WO2007125338A1 - Immunoglobulin free light chain assay - Google Patents
Immunoglobulin free light chain assay Download PDFInfo
- Publication number
- WO2007125338A1 WO2007125338A1 PCT/GB2007/001551 GB2007001551W WO2007125338A1 WO 2007125338 A1 WO2007125338 A1 WO 2007125338A1 GB 2007001551 W GB2007001551 W GB 2007001551W WO 2007125338 A1 WO2007125338 A1 WO 2007125338A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- assay
- free light
- light chain
- free
- sample
- Prior art date
Links
Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
- G01N33/6854—Immunoglobulins
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/543—Immunoassay; Biospecific binding assay; Materials therefor with an insoluble carrier for immobilising immunochemicals
- G01N33/54366—Apparatus specially adapted for solid-phase testing
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/58—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving labelled substances
- G01N33/582—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving labelled substances with fluorescent label
Definitions
- the present invention relates to the field of real-time detection of immunoglobulin free light chains in blood, or blood serum, or a dialysate fluid used during a haemodialysis process for removal of free light chains from blood serum.
- Antibody molecules also known as immunoglobulins
- the variable domains of the heavy and light chains combine to form an antigen-binding site, so that both chains contribute to the antigen-binding specificity of the antibody molecule.
- the basic tetrameric structure of antibodies comprises two heavy chains covalently linked by a disulphide bond. Each heavy chain is in turn attached to a light chain, again via a disulphide bond, to produce a substantially "Y"-shaped molecule.
- K Lambda
- ⁇ Lambda
- K Kappa
- Each chain contains approximately 220 amino acids in a single polypeptide chain that is folded into one constant and one variable domain.
- Plasma cells produce one of the five heavy chain types together with either K or ⁇ molecules.
- FLCs free light chain molecules
- the K light chains are usually found as monomers.
- the ⁇ light chains tend to form dimers.
- FIG. 1 shows the development of B-cell lineage and associated diseases. These diseases are known as malignant B-cell diseases. They are summarised in detail in the book “Serum-free Light Chain Analysis” A.R. Bradwell, available from The Binding Site Limited, Birmingham, UK (ISBN: 07044 24894). In many such diseases a plasma cell proliferates to form a monoclonal tumour of identical plasma cells. This results in production of large amounts of identical immunoglobulins and is known as monoclonal gammopathy.
- myeloma and primary systemic amyloidosis account for approximately 1.5% and 0.3% respectively of cancer deaths in the United Kingdom.
- Multiple myeloma is the second-most common form of haematological malignancy after non- Hodgkin lymphoma. In Caucasian populations the incidence is approximately 40 per million per year.
- diagnosis of MM is based on the presence of excess monoclonal plasma cells in the bone marrow, monoclonal immunoglobulins in the serum or urine and related organ or tissue impairment such as hypercalcaemia, renal insufficiency, anaemia or bone lesions.
- Normal plasma cell content of the bone marrow is about 1%, while in MM the content is typically greater than 30%, but may be over 90%.
- AL amyloidosis is a protein conformation disorder characterised by the accumulation of monoclonal free light chain fragments as amyloid deposits. Typically, these patients present with heart or renal failure but peripheral nerves and other organs may also be involved.
- Dimeric free light chains typically ⁇ , are cleared in 3-6 hours at 20% of the glomerular filtration rate, while large molecules are cleared more slowly. Removal may be prolonged to 2-3 days in MM patients in renal failure, when serum free light chains (sFLCs) are removed by the liver and other tissues (Russo et al. (2002) Am. J. Kidney Dis. 39 899-919). In contrast, IgG has a half-life of 21 days that is not affected by renal impairment.
- Each nephron contains a glomerulus with pores that allow filtration of serum molecules into its proximal tubule.
- the pore sizes are variable with a restriction in filtration commencing at about 4OkDa and being complete by 6OkDa.
- Protein molecules that pass the glomerular pores are then either absorbed unchanged or degraded in the proximal tubular cells and excreted as fragments. This is an essential mechanism to prevent loss of proteins and peptides into the urine and is very efficient.
- the exact pathway of free light chain is unknown but between 10-30g per day can be processed by the kidneys, so, under normal conditions, very little intact light chain passes beyond the proximal tubules.
- FLCs After filtration by the glomeruli, FLCs enter the proximal tubules and bind to brush-border membranes via low-affinity, high-capacity receptors called cubulins (gp280) (Winearls (2003) "Myeloma Kidney” - Ch. 17 Comprehensive Clinical Nephrology, 2 nd Ed. Eds Johnson & Feehally; Pub: Mosby). Binding provokes internalisation of the FLCs and subsequent metabolism. The concentration of the FLCs leaving the proximal tubules, therefore, depends upon the amounts in the glomerular filtrate, competition for binding uptake from other proteins and the absorptive capacity of the tubular cells.
- a reduction in the glomerular filtration rate increases serum FLC concentrations so that more is filtered by the remaining functioning nephrons.
- hyperfiltering glomeruli leak albumin and other proteins which compete with FLCs for absorption, thereby causing more to enter the distal tubules.
- FLCs entering the distal tubule normally bind to uromucoid (Tamm-Horsfall protein). This is the dominant protein in normal urine and is though to be important in preventing ascending urinary infections. It is a glycoprotein (85kDa) that aggregates into high molecular weight polymers of 20-30 units.
- Serum FLC concentrations are abnormal in >95% of patients with MM and have a wide range of concentrations, but their inherent toxicity also varies considerably, as was shown by Sanders & Brooker using isolated rat nephrons (Sanders & Brooker (1992) J. Clin. Invest. 89 630-639). The toxicity is in part related to binding with Tamm-Horsfall protein (see e.g. Winearls (1995) Kidney Int. 48 1347-1361).
- PE plasma exchange
- an assay for the real-time quantitative detection of immunoglobulin free light chain in a sample which is either a subject's blood, dialysate or ultrafiltrate used or produced during haemodialysis, haemof ⁇ ltration or haemodiafiltration of a subject's blood.
- the sample is assayed for immunoglobulin free light chains.
- real-time indicates that the assay can be carried out in close proximity to the subject such as within a hospital ward or at a bedside and that results from the assay are obtained within 30 minutes, preferably within 15 minutes, more preferably within 10 minutes.
- such an assay provides a real-time detection system for free light chains in the sample.
- a membrane used to remove FLCs from the blood serum of a subject by haemodialysis to be monitored for efficacy, such that, when the membrane becomes at least partially blocked, the resultant reduction in the rate of FLC removal can be detected.
- the membrane can then be substituted with a fresh membrane or, alternatively, the haemodialysis procedure can be stopped.
- the assay is carried out in close proximity to the subject, rather than having to be carried out in a separate laboratory facility, such that results are obtained quickly, whilst the patient is still undergoing the haemodialysis procedure.
- This may also be used to detect the effect of, for example, chemotherapy, on the production of free light chains by a patient.
- the assay is adapted to remove or lyse or otherwise destroy red blood cells in a blood sample.
- Red blood cells may interfere with the assay. This may be achieved using techniques generally known in the art.
- red blood cells may be lysed by using a detergent.
- the assay may comprise a filter to filter out the red blood cells.
- a blood sample may be filtered through the filter prior to quantitatively determining an amount of free light chain in the sample.
- the filtration step may use a filter separate to the part of the assay detecting the free light chains and a blood sample filtered prior to assaying for free light chains.
- the filter may be attached to an assay device, blood being passed directly through the assay before contacting the part of the assay arranged to determine the free light chain concentration.
- the subject is preferably a mammal and, most preferably, is a human subject.
- the assay is an immunoassay, such as a nephalometric or turbidometric assay.
- immunoassays preferably use an antiimmunoglobulin free light chain antibody to trap or detect the immunoglobulin free light chains.
- the assay comprises the steps of: a) exposing to the sample a support surface having at least one primary anti-free light chain antibody adhered thereto; b) exposing the support surface, after step (a) has been completed, to a secondary anti- free light chain antibody; and c) detecting a secondary antibody bound to a free light chain molecule.
- the invention also provides real time assay devices for use in the assay according to the invention.
- Such devices preferably comprise:
- a filter to trap red blood cells, or means to destroy or lyse such cells is preferably provided before the solid support, so that a sample is filtered prior to passing to the solid support.
- the filter, or means to destroy or lyse the cells may be as described above.
- the detection label allows the detection of the binding of the secondary antibody, preferably in a quantitative manner.
- labels are generally known in the art and include dyes, coloured particles such as gold sols or latex particles, enzymes and radio labels.
- the assay or device is an ELISA or device.
- Quantitative immunoassays are summarised, for example, in “Quantitative Immunoassay: A practical guide for assay establishment, troubleshooting, and clinical application", James T. Wu 2000, ISBN 1890883336, publ. AACC Press.
- the assay and device may use a lateral flow device of a type generally known in the art for the detection of analytes, such as pregnancy associated hormones (e.g. hCG).
- a lateral flow device of a type generally known in the art for the detection of analytes, such as pregnancy associated hormones (e.g. hCG).
- Such devices often utilise a dipstick and comprise the reagents for the assay in dehydrated form on a matrix through which the sample travels.
- Quantitative measurements may be obtained using, for example, luminescent systems with fluorescent conjugates (e.g. Cy5).
- the assay preferably comprises a dipstick or other lateral flow device.
- Debris from destroyed red blood cells may be eluted from the zone comprising antibodies used to detect the free light chain by the flow of the sample.
- a fluorescent species is conjugated to the secondary anti-free light chain antibody and acts as the label.
- the fluorescent species may emit light following the application of an energy source such as an electrical pulse or ultraviolet light. Detection of a free light chain bound to each at least one free light chain antibody may be by detection of light emitted by the fluorescent species.
- the binding of the secondary antibody may be determined using an enzyme, such as horseradish peroxidase (HRP) attached to the secondary antibody. HRP may be used to convert suitable non-coloured substrates, such as TMB, into a coloured detectable product.
- HRP horseradish peroxidase
- hemodialysis refers to a process to correct the chemical composition of blood by removing accumulated metabolic products and adding buffer in a process of diffusion through a natural or synthetic semi-permeable membrane.
- HDF hemodiafiltration
- hemodiafiltration refers to a process to remove accumulated metabolic products from blood by a combination of diffusive and convective transport through a semi-permeable membrane of high-flux type; fluid is removed by ultrafiltration and the volume of filtered fluid exceeding the desired weight loss is replaced by sterile, pyrogen-free infusion solution.
- hemofiltration refers to a process of filtering blood by a membrane with separation of plasma water and solutes with the ultrafiltrate, and retains all proteins larger than effective pore size and blood cells.
- the accumulated metabolic products are removed from the blood by the process of convective transport as a consequence of ultrafiltration through a semi-permeable membrane of high-flux type; the volume of filtered fluid exceeding the desired weight loss is replaced by sterile pyrogen-free infusion solution.
- the term "ultrafiltrate” refers to the filtered plasma water and solute and molecules (including free light chains) smaller than effective pore size.
- the at least one free light chain antibody may be a K free light chain antibody or a ⁇ free light chain antibody.
- the support surface may have at least one K free light chain antibody and at least one ⁇ free light chain antibody adhered thereto.
- the detectable element may be a fluorescent species which, more preferably, emits light following the application of an energy source such as an electrical pulse or ultraviolet light.
- a free light chain bound to each at least one free light chain antibody may be detected by detection of light emitted by the fluorescent species.
- such an assay provides a real-time detection system for free light chains in a sample.
- This allows a dialysis membrane being used during haemodialysis to remove FLCs from the blood serum of a subject to be monitored for efficacy, such that, when the membrane becomes at least partially blocked, the resultant reduction in the rate of FLC removal can be detected.
- the membrane can then be substituted with a fresh membrane or, alternatively, the haemodialysis procedure can be stopped. This also ensures that the subject does not have to tolerate the discomfort and inconvenience of haemodialysis for a longer period than is necessary.
- the assay may also be used to give an early indication of the cause of renal failure or an indication of renal failure itself.
- the invention therefore provides a method for obtaining an indication of renal failure or the cause of renal failure, comprising:
- the method preferably uses an assay according to the invention.
- High levels of FLC in the blood or urine give an indication of renal failure or the cause of renal failure.
- the assay kits of the invention may also be used to monitor the build-up of FLC due to disease or decrease in FLC due to treatment by, for example, chemotherapy.
- the subject is preferably a mammal and, most preferably, is a human subject.
- Figure 1 shows proliferative diseases which are associated with antibody producing cells.
- Figure 2 shows removal of ⁇ molecules over a 6-hour dialysis period using a Gambro HC 1100 membrane in a patient with acute renal failure from ⁇ light chain myeloma. The arrows indicate when the membrane was changed;
- Figure 3 shows efficacy of FLC removal by haemodialysis compared to plasma exchange. These are based on a mathematic model of light chain removal by dialysis using a protein leaking membrane and plasma exchange;
- Figure 4 shows that ⁇ molecules are removed more slowly by haemodialysis than K molecules by the mathematical model;
- a - Baseline (25%/day, K) B - Dialysis (4 hrs, 3/wk, K), C - Dialysis (4 hrs, 3/wk, ⁇ ), D - Dialysis (12 hrs/day, K, 2*kd), E - Dialysis (12 hrs/day, ⁇ , 2*kd).
- Figure 5 is a comparison of the reduction in sFLC in a patient with K LCMM over a 4-hour haemodialysis period, using Toray BK-P 2.1 dialyser, BBraun HIPcS 1.8 dialyser and Gambro dialyser HCO 1100;
- Figure 6 shows the use of dialysis on serum free kappa levels during treatment of MM with dexamethasone.
- Figure 7 shows the results for the Kappa (A) and Lambda (B) ELISAs at a coating concentration of 50 ⁇ g/ml.
- the mean absorbance minus the substrate blank is plotted for each concentration of antigen/sample tested. Note that concentrations are plotted on a logarithmic scale. Some results gave a slightly negative value after subtracting the substrate blank, in order to be plotted on this scale, these results were given a value of 0.001.
- FIG. 1100 The Gambro membrane (HCO 1100) is of the type disclosed in WO 2004/056460.
- the inventors compared: B Braun HiPeSlS, Asahi APS-1050, Nikkiso FLX18GWS, Idemsa 200MHP, Toray Bk21-F, Toray BG2.1U and Gambro HCIlOO dialysers.
- the efficiency of sFLC removal was determined in vitro by recirculating serum, containing 1000 mg/L of both monoclonal K and ⁇ light chains; at 400ml/min with trans-membrane pressure (TMP) kept between 300 and 400 mm Hg for haemof ⁇ ltration and at 200ml/min with TMP kept below 50mmHg for haemodialysis.
- TMP trans-membrane pressure
- the haemofiltration was stopped when production of ultraf ⁇ ltrate (UF) fluid ceased and haemodialysis was stopped after 4 hours.
- the filtered or dialysed serum, UF or dialysate, and saline wash (where appropriate) were analysed for sFLC by FreeliteTM nephelometric assays (The Binding Site Ltd, UK).
- the Gambro was the most effective dialyser at clearing both Kappa and Lambda FLC, but unlike the Toray high amounts of FLC were detected in the dialysate fluid, suggesting that the FLC actually pass through the membrane rather than adsorbing to it.
- the Gambro membrane is made according to WO 2004/056460. Table 1: Table showing the average percentage sFLC removal during haemofiltration for each dialyser.
- Table 2 Table showing the percentage sFLC removal during haemodialysis for each dialvser.
- the inventors have demonstrated in vitro the ability of dialysers to effectively clear sFLC.
- Figure 6 shows a summary of the effect of dialysis on a patient being treated for MM with dexamethasone.
- the point of dexamethasone treatment is shown by the arrows.
- a continuous line shows the effect of the dexamethasone on serum IgG. It shows a reduction in IgG levels as the MM is treated with the dexamethasone.
- Dialysis was preformed using a Gambro HCO 1100 dialysis membrane and the concentrate of serum free kappa was monitored both before and after dialysis. Dialysis was preformed on each occasion for 2 hours (6/3/06 first dialysis), 6 hours (6/3/06), 8 hours (7/3/06), 6 hours (9/3/06, 11/3/06, 13/3/06, 15/3/06), 2 hours (17/3/06), 2.5 hours (18/3/06), 4 hours (20/3/06), 6 hours (23/3/06), 3.5 hours (24/3/06) and 4 hours (26/3/06, 28/3/06), using a Gambro membrane. The decrease in serum kappa on each treatment is shown as a line between two points on each day.
- the concentration of IgG and free kappa were monitored using laboratory kits available from The Binding Site Ltd., Birmingham, UK. Other assays known in the art may be used instead of the kits.
- FreeliteTM antibodies are free K and free ⁇ specific antibodies available from The Binding Site Ltd. This involved coating anti- ⁇ and anti- ⁇ free light chain (FLC) FreeliteTM antibodies onto ELISA plates, then adding antigens and clinical samples which either should or should not bind to the antibody. Next, an enzyme-linked secondary antibody (conjugated to peroxidase) specific for each target-antigen and a substrate catalysed by peroxidase to yield a coloured product are applied to the plates. This enables the relative amounts of antigen bound to its antibody to be quantified by reading the absorbance of each well at 450nm.
- FLC anti- ⁇ and anti- ⁇ free light chain
- the FreeliteTM antibodies used are sheep-anti-human Free Kappa and sheep-anti-human Free Lambda.
- the antibody concentrations were made by dilution with 0.1 M carbonate buffer (type 188) lOO ⁇ l of each concentration was then loaded into the appropriate lanes of the plates. The plates were incubated overnight, refrigerated in a humid container. Lanes 11 and 12 on each plate were used as control lanes, so received just carbonate buffer.
- the ELISA plates were removed from the fridge and the wells were emptied of FreeliteTM antibody.
- the plate wells were then incubated in 125 ⁇ l of 50% Stabilcoat (JVC Sales & Technical Consultants GmbH, Thomasberg, Germany) for 1 hour at room temperature in a humid container. Since the ELISA plates used are highly protein-philic this step blocks any remaining binding sites for proteins, ensuring that when antigen is added it should only be able to bind specifically to the antibody and not non-specifically to the plate.
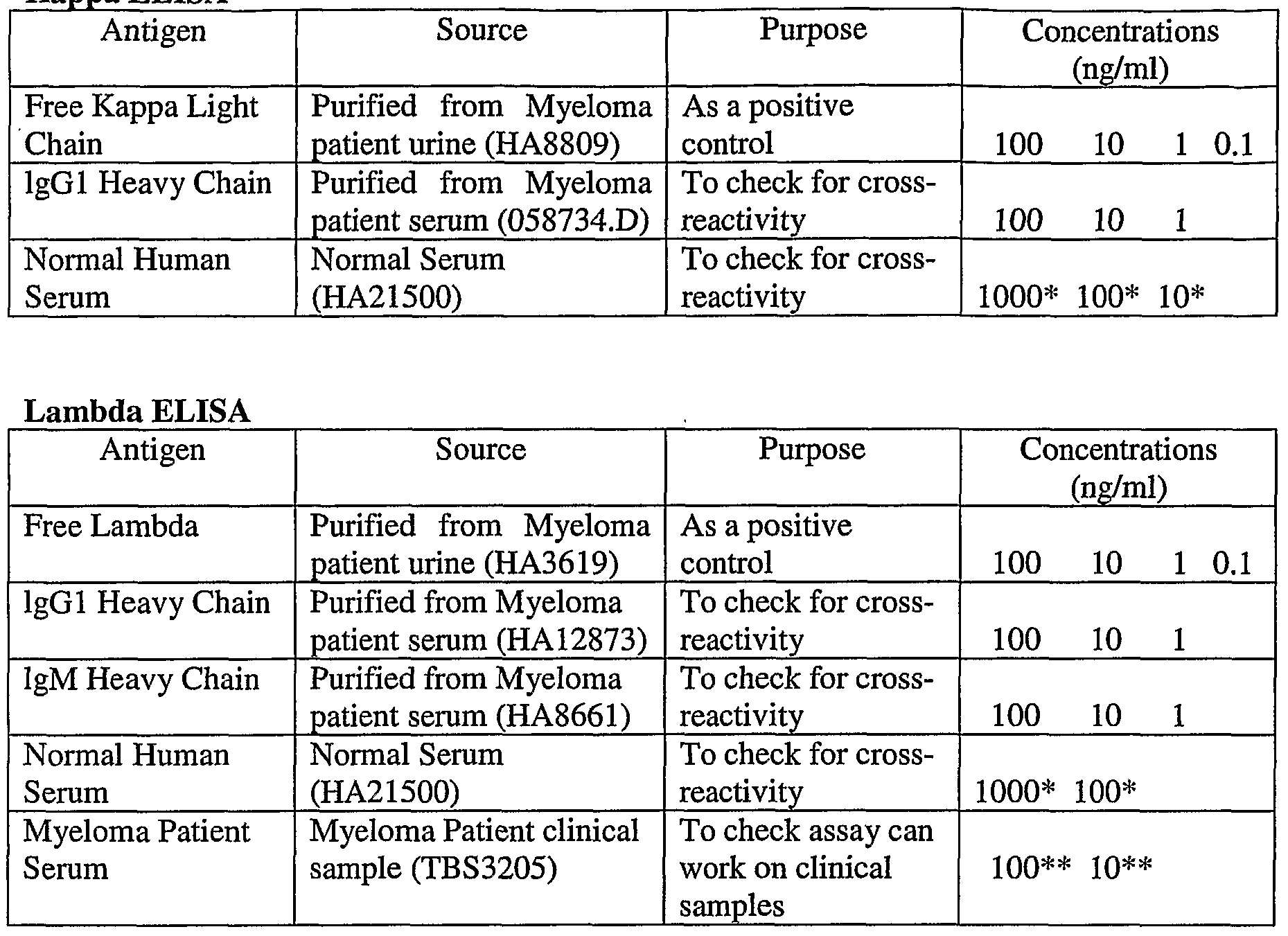
- Table 4 Table listing the type of antigen or sample used and the concentrations at which they were loaded onto the plates. * The concentrations quoted for the normal human serum refer to the approximate concentration of total IgG in that sample. ** The concentrations quoted for myeloma patient serum refer to the concentration of free Lambda in that sample.
- the antigens/samples were applied to the wells and the plates were incubated for one hour at room temperature in a humid container.
- the next stage was to add the secondary antibody.
- Affinity purified sheep-anti-human K or ⁇ antibody conjugated to peroxidase were used for the K and ⁇ plates respectively.
- the secondary antibodies were diluted to 1 in 10000 using conjugate diluent (type 56). lOO ⁇ l of the appropriate secondary antibody solution was added to the wells of each plate. Plates were then incubated at room temperature for one hour in a humid container.
- TMB solution Small Kinetic 1 Component HRP Microwell Substrate
- Stop solution orthophosphoric acid
- the plates were put into a plate reader that measures the absorbance of each well at 450nm.
- the secondary antibodies could be labelled and detected using a system such as that outlined in WO03/087800.
- molecules are labelled with, for example, isothiocyanate derivatives, for example a derivative of Tb(IH)-I chelate. Molecules with such derivatives bound can be detected by causing the chelate to enter an excited state by applying electrical pulses; as the chelate spontaneously returns to the non-excited state, ultraviolet, visible or infrared light is emitted. This light can be detected and a quantitative measure of the amount of K or ⁇ free light chains bound to their respective antibodies obtained.
- the secondary antibody can be labelled with a fluorescent probe, which fluoresces on exposure to, for example, ultraviolet light.
- a fluorescent probe which fluoresces on exposure to, for example, ultraviolet light.
Abstract
There is provided an assay for the real-time quantitative detection of immunoglobulin free light chain in a sample which is either a subject's blood, or a dialysate used during haemodialysis of a subject's blood.
Description
IMMUNOGLOBULIN FREE LIGHT CHAIN ASSAY
The present invention relates to the field of real-time detection of immunoglobulin free light chains in blood, or blood serum, or a dialysate fluid used during a haemodialysis process for removal of free light chains from blood serum.
Antibody molecules (also known as immunoglobulins) have a twofold symmetry and are composed of two identical heavy chains and two identical light chains, each containing variable and constant domains. The variable domains of the heavy and light chains combine to form an antigen-binding site, so that both chains contribute to the antigen-binding specificity of the antibody molecule. The basic tetrameric structure of antibodies comprises two heavy chains covalently linked by a disulphide bond. Each heavy chain is in turn attached to a light chain, again via a disulphide bond, to produce a substantially "Y"-shaped molecule.
There are two types of light chain: Lambda (λ) and Kappa (K). There are approximately twice as many K as λ molecules produced in humans, but this is quite different in some mammals. Each chain contains approximately 220 amino acids in a single polypeptide chain that is folded into one constant and one variable domain. Plasma cells produce one of the five heavy chain types together with either K or λ molecules. There is normally approximately 40% excess free light chain production over heavy chain synthesis. Where the light chain molecules are not bound to heavy chain molecules, they are known as "free light chain molecules" (FLCs). The K light chains are usually found as monomers. The λ light chains tend to form dimers.
There are a number of proliferative diseases associated with antibody producing cells. Figure 1 shows the development of B-cell lineage and associated diseases. These diseases are known as malignant B-cell diseases. They are summarised in detail in the book "Serum-free Light Chain Analysis" A.R. Bradwell, available from The Binding Site Limited, Birmingham, UK (ISBN: 07044 24894).
In many such diseases a plasma cell proliferates to form a monoclonal tumour of identical plasma cells. This results in production of large amounts of identical immunoglobulins and is known as monoclonal gammopathy.
Diseases such as myeloma and primary systemic amyloidosis (AL amyloidosis) account for approximately 1.5% and 0.3% respectively of cancer deaths in the United Kingdom. Multiple myeloma (MM) is the second-most common form of haematological malignancy after non- Hodgkin lymphoma. In Caucasian populations the incidence is approximately 40 per million per year. Conventionally, the diagnosis of MM is based on the presence of excess monoclonal plasma cells in the bone marrow, monoclonal immunoglobulins in the serum or urine and related organ or tissue impairment such as hypercalcaemia, renal insufficiency, anaemia or bone lesions. Normal plasma cell content of the bone marrow is about 1%, while in MM the content is typically greater than 30%, but may be over 90%.
AL amyloidosis is a protein conformation disorder characterised by the accumulation of monoclonal free light chain fragments as amyloid deposits. Typically, these patients present with heart or renal failure but peripheral nerves and other organs may also be involved.
The applicants have previously developed a sensitive assay that can detect the free K light chains and, separately, the free λ light chains (PCT/GB2006/000267). This method uses a polyclonal antibody directed towards either the free K or the free λ light chains. This is discussed in detail in the book by A.R. Bradwell, cited above. The possibility of raising such antibodies was also discussed as one of a number of different possible specificities, in WO97/17372. This form of assay has been found to successfully detect free light chain concentrations. Furthermore, the sensitivity of the technique is very high.
Bradwell A.R., et al. (Clin. & Applied Immunol. Reviews 3 (2002), 17-33) reviews serum free light chain immunoassays and their applications. Historically, urine concentrations of FLC have not been considered to accurately reflect plasma cell synthesis. Hence, there has been a move away from testing urine concentrations to serum-based FLC assays, using techniques such as nephalometry and immunofixation electrophoresis. The paper summarises the understanding in the art of FLC synthesis and metabolism with respect to renal function.
Free K and free λ are cleared by filtration through the kidneys and the rate depends on their molecular size. Monomeric free light chains, characteristically K, are cleared in 2-4 hours at 40% of the glomerular filtration rate. Dimeric free light chains, typically λ, are cleared in 3-6 hours at 20% of the glomerular filtration rate, while large molecules are cleared more slowly. Removal may be prolonged to 2-3 days in MM patients in renal failure, when serum free light chains (sFLCs) are removed by the liver and other tissues (Russo et al. (2002) Am. J. Kidney Dis. 39 899-919). In contrast, IgG has a half-life of 21 days that is not affected by renal impairment.
There are approximately 0.5 million nephrons in each human kidney. Each nephron contains a glomerulus with pores that allow filtration of serum molecules into its proximal tubule. The pore sizes are variable with a restriction in filtration commencing at about 4OkDa and being complete by 6OkDa. Protein molecules that pass the glomerular pores are then either absorbed unchanged or degraded in the proximal tubular cells and excreted as fragments. This is an essential mechanism to prevent loss of proteins and peptides into the urine and is very efficient. The exact pathway of free light chain is unknown but between 10-30g per day can be processed by the kidneys, so, under normal conditions, very little intact light chain passes beyond the proximal tubules.
After filtration by the glomeruli, FLCs enter the proximal tubules and bind to brush-border membranes via low-affinity, high-capacity receptors called cubulins (gp280) (Winearls (2003) "Myeloma Kidney" - Ch. 17 Comprehensive Clinical Nephrology, 2nd Ed. Eds Johnson & Feehally; Pub: Mosby). Binding provokes internalisation of the FLCs and subsequent metabolism. The concentration of the FLCs leaving the proximal tubules, therefore, depends upon the amounts in the glomerular filtrate, competition for binding uptake from other proteins and the absorptive capacity of the tubular cells. A reduction in the glomerular filtration rate increases serum FLC concentrations so that more is filtered by the remaining functioning nephrons. Subsequently and with increasing renal failure, hyperfiltering glomeruli leak albumin and other proteins which compete with FLCs for absorption, thereby causing more to enter the distal tubules.
FLCs entering the distal tubule normally bind to uromucoid (Tamm-Horsfall protein). This is the dominant protein in normal urine and is though to be important in preventing ascending urinary infections. It is a glycoprotein (85kDa) that aggregates into high molecular weight polymers of 20-30 units. Interestingly, it contains a short peptide motif that has a high affinity for FLCs (Ying & Sanders (2001) Am. J. Path. 158 1859-1866). Together, the two proteins form waxy casts that are more characteristically found in acute renal failure associated with light chain MM (LCMM) (see e.g. Winearls (1995) Kidney Int. 48 1347-1361). The casts obstruct tubular fluid flow, leading to disruption of the basement membrane and interstitial damage. Rising concentrations of sFLCs are filtered by the remaining functioning nephrons leading to a vicious cycle of accelerating renal damage with further increases in sFLCs. This may explain why MM patients, without apparent pre-existing renal impairment, suddenly develop catastrophic and irreversible renal injury and renal failure. The process is aggravated by other factors such as dehydration, diuretics, hypercalcaemia, infections and nephrotoxic drugs.
Serum FLC concentrations are abnormal in >95% of patients with MM and have a wide range of concentrations, but their inherent toxicity also varies considerably, as was shown by Sanders & Brooker using isolated rat nephrons (Sanders & Brooker (1992) J. Clin. Invest. 89 630-639). The toxicity is in part related to binding with Tamm-Horsfall protein (see e.g. Winearls (1995) Kidney Int. 48 1347-1361).
In spite of much effort to show otherwise, particular molecular charge and/or K or λ type are not now considered relevant to FLC toxicity. Furthermore, highly polymerised FLCs (a frequent finding in MM) are probably not nephrotoxic because they cannot readily pass through the glomeruli. This may partly account for the lack of renal damage in some patients who have very high sFLC concentrations.
The amount of sFLCs necessary to cause renal impairment was recently studied by Nowrousain et al. (Clin. Cancer Res. (2005) 11 8706-8714), who showed that the median serum concentrations associated with overflow proteinuria (and hence potential for tubular damage) was 113mg/L for K and 278mg/L for λ. These concentrations are approximately 5- to 10-fold above the normal serum concentrations and presumably relate to the maximum tubular reabsorption capacity of the proximal tubules. Since the normal daily production of FLC is ~500mg, increases of ~5g/day are likely to be nephrotoxic in many patients.
There have been several urine studies that have related urine FLC excretion rates to renal impairment. Typically, the associated renal impairment rises with increasing urine FLCs. One study showed that 5%, 17% and 39% of patients had renal impairment with excretion rates of <0.005g/day, 0.005-2g/day and >2g/day, respectively (Blade (2003) "Management of Renal, Hematologic and Infectious Complications" in: Myeloma: Biology and Management, 3rd Ed. Eds Malpas et al; Pub: Saunders). However, FLC excretion is an indicator of renal damage in addition to its cause.
The pre-renal load of FLCs is an important factor in renal toxicity. In an attempt to minimise renal damage, plasma exchange (PE) has been used to reduce the pre-renal load of serum free light chains. Zuchelli et al. (Kidney Int. (1988) 33 1175-1180) compared MM patients on peritoneal dialysis (control group) with plasma exchange (and haemodialysis in some patients). Only 2 of 14 in the control group had improved renal function, compared with 13 of 15 in the plasma exchange arm. Survival was also improved (P<0.01).
These early successes were not repeated in subsequent controlled trials. Johnson et al. (Arch Intern. Med. (1990) 150 863-869) compared 10 patients on forced diuresis with 11 who had additional plasma exchange and found no difference in outcome. Most recently, a large series was reported by Clarke et al. (Haematologica (2005) 90 (si) 117; Kidney Int., March 2006). Half of 97 patients who were on chemotherapy, haemodialysis or a combination of the two were randomly allocated to receive plasma exchange. Again, there was no statistically significant benefit from plasma exchange.
The applicants postulated that removal of serum free light chains by haemodialysis might be a way of reducing renal failure in patients with multiple myeloma (Bradwell et al. (2005) Blood 106 (11) 3482: 972a; 47th Annual Meeting of American Society of Hematology, 10-13 December 2005). The applicants have surprisingly found that a patient having excess serum free light chains can be treated by dialysis, with the result that renal failure is reduced.
Conventional dialysers have a molecular weight cut-off around 15-2OkDa so the filtration efficiency for FLCs is very low. However, some new "protein leaking" dialysers have much larger pores (Ward (2005) J. Am. Soc. Nephrol. 16 2421-2430). These membranes were developed to provide greater clearances of low molecular weight proteins and small protein-
bound solutes than do conventional high-flux dialysis membranes. A routine use for such membranes was not identified, since specific uremic toxins that are removed by protein- leaking membranes but not conventional high-flux membranes had not been identified. It was not clear whether the protein-leaking membranes offered benefits beyond those obtained with conventional high-flux membranes. In intensive care, high cut-off dialysers have been used within clinical studies to eliminate circulating sepsis-associated inflammatory mediators more effectively than with conventional dialysis membranes. Morgera, et al. show a remarkable clearance of interleukin-6 with high cut-off treatments leading to a significant decrease in circulating IL-6 levels in septic patients having acute renal failure (Morgera, et al. Intensive Care Med. (2003), 29: 1989-1995). Furthermore, the treatment lead to a restoration of immuneresponsiveness of blood cells in those patients (Morgera S., et ah, Nephrol. Dial. Transplant (2003), 18: 2570-2576). A study where patients were randomly allocated to high cut-off CVVH or high cut-off CVVHD showed that convection and diffusion did not exhibit the expected difference in terms of clearance of middle-molecular-weight proteins, whereas using diffusion instead of convection significantly reduces the loss of albumin while maintaining good cytokine clearance rates. In CVVHD mode a maximum albumin loss of 950 mg per hour in patients treated with the HCO membrane was reported (Morgera S., et al. Am. J. Kidney Dis. (2004), 43: 444-453). The applicants have now surprisingly found that such membranes can be used to effectively reduce sFLC concentrations.
Assays to measure serum free light chains have previously been laboratory-based assays for diagnosis purposes. The applicants have previously developed an immunoassay for detection of free K and λ light chains. Such assays must be conducted in a laboratory, with samples usually being sent away for analysis, with results not being available for at least several hours and, more typically, days. This has not previously been a problem. There has not previously been a need to have faster results. The applicants have now identified a need for and developed a real-time quantitative assay for detection of serum free light chains, which allows monitoring of the efficacy of dialysis treatment of patients having excess serum free light chains, whilst the dialysis is being carried out.
According to a first aspect of the invention there is provided an assay for the real-time quantitative detection of immunoglobulin free light chain in a sample which is either a subject's blood, dialysate or ultrafiltrate used or produced during haemodialysis,
haemofϊltration or haemodiafiltration of a subject's blood. The sample is assayed for immunoglobulin free light chains.
The term "real-time", as used throughout this specification, indicates that the assay can be carried out in close proximity to the subject such as within a hospital ward or at a bedside and that results from the assay are obtained within 30 minutes, preferably within 15 minutes, more preferably within 10 minutes.
Advantageously, such an assay provides a real-time detection system for free light chains in the sample. This allows a membrane used to remove FLCs from the blood serum of a subject by haemodialysis to be monitored for efficacy, such that, when the membrane becomes at least partially blocked, the resultant reduction in the rate of FLC removal can be detected. The membrane can then be substituted with a fresh membrane or, alternatively, the haemodialysis procedure can be stopped. This also ensures that the subject does not have to tolerate the discomfort and inconvenience of haemodialysis for a longer period than is necessary. In addition, the assay is carried out in close proximity to the subject, rather than having to be carried out in a separate laboratory facility, such that results are obtained quickly, whilst the patient is still undergoing the haemodialysis procedure.
Additionally, where renal failure has been identified as a symptom, it is important to be able to rapidly identify what is contributing to the renal failure. If high levels of free light chains are found then this suggests that dialysis should be urgently carried out to reduce renal damage and improve the chance of restored renal function. A delay in identifying free light chains because of a sample being sent away for analysis or because a laboratory is shut over a weekend or a holiday, can increase the damage to a patient's kidneys. The cause of the free light chains, such as the presence of myeloma may then be determined later.
This may also be used to detect the effect of, for example, chemotherapy, on the production of free light chains by a patient.
Preferably the assay is adapted to remove or lyse or otherwise destroy red blood cells in a blood sample. Red blood cells may interfere with the assay. This may be achieved using techniques generally known in the art. For example, red blood cells may be lysed by using a detergent. Alternatively the assay may comprise a filter to filter out the red blood cells. A
blood sample may be filtered through the filter prior to quantitatively determining an amount of free light chain in the sample. For example, the filtration step may use a filter separate to the part of the assay detecting the free light chains and a blood sample filtered prior to assaying for free light chains. Alternatively the filter may be attached to an assay device, blood being passed directly through the assay before contacting the part of the assay arranged to determine the free light chain concentration.
The subject is preferably a mammal and, most preferably, is a human subject.
Preferably the assay is an immunoassay, such as a nephalometric or turbidometric assay. Such assays preferably use an antiimmunoglobulin free light chain antibody to trap or detect the immunoglobulin free light chains.
Preferably, the assay comprises the steps of: a) exposing to the sample a support surface having at least one primary anti-free light chain antibody adhered thereto; b) exposing the support surface, after step (a) has been completed, to a secondary anti- free light chain antibody; and c) detecting a secondary antibody bound to a free light chain molecule.
The invention also provides real time assay devices for use in the assay according to the invention. Such devices preferably comprise:
(i) a solid support having at least one primary antiimmunoglobulin free light chain antibody adhered thereto;
(ii) a secondary antiimmunoglobulin free light chain antibody; and (iii) a detection label to detect the binding of the secondary antibody to a free light chain molecule.
A filter to trap red blood cells, or means to destroy or lyse such cells, is preferably provided before the solid support, so that a sample is filtered prior to passing to the solid support. The filter, or means to destroy or lyse the cells, may be as described above.
The detection label allows the detection of the binding of the secondary antibody, preferably in a quantitative manner. Such labels are generally known in the art and include dyes, coloured particles such as gold sols or latex particles, enzymes and radio labels.
Preferably the assay or device is an ELISA or device.
There are a number of examples in the art of suitable real time immunoassays which may be adapted to produce the real time assays and devices of the invention for detecting free light chains.
Labmaster Ltd. (Turku, Finland) produce a range of immunoassays based on their LM-CECL technology. This uses a membrane coated with antibodies to trap the analyte (in the current invention this would be K or λ free light chains). The membrane is washed and analyte is detected via a silicon chip. This technology is disclosed, for example, in WO03/087800.
Other quantitative immunoassays may also be used. Quantitative immunoassays are summarised, for example, in "Quantitative Immunoassay: A practical guide for assay establishment, troubleshooting, and clinical application", James T. Wu 2000, ISBN 1890883336, publ. AACC Press.
Indeed, the assay and device may use a lateral flow device of a type generally known in the art for the detection of analytes, such as pregnancy associated hormones (e.g. hCG). Such devices often utilise a dipstick and comprise the reagents for the assay in dehydrated form on a matrix through which the sample travels. Quantitative measurements may be obtained using, for example, luminescent systems with fluorescent conjugates (e.g. Cy5).
The assay preferably comprises a dipstick or other lateral flow device.
Debris from destroyed red blood cells may be eluted from the zone comprising antibodies used to detect the free light chain by the flow of the sample.
In a preferred embodiment, a fluorescent species is conjugated to the secondary anti-free light chain antibody and acts as the label. The fluorescent species may emit light following the
application of an energy source such as an electrical pulse or ultraviolet light. Detection of a free light chain bound to each at least one free light chain antibody may be by detection of light emitted by the fluorescent species. Alternatively the binding of the secondary antibody may be determined using an enzyme, such as horseradish peroxidase (HRP) attached to the secondary antibody. HRP may be used to convert suitable non-coloured substrates, such as TMB, into a coloured detectable product.
As used herein, the term "hemodialysis", HD, refers to a process to correct the chemical composition of blood by removing accumulated metabolic products and adding buffer in a process of diffusion through a natural or synthetic semi-permeable membrane.
As used herein, the term "hemodiafiltration", HDF, refers to a process to remove accumulated metabolic products from blood by a combination of diffusive and convective transport through a semi-permeable membrane of high-flux type; fluid is removed by ultrafiltration and the volume of filtered fluid exceeding the desired weight loss is replaced by sterile, pyrogen-free infusion solution.
As used herein, the term "hemofiltration", HF, refers to a process of filtering blood by a membrane with separation of plasma water and solutes with the ultrafiltrate, and retains all proteins larger than effective pore size and blood cells. In hemofiltration the accumulated metabolic products are removed from the blood by the process of convective transport as a consequence of ultrafiltration through a semi-permeable membrane of high-flux type; the volume of filtered fluid exceeding the desired weight loss is replaced by sterile pyrogen-free infusion solution.
As used herein, the term "ultrafiltrate" refers to the filtered plasma water and solute and molecules (including free light chains) smaller than effective pore size.
The at least one free light chain antibody may be a K free light chain antibody or a λ free light chain antibody.
The support surface may have at least one K free light chain antibody and at least one λ free light chain antibody adhered thereto.
In a preferred embodiment, the detectable element may be a fluorescent species which, more preferably, emits light following the application of an energy source such as an electrical pulse or ultraviolet light. A free light chain bound to each at least one free light chain antibody may be detected by detection of light emitted by the fluorescent species.
Advantageously, such an assay provides a real-time detection system for free light chains in a sample. This allows a dialysis membrane being used during haemodialysis to remove FLCs from the blood serum of a subject to be monitored for efficacy, such that, when the membrane becomes at least partially blocked, the resultant reduction in the rate of FLC removal can be detected. The membrane can then be substituted with a fresh membrane or, alternatively, the haemodialysis procedure can be stopped. This also ensures that the subject does not have to tolerate the discomfort and inconvenience of haemodialysis for a longer period than is necessary.
The assay may also be used to give an early indication of the cause of renal failure or an indication of renal failure itself. The invention therefore provides a method for obtaining an indication of renal failure or the cause of renal failure, comprising:
1. Providing a sample of, for example, blood or urine,
2. Measuring the amount of free light chains in the blood or urine.
The method preferably uses an assay according to the invention. High levels of FLC in the blood or urine give an indication of renal failure or the cause of renal failure.
The assay kits of the invention may also be used to monitor the build-up of FLC due to disease or decrease in FLC due to treatment by, for example, chemotherapy.
The subject is preferably a mammal and, most preferably, is a human subject.
Figure 1 shows proliferative diseases which are associated with antibody producing cells.
Embodiments of the invention will now be shown, by way of example only, with reference to the following Figures 2-6, in which:
Figure 2 shows removal of λ molecules over a 6-hour dialysis period using a Gambro HC 1100 membrane in a patient with acute renal failure from λ light chain myeloma. The arrows indicate when the membrane was changed;
Figure 3 shows efficacy of FLC removal by haemodialysis compared to plasma exchange. These are based on a mathematic model of light chain removal by dialysis using a protein leaking membrane and plasma exchange;
Figure 4 shows that λ molecules are removed more slowly by haemodialysis than K molecules by the mathematical model; A - Baseline (25%/day, K), B - Dialysis (4 hrs, 3/wk, K), C - Dialysis (4 hrs, 3/wk, λ), D - Dialysis (12 hrs/day, K, 2*kd), E - Dialysis (12 hrs/day, λ, 2*kd).
Figure 5 is a comparison of the reduction in sFLC in a patient with K LCMM over a 4-hour haemodialysis period, using Toray BK-P 2.1 dialyser, BBraun HIPcS 1.8 dialyser and Gambro dialyser HCO 1100;
Figure 6 shows the use of dialysis on serum free kappa levels during treatment of MM with dexamethasone.
Figure 7 shows the results for the Kappa (A) and Lambda (B) ELISAs at a coating concentration of 50μg/ml. The mean absorbance minus the substrate blank is plotted for each concentration of antigen/sample tested. Note that concentrations are plotted on a logarithmic scale. Some results gave a slightly negative value after subtracting the substrate blank, in order to be plotted on this scale, these results were given a value of 0.001.
Example 1
In a study of patients with chronic renal failure, the applicants found that, over a 4-hour dialysis period using a high flux polysulphonate membrane, 60% of K and 37% of λ molecules were removed.
Figure 2 shows an example of λ chain removal using Gambro HCO 1100 membranes over a 6 hour period. The arrows indicate the point in time that the membrane was changed. It shows that changing the membrane increases the efficiency of FLC removal as each membrane becomes less efficient over time. This demonstrates the need to monitor the membrane efficiency over time. The Gambro membrane (HCO 1100) is of the type disclosed in WO 2004/056460.
While serum concentrations were much lower than in MM, the results surprisingly indicate that haemodialysis is more efficient for FLC removal than previously thought and more effective than plasma exchange (Figure 3). Model calculations indicated that the prolonged use of "protein leaking" dialysers could reduce K sFLC concentrations to less than 0.5g/L in 2-3 days with -95% of the sFLC removed. Because dimeric λ molecules are considerably larger, they are removed more slowly (Figure 4).
Example 2
Introduction
A significant proportion of patients with multiple myeloma (MM) present with renal impairment, which is associated with a poor prognosis. The major cause of renal impairment in these patients is cast nephropathy resulting from the excess monoclonal serum free light chains (sFLC) overwhelming the kidney tubules reabsorptive capacity. Interest has therefore focused on methods of rapidly removing sFLC, in an attempt to prevent ongoing renal damage. Variable results have been obtained using plasmapheresis for sFLC removal in MM. We hypothesised that haemodialysis (HD) would be more efficient at removing sFLC, particularly the high-flux and the new class of super-flux dialysers that allow the removal of middle-sized molecules. The aim of this study was to investigate the capacity of several commercially available dialysers to remove sFLC in vitro.
Method
The inventors compared: B Braun HiPeSlS, Asahi APS-1050, Nikkiso FLX18GWS, Idemsa 200MHP, Toray Bk21-F, Toray BG2.1U and Gambro HCIlOO dialysers. The efficiency of sFLC removal was determined in vitro by recirculating serum, containing 1000 mg/L of both
monoclonal K and λ light chains; at 400ml/min with trans-membrane pressure (TMP) kept between 300 and 400 mm Hg for haemofϊltration and at 200ml/min with TMP kept below 50mmHg for haemodialysis. The haemofiltration was stopped when production of ultrafϊltrate (UF) fluid ceased and haemodialysis was stopped after 4 hours. The filtered or dialysed serum, UF or dialysate, and saline wash (where appropriate) were analysed for sFLC by Freelite™ nephelometric assays (The Binding Site Ltd, UK).
Results
All dialysers were able to remove sFLC from serum but with differing capacity (Tables 1 and 2). For the haemofiltration experiments, the B Braun dialyser showed the least sFLC clearance (54% and 39% for K and λ respectively) whilst the super-flux Toray BK model had the best clearance for both K and λ (88% and 73% respectively). The super-flux Toray BG model and the high-flux Asahi both cleared 71% of K, but the Asahi was more effective at λ removal (65% compared with 41%) and a significant proportion was removed to the UF (30% of K and 18% of λ). The Nikkiso and Toray dialysers showed high sFLC clearance but with only small quantities in the UF, suggesting that the adsorptive properties of these membranes are responsible for the substantial clearance demonstrated.
In vitro haemodialysis data on 3 of the membranes broadly supported the data obtained from the filtration. Kappa light chains are removed more easily than lambda, with 85%, 82% and 96% kappa removed and 72%, 78% and 94% lambda removed with the B Braun, Toray BK and Gambro dialysis membranes respectively (Figure 5). Again the adsorptive properties of the Toray are apparent since very small quantities of FLC were found in the dialysate fluid in spite of good FLC clearance from serum. Despite having the smallest surface area, the Gambro was the most effective dialyser at clearing both Kappa and Lambda FLC, but unlike the Toray high amounts of FLC were detected in the dialysate fluid, suggesting that the FLC actually pass through the membrane rather than adsorbing to it. The Gambro membrane is made according to WO 2004/056460.
Table 1: Table showing the average percentage sFLC removal during haemofiltration for each dialyser.

Table 2: Table showing the percentage sFLC removal during haemodialysis for each dialvser.

Conclusion
The inventors have demonstrated in vitro the ability of dialysers to effectively clear sFLC.
Example 3
Figure 6 shows a summary of the effect of dialysis on a patient being treated for MM with dexamethasone. The point of dexamethasone treatment is shown by the arrows. A continuous line shows the effect of the dexamethasone on serum IgG. It shows a reduction in IgG levels as the MM is treated with the dexamethasone.
At the time that the patient presented, the patient had acute renal failure. Dialysis was preformed using a Gambro HCO 1100 dialysis membrane and the concentrate of serum free kappa was monitored both before and after dialysis. Dialysis was preformed on each occasion for 2 hours (6/3/06 first dialysis), 6 hours (6/3/06), 8 hours (7/3/06), 6 hours (9/3/06, 11/3/06, 13/3/06, 15/3/06), 2 hours (17/3/06), 2.5 hours (18/3/06), 4 hours (20/3/06), 6 hours (23/3/06), 3.5 hours (24/3/06) and 4 hours (26/3/06, 28/3/06), using a Gambro membrane.
The decrease in serum kappa on each treatment is shown as a line between two points on each day.
The concentration of IgG and free kappa were monitored using laboratory kits available from The Binding Site Ltd., Birmingham, UK. Other assays known in the art may be used instead of the kits.
Further work showed that removal of free light chains could restore renal function in patients if identified early.
Towards the end of the treatment period the patient began to produce urine and no longer required dialysis, showing that dialysis could be used to treat renal failure.
Example 4
To investigate whether Freelite™ antibodies can be used in a capture-based system, K and λ ELISA plates were set up and tested. Freelite antibodies are free K and free λ specific antibodies available from The Binding Site Ltd. This involved coating anti-κ and anti-λ free light chain (FLC) Freelite™ antibodies onto ELISA plates, then adding antigens and clinical samples which either should or should not bind to the antibody. Next, an enzyme-linked secondary antibody (conjugated to peroxidase) specific for each target-antigen and a substrate catalysed by peroxidase to yield a coloured product are applied to the plates. This enables the relative amounts of antigen bound to its antibody to be quantified by reading the absorbance of each well at 450nm.
Method:
Two K and two λ ELISA plates were set up, coating the Freelite™ antibodies directly onto Highbind™ ELISA plates at the following concentrations.
Table 3: Table showing the coating concentrations of Freelite antibodies used. * Lanes 11 and 12 were used as control lanes.

The Freelite™ antibodies used are sheep-anti-human Free Kappa and sheep-anti-human Free Lambda. The antibody concentrations were made by dilution with 0.1 M carbonate buffer (type 188) lOOμl of each concentration was then loaded into the appropriate lanes of the plates. The plates were incubated overnight, refrigerated in a humid container. Lanes 11 and 12 on each plate were used as control lanes, so received just carbonate buffer.
The next day, the ELISA plates were removed from the fridge and the wells were emptied of Freelite™ antibody. The plate wells were then incubated in 125μl of 50% Stabilcoat (JVC Sales & Technical Consultants GmbH, Thomasberg, Germany) for 1 hour at room temperature in a humid container. Since the ELISA plates used are highly protein-philic this step blocks any remaining binding sites for proteins, ensuring that when antigen is added it should only be able to bind specifically to the antibody and not non-specifically to the plate.
After incubation in 50% Stabilcoat, the plates were washed in IxPBS 0.1% Tween 20 wash buffer (type 236) using an ELX Auto Strip Washer (Biotek Instruments, Winooski, Vermont, USA), which washes each well three times.
The antigens and samples tested and the concentrations at which they were applied to Highbind ELISA plates are listed in Table 4.
Table 4: Table listing the type of antigen or sample used and the concentrations at which they were loaded onto the plates. * The concentrations quoted for the normal human serum refer to the approximate concentration of total IgG in that sample. ** The concentrations quoted for myeloma patient serum refer to the concentration of free Lambda in that sample.
Ka a ELISA
0.1 M carbonate buffer was used to make the dilutions. lOOμl of each concentration of the samples/antigens were loaded into the appropriate wells of the plates.
The antigens/samples were applied to the wells and the plates were incubated for one hour at room temperature in a humid container.
After incubation, the plates were washed again in IxPBS 0.1% Tween 20 wash buffer using the ELX Auto Strip Washer.
The next stage was to add the secondary antibody. Affinity purified sheep-anti-human K or λ antibody conjugated to peroxidase were used for the K and λ plates respectively. The secondary antibodies were diluted to 1 in 10000 using conjugate diluent (type 56).
lOOμl of the appropriate secondary antibody solution was added to the wells of each plate. Plates were then incubated at room temperature for one hour in a humid container.
After incubation, the plates were washed again in IxPBS 0.1% Tween 20 wash buffer using the ELX Auto Strip Washer.
The substrate used is TMB solution (Slow Kinetic 1 Component HRP Microwell Substrate). lOOμl of TMB was added to every well on each plate. The plates were incubated for 30 minutes in a humid container in the dark. After 30 minutes, lOOμl of Stop solution (orthophosphoric acid) is added to every well on each plate. The plate was then ready to be analysed.
The plates were put into a plate reader that measures the absorbance of each well at 450nm.
Results:
The absorbance results obtained for Kappa and Lambda demonstrate that both of the Freelite antibodies are able to work effectively in an ELISA-based antigen capture system. Figure 7 shows kappa and lambda ELISAs.
None of the control wells had absorbances significantly higher than the substrate blank for each plate, so no significant absorbance can be attributed to background from any of the antigens/samples or secondary antibodies.
For Kappa the best results were seen with the coating concentrations at 50μg/ml and lOOμg/ml. Coating at lOμg/ml and lμg/ml also gave decent absorbance curves but the difference in absorbance seen between free Kappa at O.lng/ml and lOOng/ml is too small for a reliable ELISA system. Absorbances at a coating concentration of 0. lμg/ml did not yield linear curves suggesting that at this low coating concentration the assay is not sensitive enough to reliably measure free Kappa protein. The absorbances seen with the free Kappa antigen on the two different Kappa plates shows good agreement at all coating concentrations except 0. lμg/ml.
Cross-reaction with IgGl heavy chain or normal human serum is minimal, only becoming apparent at the highest antigen and coating concentrations, but the absorbances measured are still very small so would not be significant in this sort of system.
For Lambda also, the best results can be seen with the coating concentrations at 50μg/ml and lOOμg/ml. Coating at lOμg/ml and Iμg/ml yielded decent absorbance curves but the difference in absorbance seen between free Lambda at O.lng/ml and lOOng/ml is too small for a reliable ELISA system. As with Kappa absorbances, a Lambda coating concentration of O.lμg/ml did not yield linear curves suggesting that at this low coating concentration the assay is not sensitive enough to reliably measure free Lambda protein. The absorbances for free Lambda antigen and myeloma patient serum, on the two different Lambda plates, show good agreement at all coating concentrations. This indicates that this type of system can work reliably and predictably on clinical samples. Assuming the concentration of free Lambda in the clinical sample is unknown; using the free Lambda absorbance curve for a Lambda coating concentration of 50μg/ml yields a result of 18.0 g/L. The same sample analysed using the Freelite nephelometric assay on the Behring BNII analyser gives a Lambda result of 18.9g/L Cross-reaction with IgGl heavy chain is negligible. With IgM heavy chain or normal human serum cross-reaction is detectable but minimal, only becoming apparent at the highest antigen and coating concentrations, but the measured absorbances are very low so would not be significant for this system.
The skilled person will understand that alternative detection methods, to detect K or λ free light chains bound to their respective antibodies, may be used. For example, the secondary antibodies could be labelled and detected using a system such as that outlined in WO03/087800. In this disclosure, molecules are labelled with, for example, isothiocyanate derivatives, for example a derivative of Tb(IH)-I chelate. Molecules with such derivatives bound can be detected by causing the chelate to enter an excited state by applying electrical pulses; as the chelate spontaneously returns to the non-excited state, ultraviolet, visible or infrared light is emitted. This light can be detected and a quantitative measure of the amount of K or λ free light chains bound to their respective antibodies obtained.
Alternatively, the secondary antibody can be labelled with a fluorescent probe, which fluoresces on exposure to, for example, ultraviolet light. Once the sample had been exposed to the primary and secondary antibodies, the sample is further exposed to ultraviolet light.
The resulting fluorescence is detected and a quantitative measure of the amount of K or λ free light chains bound to their respective antibodies obtained.
Claims
1. Assay for the real-time quantitative detection of immunoglobulin free light chain in a sample which is either a subject's blood, a dialysate or ultrafiltrate used or produced during haemodialysis, haemofϊltration or haemodiafiltration of a subject's blood.
2. An assay according to claim 1 comprising filtering to trap or remove red blood cells, or destroying or lysing red blood cells, from a sample of blood.
3. Assay according to claim 1 or claim 2 which is an immunoassay.
4. Assay according to claim 3 which is a nephelometric or turbidometric assay.
5. Assay according to claims 1 to 3 comprising the steps of:
a) exposing to the sample a support surface having at least one primary antiimmunoglobulin free light chain antibody adhered thereto;
b) exposing the support surface, after step (a) has been completed, to a secondary antiimmunoglobulin free light chain antibody; and
c) detecting a secondary antibody bound to a free light chain molecule.
6. Assay according to claim 5 wherein a fluorescent species is conjugated to the secondary anti-free light chain antibody.
7. Assay according to claim 6 wherein the fluorescent species emits light following the application of an energy source.
8. Assay according to claim 7 wherein the fluorescent species emits light following the application of an electrical pulse.
9. Assay according to claim 7 wherein the fluorescent species emits light on exposure to ultraviolet light.
10. Assay according to any of claims 6-9 wherein detection of a free light chain bound to each at least one anti-free light chain antibody is by detection of light emitted by the fluorescent species.
11. An assay device for carrying out an assay according to any one of claims 1 to 10.
12. Assay device according to claim 11 comprising a filter to trap or remove red blood cells or means to destroy or lyse red blood cells from a sample of blood.
13. An assay device according to claim 11 or claim 12, comprising a solid support having:
(i) at least one primary antiimmunoglobulin free light chain antibody adhered thereto;
(ii) a secondary antiimmunoglobulin free light chain antibody; and
(iii) a detection label to detect the binding of the secondary antibody to a free light chain molecule.
14. An assay device according to claim 12 or claim 13, wherein the label is a fluorescent species.
15. A method of monitoring immunoglobulin free light chains to determine the effect of a treatment on the production of free light chains by a patient comprising the use of an assay, device or kit according to any of claims 1 to 14.
16. A method of obtaining an indication of renal failure or a cause of renal failure comprising:
(i) providing a sample of blood or urine; and
(ii) measuring the amount of immunoglobulin free light chains in the blood or urine.
17. A method according to claim 16, wherein the method uses an assay or an assay device according to any one of claims 1 to 14.
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| GB0608446.1 | 2006-04-27 | ||
| GB0608446A GB0608446D0 (en) | 2006-04-27 | 2006-04-27 | Assay |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2007125338A1 true WO2007125338A1 (en) | 2007-11-08 |
Family
ID=36589999
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/GB2007/001551 WO2007125338A1 (en) | 2006-04-27 | 2007-04-27 | Immunoglobulin free light chain assay |
Country Status (2)
| Country | Link |
|---|---|
| GB (1) | GB0608446D0 (en) |
| WO (1) | WO2007125338A1 (en) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2010049672A3 (en) * | 2008-10-28 | 2010-07-15 | The University Of Birmingham | Methods and products for measuring free immunoglobulin light chain molecules |
| GB2472518A (en) * | 2009-08-19 | 2011-02-09 | Binding Site Group Ltd | Free light chain assay kit for determination of likely survival of a subject |
| WO2011107965A1 (en) * | 2010-03-02 | 2011-09-09 | The Binding Site Group Limited | Kidney prognostic assay |
| US10845362B2 (en) | 2010-07-19 | 2020-11-24 | The Binding Site Group Limited | Competition assay |
Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2005249592A (en) * | 2004-03-04 | 2005-09-15 | Yamasa Shoyu Co Ltd | Method for measuring light chain of free human immunoglobrin and kit therefor |
-
2006
- 2006-04-27 GB GB0608446A patent/GB0608446D0/en not_active Ceased
-
2007
- 2007-04-27 WO PCT/GB2007/001551 patent/WO2007125338A1/en active Application Filing
Patent Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2005249592A (en) * | 2004-03-04 | 2005-09-15 | Yamasa Shoyu Co Ltd | Method for measuring light chain of free human immunoglobrin and kit therefor |
Non-Patent Citations (7)
| Title |
|---|
| ABE M ET AL: "Differences in kappa to lambda (kappa:gamma) ratios of serum and urinary free light chains", CLINICAL AND EXPERIMENTAL IMMUNOLOGY, OXFORD, GB, vol. 111, no. 2, February 1998 (1998-02-01), pages 457 - 462, XP002340750, ISSN: 0009-9104 * |
| BRADWELL A R ET AL: "HIGHLY SENSITIVE, AUTOMATED IMMUNOASSAY FOR IMMUNOGLOBULIN FREE LIGHT CHAINS IN SERUM AND URINE", CLINICAL CHEMISTRY, AMERICAN ASSOCIATION FOR CLINICAL CHEMISTRY, WASHINGTON, DC, US, vol. 47, no. 4, April 2001 (2001-04-01), pages 673 - 680, XP008063172, ISSN: 0009-9147 * |
| GMI, INC.: "Dade Behring BN II Nephelometer", January 2005 (2005-01-01), Retrieved from the Internet <URL:http://web.archive.org/web/20060408160803/http://www.gmi-inc.com/Categories/Dade+Behring+Nephelometer.htm> * |
| KATZMANN JERRY A ET AL: "Serum reference intervals and diagnostic ranges for free kappa and free lambda immunoglobulin light chains: Relative sensitivity for detection of monoclonal light chains", CLINICAL CHEMISTRY, AMERICAN ASSOCIATION FOR CLINICAL CHEMISTRY, WASHINGTON, DC, US, vol. 48, no. 9, September 2002 (2002-09-01), pages 1437 - 1444, XP002378160, ISSN: 0009-9147 * |
| KYLE, R.A., ET AL: "Long-Term Survival (10 Years or More) in 30 Patients With Primary Amyloidosis", BLOOD, vol. 93, no. 3, 1999, pages 1062 - 1066, XP002447821 * |
| THE BINDING SITE LIMITED: "Freelite TM Serum Free Light Chain Assay", 8 April 2006 (2006-04-08), XP002447820, Retrieved from the Internet <URL:http://www.bindingsite.co.uk/files/MKG239.pdf> * |
| TILLYER C R ET AL: "IMMUNOTURBIDIMETRIC ASSAY FOR ESTIMATING FREE LIGHT CHAINS OF IMMUNOGLOBULIN IN URINE AND SERUM", JOURNAL OF CLINICAL PATHOLOGY, LONDON, GB, vol. 44, no. 6, 1991, pages 466 - 471, XP008074231, ISSN: 0021-9746 * |
Cited By (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2010049672A3 (en) * | 2008-10-28 | 2010-07-15 | The University Of Birmingham | Methods and products for measuring free immunoglobulin light chain molecules |
| GB2472518A (en) * | 2009-08-19 | 2011-02-09 | Binding Site Group Ltd | Free light chain assay kit for determination of likely survival of a subject |
| GB2472518B (en) * | 2009-08-19 | 2011-11-16 | Binding Site Group Ltd | Survival prognostic assay |
| EP2467724B1 (en) * | 2009-08-19 | 2014-07-23 | The Binding Site Group Limited | Survival prognostic assay |
| EP2799879A3 (en) * | 2009-08-19 | 2015-02-18 | The Binding Site Group Limited | Survival prognostic assay |
| WO2011107965A1 (en) * | 2010-03-02 | 2011-09-09 | The Binding Site Group Limited | Kidney prognostic assay |
| CN102959399A (en) * | 2010-03-02 | 2013-03-06 | 结合点集团有限公司 | Kidney prognostic assay |
| JP2013521490A (en) * | 2010-03-02 | 2013-06-10 | ザ バインディング サイト グループ リミテッド | Kidney prognostic assay |
| US10845362B2 (en) | 2010-07-19 | 2020-11-24 | The Binding Site Group Limited | Competition assay |
Also Published As
| Publication number | Publication date |
|---|---|
| GB0608446D0 (en) | 2006-06-07 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US7875183B2 (en) | Method of removing antibody free light chains from blood | |
| Kabanda et al. | Determinants of the serum concentrations of low molecular weight proteins in patients on maintenance hemodialysis | |
| Nakayama et al. | Immunohistochemical detection of advanced glycosylation end-products in the peritoneum and its possible pathophysiological role in CAPD | |
| KR101939964B1 (en) | Methods, devices and kits for detecting or monitoring acute kidney injury | |
| TR201807542T4 (en) | Methods and compositions for the diagnosis and prognosis of renal injury and renal failure. | |
| CN113176411B (en) | Biomarker for detecting novel coronavirus infection by saliva and application thereof | |
| US20110160636A1 (en) | Device and method for inhibiting complement activation | |
| JPWO2010126055A1 (en) | Use of urinary megalin as a marker for detection of kidney damage | |
| JP3579549B2 (en) | Use as a marker for diabetes or diabetic complications | |
| Bakoush et al. | Urine excretion of protein HC in proteinuric glomerular diseases correlates to urine IgG but not to albuminuria | |
| WO2007125338A1 (en) | Immunoglobulin free light chain assay | |
| Kurki et al. | Transformation of membranous glomerulonephritis into crescentic glomerulonephritis with glomerular basement membrane antibodies: serial determinations of anti-GBM before the transformation | |
| Nakada et al. | Blood purification for hypercytokinemia | |
| Bakoush et al. | Renal function in proteinuric glomerular diseases correlates to the changes in urine IgM excretion but not to the changes in the degree of albuminuria | |
| TW202016547A (en) | Protein biomarkers for nephropathy and applications thereof | |
| Mistry et al. | Non enzymatic glycosylation of IgG and their urinary excretion in patients with diabetic nephropathy | |
| US20230173155A1 (en) | Dialysis system for treating sepsis | |
| JP6033889B2 (en) | How to determine renal function | |
| CN116802500A (en) | Methods and compositions for treating kidney injury and renal failure | |
| Lindström | Low molecular mass proteins as markers for renal function and dialysis efficiency | |
| RU2276366C1 (en) | Method for diagnosing endogenous intoxication syndrome gravity degree in chronic renal insufficiency patients | |
| JPH02293665A (en) | Method for inspecting renal disease | |
| RU2612092C1 (en) | Method for diagnostics of diabetes mellitus by level of methylglyoxal-modified low-density lipoproteids with application of monoclonal antibodies | |
| JPH05322888A (en) | Method and kit for determining free hemoglobin | |
| Papadimitriou et al. | Abstracts of The Japanese Journal of Nephrology |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 07732587 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 07732587 Country of ref document: EP Kind code of ref document: A1 |