WO2015094392A1 - Compositions and methods for treatment of glaucoma - Google Patents
Compositions and methods for treatment of glaucoma Download PDFInfo
- Publication number
- WO2015094392A1 WO2015094392A1 PCT/US2014/015797 US2014015797W WO2015094392A1 WO 2015094392 A1 WO2015094392 A1 WO 2015094392A1 US 2014015797 W US2014015797 W US 2014015797W WO 2015094392 A1 WO2015094392 A1 WO 2015094392A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- concentration
- pharmaceutical composition
- buffer
- dexmedetomidine
- composition
- Prior art date
Links
- 239000000203 mixture Substances 0.000 title claims abstract description 186
- 208000010412 Glaucoma Diseases 0.000 title claims abstract description 31
- 238000000034 method Methods 0.000 title claims abstract description 30
- 238000011282 treatment Methods 0.000 title claims description 23
- HRLIOXLXPOHXTA-NSHDSACASA-N dexmedetomidine Chemical compound C1([C@@H](C)C=2C(=C(C)C=CC=2)C)=CN=C[N]1 HRLIOXLXPOHXTA-NSHDSACASA-N 0.000 claims abstract description 71
- 229960004253 dexmedetomidine Drugs 0.000 claims abstract description 70
- 239000000048 adrenergic agonist Substances 0.000 claims abstract description 21
- 229940126157 adrenergic receptor agonist Drugs 0.000 claims abstract description 21
- FAPWRFPIFSIZLT-UHFFFAOYSA-M Sodium chloride Chemical compound [Na+].[Cl-] FAPWRFPIFSIZLT-UHFFFAOYSA-M 0.000 claims description 65
- RVGRUAULSDPKGF-UHFFFAOYSA-N Poloxamer Chemical compound C1CO1.CC1CO1 RVGRUAULSDPKGF-UHFFFAOYSA-N 0.000 claims description 53
- 229920001983 poloxamer Polymers 0.000 claims description 42
- 239000008194 pharmaceutical composition Substances 0.000 claims description 38
- 229920000858 Cyclodextrin Polymers 0.000 claims description 37
- 229960000502 poloxamer Drugs 0.000 claims description 35
- 229920002134 Carboxymethyl cellulose Polymers 0.000 claims description 32
- 239000000872 buffer Substances 0.000 claims description 31
- 235000010948 carboxy methyl cellulose Nutrition 0.000 claims description 31
- 239000001768 carboxy methyl cellulose Substances 0.000 claims description 31
- 239000008112 carboxymethyl-cellulose Substances 0.000 claims description 31
- 150000003839 salts Chemical class 0.000 claims description 31
- 239000011780 sodium chloride Substances 0.000 claims description 30
- 229960004853 betadex Drugs 0.000 claims description 28
- WHGYBXFWUBPSRW-FOUAGVGXSA-N beta-cyclodextrin Chemical compound OC[C@H]([C@H]([C@@H]([C@H]1O)O)O[C@H]2O[C@@H]([C@@H](O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O3)[C@H](O)[C@H]2O)CO)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@@H]3O[C@@H]1CO WHGYBXFWUBPSRW-FOUAGVGXSA-N 0.000 claims description 26
- 239000003623 enhancer Substances 0.000 claims description 24
- 229920002675 Polyoxyl Polymers 0.000 claims description 23
- HFHDHCJBZVLPGP-UHFFFAOYSA-N schardinger α-dextrin Chemical compound O1C(C(C2O)O)C(CO)OC2OC(C(C2O)O)C(CO)OC2OC(C(C2O)O)C(CO)OC2OC(C(O)C2O)C(CO)OC2OC(C(C2O)O)C(CO)OC2OC2C(O)C(O)C1OC2CO HFHDHCJBZVLPGP-UHFFFAOYSA-N 0.000 claims description 22
- 125000000217 alkyl group Chemical group 0.000 claims description 20
- 239000008363 phosphate buffer Substances 0.000 claims description 20
- -1 polyvinylpyrridone Polymers 0.000 claims description 18
- 229920002701 Polyoxyl 40 Stearate Polymers 0.000 claims description 16
- 229940099429 polyoxyl 40 stearate Drugs 0.000 claims description 16
- 229920002125 Sokalan® Polymers 0.000 claims description 15
- 229920001223 polyethylene glycol Polymers 0.000 claims description 14
- 235000019333 sodium laurylsulphate Nutrition 0.000 claims description 14
- 239000004094 surface-active agent Substances 0.000 claims description 12
- VZCYOOQTPOCHFL-UHFFFAOYSA-N trans-butenedioic acid Natural products OC(=O)C=CC(O)=O VZCYOOQTPOCHFL-UHFFFAOYSA-N 0.000 claims description 11
- 108060003345 Adrenergic Receptor Proteins 0.000 claims description 10
- 102000017910 Adrenergic receptor Human genes 0.000 claims description 10
- 229910019142 PO4 Inorganic materials 0.000 claims description 10
- 239000002202 Polyethylene glycol Substances 0.000 claims description 10
- 229960000686 benzalkonium chloride Drugs 0.000 claims description 10
- CADWTSSKOVRVJC-UHFFFAOYSA-N benzyl(dimethyl)azanium;chloride Chemical compound [Cl-].C[NH+](C)CC1=CC=CC=C1 CADWTSSKOVRVJC-UHFFFAOYSA-N 0.000 claims description 10
- NBIIXXVUZAFLBC-UHFFFAOYSA-K phosphate Chemical compound [O-]P([O-])([O-])=O NBIIXXVUZAFLBC-UHFFFAOYSA-K 0.000 claims description 10
- 239000010452 phosphate Substances 0.000 claims description 10
- 239000004372 Polyvinyl alcohol Substances 0.000 claims description 9
- DBMJMQXJHONAFJ-UHFFFAOYSA-M Sodium laurylsulphate Chemical compound [Na+].CCCCCCCCCCCCOS([O-])(=O)=O DBMJMQXJHONAFJ-UHFFFAOYSA-M 0.000 claims description 9
- 239000003963 antioxidant agent Substances 0.000 claims description 9
- 229920002451 polyvinyl alcohol Polymers 0.000 claims description 9
- 229920000036 polyvinylpyrrolidone Polymers 0.000 claims description 9
- 235000013855 polyvinylpyrrolidone Nutrition 0.000 claims description 9
- 229920001285 xanthan gum Polymers 0.000 claims description 9
- BTBUEUYNUDRHOZ-UHFFFAOYSA-N Borate Chemical compound [O-]B([O-])[O-] BTBUEUYNUDRHOZ-UHFFFAOYSA-N 0.000 claims description 8
- BVKZGUZCCUSVTD-UHFFFAOYSA-L Carbonate Chemical compound [O-]C([O-])=O BVKZGUZCCUSVTD-UHFFFAOYSA-L 0.000 claims description 8
- WHNWPMSKXPGLAX-UHFFFAOYSA-N N-Vinyl-2-pyrrolidone Chemical compound C=CN1CCCC1=O WHNWPMSKXPGLAX-UHFFFAOYSA-N 0.000 claims description 8
- VJHCJDRQFCCTHL-UHFFFAOYSA-N acetic acid 2,3,4,5,6-pentahydroxyhexanal Chemical compound CC(O)=O.OCC(O)C(O)C(O)C(O)C=O VJHCJDRQFCCTHL-UHFFFAOYSA-N 0.000 claims description 8
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Chemical compound O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 claims description 8
- KRKNYBCHXYNGOX-UHFFFAOYSA-K Citrate Chemical compound [O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O KRKNYBCHXYNGOX-UHFFFAOYSA-K 0.000 claims description 7
- 229920002307 Dextran Polymers 0.000 claims description 7
- 229920002678 cellulose Polymers 0.000 claims description 7
- 239000001913 cellulose Substances 0.000 claims description 7
- VZCYOOQTPOCHFL-UPHRSURJSA-N maleic acid Chemical compound OC(=O)\C=C/C(O)=O VZCYOOQTPOCHFL-UPHRSURJSA-N 0.000 claims description 7
- 229940069328 povidone Drugs 0.000 claims description 7
- 230000003078 antioxidant effect Effects 0.000 claims description 6
- 229960002086 dextran Drugs 0.000 claims description 6
- 235000010979 hydroxypropyl methyl cellulose Nutrition 0.000 claims description 6
- 229920003088 hydroxypropyl methyl cellulose Polymers 0.000 claims description 6
- FZWBNHMXJMCXLU-BLAUPYHCSA-N isomaltotriose Chemical compound O[C@@H]1[C@@H](O)[C@H](O)[C@@H](CO)O[C@@H]1OC[C@@H]1[C@@H](O)[C@H](O)[C@@H](O)[C@@H](OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C=O)O1 FZWBNHMXJMCXLU-BLAUPYHCSA-N 0.000 claims description 6
- 230000003232 mucoadhesive effect Effects 0.000 claims description 6
- QTBSBXVTEAMEQO-UHFFFAOYSA-M Acetate Chemical compound CC([O-])=O QTBSBXVTEAMEQO-UHFFFAOYSA-M 0.000 claims description 5
- AFVFQIVMOAPDHO-UHFFFAOYSA-N Methanesulfonic acid Chemical compound CS(O)(=O)=O AFVFQIVMOAPDHO-UHFFFAOYSA-N 0.000 claims description 5
- 239000001866 hydroxypropyl methyl cellulose Substances 0.000 claims description 5
- UFVKGYZPFZQRLF-UHFFFAOYSA-N hydroxypropyl methyl cellulose Chemical compound OC1C(O)C(OC)OC(CO)C1OC1C(O)C(O)C(OC2C(C(O)C(OC3C(C(O)C(O)C(CO)O3)O)C(CO)O2)O)C(CO)O1 UFVKGYZPFZQRLF-UHFFFAOYSA-N 0.000 claims description 5
- 229920000609 methyl cellulose Polymers 0.000 claims description 5
- 235000010981 methylcellulose Nutrition 0.000 claims description 5
- 239000001923 methylcellulose Substances 0.000 claims description 5
- CPELXLSAUQHCOX-UHFFFAOYSA-M Bromide Chemical compound [Br-] CPELXLSAUQHCOX-UHFFFAOYSA-M 0.000 claims description 4
- 229920001661 Chitosan Polymers 0.000 claims description 4
- FEWJPZIEWOKRBE-JCYAYHJZSA-N Dextrotartaric acid Chemical compound OC(=O)[C@H](O)[C@@H](O)C(O)=O FEWJPZIEWOKRBE-JCYAYHJZSA-N 0.000 claims description 4
- VZCYOOQTPOCHFL-OWOJBTEDSA-N Fumaric acid Chemical compound OC(=O)\C=C\C(O)=O VZCYOOQTPOCHFL-OWOJBTEDSA-N 0.000 claims description 4
- 108010010803 Gelatin Proteins 0.000 claims description 4
- CPELXLSAUQHCOX-UHFFFAOYSA-N Hydrogen bromide Chemical compound Br CPELXLSAUQHCOX-UHFFFAOYSA-N 0.000 claims description 4
- 229920000663 Hydroxyethyl cellulose Polymers 0.000 claims description 4
- 239000004354 Hydroxyethyl cellulose Substances 0.000 claims description 4
- 229920000161 Locust bean gum Polymers 0.000 claims description 4
- 229910002651 NO3 Inorganic materials 0.000 claims description 4
- NHNBFGGVMKEFGY-UHFFFAOYSA-N Nitrate Chemical compound [O-][N+]([O-])=O NHNBFGGVMKEFGY-UHFFFAOYSA-N 0.000 claims description 4
- QAOWNCQODCNURD-UHFFFAOYSA-L Sulfate Chemical compound [O-]S([O-])(=O)=O QAOWNCQODCNURD-UHFFFAOYSA-L 0.000 claims description 4
- 239000008351 acetate buffer Substances 0.000 claims description 4
- 230000002378 acidificating effect Effects 0.000 claims description 4
- 229920000615 alginic acid Polymers 0.000 claims description 4
- 235000010443 alginic acid Nutrition 0.000 claims description 4
- 239000000783 alginic acid Substances 0.000 claims description 4
- 229960001126 alginic acid Drugs 0.000 claims description 4
- 150000004781 alginic acids Chemical class 0.000 claims description 4
- WPYMKLBDIGXBTP-UHFFFAOYSA-N benzoic acid Chemical compound OC(=O)C1=CC=CC=C1 WPYMKLBDIGXBTP-UHFFFAOYSA-N 0.000 claims description 4
- 239000007979 citrate buffer Substances 0.000 claims description 4
- MRUAUOIMASANKQ-UHFFFAOYSA-N cocamidopropyl betaine Chemical compound CCCCCCCCCCCC(=O)NCCC[N+](C)(C)CC([O-])=O MRUAUOIMASANKQ-UHFFFAOYSA-N 0.000 claims description 4
- 229940073507 cocamidopropyl betaine Drugs 0.000 claims description 4
- 239000008273 gelatin Substances 0.000 claims description 4
- 229920000159 gelatin Polymers 0.000 claims description 4
- 235000019322 gelatine Nutrition 0.000 claims description 4
- 235000011852 gelatine desserts Nutrition 0.000 claims description 4
- QAOWNCQODCNURD-UHFFFAOYSA-M hydrogensulfate Chemical compound OS([O-])(=O)=O QAOWNCQODCNURD-UHFFFAOYSA-M 0.000 claims description 4
- 235000019447 hydroxyethyl cellulose Nutrition 0.000 claims description 4
- 235000010420 locust bean gum Nutrition 0.000 claims description 4
- 239000000711 locust bean gum Substances 0.000 claims description 4
- 230000000626 neurodegenerative effect Effects 0.000 claims description 4
- KDYFGRWQOYBRFD-UHFFFAOYSA-L succinate(2-) Chemical compound [O-]C(=O)CCC([O-])=O KDYFGRWQOYBRFD-UHFFFAOYSA-L 0.000 claims description 4
- 229940095064 tartrate Drugs 0.000 claims description 4
- UEUXEKPTXMALOB-UHFFFAOYSA-J tetrasodium;2-[2-[bis(carboxylatomethyl)amino]ethyl-(carboxylatomethyl)amino]acetate Chemical compound [Na+].[Na+].[Na+].[Na+].[O-]C(=O)CN(CC([O-])=O)CCN(CC([O-])=O)CC([O-])=O UEUXEKPTXMALOB-UHFFFAOYSA-J 0.000 claims description 4
- KIUKXJAPPMFGSW-DNGZLQJQSA-N (2S,3S,4S,5R,6R)-6-[(2S,3R,4R,5S,6R)-3-Acetamido-2-[(2S,3S,4R,5R,6R)-6-[(2R,3R,4R,5S,6R)-3-acetamido-2,5-dihydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-2-carboxy-4,5-dihydroxyoxan-3-yl]oxy-5-hydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-3,4,5-trihydroxyoxane-2-carboxylic acid Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@H](O[C@H]2[C@@H]([C@@H](O[C@H]3[C@@H]([C@@H](O)[C@H](O)[C@H](O3)C(O)=O)O)[C@H](O)[C@@H](CO)O2)NC(C)=O)[C@@H](C(O)=O)O1 KIUKXJAPPMFGSW-DNGZLQJQSA-N 0.000 claims description 3
- WSWCOQWTEOXDQX-MQQKCMAXSA-M (E,E)-sorbate Chemical compound C\C=C\C=C\C([O-])=O WSWCOQWTEOXDQX-MQQKCMAXSA-M 0.000 claims description 3
- 229920002907 Guar gum Polymers 0.000 claims description 3
- 235000010643 Leucaena leucocephala Nutrition 0.000 claims description 3
- 240000007472 Leucaena leucocephala Species 0.000 claims description 3
- 229920000148 Polycarbophil calcium Polymers 0.000 claims description 3
- GDSRMADSINPKSL-HSEONFRVSA-N gamma-cyclodextrin Chemical compound OC[C@H]([C@H]([C@@H]([C@H]1O)O)O[C@H]2O[C@@H]([C@@H](O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O3)[C@H](O)[C@H]2O)CO)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@@H]3O[C@@H]1CO GDSRMADSINPKSL-HSEONFRVSA-N 0.000 claims description 3
- 229940080345 gamma-cyclodextrin Drugs 0.000 claims description 3
- 239000000665 guar gum Substances 0.000 claims description 3
- 235000010417 guar gum Nutrition 0.000 claims description 3
- 229960002154 guar gum Drugs 0.000 claims description 3
- 229920002674 hyaluronan Polymers 0.000 claims description 3
- 229960003160 hyaluronic acid Drugs 0.000 claims description 3
- 229920003063 hydroxymethyl cellulose Polymers 0.000 claims description 3
- 229940031574 hydroxymethyl cellulose Drugs 0.000 claims description 3
- 235000010987 pectin Nutrition 0.000 claims description 3
- 229920001277 pectin Polymers 0.000 claims description 3
- 239000001814 pectin Substances 0.000 claims description 3
- 229960000292 pectin Drugs 0.000 claims description 3
- 229950005134 polycarbophil Drugs 0.000 claims description 3
- 229940075554 sorbate Drugs 0.000 claims description 3
- 239000008223 sterile water Substances 0.000 claims description 3
- 239000008362 succinate buffer Substances 0.000 claims description 3
- 239000000556 agonist Substances 0.000 abstract description 53
- 238000009472 formulation Methods 0.000 description 91
- 230000000694 effects Effects 0.000 description 88
- 230000004410 intraocular pressure Effects 0.000 description 86
- 230000009467 reduction Effects 0.000 description 76
- XYLJNLCSTIOKRM-UHFFFAOYSA-N Alphagan Chemical compound C1=CC2=NC=CN=C2C(Br)=C1NC1=NCCN1 XYLJNLCSTIOKRM-UHFFFAOYSA-N 0.000 description 62
- 229960003679 brimonidine Drugs 0.000 description 54
- 239000003814 drug Substances 0.000 description 53
- 229940079593 drug Drugs 0.000 description 49
- 230000000699 topical effect Effects 0.000 description 32
- 230000009885 systemic effect Effects 0.000 description 31
- 230000002829 reductive effect Effects 0.000 description 29
- 238000010521 absorption reaction Methods 0.000 description 27
- 206010015150 Erythema Diseases 0.000 description 19
- 102000005962 receptors Human genes 0.000 description 19
- 108020003175 receptors Proteins 0.000 description 19
- 208000002193 Pain Diseases 0.000 description 18
- 239000003795 chemical substances by application Substances 0.000 description 17
- KRKNYBCHXYNGOX-UHFFFAOYSA-N citric acid Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O KRKNYBCHXYNGOX-UHFFFAOYSA-N 0.000 description 17
- 230000001965 increasing effect Effects 0.000 description 17
- 206010039897 Sedation Diseases 0.000 description 14
- 230000036280 sedation Effects 0.000 description 14
- 229920001992 poloxamer 407 Polymers 0.000 description 13
- 229940044476 poloxamer 407 Drugs 0.000 description 13
- 230000008901 benefit Effects 0.000 description 12
- KCXVZYZYPLLWCC-UHFFFAOYSA-N EDTA Chemical compound OC(=O)CN(CC(O)=O)CCN(CC(O)=O)CC(O)=O KCXVZYZYPLLWCC-UHFFFAOYSA-N 0.000 description 11
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 description 11
- 239000004615 ingredient Substances 0.000 description 10
- 238000012360 testing method Methods 0.000 description 10
- 238000005259 measurement Methods 0.000 description 9
- HGASFNYMVGEKTF-UHFFFAOYSA-N octan-1-ol;hydrate Chemical compound O.CCCCCCCCO HGASFNYMVGEKTF-UHFFFAOYSA-N 0.000 description 9
- 229920000136 polysorbate Polymers 0.000 description 9
- 206010020751 Hypersensitivity Diseases 0.000 description 8
- 241000283973 Oryctolagus cuniculus Species 0.000 description 8
- 239000002253 acid Substances 0.000 description 8
- 229940003677 alphagan Drugs 0.000 description 8
- 229940097362 cyclodextrins Drugs 0.000 description 8
- 238000002474 experimental method Methods 0.000 description 8
- 230000035515 penetration Effects 0.000 description 8
- 238000005192 partition Methods 0.000 description 7
- 239000003755 preservative agent Substances 0.000 description 7
- 239000000243 solution Substances 0.000 description 7
- 239000003981 vehicle Substances 0.000 description 7
- GJSURZIOUXUGAL-UHFFFAOYSA-N Clonidine Chemical compound ClC1=CC=CC(Cl)=C1NC1=NCCN1 GJSURZIOUXUGAL-UHFFFAOYSA-N 0.000 description 6
- FBPFZTCFMRRESA-KVTDHHQDSA-N D-Mannitol Chemical compound OC[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)CO FBPFZTCFMRRESA-KVTDHHQDSA-N 0.000 description 6
- PEDCQBHIVMGVHV-UHFFFAOYSA-N Glycerine Chemical compound OCC(O)CO PEDCQBHIVMGVHV-UHFFFAOYSA-N 0.000 description 6
- 229930195725 Mannitol Natural products 0.000 description 6
- DNIAPMSPPWPWGF-UHFFFAOYSA-N Propylene glycol Chemical compound CC(O)CO DNIAPMSPPWPWGF-UHFFFAOYSA-N 0.000 description 6
- 208000026935 allergic disease Diseases 0.000 description 6
- 230000007815 allergy Effects 0.000 description 6
- 235000011175 beta-cyclodextrine Nutrition 0.000 description 6
- 229960002896 clonidine Drugs 0.000 description 6
- 201000010099 disease Diseases 0.000 description 6
- 238000013401 experimental design Methods 0.000 description 6
- 230000006872 improvement Effects 0.000 description 6
- 239000000594 mannitol Substances 0.000 description 6
- 235000010355 mannitol Nutrition 0.000 description 6
- 230000001225 therapeutic effect Effects 0.000 description 6
- 230000001052 transient effect Effects 0.000 description 6
- 239000001116 FEMA 4028 Substances 0.000 description 5
- 229920003171 Poly (ethylene oxide) Polymers 0.000 description 5
- 150000007513 acids Chemical class 0.000 description 5
- 239000002585 base Substances 0.000 description 5
- 230000036471 bradycardia Effects 0.000 description 5
- 208000006218 bradycardia Diseases 0.000 description 5
- 239000004359 castor oil Substances 0.000 description 5
- 235000019438 castor oil Nutrition 0.000 description 5
- 210000004087 cornea Anatomy 0.000 description 5
- 208000035475 disorder Diseases 0.000 description 5
- 238000011067 equilibration Methods 0.000 description 5
- ZEMPKEQAKRGZGQ-XOQCFJPHSA-N glycerol triricinoleate Natural products CCCCCC[C@@H](O)CC=CCCCCCCCC(=O)OC[C@@H](COC(=O)CCCCCCCC=CC[C@@H](O)CCCCCC)OC(=O)CCCCCCCC=CC[C@H](O)CCCCCC ZEMPKEQAKRGZGQ-XOQCFJPHSA-N 0.000 description 5
- 208000028867 ischemia Diseases 0.000 description 5
- 210000001328 optic nerve Anatomy 0.000 description 5
- 239000003961 penetration enhancing agent Substances 0.000 description 5
- 235000010482 polyoxyethylene sorbitan monooleate Nutrition 0.000 description 5
- 239000000244 polyoxyethylene sorbitan monooleate Substances 0.000 description 5
- 229950008882 polysorbate Drugs 0.000 description 5
- 229920000053 polysorbate 80 Polymers 0.000 description 5
- 229940068968 polysorbate 80 Drugs 0.000 description 5
- 229940002612 prodrug Drugs 0.000 description 5
- 239000000651 prodrug Substances 0.000 description 5
- 230000002087 whitening effect Effects 0.000 description 5
- NZAQRZWBQUIBSF-UHFFFAOYSA-N 4-(4-sulfobutoxy)butane-1-sulfonic acid Chemical class OS(=O)(=O)CCCCOCCCCS(O)(=O)=O NZAQRZWBQUIBSF-UHFFFAOYSA-N 0.000 description 4
- 101150051188 Adora2a gene Proteins 0.000 description 4
- RTZKZFJDLAIYFH-UHFFFAOYSA-N Diethyl ether Chemical compound CCOCC RTZKZFJDLAIYFH-UHFFFAOYSA-N 0.000 description 4
- 206010020565 Hyperaemia Diseases 0.000 description 4
- 230000009471 action Effects 0.000 description 4
- 239000000654 additive Substances 0.000 description 4
- 239000002738 chelating agent Substances 0.000 description 4
- 150000001875 compounds Chemical class 0.000 description 4
- 239000002537 cosmetic Substances 0.000 description 4
- GNBHRKFJIUUOQI-UHFFFAOYSA-N fluorescein Chemical compound O1C(=O)C2=CC=CC=C2C21C1=CC=C(O)C=C1OC1=CC(O)=CC=C21 GNBHRKFJIUUOQI-UHFFFAOYSA-N 0.000 description 4
- 239000012458 free base Substances 0.000 description 4
- 239000003349 gelling agent Substances 0.000 description 4
- 230000014759 maintenance of location Effects 0.000 description 4
- LXCFILQKKLGQFO-UHFFFAOYSA-N methylparaben Chemical compound COC(=O)C1=CC=C(O)C=C1 LXCFILQKKLGQFO-UHFFFAOYSA-N 0.000 description 4
- 239000002736 nonionic surfactant Substances 0.000 description 4
- WWZKQHOCKIZLMA-UHFFFAOYSA-N octanoic acid Chemical compound CCCCCCCC(O)=O WWZKQHOCKIZLMA-UHFFFAOYSA-N 0.000 description 4
- 229920001993 poloxamer 188 Polymers 0.000 description 4
- 229940044519 poloxamer 188 Drugs 0.000 description 4
- 230000002035 prolonged effect Effects 0.000 description 4
- 208000024891 symptom Diseases 0.000 description 4
- ODLHGICHYURWBS-LKONHMLTSA-N trappsol cyclo Chemical compound CC(O)COC[C@H]([C@H]([C@@H]([C@H]1O)O)O[C@H]2O[C@@H]([C@@H](O[C@H]3O[C@H](COCC(C)O)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](COCC(C)O)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](COCC(C)O)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](COCC(C)O)[C@H]([C@@H]([C@H]3O)O)O3)[C@H](O)[C@H]2O)COCC(O)C)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@@H]3O[C@@H]1COCC(C)O ODLHGICHYURWBS-LKONHMLTSA-N 0.000 description 4
- 238000009736 wetting Methods 0.000 description 4
- 102000003688 G-Protein-Coupled Receptors Human genes 0.000 description 3
- 108090000045 G-Protein-Coupled Receptors Proteins 0.000 description 3
- 206010020772 Hypertension Diseases 0.000 description 3
- 208000001953 Hypotension Diseases 0.000 description 3
- XQFRJNBWHJMXHO-RRKCRQDMSA-N IDUR Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C(I)=C1 XQFRJNBWHJMXHO-RRKCRQDMSA-N 0.000 description 3
- 229920002685 Polyoxyl 35CastorOil Polymers 0.000 description 3
- HEMHJVSKTPXQMS-UHFFFAOYSA-M Sodium hydroxide Chemical compound [OH-].[Na+] HEMHJVSKTPXQMS-UHFFFAOYSA-M 0.000 description 3
- 206010047513 Vision blurred Diseases 0.000 description 3
- 230000000996 additive effect Effects 0.000 description 3
- 239000003945 anionic surfactant Substances 0.000 description 3
- 229960002610 apraclonidine Drugs 0.000 description 3
- IEJXVRYNEISIKR-UHFFFAOYSA-N apraclonidine Chemical compound ClC1=CC(N)=CC(Cl)=C1NC1=NCCN1 IEJXVRYNEISIKR-UHFFFAOYSA-N 0.000 description 3
- AQOKCDNYWBIDND-FTOWTWDKSA-N bimatoprost Chemical compound CCNC(=O)CCC\C=C/C[C@H]1[C@@H](O)C[C@@H](O)[C@@H]1\C=C\[C@@H](O)CCC1=CC=CC=C1 AQOKCDNYWBIDND-FTOWTWDKSA-N 0.000 description 3
- 210000004027 cell Anatomy 0.000 description 3
- 230000004087 circulation Effects 0.000 description 3
- 231100000478 corneal permeability Toxicity 0.000 description 3
- 230000007423 decrease Effects 0.000 description 3
- 206010013781 dry mouth Diseases 0.000 description 3
- 239000003792 electrolyte Substances 0.000 description 3
- 230000002708 enhancing effect Effects 0.000 description 3
- 210000003560 epithelium corneal Anatomy 0.000 description 3
- 150000002148 esters Chemical class 0.000 description 3
- 239000000499 gel Substances 0.000 description 3
- 235000011187 glycerol Nutrition 0.000 description 3
- 230000036543 hypotension Effects 0.000 description 3
- 229960004716 idoxuridine Drugs 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- GGXICVAJURFBLW-CEYXHVGTSA-N latanoprost Chemical compound CC(C)OC(=O)CCC\C=C/C[C@H]1[C@@H](O)C[C@@H](O)[C@@H]1CC[C@@H](O)CCC1=CC=CC=C1 GGXICVAJURFBLW-CEYXHVGTSA-N 0.000 description 3
- 230000000324 neuroprotective effect Effects 0.000 description 3
- 201000005111 ocular hyperemia Diseases 0.000 description 3
- 229940023490 ophthalmic product Drugs 0.000 description 3
- 239000000546 pharmaceutical excipient Substances 0.000 description 3
- 229920001451 polypropylene glycol Polymers 0.000 description 3
- 230000002265 prevention Effects 0.000 description 3
- 239000000047 product Substances 0.000 description 3
- 150000003180 prostaglandins Chemical class 0.000 description 3
- 229940127293 prostanoid Drugs 0.000 description 3
- 150000003814 prostanoids Chemical class 0.000 description 3
- 230000003381 solubilizing effect Effects 0.000 description 3
- 230000007704 transition Effects 0.000 description 3
- MKPLKVHSHYCHOC-AHTXBMBWSA-N travoprost Chemical compound CC(C)OC(=O)CCC\C=C/C[C@H]1[C@@H](O)C[C@@H](O)[C@@H]1\C=C\[C@@H](O)COC1=CC=CC(C(F)(F)F)=C1 MKPLKVHSHYCHOC-AHTXBMBWSA-N 0.000 description 3
- ZORQXIQZAOLNGE-UHFFFAOYSA-N 1,1-difluorocyclohexane Chemical compound FC1(F)CCCCC1 ZORQXIQZAOLNGE-UHFFFAOYSA-N 0.000 description 2
- IWEGDQUCWQFKHS-UHFFFAOYSA-N 1-(1,3-dioxolan-2-ylmethyl)-4-(4,4,5,5-tetramethyl-1,3,2-dioxaborolan-2-yl)pyrazole Chemical compound O1C(C)(C)C(C)(C)OB1C1=CN(CC2OCCO2)N=C1 IWEGDQUCWQFKHS-UHFFFAOYSA-N 0.000 description 2
- IHPYMWDTONKSCO-UHFFFAOYSA-N 2,2'-piperazine-1,4-diylbisethanesulfonic acid Chemical compound OS(=O)(=O)CCN1CCN(CCS(O)(=O)=O)CC1 IHPYMWDTONKSCO-UHFFFAOYSA-N 0.000 description 2
- JKMHFZQWWAIEOD-UHFFFAOYSA-N 2-[4-(2-hydroxyethyl)piperazin-1-yl]ethanesulfonic acid Chemical compound OCC[NH+]1CCN(CCS([O-])(=O)=O)CC1 JKMHFZQWWAIEOD-UHFFFAOYSA-N 0.000 description 2
- AJTVSSFTXWNIRG-UHFFFAOYSA-N 2-[bis(2-hydroxyethyl)amino]ethanesulfonic acid Chemical compound OCC[NH+](CCO)CCS([O-])(=O)=O AJTVSSFTXWNIRG-UHFFFAOYSA-N 0.000 description 2
- LVQFQZZGTZFUNF-UHFFFAOYSA-N 2-hydroxy-3-[4-(2-hydroxy-3-sulfonatopropyl)piperazine-1,4-diium-1-yl]propane-1-sulfonate Chemical compound OS(=O)(=O)CC(O)CN1CCN(CC(O)CS(O)(=O)=O)CC1 LVQFQZZGTZFUNF-UHFFFAOYSA-N 0.000 description 2
- WRMNZCZEMHIOCP-UHFFFAOYSA-N 2-phenylethanol Chemical compound OCCC1=CC=CC=C1 WRMNZCZEMHIOCP-UHFFFAOYSA-N 0.000 description 2
- XCBLFURAFHFFJF-UHFFFAOYSA-N 3-[bis(2-hydroxyethyl)azaniumyl]-2-hydroxypropane-1-sulfonate Chemical compound OCCN(CCO)CC(O)CS(O)(=O)=O XCBLFURAFHFFJF-UHFFFAOYSA-N 0.000 description 2
- NIXOWILDQLNWCW-UHFFFAOYSA-N Acrylic acid Chemical compound OC(=O)C=C NIXOWILDQLNWCW-UHFFFAOYSA-N 0.000 description 2
- QGZKDVFQNNGYKY-UHFFFAOYSA-N Ammonia Chemical compound N QGZKDVFQNNGYKY-UHFFFAOYSA-N 0.000 description 2
- OYPRJOBELJOOCE-UHFFFAOYSA-N Calcium Chemical compound [Ca] OYPRJOBELJOOCE-UHFFFAOYSA-N 0.000 description 2
- 239000005635 Caprylic acid (CAS 124-07-2) Substances 0.000 description 2
- 206010010717 Conjunctival follicles Diseases 0.000 description 2
- 206010010726 Conjunctival oedema Diseases 0.000 description 2
- 206010013774 Dry eye Diseases 0.000 description 2
- AEMRFAOFKBGASW-UHFFFAOYSA-M Glycolate Chemical compound OCC([O-])=O AEMRFAOFKBGASW-UHFFFAOYSA-M 0.000 description 2
- 206010019233 Headaches Diseases 0.000 description 2
- VEXZGXHMUGYJMC-UHFFFAOYSA-N Hydrochloric acid Chemical compound Cl VEXZGXHMUGYJMC-UHFFFAOYSA-N 0.000 description 2
- 208000010038 Ischemic Optic Neuropathy Diseases 0.000 description 2
- 206010030924 Optic ischaemic neuropathy Diseases 0.000 description 2
- NBIIXXVUZAFLBC-UHFFFAOYSA-N Phosphoric acid Chemical compound OP(O)(O)=O NBIIXXVUZAFLBC-UHFFFAOYSA-N 0.000 description 2
- 229920001213 Polysorbate 20 Polymers 0.000 description 2
- WCUXLLCKKVVCTQ-UHFFFAOYSA-M Potassium chloride Chemical compound [Cl-].[K+] WCUXLLCKKVVCTQ-UHFFFAOYSA-M 0.000 description 2
- CDBYLPFSWZWCQE-UHFFFAOYSA-L Sodium Carbonate Chemical compound [Na+].[Na+].[O-]C([O-])=O CDBYLPFSWZWCQE-UHFFFAOYSA-L 0.000 description 2
- VMHLLURERBWHNL-UHFFFAOYSA-M Sodium acetate Chemical compound [Na+].CC([O-])=O VMHLLURERBWHNL-UHFFFAOYSA-M 0.000 description 2
- UIIMBOGNXHQVGW-UHFFFAOYSA-M Sodium bicarbonate Chemical compound [Na+].OC([O-])=O UIIMBOGNXHQVGW-UHFFFAOYSA-M 0.000 description 2
- 239000004480 active ingredient Substances 0.000 description 2
- 102000030621 adenylate cyclase Human genes 0.000 description 2
- 108060000200 adenylate cyclase Proteins 0.000 description 2
- 239000003732 agents acting on the eye Substances 0.000 description 2
- 125000000129 anionic group Chemical group 0.000 description 2
- 201000007058 anterior ischemic optic neuropathy Diseases 0.000 description 2
- 230000009286 beneficial effect Effects 0.000 description 2
- 230000015572 biosynthetic process Effects 0.000 description 2
- 208000010217 blepharitis Diseases 0.000 description 2
- KGBXLFKZBHKPEV-UHFFFAOYSA-N boric acid Chemical compound OB(O)O KGBXLFKZBHKPEV-UHFFFAOYSA-N 0.000 description 2
- 239000004327 boric acid Substances 0.000 description 2
- 229960002645 boric acid Drugs 0.000 description 2
- 229960001724 brimonidine tartrate Drugs 0.000 description 2
- 235000019846 buffering salt Nutrition 0.000 description 2
- 239000011575 calcium Substances 0.000 description 2
- 229910052791 calcium Inorganic materials 0.000 description 2
- 159000000007 calcium salts Chemical class 0.000 description 2
- 229960001631 carbomer Drugs 0.000 description 2
- 230000008859 change Effects 0.000 description 2
- OSASVXMJTNOKOY-UHFFFAOYSA-N chlorobutanol Chemical compound CC(C)(O)C(Cl)(Cl)Cl OSASVXMJTNOKOY-UHFFFAOYSA-N 0.000 description 2
- 229960004106 citric acid Drugs 0.000 description 2
- 150000001860 citric acid derivatives Chemical class 0.000 description 2
- 230000000052 comparative effect Effects 0.000 description 2
- SMVRDGHCVNAOIN-UHFFFAOYSA-L disodium;1-dodecoxydodecane;sulfate Chemical compound [Na+].[Na+].[O-]S([O-])(=O)=O.CCCCCCCCCCCCOCCCCCCCCCCCC SMVRDGHCVNAOIN-UHFFFAOYSA-L 0.000 description 2
- 208000002173 dizziness Diseases 0.000 description 2
- 238000012377 drug delivery Methods 0.000 description 2
- 230000004406 elevated intraocular pressure Effects 0.000 description 2
- 210000003038 endothelium Anatomy 0.000 description 2
- 210000000981 epithelium Anatomy 0.000 description 2
- BEFDCLMNVWHSGT-UHFFFAOYSA-N ethenylcyclopentane Chemical compound C=CC1CCCC1 BEFDCLMNVWHSGT-UHFFFAOYSA-N 0.000 description 2
- 229960005150 glycerol Drugs 0.000 description 2
- 231100000869 headache Toxicity 0.000 description 2
- 102000034345 heterotrimeric G proteins Human genes 0.000 description 2
- 108091006093 heterotrimeric G proteins Proteins 0.000 description 2
- BXWNKGSJHAJOGX-UHFFFAOYSA-N hexadecan-1-ol Chemical compound CCCCCCCCCCCCCCCCO BXWNKGSJHAJOGX-UHFFFAOYSA-N 0.000 description 2
- 230000001631 hypertensive effect Effects 0.000 description 2
- 239000000815 hypotonic solution Substances 0.000 description 2
- 230000006698 induction Effects 0.000 description 2
- 229910052500 inorganic mineral Inorganic materials 0.000 description 2
- 230000003834 intracellular effect Effects 0.000 description 2
- 230000007794 irritation Effects 0.000 description 2
- 229940112534 lumigan Drugs 0.000 description 2
- 235000010270 methyl p-hydroxybenzoate Nutrition 0.000 description 2
- 239000004292 methyl p-hydroxybenzoate Substances 0.000 description 2
- 229960002216 methylparaben Drugs 0.000 description 2
- 235000010755 mineral Nutrition 0.000 description 2
- 239000011707 mineral Substances 0.000 description 2
- 229920000847 nonoxynol Polymers 0.000 description 2
- 229960002446 octanoic acid Drugs 0.000 description 2
- 229940094443 oxytocics prostaglandins Drugs 0.000 description 2
- 230000036961 partial effect Effects 0.000 description 2
- 229920005862 polyol Polymers 0.000 description 2
- 150000003077 polyols Chemical class 0.000 description 2
- 235000010486 polyoxyethylene sorbitan monolaurate Nutrition 0.000 description 2
- 239000000256 polyoxyethylene sorbitan monolaurate Substances 0.000 description 2
- 229940068977 polysorbate 20 Drugs 0.000 description 2
- 230000003389 potentiating effect Effects 0.000 description 2
- 230000002335 preservative effect Effects 0.000 description 2
- 230000004224 protection Effects 0.000 description 2
- ARIWANIATODDMH-UHFFFAOYSA-N rac-1-monolauroylglycerol Chemical compound CCCCCCCCCCCC(=O)OCC(O)CO ARIWANIATODDMH-UHFFFAOYSA-N 0.000 description 2
- GHBFNMLVSPCDGN-UHFFFAOYSA-N rac-1-monooctanoylglycerol Chemical compound CCCCCCCC(=O)OCC(O)CO GHBFNMLVSPCDGN-UHFFFAOYSA-N 0.000 description 2
- 230000007115 recruitment Effects 0.000 description 2
- 230000002207 retinal effect Effects 0.000 description 2
- 210000003994 retinal ganglion cell Anatomy 0.000 description 2
- 230000001624 sedative effect Effects 0.000 description 2
- 230000035807 sensation Effects 0.000 description 2
- 239000001632 sodium acetate Substances 0.000 description 2
- 235000017281 sodium acetate Nutrition 0.000 description 2
- HRZFUMHJMZEROT-UHFFFAOYSA-L sodium disulfite Chemical compound [Na+].[Na+].[O-]S(=O)S([O-])(=O)=O HRZFUMHJMZEROT-UHFFFAOYSA-L 0.000 description 2
- 229940001584 sodium metabisulfite Drugs 0.000 description 2
- 235000010262 sodium metabisulphite Nutrition 0.000 description 2
- 235000010199 sorbic acid Nutrition 0.000 description 2
- 239000004334 sorbic acid Substances 0.000 description 2
- 229940075582 sorbic acid Drugs 0.000 description 2
- 235000011069 sorbitan monooleate Nutrition 0.000 description 2
- 239000001593 sorbitan monooleate Substances 0.000 description 2
- 229940035049 sorbitan monooleate Drugs 0.000 description 2
- 229940124597 therapeutic agent Drugs 0.000 description 2
- 230000008719 thickening Effects 0.000 description 2
- 231100000419 toxicity Toxicity 0.000 description 2
- 230000001988 toxicity Effects 0.000 description 2
- 229940113006 travatan Drugs 0.000 description 2
- 230000002792 vascular Effects 0.000 description 2
- 229940002639 xalatan Drugs 0.000 description 2
- 239000000230 xanthan gum Substances 0.000 description 2
- 235000010493 xanthan gum Nutrition 0.000 description 2
- 229940082509 xanthan gum Drugs 0.000 description 2
- PVPBHKCSQBLDEW-ZQOBQRRWSA-N (1S,3R,5R,6S,8R,10R,11S,13R,15R,16S,18R,20R,21S,23R,25R,26S,28R,30R,31S,33R,35R,36R,37R,38R,39R,40R,41R,42R,43R,44R,45R,46R,47R,48R,49R)-5,10,15,20,25,30,35-heptakis(hydroxymethyl)-2,4,7,9,12,14,17,19,22,24,27,29,32,34-tetradecaoxaoctacyclo[31.2.2.23,6.28,11.213,16.218,21.223,26.228,31]nonatetracontane-36,37,38,39,40,41,42,43,44,45,46,47,48,49-tetradecol 4-hydroxybutane-1-sulfonic acid Chemical compound OCCCCS(O)(=O)=O.OC[C@H]1O[C@@H]2O[C@@H]3[C@@H](CO)O[C@H](O[C@@H]4[C@@H](CO)O[C@H](O[C@@H]5[C@@H](CO)O[C@H](O[C@@H]6[C@@H](CO)O[C@H](O[C@@H]7[C@@H](CO)O[C@H](O[C@@H]8[C@@H](CO)O[C@H](O[C@H]1[C@H](O)[C@H]2O)[C@H](O)[C@H]8O)[C@H](O)[C@H]7O)[C@H](O)[C@H]6O)[C@H](O)[C@H]5O)[C@H](O)[C@H]4O)[C@H](O)[C@H]3O PVPBHKCSQBLDEW-ZQOBQRRWSA-N 0.000 description 1
- YKFCISHFRZHKHY-NGQGLHOPSA-N (2s)-2-amino-3-(3,4-dihydroxyphenyl)-2-methylpropanoic acid;trihydrate Chemical compound O.O.O.OC(=O)[C@](N)(C)CC1=CC=C(O)C(O)=C1.OC(=O)[C@](N)(C)CC1=CC=C(O)C(O)=C1 YKFCISHFRZHKHY-NGQGLHOPSA-N 0.000 description 1
- XOMRRQXKHMYMOC-NRFANRHFSA-N (3s)-3-hexadecanoyloxy-4-(trimethylazaniumyl)butanoate Chemical compound CCCCCCCCCCCCCCCC(=O)O[C@@H](CC([O-])=O)C[N+](C)(C)C XOMRRQXKHMYMOC-NRFANRHFSA-N 0.000 description 1
- JCIIKRHCWVHVFF-UHFFFAOYSA-N 1,2,4-thiadiazol-5-amine;hydrochloride Chemical compound Cl.NC1=NC=NS1 JCIIKRHCWVHVFF-UHFFFAOYSA-N 0.000 description 1
- WTOROJZGWRPWSM-UHFFFAOYSA-N 1-amino-4-hydroxy-3,3-bis(hydroxymethyl)butane-2-sulfonic acid Chemical compound NCC(S(O)(=O)=O)C(CO)(CO)CO WTOROJZGWRPWSM-UHFFFAOYSA-N 0.000 description 1
- ARIWANIATODDMH-AWEZNQCLSA-N 1-lauroyl-sn-glycerol Chemical compound CCCCCCCCCCCC(=O)OC[C@@H](O)CO ARIWANIATODDMH-AWEZNQCLSA-N 0.000 description 1
- RRZWKUGIZRDCPB-UHFFFAOYSA-N 2,3-dihydroxypropyl hexanoate Chemical compound CCCCCC(=O)OCC(O)CO RRZWKUGIZRDCPB-UHFFFAOYSA-N 0.000 description 1
- SXGZJKUKBWWHRA-UHFFFAOYSA-N 2-(N-morpholiniumyl)ethanesulfonate Chemical compound [O-]S(=O)(=O)CC[NH+]1CCOCC1 SXGZJKUKBWWHRA-UHFFFAOYSA-N 0.000 description 1
- IEQAICDLOKRSRL-UHFFFAOYSA-N 2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-[2-(2-dodecoxyethoxy)ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethoxy]ethanol Chemical compound CCCCCCCCCCCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCOCCO IEQAICDLOKRSRL-UHFFFAOYSA-N 0.000 description 1
- URDCARMUOSMFFI-UHFFFAOYSA-N 2-[2-[bis(carboxymethyl)amino]ethyl-(2-hydroxyethyl)amino]acetic acid Chemical compound OCCN(CC(O)=O)CCN(CC(O)=O)CC(O)=O URDCARMUOSMFFI-UHFFFAOYSA-N 0.000 description 1
- WLAMNBDJUVNPJU-UHFFFAOYSA-N 2-methylbutyric acid Chemical compound CCC(C)C(O)=O WLAMNBDJUVNPJU-UHFFFAOYSA-N 0.000 description 1
- VTZPAJGVRWKMAG-UHFFFAOYSA-N 3-(1h-imidazol-5-ylmethyl)-2,3-dihydro-1h-inden-5-ol Chemical compound C12=CC(O)=CC=C2CCC1CC1=CN=CN1 VTZPAJGVRWKMAG-UHFFFAOYSA-N 0.000 description 1
- NUFBIAUZAMHTSP-UHFFFAOYSA-N 3-(n-morpholino)-2-hydroxypropanesulfonic acid Chemical compound OS(=O)(=O)CC(O)CN1CCOCC1 NUFBIAUZAMHTSP-UHFFFAOYSA-N 0.000 description 1
- RZQXOGQSPBYUKH-UHFFFAOYSA-N 3-[[1,3-dihydroxy-2-(hydroxymethyl)propan-2-yl]azaniumyl]-2-hydroxypropane-1-sulfonate Chemical compound OCC(CO)(CO)NCC(O)CS(O)(=O)=O RZQXOGQSPBYUKH-UHFFFAOYSA-N 0.000 description 1
- VTOWJTPBPWTSMK-UHFFFAOYSA-N 4-morpholin-4-ylbutane-1-sulfonic acid Chemical compound OS(=O)(=O)CCCCN1CCOCC1 VTOWJTPBPWTSMK-UHFFFAOYSA-N 0.000 description 1
- MDVGNOCJFCALPI-UHFFFAOYSA-N 5-amino-1,4-dihydroxy-2,2-bis(hydroxymethyl)pentane-3-sulfonic acid Chemical compound NCC(O)C(S(O)(=O)=O)C(CO)(CO)CO MDVGNOCJFCALPI-UHFFFAOYSA-N 0.000 description 1
- XZIIFPSPUDAGJM-UHFFFAOYSA-N 6-chloro-2-n,2-n-diethylpyrimidine-2,4-diamine Chemical compound CCN(CC)C1=NC(N)=CC(Cl)=N1 XZIIFPSPUDAGJM-UHFFFAOYSA-N 0.000 description 1
- 239000007991 ACES buffer Substances 0.000 description 1
- 229920001450 Alpha-Cyclodextrin Polymers 0.000 description 1
- 208000019901 Anxiety disease Diseases 0.000 description 1
- 108700016232 Arg(2)-Sar(4)- dermorphin (1-4) Proteins 0.000 description 1
- 241000283690 Bos taurus Species 0.000 description 1
- COVZYZSDYWQREU-UHFFFAOYSA-N Busulfan Chemical compound CS(=O)(=O)OCCCCOS(C)(=O)=O COVZYZSDYWQREU-UHFFFAOYSA-N 0.000 description 1
- 239000004255 Butylated hydroxyanisole Substances 0.000 description 1
- 239000004322 Butylated hydroxytoluene Substances 0.000 description 1
- NLZUEZXRPGMBCV-UHFFFAOYSA-N Butylhydroxytoluene Chemical compound CC1=CC(C(C)(C)C)=C(O)C(C(C)(C)C)=C1 NLZUEZXRPGMBCV-UHFFFAOYSA-N 0.000 description 1
- 206010010719 Conjunctival haemorrhage Diseases 0.000 description 1
- 206010051625 Conjunctival hyperaemia Diseases 0.000 description 1
- 206010010741 Conjunctivitis Diseases 0.000 description 1
- 244000303965 Cyamopsis psoralioides Species 0.000 description 1
- PJWWRFATQTVXHA-UHFFFAOYSA-N Cyclohexylaminopropanesulfonic acid Chemical compound OS(=O)(=O)CCCNC1CCCCC1 PJWWRFATQTVXHA-UHFFFAOYSA-N 0.000 description 1
- 102000004127 Cytokines Human genes 0.000 description 1
- 108090000695 Cytokines Proteins 0.000 description 1
- FBPFZTCFMRRESA-FSIIMWSLSA-N D-Glucitol Natural products OC[C@H](O)[C@H](O)[C@@H](O)[C@H](O)CO FBPFZTCFMRRESA-FSIIMWSLSA-N 0.000 description 1
- FBPFZTCFMRRESA-JGWLITMVSA-N D-glucitol Chemical compound OC[C@H](O)[C@@H](O)[C@H](O)[C@H](O)CO FBPFZTCFMRRESA-JGWLITMVSA-N 0.000 description 1
- JDRSMPFHFNXQRB-CMTNHCDUSA-N Decyl beta-D-threo-hexopyranoside Chemical compound CCCCCCCCCCO[C@@H]1O[C@H](CO)C(O)[C@H](O)C1O JDRSMPFHFNXQRB-CMTNHCDUSA-N 0.000 description 1
- 206010012374 Depressed mood Diseases 0.000 description 1
- 206010012689 Diabetic retinopathy Diseases 0.000 description 1
- 208000003556 Dry Eye Syndromes Diseases 0.000 description 1
- 208000000059 Dyspnea Diseases 0.000 description 1
- 206010013975 Dyspnoeas Diseases 0.000 description 1
- 206010015958 Eye pain Diseases 0.000 description 1
- 206010015993 Eyelid oedema Diseases 0.000 description 1
- WQZGKKKJIJFFOK-GASJEMHNSA-N Glucose Natural products OC[C@H]1OC(O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-GASJEMHNSA-N 0.000 description 1
- WDZVGELJXXEGPV-YIXHJXPBSA-N Guanabenz Chemical compound NC(N)=N\N=C\C1=C(Cl)C=CC=C1Cl WDZVGELJXXEGPV-YIXHJXPBSA-N 0.000 description 1
- INJOMKTZOLKMBF-UHFFFAOYSA-N Guanfacine Chemical compound NC(=N)NC(=O)CC1=C(Cl)C=CC=C1Cl INJOMKTZOLKMBF-UHFFFAOYSA-N 0.000 description 1
- 239000007995 HEPES buffer Substances 0.000 description 1
- OWXMKDGYPWMGEB-UHFFFAOYSA-N HEPPS Chemical compound OCCN1CCN(CCCS(O)(=O)=O)CC1 OWXMKDGYPWMGEB-UHFFFAOYSA-N 0.000 description 1
- 241000282412 Homo Species 0.000 description 1
- 229920002153 Hydroxypropyl cellulose Polymers 0.000 description 1
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical group C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 1
- 102000004310 Ion Channels Human genes 0.000 description 1
- 108090000862 Ion Channels Proteins 0.000 description 1
- PWKSKIMOESPYIA-BYPYZUCNSA-N L-N-acetyl-Cysteine Chemical compound CC(=O)N[C@@H](CS)C(O)=O PWKSKIMOESPYIA-BYPYZUCNSA-N 0.000 description 1
- 239000007993 MOPS buffer Substances 0.000 description 1
- 241000124008 Mammalia Species 0.000 description 1
- 208000000112 Myalgia Diseases 0.000 description 1
- QPCDCPDFJACHGM-UHFFFAOYSA-N N,N-bis{2-[bis(carboxymethyl)amino]ethyl}glycine Chemical compound OC(=O)CN(CC(O)=O)CCN(CC(=O)O)CCN(CC(O)=O)CC(O)=O QPCDCPDFJACHGM-UHFFFAOYSA-N 0.000 description 1
- MKWKNSIESPFAQN-UHFFFAOYSA-N N-cyclohexyl-2-aminoethanesulfonic acid Chemical compound OS(=O)(=O)CCNC1CCCCC1 MKWKNSIESPFAQN-UHFFFAOYSA-N 0.000 description 1
- JOCBASBOOFNAJA-UHFFFAOYSA-N N-tris(hydroxymethyl)methyl-2-aminoethanesulfonic acid Chemical compound OCC(CO)(CO)NCCS(O)(=O)=O JOCBASBOOFNAJA-UHFFFAOYSA-N 0.000 description 1
- 206010028740 Nasal dryness Diseases 0.000 description 1
- 208000028389 Nerve injury Diseases 0.000 description 1
- DFPAKSUCGFBDDF-UHFFFAOYSA-N Nicotinamide Chemical compound NC(=O)C1=CC=CN=C1 DFPAKSUCGFBDDF-UHFFFAOYSA-N 0.000 description 1
- 208000007950 Ocular Hypotension Diseases 0.000 description 1
- 239000008118 PEG 6000 Substances 0.000 description 1
- 239000007990 PIPES buffer Substances 0.000 description 1
- 206010033557 Palpitations Diseases 0.000 description 1
- 206010034960 Photophobia Diseases 0.000 description 1
- 229920002507 Poloxamer 124 Polymers 0.000 description 1
- 229920002517 Poloxamer 338 Polymers 0.000 description 1
- 239000004698 Polyethylene Substances 0.000 description 1
- 229920001030 Polyethylene Glycol 4000 Polymers 0.000 description 1
- 229920002584 Polyethylene Glycol 6000 Polymers 0.000 description 1
- 229920002690 Polyoxyl 40 HydrogenatedCastorOil Polymers 0.000 description 1
- 229920001219 Polysorbate 40 Polymers 0.000 description 1
- 229920001214 Polysorbate 60 Polymers 0.000 description 1
- 208000003251 Pruritus Diseases 0.000 description 1
- 241000083513 Punctum Species 0.000 description 1
- 208000013738 Sleep Initiation and Maintenance disease Diseases 0.000 description 1
- DWAQJAXMDSEUJJ-UHFFFAOYSA-M Sodium bisulfite Chemical compound [Na+].OS([O-])=O DWAQJAXMDSEUJJ-UHFFFAOYSA-M 0.000 description 1
- 206010041349 Somnolence Diseases 0.000 description 1
- CZMRCDWAGMRECN-UGDNZRGBSA-N Sucrose Chemical compound O[C@H]1[C@H](O)[C@@H](CO)O[C@@]1(CO)O[C@@H]1[C@H](O)[C@@H](O)[C@H](O)[C@@H](CO)O1 CZMRCDWAGMRECN-UGDNZRGBSA-N 0.000 description 1
- 229930006000 Sucrose Natural products 0.000 description 1
- 206010043087 Tachyphylaxis Diseases 0.000 description 1
- 239000007983 Tris buffer Substances 0.000 description 1
- 206010047139 Vasoconstriction Diseases 0.000 description 1
- 206010047571 Visual impairment Diseases 0.000 description 1
- CNHUAVJGGWJXGN-UHFFFAOYSA-N [NH4+].[NH4+].CC(O)=O.CC([O-])=O.CC([O-])=O.NCCN Chemical compound [NH4+].[NH4+].CC(O)=O.CC([O-])=O.CC([O-])=O.NCCN CNHUAVJGGWJXGN-UHFFFAOYSA-N 0.000 description 1
- 230000002159 abnormal effect Effects 0.000 description 1
- JVFGXECLSQXABC-UHFFFAOYSA-N ac1l3obq Chemical compound O1C(C(C2O)O)C(COCC(C)O)OC2OC(C(C2O)O)C(COCC(C)O)OC2OC(C(C2O)O)C(COCC(C)O)OC2OC(C(C2O)O)C(COCC(C)O)OC2OC(C(C2O)O)C(COCC(C)O)OC2OC(C(O)C2O)C(COCC(O)C)OC2OC(C(C2O)O)C(COCC(C)O)OC2OC2C(O)C(O)C1OC2COCC(C)O JVFGXECLSQXABC-UHFFFAOYSA-N 0.000 description 1
- 229960004308 acetylcysteine Drugs 0.000 description 1
- 230000004913 activation Effects 0.000 description 1
- 230000009056 active transport Effects 0.000 description 1
- 230000002411 adverse Effects 0.000 description 1
- 150000001298 alcohols Chemical class 0.000 description 1
- 208000030961 allergic reaction Diseases 0.000 description 1
- HFHDHCJBZVLPGP-RWMJIURBSA-N alpha-cyclodextrin Chemical compound OC[C@H]([C@H]([C@@H]([C@H]1O)O)O[C@H]2O[C@@H]([C@@H](O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O[C@H]3O[C@H](CO)[C@H]([C@@H]([C@H]3O)O)O3)[C@H](O)[C@H]2O)CO)O[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@@H]3O[C@@H]1CO HFHDHCJBZVLPGP-RWMJIURBSA-N 0.000 description 1
- 229940043377 alpha-cyclodextrin Drugs 0.000 description 1
- 229910000147 aluminium phosphate Inorganic materials 0.000 description 1
- 229910021529 ammonia Inorganic materials 0.000 description 1
- 239000005557 antagonist Substances 0.000 description 1
- 210000002159 anterior chamber Anatomy 0.000 description 1
- 230000002924 anti-infective effect Effects 0.000 description 1
- 229940006133 antiglaucoma drug and miotics carbonic anhydrase inhibitors Drugs 0.000 description 1
- 229960005475 antiinfective agent Drugs 0.000 description 1
- 239000004599 antimicrobial Substances 0.000 description 1
- 239000003443 antiviral agent Substances 0.000 description 1
- 229940121357 antivirals Drugs 0.000 description 1
- 230000036506 anxiety Effects 0.000 description 1
- 210000001742 aqueous humor Anatomy 0.000 description 1
- 206010003119 arrhythmia Diseases 0.000 description 1
- 230000006793 arrhythmia Effects 0.000 description 1
- 238000003556 assay Methods 0.000 description 1
- 206010003549 asthenia Diseases 0.000 description 1
- 210000003050 axon Anatomy 0.000 description 1
- 230000004888 barrier function Effects 0.000 description 1
- 239000002876 beta blocker Substances 0.000 description 1
- 229940097320 beta blocking agent Drugs 0.000 description 1
- WQZGKKKJIJFFOK-VFUOTHLCSA-N beta-D-glucose Chemical compound OC[C@H]1O[C@@H](O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-VFUOTHLCSA-N 0.000 description 1
- 229960003237 betaine Drugs 0.000 description 1
- 229960002470 bimatoprost Drugs 0.000 description 1
- OWMVSZAMULFTJU-UHFFFAOYSA-N bis-tris Chemical compound OCCN(CCO)C(CO)(CO)CO OWMVSZAMULFTJU-UHFFFAOYSA-N 0.000 description 1
- 206010005159 blepharospasm Diseases 0.000 description 1
- 230000000744 blepharospasm Effects 0.000 description 1
- 230000008499 blood brain barrier function Effects 0.000 description 1
- 230000036772 blood pressure Effects 0.000 description 1
- 238000009530 blood pressure measurement Methods 0.000 description 1
- 210000001218 blood-brain barrier Anatomy 0.000 description 1
- 230000003139 buffering effect Effects 0.000 description 1
- 235000019282 butylated hydroxyanisole Nutrition 0.000 description 1
- CZBZUDVBLSSABA-UHFFFAOYSA-N butylated hydroxyanisole Chemical compound COC1=CC=C(O)C(C(C)(C)C)=C1.COC1=CC=C(O)C=C1C(C)(C)C CZBZUDVBLSSABA-UHFFFAOYSA-N 0.000 description 1
- 229940043253 butylated hydroxyanisole Drugs 0.000 description 1
- 235000010354 butylated hydroxytoluene Nutrition 0.000 description 1
- 229940095259 butylated hydroxytoluene Drugs 0.000 description 1
- 229940082484 carbomer-934 Drugs 0.000 description 1
- 125000004432 carbon atom Chemical group C* 0.000 description 1
- 239000003489 carbonate dehydratase inhibitor Substances 0.000 description 1
- HJMZMZRCABDKKV-UHFFFAOYSA-N carbonocyanidic acid Chemical compound OC(=O)C#N HJMZMZRCABDKKV-UHFFFAOYSA-N 0.000 description 1
- 150000001735 carboxylic acids Chemical class 0.000 description 1
- 239000003093 cationic surfactant Substances 0.000 description 1
- 229940083181 centrally acting adntiadrenergic agent methyldopa Drugs 0.000 description 1
- 229960000541 cetyl alcohol Drugs 0.000 description 1
- 229960004926 chlorobutanol Drugs 0.000 description 1
- 239000006071 cream Substances 0.000 description 1
- 230000003247 decreasing effect Effects 0.000 description 1
- 229940073499 decyl glucoside Drugs 0.000 description 1
- 238000009795 derivation Methods 0.000 description 1
- 210000002555 descemet membrane Anatomy 0.000 description 1
- 238000013461 design Methods 0.000 description 1
- 238000011161 development Methods 0.000 description 1
- 239000008121 dextrose Substances 0.000 description 1
- MTHSVFCYNBDYFN-UHFFFAOYSA-N diethylene glycol Chemical compound OCCOCCO MTHSVFCYNBDYFN-UHFFFAOYSA-N 0.000 description 1
- 239000003085 diluting agent Substances 0.000 description 1
- 239000012895 dilution Substances 0.000 description 1
- 238000010790 dilution Methods 0.000 description 1
- LOKCTEFSRHRXRJ-UHFFFAOYSA-I dipotassium trisodium dihydrogen phosphate hydrogen phosphate dichloride Chemical compound P(=O)(O)(O)[O-].[K+].P(=O)(O)([O-])[O-].[Na+].[Na+].[Cl-].[K+].[Cl-].[Na+] LOKCTEFSRHRXRJ-UHFFFAOYSA-I 0.000 description 1
- 231100000673 dose–response relationship Toxicity 0.000 description 1
- 239000013583 drug formulation Substances 0.000 description 1
- 210000002889 endothelial cell Anatomy 0.000 description 1
- 210000003989 endothelium vascular Anatomy 0.000 description 1
- 150000002085 enols Chemical group 0.000 description 1
- 230000003628 erosive effect Effects 0.000 description 1
- 231100000321 erythema Toxicity 0.000 description 1
- 150000002170 ethers Chemical class 0.000 description 1
- 238000011156 evaluation Methods 0.000 description 1
- 210000000744 eyelid Anatomy 0.000 description 1
- 229950006455 fadolmidine Drugs 0.000 description 1
- 230000006870 function Effects 0.000 description 1
- 230000002496 gastric effect Effects 0.000 description 1
- 229940087068 glyceryl caprylate Drugs 0.000 description 1
- 229940074046 glyceryl laurate Drugs 0.000 description 1
- KWIUHFFTVRNATP-UHFFFAOYSA-N glycine betaine Chemical compound C[N+](C)(C)CC([O-])=O KWIUHFFTVRNATP-UHFFFAOYSA-N 0.000 description 1
- 229960004553 guanabenz Drugs 0.000 description 1
- 229960002048 guanfacine Drugs 0.000 description 1
- 230000036541 health Effects 0.000 description 1
- 235000010977 hydroxypropyl cellulose Nutrition 0.000 description 1
- 239000001863 hydroxypropyl cellulose Substances 0.000 description 1
- 230000001771 impaired effect Effects 0.000 description 1
- 239000005414 inactive ingredient Substances 0.000 description 1
- 230000002757 inflammatory effect Effects 0.000 description 1
- 230000002401 inhibitory effect Effects 0.000 description 1
- 206010022437 insomnia Diseases 0.000 description 1
- 238000001990 intravenous administration Methods 0.000 description 1
- 238000005342 ion exchange Methods 0.000 description 1
- 150000002500 ions Chemical class 0.000 description 1
- 230000003447 ipsilateral effect Effects 0.000 description 1
- 230000000622 irritating effect Effects 0.000 description 1
- 230000002045 lasting effect Effects 0.000 description 1
- 229960001160 latanoprost Drugs 0.000 description 1
- PYIDGJJWBIBVIA-UYTYNIKBSA-N lauryl glucoside Chemical compound CCCCCCCCCCCCO[C@@H]1O[C@H](CO)[C@@H](O)[C@H](O)[C@H]1O PYIDGJJWBIBVIA-UYTYNIKBSA-N 0.000 description 1
- 229940048848 lauryl glucoside Drugs 0.000 description 1
- 150000002634 lipophilic molecules Chemical class 0.000 description 1
- KSMAGQUYOIHWFS-UHFFFAOYSA-N lofexidine Chemical compound N=1CCNC=1C(C)OC1=C(Cl)C=CC=C1Cl KSMAGQUYOIHWFS-UHFFFAOYSA-N 0.000 description 1
- 229960005209 lofexidine Drugs 0.000 description 1
- 230000007774 longterm Effects 0.000 description 1
- 230000001050 lubricating effect Effects 0.000 description 1
- 238000005461 lubrication Methods 0.000 description 1
- 208000002780 macular degeneration Diseases 0.000 description 1
- 229960001855 mannitol Drugs 0.000 description 1
- 239000000463 material Substances 0.000 description 1
- 230000007246 mechanism Effects 0.000 description 1
- 230000010534 mechanism of action Effects 0.000 description 1
- 238000002483 medication Methods 0.000 description 1
- 210000004379 membrane Anatomy 0.000 description 1
- 239000012528 membrane Substances 0.000 description 1
- 239000000693 micelle Substances 0.000 description 1
- 239000001788 mono and diglycerides of fatty acids Substances 0.000 description 1
- 235000019960 monoglycerides of fatty acid Nutrition 0.000 description 1
- 210000004083 nasolacrimal duct Anatomy 0.000 description 1
- 230000008764 nerve damage Effects 0.000 description 1
- 201000001119 neuropathy Diseases 0.000 description 1
- 230000007823 neuropathy Effects 0.000 description 1
- 230000004112 neuroprotection Effects 0.000 description 1
- 229960003966 nicotinamide Drugs 0.000 description 1
- 235000005152 nicotinamide Nutrition 0.000 description 1
- 239000011570 nicotinamide Substances 0.000 description 1
- 231100000957 no side effect Toxicity 0.000 description 1
- 230000004493 normal intraocular pressure Effects 0.000 description 1
- QIQXTHQIDYTFRH-UHFFFAOYSA-N octadecanoic acid Chemical compound CCCCCCCCCCCCCCCCCC(O)=O QIQXTHQIDYTFRH-UHFFFAOYSA-N 0.000 description 1
- 239000002997 ophthalmic solution Substances 0.000 description 1
- 208000020911 optic nerve disease Diseases 0.000 description 1
- 239000002357 osmotic agent Substances 0.000 description 1
- 239000003002 pH adjusting agent Substances 0.000 description 1
- LQPLDXQVILYOOL-UHFFFAOYSA-I pentasodium;2-[bis[2-[bis(carboxylatomethyl)amino]ethyl]amino]acetate Chemical compound [Na+].[Na+].[Na+].[Na+].[Na+].[O-]C(=O)CN(CC([O-])=O)CCN(CC(=O)[O-])CCN(CC([O-])=O)CC([O-])=O LQPLDXQVILYOOL-UHFFFAOYSA-I 0.000 description 1
- 229960003330 pentetic acid Drugs 0.000 description 1
- 230000010412 perfusion Effects 0.000 description 1
- 230000035699 permeability Effects 0.000 description 1
- 239000012466 permeate Substances 0.000 description 1
- 150000002978 peroxides Chemical class 0.000 description 1
- WVDDGKGOMKODPV-ZQBYOMGUSA-N phenyl(114C)methanol Chemical compound O[14CH2]C1=CC=CC=C1 WVDDGKGOMKODPV-ZQBYOMGUSA-N 0.000 description 1
- 229940067107 phenylethyl alcohol Drugs 0.000 description 1
- 229940096826 phenylmercuric acetate Drugs 0.000 description 1
- PDTFCHSETJBPTR-UHFFFAOYSA-N phenylmercuric nitrate Chemical compound [O-][N+](=O)O[Hg]C1=CC=CC=C1 PDTFCHSETJBPTR-UHFFFAOYSA-N 0.000 description 1
- 239000002953 phosphate buffered saline Substances 0.000 description 1
- 238000007539 photo-oxidation reaction Methods 0.000 description 1
- 230000000704 physical effect Effects 0.000 description 1
- 230000004962 physiological condition Effects 0.000 description 1
- 230000035479 physiological effects, processes and functions Effects 0.000 description 1
- 239000002504 physiological saline solution Substances 0.000 description 1
- 239000002798 polar solvent Substances 0.000 description 1
- 229940093448 poloxamer 124 Drugs 0.000 description 1
- 229920000573 polyethylene Polymers 0.000 description 1
- 229920000151 polyglycol Polymers 0.000 description 1
- 239000010695 polyglycol Substances 0.000 description 1
- 235000010483 polyoxyethylene sorbitan monopalmitate Nutrition 0.000 description 1
- 239000000249 polyoxyethylene sorbitan monopalmitate Substances 0.000 description 1
- 235000010989 polyoxyethylene sorbitan monostearate Nutrition 0.000 description 1
- 239000001818 polyoxyethylene sorbitan monostearate Substances 0.000 description 1
- 229940101027 polysorbate 40 Drugs 0.000 description 1
- 229940113124 polysorbate 60 Drugs 0.000 description 1
- 229940068965 polysorbates Drugs 0.000 description 1
- 229920006316 polyvinylpyrrolidine Polymers 0.000 description 1
- 239000001267 polyvinylpyrrolidone Substances 0.000 description 1
- 239000001103 potassium chloride Substances 0.000 description 1
- 235000011164 potassium chloride Nutrition 0.000 description 1
- VWUPQQFMCOQIEJ-UHFFFAOYSA-M potassium;hydrogen carbonate;hydrate Chemical compound O.[K+].OC([O-])=O VWUPQQFMCOQIEJ-UHFFFAOYSA-M 0.000 description 1
- 230000000770 proinflammatory effect Effects 0.000 description 1
- 230000000069 prophylactic effect Effects 0.000 description 1
- 238000005086 pumping Methods 0.000 description 1
- 239000008213 purified water Substances 0.000 description 1
- 238000005057 refrigeration Methods 0.000 description 1
- 238000011160 research Methods 0.000 description 1
- 230000000241 respiratory effect Effects 0.000 description 1
- 230000000979 retarding effect Effects 0.000 description 1
- 238000012552 review Methods 0.000 description 1
- 239000000932 sedative agent Substances 0.000 description 1
- 208000013220 shortness of breath Diseases 0.000 description 1
- 239000011734 sodium Substances 0.000 description 1
- 229910052708 sodium Inorganic materials 0.000 description 1
- 229910000030 sodium bicarbonate Inorganic materials 0.000 description 1
- 235000017557 sodium bicarbonate Nutrition 0.000 description 1
- 229910000029 sodium carbonate Inorganic materials 0.000 description 1
- 239000001509 sodium citrate Substances 0.000 description 1
- NLJMYIDDQXHKNR-UHFFFAOYSA-K sodium citrate Chemical compound O.O.[Na+].[Na+].[Na+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O NLJMYIDDQXHKNR-UHFFFAOYSA-K 0.000 description 1
- FQENQNTWSFEDLI-UHFFFAOYSA-J sodium diphosphate Chemical compound [Na+].[Na+].[Na+].[Na+].[O-]P([O-])(=O)OP([O-])([O-])=O FQENQNTWSFEDLI-UHFFFAOYSA-J 0.000 description 1
- 235000010267 sodium hydrogen sulphite Nutrition 0.000 description 1
- AKHNMLFCWUSKQB-UHFFFAOYSA-L sodium thiosulfate Chemical compound [Na+].[Na+].[O-]S([O-])(=O)=S AKHNMLFCWUSKQB-UHFFFAOYSA-L 0.000 description 1
- 229940001474 sodium thiosulfate Drugs 0.000 description 1
- 235000019345 sodium thiosulphate Nutrition 0.000 description 1
- 239000002904 solvent Substances 0.000 description 1
- 229940035044 sorbitan monolaurate Drugs 0.000 description 1
- 239000000600 sorbitol Substances 0.000 description 1
- 238000001228 spectrum Methods 0.000 description 1
- 239000003381 stabilizer Substances 0.000 description 1
- 238000010186 staining Methods 0.000 description 1
- 230000003637 steroidlike Effects 0.000 description 1
- 238000006467 substitution reaction Methods 0.000 description 1
- 239000005720 sucrose Substances 0.000 description 1
- 230000001629 suppression Effects 0.000 description 1
- 230000002459 sustained effect Effects 0.000 description 1
- 206010042772 syncope Diseases 0.000 description 1
- 230000001839 systemic circulation Effects 0.000 description 1
- 229960003080 taurine Drugs 0.000 description 1
- 235000019818 tetrasodium diphosphate Nutrition 0.000 description 1
- KWXLCDNSEHTOCB-UHFFFAOYSA-J tetrasodium;1,1-diphosphonatoethanol Chemical compound [Na+].[Na+].[Na+].[Na+].[O-]P(=O)([O-])C(O)(C)P([O-])([O-])=O KWXLCDNSEHTOCB-UHFFFAOYSA-J 0.000 description 1
- 238000002560 therapeutic procedure Methods 0.000 description 1
- RTKIYNMVFMVABJ-UHFFFAOYSA-L thimerosal Chemical compound [Na+].CC[Hg]SC1=CC=CC=C1C([O-])=O RTKIYNMVFMVABJ-UHFFFAOYSA-L 0.000 description 1
- 229940033663 thimerosal Drugs 0.000 description 1
- 239000012443 tonicity enhancing agent Substances 0.000 description 1
- 239000003860 topical agent Substances 0.000 description 1
- 229940126702 topical medication Drugs 0.000 description 1
- 210000001585 trabecular meshwork Anatomy 0.000 description 1
- 229960002368 travoprost Drugs 0.000 description 1
- LENZDBCJOHFCAS-UHFFFAOYSA-N tris Chemical compound OCC(N)(CO)CO LENZDBCJOHFCAS-UHFFFAOYSA-N 0.000 description 1
- PKIDNTKRVKSLDB-UHFFFAOYSA-K trisodium;2-hydroxypropane-1,2,3-tricarboxylate;hydrate Chemical compound O.[Na+].[Na+].[Na+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O PKIDNTKRVKSLDB-UHFFFAOYSA-K 0.000 description 1
- POZPMIFKBAEGSS-UHFFFAOYSA-K trisodium;2-hydroxypropane-1,2,3-tricarboxylate;trihydrate Chemical compound O.O.O.[Na+].[Na+].[Na+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O POZPMIFKBAEGSS-UHFFFAOYSA-K 0.000 description 1
- 210000001944 turbinate Anatomy 0.000 description 1
- 229920001664 tyloxapol Polymers 0.000 description 1
- MDYZKJNTKZIUSK-UHFFFAOYSA-N tyloxapol Chemical compound O=C.C1CO1.CC(C)(C)CC(C)(C)C1=CC=C(O)C=C1 MDYZKJNTKZIUSK-UHFFFAOYSA-N 0.000 description 1
- 229960004224 tyloxapol Drugs 0.000 description 1
- 230000025033 vasoconstriction Effects 0.000 description 1
- 230000024883 vasodilation Effects 0.000 description 1
- 239000004034 viscosity adjusting agent Substances 0.000 description 1
- 230000000007 visual effect Effects 0.000 description 1
- 230000004393 visual impairment Effects 0.000 description 1
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/41—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having five-membered rings with two or more ring hetero atoms, at least one of which being nitrogen, e.g. tetrazole
- A61K31/4164—1,3-Diazoles
- A61K31/4174—Arylalkylimidazoles, e.g. oxymetazolin, naphazoline, miconazole
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/08—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing oxygen, e.g. ethers, acetals, ketones, quinones, aldehydes, peroxides
- A61K47/10—Alcohols; Phenols; Salts thereof, e.g. glycerol; Polyethylene glycols [PEG]; Poloxamers; PEG/POE alkyl ethers
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/16—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite containing nitrogen, e.g. nitro-, nitroso-, azo-compounds, nitriles, cyanates
- A61K47/18—Amines; Amides; Ureas; Quaternary ammonium compounds; Amino acids; Oligopeptides having up to five amino acids
- A61K47/186—Quaternary ammonium compounds, e.g. benzalkonium chloride or cetrimide
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/30—Macromolecular organic or inorganic compounds, e.g. inorganic polyphosphates
- A61K47/36—Polysaccharides; Derivatives thereof, e.g. gums, starch, alginate, dextrin, hyaluronic acid, chitosan, inulin, agar or pectin
- A61K47/38—Cellulose; Derivatives thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0048—Eye, e.g. artificial tears
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P27/00—Drugs for disorders of the senses
- A61P27/02—Ophthalmic agents
- A61P27/06—Antiglaucoma agents or miotics
Definitions
- Glaucoma is a multifactorial disease which encompasses a spectrum ranging from elevated intraocular pressure ("IOP") to reduced vascular perfusion of the optic nerve.
- IOP intraocular pressure
- glaucoma patients require two or more drugs for satisfactory control of their intraocular pressure.
- the prostaglandins/prostanoids including Xalatan ® (latanoprost; Xalatan is a registered trademark of Pfizer Health AB), Travatan ® (travoprost; Travatan is a registered trademark of Novartis AG) and Lumigan ® (bimatoprost; Lumigan is a registered trademark of Allergan, Inc.
- the two drugs should have different mechanisms of action.
- Brimonidine a known alpha-2 (a-2) adrenergic receptor agonist, typically causes moderate peak IOP reduction of about 20-25% in ocular hypertensive eyes and 6-18% in normotensive eyes (less than 21 mm Hg). Its peak effect is within 2 hours of instillation, its duration of effect is typically less than 12 hours, and its moderate efficacy usually requires dosing of 2-3 times a day. It is one of the leading secondary drugs, with a mechanism of action of aqueous suppression that complements the prostaglandin/prostanoids uveal scleral outflow enhancement for significant additive benefit, but about equal to other second line glaucoma drugs such as beta-blockers and carbonic anhydrase inhibitors.
- brimonidine is the only commercially available a-2 agonist, proving safer and/or more effective than predecessors agonist which it has been compared, including clonidine (i.e. fewer instances of systemic hypotension and/or bradycardia), apraclonidine (i.e. fewer instances of tachyphylaxis), and dexmedetomidine (i.e. less systemic sedation, greater IOP reduction efficacy).
- clonidine i.e. fewer instances of systemic hypotension and/or bradycardia
- apraclonidine i.e. fewer instances of tachyphylaxis
- dexmedetomidine i.e. less systemic sedation, greater IOP reduction efficacy
- brimonidine may induce substantial local side effects in 10-25% of users, such as conjunctival hyperemia (i.e.
- brimonidine a-2 agonists, including brimonidine, clonidine and dexmedetomidine, induce substantial systemic effects if absorbed into the circulation, and are specifically known to increase fatigue, decrease blood pressure (i.e. hypotension) and lower the heart rate (i.e. bradycardia).
- a-2 agonists particularly the more lipophilic drugs such as clonidine and dexmedetomidine readily cross the blood brain barrier and thereby induce potent sedative effects.
- Dexmedetomidine in particular, is a potent intravenous sedative, and side effects such as drowsiness, shortness of breath, dizziness, headache, hypotension, bradycardia, and mood depression are common to all a-2 agonists depending on their degree of systemic absorption.
- Brimonidine in particular produces topical lid and conjunctival allergy, dryness, and redness in well over 10% of patients. These side effects contribute to suboptimal compliance with brimonidine, which also negatively affects treatment.
- brimonidine has been the only commercially available a-2 agonist, due to its demonstrated combination of superior IOP reduction with greatly reduced risk of systemic side effects versus all other a-2 agonists attempted for this purpose, despite its less than optimal side effect profile and modest efficacy relative to prostaglandins/prostanoids.
- compositions and methods effective for the treatment of glaucoma in a patient in need thereof are formulated to prevent sedation, eliminate or reduce redness, eliminate or reduce ocular allergy, as well as significantly reduce intraocular pressure.
- the provided compositions may also have an eye whitening effect.
- the compositions include all of the above benefits and also have neuroprotective benefits and may be used for optic nerve protection, including the treatment of neurodegenerative conditions, such as ischemic optic neuropathy, diabetic retinopathy, optic ischemia, retinal vascular ischemia, and other optic neuropathies, particularly those involving retinal ganglion cells and/or axons at or near the optic nerve lamina.
- the present invention optimizes a-2 agonist corneal permeation utilizing a highly selective a-2 agonist which is formulated to optimize intraocular penetration at a lipophilicity of preferably Log P 2.5 or greater and range of topical lipophilicity based on the pH and optional buffering of the formulation that may range from 0.73 to 3.08 (measured relative to pH as the Log D value). Further, the improved formulations allow for reduced a-1 agonist activity and reduced systemic absorption, allowing for a more lipophilic a-2 agonist for topical use. [00011]
- the preferred compositions of the invention employ selective a-2 adrenergic receptor agonists.
- the formulation preferably has the following non-
- the elastic modulus increases about 200 to 1000 fold within 1-2 seconds during the low shear force interblink period of each cycle, more preferably at least 2000 fold, and still more preferably at least 4000 fold, and where during the blink phase such modulus is less than 100, preferably less than 10, and more preferably about 0;
- the invention provides novel formulations of dexmedetomidine, which are surprisingly found to be much more effective for the treatment of glaucoma than brimonidine.
- These novel inventive formulations share some or all of the following characteristics: a) a high selectivity for a-2 over a-1 adrenergic receptors, such as 1000: 1 or greater; more preferably 1500: 1 or greater; and even more preferably 2000: 1 or greater;
- c) include an anionic cyclodextrin such as Captisol ® (Captisol is a registered trademark of Cydex Pharmaceuticals), other cyclodextrins, or other nonionic surfactants such as poloxamer or a polyoxyl alkyl at specified concentration range, and one or more specific viscosity enhancers (also interchangeably referred to as a "gelling agents").
- an anionic cyclodextrin such as Captisol ® (Captisol is a registered trademark of Cydex Pharmaceuticals)
- other cyclodextrins or other nonionic surfactants such as poloxamer or a polyoxyl alkyl at specified concentration range
- one or more specific viscosity enhancers also interchangeably referred to as a "gelling agents”
- the invention provides a pharmaceutical composition
- a pharmaceutical composition comprising: an a-2 adrenergic receptor agonist at a concentration from between about 0.0125% to about 0.125%) weight by volume, wherein said a-2 adrenergic receptor has a Log P value of 2.0 or greater and has a binding affinity of 950 fold or greater for a-2 over a-1 adrenergic receptors;
- a cyclodextrin or a poloxamer or a polyoxyl alkyl at a concentration of between 2%> and 12% weight by volume or less;
- said pharmaceutical composition has a viscosity of between 25 and 500 cps
- said pharmaceutical composition is effective for the treatment of glaucoma in a patient in need thereof.
- a preferred a-2 adrenergic receptor agonist is dexmedetomidine.
- dexmedetomidine is at a concentration from between about 0.035% and 0.12% weight by volume, more preferably at a concentration from about 0.035% to about 0.10% and more preferably between about 0.050% and 0.10% and even more preferably between about 0.060% and 0.087%.
- the salt selected from the group consisting of sodium chloride, citrate, mesylate, hydrobromide/bromide, acetate, fumarate, sulfate/bisulfate, succinate, phosphate, maleate, nitrate, tartrate, benzoate, carbonate, and pamoate.
- the salt is sodium chloride (e.g., a saline solution).
- the viscosity enhancer is selected from carboxymethyl cellulose, methylcellulose, hydroxymethyl cellulose, hydroxypropylmethyl cellulose, hydroxyethyl cellulose, polyethylene glycol, dextran, povidone, alginic acid, guar gum, acacia, Veegum ® (Veegum is a registered trademark of Vanderbilt Minerals, LLC), gelatin, chitosan, Carbopol ® (Carbopol is a registered trademark of Lubrizol Advanced Materials, Inc.), locust bean gum, acidic polycarbophil, dextran, pectin, glycerin, polysorbate, polyvinylpyrridone, polyvinyl alcohol, hyaluronic acid and combinations thereof.
- the viscosity enhancer is carboxymethyl cellulose.
- carboxymethyl cellulose is of a high blend at a concentration of between 0.1% and 1.25% weight by volume.
- the cyclodextrin, poloxamer or polyoxyl alkyl is present at concentration range of 3% to 10%> by weight; and more preferably, at 5% to 6%> by weight.
- the cyclodextrin is selected from alpha, beta or gamma chain cyclodextrins, and is selected from the group consisting of 2 hydroxypropyl beta cyclodextrin and and more preferably the sulfobutyl ether derivative of ⁇ -cyclodextrin (Captisol ® ); poloxamer is selected from the group consisting of poloxamer 407, poloxamer 188, and combinations thereof and the polyoxyl alkyl is selected from the group consisting of polyoxyl 40 stearate, polyoxyl 35 castor oil, and or polyoxyl dehydrogenated 40 castor oil.
- the pharmaceutical composition may further comprise a buffer which may be selected from, but is not limited to, the group consisting of citrate buffer, borate buffer, maleate buffer, succinate buffer, phosphate buffer, acetate buffer, sorbate buffer and carbonate buffer.
- a buffer which may be selected from, but is not limited to, the group consisting of citrate buffer, borate buffer, maleate buffer, succinate buffer, phosphate buffer, acetate buffer, sorbate buffer and carbonate buffer.
- the buffer is at a concentration between 1 mM and 100 mM, preferably between 4 millimolar and 10 millimolar.
- the a-2 agonist of the pharmaceutical composition has an octanol-water partition coefficient Log D of between about 0.70 and about 2.98, or preferably between about 1.25 and 2.50.
- the pharmaceutical compositions of the invention may further comprise a mucoadhesive, which may be present at a concentration from between about 0.05% and about 10% weight by volume.
- the mucoadhesive is selected from the group consisting of
- Carbopol ® xanthan gums, and cellulose derivatives.
- the invention also provides methods of treating glaucoma and/or posterior pole ocular neurodegenerative conditions and/or dry eye in a patient in need thereof comprising administering to said patient the pharmaceutical compositions of the invention.
- a-1 adrenergic receptor refers to a G-protein-coupled receptor
- GPCR GPCR associated with the G q heterotrimeric G-protein.
- a-2 adrenergic receptor refers to a GPCR associated with the Gi heterotrimeric G-protein.
- selective a-2 adrenergic receptor agonists encompasses all a-2 adrenergic receptor agonists which have a binding affinity of 1000 fold or greater for a-2 over a- 1 adrenergic receptors , and more preferably 1500 fold or greater.
- the term also encompasses pharmaceutically acceptable salts, esters, prodrugs, and other derivatives of selective a-2 adrenergic receptor agonists.
- diexmedetomidine encompasses, without limitation, dexmedetomidine salts, esters, prodrugs and other derivatives.
- prodrug refers to a compound that may be converted under physiological conditions to a biologically active compound.
- composition is intended to encompass a product comprising the specified ingredients in the specified amounts, as well as any product which results, directly or indirectly, from a combination of the specified ingredients in the specified amounts.
- treating and “treatment” refer to reversing, alleviating, inhibiting, or slowing the progress of the disease, disorder, or condition to which such terms apply, or one or more symptoms of such disease, disorder, or condition.
- preventing and “prevention” refer to prophylactic use to reduce the likelihood of a disease, disorder, or condition to which such term applies, or one or more symptoms of such disease, disorder, or condition. It is not necessary to achieve a 100% likelihood of prevention; it is sufficient to achieve at least a partial effect of reducing the risk of acquiring such disease, disorder, or condition.
- significant side effects refers to substantial side effects of the treatment which include at least: a) sedation of a patient such that the patient feels sedated and becomes impaired or b) visually noticeable increase in redness of a patient's eye due to hyperemia.
- immediate camentosa refers to the inflammatory sequelae of a-1 agonist topical medications, particularly following topical ocular or nasal delivery, such as the development of increased vasodilation and hyperemia, in its less severe form referred to as "rebound”.
- Poloxamer 407 and Pluronic ® F127 are used interchangeably.
- Nonionic surfactants suitable for the present invention include cyclodextrins, polyoxyl alkyls, poloxamers or combinations thereof, and may include in addition combinations with other nonionic surfactants such as polysorbates.
- Preferred embodiments include polyoxyl 40 stearate; and optionally Poloxamer 188, Poloxamer 407, Polysorbate 20, Polysorbate 80, ionically charged (e.g. anionic) beta - cyclodextrins with or without a butyrated salt (Captisol ® ), 2-hydroxypropyl beta cyclodextrin (“HPpCD”), Polyoxyl 35 castor oil, and Polyoxyl 40 hydrogenated castor oil or combinations thereof.
- nonionizing surfactant such as poloxamer, poloxamer 103, poloxamer 123, and poloxamer 124, poloxamer 407, poloxamer 188, and poloxamer 338, any poloxamer analogue or derivative, polysorbate, polysorbate 20, polysorbate 40, polysorbate 60, polysorbate 80, any polysorbate analogue or derivative, cyclodextrin, hydroxypropyl- ⁇ - cyclodextrin, hydroxypropyl- ⁇ -cyclodextrin, randomly methylated ⁇ - cyclodextrin, ⁇ -cyclodextrin sulfobutyl ether, ⁇ -cyclodextrin sulfobutyl ether or glucosyl- ⁇ - cyclodextrin, any cyclo
- TAPSO tris(hydroxymethyl)methyl]-3-amino-2-hydroxypropane sulfonic acid
- TES N- tris(hydroxymethyl) methyl-2-aminoethane sulfonic acid
- Tris 2-Amino-2-hydroxymethyl- propane-l,3-diol
- Span a registered trademark of Uniqema Americas Inc.
- an anionic surfactant such as sodium lauryl ether sulfate, sodium lauryl sulfate (“SLS”) or a combination thereof is preferred.
- compositions and methods effective for the treatment of glaucoma in a patient in need thereof are formulated to prevent sedation, eliminate or reduce redness, eliminate or reduce ocular allergy, as well as significantly reduce intraocular pressure.
- the salt selected from the group consisting of sodium chloride, citrate, mesylate, hydrobromide/bromide, acetate, fumarate, sulfate/bisulfate, succinate, phosphate, maleate, nitrate, tartrate, benzoate, carbonate, and pamoate.
- the salt is sodium chloride (e.g., a saline solution).
- the viscosity enhancer is selected from carboxymethyl cellulose, methylcellulose, hydroxymethyl cellulose, hydroxypropylmethyl cellulose, hydroxyethyl cellulose, polyethylene glycol, dextran, povidone, alginic acid, guar gum, acacia, Veegum ® , gelatin, chitosan, Carbopol ® , locust bean gum, acidic polycarbophil, dextran, pectin, povidone, polyvinylpyrridone, polyvinyl alcohol, and hyaluronic acid.
- the viscosity enhancer is carboxymethyl cellulose.
- the cyclodextrin, poloxamer or polyoxyl alkyl is present at concentration range of 3% to 10% by weight; and more preferably, at 5% to 6% by weight.
- the cyclodextrin is selected from the group consisting of alpha, beta or gamma chain cyclodextrin, more preferably 2 hydroxypropyl beta cyclodextrin, and still more preferably the sulfobutyl ether derivative of ⁇ -cyclodextrin such as Captisol ® ; poloxamer is selected from the group consisting of poloxamer 407, poloxamer 188; and the polyoxyl alkyl is selected from the group consisting polyoxyl 40 stearate, polyoxyl 35 castor oil, and or polyoxyl dehydrogenated 40 castor oil.
- poloxamers, polyoxyl alkyls and/or combinations thereof can be used for the purposes of the present invention.
- part of the invention and optimal formulation herein has as its goal to maximize the corneal residence time and permeability of dexmedetomidme to achieve the greatest intraocular absorption while minimizing systemic circulation and side effects.
- side effects include but are not limited to sedation, blurred vision and/or discomfort (e.g., stinging).
- dexmedetomidme can reduce IOP, there has been no showing to the Applicant's knowledge of dexmedetomidme at concentrations and formulations without side effects such as sedation.
- the elastic modulus increases about 100 to 1000 fold within 1-2 seconds during the low shear force interblink period of each cycle, more preferably at least 2000 fold, and where during the blink phase such modulus is less than 100, preferably less than 10, and more preferably about 0;
- the formulation must not cause excessive stinging or discomfort, reducing compliance or causing unacceptable ocular surface toxicity
- CMC carboxymethylcellulose
- Captisol ® it is also surprising, unexpected, and important for optimal corneal absorption and reduction of systemic absorption that when using Captisol ® the CMC is preferably increased to a range from about 0.90% to about 1.2% w/v to retain similar rheological properties found at 0.80%) w/v when used with poloxamers or polyoxyl alkyls.
- highly lipophilic drugs such as dexmedetomidine or other similar a-2 agonists are embedded within a nonpolar inner cell within micelles of a micellar equilibrium of the inventive formulations and thereby shielded by a polar outer shell in such configurations reducing the absorption by the lipophilic vascular endothelium relative to free floating drug in solution.
- the present invention is directed to a pharmaceutical composition
- a pharmaceutical composition comprising: i. dexmedetomidine at a concentration from about 0.0125% to about 0.125% w/v, more preferably from about 0.035% to about 0.10% w/v, most preferably from about 0.060% to about 0.087% w/v;
- a surfactant selected from polyoxyl 40 stearate, a cyclodextrin, gamma cyclodextrin and Captisol ® at a concentration from about 1% to about 15% w/v, more preferably polyoxyl 40 stearate or Captisol ® at a concentration of about 5.5% w/v;
- iii. carboxymethyl cellulose ((1% 2,500 centipoise)), at a concentration from about 0.10%) to about 1.25%) w/v, more preferably at about 0.80%> w/v if the surfactant is polyoxyl 40 stearate or from 0.90% to about 1.2% w/v if the surfactant is Captisol ® ; iv. sodium chloride at a concentration from about 0.025% to about 0.90% w/v, more preferably from about 0.25%> to about 0.50%> w/v, most preferably at about 0.037%) w/v; v. benzalkonium chloride ("BAK”) at a concentration from about 0.007% to about 0.02% w/v; preferably at 0.02% w/v;
- BAK benzalkonium chloride
- an antioxidant at a concentration from about 0.005% to about 0.05% w/v, preferaby at 0.015% w/v, preferably the antioxidant is sodium
- ethylenediaminetetraacetic acid at a concentration of about 0.015% w/v; vii. optionally a buffer at a concentration from about 1 millimolar to about 100
- a phosphate or borate buffer from about 1 to about 5 millimolar, more preferably a phosphate buffer at a concentration from about 2 to about 4 millimolar; and
- a pH from about 4.0 to about 8.0, preferably from about 6.0 to about 7.0.
- said pharmaceutical composition is effective for the treatment of glaucoma in a patient in need thereof.
- the present invention is directed to a pharmaceutical composition
- a pharmaceutical composition comprising: i. dexmedetomidine at a concentration from about 0.060% to about 0.087% w/v; ii. polyoxyl 40 stearate at a concentration of about 5.5% w/v;
- benzalkonium chloride at a concentration of about 0.02% w/v
- sodium lauryl sulfate at a concentration from about 0.01% to about 5.0% w/v, preferably at 0.50%> w/v;
- EDTA at a concentration of about 0.015% w/v
- a phosphate buffer at a concentration from about 1 to about 5
- pH of the composition is from about 6.0 to about 7.0.
- the present invention is directed to a pharmaceutical composition
- a pharmaceutical composition comprising:
- dexmedetomidine at a concentration from about 0.06% to 0.087% w/v;
- benzalkonium chloride at a concentration of about 0.02% w/v
- v. sodium lauryl sulfate at a concentration from about 0.1% to about 1.0% w/v, preferably at 0.50%> w/v;
- an antioxidant is at a concentration of about 0.015% w/v; and vii. optionally a phosphate buffer at a concentration from about 1 to about 5
- pH of the composition is from about 6.0 to about 7.0.
- the present invention is directed to a pharmaceutical composition
- a pharmaceutical composition comprising: i. dexmedetomidine at a concentration of about 0.080% w/v;
- benzalkonium chloride at a concentration of about 0.02% w/v; and wherein w/v denotes weight by volume and wherein said pharmaceutical composition is effective for the treatment of glaucoma in a patient in need thereof.
- the pharmaceutical composition may further comprise a buffer at a concentration from about 1 miUimolar to about 5 miUimolar, which may be selected from the group consisting of citrate buffer, borate buffer, maleate buffer, succinate buffer, phosphate buffer, acetate buffer, sorbate buffer and carbonate buffer, preferably from about 2 miUimolar to about 4 miUimolar and at a pH from about 5.5 to about 7.5.
- a buffer at a concentration from about 1 miUimolar to about 5 miUimolar which may be selected from the group consisting of citrate buffer, borate buffer, maleate buffer, succinate buffer, phosphate buffer, acetate buffer, sorbate buffer and carbonate buffer, preferably from about 2 miUimolar to about 4 miUimolar and at a pH from about 5.5 to about 7.5.
- the overall pH of the pharmaceutical composition is from about 6.0 to 7.0.
- the a-2 agonist of the pharmaceutical composition has an octanol-water partition coefficient Log D of between about 0.70 and about 2.20, and preferably between about 1.25 and 2.00.
- the pharmaceutical compositions of the invention may further comprise a mucoadhesive, which may be selected from the group consisting of Carbopol ® , xanthan gums, and cellulose derivatives.
- a mucoadhesive which may be selected from the group consisting of Carbopol ® , xanthan gums, and cellulose derivatives.
- other gums and/or gels, and/or viscosity enhancers can also be used for the purposes of the present invention.
- the mucoadhesive is at a concentration from between about
- inventive formulations may also optionally include other ingredients, such as corneal penetration enhancers and others.
- the invention also provides a method of treating glaucoma and/or posterior pole ocular neurodegenerative conditions in a patient in need thereof comprising administering to said patient the pharmaceutical compositions of the invention.
- inventive compositions may provide optic nerve protection, retinal ganglion cell neuroprotection, an increase in a-2 agonist concentration in the inner retinal plexiform, and additional neuroprotective benefits. They may also increase the outfiow at the trabecular meshwork which is populated with endothelial cells and believed to be populated with a-2a receptors in humans.
- compositions of the invention may be used to reduce eye redness and/or increase eye whiteness in subjects in need thereof.
- the concentration of a poloxamer, a polyoxyl alkyl, or a cyclodextrin should be within the 15% to 25% range, at which gelling effect at room temperature is known to occur by which corneal retention is prolonged but with substantial prolonged blurring on instillation of minutes or more, and/or at the physiologic range of tonicity enhancers.
- a poloxamer, a polyoxyl alkyl, or a cyclodextrin is effective in the provided combinations when it is present at 12% or less, and preferably at more than 3% but less than 10%.
- a poloxamer, a polyoxyl alkyl, or a cyclodextrin is present at a concentration of 15% or greater or much less than 2%, the compositions are surprisingly less effective or ineffective.
- viscosity enhancers at too low concentrations resulted in surprisingly more side effects and reduced efficacy, and that viscosities are reduced up to or more than 100 fold within the inventive formulations, such that a 1% CMC solution in water of 2,500 cps will be about 100 to 250 cps on initial instillation of a preferred embodiment. It has also been found that the use of viscosity enhancers by themselves (i.e., without a poloxamer, a polyoxyl alkyl or a cyclodextrin) results in much less effective formulations with prolonged blurring on instillation, greater systemic absorption, and in general less efficacy and more side effects.
- the tonicity of the provided formulations is at 0 to 200 mOsm/kg, and preferably at 50 to 150 mOsm/kg, a sustained wetting/lubricating effect will result with minimal blurring and the greater comfort for the patients.
- an ophthalmic vehicle requires 280-310 mOsm/kg, which is achieved through the use of electrolytes or polyols (e.g. mannitol).
- cyclodextrins and more preferably the sulfobutyl ether derivative of ⁇ -cyclodextrin (Captisol ® ) enhance the topical redness reduction whitening effect of the a-2 agonist, particularly dexmedetomidine; and whereby such preferred cyclodextrins further enhance intraocular pressure reduction.
- Captisol ® the sulfobutyl ether derivative of ⁇ -cyclodextrin
- compositions and methods are effective for the treatment of glaucoma.
- the compositions of the invention are formulated to prevent sedation, eliminate or reduce redness, may increase duration of therapeutic action and reduce the incidence of rebound hyperemia and/or other allergic reaction, as well as more significantly reduce intraocular pressure than prior art formulations of a-2 agonists.
- contralateral eye IOP is 90-100% of the IOP of the treated eye, due to very high systemic absorption (vs. about 10%> systemic absorption with the compositions of the present invention).
- formulations of the present invention provide the
- IOP reduction of about 40% at 4 hours in a treated eye is greater than that found for the most optimized formulation of brimonidine (Alphagan ® P at 0.1%, pH 7.4 or greater), which is about 20%> in a treated eye.
- brimonidine Alphagan ® P at 0.1%, pH 7.4 or greater
- Every 1 mm Hg reduction in IOP may result in substantial prevention of visual field loss.
- the longer duration of effect of the present invention creates a substantial effect over a 24 hour period, while a single dose of the conventional brimonidine formulations provides the IOP reduction effect for only about 12 hours or less.
- the invention also provides improved wetting and comfort, lasting up to an hour after instillation.
- the beneficial effects of the provided compositions include:
- a-2 agonists such as apraclonidine and brimonidine
- a-2 agonists such as apraclonidine and brimonidine
- a-2 agonists such as apraclonidine and
- compositions include selectivity for a-2 versus a-1 adrenergic receptors, lipophilicity, tonicity and solubility.
- the selective a-2 adrenergic receptor agonists have binding affinities (Kj) for a-2 over a-1 receptors of 1000:1 or greater; more preferably 1500: 1 or greater; and even more preferably 2000:1 or greater. It is well within a skill in the art to design an assay to determine a- 2/ ⁇ -1 functional selectivity. For example, potency, activity or EC50 at an a-2 A receptor can be determined by assaying for inhibition of adenylate cyclase activity. Furthermore, inhibition of adenylate cyclase activity can be assayed, without limitation, in PC 12 cells stably expressing an a-2 A receptor such as a human a-2 A receptor.
- potency, activity or EC50 at an a-1 A receptor can be determined by assaying for intracellular calcium.
- Intracellular calcium can be assayed, without limitation, in HEK293 cells stably expressing an a-1 A receptor, such as a bovine a-1 A receptor.
- compositions and methods of the invention include selective a-2 adrenergic receptor agonists which have K; for a-2 over a-1 receptors of 1500 fold or greater and have an octanol-water partition coefficient of about Log P 2.50 - 3.0 adjusted however for topical pH (Log D) to be between 0.75 and 3.08.
- Gut D topical pH
- Tears and intraocular fluids are physiologic at pH 7.4, which is equal to pH at Log P and, according to the precepts of the present invention, confers IOP reduction benefits.
- compositions and methods of the invention include selective a-2 adrenergic receptor agonists which have IQ for a-2 over a-1 receptors of 1000 fold or greater and are at a concentration from between about 0.0035% to about 0.035% weight by volume.
- Brimonidine, guanfacine, guanabenz, dexmedetomidine and fadolmidine are some of the sufficiently highly selective a-2 agonists to satisfy the selectivity requirement.
- these highly selective a-2 agonists only dexmedetomidine satisfies other additional preferred formulation characteristics of the present invention, such as lipophilicity.
- Other a-2 agonists, such as clonidine, may be sufficiently lipophilic but lack sufficient selectivity.
- a-2 adrenergic receptor agonist suitable for purposes of the invention is dexmedetomidine as either the HC1 salt, or as the citrate salt.
- Other salts may similarly be substituted for the HC1.
- compositions and methods of the invention include dexmedetomidine, or another selective a-2 adrenergic receptor agonist, at a concentration from between about 0.0125%) to about 0.125%) weight by volume; preferably, between about 0.025%> to about 0.125% weight by volume; more preferably between about 0.045% and about 0.10% weight by volume and even more preferably between about 0.060%) and about 0.087%.
- Lipophilicity may be measured, for example, using known measurements, such as
- Log P log Kow derivation of the octanol-water partition coefficient and/or, a closely related coefficient, XLogP3-AA. See, for example, Tiejun Cheng et al, Computation of Octanol-Water Partition Coefficients by Guiding an Additive Model with Knowledge, J. Chem. Inf. Model., 2007, 47 (6), pp 2140-2148. These measurements represent the intraocular lipophilicity value of topical drugs for intraocular delivery (i.e., once the drug permeates into the anterior chamber and is at a pH of 7.4). A person of ordinary skill in the art is well familiar with these measurements. Thus, the Log P value is the octanol-water coefficient at pH 7.4, i.e., physiologic pH.
- Log P and/or XLogP3-AA are measured when the formulation at issue is or will be at the physiologic pH of about 7.4.
- the range between +2.0 and +3.0 typically allows for the best compromise between: a) the need for a highly lipophilic drug to penetrate the lipophilic corneal epithelium, and to a lesser extent, the very thin inner corneal membrane called Descemet's membrane, and b) a highly hydrophilic drug to penetrate the stroma, which is the middle layer of the corneal "sandwich" that must be penetrated for effective ophthalmic absorption.
- the disclosed combination of a poloxamer, a viscosity enhancer and a hypotonic solution at the disclosed concentration ranges provides a delivery vehicle for dexmedetomidine (and, it is believed, for other mild to highly lipophilic drugs) that is independent of pH and largely independent of the individual drug's lipophilicity.
- the optimal pH of the provided formulations is such pH that results in a Log "D" value for the drug (the initial topical lipophilicity) of between 0.75 and 3.08, and more preferably between 0.92 and 2.98, representing the maximum pH range of 4.0 to 8.0, and the preferred pH range of 4.5 to 7.0 for optimal comfort and stability.
- inventive formulations i.e., those formulations including all of the required ingredients at the required concentrations
- the efficacy of the inventive formulations no longer appears to be reduced by any particular buffers, including phosphate buffer.
- buffers including phosphate buffer.
- specific combination of the ingredients in the inventive formulations confers this pH independence and increased solubility range on a variety of active drugs, both for glaucoma and other purposes, as well as provides increased absorption and reduced systemic side effects; including but not limited to steroidals, nonsteroidals, anti-infectives (antivirals and antimicrobials), and macular degeneration drug treatments such as anti-VEGF.
- the preferred Log P (and XLogP3-AA) values - those that define intraocular performance according to the present invention - that are suitable for the purposes of the invention are between about 1.00 and 4.50; and more preferably, between about 2.0 and 3.50. If the selectivity of a specific a-2 agonist is substantially above 1000: 1 (for example, 1500: 1), additional advantages are believed to be conferred via greater a-2 agonist binding and reduced a- 1 agonist induced ischemia. For example, optic nerve damage progression is known to be highly sensitive to circulation change and ischemia. Because the drug is used over an extended period of time, even small reductions in unintended a-1 agonist-induced ischemia may be beneficial.
- the a-2 agonist intraocular lipophilicity as represented by Log P, and selectivity as represented by the ⁇ -2: ⁇ -1 receptor recruitment ratio, appear to be very important for greater efficacy of an a-2 agonist glaucoma drug. If the selectivity is above, for example, 2000: 1, then it is possible that this agonist may be effective for the purposes of the invention at slightly reduced lipophilicity, and vice versa.
- Table 1 provides known XLogP3-AA values (a more accurate Log P) and a2/al binding affinities for several a-2 agonists.
- Table 1 demonstrates that among the listed a-2 agonists, only dexmedetomidine has an optimal combination of high lipophilicity (XLogP3-AA) and highly selective a2:al coefficient. However, it is possible that formulations including other a-2 agonists can be achieved which meet the defined requirements of the present invention in both selectivity and lipophilicity categories.
- dexmedetomidine or another selective a-2 adrenergic receptor agonist, has Log P at an intraocular pH 7.4 of about 3.10; preferably, between about 2.0 and 5.00; and more preferably between about 2.75 and 3.50.
- Log D refers to a lipophilicity value at a given pH
- this measurement is especially useful to determine the level of topical lipophilicity and resultant corneal permeability of a topical composition through the highly lipophilic corneal epithelium.
- 0.75 and about 2.20, and more particularly between about 1.00 and about 1.50, are preferred for increased corneal permeation of dexmedetomidine and other similar a-2 agonists in normal saline, preferably below the pH of 6.4 to 6.5, and that the "vehicle" of the present invention including poloxamer, viscosity enhancer and hypotonic saline or sterile water greatly reduces and likely totally eliminates such pH limitations.
- the optimal Log D value is from 0.75 to 2.2, and more preferably is about 1.00 to 2.00 at a topical pH of about 4.7 to 6.0.
- ophthalmic drugs typically require about
- tonicity enhancers including but not limited to electrolytes, particularly 0.9% NaCl, and polyols, such as mannitol, may be used to achieve the desired range.
- the inventive compositions should include a salt; a poloxamer at a concentration of 12% weight by volume or less; and a viscosity enhancer.
- a salt for example, using the provided compositions, dexmedetomidme is rendered soluble up to or beyond 0.15%.
- Solubility for dexmedetomidme and other similar drugs in its subclass is typically reduced exponentially with increasing pH.
- dexmedetomidme is only soluble in physiologic saline to about 0.025% at a highly alkaline pH. It is believed that the inventive formulations result in enhancement of solubility of dexmedetomidme, and by extension other members of its subclass, well above the 0.125% at alkaline pH.
- dexmedetomidine is more effective than prior art formulations of dexmedetomidine and more effective than brimonidine by about 200% (IOP reduction vs. time, which is the key measure of the effectiveness of IOP reduction).
- agents that improve solubility include, but are not limited to, polyanionic (multiple negatively charged) compounds, such as methylcellulose and derivatives, particularly carboxymethyl cellulose or other cellulose derivatives; hypotonic saline; sodium acetate, calcium salt, methanesulfonate (mesylate), hydrobromide/bromide, acetate, fumarate, sulfate/bisulfate, succinate, citrate, phosphate, maleate, nitrate, tartrate, benzoate, carbonate, pamoate, borate, glycolate, pivylate, sodium citrate monohydrate, sodium citrate trihydrate, sodium carbonate, sodium ethylenediaminetetraacetic acid ("EDTA”), phosphoric acid, pent
- polyanionic (multiple negatively charged) compounds such as methylcellulose and derivatives, particularly carboxymethyl cellulose or other cellulose derivatives
- hypotonic saline such as sodium acetate, calcium salt, methanesulfonate (mesylate), hydro
- the composition includes sodium citrate dehydrate at about 0.17%, and/or sodium acetate at about 0.39%; and/or calcium salt at about 0.048%.
- compositions and methods of the invention encompass all isomeric forms of the described a-2 adrenergic receptor agonists, their racemic mixtures, enol forms, solvated and unsolvated forms, analogs, prodrugs, derivatives, including but not limited to esters and ethers, and pharmaceutically acceptable salts, including acid addition salts.
- suitable acids for salt formation are hydrochloric, sulfuric, phosphoric, acetic, citric, oxalic, malonic, salicylic, malic, furmaric, succinic, ascorbic, maleic, methanesulfonic, tartaric, and other mineral carboxylic acids well known to those in the art.
- the salts may be prepared by contacting the free base form with a sufficient amount of the desired acid to produce a salt in the conventional manner.
- the free base forms may be regenerated by treating the salt with a suitable dilute aqueous base solution such as dilute aqueous hydroxide potassium carbonate, ammonia, and sodium bicarbonate.
- a suitable dilute aqueous base solution such as dilute aqueous hydroxide potassium carbonate, ammonia, and sodium bicarbonate.
- the free base forms differ from their respective salt forms somewhat in certain physical properties, such as solubility in polar solvents, but the acid salts are equivalent to their respective free base forms for purposes of the invention. (See, for example S. M. Berge, et al, "Pharmaceutical Salts," J. Pharm. Sci., 66: 1-19 (1977) which is incorporated herein by reference).
- compositions and methods of the invention include selective a-2 adrenergic receptor agonists which have binding affinities (Kj) for a-2 over a-1 receptors of 1000 fold or greater and are highly lipophilic, having an octanol-water partition coefficient of about 2.00 or greater.
- Brimonidine by comparison, has a binding affinity for a-2 over a-1 receptors of about 976 and its lipophilicity range, even when optimized by pH, is about three hundred fold less than that of dexmedetomidine, a preferred embodiment.
- compositions and methods of the invention include selective a-2 adrenergic receptor agonists which have IQ for a-2 over a-1 receptors of 1000 fold or greater and are at a concentration from between about 0.001% to about 0.035% weight by volume.
- compositions and methods of the invention include selective a-2 adrenergic receptor agonists which have K; for a-2 over a-1 receptors of 1500 fold or greater, are present at a concentration from between about 0.010% to about 0.040% weight by volume, and have pH of about 6.2 or less.
- the compositions of the invention may also include other therapeutic agents; however, the compositions are intended to be effective without the need for any other therapeutic agents, specifically including, but not limited to, a-1 antagonists.
- the invention also provides methods of treating and/or preventing glaucoma with the provided compositions.
- the provided methods lower IOP in glaucoma patients, reduce redness, and provide eye whitening.
- the provided methods may also treat ischemic optic neuropathy and other neuropathies of various etiologies due to neuroprotective effects of the provided compositions.
- compositions of the present invention are preferably formulated for a mammal, and more preferably, for a human.
- the compositions are delivered as ophthalmic solutions into the eyes.
- topical compositions which include, but are not limited to, gels and creams. They may also include additional non-therapeutic components, which include, but are not limited to, preservatives, delivery vehicles, tonicity adjustors, buffers, pH adjustors, antioxidants, tenacity adjusting agents, mucoadhesive agents, viscosity adjusting agents, and water.
- compositions of the present invention can simply dilute more concentrated solutions of selective a-2 agonists, using methods known in the art with diluent of particular gelling agents in solution, being in a preferred embodiment polyoxyl 40 stearate.
- inventive formulations may optionally include one or more of electrolytes or tonicity enhancing agents, and preferably one or more of the weak acids and/or their salts to achieve a formulated pH of 4.0 to 8.0, and more preferably 5.5 - 6.5.
- compositions of the invention may include various inactive ingredients commonly used in formulating topical compositions and that may improve stability of the formulation.
- compositions of the invention may include alcohols and/or surface active agents, including but not limited to polyglycol ether, polyethylene glycol-nonphenol ether, polyethylene glycol sorbitan monolaurate, polyethylene glycol sorbitan monooleate, polyethylene glycol sorbitanmonooleate, polyethylene glycol sterarate, polyethylene glycol polypropylene glycol ether, polyvinyl alcohol, polyvinyl pyrrolidine, PEG and its derivatives, including but not limited to PEG 4000 or PEG 6000, in a total amount of 0.05% to 5% by mass of the composition.
- alcohols and/or surface active agents including but not limited to polyglycol ether, polyethylene glycol-nonphenol ether, polyethylene glycol sorbitan monolaurate, polyethylene glycol sorbitan monooleate, polyethylene glycol sorbitanmonooleate, polyethylene glycol sterarate, polyethylene glycol polypropylene glycol ether, polyviny
- compositions of the invention may include acids or monoglycerides of fatty acids having 8 to 12 carbon atoms, which when in 0.5 - 1.5 M, and preferably equimolar concentration to the alpha 2 agonist may improve corneal permeation via ion pair formation; or antioxidants such as ion-exchange/photooxidation stabilizing agents, including but not limited to citric acid, sorbic acid, boric acid, caprylic acid, glyceryl monocaprylate, glyceryl monocaproate, glycerol monolaurate, sodium metabisulfite.
- antioxidants such as ion-exchange/photooxidation stabilizing agents, including but not limited to citric acid, sorbic acid, boric acid, caprylic acid, glyceryl monocaprylate, glyceryl monocaproate, glycerol monolaurate, sodium metabisulfite.
- compositions and methods of the present invention may include chelating agents that further improve stability, including but not limited to ethylenediaminetetraacetic acid ("EDTA”) and structurally related acids and even more preferably citric acid or its salt.
- EDTA ethylenediaminetetraacetic acid
- the chelating agents are present at a concentration of between 0.005% and 0.2%> weight/vol.
- Preservatives include, but are not limited to, benzalkonium chloride ("BAK”), methylparaben, polypropylparaben, chlorobutanol, thimerosal, phenylmercuric acetate, perborate, or phenylmercuric nitrate.
- BAK benzalkonium chloride
- methylparaben methylparaben
- polypropylparaben chlorobutanol
- thimerosal phenylmercuric acetate
- perborate phenylmercuric nitrate
- Delivery vehicles include, but are not limited to, polyvinyl alcohol, polyethylene glycol (“PEG”) and its analogues, povidone, hydroxypropyl methyl cellulose, poloxamers, carboxymethyl cellulose (“CMC”), hydroxyethyl cellulose and purified water. It is also possible to use a physiological saline solution as a major vehicle.
- Tonicity adjusters include, but are not limited to, a salt such as sodium chloride, potassium chloride, dextran, cyclodextrins, mannitol, dextrose, glycerin, or another pharmaceutically or ophthalmically acceptable tonicity adjustor.
- the tonicity modifying agents are present at a concentration of between 0.1% and 1% weight by volume.
- compositions of the present invention may comprise corneal permeation enhancing agents which include, but are not limited to, preservatives, cyclodextrins, viscosity enhancers, and ion-channel enhancing agents.
- corneal permeation enhancing agents include citrate, a citrate salt and/or other salts which increase solubility, chelating agents such as EDTA, preservatives, ion-channeling agents, cyclodextrin, or other additives which increase corneal permeability.
- a corneal permeation enhancing agent may be selected from the group consisting of BAK at 0.007%) to 0.02%> weight by volume, EDTA at 0.015%) weight by volume, caprylic acid, citric acid, boric acid, sorbic acid and/or salts, derivatives, and analogues thereof, where citric acid or its salt is a preferred embodiment.
- compositions and methods of the present invention may include additional viscosity enhancers and/or agents increasing solubility and/or stability, including but not limited to polyvinylpyrrolidone, polyethylene glycol ("PEG"), cellulose or cellulose derivatives of various molecular weights, including methylcellulose, cellulose glycolate, hydroxypropylcellulose, CMC and its salts, gelatin, sorbitol, alpha-cyclodextrin and/or other cyclodextrin derivatives, niacinamide, carbomers of various molecular weights including carbomer 934 P and 974 P, xanthan gums, alginic acid, guar gums, locust bean gum, chitosan, propylene glycol, polyvinyl alcohol, polysorbate including polysorbate 80, glycerin, mannitol, benzyl alcohol, phenylethyl alcohol, povidone, borate, acetate,
- PEG polyethylene glycol
- BAK hydroxyaminoethyl sulfate
- EDTA EDTA
- Many of the listed additives may serve more than one purpose: for example, they can serve as both preservatives and corneal permeation enhancing agents (e.g. BAK), or solubilizing, preservative, and corneal permeation enhancing agents (e.g. citrate).
- preservatives e.g. BAK
- corneal permeation enhancing agents e.g. BAK
- solubilizing, preservative, and corneal permeation enhancing agents e.g. citrate
- Buffers and pH adjusters include, but are not limited to, acetate buffers, carbonate buffers, citrate buffers, phosphate buffers and borate buffers. It is understood that various acids or bases can be used to adjust the pH of the composition as needed. pH adjusting agents include, but are not limited to, sodium hydroxide and hydrochloric acid. Antioxidants include, but are not limited to, sodium metabisulfite, sodium thiosulfate, acetylcysteine, butylated hydroxyanisole and butylated hydroxytoluene. EXAMPLE 1 Intraocular Pressure ( ⁇ ), Redness and Burning/Stinging
- a-2 agonists were unilaterally administered to a normotensive ( ⁇ 21 mm Hg) human subject.
- the subject first underwent baseline IOP testing using standard applanation tonometry via slit lamp. After fluorescein instillation, the drug was instilled as a morning dose at between about 7:00 and 9:00 AM. Preliminary measurements at 2, 3, 3.5, 4 and 4.5 hours demonstrated a substantial peak effect between about 3.45 and 4.15 hours for a preferred formulation of the invention.
- follow up IOP checks were designed to be about 4 hours after initial instillation, where instillation consisted of 1-2 drops.
- Tables 4-8 summarize studies of various formulations and excipients with dexmedetomidme.
- Table 4 demonstrates that there are significant side effects, such as sedation, when dexmedetomidme concentration is at or greater than about 0.02%
- Table 5 demonstrates substantial and surprising improvements over Table 4 and prior art studies with the preferred embodiment of dexmedetomidme.
- Bradycardia 0 0 0 0.5 0.5 0 0 0 0
- Viscosity Enhancers Xanthan Gums, Poloxamer, pH 8.
- Polysorbate 80 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050% 0.050%
- compositions with lowest side effect profile are those which contain poloxamer at about 5-6%, CMC, sodium chloride and BAK.
- the peak dose response IOP reduction for preferred embodiments of the present invention appeared to be between about 0.070% - 0.10%.
- a formulation comprising 0.08% dexmedetomidine, 5.5% polyoxyl 40 stearate,
- baseline IOP measurements were performed on a subject using applanation slit lamp tonometry following instillation of fluorescein. Then, two drops of the topical agent to be tested were applied seconds apart to the left eye, and the punctum occluded for 30 seconds. Approximately four hours later, IOP testing was again performed. Three initial readings were taken and discarded to ensure minimal patient blepharospasm, following which the next three readings were recorded and averaged. There was a washout period of several days - 1 week between tests. All baseline IOP measurements were between 15.0 - 15.5 mm Hg at 8:00 AM - 9:00 AM at the time of instillation.
- the present invention demonstrates a surprising increase in IOP reduction, nearly two-fold greater IOP reduction versus brimonidine, greater topical comfort, greater redness reduction, reduced topical side effects, and reduced systemic side effects.
- Table 9 demonstrates the results of this experiment.
- composition C dexmedetomidine at 0.01%, phosphate buffered to pH 6.4 (Composition C); and c) dexmedetomidine at 0.1% with 5% Poloxamer 407 (F127), 0.25% NaCl, CMC high blend 0.75%>, and BAK 0.02%> at pH 6.1 (Composition A) (preferred embodiment).
- Composition B (20% (16.6% 15 (6.6% (6.6% 33% reduction) reduction) reduction)
- Composition C (20% (20% (16.6% (13.4% 83% reduction) reduction) reduction)
- composition A two-fold greater IOP peak % reduction in the treated eye with the inventive formulation
- Composition B two-fold greater iOP peak % reduction in the treated eye with the inventive formulation
- composition A two-fold less IOP % reduction in the non-treated eye with the inventive formulation
- Composition B two-fold less IOP % reduction in the non-treated eye with the inventive formulation
- composition A inventive formulation
- Composition C alternative dexmedetomidine formulation
- composition A Longer duration of action to peak IOP reduction for the inventive formulation (Composition A) increasing from 2.5 hours to 4 hours vs. brimonidine (Composition B).
- a greater differential of IOP reduction between treated and non-treated eye using the inventive compositions represents a lower systemic side effect profile as it is interpreted to correlate with reduced systemic absorption of drug reaching the non-treated eye.
- IOP was measured at one or more of 4 hrs, 8 hrs, 12 hrs, 24 hrs, 32 hrs and comfort and side effect profile were qualitatively assessed.
- the tested inventive formulation achieved a peak IOP reduction effect at about 4 to 8 hours after instillation. Furthermore, in two out of three patients the IOP remained below the baseline 24 hours after instillation.
- conventional brimonidine formulations achieve a peak IOP reduction effect of only about 15-18% in normotensive eyes about 2-3 hours after instillation.
- the IOP reduction effect of the inventive formulation was much stronger: from 41.7% to 58.8% at 8 hours after instillation.
- the formulations of the invention demonstrate improved performance over brimonidine as well as other known glaucoma drugs under similar conditions of testing (1-2 days of use, normotensive eyes).
- EXAMPLE 7 Effect of Replacing the Poloxamer or Polyoxyl Alkyl Surfactant with Captisol ® Table 13. Effect of Replacing the Poloxamer or Polyoxyl Alkyl Surfactant with Captisol ®
- Hg human subject.
- the subject first underwent baseline IOP testing using standard applanation tonometry via slit lamp, which revealed a baseline IOP of about 15.0 - 16.5 (diurnal curve, depending on time of day).
- the drug was instilled as a morning dose at between about 7:00 and 9:00 AM.
- Preliminary measurements at 2, 3, 3.5, 4 and 4.5 hours demonstrated a substantial peak effect between about 3.45 and 4.15 hours for a preferred formulation of the invention.
- follow up IOP checks were designed to be about 4 hours after initial instillation, where instillation consisted of 1-2 drops.
- SLS sodium lauryl sulfate
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Veterinary Medicine (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Public Health (AREA)
- Epidemiology (AREA)
- Chemical Kinetics & Catalysis (AREA)
- General Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- Ophthalmology & Optometry (AREA)
- Oil, Petroleum & Natural Gas (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Organic Chemistry (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Inorganic Chemistry (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicinal Preparation (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Abstract
Description














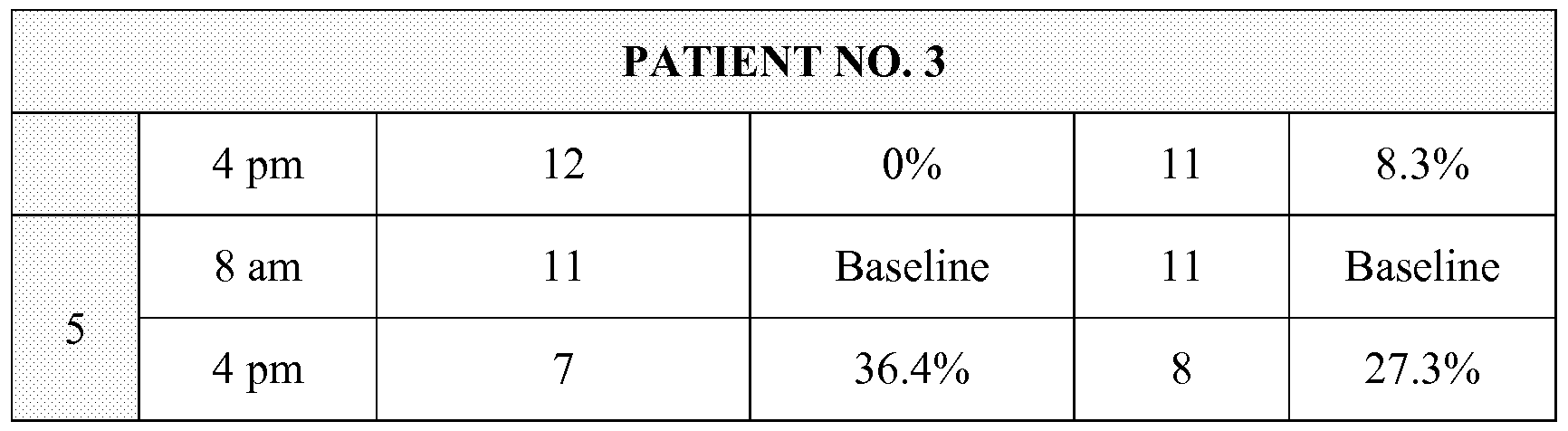

Claims
Priority Applications (6)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP14872240.8A EP3082427A4 (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for treatment of glaucoma |
| BR112016014404A BR112016014404A2 (en) | 2013-12-18 | 2014-02-11 | COMPOSITIONS AND METHODS FOR TREATMENT OF GLAUCOMA |
| JP2016560613A JP2017501224A (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for the treatment of glaucoma |
| CN201480075789.5A CN106455567A (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for treatment of glaucoma |
| CA2934453A CA2934453A1 (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for treatment of glaucoma |
| MX2016007902A MX2016007902A (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for treatment of glaucoma. |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US14/132,780 | 2013-12-18 | ||
| US14/132,780 US20140107173A1 (en) | 2011-02-03 | 2013-12-18 | Compositions and Methods for Treatment of Glaucoma |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2015094392A1 true WO2015094392A1 (en) | 2015-06-25 |
Family
ID=53403464
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2014/015797 WO2015094392A1 (en) | 2013-12-18 | 2014-02-11 | Compositions and methods for treatment of glaucoma |
Country Status (7)
| Country | Link |
|---|---|
| EP (1) | EP3082427A4 (en) |
| JP (1) | JP2017501224A (en) |
| CN (1) | CN106455567A (en) |
| BR (1) | BR112016014404A2 (en) |
| CA (1) | CA2934453A1 (en) |
| MX (1) | MX2016007902A (en) |
| WO (1) | WO2015094392A1 (en) |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2017160548A1 (en) * | 2016-03-17 | 2017-09-21 | Presbyopia Therapies, LLC | Compositions and methods for the treatment of presbyopia |
| CN115137699A (en) * | 2021-03-29 | 2022-10-04 | 四川普锐特药业有限公司 | Dexmedetomidine nasal spray with synergistic and antiseptic effects |
| US12128036B2 (en) | 2023-08-28 | 2024-10-29 | Lenz Therapeutics Operations, Inc. | Compositions and methods for storage stable ophthalmic drugs |
Families Citing this family (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN111481506B (en) * | 2019-01-25 | 2023-01-24 | 江苏恒瑞医药股份有限公司 | Pharmaceutical product comprising a nasally administrable dexmedetomidine composition |
| CN112138250B (en) * | 2019-06-28 | 2023-04-14 | 四川普锐特药业有限公司 | Medicament fluid dispenser and dexmedetomidine nasal spray device for maintaining uniform administration |
| WO2020259440A1 (en) * | 2019-06-28 | 2020-12-30 | 四川普锐特药业有限公司 | Nasal spray of dexmedetomidine, preparation method therefor and use thereof |
| CN111632025A (en) * | 2020-03-04 | 2020-09-08 | 吉林大学第一医院 | Temperature-sensitive in-situ gel for bimatoprost eyes and preparation method and application thereof |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20110189174A1 (en) * | 2010-02-01 | 2011-08-04 | Afshin Shafiee | Compositions and methods for treating, reducing, ameliorating, alleviating, or inhibiting progression of, pathogenic ocular neovascularization |
| US20110251285A1 (en) * | 2010-04-07 | 2011-10-13 | Allergan, Inc. | Combinations of preservatives for ophthalmic compositions |
| US20130079379A1 (en) * | 2011-07-14 | 2013-03-28 | Allergan, Inc. | Gel compositions of oxymetazoline and methods of use |
| US20130172357A1 (en) * | 2011-02-03 | 2013-07-04 | Eye Therapies Llc | Compositions and Methods for Treatment of Glaucoma |
| US20130296396A1 (en) * | 2003-08-07 | 2013-11-07 | Allergan, Inc. | Compositions for delivery of therapeutics into the eyes and methods for making and using same |
| US20140107173A1 (en) * | 2011-02-03 | 2014-04-17 | Gnt, Llc | Compositions and Methods for Treatment of Glaucoma |
Family Cites Families (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| GB2290964A (en) * | 1994-07-08 | 1996-01-17 | Arto Olavi Urtti | Transdermal drug delivery system |
| EP2320911B1 (en) * | 2008-08-01 | 2014-10-08 | Eye Therapies LLC | Vasoconstriction compositions and methods of use |
| US20100202979A1 (en) * | 2008-08-01 | 2010-08-12 | Gerald Horn | Compositions and methods for treatment of pulmonary diseases and conditions |
| WO2011075621A1 (en) * | 2009-12-17 | 2011-06-23 | Alpha Synergy Development, Inc. | Compositions and methods for ophthalmic delivery of nasal decongestants |
| US20120202863A1 (en) * | 2011-02-03 | 2012-08-09 | Gerald Horn | Compositions and methods for treatment of glaucoma |
| US8242158B1 (en) * | 2012-01-04 | 2012-08-14 | Hospira, Inc. | Dexmedetomidine premix formulation |
| WO2013115844A1 (en) * | 2012-02-02 | 2013-08-08 | Alpha Synergy Development, Inc. | Compositions and methods for treatment of glaucoma |
| US20140378401A1 (en) * | 2013-06-21 | 2014-12-25 | Gnt, Llc | Ophthalmic Lipophilic and Hydrophilic Drug Delivery Vehicle Formulations |
| US9089562B2 (en) * | 2013-08-28 | 2015-07-28 | Presbyopia Therapies Llc | Compositions and methods for the treatment of presbyopia |
-
2014
- 2014-02-11 CN CN201480075789.5A patent/CN106455567A/en active Pending
- 2014-02-11 MX MX2016007902A patent/MX2016007902A/en unknown
- 2014-02-11 CA CA2934453A patent/CA2934453A1/en not_active Abandoned
- 2014-02-11 WO PCT/US2014/015797 patent/WO2015094392A1/en active Application Filing
- 2014-02-11 JP JP2016560613A patent/JP2017501224A/en not_active Withdrawn
- 2014-02-11 EP EP14872240.8A patent/EP3082427A4/en not_active Withdrawn
- 2014-02-11 BR BR112016014404A patent/BR112016014404A2/en not_active IP Right Cessation
Patent Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20130296396A1 (en) * | 2003-08-07 | 2013-11-07 | Allergan, Inc. | Compositions for delivery of therapeutics into the eyes and methods for making and using same |
| US20110189174A1 (en) * | 2010-02-01 | 2011-08-04 | Afshin Shafiee | Compositions and methods for treating, reducing, ameliorating, alleviating, or inhibiting progression of, pathogenic ocular neovascularization |
| US20110251285A1 (en) * | 2010-04-07 | 2011-10-13 | Allergan, Inc. | Combinations of preservatives for ophthalmic compositions |
| US20130172357A1 (en) * | 2011-02-03 | 2013-07-04 | Eye Therapies Llc | Compositions and Methods for Treatment of Glaucoma |
| US20140107173A1 (en) * | 2011-02-03 | 2014-04-17 | Gnt, Llc | Compositions and Methods for Treatment of Glaucoma |
| US20130079379A1 (en) * | 2011-07-14 | 2013-03-28 | Allergan, Inc. | Gel compositions of oxymetazoline and methods of use |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP3082427A4 * |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2017160548A1 (en) * | 2016-03-17 | 2017-09-21 | Presbyopia Therapies, LLC | Compositions and methods for the treatment of presbyopia |
| CN115137699A (en) * | 2021-03-29 | 2022-10-04 | 四川普锐特药业有限公司 | Dexmedetomidine nasal spray with synergistic and antiseptic effects |
| CN115137699B (en) * | 2021-03-29 | 2024-05-03 | 四川普锐特药业有限公司 | Synergistic antiseptic dexmedetomidine nasal spray |
| US12128036B2 (en) | 2023-08-28 | 2024-10-29 | Lenz Therapeutics Operations, Inc. | Compositions and methods for storage stable ophthalmic drugs |
Also Published As
| Publication number | Publication date |
|---|---|
| CA2934453A1 (en) | 2015-06-25 |
| JP2017501224A (en) | 2017-01-12 |
| MX2016007902A (en) | 2016-10-28 |
| BR112016014404A2 (en) | 2017-08-08 |
| CN106455567A (en) | 2017-02-22 |
| EP3082427A4 (en) | 2017-08-02 |
| EP3082427A1 (en) | 2016-10-26 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US8445526B2 (en) | Compositions and methods for treatment of glaucoma | |
| US20140163080A1 (en) | Compositions and Methods for Treatment of Glaucoma | |
| AU2008354558B2 (en) | Stable ophthalmic formulations | |
| WO2014204791A1 (en) | Ophthalmic lipophilic and hydrophilic drug delivery vehicle formulations | |
| US20130172357A1 (en) | Compositions and Methods for Treatment of Glaucoma | |
| US10792288B2 (en) | Preservative free brimonidine and timolol solutions | |
| EP3082427A1 (en) | Compositions and methods for treatment of glaucoma | |
| US20120309720A1 (en) | Compositions and methods for treatment of glaucoma | |
| KR20140056280A (en) | Fixed dose combination of bimatoprost and brimonidine | |
| US20140107173A1 (en) | Compositions and Methods for Treatment of Glaucoma | |
| US8999938B2 (en) | Ophthalmic lipophilic drug delivery vehicle formulations | |
| JP2017503028A (en) | Compositions and methods for treating intraocular neovascularization and / or leakage | |
| CA2826644A1 (en) | Compositions and methods for treatment of glaucoma | |
| CA2863760A1 (en) | Compositions and methods for treatment of glaucoma | |
| US10058560B2 (en) | Preservative free bimatoprost and timolol solutions | |
| US20120202864A1 (en) | Compositions and Methods for Treatment of Glaucoma | |
| US20170143676A1 (en) | Compositions and Methods for Treatment of Glaucoma | |
| US20170224827A1 (en) | Stable preservative free ophthalmic formulations of opioid antagonists | |
| KR102444571B1 (en) | Opthalmic compositions comprising cetirizine and tocofersolan | |
| JP7534129B2 (en) | Multi-ingredient eye drops | |
| JP7459508B2 (en) | Mucin degeneration inhibitor and ophthalmic composition | |
| AU2010266539A1 (en) | Pharmaceutical ophthalmological liquid compositions containing propionic acid derivatives as a preservative | |
| KR20230131822A (en) | Compositions and methods for storage stable eye drops | |
| WO2023152644A1 (en) | Pharmaceutical composition of lifitegrast and loteprednol etabonate |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 14872240 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: MX/A/2016/007902 Country of ref document: MX |
|
| ENP | Entry into the national phase |
Ref document number: 2934453 Country of ref document: CA Ref document number: 2016560613 Country of ref document: JP Kind code of ref document: A |
|
| REEP | Request for entry into the european phase |
Ref document number: 2014872240 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2014872240 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: 112016014404 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: 112016014404 Country of ref document: BR Kind code of ref document: A2 Effective date: 20160617 |