WO2022255349A1 - 可溶型clec2を用いた出血性脳卒中のリスク評価法 - Google Patents
可溶型clec2を用いた出血性脳卒中のリスク評価法 Download PDFInfo
- Publication number
- WO2022255349A1 WO2022255349A1 PCT/JP2022/022077 JP2022022077W WO2022255349A1 WO 2022255349 A1 WO2022255349 A1 WO 2022255349A1 JP 2022022077 W JP2022022077 W JP 2022022077W WO 2022255349 A1 WO2022255349 A1 WO 2022255349A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- hemorrhagic stroke
- concentration
- patient
- sclec2
- soluble
- Prior art date
Links
- 208000020658 intracerebral hemorrhage Diseases 0.000 title claims abstract description 89
- 208000016988 Hemorrhagic Stroke Diseases 0.000 title claims abstract description 86
- 238000000034 method Methods 0.000 title claims abstract description 56
- 102100032529 C-type lectin domain family 1 member B Human genes 0.000 claims abstract description 45
- 101710160442 C-type lectin domain family 1 member B Proteins 0.000 claims abstract description 34
- 210000004369 blood Anatomy 0.000 claims abstract description 34
- 239000008280 blood Substances 0.000 claims abstract description 34
- 101000942284 Homo sapiens C-type lectin domain family 1 member B Proteins 0.000 claims abstract 11
- 208000032851 Subarachnoid Hemorrhage Diseases 0.000 claims description 42
- 206010008111 Cerebral haemorrhage Diseases 0.000 claims description 37
- 238000012502 risk assessment Methods 0.000 claims description 19
- 238000003018 immunoassay Methods 0.000 claims description 12
- 230000008859 change Effects 0.000 claims description 4
- 238000011984 electrochemiluminescence immunoassay Methods 0.000 claims description 3
- 230000002596 correlated effect Effects 0.000 claims 1
- 238000003745 diagnosis Methods 0.000 abstract description 17
- 238000009534 blood test Methods 0.000 abstract description 9
- 230000001502 supplementing effect Effects 0.000 abstract description 2
- 210000001772 blood platelet Anatomy 0.000 description 48
- 238000011282 treatment Methods 0.000 description 22
- 238000005259 measurement Methods 0.000 description 19
- 238000012544 monitoring process Methods 0.000 description 18
- 208000032843 Hemorrhage Diseases 0.000 description 17
- 230000000740 bleeding effect Effects 0.000 description 15
- 210000004556 brain Anatomy 0.000 description 15
- 230000010118 platelet activation Effects 0.000 description 14
- 102000004169 proteins and genes Human genes 0.000 description 14
- 108090000623 proteins and genes Proteins 0.000 description 14
- 208000024891 symptom Diseases 0.000 description 12
- 238000012360 testing method Methods 0.000 description 12
- 210000001175 cerebrospinal fluid Anatomy 0.000 description 11
- 239000000243 solution Substances 0.000 description 10
- 230000035945 sensitivity Effects 0.000 description 9
- 208000007536 Thrombosis Diseases 0.000 description 8
- 239000000090 biomarker Substances 0.000 description 7
- 239000003153 chemical reaction reagent Substances 0.000 description 7
- 230000007423 decrease Effects 0.000 description 7
- 208000001286 intracranial vasospasm Diseases 0.000 description 7
- KRKNYBCHXYNGOX-UHFFFAOYSA-N citric acid Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O KRKNYBCHXYNGOX-UHFFFAOYSA-N 0.000 description 6
- 230000015572 biosynthetic process Effects 0.000 description 5
- 210000004204 blood vessel Anatomy 0.000 description 5
- 238000007689 inspection Methods 0.000 description 5
- 241000282412 Homo Species 0.000 description 4
- FAPWRFPIFSIZLT-UHFFFAOYSA-M Sodium chloride Chemical compound [Na+].[Cl-] FAPWRFPIFSIZLT-UHFFFAOYSA-M 0.000 description 4
- 206010008118 cerebral infarction Diseases 0.000 description 4
- 239000003085 diluting agent Substances 0.000 description 4
- 230000002439 hemostatic effect Effects 0.000 description 4
- 239000004816 latex Substances 0.000 description 4
- 229920000126 latex Polymers 0.000 description 4
- 239000012528 membrane Substances 0.000 description 4
- 102000004190 Enzymes Human genes 0.000 description 3
- 108090000790 Enzymes Proteins 0.000 description 3
- 208000006011 Stroke Diseases 0.000 description 3
- 230000036772 blood pressure Effects 0.000 description 3
- 208000026106 cerebrovascular disease Diseases 0.000 description 3
- 201000010099 disease Diseases 0.000 description 3
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 description 3
- 238000011221 initial treatment Methods 0.000 description 3
- 238000009593 lumbar puncture Methods 0.000 description 3
- 230000007170 pathology Effects 0.000 description 3
- 239000003755 preservative agent Substances 0.000 description 3
- UUUHXMGGBIUAPW-UHFFFAOYSA-N 1-[1-[2-[[5-amino-2-[[1-[5-(diaminomethylideneamino)-2-[[1-[3-(1h-indol-3-yl)-2-[(5-oxopyrrolidine-2-carbonyl)amino]propanoyl]pyrrolidine-2-carbonyl]amino]pentanoyl]pyrrolidine-2-carbonyl]amino]-5-oxopentanoyl]amino]-3-methylpentanoyl]pyrrolidine-2-carbon Chemical compound C1CCC(C(=O)N2C(CCC2)C(O)=O)N1C(=O)C(C(C)CC)NC(=O)C(CCC(N)=O)NC(=O)C1CCCN1C(=O)C(CCCN=C(N)N)NC(=O)C1CCCN1C(=O)C(CC=1C2=CC=CC=C2NC=1)NC(=O)C1CCC(=O)N1 UUUHXMGGBIUAPW-UHFFFAOYSA-N 0.000 description 2
- JKMHFZQWWAIEOD-UHFFFAOYSA-N 2-[4-(2-hydroxyethyl)piperazin-1-yl]ethanesulfonic acid Chemical compound OCC[NH+]1CCN(CCS([O-])(=O)=O)CC1 JKMHFZQWWAIEOD-UHFFFAOYSA-N 0.000 description 2
- 208000030090 Acute Disease Diseases 0.000 description 2
- 102000002260 Alkaline Phosphatase Human genes 0.000 description 2
- 108020004774 Alkaline Phosphatase Proteins 0.000 description 2
- 239000003154 D dimer Substances 0.000 description 2
- KCXVZYZYPLLWCC-UHFFFAOYSA-N EDTA Chemical compound OC(=O)CN(CC(O)=O)CCN(CC(O)=O)CC(O)=O KCXVZYZYPLLWCC-UHFFFAOYSA-N 0.000 description 2
- 239000007995 HEPES buffer Substances 0.000 description 2
- 206010018852 Haematoma Diseases 0.000 description 2
- 206010019233 Headaches Diseases 0.000 description 2
- 239000007987 MES buffer Substances 0.000 description 2
- 102000004270 Peptidyl-Dipeptidase A Human genes 0.000 description 2
- 108090000882 Peptidyl-Dipeptidase A Proteins 0.000 description 2
- 102000004211 Platelet factor 4 Human genes 0.000 description 2
- 108090000778 Platelet factor 4 Proteins 0.000 description 2
- 230000001154 acute effect Effects 0.000 description 2
- 238000004458 analytical method Methods 0.000 description 2
- 238000010171 animal model Methods 0.000 description 2
- 230000003276 anti-hypertensive effect Effects 0.000 description 2
- 210000000576 arachnoid Anatomy 0.000 description 2
- 210000000601 blood cell Anatomy 0.000 description 2
- 238000004364 calculation method Methods 0.000 description 2
- 238000006243 chemical reaction Methods 0.000 description 2
- 238000013170 computed tomography imaging Methods 0.000 description 2
- 230000001419 dependent effect Effects 0.000 description 2
- 238000010586 diagram Methods 0.000 description 2
- 239000002934 diuretic Substances 0.000 description 2
- 229940030606 diuretics Drugs 0.000 description 2
- 230000000694 effects Effects 0.000 description 2
- 108010052295 fibrin fragment D Proteins 0.000 description 2
- 231100000869 headache Toxicity 0.000 description 2
- 230000002008 hemorrhagic effect Effects 0.000 description 2
- 238000003384 imaging method Methods 0.000 description 2
- 238000003317 immunochromatography Methods 0.000 description 2
- 210000004705 lumbosacral region Anatomy 0.000 description 2
- 239000003550 marker Substances 0.000 description 2
- 210000003593 megakaryocyte Anatomy 0.000 description 2
- 229940126619 mouse monoclonal antibody Drugs 0.000 description 2
- HEGSGKPQLMEBJL-RKQHYHRCSA-N octyl beta-D-glucopyranoside Chemical compound CCCCCCCCO[C@@H]1O[C@H](CO)[C@@H](O)[C@H](O)[C@H]1O HEGSGKPQLMEBJL-RKQHYHRCSA-N 0.000 description 2
- 230000036470 plasma concentration Effects 0.000 description 2
- 238000002360 preparation method Methods 0.000 description 2
- 230000002335 preservative effect Effects 0.000 description 2
- 230000008569 process Effects 0.000 description 2
- 102000005962 receptors Human genes 0.000 description 2
- 108020003175 receptors Proteins 0.000 description 2
- 238000011160 research Methods 0.000 description 2
- 238000000926 separation method Methods 0.000 description 2
- 239000011780 sodium chloride Substances 0.000 description 2
- 238000002415 sodium dodecyl sulfate polyacrylamide gel electrophoresis Methods 0.000 description 2
- BYKRNSHANADUFY-UHFFFAOYSA-M sodium octanoate Chemical compound [Na+].CCCCCCCC([O-])=O BYKRNSHANADUFY-UHFFFAOYSA-M 0.000 description 2
- 239000000758 substrate Substances 0.000 description 2
- 230000001225 therapeutic effect Effects 0.000 description 2
- 238000002560 therapeutic procedure Methods 0.000 description 2
- MZOFCQQQCNRIBI-VMXHOPILSA-N (3s)-4-[[(2s)-1-[[(2s)-1-[[(1s)-1-carboxy-2-hydroxyethyl]amino]-4-methyl-1-oxopentan-2-yl]amino]-5-(diaminomethylideneamino)-1-oxopentan-2-yl]amino]-3-[[2-[[(2s)-2,6-diaminohexanoyl]amino]acetyl]amino]-4-oxobutanoic acid Chemical compound OC[C@@H](C(O)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CCCN=C(N)N)NC(=O)[C@H](CC(O)=O)NC(=O)CNC(=O)[C@@H](N)CCCCN MZOFCQQQCNRIBI-VMXHOPILSA-N 0.000 description 1
- 206010002329 Aneurysm Diseases 0.000 description 1
- 102000008873 Angiotensin II receptor Human genes 0.000 description 1
- 108050000824 Angiotensin II receptor Proteins 0.000 description 1
- 101100339431 Arabidopsis thaliana HMGB2 gene Proteins 0.000 description 1
- 101800003265 Beta-thromboglobulin Proteins 0.000 description 1
- 201000006474 Brain Ischemia Diseases 0.000 description 1
- 102000003930 C-Type Lectins Human genes 0.000 description 1
- 108090000342 C-Type Lectins Proteins 0.000 description 1
- 229940127291 Calcium channel antagonist Drugs 0.000 description 1
- 241000282472 Canis lupus familiaris Species 0.000 description 1
- 241000700198 Cavia Species 0.000 description 1
- 208000000483 Central Nervous System Vascular Malformations Diseases 0.000 description 1
- 208000034710 Cerebral arteriovenous malformation Diseases 0.000 description 1
- 206010053942 Cerebral haematoma Diseases 0.000 description 1
- 206010008120 Cerebral ischaemia Diseases 0.000 description 1
- FBPFZTCFMRRESA-KVTDHHQDSA-N D-Mannitol Chemical compound OC[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)CO FBPFZTCFMRRESA-KVTDHHQDSA-N 0.000 description 1
- QXNVGIXVLWOKEQ-UHFFFAOYSA-N Disodium Chemical compound [Na][Na] QXNVGIXVLWOKEQ-UHFFFAOYSA-N 0.000 description 1
- 238000002965 ELISA Methods 0.000 description 1
- 102000002045 Endothelin Human genes 0.000 description 1
- 108050009340 Endothelin Proteins 0.000 description 1
- 206010017577 Gait disturbance Diseases 0.000 description 1
- 102100039289 Glial fibrillary acidic protein Human genes 0.000 description 1
- 101710193519 Glial fibrillary acidic protein Proteins 0.000 description 1
- PEDCQBHIVMGVHV-UHFFFAOYSA-N Glycerine Chemical compound OCC(O)CO PEDCQBHIVMGVHV-UHFFFAOYSA-N 0.000 description 1
- 108700010013 HMGB1 Proteins 0.000 description 1
- 101150021904 HMGB1 gene Proteins 0.000 description 1
- 206010019196 Head injury Diseases 0.000 description 1
- HTTJABKRGRZYRN-UHFFFAOYSA-N Heparin Chemical compound OC1C(NC(=O)C)C(O)OC(COS(O)(=O)=O)C1OC1C(OS(O)(=O)=O)C(O)C(OC2C(C(OS(O)(=O)=O)C(OC3C(C(O)C(O)C(O3)C(O)=O)OS(O)(=O)=O)C(CO)O2)NS(O)(=O)=O)C(C(O)=O)O1 HTTJABKRGRZYRN-UHFFFAOYSA-N 0.000 description 1
- 102100037907 High mobility group protein B1 Human genes 0.000 description 1
- 206010020772 Hypertension Diseases 0.000 description 1
- 208000004044 Hypesthesia Diseases 0.000 description 1
- 208000001953 Hypotension Diseases 0.000 description 1
- 206010061216 Infarction Diseases 0.000 description 1
- 108090001005 Interleukin-6 Proteins 0.000 description 1
- 102000004889 Interleukin-6 Human genes 0.000 description 1
- 108090001007 Interleukin-8 Proteins 0.000 description 1
- 102000004890 Interleukin-8 Human genes 0.000 description 1
- 208000002263 Intracranial Arteriovenous Malformations Diseases 0.000 description 1
- 208000008574 Intracranial Hemorrhages Diseases 0.000 description 1
- 201000008450 Intracranial aneurysm Diseases 0.000 description 1
- 206010022773 Intracranial pressure increased Diseases 0.000 description 1
- 208000032382 Ischaemic stroke Diseases 0.000 description 1
- PEEHTFAAVSWFBL-UHFFFAOYSA-N Maleimide Chemical compound O=C1NC(=O)C=C1 PEEHTFAAVSWFBL-UHFFFAOYSA-N 0.000 description 1
- 229930195725 Mannitol Natural products 0.000 description 1
- 241001465754 Metazoa Species 0.000 description 1
- 208000009433 Moyamoya Disease Diseases 0.000 description 1
- 241000699670 Mus sp. Species 0.000 description 1
- 206010028813 Nausea Diseases 0.000 description 1
- 208000012902 Nervous system disease Diseases 0.000 description 1
- 208000025966 Neurological disease Diseases 0.000 description 1
- 208000002193 Pain Diseases 0.000 description 1
- 108091005804 Peptidases Proteins 0.000 description 1
- 102100036154 Platelet basic protein Human genes 0.000 description 1
- 239000004365 Protease Substances 0.000 description 1
- 241000700159 Rattus Species 0.000 description 1
- 102100037486 Reverse transcriptase/ribonuclease H Human genes 0.000 description 1
- 206010039897 Sedation Diseases 0.000 description 1
- 229920004890 Triton X-100 Polymers 0.000 description 1
- 239000013504 Triton X-100 Substances 0.000 description 1
- 108060008682 Tumor Necrosis Factor Proteins 0.000 description 1
- 102100040247 Tumor necrosis factor Human genes 0.000 description 1
- 206010047700 Vomiting Diseases 0.000 description 1
- 230000004913 activation Effects 0.000 description 1
- 230000004520 agglutination Effects 0.000 description 1
- 230000003941 amyloidogenesis Effects 0.000 description 1
- 230000036592 analgesia Effects 0.000 description 1
- 229940035676 analgesics Drugs 0.000 description 1
- 239000000730 antalgic agent Substances 0.000 description 1
- 230000001062 anti-nausea Effects 0.000 description 1
- 108010072035 antithrombin III-protease complex Proteins 0.000 description 1
- 201000000034 arteriovenous malformations of the brain Diseases 0.000 description 1
- 210000001367 artery Anatomy 0.000 description 1
- 230000003925 brain function Effects 0.000 description 1
- 239000000872 buffer Substances 0.000 description 1
- 239000007853 buffer solution Substances 0.000 description 1
- 239000000480 calcium channel blocker Substances 0.000 description 1
- 238000005119 centrifugation Methods 0.000 description 1
- 230000003788 cerebral perfusion Effects 0.000 description 1
- 238000002591 computed tomography Methods 0.000 description 1
- 238000012790 confirmation Methods 0.000 description 1
- 230000006378 damage Effects 0.000 description 1
- 230000003247 decreasing effect Effects 0.000 description 1
- UKWLRLAKGMZXJC-QIECWBMSSA-L disodium;[4-chloro-3-[(3r,5s)-1-chloro-3'-methoxyspiro[adamantane-4,4'-dioxetane]-3'-yl]phenyl] phosphate Chemical compound [Na+].[Na+].O1OC2([C@@H]3CC4C[C@H]2CC(Cl)(C4)C3)C1(OC)C1=CC(OP([O-])([O-])=O)=CC=C1Cl UKWLRLAKGMZXJC-QIECWBMSSA-L 0.000 description 1
- 229940079593 drug Drugs 0.000 description 1
- 239000003814 drug Substances 0.000 description 1
- 238000013399 early diagnosis Methods 0.000 description 1
- ZUBDGKVDJUIMQQ-UBFCDGJISA-N endothelin-1 Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(O)=O)NC(=O)[C@H]1NC(=O)[C@H](CC=2C=CC=CC=2)NC(=O)[C@@H](CC=2C=CC(O)=CC=2)NC(=O)[C@H](C(C)C)NC(=O)[C@H]2CSSC[C@@H](C(N[C@H](CO)C(=O)N[C@@H](CO)C(=O)N[C@H](CC(C)C)C(=O)N[C@@H](CCSC)C(=O)N[C@H](CC(O)=O)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CCC(O)=O)C(=O)N2)=O)NC(=O)[C@@H](CO)NC(=O)[C@H](N)CSSC1)C1=CNC=N1 ZUBDGKVDJUIMQQ-UBFCDGJISA-N 0.000 description 1
- 238000011156 evaluation Methods 0.000 description 1
- 230000003090 exacerbative effect Effects 0.000 description 1
- 210000005046 glial fibrillary acidic protein Anatomy 0.000 description 1
- 208000035474 group of disease Diseases 0.000 description 1
- 229960002897 heparin Drugs 0.000 description 1
- 229920000669 heparin Polymers 0.000 description 1
- 208000034783 hypoesthesia Diseases 0.000 description 1
- 230000036543 hypotension Effects 0.000 description 1
- 230000001900 immune effect Effects 0.000 description 1
- 238000000338 in vitro Methods 0.000 description 1
- 238000001727 in vivo Methods 0.000 description 1
- 230000007574 infarction Effects 0.000 description 1
- 239000003112 inhibitor Substances 0.000 description 1
- 235000010355 mannitol Nutrition 0.000 description 1
- 239000000594 mannitol Substances 0.000 description 1
- 238000004519 manufacturing process Methods 0.000 description 1
- 239000000463 material Substances 0.000 description 1
- 230000007246 mechanism Effects 0.000 description 1
- 239000011859 microparticle Substances 0.000 description 1
- 208000022084 motor paralysis Diseases 0.000 description 1
- 208000010125 myocardial infarction Diseases 0.000 description 1
- 208000031225 myocardial ischemia Diseases 0.000 description 1
- 230000008693 nausea Effects 0.000 description 1
- 150000002823 nitrates Chemical class 0.000 description 1
- 231100000862 numbness Toxicity 0.000 description 1
- 230000000474 nursing effect Effects 0.000 description 1
- 238000011017 operating method Methods 0.000 description 1
- 230000036407 pain Effects 0.000 description 1
- 229940124641 pain reliever Drugs 0.000 description 1
- 239000002245 particle Substances 0.000 description 1
- 210000003446 pia mater Anatomy 0.000 description 1
- 230000002265 prevention Effects 0.000 description 1
- 238000003127 radioimmunoassay Methods 0.000 description 1
- 230000004044 response Effects 0.000 description 1
- 238000005070 sampling Methods 0.000 description 1
- 230000036280 sedation Effects 0.000 description 1
- 230000001953 sensory effect Effects 0.000 description 1
- 208000018316 severe headache Diseases 0.000 description 1
- 230000011664 signaling Effects 0.000 description 1
- 239000003998 snake venom Substances 0.000 description 1
- 230000004083 survival effect Effects 0.000 description 1
- 230000008961 swelling Effects 0.000 description 1
- 230000035488 systolic blood pressure Effects 0.000 description 1
- 210000001519 tissue Anatomy 0.000 description 1
- 238000011269 treatment regimen Methods 0.000 description 1
- 230000008673 vomiting Effects 0.000 description 1
- 238000001262 western blot Methods 0.000 description 1
Images



Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/483—Physical analysis of biological material
- G01N33/487—Physical analysis of biological material of liquid biological material
- G01N33/49—Blood
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/68—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing involving proteins, peptides or amino acids
Definitions
- the present invention relates to methods for diagnosing and monitoring hemorrhagic stroke using soluble CLEC2.
- Stroke is a group of diseases that includes ischemic stroke, which occurs when a blood vessel in the brain is clogged, that is, cerebral infarction, and hemorrhagic stroke, which occurs when a blood vessel in the brain is cut, that is, cerebral hemorrhage and subarachnoid hemorrhage. It is the second leading cause of death after ischemic heart disease. Stroke is not only a major cause of death, but it often leaves severe aftereffects even after survival, making it a major factor in the need for nursing care. , prevention, early diagnosis, prompt response after diagnosis, and a system that enables care and risk management by a wide range of medical professionals.
- Hemorrhagic stroke includes subarachnoid hemorrhage caused by rupture of an aneurysm on the surface of the brain, and cerebral hemorrhage caused by rupture of small arteries in the brain.
- a subarachnoid hemorrhage is bleeding in a blood vessel in the space between the brain and the membrane on the surface of the brain called the arachnoid. Most of the symptoms of subarachnoid hemorrhage are severe headaches, which are described as ⁇ headaches like being hit with a bat'' or ⁇ headaches you have never experienced before.'' Subarachnoid hemorrhage has a mortality rate as high as 30%, is a very serious acute disease that requires immediate treatment, and needs to be diagnosed as soon as possible.
- CT computed tomography
- D-dimer measurement was proposed in the past as an attempt to diagnose subarachnoid hemorrhage by blood test.
- the sensitivity positive rate of patients
- the sensitivity must be almost 100%, but not only cerebrospinal fluid measurement but also conventional blood test items have achieved such sensitivity. , none of which are currently in actual use.
- biomarkers for predicting complications of subarachnoid hemorrhage many biomarkers using cerebrospinal fluid samples are known. Many biomarkers in cerebrospinal fluid, such as endothelin, TNF- ⁇ , IL-8, IL-6, thrombin-antithrombin complex, and HMGB1, have been described to be associated with complications in patients with subarachnoid hemorrhage. Since it is necessary to collect cerebrospinal fluid from the lumbar spine, it has not been put to practical use. Even if it were to be carried out, it would be unrealistic to use it to observe changes over time because it would be highly invasive and impose a heavy burden on the patient.
- cerebral hemorrhage is an acute disease in which blood vessels in the brain rupture for some reason, causing bleeding into the brain. Blood clots from hemorrhage press against the brain, causing swelling in the brain and impairing brain function.
- the symptoms are said to vary depending on the site and amount of bleeding, but the symptoms vary from sensory symptoms such as headache, nausea, and vomiting to motor symptoms such as motor paralysis, numbness, and gait disturbance in the hands and feet. It is said that it is difficult to distinguish it because it includes symptoms similar to cerebral infarction.
- the amount of bleeding is large, it may be life-threatening. Like subarachnoid hemorrhage, it is often diagnosed by CT.
- Cerebral hemorrhage can be stopped by treatment such as lowering blood pressure after diagnosis, but if it does not stop, hematoma in the brain will increase and symptoms will worsen.
- An increase in hematoma can be confirmed by taking CT images many times, but as described above, it is often difficult to frequently perform CT imaging examinations using a CT examination apparatus having a certain degree of accuracy or higher.
- biomarkers for monitoring the pathology of cerebral hemorrhage S100 ⁇ , GFAP, etc. are known at the research level, but their clinical usefulness is low and they are not used in actual clinical settings. There is no test that can be easily monitored by tests or the like.
- C-type lectin-like receptor 2 (CLEC2) was identified on platelets as a receptor for the platelet-activating snake venom rhodocytin.
- CLEC2 is expressed in a platelet/megakaryocyte-specific manner in humans, and can be said to be a platelet-specific molecule. It has been reported that this sCLEC2 is released into the blood as soluble CLEC2 (hereinafter abbreviated as sCLEC2) when platelets are activated (Patent Document 1, Non-Patent Document 1).
- Hemorrhagic stroke has a high mortality rate, and since it is a serious acute stage disease that may leave sequelae even if death is avoided, it is extremely important to diagnose and start treatment as soon as possible. If typical symptoms are exhibited, a visit to a medical institution is made shortly after the onset of symptoms, and cerebral hemorrhage is confirmed by imaging tests such as CT and MRI, a diagnosis can be made based on this alone. In some cases, such as when the amount of bleeding is small or the bleeding is mild and arrives at a specialized medical institution after a long time, bleeding cannot be confirmed by CT images. In some countries and regions, medical institutions with highly sensitive CT and MRI are limited.
- a subarachnoid hemorrhage requires a highly invasive examination of the cerebrospinal fluid by lumbar puncture.
- Lumbar puncture is not performed for cerebral hemorrhage, but there is a problem that accurate diagnosis is difficult if confirmation cannot be performed with a CT image or the like.
- the initial treatment is CT, MRI, etc., and then treatment such as lowering blood pressure is started, but there is no biomarker that can monitor whether the treatment is successful and the bleeding is stopped.
- the present inventors have made intensive studies to solve the above problems. As a result, the inventors found that the blood sCLEC2 concentration in hemorrhagic stroke patients was elevated in almost all patients compared to healthy subjects, leading to the completion of the present invention. That is, the present inventors have found a method of easily diagnosing subarachnoid hemorrhage and cerebral hemorrhage by detecting hemorrhagic stroke patients with a simple blood test, which has excellent sensitivity, which is the positive rate of patients.
- the blood sCLEC2 concentration threshold for hemorrhagic stroke is preferably 137 pg/mL or less. Based on these findings, the present invention was completed as a method for evaluating the risk of hemorrhagic stroke using sCLEC2.
- the present invention provides: [1] Assess the risk of hemorrhagic stroke, including the step of measuring the concentration of soluble CLEC2 present in blood collected from patients suspected of having hemorrhagic stroke or diagnosed with hemorrhagic stroke. Method.
- a method for risk assessment of a patient suspected of having hemorrhagic stroke or a patient diagnosed with hemorrhagic stroke comprising: (1) providing a blood sample from said patient; (2) determining the concentration of soluble CLEC2 in the sample; (3) correlating the soluble CLEC2 concentration with the presence or absence of hemorrhagic stroke or likely outcome in the patient;
- the method of [1] comprising [3] A method for assessing the risk of a patient suspected of having hemorrhagic stroke or a patient diagnosed with hemorrhagic stroke, wherein the soluble CLEC2 concentration and the presence or absence of hemorrhagic stroke in the patient or wherein the step of correlating likelihood of outcome comprises assessing whether said patient is at risk based on said change in soluble CLEC2 concentration.
- [4] A method for risk assessment of a patient suspected of having hemorrhagic stroke or a patient diagnosed with hemorrhagic stroke, wherein the step of correlating soluble CLEC2 concentration with hemorrhagic stroke, wherein the threshold is 137 pg /mL, the method of [2] or [3].
- [5] A method for risk assessment of a patient suspected of having hemorrhagic stroke or a patient diagnosed with hemorrhagic stroke, comprising: (1) providing a blood sample from said patient; (2) determining the concentration of soluble CLEC2 in the sample; (3) measuring the platelet count in the sample; (4) dividing the soluble CLEC-2 concentration by the platelet count; (5) correlating the soluble CLEC2 concentration divided by the platelet count with the presence or absence of hemorrhagic stroke in the patient; The method of [1], comprising [6] A method for assessing the risk of hemorrhagic stroke in patients suspected of having hemorrhagic stroke or diagnosed with hemorrhagic stroke, wherein the value obtained by dividing the soluble CLEC2 concentration by the platelet count and the hemorrhagic The method of [5], wherein in the step of correlating stroke, said value threshold is between 0.7 and 1.0.
- [7] The method of any one of [1] to [6], wherein the hemorrhagic stroke is either subarachnoid hemorrhage or cerebral hemorrhage. [8] of [1] to [7], wherein the step of determining the soluble CLEC2 concentration is a highly sensitive immunoassay, such as a chemiluminescence immunoassay, an electrochemiluminescence immunoassay, or a fluorescence immunoassay; either way.
- a highly sensitive immunoassay such as a chemiluminescence immunoassay, an electrochemiluminescence immunoassay, or a fluorescence immunoassay; either way.
- a method for assessing the risk of hemorrhagic stroke by measuring (or determining) the soluble CLEC2 concentration (or the value obtained by dividing the soluble CLEC-2 concentration by the number of platelets) in a sample, A method of measuring (or determining) the soluble CLEC2 concentration (or the value obtained by dividing the soluble CLEC-2 concentration by the platelet count) in a sample to aid in the risk assessment of hemorrhagic stroke; A method of measuring (or determining) the soluble CLEC2 concentration (or the value obtained by dividing the soluble CLEC-2 concentration by the platelet count) in a sample for risk assessment of hemorrhagic stroke,
- An in vitro risk assessment method for hemorrhagic stroke which comprises measuring (or determining) the soluble CLEC2 concentration (or the value obtained by dividing the soluble CLEC-2 concentration by the platelet count) in a sample, use of an antibody capable of detecting the concentration of soluble CLEC2 in manufacturing a kit for evaluating the
- FIG. 4 is a diagram comparing the plasma concentration of sCLEC2 between subarachnoid hemorrhage patients and healthy subjects.
- FIG. 2 is a diagram comparing the plasma concentration of sCLEC2 between cerebral hemorrhage patients and healthy subjects. This is an example of chronological monitoring of a case of subarachnoid hemorrhage. This is an example of continuous monitoring of a case of cerebral hemorrhage.
- CLEC2 is a platelet-activating receptor belonging to the C-type lectin family, normally present in the platelet membrane, but is released into the blood following platelet activation.
- soluble CLEC2 sCLEC2
- CLEC2 or a CLEC2-derived molecule that is released from such platelets and detected in the blood.
- sCLEC2 is said to include a protein with a molecular weight of about 40 kDa, a protein with a molecular weight of about 32 kDa, a protein with a molecular weight of about 25 kDa, etc. in SDS-polyacrylamide gel electrophoresis (SDS-PAGE) under reducing conditions.
- SDS-PAGE SDS-polyacrylamide gel electrophoresis
- Non-Patent Document 1 A protein with a molecular weight of about 40 kDa and a protein with a molecular weight of about 32 kDa are present on the platelet membrane surface and are presumed to be released in a state contained in microparticles produced with platelet activation. It is considered that sugar chains are added to these.
- a protein with a molecular weight of about 25 kDa is considered to be cleaved by protease and released from platelets along with platelet activation.
- the amount of sCLEC2 as described above is measured.
- sCLEC2 may detect a protein with a molecular weight of about 40 kDa, a protein with a molecular weight of about 32 kDa, and a protein with a molecular weight of about 25 kDa collectively, or may detect only a protein with a molecular weight of about 25 kDa.
- the sCLEC2 concentration used in the present invention may be the sCLEC2 concentration alone, but preferably the value obtained by dividing the sCLEC2 concentration by the platelet count (hereinafter sometimes referred to as the C2PAC index) is used. You can In the present specification, unless otherwise specified, the sCLEC2 concentration is interpreted to include both the case of using the sCLEC2 concentration and the case of dividing the sCLEC2 concentration by the platelet count.
- the platelet count is usually measured using an automatic blood cell counter (hematometer), but a blood cell counter and a microscope are used. It is also possible to count using
- the C2PAC index which expresses the sCLEC2 concentration in plasma, for example, in pg/mL, expresses the blood platelet count, for example, in 1,000/mm 3 , and calculates the sCLEC2 concentration/platelet count.
- Any unit such as ng/mL or ng/L may be used for the concentration of sCLEC2 used in , and any unit such as 10,000/ mm3 may be used for the platelet count. Units should be used.
- sCLEC2 concentration/platelet count can take various values, but essentially the concept is the same.
- ratio calculations will often be performed using measurements from a clinical laboratory instrument that measures sCLEC2 concentrations and from a hemocytometer that measures platelet counts.
- This calculation is preferably automatically calculated on a system such as a hospital inspection system, a hospital system, or an electronic medical chart connected to both measuring instruments in daily practice.
- a connecting system may be constructed, or a machine capable of simultaneously measuring sCLEC2 concentration and platelet count may be constructed.
- you may calculate manually using both data.
- the plasma sCLEC2 concentration is divided by the blood platelet count to calculate the amount of sCLEC2 released per platelet, and this is used as an index for diagnosing thrombotic diseases
- the platelet activity is not dependent on the blood platelet count. It is preferable because it makes it possible to evaluate the degree of conversion.
- the plasma sCLEC2 concentration is expressed as pg/mL (A)
- the blood platelet count is expressed as 1,000/mm 3 (B)
- the number obtained by dividing A by B is the number of platelet activation. It can be used as an index.
- the samples used for measurement are preferably derived from humans, but samples derived from animals other than humans may be used to understand the pathology of experimental animals.
- Experimental animals include, but are not limited to, guinea pigs, rats, mice, dogs, and the like.
- the method for detecting the presence of sCLEC2 is not particularly limited, but an immunological method using an antibody that recognizes sCLEC2 is preferred.
- methods for immunologically detecting proteins include enzyme immunoassay (ELISA method), chemiluminescence immunoassay, electrochemiluminescence immunoassay, fluorescence immunoassay, radioimmunoassay, and immunochromatography. Any method can be used as long as it is an immunoassay method using a labeled antibody such as, Western blotting method, latex agglutination method, immunoturbidimetric method, or the like.
- An immunoassay method using a labeled antibody is preferably used in terms of simplicity and measurement accuracy.
- Chemiluminescence immunoassay, immunochromatography, and the like are particularly preferably used for diagnosis in the emergency area because it is desired to obtain results quickly.
- a sample is collected from the target subject (especially a patient), for example, using a blood collection tube for plasma blood collection.
- a collection tube containing citric acid, which leaves little residual platelets, is usually suitable, but a tube containing heparin or EDTA is also possible.
- a blood collection tube containing EDTA is used for blood platelet count measurement, but separate blood collection tubes may be used for simultaneous blood collection.
- Plasma sCLEC2 concentration is measured, for example, by using plasma that has been centrifuged at 2000 g for about 20 minutes, but the conditions for centrifugation are not limited to this, and a measurement system using whole blood may also be used.
- the measurement of plasma sCLEC2 concentration will be described as an example, but the present invention is not limited to this.
- hemorrhagic stroke which is the target of risk assessment, includes cerebral hemorrhage occurring inside the brain (sometimes referred to as intracerebral hemorrhage) and pia mater, which is the inner layer of the tissue covering the brain, and arachnoid membrane, which is the outer layer. It means subarachnoid hemorrhage, hemorrhage that occurs in between, but does not include cerebral hemorrhage caused by head injury.
- Known causes of cerebral hemorrhage are those derived from hypertension, cerebral aneurysm rupture, cerebral arteriovenous malformation rupture, venous sinus obstruction, dural arteriovenous fistula, amyloid deposition, moyamoya disease, and the like.
- the target cerebral hemorrhage is not limited to that caused by a specific cause.
- the blood sCLEC2 concentration value of patients suspected of having hemorrhagic stroke is compared with healthy subjects or neurological disease groups without intracerebral hemorrhage or infarction. Based on such a comparison, sCLEC2 levels can be used to diagnose hemorrhagic stroke (subarachnoid hemorrhage or intracerebral hemorrhage).
- the threshold value is set by comparing the sCLEC2 concentration in the patient-derived sample and the sCLEC2 concentration in the non-hemorrhagic stroke patient-derived sample. It may be set as appropriate and used, or may be evaluated when a significant change in sCLEC2 concentration is detected from the chronological record of sCLEC2 concentration before onset in the same patient.
- a threshold value was appropriately set by comparing the sCLEC2 concentration in the patient-derived sample and the sCLEC2 concentration in the healthy subject-derived sample.
- a method for calculating the threshold an analysis is performed to create a ROC curve (Receiver Operating Characteristic Curve) from the measured sCLEC2 value in plasma, and the sensitivity and specificity of diagnosis are both 80% or more. Concentration can be used as a threshold.
- ROC curve Receiveiver Operating Characteristic Curve
- the threshold for sCLEC2-induced hemorrhagic stroke it is preferable to select an arbitrary value of 137 pg/mL or less as the threshold for sCLEC2-induced hemorrhagic stroke.
- a similar analysis can be performed to calculate a threshold even when using a C2PAC index, which is a value obtained by dividing the sCLEC2 concentration by the platelet count.
- the threshold when using the C2PAC index can be arbitrarily set between 0.7 and 1.0.
- the blood sCLEC2 concentration increases with platelet activation, it is suggested that the blood sCLEC2 concentration is related to the formation of thrombus, and it is reported that it can be used for the diagnosis of cerebral infarction and myocardial infarction.
- hemorrhagic stroke there is no known association with hemorrhagic stroke, and it was surprising that measurement of sCLEC2 concentration would be useful for risk assessment.
- lumbar puncture and cerebrospinal fluid examination in which a needle is inserted into the lumbar vertebrae to collect cerebrospinal fluid, are performed, but these are highly invasive.
- Treatments for the diagnosis of subarachnoid hemorrhage mainly include the following treatments.
- diuretics such as mannitol and glyceol are used to reduce cerebrospinal fluid.
- careful judgment is required, such as considering the possibility of increased cerebral ischemia due to a decrease in cerebral perfusion pressure due to hypotension.
- the patient's condition can be monitored by collecting blood samples over time from a patient diagnosed with subarachnoid hemorrhage and measuring sCLEC2. Since sCLEC2 is said to represent the state of platelet activation, if sCLEC2 maintains a high value, it can be expected that bleeding will continue and the formation of a hemostatic thrombus will continue, and if the sCLEC2 value decreases, hemostatic thrombosis will occur. A decrease in formation can be expected. Cerebral vasospasm, which is a serious complication, is said to be induced by blood leaking from blood vessels, so it is important and useful to understand the state of bleeding using blood sCLEC2.
- sCLEC2 concentration can be compared before and after treatment for hemorrhagic stroke patients and used as risk prediction. For example, if the sCLEC2 concentration decreases due to treatment, platelet activation tends to be suppressed, but if the sCLEC2 concentration remains high or increases, bleeding may continue. If the treatment with antihypertensive is not effective, it is possible to provide materials for considering the selection of therapeutic methods such as further lowering blood pressure. During the process of monitoring, fluctuations in the blood platelet count may be observed, so monitoring using the C2PAC index is also more suitable for observing the patient's condition.
- sCLEC2 is said to represent the state of platelet activation, if sCLEC2 maintains a high value, it can be expected that bleeding will continue and the formation of a hemostatic thrombus will continue, and if the sCLEC2 value decreases, hemostatic thrombosis will occur. A decrease in formation can be expected. If the bleeding continues, intracerebral hematoma increases, compressing the brain and exacerbating the symptoms. Therefore, it is important and useful to understand the bleeding status using blood sCLEC2.
- sCLEC2 concentration before and after treatment for hemorrhagic stroke patients can be compared and used as risk prediction. For example, if the sCLEC2 concentration decreases due to treatment, platelet activation tends to be suppressed, but if the sCLEC2 concentration continues to be high or increases, reassessment of antihypertensive therapy can be considered. During the process of monitoring, fluctuations in the blood platelet count may be observed, so monitoring using the C2PAC index is also more suitable for observing the patient's condition.
- blood sCLEC2 concentration should be measured in patients who describe symptoms that may be suspected of hemorrhagic stroke (subarachnoid hemorrhage or cerebral hemorrhage), and if the value is in healthy subjects, etc. If the value is higher than , it can be judged that the possibility of hemorrhagic stroke is high.
- the patient's condition can be monitored by sampling blood over time from a patient diagnosed with hemorrhagic stroke, measuring the sCLEC2 concentration, and comparing the results over time.
- the correlation between the measured sCLEC2 concentration in the patient-derived sample and the possibility of hemorrhagic stroke can be determined by examining the sCLEC2 concentration in the patient-derived sample and non-hemorrhagic stroke.
- a threshold value may be appropriately set and used by comparing the sCLEC2 concentration in a human-derived sample, or from the time-lapse recording of the sCLEC2 concentration before onset in the same patient, when a significant change in the sCLEC2 concentration is detected. An evaluation may be performed.
- sCLEC2 is released into the blood with platelet activation.
- Existing platelet activation markers such as platelet factor 4 (PF4) and ⁇ -thromboglobulin ( ⁇ TG)
- PF4 platelet factor 4
- ⁇ TG ⁇ -thromboglobulin
- sCLEC2 is a signaling-dependent release mechanism that triggers platelet activation, and can be a marker that more accurately reflects platelet activation in vivo.
- CLEC2 since CLEC2 is almost exclusively expressed in the platelet/megakaryocyte system in humans, it can be a platelet-specific marker with less false positives. Therefore, by measuring sCLEC2, it becomes possible to estimate the activation state of platelets at an early stage, and it can be used for diagnosing hemorrhagic stroke and monitoring pathology.
- sCLEC2 concentration in plasma was measured as follows. (Preparation of measurement reagent and preparation of test sample) ⁇ Specimen diluent: 2% sodium octanoate and 0.5% n-octyl- ⁇ -D-glucoside (OG) using 0.1 mol/L HEPES buffer (pH 7.5) containing preservatives They were combined to obtain a specimen diluent.
- the antibody contained in the reagent was prepared as follows using the antibody described in Examples of Japanese Patent No. 6078845.
- ⁇ First antibody solution A mouse monoclonal antibody (11D5) that recognizes sCLEC2 was bound to magnetic latex particles (JSR) and dispersed in a 0.01 mol/L MES buffer solution (pH 6.0) containing a preservative. . -Second antibody solution: Another mouse monoclonal antibody (11E6) that recognizes sCLEC2 is labeled with alkaline phosphatase (ALP) by the maleimide method and dispersed in 0.01 mol/L MES buffer (pH 6.5) containing a preservative.
- ALP alkaline phosphatase
- Luminescent substrate solution 2-chloro-5-(4-methoxyspiro ⁇ 1,2-dioxetane-3,2′-(5′-chloro)-tricyclo[3.3.1.13,7]decane ⁇ - 4-yl)-1-phenylphosphate disodium (CDP-Star®: Applied Biosystems) was used.
- - B/F wash solution A buffer solution containing 0.1 mol/L citric acid (pH 6.5), 0.15 mol/L NaCl, and 0.1% Triton X-100 was used.
- ⁇ Test sample Recombinant hCLEC2 protein diluted with buffer (0.025 mol/L HEPES, 0.14 mol/L NaCl, 0.1% sodium octanoate, 0.3% BSA) Sample 1, diluted with citrated plasma, was used as test sample 2.
- a fully automatic clinical examination system STACIA registered trademark, manufactured by LSI stipulatece
- the sample diluent, the first antibody solution (magnetic latex reagent), and the second antibody solution (enzyme-labeled antibody reagent) were filled in STACIA-dedicated bottles and set in the apparatus. Measurements were carried out according to the operating method of the apparatus described below. Specifically, 40 ⁇ L of the specimen diluent was added to 10 ⁇ L of the sample and heated at 37° C. for several minutes, then 25 ⁇ L of the first antibody solution (magnetic latex reagent) was added and heated at 37° C. for several minutes.
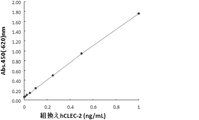
- FIG. 1 shows a standard curve prepared using the hsCLEC2 protein as a standard.
- Example 2 Measurement of sCLEC2 in plasma specimens of subarachnoid hemorrhage patients, cerebral hemorrhage patients and healthy subjects>>> Plasma sCLEC2 concentration, platelet level, and sCLEC2/platelet ratio (C2PAC index) were measured by the method of Example 1 using citrated plasma obtained from patients diagnosed with subarachnoid hemorrhage or cerebral hemorrhage by outpatient examination. (Tables 1 and 2). In addition, sCLEC concentrations in healthy subjects were also measured (Table 3).
- the measured sCLEC2 values (pg/mL) of hemorrhagic stroke patients with both subarachnoid hemorrhage and cerebral hemorrhage were significantly higher than those of healthy subjects (P ⁇ 0.0001) (Table 4). Each measured value is shown in FIG. 2 (subarachnoid hemorrhage) and FIG. 3 (cerebral hemorrhage). In addition, the upper limit of the C2PAC index measured separately for healthy subjects was 0.55.
- ⁇ Example 3 Sensitivity and specificity of diagnosis of hemorrhagic stroke (subarachnoid hemorrhage and cerebral hemorrhage) by sCLEC2>>
- the threshold is set at 120 pg/mL
- the measurement of sCLEC2 and the sCLEC2/platelet ratio (C2PAC index) are means for providing simple and accurate data for diagnosing hemorrhagic stroke.
- Example 4 Monitoring of patients with subarachnoid hemorrhage by sCLEC2>> Various test values on the 1st, 8th, and 10th days of illness in one case diagnosed with subarachnoid hemorrhage are shown (Fig. 4). sCLEC2 slightly increased from day 1 to day 8, but the platelet count also increased greatly, so the C2PAC index showed a slight downward trend.
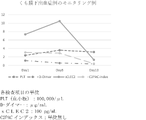
- Example 5 Monitoring of cerebral hemorrhage patients with sCLEC2>> Various test values on the 1st, 2nd, 12th, and 14th days of illness in one case diagnosed with cerebral hemorrhage are shown (FIG. 5). sCLEC2, and C2PAC index increased on day 12 and decreased on day 14, whereas D-dimer increased from day 12 to day 14.
- the measured value of blood sCLEC2 and the sCLEC2/platelet ratio in the present invention are clinical tests that can be used to diagnose hemorrhagic stroke, subarachnoid hemorrhage, and cerebral hemorrhage.
- sCLEC2 measurement is useful as a risk assessment method for hemorrhagic stroke patients because it can also be used to monitor the condition of patients with cerebral hemorrhage.
Abstract
Description
また、脳出血の病態をモニタリングするバイオマーカーとしては、S100βやGFAP等が研究レベルでは知られているが、その臨床的有用性は低く実際の臨床の場では使用されているものはないため、血液検査等で簡便にモニターできる検査はない。
これらをもとに、sCLEC2を用いた出血性脳卒中のリスク評価方法として、本発明を完成させるに至った。
[1]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者から採取した血液中に存在する、可溶型CLEC2濃度を測定する工程を含む、出血性脳卒中のリスク評価を行う方法。
[2]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、
(1)前記患者に由来する血液試料を提供する工程、
(2)前記試料中の可溶型CLEC2濃度を決定する工程、
(3)前記可溶型CLEC2濃度と、前記患者における出血性脳卒中の存在若しくは非存在、又は転帰の可能性を相関させる工程、
を含む、[1]の方法。
[3]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、前記可溶型CLEC2濃度と、前記患者における出血性脳卒中の存在若しくは非存在、又は転帰の可能性を相関させる工程が、前記可溶型CLEC2濃度の変化に基づいて、リスクを前記患者が有するかどうかを評価することを含む、[2]の方法。
[4]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、可溶型CLEC2濃度と出血性脳卒中を相関させる工程で、その閾値が137pg/mLである、[2]又は[3]の方法。
[5]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、
(1)前記患者に由来する血液試料を提供する工程、
(2)前記試料中の可溶型CLEC2濃度を決定する工程、
(3)前記試料中の血小板数を測定する工程、
(4)前記可溶型CLEC-2濃度を血小板数で除する工程、
(5)前記可溶型CLEC2濃度を血小板数で除した値と、前記患者における出血性脳卒中の存在又は非存在を相関させる工程、
を含む、[1]の方法。
[6]出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者における出血性脳卒中のリスク評価を行う方法であって、可溶型CLEC2濃度を血小板数で除した値と出血性脳卒中を相関させる工程で、前記値の閾値が0.7~1.0である、[5]の方法。
[7]出血性脳卒中が、くも膜下出血又は脳出血のいずれかである、[1]~[6]のいずれかの方法。
[8]可溶型CLEC2濃度を決定する工程が、高感度免疫測定法、例えば、化学発光免疫測定法、電気化学発光免疫測定法、蛍光免疫測定法である、[1]~[7]のいずれかの方法。
試料中の可溶型CLEC2濃度(又は可溶型CLEC-2濃度を血小板数で除した値)を測定(又は決定)する、出血性脳卒中のリスク評価を行う方法、
試料中の可溶型CLEC2濃度(又は可溶型CLEC-2濃度を血小板数で除した値)を測定(又は決定)する、出血性脳卒中のリスク評価を補助する方法、
出血性脳卒中のリスク評価のために、試料中の可溶型CLEC2濃度(又は可溶型CLEC-2濃度を血小板数で除した値)を測定(又は決定)する方法、
試料中の可溶型CLEC2濃度(又は可溶型CLEC-2濃度を血小板数で除した値)を測定(又は決定)することを特徴とする、出血性脳卒中のin vitroリスク評価方法、
可溶型CLEC2濃度を検出できる抗体の、出血性脳卒中のリスク評価用キットの製造における使用、
出血性脳卒中のリスク評価に必要な情報を提供するために、試料中の可溶型CLEC2濃度(又は可溶型CLEC-2濃度を血小板数で除した値)を測定(又は決定)する方法
が含まれる。
また、血漿中のsCLEC2濃度、又はsCLEC2濃度/血小板数と血小板活性化の程度や各種疾患との相関を示すものを、例えば、判定用閾値、あるいは、判定用閾値を算出するためのオリジナルデータ又は統計処理データなどとして使用してもよい。
血漿中sCLEC2濃度を血中血小板数で除して、血小板当たりのsCLEC2放出量を計算してこれを指標として血栓性疾患の診断を行うと、血中血小板数に依存すること無く、血小板の活性化度合いを評価することが可能となるため、好ましい。具体的には、例えば血漿中sCLEC2濃度をpg/mLで表し(A)、血中血小板数を1,000個/mm3で表し(B)、AをBで除した数字を血小板活性化の指標とすることができる。
本発明の方法において、sCLEC2による出血性脳卒中の閾値は137pg/mL以下で任意の値を選ぶことが好適である。また、更に好適な態様として、sCLEC2濃度を血小板数で除した値であるC2PACインデックスを使用した場合にも同様の解析を行って、閾値を算出することができる。C2PACインデックスを使用した場合の閾値は、0.7~1.0の間で任意に設定して使用することができる。
このような閾値を設定してリスク評価を行う場合、例えば、出血性脳卒中が疑われる頭痛の患者で、血中sCLEC2濃度がある閾値以下であれば、出血性脳卒中を否定するという使用法も可能である。
従来はくも膜下出血を疑い、画像診断で出血性脳卒中が確認できない場合には、腰椎に注射針を刺して髄液を採取する腰椎穿刺・髄液検査が行われているが、侵襲性の高い検査であり、医療従事者であればだれでもどこでも簡単に行えるものではないので、血液検査でその代替ができれば非常に簡便、有用である。もしくも膜下出血と診断された場合には、発症直後は再出血を予防するため、安静を保ち、侵襲的な検査や処置は避けることが望ましいとされていることからも、本発明の実施により侵襲性の高い検査の代替となり得ることは、好ましい。
脳出血と診断された場合に推奨される治療法としては、急性期の血圧は、早期に収縮期血圧を降下させ、7日間維持することが検討され、脳出血急性期に用いる降圧剤として、カルシウム拮抗薬、硝酸薬が選択される。また、可能であれば、患者の状態等に応じて、早期にカルシウム拮抗薬、アンジオテンシン変換酵素(ACE)阻害薬、アンジオテンシンII受容体拮抗薬(ARB)、利尿薬を用いた経口治療へ切り替えることを考慮してもよいとされている。
くも膜下出血、脳出血いずれの場合であっても、その治療は高度な経験と知識が必要とされものであり、本発明の実施が治療方針を決定する指標となることが期待される。
モニタリングの過程においては、血中血小板数の変動が見られることもあるので、C2PACインデックスを用いてモニタリングすることも患者の状態を観察するのには更に好適である。
血漿中のsCLEC2濃度を、以下のようにして測定を実施した。
(測定用試薬の作製と被検試料の調製)
・検体希釈液:防腐剤を含む0.1mol/LのHEPES緩衝液(pH7.5)を用いて、オクタン酸ナトリウム2%、n-オクチル-β-D-グルコシド(OG)0.5%になるように組み合わせて検体希釈液とした。
試薬に含まれる抗体は、特許第6078845号公報の実施例に記載の抗体を使用し、以下のように調製した。
・第1抗体溶液:磁性ラテックス粒子(JSR社)にsCLEC2を認識するマウスモノクローナル抗体(11D5)を結合させ、防腐剤を含む0.01mol/LのMES緩衝液(pH6.0)に分散させた。
・第2抗体溶液:sCLEC2を認識する別のマウスモノクローナル抗体(11E6)をマレイミド法によりアルカリホスファターゼ(ALP)標識し、防腐剤を含む0.01mol/LのMES緩衝液(pH6.5)に分散させた。
・発光基質溶液:2-クロロ-5-(4-メトキシスピロ{1,2-ジオキセタン-3,2´-(5´-クロロ)-トリシクロ[3.3.1.13,7]デカン}-4-イル)-1-フェニルホスフェート・二ナトリウム(CDP-Star(登録商標):アプライドバイオシステム社)を使用した。
・B/F洗浄液:0.1mol/Lクエン酸(pH6.5)、0.15mol/L NaCl、0.1%TritonX-100、を含む緩衝液を使用した。
・被検試料:組換えhCLEC2蛋白質を緩衝液(0.025mol/L HEPES、0.14mol/L NaCl、0.1%オクタン酸ナトリウム、0.3%BSA)を用いて希釈したものを被検試料1、クエン酸血漿を用いて希釈したものを被検試料2として使用した。
測定には、全自動臨床検査システムSTACIA(登録商標、LSIメディエンス社製)を使用した。
STACIA専用ボトルに、調製した検体希釈液、第1抗体溶液(磁性ラテックス試薬)、第2抗体溶液(酵素標識抗体試薬)をそれぞれ充填し、装置にセットした。以下前記装置の運転方法に従い測定した。
具体的には、試料10μLに検体希釈液40μLを加え、37℃で数分間加温した後、第1抗体溶液(磁性ラテックス試薬)25μLを加え、37℃で数分間加温した。次いで、B/F分離を行い、50μLの第2抗体溶液(酵素標識抗体試薬)を加え、37℃で数分間加温し、再度B/F分離を行った後、100μLの発光基質溶液を加え、37℃で数分反応後にシグナル強度(カウント)を測定した。
図1にhsCLEC2蛋白質を標準品として用いて作成した標準曲線を示した。
外来患者の診察によりくも膜下出血または脳出血と診断された患者から得られたクエン酸血漿を用いて実施例1の方法で血漿中sCLEC2濃度、血小板値、sCLEC2/血小板比(C2PACインデックス)を測定した(表1、表2)。また、健常者のsCLEC濃度についても測定を実施した(表3)。




また、別途測定したC2PACインデックスの健常者の上限値は0.55であった。
閾値を120pg/mLに設定とすると、sCLEC2の出血性脳卒中の診断能は、感度(34/34)=100%、特異度(71/71)=100%、正診率(105/105)=100%、となる(表5)。
以上のことより、sCLEC2の測定、並びにsCLEC2/血小板比(C2PACインデックス)は、出血性脳卒中の診断に対して簡便、且つ正確なデータを提供する手段となる。

くも膜下出血と診断された1症例の第1病日、第8病日、第10病日の各種検査値を示す(図4)。sCLEC2は第1病日から第8病日に若干上昇したが、血小板数も大きく上昇しているので、C2PACインデックスは若干の減少傾向を示した。
脳出血と診断された1症例の第1病日、第2病日、第12病日、第14病日の各種検査値を示す(図5)。sCLEC2、およびC2PACインデックスは第12病日に上昇し第14病日で下降したが、D-ダイマーは第12病日から第14病日にかけて上昇した。
Claims (8)
- 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者から採取した血液中に存在する、可溶型CLEC2濃度を測定する工程を含む、出血性脳卒中のリスク評価を行う方法。
- 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、
(1)前記患者に由来する血液試料を提供する工程、
(2)前記試料中の可溶型CLEC2濃度を決定する工程、
(3)前記可溶型CLEC2濃度と、前記患者における出血性脳卒中の存在若しくは非存在、又は転帰の可能性を相関させる工程、
を含む、請求項1に記載の方法。 - 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、前記可溶型CLEC2濃度と、前記患者における出血性脳卒中の存在若しくは非存在、又は転帰の可能性を相関させる工程が、前記可溶型CLEC2濃度の変化に基づいて、リスクを前記患者が有するかどうかを評価することを含む、請求項2に記載の方法。
- 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、可溶型CLEC2濃度と出血性脳卒中を相関させる工程で、その閾値が137pg/mLである、請求項2又は3に記載の方法。
- 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者のリスク評価を行う方法であって、
(1)前記患者に由来する血液試料を提供する工程、
(2)前記試料中の可溶型CLEC2濃度を決定する工程、
(3)前記試料中の血小板数を測定する工程、
(4)前記可溶型CLEC-2濃度を血小板数で除する工程、
(5)前記可溶型CLEC2濃度を血小板数で除した値と、前記患者における出血性脳卒中の存在又は非存在を相関させる工程、
を含む、請求項1に記載の方法。 - 出血性脳卒中の罹患が疑われる患者又は出血性脳卒中と診断された患者における出血性脳卒中のリスク評価を行う方法であって、可溶型CLEC2濃度を血小板数で除した値と出血性脳卒中を相関させる工程で、前記可溶型sCLEC2濃度を血小板数で除した値の閾値が0.7~1.0である、請求項5に記載の方法。
- 出血性脳卒中が、くも膜下出血又は脳出血のいずれかである、請求項1~6のいずれか一項に記載の方法。
- 可溶型CLEC2濃度を決定する工程が、高感度免疫測定法、例えば、化学発光免疫測定法、電気化学発光免疫測定法、蛍光免疫測定法である、請求項1~7のいずれか一項に記載の方法。
Priority Applications (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2023525850A JPWO2022255349A1 (ja) | 2021-05-31 | 2022-05-31 | |
| CN202280038986.4A CN117769652A (zh) | 2021-05-31 | 2022-05-31 | 使用了可溶型clec2的出血性脑卒中的风险评价方法 |
| EP22816095.8A EP4350350A1 (en) | 2021-05-31 | 2022-05-31 | Method for assessing risk of hemorrhagic stroke using soluble clec2 |
| KR1020237044828A KR20240017001A (ko) | 2021-05-31 | 2022-05-31 | 가용형 clec2를 이용한 출혈성 뇌졸중의 리스크 평가법 |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2021-091607 | 2021-05-31 | ||
| JP2021091607 | 2021-05-31 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2022255349A1 true WO2022255349A1 (ja) | 2022-12-08 |
Family
ID=84323410
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2022/022077 WO2022255349A1 (ja) | 2021-05-31 | 2022-05-31 | 可溶型clec2を用いた出血性脳卒中のリスク評価法 |
Country Status (5)
| Country | Link |
|---|---|
| EP (1) | EP4350350A1 (ja) |
| JP (1) | JPWO2022255349A1 (ja) |
| KR (1) | KR20240017001A (ja) |
| CN (1) | CN117769652A (ja) |
| WO (1) | WO2022255349A1 (ja) |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050107598A1 (en) * | 2001-12-19 | 2005-05-19 | Baum Peter R. | C-type lectin polypeptide, polynucleotide and methods of making and use thereof |
| JP2014070942A (ja) * | 2012-09-28 | 2014-04-21 | Mitsubishi Chemical Medience Corp | 可溶型clec−2に基づく血小板活性化測定方法 |
| WO2015053381A1 (ja) * | 2013-10-10 | 2015-04-16 | 幸成 加藤 | 抗ポドプラニン抗体 |
| JP2020032797A (ja) | 2018-08-28 | 2020-03-05 | スズキ株式会社 | ニーエアバッグ取付け構造 |
| JP2021003671A (ja) | 2019-06-26 | 2021-01-14 | 稔 甲斐 | 閉塞防止機能付振動篩用網及び振動篩装置 |
| WO2021172493A1 (ja) * | 2020-02-28 | 2021-09-02 | 株式会社Lsiメディエンス | 可溶型clec-2と血小板数に基づく血小板活性化測定方法 |
Family Cites Families (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPS6078845U (ja) | 1983-11-04 | 1985-06-01 | ライオン株式会社 | 食用廃油固化処理用具 |
-
2022
- 2022-05-31 JP JP2023525850A patent/JPWO2022255349A1/ja active Pending
- 2022-05-31 CN CN202280038986.4A patent/CN117769652A/zh active Pending
- 2022-05-31 EP EP22816095.8A patent/EP4350350A1/en active Pending
- 2022-05-31 KR KR1020237044828A patent/KR20240017001A/ko unknown
- 2022-05-31 WO PCT/JP2022/022077 patent/WO2022255349A1/ja active Application Filing
Patent Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050107598A1 (en) * | 2001-12-19 | 2005-05-19 | Baum Peter R. | C-type lectin polypeptide, polynucleotide and methods of making and use thereof |
| JP2014070942A (ja) * | 2012-09-28 | 2014-04-21 | Mitsubishi Chemical Medience Corp | 可溶型clec−2に基づく血小板活性化測定方法 |
| JP6078845B2 (ja) | 2012-09-28 | 2017-02-15 | 株式会社Lsiメディエンス | 可溶型clec−2に基づく血小板活性化測定方法 |
| WO2015053381A1 (ja) * | 2013-10-10 | 2015-04-16 | 幸成 加藤 | 抗ポドプラニン抗体 |
| JP2020032797A (ja) | 2018-08-28 | 2020-03-05 | スズキ株式会社 | ニーエアバッグ取付け構造 |
| JP2021003671A (ja) | 2019-06-26 | 2021-01-14 | 稔 甲斐 | 閉塞防止機能付振動篩用網及び振動篩装置 |
| WO2021172493A1 (ja) * | 2020-02-28 | 2021-09-02 | 株式会社Lsiメディエンス | 可溶型clec-2と血小板数に基づく血小板活性化測定方法 |
Non-Patent Citations (10)
| Title |
|---|
| F. KAZAMA ET AL., PLATELETS, vol. 26, no. 8, 2015, pages 711 - 719 |
| GUO MI, ZHANG HAN, LV QING-WEI, HUANG HANG-BIN, SHEN LIANG-JUN: "Higher plasma C-type lectin-like receptor 2 concentrations for prediction of higher risk of 30-day mortality in isolated severe blunt traumatic brain injury", CLINICA CHIMICA ACTA, vol. 496, 1 September 2019 (2019-09-01), AMSTERDAM, NL , pages 1 - 6, XP093010593, ISSN: 0009-8981, DOI: 10.1016/j.cca.2019.06.014 * |
| INOUE KATSUE: "CLEC-2, a platelet-activating receptor responsible for fetal angiolymphatic separation and maintenance of vascular integrity in adults", JOURNAL OF JAPANESE BIOCHEMICAL SOCIETY, vol. 89, no. 3, 25 June 2017 (2017-06-25), pages 377 - 383, XP093010568, DOI: 10.14952/SEIKAGAKU.2017.890377 * |
| INOUE KATSUE: "Development of antiplatelet drugs,anti-metastatic/neoplastic drugs, and teststargeting the novel receptor CLEC-2 on platelets", RESEARCH-ER.JP, 1 January 2013 (2013-01-01), pages 1 - 5, XP093010683, Retrieved from the Internet <URL:https://research-er.jp/projects/view/106336>> [retrieved on 20221223] * |
| MENG DANYANG, LUO MAN, LIU BEIBEI: "The Role of CLEC-2 and Its Ligands in Thromboinflammation", FRONTIERS IN IMMUNOLOGY, vol. 12, no. 688643, pages 1 - 9, XP093010598, DOI: 10.3389/fimmu.2021.688643 * |
| NAGATA MAKOTO: "Establishment of a method for measuring plasma sCLEC-2 and its clinical application aiming to prevent arterial thrombosis", GRANTS-IN-AID FOR SCIENTIFIC RESEARCH, 1 January 2013 (2013-01-01), pages 1 - 4, XP093010678 * |
| NISHIGAKI AKISATO, ICHIKAWA YUHUKO, EZAKI MINORU, YAMAMOTO AKITAKA, SUZUKI KENJI, TACHIBANA KEI, KAMON TOSHITAKA, HORIE SHOTARO, M: "Soluble C-Type Lectin-Like Receptor 2 Elevation in Patients with Acute Cerebral Infarction", JOURNAL OF CLINICAL MEDICINE, vol. 10, no. 3408, pages 1 - 8, XP093010596, DOI: 10.3390/jcm10153408 * |
| SUZUKI-INOUE KATSUE, INOUE OSAMU, OZAKI YUKIO: "Novel platelet-activating receptor CLEC-2 from discovery to prospects", JAPANESE JOURNAL OF THROMBOSIS AND HEMOSTASIS, vol. 22, no. 6, 1 December 2011 (2011-12-01), pages 348 - 362, XP093010592 * |
| SUZUKI-INOUE KATSUE: "An overview of the novel platelet activation receptor CLEC-2", JOURNAL OF THROMBOSIS AND HEMOSTASIS, vol. 20, no. 4, 1 January 2009 (2009-01-01), pages 401 - 405, XP093010676 * |
| Y. YAMASHITA ET AL., THROMBOSIS RESEARCH, vol. 178, 2019, pages 54 - 58 |
Also Published As
| Publication number | Publication date |
|---|---|
| KR20240017001A (ko) | 2024-02-06 |
| EP4350350A1 (en) | 2024-04-10 |
| JPWO2022255349A1 (ja) | 2022-12-08 |
| CN117769652A (zh) | 2024-03-26 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| D’Angelo et al. | Evaluation of a new rapid quantitative D-dimer assay in patients with clinically suspected deep vein thrombosis | |
| JP6018923B2 (ja) | 敗血症の予後の予測方法 | |
| CN101960308A (zh) | 急性肾损伤及预后推测用生物标记物以及其用途 | |
| Cai et al. | Predictive value of phosphorylated axonal neurofilament subunit H for clinical outcome in patients with acute intracerebral hemorrhage | |
| US20230168260A1 (en) | Method for measuring platelet activation based on soluble clec-2 and platelet count | |
| WO2009087190A1 (en) | Means and methods for assessing the risk of patients presenting to emergency units based on gdf-15 | |
| JP2009539080A (ja) | 急性冠状動脈症候群のリスクを有する個体の識別のためのmrp8/14レベルの使用 | |
| JP5221333B2 (ja) | 意識障害患者における病態の検出方法及び検出用キット | |
| JP5715636B2 (ja) | 循環系事象と虚血性事象を鑑別するためのNT−proANPおよびSFlt−1 | |
| JP2008547002A (ja) | Nr2ペプチドに基づく脳血管イベントを診断、及び治療する方法 | |
| WO2022255349A1 (ja) | 可溶型clec2を用いた出血性脳卒中のリスク評価法 | |
| Kong et al. | Plasma level of D-dimer is an independent diagnostic biomarker for deep venous thrombosis in patients with ischemic stroke | |
| WO2022255348A1 (ja) | 可溶型clec2を用いた急性脳血管障害のリスク評価方法 | |
| JPWO2012067151A1 (ja) | CartilageAcidicProtein1蛋白質による脳梗塞の検査方法 | |
| WO2022154045A1 (ja) | 可溶型clec2を用いた癌患者における血栓症リスクの予測方法 | |
| JP2011237402A (ja) | ガレクチン−3結合蛋白質による脳梗塞の検査方法 | |
| Abdullah et al. | Diagnostic Value of D-Dimer’s Serum Level in Patients with Cerebral Venous Thrombosis | |
| GB2563415A (en) | Combinations for use in stroke diagnosis | |
| JP7419341B2 (ja) | 心房細動の評価における循環DKK3(Dickkopf関連タンパク質3) | |
| JPWO2012067152A1 (ja) | EndothelialProteinCReceptor蛋白質による脳梗塞の検査方法 | |
| RU2602914C1 (ru) | Способ оценки степени тяжести воспалительных заболеваний органов малого таза | |
| JP2008516218A (ja) | 急性冠症候群の疑いを除外するinvitro診断方法 | |
| JP2024027767A (ja) | 可溶型clec2を用いた血小板減少性疾患の診断法 | |
| JP2023519654A (ja) | 脳卒中の評価のためのret(トランスフェクション再編成) | |
| Hsiao et al. | D-dimer assay not adequate for spontaneous intracranial hemorrhage screening |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 22816095 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2023525850 Country of ref document: JP |
|
| ENP | Entry into the national phase |
Ref document number: 20237044828 Country of ref document: KR Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2022816095 Country of ref document: EP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2022816095 Country of ref document: EP Effective date: 20240102 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2023135648 Country of ref document: RU |