WO2014144215A1 - Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use - Google Patents
Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use Download PDFInfo
- Publication number
- WO2014144215A1 WO2014144215A1 PCT/US2014/028525 US2014028525W WO2014144215A1 WO 2014144215 A1 WO2014144215 A1 WO 2014144215A1 US 2014028525 W US2014028525 W US 2014028525W WO 2014144215 A1 WO2014144215 A1 WO 2014144215A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- tendon
- composition
- accordance
- extracellular matrix
- ligament
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/52—Hydrogels or hydrocolloids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K35/00—Medicinal preparations containing materials or reaction products thereof with undetermined constitution
- A61K35/12—Materials from mammals; Compositions comprising non-specified tissues or cells; Compositions comprising non-embryonic stem cells; Genetically modified cells
- A61K35/14—Blood; Artificial blood
- A61K35/16—Blood plasma; Blood serum
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/22—Hormones
- A61K38/28—Insulins
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/14—Macromolecular materials
- A61L27/22—Polypeptides or derivatives thereof, e.g. degradation products
- A61L27/24—Collagen
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/3604—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix characterised by the human or animal origin of the biological material, e.g. hair, fascia, fish scales, silk, shellac, pericardium, pleura, renal tissue, amniotic membrane, parenchymal tissue, fetal tissue, muscle tissue, fat tissue, enamel
- A61L27/3633—Extracellular matrix [ECM]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/3641—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix characterised by the site of application in the body
- A61L27/3645—Connective tissue
- A61L27/3662—Ligaments, tendons
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/3683—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix subjected to a specific treatment prior to implantation, e.g. decellularising, demineralising, grinding, cellular disruption/non-collagenous protein removal, anti-calcification, crosslinking, supercritical fluid extraction, enzyme treatment
- A61L27/3687—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix subjected to a specific treatment prior to implantation, e.g. decellularising, demineralising, grinding, cellular disruption/non-collagenous protein removal, anti-calcification, crosslinking, supercritical fluid extraction, enzyme treatment characterised by the use of chemical agents in the treatment, e.g. specific enzymes, detergents, capping agents, crosslinkers, anticalcification agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3804—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by specific cells or progenitors thereof, e.g. fibroblasts, connective tissue cells, kidney cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3804—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by specific cells or progenitors thereof, e.g. fibroblasts, connective tissue cells, kidney cells
- A61L27/3834—Cells able to produce different cell types, e.g. hematopoietic stem cells, mesenchymal stem cells, marrow stromal cells, embryonic stem cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3839—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by the site of application in the body
- A61L27/3843—Connective tissue
- A61L27/386—Ligaments, tendons
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/54—Biologically active materials, e.g. therapeutic substances
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/58—Materials at least partially resorbable by the body
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/20—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices containing or releasing organic materials
- A61L2300/252—Polypeptides, proteins, e.g. glycoproteins, lipoproteins, cytokines
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/40—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a specific therapeutic activity or mode of action
- A61L2300/402—Anaestetics, analgesics, e.g. lidocaine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/40—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a specific therapeutic activity or mode of action
- A61L2300/404—Biocides, antimicrobial agents, antiseptic agents
- A61L2300/406—Antibiotics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/40—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a specific therapeutic activity or mode of action
- A61L2300/412—Tissue-regenerating or healing or proliferative agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/40—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a specific therapeutic activity or mode of action
- A61L2300/412—Tissue-regenerating or healing or proliferative agents
- A61L2300/414—Growth factors
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/40—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a specific therapeutic activity or mode of action
- A61L2300/45—Mixtures of two or more drugs, e.g. synergistic mixtures
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2300/00—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices
- A61L2300/60—Biologically active materials used in bandages, wound dressings, absorbent pads or medical devices characterised by a special physical form
- A61L2300/64—Animal cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2400/00—Materials characterised by their function or physical properties
- A61L2400/06—Flowable or injectable implant compositions
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/10—Materials or treatment for tissue regeneration for reconstruction of tendons or ligaments
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/40—Preparation and treatment of biological tissue for implantation, e.g. decellularisation, cross-linking
Definitions
- the invention relates generally to the treatment of ligament and tendon injuries.
- the invention provides an injectable tendon-derived composition for the minimally invasive, in-situ repair of ligament and tendon injuries such as tears that result acutely from trauma or chronically from tendon or ligament overuse.
- the tendon-derived composition is applied in solubilized form and polymerizes upon administration to the defect of an injured ligament or tendon, where it fills out and conforms to the defect, thereby creating a scaffold which attracts and guides the recruitment of new tenoblasts, tenocytes and fibroblasts inside the defect for repair and regeneration of the injured ligament or tendon.
- Tendons and ligaments are strong bands of fibrous connective tissue that consist to a great part of collagen fibers. While tendons connect muscle to bone, ligaments connect bone to bone across a joint. The point of connection between muscle and tendon is the myotendinous junction or also called tendon-muscle insertion, and the point of connection between tendon and bone is the osteotendmous junction.
- the osteotendmous junction where collagen fibrils from the tendon insert into the bone matrix, is a site of frequently occurring tendinopathies that are commonly caused by tendon overuse.
- Tendon overuse leads to significant histological and biochemical changes that alter the biomechanical and material properties in tendons and ligaments (Arya & Kulig, 2010), causing accumulative microscopic tears that ultimately result in complete tears. Tears may be graded as minimal (1st degree), moderate to severe (2nd degree), or complete (3rd degree). Such injuries are most commonly seen in the rotator cuff, Achilles tendon, quadriceps tendon, and patella tendon as well as in medial and lateral epicondylitis of the elbow.
- ligaments limit the mobility of a joint or prevent certain movements altogether.
- Ligaments are elastic and lengthen under tension, unlike tendons, which are inelastic.
- the present invention provides a composition comprising decellularized extracellular matrix derived from tendon connective tissue for in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject.
- the composition is in an injectable form below 25 degree Celsius and polymerizes to a hydrogel upon administration into the subject's area of injured ligament or tendon where it is effective in repairing and regenerating said injured ligament or tendon.
- the resulting hydrogel forms in situ a support structure which facilitates infiltration of the subject's own fibroblasts, tenoblasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon.
- a one-time administration of the hydrogel is sufficient for treatment, in other embodiments repeated administration may be needed.
- the tendon connective tissue is selected from a human donor; in other embodiments, the tendon connective tissue is selected from an animal donor such as a pig.
- the composition creates, upon gelation, a structure suitable for infiltration of host cells such as fibroblasts, tenoblasts and tenocytes.
- cells such as stem cells, progenitor cells or fibroblasts, and/or therapeutic agents such as growth factors and/or platelet-rich plasma can be added to the composition prior to administration to increase its in-situ therapeutic benefit for tendon or ligament repair and regeneration.
- the therapeutic agent is a small molecule or protein exhibiting antibacterial effects or analgesic effects in order to ameliorate pain or a risk of infection that may occur concomitant with the tendon or ligament injury.
- the invention provides a method for in-situ repair and regeneration of an injured tendon or ligament in a mammalian subject, which involves the administration of a composition comprising decellularized extracellular matrix derived from tendon connective tissue to the area of injured tendon or ligament.
- the composition is in an injectable form below 25 degree Celsius and polymerizes to a hydrogel upon administration into the subject's area of injured ligament or tendon where it is effective in repairing and regenerating said injured ligament or tendon.
- the resulting hydrogel forms in situ a support structure which facilitates infiltration of the subject's own fibroblasts, tenob lasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon.
- a one-time administration of the hydrogel is sufficient for treatment, in other embodiments repeated administration may be needed.
- the invention provides a method of producing a composition comprising decellularized extracellular matrix derived from tendon connective tissue for in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject.
- the tendon extracellular matrix is derived from an allogeneic source such as a human.
- the tendon extracellular matrix is derived from a xenogeneic source such as a pig.
- FIG 1 illustrates, as detailed in Example 1, the determination of successful digestion of the tendon extracellular matrix (ECM) solution as a function of time, pH during the digestion and concentration of tendon powder (see also Table 1).
- the digestion of the ECM solution was observed at 20x magnification every 12h.
- the degree of digestion was recorded as under, right or over (change to underdigested, adequate, and overdigested) based on homogeneity (adequate), degree of remaining tendon flakes (underdigested) and single collagen fibers (adequate). This estimation corresponded well to gelation of the ECM solution at 37°C, (-) no gelation, (+/-) weak gelation, (+) gelation.
- FIG. 2 illustrates, as detailed in Example 1, the production of injectable (25G cannula) tendon extracellular matrix (ECM) solution from ground tendon (A) and enzymatic digestion (B, enzyme used here was pepsin) at low pH and, subsequently, the formation of the hydrogel (C) following incubation for 20 minutes at 37° C. (D) shows the hydrogel poured and gelled on a petri dish.
- ECM extracellular matrix
- B enzyme used here was pepsin
- Figure 3 shows the result of a proteomic analysis of an extracellular matrix solution, which was prepared as described in Example 1 , via mass spectrometry, where the amount of detected proteins (collagens and extracellular matrix proteins) is presented as percentage of total content (%).
- Figure 4A illustrates the measurement of rheo logical data from one representative sample of tendon hydrogel, as further described in Example 1 , as a measurement of its mechanical properties; triplicates of the storage (G') and loss (G") moduli for the tendon hydrogel are shown: G' at 1 rad/s is 217 and G" is 28 in this sample (average G' is 213.1 and G" 27.1).
- Figure 4B shows a kinetic determination of hydrogel formation (in triplicates) as a function of temperature, as further described in Example 1.
- the temperature was slowly increased from 25 to 37°C, with a 2°C increase per minute. Note that the moduli of the solution remained low (i.e. weak) and did not change during this time.
- the moduli of the solution remained low (i.e. weak) and did not change during this time.
- the moduli of the solution remained low (i.e. weak) and did not change during this time.
- panel B the moduli of the solution remained low (i.e. weak) and did not change during this time.
- Figure 6 illustrates scanning electron microscope images of gels with cells, harvested 1 (lwk) and 2 (2wk) weeks after in vivo application, as further explained in Example 1.
- Collagen fibrils often have a linear arrangement with collagen defined as a porous network or linear bundles interspaced with cavities (2wk, H). Collagen bundles are highly regular with a clear longitudinal orientation along the underlying muscular surface (shown in lwk, A). Cells follow this linear arrangement in surface view (lwk, C and 2wk, F). Cells are closely adherent to fibers (B), and there is an apparent integration of the gel patch with the surrounding tissue (2wk, E). Cells grow invasively into the collagen scaffold (lwk, D; 2wk, G) and become increasingly aligned and confluent, and integrated with the gel scaffold.
- Figure 7 illustrates, as further explained in Example 1, the percutaneous administration of tendon extracellular matrix solution (1 ml per injection site, 4 sites per 350 g rat) into the back of immune-competent Wistar rats and subsequent tendon hydrogel (G) formation in the subcutaneous space that surrounded the site of administration.
- the top panel indicates where in the rats the extracellular matrix solution was injected.
- the gel was consistently confined to the subcutaneous space beneath the panniculus carnosus, subcutaneous fat (SC) and underlying para- spinal muscle (M).
- Hematoxylin and eosin (H&E) histological analysis shows the gel (G) with vast cellular ingrowth from surrounding tissues already at 3 days post injection.
- Figure 8 illustrates, on the very left, the position and size of an exemplary tendon-derived hydrogel 7 days following percutaneous injection into the back of a Wistar rat, as further explained in Example 1.
- the other panels show representative examples of tendon-derived hydrogel explants that were isolated from Wistar rats at 7, 14 and 28 days after percutaneous injection. The explants are shown with skin, panniculus carnosus, and subcutaneous fat removed.
- Figure 9 shows, as further explained in Example 1, the results from Hematoxylin and eosin (H&E) histological analysis of exemplary tendon-derived hydrogels at 2 and 4 weeks following injection into Wistar rats; panel A shows at 20x magnification after two weeks and panel B at 40x magnification after two weeks. The invasion of cells from surrounding tissues into the superficial aspects of the gel as well as the longitudinally aligned fibroblast cells in the centre are notable. Panel C shows at 20x magnification after four weeks and panel D at 40x magnification after four weeks. Note that, at four weeks, the elongated fibroblasts are more homogenously distributed throughout the tendon-derived hydrogel. No signs of capsule formation are present around the gel, indicating integration with surrounding connective tissue.
- H&E Hematoxylin and eosin
- Figure 10 shows, as further explained in Example 1, results from various staining experiments with tendon-derived hydrogel three days following percutaneous administration into Wistar rats.
- A H&E staining of superficial aspects of tendon-derived hydrogel and para-spinus muscle.
- Corresponding counterstain of adjacent sections with PI B
- B IHC of CD68+ cells
- C showing invasion of CD 68+ macrophages into the gel (all 20x).
- Figure 11 shows exemplary tendon-derived hydrogels, where the tendon extracellular matrix solution was seeded with multipotent adipo- derived stem cells (ASCs) prior to gelation.
- ASCs multipotent adipo- derived stem cells
- the cells proliferated on the surface and infiltrated the gel, as detailed in panels A-F (with 20x magnification).
- Panel A shows polymerized gel with cells in culture 5 days post reseeding; live/dead stain of the same piece of gel; panel B shows the live cells in green and panel C shows dead cells in red.
- Panel D shows SYTO green stain of cells on gel surface, panel E H&E histological analysis of cryosection and panel F corresponding SYTO green analysis.
- Figure 12 shows results from decellularizing porcine tendon tissue, as further detailed in Example 2.
- Figure 12A H&E staining of native (A) and treated (B) porcine tendon at 20X magnification. In contrast to the native tendon, no cells can be observed between fibrous connective tissue.
- Figure 12B SytoGreen 11 fluorescent staining of native (A) and treated (B) porcine tendon at 20X magnification. Decellularization is confirmed by the absence of fluorescent nuclei in the treated specimen.
- Figure 13 illustrates, as detailed in Example 2, the determination of successful digestion of porcine tendon extracellular matrix versus human tendon extracellular matrix based on homogeneity, degree of remaining tendon flakes and single collagen fibers. The degree of digestion was recorded as underdigestion, proper digestion or overdigestion.
- Figure 14 illustrates the approximate protein composition of porcine tendon powder.
- Collagen IV and Collagen I were the predominant proteins found in the sample.
- Other peptides included tenascin, vimentin, fibromodulin, decorin, and other extracellular proteins.
- Figure 15 illustrates the rheo logical properties of 2% human and 1% porcine tendon- derived extracellular matrix solutions as indicated by the storage (G') and the loss (G") moduli representing the elastic and viscous properties, respectively.
- Panel A shows frequency sweeps, i.e. testing of the elastic and viscous properties at different oscillation frequencies, of human and porcine tendon-derived matrix at 25°C.
- Panel B shows frequency sweeps of human and porcine tendon-derived matrix at 37°C.
- Panel C shows temperature sweeps of human and porcine tendon-derived matrix, where the elastic and viscous properties were tested at different temperatures.
- Panel D shows time sweeps of human and porcine tendon-derived matrix at 37°C, where the elastic and viscous properties were tested over time.
- Figure 16 shows the morphology of human adipo-derived stem cells seeded within 2% human (A) and 1% porcine (B) tendon extracellular matrix solutions. Spindle-shaped cells can be seen throughout each extracellular matrix solution.
- Figure 17 shows results from the Live/Dead Assay, as further detailed in Example 2.
- the ratio of viable to non-viable cells remained low for human adipo-derived stem cells within human and porcine tendon-derived hydrogels. Viable cells are seen as green and non-viable cells are seen as red.
- Figure 18 illustrates the proliferation of human adipo-derived stem cells in human and porcine hydrogel at 3, 5, 7, and 10 days. No difference in proliferation exists at any time point.
- Figure 19 illustrates the set up of the studies, as detailed in Example 3, where Achilles tendon defects were created in Wistar rats by removing 50% of the Achilles tendon substance in each leg. The resulting defects were filled: on the left side with 2% solubilized tendon-derived extracellular matrix that gelated once administered by injection into the defect at body temperature (37°C) and filled out the gap that was created by the removal of 50% tendon substance that had produced the defect; on the right side, the defect was filled with saline as control.
- Figure 20 shows the results of the study described in Figure 19 and Example 3, where the biomechanical properties of rats' Achilles tendon that was treated with solubilized tendon- derived extracellular matrix that gelated in-situ are compared to rats' Achilles tendon whose defect was treated with saline as control.
- Figure 21 shows results from H&E staining after 4 weeks of saline versus tendon hydrogel treatment.
- H&E sections of saline (A) and gel (B) treatment at 4 weeks show typical wound trough morphologies and population by host cells in both groups.
- Corresponding Picro- sirius Red stains (C/saline & D/gel) show a difference in collagen content between the treatment groups.
- the wound troughs of the saline-treated tendons primarily contain collagen III
- the wound troughs of the gel-treated tendons show higher concentrations of collagen I.
- T tendon
- * wound trough.
- the practice of the present invention may employ conventional techniques of chemistry, cell biology, immunology, biochemistry, as well as of bone, joint, plastic and reconstructive surgery, which are within the capabilities of a person of ordinary skill in the art. Such techniques are fully explained in the literature. For definitions, terms of art and standard methods known in the art, see, for example, 'Current Protocols in Cell Biology', John Wiley & Sons (2007);
- administration refers to introducing a composition, such as a tendon-derived extracellular matrix solution that polymerizes, i.e. gelates, at physiological temperature (body temperature, 37°C), of the present disclosure into a subject.
- a composition such as a tendon-derived extracellular matrix solution that polymerizes, i.e. gelates, at physiological temperature (body temperature, 37°C)
- body temperature 37°C
- One preferred route of administration is to administer locally, meaning directly to the injured tendon or ligament via a needle or via an incision through the skin, i.e. percutaneously, so that the composition is not systemically distributed throughout the body.
- subject refers to the host or recipient of the compositions of the present invention and includes humans as well as other mammals such as horses, cows, dogs.
- Donor refers to a mammalian cadaveric source for tendon connective tissue, as described herein, which can be from a human or animal source.
- Tendon connective tissue that was harvested from a donor can be "allogeneic", i.e., derived from a non- genetically identical member of the same species and, thus, be isolated from one subject and transferred, for example by injection, infusion or grafting, to another subject, particularly from one human to another human.
- Tendon connective tissue that was harvested from a donor can, furthermore, also be obtained from animal sources for use in the methods and compositions of the present invention.
- the tissues are "xenogeneic", i.e., from a member of a different species.
- Preferred sources of xenogeneic connective tissues are pigs, horses, cows, sheep, rodents and dogs. In either case, all connective tissues are obtained from a fresh-frozen cadaveric donor. To obtain such connective tissues from a cadaveric donor, standard biopsy techniques known in the art may be employed.
- "Therapeutically effective amount" refers to an amount that provides the desired therapeutic effect of tendon or ligament tissue repair and regeneration in a mammalian subject.
- area of tendon or ligament injury refers to the site of the defect and designates (i) the actual site of the tendon or ligament injury as well as (ii) the zone that is directly adjacent to or surrounding of the actual site of the tendon or ligament injury.
- An injectable composition refers to any material that can be made liquid enough or solubilized enough to be injected into a defect, i.e. an area of ligament or tendon injury, including an emulsion, liquid, particles and powder.
- Decellularization refers to the substantial (at least 75%), nearly complete (at least 95%) or complete removal of cellular components of tendon connective tissue by the use of physical and chemical means, or any combination thereof. It is understood that it is not necessarily preferred to achieve a maximally possible decellularization, if doing so negatively affects the biomechanical properties of the connective tissue. The optimum degree of decellularization will depend upon the biomechanical properties of the tissue and its intended use.
- the storage (G') and loss (G") moduli for tendon hydrogels of the present invention represent the elastic and viscous properties of the gel.
- Tedon-muscle insertions refers to the site of connection between tendon and muscle and is also called the tendon junction site or myotendinous junction.
- the "osteotendinous junction" is the site of connection between tendon and bone and is also called the tendon insertion site.
- Embodiments of the present invention provide methods and compositions comprising decellularized extracellular matrix derived from tendon connective tissue for the minimally invasive, in-situ repair and regeneration of ligament and tendon injuries such as tears that resulted acutely from trauma or chronically from tendon or ligament overuse in a mammalian subject.
- the composition is in an injectable form below 25° Celsius and polymerizes upon administration to the defect of an injured ligament or tendon in a mammalian subject, where it fills out and conforms to the defect, thereby creating a three-dimensional tendon scaffold which attracts and facilitates migration of surrounding hosts cells into the scaffold microenvironment.
- composition can also be supplemented with exogenous cells and/or therapeutic agents prior to administration to increase its in-situ therapeutic benefit for tendon or ligament repair and regeneration. Repair and regeneration of the injured ligament or tendon is ultimately achieved, when the tendon scaffold is replaced with the regenerated tissue.
- Tendons are strong bands of fibrous connective tissue that connect muscle to bone and are composed of parallel arrays of collagen fibers (mostly type 1 collagen) and elastin embedded in a proteoglycan-water matrix.
- the point of connection between muscle and tendon is the myotendinous junction, while the point of connection between tendon and bone is the
- tendons which are typically classified as flexors (flexing or bending a joint) or extensors (extending or straightening a joint) are to withstand tension and to allow transmission of forces created in the muscle to the bone, thus making joint and limb movements possible (Sharma & Maffulli, 2005; Kannus, 2000). This is made possible by a complex macro- and microstructure of tendons and tendon fibers, where collagen is arranged in hierarchical levels of increasing complexity, beginning with
- tropocollagen a triple-helix polypeptide chain, which unites into fibrils, fibers (primary bundles), fascicles (secondary bundles), tertiary bundles, and the tendon itself. Soluble tropocollagen molecules form cross-links to create insoluble collagen molecules, which aggregate to form collagen fibrils.
- a collagen fiber is the smallest tendon unit that can be tested mechanically and is visible under light microscopy. Although collagen fibers are mainly oriented longitudinally, fibers also run transversely and horizontally, forming spirals and plaits (Sharma & Maffulli, 2005).
- Healthy tendons have a fibro-elastic texture and show strong resistance to mechanical challenges.
- tendons are exposed to longitudinal as well as transversal and rotational forces, whereby the complex three-dimensional architecture of tendons provides critical support to prevent damage and disconnection of fibers.
- Muscles designed to create powerful, resistive forces such as the quadriceps and triceps brachii muscles, have short and broad tendons, while those that have to carry out subtle and delicate movements, like the finger flexor tendons, have long and thin tendons (Kannus, 2000).
- Intrasynovial tendons of the hand and the feet are surrounded by tendon sheaths or similar networks of connective tissue that contain the vascular, lymphatic and nerve supply to the tendon and whose main function is to minimize the friction between the tendon and its surroundings. Since proper movement and gliding of the tendon determines its efficiency, the tendon needs to be able to move freely and in an uninhibited manner.
- Tendon sheaths have two layers, an outer, fibrotic sheath, which consists of collagen fibrils and fibers, as well as an inner, synovial sheath, which consists of two sheets of synovial lining cells.
- synovial lining cells contain a thin film of fluid which is similar to the composition of the synovial fluid of a joint and which improves lubrication.
- the synovial lining cells are covered with fine collagen fibrils ('Human Tendons', by Laszlo Jozsa & Pekka Kannus, Human Kinetics (1997)). Synovial tendon sheaths are found in areas that often experience increased mechanical stress such as tendons of the hands and feet, where efficient lubrication is important (Sharma & Maffulli, 2006).
- the tendon extracellular matrix consists of collagen fibers, elastic fibers, ground substance and inorganic components such as copper, manganese and calcium.
- the tendinous ground substance, which surrounds the collagen, consists of macromolecules such as
- proteoglycans and glycosaminoglycans (GAGs), structural glycoproteins, and a wide variety of other smaller molecules.
- GAGs glycosaminoglycans
- the proteoglycans and glycosaminoglycans have a considerable capacity to bind water and are important for the biomechanical properties of tendon against shear and compressive forces.
- Tenoblasts and tenocytes lie between the collagen fibers along the axis of tendon and are its major cellular components. Tenoblasts are immature tenocytes with higher metabolic rates that eventually mature into tenocytes. Chondrocytes are located at the sites of attachment and insertion into bone. Synovial cells of the tendon sheath as well as vascular cells form the remaining cellular components of a tendon. Tendons receive their blood supply from blood vessels entering from the myotendinous and osteotendinous junctions, the intratendinous vascular network and the synovial sheath.
- Tenocytes synthesize collagen and all components of the extracellular matrix and are active in energy production, which can be aerobic as well as anaerobic. Compared to skeletal muscles, tendons and ligaments have a low metabolic rate, low oxygen consumption and a fairly well developed anaerobic energy production capacity. On the upside, a low metabolic rate allows tendons to maintain tension for prolonged periods without becoming ischemic and necrotic. On the downside, a low metabolic rate means that tendon injuries take a long time to heal.
- Tendons transmit force from muscle to bone, while at the same time acting as a buffer by absorbing external forces to limit tearing and other damage to the muscle.
- tendons have, by necessity, to exhibit high mechanical strength, good flexibility and high elasticity.
- the biomechanical properties of tendons are dependent on the collagen fiber diameter, fiber orientation, and collagen content.
- Tendons subject to multidirectional forces display collagen fiber bundles that lack regular orientation and the connective tissue is irregularly arranged.
- tendons subject to unidirectional strain display collagen fiber bundles with mostly parallel orientation.
- the mechanical behavior of collagen depends on the number and types of intra- and intermolecular bonds.
- the tensile strength of a tendon is a function of its thickness and its collagen content.
- test parameters that can be inferred from such tensile testing include stiffness, maximum load, and strain to maximal load.
- the tendon or ligament tissue is elongated at a set rate, while the changes in force are recorded. The force is then plotted against displacement.
- Methods for testing of biomechanical properties include compression and tension testing. Exemplary methods that find wide-spread use for
- biomechanical strength testing include (a) Ultimate Failure Load. Ultimate Failure Load represents the maximum load (pull force on the tendon) that the tendon can withstand before breaking, measured in Newton (N). (b) Ultimate Tensile Stress. Ultimate Tensile Stress is a relative measurement that takes the physical properties of the graft into account. It is measured in N/mm 2 as the load per cross-sectional area of the tendon or ligament in question, (c) Stiffness. Stiffness represents the rigidity of the tendon that is the extent to which it resists deformation in response to the applied pull force at testing.
- Finger flexor tendons Flexor pollicis longus tendon, flexor digitorum superficialis tendons and fiexor digitorum profundus tendons belong to the group of finger flexor tendons.
- Flexor tendons of the lower arm Flexor carpi radialis tendon, palmaris longus tendon, flexor carpi ulnaris tendon and the common flexor tendon are flexor tendons of the forearm.
- the common flexor tendon is a tendon shared by a number of superficial flexor muscles in the forearm and attaches to the medial epicondyle of the humerus. Overuse of the common flexor tendon can lead to medial epicondylitis or golfer's elbow.
- the common fiexor tendon serves as the origin for a number of superficial muscles of the anterior compartment of the forearm such as the palmaris longus (a small tendon between the flexor carpi radialis and the flexor carpi ulnaris) or flexor digitorum superficialis (an extrinsic flexor muscle of the fingers at the proximal interphalangeal joints).
- the flexor digitorum profundus is another muscle in the forearm that flexes the fingers. It is an extrinsic hand muscle because it acts on the hand, while its muscle is located in the forearm and is a flexor of the wrist, midcarpal, metacarpophalangeal and interphalangeal joints.
- Finger extensor tendons Extensor digiti minimi tendon, extensor digitorum communis tendons, extensor indicis tendon, extensor pollicis brevis tendon and extensor pollicis longus tendon belong to the group of finger extensor tendons.
- Extensor tendons of the forearm Extensor carpi ulnaris tendon; Extensor carpi radialis brevis tendon, extensor carpi radialis longus tendon and the common extensor tendon are extensor tendons of the forearm.
- the common extensor tendon originates from the lateral epicondyle and is often injured due to overuse, leading to lateral epicondylitis or tennis elbow.
- the Achilles tendon also called tendocalcaneus, is part of the posterior leg and is the thickest and strongest tendon in the body. It connects the superficial muscles of the posterior leg, plantaris, soleus and gastrocnemius (calf muscle) to the calcaneus (heel) bone. Albeit it is the largest and strongest tendon in the human body, the Achilles tendon is highly susceptible to acute and chronic injuries during athletic activities, since it needs to fulfill high functional demands during sports such as soccer, track and field, tennis, basketball and so forth. During sprinting exercises, the Achilles tendon is exposed to tensile forces that are about 10-12 times the body weight of the sprinting individual, while during jumping or cycling the tensile forces are about 6- 8 times of the body weight.
- semimembranosis tendon are flexor tendons of the thigh.
- Semitendinosus is one of the hamstring muscles and functions both as flexor and extensor by helping to extend the hip joint and to flex the knee joint; it also helps to medially rotate the knee.
- Patellar tendon and quadriceps tendon are embedded in and held in place by the patellar tendon on the tibial side (side of shin bone) and the quadriceps tendon on the femoral side (side of the thigh bone).
- the top of the patella attaches to the quadriceps muscle via the quadriceps tendon and the bottom of the patella attaches to the tibia via the patellar tendon,
- Flexor tendons of the leg Flexor digitorum longus tendons, flexor hallucis longus tendons, and tibialis posterior tendon are flexor tendons of the leg. Flexor digitorum longus, one of the muscles of the posterior compartment of the leg, functions to curl the toes and to stabilize the lower leg, while flexor hallucis longus, another muscle of the posterior compartment, performs plantar flexion of the big toe alone (downward movement of the toes). Tibialis anterior is situated on the lateral side of the tibia; it is thick, fleshy above, tendinous below and acts to dorsiflex (turn upward) and invert the foot.
- Tibialis posterior a muscle of the posterior compartment of the leg, is the main stabilizing muscle of the lower leg and assists with foot inversion and ankle plantar flexion.
- Peroneus longus, and peroneus brevis are everters of the foot that secondarily plantarflex at the ankle.
- Flexor tendons of the foot are flexor tendons of the foot.
- the flexor digitorum longus and brevis, flexor hallucis longus and brevis, and flexor digiti minimi brevis tendon are flexor tendons of the foot.
- Extensor tendons of the leg Extensor digitorum longus tendons and extensor hallucis longus tendon are extensor tendons of the leg.
- the extensor digitorum longus tendons are located at the lateral part of the front leg and act to dorsiflex the foot as well as the toes and invert the foot.
- the extensor hallucis longus is part of the anterior leg and functions to extend the big toe, dorsiflex the foot, and assists with foot inversion.
- Tibialis anterior and peroneus tertius are extensor tendons of the leg that dorsiflex the foot at the ankle.
- Extensor tendons of the foot Extensor digitorum longus and brevis tendons as well as extensor hallucis longus and brevis tendons are extensor tendons of the foot.
- the extensor digitorum brevis is a muscle on the dorsal (upper) part of the foot that functions to extend the smaller toes, while the extensor hallucis brevis, which is a muscle of the dorsum of the foot, acts to extend the big toe.
- tendon disorders such as tendon injuries and tendinopathies occur frequently and in any age group, leading to weeks and months of pain, impaired physical activity and lengthy treatment that can range from physical therapy to surgical rehabilitation.
- Tendons and ligaments have an about 7.5 lower oxygen consumption than skeletal muscles due to a low metabolic rate and capacity to generate energy anaerobically which makes tendons and ligaments well suited to withstand and maintain tension.
- the low metabolic rate also means that the healing process is slower than in skeletal muscle (Sharma & Maffulli, 2005).
- Tendon injuries can be (i) acute strain injuries, tendon tears or full ruptures of the muscle- tendon units due to sudden, spontaneous impacts or laceration by a sharp object or (ii) chronic injuries (tendinopathies) due to tendon overuse without proper recovery time between uses and possible subsequent degeneration of the tendon tissue.
- acute tensile overload situations and overuse cause injuries to the musculotendinous junction, which manifest as sprains, strains and rupture, while injuries to the osteotendinous junction lead to avulsion fractures, bone detachment injuries and chronic enthesopathies, i.e. disorders of the tendon-bone attachment.
- Tendon injuries manifest themselves usually through pain, particularly during sports-related activities which might have contributed to the injury at the first place, then focal tenderness with pain radiating from particular trigger points and decreased strength and ability to move.
- Tendon injuries that frequently occur in the course of sports activities and for which the methods and compositions of the present invention are particularly well suited, include (i) Achilles tendon injuries, generally due to the performance of high- force movements and spontaneous change of directionality, as it is the case in soccer, track and field or tennis (Kannus & Natri, 2007); (ii) rotator cuff injuries, usually caused by motions that require forceful pulling motions or repetitive overhead motions, as they occur in sports activities such as tennis, martial arts, boxing, swimming, golf, cheerleading or throwing activities; (iii) common flexor tendon injuries such as medial epicondylitis of the elbow, the so-called 'golfer's elbow', and common extensor tendon injuries such as lateral epicondylitis of the elbow, the so-called 'tennis elbow'; (iv) patellar tendon and quadriceps tendon injuries that are concomitant with patellar dislocation that often occurs during sports activities that involve sudden and force
- Hamstring or medial collateral and lateral collateral ligaments, anterior or posterior cruciate ligaments of the knee are examples of important ligaments of the body.
- Ligaments similar to tendons, are strong bands of fibrous connective tissue consisting of fibers made mainly out of type 1 collagen. In contrast to tendons, which connect muscle to bone, ligaments connect bones to other bones across a joint. Some ligaments limit the mobility of a joint or prevent certain movements altogether. Ligaments are elastic and lengthen under tension, unlike tendons, which are inelastic.
- Capsular ligaments are part of the articular capsule that surrounds synovial joints. They act as mechanical reinforcements. Extra-capsular ligaments provide joint stability. Intra-capsular ligaments, also provide stability, but permit a far larger range of motion. Cruciate ligaments occur in pairs (anterior and posterior).
- Ligaments of the head, neck and chest include the cricothyroid ligament, periodontal ligament and suspensory ligament of the lens, which all are ligaments of the head and neck, while the suspensory ligament of the breast is a ligament of the human thorax.
- the metacarpophalangeal joints are ligaments of the human hand.
- the palmar radiocarpal ligament, dorsal radiocarpal ligament, ulnar collateral ligament and radial collateral ligament are ligaments of the human wrist.
- the acromioclavicular ligaments surround and support the acromioclavicular joint which is the connection between the scapula and the clavicle.
- the coracoclavicular ligaments hold the clavicle down by attaching it to a bony knob on the scapula called the coracoid process.
- the scapho lunate interosseous ligament is a broad ligament connecting the scaphoid bone to the lunate bone.
- Ligaments of the lower extremities include the anterior cruciate ligament (ACL), lateral collateral ligament (LCL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), which all are main ligaments of the human knee.
- ACL anterior cruciate ligament
- LCL lateral collateral ligament
- PCL posterior cruciate ligament
- MCL medial collateral ligament
- the ACL is referred to as the cranial cruciate ligament (CrCL)
- the PCL is referred to as the caudal cruciate ligament (CaCL).
- the anterior sacroiliac ligament, the posterior sacroiliac ligament, the sacrotuberous ligament, the sacrospinous ligament, the inferior pubic ligament, the superior pubic ligament and the suspensory ligament of the penis are ligaments of the human pelvis.
- Ligament injuries which are often acquired during weight-bearing sports activities such as downhill skiing, running, jumping and the like, can lead to instability of the joint that the ligament is supposed to stabilize. Instability of a joint can lead to cartilage wear over time and eventually to osteoarthritis. Therefore ligament injuries need to be taken seriously and repaired.
- thermosensitivity and solid-liquid characteristics of the tendon extracellular matrix solution being liquid at a cold temperature up to room temperature (4-25°C) and gelating at physiological body temperature, at around 37°C, allow easy and quick administration of the solution via injection or infusion, while the gelation in situ, upon administration into the area of the tendon or ligament defect, i.e. the site of injury, of a subject allows the formation of a three- dimensional tendon support scaffold.
- this resulting tendon support scaffold/tendon hydrogel is based on decellularized materials from tendon tissue, it replaces 'like with like', since the scaffold already possesses the mix of non-cellular components that matches that of the native tissue (tendon or ligament) such as various types of collagen fibers, hyaluronic acid, fibronectin, laminin, carbohydrate polymers, polysaccharides and sulfates.
- the administration of the solubilized tendon-derived extracellular matrix into the area of ligament or tendon defect or injury is preferably carried out via injection with a needle (for example, 25 gauge). It is considered a minimally invasive procedure, since it does not require a surgical procedure (including anesthesia) and can be carried out during an office visit. This ensures quick attendance to the tendon or ligament injury and, consequently, accelerates a subject's recovery from the injury.
- the solubilized tendon-derived extracellular matrix conforms to the three- dimensional space of the tendon or ligament defect that resulted from the injury and so facilitates in situ regeneration by means of three-dimensional (3D) guided tissue regeneration, accelerating ligament and tendon healing, as shown in Example 2.
- 3D three-dimensional
- the repair and regeneration of the tissue defect in the injured ligament or tendon is aided by the three-dimensional support scaffold of the tendon-derived hydrogel ('tendon hydrogel').
- the tendon-derived hydrogel provides a supportive nanostructure for renewed organization of collagen fibers that became disorganized during the tendon or ligament injury.
- the tendon-derived hydrogel furthermore, creates a structure suitable for host cell infiltration, i.e. infiltration of fibroblasts, tenoblasts and tenocytes from the host, and tissue regeneration.
- cells such as stem cells, progenitor cells or fibroblasts, and therapeutic agents can be added to the solubilized tendon-derived extracellular matrix prior to injection and prior to gelation in order to increase its in-situ therapeutic benefit for tissue regeneration.
- the therapeutic agent can be a growth factor such as basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), insulin-like growth factors 1 and 2 (IGF-1 and IGF -2), platelet derived growth factor (PDGF), or stromal cell derived factor (SDF-1).
- bFGF basic fibroblast growth factor
- VEGF vascular endothelial growth factor
- HGF hepatocyte growth factor
- IGF-1 and IGF-2 insulin-like growth factors 1 and 2
- PDGF platelet derived growth factor
- SDF-1 stromal cell derived factor
- growth factors can be supplemented through autologous platelet-rich plasma (PRP) enrichment of the tendon-derived hydrogel to stimulate and accelerate tissue regeneration.
- PRP refers to autologous plasma with platelet concentrations at particular levels above baseline values (Hall et al., 2009).
- the therapeutic agent is a small molecule or protein exhibiting antibacterial effects in order to ameliorate a risk of infection that may occur concomitant with the tendon or ligament injury.
- antibiotics suitable as therapeutic agents include (i) aminoglycosides such as gentamicin, streptomycin, tobramycin, (ii) glycopeptides such as vancomycin, (iii) lincosamides such as clindamycin, (iv) macrolides such as azithromycin, (v) polypeptides such as bacitracin, (vi) quinolones such as ciprofloxacin, (vii) tetracyclines such as doxycycline, tetracycline, and other categories of antibiotics that can be administered into the defect, either combined with the tendon-derived extracellular matrix solution, administered prior to the administration of the tendon-derived extracellular matrix or administered after the tendon- derived extracellular matrix has been administered, and can exert a localized effect.
- the therapeutic agent is a small molecule or protein exhibiting analgesic effects in order to ameliorate pain that may occur concomitant with the tendon or ligament injury.
- analgesics suitable as therapeutic agents include (i) non-steroidal anti-inflammatory agents such as ibuprofen and naproxen as well as (ii) local anesthetics such as lidocaine and bupivacaine.
- compositions such as the described tendon-derived hydrogels that support the healing process and that can be administered to the injured tissue without a major surgical step, as described in the present invention, are of high utility and benefit.
- solubilized tendon- derived extracellular matrix Due to its thermosensitive properties solubilized tendon- derived extracellular matrix remains liquid and injectable in the temperature range of about 4-25 °C.
- solubilized tendon extracellular matrix Upon injection of the solubilized tendon-derived extracellular matrix into a bodily space such as into the area of a ligament or tendon injury, the solubilized tendon extracellular matrix - at the body temperature of about 37°C - gelates within minutes into a tendon-derived hydrogel, as described in Examples 1 and 2.
- the hydrogel then fills out and conforms to the defect. It, thus, creates a scaffold which attracts and guides the settling of new tenoblasts, tenocytes and fibroblasts inside the defect for repair and regeneration of the injured ligament or tendon.
- a one-time administration of a therapeutically effective amount of a tendon-derived hydrogel might be sufficient to treat the defect.
- repeated administration of therapeutically effective amounts of a tendon-derived hydrogel, within the time period of several days, weeks or months, might be needed to treat the defect.
- repeated administration of therapeutically effective amounts of a tendon-derived hydrogel, within the time period of several days, weeks or months might be carried out to improve clinical efficacy.
- composition for in-situ repair and regeneration of an injured ligament or tendon comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel at physiological temperature
- FDS tendons were transected 2cm proximal to the chiasma
- FDP and FPL tendons were transected 1cm proximal to the osteotendinous junction.
- the tendons were then decellularized following a previously reported protocol (Pridgen BC et al, 2011).
- scaffolds were treated with 0.1% ethylenediamine-tetraacetic acid (EDTA) for 4 hours followed by 0.1% sodium dodecyl sulfate (SDS) in 0.1% EDTA for 24 hours at room temperature with constant agitation. Scaffolds were washed in PBS (also referred to as saline herein) and stored at -80°C.
- EDTA ethylenediamine-tetraacetic acid
- SDS sodium dodecyl sulfate
- the frozen decellularized material was then lyophilized, and thereafter cut into smaller tendon pieces and milled into a fine powder using a Wiley Mini Mill (Thomas Scientific, Sedesboro, NJ, USA). The powder was stored at 4°C until needed for use.
- a DNA assay along with routine H&E histology and SYTO green- fluorescent nucleic acid staining was used to quantify the effectiveness of decellularization of tendons. This is described in detail in a previous publication (Pridgen et al., 2011). In short, DNA was extracted from lyophilized tendons using a DNeasy kit (QIAGEN).
- the concentration of the extract was determined using an ultra-violet spectrophotometer (Biophotometer 22331 ; Eppendorf) at a wavelength of 260 nm.
- the concentration of the samples was calculated by software on the spectrophotometer using a known extinction coefficient for dsDNA.
- Extracellular matrix (ECM) gel formation The powder of decellularized and lyophilized ground tendons, which was produced as described above, was then solubilized and enzymatically digested by adding a lmg/ml solution of pepsin (Sigma, St Louis, MO) in HC1 and water such that the final concentration of material was 10, 20 and 30 mg/ml (1-3% respectively, dry weight).
- pepsin Sigma, St Louis, MO
- Optimal pH for pepsin digestion was explored and set to pH 2.2 (Bohak, 1969). Increasing molarity of HC1 is needed to accomplish optimal digestion with increasing
- the material was digested for up to 72h (12, 24, 36, 48 and 72h) at room temperature with constant stirring.
- the extracellular matrix solution (ECM solution) was checked for pH and homogeneity under a microscope every 12h to optimize the conditions for digestion.
- the digestion time was set to 24h to ensure complete digestion.
- the salt concentration was adjusted with the addition of lOx PBS (1/10 of final neutralized volume), while cooled on ice.
- Pepsin activity was then completely reversed by adding of NaOH to increase the pH >8, before the final solution pH was neutralized to a pH of 7.4 by addition of HC1.
- the final mixture was then ready for injection or in vitro experiments. When placed in an incubator at 37°C it was allowed to gel for 20-60 minutes at 37°C. Gelation was confirmed macroscopically and with rheology (see below and Figure 1).
- Samples were prepared using a FASP (Filter aided proteome preparation) (Wisniewski et al, 2009) protocol, where the sample was solubilized in SDS, DTT and Tris-HCL and digested overnight by trypsin.
- the peptides were loaded onto a self-packed fused silica CI 8 analytical column, interfaced by a Bruker Michrom Advance (Auburn, CA, USA) source with a flow rate of 600 nL/min and a spray voltage of 1.7kV.
- the mass spectrometer was a LTQ Orbitrap Velos, Thermo Scientific (Vancouver, Canada), set in data dependent acquisition mode fragmenting the top 12 most intense precursor ions.
- the RAW data was converted to mzXML format and database searched against the human uniprot-sprot database using Sequest on a Sorcerer platform.
- the data was visualized using Scaffold 3, Proteome Software (Portland, OR, USA).
- Rheology storage modulus, temperature characteristics.
- Rheo logical measurements were made using a TA Instruments ARG2 Rheometer. Two parallel steel plates (40 mm diameter) at lOOum gap height were used on 500 ⁇ of tendon-derived hydrogel in different concentrations, performed 24 hours after the extracellular matrix solution was allowed to gelate. The setup was such that the sample completely filled the gap between the rheology plates.
- the storage modulus (G') and loss modulus (G") over frequencies of 0.1-10 rad s-1 (frequency sweep) were recorded for every gel condition in triplicate and plotted.
- the peltier probes of the rheometer were preheated to 25°C.
- ASCs adipo-derived stem cells
- ADSC-BM medium Lionza, Walkers ville,MD, USA
- FCS adipo-derived stem cells
- Cells were grown to confluence at 37°C in a humidified tissue culture chamber with 5% carbon dioxide.
- Reseeding of the ECM solution was performed both onto preformed gel (a), and by mixing cells into the ECM solution before gelation (b).
- the ECM solution was first allowed to gel for lh in a 48 well plate at 37°C.
- a cell suspension containing 5xl0 4 cells/0.2ml was placed on top of the preformed gel, and incubated overnight, (b) Seeding was also performed by mixing a cell suspension of 5xl0 4 cells/0.2ml with 0.5 ml ECM solution. The mix was placed in a 48 well plate and allowed to gel for lh at 37°C, then 0.5 ml medium was added. Cell culture medium was changed every other day for both seeding protocols. Cells were stained with SYTO Green or using a live dead assay on day 5 to check for viability on the gel surface and inside the gel.
- a mouse anti-rat CD68 primary antibody was used (Santa Cruz Biotechnology). Rat spleen was used as a positive control. Sections were also counter- stained with Propidium Iodine (PI) to assess for cell infiltration. Whole tissue mounts were divided longitudinally and immersed in SYTO green (Invitrogen) nucleic acid stain at 1 :2000 dilution in DI water for 20min. Reseeded gels were then placed on coverslips and imaged.
- SYTO green Invitrogen
- Live/Dead assay (Invitrogen) was performed on reseeded gels at 5 days, on constructs where adipo-derived stem cells (ASCs) had been premixed with solubilized tendon extracellular matrix prior to gelation at 37°C. This assay was performed to assess the ratio of viable to nonviable cells. Gels 5 days post reseeding were labeled with Live/Dead stain and incubated for 20 minutes.
- ASCs adipo-derived stem cells
- Hydrogels were successfully prepared from decellularized and ground human tendons (Human flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS) and flexor pollicis longus (FPL) tendons), that had been harvested from human cadavers and immediately fresh frozen at - 80°C and reconstituted to obtain solubilized tendon extracellular matrices with concentrations ranging from 1-3% (v/v). Increasing extracellular matrix concentration provided a more rigid gel structure that was easier to handle. The 2% solubilized tendon extracellular matrix produced a gel that showed an optimal balance between handling properties, structural rigidity and permeability to seeded cells. Therefore, experiments on reseeding, storage and in vivo experiments were preferably conducted using the 2% solubilized tendon extracellular matrix concentration.
- FDP Human flexor digitorum profundus
- FDS flexor digitorum superficialis
- FPL flexor pollicis longus
- Optimal HC1 molarity and digestion time [in minutes] was determined based on microscopic appearance of the degree of ECM digestion (see Table 1 and Figure 1). Table 1. Optimal pH for pepsin digestion was explored. Increasing molarity (N) of hydrochloric acid (HC1) is needed to accomplish optimal digestion with increasing concentration of tendon powder. This is an essential step in the gel making process as complete digestion of the decellularized lyophilized powder is needed for the extracellular matrix (ECM) solution to hold its thermoregulatory gelation properties so that it is liquid at 4-25°C and gelates at around 37°C.
- ECM extracellular matrix
- the ECM solution can thus be stored for extended periods of time in its soluble and injectable form in cold temperature, and "activated" at the time of injection to form a gel in situ at body temperature.
- Both the storage modulus (G') and the loss modulus (G") were also shown to increase as a function of time at 37°C.
- the change in tendon extracellular matrix solution moduli was depicted as a sigmoidal shaped increase, initiated approximately after 15 minutes, with a plateau that was reached after 20 minutes (Figure 4b, right graph). 20 minutes corresponded well to the time it takes for the tendon extracellular matrix solution to completely form a gel in vitro, as observed macroscopically.
- Figure 1 OB is a nuclear counterstain that stains all live cells in an adjacent section whereas 11C is an immune -histochemical stain of CD68+ macrophages.
- cell ingrowth was preferentially seen in the superficial parts of the gel, as depicted in Figure 9.
- CD68+ cells continued to populate the full thickness of the gel at all time points.
- histology displayed increasing numbers of spindle shaped elongated fibroblast cells, on its surface as well as centrally ( Figures 9 A and B).
- ASCs Multipotent adipo-derived stem cells
- tendon- derived extracellular matrix solution proliferated on the surface and infiltrated the gel.
- Spindle shaped cells were observed both on the gel surface as well as within the gels, with a regular distribution throughout the gel.
- Live/dead staining and SYTO green staining on whole tissue mounts of gels confirmed that reseeded cells were homogenously distributed throughout the gel.
- the fraction of nonviable cells remained low, indicating that the tendon extracellular matrix hydrogel appears well suited for delivery of cells, such as multipotent adipoderived stem cells, to the area of tendon injury in order to speed up tendon tissue repair and regeneration (Figure 11).
- the resulting tendon hydrogel forms a mesh of collagen fibers and collagen fiber bundels characterized by a highly regular linear pattern and orientation in longitudinal fashion along the underlying muscular surface.
- the regular pattern and longitudinal orientation is instrumental in rebuilding the injured tendon or ligament in a way that it regains the structural, biomechanical and functional characteristics of a normal, healthy tendon or ligament with its full range of motion and tensile strength.
- Capsule formation would have indicated that the body reacted to the extracellular matrix as being foreign tissue.
- EXAMPLE 2 INJECTABLE PORCINE TENDON HYDROGEL AS A SCAFFOLD FOR IN-SITU GUIDED TISSUE REGENERATION IN THE MUSCULOSKELETAL SYSTEM
- Flexor tendons were harvested from fresh cadaveric forearms, as described in example 1. These tendons were meticulously debrided of remaining synovial material and muscle tissue. Flexor digitorum superficialis tendons were transected 2 cm proximal to the chiasma, while flexor digitorum profundus and flexor pollicis longus tendons were transected 1 cm proximal to the osteotendinous insertion.
- Harvested tendons were subsequently cut into 1 cm segments and treated with 0.1% ethylenediaminetetraacetic acid (EDTA) for 4 hours and then washed in 0.1% sodium dodecyl sulfate (SDS) in 0.1 % EDTA for 24 hours at ambient temperature with constant agitation. Tendon was then rinsed in IX PBS for 4 hours and stored at -80°C.
- EDTA ethylenediaminetetraacetic acid
- SDS sodium dodecyl sulfate
- concentration of dsDNA present within samples was then extrapolated using a known extinction coefficient for the molecule.
- Rheology storage modulus, temperature characteristics.
- Rheo logical studies were performed with a TA Instruments ARG2 Rheometer. Extracellular matrix solution samples were dispensed (500 ⁇ ) onto two parallel steel plates (40 mm diameter) at a gap height of 100 ⁇ , which allowed the solution to completely spread to the edge of the probe. Excess solution was gently wiped away. Using a barrier for containment, silicone oil was used to prevent evaporation of the sample.
- the storage modulus (G') and loss modulus (G") were measured for range of frequencies (0.1-10 rad s "1 ) at 25°C and 37°C (frequency sweep).
- the samples were then subjected to increasing temperatures ranging from 25°C up to 37°C at a rate of 2°C per minute with a frequency 1 rad s "1 (temperature sweep). The temperature was then held at 37°C for 30 minutes, until the hydrogel had formed, and the storage and loss moduli were measured (time sweep).
- Tetrazolium dye Cell Titer 96 Aqueous Non-radioactive Cell Proliferation Assay, Promega, Madison, WI, USA
- Tetrazolium dye Cell Titer 96 Aqueous Non-radioactive Cell Proliferation Assay, Promega, Madison, WI, USA
- the contents of individual wells were transferred to microcentrifuge tubes and spun at 5000 g for 2 minutes to pellet hydrogel and cells. The supernatant was then collected and plated for reading.
- Proliferation was represented by absorbance values (optical density, O.D.) of the supernatant at 490 nm using an Epoch spectrophotometer (BioTek, Winooski, VT, USA).
- ECM gel formation - digestion time and concentration Human tendon hydrogel at a concentration of 20 mg/ml (2%) was successfully prepared based on methods and optimization experiments outlined in Example 1. Porcine tendon extracellular matrix solutions ranging from 10 mg/ml (1%) to 20 mg ml "1 (2%) were evaluated, and the 1%> porcine solution was chosen for rheological, biocompatibility, and proliferation studies, because of its superior handling properties, cellular proliferation profile, and structural integrity in comparison to other concentrations.
- porcine tendon extracellular matrix solutions Storage of porcine tendon extracellular matrix solutions.
- the porcine tendon- derived extracellular matrix solutions gradually lost their ability to form gels over ensuing weeks unless the samples were stored at pH 2.2.
- pH 2.2 liquefied porcine tendon extracellular matrix solutions can be stored for prolonged periods, with unchanged gelation properties following neutralization to pH 7.4.
- Extracellular matrix solutions obtained from pig tendon proved to have a higher viscosity than extracellular matrix solutions obtained from human tendon and, therefore, a 1% extracellular matrix solution from pig tendon was found most useful to use with respect to ease of handling in liquid format.
- the extracellular matrix solution from pig tendon was liquid at temperatures below 25°C (4-25°C) and polymerized when the temperature was increased to physiological levels (37°C).
- extracellular matrix solution from pig tendon was seeded with human adipo-derived stem cells, standard cellular proliferation of the cells was observed without any significant difference between cellular proliferation in extracellular matrix solution from human versus pig tendon.
- porcine tendon extracellular matrix can be seeded with human cells that would persist, in the polymerized form of the porcine tendon hydrogel, at the site of tendon or ligament injury of a mammalian subject and would sustain the growth of such cells.
- the extracellular matrix solution from pig tendon holds the potential to be useful as an injectable composition for promoting the in-situ repair and regeneration of injured ligaments and tendons in a mammalian subject.
- Method for in-situ repair and regeneration of an injured tendon in a mammalian subject comprising administering to said subject su ffering from an injured tendon a therapeutically effective amount of a composition into said subject's area of injured tendon, said composition comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon
- Extracellular ECM gel formation The extracellular matrix material was
- Achilles tendon injuries were produced in 36 Wistar rats (mean weight 350 g) by surgical removal of part of the Achilles tendon substance (about half of the tendon substance was removed). All animals were kept anesthetized with isofluorane in a prone position. A slightly curved 1 cm incision was made lateral to the Achilles tendon to create a skin flap, ensuring that the Achilles tendon defect would not be created immediately under the skin wound. Great care was taken not to harm the sural nerve or large vessels in the dissection.
- Two surgical blades (size 15, Fisher Scientific) bonded with cyanoacrylate were used to make parallel incisions in the tendon 0.5 mm apart and 5 mm long, spanning from the TBI at the calcaneus to mid-tendon (Figure 19). This was performed under magnification using an operating microscope (Zeiss Opthalmic Surgical/Operative Microscope OPMI 6-SDFC, West Germany). Microscissors were used to remove the scored sections, such that a full-thickness defect was created mid-substance (within the middle of the tendon longitudinally). A pair-matched design was employed to compare the gel effect on one leg to a saline control on the other leg.
- the defect that resulted from the partial Achilles tendon removal on the rats' one side was filled with 0.05 mL of injectable, solubilized extracellular matrix (2%), which was solubilized as described above and which gelated in situ at the site of injection as described in Example 1; the defect on the rats' corresponding other leg was filled with 0.05 mL of PBS ( Figure 19.
- the wound was closed with 4-0 resorbable Vicryl stitches.
- the rats had received an intravenous injection of 0.05 mg/kg buprenorphine (Buprenex) for pain management, and an intravenous injection of 20 mg/kg enrofloxacin (Baytril) as antibiotic prophylaxis. All animals, including the control animals, were given the same per-operative treatment and medication.
- Biomechanical testing was carried out with the Mini Bionix testing system (MTS Systems, Eden Prairie, MN, USA), using a 50-lb load cell. Tendons were harvested still attached to the rat foot. Muscle was completely removed from the tendon such that the tendon-muscle insertions (proximal extent of the tendon, where it inserts into the gastrocnemius muscle) were exposed. A custom rig was used to secure the foot while the tendon- muscle insertions were clamped between sandpaper and cyanoacrylate. Orthogonal photographs together with a known scale (digital caliper) were obtained using a digital camera (8.2 megapixel Canon EOS 30D, Tokyo, Japan) at a fixed distance to measure two dimensions of the tendon.
- MTS Systems Eden Prairie, MN, USA
- the cross-sectional area was calculated using an elliptical assumption (ImageJ software, NIH) and used to calculate the ultimate tensile stress (UTS). Tendons were stretched at a rate of 0.5 mm/sec until failure. The ultimate failure load (UFL) was recorded; UTS was computed from UFL and cross-sectional area data; stiffness was determined from force/displacement curves. These curves were obtained by computer registering the MTS forces. The treatment groups were compared using a paired Student's t-Test.
- Tendon-derived extracellular matrix solution is liquid at or below room temperature (4 - 25 degree Celsius), but, upon administration into a mammalian subject, such as a rat, at the site of tendon injury forms right there, in situ, at physiological temperature, a tendon hydrogel.
- the Achilles tendons that were treated with the hydrogel were significantly stronger after four weeks than the Achilles tendons that were filled with saline only ('saline-treated', see Figure 20).
- An ultimate failure load (strength) of 74.8N of the gel-treated tendons compared to 58.4N was seen at 4 weeks following the administration of the tendon-derived extracellular matrix hydrogel.
- the gel-treated tendons were found to be as strong and possessing the same stiffness as native tendons according to previously assessed values for native tendons, namely 74.8 ⁇ 11.6N gel-treated tendon versus 75.7 ⁇ 18.5 native tendon for strength and 17.9 ⁇ 3.5 gel-treated tendon versus 17.9 ⁇ 5.5 native tendon for stiffness).
- the gel gradually degrades over a period of about four weeks, its full benefits should occur early, likely peak at the 4-week time point, as was observed in the described studies, and decrease over the remaining healing period up to 8 weeks.
- the tendons of both the gel-treated and the saline-treated groups were found to be primarily composed of the robust collagen I and had no further differences in strength.
- This accelerated rebuilding and healing process can be furthermore supported and enhanced by adding (i) external cells such as stem cells, progenitor cells and fibroblasts, (ii) growth factors such as insulin-like growth factor-I (IGF-I), transforming growth factor beta (TGFbeta), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and basic fibroblast growth factor (bFGF) and/or (iii) platelet-rich plasma to the tendon-derived extracellular matrix solution prior to injection into the area of ligament or tendon injury.
- IGF-I insulin-like growth factor-I
- TGFbeta transforming growth factor beta
- VEGF vascular endothelial growth factor
- PDGF platelet-derived growth factor
- bFGF basic fibroblast growth factor
- TBI tendon bone insertion
- Method for in-situ repair and regeneration of an injured ligament in a mammalian subject comprising administering to said subject suffering from an injured ligament a therapeutically effective amount of a composition into said subject's area of injured ligament, said composition comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon administration into subject's area of injured ligament
- Adipose-derived stem cells characterization and current application in orthopaedic tissue repair. Exp Biol Med 234(1): 1-9. Epub 2008/12/26.
- Adipose-derived stem cells enhance primary tendon repair:
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- Biomedical Technology (AREA)
- Medicinal Chemistry (AREA)
- Animal Behavior & Ethology (AREA)
- Epidemiology (AREA)
- General Health & Medical Sciences (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Transplantation (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Dermatology (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Cell Biology (AREA)
- Zoology (AREA)
- Botany (AREA)
- Pharmacology & Pharmacy (AREA)
- Molecular Biology (AREA)
- Developmental Biology & Embryology (AREA)
- Hematology (AREA)
- Immunology (AREA)
- Urology & Nephrology (AREA)
- Vascular Medicine (AREA)
- Rehabilitation Therapy (AREA)
- Orthopedic Medicine & Surgery (AREA)
- Rheumatology (AREA)
- Virology (AREA)
- Biotechnology (AREA)
- Biophysics (AREA)
- Dispersion Chemistry (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Gastroenterology & Hepatology (AREA)
- Endocrinology (AREA)
- General Chemical & Material Sciences (AREA)
- Diabetes (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Materials For Medical Uses (AREA)
- Medicines Containing Material From Animals Or Micro-Organisms (AREA)
Abstract
The invention provides an injectable composition and method for the minimally invasive, in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject. The composition is also useful for the delivery of growth factors, therapeutic agents and cells into the area of tendon or ligament injury.
Description
INJECTABLE COMPOSITION FOR IN-SITU REPAIR AND REGENERATION OF AN INJURED LIGAMENT OR TENDON AND METHODS OF USE
1. CROSS-REFERENCE TO RELATED APPLICATION
[0001] This application claims priority and other benefits from U.S. Provisional Patent Application Ser. No. 61/789,336 filed March 15, 2013, entitled "Injectable tendon hydrogel as a scaffold for in-situ guided tendon and ligament repair and regeneration and methods of use". Its entire content is specifically incorporated herein by reference.
2. TECHNICAL FIELD OF THE INVENTION
[0002] The invention relates generally to the treatment of ligament and tendon injuries.
Particularly, the invention provides an injectable tendon-derived composition for the minimally invasive, in-situ repair of ligament and tendon injuries such as tears that result acutely from trauma or chronically from tendon or ligament overuse. The tendon-derived composition is applied in solubilized form and polymerizes upon administration to the defect of an injured ligament or tendon, where it fills out and conforms to the defect, thereby creating a scaffold which attracts and guides the recruitment of new tenoblasts, tenocytes and fibroblasts inside the defect for repair and regeneration of the injured ligament or tendon.
3. BACKGROUND
[0003] Tendons and ligaments are strong bands of fibrous connective tissue that consist to a great part of collagen fibers. While tendons connect muscle to bone, ligaments connect bone to bone across a joint. The point of connection between muscle and tendon is the myotendinous junction or also called tendon-muscle insertion, and the point of connection between tendon and bone is the osteotendmous junction. The osteotendmous junction, where collagen fibrils from the tendon insert into the bone matrix, is a site of frequently occurring tendinopathies that are commonly caused by tendon overuse. Tendon overuse leads to significant histological and biochemical changes that alter the biomechanical and material properties in tendons and
ligaments (Arya & Kulig, 2010), causing accumulative microscopic tears that ultimately result in complete tears. Tears may be graded as minimal (1st degree), moderate to severe (2nd degree), or complete (3rd degree). Such injuries are most commonly seen in the rotator cuff, Achilles tendon, quadriceps tendon, and patella tendon as well as in medial and lateral epicondylitis of the elbow.
[0004] Some ligaments limit the mobility of a joint or prevent certain movements altogether. Ligaments are elastic and lengthen under tension, unlike tendons, which are inelastic.
[0005] Sports medicine specialists are frequently faced with the need to repair and regenerate ligaments and tendons that are injured in ways that result in tears during everyday activities involving high-impact repetitive movements such as running, playing soccer or golf. Readily available materials for quick and efficient, minimally invasive administration and treatment are, therefore, needed. The methods and compositions of the present invention address this need.
4. SUMMARY OF THE INVENTION
[0006] In one aspect, the present invention provides a composition comprising decellularized extracellular matrix derived from tendon connective tissue for in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject. The composition is in an injectable form below 25 degree Celsius and polymerizes to a hydrogel upon administration into the subject's area of injured ligament or tendon where it is effective in repairing and regenerating said injured ligament or tendon. In certain embodiments, the resulting hydrogel forms in situ a support structure which facilitates infiltration of the subject's own fibroblasts, tenoblasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon. In some embodiments, a one-time administration of the hydrogel is sufficient for treatment, in other embodiments repeated administration may be needed.
[0007] In certain embodiments, the tendon connective tissue is selected from a human donor; in other embodiments, the tendon connective tissue is selected from an animal donor such as a pig.
[0008] In some embodiments, the composition creates, upon gelation, a structure suitable for infiltration of host cells such as fibroblasts, tenoblasts and tenocytes. In other embodiments, cells such as stem cells, progenitor cells or fibroblasts, and/or therapeutic agents such as growth factors and/or platelet-rich plasma can be added to the composition prior to administration to
increase its in-situ therapeutic benefit for tendon or ligament repair and regeneration. In other embodiments, the therapeutic agent is a small molecule or protein exhibiting antibacterial effects or analgesic effects in order to ameliorate pain or a risk of infection that may occur concomitant with the tendon or ligament injury.
[0009] In a further aspect, the invention provides a method for in-situ repair and regeneration of an injured tendon or ligament in a mammalian subject, which involves the administration of a composition comprising decellularized extracellular matrix derived from tendon connective tissue to the area of injured tendon or ligament. The composition is in an injectable form below 25 degree Celsius and polymerizes to a hydrogel upon administration into the subject's area of injured ligament or tendon where it is effective in repairing and regenerating said injured ligament or tendon. In certain embodiments, the resulting hydrogel forms in situ a support structure which facilitates infiltration of the subject's own fibroblasts, tenob lasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon. In some embodiments, a one-time administration of the hydrogel is sufficient for treatment, in other embodiments repeated administration may be needed.
[0010] In another aspect, the invention provides a method of producing a composition comprising decellularized extracellular matrix derived from tendon connective tissue for in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject. In some embodiments, the tendon extracellular matrix is derived from an allogeneic source such as a human. In other embodiments, the tendon extracellular matrix is derived from a xenogeneic source such as a pig.
[0011] The above summary is not intended to include all features and aspects of the present invention nor does it imply that the invention must include all features and aspects discussed in this summary.
5. INCORPORATION BY REFERENCE
[0012] All publications mentioned in this specification are herein incorporated by reference to the same extent as if each individual publication was specifically and individually indicated to be
incorporated by reference.
6. BRIEF DESCRIPTION OF THE DRAWINGS
[0013] The accompanying drawings illustrate embodiments of the invention and, together with the description, serve to explain the invention. These drawings are offered by way of illustration and not by way of limitation; it is emphasized that the various features of the drawings may not be to-scale.
[0014] Figure 1 illustrates, as detailed in Example 1, the determination of successful digestion of the tendon extracellular matrix (ECM) solution as a function of time, pH during the digestion and concentration of tendon powder (see also Table 1). The digestion of the ECM solution was observed at 20x magnification every 12h. The degree of digestion was recorded as under, right or over (change to underdigested, adequate, and overdigested) based on homogeneity (adequate), degree of remaining tendon flakes (underdigested) and single collagen fibers (adequate). This estimation corresponded well to gelation of the ECM solution at 37°C, (-) no gelation, (+/-) weak gelation, (+) gelation. In conclusion, optimal digestion is needed in order to obtain favorable gelation characteristics and the desired thermo-sensitivity of the ECM solution, which makes possible the administration of the tendon extracellular matrix in solubilized form at a temperature that is considerably lower than body temperature (assuming 37° Celsius as physiological or body temperature), preferably at 4° Celsius and within a range of 4-25° Celsius, followed, upon administration into a defect, by gelation at body temperature.
[0015] Figure 2 illustrates, as detailed in Example 1, the production of injectable (25G cannula) tendon extracellular matrix (ECM) solution from ground tendon (A) and enzymatic digestion (B, enzyme used here was pepsin) at low pH and, subsequently, the formation of the hydrogel (C) following incubation for 20 minutes at 37° C. (D) shows the hydrogel poured and gelled on a petri dish.
[0016] Figure 3 shows the result of a proteomic analysis of an extracellular matrix solution, which was prepared as described in Example 1 , via mass spectrometry, where the amount of detected proteins (collagens and extracellular matrix proteins) is presented as percentage of total content (%).
[0017] Figure 4A illustrates the measurement of rheo logical data from one representative sample of tendon hydrogel, as further described in Example 1 , as a measurement of its mechanical properties; triplicates of the storage (G') and loss (G") moduli for the tendon hydrogel are shown: G' at 1 rad/s is 217 and G" is 28 in this sample (average G' is 213.1 and G" 27.1).
[0018] Figure 4B shows a kinetic determination of hydrogel formation (in triplicates) as a function of temperature, as further described in Example 1. In panel A, the temperature was slowly increased from 25 to 37°C, with a 2°C increase per minute. Note that the moduli of the solution remained low (i.e. weak) and did not change during this time. In panel B, the
temperature was kept constant at 37°C, and the tendon ECM solution was allowed to gelate without further increases in temperature. Both the storage modulus (G') and the loss modulus (G") increased as a function of time, depicted as a sigmoidal shaped increase. This process was initiated approximately after 15 minutes at 37°C, with a plateau that was reached after 20 minutes. Thus, solubilized tendon extracellular matrix remained liquid at temperatures below 37°C, however, it started to change its viscoelastic properties from 37° Celsius on, at which point it polymerized into a gel. This change occurs at approximately 20 minutes, which also corresponds to the time it takes for the tendon ECM solution to completely form a gel in vitro, as observed macroscopically.
[0019] In Figure 5, scanning electron microscope (SEM) images of in-vitro polymerization of the tendon hydrogel illustrate that improved fiber definition correlated with increased
temperature, and nanoscale collagen features at 37°C, as described in Example 1.
[0020] Figure 6 illustrates scanning electron microscope images of gels with cells, harvested 1 (lwk) and 2 (2wk) weeks after in vivo application, as further explained in Example 1. Collagen fibrils often have a linear arrangement with collagen defined as a porous network or linear bundles interspaced with cavities (2wk, H). Collagen bundles are highly regular with a clear longitudinal orientation along the underlying muscular surface (shown in lwk, A). Cells follow this linear arrangement in surface view (lwk, C and 2wk, F). Cells are closely adherent to fibers (B), and there is an apparent integration of the gel patch with the surrounding tissue (2wk, E). Cells grow invasively into the collagen scaffold (lwk, D; 2wk, G) and become increasingly aligned and confluent, and integrated with the gel scaffold.
[0021] Figure 7 illustrates, as further explained in Example 1, the percutaneous administration of tendon extracellular matrix solution (1 ml per injection site, 4 sites per 350 g rat) into the back of
immune-competent Wistar rats and subsequent tendon hydrogel (G) formation in the subcutaneous space that surrounded the site of administration. The top panel indicates where in the rats the extracellular matrix solution was injected. The gel was consistently confined to the subcutaneous space beneath the panniculus carnosus, subcutaneous fat (SC) and underlying para- spinal muscle (M). Hematoxylin and eosin (H&E) histological analysis (with a magnification of 20x), bottom, shows the gel (G) with vast cellular ingrowth from surrounding tissues already at 3 days post injection.
[0022] Figure 8 illustrates, on the very left, the position and size of an exemplary tendon-derived hydrogel 7 days following percutaneous injection into the back of a Wistar rat, as further explained in Example 1. The other panels show representative examples of tendon-derived hydrogel explants that were isolated from Wistar rats at 7, 14 and 28 days after percutaneous injection. The explants are shown with skin, panniculus carnosus, and subcutaneous fat removed.
[0023] Figure 9 shows, as further explained in Example 1, the results from Hematoxylin and eosin (H&E) histological analysis of exemplary tendon-derived hydrogels at 2 and 4 weeks following injection into Wistar rats; panel A shows at 20x magnification after two weeks and panel B at 40x magnification after two weeks. The invasion of cells from surrounding tissues into the superficial aspects of the gel as well as the longitudinally aligned fibroblast cells in the centre are notable. Panel C shows at 20x magnification after four weeks and panel D at 40x magnification after four weeks. Note that, at four weeks, the elongated fibroblasts are more homogenously distributed throughout the tendon-derived hydrogel. No signs of capsule formation are present around the gel, indicating integration with surrounding connective tissue.
[0024] Figure 10 shows, as further explained in Example 1, results from various staining experiments with tendon-derived hydrogel three days following percutaneous administration into Wistar rats. (A) H&E staining of superficial aspects of tendon-derived hydrogel and para-spinus muscle. Corresponding counterstain of adjacent sections with PI (B) and IHC of CD68+ cells (C) showing invasion of CD 68+ macrophages into the gel (all 20x).
[0025] Figure 11, as further explained in Example 1, shows exemplary tendon-derived hydrogels, where the tendon extracellular matrix solution was seeded with multipotent adipo- derived stem cells (ASCs) prior to gelation. The cells proliferated on the surface and infiltrated the gel, as detailed in panels A-F (with 20x magnification). Panel A shows polymerized gel with cells in culture 5 days post reseeding; live/dead stain of the same piece of gel; panel B shows the
live cells in green and panel C shows dead cells in red. Panel D shows SYTO green stain of cells on gel surface, panel E H&E histological analysis of cryosection and panel F corresponding SYTO green analysis.
[0026] Figure 12 shows results from decellularizing porcine tendon tissue, as further detailed in Example 2. Figure 12A: H&E staining of native (A) and treated (B) porcine tendon at 20X magnification. In contrast to the native tendon, no cells can be observed between fibrous connective tissue. Figure 12B: SytoGreen 11 fluorescent staining of native (A) and treated (B) porcine tendon at 20X magnification. Decellularization is confirmed by the absence of fluorescent nuclei in the treated specimen.
[0027] Figure 13 illustrates, as detailed in Example 2, the determination of successful digestion of porcine tendon extracellular matrix versus human tendon extracellular matrix based on homogeneity, degree of remaining tendon flakes and single collagen fibers. The degree of digestion was recorded as underdigestion, proper digestion or overdigestion.
[0028] Figure 14 illustrates the approximate protein composition of porcine tendon powder. Collagen IV and Collagen I were the predominant proteins found in the sample. Other peptides included tenascin, vimentin, fibromodulin, decorin, and other extracellular proteins.
[0029] Figure 15 illustrates the rheo logical properties of 2% human and 1% porcine tendon- derived extracellular matrix solutions as indicated by the storage (G') and the loss (G") moduli representing the elastic and viscous properties, respectively. Panel A shows frequency sweeps, i.e. testing of the elastic and viscous properties at different oscillation frequencies, of human and porcine tendon-derived matrix at 25°C. Panel B shows frequency sweeps of human and porcine tendon-derived matrix at 37°C. Panel C shows temperature sweeps of human and porcine tendon-derived matrix, where the elastic and viscous properties were tested at different temperatures. Panel D shows time sweeps of human and porcine tendon-derived matrix at 37°C, where the elastic and viscous properties were tested over time.
[0030] Figure 16 shows the morphology of human adipo-derived stem cells seeded within 2% human (A) and 1% porcine (B) tendon extracellular matrix solutions. Spindle-shaped cells can be seen throughout each extracellular matrix solution.
[0031] Figure 17 shows results from the Live/Dead Assay, as further detailed in Example 2. The ratio of viable to non-viable cells remained low for human adipo-derived stem cells within
human and porcine tendon-derived hydrogels. Viable cells are seen as green and non-viable cells are seen as red.
[0032] Figure 18 illustrates the proliferation of human adipo-derived stem cells in human and porcine hydrogel at 3, 5, 7, and 10 days. No difference in proliferation exists at any time point.
[0033] Figure 19 illustrates the set up of the studies, as detailed in Example 3, where Achilles tendon defects were created in Wistar rats by removing 50% of the Achilles tendon substance in each leg. The resulting defects were filled: on the left side with 2% solubilized tendon-derived extracellular matrix that gelated once administered by injection into the defect at body temperature (37°C) and filled out the gap that was created by the removal of 50% tendon substance that had produced the defect; on the right side, the defect was filled with saline as control.
[0034] Figure 20 shows the results of the study described in Figure 19 and Example 3, where the biomechanical properties of rats' Achilles tendon that was treated with solubilized tendon- derived extracellular matrix that gelated in-situ are compared to rats' Achilles tendon whose defect was treated with saline as control.
[0035] Figure 21 shows results from H&E staining after 4 weeks of saline versus tendon hydrogel treatment. H&E sections of saline (A) and gel (B) treatment at 4 weeks show typical wound trough morphologies and population by host cells in both groups. Corresponding Picro- sirius Red stains (C/saline & D/gel) show a difference in collagen content between the treatment groups. Whereas the wound troughs of the saline-treated tendons primarily contain collagen III, the wound troughs of the gel-treated tendons show higher concentrations of collagen I. T = tendon, * = wound trough.
7. DEFINITIONS
[0036] Before describing detailed embodiments of the invention, it will be useful to set forth definitions that are utilized in describing the present invention.
[0037] The practice of the present invention may employ conventional techniques of chemistry, cell biology, immunology, biochemistry, as well as of bone, joint, plastic and reconstructive surgery, which are within the capabilities of a person of ordinary skill in the art. Such techniques
are fully explained in the literature. For definitions, terms of art and standard methods known in the art, see, for example, 'Current Protocols in Cell Biology', John Wiley & Sons (2007);
'Human Tendons', by Laszlo Jozsa & Pekka Kannus, Human Kinetics (1997). Each of these general texts is herein incorporated by reference.
[0038] Unless defined otherwise, all technical and scientific terms used herein have the same meaning as commonly understood by a person of ordinary skill in the art to which this invention belongs. The following definitions are intended to also include their various grammatical forms, where applicable. As used herein, the singular forms "a" and "the" include plural referents, unless the context clearly dictates otherwise.
[0039] The term "administration", as used herein, refers to introducing a composition, such as a tendon-derived extracellular matrix solution that polymerizes, i.e. gelates, at physiological temperature (body temperature, 37°C), of the present disclosure into a subject. One preferred route of administration is to administer locally, meaning directly to the injured tendon or ligament via a needle or via an incision through the skin, i.e. percutaneously, so that the composition is not systemically distributed throughout the body.
[0040] The term "subject" refers to the host or recipient of the compositions of the present invention and includes humans as well as other mammals such as horses, cows, dogs.
[0041] "Donor", as used herein, refers to a mammalian cadaveric source for tendon connective tissue, as described herein, which can be from a human or animal source. Tendon connective tissue that was harvested from a donor can be "allogeneic", i.e., derived from a non- genetically identical member of the same species and, thus, be isolated from one subject and transferred, for example by injection, infusion or grafting, to another subject, particularly from one human to another human. Tendon connective tissue that was harvested from a donor can, furthermore, also be obtained from animal sources for use in the methods and compositions of the present invention. In such a case, the tissues are "xenogeneic", i.e., from a member of a different species. Preferred sources of xenogeneic connective tissues are pigs, horses, cows, sheep, rodents and dogs. In either case, all connective tissues are obtained from a fresh-frozen cadaveric donor. To obtain such connective tissues from a cadaveric donor, standard biopsy techniques known in the art may be employed.
[0042] "Therapeutically effective amount", as used herein, refers to an amount that provides the desired therapeutic effect of tendon or ligament tissue repair and regeneration in a mammalian subject.
[0043] The term "area of tendon or ligament injury", as used herein, refers to the site of the defect and designates (i) the actual site of the tendon or ligament injury as well as (ii) the zone that is directly adjacent to or surrounding of the actual site of the tendon or ligament injury.
[0044] An injectable composition, as used herein, refers to any material that can be made liquid enough or solubilized enough to be injected into a defect, i.e. an area of ligament or tendon injury, including an emulsion, liquid, particles and powder.
[0045] "Decellularization", as used herein, refers to the substantial (at least 75%), nearly complete (at least 95%) or complete removal of cellular components of tendon connective tissue by the use of physical and chemical means, or any combination thereof. It is understood that it is not necessarily preferred to achieve a maximally possible decellularization, if doing so negatively affects the biomechanical properties of the connective tissue. The optimum degree of decellularization will depend upon the biomechanical properties of the tissue and its intended use.
[0046] The storage (G') and loss (G") moduli for tendon hydrogels of the present invention represent the elastic and viscous properties of the gel.
[0047] "Tendon-muscle insertions", as used herein, refers to the site of connection between tendon and muscle and is also called the tendon junction site or myotendinous junction.
[0048] The "osteotendinous junction"is the site of connection between tendon and bone and is also called the tendon insertion site.
8. DETAILED DESCRIPTION
[0049] Embodiments of the present invention provide methods and compositions comprising decellularized extracellular matrix derived from tendon connective tissue for the minimally invasive, in-situ repair and regeneration of ligament and tendon injuries such as tears that resulted acutely from trauma or chronically from tendon or ligament overuse in a mammalian subject. The composition is in an injectable form below 25° Celsius and polymerizes upon
administration to the defect of an injured ligament or tendon in a mammalian subject, where it fills out and conforms to the defect, thereby creating a three-dimensional tendon scaffold which attracts and facilitates migration of surrounding hosts cells into the scaffold microenvironment. The composition can also be supplemented with exogenous cells and/or therapeutic agents prior to administration to increase its in-situ therapeutic benefit for tendon or ligament repair and regeneration. Repair and regeneration of the injured ligament or tendon is ultimately achieved, when the tendon scaffold is replaced with the regenerated tissue.
8.1 TENDONS
8.1.1 Tendon Composition
[0050] Tendons are strong bands of fibrous connective tissue that connect muscle to bone and are composed of parallel arrays of collagen fibers (mostly type 1 collagen) and elastin embedded in a proteoglycan-water matrix. The point of connection between muscle and tendon is the myotendinous junction, while the point of connection between tendon and bone is the
osteotendinous junction. Most muscles have a single tendon distally, although some muscles have both a proximal and distal tendon. The basic functions of tendons, which are typically classified as flexors (flexing or bending a joint) or extensors (extending or straightening a joint) are to withstand tension and to allow transmission of forces created in the muscle to the bone, thus making joint and limb movements possible (Sharma & Maffulli, 2005; Kannus, 2000). This is made possible by a complex macro- and microstructure of tendons and tendon fibers, where collagen is arranged in hierarchical levels of increasing complexity, beginning with
tropocollagen, a triple-helix polypeptide chain, which unites into fibrils, fibers (primary bundles), fascicles (secondary bundles), tertiary bundles, and the tendon itself. Soluble tropocollagen molecules form cross-links to create insoluble collagen molecules, which aggregate to form collagen fibrils. A collagen fiber is the smallest tendon unit that can be tested mechanically and is visible under light microscopy. Although collagen fibers are mainly oriented longitudinally, fibers also run transversely and horizontally, forming spirals and plaits (Sharma & Maffulli, 2005).
[0051] Healthy tendons have a fibro-elastic texture and show strong resistance to mechanical challenges. During various phases of movement, tendons are exposed to longitudinal as well as transversal and rotational forces, whereby the complex three-dimensional architecture of tendons
provides critical support to prevent damage and disconnection of fibers. Muscles designed to create powerful, resistive forces such as the quadriceps and triceps brachii muscles, have short and broad tendons, while those that have to carry out subtle and delicate movements, like the finger flexor tendons, have long and thin tendons (Kannus, 2000). Intrasynovial tendons of the hand and the feet are surrounded by tendon sheaths or similar networks of connective tissue that contain the vascular, lymphatic and nerve supply to the tendon and whose main function is to minimize the friction between the tendon and its surroundings. Since proper movement and gliding of the tendon determines its efficiency, the tendon needs to be able to move freely and in an uninhibited manner. Tendon sheaths have two layers, an outer, fibrotic sheath, which consists of collagen fibrils and fibers, as well as an inner, synovial sheath, which consists of two sheets of synovial lining cells. These lining cells contain a thin film of fluid which is similar to the composition of the synovial fluid of a joint and which improves lubrication. The synovial lining cells are covered with fine collagen fibrils ('Human Tendons', by Laszlo Jozsa & Pekka Kannus, Human Kinetics (1997)). Synovial tendon sheaths are found in areas that often experience increased mechanical stress such as tendons of the hands and feet, where efficient lubrication is important (Sharma & Maffulli, 2006).
[0052] The tendon extracellular matrix consists of collagen fibers, elastic fibers, ground substance and inorganic components such as copper, manganese and calcium. The tendinous ground substance, which surrounds the collagen, consists of macromolecules such as
proteoglycans and glycosaminoglycans (GAGs), structural glycoproteins, and a wide variety of other smaller molecules. The proteoglycans and glycosaminoglycans have a considerable capacity to bind water and are important for the biomechanical properties of tendon against shear and compressive forces.
8.1.2 Tendon Composition
[0053] Tenoblasts and tenocytes lie between the collagen fibers along the axis of tendon and are its major cellular components. Tenoblasts are immature tenocytes with higher metabolic rates that eventually mature into tenocytes. Chondrocytes are located at the sites of attachment and insertion into bone. Synovial cells of the tendon sheath as well as vascular cells form the remaining cellular components of a tendon. Tendons receive their blood supply from blood
vessels entering from the myotendinous and osteotendinous junctions, the intratendinous vascular network and the synovial sheath.
[0054] Tenocytes synthesize collagen and all components of the extracellular matrix and are active in energy production, which can be aerobic as well as anaerobic. Compared to skeletal muscles, tendons and ligaments have a low metabolic rate, low oxygen consumption and a fairly well developed anaerobic energy production capacity. On the upside, a low metabolic rate allows tendons to maintain tension for prolonged periods without becoming ischemic and necrotic. On the downside, a low metabolic rate means that tendon injuries take a long time to heal.
8.1.3 Tendon Biomechanics
[0055] Tendons transmit force from muscle to bone, while at the same time acting as a buffer by absorbing external forces to limit tearing and other damage to the muscle. As a consequence, tendons have, by necessity, to exhibit high mechanical strength, good flexibility and high elasticity. The biomechanical properties of tendons are dependent on the collagen fiber diameter, fiber orientation, and collagen content. Tendons subject to multidirectional forces display collagen fiber bundles that lack regular orientation and the connective tissue is irregularly arranged. In contrast, tendons subject to unidirectional strain display collagen fiber bundles with mostly parallel orientation. The mechanical behavior of collagen depends on the number and types of intra- and intermolecular bonds. The tensile strength of a tendon is a function of its thickness and its collagen content.
8.1.4 Tests To Assess the Strengths of Tendons and also Ligaments
[0056] In- vitro assessments. The biomechanical properties of an isolated tendon or ligament are tested in various in vitro tests. Test parameters that can be inferred from such tensile testing include stiffness, maximum load, and strain to maximal load. For the testing, the tendon or ligament tissue is elongated at a set rate, while the changes in force are recorded. The force is then plotted against displacement. Methods for testing of biomechanical properties include compression and tension testing. Exemplary methods that find wide-spread use for
biomechanical strength testing include (a) Ultimate Failure Load. Ultimate Failure Load represents the maximum load (pull force on the tendon) that the tendon can withstand before
breaking, measured in Newton (N). (b) Ultimate Tensile Stress. Ultimate Tensile Stress is a relative measurement that takes the physical properties of the graft into account. It is measured in N/mm2 as the load per cross-sectional area of the tendon or ligament in question, (c) Stiffness. Stiffness represents the rigidity of the tendon that is the extent to which it resists deformation in response to the applied pull force at testing.
[0057] In- vivo assessment in subjects following tissue repair and regeneration using an injectable tendon hydrogel, as described herein. The assessment includes clinical evaluation of parameters such as 1) absence of pain, 2) speed of recovery to resume all-day activities such as walking and going up/down stairs as well as recreational sports such as running and biking, 3) less need for immobilization after injuries allowing for earlier active mobilization, and 4) strength and range of motion over affected joints. These variables, along with subjects' subjective satisfaction will be assessed in randomized clinical trials comparing the gel to conventional methods of treatment.
8.1.5 Tendons In The Upper Extremities
[0058] Finger flexor tendons. Flexor pollicis longus tendon, flexor digitorum superficialis tendons and fiexor digitorum profundus tendons belong to the group of finger flexor tendons.
[0059] Flexor tendons of the lower arm. Flexor carpi radialis tendon, palmaris longus tendon, flexor carpi ulnaris tendon and the common flexor tendon are flexor tendons of the forearm. The common flexor tendon is a tendon shared by a number of superficial flexor muscles in the forearm and attaches to the medial epicondyle of the humerus. Overuse of the common flexor tendon can lead to medial epicondylitis or golfer's elbow.
[0060] The common fiexor tendon serves as the origin for a number of superficial muscles of the anterior compartment of the forearm such as the palmaris longus (a small tendon between the flexor carpi radialis and the flexor carpi ulnaris) or flexor digitorum superficialis (an extrinsic flexor muscle of the fingers at the proximal interphalangeal joints). The flexor digitorum profundus is another muscle in the forearm that flexes the fingers. It is an extrinsic hand muscle because it acts on the hand, while its muscle is located in the forearm and is a flexor of the wrist, midcarpal, metacarpophalangeal and interphalangeal joints.
[0061] Finger extensor tendons. Extensor digiti minimi tendon, extensor digitorum communis tendons, extensor indicis tendon, extensor pollicis brevis tendon and extensor pollicis longus tendon belong to the group of finger extensor tendons. The abductor pollicis longus tendon, also found in the extensor group, is included in this category.
[0062] Tendons of the arm and shoulder. The tendons of the rotator cuff muscles help to stabilize the shoulder, while the biceps tendon helps to bend the elbow and rotate the arm.
[0063] Extensor tendons of the forearm. Extensor carpi ulnaris tendon; Extensor carpi radialis brevis tendon, extensor carpi radialis longus tendon and the common extensor tendon are extensor tendons of the forearm. The common extensor tendon originates from the lateral epicondyle and is often injured due to overuse, leading to lateral epicondylitis or tennis elbow.
8.1.6 Tendons In The Lower Extremities
[0064] The Achilles tendon, also called tendocalcaneus, is part of the posterior leg and is the thickest and strongest tendon in the body. It connects the superficial muscles of the posterior leg, plantaris, soleus and gastrocnemius (calf muscle) to the calcaneus (heel) bone. Albeit it is the largest and strongest tendon in the human body, the Achilles tendon is highly susceptible to acute and chronic injuries during athletic activities, since it needs to fulfill high functional demands during sports such as soccer, track and field, tennis, basketball and so forth. During sprinting exercises, the Achilles tendon is exposed to tensile forces that are about 10-12 times the body weight of the sprinting individual, while during jumping or cycling the tensile forces are about 6- 8 times of the body weight.
[0065] Flexor tendons of the thigh. The semitendinosis tendon, gracilis tendon,
semimembranosis tendon are flexor tendons of the thigh. Semitendinosus is one of the hamstring muscles and functions both as flexor and extensor by helping to extend the hip joint and to flex the knee joint; it also helps to medially rotate the knee.
[0066] Patellar tendon and quadriceps tendon. The patella, also known as the knee cap, is embedded in and held in place by the patellar tendon on the tibial side (side of shin bone) and the quadriceps tendon on the femoral side (side of the thigh bone). The top of the patella attaches to
the quadriceps muscle via the quadriceps tendon and the bottom of the patella attaches to the tibia via the patellar tendon,
[0067] Flexor tendons of the leg. Flexor digitorum longus tendons, flexor hallucis longus tendons, and tibialis posterior tendon are flexor tendons of the leg. Flexor digitorum longus, one of the muscles of the posterior compartment of the leg, functions to curl the toes and to stabilize the lower leg, while flexor hallucis longus, another muscle of the posterior compartment, performs plantar flexion of the big toe alone (downward movement of the toes). Tibialis anterior is situated on the lateral side of the tibia; it is thick, fleshy above, tendinous below and acts to dorsiflex (turn upward) and invert the foot. Tibialis posterior, a muscle of the posterior compartment of the leg, is the main stabilizing muscle of the lower leg and assists with foot inversion and ankle plantar flexion. Peroneus longus, and peroneus brevis are everters of the foot that secondarily plantarflex at the ankle.
[0068] Flexor tendons of the foot. The flexor digitorum longus and brevis, flexor hallucis longus and brevis, and flexor digiti minimi brevis tendon are flexor tendons of the foot.
[0069] Extensor tendons of the leg. Extensor digitorum longus tendons and extensor hallucis longus tendon are extensor tendons of the leg. The extensor digitorum longus tendons are located at the lateral part of the front leg and act to dorsiflex the foot as well as the toes and invert the foot. The extensor hallucis longus is part of the anterior leg and functions to extend the big toe, dorsiflex the foot, and assists with foot inversion. Tibialis anterior and peroneus tertius are extensor tendons of the leg that dorsiflex the foot at the ankle.
[0070] Extensor tendons of the foot. Extensor digitorum longus and brevis tendons as well as extensor hallucis longus and brevis tendons are extensor tendons of the foot. The extensor digitorum brevis is a muscle on the dorsal (upper) part of the foot that functions to extend the smaller toes, while the extensor hallucis brevis, which is a muscle of the dorsum of the foot, acts to extend the big toe.
8.1.7 Acute Tendon Injuries and Chronic Tendon Injuries (Tendinopathies)
[0071] Particularly currently in an exercise-conscious and sports enthusiastic society, tendon disorders such as tendon injuries and tendinopathies occur frequently and in any age group, leading to weeks and months of pain, impaired physical activity and lengthy treatment that can
range from physical therapy to surgical rehabilitation. Tendons and ligaments have an about 7.5 lower oxygen consumption than skeletal muscles due to a low metabolic rate and capacity to generate energy anaerobically which makes tendons and ligaments well suited to withstand and maintain tension. The low metabolic rate, however, also means that the healing process is slower than in skeletal muscle (Sharma & Maffulli, 2005).
[0072] Tendon injuries can be (i) acute strain injuries, tendon tears or full ruptures of the muscle- tendon units due to sudden, spontaneous impacts or laceration by a sharp object or (ii) chronic injuries (tendinopathies) due to tendon overuse without proper recovery time between uses and possible subsequent degeneration of the tendon tissue. Generally, acute tensile overload situations and overuse cause injuries to the musculotendinous junction, which manifest as sprains, strains and rupture, while injuries to the osteotendinous junction lead to avulsion fractures, bone detachment injuries and chronic enthesopathies, i.e. disorders of the tendon-bone attachment.
[0073] Tendon injuries manifest themselves usually through pain, particularly during sports- related activities which might have contributed to the injury at the first place, then focal tenderness with pain radiating from particular trigger points and decreased strength and ability to move.
[0074] Tendon injuries, that frequently occur in the course of sports activities and for which the methods and compositions of the present invention are particularly well suited, include (i) Achilles tendon injuries, generally due to the performance of high- force movements and spontaneous change of directionality, as it is the case in soccer, track and field or tennis (Kannus & Natri, 2007); (ii) rotator cuff injuries, usually caused by motions that require forceful pulling motions or repetitive overhead motions, as they occur in sports activities such as tennis, martial arts, boxing, swimming, golf, cheerleading or throwing activities; (iii) common flexor tendon injuries such as medial epicondylitis of the elbow, the so-called 'golfer's elbow', and common extensor tendon injuries such as lateral epicondylitis of the elbow, the so-called 'tennis elbow'; (iv) patellar tendon and quadriceps tendon injuries that are concomitant with patellar dislocation that often occurs during sports activities that involve sudden and forceful knee rotation, such it is the case in soccer, tennis, basketball and martial arts.
8.1.8 Healing Process in Tendons: need to maintain normal and organized tendon tissue
[0075] Dependent on the extent of the injury, likely excluding a healing in cases of complete ruptures, tendons have a capacity to heal on their own. The process of tendon healing occurs in several phases. After the initial inflammatory phase within the first 24-72 hours, the remodeling phase begins within an increased collagen synthesis. After approximately six weeks, the modeling stage begins with high collagen synthesis and high tenocyte metabolism, in the course of which the injured tissue becomes filled with disorganized tissue and gradually changes from cellular to fibrous and eventually to scar-like tissue. As a consequence, the structural
organization and the mechanical properties of the healing tissue are altered and the tendon's capability to withstand force is compromised. Although the tensile strength of the healing tendon reportedly improves over time, it does not return to its original levels for about one year or longer (Lin et al, 2004).
[0076] Not only is clinical tendon repair and regeneration, for which the methods and compositions of the present invention are well suited, important to accelerate a subject's recovery and ability to use the healed tendon, it is also critical to rebuild the injured tendon in a way that it regains the structural and functional characteristics of a normal, healthy tendon with its full range of motion and tensile strength.
8.2 LIGAMENTS
[0077] Hamstring or medial collateral and lateral collateral ligaments, anterior or posterior cruciate ligaments of the knee are examples of important ligaments of the body.
[0078] Ligaments, similar to tendons, are strong bands of fibrous connective tissue consisting of fibers made mainly out of type 1 collagen. In contrast to tendons, which connect muscle to bone, ligaments connect bones to other bones across a joint. Some ligaments limit the mobility of a joint or prevent certain movements altogether. Ligaments are elastic and lengthen under tension, unlike tendons, which are inelastic.
[0079] Capsular ligaments are part of the articular capsule that surrounds synovial joints. They act as mechanical reinforcements. Extra-capsular ligaments provide joint stability. Intra-capsular ligaments, also provide stability, but permit a far larger range of motion. Cruciate ligaments occur in pairs (anterior and posterior).
8.2.1 Ligaments of the head, neck and chest
[0080] Ligaments of the head, neck and chest, include the cricothyroid ligament, periodontal ligament and suspensory ligament of the lens, which all are ligaments of the head and neck, while the suspensory ligament of the breast is a ligament of the human thorax.
8.2.2. Ligaments of the upper extremities
[0081] The radial and ulnar collateral ligaments of the interphalangeal and
metacarpophalangeal joints are ligaments of the human hand. The palmar radiocarpal ligament, dorsal radiocarpal ligament, ulnar collateral ligament and radial collateral ligament are ligaments of the human wrist. The acromioclavicular ligaments surround and support the acromioclavicular joint which is the connection between the scapula and the clavicle. The coracoclavicular ligaments hold the clavicle down by attaching it to a bony knob on the scapula called the coracoid process. The scapho lunate interosseous ligament is a broad ligament connecting the scaphoid bone to the lunate bone. There are multiple additional intrinsic and extrinsic wrist ligaments that contribute to stability of the wrist.
8.2.3. Ligaments of the lower extremities
[0082] Ligaments of the lower extremities include the anterior cruciate ligament (ACL), lateral collateral ligament (LCL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), which all are main ligaments of the human knee. In the quadruped from, the ACL is referred to as the cranial cruciate ligament (CrCL), while the PCL is referred to as the caudal cruciate ligament (CaCL).
8.2.4 Ligaments of the pelvis
[0083] The anterior sacroiliac ligament, the posterior sacroiliac ligament, the sacrotuberous ligament, the sacrospinous ligament, the inferior pubic ligament, the superior pubic ligament and the suspensory ligament of the penis are ligaments of the human pelvis.
8.2.5 Ligament injuries and problem in ligament repair
[0084] Ligament injuries, which are often acquired during weight-bearing sports activities such as downhill skiing, running, jumping and the like, can lead to instability of the joint that the
ligament is supposed to stabilize. Instability of a joint can lead to cartilage wear over time and eventually to osteoarthritis. Therefore ligament injuries need to be taken seriously and repaired.
8.3 TENDON-DERIVED EXTRACELLULAR MATRIX HYDROGEL FOR TISSUE REPAIR AND REGENERATION
[0085] The thermosensitivity and solid-liquid characteristics of the tendon extracellular matrix solution, being liquid at a cold temperature up to room temperature (4-25°C) and gelating at physiological body temperature, at around 37°C, allow easy and quick administration of the solution via injection or infusion, while the gelation in situ, upon administration into the area of the tendon or ligament defect, i.e. the site of injury, of a subject allows the formation of a three- dimensional tendon support scaffold. Since this resulting tendon support scaffold/tendon hydrogel is based on decellularized materials from tendon tissue, it replaces 'like with like', since the scaffold already possesses the mix of non-cellular components that matches that of the native tissue (tendon or ligament) such as various types of collagen fibers, hyaluronic acid, fibronectin, laminin, carbohydrate polymers, polysaccharides and sulfates.
[0086] The administration of the solubilized tendon-derived extracellular matrix into the area of ligament or tendon defect or injury is preferably carried out via injection with a needle (for example, 25 gauge). It is considered a minimally invasive procedure, since it does not require a surgical procedure (including anesthesia) and can be carried out during an office visit. This ensures quick attendance to the tendon or ligament injury and, consequently, accelerates a subject's recovery from the injury.
[0087] Upon gelation, the solubilized tendon-derived extracellular matrix conforms to the three- dimensional space of the tendon or ligament defect that resulted from the injury and so facilitates in situ regeneration by means of three-dimensional (3D) guided tissue regeneration, accelerating ligament and tendon healing, as shown in Example 2. Thus, the repair and regeneration of the tissue defect in the injured ligament or tendon is aided by the three-dimensional support scaffold of the tendon-derived hydrogel ('tendon hydrogel').
[0088] Furthermore, upon gelation and adaption/conformation to the 3D space of the tendon or ligament defect, the tendon-derived hydrogel provides a supportive nanostructure for renewed organization of collagen fibers that became disorganized during the tendon or ligament injury. The tendon-derived hydrogel, furthermore, creates a structure suitable for host cell infiltration,
i.e. infiltration of fibroblasts, tenoblasts and tenocytes from the host, and tissue regeneration. Likewise, cells such as stem cells, progenitor cells or fibroblasts, and therapeutic agents can be added to the solubilized tendon-derived extracellular matrix prior to injection and prior to gelation in order to increase its in-situ therapeutic benefit for tissue regeneration.
[0089] In certain embodiments, the therapeutic agent can be a growth factor such as basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), insulin-like growth factors 1 and 2 (IGF-1 and IGF -2), platelet derived growth factor (PDGF), or stromal cell derived factor (SDF-1).
[0090] Alternatively, growth factors can be supplemented through autologous platelet-rich plasma (PRP) enrichment of the tendon-derived hydrogel to stimulate and accelerate tissue regeneration. PRP refers to autologous plasma with platelet concentrations at particular levels above baseline values (Hall et al., 2009).
[0091] In other embodiments, the therapeutic agent is a small molecule or protein exhibiting antibacterial effects in order to ameliorate a risk of infection that may occur concomitant with the tendon or ligament injury. Examples of antibiotics suitable as therapeutic agents include (i) aminoglycosides such as gentamicin, streptomycin, tobramycin, (ii) glycopeptides such as vancomycin, (iii) lincosamides such as clindamycin, (iv) macrolides such as azithromycin, (v) polypeptides such as bacitracin, (vi) quinolones such as ciprofloxacin, (vii) tetracyclines such as doxycycline, tetracycline, and other categories of antibiotics that can be administered into the defect, either combined with the tendon-derived extracellular matrix solution, administered prior to the administration of the tendon-derived extracellular matrix or administered after the tendon- derived extracellular matrix has been administered, and can exert a localized effect.
[0092] In further embodiments, the therapeutic agent is a small molecule or protein exhibiting analgesic effects in order to ameliorate pain that may occur concomitant with the tendon or ligament injury. Examples of analgesics suitable as therapeutic agents include (i) non-steroidal anti-inflammatory agents such as ibuprofen and naproxen as well as (ii) local anesthetics such as lidocaine and bupivacaine.
8.4 UTILITY OF INJECTABLE TENDON-DERIVED EXTRACELLULAR MATRIX THAT GELATES IN SITU TO A TENDON-DERIVED HYDROGEL FOR IN-SITU TENDON AND LIGAMENT REPAIR AND REGENERATION
[0093] Since tendon disorders such as tendon injuries as well as tendinopathies and ligament injuries occur frequently and in any age group, and lead to weeks and months of pain, impaired physical activity and lengthy treatment, ranging from physical therapy to surgical rehabilitation, compositions such as the described tendon-derived hydrogels that support the healing process and that can be administered to the injured tissue without a major surgical step, as described in the present invention, are of high utility and benefit. This is evidenced by a shortened healing time as well as tissue (tendon and ligament) regeneration that enables to regain the original strength of the tendon and ligaments. Due to its thermosensitive properties solubilized tendon- derived extracellular matrix remains liquid and injectable in the temperature range of about 4-25 °C. Upon injection of the solubilized tendon-derived extracellular matrix into a bodily space such as into the area of a ligament or tendon injury, the solubilized tendon extracellular matrix - at the body temperature of about 37°C - gelates within minutes into a tendon-derived hydrogel, as described in Examples 1 and 2.
[0094] The hydrogel then fills out and conforms to the defect. It, thus, creates a scaffold which attracts and guides the settling of new tenoblasts, tenocytes and fibroblasts inside the defect for repair and regeneration of the injured ligament or tendon.
[0095] In some cases of ligament or tendon injury, a one-time administration of a therapeutically effective amount of a tendon-derived hydrogel might be sufficient to treat the defect. In other cases, repeated administration of therapeutically effective amounts of a tendon-derived hydrogel, within the time period of several days, weeks or months, might be needed to treat the defect. In further cases, repeated administration of therapeutically effective amounts of a tendon-derived hydrogel, within the time period of several days, weeks or months, might be carried out to improve clinical efficacy.
[0096] As will be apparent to those of skill in the art upon reading this disclosure, each of the individual embodiments described and illustrated herein has discrete components and features which may be readily separated from or combined with the features of any of the other several embodiments without departing from the scope or spirit of the present invention. Any recited method can be carried out in the order of events recited or in any other order which is logically possible. In the following, experimental procedures and examples will be described to illustrate parts of the invention.
9. EXAMPLES
[0097] The following examples are put forth as to provide those of ordinary skill in the art with a complete disclosure and description of how to make and use the present invention; they are not intended to limit the scope of what the inventors regard as their invention. Unless indicated otherwise, parts are parts by weight, molecular weight is average molecular weight, temperature is in degrees Centigrade, and pressure is at or near atmospheric.
I. Composition for in-situ repair and regeneration of an injured ligament or tendon comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel at physiological temperature
EXAMPLE 1: INJECTABLE HUMAN TENDON-DERIVED HYDROGEL AS A
SCAFFOLD FOR IN-SITU GUIDED TISSUE REGENERATION IN THE
MUSCULOSKELETAL SYSTEM
1.1 EXPERIMENTAL PROCEDURES
[0098] Tissue decellularization and material processing. Human flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS) and flexor pollicis longus (FPL) tendons were harvested from fresh-frozen human cadaveric forearms (Science Care, Phoenix, Arizona).
Epitenon, synovial sheath, and muscle tissue were meticulously debrided. Distally, FDS tendons were transected 2cm proximal to the chiasma, and FDP and FPL tendons were transected 1cm proximal to the osteotendinous junction. The tendons were then decellularized following a previously reported protocol (Pridgen BC et al, 2011). In brief, scaffolds were treated with 0.1% ethylenediamine-tetraacetic acid (EDTA) for 4 hours followed by 0.1% sodium dodecyl sulfate (SDS) in 0.1% EDTA for 24 hours at room temperature with constant agitation. Scaffolds were washed in PBS (also referred to as saline herein) and stored at -80°C. The decellularization protocol was used as sole sterilizing agent in these experiments.
[0099] The frozen decellularized material was then lyophilized, and thereafter cut into smaller tendon pieces and milled into a fine powder using a Wiley Mini Mill (Thomas Scientific,
Sedesboro, NJ, USA). The powder was stored at 4°C until needed for use. A DNA assay along with routine H&E histology and SYTO green- fluorescent nucleic acid staining was used to quantify the effectiveness of decellularization of tendons. This is described in detail in a previous publication (Pridgen et al., 2011). In short, DNA was extracted from lyophilized tendons using a DNeasy kit (QIAGEN). The concentration of the extract was determined using an ultra-violet spectrophotometer (Biophotometer 22331 ; Eppendorf) at a wavelength of 260 nm. The concentration of the samples was calculated by software on the spectrophotometer using a known extinction coefficient for dsDNA.
[00100] Extracellular matrix (ECM) gel formation. The powder of decellularized and lyophilized ground tendons, which was produced as described above, was then solubilized and enzymatically digested by adding a lmg/ml solution of pepsin (Sigma, St Louis, MO) in HC1 and water such that the final concentration of material was 10, 20 and 30 mg/ml (1-3% respectively, dry weight). Optimal pH for pepsin digestion was explored and set to pH 2.2 (Bohak, 1969). Increasing molarity of HC1 is needed to accomplish optimal digestion with increasing
concentration of tendon powder (see Table 1). The material was digested for up to 72h (12, 24, 36, 48 and 72h) at room temperature with constant stirring. The extracellular matrix solution (ECM solution) was checked for pH and homogeneity under a microscope every 12h to optimize the conditions for digestion. For the in vivo experiments and reseeding of 2%> gels in vitro, the digestion time was set to 24h to ensure complete digestion. After complete and optimal digestion was confirmed, the salt concentration was adjusted with the addition of lOx PBS (1/10 of final neutralized volume), while cooled on ice. Pepsin activity was then completely reversed by adding of NaOH to increase the pH >8, before the final solution pH was neutralized to a pH of 7.4 by addition of HC1. The final mixture was then ready for injection or in vitro experiments. When placed in an incubator at 37°C it was allowed to gel for 20-60 minutes at 37°C. Gelation was confirmed macroscopically and with rheology (see below and Figure 1).
[00101] Optimal storage conditions of the ECM solution was explored. The ECM solution was stored as neutralized samples with a pH 7.4, and as acidic samples with a pH 2.2 under different conditions (4°, -80° and lyophilized). The acidic samples were neutralized after storage, but prior to gelation at 37°. Gelation was observed on day 1, 7, and 10 over 30 minutes and recorded as (-) no gelation, (+/-) weak gelation, (+) gelation.
[00102] Evaluation by Mass Spectrometry. Samples were prepared using a FASP (Filter aided proteome preparation) (Wisniewski et al, 2009) protocol, where the sample was solubilized in SDS, DTT and Tris-HCL and digested overnight by trypsin. The peptides were loaded onto a self-packed fused silica CI 8 analytical column, interfaced by a Bruker Michrom Advance (Auburn, CA, USA) source with a flow rate of 600 nL/min and a spray voltage of 1.7kV. The mass spectrometer was a LTQ Orbitrap Velos, Thermo Scientific (Vancouver, Canada), set in data dependent acquisition mode fragmenting the top 12 most intense precursor ions. The RAW data was converted to mzXML format and database searched against the human uniprot-sprot database using Sequest on a Sorcerer platform. The data was visualized using Scaffold 3, Proteome Software (Portland, OR, USA).
[00103] Rheology: storage modulus, temperature characteristics. Rheo logical measurements were made using a TA Instruments ARG2 Rheometer. Two parallel steel plates (40 mm diameter) at lOOum gap height were used on 500 μΐ of tendon-derived hydrogel in different concentrations, performed 24 hours after the extracellular matrix solution was allowed to gelate. The setup was such that the sample completely filled the gap between the rheology plates. For each condition, the storage modulus (G') and loss modulus (G") over frequencies of 0.1-10 rad s-1 (frequency sweep) were recorded for every gel condition in triplicate and plotted. To document gelation properties at increasing temperature (temperature sweep), the peltier probes of the rheometer were preheated to 25°C. Measurements of samples of extracellular matrix solution that had not been allowed to gelate were recorded at 1 rad sec-1 at increasing temperature, 2°C per minute until 37°C was reached. Temperature was maintained at 37°C for 24 minutes until the gel had polymerized and the modulus had stabilized.
[00104] Scanning electron microscopy. Samples were fixed from 24hrs to 4 days at 4°C with 4% paraformaldehyde and 2% glutaraldehyde in 0.1M sodium cacodylate buffer (pH 7.2), rinsed in the same buffer and post- fixed for lhr with 1% aqueous Os04. After dehydration in an ascending ethanol series (50, 70, 90, 100 %; 15min each) samples were dried with liquid C02 in a Tousimis Autosamdri-815B apparatus (Tousimis, Rockville, MD, USA), mounted on adhesive copper tape on 15mm aluminum stubs (Ted Pella, Redding, CA), and sputter-coated with 50A of Au/Pd using a Denton Deskll Sputter Coater. Visualization was performed with a Hitachi S- 3400N Variable Pressure (VP) SEM operated at 15kV, working distance 7-8mm, and secondary electron (SE) detection under high- vacuum conditions (<lPa). High-resolution images of
collagen fibrils were captured with a Zeiss Sigma Field Emission SEM operated at 3kV and using Inlens SE detection. For VP-SEM application scaffolds with and without cells were visualized fully hydrated with variable pressure (50-60Pa) and coldstage control (-25°C) after aldehyde-fixation, and additional osmication of scaffolds with cells was performed (Joubert, 2009).
[00105] Cell Culture and Scaffold Reseeding. Commercially obtained adipo-derived stem cells (ASCs) (up to passage 4, Poietics PT-5006 cryopreserved adipoderived stem cells, Lonza, Walkersville,MD, USA) were cultured in ADSC-BM medium (Lonza, Walkers ville,MD, USA) augmented with 10% FCS. Cells were grown to confluence at 37°C in a humidified tissue culture chamber with 5% carbon dioxide. Reseeding of the ECM solution was performed both onto preformed gel (a), and by mixing cells into the ECM solution before gelation (b). (a) The ECM solution was first allowed to gel for lh in a 48 well plate at 37°C. A cell suspension containing 5xl04 cells/0.2ml was placed on top of the preformed gel, and incubated overnight, (b) Seeding was also performed by mixing a cell suspension of 5xl04 cells/0.2ml with 0.5 ml ECM solution. The mix was placed in a 48 well plate and allowed to gel for lh at 37°C, then 0.5 ml medium was added. Cell culture medium was changed every other day for both seeding protocols. Cells were stained with SYTO Green or using a live dead assay on day 5 to check for viability on the gel surface and inside the gel.
[00106] In vivo application. 8 Wistar rats (mean weight 280g) were used as recipients for injections of solubilized tendon extracellular matrix for subsequent gelation in situ, i.e. at and around the injection site. The rats were anesthetized with isofluorane in a prone position. Dorsal hair was shaved and the animals were marked with a permanent marker to assign four injection sites. Under sterile conditions, 1ml of 2% solubilized tendon extracellular matrix was injected subcutaneously with a 25G needle and syringe (Figure 7) for subsequent gelation in situ. After the injections, all animals were housed at 21°C in a 12-hour light and dark cycle and were given food and water ad libitum.
[00107] Gel specimens were harvested at 3 days, 7 days, 14 days and 21 days. One sample at each time point was used for measurement of size and subsequent SEM. The three other samples were used for histology. Formalin- fixed, paraffin-embedded (FFPE) sections (5μιη) were stained with hematoxylin and eosin (H&E, Sigma) for assessment of seeding efficacy and scaffold
morphology. All histological images were taken with an inverted microscope (Nikon TS100, Nikon, Melville, NY).
[00108] For macrophage staining, a mouse anti-rat CD68 primary antibody was used (Santa Cruz Biotechnology). Rat spleen was used as a positive control. Sections were also counter- stained with Propidium Iodine (PI) to assess for cell infiltration. Whole tissue mounts were divided longitudinally and immersed in SYTO green (Invitrogen) nucleic acid stain at 1 :2000 dilution in DI water for 20min. Reseeded gels were then placed on coverslips and imaged.
Separate images were obtained for the outer convex scaffold surface and the inner cut (core) surface.
[00109] Live/Dead assay (Invitrogen) was performed on reseeded gels at 5 days, on constructs where adipo-derived stem cells (ASCs) had been premixed with solubilized tendon extracellular matrix prior to gelation at 37°C. This assay was performed to assess the ratio of viable to nonviable cells. Gels 5 days post reseeding were labeled with Live/Dead stain and incubated for 20 minutes.
1.2 TENDON EXTRACELLULAR MATRIX (ECM) GEL FORMATION:
PH AND DIGESTION TIME
[00110] Hydrogels were successfully prepared from decellularized and ground human tendons (Human flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS) and flexor pollicis longus (FPL) tendons), that had been harvested from human cadavers and immediately fresh frozen at - 80°C and reconstituted to obtain solubilized tendon extracellular matrices with concentrations ranging from 1-3% (v/v). Increasing extracellular matrix concentration provided a more rigid gel structure that was easier to handle. The 2% solubilized tendon extracellular matrix produced a gel that showed an optimal balance between handling properties, structural rigidity and permeability to seeded cells. Therefore, experiments on reseeding, storage and in vivo experiments were preferably conducted using the 2% solubilized tendon extracellular matrix concentration.
[00111] Optimal HC1 molarity and digestion time [in minutes] was determined based on microscopic appearance of the degree of ECM digestion (see Table 1 and Figure 1).
Table 1. Optimal pH for pepsin digestion was explored. Increasing molarity (N) of hydrochloric acid (HC1) is needed to accomplish optimal digestion with increasing concentration of tendon powder. This is an essential step in the gel making process as complete digestion of the decellularized lyophilized powder is needed for the extracellular matrix (ECM) solution to hold its thermoregulatory gelation properties so that it is liquid at 4-25°C and gelates at around 37°C.
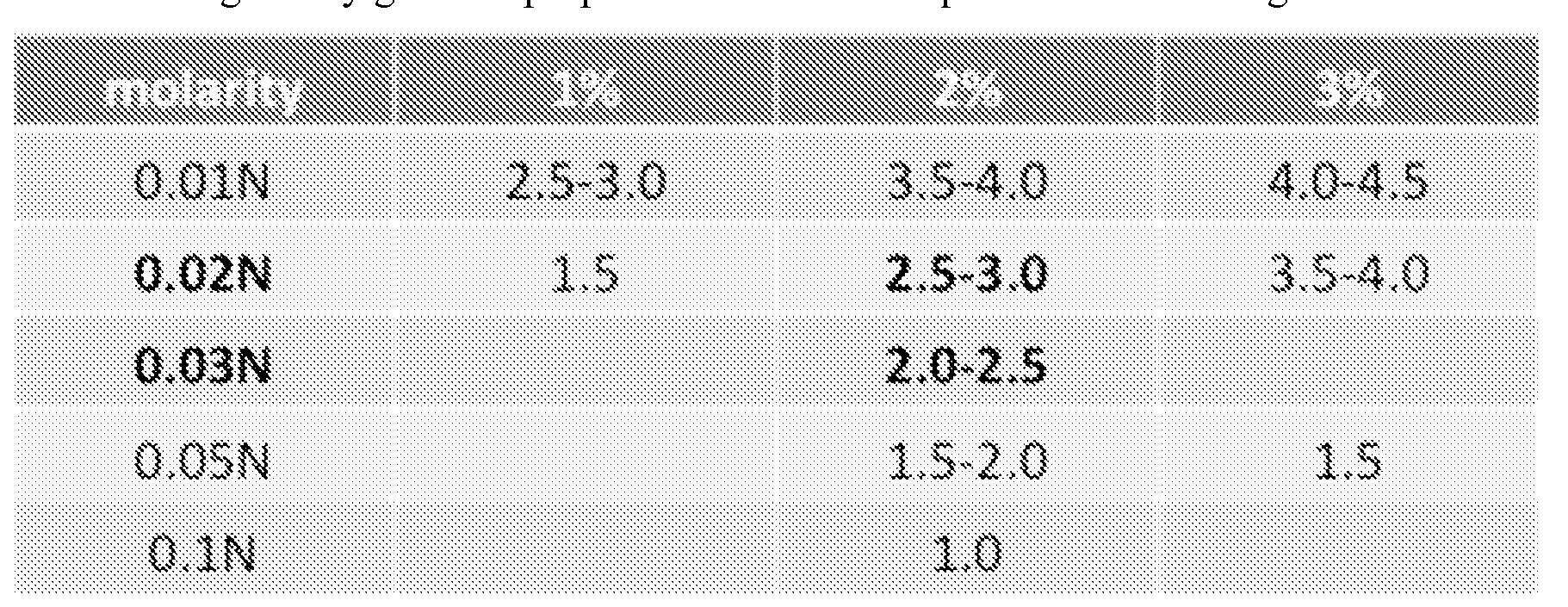
[00112] The optimal conditions consisted of the ECM powder digested over 24h at pH around 2.2, with gelation macroscopically complete after 20 minutes in 37°C (Figure 2). Once solubilized, the tendon extracellular matrix solution remained liquid at 4°C. To induce gelation in vitro, samples of solubilized tendon extracellular matrix were placed in an incubation chamber at 37°C. Gelation was observed macroscopically within 20 minutes. The tendon extracellular matrix solution showed a gradual decrease in gelation characteristics after storage at various conditions over time, unless the samples were stored at about pH 2.2. At pH 2.2, the solubilized tendon extracellular matrix could be stored for prolonged periods, with unchanged gelation properties following neutralization to pH 7.4 (Table 2).
Table 2. Comparison of tendon extracellular matrix gelation properties stored at pH 2.2 v. pH 7.4

[00113] Mass spectrometry. Proteome analysis of the tendon-derived extracellular matrix solution and resulting tendon-derived hydrogel through filter-aided sample preparation (FASP) and mass spectroscopy yielded identification of the most abundant 150 proteins, of which Collagens represented more than 55% of the sample (Figure 3). Collagen 1 A2 was the most prominent protein (42% of total content) followed by Collagen 1A1 (15%). All other proteins had a less than 5% representation in the assay. The 16 proteins with highest representation are listed in Figure 3.
[00114] Rheology. The rheo logical properties of the tendon extracellular matrix solution were determined through triplicates of the storage (G') and loss (G") moduli as shown in Figure 4a. G' at 1 rad/s was 213.1±19.9 and G" 27.1±2.4. A temperature sweep was performed to evaluate the effect of temperature and time on modulus. Both the storage modulus G' and the loss modulus G" remained stable, approximately one order of magnitude lower than after gelation (Figure 4b) as the temperature was slowly increased from 25°C to 37°C. At 37°C, the tendon extracellular matrix solution was allowed to gel without further increases in temperature. The fact that the tendon extracellular matrix solution only forms a tendon hydrogel at body temperature is a key feature of this hydrogel. The ECM solution can thus be stored for extended periods of time in its soluble and injectable form in cold temperature, and "activated" at the time of injection to form a gel in situ at body temperature. Both the storage modulus (G') and the loss modulus (G") were also shown to increase as a function of time at 37°C. The change in tendon extracellular matrix
solution moduli was depicted as a sigmoidal shaped increase, initiated approximately after 15 minutes, with a plateau that was reached after 20 minutes (Figure 4b, right graph). 20 minutes corresponded well to the time it takes for the tendon extracellular matrix solution to completely form a gel in vitro, as observed macroscopically.
[00115] Scanning electron microscopy (SEM). Scanning electron microscopy of specimens showed a distinct correlation between temperature and fiber definition. At lower temperatures (4 and 25 °C), collagen fibers were only partially developed, and individual fibers were aggregated by amorphous clumps, with less aggregation at ambient temperature than at 4°C. At 37°C, fibers became characterized as individual strands, which were well defined and often aligned as bundles with porosity conducive to fluid flow and gas exchange (Figure 5). After injection of tendon extracellular matrix solution into Wistar rats and subsequent gelation into tendon hydrogel that formed a supportive scaffold structure, as detailed in Examples 1 and 3, the collagen fibers retained their linearity, and aggregates of fibers were similarly aligned with well- defined individual fibrils in which typical collagen 'D banded morphology' was evident at high magnification (FESEM image). Furthermore, these resulting supportive scaffold structures supported cell growth, and invasion of the scaffolds with cells increased over time, as was observed, when comparing in vivo samples one and two weeks following the administration of the tendon extracellular matrix solution. Cells supported by the collagen scaffold became aligned with collagen fibers (Figure 6).
[00116] In vivo - gel volume. Wistar rats tolerated the tendon extracellular matrix solution injections well, and no adverse effects were observed. The initial prominent subcutaneous mass (Figure 7) gradually decreased over the first postoperative hour as the tendon extracellular matrix gelated and conformed to the available subcutaneous space (Figure 7). Explants of the tendon extracellular matrix hydrogel at 7, 14 and 28 days showed a gradual decrease in size and weight. It became difficult to distinguish gel from connective tissue that had grown into the gel at 4 weeks (Figure 8). Tissue ingrowth and regeneration at the site of injection was seen, with no evidence of capsule formation that would have indicated that the body reacted to the gel as being foreign tissue. This further exemplifies the good biocompatibility seen with the gel in vivo (Figure 9).
[00117] In vivo - histology. The tendon extracellular matrix gels were consistently confined to the subcutaneous space beneath the panniculus carnosus, subcutaneous fat and underlying
para-spinus muscles (Figure 7). All gels remained as a coherent entity with no sign of capsule formation at any time point. After 4 weeks, ongoing degradation and regeneration caused the gel to merge with the surrounding tissue (Figures 9 C and D). Interestingly, the collagen bundles were highly regular and oriented in longitudinal fashion along the underlying muscular surface. The same pattern was found on SEM. Cellular infiltration was documented at 3, 7, 14, and 28 days. Figure 10A illustrates CD 68+ macrophage infiltration of the gel from surrounding fat and muscle tissue at 3 days. Figure 1 OB is a nuclear counterstain that stains all live cells in an adjacent section whereas 11C is an immune -histochemical stain of CD68+ macrophages. At the early time points, cell ingrowth was preferentially seen in the superficial parts of the gel, as depicted in Figure 9. However CD68+ cells continued to populate the full thickness of the gel at all time points. At 14 days, histology displayed increasing numbers of spindle shaped elongated fibroblast cells, on its surface as well as centrally (Figures 9 A and B).
[00118] In vitro - histology. Multipotent adipo-derived stem cells (ASCs) mixed with tendon- derived extracellular matrix solution proliferated on the surface and infiltrated the gel. Spindle shaped cells were observed both on the gel surface as well as within the gels, with a regular distribution throughout the gel. Live/dead staining and SYTO green staining on whole tissue mounts of gels confirmed that reseeded cells were homogenously distributed throughout the gel. The fraction of nonviable cells remained low, indicating that the tendon extracellular matrix hydrogel appears well suited for delivery of cells, such as multipotent adipoderived stem cells, to the area of tendon injury in order to speed up tendon tissue repair and regeneration (Figure 11).
[00119] Utility of the described injectable extracellular matrix solution that gelates in situ to a tendon hydrogel. The described tendon-derived hydrogel offers the advantage that it can be readily delivered as injectable extracellular matrix solution through a direct injection into the area of the tendon or ligament injury.
[00120] Upon injection of the tendon-derived extracellular matrix solution, at a temperature (4-25°C) where the solution is fully liquid, into an area of tendon or ligament injury and subsequent gelation at physiological body temperature (37°C), the resulting tendon hydrogel forms a mesh of collagen fibers and collagen fiber bundels characterized by a highly regular linear pattern and orientation in longitudinal fashion along the underlying muscular surface. The regular pattern and longitudinal orientation is instrumental in rebuilding the injured tendon or
ligament in a way that it regains the structural, biomechanical and functional characteristics of a normal, healthy tendon or ligament with its full range of motion and tensile strength.
[00121] Seeding of the tendon-derived extracellular matrix solution with rat adipoderived stem cells did not affect the biocompatibility of the resulting tendon hydrogel upon
administration into rats, as evidenced by the lack of capsule formation. Capsule formation would have indicated that the body reacted to the extracellular matrix as being foreign tissue.
EXAMPLE 2: INJECTABLE PORCINE TENDON HYDROGEL AS A SCAFFOLD FOR IN-SITU GUIDED TISSUE REGENERATION IN THE MUSCULOSKELETAL SYSTEM
2.1 EXPERIMENTAL PROCEDURES
[00122] Tissue decellularization and material processing for the manufacture of human tendon hydrogel. Flexor tendons were harvested from fresh cadaveric forearms, as described in example 1. These tendons were meticulously debrided of remaining synovial material and muscle tissue. Flexor digitorum superficialis tendons were transected 2 cm proximal to the chiasma, while flexor digitorum profundus and flexor pollicis longus tendons were transected 1 cm proximal to the osteotendinous insertion. Harvested tendons were subsequently cut into 1 cm segments and treated with 0.1% ethylenediaminetetraacetic acid (EDTA) for 4 hours and then washed in 0.1% sodium dodecyl sulfate (SDS) in 0.1 % EDTA for 24 hours at ambient temperature with constant agitation. Tendon was then rinsed in IX PBS for 4 hours and stored at -80°C.
[00123] Tissue decellularization and material processing for the manufacture of porcine tendon hydrogel. Tendon was harvested from the dorsal and volar regions of fresh pig hindlimbs and meticulously debrided from remaining synovial material and muscle tissue. Harvested tendon was cut into 1 cm segments and treated with 0.2% ethylenediaminetetraacetic acid (EDTA) for 4 hours followed by 0.2% sodium dodecyl sulfate (SDS) in 0.2% EDTA for 24 hours at ambient temperature with constant agitation. Tendon was then rinsed in IX PBS for 4 hours and stored at -80°C.
[00124] The frozen, decellularized tendons derived from human and porcine sources were lyophilized for 48 hours (Labconco, Kansas City, MO, USA), and milled into a fine powder
using a Wiley Mini Mill, filter size 80 (Thomas Scientific, Sedesboro, NJ, USA). The tendon powders were stored at 4°C until use.
[00125] Confirmation of Decellularization. To confirm decellularization of human as well as porcine tendon powders, cell visualization via routine H&E staining and SytoGreen 11 fluorescent staining was performed. In addition, DNeasy Assay was used to quantify the amount of nucleic acid present in decellularized samples. First, DNA was extracted from decellularized freeze-dried human as well as porcine tendon. Using the absorbance peak at 260 nm as a proxy, the concentration of dsDNA present in the extract was quantified using an ultraviolet
spectrophotometer (Biophotometer 22331; Eppendorf, Hauppauge, NY, USA). The
concentration of dsDNA present within samples was then extrapolated using a known extinction coefficient for the molecule.
[00126] Gel formation from extracellular matrix solution. Based on previous optimization experiments, as described in example 1 , human tendon powder was enzymatically digested by the addition of 1 mg ml"1 pepsin in a 0.02M HCl solution to obtain a final concentration of 20 mg ml"1 or 2%. The material was digested for 24 hours at ambient (room) temperature with constant stirring to ensure homogeneity. Analogously to the described method of digestion of human tendon powder, porcine tendon powder was digested by the addition of 0.1 mg ml"1 pepsin in a 0.01M HCl solution. Final concentrations of the material were 10, 15, and 20 mg ml"1 or 1, 1.5, and 2% respectively. The material was digested for up to 24 hours at ambient temperature with constant stirring. Microscopic observation of the resulting extracellular matrix solution demonstrated that optimal digestion of milled porcine tendon powder occurred at about 1 hour of stirring.
[00127] Prior to use, human and porcine tendon extracellular matrix solutions, respectively, were cooled on ice. Pepsin was denatured by the addition of 1M NaOH until the pH of the mixture reached 8.5. The pH was subsequently adjusted to 7.4 by the addition of 1M HCl. The salinity of the solution was also adjusted to physiologic levels by the addition of 10X PBS in a 1 : 10 fashion (1 ml 1 OX PBS per 10 ml gel).
[00128] Storage of Gel. Human and porcine tendon extracellular matrix solutions, respectively, were stored at 4°C following digestion until use. The extracellular matrix solutions were left acidified at pH 2 until the time of the experiment. At that point, solutions were alkalized to denature pepsin and then brought to physiologic pH as described above.
[00129] Mass Spectrometry. Mass spectrometry (LTQ Orbitrap Velos, Thermo Scientific, Vancouver, Canada) was performed on milled decellularized porcine tendon prior to pepsin digestion. Analytic samples were prepared using a FASP (Wisniewski et al, 2009) protocol. A small amount of the tendon powder was solubilized in SDS, DTT and Tris-HCL, and digested overnight by trypsin. The resulting peptide fragments were then loaded onto a self- packed fused silica CI 8 analytical column with a Bruker Michrom Advance interface (Auburn, CA, USA). A flow rate of 600 nL/min and a spray voltage of 1.7kV were utilized. The mass spectrometer was set in data dependent acquisition mode and the 12 most intense precursor ions were detected. The data was converted to mzXML format and searched against the human uniprot-sprot database using Sequest on a Sorcerer platform. Scaffold 3 (Proteome Software, Portland, OR, USA) was used to analyze the data.
[00130] Rheology: storage modulus, temperature characteristics. Rheo logical studies were performed with a TA Instruments ARG2 Rheometer. Extracellular matrix solution samples were dispensed (500 μΐ) onto two parallel steel plates (40 mm diameter) at a gap height of 100 μιη, which allowed the solution to completely spread to the edge of the probe. Excess solution was gently wiped away. Using a barrier for containment, silicone oil was used to prevent evaporation of the sample. The storage modulus (G') and loss modulus (G") were measured for range of frequencies (0.1-10 rad s"1) at 25°C and 37°C (frequency sweep). The samples were then subjected to increasing temperatures ranging from 25°C up to 37°C at a rate of 2°C per minute with a frequency 1 rad s"1 (temperature sweep). The temperature was then held at 37°C for 30 minutes, until the hydrogel had formed, and the storage and loss moduli were measured (time sweep).
[00131] Live/Dead Assay of Human Adipo-derived Stem Cells Reseeded on Human or Porcine Tendon Hydrogels. Human adipo-derived stem cells (ASCs) were gently mixed with human and porcine tendon-derived extracellular matrix solutions, respectively, and incubated at 37°C. A Live/Dead assay (Promega, Madison, WI, USA) was performed on the subsequently polymerized human and porcine hydrogels 7 days after seeding to assess the ratio of viable to nonviable cells. Cell-seeded tendon hydrogels were gently mixed with the staining agents and incubated per standard protocol.
[00132] Cell Proliferation of Reseeded ASCs. Cell proliferation in human and porcine tendon hydrogels, respectively, was evaluated by the MTS colorimetric assay. Human adipo-derived
stem cells (up to passage 4, Poietics PT-5006 cryopreserved adipoderived stem cells, Lonza, Walkersville, MD, USA) were cultured in fetal bovine serum (Gibco, Life Technologies, Grand Island, NY, USA) supplemented ADSC-BM medium (Lonza, Walkersville, MD, USA). ASCs were grown until 90% confluence at 37°C in humidified tissue culture chamber with 5% C02 content. The tendon hydrogels were seeded with ASCs and cell proliferation was measured at 3, 5, 7, and 10 days thereafter. Tetrazolium dye (Cell Titer 96 Aqueous Non-radioactive Cell Proliferation Assay, Promega, Madison, WI, USA) was directly added to wells in a 1 : 10 fashion, gently mixed, and allowed to incubate at 37°C for 30 minutes. The contents of individual wells were transferred to microcentrifuge tubes and spun at 5000 g for 2 minutes to pellet hydrogel and cells. The supernatant was then collected and plated for reading. Proliferation was represented by absorbance values (optical density, O.D.) of the supernatant at 490 nm using an Epoch spectrophotometer (BioTek, Winooski, VT, USA).
2.2 TENDON-DERIVED PORCINE HYDROGEL: COMPARISON TO TENDON- DERIVED HUMAN HYDROGEL
[00133] Manufacture of Human and Porcine Gel. Human tendon was successfully decellularized, as described supra. The decellularization protocol for human tendon was unsuited to remove cells from porcine tendon and was, therefore, step-wise altered until decellularization in porcine tendon was achieved with 0.2% EDTA followed by 0.2% EDTA in 0.2% SDS, as confirmed by H&E staining (Figure 12a) and SytoGreen 11 fluorescent staining (Figure 12b). DNeasy Assay yielded a concentration of 132 ng dsDNA per mg decellularized tendon, a value similar to that obtained from decellularized human tendon (Pridgen et al., 2011).
[00134] ECM gel formation - digestion time and concentration. Human tendon hydrogel at a concentration of 20 mg/ml (2%) was successfully prepared based on methods and optimization experiments outlined in Example 1. Porcine tendon extracellular matrix solutions ranging from 10 mg/ml (1%) to 20 mg ml"1 (2%) were evaluated, and the 1%> porcine solution was chosen for rheological, biocompatibility, and proliferation studies, because of its superior handling properties, cellular proliferation profile, and structural integrity in comparison to other concentrations.
[00135] Details of digestion. Human tendon-derived extracellular matrix solution was digested for 24 hours with 1 mg/ml pepsin, whereas porcine tendon extracellular matrix solution
was digested for only 1 hour with 0.1 mg/ml pepsin. The extent of digestion was assessed microscopically, as described in Example 1. Figure 13 details human and porcine gel samples that have undergone over-, under-, and optimal digestion.
[00136] Storage of porcine tendon extracellular matrix solutions. The porcine tendon- derived extracellular matrix solutions gradually lost their ability to form gels over ensuing weeks unless the samples were stored at pH 2.2. At pH 2.2, liquefied porcine tendon extracellular matrix solutions can be stored for prolonged periods, with unchanged gelation properties following neutralization to pH 7.4.
[00137] Mass Spectrometry. Proteome analysis of porcine tendon powder was performed following filter-aided sample preparation (FASP) and mass spectroscopy, which yielded 150 of the most abundant proteins in the sample. The 15 most abundant proteins are illustrated in Figure 14. Collagen represented the most predominant protein family, constituting 32.3% of the total sample. Collagen 6 A3 was the most abundant single protein in the sample (17.1% of the total content) followed by Collagen 6A2 (9.2%). A number of other extracellular matrix proteins were also found in the sample.
[00138] Rheology. The rheo logical properties of 2% human and 1% porcine tendon-derived extracellular matrix solutions and their subsequently formed tendon hydrogels were determined using triplicates of the storage (G') and loss moduli (G"). Representative samples are shown in (Figure 15). Frequency sweeps were performed to demonstrate the elastic and viscous tendencies of the samples at a range of angular frequencies as shown in Figure 15A and 15B. At 25°C, G' at 1 rad/s was found to be 177.9 and 137.9, while G" was 27.6 and 34.1 for human and porcine samples, respectively. At 37°C, G' at 1 rad/s was found to be 236.0 and 113.2, while G" was 22.5 and 12.4 for human and porcine samples, respectively.
[00139] To determine the effect of temperature on G' and G", a temperature sweep was performed (Figure 15C). As the temperature increased from 25°C to 37°C at a rate of 2°C per minute, the storage modulus for the human tendon extracellular matrix solutions increased from 180.6 to 208.3. Yet, the storage modulus for the porcine tendon extracellular matrix solutions decreased from 139.8 to 108.0. Once the temperature reached 37°C, the extracellular matrix solutions were monitored without further increases in temperature via a time sweep. In both human and porcine samples, the storage modulus (G') minimally increased, while the loss modulus (G") minimally decreased as a function of time, as depicted in Figure 15D.
[00140] In vitro - Live/Dead Staining and Cell Morphology. Human adipo-derived stem cells were gently suspended within porcine and human tendon-derived extracellular matrix solutions, respectively, and proliferated within the subsequently formed hydrogels for 7 days at 37°C. For human and porcine samples alike, spindle shaped cells were observed (Figure 16), displaying an even distribution throughout the solution. Over the course of 7 days, the fraction of nonviable cells remained low as assessed visually by the live/dead assay (Figure 17).
[00141] Cellular Proliferation . Human adipo-derived stem cells were seeded within human and porcine tendon-derived extracellular matrix solutions, respectively, and incubated at 37°C where human and porcine tendon hydrogels, respectively, formed. At days 3, 5, 7, and 10 after seeding, there was no significant difference between the proliferation of cells within the human and porcine tendon hydrogel samples, respectively, as determined by tetrazolium dye assay (Figure 18).
[00142] Utility of the described injectable extracellular matrix solution derived from porcine tendon material. An animal source for the tendon extracellular matrix is beneficial with respect to lower costs and higher availability in comparison to obtaining the connective tissue from a human cadaver. Also, the use of animal tissue might possibly raise less ethical concerns than the harvesting of tendon tissue from a human cadaver.
[00143] Since the connective tissue found in pig tendon is denser than that in human tendon, the decellularization process is more difficult for pig tendon than for human. However, once decellularization is achieved in pig tendon, the resulting powder requires then less time and amount of digesting enzyme to achieve full digestion, compared to human tendon.
[00144] Extracellular matrix solutions obtained from pig tendon proved to have a higher viscosity than extracellular matrix solutions obtained from human tendon and, therefore, a 1% extracellular matrix solution from pig tendon was found most useful to use with respect to ease of handling in liquid format.
[00145] Like extracellular matrix solution from human tendon, the extracellular matrix solution from pig tendon was liquid at temperatures below 25°C (4-25°C) and polymerized when the temperature was increased to physiological levels (37°C). When extracellular matrix solution from pig tendon was seeded with human adipo-derived stem cells, standard cellular proliferation of the cells was observed without any significant difference between cellular proliferation in extracellular matrix solution from human versus pig tendon. This provides evidence that porcine
tendon extracellular matrix can be seeded with human cells that would persist, in the polymerized form of the porcine tendon hydrogel, at the site of tendon or ligament injury of a mammalian subject and would sustain the growth of such cells. As such, the extracellular matrix solution from pig tendon holds the potential to be useful as an injectable composition for promoting the in-situ repair and regeneration of injured ligaments and tendons in a mammalian subject.
II. Method for in-situ repair and regeneration of an injured tendon in a mammalian subject, comprising administering to said subject su ffering from an injured tendon a therapeutically effective amount of a composition into said subject's area of injured tendon, said composition comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon
administration into subject's area of injured tendon
EXAMPLE 3: INJECTABLE TENDON HYDROGEL AUGMENTS TENDON HEALING IN AN RAT ACHILLES TEND ON INJURY MODEL
3.1 EXPERIMENTAL PROCEDURES
[00146] Tissue decellularization and material processing to obtain decellularized and lyophilized extracellular matrix material for the subsequent preparation of a tendon
(hydro)gel. Human flexor digitorum profundus (FDP), flexor digitorum superficialis (FDS) and flexor pollicis longus (FPL) tendons were harvested from fresh-frozen human cadaveric forearms and processed as described in Example 1.
[00147] Extracellular ECM gel formation . The extracellular matrix material was
enzymatically digested by adding a 1 mg/ml solution of pepsin (Sigma, St Louis, MO) in 0.02 M HC1 and sterile water such that the final concentration of material was 20 mg/ml, and pH was 2.2. The material was digested for 24 hours at room temperature with constant stirring. While the resulting liquid cooled on ice, the pH was first raised to 8 using NaOH to deactivate the pepsin, then lowered to 7.4. Salt concentration was adjusted using lOx PBS to achieve an isotonic solution.
[00148] Surgical procedure and treatment. Acute, bilateral Achilles tendon injuries were produced in 36 Wistar rats (mean weight 350 g) by surgical removal of part of the Achilles tendon substance (about half of the tendon substance was removed). All animals were kept anesthetized with isofluorane in a prone position. A slightly curved 1 cm incision was made lateral to the Achilles tendon to create a skin flap, ensuring that the Achilles tendon defect would not be created immediately under the skin wound. Great care was taken not to harm the sural nerve or large vessels in the dissection. Two surgical blades (size 15, Fisher Scientific) bonded with cyanoacrylate were used to make parallel incisions in the tendon 0.5 mm apart and 5 mm long, spanning from the TBI at the calcaneus to mid-tendon (Figure 19). This was performed under magnification using an operating microscope (Zeiss Opthalmic Surgical/Operative Microscope OPMI 6-SDFC, West Germany). Microscissors were used to remove the scored sections, such that a full-thickness defect was created mid-substance (within the middle of the tendon longitudinally). A pair-matched design was employed to compare the gel effect on one leg to a saline control on the other leg.
[00149] The defect that resulted from the partial Achilles tendon removal on the rats' one side was filled with 0.05 mL of injectable, solubilized extracellular matrix (2%), which was solubilized as described above and which gelated in situ at the site of injection as described in Example 1; the defect on the rats' corresponding other leg was filled with 0.05 mL of PBS (Figure 19. The wound was closed with 4-0 resorbable Vicryl stitches. Preoperatively, the rats had received an intravenous injection of 0.05 mg/kg buprenorphine (Buprenex) for pain management, and an intravenous injection of 20 mg/kg enrofloxacin (Baytril) as antibiotic prophylaxis. All animals, including the control animals, were given the same per-operative treatment and medication.
[00150] At 2, 4 and 8 weeks following the procedure of removing tendon and filling with extracellular matrix or saline, 12 rats were sacrificed per time point and the Achilles tendons on both legs of the rats were harvested. The time points were determined based on the results of a pilot study which had been conducted with 1 week, 2 weeks, and 4 weeks time points. The 1- week time point was eliminated to minimize any effects of variation in the surgical procedure, and the 8 week time point was added to observe a longer healing period. The rats were sacrificed via carbon dioxide inhalation and subsequent lung puncture. From the 12 rats per time point, ten
at each time point were used for biomechanical testing, while the other two were used for histology.
[00151] Biomechanical testing. Biomechanical testing was carried out with the Mini Bionix testing system (MTS Systems, Eden Prairie, MN, USA), using a 50-lb load cell. Tendons were harvested still attached to the rat foot. Muscle was completely removed from the tendon such that the tendon-muscle insertions (proximal extent of the tendon, where it inserts into the gastrocnemius muscle) were exposed. A custom rig was used to secure the foot while the tendon- muscle insertions were clamped between sandpaper and cyanoacrylate. Orthogonal photographs together with a known scale (digital caliper) were obtained using a digital camera (8.2 megapixel Canon EOS 30D, Tokyo, Japan) at a fixed distance to measure two dimensions of the tendon. The cross-sectional area was calculated using an elliptical assumption (ImageJ software, NIH) and used to calculate the ultimate tensile stress (UTS). Tendons were stretched at a rate of 0.5 mm/sec until failure. The ultimate failure load (UFL) was recorded; UTS was computed from UFL and cross-sectional area data; stiffness was determined from force/displacement curves. These curves were obtained by computer registering the MTS forces. The treatment groups were compared using a paired Student's t-Test.
[00152] Histological analysis. Formalin- fixed, paraffin-embedded sections (6 μιη) were stained with hematoxylin and eosin to assess tendon morphology. Adjacent slides were stained with Picro-sirius Red solution to assess collagen I and collagen III content. All images were taken with a Leica DM5000B fluorescent microscope, with a polarizing filter for Picro-sirius Red stains.
3.2 COMPARATIVE RESULTS FOR IN-VIVO GUIDED TENDON REGENERATION USING INJECTABLE TENDON-DERIVED EXTRACELLULAR MATRIX SOLUTION, THAT GELATES IN SITU TO TENDON HYDROGEL, VERSUS SALINE CONTROL
[00153] Biomechanical properties. One animal from each time point was excluded because of tendons slipping out of the clamp during testing and losing their tendon-muscle insertions. At 2 weeks, the majority of ruptures occurred in the mid substance of the tendon. At 4 and 8 weeks, ruptures were more common at the tendon-bone insertion.
[00154] There was no significant difference in UFL (p = 0.151), UTS (p = 0.424), and stiffness (p = 0.760) between the gel and PBS treatments at the early 2-week time point. However at 4 weeks, tendons treated with gel had UFLs that were 28% stronger on average than those treated with PBS (74.8±11.6 N for gel-treated vs. 58.4±14.2 N treated with PBS, p = 0.016) (Figure 20); at this time point, the tendons that had been treated with tendon hydrogel had already reached near-native strength. There remained no significant difference in UTS (p = 0.634) and stiffness (p = 0.082). By 8 weeks there was no longer a significant difference in UFL (p = 0.156) between treatments, since near-native strength had already been achieved at the 4- weeks timepoint. There remained no significant difference in UTS (p = 0.385) and stiffness (p = 0.748).
[00155] Histological results. Cross-sections of both treatment groups (gel treatment vs. treatment with PBS) showed similar injury morphologies at 2 and 4 weeks, where the wound defect was clearly visible between tendon portions. By 8 weeks, the wound space was indiscernible from healing tendon tissue. No capsule formation was observed which would have indicated that the body reacted to the gel as being foreign tissue; rather, the gel might have acted to facilitate infiltration by the host cells. At 2 weeks, Picro-sirius Red staining revealed a very strong presence of collagen I in the wound trough of tendons treated with gel that is absent in those treated with saline. By 4 weeks, a noticeable difference in the collagen content of the injury troughs could be observed suggesting that the gel might have promoted early collagen I formation within the trough. The collagen I at this time point is aligned with the healing collagen III and does not match the morphology of the digested, unaligned collagen I seen at 2 weeks. At 8 weeks, the collagen content of the healing areas was indistinguishable in both, the gel-treated and the PBS-treated, groups.
[00156] Utility of the described injectable tendon-derived extracellular matrix solution that gelates in situ to tendon hydrogel. Comparing the Achilles tendon repair and regeneration process during the first eight weeks following acute, bilateral Achilles tendon injuries (by partial removal of the Achilles tendon) in a rat model illustrates that the application of tendon-derived extracellular matrix solution to the site of injury supported and accelerated the tendon healing process, as measured by superior biomechanical function at 4 weeks after injury in comparison to the application of saline, as control. Tendon-derived extracellular matrix solution is liquid at or below room temperature (4 - 25 degree Celsius), but, upon administration into a mammalian
subject, such as a rat, at the site of tendon injury forms right there, in situ, at physiological temperature, a tendon hydrogel. The Achilles tendons that were treated with the hydrogel ('gel- treated') were significantly stronger after four weeks than the Achilles tendons that were filled with saline only ('saline-treated', see Figure 20). An ultimate failure load (strength) of 74.8N of the gel-treated tendons compared to 58.4N was seen at 4 weeks following the administration of the tendon-derived extracellular matrix hydrogel. This corresponded to an about 28% higher strength in the gel-treated group compared to the saline-treated group. In fact, at that 4-weeks time point, the gel-treated tendons were found to be as strong and possessing the same stiffness as native tendons according to previously assessed values for native tendons, namely 74.8 ± 11.6N gel-treated tendon versus 75.7 ± 18.5 native tendon for strength and 17.9 ± 3.5 gel-treated tendon versus 17.9 ± 5.5 native tendon for stiffness).
[00157] Furthermore, a histological evaluation of the gel-treated versus saline-treated tendons revealed cellular ingrowth in the gel-treated tendon which was not observable in the saline- treated controls: at the same 4-week time point, where gel-treated tendons were found about 28% stronger than saline-treated controls, it was observed that early collagen I had formed in the gel- treated tendons, whereby such early collagen I was aligned with healing collagen III fibers. Picro-sirius Red staining of the gel-treated and saline-treated tendons at the 4-week time point showed a considerably higher collagen I: collagen III ratio in the gel-treated tendons compared to saline -treated controls (see Figure 21).
[00158] While collagen III fibers typically occur during the second healing phase of collagen proliferation, as described earlier, the formation of early collagen I is not typical and was primarly observed in gel-treated tendons. The formation of early collagen I and its alignment with healing collagen III, therefore, indicates that the presence of the tendon hydrogel induced the infiltration of host cells into the site of tendon injury and, thus, exerted biological and chemical cues onto the cellular environment. The fact that collagen I fibers are more robust then the thinner collagen III fibers might explain the superior strength of gel-treated tendons at the 4- week time point.
[00159] Ancillary investigations of the described tendon hydrogels that were detailed in Example 1 had revealed that the hydrogel was well tolerated by a mammalian subject such as a rat, that it did not form a capsule and, of particular noteworthiness, that it gradually degraded over a period of about four weeks. This lends very reasonable support to the described
observation in the acute, bilateral Achilles tendon injury rat model, where - after four weeks - gel-treated tendons proved to be 28% stronger than controls and infiltrated with supporting host cells which accelerated the healing process in comparison to saline-treated controls.
[00160] Since the gel gradually degrades over a period of about four weeks, its full benefits should occur early, likely peak at the 4-week time point, as was observed in the described studies, and decrease over the remaining healing period up to 8 weeks. At the 8-week time point, the tendons of both the gel-treated and the saline-treated groups were found to be primarily composed of the robust collagen I and had no further differences in strength.
[00161] In the clinical setting, administration of such an injectable extracellular matrix solution that gelates in situ could improve tending healing in a mammalian subject by accelerating the healing process, providing increased strength to the healing tendon and, thus, allowing for more rapid mobilization and weight-bearing of the injured tendon. This applies to cases of extensive, traumatic tendon injuries which require surgery; here, the administration of such an injectable extracellular matrix solution that gelates in situ following the surgery would support and accelerate healing. Furthermore, the administration of injectable extracellular matrix solution that gelates in situ would support and accelerate healing in cases of microscopic tendon injuries that are characterized by tears, but not full ruptures of tendon and usually don't require surgical intervention. The mere administration of injectable extracellular matrix solution that gelates in situ might be sufficient to regenerate the microscopically injured tendon to its native strength.
[00162] This accelerated rebuilding and healing process can be furthermore supported and enhanced by adding (i) external cells such as stem cells, progenitor cells and fibroblasts, (ii) growth factors such as insulin-like growth factor-I (IGF-I), transforming growth factor beta (TGFbeta), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and basic fibroblast growth factor (bFGF) and/or (iii) platelet-rich plasma to the tendon-derived extracellular matrix solution prior to injection into the area of ligament or tendon injury. As detailed in example 1 , seeding of the tendon-derived extracellular matrix solution with rat adipoderived stem cells did not affect the biocompatibility of the resulting tendon hydrogel upon administration into rats, as evidenced by the lack of capsule formation.
Table 3. Comparison of biomechanical properties of tendon-derived hydrogel-treated (gel-
treated) versus saline-treated tendons

TBI = tendon bone insertion ns = non significant * = p<0.05
HI. Method for in-situ repair and regeneration of an injured ligament in a mammalian subject, comprising administering to said subject suffering from an injured ligament a therapeutically effective amount of a composition into said subject's area of injured ligament, said composition comprising decellularized extracellular matrix derived from tendon
connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon administration into subject's area of injured ligament
EXAMPLE 4: INJECTABLE TENDON HYDROGEL TO TREAT LIGAMENT IN JURIES
[00163] Tendon overuse in both professional and recreational settings gradually alters the biomechanical properties of both tendons and ligaments. Both of these tissues have structural properties and a tissue composition that is very similar. Structural changes seen at injuries typically first present as microscopic tears that, after a period of accumulation, may lead to full- thickness injuries. Common ligament injuries include the ligaments of the wrist, base of thumb, elbow and shoulder. The tendon hydrogel contains the appropriate extracellular matrices (ECMs) of ligaments and therefore, the healing of a ligamentous injury may also be augmented by the introduction of a tendon-derived hydrogel into the injury site.
[00164] Although the foregoing invention and its embodiments have been described in some detail by way of illustration and example for purposes of clarity of understanding, it is readily apparent to those of ordinary skill in the art in light of the teachings of this invention that certain changes and modifications may be made thereto without departing from the spirit or scope of the appended claims. Accordingly, the preceding merely illustrates the principles of the invention. It will be appreciated that those skilled in the art will be able to devise various arrangements which, although not explicitly described or shown herein, embody the principles of the invention and are included within its spirit and scope.
10. REFERENCES
Adair-Kirk TL & Senior RM (2008). Fragments of extracellular matrix as mediators of inflammation. The international journal of biochemistry & cell biology. 40(6-7):l 101-10.
Andersson T et al. (2012). Growth hormone does not stimulate early healing in rat tendons.
International journal of sports medicine 33(3):240-3.
Archambault JM et al. (2007). Rat supraspinatus tendon expresses cartilage markers with overuse. J Orthop Res. 25(5):617-24.
Arya S & Kulig K (2010). Tendinopathy alters mechanical and material properties of the Achilles tendon. J Appl Physiol. 108(3):670-5.
Beck J et al. (2012). The biomechanical and histologic effects of platelet-rich plasma on rat rotator cuff repairs. Am J Sports Med. 40(9):2037-44.
Bohak Z (1969). Purification and characterization of chicken pepsinogen and chicken pepsin. The Journal of biological chemistry. 244(17):4638-48.
Brennan EP et al (2006). Antibacterial activity within degradation products of biological scaffolds composed of extracellular matrix. Tissue Eng. 2006;12(10):2949-55.
Chong AK et al. (2007). Bone marrow-derived mesenchymal stem cells influence early tendon healing in a rabbit achilles tendon model. J Bone Joint Surg Am. 89(1):74-81.
Daamen WF et al (2003). Preparation and evaluation of molecularly-defmed collagen-elastin glycosaminoglycan scaffolds for tissue engineering. Biomaterials 24(22):4001-9.
Davis GE et al (2000). Regulation of tissue injury responses by the exposure of matricryptic sites within extracellular matrix molecules. The American journal of pathology. 156(5): 1489-98. Epub 2000/05/04.
DeQuach JA et al (2011). Decellularized porcine brain matrix for cell culture and tissue engineering scaffolds. Tissue Eng Part A 17(21-22):2583-92.
DeQuach JA et al (2012). Injectable skeletal muscle matrix hydrogel promotes
neovascularization and muscle cell infiltration in a hindlimb ischemia model. European cells &
materials 23:400-12; discussion 12.
Freytes DO et al (2008). Preparation and rheological characterization of a gel form of the porcine urinary bladder matrix. Biomaterials 29(11): 1630-7.
Garg T et al. (2012). Scaffold: a novel carrier for cell and drug delivery. Critical reviews in therapeutic drug carrier systems 29(1): 1-63.
Gimbel JA et al. (2004). Supraspinatus tendon organizational and mechanical properties in a chronic rotator cuff tear animal model. J Biomech. 37(5):739-49.
Gimble JM et al (2007). Adipose-derived stem cells for regenerative medicine. Circ Res.
100(9): 1249-60.
Hall MP et al. (2009). Platelet-rich Plasma: Current Concepts and Application in Sports
Medicine. J Am Acad Orthop Surg 17(10):602-608.
Hamada Y et al. (2012). The preparation of PLLA/calcium phosphate hybrid composite and its evaluation of biocompatibility. Dental materials journal 31(6): 1087-96.
Huss FR et al. (2010. Use of macroporous gelatine spheres as a biodegradable scaffold for guided tissue regeneration of healthy dermis in humans: an in vivo study. J Plast Reconstr Aesthet Surg. 63(5):848-57.
Johnson TD et al (2011). Tailoring material properties of a nano fibrous extracellular matrix derived hydrogel. Nanotechnology 22(49):494015.
Joubert L-M (2009). Visualization of Hydrogels with Variable -Pressure SEM. Microsc
Microanal. l5(Suppl. 2): 1308.
Kampa RJ & Connell DA (2010). Treatment of tendinopathy: is there a role for autologous whole blood and platelet rich plasma injection? International journal of clinical practice
64(13): 1813-23.
Kannus, P (2000). Structure of the tendon connective tissue. ScandJ Med Sci Sports 10:312-320.
Kannus P & Natri A (2007). Etiology and pathophysiology of tendon ruptures in sports.
Scandinavian Journal of Medicine & Science in Sports 7: 107-112.
Kenne L et al. (2013). Modification and cross-linking parameters in hyaluronic acid hydrogels definitions and analytical methods. Carbohydrate polymers 91(l):410-8.
Khan KM et al. (1999). Histopathology of common tendinopathies. Update and implications for clinical management. Sports Med. 27(6):393-408.
Kim JK et al. (2007). Preparation and properties of collagen/modified hyaluronic acid hydrogel for biomedical application. Journal of nanoscience and nanotechnology 7(11):3852-6.
Kurtz CA (1999). Insulin- like growth factor I accelerates functional recovery from Achilles tendon injury in a rat model. Am J Sports Med. 27(3):363-9.
Lin TW et al. (2004). Biomechanics of tendon injury and repair. Journal of Biomechanics 37 (6), p. 865-877.
Longo UG et al. (2008). Histopathology of the supraspinatus tendon in rotator cuff tears. Am J Sports Med. 36(3):533-8.
Longo UG et al. (2011). Tissue engineered biological augmentation for tendon healing: a systematic review. British medical bulletin 98:31-59.
Lu F et al. (2008). Improved viability of random pattern skin flaps through the use of adipose derived stem cells. Plast Reconstr Surg. 121(l):50-8. Epub 2008/01/08.
Martinello T et al. (2012). Successful recellularization of human tendon scaffolds using adipose derived mesenchymal stem cells and collagen gel. Journal of tissue engineering and regenerative medicine, epub June 19, 2012.
Meyers SA et al (1989). Effect of hyaluronic acid/chondroitin sulfate on healing of full-thickness tendon lacerations in rabbits. J Orthop Res. 7(5):683-9.
Mott JD & Werb Z (2004). Regulation of matrix biology by matrix metalloproteinases. Current opinion in cell biology. 16(5):558-64.
Nakaji-Hirabayashi T et al (2012). Improvement of neural stem cell survival in collagen hydrogels by incorporating laminin-derived cell adhesive polypeptides. Bioconjugate chemistry 23(2):212-21.
Neviaser A et al. (2012). Basic mechanisms of tendon fatigue damage. J Shoulder Elbow Surg. 21(2): 158-63.
Ngo M et al. (2001). Differential expression of transforming growth factor-beta receptors in a rabbit zone II flexor tendon wound healing model. Plast Reconstr Surg. 108(5): 1260-7.
Noth U et al (2005). Anterior cruciate ligament constructs fabricated from human mesenchymal stem cells in a collagen type I hydrogel. Cytotherapy 7(5):447-55.
Okamoto N (2010). Treating Achilles tendon rupture in rats with bone -marrow-cell
transplantation therapy. J Bone Joint Surg Am. 92(17):2776-84.
Peng KT et al. (2010). Treatment of osteomyelitis with teicoplanin-encapsulated biodegradable thermosensitive hydrogel nanoparticles. Biomaterials 31(19):5227-36.
Pittenger MF et al (1999). Multilineage potential of adult human mesenchymal stem cells.
Science 284(5411): 143-7. Epub 1999/04/02.
Pridgen BC et al (2011). Flexor Tendon Tissue Engineering: Acellularization of Human Flexor Tendons With Preservation of Biomechanical Properties and Biocompatibility. Tissue Eng Part C Methods. 17(8):810-28.
Sato D et al. (2012). Effect of platelet-rich plasma with fibrin matrix on healing of intrasynovial flexor tendons. J Hand Surg Am. 37(7): 1356-63.
Seif-Naraghi SB et al (2010). Design and characterization of an injectable pericardial matrix gel: a potentially autologous scaffold for cardiac tissue engineering. Tissue Eng Part A 16(6):2017-
Seif-Naraghi SB et al. (2012). Injectable extracellular matrix derived hydrogel provides a platform for enhanced retention and delivery of a heparin-binding growth factor. Acta biomaterialia. 8(10):3695-703.
Sharma P & Maffulli N (2005).Tendon injury and tendinopathy: healing and repair. J Bone Joint Surg Am 87: 187-202.
Sharma P & Maffulli N (2006). Biology of tendon injury: healing, modeling and remodeling. J Musculoskelet Neuronal Interact 6(2) : 181 - 190.
Singelyn JM et al (2009). Naturally derived myocardial matrix as an injectable scaffold for cardiac tissue engineering. Biomaterials 30(29):5409-16.
Singelyn JM et al (2012). Catheter-deliverable hydrogel derived from decellularized ventricular extracellular matrix increases endogenous cardiomyocytes and preserves cardiac function post myocardial infarction. J Am Coll Cardiol. 59(8):751-63.
Stabenfeldt SE & LaPlaca MC (2011). Variations in rigidity and ligand density influence neuronal response in methylcellulose-laminin hydrogels. Acta biomaterialia 7(12):4102-8.
Suri S & Schmidt CE (2010). Cell-laden hydrogel constructs of hyaluronic acid, collagen, and laminin for neural tissue engineering. Tissue Eng Part A 16(5): 1703-16.
Tapp H et al. (2009). Adipose-derived stem cells: characterization and current application in orthopaedic tissue repair. Exp Biol Med 234(1): 1-9. Epub 2008/12/26.
Tobita M et al (2008). Periodontal tissue regeneration with adipose-derived stem cells. Tissue Eng Part A 14(6):945-53.
Uysal CA et al (2012). Adipose-derived stem cells enhance primary tendon repair:
Biomechanical and immunohistochemical evaluation. J Plast Reconstr Aesthet Surg.
65(12) : 1712-9.
Valentin JE et al (2009). Macrophage participation in the degradation and remodeling of extracellular matrix scaffolds. Tissue Eng Part A. 15(7): 1687-94.
Virchenko O & Aspenberg P (2006). How can one platelet injection after tendon injury lead to a stronger tendon after 4 weeks? Interplay between early regeneration and mechanical stimulation. Acta orthopaedica 77(5):806-12.
Wisniewski JR et al (2009). Universal sample preparation method for proteome analysis. Nature methods. 6(5):359-62. Epub 2009/04/21.
Wolf MT et al (2012). A hydrogel derived from decellularized dermal extracellular matrix. Biomaterials 33(29):7028-38.
Yan XM et al (2012). Improved synthesis of hyaluronic acid hydrogel and its effect on tissue augmentation. Journal of biomaterials applications 27(2): 179-86.
Young RG et al. (1998). Use of mesenchymal stem cells in a collagen matrix for Achilles tendon repair. J Orthop Res. 16(4):406-13.
Zhang X et al. (2012). Structural study and preliminary biological evaluation on the collagen hydrogel crosslinked by gamma-irradiation. J Biomed Mater Res A. 100(11):2960-9.
Zuk PA et al (2001). Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng. 7(2):211-28. Epub 2001/04/17.
Claims
1. A composition for in-situ repair and regeneration of an injured ligament or tendon in a mammalian subject, comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon administration into said subject's area of injured ligament or tendon, whereby said composition is effective in repairing and regenerating said injured ligament or tendon by forming in situ a support structure which facilitates infiltration of said subject's own fibroblasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon.
2. The composition in accordance to Claim 1, wherein said tendon connective tissue is obtained from an allogeneic source.
3. The composition in accordance to Claim 2, wherein said allogeneic source is human.
4. The composition in accordance to Claim 1, wherein said tendon connective tissue is obtained from a xenogeneic source.
5. The composition in accordance to Claim 4, wherein said xenogeneic source is porcine.
6. The composition in accordance to Claim 1, further comprising cells selected from the group consisting of stem cells, progenitor cells and fibroblasts.
7. The composition in accordance to Claim 1, further comprising a therapeutic agent.
8. The composition in accordance to Claim 6, further comprising a therapeutic agent.
9. The composition in accordance to Claim 7, wherein said therapeutic agent is selected from the group consisting of growth factors, analgesics, antibiotics and platelet-rich plasma.
10. The composition in accordance to Claim 8, wherein said therapeutic agent is selected from the group consisting of growth factors, analgesics, antibiotics and platelet-rich plasma.
11. The composition in accordance to Claim 1 , wherein said composition is administered once.
12. The composition in accordance to Claim 1, wherein said composition is administered more than once.
13. The composition in accordance to Claim 1, wherein said injured tendon is one of Achilles tendon, rotator cuff, patella tendon, common flexor tendon or common extensor tendon.
14. The composition in accordance to any of Claims 1, 6, 7 or 8, wherein the composition is an injectable decellularized extracellular matrix derived from human tendon connective tissue.
15. The composition in accordance to any of Claims 1, 6, 7 or 8, wherein the composition is an injectable decellularized extracellular matrix derived from porcine tendon connective tissue.
16. A method for in-situ repair and regeneration of an injured tendon or ligament in a
mammalian subject, comprising administering to said subject suffering from an injured ligament or tendon a therapeutically effective amount of a the composition of Claim 1 into said subject's area of injured ligament or tendon, said composition comprising decellularized extracellular matrix derived from tendon connective tissue, said composition being in injectable form below 25 degree Celsius and forming a gel upon administration into subject's area of injured ligament or tendon, whereby said
composition is effective in repairing and regenerating said injured ligament or tendon by forming in situ a support structure which facilitates infiltration of said subject's own fibroblasts and tenocytes into said support structure and, thereby, facilitates in-situ repair and regeneration of injured ligament or tendon.
17. The method in accordance to Claim 16, wherein said tendon connective tissue is obtained from an allogeneic source.
18. The method in accordance to Claim 17, wherein said allogeneic source is human.
19. The method in accordance to Claim 16, wherein said tendon connective tissue is obtained from a xenogeneic source.
20. The method in accordance to Claim 19, wherein said xenogeneic source is porcine.
21. The method in accordance to Claim 16, wherein said composition further comprises cells selected from the group consisting of stem cells, progenitor cells and fibroblasts.
22. The method in accordance to Claim 16, wherein said composition further comprises a therapeutic agent.
23. The method in accordance to Claim 21, wherein said composition further comprises a therapeutic agent.
24. The method in accordance to Claim 22, wherein said therapeutic agent is selected from the group consisting of growth factors, analgesics, antibiotics and platelet-rich plasma.
25. The method in accordance to Claim 23, wherein said therapeutic agent is selected from the group consisting of growth factors, analgesics, antibiotics and platelet-rich plasma.
26. The method in accordance to Claim 16, wherein said composition is administered once.
27. The method in accordance to Claim 16, wherein said composition is administered more than once.
28. The method in accordance to Claim 16, wherein said injured tendon is one of Achilles tendon, rotator cuff, patella tendon, common flexor tendon or common extensor tendon.
29. The method in accordance to any of Claims 16, 21, 22 or 23, wherein the composition is an injectable decellularized extracellular matrix derived from human tendon connective tissue.
30. The method in accordance to any of Claims 16, 21, 22 or 23, wherein the composition is an injectable decellularized extracellular matrix derived from porcine tendon connective tissue.
31. A method of producing a composition comprising decellularized tendon extracellular matrix, said method comprising: (a) processing tendon connective tissue that was obtained from a donor to remove cellular components to obtain decellularized tendon extracellular matrix; (c) grinding and enzymatically treating said tendon extracellular matrix.
32. The method in accordance to Claim 31, wherein said decellularized tendon extracellular matrix is derived from an allogeneic source.
33. The method in accordance to Claim 32, wherein said allogeneic source is human.
34. The method in accordance to Claim 31, wherein said decellularized tendon extracellular matrix is derived from an xenogeneic source.
35. The method in accordance to Claim 34, wherein said xenogeneic source is porcine.
Priority Applications (3)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP14763616.1A EP2968417A4 (en) | 2013-03-15 | 2014-03-14 | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use |
| US14/855,034 US9925308B2 (en) | 2013-03-15 | 2015-09-15 | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use |
| US15/837,300 US10857265B2 (en) | 2013-03-15 | 2017-12-11 | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201361789336P | 2013-03-15 | 2013-03-15 | |
| US61/789,336 | 2013-03-15 |
Related Child Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| US14/855,034 Continuation-In-Part US9925308B2 (en) | 2013-03-15 | 2015-09-15 | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2014144215A1 true WO2014144215A1 (en) | 2014-09-18 |
Family
ID=51537646
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2014/028525 WO2014144215A1 (en) | 2013-03-15 | 2014-03-14 | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use |
Country Status (3)
| Country | Link |
|---|---|
| US (2) | US9925308B2 (en) |
| EP (1) | EP2968417A4 (en) |
| WO (1) | WO2014144215A1 (en) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN111346262A (en) * | 2020-03-17 | 2020-06-30 | 四川大学 | Injectable calcium-phosphorus ceramic for promoting healing of tendon and bone and preparation method and application thereof |
| US11179494B2 (en) | 2014-12-15 | 2021-11-23 | Northeastern University | Collagenous tissue repair device |
| EP3755267A4 (en) * | 2018-02-22 | 2021-11-24 | University of Pittsburgh - of the Commonwealth System of Higher Education | Extracts for the regeneration of ligaments |
| US11389566B2 (en) | 2016-03-14 | 2022-07-19 | Regentys Corporation | Method and composition for treating inflammatory bowel disease |
Families Citing this family (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2017008035A1 (en) * | 2015-07-08 | 2017-01-12 | The Trustees Of The University Of Pennesylvania | Decellularized organ-derived tissue engineering scaffolds |
| WO2017096148A1 (en) * | 2015-12-03 | 2017-06-08 | Katz Robert S | Methods and systems for diagnosing and treating fibromyalgia |
| CA3075099A1 (en) | 2017-10-18 | 2019-04-25 | Lifecell Corporation | Adipose tissue products and methods of production |
| US11246994B2 (en) * | 2017-10-19 | 2022-02-15 | Lifecell Corporation | Methods for introduction of flowable acellular tissue matrix products into a hand |
| EP3697462B1 (en) | 2017-10-19 | 2023-07-12 | LifeCell Corporation | Flowable acellular tissue matrix products and methods of production |
| CN114040730A (en) * | 2018-12-20 | 2022-02-11 | 斯特曼诊所及斯德曼菲利庞研究院 | Acellular tendon matrix method and application thereof |
| KR20210142003A (en) * | 2019-03-13 | 2021-11-23 | 유니버시티 오브 피츠버그 - 오브 더 커먼웰쓰 시스템 오브 하이어 에듀케이션 | Acoustic extracellular matrix hydrogels and uses thereof |
| CN113546217A (en) * | 2021-07-15 | 2021-10-26 | 中山大学 | Modified acellular myocardial matrix gel and preparation method thereof |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20120114755A1 (en) * | 2009-06-22 | 2012-05-10 | Mayo Foundation For Medical Education And Research | Methods and materials for tissue repair |
| US20120264190A1 (en) * | 2009-12-21 | 2012-10-18 | The Regents Of The University Of California | Decellularized and Delipidized Extracellular Matrix and Methods of Use |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CA2710207C (en) * | 2007-12-21 | 2017-06-06 | Rti Biologics, Inc. | Osteoinductive putties and methods of making and using such putties |
| US8894707B2 (en) * | 2009-03-06 | 2014-11-25 | Mayo Foundation For Medical Education And Research | Tendon or ligament tissue engineering |
-
2014
- 2014-03-14 EP EP14763616.1A patent/EP2968417A4/en not_active Withdrawn
- 2014-03-14 WO PCT/US2014/028525 patent/WO2014144215A1/en active Application Filing
-
2015
- 2015-09-15 US US14/855,034 patent/US9925308B2/en active Active
-
2017
- 2017-12-11 US US15/837,300 patent/US10857265B2/en active Active
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20120114755A1 (en) * | 2009-06-22 | 2012-05-10 | Mayo Foundation For Medical Education And Research | Methods and materials for tissue repair |
| US20120264190A1 (en) * | 2009-12-21 | 2012-10-18 | The Regents Of The University Of California | Decellularized and Delipidized Extracellular Matrix and Methods of Use |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP2968417A4 * |
Cited By (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11179494B2 (en) | 2014-12-15 | 2021-11-23 | Northeastern University | Collagenous tissue repair device |
| US11389566B2 (en) | 2016-03-14 | 2022-07-19 | Regentys Corporation | Method and composition for treating inflammatory bowel disease |
| EP3755267A4 (en) * | 2018-02-22 | 2021-11-24 | University of Pittsburgh - of the Commonwealth System of Higher Education | Extracts for the regeneration of ligaments |
| US12070475B2 (en) | 2018-02-22 | 2024-08-27 | University of Pittsburgh—of the Commonwealth System of Higher Education | Extracts for the regeneration of ligaments |
| CN111346262A (en) * | 2020-03-17 | 2020-06-30 | 四川大学 | Injectable calcium-phosphorus ceramic for promoting healing of tendon and bone and preparation method and application thereof |
| CN111346262B (en) * | 2020-03-17 | 2022-02-01 | 四川大学 | Injectable calcium-phosphorus ceramic for promoting healing of tendon and bone and preparation method and application thereof |
Also Published As
| Publication number | Publication date |
|---|---|
| US9925308B2 (en) | 2018-03-27 |
| US20160166735A1 (en) | 2016-06-16 |
| US10857265B2 (en) | 2020-12-08 |
| EP2968417A1 (en) | 2016-01-20 |
| US20180133369A1 (en) | 2018-05-17 |
| EP2968417A4 (en) | 2016-09-14 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US10857265B2 (en) | Injectable composition for in-situ repair and regeneration of an injured ligament or tendon and methods of use | |
| Spang et al. | Extracellular matrix hydrogel therapies: In vivo applications and development | |
| Chen et al. | An asymmetric chitosan scaffold for tendon tissue engineering: In vitro and in vivo evaluation with rat tendon stem/progenitor cells | |
| Huang et al. | A functional biphasic biomaterial homing mesenchymal stem cells for in vivo cartilage regeneration | |
| Shen et al. | Long-term effects of knitted silk–collagen sponge scaffold on anterior cruciate ligament reconstruction and osteoarthritis prevention | |
| Wu et al. | An injectable extracellular matrix derived hydrogel for meniscus repair and regeneration | |
| Kim et al. | Nature-derived aloe vera gel blended silk fibroin film scaffolds for cornea endothelial cell regeneration and transplantation | |
| Zheng et al. | A review of recent progress on collagen‐based biomaterials | |
| Yuan et al. | AMECM/DCB scaffold prompts successful total meniscus reconstruction in a rabbit total meniscectomy model | |
| Sheng et al. | Electrospun PCL/Gel-aligned scaffolds enhance the biomechanical strength in tendon repair | |
| Narayanan et al. | Biomimetic glycosaminoglycan-based scaffolds improve skeletal muscle regeneration in a Murine volumetric muscle loss model | |
| US10729534B2 (en) | Methods of treating a musculoskeletal tissue interface injury using decellularized composite tissue bioscaffolds | |
| Moshiri et al. | Role of tissue-engineered artificial tendon in healing of a large Achilles tendon defect model in rabbits | |
| Hao et al. | Biofabrication of cell-free dual drug-releasing biomimetic scaffolds for meniscal regeneration | |
| Zhang et al. | Tissue-adhesive paint of silk microparticles for articular surface cartilage regeneration | |
| AU2017254864A1 (en) | Biomaterial for articular cartilage maintenance and treatment of arthritis | |
| KR101536134B1 (en) | soft tissue recovery matrix a method of manufacturing | |
| Yan et al. | 3D-bioprinted silk fibroin-hydroxypropyl cellulose methacrylate porous scaffold with optimized performance for repairing articular cartilage defects | |
| Qiu et al. | A lubricant and adhesive hydrogel cross-linked from hyaluronic acid and chitosan for articular cartilage regeneration | |
| Chen et al. | Hyaluronic acid/platelet rich plasma-infused core-shell nanofiber membrane to prevent postoperative tendon adhesion and promote tendon healing | |
| Peng et al. | Natural biopolymer scaffold for meniscus tissue engineering | |
| Dai et al. | Enhanced osteochondral repair with hyaline cartilage formation using an extracellular matrix-inspired natural scaffold | |
| Yuan et al. | Kartogenin releasing decellularized umbilical cord Wharton's jelly scaffold promotes rotator cuff fibrocartilaginous interface regeneration | |
| Hou et al. | Biomimetic melatonin-loaded silk fibroin/GelMA scaffold strengthens cartilage repair through retrieval of mitochondrial functions | |
| Anjum et al. | Exploring polysaccharide and protein-enriched decellularized matrix scaffolds for tendon and ligament repair: a review |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 14763616 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REEP | Request for entry into the european phase |
Ref document number: 2014763616 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2014763616 Country of ref document: EP |