WO2018080591A1 - Methods of treatment with deuterated cftr potentiators - Google Patents
Methods of treatment with deuterated cftr potentiators Download PDFInfo
- Publication number
- WO2018080591A1 WO2018080591A1 PCT/US2017/029920 US2017029920W WO2018080591A1 WO 2018080591 A1 WO2018080591 A1 WO 2018080591A1 US 2017029920 W US2017029920 W US 2017029920W WO 2018080591 A1 WO2018080591 A1 WO 2018080591A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- compound
- fat
- administered
- food
- ivacaftor
- Prior art date
Links
- 0 CC(C)(C)c(cc(C(*)(*)*)c(O)c1)c1NC(C1=CNc2ccccc2C1=O)=O Chemical compound CC(C)(C)c(cc(C(*)(*)*)c(O)c1)c1NC(C1=CNc2ccccc2C1=O)=O 0.000 description 7
- CTRCOIVJCBPCPX-UHFFFAOYSA-N O=CC1=CNc2ccccc2C1=O Chemical compound O=CC1=CNc2ccccc2C1=O CTRCOIVJCBPCPX-UHFFFAOYSA-N 0.000 description 2
- XKFZZNZOVWDTLZ-UHFFFAOYSA-N CC(C)(C)C(C(C1)O)=CC(C(C)(C)C)=C1N[NH+](C(CNc1ccccc11)C1=O)[O-] Chemical compound CC(C)(C)C(C(C1)O)=CC(C(C)(C)C)=C1N[NH+](C(CNc1ccccc11)C1=O)[O-] XKFZZNZOVWDTLZ-UHFFFAOYSA-N 0.000 description 1
- GYGZOWDMDIEGDR-CYYJNZCTSA-N CC(C)(C)C(CC(C(C)(C)CO)C(O)=C1)=C1/N=N/C(CNC1C2=CC=C(C)C1)C2=O Chemical compound CC(C)(C)C(CC(C(C)(C)CO)C(O)=C1)=C1/N=N/C(CNC1C2=CC=C(C)C1)C2=O GYGZOWDMDIEGDR-CYYJNZCTSA-N 0.000 description 1
- IQZBXTSJIFWXKJ-FNORWQNLSA-N CC(C)N/C=C(\C)/[NH+](C)[O-] Chemical compound CC(C)N/C=C(\C)/[NH+](C)[O-] IQZBXTSJIFWXKJ-FNORWQNLSA-N 0.000 description 1
- NDJBTCJUHWEZRA-UHFFFAOYSA-N CCC(NC=C)=C Chemical compound CCC(NC=C)=C NDJBTCJUHWEZRA-UHFFFAOYSA-N 0.000 description 1
- GSODXYSLVMIJHU-PKPIPKONSA-N C[C@@H]1C(N)=CC1C(C)(C)C Chemical compound C[C@@H]1C(N)=CC1C(C)(C)C GSODXYSLVMIJHU-PKPIPKONSA-N 0.000 description 1
- XGMVMMJKUXZBKN-UHFFFAOYSA-N O=CC(CNC1=CCCC=C11)C1=O Chemical compound O=CC(CNC1=CCCC=C11)C1=O XGMVMMJKUXZBKN-UHFFFAOYSA-N 0.000 description 1
Classifications
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07B—GENERAL METHODS OF ORGANIC CHEMISTRY; APPARATUS THEREFOR
- C07B59/00—Introduction of isotopes of elements into organic compounds ; Labelled organic compounds per se
- C07B59/002—Heterocyclic compounds
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/47—Quinolines; Isoquinolines
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07D—HETEROCYCLIC COMPOUNDS
- C07D215/00—Heterocyclic compounds containing quinoline or hydrogenated quinoline ring systems
- C07D215/02—Heterocyclic compounds containing quinoline or hydrogenated quinoline ring systems having no bond between the ring nitrogen atom and a non-ring member or having only hydrogen atoms or carbon atoms directly attached to the ring nitrogen atom
- C07D215/16—Heterocyclic compounds containing quinoline or hydrogenated quinoline ring systems having no bond between the ring nitrogen atom and a non-ring member or having only hydrogen atoms or carbon atoms directly attached to the ring nitrogen atom with hetero atoms or with carbon atoms having three bonds to hetero atoms with at the most one bond to halogen, e.g. ester or nitrile radicals, directly attached to ring carbon atoms
- C07D215/48—Carbon atoms having three bonds to hetero atoms with at the most one bond to halogen
- C07D215/54—Carbon atoms having three bonds to hetero atoms with at the most one bond to halogen attached in position 3
- C07D215/56—Carbon atoms having three bonds to hetero atoms with at the most one bond to halogen attached in position 3 with oxygen atoms in position 4
Definitions
- ADME absorption, distribution, metabolism and/or excretion
- ADME limitation that affects many medicines is the formation of toxic or biologically reactive metabolites.
- some patients receiving the drug may experience toxicities, or the safe dosing of such drugs may be limited such that patients receive a suboptimal amount of the active agent.
- modifying dosing intervals or formulation approaches can help to reduce clinical adverse effects, but often the formation of such undesirable metabolites is intrinsic to the metabolism of the compound.
- a metabolic inhibitor will be co- administered with a drug that is cleared too rapidly.
- a drug that is cleared too rapidly.
- the FDA recommends that these drugs be co-dosed with ritonavir, an inhibitor of cytochrome P450 enzyme 3A4 (CYP3A4), the enzyme typically responsible for their metabolism (see Kempf, D.J. et al., Antimicrobial agents and chemotherapy, 1997, 41(3): 654-60).
- CYP3A4 cytochrome P450 enzyme 3A4
- Ritonavir causes adverse effects and adds to the pill burden for HIV patients who must already take a combination of different drugs.
- the CYP2D6 inhibitor quinidine has been added to dextromethorphan for the purpose of reducing rapid CYP2D6 metabolism of dextromethorphan in a treatment of pseudobulbar affect.
- a potentially attractive strategy for improving a drug's metabolic properties is deuterium modification.
- Deuterium is a safe, stable, non-radioactive isotope of hydrogen. Compared to hydrogen, deuterium forms stronger bonds with carbon. In select cases, the increased bond strength imparted by deuterium can positively impact the ADME properties of a drug, creating the potential for improved drug efficacy, safety, and/or tolerability.
- the size and shape of deuterium are essentially identical to those of hydrogen, replacement of hydrogen by deuterium would not be expected to affect the biochemical potency and selectivity of the drug as compared to the original chemical entity that contains only hydrogen.
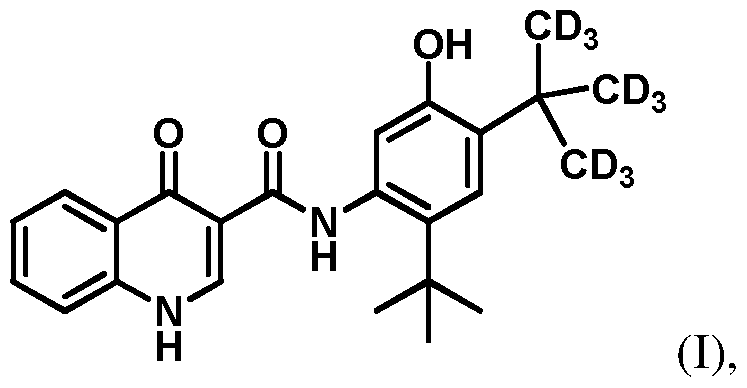
- This disclosure relates to deuterated derivatives of ivacaftor, and pharmaceutically acceptable salts thereof.
- This disclosure also relates to compositions comprising a deuterated derivatives of ivacaftor and the use of such compositions in methods of treating diseases and conditions that are beneficially treated by administering a CFTR (cystic fibrosis
- Ivacaftor also known as VX-770 and by the chemical name, N-(2,4-di-tert-butyl-5- hydroxyphenyl)-4-oxo-l,4-dihydroquinoline-3-carboxamide, acts as a CFTR potentiator.
- Results from phase III trials of ivacaftor in patients with cystic fibrosis carrying at least one copy of the G551D-CFTR mutation demonstrated marked levels of improvement in lung function and other key indicators of the disease including sweat chloride levels, likelihood of pulmonary exacerbations and body weight. Ivacaftor was approved by the FDA in 2012 for the treatment of cystic fibrosis in patients who have the G551D-CFTR mutation.
- ivacaftor was approved for treating cystic fibrosis in patients who have one of eight additional mutations (G178R, S549N, S549R, G551S, G1244E, S 1251N, S 1255P and G1349D) in the CFTR gene.
- ivacaftor was approved for treating cystic fibrosis in patients who have one of 10 mutations in the CFTR gene (G551D, G1244E, G1349D, G178R, G551S, S 125 IN, S 1255P, S549N, S549R and R117H).
- Ivacaftor was granted fast track designation and orphan drug designation by the FDA in 2006 and 2007, respectively, and is marketed under the tradename Kalydeco®. Ivacaftor is also approved in combination with VX-809 (also known as lumacaftor, a CFTR corrector) for the oral treatment of cystic fibrosis patients who carry the more common AF508-CFTR mutation; the combination is marketed under the tradename Orkambi®.
- VX-809 also known as lumacaftor, a CFTR corrector
- ivacaftor including Compound (I), also referred to as CTP-656, D9-ivacaftor or Compound 106) have an enhanced metabolic profile when administered to a subject, as compared to ivacaftor.
- the parent to metabolite ratio of Compound (I) is greater than the ratio found for ivacaftor.
- Compound (I) is represented by the following structural formula:
- this disclosure provides a method for treating conditions that can be treated by compounds that potentiate the activity of CFTR.
- this disclosure provides a method of treating a condition that is mediated by CFTR in a subject comprising orally administering to the subject an effective amount of Com ound (I):
- the amount of Compound (I), or a pharmaceutically acceptable salt thereof is in the range of about 50 mg to about 200 mg, for example, about 50 mg, about 60 mg, about 70 mg, about 80 mg, about 90 mg, about 100 mg, about 110 mg, about 120 mg, about 130 mg, about 140 mg, about 150 mg, about 160 mg, about 170 mg, about 180 mg, about 190 mg, or about 200 mg.
- the subject is a human. In one embodiment, the subject is a human 6 years of age or older. Compound (I), or a
- the method comprises administering to a subject an amount of Compound (I), or a pharmaceutically acceptable salt thereof, once a day, wherein the amount of Compound (I), or a
- pharmaceutically acceptable salt thereof is in the range of about 25 mg to about 75 mg, for example, about 25 mg, about 37.5 mg, about 50 mg, about 62.5 mg, or about 75 mg, wherein the subject is a human 2 to less than 6 years of age and less than 14 kg; or alternatively, is a human 2 to less than 6 years of age and 14 kg or greater.
- the dose for the human 2 to less than 6 years of age and less than 14 kg is 25 mg.
- the dose for the human 2 to less than 6 years of age and greater than 14 kg is 37.5 mg.
- Compound (I), or a pharmaceutically acceptable salt thereof is administered orally at any of the foregoing dosages.
- the Compound (I), or a pharmaceutically acceptable salt thereof is administered orally at any of the foregoing dosages in a pharmaceutical formulation which is a granule.
- the compound is Compound (I).
- a second aspect is Compound (I), or a pharmaceutically acceptable salt thereof, for treating conditions that can be treated by compounds that potentiate the activity of CFTR.
- the compound may be administered as disclosed herein, i.e., by administering Compound (I) with food containing less than 60 g of fat.
- a third aspect is the use of Compound (I), or a pharmaceutically acceptable salt thereof, for the manufacture of a medicament for treating conditions that can be treated by compounds that potentiate the activity of CFTR.
- the compound may be administered as disclosed herein, as disclosed herein, i.e., by administering Compound (I) with food containing less than 60 g of fat, e.g., in an amount in the range of 50 mg to 200 mg, once per day.
- a fourth aspect is a pharmaceutical composition comprising a pharmaceutically acceptable carrier or diluent and about 50 mg to about 200 mg of Compound (I), or a pharmaceutically acceptable salt thereof.
- the pharmaceutical composition comprises about 50 mg, about 60 mg, about 70 mg, about 80 mg, about 90 mg, about 100 mg, about 110 mg, about 120 mg, about 130 mg, about 140 mg, about 150 mg, about 160 mg, about 170 mg, about 180 mg, about 190 mg, or about 200 mg of Compound (I), or a pharmaceutically acceptable salt thereof. More specifically, for example, the pharmaceutical composition comprises about 75, about 100, or about 150 mg of Compound I to be administered once per day. In a particular embodiment, the pharmaceutical composition comprises about 100 - about 150 mg of Compound I to be administered once per day. In a particular embodiment, the pharmaceutical composition comprises about 100 mg of
- the pharmaceutical composition is a tablet.
- An alternative fourth aspect is a pharmaceutical composition comprising a pharmaceutically acceptable carrier or diluent and about 25 mg to about 75 mg of Compound (I), or a pharmaceutically acceptable salt thereof. Specifically, the
- composition comprises about 25 mg, about 37.5 mg, about 50 mg, about 62.5 mg, or about 75 mg of Compound (I), or a pharmaceutically acceptable salt thereof.
- the pharmaceutical composition is a granule.
- this disclosure provides a compound as disclosed herein (e.g. , compound (I) or a pharmaceutically acceptable salt thereof) or a composition comprising an effective amount of Compound (I) (or a pharmaceutically acceptable salt thereof) for use in treating a condition that is mediated by CFTR in a subject, wherein the compound is administered with food containing less than 60 g of fat.
- the condition that is mediated by CFTR is cystic fibrosis.
- Figure 1A depicts the mean plasma concentration (ng/mL) for CTP-656 and ivacaftor in the single ascending dose study.
- Figure IB depicts the mean plasma concentration (ng/mL) for CTP-656 and ivacaftor in the single ascending dose study.
- Figure 2 depicts the mean plasma concentration (ng/mL) for CTP-656 and ivacaftor following a 150 mg oral dose.
- Figure 3 depicts the parent verses metabolite pharmacokinetic profile for (a) CTP-656 and (b) Ivacaftor (Kalydeco) following a 150 mg oral dose.
- Figure 4A depicts the peak current potentiated by sequential additions of test articles.
- Figure 4B depicts the AUC of potentiator response.
- Figure 4C depicts the AIsc of potentiator response for ivacaftor, CTP-656, and D18- ivacaftor.
- Figure 5 is a schematic of the single ascending dose study.
- Figure 6 is a scheme of the metabolites of ivacaftor and CTP-656.
- Figure 7A is a schematic of the crossover study for D9-ivacaftor and D18-ivacaftor.
- Figure 7B depicts the mean plasma concentration (ng/mL) for D9-ivacaftor and D18- ivacaftor following a 25 mg oral dose.
- Figure 8 shows a schematic of the design of a multiple-ascending dose trial for CTP- 656 (D9-ivacaftor).
- Part A single dose pharmacokinetic comparison (with crossover) of 150 mg CTP-656 (2x 75 mg tablets) versus 150 mg ivacaftor.
- Part B assessment of three doses of CTP-656 (75 mg, 150 mg, and 225 mg or placebo, dosed once daily for seven days.
- Figure 9 is a graph showing the plasma concentration of CTP-656 and ivacaftor after a single dose of CTP-656 or ivacaftor.
- Figure 10 is a graph showing the plasma concentration of CTP-656 and metabolites (left panel) and a graph showing the plasma concentration of ivacaftor and metabolites (right panel) after a single dose of CTP-656 or ivacaftor.
- Figure 11 is a graph showing the plasma concentration of CTP-656 and metabolites after multiple dosing (once per day for seven days) of CTP-656.
- Figure 12 depicts a food-effect study for CTP-656: (A) schematic of the design of the food-effect study; (B) a graph showing the mean plasma concentration of CTP-656 in the food-effect study; (C) a table showing pharmacokinetic (PK) parameters for CTP-656 in the food-effect study.
- A schematic of the design of the food-effect study
- B a graph showing the mean plasma concentration of CTP-656 in the food-effect study
- C a table showing pharmacokinetic (PK) parameters for CTP-656 in the food-effect study.
- treat means decrease, suppress, attenuate, diminish, arrest, or stabilize the development or progression of a disease (e.g. , a disease or disorder delineated herein), lessen the severity of the disease or improve the symptoms associated with the disease.
- a disease e.g. , a disease or disorder delineated herein
- Disease means any condition or disorder that damages or interferes with the normal function of a cell, tissue, or organ.
- Disease means any condition or disorder that damages or interferes with the normal function of a cell, tissue, or organ.
- any atom not specifically designated as a particular isotope is meant to represent any stable isotope of that atom.
- a position is designated specifically as “H” or “hydrogen”
- the position is understood to have hydrogen at its natural abundance isotopic composition.
- a position is designated specifically as “D” or “deuterium”
- the position is understood to have deuterium at an abundance that is at least 3000 times greater than the natural abundance of deuterium, which is 0.015% (i.e., at least 45% incorporation of deuterium).
- isotopic enrichment factor means the ratio between the isotopic abundance and the natural abundance of a specified isotope.
- a compound of this invention i.e., Compound I has an isotopic enrichment factor for each designated deuterium atom of at least 3500 (52.5% deuterium incorporation at each designated deuterium atom), at least 4000 (60% deuterium
- isotopologue refers to a species in which the chemical structure differs from Compound (I) only in the isotopic composition thereof.
- a compound represented by a particular chemical structure containing indicated deuterium atoms will also contain lesser amounts of isotopologues having hydrogen atoms at one or more of the designated deuterium positions in that structure.
- the relative amount of such isotopologues in a compound of this invention will depend upon a number of factors including the isotopic purity of deuterated reagents used to make the compound and the efficiency of incorporation of deuterium in the various synthesis steps used to prepare the compound.
- the invention also provides salts of Compound (I).
- a salt of a compound of this invention is formed between an acid and a basic group of the compound, such as an amino functional group, or a base and an acidic group of the compound, such as a carboxyl functional group.
- the compound is a pharmaceutically acceptable acid addition salt.
- pharmaceutically acceptable refers to a component that is, within the scope of sound medical judgment, suitable for use in contact with the tissues of humans and other mammals without undue toxicity, irritation, allergic response and the like, and are commensurate with a reasonable benefit/risk ratio.
- pharmaceutically acceptable salt means any non-toxic salt that, upon administration to a recipient, is capable of providing, either directly or indirectly, a compound of this invention.
- pharmaceutically acceptable counterion is an ionic portion of a salt that is not toxic when released from the salt upon administration to a recipient.
- Acids commonly employed to form pharmaceutically acceptable salts include inorganic acids such as hydrogen bisulfide, hydrochloric acid, hydrobromic acid, hydroiodic acid, sulfuric acid and phosphoric acid, as well as organic acids such as para-toluenesulfonic acid, salicylic acid, tartaric acid, bitartaric acid, ascorbic acid, maleic acid, besylic acid, fumaric acid, gluconic acid, glucuronic acid, formic acid, glutamic acid, methanesulfonic acid, ethanesulfonic acid, benzenesulfonic acid, lactic acid, oxalic acid, para- bromophenylsulfonic acid, carbonic acid, succinic acid, citric acid, benzoic acid and acetic acid, as well as related inorganic and organic acids.
- Such pharmaceutically acceptable salts thus include sulfate, pyrosulfate, bisulfate, sulfite, bisulfite
- stable compounds refers to compounds which possess stability sufficient to allow for their manufacture and which maintain the integrity of the compound for a sufficient period of time to be useful for the purposes detailed herein (e.g. , formulation into therapeutic products, intermediates for use in production of therapeutic compounds, isolatable or storable intermediate compounds, treating a disease or condition responsive to therapeutic agents).
- bioequivalent means a drug product showing the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in a pharmaceutical equivalent to the drug product becomes available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study, wherein "significant difference” means that the 90%
- Substituted with deuterium refers to the replacement of one or more hydrogen atoms with a corresponding number of deuterium atoms.
- this disclosure relates to methods of use of Compound (I), or a pharmaceutically acceptable salt thereof, involving certain dosing regimens and certain pharmaceutical compositions comprising Compound (I), or a pharmaceutically acceptable salt thereof.
- the pharmaceutical compositions and dosing regimens are useful for treating conditions mediated by CFTR (cystic fibrosis transmembrane conductance regulator).
- CFTR cystic fibrosis transmembrane conductance regulator
- compositions and methods are useful for treating conditions that can be treated by compounds that potentiate the activity of CFTR.
- the prescribing information for ivacaftor 150 mg tablets indicates that one 150 tablet should be taken orally every 12 hours with fat-containing food. It has now been found that Compound (I), as described herein, can be administered with food having low, moderate, or high fat content, and the patient's exposure to CTP-656 is similar regardless of the fat content of a meal.
- the disclosure provides methods for treating conditions that can be treated by compounds that potentiate the activity of CFTR.
- the disclosure provides a method of treating a condition that is mediated by CFTR in a subject comprising orally administering to the subject an effective amount of Compound (I):
- Compound (I) is administered to the subject with food containing less than 60 g of fat.
- Compound (I) can be administered as a pharmaceutical composition, e.g. , together with carrier, fillers, excipients, and the like.
- the condition is cystic fibrosis.
- Compound (I), or a pharmaceutically acceptable salt thereof is administered once per day.
- the Compound (I) is administered in a pharmaceutical formulation which is a tablet.
- the Compound (I) is administered in a pharmaceutical formulation which is a granule.
- the Compound (I) is administered as a pharmaceutical composition, and the drug loading of Compound (I), or pharmaceutical salt thereof, in the composition (that is, the ratio of the weight of the Compound (I) (or pharmaceutical salt thereof) to the total weight of the composition (which includes carriers, fillers, excipients, and the like)) is not greater than 25%, or not greater than 20%, or not greater than 15%.
- the drug loading of Compound (I) (or pharmaceutical salt thereof) in the composition is between about 10% and 15%, or between about 13% and 15%.
- the drug loading of Compound (I) (or pharmaceutical salt thereof) in the composition is about 13% to about 14%, or 13.5% to 14%, or 13.6% to 13.8%.
- any atom not designated as deuterium in Compound (I) is present at its natural isotopic abundance.
- the plasma concentration of Compound (I) in the subject at 8 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 8 hours when the Compound (I) is administered without food.
- the plasma concentration of Compound (I) in the subject at 16 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 16 hours when the Compound (I) is administered without food.
- the plasma concentration of Compound (I) in the subject at 24 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 24 hours when the Compound (I) is administered without food.
- the subject is a human adult or a human pediatric patient 6 years and older.
- the food contains less than about 30 g of fat.
- the food contains less than about 20 g of fat.
- the food contains less than about 10 g of fat.
- the food contains between about 0 and about 50 g of fat.
- the food contains between essentially no fat, i.e. is substantially fat-free.
- the food contains between about 5 and about 20 g of fat.
- the food contains about 7 g of fat. In certain of the above embodiments, the food contains about 20 g of fat.
- the food is low-fat food or a low-fat meal.
- Low-fat food or a “low-fat meal” includes food or a meal having less than about 10 g of total fat (e.g. , about 7 g total fat or less).
- the food is moderate-fat food or a moderate-fat meal.
- Moderate-fat food or a “moderate-fat meal” includes food or a meal having between about 10 g of total fat and about 30 g total fat (e.g., about 15 g to about 25 g of total fat, or about 20 g total fat).
- the food is a small meal.
- the food comprises cheese and/or crackers.
- the condition is cystic fibrosis and the subject has one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S 125 IN, S 1255P, S549N, S549R, and R117H.
- Compound I can be administered once per day. More specifically, for example, 75, 100, or 150 mg of Compound I can be administered once per day. In a particular embodiment, 100 - 150 mg of Compound I can be administered once per day. In a particular embodiment, 100 mg of Compound I can be administered once per day. In particular embodiments, the subject is a human.
- the method comprises administering to a subject an amount of Compound (I), or a pharmaceutically acceptable salt thereof, once a day, wherein the amount of Compound (I), or a pharmaceutically acceptable salt thereof, is in the range of 25 mg to 75 mg, for example, 25 mg, 37.5 mg, 50 mg, 62.5 mg, or 75 mg, wherein the subject is a human 2 to less than 6 years of age and less than 14 kg; or alternatively, is a human 2 to less than 6 years of age and 14 kg or greater.
- the dose for the human 2 to less than 6 years of age and less than 14 kg is 25 mg.
- the dose for the human 2 to less than 6 years of age and greater than 14 kg is 37.5 mg.
- Compound I can be administered immediately before, concurrently with, or immediately after (e.g. , within 30 minutes after) the
- Compound I can be administered to the subject with food without a pre-specified fat level or without requiring a high fat content, e.g., a food or meal containing less than 60 g of fat.
- the disclosure provides a kit for use in treating a condition that is mediated by CFTR in a subject.
- the kit comprises an effective amount of Compound (I), or a pharmaceutical composition comprising an effective amount of Compound (I):
- the pharmaceutical composition can include carriers, fillers, excipients, and the like.
- the condition is cystic fibrosis.
- Compound (I), or a pharmaceutically acceptable salt thereof is administered once per day.
- the Compound (I) is administered in a pharmaceutical formulation which is a tablet.
- the Compound (I) is administered in a pharmaceutical formulation which is a granule.
- the drug loading of Compound (I) (or pharmaceutical salt thereof) in the composition is not greater than 25%, or not greater than 20%, or not greater than 15%. In certain embodiments, the drug loading of Compound (I) (or pharmaceutical salt thereof) in the composition is between about 10% and 15%, or between about 13% and 15%. In certain embodiments, the drug loading of Compound (I) (or pharmaceutical salt thereof) in the composition is about 13% to about 14%, or 13.5% to 14%, or 13.6% to 13.8%.
- any atom not designated as deuterium in Compound (I) is present at its natural isotopic abundance.
- the plasma concentration of Compound (I) in the subject at 8 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 8 hours when the Compound (I) is administered without food.
- the plasma concentration of Compound (I) in the subject at 16 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 16 hours when the Compound (I) is administered without food.
- the plasma concentration of Compound (I) in the subject at 24 hours after administration is about 1.5 - 2-fold greater than the plasma concentration of Compound (I) at 24 hours when the Compound (I) is administered without food.
- the subject is a human adult or a human pediatric patient 6 years and older.
- the food contains less than about 30 g of fat.
- the food contains less than about 20 g of fat.
- the food contains less than about 10 g of fat.
- the food contains between about 0 and about 50 g of fat.
- the food contains between essentially no fat, i.e. is substantially fat-free.
- the food contains between about 5 and about 20 g of fat.
- the food contains about 7 g of fat. In certain of the above embodiments, the food contains about 20 g of fat.
- the food is low-fat food or a low-fat meal.
- Low-fat food or a “low-fat meal” includes food or a meal having less than about 10 g of total fat (e.g. , about 7 g total fat or less).
- the food is moderate-fat food or a moderate-fat meal.
- Moderate-fat food or a “moderate-fat meal” includes food or a meal having between about 10 g of total fat and about 30 g total fat (e.g., about 15 g to about 25 g of total fat, or about 20 g total fat).
- the food is a small meal.
- the food comprises cheese and/or crackers.
- the condition is cystic fibrosis and the subject has one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S 125 IN, S 1255P, S549N, S549R, and R117H.
- Compound I can be administered once per day. More specifically, for example, 75, 100, or 150 mg of Compound I can be administered once per day. In a particular embodiment, 100 - 150 mg of Compound I can be administered once per day. In a particular embodiment, 100 mg of Compound I can be administered once per day. In particular embodiments, the subject is a human.
- Compound (I), or a pharmaceutically acceptable salt thereof is administered once a day, wherein the amount of Compound (I), or a pharmaceutically acceptable salt thereof, is in the range of 25 mg to 75 mg, for example, 25 mg, 37.5 mg, 50 mg, 62.5 mg, or 75 mg, wherein the subject is a human 2 to less than 6 years of age and less than 14 kg; or alternatively, is a human 2 to less than 6 years of age and 14 kg or greater.
- the dose for the human 2 to less than 6 years of age and less than 14 kg is 25 mg.
- the dose for the human 2 to less than 6 years of age and greater than 14 kg is 37.5 mg.
- Compound I can be administered immediately before, concurrently with, or immediately after (e.g. , within 30 minutes after) the
- Conditions treatable by the methods and kits disclosed herein include cystic fibrosis, Hereditary emphysema, Hereditary hemochromatosis, Coagulation- Fibrinolysis deficiencies, such as Protein C deficiency, Type 1 hereditary angioedema, Lipid processing deficiencies, such as Familial hypercholesterolemia, Type 1 chylomicronemia, Abetalipoproteinemia, Lysosomal storage diseases, such as I-cell disease/Pseudo-Hurler, Mucopolysaccharidoses, Sandhof/T ay-Sachs, Crigler-Najjar type II, Polyendocrinopathy/Hyperinsulemia, Diabetes mellitus, Laron dwarfism, Myleoperoxidase deficiency, Primary hypoparathyroidism, Melanoma, Glycanosis CDG type 1, Hereditary emphysema, Congenital hyperthyroidism, Osteogenesis imperfect
- the condition is cystic fibrosis in a subject such as a human patient in need thereof.
- the condition is chronic obstructive pulmonary disease in a subject such as a human patient in need thereof.
- the subject is a human patient having the G551D-CFTR mutation.
- the subject is a human patient having one of the following mutations in the CFTR gene: G178R, S549N, S549R, G551S, G1244E, S 125 IN, S 1255P or G1349D.
- the subject is a human patient having one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S 125 IN, S 1255P, S549N, S549R and Rl 17H.
- the compound is administered orally once a day.
- the compound is administered optionally in combination with a second agent.
- the subject is a human patient having the AF508-CFTR mutation.
- second agents include CFTR correctors, such as lumacaftor (VX-809) or tezacaftor (VX-661). In some embodiments wherein
- Compound (I), or a pharmaceutically acceptable salt thereof is administered optionally in combination with a second agent, the amount of Compound (I), or a pharmaceutically acceptable salt thereof, is administered once daily at 50 mg to 200 mg each time, for example, about 50 mg, 60 mg, 70 mg, 80 mg, 90 mg, 100 mg, 110 mg, 120 mg, 130 mg, 140 mg, 150 mg, 160 mg, 170 mg, 180 mg, 190 mg, or about 200 mg.
- the amount of Compound (I), or a pharmaceutically acceptable salt thereof is administered once daily at 25 mg to 75 mg each time, for example, about 25 mg, 37.5 mg, 50 mg, 62.5 mg, or about 75 mg.
- Effective doses will also vary, as recognized by those skilled in the art, depending on the diseases treated, the severity of the disease, the route of administration, the sex, age and general health condition of the subject, excipient usage, the possibility of co-usage with other therapeutic treatments such as use of other agents and the judgment of the treating physician.
- an effective amount of the second therapeutic agent is between about 20% and 100% of the dosage normally utilized in a monotherapy regime using just that agent.
- an effective amount is between about 70% and 100% of the normal monotherapeutic dose.
- the normal monotherapeutic dosages of these second therapeutic agents are well known in the art. See, e.g., Wells et al., eds., Pharmacotherapy Handbook, 2nd Edition, Appleton and Lange, Stamford, Conn. (2000); PDR Pharmacopoeia, Tarascon Pocket Pharmacopoeia 2000, Deluxe Edition, Tarascon Publishing, Loma Linda, Calif. (2000), each of which references are incorporated herein by reference in their entirety.
- Compound (I) or a pharmaceutically acceptable salt thereof, synergistic improvements in efficacy, improved ease of administration or use and/or reduced overall expense of compound preparation or formulation.
- any of the above methods of treatment comprises the further step of co -administering to the subject in need thereof one or more second therapeutic agents.
- the choice of second therapeutic agent may be made from any second therapeutic agent known to be useful for co-administration with ivacaftor.
- the choice of second therapeutic agent is also dependent upon the particular disease or condition to be treated. Examples of second therapeutic agents that may be employed in the methods of this invention are those set forth above for use in combination compositions comprising Compound (I), or a
- the combination therapies of this invention include co- administering a Compound (I), or a pharmaceutically acceptable salt thereof, or a pharmaceutically acceptable salt thereof and a second therapeutic agent such as VX-809 (lumacaftor) or VX- 661 (tezacaftor), to a subject in need thereof for treatment.
- the subject is a human patient having the AF508-CFTR mutation (in particular, a human patient homozygous for the F508del mutation).
- co- administered means that the second therapeutic agent may be administered together with Compound (I), or a pharmaceutically acceptable salt thereof, as part of a single dosage form (such as a composition of this invention comprising a compound of the invention and an second therapeutic agent as described above) or as separate, multiple dosage forms.
- the additional agent may be administered prior to, consecutively with, or following the administration of Compound (I), or a pharmaceutically acceptable salt thereof.
- both Compound (I), or a pharmaceutically acceptable salt thereof, and the second therapeutic agent(s) are administered by conventional methods.
- composition of this invention comprising both Compound (I), or a pharmaceutically acceptable salt thereof, and a second therapeutic agent
- administration of a composition of this invention, comprising both Compound (I), or a pharmaceutically acceptable salt thereof, and a second therapeutic agent, to a subject does not preclude the separate administration of that same therapeutic agent, any other second therapeutic agent or Compound (I), or a pharmaceutically acceptable salt thereof, to said subject at another time during a course of treatment.
- Effective amounts of these second therapeutic agents are well known to those skilled in the art and guidance for dosing may be found in patents and published patent applications referenced herein, as well as in Wells et al., eds., Pharmacotherapy Handbook, 2nd Edition, Appleton and Lange, Stamford, Conn.
- the effective amount of the second therapeutic agent is less than its effective amount would be where Compound (I), or a pharmaceutically acceptable salt thereof, is not administered. In this way, undesired side effects associated with high doses of either agent may be minimized.
- Other potential advantages including without limitation improved dosing regimens and/or reduced drug cost
- the invention provides the use of Compound (I), or a
- Another aspect of the invention is Compound (I), or a pharmaceutically acceptable salt thereof, for use in the treatment or prevention in a subject of a disease, disorder or symptom thereof delineated herein.
- any atom not designated as deuterium is present at its natural isotopic abundance in Compound (I), or a pharmaceutically acceptable salt thereof.
- Such methods can be carried out utilizing corresponding deuterated and optionally, other isotope-containing reagents and/or intermediates to synthesize the compounds delineated herein, or invoking standard synthetic protocols known in the art for introducing isotopic atoms to a chemical structure.
- compositions comprising an effective amount of Compound (I), or a pharmaceutically acceptable salt thereof; and a
- the carrier(s) are "acceptable” in the sense of being compatible with the other ingredients of the formulation and, in the case of a pharmaceutically acceptable carrier, not deleterious to the recipient thereof in an amount used in the medicament.
- Pharmaceutically acceptable carriers, adjuvants and vehicles that may be used in the pharmaceutical compositions of this invention include, but are not limited to, ion exchangers, alumina, aluminum stearate, lecithin, serum proteins, such as human serum albumin, buffer substances such as phosphates, glycine, sorbic acid, potassium sorbate, partial glyceride mixtures of saturated vegetable fatty acids, water, salts or electrolytes, such as protamine sulfate, disodium hydrogen phosphate, potassium hydrogen phosphate, sodium chloride, zinc salts, colloidal silica, magnesium trisilicate, polyvinyl pyrrolidone, cellulose-based substances, polyethylene glycol, sodium carboxymethylcellulose, polyacrylates, waxes, polyethylene-polyoxypropylene-block polymers, polyethylene glycol and wool fat.
- ion exchangers alumina, aluminum stearate, lecithin
- serum proteins such as human serum albumin
- buffer substances such as phosphat
- the solubility and bioavailability of the compounds of the present invention in pharmaceutical compositions may be enhanced by methods well-known in the art.
- One method includes the use of lipid excipients in the formulation. See “Oral Lipid- Based Formulations: Enhancing the Bioavailability of Poorly Water-Soluble Drugs (Drugs and the Pharmaceutical Sciences),” David J. Hauss, ed. Informa Healthcare, 2007; and “Role of Lipid Excipients in Modifying Oral and Parenteral Drug Delivery: Basic Principles and Biological Examples," Kishor M. Wasan, ed. Wiley-Interscience, 2006.
- Another known method of enhancing bioavailability is the use of an amorphous form of a compound of this invention optionally formulated with a poloxamer, such as LUTROLTM and PLURONICTM (BASF Corporation), or block copolymers of ethylene oxide and propylene oxide. See United States patent 7,014,866; and United States patent publications 20060094744 and 20060079502.
- compositions of the invention include those suitable for oral administration.
- Other formulations may conveniently be presented in unit dosage form, e.g. , tablets, sustained release capsules, granules, and in liposomes, and may be prepared by any methods well known in the art of pharmacy. See, for example, Remington: The Science and Practice of Pharmacy, Lippincott Williams & Wilkins, Baltimore, MD (20th ed. 2000).
- Such preparative methods include the step of bringing into association with the molecule to be administered ingredients such as the carrier that constitutes one or more accessory ingredients.
- the compositions are prepared by uniformly and intimately bringing into association the active ingredients with liquid carriers, liposomes or finely divided solid carriers, or both, and then, if necessary, shaping the product.
- the compound is administered orally.
- compositions of the present invention suitable for oral administration may be presented as discrete units such as capsules, sachets, or tablets each containing a predetermined amount of the active ingredient; a powder or granules; a solution or a suspension in an aqueous liquid or a non-aqueous liquid; an oil-in-water liquid emulsion; a water-in-oil liquid emulsion; packed in liposomes; or as a bolus, etc.
- Soft gelatin capsules can be useful for containing such suspensions, which may beneficially increase the rate of compound absorption.
- the compound is administered orally as a tablet.
- the compound is administered orally as a granule.
- carriers that are commonly used include lactose and corn starch.
- Lubricating agents such as magnesium stearate, are also typically added.
- useful diluents include lactose and dried cornstarch.
- the active ingredient is combined with emulsifying and suspending agents. If desired, certain sweetening and/or flavoring and/or coloring agents may be added.
- the composition is in the form of a tablet.
- exemplary formulations for the tablet are disclosed in US. Patent No. 8,754,224, the teachings of which are herein incorporated by reference.
- the tablet contains 150 mg of Compound (I), or a pharmaceutically acceptable salt thereof, and the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate.
- the tablet film coat contains carnauba wax, FD&C Blue #2, PEG 3350, polyvinyl alcohol, talc, and titanium dioxide.
- the tablet is printed with a printing ink; the printing ink may contain ammonium hydroxide, iron oxide black, propylene glycol, and shellac.
- the tablet contains 75 mg of Compound I (CTP-656, D9-ivacaftor), together with the following inactive ingredients:
- microcrystalline cellulose lactose monohydrate, colloidal silicon dioxide, croscarmellose sodium, magnesium stearate, and sodium lauryl sulfate.
- Multiple tablets may be administered to provide a suitable once-daily dose (e.g., two 75 mg tablets administered together for a 150 mg once-daily dose).
- the tablet comprises granules compressed with extra-granular material; the granules comprise about 17.1 percent (by weight of the tablet) of an amorphous dispersion of Compound I (wherein the amorphous dispersion comprises about 80% substantially amorphous Compound I by weight of the dispersion, hypromellose acetate succinate (HPMCAS) (about 19.5 percent by weight of the dispersion) and sodium laurel sulfate (about 0.5 percent by weight of the dispersion)), a compression aid such as microcrystalline cellulose (e.g.
- the extracellular matrix comprises a disintegrant such as croscarmellose sodium (e.g., croscarmellose sodium (e.g., Ac-di-sol) (about 1.50 percent by weight of the tablet) and a lubricant such as Hyqual magnesium stearate (about 0.20 percent by weight of the tablet), and the extracellular matrix comprises a disintegrant such as croscarmellose sodium (e.g.
- a glidant such as colloidal silicon dioxide (about 0.50 percent by weight of the tablet) and additional lubricant such as magnesium stearate (e.g. , Hyqual (about 0.80 percent by weight of the tablet).
- the invention provides a pharmaceutical composition
- a pharmaceutical composition comprising about 17.1 wt % of a solid dispersion by weight of the composition, wherein the dispersion comprises about 80 wt % of substantially amorphous Compound I (CTP-656) by weight of the dispersion, about 19.5 wt % of hypromellose acetate succinate (HPMCAS) by weight of the dispersion, and about 0.5 wt % SLS by weight of the dispersion; about 39.0 wt % of microcrystalline cellulose by weight of the composition; about 38.9 wt % of lactose monohydrate by weight of the composition; about 3 wt % of sodium
- the tablet comprises 75 mg of Compound I (CTP-656). In other embodiments, the tablet comprises 100 mg of Compound I (CTP-656). In still other embodiments, the tablet comprises 150 mg of Compound I (CTP-656).
- the granule is enclosed in a unit-dose packet containing 25 mg, 50 mg or 75 mg of Compound (I), or a pharmaceutically acceptable salt thereof.
- Each unit-dose packet of Compound (I) oral granules contains 25 mg of Compound (I), 50 mg of Compound (I) or 75 mg of Compound (I) and the following inactive
- the composition is in the form of a granule.
- exemplary formulations for the granule are disclosed in US. Patent No. 8,883,206, the teachings of which are herein incorporated by reference.
- a composition of this invention further comprises a second therapeutic agent.
- the second therapeutic agent may be selected from any compound or therapeutic agent known to have or that demonstrates advantageous properties when administered with a compound having the same mechanism of action as ivacaftor.
- the second therapeutic agent is an agent useful in the treatment of a variety of conditions, including cystic fibrosis, Hereditary emphysema, Hereditary hemochromatosis, Coagulation-Fibrinolysis deficiencies, such as Protein C deficiency, Type 1 hereditary angioedema, Lipid processing deficiencies, such as Familial hypercholesterolemia, Type 1 chylomicronemia, Abetalipoproteinemia, Lysosomal storage diseases, such as I-cell disease/Pseudo-Hurler, Mucopolysaccharidoses, Sandhof/T ay-Sachs, Crigler-Najjar type II, Polyendocrinopathy/Hyperinsulemia, Diabetes mellitus, Laron dwarfism, Myleoperoxidase deficiency, Primary hypoparathyroidism, Melanoma, Glycanosis CDG type 1, Hereditary emphysema, Congenital
- hypofibrinogenemia ACT deficiency
- Diabetes insipidus DI
- Neurophyseal DI Neprogenic DI
- Charcot-Marie Tooth syndrome Perlizaeus-Merzbacher disease
- neurodegenerative diseases such as Alzheimer's disease, Parkinson's disease, Amyotrophic lateral sclerosis, Progressive supranuclear palsy, Pick's disease, several polyglutamine neurological disorders asuch as Huntington, Spinocerebullar ataxia type I, Spinal and bulbar muscular atrophy, Dentatorubal pallidoluysian, and Myotonic dystrophy, as well as Spongiform
- encephalopathies such as Hereditary Creutzfeldt- Jakob disease, Fabry disease, Straussler- Scheinker syndrome, COPD, dry-eye disease, Sjogren's disease, and a bile duct disorder or a kidney ion channel disorder, including, but not limited to, Bartter's syndrome and Dent's disease.
- the second therapeutic agent is an agent useful in the treatment of cystic fibrosis.
- the second therapeutic agent is an agent useful in the treatment of cystic fibrosis in a human patient having the G551D-CFTR mutation.
- the second therapeutic agent is an agent useful in the treatment of cystic fibrosis in a human patient having any of the following mutations in the CFTR gene: G178R, S549N, S549R, G551S, G1244E, S 125 IN, S 1255P or G1349D.
- the second therapeutic agent is an agent useful in the treatment of cystic fibrosis in a human patient having any of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S 125 IN, S 1255P, S549N, S549R and R117H.
- the second therapeutic agent is VX-809 (lumacaftor) or VX-661 (tezacaftor).
- the subject is a human patient having the AF508-CFTR mutation (in particular, a human patient homozygous for the F508del mutation).
- the invention provides separate dosage forms of Compound (I), or a pharmaceutically acceptable salt thereof, and one or more of any of the above- described second therapeutic agents, wherein Compound (I), or a pharmaceutically acceptable salt thereof, and second therapeutic agent are associated with one another.
- the term "associated with one another" as used herein means that the separate dosage forms are packaged together or otherwise attached to one another such that it is readily apparent that the separate dosage forms are intended to be sold and administered together (within less than 24 hours of one another, consecutively or simultaneously).
- Compound (I), or a pharmaceutically acceptable salt thereof is present in an effective amount.
- effective amount refers to an amount which, when administered in a proper dosing regimen, is sufficient to treat the target disorder.
- the product comprises: a) an oral dosage form com rising an effective amount of Compound (I):
- the prescribing information includes: i) dosage and administration information for adults and pediatric patients 6 years and older instructing the administration of 50-200 mg of Compound (I) taken orally with food containing less than 60 g of fat.
- the oral dosage form comprises about 75, about 100, or about 150 mg of Compound I.
- the prescribing information instructs the oral administration of Compound (I) once per day.
- the prescribing information instructs the oral administration of
- the prescribing information instructs the oral administration of Compound (I) with food containing less than 30 g of fat, or less than 20 g of fat, or less than 10 g of fat.
- the prescribing information instructs the oral administration of Compound (I) with food containing between 0 and 50 g of fat, or between 5 and 20 g of fat. In certain embodiments, the prescribing information instructs the oral administration of Compound (I) with food containing about 7 g of fat. In certain embodiments, the prescribing information instructs the oral administration of Compound (I) with food containing about 20 g of fat. In certain embodiments, the prescribing information instructs the oral administration of Compound (I) with food containing about low-fat food or a low-fat meal.
- the prescribing information instructs the oral administration of Compound (I) with moderate-fat food or a moderate-fat meal. In certain embodiments, the prescribing information instructs the oral administration of Compound (I) with a small meal. In certain embodiments, the pharmaceutical product is used in the claimed methods and the claimed kit as described above.
- the food comprises cheese.
- the oral dosage form comprises a pharmaceutical composition of Compound (I) with a pharmaceutically acceptable carrier.
- the objective of the study was to compare the pharmacokinetics of single ascending doses (75, 150, and 300 mg) of CTP-656, to compare the pharmacokinetics of a single dose of 150 mg CTP-656 and 150 mg Kalydeco and to assess the safety and tolerability of CTP-656.
- T max for CTP-656 was similar between each of the treatments, with the apparent terminal half- life of 14- 17 hours.
- the apparent terminal half-life of 150 mg of Kalydeco ® (11.18 hours) was shorter than for CTP-656.
- CTP-656 has potential to show efficacy at doses in the range of 50-200 mg QD (once daily).
- the parent-to-Ml ratio of C max and C 2 4hr for CTP-656/D8-M1 are 2.1 and 2.2, respectively, compared to 0.54 and 0.55, respectively, for ivacaftor/Ml.
- the parent-to-M6 ratio of AUCo-24hr for CTP-656/D6-M6 is 4.0, compared to 1.5 for the ratio of ivacaftor to M6.
- the parent-to-M6 ratio of C max and C 2 4hr for CTP-656/D6-M6 are 4.3 and 2.5 respectively, compared to 1.4 and 0.97, respectively, for ivacaftor/M6.
- CTP-656 is the most abundant species in plasma at all times measured, in contrast to ivacaftor (b), where the Ml metabolite predominates after 2 hours, and the level of the M6 metabolite reaches the level of ivacaftor after about 8 hours.
- the most pharmacologically-active species i.e., the parent
- the most abundant species for CTP-656 is the most abundant species for CTP-656, but not for ivacaftor.
- CTP-656 demonstrated a superior pharmacokinetic profile compared to Kalydeco, the current standard of care for treatment of cystic fibrosis patients. Results of the Phase 1 trial also showed that CTP-656 was well-tolerated and its safety profile was comparable to Kalydeco. In the Phase 1 cross-over comparison of CTP-656 and Kalydeco, CTP-656 demonstrated a superior pharmacokinetic profile compared to Kalydeco including a reduced rate of clearance, longer half-life, substantially increased exposure and greater plasma levels at 24 hours.
- Test articles were applied in an additive and sequential manner to epithelia at 0.0008 ⁇ , 0.004 ⁇ , 0.02 ⁇ , and 0.1 ⁇ along with 0.5 ⁇ , 2.0 ⁇ , 0.5 ⁇ , and 2.5 ⁇ ⁇ additions of the DMSO vehicle. Values are the means of responses from each test concentration applied to six epithelia. ( Figure 4B and Figure 4C).
- CTP-656 (D9-ivacaftor) (17.1% by weight of an 80% amorphous dispersion (the dispersion contains 80% of Compound I by weight of the dispersion, hypromellose acetate succinate (HPMCAS) (about 19.5 percent by weight of the dispersion) and sodium laurel sulfate (about 0.5 percent by weight of the dispersion)) was blended with microcrystalline cellulose (Avicel PH101) (39.00 percent by weight), lactose monohydrate 316 (38.9 percent by weight) sodium lauryl sulfate (0.50 percent by weight), croscarmellose sodium (Ac-di-sol) (1.50 percent by weight) and Hyqual magnesium stearate (0.20 percent by weight) in a bottle blender.
- HPMCAS hypromellose acetate succinate
- sodium laurel sulfate about 0.5 percent by weight of the dispersion
- the blend was compacted and milled to form granules, which are sieved through #20 and #80 mesh sieves.
- the granules and remaining fines are blended with additional croscarmellose sodium (Ac-di-sol) (1.50 percent by weight), colloidal silicon dioxide (0.50 percent by weight) and additional Hyqual magnesium stearate (0.80 percent by weight), and the final blend compressed into tablets using a rotary press.
- Each tablet contains 75 mg CTP- 656 (D9-ivacaftor).
- CTP-656 Figure 8, right panel.
- the objective of the study was to compare the safety, tolerability, and pharmacokinetics of D9-ivacaftor at three doses for seven days, compared to placebo.
- Doses of D9-ivacaftor (CTP-656) and placebo were administered as tablets (the D9- ivacaftor was administered as one, two or three 75 mg tablets, for doses of 75 mg, 150 mg, or
- CTP-656 D9-ivacaftor
- All doses of D9-ivacaftor (CTP-656) were administered to fed subjects (high fat breakfast; about 60 g fat)) (8 subjects per sequence received CTP-656, two subjects per sequence received placebo). There was a 7 day washout between doses. Blood samples were taken at intervals and the plasma concentration of CTP-656.
- the food-effect study was an open-label, single-dose, crossover study. Subjects fasted overnight prior to randomization in a 1: 1: 1 ratio to one of three sequences (Fig. 12A). All subjects received a single dose of 150 mg of CTP-656 (two 75 mg tablets, prepared as in Example 5) either under fasting conditions or 30 minutes following the start of a low-fat (about 7 g of fat) or moderate-fat (about 20 g of fat) meal. The plasma concentrations of CTP-656 and certain metabolites were measured as applicable.
Abstract
Description










Claims


Priority Applications (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| AU2017352206A AU2017352206B2 (en) | 2016-10-27 | 2017-04-27 | Methods of treatment with deuterated CFTR potentiators |
| CA3041819A CA3041819A1 (en) | 2016-10-27 | 2017-04-27 | Methods of treatment with deuterated cftr potentiators |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201662413941P | 2016-10-27 | 2016-10-27 | |
| US62/413,941 | 2016-10-27 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2018080591A1 true WO2018080591A1 (en) | 2018-05-03 |
Family
ID=62023876
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2017/029920 WO2018080591A1 (en) | 2016-10-27 | 2017-04-27 | Methods of treatment with deuterated cftr potentiators |
Country Status (3)
| Country | Link |
|---|---|
| AU (1) | AU2017352206B2 (en) |
| CA (1) | CA3041819A1 (en) |
| WO (1) | WO2018080591A1 (en) |
Cited By (26)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10479766B2 (en) | 2011-05-18 | 2019-11-19 | Verex Pharmaceuticals (Europe) Limited | Deuterated CFTR potentiators |
| WO2020102346A1 (en) | 2018-11-14 | 2020-05-22 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| US10759721B2 (en) | 2015-09-25 | 2020-09-01 | Vertex Pharmaceuticals (Europe) Limited | Deuterated CFTR potentiators |
| WO2020206080A1 (en) | 2019-04-03 | 2020-10-08 | Vertex Pharmaceuticals Incorporated | Cystic fibrosis transmembrane conductance regulator modulating agents |
| WO2020214921A1 (en) | 2019-04-17 | 2020-10-22 | Vertex Pharmaceuticals Incorporated | Solid forms of modulators of cftr |
| WO2021030555A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2021030552A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Crystalline forms of cftr modulators |
| WO2021030556A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022032068A1 (en) | 2020-08-07 | 2022-02-10 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022036060A1 (en) | 2020-08-13 | 2022-02-17 | Vertex Pharmaceuticals Incorporated | Crystalline forms of cftr modulators |
| WO2022076625A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076618A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076624A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076621A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076627A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076628A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076626A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076629A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076622A2 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022125826A1 (en) | 2020-12-10 | 2022-06-16 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| US11708331B2 (en) | 2017-12-01 | 2023-07-25 | Vertex Pharmaceuticals Incorporated | Processes for making modulators of cystic fibrosis transmembrane conductance regulator |
| WO2023150237A1 (en) | 2022-02-03 | 2023-08-10 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| WO2023154291A1 (en) | 2022-02-08 | 2023-08-17 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2023196429A1 (en) | 2022-04-06 | 2023-10-12 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2023224931A1 (en) | 2022-05-16 | 2023-11-23 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| US11866450B2 (en) | 2018-02-15 | 2024-01-09 | Vertex Pharmaceuticals Incorporated | Modulators of Cystic Fibrosis Transmembrane Conductance regulator, pharmaceutical compositions, methods of treatment, and process for making the modulators |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20140221424A1 (en) * | 2013-01-30 | 2014-08-07 | Vertex Pharmaceuticals Incorporated | Pharmaceutical compositions for use in the treatment of cystic fibrosis |
| US20150099780A1 (en) * | 2011-05-18 | 2015-04-09 | Concert Pharmaceuticals, Inc. | Deuterated cftr potentiators |
| WO2015063041A1 (en) * | 2013-10-28 | 2015-05-07 | Nestec S.A. | Monoacylglycerols and fat-soluble nutrients for use in the treatment of maldigestion |
-
2017
- 2017-04-27 WO PCT/US2017/029920 patent/WO2018080591A1/en active Application Filing
- 2017-04-27 CA CA3041819A patent/CA3041819A1/en active Pending
- 2017-04-27 AU AU2017352206A patent/AU2017352206B2/en active Active
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20150099780A1 (en) * | 2011-05-18 | 2015-04-09 | Concert Pharmaceuticals, Inc. | Deuterated cftr potentiators |
| US20140221424A1 (en) * | 2013-01-30 | 2014-08-07 | Vertex Pharmaceuticals Incorporated | Pharmaceutical compositions for use in the treatment of cystic fibrosis |
| WO2015063041A1 (en) * | 2013-10-28 | 2015-05-07 | Nestec S.A. | Monoacylglycerols and fat-soluble nutrients for use in the treatment of maldigestion |
Cited By (31)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10479766B2 (en) | 2011-05-18 | 2019-11-19 | Verex Pharmaceuticals (Europe) Limited | Deuterated CFTR potentiators |
| US10894773B2 (en) | 2011-05-18 | 2021-01-19 | Vertex Pharmaceuticals (Europe) Limited | Deuterated CFTR potentiators |
| US10759721B2 (en) | 2015-09-25 | 2020-09-01 | Vertex Pharmaceuticals (Europe) Limited | Deuterated CFTR potentiators |
| US11708331B2 (en) | 2017-12-01 | 2023-07-25 | Vertex Pharmaceuticals Incorporated | Processes for making modulators of cystic fibrosis transmembrane conductance regulator |
| US11866450B2 (en) | 2018-02-15 | 2024-01-09 | Vertex Pharmaceuticals Incorporated | Modulators of Cystic Fibrosis Transmembrane Conductance regulator, pharmaceutical compositions, methods of treatment, and process for making the modulators |
| WO2020102346A1 (en) | 2018-11-14 | 2020-05-22 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| EP4218754A2 (en) | 2018-11-14 | 2023-08-02 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| WO2020206080A1 (en) | 2019-04-03 | 2020-10-08 | Vertex Pharmaceuticals Incorporated | Cystic fibrosis transmembrane conductance regulator modulating agents |
| EP4335498A1 (en) | 2019-04-03 | 2024-03-13 | Vertex Pharmaceuticals Incorporated | Cystic fibrosis transmembrane conductance regulator modulating agents |
| WO2020214921A1 (en) | 2019-04-17 | 2020-10-22 | Vertex Pharmaceuticals Incorporated | Solid forms of modulators of cftr |
| US11591350B2 (en) | 2019-08-14 | 2023-02-28 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2021030555A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| US11873300B2 (en) | 2019-08-14 | 2024-01-16 | Vertex Pharmaceuticals Incorporated | Crystalline forms of CFTR modulators |
| WO2021030552A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Crystalline forms of cftr modulators |
| WO2021030556A1 (en) | 2019-08-14 | 2021-02-18 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022032068A1 (en) | 2020-08-07 | 2022-02-10 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022036060A1 (en) | 2020-08-13 | 2022-02-17 | Vertex Pharmaceuticals Incorporated | Crystalline forms of cftr modulators |
| WO2022076628A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076621A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076622A2 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076626A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076625A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076627A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076629A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076618A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022076624A1 (en) | 2020-10-07 | 2022-04-14 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2022125826A1 (en) | 2020-12-10 | 2022-06-16 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| WO2023150237A1 (en) | 2022-02-03 | 2023-08-10 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
| WO2023154291A1 (en) | 2022-02-08 | 2023-08-17 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2023196429A1 (en) | 2022-04-06 | 2023-10-12 | Vertex Pharmaceuticals Incorporated | Modulators of cystic fibrosis transmembrane conductance regulator |
| WO2023224931A1 (en) | 2022-05-16 | 2023-11-23 | Vertex Pharmaceuticals Incorporated | Methods of treatment for cystic fibrosis |
Also Published As
| Publication number | Publication date |
|---|---|
| AU2017352206A1 (en) | 2019-05-16 |
| CA3041819A1 (en) | 2018-05-03 |
| AU2017352206B2 (en) | 2022-03-03 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| AU2022201135B2 (en) | Administration of deuterated cftr potentiators | |
| AU2017352206B2 (en) | Methods of treatment with deuterated CFTR potentiators | |
| US20210052570A1 (en) | Methods of treatment with deuterated cftr potentiators | |
| US10738036B2 (en) | Deuterated CFTR modulators | |
| US20150315152A2 (en) | Pharmaceutical Compositions for the Treatment of CFTR-Mediated Disorders | |
| EP3235812A1 (en) | Deuterated derivatives of ivacaftor | |
| AU2017261286B2 (en) | Treatment of hair loss disorders with deuterated JAK inhibitors | |
| OA19045A (en) | Administration of deuterated CFTR potentiators. | |
| AU2017217806A1 (en) | Deuterium-modified CFTR modulators |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 17865794 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 3041819 Country of ref document: CA |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2017352206 Country of ref document: AU Date of ref document: 20170427 Kind code of ref document: A |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 17865794 Country of ref document: EP Kind code of ref document: A1 |