RU2611398C1 - Method of increasing the efficiency of treatment of patients with tuberculosis - Google Patents
Method of increasing the efficiency of treatment of patients with tuberculosis Download PDFInfo
- Publication number
- RU2611398C1 RU2611398C1 RU2015135174A RU2015135174A RU2611398C1 RU 2611398 C1 RU2611398 C1 RU 2611398C1 RU 2015135174 A RU2015135174 A RU 2015135174A RU 2015135174 A RU2015135174 A RU 2015135174A RU 2611398 C1 RU2611398 C1 RU 2611398C1
- Authority
- RU
- Russia
- Prior art keywords
- treatment
- adherence
- points
- medication adherence
- stens
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/435—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with one nitrogen as the only ring hetero atom
- A61K31/47—Quinolines; Isoquinolines
- A61K31/473—Quinolines; Isoquinolines ortho- or peri-condensed with carbocyclic ring systems, e.g. acridines, phenanthridines
Abstract
Description
Изобретение относится к медицине, а именно к фтизиатрии, и может быть использовано для повышения эффективности лечения больного туберкулезом.The invention relates to medicine, namely to TB, and can be used to increase the effectiveness of the treatment of a patient with tuberculosis.
Соблюдение принципа отечественной медицины лечить больного, а не болезнь, отражает объективно существующую связь между психоэмоциональным статусом больного и его заболеванием. В эпоху химиотерапии при лечении больных туберкулезом главное внимание уделяется медикаментозным методам, личностные же и индивидуальные психоэмоциональные факторы в построении стратегии лечения и реабилитации учитываются существенно в меньшей степени. В единичных исследованиях установлена связь между состоянием психоэмоциональной сферы больного туберкулезом и течением заболевания [Стрельцов В.А., Баранова В.Г., Столбун Ю.В. Необходимость оценки психологического статуса больных туберкулезом легких // Туберкулез и болезни легких. 2011. - №5. - С. 176-177; Филиппова Т.П. Патогенетически направленная коррекция адаптационных реакций организма в лечении впервые выявленных больных с вторичными формами туберкулеза легких. Автореф. дис. доктор. - М. - 2008. 28 с.]. Между тем специфическая антибактериальная терапия не всегда является залогом успеха в лечении больных туберкулезом [Шилова М.В. Организация противотуберкулезной помощи в России и пути модернизации организационно-методического управления диспансерным наблюдением больных туберкулезом в современных эпидемических и социально-экономических условиях // Туберкулез и болезни легких. - 2011. - №5. - С. 236-237]. Низкую эффективность лечения трудно объяснить только формированием лекарственной устойчивости возбудителя или неправильной терапией. Значительное влияние при этом имеет нарушение больными режима лечения вследствие отсутствия у них приверженности лечению. Истинные причины низкой приверженности остаются нераспознанными и нередко опровергают современные терапевтические методики. В частности остаются неясными психологические мотивы отказа больных от лечения.Compliance with the principle of domestic medicine to treat a patient, and not a disease, reflects the objectively existing relationship between the psycho-emotional status of the patient and his disease. In the era of chemotherapy in the treatment of tuberculosis patients, the main attention is paid to medical methods, while personal and individual psychoemotional factors are taken into account to a lesser extent in the construction of a treatment and rehabilitation strategy. In single studies, a relationship has been established between the state of the psycho-emotional sphere of a patient with tuberculosis and the course of the disease [Streltsov V.A., Baranova V.G., Stolbun Yu.V. The need to assess the psychological status of patients with pulmonary tuberculosis // Tuberculosis and lung disease. 2011. - No. 5. - S. 176-177; Filippova T.P. Pathogenetically directed correction of the body's adaptive reactions in the treatment of newly diagnosed patients with secondary forms of pulmonary tuberculosis. Abstract. dis. doctor. - M. - 2008.28 p.]. Meanwhile, specific antibiotic therapy is not always the key to success in the treatment of tuberculosis patients [Shilova M.V. The organization of tuberculosis care in Russia and ways of modernizing the organizational and methodological management of dispensary observation of tuberculosis patients in modern epidemic and socio-economic conditions // Tuberculosis and lung diseases. - 2011. - No. 5. - S. 236-237]. The low effectiveness of the treatment is difficult to explain only by the formation of drug resistance of the pathogen or improper therapy. In this case, a violation of the treatment regimen due to their lack of adherence has a significant effect. The true causes of low adherence remain unrecognized and often refute modern therapeutic techniques. In particular, the psychological motives of patients refusing treatment remain unclear.
Приверженность лечению или степень соответствия между поведением пациента и рекомендациями рассматривается очень часто в современной медицине как проблема комплаенса (от англ. patient compliance) и является одним из основных принципов лечения в настоящее время. Многие больные туберкулезом не всегда выполняют непонятные им рекомендации на протяжении длительного времени, что ведет к нарушению режимов лечения, и тем самым, снижению его эффективности [Богородская Е.М., Смердин С.В., Стерликов С.А. Организационные аспекты лечения больных туберкулезом в современных социально-экономических условиях. - М.: Нью-Терра. - 2011. - 216 с.]. На формирование приверженности лечению оказывают влияние факторы, связанные с психологическими особенностями личности больного, клинической картиной заболевания (форма, длительность осложнения, рецидивы заболевания), характером отношений с родными и близкими, результатами лечения, уровнем компетентности медицинского персонала и организации оказания медицинской помощи. Известно, что при повышении приверженности эффективность лечения больных возрастает на 30-40% [Кравченко С.С. Проблема повышения комплаентности пациентов во фтизиатрии, 20.01.11. URL: www.spellsystems.ru].Adherence to treatment or the degree of correspondence between patient behavior and recommendations is often considered in modern medicine as a compliance problem (from the English. Patient compliance) and is one of the basic principles of treatment at present. Many patients with tuberculosis do not always comply with incomprehensible recommendations for a long time, which leads to a disruption in treatment regimens, and thereby to a decrease in its effectiveness [Bogorodskaya EM, Smerdin SV, Sterlikov SA Organizational aspects of the treatment of tuberculosis patients in modern socio-economic conditions. - M .: New Terra. - 2011. - 216 p.]. The formation of adherence to treatment is influenced by factors related to the psychological characteristics of the patient’s personality, the clinical picture of the disease (form, duration of the complication, relapse of the disease), the nature of relations with relatives and friends, the results of treatment, the level of competence of medical personnel and the organization of medical care. It is known that with increasing commitment, the effectiveness of treatment of patients increases by 30-40% [S. Kravchenko The problem of increasing patient compliance in phthisiology, 01/20/11. URL: www.spellsystems.ru].
В связи с этим является актуальным внедрение во фтизиатрическую практику методов коррекции режима химиотерапии с учетом состояния приверженности больного лечению с целью повышения сотрудничества с медицинским персоналом, что в конечном итоге усиливает контроль лечения и повышает эффективность реабилитации.In this regard, the introduction of chemotherapy regimen correction methods into the phthisiatric practice, taking into account the patient’s adherence to treatment with the aim of increasing cooperation with medical personnel, which ultimately strengthens treatment control and increases the effectiveness of rehabilitation, is relevant.
Известны методы определения комплаенса, такие как метод рибофлавинового маркера, когда к исследуемому препарату и к плацебо добавляли рибофлавин и проводили экспресс-контроль его содержания в моче и тем самым осуществляли контроль приема назначенных препаратов [Крупицкий Е.М., Борцов А.В. Применение принципов доказательной медицины при проведении клинических исследований в наркологии // Обозрение психиатр. и мед. психол. 2005; 2 (1)]. У больных шизофренией использовали шкалу установки на лечение DAI (Disease Attitude Inventory) [Hogan T et al. A self-report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity // Psychol. Med. - 1983. - №13. - P. 177-183].Known methods for determining compliance, such as the riboflavin marker method, when riboflavin was added to the test drug and placebo and express control of its content in the urine was performed, and thus, the administration of prescribed drugs was monitored [Krupitsky EM, Bortsov A.V. Application of the principles of evidence-based medicine in conducting clinical trials in narcology // Review of a psychiatrist. and honey. psychol. 2005; 2 (1)]. In patients with schizophrenia, a DAI (Disease Attitude Inventory) treatment scale was used [Hogan T et al. A self-report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity // Psychol. Med. - 1983. - No. 13. - P. 177-183].
За прототип взят способ повышения эффективности лечения в зависимости от уровня и методов информационно-образовательной работы среди больных туберкулезом [Пьянзова Т.В. Влияние информационно-образовательной работы с впервые выявленными больными туберкулезом на эффективность лечения // Туберкулез и болезни легких. - 2009. - №10. - С. 32-36]. Исследовали психологический статус стандартизированным методом исследования личности (СМОЛ) [Зайцев В.П., 1981], представляющий собой модификацию Миннесотского многоаспектного личностного опросника (ММР1) [Собчик Л.Н., 2001] и выявляли усредненный профиль по Уэлшу, затем по специальной системе определяли уровень потенциала преодоления болезни у больных впервые выявленным туберкулезом легких. В зависимости от уровня потенциала выявляли лиц с высокой и низкой приверженностью лечению еще до начала химиотерапии и с целью повышения эффективности лечения применяли систему информационно-образовательного воздействия.The prototype is a way to increase the effectiveness of treatment, depending on the level and methods of information and educational work among patients with tuberculosis [Pyanzova T.V. The effect of information and educational work with newly diagnosed patients with tuberculosis on the effectiveness of treatment // Tuberculosis and pulmonary diseases. - 2009. - No. 10. - S. 32-36]. The psychological status was examined using the standardized personality research method (SMOL) [Zaitsev VP, 1981], which is a modification of the Minnesota multi-aspect personality questionnaire (MMP1) [Sobchik LN, 2001] and the average profile was determined according to Welch, then using a special system we determined the level of overcoming the disease in patients with newly diagnosed pulmonary tuberculosis. Depending on the level of potential, individuals with high and low adherence to treatment were identified even before the start of chemotherapy and in order to increase the effectiveness of treatment, an information-educational impact system was used.
Недостатком известного способа является то, что, во-первых, известный способ технически сложный, содержит сложные вопросы, ответы на которые требуют достаточно высокого уровня интеллекта, отсутствующего у большинства обездоленных, социально-дезадаптированных больных туберкулезом.The disadvantage of this method is that, firstly, the known method is technically complex, contains complex questions, the answers to which require a sufficiently high level of intelligence, which is absent in most disadvantaged, socially maladaptive patients with tuberculosis.
Во-вторых, способ рекомендован и апробирован только для больных впервые выявленным туберкулезом легких.Secondly, the method is recommended and tested only for patients with newly diagnosed pulmonary tuberculosis.
В-третьих, известный способ предусматривает применение для повышения эффективности лечения путем повышения приверженности только систему информационно-образовательного воздействия.Thirdly, the known method provides for the application to increase the effectiveness of treatment by increasing adherence to only the information-educational impact system.
Техническим результатом изобретения является повышение эффективности лечения больных туберкулезом, за счет определения степени приверженности больного лечению с целью дальнейшей коррекции лечения.The technical result of the invention is to increase the effectiveness of treatment of patients with tuberculosis by determining the degree of adherence to treatment with the aim of further correction of treatment.
Технический результат достигается тем, что определяют степень приверженности больного лечению, путем его анкетирования, которое проводят в начале основного курса лечения, путем определения стена, прогнозируют состояние приверженности и при неблагоприятном прогнозе проводят коррекцию режима химиотерапии путем изменения методов введения этиотропных препаратов с назначением преимущественно парентерального и ингаляционного способа, назначения иммуномодулятора Циклоферон и методов психотерапевтического воздействия.The technical result is achieved by determining the degree of adherence of the patient to the treatment, by questioning it, which is carried out at the beginning of the main course of treatment, by determining the wall, predicting the state of adherence and, if the prognosis is poor, adjusting the chemotherapy regimen by changing the methods of administering etiotropic drugs with mainly parenteral and inhalation method, the appointment of the immunomodulator Cycloferon and methods of psychotherapeutic effects.
В начале основного курса химиотерапии проводится определение степени приверженности лечению путем использования тест-анкеты из 80 вопросов, подсчета баллов по положительным ответам из указанных 35 и по отрицательным ответам из 30 указанных вопросов, перевода суммы «сырых» баллов в стены с последующим прогнозированием состояния приверженности больного. При неблагоприятном прогнозе проводится коррекция режима химиотерапии путем изменения методов введения этиотропных препаратов с назначением преимущественно парентерального и ингаляционного способа с целью усиления контроля лечения и повышения мотивации пациента, назначения иммуномодулятора Циклоферон и методов психотерапевтического воздействия.At the beginning of the main chemotherapy course, the degree of adherence to treatment is determined by using a test questionnaire of 80 questions, scoring for positive answers from the indicated 35 and negative answers from 30 of the indicated questions, transferring the amount of “raw” points to the walls, followed by predicting the patient’s adherence . In case of an unfavorable prognosis, the chemotherapy regimen is corrected by changing the methods of administering etiotropic drugs with the appointment of the predominantly parenteral and inhalation methods in order to strengthen the control of treatment and increase patient motivation, the appointment of the Cycloferon immunomodulator and methods of psychotherapeutic intervention.
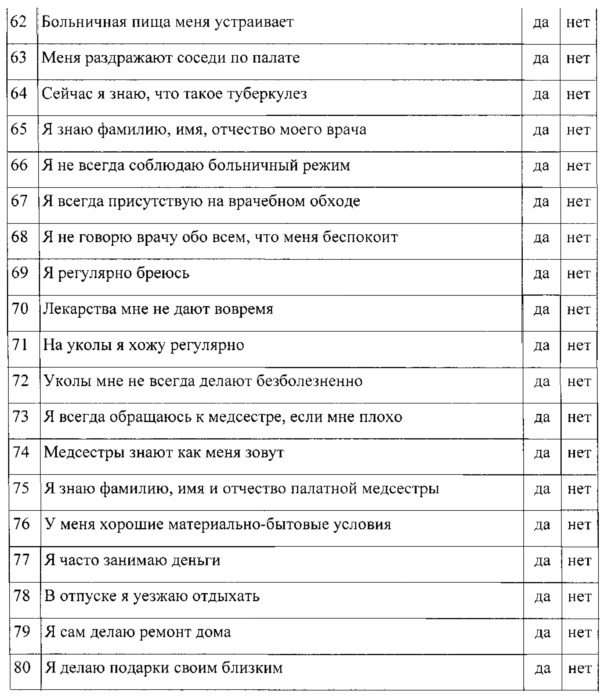
Изначально проводится опрос по разработанной анкете (Приложение 1), которая составлена таким образом, чтобы выявить не только объективные факторы, мешающие лечению, например, побочное действие лекарств, или не сложившийся профессиональный контакт с медперсоналом, но и дать оценку субъективным факторам, которые препятствуют лечению, таким как стресс, фрустрация, стигматизация, внушаемость, пристрастие к алкоголю. Анкета содержит 80 вопросов, предназначена для самостоятельного заполнения больными при их добровольном согласии на тестирование. Вначале анкеты в кратком вступлении больной вводится в ситуацию опроса и стимулируется его интерес к общению. Вопросы простые и доступные по смыслу и технике заполнения. К середине опроса вместе с активизацией внимания и интереса респондентов увеличивается сложность и острота вопросов, используются психологические приемы, активизирующие внимание больного.Initially, a survey is conducted on the developed questionnaire (Appendix 1), which is designed in such a way as to identify not only objective factors that interfere with treatment, for example, side effects of drugs, or unstable professional contact with medical staff, but also evaluate subjective factors that interfere with treatment such as stress, frustration, stigmatization, suggestibility, addiction to alcohol. The questionnaire contains 80 questions, intended for self-completion by patients with their voluntary consent to testing. At the beginning of the questionnaire, in a brief introduction, the patient is introduced into the survey situation and his interest in communication is stimulated. Questions are simple and accessible in meaning and filling technique. By the middle of the survey, along with increased attention and interest of respondents, the complexity and severity of the questions increases, psychological techniques that activate the patient's attention are used.
Язык анкеты свободен от частых клише, газетных штампов, стереотипных оборотов, приближен к разговорной речи больных туберкулезом, учитывает преобладание социально-дезадаптированных лиц и оперирует ситуациями, достаточно близкими и понятными респондентам. Респондент не решает в ходе анкетирования сложных задач, отнимающих у него много времени, поэтому количество вопросов ограничено - 80, а ответы на них требуют не более 20-25 минут.The language of the questionnaire is free from frequent cliches, newspaper cliches, stereotypical turns, is close to colloquial speech of patients with tuberculosis, takes into account the predominance of socially maladaptive persons and operates with situations that are quite close and understandable to respondents. During the questionnaire, the respondent does not solve complex tasks that take up a lot of his time, therefore the number of questions is limited to 80, and the answers to them require no more than 20-25 minutes.
При оценке результатов опроса изначально анализируется искренность, или достоверность ответов респондентов, их установка на сотрудничество с медицинским персоналом. 15 вопросов анкеты составляют шкалу искренности пациентов и в случае набора 10 и более баллов по этой шкале результаты не учитываются и с больным проводятся отдельные беседы-тренинги. В остальных случаях далее определяется степень приверженности лечению, включающая 35 вопросов анкеты с положительными и 30 вопросов с отрицательными ответами, составляющие «сырые» баллы, по которым выделяют стены. При сумме от 35 и выше баллов - 1 и 2 стены, отмечается неудовлетворительная приверженность лечению; склонность к частым нарушениям больничного режима, отсутствие эффекта лечения, частые рецидивы и обострения. При сумме 16-34 баллов - 3-5 стены, отмечается удовлетворительная приверженность лечению; в экстремальных ситуациях умеренные нарушения больничного режима, плохие результаты терапии, редкие рецидивы и обострения. При сумме 4-15 баллов - 6-8 стены, определяется хорошая приверженность лечению; возможны единичные кратковременные нарушения больничного режима в экстремальных ситуациях, низкая вероятность рецидивов и обострений. При сумме до 3 баллов - 9-10 стены, отмечается высокая приверженность к лечению; низкая вероятность нарушений больничного режима, высокая эффективность лечения.When evaluating the results of the survey, the sincerity, or reliability of the answers of the respondents, their installation for cooperation with medical personnel is initially analyzed. 15 questions on the questionnaire constitute a scale of patient sincerity, and if 10 or more points are scored on this scale, the results are not taken into account and separate training sessions are held with the patient. In other cases, the degree of adherence to treatment is further determined, which includes 35 questions of the questionnaire with positive and 30 questions with negative answers, which make up the "raw" points for which the walls are highlighted. With an amount of 35 or more points - 1 and 2 walls, an unsatisfactory adherence to treatment is noted; tendency to frequent violations of the hospital regimen, lack of treatment effect, frequent relapses and exacerbations. With the sum of 16-34 points - 3-5 walls, a satisfactory adherence to treatment is noted; in extreme situations, moderate violations of the hospital regime, poor therapy results, rare relapses and exacerbations. With a sum of 4-15 points - 6-8 walls, a good adherence to treatment is determined; single short-term violations of the hospital regime in extreme situations, low probability of relapse and exacerbations are possible. With a sum of up to 3 points - 9-10 walls, there is a high commitment to treatment; low probability of violations of the hospital regime, high treatment efficiency.
Следующим этапом является диагностика факторов: стресс, фрустрация, внушаемость, пристрастие к алкоголю, социально-психологический статус, побочные реакции на лечение, отсутствие эффекта лечения, не сложившиеся взаимоотношения с мед. персоналом и экономическое неблагополучие. Для определения данных факторов выделены 10 шкал вопросов с положительными или отрицательными ответами.The next stage is the diagnosis of factors: stress, frustration, suggestibility, addiction to alcohol, socio-psychological status, adverse reactions to treatment, the lack of treatment effect, not established relationship with honey. staff and economic distress. To determine these factors, 10 scales of questions with positive or negative answers are highlighted.
В процессе анкетирования и последующих бесед реализуется «сценарий», представляющий собой своеобразный психофизиологический тренинг больного. Известно, что согласно закону апперцепции, понимание испытуемым вопросов происходит опосредованно, путем пропускания их сквозь призму личного опыта, вызывающего индивидуальные ответные реакции и их дифференциальные различия, учитывается влияние социокультурного фактора и социально-психологические особенности пациента. Таким образом, отношение больного к себе и своему лечению может изменяться, что влияет на степень его приверженности.In the process of questioning and subsequent conversations, a “scenario” is realized, which is a kind of psychophysiological training of the patient. It is known that, according to the law of apperception, subjects' understanding of issues occurs indirectly, by passing them through the prism of personal experience that causes individual responses and their differential differences, the influence of the sociocultural factor and socio-psychological characteristics of the patient are taken into account. Thus, the patient’s attitude to himself and his treatment can change, which affects the degree of his adherence.
На заключительном этапе определяется прогноз приверженности лечению с учетом стенов. При неблагоприятном прогнозе (1-5 стен) проводится коррекция режима химиотерапии путем изменения методов введения этиотропных препаратов с назначением преимущественно парентерального и ингаляционного способа с целью усиления контроля лечения и повышения мотивации пациента, назначения иммуномодулятора Циклоферон и методов психотерапевтического воздействия.At the final stage, the prognosis of treatment adherence to the walls is determined. In case of an unfavorable prognosis (walls 1-5), the chemotherapy regimen is corrected by changing the methods of administering etiotropic drugs with the appointment of a predominantly parenteral and inhalation method in order to strengthen the control of treatment and increase patient motivation, the appointment of Cycloferon immunomodulator and methods of psychotherapeutic effects.
Примеры клинического использования.Examples of clinical use.
Пример 1. Мужчина 24 лет, студент, поступил в клинику с впервые выявленным инфильтративным туберкулезом в нижней доле левого легкого в фазе распада, МБТ+. После установления диагноза и назначения лечения выполнена оценка степени приверженности лечению согласно предлагаемой методике, которая оказалась в пределах 20 баллов - 5 стен. Установлена удовлетворительная приверженность и прогнозированы в экстремальных ситуациях умеренные нарушений больничного режима, плохие результаты терапии. Дальнейший анализ анкеты показал, что на снижение приверженности лечению влияют такие факторы как фрустрация и легкая внушаемость: 5 и 6 баллов соответственно. С целью психологической и медикаментозной коррекции проведены беседы, назначены седативные средства, инъекционное введение основных противотуберкулезных препаратов: изониазида и рифампицина и курс иммуномодулирующей терапии препаратом циклоферон. Повторная оценка степени приверженности лечению через 6 недель показала результаты в пределах 9 баллов - 7 стен и был установлен благоприятный прогноз с возможными единичными и кратковременными нарушениями больничного режима в экстремальных ситуациях и низкой вероятностью рецидивов и обострений. Неблагоприятные факторы приверженности больного лечению обнаружены по шкалам фрустрации и социально-экономического положения. В беседах выяснено, что студент боится быть «отчисленным» и потеряет год, что неблагоприятно скажется на экономическом положении его семьи. Беседа с родителями позволила уменьшить действие этих неблагоприятных факторов. К моменту окончания интенсивной фазы лечения зарубцевалась полость распада и прекратилось бактериовыделение. Больной выписан для продолжения лечения в амбулаторных условиях. Санаторное лечение перенесено на летний период.Example 1. A man of 24 years old, a student, was admitted to the clinic with the first detected infiltrative tuberculosis in the lower lobe of the left lung in the decay phase, MBT +. After establishing a diagnosis and prescribing treatment, an assessment was made of the degree of adherence to treatment according to the proposed methodology, which turned out to be within 20 points - 5 walls. Satisfactory adherence was established and moderate conditions of a hospital regimen and poor therapy results were predicted in extreme situations. Further analysis of the questionnaire showed that factors such as frustration and easy suggestibility influence the decrease in adherence to treatment: 5 and 6 points, respectively. For the purpose of psychological and medical correction, discussions were held, sedatives were prescribed, injection of the main anti-TB drugs: isoniazid and rifampicin and a course of immunomodulating therapy with cycloferon. A repeated assessment of the degree of adherence to treatment after 6 weeks showed results within 9 points - 7 walls and a favorable prognosis was established with possible single and short-term violations of the hospital regime in extreme situations and a low probability of relapse and exacerbations. Adverse factors of patient adherence to treatment were found on the scales of frustration and socio-economic status. In the conversations it was found out that the student is afraid of being “expelled” and will lose a year, which will adversely affect the economic situation of his family. A conversation with parents made it possible to reduce the effects of these adverse factors. By the end of the intensive phase of treatment, the decay cavity had healed and bacterial excretion stopped. The patient was discharged to continue treatment on an outpatient basis. Sanatorium treatment was postponed to the summer period.
Пример 2. Мужчина, 45 лет, поступил в стационар с диагнозом: Диссеминированный туберкулез легких, фаза инфильтрации и распада, МБТ+. Ранее неоднократно лечился по поводу туберкулеза, однако ввиду пристрастия к алкоголю прерывал курсы химиотерапии. При поступлении проведена оценка степени приверженности лечению, согласно разработанной методике (37 баллов - 2 стен). Установлен неблагоприятный прогноз. Анализ анкеты показал, что на снижение приверженности влияют такие факторы как фрустрация и пристрастие к алкоголю: 7 и 8 баллов соответственно. С целью повышения эффективности лечения в режиме 2Б осуществлялось инъекционное введение рифампицина, курс санационных бронхоскопий с эндобронхиальным введением изониазида и капреомицина, курс иммуномодулирующей терапии препаратом циклоферон и проведены беседы психотерапевтической направленности с привлечением психолога и нарколога. Повторная оценка приверженности лечению через 6 недель показала результаты: сумма «сырых» баллов 13-6 стен и изменен прогноз. При обследовании отмечается положительная динамика в виде частичного рассасывания очагов и уменьшения компонента инфильтрации, уменьшение размеров полости распада. Больной выписан с положительным результатом через 6 месяцев после прекращения бактериовыделения и рубцевания полости.Example 2. A man, 45 years old, was admitted to the hospital with a diagnosis of Disseminated pulmonary tuberculosis, phase of infiltration and decay, MBT +. Previously, he was repeatedly treated for tuberculosis, however, due to addiction to alcohol, he interrupted chemotherapy courses. Upon admission, an assessment of the degree of adherence to treatment was carried out according to the developed technique (37 points - 2 walls). An unfavorable prognosis has been established. The analysis of the questionnaire showed that such factors as frustration and addiction to alcohol influence the decrease in adherence: 7 and 8 points, respectively. In order to increase the effectiveness of treatment in regimen 2B, rifampicin was injected, a course of debridement bronchoscopy with endobronchial administration of isoniazid and capreomycin was administered, a course of immunomodulating therapy with cycloferon was conducted, and psychotherapeutic discussions were conducted with the participation of a psychologist and narcologist. A reassessment of treatment adherence after 6 weeks showed results: the sum of the “raw” points of 13-6 walls and the prognosis changed. During the examination, there is a positive dynamics in the form of partial resorption of foci and a decrease in the component of infiltration, a decrease in the size of the decay cavity. The patient was discharged with a positive result 6 months after the cessation of bacterial excretion and scarring of the cavity.
Таким образом, диагностика степени и прогноза приверженности лечению позволят своевременно назначить необходимую корригирующую медикаментозную и психотерапию, сократить длительность лечения и повысить его эффективность. Это уменьшит сроки рубцевания мелких каверн, а значит и сроки пребывания больных в стационере, предупредит образование кавернозных форм туберкулеза легких и улучшит эпидемиологическую ситуацию в регионе.Thus, the diagnosis of the degree and prognosis of adherence to treatment will allow timely prescribing of the necessary corrective medication and psychotherapy, reduce the duration of treatment and increase its effectiveness. This will reduce the time of scarring of small caverns, and hence the duration of patients in the hospital, prevent the formation of cavernous forms of pulmonary tuberculosis and improve the epidemiological situation in the region.
Приложение 1Annex 1



Оценка приверженности по шкаламScale adherence rating
80 пунктов опросника сгруппированы в десять шкал: стресс, фрустрация, стигматизация, внушаемость, пристрастие к алкоголю, социально-психологический статус, побочные реакции на лечение, отсутствие эффекта лечения, взаимоотношения с медперсоналом, экономическое неблагополучие. Показатели каждой шкалы варьируют между 0 и 10, где 0 представляет высокий комплаенс по данной шкале. Все шкалы формируют два показателя: субъективные и объективные факторы, влияющие на комплаенс.80 points of the questionnaire are grouped into ten scales: stress, frustration, stigmatization, suggestibility, addiction to alcohol, socio-psychological status, adverse reactions to treatment, lack of treatment effect, relationships with medical staff, economic distress. The performance of each scale varies between 0 and 10, where 0 represents high compliance on this scale. All scales form two indicators: subjective and objective factors affecting compliance.
Результаты представляются в виде оценок в баллах по каждой из 10 шкал, составленных таким образом, что более высокая оценка указывает на более низкий уровень комплаенса. Количественно оцениваются следующие показатели:The results are presented as scores on each of 10 scales, designed in such a way that a higher score indicates a lower level of compliance. The following indicators are quantified:
1. Стресс, неадекватная адаптация пациентов, обусловленная индивидуально-типовыми различиями, ведет к изменениям психофизиологических показателей и самооценок, объективно отражающих их общее психическое состояние в новых условиях противотуберкулезного стационара, ограничивает выполнение ими врачебных назначений (уклонение от приема препаратов, нарушения режима, упор на нетрадиционные методы лечения, злоупотребление алкоголем), затрудняет процесс излечения и ухудшает здоровье.1. Stress, inadequate adaptation of patients due to individual type differences, leads to changes in psychophysiological indicators and self-esteem, objectively reflecting their general mental state in the new conditions of the TB hospital, restricts their medical appointments (avoidance of taking drugs, violation of the regime, focus on non-traditional methods of treatment, alcohol abuse), complicates the healing process and worsens health.
2. Фрустрация возникает у больных в стационаре и проявляется в ряде, таких эмоциональных процессов, как разочарование, тревога, раздражение, отчаяние при отсутствии быстрого наступления положительного эффекта лечения, и, хотя в состоянии фрустрации могут продолжать борьбу за получение желаемого, но, если они не знают точно, что нужно сделать для достижения успеха, фрустрация может переходить в агрессию, направленную внутрь или вовне организма.2. Frustration occurs in patients in the hospital and manifests itself in a number of emotional processes such as disappointment, anxiety, irritation, despair in the absence of a rapid onset of the positive effect of treatment, and although in a state of frustration they can continue the struggle to get what they want, but if they they don’t know exactly what needs to be done to succeed, frustration can turn into aggression directed inside or outside the body.
3. Стигматизация - это процесс выделения больных туберкулезом среди других индивидов на основании их эпидемиологической опасности и дискриминация по отношению к ним, нарушающая привычные социальные связи, дружеские и семейные взаимоотношения, которые могут стать стойким препятствием на пути излечения таких пациентов.3. Stigmatization is the process of distinguishing tuberculosis patients from other individuals on the basis of their epidemiological danger and discrimination against them, violating the usual social ties, friendships and family relationships, which can become a persistent obstacle to the cure of such patients.
4. Внушаемость - повышенная податливость по отношению к побуждениям, которые спровоцированы домочадцами, "бывалыми" соседями по палате, недоброжелателями, некритическая готовность подчиниться, склонность заражаться чужими настроениями и перенимать привычки. Повышенная внушаемость характеризует больных с относительно низким уровнем интеллектуального развития и несформированным логическим мышлением, входящим в структуру критичности. Определенные условия, такие как заболевания, стресс, дефицит времени, недостаток компетентности и групповое давление, могут провоцировать повышение степени индивидуальной внушаемости.4. Suggestibility - increased compliance with the motives that are provoked by household members, “experienced” roommates, ill-wishers, uncritical willingness to obey, a tendency to become infected with other people's moods and adopt habits. Increased suggestibility characterizes patients with a relatively low level of intellectual development and unformed logical thinking, which is part of the criticality structure. Certain conditions, such as illness, stress, lack of time, lack of competence and group pressure, can trigger an increase in individual suggestibility.
5. Пристрастие к алкоголю, заболевание, разновидность токсикомании, характеризующееся болезненным пристрастием к алкоголю (этиловому спирту), с психической и физической зависимостью от него и негативными последствиями, которые могут выражаться психическими и физическими расстройствами, а также нарушениями социальных отношений пациента, страдающего этим заболеванием.5. Addiction to alcohol, a disease, a form of substance abuse, characterized by a painful addiction to alcohol (ethyl alcohol), with mental and physical dependence on it and negative consequences, which can be expressed by mental and physical disorders, as well as violations of social relations of a patient suffering from this disease .
6. Социально-психологический статус подразумевает личность больного не только как индивидуальность, но и как определенный социально-психологический тип, который характеризуют ментальность, социальная активность, ценностные ориентации, позиции, определяющие линию поведения в условиях конкретной социально-психологической среды противотуберкулезного стационара, в которой внешние социальные воздействия и связи трансформируются во внутренние мотивы и отношения самой личности.6. Socio-psychological status implies the patient’s personality not only as an individual, but also as a specific socio-psychological type, which is characterized by mentality, social activity, value orientations, positions that determine the line of behavior in a particular socio-psychological environment of a TB hospital, in which external social influences and connections are transformed into internal motives and relationships of the individual.
7. Побочные реакции на лечение, установленные при предварительном испытании и известные уже при выпуске лекарств, не охватывают всех возможных проявлений их токсического действия и при их использовании возможны неизвестные побочные эффекты способные оказать неблагоприятное действие на комплаенс.7. Adverse reactions to treatment, established during the preliminary test and already known at the time of drug release, do not cover all possible manifestations of their toxic effects and, when used, unknown side effects are possible that can have an adverse effect on compliance.
8. Отсутствие эффекта лечения характеризует настроение, наличие депрессии, тревоги, общий низкий показатель положительных эмоций. Его показатели свидетельствуют о наличии депрессивных, тревожных переживаний, психическом неблагополучии.8. The absence of a treatment effect characterizes mood, the presence of depression, anxiety, and a general low indicator of positive emotions. His indicators indicate the presence of depressive, anxious experiences, mental distress.
9. Несложившиеся взаимоотношения с медперсоналом: когда доверие перестает быть основой отношений между врачом и больным, построенным на сотрудничестве, включающем поддержку, понимание, уважение и сочувствие.9. Unfolding relationships with medical staff: when trust ceases to be the basis of the relationship between the doctor and the patient, built on cooperation, which includes support, understanding, respect and sympathy.
10. Экономическое неблагополучие - это низкий социальный статус больного, не позволяющий справляться с функциями в какой-либо из сфер жизнедеятельности или нескольких одновременно. Адаптивные способности экономически неблагополучной семьи существенно снижены, процесс излечения заболевших протекает с большими трудностями.10. Economic trouble - this is the low social status of the patient, not allowing to cope with the functions in any of the spheres of life or several at the same time. Adaptive abilities of economically dysfunctional families are significantly reduced; the process of curing the sick proceeds with great difficulties.
Шкалы группируются в два показателя «субъективные факторы комплаенса» и «объективные факторы комплаенса»:Scales are grouped into two indicators: “subjective compliance factors” and “objective compliance factors”:
1. Субъективные факторы комплаенса1. Subjective compliance factors
Составляющие шкалы:Component scales:
- Стресс- stress
- Фрустрация- Frustration
- Стигматизация- stigmatization
- Внушаемость- Suggestibility
- Пристрастие к алкоголю- Addiction to alcohol
2. Объективные факторы комплаенса2. Objective compliance factors
Составляющие шкалы:Component scales:
- Социально-психологический статус- Socio-psychological status
- Побочные реакции на лечение- Adverse reactions to treatment
- Отсутствие эффекта лечения- Lack of treatment effect
- Несложившиеся взаимоотношения с медперсоналом- Unworthy relationships with medical staff
- Экономическое неблагополучие- Economic trouble
Каждый положительный или отрицательный ответ, совпадающий с ответом в таблице, соответствует 1 баллу. Преобладающие суммы баллов указывают на субъективные или объективные факторы низкого комплаенса и направления, в которых предполагается психологическая или медикаментозная помощь.Each positive or negative answer that matches the answer in the table corresponds to 1 point. The prevailing scores indicate subjective or objective factors of low compliance and the direction in which psychological or medical assistance is expected.





Claims (1)
Priority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015135174A RU2611398C1 (en) | 2015-08-19 | 2015-08-19 | Method of increasing the efficiency of treatment of patients with tuberculosis |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2015135174A RU2611398C1 (en) | 2015-08-19 | 2015-08-19 | Method of increasing the efficiency of treatment of patients with tuberculosis |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| RU2611398C1 true RU2611398C1 (en) | 2017-02-21 |
| RU2015135174A RU2015135174A (en) | 2017-02-27 |
Family
ID=58453859
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2015135174A RU2611398C1 (en) | 2015-08-19 | 2015-08-19 | Method of increasing the efficiency of treatment of patients with tuberculosis |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2611398C1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2808910C1 (en) * | 2023-01-19 | 2023-12-05 | Алексей Георгиевич Наумов | Method of increasing adherence to anti-tuberculosis therapy |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2297846C2 (en) * | 2005-03-15 | 2007-04-27 | Государственное учреждение Научный центр Клинической и Экспериментальной медицины Сибирского Отделения Российской академии медицинских наук (ГУ НЦ КЭМ СО РАМН) | Method for treatment of focal and infiltrative pulmonary tuberculosis |
| WO2008057606A2 (en) * | 2006-11-08 | 2008-05-15 | Astrazeneca Ab | Predicting patient compliance with medical treatment |
| WO2012103119A1 (en) * | 2011-01-24 | 2012-08-02 | Activbiotics Pharma, Llc | Compositions for administering rifalazil and other anti-tuberculosis agents in unit dosage form for oral administration |
-
2015
- 2015-08-19 RU RU2015135174A patent/RU2611398C1/en not_active IP Right Cessation
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2297846C2 (en) * | 2005-03-15 | 2007-04-27 | Государственное учреждение Научный центр Клинической и Экспериментальной медицины Сибирского Отделения Российской академии медицинских наук (ГУ НЦ КЭМ СО РАМН) | Method for treatment of focal and infiltrative pulmonary tuberculosis |
| WO2008057606A2 (en) * | 2006-11-08 | 2008-05-15 | Astrazeneca Ab | Predicting patient compliance with medical treatment |
| WO2012103119A1 (en) * | 2011-01-24 | 2012-08-02 | Activbiotics Pharma, Llc | Compositions for administering rifalazil and other anti-tuberculosis agents in unit dosage form for oral administration |
Non-Patent Citations (1)
| Title |
|---|
| ПЬЯНЗОВА Т.В. Влияние информационно-образовательной работы с впервые выявленными больными туберкулезом на эффективность лечения.Автореф.дисс.к.м.н., Новосибирск - 2010, с. 1-22. * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2808910C1 (en) * | 2023-01-19 | 2023-12-05 | Алексей Георгиевич Наумов | Method of increasing adherence to anti-tuberculosis therapy |
Also Published As
| Publication number | Publication date |
|---|---|
| RU2015135174A (en) | 2017-02-27 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Etminan et al. | Oral fluoroquinolones and the risk of retinal detachment | |
| Woodbury-Smith et al. | Autism spectrum disorder (ASD) and unlawful behaviour: Where do we go from here? | |
| Sharshar et al. | Brainstem responses can predict death and delirium in sedated patients in intensive care unit | |
| Arpa | Women who use drugs: Issues, needs, responses, challenges and implications for policy and practice | |
| Usher | Taking neuroleptic medications as the treatment for schizophrenia: A phenomenological study | |
| Lakoff | The right patients for the drug: Managing the placebo effect in antidepressant trials | |
| Norris et al. | Cognitive mediation of alcohol's effects on women's in-the-moment sexual decision making. | |
| Stappenbeck et al. | In-the-moment dissociation, emotional numbing, and sexual risk: The influence of sexual trauma history, trauma symptoms, and alcohol intoxication. | |
| Feldman et al. | Randomized controlled trial of a scoring aid to improve Glasgow Coma Scale scoring by emergency medical services providers | |
| Marcotte et al. | Evaluation of field sobriety tests for identifying drivers under the influence of cannabis: a randomized clinical trial | |
| Kim et al. | Effect of self-treatment of recurrent benign paroxysmal positional vertigo: a randomized clinical trial | |
| Larson et al. | Memory deficits, postconcussive complaints, and posttraumatic stress disorder in a volunteer sample of veterans. | |
| RU2611398C1 (en) | Method of increasing the efficiency of treatment of patients with tuberculosis | |
| Vertigan et al. | The role of sensory dysfunction in the development of voice disorders, chronic cough and paradoxical vocal fold movement | |
| Rader et al. | Psychological correlates of unwanted pregnancy. | |
| Lamberg | Venus orbits closer to pain than Mars, Rx for one sex may not benefit the other | |
| Mohamed et al. | Quality of life and its relation with treatment compliance among schizophrenic patients | |
| Soroka et al. | Between self-stigma and the will of recovery. Difficulties in accepting a psychiatric diagnosis–case study | |
| Wijdicks | Examining Neurocritical Patients | |
| JUTTE et al. | Rehabilitation psychology insights for treatment of critical illness survivors | |
| Smith et al. | Schizophrenia and other psychotic disorders | |
| RU2808910C1 (en) | Method of increasing adherence to anti-tuberculosis therapy | |
| Banks | The role of neuropsychological testing and evaluation: when to refer | |
| Staab | Psychological Morbidity in Patients with Vestibular Disorders | |
| Vechiu et al. | A Brief Description of the Disorders |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees |
Effective date: 20170820 |