WO2018011796A1 - Early diagnosis of infections - Google Patents
Early diagnosis of infections Download PDFInfo
- Publication number
- WO2018011796A1 WO2018011796A1 PCT/IL2017/050781 IL2017050781W WO2018011796A1 WO 2018011796 A1 WO2018011796 A1 WO 2018011796A1 IL 2017050781 W IL2017050781 W IL 2017050781W WO 2018011796 A1 WO2018011796 A1 WO 2018011796A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- infection
- trail
- subject
- bacterial
- viral
- Prior art date
Links
- 208000015181 infectious disease Diseases 0.000 title claims abstract description 142
- 238000013399 early diagnosis Methods 0.000 title description 4
- 238000000034 method Methods 0.000 claims abstract description 164
- 208000024891 symptom Diseases 0.000 claims abstract description 54
- 102100024598 Tumor necrosis factor ligand superfamily member 10 Human genes 0.000 claims description 149
- 101710097160 Tumor necrosis factor ligand superfamily member 10 Proteins 0.000 claims description 148
- 208000035143 Bacterial infection Diseases 0.000 claims description 103
- 208000022362 bacterial infectious disease Diseases 0.000 claims description 103
- 208000036142 Viral infection Diseases 0.000 claims description 81
- 230000009385 viral infection Effects 0.000 claims description 70
- 108010074051 C-Reactive Protein Proteins 0.000 claims description 60
- 102100032752 C-reactive protein Human genes 0.000 claims description 60
- 102000004889 Interleukin-6 Human genes 0.000 claims description 45
- 108090001005 Interleukin-6 Proteins 0.000 claims description 45
- 229940100601 interleukin-6 Drugs 0.000 claims description 45
- 108090000623 proteins and genes Proteins 0.000 claims description 42
- 108010048233 Procalcitonin Proteins 0.000 claims description 40
- CWCXERYKLSEGEZ-KDKHKZEGSA-N procalcitonin Chemical compound C([C@@H](C(=O)N1CCC[C@H]1C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@H](C(=O)N[C@@H](C)C(=O)N[C@@H]([C@@H](C)CC)C(=O)NCC(=O)N[C@@H](C(C)C)C(=O)NCC(=O)N[C@@H](C)C(=O)N1[C@@H](CCC1)C(=O)NCC(O)=O)[C@@H](C)O)NC(=O)[C@@H](NC(=O)[C@H](CC=1NC=NC=1)NC(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@H](CCCCN)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@@H](NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@@H](NC(=O)CNC(=O)[C@H](CC(C)C)NC(=O)[C@H](CCSC)NC(=O)[C@H]1NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CO)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CC(N)=O)NC(=O)CNC(=O)[C@@H](N)CSSC1)[C@@H](C)O)[C@@H](C)O)[C@@H](C)O)C1=CC=CC=C1 CWCXERYKLSEGEZ-KDKHKZEGSA-N 0.000 claims description 40
- 229920001184 polypeptide Polymers 0.000 claims description 34
- 102000004196 processed proteins & peptides Human genes 0.000 claims description 34
- 108090000765 processed proteins & peptides Proteins 0.000 claims description 34
- 102000004169 proteins and genes Human genes 0.000 claims description 34
- 230000001717 pathogenic effect Effects 0.000 claims description 33
- 244000052769 pathogen Species 0.000 claims description 29
- 230000003115 biocidal effect Effects 0.000 claims description 23
- 230000005713 exacerbation Effects 0.000 claims description 23
- 239000003242 anti bacterial agent Substances 0.000 claims description 21
- 210000004369 blood Anatomy 0.000 claims description 21
- 239000008280 blood Substances 0.000 claims description 21
- 208000006545 Chronic Obstructive Pulmonary Disease Diseases 0.000 claims description 18
- 210000002966 serum Anatomy 0.000 claims description 16
- 238000003018 immunoassay Methods 0.000 claims description 15
- 101001076418 Homo sapiens Interleukin-1 receptor type 1 Proteins 0.000 claims description 12
- 102100026016 Interleukin-1 receptor type 1 Human genes 0.000 claims description 12
- 238000011269 treatment regimen Methods 0.000 claims description 12
- 208000006673 asthma Diseases 0.000 claims description 11
- 241000725643 Respiratory syncytial virus Species 0.000 claims description 10
- 230000002458 infectious effect Effects 0.000 claims description 10
- 206010037660 Pyrexia Diseases 0.000 claims description 9
- 108010074328 Interferon-gamma Proteins 0.000 claims description 8
- 102000008070 Interferon-gamma Human genes 0.000 claims description 8
- 229960003130 interferon gamma Drugs 0.000 claims description 7
- 210000004027 cell Anatomy 0.000 claims description 6
- 241000709661 Enterovirus Species 0.000 claims description 5
- 206010022000 influenza Diseases 0.000 claims description 5
- 210000004698 lymphocyte Anatomy 0.000 claims description 5
- 239000003443 antiviral agent Substances 0.000 claims description 4
- 210000001616 monocyte Anatomy 0.000 claims description 4
- 102000004420 Creatine Kinase Human genes 0.000 claims description 3
- 108010042126 Creatine kinase Proteins 0.000 claims description 3
- 241001505901 Streptococcus sp. 'group A' Species 0.000 claims description 3
- 101001076407 Homo sapiens Interleukin-1 receptor antagonist protein Proteins 0.000 claims description 2
- 206010061372 Streptococcal infection Diseases 0.000 claims description 2
- 210000003714 granulocyte Anatomy 0.000 claims description 2
- 238000012360 testing method Methods 0.000 description 71
- 239000000523 sample Substances 0.000 description 70
- 230000001580 bacterial effect Effects 0.000 description 58
- 241000699666 Mus <mouse, genus> Species 0.000 description 55
- 230000003612 virological effect Effects 0.000 description 55
- 239000000090 biomarker Substances 0.000 description 52
- 238000003556 assay Methods 0.000 description 41
- 230000035945 sensitivity Effects 0.000 description 36
- 238000001514 detection method Methods 0.000 description 32
- 238000011282 treatment Methods 0.000 description 32
- 208000003322 Coinfection Diseases 0.000 description 31
- 239000012491 analyte Substances 0.000 description 30
- 201000010099 disease Diseases 0.000 description 22
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 description 22
- 230000036541 health Effects 0.000 description 21
- 238000004458 analytical method Methods 0.000 description 20
- 238000005259 measurement Methods 0.000 description 20
- 241000894006 Bacteria Species 0.000 description 19
- 208000035473 Communicable disease Diseases 0.000 description 18
- 102000004190 Enzymes Human genes 0.000 description 16
- 108090000790 Enzymes Proteins 0.000 description 16
- 238000004422 calculation algorithm Methods 0.000 description 16
- 102100025248 C-X-C motif chemokine 10 Human genes 0.000 description 15
- 230000003287 optical effect Effects 0.000 description 14
- 230000004044 response Effects 0.000 description 14
- 101710098275 C-X-C motif chemokine 10 Proteins 0.000 description 13
- 230000006870 function Effects 0.000 description 13
- 239000000463 material Substances 0.000 description 13
- PCHJSUWPFVWCPO-UHFFFAOYSA-N gold Chemical compound [Au] PCHJSUWPFVWCPO-UHFFFAOYSA-N 0.000 description 12
- 239000012528 membrane Substances 0.000 description 12
- 206010057190 Respiratory tract infections Diseases 0.000 description 11
- 241000700605 Viruses Species 0.000 description 11
- 239000003814 drug Substances 0.000 description 11
- 239000002245 particle Substances 0.000 description 11
- 238000003752 polymerase chain reaction Methods 0.000 description 11
- 230000001154 acute effect Effects 0.000 description 10
- 229940088710 antibiotic agent Drugs 0.000 description 10
- 239000003153 chemical reaction reagent Substances 0.000 description 10
- 238000003745 diagnosis Methods 0.000 description 10
- 238000002405 diagnostic procedure Methods 0.000 description 10
- 238000000926 separation method Methods 0.000 description 10
- 238000012706 support-vector machine Methods 0.000 description 10
- 206010046306 Upper respiratory tract infection Diseases 0.000 description 9
- 238000007635 classification algorithm Methods 0.000 description 9
- 208000035850 clinical syndrome Diseases 0.000 description 9
- 238000005516 engineering process Methods 0.000 description 9
- 239000002105 nanoparticle Substances 0.000 description 9
- 238000002560 therapeutic procedure Methods 0.000 description 9
- 230000000845 anti-microbial effect Effects 0.000 description 8
- 239000000427 antigen Substances 0.000 description 8
- 108091007433 antigens Proteins 0.000 description 8
- 102000036639 antigens Human genes 0.000 description 8
- 238000006243 chemical reaction Methods 0.000 description 8
- 229940079593 drug Drugs 0.000 description 8
- 108091023037 Aptamer Proteins 0.000 description 7
- 208000031662 Noncommunicable disease Diseases 0.000 description 7
- 230000001419 dependent effect Effects 0.000 description 7
- 230000000694 effects Effects 0.000 description 7
- 229910052737 gold Inorganic materials 0.000 description 7
- 239000010931 gold Substances 0.000 description 7
- 230000001965 increasing effect Effects 0.000 description 7
- 239000000203 mixture Substances 0.000 description 7
- 238000010606 normalization Methods 0.000 description 7
- 230000008569 process Effects 0.000 description 7
- 239000000758 substrate Substances 0.000 description 7
- 208000019206 urinary tract infection Diseases 0.000 description 7
- 208000037581 Persistent Infection Diseases 0.000 description 6
- 238000013459 approach Methods 0.000 description 6
- 230000008901 benefit Effects 0.000 description 6
- 238000009826 distribution Methods 0.000 description 6
- 239000012530 fluid Substances 0.000 description 6
- 229940127121 immunoconjugate Drugs 0.000 description 6
- 210000000265 leukocyte Anatomy 0.000 description 6
- 238000007403 mPCR Methods 0.000 description 6
- 239000000047 product Substances 0.000 description 6
- 238000003860 storage Methods 0.000 description 6
- 108091032973 (ribonucleotides)n+m Proteins 0.000 description 5
- 241000282414 Homo sapiens Species 0.000 description 5
- 238000013528 artificial neural network Methods 0.000 description 5
- 239000011324 bead Substances 0.000 description 5
- 230000027455 binding Effects 0.000 description 5
- 238000011976 chest X-ray Methods 0.000 description 5
- 238000010276 construction Methods 0.000 description 5
- 239000000975 dye Substances 0.000 description 5
- 230000006872 improvement Effects 0.000 description 5
- 239000007788 liquid Substances 0.000 description 5
- 238000007477 logistic regression Methods 0.000 description 5
- 238000007726 management method Methods 0.000 description 5
- 239000011159 matrix material Substances 0.000 description 5
- 238000002360 preparation method Methods 0.000 description 5
- 238000007637 random forest analysis Methods 0.000 description 5
- 239000000243 solution Substances 0.000 description 5
- 239000000126 substance Substances 0.000 description 5
- 241000701161 unidentified adenovirus Species 0.000 description 5
- OKTJSMMVPCPJKN-UHFFFAOYSA-N Carbon Chemical compound [C] OKTJSMMVPCPJKN-UHFFFAOYSA-N 0.000 description 4
- 206010024971 Lower respiratory tract infections Diseases 0.000 description 4
- 239000000020 Nitrocellulose Substances 0.000 description 4
- 241000283973 Oryctolagus cuniculus Species 0.000 description 4
- 150000001413 amino acids Chemical group 0.000 description 4
- 229910052799 carbon Inorganic materials 0.000 description 4
- 230000008859 change Effects 0.000 description 4
- 230000000295 complement effect Effects 0.000 description 4
- 238000013500 data storage Methods 0.000 description 4
- 238000002372 labelling Methods 0.000 description 4
- 230000000670 limiting effect Effects 0.000 description 4
- 239000007791 liquid phase Substances 0.000 description 4
- 238000004519 manufacturing process Methods 0.000 description 4
- 239000003550 marker Substances 0.000 description 4
- 230000002906 microbiologic effect Effects 0.000 description 4
- 244000005700 microbiome Species 0.000 description 4
- 230000004048 modification Effects 0.000 description 4
- 238000012986 modification Methods 0.000 description 4
- 208000010125 myocardial infarction Diseases 0.000 description 4
- 229920001220 nitrocellulos Polymers 0.000 description 4
- 230000002829 reductive effect Effects 0.000 description 4
- 239000007787 solid Substances 0.000 description 4
- 230000009885 systemic effect Effects 0.000 description 4
- 238000010863 targeted diagnosis Methods 0.000 description 4
- 210000002700 urine Anatomy 0.000 description 4
- 241000283707 Capra Species 0.000 description 3
- 206010013975 Dyspnoeas Diseases 0.000 description 3
- 238000008157 ELISA kit Methods 0.000 description 3
- 241000588724 Escherichia coli Species 0.000 description 3
- 241000711549 Hepacivirus C Species 0.000 description 3
- 241000701044 Human gammaherpesvirus 4 Species 0.000 description 3
- 241000725303 Human immunodeficiency virus Species 0.000 description 3
- 108010050904 Interferons Proteins 0.000 description 3
- 102000014150 Interferons Human genes 0.000 description 3
- 206010036790 Productive cough Diseases 0.000 description 3
- 230000004075 alteration Effects 0.000 description 3
- 239000012472 biological sample Substances 0.000 description 3
- 238000004820 blood count Methods 0.000 description 3
- 238000003759 clinical diagnosis Methods 0.000 description 3
- 239000003086 colorant Substances 0.000 description 3
- 230000002860 competitive effect Effects 0.000 description 3
- 150000001875 compounds Chemical class 0.000 description 3
- 238000004590 computer program Methods 0.000 description 3
- 230000021615 conjugation Effects 0.000 description 3
- 230000007423 decrease Effects 0.000 description 3
- 230000003111 delayed effect Effects 0.000 description 3
- 230000006866 deterioration Effects 0.000 description 3
- 230000007717 exclusion Effects 0.000 description 3
- 239000007850 fluorescent dye Substances 0.000 description 3
- 230000002496 gastric effect Effects 0.000 description 3
- 230000028993 immune response Effects 0.000 description 3
- 229940079322 interferon Drugs 0.000 description 3
- 238000011835 investigation Methods 0.000 description 3
- 239000006249 magnetic particle Substances 0.000 description 3
- 238000010369 molecular cloning Methods 0.000 description 3
- 210000000440 neutrophil Anatomy 0.000 description 3
- 230000007918 pathogenicity Effects 0.000 description 3
- 230000026731 phosphorylation Effects 0.000 description 3
- 238000006366 phosphorylation reaction Methods 0.000 description 3
- 210000002381 plasma Anatomy 0.000 description 3
- 239000002096 quantum dot Substances 0.000 description 3
- PYWVYCXTNDRMGF-UHFFFAOYSA-N rhodamine B Chemical compound [Cl-].C=12C=CC(=[N+](CC)CC)C=C2OC2=CC(N(CC)CC)=CC=C2C=1C1=CC=CC=C1C(O)=O PYWVYCXTNDRMGF-UHFFFAOYSA-N 0.000 description 3
- 238000001179 sorption measurement Methods 0.000 description 3
- 210000003802 sputum Anatomy 0.000 description 3
- 208000024794 sputum Diseases 0.000 description 3
- 238000007619 statistical method Methods 0.000 description 3
- 230000001225 therapeutic effect Effects 0.000 description 3
- 230000032258 transport Effects 0.000 description 3
- FMZXNVLFJHCSAF-DNVCBOLYSA-N (6R,7R)-3-[(4-carbamoyl-1-pyridin-1-iumyl)methyl]-8-oxo-7-[(1-oxo-2-thiophen-2-ylethyl)amino]-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound C1=CC(C(=O)N)=CC=[N+]1CC1=C(C([O-])=O)N2C(=O)[C@@H](NC(=O)CC=3SC=CC=3)[C@H]2SC1 FMZXNVLFJHCSAF-DNVCBOLYSA-N 0.000 description 2
- 229920000936 Agarose Polymers 0.000 description 2
- BPYKTIZUTYGOLE-IFADSCNNSA-N Bilirubin Chemical compound N1C(=O)C(C)=C(C=C)\C1=C\C1=C(C)C(CCC(O)=O)=C(CC2=C(C(C)=C(\C=C/3C(=C(C=C)C(=O)N\3)C)N2)CCC(O)=O)N1 BPYKTIZUTYGOLE-IFADSCNNSA-N 0.000 description 2
- 241000124740 Bocaparvovirus Species 0.000 description 2
- UQLLWWBDSUHNEB-CZUORRHYSA-N Cefaprin Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC(=O)C)C(O)=O)C(=O)CSC1=CC=NC=C1 UQLLWWBDSUHNEB-CZUORRHYSA-N 0.000 description 2
- 102000019034 Chemokines Human genes 0.000 description 2
- 108010012236 Chemokines Proteins 0.000 description 2
- 241001647372 Chlamydia pneumoniae Species 0.000 description 2
- 206010011224 Cough Diseases 0.000 description 2
- 102000004127 Cytokines Human genes 0.000 description 2
- 108090000695 Cytokines Proteins 0.000 description 2
- 241000701022 Cytomegalovirus Species 0.000 description 2
- 206010061818 Disease progression Diseases 0.000 description 2
- 208000000059 Dyspnea Diseases 0.000 description 2
- 238000002965 ELISA Methods 0.000 description 2
- XQSPYNMVSIKCOC-NTSWFWBYSA-N Emtricitabine Chemical compound C1=C(F)C(N)=NC(=O)N1[C@H]1O[C@@H](CO)SC1 XQSPYNMVSIKCOC-NTSWFWBYSA-N 0.000 description 2
- 241000194032 Enterococcus faecalis Species 0.000 description 2
- 241000283073 Equus caballus Species 0.000 description 2
- ULGZDMOVFRHVEP-RWJQBGPGSA-N Erythromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)C(=O)[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 ULGZDMOVFRHVEP-RWJQBGPGSA-N 0.000 description 2
- 238000003794 Gram staining Methods 0.000 description 2
- 108010043121 Green Fluorescent Proteins Proteins 0.000 description 2
- 102000004144 Green Fluorescent Proteins Human genes 0.000 description 2
- 208000005176 Hepatitis C Diseases 0.000 description 2
- 101000610604 Homo sapiens Tumor necrosis factor receptor superfamily member 10B Proteins 0.000 description 2
- 101000798130 Homo sapiens Tumor necrosis factor receptor superfamily member 11B Proteins 0.000 description 2
- 241000589242 Legionella pneumophila Species 0.000 description 2
- 208000019693 Lung disease Diseases 0.000 description 2
- 241000736262 Microbiota Species 0.000 description 2
- 241000202934 Mycoplasma pneumoniae Species 0.000 description 2
- 241001263478 Norovirus Species 0.000 description 2
- 208000002606 Paramyxoviridae Infections Diseases 0.000 description 2
- 241001494479 Pecora Species 0.000 description 2
- JGSARLDLIJGVTE-MBNYWOFBSA-N Penicillin G Chemical compound N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)CC1=CC=CC=C1 JGSARLDLIJGVTE-MBNYWOFBSA-N 0.000 description 2
- 206010035664 Pneumonia Diseases 0.000 description 2
- 241000700159 Rattus Species 0.000 description 2
- 108020004511 Recombinant DNA Proteins 0.000 description 2
- 208000036071 Rhinorrhea Diseases 0.000 description 2
- 206010039101 Rhinorrhoea Diseases 0.000 description 2
- 241000702670 Rotavirus Species 0.000 description 2
- 241000193998 Streptococcus pneumoniae Species 0.000 description 2
- 101710120037 Toxin CcdB Proteins 0.000 description 2
- 108060008682 Tumor Necrosis Factor Proteins 0.000 description 2
- 102100040112 Tumor necrosis factor receptor superfamily member 10B Human genes 0.000 description 2
- 102100032236 Tumor necrosis factor receptor superfamily member 11B Human genes 0.000 description 2
- 238000010521 absorption reaction Methods 0.000 description 2
- 229960004150 aciclovir Drugs 0.000 description 2
- MKUXAQIIEYXACX-UHFFFAOYSA-N aciclovir Chemical compound N1C(N)=NC(=O)C2=C1N(COCCO)C=N2 MKUXAQIIEYXACX-UHFFFAOYSA-N 0.000 description 2
- 230000009471 action Effects 0.000 description 2
- 239000003463 adsorbent Substances 0.000 description 2
- 210000004102 animal cell Anatomy 0.000 description 2
- 230000000840 anti-viral effect Effects 0.000 description 2
- 238000003491 array Methods 0.000 description 2
- 244000309743 astrovirus Species 0.000 description 2
- 229960000074 biopharmaceutical Drugs 0.000 description 2
- 238000001574 biopsy Methods 0.000 description 2
- 210000000601 blood cell Anatomy 0.000 description 2
- 239000000872 buffer Substances 0.000 description 2
- 229960003972 cefacetrile Drugs 0.000 description 2
- RRYMAQUWDLIUPV-BXKDBHETSA-N cefacetrile Chemical compound S1CC(COC(=O)C)=C(C(O)=O)N2C(=O)[C@@H](NC(=O)CC#N)[C@@H]12 RRYMAQUWDLIUPV-BXKDBHETSA-N 0.000 description 2
- FUBBGQLTSCSAON-PBFPGSCMSA-N cefaloglycin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)COC(=O)C)C(O)=O)=CC=CC=C1 FUBBGQLTSCSAON-PBFPGSCMSA-N 0.000 description 2
- 229950004030 cefaloglycin Drugs 0.000 description 2
- 229960000603 cefalotin Drugs 0.000 description 2
- 229960004350 cefapirin Drugs 0.000 description 2
- 229960001139 cefazolin Drugs 0.000 description 2
- MLYYVTUWGNIJIB-BXKDBHETSA-N cefazolin Chemical compound S1C(C)=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)CN3N=NN=C3)[C@H]2SC1 MLYYVTUWGNIJIB-BXKDBHETSA-N 0.000 description 2
- 229960002588 cefradine Drugs 0.000 description 2
- 229940036735 ceftaroline Drugs 0.000 description 2
- ZCCUWMICIWSJIX-NQJJCJBVSA-N ceftaroline fosamil Chemical compound S([C@@H]1[C@@H](C(N1C=1C([O-])=O)=O)NC(=O)\C(=N/OCC)C=2N=C(NP(O)(O)=O)SN=2)CC=1SC(SC=1)=NC=1C1=CC=[N+](C)C=C1 ZCCUWMICIWSJIX-NQJJCJBVSA-N 0.000 description 2
- 229920002678 cellulose Polymers 0.000 description 2
- 239000001913 cellulose Substances 0.000 description 2
- 229940106164 cephalexin Drugs 0.000 description 2
- ZAIPMKNFIOOWCQ-UEKVPHQBSA-N cephalexin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)C)C(O)=O)=CC=CC=C1 ZAIPMKNFIOOWCQ-UEKVPHQBSA-N 0.000 description 2
- VUFGUVLLDPOSBC-XRZFDKQNSA-M cephalothin sodium Chemical compound [Na+].N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC(=O)C)C([O-])=O)C(=O)CC1=CC=CS1 VUFGUVLLDPOSBC-XRZFDKQNSA-M 0.000 description 2
- RDLPVSKMFDYCOR-UEKVPHQBSA-N cephradine Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)C)C(O)=O)=CCC=CC1 RDLPVSKMFDYCOR-UEKVPHQBSA-N 0.000 description 2
- 239000007795 chemical reaction product Substances 0.000 description 2
- 230000001684 chronic effect Effects 0.000 description 2
- MYSWGUAQZAJSOK-UHFFFAOYSA-N ciprofloxacin Chemical compound C12=CC(N3CCNCC3)=C(F)C=C2C(=O)C(C(=O)O)=CN1C1CC1 MYSWGUAQZAJSOK-UHFFFAOYSA-N 0.000 description 2
- 239000005515 coenzyme Substances 0.000 description 2
- 239000002131 composite material Substances 0.000 description 2
- 230000036757 core body temperature Effects 0.000 description 2
- 230000002596 correlated effect Effects 0.000 description 2
- DDRJAANPRJIHGJ-UHFFFAOYSA-N creatinine Chemical compound CN1CC(=O)NC1=N DDRJAANPRJIHGJ-UHFFFAOYSA-N 0.000 description 2
- 239000013078 crystal Substances 0.000 description 2
- 238000013523 data management Methods 0.000 description 2
- 238000003066 decision tree Methods 0.000 description 2
- WHBIGIKBNXZKFE-UHFFFAOYSA-N delavirdine Chemical compound CC(C)NC1=CC=CN=C1N1CCN(C(=O)C=2NC3=CC=C(NS(C)(=O)=O)C=C3C=2)CC1 WHBIGIKBNXZKFE-UHFFFAOYSA-N 0.000 description 2
- 230000005750 disease progression Effects 0.000 description 2
- NOPFSRXAKWQILS-UHFFFAOYSA-N docosan-1-ol Chemical compound CCCCCCCCCCCCCCCCCCCCCCO NOPFSRXAKWQILS-UHFFFAOYSA-N 0.000 description 2
- 238000001035 drying Methods 0.000 description 2
- 229940032049 enterococcus faecalis Drugs 0.000 description 2
- 230000002255 enzymatic effect Effects 0.000 description 2
- 230000005284 excitation Effects 0.000 description 2
- 238000000684 flow cytometry Methods 0.000 description 2
- GNBHRKFJIUUOQI-UHFFFAOYSA-N fluorescein Chemical compound O1C(=O)C2=CC=CC=C2C21C1=CC=C(O)C=C1OC1=CC(O)=CC=C21 GNBHRKFJIUUOQI-UHFFFAOYSA-N 0.000 description 2
- 238000009472 formulation Methods 0.000 description 2
- 239000012634 fragment Substances 0.000 description 2
- 229960003170 gemifloxacin Drugs 0.000 description 2
- ZRCVYEYHRGVLOC-HYARGMPZSA-N gemifloxacin Chemical compound C1C(CN)C(=N/OC)/CN1C(C(=C1)F)=NC2=C1C(=O)C(C(O)=O)=CN2C1CC1 ZRCVYEYHRGVLOC-HYARGMPZSA-N 0.000 description 2
- 239000003365 glass fiber Substances 0.000 description 2
- 239000005090 green fluorescent protein Substances 0.000 description 2
- 238000003384 imaging method Methods 0.000 description 2
- 230000008105 immune reaction Effects 0.000 description 2
- 238000003119 immunoblot Methods 0.000 description 2
- 238000010166 immunofluorescence Methods 0.000 description 2
- 238000000338 in vitro Methods 0.000 description 2
- 239000012678 infectious agent Substances 0.000 description 2
- 230000001524 infective effect Effects 0.000 description 2
- 230000002757 inflammatory effect Effects 0.000 description 2
- 239000004615 ingredient Substances 0.000 description 2
- 238000012125 lateral flow test Methods 0.000 description 2
- 229920000126 latex Polymers 0.000 description 2
- 239000004816 latex Substances 0.000 description 2
- 229940115932 legionella pneumophila Drugs 0.000 description 2
- 239000003446 ligand Substances 0.000 description 2
- 210000004185 liver Anatomy 0.000 description 2
- 238000012423 maintenance Methods 0.000 description 2
- 238000007620 mathematical function Methods 0.000 description 2
- 238000001840 matrix-assisted laser desorption--ionisation time-of-flight mass spectrometry Methods 0.000 description 2
- 230000001404 mediated effect Effects 0.000 description 2
- 230000035772 mutation Effects 0.000 description 2
- NQDJXKOVJZTUJA-UHFFFAOYSA-N nevirapine Chemical compound C12=NC=CC=C2C(=O)NC=2C(C)=CC=NC=2N1C1CC1 NQDJXKOVJZTUJA-UHFFFAOYSA-N 0.000 description 2
- 230000008520 organization Effects 0.000 description 2
- 230000037361 pathway Effects 0.000 description 2
- 239000012071 phase Substances 0.000 description 2
- ZJAOAACCNHFJAH-UHFFFAOYSA-N phosphonoformic acid Chemical compound OC(=O)P(O)(O)=O ZJAOAACCNHFJAH-UHFFFAOYSA-N 0.000 description 2
- 102000054765 polymorphisms of proteins Human genes 0.000 description 2
- 230000004481 post-translational protein modification Effects 0.000 description 2
- 230000005180 public health Effects 0.000 description 2
- 230000002285 radioactive effect Effects 0.000 description 2
- 230000009467 reduction Effects 0.000 description 2
- 238000011160 research Methods 0.000 description 2
- 230000000241 respiratory effect Effects 0.000 description 2
- 238000012552 review Methods 0.000 description 2
- 239000012488 sample solution Substances 0.000 description 2
- 238000012216 screening Methods 0.000 description 2
- 230000000405 serological effect Effects 0.000 description 2
- 239000011734 sodium Substances 0.000 description 2
- 238000000638 solvent extraction Methods 0.000 description 2
- 241000894007 species Species 0.000 description 2
- 238000010561 standard procedure Methods 0.000 description 2
- 238000013517 stratification Methods 0.000 description 2
- 229940031000 streptococcus pneumoniae Drugs 0.000 description 2
- UCSJYZPVAKXKNQ-HZYVHMACSA-N streptomycin Chemical compound CN[C@H]1[C@H](O)[C@@H](O)[C@H](CO)O[C@H]1O[C@@H]1[C@](C=O)(O)[C@H](C)O[C@H]1O[C@@H]1[C@@H](NC(N)=N)[C@H](O)[C@@H](NC(N)=N)[C@H](O)[C@H]1O UCSJYZPVAKXKNQ-HZYVHMACSA-N 0.000 description 2
- 229960005240 telavancin Drugs 0.000 description 2
- ONUMZHGUFYIKPM-MXNFEBESSA-N telavancin Chemical compound O1[C@@H](C)[C@@H](O)[C@](NCCNCCCCCCCCCC)(C)C[C@@H]1O[C@H]1[C@H](OC=2C3=CC=4[C@H](C(N[C@H]5C(=O)N[C@H](C(N[C@@H](C6=CC(O)=C(CNCP(O)(O)=O)C(O)=C6C=6C(O)=CC=C5C=6)C(O)=O)=O)[C@H](O)C5=CC=C(C(=C5)Cl)O3)=O)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](NC(=O)[C@@H](CC(C)C)NC)[C@H](O)C3=CC=C(C(=C3)Cl)OC=2C=4)O[C@H](CO)[C@@H](O)[C@@H]1O ONUMZHGUFYIKPM-MXNFEBESSA-N 0.000 description 2
- 108010089019 telavancin Proteins 0.000 description 2
- 238000012549 training Methods 0.000 description 2
- 230000009466 transformation Effects 0.000 description 2
- 238000000844 transformation Methods 0.000 description 2
- 102000003390 tumor necrosis factor Human genes 0.000 description 2
- 230000002485 urinary effect Effects 0.000 description 2
- 239000013598 vector Substances 0.000 description 2
- 238000011179 visual inspection Methods 0.000 description 2
- HBOMLICNUCNMMY-XLPZGREQSA-N zidovudine Chemical compound O=C1NC(=O)C(C)=CN1[C@@H]1O[C@H](CO)[C@@H](N=[N+]=[N-])C1 HBOMLICNUCNMMY-XLPZGREQSA-N 0.000 description 2
- VCOPTHOUUNAYKQ-WBTCAYNUSA-N (3s)-3,6-diamino-n-[[(2s,5s,8e,11s,15s)-15-amino-11-[(6r)-2-amino-1,4,5,6-tetrahydropyrimidin-6-yl]-8-[(carbamoylamino)methylidene]-2-(hydroxymethyl)-3,6,9,12,16-pentaoxo-1,4,7,10,13-pentazacyclohexadec-5-yl]methyl]hexanamide;(3s)-3,6-diamino-n-[[(2s,5s,8 Chemical compound N1C(=O)\C(=C/NC(N)=O)NC(=O)[C@H](CNC(=O)C[C@@H](N)CCCN)NC(=O)[C@H](C)NC(=O)[C@@H](N)CNC(=O)[C@@H]1[C@@H]1NC(N)=NCC1.N1C(=O)\C(=C/NC(N)=O)NC(=O)[C@H](CNC(=O)C[C@@H](N)CCCN)NC(=O)[C@H](CO)NC(=O)[C@@H](N)CNC(=O)[C@@H]1[C@@H]1NC(N)=NCC1 VCOPTHOUUNAYKQ-WBTCAYNUSA-N 0.000 description 1
- CNPVJJQCETWNEU-CYFREDJKSA-N (4,6-dimethyl-5-pyrimidinyl)-[4-[(3S)-4-[(1R)-2-methoxy-1-[4-(trifluoromethyl)phenyl]ethyl]-3-methyl-1-piperazinyl]-4-methyl-1-piperidinyl]methanone Chemical compound N([C@@H](COC)C=1C=CC(=CC=1)C(F)(F)F)([C@H](C1)C)CCN1C(CC1)(C)CCN1C(=O)C1=C(C)N=CN=C1C CNPVJJQCETWNEU-CYFREDJKSA-N 0.000 description 1
- SGKRLCUYIXIAHR-AKNGSSGZSA-N (4s,4ar,5s,5ar,6r,12ar)-4-(dimethylamino)-1,5,10,11,12a-pentahydroxy-6-methyl-3,12-dioxo-4a,5,5a,6-tetrahydro-4h-tetracene-2-carboxamide Chemical compound C1=CC=C2[C@H](C)[C@@H]([C@H](O)[C@@H]3[C@](C(O)=C(C(N)=O)C(=O)[C@H]3N(C)C)(O)C3=O)C3=C(O)C2=C1O SGKRLCUYIXIAHR-AKNGSSGZSA-N 0.000 description 1
- FFTVPQUHLQBXQZ-KVUCHLLUSA-N (4s,4as,5ar,12ar)-4,7-bis(dimethylamino)-1,10,11,12a-tetrahydroxy-3,12-dioxo-4a,5,5a,6-tetrahydro-4h-tetracene-2-carboxamide Chemical compound C1C2=C(N(C)C)C=CC(O)=C2C(O)=C2[C@@H]1C[C@H]1[C@H](N(C)C)C(=O)C(C(N)=O)=C(O)[C@@]1(O)C2=O FFTVPQUHLQBXQZ-KVUCHLLUSA-N 0.000 description 1
- SOVUOXKZCCAWOJ-HJYUBDRYSA-N (4s,4as,5ar,12ar)-9-[[2-(tert-butylamino)acetyl]amino]-4,7-bis(dimethylamino)-1,10,11,12a-tetrahydroxy-3,12-dioxo-4a,5,5a,6-tetrahydro-4h-tetracene-2-carboxamide Chemical compound C1C2=C(N(C)C)C=C(NC(=O)CNC(C)(C)C)C(O)=C2C(O)=C2[C@@H]1C[C@H]1[C@H](N(C)C)C(=O)C(C(N)=O)=C(O)[C@@]1(O)C2=O SOVUOXKZCCAWOJ-HJYUBDRYSA-N 0.000 description 1
- GUXHBMASAHGULD-SEYHBJAFSA-N (4s,4as,5as,6s,12ar)-7-chloro-4-(dimethylamino)-1,6,10,11,12a-pentahydroxy-3,12-dioxo-4a,5,5a,6-tetrahydro-4h-tetracene-2-carboxamide Chemical compound C1([C@H]2O)=C(Cl)C=CC(O)=C1C(O)=C1[C@@H]2C[C@H]2[C@H](N(C)C)C(=O)C(C(N)=O)=C(O)[C@@]2(O)C1=O GUXHBMASAHGULD-SEYHBJAFSA-N 0.000 description 1
- MMQXRUYUBYWTDP-KEIGCJKLSA-N (5s,6r,7r)-3-(acetyloxymethyl)-7-[[(2z)-2-(2-amino-1,3-thiazol-4-yl)-2-methoxyiminoacetyl]amino]-5,8-dioxo-5$l^{4}-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound N([C@@H]1C(N2[C@@H]1[S@](CC(COC(C)=O)=C2C(O)=O)=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 MMQXRUYUBYWTDP-KEIGCJKLSA-N 0.000 description 1
- YBHZVPYSEUQIII-DYJQDLSISA-N (6r,7r)-3-(acetyloxymethyl)-7-[[(2z)-2-(furan-2-yl)-2-methoxyiminoacetyl]amino]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound N([C@@H]1C(N2C(=C(COC(C)=O)CS[C@@H]21)C(O)=O)=O)C(=O)\C(=N/OC)C1=CC=CO1 YBHZVPYSEUQIII-DYJQDLSISA-N 0.000 description 1
- OCLRGULJISNUQS-OXQOHEQNSA-N (6r,7r)-3-(acetyloxymethyl)-7-[[3-(2-chlorophenyl)-5-methyl-1,2-oxazole-4-carbonyl]amino]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC(=O)C)C(O)=O)C(=O)C1=C(C)ON=C1C1=CC=CC=C1Cl OCLRGULJISNUQS-OXQOHEQNSA-N 0.000 description 1
- QFTZCQVZVRVDTD-DNVCBOLYSA-N (6r,7r)-3-methyl-8-oxo-7-[[2-[4-(1,4,5,6-tetrahydropyrimidin-2-yl)phenyl]acetyl]amino]-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)C)C(O)=O)C(=O)CC(C=C1)=CC=C1C1=NCCCN1 QFTZCQVZVRVDTD-DNVCBOLYSA-N 0.000 description 1
- XSPUSVIQHBDITA-KXDGEKGBSA-N (6r,7r)-7-[[(2e)-2-(2-amino-1,3-thiazol-4-yl)-2-methoxyiminoacetyl]amino]-3-[(5-methyltetrazol-2-yl)methyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)/C(=N/OC)C=2N=C(N)SC=2)CC=1CN1N=NC(C)=N1 XSPUSVIQHBDITA-KXDGEKGBSA-N 0.000 description 1
- RULITNAIJFZYLO-UEKVPHQBSA-N (6r,7r)-7-[[(2r)-2-amino-2-(3-chloro-4-hydroxyphenyl)acetyl]amino]-3-methyl-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)C)C(O)=O)=CC=C(O)C(Cl)=C1 RULITNAIJFZYLO-UEKVPHQBSA-N 0.000 description 1
- SBUCDZYLTRYMFG-PBFPGSCMSA-N (6r,7r)-7-[[(2r)-2-amino-2-(4-hydroxyphenyl)acetyl]amino]-3-[(5-methyl-1,3,4-thiadiazol-2-yl)sulfanylmethyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound S1C(C)=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)[C@H](N)C=3C=CC(O)=CC=3)[C@H]2SC1 SBUCDZYLTRYMFG-PBFPGSCMSA-N 0.000 description 1
- WDLWHQDACQUCJR-ZAMMOSSLSA-N (6r,7r)-7-[[(2r)-2-azaniumyl-2-(4-hydroxyphenyl)acetyl]amino]-8-oxo-3-[(e)-prop-1-enyl]-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)/C=C/C)C(O)=O)=CC=C(O)C=C1 WDLWHQDACQUCJR-ZAMMOSSLSA-N 0.000 description 1
- VDFFPBOAOLQAJV-SUYBPPKGSA-N (6r,7r)-7-[[(2r)-2-hydroxy-2-phenylacetyl]amino]-3-[(5-methyl-1,3,4-thiadiazol-2-yl)sulfanylmethyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound S1C(C)=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)[C@H](O)C=3C=CC=CC=3)[C@H]2SC1 VDFFPBOAOLQAJV-SUYBPPKGSA-N 0.000 description 1
- MMRINLZOZVAPDZ-LSGRDSQZSA-N (6r,7r)-7-[[(2z)-2-(2-amino-1,3-thiazol-4-yl)-2-methoxyiminoacetyl]amino]-3-[(1-methylpyrrolidin-1-ium-1-yl)methyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid;chloride Chemical compound Cl.S([C@@H]1[C@@H](C(N1C=1C([O-])=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1C[N+]1(C)CCCC1 MMRINLZOZVAPDZ-LSGRDSQZSA-N 0.000 description 1
- YWKJNRNSJKEFMK-PQFQYKRASA-N (6r,7r)-7-[[(2z)-2-(2-amino-1,3-thiazol-4-yl)-2-methoxyiminoacetyl]amino]-8-oxo-3-(5,6,7,8-tetrahydroquinolin-1-ium-1-ylmethyl)-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound N([C@@H]1C(N2C(=C(C[N+]=3C=4CCCCC=4C=CC=3)CS[C@@H]21)C([O-])=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 YWKJNRNSJKEFMK-PQFQYKRASA-N 0.000 description 1
- CUCFRCCRYQDMNM-PXIRVSTKSA-N (6r,7r)-7-[[(2z)-2-(2-amino-1,3-thiazol-5-yl)-2-(2-oxopyrrolidin-3-yl)oxyiminoacetyl]amino]-8-oxo-3-(pyridin-1-ium-1-ylmethyl)-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound S1C(N)=NC=C1C(\C(=O)N[C@@H]1C(N2C(=C(C[N+]=3C=CC=CC=3)CS[C@@H]21)C([O-])=O)=O)=N\OC1C(=O)NCC1 CUCFRCCRYQDMNM-PXIRVSTKSA-N 0.000 description 1
- ZWTPTPWLMRXLJE-WIYYLYMNSA-N (6r,7r)-7-[[2-(3-chlorophenyl)acetyl]amino]-3-[(4,4-dimethylpiperazin-4-ium-1-carbothioyl)sulfanylmethyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate Chemical compound C1C[N+](C)(C)CCN1C(=S)SCC1=C(C([O-])=O)N2C(=O)[C@@H](NC(=O)CC=3C=C(Cl)C=CC=3)[C@H]2SC1 ZWTPTPWLMRXLJE-WIYYLYMNSA-N 0.000 description 1
- JXHWKLWIYBATLL-GMIKGCRTSA-N (6r,7r)-7-[[2-[(z)-2-cyanoethenyl]sulfanylacetyl]amino]-3-[(1-methyltetrazol-5-yl)sulfanylmethyl]-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound CN1N=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)CS\C=C/C#N)[C@H]2SC1 JXHWKLWIYBATLL-GMIKGCRTSA-N 0.000 description 1
- UQWYUAURRDNBKR-BXUZGUMPSA-N (6r,7r)-8-oxo-7-[(2-thiophen-2-ylacetyl)amino]-3-(1h-1,2,4-triazol-5-ylsulfanylmethyl)-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid Chemical compound O=C([C@@H](NC(=O)CC=1SC=CC=1)[C@H]1SC2)N1C(C(=O)O)=C2CSC1=NC=NN1 UQWYUAURRDNBKR-BXUZGUMPSA-N 0.000 description 1
- RXZBMPWDPOLZGW-XMRMVWPWSA-N (E)-roxithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)C(=N/OCOCCOC)/[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 RXZBMPWDPOLZGW-XMRMVWPWSA-N 0.000 description 1
- QKDHBVNJCZBTMR-LLVKDONJSA-N (R)-temafloxacin Chemical compound C1CN[C@H](C)CN1C(C(=C1)F)=CC2=C1C(=O)C(C(O)=O)=CN2C1=CC=C(F)C=C1F QKDHBVNJCZBTMR-LLVKDONJSA-N 0.000 description 1
- XUBOMFCQGDBHNK-JTQLQIEISA-N (S)-gatifloxacin Chemical compound FC1=CC(C(C(C(O)=O)=CN2C3CC3)=O)=C2C(OC)=C1N1CCN[C@@H](C)C1 XUBOMFCQGDBHNK-JTQLQIEISA-N 0.000 description 1
- UBCHPRBFMUDMNC-UHFFFAOYSA-N 1-(1-adamantyl)ethanamine Chemical compound C1C(C2)CC3CC2CC1(C(N)C)C3 UBCHPRBFMUDMNC-UHFFFAOYSA-N 0.000 description 1
- YLDCUKJMEKGGFI-QCSRICIXSA-N 4-acetamidobenzoic acid;9-[(2r,3r,4s,5r)-3,4-dihydroxy-5-(hydroxymethyl)oxolan-2-yl]-3h-purin-6-one;1-(dimethylamino)propan-2-ol Chemical compound CC(O)CN(C)C.CC(O)CN(C)C.CC(O)CN(C)C.CC(=O)NC1=CC=C(C(O)=O)C=C1.CC(=O)NC1=CC=C(C(O)=O)C=C1.CC(=O)NC1=CC=C(C(O)=O)C=C1.O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1C(NC=NC2=O)=C2N=C1 YLDCUKJMEKGGFI-QCSRICIXSA-N 0.000 description 1
- WZRJTRPJURQBRM-UHFFFAOYSA-N 4-amino-n-(5-methyl-1,2-oxazol-3-yl)benzenesulfonamide;5-[(3,4,5-trimethoxyphenyl)methyl]pyrimidine-2,4-diamine Chemical compound O1C(C)=CC(NS(=O)(=O)C=2C=CC(N)=CC=2)=N1.COC1=C(OC)C(OC)=CC(CC=2C(=NC(N)=NC=2)N)=C1 WZRJTRPJURQBRM-UHFFFAOYSA-N 0.000 description 1
- YVMBAUWDIGJRNY-BESUKNQGSA-N 4o8o7q7iu4 Chemical compound C1C(=O)C[C@H](O)\C=C(/C)\C=C\CNC(=O)\C=C\[C@@H](C)[C@@H](C(C)C)OC(=O)C2=CCCN2C(=O)C2=COC1=N2.N([C@@H]1C(=O)N[C@@H](C(N2CCC[C@H]2C(=O)N(C)[C@@H](CC=2C=CC(=CC=2)N(C)C)C(=O)N2CCC(=O)C[C@H]2C(=O)N[C@H](C(=O)O[C@@H]1C)C=1C=CC=CC=1)=O)CC)C(=O)C1=NC=CC=C1O YVMBAUWDIGJRNY-BESUKNQGSA-N 0.000 description 1
- WUWFMDMBOJLQIV-UHFFFAOYSA-N 7-(3-aminopyrrolidin-1-yl)-1-(2,4-difluorophenyl)-6-fluoro-4-oxo-1,4-dihydro-1,8-naphthyridine-3-carboxylic acid Chemical compound C1C(N)CCN1C(C(=C1)F)=NC2=C1C(=O)C(C(O)=O)=CN2C1=CC=C(F)C=C1F WUWFMDMBOJLQIV-UHFFFAOYSA-N 0.000 description 1
- MPORYQCGWFQFLA-ONPDANIMSA-N 7-[(7s)-7-amino-5-azaspiro[2.4]heptan-5-yl]-8-chloro-6-fluoro-1-[(1r,2s)-2-fluorocyclopropyl]-4-oxoquinoline-3-carboxylic acid;trihydrate Chemical compound O.O.O.C([C@H]1N)N(C=2C(=C3C(C(C(C(O)=O)=CN3[C@H]3[C@H](C3)F)=O)=CC=2F)Cl)CC11CC1.C([C@H]1N)N(C=2C(=C3C(C(C(C(O)=O)=CN3[C@H]3[C@H](C3)F)=O)=CC=2F)Cl)CC11CC1 MPORYQCGWFQFLA-ONPDANIMSA-N 0.000 description 1
- GSDSWSVVBLHKDQ-UHFFFAOYSA-N 9-fluoro-3-methyl-10-(4-methylpiperazin-1-yl)-7-oxo-2,3-dihydro-7H-[1,4]oxazino[2,3,4-ij]quinoline-6-carboxylic acid Chemical compound FC1=CC(C(C(C(O)=O)=C2)=O)=C3N2C(C)COC3=C1N1CCN(C)CC1 GSDSWSVVBLHKDQ-UHFFFAOYSA-N 0.000 description 1
- DPSPPJIUMHPXMA-UHFFFAOYSA-N 9-fluoro-5-methyl-1-oxo-6,7-dihydro-1H,5H-pyrido[3,2,1-ij]quinoline-2-carboxylic acid Chemical compound C1CC(C)N2C=C(C(O)=O)C(=O)C3=C2C1=CC(F)=C3 DPSPPJIUMHPXMA-UHFFFAOYSA-N 0.000 description 1
- 240000005020 Acaciella glauca Species 0.000 description 1
- 102000002260 Alkaline Phosphatase Human genes 0.000 description 1
- 108020004774 Alkaline Phosphatase Proteins 0.000 description 1
- 241000272525 Anas platyrhynchos Species 0.000 description 1
- 241000272814 Anser sp. Species 0.000 description 1
- WZPBZJONDBGPKJ-UHFFFAOYSA-N Antibiotic SQ 26917 Natural products O=C1N(S(O)(=O)=O)C(C)C1NC(=O)C(=NOC(C)(C)C(O)=O)C1=CSC(N)=N1 WZPBZJONDBGPKJ-UHFFFAOYSA-N 0.000 description 1
- 102000007592 Apolipoproteins Human genes 0.000 description 1
- 108010071619 Apolipoproteins Proteins 0.000 description 1
- 200000000007 Arterial disease Diseases 0.000 description 1
- AXRYRYVKAWYZBR-UHFFFAOYSA-N Atazanavir Natural products C=1C=C(C=2N=CC=CC=2)C=CC=1CN(NC(=O)C(NC(=O)OC)C(C)(C)C)CC(O)C(NC(=O)C(NC(=O)OC)C(C)(C)C)CC1=CC=CC=C1 AXRYRYVKAWYZBR-UHFFFAOYSA-N 0.000 description 1
- 108010019625 Atazanavir Sulfate Proteins 0.000 description 1
- 108010001478 Bacitracin Proteins 0.000 description 1
- 208000031729 Bacteremia Diseases 0.000 description 1
- 201000001178 Bacterial Pneumonia Diseases 0.000 description 1
- MGQLHRYJBWGORO-LLVKDONJSA-N Balofloxacin Chemical compound C1[C@H](NC)CCCN1C1=C(F)C=C2C(=O)C(C(O)=O)=CN(C3CC3)C2=C1OC MGQLHRYJBWGORO-LLVKDONJSA-N 0.000 description 1
- 241000588832 Bordetella pertussis Species 0.000 description 1
- 241000283690 Bos taurus Species 0.000 description 1
- 206010006187 Breast cancer Diseases 0.000 description 1
- 208000026310 Breast neoplasm Diseases 0.000 description 1
- 102100028990 C-X-C chemokine receptor type 3 Human genes 0.000 description 1
- QAGYKUNXZHXKMR-UHFFFAOYSA-N CPD000469186 Natural products CC1=C(O)C=CC=C1C(=O)NC(C(O)CN1C(CC2CCCCC2C1)C(=O)NC(C)(C)C)CSC1=CC=CC=C1 QAGYKUNXZHXKMR-UHFFFAOYSA-N 0.000 description 1
- 101001120790 Caenorhabditis elegans UDP-N-acetylglucosamine-peptide N-acetylglucosaminyltransferase Proteins 0.000 description 1
- 241000282836 Camelus dromedarius Species 0.000 description 1
- 241000589876 Campylobacter Species 0.000 description 1
- 108010065839 Capreomycin Proteins 0.000 description 1
- 241000700199 Cavia porcellus Species 0.000 description 1
- GNWUOVJNSFPWDD-XMZRARIVSA-M Cefoxitin sodium Chemical compound [Na+].N([C@]1(OC)C(N2C(=C(COC(N)=O)CS[C@@H]21)C([O-])=O)=O)C(=O)CC1=CC=CS1 GNWUOVJNSFPWDD-XMZRARIVSA-M 0.000 description 1
- 108010075016 Ceruloplasmin Proteins 0.000 description 1
- 102100023321 Ceruloplasmin Human genes 0.000 description 1
- 108010008978 Chemokine CXCL10 Proteins 0.000 description 1
- 241001185363 Chlamydiae Species 0.000 description 1
- VWFCHDSQECPREK-LURJTMIESA-N Cidofovir Chemical compound NC=1C=CN(C[C@@H](CO)OCP(O)(O)=O)C(=O)N=1 VWFCHDSQECPREK-LURJTMIESA-N 0.000 description 1
- 206010010071 Coma Diseases 0.000 description 1
- 206010010356 Congenital anomaly Diseases 0.000 description 1
- 241000711573 Coronaviridae Species 0.000 description 1
- 241000606678 Coxiella burnetii Species 0.000 description 1
- 206010011376 Crepitations Diseases 0.000 description 1
- 241000724252 Cucumber mosaic virus Species 0.000 description 1
- 108010069514 Cyclic Peptides Proteins 0.000 description 1
- 102000001189 Cyclic Peptides Human genes 0.000 description 1
- DYDCUQKUCUHJBH-UWTATZPHSA-N D-Cycloserine Chemical compound N[C@@H]1CONC1=O DYDCUQKUCUHJBH-UWTATZPHSA-N 0.000 description 1
- DYDCUQKUCUHJBH-UHFFFAOYSA-N D-Cycloserine Natural products NC1CONC1=O DYDCUQKUCUHJBH-UHFFFAOYSA-N 0.000 description 1
- 108010013198 Daptomycin Proteins 0.000 description 1
- FMTDIUIBLCQGJB-UHFFFAOYSA-N Demethylchlortetracyclin Natural products C1C2C(O)C3=C(Cl)C=CC(O)=C3C(=O)C2=C(O)C2(O)C1C(N(C)C)C(O)=C(C(N)=O)C2=O FMTDIUIBLCQGJB-UHFFFAOYSA-N 0.000 description 1
- 108700022150 Designed Ankyrin Repeat Proteins Proteins 0.000 description 1
- 206010012735 Diarrhoea Diseases 0.000 description 1
- BXZVVICBKDXVGW-NKWVEPMBSA-N Didanosine Chemical compound O1[C@H](CO)CC[C@@H]1N1C(NC=NC2=O)=C2N=C1 BXZVVICBKDXVGW-NKWVEPMBSA-N 0.000 description 1
- 206010059866 Drug resistance Diseases 0.000 description 1
- 238000012286 ELISA Assay Methods 0.000 description 1
- XPOQHMRABVBWPR-UHFFFAOYSA-N Efavirenz Natural products O1C(=O)NC2=CC=C(Cl)C=C2C1(C(F)(F)F)C#CC1CC1 XPOQHMRABVBWPR-UHFFFAOYSA-N 0.000 description 1
- 108010032976 Enfuvirtide Proteins 0.000 description 1
- 241000283074 Equus asinus Species 0.000 description 1
- 208000010201 Exanthema Diseases 0.000 description 1
- 241000282326 Felis catus Species 0.000 description 1
- 241000192125 Firmicutes Species 0.000 description 1
- UIOFUWFRIANQPC-JKIFEVAISA-N Floxacillin Chemical compound N([C@@H]1C(N2[C@H](C(C)(C)S[C@@H]21)C(O)=O)=O)C(=O)C1=C(C)ON=C1C1=C(F)C=CC=C1Cl UIOFUWFRIANQPC-JKIFEVAISA-N 0.000 description 1
- 241000287828 Gallus gallus Species 0.000 description 1
- 208000005577 Gastroenteritis Diseases 0.000 description 1
- 229930182566 Gentamicin Natural products 0.000 description 1
- CEAZRRDELHUEMR-URQXQFDESA-N Gentamicin Chemical compound O1[C@H](C(C)NC)CC[C@@H](N)[C@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H](NC)[C@@](C)(O)CO2)O)[C@H](N)C[C@@H]1N CEAZRRDELHUEMR-URQXQFDESA-N 0.000 description 1
- AIJTTZAVMXIJGM-UHFFFAOYSA-N Grepafloxacin Chemical compound C1CNC(C)CN1C(C(=C1C)F)=CC2=C1C(=O)C(C(O)=O)=CN2C1CC1 AIJTTZAVMXIJGM-UHFFFAOYSA-N 0.000 description 1
- 241000606768 Haemophilus influenzae Species 0.000 description 1
- 206010019233 Headaches Diseases 0.000 description 1
- 241000700721 Hepatitis B virus Species 0.000 description 1
- 101000916050 Homo sapiens C-X-C chemokine receptor type 3 Proteins 0.000 description 1
- 101000858088 Homo sapiens C-X-C motif chemokine 10 Proteins 0.000 description 1
- 101000942118 Homo sapiens C-reactive protein Proteins 0.000 description 1
- 101000922020 Homo sapiens Cysteine and glycine-rich protein 1 Proteins 0.000 description 1
- 101000844686 Homo sapiens Thioredoxin reductase 1, cytoplasmic Proteins 0.000 description 1
- 101000835093 Homo sapiens Transferrin receptor protein 1 Proteins 0.000 description 1
- 101000610609 Homo sapiens Tumor necrosis factor receptor superfamily member 10D Proteins 0.000 description 1
- 108010001336 Horseradish Peroxidase Proteins 0.000 description 1
- 241000711467 Human coronavirus 229E Species 0.000 description 1
- 241000482741 Human coronavirus NL63 Species 0.000 description 1
- 241001428935 Human coronavirus OC43 Species 0.000 description 1
- 241000342334 Human metapneumovirus Species 0.000 description 1
- 206010020751 Hypersensitivity Diseases 0.000 description 1
- XQFRJNBWHJMXHO-RRKCRQDMSA-N IDUR Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C(I)=C1 XQFRJNBWHJMXHO-RRKCRQDMSA-N 0.000 description 1
- -1 IP- 10 Proteins 0.000 description 1
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical compound C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 1
- 108010054477 Immunoglobulin Fab Fragments Proteins 0.000 description 1
- 102000001706 Immunoglobulin Fab Fragments Human genes 0.000 description 1
- 241000712431 Influenza A virus Species 0.000 description 1
- 241000713196 Influenza B virus Species 0.000 description 1
- 241001500351 Influenzavirus A Species 0.000 description 1
- 241001500350 Influenzavirus B Species 0.000 description 1
- 229930010555 Inosine Natural products 0.000 description 1
- UGQMRVRMYYASKQ-KQYNXXCUSA-N Inosine Chemical compound O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1C2=NC=NC(O)=C2N=C1 UGQMRVRMYYASKQ-KQYNXXCUSA-N 0.000 description 1
- 108010014726 Interferon Type I Proteins 0.000 description 1
- 102000002227 Interferon Type I Human genes 0.000 description 1
- JUZNIMUFDBIJCM-ANEDZVCMSA-N Invanz Chemical compound O=C([C@H]1NC[C@H](C1)SC=1[C@H](C)[C@@H]2[C@H](C(N2C=1C(O)=O)=O)[C@H](O)C)NC1=CC=CC(C(O)=O)=C1 JUZNIMUFDBIJCM-ANEDZVCMSA-N 0.000 description 1
- KJHKTHWMRKYKJE-SUGCFTRWSA-N Kaletra Chemical compound N1([C@@H](C(C)C)C(=O)N[C@H](C[C@H](O)[C@H](CC=2C=CC=CC=2)NC(=O)COC=2C(=CC=CC=2C)C)CC=2C=CC=CC=2)CCCNC1=O KJHKTHWMRKYKJE-SUGCFTRWSA-N 0.000 description 1
- 241000087799 Koma Species 0.000 description 1
- OUYCCCASQSFEME-QMMMGPOBSA-N L-tyrosine Chemical compound OC(=O)[C@@H](N)CC1=CC=C(O)C=C1 OUYCCCASQSFEME-QMMMGPOBSA-N 0.000 description 1
- XAGMUUZPGZWTRP-ZETCQYMHSA-N LSM-5745 Chemical compound C([C@@H](N1C2=C(C(C(C(O)=O)=C1)=O)C=C1F)C)OC2=C1C1(N)CC1 XAGMUUZPGZWTRP-ZETCQYMHSA-N 0.000 description 1
- 241000589248 Legionella Species 0.000 description 1
- 208000007764 Legionnaires' Disease Diseases 0.000 description 1
- GSDSWSVVBLHKDQ-JTQLQIEISA-N Levofloxacin Chemical compound C([C@@H](N1C2=C(C(C(C(O)=O)=C1)=O)C=C1F)C)OC2=C1N1CCN(C)CC1 GSDSWSVVBLHKDQ-JTQLQIEISA-N 0.000 description 1
- OJMMVQQUTAEWLP-UHFFFAOYSA-N Lincomycin Natural products CN1CC(CCC)CC1C(=O)NC(C(C)O)C1C(O)C(O)C(O)C(SC)O1 OJMMVQQUTAEWLP-UHFFFAOYSA-N 0.000 description 1
- 108060001084 Luciferase Proteins 0.000 description 1
- 239000005089 Luciferase Substances 0.000 description 1
- 241000124008 Mammalia Species 0.000 description 1
- 201000009906 Meningitis Diseases 0.000 description 1
- 241000351643 Metapneumovirus Species 0.000 description 1
- 241001430197 Mollicutes Species 0.000 description 1
- MSFSPUZXLOGKHJ-UHFFFAOYSA-N Muraminsaeure Natural products OC(=O)C(C)OC1C(N)C(O)OC(CO)C1O MSFSPUZXLOGKHJ-UHFFFAOYSA-N 0.000 description 1
- 208000000112 Myalgia Diseases 0.000 description 1
- 208000001572 Mycoplasma Pneumonia Diseases 0.000 description 1
- 201000008235 Mycoplasma pneumoniae pneumonia Diseases 0.000 description 1
- 102100030856 Myoglobin Human genes 0.000 description 1
- 108010062374 Myoglobin Proteins 0.000 description 1
- KJHOZAZQWVKILO-UHFFFAOYSA-N N-(diaminomethylidene)-4-morpholinecarboximidamide Chemical compound NC(N)=NC(=N)N1CCOCC1 KJHOZAZQWVKILO-UHFFFAOYSA-N 0.000 description 1
- 206010028813 Nausea Diseases 0.000 description 1
- 229930193140 Neomycin Natural products 0.000 description 1
- 206010028980 Neoplasm Diseases 0.000 description 1
- 102000005348 Neuraminidase Human genes 0.000 description 1
- 108010006232 Neuraminidase Proteins 0.000 description 1
- 108091028043 Nucleic acid sequence Proteins 0.000 description 1
- 108091034117 Oligonucleotide Proteins 0.000 description 1
- 108700020796 Oncogene Proteins 0.000 description 1
- 206010068319 Oropharyngeal pain Diseases 0.000 description 1
- 206010033078 Otitis media Diseases 0.000 description 1
- 108090000854 Oxidoreductases Proteins 0.000 description 1
- 102000004316 Oxidoreductases Human genes 0.000 description 1
- KYGZCKSPAKDVKC-UHFFFAOYSA-N Oxolinic acid Chemical compound C1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC2=C1OCO2 KYGZCKSPAKDVKC-UHFFFAOYSA-N 0.000 description 1
- 239000004100 Oxytetracycline Substances 0.000 description 1
- UOZODPSAJZTQNH-UHFFFAOYSA-N Paromomycin II Natural products NC1C(O)C(O)C(CN)OC1OC1C(O)C(OC2C(C(N)CC(N)C2O)OC2C(C(O)C(O)C(CO)O2)N)OC1CO UOZODPSAJZTQNH-UHFFFAOYSA-N 0.000 description 1
- JNTOCHDNEULJHD-UHFFFAOYSA-N Penciclovir Chemical compound N1C(N)=NC(=O)C2=C1N(CCC(CO)CO)C=N2 JNTOCHDNEULJHD-UHFFFAOYSA-N 0.000 description 1
- 229930195708 Penicillin V Natural products 0.000 description 1
- 108010013639 Peptidoglycan Proteins 0.000 description 1
- 241000009328 Perro Species 0.000 description 1
- 206010057249 Phagocytosis Diseases 0.000 description 1
- 201000007100 Pharyngitis Diseases 0.000 description 1
- 241000233805 Phoenix Species 0.000 description 1
- 102000004160 Phosphoric Monoester Hydrolases Human genes 0.000 description 1
- 108090000608 Phosphoric Monoester Hydrolases Proteins 0.000 description 1
- 108010093965 Polymyxin B Proteins 0.000 description 1
- 239000004793 Polystyrene Substances 0.000 description 1
- ZLMJMSJWJFRBEC-UHFFFAOYSA-N Potassium Chemical compound [K] ZLMJMSJWJFRBEC-UHFFFAOYSA-N 0.000 description 1
- 108010079780 Pristinamycin Proteins 0.000 description 1
- RLNUPSVMIYRZSM-UHFFFAOYSA-N Pristinamycin Natural products CC1OC(=O)C(C=2C=CC=CC=2)NC(=O)C2CC(=O)CCN2C(=O)C(CC=2C=CC(=CC=2)N(C)C)CCN(C)C(=O)C2CCCN2C(=O)C(CC)NC(=O)C1NC(=O)C1=NC=CC=C1O RLNUPSVMIYRZSM-UHFFFAOYSA-N 0.000 description 1
- PWNMXPDKBYZCOO-UHFFFAOYSA-N Prulifloxacin Chemical compound C1=C2N3C(C)SC3=C(C(O)=O)C(=O)C2=CC(F)=C1N(CC1)CCN1CC=1OC(=O)OC=1C PWNMXPDKBYZCOO-UHFFFAOYSA-N 0.000 description 1
- CZPWVGJYEJSRLH-UHFFFAOYSA-N Pyrimidine Chemical compound C1=CN=CN=C1 CZPWVGJYEJSRLH-UHFFFAOYSA-N 0.000 description 1
- 206010037688 Q fever Diseases 0.000 description 1
- ZVGNESXIJDCBKN-WUIGKKEISA-N R-Tiacumicin B Natural products O([C@@H]1[C@@H](C)O[C@H]([C@H]([C@H]1O)OC)OCC1=CC=CC[C@H](O)C(C)=C[C@@H]([C@H](C(C)=CC(C)=CC[C@H](OC1=O)[C@@H](C)O)O[C@H]1[C@H]([C@@H](O)[C@H](OC(=O)C(C)C)C(C)(C)O1)O)CC)C(=O)C1=C(O)C(Cl)=C(O)C(Cl)=C1CC ZVGNESXIJDCBKN-WUIGKKEISA-N 0.000 description 1
- 108091030071 RNAI Proteins 0.000 description 1
- 238000011529 RT qPCR Methods 0.000 description 1
- 208000037656 Respiratory Sounds Diseases 0.000 description 1
- 241001325464 Rhinovirus A Species 0.000 description 1
- 241001325459 Rhinovirus B Species 0.000 description 1
- IWUCXVSUMQZMFG-AFCXAGJDSA-N Ribavirin Chemical compound N1=C(C(=O)N)N=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](CO)O1 IWUCXVSUMQZMFG-AFCXAGJDSA-N 0.000 description 1
- NCDNCNXCDXHOMX-UHFFFAOYSA-N Ritonavir Natural products C=1C=CC=CC=1CC(NC(=O)OCC=1SC=NC=1)C(O)CC(CC=1C=CC=CC=1)NC(=O)C(C(C)C)NC(=O)N(C)CC1=CSC(C(C)C)=N1 NCDNCNXCDXHOMX-UHFFFAOYSA-N 0.000 description 1
- NJCJBUHJQLFDSW-UHFFFAOYSA-N Rufloxacin Chemical compound C1CN(C)CCN1C1=C(F)C=C2C(=O)C(C(O)=O)=CN3CCSC1=C32 NJCJBUHJQLFDSW-UHFFFAOYSA-N 0.000 description 1
- 240000004808 Saccharomyces cerevisiae Species 0.000 description 1
- 241000607142 Salmonella Species 0.000 description 1
- 206010040070 Septic Shock Diseases 0.000 description 1
- MTCFGRXMJLQNBG-UHFFFAOYSA-N Serine Natural products OCC(N)C(O)=O MTCFGRXMJLQNBG-UHFFFAOYSA-N 0.000 description 1
- 241000607768 Shigella Species 0.000 description 1
- 108010003723 Single-Domain Antibodies Proteins 0.000 description 1
- 241000191967 Staphylococcus aureus Species 0.000 description 1
- 208000006011 Stroke Diseases 0.000 description 1
- NHUHCSRWZMLRLA-UHFFFAOYSA-N Sulfisoxazole Chemical compound CC1=NOC(NS(=O)(=O)C=2C=CC(N)=CC=2)=C1C NHUHCSRWZMLRLA-UHFFFAOYSA-N 0.000 description 1
- 241000282898 Sus scrofa Species 0.000 description 1
- 102000046283 TNF-Related Apoptosis-Inducing Ligand Human genes 0.000 description 1
- 108700012411 TNFSF10 Proteins 0.000 description 1
- 108010053950 Teicoplanin Proteins 0.000 description 1
- 239000004098 Tetracycline Substances 0.000 description 1
- WKDDRNSBRWANNC-UHFFFAOYSA-N Thienamycin Natural products C1C(SCCN)=C(C(O)=O)N2C(=O)C(C(O)C)C21 WKDDRNSBRWANNC-UHFFFAOYSA-N 0.000 description 1
- AYFVYJQAPQTCCC-UHFFFAOYSA-N Threonine Natural products CC(O)C(N)C(O)=O AYFVYJQAPQTCCC-UHFFFAOYSA-N 0.000 description 1
- 239000004473 Threonine Substances 0.000 description 1
- HJLSLZFTEKNLFI-UHFFFAOYSA-N Tinidazole Chemical compound CCS(=O)(=O)CCN1C(C)=NC=C1[N+]([O-])=O HJLSLZFTEKNLFI-UHFFFAOYSA-N 0.000 description 1
- SUJUHGSWHZTSEU-UHFFFAOYSA-N Tipranavir Natural products C1C(O)=C(C(CC)C=2C=C(NS(=O)(=O)C=3N=CC(=CC=3)C(F)(F)F)C=CC=2)C(=O)OC1(CCC)CCC1=CC=CC=C1 SUJUHGSWHZTSEU-UHFFFAOYSA-N 0.000 description 1
- 241000245032 Trillium Species 0.000 description 1
- 108060008683 Tumor Necrosis Factor Receptor Proteins 0.000 description 1
- 102100040110 Tumor necrosis factor receptor superfamily member 10D Human genes 0.000 description 1
- XSQUKJJJFZCRTK-UHFFFAOYSA-N Urea Chemical compound NC(N)=O XSQUKJJJFZCRTK-UHFFFAOYSA-N 0.000 description 1
- HDOVUKNUBWVHOX-QMMMGPOBSA-N Valacyclovir Chemical compound N1C(N)=NC(=O)C2=C1N(COCCOC(=O)[C@@H](N)C(C)C)C=N2 HDOVUKNUBWVHOX-QMMMGPOBSA-N 0.000 description 1
- WPVFJKSGQUFQAP-GKAPJAKFSA-N Valcyte Chemical compound N1C(N)=NC(=O)C2=C1N(COC(CO)COC(=O)[C@@H](N)C(C)C)C=N2 WPVFJKSGQUFQAP-GKAPJAKFSA-N 0.000 description 1
- 108010059993 Vancomycin Proteins 0.000 description 1
- OIRDTQYFTABQOQ-UHTZMRCNSA-N Vidarabine Chemical compound C1=NC=2C(N)=NC=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1O OIRDTQYFTABQOQ-UHTZMRCNSA-N 0.000 description 1
- 108010015940 Viomycin Proteins 0.000 description 1
- OZKXLOZHHUHGNV-UHFFFAOYSA-N Viomycin Natural products NCCCC(N)CC(=O)NC1CNC(=O)C(=CNC(=O)N)NC(=O)C(CO)NC(=O)C(CO)NC(=O)C(NC1=O)C2CC(O)NC(=N)N2 OZKXLOZHHUHGNV-UHFFFAOYSA-N 0.000 description 1
- WREGKURFCTUGRC-POYBYMJQSA-N Zalcitabine Chemical compound O=C1N=C(N)C=CN1[C@@H]1O[C@H](CO)CC1 WREGKURFCTUGRC-POYBYMJQSA-N 0.000 description 1
- ZWBTYMGEBZUQTK-PVLSIAFMSA-N [(7S,9E,11S,12R,13S,14R,15R,16R,17S,18S,19E,21Z)-2,15,17,32-tetrahydroxy-11-methoxy-3,7,12,14,16,18,22-heptamethyl-1'-(2-methylpropyl)-6,23-dioxospiro[8,33-dioxa-24,27,29-triazapentacyclo[23.6.1.14,7.05,31.026,30]tritriaconta-1(32),2,4,9,19,21,24,26,30-nonaene-28,4'-piperidine]-13-yl] acetate Chemical compound CO[C@H]1\C=C\O[C@@]2(C)Oc3c(C2=O)c2c4NC5(CCN(CC(C)C)CC5)N=c4c(=NC(=O)\C(C)=C/C=C/[C@H](C)[C@H](O)[C@@H](C)[C@@H](O)[C@@H](C)[C@H](OC(C)=O)[C@@H]1C)c(O)c2c(O)c3C ZWBTYMGEBZUQTK-PVLSIAFMSA-N 0.000 description 1
- DLGSOJOOYHWROO-WQLSENKSSA-N [(z)-(1-methyl-2-oxoindol-3-ylidene)amino]thiourea Chemical compound C1=CC=C2N(C)C(=O)\C(=N/NC(N)=S)C2=C1 DLGSOJOOYHWROO-WQLSENKSSA-N 0.000 description 1
- JLCPHMBAVCMARE-UHFFFAOYSA-N [3-[[3-[[3-[[3-[[3-[[3-[[3-[[3-[[3-[[3-[[3-[[5-(2-amino-6-oxo-1H-purin-9-yl)-3-[[3-[[3-[[3-[[3-[[3-[[5-(2-amino-6-oxo-1H-purin-9-yl)-3-[[5-(2-amino-6-oxo-1H-purin-9-yl)-3-hydroxyoxolan-2-yl]methoxy-hydroxyphosphoryl]oxyoxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(5-methyl-2,4-dioxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxyoxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(5-methyl-2,4-dioxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(4-amino-2-oxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(5-methyl-2,4-dioxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(5-methyl-2,4-dioxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(4-amino-2-oxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(4-amino-2-oxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(4-amino-2-oxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(6-aminopurin-9-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-5-(4-amino-2-oxopyrimidin-1-yl)oxolan-2-yl]methyl [5-(6-aminopurin-9-yl)-2-(hydroxymethyl)oxolan-3-yl] hydrogen phosphate Polymers Cc1cn(C2CC(OP(O)(=O)OCC3OC(CC3OP(O)(=O)OCC3OC(CC3O)n3cnc4c3nc(N)[nH]c4=O)n3cnc4c3nc(N)[nH]c4=O)C(COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3COP(O)(=O)OC3CC(OC3CO)n3cnc4c(N)ncnc34)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3ccc(N)nc3=O)n3cnc4c(N)ncnc34)n3cnc4c(N)ncnc34)n3cc(C)c(=O)[nH]c3=O)n3cc(C)c(=O)[nH]c3=O)n3ccc(N)nc3=O)n3cc(C)c(=O)[nH]c3=O)n3cnc4c3nc(N)[nH]c4=O)n3cnc4c(N)ncnc34)n3cnc4c(N)ncnc34)n3cnc4c(N)ncnc34)n3cnc4c(N)ncnc34)O2)c(=O)[nH]c1=O JLCPHMBAVCMARE-UHFFFAOYSA-N 0.000 description 1
- GLWHPRRGGYLLRV-XLPZGREQSA-N [[(2s,3s,5r)-3-azido-5-(5-methyl-2,4-dioxopyrimidin-1-yl)oxolan-2-yl]methoxy-hydroxyphosphoryl] phosphono hydrogen phosphate Chemical compound O=C1NC(=O)C(C)=CN1[C@@H]1O[C@H](COP(O)(=O)OP(O)(=O)OP(O)(O)=O)[C@@H](N=[N+]=[N-])C1 GLWHPRRGGYLLRV-XLPZGREQSA-N 0.000 description 1
- 229960004748 abacavir Drugs 0.000 description 1
- MCGSCOLBFJQGHM-SCZZXKLOSA-N abacavir Chemical compound C=12N=CN([C@H]3C=C[C@@H](CO)C3)C2=NC(N)=NC=1NC1CC1 MCGSCOLBFJQGHM-SCZZXKLOSA-N 0.000 description 1
- 230000002159 abnormal effect Effects 0.000 description 1
- 239000000654 additive Substances 0.000 description 1
- 229960001997 adefovir Drugs 0.000 description 1
- WOZSCQDILHKSGG-UHFFFAOYSA-N adefovir depivoxil Chemical compound N1=CN=C2N(CCOCP(=O)(OCOC(=O)C(C)(C)C)OCOC(=O)C(C)(C)C)C=NC2=C1N WOZSCQDILHKSGG-UHFFFAOYSA-N 0.000 description 1
- 230000002411 adverse Effects 0.000 description 1
- DKNWSYNQZKUICI-UHFFFAOYSA-N amantadine Chemical compound C1C(C2)CC3CC2CC1(N)C3 DKNWSYNQZKUICI-UHFFFAOYSA-N 0.000 description 1
- 229960003805 amantadine Drugs 0.000 description 1
- 229960004821 amikacin Drugs 0.000 description 1
- LKCWBDHBTVXHDL-RMDFUYIESA-N amikacin Chemical compound O([C@@H]1[C@@H](N)C[C@H]([C@@H]([C@H]1O)O[C@@H]1[C@@H]([C@@H](N)[C@H](O)[C@@H](CO)O1)O)NC(=O)[C@@H](O)CCN)[C@H]1O[C@H](CN)[C@@H](O)[C@H](O)[C@H]1O LKCWBDHBTVXHDL-RMDFUYIESA-N 0.000 description 1
- 229960003022 amoxicillin Drugs 0.000 description 1
- LSQZJLSUYDQPKJ-NJBDSQKTSA-N amoxicillin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@H]3SC([C@@H](N3C2=O)C(O)=O)(C)C)=CC=C(O)C=C1 LSQZJLSUYDQPKJ-NJBDSQKTSA-N 0.000 description 1
- 229960000723 ampicillin Drugs 0.000 description 1
- AVKUERGKIZMTKX-NJBDSQKTSA-N ampicillin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@H]3SC([C@@H](N3C2=O)C(O)=O)(C)C)=CC=CC=C1 AVKUERGKIZMTKX-NJBDSQKTSA-N 0.000 description 1
- 230000003321 amplification Effects 0.000 description 1
- 229960001830 amprenavir Drugs 0.000 description 1
- YMARZQAQMVYCKC-OEMFJLHTSA-N amprenavir Chemical compound C([C@@H]([C@H](O)CN(CC(C)C)S(=O)(=O)C=1C=CC(N)=CC=1)NC(=O)O[C@@H]1COCC1)C1=CC=CC=C1 YMARZQAQMVYCKC-OEMFJLHTSA-N 0.000 description 1
- 229940121357 antivirals Drugs 0.000 description 1
- 208000028922 artery disease Diseases 0.000 description 1
- 229960003277 atazanavir Drugs 0.000 description 1
- AXRYRYVKAWYZBR-GASGPIRDSA-N atazanavir Chemical compound C([C@H](NC(=O)[C@@H](NC(=O)OC)C(C)(C)C)[C@@H](O)CN(CC=1C=CC(=CC=1)C=1N=CC=CC=1)NC(=O)[C@@H](NC(=O)OC)C(C)(C)C)C1=CC=CC=C1 AXRYRYVKAWYZBR-GASGPIRDSA-N 0.000 description 1
- 229940068561 atripla Drugs 0.000 description 1
- 229960004099 azithromycin Drugs 0.000 description 1
- MQTOSJVFKKJCRP-BICOPXKESA-N azithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)N(C)C[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 MQTOSJVFKKJCRP-BICOPXKESA-N 0.000 description 1
- WZPBZJONDBGPKJ-VEHQQRBSSA-N aztreonam Chemical compound O=C1N(S([O-])(=O)=O)[C@@H](C)[C@@H]1NC(=O)C(=N/OC(C)(C)C(O)=O)\C1=CSC([NH3+])=N1 WZPBZJONDBGPKJ-VEHQQRBSSA-N 0.000 description 1
- 229960003644 aztreonam Drugs 0.000 description 1
- 229960002699 bacampicillin Drugs 0.000 description 1
- PFOLLRNADZZWEX-FFGRCDKISA-N bacampicillin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)[C@H](C(S3)(C)C)C(=O)OC(C)OC(=O)OCC)=CC=CC=C1 PFOLLRNADZZWEX-FFGRCDKISA-N 0.000 description 1
- 229960003071 bacitracin Drugs 0.000 description 1
- 229930184125 bacitracin Natural products 0.000 description 1
- CLKOFPXJLQSYAH-ABRJDSQDSA-N bacitracin A Chemical compound C1SC([C@@H](N)[C@@H](C)CC)=N[C@@H]1C(=O)N[C@@H](CC(C)C)C(=O)N[C@H](CCC(O)=O)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H]1C(=O)N[C@H](CCCN)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@H](CC=2C=CC=CC=2)C(=O)N[C@@H](CC=2N=CNC=2)C(=O)N[C@H](CC(O)=O)C(=O)N[C@@H](CC(N)=O)C(=O)NCCCC1 CLKOFPXJLQSYAH-ABRJDSQDSA-N 0.000 description 1
- 244000052616 bacterial pathogen Species 0.000 description 1
- 229950000805 balofloxacin Drugs 0.000 description 1
- 238000013476 bayesian approach Methods 0.000 description 1
- 230000006399 behavior Effects 0.000 description 1
- 229960004024 besifloxacin Drugs 0.000 description 1
- QFFGVLORLPOAEC-SNVBAGLBSA-N besifloxacin Chemical compound C1[C@H](N)CCCCN1C1=C(F)C=C2C(=O)C(C(O)=O)=CN(C3CC3)C2=C1Cl QFFGVLORLPOAEC-SNVBAGLBSA-N 0.000 description 1
- 230000000975 bioactive effect Effects 0.000 description 1
- 230000008436 biogenesis Effects 0.000 description 1
- 230000008236 biological pathway Effects 0.000 description 1
- 230000015572 biosynthetic process Effects 0.000 description 1
- 239000002981 blocking agent Substances 0.000 description 1
- 230000000903 blocking effect Effects 0.000 description 1
- 238000009640 blood culture Methods 0.000 description 1
- 230000036765 blood level Effects 0.000 description 1
- 210000001772 blood platelet Anatomy 0.000 description 1
- 230000036760 body temperature Effects 0.000 description 1
- 206010006451 bronchitis Diseases 0.000 description 1
- 229940124630 bronchodilator Drugs 0.000 description 1
- 239000000168 bronchodilator agent Substances 0.000 description 1
- 239000007853 buffer solution Substances 0.000 description 1
- 201000011510 cancer Diseases 0.000 description 1
- 229960004602 capreomycin Drugs 0.000 description 1
- 239000004202 carbamide Substances 0.000 description 1
- 229960003669 carbenicillin Drugs 0.000 description 1
- FPPNZSSZRUTDAP-UWFZAAFLSA-N carbenicillin Chemical compound N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)C(C(O)=O)C1=CC=CC=C1 FPPNZSSZRUTDAP-UWFZAAFLSA-N 0.000 description 1
- 229960005361 cefaclor Drugs 0.000 description 1
- QYIYFLOTGYLRGG-GPCCPHFNSA-N cefaclor Chemical compound C1([C@H](C(=O)N[C@@H]2C(N3C(=C(Cl)CS[C@@H]32)C(O)=O)=O)N)=CC=CC=C1 QYIYFLOTGYLRGG-GPCCPHFNSA-N 0.000 description 1
- 229960004841 cefadroxil Drugs 0.000 description 1
- NBFNMSULHIODTC-CYJZLJNKSA-N cefadroxil monohydrate Chemical compound O.C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)C)C(O)=O)=CC=C(O)C=C1 NBFNMSULHIODTC-CYJZLJNKSA-N 0.000 description 1
- 229950005258 cefalonium Drugs 0.000 description 1
- GOFCPYKUMJBHBH-RHSMWYFYSA-N cefaloram Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC(=O)C)C(O)=O)C(=O)CC1=CC=CC=C1 GOFCPYKUMJBHBH-RHSMWYFYSA-N 0.000 description 1
- 229950001373 cefaloram Drugs 0.000 description 1
- 229960003866 cefaloridine Drugs 0.000 description 1
- CZTQZXZIADLWOZ-CRAIPNDOSA-N cefaloridine Chemical compound O=C([C@@H](NC(=O)CC=1SC=CC=1)[C@H]1SC2)N1C(C(=O)[O-])=C2C[N+]1=CC=CC=C1 CZTQZXZIADLWOZ-CRAIPNDOSA-N 0.000 description 1
- 229960003012 cefamandole Drugs 0.000 description 1
- OLVCFLKTBJRLHI-AXAPSJFSSA-N cefamandole Chemical compound CN1N=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)[C@H](O)C=3C=CC=CC=3)[C@H]2SC1 OLVCFLKTBJRLHI-AXAPSJFSSA-N 0.000 description 1
- 229950000042 cefaparole Drugs 0.000 description 1
- 229960002420 cefatrizine Drugs 0.000 description 1
- ACXMTAJLYQCRGF-PBFPGSCMSA-N cefatrizine Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)[C@H](N)C=2C=CC(O)=CC=2)CC=1CSC1=CN=N[N]1 ACXMTAJLYQCRGF-PBFPGSCMSA-N 0.000 description 1
- HGXLJRWXCXSEJO-GMSGAONNSA-N cefazaflur Chemical compound CN1N=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)CSC(F)(F)F)[C@H]2SC1 HGXLJRWXCXSEJO-GMSGAONNSA-N 0.000 description 1
- 229950004359 cefazaflur Drugs 0.000 description 1
- 229960005312 cefazedone Drugs 0.000 description 1
- VTLCNEGVSVJLDN-MLGOLLRUSA-N cefazedone Chemical compound S1C(C)=NN=C1SCC1=C(C(O)=O)N2C(=O)[C@@H](NC(=O)CN3C=C(Cl)C(=O)C(Cl)=C3)[C@H]2SC1 VTLCNEGVSVJLDN-MLGOLLRUSA-N 0.000 description 1
- 229950002706 cefcanel Drugs 0.000 description 1
- 229960002966 cefcapene Drugs 0.000 description 1
- HJJRIJDTIPFROI-NVKITGPLSA-N cefcapene Chemical compound N([C@@H]1C(N2C(=C(COC(N)=O)CS[C@@H]21)C(O)=O)=O)C(=O)\C(=C/CC)C1=CSC(N)=N1 HJJRIJDTIPFROI-NVKITGPLSA-N 0.000 description 1
- JUVHVMCKLDZLGN-TVNFHGJBSA-N cefclidin Chemical compound N([C@@H]1C(N2C(=C(C[N+]34CCC(CC3)(CC4)C(N)=O)CS[C@@H]21)C([O-])=O)=O)C(=O)\C(=N/OC)C1=NSC(N)=N1 JUVHVMCKLDZLGN-TVNFHGJBSA-N 0.000 description 1
- HOGISBSFFHDTRM-GHXIOONMSA-N cefdaloxime Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC)C(O)=O)C(=O)C(=N/O)\C1=CSC(N)=N1 HOGISBSFFHDTRM-GHXIOONMSA-N 0.000 description 1
- 229950006550 cefdaloxime Drugs 0.000 description 1
- 229960003719 cefdinir Drugs 0.000 description 1
- RTXOFQZKPXMALH-GHXIOONMSA-N cefdinir Chemical compound S1C(N)=NC(C(=N\O)\C(=O)N[C@@H]2C(N3C(=C(C=C)CS[C@@H]32)C(O)=O)=O)=C1 RTXOFQZKPXMALH-GHXIOONMSA-N 0.000 description 1
- 229960004069 cefditoren Drugs 0.000 description 1
- KMIPKYQIOVAHOP-YLGJWRNMSA-N cefditoren Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1\C=C/C=1SC=NC=1C KMIPKYQIOVAHOP-YLGJWRNMSA-N 0.000 description 1
- 229950007281 cefedrolor Drugs 0.000 description 1
- 229950009347 cefempidone Drugs 0.000 description 1
- 229960002100 cefepime Drugs 0.000 description 1
- 229960004041 cefetamet Drugs 0.000 description 1
- MQLRYUCJDNBWMV-GHXIOONMSA-N cefetamet Chemical compound N([C@@H]1C(N2C(=C(C)CS[C@@H]21)C(O)=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 MQLRYUCJDNBWMV-GHXIOONMSA-N 0.000 description 1
- 229950003098 cefetrizole Drugs 0.000 description 1
- 229950007546 cefivitril Drugs 0.000 description 1
- 229960002129 cefixime Drugs 0.000 description 1
- OKBVVJOGVLARMR-QSWIMTSFSA-N cefixime Chemical compound S1C(N)=NC(C(=N\OCC(O)=O)\C(=O)N[C@@H]2C(N3C(=C(C=C)CS[C@@H]32)C(O)=O)=O)=C1 OKBVVJOGVLARMR-QSWIMTSFSA-N 0.000 description 1
- XAKKNLNAJBNLPC-MAYKBZFQSA-N cefluprenam Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)/C=C/C[N+](C)(CC)CC(N)=O)C([O-])=O)C(=O)C(=N/OCF)\C1=NSC(N)=N1 XAKKNLNAJBNLPC-MAYKBZFQSA-N 0.000 description 1
- 229950001334 cefluprenam Drugs 0.000 description 1
- UEQVTKSAEXANEZ-YCRCPZNHSA-N cefmatilen Chemical compound S1C(N)=NC(C(=N\O)\C(=O)N[C@@H]2C(N3C(=C(SCSC4=NNN=C4)CS[C@@H]32)C(O)=O)=O)=C1 UEQVTKSAEXANEZ-YCRCPZNHSA-N 0.000 description 1
- 229950008727 cefmatilen Drugs 0.000 description 1
- 229960003791 cefmenoxime Drugs 0.000 description 1
- HJJDBAOLQAWBMH-YCRCPZNHSA-N cefmenoxime Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC1=NN=NN1C HJJDBAOLQAWBMH-YCRCPZNHSA-N 0.000 description 1
- 229960003585 cefmetazole Drugs 0.000 description 1
- SNBUBQHDYVFSQF-HIFRSBDPSA-N cefmetazole Chemical compound S([C@@H]1[C@@](C(N1C=1C(O)=O)=O)(NC(=O)CSCC#N)OC)CC=1CSC1=NN=NN1C SNBUBQHDYVFSQF-HIFRSBDPSA-N 0.000 description 1
- 229960001958 cefodizime Drugs 0.000 description 1
- XDZKBRJLTGRPSS-BGZQYGJUSA-N cefodizime Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC1=NC(C)=C(CC(O)=O)S1 XDZKBRJLTGRPSS-BGZQYGJUSA-N 0.000 description 1
- 229960004489 cefonicid Drugs 0.000 description 1
- DYAIAHUQIPBDIP-AXAPSJFSSA-N cefonicid Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)[C@H](O)C=2C=CC=CC=2)CC=1CSC1=NN=NN1CS(O)(=O)=O DYAIAHUQIPBDIP-AXAPSJFSSA-N 0.000 description 1
- 229960004682 cefoperazone Drugs 0.000 description 1
- GCFBRXLSHGKWDP-XCGNWRKASA-N cefoperazone Chemical compound O=C1C(=O)N(CC)CCN1C(=O)N[C@H](C=1C=CC(O)=CC=1)C(=O)N[C@@H]1C(=O)N2C(C(O)=O)=C(CSC=3N(N=NN=3)C)CS[C@@H]21 GCFBRXLSHGKWDP-XCGNWRKASA-N 0.000 description 1
- ZINFAXPQMLDEEJ-GFVOIPPFSA-N cefoselis Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CN1C=CC(=N)N1CCO ZINFAXPQMLDEEJ-GFVOIPPFSA-N 0.000 description 1
- 229950001580 cefoselis Drugs 0.000 description 1
- 229960004261 cefotaxime Drugs 0.000 description 1
- AZZMGZXNTDTSME-JUZDKLSSSA-M cefotaxime sodium Chemical compound [Na+].N([C@@H]1C(N2C(=C(COC(C)=O)CS[C@@H]21)C([O-])=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 AZZMGZXNTDTSME-JUZDKLSSSA-M 0.000 description 1
- 229960005495 cefotetan Drugs 0.000 description 1
- SRZNHPXWXCNNDU-RHBCBLIFSA-N cefotetan Chemical compound N([C@]1(OC)C(N2C(=C(CSC=3N(N=NN=3)C)CS[C@@H]21)C(O)=O)=O)C(=O)C1SC(=C(C(N)=O)C(O)=O)S1 SRZNHPXWXCNNDU-RHBCBLIFSA-N 0.000 description 1
- 229960003391 cefovecin Drugs 0.000 description 1
- ZJGQFXVQDVCVOK-MSUXKOGISA-N cefovecin Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)/C(=N/OC)C=2N=C(N)SC=2)CC=1[C@@H]1CCCO1 ZJGQFXVQDVCVOK-MSUXKOGISA-N 0.000 description 1
- 229950002823 cefoxazole Drugs 0.000 description 1
- 229960002682 cefoxitin Drugs 0.000 description 1
- 229960002642 cefozopran Drugs 0.000 description 1
- QDUIJCOKQCCXQY-WHJQOFBOSA-N cefozopran Chemical compound N([C@@H]1C(N2C(=C(CN3C4=CC=CN=[N+]4C=C3)CS[C@@H]21)C([O-])=O)=O)C(=O)\C(=N/OC)C1=NSC(N)=N1 QDUIJCOKQCCXQY-WHJQOFBOSA-N 0.000 description 1
- LNZMRLHZGOBKAN-KAWPREARSA-N cefpimizole Chemical compound N1=CNC(C(=O)N[C@@H](C(=O)N[C@@H]2C(N3C(=C(C[N+]=4C=CC(CCS(O)(=O)=O)=CC=4)CS[C@@H]32)C([O-])=O)=O)C=2C=CC=CC=2)=C1C(=O)O LNZMRLHZGOBKAN-KAWPREARSA-N 0.000 description 1
- 229950004036 cefpimizole Drugs 0.000 description 1
- DKOQGJHPHLTOJR-WHRDSVKCSA-N cefpirome Chemical compound N([C@@H]1C(N2C(=C(C[N+]=3C=4CCCC=4C=CC=3)CS[C@@H]21)C([O-])=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 DKOQGJHPHLTOJR-WHRDSVKCSA-N 0.000 description 1
- 229960000466 cefpirome Drugs 0.000 description 1
- 229960005090 cefpodoxime Drugs 0.000 description 1
- WYUSVOMTXWRGEK-HBWVYFAYSA-N cefpodoxime Chemical compound N([C@H]1[C@@H]2N(C1=O)C(=C(CS2)COC)C(O)=O)C(=O)C(=N/OC)\C1=CSC(N)=N1 WYUSVOMTXWRGEK-HBWVYFAYSA-N 0.000 description 1
- 229960002580 cefprozil Drugs 0.000 description 1
- 229950009592 cefquinome Drugs 0.000 description 1
- 229950003685 cefrotil Drugs 0.000 description 1
- 229960003844 cefroxadine Drugs 0.000 description 1
- RDMOROXKXONCAL-UEKVPHQBSA-N cefroxadine Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)OC)C(O)=O)=CCC=CC1 RDMOROXKXONCAL-UEKVPHQBSA-N 0.000 description 1
- OFKRKCHCYWQZLY-XHBSWPGZSA-N cefsumide Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)C(=C(CS3)C)C(O)=O)=CC=CC(NS(C)(=O)=O)=C1 OFKRKCHCYWQZLY-XHBSWPGZSA-N 0.000 description 1
- 229950010594 cefsumide Drugs 0.000 description 1
- 229960000484 ceftazidime Drugs 0.000 description 1
- NMVPEQXCMGEDNH-TZVUEUGBSA-N ceftazidime pentahydrate Chemical compound O.O.O.O.O.S([C@@H]1[C@@H](C(N1C=1C([O-])=O)=O)NC(=O)\C(=N/OC(C)(C)C(O)=O)C=2N=C(N)SC=2)CC=1C[N+]1=CC=CC=C1 NMVPEQXCMGEDNH-TZVUEUGBSA-N 0.000 description 1
- 229950000679 cefteram Drugs 0.000 description 1
- 229960004366 ceftezole Drugs 0.000 description 1
- DZMVCVMFETWNIU-LDYMZIIASA-N ceftezole Chemical compound O=C([C@@H](NC(=O)CN1N=NN=C1)[C@H]1SC2)N1C(C(=O)O)=C2CSC1=NN=CS1 DZMVCVMFETWNIU-LDYMZIIASA-N 0.000 description 1
- 229960004086 ceftibuten Drugs 0.000 description 1
- UNJFKXSSGBWRBZ-BJCIPQKHSA-N ceftibuten Chemical compound S1C(N)=NC(C(=C\CC(O)=O)\C(=O)N[C@@H]2C(N3C(=CCS[C@@H]32)C(O)=O)=O)=C1 UNJFKXSSGBWRBZ-BJCIPQKHSA-N 0.000 description 1
- 229960005229 ceftiofur Drugs 0.000 description 1
- ZBHXIWJRIFEVQY-IHMPYVIRSA-N ceftiofur Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC(=O)C1=CC=CO1 ZBHXIWJRIFEVQY-IHMPYVIRSA-N 0.000 description 1
- WJXAHFZIHLTPFR-JLRJEBFFSA-N ceftiolene Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1\C=C\SC1=NNC(=O)C(=O)N1CC=O WJXAHFZIHLTPFR-JLRJEBFFSA-N 0.000 description 1
- 229950008880 ceftiolene Drugs 0.000 description 1
- 229950007152 ceftioxide Drugs 0.000 description 1
- 229960001991 ceftizoxime Drugs 0.000 description 1
- NNULBSISHYWZJU-LLKWHZGFSA-N ceftizoxime Chemical compound N([C@@H]1C(N2C(=CCS[C@@H]21)C(O)=O)=O)C(=O)\C(=N/OC)C1=CSC(N)=N1 NNULBSISHYWZJU-LLKWHZGFSA-N 0.000 description 1
- VOAZJEPQLGBXGO-SDAWRPRTSA-N ceftobiprole Chemical compound S1C(N)=NC(C(=N\O)\C(=O)N[C@@H]2C(N3C(=C(\C=C/4C(N([C@H]5CNCC5)CC\4)=O)CS[C@@H]32)C(O)=O)=O)=N1 VOAZJEPQLGBXGO-SDAWRPRTSA-N 0.000 description 1
- 229950004259 ceftobiprole Drugs 0.000 description 1
- 229960004755 ceftriaxone Drugs 0.000 description 1
- VAAUVRVFOQPIGI-SPQHTLEESA-N ceftriaxone Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC1=NC(=O)C(=O)NN1C VAAUVRVFOQPIGI-SPQHTLEESA-N 0.000 description 1
- 229950010799 cefuracetime Drugs 0.000 description 1
- 229960001668 cefuroxime Drugs 0.000 description 1
- JFPVXVDWJQMJEE-IZRZKJBUSA-N cefuroxime Chemical compound N([C@@H]1C(N2C(=C(COC(N)=O)CS[C@@H]21)C(O)=O)=O)C(=O)\C(=N/OC)C1=CC=CO1 JFPVXVDWJQMJEE-IZRZKJBUSA-N 0.000 description 1
- CXHKZHZLDMQGFF-ZSDSSEDPSA-N cefuzonam Chemical compound S([C@@H]1[C@@H](C(N1C=1C(O)=O)=O)NC(=O)\C(=N/OC)C=2N=C(N)SC=2)CC=1CSC1=CN=NS1 CXHKZHZLDMQGFF-ZSDSSEDPSA-N 0.000 description 1
- 229950000807 cefuzonam Drugs 0.000 description 1
- 238000000423 cell based assay Methods 0.000 description 1
- 238000004113 cell culture Methods 0.000 description 1
- 210000002421 cell wall Anatomy 0.000 description 1
- 230000001413 cellular effect Effects 0.000 description 1
- 210000001175 cerebrospinal fluid Anatomy 0.000 description 1
- 230000005465 channeling Effects 0.000 description 1
- 238000012512 characterization method Methods 0.000 description 1
- NPGNOVNWUSPMDP-UTEPHESZSA-N chembl1650818 Chemical compound N(/[C@H]1[C@@H]2N(C1=O)[C@H](C(S2)(C)C)C(=O)OCOC(=O)C(C)(C)C)=C\N1CCCCCC1 NPGNOVNWUSPMDP-UTEPHESZSA-N 0.000 description 1
- DDTDNCYHLGRFBM-YZEKDTGTSA-N chembl2367892 Chemical compound CC(=O)N[C@H]1[C@@H](O)[C@H](O)[C@H](CO)O[C@H]1O[C@@H]([C@H]1C(N[C@@H](C2=CC(O)=CC(O[C@@H]3[C@H]([C@H](O)[C@H](O)[C@@H](CO)O3)O)=C2C=2C(O)=CC=C(C=2)[C@@H](NC(=O)[C@@H]2NC(=O)[C@@H]3C=4C=C(O)C=C(C=4)OC=4C(O)=CC=C(C=4)[C@@H](N)C(=O)N[C@H](CC=4C=C(Cl)C(O5)=CC=4)C(=O)N3)C(=O)N1)C(O)=O)=O)C(C=C1Cl)=CC=C1OC1=C(O[C@H]3[C@H]([C@@H](O)[C@H](O)[C@H](CO)O3)NC(C)=O)C5=CC2=C1 DDTDNCYHLGRFBM-YZEKDTGTSA-N 0.000 description 1
- 239000003795 chemical substances by application Substances 0.000 description 1
- 229960005091 chloramphenicol Drugs 0.000 description 1
- WIIZWVCIJKGZOK-RKDXNWHRSA-N chloramphenicol Chemical compound ClC(Cl)C(=O)N[C@H](CO)[C@H](O)C1=CC=C([N+]([O-])=O)C=C1 WIIZWVCIJKGZOK-RKDXNWHRSA-N 0.000 description 1
- 229960000724 cidofovir Drugs 0.000 description 1
- 229960003405 ciprofloxacin Drugs 0.000 description 1
- 229960002626 clarithromycin Drugs 0.000 description 1
- AGOYDEPGAOXOCK-KCBOHYOISA-N clarithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H](O)[C@@H](C)C(=O)[C@H](C)C[C@](C)([C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)OC)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 AGOYDEPGAOXOCK-KCBOHYOISA-N 0.000 description 1
- 238000013145 classification model Methods 0.000 description 1
- QGPKADBNRMWEQR-UHFFFAOYSA-N clinafloxacin Chemical compound C1C(N)CCN1C1=C(F)C=C2C(=O)C(C(O)=O)=CN(C3CC3)C2=C1Cl QGPKADBNRMWEQR-UHFFFAOYSA-N 0.000 description 1
- 229950001320 clinafloxacin Drugs 0.000 description 1
- 229960002227 clindamycin Drugs 0.000 description 1
- KDLRVYVGXIQJDK-AWPVFWJPSA-N clindamycin Chemical compound CN1C[C@H](CCC)C[C@H]1C(=O)N[C@H]([C@H](C)Cl)[C@@H]1[C@H](O)[C@H](O)[C@@H](O)[C@@H](SC)O1 KDLRVYVGXIQJDK-AWPVFWJPSA-N 0.000 description 1
- 229960003326 cloxacillin Drugs 0.000 description 1
- LQOLIRLGBULYKD-JKIFEVAISA-N cloxacillin Chemical compound N([C@@H]1C(N2[C@H](C(C)(C)S[C@@H]21)C(O)=O)=O)C(=O)C1=C(C)ON=C1C1=CC=CC=C1Cl LQOLIRLGBULYKD-JKIFEVAISA-N 0.000 description 1
- 229940047766 co-trimoxazole Drugs 0.000 description 1
- 229940014461 combivir Drugs 0.000 description 1
- 239000000470 constituent Substances 0.000 description 1
- 239000013068 control sample Substances 0.000 description 1
- 239000003246 corticosteroid Substances 0.000 description 1
- 229960001334 corticosteroids Drugs 0.000 description 1
- 229940109239 creatinine Drugs 0.000 description 1
- 238000002790 cross-validation Methods 0.000 description 1
- 238000007821 culture assay Methods 0.000 description 1
- 238000013211 curve analysis Methods 0.000 description 1
- 229960003077 cycloserine Drugs 0.000 description 1
- 230000002380 cytological effect Effects 0.000 description 1
- DOAKLVKFURWEDJ-QCMAZARJSA-N daptomycin Chemical compound C([C@H]1C(=O)O[C@H](C)[C@@H](C(NCC(=O)N[C@@H](CCCN)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@H](C)C(=O)N[C@@H](CC(O)=O)C(=O)NCC(=O)N[C@H](CO)C(=O)N[C@H](C(=O)N1)[C@H](C)CC(O)=O)=O)NC(=O)[C@H](CC(O)=O)NC(=O)[C@@H](CC(N)=O)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)CCCCCCCCC)C(=O)C1=CC=CC=C1N DOAKLVKFURWEDJ-QCMAZARJSA-N 0.000 description 1
- 229960005484 daptomycin Drugs 0.000 description 1
- 229960005107 darunavir Drugs 0.000 description 1
- CJBJHOAVZSMMDJ-HEXNFIEUSA-N darunavir Chemical compound C([C@@H]([C@H](O)CN(CC(C)C)S(=O)(=O)C=1C=CC(N)=CC=1)NC(=O)O[C@@H]1[C@@H]2CCO[C@@H]2OC1)C1=CC=CC=C1 CJBJHOAVZSMMDJ-HEXNFIEUSA-N 0.000 description 1
- 238000013480 data collection Methods 0.000 description 1
- 230000034994 death Effects 0.000 description 1
- 230000003247 decreasing effect Effects 0.000 description 1
- 230000007812 deficiency Effects 0.000 description 1
- 230000002950 deficient Effects 0.000 description 1
- 229960005319 delavirdine Drugs 0.000 description 1
- 229960002398 demeclocycline Drugs 0.000 description 1
- 230000008021 deposition Effects 0.000 description 1
- 238000009795 derivation Methods 0.000 description 1
- 238000013461 design Methods 0.000 description 1
- 238000011161 development Methods 0.000 description 1
- 230000018109 developmental process Effects 0.000 description 1
- 206010012601 diabetes mellitus Diseases 0.000 description 1
- 229960001585 dicloxacillin Drugs 0.000 description 1
- YFAGHNZHGGCZAX-JKIFEVAISA-N dicloxacillin Chemical compound N([C@@H]1C(N2[C@H](C(C)(C)S[C@@H]21)C(O)=O)=O)C(=O)C1=C(C)ON=C1C1=C(Cl)C=CC=C1Cl YFAGHNZHGGCZAX-JKIFEVAISA-N 0.000 description 1
- 229960002656 didanosine Drugs 0.000 description 1
- 229960004100 dirithromycin Drugs 0.000 description 1
- WLOHNSSYAXHWNR-NXPDYKKBSA-N dirithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)O[C@@H]([C@@]([C@H]2O[C@H](COCCOC)N[C@H]([C@@H]2C)[C@H](C)C[C@@](C)(O)[C@H](O[C@H]2[C@@H]([C@H](C[C@@H](C)O2)N(C)C)O)[C@H]1C)(C)O)CC)[C@H]1C[C@@](C)(OC)[C@@H](O)[C@H](C)O1 WLOHNSSYAXHWNR-NXPDYKKBSA-N 0.000 description 1
- 229960000735 docosanol Drugs 0.000 description 1
- 229960002542 dolutegravir Drugs 0.000 description 1
- RHWKPHLQXYSBKR-BMIGLBTASA-N dolutegravir Chemical compound C([C@@H]1OCC[C@H](N1C(=O)C1=C(O)C2=O)C)N1C=C2C(=O)NCC1=CC=C(F)C=C1F RHWKPHLQXYSBKR-BMIGLBTASA-N 0.000 description 1
- 229960000895 doripenem Drugs 0.000 description 1
- AVAACINZEOAHHE-VFZPANTDSA-N doripenem Chemical compound C=1([C@H](C)[C@@H]2[C@H](C(N2C=1C(O)=O)=O)[C@H](O)C)S[C@@H]1CN[C@H](CNS(N)(=O)=O)C1 AVAACINZEOAHHE-VFZPANTDSA-N 0.000 description 1
- 229960003722 doxycycline Drugs 0.000 description 1
- 230000009977 dual effect Effects 0.000 description 1
- 229960002030 edoxudine Drugs 0.000 description 1
- XACKNLSZYYIACO-DJLDLDEBSA-N edoxudine Chemical compound O=C1NC(=O)C(CC)=CN1[C@@H]1O[C@H](CO)[C@@H](O)C1 XACKNLSZYYIACO-DJLDLDEBSA-N 0.000 description 1
- 229960003804 efavirenz Drugs 0.000 description 1
- XPOQHMRABVBWPR-ZDUSSCGKSA-N efavirenz Chemical compound C([C@]1(C2=CC(Cl)=CC=C2NC(=O)O1)C(F)(F)F)#CC1CC1 XPOQHMRABVBWPR-ZDUSSCGKSA-N 0.000 description 1
- 238000000835 electrochemical detection Methods 0.000 description 1
- 239000003792 electrolyte Substances 0.000 description 1
- 229960000366 emtricitabine Drugs 0.000 description 1
- 230000002124 endocrine Effects 0.000 description 1
- 229960002062 enfuvirtide Drugs 0.000 description 1
- PEASPLKKXBYDKL-FXEVSJAOSA-N enfuvirtide Chemical compound C([C@@H](C(=O)N[C@@H](CO)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](C)C(=O)N[C@@H](CO)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC=1C=CC=CC=1)C(N)=O)NC(=O)[C@@H](NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CO)NC(=O)[C@@H](NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(C)=O)[C@@H](C)O)[C@@H](C)CC)C1=CN=CN1 PEASPLKKXBYDKL-FXEVSJAOSA-N 0.000 description 1
- 229960002549 enoxacin Drugs 0.000 description 1
- IDYZIJYBMGIQMJ-UHFFFAOYSA-N enoxacin Chemical compound N1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC(F)=C1N1CCNCC1 IDYZIJYBMGIQMJ-UHFFFAOYSA-N 0.000 description 1
- 229960000980 entecavir Drugs 0.000 description 1
- YXPVEXCTPGULBZ-WQYNNSOESA-N entecavir hydrate Chemical compound O.C1=NC=2C(=O)NC(N)=NC=2N1[C@H]1C[C@H](O)[C@@H](CO)C1=C YXPVEXCTPGULBZ-WQYNNSOESA-N 0.000 description 1
- 238000006911 enzymatic reaction Methods 0.000 description 1
- 238000001952 enzyme assay Methods 0.000 description 1
- YJGVMLPVUAXIQN-UHFFFAOYSA-N epipodophyllotoxin Natural products COC1=C(OC)C(OC)=CC(C2C3=CC=4OCOC=4C=C3C(O)C3C2C(OC3)=O)=C1 YJGVMLPVUAXIQN-UHFFFAOYSA-N 0.000 description 1
- 210000002919 epithelial cell Anatomy 0.000 description 1
- 229960002770 ertapenem Drugs 0.000 description 1
- 210000003743 erythrocyte Anatomy 0.000 description 1
- 229960003276 erythromycin Drugs 0.000 description 1
- 238000011156 evaluation Methods 0.000 description 1
- 201000005884 exanthem Diseases 0.000 description 1
- 229960004396 famciclovir Drugs 0.000 description 1
- GGXKWVWZWMLJEH-UHFFFAOYSA-N famcyclovir Chemical compound N1=C(N)N=C2N(CCC(COC(=O)C)COC(C)=O)C=NC2=C1 GGXKWVWZWMLJEH-UHFFFAOYSA-N 0.000 description 1
- 230000009795 fibrotic process Effects 0.000 description 1
- 229960000628 fidaxomicin Drugs 0.000 description 1
- ZVGNESXIJDCBKN-UUEYKCAUSA-N fidaxomicin Chemical compound O([C@@H]1[C@@H](C)O[C@H]([C@H]([C@H]1O)OC)OCC\1=C/C=C/C[C@H](O)/C(C)=C/[C@@H]([C@H](/C(C)=C/C(/C)=C/C[C@H](OC/1=O)[C@@H](C)O)O[C@H]1[C@H]([C@@H](O)[C@H](OC(=O)C(C)C)C(C)(C)O1)O)CC)C(=O)C1=C(O)C(Cl)=C(O)C(Cl)=C1CC ZVGNESXIJDCBKN-UUEYKCAUSA-N 0.000 description 1
- 238000001914 filtration Methods 0.000 description 1
- 229960004273 floxacillin Drugs 0.000 description 1
- 229960000702 flumequine Drugs 0.000 description 1
- 229960001447 fomivirsen Drugs 0.000 description 1
- XCWFZHPEARLXJI-UHFFFAOYSA-N fomivirsen Chemical compound C1C(N2C3=C(C(NC(N)=N3)=O)N=C2)OC(CO)C1OP(O)(=S)OCC1OC(N(C)C(=O)\N=C(\N)C=C)CC1OP(O)(=S)OCC1OC(N2C3=C(C(NC(N)=N3)=O)N=C2)CC1OP(O)(=S)OCC1OC(N2C(NC(=O)C(C)=C2)=O)CC1OP(O)(=S)OCC1OC(N2C(NC(=O)C(C)=C2)=O)CC1OP(O)(=S)OCC1OC(N2C(NC(=O)C(C)=C2)=O)CC1OP(O)(=S)OCC1OC(N2C3=C(C(NC(N)=N3)=O)N=C2)CC1OP(O)(=S)OCC1OC(N2C(N=C(N)C=C2)=O)CC1OP(O)(=S)OCC(C(C1)OP(S)(=O)OCC2C(CC(O2)N2C(N=C(N)C=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(N=C(N)C=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(N=C(N)C=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C(NC(=O)C(C)=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C3=C(C(NC(N)=N3)=O)N=C2)OP(O)(=S)OCC2C(CC(O2)N2C(N=C(N)C=C2)=O)OP(O)(=S)OCC2C(CC(O2)N2C3=C(C(NC(N)=N3)=O)N=C2)O)OC1N1C=C(C)C(=O)NC1=O XCWFZHPEARLXJI-UHFFFAOYSA-N 0.000 description 1
- 229960003142 fosamprenavir Drugs 0.000 description 1
- MLBVMOWEQCZNCC-OEMFJLHTSA-N fosamprenavir Chemical compound C([C@@H]([C@H](OP(O)(O)=O)CN(CC(C)C)S(=O)(=O)C=1C=CC(N)=CC=1)NC(=O)O[C@@H]1COCC1)C1=CC=CC=C1 MLBVMOWEQCZNCC-OEMFJLHTSA-N 0.000 description 1
- 229960005102 foscarnet Drugs 0.000 description 1
- 229940112424 fosfonet Drugs 0.000 description 1
- 230000004927 fusion Effects 0.000 description 1
- 229940125777 fusion inhibitor Drugs 0.000 description 1
- 229960002963 ganciclovir Drugs 0.000 description 1
- IRSCQMHQWWYFCW-UHFFFAOYSA-N ganciclovir Chemical compound O=C1NC(N)=NC2=C1N=CN2COC(CO)CO IRSCQMHQWWYFCW-UHFFFAOYSA-N 0.000 description 1
- 229960003923 gatifloxacin Drugs 0.000 description 1
- 230000009368 gene silencing by RNA Effects 0.000 description 1
- 230000002068 genetic effect Effects 0.000 description 1
- 229960002518 gentamicin Drugs 0.000 description 1
- 230000013595 glycosylation Effects 0.000 description 1
- 238000006206 glycosylation reaction Methods 0.000 description 1
- ZBKIUFWVEIBQRT-UHFFFAOYSA-N gold(1+) Chemical compound [Au+] ZBKIUFWVEIBQRT-UHFFFAOYSA-N 0.000 description 1
- 229960000642 grepafloxacin Drugs 0.000 description 1
- 229940047650 haemophilus influenzae Drugs 0.000 description 1
- 231100000869 headache Toxicity 0.000 description 1
- 230000005802 health problem Effects 0.000 description 1
- 230000003862 health status Effects 0.000 description 1
- 239000012456 homogeneous solution Substances 0.000 description 1
- 102000051143 human CRP Human genes 0.000 description 1
- 229960000374 ibacitabine Drugs 0.000 description 1
- WEVJJMPVVFNAHZ-RRKCRQDMSA-N ibacitabine Chemical compound C1=C(I)C(N)=NC(=O)N1[C@@H]1O[C@H](CO)[C@@H](O)C1 WEVJJMPVVFNAHZ-RRKCRQDMSA-N 0.000 description 1
- 229960004716 idoxuridine Drugs 0.000 description 1
- 229960002182 imipenem Drugs 0.000 description 1
- ZSKVGTPCRGIANV-ZXFLCMHBSA-N imipenem Chemical compound C1C(SCC\N=C\N)=C(C(O)=O)N2C(=O)[C@H]([C@H](O)C)[C@H]21 ZSKVGTPCRGIANV-ZXFLCMHBSA-N 0.000 description 1
- 229960002751 imiquimod Drugs 0.000 description 1
- DOUYETYNHWVLEO-UHFFFAOYSA-N imiquimod Chemical compound C1=CC=CC2=C3N(CC(C)C)C=NC3=C(N)N=C21 DOUYETYNHWVLEO-UHFFFAOYSA-N 0.000 description 1
- 210000001822 immobilized cell Anatomy 0.000 description 1
- 230000002519 immonomodulatory effect Effects 0.000 description 1
- 210000000987 immune system Anatomy 0.000 description 1
- 230000003053 immunization Effects 0.000 description 1
- 238000002649 immunization Methods 0.000 description 1
- 230000000984 immunochemical effect Effects 0.000 description 1
- 230000007233 immunological mechanism Effects 0.000 description 1
- 238000013198 immunometric assay Methods 0.000 description 1
- 238000001114 immunoprecipitation Methods 0.000 description 1
- 230000001506 immunosuppresive effect Effects 0.000 description 1
- 229960001936 indinavir Drugs 0.000 description 1
- CBVCZFGXHXORBI-PXQQMZJSSA-N indinavir Chemical compound C([C@H](N(CC1)C[C@@H](O)C[C@@H](CC=2C=CC=CC=2)C(=O)N[C@H]2C3=CC=CC=C3C[C@H]2O)C(=O)NC(C)(C)C)N1CC1=CC=CN=C1 CBVCZFGXHXORBI-PXQQMZJSSA-N 0.000 description 1
- 230000002401 inhibitory effect Effects 0.000 description 1
- 238000013101 initial test Methods 0.000 description 1
- 230000000977 initiatory effect Effects 0.000 description 1
- 208000014674 injury Diseases 0.000 description 1
- 229960003786 inosine Drugs 0.000 description 1
- 238000007689 inspection Methods 0.000 description 1
- 229940124524 integrase inhibitor Drugs 0.000 description 1
- 239000002850 integrase inhibitor Substances 0.000 description 1
- 230000003993 interaction Effects 0.000 description 1
- 108010018844 interferon type III Proteins 0.000 description 1
- 229940028894 interferon type ii Drugs 0.000 description 1
- 230000000968 intestinal effect Effects 0.000 description 1
- 230000003834 intracellular effect Effects 0.000 description 1
- 150000002500 ions Chemical class 0.000 description 1
- 229960000318 kanamycin Drugs 0.000 description 1
- 229930027917 kanamycin Natural products 0.000 description 1
- SBUJHOSQTJFQJX-NOAMYHISSA-N kanamycin Chemical compound O[C@@H]1[C@@H](O)[C@H](O)[C@@H](CN)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H](N)[C@H](O)[C@@H](CO)O2)O)[C@H](N)C[C@@H]1N SBUJHOSQTJFQJX-NOAMYHISSA-N 0.000 description 1
- 229930182823 kanamycin A Natural products 0.000 description 1
- 238000000021 kinase assay Methods 0.000 description 1
- 229960001627 lamivudine Drugs 0.000 description 1
- JTEGQNOMFQHVDC-NKWVEPMBSA-N lamivudine Chemical compound O=C1N=C(N)C=CN1[C@H]1O[C@@H](CO)SC1 JTEGQNOMFQHVDC-NKWVEPMBSA-N 0.000 description 1
- 229960003376 levofloxacin Drugs 0.000 description 1
- OJMMVQQUTAEWLP-KIDUDLJLSA-N lincomycin Chemical compound CN1C[C@H](CCC)C[C@H]1C(=O)N[C@H]([C@@H](C)O)[C@@H]1[C@H](O)[C@H](O)[C@@H](O)[C@@H](SC)O1 OJMMVQQUTAEWLP-KIDUDLJLSA-N 0.000 description 1
- 229960005287 lincomycin Drugs 0.000 description 1
- 238000012886 linear function Methods 0.000 description 1
- 238000012417 linear regression Methods 0.000 description 1
- 229960003907 linezolid Drugs 0.000 description 1
- TYZROVQLWOKYKF-ZDUSSCGKSA-N linezolid Chemical compound O=C1O[C@@H](CNC(=O)C)CN1C(C=C1F)=CC=C1N1CCOCC1 TYZROVQLWOKYKF-ZDUSSCGKSA-N 0.000 description 1
- 150000002632 lipids Chemical class 0.000 description 1
- 229960002422 lomefloxacin Drugs 0.000 description 1
- ZEKZLJVOYLTDKK-UHFFFAOYSA-N lomefloxacin Chemical compound FC1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC(F)=C1N1CCNC(C)C1 ZEKZLJVOYLTDKK-UHFFFAOYSA-N 0.000 description 1
- 230000007774 longterm Effects 0.000 description 1
- 229960004525 lopinavir Drugs 0.000 description 1
- CJPLEFFCVDQQFZ-UHFFFAOYSA-N loviride Chemical compound CC(=O)C1=CC=C(C)C=C1NC(C(N)=O)C1=C(Cl)C=CC=C1Cl CJPLEFFCVDQQFZ-UHFFFAOYSA-N 0.000 description 1
- 229950006243 loviride Drugs 0.000 description 1
- 210000004072 lung Anatomy 0.000 description 1
- 210000002540 macrophage Anatomy 0.000 description 1
- 230000036210 malignancy Effects 0.000 description 1
- 229960004710 maraviroc Drugs 0.000 description 1
- GSNHKUDZZFZSJB-QYOOZWMWSA-N maraviroc Chemical compound CC(C)C1=NN=C(C)N1[C@@H]1C[C@H](N2CC[C@H](NC(=O)C3CCC(F)(F)CC3)C=3C=CC=CC=3)CC[C@H]2C1 GSNHKUDZZFZSJB-QYOOZWMWSA-N 0.000 description 1
- 238000010339 medical test Methods 0.000 description 1
- 238000002483 medication Methods 0.000 description 1
- 229960002260 meropenem Drugs 0.000 description 1
- DMJNNHOOLUXYBV-PQTSNVLCSA-N meropenem Chemical compound C=1([C@H](C)[C@@H]2[C@H](C(N2C=1C(O)=O)=O)[C@H](O)C)S[C@@H]1CN[C@H](C(=O)N(C)C)C1 DMJNNHOOLUXYBV-PQTSNVLCSA-N 0.000 description 1
- 229960003152 metisazone Drugs 0.000 description 1
- 229960000282 metronidazole Drugs 0.000 description 1
- VAOCPAMSLUNLGC-UHFFFAOYSA-N metronidazole Chemical compound CC1=NC=C([N+]([O-])=O)N1CCO VAOCPAMSLUNLGC-UHFFFAOYSA-N 0.000 description 1
- 229960000198 mezlocillin Drugs 0.000 description 1
- YPBATNHYBCGSSN-VWPFQQQWSA-N mezlocillin Chemical compound N([C@@H](C(=O)N[C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C=1C=CC=CC=1)C(=O)N1CCN(S(C)(=O)=O)C1=O YPBATNHYBCGSSN-VWPFQQQWSA-N 0.000 description 1
- 238000002493 microarray Methods 0.000 description 1
- 230000000813 microbial effect Effects 0.000 description 1
- 244000000010 microbial pathogen Species 0.000 description 1
- 239000004005 microsphere Substances 0.000 description 1
- 229960004023 minocycline Drugs 0.000 description 1
- 239000003068 molecular probe Substances 0.000 description 1
- 229960005389 moroxydine Drugs 0.000 description 1
- 229960003702 moxifloxacin Drugs 0.000 description 1
- FABPRXSRWADJSP-MEDUHNTESA-N moxifloxacin Chemical compound COC1=C(N2C[C@H]3NCCC[C@H]3C2)C(F)=CC(C(C(C(O)=O)=C2)=O)=C1N2C1CC1 FABPRXSRWADJSP-MEDUHNTESA-N 0.000 description 1
- 210000003097 mucus Anatomy 0.000 description 1
- 238000000491 multivariate analysis Methods 0.000 description 1
- 210000003205 muscle Anatomy 0.000 description 1
- 208000015001 muscle soreness Diseases 0.000 description 1
- 229960003808 nadifloxacin Drugs 0.000 description 1
- JYJTVFIEFKZWCJ-UHFFFAOYSA-N nadifloxacin Chemical compound FC1=CC(C(C(C(O)=O)=C2)=O)=C3N2C(C)CCC3=C1N1CCC(O)CC1 JYJTVFIEFKZWCJ-UHFFFAOYSA-N 0.000 description 1
- 229960000515 nafcillin Drugs 0.000 description 1
- GPXLMGHLHQJAGZ-JTDSTZFVSA-N nafcillin Chemical compound C1=CC=CC2=C(C(=O)N[C@@H]3C(N4[C@H](C(C)(C)S[C@@H]43)C(O)=O)=O)C(OCC)=CC=C21 GPXLMGHLHQJAGZ-JTDSTZFVSA-N 0.000 description 1
- 229960000210 nalidixic acid Drugs 0.000 description 1
- MHWLWQUZZRMNGJ-UHFFFAOYSA-N nalidixic acid Chemical compound C1=C(C)N=C2N(CC)C=C(C(O)=O)C(=O)C2=C1 MHWLWQUZZRMNGJ-UHFFFAOYSA-N 0.000 description 1
- 239000002086 nanomaterial Substances 0.000 description 1
- 230000008693 nausea Effects 0.000 description 1
- 230000001338 necrotic effect Effects 0.000 description 1
- 239000013642 negative control Substances 0.000 description 1
- 229960000884 nelfinavir Drugs 0.000 description 1
- QAGYKUNXZHXKMR-HKWSIXNMSA-N nelfinavir Chemical compound CC1=C(O)C=CC=C1C(=O)N[C@H]([C@H](O)CN1[C@@H](C[C@@H]2CCCC[C@@H]2C1)C(=O)NC(C)(C)C)CSC1=CC=CC=C1 QAGYKUNXZHXKMR-HKWSIXNMSA-N 0.000 description 1
- 229960004927 neomycin Drugs 0.000 description 1
- 229960000808 netilmicin Drugs 0.000 description 1
- ZBGPYVZLYBDXKO-HILBYHGXSA-N netilmycin Chemical compound O([C@@H]1[C@@H](N)C[C@H]([C@@H]([C@H]1O)O[C@@H]1[C@]([C@H](NC)[C@@H](O)CO1)(C)O)NCC)[C@H]1OC(CN)=CC[C@H]1N ZBGPYVZLYBDXKO-HILBYHGXSA-N 0.000 description 1
- 229960000689 nevirapine Drugs 0.000 description 1
- 229940101771 nexavir Drugs 0.000 description 1
- 229960000564 nitrofurantoin Drugs 0.000 description 1
- NXFQHRVNIOXGAQ-YCRREMRBSA-N nitrofurantoin Chemical compound O1C([N+](=O)[O-])=CC=C1\C=N\N1C(=O)NC(=O)C1 NXFQHRVNIOXGAQ-YCRREMRBSA-N 0.000 description 1
- 229960001180 norfloxacin Drugs 0.000 description 1
- OGJPXUAPXNRGGI-UHFFFAOYSA-N norfloxacin Chemical compound C1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC(F)=C1N1CCNCC1 OGJPXUAPXNRGGI-UHFFFAOYSA-N 0.000 description 1
- 239000000101 novel biomarker Substances 0.000 description 1
- 238000010899 nucleation Methods 0.000 description 1
- 238000003199 nucleic acid amplification method Methods 0.000 description 1
- 238000007899 nucleic acid hybridization Methods 0.000 description 1
- 108020004707 nucleic acids Proteins 0.000 description 1
- 102000039446 nucleic acids Human genes 0.000 description 1
- 150000007523 nucleic acids Chemical class 0.000 description 1
- 230000000414 obstructive effect Effects 0.000 description 1
- 229960001699 ofloxacin Drugs 0.000 description 1
- 238000002515 oligonucleotide synthesis Methods 0.000 description 1
- VSZGPKBBMSAYNT-RRFJBIMHSA-N oseltamivir Chemical compound CCOC(=O)C1=C[C@@H](OC(CC)CC)[C@H](NC(C)=O)[C@@H](N)C1 VSZGPKBBMSAYNT-RRFJBIMHSA-N 0.000 description 1
- 229960003752 oseltamivir Drugs 0.000 description 1
- 229960001019 oxacillin Drugs 0.000 description 1
- UWYHMGVUTGAWSP-JKIFEVAISA-N oxacillin Chemical compound N([C@@H]1C(N2[C@H](C(C)(C)S[C@@H]21)C(O)=O)=O)C(=O)C1=C(C)ON=C1C1=CC=CC=C1 UWYHMGVUTGAWSP-JKIFEVAISA-N 0.000 description 1
- 229960000321 oxolinic acid Drugs 0.000 description 1
- 229960000625 oxytetracycline Drugs 0.000 description 1
- IWVCMVBTMGNXQD-PXOLEDIWSA-N oxytetracycline Chemical compound C1=CC=C2[C@](O)(C)[C@H]3[C@H](O)[C@H]4[C@H](N(C)C)C(O)=C(C(N)=O)C(=O)[C@@]4(O)C(O)=C3C(=O)C2=C1O IWVCMVBTMGNXQD-PXOLEDIWSA-N 0.000 description 1
- 235000019366 oxytetracycline Nutrition 0.000 description 1
- LSQZJLSUYDQPKJ-UHFFFAOYSA-N p-Hydroxyampicillin Natural products O=C1N2C(C(O)=O)C(C)(C)SC2C1NC(=O)C(N)C1=CC=C(O)C=C1 LSQZJLSUYDQPKJ-UHFFFAOYSA-N 0.000 description 1
- 229960001914 paromomycin Drugs 0.000 description 1
- UOZODPSAJZTQNH-LSWIJEOBSA-N paromomycin Chemical compound N[C@@H]1[C@@H](O)[C@H](O)[C@H](CN)O[C@@H]1O[C@H]1[C@@H](O)[C@H](O[C@H]2[C@@H]([C@@H](N)C[C@@H](N)[C@@H]2O)O[C@@H]2[C@@H]([C@@H](O)[C@H](O)[C@@H](CO)O2)N)O[C@@H]1CO UOZODPSAJZTQNH-LSWIJEOBSA-N 0.000 description 1
- 239000013610 patient sample Substances 0.000 description 1
- 238000003909 pattern recognition Methods 0.000 description 1
- 229960002625 pazufloxacin Drugs 0.000 description 1
- 229960004236 pefloxacin Drugs 0.000 description 1
- FHFYDNQZQSQIAI-UHFFFAOYSA-N pefloxacin Chemical compound C1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC(F)=C1N1CCN(C)CC1 FHFYDNQZQSQIAI-UHFFFAOYSA-N 0.000 description 1
- 108010092853 peginterferon alfa-2a Proteins 0.000 description 1
- 229960003930 peginterferon alfa-2a Drugs 0.000 description 1
- 229960001179 penciclovir Drugs 0.000 description 1
- 229940056360 penicillin g Drugs 0.000 description 1
- 229940056367 penicillin v Drugs 0.000 description 1
- XRQDFNLINLXZLB-CKIKVBCHSA-N peramivir Chemical compound CCC(CC)[C@H](NC(C)=O)[C@@H]1[C@H](O)[C@@H](C(O)=O)C[C@H]1NC(N)=N XRQDFNLINLXZLB-CKIKVBCHSA-N 0.000 description 1
- 229960001084 peramivir Drugs 0.000 description 1
- 230000008782 phagocytosis Effects 0.000 description 1
- 230000000144 pharmacologic effect Effects 0.000 description 1
- BPLBGHOLXOTWMN-MBNYWOFBSA-N phenoxymethylpenicillin Chemical compound N([C@H]1[C@H]2SC([C@@H](N2C1=O)C(O)=O)(C)C)C(=O)COC1=CC=CC=C1 BPLBGHOLXOTWMN-MBNYWOFBSA-N 0.000 description 1
- XUYJLQHKOGNDPB-UHFFFAOYSA-N phosphonoacetic acid Chemical compound OC(=O)CP(O)(O)=O XUYJLQHKOGNDPB-UHFFFAOYSA-N 0.000 description 1
- 230000035790 physiological processes and functions Effects 0.000 description 1
- 229960001732 pipemidic acid Drugs 0.000 description 1
- JOHZPMXAZQZXHR-UHFFFAOYSA-N pipemidic acid Chemical compound N1=C2N(CC)C=C(C(O)=O)C(=O)C2=CN=C1N1CCNCC1 JOHZPMXAZQZXHR-UHFFFAOYSA-N 0.000 description 1
- 229960002292 piperacillin Drugs 0.000 description 1
- WCMIIGXFCMNQDS-IDYPWDAWSA-M piperacillin sodium Chemical compound [Na+].O=C1C(=O)N(CC)CCN1C(=O)N[C@H](C=1C=CC=CC=1)C(=O)N[C@@H]1C(=O)N2[C@@H](C([O-])=O)C(C)(C)S[C@@H]21 WCMIIGXFCMNQDS-IDYPWDAWSA-M 0.000 description 1
- 229960004444 piromidic acid Drugs 0.000 description 1
- RCIMBBZXSXFZBV-UHFFFAOYSA-N piromidic acid Chemical compound N1=C2N(CC)C=C(C(O)=O)C(=O)C2=CN=C1N1CCCC1 RCIMBBZXSXFZBV-UHFFFAOYSA-N 0.000 description 1
- 229960003342 pivampicillin Drugs 0.000 description 1
- ZEMIJUDPLILVNQ-ZXFNITATSA-N pivampicillin Chemical compound C1([C@@H](N)C(=O)N[C@H]2[C@@H]3N(C2=O)[C@H](C(S3)(C)C)C(=O)OCOC(=O)C(C)(C)C)=CC=CC=C1 ZEMIJUDPLILVNQ-ZXFNITATSA-N 0.000 description 1
- 229960004212 pivmecillinam Drugs 0.000 description 1
- 229960000471 pleconaril Drugs 0.000 description 1
- KQOXLKOJHVFTRN-UHFFFAOYSA-N pleconaril Chemical compound O1N=C(C)C=C1CCCOC1=C(C)C=C(C=2N=C(ON=2)C(F)(F)F)C=C1C KQOXLKOJHVFTRN-UHFFFAOYSA-N 0.000 description 1
- 229960001237 podophyllotoxin Drugs 0.000 description 1
- YJGVMLPVUAXIQN-XVVDYKMHSA-N podophyllotoxin Chemical compound COC1=C(OC)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@H](O)[C@@H]3[C@@H]2C(OC3)=O)=C1 YJGVMLPVUAXIQN-XVVDYKMHSA-N 0.000 description 1
- YVCVYCSAAZQOJI-UHFFFAOYSA-N podophyllotoxin Natural products COC1=C(O)C(OC)=CC(C2C3=CC=4OCOC=4C=C3C(O)C3C2C(OC3)=O)=C1 YVCVYCSAAZQOJI-UHFFFAOYSA-N 0.000 description 1
- 229920000728 polyester Polymers 0.000 description 1
- 229920000642 polymer Polymers 0.000 description 1
- 229920000024 polymyxin B Polymers 0.000 description 1
- 229960005266 polymyxin b Drugs 0.000 description 1
- 108091033319 polynucleotide Proteins 0.000 description 1
- 102000040430 polynucleotide Human genes 0.000 description 1
- 239000002157 polynucleotide Substances 0.000 description 1
- 229920002223 polystyrene Polymers 0.000 description 1
- 239000011148 porous material Substances 0.000 description 1
- 239000013641 positive control Substances 0.000 description 1
- 230000001374 post-anti-biotic effect Effects 0.000 description 1
- 238000012805 post-processing Methods 0.000 description 1
- 229910052700 potassium Inorganic materials 0.000 description 1
- 239000011591 potassium Substances 0.000 description 1
- 238000003825 pressing Methods 0.000 description 1
- 230000002265 prevention Effects 0.000 description 1
- 229960003961 pristinamycin Drugs 0.000 description 1
- DAIKHDNSXMZDCU-OUDXUNEISA-N pristinamycin-IIA Natural products CC(C)[C@H]1OC(=O)C2=CCCN2C(=O)c3coc(CC(=O)C[C@H](O)C=C(C)C=CCNC(=O)C=C[C@@H]1C)n3 DAIKHDNSXMZDCU-OUDXUNEISA-N 0.000 description 1
- JOOMGSFOCRDAHL-XKCHLWDXSA-N pristinamycin-IIB Natural products CC(C)[C@@H]1OC(=O)[C@H]2CCCN2C(=O)c3coc(CC(=O)C[C@@H](O)C=C(C)C=CCNC(=O)C=C[C@H]1C)n3 JOOMGSFOCRDAHL-XKCHLWDXSA-N 0.000 description 1
- 238000012545 processing Methods 0.000 description 1
- 238000004393 prognosis Methods 0.000 description 1
- 208000037821 progressive disease Diseases 0.000 description 1
- 230000002035 prolonged effect Effects 0.000 description 1
- 238000000159 protein binding assay Methods 0.000 description 1
- 238000012514 protein characterization Methods 0.000 description 1
- 238000001742 protein purification Methods 0.000 description 1
- 229960001224 prulifloxacin Drugs 0.000 description 1
- 238000004451 qualitative analysis Methods 0.000 description 1
- 238000011002 quantification Methods 0.000 description 1
- 229960005442 quinupristin Drugs 0.000 description 1
- WTHRRGMBUAHGNI-LCYNINFDSA-N quinupristin Chemical compound N([C@@H]1C(=O)N[C@@H](C(N2CCC[C@H]2C(=O)N(C)[C@@H](CC=2C=CC(=CC=2)N(C)C)C(=O)N2C[C@@H](CS[C@H]3C4CCN(CC4)C3)C(=O)C[C@H]2C(=O)N[C@H](C(=O)O[C@@H]1C)C=1C=CC=CC=1)=O)CC)C(=O)C1=NC=CC=C1O WTHRRGMBUAHGNI-LCYNINFDSA-N 0.000 description 1
- 108700028429 quinupristin Proteins 0.000 description 1
- 229960004742 raltegravir Drugs 0.000 description 1
- CZFFBEXEKNGXKS-UHFFFAOYSA-N raltegravir Chemical compound O1C(C)=NN=C1C(=O)NC(C)(C)C1=NC(C(=O)NCC=2C=CC(F)=CC=2)=C(O)C(=O)N1C CZFFBEXEKNGXKS-UHFFFAOYSA-N 0.000 description 1
- 206010037844 rash Diseases 0.000 description 1
- 102000005962 receptors Human genes 0.000 description 1
- 108020003175 receptors Proteins 0.000 description 1
- 235000003499 redwood Nutrition 0.000 description 1
- 230000029058 respiratory gaseous exchange Effects 0.000 description 1
- 210000001995 reticulocyte Anatomy 0.000 description 1
- 229960000329 ribavirin Drugs 0.000 description 1
- HZCAHMRRMINHDJ-DBRKOABJSA-N ribavirin Natural products O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1N=CN=C1 HZCAHMRRMINHDJ-DBRKOABJSA-N 0.000 description 1
- 229960000885 rifabutin Drugs 0.000 description 1
- 229960001225 rifampicin Drugs 0.000 description 1
- JQXXHWHPUNPDRT-WLSIYKJHSA-N rifampicin Chemical compound O([C@](C1=O)(C)O/C=C/[C@@H]([C@H]([C@@H](OC(C)=O)[C@H](C)[C@H](O)[C@H](C)[C@@H](O)[C@@H](C)\C=C\C=C(C)/C(=O)NC=2C(O)=C3C([O-])=C4C)C)OC)C4=C1C3=C(O)C=2\C=N\N1CC[NH+](C)CC1 JQXXHWHPUNPDRT-WLSIYKJHSA-N 0.000 description 1
- 229960002599 rifapentine Drugs 0.000 description 1
- WDZCUPBHRAEYDL-GZAUEHORSA-N rifapentine Chemical compound O([C@](C1=O)(C)O/C=C/[C@@H]([C@H]([C@@H](OC(C)=O)[C@H](C)[C@H](O)[C@H](C)[C@@H](O)[C@@H](C)\C=C\C=C(C)/C(=O)NC=2C(O)=C3C(O)=C4C)C)OC)C4=C1C3=C(O)C=2\C=N\N(CC1)CCN1C1CCCC1 WDZCUPBHRAEYDL-GZAUEHORSA-N 0.000 description 1
- 229960000888 rimantadine Drugs 0.000 description 1
- 238000012502 risk assessment Methods 0.000 description 1
- 229960000311 ritonavir Drugs 0.000 description 1
- NCDNCNXCDXHOMX-XGKFQTDJSA-N ritonavir Chemical compound N([C@@H](C(C)C)C(=O)N[C@H](C[C@H](O)[C@H](CC=1C=CC=CC=1)NC(=O)OCC=1SC=NC=1)CC=1C=CC=CC=1)C(=O)N(C)CC1=CSC(C(C)C)=N1 NCDNCNXCDXHOMX-XGKFQTDJSA-N 0.000 description 1
- 239000003419 rna directed dna polymerase inhibitor Substances 0.000 description 1
- 229960003889 rosoxacin Drugs 0.000 description 1
- XBPZXDSZHPDXQU-UHFFFAOYSA-N rosoxacin Chemical compound C1=C2N(CC)C=C(C(O)=O)C(=O)C2=CC=C1C1=CC=NC=C1 XBPZXDSZHPDXQU-UHFFFAOYSA-N 0.000 description 1
- 229960005224 roxithromycin Drugs 0.000 description 1
- 229960004062 rufloxacin Drugs 0.000 description 1
- 210000003296 saliva Anatomy 0.000 description 1
- 150000003839 salts Chemical class 0.000 description 1
- 229960001852 saquinavir Drugs 0.000 description 1
- QWAXKHKRTORLEM-UGJKXSETSA-N saquinavir Chemical compound C([C@@H]([C@H](O)CN1C[C@H]2CCCC[C@H]2C[C@H]1C(=O)NC(C)(C)C)NC(=O)[C@H](CC(N)=O)NC(=O)C=1N=C2C=CC=CC2=CC=1)C1=CC=CC=C1 QWAXKHKRTORLEM-UGJKXSETSA-N 0.000 description 1
- 210000000582 semen Anatomy 0.000 description 1
- 238000012764 semi-quantitative analysis Methods 0.000 description 1
- 230000036303 septic shock Effects 0.000 description 1
- 238000004904 shortening Methods 0.000 description 1
- 208000013220 shortness of breath Diseases 0.000 description 1
- 230000011664 signaling Effects 0.000 description 1
- 229910052709 silver Inorganic materials 0.000 description 1
- 239000004332 silver Substances 0.000 description 1
- 201000009890 sinusitis Diseases 0.000 description 1
- 229960003177 sitafloxacin Drugs 0.000 description 1
- 150000003384 small molecules Chemical class 0.000 description 1
- 229910052708 sodium Inorganic materials 0.000 description 1
- 229960002063 sofosbuvir Drugs 0.000 description 1
- TTZHDVOVKQGIBA-IQWMDFIBSA-N sofosbuvir Chemical compound N1([C@@H]2O[C@@H]([C@H]([C@]2(F)C)O)CO[P@@](=O)(N[C@@H](C)C(=O)OC(C)C)OC=2C=CC=CC=2)C=CC(=O)NC1=O TTZHDVOVKQGIBA-IQWMDFIBSA-N 0.000 description 1
- 229960004954 sparfloxacin Drugs 0.000 description 1
- DZZWHBIBMUVIIW-DTORHVGOSA-N sparfloxacin Chemical compound C1[C@@H](C)N[C@@H](C)CN1C1=C(F)C(N)=C2C(=O)C(C(O)=O)=CN(C3CC3)C2=C1F DZZWHBIBMUVIIW-DTORHVGOSA-N 0.000 description 1
- 230000009870 specific binding Effects 0.000 description 1
- 239000012798 spherical particle Substances 0.000 description 1
- 210000000130 stem cell Anatomy 0.000 description 1
- 239000011232 storage material Substances 0.000 description 1
- 229960005322 streptomycin Drugs 0.000 description 1
- XXUZFRDUEGQHOV-UHFFFAOYSA-J strontium ranelate Chemical compound [Sr+2].[Sr+2].[O-]C(=O)CN(CC([O-])=O)C=1SC(C([O-])=O)=C(CC([O-])=O)C=1C#N XXUZFRDUEGQHOV-UHFFFAOYSA-J 0.000 description 1
- 229960000654 sulfafurazole Drugs 0.000 description 1
- 229960005158 sulfamethizole Drugs 0.000 description 1
- VACCAVUAMIDAGB-UHFFFAOYSA-N sulfamethizole Chemical compound S1C(C)=NN=C1NS(=O)(=O)C1=CC=C(N)C=C1 VACCAVUAMIDAGB-UHFFFAOYSA-N 0.000 description 1
- 229960005404 sulfamethoxazole Drugs 0.000 description 1
- JLKIGFTWXXRPMT-UHFFFAOYSA-N sulphamethoxazole Chemical compound O1C(C)=CC(NS(=O)(=O)C=2C=CC(N)=CC=2)=N1 JLKIGFTWXXRPMT-UHFFFAOYSA-N 0.000 description 1
- 230000004083 survival effect Effects 0.000 description 1
- 210000004243 sweat Anatomy 0.000 description 1
- 230000035900 sweating Effects 0.000 description 1
- 230000000946 synaptic effect Effects 0.000 description 1
- NHKZSTHOYNWEEZ-AFCXAGJDSA-N taribavirin Chemical compound N1=C(C(=N)N)N=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](CO)O1 NHKZSTHOYNWEEZ-AFCXAGJDSA-N 0.000 description 1
- 229950006081 taribavirin Drugs 0.000 description 1
- 229960001608 teicoplanin Drugs 0.000 description 1
- 229960003250 telithromycin Drugs 0.000 description 1
- LJVAJPDWBABPEJ-PNUFFHFMSA-N telithromycin Chemical compound O([C@@H]1[C@@H](C)C(=O)[C@@H](C)C(=O)O[C@@H]([C@]2(OC(=O)N(CCCCN3C=C(N=C3)C=3C=NC=CC=3)[C@@H]2[C@@H](C)C(=O)[C@H](C)C[C@@]1(C)OC)C)CC)[C@@H]1O[C@H](C)C[C@H](N(C)C)[C@H]1O LJVAJPDWBABPEJ-PNUFFHFMSA-N 0.000 description 1
- 229960004576 temafloxacin Drugs 0.000 description 1
- 229960004556 tenofovir Drugs 0.000 description 1
- SGOIRFVFHAKUTI-ZCFIWIBFSA-N tenofovir (anhydrous) Chemical compound N1=CN=C2N(C[C@@H](C)OCP(O)(O)=O)C=NC2=C1N SGOIRFVFHAKUTI-ZCFIWIBFSA-N 0.000 description 1
- 229960001355 tenofovir disoproxil Drugs 0.000 description 1
- JFVZFKDSXNQEJW-CQSZACIVSA-N tenofovir disoproxil Chemical compound N1=CN=C2N(C[C@@H](C)OCP(=O)(OCOC(=O)OC(C)C)OCOC(=O)OC(C)C)C=NC2=C1N JFVZFKDSXNQEJW-CQSZACIVSA-N 0.000 description 1
- VCMJCVGFSROFHV-WZGZYPNHSA-N tenofovir disoproxil fumarate Chemical compound OC(=O)\C=C\C(O)=O.N1=CN=C2N(C[C@@H](C)OCP(=O)(OCOC(=O)OC(C)C)OCOC(=O)OC(C)C)C=NC2=C1N VCMJCVGFSROFHV-WZGZYPNHSA-N 0.000 description 1
- IWVCMVBTMGNXQD-UHFFFAOYSA-N terramycin dehydrate Natural products C1=CC=C2C(O)(C)C3C(O)C4C(N(C)C)C(O)=C(C(N)=O)C(=O)C4(O)C(O)=C3C(=O)C2=C1O IWVCMVBTMGNXQD-UHFFFAOYSA-N 0.000 description 1
- 229960002180 tetracycline Drugs 0.000 description 1
- 229930101283 tetracycline Natural products 0.000 description 1
- 235000019364 tetracycline Nutrition 0.000 description 1
- 150000003522 tetracyclines Chemical class 0.000 description 1
- 238000011285 therapeutic regimen Methods 0.000 description 1
- ANRHNWWPFJCPAZ-UHFFFAOYSA-M thionine Chemical compound [Cl-].C1=CC(N)=CC2=[S+]C3=CC(N)=CC=C3N=C21 ANRHNWWPFJCPAZ-UHFFFAOYSA-M 0.000 description 1
- 229960004659 ticarcillin Drugs 0.000 description 1
- OHKOGUYZJXTSFX-KZFFXBSXSA-N ticarcillin Chemical compound C=1([C@@H](C(O)=O)C(=O)N[C@H]2[C@H]3SC([C@@H](N3C2=O)C(O)=O)(C)C)C=CSC=1 OHKOGUYZJXTSFX-KZFFXBSXSA-N 0.000 description 1
- 229960004089 tigecycline Drugs 0.000 description 1
- 229960005053 tinidazole Drugs 0.000 description 1
- 229960000838 tipranavir Drugs 0.000 description 1
- SUJUHGSWHZTSEU-FYBSXPHGSA-N tipranavir Chemical compound C([C@@]1(CCC)OC(=O)C([C@H](CC)C=2C=C(NS(=O)(=O)C=3N=CC(=CC=3)C(F)(F)F)C=CC=2)=C(O)C1)CC1=CC=CC=C1 SUJUHGSWHZTSEU-FYBSXPHGSA-N 0.000 description 1
- 210000001519 tissue Anatomy 0.000 description 1
- 229960000707 tobramycin Drugs 0.000 description 1
- NLVFBUXFDBBNBW-PBSUHMDJSA-N tobramycin Chemical compound N[C@@H]1C[C@H](O)[C@@H](CN)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O[C@@H]2[C@@H]([C@@H](N)[C@H](O)[C@@H](CO)O2)O)[C@H](N)C[C@@H]1N NLVFBUXFDBBNBW-PBSUHMDJSA-N 0.000 description 1
- 229950008187 tosufloxacin Drugs 0.000 description 1
- 238000013518 transcription Methods 0.000 description 1
- 230000035897 transcription Effects 0.000 description 1
- 238000012546 transfer Methods 0.000 description 1
- 238000013519 translation Methods 0.000 description 1
- 230000008733 trauma Effects 0.000 description 1
- 229960003962 trifluridine Drugs 0.000 description 1
- VSQQQLOSPVPRAZ-RRKCRQDMSA-N trifluridine Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C(C(F)(F)F)=C1 VSQQQLOSPVPRAZ-RRKCRQDMSA-N 0.000 description 1
- 229940111527 trizivir Drugs 0.000 description 1
- 229960000832 tromantadine Drugs 0.000 description 1
- UXQDWARBDDDTKG-UHFFFAOYSA-N tromantadine Chemical compound C1C(C2)CC3CC2CC1(NC(=O)COCCN(C)C)C3 UXQDWARBDDDTKG-UHFFFAOYSA-N 0.000 description 1
- 229960000497 trovafloxacin Drugs 0.000 description 1
- WVPSKSLAZQPAKQ-CDMJZVDBSA-N trovafloxacin Chemical compound C([C@H]1[C@@H]([C@H]1C1)N)N1C(C(=CC=1C(=O)C(C(O)=O)=C2)F)=NC=1N2C1=CC=C(F)C=C1F WVPSKSLAZQPAKQ-CDMJZVDBSA-N 0.000 description 1
- 229940008349 truvada Drugs 0.000 description 1
- 102000003298 tumor necrosis factor receptor Human genes 0.000 description 1
- OUYCCCASQSFEME-UHFFFAOYSA-N tyrosine Natural products OC(=O)C(N)CC1=CC=C(O)C=C1 OUYCCCASQSFEME-UHFFFAOYSA-N 0.000 description 1
- 229960004626 umifenovir Drugs 0.000 description 1
- KCFYEAOKVJSACF-UHFFFAOYSA-N umifenovir Chemical compound CN1C2=CC(Br)=C(O)C(CN(C)C)=C2C(C(=O)OCC)=C1CSC1=CC=CC=C1 KCFYEAOKVJSACF-UHFFFAOYSA-N 0.000 description 1
- 241001515965 unidentified phage Species 0.000 description 1
- 229940093257 valacyclovir Drugs 0.000 description 1
- 229960002149 valganciclovir Drugs 0.000 description 1
- 238000010200 validation analysis Methods 0.000 description 1
- 229960003165 vancomycin Drugs 0.000 description 1
- MYPYJXKWCTUITO-LYRMYLQWSA-N vancomycin Chemical compound O([C@@H]1[C@@H](O)[C@H](O)[C@@H](CO)O[C@H]1OC1=C2C=C3C=C1OC1=CC=C(C=C1Cl)[C@@H](O)[C@H](C(N[C@@H](CC(N)=O)C(=O)N[C@H]3C(=O)N[C@H]1C(=O)N[C@H](C(N[C@@H](C3=CC(O)=CC(O)=C3C=3C(O)=CC=C1C=3)C(O)=O)=O)[C@H](O)C1=CC=C(C(=C1)Cl)O2)=O)NC(=O)[C@@H](CC(C)C)NC)[C@H]1C[C@](C)(N)[C@H](O)[C@H](C)O1 MYPYJXKWCTUITO-LYRMYLQWSA-N 0.000 description 1
- MYPYJXKWCTUITO-UHFFFAOYSA-N vancomycin Natural products O1C(C(=C2)Cl)=CC=C2C(O)C(C(NC(C2=CC(O)=CC(O)=C2C=2C(O)=CC=C3C=2)C(O)=O)=O)NC(=O)C3NC(=O)C2NC(=O)C(CC(N)=O)NC(=O)C(NC(=O)C(CC(C)C)NC)C(O)C(C=C3Cl)=CC=C3OC3=CC2=CC1=C3OC1OC(CO)C(O)C(O)C1OC1CC(C)(N)C(O)C(C)O1 MYPYJXKWCTUITO-UHFFFAOYSA-N 0.000 description 1
- 229950009860 vicriviroc Drugs 0.000 description 1
- 229960003636 vidarabine Drugs 0.000 description 1
- GXFAIFRPOKBQRV-GHXCTMGLSA-N viomycin Chemical compound N1C(=O)\C(=C\NC(N)=O)NC(=O)[C@H](CO)NC(=O)[C@H](CO)NC(=O)[C@@H](NC(=O)C[C@@H](N)CCCN)CNC(=O)[C@@H]1[C@@H]1NC(=N)N[C@@H](O)C1 GXFAIFRPOKBQRV-GHXCTMGLSA-N 0.000 description 1
- 229950001272 viomycin Drugs 0.000 description 1
- 239000002699 waste material Substances 0.000 description 1
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Substances O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 description 1
- 229960000523 zalcitabine Drugs 0.000 description 1
- 229960001028 zanamivir Drugs 0.000 description 1
- ARAIBEBZBOPLMB-UFGQHTETSA-N zanamivir Chemical compound CC(=O)N[C@@H]1[C@@H](N=C(N)N)C=C(C(O)=O)O[C@H]1[C@H](O)[C@H](O)CO ARAIBEBZBOPLMB-UFGQHTETSA-N 0.000 description 1
- 229960002555 zidovudine Drugs 0.000 description 1
Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/569—Immunoassay; Biospecific binding assay; Materials therefor for microorganisms, e.g. protozoa, bacteria, viruses
- G01N33/56911—Bacteria
- G01N33/56944—Streptococcus
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P31/00—Antiinfectives, i.e. antibiotics, antiseptics, chemotherapeutics
- A61P31/04—Antibacterial agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P31/00—Antiinfectives, i.e. antibiotics, antiseptics, chemotherapeutics
- A61P31/12—Antivirals
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/5005—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving human or animal cells
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/531—Production of immunochemical test materials
- G01N33/532—Production of labelled immunochemicals
- G01N33/535—Production of labelled immunochemicals with enzyme label or co-enzymes, co-factors, enzyme inhibitors or enzyme substrates
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/543—Immunoassay; Biospecific binding assay; Materials therefor with an insoluble carrier for immobilising immunochemicals
- G01N33/544—Immunoassay; Biospecific binding assay; Materials therefor with an insoluble carrier for immobilising immunochemicals the carrier being organic
- G01N33/545—Synthetic resin
- G01N33/547—Synthetic resin with antigen or antibody attached to the carrier via a bridging agent
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/569—Immunoassay; Biospecific binding assay; Materials therefor for microorganisms, e.g. protozoa, bacteria, viruses
- G01N33/56911—Bacteria
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/569—Immunoassay; Biospecific binding assay; Materials therefor for microorganisms, e.g. protozoa, bacteria, viruses
- G01N33/56983—Viruses
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6863—Cytokines, i.e. immune system proteins modifying a biological response such as cell growth proliferation or differentiation, e.g. TNF, CNF, GM-CSF, lymphotoxin, MIF or their receptors
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6863—Cytokines, i.e. immune system proteins modifying a biological response such as cell growth proliferation or differentiation, e.g. TNF, CNF, GM-CSF, lymphotoxin, MIF or their receptors
- G01N33/6869—Interleukin
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6893—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids related to diseases not provided for elsewhere
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/52—Assays involving cytokines
- G01N2333/521—Chemokines
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/52—Assays involving cytokines
- G01N2333/525—Tumor necrosis factor [TNF]
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/52—Assays involving cytokines
- G01N2333/54—Interleukins [IL]
- G01N2333/5412—IL-6
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/575—Hormones
- G01N2333/5753—Calcitonin gene related peptide
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/70578—NGF-receptor/TNF-receptor superfamily, e.g. CD27, CD30 CD40 or CD95
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/70596—Molecules with a "CD"-designation not provided for elsewhere in G01N2333/705
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/715—Assays involving receptors, cell surface antigens or cell surface determinants for cytokines; for lymphokines; for interferons
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/715—Assays involving receptors, cell surface antigens or cell surface determinants for cytokines; for lymphokines; for interferons
- G01N2333/7151—Assays involving receptors, cell surface antigens or cell surface determinants for cytokines; for lymphokines; for interferons for tumor necrosis factor [TNF]; for lymphotoxin [LT]
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2333/00—Assays involving biological materials from specific organisms or of a specific nature
- G01N2333/435—Assays involving biological materials from specific organisms or of a specific nature from animals; from humans
- G01N2333/705—Assays involving receptors, cell surface antigens or cell surface determinants
- G01N2333/715—Assays involving receptors, cell surface antigens or cell surface determinants for cytokines; for lymphokines; for interferons
- G01N2333/7155—Assays involving receptors, cell surface antigens or cell surface determinants for cytokines; for lymphokines; for interferons for interleukins [IL]
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/26—Infectious diseases, e.g. generalised sepsis
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/60—Complex ways of combining multiple protein biomarkers for diagnosis
Definitions
- a method of determining a treatment regimen in a subject showing symptoms of a pathogenic infection comprising measuring the amount of TRAIL in a blood sample, the blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of the TRAIL is below a first predetermined level, the subject is recommended an anti-bacterial agent.
- a method of diagnosing an infection in a subject showing symptoms of an infection comprising measuring the amount of IP10 in a blood sample being derived from the subject no more than two days following symptom onset, wherein the amount of the IPIO is indicative of the infection.
- the infection type comprises a pathogenic infection or a non-pathogenic infection.
- the symptoms of an infection comprise fever.
- the treating comprises administering to the subject a therapeutically effective amount of an anti-bacterial agent.
- FIG. 4 Distribution of major clinical syndromes of the infectious disease patients enrolled in the clinical study.
- FIG. 7 Pathogen isolated from infectious disease patients enrolled in the clinical study
- a bacterial infection may be ruled out if the polypeptide concentration of TRAIL determined is higher than a pre-determined first threshold value.
- the method further includes determining if a subject has a viral infection (i.e., ruling in a viral infection). A viral infection is ruled in if the polypeptide concentration of TRAIL is higher than a pre-determined second threshold value.
- Additional polypeptides that may be analyzed for the early detection of bacterial infections include but are not limited to CRP and IP10.
- CRP and IP10 CRP and IP 10.
- TRAIL and CRP may be measured
- TRAIL and IP 10 may be measured or TRAIL
- CRP and IP 10 may be measured.
- Information regarding CRP and IP 10 is provided in Table 2, herein below.
- concentrations of each of the above identified polypeptides may be combined (e.g. by way of a pre-determined mathematical function) to compute a score and the score may be compared to a predetermined reference value as further described herein below.
- Acyclovir Adefovir; Amantadine; Amprenavir; Ampligen; Arbidol; Atazanavir; Atripla;
- Suitable sources for antibodies for the detection of determinants include commercially available sources such as, for example, Abazyme, Abnova, AssayPro, Affinity Biologicals, AntibodyShop, Aviva bioscience, Biogenesis, Biosense Laboratories, Calbiochem, Cell Sciences, Chemicon International, Chemokine, Clontech, Cytolab, DAKO, Diagnostic BioSystems, eBioscience, Endocrine Technologies, Enzo Biochem, Eurogentec, Fusion Antibodies, Genesis Biotech, GloboZymes, Haematologic Technologies, Immunodetect, Immunodiagnostik, Immunometrics, Immunostar, Immunovision, Biogenex, Invitrogen, Jackson ImmunoResearch Laboratory, KMI Diagnostics, Koma Biotech, LabFrontier Life Science Institute, Lee Laboratories, Lifescreen, Maine Biotechnology Services, Mediclone, MicroPharm Ltd., ModiQuest, Molecular Innovations, Molecular Probes, Neoclone, Neuromics, New England Biolabs, Novocastra,
- the patient medical background conditions such as chronic lung diseases and diabetes may affect its immune response to infection that is reflected by changes in diagnostic accuracy of immune-based diagnostics (see Example 1, herein below).
- information regarding the patient background clinical conditions could potentially be integrated with protein biomarker classifiers predicted outcome in order to improve patient diagnosis.
- kits may contain in separate containers antibodies (either already bound to a solid matrix or packaged separately with reagents for binding them to the matrix), control formulations (positive and/or negative), and/or a detectable label such as fluorescein, green fluorescent protein, rhodamine, cyanine dyes, Alexa dyes, lucif erase, radiolabels, among others.
- the detectable label may be attached to a secondary antibody which binds to the Fc portion of the antibody which recognizes the determinant.
- Instructions e.g., written, tape, VCR, CD-ROM, etc.
- for carrying out the assay may be included in the kit.
- the health-related data management system used in some aspects of the invention may also be considered to be implemented as a computer-readable storage medium, configured with a computer program, where the storage medium so configured causes a computer to operate in a specific and predefined manner to perform various functions described herein.
- numeric result of a classifier formula itself may be transformed post-processing by its reference to an actual clinical population and study results and observed endpoints, in order to calibrate to absolute risk and provide confidence intervals for varying numeric results of the classifier or risk formula.
- ways (and formulations) to combine two biomarkers into one predictive score For example, using dual cutoffs - one for each biomarker, generates a quadrary separation pattern that can separate between bacterial, viral and mixed (bacterial-viral co-infection) patients.
- “Accuracy” refers to the degree of conformity of a measured or calculated quantity (a test reported value) to its actual (or true) value. Clinical accuracy relates to the proportion of true outcomes (true positives (TP) or true negatives (TN) versus misclassified outcomes (false positives (FP) or false negatives (FN)), and may be stated as a sensitivity, specificity, positive predictive values (PPV) or negative predictive values (NPV), Matheus correlation coefficient (MCC), or as a likelihood, odds ratio, Receiver Operating Characteristic (ROC) curve, Area Under the Curve (AUC) among other measures.
- TP true positives
- TN true negatives
- FP false negatives
- MPC Matheus correlation coefficient
- ROC Receiver Operating Characteristic
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Immunology (AREA)
- Engineering & Computer Science (AREA)
- Molecular Biology (AREA)
- Chemical & Material Sciences (AREA)
- Biomedical Technology (AREA)
- Hematology (AREA)
- Urology & Nephrology (AREA)
- Cell Biology (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Analytical Chemistry (AREA)
- Food Science & Technology (AREA)
- Microbiology (AREA)
- Physics & Mathematics (AREA)
- Biotechnology (AREA)
- Biochemistry (AREA)
- General Physics & Mathematics (AREA)
- Pathology (AREA)
- Virology (AREA)
- Tropical Medicine & Parasitology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Organic Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Oncology (AREA)
- Communicable Diseases (AREA)
- Investigating Or Analysing Biological Materials (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
Abstract
Methods of determining infection type are disclosed. In one embodiment, the method comprises measuring the amount of TRAIL and/or IP10 no more than two days from symptom onset.
Description
EARLY DIAGNOSIS OF INFECTIONS
FIELD AND BACKGROUND OF THE INVENTION
The present invention, in some embodiments thereof, relates to the identification of signatures and determinants associated with bacterial and viral infections. More specifically, it was discovered that the protein TRAIL is a particularly accurate determinant when it is analyzed less than two days following symptom onset.
Antibiotics are the world's most prescribed class of drugs with a 25-30 billion $US global market. Antibiotics are also the world's most misused drug with a significant fraction of all drugs (40-70%) being wrongly prescribed.
One type of antibiotic misuse is when the drug is administered in case of a nonbacterial disease, such as a viral infection, for which antibiotics are ineffective. For example, according to the USA center for disease control and prevention CDC, over 60 Million wrong antibiotic prescriptions are given annually to treat flu in the US. The health-care and economic consequences of the antibiotic over-prescriptions include: (i) the cost of antibiotics that are unnecessarily prescribed globally, estimated at >$10 billion annually; (ii) side effects resulting from unnecessary antibiotics treatment are reducing quality of healthcare, causing complications and prolonged hospitalization (e.g. allergic reactions, Antibiotics-associated diarrhea, intestinal yeast etc.) and (iii) the emergence of resistant strains of bacteria as a result of the overuse.
Resistance of microbial pathogens to antibiotics is increasing world-wide at an accelerating rate ("CDC - Get Smart: Fast Facts About Antibiotic Resistance" 2013; "European Surveillance of Antimicrobial Consumption Network (ESAC-Net)" 2014; "CDC - About Antimicrobial Resistance" 2013; "Threat Report 2013 I Antimicrobial Resistance I CDC" 2013), with a concomitant increase in morbidity and mortality associated with infections caused by antibiotic resistant pathogens ("Threat Report 2013 I Antimicrobial Resistance I CDC" 2013). At least 2 million people are infected with antibiotic resistant bacteria each year in the US alone, and at least 23,000 people die as a direct result of these infections ("Threat Report 2013 I Antimicrobial Resistance I CDC" 2013). In the European Union, an estimated 400,000 patients present with resistant bacterial strains each year, of which 25,000 patients die ("WHO Europe -Data and Statistics" 2014). Consequently, the World Health Organization has warned that
therapeutic coverage will be insufficient within 10 years, placing the world at risk of entering a "post- antibiotic era", in which antibiotics will no longer be effective against infectious diseases ("WHO I Antimicrobial Resistance" 2013). The CDC considers this phenomenon "one of the world's most pressing health problems in the 21st century" ("CDC - About Antimicrobial Resistance" 2013).
Antibiotic under-prescription is not uncommon either. For example, up to 15% of adult bacterial pneumonia-hospitalized patients in the US receive delayed or no Abx treatment, even though in these instances early treatment can save lives and reduce complications.
Technologies for infectious disease diagnostics have the potential to reduce the associated health and financial burden associated with antibiotics misuse. Ideally, such a technology should: (i) accurately differentiate between a bacterial and viral infections; (ii) be rapid (within minutes); (iii) be able to differentiate between pathogenic and nonpathogenic bacteria that are part of the body's natural flora; (iv) differentiate between mixed co-infections and pure viral infections and (v) be applicable in cases where the pathogen is inaccessible (e.g. sinusitis, pneumonia, otitis-media, bronchitis, etc).
Correct identification of bacterial patients is of high importance as these patients require antibiotic treatment and in some cases more aggressive management (hospitalization, additional diagnostic tests etc). Misclassification of bacterial patients increases the chance of morbidity and mortality. Therefore, increasing the sensitivity of a diagnostic test that distinguishes between bacterial and viral infections is desired, even at a cost of reduced specificity.
Additional background art includes US Patent Application No. 20080171323, WO2011/132086 and WO2013/117746. SUMMARY OF THE INVENTION
According to an aspect of some embodiments of the present invention there is provided a method of ruling in a bacterial infection in a subject showing symptoms of an infection, the method comprising measuring the amount of TRAIL in a blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of the TRAIL is below a first predetermined level, a bacterial infection is ruled in.
According to an aspect of some embodiments of the present invention there is provided a method of determining a treatment regimen in a subject showing symptoms of a pathogenic infection comprising measuring the amount of TRAIL in a blood sample, the blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of the TRAIL is below a first predetermined level, the subject is recommended an anti-bacterial agent.
According to an aspect of some embodiments of the present invention there is provided a method of classifying an infection type of a subject comprising:
(a) analyzing for the presence of specific pathogen in a sample of the subject; and
(b) measuring the amount of TRAIL in a sample of the subject, wherein the presence of the specific pathogen and the amount of TRAIL is indicative of the infection type.
According to an aspect of some embodiments of the present invention there is provided a method of distinguishing between an infectious exacerbation state and a noninfectious exacerbation state of chronic obstructive pulmonary disease (COPD) or asthma of a subject comprising measuring the amount of TNF-related apoptosis- inducing ligand (TRAIL) in a blood sample derived from the subject, wherein the amount is indicative of the infectivity of the exacerbation state of COPD or asthma.
According to an aspect of some embodiments of the present invention there is provided a method of treating a subject showing symptoms of an infection comprising:
(a) determining a treatment regimen as described herein and;
(b) treating the subject according to the results of the determining.
According to an aspect of some embodiments of the present invention there is provided a method of diagnosing an infection in a subject showing symptoms of an infection, the method comprising measuring the amount of IP10 in a blood sample being derived from the subject no more than two days following symptom onset, wherein the amount of the IPIO is indicative of the infection.
According to some embodiments of the invention, the bacterial infection is a group a streptococcal infection.
According to some embodiments of the invention, the amount of TRAIL is above a second predetermined level, a viral infection is ruled in.
According to some embodiments of the invention, the amount of TRAIL is above a second predetermined level, the subject is recommended an anti-viral agent.
According to some embodiments of the invention, the specific pathogen is selected from the group consisting of Influenza, Respiratory syncytial virus (RSV), Rhinovirus and Group A Streptococcus.
According to some embodiments of the invention, the infection type comprises a pathogenic infection or a non-pathogenic infection.
According to some embodiments of the invention, step (a) is effected following step (b).
According to some embodiments of the invention, step (b) is effected following step (a).
According to some embodiments of the invention, the level is 70 pg/ml.
According to some embodiments of the invention, the subject has a normal level of creatine kinase.
According to some embodiments of the invention, the first predetermined level and the second predetermined level are identical.
According to some embodiments of the invention, the first predetermined level and the second predetermined level are non-identical.
According to some embodiments of the invention, the symptoms of an infection comprise fever.
According to some embodiments of the invention, the symptoms of a pathogenic infection comprise fever.
According to some embodiments of the invention, the sample is derived from the subject no more than one day following symptom onset.
According to some embodiments of the invention, the sample is whole blood or a fraction thereof.
According to some embodiments of the invention, the fraction comprises serum. According to some embodiments of the invention, the blood fraction sample comprises cells selected from the group consisting of lymphocytes, monocytes and granulocytes.
According to some embodiments of the invention, the method further comprises analyzing a level of C-reactive protein (CRP) and/or Interferon gamma-induced protein 10 (IPIO).
According to some embodiments of the invention, the method further comprises analyzing a level of a polypeptide selected from the group consisting of Interferon gamma-induced protein 10 (IPIO), Interleukin 6 (IL-6), and Interleukin 1 receptor, type I (ILIRA).
According to some embodiments of the invention, the method further comprises analyzing a level of a polypeptide selected from the group consisting of Interferon gamma- induced protein 10 (IP10), Interleukin 6 (IL-6), Interleukin 1 receptor, type I (ILIRA), C-reactive protein (CRP) and procalcitonin (PCT).
According to some embodiments of the invention, the TRAIL is measured using a lateral flow immunoassay.
According to some embodiments of the invention, the TRAIL is measured using an antibody which binds specifically to TRAIL.
According to some embodiments of the invention, the antibody is a monoclonal antibody.
According to some embodiments of the invention, the treating comprises administering to the subject a therapeutically effective amount of an anti-bacterial agent.
According to some embodiments of the invention, the anti-bacterial agent is an antibiotic.
According to some embodiments of the invention, when the amount is above a predetermined level a viral infection is ruled in.
According to some embodiments of the invention, when the amount is below a predetermined level, an infection is ruled out.
According to some embodiments of the invention, the method further comprises analyzing a level of a polypeptide selected from the group consisting of TRAIL, Interleukin 6 (IL-6), and Interleukin 1 receptor, type I (ILIRA).
According to some embodiments of the invention, the method further comprises analyzing a level of a polypeptide selected from the group consisting of Interferon
gamma- induced protein 10 (IP 10), Interleukin 6 (IL-6), Interleukin 1 receptor, type I (IL1RA), C-reactive protein (CRP) and procalcitonin (PCT).
Unless otherwise defined, all technical and/or scientific terms used herein have the same meaning as commonly understood by one of ordinary skill in the art to which the invention pertains. Although methods and materials similar or equivalent to those described herein can be used in the practice or testing of embodiments of the invention, exemplary methods and/or materials are described below. In case of conflict, the patent specification, including definitions, will control. In addition, the materials, methods, and examples are illustrative only and are not intended to be necessarily limiting. BRIEF DESCRIPTION OF THE SEVERAL VIEWS OF THE DRAWINGS
Some embodiments of the invention are herein described, by way of example only, with reference to the accompanying drawings. With specific reference now to the drawings in detail, it is stressed that the particulars shown are by way of example and for purposes of illustrative discussion of embodiments of the invention. In this regard, the description taken with the drawings makes apparent to those skilled in the art how embodiments of the invention may be practiced.
In the drawings:
FIG. 1: Clinical study workflow.
FIG. 2: Distribution of age and gender of the patients enrolled in the clinical study.
FIG. 3: Distribution of physiological systems of the infectious disease patients enrolled in the clinical study.
FIG. 4: Distribution of major clinical syndromes of the infectious disease patients enrolled in the clinical study.
FIG. 5: Distribution of maximal body temperatures of the infectious disease patients enrolled in the clinical study.
FIG. 6: Distribution of time from initiation of symptoms of the infectious disease patients enrolled in the clinical study.
FIG. 7: Pathogen isolated from infectious disease patients enrolled in the clinical study
FIG. 8: TRAIL is differentially expressed in bacterial, viral and non-infectious patients (n = 765). Red line and circle correspond to group median and average respectively.
FIG. 9: Serum TRAIL levels of pediatric patients presenting with different infection types.
Blue boxes present first to third quartiles. Red line corresponds to group median. RSV - Respiratory syncytial virus; hMPV - human Metapneumovirus; Enteric viruses include: Rota Virus, Astrovirus, Enteric Adenovirus, Norovirus G I and G II.
FIG. 10: TRAIL is a useful marker for early diagnosis of bacterial and viral infections. Average serum levels of TRAIL, CRP, PCT, IP- 10, IL-6 and the TRAIL- CRP-IP-10 signature score at different days from symptoms onset in bacterial and viral patients.
FIG. 11: TRAIL levels are reduced in patients with bacterial- viral co-infection (mixed), similar to patients with pure bacterial infections. Serum TRAIL levels of patients with different infection types as indicated.
DESCRIPTION OF SPECIFIC EMBODIMENTS OF THE INVENTION
The present invention, in some embodiments thereof, relates to the identification of signatures and determinants associated with infections.
Before explaining at least one embodiment of the invention in detail, it is to be understood that the invention is not necessarily limited in its application to the details set forth in the following description or exemplified by the Examples. The invention is capable of other embodiments or of being practiced or carried out in various ways.
Correct identification of bacterial patients is of high importance as these patients require antibiotic treatment and in some cases more aggressive management (hospitalization, additional diagnostic tests etc). Misclassification of bacterial patients increases the chance of morbidity and mortality. The clinical challenge is to distinguish between these patients from patients with viral infection that have similar symptoms but do not require antibiotic treatment. Circulating host-proteins, such as C-reactive protein (CRP), are routinely used to support diagnosis of infection. The blood levels of these biomarkers are moderately elevated in response to viral infections and to higher extent in response to bacterial infections, with some degree of overlapping. Moreover, some
virus type (e.g., adenovirus and influenza), can cause a significant increase in CRP levels, similar to various bacterial infections. The present inventors previously identified TNF-related apoptosis-inducing ligand (TRAIL), as a novel biomarker that can accurately distinguish between bacterial and viral infections. Unlike known biomarkers, TRAIL has unique dynamics in response to infections as its serum levels decrease in response to bacterial infections and increase in response to viral infections (Figure 8). For example, in a sub-cohort of 233 febrile children (78 bacterial and 155 viral) and 15 non-infectious controls, TRAIL levels were increased in viral patients and decreased in bacterial patients as compared to controls (average+SD [pg/ml]: bacterial 44+32; viral 153+110; controls 78+29; Figure 9). The difference between TRAIL levels in viral and bacterial patients was statistically significant for all 11 evaluated viral strains (test p-value<0.001; Figure 9).
Delayed or no antibiotic treatment in cases of bacterial disease is very common (24%-40% of all bacterial infections), and can lead to disease-related complications resulting in increased rates of morbidity and mortality. Thus, timely identification of patients with bacterial infection is of great importance to guide correct patient management. The present inventors therefore, evaluated the performance of TRAIL in different stages of disease progression. Importantly, it was found that TRAIL levels are already significantly different in patients with bacterial infections at the first days following symptoms onset (Figure 10). This is compared to currently used biomarkers such as CRP or Procalcitonin (PCT) that reach their maximal differential expression between bacterial and viral patients, only 2-3 days after symptoms onset (Figure 10). Moreover, the accuracy levels of TRAIL in distinguishing between patients with bacterial and viral infections were higher in the first days following symptoms onset using different TRAIL cutoffs (Tables 5A and B).
Thus, according to a first aspect of the present invention there is provided a method of ruling in a bacterial infection in a subject showing symptoms of an infection, the method comprising measuring the amount of TRAIL in a blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of the TRAIL is below a first predetermined level, a bacterial infection is ruled in.
The present inventors have also shown that IP 10 levels are already significantly different in patients with infections at the first days following symptoms onset (Figure 10).
According to a particular embodiment, the bacterial infection is a Group A streptococcal bacterial infection.
According to another aspect of the present invention there is provided a method of determining a treatment regimen in a subject showing symptoms of a pathogenic infection comprising measuring the amount of TRAIL in a blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of the TRAIL is below a first predetermined level, the subject is recommended an anti-bacterial agent.
The methods disclosed herein are used to identify subjects with an infection or a specific infection type. By type of infection it is meant to include bacterial infections, viral infections, mixed infections (bacterial and viral co-infection), no infection (i.e., non-infectious). In a particular embodiment, the methods disclosed are used to rule in a bacterial infection. In further embodiments, the methods disclosed are used to rule in a viral infection or rule out a viral infection. Some methods of the invention are used to distinguish subjects having a bacterial infection, a viral infection, a mixed infection (i.e., bacterial and viral co-infection), patients with a non-infectious disease and healthy individuals. Some methods of the present invention can also be used to monitor or select a treatment regimen for a subject who has an infection
In various aspects the method distinguishes a bacterially infected subject from either a subject with non-infectious disease or a healthy subject; a bacterially infected subject from a virally infected subject; a bacterially infected subject from a subject having both a viral and bacterial infection (mixed infection) and a virally infected subject from a subject having both a viral and bacterial infection.
A mixed infected subject refers to a subject having a bacterial and viral co- infection.
In another embodiment, the method is used to discriminate between bacterial and viral etiologies of chronic obstructive pulmonary disease (COPD) exacerbation.
In still another embodiment, the method is used to distinguish between an infective exacerbation state of chronic obstructive pulmonary disease (COPD) and a non-infective exacerbation state of COPD, as further described herein below.
In further embodiments, the method is used in conjunction with an assay to determine the presence of a specific virus/bacteria, as further described herein below.
The infection may be an acute or chronic infection.
A chronic infection is an infection that develops slowly and lasts a long time. Viruses that may cause a chronic infection include Hepatitis C and HIV. One difference between acute and chronic infection is that during acute infection the immune system often produces IgM+ antibodies against the infectious agent, whereas the chronic phase of the infection is usually characteristic of IgM-/IgG+ antibodies. In addition, acute infections cause immune mediated necrotic processes while chronic infections often cause inflammatory mediated fibrotic processes and scaring (e.g. Hepatitis C in the liver). Thus, acute and chronic infections may elicit different underlying immunological mechanisms.
As used herein, the term "infection" refers to a state caused by an infectious agent of viral or bacterial origin. The bacterial infection may be the result of gram- positive, gram-negative bacteria or atypical bacteria.
The term "Gram-positive bacteria" are bacteria that are stained dark blue by Gram staining. Gram-positive organisms are able to retain the crystal violet stain because of the high amount of peptidoglycan in the cell wall.
The term "Gram- negative bacteria" are bacteria that do not retain the crystal violet dye in the Gram staining protocol.
The term "Atypical bacteria" are bacteria that do not fall into one of the classical "Gram" groups. They are usually, though not always, intracellular bacterial pathogens. They include, without limitations, Mycoplasmas spp., Legionella spp. Rickettsiae spp., and Chlamydiae spp.
By "ruling in" an infection it is meant that the subject has that type of infection. By "ruling out" an infection it is meant that the subject does not have that type of infection.
The subjects of this aspect of the present invention may present with a variety of pathogens including, but not limited to Adenovirus, Coronavirus, Parainfluenza virus,
Influenza A virus, Influenza B virus, Respiratory syncytial virus A/B, Chlamydophila pneumoniae, Mycoplasma pneumoniae, Legionella pneumophila, Rota Virus, Staphylococcus aureus, Streptococcus pneumoniae, Astrovirus, Enteric Adenovirus, Norovirus G I and G II, Bocavirus 1/2/3/4, Enterovirus, CMV virus, EBV virus, Group A Strep, or Escherichia coli.
Exemplary pathogens contemplated by the present invention include, but are not limited to influenza, respiratory syncytial virus (RSV), rhinovirus and Group A Streptococcus.
The subjects (e.g. children) may present with a particular clinical syndrome - for example, low respiratory tract infection (LRTI) infection, upper respiratory tract infection (URTI), fever without identifiable source (FWS), or a serious bacterial infection (SBI) such as UTI (urinary tract infections), septic shock, bacteremia, pneumonia or meningitis.
"Measuring" or "measurement," or alternatively "detecting" or "detection," means assessing the presence, absence, quantity or amount (which can be an effective amount) of the determinant within a clinical or subject-derived sample, including the derivation of qualitative or quantitative concentration levels of such determinants.
A "sample" in the context of the present invention is a biological sample isolated from a subject and can include, by way of example and not limitation, whole blood, serum, plasma, saliva, mucus, breath, urine, CSF, sputum, sweat, stool, hair, seminal fluid, biopsy, rhinorrhea, tissue biopsy, cytological sample, platelets, reticulocytes, leukocytes, epithelial cells, or whole blood cells.
In a particular embodiment, the sample is a blood sample - e.g. serum or a sample comprising blood cells. In a particular embodiment, the sample is depleted of red blood cells.
According to this aspect of the present invention, the sample is derived from the subject no more than 72 hours, no more than 60 hours, no more than 48 hours, no more than 36 hours, no more than one 24 hours or even no more than 12 hours following symptom onset.
The sample may be fresh or frozen.
A "subject" in the context of the present invention may be a mammal (e.g. a human, dog, cat, horse, cow, sheep, pig, goat). According to another embodiment, the
subject is a bird (e.g. chicken, turkey, duck or goose). According to a particular embodiment, the subject is a human. The subject may be male or female. The subject may be an adult (e.g. older than 18, 21, or 22 years or a child (e.g. younger than 18, 21 or 22 years). In another embodiment, the subject is an adolescent (between 12 and 21 years), an infant (29 days to less than 2 years of age) or a neonate (birth through the first 28 days of life).
Exemplary symptoms which the subject may present include but are not limited to fever, nausea, headache, sore throat, runny nose, rash and/or muscle soreness.
According to a particular embodiment, the subject does not show signs of having had a heart attack (e.g. has a normal level of creatine kinase, troponin or serum myoglobin, and/or has a normal ECG or EKG).
According to one aspect of the present invention, the level of the polypeptide TRAIL is used to rule in a bacterial infection.
TRAIL: The protein encoded by this gene is a cytokine that belongs to the tumor necrosis factor (TNF) ligand family. The present invention contemplates measuring either the soluble and/or the membrane form of this protein. In one embodiment, only the soluble form of this protein is measured. Additional names of the gene include without limitations AP02L, TNF-related apoptosis-inducing ligand, TNFSFIO and CD253. This protein binds to several members of the TNF receptor superfamily such as TNFRS F 10 A/TR AILR 1 , TNFRSF10B/TRAILR2, TNFRS F 1 OC/TR AILR3 , TNFRS F10D/TRAILR4, and possibly also to TNFRSF11B/OPG.
Additional information concerning TRAIL is provided in Table 1, herein below. Table 1

Exemplary amino acid sequences of TRAIL are set forth in SEQ ID NOs
In a particular embodiment, TRAIL is the protein that is recognized by the antibody of the kit R&D systems, Human TR AIL/TNFS F 10 Quantikine ELISA Kit catalog # DTRL00.
The level of TRAIL increases in viral infections (as compared to non-infectious diseases), and decreases in bacterial infections (as compared to non-infectious diseases).
Thus, when the level of TRAIL is above a predetermined level, it is indicative that the infection is a viral infection and a viral infection may be ruled in (or a bacterial infection may be ruled out).
When the level of TRAIL is below a predetermined level, it is indicative that the infection is a bacterial infection and a bacterial infection may be ruled in (or a viral infection may be ruled out).
For example, a bacterial infection may be ruled out if the polypeptide concentration of TRAIL determined is higher than a pre-determined first threshold value. Optionally, the method further includes determining if a subject has a viral infection (i.e., ruling in a viral infection). A viral infection is ruled in if the polypeptide concentration of TRAIL is higher than a pre-determined second threshold value.
In another specific embodiment the invention includes determining if a subject does not have a viral infection (i.e. ruling out a viral infection). A viral infection is ruled out if the polypeptide concentration of TRAIL determined is lower than a pre- determined first threshold value. Optionally, the method further includes determining if a subject has a bacterial infection (i.e., ruling in a bacterial infection). A bacterial infection is ruled in if the polypeptide concentration of TRAIL is lower than a predetermined second threshold value.
More specifically, TRAIL levels of 100-1000 pg/ml are usually indicative of a viral infection, while 0-85 pg/ml are usually indicative of a bacterial infection. Bacterial infection can usually be ruled in if TRAIL levels are lower than 85 pg/ml, 70 pg/ml, 60 pg/ml or more preferably 50, 40, 30 or 20 pg/ml, and ruled out if TRAIL levels are higher than 100, 120, 140 or preferably 150 pg/ml.
Additional polypeptides that may be analyzed for the early detection of bacterial infections include but are not limited to CRP and IP10. Thus TRAIL and CRP may be measured, TRAIL and IP 10 may be measured or TRAIL, CRP and IP 10 may be measured.
Information regarding CRP and IP 10 is provided in Table 2, herein below.
Table 2

CRP: C-reactive protein; additional aliases of CRP include without limitation RPl l-419N10.4 and PTXl.
An exemplary amino acid sequence of human CRP is set forth below in SEQ ID
NO: 1.
The level of CRP typically increases in infections (as compared to noninfectious diseases), with the level of CRP being higher in bacterial infections as opposed to viral infections.
Thus, when the level of CRP is above a predetermined level, it is indicative that the infection is a bacterial infection and a bacterial infection may be ruled in (or a viral infection may be ruled out).
When the level of CRP is below a predetermined level, it is indicative that the infection is a viral infection and a viral infection may be ruled in (or a bacterial infection may be ruled out).
CRP levels of 0-40 μg/ml are usually indicative of a viral infection, while 40- 400 μg/ml are usually indicative of a bacterial infection. Bacterial infection can usually be ruled in if CRP levels are higher than 50, 60, 70 or more preferably 80 μg/ml, and ruled out if CRP levels are lower than 30 and more preferably 20 μg/ml.
IP10: This gene encodes a chemokine of the CXC subfamily and ligand for the receptor CXCR3. Additional names of the gene include without limitations: CXCLIO, Gamma-IPIO, INP10 and chemokine (C-X-C motif) ligand 10.
An exemplary amino acid sequence of human IP10 is set forth in SEQ ID NO:
In a particular embodiment, IP 10 is the protein that is recognized by the antibody of the kit (R&D systems, Human CXCLlO/IP-10 Quantikine ELISA Kit catalog * DIP 100).
The level of IP10 increases in infections (as compared to non-infectious diseases), with the level of IP10 being higher in viral infections as opposed to bacterial infections.
Thus, when the level of IP10 is above a predetermined level, it is indicative that the infection is a viral infection and a viral infection may be ruled in (or a bacterial infection may be ruled out).
When the level of IP 10 is below a predetermined level, it is indicative that the infection is a bacterial infection and a bacterial infection may be ruled in (or a viral infection may be ruled out).
IP- 10 levels of 300-2000 pg/ml are usually indicative of a viral infection, while
160-860 pg/ml are usually indicative of a bacterial infection.
Since IP- 10 levels have been shown to be significantly different in patients with infections at the first days following symptoms onset (Figure 10), the present inventors further contemplate that IP- 10 alone can be used as a marker of early infection.
The concentrations of each of the above identified polypeptides may be combined (e.g. by way of a pre-determined mathematical function) to compute a score and the score may be compared to a predetermined reference value as further described herein below.
Further information on generating pre-determined mathematical functions in general and for CRP, IP 10 and TRAIL in particular are provided in International Patent Application IL2015/050823, the contents of which are incorporated herein by reference.
Statistical classification algorithms which may be used to calculate the score include, but are not limited to Support Vector Machine (SVM), Logistic Regression (LogReg), Neural Network, Bayesian Network, and a Hidden Markov Model.
A reference value can be relative to a number or value derived from population studies, including without limitation, such subjects having the same infection, subject having the same or similar age range, subjects in the same or similar ethnic group, or relative to the starting sample of a subject undergoing treatment for an infection. Such reference values can be derived from statistical analyses and/or risk prediction data of
populations obtained from mathematical algorithms and computed indices of infection. Reference determinant indices can also be constructed and used using algorithms and other methods of statistical and structural classification.
In one embodiment of the present invention, the reference value is the amount (i.e. level) of determinants in a control sample derived from one or more subjects who do not have an infection (i.e., healthy, and or non-infectious individuals). In a further embodiment, such subjects are monitored and/or periodically retested for a diagnostically relevant period of time ("longitudinal studies") following such test to verify continued absence of infection. Such period of time may be one day, two days, two to five days, five days, five to ten days, ten days, or ten or more days from the initial testing date for determination of the reference value. Furthermore, retrospective measurement of determinants in properly banked historical subject samples may be used in establishing these reference values, thus shortening the study time required.
A reference value can also comprise the amounts of determinants derived from subjects who show an improvement as a result of treatments and/or therapies for the infection. A reference value can also comprise the amounts of determinants derived from subjects who have confirmed infection by known techniques.
An example of a bacterially infected reference value index value is the mean or median concentrations of that determinant in a statistically significant number of subjects having been diagnosed as having a bacterial infection.
An example of a virally infected reference value is the mean or median concentrations of that determinant in a statistically significant number of subjects having been diagnosed as having a viral infection.
In another embodiment, the reference value is an index value or a baseline value. An index value or baseline value is a composite sample of an effective amount of determinants from one or more subjects who do not have an infection. A baseline value can also comprise the amounts of determinants in a sample derived from a subject who has shown an improvement in treatments or therapies for the infection. In this embodiment, to make comparisons to the subject-derived sample, the amounts of determinants are similarly calculated and compared to the index value. Optionally, subjects identified as having an infection, are chosen to receive a therapeutic regimen to slow the progression or eliminate the infection.
Additionally, the amount of the determinant can be measured in a test sample and compared to the "normal control level," utilizing techniques such as reference limits, discrimination limits, or risk defining thresholds to define cutoff points and abnormal values. The "normal control level" means the level of one or more determinants or combined determinant indices typically found in a subject not suffering from an infection. Such normal control level and cutoff points may vary based on whether a determinant is used alone or in a formula combining with other determinants into an index. Alternatively, the normal control level can be a database of determinant patterns from previously tested subjects.
The effectiveness of a treatment regimen can be monitored by detecting a determinant in an effective amount (which may be one or more) of samples obtained from a subject over time and comparing the amount of determinants detected. For example, a first sample can be obtained prior to the subject receiving treatment and one or more subsequent samples are taken after or during treatment of the subject.
For example, the methods of the invention can be used to discriminate between bacterial, viral and mixed infections (i.e. bacterial and viral co-infections). This will allow patients to be stratified and treated accordingly.
In a specific embodiment of the invention a treatment recommendation (i.e., selecting a treatment regimen) for a subject is provided by identifying the type infection (i.e., bacterial, viral, mixed infection or no infection) in the subject according to the method of any of the disclosed methods and recommending that the subject receive an antibiotic treatment if the subject is identified as having bacterial infection or a mixed infection; or an anti- viral treatment is if the subject is identified as having a viral infection.
Examples of antibiotics contemplated by the present invention include, but are not limited to Daptomycin; Gemifloxacin; Telavancin; Ceftaroline; Fidaxomicin; Amoxicillin; Ampicillin; Bacampicillin; Carbenicillin; Cloxacillin; Dicloxacillin; Flucloxacillin; Mezlocillin; Nafcillin; Oxacillin; Penicillin G; Penicillin V; Piperacillin; Pivampicillin; Pivmecillinam; Ticarcillin; Aztreonam; Imipenem; Doripenem; Meropenem; Ertapenem; Clindamycin; Lincomycin; Pristinamycin; Quinupristin; Cefacetrile (cephacetrile); Cefadroxil (cefadroxyl); Cef alexin (cephalexin); Cefaloglycin (cephaloglycin); Cefalonium (cephalonium); Cefaloridine (cephaloradine); Cefalotin
(cephalothin); Cefapirin (cephapirin); Cefatrizine; Cefazaflur; Cefazedone; Cefazolin
(cephazolin);Cefradine (cephradine); Cefroxadine; Ceftezole; Cefaclor; Cefamandole;
Cefmetazole; Cefonicid; Cefotetan; Cefoxitin; Cefprozil (cefproxil); Cefuroxime;
Cefuzonam; Cefcapene; Cefdaloxime; Cefdinir; Cefditoren; Cefetamet; Cefixime; Cefmenoxime; Cefodizime; Cefotaxime; Cefpimizole; Cefpodoxime; Cefteram;
Ceftibuten; Ceftiofur; Ceftiolene; Ceftizoxime; Ceftriaxone; Cefoperazone; Ceftazidime;
Cefclidine; Cefepime; Cefluprenam; Cefoselis; Cefozopran; Cefpirome; Cefquinome;
Fifth Generation; Ceftobiprole; Ceftaroline; Not Classified; Cefaclomezine; Cefaloram;
Cefaparole; Cefcanel; Cefedrolor; Cefempidone; Cefetrizole; Cefivitril; Cefmatilen; Cefmepidium; Cefovecin; Cefoxazole; Cefrotil; Cefsumide; Cefuracetime; Ceftioxide;
Azithromycin; Erythromycin; Clarithromycin; Dirithromycin; Roxithromycin;
Telithromycin; Amikacin; Gentamicin; Kanamycin; Neomycin; Netilmicin;
Paromomycin; Streptomycin; Tobramycin; Flumequine; Nalidixic acid; Oxolinic acid;
Piromidic acid; Pipemidic acid; Rosoxacin; Ciprofloxacin; Enoxacin; Lomefloxacin; Nadifloxacin; Norfloxacin; Ofloxacin; Pefloxacin; Rufloxacin; Balofloxacin;
Gatifloxacin; Grepafloxacin; Levofloxacin; Moxifloxacin; Pazufloxacin; Sparfloxacin;
Temafloxacin; Tosufloxacin; Besifloxacin; Clinafloxacin; Gemifloxacin; Sitafloxacin;
Trovafloxacin; Prulifloxacin; Sulfamethizole; Sulfamethoxazole; Sulfisoxazole;
Trimethoprim-Sulfamethoxazole; Demeclocycline; Doxycycline; Minocycline; Oxytetracycline; Tetracycline; Tigecycline; Chloramphenicol; Metronidazole;
Tinidazole; Nitrofurantoin; Vancomycin; Teicoplanin; Telavancin; Linezolid;
Cycloserine 2; Rifampin; Rifabutin; Rifapentine; Bacitracin; Polymyxin B; Viomycin;
Capreomycin.
If a viral infection is ruled in, the subject may be treated with an antiviral agent. Examples of antiviral agents include, but are not limited to Abacavir; Aciclovir;
Acyclovir; Adefovir; Amantadine; Amprenavir; Ampligen; Arbidol; Atazanavir; Atripla;
Balavir; Boceprevirertet; Cidofovir; Combivir; Dolutegravir; Darunavir; Delavirdine;
Didanosine; Docosanol; Edoxudine; Efavirenz; Emtricitabine; Enfuvirtide; Entecavir;
Ecoliever; Famciclovir; Fomivirsen; Fos amprenavir; Foscarnet; Fosfonet; Fusion inhibitor; Ganciclovir; Ibacitabine; Imunovir; Idoxuridine; Imiquimod; Indinavir;
Inosine; Integrase inhibitor; Interferon type III; Interferon type II; Interferon type I;
Interferon; Lamivudine; Lopinavir; Loviride; Maraviroc; Moroxydine; Methisazone;
Nelfinavir; Nevirapine; Nexavir; Oseltamivir; Peginterferon alfa-2a; Penciclovir; Peramivir; Pleconaril; Podophyllo toxin; Raltegravir; Reverse transcriptase inhibitor; Ribavirin; Rimantadine; Ritonavir; Pyramidine; Saquinavir; Sofosbuvir; StavudineTelaprevir; Tenofovir; Tenofovir disoproxil; Tipranavir; Trifluridine; Trizivir; Tromantadine; Truvada; traporved; Valaciclovir; Valganciclovir; Vicriviroc; Vidarabine; Viramidine; Zalcitabine; Zanamivir; Zidovudine; RNAi antiviralsmonoclonal antibody respigams; neuraminidase blocking agents.
In another embodiment, the methods of the invention can be used to prompt additional targeted diagnosis such as pathogen specific PCRs, chest-X-ray, cultures etc. For example, a diagnosis that indicates a viral infection according to embodiments of this invention, may prompt the usage of additional viral specific multiplex-PCRs, whereas a diagnosis that indicates a bacterial infection according to embodiments of this invention may prompt the usage of a bacterial specific multiplex-PCR. Thus, one can reduce the costs of unwarranted expensive diagnostics.
In a specific embodiment, a diagnostic test recommendation for a subject is provided by identifying the infection type (i.e., bacterial, viral, mixed infection or no infection) in the subject according to any of the disclosed methods and recommending a test to determine the source of the bacterial infection if the subject is identified as having a bacterial infection or a mixed infection; or a test to determine the source of the viral infection if the subject is identified as having a viral infection.
As well as measuring the polypeptide determinants mentioned herein above, the present inventors contemplate measuring at least one, two, three, four, five, six, seven, eight, nine, ten or more additional (non-identical) determinants (polypeptide, RNA or other), wherein the at least one additional determinant is set forth in US Patent Application No. 20080171323, WO2011/132086 and WO2013/117746 and PCT Application IL 2015/051024 and PCT Application IL 2015/051201 and Provisional Application No. 62/302,849 the contents of each are incorporated herein by reference. Other polypeptide determinants contemplated by the present inventors are the polypeptide counterparts of the RNA determinants described therein.
In one embodiment, at least of the additional determinants is set forth in Table 3 herein below.
Table 3
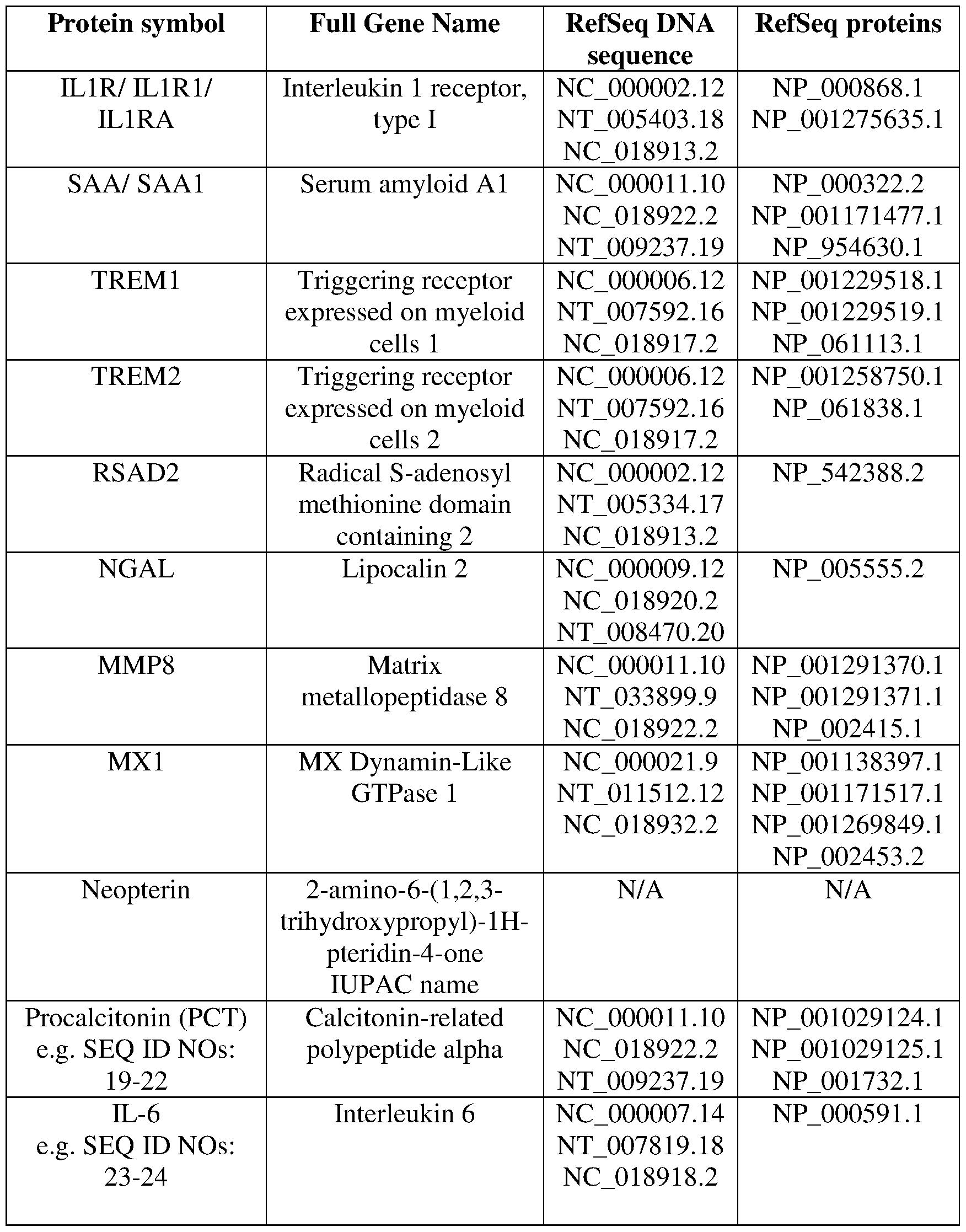
More specifically, as well as analyzing TRAIL polypeptide, at least one, at least two, at least three, at least four of the following polypeptides may be analyzed: Interferon gamma-induced protein 10 (IP10), Interleukin 6 (IL-6), and Interleukin 1 receptor, type I (ILIRA). In another embodiment CRP and/or PCT may also be analyzed.
More specifically, as well as analyzing IP 10 polypeptide, at least one, at least two, at least three, at least four of the following polypeptides may be analyzed: TRAIL,
Interleukin 6 (IL-6), and Interleukin 1 receptor, type I (ILIRA). In another embodiment
CRP and/or PCT may also be analyzed.
Contemplated combinations of polypeptides include, but are not limited to:
TRAIL+ IP-10,
TRAIL+ CRP,
TRAIL+ PCT,
TRAIL+ ILIRa,
TRAIL+ IL-6,
IP- 10+ CRP,
IP- 10+ PCT,
IP- 10+ ILIRa,
IP- 10+ IL-6,
TRAIL+ IP-10+ CRP,
TRAIL+IP-10+ PCT,
TRAIL+ IP-10+ILlRa,
TRAIL+ IP-10+ IL-6,
TRAIL+CRP+ PCT,
TRAIL+CRP+ ILIRa,
TRAIL+CRP+ IL-6,
TRAIL+ PCT+ ILIRa,
TRAIL+ PCT+IL-6,
TRAIL+ ILlRa+ IL-6,
IP-10+CRP+ PCT,
IP- 10+CRP+ ILIRa,
IP-lO+CRP+ IL-6,
IP- 10+ PCT+ILIRa,
IP- 10+ PCT+ IL-6,
IP-10+ ILlRa+ IL-6,
TRAIL+ IP- 10+ CRP+ PCT,
TRAIL+ IP- 10+ CRP+ ILIRa,
TRAIL+ IP- 10+ CRP+ IL-6,
TRAIL+ IP-10+ PCT+ ILIRa,
TRAIL+ IP-10+ PCT+ IL-6,
TRAIL+ IP- 10+ ILlRa+ IL-6,
TRAIL+ CRP+ PCT+ ILIRa,
TRAIL+ CRP+ PCT+ IL-6,
TRAIL+ CRP+ ILlRa+ IL-6,
TRAIL+ PCT+ ILlRa+ IL-6,
IP- 10+ CRP+ PCT+ ILIRa,
IP-10+ CRP+ PCT+ IL-6,
IP- 10+ CRP+ ILlRa+ IL-6,
IP- 10+ PCT+ ILlRa+ IL-6,
TRAIL+ IP- 10+ CRP+ PCT+ ILIRa,
TRAIL+ IP- 10+ CRP+ PCT, IL-6,
TRAIL+ IP- 10+ CRP+ ILlRa+ IL-6,
TRAIL+ IP- 10+ PCT+ ILlRa+ IL-6,
TRAIL+ CRP+ PCT+ ILlRa+ IL-6,
IP- 10+ CRP+ PCT+ ILlRa+ IL-6,
TRAIL+ IP-10+ CRP+ PCT+ ILlRa+ IL-6,
According to this aspect of the present invention, in order to distinguish between the different infection types (or to rule in a bacterial infection), no more than
30 determinants are measured, no more than 25 determinants are measured, no more than 20 determinants are measured, no more than 15 determinants are measured, no more than 10 determinants are measured, no more than 5 determinants are measured, no more than 4 determinants are measured, no more than 3 determinants are measured, no more than 2 determinants are measured or only TRAIL is measured.
Other determinants that may be measured according to aspects of the present invention include pathogen (bacterial or viral) specific RNA or polypeptide determinants. This may be carried out in order to aid in identification of a specific pathogen. The measurements may be effected simultaneously with the above-described measurements or consecutively.
According to another aspect of the present invention there is provided a method of distinguishing between an infectious exacerbation state and a non-infectious exacerbation state of chronic obstructive pulmonary disease (COPD) or asthma of a subject comprising measuring the amount of TNF-related apoptosis-inducing ligand (TRAIL) in a blood sample derived from the subject, wherein the amount is indicative of the infectivity of the exacerbation state of COPD or asthma.
Chronic obstructive pulmonary disease (COPD) is an obstructive, inflammatory lung disease characterized by long-term poor airflow. The main symptoms include shortness of breath and cough with sputum production. COPD is a progressive disease, worsening over time.
An exacerbation of COPD is defined as an event in the natural course of the disease characterized by a change in the patient's baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variations; it is typically acute in onset; and may warrant a change in regular medication. The exacerbation may present with signs of increased work of breathing such as fast breathing, a fast heart rate, sweating, active use of muscles in the neck, a bluish tinge to the skin, and confusion or combative behavior in very severe exacerbations. Crackles may also be heard over the lungs on examination with a stethoscope.
The method of this aspect of the present invention seeks to direct preventative therapies, differentiate stable disease from exacerbation, exacerbation of COPD or asthma from other causes of symptom deterioration and discriminate between bacterial and viral etiologies of exacerbation in order to guide correct treatment. At present exacerbation is a clinical diagnosis of exclusion, leading to both under- and over- treatment of patients and therefore excess morbidity and healthcare cost.
In some embodiments of the present invention, TRAIL serum levels is associated with bacterial, viral or mixed infection in COPD patients. Thus, it can distinguish between infection-related exacerbations from other causes of symptom deterioration in COPD patients. In yet another embodiment, it can distinguish between bacterial and viral etiologies of exacerbation in COPD patients, which in turn allows for the selection of an appropriate treatment regimen (e.g. antibiotic treatment in the case of bacterial infection; or inhaled bronchodilators or corticosteroids in the case of a non-bacterial
infection). In yet another embodiment, it can distinguish between mixed bacterial-viral co-infection and a pure viral infection in COPD patients.
In some embodiments of the present invention, TRAIL serum levels is associated with bacterial, viral or mixed infection in asthmatic patients. Thus, it can distinguish between infection-related exacerbations from other causes of symptom deterioration in asthmatic patients. In yet another embodiment, it can distinguish between bacterial and viral etiologies of exacerbation in asthmatic patients, which in turn allows for the selection of an appropriate treatment regimen. In yet another embodiment, it can distinguish between mixed bacterial-viral co-infection and a pure viral infection in asthmatic patients.
As mentioned, the assay of the present invention may also be carried out in conjunction with additional microbial tests such as nucleic acid amplification-based tests (NAAT) which analyze for the presence of a specific pathogen.
Testing for the presence of particular pathogens may suffer from reduced clinical utility because such tests cannot not distinguish between pathogenic strains of microorganisms and potential colonizers, which can be present as part of the natural microbiota without causing an infection. A biomarker that is able to distinguish between carriage and pathogenicity of a detected microorganism could serve as a complementary diagnostic with high clinical value. The combination of the two types of diagnostics offers the physician valuable information that can guide correct patient treatment. For example qPCR detection of specific bacteria together with biomarker-based conformation of pathogenicity empower the physician prescribing the correct antibiotic type. On the other hand, identification of specific bacteria but with biomarker-based conformation of carriage could prevent the doctor from prescribing unnecessary antibiotic treatment. Biomarkers that are based on the patient immune response to infection are not sensitive to bacterial or viral carriage (of microorganisms that are part of the body natural microbiota) as these do to evoke an immune response. Therefore, they are ideal candidates to serve as complementary diagnostic to methods that target the pathogen (NAAT based, culture etc.). Another significant limitation of diagnostic test that target the pathogen is the difficulty in identifying mixed bacterial and viral co- infections. For example, identifying a respiratory viral strain by NAAT-based methods (e.g., PCR), can lead the doctor to avoid antibiotic treatment. However, in many cases,
there is a secondary bacterial infection on top of the viral infection that can result in morbidity and mortality if left untreated. Host-based biomarkers that can indicate a potential secondary bacterial infection in case of identified primary viral infection can complement the targeted diagnostics and guide the doctor to prescribe appropriate antibiotic treatment. As illustrated in the Examples section, the present inventors demonstrated that TRAIL levels go down in patients with mixed infections similar to patients with pure bacterial infections (Figure 11). Thus, TRAIL can be used as an effective biomarker for guiding antibiotic treatment in cases of bacterial-viral co- infection as a complement to targeted diagnostics.
Thus, according to still another aspect of the present invention there is provided a method of classifying an infection type of a subject comprising:
(a) analyzing for the presence of specific pathogen in a sample of the subject; and
(b) measuring the amount of TRAIL in a sample of the subject, wherein the presence of the specific pathogen and the amount of TRAIL is indicative of the infection type.
Methods for analyzing for a specific pathogen may comprise the use polynucleotide base assays (e.g. PCR based assays) that are capable of detecting a gene product that is specific to that pathogen type. Other methods include culture assays as known in the art.
According to this aspect of the present invention the TRAIL may be measured at the RNA level or the protein level, as further described herein.
In particular embodiments, determining the amount of TRAIL is effected following a positive result for the presence of the specific pathogen. In this set up, the level of TRAIL may be used to distinguish between carriage and pathogenicity of an identified microorganism (bacteria or virus).
In other embodiments, TRAIL is used to distinguish between mixed bacterial- viral co-infection and a pure viral infection following identification of a viral strain in a patient sample.
In some embodiments, measuring the RNA or protein levels of TRAIL can be performed simultaneously on the same apparatus as the targeted diagnosis.
In other embodiments, measuring TRAIL levels can be used to prompt additional targeted diagnosis such as pathogen specific PCRs. For example, a diagnosis that indicates a viral infection according to embodiments of this invention, may prompt the usage of additional viral specific multiplex-PCRs, whereas a diagnosis that indicates a bacterial infection according to embodiments of this invention may prompt the usage of a bacterial specific multiplex-PCR. Thus, one can reduce the costs of unwarranted expensive diagnostics.
For all the aspects described herein, methods of measuring the levels of polypeptides are well known in the art and include, e.g., immunoassays based on antibodies to proteins, aptamers or molecular imprints.
The polypeptide determinants can be detected in any suitable manner, but are typically detected by contacting a sample from the subject with an antibody, which binds the determinant and then detecting the presence or absence of a reaction product. The antibody may be monoclonal, polyclonal, chimeric, or a fragment of the foregoing, as discussed in detail above, and the step of detecting the reaction product may be carried out with any suitable immunoassay. The sample from the subject is typically a biological sample as described above, and may be the same sample of biological sample used to conduct the method described above.
In one embodiment, the antibody which specifically binds the determinant is attached (either directly or indirectly) to a signal producing label, including but not limited to a radioactive label, an enzymatic label, a hapten, a reporter dye or a fluorescent label.
Immunoassays carried out in accordance with some embodiments of the present invention may be homogeneous assays or heterogeneous assays. In a homogeneous assay the immunological reaction usually involves the specific antibody (e.g., anti- determinant antibody), a labeled analyte, and the sample of interest. The signal arising from the label is modified, directly or indirectly, upon the binding of the antibody to the labeled analyte. Both the immunological reaction and detection of the extent thereof can be carried out in a homogeneous solution. Immunochemical labels, which may be employed, include free radicals, radioisotopes, fluorescent dyes, enzymes, bacteriophages, or coenzymes.
In a heterogeneous assay approach, the reagents are usually the sample, the antibody, and means for producing a detectable signal. Samples as described above may be used. The antibody can be immobilized on a support, such as a bead (such as protein A and protein G agarose beads), plate or slide, and contacted with the specimen suspected of containing the antigen in a liquid phase. The support is then separated from the liquid phase and either the support phase or the liquid phase is examined for a detectable signal employing means for producing such signal. The signal is related to the presence of the analyte in the sample. Means for producing a detectable signal include the use of radioactive labels, fluorescent labels, or enzyme labels. For example, if the antigen to be detected contains a second binding site, an antibody which binds to that site can be conjugated to a detectable group and added to the liquid phase reaction solution before the separation step. The presence of the detectable group on the solid support indicates the presence of the antigen in the test sample. Examples of suitable immunoassays are oligonucleotides, immunoblotting, immunofluorescence methods, immunoprecipitation, chemiluminescence methods, electrochemiluminescence (ECL) or enzyme-linked immunoassays.
Those skilled in the art will be familiar with numerous specific immunoassay formats and variations thereof which may be useful for carrying out the method disclosed herein. See generally E. Maggio, Enzyme-Immunoassay, (1980) (CRC Press, Inc., Boca Raton, Fla.); see also U.S. Pat. No. 4,727,022 to Skold et al., titled "Methods for Modulating Ligand-Receptor Interactions and their Application," U.S. Pat. No. 4,659,678 to Forrest et al., titled "Immunoassay of Antigens," U.S. Pat. No. 4,376,110 to David et al., titled "Immunometric Assays Using Monoclonal Antibodies," U.S. Pat. No. 4,275,149 to Litman et al., titled "Macromolecular Environment Control in Specific Receptor Assays," U.S. Pat. No. 4,233,402 to Maggio et al., titled "Reagents and Method Employing Channeling," and U.S. Pat. No. 4,230,767 to Boguslaski et al., titled "Heterogenous Specific Binding Assay Employing a Coenzyme as Label. "The determinant can also be detected with antibodies using flow cytometry. Those skilled in the art will be familiar with flow cytometric techniques which may be useful in carrying out the methods disclosed herein(Shapiro 2005). These include, without limitation, Cytokine Bead Array (Becton Dickinson) and Luminex technology.
Antibodies can be conjugated to a solid support suitable for a diagnostic assay (e.g., beads such as protein A or protein G agarose, microspheres, plates, slides or wells formed from materials such as latex or polystyrene) in accordance with known techniques, such as passive binding. Antibodies as described herein may likewise be conjugated to detectable labels or groups such as radiolabels (e.g., 35 S, 125 I, 131 I), enzyme labels (e.g., horseradish peroxidase, alkaline phosphatase), and fluorescent labels (e.g., fluorescein, Alexa, green fluorescent protein, rhodamine) in accordance with known techniques.
Antibodies can also be useful for detecting post-translational modifications of determinant proteins, polypeptides, mutations, and polymorphisms, such as tyrosine phosphorylation, threonine phosphorylation, serine phosphorylation, glycosylation (e.g., O-GlcNAc). Such antibodies specifically detect the phosphorylated amino acids in a protein or proteins of interest, and can be used in immunoblotting, immunofluorescence, and ELISA assays described herein. These antibodies are well-known to those skilled in the art, and commercially available. Post-translational modifications can also be determined using metastable ions in reflector matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF) (Wirth U. and Muller D. 2002).
For determinant-proteins, polypeptides, mutations, and polymorphisms known to have enzymatic activity, the activities can be determined in vitro using enzyme assays known in the art. Such assays include, without limitation, kinase assays, phosphatase assays, reductase assays, among many others. Modulation of the kinetics of enzyme activities can be determined by measuring the rate constant KM using known algorithms, such as the Hill plot, Michaelis-Menten equation, linear regression plots such as Lineweaver-Burk analysis, and Scatchard plot.
In particular embodiments, the antibodies of the present invention are monoclonal antibodies.
Suitable sources for antibodies for the detection of determinants include commercially available sources such as, for example, Abazyme, Abnova, AssayPro, Affinity Biologicals, AntibodyShop, Aviva bioscience, Biogenesis, Biosense Laboratories, Calbiochem, Cell Sciences, Chemicon International, Chemokine, Clontech, Cytolab, DAKO, Diagnostic BioSystems, eBioscience, Endocrine
Technologies, Enzo Biochem, Eurogentec, Fusion Antibodies, Genesis Biotech, GloboZymes, Haematologic Technologies, Immunodetect, Immunodiagnostik, Immunometrics, Immunostar, Immunovision, Biogenex, Invitrogen, Jackson ImmunoResearch Laboratory, KMI Diagnostics, Koma Biotech, LabFrontier Life Science Institute, Lee Laboratories, Lifescreen, Maine Biotechnology Services, Mediclone, MicroPharm Ltd., ModiQuest, Molecular Innovations, Molecular Probes, Neoclone, Neuromics, New England Biolabs, Novocastra, Novus Biologicals, Oncogene Research Products, Orbigen, Oxford Biotechnology, Panvera, PerkinElmer Life Sciences, Pharmingen, Phoenix Pharmaceuticals, Pierce Chemical Company, Polymun Scientific, Polysiences, Inc., Promega Corporation, Proteogenix, Protos Immunoresearch, QED Biosciences, Inc., R&D Systems, Repligen, Research Diagnostics, Roboscreen, Santa Cruz Biotechnology, Seikagaku America, Serological Corporation, Serotec, SigmaAldrich, StemCell Technologies, Synaptic Systems GmbH, Technopharm, Terra Nova Biotechnology, TiterMax, Trillium Diagnostics, Upstate Biotechnology, US Biological, Vector Laboratories, Wako Pure Chemical Industries, and Zeptometrix. However, the skilled artisan can routinely make antibodies, against any of the polypeptide determinants described herein.
The presence of a label can be detected by inspection, or a detector which monitors a particular probe or probe combination is used to detect the detection reagent label. Typical detectors include spectrophotometers, phototubes and photodiodes, microscopes, scintillation counters, cameras, film and the like, as well as combinations thereof. Those skilled in the art will be familiar with numerous suitable detectors that widely available from a variety of commercial sources and may be useful for carrying out the method disclosed herein. Commonly, an optical image of a substrate comprising bound labeling moieties is digitized for subsequent computer analysis. See generally The Immunoassay Handbook [The Immunoassay Handbook. Third Edition. 2005].
Traditional laboratory risk factors and additional clinical parameters may also be measured together with the above-described polypeptides to further increase the accuracy of the signatures.
"Traditional laboratory risk factors" encompass biomarkers isolated or derived from subject samples and which are currently evaluated in the clinical laboratory and used in traditional global risk assessment algorithms, such as absolute neutrophil count
(abbreviated ANC), absolute lymphocyte count (abbreviated ALC), white blood count (abbreviated WBC), neutrophil % (defined as the fraction of white blood cells that are neutrophils and abbreviated Neu (%)), lymphocyte % (defined as the fraction of white blood cells that are lymphocytes and abbreviated Lym (%)), monocyte % (defined as the fraction of white blood cells that are monocytes and abbreviated Mon (%)),Sodium (abbreviated Na), Potassium (abbreviated K), Bilirubin (abbreviated Bili).
"Clinical parameters" encompass all non-sample or non-analyte biomarkers of subject health status or other characteristics, such as, without limitation, age (Age), ethnicity (RACE), gender (Sex), core body temperature (abbreviated "temperature"), maximal core body temperature since initial appearance of symptoms (abbreviated "maximal temperature"), time from initial appearance of symptoms (abbreviated "time from symptoms") or family history (abbreviated FamHX).
The patient medical background conditions such as chronic lung diseases and diabetes may affect its immune response to infection that is reflected by changes in diagnostic accuracy of immune-based diagnostics (see Example 1, herein below). Thus, information regarding the patient background clinical conditions could potentially be integrated with protein biomarker classifiers predicted outcome in order to improve patient diagnosis.
Kits
Some aspects of the invention also include a determinant-detection reagent such as antibodies packaged together in the form of a kit. The kit may contain in separate containers antibodies (either already bound to a solid matrix or packaged separately with reagents for binding them to the matrix), control formulations (positive and/or negative), and/or a detectable label such as fluorescein, green fluorescent protein, rhodamine, cyanine dyes, Alexa dyes, lucif erase, radiolabels, among others. The detectable label may be attached to a secondary antibody which binds to the Fc portion of the antibody which recognizes the determinant. Instructions (e.g., written, tape, VCR, CD-ROM, etc.) for carrying out the assay may be included in the kit.
The kits of this aspect of the present invention may comprise additional components that aid in the detection of the determinants such as enzymes, salts, buffers etc. necessary to carry out the detection reactions.
For example, determinant detection reagents (e.g. antibodies) can be immobilized on a solid matrix such as a porous strip or an array to form at least one determinant detection site. The measurement or detection region of the porous strip may include a plurality of sites. A test strip may also contain sites for negative and/or positive controls. Alternatively, control sites can be located on a separate strip from the test strip. Optionally, the different detection sites may contain different amounts of immobilized detection reagents, e.g., a higher amount in the first detection site and lesser amounts in subsequent sites. Upon the addition of test sample, the number of sites displaying a detectable signal provides a quantitative indication of the amount of determinants present in the sample. The detection sites may be configured in any suitably detectable shape and are typically in the shape of a bar or dot spanning the width of a test strip.
Examples of "Monoclonal antibodies for measuring TRAIL", include without limitation: Mouse, Monoclonal (55B709-3) IgG; Mouse, Monoclonal (2E5) IgGl; Mouse, Monoclonal (2E05) IgGl; Mouse, Monoclonal (M912292) IgGl kappa; Mouse, Monoclonal (IIIF6) IgG2b; Mouse, Monoclonal (2E1-1B9) IgGl; Mouse, Monoclonal (RIK-2) IgGl, kappa; Mouse, Monoclonal M181 IgGl; Mouse, Monoclonal VI10E IgG2b; Mouse, Monoclonal MAB375 IgGl; Mouse, Monoclonal MAB687 IgGl; Mouse, Monoclonal HS501 IgGl; Mouse, Monoclonal clone 75411.11 Mouse IgGl; Mouse, Monoclonal T8175-50 IgG; Mouse, Monoclonal 2B2.108 IgGl; Mouse, Monoclonal B-T24 IgGl ; Mouse, Monoclonal 55B709.3 IgGl; Mouse, Monoclonal D3 IgGl; Goat, Monoclonal C19 IgG; Rabbit, Monoclonal H257 IgG; Mouse, Monoclonal 500-M49 IgG; Mouse, Monoclonal 05-607 IgG; Mouse, Monoclonal B-T24 IgGl; Rat, Monoclonal (N2B2), IgG2a, kappa; Mouse, Monoclonal (1A7-2B7), IgGl; Mouse, Monoclonal (55B709.3), IgG and Mouse, Monoclonal B-S23* IgGl.
Soluble TRAIL and membrane TRAIL can be distinguished by using different measuring techniques and samples. For example, Soluble TRAL can be measured without limitation in cell free samples such as serum or plasma, using without limitation lateral flow immunoassay (LFIA), as further described herein below. Membrane TRAIL can be measured in samples that contain cells using cell based assays including without limitation flow cytometry, ELISA, and other immunoassays.
Lateral Flow Immunoassays (LFIA): This is a technology which allows rapid measurement of analytes at the point of care (POC) and its underlying principles are described below. According to one embodiment, LFIA is used in the context of a handheld device.
The technology is based on a series of capillary beds, such as pieces of porous paper or sintered polymer. Each of these elements has the capacity to transport fluid (e.g., urine) spontaneously. The first element (the sample pad) acts as a sponge and holds an excess of sample fluid. Once soaked, the fluid migrates to the second element (conjugate pad) in which the manufacturer has stored the so-called conjugate, a dried format of bio-active particles (see below) in a salt-sugar matrix that contains everything to guarantee an optimized chemical reaction between the target molecule (e.g., an antigen) and its chemical partner (e.g., antibody) that has been immobilized on the particle's surface. While the sample fluid dissolves the salt-sugar matrix, it also dissolves the particles and in one combined transport action the sample and conjugate mix while flowing through the porous structure. In this way, the analyte binds to the particles while migrating further through the third capillary bed. This material has one or more areas (often called stripes) where a third molecule has been immobilized by the manufacturer. By the time the sample-conjugate mix reaches these strips, analyte has been bound on the particle and the third 'capture' molecule binds the complex.
After a while, when more and more fluid has passed the stripes, particles accumulate and the stripe-area changes color. Typically there are at least two stripes: one (the control) that captures any particle and thereby shows that reaction conditions and technology worked fine, the second contains a specific capture molecule and only captures those particles onto which an analyte molecule has been immobilized. After passing these reaction zones the fluid enters the final porous material, the wick, that simply acts as a waste container. Lateral Flow Tests can operate as either competitive or sandwich assays.
Different formats may be adopted in LFIA. Strips used for LFIA contain four main components. A brief description of each is given before describing format types.
Sample application pad: It is made of cellulose and/or glass fiber and sample is applied on this pad to start assay. Its function is to transport the sample to other components of lateral flow test strip (LFTS). Sample pad should be capable of
transportation of the sample in a smooth, continuous and homogenous manner. Sample application pads are sometimes designed to pretreat the sample before its transportation. This pretreatment may include separation of sample components, removal of interferences, adjustment of pH, etc.
Conjugate pad: It is the place where labeled biorecognition molecules are dispensed. Material of conjugate pad should immediately release labeled conjugate upon contact with moving liquid sample. Labeled conjugate should stay stable over entire life span of lateral flow strip. Any variations in dispensing, drying or release of conjugate can change results of assay significantly. Poor preparation of labeled conjugate can adversely affect sensitivity of assay. Glass fiber, cellulose, polyesters and some other materials are used to make conjugate pad for LFIA. Nature of conjugate pad material has an effect on release of labeled conjugate and sensitivity of assay.
Nitrocellulose membrane: It is highly critical in determining sensitivity of LFIA. Nitrocellulose membranes are available in different grades. Test and control lines are drawn over this piece of membrane. So an ideal membrane should provide support and good binding to capture probes (antibodies, aptamers etc.). Nonspecific adsorption over test and control lines may affect results of assay significantly, thus a good membrane will be characterized by lesser non-specific adsorption in the regions of test and control lines. Wicking rate of nitrocellulose membrane can influence assay sensitivity. These membranes are easy to use, inexpensive, and offer high affinity for proteins and other biomolecules. Proper dispensing of bioreagents, drying and blocking play a role in improving sensitivity of assay.
Adsorbent pad: It works as sink at the end of the strip. It also helps in maintaining flow rate of the liquid over the membrane and stops back flow of the sample. Adsorbent capacity to hold liquid can play an important role in results of assay.
All these components are fixed or mounted over a backing card. Materials for backing card are highly flexible because they have nothing to do with LFIA except providing a platform for proper assembling of all the components. Thus backing card serves as a support and it makes easy to handle the strip.
Major steps in LFIA are (i) preparation of antibody against target analyte (ii) preparation of label (iii) labeling of biorecognition molecules (iv) assembling of all
components onto a backing card after dispensing of reagents at their proper pads (v) application of sample and obtaining results.
Sandwich format: In a typical format, label (Enzymes or nanoparticles or fluorescence dyes) coated antibody or aptamer is immobilized at conjugate pad. This is a temporary adsorption which can be flushed away by flow of any buffer solution. A primary antibody or aptamer against target analyte is immobilized over test line. A secondary antibody or probe against labeled conjugate antibody/aptamer is immobilized at control zone.
Sample containing the analyte is applied to the sample application pad and it subsequently migrates to the other parts of strip. At conjugate pad, target analyte is captured by the immobilized labeled antibody or aptamer conjugate and results in the formation of labeled antibody conjugate/analyte complex. This complex now reaches at nitrocellulose membrane and moves under capillary action. At test line, label antibody conjugate/analyte complex is captured by another antibody which is primary to the analyte. Analyte becomes sandwiched between labeled and primary antibodies forming labeled antibody conjugate/analyte/primary antibody complex. Excess labeled antibody conjugate will be captured at control zone by secondary antibody. Buffer or excess solution goes to absorption pad. Intensity of color at test line corresponds to the amount of target analyte and is measured with an optical strip reader or visually inspected. Appearance of color at control line ensures that a strip is functioning properly.
Competitive format: Such a format suits best for low molecular weight compounds which cannot bind two antibodies simultaneously. Absence of color at test line is an indication for the presence of analyte while appearance of color both at test and control lines indicates a negative result. Competitive format has two layouts. In the first layout, solution containing target analyte is applied onto the sample application pad and prefixed labeled biomolecule (antibody/aptamer) conjugate gets hydrated and starts flowing with moving liquid. Test line contains pre-immobilized antigen (same analyte to be detected) which binds specifically to label conjugate. Control line contains pre- immobilized secondary antibody which has the ability to bind with labeled antibody conjugate. When liquid sample reaches at the test line, pre-immobilized antigen will bind to the labeled conjugate in case target analyte in sample solution is absent or present in such a low quantity that some sites of labeled antibody conjugate were
vacant. Antigen in the sample solution and the one which is immobilized at test line of strip compete to bind with labeled conjugate. In another layout, labeled analyte conjugate is dispensed at conjugate pad while a primary antibody to analyte is dispensed at test line. After application of analyte solution a competition takes place between analyte and labeled analyte to bind with primary antibody at test line.
Multiplex detection format: Multiplex detection format is used for detection of more than one target species and assay is performed over the strip containing test lines equal to number of target species to be analyzed. It is highly desirable to analyze multiple analytes simultaneously under same set of conditions. Multiplex detection format is very useful in clinical diagnosis where multiple analytes which are interdependent in deciding about the stage of a disease are to be detected. Lateral flow strips for this purpose can be built in various ways i.e. by increasing length and test lines on conventional strip, making other structures like stars or T-shapes. Shape of strip for LFIA will be dictated by number of target analytes. Miniaturized versions of LFIA based on microarrays for multiplex detection of DNA sequences have been reported to have several advantages such as less consumption of test reagents, requirement of lesser sample volume and better sensitivity.
Labels: Any material that is used as a label should be detectable at very low concentrations and it should retain its properties upon conjugation with biorecognition molecules. This conjugation is also expected not to change features of biorecognition probes. Ease in conjugation with biomolecules and stability over longer period of time are desirable features for a good label. Concentrations of labels down to 1(Γ9 M are optically detectable. After the completion of assay, some labels generate direct signal (as color from gold colloidal) while others require additional steps to produce analytical signal (as enzymes produce detectable product upon reaction with suitable substrate). Hence the labels which give direct signal are preferable in LFA because of less time consumption and reduced procedure.
Gold nanoparticles: Colloidal gold nanoparticles are the most commonly used labels in LFA. Colloidal gold is inert and gives very perfect spherical particles. These particles have very high affinity toward biomolecules and can be easily functionalized. Optical properties of gold nanoparticles are dependent on size and shape. Size of particles can be tuned by use of suitable chemical additives. Their unique features
include environment friendly preparation, high affinity toward proteins and biomolecules, enhanced stability, exceptionally higher values for charge transfer and good optical signaling. Optical signal of gold nanoparticles in colorimetric LFA can be amplified by deposition of silver, gold nanoparticles and enzymes.
Magnetic particles and aggregates : Colored magnetic particles produce color at the test line which is measured by an optical strip reader but magnetic signals coming from magnetic particles can also be used as detection signals and recorded by a magnetic assay reader. Magnetic signals are stable for longer time compared to optical signals and they enhance sensitivity of LFA by 10 to 1000 folds.
Fluorescent and luminescent materials: Fluorescent molecules are widely used in LFA as labels and the amount of fluorescence is used to quantitate the concentration of analyte in the sample. Detection of proteins is accomplished by using organic fluorophores such as rhodamine as labels in LFA.
Current developments in nanomaterial have headed to manufacture of quantum dots which display very unique electrical and optical properties. These semiconducting particles are not only water soluble but can also be easily combined with biomolecules because of closeness in dimensions. Owing to their unique optical properties, quantum dots have come up as a substitute to organic fluorescent dyes. Like gold nanoparticles QDs show size dependent optical properties and a broad spectrum of wavelengths can be monitored. Single light source is sufficient to excite quantum dots of all different sizes. QDs have high photo stability and absorption coefficients.
Upconverting phosphors (UCP) are characterized by their excitation in infra-red region and emission in high energy visible region. Compared to other fluorescent materials, they have a unique advantage of not showing any auto fluorescence. Because of their excitation in IR regions, they do not photo degrade biomolecules. A major advantage lies in their production from easily available bulk materials. Although difference in batch to batch preparation of UCP reporters can affect sensitivity of analysis in LFA, it was observed that they can enhance sensitivity of analytical signal by 10 to 100 folds compared to gold nanoparticles or colored latex beads, when analysis is carried out under same set of biological conditions.
Enzymes: Enzymes are also employed as labels in LFA. But they increase one step in LFA which is application of suitable substrate after complete assay. This
substrate will produce color at test and control lines as a result of enzymatic reaction. In case of enzymes, selection of suitable enzyme substrate combination is one necessary requirement in order to get a colored product for strip reader or electroactive product for electrochemical detection. In other words, sensitivity of detection is dependent on enzyme substrate combination.
Colloidal carbon: Colloidal carbon is comparatively inexpensive label and its production can be easily scaled up. Because of their black color, carbon NPs can be easily detected with high sensitivity. Colloidal carbon can be functionalized with a large variety of biomolecules for detection of low and high molecular weight analytes.
Detection systems: In case of gold nanoparticles or other color producing labels, qualitative or semi-quantitative analysis can be done by visual inspection of colors at test and control lines. The major advantage of visual inspection is rapid qualitative answer in "Yes" or "NO". Such quick replies about presence of an analyte in clinical analysis have very high importance. Such tests help doctors to make an immediate decision near the patients in hospitals in situations where test results from central labs cannot be waited for because of huge time consumption. But for quantification, optical strip readers are employed for measurement of the intensity of colors produced at test and control lines of strip. This is achieved by inserting the strips into a strip reader and intensities are recorded simultaneously by imaging softwares. Optical images of the strips can also be recorded with a camera and then processed by using a suitable software. Procedure includes proper placement of strip under the camera and a controlled amount of light is thrown on the areas to be observed. Such systems use monochromatic light and wavelength of light can be adjusted to get a good contrast among test and control lines and background. In order to provide good quantitative and reproducible results, detection system should be sensitive to different intensities of colors. Optical standards can be used to calibrate an optical reader device. Automated systems have advantages over manual imaging and processing in terms of time consumption, interpretation of results and adjustment of variables.
In case of fluorescent labels, a fluorescence strip reader is used to record fluorescence intensity of test and control lines. Fluorescence brightness of test line increased with an increase in nitrated ceruloplasmin concentration in human serum when it was detected with a fluorescence strip reader. A photoelectric sensor was also
used for detection in LFIA where colloidal gold is exposed to light emitting diode and resulting photoelectrons are recorded. Chemiluminescence which results from reaction of enzyme and substrate is measured as a response to amount of target analyte. Magnetic strip readers and electrochemical detectors are also reported as detection systems in LFTS but they are not very common. Selection of detector is mainly determined by the label employed in analysis.
Examples of "Monoclonal antibodies for measuring CRP", include without limitation: Mouse, Monoclonal (108-2A2); Mouse, Monoclonal (108-7G41D2); Mouse, Monoclonal (12D-2C-36), IgGl; Mouse, Monoclonal (1G1), IgGl; Mouse, Monoclonal (5A9), IgG2a kappa; Mouse, Monoclonal (63F4), IgGl; Mouse, Monoclonal (67A1), IgGl; Mouse, Monoclonal (8B-5E), IgGl; Mouse, Monoclonal (B893M), IgG2b, lambda; Mouse, Monoclonal (CI), IgG2b; Mouse, Monoclonal (C11F2), IgG; Mouse, Monoclonal (C2), IgGl; Mouse, Monoclonal (C3), IgGl; Mouse, Monoclonal (C4), IgGl; Mouse, Monoclonal (C5), IgG2a; Mouse, Monoclonal (C6), IgG2a; Mouse, Monoclonal (C7), IgGl; Mouse, Monoclonal (CRP103), IgG2b; Mouse, Monoclonal (CRP11), IgGl; Mouse, Monoclonal (CRP135), IgGl; Mouse, Monoclonal (CRP169), IgG2a; Mouse, Monoclonal (CRP30), IgGl; Mouse, Monoclonal (CRP36), IgG2a; Rabbit, Monoclonal (EPR283Y), IgG; Mouse, Monoclonal (KT39), IgG2b; Mouse, Monoclonal (N-a), IgGl; Mouse, Monoclonal (N1G1), IgGl; Monoclonal (P5A9AT); Mouse, Monoclonal (S5G1), IgGl; Mouse, Monoclonal (SB78c), IgGl; Mouse, Monoclonal (SB78d), IgGl and Rabbit, Monoclonal (Y284), IgG.
Polyclonal antibodies for measuring determinants include without limitation antibodies that were produced from sera by active immunization of one or more of the following: Rabbit, Goat, Sheep, Chicken, Duck, Guinea Pig, Mouse, Donkey, Camel, Rat and Horse.
Examples of detection agents, include without limitation: scFv, dsFv, Fab, sVH, F(ab')2, Cyclic peptides, Haptamers, A single-domain antibody, Fab fragments, Single- chain variable fragments, Affibody molecules, Affilins, Nanofitins, Anticalins, Avimers, DARPins, Kunitz domains, Fynomers and Monobody.
In particular embodiments, the kit does not comprise a number of antibodies that specifically recognize more than 50, 20 15, 10, 9, 8, 7, 6, 5 or 4 polypeptides.
In other embodiments, the array of the present invention does not comprise a number of antibodies that specifically recognize more than 50, 20 15, 10, 9, 8, 7, 6, 5 or 4 polypeptides.
Some aspects of the present invention can also be used to screen patient or subject populations in any number of settings. For example, a health maintenance organization, public health entity or school health program can screen a group of subjects to identify those requiring interventions, as described above, or for the collection of epidemiological data. Insurance companies (e.g., health, life or disability) may screen applicants in the process of determining coverage or pricing, or existing clients for possible intervention. Data collected in such population screens, particularly when tied to any clinical progression to conditions like infection, will be of value in the operations of, for example, health maintenance organizations, public health programs and insurance companies. Such data arrays or collections can be stored in machine- readable media and used in any number of health-related data management systems to provide improved healthcare services, cost effective healthcare, improved insurance operation, etc. See, for example, U.S. Patent Application No. 2002/0038227; U.S. Patent Application No. US 2004/0122296; U.S. Patent Application No. US 2004/ 0122297; and U.S. Patent No. 5,018,067. Such systems can access the data directly from internal data storage or remotely from one or more data storage sites as further detailed herein.
A machine-readable storage medium can comprise a data storage material encoded with machine-readable data or data arrays which, when using a machine programmed with instructions for using the data, is capable of use for a variety of purposes. Measurements of effective amounts of the biomarkers of the invention and/or the resulting evaluation of risk from those biomarkers can be implemented in computer programs executing on programmable computers, comprising, inter alia, a processor, a data storage system (including volatile and non-volatile memory and/or storage elements), at least one input device, and at least one output device. Program code can be applied to input data to perform the functions described above and generate output information. The output information can be applied to one or more output devices, according to methods known in the art. The computer may be, for example, a personal computer, microcomputer, or workstation of conventional design.
Each program can be implemented in a high level procedural or object oriented programming language to communicate with a computer system. However, the programs can be implemented in assembly or machine language, if desired. The language can be a compiled or interpreted language. Each such computer program can be stored on a storage media or device (e.g., ROM or magnetic diskette or others as defined elsewhere in this disclosure) readable by a general or special purpose programmable computer, for configuring and operating the computer when the storage media or device is read by the computer to perform the procedures described herein. The health-related data management system used in some aspects of the invention may also be considered to be implemented as a computer-readable storage medium, configured with a computer program, where the storage medium so configured causes a computer to operate in a specific and predefined manner to perform various functions described herein.
The polypeptide determinants of the present invention, in some embodiments thereof, can be used to generate a "reference determinant profile" of those subjects who do not have an infection. The determinants disclosed herein can also be used to generate a "subject determinant profile" taken from subjects who have an infection. The subject determinant profiles can be compared to a reference determinant profile to diagnose or identify subjects with an infection. The subject determinant profile of different infection types can be compared to diagnose or identify the type of infection. The reference and subject determinant profiles of the present invention, in some embodiments thereof, can be contained in a machine-readable medium, such as but not limited to, analog tapes like those readable by a VCR, CD-ROM, DVD-ROM, USB flash media, among others. Such machine-readable media can also contain additional test results, such as, without limitation, measurements of clinical parameters and traditional laboratory risk factors. Alternatively or additionally, the machine-readable media can also comprise subject information such as medical history and any relevant family history. The machine-readable media can also contain information relating to other disease-risk algorithms and computed indices such as those described herein.
The effectiveness of a treatment regimen can be monitored by detecting a determinant in an effective amount (which may be one or more) of samples obtained from a subject over time and comparing the amount of determinants detected. For
example, a first sample can be obtained prior to the subject receiving treatment and one or more subsequent samples are taken after or during treatment of the subject.
For example, the methods of the invention can be used to discriminate between bacterial, viral and mixed infections (i.e. bacterial and viral co-infections.) This will allow patients to be stratified and treated accordingly.
In a specific embodiment of the invention a treatment recommendation (i.e., selecting a treatment regimen) for a subject is provided by identifying the type infection (i.e., bacterial, viral, mixed infection or no infection) in the subject according to the method of any of the disclosed methods and recommending that the subject receive an antibiotic treatment if the subject is identified as having bacterial infection or a mixed infection; or an anti-viral treatment is if the subject is identified as having a viral infection.
In another embodiment, the methods of the invention can be used to prompt additional targeted diagnosis such as pathogen specific PCRs, chest-X-ray, cultures etc. For example, a diagnosis that indicates a viral infection according to embodiments of this invention, may prompt the usage of additional viral specific multiplex-PCRs, whereas a diagnosis that indicates a bacterial infection according to embodiments of this invention may prompt the usage of a bacterial specific multiplex-PCR. Thus, one can reduce the costs of unwarranted expensive diagnostics.
In a specific embodiment, a diagnostic test recommendation for a subject is provided by identifying the infection type (i.e., bacterial, viral, mixed infection or no infection) in the subject according to any of the disclosed methods and recommending a test to determine the source of the bacterial infection if the subject is identified as having a bacterial infection or a mixed infection; or a test to determine the source of the viral infection if the subject is identified as having a viral infection.
Performance and Accuracy Measures of the Invention.
The performance and thus absolute and relative clinical usefulness of the invention may be assessed in multiple ways as noted above. Amongst the various assessments of performance, some aspects of the invention are intended to provide accuracy in clinical diagnosis and prognosis. The accuracy of a diagnostic or prognostic test, assay, or method concerns the ability of the test, assay, or method to distinguish between subjects having an infection is based on whether the subjects have, a
"significant alteration" (e.g., clinically significant and diagnostically significant) in the levels of a determinant. By "effective amount" it is meant that the measurement of an appropriate number of determinants (which may be one or more) to produce a "significant alteration" (e.g. level of expression or activity of a determinant) that is different than the predetermined cut-off point (or threshold value) for that determinant (s) and therefore indicates that the subject has an infection for which the determinant (s) is an indication. The difference in the level of determinant is preferably statistically significant. As noted below, and without any limitation of the invention, achieving statistical significance, and thus the preferred analytical, diagnostic, and clinical accuracy, may require that combinations of several determinants be used together in panels and combined with mathematical algorithms in order to achieve a statistically significant determinant index.
In the categorical diagnosis of a disease state, changing the cut point or threshold value of a test (or assay) usually changes the sensitivity and specificity, but in a qualitatively inverse relationship. Therefore, in assessing the accuracy and usefulness of a proposed medical test, assay, or method for assessing a subject's condition, one should always take both sensitivity and specificity into account and be mindful of what the cut point is at which the sensitivity and specificity are being reported because sensitivity and specificity may vary significantly over the range of cut points. One way to achieve this is by using the Matthews correlation coefficient (MCC) metric, which depends upon both sensitivity and specificity. Use of statistics such as area under the ROC curve (AUC), encompassing all potential cut point values, is preferred for most categorical risk measures when using some aspects of the invention, while for continuous risk measures, statistics of goodness-of-fit and calibration to observed results or other gold standards, are preferred.
By predetermined level of predictability it is meant that the method provides an acceptable level of clinical or diagnostic accuracy. Using such statistics, an "acceptable degree of diagnostic accuracy", is herein defined as a test or assay (such as the test used in some aspects of the invention for determining the clinically significant presence of determinants, which thereby indicates the presence an infection type) in which the AUC (area under the ROC curve for the test or assay) is at least 0.60, desirably at least 0.65,
more desirably at least 0.70, preferably at least 0.75, more preferably at least 0.80, and most preferably at least 0.85.
By a "very high degree of diagnostic accuracy", it is meant a test or assay in which the AUC (area under the ROC curve for the test or assay) is at least 0.75, 0.80, desirably at least 0.85, more desirably at least 0.875, preferably at least 0.90, more preferably at least 0.925, and most preferably at least 0.95.
Alternatively, the methods predict the presence or absence of an infection or response to therapy with at least 75% total accuracy, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater total accuracy.
Alternatively, the methods predict the presence of a bacterial infection or response to therapy with at least 75% sensitivity, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater sensitivity.
Alternatively, the methods predict the presence of a viral infection or response to viral therapy with at least 75% specificity, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater specificity.
Alternatively, the methods rule out the presence of a bacterial infection or rule in a viral infection with at least 75% NPV, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater NPV.Alternatively, the methods rule in the presence of a bacterial infection or rule out a viral infection with at least 75% PPV, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater PPV.
Alternatively, the methods predict the presence of a viral infection or response to therapy with at least 75% specificity, more preferably 80%, 85%, 90%, 95%, 97%, 98%, 99% or greater specificity. Alternatively, the methods predict the presence or absence of an infection or response to therapy with an MCC larger than 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9 or 1.0.
In general, alternative methods of determining diagnostic accuracy are commonly used for continuous measures, when a disease category has not yet been clearly defined by the relevant medical societies and practice of medicine, where thresholds for therapeutic use are not yet established, or where there is no existing gold standard for diagnosis of the pre-disease. For continuous measures of risk, measures of diagnostic accuracy for a calculated index are typically based on curve fit and calibration between the predicted continuous value and the actual observed values (or a historical index
calculated value) and utilize measures such as R squared, Hosmer- Lemeshow -value statistics and confidence intervals. It is not unusual for predicted values using such algorithms to be reported including a confidence interval (usually 90% or 95% CI) based on a historical observed cohort's predictions, as in the test for risk of future breast cancer recurrence commercialized by Genomic Health, Inc. (Redwood City, California).
In general, by defining the degree of diagnostic accuracy, i.e., cut points on a ROC curve, defining an acceptable AUC value, and determining the acceptable ranges in relative concentration of what constitutes an effective amount of the determinants of the invention allows for one of skill in the art to use the determinants to identify, diagnose, or prognose subjects with a pre-determined level of predictability and performance.
Furthermore, other unlisted biomarkers will be very highly correlated with the determinants (for the purpose of this application, any two variables will be considered to be "very highly correlated" when they have a Coefficient of Determination (R ) of 0.5 or greater). Some aspects of the present invention encompass such functional and statistical equivalents to the aforementioned determinants. Furthermore, the statistical utility of such additional determinants is substantially dependent on the cross- correlation between multiple biomarkers and any new biomarkers will often be required to operate within a panel in order to elaborate the meaning of the underlying biology.
One or more of the listed determinants can be detected in the practice of the present invention, in some embodiments thereof. For example, two (2), three (3), four (4), five (5), ten (10), fifteen (15), twenty (20), forty (40), or more determinants can be detected.
In some aspects, all determinants listed herein can be detected. Preferred ranges from which the number of determinants can be detected include ranges bounded by any minimum selected from between one and, particularly two, three, four, five, six, seven, eight, nine ten, twenty, or forty. Particularly preferred ranges include two to five (2-5), two to ten (2-10), two to twenty (2-20), or two to forty (2-40).
Construction of determinant Panels
Groupings of determinants can be included in "panels", also called "determinant- signatures", "determinant signatures", or "multi-determinant signatures." A "panel" within the context of the present invention means a group of biomarkers (whether they
are determinants, clinical parameters, or traditional laboratory risk factors) that includes one or more determinants. A panel can also comprise additional biomarkers, e.g., clinical parameters, traditional laboratory risk factors, known to be present or associated with infection, in combination with a selected group of the determinants listed herein.
As noted above, many of the individual determinants, clinical parameters, and traditional laboratory risk factors listed, when used alone and not as a member of a multi-biomarker panel of determinants, have little or no clinical use in reliably distinguishing individual normal subjects, subjects at risk for having an infection (e.g., bacterial, viral or co-infection), and thus cannot reliably be used alone in classifying any subject between those three states. Even where there are statistically significant differences in their mean measurements in each of these populations, as commonly occurs in studies which are sufficiently powered, such biomarkers may remain limited in their applicability to an individual subject, and contribute little to diagnostic or prognostic predictions for that subject. A common measure of statistical significance is the p-value, which indicates the probability that an observation has arisen by chance alone; preferably, such p-values are 0.05 or less, representing a 5% or less chance that the observation of interest arose by chance. Such p-values depend significantly on the power of the study performed.
Despite this individual determinant performance, and the general performance of formulas combining only the traditional clinical parameters and few traditional laboratory risk factors, the present inventors have noted that certain specific combinations of two or more determinants can also be used as multi-biomarker panels comprising combinations of determinants that are known to be involved in one or more physiological or biological pathways, and that such information can be combined and made clinically useful through the use of various formulae, including statistical classification algorithms and others, combining and in many cases extending the performance characteristics of the combination beyond that of the individual determinants. These specific combinations show an acceptable level of diagnostic accuracy, and, when sufficient information from multiple determinants is combined in a trained formula, they often reliably achieve a high level of diagnostic accuracy transportable from one population to another.
The general concept of how two less specific or lower performing determinants are combined into novel and more useful combinations for the intended indications, is a key aspect of some embodiments of the invention. Multiple biomarkers can yield significant improvement in performance compared to the individual components when proper mathematical and clinical algorithms are used; this is often evident in both sensitivity and specificity, and results in a greater AUC or MCC. Significant improvement in performance could mean an increase of 1%, 2%, 3%, 4%, 5%, 8%, 10% or higher than 10% in different measures of accuracy such as total accuracy, AUC, MCC, sensitivity, specificity, PPV or NPV. Secondly, there is often novel unperceived information in the existing biomarkers, as such was necessary in order to achieve through the new formula an improved level of sensitivity or specificity. This hidden information may hold true even for biomarkers which are generally regarded to have suboptimal clinical performance on their own. In fact, the suboptimal performance in terms of high false positive rates on a single biomarker measured alone may very well be an indicator that some important additional information is contained within the biomarker results - information which would not be elucidated absent the combination with a second biomarker and a mathematical formula.
On the other hand, it is often useful to restrict the number of measured diagnostic determinants (e.g., protein biomarkers), as this allows significant cost reduction and reduces required sample volume and assay complexity. Accordingly, even when two signatures have similar diagnostic performance (e.g., similar AUC or sensitivity), one which incorporates fewer proteins could have significant utility and ability to reduce to practice. For example, a signature that includes 5 proteins compared to 10 proteins and performs similarly has many advantages in real world clinical setting and thus is desirable. Therefore, there is value and invention in being able to reduce the number of proteins incorporated in a signature while retaining similar levels of accuracy. In this context similar levels of accuracy could mean plus or minus 1%, 2%, 3%, 4%, 5%, 8%, or 10% in different measures of accuracy such as total accuracy, AUC, MCC, sensitivity, specificity, PPV or NPV; a significant reduction in the number of genes of a signature includes reducing the number of genes by 2, 3, 4, 5, 6, 7, 8, 9, 10 or more than 10 genes.
Several statistical and modeling algorithms known in the art can be used to both assist in determinant selection choices and optimize the algorithms combining these choices. Statistical tools such as factor and cross-biomarker correlation/covariance analyses allow more rationale approaches to panel construction. Mathematical clustering and classification tree showing the Euclidean standardized distance between the determinants can be advantageously used. Pathway informed seeding of such statistical classification techniques also may be employed, as may rational approaches based on the selection of individual determinants based on their participation across in particular pathways or physiological functions.
Ultimately, formula such as statistical classification algorithms can be directly used to both select determinants and to generate and train the optimal formula necessary to combine the results from multiple determinants into a single index. Often, techniques such as forward (from zero potential explanatory parameters) and backwards selection (from all available potential explanatory parameters) are used, and information criteria, such as AIC or BIC, are used to quantify the tradeoff between the performance and diagnostic accuracy of the panel and the number of determinants used. The position of the individual determinant on a forward or backwards selected panel can be closely related to its provision of incremental information content for the algorithm, so the order of contribution is highly dependent on the other constituent determinants in the panel.
Construction of Clinical Algorithms
Any formula may be used to combine determinant results into indices useful in the practice of the invention. As indicated above, and without limitation, such indices may indicate, among the various other indications, the probability, likelihood, absolute or relative risk, time to or rate of conversion from one to another disease states, or make predictions of future biomarker measurements of infection. This may be for a specific time period or horizon, or for remaining lifetime risk, or simply be provided as an index relative to another reference subject population.
Although various preferred formula are described here, several other model and formula types beyond those mentioned herein and in the definitions above are well known to one skilled in the art. The actual model type or formula used may itself be selected from the field of potential models based on the performance and diagnostic
accuracy characteristics of its results in a training population. The specifics of the formula itself may commonly be derived from determinant results in the relevant training population. Amongst other uses, such formula may be intended to map the feature space derived from one or more determinant inputs to a set of subject classes (e.g. useful in predicting class membership of subjects as normal, having an infection), to derive an estimation of a probability function of risk using a Bayesian approach, or to estimate the class -conditional probabilities, then use Bayes' rule to produce the class probability function as in the previous case.
Preferred formulas include the broad class of statistical classification algorithms, and in particular the use of discriminant analysis. The goal of discriminant analysis is to predict class membership from a previously identified set of features. In the case of linear discriminant analysis (LDA), the linear combination of features is identified that maximizes the separation among groups by some criteria. Features can be identified for LDA using an eigengene based approach with different thresholds (ELDA) or a stepping algorithm based on a multivariate analysis of variance (MANOVA). Forward, backward, and stepwise algorithms can be performed that minimize the probability of no separation based on the Ho telling- Lawley statistic.
Eigengene-based Linear Discriminant Analysis (ELDA) is a feature selection technique developed by Shen et al. (2006). The formula selects features (e.g. biomarkers) in a multivariate framework using a modified eigen analysis to identify features associated with the most important eigenvectors. "Important" is defined as those eigenvectors that explain the most variance in the differences among samples that are trying to be classified relative to some threshold.
A support vector machine (SVM) is a classification formula that attempts to find a hyperplane that separates two classes. This hyperplane contains support vectors, data points that are exactly the margin distance away from the hyperplane. In the likely event that no separating hyperplane exists in the current dimensions of the data, the dimensionality is expanded greatly by projecting the data into larger dimensions by taking non-linear functions of the original variables (Venables and Ripley, 2002). Although not required, filtering of features for SVM often improves prediction. Features (e.g., biomarkers) can be identified for a support vector machine using a non- parametric Kruskal-Wallis (KW) test to select the best univariate features. A random
forest (RF, Breiman, 2001) or recursive partitioning (RPART, Breiman et al., 1984) can also be used separately or in combination to identify biomarker combinations that are most important. Both KW and RF require that a number of features be selected from the total. RPART creates a single classification tree using a subset of available biomarkers.
Other formula may be used in order to pre-process the results of individual determinant measurements into more valuable forms of information, prior to their presentation to the predictive formula. Most notably, normalization of biomarker results, using either common mathematical transformations such as logarithmic or logistic functions, as normal or other distribution positions, in reference to a population's mean values, etc. are all well known to those skilled in the art. Of particular interest are a set of normalizations based on clinical-determinants such as time from symptoms, gender, race, or sex, where specific formula are used solely on subjects within a class or continuously combining a clinical-determinants as an input. In other cases, analyte-based biomarkers can be combined into calculated variables which are subsequently presented to a formula.
In addition to the individual parameter values of one subject potentially being normalized, an overall predictive formula for all subjects, or any known class of subjects, may itself be recalibrated or otherwise adjusted based on adjustment for a population's expected prevalence and mean biomarker parameter values, according to the technique outlined in D'Agostino et al., (2001) JAMA 286: 180-187, or other similar normalization and recalibration techniques. Such epidemiological adjustment statistics may be captured, confirmed, improved and updated continuously through a registry of past data presented to the model, which may be machine readable or otherwise, or occasionally through the retrospective query of stored samples or reference to historical studies of such parameters and statistics. Additional examples that may be the subject of formula recalibration or other adjustments include statistics used in studies by Pepe, M.S. et al., 2004 on the limitations of odds ratios; Cook, N.R., 2007 relating to ROC curves. Finally, the numeric result of a classifier formula itself may be transformed post-processing by its reference to an actual clinical population and study results and observed endpoints, in order to calibrate to absolute risk and provide confidence intervals for varying numeric results of the classifier or risk formula.
There are various ways (and formulations) to combine two biomarkers into one predictive score. For example, using dual cutoffs - one for each biomarker, generates a quadrary separation pattern that can separate between bacterial, viral and mixed (bacterial-viral co-infection) patients. For some biomarkers, adding another cutoff also enables the identification of healthy patients by generating a separation pattern composed of six units. Alternatively, the separation between bacterial and viral patients could be based on the ratio between the two biomarkers. Using a defined cutoff for the ratio between the two biomarkers generates a line that separates between bacterial and viral zones.
Another way to combine two biomarkers is using statistical classification algorithms that can generate various unique separation hyperplanes that distinguish between two groups of patients with high levels of accuracy in a cutoff independent manner. Importantly, cutoff independent models (generated for example using statistical classification algorithms) can provide a likelihood score (e.g., 90% chance for bacterial infection) compared to a binary result (bacterial or viral result only) obtained using defined cutoffs and a quadrary/six units separation patterns. Thus, it can provide additional clinical information that can guide correct patient management. Examples for statistical classification algorithms include Artificial Neural Networks (ANN), Support Vector Machines (SVM), Bayesian Networks (BN), K-Nearest Neighbor (KNN) and Logistic Regression.
Thus, certain embodiments of this invention include combining two polypeptides, the first being TRAIL and the second being selected from the list of polypeptides that includes for example CRP, PCT, IL-6, IP-10, MXl, ILIRA for early ruling in of bacterial infections.
In another embodiment, the separation is based on the ratio between the two biomarkers using a defined cutoff.
In yet another embodiment, the combination of the two biomarkers is performed in a cutoff independent manner using statistical classification algorithms.
Some determinants may exhibit trends that depends on the patient age (e.g. the population baseline may rise or fall as a function of age). One can use an 'Age dependent normalization or stratification' scheme to adjust for age related differences. Performing age dependent normalization, stratification or distinct mathematical
formulas can be used to improve the accuracy of determinants for differentiating between different types of infections. For example, one skilled in the art can generate a function that fits the population mean levels of each determinant as function of age and use it to normalize the determinant of individual subjects levels across different ages. Another example is to stratify subjects according to their age and determine age specific thresholds or index values for each age group independently.
In the context of the present invention the following statistical terms may be used:
"TP" is true positive, means positive test result that accurately reflects the tested-for activity. For example in the context of the present invention a TP, is for example but not limited to, truly classifying a bacterial infection as such.
"TN" is true negative, means negative test result that accurately reflects the tested-for activity. For example in the context of the present invention a TN, is for example but not limited to, truly classifying a viral infection as such.
"FN" is false negative, means a result that appears negative but fails to reveal a situation. For example in the context of the present invention a FN, is for example but not limited to, falsely classifying a bacterial infection as a viral infection.
"FP" is false positive, means test result that is erroneously classified in a positive category. For example in the context of the present invention a FP, is for example but not limited to, falsely classifying a viral infection as a bacterial infection.
"Sensitivity" is calculated by TP/(TP+FN) or the true positive fraction of disease subjects.
"Specificity" is calculated by TN/(TN+FP) or the true negative fraction of non- disease or normal subjects.
"Total accuracy" is calculated by (TN + TP)/(TN + FP +TP + FN).
"Positive predictive value" or "PPV" is calculated by TP/(TP+FP) or the true positive fraction of all positive test results. It is inherently impacted by the prevalence of the disease and pre-test probability of the population intended to be tested.
"Negative predictive value" or "NPV" is calculated by TN/(TN + FN) or the true negative fraction of all negative test results. It also is inherently impacted by the prevalence of the disease and pre-test probability of the population intended to be tested. See, e.g., O'Marcaigh AS, Jacobson RM, "Estimating The Predictive Value Of
A Diagnostic Test, How To Prevent Misleading Or Confusing Results," Clin. Ped. 1993, 32(8): 485-491, which discusses specificity, sensitivity, and positive and negative predictive values of a test, e.g., a clinical diagnostic test.
"MCC" (Mathwes Correlation coefficient) is calculated as follows: MCC = (TP * TN - FP * FN) / {(TP + FN) * (TP + FP) * (TN + FP) * (TN + FN)}A0.5 where TP, FP, TN, FN are true-positives, false-positives, true-negatives, and false-negatives, respectively. Note that MCC values range between -1 to +1, indicating completely wrong and perfect classification, respectively. An MCC of 0 indicates random classification. MCC has been shown to be a useful for combining sensitivity and specificity into a single metric (Baldi, Brunak et al. 2000). It is also useful for measuring and optimizing classification accuracy in cases of unbalanced class sizes (Baldi, Brunak et al. 2000).
Often, for binary disease state classification approaches using a continuous diagnostic test measurement, the sensitivity and specificity is summarized by a Receiver Operating Characteristics (ROC) curve according to Pepe et al., "Limitations of the Odds Ratio in Gauging the Performance of a Diagnostic, Prognostic, or Screening Marker," Am. J. Epidemiol 2004, 159 (9): 882-890, and summarized by the Area Under the Curve (AUC) or c-statistic, an indicator that allows representation of the sensitivity and specificity of a test, assay, or method over the entire range of test (or assay) cut points with just a single value. See also, e.g., Shultz, "Clinical Interpretation Of Laboratory Procedures," chapter 14 in Teitz, Fundamentals of Clinical Chemistry, Burtis and Ashwood (eds.), 4th edition 1996, W.B. Saunders Company, pages 192-199; and Zweig et al., "ROC Curve Analysis: An Example Showing The Relationships Among Serum Lipid And Apolipoprotein Concentrations In Identifying Subjects With Coronory Artery Disease," Clin. Chem., 1992, 38(8): 1425-1428. An alternative approach using likelihood functions, odds ratios, information theory, predictive values, calibration (including goodness-of-fit), and reclassification measurements is summarized according to Cook, "Use and Misuse of the Receiver Operating Characteristic Curve in Risk Prediction," Circulation 2007, 115: 928-935.
"Accuracy" refers to the degree of conformity of a measured or calculated quantity (a test reported value) to its actual (or true) value. Clinical accuracy relates to the proportion of true outcomes (true positives (TP) or true negatives (TN) versus
misclassified outcomes (false positives (FP) or false negatives (FN)), and may be stated as a sensitivity, specificity, positive predictive values (PPV) or negative predictive values (NPV), Matheus correlation coefficient (MCC), or as a likelihood, odds ratio, Receiver Operating Characteristic (ROC) curve, Area Under the Curve (AUC) among other measures.
A "formula," "algorithm," or "model" is any mathematical equation, algorithmic, analytical or programmed process, or statistical technique that takes one or more continuous or categorical inputs (herein called "parameters") and calculates an output value, sometimes referred to as an "index" or "index value". Non-limiting examples of "formulas" include sums, ratios, and regression operators, such as coefficients or exponents, biomarker value transformations and normalizations (including, without limitation, those normalization schemes based on clinical-determinants, such as gender, age, or ethnicity), rules and guidelines, statistical classification models, and neural networks trained on historical populations. Of particular use in combining determinants are linear and non-linear equations and statistical classification analyses to determine the relationship between levels of determinants detected in a subject sample and the subject's probability of having an infection or a certain type of infection. In panel and combination construction, of particular interest are structural and syntactic statistical classification algorithms, and methods of index construction, utilizing pattern recognition features, including established techniques such as cross-correlation, Principal Components Analysis (PCA), factor rotation, Logistic Regression (LogReg), Linear Discriminant Analysis (LDA), Eigengene Linear Discriminant Analysis (ELDA), Support Vector Machines (SVM), Random Forest (RF), Recursive Partitioning Tree (RPART), as well as other related decision tree classification techniques, Shrunken Centroids (SC), StepAIC, Kth-Nearest Neighbor, Boosting, Decision Trees, Neural Networks, Bayesian Networks, and Hidden Markov Models, among others. Other techniques may be used in survival and time to event hazard analysis, including Cox, Weibull, Kaplan-Meier and Greenwood models well known to those of skill in the art. Many of these techniques are useful either combined with a determinant selection technique, such as forward selection, backwards selection, or stepwise selection, complete enumeration of all potential panels of a given size, genetic algorithms, or they may themselves include biomarker selection methodologies in their
own technique. These may be coupled with information criteria, such as Akaike's Information Criterion (AIC) or Bayes Information Criterion (BIC), in order to quantify the tradeoff between additional biomarkers and model improvement, and to aid in minimizing overfit. The resulting predictive models may be validated in other studies, or cross-validated in the study they were originally trained in, using such techniques as Bootstrap, Leave-One-Out (LOO) and 10-Fold cross-validation (10-Fold CV). At various steps, false discovery rates may be estimated by value permutation according to techniques known in the art. A "health economic utility function" is a formula that is derived from a combination of the expected probability of a range of clinical outcomes in an idealized applicable patient population, both before and after the introduction of a diagnostic or therapeutic intervention into the standard of care. It encompasses estimates of the accuracy, effectiveness and performance characteristics of such intervention, and a cost and/or value measurement (a utility) associated with each outcome, which may be derived from actual health system costs of care (services, supplies, devices and drugs, etc.) and/or as an estimated acceptable value per quality adjusted life year (QALY) resulting in each outcome. The sum, across all predicted outcomes, of the product of the predicted population size for an outcome multiplied by the respective outcome's expected utility is the total health economic utility of a given standard of care. The difference between (i) the total health economic utility calculated for the standard of care with the intervention versus (ii) the total health economic utility for the standard of care without the intervention results in an overall measure of the health economic cost or value of the intervention. This may itself be divided amongst the entire patient group being analyzed (or solely amongst the intervention group) to arrive at a cost per unit intervention, and to guide such decisions as market positioning, pricing, and assumptions of health system acceptance. Such health economic utility functions are commonly used to compare the cost-effectiveness of the intervention, but may also be transformed to estimate the acceptable value per QALY the health care system is willing to pay, or the acceptable cost-effective clinical performance characteristics required of a new intervention.
For diagnostic (or prognostic) interventions of the invention, as each outcome
(which in a disease classifying diagnostic test may be a TP, FP, TN, or FN) bears a different cost, a health economic utility function may preferentially favor sensitivity
over specificity, or PPV over NPV based on the clinical situation and individual outcome costs and value, and thus provides another measure of health economic performance and value which may be different from more direct clinical or analytical performance measures. These different measurements and relative trade-offs generally will converge only in the case of a perfect test, with zero error rate (a.k.a., zero predicted subject outcome misclassifications or FP and FN), which all performance measures will favor over imperfection, but to differing degrees.
"Analytical accuracy" refers to the reproducibility and predictability of the measurement process itself, and may be summarized in such measurements as coefficients of variation (CV), Pearson correlation, and tests of concordance and calibration of the same samples or controls with different times, users, equipment and/or reagents. These and other considerations in evaluating new biomarkers are also summarized in Vasan, 2006.
"Performance" is a term that relates to the overall usefulness and quality of a diagnostic or prognostic test, including, among others, clinical and analytical accuracy, other analytical and process characteristics, such as use characteristics (e.g., stability, ease of use), health economic value, and relative costs of components of the test. Any of these factors may be the source of superior performance and thus usefulness of the test, and may be measured by appropriate "performance metrics," such as AUC and MCC, time to result, shelf life, etc. as relevant.
By "statistically significant", it is meant that the alteration is greater than what might be expected to happen by chance alone (which could be a "false positive"). Statistical significance can be determined by any method known in the art. Commonly used measures of significance include the p-value, which presents the probability of obtaining a result at least as extreme as a given data point, assuming the data point was the result of chance alone. A result is often considered highly significant at a p-value of 0.05 or less.
In the context of the present invention the following abbreviations may be used: Antibiotics (Abx), Adverse Event (AE), Arbitrary Units (A.U.), Complete Blood Count (CBC), Case Report Form (CRF), Chest X-Ray (CXR), Electronic Case Report Form (eCRF), Food and Drug Administration (FDA), Good Clinical Practice (GCP), Gastrointestinal (GI), Gastroenteritis (GE), International Conference on Harmonization
(ICH), Infectious Disease (ID), In vitro diagnostics (IVD), Lower Respiratory Tract Infection (LRTI), Myocardial infarction (MI), Polymerase chain reaction (PCR), Per- oss (P.O), Per-rectum (P.R), Standard of Care (SoC), Standard Operating Procedure (SOP), Urinary Tract Infection (UTI), Upper Respiratory Tract Infection (URTI).
As used herein the term "about" refers to ± 10 %.
The terms "comprises", "comprising", "includes", "including", "having" and their conjugates mean "including but not limited to".
The term "consisting of means "including and limited to".
The term "consisting essentially of" means that the composition, method or structure may include additional ingredients, steps and/or parts, but only if the additional ingredients, steps and/or parts do not materially alter the basic and novel characteristics of the claimed composition, method or structure.
As used herein, the singular form "a", "an" and "the" include plural references unless the context clearly dictates otherwise. For example, the term "a compound" or "at least one compound" may include a plurality of compounds, including mixtures thereof.
Throughout this application, various embodiments of this invention may be presented in a range format. It should be understood that the description in range format is merely for convenience and brevity and should not be construed as an inflexible limitation on the scope of the invention. Accordingly, the description of a range should be considered to have specifically disclosed all the possible subranges as well as individual numerical values within that range. For example, description of a range such as from 1 to 6 should be considered to have specifically disclosed subranges such as from 1 to 3, from 1 to 4, from 1 to 5, from 2 to 4, from 2 to 6, from 3 to 6 etc., as well as individual numbers within that range, for example, 1, 2, 3, 4, 5, and 6. This applies regardless of the breadth of the range.
Whenever a numerical range is indicated herein, it is meant to include any cited numeral (fractional or integral) within the indicated range. The phrases "ranging/ranges between" a first indicate number and a second indicate number and "ranging/ranges from" a first indicate number "to" a second indicate number are used herein interchangeably and are meant to include the first and second indicated numbers and all the fractional and integral numerals therebetween.
As used herein the term "method" refers to manners, means, techniques and procedures for accomplishing a given task including, but not limited to, those manners, means, techniques and procedures either known to, or readily developed from known manners, means, techniques and procedures by practitioners of the chemical, pharmacological, biological, biochemical and medical arts.
As used herein, the term "treating" includes abrogating, substantially inhibiting, slowing or reversing the progression of a condition, substantially ameliorating clinical or aesthetical symptoms of a condition or substantially preventing the appearance of clinical or aesthetical symptoms of a condition.
It is appreciated that certain features of the invention, which are, for clarity, described in the context of separate embodiments, may also be provided in combination in a single embodiment. Conversely, various features of the invention, which are, for brevity, described in the context of a single embodiment, may also be provided separately or in any suitable subcombination or as suitable in any other described embodiment of the invention. Certain features described in the context of various embodiments are not to be considered essential features of those embodiments, unless the embodiment is inoperative without those elements.
Although the invention has been described in conjunction with specific embodiments thereof, it is evident that many alternatives, modifications and variations will be apparent to those skilled in the art. Accordingly, it is intended to embrace all such alternatives, modifications and variations that fall within the spirit and broad scope of the appended claims.
All publications, patents and patent applications mentioned in this specification are herein incorporated in their entirety by reference into the specification, to the same extent as if each individual publication, patent or patent application was specifically and individually indicated to be incorporated herein by reference. In addition, citation or identification of any reference in this application shall not be construed as an admission that such reference is available as prior art to the present invention. To the extent that section headings are used, they should not be construed as necessarily limiting.
Various embodiments and aspects of the present invention as delineated hereinabove and as claimed in the claims section below find experimental support in the following examples.
EXAMPLES
Reference is now made to the following examples, which together with the above descriptions illustrate some embodiments of the invention in a non limiting fashion.
Generally, the nomenclature used herein and the laboratory procedures utilized in the present invention include molecular, biochemical, microbiological and recombinant DNA techniques. Such techniques are thoroughly explained in the literature. See, for example, "Molecular Cloning: A laboratory Manual" Sambrook et al., (1989); "Current Protocols in Molecular Biology" Volumes I-III Ausubel, R. M., ed. (1994); Ausubel et al., "Current Protocols in Molecular Biology", John Wiley and Sons, Baltimore, Maryland (1989); Perbal, "A Practical Guide to Molecular Cloning", John Wiley & Sons, New York (1988); Watson et al., "Recombinant DNA", Scientific American Books, New York; Birren et al. (eds) "Genome Analysis: A Laboratory Manual Series", Vols. 1-4, Cold Spring Harbor Laboratory Press, New York (1998); methodologies as set forth in U.S. Pat. Nos. 4,666,828; 4,683,202; 4,801,531; 5,192,659 and 5,272,057; "Cell Biology: A Laboratory Handbook", Volumes I-III Cellis, J. E., ed. (1994); "Culture of Animal Cells - A Manual of Basic Technique" by Freshney, Wiley- Liss, N. Y. (1994), Third Edition; "Current Protocols in Immunology" Volumes I-III Coligan J. E., ed. (1994); Stites et al. (eds), "Basic and Clinical Immunology" (8th Edition), Appleton & Lange, Norwalk, CT (1994); Mishell and Shiigi (eds), "Selected Methods in Cellular Immunology", W. H. Freeman and Co., New York (1980); available immunoassays are extensively described in the patent and scientific literature, see, for example, U.S. Pat. Nos. 3,791,932; 3,839,153; 3,850,752; 3,850,578; 3,853,987; 3,867,517; 3,879,262; 3,901,654; 3,935,074; 3,984,533; 3,996,345; 4,034,074; 4,098,876; 4,879,219; 5,011,771 and 5,281,521; "Oligonucleotide Synthesis" Gait, M. J., ed. (1984); "Nucleic Acid Hybridization" Hames, B. D., and Higgins S. J., eds. (1985); "Transcription and Translation" Hames, B. D., and Higgins S. J., eds. (1984); "Animal Cell Culture" Freshney, R. I., ed. (1986); "Immobilized Cells and Enzymes" IRL Press, (1986); "A Practical Guide to Molecular Cloning" Perbal, B., (1984) and "Methods in Enzymology" Vol. 1-317, Academic Press; "PCR Protocols: A Guide To Methods And Applications", Academic Press, San Diego, CA (1990); Marshak et al., "Strategies for Protein Purification and Characterization - A Laboratory Course Manual" CSHL Press (1996); all of which are incorporated by
reference as if fully set forth herein. Other general references are provided throughout this document. The procedures therein are believed to be well known in the art and are provided for the convenience of the reader. All the information contained therein is incorporated herein by reference.
Methods
Study population: 1002 patients with suspected acute infectious disease and non-infectious controls were prospectively recruited between August 2009 and November 2013 from Hillel-Yaffe and Bnai-Zion Medical Centers, Israel (NCT01917461). The study was approved by the Hillel-Yaffe Medical Center Institutional Review Board, and the Bnai-Zion Medical Center Institutional Review Board. The study was conducted according to the guidelines and recommendations of Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from each participant or legal guardian, as applicable.
Pediatric patients (<18 years) were recruited from pediatric emergency departments (PED), pediatric wards and surgical departments, and adults (>18 years) from emergency departments (ED), internal medicine departments and surgical departments. Informed consent was obtained from each participant or legal guardian, as applicable. Inclusion criteria for the infectious disease cohort included: clinical suspicion of an acute infectious disease, peak fever >37.5°C since symptoms onset, and duration of symptoms <12 days. Inclusion criteria for the control group included: clinical impression of a non-infectious disease (e.g. trauma, stroke and myocardial infarction), or healthy subjects. Exclusion criteria included: evidence of any episode of acute infectious disease in the two weeks preceding enrollment; diagnosed congenital immune deficiency; current treatment with immunosuppressive or immunomodulatory therapy; active malignancy, proven or suspected human immunodeficiency virus (HIV)- 1, hepatitis B virus (HBV), or hepatitis C virus (HCV) infection. Importantly, in order to enable broad generalization, antibiotic treatment at enrollment did not cause exclusion from the study.
Enrollment process and data collection: For each patient, the following baseline variables were recorded: demographics, physical examination, medical history (e.g. main complaints, underlying diseases, chronically-administered medications, comorbidities, time of symptom onset, and peak temperature), complete blood count
(CBC) obtained at enrollment, and chemistry panel (e.g. creatinine, urea, electrolytes, and liver enzymes). A nasal swab was obtained from each patient for further microbiological investigation, and a blood sample was obtained for protein screening and validation. Additional samples were obtained as deemed appropriate by the physician (e.g. urine and stool samples in cases of suspected urinary tract infection [UTI], and gastroenteritis [GI] respectively). Radiological tests were obtained at the discretion of the physician (e.g. chest X-ray for suspected lower respiratory tract infection [LRTI]). Thirty days after enrollment, disease course and response to treatment were recorded. All information was recorded in a custom electronic case report form (eCRF).
Microbiological investigation: Patients underwent two multiplex-PCR diagnostic assays from nasal swab samples: (i) Seeplex® RV15 (n=713), for detection of parainfluenza virus 1, 2, 3, and 4, coronavirus 229E/NL63, adenovirus A/B/C/D/E, bocavirus 1/2/3/4, influenza virus A and B, metapneumovirus, coronavirus OC43, rhinovirus A/B/C, respiratory syncytial virus A and B, and Enterovirus, and (ii) Seeplex® PB6 (n=633) for detection of Streptococcus pneumoniae, Haemophilus influenzae, Chlamydophila pneumoniae, Legionella pneumophila, Bordetella pertussis, and Mycoplasma pneumoniae. Multiplex-PCR assays were performed by a certified service laboratory. Patients were also tested for additional pathogens according to their suspected clinical syndrome, including: blood culture (n=420), urine culture (n=188) and stool culture for Shigella spp., Campylobacter spp. and Salmonella spp. (n=66); serological testing (IgM and/or IgG) for cytomegalovirus (CMV), Epstein-Barr virus (EBV), Mycoplasma Pneumonia, and Coxiella burnetii (Q-Fever) (n=167, n=130, n=206 and n=41 respectively).
Establishing the reference standard: A rigorous composite reference standard was created following recommendations of the Standards for Reporting of Diagnostic Accuracy (STARD; Figure l).1 First, a thorough clinical and microbiological investigation was performed for each patient as described above. Then, all the data collected throughout the disease course was reviewed by a panel of three physicians. For adult patients (>18 years) the panel included the attending physician and two infectious disease specialists, while for children and adolescents (<18 years) it included the attending pediatrician, an infectious disease expert and a senior attending
pediatrician. Each panel member assigned one of the following diagnostic labels to each patient: (i) bacterial; (ii) viral; (iii) no apparent infectious disease or healthy (controls); and (iv) mixed infections (bacteria plus virus). Importantly, the panel members were blinded to the labeling of their peers and to the results of the signature.
Samples, procedures and protein measurements: Venous blood samples were stored at 4 °C for up to 5 hours on site and subsequently fractionated into plasma, serum and total leukocytes and stored at -80 °C. Nasal swabs and stool samples were stored at 4 °C for up to 72 hours and subsequently transported to a certified service laboratory for multiplex PCR-based assay. TRAIL protein was measured using commercial ELISA kits (MeMed Diagnostics).
Statistical analysis: The primary analysis was based on area under the receiver operating characteristics curve (AUC), Sensitivity (TP/P), Specificity (TN/N), Positive predictive value (PPV = TP / [TP+FP]), Negative predictive value (NPV = TN / [TN+FN]), where P, N, TP and TN correspond to positives (bacterial patients), negatives (viral patients), true positives (correctly diagnosed bacterial patients), and true negatives (correctly diagnosed viral patients), respectively. Statistical analysis was performed with MATLAB.
RESULTS
Patient characteristics: Three physicians independently assigned a label to each patient (either bacterial, viral, controls, or indeterminate). 98 patients were labeled as indeterminate, because the physicians could not establish disease etiology or there was no majority labeling. A detailed characterization of the analyzed cohort is depicted in FIGs. 2-7. Briefly, the cohort was balanced with respect to gender (47% females, 53% males) and included 56% pediatric patients (<18 years) and 44% adults (>18 years). Patients presented with a wide range of clinical syndromes (e.g. RTI, UTI, and systemic infections), maximal temperatures (36-41.5°C), and time from symptoms onset (0-12 days). Altogether, 56 pathogen species were detected that are responsible for the vast majority of acute infectious diseases in the Western world.
TRAIL as a diagnostic marker for diagnosing bacterial infections TRAIL is a valuable biomarker for distinguishing between bacterial and viral infections as unlike known biomarkers, the serum levels of TRAIL decrease in response to bacterial infections and increase in response to viral infections (Figure 8). The
accuracy levels of TRAIL in distinguishing between bacterial and viral infections depend on the cutoff that is used. Table 4 presents the measures of accuracy in two exemplary TRAIL cutoffs (70 and 85 pg/ml). Table 4. Measures of accuracy of TRAIL in distinguishing between patients with bacterial (n=319) and viral (n=334) infections, using different cutoffs as indicated.

The present inventors further evaluated the ability of TRAIL to distinguish between bacterial and viral infections in various patient sub-groups. Patients were stratified according to several categories (i.e., clinical syndrome; specific pathogen; and age), and measures of accuracy were calculated for TRAIL using exemplary cutoffs.
Examples of Specific pathogens
TRAIL presented superior performances in disguising between E.coli, Group A Strep, or Enterococcus faecalis and viruses affecting the same physiological system in the exemplary TRAIL cutoffs that were evaluated (Tables 5 and 6). Table 5. Measures of accuracy of TRAIL in distinguishing between patients with viral and different bacterial infections as indicated (TRAIL cutoffs 70 pg/ml).
Bacteria was compared to virus affecting the same physiological system as indicated.
Physiological
Bacteria Sensitivity Specificity
system
Urinary,
E.coli 0.89 0.83
systemic
Group A Strep 0.93 0.79 Respiratory,
systemic, skin
Urinary,
Enterococcus faecalis 1.00 0.83
systemic
Table 6. Measures of accuracy of TRAIL in distinguishing between patients with viral and different bacterial infections as indicated (TRAIL cutoff 85 pg/ml). Bacteria was compared to virus affecting the same physiological system as indicated.

Examples of Clinical syndromes
TRAIL presented superior performances in disguising between bacterial and viral infections in patients with various clinical syndromes including serious bacterial infection (SBI), upper respiratory tract infection (UTRI), lower respiratory tract infection (LRTI), and fever without source (FWS; Table 7).
Table 7. Measures of accuracy of TRAIL (cutoff 85 pg/ml) in distinguishing between viral and bacterial infections in patients presented with different clinical syndromes as indicated (SBI - serious bacterial infection; UTRI - upper respiratory tract infection; LRTI - lower respiratory tract infection; FWS - fever without source).
Clinical syndrome Sensitivity Specificity
SBI 0.90 0.47
URTI 0.97 0.66
LRTI 0.85 0.53
FWS 0.92 0.72
Age
TRAIL accuracy measures exhibit some level of difference. For example, sensitivity of TRAIL was higher in the adults group (>18 years old), while the specificity was higher in the pediatric group (<18 years old; Table 8; TRAIL cutoff 70 pg/ml).
Table 8. Measures of accuracy of TRAIL (cutoff 70 pg/ml) in distinguishing between viral and bacterial infections in adult (n=251) and pediatric (n=402) patients as indicated.

TRAIL is particularly useful for early diagnosis of bacterial infections
Delayed or no antibiotic treatment in cases of bacterial disease is very common (24%-40% of all bacterial infections) , and can lead to disease-related complications resulting in increased rates of morbidity and mortality 8—10. Thus, timely identification of patients with bacterial infection is of great importance to guide correct patient management. The present inventors therefore, evaluated the performance of TRAIL in different stages of disease progression. Interestingly, it was found that TRAIL levels are already significantly different in patients with bacterial and viral infection at the first days from symptoms onset (Figure 10). Moreover, the accuracy levels of TRAIL in distinguishing between patients with bacterial and viral infections were higher in the first days following symptoms onset using different TRAIL cutoffs (Tables 9 and 10).
Table 9. Measures of accuracy of TRAIL (cutoff 85 pg/ml) in distinguishing between viral and bacterial infections in different days from symptoms onset as indicated.
Days 0-1 Days >1 Days 0-2 Days >2
Sensitivity 0.93 0.89 0.92 0.89
Specificity 0.67 0.66 0.69 0.64
Table 10. Measures of accuracy of TRAIL (cutoff 70 pg/tnl) in distinguishing between viral and bacterial infections in different days from symptoms onset as indicated.

Although the invention has been described in conjunction with specific embodiments thereof, it is evident that many alternatives, modifications and variations will be apparent to those skilled in the art. Accordingly, it is intended to embrace all such alternatives, modifications and variations that fall within the spirit and broad scope of the appended claims.
All publications, patents and patent applications mentioned in this specification are herein incorporated in their entirety by reference into the specification, to the same extent as if each individual publication, patent or patent application was specifically and individually indicated to be incorporated herein by reference. In addition, citation or identification of any reference in this application shall not be construed as an admission that such reference is available as prior art to the present invention. To the extent that section headings are used, they should not be construed as necessarily limiting.
REFERENCES
1. Bossuyt, P. M. et al. The STARD Statement for Reporting Studies of Diagnostic Accuracy: Explanation and Elaboration. Ann Intern Med 138, W1-W12 (2003).
2. Kunze, W., Beier, D. & Groeger, K. Adenovirus Respiratory Infections In Children. Do They Mimic Bacterial Infections? (2010).
3. Oved, K. et al. A Novel Host-Proteome Signature for Distinguishing between Acute Bacterial and Viral Infections. PLoS ONE 10, e0120012 (2015).
4. Craig, J. C. et al. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ 340, (2010).
5. Dedier, J., Singer, D. E., Chang, Y., Moore, M. & Atlas, S. J. Processes of care, illness severity, and outcomes in the management of community-acquired pneumonia at academic hospitals. Arch. Intern. Med. 161, 2099-2104 (2001).
6. Caterino, J. M., Hiestand, B. C. & Martin, D. R. Quality of care in elder emergency department patients with pneumonia: a prospective cohort study. BMC Emerg Med 8, 6 (2008).
7. Houck, P. M. Timing of antibiotic administration and outcomes for medicare patients hospitalized with community- acquired pneumonia. Arch Intern Med 164, 637-644 (2004).
8. Zwart, S. et al. Penicillin for acute sore throat: randomised double blind trial of seven days versus three days treatment or placebo in adults. BMJ 320, 150-154 (2000).
9. Little, P. Delayed prescribing of antibiotics for upper respiratory tract infection. BMJ 331, 301-302 (2005).
10. Spiro, D. M. et al. Wait-and-see prescription for the treatment of acute otitis media: a randomized controlled trial. JAMA 296, 1235-1241 (2006).
11. Fauci AS & Marston HD. The perpetual challenge of antimicrobial resistance. JAMA (2014). doi: 10.1001/jama.2014.2465.
12. CDC - Get Smart: Fast Facts About Antibiotic Resistance. (2011). Available at: www(dot)cdc(dot)gov/getsmart/antibiotic-use/fast-facts(dot)html. (Accessed: 21st November 2011).
13. CDC - About Antimicrobial Resistance. (2011). Available at: www(dot)cdc(dot)gov/drugresistance/about(dot)html. (Accessed: 21st November 2011).
14. Niemz, A., Ferguson, T. M. & Boyle, D. S. Point-of-care nucleic acid testing for infectious diseases. Trends Biotechnol. 29, 240-250 (2011).
15. Craw, P. & Balachandran, W. Isothermal nucleic acid amplification technologies for point-of-care diagnostics: a critical review. Lab Chip 12, 2469-2486 (2012).
16. Kim, K. H., Shin, J. H. & Kim, S. Y. The Clinical Significance of Nasopharyngeal Carriages in Immunocompromised Children as Assessed. The Korean Journal of Hematology 44, 220 (2009).
17. Shin, J. H., Han, H. Y. & Kim, S. Y. Detection of nasopharyngeal carriages in children by multiplex reverse transcriptase-polymerase chain reaction. Korean Journal of Pediatrics 52, 1358 (2009).
18. Jung, C. L., Lee, M. A. & Chung, W. S. Clinical Evaluation of the Multiplex PCR Assay for the Detection of Bacterial Pathogens in Respiratory Specimens from Patients with Pneumonia. Korean Journal of Clinical Microbiology 13, 40 (2010).
19. Rhedin, S. et al. Clinical Utility of PCR for Common Viruses in Acute Respiratory Illness. Pediatrics peds.2013-3042 (2014). doi: 10.1542/peds.2013-3042.
20. Bogaert, D., De Groot, R. & Hermans, P. W. M. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis 4, 144- 154 (2004).
21. Spuesens, E. B. M. et al. Carriage of Mycoplasma pneumoniae in the Upper Respiratory Tract of Symptomatic and Asymptomatic Children: An Observational Study. PLoS Med 10, el001444 (2013).
22. Salvi, S. The silent epidemic of COPD in Africa. Lancet Glob Health 3, e6-7 (2015).
23. GOLD - the Global initiative for chronic Obstructive Lung Disease. Available at: www(dot)goldcopd(dot)org/guidelines-global-strategy-for-diagnosis- management(dot)html. (Accessed: 15th April 2015).
24. WHO I The top 10 causes of death. WHO Available at: www(dot)who(dot)int/mediacentre/factsheets/fs310/en/. (Accessed: 17th March 2015).
25. Global Problems, Smart Solutions. Cambridge University Press Available at:
www(dot)cambridge(dot)org/il/academic/subjects/economics/public-economics- and-public-policy/global-problems-smart-solutions-costs-and-benefits. (Accessed: 15th April 2015).
26. Hoogendoorn, M. Economic impact of COPD: Empirical and model- based studies on the cost-effectiveness of treatment options. Journal of Neurophysiology - J NEUROPHYSIOL (2011).
27. Hurst, J. R. et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 363, 1128-1138 (2010).
28. Kim, V. et al. Airway wall thickness is increased in COPD patients with bronchodilator responsiveness. Respir. Res. 15, 84 (2014).
29. Bhowmik, A., Seemungal, T. A., Sapsford, R. J. & Wedzicha, J. A. Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations. Thorax 55, 114-120 (2000).
30. Molyneaux, P. L. et al. Outgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 188, 1224-1231 (2013).
31. Taylor, A. E. et al. Defective macrophage phagocytosis of bacteria in COPD. Eur. Respir. J. 35, 1039-1047 (2010).
32. Sethi, S., Evans, N., Grant, B. J. B. & Murphy, T. F. New strains of bacteria and exacerbations of chronic obstructive pulmonary disease. N. Engl. J. Med. 347, 465-471 (2002).
33. Lin, C.-L. et al. MAnnose-binding lectin gene polymorphism contributes to recurrence of infective exacerbation in patients with copd. Chest 139, 43-51 (2011).
Claims
1. A method of ruling in a bacterial infection in a subject showing symptoms of an infection, the method comprising measuring the amount of TRAIL in a blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of said TRAIL is below a first predetermined level, a bacterial infection is ruled in.
2. The method of claim 1, wherein said bacterial infection is a group a streptococcal infection.
3. The method of claim 1, wherein when the amount of said TRAIL is above a second predetermined level, a viral infection is ruled in.
4. A method of determining a treatment regimen in a subject showing symptoms of a pathogenic infection comprising measuring the amount of TRAIL in a blood sample, said blood sample being derived from the subject no more than two days following symptom onset, wherein when the amount of said TRAIL is below a first predetermined level, the subject is recommended an anti-bacterial agent.
5. The method of claim 4, wherein when the amount of said TRAIL is above a second predetermined level, the subject is recommended an anti-viral agent.
6. A method of classifying an infection type of a subject comprising:
(a) analyzing for the presence of specific pathogen in a sample of the subject; and
(b) measuring the amount of TRAIL in a sample of the subject, wherein the presence of said specific pathogen and the amount of TRAIL is indicative of the infection type.
7. The method of claim 6, wherein said specific pathogen is selected from the group consisting of Influenza, Respiratory syncytial virus (RSV), Rhinovirus and Group A Streptococcus.
8. The method of claim 6, wherein said infection type comprises a pathogenic infection or a non-pathogenic infection.
9. The method of claim 6, wherein step (a) is effected following step (b).
10. The method of claim 6, wherein step (b) is effected following step (a).
11. A method of distinguishing between an infectious exacerbation state and a non-infectious exacerbation state of chronic obstructive pulmonary disease (COPD) or asthma of a subject comprising measuring the amount of TNF-related apoptosis- inducing ligand (TRAIL) in a blood sample derived from the subject, wherein said amount is indicative of the infectivity of the exacerbation state of COPD or asthma.
12. The method of claims 1 or 4, wherein said level is 70 pg/ml.
13. The method of any one of claims 1, 4, 6 or 11, wherein the subject has a normal level of creatine kinase.
14. The method of claims 3 or 5, wherein said first predetermined level and said second predetermined level are identical.
15. The method of claims 3 or 5, wherein said first predetermined level and said second predetermined level are non-identical.
16. The method of claim 1, wherein said symptoms of an infection comprise fever.
17. The method of claim 4, wherein said symptoms of a pathogenic infection comprise fever.
18. The method of any one of claims 1, 4, 6 or 11, wherein the sample is derived from the subject no more than one day following symptom onset.
19. The method of any one of claims 1, 4, 6 or 11, wherein the sample is whole blood or a fraction thereof.
20. The method of claim 19, wherein said fraction comprises serum.
21. The method of claim 19, wherein said blood fraction sample comprises cells selected from the group consisting of lymphocytes, monocytes and granulocytes.
22. The method of any one of claims 1-21, further comprising analyzing a level of C-reactive protein (CRP) and/or Interferon gamma-induced protein 10 (IP10).
23. The method of any one of claims 1-21, further comprising analyzing a level of a polypeptide selected from the group consisting of Interferon gamma-induced protein 10 (IP10), Interleukin 6 (IL-6), and Interleukin 1 receptor, type I (ILIRA).
24. The method of any one of claims 1-21, further comprising analyzing a level of a polypeptide selected from the group consisting of Interferon gamma-induced protein 10 (IP10), Interleukin 6 (IL-6), Interleukin 1 receptor, type I (ILIRA), C- reactive protein (CRP) and procalcitonin (PCT).
25. The method of any one of claims 1-21, wherein said TRAIL is measured using a lateral flow immunoassay.
26. The method of any one of claims 1-25, wherein said TRAIL is measured using an antibody which binds specifically to TRAIL.
27. The method of claim 26, wherein said antibody is a monoclonal antibody.
28. A method of treating a subject showing symptoms of an infection comprising:
(a) determining a treatment regimen according to claim 4 and;
(b) treating the subject according to the results of the determining.
29. The method of claim 28, wherein said treating comprises administering to the subject a therapeutically effective amount of an anti-bacterial agent.
30. The method of claims 4 or 28, wherein said anti-bacterial agent is an antibiotic.
31. A method of diagnosing an infection in a subject showing symptoms of an infection, the method comprising measuring the amount of IP 10 in a blood sample being derived from the subject no more than two days following symptom onset, wherein the amount of said IPIO is indicative of the infection.
32. The method of claim 31, wherein when the amount is above a predetermined level a viral infection is ruled in.
33. The method of claim 31, wherein when the amount is below a predetermined level, an infection is ruled out.
34. The method of any one of claims 31-33, further comprising analyzing a level of a polypeptide selected from the group consisting of TRAIL, Interleukin 6 (IL- 6), and Interleukin 1 receptor, type I (IL1RA).
35. The method of any one of claims 31-33, further comprising analyzing a level of a polypeptide selected from the group consisting of Interferon gamma-induced
protein 10 (IP10), Interleukin 6 (IL-6), Interleukin 1 receptor, type I (ILIRA), C- reactive protein (CRP) and procalcitonin (PCT).
Priority Applications (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP22204952.0A EP4184167A1 (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infections |
| US16/316,631 US11340223B2 (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infections |
| CN201780055347.8A CN109804245B (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infection |
| EP17827122.7A EP3482201B1 (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infections |
| US17/717,200 US12055545B2 (en) | 2016-07-10 | 2022-04-11 | Early diagnosis of infections |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201662360420P | 2016-07-10 | 2016-07-10 | |
| US62/360,420 | 2016-07-10 |
Related Child Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US16/316,631 A-371-Of-International US11340223B2 (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infections |
| US17/717,200 Continuation US12055545B2 (en) | 2016-07-10 | 2022-04-11 | Early diagnosis of infections |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2018011796A1 true WO2018011796A1 (en) | 2018-01-18 |
Family
ID=60952344
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/IL2017/050781 WO2018011796A1 (en) | 2016-07-10 | 2017-07-10 | Early diagnosis of infections |
Country Status (4)
| Country | Link |
|---|---|
| US (2) | US11340223B2 (en) |
| EP (2) | EP4184167A1 (en) |
| CN (1) | CN109804245B (en) |
| WO (1) | WO2018011796A1 (en) |
Cited By (12)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10209260B2 (en) | 2017-07-05 | 2019-02-19 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| US10303846B2 (en) | 2014-08-14 | 2019-05-28 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US10502739B2 (en) | 2012-02-09 | 2019-12-10 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| US10859574B2 (en) | 2014-10-14 | 2020-12-08 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections in non-human subjects and methods of use thereof |
| WO2020251460A1 (en) * | 2019-06-14 | 2020-12-17 | Delaval Holding Ab | System for determining validity of a lateral flow test result |
| US11131671B2 (en) | 2016-07-10 | 2021-09-28 | Memed Diagnostics Ltd. | Protein signatures for distinguishing between bacterial and viral infections |
| WO2021204984A1 (en) | 2020-04-09 | 2021-10-14 | B.R.A.H.M.S Gmbh | Biomarkers for the diagnosis of respiratory tract infections |
| US11340223B2 (en) | 2016-07-10 | 2022-05-24 | Memed Diagnostics Ltd. | Early diagnosis of infections |
| US11353456B2 (en) | 2016-09-29 | 2022-06-07 | Memed Diagnostics Ltd. | Methods of risk assessment and disease classification for appendicitis |
| US11385241B2 (en) | 2016-09-29 | 2022-07-12 | Memed Diagnostics Ltd. | Methods of prognosis and treatment |
| US11466331B2 (en) | 2016-03-03 | 2022-10-11 | Memed Diagnostics Ltd. | RNA determinants for distinguishing between bacterial and viral infections |
| CN115691827A (en) * | 2023-01-04 | 2023-02-03 | 成都信通网易医疗科技发展有限公司 | Method and storage medium for determining suspected infected patient |
Families Citing this family (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP3817005A1 (en) * | 2019-11-01 | 2021-05-05 | Koninklijke Philips N.V. | System for infection diagnosis |
| WO2022169842A1 (en) * | 2021-02-02 | 2022-08-11 | Revelation Biosciences, Inc. | Rapid detection kits and methods for diagnosing infections of the respiratory tract |
Citations (38)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US3791932A (en) | 1971-02-10 | 1974-02-12 | Akzona Inc | Process for the demonstration and determination of reaction components having specific binding affinity for each other |
| US3839153A (en) | 1970-12-28 | 1974-10-01 | Akzona Inc | Process for the detection and determination of specific binding proteins and their corresponding bindable substances |
| US3850578A (en) | 1973-03-12 | 1974-11-26 | H Mcconnell | Process for assaying for biologically active molecules |
| US3850752A (en) | 1970-11-10 | 1974-11-26 | Akzona Inc | Process for the demonstration and determination of low molecular compounds and of proteins capable of binding these compounds specifically |
| US3853987A (en) | 1971-09-01 | 1974-12-10 | W Dreyer | Immunological reagent and radioimmuno assay |
| US3867517A (en) | 1971-12-21 | 1975-02-18 | Abbott Lab | Direct radioimmunoassay for antigens and their antibodies |
| US3879262A (en) | 1972-05-11 | 1975-04-22 | Akzona Inc | Detection and determination of haptens |
| US3901654A (en) | 1971-06-21 | 1975-08-26 | Biological Developments | Receptor assays of biologically active compounds employing biologically specific receptors |
| US3935074A (en) | 1973-12-17 | 1976-01-27 | Syva Company | Antibody steric hindrance immunoassay with two antibodies |
| US3984533A (en) | 1975-11-13 | 1976-10-05 | General Electric Company | Electrophoretic method of detecting antigen-antibody reaction |
| US3996345A (en) | 1974-08-12 | 1976-12-07 | Syva Company | Fluorescence quenching with immunological pairs in immunoassays |
| US4034074A (en) | 1974-09-19 | 1977-07-05 | The Board Of Trustees Of Leland Stanford Junior University | Universal reagent 2-site immunoradiometric assay using labelled anti (IgG) |
| US4098876A (en) | 1976-10-26 | 1978-07-04 | Corning Glass Works | Reverse sandwich immunoassay |
| US4230767A (en) | 1978-02-08 | 1980-10-28 | Toyo Boseki Kabushiki Kaisha | Heat sealable laminated propylene polymer packaging material |
| US4233402A (en) | 1978-04-05 | 1980-11-11 | Syva Company | Reagents and method employing channeling |
| US4275149A (en) | 1978-11-24 | 1981-06-23 | Syva Company | Macromolecular environment control in specific receptor assays |
| US4376110A (en) | 1980-08-04 | 1983-03-08 | Hybritech, Incorporated | Immunometric assays using monoclonal antibodies |
| US4659678A (en) | 1982-09-29 | 1987-04-21 | Serono Diagnostics Limited | Immunoassay of antigens |
| US4666828A (en) | 1984-08-15 | 1987-05-19 | The General Hospital Corporation | Test for Huntington's disease |
| US4683202A (en) | 1985-03-28 | 1987-07-28 | Cetus Corporation | Process for amplifying nucleic acid sequences |
| US4727022A (en) | 1984-03-14 | 1988-02-23 | Syntex (U.S.A.) Inc. | Methods for modulating ligand-receptor interactions and their application |
| US4801531A (en) | 1985-04-17 | 1989-01-31 | Biotechnology Research Partners, Ltd. | Apo AI/CIII genomic polymorphisms predictive of atherosclerosis |
| US4879219A (en) | 1980-09-19 | 1989-11-07 | General Hospital Corporation | Immunoassay utilizing monoclonal high affinity IgM antibodies |
| US5011771A (en) | 1984-04-12 | 1991-04-30 | The General Hospital Corporation | Multiepitopic immunometric assay |
| US5018067A (en) | 1987-01-12 | 1991-05-21 | Iameter Incorporated | Apparatus and method for improved estimation of health resource consumption through use of diagnostic and/or procedure grouping and severity of illness indicators |
| US5192659A (en) | 1989-08-25 | 1993-03-09 | Genetype Ag | Intron sequence analysis method for detection of adjacent and remote locus alleles as haplotypes |
| US5272057A (en) | 1988-10-14 | 1993-12-21 | Georgetown University | Method of detecting a predisposition to cancer by the use of restriction fragment length polymorphism of the gene for human poly (ADP-ribose) polymerase |
| US5281521A (en) | 1992-07-20 | 1994-01-25 | The Trustees Of The University Of Pennsylvania | Modified avidin-biotin technique |
| US20020038227A1 (en) | 2000-02-25 | 2002-03-28 | Fey Christopher T. | Method for centralized health data management |
| US20040122296A1 (en) | 2002-12-18 | 2004-06-24 | John Hatlestad | Advanced patient management for triaging health-related data |
| US20040122297A1 (en) | 2002-12-18 | 2004-06-24 | Stahmann Jeffrey E. | Advanced patient management for identifying, displaying and assisting with correlating health-related data |
| US20080171323A1 (en) | 2006-08-11 | 2008-07-17 | Baylor Research Institute | Gene Expression Signatures in Blood Leukocytes Permit Differential Diagnosis of Acute Infections |
| WO2011132086A2 (en) | 2010-04-21 | 2011-10-27 | MeMed Diagnostics, Ltd. | Signatures and determinants for distinguishing between a bacterial and viral infection and methods of use thereof |
| WO2013117746A1 (en) | 2012-02-09 | 2013-08-15 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| WO2016059636A1 (en) | 2014-10-14 | 2016-04-21 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections in non-human subjects and methods of use thereof |
| WO2016079219A1 (en) | 2014-11-19 | 2016-05-26 | Koninklijke Philips N.V. | Diagnostic method employing hnl |
| WO2016092554A1 (en) | 2014-12-11 | 2016-06-16 | Memed Diagnostics Ltd. | Marker combinations for diagnosing infections and methods of use thereof |
| WO2017221255A1 (en) | 2016-06-23 | 2017-12-28 | Memed Diagnostics Ltd. | Measuring trail by lateral flow immunoassay |
Family Cites Families (119)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| DE4322330A1 (en) | 1992-08-31 | 1994-03-03 | Behringwerke Ag | Use of the IL-4 receptor for the therapy, prophylaxis and diagnosis of allergic, viral, parasitic and bacterial diseases as well as fungal infections |
| DE4227454C1 (en) | 1992-08-19 | 1994-02-03 | Henning Berlin Gmbh | Process for early detection, for the detection of the severity as well as for the therapy-accompanying assessment of the course of sepsis as well as means for carrying out the process |
| SE9401351D0 (en) | 1994-04-21 | 1994-04-21 | Venge | A method of diagnosis |
| US5910421A (en) | 1995-12-21 | 1999-06-08 | University Of Florida | Rapid diagnostic method for distinguishing allergies and infections |
| US6077665A (en) | 1996-05-07 | 2000-06-20 | The Board Of Trustees Of The Leland Stanford Junior University | Rapid assay for infection in neonates |
| JP2002508933A (en) | 1997-12-24 | 2002-03-26 | ダイアテック・ピーティワイ・リミテッド | Bifunctional molecule |
| EP1080233A4 (en) | 1998-05-18 | 2003-02-05 | Apoptosis Technology Inc | Compounds, screening methods, and uses involving anti-apoptotic genes and gene products |
| DE19847690A1 (en) | 1998-10-15 | 2000-04-20 | Brahms Diagnostica Gmbh | Diagnosing sepsis and severe infections, useful for assessing severity and progress of treatment, by measuring content of peptide prohormone or their derived fragments |
| US6709855B1 (en) | 1998-12-18 | 2004-03-23 | Scios, Inc. | Methods for detection and use of differentially expressed genes in disease states |
| CA2702148C (en) | 1999-01-06 | 2014-03-04 | Genenews Inc. | Method of profiling gene expression in a human subject having an infectious disease |
| EP1206529B1 (en) | 1999-08-24 | 2006-11-29 | Glycozym ApS | UDP-N-ACETYLGLUCOSAMINE: GALACTOSE-BETA 1,3-N-ACETYLGALACTOSAMINE-ALPHA-R/(GlcNAc to GalNAc) BETA 1,6-N-ACETYLGLUCOSAMINYLTRANSFERASE, C2GnT3 |
| IL132687A0 (en) | 1999-11-01 | 2001-03-19 | Keren Mechkarim Ichilov Pnimit | System and method for evaluating body fluid samples |
| US7668661B2 (en) | 2000-04-28 | 2010-02-23 | Siemens Healthcare Diagnostics Inc. | Liver disease-related methods and systems |
| EP1375672A4 (en) | 2001-03-27 | 2005-02-16 | Toshiba Kk | Method of detecting nucleic acid relating to disease |
| US7713705B2 (en) * | 2002-12-24 | 2010-05-11 | Biosite, Inc. | Markers for differential diagnosis and methods of use thereof |
| DE10119804A1 (en) | 2001-04-23 | 2002-10-24 | Brahms Ag | New peptides produced in primates during inflammation and sepsis, useful for diagnosis and treatment of these diseases, and their related antibodies |
| US7115717B2 (en) | 2001-05-18 | 2006-10-03 | Kirin Beer Kabushiki Kaisha | Anti-TRAIL-R antibodies |
| FI115165B (en) | 2001-06-04 | 2005-03-15 | Aboatech Ab Oy | Method for determining the quality of infection |
| DE10130985B4 (en) | 2001-06-27 | 2004-03-18 | B.R.A.H.M.S Ag | Procedure for the diagnosis of sepsis and severe infections by determining soluble cytokeratin 1 fragments |
| US20040209307A1 (en) | 2001-08-20 | 2004-10-21 | Biosite Incorporated | Diagnostic markers of stroke and cerebral injury and methods of use thereof |
| EP1318407B1 (en) | 2001-12-07 | 2004-09-29 | B.R.A.H.M.S Aktiengesellschaft | Use of aldose-1-epimerase (mutarotase) for the diagnosis of infections and sepsis |
| EP1317902B1 (en) | 2001-12-10 | 2005-11-09 | Kabushiki Gaisha K-and-S | Biological data observation apparatus |
| US20040038201A1 (en) | 2002-01-22 | 2004-02-26 | Whitehead Institute For Biomedical Research | Diagnostic and therapeutic applications for biomarkers of infection |
| KR20040105784A (en) | 2002-03-22 | 2004-12-16 | 교와 메덱스 가부시키가이샤 | Method of judging viral infection |
| US7485298B2 (en) | 2002-05-23 | 2009-02-03 | Michael Powell | Diagnosis and treatment of human dormancy-related sequellae |
| EP1552021A4 (en) | 2002-06-11 | 2006-06-14 | Idaho Res Foundation | Type i interferon-inducible proteins to detect viral infection |
| US8563476B2 (en) | 2002-11-15 | 2013-10-22 | Morehouse School Of Medicine | Anti-CXCL9, anti-CXCL10, anti-CXCL11, anti-CXCL13, anti-CXCR3 and anti-CXCR5 agents for inflammatory disorders |
| CA2528162A1 (en) | 2003-06-04 | 2004-12-16 | The Government Of The United States As Represented By The Secretary Of T He Department Of Health And Human Services, Centers For Disease Control | Pni microarray and uses |
| WO2005033327A2 (en) | 2003-09-29 | 2005-04-14 | Biosite Incorporated | Methods and compositions for the diagnosis of sepsis |
| JP2005106694A (en) | 2003-09-30 | 2005-04-21 | Mochida Pharmaceut Co Ltd | Early detection of blood poisoning and evaluation on seriousness |
| GB0401730D0 (en) | 2004-01-27 | 2004-03-03 | Bioxell Spa | Diagnosis method |
| US8906630B2 (en) | 2004-02-27 | 2014-12-09 | The Trustees Of The University Of Pennsylvania | Assays for detecting pathogenic respiratory bacteria |
| US7892539B2 (en) | 2004-03-24 | 2011-02-22 | The Regents Of The University Of California | Modulation of an innate immune response by altering TRIAL-R signaling |
| US8155993B2 (en) | 2004-06-15 | 2012-04-10 | Janssen Pharmaceutica, N.V. | Apparatus and methods for assessing a pharmaceutical product |
| CA2614507A1 (en) | 2004-07-09 | 2006-08-17 | Amaox, Ltd. | Immune cell biosensors and methods of using same |
| US7572640B2 (en) | 2004-09-28 | 2009-08-11 | Singulex, Inc. | Method for highly sensitive detection of single protein molecules labeled with fluorescent moieties |
| US20060078998A1 (en) | 2004-09-28 | 2006-04-13 | Singulex, Inc. | System and methods for sample analysis |
| CN101218355A (en) | 2004-11-05 | 2008-07-09 | 海军秘书处代表的美国政府 | Diagnosis and prognosis of infectious diesease clinical phenotypes and other physiologic states using host gene expresion biomarkers in blood |
| WO2007018574A2 (en) | 2004-11-10 | 2007-02-15 | The United States Of America As Represented By The Secretary Of The Navy | Diagnostic assay for rickettsia prowazekii disease by detection of responsive gene expression |
| CN101208602A (en) | 2005-04-15 | 2008-06-25 | 贝克顿迪金森公司 | Diagnosis of sepsis |
| EP1869463A4 (en) | 2005-04-15 | 2010-05-05 | Becton Dickinson Co | Diagnosis of sepsis |
| US20070015172A1 (en) | 2005-06-01 | 2007-01-18 | Z-Biomed, Inc. | Expression profiles for microbial infection |
| UA78641C2 (en) | 2005-08-29 | 2007-04-10 | Open Joint Stock Company Conce | A process for the preparation of carbamide-formaldehyde resin |
| DE102005050933A1 (en) | 2005-10-21 | 2007-04-26 | Justus-Liebig-Universität Giessen | Invention relating to expression profiles for the prediction of septic states |
| CN101374964B (en) | 2005-12-09 | 2013-07-17 | 贝勒研究院 | Module-level analysis of peripheral blood leukocyte transcriptional profiles |
| GB0601959D0 (en) | 2006-01-31 | 2006-03-15 | King S College London | Sepsis test |
| US20070184460A1 (en) | 2006-02-09 | 2007-08-09 | Wei-Mei Ching | Diagnostic assay for Orientia tsutsugamushi by detection of responsive gene expression |
| RU2008146518A (en) | 2006-04-26 | 2010-06-10 | Вертекс Фармасьютикалз Инкорпорейтед (Us) | BIOMARKERS OF INFECTION Caused by the Hepatitis C Virus |
| AU2012244350B2 (en) * | 2006-09-05 | 2013-08-15 | Statens Serum Institut | Ip-10 based immunological monitoring |
| ATE504000T1 (en) | 2006-09-05 | 2011-04-15 | Hvidovre Hospital | IP-10 BASED IMMUNOLOGICAL MONITORING |
| EP2078201A2 (en) | 2006-10-05 | 2009-07-15 | Agency for Science, Technology and Research | Dengue diagnosis and treatment |
| US20100143372A1 (en) | 2006-12-06 | 2010-06-10 | Medimmune, Llc | Interferon alpha-induced pharmacodynamic markers |
| DE102006060112A1 (en) | 2006-12-20 | 2008-06-26 | Brahms Aktiengesellschaft | Diagnosis and risk stratification using the new marker CT-proADM |
| CN101617056A (en) | 2006-12-21 | 2009-12-30 | 伊诺基因卡尔生物技术私人有限公司 | The method of early diagnosis of Epstein-Barr virus associated cancer and separately reagent and test kit |
| EP2102370A4 (en) | 2007-01-11 | 2010-01-13 | Univ Duke | Method of monitoring hiv infection |
| US8293489B2 (en) | 2007-01-31 | 2012-10-23 | Henkin Robert I | Methods for detection of biological substances |
| BRPI0808150A2 (en) | 2007-02-28 | 2014-07-01 | Procter & Gamble | METHODS AND TARGETS FOR IDENTIFYING COMPOUNDS FOR REGULATING RHINOVIRUS INFECTION |
| DE102007009751A1 (en) | 2007-02-28 | 2008-09-04 | B.R.A.H.M.S Aktiengesellschaft | Diagnostic immunoassay for procalcitonin in a biological sample from a patient comprises selectively determining full-length procalcitonin 1-116 |
| CA2689306C (en) | 2007-06-01 | 2019-01-15 | Council Of Scientific & Industrial Research | A novel method for simultaneous detection and discrimination of bacterial, fungal, parasitic and viral infections of eye and central nervous system |
| RU2352948C1 (en) | 2007-06-15 | 2009-04-20 | Государственное образовательное учреждение высшего профессионального образования "КРАСНОЯРСКАЯ ГОСУДАРСТВЕННАЯ МЕДИЦИНСКАЯ АКАДЕМИЯ ФЕДЕРАЛЬНОГО АГЕНТСТВА ПО ЗДРАВООХРАНЕНИЮ И СОЦИАЛЬНОМУ РАЗВИТИЮ" | Method of outcome forecast of disease of patients with urgent surgical pathology of organs of abdominal cavity |
| IL184478A (en) | 2007-07-08 | 2017-07-31 | Hadasit Medical Res Services & Development Ltd | Compositions, methods and kits for the diagnosis of carriers of mutations in the brca1 and brca2 genes and early diagnosis of cancerous disorders associated with mutations in brca1 and brca2 genes |
| DE102007035640A1 (en) | 2007-07-27 | 2009-01-29 | Lkh-Kunststoffwerk Gmbh & Co. Kg | plunger |
| EP2020603A1 (en) | 2007-08-03 | 2009-02-04 | BRAHMS Aktiengesellschaft | Method for risk stratification in stable coronary artery disease |
| ATE533061T1 (en) | 2007-08-03 | 2011-11-15 | Brahms Gmbh | METHOD FOR DIAGNOSING BACTERIAL INFECTIONS |
| TW200920358A (en) | 2007-08-13 | 2009-05-16 | Lundbeck & Co As H | Method of treating stress-mediated depression |
| WO2009025743A2 (en) | 2007-08-17 | 2009-02-26 | University Of Massachusetts Medical School | Use of trail compositions as antiviral agents |
| EP2071334A1 (en) | 2007-12-14 | 2009-06-17 | Transmedi SA | Compositions and methods of detecting TIABS |
| WO2009100907A1 (en) | 2008-02-14 | 2009-08-20 | Dianeering Diagnostics Engineering And Research Gmbh | Means and methods for assessing the risk of patients presenting to emergency departments based on very low concentrations of troponin i or t or using a combination of markers |
| US8293880B2 (en) | 2008-03-25 | 2012-10-23 | University Of Southern California | Prognostic panel for urinary bladder cancer |
| JP2011519551A (en) | 2008-04-21 | 2011-07-14 | ノバルティス・フォルシュングスシュティフトゥング・ツヴァイクニーダーラッスング・フリードリッヒ・ミーシェー・インスティトゥート・フォー・バイオメディカル・リサーチ | Antiviral treatment |
| US9910036B2 (en) | 2008-05-20 | 2018-03-06 | Rapid Pathogen Screening, Inc. | Method and device for combined detection of viral and bacterial infections |
| EP2796878A1 (en) | 2008-05-23 | 2014-10-29 | Biocartis NV | New biomarkers for diagnosis, prediction and/or prognosis of sepsis and uses thereof |
| EA201170088A1 (en) | 2008-06-25 | 2011-10-31 | Бейлор Рисёч Инститьют | TRANSCRIPTION SIGNATURE OF BLOOD INFECTION MYCOBACTERIUM TUBERCULOSIS |
| CN102257386B (en) | 2008-10-24 | 2014-12-31 | B.R.A.H.M.S有限公司 | Prognosis and risk assessment in stroke patients by determining the level of marker peptides |
| TW201021778A (en) | 2008-11-12 | 2010-06-16 | Alcon Res Ltd | Intraocular lens delivery device with a multi-part plunger tip |
| EP2730662A1 (en) | 2008-11-12 | 2014-05-14 | Caris Life Sciences Luxembourg Holdings | Methods and systems of using exosomes for determining phenotypes |
| UA92843C2 (en) | 2009-05-21 | 2010-12-10 | Институт Технической Теплофизики Национальной Академии Наук Украины | Process for the preparation of food coloring powder from table beet |
| WO2010138618A1 (en) | 2009-05-26 | 2010-12-02 | Duke University | Molecular predictors of fungal infection |
| EP2438447B1 (en) | 2009-06-05 | 2015-02-18 | B.R.A.H.M.S GmbH | Detection of bacterial infections in subjects suffering from dyspnea. |
| US20110065136A1 (en) | 2009-08-07 | 2011-03-17 | Rules-Based Medicine, Inc. | Methods and Devices for Detecting Glomerulonephritis and Associated Disorders |
| JP5667353B2 (en) | 2009-09-25 | 2015-02-12 | シスメックス株式会社 | Blood cell counter, diagnosis support apparatus, diagnosis support method, and computer program |
| JP5722587B2 (en) * | 2009-10-13 | 2015-05-20 | ベー.エル.アー.ハー.エム.エス ゲゼルシャフト ミット ベシュレンクテル ハフツング | Procalcitonin and antibiotic treatment guidance for the diagnosis of bacterial infection in patients with acute stroke or transient ischemic attack |
| CA2777800C (en) | 2009-10-15 | 2019-11-12 | Crescendo Bioscience | Biomarkers and methods for measuring and monitoring inflammatory disease activity |
| CN102762743A (en) | 2009-12-09 | 2012-10-31 | 阿维埃尔公司 | Biomarker assay for diagnosis and classification of cardiovascular disease |
| US20110312534A1 (en) | 2010-03-05 | 2011-12-22 | Erasmus University Medical Center Rotterdam | Method for prediction of human iris color |
| JP5916130B2 (en) | 2010-05-31 | 2016-05-11 | 国立大学法人徳島大学 | Examination method of disease severity |
| GB2482187A (en) | 2010-07-23 | 2012-01-25 | Univ Exeter | Predicting response to surgery |
| US8877212B2 (en) | 2011-02-07 | 2014-11-04 | Trudeau Institute | Use of an IL12 receptor-beta 1 splice variant to diagnose active tuberculosis |
| RU2476887C2 (en) | 2011-03-29 | 2013-02-27 | Учреждение Российской академии медицинских наук Дальневосточный научный центр физиологии и патологии дыхания Сибирского отделения РАМН | Method for prediction of developing complications in patients with community-acquired pneumonia |
| AU2012274461A1 (en) | 2011-06-20 | 2014-01-16 | Kyowa Hakko Kirin Co., Ltd. | Anti-erbB3 antibody |
| EP2756103A4 (en) | 2011-09-12 | 2015-06-03 | Univ Vanderbilt | Characterizing multiple sclerosis |
| JP5842107B2 (en) | 2011-10-19 | 2016-01-13 | パナソニックIpマネジメント株式会社 | Cardiodynamic measurement device |
| ES2656150T3 (en) | 2011-11-14 | 2018-02-23 | Universitätsklinikum Jena | Diagnosis of sepsis and systemic inflammatory response syndrome |
| CN104159616B (en) | 2012-03-08 | 2017-10-31 | 托门医学股份公司 | It is used for the chewing gum for diagnosing inflammatory tissue in dental applications |
| EP2637023A1 (en) | 2012-03-08 | 2013-09-11 | B.R.A.H.M.S GmbH | Prediction of outcome in patients with chronic obstructive pulmonary disease |
| CN114042171A (en) | 2012-03-30 | 2022-02-15 | 文森医学公司 | Bacterial imaging agents and methods of use thereof |
| GB201211982D0 (en) | 2012-07-05 | 2012-08-22 | Isis Innovation | Biomarker |
| EP2872891B1 (en) | 2012-07-10 | 2019-03-13 | Nepean Blue Mountains Local Health District | Risk stratification in influenza |
| FR2996003B1 (en) | 2012-09-25 | 2014-10-17 | Commissariat Energie Atomique | METHOD FOR SPECIFICALLY DETECTION IN SAMPLE MATRIX METALLOPROTEASE (MMP) OF INTEREST ONLY IN ACTIVE FORM |
| US20140127827A1 (en) | 2012-11-05 | 2014-05-08 | Gwangju Institute Of Science And Technology | Method for detection of antigen using fluorescence resonance energy transfer immunoassay |
| BR112015012616A2 (en) | 2012-11-30 | 2017-09-12 | Applied Proteomics Inc | method for assessing the presence or risk of colon tumors |
| RU2015135359A (en) | 2013-01-22 | 2017-03-02 | Имикрок, С.Л. | FAST METHOD FOR DETECTING PATHOGENS |
| JP2016514291A (en) | 2013-01-29 | 2016-05-19 | モレキュラー ヘルス ゲーエムベーハー | System and method for clinical decision support |
| US10689701B2 (en) | 2013-03-15 | 2020-06-23 | Duke University | Biomarkers for the molecular classification of bacterial infection |
| JP6185142B2 (en) | 2013-03-15 | 2017-08-23 | ボストン サイエンティフィック ニューロモデュレイション コーポレイション | Clinical response data mapping |
| US10794917B2 (en) | 2013-09-20 | 2020-10-06 | Astute Medical, Inc. | Methods and compositions for diagnosis and prognosis of appendicitis and differentiation of causes of abdominal pain |
| WO2015048098A1 (en) | 2013-09-24 | 2015-04-02 | Washington University | Diagnostic methods for infectious disease using endogenous gene expression |
| CN111624346A (en) | 2014-08-14 | 2020-09-04 | 米密德诊断学有限公司 | Kit for predicting and/or determining prognosis |
| KR20160072626A (en) | 2014-12-15 | 2016-06-23 | 전북대학교산학협력단 | Rapid diagnostic Kit for detecting sepsis factor IL-6 |
| WO2017072777A1 (en) | 2015-11-01 | 2017-05-04 | Elminda Ltd. | Method and system for estimating potential distribution on cortical surface |
| CN114959084A (en) | 2016-03-03 | 2022-08-30 | 米密德诊断学有限公司 | Analysis of RNA for diagnosis of infection type |
| CA3015046A1 (en) | 2016-03-03 | 2017-09-08 | Memed Diagnostics Ltd. | Rna determinants for distinguishing between bacterial and viral infections |
| EP4184167A1 (en) | 2016-07-10 | 2023-05-24 | MeMed Diagnostics Ltd. | Early diagnosis of infections |
| EP4141448A1 (en) | 2016-07-10 | 2023-03-01 | MeMed Diagnostics Ltd. | Protein signatures for distinguishing between bacterial and viral infections |
| WO2018052137A1 (en) | 2016-09-16 | 2018-03-22 | 株式会社オンチップ・バイオテクノロジーズ | Fine particle dispensing device, fine particle analysis device, reaction detection device, and method using said devices |
| WO2018060998A1 (en) | 2016-09-29 | 2018-04-05 | Memed Diagnostics Ltd. | Methods of prognosis and treatment |
| CN110073220A (en) | 2016-09-29 | 2019-07-30 | 米密德诊断学有限公司 | The method of risk assessment and classification of diseases |
| US10209260B2 (en) | 2017-07-05 | 2019-02-19 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| US20220329345A1 (en) | 2021-04-08 | 2022-10-13 | Infinidome Ltd. | Adjustable null steering in a stationary network |
-
2017
- 2017-07-10 EP EP22204952.0A patent/EP4184167A1/en active Pending
- 2017-07-10 CN CN201780055347.8A patent/CN109804245B/en active Active
- 2017-07-10 WO PCT/IL2017/050781 patent/WO2018011796A1/en unknown
- 2017-07-10 EP EP17827122.7A patent/EP3482201B1/en active Active
- 2017-07-10 US US16/316,631 patent/US11340223B2/en active Active
-
2022
- 2022-04-11 US US17/717,200 patent/US12055545B2/en active Active
Patent Citations (39)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US3850752A (en) | 1970-11-10 | 1974-11-26 | Akzona Inc | Process for the demonstration and determination of low molecular compounds and of proteins capable of binding these compounds specifically |
| US3839153A (en) | 1970-12-28 | 1974-10-01 | Akzona Inc | Process for the detection and determination of specific binding proteins and their corresponding bindable substances |
| US3791932A (en) | 1971-02-10 | 1974-02-12 | Akzona Inc | Process for the demonstration and determination of reaction components having specific binding affinity for each other |
| US3901654A (en) | 1971-06-21 | 1975-08-26 | Biological Developments | Receptor assays of biologically active compounds employing biologically specific receptors |
| US3853987A (en) | 1971-09-01 | 1974-12-10 | W Dreyer | Immunological reagent and radioimmuno assay |
| US3867517A (en) | 1971-12-21 | 1975-02-18 | Abbott Lab | Direct radioimmunoassay for antigens and their antibodies |
| US3879262A (en) | 1972-05-11 | 1975-04-22 | Akzona Inc | Detection and determination of haptens |
| US3850578A (en) | 1973-03-12 | 1974-11-26 | H Mcconnell | Process for assaying for biologically active molecules |
| US3935074A (en) | 1973-12-17 | 1976-01-27 | Syva Company | Antibody steric hindrance immunoassay with two antibodies |
| US3996345A (en) | 1974-08-12 | 1976-12-07 | Syva Company | Fluorescence quenching with immunological pairs in immunoassays |
| US4034074A (en) | 1974-09-19 | 1977-07-05 | The Board Of Trustees Of Leland Stanford Junior University | Universal reagent 2-site immunoradiometric assay using labelled anti (IgG) |
| US3984533A (en) | 1975-11-13 | 1976-10-05 | General Electric Company | Electrophoretic method of detecting antigen-antibody reaction |
| US4098876A (en) | 1976-10-26 | 1978-07-04 | Corning Glass Works | Reverse sandwich immunoassay |
| US4230767A (en) | 1978-02-08 | 1980-10-28 | Toyo Boseki Kabushiki Kaisha | Heat sealable laminated propylene polymer packaging material |
| US4233402A (en) | 1978-04-05 | 1980-11-11 | Syva Company | Reagents and method employing channeling |
| US4275149A (en) | 1978-11-24 | 1981-06-23 | Syva Company | Macromolecular environment control in specific receptor assays |
| US4376110A (en) | 1980-08-04 | 1983-03-08 | Hybritech, Incorporated | Immunometric assays using monoclonal antibodies |
| US4879219A (en) | 1980-09-19 | 1989-11-07 | General Hospital Corporation | Immunoassay utilizing monoclonal high affinity IgM antibodies |
| US4659678A (en) | 1982-09-29 | 1987-04-21 | Serono Diagnostics Limited | Immunoassay of antigens |
| US4727022A (en) | 1984-03-14 | 1988-02-23 | Syntex (U.S.A.) Inc. | Methods for modulating ligand-receptor interactions and their application |
| US5011771A (en) | 1984-04-12 | 1991-04-30 | The General Hospital Corporation | Multiepitopic immunometric assay |
| US4666828A (en) | 1984-08-15 | 1987-05-19 | The General Hospital Corporation | Test for Huntington's disease |
| US4683202B1 (en) | 1985-03-28 | 1990-11-27 | Cetus Corp | |
| US4683202A (en) | 1985-03-28 | 1987-07-28 | Cetus Corporation | Process for amplifying nucleic acid sequences |
| US4801531A (en) | 1985-04-17 | 1989-01-31 | Biotechnology Research Partners, Ltd. | Apo AI/CIII genomic polymorphisms predictive of atherosclerosis |
| US5018067A (en) | 1987-01-12 | 1991-05-21 | Iameter Incorporated | Apparatus and method for improved estimation of health resource consumption through use of diagnostic and/or procedure grouping and severity of illness indicators |
| US5272057A (en) | 1988-10-14 | 1993-12-21 | Georgetown University | Method of detecting a predisposition to cancer by the use of restriction fragment length polymorphism of the gene for human poly (ADP-ribose) polymerase |
| US5192659A (en) | 1989-08-25 | 1993-03-09 | Genetype Ag | Intron sequence analysis method for detection of adjacent and remote locus alleles as haplotypes |
| US5281521A (en) | 1992-07-20 | 1994-01-25 | The Trustees Of The University Of Pennsylvania | Modified avidin-biotin technique |
| US20020038227A1 (en) | 2000-02-25 | 2002-03-28 | Fey Christopher T. | Method for centralized health data management |
| US20040122296A1 (en) | 2002-12-18 | 2004-06-24 | John Hatlestad | Advanced patient management for triaging health-related data |
| US20040122297A1 (en) | 2002-12-18 | 2004-06-24 | Stahmann Jeffrey E. | Advanced patient management for identifying, displaying and assisting with correlating health-related data |
| US20080171323A1 (en) | 2006-08-11 | 2008-07-17 | Baylor Research Institute | Gene Expression Signatures in Blood Leukocytes Permit Differential Diagnosis of Acute Infections |
| WO2011132086A2 (en) | 2010-04-21 | 2011-10-27 | MeMed Diagnostics, Ltd. | Signatures and determinants for distinguishing between a bacterial and viral infection and methods of use thereof |
| WO2013117746A1 (en) | 2012-02-09 | 2013-08-15 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| WO2016059636A1 (en) | 2014-10-14 | 2016-04-21 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections in non-human subjects and methods of use thereof |
| WO2016079219A1 (en) | 2014-11-19 | 2016-05-26 | Koninklijke Philips N.V. | Diagnostic method employing hnl |
| WO2016092554A1 (en) | 2014-12-11 | 2016-06-16 | Memed Diagnostics Ltd. | Marker combinations for diagnosing infections and methods of use thereof |
| WO2017221255A1 (en) | 2016-06-23 | 2017-12-28 | Memed Diagnostics Ltd. | Measuring trail by lateral flow immunoassay |
Non-Patent Citations (49)
| Title |
|---|
| "Global Problems, Smart Solutions", 15 April 2015, CAMBRIDGE UNIVERSITY PRESS |
| "Immobilized Cells and Enzymes", 1986, IRL PRESS |
| "Nucleic Acid Hybridization", 1985 |
| "PCR Protocols: A Guide To Methods And Applications", vol. 1-317, 1990, ACADEMIC PRESS |
| "Transcription and Translation", 1984 |
| BHOWMIK, A.SEEMUNGAL, T. A.SAPSFORD, R. J.WEDZICHA, J. A.: "Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations", THORAX, vol. 55, 2000, pages 114 - 120 |
| BOGAERT, D.DE GROOT, R.HERMANS, P. W. M.: "Streptococcus pneumoniae colonisation: the key to pneumococcal disease", LANCET INFECT DIS, vol. 4, 2004, pages 144 - 154, XP004808691, DOI: 10.1016/S1473-3099(04)00938-7 |
| BOSSUYT, P. M. ET AL.: "The STARD Statement for Reporting Studies of Diagnostic Accuracy: Explanation and Elaboration", ANN INTERN MED, vol. 138, 2003, pages W1 - W12 |
| CATERINO, J. M.HIESTAND, B. C.MARTIN, D. R.: "Quality of care in elder emergency department patients with pneumonia: a prospective cohort study", BMC EMERG MED, vol. 8, 2008, pages 6, XP021033955 |
| CDC - ABOUT ANTIMICROBIAL RESISTANCE, 21 November 2011 (2011-11-21), Retrieved from the Internet <URL:www(dot)cdc(dot)gov/drugresistance/about(dot)html> |
| CDC - GET SMART: FAST FACTS ABOUT ANTIBIOTIC RESISTANCE, pages 20111121, Retrieved from the Internet <URL:www(dot)cdc(dot)gov/getsmart/antibiotic-use/fast-facts(dot)html> |
| COOK: "Use and Misuse of the Receiver Operating Characteristic Curve in Risk Prediction", CIRCULATION, vol. 115, 2007, pages 928 - 935 |
| CRAIG, J. C. ET AL.: "The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses", BMJ, vol. 340, 2010 |
| CRAW, P.BALACHANDRAN, W.: "Isothermal nucleic acid amplification technologies for point-of-care diagnostics: a critical review", LAB CHIP, vol. 12, 2012, pages 2469 - 2486 |
| D'AGOSTINO ET AL., JAMA, vol. 286, 2001, pages 180 - 187 |
| DEDIER, J.SINGER, D. E.CHANG, Y.MOORE, M.ATLAS, S. J.: "Processes of care, illness severity, and outcomes in the management of community-acquired pneumonia at academic hospitals", ARCH. INTERN. MED., vol. 161, 2001, pages 2099 - 2104 |
| E. MAGGIO: "Selected Methods in Cellular Immunology", 1980, W. H. FREEMAN AND CO. |
| FAUCI ASMARSTON HD: "The perpetual challenge of antimicrobial resistance", JAMA, 2014 |
| FRESHNEY: "Culture of Animal Cells - A Manual of Basic Technique", vol. I-III, 1994, APPLETON & LANGE |
| GOLD - THE GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE, 15 April 2015 (2015-04-15), Retrieved from the Internet <URL:www(dot)goldcopd(dot)org/guidelines-global-strategy-for-diagnosis-management(dot)html> |
| HOOGENDOORN, M.: "Economic impact of COPD: Empirical and model-based studies on the cost-effectiveness of treatment options", JOURNAL OF NEUROPHYSIOLOGY - J NEUROPHYSIOL, 2011 |
| HOUCK, P. M.: "Timing of antibiotic administration and outcomes for medicare patients hospitalized with community-acquired pneumonia", ARCH INTERN MED, vol. 164, 2004, pages 637 - 644 |
| HURST, J. R. ET AL.: "Susceptibility to exacerbation in chronic obstructive pulmonary disease", N. ENGL. J. MED., vol. 363, 2010, pages 1128 - 1138 |
| JUNG, C. L.LEE, M. A.CHUNG, W. S.: "Clinical Evaluation of the Multiplex PCR Assay for the Detection of Bacterial Pathogens in Respiratory Specimens from Patients with Pneumonia", KOREAN JOURNAL OF CLINICAL MICROBIOLOGY, vol. 13, 2010, pages 40 |
| KIM, K. H.SHIN, J. H.KIM, S. Y.: "The Clinical Significance of Nasopharyngeal Carriages in Immunocompromised Children as Assessed", THE KOREAN JOURNAL OF HEMATOLOGY, vol. 44, 2009, pages 220 |
| KIM, V. ET AL.: "Airway wall thickness is increased in COPD patients with bronchodilator responsiveness", RESPIR. RES., vol. 15, 2014, pages 84, XP021192638, DOI: 10.1186/s12931-014-0084-3 |
| KUNZE, W.BEIER, D.GROEGER, K.: "Adenovirus Respiratory Infections In Children", DO THEY MIMIC BACTERIAL INFECTIONS?, 2010 |
| LIN, C.-L. ET AL.: "MAnnose-binding lectin gene polymorphism contributes to recurrence of infective exacerbation in patients with copd", CHEST, vol. 139, 2011, pages 43 - 51 |
| LITTLE, P.: "Delayed prescribing of antibiotics for upper respiratory tract infection", BMJ, vol. 331, 2005, pages 301 - 302 |
| MARSHAK ET AL.: "Strategies for Protein Purification and Characterization - A Laboratory Course Manual", 1996, CSHL PRESS |
| MOLYNEAUX, P. L. ET AL.: "Outgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary disease", AM. J. RESPIR. CRIT. CARE MED., vol. 188, 2013, pages 1224 - 1231, XP055204730, DOI: 10.1164/rccm.201302-0341OC |
| NIEMZ, A.FERGUSON, T. M.BOYLE, D. S.: "Point-of-care nucleic acid testing for infectious diseases", TRENDS BIOTECHNOL, vol. 29, 2011, pages 240 - 250, XP028194817, DOI: 10.1016/j.tibtech.2011.01.007 |
| O'MARCAIGH ASJACOBSON RM: "Estimating The Predictive Value Of A Diagnostic Test, How To Prevent Misleading Or Confusing Results", CLIN. PED., vol. 32, no. 8, 1993, pages 485 - 491 |
| OVED, K. ET AL.: "A Novel Host-Proteome Signature for Distinguishing between Acute Bacterial and Viral Infections", PLOS ONE, vol. 10, no. 3, 2015, pages e0120012 |
| PEPE ET AL.: "Limitations of the Odds Ratio in Gauging the Performance of a Diagnostic, Prognostic, or Screening Marker", AM. J. EPIDEMIOL, vol. 159, no. 9, 2004, pages 882 - 890, XP055013965, DOI: 10.1093/aje/kwh101 |
| PERBAL, B.: "A Practical Guide to Molecular Cloning", 1984, JOHN WILEY & SONS |
| RHEDIN, S. ET AL.: "Clinical Utility of PCR for Common Viruses in Acute Respiratory Illness", PEDIATRICS PEDS, 2014, pages 2013 - 3042 |
| SALVI, S.: "The silent epidemic of COPD in Africa", LANCET GLOB HEALTH, vol. 3, 2015, pages e6 - 7 |
| SAMBROOK ET AL.: "Current Protocols in Molecular Biology", 1989, JOHN WILEY AND SONS |
| SETHI, S.EVANS, N.GRANT, B. J. B.MURPHY, T. F.: "New strains of bacteria and exacerbations of chronic obstructive pulmonary disease", N. ENGL. J. MED., vol. 347, 2002, pages 465 - 471, XP008153479, DOI: 10.1056/NEJMoa012561 |
| SHIN, J. H.HAN, H. Y.KIM, S. Y.: "Detection of nasopharyngeal carriages in children by multiplex reverse transcriptase-polymerase chain reaction", KOREAN JOURNAL OF PEDIATRICS, vol. 52, 2009, pages 1358 |
| SHULTZ: "Teitz, Fundamentals of Clinical Chemistry", 1996, W.B. SAUNDERS COMPANY, article "Clinical Interpretation Of Laboratory Procedures", pages: 192 - 199 |
| SPIRO, D. M. ET AL.: "Wait-and-see prescription for the treatment of acute otitis media: a randomized controlled trial", JAMA, vol. 296, 2006, pages 1235 - 1241 |
| SPUESENS, E. B. M. ET AL.: "Carriage of Mycoplasma pneumoniae in the Upper Respiratory Tract of Symptomatic and Asymptomatic Children: An Observational Study", PLOS MED, vol. 10, 2013, pages e1001444 |
| TAYLOR, A. E. ET AL.: "Defective macrophage phagocytosis of bacteria in COPD", EUR. RESPIR. J., vol. 35, 2010, pages 1039 - 1047 |
| WATSON ET AL.: "Genome Analysis: A Laboratory Manual Series", vol. 1-4, 1998, COLD SPRING HARBOR LABORATORY PRESS |
| WHO: "The top 10 causes of death", 17 March 2015, WHO |
| ZWART, S. ET AL.: "Penicillin for acute sore throat: randomised double blind trial of seven days versus three days treatment or placebo in adults", BMJ, vol. 320, 2000, pages 150 - 154 |
| ZWEIG ET AL.: "ROC Curve Analysis: An Example Showing The Relationships Among Serum Lipid And Apolipoprotein Concentrations In Identifying Subjects With Coronory Artery Disease", CLIN. CHEM., vol. 38, no. 8, 1992, pages 1425 - 1428 |
Cited By (19)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10502739B2 (en) | 2012-02-09 | 2019-12-10 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| US11175291B2 (en) | 2012-02-09 | 2021-11-16 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| US11450406B2 (en) | 2014-08-14 | 2022-09-20 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US12131807B2 (en) | 2014-08-14 | 2024-10-29 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US11081206B2 (en) | 2014-08-14 | 2021-08-03 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US10303846B2 (en) | 2014-08-14 | 2019-05-28 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US11776658B2 (en) | 2014-08-14 | 2023-10-03 | Memed Diagnostics Ltd. | Computational analysis of biological data using manifold and a hyperplane |
| US10859574B2 (en) | 2014-10-14 | 2020-12-08 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections in non-human subjects and methods of use thereof |
| US11466331B2 (en) | 2016-03-03 | 2022-10-11 | Memed Diagnostics Ltd. | RNA determinants for distinguishing between bacterial and viral infections |
| US11131671B2 (en) | 2016-07-10 | 2021-09-28 | Memed Diagnostics Ltd. | Protein signatures for distinguishing between bacterial and viral infections |
| US12055545B2 (en) | 2016-07-10 | 2024-08-06 | Memed Diagnostics Ltd. | Early diagnosis of infections |
| US11340223B2 (en) | 2016-07-10 | 2022-05-24 | Memed Diagnostics Ltd. | Early diagnosis of infections |
| US12044681B2 (en) | 2016-07-10 | 2024-07-23 | Memed Diagnostics Ltd. | Protein signatures for distinguishing between bacterial and viral infections |
| US11385241B2 (en) | 2016-09-29 | 2022-07-12 | Memed Diagnostics Ltd. | Methods of prognosis and treatment |
| US11353456B2 (en) | 2016-09-29 | 2022-06-07 | Memed Diagnostics Ltd. | Methods of risk assessment and disease classification for appendicitis |
| US10209260B2 (en) | 2017-07-05 | 2019-02-19 | Memed Diagnostics Ltd. | Signatures and determinants for diagnosing infections and methods of use thereof |
| WO2020251460A1 (en) * | 2019-06-14 | 2020-12-17 | Delaval Holding Ab | System for determining validity of a lateral flow test result |
| WO2021204984A1 (en) | 2020-04-09 | 2021-10-14 | B.R.A.H.M.S Gmbh | Biomarkers for the diagnosis of respiratory tract infections |
| CN115691827A (en) * | 2023-01-04 | 2023-02-03 | 成都信通网易医疗科技发展有限公司 | Method and storage medium for determining suspected infected patient |
Also Published As
| Publication number | Publication date |
|---|---|
| EP4184167A1 (en) | 2023-05-24 |
| EP3482201A1 (en) | 2019-05-15 |
| US20190242895A1 (en) | 2019-08-08 |
| CN109804245A (en) | 2019-05-24 |
| CN109804245B (en) | 2022-10-25 |
| US12055545B2 (en) | 2024-08-06 |
| US11340223B2 (en) | 2022-05-24 |
| EP3482201A4 (en) | 2020-02-19 |
| EP3482201B1 (en) | 2022-12-14 |
| US20220236269A1 (en) | 2022-07-28 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US12055545B2 (en) | Early diagnosis of infections | |
| US12044681B2 (en) | Protein signatures for distinguishing between bacterial and viral infections | |
| US11776658B2 (en) | Computational analysis of biological data using manifold and a hyperplane | |
| Lucas et al. | Delayed production of neutralizing antibodies correlates with fatal COVID-19 | |
| US20220326238A1 (en) | Methods of risk assessment and disease classification | |
| EP3504553B1 (en) | System and method for analysis of biological data | |
| EP3519833B1 (en) | Methods of prognosis and treatment | |
| Cheng et al. | A review of current effective COVID-19 testing methods and quality control | |
| US20240369552A1 (en) | Early diagnosis of infections | |
| WO2023275876A1 (en) | Method and system for analyzing biological data |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 17827122 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2017827122 Country of ref document: EP Effective date: 20190211 |