include any one or more of the following: tumor shrinkage (in terms of weight and/or volume); a decrease in the number of individual tumor colonies; tumor elimination; and progression-free survival. Change in tumor size may be determined by any suitable method such as imaging. Various diagnostic imaging modalities can be employed, such as computed tomography (CT scan), dual energy CDT, positron emission tomography and MRI.
[00149] With regard to the frequency and schedule of administering the neoantigen- based DNA cancer vaccine and the T cell expander, optionally combined with a checkpoint inhibitor, one of ordinary skill in the art will be able to determine an appropriate frequency for each of the components of the combination. For example, in a treatment cycle, a clinician can decide to administer the neoantigen-based DNA cancer vaccine, either as a single dose or in a series of doses, e.g., over the course of several days or weeks. The T cell expander is administered, either concurrently with the neoantigen-based DNA cancer vaccine, prior to vaccination, or following administration of the cancer vaccine. Preferably, and in some treatment modalities, the T cell expander, e.g., RSL AIL-2, is administered following the vaccination induction period. Based upon the long acting nature of the illustrative T cell expander, RSL AIL-2, such composition may be administered relatively infrequently (e.g., once every four weeks, once every three weeks, once every two weeks, one every 8-10 days, once every week, etc.).
[00150] In a preferred dosing regimen, dosing of the neoepitope-specific DNA-based cancer vaccine and the T cell expander are scheduled to align or substantially align the peak T cell responses of both therapeutic agents, to thereby achieve an optimized (and preferably synergistic) response.
[00151] For example, in one or more embodiments, initial administration of a T cell expander such as RSLAIL-2 is subsequent to one or more administrations of a neoepitope-
specific DNA-based cancer vaccine, and is preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander.
[00152] In some embodiments, a treatment protocol includes a time period for screening and manufacture of a therapeutic neoantigen-based DNA cancer vaccine against tumor-specific neoantigens, a vaccination induction period where the anticancer vaccine is administered, and a vaccination maintenance period where a T cell expander is administered. During the vaccination maintenance period, the anticancer vaccine is preferably administered one or more times concurrently with or separate from the T cell expander. Prior to administration, the anticancer vaccine may be prepared by any means as known in the art. In some embodiments, the anticancer vaccine against tumor-specific neoantigens is prepared by sequencing the genome, or exome of a tumor; identifying tumor neoantigens comprising neoepitopes from the tumor; and selecting neoepitopes based on a predicted antigenicity. An exemplary method of preparing such an anticancer vaccine is described in U.S. Patent Publication No. 2019/0022202, the methods of preparation being incorporated by reference herein. After screening the tumor and manufacture of the anticancer vaccine, e.g. from about 12-16 weeks, more preferably from about 6-10 weeks, or from 6-8 weeks, the neoantigen- based DNA cancer vaccine against tumor-specific neoantigens and/or T cell expander are administered according to a dosing schedule or protocol that provides a peak response for one or both of the anticancer vaccine and the T cell expander. The neoantigen-based DNA cancer vaccine may initially be administered for a period of time (e.g. 4-8 weeks or longer) as a vaccination induction. The patient may be vaccinated one or more times with the neoantigen- based DNA cancer vaccine during the induction period. After the induction period, the T cell expander is administered one or more times with or without administration of additional or maintenance anticancer vaccine. The T cell expander and/or the neoantigen-based DNA cancer vaccine may be administered for a period of time as needed for treatment (e.g. 1-12 months or longer). An exemplary administration schedule for treatment is provided below:
[00153] Table 1. Exemplary Administration Schedule

[00154] Exemplary lengths of time associated with the course of therapy include about one week; about two weeks; about three weeks; about four weeks; about five weeks; about six weeks; about seven weeks; about eight weeks; about nine weeks; about ten weeks; about eleven weeks; about twelve weeks; about thirteen weeks; about fourteen weeks; about fifteen weeks; about sixteen weeks; about seventeen weeks; about eighteen weeks; about nineteen weeks; about twenty weeks; about twenty-one weeks; about twenty-two weeks; about twenty- three weeks; about twenty four weeks; about seven months; about eight months; about nine months; about ten months; about eleven months; about twelve months; about thirteen months; about fourteen months; about fifteen months; about sixteen months; about seventeen months; about eighteen months; about nineteen months; about twenty months; about twenty one months; about twenty-two months; about twenty-three months; about twenty-four months; about thirty months; about three years; about four years and about five years.
[00155] The treatment methods described herein are typically continued for as long as the clinician overseeing the patient's care deems the treatment method to be effective, i.e., that the patient is responding to treatment, including no further progression of the disease, e.g., cancer. Non-limiting parameters that indicate the treatment method is effective may include one or more of the following: tumor shrinkage (in terms of weight and/or volume and/or visual appearance); a decrease in the number of individual tumor colonies; tumor elimination; progression-free survival; appropriate response by a suitable tumor marker (if applicable), increased number of NK (natural killer) cells, increased number of T cells, increased number of memory T cells, increased number of central memory T cells, reduced numbers of regulatory T cells such as CD4+ Tregs, CD25+ Tregs, and FoxP3+ Tregs.
[00156] The methods provided herein are useful for (among other things) treating a patient with cancer. For example, patients may be responsive to the neoantigen-based DNA alone, as well as the combination with the T cell expander, optionally with a checkpoint inhibitor (CPI), but are more responsive to administration of the combination. By way of further example, patients may be non-responsive or only marginally responsive to the neoantigen-based DNA cancer vaccine, or the T cell expander, or the checkpoint inhibitor, but are more responsive to the combination. By way of still further example, patients may be non-responsive to the neoantigen-based DNA cancer vaccine or to the T cell expander or to the checkpoint inhibitor alone, but are responsive to the combination.
[00157] Administration, e.g., of the neoantigen-based DNA cancer vaccine and/or the T cell expander (e.g., RSLAIL-2) and/or the checkpoint inhibitor is typically via injection. Other modes of administration are also contemplated, such as pulmonary, nasal, buccal, rectal, sublingual and transdermal. As used herein, the term "parenteral" includes subcutaneous, intravenous, intra-arterial, intratumoral, intralymphatic, intraperitoneal, intracardiac, intrathecal, and intramuscular injection, as well as infusion injections.
[00158] The presently described methods, combinations, compositions and the like can be used to treat a patient suffering from any condition that can be remedied or prevented by the methods provided herein, such as cancer. Exemplary conditions are cancers, such as, for example, fibrosarcoma, myxosarcoma, liposarcoma, chondrosarcoma, osteogenic sarcoma, chordoma, angiosarcoma, endotheliosarcoma, lymphangiosarcoma,
lymphangioendotheliosarcoma, synovioma, mesothelioma, Ewing's tumor, leiomyosarcoma, rhabdomyosarcoma, colon carcinoma, pancreatic cancer, brain cancer, breast cancer, ovarian cancer, prostate cancer, squamous cell cancer, basal cell cancer, adenocarcinoma, sweat gland cancer, sebaceous gland cancer, papillary cancer, papillary adenocarcinomas,
cystadenocarcinoma, medullary cancer, bronchogenic cancer, renal cell cancer, hepatoma, bile duct cancer, choriocarcinoma, seminoma, embryonal cancer, Wilms' tumor, cervical cancer, Hodgkin lymphoma, non-Hodgkin lymphoma, testicular cancer, lung cancer, small cell lung cancer, brain cancer, bladder cancer, epithelial cancer, glioma, astrocytoma, medulloblastoma, craniopharyngioma, ependymoma, pinealoma, hemangioblastoma, acoustic neuroma, oligodendroglioma, meningioma, melanoma, multiple myeloma, neuroblastoma, retinoblastoma and leukemias.
[00159] In some particular embodiments, the cancer to be treated is a solid cancer, such as for example, breast cancer, ovarian cancer, colon cancer, prostate cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer, non-small cell lung cancer, pancreatic cancer, thyroid cancers, kidney cancer, cancer of the bile duct, brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer, esophageal cancer, Hodgkin's disease and adrenocortical cancer.
[00160] The present methods, combinations and compositions are useful for enhancing the therapeutic effectiveness of a neoantigen-based DNA cancer vaccine, for example, by improving the subject’s immune response to the neoantigen-based DNA cancer vaccine composition. An enhanced response may be evaluated at any suitable time point during treatment, after a single round of treatment, after 2-3 cycles of treatment, etc., and by any of a number of suitable methods, including shrinkage of a tumor (partial response), i.e., an evaluation of tumor size or volume, disappearance of a tumor, a reduction in disease progression (cancer has not progressed), and analysis of one or more tumor test markers if appropriate. The methods, kits, compositions and the like provided herein are also useful for reducing tumor growth or size (or volume) in a subject undergoing treatment. Treatment by administering a therapeutically combination as described herein is effective, in one or more embodiments, to reduce tumor growth or size in the subject. For example, in some embodiments, one or more cycles of treatment is effective to reduce tumor size by about 25%, or by about 30%, or by about 40%, or by about 50%, or even by about 60%, or by about 70% or more when compared to the size of the tumor prior to treatment.
[00161] In yet some further embodiments, the methods, compositions and the like provided herein are effective to inhibit accumulation of regulatory T cells (Tregs) in a subject undergoing treatment for cancer. In yet some further embodiments, the methods, compositions and the like provided herein are effective to stimulate T cell and/or NK cell activity and/or proliferation in a subject. In some embodiments, the method is effective, for example, when evaluated in a cancer mouse model of the corresponding cancer, for increasing the number of CD8+ T cells and/or CD4 T cells in the subject when compared to vaccination with a neoantigen-based DNA cancer vaccine alone. For example, the subject’s CD8+ T cells may be increased by 2-fold or more, or 3-fold or more, or even 4-fold or more, when compared to treatment with the neoantigen-based DNA cancer vaccine alone. The treatment may, in some embodiments, be effective to increase the subject’s CD8+ T cells or
CD4 T cells against the neoantigens by at least 2-fold or more, or 3 -fold or more, or even 4- fold or more, or 5-fold or more, or 6-fold or more when compared to an untreated subject.
[00162] In turning to the Examples, the supporting preclinical studies provide an indication of the synergistic effect arising from the administration of a neoantigen-based DNA cancer vaccine when accompanied by administration of the exemplary T cell expander, RSLAIL-2, and optionally, a checkpoint inhibitor.
[00163] As illustrated in Example 1, it was discovered that administration of the exemplary T cell expander, RSLAIL-2, in combination with an exemplary individualized anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, e.g., VB4011, is effective to not only increase the frequency, but to also increase the total numbers of neoepitope-specific T cells when evaluated in a preclinical melanoma model in mice.
[00164] Thus, vaccination with the therapeutic neoepitope-specific DNA-based cancer vaccine is effective to induce a neoepitope-specific T cell response, which is then further expanded by administration of a T cell expander such as RSLAIL-2, effective to further expand the existing T cell population unspecifically. By aligning or substantially aligning the peak T cell responses of both therapeutic agents, i.e., the neoepitope-specific DNA-based cancer vaccine and the T cell expander, an optimized (and preferably synergistic) response could be achieved. See, for example, the results shown in FIGs. 5A and 5B, which support as a preferred approach based upon this preclinical cancer model, administration of a T cell expander such as RSLAIL-2 subsequent to one or more administrations of a neoepitope- specific DNA-based cancer vaccine, and preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander. For example, in the doublet combination, and based only on a single initial administration of the vaccine, an optimal response was observed when administration of the T cell expander, RSLAIL-2, occurred 11 days following administration of the vaccine. Thus, these results indicate that an optimized response can be achieved by strategic alignment of dosing of each therapeutic agent based upon its peak T cell response following
administration. As illustrated in Fig. 5B, the timing of administration of the T cell expander, RSLAIL-2, relative to the timing of administration of a second dose of the neoepitope- specific DNA-based cancer vaccine affected the T cell response. That is to say, as shown in FIG. 5B, administration of RSLAIL-2 at a period of time following administration of a
second dose of the vaccine, in this case, 3 days later, resulted in a notable enhancement of the specific T cell response.
[00165] FIG. 5C provides the results of administering RSLAIL-2 at various stages of the exemplary vaccination schedule, e.g., same day administration of the 3rd vaccine dose and RSLAIL-2, as well as administration of the 3rd vaccine dose with delayed administration of RSLAIL-2. If two or more vaccinations, RSLAIL-2 administration was delayed by 3 days; in the case of a single vaccination, administration of RSLAIL-2 was delayed 7, 11 or 14 days. Based upon these results in this preclinical B16 model, it appears that administration of the T cell expander, RSLAIL-2, with a second dose of the neoantigen-based DNA cancer vaccine modestly synergizes the specific T cell response, and that in this same model, administration of RSLAIL-2 with the 3rd dose of vaccine does appear to synergistically effect the specific T cell response to a similar extent whether administered on the same day or delayed. Based upon these results, it appears that it may be preferable to administer a T cell expander such as RSLAIL-2 following the neoepitope-specific DNA-based cancer vaccine induction phase (e.g., following more than one vaccination, e.g., following 2 or 3 or 4 or more vaccinations) to thereby synergize or at least maximize the specific T cell response, preferably with reduced sensitivity to timing of administration of the T cell expander.
[00166] As described in Example 2, studies were also undertaken to investigate whether the T cell expander, (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9- yl)methyl N-carbamate)6avginterleukin-2 (“RLSAIL-2”), could boost the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary
immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO, in vaccination studies conducted in a colon cancer CT 26 mouse tumor model, and to evaluate the extent of any enhanced neoepitope-specific T cell responses. These data clearly demonstrate, and confirm in yet a further and different preclinical mouse model, that RSLAIL-2 strongly synergizes neoepitope-specific IFN-g T cell responses in VB4061 vaccinated mice, thus further validating the approach provided herein at improving clinical outcomes in patients by eliciting a strong, neoantigen-focused immune response by virtue of administering a combination of an individualized DNA-based neoantigen vaccine in combination with a T cell enhancer such as RSLAIL-2. More particularly, when evaluated in a colon cancer CT 26 mouse tumor model, the combination of the exemplary neoepitope cancer vaccine,
VB10.NEO, and the T cell expander, RSLAIL-2, significantly synergizes to boost
neoepitope-specific T cells responses, resulting in up to 5-fold increase in the number of neoepitope-specific T cell responses compared to VBIO.NEO monotherapy. Moreover, in these experiments, mice were injected with tumor cells to mimic a tumor-bearing clinical setting. It was observed that the combination of VB4061 + RSL AIL-2 was effective to increase both the breadth (more neoepitopes) and depth (stronger response to each neoepitope) of the neoepitope-specific T cell responses.
[00167] The unexpected advantages of the combination therapy are further demonstrated in Example 3, which explores whether the T cell expander, RSLAIL-2, could increase tumor protective immune responses in VB4061 and anti-PD-1 antibody vaccinated mice (as illustrative of a subject undergoing cancer treatment with a checkpoint inhibitor further combined with administration of an individualized neoantigen-based DNA cancer vaccine) in a CT26 tumor model. Treatment with VB4061 alone and in combination with anti-PD-1 induces tumor protective responses (data not shown). However, in the study described in Example 3, it was confirmed that vaccination could induce tumor protective immune responses (FIGs. 4A-4D). Moreover, the results further illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-lwas further and notably boosted when administered in combination with the T cell expander, RSLAIL-2. Reduced tumor growth was observed in the triple-therapy VB4061 + anti-PD-1 antibody + RSLAIL-2 treated group, where 50% of triple-treated mice remained tumor free and never did establish tumors. In contrast, only 20% of mice receiving VB4061 + anti-PD-1 antibody without RSLAIL-2 (FIG. 4B) were protected. In both treatment arms, tumor regression of established tumors was observed, and overall survival was 70% and 80% in each of the VB4061 + anti-PD-1, and VB4061 + anti-PD-1 + RSLAIL-2 treated groups, respectively (FIG. 4C). In the re challenge experiment both treatment groups were fully protective against the lethal dose of CT26 cells and both groups were statistically different from the control group both in tumor growth and in overall survival.
[00168] Tumor protection as observed in mice vaccinated with VB4061 + anti-PDl and was further strengthened when combined with a T cell expander, i.e., RSLAIL-2. These results demonstrate that the integration of these unique and non-overlapping mechanisms can be used to create an effective treatment of established tumors. In mice re-challenged with a lethal dose of tumor cells, both treatment groups were fully protected, demonstrating that the therapy induced long-lasting and tumor protective memory immune responses.
[00169] Tumor length for untreated mice (control) and mice treated with VB4061 + anti-PD-1 + RSLAIL-2 groups was further monitored regularly by measuring the tumor length size (mm) using an electronic caliper. In this study, it was confirmed that vaccination could induce tumor regression and stabilization in a CT26 colon carcinoma mouse model (FIGs. 7A-7B). The results of this experiment illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-1 was further boosted when administered in
combination with RSLAIL-2. As shown in Fig. 7B, vaccination of mice with VB4061 and a checkpoint inhibitor, anti-PD-1, in combination with administration of RSLAIL-2 resulted in rapid, complete and long lasting tumor regression in mice with relatively small tumors (e.g. tumors less than about 5-6 mm) as well as long lasting stabilization of larger tumors (e.g. tumors larger than about 5-6 mm and even larger than about 10 mm).
[00170] All articles, books, patents, patent publications and other publications referenced herein are expressly incorporated herein by reference in their entireties. In the event of an inconsistency between the teachings of this specification and the art incorporated by reference, the meaning of the teachings and definitions in this specification shall prevail (particularly with respect to terms used in the claims appended herein). For example, where the present application and a publication incorporated by reference defines the same term differently, the definition of the term shall be preserved within the teachings of the document from which the definition is located.
EXAMPLES
[00171] It is to be understood that the foregoing description as well as the examples that follow are intended to illustrate and not limit the scope of the invention(s) provided herein. Other aspects, advantages and modifications within the scope of the invention will be apparent to those skilled in the art to which the invention pertains.
Materials and Methods
[00172] (2.7-(bis-methoxyPEGiokd-carboxyamide)(9h-fluorene-9-yl)methyl N- carbamate)6avginterleukin-2 : Recombinant human IL-2 having an amino acid sequence identical to that of aldesleukin (des-alanyl-1, serine-125 human interleukin-2) was cloned and expressed and used to prepare the exemplary T cell expander, (2,7-(bis-methoxyPEGiokD- carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2 (CAS No. 1939126- 74-5), also referred to bempegaldesleukin, or more generally in these examples as,“RSLAIL-
2”. The preparation of (2,7-(bis-methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2 is described, e.g., in WO 2018/132496 (Example 19); Example 20 describes the molecule’s receptor bias/selectivity. For the precbnical studies, RSLAIL-2 was diluted in dilution buffer to a concentration of 0.1 mg/ml and the volume determined to arrive at a final dose of 0.8 mg/kg, based upon the weight of the mouse, and injected into the tail vein of the mice. For clinical studies, RSLAIL-2 is provided as a sterile white to yellow lyophilized powder for reconstitution as described in Example 4.
[00173] VBIO.NEO (neoantigen-based therapeutic DNA vaccine for precbnical
studies). In the precbnical studies described below, control plasmid VB1026, and two
VBIO.NEO pDNA constructs, VB4011 and VB4061, were used as illustrative neoantigen- based DNA anticancer vaccines. The pDNA constructs, VB4011 and VB4061, encode 10 neoepitopes from B16 and 20 neoepitopes from CT26, respectively, as described in Table 2 below. Vaccination of mice was performed in combination with electroporation. The
different functional elements of the pVBlO.NEO plasmids are shown in FIG. 13.
[00174] Anti-PD-1 antibody (precbnical experiments): InVivoMAb anti-mouse PD- 1, Clone RMP1-14. Cat no: BE0146 (Bio X Cell®).
[00175] Table 2. VBIO.NEO pDNA plasmid Description
Designation Plasmid Targeting unit Dimerization unit Antigen unit
pUMVC4a with human MIP- la human hinge + Empty
signal peptide CH3 IgG3
VB1026
LD78
pUMVC4a with human MIP- la human hinge + B-pepMl-M10. Each peptide is
VB4011
signal peptide CH3 IgG3 separated by a 10 amino acid
(VBIO.NEO
LD78 linker (GGGGS)2
B16-X)
pUMVC4a with human MIP- la human hinge + C-pepM86-M 106-M 125 -M 115 - signal peptide CH3 IgG3 M92-M2-M8-M 103 -M 1 -M75 -
VB4061
LD78 M 104-M65 -M88-M69-M 10-
(VBIO.NEO
M108-M30-M114-M7-M112.
CT26-XX)
Each peptide is separated by a 10 amino acid linker (GGGGSE
[00176] The amino acid sequence of VB4011 corresponds to SEQ ID NO: 1 (FIG. 1).
The amino acid sequence of VB4061 corresponds to SEQ ID NO:2 (FIG. 8). A listing of the
twenty neoepitopes included in the VB4061 mouse construct is shown in FIG. 9 and correspond to SEQ ID NOs:3-22. A listing of the ten individual neoepitopes included in the VB4011 construct is shown in FIG. 10 and correspond to SEQ ID NOs:23-32. Methods for construction and expression of the above exemplary vaccibody vaccines is described in U.S. Patent Publication No. 2019/0022202, the contents of which is expressly incorporated herein in its entirety.
[00177] Harvest of spleens isolation of splenocvtes. and CD4+ or CD8+ T cell depleted splenocvtes: The mice were sacrificed, and the spleens were harvested aseptically. Spleens from individual mice were meshed through a 70 mM tissue filter to isolate single splenocytes. Splenocytes were washed once in culture medium re-suspended in lx ACK buffer to lyse red blood cells. After washings, cells were resuspended in culture medium and counted. For depletion of either the CD4+ or CD8+ splenocytes, DYNABEADS® Mouse CD4 (L3T4) or DYNABEADS® Mouse CD8 (Lyt2) were used according to the
manufacture’s instruction.
[00178] IFN-Y ELISpot assay: Briefly, splenocytes, CD4+ or CD8+ T cell depleted splenocytes were re-suspended to a cell concentration of 6xl05 cells. The cells were plated in triplicates (if limited number of cells duplicates were used) and re-stimulated for 24 hours with 2 pg/ml of individual peptides corresponding to the neoepitopes in the original VB10.NEO constructs (Table 2) used during vaccination. Immunogenicity was analyzed by IFN-g ELISpot Plus kit (Mabtech AB, Sweden) following the manufacturer’s instructions. Spot-forming units (SPU) were counted in a CTL ELISpot reader, ImmunoSpot 5.0.3 from Cellular Technology. Results are shown as number of IFN-g + spots/106 splenocytes or as IFN-g + spots /spleen.
[00179] Subcutaneous tumor challenge with the CT26 colon cancer cell line: Briefly, CT26 tumor cells (# CRL-2638, ATCC) were cultured in bottles with culture medium (RPMI 1640, 10 mM HEPES, 1 mM sodium pyruvate, 1% non-essential amino acid solution, 1% penicillin/streptomycin, 10% FBS). Prior to injection, the cells were washed twice in lx PBS while still adherent to the flask and then trypsin treated, washed and resuspended in lx PBS to a final concentration of 5xl05 cell/ml. BALB/cJRj mice were injected s.c. in the left thigh with 100 pi of 5xl04 CT26 cells.
[00180] VBIO.NEO (neoantigen-based therapeutic DNA vaccine for clinical studies'). The personalized neoantigenic vaccine, pVBlO.NEO, is a non-replicative, non-integrating, genetically stable and non-pathogenic naked, covalently closed, circular and supercoiled double-stranded deoxyribonucleic acid (DNA) plasmid of 6297-7407 base pairs, dependent on the number of neoepitopes included in the personalized human vaccine. The DNA plasmid is based on the pUMVC4a vector backbone encoding a single recombinant homodimer protein that includes three modules: the targeting, the dimerization and the neoepitope antigenic module. The targeting module encodes the human chemokine macrophage inflammatory protein- 1 alpha (hMIP-la), which binds to its cognate receptors on the cell surface of antigen presenting cells (APCs), while the dimerization module encodes the upper and lower hinge regions and the constant heavy chain 3 (CH3) domain from human IgG3. The lower hinge region links two vaccibody monomers by disulfide bridges and the CH3 domain contributes to dimerization by hydrophobic interactions. The upper hinge region facilitates flexible bivalent binding of the targeting module to its cognate receptors to thereby enhance the immunogenicity of the vaccine.
[00181] The neoepitope antigenic module consists of multiple (10-20) patient-specific neoepitopes including the somatic mutation/alteration spanning a total length of several (14 - 27) amino acids to form the neoepitope sequence and linked together by 10 amino acid flexible glycine/serine-rich linkers. The glycine/serine rich linkers typically change from construct to construct for the individualized vaccines based upon an evaluation of junctional sequences, such that a selected linker will typically excludes a junctional epitope that resembles a sequence found in the human preoteome. The neoepitope antigenic module is linked to the natural human chemokine macrophage inflammatory protein- la (targeting module) via a dimerization module derived from human IgG3 as described above. The transcript is translated to a 603-973 amino acid-containing protein of approximately 100 kDa, which forms an approximately 200 kDa dimeric protein.
[00182] Once delivered by i.m. administration to a patient, pVBlO. NEO is taken up by cells and leads to local and transient production, and secretion of the VBIO.NEO protein. The structure of the encoded protein is designed and selected to support the induction of strong cellular immune responses against patient-specific neoantigens.
[00183] The pVBlO.NEO DNA backbone sequence (with a general indicator for the neoepitope antigenic module) is shown in FIG. 12 and provided as SEQ ID NO: 77. The different functional elements of the pVBlO.NEO plasmids are shown in FIG. 13.
EXAMPLE 1
COMBINATION THERAPY WITH VB10.NEO NEOANTIGEN DNA VACCINE AND (2,7-(BIS-METHOXYPEGIOKD-CARBOXYAMIDE)(9H-FLUORENE-9-YL)METHYL N-CARBAMATE)6AVGINTERLEUKIN-2 IN A MOUSE MODEL OF MELANOMA
(B16)
[00184] Studies were undertaken to investigate whether the T cell expander, (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2, could boost the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VB10.NEO, in vaccination studies conducted in a melanoma B16 mouse tumor model, and to evaluate the extent of any enhanced neoepitope-specific T cell responses.
[00185] 15 female C57BL/6 mice were obtained from Janvier Laboratories. Overview of the study design and vaccination schedule is shown in Table 3.
[00186] B16 model: C56B1/6 mice were vaccinated 3x at day 0, 21 and 35 with either
20 pg control pDNA VB1026 or 20 pg VB4011. RSLAIL-2 (0.8 mg/kg) was administered i.v. on the same day as the third VB4011 vaccination. Immunogenicity was measured by IFN-g ELISpot at day 42 after the first VB4011 vaccination (day 7 after third vaccination).
Table 3. B16 Mouse Model Vaccination Schedule pDNA, 20 pg RSLAIL-2
Number of ELISpot
(day 0, 21, 35) (0.8 mg/kg) mice
5 VB1026 Day 42
5 VB4011 Day 42
5 VB4011 Day 35 Day 42
[00187] Other vaccination/administration schedules were also explored, as described further herein.
[00188] ELISpot Results in the B16 Melanoma Mouse Model: Administration of RSLAIL-2 in combination with VB4011 was effective to boost neoepitope-specific IFN-g T cell responses as shown in FIG. 2A and Table 4). In VB4011 vaccinated mice, the neoepitopes M2, M3, M4, M7, M9 and M10 were immunogenic (Table 4 (immunogenic responses shown in grey boxes) and FIG. 2A). For splenocytes isolated from VB4011 + RSLAIL-2-treated mice, the neoepitopes M2, M4, M6, M7, M9 and M10 were immunogenic. For the neoepitopes that were immunogenic in both treatment arms, a stronger immune response was observed in mice treated with the VB4011 + RSLAIL-2 combination therapy compared to VB4011 monotherapy.
[00189] The criterium for an immunogenic epitope was defined as >25 IFN-g + spots/106 cells and > IFN-g + spots/106 cells than average negative control (pDNA VB1026) +2xSD. However, in this experiment since splenocytes were pooled (5 mice), 2xSD could not be used.
Table 4. Number of IFN-g + spots (SPU) from pooled splenocytes (N=5) from VB4011 vaccinated mice alone or in combination with RSLAIL-2 when re-stimulated with peptides corresponding to the neoepitopes encoded in the VB4011 vaccine (B16 Melanoma Model)
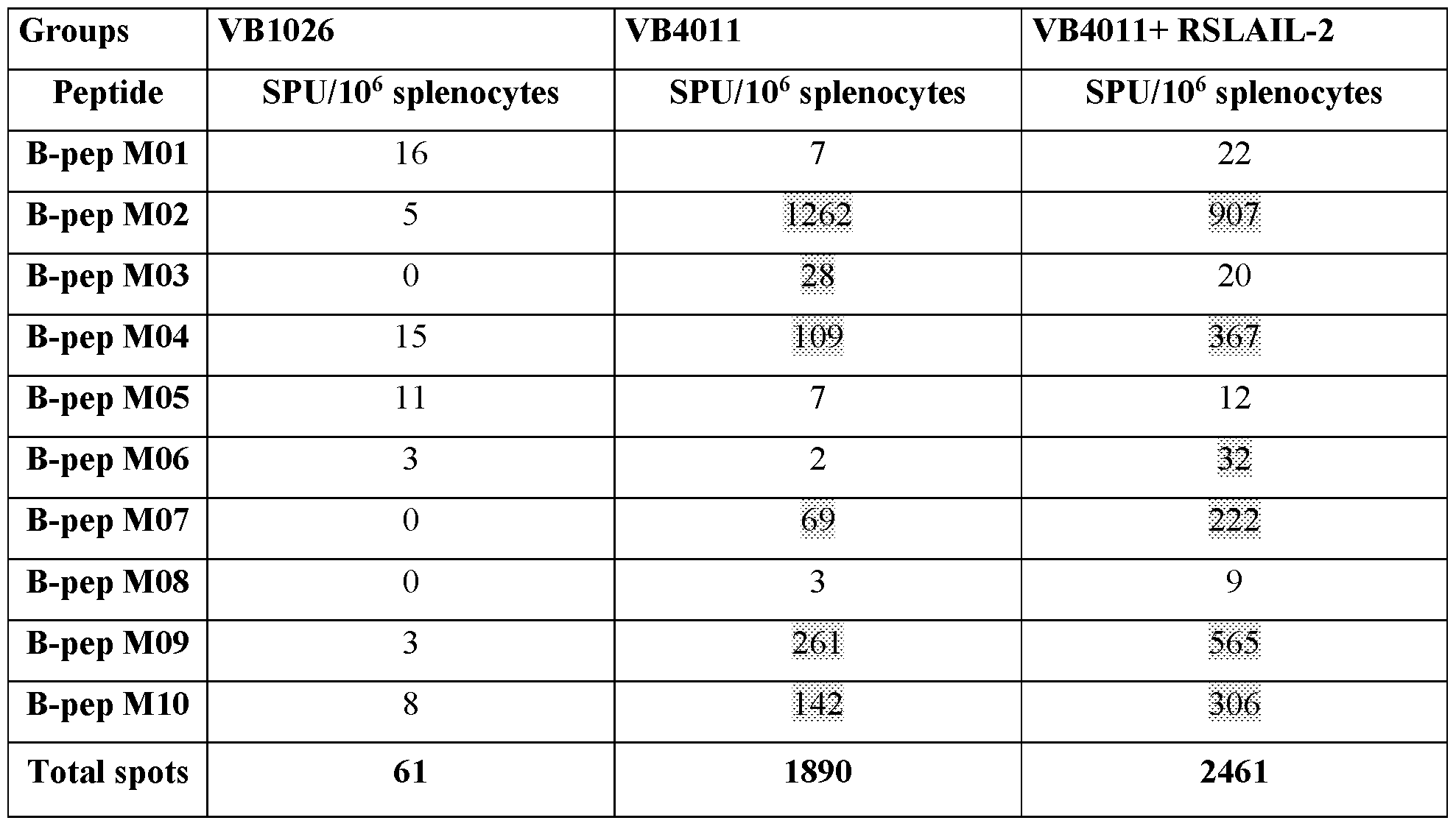
reported as 0. Criteria of an immunogenic epitope was defined as >25 SPU/106 cells.
Epitopes determined to be immunogenic are boxed in grey.
[00191] Reporting IFN-g + spots/106 cells demonstrates that the frequency of
neoepitope-specific T cells increased in mice treated with RSLAIL-2 + VB4011 (doublet). In the doublet-treated mice, it was observed that spleens were enlarged typically 2-3-fold when compared to VB4011 vaccinated mice (Table 5). Thus, in mice treated with the VB4011 - RSLAIL-2 combination, the total number of neoepitope-specific T cells also increased. To accommodate this increase, the total number of IFN-g + secreting T cells (SPU) per spleen was calculated (Table 5), and as a result, a 3.7-fold increase of neoepitope-specific T cells was determined (see also FIG. 2B). This increase was evident for both CD8+ T cells and
CD4+ T cells (FIGs. 2C and 2D, respectively). This finding demonstrates that administration of RSLAIL-2 in combination with VB4011 is effective to not only increase the frequency, but to also increase the total numbers of neoepitope-specific T cells in a preclinical melanoma model in mice.
Table 5. Total number of splenocytes in treated mice (B16 melanoma model)
Group # Total # Average # Total Total Total CD4+ Total CD8+ spleen cells/group cells/spleen SPU/106 SPU/spleen SPU/spleen SPU/spleen _ s _ cells _
VB1026 5 3.94xl08 7.87xl07 61 4798 2564 0
. YB401 1.5.3.63 10s .7.26 10 . . .1890 137281. 35341. 56752.
. VIS 101 1 .5.1 .04 10'' .2.07 10s 2461 509954 143880. 197003.
+
RSLAIL-
2
[00192] Additional studies: Prior to and subsequent to arriving at the study protocol described above, alternative dosing schedules were explored. It was hypothesized that in order to achieve a particularly strong and durable T cell response as a result of the subject combination therapy, administration of RSLAIL-2 would preferably occur following
establishment of a neoepitope specific T vaccine-induced T cell response, that is, following vaccination (i.e., of a first, second, or subsequent dose of the vaccine). Thus, vaccination
with the therapeutic neoepitope-specific DNA-based cancer vaccine is effective to induce a neoepitope-specific T cell response, which is then further expanded by administration of a T cell expander such as RSLAIL-2, effective to further expand the existing T cell population unspecifically. Studies revealed that by aligning or substantially aligning the peak T cell responses of both therapeutic agents, i.e., the neoepitope-specific DNA-based cancer vaccine and the T cell expander, an optimized (and preferably synergistic) response could be achieved. See, for example, the results shown in FIGs. 5A and 5B, which support, based upon this preclinical cancer model, administration of a T cell expander such as RSLAIL-2 subsequent to one or more administrations of a neoepitope-specific DNA-based cancer vaccine, and preferably in a manner in which peak T cell responses due to administration of each immunotherapeutic agent are substantially matched, particularly following initial or early rounds of vaccination and/or administration of the T cell expander. For example, in the doublet combination, and based only on a single initial administration of the vaccine, an optimal response was observed when administration of the T cell expander, RSLAIL-2, occurred 11 days following administration of the vaccine. Thus, these results indicate that an optimized response can be achieved by strategic alignment of dosing of each therapeutic agent based upon its peak T cell response following administration. As illustrated in Fig. 5B, the timing of administration of the T cell expander, RSLAIL-2, relative to the timing of administration of a second dose of the neoepitope-specific DNA-based cancer vaccine affected the T cell response. That is to say, as shown in FIG. 5B, administration of RSLAIL- 2 at a period of time following administration of a second dose of the vaccine, in this case, 3 days later, resulted in a notable enhancement of the specific T cell response.
[00193] In further exploring the dosing schedule, FIG. 5C provides the results of administering RSLAIL-2 at various stages of the vaccination schedule, e.g., same day administration of the 3rd vaccine dose and RSLAIL-2, as well as administration of the 3rd vaccine dose with delayed administration of RSLAIL-2. If two or more vaccinations, RSLAIL-2 administration was delayed by 3 days; in the case of a single vaccination, administration of RSLAIL-2 was delayed 7, 11 or 14 days. Based upon these results in the B16 model, it appears that administration of the T cell expander, RSLAIL-2, with a second dose of the vaccine modestly synergizes the specific T cell response, and that in this same model, administration of RSLAIL-2 with the 3rd dose of vaccine does appear to
synergistically effect the specific T cell response to a similar extent whether administered on the same day or delayed. Based upon these results, it appears that it may be preferable to
administer a T cell expander such as RSLAIL-2 following the neoepitope-specific DNA- based cancer vaccine induction phase (e.g., following more than one vaccination, e.g.,
following 2 or 3 or 4 or more vaccinations) to thereby synergize the specific T cell response, preferably with reduced sensitivity to timing of administration of the T cell expander.
EXAMPLE 2
COMBINATION THERAPY WITH VBIO.NEO NEOANTIGEN DNA VACCINE AND (2,7-(BIS-METHOXYPEGIOKD-CARBOXYAMIDE)(9H-FLUORENE-9-YL)METHYL N-CARBAMATE)6AVGINTERLEUKIN-2 IN MOUSE MODEL OF COLON CANCER
(CT26)
[00194] Studies were undertaken to investigate whether the T cell expander, (2,7-(bis- methoxyPEGiokD-carboxyamide)(9H-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2, could boost the neoepitope-specific IFN-g T cell response when administered in combination with an exemplary immunotherapeutic DNA-based neoantigen vaccine, VBIO.NEO, in vaccination studies conducted in a colon cancer CT 26 mouse tumor model, and to evaluate the extent of any enhanced neoepitope-specific T cell responses.
[00195] 20 female BALB/cJRj mice were obtained from Janvier Laboratories.
Overview of the study design and vaccination schedule is shown in Table 5.
[00196] CT26 model: In the CT26 model, BALB/c mice were vaccinated lx with either 50 pg control pDNA VB1026 or 50 pg VB4061. RSLAIL-2 (0.8 mg/kg) was
administered i.v. at day 7 post VB4061 vaccination. To mimic a tumor-setting during
vaccination, 5x104 CT26 tumor cells were injected 7 days prior to pDNA (VB1026 or
VB4061) vaccination. Immunogenicity was measured by IFN-g ELISpot at day 14 post
VB4061 vaccination.
Table 6. CT26 Mouse Model Vaccination Schedule
5xl04 CT26 RSLAIL-2
Number of mice pDNA 50 mg ELISpot tumor cells (0.8 mg/kg)
5 Day 0* VB1026 day 7 Day 21
5 Day 0 VB4061 day 7 Day 21
5 Day 0 Day 14 Day 21
5 Day 0 VB4061 day 7 Day 14 Day 21 may also consider tumor day as occurring on day (-)7, vaccination occurring on day 0 and administration of RSLAIL-2 on day 7.
[00197] Other vaccination/administration schedules were also explored.
[00198] ELISpot in CT26 colon cancer model: In line with the strong synergism observed in the exemplary B16 melanoma model described in Example 1 above, the neoepitope-specific IFN-g T cell responses were also significantly elevated for the combination of VB4061 and RSLAIL-2 in the CT26 mouse tumor model (FIGs. 3A-3D and Table 7).
[00199] In mice vaccinated with VB4061, immune responses against the neoepitopes Ml, M30, Ml 03 and Ml 06 were elicited (FIG. 3A and Table 7, immunogenic epitopes are indicated in grey boxes). In contrast, in mice treated with VB4061 + RSLAIL-2, 6 more neoepitopes induced immune responses (M2, M8, M65, Ml 12 and Ml 25). The splenocytes isolated from RSLAIL-2 monotherapy-treated mice elicited immune responses only against the neoepitope Ml 12.
[00200] These data clearly demonstrate, and confirm in yet a further and different preclinical mouse model, that RSLAIL-2 strongly synergizes neoepitope-specific IFN-g T cell responses in VB4061 vaccinated mice, thus further validating the approach provided herein at improving clinical outcomes in patients by eliciting a strong, neoantigen-focused immune response by virtue of administering a combination of an individualized DNA-based neoantigen vaccine in combination with a T cell enhancer such as RSLAIL-2. Moreover, in these experiments, mice were injected with tumor cells to mimic a tumor-bearing clinical setting. It was observed that the combination of VB4061 + RSLAIL-2 was effective to increase both the breadth (more neoepitopes) and depth (stronger response to each neoepitope) of the neoepitope-specific T cell responses.
[00201] Splenocytes of individual mice were analyzed in the ELISpot assay and the criteria for an immunogenic epitope was defined to be >25 IFN-g + spots/106 cells and > average negative control (VB1026) +2xSD (Table 7, the numbers of average negative control (VB1026+2xSD) are shadowed in the second column.
[00202] The numbers represent duplicates of individual mice in ELISpot and presented as SPU/106 splenocytes. The average number of SPU in the medium control was subtracted from the average of SPU elicited against each neoepitope for each sample. Samples with spot counts <0 are reported as 0. An immunogenic epitope is defined as>25 SPU/106 splenocytes
and > average negative control (VB1026) +2xSD. Epitopes deemed immunogenic are indicated by a grey box.
Table 7. Number of IFN-g + cells (SPU) from splenocytes isolated from VB4061 vaccinated mice with or without RSLAIL-2 when re-stimulated with peptides corresponding to the neoepitopes encoded in the VB4061 vaccine

observed to have spleens that were enlarged by about 2-3 fold when compared to mice
vaccinated with VB4061 (Table 8). Just as in the case for the B 16 model, total number of
IFN-g + secreting T cells per spleen was calculated. A 4-fold increase in total number of neoepitope-specific T cells was observed in RSLAIL-2 + VB4061 treated mice (FIG. 3B).
[00204] The synergistic effect of RSLAIL-2 in combination with VB4061 was even more profound on CD8+ T cell restricted neoepitopes, which increased 6-fold in the combo- treated group (see FIGs. 3C and 3D). The induced activation of effector CD8+ T cells aligns with the mechanism of RSLAIL-2, which has been shown to specifically signal through the
IL-2RBy. which has been shown to promote expansion and activation of tumor-killing
lymphocytes, such as NK and effector CD8+ T cells above CD4+ T cells, due to their
different expression of IL-2R chains. The results for each of the CT26 tumor model study groups on the total CD4+ T cell response is shown in FIG. 3D, which showed a 2.5 fold
increase in the combo-treated group.
Table 8. Total number of splenocytes and T cell responses (SPU) per spleen
Group # Total # Average # Total SPU/106 Total Total CD4+ Total CD8+ spleens cells/group cells/spleen cells SPU/spleen SPU /spleen SPU /spleen
VB1026 5 1.125 xlO9 2.25xl08 58 13064 19600 4500
VB4061 5 8.1x10s 1.62xl08 453 73549 66600 30400
RSLAIL
5 1.69 xlO9 3.38 xlO8 182 61501 15200 8110
-2
VB4061
+
5 1.48 xlO9 2.96xl08 891 264092 145000 182000
RSLAIL
-2
[00205] Based at least upon the results described above, the combination of the
exemplary neoepitope cancer vaccine, VB10.NEO, and RSLAIL-2 significantly synergizes to boost neoepitope-specific T cells responses, resulting in up to 5-fold increase in the number of neoepitope-specific T cell responses compared to VB10.NEO monotherapy. Mice treated with VB10.NEO in combination with RSLAIL-2 exhibited a stronger response to each
neoepitope, and also to more neoepitopes, demonstrating that the combination increased both
the breadth and depth of the immune response. In addition, both frequency and total number of neoepitope-specific T cells were elevated. Moreover, the synergistic effect was even more profound on the CD8+ T cell responses compared with CD4+ T cell responses supporting the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses.
EXAMPLE 3
COMBINATION THERAPY WITH VB10.NEO NEOANTIGEN DNA VACCINE AND (2,7-(BIS-METHOXYPEGIOKD-CARBOXYAMIDE)(9H-FLUORENE-9-YL)METHYL
N-CARBAMATE)6AVGINTERLEUKIN-2 AND AN ANTI-PD-1 ANTIBODY IN A
CT26 COLON CANCER MOUSE MODEL
[00206] This experiment was carried out to explore whether RSLAIL-2 could increase tumor protective immune responses in VB4061 and anti-PD-1 antibody-vaccinated mice in a CT26 tumor model. The exemplary therapeutic neoantigen DNA vaccine employed,
VB4061, encodes 20 neoepitopes from CT26 as shown above in Table 2 above and in FIGs. 7 and 8.
[00207] In this study, 36 female BALB/cJRj mice were obtained from Janvier
Laboratories. All Balb/c mice were challenged with a lethal dose of 5xl04 CT26 tumor cells at day 0. 50 pg VB4061 was administered intramuscularly (i.m.) with electroporation at day 0, 3, 7, 10, 14, 27 and 64. 200 pg of an anti-PD-1 antibody was injected intraperitoneally
(i.p.) Q7d starting at day 7, and 0.8 mg/kg RSLAIL-2 was injected intravenously (i.v.) Q9d starting at day 18. VB1026 (as described in Table 2) was used as a negative control and
administrated on the same days as VB4061. The pDNA plasmids used in this study are
shown in Table 2 and the vaccination protocol is shown in Table 9.
Table 9. Therapeutic Vaccination Schedule
Number CT26 tumor RSLAIL-2 Anti-PD-1 Ab pDNA 50 mg
cells (0.8 mg/kg) 200 mg of mice
10 Day 0
and d27
VB4061 dO, d3, d7, dlO, Start day 7, and
10 Day 0
dl4, d27 and d64 then q7d
VB4061 dO, d3, d7, dlO, Start day 18 and Start day 7 and
10 Day 0
dl4, d27 and d64 then q9d then q7d
[00208] At day 56 post tumor cell injection, the tumor free mice who had been treated with VB4061 + anti-PD-1 Ab (n=6) or with the triple combination VB4061 + anti -PD- 1 Ab + RSLAIL-2 (n=7) were re-challenged with a second lethal dose of 5x104 CT26 tumor cells. Naive Balb/c mice (n=6) were included as a control for growth of the tumor cells in vivo. No further vaccinations were performed.
[00209] Tumor growth of the CT26 cells was monitored regularly by measuring the body weight and the tumor volume size using an electronic caliper. The health condition of the mice was followed closely according to a score sheet. Mice were sacrificed before the tumors reached >10% of the body weight.
[00210] VB4061 alone and in combination with anti-PD-1 induces tumor protective responses (data not shown). In this study, it was confirmed that vaccination could induce tumor protective immune responses (FIGs. 4A-4D). Moreover, the results of this experiment illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-1 was further boosted when administered in combination with RSLAIL-2. Tumor growth, tumor take and overall survival are shown in FIGs. 4A-4C.
[00211] Re-challenge: The Balb/c mice in both treatment arms that were tumor-free on day 56 were re-challenged with a second lethal dose of 5xl04 CT26 tumor cells without further treatment. Naive Balb/c mice (n=6) were included as a control to monitor tumor growth. The mice were observed for tumor growth up to day 71 after re-challenge. All 6 control mice rapidly developed tumors and were sacrificed. In contrast, all mice pre-treated with VB4061 + anti-PD-1 or VB4061 + anti-PD-1 + RSLAIL-2 were fully protected against the second lethal dose of CT26 tumor cells - demonstrating induction of protective memory immune responses (FIG. 4D).
[00212] Statistical analysis: The tumor growth curves in both treatment groups (FIG. 4A) were statistically different from the control group, however, the two treatment groups were not statistically different (Table 10).
Table 10. Statistical analysis (Dunnett’s multiple comparisons test from two-way ANOVA) of tumor growth for the treatment groups
(Multiple comparisons of the tumor growth (mean values) of the respective groups (analyzed by Graph Pad Prism 6.05)

[00213] Reduced tumor growth was observed in the triple-therapy VB4061 + anti-PD- 1 Ab + RSL AIL-2 treated group, where 50% of triple-treated mice remained tumor free and never did establish tumors. In contrast, only 20% of mice receiving VB4061 + anti-PD-1 antibody without RSLAIL-2 (FIG. 4B) were protected. Despite numeric differences between the treatment groups, statistical analysis using the Mantel-Cox test resulted in a P value of P=0.2083 (Table 11).
[00214] In both treatment arms, tumor regression of established tumors was observed, and overall survival was 70% and 80% in each of the VB4061 + anti-PD-1, and VB4061 + anti-PD-1 + RSLAIL-2 treated groups, respectively (FIG. 4C). Statistical analysis using the Mantel-Cox test of the survival curves for the two treatment arms showed no statistically significant difference in these two groups, although both treatment arms reached significance when compared to the control group (Table 11).
Table 11. Statistical analysis (Mantel-Cox test) of the treatment groups: Tumor growth and overall survival in primary tumor challenge

ns = not significant and ||||| = P < 0.0001. Analysis was performed in Graph Pad Prism 6.05
[00215] In the re-challenge experiment both treatment groups were fully protective against the lethal dose of CT26 cells and both groups were statistically different from the control group both in tumor growth and in overall survival (Table 12).
Table 12. Statistical analysis (Mantel-Cox test) of the treatment groups: Tumor growth and overall survival in re-challenge

[00216] Tumor protection as observed in mice vaccinated with VB4061 + anti-PDl, and was further strengthened when combined with a T cell expander, i.e., RSLAIL-2. These results demonstrate that the integration of these unique and non-overlapping mechanisms can be used to create an effective treatment of established tumors. In mice re-challenged with a lethal dose of tumor cells, both treatment groups were fully protected, demonstrating that the therapy induced long-lasting and tumor protective memory immune responses.
[00217] In ongoing tumor challenge experiments in mice, it appears that tumor burden upon initiation of treatment with RSLAIL-2 may be predictive of response - e.g., a complete
response was observed for greater numbers of mice when the tumor size was less than 6 mm upon administration of a first dose of RSLAIL-2.
[00218] Tumor length for untreated mice (control) and mice treated with VB4061 + anti-PD-1 + RSLAIL-2 groups was further monitored regularly by measuring the tumor length size (mm) using an electronic caliper. In this study, it was confirmed that vaccination could induce tumor regression and stabilization in a CT26 colon carcinoma mouse model (FIGs. 7A-7B). The results of this experiment illustrate that tumor protection in mice vaccinated with VB4061 and anti-PD-1 was further boosted when administered in combination with RSLAIL-2. As shown in Fig. 7B, vaccination of mice with VB4061 and anti-PD-1 in combination with administration of RSLAIL-2 resulted in rapid, complete and long lasting tumor regression in mice with relatively small tumors (e.g. tumors less than about 5-6 mm) as well as long lasting stabilization of larger tumors (e.g. tumors larger than about 5-6 mm and even larger than about 10 mm).
EXAMPLE 4
PHASE 1/2A STUDY IN HUMANS WITH INDIVIDUALIZED VB10.NEO NEOANTIGEN DNA VACCINE ALONE OR WITH (2,7-(BIS-METHOXYPEGIOKD- CARBOXYAMIDE)(9H-FLUORENE-9-YL)METHYL N- CARBAMATE)6AVGINTERLEUKIN-2 IN PATIENTS WITH LOCALLY ADVANCED OR METASTATIC MELANOMA, NSCLC, CLEAR RENAL CELL CARCINOMA, UROTHELIAL CANCER OR SQUAMOUS CELL CARCINOMA OF THE HEAD AND NECK, WHO DID NOT REACH COMPLETE RESPONSES WITH CURRENT
STANDARD OF CARE IMMUNE CHECKPOINT BLOCKADE
[00219] Objectives: The primary objective of this Phase l/2a study is to assess the safety/tolerability of (i) multiple doses of 3 mg VB10.NEO immunotherapy and of (ii) multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2. Secondary objectives include (i) assessment of the immunogenicity of multiple doses of 3 mg VB10.NEO immunotherapy and of multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2, and (ii) additional preliminary assessments of the efficacy of multiple doses of 3 mg VB10.NEO immunotherapy and of multiple doses of 3 mg VB10.NEO immunotherapy in combination with 0.006 mg/kg RSLAIL-2. Additional exploratory objects include, for example, an investigation of the immune signature alterations during therapy, and exploration of the correlation between immunological response and clinical efficacy after VB10.NEO immunotherapy alone or in combination with RSLAIL-2.
[00220] Rationale: Pre-clinical studies (above) have shown that the combination of VBIO.NEO and RSL AIL-2 synergizes to boost neoepitope-specific T cells responses, resulting in a 5-fold increase in the number of neoepitope-specific T cell responses compared to VBIO.NEO alone. Mice treated with VBIO.NEO in combination with RSLAIL-2 showed both a stronger response to each neoepitope and to increased numbers of neoepitopes, showing that both the breadth and depth of the immune response were elevated. The combination showed an even more evident effect on CD8+ T cell responses as the combination elicited a neoepitope-specific CD8+ T cell response to more neoepitopes compared to either drug when administrated alone, further strengthening the combination’s ability to induce strong neoepitope-specific CD8+ T cell responses. In a therapeutic tumor model, an increased number of complete responders was observed in mice treated with the triple combination of VBIO.NEO, RSLAIL-2 and a checkpoint inhibitor, an anti -PD- 1 antibody, demonstrating the strong rationale for bringing together these unique and non overlapping mechanisms that have been shown in preclinical models to create an effective treatment of established tumors.
[00221] This trial investigates the safety, immunogenicity and efficacy of multiple doses of VBIO.NEO in combination with RSLAIL-2 on the background of checkpoint inhibition in patients with locally advanced or metastatic solid tumors. In the combination arm, patients receive VBIO.NEO vaccinations and 0.006 mg/kg IV RSLAIL-2 with the first dose being administered 11 weeks after initiation of VBIO.NEO vaccinations. More particularly, this open-label first-in-human phase l/2a study is designed to evaluate the safety and efficacy of multiple dosing with individualised VBIO.NEO or VBIO.NEO and RSLAIL- 2 immunotherapy in combination, in patients with locally advanced or metastatic solid tumors including melanoma, NSCLC (non-small cell lung cancer), clear-cell RCC (renal cell cancer), urothelial cancer or SCCHN (squamous cell carcinoma of the head and neck), who did not reach complete responses with current standard of care (i.e., checkpoint inhibitor therapy, CPI). CPI standard of care includes, e.g., nivolumab, pembrolizumab or atezolizumab. This study protocol may be amended during the course of the study.
[00222] Part A of the study consists of 6 arms in 5 different tumor entities. All patients are administered VBIO.NEO on the background of CPI therapy. Patients receive CPI at least from the commencement of vaccine manufacturing (arms 1, 5 A and 5B) or for additional > 12 weeks (arms 2-4). Arm 5 (SCCHN) is divided into arm 5 A and arm 5B. Arm
5 A is administered VBIO.NEO whereas arm 5B receives the combination of VBIO.NEO and RSLAIL-2.
• Arm 1 Melanoma VBIO.NEO
• Arm 2 NSCLC VBIO.NEO
• Arm 3 RCC VBIO.NEO
• Arm 4 Urothelial cancer VBIO.NEO
• Arm 5A SCCHN VBIO.NEO
• Arm 5B SCCHN VBIO.NEO + RSLAIL-2 (combination)
[00223] Up to 10 patients are treated in each arm in the first phase (part A) of the study.
[00224] Part B of the study will be opened after a certain number of patients have been enrolled and analysed in part A. The expansion part B will include up to 3 tumor-specific expansion cohorts.
[00225] The study is divided into 3 periods: a screening and manufacturing period, a treatment period, and a long-term follow-up period.
[00226] The neoantigenic vaccine, pVBlO.NEO, is a non-replicative, non-integrating, genetically stable and non-pathogenic naked, covalently closed, circular and supercoiled double-stranded deoxyribonucleic acid (DNA) plasmid of 6297-7407 base pairs, dependent on the number of neoepitopes included in the personalized vaccine. It encodes a single recombinant homodimer protein consisting of 3 modules: the targeting, the dimerization and the neoepitope antigenic module. The latter consists of multiple (10-20) patient-specific neoepitopes including the somatic mutation/alteration spanning a total length of several (14 - 27) amino acids to form the neoepitope sequence and linked together by 10 amino acid flexible glycine/serine-rich linkers. The neoepitope antigenic module is linked to the natural human chemokine macrophage inflammatory protein- la (targeting module) via a dimerization module derived from human IgG3. The transcript is translated to a 603-973 amino acid-containing protein of approximately 100 kDa, which forms an approximately 200 kDa dimeric protein. See FIG. 12.
[00227] The glycine/serine-rich linkers used between the neoepitopes typically change from construct to construct for the different patient vaccines based upon evaluation of
junctional sequences such that a preferred linker is one that excludes a junctional epitope that resembles a sequence found in the human genome. Illustrative linkers that may be used between the neoepitopes include those provided in SEQ ID NOs:67-76.
[00228] Screening, manufacturing, and delivery of VBIO.NEO vaccine: VBIO.NEO is supplied as a sterile, ready to use solution at a concentration of 3 mg/mL in phosphate buffered saline pH 7.4 in 2 mL sterile cyclo-olefin copolymer vials. The vials are stored at - 20°C (± 5°C). The vaccine is administered using a needle-free injection system,
PHARMAJET® Stratis 0.5 mL Needle Free Injection System.
[00229] To prepare the individualized vaccine, neoepitopes are selected based on qualified algorithms identifying immunogenic neoepitopes with low risk of inducing autoimmunity. The individual VBIO.NEO vaccine is then synthesized; it is estimated that the process from tumor sampling to administration will take approximately 12 to 16 weeks, preferably from 6-10 weeks, and more preferably from 4-6 weeks. The vaccinations are given by intramuscular injection.
[00230] Patients who fulfil all eligibility criteria (e.g. have a life expectancy of > 6 months and an ongoing good performance status (Eastern Cooperative Oncology Group [ECOG] performance status < 1) are acceptable to enter the trial.
[00231] Arm 1-4: Patients screened must have been receiving for at least 12 weeks a checkpoint inhibitor (anti-PD-1 or anti-PD-Ll) as the patient’s standard of care and according to currently approved indications.
[00232] Arms 5 A and 5B: Patients can be screened as long as CPI treatments have been started as the patient’s standard of care for SCCHN.
[00233] At the screening visit, eligible patients provide a blood sample and at least 1 tumor specimen. The blood sample and the tumor specimen are mandatory. Once an adequate tumor specimen is available, the patient is enrolled, and the individualized neoantigen vaccine manufacturing period starts (approximately 12-16 weeks).
[00234] The blood and tissue samples are included into the exome-sequencing program where the exome sequenced from the blood and the tumor sample/s are compared to identify the patients’ individual somatic tumor-specific mutations (neoepitopes). The blood and tissue
samples are included into the exome-sequencing program where the exome sequenced from the blood and the screening tumor sample/s are compared to identify the patient’s individual somatic tumor-specific mutations (neoepitopes). Neoepitopes found in more than one sample (fresh biopsies, available archival tumor specimens and cell free (cf)DNA from blood) are preferentially selected when designing/assembling the VBIO.NEO vaccine.
[00235] The tumor samples are subjected to RNA sequencing to select neoepitopes found in expressed proteins in the tumor. In addition, the blood sample is used for HLA typing to select neoepitopes that bind the individual patient’s HLA molecules. Vaccinations with individualized VBIO.NEO immunotherapy are commenced as soon as the patient- specific VBIO.NEO vaccine is available and if the patient-specific vaccine meets all pre specified product-release criteria after manufacturing.
[00236] RSLAIL-2, provided as a lyophilized powder, is reconstituted by the clinician prior to administration, and each patient’s dose is determined by the patient’s weight in kilograms. RSLAIL-2 is administered IV over 30 (± 5) minutes at a starting dose of
0.006 mg/kg according to dosing schedule. Except for the first dose, RSLAIL-2 is administered on the same day as VBIO.NEO. The vaccination occurs first, and the RSLAIL- 2 administration occurs 2 hours later. If treatment with CPI occurs on the same day, then the dosing is in the following order with the time interval between: (1) VBIO.NEO (wait 2 hours); (2) RSLAIL-2 (wait 30 minutes) (3) CPI.
[00237] Dose delays and reductions are permitted for RSLAIL-2. Administration of RSLAIL-2 may be delayed or the dose reduced to 0.003 mg/kg based on observed drug- related toxicities. If the RSLAIL-2 dose is reduced to 0.003 mg/kg, the dose level should remain at this level throughout the remainder of the study.
[00238] During the personalized vaccine manufacturing period, imaging procedures (computerized tomography/magnetic resonance imaging, e.g., CT/MRI, are performed as part of the standard patient care and the latest imaging procedure serves as baseline for efficacy assessment. Patients with complete response or patients who have discontinued CPI treatment prior to the start of the treatment period or patients that have started with another anti-cancer treatment will still have the possibility to receive VBIO.NEO (and RSLAIL-2 for arm 5B) upon agreement with the investigator and sponsor once the manufacturing of the vaccine is completed.
[00239] VBIO.NEO (all arms): Vaccinations start at visit 1. Patients will have received CPI at least from the start of manufacturing (arms 5 A and 5B) or for additional > 12 weeks (arms 1-4). Patients receive a maximum of 14 vaccinations of each 3 mg VBIO.NEO at pre-specified time points for up to 1 year from first vaccination in addition to CPI. The VBIO.NEO vaccine is added to this continuing CPI treatment and will not replace, omit, postpone or terminate the standard therapy. In the vaccination induction period, patients receive 3 vaccinations of 3 mg VBIO.NEO Q3W in addition to their CPI. From week 10, patients will receive maintenance treatment with vaccinations Q4W for up to 1 year from the first vaccination in addition to their CPI.
[00240] RSLAIL-2 (arm 5B): Dosing with RSLAIL-2 starts at week 11 (visit 8A), 1 week after the fourth VBIO.NEO vaccination and when VBIO.NEO is expected to have created a robust neoantigen-specific T cell response. Patients with SCCHN who are enrolled into arm 5A can, if willing to and fulfil all inclusion criteria for arm 5B, move into arm 5B (upon investigator’s and sponsor’s agreement) and start treatment with RSLAIL-2 at week 11 or 1 week after any later VBIO.NEO vaccination visit in the maintenance period up to week 34 (i.e. VBIO.NEO dose 10, week 18 + 1 week). Patients who have received at least 1 dose of VBIO.NEO vaccination are eligible for RSLAIL-2 administration.
[00241] Patients in arm 5B receive 0.006 mg/kg IV RSLAIL-2 in addition to
VBIO.NEO and CPI. The first 2 doses of RSLAIL-2 4 are administered in a Q3W interval and following doses in Q4W intervals. Treatment continues until end of treatment (EoT) at visit 18 (week 50). Depending on the time point of the RSLAIL-2 start, patients receive a maximum of 11 doses of RSLAIL-2. Except for the first RSLAIL-2 dose, all following doses are administrated on the same day as VBIO.NEO.
Biopsy and blood procedures:
[00242] Arms 1-4: To capture changes between screening and the first VBIO.NEO vaccination as well as in response to VBIO.NEO vaccination, up to 3 biopsies are taken at visit 1 (first VBIO.NEO vaccination) and 1 biopsy at visit 10 (week 18). This leads to a total maximum of 10 biopsies (3 at screening, 3 at visit 1, 1 at visit 10, and up to 3 additional biopsies at any timepoint after the first vaccination).
[00243] Arms 5A and 5B: To characterize changes before and after RSLAIL-2 administration, patients are asked to provide optional biopsies within 7 days prior and 15-21
days after the first administration of RSLAIL-2. In addition, biopsies can be taken at visit 1. At each of these time points, up to 3 biopsies are taken. This leads to a total maximum of 13 biopsies (3 at screening, 3 at visit 1, 3 at 1 week prior to the first RSLAIL-2 dose, 3 at 15-21 days after the first administration, and 1 additional biopsy at any timepoint after the first vaccination).
[00244] If a patient undergoes resection during the trial for any cause, tumor material is be secured for further analysis.
[00245] All biopsies described above are optional and should be taken only with the patient’s consent and with a safely accessible lesion which would not place the patient at an unjustifiable risk, in the opinion of the investigator. The investigator will decide which tumor lesions are preferable and whether CT-guided biopsies are needed to secure high-quality samples with sufficient tumour cell content. To minimize the radiation burden to the patients, CT-guided biopsies are restricted to a maximum of 5 biopsies during the course of this study.
[00246] All arms: Blood samples are taken at screening, visit 2, 8, 10, 13 and 18 for isolation of cfDNA for exome sequencing and monitoring of patient-specific tumor-mutations in plasma during treatment
[00247] All arms: Blood samples (peripheral blood monocytic cell [PBMC]) will be taken at visit 1 (baseline), visit 8A (week 11), visit 11 (week 22), visit 14 (week 34), and visit 19 (30 days after last vaccination) in order to quantify peripheral neoepitope-specific T cell responses. For patients who terminate participation or discontinue treatment before week 50, a blood sample for PBMC is taken at the follow-up visit at 30 days after the last vaccination.
[00248] In arms 5A and 5B, an additional blood sample (PBMC) is taken at visit 8B/week 12. This sample is used to quantify peripheral neoepitope-specific T cell responses induced by the T cell expander, RSLAIL-2.
[00249] In arms 5A and 5B, blood samples are taken 7-14 days after the third
VB10.NEO vaccination (visit 7A/week 7) and 7 days after first RSLAIL-2 administration (visit 8B/week 12) in order to fine characterize neoepitope-specific T cells. Functional analyses may include, for example, flow cytometry, ELISpot, enzyme-linked immunosorbent
assay, and cytotox assays and will be compared with T cell clones isolated from tumor tissue/specimens.
[00250] Efficacy to treatment is assessed as follows. Tumor response to VB10.NEO and RSLAIL-2 is assessed by means of iRECIST at regular intervals according to standard of practice. The imaging procedure is performed as part of the standard patient care and the patient is not exposed to any further radiation due to participation in this study.
[00251] Due to a 12- to 16-week manufacturing period of VB10.NEO, at least 2 imaging procedures, performed as standard practice, should be available before the start of treatment, where the latter of the two is within 4 weeks of visit 1.
[00252] The imaging performed within 4 weeks of visit 1 is the baseline for tumor assessments according to iRECIST. For arm 5B, an imaging assessment should preferably be carried out as close as possible prior to the first dose of RSLAIL-2.
[00253] The same method of assessment (imaging modality, e.g., MRI or CT) is ideally be used to characterise each identified and reported lesion at baseline and during all follow-up examinations for an individual patient according to the individual site's practices of standard of care.
[00254] Efficacy analysis: Early signs of efficacy of VB10.NEO immunotherapy alone or in combination with RSLAIL-2 will be based on Overall Response Rate (ORR), Duration of response (DOR), Progression-free survival (PFS), Overall survival (OS).
Efficacy analyses will be done separately for each tumor entity-specific cohort in part A and part B. The efficacy endpoints will be analyzed descriptively including 95% confidence intervals for proportions wherever applicable. The DOR, PFS and OS will be analyzed using the Kaplan-Meier product-limit method.
[00255] Additional assessments to be conducted include vital signs (body temperature, oxygenation, pulse rate, and systolic and diastolic BP, monitoring of BP, pulse and ECG, as well as blood assessments. Blood analysis includes the following: differential leukocyte analysis, haemoglobin, haematocrit, red blood cell count, platelet count, urea, calcium, chloride, phosphorus-inorganic, potassium, sodium, creatinine, uric acid, C-reactive protein, ALT, AST, gamma glutamyltransferase, bilirubin, lipase, alkaline phosphatase, lactate dehydrogenase, thyroid stimulating hormone (TSH), free triiodothyronine (fT3), free
thyroxine (fT4), glucose, protein, albumin, partial thromboplastin time, international normalized ratio, cholesterol, triglycerides, cholinesterase, creatine kinase. Serum will also be collected and frozen to assess if needed. Urinalysis will also be conducted. Blood samples will also be collected for isolation and cryopreservation of PBMCs.
[00256] The peripheral immune response of the individualized VBIO.NEO vaccine strategy will be measured by IFN-g enzyme-linked immunospot assay (ELISpot), a surrogate for T cell activity. The immune response to each neoepitope included in the vaccines will be assessed individually. For patients with sufficient PBMC, further analysis may be performed by flow cytometry analysis of cellular surface markers, tetramer analysis and intracellular cytokine staining to characterize the T cell profile. In addition, further analysis of the T cell receptor (TCR) repertoire may be performed by TCR sequencing.
Claims
1. A method for treating a subj ect having cancer, comprising:
administering to the subject, (i) an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, and (ii) a compound effective to
stimulate/expand production of T cells.
2. A method for treating a subject having cancer, comprising:
administering to the subject, (i) an anticancer DNA vaccine directed to a plurality of neoepitopes from tumor neoantigens, (ii) a compound effective to stimulate/expand production of T cells, and (iii) a checkpoint inhibitor.
3. The method of claim 1 or 2, wherein the neoepitopes comprised in the vaccine are presented to the immune system as a vaccibody dimeric protein.
4. The method of any previous claim, wherein the anticancer DNA vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding (i) a targeting unit, such as for example, hMIP-la, (ii) a dimerization unit, such as, for example, hi and h4 and CH3 domains of hIgG3 (iii) a first linker, and (iv) an antigenic unit.
5. The method of claim 4, wherein said antigenic unit comprises n-1 antigenic subunits.
6. The method of claim 5, wherein each subunit comprises at least a part of a cancer neoepitope sequence and a second linker, and said antigenic unit further comprising a final cancer neoepitope sequence.
7. The method of claim 5 or 6, wherein n is an integer of from 3 to 50.
8. The method of any one of claims 1-3, wherein the anticancer DNA vaccine comprises an immunologically effective amount of a DNA polynucleotide comprising a nucleotide sequence encoding an antigenic unit.
9. The method of claim 8, wherein said antigenic unit comprises n-1 antigenic subunits.
10. The method of claim 8 or 9, wherein each subunit comprises at least a part of a cancer neoepitope sequence and a linker, and said antigenic unit further comprises a final cancer neoepitope sequence.
11. The method of claim 9 or 10, wherein n is an integer of from 3 to 50.
12. The method of any previous claim, wherein the anticancer DNA vaccine is a
vaccibody DNA vaccine comprising from 10 to 50 neoepitopes.
13. The method of any previous claim, wherein the anticancer DNA vaccine is a
vaccibody DNA vaccine comprising from 15 to 40 neoepitopes.
14. The method of any of one of claims 4 to 13, wherein the first and/or the second linker is an amino acid linker, for example a glycine/serine rich linker and/or a linker selected from SEQ ID NO:67-76.
15. The method of any previous claim, wherein the anticancer DNA vaccine comprises a DNA polynucleotide sequence that is human (such as e.g., the plasmid backbone sequence of SEQ ID NO:77 or having 95 percent or greater sequence identity thereto, excluding the antigenic unit).
16. The method of any previous claim, wherein the administering is effective to enhance specific clonal T cell expansion to vaccine neoepitopes over that achieved upon administration of the anti cancer DNA vaccine in the absence of the compound effective to stimulate/expand production of T cells that is greater than additive.
17. The method of any previous claim, wherein the compound effective to
stimulate/expand production of T cells is a prodrug of an interleukin-2 (IL-2), wherein the IL-2 is modified by releasable covalent attachment of multiple polyethylene glycol moieties.
18. The method of claim 17, wherein the IL-2 is an interleukin-2 receptor beta (IL-2R{1) selective agonist.
19. The method of claim 17 or 18, wherein the IL-2 is aldesleukin.
20. The method of any one of claims 1 to 16, wherein the compound effective to
stimulate/expand production of T cells is an IL-2R{l-selective agonist of Formula (I),

Formula (I), wherein IL-2 is interleukin-2,
-NH-IL-2 is an amino group of interleukin-2,
each integer (n) has a value from about 200-300;
or pharmaceutically acceptable salt forms thereof.
21. The method of any one of claims 1 to 16, wherein the compound effective to stimulate/expand production of T cells is (2,7-(bis-methoxyPEGiokd- carboxyamide)(9h-fluorene-9-yl)methyl N-carbamate)6avginterleukin-2.
22. The method of any previous claim, wherein the cancer comprises a cancerous tumor.
23. The method of any previous claim, wherein, administration of the anticancer DNA vaccine and the compound effective to stimulate/expand production of T cells is effective to increase the numbers of vaccine-induced T cells in the tumor over such T cells determined upon following administration of one or more doses of the anticancer DNA vaccine alone, when evaluated in either a clinical or a preclinical setting.
24. The method of any previous claim, wherein the cancer is a solid cancer.
25. The method of any previous claim, wherein the cancer is selected from the group consisting of breast cancer, ovarian cancer, colon cancer, prostate cancer, bone cancer, colorectal cancer, gastric cancer, lymphoma, malignant melanoma, liver cancer, small cell lung cancer, non-small cell lung cancer, pancreatic cancer, thyroid cancers, kidney cancer, renal cell carcinoma, cancer of the bile duct, cancer of the head and neck, squamous cell carcinomas of the head and neck, brain cancer, cervical cancer, maxillary sinus cancer, bladder cancer, urothelial carcinoma, esophageal cancer, Hodgkin's disease and adrenocortical cancer.
26. The method of any previous claim, wherein the cancer is melanoma or colon cancer.
27. The method of any one of claims 1 or 3-26, wherein the anti cancer DNA vaccine and the T cell expander are administered concurrently or sequentially.
28. The method of any one of claims 1 or 3-27, wherein the anti cancer DNA vaccine and the T cell expander are administered via the same or different routes of
administration.
29. The method of any one of claims 1 or 3-28, wherein the anticancer DNA vaccine and the T cell expander are administered on the same day, on different days, or, a mixture of both the same and different days.
30. The method of any one of claims 2-26, wherein the anticancer DNA vaccine, the T cell expander and/or the checkpoint inhibitor are administered concurrently, sequentially or a combination of concurrently and sequentially.
31. The method of any one of claims 2-26 or 30, wherein the anticancer DNA vaccine, the T cell expander and/or the checkpoint inhibitor are administered via the same or different routes of administration.
32. The method of any one of claims 2-26 or 30-31, wherein the anticancer DNA vaccine, the T cell expander and/or the checkpoint inhibitor are administered on the same day, on different days, or, a mixture of both the same and different days.
33. The method of any previous claim, wherein said administration comprises a single cycle of administration or multiple cycles of administration.
34. The method of any previous claim, wherein said administration comprises
administering one or more doses of each or both of the anticancer DNA vaccine and the compound effective to stimulate/expand production of T cells.
35. The method of any one of claims 2-26 or 30-34, wherein said administration
comprises administering one or more doses of each, a combination of, or all of the anticancer DNA vaccine, the compound effective to stimulate/expand production of T cells, and/or the checkpoint inhibitor.
36. The method of any previous claim, wherein the compound effective to
stimulate/expand production of T cells is administered following administration of the anticancer DNA vaccine.
37. The method of any previous claim, wherein the compound effective to
stimulate/expand production of T cells is administered following an anti cancer DNA vaccine induction phase, wherein such induction phase may span one or more administrations of the anticancer DNA vaccine.
38. The method of claim 37, wherein the induction phase comprises 1, 2, 3 or more
administrations of the anticancer DNA vaccine over a given time period.
39. The method of claim 37 or 38, wherein the compound effective to stimulate/expand production of T cells is administered following one or more vaccinations, at which the neoepitope-specific T cell response has substantially levelled off, that is, is no longer significantly increasing.
40. The method of any one of claims 37 to 39, wherein the compound effective to
stimulate/expand production of T cells is administered after a neoepitope-specific T cell response has reached a maximum.
41. The method of claim 40, wherein the compound effective to stimulate/expand
production of T cells is administered after a neoepitope-specific T cell response has reached +25% of its maximum, or is within + 15% of its maximum, or is within about + 10% of its maximum.
42. The method of any previous claim, wherein administering comprises administering each of the anticancer DNA vaccine and the compound effective to stimulate/expand
production of T cells to align or substantially align the peak T cell responses of both the anticancer DNA vaccine and the compound effective to stimulate/expand production of T cells to thereby provide an optimized T cell response.
43. The method of any previous claim, wherein the compound effective to
stimulate/expand production of T cells is administered at a period of time following administration of one or more doses of the anticancer DNA vaccine.
44. The method of claim 43, wherein the compound effective to stimulate/expand
production of T cells is administered following 1-5 doses of the anticancer DNA vaccine.
45. The method of any previous claim, wherein said administering comprises
administering the compound effective to stimulate/expand production of T cells is administered 5-10 days following 1-5 doses of the anticancer DNA vaccine, and or following 1-4 doses of the anti cancer DNA vaccine, or following 1-3 doses of the anticancer DNA vaccine.
46. The method of claim 44 or 45, wherein administration of the anticancer DNA vaccine and the anticancer DNA vaccine is effective to provide an enhancement of the specific T cell response.
47. The method of any one of claims 44 to 46, wherein the compound effective to
stimulate/expand production of T cells is administered following 2 or 3 doses of the anticancer DNA vaccine.
48. The method of any one of claims 37 to 47, wherein the vaccine induction period comprises more than one vaccination, each subsequent vaccination separated by 1 week, 2 weeks, 3 weeks, 4 weeks, 5 weeks, 6 weeks or more following the first administration of the anticancer DNA vaccine.
49. The method of claim 48, wherein each subsequent vaccination is separated by 3 or 4 weeks following the first administration of the anticancer DNA vaccine.
50. The method of any one of claims 37 to 49, wherein the vaccine induction period comprises 3 vaccinations, each separated by from 1-6 weeks.
51. The method of any one of claims 2-26 or 30-50, wherein the checkpoint inhibitor is an anti-PD-1 antibody.
52. The method of any one of claims 2-26 or 30-51, wherein the checkpoint inhibitor is administered, for one or for multiple rounds (i) on the same day as the anticancer DNA vaccine, (ii) on the same day as the compound effective to stimulate/expand production of T cells, (iii) following administering of the anticancer DNA vaccine,
(iv) following administering of the compound effective to stimulate/expand production of T cells, (v) following administering of the anticancer DNA vaccine but before administering the compound effective to stimulate/expand production of T cells, or (vi) on the same day as the anticancer DNA vaccine and the compound effective to stimulate/expand production of T cells following administering of the anticancer DNA vaccine and the compound effective to stimulate/expand production of T cells, where the compound is administered after the vaccine.
53. The method of any one of claims 2-26 or 30-52, wherein administering the checkpoint inhibitor comprises administering the checkpoint inhibitor more than once over a course of treatment.
54. The method of any one of claims 2-26 or 30-50, wherein administering comprises administering the vaccine, the compound and the checkpoint inhibitor in the same day in order of the vaccine, the compound and the checkpoint inhibitor.
55. The method of any previous claim, wherein the cancer comprises a cancerous tumor and said administering is effective to reduce the size of the cancerous tumor when compared to the size of the tumor prior to treatment.
56. The method of any previous claim, wherein the cancer comprises a cancerous tumor, and said administering is effective to reduce the size of the cancerous tumor by at least about 30%, by at least about 40%, by at least about 50%, by at least about 60%, by at least about 70%, by at least about 80%, by at least about 90%, or to result in complete tumor regression, when compared to the size of the tumor prior to the administering.
57. The method of any previous claim, wherein the cancer comprises a cancerous tumor, and said administering is effective to result in complete tumor regression.
Priority Applications (3)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CN202080025990.8A CN113631185A (en) | 2019-02-27 | 2020-02-27 | Immunotherapeutic combinations for the treatment of cancer |
| EP20763489.0A EP3930747A4 (en) | 2019-02-27 | 2020-02-27 | Immunotherapeutic combination for treating cancer |
| JP2021550014A JP2022521792A (en) | 2019-02-27 | 2020-02-27 | Immunotherapeutic combination to treat cancer |
Applications Claiming Priority (8)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201962811459P | 2019-02-27 | 2019-02-27 | |
| US62/811,459 | 2019-02-27 | ||
| US201962825487P | 2019-03-28 | 2019-03-28 | |
| US62/825,487 | 2019-03-28 | ||
| US201962838180P | 2019-04-24 | 2019-04-24 | |
| US62/838,180 | 2019-04-24 | ||
| US201962881832P | 2019-08-01 | 2019-08-01 | |
| US62/881,832 | 2019-08-01 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2020176797A1 true WO2020176797A1 (en) | 2020-09-03 |
Family
ID=72238533
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2020/020224 WO2020176797A1 (en) | 2019-02-27 | 2020-02-27 | Immunotherapeutic combination for treating cancer |
Country Status (4)
| Country | Link |
|---|---|
| EP (1) | EP3930747A4 (en) |
| JP (1) | JP2022521792A (en) |
| CN (1) | CN113631185A (en) |
| WO (1) | WO2020176797A1 (en) |
Cited By (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2021219897A1 (en) | 2020-05-01 | 2021-11-04 | Vaccibody As | Betacoronavirus prophylaxis and therapy |
| WO2022200590A1 (en) | 2021-03-26 | 2022-09-29 | Nykode Therapeutics ASA | Therapeutic combination for treating cancer |
| WO2022233851A1 (en) | 2021-05-03 | 2022-11-10 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of infectious diseases |
| WO2022238432A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Co-expression of constructs and immunoinhibitory compounds |
| WO2022238420A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Co-expression of constructs and immunostimulatory compounds |
| WO2022238363A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of infectious diseases |
| WO2022238395A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Tolerance-inducing constructs and compositions and their use for the treatment of immune disorders |
| WO2022238381A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Immunotherapy constructs for treatment of disease |
| WO2022238402A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Tolerance-inducing constructs and composition and their use for the treatment of immune disorders |
| WO2023079001A1 (en) | 2021-11-03 | 2023-05-11 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of diseases caused by sars-cov-2 |
Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2016191545A1 (en) * | 2015-05-26 | 2016-12-01 | Advaxis, Inc. | Personalized delivery vector-based immunotherapy and uses thereof |
| WO2017173321A1 (en) * | 2016-03-31 | 2017-10-05 | Neon Therapeutics, Inc. | Neoantigens and methods of their use |
| WO2018039567A1 (en) * | 2016-08-25 | 2018-03-01 | Nantomics, Llc | Immunotherapy markers and uses therefor |
| WO2018234506A2 (en) * | 2017-06-21 | 2018-12-27 | Transgene Sa | Personalized vaccine |
| US20190022202A1 (en) * | 2016-01-08 | 2019-01-24 | Vaccibody As | Therapeutic anticancer neoepitope vaccine |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20170216403A1 (en) * | 2014-08-12 | 2017-08-03 | Massachusetts Institute Of Technology | Synergistic tumor treatment with il-2, a therapeutic antibody, and an immune checkpoint blocker |
| WO2018089669A2 (en) * | 2016-11-10 | 2018-05-17 | Nektar Therapeutics | Immunotherapeutic tumor treatment method |
-
2020
- 2020-02-27 EP EP20763489.0A patent/EP3930747A4/en not_active Withdrawn
- 2020-02-27 JP JP2021550014A patent/JP2022521792A/en active Pending
- 2020-02-27 CN CN202080025990.8A patent/CN113631185A/en active Pending
- 2020-02-27 WO PCT/US2020/020224 patent/WO2020176797A1/en unknown
Patent Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2016191545A1 (en) * | 2015-05-26 | 2016-12-01 | Advaxis, Inc. | Personalized delivery vector-based immunotherapy and uses thereof |
| US20190022202A1 (en) * | 2016-01-08 | 2019-01-24 | Vaccibody As | Therapeutic anticancer neoepitope vaccine |
| WO2017173321A1 (en) * | 2016-03-31 | 2017-10-05 | Neon Therapeutics, Inc. | Neoantigens and methods of their use |
| WO2018039567A1 (en) * | 2016-08-25 | 2018-03-01 | Nantomics, Llc | Immunotherapy markers and uses therefor |
| WO2018234506A2 (en) * | 2017-06-21 | 2018-12-27 | Transgene Sa | Personalized vaccine |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP3930747A4 * |
Cited By (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2021219897A1 (en) | 2020-05-01 | 2021-11-04 | Vaccibody As | Betacoronavirus prophylaxis and therapy |
| WO2022200590A1 (en) | 2021-03-26 | 2022-09-29 | Nykode Therapeutics ASA | Therapeutic combination for treating cancer |
| WO2022233851A1 (en) | 2021-05-03 | 2022-11-10 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of infectious diseases |
| WO2022238432A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Co-expression of constructs and immunoinhibitory compounds |
| WO2022238420A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Co-expression of constructs and immunostimulatory compounds |
| WO2022238363A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of infectious diseases |
| WO2022238395A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Tolerance-inducing constructs and compositions and their use for the treatment of immune disorders |
| WO2022238381A2 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Immunotherapy constructs for treatment of disease |
| WO2022238402A1 (en) | 2021-05-10 | 2022-11-17 | Nykode Therapeutics ASA | Tolerance-inducing constructs and composition and their use for the treatment of immune disorders |
| WO2023079001A1 (en) | 2021-11-03 | 2023-05-11 | Nykode Therapeutics ASA | Immunogenic constructs and vaccines for use in the prophylactic and therapeutic treatment of diseases caused by sars-cov-2 |
Also Published As
| Publication number | Publication date |
|---|---|
| EP3930747A1 (en) | 2022-01-05 |
| EP3930747A4 (en) | 2023-04-05 |
| JP2022521792A (en) | 2022-04-12 |
| CN113631185A (en) | 2021-11-09 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| EP3930747A1 (en) | Immunotherapeutic combination for treating cancer | |
| US20200368321A1 (en) | Il-2rbeta-selective agonists in combination with an anti-ctla-4 antibody or an anti-pd-1 antibody | |
| US20190275133A1 (en) | Immunotherapeutic tumor treatment method | |
| US11318164B2 (en) | Immunotherapeutic treatment method using an interleukin-2 receptor beta-selective agonist in combination with adoptive cell transfer therapy | |
| JP2019505512A (en) | Anti-cancer neoepitope vaccine for treatment | |
| KR20180093123A (en) | Novel peptides, combination of peptides and scaffolds for use in immunotherapeutic treatment of various cancers | |
| JP2013028619A (en) | Method to elicit, enhance and sustain immune response against mhc class i-restricted epitope, for prophylactic or therapeutic purpose | |
| US20210154277A1 (en) | Immunotherapeutic combination for treating cancer | |
| US20200317784A1 (en) | Methods and compositions for treating cancer by modifying multiple arms of the immune system | |
| US9920378B2 (en) | Allogeneic autophagosome-enriched composition for the treatment of disease | |
| KR20210090203A (en) | Long acting interleukin-15 receptor agonists in combination with another pharmacologically active agent | |
| US20180128833A1 (en) | Methods of treating with tumor membrane vesicle-based immunotherapy and predicting therapeutic response thereto | |
| KR20140131925A (en) | Autologous cancer cell vaccine | |
| JP2022130623A (en) | Vaccination with mica/b alpha 3 domain for treatment of cancer |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 20763489 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2021550014 Country of ref document: JP Kind code of ref document: A |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2020763489 Country of ref document: EP Effective date: 20210927 |