CN111032090A - Patch implant composition for cell implantation - Google Patents
Patch implant composition for cell implantation Download PDFInfo
- Publication number
- CN111032090A CN111032090A CN201880050902.2A CN201880050902A CN111032090A CN 111032090 A CN111032090 A CN 111032090A CN 201880050902 A CN201880050902 A CN 201880050902A CN 111032090 A CN111032090 A CN 111032090A
- Authority
- CN
- China
- Prior art keywords
- cells
- implant
- patch
- cell
- tissue
- Prior art date
- Legal status (The legal status is an assumption and is not a legal conclusion. Google has not performed a legal analysis and makes no representation as to the accuracy of the status listed.)
- Pending
Links
- 239000007943 implant Substances 0.000 title claims abstract description 397
- 238000002513 implantation Methods 0.000 title abstract description 92
- 239000000203 mixture Substances 0.000 title abstract description 66
- 210000004027 cell Anatomy 0.000 claims abstract description 797
- 238000000034 method Methods 0.000 claims abstract description 176
- 108010000684 Matrix Metalloproteinases Proteins 0.000 claims abstract description 172
- 102000002274 Matrix Metalloproteinases Human genes 0.000 claims abstract description 171
- 239000000758 substrate Substances 0.000 claims abstract description 145
- 210000000056 organ Anatomy 0.000 claims abstract description 102
- 210000002919 epithelial cell Anatomy 0.000 claims abstract description 96
- 239000012620 biological material Substances 0.000 claims abstract description 79
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 claims abstract description 39
- 239000012528 membrane Substances 0.000 claims abstract description 36
- 201000010099 disease Diseases 0.000 claims abstract description 27
- 210000000130 stem cell Anatomy 0.000 claims description 263
- 210000001519 tissue Anatomy 0.000 claims description 215
- 239000000017 hydrogel Substances 0.000 claims description 153
- 210000004185 liver Anatomy 0.000 claims description 128
- 229920002674 hyaluronan Polymers 0.000 claims description 99
- 230000005012 migration Effects 0.000 claims description 70
- 238000013508 migration Methods 0.000 claims description 70
- 239000000463 material Substances 0.000 claims description 63
- 210000003494 hepatocyte Anatomy 0.000 claims description 55
- 210000000496 pancreas Anatomy 0.000 claims description 54
- 239000002243 precursor Substances 0.000 claims description 51
- 239000002609 medium Substances 0.000 claims description 45
- 210000002901 mesenchymal stem cell Anatomy 0.000 claims description 41
- 230000004069 differentiation Effects 0.000 claims description 36
- 210000004379 membrane Anatomy 0.000 claims description 35
- 210000004500 stellate cell Anatomy 0.000 claims description 34
- 210000003038 endothelium Anatomy 0.000 claims description 33
- 239000001963 growth medium Substances 0.000 claims description 31
- 210000003734 kidney Anatomy 0.000 claims description 27
- 230000004888 barrier function Effects 0.000 claims description 23
- 208000016222 Pancreatic disease Diseases 0.000 claims description 22
- 208000017169 kidney disease Diseases 0.000 claims description 21
- 230000035800 maturation Effects 0.000 claims description 20
- 108010088571 Membrane-Associated Matrix Metalloproteinases Proteins 0.000 claims description 17
- 102000008887 Membrane-Associated Matrix Metalloproteinases Human genes 0.000 claims description 17
- 102000015632 Secreted Matrix Metalloproteinases Human genes 0.000 claims description 17
- 108010063696 Secreted Matrix Metalloproteinases Proteins 0.000 claims description 17
- 210000004738 parenchymal cell Anatomy 0.000 claims description 15
- 230000000735 allogeneic effect Effects 0.000 claims description 14
- 210000003205 muscle Anatomy 0.000 claims description 14
- 210000001691 amnion Anatomy 0.000 claims description 13
- 210000001035 gastrointestinal tract Anatomy 0.000 claims description 13
- 210000004072 lung Anatomy 0.000 claims description 13
- 210000003445 biliary tract Anatomy 0.000 claims description 12
- 208000035475 disorder Diseases 0.000 claims description 12
- 210000003566 hemangioblast Anatomy 0.000 claims description 12
- 210000000936 intestine Anatomy 0.000 claims description 12
- 210000004153 islets of langerhan Anatomy 0.000 claims description 12
- 206010016654 Fibrosis Diseases 0.000 claims description 11
- 210000004204 blood vessel Anatomy 0.000 claims description 11
- 239000011248 coating agent Substances 0.000 claims description 11
- 238000000576 coating method Methods 0.000 claims description 11
- 208000024691 pancreas disease Diseases 0.000 claims description 11
- 229920002994 synthetic fiber Polymers 0.000 claims description 11
- 230000002792 vascular Effects 0.000 claims description 11
- 210000000481 breast Anatomy 0.000 claims description 10
- 210000002216 heart Anatomy 0.000 claims description 10
- 208000019423 liver disease Diseases 0.000 claims description 10
- 210000001541 thymus gland Anatomy 0.000 claims description 10
- 210000004291 uterus Anatomy 0.000 claims description 10
- 208000018522 Gastrointestinal disease Diseases 0.000 claims description 9
- 210000004556 brain Anatomy 0.000 claims description 9
- 208000014674 injury Diseases 0.000 claims description 9
- 210000002307 prostate Anatomy 0.000 claims description 9
- 210000003491 skin Anatomy 0.000 claims description 9
- 210000000278 spinal cord Anatomy 0.000 claims description 9
- 210000001685 thyroid gland Anatomy 0.000 claims description 9
- 230000008733 trauma Effects 0.000 claims description 9
- 208000010643 digestive system disease Diseases 0.000 claims description 8
- 208000018685 gastrointestinal system disease Diseases 0.000 claims description 8
- 210000002435 tendon Anatomy 0.000 claims description 8
- 210000000845 cartilage Anatomy 0.000 claims description 7
- 208000019425 cirrhosis of liver Diseases 0.000 claims description 7
- 230000004761 fibrosis Effects 0.000 claims description 7
- 230000002401 inhibitory effect Effects 0.000 claims description 7
- 230000004203 pancreatic function Effects 0.000 claims description 7
- 210000002826 placenta Anatomy 0.000 claims description 7
- 210000003932 urinary bladder Anatomy 0.000 claims description 7
- 210000000988 bone and bone Anatomy 0.000 claims description 6
- 230000003871 intestinal function Effects 0.000 claims description 6
- 210000002747 omentum Anatomy 0.000 claims description 6
- 230000003907 kidney function Effects 0.000 claims description 5
- 208000032843 Hemorrhage Diseases 0.000 claims description 4
- 230000007882 cirrhosis Effects 0.000 claims description 4
- 230000003908 liver function Effects 0.000 claims description 4
- 210000004923 pancreatic tissue Anatomy 0.000 claims description 4
- 208000011580 syndromic disease Diseases 0.000 claims description 4
- 239000004758 synthetic textile Substances 0.000 claims description 4
- 208000009304 Acute Kidney Injury Diseases 0.000 claims description 3
- 208000022309 Alcoholic Liver disease Diseases 0.000 claims description 3
- 206010003827 Autoimmune hepatitis Diseases 0.000 claims description 3
- 208000008439 Biliary Liver Cirrhosis Diseases 0.000 claims description 3
- 208000033222 Biliary cirrhosis primary Diseases 0.000 claims description 3
- 206010008609 Cholangitis sclerosing Diseases 0.000 claims description 3
- 206010009657 Clostridium difficile colitis Diseases 0.000 claims description 3
- 208000015943 Coeliac disease Diseases 0.000 claims description 3
- 206010009900 Colitis ulcerative Diseases 0.000 claims description 3
- 206010010317 Congenital absence of bile ducts Diseases 0.000 claims description 3
- 208000011231 Crohn disease Diseases 0.000 claims description 3
- 201000003883 Cystic fibrosis Diseases 0.000 claims description 3
- 206010058314 Dysplasia Diseases 0.000 claims description 3
- 206010016202 Familial Amyloidosis Diseases 0.000 claims description 3
- 208000005577 Gastroenteritis Diseases 0.000 claims description 3
- 206010017993 Gastrointestinal neoplasms Diseases 0.000 claims description 3
- 208000009139 Gilbert Disease Diseases 0.000 claims description 3
- 208000022412 Gilbert syndrome Diseases 0.000 claims description 3
- 206010018364 Glomerulonephritis Diseases 0.000 claims description 3
- 208000032007 Glycogen storage disease due to acid maltase deficiency Diseases 0.000 claims description 3
- 206010053185 Glycogen storage disease type II Diseases 0.000 claims description 3
- 206010072579 Granulomatosis with polyangiitis Diseases 0.000 claims description 3
- 208000018565 Hemochromatosis Diseases 0.000 claims description 3
- 206010019799 Hepatitis viral Diseases 0.000 claims description 3
- 208000002972 Hepatolenticular Degeneration Diseases 0.000 claims description 3
- 208000010159 IgA glomerulonephritis Diseases 0.000 claims description 3
- 206010021263 IgA nephropathy Diseases 0.000 claims description 3
- 208000022559 Inflammatory bowel disease Diseases 0.000 claims description 3
- 208000008839 Kidney Neoplasms Diseases 0.000 claims description 3
- 208000005777 Lupus Nephritis Diseases 0.000 claims description 3
- 206010065673 Nephritic syndrome Diseases 0.000 claims description 3
- 206010029164 Nephrotic syndrome Diseases 0.000 claims description 3
- 206010033627 Pancreatic injury Diseases 0.000 claims description 3
- 208000035467 Pancreatic insufficiency Diseases 0.000 claims description 3
- 206010061902 Pancreatic neoplasm Diseases 0.000 claims description 3
- 206010033645 Pancreatitis Diseases 0.000 claims description 3
- 208000008469 Peptic Ulcer Diseases 0.000 claims description 3
- 108010071690 Prealbumin Proteins 0.000 claims description 3
- 208000012654 Primary biliary cholangitis Diseases 0.000 claims description 3
- 208000003100 Pseudomembranous Enterocolitis Diseases 0.000 claims description 3
- 206010037128 Pseudomembranous colitis Diseases 0.000 claims description 3
- 206010038389 Renal cancer Diseases 0.000 claims description 3
- 208000033626 Renal failure acute Diseases 0.000 claims description 3
- 102000009190 Transthyretin Human genes 0.000 claims description 3
- 201000006704 Ulcerative Colitis Diseases 0.000 claims description 3
- 208000018839 Wilson disease Diseases 0.000 claims description 3
- 201000011040 acute kidney failure Diseases 0.000 claims description 3
- 208000006682 alpha 1-Antitrypsin Deficiency Diseases 0.000 claims description 3
- 206010002022 amyloidosis Diseases 0.000 claims description 3
- 201000005271 biliary atresia Diseases 0.000 claims description 3
- 230000001684 chronic effect Effects 0.000 claims description 3
- 206010012601 diabetes mellitus Diseases 0.000 claims description 3
- 210000002249 digestive system Anatomy 0.000 claims description 3
- 230000004064 dysfunction Effects 0.000 claims description 3
- 210000000750 endocrine system Anatomy 0.000 claims description 3
- 208000006275 fascioliasis Diseases 0.000 claims description 3
- 210000004996 female reproductive system Anatomy 0.000 claims description 3
- 230000002496 gastric effect Effects 0.000 claims description 3
- 201000004502 glycogen storage disease II Diseases 0.000 claims description 3
- 208000006454 hepatitis Diseases 0.000 claims description 3
- 231100000283 hepatitis Toxicity 0.000 claims description 3
- 208000017105 hereditary amyloidosis Diseases 0.000 claims description 3
- 208000009326 ileitis Diseases 0.000 claims description 3
- 210000001613 integumentary system Anatomy 0.000 claims description 3
- 208000002551 irritable bowel syndrome Diseases 0.000 claims description 3
- 201000010982 kidney cancer Diseases 0.000 claims description 3
- 201000007270 liver cancer Diseases 0.000 claims description 3
- 208000014018 liver neoplasm Diseases 0.000 claims description 3
- 210000005228 liver tissue Anatomy 0.000 claims description 3
- 210000004324 lymphatic system Anatomy 0.000 claims description 3
- 210000004995 male reproductive system Anatomy 0.000 claims description 3
- 208000015486 malignant pancreatic neoplasm Diseases 0.000 claims description 3
- 210000002346 musculoskeletal system Anatomy 0.000 claims description 3
- 201000008383 nephritis Diseases 0.000 claims description 3
- 210000000653 nervous system Anatomy 0.000 claims description 3
- 208000008338 non-alcoholic fatty liver disease Diseases 0.000 claims description 3
- 201000002528 pancreatic cancer Diseases 0.000 claims description 3
- 208000008443 pancreatic carcinoma Diseases 0.000 claims description 3
- 208000011906 peptic ulcer disease Diseases 0.000 claims description 3
- 239000011148 porous material Substances 0.000 claims description 3
- 201000000742 primary sclerosing cholangitis Diseases 0.000 claims description 3
- 210000005084 renal tissue Anatomy 0.000 claims description 3
- 210000002345 respiratory system Anatomy 0.000 claims description 3
- 208000010157 sclerosing cholangitis Diseases 0.000 claims description 3
- 210000005070 sphincter Anatomy 0.000 claims description 3
- 230000002485 urinary effect Effects 0.000 claims description 3
- 201000001862 viral hepatitis Diseases 0.000 claims description 3
- 208000024985 Alport syndrome Diseases 0.000 claims 1
- 206010010539 Congenital megacolon Diseases 0.000 claims 1
- 208000004592 Hirschsprung disease Diseases 0.000 claims 1
- 208000003215 hereditary nephritis Diseases 0.000 claims 1
- 239000007787 solid Substances 0.000 abstract description 23
- 230000010354 integration Effects 0.000 abstract description 14
- 210000002782 epithelial mesenchymal cell Anatomy 0.000 abstract description 9
- 230000003319 supportive effect Effects 0.000 abstract description 6
- 230000007246 mechanism Effects 0.000 abstract description 2
- 230000003100 immobilizing effect Effects 0.000 abstract 1
- 239000010410 layer Substances 0.000 description 105
- KIUKXJAPPMFGSW-DNGZLQJQSA-N (2S,3S,4S,5R,6R)-6-[(2S,3R,4R,5S,6R)-3-Acetamido-2-[(2S,3S,4R,5R,6R)-6-[(2R,3R,4R,5S,6R)-3-acetamido-2,5-dihydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-2-carboxy-4,5-dihydroxyoxan-3-yl]oxy-5-hydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-3,4,5-trihydroxyoxane-2-carboxylic acid Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@H](O[C@H]2[C@@H]([C@@H](O[C@H]3[C@@H]([C@@H](O)[C@H](O)[C@H](O3)C(O)=O)O)[C@H](O)[C@@H](CO)O2)NC(C)=O)[C@@H](C(O)=O)O1 KIUKXJAPPMFGSW-DNGZLQJQSA-N 0.000 description 97
- 229960003160 hyaluronic acid Drugs 0.000 description 90
- 210000002220 organoid Anatomy 0.000 description 89
- 239000005090 green fluorescent protein Substances 0.000 description 55
- 102000004144 Green Fluorescent Proteins Human genes 0.000 description 49
- 108010043121 Green Fluorescent Proteins Proteins 0.000 description 49
- 230000014509 gene expression Effects 0.000 description 42
- 108090000623 proteins and genes Proteins 0.000 description 42
- 238000010186 staining Methods 0.000 description 37
- NOESYZHRGYRDHS-UHFFFAOYSA-N insulin Chemical compound N1C(=O)C(NC(=O)C(CCC(N)=O)NC(=O)C(CCC(O)=O)NC(=O)C(C(C)C)NC(=O)C(NC(=O)CN)C(C)CC)CSSCC(C(NC(CO)C(=O)NC(CC(C)C)C(=O)NC(CC=2C=CC(O)=CC=2)C(=O)NC(CCC(N)=O)C(=O)NC(CC(C)C)C(=O)NC(CCC(O)=O)C(=O)NC(CC(N)=O)C(=O)NC(CC=2C=CC(O)=CC=2)C(=O)NC(CSSCC(NC(=O)C(C(C)C)NC(=O)C(CC(C)C)NC(=O)C(CC=2C=CC(O)=CC=2)NC(=O)C(CC(C)C)NC(=O)C(C)NC(=O)C(CCC(O)=O)NC(=O)C(C(C)C)NC(=O)C(CC(C)C)NC(=O)C(CC=2NC=NC=2)NC(=O)C(CO)NC(=O)CNC2=O)C(=O)NCC(=O)NC(CCC(O)=O)C(=O)NC(CCCNC(N)=N)C(=O)NCC(=O)NC(CC=3C=CC=CC=3)C(=O)NC(CC=3C=CC=CC=3)C(=O)NC(CC=3C=CC(O)=CC=3)C(=O)NC(C(C)O)C(=O)N3C(CCC3)C(=O)NC(CCCCN)C(=O)NC(C)C(O)=O)C(=O)NC(CC(N)=O)C(O)=O)=O)NC(=O)C(C(C)CC)NC(=O)C(CO)NC(=O)C(C(C)O)NC(=O)C1CSSCC2NC(=O)C(CC(C)C)NC(=O)C(NC(=O)C(CCC(N)=O)NC(=O)C(CC(N)=O)NC(=O)C(NC(=O)C(N)CC=1C=CC=CC=1)C(C)C)CC1=CN=CN1 NOESYZHRGYRDHS-UHFFFAOYSA-N 0.000 description 34
- 239000002775 capsule Substances 0.000 description 32
- 238000002054 transplantation Methods 0.000 description 32
- 239000011159 matrix material Substances 0.000 description 28
- 230000008569 process Effects 0.000 description 26
- 230000006872 improvement Effects 0.000 description 23
- 210000002966 serum Anatomy 0.000 description 23
- WZUVPPKBWHMQCE-UHFFFAOYSA-N Haematoxylin Chemical compound C12=CC(O)=C(O)C=C2CC2(O)C1C1=CC=C(O)C(O)=C1OC2 WZUVPPKBWHMQCE-UHFFFAOYSA-N 0.000 description 22
- 238000003556 assay Methods 0.000 description 22
- 210000004940 nucleus Anatomy 0.000 description 22
- 238000003364 immunohistochemistry Methods 0.000 description 21
- 102000010834 Extracellular Matrix Proteins Human genes 0.000 description 20
- 108010037362 Extracellular Matrix Proteins Proteins 0.000 description 20
- 241001465754 Metazoa Species 0.000 description 20
- 210000001835 viscera Anatomy 0.000 description 20
- 230000000694 effects Effects 0.000 description 19
- 210000002744 extracellular matrix Anatomy 0.000 description 19
- 102000004169 proteins and genes Human genes 0.000 description 18
- 238000001356 surgical procedure Methods 0.000 description 18
- 229920002683 Glycosaminoglycan Polymers 0.000 description 17
- 102000004877 Insulin Human genes 0.000 description 17
- 108090001061 Insulin Proteins 0.000 description 17
- 230000024245 cell differentiation Effects 0.000 description 17
- 229940125396 insulin Drugs 0.000 description 17
- 230000006870 function Effects 0.000 description 16
- 239000003102 growth factor Substances 0.000 description 16
- 238000002347 injection Methods 0.000 description 16
- 239000007924 injection Substances 0.000 description 16
- 238000004519 manufacturing process Methods 0.000 description 16
- 108020004999 messenger RNA Proteins 0.000 description 16
- 235000018102 proteins Nutrition 0.000 description 16
- 108010029485 Protein Isoforms Proteins 0.000 description 15
- 102000001708 Protein Isoforms Human genes 0.000 description 15
- 239000006285 cell suspension Substances 0.000 description 15
- 230000001413 cellular effect Effects 0.000 description 15
- 238000012360 testing method Methods 0.000 description 15
- 102000009027 Albumins Human genes 0.000 description 14
- 108010088751 Albumins Proteins 0.000 description 14
- -1 NANOG Proteins 0.000 description 14
- 241000282887 Suidae Species 0.000 description 14
- 239000000499 gel Substances 0.000 description 14
- 238000007634 remodeling Methods 0.000 description 14
- 102000008186 Collagen Human genes 0.000 description 13
- 108010035532 Collagen Proteins 0.000 description 13
- 102000004127 Cytokines Human genes 0.000 description 13
- 108090000695 Cytokines Proteins 0.000 description 13
- 210000000648 angioblast Anatomy 0.000 description 13
- 229920001436 collagen Polymers 0.000 description 13
- 238000004091 panning Methods 0.000 description 13
- 101001013150 Homo sapiens Interstitial collagenase Proteins 0.000 description 12
- 102000000380 Matrix Metalloproteinase 1 Human genes 0.000 description 12
- 230000002062 proliferating effect Effects 0.000 description 12
- 102000018651 Epithelial Cell Adhesion Molecule Human genes 0.000 description 11
- 108010066687 Epithelial Cell Adhesion Molecule Proteins 0.000 description 11
- 239000007640 basal medium Substances 0.000 description 11
- 230000000670 limiting effect Effects 0.000 description 11
- 230000007935 neutral effect Effects 0.000 description 11
- 102000040430 polynucleotide Human genes 0.000 description 11
- 108091033319 polynucleotide Proteins 0.000 description 11
- 239000002157 polynucleotide Substances 0.000 description 11
- 230000008093 supporting effect Effects 0.000 description 11
- 102100026802 72 kDa type IV collagenase Human genes 0.000 description 10
- 102000016289 Cell Adhesion Molecules Human genes 0.000 description 10
- 108010067225 Cell Adhesion Molecules Proteins 0.000 description 10
- 101000627872 Homo sapiens 72 kDa type IV collagenase Proteins 0.000 description 10
- 101000610551 Homo sapiens Prominin-1 Proteins 0.000 description 10
- 102100024616 Platelet endothelial cell adhesion molecule Human genes 0.000 description 10
- 102100040120 Prominin-1 Human genes 0.000 description 10
- 229940024606 amino acid Drugs 0.000 description 10
- 235000001014 amino acid Nutrition 0.000 description 10
- 150000001413 amino acids Chemical class 0.000 description 10
- QVGXLLKOCUKJST-UHFFFAOYSA-N atomic oxygen Chemical compound [O] QVGXLLKOCUKJST-UHFFFAOYSA-N 0.000 description 10
- LOKCTEFSRHRXRJ-UHFFFAOYSA-I dipotassium trisodium dihydrogen phosphate hydrogen phosphate dichloride Chemical compound P(=O)(O)(O)[O-].[K+].P(=O)(O)([O-])[O-].[Na+].[Na+].[Cl-].[K+].[Cl-].[Na+] LOKCTEFSRHRXRJ-UHFFFAOYSA-I 0.000 description 10
- 229910052760 oxygen Inorganic materials 0.000 description 10
- 239000001301 oxygen Substances 0.000 description 10
- 239000002953 phosphate buffered saline Substances 0.000 description 10
- 230000001052 transient effect Effects 0.000 description 10
- 108010063198 6-phospho-beta-galactosidase Proteins 0.000 description 9
- 102100041030 Pancreas/duodenum homeobox protein 1 Human genes 0.000 description 9
- 241000282898 Sus scrofa Species 0.000 description 9
- 230000001464 adherent effect Effects 0.000 description 9
- 230000015572 biosynthetic process Effects 0.000 description 9
- 210000002889 endothelial cell Anatomy 0.000 description 9
- 230000003511 endothelial effect Effects 0.000 description 9
- 229940088597 hormone Drugs 0.000 description 9
- 239000005556 hormone Substances 0.000 description 9
- 238000010166 immunofluorescence Methods 0.000 description 9
- 102000012422 Collagen Type I Human genes 0.000 description 8
- 108010022452 Collagen Type I Proteins 0.000 description 8
- 102000003745 Hepatocyte Growth Factor Human genes 0.000 description 8
- 108090000100 Hepatocyte Growth Factor Proteins 0.000 description 8
- 101710183548 Pyridoxal 5'-phosphate synthase subunit PdxS Proteins 0.000 description 8
- BUGBHKTXTAQXES-UHFFFAOYSA-N Selenium Chemical compound [Se] BUGBHKTXTAQXES-UHFFFAOYSA-N 0.000 description 8
- 102000004338 Transferrin Human genes 0.000 description 8
- 108090000901 Transferrin Proteins 0.000 description 8
- 238000004458 analytical method Methods 0.000 description 8
- 230000002500 effect on skin Effects 0.000 description 8
- YQGOJNYOYNNSMM-UHFFFAOYSA-N eosin Chemical compound [Na+].OC(=O)C1=CC=CC=C1C1=C2C=C(Br)C(=O)C(Br)=C2OC2=C(Br)C(O)=C(Br)C=C21 YQGOJNYOYNNSMM-UHFFFAOYSA-N 0.000 description 8
- 210000003999 epithelial cell of bile duct Anatomy 0.000 description 8
- 210000004907 gland Anatomy 0.000 description 8
- 108090000765 processed proteins & peptides Proteins 0.000 description 8
- 239000000523 sample Substances 0.000 description 8
- 238000007920 subcutaneous administration Methods 0.000 description 8
- 208000024891 symptom Diseases 0.000 description 8
- 239000012581 transferrin Substances 0.000 description 8
- 230000009261 transgenic effect Effects 0.000 description 8
- OYPRJOBELJOOCE-UHFFFAOYSA-N Calcium Chemical compound [Ca] OYPRJOBELJOOCE-UHFFFAOYSA-N 0.000 description 7
- 101000990912 Homo sapiens Matrilysin Proteins 0.000 description 7
- 102100030417 Matrilysin Human genes 0.000 description 7
- 108091023040 Transcription factor Proteins 0.000 description 7
- 102000040945 Transcription factor Human genes 0.000 description 7
- 210000000013 bile duct Anatomy 0.000 description 7
- 239000011575 calcium Substances 0.000 description 7
- 229910052791 calcium Inorganic materials 0.000 description 7
- 230000011748 cell maturation Effects 0.000 description 7
- 238000012258 culturing Methods 0.000 description 7
- 239000012530 fluid Substances 0.000 description 7
- 235000021588 free fatty acids Nutrition 0.000 description 7
- 125000003729 nucleotide group Chemical group 0.000 description 7
- 235000015097 nutrients Nutrition 0.000 description 7
- 229920001432 poly(L-lactide) Polymers 0.000 description 7
- 229920001223 polyethylene glycol Polymers 0.000 description 7
- 239000000047 product Substances 0.000 description 7
- 229910052711 selenium Inorganic materials 0.000 description 7
- 239000011669 selenium Substances 0.000 description 7
- 210000002536 stromal cell Anatomy 0.000 description 7
- 239000000126 substance Substances 0.000 description 7
- 239000013589 supplement Substances 0.000 description 7
- 239000000725 suspension Substances 0.000 description 7
- 229940045997 vitamin a Drugs 0.000 description 7
- 102100023635 Alpha-fetoprotein Human genes 0.000 description 6
- 108091003079 Bovine Serum Albumin Proteins 0.000 description 6
- 102000004190 Enzymes Human genes 0.000 description 6
- 108090000790 Enzymes Proteins 0.000 description 6
- 102000015779 HDL Lipoproteins Human genes 0.000 description 6
- 108010010234 HDL Lipoproteins Proteins 0.000 description 6
- 101001063456 Homo sapiens Leucine-rich repeat-containing G-protein coupled receptor 5 Proteins 0.000 description 6
- 102100031036 Leucine-rich repeat-containing G-protein coupled receptor 5 Human genes 0.000 description 6
- 102100035423 POU domain, class 5, transcription factor 1 Human genes 0.000 description 6
- 238000003559 RNA-seq method Methods 0.000 description 6
- 108010073929 Vascular Endothelial Growth Factor A Proteins 0.000 description 6
- 102000005789 Vascular Endothelial Growth Factors Human genes 0.000 description 6
- 108010019530 Vascular Endothelial Growth Factors Proteins 0.000 description 6
- 238000004113 cell culture Methods 0.000 description 6
- 230000012292 cell migration Effects 0.000 description 6
- 238000004132 cross linking Methods 0.000 description 6
- 230000009089 cytolysis Effects 0.000 description 6
- 238000009826 distribution Methods 0.000 description 6
- 239000003814 drug Substances 0.000 description 6
- 210000001671 embryonic stem cell Anatomy 0.000 description 6
- 229940088598 enzyme Drugs 0.000 description 6
- 239000007850 fluorescent dye Substances 0.000 description 6
- 210000003897 hepatic stem cell Anatomy 0.000 description 6
- 238000001727 in vivo Methods 0.000 description 6
- 150000002632 lipids Chemical class 0.000 description 6
- 239000003550 marker Substances 0.000 description 6
- 229920000642 polymer Polymers 0.000 description 6
- 102000013142 Amylases Human genes 0.000 description 5
- 108010065511 Amylases Proteins 0.000 description 5
- BPYKTIZUTYGOLE-IFADSCNNSA-N Bilirubin Chemical compound N1C(=O)C(C)=C(C=C)\C1=C\C1=C(C)C(CCC(O)=O)=C(CC2=C(C(C)=C(\C=C/3C(=C(C=C)C(=O)N\3)C)N2)CCC(O)=O)N1 BPYKTIZUTYGOLE-IFADSCNNSA-N 0.000 description 5
- 241000255789 Bombyx mori Species 0.000 description 5
- IAJILQKETJEXLJ-UHFFFAOYSA-N Galacturonsaeure Natural products O=CC(O)C(O)C(O)C(O)C(O)=O IAJILQKETJEXLJ-UHFFFAOYSA-N 0.000 description 5
- HTTJABKRGRZYRN-UHFFFAOYSA-N Heparin Chemical compound OC1C(NC(=O)C)C(O)OC(COS(O)(=O)=O)C1OC1C(OS(O)(=O)=O)C(O)C(OC2C(C(OS(O)(=O)=O)C(OC3C(C(O)C(O)C(O3)C(O)=O)OS(O)(=O)=O)C(CO)O2)NS(O)(=O)=O)C(C(O)=O)O1 HTTJABKRGRZYRN-UHFFFAOYSA-N 0.000 description 5
- 101001011906 Homo sapiens Matrix metalloproteinase-14 Proteins 0.000 description 5
- 101000603702 Homo sapiens Neurogenin-3 Proteins 0.000 description 5
- JVTAAEKCZFNVCJ-REOHCLBHSA-N L-lactic acid Chemical compound C[C@H](O)C(O)=O JVTAAEKCZFNVCJ-REOHCLBHSA-N 0.000 description 5
- 102100030216 Matrix metalloproteinase-14 Human genes 0.000 description 5
- 102100038553 Neurogenin-3 Human genes 0.000 description 5
- 108091008605 VEGF receptors Proteins 0.000 description 5
- 102000009484 Vascular Endothelial Growth Factor Receptors Human genes 0.000 description 5
- HCHKCACWOHOZIP-UHFFFAOYSA-N Zinc Chemical compound [Zn] HCHKCACWOHOZIP-UHFFFAOYSA-N 0.000 description 5
- 210000000170 cell membrane Anatomy 0.000 description 5
- 238000002659 cell therapy Methods 0.000 description 5
- 238000007906 compression Methods 0.000 description 5
- 230000006835 compression Effects 0.000 description 5
- 238000005138 cryopreservation Methods 0.000 description 5
- 238000013461 design Methods 0.000 description 5
- 239000003599 detergent Substances 0.000 description 5
- 125000004386 diacrylate group Chemical group 0.000 description 5
- 210000001198 duodenum Anatomy 0.000 description 5
- 210000000981 epithelium Anatomy 0.000 description 5
- 210000000232 gallbladder Anatomy 0.000 description 5
- 238000001879 gelation Methods 0.000 description 5
- 230000012010 growth Effects 0.000 description 5
- 230000002440 hepatic effect Effects 0.000 description 5
- 230000001976 improved effect Effects 0.000 description 5
- 102000006495 integrins Human genes 0.000 description 5
- 108010044426 integrins Proteins 0.000 description 5
- 239000007788 liquid Substances 0.000 description 5
- 108010082117 matrigel Proteins 0.000 description 5
- DWCZIOOZPIDHAB-UHFFFAOYSA-L methyl green Chemical compound [Cl-].[Cl-].C1=CC(N(C)C)=CC=C1C(C=1C=CC(=CC=1)[N+](C)(C)C)=C1C=CC(=[N+](C)C)C=C1 DWCZIOOZPIDHAB-UHFFFAOYSA-L 0.000 description 5
- 230000004048 modification Effects 0.000 description 5
- 238000012986 modification Methods 0.000 description 5
- 238000002360 preparation method Methods 0.000 description 5
- 239000012679 serum free medium Substances 0.000 description 5
- 230000011664 signaling Effects 0.000 description 5
- 235000002639 sodium chloride Nutrition 0.000 description 5
- 239000000243 solution Substances 0.000 description 5
- 210000000603 stem cell niche Anatomy 0.000 description 5
- 230000004083 survival effect Effects 0.000 description 5
- 230000009466 transformation Effects 0.000 description 5
- 239000011701 zinc Substances 0.000 description 5
- 229910052725 zinc Inorganic materials 0.000 description 5
- SQDAZGGFXASXDW-UHFFFAOYSA-N 5-bromo-2-(trifluoromethoxy)pyridine Chemical compound FC(F)(F)OC1=CC=C(Br)C=N1 SQDAZGGFXASXDW-UHFFFAOYSA-N 0.000 description 4
- 108700028369 Alleles Proteins 0.000 description 4
- 239000004382 Amylase Substances 0.000 description 4
- 241001260012 Bursa Species 0.000 description 4
- RYGMFSIKBFXOCR-UHFFFAOYSA-N Copper Chemical compound [Cu] RYGMFSIKBFXOCR-UHFFFAOYSA-N 0.000 description 4
- 108010079245 Cystic Fibrosis Transmembrane Conductance Regulator Proteins 0.000 description 4
- 102000012605 Cystic Fibrosis Transmembrane Conductance Regulator Human genes 0.000 description 4
- 241000150534 El Moro Canyon orthohantavirus Species 0.000 description 4
- LFQSCWFLJHTTHZ-UHFFFAOYSA-N Ethanol Chemical compound CCO LFQSCWFLJHTTHZ-UHFFFAOYSA-N 0.000 description 4
- 102000018233 Fibroblast Growth Factor Human genes 0.000 description 4
- 108050007372 Fibroblast Growth Factor Proteins 0.000 description 4
- 102000003693 Hedgehog Proteins Human genes 0.000 description 4
- 108090000031 Hedgehog Proteins Proteins 0.000 description 4
- 229920002971 Heparan sulfate Polymers 0.000 description 4
- 101710123134 Ice-binding protein Proteins 0.000 description 4
- 101710082837 Ice-structuring protein Proteins 0.000 description 4
- 108010076876 Keratins Proteins 0.000 description 4
- 108010069196 Neural Cell Adhesion Molecules Proteins 0.000 description 4
- 101710126211 POU domain, class 5, transcription factor 1 Proteins 0.000 description 4
- 239000012980 RPMI-1640 medium Substances 0.000 description 4
- 238000011529 RT qPCR Methods 0.000 description 4
- 101710107540 Type-2 ice-structuring protein Proteins 0.000 description 4
- 230000003187 abdominal effect Effects 0.000 description 4
- IAJILQKETJEXLJ-QTBDOELSSA-N aldehydo-D-glucuronic acid Chemical compound O=C[C@H](O)[C@@H](O)[C@H](O)[C@H](O)C(O)=O IAJILQKETJEXLJ-QTBDOELSSA-N 0.000 description 4
- 235000019418 amylase Nutrition 0.000 description 4
- 238000013459 approach Methods 0.000 description 4
- 210000001130 astrocyte Anatomy 0.000 description 4
- 229940098773 bovine serum albumin Drugs 0.000 description 4
- 238000012512 characterization method Methods 0.000 description 4
- 239000003153 chemical reaction reagent Substances 0.000 description 4
- 229910052802 copper Inorganic materials 0.000 description 4
- 239000010949 copper Substances 0.000 description 4
- 239000003431 cross linking reagent Substances 0.000 description 4
- 210000000805 cytoplasm Anatomy 0.000 description 4
- 210000001900 endoderm Anatomy 0.000 description 4
- 238000005516 engineering process Methods 0.000 description 4
- 229940126864 fibroblast growth factor Drugs 0.000 description 4
- 238000007667 floating Methods 0.000 description 4
- 230000004927 fusion Effects 0.000 description 4
- 230000030279 gene silencing Effects 0.000 description 4
- 230000002068 genetic effect Effects 0.000 description 4
- 229920000669 heparin Polymers 0.000 description 4
- 229960002897 heparin Drugs 0.000 description 4
- JYGXADMDTFJGBT-VWUMJDOOSA-N hydrocortisone Chemical compound O=C1CC[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 JYGXADMDTFJGBT-VWUMJDOOSA-N 0.000 description 4
- 238000001802 infusion Methods 0.000 description 4
- 210000003228 intrahepatic bile duct Anatomy 0.000 description 4
- 230000009545 invasion Effects 0.000 description 4
- 210000003292 kidney cell Anatomy 0.000 description 4
- 238000012423 maintenance Methods 0.000 description 4
- 230000003278 mimic effect Effects 0.000 description 4
- 150000007523 nucleic acids Chemical group 0.000 description 4
- 239000002773 nucleotide Substances 0.000 description 4
- 210000000277 pancreatic duct Anatomy 0.000 description 4
- 229920000671 polyethylene glycol diacrylate Polymers 0.000 description 4
- 229920001184 polypeptide Polymers 0.000 description 4
- 102000004196 processed proteins & peptides Human genes 0.000 description 4
- 230000035755 proliferation Effects 0.000 description 4
- 230000002829 reductive effect Effects 0.000 description 4
- 150000003839 salts Chemical class 0.000 description 4
- 239000003894 surgical glue Substances 0.000 description 4
- 230000001960 triggered effect Effects 0.000 description 4
- VBEQCZHXXJYVRD-GACYYNSASA-N uroanthelone Chemical compound C([C@@H](C(=O)N[C@H](C(=O)N[C@@H](CS)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CS)C(=O)N[C@H](C(=O)N[C@@H]([C@@H](C)CC)C(=O)NCC(=O)N[C@@H](CC=1C=CC(O)=CC=1)C(=O)N[C@@H](CO)C(=O)NCC(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CS)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(O)=O)C(C)C)[C@@H](C)O)NC(=O)[C@H](CO)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CO)NC(=O)[C@H](CCC(O)=O)NC(=O)[C@@H](NC(=O)[C@H](CC=1NC=NC=1)NC(=O)[C@H](CCSC)NC(=O)[C@H](CS)NC(=O)[C@@H](NC(=O)CNC(=O)CNC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CS)NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)CNC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CO)NC(=O)[C@H](CO)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](CS)NC(=O)CNC(=O)[C@H]1N(CCC1)C(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CO)NC(=O)[C@@H](N)CC(N)=O)C(C)C)[C@@H](C)CC)C1=CC=C(O)C=C1 VBEQCZHXXJYVRD-GACYYNSASA-N 0.000 description 4
- 229940088594 vitamin Drugs 0.000 description 4
- 239000011782 vitamin Substances 0.000 description 4
- 235000013343 vitamin Nutrition 0.000 description 4
- 229930003231 vitamin Natural products 0.000 description 4
- ZCYVEMRRCGMTRW-UHFFFAOYSA-N 7553-56-2 Chemical compound [I] ZCYVEMRRCGMTRW-UHFFFAOYSA-N 0.000 description 3
- CSCPPACGZOOCGX-UHFFFAOYSA-N Acetone Chemical compound CC(C)=O CSCPPACGZOOCGX-UHFFFAOYSA-N 0.000 description 3
- 102000007469 Actins Human genes 0.000 description 3
- 108010085238 Actins Proteins 0.000 description 3
- 102100036475 Alanine aminotransferase 1 Human genes 0.000 description 3
- 108010082126 Alanine transaminase Proteins 0.000 description 3
- 206010002091 Anaesthesia Diseases 0.000 description 3
- 108010003415 Aspartate Aminotransferases Proteins 0.000 description 3
- 102000004625 Aspartate Aminotransferases Human genes 0.000 description 3
- 102100031650 C-X-C chemokine receptor type 4 Human genes 0.000 description 3
- 229920001287 Chondroitin sulfate Polymers 0.000 description 3
- 102000029816 Collagenase Human genes 0.000 description 3
- 108060005980 Collagenase Proteins 0.000 description 3
- 102000007644 Colony-Stimulating Factors Human genes 0.000 description 3
- 108010071942 Colony-Stimulating Factors Proteins 0.000 description 3
- 108050001175 Connexin Proteins 0.000 description 3
- IAZDPXIOMUYVGZ-UHFFFAOYSA-N Dimethylsulphoxide Chemical compound CS(C)=O IAZDPXIOMUYVGZ-UHFFFAOYSA-N 0.000 description 3
- 241000283074 Equus asinus Species 0.000 description 3
- 241000283073 Equus caballus Species 0.000 description 3
- 102000051325 Glucagon Human genes 0.000 description 3
- 108060003199 Glucagon Proteins 0.000 description 3
- 101000922348 Homo sapiens C-X-C chemokine receptor type 4 Proteins 0.000 description 3
- 101000990902 Homo sapiens Matrix metalloproteinase-9 Proteins 0.000 description 3
- 101001069749 Homo sapiens Prospero homeobox protein 1 Proteins 0.000 description 3
- 102100033420 Keratin, type I cytoskeletal 19 Human genes 0.000 description 3
- 102000011782 Keratins Human genes 0.000 description 3
- YQEZLKZALYSWHR-UHFFFAOYSA-N Ketamine Chemical compound C=1C=CC=C(Cl)C=1C1(NC)CCCCC1=O YQEZLKZALYSWHR-UHFFFAOYSA-N 0.000 description 3
- 102100030412 Matrix metalloproteinase-9 Human genes 0.000 description 3
- OKKJLVBELUTLKV-UHFFFAOYSA-N Methanol Chemical compound OC OKKJLVBELUTLKV-UHFFFAOYSA-N 0.000 description 3
- 206010028851 Necrosis Diseases 0.000 description 3
- 108010025020 Nerve Growth Factor Proteins 0.000 description 3
- 102000001068 Neural Cell Adhesion Molecules Human genes 0.000 description 3
- 240000008881 Oenanthe javanica Species 0.000 description 3
- 241000283973 Oryctolagus cuniculus Species 0.000 description 3
- 102000035195 Peptidases Human genes 0.000 description 3
- 108091005804 Peptidases Proteins 0.000 description 3
- 239000002202 Polyethylene glycol Substances 0.000 description 3
- 102100033880 Prospero homeobox protein 1 Human genes 0.000 description 3
- 239000004365 Protease Substances 0.000 description 3
- 241000220317 Rosa Species 0.000 description 3
- 101150106167 SOX9 gene Proteins 0.000 description 3
- 102100037192 Sal-like protein 4 Human genes 0.000 description 3
- 102000003673 Symporters Human genes 0.000 description 3
- 108090000088 Symporters Proteins 0.000 description 3
- 108700019146 Transgenes Proteins 0.000 description 3
- GLNADSQYFUSGOU-GPTZEZBUSA-J Trypan blue Chemical compound [Na+].[Na+].[Na+].[Na+].C1=C(S([O-])(=O)=O)C=C2C=C(S([O-])(=O)=O)C(/N=N/C3=CC=C(C=C3C)C=3C=C(C(=CC=3)\N=N\C=3C(=CC4=CC(=CC(N)=C4C=3O)S([O-])(=O)=O)S([O-])(=O)=O)C)=C(O)C2=C1N GLNADSQYFUSGOU-GPTZEZBUSA-J 0.000 description 3
- 230000037005 anaesthesia Effects 0.000 description 3
- 239000000427 antigen Substances 0.000 description 3
- 108091007433 antigens Proteins 0.000 description 3
- 102000036639 antigens Human genes 0.000 description 3
- 230000008901 benefit Effects 0.000 description 3
- MSWZFWKMSRAUBD-UHFFFAOYSA-N beta-D-galactosamine Natural products NC1C(O)OC(CO)C(O)C1O MSWZFWKMSRAUBD-UHFFFAOYSA-N 0.000 description 3
- 210000000941 bile Anatomy 0.000 description 3
- 239000000090 biomarker Substances 0.000 description 3
- 239000000872 buffer Substances 0.000 description 3
- 230000008859 change Effects 0.000 description 3
- 238000006243 chemical reaction Methods 0.000 description 3
- 229940059329 chondroitin sulfate Drugs 0.000 description 3
- 229960002424 collagenase Drugs 0.000 description 3
- 239000002299 complementary DNA Substances 0.000 description 3
- 235000014113 dietary fatty acids Nutrition 0.000 description 3
- 150000002016 disaccharides Chemical group 0.000 description 3
- 229940079593 drug Drugs 0.000 description 3
- 239000000975 dye Substances 0.000 description 3
- 238000002474 experimental method Methods 0.000 description 3
- 229930195729 fatty acid Natural products 0.000 description 3
- 239000000194 fatty acid Substances 0.000 description 3
- 150000004665 fatty acids Chemical class 0.000 description 3
- 210000004602 germ cell Anatomy 0.000 description 3
- MASNOZXLGMXCHN-ZLPAWPGGSA-N glucagon Chemical compound C([C@@H](C(=O)N[C@H](C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H]([C@@H](C)O)C(O)=O)C(C)C)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@H](C)NC(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CO)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CCCCN)NC(=O)[C@H](CO)NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CO)NC(=O)[C@@H](NC(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@@H](NC(=O)CNC(=O)[C@H](CCC(N)=O)NC(=O)[C@H](CO)NC(=O)[C@@H](N)CC=1NC=NC=1)[C@@H](C)O)[C@@H](C)O)C1=CC=CC=C1 MASNOZXLGMXCHN-ZLPAWPGGSA-N 0.000 description 3
- 229960004666 glucagon Drugs 0.000 description 3
- 229940097043 glucuronic acid Drugs 0.000 description 3
- 210000003958 hematopoietic stem cell Anatomy 0.000 description 3
- 210000005161 hepatic lobe Anatomy 0.000 description 3
- 230000001506 immunosuppresive effect Effects 0.000 description 3
- 238000000338 in vitro Methods 0.000 description 3
- 210000004263 induced pluripotent stem cell Anatomy 0.000 description 3
- 239000011630 iodine Substances 0.000 description 3
- 229910052740 iodine Inorganic materials 0.000 description 3
- 238000002955 isolation Methods 0.000 description 3
- 229960003299 ketamine Drugs 0.000 description 3
- 238000002372 labelling Methods 0.000 description 3
- 210000000651 myofibroblast Anatomy 0.000 description 3
- 230000017074 necrotic cell death Effects 0.000 description 3
- 102000039446 nucleic acids Human genes 0.000 description 3
- 108020004707 nucleic acids Proteins 0.000 description 3
- 238000011176 pooling Methods 0.000 description 3
- 238000003259 recombinant expression Methods 0.000 description 3
- 230000004044 response Effects 0.000 description 3
- 230000028327 secretion Effects 0.000 description 3
- FVAUCKIRQBBSSJ-UHFFFAOYSA-M sodium iodide Chemical compound [Na+].[I-] FVAUCKIRQBBSSJ-UHFFFAOYSA-M 0.000 description 3
- 239000011343 solid material Substances 0.000 description 3
- 210000001082 somatic cell Anatomy 0.000 description 3
- 241000894007 species Species 0.000 description 3
- 230000006641 stabilisation Effects 0.000 description 3
- 238000011105 stabilization Methods 0.000 description 3
- 238000010257 thawing Methods 0.000 description 3
- 238000002560 therapeutic procedure Methods 0.000 description 3
- 238000012546 transfer Methods 0.000 description 3
- 108010047303 von Willebrand Factor Proteins 0.000 description 3
- 102100036537 von Willebrand factor Human genes 0.000 description 3
- 229960001134 von willebrand factor Drugs 0.000 description 3
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Substances O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 description 3
- BPICBUSOMSTKRF-UHFFFAOYSA-N xylazine Chemical compound CC1=CC=CC(C)=C1NC1=NCCCS1 BPICBUSOMSTKRF-UHFFFAOYSA-N 0.000 description 3
- 229960001600 xylazine Drugs 0.000 description 3
- MSWZFWKMSRAUBD-IVMDWMLBSA-N 2-amino-2-deoxy-D-glucopyranose Chemical compound N[C@H]1C(O)O[C@H](CO)[C@@H](O)[C@@H]1O MSWZFWKMSRAUBD-IVMDWMLBSA-N 0.000 description 2
- 206010067484 Adverse reaction Diseases 0.000 description 2
- 102000002260 Alkaline Phosphatase Human genes 0.000 description 2
- 108020004774 Alkaline Phosphatase Proteins 0.000 description 2
- 244000105975 Antidesma platyphyllum Species 0.000 description 2
- CIWBSHSKHKDKBQ-JLAZNSOCSA-N Ascorbic acid Chemical compound OC[C@H](O)[C@H]1OC(=O)C(O)=C1O CIWBSHSKHKDKBQ-JLAZNSOCSA-N 0.000 description 2
- 241000283690 Bos taurus Species 0.000 description 2
- 208000007257 Budd-Chiari syndrome Diseases 0.000 description 2
- 102100032912 CD44 antigen Human genes 0.000 description 2
- 206010008635 Cholestasis Diseases 0.000 description 2
- 241000252203 Clupea harengus Species 0.000 description 2
- 102000010970 Connexin Human genes 0.000 description 2
- 238000000116 DAPI staining Methods 0.000 description 2
- 108020004414 DNA Proteins 0.000 description 2
- RTZKZFJDLAIYFH-UHFFFAOYSA-N Diethyl ether Chemical compound CCOCC RTZKZFJDLAIYFH-UHFFFAOYSA-N 0.000 description 2
- 208000005189 Embolism Diseases 0.000 description 2
- 102400001368 Epidermal growth factor Human genes 0.000 description 2
- 101800003838 Epidermal growth factor Proteins 0.000 description 2
- 108090000379 Fibroblast growth factor 2 Proteins 0.000 description 2
- 102000003974 Fibroblast growth factor 2 Human genes 0.000 description 2
- 102100037362 Fibronectin Human genes 0.000 description 2
- 108010067306 Fibronectins Proteins 0.000 description 2
- WSFSSNUMVMOOMR-UHFFFAOYSA-N Formaldehyde Chemical compound O=C WSFSSNUMVMOOMR-UHFFFAOYSA-N 0.000 description 2
- DHMQDGOQFOQNFH-UHFFFAOYSA-N Glycine Chemical compound NCC(O)=O DHMQDGOQFOQNFH-UHFFFAOYSA-N 0.000 description 2
- 229920002527 Glycogen Polymers 0.000 description 2
- 208000024869 Goodpasture syndrome Diseases 0.000 description 2
- 102100022057 Hepatocyte nuclear factor 1-alpha Human genes 0.000 description 2
- 101000868273 Homo sapiens CD44 antigen Proteins 0.000 description 2
- 101001045751 Homo sapiens Hepatocyte nuclear factor 1-alpha Proteins 0.000 description 2
- 101000998011 Homo sapiens Keratin, type I cytoskeletal 19 Proteins 0.000 description 2
- 101001054921 Homo sapiens Lymphatic vessel endothelial hyaluronic acid receptor 1 Proteins 0.000 description 2
- 101000972278 Homo sapiens Mucin-6 Proteins 0.000 description 2
- 101000740178 Homo sapiens Sal-like protein 4 Proteins 0.000 description 2
- 101000687905 Homo sapiens Transcription factor SOX-2 Proteins 0.000 description 2
- 206010062016 Immunosuppression Diseases 0.000 description 2
- 108090000723 Insulin-Like Growth Factor I Proteins 0.000 description 2
- 102000014429 Insulin-like growth factor Human genes 0.000 description 2
- 102000015696 Interleukins Human genes 0.000 description 2
- 108010063738 Interleukins Proteins 0.000 description 2
- PIWKPBJCKXDKJR-UHFFFAOYSA-N Isoflurane Chemical compound FC(F)OC(Cl)C(F)(F)F PIWKPBJCKXDKJR-UHFFFAOYSA-N 0.000 description 2
- 102100023974 Keratin, type II cytoskeletal 7 Human genes 0.000 description 2
- 108010070507 Keratin-7 Proteins 0.000 description 2
- 102000004058 Leukemia inhibitory factor Human genes 0.000 description 2
- 108090000581 Leukemia inhibitory factor Proteins 0.000 description 2
- 102100026849 Lymphatic vessel endothelial hyaluronic acid receptor 1 Human genes 0.000 description 2
- 241000124008 Mammalia Species 0.000 description 2
- 102100022493 Mucin-6 Human genes 0.000 description 2
- 101100043050 Mus musculus Sox4 gene Proteins 0.000 description 2
- 101100096242 Mus musculus Sox9 gene Proteins 0.000 description 2
- OVRNDRQMDRJTHS-UHFFFAOYSA-N N-acelyl-D-glucosamine Natural products CC(=O)NC1C(O)OC(CO)C(O)C1O OVRNDRQMDRJTHS-UHFFFAOYSA-N 0.000 description 2
- 102000015336 Nerve Growth Factor Human genes 0.000 description 2
- 208000007256 Nevus Diseases 0.000 description 2
- 108010038512 Platelet-Derived Growth Factor Proteins 0.000 description 2
- 102000010780 Platelet-Derived Growth Factor Human genes 0.000 description 2
- 108010067787 Proteoglycans Proteins 0.000 description 2
- 102000016611 Proteoglycans Human genes 0.000 description 2
- 108010071390 Serum Albumin Proteins 0.000 description 2
- 102000007562 Serum Albumin Human genes 0.000 description 2
- 229920002472 Starch Polymers 0.000 description 2
- QJJXYPPXXYFBGM-LFZNUXCKSA-N Tacrolimus Chemical compound C1C[C@@H](O)[C@H](OC)C[C@@H]1\C=C(/C)[C@@H]1[C@H](C)[C@@H](O)CC(=O)[C@H](CC=C)/C=C(C)/C[C@H](C)C[C@H](OC)[C@H]([C@H](C[C@H]2C)OC)O[C@@]2(O)C(=O)C(=O)N2CCCC[C@H]2C(=O)O1 QJJXYPPXXYFBGM-LFZNUXCKSA-N 0.000 description 2
- 102100024270 Transcription factor SOX-2 Human genes 0.000 description 2
- 108010009583 Transforming Growth Factors Proteins 0.000 description 2
- 102000009618 Transforming Growth Factors Human genes 0.000 description 2
- 108060008682 Tumor Necrosis Factor Proteins 0.000 description 2
- DFPAKSUCGFBDDF-ZQBYOMGUSA-N [14c]-nicotinamide Chemical compound N[14C](=O)C1=CC=CN=C1 DFPAKSUCGFBDDF-ZQBYOMGUSA-N 0.000 description 2
- 210000001015 abdomen Anatomy 0.000 description 2
- 238000010521 absorption reaction Methods 0.000 description 2
- 230000009471 action Effects 0.000 description 2
- 230000004913 activation Effects 0.000 description 2
- 238000004115 adherent culture Methods 0.000 description 2
- 230000006838 adverse reaction Effects 0.000 description 2
- AEMOLEFTQBMNLQ-WAXACMCWSA-N alpha-D-glucuronic acid Chemical compound O[C@H]1O[C@H](C(O)=O)[C@@H](O)[C@H](O)[C@H]1O AEMOLEFTQBMNLQ-WAXACMCWSA-N 0.000 description 2
- 108010026331 alpha-Fetoproteins Proteins 0.000 description 2
- 239000003242 anti bacterial agent Substances 0.000 description 2
- 229940088710 antibiotic agent Drugs 0.000 description 2
- 210000000227 basophil cell of anterior lobe of hypophysis Anatomy 0.000 description 2
- 238000005452 bending Methods 0.000 description 2
- 230000009286 beneficial effect Effects 0.000 description 2
- 229960000074 biopharmaceutical Drugs 0.000 description 2
- 210000004369 blood Anatomy 0.000 description 2
- 239000008280 blood Substances 0.000 description 2
- 230000037396 body weight Effects 0.000 description 2
- 150000001720 carbohydrates Chemical class 0.000 description 2
- 235000014633 carbohydrates Nutrition 0.000 description 2
- 230000021164 cell adhesion Effects 0.000 description 2
- 239000002771 cell marker Substances 0.000 description 2
- 230000003833 cell viability Effects 0.000 description 2
- 231100000359 cholestasis Toxicity 0.000 description 2
- 230000007870 cholestasis Effects 0.000 description 2
- 210000003459 common hepatic duct Anatomy 0.000 description 2
- 239000002131 composite material Substances 0.000 description 2
- 230000007423 decrease Effects 0.000 description 2
- 230000003247 decreasing effect Effects 0.000 description 2
- 230000001419 dependent effect Effects 0.000 description 2
- AVJBPWGFOQAPRH-FWMKGIEWSA-L dermatan sulfate Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@H](OS([O-])(=O)=O)[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@H](O)[C@H](C([O-])=O)O1 AVJBPWGFOQAPRH-FWMKGIEWSA-L 0.000 description 2
- 238000010790 dilution Methods 0.000 description 2
- 239000012895 dilution Substances 0.000 description 2
- 239000002552 dosage form Substances 0.000 description 2
- 230000034431 double-strand break repair via homologous recombination Effects 0.000 description 2
- 238000007459 endoscopic retrograde cholangiopancreatography Methods 0.000 description 2
- 229940116977 epidermal growth factor Drugs 0.000 description 2
- 210000003527 eukaryotic cell Anatomy 0.000 description 2
- 238000011156 evaluation Methods 0.000 description 2
- 230000001747 exhibiting effect Effects 0.000 description 2
- 239000013604 expression vector Substances 0.000 description 2
- 210000003722 extracellular fluid Anatomy 0.000 description 2
- 239000000284 extract Substances 0.000 description 2
- 239000012091 fetal bovine serum Substances 0.000 description 2
- 230000001605 fetal effect Effects 0.000 description 2
- 238000000684 flow cytometry Methods 0.000 description 2
- 235000013305 food Nutrition 0.000 description 2
- 210000000609 ganglia Anatomy 0.000 description 2
- 238000012239 gene modification Methods 0.000 description 2
- 102000054766 genetic haplotypes Human genes 0.000 description 2
- 230000005017 genetic modification Effects 0.000 description 2
- 235000013617 genetically modified food Nutrition 0.000 description 2
- 229960002442 glucosamine Drugs 0.000 description 2
- 102000006602 glyceraldehyde-3-phosphate dehydrogenase Human genes 0.000 description 2
- 108020004445 glyceraldehyde-3-phosphate dehydrogenase Proteins 0.000 description 2
- 229940096919 glycogen Drugs 0.000 description 2
- 235000009424 haa Nutrition 0.000 description 2
- 230000003394 haemopoietic effect Effects 0.000 description 2
- 230000036541 health Effects 0.000 description 2
- 235000019514 herring Nutrition 0.000 description 2
- 229940099552 hyaluronan Drugs 0.000 description 2
- KIUKXJAPPMFGSW-MNSSHETKSA-N hyaluronan Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@@H](O)C1O[C@H]1[C@H](O)[C@@H](O)[C@H](O[C@H]2[C@@H](C(O[C@H]3[C@@H]([C@@H](O)[C@H](O)[C@H](O3)C(O)=O)O)[C@H](O)[C@@H](CO)O2)NC(C)=O)[C@@H](C(O)=O)O1 KIUKXJAPPMFGSW-MNSSHETKSA-N 0.000 description 2
- 229960000890 hydrocortisone Drugs 0.000 description 2
- 239000001257 hydrogen Substances 0.000 description 2
- 229910052739 hydrogen Inorganic materials 0.000 description 2
- 230000006698 induction Effects 0.000 description 2
- 239000004615 ingredient Substances 0.000 description 2
- 229910052500 inorganic mineral Inorganic materials 0.000 description 2
- 230000003993 interaction Effects 0.000 description 2
- 230000008611 intercellular interaction Effects 0.000 description 2
- 229940047122 interleukins Drugs 0.000 description 2
- 230000000968 intestinal effect Effects 0.000 description 2
- 210000002490 intestinal epithelial cell Anatomy 0.000 description 2
- JEIPFZHSYJVQDO-UHFFFAOYSA-N iron(III) oxide Inorganic materials O=[Fe]O[Fe]=O JEIPFZHSYJVQDO-UHFFFAOYSA-N 0.000 description 2
- 229960002725 isoflurane Drugs 0.000 description 2
- 210000005229 liver cell Anatomy 0.000 description 2
- 239000012092 media component Substances 0.000 description 2
- 230000031864 metaphase Effects 0.000 description 2
- HPNSFSBZBAHARI-UHFFFAOYSA-N micophenolic acid Natural products OC1=C(CC=C(C)CCC(O)=O)C(OC)=C(C)C2=C1C(=O)OC2 HPNSFSBZBAHARI-UHFFFAOYSA-N 0.000 description 2
- 230000001617 migratory effect Effects 0.000 description 2
- 235000010755 mineral Nutrition 0.000 description 2
- 239000011707 mineral Substances 0.000 description 2
- 238000002156 mixing Methods 0.000 description 2
- 238000010369 molecular cloning Methods 0.000 description 2
- HPNSFSBZBAHARI-RUDMXATFSA-N mycophenolic acid Chemical compound OC1=C(C\C=C(/C)CCC(O)=O)C(OC)=C(C)C2=C1C(=O)OC2 HPNSFSBZBAHARI-RUDMXATFSA-N 0.000 description 2
- 239000013642 negative control Substances 0.000 description 2
- 229940053128 nerve growth factor Drugs 0.000 description 2
- 206010033675 panniculitis Diseases 0.000 description 2
- 230000003076 paracrine Effects 0.000 description 2
- 230000014306 paracrine signaling Effects 0.000 description 2
- 239000012188 paraffin wax Substances 0.000 description 2
- 230000001717 pathogenic effect Effects 0.000 description 2
- 230000037361 pathway Effects 0.000 description 2
- 239000008188 pellet Substances 0.000 description 2
- 239000000816 peptidomimetic Substances 0.000 description 2
- 229920003023 plastic Polymers 0.000 description 2
- 239000004033 plastic Substances 0.000 description 2
- 229920001282 polysaccharide Polymers 0.000 description 2
- 239000005017 polysaccharide Substances 0.000 description 2
- 238000011002 quantification Methods 0.000 description 2
- 230000010076 replication Effects 0.000 description 2
- 238000011160 research Methods 0.000 description 2
- 238000012552 review Methods 0.000 description 2
- 239000007320 rich medium Substances 0.000 description 2
- OARRHUQTFTUEOS-UHFFFAOYSA-N safranin Chemical compound [Cl-].C=12C=C(N)C(C)=CC2=NC2=CC(C)=C(N)C=C2[N+]=1C1=CC=CC=C1 OARRHUQTFTUEOS-UHFFFAOYSA-N 0.000 description 2
- 238000001338 self-assembly Methods 0.000 description 2
- 238000000926 separation method Methods 0.000 description 2
- 239000012090 serum-supplement Substances 0.000 description 2
- ZIQRIAYNHAKDDU-UHFFFAOYSA-N sodium;hydroiodide Chemical compound [Na].I ZIQRIAYNHAKDDU-UHFFFAOYSA-N 0.000 description 2
- 208000035736 spondylodysplastic type Ehlers-Danlos syndrome Diseases 0.000 description 2
- 230000002269 spontaneous effect Effects 0.000 description 2
- 235000019698 starch Nutrition 0.000 description 2
- 239000008107 starch Substances 0.000 description 2
- 238000011476 stem cell transplantation Methods 0.000 description 2
- 210000004304 subcutaneous tissue Anatomy 0.000 description 2
- 230000019635 sulfation Effects 0.000 description 2
- 238000005670 sulfation reaction Methods 0.000 description 2
- 230000008961 swelling Effects 0.000 description 2
- 229960001967 tacrolimus Drugs 0.000 description 2
- QJJXYPPXXYFBGM-SHYZHZOCSA-N tacrolimus Natural products CO[C@H]1C[C@H](CC[C@@H]1O)C=C(C)[C@H]2OC(=O)[C@H]3CCCCN3C(=O)C(=O)[C@@]4(O)O[C@@H]([C@H](C[C@H]4C)OC)[C@@H](C[C@H](C)CC(=C[C@@H](CC=C)C(=O)C[C@H](O)[C@H]2C)C)OC QJJXYPPXXYFBGM-SHYZHZOCSA-N 0.000 description 2
- 210000004876 tela submucosa Anatomy 0.000 description 2
- 238000013518 transcription Methods 0.000 description 2
- 230000035897 transcription Effects 0.000 description 2
- 102000003390 tumor necrosis factor Human genes 0.000 description 2
- 239000013598 vector Substances 0.000 description 2
- 230000035899 viability Effects 0.000 description 2
- 210000002417 xiphoid bone Anatomy 0.000 description 2
- RZLVQBNCHSJZPX-UHFFFAOYSA-L zinc sulfate heptahydrate Chemical compound O.O.O.O.O.O.O.[Zn+2].[O-]S([O-])(=O)=O RZLVQBNCHSJZPX-UHFFFAOYSA-L 0.000 description 2
- LEBVLXFERQHONN-UHFFFAOYSA-N 1-butyl-N-(2,6-dimethylphenyl)piperidine-2-carboxamide Chemical compound CCCCN1CCCCC1C(=O)NC1=C(C)C=CC=C1C LEBVLXFERQHONN-UHFFFAOYSA-N 0.000 description 1
- MSWZFWKMSRAUBD-GASJEMHNSA-N 2-amino-2-deoxy-D-galactopyranose Chemical compound N[C@H]1C(O)O[C@H](CO)[C@H](O)[C@@H]1O MSWZFWKMSRAUBD-GASJEMHNSA-N 0.000 description 1
- NEWKHUASLBMWRE-UHFFFAOYSA-N 2-methyl-6-(phenylethynyl)pyridine Chemical compound CC1=CC=CC(C#CC=2C=CC=CC=2)=N1 NEWKHUASLBMWRE-UHFFFAOYSA-N 0.000 description 1
- BUOYTFVLNZIELF-UHFFFAOYSA-N 2-phenyl-1h-indole-4,6-dicarboximidamide Chemical compound N1C2=CC(C(=N)N)=CC(C(N)=N)=C2C=C1C1=CC=CC=C1 BUOYTFVLNZIELF-UHFFFAOYSA-N 0.000 description 1
- MCSXGCZMEPXKIW-UHFFFAOYSA-N 3-hydroxy-4-[(4-methyl-2-nitrophenyl)diazenyl]-N-(3-nitrophenyl)naphthalene-2-carboxamide Chemical compound Cc1ccc(N=Nc2c(O)c(cc3ccccc23)C(=O)Nc2cccc(c2)[N+]([O-])=O)c(c1)[N+]([O-])=O MCSXGCZMEPXKIW-UHFFFAOYSA-N 0.000 description 1
- FHVDTGUDJYJELY-UHFFFAOYSA-N 6-{[2-carboxy-4,5-dihydroxy-6-(phosphanyloxy)oxan-3-yl]oxy}-4,5-dihydroxy-3-phosphanyloxane-2-carboxylic acid Chemical compound O1C(C(O)=O)C(P)C(O)C(O)C1OC1C(C(O)=O)OC(OP)C(O)C1O FHVDTGUDJYJELY-UHFFFAOYSA-N 0.000 description 1
- 108010005465 AC133 Antigen Proteins 0.000 description 1
- 102000005908 AC133 Antigen Human genes 0.000 description 1
- 102100027211 Albumin Human genes 0.000 description 1
- 239000012103 Alexa Fluor 488 Substances 0.000 description 1
- 239000012109 Alexa Fluor 568 Substances 0.000 description 1
- 108010053481 Antifreeze Proteins Proteins 0.000 description 1
- 102000010637 Aquaporins Human genes 0.000 description 1
- 108010063290 Aquaporins Proteins 0.000 description 1
- JEBFVOLFMLUKLF-IFPLVEIFSA-N Astaxanthin Natural products CC(=C/C=C/C(=C/C=C/C1=C(C)C(=O)C(O)CC1(C)C)/C)C=CC=C(/C)C=CC=C(/C)C=CC2=C(C)C(=O)C(O)CC2(C)C JEBFVOLFMLUKLF-IFPLVEIFSA-N 0.000 description 1
- 244000063299 Bacillus subtilis Species 0.000 description 1
- 235000014469 Bacillus subtilis Nutrition 0.000 description 1
- 241001436672 Bhatia Species 0.000 description 1
- 101100284398 Bos taurus BoLA-DQB gene Proteins 0.000 description 1
- 238000010356 CRISPR-Cas9 genome editing Methods 0.000 description 1
- 108010061299 CXCR4 Receptors Proteins 0.000 description 1
- 102000012000 CXCR4 Receptors Human genes 0.000 description 1
- 241000282465 Canis Species 0.000 description 1
- 241000283707 Capra Species 0.000 description 1
- 229920002134 Carboxymethyl cellulose Polymers 0.000 description 1
- 108090000994 Catalytic RNA Proteins 0.000 description 1
- 102000053642 Catalytic RNA Human genes 0.000 description 1
- 229920002157 Cellulin Polymers 0.000 description 1
- 241000282693 Cercopithecidae Species 0.000 description 1
- 108091006146 Channels Proteins 0.000 description 1
- 102100035294 Chemokine XC receptor 1 Human genes 0.000 description 1
- 102000019034 Chemokines Human genes 0.000 description 1
- 108010012236 Chemokines Proteins 0.000 description 1
- 101800001982 Cholecystokinin Proteins 0.000 description 1
- 102100025841 Cholecystokinin Human genes 0.000 description 1
- 108010059480 Chondroitin Sulfate Proteoglycans Proteins 0.000 description 1
- 102000005598 Chondroitin Sulfate Proteoglycans Human genes 0.000 description 1
- 108010077544 Chromatin Proteins 0.000 description 1
- 102000001187 Collagen Type III Human genes 0.000 description 1
- 108010069502 Collagen Type III Proteins 0.000 description 1
- 102000004266 Collagen Type IV Human genes 0.000 description 1
- 108010042086 Collagen Type IV Proteins 0.000 description 1
- 102000012432 Collagen Type V Human genes 0.000 description 1
- 108010022514 Collagen Type V Proteins 0.000 description 1
- 102000002734 Collagen Type VI Human genes 0.000 description 1
- 108010043741 Collagen Type VI Proteins 0.000 description 1
- 102000001191 Collagen Type VIII Human genes 0.000 description 1
- 108010069526 Collagen Type VIII Proteins 0.000 description 1
- 102000030746 Collagen Type X Human genes 0.000 description 1
- 108010022510 Collagen Type X Proteins 0.000 description 1
- 206010011224 Cough Diseases 0.000 description 1
- QASFUMOKHFSJGL-LAFRSMQTSA-N Cyclopamine Chemical compound C1C=C2C[C@@H](O)CC[C@]2(C)[C@@H](CC2=C3C)[C@@H]1[C@@H]2CC[C@@]13O[C@@H]2C[C@H](C)CN[C@H]2[C@H]1C QASFUMOKHFSJGL-LAFRSMQTSA-N 0.000 description 1
- 102000016911 Deoxyribonucleases Human genes 0.000 description 1
- 108010053770 Deoxyribonucleases Proteins 0.000 description 1
- 229920000045 Dermatan sulfate Polymers 0.000 description 1
- 229920002307 Dextran Polymers 0.000 description 1
- 238000002965 ELISA Methods 0.000 description 1
- 241000196324 Embryophyta Species 0.000 description 1
- 102000005593 Endopeptidases Human genes 0.000 description 1
- 108010059378 Endopeptidases Proteins 0.000 description 1
- 102000003951 Erythropoietin Human genes 0.000 description 1
- 108090000394 Erythropoietin Proteins 0.000 description 1
- 241000282324 Felis Species 0.000 description 1
- 101100058548 Felis catus BMI1 gene Proteins 0.000 description 1
- 102100028071 Fibroblast growth factor 7 Human genes 0.000 description 1
- 108090000385 Fibroblast growth factor 7 Proteins 0.000 description 1
- 108010022355 Fibroins Proteins 0.000 description 1
- 241000287828 Gallus gallus Species 0.000 description 1
- 108010010803 Gelatin Proteins 0.000 description 1
- 239000004471 Glycine Substances 0.000 description 1
- 108010017213 Granulocyte-Macrophage Colony-Stimulating Factor Proteins 0.000 description 1
- 102100039620 Granulocyte-macrophage colony-stimulating factor Human genes 0.000 description 1
- 102000008055 Heparan Sulfate Proteoglycans Human genes 0.000 description 1
- 206010019663 Hepatic failure Diseases 0.000 description 1
- 108010049606 Hepatocyte Nuclear Factors Proteins 0.000 description 1
- 102000008088 Hepatocyte Nuclear Factors Human genes 0.000 description 1
- 102100029087 Hepatocyte nuclear factor 6 Human genes 0.000 description 1
- 102100031000 Hepatoma-derived growth factor Human genes 0.000 description 1
- 108010033040 Histones Proteins 0.000 description 1
- 101150068639 Hnf4a gene Proteins 0.000 description 1
- 241000282412 Homo Species 0.000 description 1
- 101000804783 Homo sapiens Chemokine XC receptor 1 Proteins 0.000 description 1
- 101001002170 Homo sapiens Glutamine amidotransferase-like class 1 domain-containing protein 3, mitochondrial Proteins 0.000 description 1
- 101000988619 Homo sapiens Hepatocyte nuclear factor 6 Proteins 0.000 description 1
- 101001083798 Homo sapiens Hepatoma-derived growth factor Proteins 0.000 description 1
- 101000599852 Homo sapiens Intercellular adhesion molecule 1 Proteins 0.000 description 1
- 101000971533 Homo sapiens Killer cell lectin-like receptor subfamily G member 1 Proteins 0.000 description 1
- 101001139134 Homo sapiens Krueppel-like factor 4 Proteins 0.000 description 1
- 101000981765 Homo sapiens Leucine-rich repeat-containing G-protein coupled receptor 6 Proteins 0.000 description 1
- 101001094700 Homo sapiens POU domain, class 5, transcription factor 1 Proteins 0.000 description 1
- 101000612089 Homo sapiens Pancreas/duodenum homeobox protein 1 Proteins 0.000 description 1
- 101000595923 Homo sapiens Placenta growth factor Proteins 0.000 description 1
- 101001100327 Homo sapiens RNA-binding protein 45 Proteins 0.000 description 1
- 101000738771 Homo sapiens Receptor-type tyrosine-protein phosphatase C Proteins 0.000 description 1
- 101000716102 Homo sapiens T-cell surface glycoprotein CD4 Proteins 0.000 description 1
- 101000843556 Homo sapiens Transcription factor HES-1 Proteins 0.000 description 1
- 101000979205 Homo sapiens Transcription factor MafA Proteins 0.000 description 1
- 101000652332 Homo sapiens Transcription factor SOX-1 Proteins 0.000 description 1
- 108091006905 Human Serum Albumin Proteins 0.000 description 1
- 102000008100 Human Serum Albumin Human genes 0.000 description 1
- XQFRJNBWHJMXHO-RRKCRQDMSA-N IDUR Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(=O)NC(=O)C(I)=C1 XQFRJNBWHJMXHO-RRKCRQDMSA-N 0.000 description 1
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical compound C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 1
- 102100037877 Intercellular adhesion molecule 1 Human genes 0.000 description 1
- 102000014150 Interferons Human genes 0.000 description 1
- 108010050904 Interferons Proteins 0.000 description 1
- 102100033421 Keratin, type I cytoskeletal 18 Human genes 0.000 description 1
- 102100023972 Keratin, type II cytoskeletal 8 Human genes 0.000 description 1
- 108010066327 Keratin-18 Proteins 0.000 description 1
- 108010066302 Keratin-19 Proteins 0.000 description 1
- 108010070511 Keratin-8 Proteins 0.000 description 1
- 102100021457 Killer cell lectin-like receptor subfamily G member 1 Human genes 0.000 description 1
- 102100020677 Krueppel-like factor 4 Human genes 0.000 description 1
- 102100024140 Leucine-rich repeat-containing G-protein coupled receptor 6 Human genes 0.000 description 1
- 102000004882 Lipase Human genes 0.000 description 1
- 108090001060 Lipase Proteins 0.000 description 1
- 239000004367 Lipase Substances 0.000 description 1
- 102000008072 Lymphokines Human genes 0.000 description 1
- 108010074338 Lymphokines Proteins 0.000 description 1
- 108010076557 Matrix Metalloproteinase 14 Proteins 0.000 description 1
- 102000005741 Metalloproteases Human genes 0.000 description 1
- 108010006035 Metalloproteases Proteins 0.000 description 1
- 206010027476 Metastases Diseases 0.000 description 1
- 102000036436 Metzincins Human genes 0.000 description 1
- 108091007161 Metzincins Proteins 0.000 description 1
- 102000013967 Monokines Human genes 0.000 description 1
- 108010050619 Monokines Proteins 0.000 description 1
- 241001529936 Murinae Species 0.000 description 1
- OVRNDRQMDRJTHS-RTRLPJTCSA-N N-acetyl-D-glucosamine Chemical compound CC(=O)N[C@H]1C(O)O[C@H](CO)[C@@H](O)[C@@H]1O OVRNDRQMDRJTHS-RTRLPJTCSA-N 0.000 description 1
- OVRNDRQMDRJTHS-FMDGEEDCSA-N N-acetyl-beta-D-glucosamine Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O OVRNDRQMDRJTHS-FMDGEEDCSA-N 0.000 description 1
- 238000011887 Necropsy Methods 0.000 description 1
- 206010028980 Neoplasm Diseases 0.000 description 1
- 102000007072 Nerve Growth Factors Human genes 0.000 description 1
- 102100027347 Neural cell adhesion molecule 1 Human genes 0.000 description 1
- 108050003738 Neural cell adhesion molecule 1 Proteins 0.000 description 1
- 102100023616 Neural cell adhesion molecule L1-like protein Human genes 0.000 description 1
- 101100519293 Neurospora crassa (strain ATCC 24698 / 74-OR23-1A / CBS 708.71 / DSM 1257 / FGSC 987) pdx-1 gene Proteins 0.000 description 1
- 108020004711 Nucleic Acid Probes Proteins 0.000 description 1
- 108091028043 Nucleic acid sequence Proteins 0.000 description 1
- 108010047956 Nucleosomes Proteins 0.000 description 1
- 239000004677 Nylon Substances 0.000 description 1
- 108010068425 Octamer Transcription Factor-3 Proteins 0.000 description 1
- 108091034117 Oligonucleotide Proteins 0.000 description 1
- 241000366596 Osiris Species 0.000 description 1
- 238000012408 PCR amplification Methods 0.000 description 1
- 235000021314 Palmitic acid Nutrition 0.000 description 1
- 235000021319 Palmitoleic acid Nutrition 0.000 description 1
- 102000016387 Pancreatic elastase Human genes 0.000 description 1
- 108010067372 Pancreatic elastase Proteins 0.000 description 1
- 238000010220 Pearson correlation analysis Methods 0.000 description 1
- 241000233805 Phoenix Species 0.000 description 1
- 102100035194 Placenta growth factor Human genes 0.000 description 1
- 102000004211 Platelet factor 4 Human genes 0.000 description 1
- 108090000778 Platelet factor 4 Proteins 0.000 description 1
- 239000004743 Polypropylene Substances 0.000 description 1
- 108010007568 Protamines Proteins 0.000 description 1
- 102000007327 Protamines Human genes 0.000 description 1
- 102100038823 RNA-binding protein 45 Human genes 0.000 description 1
- 108091030071 RNAI Proteins 0.000 description 1
- 102100037422 Receptor-type tyrosine-protein phosphatase C Human genes 0.000 description 1
- 108020004511 Recombinant DNA Proteins 0.000 description 1
- 108091028664 Ribonucleotide Proteins 0.000 description 1
- 101710192312 Sal-like protein 4 Proteins 0.000 description 1
- 102100037505 Secretin Human genes 0.000 description 1
- 108010086019 Secretin Proteins 0.000 description 1
- 102100028927 Secretin receptor Human genes 0.000 description 1
- 206010039897 Sedation Diseases 0.000 description 1
- 241000607720 Serratia Species 0.000 description 1
- 235000021355 Stearic acid Nutrition 0.000 description 1
- 238000000692 Student's t-test Methods 0.000 description 1
- 108090000054 Syndecan-2 Proteins 0.000 description 1
- 102100036011 T-cell surface glycoprotein CD4 Human genes 0.000 description 1
- 102000036693 Thrombopoietin Human genes 0.000 description 1
- 108010041111 Thrombopoietin Proteins 0.000 description 1
- AUYYCJSJGJYCDS-LBPRGKRZSA-N Thyrolar Chemical compound IC1=CC(C[C@H](N)C(O)=O)=CC(I)=C1OC1=CC=C(O)C(I)=C1 AUYYCJSJGJYCDS-LBPRGKRZSA-N 0.000 description 1
- 108010048992 Transcription Factor 4 Proteins 0.000 description 1
- 102100023489 Transcription factor 4 Human genes 0.000 description 1
- 102100030798 Transcription factor HES-1 Human genes 0.000 description 1
- 102100030248 Transcription factor SOX-1 Human genes 0.000 description 1
- 108020004566 Transfer RNA Proteins 0.000 description 1
- 102100023935 Transmembrane glycoprotein NMB Human genes 0.000 description 1
- 108020004417 Untranslated RNA Proteins 0.000 description 1
- 102000039634 Untranslated RNA Human genes 0.000 description 1
- 101710181748 Venom protease Proteins 0.000 description 1
- 108010067390 Viral Proteins Proteins 0.000 description 1
- 102000013814 Wnt Human genes 0.000 description 1
- 108050003627 Wnt Proteins 0.000 description 1
- 102000036859 Zinc-dependent proteases Human genes 0.000 description 1
- 108091006973 Zinc-dependent proteases Proteins 0.000 description 1
- 238000012084 abdominal surgery Methods 0.000 description 1
- 230000002159 abnormal effect Effects 0.000 description 1
- 238000005299 abrasion Methods 0.000 description 1
- 239000002253 acid Substances 0.000 description 1
- 210000000577 adipose tissue Anatomy 0.000 description 1
- 230000002411 adverse Effects 0.000 description 1
- 230000002776 aggregation Effects 0.000 description 1
- 238000004220 aggregation Methods 0.000 description 1
- 238000007605 air drying Methods 0.000 description 1
- 229940072056 alginate Drugs 0.000 description 1
- 229920000615 alginic acid Polymers 0.000 description 1
- 235000010443 alginic acid Nutrition 0.000 description 1
- SHGAZHPCJJPHSC-YCNIQYBTSA-N all-trans-retinoic acid Chemical compound OC(=O)\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C SHGAZHPCJJPHSC-YCNIQYBTSA-N 0.000 description 1
- 235000020661 alpha-linolenic acid Nutrition 0.000 description 1
- 210000004381 amniotic fluid Anatomy 0.000 description 1
- 230000003321 amplification Effects 0.000 description 1
- 230000033115 angiogenesis Effects 0.000 description 1
- 210000004102 animal cell Anatomy 0.000 description 1
- 230000002528 anti-freeze Effects 0.000 description 1
- 230000000890 antigenic effect Effects 0.000 description 1
- 210000000709 aorta Anatomy 0.000 description 1
- 235000010323 ascorbic acid Nutrition 0.000 description 1
- 229960005070 ascorbic acid Drugs 0.000 description 1
- 239000011668 ascorbic acid Substances 0.000 description 1
- MQZIGYBFDRPAKN-ZWAPEEGVSA-N astaxanthin Chemical compound C([C@H](O)C(=O)C=1C)C(C)(C)C=1/C=C/C(/C)=C/C=C/C(/C)=C/C=C/C=C(C)C=CC=C(C)C=CC1=C(C)C(=O)[C@@H](O)CC1(C)C MQZIGYBFDRPAKN-ZWAPEEGVSA-N 0.000 description 1
- 229940022405 astaxanthin Drugs 0.000 description 1
- 235000013793 astaxanthin Nutrition 0.000 description 1
- 239000001168 astaxanthin Substances 0.000 description 1
- 208000006673 asthma Diseases 0.000 description 1
- 230000003140 astrocytic effect Effects 0.000 description 1
- 238000011888 autopsy Methods 0.000 description 1
- 239000000987 azo dye Substances 0.000 description 1
- 230000001580 bacterial effect Effects 0.000 description 1
- 210000002469 basement membrane Anatomy 0.000 description 1
- 210000000741 bile canaliculi Anatomy 0.000 description 1
- 238000002306 biochemical method Methods 0.000 description 1
- 239000000560 biocompatible material Substances 0.000 description 1
- 239000013060 biological fluid Substances 0.000 description 1
- 230000031018 biological processes and functions Effects 0.000 description 1
- 230000033228 biological regulation Effects 0.000 description 1
- 229920001222 biopolymer Polymers 0.000 description 1
- 230000000740 bleeding effect Effects 0.000 description 1
- 230000000903 blocking effect Effects 0.000 description 1
- 238000009534 blood test Methods 0.000 description 1
- 108091005948 blue fluorescent proteins Proteins 0.000 description 1
- 210000001185 bone marrow Anatomy 0.000 description 1
- 210000004271 bone marrow stromal cell Anatomy 0.000 description 1
- 229960003150 bupivacaine Drugs 0.000 description 1
- 238000010805 cDNA synthesis kit Methods 0.000 description 1
- 229940069978 calcium supplement Drugs 0.000 description 1
- 201000011510 cancer Diseases 0.000 description 1
- 230000023852 carbohydrate metabolic process Effects 0.000 description 1
- 235000021256 carbohydrate metabolism Nutrition 0.000 description 1
- 229940077731 carbohydrate nutrients Drugs 0.000 description 1
- 239000001768 carboxy methyl cellulose Substances 0.000 description 1
- 235000010948 carboxy methyl cellulose Nutrition 0.000 description 1
- 239000008112 carboxymethyl-cellulose Substances 0.000 description 1
- 230000015556 catabolic process Effects 0.000 description 1
- 239000006143 cell culture medium Substances 0.000 description 1
- 230000003915 cell function Effects 0.000 description 1
- 230000010261 cell growth Effects 0.000 description 1
- 238000005119 centrifugation Methods 0.000 description 1
- 239000003795 chemical substances by application Substances 0.000 description 1
- 235000013330 chicken meat Nutrition 0.000 description 1
- 229940107137 cholecystokinin Drugs 0.000 description 1
- KXKPYJOVDUMHGS-OSRGNVMNSA-N chondroitin sulfate Chemical compound CC(=O)N[C@H]1[C@H](O)O[C@H](OS(O)(=O)=O)[C@H](O)[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@H](O)[C@@H](C(O)=O)O1 KXKPYJOVDUMHGS-OSRGNVMNSA-N 0.000 description 1
- 210000003483 chromatin Anatomy 0.000 description 1
- 230000015271 coagulation Effects 0.000 description 1
- 238000005345 coagulation Methods 0.000 description 1
- 229940096422 collagen type i Drugs 0.000 description 1
- 229940047120 colony stimulating factors Drugs 0.000 description 1
- 230000000295 complement effect Effects 0.000 description 1
- 150000001875 compounds Chemical class 0.000 description 1
- 238000002591 computed tomography Methods 0.000 description 1
- 238000012790 confirmation Methods 0.000 description 1
- 238000001218 confocal laser scanning microscopy Methods 0.000 description 1
- 230000021615 conjugation Effects 0.000 description 1
- 239000000994 contrast dye Substances 0.000 description 1
- 238000007796 conventional method Methods 0.000 description 1
- 239000003246 corticosteroid Substances 0.000 description 1
- 229960001334 corticosteroids Drugs 0.000 description 1
- QASFUMOKHFSJGL-UHFFFAOYSA-N cyclopamine Natural products C1C=C2CC(O)CCC2(C)C(CC2=C3C)C1C2CCC13OC2CC(C)CNC2C1C QASFUMOKHFSJGL-UHFFFAOYSA-N 0.000 description 1
- 230000001086 cytosolic effect Effects 0.000 description 1
- 238000013016 damping Methods 0.000 description 1
- 230000034994 death Effects 0.000 description 1
- 230000007547 defect Effects 0.000 description 1
- 239000007857 degradation product Substances 0.000 description 1
- 239000005547 deoxyribonucleotide Substances 0.000 description 1
- 125000002637 deoxyribonucleotide group Chemical group 0.000 description 1
- 229940051593 dermatan sulfate Drugs 0.000 description 1
- 238000001514 detection method Methods 0.000 description 1
- 238000001784 detoxification Methods 0.000 description 1
- 238000011161 development Methods 0.000 description 1
- 230000018109 developmental process Effects 0.000 description 1
- 235000005911 diet Nutrition 0.000 description 1
- 230000037213 diet Effects 0.000 description 1
- 235000015872 dietary supplement Nutrition 0.000 description 1
- 230000009274 differential gene expression Effects 0.000 description 1
- 238000009792 diffusion process Methods 0.000 description 1
- 230000029087 digestion Effects 0.000 description 1
- 239000000539 dimer Substances 0.000 description 1
- 239000006185 dispersion Substances 0.000 description 1
- 238000004090 dissolution Methods 0.000 description 1
- 150000002019 disulfides Chemical class 0.000 description 1
- 238000004043 dyeing Methods 0.000 description 1
- 230000002900 effect on cell Effects 0.000 description 1
- 239000013013 elastic material Substances 0.000 description 1
- 230000008030 elimination Effects 0.000 description 1
- 238000003379 elimination reaction Methods 0.000 description 1
- 230000010102 embolization Effects 0.000 description 1
- 230000002124 endocrine Effects 0.000 description 1
- 210000003890 endocrine cell Anatomy 0.000 description 1
- 229940066758 endopeptidases Drugs 0.000 description 1
- 238000009558 endoscopic ultrasound Methods 0.000 description 1
- 239000002158 endotoxin Substances 0.000 description 1
- 238000010201 enrichment analysis Methods 0.000 description 1
- 210000003743 erythrocyte Anatomy 0.000 description 1
- 229940105423 erythropoietin Drugs 0.000 description 1
- 150000002148 esters Chemical class 0.000 description 1
- 230000029142 excretion Effects 0.000 description 1
- 238000010195 expression analysis Methods 0.000 description 1
- 210000002603 extrahepatic bile duct Anatomy 0.000 description 1
- 239000004744 fabric Substances 0.000 description 1
- 230000002550 fecal effect Effects 0.000 description 1
- 238000000855 fermentation Methods 0.000 description 1
- 230000004151 fermentation Effects 0.000 description 1
- 102000013373 fibrillar collagen Human genes 0.000 description 1
- 108060002894 fibrillar collagen Proteins 0.000 description 1
- 230000003176 fibrotic effect Effects 0.000 description 1
- 102000034287 fluorescent proteins Human genes 0.000 description 1
- 108091006047 fluorescent proteins Proteins 0.000 description 1
- 238000009472 formulation Methods 0.000 description 1
- 239000012634 fragment Substances 0.000 description 1
- 108020001507 fusion proteins Proteins 0.000 description 1
- 102000037865 fusion proteins Human genes 0.000 description 1
- 230000005021 gait Effects 0.000 description 1
- 229930182830 galactose Natural products 0.000 description 1
- 239000007789 gas Substances 0.000 description 1
- 239000008273 gelatin Substances 0.000 description 1
- 229920000159 gelatin Polymers 0.000 description 1
- 235000019322 gelatine Nutrition 0.000 description 1
- 235000011852 gelatine desserts Nutrition 0.000 description 1
- 230000009368 gene silencing by RNA Effects 0.000 description 1
- 238000010353 genetic engineering Methods 0.000 description 1
- 239000011521 glass Substances 0.000 description 1
- 239000003292 glue Substances 0.000 description 1
- 150000004676 glycans Chemical class 0.000 description 1
- 230000023597 hemostasis Effects 0.000 description 1
- 239000000833 heterodimer Substances 0.000 description 1
- 230000007768 histopathological growth pattern Effects 0.000 description 1
- 235000012907 honey Nutrition 0.000 description 1
- 238000009396 hybridization Methods 0.000 description 1
- GTDOPRQDTRLYAL-UHFFFAOYSA-N hydrogen peroxide;methanol Chemical compound OC.OO GTDOPRQDTRLYAL-UHFFFAOYSA-N 0.000 description 1
- 229960004716 idoxuridine Drugs 0.000 description 1
- 210000003111 iliac vein Anatomy 0.000 description 1
- 210000001822 immobilized cell Anatomy 0.000 description 1
- 230000002163 immunogen Effects 0.000 description 1
- 230000002055 immunohistochemical effect Effects 0.000 description 1
- 238000011532 immunohistochemical staining Methods 0.000 description 1
- 239000003018 immunosuppressive agent Substances 0.000 description 1
- 229940124589 immunosuppressive drug Drugs 0.000 description 1
- 238000005470 impregnation Methods 0.000 description 1
- 238000011065 in-situ storage Methods 0.000 description 1
- 230000002779 inactivation Effects 0.000 description 1
- 238000010348 incorporation Methods 0.000 description 1
- 238000011534 incubation Methods 0.000 description 1
- 230000004054 inflammatory process Effects 0.000 description 1
- 239000003999 initiator Substances 0.000 description 1
- 230000009027 insemination Effects 0.000 description 1
- 102000028416 insulin-like growth factor binding Human genes 0.000 description 1
- 108091022911 insulin-like growth factor binding Proteins 0.000 description 1
- 229940047124 interferons Drugs 0.000 description 1
- 210000004347 intestinal mucosa Anatomy 0.000 description 1
- 238000010253 intravenous injection Methods 0.000 description 1
- OGQSCIYDJSNCMY-UHFFFAOYSA-H iron(3+);methyl-dioxido-oxo-$l^{5}-arsane Chemical compound [Fe+3].[Fe+3].C[As]([O-])([O-])=O.C[As]([O-])([O-])=O.C[As]([O-])([O-])=O OGQSCIYDJSNCMY-UHFFFAOYSA-H 0.000 description 1
- 235000015110 jellies Nutrition 0.000 description 1
- 239000008274 jelly Substances 0.000 description 1
- 231100000636 lethal dose Toxicity 0.000 description 1
- 210000004901 leucine-rich repeat Anatomy 0.000 description 1
- 210000000265 leukocyte Anatomy 0.000 description 1
- 239000003446 ligand Substances 0.000 description 1
- 235000020778 linoleic acid Nutrition 0.000 description 1
- 235000019421 lipase Nutrition 0.000 description 1
- 231100000835 liver failure Toxicity 0.000 description 1
- 208000007903 liver failure Diseases 0.000 description 1
- 238000007449 liver function test Methods 0.000 description 1
- 230000007774 longterm Effects 0.000 description 1
- 210000004880 lymph fluid Anatomy 0.000 description 1
- 210000004962 mammalian cell Anatomy 0.000 description 1
- 238000013507 mapping Methods 0.000 description 1
- 238000005259 measurement Methods 0.000 description 1
- 230000001404 mediated effect Effects 0.000 description 1
- 210000000713 mesentery Anatomy 0.000 description 1
- 230000004060 metabolic process Effects 0.000 description 1
- 230000009401 metastasis Effects 0.000 description 1
- WSFSSNUMVMOOMR-NJFSPNSNSA-N methanone Chemical compound O=[14CH2] WSFSSNUMVMOOMR-NJFSPNSNSA-N 0.000 description 1
- 238000001000 micrograph Methods 0.000 description 1
- VYQNWZOUAUKGHI-UHFFFAOYSA-N monobenzone Chemical compound C1=CC(O)=CC=C1OCC1=CC=CC=C1 VYQNWZOUAUKGHI-UHFFFAOYSA-N 0.000 description 1
- 239000000178 monomer Substances 0.000 description 1
- 230000000877 morphologic effect Effects 0.000 description 1
- 230000035772 mutation Effects 0.000 description 1
- 229940014456 mycophenolate Drugs 0.000 description 1
- 229960000951 mycophenolic acid Drugs 0.000 description 1
- VMGAPWLDMVPYIA-HIDZBRGKSA-N n'-amino-n-iminomethanimidamide Chemical compound N\N=C\N=N VMGAPWLDMVPYIA-HIDZBRGKSA-N 0.000 description 1
- 229950006780 n-acetylglucosamine Drugs 0.000 description 1
- 239000005445 natural material Substances 0.000 description 1
- 210000001178 neural stem cell Anatomy 0.000 description 1
- 210000002569 neuron Anatomy 0.000 description 1
- 239000003900 neurotrophic factor Substances 0.000 description 1
- 210000000440 neutrophil Anatomy 0.000 description 1
- 238000003199 nucleic acid amplification method Methods 0.000 description 1
- 238000007899 nucleic acid hybridization Methods 0.000 description 1
- 239000002853 nucleic acid probe Substances 0.000 description 1
- 210000001623 nucleosome Anatomy 0.000 description 1
- 229920001778 nylon Polymers 0.000 description 1
- QIQXTHQIDYTFRH-UHFFFAOYSA-N octadecanoic acid Chemical class CCCCCCCCCCCCCCCCCC(O)=O QIQXTHQIDYTFRH-UHFFFAOYSA-N 0.000 description 1
- 235000021313 oleic acid Nutrition 0.000 description 1
- ZQPPMHVWECSIRJ-KTKRTIGZSA-N oleic acid group Chemical group C(CCCCCCC\C=C/CCCCCCCC)(=O)O ZQPPMHVWECSIRJ-KTKRTIGZSA-N 0.000 description 1
- 238000002515 oligonucleotide synthesis Methods 0.000 description 1
- 230000003287 optical effect Effects 0.000 description 1
- 239000003960 organic solvent Substances 0.000 description 1
- 230000010355 oscillation Effects 0.000 description 1
- IPCSVZSSVZVIGE-UHFFFAOYSA-N palmitic acid group Chemical group C(CCCCCCCCCCCCCCC)(=O)O IPCSVZSSVZVIGE-UHFFFAOYSA-N 0.000 description 1
- 230000015031 pancreas development Effects 0.000 description 1
- 230000036961 partial effect Effects 0.000 description 1
- 229960001412 pentobarbital Drugs 0.000 description 1
- WEXRUCMBJFQVBZ-UHFFFAOYSA-N pentobarbital Chemical compound CCCC(C)C1(CC)C(=O)NC(=O)NC1=O WEXRUCMBJFQVBZ-UHFFFAOYSA-N 0.000 description 1
- 230000009984 peri-natal effect Effects 0.000 description 1
- 230000002093 peripheral effect Effects 0.000 description 1
- 102000013415 peroxidase activity proteins Human genes 0.000 description 1
- 108040007629 peroxidase activity proteins Proteins 0.000 description 1
- 238000013310 pig model Methods 0.000 description 1
- 210000005152 placental membrane Anatomy 0.000 description 1
- 239000013612 plasmid Substances 0.000 description 1
- 210000001778 pluripotent stem cell Anatomy 0.000 description 1
- 238000006116 polymerization reaction Methods 0.000 description 1
- 229920001155 polypropylene Polymers 0.000 description 1
- OXCMYAYHXIHQOA-UHFFFAOYSA-N potassium;[2-butyl-5-chloro-3-[[4-[2-(1,2,4-triaza-3-azanidacyclopenta-1,4-dien-5-yl)phenyl]phenyl]methyl]imidazol-4-yl]methanol Chemical compound [K+].CCCCC1=NC(Cl)=C(CO)N1CC1=CC=C(C=2C(=CC=CC=2)C2=N[N-]N=N2)C=C1 OXCMYAYHXIHQOA-UHFFFAOYSA-N 0.000 description 1
- 230000003389 potentiating effect Effects 0.000 description 1
- 238000012545 processing Methods 0.000 description 1
- 210000003689 pubic bone Anatomy 0.000 description 1
- 238000003908 quality control method Methods 0.000 description 1
- 238000004445 quantitative analysis Methods 0.000 description 1
- 238000010791 quenching Methods 0.000 description 1
- 230000000171 quenching effect Effects 0.000 description 1
- 230000035802 rapid maturation Effects 0.000 description 1
- 239000002994 raw material Substances 0.000 description 1
- 102000005962 receptors Human genes 0.000 description 1
- 108020003175 receptors Proteins 0.000 description 1
- 239000001044 red dye Substances 0.000 description 1
- 230000009467 reduction Effects 0.000 description 1
- 230000008929 regeneration Effects 0.000 description 1
- 238000011069 regeneration method Methods 0.000 description 1
- 230000001105 regulatory effect Effects 0.000 description 1
- 102000037983 regulatory factors Human genes 0.000 description 1
- 108091008025 regulatory factors Proteins 0.000 description 1
- BOLDJAUMGUJJKM-LSDHHAIUSA-N renifolin D Natural products CC(=C)[C@@H]1Cc2c(O)c(O)ccc2[C@H]1CC(=O)c3ccc(O)cc3O BOLDJAUMGUJJKM-LSDHHAIUSA-N 0.000 description 1
- 230000029058 respiratory gaseous exchange Effects 0.000 description 1
- 230000008458 response to injury Effects 0.000 description 1
- 230000000284 resting effect Effects 0.000 description 1
- 230000000717 retained effect Effects 0.000 description 1
- 210000001995 reticulocyte Anatomy 0.000 description 1
- 229930002330 retinoic acid Natural products 0.000 description 1
- 238000000518 rheometry Methods 0.000 description 1
- 239000002336 ribonucleotide Substances 0.000 description 1
- 125000002652 ribonucleotide group Chemical group 0.000 description 1
- 108020004418 ribosomal RNA Proteins 0.000 description 1
- 108091092562 ribozyme Proteins 0.000 description 1
- 235000002020 sage Nutrition 0.000 description 1
- 238000007789 sealing Methods 0.000 description 1
- 229960002101 secretin Drugs 0.000 description 1
- OWMZNFCDEHGFEP-NFBCVYDUSA-N secretin human Chemical compound C([C@@H](C(=O)N[C@H](C(=O)N[C@@H](CO)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCC(O)=O)C(=O)NCC(=O)N[C@@H](C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCC(N)=O)C(=O)NCC(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](C(C)C)C(N)=O)[C@@H](C)O)NC(=O)[C@@H](NC(=O)CNC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CO)NC(=O)[C@@H](N)CC=1NC=NC=1)[C@@H](C)O)C1=CC=CC=C1 OWMZNFCDEHGFEP-NFBCVYDUSA-N 0.000 description 1
- 108700027603 secretin receptor Proteins 0.000 description 1
- 230000003248 secreting effect Effects 0.000 description 1
- 230000036280 sedation Effects 0.000 description 1
- 238000010187 selection method Methods 0.000 description 1
- 230000000405 serological effect Effects 0.000 description 1
- IZTQOLKUZKXIRV-YRVFCXMDSA-N sincalide Chemical compound C([C@@H](C(=O)N[C@@H](CCSC)C(=O)NCC(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CC=1C=CC=CC=1)C(N)=O)NC(=O)[C@@H](N)CC(O)=O)C1=CC=C(OS(O)(=O)=O)C=C1 IZTQOLKUZKXIRV-YRVFCXMDSA-N 0.000 description 1
- 239000002356 single layer Substances 0.000 description 1
- 239000003998 snake venom Substances 0.000 description 1
- 239000011734 sodium Substances 0.000 description 1
- 229910052708 sodium Inorganic materials 0.000 description 1
- 235000009518 sodium iodide Nutrition 0.000 description 1
- YWIVKILSMZOHHF-QJZPQSOGSA-N sodium;(2s,3s,4s,5r,6r)-6-[(2s,3r,4r,5s,6r)-3-acetamido-2-[(2s,3s,4r,5r,6r)-6-[(2r,3r,4r,5s,6r)-3-acetamido-2,5-dihydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-2-carboxy-4,5-dihydroxyoxan-3-yl]oxy-5-hydroxy-6-(hydroxymethyl)oxan-4-yl]oxy-3,4,5-trihydroxyoxane-2- Chemical class [Na+].CC(=O)N[C@H]1[C@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O[C@H]1[C@H](O)[C@@H](O)[C@H](O[C@H]2[C@@H]([C@@H](O[C@H]3[C@@H]([C@@H](O)[C@H](O)[C@H](O3)C(O)=O)O)[C@H](O)[C@@H](CO)O2)NC(C)=O)[C@@H](C(O)=O)O1 YWIVKILSMZOHHF-QJZPQSOGSA-N 0.000 description 1
- 230000003381 solubilizing effect Effects 0.000 description 1
- 230000000392 somatic effect Effects 0.000 description 1
- 230000003595 spectral effect Effects 0.000 description 1
- 210000000952 spleen Anatomy 0.000 description 1
- 230000010473 stable expression Effects 0.000 description 1
- 229910001220 stainless steel Inorganic materials 0.000 description 1
- 239000010935 stainless steel Substances 0.000 description 1
- 238000003756 stirring Methods 0.000 description 1
- 210000002784 stomach Anatomy 0.000 description 1
- 239000012536 storage buffer Substances 0.000 description 1
- 238000005728 strengthening Methods 0.000 description 1
- 235000000346 sugar Nutrition 0.000 description 1
- 150000008163 sugars Chemical class 0.000 description 1
- 230000009469 supplementation Effects 0.000 description 1
- 108010070228 surgisis Proteins 0.000 description 1
- 238000003786 synthesis reaction Methods 0.000 description 1
- 238000012353 t test Methods 0.000 description 1
- 230000001225 therapeutic effect Effects 0.000 description 1
- 210000001578 tight junction Anatomy 0.000 description 1
- 230000036962 time dependent Effects 0.000 description 1
- 239000003106 tissue adhesive Substances 0.000 description 1
- 230000000699 topical effect Effects 0.000 description 1
- 239000011573 trace mineral Substances 0.000 description 1
- 235000013619 trace mineral Nutrition 0.000 description 1
- 238000012549 training Methods 0.000 description 1
- 238000013519 translation Methods 0.000 description 1
- 108091007466 transmembrane glycoproteins Proteins 0.000 description 1
- 230000032258 transport Effects 0.000 description 1
- 229960001727 tretinoin Drugs 0.000 description 1
- 210000005239 tubule Anatomy 0.000 description 1
- 238000002604 ultrasonography Methods 0.000 description 1
- 210000003954 umbilical cord Anatomy 0.000 description 1
- 238000012795 verification Methods 0.000 description 1
- 239000003190 viscoelastic substance Substances 0.000 description 1
- 239000011345 viscous material Substances 0.000 description 1
- 239000011800 void material Substances 0.000 description 1
- 239000002699 waste material Substances 0.000 description 1
- 239000001993 wax Substances 0.000 description 1
Images




















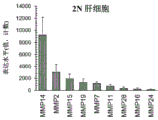
















Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3886—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells comprising two or more cell types
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/14—Macromolecular materials
- A61L27/20—Polysaccharides
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/14—Macromolecular materials
- A61L27/22—Polypeptides or derivatives thereof, e.g. degradation products
- A61L27/227—Other specific proteins or polypeptides not covered by A61L27/222, A61L27/225 or A61L27/24
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/14—Macromolecular materials
- A61L27/26—Mixtures of macromolecular compounds
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/28—Materials for coating prostheses
- A61L27/34—Macromolecular materials
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/3604—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix characterised by the human or animal origin of the biological material, e.g. hair, fascia, fish scales, silk, shellac, pericardium, pleura, renal tissue, amniotic membrane, parenchymal tissue, fetal tissue, muscle tissue, fat tissue, enamel
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/3641—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix characterised by the site of application in the body
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3804—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by specific cells or progenitors thereof, e.g. fibroblasts, connective tissue cells, kidney cells
- A61L27/3813—Epithelial cells, e.g. keratinocytes, urothelial cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3804—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by specific cells or progenitors thereof, e.g. fibroblasts, connective tissue cells, kidney cells
- A61L27/3834—Cells able to produce different cell types, e.g. hematopoietic stem cells, mesenchymal stem cells, marrow stromal cells, embryonic stem cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/36—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix
- A61L27/38—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells
- A61L27/3839—Materials for grafts or prostheses or for coating grafts or prostheses containing ingredients of undetermined constitution or reaction products thereof, e.g. transplant tissue, natural bone, extracellular matrix containing added animal cells characterised by the site of application in the body
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/52—Hydrogels or hydrocolloids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/54—Biologically active materials, e.g. therapeutic substances
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/56—Porous materials, e.g. foams or sponges
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L27/00—Materials for grafts or prostheses or for coating grafts or prostheses
- A61L27/50—Materials characterised by their function or physical properties, e.g. injectable or lubricating compositions, shape-memory materials, surface modified materials
- A61L27/58—Materials at least partially resorbable by the body
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P1/00—Drugs for disorders of the alimentary tract or the digestive system
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P1/00—Drugs for disorders of the alimentary tract or the digestive system
- A61P1/16—Drugs for disorders of the alimentary tract or the digestive system for liver or gallbladder disorders, e.g. hepatoprotective agents, cholagogues, litholytics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P1/00—Drugs for disorders of the alimentary tract or the digestive system
- A61P1/18—Drugs for disorders of the alimentary tract or the digestive system for pancreatic disorders, e.g. pancreatic enzymes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P13/00—Drugs for disorders of the urinary system
- A61P13/12—Drugs for disorders of the urinary system of the kidneys
-
- C—CHEMISTRY; METALLURGY
- C08—ORGANIC MACROMOLECULAR COMPOUNDS; THEIR PREPARATION OR CHEMICAL WORKING-UP; COMPOSITIONS BASED THEREON
- C08L—COMPOSITIONS OF MACROMOLECULAR COMPOUNDS
- C08L5/00—Compositions of polysaccharides or of their derivatives not provided for in groups C08L1/00 or C08L3/00
- C08L5/08—Chitin; Chondroitin sulfate; Hyaluronic acid; Derivatives thereof
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N5/00—Undifferentiated human, animal or plant cells, e.g. cell lines; Tissues; Cultivation or maintenance thereof; Culture media therefor
- C12N5/06—Animal cells or tissues; Human cells or tissues
- C12N5/0602—Vertebrate cells
- C12N5/0652—Cells of skeletal and connective tissues; Mesenchyme
- C12N5/0662—Stem cells
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N5/00—Undifferentiated human, animal or plant cells, e.g. cell lines; Tissues; Cultivation or maintenance thereof; Culture media therefor
- C12N5/06—Animal cells or tissues; Human cells or tissues
- C12N5/0602—Vertebrate cells
- C12N5/0652—Cells of skeletal and connective tissues; Mesenchyme
- C12N5/0662—Stem cells
- C12N5/0668—Mesenchymal stem cells from other natural sources
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N5/00—Undifferentiated human, animal or plant cells, e.g. cell lines; Tissues; Cultivation or maintenance thereof; Culture media therefor
- C12N5/06—Animal cells or tissues; Human cells or tissues
- C12N5/0602—Vertebrate cells
- C12N5/067—Hepatocytes
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N5/00—Undifferentiated human, animal or plant cells, e.g. cell lines; Tissues; Cultivation or maintenance thereof; Culture media therefor
- C12N5/06—Animal cells or tissues; Human cells or tissues
- C12N5/0602—Vertebrate cells
- C12N5/0676—Pancreatic cells
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/22—Materials or treatment for tissue regeneration for reconstruction of hollow organs, e.g. bladder, esophagus, urether, uterus
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/26—Materials or treatment for tissue regeneration for kidney reconstruction
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/28—Materials or treatment for tissue regeneration for liver reconstruction
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61L—METHODS OR APPARATUS FOR STERILISING MATERIALS OR OBJECTS IN GENERAL; DISINFECTION, STERILISATION OR DEODORISATION OF AIR; CHEMICAL ASPECTS OF BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES; MATERIALS FOR BANDAGES, DRESSINGS, ABSORBENT PADS OR SURGICAL ARTICLES
- A61L2430/00—Materials or treatment for tissue regeneration
- A61L2430/34—Materials or treatment for tissue regeneration for soft tissue reconstruction
-
- C—CHEMISTRY; METALLURGY
- C12—BIOCHEMISTRY; BEER; SPIRITS; WINE; VINEGAR; MICROBIOLOGY; ENZYMOLOGY; MUTATION OR GENETIC ENGINEERING
- C12N—MICROORGANISMS OR ENZYMES; COMPOSITIONS THEREOF; PROPAGATING, PRESERVING, OR MAINTAINING MICROORGANISMS; MUTATION OR GENETIC ENGINEERING; CULTURE MEDIA
- C12N2506/00—Differentiation of animal cells from one lineage to another; Differentiation of pluripotent cells
- C12N2506/13—Differentiation of animal cells from one lineage to another; Differentiation of pluripotent cells from connective tissue cells, from mesenchymal cells
- C12N2506/1346—Differentiation of animal cells from one lineage to another; Differentiation of pluripotent cells from connective tissue cells, from mesenchymal cells from mesenchymal stem cells
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Engineering & Computer Science (AREA)
- Biomedical Technology (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Public Health (AREA)
- Veterinary Medicine (AREA)
- Animal Behavior & Ethology (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Transplantation (AREA)
- Dermatology (AREA)
- Epidemiology (AREA)
- Zoology (AREA)
- Cell Biology (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Organic Chemistry (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Botany (AREA)
- Biotechnology (AREA)
- Genetics & Genomics (AREA)
- Wood Science & Technology (AREA)
- Urology & Nephrology (AREA)
- Developmental Biology & Embryology (AREA)
- Microbiology (AREA)
- Biochemistry (AREA)
- General Engineering & Computer Science (AREA)
- Dispersion Chemistry (AREA)
- Vascular Medicine (AREA)
- Pharmacology & Pharmacy (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- General Chemical & Material Sciences (AREA)
- Molecular Biology (AREA)
- Hematology (AREA)
- Rheumatology (AREA)
- Gastroenterology & Hepatology (AREA)
- Polymers & Plastics (AREA)
- Medicines Containing Material From Animals Or Micro-Organisms (AREA)
- Materials For Medical Uses (AREA)
Abstract
The present invention provides compositions and methods for transplanting cells into a solid organ by an implantation strategy. These methods and compositions are useful for repairing diseased organs or for modeling disease states in experimental hosts. The method involves attaching a patch implant, a "bandage-like" covering, to the surface of a tissue or organ, the "bandage-like" covering containing epithelial cells as well as mesenchymal cells during supportive early lineage. The cells are incorporated into a gel-forming biomaterial that is prepared under serum-free, defined conditions that collectively support the sternness of the donor cells. The implant is covered with a biodegradable, biocompatible, bioresorbable substrate for immobilizing the implant at a target site. The cells in the implant migrate to and throughout the tissue such that they are evenly dispersed within the recipient (host) tissue within two weeks. The mechanism of donor cell implantation and integration into the organ or tissue involves multiple membrane-associated and secreted forms of MMPs.
Description
Cross Reference to Related Applications
This patent application claims priority from us patent application No. 62/518,380 filed on 12.6.2017 and us patent application No. 62/664,694 filed on 30.4.2018 in accordance with clause 119 (e) of the american codex 35, the contents of which are hereby incorporated by reference in their entirety.
Technical Field
The present invention relates generally to the field of cell transplantation or tissue implantation. And more particularly to implantation from, and in particular to implantation into, a solid organ or tissue. The present invention relates to compositions and methods for providing strategies for rapid transplantation, implantation and integration of cells into solid organs and tissues to treat diseases or conditions of the solid organs or tissues, or to establish model systems for diseases. A representative example of this potential is cell therapy for the treatment of liver or pancreatic diseases.
Background
There has long been a need for implantation strategies for cells from solid organs, other than for hematopoietic cell transplantation or for mesenchymal stem/progenitor cell transplantation. Turner, R. et al, transplantation90,807-810 (2010); gattinini, L. et al Nature Medicine 23,18-27 (2017); trousnon A. et al, CellStem Cell 17,11-22 (2015); sun B.K. et al Science 346,941-945 (2014); lainas, P. et al JHEPATAL 49, 354-. Transplantation of hematopoietic and mesenchymal cells is typically performed by cellular delivery through the vascular groove and, due to microenvironment signaling (a process called "homing"), depends on activation of adhesion molecules in the transplanted cells when in the relevant target site. The method for skin (using a similar method for an ocular target) employs an implantation method in which cells are applied directly to the target site. Sun B.K. et al Science 346,941-945 (2014). Many methods of implantation for the skin are available for cells from solid internal organs, but require extensive modification to adapt the cells to the microenvironment of these internal organs. The implant must counter the mechanical forces exerted by the interaction of the tissue and organ with each other; examples include the effect of the lungs during respiration, or the compression of the diaphragm by the liver, or the transient effect of mechanical forces exerted by the intestinal tract on adjacent tissues during food processing. Implants, especially those for internal organs, are challenging to design due to issues with respect to size, shape, and complexity of the organ structure in addition to significant dynamic mechanical forces.
For decades, cell therapy for cells from solid organs other than skin has been attempted using transplantation via the vascular route or by direct injection into tissues. When delivered by any of these strategies, most transplanted cells die or are transported to ectopic sites where they can survive for months and form tissue at inappropriate sites, potentially causing clinical adverse reactions. Turner, R. et al transfer 90,807-810 (2010); lanzoni, G, et al, Stem Cells 31,2047-2060 (2013). Implantation of the liver can be improved by coating the cells with hyaluronic acid and delivering them to the liver via the blood vessels; the improvement in implantation efficiency is due to the natural clearance process of hyaluronic acid by the liver. Nevi et al Stem Cell Research & Therapy 8,68, 2017. However, these improvements are still not as effective as the improvements of the implantation strategy and, importantly, still allow delivery of cells to ectopic sites.
There remains a need for improved methods of implantation of cells into solid organs. The present disclosure satisfies this need and provides related advantages.
Disclosure of Invention
For a long time, there is a continuing need for implantation strategies for cells from solid organs (Turner, r. et al, Transplantation90,807-810 (2010)), other than for hematopoietic cell, mesenchymal stem cell Transplantation or for skin. Transplantation of hematopoietic and mesenchymal cells is typically via the vascular sulcus and depends on activation of adhesion molecules in the relevant target site due to microenvironment signaling, a process called "homing". The method for skin uses an implantation method in which cells are applied directly to a target site.
Transplantation of cells from solid organs other than the skin has long been used for vascular delivery. This is illogical, as the adhesion molecules on these cells are always active and lead to rapid (a few seconds) cell aggregation that can produce life-threatening emboli. Even with successful embolization control to minimize health risks, cell engraftment efficiency is low (only-20%) for adult cells and even lower (< 5%) for stem/progenitor cells. Most transplanted cells die or are transported to ectopic sites where they can survive for months and form tissue at inappropriate sites, potentially causing clinical adverse reactions. A small fraction of the cells implanted at the target site slowly integrate, taking weeks to months to become a significant part of the tissue. Implantation in the liver would be improved if the cells were coated with hyaluronic acid and delivered via the blood vessels due to hyaluronic acid clearance of the tissue (e.g. of the liver). (Nevi et al, StemShell Research & Therapy 8,68, 2017).
Applicants propose a distinct approach, one that was found to be even more successful than coating cells with hyaluronic acid: implants are placed directly on the surface of a target site and when they are under conditions that enhance the transplanted biological material, the unique phenotypic traits of the transplanted biological material and certain cells are used. This is similar in some respects to the strategy for cell therapy of the skin, but requires substantial modification to the internal organs due to mechanical action, wear or compression of organs in close proximity to each other, and due to the unique fluid microenvironment around a particular organ and the size, structure and complexity of the organs.
Described herein are novel patch implant compositions and methods for the transplantation of cells to tissues and solid organs. In some embodiments, the methods and implants are applicable to internal organs, and their design characteristics depend on the level of maturation of the cells, particularly whether the cells are stem cells or mature cells. In some embodiments, disclosed herein are donor cells (optionally autologous or allogeneic cells) for patch implants, optionally incorporated into the implant biomaterial as a cell mixture or organoid form, aggregates of epithelial stem cells, and their natural lineage-appropriate mesenchymal cell partner, e.g., mesenchymal stem/progenitor cells, such as early lineage mesenchymal cells (ELSMCs). In some embodiments, the donor cell is a somatic cell that is incorporated into the implant material as a cell suspension of somatic epithelium and is paired with mesenchymal stem/progenitor cells (optionally ELSMCs) in a ratio designed to optimize the expression of membrane-associated and/or secreted Matrix Metalloproteinases (MMPs) of the stem/progenitor cells. In some embodiments, other important variables are the implantation of the biomaterial and the substrate material, which are required to be neutral in their effect on the differentiation of the donor cells.
Aspects of the present disclosure relate to a patch implant for retaining and maintaining a single cell population or a mixed population of cell populations, the patch implant comprising (a) a single cell type or a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), or comprising MMPs from another source (e.g., purified or recombinant MMPs), the cell population or mixed population being supported in a culture medium present in a hydrogel matrix having sufficient viscoelastic properties to allow migration of the mixed population (optionally, within or away from the hydrogel and/or within or away from the patch implant); (b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in the direction of the substrate; and optionally (c) a hydrogel overlaid on a serosal (i.e., exterior) surface of the substrate, the serosal surface being opposite the surface contacting the mixed population and, in embodiments in which the patch implant is tethered to the target site, opposite the side contacting the target site (e.g., organ or tissue). In some embodiments, the layer prevents or inhibits adhesion by, or with, other tissues or organs. In some embodiments, the patch implant is configured to maintain and maintain the mixed population while inhibiting differentiation or further maturation of the at least one early lineage stage cell type to a late lineage stage that is no longer capable of expressing membrane-associated and/or secreted MMPs. The patch implant may be a single layer plus a substrate or multiple layers.
In some embodiments, the substrate is porous or non-porous. In some embodiments, the substrate comprises a porous mesh, scaffold, or membrane. In some embodiments, the substrate comprises a filament; a synthetic fabric; or natural materials (such as amnion, placenta or omentum); or a combination thereof. In some embodiments, the substrate comprises a porous mesh infused with a hydrogel. In further embodiments, such infusion prevents migration of cells away from the target organ or tissue. In some embodiments, the substrate comprises a solid material.
In some embodiments, one or more of the hydrogels comprises hyaluronic acid.
In some embodiments, the culture medium comprises a Kubota's medium or another medium that supports stem cells and is capable of maintaining a dry quality.
In some embodiments, the mixed population comprises mesenchymal cells and epithelial cells. In some embodiments, the epithelial cells can be ectodermal, endodermal, or mesodermal cells. In some embodiments, the mesenchymal cells comprise Early Lineage Stage Mesenchymal Cells (ELSMCs). In some embodiments, the ELSMC includes one or more of a hemangioblast, a precursor of endothelium, a precursor of stellate cells, and a Mesenchymal Stem Cell (MSC). In some embodiments, the epithelial cells comprise epithelial stem cells. In some embodiments, the epithelial cells comprise biliary stem cells (BTSCs). In some embodiments, the epithelial cells comprise committed and/or mature epithelial cells. In some embodiments, the committed and/or mature epithelial cells comprise mature parenchymal cells. In some embodiments, the mature parenchymal cells include one or more of hepatocytes, cholangiocytes, and islet cells. In some embodiments, the mesenchymal cells and epithelial cells both comprise stem cells.
In a certain embodiment, the mixed population comprises autologous cells and/or allogeneic cells.
In some embodiments, one or more cell types are genetically modified.
Additional aspects relate to methods of using the disclosed patch implant compositions. Accordingly, provided herein is a method of implanting cells into a target tissue, the method comprising, consisting of, or consisting essentially of contacting the target tissue with the patch implant disclosed above.
In some embodiments of the method, the target tissue is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, gastrointestinal tract, lung, prostate, breast, brain, bladder, spinal cord, skin and subcutaneous dermal tissue, uterus, kidney, muscle, blood vessel, heart, cartilage, tendon, and skeletal tissue. In some embodiments of the method, the target tissue is liver tissue. In some embodiments of the method, the target tissue is pancreatic tissue. In some embodiments of the method, the target tissue is biliary tissue. In some embodiments of the method, the target tissue is a gastrointestinal tract tissue. In some embodiments, the tissue is diseased, damaged, or has a disorder. In some embodiments of the method, the target tissue is kidney tissue.
In some embodiments of the method, the target tissue is an organ. In some embodiments of the method, the organ is an organ of the musculoskeletal system, digestive system, respiratory system, urinary system, female reproductive system, male reproductive system, endocrine system, circulatory system, lymphatic system, nervous system, or integumentary system. In some embodiments of the method, the organ is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, stomach, intestine, lung, prostate, breast, brain, bladder, spinal cord, skin and subcutaneous dermal tissue, uterus, kidney, muscle, blood vessel, heart, cartilage, tendon, and bone. In some embodiments, the organ is diseased, damaged, or has a disorder.
In some embodiments of the method, the liver disease or disorder is liver fibrosis, cirrhosis, hemochromatosis, liver cancer, biliary atresia, nonalcoholic fatty liver disease, hepatitis, viral hepatitis, autoimmune hepatitis, fascioliasis, alcoholic liver disease, α 1-antitrypsin deficiency, glycogen storage disease type II, transthyretin-associated hereditary amyloidosis, Gilbert's syndrome, primary biliary cirrhosis, primary sclerosing cholangitis, bade-Chiari syndrome, liver trauma, or Wilson's disease.
In other aspects, provided herein are methods of treating a subject having a pancreatic disease or disorder, comprising, consisting of, or consisting essentially of contacting a pancreas of the subject with the patch implant disclosed above. In some embodiments of the method, the pancreatic disease or disorder is diabetes, pancreatic exocrine insufficiency, pancreatitis, pancreatic cancer, Oddi (Oddi) sphincter dysfunction, cystic fibrosis, pancreatic division, cricoid pancreas, pancreatic trauma, or pancreatic ductal hemorrhage.
In other aspects, provided herein are methods of treating a subject having a disease or disorder of the gastrointestinal tract, comprising, consisting of, or consisting essentially of contacting one or more intestines of the subject with a patch implant disclosed above. In some embodiments, the gastrointestinal disease or disorder is gastroenteritis, gastrointestinal cancer, ileitis, inflammatory bowel disease, Crohn's disease, ulcerative colitis, irritable bowel syndrome, peptic ulcer disease, celiac disease, fibrosis, vascular dysplasia, hirschsprong's disease, pseudomembranous colitis, or gastrointestinal trauma.
In some aspects, provided herein are methods of treating a subject having a kidney disease or disorder, the method comprising, consisting of, or consisting essentially of contacting one or more kidneys of the subject with a patch implant disclosed above. In some embodiments of the method, the kidney disease or disorder is nephritis, nephropathy, nephritic syndrome, nephrotic syndrome, chronic nephropathy, acute kidney injury, kidney trauma, cystic nephropathy, polycystic nephropathy, glomerulonephritis, IgA nephropathy, lupus nephritis, kidney cancer, Alport (Alport) syndrome, amyloidosis, Goodpasture's syndrome, or Wegener's granulomatosis.
Drawings
Fig. 1A-1D provide information about porcine donor cells for patch implants. Fig. 1A is a schematic illustration of the process and estimated time required to prepare the organoid, assemble the patch implant and perform the surgery. In fig. 1B, donor cells for stem cell patch implants were isolated from cell suspensions from biliary tissue of transgenic pigs; the cells were made organoid in serum-free bottom tower medium and on low-adherence culture dishes. Biliary stem cells (BTSCs) and their early lineage mesenchymal cell (ELSMC) partners, angioblasts, and organoids of endothelial and stellate cell precursors. They are shown in phase contrast micrographs in comparison to cells displaying transgenic, Green Fluorescent Protein (GFP) expression. ). All cells of the aggregate were green in color, as the transgene was present in both epithelial and mesenchymal cells. The transgene is coupled to the histone (H-2B) locus. Paraffin embedding, sectioning and histology of stem cell organoids stained with hematoxylin/eosin. (d) Enlargement of organoids of BTSC and ELSMC. Figure 1C shows Immunohistochemistry (IHC) showing expression of stem cells, liver and pancreatic markers, indicating that these cells are precursors to both liver and pancreas. The IHC assay identifies the outer layer by a metaphase stem cell marker, such as EpCAM, and identifies the inner cells that express very primitive genes, such as pluripotency genes and endoderm transcription factors (e.g., SOX17, SOX9, PDX 1). Figure 1D is a representative qRT-PCR assay to assess expression of various genes in organoids, indicating that the cells are stem cells or early progenitor cells. Controls were mature hepatocytes from piglet liver.
Fig. 2A-2F provide information about the major components of the patch implant. Fig. 2A is a schematic illustration of a patch implant fixed to a pig liver, the right figure being the composition of the implant. Early lineage stage cells of both epithelial and mesenchymal cells are the source of Matrix Metalloproteinases (MMPs) that are key regulatory factors for the production of engraftment. The matrix component of the implant biomaterial on which the donor cells are placed is soft (-100 Pa) and is not (or minimally) sulfated, such as a hyaluronic acid hydrogel. The structure of the implant is made up of a layer of biomaterial and cells tethered to the target site. The media components are free of serum, growth factors and cytokines that affect donor cell differentiation and should be tailored for survival and expansion of cells at the early lineage stage (such as stem/progenitor cells). The substrate has sufficient tensile strength for surgical procedures, but is neutral in its effect on donor cell differentiation (cells in which type I collagen should be avoided). The substrate dip is coated with a thicker 10 × hydrogel (-700 Pa) to act as a barrier to direct migration of donor cells to the target tissue and minimize adhesion. After attachment to the target site, a 2 × HA hydrogel (sufficiently fluid to coat or coat on the serosal surface) is added and used to further minimize adhesion. Fig. 2B depicts an implant secured to the liver or pancreas of a host. Fig. 2C is a schematic view of an implant showing the layers that make up the implant composition. Figure 2D depicts the results of an assay that empirically evaluates the rheological or viscoelastic properties (shear and compressive mechanical forces) of a particular hydrogel layer. Figure 2E provides a formulation of the viscoelastic properties of a 3-layer hydrogel. Fig. 2F is a close-up view of a patch implant sutured to the surface of a pig liver.
Fig. 3A-3D depict Immunohistochemical (IHC) and histological results of liver patch implants. Fig. 3A shows the trichromatic dyeing results at one week of the patch implant. Trichrome recognises collagen (blue), cytoplasm (red) and nucleus (black) and is used to recognise the Glisson's capsule (usually adjacent the surface of the liver lobule) and adhesions (at the serosal surface of the implant). There is a high level of blue staining in the layer at the serosal surface, which means adhesion to the implant. Additionally, the implant separates from the host tissue at the interface between the substrate and the host; this is often the case because of the large number of MMPs generated at this interface. The remodeling zone provides evidence of loss of the classical lobular structure of the liver; they create regions: wherein donor cells migrate to the tissue and alter host tissue architecture in parallel. In the low magnification image (a), trichrome staining of the implant placed on the liver confirmed that extensive remodelling of the gleason bursa occurred and generally led to separation between the implant and the host liver. In the high magnification image (b), the remodelling zone is very broad and consists of a region (c) near the implant where the liver leaflet structure is completely missing and a region (d) within the remaining liver leaflets which is destroyed during the remodelling process. Fig. 3B shows the trichromatic staining results at three weeks of patch implant. The hyaluronic acid in the implant has been resorbed, leaving only the substrate (a). With resorption of HA, the glisson bursa reappears (b) and the liver lobules near the implant stabilize again to their typical histological pattern, such as lobules and acini of the liver. (b) The arrow in (b) indicates the re-appearance of collagen during the re-formation of the Gleason's capsule. Fig. 3C and 3D show hematoxylin/eosin staining results of sections from the implant one week after implantation (C) and two weeks after implantation (D). The upper graph is 40X. The parts in the figures (a, b, c) are enlarged views enlarged by 100 ×; the rectangular chart below each of these magnifications is magnified 200 x. The figure shows 3 sites of the implant: (a) a site within the substrate and associated implant biomaterial; (b) a site at the interface between the implant and the host tissue; and (c) sites within the liver lobules. Hematoxylin/eosin staining yields images that help understand the implantation and migration processes that combine the characteristics of inflammatory processes.
Figures 4A-4C show the fate of implantation, migration and rapid maturation to adults within a week. Fig. 4A is a low magnification view of a patch implant on the surface of a pig liver after one week. The dashed line represents the interface between the implant and the host liver. Donor GFP + cells were visualized by labeling with antibodies to GFP and a secondary antibody conjugated to a Red fluorescent probe Novo Red (the nucleus was pink; white arrows indicate regions with large numbers of donor GFP + stem cells). Staining of the nuclei blue with 4, 6-diamidino-2-phenylindole (DAPI) enables identification of host cells with blue nuclei only and donor cells with pink nuclei (merged images of DAPI and Novo Red). Host tissue (a) hyaluronic acid extending to the implant (HA, black background); tissue near the basement occasionally contains organoids (insets), but most donor cells are dispersed in single cells; a large number of dispersed donor GFP + stem cells were visible throughout the host tissue (b). There is no evidence of the presence of the Gleason's capsule in this region constituting the remodeled region. FIG. 4B shows that implantation and migration of donor cells is rapid; within one week, all donor cells were in the host liver; there were donor cells both near the implant site and on opposite sides of the liver lobe (estimated distance from the implant was at least 1.5 cm). An ongoing study is to analyze the more distant regions of piglet liver (i.e. other lobes of the liver) to more accurately define how far donor cells can migrate within a defined period of time. Donor cells (pink nuclei) near the host mature hepatocyte lobule (forest green autofluorescence from lipofuscin) on the side of the liver lobes remote from the implant site are shown. Figure 4C shows the fate of donor cell maturation to adults that occurs in parallel with reabsorbed HA. An enlargement of the region (a) containing donor GFP + cells (single cells with pink nuclei) near the host hepatocytes (forest green in color (autofluorescence of lipofuscin)), which are readily distinguishable from the hepatocytes of mature donor source (b) (light purple in color) (combined images of pink-GFP, blue-DAPI, and green-lipofuscin), that is, they are lineage restricted from donor GFP + stem cells. By other IHC assays (data not shown), the leuchun green cells in the plates of both host and donor hepatocytes were demonstrated to be endothelial and stellate cells.
Fig. 5A-5C compare the engraftment and maturation of cells in liver patch implants one and two weeks after transplantation. Fig. 5A is an examination of pig liver 1 week after patch implantation. Immunohistochemistry of pan-cytokeratin (pCK) and Sox9 was performed on consecutive 3- μm sections using collagen-stained azo dye sirius red dye; and Immunofluorescence (IF) staining. At the patch implant site, the implanted donor cells coalesce with the liver lobules. In the upper panel (original magnification ═ 5 ×), the patch implant is composed of mesenchymal and epithelial pCK+Cells (arrows). In the middle panel, a higher magnification (20 ×) is provided. Epithelial cells show a typical immunophenotype of biliary stem cells (BTSCs) expressing biliary cytokeratin (pCK) and the endodermal stem cell marker Sox 9. The BTSCs within the patch implant are arranged into cell strings that reassemble the bile canaliculus (arrows) and maintain direct continuity with the hepatocyte plates of the adjacent liver lobules (wedge symbols). Host hepatocytes in the lobules were pCK and Sox9 negative. In the lower panel (original magnification ═ 20 ×), immunofluorescence of GFP allowed the identification of single implanted cells and their progeny. Hepatocytes in the leaflets adjacent to the patch implant were GFP positive, indicating that these cells are donor cell-derived cells that have substantially merged with the host liver. At the interface between the patch implant and the liver leaflets, pCK+/GFP+GFP in tubules (i.e. biliary epithelial cells of donor origin) and leaflets+/pCK-Cells (donor-derived hepatocytes) maintained direct continuity (wedge symbols), indicating that the engrafted cells matured into the lives of hepatocytesAnd (6) carrying out transportation. Fig. 5B is an examination of pig liver 2 weeks after patch implantation. IF staining revealed GFP+Cells are present within leaflets remote from the implantation site they are evenly dispersed so they are in a mixture of host cells (cells with blue nuclei from DAPI) and donor cells (blue and GFP-labeled red pooled pink/purple nuclei of DAPI) they co-express mature hepatocyte markers such as Hepatocyte Nuclear Factor (HNF)4 α (mixture of green and pink/purple nuclei) and albumin (green cytoplasm and pink/purple nuclei) individual or pooled channels are included nuclei are shown in blue (DAPI) original magnification: 40 x fig. 5C is an assessment of pig liver one week after patch implantation showing a region of broad remodeling at the interface between patch implant and host tissue the sections in the low magnification map and the enlarged leaflets of fig. 1 are hematoxylin/eosin (light staining), the sections in fig. 2 are stained with Vector-SG providing blue sections/grey, the sections in blue section stain fetal protamine protein, the background is hematoxylin/eosin, 5 is a section of hematoxylin the liver, and the sections in which are shown by Vector-SG, provide blue sections of stained for which the blue section/grey, the background is indicative of the presence of a change in the donor cell status of a, such as a sign of a change in the donor cells, and thus the status of the absence of the presence of a marker of a host cell in the mature liver.
Fig. 6A-6D provide information about a patch implant of stem cell organoids tethered to the pancreas fig. 6A is a low magnification (panoramic scan) map of GFP + donor cells implanted into the submucosa (region containing the bunner's glands) of the majority of the pancreas and duodenum fig. GFP (green), insulin (red), DAPI (blue) donor-derived GFP + cells appear near the site where the implant is located and show integration into the pancreatic parenchyma in the patch implant site fig. 6B shows that the donor cells mature into functional islets at high magnification fig. 6B shows that donor cells are from donor-derived β cells (yellow-from the combined color of GFP and insulin-stained red) are observed at high magnification in combination with host/insulin + (red) cells in the pancreatic parenchyma (yellow-from the combined color of GFP and insulin-stained red) β in combination with host/insulin-derived from the pancreatic parenchyma, and the high magnification map of the extracellular secretion of pancreatic cells from the pancreatic parenchyma, the high magnification of the starch-derived from the parenchyma of the kidney cells, the patch implant cells are shown in a continuous magnification map of the presence of GFP (blue) and the high magnification of the focus of the starch-derived from the parenchyma of the kidney cells in the pancreas, the patch implant, the patch, the high magnification map shows that the absence of the kidney cells in the kidney cells and the high magnification of the patch.
FIGS. 7A-7H provide a characterization of Matrix Metalloproteases (MMPs). MMPs consist of calcium-dependent, zinc-containing enzymes that solubilize a large gene family of extracellular matrix components. At least 24 isoforms are known in pigs, one subset of which are secreted factors (e.g., MMP1, MMP2, MMP7, MMP9) and another subset of which are membrane-associated factors (e.g., MMP14, MMP 15). MMP1 was identified by IHC, particularly in the remodeled region, but could not be identified by RNA-seq, as the annotated form of porcine MMP1 has not been available for RNA seq analysis. Fig. 7A, 7B, 7C, and 7D show that isoforms of secretory and membrane-associated species are expressed by both stem/progenitor cells and mature cells. Quantification of expression levels indicated that the membrane-associated forms were similar for both stem/progenitor and mature cells (note the comparison in fig. 7D). In contrast, the secreted form is expressed at very high levels in stem/progenitor cells and at low or negligible levels in mature cell types. The cell population of adult cells analyzed was isolated from a suspension of piglet liver and biliary tissue and consisted of CD45+ cells (hematopoietic cells), CD146+ cells (stellate cells), CD31+ cells (endothelium), EpCAM +/CD 45-cells (adult diploid hepatocytes and biliary epithelium). These EpCAM +/CD 45-cells are mature parenchymal cells present in the livers of piglets. BTSCs were isolated from biliary lines by the protocol given in the examples. Figure 7E shows representative MMP expression in the remodeled region with BTSC/ELSMC implant. In sections of the patch implant adjacent to the BTSC/ELSMC, staining was performed with a trichrome representing the remodeled area (bracket). This region appears as a linear band in red and blue, with cellular and matrix components undergoing lysis by the MMP "sea". The strip ends at the edge of the leaflet, which is largely still intact, but begins to "wear out" at the boundary due to the action of MMPs derived from invading cells. FIG. 7F shows a representative image of an IHC assay for MMP1(Novo-red +). Methyl green is background staining. The lobular/acinar structures of the liver are solubilized in the wavy coil of the cell and are marked by the strong expression of MMP1 (the secreted isoform of MMP). FIG. 7G shows sections stained for MMP2(Novo-red +). Hematoxylin is background staining. The lobular/acinar structure of the liver has disappeared and has been replaced by a mixture of cells with strong staining for MMP2 (russet). Fig. 7H shows the ongoing remodeling process within the liver lobules. Liver lobules have become bands of cells scattered among invading cells; MMP2+ expression (rust color) was very high and contributed to the loss of leaflet/acinar structure. With clearance of hyaluronic acid (2-3 weeks), leaflet structure reappears.
Fig. 8 is a schematic illustration of the implantation and integration phenomena in the liver and on the pancreas.
Fig. 9A-9E provide information about a patch implant of mature (adult) hepatocytes collocated with Mature Mesenchymal Cells (MMC), such as endothelial or stellate cells. These patch implants cannot be implanted. Implantation is achievable if hepatocytes are paired with early lineage mesenchymal cells (ELSMCs), here porcine Mesenchymal Stem Cells (MSCs). Implantation occurs if present with an ELSMC, but is limited to the area near implantation. Figure 9A shows trichrome staining of normal pig liver. The bars are 200 μm for the low magnification plot (a) and 50 μm for the high magnification plot (b). Note the boundary between collagen in the grignard capsule and the liver acinus. Fig. 9B shows trichrome staining of a normal adult hepatocyte patch implant paired with Mature Mesenchymal Cells (MMC), endothelium and stellate cells, which was not implantable. In the low magnification plot (a), note that the Gleason's capsule is intact and the cells are still on top of the capsule. (b) At high magnification, there is evidence that the cells have some degree of remodeling (plasticity phenomenon) in the lobules next to the implant (a patchy red color within the hepatocytes). This plasticity is thought to be due to membrane-associated MMPs known to be present on both stem and adult cells. Fig. 9C shows IHC assay for a patch implant of normal adult hepatocytes collocated with Mature Mesenchymal Cells (MMC). Sections were stained with antibodies to RBMY-1, hematoxylin as a counterstain. The Gleason's capsule is intact, as are the boundary regions between the leaflets. At high magnification (b), apparently no implantation occurred. (d) A negative control for non-specific staining (staining without primary antibody) is indicated. Fig. 9D shows the trichrome staining of a normal adult hepatocyte paired with ELSMC patch implant, here a porcine Mesenchymal Stem Cell (MSC) that functions as a cell source for MMPs. The implant separates at the interface between the implant and the host tissue. Brackets indicate remodeling regions. Note that the liver leaflets have lost the stroma that normally constitutes the boundary zone between them and wear occurs at the edges. In high magnification (a) donor cells are visible throughout the image (light red, while donor cells in the center of the leaflet are dark red); (b) in (b) is an enlarged view showing the area under the patch and in (c) where the gleason bursa is significantly thinner (compared to the area to the left of the box). There is significant extensive remodeling in cells adjacent to the implant (c). Fig. 9E shows a patch implant of hepatocytes collocated with ELSMCs (porcine MSCs) after one week. Sections (a) were stained with antibodies to RBMY-1 (brown) and methyl green as counterstain. The donor cells engraft (rust red areas) and mature into adult parenchymal cells in the acini near the implant. Section (b) shows a magnified view of the image near the rest of the thinned grignard capsule showing that the donor cells (dark brown nuclei) are evenly dispersed in the host cells (nuclei are methyl green in color). Section (c) is a negative control for (b). Sections (d) were stained with antibodies against GFP (coupled with Novus red, producing russet brown) with methyl green as counterstain. Most of the cells have been engrafted and formed a deep red band of donor (mature) hepatocytes within the host hepatic acinus. The Gleason's capsule remained but the thickness was reduced. No migration beyond the liver region near the implant was observed within the three week time frame of the experiment.
Fig. 10 is a schematic comparing the implantation of stem cells with adult cells.
FIG. 11 shows evidence that the implantation process involves migration of cells a considerable distance within the host tissue. Organoids one week after transplantation for BTSC/ELSMC implants are shown here. A schematic of the liver divided into 8 different regions is used to represent the regions that were used to assess the presence of donor cells. Sections were prepared from regions 1-8 and then stained to identify donor cells. The table summarizes the findings, which show the distance between the implant and each zone and the replication of the GFP + cells present. The image on the left of the table is a scan of a representative slice from each region. Dark brown staining was strongest in 6 near the implant and became lighter with increasing distance from the implant, zone 1 was lightest.
FIGS. 12A-12E provide evidence of donor cell migration throughout the host liver. GFP + cells were stained with Novo-red (russet brown); host cells were stained with methyl green. Fig. 12A is a low magnification view of the interface of the implant and the host liver. Separation of the implant from the host liver is usually visible (note that this is also true in fig. 3); and have been shown to be associated with abnormally high levels of secreted MMPs. Enlarged views of regions (a) and (b) are given below. Note the areas in the low magnification plot and in the magnified plot of (b) where the staining was speckled and these areas showed a hazy appearance and were confirmed due to the hyaluronic acid level in the tissue. Fig. 12B depicts the intermediate zone to which the cells migrated. The donor cells are in the entire tissue in both the bile duct and acinar parenchyma. FIG. 12C shows the distant zone to which the cells migrate. Note that only bile ducts were stained. Fig. 12D provides an enlarged view showing donor cells in the bile duct. FIGS. 12E and 12F provide essentially enlarged views showing donor cells with GFP markers in the nucleus.
Fig. 13 shows the ill-conditions obtained for a patch implant with certain substrates (see also table 1 and table 2). These include necrosis, adhesions, and finding sites where cholestasis occurs when the implant is placed too close to some tubes so that swelling causes the tubes to become blocked.
Fig. 14 shows a graph of two lineage stages for epithelial cells (fig. 14A) and mesenchymal cells (fig. 14B) and corresponding biomarker profiles.
FIG. 15 shows organoids of kidney implanted H2B-GFP + BTSC/ELSMC patches. Evaluation was performed 1 week after implantation. Panel a shows trichrome staining of implanted kidneys. The kidney was prepared in a transection fashion to expose the deeper layers with the "V" shaped implant. The lower half "V" stained bright blue is the implanted side on the kidney; the upper half "V" of the figure is a layer deeper than the implanted layer. Panel B shows H & E staining for the same section of implanted kidney. Panel C is a higher magnification view of a patch implanted kidney. The renal capsule under the implant relaxes in a manner similar to that in the liver (from dissolution by MMPs). Panel D shows IHC staining of GFP + cells (dark red) implanted in the kidney at the layer under the patch. Panel E shows the implantation of GFP + cells (dark red) in the deeper layers of the kidney. Necropsy reports indicated the absence of necrosis in the implanted kidney or elsewhere in the animal receiving the patch implant.
Description of the attached tables
Table 1 provides a summary of surgical or other methods for a patch implant.
Table 2 provides a comparison of substrates tested against exemplary patch implants.
Table 3 provides a summary of the antibodies used in the examples for IHC and IF.
Table 4 provides a summary of the primers used for the qRT-PCR assay.
Detailed Description
Embodiments in accordance with the present disclosure are described more fully hereinafter. However, aspects of the present disclosure may be embodied in different forms and should not be construed as limited to the embodiments set forth herein. Rather, these embodiments are provided so that this disclosure will be thorough and complete, and will fully convey the scope of the invention to those skilled in the art. All publications, patent applications, patents, and other references mentioned herein are incorporated by reference in their entirety.
Unless defined otherwise, all terms (including technical and scientific terms) used herein have the same meaning as commonly understood by one of ordinary skill in the art to which this invention belongs. It will be further understood that terms, such as those defined in commonly used dictionaries, should be interpreted as having a meaning that is consistent with their meaning in the context of this patent application and the relevant art and will not be interpreted in an idealized or overly formal sense unless expressly so defined herein. Although not explicitly defined below, such terms should be interpreted according to their usual meaning.
The practice of the present technology will employ, unless otherwise indicated, conventional techniques of tissue culture, immunology, molecular biology, microbiology, cell biology, and recombinant DNA, which are within the skill of the art. See, e.g., Sambrook and Russell eds (2012) Molecular Cloning, A Laboratory Manual, 4 th edition; ausubel et al eds (2012) Current Protocols in Molecular Biology series; methods in Enzymology series (Academic Press, Inc., N.Y.); MacPherson et al (1991) PCR 1: A Practical Approach (IRL Press at Oxford University Press); MacPherson et al (1995) PCR 2: A practical Aproach; harlow and Lane eds (2014) Antibodies, A Laboratory Manual, 2 nd edition; freshney (2011) Culture of Animal Cells A Manual of Basic Technique, 6 th edition; gait, eds (1984) Oligonucleotide Synthesis; U.S. Pat. nos. 4,683,195; hames and Higgins eds (1985) nucleic Hybridization; anderson (1999) Nucleic Acid Hybridization; hames and Higgins eds (1984) Transcription and transformation; immobilized Cells and Enzymes (IRL Press (1986)); perbal (1984) A Practical Guide to Molecular Cloning; miller and Calos eds (1987) Gene Transfer Vectors for Mammalian Cells (Cold Spring harbor laboratory); makrides eds (2003) Gene Transfer and Expression in Mammarian Cells; mayer and Walker eds (1987) biochemical Methods in Cell and Molecular Biology (Academic Press, London); and Herzenberg et al (1996) Weir's Handbook of Experimental Immunology.
Unless the context indicates otherwise, it is specifically intended that the various features of the invention described herein can be used in any combination. Furthermore, the present disclosure also contemplates that, in some embodiments, any feature or combination of features set forth herein may be excluded or omitted. For illustration purposes, if the specification states that the complex comprises components A, B and C, it is specifically intended that either of A, B or C, or a combination thereof, may be omitted and discarded, either individually or in any combination.
All numerical designations, such as pH, temperature, time, concentration, and molecular weight, including ranges, are approximate and vary by increments (+) or (-) of 1.0 or 0.1, or by +/-15%, or 10%, or 5%, or 2%, as the case may be. It is to be understood that all numerical designations are preceded by the term "about," although this is not always explicitly stated. It is also to be understood that, although not always explicitly indicated, the reagents described herein are exemplary only and that equivalents of such reagents are known in the art.
Definition of
As used in the description of the invention and the appended claims, the singular forms "a", "an", and "the" are intended to include the plural forms as well, unless the context clearly indicates otherwise.
As used herein, the term "about," when referring to a measurable value, such as an amount or concentration (e.g., the percentage of collagen in the total protein in a biomatrix scaffold), etc., is meant to encompass variations of 20%, 10%, 5%, 1%, 0.5%, or even 0.1% of the specified amount.
When used to describe the selection of any component, range, dosage form, etc., the terms or "acceptable", "effective" or "sufficient" disclosed herein mean that the component, range, dosage form, etc., is suitable for the purposes disclosed.
Also as used herein, "and/or" means and covers any and all possible combinations of one or more of the associated listed items, as well as the absence of a combination when interpreted in an alternative manner ("or").
As used herein, the term "comprising" means that the compositions and methods include the recited elements, but do not exclude other elements. As used herein, the transitional phrase "consisting essentially of … …" (and grammatical variations) should be interpreted as encompassing the recited or steps, as well as "those material steps that do not materially affect one or more of the basic and novel features of the recited embodiments. See, Inre Herz,537F.2d 549,551-52,190U.S.P.Q.461,463(CCPA1976) (all highlighted above); see also MPEP § 2111.03. As used herein, the term "consisting essentially of … …" should not be construed as equivalent to "comprising". "consisting of … …" shall mean excluding more than trace amounts of other ingredient elements and the essential method steps for administering the compositions disclosed herein. Aspects defined by each of these transitional terms are within the scope of the present disclosure.
As used herein, the term "patch implant" refers to a composition of cells embedded or contained in a suitable biological material to allow for the transplantation of donor cells (allogeneic or autologous) to a host. In some embodiments, the term refers to a composition of cells embedded or contained in an appropriate biological material to allow for the transplantation of donor cells to a host. The biomaterial is a biomaterial that can be prepared under specified conditions (e.g., culture medium of purified free fatty acids complexed with purified albumin-plus-lipoprotein carrier molecules such as high density lipoproteins) including (optionally cured) in a soft gel (less than 200Pa, optionally about 100Pa) and covered with a substrate having sufficient tensile strength to allow surgical attachment or tethering to the host's tissues or organs, but with chemical properties that have minimal impact on donor cell differentiation, optionally supplemented with basal media and/or nutrient factors, vitamins, amino acids, carbohydrates, minerals, insulin, transferrin/Fe, and/or lipids. Supplements containing factors that may drive differentiation of cells, especially mesenchymal cells during Early Lineages (ELSMCs), should be avoided; these factors include serum, growth factors and cytokines that affect ELSMC, as well as mature matrix components (e.g., type I collagen).
As used herein, the term "substrate" refers to a material that is a substrate or barrier on the surface of the patch implant that is capable of tethering the implant to the target site and/or facilitating the migration of cells therein to the target site and/or preventing or inhibiting the migration of cells to the substrate. The substrate is or includes a "biodegradable, biocompatible material", "biocompatible, biodegradable material" or any variant thereof, referring to such materials: (i) is biocompatible with respect to the subject to whom the material is transplanted, (ii) exhibits mechanical elasticity to withstand compressive and shear forces (particularly one of the interior) occurring on organs and tissues, which in turn allows the material to function as surgical tissue, and (iii) has a neutral or minimal effect on the state of differentiation of cells contacting the material. In some embodiments, the substrate of the patch implant comprises such a material. In such embodiments, the mechanical elasticity of (ii) should be such that the substrate can tether the implant to the target site. In further such embodiments, the substrate directs migration of cells toward the target site-for example, by affecting differentiation of those cells that migrate in a direction away from the target site or by physically impeding the migration. In this regard, suitable materials include, but are not limited to, Seri-Silk (optionally profiled Seri-Silk or derivatives thereof), amniotic membrane (e.g., the fetal side-facing amniotic membrane) or extracts thereof, and/or patches or fabrics composed of PGA and/or PLLA. Non-limiting examples of suitable synthetic material patches include woven patches composed of 91% PGA-9% PLLA copolymer, woven patches composed of 91% PGA-9% PLLA copolymerWoven patch or a nonwoven patch consisting of 100% PGA. More generally, suitable substrates may include silk forms of silk moth (such as Seri)RSurgical silk stents (Sofregen, New York, NY)), other derivatives of silk moth and synthetic fabrics (such as polyglycolic acid-poly-L-lactic acid copolymer (PGA/PLLA) forms).
In some embodiments, the substrate is also bioresorbable. As used herein, "bioresorbable" refers to a material that can be broken down by the body of the host or recipient of the implant and does not require mechanical removal. In some embodiments, the bioresorbable substrate is bioresorbable in the range of about 2 to about 10 weeks, about 2 to about 20 weeks, about 2 to about 52 weeks, about 4 to about 16 weeks, about 4 to about 12 weeks, or about 4 to about 8 weeks. In some embodiments, the bioresorbable substrate is coated with a coating for about 4 to about 8 weeks; is bioresorbable in the range of about 4 to about 12 weeks, about 4 to about 16 weeks, about 4 to about 20 weeks, and about 4 to about 52 weeks.
As used herein, the biomaterial of the implant and the biomaterial of the implant independent of the substrate include biomaterials that can form a hydrogel. The term "gel" refers to a solid, gelatinous material that can have properties ranging from soft and weak to hard and tough. A gel is defined as a crosslinked system that is substantially dilute and exhibits a non-flowing state when in a steady state. Gels are mostly liquids by weight, however, they behave like solids due to the three-dimensional cross-linked network within liquids. It is the cross-linking within the fluid that gives the gel structure (stiffness, consistency, mechanical or viscoelastic properties) and contributes to the adhesiveness of the gel. Thus, a gel is a dispersion of liquid molecules within a solid, where the solid is the continuous phase and the liquid is the discontinuous phase. "hydrogel," also referred to herein as a "hydrogel matrix," is a non-limiting example of a gel composed of a macromolecular polymer gel constructed from a network of polymer chains. Hydrogels are synthesized from hydrophilic monomers or hydrophilic dimers (e.g., in the case of hyaluronic acid) by chain growth or step growth and network formation. The network structure and void defects enhance the ability of the hydrogel to absorb large amounts of water via hydrogen bonding. Thus, hydrogels produce the characteristic strong yet elastic mechanical properties. When old bonds within a material break, they are able to undergo spontaneous formation of new bonds. The structure of the hydrogel and electrostatic attraction drive the formation of new bonds through non-covalent hydrogen bonds.
Biomaterials used in implants have mechanical properties, consistency, which can be more strictly defined as the viscoelastic properties of the biomaterial. See https:// en. wikipedia. org/wiki/Viscoelasticity. Implant Biomaterials to facilitate implantation must be very soft (e.g., about 100Pa), allowing the donor cells to remain in immature conditions (Lozoya et al, Biomaterials 2011; 32(30):7389 and 7402), so membrane-associated and/or secreted forms of MMP can be produced.
As used herein, the term "viscoelastic" refers to the property of a material that exhibits both viscous and elastic characteristics when undergoing deformation. Viscous materials are able to resist shear flow like honey and are linearly strained over time when stress is applied. Elastic materials are strained when stretched and quickly recover their original state once the stress is removed. Viscoelastic materials have elements of both properties and therefore exhibit time-dependent strain. Elasticity is generally a result of stretching of bonds along crystalline planes in ordered solids, while viscosity is a result of diffusion of atoms or molecules within the amorphous material. While there are many instruments that test the mechanical and viscoelastic responses of materials, Broadband Viscoelastic Spectrometers (BVS) and Resonant Ultrasonic Spectrometers (RUS) are more commonly used to test viscoelastic behavior because they can be used above and below ambient temperatures and are more specific for testing viscoelastic properties. Both instruments employ damping mechanisms at various frequencies and time ranges, without requiring time-temperature superposition. The use of BVS and RUS to study the mechanical properties of a material is important to understand how a material exhibiting viscoelastic properties performs.
As used herein, the term "hyaluronic acid" (hyaluronan or hyaluronan acid) refers to a polymer of disaccharide units consisting of glucosamine and glucuronic acid [1-3] linked by β 1-4, β 1-3 bonds and salts thereof the term hyaluronic acid thus refers to both the natural and synthetic forms of hyaluronic acid, a water-soluble polysaccharide of naturally occurring Hyaluronic Acid (HA), disaccharide units comprising D-glucuronic acid (GlcUA) and N-acetyl-D-glucosamine (GlcNAc), which are alternately linked to form a linear polymer, a high molecular weight HA may comprise 100 to 10,000 disaccharide units.
Other glycosaminoglycans (GAGs) may also be used in the hydrogel. These glycosaminoglycans include Chondroitin Sulfate (CS) and Dermatan Sulfate (DS) forms, polymers of glucuronic acid and galactosamine, and polymers of Heparan Sulfate (HS) and Heparin (HP), glucuronic acid and glucosamine. The degree and pattern of sulfation of these GAGs is of critical importance, as the sulfation pattern determines the formation of complexes with multiple families of proteins (e.g., coagulation proteins, growth factors, cytokines, neutrophils). See, e.g., Powell AK, Yates EA, Fernig DG, Turnbull JE. interactions of heparin/heparin sulfate with proteins, aprazal of structural factors and Experimental protocols, Glycobiology, 2004, month 4; 14(4):17R-30R ] those suitable for optimizing implanted patch implants include hyaluronic acid, non-sulfated GAGs and minimally sulfated GAGs (such as the Chondroitin sulfate form present in the stem cell niche), such as Karumbaiah L et al, Chondrotin Sulfate Glycoamino glyco-polysaccharides Hydrogels Create endogenesis Niches for Neural Stem cells bioconjugate Chem.2015.12, 16; 26(12) 2336-49 and Hayes AJ et al, Chondroitin sulfate as reactive biologizers for isolation of insulating porous promoter cells.J. Histochem Cytochem.2008, 2 months; 56(2) 125-38 (incorporated herein by reference).
As used herein, the term "cell" refers to one or more cells in an implant. The cells of the present disclosure are eukaryotic cells. In some embodiments, the cell is of animal origin, optionally from a human organ, and may be a stem cell, a mature somatic cell, a progenitor cell, or an intermediate cell in the lineage stage from a stem cell to a mature cell. The term "cell population" or "cell" refers to a combination of one or more cells of the same or different origin, of the same or different cell types; the term is used interchangeably herein with the term "donor cell," which means a cell that may be autologous or allogeneic. In some embodiments, the cell population may be derived from a cell line, from freshly isolated cells, or in some embodiments, the cell population may be derived from a portion of an organ or tissue, optionally from a donor or recipient.
The term "stem cell" refers to a population of cells that can self-replicate (produce the same daughter cells as the mother cells) and have the ability to differentiate multiple times (i.e., can produce more than one type of adult cell). As used herein, the term "progenitor cell" or "precursor" is defined broadly to encompass the progeny of a stem cell and its progeny. Progenitor cells are populations of cells that may have multi-, bi-or mono-differentiation properties, but minimal, if any, self-replicating capacity. Committed progenitors are progenitors that have unidifferentiation properties and can differentiate into specific lineages, resulting in only one mature cell type. Non-limiting examples of stem cells include, but are not limited to, Embryonic Stem (ES) cells, Induced Pluripotent Stem (iPS) cells, germ layer stem cells, defined stem cells (ectodermal, mesodermal or endodermal), perinatal stem cells, amniotic fluid derived stem cells, Mesenchymal Stem Cells (MSCs), hemangioblasts, and those derived from umbilical cord, Wharton's glue and/or placenta. Intermediate cells between stem cells and committed progenitors include populations of cells such as hepatoblasts and pancreatic duct progenitors, as well as other forms of transient proliferative cells that may have multi-differentiation potential, but broad proliferative potential, but more limited, if any, self-replicating capacity.
The term "mesenchymal cells" refers to cells derived from the mesenchyme, including but not limited to angioblasts, precursors of endothelium, precursors of stellate cells, endothelium, stellate cells, stromal cells, various subpopulations of mature and progenitor cells, and Mesenchymal Stem Cells (MSCs), which are multipotential stromal cells, and various subpopulations of mature and progenitor mesenchymal cells. MSCs are populations of Cells prepared from tissues by culture selection processes (Cathey et al Stem Cells 2018; PMID: 29732653; Graceb et al Biochimie2018: PMID 29698670; Caplan AI. Stem Cells int.2015; PMID: 26273305. mature mesenchymal Cells are of at least two general classes, (a) mature mesenchymal Cells (astrocytes/stromal Cells) that produce and are surrounded by extracellular matrix forms comprising fibrillar collagen (e.g., type I collagen, type III collagen, type V collagen) and related matrix components (fibronectin, chondroitin sulfate proteoglycans, dermatan sulfate proteoglycans) and binding signals that form complexes (e.g., growth factors, cytokines) and binding signals that form complexes with Cells of the generally linear (stringy) cell population Tendon, stroma, and myofibroblasts. (b) Mature mesenchymal cells, such as endothelium, produce and are surrounded by extracellular matrix forms comprising network-like collagens (e.g., type IV collagen, type VI collagen, type VIII collagen, type X collagen) and associated matrix molecules (fibronectin, heparan sulfate proteoglycans, heparin proteoglycans) and binding signals (e.g., growth factors, cytokines) that are collectively associated with cells with more squamous or cubic or cobblestone morphology. Non-limiting examples of such cells include endothelium and myoepithelium.
Precursors of these mesenchymal cell types include, but are not limited to, angioblasts, which have pluripotency and can differentiate into endothelial lineages (their advanced stages are fenestrated endothelium) or stellate cells (their advanced stages are myofibroblasts (stroma). MSCs can optionally be prepared by culture selection methods (Cathy et al Stem Cells 2018; PMID: 29732653; Graceb et al Biochimie2018: PMID 29698670; Caplan AI. Stem Cells int.2015; PMID: 26273305).
The term "epithelial cell expansion" is associated with the diameter of epithelial cell colonies that typically form colonies of cubic or cobblestone morphology, and estimates of growth are associated with complexes of the diameters of the cells of the colonies. In contrast, estimates of growth of mesenchymal cell colonies correlate with the density of the colonies, as mesenchymal cells are more mobile and mobile, and colony density is a reflection of the net total number of cells remaining within the colony boundary.
The term "epithelial cells" refers to cells derived from the epithelium, specialized cells that provide multiple functions required for the tissue and/or the whole body of the host. They are believed to have the ability to migrate as precursors or immature cells; as they mature, they become quiescent and form squamous or cobblestone-like or columnar polarized cells with apical, basal and lateral faces, and bind to each other through various junctions (connexins, tight junctions, adherence). Their amplification potential is expressed in the diameter of the colony (rather than in density). Mature epithelial cells provide a variety of functions, such as specialized product secretion or contributing to metabolism (hepatocytes, cholangiocytes), detoxification (hepatocytes), enzyme production (acinar cells), endocrine factor production (e.g., pancreatic islets or other endocrine cells), electrical activity (neuronal cells), and absorption (intestinal cells).
The term "biliary stem cell" (BTSC) refers to an epithelial stem cell present throughout the biliary system and located extramurally and intramurally as well as intracryptic Pericholecystal (PBG), bulonna glands of the gallbladder villus. They have the ability to convert to committed liver and/or pancreatic progenitors. Liver offspring enter hepatic sinusoids via herring's canal; pancreatic progenitor cells are present within the Pancreatic Ductal Gland (PDG), localized to regions of the biliary system within the pancreas.
To date, at least 7 subpopulations of stem cell populations have been identified by overlapping traits, ranging from extremely primitive BTSCs to stem cell populations that can be defined as liver stem cells or pancreatic stem cells. A description of these known matters is given below. The most primitive cells are found in both extramural peribiliary glands-cells tethered to the surface of the bile duct-and intramural peribiliary glands-cells found within the wall of the bile duct. The intramural pericholecystal glands (PBGs) near the fibromuscular layer in the center of the bile duct wall can also be considered as crypts (parallel to the intestinal crypts), where niches for the most primitive stem cell population are present. A large number of PBGs within the biliary network are present within the hepatopancreatic common duct and within the large intrahepatic bile ducts. PBG is not present in the gallbladder, and the stem cell niche within the gallbladder is the bottom of the gallbladder villi containing a metaphase to late stem cell population (precursors of liver stem cells). BTSC are precursors to both the liver and pancreas. They produce liver stem cells (precursors of the liver) and pancreatic stem cells (precursors of the pancreas), and these stem cells are present in the entire biliary system, but the number is affected by the proximity of the liver or of the pancreas. Thus, a small number of pancreatic stem cells and a large number of liver stem cells are localized in the PBGs of the large intrahepatic bile ducts, while a small number of liver stem cells and a large number of pancreatic stem cells are localized in the PBGs of the hepatopancreatic common duct.
A summary of genetic markers is provided in the figures, generally, all BTSC subpopulations express general biomarkers including endodermal transcription factors for both liver and pancreas (e.g., SOX9, SOX17, PDX1), pluripotency genes (e.g., OCT4, SOX 4, NANOG, SALL4, KLF4/KLF 4, BMI-1), one or more of the hyaluronic acid receptor isoforms (standard and/or variant isoforms) of CD4, CXCR4, and cytokeratin 8 and cytokeratin 18. the stem cell subpopulations within the biliary and PBG include (1) bunner gland stem cells in the submucosa of the duodenum, which express 4, TRA-160 and 181, and which have a trait that is distinguishable from stem cells in the intestinal tract, (2) LG intramural lineages (36SC) which express sodium iodide in the same direction as pancreatic reticulocytes (NIS) and are absent in 4, and are found in the bile duct epithelial stem cells of the liver, and have a high or a pancreatic endothelial cell adhesion to pancreatic epithelial cells (PBACH), and are found in the liver epithelial stem cells of the liver, and are found in the liver epithelial cells of the liver, and are found in the liver.
Notably, when the liver stem cells and pancreatic stem cells are in an early developmental stage (e.g., as ESCs or other cells), they may also be present in their respective organ of origin, and any of those cells disclosed herein may alternatively be produced by induction (i.e., as ipscs).
As used herein, the term "supportive" is used to describe cells that are capable of assisting cells to proliferate from another lineage stage or to assist neighboring cells by producing "paracrine signals," which are factors that are active in terms of survival, expansion, migration, differentiation, and maturation in terms of effects on neighboring cells. For example, supportive mesenchymal cells may be defined by their ability to affect epithelial cells, optionally by secretion of Matrix Metalloproteinases (MMPs) and/or one or more paracrine signals or growth factors. Many of these cells have been outlined in recent reviews. (Cathey et al Stem Cells 2018; PMID: 29732653; Graceb et al Biochimie2018: PMID 2969870; Caplan AI. Stem Cells int.2015; PMID: 26273305).
For hepatic stem cells or biliary stem cells, these partners consist of hemangioblasts (CD117+, CD133+, VEGFr +, CD31 negative) and their direct progeny, precursors of the endothelium (CD133+, VEGFr +, CD31+, wecker factor (vWF +)) and precursors of the stellate cells (CD146+, ICAM-1+, α -smooth muscle actin + (ASMA), vitamin a negative), which can be mimicked, in part and/or to some extent, by the use of Mesenchymal Stem Cells (MSCs), such as but not limited to stem cells derived from bone marrow or adipose tissue.
Intermediate cells in the lineage network are termed "transient proliferating cells," which are cells that can have bi-differentiation (or multi-differentiation) potential, have substantial proliferation potential but exhibit little, if any, true self-replication, have low to moderate (or even no) pluripotency gene expression, and express traits indicative of fate directed to the liver (e.g., albumin, alpha-fetoprotein) or pancreas (e.g., insulin, MUC6, amylase). These cells include hepatoblasts (the network produces the liver) and pancreatic duct progenitors (the network produces the pancreas).
As used herein, the term "pancreatic ductal progenitor cells" refers to the bilaterally competent cells present within the Pancreatic Ductal Gland (PDG) within the pancreas and producing acinar cells and islets in our study, we found that they express SOX9, PDX1, PTF1a, HNF1 β, EpCAM, LGR5, ICAM-1, CD44, and a subset that express NGN3 or MUC6 or amylase, which are also widely characterized in other studies, see, e.g., Rezanejad H, Ouziel-Yahalom L, KeyKezer CA, Sullivan BA, Hollie-Lock J, Li WC, Guo L, Deng S, Lei J, Markmann J, Bonner-Weir S.738 heterology of SOX9and HNF1 β. Cell pages 3. 13; 10. mu. 13. Rep.) (725.
As used herein, the term "hepatoblasts" refers to bilaterally competent liver cells that can give rise to the hepatocyte and cholangiocyte lineages and are present in PBGs in or near the canals of herring or within the large intrahepatic bile ducts, they have extraordinary proliferation (i.e., expansion) capacity, but very low, if any, self-replicating capacity relative to observations in hepatic stem cells or BTSCs, these cells are characterized by overlapping, but distinct from biomarker profiles of hepatic stem cells or biliary stem cells, they express SOX9, low (or even negligible) levels of SOX17, high levels of LGR5, HNF4- α, and EpCAM, which are predominantly present at the plasma membrane and express P450a7, cytokeratin 7, secretin receptors, stable expression of albumin in all hepatoblasts, high levels of formazan protein (AFP), intercellular adhesion molecule (ICAM-1) but not NCAM-1, and negligible or non-pluripotent gene expression (e.g. multiple gene expression of clon P735, KL 3, e.g. nank 3, KL 3, and no substantial marker such as nax 355631, KL.
As used herein, the term "committed progenitor" refers to a single differentiated competent progenitor cell that produces a single cell type (e.g., committed hepatocyte progenitor cells). In some embodiments, they do not express pluripotency genes. Committed hepatocyte progenitors are identified by the expression of albumin, AFP, glycogen, ICAM-1, various enzymes involved in glycogen synthesis, and gap junction genes (connexin 28). These cells produce hepatocytes. The committed biliary (or cholangioepithelial) progenitor cells give rise to biliary epithelial cells and are identified by the expression of EpCAM, cytokeratin 7 and cytokeratin 19, aquaporins, CFTR (cystic fibrosis transmembrane conductance regulator) and membrane pumps associated with bile production. In some embodiments, the committed islet progenitor cells express insulin, glucagon, and other islet hormones, albeit at very low levels; as it matures, the level of islet hormone expression increases, but certain cells preferentially express certain hormones.
As used herein, the term "aggregate" refers to a plurality of cells that are aggregated together. The size and shape of the aggregates may vary, or the size and/or shape may be substantially uniform. The cell aggregates used herein may have various shapes such as spheres, cylinders (preferably equal in height and diameter) or rods, and the like. In one embodiment of the present disclosure, it is generally preferred that the aggregates be spherical or cylindrical, although other shaped aggregates can be used. The term "non-aggregated" refers to single or unicellular stem and/or progenitor or mature cells. In some embodiments, the compositions provided herein can comprise substantially aggregated cells, substantially non-aggregated cells, or mixtures thereof.
The term "organoid" refers herein to a specific cell aggregate of donor epithelial cells and mesenchymal cells that self-assemble by the simple panning process described herein. In some embodiments, the mesenchymal cell is a supporting mesenchymal cell. In some embodiments, organoids are formed following culture on low-adherence culture dishes under defined serum-free conditions tailored for multiple lineage stages of aggregated cells in suspension. Other studies have also used specific matrix extracts (such as Matrigel) to prepare organoids. Indeed, this material is known to be an industry standard. See Hindley et al dev.biology 2016; 420:251-261. PMID 27364469. For the use of these organoids in the patch implants described in the present invention, the described conditions for maintaining these organoids would not be successful. Factors such as those present in Matrigel will prevent or substantially reduce MMP production by the cells required for success of these patch implants. Furthermore, Matrigel cannot be used as a component of conditions under which cells are clinically used for human or veterinary purposes.
The term "culture" or "cell culture" means the maintenance of cells in an artificial in vitro environment. "cell culture system" is used herein to refer to culture conditions under which a population of cells can be grown ex vivo (outside the body).
"Medium" is used herein to refer to a nutrient solution used for cell culture, growth, or proliferation. The medium may be characterized by functional properties such as: such as, but not limited to, the ability to maintain the cells in a particular state (e.g., pluripotent, proliferative, resting, etc.) to mature cells-in some cases, specifically, the ability to promote differentiation of progenitor cells into cells of a particular lineage. A non-limiting example of a culture medium is Serum Supplemented Medium (SSM), which is any basal medium supplemented with a certain level (typically about 10% to about 20%) of serum. The serum may be autologous (same species as the cells), or more commonly serum from animals that are routinely slaughtered for commercial purposes (e.g., chickens, cows, pigs, etc.). Notably, embodiments of the invention directed to stem cells employ media that avoid binding to serum and/or serum components that drive differentiation. The depot column medium is a serum-free medium designed for endodermal stem/progenitor cells, comprising a basal medium (nutrients, amino acids, vitamins, salts, carbohydrates), free of copper, containing a small amount (<0.5mM) of calcium, supplemented with selenium, zinc, insulin, transferrin, lipids, but free of cytokines or growth factors. Other media that support stem cells have been found to be useful, but they must avoid any factor that causes cell differentiation, as the maturation process will result in silencing of membrane-associated and/or secreted MMP production.
The basal medium is a buffer for cell culture and is composed of various nutrients in a composition of amino acids, sugars, lipids, vitamins, minerals, salts, trace elements, and chemical components that mimic the interstitial fluid around the cells. Furthermore, the cell culture medium is usually composed of a basal medium supplemented with a small amount (usually 2% -10%) of serum. For the implantation techniques described herein, the conditions are used to maintain the cells as stem cells or early progenitor cells, so serum or any typical supplement that might drive the cells toward mature cell fate should be avoided. In addition to conventional basal media, there are various nutritional supplements, lipids (a mixture of free fatty acids complexed with albumin and carrier molecules such as high density lipoproteins). Only two hormones/growth factors were added: insulin (required for carbohydrate metabolism) and transferrin (required as the Fe carrier for polymerase). The depot column medium is a serum-free medium designed for endodermal stem/progenitor cells comprising a basal medium, containing no copper, a small amount (<0.5mM) of calcium, supplemented with zinc, selenium, insulin, transferrin, lipids, but no cytokines or growth factors. The use of other growth factors and cytokines, especially serum, should be avoided as they induce donor cell differentiation, thereby minimizing the production of MMPs required for implantation and migration processes.
As used herein, "depot column medium" refers to any medium that is free of copper, calcium (<0.5mM), selenium, zinc, insulin, transferrin/Fe, a mixture of free fatty acids bound to purified albumin, and optionally also contains High Density Lipoprotein (HDL). In some embodiments, the depot tower medium comprises any medium (e.g., RPMI1640 or DMEM-F12) that is copper-free, contains a small amount of calcium (e.g., 0.3mM),. about.10-9M selenium,. about.0.1% bovine serum albumin or human serum albumin (highly purified and free of fatty acids),. about.4.5 mM nicotinamide,. about.0.1 nM zinc sulfate heptahydrate,. about.10-8M hydrocortisone (an optional component for liver precursors but not pancreas precursors),. about.5 μ g/ml transferrin/Fe,. about.5 μ g/ml insulin,. about.10 μ g/ml high density lipoprotein, and a mixture of purified free fatty acids (added after the free fatty acids are bound to the purified serum albumin). The free fatty acid mixture consists of-100 mM of each of palmitic, palmitoleic, oleic, linoleic, linolenic, and stearic acids. Non-limiting exemplary methods for preparing the media have been disclosed elsewhere, for example, Kubota H, Reid LM, proc.nat.acad.scienn. (USA) 2000; 97: 12132-.
Thus, in some embodiments, the conditions of these patch implants are reversed from conventional use of medium supplemented with small amounts (typically 2% -10%) of serum. Serum has long been added to provide the necessary signaling molecules (hormones, growth factors, cytokines) required to drive biological processes (e.g., proliferation, differentiation). In some embodiments, serum is not included to avoid differentiation of cells and/or to avoid inactivation or silencing of MMP production (particularly in secreted form).
As used herein, the term "effective amount" (or effective amount) refers to an amount sufficient to treat a disease state or condition (e.g., liver disease or pancreatic disease). An effective amount may be administered in one or more administrations, applications or doses. Such delivery depends on many variables, including the time period over which the individual dosage units are used, the bioavailability of the composition, the route of administration, and the like. It will be understood, however, that the specific amount of the composition for any particular patient will depend upon a variety of factors including the activity of the specific agent employed, the age, body weight, general health, sex and diet of the patient, the time of administration, the rate of excretion, the composition combination, the severity of the particular disease being treated (e.g., liver or pancreatic disease), and the mode of administration.
The terms "equivalent" or "biological equivalent" when referring to a particular molecule, biological material, or cellular material are used interchangeably and refer to those substances having minimal homology while still maintaining the desired structure or function.
As used herein, the term "expression" refers to the process of transcription of a polynucleotide into mRNA and/or the subsequent translation of the transcribed mRNA into a peptide, polypeptide, or protein, and if the polynucleotide is derived from genomic DNA, expression may include splicing of the mRNA in eukaryotic cells. The expression level of a gene can be determined by measuring the amount of mRNA or protein in a cell or tissue sample; in addition, the expression levels of multiple genes can be determined to establish an expression profile for a particular sample.
As used herein, the term "function" may be used to modify any molecule, biological material, or cellular material to achieve a particular specified effect.
As used herein, the term "gene" is meant to broadly include any nucleic acid sequence that is transcribed into an RNA molecule, whether the RNA is coding (e.g., mRNA) or non-coding (e.g., ncRNA).
As used herein, the term "produce" and equivalents thereof (e.g., generating, generated, etc.) are used interchangeably when referring to method steps for producing organoids of the present disclosure.
As used herein, the term "isolated" refers to a molecule or biological or cellular material that is substantially free of other materials.
The terms "nucleic acid", "polynucleotide" and "oligonucleotide" are used interchangeably to refer to a polymeric form of nucleotides of any length, i.e., deoxyribonucleotides or ribonucleotides or their analogs. The polynucleotide may have any three-dimensional (3D) structure and may perform any known or unknown function. The following are non-limiting examples of polynucleotides: a gene or gene fragment (e.g., a probe, primer, EST, or SAGE tag), an exon, an intron, messenger RNA (mrna), transfer RNA, ribosomal RNA, RNAi, ribozyme, cDNA, recombinant polynucleotide, branched polynucleotide, plasmid, vector, isolated DNA having any sequence, isolated RNA having any sequence, nucleic acid probe, and primer.
Polynucleotides may include modified nucleotides, such as methylated nucleotides and nucleotide analogs. Modification of the nucleotide structure, if present, may be performed before or after polynucleotide assembly. The sequence of nucleotides may be interrupted by non-nucleotide components. The polynucleotide may be further modified after polymerization, such as by conjugation with a labeling component. The term also refers to both double-stranded and single-stranded molecules. Unless otherwise indicated or required, any aspect of the technology (i.e., polynucleotide technology) encompasses the double-stranded form as well as each of the two complementary single-stranded forms known or predicted to constitute the double-stranded form.
The terms "protein," "peptide," and "polypeptide" are used interchangeably and refer in the broadest sense to a compound that is an amino acid, amino acid analog, or peptidomimetic of two or more subunits. The subunits may be linked by peptide bonds. In another aspect, the subunits may be linked by other linkages (e.g., ester, ether, etc.). The protein or peptide must contain at least two amino acids, and there is no limitation on the maximum number of amino acids that can constitute the sequence of the protein or peptide. As used herein, the term "amino acid" refers to natural and/or unnatural or synthetic amino acids, including glycine as well as both D and L optical isomers, amino acid analogs, and peptidomimetics.
As used herein, the terms "subject" and "patient" are used interchangeably and are intended to mean any animal. In some embodiments, the subject may be a mammal. In some embodiments, the mammal is a bovine, equine, porcine, canine, feline, simian, murine, human, or rat. In some embodiments, the subject is a human.
The term "tissue" is used herein to refer to the tissue of a living or dead organism, or any tissue derived from or designed to mimic a living or dead organism. The tissue may be healthy, diseased, wounded, damaged, and/or have a genetic mutation. As used herein, the term "native tissue" or "biological tissue" and variations thereof refer to biological tissue that, when derived from an organism, exists in a native state or an unmodified state. "micro-organ" refers to a portion of a "bioengineered tissue" that mimics a "native tissue".
A biological tissue may include any single tissue (e.g., a collection of cells that may be interconnected) or a group of tissues that constitute an organ or portion or region of an organism. The tissue may comprise a homogeneous cellular material, or it may be a composite structure, such as that present in a region of the body comprising the breast, which may comprise, for example, lung tissue, skeletal tissue, and/or muscle tissue. Exemplary tissues include, but are not limited to, those derived from liver, pancreas, biliary system, lung, intestine, thyroid, thymus, bladder, kidney, prostate, uterus, breast, skin and subcutaneous dermal tissues, brain, spinal cord, blood vessels (e.g., aorta, iliac veins), heart, muscle, including any combination thereof.
As used herein, "treating" (or treating) a disease in a subject refers to (1) preventing the appearance of symptoms or disease in a subject susceptible to or not yet exhibiting symptoms of the disease; (2) inhibiting or arresting the development of the disease; or (3) ameliorating or causing regression of the disease or symptoms of the disease. As understood in the art, "treatment" is a method for obtaining beneficial or desired results, including clinical results. For purposes of the present technology, beneficial or desired results can include, but are not limited to, one or more of alleviation or amelioration of one or more symptoms, diminishment of extent of a disorder (including disease), stabilization of state of a disorder (including disease) (i.e., not worsening), delay or slowing of a disorder (including disease), progression, amelioration or palliation of a disorder (including disease), state, and detectable or undetectable remission (partial or complete).
Abbreviations
AFP, alpha-fetoprotein; ALB, albumin; BTSC, biliary stem cells; CD, common determinant; CD44, hyaluronic acid receptor; CD133, prominin; CFTR, cystic fibrosis transmembrane conductance regulator; CK, cytokeratin; CXCR4, CXC-chemokine receptor 4 (also known as fusion viral protein or CD 184; also known as platelet factor 4); EGF, epidermal growth factor; ELSMC, early lineage mesenchymal cells, consisting of angioblasts and their progeny, precursors of the endothelium and precursors of the stellate cells; EpCAM, epithelial cell adhesion molecule; FGF, fibroblast growth factor; HB, hepatoblasts; HGF, hepatocyte growth factor; HpSC, liver stem cells; KM, depot column medium, a serum-free medium designed for endoderm stem cells; KRT, cytokeratin gene; LGR5, G protein-coupled receptor 5 containing leucine-rich repeats that binds to R-spondin; MMPs, matrix metalloproteinases, a large family of proteases associated with the lysis, cell migration and regeneration reactions of the extracellular matrix; NANOG, a transcription factor critically involved in self-renewal; NCAM, neural cell adhesion molecule; NIS, sodium/iodine symporter; OCT4, (octamer-binding transcription factor 4) also known as POU5F1(POU domain, class 5, transcription factor 1), a gene expressed by stem cells; PDX1, pancreatic and duodenal homeobox 1, transcription factors critical to pancreatic development; PBG, pericholecystal gland, stem cell niche for biliary stem cells; SALL4, Sal-like protein 4, was found to be important for the autonomous replication of stem cells; SOX, Sry related HMG box; SOX2, a transcription factor important for maintaining self-renewal, or pluripotency of embryonic stem cells and defined stem cells. SOX9, a transcription factor associated with endosymous tissues (liver, intestine and pancreas); SOX17, a transcription factor important for liver differentiation; VEGF, vascular endothelial growth factor; vWF, von willebrand factor.
Embodiments of the present disclosure
In the examples provided herein, applicants have created patch implants, a novel method for transplanting cells into an internal organ, the design characteristics of which depend on whether the cells are stem or mature cells. Applicants demonstrate herein these methods wherein an implant of biliary stem cells (BTSCs), precursors of liver and pancreas, is transplanted into the liver or pancreas. The host used to develop these methods is a breed of domestic pigs (Sus scrofa therapeutics). They are the major animal species used for transformation studies, surgical models and procedural training, and are increasingly used as a replacement for monkeys in preclinical studies.
Organoids containing organoids are placed on a Seri-silk substrate (mesh material), impregnated on the plasma membrane side of the Seri-silk substrate with a thicker HA hydrogel (-700 Pa) that is surgically or tethered to the surface of the liver or pancreas, the implant causes remodeling of the organ capsule and adjacent tissues, and optionally distant parenchymal tissue, followed by merging of donor cells and host cells, by two weeks the donor cells have matured to a functional adult fate, such as hepatocytes (albumin) or islets of langerhans (β cellulin), by three weeks the histology of the organ capsule and normal tissues is restored.
These results of these examples are in contrast to past work on cell transplantation from solid organs to internal organs, where transplantation was achieved by direct injection or by cell delivery via a vascular route (see reviews by Bhatia et al, Lanzoni et al, Weber, etc.). Past transplantation methods have produced small numbers of cells to be implanted, with a potentially life-threatening risk of embolism, and significant levels of ectopic cell distribution. These problems can result in minimal or incomplete use of cell therapies directed to internal solid organs.
The patch implant strategy provides an alternative approach to cell therapy that is capable of delivering a sufficient number of cells and integrating them into the tissue, thereby significantly restoring one or more functions. These examples demonstrate safety provided that the biomaterials and substrate support used maintain the immature state of some or all of the donor cells, so a relevant pool of MMPs can be generated. A common cause of failure is any factor that causes donor cell differentiation. Without being bound by theory, it is contemplated herein that purified MMPs can be incorporated into implant biomaterials and/or that cells can be transformed using recombinant expression systems or other genetic modification techniques to secrete MMPs as an alternative to providing cells in a naturally occurring essential MMP implant. In such embodiments, the combination of MMPs bound to or transduced via the construct should include those identified in the expression profile provided in the examples below.
Composition of patch implant
Aspects disclosed herein relate to patch implants comprising a layer comprising a single cell population or two or more cell populations (e.g., donor cells that may be autologous or allogeneic) and a source of MMPs and a substrate comprising a biocompatible, biodegradable material that can be used to tether the implant to a target site. In some embodiments, the one or more cell populations comprise a population of epithelial cells and a population of mesenchymal cells. In some embodiments, the cell population must be maintained in a particular state or "lineage stage" as part of the implant, meaning that they do not differentiate or mature further until incorporation into the organ. This can be achieved by maintaining a balance of variables relating to cell origin, MMP content, culture medium used and substrate quality. Each of these aspects is described in more detail below.
Without being bound by theory, it is believed that patch implants with (1) an optimal population or mixture of cells in culture medium and hydrogel-such as donor epithelial cells and a supporting mesenchymal stem/progenitor cell population that produces membrane-associated and/or secreted MMPs-that do not result in differentiation of the supporting mesenchymal stem/progenitor cell population or contain the appropriate MMPs, and (2) a substrate suitable for tethering the implant to a target site and preventing migration of cells in the implant towards the substrate, away from the target site, can be achieved successfully.
Exemplary cells
Without being bound by theory, the cells may be of any mature lineage stage, including Embryonic Stem (ES) cells, Induced Pluripotent Stem (iPS) cells, defined stem cells, committed progenitor cells, transient proliferating cells, or mature cells. However, in certain embodiments, the source of MMPs must be present in the patch implant. Thus, a cellular source of MMPs for patch implants is contemplated herein. Such cell sources must be in an early lineage stage capable of expressing membrane-associated and/or secreted matrix metalloproteinases. A non-limiting example of such an early lineage stage is early lineage stage mesenchymal stem cells (ESMLC).
In some embodiments, the cells to be implanted are epithelial cells collocated with mesenchymal cells. In some embodiments, the epithelial cells comprise epithelial stem cells. In some embodiments, the epithelial cells comprise committed and/or mature epithelial cells. In some embodiments, the committed and/or mature epithelial cells comprise mature parenchymal cells. In some embodiments, the mature parenchymal cells include one or more of hepatocytes, cholangiocytes, or islet cells. In some embodiments, the mesenchymal cells comprise ELSMC. In some embodiments, the ELSMC includes one or more of angioblasts, precursors of endothelium, precursors of stellate cells, and MSCs. In some embodiments, the epithelial cells and mesenchymal cells are lineage-collocated with each other. In some embodiments, the epithelial cells and mesenchymal cells are not lineage stage partners of each other, e.g., are not at about the same lineage stage or maturation stage, respectively. In some embodiments, the epithelial cell is a mature cell. In some embodiments, the mesenchymal cells are ELSMCs.
In some embodiments, at least one of the epithelial cells and the mesenchymal cells are derived from a donor. In some embodiments, the donor is a subject in need of tissue transplantation. In some embodiments, the donor is a source of healthy cells for tissue transplantation. In some embodiments, at least one of the epithelial cells and the mesenchymal cells is autologous to the intended recipient of the patch implant. In some embodiments, all cells (i.e., epithelial and mesenchymal cells) are autologous to the intended recipient of the implant. In some embodiments, the donor of the cells may be a donor other than the recipient (allogeneic), or may also be a subject with an internal organ that is diseased or dysfunctional (autologous), optionally wherein the donor is obtained from a portion of the internal organ that is not diseased or dysfunctional and/or has been genetically modified to restore function to the cells.
In another aspect, the mesenchymal cells are a lineage stage partner of the donor cell, e.g., at a comparable or corresponding lineage stage. In another aspect, the mesenchymal cells are not a suitable partner for the lineage stage of the donor cell. The mesenchymal lineage stage cells can be angioblasts, early lineage stage precursors of endothelial and/or stellate cells, mesenchymal stem cells, endothelial or stellate cells or derivatives of these cell populations.
For stem cell transplantation, epithelial cells should be paired with natural lineage-partner mesenchymal cells (precursors of angioblasts and/or endothelial or stellate cells). For adult epithelial cells, suitable partners include early lineage mesenchymal cells (ELSMCs) consisting of precursors of angioblasts and/or astrocytes and endothelial cells. Applicants have shown that implantation can be achieved using preparations of Mesenchymal Stem Cells (MSCs) in combination with adult cells. In some embodiments, certain MSCs may be preferred over other MSCs. Without being bound by theory, it is believed that the implant can be optimized by selecting a cell combination that requires minimal, if any, cell culture and that will avoid serum and matrix components that can drive cell differentiation. Without being bound by theory, it is also understood that the epithelial-mesenchymal relationship is important because paracrine signaling supports MMP production. However, mature epithelial cells that are collocated with mature endothelium will survive the implant and will be functional cells, but cannot be implanted. Thus, if mature epithelial cells are paired with a mature matrix to form an implant, the resulting implant may be fibrotic.
For treatment of diseased or dysfunctional organs, the cells may be from a donor other than the recipient (allograft), or may also be autograft, and so from a subject with a diseased or dysfunctional condition internal organ, optionally wherein obtained from a portion of the internal organ that has not been diseased or dysfunctional and/or to which the cells have been genetically modified to restore function.
For establishing a model system for studying disease, the cells may be cells that have the disease and are transplanted onto/into normal tissue in an experimental host.
In some embodiments, the epithelial cells may be stem cells combined with supporting mesenchymal cells (optionally ELSMCs) to form organoids (optionally self-assembled). These organoids may be embedded or contained in the hyaluronic acid hydrogel. The stem cells and/or progenitor cells of the present disclosure can include any stem cells and/or progenitor cells known in the art, including, for example, Embryonic Stem Cells (ESCs), Embryonic Germ Cells (EGCs), induced pluripotent stem cells (ipscs), Pancreatic Stem Cells (PSCs), hepatic stem cells (hpscs), biliary stem cells (BTSCs), hepatoblasts, pancreatic ductal progenitors, committed pancreatic progenitors, or committed hepatic progenitors. In some embodiments, the cell population includes only stem cells, such as pancreatic stem cells, liver stem cells, biliary stem cells (BTSCs), or buna-na stem cells. In other embodiments, the cells comprise only a subset of the multi-differentiation competent progenitor cells, such as hepatoblasts or pancreatic duct progenitor cells, or the implant may contain committed mono-differentiation competent progenitor cells (e.g., hepatocytes or biliary or pancreatic islet or acinar committed progenitor cells). In other embodiments, the cells comprise a mixture of stem cells and progenitor cells.
If adult epithelial cells are used, they can be mixed with ELSMCs in relevant ratios into the implant biomaterial. The ratio of the cell mixture can be determined to mimic the target tissue. Alternatively or additionally, the ratio may be determined by self-assembly of organoids. Organoids or cell mixtures are embedded in soft implant biomaterials (such as soft hyaluronic acid hydrogels). If stem cells are implanted, the stem cells and/or progenitor cells of the present disclosure can include any stem cells and/or progenitor cells known in the art, including, for example, Embryonic Stem Cells (ESCs), Embryonic Germ Cells (EGCs), Induced Pluripotent Stem Cells (iPSCs), Blanca stem cells (BGSCs), biliary stem cells (BTSCs), Pancreatic Stem Cells (PSCs), hepatic stem cells (HpSCs), transient proliferative cells (e.g., hepatoblasts or pancreatic duct progenitors), and committed mono-differentiated functional progenitors (e.g., committed pancreatic progenitors or hepatocyte progenitors or biliary epithelial progenitors). In some embodiments, the population of cells comprises only stem cells. In other embodiments, the cells comprise only a subpopulation of progenitor cells. In other embodiments, the cells comprise a mixture of stem cells and progenitor cells or a mixture of stem/progenitor cells and more mature cells. In yet other embodiments, a chimeric mixture of adult cells (e.g., hepatocytes, biliary epithelial cells, intestinal epithelial cells, pancreatic islets) and ELSMCs may be present.
Non-limiting examples include the use of a combination of assays that define self-replicating capacity and assays that demonstrate multi-differentiation capacity by morphological analysis, by gene and/or protein expression, cell surface markers, and the like, in some embodiments, stem cells and/or progenitor cells express at least one marker indicative of early liver cell lineage cells (e.g., SOX17, HNF-4 α, HNF6, HES1, CK19) and at least one marker indicative of early pancreatic cell lineage (e.g., PDX1, PROX1, NGN3, HNF β) for example, various combinations of pluripotent stem cell expression, such as SOX 4, clonx 4642, noc 364642, and SOX/or KLF 4642 may be identified by SOX9, SOX17, PDX1, CD133, NCAM, sonic hedgehog factor (sonic hedgehog) (SHH), sodium iodine symporter (NIS), nrr 8, CD 6866, OCT 44, and various combinations of these.
Thus, they will express one or more markers common to both the liver and pancreatic lineages (e.g., SOX9, LGR5/LGR6, EpCAM, CD133, CK19) and one or more markers of the early pancreatic lineage (e.g., SOX1, PROX1, NGN3, HNF β 1) for example, one or more markers of the early pancreatic lineage (e.g., PDX1, PROX1, NGN3, HNF β 1) may be identified by SOX9, SOX17, PDX1, CD133, NCAM, sonic hedgehog factor (sonic hedgehog) (SHH), sodium iodine symporter (lgs), LGR5, nir 6, and various pluripotent genes (e.g., OCT4, SALL 5845, nang) for example, klx 4624, kl 2, or a combination thereof.
Generation of mature cell types
The stem and/or progenitor cells can also differentiate into more mature cell types, if desired. This can be done in vitro by spontaneous differentiation and/or by direct differentiation. Direct differentiation may involve genetically modifying stem and/or progenitor cells to express a gene of interest or a combination thereof using defined media.
Non-limiting examples of defined media for differentiating cells include hormone-defined media (HDM) for differentiating endoderm stem cells into adult fates. Supplements can be added to the depot tower medium to produce serum-free, hormone-defined media (HDM) that facilitate the differentiation of normal hepatic or biliary stem cells to a specific adult fate. These supplements include calcium supplement to achieve a concentration equal to or greater than 0.6mM, 1nM triiodothyronine(T3)、10-12M copper, 10nM hydrocortisone and 20ng/ml basic fibroblast growth factor (bFGF). The other medium conditions than those required for the selective production of hepatocytes (HDM-H) and cholangioepithelial cells (HDM-C) and pancreatic islets (HDM-P) were:
1) HDM-H: further supplemented with 7 μ g/L glucagon, 2g/L galactose, 10ng/ml Epidermal Growth Factor (EGF) and 20ng/ml Hepatocyte Growth Factor (HGF);
2) HDM-C: further supplemented with 20ng/ml Vascular Endothelial Growth Factor (VEGF) and 10ng/ml HGF; and
3) HDM-P: prepared without corticosteroids and further supplemented with 1% B27, 0.1mM ascorbic acid, 0.25 μ M cyclopamine, 1 μ M retinoic acid, 20ng/ml FGF-7 for 4 days, then replaced with the following supplements: 50ng/ml exenatide-4 and 20ng/ml HGF, induced for another 6 days.
The HDMs provided herein can be supplemented with additional growth factors, including, but not limited to, Wnt signaling, Epidermal Growth Factor (EGF), Fibroblast Growth Factor (FGF), Hepatocyte Growth Factor (HGF), insulin-like growth factor (IGF), Transforming Growth Factor (TGF), Nerve Growth Factor (NGF), neurotrophic factors, various interleukins, Leukemia Inhibitory Factor (LIF), Vascular Endothelial Growth Factor (VEGF), platelet-derived growth factor (PDGF), Stem Cell Factor (SCF), Colony Stimulating Factor (CSF), GM-CSF, erythropoietin, thrombopoietin, heparin-binding growth factor, IGF binding protein, and/or placental growth factor.
The HDMs provided herein can be supplemented with cytokines including, but not limited to, interleukins, lymphokines, monokines, colony stimulating factors, chemokines, interferons, and Tumor Necrosis Factor (TNF).
Applicants have shown that hyaluronic acid can affect stem and/or progenitor cells to express factors of key cell adhesion molecules required to modulate cell anchorage and cell-cell interactions, and to prevent internalization of those anchorage factors by stem and/or progenitor cells following cell suspension preparation, cryopreservation or transplantation non-limiting examples of such anchorage factors include integrins, which are large families of heterodimeric transmembrane glycoproteins that function to attach cells to extracellular matrix proteins of basement membranes, ligands on other cells, and soluble ligands-integrins contain large and small subunits, referred to as α and β, respectively-such subunits form β 0 αβ heterodimers, and at least 18 β and eight αβ subunits are known in humans, can produce 24 heterodimer integrations-in some embodiments, stem and/or progenitor cells express high levels of integrin subunits, such as ITG β, ITG β, ITG 3642, ITG 3653, ITG 3664, ITG B, ITG β, ITG 72, B, ITG β, and the like in embodiments of the cell ITG 3, itp 3, and B, ITG β, ITG 3.
In some embodiments, the stem cells and/or progenitor cells of the present disclosure differ from naturally occurring stem cells and/or progenitor cells at least in that they express the integrin subunit in an amount that is at least 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, 100%, 200% more than the amount of integrin subunit in the unmodified stem cells and/or progenitor cells. It is contemplated that an increase in integrin subunits can facilitate attachment of stem cells and/or progenitor cells to form cell-cell interactions, and prevent internalization of stem cells and/or progenitor cells if desired.
MMP
MMPs are one of the key factors that facilitate implantation and integration. MMPs consist of many isoforms (at least 28; in pigs, 24 isoforms are known), some are secreted (e.g., MMP1, MMP2, MMP7, MMP9), and others are plasma membrane associated (e.g., MMP14, MMP 15). Without being bound by theory, it is believed that a mixture of these isoforms is necessary for implantation, especially a mixture of secreted forms. All cells studied produced different amounts of secreted and membrane-associated forms, but stem/progenitor cells produced very high levels of secreted forms. Implantation depends on these secreted MMPs (membrane-associated forms have some known synergy). The cellular source of these isoforms is a practical way to provide the necessary MMPs to achieve implantation. As an alternative approach, applicants contemplate the genetic engineering of purified/recombinant forms of MMPs into implant biomaterials for binding to and/or cells in the implant to produce the necessary MMPs.
Cells can be successfully implanted so long as there is a source (ideally a cellular source) of a plurality of Matrix Metalloproteinases (MMPs), optionally in one or both of secreted and membrane-associated forms. MMPs are produced by all cell types (both immature and mature), but they differ in which isoform is produced and how the expression level of a particular MMP is. Representative secreted forms include MMP1, MMP2, MMP7, and MMP 9. Representative membrane-associated forms include MMP14 and MMP 15. It has been empirically found that the highest yield of secreted MMPs is produced by early lineage stage cells, stem cells and early progenitor cells. The biomaterial of the implant supports the ability of epithelial and mesenchymal cells to produce these various forms of Matrix Metalloproteinases (MMPs) that lyse the surrounding organ or tissue And allows cells to migrate by solubilizing various forms of extracellular matrix components.
And allows cells to migrate by solubilizing various forms of extracellular matrix components.
More generally, Matrix Metalloproteinases (MMPs) are a large family of zinc-dependent proteases that are involved in the breakdown and regulation of extracellular matrix components, and in transplantation, invasion, angiogenesis, vascularization and migration in both normal and pathogenic processes. There are at least 28 isoforms, including matrix protease, snake venom protease, astaxanthin, serratia protease, and the like. Their role in normal processes (such as transplants of the placenta) and pathogenic processes (such as invasion and metastasis of cancer) has been characterized.
The studies described herein provide evidence for novel effects of MMPs that contribute to the engraftment, migration and integration of transplanted cells. Stem/progenitor cells (both epithelial and mesenchymal) express multiple MMP isoforms that are particularly effective in these effects. Maturation of the cells results in silencing of the expression of one or more potent stem/progenitor-related MMPs, thereby reducing invasion and migration processes. Adult cells also express MMPs, mainly membrane-bound MMPs (MT-MMPs), which are involved in plastic processes, but not in the overall implantation and integration of cells into tissues. However, there is some synergy between MT-MMP and secreted forms. The net sum of this recognition is that, among other features, the implant biomaterial, substrate and other conditions must be one that optimizes the expression of various MMPs (such as secreted MMPs) so that implantation and migration processes can occur. Therefore, factors driving differentiation of transplanted cells will silence the complex MMP response in parallel. This recognition means that factors to be avoided include serum (which drives differentiation), soluble signals that drive differentiation (e.g., certain growth factors, cytokines, and hormones); extracellular matrix components that drive differentiation (e.g., collagen, adhesion molecules, highly sulfated glycosaminoglycans/proteoglycans); and mechanical forces (viscoelastic properties, which drive differentiation) that contribute to the consistency of the implant.
In some embodiments, the one or more cells in the mixture are a source of secreted and/or membrane-associated MMPs. Secreted MMPs may optionally be naturally produced by one or more of epithelial or mesenchymal cells, or optionally result from transformation of one or more of epithelial or mesenchymal cells with a recombinant expression vector or genetic editing for MMP production. In some embodiments, such as but not limited to embodiments involving a population of stem/progenitor cells that natively secrete MMPs, the variable that silences MMP expression-optionally membrane-associated and/or secreted MMP expression-is controlled in the patch implant. Non-limiting examples of such variables include variables that lead to stem/progenitor cell maturation such as, but not limited to, serum supplements to culture media or implant biomaterials, hormones or other soluble signals that affect differentiation of epithelial and/or mesenchymal cells, oxygen levels (since anaerobic conditions keep cells in an immature state, while higher oxygen levels promote differentiation), and the consistency of the implant material (since consistency or mechanical forces (such as shear forces) and compression can drive differentiation).
For stem cell implants, epithelial cells and their mesenchymal counterparts are optimally stem or progenitor cells, as both provide contributions from multiple types of MMPs. For implantation into adult cells, MMPs of epithelial or mesenchymal cells should optimally provide a cellular source of membrane-associated and/or secreted MMPs, e.g. optionally using ELSMC as a cellular source of membrane-associated and/or secreted MMPs. Thus, implants in which both epithelial and mesenchymal cells are mature cell types cannot be successfully implanted. Epithelial cells may survive and proliferate and function if they have mature endothelium, but cannot be implanted; if a mature matrix is present, fibrosis of the implant may occur.
In summary, implantation will occur if the epithelial-mesenchymal cell partner is a stem/progenitor cell, or if at least one of the epithelial or mesenchymal cells is a stem cell, for example optionally using ELSMC as a source of matrix-associated and/or secreted isoforms of Matrix Metalloproteinases (MMPs), or if purified/recombinant forms of those MMPs are provided in the implant biomaterial. The early lineage mesenchymal cells (ELSMCs) suitable for use in patch implants may be hemangioblasts, precursors of endothelium, early lineage endothelium, precursors of stellate cells, early stellate cells or Mesenchymal Stem Cells (MSCs) or mixtures thereof.
Thus, contemplated herein are compositions for use as patch implants comprising at least a population of cells (e.g., epithelial and mesenchymal cells) and a source of MMPs (i.e., a population of cells in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), optionally supported by the conditions of the culture medium and/or hydrogel).
Media Components
For use in combination with the sources of cells and MMPs disclosed herein, any medium (including nutrients, vitamins, salts, etc.) plus key soluble factors (such as insulin, transferrin/Fe and lipids, which are found to be useful for expansion and/or survival of stem/progenitor cells) can be used. All factors that lead to cell maturation must be avoided as maturation will lead to reduced or silenced MMP expression. Factors to be avoided include serum, soluble signals to drive differentiation, extracellular matrix components to drive differentiation, and consistency or mechanical forces (compression, abrasion). A non-limiting example of such a medium is a depot column medium.
Thus, contemplated herein are compositions for use as patch implants comprising at least a population of cells and a source of MMPs (e.g., a population of cells in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a suitable culture medium or purified MMPs). A non-limiting example of a suitable medium is a depot column medium. Other stem cell media, such as those used for Embryonic Stem (ES) cells or Induced Pluripotent Stem (iPS) cells, are equally suitable provided that they do not contain soluble or matrix signals that drive differentiation of the cells, are a source of MMPs, or are present or include MMPs from other sources.
Hydrogels
The patch implant comprises one or more hydrogel components. In some aspects, biomaterials that can form hydrogels or parallel insoluble complexes (e.g., non-collagenous gelatin) include hyaluronic acid, thiol-modified hyaluronic acid, other glycosaminoglycans (GAGs), or combinations thereof. The trigger for curing may be any factor that initiates crosslinking of the matrix components or gelling of those components where gelling may occur. The cross-linking agent may comprise a poly (ethylene glycol) (PEG) or PEG-diacrylate (PEGDA) hydrogel or disulfide bond-containing derivatives thereof. Notably, the biomaterial included in the hydrogel should be selected for its ability to support the dryness of the disclosed cell population or populations used in patch implants (e.g., ELSMCs).
Matrix components that support maintenance of dryness can be used, but components that drive differentiation cannot be used. Non-limiting examples of supportive components include hyaluronic acid or non-sulfated (or minimally sulfated) glycosaminoglycans. These components are particularly useful because they can be "tuned", i.e. modified, to have different levels of consistency (optionally measured as viscoelasticity). Thus, in some aspects, the cell population (optionally cells of an isolated internal organ) may be solidified ex vivo within the biological material prior to introducing the cells into the host, or in the alternative, injected with a fluid substance and allowed to solidify in vivo.
Very soft (e.g., -100 Pa) hydrogels are ideal for maintaining the immature state of the donor cells. A more dense (e.g., >500Pa) version can be used to mature cells enough to cut MMP production, thereby blocking migration. The thicker version may also minimize adhesion of adjacent tissues. In certain embodiments, the cell population and the source of MMPs, optionally another cell population (i.e., a cell population at an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs)).
Without being bound by theory, it is believed that the presence of the extracellular matrix form in the amniotic membrane can maintain the donor cells in an immature state. Thus, it is contemplated that amniotic membrane may be used for the hydrogel, and optionally as an alternative biocompatible, biodegradable material.
Notably, materials known to trigger maturation comprise certain components derived from the mature extracellular matrix, such as, but not limited to, type I collagen. These materials should be excluded from all elements of the patch implant, including but not limited to cells, hydrogels, culture media, substrates, and/or any additional components.
Thus, contemplated herein are compositions for patch implants comprising at least a population of cells and a source of MMPs (i.e., a population of cells in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a suitable medium and contained in a hydrogel).
As described above, consistency may drive the ability of cells to differentiate. Additional thick hydrogels may have an effect on cell migration ability. Since the cells have to migrate into the organ, the hydrogel comprising the cells should have sufficient viscoelastic properties to allow said cells to migrate optionally within or away from the hydrogel and/or patch implant. Non-limiting examples of such viscoelasticity include, but are not limited to, viscoelasticity in the range of about 50 to about 100Pa or about 250Pa, for example, at least about 50Pa, at least about 100Pa, at least about 150Pa, at least about 200Pa, at most about 250Pa, at most about 200Pa, at most about 150Pa, at most about 100Pa, and/or any single value therebetween, such as, but not limited to, about 50Pa, about 100Pa, about 150Pa, about 200Pa, and about 250 Pa.
Without being bound by theory, it is believed that as cells migrate from the patch implant to the target organ or tissue, they migrate with some of the hydrogel with which they are associated or with which they are coated. The hydrogel isolates the cells from signals in the tissue microenvironment that affect cell differentiation or maturation and maintain the cells in an immature state. This facilitates cell migration throughout the parenchymal tissue. As the hyaluronic acid in the hydrogel is gradually degraded and removed, the cells begin to differentiate or mature and turn on adult cell function.
Method of producing organoids
Without being bound by theory, it has been determined that early lineage cells can have a high success rate of implantation when incorporated into organoids or aggregates. Such tissue may optionally comprise early lineage stage epithelial and mesenchymal cells.
Accordingly, provided herein is a method of forming an organoid, the method comprising, consisting of, or consisting essentially of culturing a mixture of epithelial and mesenchymal cells in a vessel suitable for tissue culture and in the presence of a culture medium, removing adherent mature cells on the surface of the vessel by panning, and recovering a self-assembled organoid from a cell suspension in the culture medium. Also disclosed herein are compositions comprising the organoids so produced.
In some embodiments, the procedure involves panning to remove mature cells by allowing the cells to selectively, rapidly (15-30 minutes) adhere to a conventional culture dish under serum-free conditions at 37 ℃ because even under these conditions, mature cells express various matrix components that make the cells adhere. Multiple rounds (e.g., 4-5 rounds) of this panning process can enrich for early lineage stage cells in the cell suspension. The cell suspension was then transferred to a low-adherence culture dish, placed again in serum-free medium (designed for early lineage cells) and placed in an incubator overnight at 37 ℃. The conditions promote the self-assembly of lineage-matched epithelial and mesenchymal cells into organoids. Organoids can be obtained from a mixture of early epithelial (ES cells, iPS cells, defined stem cells, transient proliferative cells, progenitor cells) and early mesenchymal cells (angioblasts, precursors of endothelium, precursors of stellate cells).
Mixtures of adult epithelial cells and mature mesenchymal cells and chimeric mixtures of mature epithelial cells and early lineage mesenchymal cells (ELSMCs) do not typically produce organoids, but can be used as a mixture of cells in suspension in an implant biomaterial. If the mature epithelium (e.g., hepatocytes, cholangiocytes, islets, acinar cells, intestinal epithelial cells, etc.) is paired with mature mesenchymal cells (e.g., endothelium, stellate cells, stromal cells, myofibroblasts), the mixture will not trigger successful integration of the implant into the target site or organ, but will remain on the surface of the organ or tissue. If a chimeric mixture comprising somatic cells and stem/progenitor cells (e.g., mature hepatocytes and hemangioblasts) is used, implantation does not occur because there is a source of MMPs that allow for cell implantation and migration.
In another aspect, the cells of the isolated internal organ may be solidified ex vivo within the biomaterial prior to introducing the cells into the host, or in the alternative, injected with a fluid substance and allowed to solidify in vivo into the implant. Preferably, the cells are introduced at or near diseased or dysfunctional tissue and may be introduced via injection or implanted onto/into the tissue, or introduced using a suitable surgical method.
In another aspect, biomaterials that can form hydrogels or parallel insoluble complexes can include hyaluronic acid, thiol-modified hyaluronic acid, other glycosaminoglycans (GAGs). The trigger for curing may be any factor that initiates crosslinking of the matrix components or gelling of those components where gelling may occur. The cross-linking agent may comprise a poly (ethylene glycol) (PEG) or PEG-diacrylate (PEGDA) hydrogel or disulfide bond-containing derivatives thereof.
In another aspect, the present disclosure provides a method of forming an organoid by culturing a first type of cell (epithelial) with one or more second type of cell (mesenchymal), wherein the second type of cell is in a mature stage that is a suitable lineage partner for the first type of cell. In some embodiments, this may be achieved by: removing mature cells adherent to the culture dish by panning; transferring the nonadherent cells to a low-adherence culture dish and placing the nonadherent cells in a proper culture medium; and recovering the organoids self-assembled under these conditions. The first type of cell may be an epithelial stem cell, a committed progenitor of an epithelial cell, or a mature cell (e.g., a hepatocyte). The second type of cell may be a stem cell of mesenchymal lineage (e.g., hemangioblast, mesenchymal stem cell), a progenitor cell of these lineages (e.g., endothelial or astrocytic progenitor cell), or a mixture of mesenchymal cells during early lineage. It is essential that this formation does not occur under all conditions. For example, culturing in Matrigel does not produce organoids suitable for successful patch implantation. Although Matrigel-prepared organoids can be implanted, the extent of implantation will be reduced relative to organoids prepared under defined conditions. Furthermore, Matrigel cannot be used as a component of the conditions to be used in clinical products.
In another aspect, the present disclosure provides a method for implanting cells into an organ, the method comprising contacting a patch implant, the patch implant comprising a plurality of layers, the plurality of layers comprising a biocompatible, biodegradable substrate, the substrate being neutral in effect on donor cell differentiation; a second layer comprising one or more biological materials (such as hyaluronic acid) that can be cured, such as a hydrogel; a mixture of epithelial cells and supporting mesenchymal cells bound to the solidified biomaterial; and attaching the bandage-like structure to the target site by suture or surgical glue. Adding a layer of cured biomaterial to the serosal surface of the substrate, the cured biomaterial being prepared to achieve 400Pa or more at a level at least twice the level present in the soft biomaterial to which the donor cells are bound. Cells within the patch implant are able to implant and migrate into and throughout tissues/organs, which then mature into an associated adult fate depending on the microenvironment they are in. Higher pascal levels of biomaterial embedded or contained into the porous substrate can prevent cell migration in the wrong direction, and biomaterial added to the serosal surface of the implant can minimize cell adhesion to other organs and tissues.
Organoids
According to one embodiment disclosed herein, organoids, floating aggregates of biliary stem cells (hereinafter "BTSCs"), and mesenchymal cells during early lineage (hereinafter "ELMC") have proven to be the most successful methods of incorporating cells into implants. Disclosed herein are the following: BTSCs and ELMCs can be self-selected to be organoids by panning to remove mature star/stromal cells, and this has proven to be more efficient and effective in establishing appropriate epithelial-mesenchymal partners for the lineage stage of the implant. In another aspect, the present disclosure provides a method of forming an organoid by culturing a first type of cell with a second type of cell, wherein the second type of cell is a lineage-appropriate partner of the first type of cell, removing mature cells adherent to a culture dish by panning, and recovering the self-assembled organoid from the cultured suspension. The first type of cell may be an epithelial stem cell or a committed epithelial cell. The second type of cell may be a cell of mesenchymal lineage, a mesenchymal stem cell or a mesenchymal cell during early lineage. Other aspects relate to self-assembled organoids and uses thereof.
In some embodiments, the donor cell and/or the supporting mesenchymal cell express a matrix metalloproteinase (hereinafter referred to as MMP). Without being bound by theory, it is believed that MMPs allow for pooling of donor and host cells, as well as lysis of the gleason's capsule (or equivalent capsule around a tissue or organ). The disclosure herein provides the expression that, in some embodiments, early stem cells or ELMCs express high levels of MMPs, while mature hepatocytes express low levels of MMPs. In some embodiments, the collocation of mature hepatocytes with mature sinusoidal endothelium (CD31+ + +, VEGF receptor +, collagen IV + and CD117 negative) and those for adult biliary epithelial cells associated with mature stellate and stromal cells (ICAM-1+, ASMA +, vitamin a + +, collagen I +) results in cell aggregates that remain on the surface of the organ and are not effectively engrafted. In some embodiments, implantation of mature epithelial cells requires that they be paired with immature mesenchymal cells that produce MMPs necessary for implantation and migration.
According to one embodiment disclosed herein, floating aggregates of organoids, stem/progenitor cells (such as BTSCs and ELSMCs) are demonstrated to be the most successful cell presentation for patch implantation success. Disclosed herein are the following: BTSCs and ELSMCs can be self-selected to be organoids by: mature mesenchymal cells were removed by standard panning procedures against cells adherent to conventional culture dishes under serum-free conditions, and the remaining cells (those that were not adherent) were then cultured in low-adherence culture dishes and in serum-free defined medium. Organoids self-assemble under these conditions.
In another aspect, the present disclosure provides a method of forming an organoid by culturing a first type of cell (epithelial) with a second type of cell (mesenchymal), wherein the second type of cell is a lineage-appropriate partner of the first type of cell, removing mature cells adherent to a conventional culture dish by a panning procedure, and recovering the self-assembled organoid from a culture suspension on a low-adherent culture dish. The first type of cell may be an epithelial stem cell, a transient proliferative cell, a committed epithelial progenitor cell. The second type of cell may be a stem cell of a mesenchymal cell, a transient proliferative cell or a committed mesenchymal progenitor cell.
In some embodiments, the donor cell and/or the supporting mesenchymal cell express a matrix metalloproteinase (hereinafter referred to as MMP). Without being bound by theory, it is believed that MMPs cause lysis of the capsule around the tissue or organ and allow for pooling of donor and host cells. The disclosure herein provides the expression that, in some embodiments, early stem cells or ELMCs express high levels of MMPs, while mature hepatocytes express low levels of MMPs. In some embodiments, the collocation of mature hepatocytes with mature sinusoidal endothelium (CD31+ + +, VEGF receptor +, collagen IV + and CD117 negative) and those for adult biliary epithelial cells associated with mature stellate and stromal cells (ICAM-1+, ASMA +, vitamin a + +, collagen I +) results in cell aggregates that remain on the surface of the organ and are not effectively engrafted. In some embodiments, implantation of mature epithelial cells requires that they be paired with immature mesenchymal cells that produce MMPs necessary for implantation and migration.
According to one embodiment disclosed herein, floating aggregates of organoids, stem/progenitor cells (such as BTSCs and ELSMCs) are demonstrated to be the most successful cell presentation for patch implantation success. Disclosed herein are the following: BTSCs and ELSMCs can be self-selected to be organoids by: mature mesenchymal cells were removed by standard panning procedures against cells adherent to conventional culture dishes under serum-free conditions, and the remaining cells (those that were not adherent) were then cultured in low-adherence culture dishes and in serum-free defined medium. Organoids self-assemble under these conditions.
In another aspect, the present disclosure provides a method of forming an organoid by culturing a first type of cell (epithelial) with a second type of cell (mesenchymal), wherein the second type of cell is a lineage-appropriate partner of the first type of cell, removing mature cells adherent to a conventional culture dish by a panning procedure, and recovering the self-assembled organoid from a culture suspension on a low-adherent culture dish. The first type of cell may be an epithelial stem cell, a transient proliferative cell, a committed epithelial progenitor cell. The second type of cell may be a stem cell of a mesenchymal cell, a transient proliferative cell or a committed mesenchymal progenitor cell.
In some embodiments, for the patch implantation strategy to be successful, the donor cells and/or supporting mesenchymal cells must express multiple matrix metalloproteinases (hereinafter MMPs), particularly secreted forms of MMPs. Without being bound by theory, it is believed that the various isoforms of MMPs allow for the lysis of the bursa around the organ or tissue, followed by rapid migration of the donor cells to the host tissue. The disclosure herein provides the expression that early epithelial stem cells and/or ELSMCs express high levels of membrane-associated and/or secreted MMPs, whereas mature cells (e.g., hepatocytes) express low levels of secreted MMPs, even though they also express plasma membrane-associated MMPs. Implantation of such adult cells (e.g., hepatocytes, biliary epithelium, islets, intestinal epithelium, etc.) requires the following: the mesenchymal partner is the cellular source of MMPs (especially secreted forms of MMPs) if implantation is to take place. An alternative is to provide the relevant isoforms of MMPs in the biomaterial of the implant, i.e. their purified forms.
According to the present disclosure, the number of cells that can be implanted using a patch implant is very large (>108) And depends on the size of the implant, the number and size of the organoids (or the number of cells-if not part of an organoid) (whether the donor cells are stem cells or mature cells), and the expression of secreted and membrane-associated MMPs (from epithelial and/or from mesenchymal cells). These findings are quite different from the limited number of cells that can be used for vascular delivery or injection implantation (e.g., 10)5-106)。
Disclosed herein are the following: preparing the implant includes mixing the cells with a suitable biomaterial that can be rendered insoluble and keep the cells localized at the target site. In another aspect, the cells of the isolated internal organ may be solidified ex vivo within the biological material prior to introducing the cells into the host, or in the alternative, injected with a fluid substance and allowed to solidify in vivo. In another aspect, the biomaterial that can form a hydrogel or parallel insoluble complex can include hyaluronic acid or other non-sulfated or minimally sulfated glycosaminoglycans, thiol-modified sodium hyaluronate, or plant-derived materials (e.g., alginate). The trigger for curing may be any factor that initiates crosslinking of the matrix components or gelling of those components where gelling may occur. The crosslinking agent may comprise polyethylene glycol diacrylate or a disulfide bond-containing derivative thereof. Preferably, the insoluble complex of cells and biological material has a viscoelasticity in the range of about 0.1 to 200Pa, preferably about 0.1 to about 1Pa, about 1 to about 10Pa, about 10-100Pa, or about 100 to about 200.
Preferably, the cells are introduced at or near diseased or dysfunctional tissue and may be introduced via injection or surgical delivery. Without being bound by theory, it is hypothesized herein that a thicker HA hydrogel (e.g., >500Pa) triggers cell differentiation and decreases engraftment, due in part to decreased expression of MMPs with maturation and a parallel decrease in migratory capacity.
Substrate
There are a number of options for a biocompatible, biodegradable substrate that is neutral to the mature state of the donor cells. They include silk forms of silk moth (such as Seri)RSurgical Silk stents or profiled Seri-Silk (Sofregen, New York, NY)), other derivatives of Silk of bombyx mori, amnion derivatives, omentum, placenta, and synthetic fabrics or materials (such as in the form of polyglycolic acid-poly-L-lactic acid copolymer (PGA/PLLA)). The key to the effectiveness of the substrate is that it has minimal impact on the differentiation of the donor cells. Thus, many basal forms used clinically cannot be used for patch implantation because they are composed of components that induce donor cell differentiation (e.g., mature-type forms of extracellular matrix).
The substrate must have sufficient tensile strength to allow the implant to be attached to the target site by sutures or by surgical glue. It should consist of biocompatible, biodegradable materials that can degrade within months, but the degradation products do not change the maturation state of the donor cells. Thus, the product should have minimal impact on pH or other aspects of the environment. The substrate must also be able to conform to the surface of the target site; the flexible substrate will facilitate the use of the implant at a site of significant bending. Seri-Silk is a non-limiting example of a suitable material for the substrate. Amnion-derived substitutes for materials suitable for use as substrates are also contemplated, such as, but not limited to, amnion-derived materials produced by Osiris Therapeutics, Inc (Columbia, MD).
The substrate may be derived from a porous scaffold, such as Seri-silk, or a non-porous membrane, such as an amniotic membrane or a placental membrane or omentum, or may be a porous or non-porous synthetic fabric, or a combination thereof. If the substrate is porous, it is sealed using a biomaterial infusion/impregnation to inhibit migration of the cell population in the direction of the substrate (i.e., away from the target site, or through the substrate). As defined above, the key features of the base material are biocompatibility, biodegradability neutral, and sufficient tensile strength as described above. In addition, the material may optionally be bioresorbable.
The substrate may be further optimized according to the application. For example, in some embodiments, if the patch implant includes a substrate designed to survive under the influence of the air drying effect, it may be applied to the skin and subcutaneous dermal tissue.
The hydrogel matrix disclosed above may also be used in other parts of a patch implant. For example, if the biocompatible, biodegradable substrate is porous, a hydrogel may be used to inhibit migration of the cell population in the direction of the substrate. Such hydrogels require higher viscoelasticity than hydrogels, e.g., between 1.5 and 15 times higher, e.g., 2 times higher. Non-limiting examples of suitable viscoelastics include, but are not limited to, viscoelastic properties in the range of from about 250 to about 600Pa, such as at least about 250Pa, at least about 300Pa, at least about 350Pa, at least about 400Pa, at least about 450Pa, at least about 500Pa, at least about 550Pa, at most about 600Pa, at most about 550Pa, at most about 500Pa, at most about 450Pa, at most about 400Pa, at most about 350Pa, at most about 200Pa, and/or any single value therebetween, such as, but not limited to, about 250Pa, about 300Pa, about 350Pa, about 400Pa, about 450Pa, about 500Pa, about 550Pa, and about 600 Pa. Other non-limiting examples of suitable viscoelastics include, but are not limited to, viscoelastics in the range of from about 600 to about 800Pa, such as at least about 600Pa, at least about 650Pa, at least about 700Pa, at least about 750Pa, at most about 800Pa, at most about 750Pa, at most about 700Pa, at most about 650Pa, at most about 600Pa, and/or any single value therebetween, such as, but not limited to, viscoelastics of about 600Pa, about 650Pa, about 700Pa, about 750Pa, and about 800 Pa. Additional non-limiting examples include a range of about 250Pa to about 800 Pa.
Still further, the hydrogels disclosed herein may be used as a coating to prevent adhesion on the serosal surface of the substrate, which is opposite the substrate side of the adjacent cells. Such hydrogels may have viscoelasticity between that suitable for use with cell-containing hydrogels and suitable sealing substrates. Non-limiting examples of suitable viscoelastics include, but are not limited to, viscoelastics in the range of from about 250 to about 400Pa or about 500Pa, e.g., at least about 250Pa, at least about 300Pa, at least about 350Pa, at least about 400Pa, at least about 450Pa, at most about 500Pa, at most about 450Pa, at most about 400Pa, at most about 350Pa, at most about 200Pa, and/or any single value therebetween, such as, but not limited to, viscoelastics of about 250Pa, about 300Pa, about 350Pa, about 400Pa, about 450Pa, and about 500 Pa.
Implant, general description
In general, patch implants can be designed using the aforementioned methods and components for transplantation of donor (allogeneic or autologous) cells to a solid organ or tissue, as well as conditions to maintain and maintain the donor cells in an early mature lineage stage. In particular, patch implants for the transplantation of donor cells (allogeneic or autologous) into a solid organ or tissue, as well as conditions that maintain and maintain some or all of the donor cells in the early mature lineage stage, are contemplated. In some embodiments, the donor cell is a mixture of epithelial and mesenchymal cells. In some embodiments, both donor cell populations are stem/progenitor cells. In some embodiments, the epithelial cells are mature cells (e.g., hepatocytes, islets, etc.) and the mesenchymal cells are stem/progenitor cells. In some embodiments, the conditions of the implant biomaterial, such as the culture medium and the matrix components, maintain both donor cell populations, or at least the mesenchymal cell population, as stem/progenitor cells. In some embodiments, the culture medium comprises a basal medium and a soluble signal. In further embodiments, the basal medium and soluble signal support sternness maintenance in both donor populations or at least in the mesenchymal cell population. In some embodiments, the matrix (optionally including extracellular matrix components) and its consistency level support the maintenance of the sternness of the donor population or at least the mesenchymal cell population. In some embodiments, the matrix comprises hyaluronic acid, optionally prepared as a soft hydrogel having a viscoelasticity of about 50Pa to about 150 Pa. In some embodiments, the patch implant includes a substrate having sufficient mechanical strength to tether the implant to the target site, and is composed of a biocompatible, biodegradable material that does not significantly alter the mature lineage stage of the donor cells. Optionally, without further modification, the substrate itself should be sufficient to protect the layer containing donor cells that do not significantly affect the mature lineage stage of the donor cells. In some embodiments, the substrate is a mesh or scaffold and is further impregnated with a biomaterial (such as hyaluronic acid) that has sufficiently high viscoelastic properties to allow sufficient maturation of any cells that migrate thereto, thereby eliminating migration of donor cells in directions other than toward the target site. In some embodiments, the viscoelastic properties are about 500Pa or greater. In some embodiments, the serological surface of the implant is coated with a biomaterial to minimize adhesion from adjacent tissues or organs. In some embodiments, the biomaterials have a viscoelasticity of about 200Pa to about 300 Pa.
The proposed substrate is envisioned to be elastic enough to withstand mechanical forces, capable of tethering to a target organ or tissue, and flexible enough to tether into a position with bending. Any biomaterial (other than hydrogel) may also be employed, provided that the biomaterial is capable of retaining and maintaining a cell population and has viscoelastic properties sufficient to allow migration of the cell population within or away from the patch implant.
In another embodiment, a patch implant may be used to hold and maintain a cell population and include: (a) a population of cells (optionally a population of cells of a single type) supported in a culture medium in a hydrogel or other biological material having sufficient viscoelastic properties to allow migration of cells within or away from the patch implant; and (b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of a cell population in the direction of the substrate (or to provide a barrier to migration of the cell population).
It is important to note that MMPs can be membrane-associated and/or secreted MMPs; they may be provided by MMP producing cells, derived from these cells, or they may be added to the composition of interest (e.g., a purified or recombinantly produced composition).
In another embodiment, a covering or coating for a patch implant or tissue is provided that includes a hydrogel or other biomaterial having sufficient viscoelasticity and elasticity to withstand the mechanical forces applied against the covering or coating (from or by other tissues and organs). By using a covering or coating, a method for inhibiting or preventing the formation of adhesions (which may involve or result from mechanical forces or contact from other organs and tissues) is provided, which comprises covering or coating a surface with hydrogel or other comparable biological material.
In yet another embodiment, a method of implanting cells into a target tissue is provided, the method comprising contacting the target tissue with a patch implant comprising: (a) a population of cells, including at least one population having an early lineage stage, including a single type or multiple types of cells supported in a hydrogel or other biological material having rheological properties (e.g., viscoelasticity) sufficient to allow the cells of the population to migrate within or away from the patch implant; and (b) a substrate comprising a biocompatible, biodegradable material having rheological properties (e.g., viscoelasticity) sufficient to inhibit migration of cells of a population in the direction of the substrate (or to provide a barrier to migration of cells of a population), the patch implant being configured to retain and maintain the population of cells while inhibiting differentiation or further maturation of the at least one population having an early lineage stage to a late lineage stage. In another embodiment, there is provided a method of: wherein a population with an early lineage stage is capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs). In another embodiment, the cell does not have this capability, but MMPs from other sources (e.g., recombinant) are present or included.
Implants with cellular sources of MMPs
Aspects of the present disclosure relate to a patch implant for retaining and maintaining a mixed population of cells, the patch implant comprising (a) a mixed population of two or more cell types, at least one type of which is at an early lineage stage capable of expressing secreted and/or membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), the mixed population being supported in a culture medium present in a hydrogel matrix having sufficient viscoelastic properties to allow migration of the mixed population (optionally, within or away from the hydrogel and/or within or away from the patch implant); (b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in the direction of the substrate; and optionally (c) a hydrogel overlying a serosal (i.e., external) surface of the substrate, the serosal surface opposite the surface contacting the mixed population and, in embodiments where the patch implant is tethered to a target site, opposite the side contacting the target site (e.g., (organ or tissue) — in some embodiments, this layer prevents or inhibits adhesions by, or prevents or inhibits adhesions with, other tissues or organs.
In some embodiments, the implant may contain only one cell type, such as Embryonic Stem (ES) cells or Induced Pluripotent Stem (iPS) cells. Success can be achieved as long as these cells are a cellular source of MMPs, or other sources, such as purified (e.g., recombinant) forms of MMPs, are added to the implant.
In some embodiments, the substrate is porous or non-porous. In some embodiments, the substrate comprises a porous and/or non-porous mesh, scaffold, or membrane. In some embodiments, the substrate comprises a filament; a synthetic fabric; or a natural material (such as amnion, placenta or omentum or derivatives thereof); or a combination thereof. In some embodiments, the substrate comprises a porous mesh infused with a hydrogel or other biological material that is used to convert to a barrier. In further embodiments, such infusion prevents migration of cells away from the target organ or tissue. In some embodiments, the substrate comprises a solid material.
In some embodiments, one or more of the hydrogels comprises hyaluronic acid.
In some embodiments, the culture medium comprises a depot column medium or another medium that supports stem cells and is capable of maintaining a dry quality.
In some embodiments, the mixed population comprises mesenchymal cells and epithelial cells. In some embodiments, the epithelial cells can be ectodermal, endodermal, or mesodermal cells. In some embodiments, the mesenchymal cells comprise Early Lineage Stage Mesenchymal Cells (ELSMCs). In some embodiments, the ELSMC includes one or more of a hemangioblast, a precursor of endothelium, a precursor of stellate cells, and a Mesenchymal Stem Cell (MSC). In some embodiments, the epithelial cells comprise epithelial stem cells. In some embodiments, the epithelial cells comprise biliary stem cells (BTSCs). In some embodiments, the epithelial cells comprise committed and/or mature epithelial cells. In some embodiments, the committed and/or mature epithelial cells comprise mature parenchymal cells. In some embodiments, the mature parenchymal cells include one or more of hepatocytes, cholangiocytes, and islet cells. In some embodiments, the mesenchymal cells and epithelial cells both comprise stem cells.
In a certain embodiment, the mixed population comprises autologous cells and/or allogeneic cells.
In some embodiments, one or more cell types are genetically modified.
"layered" implant
In some embodiments, the patch implant is considered a multi-layered implant. For example, provided herein are patch implants comprising, consisting of, or consisting essentially of a plurality of layers, the plurality of layers comprising at least: (a) a soft hydrogel first layer comprising donor cells, optionally epithelial and/or mesenchymal cells; (b) a thickened hydrogel second layer; and (c) a third layer comprising a biocompatible, biodegradable substrate. In some embodiments, particularly where the third layer is porous, the second layer is incorporated into, impregnated into, and/or infused into the third layer. In some embodiments, the patch implant further comprises a fourth layer of hydrogel. In some embodiments of the patch implant, the fourth layer is coated or painted onto the serosal surface of the implant. In some embodiments of the patch implant, the first layer is adapted to directly contact the target tissue or organ.
As used herein, "soft" refers to a hydrogel layer that exhibits a low level of internal pressure as quantitatively determined by the pascal (Pa) assay. One pascal is defined as one newton per square meter. In some embodiments, the softer layer has a viscosity of from about 10Pa to about 300Pa, from about 50Pa to about 250Pa, from about 100Pa to about 250Pa, from about 50Pa to about 200Pa, from about 150Pa to about 200Pa, or from about 100Pa to about 200 Pa. In a particular embodiment, the soft hydrogel layer has a viscosity of less than or about equal to 200 Pa.
As used herein, "thick" refers to a hydrogel layer that exhibits a high level of internal pressure as quantitatively determined by the pascal (Pa) assay. In some embodiments, the thick stock layer has a viscosity of about 300Pa to about 3000Pa, about 300Pa to about 1000Pa, about 400Pa to about 750Pa, about 400Pa to about 550Pa, about 450Pa to about 600Pa, or about 500Pa to about 600 Pa. In a particular embodiment, the thick hydrogel layer has a viscosity greater than or about equal to 500 Pa.
Preferably, for the first layer of the layered implant, the insoluble complex of cells and biomaterial has a viscosity or viscoelasticity in the range of about 0.1 to 200Pa, preferably about 0.1 to about 1Pa, about 1 to about 10Pa, about 10 to 100Pa, or about 100 to about 200, or about 50 to about 250Pa, or about 200 Pa. Preferably, for the first layer of the layered implant, the insoluble complex of cells and biological material has a viscoelasticity in the range of about 0.1 to 200Pa, preferably about 0.1 to about 1Pa, about 1 to about 10Pa, about 10 to 100Pa, or about 100 to about 200.
In some embodiments, the one or more cells in the mixture are a source of secreted and/or membrane-associated MMPs. In some embodiments, such as but not limited to those involving stem/progenitor cell populations that naturally secrete MMPs, the variable that silences MMP expression-optionally secreted MMP expression-is controlled in the patch implant. Non-limiting examples of such variables include variables that lead to stem/progenitor cell maturation such as, but not limited to, serum supplements to culture media or implant biomaterials, hormones or other soluble signals that affect differentiation of epithelial and/or mesenchymal cells, oxygen levels (since anaerobic conditions keep cells in an immature state, while higher oxygen levels promote differentiation), and rigidity of implant materials (since mechanical forces (such as shear forces) and compression can drive differentiation).
In some embodiments of the patch implant, the viscosity of the first layer is about 50 to about 250 Pa. In some embodiments of the patch implant, the viscosity of the first layer is about 200 Pa. In some embodiments of the patch implant, the second layer has a viscosity of about 250Pa to about 600 Pa. In some embodiments of the patch implant, the viscosity of the second layer is about 500 Pa. In some embodiments of the patch implant, the viscosity of the fourth layer is from about 250 to about 500 Pa. In some embodiments of the patch implant, the viscosity of the fourth layer is about 400 Pa. In some embodiments of the patch implant, the viscosity of the second layer is greater than the viscosity of the 1 st layer. In some embodiments of the patch implant, the viscosity of the second layer is about 1.5 to about 15 times greater than the viscosity of the first layer. In some embodiments of the patch implant, the second layer has a viscosity of about 2 times greater than the first layer.
In one embodiment, the patch implant comprises, consists of, or consists essentially of a plurality of layers, starting from where it contacts the target site, and consisting of: donor cells embedded in a soft (<200Pa) hydrogel prepared in serum-free defined medium (these cells will engraft and migrate into the tissue); a second layer of hydrogel prepared in the same medium and triggered to have a higher consistency (e.g., -500 Pa or higher) to provide a barrier to migration of donor cells in any direction other than towards the target tissue; a third layer of biocompatible, biodegradable, bioresorbable substrate that is neutral in its effect on the maturation state of the donor cells and that can be used intra-operatively or by other means to tether the implant to the target site; and a final layer of hydrogel having a consistency intermediate between that of the soft hydrogel and the very thick hydrogel and being sufficiently fluid to coat or coat a surface to minimize adhesion near tissue.
In some embodiments of the patch implant, the first layer and the second layer each comprise one or more hyaluronic acids. In some embodiments of the patch implant, the fourth layer comprises one or more hyaluronic acids.
In some embodiments of the patch implant, the epithelial cells and mesenchymal cells form one or more aggregates. In some embodiments of the patch implant, the one or more aggregates are organoids. In some embodiments of the patch implant, the epithelial cells comprise epithelial stem cells. In some embodiments of the patch implant, the epithelial cells comprise biliary epithelial cells. In some embodiments of the patch implant, the epithelial cells comprise committed and/or mature epithelial cells. In some embodiments of the patch implant, the committed and/or mature epithelial cells comprise mature parenchymal cells. In some embodiments of the patch implant, the mature parenchymal cells comprise one or more of hepatocytes, cholangiocytes, and islet cells.
In some embodiments of the patch implant, the mesenchymal cells are supportive mesenchymal cells. In some embodiments of the patch implant, the mesenchymal cells comprise early lineage mesenchymal cells (ELSMCs). In some embodiments of the patch implant, the ELSMC includes one or more selected from the group consisting of angioblasts, precursors of endothelium, precursors of stellate cells, and Mesenchymal Stem Cells (MSCs).
In some embodiments of the patch implant, the epithelial cells and the mesenchymal cells are not lineage-collocated with each other. In some embodiments of the patch implant, the epithelial cells are mature cells. In some embodiments of the patch implant, the mesenchymal cells are ELSMCs.
In some embodiments of the patch implant, at least one of the epithelial cells and the mesenchymal cells are derived from a donor. In some embodiments, the donor is a subject in need of tissue transplantation. In some embodiments, the donor is a source of healthy cells for tissue transplantation. In some embodiments of the patch implant, at least one of the epithelial cells and the mesenchymal cells are autologous to the intended recipient of the patch implant. In some embodiments, all cells (i.e., epithelial and mesenchymal cells) are autologous to the intended recipient of the implant. In some embodiments, the donor of the cells may be a donor other than the recipient (allogeneic), or may also be a subject with an internal organ that is diseased or dysfunctional (autologous), optionally wherein the donor is obtained from a portion of the internal organ that is not diseased or dysfunctional and/or has been genetically modified to restore function to the cells. For establishing a model system for studying disease, the donor cells may be cells that have the disease and are transplanted onto/into normal tissue in the experimental host.
In some embodiments of the patch implant, at least one of the epithelial cells or mesenchymal cells are modified. In some embodiments, all cells are modified. In some embodiments, the modification is a genetic modification. In some embodiments, the one or more cells are modified to express a therapeutic nucleic acid or polypeptide. In some embodiments, the one or more cells are modified to express a wild-type allele of a nucleic acid or polypeptide.
In some embodiments of the patch implant, the biocompatible, biodegradable substrate is bioresorbable. In some embodiments of the patch implant, the biocompatible, biodegradable substrate comprises a porous material. In some embodiments of the patch implant, the biocompatible, biodegradable substrate comprises a scaffold or a membrane. In some embodiments of the patch implant, the scaffold or membrane comprises silk, amniotic membrane, synthetic fabric, or a combination thereof. In some embodiments, the biocompatible, biodegradable substrate does not include any factors that induce or prevent cell differentiation. In some embodiments of the patch implant, the biocompatible, biodegradable substrate does not include one or more components derived from the mature extracellular matrix. In some embodiments of the patch implant, the component derived from the mature extracellular matrix is type I collagen.
In some embodiments of the patch implant, the patch implant further comprises one or more Matrix Metalloproteinases (MMPs). In some embodiments of the patch implant, the MMPs are membrane-associated MMPs. In some embodiments of the patch implant, the membrane-associated MMPs are provided by one or more of epithelial cells or mesenchymal cells. In some embodiments of the patch implant, the MMP is a secreted MMP. Secreted MMPs may optionally be naturally produced by one or more of epithelial or mesenchymal cells, or optionally be produced as a result of transformation of one or more of epithelial or mesenchymal cells with a recombinant expression vector for MMP production.
In some aspects, provided herein are patch implants comprising, consisting of, or consisting essentially of a plurality of layers, the plurality of layers comprising at least: a soft hydrogel first layer comprising biliary stem cells; a thickened hydrogel second layer; and a third layer comprising a biocompatible, biodegradable substrate.
In one embodiment, the patch implant is composed of layers of material and cells that together form a "bandage-like implant" that can be surgically or otherwise tethered to a target site. The first layer next to the target site comprises a soft hydrogel (less than 200Pa) seeded with a mixture of epithelial cells and supporting mesenchymal cells suspended in defined serum-free nutrient-rich medium designed for the expansion and/or survival of the cells; the second layer contains a hydrogel that is prepared in the same medium but gels to a thicker level (i.e., higher pascal level) and forms a barrier that blocks migration of cells in directions other than the target site; the third level comprises a biocompatible, biodegradable substrate that does not affect or minimally affects the level of differentiation of the donor cells, but acts as a mechanical support structure for the patch; a fourth layer consisting of a coatable hydrogel (such as hyaluronic acid in addition) having a consistency level intermediate between that of the soft hydrogel and the thick hydrogel and serving to minimize adhesion from cells from adjacent tissues to the implant. Hydrogels must be composed of biocompatible, biodegradable and "tunable" (meaning controllable with respect to consistency) materials. One successful material for hydrogels is thiol-modified hyaluronic acid, which can be triggered to form hydrogels when exposed to oxygen and/or poly (ethylene glycol) diacrylate (PEGDA), and can be easily "tuned" by the precise ratio of hyaluronic acid and PEGDA concentrations (and/or oxygen levels).
In another embodiment, the patch implant includes multiple layers. The first layer next to the target site is a soft hydrogel, which is a minimally sulfated or non-sulfated GAG or other non-sulfated or neutral biomaterial that can be gelled or solidified and in the middle can place the donor cell. The second layer of hydrogel or biomaterial is thicker and incorporates a substrate, i.e., a biocompatible, biodegradable, bioresorbable substrate that allows the patch to be handled for surgery or other purposes and acts as a barrier to forcing cells to migrate toward the target tissue, in/on or within. The serosal side of the substrate is surgically coated with a biomaterial, such as hyaluronic acid (or other minimally sulfated or non-sulfated GAGs or other materials that may gel or solidify), and wherein the pascal level is at least twice that present in the soft biomaterial layer; this serves the purpose of minimizing adhesions from adjacent tissue. The patch implant is tethered to the target organ or tissue and the cells are able to migrate to and fully incorporate into the tissue or organ.
In a particular embodiment, the patch implant comprises a first layer of soft biomaterial (<200Pa), such as soft hyaluronic acid hydrogel, in between which are placed donor cells to be transplanted in serum-free defined medium, tailored for the lineage stage of the cells. This layer is placed on a thicker layer (e.g., a thicker hydrogel) that acts as a barrier to force donor cells to be directed during migration to the target tissue. The thicker layer is prepared in advance on a substrate (i.e., a biocompatible, biodegradable substrate that allows the patch to be processed for surgery or other procedures to secure the patch to the target site). The last layer is a biomaterial with a consistency between that against the donor cells on the target tissue side and that against the barrier. This layer is added to the serosal side of the implant at the time of surgery and serves to minimize adhesions from adjacent tissue. The biocompatible, biodegradable substrate may be Seri-silk or derivatives thereof.
Methods of use and delivery of patch implants
Aspects of the present disclosure relate to compositions and methods for implanting cells into an organ. The task of transplanting cells from a solid organ to an internal organ typically uses direct injection or delivery of cells via the vascular pathway. Lanzoni, G, et al, Stem Cells 31,2047-2060 (2013). These transplantation methods produce small numbers of cells that are transplanted to the target site and carry the risk of potentially life-threatening emboli. If the cells are delivered by "injection implantation", in which the cells are suspended in or coated with hyaluronic acid, and then co-injected with an initiator (PEGDA) that causes the hyaluronic acid to gel in situ, the cells are then injected in situGrafting was improved as described in Turner R et al Hepatology 57,775- & 784 (2013). The injection implantation method provides a strategy for localizing cells to a specific site, although in small numbers, typically 105-107、106-107Or 105-106Individual cells/injection site. This strategy eliminates or minimizes ectopic cell distribution and optimizes cell integration in the site. However, if mature functional cells are used, they may be highly immunogenic, which requires long-term immunosuppression. In addition, the number of cells that can be injected may not be sufficient to achieve the necessary clinical results.
The "patch implantation" strategy described herein overcomes these obstacles and problems. In some embodiments, a "bandage-like" implant is surgically or otherwise tethered to the surface of an organ or tissue; the conditions of the implant allow cells to be fully implanted in the site, migrate throughout the organ/tissue, and then mature into the relevant adult cell type. The large number of cells is formed or determined by the size of the patch, the number or mixture of cells within the implant, and the source of the various forms of MMP (ideally a cellular source of MMPs) ((ii))>108Individual cells). Furthermore, in some embodiments, the use of organoids aids in the ability to store donor cells, and the manner in which organoids are cryopreserved under defined serum-free conditions is more conducive to such ability.
The patch implant compositions provided herein relate to the direct implantation of cells into a tissue or solid organ. The method is safe, avoids embolism and ectopic cell distribution, and optimizes cell number implantation and distribution in and throughout the tissue.
Accordingly, provided herein is a method of implanting cells into a target tissue, the method comprising, consisting of, or consisting essentially of contacting the target tissue with the patch implant disclosed above.
In some embodiments of the method, the target tissue is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, gastrointestinal tract, lung, prostate, breast, brain, bladder, spinal cord, skin and subcutaneous dermal tissue, uterus, kidney, muscle, blood vessel, heart, cartilage, tendon, and skeletal tissue. In some embodiments of the method, the target tissue is liver tissue. In some embodiments of the method, the target tissue is pancreatic tissue. In some embodiments of the method, the target tissue is biliary tissue. In some embodiments of the method, the target tissue is a gastrointestinal tract tissue. In some embodiments, the tissue is diseased, damaged, or has a disorder. In some embodiments of the method, the target tissue is kidney tissue.
In some embodiments of the method, the target tissue is an organ. In some embodiments of the method, the organ is an organ of the musculoskeletal system, digestive system, respiratory system, urinary system, female reproductive system, male reproductive system, endocrine system, circulatory system, lymphatic system, nervous system, or integumentary system. In some embodiments of the method, the organ is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, gastrointestinal tract, lung, prostate, breast, brain, bladder, spinal cord, skin and subcutaneous dermal tissue, uterus, kidney, muscle, blood vessels, heart, cartilage, tendons, and bone. In some embodiments, the organ is diseased, damaged, or has a disorder.
In some embodiments of the method, the liver disease or disorder is liver fibrosis, cirrhosis, hemochromatosis, liver cancer, biliary atresia, nonalcoholic fatty liver disease, hepatitis, viral hepatitis, autoimmune hepatitis, fascioliasis, alcoholic liver disease, α 1-antitrypsin deficiency, glycogen storage disease type II, transthyretin-associated hereditary amyloidosis, Gilbert's syndrome, primary biliary cirrhosis, primary sclerosing cholangitis, bade-Chiari syndrome, liver trauma, or Wilson's disease.
In other aspects, provided herein are methods of treating a subject having a pancreatic disease or disorder, comprising, consisting of, or consisting essentially of contacting a pancreas of the subject with the patch implant disclosed above. In some embodiments of the method, the pancreatic disease or disorder is diabetes, pancreatic exocrine insufficiency, pancreatitis, pancreatic cancer, Oddi (Oddi) sphincter dysfunction, cystic fibrosis, pancreatic division, cricoid pancreas, pancreatic trauma, or pancreatic ductal hemorrhage.
In other aspects, provided herein are methods of treating a subject having a disease or disorder of the gastrointestinal tract, comprising, consisting of, or consisting essentially of contacting one or more intestines of the subject with a patch implant disclosed above. In some embodiments, the gastrointestinal disease or disorder is gastroenteritis, gastrointestinal cancer, ileitis, inflammatory bowel disease, Crohn's disease, ulcerative colitis, irritable bowel syndrome, peptic ulcer disease, celiac disease, fibrosis, vascular dysplasia, hirschsprong's disease, pseudomembranous colitis, or gastrointestinal trauma.
In some aspects, provided herein are methods of treating a subject having a kidney disease or disorder, the method comprising, consisting of, or consisting essentially of contacting one or more kidneys of the subject with a patch implant disclosed above. In some embodiments of the method, the kidney disease or disorder is nephritis, nephropathy, nephritic syndrome, nephrotic syndrome, chronic nephropathy, acute kidney injury, kidney trauma, cystic nephropathy, polycystic nephropathy, glomerulonephritis, IgA nephropathy, lupus nephritis, kidney cancer, Alport (Alport) syndrome, amyloidosis, Goodpasture's syndrome, or Wegener's granulomatosis.
In some embodiments of the method of therapy, at least one of the epithelial cells and the mesenchymal cells are derived from a donor. In some embodiments, the donor is a subject in need of tissue transplantation. In some embodiments, the donor is a source of healthy cells for tissue transplantation. In some embodiments, at least one of the epithelial cells and the mesenchymal cells is autologous to the intended recipient of the patch implant. In some embodiments, all cells (i.e., epithelial and mesenchymal cells) are autologous to the intended recipient of the implant. In some embodiments, the donor of the cells may be a donor other than the recipient (allogeneic), or may also be a subject with an internal organ that is diseased or dysfunctional (autologous), optionally wherein the donor is obtained from a portion of the internal organ that is not diseased or dysfunctional and/or has been genetically modified to restore function to the cells.
In some embodiments, the patch implant used in the method disclosed above is a patch implant comprising a plurality of layers, the plurality of layers comprising at least: a hydrogel first layer comprising epithelial cells and mesenchymal cells; a second layer of hydrogel; a third layer comprising a biocompatible, biodegradable substrate; and optionally a fourth layer of hydrogel. In some embodiments, the method further comprises allowing cells contained in the patch implant to incorporate into the tissue. In some embodiments of the method, the hydrogel first layer is soft. In some embodiments of the method, the hydrogel second layer is a thick. In some embodiments of the method, the mesenchymal cells are supportive mesenchymal cells.
In another aspect, the present disclosure provides a method for implanting cells into an organ, the method comprising the use of a patch implant (i.e., a bandage-like composite having multiple layers of materials and cells) that together may be surgically or otherwise tethered to a target site. The first layer next to the target site comprises a soft hydrogel (less than 200Pa) seeded with a mixture of epithelial cells and supporting mesenchymal cells suspended in defined serum-free nutrient-rich medium designed for the expansion and/or survival of the cells; the second layer contains a hydrogel that is prepared in the same medium but gels to a thicker level (i.e., higher pascal level) and forms a barrier that blocks migration of cells in directions other than the target site; the third level comprises a biocompatible, biodegradable substrate that does not affect or minimally affects the level of differentiation of the donor cells, and is therefore "neutral"; a fourth layer consisting of a coatable hydrogel (such as hyaluronic acid in addition) having a consistency level intermediate between that of the soft hydrogel and the thick hydrogel and serving to minimize adhesion from cells from adjacent tissues to the implant. Hydrogels must be composed of biocompatible, biodegradable and "tunable" (meaning controllable with respect to consistency) materials. One successful material for hydrogels is thiol-modified hyaluronic acid, which can be triggered to form hydrogels when exposed to oxygen and/or poly (ethylene glycol) diacrylate (PEGDA), and can be easily "tuned" by the precise ratio of hyaluronic acid and PEGDA concentrations (and/or oxygen levels). The cells produce a variety of Matrix Metalloproteinases (MMPs) under the conditions of the biomaterial of the implant that facilitate implantation, migration and integration of the donor cells into the recipient's tissue. The microenvironment of the recipient tissue determines the adult fate of the transplanted cells.
In another aspect, the present disclosure provides a method for implanting cells into an organ, the method comprising contacting a patch implant, the patch implant comprising a plurality of layers, the plurality of layers comprising at least a first layer comprising a biocompatible, biodegradable substrate, a second layer comprising one or more hyaluronic acids comprising a mixture of epithelial cells and supporting mesenchymal cells, and a third layer comprising one or more hyaluronic acids, wherein the layer with cells embedded in the middle is soft (less than 200 Pa); the layers associated with the substrate are thicker (-500 Pa or greater); the pascal level of the third layer is intermediate and helps to minimize adhesion near the tissue or organ. In yet another aspect, the cells can be implanted in an organ selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, intestine, lung, prostate, breast, brain, spinal cord, ganglia, skin and subcutaneous dermal tissue, uterus, bone, thymus, intestine, uterus, bone, kidney, muscle, blood vessels, or heart.
In yet another aspect, the cells may be implanted in an organ selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, intestine, lung, prostate, breast, brain, spinal cord, ganglia, skin and subcutaneous dermal tissue, uterus, bone, tendons, cartilage, kidney, muscle, blood vessels, or heart.
Non-limiting examples of patch implants suitable for use in the methods disclosed herein are patch implants comprising: (a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing secreted and/or membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), the mixed population being supported in a culture medium present in a hydrogel matrix having sufficient viscoelastic properties to allow migration of the mixed population (optionally, within or away from the hydrogel and/or within or away from the patch implant); (b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in the direction of the substrate or to provide a barrier to said migration; and optionally (c) a hydrogel overlying a serosal (i.e., external) surface of the substrate, the serosal surface opposite the surface contacting the mixed population and, in embodiments where the patch implant is tethered to a target site, opposite the side contacting the target site (e.g., (organ or tissue) — in some embodiments, this layer prevents or inhibits adhesions by, or prevents or inhibits adhesions with, other tissues or organs.
In some embodiments, the substrate is porous or non-porous. In some embodiments, the substrate comprises a porous mesh, scaffold, or membrane. In some embodiments, the substrate comprises a filament; a synthetic fabric; or natural materials (such as amnion, placenta or omentum); or a combination thereof. In some embodiments, the substrate comprises a porous mesh infused with a hydrogel. In further embodiments, such infusion prevents migration of cells away from the target organ or tissue. In some embodiments, the substrate comprises a solid material.
In some embodiments, the patch implant further comprises a hydrogel superimposed on a serosal surface of the substrate, the serosal surface being opposite the surface contacting the single cell or mixed population of cells.
In some embodiments, one or more of the hydrogels comprises hyaluronic acid.
In some embodiments, the culture medium comprises a depot column medium or another medium that supports stem cells and is capable of maintaining a dry quality.
In some embodiments, the mixed population comprises mesenchymal cells and epithelial cells. In some embodiments, the epithelial cells can be ectodermal, endodermal, or mesodermal cells. In some embodiments, the mesenchymal cells comprise Early Lineage Stage Mesenchymal Cells (ELSMCs). In some embodiments, the ELSMC includes one or more of a hemangioblast, a precursor of endothelium, a precursor of stellate cells, and a Mesenchymal Stem Cell (MSC). In some embodiments, the epithelial cells comprise epithelial stem/progenitor cells. In some embodiments, the epithelial cells comprise biliary stem cells (BTSCs). In some embodiments, the epithelial cells comprise committed and/or mature epithelial cells. In some embodiments, the committed and/or mature epithelial cells comprise mature parenchymal cells. In some embodiments, the mature parenchymal cells include one or more of hepatocytes, cholangiocytes, and islet cells. In some embodiments, the mesenchymal cells and epithelial cells both comprise stem cells.
In a certain embodiment, the mixed population comprises autologous cells and/or allogeneic cells.
In some embodiments, one or more cell types are genetically modified.
Examples
The following examples are non-limiting and illustrate procedures that may be used in various circumstances to effect the present disclosure. In addition, all references disclosed below are incorporated by reference in their entirety.
Example 1: pig model for patch implant verification
Animal(s) production
Animals used as hosts or as donors of cells were maintained in facilities of the NCSU (Raleigh, NC) veterinary college. Surgery, autopsy, and collection of all biological fluids and tissues are performed in these facilities. All procedures were approved by the NCSU IACUC committee. Pigs used as recipients were a mixture of six different breeds: six breed hybrids consisting of Yorkshires, Large Whits, Landraces (from sows), Durocs, Spots, and Pietrans (from boars). These highly heterogeneous genetic backgrounds are desirable because they correspond to heterogeneous genetic constructs of the human population. The host animals were all female, approximately six weeks of age, weighing-15 kg.
There are two classes of host animals, a) male pigs (approximately six weeks of age, weighing-15 kg) were used as donors for cell transplantation to female pigs, b) transgenic donor animals carrying a GFP transgene the GFP + donor animals were obtained by crossing transgenic H2B-GFP male pigs with wild type gilts by standard artificial insemination the model was developed via IRES-pH2B-eGFP to endogenous β -Actin (ACTB) locus CRISPR-Cas9 mediated Homology Directed Repair (HDR).
For each donor and recipient animal, the porcine leukocyte antigen class I (SLA-I) and class II (SLA-II) loci have been PCR amplified using primers designed to amplify known alleles in these regions according to a PCR sequence-specific primer strategy. The system consists of amplifying the gene loci of SLA-1, SLA-2 and SLA-353And 47 discriminatory SLA-I primer sets for amplifying DRB1, DQB1 and DQA loci. These primer sets have been developed to differentiate alleles by groups sharing similar sequence motifs, and have been readily and unambiguously shown to detect known SLA-I and SLA-II alleles. When used together, these primer sets are effective in providing a haplotype for each test animal, thereby providing an assay that readily confirms the matched or mismatched haplotypes in the donor and recipient animals.
Culture media and solutions
All media were sterile filtered (0.22 μm filter) and stored at 4 ℃ protected from light prior to use. Basal medium and Fetal Bovine Serum (FBS) were purchased from GIBCO/Invitrogen. All growth factors were purchased from R & D Systems. All other reagents were obtained from Sigma, except as already indicated.
The cell detergent was formulated with 599ml basal medium (e.g., RPMI 1640; Gibco # 11875-. It is used to wash tissue and cells during treatment.
A collagenase buffer consisting of 100ml of a cell detergent supplemented with collagenase (Sigma # C5138) (final concentration of 600U/ml (R145125 mg) for biliary (bile duct) tissue and 300U/ml (12.5mg) for organ parenchymal tissue (liver, pancreas)) was prepared.
Stock tower medium (defined serum-free medium designed for endodermal stem/progenitor cells) was used to prepare cell suspensions, organoids, and HA hydrogels. The medium was composed of copper-free, small amount of calcium (0.3mM), 1nM selenium, 0.1% bovine serum albumin (purified)No fatty acid; fraction V), 4.5mM nicotinamide, 0.1nM zinc sulfate heptahydrate, 5 μ g/ml transferrin/Fe, 5 μ g/ml insulin, 10 μ g/ml high density lipoprotein and a mixture of purified free fatty acids (provided in complex with fatty acid free, highly purified albumin) in any basal medium (here RPMI 1640). Its preparation is detailed in a summary of the methods57. In addition, it is commercially available from Phoenix Songs Biologicals (Branford, CT).
Soluble long-chain form of HA (Sigma catalog #52747) is used for organoid culture stabilization and cryopreservation. Those HA (thiol-modified HA) used to prepare hydrogels were obtained from Glycosan biosciences, a subsidiary of Biotime. These thiol-modified HA components were prepared by proprietary bacterial fermentation processes using Bacillus subtilis as host in ISO 9001:2000 process (www.biopolymer.novozymes.com /). These components are sold under the trade name Novozymes Produced and 100% free of animal derived raw materials and organic solvent residues. Animal derived ingredients are not used for production and the protein levels are very low and endotoxin free. Production follows the criteria established in the European Pharmacopoeia (European Pharmacopeia). HA hydrogels were prepared using Glycosil (C.) (II: (C.))
Produced and 100% free of animal derived raw materials and organic solvent residues. Animal derived ingredients are not used for production and the protein levels are very low and endotoxin free. Production follows the criteria established in the European Pharmacopoeia (European Pharmacopeia). HA hydrogels were prepared using Glycosil (C.) (II: (C.)) HA, ESI BIO-CG313) thiol-modified HA, which can be used to trigger Glycosil formation of disulfides using polyethylene glycol diacrylate (PEGDA). Degassed water was used in 1% Phosphate Buffered Saline (PBS) or in our case in the stock column medium
HA, ESI BIO-CG313) thiol-modified HA, which can be used to trigger Glycosil formation of disulfides using polyethylene glycol diacrylate (PEGDA). Degassed water was used in 1% Phosphate Buffered Saline (PBS) or in our case in the stock column medium Reverting to a 1% solution of thiolated HA. On reconstitution, it remains in the liquid state for several hours, but if exposed to oxygen, it may undergo some gelation. If Glycosil is treated with a crosslinking agent (such as PEGDA) that causes gelation to occur within minutes, there is no temperature or pH changeMore precise gelation occurs in the case of chemical gelation.
Reverting to a 1% solution of thiolated HA. On reconstitution, it remains in the liquid state for several hours, but if exposed to oxygen, it may undergo some gelation. If Glycosil is treated with a crosslinking agent (such as PEGDA) that causes gelation to occur within minutes, there is no temperature or pH changeMore precise gelation occurs in the case of chemical gelation.
The level of crosslinking determines the consistency level and can be precisely defined by the ratio of thiol-modified HA to PEGDA. In previous studies, stem cell populations were tested in HA hydrogels of different consistency levels, and it was found that they remained antigenic and functional (i.e. in terms of migratory capacity) stem cells only at consistency levels of less than 200Pa23. We used this finding to design an implant of hyaluronic acid hydrogel with a very soft layer and a thicker layer on the serosal side to form a barrier to migration in directions other than the target tissue, as well as to minimize adhesion from cells near the tissue. The 3 hydrogel patterns with different consistency levels are characterized in fig. 2, i.e. including a characterization of the direct measurement of the rheological properties. The thickest barrier of 10 × HA hydrogel (consistency 760Pa) is prepared in advance on a substrate and can be stored at ultra low temperature if necessary. At the time of surgery, donor cells were prepared in soft 1 × HA hydrogel (consistency ═ 60 Pa); placed in a thicker 10 × hydrogel (already on the substrate); and the patch is tethered to the target site. After tethering, use the disc with BD Micro-FineTMNORM-JECT 4010.200V0 plastic syringe with permanently attached needle IV coats or coats the serosal side of the implant with 2 XHA hydrogel (consistency 106 Pa).
Stress-controlled cone-plate rheometers (TA Instruments, AR-G2, 40mm cone diameter, 1 ° angle) were used to determine the large-scale rheological properties of the hydrogels. The gel was living polymerized on a rheometer while oscillating at a frequency of 1rad/s and a stress amplitude of 0.6Pa and the modulus was continuously monitored to inquire whether the crosslinking reaction was sufficiently complete. Once equilibrated, the hydrogel can be subjected to an oscillation frequency sweep (stress amplitude: 0.6Pa, frequency range: 0.01-100 Hz). The viscoelastic (rheological) properties of the 3 hyaluronic acid hydrogels used are summarized in fig. 2.
The most commonly used donor cells were derived from transgenic H2B-GFP pigs as described above. They offer significant advantages for cell transplantation studies because all cells are labeled with GFP. The use of fluorescent proteins as molecular tags allows for tracking of donor cells in migration and implantation after transplantation. The fusion protein targets nucleosomes, thereby generating a nuclear/chromatin GFP signal. In the described implants, stem cells express GFP throughout the nucleus, but those lineages restricted to adult cell types may have GFP in the cytoplasm or nucleus. Note that cytoplasmic GFP levels were particularly high in the first week and decreased over time. This is because the implantation/invasion/integration process results in an effect on the cells, which may result in the presence of H2B-linked GFP in the cytoplasm. This does not mean that the cells are dying, but rather that they respond to high levels of MMPs and associated signaling as part of the remodeling region. Indeed, the GFP + cells examined were apparently viable and proliferating, all of which expressed various adult functions (e.g. albumin, HNF4a, AFP, insulin, glucagon or amylase).
As described in more detail in the characterization of implants, autofluorescence of both the basement (spring green) and lipofuscin (dark forest green) in mature hepatocytes poses a challenge in view of the wavelength overlap with GFP. Therefore, applicants used antibodies to GFP and secondary antibodies to antibodies with red fluorescent probes to convert the GFP + signal to pink or rose. This resulted in the stem cells being recognized as minicells with pink nuclei (a combination of blue DAPI staining of the nuclei and antibody-labeled rose GFP + labeling). Any donor cells that matured into hepatocytes were identified as having a combined color of light purple from green autofluorescence (lipofuscin), blue (DAPI), and rose (GFP) (fig. 4).
Porcine extrahepatic biliary tissue (gallbladder, common duct, hepatic duct) was obtained from transgenic pigs. Tissues were beaten with a sterile stainless steel hammer to remove parenchymal cells, taking care to maintain the intra-hepatic and extra-hepatic bile duct connections. The bile lines were then washed with "cell wash" buffer supplemented with antibiotics, 0.1% serum albumin and 1nM selenium (10)-9M) sterile, serum-free basal medium. The biliary lines were then mechanically separated with a cross scalpel and aggregates were dispersed enzymatically in a cell suspension in RPMI-1640 supplemented with 0.1% Bovine Serum Albumin (BSA), 1nM selenium, 300U/ml type IV collagenase, 0.3mg/ml deoxyribonuclease (dnase) and antibiotics. Xiaoxiao (medicine for eliminating cough and asthma)The reaction is carried out at 32 ℃ for 30-60 minutes under continuous stirring. Most tissues required two rounds of digestion followed by centrifugation at 1100rpm at 4 ℃. The cell pellet was combined and resuspended in cell detergent. The cell suspension was centrifuged at 30G for 5 minutes at 4 ℃ to remove erythrocytes. The cell pellet was resuspended in cell detergent, filtered through a 40 μm nylon cell strainer (Becton Dickenson Falcon #352340), and washed with fresh cell detergent. Cell numbers were determined and viability was assessed using trypan blue. Cell viability greater than 90% -95% was routinely observed.
Mesenchymal cells collocated with BTSCs are subpopulations free of MHC antigens, with low side scatter, and can be identified as angioblasts (CD117+, CD133+, VEGF receptor + and CD31 negative), precursors of endothelium (CD133+, VEGF receptor + and CD31+) and precursors of astrocytes (CD146+, ICAM1+, VCAM +, α -smooth muscle actin (ASMA) + and vitamin a negative), these 3 subpopulations are collectively referred to as early lineage-stage mesenchymal cells (ELSMC), adult hepatocytes are associated with mature sinusoidal endothelium (CD31+ + +, IV protein +, VEGF receptor + and CD117 collagen negative) and biliary epithelial cells associated with mature astrocytes (ICAM-1+, ASMA +, vitamin a + +, I protein +).
The cell suspension was added to serum-free bank tower medium in a multi-well flat bottom cell culture plate (Corning #353043) and incubated at 37 ℃ for-one hour to promote adherence of mature mesenchymal cells. Mature mesenchymal cells adhere to the culture dish within 10-15 minutes, even if the medium is serum-free. The cells remaining in suspension were transferred to another dish and incubated again for up to one hour. This step is repeated to eliminate most of the mature mesenchymal cells. After removal of mature mesenchymal cells, the remaining floating cells were depleted by-2X 105Individual cells/well were seeded in serum-free, bottom-of-the-pool column medium in Corning's ultra-low-adherence culture dish (Corning #3471) and incubated at 37 ℃ in a CO2 incubatorIncubate overnight. Organoids consisted of biliary stem cells (BTSCs) and overnight formed ELMSCs (fig. 1). These organoid cultures survived for weeks in the stock tower medium, especially in the case of medium supplementation (0.1%) with the soluble form of HA (Sigma); they may also be stored at ultra low temperatures as described below. We obtained-1.5X 10 from per gram of neonatal porcine biliary tissue7And (4) cells. In 6-hole ultra-low wall-mounted panels, we use 3-6X 105Cells/well and incubated in serum-free depot column medium. Cells produce on average 6000 to 20,000 small organoids (-50-100 cells/organoid/well). For implants, we use at least 100,000 organoids ((ii))>107Individual cells). Depending on the size of the substrate, applicants were able to increase the number of organoids in the implant up to 108An organoid (i.e., -10)9Individual cells) or further embedded in-1 ml of soft hyaluronic acid hydrogel on a 3cm x 4.5cm substrate.
Isolated stem cell organoids were stored in CS10 at ultra low temperature, CS10 was an isotonic ultra low temperature storage buffer containing anti-freeze factor, dextran and DMSO (Bioliffe, Seattle, Washington; https:// www.stemcell.com/products/cryostor-CS10. html). Cell viability was further improved by 0.1% HA supplement (Sigma # 52747). Cryopreservation was performed using a cryoMedTM programmable freezer. The viability upon thawing is greater than 90%, and the cells after thawing are able to adhere to the wall, thereby expanding ex vivo and in vivo and producing the desired mature cells in vitro and in vivo.
Cell isolation and implant assembly are characterized in the schematic of fig. 1, the details of which are summarized in fig. 2. The implants were formed by using a substrate (table 1) on which the stem cell organoids embedded in a soft hyaluronic acid hydrogel were placed. These implants can be easily prepared in advance and maintained overnight in a petri dish in an incubator. The implant appeared stable at the target site throughout the experiment. Cryopreservation of organoids can be easily achieved, but is not necessarily the case when in soft hydrogels. This means that the organoids must be embedded in a soft hydrogel prior to surgery.
Surgery
Anesthesia was induced by administration of either a combination of intravenously injected ketamine/xylazine (2-3 mg/kg body weight each) or intramuscularly injected 20mg/kg ketamine plus 2gm/kg xylazine and maintained by administration of oxygen and isoflurane via a closed loop gas anesthesia unit.
The animals were placed in a dorsal position and the abdomen was excised from the xiphoid process to the pubic bone. The skin was prepared aseptically by alternating iodine swabbing and alcohol solutions. After entering the operating room, the preparation of the skin is repeated using sterile techniques, covering the area with a topical iodine solution, and then a sterile surgical drape. The surgeon uses appropriate aseptic techniques. A medial abdominal incision was made through the skin, through the subcutaneous tissue and the linea alba, starting from the xiphoid process and extending 8-12cm caudally. The left liver was split exposed and a 3 x 4.5cm patch implant containing 1 xha (-60 Pa) was applied to the abdominal surface of the liver, the embedded organoids were placed on a substrate containing 10 xha (-760 Pa) and the patch was placed in direct contact with the surface of the liver capsule. The patch implant was sutured to the liver using 4-6 simple, interrupted 4-0 polypropylene sutures. The exposed surface of the implant was then treated with 2ml of a 2 × HA hydrogel (-106 Pa) at a consistency level sufficient to allow it to coat or coat the serosal side of the implant; it is used to minimize adhesion from adjacent tissue. After placement of the surgical implant, the white line was closed by a simple continuous suture using 0-PDS. The white line was blocked with 2mg/kg 0.5% bupivacaine injected intramuscularly. The subcutaneous tissue and skin were closed with continuous 2-0PDS and 3-0Monocryl sutures, respectively. The tissue adhesive is placed on the skin surface.
The implant graft from the transgenic pig to the recipient is allogeneic, so immunosuppression is required. The immunosuppressive regimen used was one established by others. Starting 24 hours prior to surgery, all pigs received oral doses of the immunosuppressive drugs Tacrolimus (Tacrolimus) (0.5mg/kg) and mycophenolic acid (Mycophenolate) (500mg) twice daily. The drug was administered continuously throughout the experiment. These drugs can be easily administered to animals if they are mixed with foods that the animals like.
All animals were euthanized humanely by ketamine/xylazine sedation and isoflurane anesthesia at the indicated time points, followed by intravenous injection of a lethal dose of sodium pentobarbital. After confirmation of death, the cadavers were carefully dissected, removed and placed in cooled depot tower medium for transport to the laboratory. In addition to the liver, lungs, heart, kidneys and spleen were collected and fixed in 10% neutral formalin.
Characterization of implants
After 48+ hours of fixation, the tissue samples were placed in 70% ethanol in marker cassettes and processed in a LeicaASP300S tissue processor at 60 degrees for approximately 10 hours with long cycles. After the overnight treatment was completed, the samples were embedded using a LeicaEG1160 embedding machine. The mold is filled with wax and the sample is placed in the correct orientation for collection of the desired slices. The cartridge is cooled until the block and tissue sample can be removed from the mold as a unit. The blocks were cut into 5 micron sections using a Leica RM2235 microtome; the sections were floated in a water bath and placed on glass slides. Slides were allowed to air dry overnight before staining. Sections were stained with hematoxylin and eosin (H & E; reagents #7211 and #7111) or Masson's trichrome (Masson's trichrome stain: blue collagen kit #87019) using Richard Allan scientific histology products following the manufacturer's recommended protocol; this scheme has been programmed into a Leica Autostainer XL.
Tissues were embedded and frozen in OCT and snap frozen at-20 ℃ for frozen sectioning. The frozen sections were IHC stained according to the protocol described above. For immunofluorescence, frozen sections were thawed at room temperature for 1 hour and then fixed in 10% buffered formaldehyde, acetone or methanol according to antibody instructions. After fixation, sections were washed 3 times in 1% Phosphate Buffered Saline (PBS) and then blocked with 2.5% horse serum in PBS for 1 hour at room temperature. Primary antibody diluted in 10% goat serum in PBS was added and incubated overnight at 4 ℃. The following morning, sections were washed 3 times with PBS and incubated with secondary antibody diluted in 2.5% horse serum in PBS for 2 hours at room temperature. Images were acquired using a Zeiss CLSM 710 spectral confocal laser scanning microscope (Carl Zeiss microcopy). The antibodies are listed in table 3.
For the images in FIG. 5, sections (3 μm) were stained with hematoxylin-eosin and sirius red according to standard protocols for immunohistochemistry endogenous peroxidase activity was blocked by incubation for 30min in methanol hydrogen peroxide (2.5%), as described by the supplier, the sections were incubated at room temperature with primary antibodies (pan keratin, Dako, code: Z0622, dilution: 1: 100; Sox9, Millipore, code: AB5535, dilution: 1:200) overnight at 4 ℃, the samples were washed twice with PBS for 5min, with biotinylated secondary antibodies (LSA B + System-HRP, code K0690; Dako, Glostrip, Denmark, then with streptavidin-HRP (B + System-HRP), code K0690, and the sections were examined by staining with a confocal microscope (Involu) with a fluorescent microscope (Involu-ELISA, Involu-20) and examined by staining with a fluorescent staining procedure with a rabbit-rabbit staining procedure (Involuol) as well as a staining procedure, staining with a staining procedure No. 20, staining with a staining procedure No. 5-20, staining procedure No. 5, No. 4, and No. 5, No. 4, No. 5, No. 4, No. 5, No. 1, No. 4, No. 1, No. 4, No. 1, No. 5, No. 1, No. 4, No. 1, No. 4, No. 1, No. 4, No.
Frozen sections are problematic in view of the high autofluorescence of hepatocytes (lipofuscin) and the fluorescence of the Seri-Silk substrate. Applicants have achieved greater success by preparing paraffin sections and staining GFP with rabbit polyclonal antibodies to GFP (Novus Biologicals, NE 600-308); the rabbit anti-GFP antibody was used in combination with a donkey anti-rabbit IgG H & L secondary antibody (Alexa Fluor 568; ab175470, Invitrogen), while the donkey anti-goat IgG Alexa Fluor 488 antibody was used to exclude non-specific staining of liver autofluorescence. Autofluorescence was reduced by quenching with a dye including trypan blue. Trypan blue was dissolved in PBS at 0.4% for tissue/cells. This significantly reduces the background.
Total RNA was extracted from organoids or implants using trizol (invitrogen). First strand cDNA synthesized using Primescript 1 st strand cDNA Synthesis kit (Takara) was used as a template for PCR amplification. Quantitative analysis of mRNA levels was performed using Faststart Universal Probe template (Roche Diagnostics) with the ABI PRISM 7900HT sequence detection System (Applied Biosystems). Primers were designed at the Universal Probe library assay Design Center (Universal Probe library Design Center) (Roche Applied Science). The primer sequences are listed in table 4. The primers were annealed at 50 ℃ for 2min and treated at 95 ℃ for 10min, followed by 40 cycles of 95 ℃ (15s) and 60 ℃ (1 min). Expression of glyceraldehyde-3-phosphate dehydrogenase (GAPDH) is commonly used as a control and standard.
RNA was purified from cells using Qiagen RNeasy kit and RNA Integrity (RIN) analysis was performed using Agilent2000 bioanalyzer. cDNA libraries were generated using Illumina TruSeq standard mRNA preparation kit and sequenced on Illumina HiSeq 2500 platform. Two samples per lane were sequenced, and for all samples (one flow cell), these samples occupied a total of 8 lanes. Quality control analysis was done using FastQ. Mapping of sequence reads to the human genome (hg19) was performed by mapspice 2 using default parameters. Transcript quantification was performed by RSEM analysis, and DESeq was used to normalize gene expression and identify differentially expressed genes. Mapscice 2 was also used to detect candidate fusion transcripts. The fusion identification is based on the depth and complexity of the reads that span the candidate fusion connection points. Pearson's correlation analysis was used to compare gene expression profiles and hierarchical clustering was performed in R. Hierarchical clustering was performed according to the differential stabilization transformation provided in the DESeq package. The Pathway enrichment Analysis was performed using Ingenity Path Analysis (IPA) software. Differential gene expression analysis was performed only on genes with minimum mean normalized counts >50 in at least one category.
The Student's two-tailed t-test was used to calculate statistically significant differences between samples, with results expressed as mean ± Standard Deviation (SD). P values less than 0.05 were considered statistically significant.
Results
In previous studies on injection implantation, it was found that implantation required co-transplantation of epithelial cells with a suitable mesenchymal cell partner for their lineage stage for liver stem cells and biliary stem cells, these mesenchymal cells consisted of angioblasts (CD117+, CD133+, VEGFr +, CD31 negative) and their direct progeny, precursors of endothelium (CD133+, VEGFr +, CD31+, weweber's factor +) and precursors of stellate cells (CD146+, ICAM-1+, α -smooth muscle + (ASMA), vitamin a negative).
In previous studies, applicants achieved the isolation of matched epithelial and mesenchymal cell phases using multi-parameter flow cytometry to determine the ratios of lineage stage partners of epithelial and mesenchymal cells in cell suspensions, and then use those ratios by immunoselection of the cells. In these studies, applicants found that it was more effective to cull the cell suspension of mature mesenchymal cells by repeating the panning procedure and then culturing the remaining cell suspension on low-adherence culture dishes and in serum-free bank media for 6-8 hours. Organoids self-assemble, containing approximately 50-100 cells per aggregate. Marker analysis indicated that BTSCs collocated with ELSMC (fig. 1). As summarized in the schematic illustration of fig. 1A, they can be used immediately or cryopreserved under defined conditions previously determined and thawed as needed for implantation. Immunofluorescence (IF), qRT-PCR and RNA-seq were used to characterize the organoids of BTSC/ELSMCs and showed classical behavior of expressing BTSC (FIG. 1) and ELSMCs (data not shown). BTSCs in organoids do not express mature liver or pancreas genes, but express low levels of pluripotency genes (e.g., OCT4, SOX2) and endoderm stem cell genes (e.g., EpCAM, SOX 9, SOX17, PDX1, LGR5, CXCR4, MAFA, NGN3, and NIS). Representative qRT-PCR assays confirmed findings from IF and from IHC against cells prior to transplantation (fig. 1D). IHC assays indicate that more primitive cells (e.g., cells expressing pluripotency genes) are distributed in the interior of organoids and in the peripheral, late maturation lineage (e.g., EpCAM or albumin expressing cells) (fig. 1C).
The results from the patch implants were compared to those from the injection implants by a previously established method consisting of cell injection and localized to the site by triggering hyaluronic acid gelation within minutes using polyethylene glycol diacrylate (PEGDA). Injection of the implant into the porcine liver parenchyma resulted in essentially 100% implantation, but had minimal (if any) migration and integration into host tissues slowly occurred over several weeks (data not shown). These findings are similar to those previously observed with injected implants of liver stem cells17. Injection of the implant through the large tube into the mesentery near the hepatic duct/portal branch immediately caudal to the liver lobes was feasible, but resulted in smaller ones being blocked by swelling of the HA hydrogel and resulted in cholestasis (fig. 13). The success of patch implants has given us up further work with injection implantation strategies.
The composition of the implant against stem cells involved conditions using Hyaluronic Acid (HA) hydrogel with 3 distinct layers, where the precise concentration of HA and PEGDA was used to achieve consistency levels assessed by rheometry (fig. 2C). Donor cells were embedded in a soft HA layer (-100 Pa) and placed against the liver/pancreas surface; at this pointIn these studies, the soft hydrogel maintained the dry state23Prove important for implantation. This layer is placed on top of a thick (10 ×; -700 Pa) HA layer, prepared in advance on a substrate and acting as a barrier to migration. The patch is attached to the target site using sutures or surgical glue. The 2 xha hydrogel is soft enough (consistency ═ 200Pa) to allow coating or application to the serosal surface of the implant at the time of surgery and to minimize adhesion near the tissue.
The patch implant is placed on the surface of the liver, i.e. the surface of the gleason's capsule or pancreatic capsule, and attached on the corners by sutures or by surgical glue (fig. 2F). The consistency of Seri-Silk results in the implant being placed at the site of least flexure and away from the site of greater mechanical force (e.g., near the septum). In an implant implanted in the pancreas, the implant is wedged between the duodenum and the pancreas.
An attempt was then made to forego the only patch implant variant after surgical removal of the capsule completely. Given the adverse effects of serum on donor cells, excessive bleeding avoids future use in hosts with altered hemostasis associated with liver failure, or even in normal hosts. Without such work to alter the organ capsule, the patch implant is easy to perform a surgical procedure.
A number of substrates were tried, with emphasis on the substrates used clinically in abdominal surgery (tables 1 and 2). In addition to Seri-Silk, can cause problems that can lead to their removal for further consideration. These problems include fragility (e.g., Seprafilm, Retroglyde); induction of necrosis or fibrosis and significant levels of adhesions (e.g., Surgisis, Vetrix); and Seri-Silk sponge type of severe adhesion formation or any substrate with an abdominal supplement of carboxymethyl cellulose ("belly jelly"). Of those tested, the SERI procedure Silk24-26(Allergan, inc. irvine, CA) provides the best combination of mechanical support and minimal adhesion, the effect being further enhanced by application of 2 x HA to the serosal surface of SeriSilk after attachment to the target site. This product was a purified fibroin of silk moth silk and was developed by David Kaplan (Tuft's University, Boston, MA). Shen-Shi-an exercise for strengthening the muscles and jointsApplicants found it to be thick, a property that was found to be useful for surgical manipulation and placement on flat/thick organs such as the liver. The consistency makes it difficult to apply to sites that have significant bends or require flexibility. In addition, its consistency proved to be neutral with respect to maturation against donor cells, which finding made the substrate useful for patch implants. In the 3-week implants, the Seri-Silk was encapsulated by collagen bands, indicating a mild foreign body response. Evaluation of other candidate substrates (such as synthetic fabrics) is ongoing.
Evidence of remodeling in the first week after surgery was verified using trichrome staining (fig. 3, 7) or safranin O, which has a dye that stains collagen and other extracellular matrix components. Images of implants stained with trichrome (fig. 3A-B) were compared to images of the same sites and stained with hematoxylin/eosin (fig. 3C-D). The reconstruction of the Gleason's capsule and lobule occurred at 3 weeks in parallel with the absorption of HA. The band including the remodeled region was very large (fig. 3-5, 7).
Donor cells derived from transgenic GFP + pigs can be readily identified by GFP expression as determined by IHC assay. In the pancreas, donor cells were identified by green fluorescence. However, in the liver, the autofluorescence of lipofuscin in hepatocytes peaks at a wavelength that overlaps with the autofluorescence of GFP. Therefore, we identified donor cells in the liver with antibodies to GFP (rabbit anti-GFP antibody; Novus, NB600-308) and coupled to a secondary antibody with a red fluorescent probe (donkey anti-rabbit 555, Invitrogen) so that the donor cells had pink nuclei (red fluorescent probe plus blue DAPI). Host cells could be identified due to their blue nuclei (DAPI staining), but these host cells did not express GFP (fig. 4).
Liver lobules of mature hepatocytes were forest green of autofluorescence (lipofuscin) (fig. 4B). Donor GFP + cells that had matured into aggregates of hepatocytes were light purple with pink nuclei (fig. 4C), because of the combined color of red fluorescent probe from GFP, blue from DAPI, and autofluorescence dark green from lipofuscin, host or donor-derived hepatocytes clustered around host mesenchymal cells (endothelium, stellate cells) with bright yellow/green autofluorescence, we believe due to vitamin a in mature stellate cells (fig. 4C); IHC data for endothelial and stellate cells are not shown.
Within one week, patch implants of BTSC/ELSMC organoids resulted in remodeling of the organ capsule and adjacent leaflets, followed by pooling of host and donor cells (fig. 3-5, 7). The finger-like extension of the donor cells extends to the liver lobules of the host tissue; in parallel, the host cells extended to the HA of the implant (fig. 4). In the case of the pancreas, the implant was wedged between the pancreas and the duodenum, and one week after surgery, implantation of donor cells occurred in the submucosal bunloner glands of the pancreas and duodenum (fig. 6). Cell integration in the large liver (or pancreas) area is complete at 2 weeks, when the HA layer is mostly taken up; donor cells have lineages restricted to adult hepatic parenchymal fates (cholangioepithelial and hepatocyte fates) (fig. 5) or pancreatic fates (fig. 6).
At 3 weeks, the HA layer is completely absorbed, leaving only the basement, which correlates with the histological structure of the organ capsule and tissue near the capsule (FIGS. 3, 5, 6) or the reproduction of the pancreatic capsule and pancreatic histological structure (FIG. 6). in the pancreas, mature cells are identified by functional markers including insulin against pancreatic islet cells (β cells) and amylase against acinar cells.
At one week, the implantation efficiency was close to 100% for both the liver and the pancreas, as all identified donor cells were found to be viable and within the liver or pancreas; not in the remnants of the implant on the organ capsule; and with negligible or no evidence of ectopic cell distribution in other organs (e.g., lungs).
The migration rate of donor cells through the liver and through the pancreas in BTSC/ELSMC implants was demonstrated to be very high, resulting in donor cells in most regions of the organ (liver or pancreas) at the end of one week and uniformly dispersed cells throughout the tissue (liver/pancreas) at 2-3 weeks (fig. 3-6).
Elevated expression of various MMPs, enzymes known to solubilize extracellular matrix components and to be associated with cell migration, is associated with lysis and remodeling of the glehnson capsule (or pancreatic capsule) and adjacent liver lobules (or pancreatic tissue) and with mass implantation. Data from RNA-seq studies and IHC assays for MMP expressed by stem/progenitor cells and adult cells are summarized in fig. 7. BTSCs express high levels of multiple MMPs, including secreted forms (e.g., MMP2, MMP7) and membrane-associated forms (e.g., MMP14 and MMP 15). Precursors of ELSMC, endothelium and stellate cells also contribute to a variety of MMPs.
The findings from the RNA-seq data were confirmed by IHC assay for protein encoded by MMP gene (fig. 7). The IHC assay confirms the presence of secreted forms of MMPs (e.g., MMP1, MMP2, MMP7, MMP9), especially in the remodeling region. Protein expression of MMP1 is present in BTSC/ELSMC organoids and in the remodeled region of implants; however, the existing database of RNA-seq discovery results does not include MMP1 due to the lack of annotated species of porcine MMP1 to be used for analysis. Therefore, its expression was recognized based on IHC assay.
The variables that lead to donor cell differentiation led to silencing of MMP expression, particularly in the secreted form, and in parallel the loss of potential for engraftment and migration (data not shown). These factors include serum, various soluble regulatory signals (growth factors, cytokines, hormones) known to affect the differentiation of donor cells, extracellular matrix components (whether in the hydrogel or in the basement (especially collagen type I-containing basement)), and the consistency of the HA hydrogel (i.e., Pa levels). Fibrosis of the implant occurs if the differentiation of the ELSMC preferentially progresses to the matrix; the implant retained viable cells and tissue if advanced to the endothelium, but remained on the surface of the organ capsule (data not shown).
Organoids of BTSC/ELSMC have proven to be the most successful arrangement for cells for implantation. In the past, we used unique surface antigens to co-transplant epithelial-mesenchymal partners by immunoselection of the epithelial-mesenchymal partner from a cell suspension by flow cytometry, and then mixed the epithelial-mesenchymal partners according to the ratio present in the cell suspension of freshly isolated tissue17. Here, we have found that, in this case,self-selection of mature mesenchymal cells as organoids after their removal by panning proves to be more efficient and effective in establishing lineage-appropriate epithelial-mesenchymal partners (with associated paracrine signaling for the implant) and in generating organoids under defined (serum-free) conditions (enabling their easy and safe cryopreservation).
The initial design of the implant involves mixing the cells with a suitable biomaterial that can be rendered insoluble and keep the cells localized to the target site. For implants, the ideal biomaterial HAs been shown to be a non-sulfated or minimally sulfated glycosaminoglycan (GAG), such as Hyaluronic Acid (HA), present in all stem cell niches, the receptor for HA having the classic stem cell trait. Maintaining the cells as stem/progenitor cells optimizes the expression of secreted and membrane-associated MMPs that are effective for implantation.
Evidence of the implantation process is particularly evident in the remodeled region, which occurs at the interface of the implant and host tissue. To verify the findings of remodeling, trichrome staining with dyes staining extracellular matrix components and safranin O were used and analyzed in parallel with hematoxylin/eosin stained adjacent sections (fig. 3, 7). It demonstrates remodeling of the organ capsule and adjacent tissue within one week after surgery. At 3 weeks post-surgery, these assays indicated histological reconstruction of organ capsules and normal tissue after HA clearance. The remodelling zone was very large (figures 3, 7), especially one week post surgery, and was shown to be involved in multiple forms of MMP (figure 7).
Although there are many sources and types of HA, the most useful is the thiol-modified HA established by Glenn Prestwich (University of utah, Salt Lake City, UT), which can be triggered by PEGDA to form hydrogels with precise biochemical and mechanical properties. These properties of HA confer perfect elasticity, allowing an implant to capture all soluble signals in blood, lymph or interstitial fluid, and minimizing maturation of donor cells until implantation and migration occur. The ability to alter rheological factors by simple changes in HA and PEGDA concentrations HAs been suggested in directing cell migration and minimizing adhesionProviding additional advantages. Soft HA hydrogels (i.e., hydrogels that mimic properties in the stem cell niche) are allowed to express stem/progenitor cell-associated MMP libraries. Therefore, the mechanical properties of HA (which have been studied for many years in terms of the function of skeletal tissue) are also important in managing the implantation strategy23。
Patch implants containing stem/progenitor cells resulted in the surprising phenomenon of "thawing" of the implant into the tissue within a few days, followed by a combination of donor and host cells, and a distribution of cells over a large area of the organ over one to two weeks. Thereafter, donor cell maturation and organ capsule restoration occurred in parallel with tissue clearance of HA.
The implantation and integration processes are associated with the expression of a variety of MMPs, a family of calcium-dependent, zinc-containing endopeptidases that degrade extracellular matrix components. Using RNA-seq studies, we found patterns of stem/progenitor cell-associated MMPs consisting of high levels of secreted forms (e.g., MMP2, MMP7) and membrane-associated forms (e.g., MMP14, MMP 15). IHC assays indicate that protein levels of secreted MMPs (e.g. MMP1, MMP2, MMP7) were found to be abundantly expressed in the remodeled region (figure 7). Conditions leading to donor cell differentiation (soluble growth factors, cytokines, serum, matrix components, mechanical forces) result in a reduction of MMPs (especially secreted forms) and elimination of the parallel implantation process.
The biomaterial of the implant (HA in particular) HAs been shown to maintain the dry character of the cells ex vivo and in vivo. Since the implant does not contain known signals that can trigger fate determination, donor cell maturation is a finding of a unique adult fate, depending on whether the implant is placed on the liver or pancreas, suggesting that the local microenvironment of the host tissue is a logical source of relevant factors for the maturation process.
A large number of implantable cells (>108) And depends on the size of the implant, the number of cells and the secreted MMP pool associated with the plasma membrane. These findings are associated with a limited number of cells (e.g., 10) that can be used for vascular delivery or injection implantation5-106) The opposite is true.
Patch implants are a safety strategy by which large numbers of cells can be transplanted into solid organs, including internal organs, and may prove useful for the treatment of patients, especially where implantation can occur adequately in disease conditions. Although there are the following problems: in the case of fibrosis of the tissue or the effects of cirrhosis, abnormal implantation may occur. Accordingly, provided herein are embodiments of determining the efficacy of a patch implant for a method aspect.
Example 2: treatment of liver disease.
This example describes one exemplary method of treating a subject having a liver disease or disorder using a patch implant. Donor cells were prepared as organoids of biliary stem cells (BTSCs), liver and pancreas precursors, aggregates of Early Lineage Stage Mesenchymal Cells (ELSMCs) consisting of angioblasts and their early lineage stage progeny, precursors of endothelium and precursors of stellate cells as described herein. The BTSC/ELSMC organoids were embedded in a soft hyaluronic acid hydrogel (<200Pa) placed on a substrate tethered to a target site of the liver of a subject.
Following administration of the patch implant, the subject is monitored for improvement in liver function. Commonly used tests to examine liver function include, but are not limited to, alanine Aminotransferase (ALT), aspartate Aminotransferase (AST), alkaline phosphatase (ALP), albumin, and bilirubin tests. The ALT and AST tests measure enzymes released by the liver in response to injury or disease. The albumin and bilirubin test measures how the liver produces albumin (protein) and how bilirubin is processed (waste product of the blood). It is expected that after about 2 weeks to about 36 weeks, an improvement in liver function will be detected. The improvement is determined by detecting an improvement in the value of one or more liver function tests relative to the value prior to implant administration and/or an improvement or amelioration of one or more symptoms of the liver disease or disorder.
Example 3: treatment of pancreatic diseases.
This example describes one exemplary method of treating a subject having a pancreatic disease or disorder using a patch implant. Donor cells were prepared as organoids of biliary stem cells (BTSCs), aggregates of Early Lineage Stage Mesenchymal Cells (ELSMCs) consisting of hemangioblasts and their early lineage stage progeny, precursors of endothelium and precursors of stellate cells as described herein. The BTSC/ELSMC organoids were embedded in a soft hyaluronic acid hydrogel (<200Pa) placed on a substrate tethered to a target site of the pancreas of the subject.
Following administration of the patch implant, the subject is monitored for an improvement in pancreatic function. Commonly used tests to examine pancreatic function include, but are not limited to, blood tests for levels of pancreatic enzymes amylase and lipase, direct pancreatic function tests after administration of secretin or cholecystokinin, fecal elastase tests, CT scans with contrast dyes, abdominal ultrasound, Endoscopic Retrograde Cholangiopancreatography (ERCP), endoscopic ultrasound, and magnetic resonance cholangiopancreatography. It is expected that after about 2 to about 36 weeks, an improvement in pancreatic function will be detected. The improvement is determined by detecting an improvement in one or more pancreatic function tests relative to the value prior to implant administration and/or an improvement or amelioration of one or more symptoms of the pancreatic disease or disorder.
Example 4: treatment of kidney disease.
This example describes one exemplary method of treating a subject having a renal disease or disorder using a patch implant. Donor cells were prepared as organoids of biliary stem cells (BTSCs), aggregates of Early Lineage Stage Mesenchymal Cells (ELSMCs) consisting of hemangioblasts and their early lineage stage progeny, precursors of endothelium and precursors of stellate cells as described herein. The BTSC/ELSMC organoids were embedded in a soft hyaluronic acid hydrogel (<200Pa) placed on a substrate tethered to a target site of the subject's kidney.
Following administration of the patch implant, the subject is monitored for an improvement in renal function. Commonly used tests to examine pancreatic function include, but are not limited to, clinically relevant endpoints of renal function known in the art. It is expected that an improvement in renal function will be detected after about 2 weeks to about 36 weeks. The improvement is determined by detecting an improvement in the value of one or more renal function tests relative to the value prior to implant administration and/or an improvement or amelioration of one or more symptoms of the pancreatic disease or disorder.
Example 5: treatment of gastrointestinal disorders.
This example describes one exemplary method of using a patch implant to treat a subject having a disease or disorder of the gastrointestinal tract. Donor cells were prepared as organoids of biliary stem cells (BTSCs), aggregates of Early Lineage Stage Mesenchymal Cells (ELSMCs) consisting of hemangioblasts and their early lineage stage progeny, precursors of endothelium and precursors of stellate cells as described herein. The BTSC/ELSMC organoids are embedded in a soft hyaluronic acid hydrogel (<200Pa) placed on a substrate tethered to a target site of the intestine of a subject.
Following administration of the patch implant, the subject is monitored for an improvement in intestinal function. Commonly used tests to examine bowel function include, but are not limited to, clinically relevant endpoints of bowel function known in the art. It is expected that after about 2 weeks to about 36 weeks, an improvement in bowel function will be detected. The improvement is determined by detecting an improvement in the value of one or more bowel function tests relative to the value prior to administration of the implant and/or an improvement or amelioration of one or more symptoms of the gastrointestinal disease or disorder.
Specification accessory
Tables 1-4 Patch Grafts (Patch implants) 2018





Claims (47)
1. A patch implant for retaining and maintaining a mixed cell population, the patch implant comprising:
(a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population within or away from the patch implant; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in the direction of the substrate or barrier,
the patch implant is configured to maintain and maintain the mixed population while inhibiting differentiation or further maturation of the at least one early lineage stage cell type to a late lineage stage that is no longer capable of expressing membrane-associated and/or secreted MMPs.
2. The patch implant of claim 1, wherein the substrate comprises a porous mesh infused with a hydrogel.
3. The patch implant of claim 1, further comprising:
(c) a hydrogel superimposed on a serosal surface of the substrate, the serosal surface being opposite the surface contacting the mixed population.
4. The patch implant of claim 1, wherein the hydrogel of element (a) comprises one or more hyaluronic acids.
5. The patch implant of claim 2, wherein the hydrogel of element (b) comprises one or more hyaluronic acids.
6. The patch implant of claim 3, wherein the hydrogel of element (c) comprises one or more hyaluronic acids.
7. The patch implant of claim 1, wherein the culture medium comprises a depot tower medium or other medium that supports "dryness".
8. The patch implant of claim 1, wherein the mixed population comprises mesenchymal cells and epithelial cells.
9. The patch implant of claim 8, wherein the mesenchymal cells comprise early lineage mesenchymal cells (ELSMCs).
10. The patch implant of claim 9, wherein the ELSMC includes one or more of a hemangioblast, a precursor of endothelium, or a precursor of stellate cells or Mesenchymal Stem Cells (MSCs).
11. The patch implant of claim 8, wherein the epithelial cells comprise epithelial stem cells.
12. The patch implant of claim 8, wherein the epithelial cells comprise biliary stem cells (BTSCs).
13. A patch implant as in claim 8, wherein the epithelial cells comprise committed and/or mature epithelial cells.
14. A patch implant as claimed in claim 13, wherein the oriented and/or mature epithelial cells comprise mature parenchymal cells.
15. The patch implant of claim 14, wherein the mature parenchymal cells include one or more of hepatocytes, cholangiocytes, and islet cells.
16. The patch implant of claim 8, wherein both the mesenchymal cells and epithelial cells comprise stem cells.
17. The patch implant of claim 1, wherein the mixed population comprises autologous and/or allogeneic cells.
18. The patch implant of claim 1, wherein one or more cell types are genetically modified.
19. The patch implant of claim 1, wherein the substrate comprises a porous mesh, scaffold, or membrane.
20. The patch implant of claim 1, wherein the substrate comprises a non-porous material.
21. A patch implant according to claim 20, wherein the non-porous material is selected from silk, amnion, placenta, omentum, synthetic fabrics, derivatives of the foregoing, or combinations thereof.
22. The patch implant of claim 1, wherein the substrate has sufficient elasticity to withstand mechanical forces, is capable of tethering to a target organ or tissue, and has sufficient flexibility to tether to a position having a bend.
23. The patch implant of claim 1, wherein any biomaterial (other than hydrogel) may be employed, provided that the biomaterial is capable of retaining and maintaining the cell population and has rheological properties (e.g., viscoelasticity) sufficient to allow the cell population to migrate within or away from the patch implant.
24. A patch implant for retaining and maintaining a cell population, the patch implant comprising:
(a) a population of cells (optionally a population of cells of a single type) supported in a culture medium in a hydrogel or other biomaterial having rheological properties (e.g., viscoelasticity) sufficient to allow the cells to migrate within or away from the patch implant; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration (or provide a barrier to migration) of the population of cells in the direction of the substrate.
25. A covering or coating for a patch implant or tissue comprising a hydrogel or other biomaterial having sufficient viscoelastic and elastic properties to withstand mechanical forces, including such forces as from other tissues and organs.
26. A method of preventing adhesions involving or resulting from mechanical forces or contact from other organs and tissues, the method comprising covering or coating a surface with hydrogel or other comparable biological material.
27. A method of implanting cells into a target tissue, the method comprising contacting the target tissue with a patch implant comprising:
(a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population toward and into a target tissue; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population away from a target tissue and through the substrate or barrier.
28. The method of claim 27, further comprising allowing the cells contained in the patch implant to incorporate into the tissue.
29. The method of claim 27, wherein the target tissue is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, gastrointestinal tract, lung, prostate, breast, brain, bladder, spinal cord, skin, uterus, kidney, muscle, blood vessel, heart, cartilage, tendon, and skeletal tissue.
30. The method of claim 29, wherein the target tissue is liver tissue.
31. The method of claim 29, wherein the target tissue is pancreatic tissue.
32. The method of claim 29, wherein the target tissue is biliary tissue.
33. The method of claim 29, wherein the target tissue is a gastrointestinal tract tissue.
34. The method of claim 29, wherein the target tissue is kidney tissue.
35. The method of claim 29, wherein the target tissue is an organ.
36. The method of claim 35, wherein the organ is an organ of the musculoskeletal system, digestive system, respiratory system, urinary system, female reproductive system, male reproductive system, endocrine system, circulatory system, lymphatic system, nervous system, or integumentary system.
37. The method of claim 35, wherein the organ is selected from the group consisting of liver, pancreas, biliary system, thyroid, thymus, intestine, lung, prostate, breast, brain, bladder, spinal cord, skin, uterus, kidney, muscle, blood vessel, heart, cartilage, tendon, and bone.
38. A method of implanting cells into a target tissue, the method comprising contacting the target tissue with a patch implant comprising:
(a) a population of cells, including one having an early lineage stage, the population comprising a single type or multiple types of cells supported in a culture medium in a hydrogel or other biological material having rheological properties (e.g., viscoelasticity) sufficient to allow the cells of the population to migrate within or away from the patch implant; and
(b) a substrate comprising a biocompatible, biodegradable material having rheological properties (e.g., viscoelasticity) sufficient to inhibit migration (or provide a barrier to migration) of cells of the population in the direction of the substrate,
the patch implant is configured to hold and maintain the cell population while inhibiting differentiation or further maturation of the one population having an early lineage stage to a later lineage stage.
39. The method of claim 38, wherein the one population with an early lineage stage is capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs).
40. A method of treating a subject having a liver disease or disorder, the method comprising contacting the liver of the subject with a patch implant comprising: (a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population toward and into a target tissue; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in a direction away from the target tissue and through the substrate or barrier, an
Allowing the cells contained in the patch implant to bind into the liver, thereby restoring a certain liver function.
41. The method of claim 40, wherein the liver disease or disorder is liver fibrosis, cirrhosis, hemochromatosis, liver cancer, biliary atresia, nonalcoholic fatty liver disease, hepatitis, viral hepatitis, autoimmune hepatitis, fascioliasis, alcoholic liver disease, α 1-antitrypsin deficiency, glycogen storage disease type II, transthyretin-associated hereditary amyloidosis, Gilbert's syndrome, primary biliary cirrhosis, primary sclerosing cholangitis, Padd-Guillai syndrome, liver trauma, or Wilson's disease.
42. A method of treating a subject having a pancreatic disease or disorder, the method comprising contacting a pancreas of the subject with a patch implant comprising: (a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population toward and into a target tissue; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in a direction away from the target tissue and through the substrate or barrier, an
Allowing the cells contained in the patch implant to bind into the pancreas, thereby restoring certain pancreatic function.
43. The method of claim 42, wherein the pancreatic disease or disorder is diabetes, pancreatic exocrine insufficiency, pancreatitis, pancreatic cancer, Oddi (Oddi) sphincter dysfunction, cystic fibrosis, pancreatic division, cricoid pancreas, pancreatic trauma, or pancreatic ductal hemorrhage.
44. A method of treating a subject having a disease or disorder of the gastrointestinal tract, the method comprising contacting one or more intestines of the subject with a patch implant comprising: (a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population toward and into a target tissue; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in a direction away from the target tissue and through the substrate or barrier, an
Allowing the cells contained in the patch implant to bind into the intestine, thereby restoring certain intestinal function.
45. The method of claim 44, wherein the gastrointestinal disease or disorder is gastroenteritis, gastrointestinal cancer, ileitis, inflammatory bowel disease, Crohn's disease, ulcerative colitis, irritable bowel syndrome, peptic ulcer disease, celiac disease, fibrosis, vascular dysplasia, Hirschsprung's disease, pseudomembranous colitis, or gastrointestinal trauma.
46. A method of treating a subject having a kidney disease or disorder, the method comprising contacting one or more kidneys of the subject with a patch implant comprising: (a) a mixed population of two or more cell types, at least one type of which is in an early lineage stage capable of expressing membrane-associated and/or secreted Matrix Metalloproteinases (MMPs), supported in a culture medium in a hydrogel having sufficient viscoelastic properties to allow migration of the mixed population toward and into a target tissue; and
(b) a substrate comprising a biocompatible, biodegradable material having sufficient viscoelastic properties to inhibit migration of the mixed population in a direction away from the target tissue and through the substrate or barrier, an
Allowing said cells contained in said patch implant to bind into said kidney, thereby restoring a certain kidney function.
47. The method of claim 46, wherein the kidney disease or disorder is nephritis, nephropathy, nephritic syndrome, nephrotic syndrome, chronic nephropathy, acute kidney injury, kidney trauma, cystic nephropathy, polycystic nephropathy, glomerulonephritis, IgA nephropathy, lupus nephritis, kidney cancer, Alport syndrome, amyloidosis, Goodpastel's syndrome, or Wegener's granulomatosis.
Applications Claiming Priority (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201762518380P | 2017-06-12 | 2017-06-12 | |
| US62/518,380 | 2017-06-12 | ||
| US201862664694P | 2018-04-30 | 2018-04-30 | |
| US62/664,694 | 2018-04-30 | ||
| PCT/US2018/036960 WO2018231726A1 (en) | 2017-06-12 | 2018-06-11 | Patch graft compositions for cell engraftment |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| CN111032090A true CN111032090A (en) | 2020-04-17 |
Family
ID=64562760
Family Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| CN201880050902.2A Pending CN111032090A (en) | 2017-06-12 | 2018-06-11 | Patch implant composition for cell implantation |
| CN202080049127.6A Pending CN114040786A (en) | 2017-06-12 | 2020-05-22 | Patch transplantation of stem/progenitor cells into solid organs |
Family Applications After (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| CN202080049127.6A Pending CN114040786A (en) | 2017-06-12 | 2020-05-22 | Patch transplantation of stem/progenitor cells into solid organs |
Country Status (13)
| Country | Link |
|---|---|
| US (10) | US11738117B2 (en) |
| EP (2) | EP3638310A4 (en) |
| JP (2) | JP7539832B2 (en) |
| KR (1) | KR20200028391A (en) |
| CN (2) | CN111032090A (en) |
| AU (2) | AU2018282728A1 (en) |
| BR (2) | BR112019026444A2 (en) |
| CA (2) | CA3066710A1 (en) |
| IL (2) | IL296689B1 (en) |
| MX (1) | MX2019014912A (en) |
| SG (1) | SG11201911701SA (en) |
| TW (1) | TW201902467A (en) |
| WO (2) | WO2018231726A1 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN111939312A (en) * | 2020-07-03 | 2020-11-17 | 中国科学院大学温州研究院(温州生物材料与工程研究所) | Dual-crosslinked multifunctional hydrogel dressing and preparation and application thereof |
| CN114732832A (en) * | 2022-04-08 | 2022-07-12 | 宁夏医科大学总医院 | Implantable article for preventing intrauterine adhesion |
Families Citing this family (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CA3032160C (en) | 2016-08-24 | 2024-05-28 | Arthrex, Inc. | Tissue hybrid for use in repairing, reconstructing or regenerating musculoskeletal degenerative processes or injuries |
| WO2018231726A1 (en) * | 2017-06-12 | 2018-12-20 | The University Of North Carolina At Chapel Hill | Patch graft compositions for cell engraftment |
| WO2020154632A1 (en) * | 2019-01-24 | 2020-07-30 | North Carolina State University | Transgenic models for stem cell therapies |
| US11511017B2 (en) | 2019-03-12 | 2022-11-29 | Arthrex, Inc. | Ligament reconstruction |
| CN109938876A (en) * | 2019-04-02 | 2019-06-28 | 青岛市城阳区人民医院 | A kind of method of 3D printing production stomach and intestine nursing film |
| CN110384823B (en) * | 2019-07-19 | 2021-08-03 | 大连医科大学 | Bionic liver lobule based on silk fibroin scaffold and construction method |
| CN113350564B (en) * | 2021-05-20 | 2023-03-10 | 诺一迈尔(苏州)生命科技有限公司 | Biodegradable tissue adhesive patch and preparation method thereof |
| KR20230052666A (en) | 2021-10-13 | 2023-04-20 | 서울대학교산학협력단 | Epithelial cell tube for tracheal transplantation |
| IT202100027047A1 (en) * | 2021-10-21 | 2023-04-21 | The Wave Innovation Group Srls | HETEROGENOUS COMPOSITION WITH LAYERED PHASES OF HYALURONIC ACID AND ITS INTRARTICULAR USE |
| US20240307706A1 (en) * | 2023-03-15 | 2024-09-19 | Jill Kelley | Device and method for supporting tissue undergoing radiation |
Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20040136968A1 (en) * | 2002-09-27 | 2004-07-15 | Verigen Ag | Autologous cells on a support matrix for tissue repair |
| JP2004210713A (en) * | 2002-12-27 | 2004-07-29 | Asahi Kasei Corp | Medical cell preparation derived from placenta |
| US20080044900A1 (en) * | 2005-12-13 | 2008-02-21 | Mooney David J | Scaffolds for cell transplantation |
| US20080248005A1 (en) * | 2005-10-21 | 2008-10-09 | Cellresearch Corporation Pte Ltd | Isolation and Cultivation of Stem/Progenitor Cells From the Amniotic Membrane of Umbilical Cord and Uses of Cells Differentiated Therefrom |
| US20120225814A1 (en) * | 2009-11-10 | 2012-09-06 | The Johns Hopkins University | Hydrogel-based vascular lineage cell growth media and uses thereof |
| CN103249404A (en) * | 2010-07-02 | 2013-08-14 | 北卡罗来纳-查佩尔山大学 | Biomatrix scaffolds |
| CN105264065A (en) * | 2013-03-13 | 2016-01-20 | 北卡罗来纳大学教堂山分校 | Method of treating pancreatic and liver conditions by transplantation of stem cells into bile duct walls |
Family Cites Families (24)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4683195A (en) | 1986-01-30 | 1987-07-28 | Cetus Corporation | Process for amplifying, detecting, and/or-cloning nucleic acid sequences |
| US20090324607A1 (en) * | 2001-09-07 | 2009-12-31 | Yeda Research And Development Co. Ltd. | Therapeutic Transplantation Using Developing, Human or Porcine, Renal or Hepatic, Grafts |
| US8404229B2 (en) * | 2001-12-07 | 2013-03-26 | Cytori Therapeutics, Inc. | Methods of using adipose derived stem cells to treat acute tubular necrosis |
| US7396537B1 (en) | 2002-02-28 | 2008-07-08 | The Trustees Of The University Of Pennsylvania | Cell delivery patch for myocardial tissue engineering |
| US20060140914A1 (en) * | 2002-10-31 | 2006-06-29 | The General Hospital Corporation | Repairing or replacing tissues or organs |
| WO2005112888A2 (en) * | 2004-05-20 | 2005-12-01 | Mentor Corporation | Methods for making injectable polymer hydrogels |
| US7402172B2 (en) | 2004-10-13 | 2008-07-22 | Boston Scientific Scimed, Inc. | Intraluminal therapeutic patch |
| WO2006113642A1 (en) * | 2005-04-18 | 2006-10-26 | Duke University | Three-dimensional fiber scaffolds for tissue engineering |
| BRPI0808696A2 (en) | 2007-03-06 | 2015-06-23 | Univ North Carolina | Hyuronan complexes, other matrix components, hormones and growth factors for cell maintenance, expansion and / or differentiation |
| WO2010032242A1 (en) | 2008-09-17 | 2010-03-25 | Beta O2 Technologies Ltd. | Optimization of alginate encapsulation of islets for transplantation |
| EP2358410B1 (en) | 2008-10-17 | 2015-08-05 | Sofradim Production | Implant for visceral surgery |
| US8470355B2 (en) * | 2009-10-01 | 2013-06-25 | Covidien Lp | Mesh implant |
| MX354068B (en) * | 2010-01-14 | 2018-02-09 | Organogenesis Inc | Bioengineered tissue constructs and methods for producing and using thereof. |
| RU2736955C2 (en) * | 2010-05-07 | 2020-11-23 | Юниверсити Оф Норт Каролина Эт Чепел Хилл | Method of grafting liver cells to a subject with liver disease or dysfunction |
| KR101703095B1 (en) | 2010-06-17 | 2017-02-06 | 워싱톤 유니버시티 | Biomedical patches with aligned fibers |
| EP2593117B1 (en) | 2010-07-12 | 2019-03-20 | University of Southern California | Biocompatible substrate for facilitating interconnections between stem cells and target tissues and methods for implanting same |
| EP2596332B1 (en) | 2010-07-21 | 2019-08-28 | F.Hoffmann-La Roche Ag | Increase of usable dynamic range in photometry |
| US10233420B2 (en) * | 2010-09-01 | 2019-03-19 | Regents Of The University Of Minnesota | Methods of recellularizing a tissue or organ for improved transplantability |
| WO2012101181A1 (en) * | 2011-01-25 | 2012-08-02 | Université Catholique de Louvain | Compositions and methods for cell transplantation |
| US20160030640A1 (en) * | 2013-03-15 | 2016-02-04 | New York Society For The Ruptured And Crippled Maintaining The Hospital For Special Surgery | Carbon nanotubes and graphene patches and implants for biological tissue |
| EP3620514A1 (en) | 2013-08-28 | 2020-03-11 | Promethera Biosciences S.A. / N.V. | Method for producing adult liver progenitor cells |
| WO2016195605A1 (en) | 2015-05-29 | 2016-12-08 | Koc Universitesi | Pre-operative development of patient-specific vascular patch graft prototypes for pediatric and neonatal patients |
| US20170369849A1 (en) * | 2016-05-11 | 2017-12-28 | The University Of North Carolina At Chapel Hill | Compositions and methods for bioengineered tissues |
| WO2018231726A1 (en) | 2017-06-12 | 2018-12-20 | The University Of North Carolina At Chapel Hill | Patch graft compositions for cell engraftment |
-
2018
- 2018-06-11 WO PCT/US2018/036960 patent/WO2018231726A1/en unknown
- 2018-06-11 IL IL296689A patent/IL296689B1/en unknown
- 2018-06-11 CA CA3066710A patent/CA3066710A1/en active Pending
- 2018-06-11 SG SG11201911701SA patent/SG11201911701SA/en unknown
- 2018-06-11 EP EP18817374.4A patent/EP3638310A4/en active Pending
- 2018-06-11 KR KR1020207000811A patent/KR20200028391A/en not_active Application Discontinuation
- 2018-06-11 TW TW107120078A patent/TW201902467A/en unknown
- 2018-06-11 BR BR112019026444-2A patent/BR112019026444A2/en unknown
- 2018-06-11 AU AU2018282728A patent/AU2018282728A1/en active Pending
- 2018-06-11 MX MX2019014912A patent/MX2019014912A/en unknown
- 2018-06-11 CN CN201880050902.2A patent/CN111032090A/en active Pending
- 2018-06-11 JP JP2020517773A patent/JP7539832B2/en active Active
- 2018-06-12 US US16/006,448 patent/US11738117B2/en active Active
- 2018-06-12 US US16/006,464 patent/US11129923B2/en active Active
- 2018-06-12 US US16/006,496 patent/US11446412B2/en active Active
- 2018-06-12 US US16/006,482 patent/US20180361028A1/en active Pending
- 2018-06-12 US US16/006,460 patent/US20180353651A1/en active Pending
- 2018-06-12 US US16/006,504 patent/US20180353653A1/en not_active Abandoned
-
2019
- 2019-05-24 US US16/422,086 patent/US20190388584A1/en active Pending
- 2019-12-03 IL IL271146A patent/IL271146B2/en unknown
-
2020
- 2020-05-22 CA CA3140912A patent/CA3140912A1/en active Pending
- 2020-05-22 JP JP2021569288A patent/JP2022532926A/en active Pending
- 2020-05-22 CN CN202080049127.6A patent/CN114040786A/en active Pending
- 2020-05-22 BR BR112021023571A patent/BR112021023571A2/en not_active Application Discontinuation
- 2020-05-22 EP EP20812950.2A patent/EP3976122A4/en active Pending
- 2020-05-22 AU AU2020283472A patent/AU2020283472A1/en active Pending
- 2020-05-22 WO PCT/US2020/034250 patent/WO2020242952A1/en unknown
-
2021
- 2021-08-10 US US17/398,982 patent/US20220211911A1/en active Pending
-
2022
- 2022-07-18 US US17/867,135 patent/US20220347350A1/en active Pending
-
2023
- 2023-08-28 US US18/239,036 patent/US20240082461A1/en active Pending
Patent Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20040136968A1 (en) * | 2002-09-27 | 2004-07-15 | Verigen Ag | Autologous cells on a support matrix for tissue repair |
| JP2004210713A (en) * | 2002-12-27 | 2004-07-29 | Asahi Kasei Corp | Medical cell preparation derived from placenta |
| US20080248005A1 (en) * | 2005-10-21 | 2008-10-09 | Cellresearch Corporation Pte Ltd | Isolation and Cultivation of Stem/Progenitor Cells From the Amniotic Membrane of Umbilical Cord and Uses of Cells Differentiated Therefrom |
| US20080044900A1 (en) * | 2005-12-13 | 2008-02-21 | Mooney David J | Scaffolds for cell transplantation |
| US20120225814A1 (en) * | 2009-11-10 | 2012-09-06 | The Johns Hopkins University | Hydrogel-based vascular lineage cell growth media and uses thereof |
| CN103249404A (en) * | 2010-07-02 | 2013-08-14 | 北卡罗来纳-查佩尔山大学 | Biomatrix scaffolds |
| CN105264065A (en) * | 2013-03-13 | 2016-01-20 | 北卡罗来纳大学教堂山分校 | Method of treating pancreatic and liver conditions by transplantation of stem cells into bile duct walls |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN111939312A (en) * | 2020-07-03 | 2020-11-17 | 中国科学院大学温州研究院(温州生物材料与工程研究所) | Dual-crosslinked multifunctional hydrogel dressing and preparation and application thereof |
| CN111939312B (en) * | 2020-07-03 | 2022-04-12 | 中国科学院大学温州研究院(温州生物材料与工程研究所) | Dual-crosslinked multifunctional hydrogel dressing and preparation and application thereof |
| CN114732832A (en) * | 2022-04-08 | 2022-07-12 | 宁夏医科大学总医院 | Implantable article for preventing intrauterine adhesion |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US20220347350A1 (en) | Patch graft compositions for cell engraftment | |
| US9492484B2 (en) | Cardiosphere derived cell population and methods of use | |
| US20200080061A1 (en) | Compositions and methods for bioengineered tissues | |
| JP2023126246A (en) | Vascular organoid, methods of producing and using organoid | |
| EP2970879B1 (en) | Method of treating liver conditions by transplantation of stem cells into bile duct walls | |
| Zhang et al. | Patch grafting, strategies for transplantation of organoids into solid organs such as liver | |
| Adil et al. | Recellularization of bioengineered scaffolds for vascular composite allotransplantation | |
| US20200360563A1 (en) | Methods for Vascular Construction and Products Therefrom | |
| RU2828021C2 (en) | Cell transplant composition | |
| TW201741451A (en) | Compositions and methods for bioengineered tissues |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| PB01 | Publication | ||
| PB01 | Publication | ||
| SE01 | Entry into force of request for substantive examination | ||
| SE01 | Entry into force of request for substantive examination | ||
| REG | Reference to a national code |
Ref country code: HK Ref legal event code: DE Ref document number: 40028185 Country of ref document: HK |